
Neoangiogenesis after direct intramyocardial implantation of bone marrow-derived stem cells in a...
7
Central European Journal of Medicine Neoangiogenesis after direct intramyocardial implantation of bone marrow-derived stem cells in a patient with severe coronary artery disease ineligible for percutaneous or surgical revascularization * E-mail: [email protected] Received 6 September 2008; Accepted 20 March 2009 Abstract: Bone marrow-derived stem cells (BMSC) may be an alternative for the treatment of patients with severe coronary artery disease ineli- gible for either percutaneous or surgical revascularization. This case report presents a 65-year-old male patient with untreatable angina pectoris (Canadian Cardiovascular Society Class III) and severe coronary artery disease. A mixture of BMSC containing approximately 3x106 CD34+ cells was directly injected into preoperatively determined ischemic regions of the myocardium by median sternotomy. At baseline, at 3 months, and at 1 year of follow-up, echocardiography (demonstrating wall motions of 16 segments), single-photon emission computed tomography, and coronary angiography (at baseline and at 1 year) were performed to assess myocardial perfu- sion, left ventricular (LV) function and coronary anatomy. The patient reached Canadian Cardiovascular Society Class I after 6 months of cell implantation. The ejection fraction increased from 34% to 37% at the third month and 40% at 1 year of follow-up. At 1 year of follow-up, preoperatively akinetic mid-base septum and anteroseptal regions progressed to mild hipokinesia and severe hypokinetic mid-base-apical anterior regions and apical lateral-inferior regions became normokinesia. Single-photon emission computed tomog- raphy revealed a visible improvement in anterior and lateral segments at 1 year of follow-up. Coronary angiography showed newly developed collateral arteries at 1 year of follow-up. BMSC transplantation in a patient with severe coronary artery disease resulted in increase of LV ejection fraction, an increase of the perfusion of ischemic myocardial regions, and improvement in wall motion defects without any adverse events. © Versita Warsaw and Springer-Verlag Berlin Heidelberg. Keywords: Coronary artery disease • Stem cells • Myocardial regeneration • Angiogenesis • Myocardial injury 1 Department of Cardiovascular Surgery, Istanbul University, Istanbul Medical Faculty, 34093, Capa, Istanbul, Turkey 2 Department of Haematology, Istanbul University, Istanbul Medical Faculty, 34093, Capa, Istanbul, Turkey Bugra Harmandar 1* , Turkan Tansel 1 , Ertan Onursal 1 , Nuray Gurses 2 , Sevgi Besisik 2 , Deniz Sargin 2 Research Article 1. Introduction Myocardial stem cell transplantation has been suggested for the generation of new blood vessels (neoangiogenesis) in ischemic myocardium and might be useful in patients with severe coronary artery disease that are ineligible for other types of revascularization [1-4]. If the ischemic myocardial territory cannot be reached via transcoronary due to severe coronary artery disease, stem cells cannot be delivered by a percutaneous route. In such patients, transepicardial (intramyocardial) or transendocardial routes are used for stem cell transplantation [4-6]. In the present study, unselected bone marrow-derived stem cells were transplanted to the ischemic regions of myocardium via direct intramyocardial injection in a patient with severe coronary artery disease that was ineligible for other types of revascularization and was refractory to conventional medical treatments. Cent. Eur. J. Med. • 4(3) • 2009 • 279-285 DOI: 10.2478/s11536-009-0035-4 279
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of Neoangiogenesis after direct intramyocardial implantation of bone marrow-derived stem cells in a...

Central European Journal of Medicine
Neoangiogenesis after direct intramyocardial implantation of bone marrow-derived stem cells in a patient with severe coronary artery disease ineligible for percutaneous or surgical revascularization
* E-mail: [email protected]
Received 6 September 2008; Accepted 20 March 2009
Abstract: Bone marrow-derived stem cells (BMSC) may be an alternative for the treatment of patients with severe coronary artery disease ineli-gible for either percutaneous or surgical revascularization. This case report presents a 65-year-old male patient with untreatable angina pectoris (Canadian Cardiovascular Society Class III) and severe coronary artery disease. A mixture of BMSC containing approximately 3x106 CD34+ cells was directly injected into preoperatively determined ischemic regions of the myocardium by median sternotomy. At baseline, at 3 months, and at 1 year of follow-up, echocardiography (demonstrating wall motions of 16 segments), single-photon emission computed tomography, and coronary angiography (at baseline and at 1 year) were performed to assess myocardial perfu-sion, left ventricular (LV) function and coronary anatomy. The patient reached Canadian Cardiovascular Society Class I after 6 months of cell implantation. The ejection fraction increased from 34% to 37% at the third month and 40% at 1 year of follow-up. At 1 year of follow-up, preoperatively akinetic mid-base septum and anteroseptal regions progressed to mild hipokinesia and severe hypokinetic mid-base-apical anterior regions and apical lateral-inferior regions became normokinesia. Single-photon emission computed tomog-raphy revealed a visible improvement in anterior and lateral segments at 1 year of follow-up. Coronary angiography showed newly developed collateral arteries at 1 year of follow-up. BMSC transplantation in a patient with severe coronary artery disease resulted in increase of LV ejection fraction, an increase of the perfusion of ischemic myocardial regions, and improvement in wall motion defects without any adverse events.
