
Sniffing enables communication and environmental control for the severely disabled
Upload
independentCategory
view
0download
0
Spinal Cord Stimulation for SeverelyIschemic Limbs
CARLOS TULIO SAMPERE. JORGE ALBERTO GUASCH, GARLOS MARIAPALADINO. MANUEL S A N C H E Z G A S A L O N G U E , andBENJAMIN ELENGWAJG
From the Department of Vascular Surgery, Cardiovascular School Cosme Argerich Hospital,Buenos Aires, Argentina.
SAMPERE, C.T., ET AL.: Spinal cord stimulation for severely ischemic limbs. Severe atherosclerosis ofthe lower limbs causes rest pain, skin ulcerations and gangrene. In such situations and when standardsurgical treatment had failed or it is impossible to employ, spinal cord stimulation (SCSJ seems to he ofvalue. Since April 1985, we have used this technique on 19 patients. The results have been beneficial in70.6% of the cases and have shown some evidence of increasing cutaneous flow. However, randomizedseries are required before accepting it as having a special place in the fight against atherosclerotic disease.(PACE, Vol. 12, February 1989}
atherosclerosis, severe ischemic, spinal cord stimulation
Introduction
The rate of blood flow to the tissues of anypart of the body is determined by the head ofpressure driving blood through it and the sum ofthe resistances of the vasculature of tbe part. Thefollowing formula from Pouiseuille's law ex-presses tbese relationsbips in a simple formwhere Q is the flow. Pa and Pv tbe arterial andvenous pressures, Rf and Rp the functional andpatbological resistances.'
Q =P a - P v
Rf + Rp
Any tberapeutic measure to be effective musteither increase the pressure gradient perfusingthe iscbemic part or decrease the resistances. Tbeformer is achieved easily with a successful bypassand the latter may be obtained witb sympathec-tomy, vasodilator drugs and more recently withspinal cord stimulation (SCS).̂
Address for reprints: Dr, C.T. Sampere. Cosme Argerich Hospi-tal, Alte. Brown 240 (1155) Buenos Aires. Argentina.
Received October 7. 1988; accepted October 10, 1988.
This technique has been employed in angio-spastic diseases or in atherosclerosis when thereare obstacles for direct revascularization.^ •* Tbepurpose of tbis article is to present preliminaryobservations on 19 patients who received SCS.
Material and Methods
From April 1985 to July 1987, 19 patientswere selected to be treated by SCS (Tables I and IIsummarize the clinical data). Tbe average age was69 and tbere were 17 men and two women. All ofthem had a severe chronic iscbemia due to atb-erosclerotic symptomatic disease. Nine were dia-betics, four bad coronary disease, and tbree badsuffered cerebrovascular disorders. All of the pa-tients complained of either intermittent or perma-nent rest pain. Moreover, they suffered from skinlesions in several forms and sizes (Table II). Insome cases skin lesions were small (#3, 6, 8, 13,15, 16) but in others (#7, 9, 10, 11, 12, 18) lesionsspread over a wide area of soft tissues and fourcases (#2, 4, 7, 12) had digital gangrene.
All patients bad signs and symptoms that sta-bilized at least 6 months before tbe study. All butone patient had given up smoking. Angiograms
PACE. Vol. 12 February 1989 273

SAMPERE, ET AL.
PatientNumber
2346789
10111213141516171819
Age
5674618054797777706457706471115585
Patients
Sex
MM
LJ.
MMMFMMMMMFMMMM
Table 1.
Treated with SCS
Diabetes
YesYesYesYesNoNoYesNoYesYesNoYesNoNoNoNoNo
Previous V.Surgery (N")
23
——1
——1
—13
——112—
VascularOcclusion
f.p.t.f.p.t.t.f.p.t.f.p.tf.p.t.f.p.tt.f.p.t.f.p.t.f.p.t.f.p.t.f.p.t.f.p.t.f.p.t.f.p.t.f.p.t.
f.p.t.: femoro popliteal tibialt.: tibial
were performed in all of them; in 17 patients vas-cular surgery was considered impossible and intwo the prognosis was poor. Prior direct vascularsurgery had failed in nine patients, three of whomhad had lumbar sympathectomy.
Systolic blood pressures ofthe first toe, ankleand arm were measured by Doppler technique.
When possible, walking time was assessed ona treadmill at 2 mph up a 12% grade. These stud-ies were repeated every 3 months during the pe-riod of follow-up. Last year we began to use laserDoppler velocimetry. The probe was placed on atoe and capillary flow was continuously recordedduring 3 to 5 hours. Furthermore, changes during"gasp" and Valsalva maneuver were investi-gated.^ Capillary pulse reappearance was also as-sessed after 3 minutes occlusion by a cuff justbelow the knee.
