N-Acetylaspartate Concentration in the Anterior Cingulate of Maltreated Children and Adolescents...
10
N-acetyl aspartate concentration in the anterior cingulate cortex in patients with schizophrenia: A study of clinical and neuropsychological correlates and preliminary exploration of cognitive behaviour therapy effects Preethi Premkumar a , Vivek A. Parbhakar a , Dominic Fannon a,b , David Lythgoe c , Steven C. Williams c , Elizabeth Kuipers a,d , Veena Kumari a, ⁎ a Department of Psychology, Institute of Psychiatry, King's College London, London, United Kingdom b Division of Psychological Medicine and Psychiatry, Institute of Psychiatry, King's College London, London, United Kingdom c Centre for Neuroimaging Sciences, Institute of Psychiatry, King's College London, London, United Kingdom d NIHR Biomedical Research Centre for Mental Health, South London and Maudsley NHS Foundation Trust, London, London, United Kingdom abstract article info Article history: Received 15 October 2009 Received in revised form 18 February 2010 Accepted 18 February 2010 Keywords: Chemical shift imaging Cognitive behaviour therapy Neuropsychological function Magnetic resonance spectroscopy Metabolism Symptoms This study investigated the clinical and neuropsychological correlates of N-acetyl aspartate (NAA) concentration in the anterior cingulate cortex (ACC) in schizophrenia, and explored whether ACC NAA concentration is sensitive to symptom change following cognitive behaviour therapy for psychosis (CBTp). Participants comprised 30 patients and 15 healthy controls who underwent magnetic resonance spectroscopy of the ACC and were assessed on frontal lobe based neuropsychological tasks. Twenty-four (of 30) patients were followed-up; 11 subsequently received 8–9 months of CBTp in addition to standard care (CBTp + SC) and 13 received SC only. At baseline (i) NAA and Cr concentrations were lower in patients compared to controls, (ii) in patients, NAA concentration correlated inversely with positive symptoms and general psychopathology (positive symptoms explained 21% of the variance; total variance explained = 25%) and Cho concentration correlated inversely with positive symptoms, and (iii) in controls, NAA concentration correlated positively with working and short-term memory and Cr concentration inversely with executive function. NAA concentration tended to increase in CBTp + SC patients at follow-up (n = 7 with usable data) concomitant with improvement in positive symptoms. NAA concentration may be more closely associated with symptoms and symptom change than frontal lobe based neuropsychological function in schizophrenia, perhaps because the latter is relatively stable during the long-term illness course. © 2010 Elsevier Ireland Ltd. All rights reserved. 1. Introduction Schizophrenia is often characterised by a profile of clinical and neuropsychological impairment that is consistent with a frontal lobe based pathology (Weinberger et al., 1994). Structurally, grey matter (GM) reduction in the anterior cingulate cortex (ACC) has been observed in patients with schizophrenia (Baiano et al., 2007; Fornito et al., 2008), though such reductions are not limited to the ACC (see Honea et al., 2005, for a meta-analytic review of GM reductions in schizophrenia). A further mode of investigating the neuropathology of schizo- phrenia is at the neurochemical level. N-acetyl aspartate (NAA) loss and impaired mitochondrial function are characteristic of several neurodegenerative diseases, including Alzheimer's Disease and multiple sclerosis (Perry et al., 2002; Rutten et al., 2003). These findings suggest that NAA concentration may be an indicator of mitochondrial function. N-methyl D-aspartate (NMDA) receptor activation coupled with Ca2+ cellular influx has been reported to increase neuronal release of NAA and delay nerve cell death (Tranberg et al., 2004). NAA concentration thus may also be an indicator of NMDA function and neuronal longevity. Interestingly, NMDA gluta- mate receptor dysfunction has been suggested to sub-serve many abnormalities associated with schizophrenia (Moghaddam, 2003). It has been reported that inhibitors of NMDA function, such as phencyclidine or ketamine, precipitate symptoms of schizophrenia in healthy people and exacerbate symptoms in patients with schizophrenia (Adler et al., 1999; Krystal et al., 1994; Lahti et al., 1995; Malhotra et al., 1997). Ketamine is also found to cause disruptions in working memory in both healthy and schizophrenia populations (Adler et al., 1999), indicating that deficient activation of NMDA receptors may be crucially involved in neuropsychological deficits commonly observed in patients with schizophrenia. Choline (Cho) and creatine/phosphocreatine (Cr) concentrations may also be important to neuronal integrity. Cho is involved in the synthesis of Psychiatry Research: Neuroimaging 182 (2010) 251–260 ⁎ Corresponding author. PO78, Institute of Psychiatry, De Crespigny Park, London SE5 8AF, United Kingdom. Tel.: +44 207 848 0233; fax: +44 207 848 0860. E-mail address: [email protected] (V. Kumari). 0925-4927/$ – see front matter © 2010 Elsevier Ireland Ltd. All rights reserved. doi:10.1016/j.pscychresns.2010.02.008 Contents lists available at ScienceDirect Psychiatry Research: Neuroimaging journal homepage: www.elsevier.com/locate/psychresns
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of N-Acetylaspartate Concentration in the Anterior Cingulate of Maltreated Children and Adolescents...
