
Direct Freeform Fabrication of Seeded Hydrogels in Arbitrary Geometries
e u r o p e a n j o u r n a l o f p h a r m a c e u t i c a l s c i e n c e s 2 9 ( 2 0 0 6 ) 183–197
avai lab le at www.sc iencedi rec t .com
journa l homepage: www.e lsev ier .com/ locate /e jps
Nanoscale analysis of protein and peptide absorption:Insulin absorption using complexation and pH-sensitivehydrogels as delivery vehicles
Nicholas A. Peppasa,b,c,∗, Nikhil J. Kavimandana
a Department of Chemical Engineering, University of Texas at Austin, Austin, TX 78712, USAb Department of Biomedical Engineering, University of Texas at Austin, Austin, TX 78712, USAc Division of Pharmaceutics, University of Texas at Austin, Austin, TX 78712-1062, USA
a r t i c l e i n f o
Article history:
Received 24 March 2006
Accepted 24 April 2006
Published on line 10 May 2006
Keywords:
Nanotechnology
Protein delivery
Nanoparticles
a b s t r a c t
Recent advances in the discovery and delivery of drugs to cure chronic diseases are achieved
by combination of intelligent material design with advances in nanotechnology. Since many
drugs act as protagonists or antagonists to different chemicals in the body, a delivery system
that can respond to the concentrations of certain molecules in the body is invaluable. For this
purpose, intelligent therapeutics or “smart drug delivery” calls for the design of the newest
generation of sensitive materials based on molecular recognition. Biomimetic polymeric
networks can be prepared by designing interactions between the building blocks of biocom-
patible networks and the desired specific ligands and by stabilizing these interactions by a
three-dimensional structure. These structures are at the same time flexible enough to allow
for diffusion of solvent and ligand into and out of the networks. Synthetic networks that can
be designed to recognize and bind biologically significant molecules are of great importance
and influence a number of emerging technologies. These synthetic materials can be used
as unique systems or incorporated into existing drug delivery technologies that can aid in
the removal or delivery of biomolecules and restore the natural profiles of compounds in
Here we evaluate critically novel methods for administra-
the body.
1. Introduction
Major innovations in the drug delivery field have surfaced inrecent years. Oral administration of therapeutic agents is thepreferred means of delivering drugs because of ease of admin-istration, low cost and high patient compliance. However, for-mulating a drug for oral delivery is a complicated process. Poorintrinsic protein permeability as a result of large molecular
weight, degradation by proteolytic enzymes in the stomachand in the small intestine, and chemical instability are someof the major hurdles for developing effective formulations for∗ Corresponding author. Tel.: +1 512 471 6644; fax: +1 512 471 8227.E-mail address: [email protected] (N.A. Peppas).
0928-0987/$ – see front matter © 2006 Elsevier B.V. All rights reserved.doi:10.1016/j.ejps.2006.04.014
© 2006 Elsevier B.V. All rights reserved.
delivery of peptides and proteins. Although there are severalsuccess stories in the development and commercialization oforal dosage forms for small molecules, very few oral deliverysystems have been developed for proteins and peptides. Theoral formulation of cyclosporin (Tan et al., 1995) is one of thevery few examples of successful development of oral formu-lations for peptide drugs.
tion of insulin for the treatment of diabetes. Since its initialadministration to humans in 1922, insulin has been the cor-nerstone of type 1 diabetes. Conventionally, insulin is admin-

u t
184 e u r o p e a n j o u r n a l o f p h a r m a c eistered by subcutaneous injections which mimic, as close aspossible, secretion of insulin by healthy pancreas. However,due to compliance-related issues and other complications,more acceptable delivery systems are highly desirable. Specialattention is given to oral insulin delivery which is the focus ofthis work.
1.1. Diabetes mellitus
Diabetes is characterized by the body’s inability to produceor properly use insulin. Diabetes mellitus is a metabolic dis-order of multiple aetiology characterized by chronic hyper-glycaemia with disturbances of carbohydrate, fat and pro-tein metabolism resulting from defects in insulin secretion,insulin action or both. There are 18.2 million people in theUnited States, or 6.3% of the population, who have diabetes(McCarthy, 2004). Diabetes mellitus is occurring in epidemicproportions in many developing and newly industrializedcountries (Simpson et al., 2003). Globally, it is now one of themost common non-communicable diseases and is the fourthor fifth leading cause of death in most developed countries(Park, 2004). The global burden of diabetes is estimated to risefrom about 118 million in 1995 to 220 million in 2010 and 300million in 2025 (Amos et al., 1997; King et al., 1998).
The aetiological types of diabetes are designated as type1, type 2 diabetes and other specific types of diabetes result-ing from genetic defects of �-cell function, genetic defects ininsulin action, endocrinopathies (resulting from over secre-tion of insulin antagonizing hormones), infections and drug-or chemically induced diabetes. Further, in nearly 3–5% ofall pregnancies, women develop gestational diabetes (Anon.,1999; Gabbe and Graves, 2003).
Type 1 diabetes can be classified as autoimmune dia-betes mellitus or idiopathic type 1 diabetes. Autoimmune dia-betes mellitus is characterized by the autoimmune-mediateddestruction of the insulin secreting pancreatic �-cells. Indi-viduals suffering from this form of type 1 diabetes typicallybecome dependent on insulin for survival and are at a risk ofketoacidosis, a condition resulting from extremely high levelsof blood glucose (over 249 mg/dl) wherein the body begins toburn fat and muscle for energy which causes release of ketonebodies in the bloodstream. Idiopathic type 1 diabetes is a dia-betes of unknown origin. Some of the patients suffering fromthis disease have permanent insulin deficiency and are proneto ketoacidosis, but this form of diabetes shows no evidenceof autoimmunity (McCarthy, 2004).
Type 2 is the most common form of diabetes and is charac-terized by disorders of insulin action and insulin secretion,either of which may be the predominant feature. Individu-als suffering from this form of diabetes are typically resis-tant to the action of insulin (Lillioja et al., 1993). Nearly 16million individuals in the United States have type 2 diabeteswhile about one-third of those people are not aware that theyhave the disease (McCarthy, 2004). This is primarily becausethe hyperglycemia is often not severe enough to be symp-tomatic. Ketoacidosis is relatively infrequent in this type of
diabetes. Nevertheless, individuals suffering from this form ofdiabetes are at increased risk of developing macrovascular andmicrovascular complications. If untreated, type 2 diabetes cancause serious complications, including kidney failure, blind-i c a l s c i e n c e s 2 9 ( 2 0 0 6 ) 183–197
ness, heart attack and lower-limb amputation (Anthony et al.,2004). Fortunately, in many cases, type 2 diabetes can be ade-quately controlled through a combination of proper nutritionand exercise. However, some people with type 2 diabetes dorequire oral medications or insulin injections.
To determine if a patient is normal, pre-diabetic or diabetic,health care providers conduct a fasting plasma glucose test(FPG) or an oral glucose tolerance test (OGTT) (Genuth et al.,2003). Either test can be used to diagnose pre-diabetes or dia-betes. Pre-diabetes, characterized by a glucose level betweenthat of a healthy individual and a diabetic patient, is also calledimpaired glucose tolerance (IGT) or impaired fasting glucose(IFG) (Benjamin et al., 2003).
The FPG test is easier, faster and less expensive to perform.With the FPG test, a fasting blood glucose level between 100and 125 mg/dl indicates pre-diabetes. A person with a fastingblood glucose level of 126 mg/dl or higher is considered dia-betic (Genuth et al., 2003).
In the OGTT test, a person’s blood glucose level is mea-sured after a fast and 2 h after drinking a glucose-rich beverage(2-h PG value). Two-hour blood glucose level of 140–199 mg/dlsignals pre-diabetes, whereas the 2-h blood glucose level of>200 mg/dl, signals diabetes (Genuth et al., 2003). Although theOGTT (which consists of an FPG and 2-h PG value) is recog-nized as a valid way to diagnose diabetes, the use of the testfor diagnostic purposes in clinical practice is limited becauseof its inconvenience, less reproducibility, greater cost (Genuthet al., 2003; Stern et al., 2002).
Curative therapy for diabetes mellitus mainly impliesreplacement of functional insulin-producing pancreatic betacells, with pancreas or islet-cell transplants. This is the onlyreplacement therapy that can improve metabolic control otherthan conventional and intensive insulin therapy (de Groot etal., 2004). Transplantation can be performed either by implan-tation of the pancreatic organ or by implantation of only thepancreatic islets of Langerhans. Until recently, pancreas trans-plantation was considered to be the only viable procedure forautonomous regulation of glucose level (de Groot et al., 2004;McChesney, 1999). However, to avoid pancreatic graft rejection,transplantation has to be coupled with lifelong immunosup-pression which itself can cause severe side effect as increasedsusceptibility to viral, fungal and bacterial infections, andincreased risk for the development of malignancies (de Grootet al., 2004; Penn, 2000; Vial and Descotes, 2003).
Islet transplants are beneficial compared to implantationof pancreatic organ since they avoid the need for major sur-gical procedures. A small mass of islet cells can be deliv-ered to the liver through intraportal infusion. The procedurefor islet cell transplantation was initially successful in smallanimal models, but was not effective in humans (Ballingerand Lacy, 1972; Street et al., 2004). However, Shapiro et al.(2000) recently developed a new immunosuppressive regimenand reported a 100% success rate in achieving insulin inde-pendence through islet transplantation in seven long-termdiabetic patients. Unfortunately, like pancreatic graft trans-plants, islet transplantation also suffers from the necessity of
lifelong immunosuppression. Another limitation of islet celltransplantation procedures is the need for adequate supplyof donor islet cells. One solution to this problem that is cur-rently an area of active research is differentiation of embryonic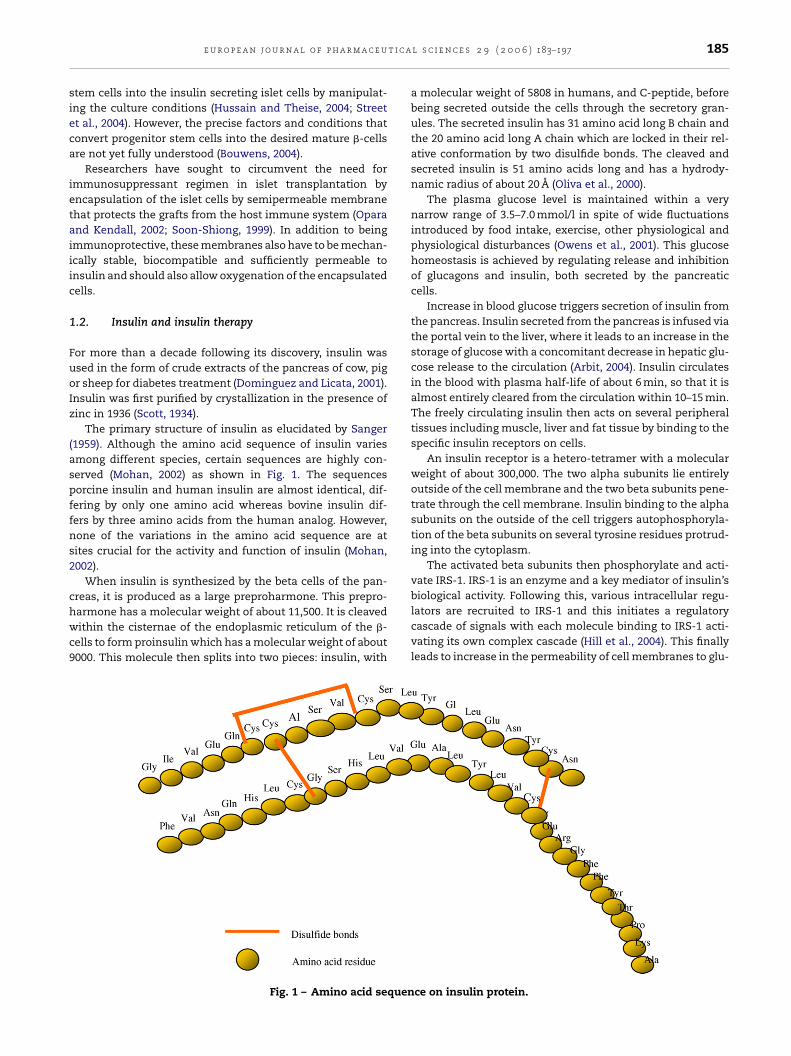
t i c a
sieca
ietaiiic
1
FuoIz
(aspffns2
chwc9
e u r o p e a n j o u r n a l o f p h a r m a c e u
tem cells into the insulin secreting islet cells by manipulat-ng the culture conditions (Hussain and Theise, 2004; Streett al., 2004). However, the precise factors and conditions thatonvert progenitor stem cells into the desired mature �-cellsre not yet fully understood (Bouwens, 2004).
