Near-total human face transplantation for a severely disfigured patient in the USA
7
Articles www.thelancet.com Vol 374 July 18, 2009 203 Near-total human face transplantation for a severely disfigured patient in the USA Maria Siemionow, Frank Papay, Daniel Alam, Steven Bernard, Risal Djohan, Chad Gordon, Mark Hendrickson, Robert Lohman, Bijan Eghtesad, Kathy Coffman, Eric Kodish, Carmen Paradis, Robin Avery, John Fung Summary Background Multiple reconstructive procedures are common for the reconstruction of complex facial deformities of skin, soft tissues, bony structures, and functional subunits, such as the nose, lips, and eyelids. However, the results have been unsatisfactory. An innovative approach entailing a single surgical procedure of face allograft transplantation is a viable alternative and gives improved results. Methods On Dec 9, 2008, a 45-year-old woman with a history of severe midface trauma underwent near-total face transplantation in which 80% of her face was replaced with a tailored composite tissue allograft. We addressed issues of immunosuppressive therapy, psychological and ethical outcomes, and re-integration of the patient into society. Findings After the operation, the patient did well physically and psychologically, and tolerated immunosuppression without any major complication. Routine biopsy on day 47 after transplantation showed rejection of graft mucosa; however, a single bolus of corticosteroids reversed rejection. During the first 3 weeks after transplantation, the patient accepted her new face; 6 months after surgery, the functional outcome has been excellent. In contrast to her status before transplantation, the patient can now breathe through her nose, smell, taste, speak intelligibly, eat solid foods, and drink from a cup. Interpretation We show the feasibility of reconstruction of severely disfigured patients in a single surgical procedure using composite face allotransplantation. Therefore, this should be taken in consideration as an early option for severely disfigured patients. Funding None. Introduction The face is the physical foundation of attractiveness and identity, and has a major role in social interactions. Consequently, severe facial disfigurement—traumatic, inborn, or acquired—exposes a person to the stigma of being different. Therefore, the person becomes socially and emotionally withdrawn. However, this is an anatomical problem, not a technical one. The human face is unique in structure and function, and in the specificity of its tissues and functional subunits, such as the nose, lips, and eyelids—none of which can be borrowed from another part of the body. To address the technical challenges to give disfigured patients normal- looking faces, we devoted the past 20 years to the study of the surgical feasibility and immunological aspects of different composite tissue allografts, including limb and face transplants. 1–12 We report the results at 6 months after surgery of this near-total face transplantation in the USA, and address the functional, psychological, and ethical challenges encountered. Methods The patient The patient was a 45-year-old woman who, in September, 2004, sustained severe facial trauma to her midface from a close-range shotgun blast (figure 1). Her facial deformities included absence of nose, nasal lining and underlying bone; contracted remnants of the upper lip; loss of orbicularis oris and orbicularis oculi muscle functions; distorted and scarred lower eyelids with ectropion; right-eye enucleation supported by eye prosthesis; and facial nerve deficit manifested in the lack of midface function (figure 2). As a result of this trauma, the patient could not drink from a cup and her speech was slurred because of the palatal defect. Destruction of her nasal passage deprived her of the sense of smell. She could not eat solid foods, and received most of her nutrition via percutaneous epigastric tube. 2 months after trauma, she was referred to the Cleveland Clinic (OH, USA) for conventional reconstruction of her serious facial disfiguration, and she was informed of the complex reconstruction necessary to restore impaired structures and functions. Before face transplantation, the patient had undergone 23 major autologous reconstructive operations that included correction of: bone defect by free fibula and split-calvaria/rib grafts; soft-tissue defect by anterolateral free flap, temporalis muscle flap, paramedian forehead flap, and radial forearm free flap; and skin defect by multiple split-thickness skin grafts. Unfortunately, these operations failed to restore disfigured structures and functions. Therefore, the patient suffered humiliation in public situations. Lancet 2009; 374: 203–09 Published Online July 15, 2009 DOI:10.1016/S0140- 6736(09)61155-7 See Comment page 177 Cleveland Clinic, Cleveland, OH, USA (Prof M Siemionow MD); Dermatology and Plastic Surgery Institute (F Papay MD, S Bernard MD, R Djohan MD, C Gordon DO, M Hendrickson MD, R Lohman MD); Head and Neck Institute (D Alam MD); Digestive Disease Institute (B Eghtesad MD, Prof J Fung MD); Neurological Institute (K Coffman MD); Bioethics Department (Prof E Kodish MD, C Paradis MD); Medicine Institute (Prof R Avery MD); and Surgical Institute, Cleveland, OH, USA (Prof J Fung) Correspondence to: Prof Maria Siemionow, Cleveland Clinic, 9500 Euclid Avenue, Desk A-60, Cleveland, OH 44195, USA [email protected]
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Near-total human face transplantation for a severely disfigured patient in the USA

Articles
www.thelancet.com Vol 374 July 18, 2009 203
Near-total human face transplantation for a severely disfi gured patient in the USAMaria Siemionow, Frank Papay, Daniel Alam, Steven Bernard, Risal Djohan, Chad Gordon, Mark Hendrickson, Robert Lohman, Bijan Eghtesad, Kathy Coff man, Eric Kodish, Carmen Paradis, Robin Avery, John Fung
SummaryBackground Multiple reconstructive procedures are common for the reconstruction of complex facial deformities of skin, soft tissues, bony structures, and functional subunits, such as the nose, lips, and eyelids. However, the results have been unsatisfactory. An innovative approach entailing a single surgical procedure of face allograft transplantation is a viable alternative and gives improved results.