The stimulator implant (Itrel, TM; Medtronic,Minneapolis, MN, USA.) was carried out in twostages separated by a trial period: (a) Lead im-plant: it was inserted percutaneously and a moni-toring cable was left connected to a temporarypacemaker. The trial period usually lasted from 3
to 7 days and the decision to internalize was basedupon the extent of pain relief, signs of flow in-crease, if any, and patient acceptance of stimula-tion; (b) Internalization: the pulse generator wasplaced in a subcutaneous pouch. There was nopain relief in two cases during the trial period andthe pulse generator was not implanted (#1 and 5).The follow-up ranged from 2 to 27 months.
Results
We classified the SCS results as: (a) null; (b)good or (c) excellent. We define these terms as:null: when there is neither pain relief nor lesionimprovement; good: when symptoms decrease75% and skin lesions improve; excellent: whensymptoms and signs disappear.
In five patients the results were null (TableIII], three of them underwent major amputationsduring the follow-up period and in one patient asaphenous bypass to an isolated popliteal arterywas performed successfully as a last resource forlimb salvage. The last one died from a stroke.Nine patients had good results (Table IV). Two
274 February 1989 PACE, Vol. 12

SPINAL CORD STIMULATION
Patient
234
6
7
8
910
11
12
13141516171819
Rest Pain
IntermittentPermanentPermanent
Permanent
Permanent
Permanent
PermanentPermanent
Intermittent
Permanent
PermanentIntermittentIntermittentIntermittentPermanentPermanentPermanent
N
(3)(2)(2)(1)
(3)
0)(1)
(3)
( - )
(1)(1)(1)(1)
Table II.
Characteristics of the Patients
Ulcers
1.4. 12.91.40.1
—
0.33,0.53611.51. 1.5
61510.1
—30
—
Gangrene
Vtoe—
Ill toe
—
II toeIII toe + Mt.
—
——
—
IV toeV toe + Mt.
——————
1 toe
B.P. toe
25—40
20
—
20
40
—
45
30505045———
A/AI
0.350.310.35
0.61'*'
0.30
0.61***
0.300.35
0.37
0.35
0.360.400.430.30
—0.410.27
Photop.Waves
YesNoNo
No
No
No
NoNo
No
Yes
YesNoYesNoNoYesNo
B.P. toe: blood pressure toe; A/A I: ankle/arm index; ('): calcified arteries; Mt.: metatarsal; Photop. Waves:Photopletismographic waves.
died from cardiac disease, and one after colonicsurgery. The results were excellent in three cases(Table V) including one who suffered the ampu-
tation of two toes. In four patients walking timeincreased 5 to 8 minutes over the preceding dura-tion.
Patient
7
91 0 "
11
12
Pain Relief
25-50%
0-25%50-75%
25-50%
0-25%
Table III.
"Null" Results
Ulcer Gangrene
•
*
^^ •
Follow Up (months)
Above knee 2Amputation+ Stroke 3Above knee 7AmputationIsolated popliteal 5BypassAbove knee 2Amputation
no change* progressed to femoropopliteal occlusion
PACE. Vol. 12 February 1989 275

SAMPERE, ET AL.
Patient
3468
1 3 "14171819
Pain Relief
75-100%75-100%75-100%75-100%75-100%75-100%75-100%75-100%75-100%
Table IV.