Psychiatry Research Neuroimaging 182 (2010) 251ndash260
Contents lists available at ScienceDirect
Psychiatry Research Neuroimaging
j ourna l homepage wwwe lsev ie rcom locate psychresns
N-acetyl aspartate concentration in the anterior cingulate cortex in patients withschizophrenia A study of clinical and neuropsychological correlates and preliminaryexploration of cognitive behaviour therapy effects
Preethi Premkumara Vivek A Parbhakara Dominic Fannonab David Lythgoec Steven C WilliamscElizabeth Kuipersad Veena KumariaaDepartment of Psychology Institute of Psychiatry Kings College London London United KingdombDivision of Psychological Medicine and Psychiatry Institute of Psychiatry Kings College London London United KingdomcCentre for Neuroimaging Sciences Institute of Psychiatry Kings College London London United KingdomdNIHR Biomedical Research Centre for Mental Health South London and Maudsley NHS Foundation Trust London London United Kingdom
Corresponding author PO78 Institute of Psychiatry8AF United Kingdom Tel +44 207 848 0233 fax +4
E-mail address vkumariiopkclacuk (V Kumari)
0925-4927$ ndash see front matter copy 2010 Elsevier Irelanddoi101016jpscychresns201002008
a b s t r a c t
a r t i c l e i n f o
Article historyReceived 15 October 2009Received in revised form 18 February 2010Accepted 18 February 2010
KeywordsChemical shift imagingCognitive behaviour therapyNeuropsychological functionMagnetic resonance spectroscopyMetabolismSymptoms
This study investigated the clinical and neuropsychological correlates of N-acetyl aspartate (NAA)concentration in the anterior cingulate cortex (ACC) in schizophrenia and explored whether ACC NAAconcentration is sensitive to symptom change following cognitive behaviour therapy for psychosis (CBTp)Participants comprised 30 patients and 15 healthy controls who underwent magnetic resonance spectroscopyof the ACC and were assessed on frontal lobe based neuropsychological tasks Twenty-four (of 30) patientswere followed-up 11 subsequently received 8ndash9 months of CBTp in addition to standard care (CBTp+SC)and 13 received SC only At baseline (i) NAA and Cr concentrations were lower in patients compared tocontrols (ii) in patients NAA concentration correlated inversely with positive symptoms and generalpsychopathology (positive symptoms explained 21 of the variance total variance explained=25) and Choconcentration correlated inverselywith positive symptoms and (iii) in controls NAA concentration correlatedpositively with working and short-termmemory and Cr concentration inversely with executive function NAAconcentration tended to increase in CBTp+SC patients at follow-up (n=7with usable data) concomitantwithimprovement in positive symptoms NAA concentration may be more closely associated with symptoms andsymptom change than frontal lobe based neuropsychological function in schizophrenia perhaps because thelatter is relatively stable during the long-term illness course
De Crespigny Park London SE54 207 848 0860
Ltd All rights reserved
copy 2010 Elsevier Ireland Ltd All rights reserved
1 Introduction
Schizophrenia is often characterised by a profile of clinical andneuropsychological impairment that is consistent with a frontal lobebased pathology (Weinberger et al 1994) Structurally grey matter(GM) reduction in the anterior cingulate cortex (ACC) has beenobserved in patients with schizophrenia (Baiano et al 2007 Fornitoet al 2008) though such reductions are not limited to the ACC (seeHonea et al 2005 for a meta-analytic review of GM reductions inschizophrenia)
A further mode of investigating the neuropathology of schizo-phrenia is at the neurochemical level N-acetyl aspartate (NAA) lossand impaired mitochondrial function are characteristic of severalneurodegenerative diseases including Alzheimers Disease andmultiple sclerosis (Perry et al 2002 Rutten et al 2003) These
findings suggest that NAA concentration may be an indicator ofmitochondrial function N-methyl D-aspartate (NMDA) receptoractivation coupled with Ca2+ cellular influx has been reported toincrease neuronal release of NAA and delay nerve cell death (Tranberget al 2004) NAA concentration thus may also be an indicator ofNMDA function and neuronal longevity Interestingly NMDA gluta-mate receptor dysfunction has been suggested to sub-serve manyabnormalities associated with schizophrenia (Moghaddam 2003) Ithas been reported that inhibitors of NMDA function such asphencyclidine or ketamine precipitate symptoms of schizophreniain healthy people and exacerbate symptoms in patients withschizophrenia (Adler et al 1999 Krystal et al 1994 Lahti et al1995 Malhotra et al 1997) Ketamine is also found to causedisruptions in working memory in both healthy and schizophreniapopulations (Adler et al 1999) indicating that deficient activation ofNMDA receptors may be crucially involved in neuropsychologicaldeficits commonly observed in patients with schizophrenia Choline(Cho) and creatinephosphocreatine (Cr) concentrations may also beimportant to neuronal integrity Cho is involved in the synthesis of