Methods On Dec 9, 2008, a 45-year-old woman with a history of severe midface trauma underwent near-total face transplantation in which 80% of her face was replaced with a tailored composite tissue allograft. We addressed issues of immunosuppressive therapy, psychological and ethical outcomes, and re-integration of the patient into society.
Findings After the operation, the patient did well physically and psychologically, and tolerated immunosuppression without any major complication. Routine biopsy on day 47 after transplantation showed rejection of graft mucosa; however, a single bolus of corticosteroids reversed rejection. During the fi rst 3 weeks after transplantation, the patient accepted her new face; 6 months after surgery, the functional outcome has been excellent. In contrast to her status before transplantation, the patient can now breathe through her nose, smell, taste, speak intelligibly, eat solid foods, and drink from a cup.
Interpretation We show the feasibility of reconstruction of severely disfi gured patients in a single surgical procedure using composite face allotransplantation. Therefore, this should be taken in consideration as an early option for severely disfi gured patients.
Funding None.
IntroductionThe face is the physical foundation of attractiveness and identity, and has a major role in social interactions. Consequently, severe facial disfi gurement—traumatic, inborn, or acquired—exposes a person to the stigma of being diff erent. Therefore, the person becomes socially and emotionally withdrawn. However, this is an anatomical problem, not a technical one. The human face is unique in structure and function, and in the specifi city of its tissues and functional subunits, such as the nose, lips, and eyelids—none of which can be borrowed from another part of the body. To address the technical challenges to give disfi gured patients normal-looking faces, we devoted the past 20 years to the study of the surgical feasibility and immunological aspects of diff erent composite tissue allografts, including limb and face transplants.1–12
We report the results at 6 months after surgery of this near-total face transplantation in the USA, and address the functional, psychological, and ethical challenges encountered.
MethodsThe patientThe patient was a 45-year-old woman who, in September, 2004, sustained severe facial trauma to her midface from a close-range shotgun blast (fi gure 1). Her facial
deformities included absence of nose, nasal lining and underlying bone; contracted remnants of the upper lip; loss of orbicularis oris and orbicularis oculi muscle functions; distorted and scarred lower eyelids with ectropion; right-eye enucleation supported by eye prosthesis; and facial nerve defi cit manifested in the lack of midface function (fi gure 2). As a result of this trauma, the patient could not drink from a cup and her speech was slurred because of the palatal defect. Destruction of her nasal passage deprived her of the sense of smell. She could not eat solid foods, and received most of her nutrition via percutaneous epigastric tube.
2 months after trauma, she was referred to the Cleveland Clinic (OH, USA) for conventional reconstruction of her serious facial disfi guration, and she was informed of the complex reconstruction necessary to restore impaired structures and functions. Before face transplantation, the patient had undergone 23 major autologous reconstructive operations that included correction of: bone defect by free fi bula and split-calvaria/rib grafts; soft-tissue defect by anterolateral free fl ap, temporalis muscle fl ap, paramedian forehead fl ap, and radial forearm free fl ap; and skin defect by multiple split-thickness skin grafts. Unfortunately, these operations failed to restore disfi gured structures and functions. Therefore, the patient suff ered humiliation in public situations.