"Good" Results
Ulcer Gangrene
healing —healing *healing —healing —healing —healing —
— —healing —
*
Follow Up (months)
+ Myocardial infarct. 14+ Arrhythmias
AliveAliveAliveAlive
+ Colonic surgeryAliveAlive
3181788332
no change' redo 6 months
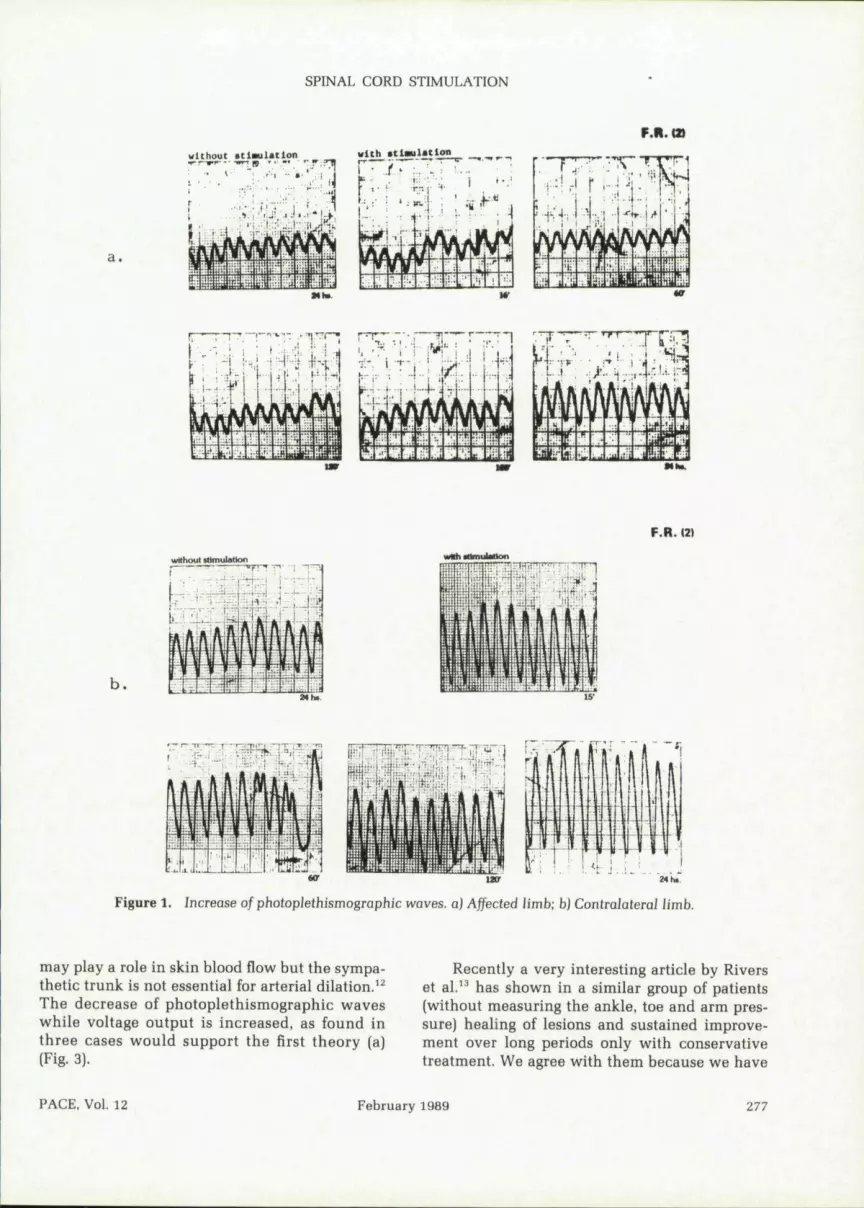
There were no changes of the ankle, arm andtoe pressure. Two out of four limbs where photo-plethismographic waves were able to be obtainedshowed a slight increase in this measurement.These results were best recorded from the contra-lateral limb that was usually less affected (Fig. 1).
No variation was registered with laserDoppler velocimetry (#16,17,19) neither in capil-lary flow nor during "gasp" and Valsalva maneu-ver, however, increase in capillary pulse reap-pearance time was observed in these three casesafter 20-30 days of SCS (Fig. 2). This new testseems to be of value, although further research isneeded before accepting it as reliable.
Discussion
SCS was beneficial in 70.6% of the cases, andthese results are similar to those of Augustinson.^Although SCS was not useful in the remaining29.4% of the patients, we can expect a decrease,
because according to Broseta'* we now indicatethis procedure to patients whose ulcers are lessthan 3 cm^ and whose digital gangrene is limitedto one or two toes.
One of the main demonstrated advantages ofSCS has been pain relief^ •"'" while healing of le-sions by vasodilation occurs slowly in atherio-sclerotic patients^ •* as was observed in our cases.
It is not known whether the pain relief andautonomic effects are due to the same mechanismor if they are two different actions.^ We couldshow some evidence of flow increase as wasmentioned above. In angiospastic disorders andvasculitis the results are better.^•''•'"
In 1986, we treated a Martorell ulcer by thisprocedure.^' The patient is in his 25th month offollow-up and recurrence of the lesion bas notoccured.
SCS may improve blood perfusion through (a)sensory masking, (b) vasoconstrictor blockage, or(c) antidromic vasodilation. Prostagiandin release
276
Patient
2
1516
* healing
Pain Relief
100%
75-100%100%
Table V.