252 P Premkumar et al Psychiatry Research Neuroimaging 182 (2010) 251ndash260
membrane phospholipids (for review see Ross and Sachdev 2004)while Cr helps maintain the energy homeostasis within the nervecell (Andres et al 2008) The evidence suggests that Cr may alsohave direct effects on neuropsychological function For example oralsupplements of Cr increased intelligence working memory perfor-mance (Rae et al 2003) and executive function (McMorris et al2007 2006)
Previous studies have reported using magnetic resonance spec-troscopy (MRS) lower ACC NAA level in patients with schizophreniaespecially in those treated with typical antipsychotic drugs comparedwith healthy participants (Braus et al 2002 Deicken et al 2000Ende et al 2000 Sanches et al 2008 Tayoshi et al 2009Wood et al2007 Yamasue et al 2002 see Appendix A for detailed information)Within this patient population ACC NAA concentration is reported tobe inversely associated with illness duration in some studies (Brauset al 2002 Ende et al 2000 Theberge et al 2003) but not others(Deicken et al 1997 Tayoshi et al 2009 Theberge et al 2004Woodet al 2007 Yamasue et al 2002) NAA reductions have been reportedin antipsychotic drug-naiumlve first-episode patients and treatment mayincrease NAA levels in both recent-onset cases and patients withchronic illness (Braus et al 2002 Fannon et al 2003) NAAconcentration is positively associated with duration on atypicalantipsychotic medication in long-term patients (Braus et al 2002)and inversely correlated with the duration of positive symptoms infirst-episode neuroleptic-naiumlve patients (Theberge et al 2004) Morerecently Tayoshi et al (2009) observed no association between NAAconcentration and symptoms but reported a positive associationbetween NAA concentration andWisconsin Card Sorting Test (WCST)performance the latter finding was also present in two earlier studies(Braus et al 2002 Ohrmann et al 2008)
Neuropsychologically the ACC is involved in components of thecentral executive that facilitate working memory (Osaka et al 2004Smith and Jonides 1999) including encoding of semantic information(Kaneda and Osaka 2008) and reported to be deactivated inschizophrenia patients compared with healthy participants duringthe stimulus encoding phase of a working memory task (Schlosser etal 2008) A further role of the ACC is in emotional decision-makingwhere there is a relationship between an action and the reinforce-ment value of its outcome (Rushworth et al 2004 Walton et al2007) The ACC is involved in updating and integrating recentinformation to existing information on reward value of outcome interms of predicting future outcome (Behrens et al 2007 Kennerleyet al 2008)
The present study has two parts cross-sectional and longitudinalCross-sectionally the study aimed to compare the ACC NAAconcentrations in patients with schizophrenia and healthy partici-pants and to determine their clinical andor neuropsychologicalcorrelates it also explored these effects in Cho and Cr All except forthree recent studies that examined these metabolites in patients withschizophrenia (Ohrmann et al 2008 Sanches et al 2008 Tayoshiet al 2009) had a smaller sample size than that in our investigationand none undertook a comprehensive examination of metaboliteconcentration relationships with clinical symptoms and neuropsy-chological functions We hypothesized that (1) NAA concentrationwould be reduced in patients compared with healthy participants dueto impaired neuronal function (2) in patients NAA concentrationwould be associated inversely with illness duration (Braus et al 2002Ende et al 2000 Theberge et al 2003) and symptoms on the Positiveand Negative Syndrome Scale (Wood et al 2007) and (3) NAAconcentration would be positively associated with neuropsycholog-ical measures that involve the ACC namely working memory conflictdetection and decision-making (Behrens et al 2007 Carter and vanVeen 2007 Osaka et al 2004 Peterson et al 1999 Smith andJonides 1999 Walton et al 2007) both in healthy participants andpatients though such relationships may be weaker in patientsbecause they as mentioned earlier engage the ACC at a less-than-