© Versita Warsaw and Springer-Verlag Berlin Heidelberg.
Keywords: Coronary artery disease • Stem cells • Myocardial regeneration • Angiogenesis • Myocardial injury
1 Department of Cardiovascular Surgery, Istanbul University, Istanbul Medical Faculty, 34093, Capa, Istanbul, Turkey
2 Department of Haematology, Istanbul University, Istanbul Medical Faculty, 34093, Capa, Istanbul, Turkey
Bugra Harmandar1*, Turkan Tansel1, Ertan Onursal1, Nuray Gurses2, Sevgi Besisik2, Deniz Sargin2
Research Article
1. IntroductionMyocardial stem cell transplantation has been suggested for the generation of new blood vessels (neoangiogenesis) in ischemic myocardium and might be useful in patients with severe coronary artery disease that are ineligible for other types of revascularization [1-4]. If the ischemic myocardial territory cannot be reached via transcoronary due to severe coronary
artery disease, stem cells cannot be delivered by a percutaneous route. In such patients, transepicardial (intramyocardial) or transendocardial routes are used for stem cell transplantation [4-6]. In the present study, unselected bone marrow-derived stem cells were transplanted to the ischemic regions of myocardium via direct intramyocardial injection in a patient with severe coronary artery disease that was ineligible for other types of revascularization and was refractory to conventional medical treatments.
Cent. Eur. J. Med. • 4(3) • 2009 • 279-285 DOI: 10.2478/s11536-009-0035-4
279
Neoangiogenesis after direct intramyocardial implantation of bone marrow-derived stem cells in a patient with severe coronary artery
disease ineligible for percutaneous or surgical revascularization
2. Material and MethodsOne patient with severe coronary artery disease who was ineligible for surgical or percutaneous revascularization was enrolled in the study. Pre and postoperative data regarding myocardial function and perfusion was assessed and compared with echocardiography, myocardial perfusion scintigraphy and coronary angiography.
2.1. Preparation of stem cellsOne day before the operation, 40 ml of bone marrow was aspirated from the iliac crest, split into four parts and transferred into 50-ml polypropylene centrifuge tubes containing 25 ml of Ficoll. Following centrifugation at 1050 x g for 20 min at 10°C, the buffy-coat layer was collected and mixed with 50 ml of stem cell growth medium. After centrifugation at 544 x g for 10 min at 10°C, the supernatant was discarded and the pellet was resuspended in 50 ml of stem cell growth medium. After a second centrifugation, the pellet was collected and resuspended in 15 ml of stem cell growth medium, put into a Teflon bag, and incubated overnight. The solution was transferred back to a 50-ml polypropylene centrifuge tube and centrifuged at 544 x g for 10 min at 10°C. The supernatant was discarded and the pellet was mixed with 15 ml 0.9% saline. Microbiologic testing confirmed that sample was sterile (i.e., not contaminated with microorganisms). Cell numbers were counted by using CD34 [Anti-HPCA-2] PE 345802 and CD45 FITC 345808. Cell viability was tested by microscopic examination (Table 1).
2.2. Stem cell implantationThe operation was performed through median sternotomy. Intraoperatively, the LAD coronary artery was found to be very thin and poorly diffused with stiff plaques. The right coronary artery was rudimentary and underdeveloped. The physical characteristics of the LAD and the radiological image showing inadequate distal
filling indicated that the coronary artery was not operable. Coronary artery bypass grafting was not performed.
Nine ml of mononuclear stem cell suspension was injected into the anterior, anterolateral, apical regions of the left ventricle and around the distal LAD. The areas of injection were preoperatively determined to be ischemic according to the results of myocardial perfusion scintigraphy. For each transepicardial injection, 0.5 ml of suspension was injected 2 mm into the external surface of the myocardium.