"Excellent" Results
Ulcer Gangrene
— IV-V toeResection"
healed —healed —
February 1989
Follow Up
Alive
AliveAlive
(months)
26
66
PACE, Vol. 12
SPINAL CORD STIMULATION
a.
M b *
Ml*.
F.R. (2t
b .
without tUmulatlon
Uff
Figure 1. Increase of pholoplethismographic waves, a) Affected iimb; h) Contralaterai Jimb.
may play a role in skin blood flow but the sympa-thetic trunk is not essential for arterial dilation.^^The decrease of photoplethismographic waveswhile voltage output is increased, as found inthree cases would support the first theory (a)(Fig. 3).
Recently a very interesting article by Riverset al." has shown in a similar group of patients(without measuring the ankle, toe and arm pres-sure) healing of lesions and sustained improve-ment over long periods only with conservativetreatment. We agree with them because we have
PACE, Vol. 12 February 1989 277

SAMPERE, ET AL.
27/1/87 preoperatlve
v.O. 3*1 3.5'
B.L (16)
•4
V.O.- vascular occlusion
Figure 2. Capillary pulse reappearance time (Laser Doppier).
Figure 3. The decrease of pbotopletismographic waves while voltage output is increased.
observed several of these cases and because ofthis we waited for 6 months as it is previouslymentioned.
So SCS may allow patients to live withoutpain while waiting for the disease to run itscourse.
We look forward to randomized controlledseries in which the new treatment would becompared in a series of patients some of whom
References
1. Strandness DE, Summer D. Hemodynamics forSurgeons. New York, Grune and Stratton. 1975,pp. 290-291.
2. Myklebust }B, Cusik J, Zyvdoskyi M. Muscle blood
would receive no treatment and where theywould be categorized according to the Committeeon Reporting Standards (I.S.C.S.).̂ "
Based on the reasons given above, we thinkthat SCS has a special place in the fight againstvasospastic and atherosclerotic disease of thelimbs. We believe it is promising in patients withsevere ischemia where other procedures havefailed or cannot be employed.
flow alteration with spinal cord stimulation. Pro-ceed. 14th Meeting of Neuroelectric Society,Athens, June 1985.
3. Augustinsson L. Epidural spinal electrical stimu-
278 February 1989 PACE, Vol. 12

SPINAL CORD STIMULATION
lation in peripheral vascular disease. PACE 1987; 10.10(l):205-206.Broseta }. Garcia A, Ingelmo A, et al. Estimulacionmedular cronica en la insuficiencia arterialperiferica. Estudio cooperativo. Angiologia 1985;37(2):70-85.Low PA, Neumann C, Dyck PJ, et al. Evaluation of 11.skin vasodiiator reflexes by using Laser Dopplervelocimetry. Mayo Clin Proc 1983; 58:583-589.Cook AW. Vascular disease of extremities, electri- 12.cal stimulation of spinal cord. NY St | Medicai1976; 76:366-368.Meglio M, Cioni B. Personal experience with spi- 13,nal cord stimulation in chronic pain management.App Neurophysiol 1982; 45:195-200.Shealy CN, Mortimer ]T, Hagfors NR: Dorsalcolumn stimulation. J Neurosurg 1970; 32:560- 14.565,Tallis RC. lllis LS. Sedwick EM, et al. Spinal cordstimulation in peripheral vascular disease. JNeurol Neurosurg Psychiatry 1983; 46:478-484.
Sampere CT, Cuasch |A, Paladino C. et al. La esti-mulacion electrica epidural en la isquemiacronica de los miembros inferiores. AmericanChapter International Society for CardiovascuiarSurgery. Uruguay, Punta del Este, Decembre,1986.Sampere CT, Cuasch JA, Paladino C, et al. La ul-cera isquemica hipertensiva. Un nuevo enfoqueterapeutico. Rev Arg Cir 1986; 51:207-209.Dooley D. Kasprak M. Modification of blood flowto the extremities by electrical stimulation of thenervous system. So Med ] 1976; 60(10):1309-1311.Rivers SP, Veith EJ, Ascer E, et al. Successful con-servative therapy of severe iimb-threatening isch-emia: The value of non-sympathectomy. Surgery1986; 99:759-762.Rutherford RB, Elanigan DP, Gupta SK, et al. Sug-gested standards for reports deaiing with lowerextremity ischemia. Vase Surg 1986; 4:80-94.
PACE, Vol. 12 February 1989 279
Copyright © 2022 FDOKUMEN




