normal level during relevant tasks We expected that the clinical orneuropsychological correlates of metabolite concentration would beattenuated or abolished after controlling for ACC grey matter (GM)concentration (Yamasue et al 2002) as GM concentration mayinfluence metabolite availability
Longitudinally the study aimed to determine the effect ofcognitive behavioural therapy for psychosis (CBTp) on metaboliteconcentration A sub-sample of the patients in the present investiga-tion went on to receive CBTp in addition to their standard care Thestudy therefore also examined whether (i) baseline metaboliteconcentration predicted symptom change following CBTp+SC and(ii) there was a change in metabolite concentration in patients whoreceived CBTp in addition to standard care We hypothesized that inthis sub-sample NAA concentration would increase coincident with areduced level of symptoms following CBTp
2 Materials and method
21 Participants and design
The study involved 30 patients with schizophrenia and 15 healthyparticipants all of whom underwent MRS of the ACC at study entryThe patient and control groups were matched on average for age andgender (Table 2) All patients were assessed by a ConsultantPsychiatrist (DF) for clinical diagnosis using the Structured ClinicalInterview for DSM-IV Axis I disorder (First et al 2002) and symptomseverity using the Positive and Negative Syndrome Scale (PANSS Kayet al 1987) All patients were recruited from the South London andMaudsley NHS Foundation Trust as part of a larger project investi-gating the functional neuroimaging correlates and predictors of CBTp(the MRS component was added to the larger project) had been onstable doses of antipsychotic medication for at least 2 years and onthe current antipsychotic drug for at least 3months before taking part
Of the 30 patients at study entry (baseline) 11 patients sub-sequently received CBTp+SC in a specialist clinical service [Psycho-logical Interventions Clinic for Outpatients with Psychosis (PICuP)South London and Maudsley NHS Foundation Trust (SLAM)] inaddition to their standard care and 13 patients continued to receivestandard care only (SC controls) all of these 24 patients (i) received arating of ge60 on the PANSS (ii) reported at least one positivelsquodistressingrsquo symptom of schizophrenia and (iii) wished to receiveCBTp (if available only about 10ndash20 of eligible SLAM patients wereaccepted for CBTp with the existing resources availability was theonly criterion that determined whether or not eligible patientsreceived CBTp) Eight of 11 CBTp+SC patients and 12 of 13 SCcontrol patients were assessed for symptom severity at follow-up ofwhom seven and four patients respectively underwent MRS atfollow-up Six (of 30) patients had low symptom severity at baselinethey were considered to be responsive to antipsychotic treatment bytheir long-term treating clinicians (SC responsive) these patientswere not followed up
The patients in the CBTp+SC and SC control groups wererecruited from the same geographical area were identified by localConsultant Psychiatrists as suitable for CBTp and wished to receiveCBTp in addition to their usual care Allocation to CBTp+SC and SCcontrol groups was not randomised but followed a cohort case-controlled design Patients who were referred to and accepted forCBTp by the Psychological Interventions Clinic for Outpatientswith Psychosis (PICuP) SLAM NHS Foundation Trust went into theCBTp+SC group Others who matched demographically (age andnumber of years in education) and clinically (illness duration andPANSS symptoms) as much as possible those accepted for CBTp bythe PICuP were studied as part of the SC control group over thesame interval as the CBTp+SC group patients SC consisted of casemanagement offered by the case management team for a particulargeographical area Most patients (80) were on a single antipsychotic
253P Premkumar et al Psychiatry Research Neuroimaging 182 (2010) 251ndash260
drug (see Table 2) Of the 12 patients on olanzapine one patient alsotook aripiprazole and a further patient also took trifluoperazine Of thesix patients on clozapine one patient also took quetiapine and afurther patient also took amisulperide Of the two patients onhaloperidol one patient was also on sulperide and the other patienton pipotiazine In addition to antipsychotic drug treatment fourpatients were receiving anti-cholinergics