Lancet 2009; 374: 203–09
Published OnlineJuly 15, 2009DOI:10.1016/S0140-6736(09)61155-7
See Comment page 177
Cleveland Clinic, Cleveland, OH, USA (Prof M Siemionow MD); Dermatology and Plastic Surgery Institute (F Papay MD, S Bernard MD, R Djohan MD, C Gordon DO, M Hendrickson MD, R Lohman MD); Head and Neck Institute (D Alam MD); Digestive Disease Institute (B Eghtesad MD, Prof J Fung MD); Neurological Institute (K Coff man MD); Bioethics Department (Prof E Kodish MD, C Paradis MD); Medicine Institute (Prof R Avery MD); and Surgical Institute, Cleveland, OH, USA (Prof J Fung)
Correspondence to:Prof Maria Siemionow, Cleveland Clinic, 9500 Euclid Avenue, Desk A-60, Cleveland, OH 44195, [email protected]

Articles
204 www.thelancet.com Vol 374 July 18, 2009
Almost 4 years after her trauma—in August, 2008—the patient was presented with the option of composite tissue allotransplantation as a last-attempt therapeutic alternative for reconstructing her face so that she would regain a normal appearance and potentially have some or all of her lost facial functions restored.
Institutional Review Board approved the face transplantation on Nov 15, 2004. Between that time and Dec 9, 2008, when we did the procedure, three partial face transplantations were reported.13–15 As part of the process for Institutional Review Board approval, the patient was comprehensively assessed by a multi disci-plinary team of specialists, including plastic surgeons, otolaryngo logists, transplant surgeons, anaesthesi-ologists, transplant psychia trists, bioethicists, dentists, transplant infectious-disease specialists, and immun-ologists. The assessment showed that the patient was psycho logically stable, ethically suitable and informed, and in satisfactory general health.
After the entire multidisciplinary team unanimously agreed to proceed with face allotransplantation, she was given informed consent that this is a potentially life-threatening procedure with serious complications, such as severe infections, diabetes, kidney failure, lymphoma, and bone necrosis. After we established that she fully understood the risks and benefi ts, the patient, in the presence of a witness and the face transplant project leader, signed the informed consent to proceed with face allograft transplantation. The act of signing was videorecorded.
After all the preliminary steps had been implemented, in the third quarter of 2008, the patient was listed with a local organ procurement organisation—LifeBanc of Cleveland (OH, USA)—which, on the basis of our protocol submitted in 2004, granted us approval in January, 2007, to do the procedure.
The donorThe donor was a brain-dead woman who matched the patient in age, race, and skin complexion. The transplant coordinator received from the donor’s family the informed consent to recover and transplant the donor’s face. The donor’s blood group was A and the recipient’s was AB. The donor and recipient shared two major human leucocyte antigens (HLA) (donor: HLA A 11,23; B 44,64; Cw 5,8; DR 7,16; DRw51; DQ5,9; recipient: HLA A 1,29; B 8,44; Cw 7,16; DR 7,17; DRw52; DQ2). The patient had no anti-HLA reactive antibodies and retrospective cross-match was negative. The donor was cytomegalovirus positive, and the recipient cyto megalovirus negative.
ProcedureThe face transplant was done in December, 2008. An eight-surgeon team, consisting of seven attending staff and one fellow, worked simultaneously in two operating rooms. One team prepared the recipient, while the second team recovered the donor facial allograft (fi gure 3). The entire procedure required 22 h.
Surgery on the recipient started with an outline of the template of required tissues from the donor, and with the revision of bilateral neck vessels of posterior facial veins and external jugular veins, and common facial, external carotid, and common carotid arteries. This part was undertaken to make sure that no vascular territories had been violated because of previous surgeries. Bilateral superfi cial parotid glands were then dissected to identify the facial nerve trunks. In preparation for donor allograft, inset the soft tissue, bones, and hardware such as plates and screws from previous reconstructions (including multiple cranial grafts) and autogenous bone grafts (including a free fi bula) were all removed.
Surgery on the donor started after we confi rmed that the recipient’s vascular territories were intact. Recovery of the graft proceeded according to the defect template tested in mock transplants in the cadaver laboratory, and reconfi rmation of the three-dimensional graft architecture and size was based on stereolythic print estimates from the CT angiogram.