Researchers have sought to circumvent the need formmunosuppressant regimen in islet transplantation byncapsulation of the islet cells by semipermeable membranehat protects the grafts from the host immune system (Oparand Kendall, 2002; Soon-Shiong, 1999). In addition to beingmmunoprotective, these membranes also have to be mechan-cally stable, biocompatible and sufficiently permeable tonsulin and should also allow oxygenation of the encapsulatedells.
.2. Insulin and insulin therapy
or more than a decade following its discovery, insulin wassed in the form of crude extracts of the pancreas of cow, pigr sheep for diabetes treatment (Dominguez and Licata, 2001).nsulin was first purified by crystallization in the presence ofinc in 1936 (Scott, 1934).
The primary structure of insulin as elucidated by Sanger1959). Although the amino acid sequence of insulin variesmong different species, certain sequences are highly con-erved (Mohan, 2002) as shown in Fig. 1. The sequencesorcine insulin and human insulin are almost identical, dif-ering by only one amino acid whereas bovine insulin dif-ers by three amino acids from the human analog. However,one of the variations in the amino acid sequence are atites crucial for the activity and function of insulin (Mohan,002).
When insulin is synthesized by the beta cells of the pan-reas, it is produced as a large preproharmone. This prepro-
armone has a molecular weight of about 11,500. It is cleavedithin the cisternae of the endoplasmic reticulum of the �-ells to form proinsulin which has a molecular weight of about000. This molecule then splits into two pieces: insulin, with
Fig. 1 – Amino acid sequen
l s c i e n c e s 2 9 ( 2 0 0 6 ) 183–197 185
a molecular weight of 5808 in humans, and C-peptide, beforebeing secreted outside the cells through the secretory gran-ules. The secreted insulin has 31 amino acid long B chain andthe 20 amino acid long A chain which are locked in their rel-ative conformation by two disulfide bonds. The cleaved andsecreted insulin is 51 amino acids long and has a hydrody-namic radius of about 20 A (Oliva et al., 2000).
The plasma glucose level is maintained within a verynarrow range of 3.5–7.0 mmol/l in spite of wide fluctuationsintroduced by food intake, exercise, other physiological andphysiological disturbances (Owens et al., 2001). This glucosehomeostasis is achieved by regulating release and inhibitionof glucagons and insulin, both secreted by the pancreaticcells.
Increase in blood glucose triggers secretion of insulin fromthe pancreas. Insulin secreted from the pancreas is infused viathe portal vein to the liver, where it leads to an increase in thestorage of glucose with a concomitant decrease in hepatic glu-cose release to the circulation (Arbit, 2004). Insulin circulatesin the blood with plasma half-life of about 6 min, so that it isalmost entirely cleared from the circulation within 10–15 min.The freely circulating insulin then acts on several peripheraltissues including muscle, liver and fat tissue by binding to thespecific insulin receptors on cells.
An insulin receptor is a hetero-tetramer with a molecularweight of about 300,000. The two alpha subunits lie entirelyoutside of the cell membrane and the two beta subunits pene-trate through the cell membrane. Insulin binding to the alphasubunits on the outside of the cell triggers autophosphoryla-tion of the beta subunits on several tyrosine residues protrud-ing into the cytoplasm.
The activated beta subunits then phosphorylate and acti-vate IRS-1. IRS-1 is an enzyme and a key mediator of insulin’sbiological activity. Following this, various intracellular regu-
lators are recruited to IRS-1 and this initiates a regulatorycascade of signals with each molecule binding to IRS-1 acti-vating its own complex cascade (Hill et al., 2004). This finallyleads to increase in the permeability of cell membranes to glu-ce on insulin protein.

u t i c
186 e u r o p e a n j o u r n a l o f p h a r m a c ecose and glucose uptake increases. This increased uptake ofglucose due to insulin binding occurs in the muscle cells, adi-pose cells and other types of cells in the body constitutingabout 80% of all the cells.
In addition to its role in uptake of glucose, insulin alsostimulates conversion of carbohydrate or proteins to fat (lipo-genesis), and increases amino acid transport into cells. It alsostimulates growth, DNA synthesis and cell replication.
In the absence of curative therapy for the treatment ofdiabetes, insulin replacement therapy is required for all peo-ple with type 1 diabetes (McAulay and Frier, 2003). Benefitsof insulin therapy in patients with type 2 diabetes are alsowell recognized now (Group, 1998; Malmberg, 1997; Ohkuboet al., 1995). Intensive glucose control delays the onset andretards the progression of microvascular and macrovascu-lar diseases in patients with type 2 diabetes (Mudaliar andEdelman, 2001). Insulin therapy is, therefore, central to man-agement of patients with diabetes. With the development andapproval of recombinant technologies for insulin production,human insulin could be made biosynthetically which becamethe preferred method of insulin production. This also led to thedevelopment of mutant insulin analogues having improvedpharmacokinetic properties for subcutaneous administration(Barnett and Owens, 1997; Bolli et al., 1999; Brange andVolund, 1999). However, for over 80 years injection or infu-sion of insulin into the subcutaneous (s.c.) tissue has been theonly route of insulin delivery used in clinical practice. Thismimics, as close as possible, secretion of insulin by healthypancreas.
Recent developments of improved injection devices, suchas insulin pens, and very sharp needles, have reduced thepain associated with the injection therapy to a considerableextent. But even with these developments, injection ther-apy still requires the handling of a device and is associ-ated with pain. This often results in low patience compli-ance to the therapy. Clinical studies have shown that becauseof the non-compliance-related issues, even on insulin treat-ment, a significant percentage of patients fail to attain last-ing glycemic control (Arbit, 2004). Furthermore, this route ofinsulin administration has associated side effects, such ashyperinsulinemia and localized deposition of insulin that leadto local hypertrophy and fat deposits at injection sites (Skyler,1986).
2. Alternative routes of insulinadministration
The current recommended intensive insulin therapy regi-mens involve multiple subcutaneous insulin injections every-day. These increases compliance constrains on patients toa great extent and reduce the overall efficacy of treatment.Hence, as discussed above, non-invasive insulin formulationsthat mimic physiological secretion of insulin as a means ofmaintaining the glucose homeostasis are highly desirable.Recent advances in alternative routes of administration as an
approach to improve insulin therapy are discussed here. Inves-tigated delivery systems for insulin therapy mainly includetransdermal, nasal, buccal, pulmonary and oral delivery sys-tems.a l s c i e n c e s 2 9 ( 2 0 0 6 ) 183–197
2.1. Transdermal delivery
Large, hydrophilic macromolecules such as insulin cannot effi-ciently permeate the skin. This skin impermeability is mainlydue to the intercellular lipid layer of the stratum corneum(Foldvari, 2000). Thus, the delivery approaches targeted atimproving the transdermal delivery of drugs involve break-ing down or removing the lipid barrier by chemical, electricalor physical methods (Owens et al., 2003). Iontophoresis, low-frequency ultrasound or chemical agents acting as vesiclesare some of the methodologies investigated. In Iontophoresis,low-level electric current is used to enhance the permeabilityof the drug across the stratum corneum and the permeabilityof insulin depends on the net charge of the insulin molecule(Langkjaer et al., 1998; Stephen et al., 1984). However, thepotential of this methodology has only been demonstrated inanimal studies and the amount of insulin transferred acrossthe skin was barely enough to meet basal insulin requirement(Owens et al., 2003).
Low-frequency ultrasound (20–150 kHz) has been shown tobe more effective by causing several-fold increase in macro-molecular permeability (Mitragotri et al., 1995). However, evenwith this technique, insulin delivery rates may not be suffi-cient for physiological replacement of insulin (Cefalu, 2004).Combined use of iontophoresis and ultrasound has been pro-posed as an approach for increasing macromolecular transferacross the skin barrier (Le et al., 2000).
Another approach involves incorporating insulin into vesi-cles made of soybean phosphatidylcholine, called transfer-somes. Transfersomes are highly deformable and as a resultare able to pass through pores smaller than their size with per-meability similar to water (Cevc et al., 1998). It was observedthat transformers transport insulin with 50% bioefficiencycompared to subcutaneous injection. However, more recentstudies have been unable to reproduce these findings (Owenset al., 2003). Despite a number of techniques that have beeninvestigated, so far, dermal insulin methodologies have notresulted in reproducible and acceptable transfer of insulinacross the highly efficient skin barrier (Owens et al., 2003).
2.2. Intranasal delivery
The nasal mucosa is characterized by large surface area fordrug absorption (about 150 cm2), high coverage density of theepithelium by microvilli, and a rich, vascularized subepithe-lium (Owens, 2002). The drugs entering through this routedirectly enter the systemic circulation, thus avoiding hepaticfirst-pass metabolism. Nasal absorption also provides for rapidattainment of therapeutic blood levels, and quicker onset ofpharmacological activity (Kissel and Werner, 1998). The mainbarriers to absorption include the very active mucociliaryclearance, enzyme activity, low permeability and low pH ofthe nasal epithelium. In addition, little information is avail-able on the influence of nasal pathology on the efficacy ofinsulin administration (Hayakawa et al., 1989; Owens, 2002).Small molecular weight molecules such as oxytocin (MW 1007)
and calcitonin (MW 3431) have been successfully delivered viathe nasal route (Sayani and Chien, 1996), but reproducible andreliable intranasal delivery methodology for insulin has notbeen developed.
t i c a
vtkba(wa
pair1rftacp
pttai
2
BfobtkpcihaTaciVvcdit1
sohmaig
e u r o p e a n j o u r n a l o f p h a r m a c e u
The observed low bioavailability of insulin administeredia the intranasal route often necessitates use of absorp-ion enhancers. However, many of these enhancers have beennown to cause damage to the nasal mucosa. Use of lecithin,ile salts or laureth-9 as absorption enhancers for nasalbsorption enhancement caused nasal irritation in patientsCefalu, 2004; Gordon et al., 1985; Salzman et al., 1985). Even
ith the use of absorption enhancers, reproducible and reli-ble insulin delivery has not been achieved.
Intranasal insulin administration with a medium-chainhospholipid (didecanoyl-l-alpha-phosphatidylcholine) as anbsorption enhancer was observed to cause rapid increasen the serum insulin concentration in healthy individuals,eaching glucose reducing peak in 20–45 min (Drejer et al.,992; Nolte et al., 1990). Pharmacological bioavailability, cor-ected for the endogenously produced insulin for the nasalormulation, was 8.3% relative to an intravenous bolus injec-ion (Drejer et al., 1992). Administered insulin also exhibited
faster time-course of absorption when compared to sub-utaneous injection. This makes intranasal administration aarticularly attractive option for prandial insulin replacement.
However, subsequent studies failed to confirm these initialositive results (Heinemann et al., 2001). Potential damage tohe nasal mucosa and nasal irritation, especially in the long-erm treatment regimen and high rates of treatment failurere the main obstacles in clinical application of intranasalnsulin delivery (Cefalu, 2004; Owens et al., 2003).
.3. Buccal delivery
uccal mucosa offers an interesting portal of administrationor both systemic and local delivery of therapeutic agents. Theral mucosa consists of a non-keratinized area (sublingual anduccal mucosa) and the keratinized area (the gum or gingiva,he palatal mucosa and the inner side of the lips). The non-eratinized regions are generally more permeable as com-ared to the keratinized areas (Veuillez et al., 2001). The oralavity has a large surface area for absorption (100–200 cm2),s richly vascularized and has little proteolytic activity. Itas fewer proteolytic enzymes than the oral, nasal, vaginalnd rectal administration areas (Lee and Yamamoto, 1989).he predominant peptidases found in the buccal mucosa areminopeptidases. The proteolytic enzymes such as trypsin,hymotrypsin and pepsin, which are present in the gastric andntestinal fluids, are largely absent (Stratford and Lee, 1986;euillez et al., 2001). The factors limiting insulin absorptionia the buccal route are the relatively thick multi-layered buc-al barrier, the high rate of mucus turnover and the proteolyticegradation. Strategies investigated to improve absorption of
nsulin include use of absorption enhancers, bioadhesive sys-ems and enzyme inhibitors (Aungst and Rogers, 1988; Nagai,986; Veuillez et al., 2001).
Recently, Generex (Guevara-Aguirre et al., 2004) demon-trated efficacy of a buccal insulin delivery system based on anral insulin spray which administers insulin in the form of aigh velocity, fine particle aerosol directly into the patient’s
outh. The particles consist of mixed micelles made frombsorption enhancers that encapsulate insulin. The fast mov-ng, fine particles are able to penetrate a thin membrane thatuards the surface area in direct contact with the blob circu-
l s c i e n c e s 2 9 ( 2 0 0 6 ) 183–197 187
lation. Combined with the effect of absorption enhancers, thepenetrating particles cause a rapid increase in the uptake ofinsulin into the systemic circulation (Modi et al., 2002). Theadministered insulin appears in the circulation within 10 minof application. Bioavailability of 7–8% was determined in aproof-of-concept study involving type 2 diabetic patients andthe insulin peak was reached in about 30 min after application.The subcutaneously injected insulin reached the absorptionpeak in about 60 min (Guevara-Aguirre et al., 2004). More clin-ical and toxicological data is required to establish the efficacyof this system.