CBTp followed the procedure developed by Fowler et al (1995)Therapy sessions were conducted on a weekly or fortnightly basis aspreferred by the patient Patients received an average of 16 sessionsAll CBT interventions were formulation-driven and focused on thetherapy goals of the patient The therapists were supervised by one ofthe investigators (EK) who has extensive experience of CBTp
The study procedures were approved by the ethics committee ofthe Institute of Psychiatry and the South London and Maudsley NHSFoundation Trust London All participants provided written informedconsent to their participation and were compensated for their timeand travel
22 Neuropsychological assessments
All patients and 13 healthy participants were assessed onneuropsychological measures (described in Table 1) that areconsidered to recruit the ACC and found to reveal performancedeficits in executive function workingshort-term memory attentionand emotional decision-making in schizophrenia
23 Magnetic resonance spectroscopy data acquisition and processing
Images were acquired using a 15 Tesla GE NVi Signa System(General Electric Milwaukee WI USA) at the Maudsley HospitalSouth London A quadrature birdcage head coil was used for RFtransmission and reception Initially a series of fast gradient echoscout images were acquired in order to orient subsequent imagesrelative to the anterior commissureposterior commissure line andthe interhemispheric fissure Subsequently the whole brain wasscanned with a 3-D inversion recovery prepared fast spoiled GRASST1-weighted dataset Chemical shift images were acquired from aPRESS excited volume in a 15 cm thick slab through the anteriorcommissure correspondingwith the dorsal ACC with a nominal voxelsize of 15 cm3 (24times24 phase-encode steps over a 24 cm FOV) Tominimise relaxation effects a short TE of 35 ms was used and arelatively long TR of 2 s
Only metabolite information with a fitting error (percent standarddeviation) of b20 was included in the final analysis (Ohrmann et al
Table 1Battery of neuropsychological measures
Neuropsychological test Variables used in analysis
Executive functionBrixton Test (Burgess and Shallice 1997) Perseverative errorsWisconsin Card Sorting Test (WCST)(Heaton et al 1993)
Perseverative errors
Workingshort-term memoryLetter number test (Gold et al 1997) Total number of items correctWechsler Memory ScalemdashRevised (WMS-R) LogicalMemory (Wechsler 1987)mdashImmediate recall
Unit recall scaled score
Hopkins Verbal Learning Test(Shapiro et al 1999)
Total number of items freelyrecalled
AttentionContinuous Performance Testmdashidentical pairs(Cornblatt et al 1988)
Discriminability
Emotional decision-makingIowa Gambling Task (Bechara et al 1994) Overall learning
(block 5 minus block 1)
2008) Absolute concentrations of NAA Cho and Cr were measured inmillimolars in all participants using the LCmodel (McLean et al 2000Provencher 1993) For each MRS voxel the proportions of GM whitematter and cerebrospinal fluid (CSF) were calculated by segmentingthe Spoiled Gradient Recalled (SPGR) image (Fig 1) This allowscorrection for CSF contamination within each voxel and extrapolationto concentrations for pure GM (McLean et al 2000) Metaboliteconcentration was calculated as a function of CSF concentrationwithin each voxel using the following formula
Metabolite value=eth1minusCSF concentrationTHORN
100
NAA Cho and Cr absolute concentration estimates in millimolarsare reported rather than metabolite peak ratios such as NAAChoNAACr and ChoCr because absolute concentrations of individualmetabolites are not influenced by fluctuations in the concentration ofthe reference metabolite Metabolite ratios are believed to account foralterations in the Cr reference peak which invalidate its usefulness asan internal reference for the other metabolite peaks of the protonspectrum (Deicken et al 1997)
24 Statistical analysis
241 Cross-sectional analysis
2411 Group comparison of metabolite concentration Differencesbetween patient (across all patients) and healthy participant groupsin metabolite concentration and GM concentration age years ofeducation and clinical and neuropsychological variables wereexamined using analysis of variance (ANOVA) For the neuropsycho-logical variables showing a non-normal distribution (Brixton persev-erative errors) MannndashWhitney U tests were performed A chi-squared test examined group differences in gender distribution