Briefl y, the composite tissue facial allograft was pedicled on bilateral common facial arteries, external jugular veins, and left posterior facial vein. The allograft was designed to cover the recipient’s anterior craniofacial skeleton, and it included about 80% of the surface area of the anterior face. It was based on a Le Fort III composite tissue allograft containing total nose, lower eyelids, upper lip, total infraorbital fl oor, bilateral zygomas, and anterior maxilla with incisors, and included total alveolus, anterior
A B
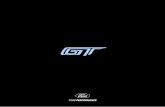
Figure 1: CT scan(A) Gunshot injury to the patient’s face before surgery, showing substantial damage of the entire front and midface skeleton, with remnants of infraorbital fl oor and nasal, zygomatic, and maxillary bones mixed with the metal pieces. (B) At 3 months after transplantation, showing complete restoration of the craniofacial defect by replacement of all missing bony components of facial skeleton and soft tissues of the patient with the composite facial allograft from the donor.

Articles
www.thelancet.com Vol 374 July 18, 2009 205
hard palate, and bilateral parotid glands. The graft was then transferred to the recipient for the fi nal inset. The allotransplant inset to the recipient started with the adjustments of a Le Fort III composite allograft to the recipient’s skeletal defect. Once bone components of the facial allograft were secured and stable, we then proceeded with bilateral microvascular anastomoses of both arteries and veins.
This procedure was fi rst started on the left side. The left facial common artery was anastomosed to the left recipient facial common artery; the left external jugular vein from the donor was connected to the left recipient external jugular vein; and the left posterior facial vein was connected to the recipient left posterior facial vein. After 2 h and 40 min of total ischaemia time, the allograft skin and the internal anterior mucosa of the alveolus, hard palate, and intranasal mucosa all suddenly pinked up, confi rming the graft’s viability on just the unilateral anastomoses.
Microvascular anastomoses continued to the right side. The right common facial artery was anastomosed to the right common facial artery of the recipient. The donor’s right facial vein was attached to the right recipient facial vein. After release of clamps the graft remained well perfused.
Once the craniofacial skeleton was intact, the bilateral facial nerves were connected using standard epineural repair. First, the donor’s vagus nerve, taken as an interpositional graft, was attached to the upper division of the trunk of the right side of the recipient’s facial nerve. On the left side, the donor’s hypoglossal nerve, used as an interpositional graft, was attached to the upper division of the trunk on the recipient facial nerve. Both grafts were connected to the main trunk of the donor nerve. Then, bilateral Medpor polyethylene facial implants (Porex Surgical Inc, USA) were used to reconstruct orbital fl oors. Finally, the lower eyelids, including the recipient’s conjunctiva and lash lines, were reconstructed bilaterally using donor eyelid skin. The composite facial allograft inset was completed after skin closure.
MedicationInduction of immunosuppression was carried out with rabbit anti-thymocyte globulin (1·2 mg/kg intravenously once a day for 9 days) in combination with methylpredni-solone 1000 mg bolus intravenously on the day of transplant, and rapidly tapered thereafter (fi gure 4). The immunosuppressive regimen was maintained with
A B C D E
F G H I J
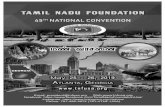
Figure 2: Patient outcome after face transplantationPatient views before transplantation: front (A), left semiprofi le and profi le (B and C) and right semiprofi le and profi le (D and E), indicating severe tridimensional craniofacial defect with missing nose, upper lip, and lower eyelids contracted by massive scar tissue. Patient after face transplantation front (F), left semiprofi le and profi le (G and H) and right semiprofi le and profi le (I and J), presenting successful reconstruction of the facial defect with restoration of major functional and aesthetic subunits of nose, upper lip, and lower eyelids leading to satisfactory aesthetic outcome at 6 months after transplantation.