2.4. Pulmonary delivery
The respiratory tract offers a high area for drug absorption, athin epithelial membrane and a rich vasculature. It also lackseffective mucociliary clearance and is highly immunotolerant.In addition, this route of administration also eliminates thefirst-pass hepatic metabolism (Heinemann et al., 2001). Thismakes the lungs an attractive option for drug delivery (Owens,2002; Patton et al., 1999). Inhalers are typically used for pul-monary insulin delivery, which enables the drug to reach thedeep-lung, from where it can be quickly absorbed into thecirculation. The factors that need to be controlled for opti-mizing insulin delivery include the type of propellant used,the air flow speed, the losses within the device, the parti-cle size and drug deposition into the throat and bronchialtubes (Cefalu, 2004). Particle size and velocity greatly influ-ence the deep-lung deposition of the inhaled protein (Patton etal., 1999). Several pulmonary insulin delivery systems includ-ing Exubera, jointly developed by Nektar Therapeutics, Pfizerand Aventis, the AERx, developed by Aradigm Corporationand Novo Nordisk and AIR developed by Alkermes and EliLilly, are in development and in phase III testing [42-Cefalu].Two of these devices, Exubera and AERx are in phase III test-ing and show efficacy comparable to subcutaneous insulin(Cefalu, 2004; Hermansen et al., 2004; Skyler et al., 2001). Insome studies however, it was observed that patients treatedwith inhaled insulin had increased insulin antibody levels,but these levels thus far have not been related to any signifi-cant clinical change (Cefalu, 2004; Stoever and Palmer, 2002).Adverse effects of the treatment on pulmonary function arealso a cause of concern (Cefalu et al., 2002). Safety and tol-erability issues need to be addressed for this treatment to beclinically applicable.
3. Oral protein delivery
Of all the routes of delivering drugs, the oral route is themost desirable. This route of administration results in higherpatient compliance than any other route of administration. Ifsuccessful, this delivery system will solve the current non-compliance-related problems associated with insulin injec-tions. The ease of this delivery system has led to severalattempts to develop oral insulin formulations (Heinemann et
al., 2001). Another great advantage of this route of administra-tion is that insulin delivered via the oral route mimics moreclosely the endogenous secretion of insulin. Insulin absorbedfrom the intestinal epithelium reaches the liver through the
u t i c
188 e u r o p e a n j o u r n a l o f p h a r m a c eportal vein and can have a direct effect on the hepatic glucoseproduction. This mode of distribution is highly appropriate,since the liver plays an important role in maintaining glu-cose homeostasis in the bloodstream, taking up and storingthe energy in carbohydrates in the form of glycogen. Par-enterally administered insulin mainly targets the peripheraltissue rather than the liver with pharmacokinetics that do notreplicate the normal dynamics of endogenous insulin release(Arbit, 2004).
3.1. Oral delivery of insulin
Oral delivery formulation for insulin is highly desirable froma patient compliance point of view and other considerationsdiscussed above. However, only a small portion of insulinadministered orally reaches the blood stream, mainly due toextensive degradation of the protein in the gastrointestinaltract. Further, large size and hydrophilicity of the moleculegreatly limits its transport across the intestinal epithelium.No specific transport mechanism is present for the passage ofinsulin cross the intestinal cell monolayer. Insulin moleculesthat are unable to cross the intestinal barrier thus get fur-ther exposed to the intestinal proteolytic activity, this in turnreduces the bioavailability of the protein. Owing to these fac-tors, less than 0.5% of the orally administered insulin typicallyreaches the systemic circulation.
For many years researchers have tried to find a solution tothese problems and in effect increase the oral bioavailabilityof insulin. The investigated approaches include use of per-meation enhancers, protease inhibitors (Bernkop-Schnurch,1998; Fasano and Uzzau, 1997; Morishita et al., 1993) or con-comitant administration of permeation enhancers and pro-tease inhibitors, chitosan coatings to stabilize the protein andimprove cellular permeability (Wu et al., 2004), entrapment ofinsulin within microparticles (Sajeesh and Sharma, 2004) andprotein modification to make it resistant to proteolytic attackand more permeable across the epithelium (Clement et al.,2004; Xia et al., 2000).
Degradation of proteins during their transit from mouth,the pharynx and the esophagus is minimal. The secretionsof the salivary glands contain mucus, amylase and lysozyme.Digestion in the mouth is limited to initiation of polysaccha-rides hydrolysis into disaccharides by amylase. No absorp-tion of food material occurs in the mouth. The secretionsof esophagus are entirely mucoid in character and maintaina well-lubricated esophageal lumen. Mucus secreted by theesophagus protects the esophageal wall from damage due tofood. The entire movement of food through the pharynx andesophagus takes between 6 and 10 s.
After traveling through the esophagus the food reaches thestomach where it is stored and digestion of the ingested foodbegins. Based on anatomical and histological characteristics,the stomach is divided into the fundus (part of stomach thatlies above the esophageal opening), the body (middle portion)and the antrum (lowermost part of the stomach characterizedby thick muscles). The three regions coordinate and control
the motility function of stomach. The digestive juices of thestomach are mainly secreted by gastric (or oxyntic) glands.These glands are responsible for secretion of hydrochloric acidand pepsinogen and mucus along with other components.a l s c i e n c e s 2 9 ( 2 0 0 6 ) 183–197
Other exocrine glands present in the gastric mucosa arethe pyloric glands. These mainly secrete mucus and somepepsinogen. The oxyntic glands are mainly present in on theinside surface of the body on the fundus (oxyntic mucosa)whereas the pyloric glands are present in the pyloric glandarea lining the antral surface. Pepsinogen, the inactive pre-cursor of pepsin, is converted into pepsin by the HCl secretedby the oxyntic glands. This then leads to autocatalytic conver-sion of pepsinogen into pepsin, which is the main digestiveenzyme of the stomach. Pepsin is active at low pH but is rapidlyinactivated above pH 5.0. Pepsin acts at specific amide bondswithin protein molecules and convert them into smaller pep-tide fragments.
It is most efficient in cleaving amino acid linkages involv-ing the aromatic amino acids, phenylalanine, tryptophan andtyrosine.
No absorption of foodstuff takes place through the stom-ach. Food components digested in the stomach are still largefragments and hence cannot get absorbed through the gas-tric mucosa. Most of the digestion and absorption occurs inthe small intestine. The small intestine is divided into threesections: the duodenum, the jejunum and the ileum (Ganong,1995). The small intestine secretions themselves do not con-tribute significantly to the process of digestion. Althoughthe intestinal cells do secrete digestive enzymes (such asaminopeptidase), they mainly act in the brush border of theepithelial cells. The exocrine glands in the small intestinemainly secrete mucus that lines the inside of the intestinalwall. Protein digestion activity of the small intestine mainlycomes from the pancreatic secretions.
The gastric contents, on emptying into the upper portionof the small intestine (duodenum), mix with the juices inthe small intestine and also with the secretions of the pan-creas. The secretions of the pancreas come from the exocrinepancreatic acinar cells. These cells form sac-like structureswith the duct cells forming channels leading to the pancre-atic duct. The secretions of the pancreas mix with the bileduct coming from the liver before mixing into the intestinalcontents.
The acinar cells are responsible for the secretion of prote-olytic enzymes (protein digestion), pancreatic amylase (car-bohydrate digestion) and pancreatic lipase (fat digestion).The duct cells secrete large amounts of sodium bicarbonate(NaHCO3) that neutralizes the acidity of the contents emptiedby the stomach. The proteolytic enzyme secretions from thepancreas contain trypsinogen, chymotrypsinogen and pro-carboxypeptidase. Trypsinogen is converted by an autocat-alytic reaction to its active form, trypsin, by an enzyme calledenterokinase present in the wall of the duodenum. Trypsinthen converts chymotrypsin and procarboxypeptidase intotheir active analogues. Trypsin is the most abundant of thethree enzymes.
Each of these enzymes acts on specific amino acid linkagesand convert the peptide fragments (formed by pepsin diges-tion) into small peptides and amino acids. Trypsin cleaves thepeptide bonds where the carboxyl group comes from arginine
or lysine residue, whereas chymotrypsin specifically breaksthe peptide bonds where the carboxyl group is donated bytyrosine, phenylalanine, tryptophan, methionine or leucine.Due to the high specificity of trypsin for amino acid linkages,
t i c a l s c i e n c e s 2 9 ( 2 0 0 6 ) 183–197 189
ip
3
TontasnTaifasitTsaaaal
lcenaimtr
cccEiarhti
atdNomatcst
those approaches where the protein molecule is modified, typ-
e u r o p e a n j o u r n a l o f p h a r m a c e u
t is commonly used as a reagent in unambiguous cleavage ofroteins.
.2. The intestinal epithelial cell barrier
he epithelial tissue consists of cells specialized in exchangef materials between the external environment and the inter-al host milieu. Since these cells form the boundary betweenhe external and the internal environment, the transportcross these cells is highly regulated and passage of onlyelective components is allowed. Most of the absorption ofutrients is completed in the duodenum and the jejunum.he small intestinal absorptive epithelium is remarkably welldapted for absorption of nutrients from the lumen. Thenner surface of the intestine forms macroscopic circularolds, called valvulae conniventes that increase the surfacerea for absorption three-fold. Each of these folds has micro-copic finger-like projections called villi that result in a 10-foldncrease in the surface area. The villus surface is covered byhe absorptive epithelial cells along with some mucous cells.he epithelial cells form hair-like projections on the luminalide called the microvilli that further increase the absorptiverea 20-fold. Enzymatic secretions of the small intestine arective within these brush borders. Thus, these macroscopicnd microscopic projections together increase the surfacerea nearly 600-fold compared to a hollow cylinder of simi-ar dimensions or about 250 m2.
Nutrients, such as amino acids and sugars, enter the circu-ation by crossing the epithelium covering the villi. Each villusontains a blunt-ended lymphatic capillary bed and a blunt-nded lymphatic vessel called the central lacteal. It also has aetwork of capillaries which absorb the molecules transportedcross the epithelial cells. The intestinal capillaries convergento venules and the hepatic portal vein that take the absorbed
olecules to the liver. Fats, instead of being transported intohe capillaries, are absorbed into the lymphatic vessels thatapidly flow into the blood via the thoracic duct.
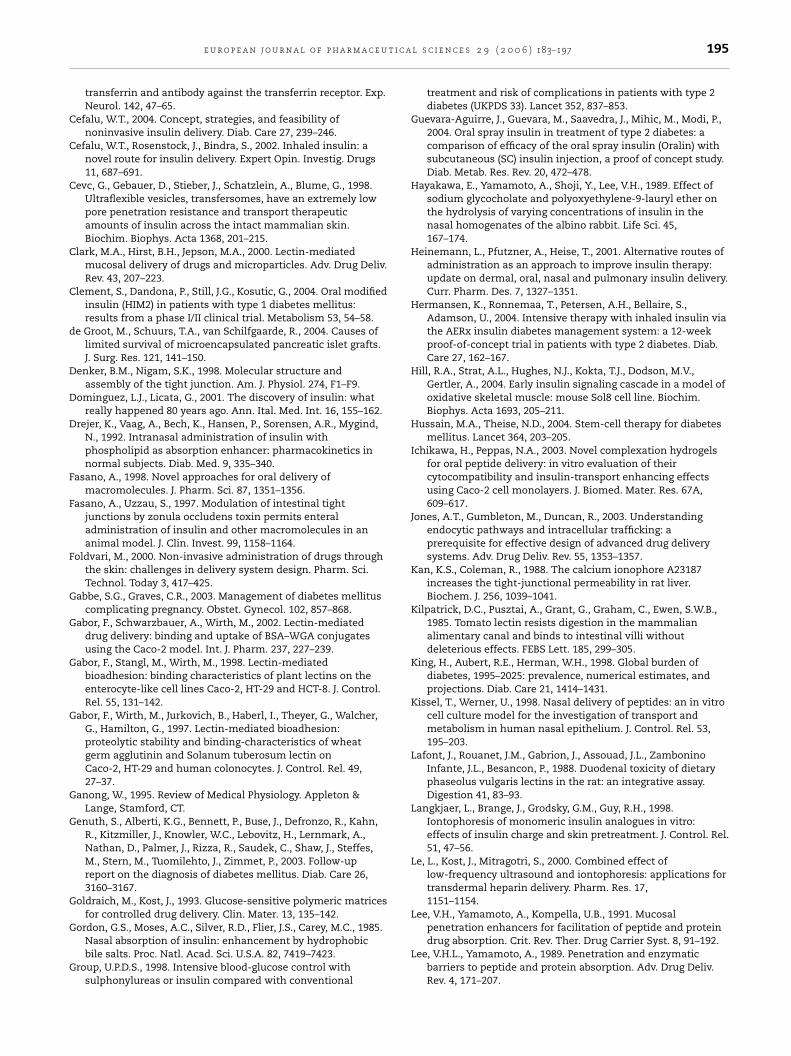
The small intestinal epithelium is highly differentiated andonsists of six distinct cell types: the enterocytes or absorptiveells, mucin-producing goblet cells, endocrine cells, panethells, M cells and tuft and cup cells (Madara and Trier, 1986).pithelial cells are the most common type of cells in thentestinal cell monolayer. The epithelial cells are organizeds polarized monolayer, which provides a permeability bar-ier between two distinct environments. Disruption of thisighly regulated polarized cell barrier can cause passage ofoxic luminal contents to the systemic circulation as shownn Fig. 2.