3. ResultsThe patient was a 65-year-old male suffering from chronic angina pectoris that had been gradually worsening for the past 5 years. At the start of this study, he was in Canadian Cardiovascular Society (CCS) Class III despite medical treatment with long-acting nitrates, b-blockers, and calcium channel agents. He had a history of smoking and peripheral arterial occlusive disease. Coronary angiography revealed a total occlusion in left anterior descending (LAD) coronary artery with inadequate distal filling after branching to a thin diagonal artery and 95% stenosis in a rudimentary right coronary artery. The circumflex coronary artery was dominant and appeared to be normal (Figure 1). Nuclear imaging (gated technetium-99m single-photon emission computed tomography [SPECT]) revealed ischemia in the anterior, anterolateral, and inferior regions of left ventricle. The patient was considered ineligible for percutaneous or surgical revascularization by cardiologists. Despite the angiography results, the cardiac surgery team sought a suitable area of the LAD for coronary bypass grafting. Implantation of bone marrow-derived stem cells and coronary artery bypass grafting for LAD were therefore considered. Accordingly, median sternotomy was selected as the surgical approach.
Echocardiography for 16 segments of left ventricle was performed using the protocol suggested by the American Society of Echocardiography (7). Segmental wall motion defects were detected and compared with subsequent echocardiographies postoperatively on day 7, month 3, and month 12 (Table 2). Left ventricular ejection fraction, left ventricular end-diastolic, end-systolic diameter and volumes were calculated (Table 3).
The patient underwent SPECT myocardial perfusion scintigraphy following a 1-day rest. The perfusion of each segment was classified (Table 4) as normal perfusion, mildly decreased perfusion, moderately decreased perfusion, severely decreased perfusion and aperfusion. Preoperative SPECT data were compared
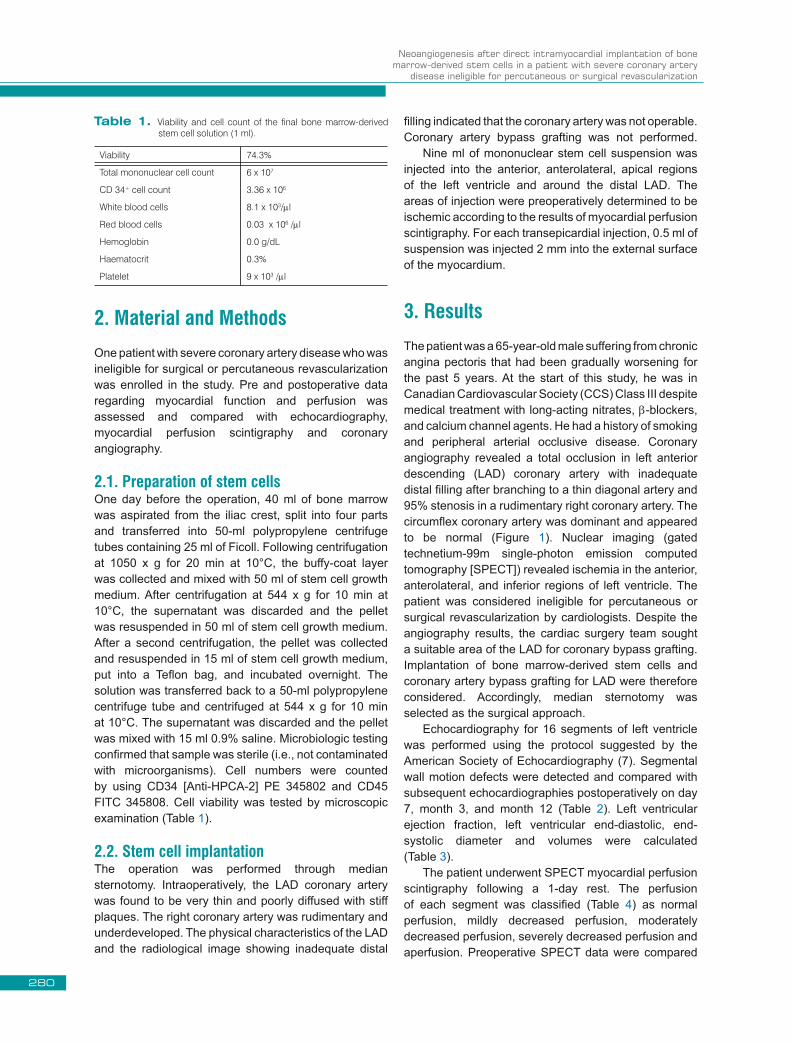
Viability 74.3%
Total mononuclear cell count 6 x 107
CD 34+ cell count 3.36 x 106
White blood cells 8.1 x 103/ml
Red blood cells 0.03 x 106 /ml
Hemoglobin 0.0 g/dL
Haematocrit 0.3%
Platelet 9 x 103 /ml
Table 1. Viability and cell count of the final bone marrow-derived stem cell solution (1 ml).