Articles
206 www.thelancet.com Vol 374 July 18, 2009
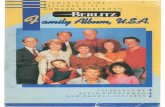
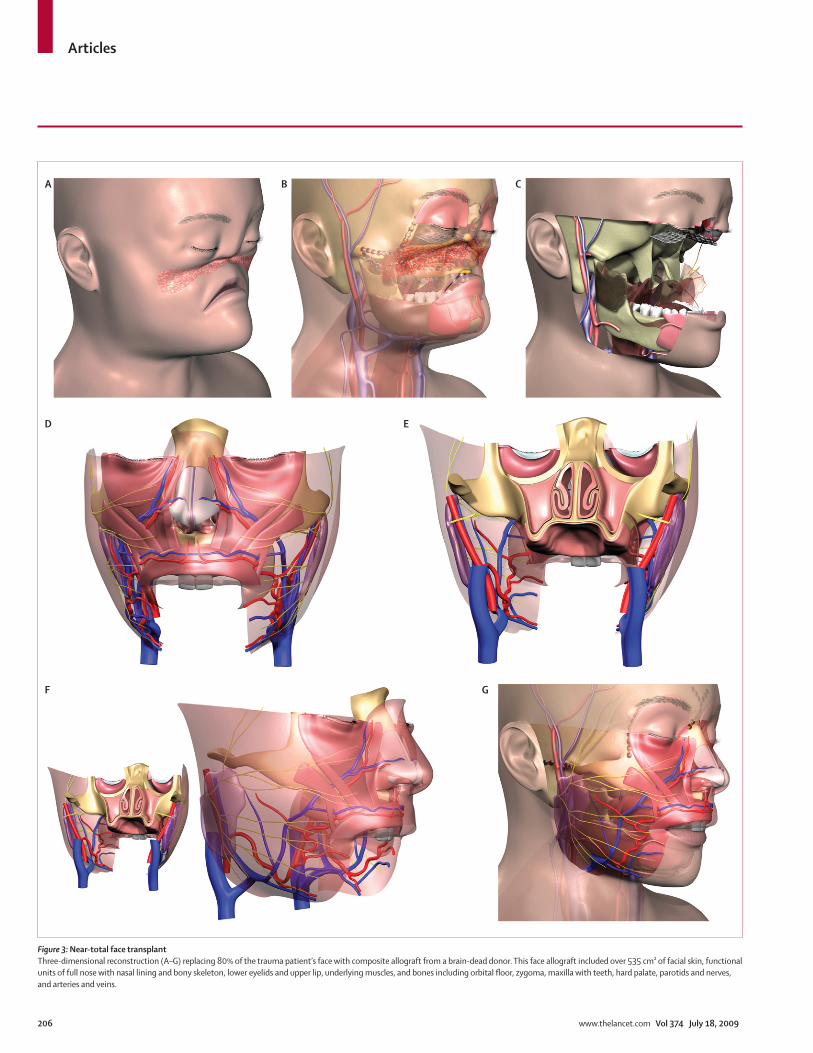
Figure 3: Near-total face transplantThree-dimensional reconstruction (A–G) replacing 80% of the trauma patient’s face with composite allograft from a brain-dead donor. This face allograft included over 535 cm² of facial skin, functional units of full nose with nasal lining and bony skeleton, lower eyelids and upper lip, underlying muscles, and bones including orbital fl oor, zygoma, maxilla with teeth, hard palate, parotids and nerves, and arteries and veins.
A B C
F
D E
G

Articles
www.thelancet.com Vol 374 July 18, 2009 207
tacrolimus, mycophenolate mofetil, and low-dose oral prednisone. Tacrolimus was dosed to get a blood trough level of 12–15 ng/mL for the fi rst 3 months and 10–12 ng/mL thereafter. Mycophenolate mofetil dosage was determined by the patient’s white blood cell count, and will be discontinued at 6 months after trans-plantation (fi gure 4).
Prophylaxis for cytomegalovirus and Pneumocystis jerovici included ganciclovir (5 mg/kg intravenously twice a day) for 8 weeks followed by valganciclovir (900 mg twice a day) for 5 months, and trimethoprim- sulfametho xazole (160 mg/800 mg three times per week) thereafter.
Immunological monitoring included complete blood count once a day, with diff erential, daily tacrolimus level, and weekly lymphocyte ATP function assay (Cylex ImmunKnow, IBT Labs Lenexa Kansas, KS, USA), virtual cross-match for all mismatched antigens, and short tandem repeat assay (AmpFLSTR Profi ler Plus, Applied Biosystems, Foster City, CA, USA). Soon after transplan tation, we observed reactivity in the region DQ9, which rapidly declined to undetectable and remained undetectable until now.
The patient was also examined with mucosa and skin biopsy every week for the fi rst 10 weeks, then twice a month for 2 months, and once a month thereafter.
PhysiotherapyPhysiotherapy and speech therapy began 48 h after surgery, once a day for the fi rst 6 weeks, then three times per week during follow-up. Rehabilitation consisted of supervised controlled passive and active motion exercises, assessment of mastication, smell, speech, swallowing of solid foods, and facial expression, gentle massage, sensory re-education, and re-education in facial acceptance.