The epithelial cells are circumferentially tied to onenother by intercellular junctional complexes. These includehe tight junctions or zonula occludens, zonula adherens andesmosomes (Anderson and Van Itallie, 1995; Denker andigam, 1998). The tight junctions, which appear as a seriesf fusion points involving the outer leaflets of the plasmaembranes, attach the adjacent cells to one another at the
pical region of the cells. A century ago, these complexes were
hought to be absolute and unregulated barriers in the para-ellular space (Anderson and Van Itallie, 1995). Physiologicaltudies of the past several decades have shown the tight junc-ions to be dynamic structures, able to respond to extracellularFig. 2 – Transport pathways through the cell monolayer.
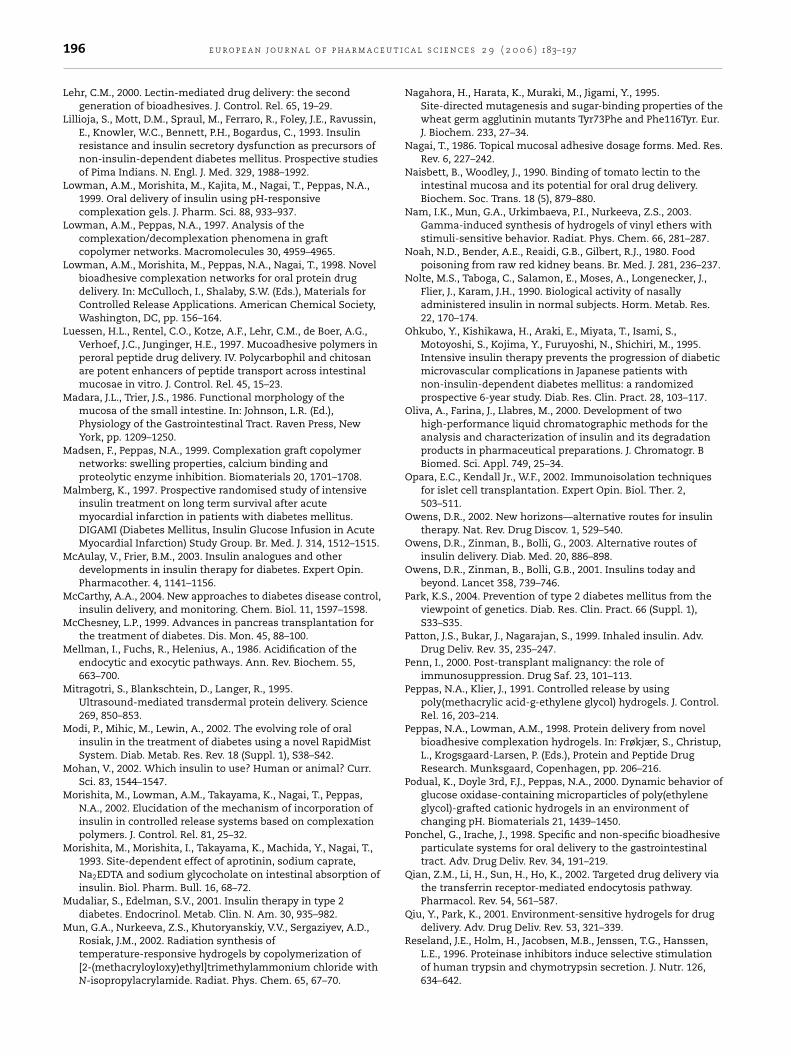
environmental changes. They are composed of the transmem-brane proteins occludin and claudin, and cytoplasmic plaqueproteins zonula occludens (ZO)-1, ZO-2, ZO-3, cingulin and7H6 (Anderson and Van Itallie, 1995).
Next to the tight junction lies the adherens junction, inwhich cadherins act as adhesion receptors as indicated inFig. 3. The cadherins are a group of functionally related gly-coproteins responsible for the calcium-dependent cell-to-celladhesion.
The transcellular pathway is limited to those moleculeswhich have specific mechanisms of active or facilitated trans-port, such as receptors-mediated endocytosis, wherein themolecules recognize specific receptors presented on the cellsurface and get endocytosed in the form of endocytotic vesi-cles. The absorption of large and hydrophilic macromoleculesis almost exclusively limited to the paracellular pathway,which consists of aqueous pores created by the cellulartight junctions (Madara and Trier, 1986). However, under nor-mal conditions, this pathway is restricted to molecules withmolecular radii less than 11 A (Fasano, 1998).
The development of efficacious delivery systems based onwell-regulated modulation of the tight junctions by absorptionenhancers has not been very successful, mainly due to lackof comprehensive understanding of the function of the tightjunctions.
3.3. Strategies for enhancing the protein oralbioavailability
The strategies for enhancing the oral bioavailability of pro-teins can mainly be categorized into two subsets. The firstsubset includes approaches that aim at reversibly changingthe intestinal environment so as to make it more favorable forthe stability and transport of the protein molecule across theintestinal epithelium. The term ‘intestinal environment’ is usedhere to include the lumen of the stomach and the intestine,and the intestinal epithelium. The second subset includes
ically by covalent modifications, so that it can better resistthe proteolytic degradation and can permeate the intestinalepithelium effectively. Some specific examples each of theseapproaches are discussed below.

190 e u r o p e a n j o u r n a l o f p h a r m a c e u t i c a l s c i e n c e s 2 9 ( 2 0 0 6 ) 183–197
Fig. 3 – Representation of the protein components of the apical junction complex, the tight junction and the adherens
junctions in a highly polarized epithelial cell.3.3.1. Changing the intestinal milieu for improvedabsorptionAs pointed out earlier, the reduced bioavailability of proteinsfrom the oral route is mainly due to their extensive degrada-tion in the gastric and intestinal fluids and to some extent, inthe brush border of the epithelial cells, and also due to theirlimited permeability across the intestinal epithelial barrier.Thus, inhibition of the degradative functions of the proteolyticenzymes or an overall increase in the paracellular or transcel-lular permeability of the epithelium may result in significantincrease in the bioavailability of orally administered proteins.Some approaches based on this methodology are highlightedhere.
3.3.2. Permeation enhancers, protease inhibitors and thezonula occludens toxinPermeation enhancers and protease inhibitors have beenextensively studied to overcome the barriers to oral proteinand peptide delivery. Penetration enhancers act on the intesti-nal epithelium and increase the permeability of the mem-brane by either the paracellular or the transcellular pathway.Representative examples of this class of compounds includesubstances like surfactants, fatty acids, bile salts and chela-tors such as ethylene diamine tetra acetate (EDTA). Manygel-forming polymers such as polycarbophil, also act as per-meation enhancers by binding the extracellular Ca2+. Fattyacids, bile salts and surfactants mostly increase the fluidityof the lipid bilayer of the cell membranes thus making themmore permeable. Local toxicity to the epithelium in the gas-trointestinal tract is a major concern in using these systemsin pharmaceutical products.
Intracellular Ca2+ plays an important role in regulating thetight junctional permeability (Kan and Coleman, 1988). Thus,
compounds, such as EDTA, that can bind the extracellularCa2+ thus lowering the intracellular Ca2+ concentration, canact as permeation enhancers by rendering the paracellularpathway more permeable. Some of these enhancers, however,can locally damage the intestinal mucosa and even enter thesystemic circulation, leading to systemic toxic effects. Thus,damage to the epithelium and changes in the intestinal mor-phology, especially in the long-term multi-dosing regimen, aswould be required in diabetes treatment, are major concernsin clinical use of these agents. Another disadvantage of thesecompounds is their non-specificity in permeation enhance-ment. Increased permeability of the epithelium may also allowtoxins and biological pathogens in the intestinal lumen to passinto the systemic circulation.
Aprotinin, soybean trypsin inhibitors and polycarbophil arerepresentative examples of protease inhibitors. By formingreversible stoichiometric enzyme inhibitor complexes, apro-tinin acts as an inhibitor of human trypsin and chymotrypsin.Concomitant administration of insulin with aprotinin andsoybean trypsin inhibitors has been shown to induce hypo-glycemic effect (Bernkop-Schnurch, 1998; Morishita et al.,1993). Polyacrylates such as Carbopol 934P and polycarbophil,which are typically used as bioadhesives, are also known toinhibit the activity of trypsin and chymotrypsin in a calcium-dependent manner (Luessen et al., 1997; Madsen and Peppas,1999). Bai et al. (1996) showed that in situ absorption of insulinwas improved by carbomer polymers and also induced a sig-nificant decline in blood glucose levels.
However, these enzyme inhibitors have a toxic potentialcaused by the inhibition of digestive enzymes, which canfurther cause incomplete digestion of the nutritive proteins.In addition, the inhibitory action can cause increased secre-tion of these enzymes by a feed-back regulation (Bernkop-Schnurch, 1998; Reseland et al., 1996). Studies have shown thatthis feed-back regulation leads to both hypertrophy and hyper-plasia of the pancreas. Prolonged administration of soybeantrypsin inhibitor can lead to invasive carcinoma (Bernkop-
Schnurch, 1998).One of the recent additions to the class of absorptionenhancers is zonula occludens toxin (Zot), a protein secretedby Vibrio cholerae (Baudry et al., 1992). This toxin induces mod-
t i c a l s c i e n c e s 2 9 ( 2 0 0 6 ) 183–197 191
ifitaittaagaisa
thsc
3d
MsstNrpnitwrte
wgtpaepgw
ipabactghpim
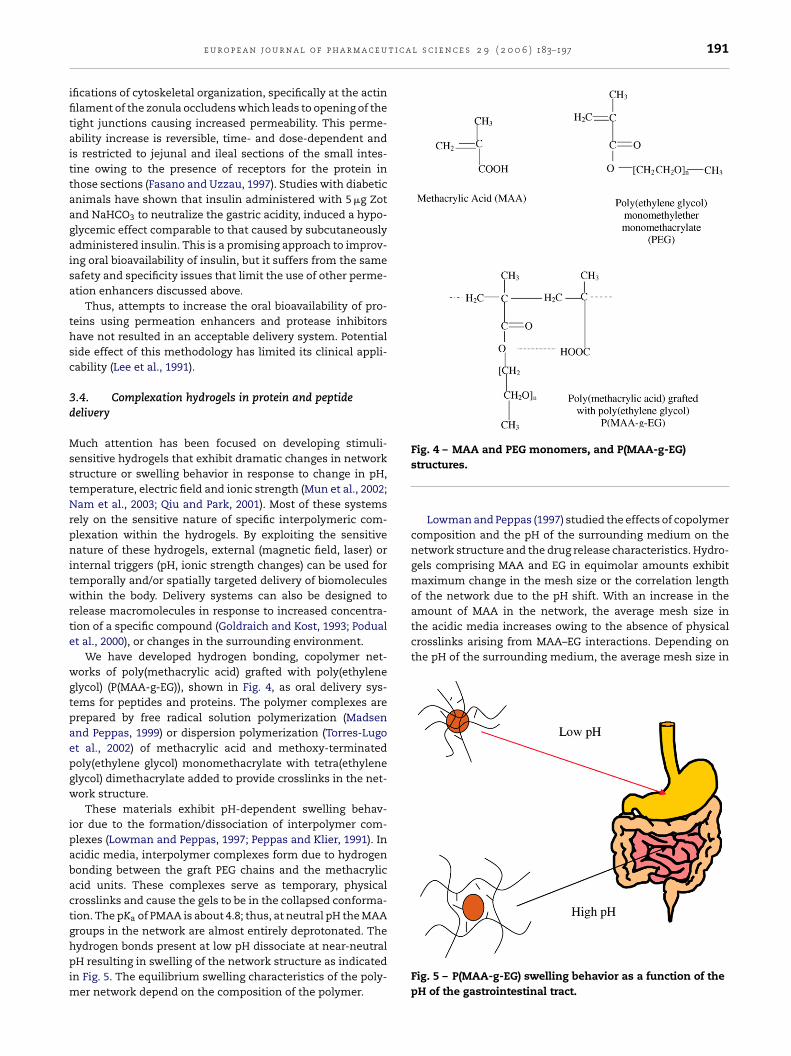
Fig. 4 – MAA and PEG monomers, and P(MAA-g-EG)
amount of MAA in the network, the average mesh size inthe acidic media increases owing to the absence of physicalcrosslinks arising from MAA–EG interactions. Depending onthe pH of the surrounding medium, the average mesh size in
e u r o p e a n j o u r n a l o f p h a r m a c e u
fications of cytoskeletal organization, specifically at the actinlament of the zonula occludens which leads to opening of theight junctions causing increased permeability. This perme-bility increase is reversible, time- and dose-dependent ands restricted to jejunal and ileal sections of the small intes-ine owing to the presence of receptors for the protein inhose sections (Fasano and Uzzau, 1997). Studies with diabeticnimals have shown that insulin administered with 5 �g Zotnd NaHCO3 to neutralize the gastric acidity, induced a hypo-lycemic effect comparable to that caused by subcutaneouslydministered insulin. This is a promising approach to improv-ng oral bioavailability of insulin, but it suffers from the sameafety and specificity issues that limit the use of other perme-tion enhancers discussed above.