280

B. Harmandar et al.
Preoperative Postoperative 7th day Postoperative 3rd month Postoperative 12th month
Anterior Mid Severe hypokinetic Severe hypokinetic Mild Hypokinetic Normokinetic
Base Severe hypokinetic Severe hypokinetic Mild Hypokinetic Normokinetic
Apical Severe hypokinetic Severe hypokinetic Mild Hypokinetic Normokinetic
Antero-septal Mid Akinetic Dyskinetic Mild Hypokinetic Mild Hypokinetic
Base Akinetic Akinetic Mild Hypokinetic Mild Hypokinetic
Apical Normokinetic Normokinetic Normokinetic Normokinetic
Septum Mid Akinetic Dyskinetic Mild Hypokinetic Mild Hypokinetic
Base Akinetic Akinetic Mild Hypokinetic Mild Hypokinetic
Lateral Mid Normokinetic Normokinetic Normokinetic Normokinetic
Base Normokinetic Normokinetic Normokinetic Normokinetic
Apical Severe hypokinetic Severe hypokinetic Severe hypokinetic Normokinetic
İnferior Mid Normokinetic Normokinetic Normokinetic Normokinetic
Base Normokinetic Normokinetic Normokinetic Normokinetic
Apical Severe hypokinetic Severe hypokinetic Severe hypokinetic Normokinetic
Posterior Mid Normokinetic Normokinetic Normokinetic Normokinetic
Base Normokinetic Normokinetic Normokinetic Normokinetic
Table 2. Preoperative and postoperative echocardiographic data demonstrating wall motion status for 16 segments of the left ventricle.
Preoperative Postoperative 7th day Postoperative 3rd month Postoperative 12th month
EF (%) 34 34 37 40
LVEDD (cm) 5,4 5,4 5,4 5,4
LVESD (cm) 3,6 3,6 3,5 3,6
LVEDV (ml) 141 141 141 141
LVESV (ml) 54 54 48 52
Table 3. Preoperative and postoperative echocardiographic data demonstrating ejection fraction, end-diastolic, and end-systolic diameters and volumes of the left ventricle.
EF: Ejection fraction, LVEDD: Left ventricular end-diastolic diameter, LVESD: Left ventricular end-systolic diameter, LVEDV: Left ventricular end-diastolic volume, LVESV: Left ventricular end-systolic volume.
Figure 1. Preoperative and postoperative (month 12) angiographies. a. Total occlusion in left anterior descending (LAD) coronary artery with inadequate distal filling. b. Thin diagonal artery. c. Dominant and normal circumflex coronary artery. *Newly developed widespread collateral arteries.
281

Neoangiogenesis after direct intramyocardial implantation of bone marrow-derived stem cells in a patient with severe coronary artery
disease ineligible for percutaneous or surgical revascularization
with postoperative scintigraphies at three months and 1 year after surgery (Figure 2).
The results of postoperative echocardiography (day 7 and months 3 and 12), 99mTc-SPECT myocardial perfusion scintigraphy (months 3 and 12), 24-hour ECG monitoring (day 7 and months 3 and 12), and coronary angiography (month 12) were compared with preoperative data.