Psychological carePsychological support was given once a day during the fi rst 6 weeks, then three times per week. Baseline rating scales were done for anxiety, depression, and quality of life. Further issues were investigated with the perception of teasing scale, Rosenberg’s self-esteem scale, the body esteem scale for adolescents and adults, fear of negative appearance evaluation scale, physical appearance state and trait anxiety scale, and the body-self relations questionnaire (appearance evaluation subscale).
Thymoglobulin
mg/
kg
0·0
0·2
0·4
0·6
0·8
1·0
1·2
1·4
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
A
Tacrolimus
0
0 3 6 9 12 15 18 21 27
Days after transplantation30 33 38 46 52 55 69 90 111
132157
2
4
6
8
10
12
14
16
18
mg/
day
DSteroids
Days after transplantation
020406080
100120140160180200220
Solumedrol 1000 mg at day 0 and day 47
Solumedrol mg/dayMethylprednisolone
0 3 6 9 12 15 18 21 27 30 33 38 46 52 55 69 90 111132
157
Topical steroids
mg/
day
C
MMF
0
500
1000
1500
2000
2500
mg/
day
B
Figure 4: Immunosuppressive treatment and maintenance therapy(A) Induction therapy with thymoglobulin (1·2 mg/kg per day) was given for 9 days. (B) Mycophenolate mofetil (MMF) (2000 mg per day) was tapered over the fi rst 3 months and maintained at 1000 mg per day. (C) Solumedrol (fi rst dose 1000 mg tapered to 40 mg at day 6 after transplantation, and down to 5 mg over 3 months). One episode of acute rejection at day 47 after transplantation was treated with a single bolus of 1000 mg methylprednisolone, which reversed the rejection in 3 days with no further acute rejection episode. (D) Tacrolimus was dosed to get blood trough concentration at 12–15 ng/mL for the fi rst 3 months and 10–12 ng/mL thereafter.

Articles
208 www.thelancet.com Vol 374 July 18, 2009
Ethics consultationBecause of the novelty of the procedure, ethics consultants helped the patient to confront and clarify issues, such as her motivation; risks and benefi ts of the procedure, and of anti-rejection medication; the research nature of the endeavour; and the unique risks of being a pioneering patient in face transplant, including the possibility of media attention. Because the procedure was innovative, exposure to the media was prevented by 24-h security personnel at the entrance to the patient’s room. The patient was advised to consider retaining a lawyer or civilian advocate who could represent and advise her regarding challenges she could encounter after transplantation, such as interest by the media and issues connected with, for example, family and fi nances.
ResultsThe initial course after operation was uneventful, and the patient’s general condition remained very good throughout her hospital stay. The patient accepted her face within the fi rst weeks after transplantation. The immunosuppressive regimen after transplantation (fi gure 4) is similar to that in previously published cases, except that we did not use donor bone marrow infusion, phototherapy, or irradiation.16–18
Transient leucopenia below accepted levels was encountered briefl y during the third week after operation. This state required maintaining ganciclovir for 48 h and lowering mycophenolate mofetil dosage. So far, no signs of cytomegalovirus or other opportunistic infection exist, and no new-onset diabetes or renal insuffi ciency, confi rmed by normal, stable creatinine concentrations over the 6 months.
No clinical signs of rejection were observed at any time after transplantation. A routine biopsy on day 47 showed rejection of the graft mucosa, showing mild perivascular and focal interface infl ammation with keratinocyte apoptosis (Banff III/IV) but no evidence of skin rejection (Banff 0/IV). A single bolus of 1 g of methylprednisolone reversed rejection, which was confi rmed by normal biopsy 3 days later. Routine biopsies at 5 months after transplantation showed no clinical evidence of skin or graft rejection but occasional histological signs of mucosa rejection (Banff II/IV) at days 63, 77, and 91.The patient was not treated for this.
Rehabilitation (static and dynamic exercises) was done every day until the patient was discharged from the hospital.
Quantitative neurosensory testing was assessed with two-point sensory discrimination of the facial skin and was tested with the pressure-specifi ed sensory device (Sensory Management Services LLC, Baltimore, MD, USA) and by clinical assessment of two-point sensory discrimination with Disk-Criminator (Kom Kare Company, Middletown, OH, USA). At 6 months, sensory discrimination returned to the entire facial skin, as measured by pressure-specifi ed sensory device presence
of two-point sensory discrimination at the area under the lower eyelids, upper lip, and the tip of the nose on the both sides of the graft.
Motor recovery—assessed by repose, pucker, smile, and pronunciation of the vowels a, e, i , o, and u—is slow but progressing, as shown by improved facial mimetics with symmetric smiling and upper lip occlusion. The patient’s upper lip and lower eyelid movements remain imperfect but it is too early to expect complete motor recovery.