Thus, attempts to increase the oral bioavailability of pro-eins using permeation enhancers and protease inhibitorsave not resulted in an acceptable delivery system. Potentialide effect of this methodology has limited its clinical appli-ability (Lee et al., 1991).
.4. Complexation hydrogels in protein and peptideelivery
uch attention has been focused on developing stimuli-ensitive hydrogels that exhibit dramatic changes in networktructure or swelling behavior in response to change in pH,emperature, electric field and ionic strength (Mun et al., 2002;am et al., 2003; Qiu and Park, 2001). Most of these systems
ely on the sensitive nature of specific interpolymeric com-lexation within the hydrogels. By exploiting the sensitiveature of these hydrogels, external (magnetic field, laser) or
nternal triggers (pH, ionic strength changes) can be used foremporally and/or spatially targeted delivery of biomoleculesithin the body. Delivery systems can also be designed to
elease macromolecules in response to increased concentra-ion of a specific compound (Goldraich and Kost, 1993; Podualt al., 2000), or changes in the surrounding environment.
We have developed hydrogen bonding, copolymer net-orks of poly(methacrylic acid) grafted with poly(ethylene
lycol) (P(MAA-g-EG)), shown in Fig. 4, as oral delivery sys-ems for peptides and proteins. The polymer complexes arerepared by free radical solution polymerization (Madsennd Peppas, 1999) or dispersion polymerization (Torres-Lugot al., 2002) of methacrylic acid and methoxy-terminatedoly(ethylene glycol) monomethacrylate with tetra(ethylenelycol) dimethacrylate added to provide crosslinks in the net-ork structure.
These materials exhibit pH-dependent swelling behav-or due to the formation/dissociation of interpolymer com-lexes (Lowman and Peppas, 1997; Peppas and Klier, 1991). Incidic media, interpolymer complexes form due to hydrogenonding between the graft PEG chains and the methacryliccid units. These complexes serve as temporary, physicalrosslinks and cause the gels to be in the collapsed conforma-ion. The pKa of PMAA is about 4.8; thus, at neutral pH the MAAroups in the network are almost entirely deprotonated. The
ydrogen bonds present at low pH dissociate at near-neutralH resulting in swelling of the network structure as indicatedn Fig. 5. The equilibrium swelling characteristics of the poly-er network depend on the composition of the polymer.
structures.
Lowman and Peppas (1997) studied the effects of copolymercomposition and the pH of the surrounding medium on thenetwork structure and the drug release characteristics. Hydro-gels comprising MAA and EG in equimolar amounts exhibitmaximum change in the mesh size or the correlation lengthof the network due to the pH shift. With an increase in the
Fig. 5 – P(MAA-g-EG) swelling behavior as a function of thepH of the gastrointestinal tract.
u t i c a l s c i e n c e s 2 9 ( 2 0 0 6 ) 183–197
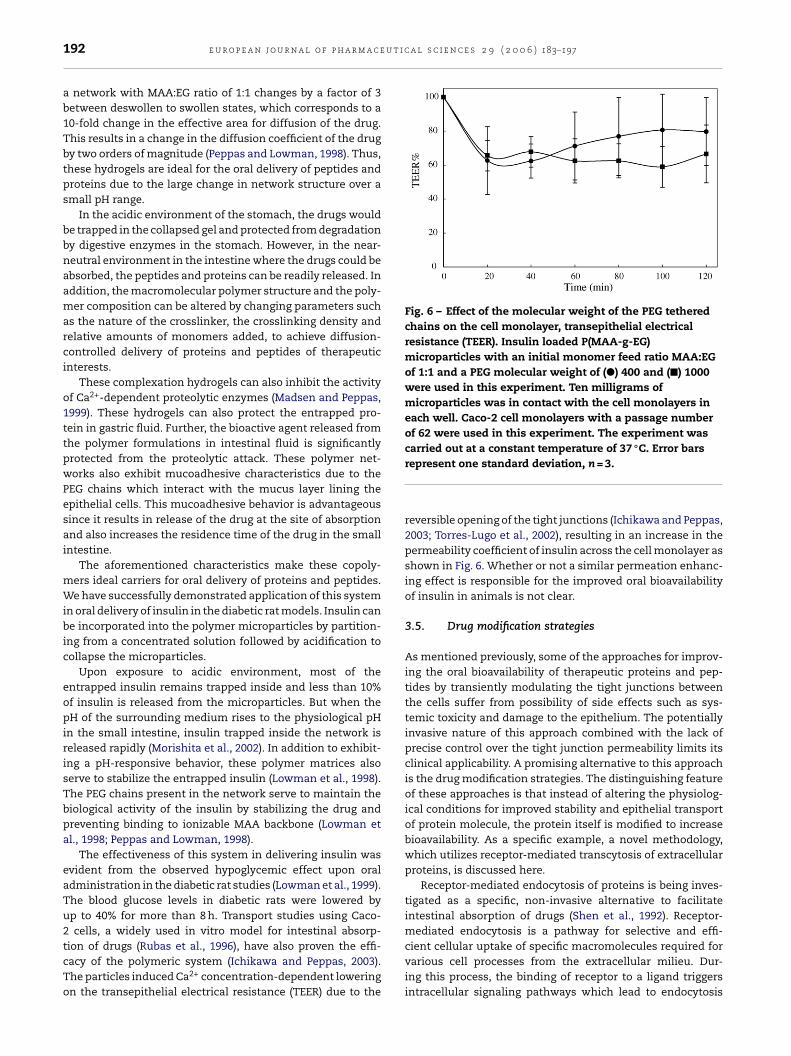
Fig. 6 – Effect of the molecular weight of the PEG tetheredchains on the cell monolayer, transepithelial electricalresistance (TEER). Insulin loaded P(MAA-g-EG)microparticles with an initial monomer feed ratio MAA:EGof 1:1 and a PEG molecular weight of (�) 400 and (�) 1000were used in this experiment. Ten milligrams ofmicroparticles was in contact with the cell monolayers ineach well. Caco-2 cell monolayers with a passage numberof 62 were used in this experiment. The experiment wascarried out at a constant temperature of 37 ◦C. Error bars
192 e u r o p e a n j o u r n a l o f p h a r m a c e
a network with MAA:EG ratio of 1:1 changes by a factor of 3between deswollen to swollen states, which corresponds to a10-fold change in the effective area for diffusion of the drug.This results in a change in the diffusion coefficient of the drugby two orders of magnitude (Peppas and Lowman, 1998). Thus,these hydrogels are ideal for the oral delivery of peptides andproteins due to the large change in network structure over asmall pH range.
In the acidic environment of the stomach, the drugs wouldbe trapped in the collapsed gel and protected from degradationby digestive enzymes in the stomach. However, in the near-neutral environment in the intestine where the drugs could beabsorbed, the peptides and proteins can be readily released. Inaddition, the macromolecular polymer structure and the poly-mer composition can be altered by changing parameters suchas the nature of the crosslinker, the crosslinking density andrelative amounts of monomers added, to achieve diffusion-controlled delivery of proteins and peptides of therapeuticinterests.
These complexation hydrogels can also inhibit the activityof Ca2+-dependent proteolytic enzymes (Madsen and Peppas,1999). These hydrogels can also protect the entrapped pro-tein in gastric fluid. Further, the bioactive agent released fromthe polymer formulations in intestinal fluid is significantlyprotected from the proteolytic attack. These polymer net-works also exhibit mucoadhesive characteristics due to thePEG chains which interact with the mucus layer lining theepithelial cells. This mucoadhesive behavior is advantageoussince it results in release of the drug at the site of absorptionand also increases the residence time of the drug in the smallintestine.
The aforementioned characteristics make these copoly-mers ideal carriers for oral delivery of proteins and peptides.We have successfully demonstrated application of this systemin oral delivery of insulin in the diabetic rat models. Insulin canbe incorporated into the polymer microparticles by partition-ing from a concentrated solution followed by acidification tocollapse the microparticles.
Upon exposure to acidic environment, most of theentrapped insulin remains trapped inside and less than 10%of insulin is released from the microparticles. But when thepH of the surrounding medium rises to the physiological pHin the small intestine, insulin trapped inside the network isreleased rapidly (Morishita et al., 2002). In addition to exhibit-ing a pH-responsive behavior, these polymer matrices alsoserve to stabilize the entrapped insulin (Lowman et al., 1998).The PEG chains present in the network serve to maintain thebiological activity of the insulin by stabilizing the drug andpreventing binding to ionizable MAA backbone (Lowman etal., 1998; Peppas and Lowman, 1998).
The effectiveness of this system in delivering insulin wasevident from the observed hypoglycemic effect upon oraladministration in the diabetic rat studies (Lowman et al., 1999).The blood glucose levels in diabetic rats were lowered byup to 40% for more than 8 h. Transport studies using Caco-2 cells, a widely used in vitro model for intestinal absorp-
tion of drugs (Rubas et al., 1996), have also proven the effi-cacy of the polymeric system (Ichikawa and Peppas, 2003).The particles induced Ca2+ concentration-dependent loweringon the transepithelial electrical resistance (TEER) due to therepresent one standard deviation, n = 3.
reversible opening of the tight junctions (Ichikawa and Peppas,2003; Torres-Lugo et al., 2002), resulting in an increase in thepermeability coefficient of insulin across the cell monolayer asshown in Fig. 6. Whether or not a similar permeation enhanc-ing effect is responsible for the improved oral bioavailabilityof insulin in animals is not clear.
3.5. Drug modification strategies
As mentioned previously, some of the approaches for improv-ing the oral bioavailability of therapeutic proteins and pep-tides by transiently modulating the tight junctions betweenthe cells suffer from possibility of side effects such as sys-temic toxicity and damage to the epithelium. The potentiallyinvasive nature of this approach combined with the lack ofprecise control over the tight junction permeability limits itsclinical applicability. A promising alternative to this approachis the drug modification strategies. The distinguishing featureof these approaches is that instead of altering the physiolog-ical conditions for improved stability and epithelial transportof protein molecule, the protein itself is modified to increasebioavailability. As a specific example, a novel methodology,which utilizes receptor-mediated transcytosis of extracellularproteins, is discussed here.
Receptor-mediated endocytosis of proteins is being inves-tigated as a specific, non-invasive alternative to facilitateintestinal absorption of drugs (Shen et al., 1992). Receptor-mediated endocytosis is a pathway for selective and effi-
cient cellular uptake of specific macromolecules required forvarious cell processes from the extracellular milieu. Dur-ing this process, the binding of receptor to a ligand triggersintracellular signaling pathways which lead to endocytosis
t i c a
oct(tttitir
rsddeoprtcaeclc
3
ToirmSba(
t(bTbitaamts
hcFtigs
e u r o p e a n j o u r n a l o f p h a r m a c e u
f the receptor–ligand complex in membrane-derived vesi-les. After endocytosis, the receptor–ligand complex encoun-ers the acidic pH in the early endosomal compartmentsMellman et al., 1986), which may lead to: (i) uncoupling ofhe ligand–receptor complex due to changes in the conforma-ion of receptor proteins followed by recycling of the recep-or to the cell membrane, or (ii) degradation of the receptorn lysosomes. The endocytosed ligands that dissociate fromheir receptors in the early endosomes are usually degradedn the lysosomes. Some ligands, however, remain bound to theeceptors and hence share the fate of their bound receptors.
Depending on the specific type of the receptor proteins, theeceptors along with the bound ligand may be recycled to theame plasma membrane domain from which they came, getegraded in the lysosomes, or get transported to a differentomain of the membrane, as in the polarized epithelial andndothelial cells. The last process is called transcytosis and isf particular interest from drug delivery standpoint. By cou-ling therapeutic proteins to the ligand molecules that canecognize specific receptors on the epithelial cell monolayers,ranscellular delivery of these macromolecular biopharma-euticals may be achieved. Since only those molecules thatre conjugated to the ligands are transcytosed, this processliminates the potential side effects associated to the unspe-ific transport by the paracellular pathway. Transferrin andectin receptor-mediated protein delivery systems are dis-ussed here.