No complications were encountered intraoperatively. The patient’s hemodynamics were stable, and there was no bleeding from the sites of injection, cardiac arrhythmia, fever, or pleural effusion during hospitalization. The postoperative early period was uneventful. Comparison
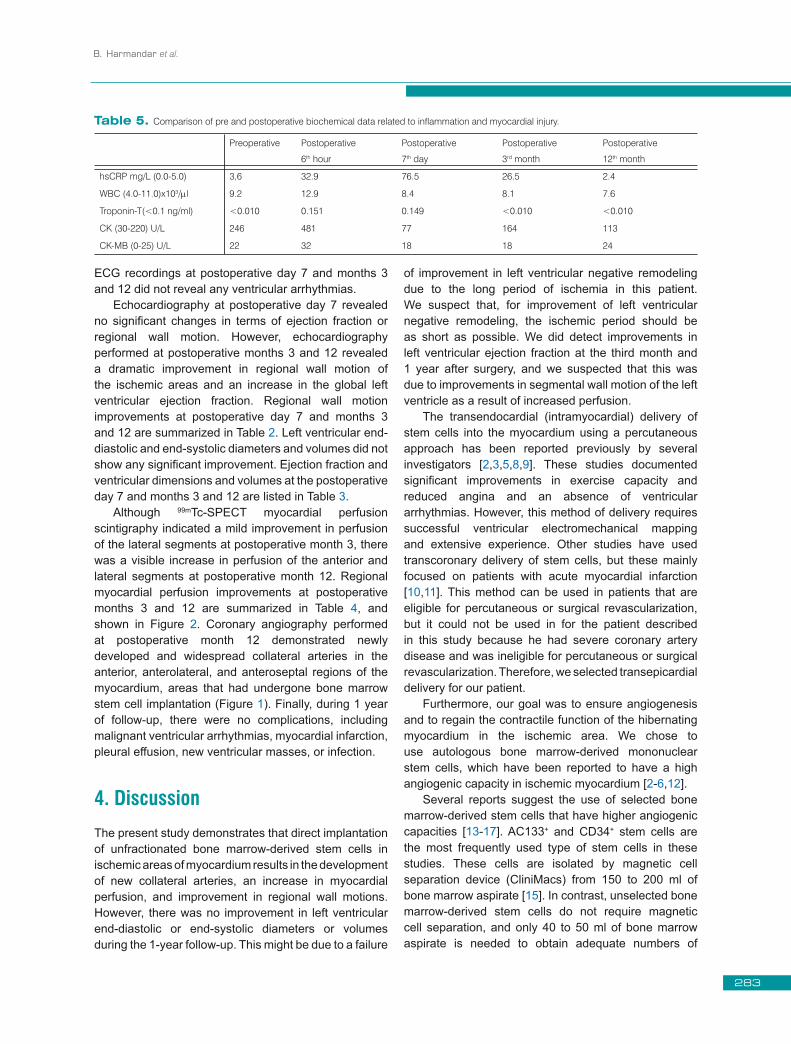
of pre- and post-operative laboratory results, including troponin-T, creatine kinase, and creatine kinase – MB levels, indicated a lack of myocardial injury. C-reactive protein levels, however, increased until postoperative day 7 and then decreased gradually. Leukocyte counts were within normal ranges. Blood cultures were sterile and no infection was detected. Sterile inflammation due to cell inoculation was suspected. Biochemical data related to inflammation and myocardial injury are shown in Table 5. The patient was discharged at postoperative day 10 with a good hemodynamic status. Six months after cell implantation, the patient had improved from CCS angina class 3 to class 1. Postoperative 24-hour
Preoperative Postoperative 3rd month Postoperative 12th month
Anterior Mid Normal Perfusion Normal Perfusion Normal Perfusion
Base Normal Perfusion Normal Perfusion Normal Perfusion
Apical Aperfusion Aperfusion Mild hipoperfusion
Antero-lateral Mid Aperfusion Severe hipoperfusion Mild hipoperfusion
Base Normal Perfusion Normal Perfusion Normal Perfusion
Apical Aperfusion Severe hipoperfusion Mild hipoperfusion
Septum Mid Normal Perfusion Normal Perfusion Normal Perfusion
Base Normal Perfusion Normal Perfusion Normal Perfusion
Apical Severe hipoperfusion Mild hipoperfusion Normal Perfusion
Lateral Mid Aperfusion Severe hipoperfusion Mild hipoperfusion
Base Aperfusion Severe hipoperfusion Mild hipoperfusion
Apical Aperfusion Severe hipoperfusion Mild hipoperfusion
İnferior Mid Normal Perfusion Normal Perfusion Normal Perfusion
Base Normal Perfusion Normal Perfusion Normal Perfusion
Apical Aperfusion Aperfusion Mild hipoperfusion
İnfero-lateral Mid Aperfusion Severe hipoperfusion Mild hipoperfusion
Base Normal Perfusion Normal Perfusion Normal Perfusion
Apical Aperfusion Severe hipoperfusion Mild hipoperfusion
Table 4. Preoperative and postoperative SPECT data demonstrating perfusion status of the left ventricle.
Figure 2. Preoperative and postoperative months 3 - 12 99mTc-MIBI myocardial perfusion scintigraphies. At month 3, there was a mild improvement in perfusion of the lateral segments, and at month 12, there was a significant increase in perfusion of the anterior and lateral segments.
282
B. Harmandar et al.
ECG recordings at postoperative day 7 and months 3 and 12 did not reveal any ventricular arrhythmias.