Functional recovery of this three-dimensional facial defect is excellent, with major functions, which the patient had lacked for 4 years before transplantation, restored. Transplanted nasal passages restored her sense of smell, and she can now eat solid foods without the need of gastric-tube parenteral feeding. Restoration of her upper lip enables her to drink from a cup, and her speech is intelligible because of hard palate reconstruction with composite allograft and palatal obturator support. Aesthetic outcome will be improved by excision of the redundant skin, which is planned about 1 year after transplantation. Finally, because scarred and contracted tissues within the face were removed, the patient reports pain reduction from a chronic pain level of 8 out of 10 before transplantation to 1 out of 10 after trans-plantation.
Psychologically, the patient is doing well. She has no symptoms of depression or post-traumatic stress disorder. Our team’s transplant psychiatrist saw her once a day during the fi rst 6 weeks, then three times per week during the fi rst 3 months, and then once a week (between 3 and 5 months) and once a month thereafter (6 months and after), and this support has contributed to her exceptional recovery.
At 3 weeks after transplantation, after seeing her face for the fi rst time, the patient reacted favourably and rated her appearance as 5 out of 10, the same as before her injury. By week 14, on the psychosocial adjustment to illness scale (PAIS), the most notable change was a remarkable decrease in worrying about changes in her looks that made her feel less attractive, from extremely to a little bit. At 5 months after transplantation, she rates her self-appearance as 8 out of 10. Since surgery, she has recovered self-confi dence, and looks forward to rebuilding her social life and to helping others who have been similarly disabled by trauma.
DiscussionConventional reconstructive techniques should be the main option when the surgical goal is skin coverage. However, we have shown that in such extreme cases, face transplantation, although innovative, is a practicable alternative and should be taken into consideration as an early option, if only to spare a patient years of continued disfi gurement, social ostracism, and the cumulative fi nancial burden of multiple reconstructions. In 2004, we received the Institutional Review Board approval to

Articles
www.thelancet.com Vol 374 July 18, 2009 209
proceed with face transplantation and, from the start, we faced many challenges.
One of the most complex issues was the selection of a candidate with severe facial trauma who had tried all conventional means of reconstruction, yet was left with substantial functional defi cits. After fi nding the right candidate and obtaining consent for surgery, we confronted the second major challenge of doing a near-total face transplantation, consisting of a very complex three-dimensional reconstruction, in which over 80% of facial skin was replaced, and major anatomical structures and physiological functions were restored. The results were: new nasal cavity for breathing and smelling; reconstruction of the lower eyelids; a new palate to restore the ability to speak intelligibly and to masticate satisfactorily; and reconstruction of the upper lip to restore the ability to drink from a cup. The fi nal challenge after our successful transplantation with excellent functional outcome was to rethink our approach of selection only of candidates who had exhausted conventional means of transplantation and to consider presenting face transplantation as an early alternative for patients with massive three-dimensional craniofacial defects and multifunctional defi cits.
Our procedure was innovative for: the complexity of the surgery; unique long-term quantitative psychological assessment; extended ethical follow-up; patient’s security after transplantation; and providing access to a patient advocate to represent the patient in the challenges she could meet after transplantation (eg, interest from the media and issues with the family and fi nances). Complexity of guidelines for face transplantation was extensively studied.19
However, ethical challenges remain for patient selection, continuation of medical support, and appre-ciation of the moral, professional, and fi nancial responsibilities towards the patient. All these aspects should be taken into account before a novel, and still experimental, procedure is undertaken. The nature of these challenges will diff er depending on the geographical, cultural, and economic conditions under which facial allotransplantation is done. Nevertheless, in complex physically and functionally disabling cases, the patient’s ethical right to make decisions should be respected, after being informed of the risks and benefi ts of the procedure and of the need for life-long immunosuppression.
Contributors MS (lead surgeon) developed the Institutional Review Board protocol
and consent form protocol; developed protocol for Organ Procurement
Organisation approval; developed mock transplantation protocol in
anatomy laboratory; collected, reviewed, and summarised data; and
wrote the manuscript. FP, DA, SB, RD, MH, and RL participated in
preoperative assessment, preoperative mock transplantations in anatomy
laboratory, and in postoperative care of the patient. CG participated in
the preoperative assessment, preoperative mock transplantations in
anatomy laboratory, in postoperative care of the patient, and collected
and summarised clinical data for the manuscript. BE participated in
preoperative assessment of the patient and in monitoring the
immunnosupression protocol; collected and summarised
immunological data for the manuscript, and participated in
postoperative care of the patient. KC participated in preoperative
evaluation and postoperative psychiatric care of the patient. EK and
CP were involved in ethical aspects both before and after surgery.