2412 Clinical correlates of metabolite concentration Pearson andpartial correlations controlling for GM concentration or Spearmancorrelations for clinical variables with a non-normal distribution(antipsychotic medication level) were performed between clinicalvariables and metabolite concentrations The clinical variables were
Fig 1 A Spoiled Gradient Recalled (SPGR) brain image in the axial slice in a controlsubject The square indicates the volume of interest (VOI) 15times15times15 cm3 voxel inthe anterior cingulate cortex Within the VOI each tissue (cerebrospinal fluid greymatter and white matter) was segmented
254 P Premkumar et al Psychiatry Research Neuroimaging 182 (2010) 251ndash260
PANSS symptoms illness duration (defined as the difference betweenthe age at onset of psychotic symptoms as reported by the patient andwhere possible confirmed with other sources and age at the time ofbaseline assessments) and antipsychotic medication level (in chlor-promazine equivalents) Spearman correlations were performed toexamine the relationship between metabolite values and individualPANSS items in those subscales that were found to have a significantassociation with metabolite values
2413 Neuropsychological correlates of metabolite concentrationPearson and partial correlations controlling for GM concentration orSpearman correlations for neuropsychological variables with a non-normal distribution (Brixton perseverative errors) were performedbetween neuropsychological performance measures and metaboliteconcentration in patient and healthy participant groups
2414 Multiple regression of clinical andor neuropsychological correlateson metabolite concentration Significant clinical andor neuropsycholog-ical variables that had a normal distribution were entered into themultiple regression model using a stepwise method (to estimate theeffect of individual predictors on variability of criterion variable) andusing a forced-entry method (to explain the combined effect ofpredictors on the variability of the criterion variable)
242 Longitudinal analysis
2421 Group comparison of metabolite concentration Due to the smallsample sizes differences between CBTp+SC SC control and SCresponsive patient groups in age education clinical variables andbaseline metabolite and GM concentrations were examined using non-parametric analyses namely the Kruskal-Wallis test A chi-squared testdetermined group differences in gender distribution
2422 Metabolite concentration as a predictor of symptom changefollowing CBTpSpearman correlationswere performed in the CBTp+SCpatients who were followed up (n=8) between baseline metaboliteconcentrations and residual PANSS symptom change scores frombaseline to follow-up
2423 Change in symptom severity and metabolite concentrationfollowing CBTp Due to the small sample sizes (CBTp+SC n=7 andSC control n=4) changes in symptom severity metabolite and GMconcentrations from baseline to follow-up in the patient groups wereexamined using the Wilcoxon Signed Rank test
All analyses were performed in SPSS windows (version 15) Alphalevel for testing significance of effects was maintained at Pb005 Wechose not to apply the Bonferroni method of adjusting the P valuebecause we expected the size of the relationship between MRS valuesand symptomsneuropsychological functions to be small or at bestmodest given that symptoms in schizophrenia are unlikely to have asingle aetiology and successful task performance on most neuropsy-chological tasks would recruit additional brain regions
3 Results
31 Cross-sectional analysis
311 Group differences in demographic and neuropsychological variablesPatient and healthy participant groups did not differ in gender and
age Patients had fewer years in education and showed deficientperformance on most neuropsychological measures relative tohealthy participants (Table 2)
312 Group differences in metabolite concentration in the ACCNAA Cr and GM concentrations were lower in the patient
compared with the healthy participant group (Table 3)
313 Clinical correlates of metabolite concentrationNAA concentration correlated inversely with positive symptoms
general psychopathology and total symptoms (Table 4) Thesecorrelations remained significant after controlling for GM NAAconcentration correlated inversely with negative symptoms onlyafter controlling for GM PANSS item-wise correlations revealed thatNAA concentration was inversely correlated with delusions disorga-nisation and persecution items of the positive syndrome subscalepassive social withdrawal and stereotyped thinking items of thenegative syndrome subscale and somatic concern and preoccupationitems of the general psychopathology subscale