Echocardiography at postoperative day 7 revealed no significant changes in terms of ejection fraction or regional wall motion. However, echocardiography performed at postoperative months 3 and 12 revealed a dramatic improvement in regional wall motion of the ischemic areas and an increase in the global left ventricular ejection fraction. Regional wall motion improvements at postoperative day 7 and months 3 and 12 are summarized in Table 2. Left ventricular end-diastolic and end-systolic diameters and volumes did not show any significant improvement. Ejection fraction and ventricular dimensions and volumes at the postoperative day 7 and months 3 and 12 are listed in Table 3.
Although 99mTc-SPECT myocardial perfusion scintigraphy indicated a mild improvement in perfusion of the lateral segments at postoperative month 3, there was a visible increase in perfusion of the anterior and lateral segments at postoperative month 12. Regional myocardial perfusion improvements at postoperative months 3 and 12 are summarized in Table 4, and shown in Figure 2. Coronary angiography performed at postoperative month 12 demonstrated newly developed and widespread collateral arteries in the anterior, anterolateral, and anteroseptal regions of the myocardium, areas that had undergone bone marrow stem cell implantation (Figure 1). Finally, during 1 year of follow-up, there were no complications, including malignant ventricular arrhythmias, myocardial infarction, pleural effusion, new ventricular masses, or infection.
4. DiscussionThe present study demonstrates that direct implantation of unfractionated bone marrow-derived stem cells in ischemic areas of myocardium results in the development of new collateral arteries, an increase in myocardial perfusion, and improvement in regional wall motions. However, there was no improvement in left ventricular end-diastolic or end-systolic diameters or volumes during the 1-year follow-up. This might be due to a failure
of improvement in left ventricular negative remodeling due to the long period of ischemia in this patient. We suspect that, for improvement of left ventricular negative remodeling, the ischemic period should be as short as possible. We did detect improvements in left ventricular ejection fraction at the third month and 1 year after surgery, and we suspected that this was due to improvements in segmental wall motion of the left ventricle as a result of increased perfusion.
The transendocardial (intramyocardial) delivery of stem cells into the myocardium using a percutaneous approach has been reported previously by several investigators [2,3,5,8,9]. These studies documented significant improvements in exercise capacity and reduced angina and an absence of ventricular arrhythmias. However, this method of delivery requires successful ventricular electromechanical mapping and extensive experience. Other studies have used transcoronary delivery of stem cells, but these mainly focused on patients with acute myocardial infarction [10,11]. This method can be used in patients that are eligible for percutaneous or surgical revascularization, but it could not be used in for the patient described in this study because he had severe coronary artery disease and was ineligible for percutaneous or surgical revascularization. Therefore, we selected transepicardial delivery for our patient.
Furthermore, our goal was to ensure angiogenesis and to regain the contractile function of the hibernating myocardium in the ischemic area. We chose to use autologous bone marrow-derived mononuclear stem cells, which have been reported to have a high angiogenic capacity in ischemic myocardium [2-6,12].
Several reports suggest the use of selected bone marrow-derived stem cells that have higher angiogenic capacities [13-17]. AC133+ and CD34+ stem cells are the most frequently used type of stem cells in these studies. These cells are isolated by magnetic cell separation device (CliniMacs) from 150 to 200 ml of bone marrow aspirate [15]. In contrast, unselected bone marrow-derived stem cells do not require magnetic cell separation, and only 40 to 50 ml of bone marrow aspirate is needed to obtain adequate numbers of
Preoperative Postoperative
6th hour
Postoperative
7th day
Postoperative
3rd month
Postoperative
12th month
hsCRP mg/L (0.0-5.0) 3,6 32.9 76.5 26.5 2.4
WBC (4.0-11.0)x103/ml 9.2 12.9 8.4 8.1 7.6
Troponin-T(<0.1 ng/ml) <0.010 0.151 0.149 <0.010 <0.010
CK (30-220) U/L 246 481 77 164 113
CK-MB (0-25) U/L 22 32 18 18 24
Table 5. Comparison of pre and postoperative biochemical data related to inflammation and myocardial injury.
283

Neoangiogenesis after direct intramyocardial implantation of bone marrow-derived stem cells in a patient with severe coronary artery
disease ineligible for percutaneous or surgical revascularization
mononuclear stem cells. Previous studies reported that neoangiogenesis can be induced using 4 x 106 to 2.2 x 109 stem cells [2-6,14,15]. Similarly, in the current study, we used approximately 3 x 106 cells, but in contrast to the previous studies where the cells were contained in a 10-ml suspension, the stem cell solution used here could be concentrated to a volume of 1 ml. However, with such a low volume, it is difficult to inject equal amounts into large areas of the left ventricle. Finally, unlike the previous preparations of magnetically selected cells, the cell suspension used here contained several different types of stem cells that could have contributed to primarily to neoangiogenesis but also to myocardial regeneration and contractility [12,13]. Meanwhile, several reports have demonstrated that there are no significant differences between selected and unselected bone marrow-derived stem cells [10,18-20]. Thus, unselected bone marrow-derived stem cells may also be preferred for promoting neoangiogenesis because of their easy preparation and relative cost effectiveness.