RA participated in preoperative assessment, monitored antiviral,
antibacterial, and antifungal protocols, and participated in postoperative
care of the patient. JF participated in preoperative assessment and in
monitoring immunosuppression protocol; and participated in
postoperative care of the patient. All authors contributed to the fi nal
version of the paper.
Confl icts of interest We declare that we have no confl icts of interest.
References1 Siemionow M, Gozel-Ulusal B, Engin Ulusal A, Ozmen S, Izycki D,
Zins JE. Functional tolerance following face transplantation in the rat. Transplantation 2003; 75: 1607–09.
2 Siemionow M, Ortak T. Izycki D, et al. Induction of tolerance in composite-tissue allografts. Transplantation 2002; 74: 1211–17.
3 Gozel-Ulusal B, Ulusal AE, Ozmen S, Zins JE, Siemionow MZ. A new composite facial and scalp transplantation model in rats. Plast Reconstr Surg 2003; 112: 1302–11.
4 Demir Y, Ozmen S, Klimczak A, Mukherjee AL, Siemionow M. Tolerance induction in composite facial allograft transplantation in the rat model. Plast Reconstr Surg 2004; 114: 1790–801.
5 Siemionow M, Demir Y, Mukherjee A, Klimczak A. Development and maintenance of donor-specifi c chimerism in semi-allogenic and fully major histocompatibility complex mismatched facial allograft transplants. Transplantation 2005; 79: 558–67.
6 Unal S, Agaoglu G, Zins J, Siemionow M. New surgical approach in facial transplantation extends survival of allograft recipients. Ann Plast Surg 2005; 55: 297–303.
7 Yazici I, Unal S, Siemionow M. Composite hemiface/calvaria transplantation model in rats. Plast Reconstr Surg 2006; 118: 1321–27.
8 Yazici I, Carnevale K, Klimczak A, Siemionow M. A new rat model of maxilla allotransplantation. Ann Plast Surg 2007; 58: 338–44.
9 Siemionow M, Unal S, Agaoglu G, Sari A. A cadaver study in preparation for facial allograft transplantation in humans: part I. What are alternative sources for total facial defect coverage? Plast Reconstr Surg 2006; 117: 864–72.
10 Siemionow M. Agaoglu G, Unal S. A cadaver study in preparation for facial allograft transplantation in humans: part II. Mock facial transplantation. Plast Reconstr Surg 2006; 117: 876–85.
11 Siemionow M, Agaoglu G. The issue of facial appearance and identity transfer after mock transplantation: a cadaver study in preparation for facial allograft transplantation in humans. J Reconstr Microsurg 2006; 22: 329–34.
12 Siemionow M, Papay F, Kulahci Y, et al. Coronal-posterior approach for face/scalp fl ap harvesting in preparation for face transplantation. J Reconstr Microsurg 2006; 22: 399–405.
13 Devauchelle B, Badet L, Lengelé B, et al. First human face allograft: early report. Lancet 2006; 368: 203–09.
14 Guo S, Han Y, Zhang X, et al. Human facial allotransplantaion: a 2-year follow-up study. Lancet 2008; 372: 631–38.
15 Lantieri L, Meningaud JP, Grimbert P, et al. Repair of the lower and middle parts of the face by composite tissue allotransplantation in a patient with massive plexiform neurofi broma: a 1-year follow-up study. Lancet 2008; 372: 639–45.
16 Dubernard JM, Lengele B, Morelon E, et al. Outcomes 18 months after the fi rst human partial face transplantation. N Engl J Med 2007; 357: 2451–60.
17 Meningaud JP, Paraskevas A, Ingallina F, Bouhana E, Lantieri L. Face transplant graft procurement: a preclinical and clinical study. Plast Reconstr Surg 2008; 122: 1383–89.
18 Chenggang Y, Yan H. Xudong Z, et al. Some issues in facial transplantation. Am J Transplant 2008; 8: 2169–72.
19 Morris P, Bradley A, Doyal L, et al. Face transplantation: a review of the technical, immunological, psychological and clinical issues with recoomendations for good practice. Transplantation 2007; 83: 109–28.