.6. Transferrin-mediated drug delivery
ransferrin is a single-chain protein with molecular weightf approximately ∼80 kDa (Singh, 1999). Serum transferrin is
nvolved in uptake of iron by the cells and tissues. Transfer-in receptors (TfRs) have been widely explored for receptor-
ediated delivery of anticancer agents (Beyer et al., 1998;ingh, 1999), in enhancing the transport of drugs across thelood brain barrier (Broadwell et al., 1996; Qian et al., 2002),nd more recently, across the epithelial cells of the intestineXia et al., 2000).
TfR is a homodimer expressed by many cell types includinghe human intestinal cells. TfR binds iron-bound transferrinholo-transferrin) on the cell surface. This binding is sensedy the cells which results in an uptake of the Tf–TfR complex.riggered by the change in the endosomal pH, the ligand-ound transferrin then looses its bound iron and the complex
s recycled to the cell surface where iron-free transferrin (apo-ransferrin) is released. In polarized cells such as the epithelialnd endothelial cells, transferrin can be transcytosed from thepical to the basolateral membrane (Jones et al., 2003). Thisechanism is exploited in TfR-mediated drug delivery across
he blood brain barrier as well as the epithelial barrier of themall intestine.
Transferrin receptors are present at high densities inuman GI epithelium (Banerjee et al., 1986), and transferrinan resist tryptic and chymotryptic degradation (Azari andeeney, 1958). Shen and co-workers (Wan et al., 1992) were
he first to utilize the potential of TfR-mediated transport inmproving oral delivery of therapeutic agents. They conju-ated transferrin to insulin via disulfide linkages and demon-trated that the conjugation resulted in 5–15-fold increasel s c i e n c e s 2 9 ( 2 0 0 6 ) 183–197 193
in insulin transport across Caco-2 cell monolayer (Shah andShen, 1996). As pointed out earlier, since this enhancement isspecific for the conjugated protein, viz. insulin, and takes placewithout causing the tight junctions to open even momentar-ily, this approach is most desirable in terms of toxicity anddamage to the epithelium.
Following successful in vitro studies, Shen and co-workers(Xia et al., 2000) demonstrated that insulin–transferrin conju-gate, when administered orally to diabetic rats, caused slowbut prolonged hypoglycemic effect. In–Tf conjugate after oraladministration as well as after subcutaneous injection causeda delayed but prolonged glucose reducing activity as com-pared to native insulin after subcutaneous injection. Subcuta-neously administered In–Tf conjugate maintained low bloodglucose levels for at least four times longer than unconjugatedinsulin. While this might be beneficial in terms of the fre-quency of dosage, the reasons behind this behavior is not fullyunderstood.
The authors have also presented data suggesting that thedisulfide linkage between the two proteins can be reducedin the liver following its absorption into the portal vein. Theapproach thus makes use of transferrin for overcoming thetransport barrier of the small intestine after which free insulincan be released to perform its physiological system.
The observation that the intact conjugate is able to reachthe systemic circulation intact, suggests that the insulin con-jugated to transferrin is able to overcome proteolytic attackduring transit in the GI tract and across the epithelial cells. Invitro studies with simulated gastric and intestinal fluids canshed light on the conjugates ability to shield insulin from pro-teolytic attack.
3.7. Lectin-mediated drug delivery
Lectins are a class of structurally diverse proteins of non-immune origin that are characterized by their ability to specifi-cally bind carbohydrates (Rini, 1995). They are primarily foundin seeds, but are also present in animals, plants and microor-ganisms. Lectins have been studied widely for oral deliveryapplications because of their relatively good resistance to theacidic pH and enzymatic degradation and presence of bindingsites in the gastrointestinal tract (Gabor et al., 1997; Naisbettet al., 1990). While some lectins such as phaseolus vulgarisagglutinin (PHA) from raw kidney beans have been known tocause dietary toxicity (Lafont et al., 1988; Noah et al., 1980) andare unsuitable for drug delivery applications, variety of otherlectins such as wheat germ agglutinin (WGA) Triticum vulgare(Gabor et al., 1997) and tomato lectin (TL) from Lycopersicumesculentum (Kilpatrick et al., 1985) are natural component ofour diet and bind to intestinal mucosa without any obviousdeleterious effects.
Use of lectins in improving the residence time of the drugcarrier particulate systems has been the subject of a num-ber of excellent reviews (Clark et al., 2000; Lehr, 2000; Poncheland Irache, 1998; Woodley, 2001). Recent work on the use ofWGA–protein conjugates for improving the uptake and tran-
scytosis of proteins across the epithelial cell barrier of the gutis discussed here.WGA is a dimeric protein with two subunits contain-ing two or four carbohydrate-combining sites (Nagahora

u t i c
r
194 e u r o p e a n j o u r n a l o f p h a r m a c e
et al., 1995). It specifically binds N-acetylglucosamine andsialic acid residues. Wheat germ contains approximately300 mg WGA/kg and hence the peroral toxicity that can resultfrom long-term oral administration of WGA may be negligible(Gabor et al., 2002). Further the lectin can resist degradationdue to proteolytic attack upon exposure to the gastrointesti-nal enzymes (Gabor et al., 1997). These characteristics andthe presence of N-acetylglucosamine containing oligosaccha-rides in the glycocalyx of the intestinal mucosa make WGA apromising candidate for enhancing oral bioavailability of drugcandidates.
Binding studies of WGA using Caco-2 cells, mucus-producing HT-29 cells and HT-8 cells have revealed that itexhibits low non-specific proteinaceous binding to the cell sur-faces and high affinity for oligosaccharides present on the cellsurfaces (Gabor et al., 1998). In an interesting study, Gabor etal. (2002) examined whether WGA can improve the bindingand uptake of a model fluorescently labeled BSA (F-BSA), bythe Caco-2 cells. They observed that WGA in the conjugatedform was able to bind specifically to the oligosaccharides onthe cell surface and the conjugate was uptaken by the cells byan energy-dependent mechanism.
This is an important result since it demonstrates the poten-tial of lectin-mediated delivery in improving the transcellulartransport of proteins across the epithelium. However, thereare concerns about the cellular fate of the uptaken conjugate.The conjugate accumulated within lysosomal compartmentwhere it was degraded. The degraded products diffused intothe cytosol and finally appeared in the extracellular medium.Thus, even though lectins can resist degradation due to pro-teolytic attack, the conjugated protein drug is still susceptibleto degradation by the enzymes in the lysosomes. In addition,the stability of such conjugates in the gastrointestinal envi-ronment is an unaddressed issue.
One important consideration here is the size of the proteinunder consideration that is conjugated to the lectin. WGA is147 kDa, whereas BSA is 68 kDa protein. Since BSA is a largemolecule, the lectin may not be able to protect bound proteinby creating a steric hindrance to the proteolytic attack. But ifa smaller protein such as insulin (5.8 kDa with hydrodynamicradius of approximately 20 A) is conjugated to WGA, the lectinmight shield the bound protein from proteolytic attack andhence improve its stability during transit in the GI tract andthrough the cellular barrier.
4. Conclusions
A variety of approaches have emerged in the recent pastfor designing oral delivery systems for therapeutic proteinsand peptides, although a clinically viable solution to thislong standing problem still alludes the scientific community.These approaches come from such diverse research disci-plines as biomaterials, conjugation chemistry, nanotechnol-ogy, cell biology and employ different methodologies for solv-
ing the same problem. Some of these strategies have distin-guishing beneficial characteristics that make them good can-didates for oral protein delivery. Interfacing different strate-gies to combine the benefits of novel approaches is an inter-esting new possibility.a l s c i e n c e s 2 9 ( 2 0 0 6 ) 183–197
Acknowledgment
This work was supported by grant R01 EB000246 from theNational Institutes of Health of the USA. We kindly acknowl-edge technical support by our colleague Dr. Jennifer Lopez whodrew Figs. 1–3.
e f e r e n c e s
Anon., 1999. Definition, Diagnosis and Classification of DiabetesMellitus and its Complications. Report of a WHOConsultation, Part 1: Diagnosis and Classification of DiabetesMellitus. World Health Organization, Geneva.
Amos, A.F., McCarty, D.J., Zimmet, P., 1997. The rising globalburden of diabetes and its complications: estimates andprojections to the year 2010. Diab. Med. 14 (Suppl. 5), S1–S85.
Anderson, J.M., Van Itallie, C.M., 1995. Tight junctions and themolecular basis for regulation of paracellular permeability.Am. J. Physiol. 269, G467–G475.
Anthony, S., Odgers, T., Kelly, W., 2004. Health promotion andhealth education about diabetes mellitus. J. R. Soc. Health 124,70–73.
Arbit, E., 2004. The physiological rationale for oral insulinadministration. Diab. Technol. Ther. 6, 510–517.
Aungst, B.J., Rogers, N.J., 1988. Site dependence ofabsorption-promoting actions of laureth-9, Na salicylate,Na2EDTA, and aprotinin on rectal, nasal, and buccal insulindelivery. Pharm. Res. 5, 305–308.
Azari, P.R., Feeney, R.E., 1958. Resistance of metal complexes ofconalbumin and transferrin to proteolysis and to thermaldenaturation. J. Biol. Chem. 232, 293–302.
Bai, J.P., Chang, L.L., Guo, J.H., 1996. Effects of polyacrylicpolymers on the degradation of insulin and peptide drugs bychymotrypsin and trypsin. J. Pharm. Pharmacol. 48, 17–21.
Ballinger, W.F., Lacy, P.E., 1972. Transplantation of intactpancreatic islets in rats. Surgery 72, 175–186.
Banerjee, D., Flanagan, P.R., Cluett, J., Valberg, L.S., 1986.Transferrin receptors in the human gastrointestinal tract.Relationship to body iron stores. Gastroenterology 91, 861–869.
Barnett, A.H., Owens, D.R., 1997. Insulin analogues. Lancet 349,47–51.
Baudry, B., Fasano, A., Ketley, J., Kaper, J.B., 1992. Cloning of a gene(zot) encoding a new toxin produced by Vibrio cholerae. Infect.Immun. 60, 428–434.
Benjamin, S.M., Valdez, R., Geiss, L.S., Rolka, D.B., Narayan, K.M.,2003. Estimated number of adults with prediabetes in the USin 2000: opportunities for prevention. Diab. Care 26, 645–649.
Bernkop-Schnurch, A., 1998. The use of inhibitory agents toovercome the enzymatic barrier to perorally administeredtherapeutic peptides and proteins. J. Control. Rel. 52, 1–16.
Beyer, U., Roth, T., Schumacher, P., Maier, G., Unold, A., Frahm,A.W., Fiebig, H.H., Unger, C., Kratz, F., 1998. Synthesis and invitro efficacy of transferrin conjugates of the anticancer drugchlorambucil. J. Med. Chem. 41, 2701–2708.
Bolli, G.B., Di Marchi, R.D., Park, G.D., Pramming, S., Koivisto, V.A.,1999. Insulin analogues and their potential in themanagement of diabetes mellitus. Diabetologia 42, 1151–1167.
Bouwens, L., 2004. Islet morphogenesis and stem cell markers.Cell Biochem. Biophys. 40, 81–88.