Recent studies report the use of minimally invasive techniques for the injection of stem cells into myocardium [15-16]. Because we wanted to perform coronary bypass grafting to the target vessel, we planned on using median
sternotomy. However, intraoperatively, the coronary arteries were judged to be ineligible for coronary bypass grafting, so we performed only stem cell implantation.
In conclusion, we show that the direct implantation of unfractionated bone marrow-derived stem cells in ischemic areas of myocardium is feasible for inducing therapeutic angiogenesis and improving myocardial perfusion. The preliminary results presented here are in agreement with previous studies in which stem cells were delivered via transepicardial [6,15,16] or transendocardial [2,3,5] routes. The uncomplicated postoperative period of this patient suggests that the procedure is safe. These findings indicate that transepicardial implantation of bone marrow-derived stem cells is a potential alternative in patients with severe ischemic heart disease that are ineligible for surgical or interventional revascularization.
References
[1] Wollert KC, Drexler H. Clinical applications of stem cells for the heart. Circ Res 2005 Feb 4;96(2):151-63
[2] Fuchs S, Satler LF, Kornowski R, Okubagzi P, Weisz G, Baffour R, Waksman R, Weissman NJ, Cerqueira M, Leon MB, Epstein SE. Cathater-based autologous bone marrow myocardial injection in no-option patients with advanced coronary artery disease: a feasibility study. J Am Coll Cardiol 2003 May 21;41(10):1721-4
[3] Perin EC, Dohmann HF, Borojevic R, Silva SA, Sousa AL, Silva GV, Mesquita CT, Belém L, Vaughn WK, Rangel FO, Assad JA, Carvalho AC, Branco RV, Rossi MI, Dohmann HJ, Willerson JT. Improved exercise capacity and ischemia 6 and 12 months after transendocardial injection of autologous bone marrow mononuclear cells for ischemic cardiomyopathy. Circulation 2004 Sep 14;110(11 Suppl 1):II213-8
[4] Perin EC, Dohmann HF, Borojevic R, Silva SA, Sousa AL, Mesquita CT, Rossi MI, Carvalho AC, Dutra HS, Dohmann HJ, Silva GV, Belém L, Vivacqua R, Rangel FO, Esporcatte R, Geng YJ, Vaughn WK, Assad JA, Mesquita ET, Willerson JT. Transendocardial, autologous bone marrow cell transplantation for severe, chronic ischemic heart
failure. Circulation 2003 May 13;107(18):2294-302[5] Tse HF, Kwong YL, Chan JK, Lo G, Ho CL, Lau
CP. Angiogenesis in ischaemic myocardium by intramyocardial autologous bone marrow mononuclear cell implantation. Lancet 2003 Jan 4;361(9351):47
[6] Hamano K, Nishida M, Hirata K, Mikamo A, Li TS, Harada M, Miura T, Matsuzaki M, Esato K. Local implantation of autologous bone marrow cells for therapeutic angiogenesis in patients with ischemic heart disease: clinical trial and preliminary results. Jpn Circ J 2001 Sep;65(9):845-7
[7] Schiller NB, Shah PM, Crawford M, DeMaria A, Devereux R, Feigenbaum H, Gutgesell H, Reichek N, Sahn D, Schnittger I, et al. Recommendations for quantitation of the left ventricle by two-dimensional echocardiography. American Society of Echocardiography Committee on Standards, Subcommittee on Quantitation of Two-Dimensional Echocardiograms. J Am Soc Echocardiogr. 1989 Sep-Oct;2(5):358-67
[8] Beeres SL, Bax JJ, Kaandorp TA, Zeppenfeld K, Lamb HJ, Dibbets-Schneider P, Stokkel MP, Fibbe WE, de Roos A, van der Wall EE, Schalij MJ, Atsma DE. Usefulness of intramyocardial injection of autologous bone marrow-derived mononuclear cells
284