Brange, J., Volund, A., 1999. Insulin analogs with improved
pharmacokinetic profiles. Adv. Drug Deliv. Rev. 35, 307–335.Broadwell, R.D., Baker-Cairns, B.J., Friden, P.M., Oliver, C., Villegas,J.C., 1996. Transcytosis of protein through the mammaliancerebral epithelium and endothelium. III. Receptor-mediatedtranscytosis through the blood–brain barrier of blood-borne
t i c a
C
C
C
C
C
d
D
D
D
F
F
F
G
G
G
G
G
G
G
G
G
e u r o p e a n j o u r n a l o f p h a r m a c e u
transferrin and antibody against the transferrin receptor. Exp.Neurol. 142, 47–65.
efalu, W.T., 2004. Concept, strategies, and feasibility ofnoninvasive insulin delivery. Diab. Care 27, 239–246.
efalu, W.T., Rosenstock, J., Bindra, S., 2002. Inhaled insulin: anovel route for insulin delivery. Expert Opin. Investig. Drugs11, 687–691.
evc, G., Gebauer, D., Stieber, J., Schatzlein, A., Blume, G., 1998.Ultraflexible vesicles, transfersomes, have an extremely lowpore penetration resistance and transport therapeuticamounts of insulin across the intact mammalian skin.Biochim. Biophys. Acta 1368, 201–215.
lark, M.A., Hirst, B.H., Jepson, M.A., 2000. Lectin-mediatedmucosal delivery of drugs and microparticles. Adv. Drug Deliv.Rev. 43, 207–223.
lement, S., Dandona, P., Still, J.G., Kosutic, G., 2004. Oral modifiedinsulin (HIM2) in patients with type 1 diabetes mellitus:results from a phase I/II clinical trial. Metabolism 53, 54–58.
e Groot, M., Schuurs, T.A., van Schilfgaarde, R., 2004. Causes oflimited survival of microencapsulated pancreatic islet grafts.J. Surg. Res. 121, 141–150.
enker, B.M., Nigam, S.K., 1998. Molecular structure andassembly of the tight junction. Am. J. Physiol. 274, F1–F9.
ominguez, L.J., Licata, G., 2001. The discovery of insulin: whatreally happened 80 years ago. Ann. Ital. Med. Int. 16, 155–162.
rejer, K., Vaag, A., Bech, K., Hansen, P., Sorensen, A.R., Mygind,N., 1992. Intranasal administration of insulin withphospholipid as absorption enhancer: pharmacokinetics innormal subjects. Diab. Med. 9, 335–340.
asano, A., 1998. Novel approaches for oral delivery ofmacromolecules. J. Pharm. Sci. 87, 1351–1356.
asano, A., Uzzau, S., 1997. Modulation of intestinal tightjunctions by zonula occludens toxin permits enteraladministration of insulin and other macromolecules in ananimal model. J. Clin. Invest. 99, 1158–1164.
oldvari, M., 2000. Non-invasive administration of drugs throughthe skin: challenges in delivery system design. Pharm. Sci.Technol. Today 3, 417–425.
abbe, S.G., Graves, C.R., 2003. Management of diabetes mellituscomplicating pregnancy. Obstet. Gynecol. 102, 857–868.
abor, F., Schwarzbauer, A., Wirth, M., 2002. Lectin-mediateddrug delivery: binding and uptake of BSA–WGA conjugatesusing the Caco-2 model. Int. J. Pharm. 237, 227–239.
abor, F., Stangl, M., Wirth, M., 1998. Lectin-mediatedbioadhesion: binding characteristics of plant lectins on theenterocyte-like cell lines Caco-2, HT-29 and HCT-8. J. Control.Rel. 55, 131–142.
abor, F., Wirth, M., Jurkovich, B., Haberl, I., Theyer, G., Walcher,G., Hamilton, G., 1997. Lectin-mediated bioadhesion:proteolytic stability and binding-characteristics of wheatgerm agglutinin and Solanum tuberosum lectin onCaco-2, HT-29 and human colonocytes. J. Control. Rel. 49,27–37.
anong, W., 1995. Review of Medical Physiology. Appleton &Lange, Stamford, CT.
enuth, S., Alberti, K.G., Bennett, P., Buse, J., Defronzo, R., Kahn,R., Kitzmiller, J., Knowler, W.C., Lebovitz, H., Lernmark, A.,Nathan, D., Palmer, J., Rizza, R., Saudek, C., Shaw, J., Steffes,M., Stern, M., Tuomilehto, J., Zimmet, P., 2003. Follow-upreport on the diagnosis of diabetes mellitus. Diab. Care 26,3160–3167.
oldraich, M., Kost, J., 1993. Glucose-sensitive polymeric matricesfor controlled drug delivery. Clin. Mater. 13, 135–142.
ordon, G.S., Moses, A.C., Silver, R.D., Flier, J.S., Carey, M.C., 1985.
Nasal absorption of insulin: enhancement by hydrophobicbile salts. Proc. Natl. Acad. Sci. U.S.A. 82, 7419–7423.roup, U.P.D.S., 1998. Intensive blood-glucose control withsulphonylureas or insulin compared with conventional
l s c i e n c e s 2 9 ( 2 0 0 6 ) 183–197 195
treatment and risk of complications in patients with type 2diabetes (UKPDS 33). Lancet 352, 837–853.
Guevara-Aguirre, J., Guevara, M., Saavedra, J., Mihic, M., Modi, P.,2004. Oral spray insulin in treatment of type 2 diabetes: acomparison of efficacy of the oral spray insulin (Oralin) withsubcutaneous (SC) insulin injection, a proof of concept study.Diab. Metab. Res. Rev. 20, 472–478.
Hayakawa, E., Yamamoto, A., Shoji, Y., Lee, V.H., 1989. Effect ofsodium glycocholate and polyoxyethylene-9-lauryl ether onthe hydrolysis of varying concentrations of insulin in thenasal homogenates of the albino rabbit. Life Sci. 45,167–174.
Heinemann, L., Pfutzner, A., Heise, T., 2001. Alternative routes ofadministration as an approach to improve insulin therapy:update on dermal, oral, nasal and pulmonary insulin delivery.Curr. Pharm. Des. 7, 1327–1351.
Hermansen, K., Ronnemaa, T., Petersen, A.H., Bellaire, S.,Adamson, U., 2004. Intensive therapy with inhaled insulin viathe AERx insulin diabetes management system: a 12-weekproof-of-concept trial in patients with type 2 diabetes. Diab.Care 27, 162–167.
Hill, R.A., Strat, A.L., Hughes, N.J., Kokta, T.J., Dodson, M.V.,Gertler, A., 2004. Early insulin signaling cascade in a model ofoxidative skeletal muscle: mouse Sol8 cell line. Biochim.Biophys. Acta 1693, 205–211.
Hussain, M.A., Theise, N.D., 2004. Stem-cell therapy for diabetesmellitus. Lancet 364, 203–205.
Ichikawa, H., Peppas, N.A., 2003. Novel complexation hydrogelsfor oral peptide delivery: in vitro evaluation of theircytocompatibility and insulin-transport enhancing effectsusing Caco-2 cell monolayers. J. Biomed. Mater. Res. 67A,609–617.
Jones, A.T., Gumbleton, M., Duncan, R., 2003. Understandingendocytic pathways and intracellular trafficking: aprerequisite for effective design of advanced drug deliverysystems. Adv. Drug Deliv. Rev. 55, 1353–1357.
Kan, K.S., Coleman, R., 1988. The calcium ionophore A23187increases the tight-junctional permeability in rat liver.Biochem. J. 256, 1039–1041.
Kilpatrick, D.C., Pusztai, A., Grant, G., Graham, C., Ewen, S.W.B.,1985. Tomato lectin resists digestion in the mammalianalimentary canal and binds to intestinal villi withoutdeleterious effects. FEBS Lett. 185, 299–305.
King, H., Aubert, R.E., Herman, W.H., 1998. Global burden ofdiabetes, 1995–2025: prevalence, numerical estimates, andprojections. Diab. Care 21, 1414–1431.
Kissel, T., Werner, U., 1998. Nasal delivery of peptides: an in vitrocell culture model for the investigation of transport andmetabolism in human nasal epithelium. J. Control. Rel. 53,195–203.
Lafont, J., Rouanet, J.M., Gabrion, J., Assouad, J.L., ZamboninoInfante, J.L., Besancon, P., 1988. Duodenal toxicity of dietaryphaseolus vulgaris lectins in the rat: an integrative assay.Digestion 41, 83–93.
Langkjaer, L., Brange, J., Grodsky, G.M., Guy, R.H., 1998.Iontophoresis of monomeric insulin analogues in vitro:effects of insulin charge and skin pretreatment. J. Control. Rel.51, 47–56.
Le, L., Kost, J., Mitragotri, S., 2000. Combined effect oflow-frequency ultrasound and iontophoresis: applications fortransdermal heparin delivery. Pharm. Res. 17,1151–1154.
Lee, V.H., Yamamoto, A., Kompella, U.B., 1991. Mucosalpenetration enhancers for facilitation of peptide and protein
drug absorption. Crit. Rev. Ther. Drug Carrier Syst. 8, 91–192.Lee, V.H.L., Yamamoto, A., 1989. Penetration and enzymaticbarriers to peptide and protein absorption. Adv. Drug Deliv.Rev. 4, 171–207.
u t i c
196 e u r o p e a n j o u r n a l o f p h a r m a c eLehr, C.M., 2000. Lectin-mediated drug delivery: the secondgeneration of bioadhesives. J. Control. Rel. 65, 19–29.
Lillioja, S., Mott, D.M., Spraul, M., Ferraro, R., Foley, J.E., Ravussin,E., Knowler, W.C., Bennett, P.H., Bogardus, C., 1993. Insulinresistance and insulin secretory dysfunction as precursors ofnon-insulin-dependent diabetes mellitus. Prospective studiesof Pima Indians. N. Engl. J. Med. 329, 1988–1992.
Lowman, A.M., Morishita, M., Kajita, M., Nagai, T., Peppas, N.A.,1999. Oral delivery of insulin using pH-responsivecomplexation gels. J. Pharm. Sci. 88, 933–937.
Lowman, A.M., Peppas, N.A., 1997. Analysis of thecomplexation/decomplexation phenomena in graftcopolymer networks. Macromolecules 30, 4959–4965.
Lowman, A.M., Morishita, M., Peppas, N.A., Nagai, T., 1998. Novelbioadhesive complexation networks for oral protein drugdelivery. In: McCulloch, I., Shalaby, S.W. (Eds.), Materials forControlled Release Applications. American Chemical Society,Washington, DC, pp. 156–164.
Luessen, H.L., Rentel, C.O., Kotze, A.F., Lehr, C.M., de Boer, A.G.,Verhoef, J.C., Junginger, H.E., 1997. Mucoadhesive polymers inperoral peptide drug delivery. IV. Polycarbophil and chitosanare potent enhancers of peptide transport across intestinalmucosae in vitro. J. Control. Rel. 45, 15–23.
Madara, J.L., Trier, J.S., 1986. Functional morphology of themucosa of the small intestine. In: Johnson, L.R. (Ed.),Physiology of the Gastrointestinal Tract. Raven Press, NewYork, pp. 1209–1250.
Madsen, F., Peppas, N.A., 1999. Complexation graft copolymernetworks: swelling properties, calcium binding andproteolytic enzyme inhibition. Biomaterials 20, 1701–1708.
Malmberg, K., 1997. Prospective randomised study of intensiveinsulin treatment on long term survival after acutemyocardial infarction in patients with diabetes mellitus.DIGAMI (Diabetes Mellitus, Insulin Glucose Infusion in AcuteMyocardial Infarction) Study Group. Br. Med. J. 314, 1512–1515.
McAulay, V., Frier, B.M., 2003. Insulin analogues and otherdevelopments in insulin therapy for diabetes. Expert Opin.Pharmacother. 4, 1141–1156.
McCarthy, A.A., 2004. New approaches to diabetes disease control,insulin delivery, and monitoring. Chem. Biol. 11, 1597–1598.
McChesney, L.P., 1999. Advances in pancreas transplantation forthe treatment of diabetes. Dis. Mon. 45, 88–100.
Mellman, I., Fuchs, R., Helenius, A., 1986. Acidification of theendocytic and exocytic pathways. Ann. Rev. Biochem. 55,663–700.
Mitragotri, S., Blankschtein, D., Langer, R., 1995.Ultrasound-mediated transdermal protein delivery. Science269, 850–853.
Modi, P., Mihic, M., Lewin, A., 2002. The evolving role of oralinsulin in the treatment of diabetes using a novel RapidMistSystem. Diab. Metab. Res. Rev. 18 (Suppl. 1), S38–S42.
Mohan, V., 2002. Which insulin to use? Human or animal? Curr.Sci. 83, 1544–1547.
Morishita, M., Lowman, A.M., Takayama, K., Nagai, T., Peppas,N.A., 2002. Elucidation of the mechanism of incorporation ofinsulin in controlled release systems based on complexationpolymers. J. Control. Rel. 81, 25–32.
Morishita, M., Morishita, I., Takayama, K., Machida, Y., Nagai, T.,1993. Site-dependent effect of aprotinin, sodium caprate,Na2EDTA and sodium glycocholate on intestinal absorption ofinsulin. Biol. Pharm. Bull. 16, 68–72.
Mudaliar, S., Edelman, S.V., 2001. Insulin therapy in type 2diabetes. Endocrinol. Metab. Clin. N. Am. 30, 935–982.
Mun, G.A., Nurkeeva, Z.S., Khutoryanskiy, V.V., Sergaziyev, A.D.,
Rosiak, J.M., 2002. Radiation synthesis oftemperature-responsive hydrogels by copolymerization of[2-(methacryloyloxy)ethyl]trimethylammonium chloride withN-isopropylacrylamide. Radiat. Phys. Chem. 65, 67–70.a l s c i e n c e s 2 9 ( 2 0 0 6 ) 183–197
Nagahora, H., Harata, K., Muraki, M., Jigami, Y., 1995.Site-directed mutagenesis and sugar-binding properties of thewheat germ agglutinin mutants Tyr73Phe and Phe116Tyr. Eur.J. Biochem. 233, 27–34.
Nagai, T., 1986. Topical mucosal adhesive dosage forms. Med. Res.Rev. 6, 227–242.
Naisbett, B., Woodley, J., 1990. Binding of tomato lectin to theintestinal mucosa and its potential for oral drug delivery.Biochem. Soc. Trans. 18 (5), 879–880.