B. Harmandar et al.
in patients with severe angina pectoris and stress-induced myocardial ischemia. Am J Cardiol. 2006 May 1;97(9):1326-31
[9] Briguori C, Reimers B, Sarais C, Napodano M, Pascotto P, Azzarello G, Bregni M, Porcellini A, Vinante O, Zanco P, Peschle C, Condorelli G, Colombo A. Direct intramyocardial percutaneous delivery of autologous bone marrow in patients with refractory myocardial angina. Am Heart J. 2006 Mar;151(3):674-80
[10] Schächinger V, Assmus B, Britten MB, Honold J, Lehmann R, Teupe C, Abolmaali ND, Vogl TJ, Hofmann WK, Martin H, Dimmeler S, Zeiher AM. Transplantation of progenitor cells and regeneration enhancement in acute myocardial infarction: final one-year results of the TOPCARE-AMI Trial. J Am Coll Cardiol. 2004 Oct 19;44(8):1690-9.
[11] Meyer GP, Wollert KC, Lotz J, Steffens J, Lippolt P, Fichtner S, Hecker H, Schaefer A, Arseniev L, Hertenstein B, Ganser A, Drexler H. Intracoronary bone marrow cell transfer after myocardial infarction: eighteen months' follow-up data from the randomized, controlled BOOST (BOne marrOw transfer to enhance ST-elevation infarct regeneration) trial. Circulation. 2006 Mar 14;113(10):1287-94
[12] Orlic D, Kajstura J, Chimenti S, Jakoniuk I, Anderson SM, Li B, Pickel J, McKay R, Nadal-Ginard B, Bodine DM, Leri A, Anversa P. Bone marrow cells regenerate infarcted myocardium. Nature 2001 Apr 5;410(6829):701-5.
[13] Stamm C, Westphal B, Kleine HD, Petzsch M, Kittner C, Klinge H, Schümichen C, Nienaber CA, Freund M, Steinhoff G. Autologous bone-marrow stem-cell transplantation for myocardial regeneration. Lancet 2003 Jan 4;361(9351):45-6.
[14] Stamm C, Kleine HD, Choi YH, Dunkelmann S, Lauffs JA, Lorenzen B, David A, Liebold A, Nienaber C, Zurakowski D, Freund M, Steinhoff G. Intramyocardial delivery of CD133+ bone marrow cells and coronary artery bypass grafting for chronic ischemic heart disease: safety and efficacy studies. J Thorac Cardiovasc Surg. 2007 Mar;133(3):717-25
[15] Pompilio G, Steinhoff G, Liebold A, Pesce M, Alamanni F, Capogrossi MC, Biglioli P. Direct minimally invasive intramyocardial injection of bone marrow-derived AC133+ stem cells in patients with refractory ischemia: preliminary results. Thorac Cardiovasc Surg. 2008 Mar;56(2):71-6
[16] Klein HM, Ghodsizad A, Marktanner R, Poll L, Voelkel T, Mohammad Hasani MR, Piechaczek C, Feifel N, Stockschlaeder M, Burchardt ER, Kar BJ, Gregoric I, Gams E. Intramyocardial implantation of CD133+ stem cells improved cardiac function without bypass surgery. Heart Surg Forum. 2007;10(1):E66-9
[17] Archundia A, Aceves JL, López-Hernández M, Alvarado M, Rodriguez E, Díaz Quiroz G, Páez A, Rojas FM, Montaño LF. Direct cardiac injection of G-CSF mobilized bone-marrow stem-cells improves ventricular function in old myocardial infarction. Life Sci. 2005 Dec 5;78(3):279-83. Epub 2005 Sep 23
[18] Strauer BE, Brehm M, Zeus T, Köstering M, Hernandez A, Sorg RV, Kögler G, Wernet P. Repair of infarcted myocardium by autologous intracoronary mononuclear bone marrow cell transplantation in humans. Circulation. 2002 Oct 8;106(15):1913-8
[19] Fernández-Avilés F, San Román JA, García-Frade J, Fernández ME, Peñarrubia MJ, de la Fuente L, Gómez-Bueno M, Cantalapiedra A, Fernández J, Gutierrez O, Sánchez PL, Hernández C, Sanz R, García-Sancho J, Sánchez A. Experimental and clinical regenerative capability of human bone marrow cells after myocardial infarction. Circ Res. 2004 Oct 1;95(7):742-8. Epub 2004 Sep 9
[20] Kuethe F, Richartz BM, Sayer HG, Kasper C, Werner GS, Höffken K, Figulla HR. Lack of regeneration of myocardium by autologous intracoronary mononuclear bone marrow cell transplantation in humans with large anterior myocardial infarctions. Int J Cardiol. 2004 Oct;97(1):123-7
285




