Nam, I.K., Mun, G.A., Urkimbaeva, P.I., Nurkeeva, Z.S., 2003.Gamma-induced synthesis of hydrogels of vinyl ethers withstimuli-sensitive behavior. Radiat. Phys. Chem. 66, 281–287.
Noah, N.D., Bender, A.E., Reaidi, G.B., Gilbert, R.J., 1980. Foodpoisoning from raw red kidney beans. Br. Med. J. 281, 236–237.
Nolte, M.S., Taboga, C., Salamon, E., Moses, A., Longenecker, J.,Flier, J., Karam, J.H., 1990. Biological activity of nasallyadministered insulin in normal subjects. Horm. Metab. Res.22, 170–174.
Ohkubo, Y., Kishikawa, H., Araki, E., Miyata, T., Isami, S.,Motoyoshi, S., Kojima, Y., Furuyoshi, N., Shichiri, M., 1995.Intensive insulin therapy prevents the progression of diabeticmicrovascular complications in Japanese patients withnon-insulin-dependent diabetes mellitus: a randomizedprospective 6-year study. Diab. Res. Clin. Pract. 28, 103–117.
Oliva, A., Farina, J., Llabres, M., 2000. Development of twohigh-performance liquid chromatographic methods for theanalysis and characterization of insulin and its degradationproducts in pharmaceutical preparations. J. Chromatogr. BBiomed. Sci. Appl. 749, 25–34.
Opara, E.C., Kendall Jr., W.F., 2002. Immunoisolation techniquesfor islet cell transplantation. Expert Opin. Biol. Ther. 2,503–511.
Owens, D.R., 2002. New horizons—alternative routes for insulintherapy. Nat. Rev. Drug Discov. 1, 529–540.
Owens, D.R., Zinman, B., Bolli, G., 2003. Alternative routes ofinsulin delivery. Diab. Med. 20, 886–898.
Owens, D.R., Zinman, B., Bolli, G.B., 2001. Insulins today andbeyond. Lancet 358, 739–746.
Park, K.S., 2004. Prevention of type 2 diabetes mellitus from theviewpoint of genetics. Diab. Res. Clin. Pract. 66 (Suppl. 1),S33–S35.
Patton, J.S., Bukar, J., Nagarajan, S., 1999. Inhaled insulin. Adv.Drug Deliv. Rev. 35, 235–247.
Penn, I., 2000. Post-transplant malignancy: the role ofimmunosuppression. Drug Saf. 23, 101–113.
Peppas, N.A., Klier, J., 1991. Controlled release by usingpoly(methacrylic acid-g-ethylene glycol) hydrogels. J. Control.Rel. 16, 203–214.
Peppas, N.A., Lowman, A.M., 1998. Protein delivery from novelbioadhesive complexation hydrogels. In: Frøkjær, S., Christup,L., Krogsgaard-Larsen, P. (Eds.), Protein and Peptide DrugResearch. Munksgaard, Copenhagen, pp. 206–216.
Podual, K., Doyle 3rd, F.J., Peppas, N.A., 2000. Dynamic behavior ofglucose oxidase-containing microparticles of poly(ethyleneglycol)-grafted cationic hydrogels in an environment ofchanging pH. Biomaterials 21, 1439–1450.
Ponchel, G., Irache, J., 1998. Specific and non-specific bioadhesiveparticulate systems for oral delivery to the gastrointestinaltract. Adv. Drug Deliv. Rev. 34, 191–219.
Qian, Z.M., Li, H., Sun, H., Ho, K., 2002. Targeted drug delivery viathe transferrin receptor-mediated endocytosis pathway.Pharmacol. Rev. 54, 561–587.
Qiu, Y., Park, K., 2001. Environment-sensitive hydrogels for drugdelivery. Adv. Drug Deliv. Rev. 53, 321–339.
Reseland, J.E., Holm, H., Jacobsen, M.B., Jenssen, T.G., Hanssen,L.E., 1996. Proteinase inhibitors induce selective stimulationof human trypsin and chymotrypsin secretion. J. Nutr. 126,634–642.
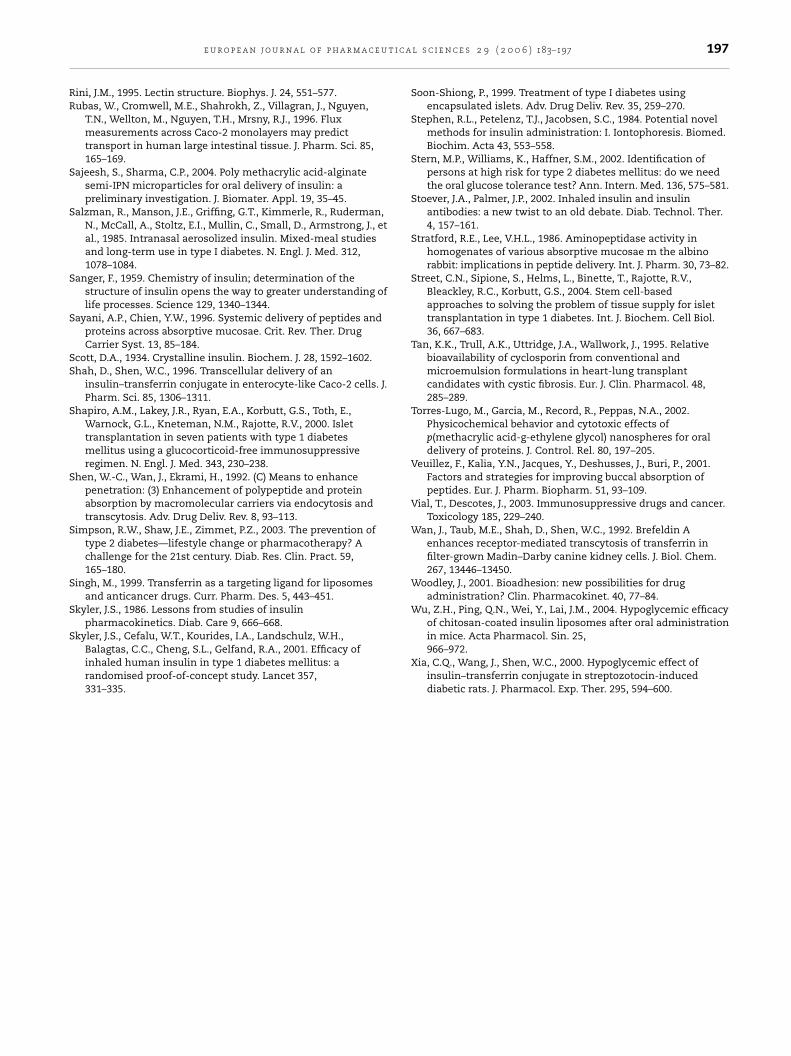
t i c a
RR
S
S
S
S
SS
S
S
S
S
S
S
e u r o p e a n j o u r n a l o f p h a r m a c e u
ini, J.M., 1995. Lectin structure. Biophys. J. 24, 551–577.ubas, W., Cromwell, M.E., Shahrokh, Z., Villagran, J., Nguyen,
T.N., Wellton, M., Nguyen, T.H., Mrsny, R.J., 1996. Fluxmeasurements across Caco-2 monolayers may predicttransport in human large intestinal tissue. J. Pharm. Sci. 85,165–169.
ajeesh, S., Sharma, C.P., 2004. Poly methacrylic acid-alginatesemi-IPN microparticles for oral delivery of insulin: apreliminary investigation. J. Biomater. Appl. 19, 35–45.
alzman, R., Manson, J.E., Griffing, G.T., Kimmerle, R., Ruderman,N., McCall, A., Stoltz, E.I., Mullin, C., Small, D., Armstrong, J., etal., 1985. Intranasal aerosolized insulin. Mixed-meal studiesand long-term use in type I diabetes. N. Engl. J. Med. 312,1078–1084.
anger, F., 1959. Chemistry of insulin; determination of thestructure of insulin opens the way to greater understanding oflife processes. Science 129, 1340–1344.
ayani, A.P., Chien, Y.W., 1996. Systemic delivery of peptides andproteins across absorptive mucosae. Crit. Rev. Ther. DrugCarrier Syst. 13, 85–184.
cott, D.A., 1934. Crystalline insulin. Biochem. J. 28, 1592–1602.hah, D., Shen, W.C., 1996. Transcellular delivery of an
insulin–transferrin conjugate in enterocyte-like Caco-2 cells. J.Pharm. Sci. 85, 1306–1311.
hapiro, A.M., Lakey, J.R., Ryan, E.A., Korbutt, G.S., Toth, E.,Warnock, G.L., Kneteman, N.M., Rajotte, R.V., 2000. Islettransplantation in seven patients with type 1 diabetesmellitus using a glucocorticoid-free immunosuppressiveregimen. N. Engl. J. Med. 343, 230–238.
hen, W.-C., Wan, J., Ekrami, H., 1992. (C) Means to enhancepenetration: (3) Enhancement of polypeptide and proteinabsorption by macromolecular carriers via endocytosis andtranscytosis. Adv. Drug Deliv. Rev. 8, 93–113.
impson, R.W., Shaw, J.E., Zimmet, P.Z., 2003. The prevention oftype 2 diabetes—lifestyle change or pharmacotherapy? Achallenge for the 21st century. Diab. Res. Clin. Pract. 59,165–180.
ingh, M., 1999. Transferrin as a targeting ligand for liposomesand anticancer drugs. Curr. Pharm. Des. 5, 443–451.
kyler, J.S., 1986. Lessons from studies of insulinpharmacokinetics. Diab. Care 9, 666–668.
kyler, J.S., Cefalu, W.T., Kourides, I.A., Landschulz, W.H.,Balagtas, C.C., Cheng, S.L., Gelfand, R.A., 2001. Efficacy ofinhaled human insulin in type 1 diabetes mellitus: arandomised proof-of-concept study. Lancet 357,331–335.
l s c i e n c e s 2 9 ( 2 0 0 6 ) 183–197 197
Soon-Shiong, P., 1999. Treatment of type I diabetes usingencapsulated islets. Adv. Drug Deliv. Rev. 35, 259–270.
Stephen, R.L., Petelenz, T.J., Jacobsen, S.C., 1984. Potential novelmethods for insulin administration: I. Iontophoresis. Biomed.Biochim. Acta 43, 553–558.
Stern, M.P., Williams, K., Haffner, S.M., 2002. Identification ofpersons at high risk for type 2 diabetes mellitus: do we needthe oral glucose tolerance test? Ann. Intern. Med. 136, 575–581.
Stoever, J.A., Palmer, J.P., 2002. Inhaled insulin and insulinantibodies: a new twist to an old debate. Diab. Technol. Ther.4, 157–161.
Stratford, R.E., Lee, V.H.L., 1986. Aminopeptidase activity inhomogenates of various absorptive mucosae m the albinorabbit: implications in peptide delivery. Int. J. Pharm. 30, 73–82.
Street, C.N., Sipione, S., Helms, L., Binette, T., Rajotte, R.V.,Bleackley, R.C., Korbutt, G.S., 2004. Stem cell-basedapproaches to solving the problem of tissue supply for islettransplantation in type 1 diabetes. Int. J. Biochem. Cell Biol.36, 667–683.
Tan, K.K., Trull, A.K., Uttridge, J.A., Wallwork, J., 1995. Relativebioavailability of cyclosporin from conventional andmicroemulsion formulations in heart-lung transplantcandidates with cystic fibrosis. Eur. J. Clin. Pharmacol. 48,285–289.
Torres-Lugo, M., Garcia, M., Record, R., Peppas, N.A., 2002.Physicochemical behavior and cytotoxic effects ofp(methacrylic acid-g-ethylene glycol) nanospheres for oraldelivery of proteins. J. Control. Rel. 80, 197–205.
Veuillez, F., Kalia, Y.N., Jacques, Y., Deshusses, J., Buri, P., 2001.Factors and strategies for improving buccal absorption ofpeptides. Eur. J. Pharm. Biopharm. 51, 93–109.
Vial, T., Descotes, J., 2003. Immunosuppressive drugs and cancer.Toxicology 185, 229–240.
Wan, J., Taub, M.E., Shah, D., Shen, W.C., 1992. Brefeldin Aenhances receptor-mediated transcytosis of transferrin infilter-grown Madin–Darby canine kidney cells. J. Biol. Chem.267, 13446–13450.
Woodley, J., 2001. Bioadhesion: new possibilities for drugadministration? Clin. Pharmacokinet. 40, 77–84.
Wu, Z.H., Ping, Q.N., Wei, Y., Lai, J.M., 2004. Hypoglycemic efficacyof chitosan-coated insulin liposomes after oral administration
in mice. Acta Pharmacol. Sin. 25,966–972.Xia, C.Q., Wang, J., Shen, W.C., 2000. Hypoglycemic effect ofinsulin–transferrin conjugate in streptozotocin-induceddiabetic rats. J. Pharmacol. Exp. Ther. 295, 594–600.
Copyright © 2022 FDOKUMEN




