Cho concentration correlated inversely with positive and totalsymptoms After controlling for GM concentration Cho concentrationcorrelated with total symptoms but not positive symptoms Choconcentration correlated inversely with negative symptoms at a trendlevel only after controlling for GM concentration PANSS item-wisecorrelations revealed that Cho concentration was inversely correlatedwith disorganisation and hostility items of the positive syndromesubscale passive social withdrawal item of the negative syndromesubscale and somatic concern item of the general psychopathologysubscale Cho concentration correlated positively with antipsychoticmedication dosage Cr concentration did not correlate with anyclinical variable
314 Neuropsychological correlates of metabolite concentrationPatients A positive correlation between NAA concentration and
working memory as assessed by the letter number test emerged onlyafter controlling for GM concentration (Table 5)
Healthy participants NAA concentration correlated positively withworking memory as assessed by the letter number test and short-term memory as assessed by the Hopkins verbal learning test thoughthese correlations were reduced to a trend level of significance aftercontrolling for GM concentration (Table 5) Cho concentrationcorrelated inversely with short-term memory as assessed by theWechsler Memory ScalemdashRevised (WMS-R) logical memory imme-diate recall test after controlling for GM concentration Cr concentra-tion correlated inversely with executive function as assessed byBrixton perseverative errors
315 Multiple regression of clinical andor neuropsychologicalcorrelates of metabolite concentration
Patients In the stepwise regression model with NAA concentra-tion as the criterion variable positive symptoms proved to be asignificant predictor (r=minus0489 P=0006) The model explained 21of the variance in NAA concentration In the forced-entry regressionmodel the predictors (positive symptoms general psychopathologyand letter number test) explained 25 of the variance in NAAconcentration
Healthy participants In the stepwise regression model with NAAconcentration as the criterion variable short-term memory asassessed by the Hopkins verbal learning test was a significantpredictor (r=0576 P=0039) The model explained 27 of thevariance in NAA concentration In the forced-entry regression modelthe predictors (Hopkins verbal learning test and letter number test)explained 27 of the model
32 Longitudinal analysis
321 Metabolite concentration differences at baseline between patientsub-groups
NAA concentration tended to differ between patient groups atbaseline mainly due to greater concentration in the low-symptomSC-responsive group (Table 6)
Table 2Demographic clinical and neuropsychological characteristics of patients and healthy participants groups
Characteristic Patients Healthy participants Test χ2 (df) P
Gender malefemale (n) 246 132 Chi-squared 0304 (1) 0581mean SD mean SD F or z (df)
Age in years 3640 864 3540 1334 ANOVA 0092 (143) 0763Years in education 1383 215 1561 323 ANOVA 4555 (141) 0039Illness duration years 1298 894
Symptoms (PANSS)Positive 1693 395Negative 1787 452General psychopathology 3170 639Total 6650 1317Medication level (chlorpromazine equivalents) 50267 32788Medication type (n)
Olanzapine 12Clozapine 6Risperidone 5Aripiprazole 2Flupentixol 2Amisulperide 1Haloperidol 2
Neuropsychological functionBrixton perseverative errors 050 078 031 048 MannndashWhitney U minus0552 (141) 0648WCST perseverative errors 1817 886 1175 751 ANOVA 4870 (140) 0033Letter number test number correct 1380 380 1692 296 ANOVA 6925 (141) 0012WMS logical memory immediate unit recalled 710 258 969 333 ANOVA 7533 (140) 0009Hopkins total freely recalled 2186 538 2692 517 ANOVA 8122 (140) 0007CPT discriminability 029 059 187 100 ANOVA 14257 (139) 0001IGT overall learning 280 1183 892 1473 ANOVA 2092 (141) 0156
255P Premkumar et al Psychiatry Research Neuroimaging 182 (2010) 251ndash260
33 Metabolite concentration correlates of symptom change followingCBTp
In the CBTp+SC group metabolite concentration at baseline wasnot associated with symptom change following CBTp (SupplementaryTable)
34 Symptom severity and metabolite concentration change frombaseline to follow-up in CBTp+SC and SC control groups
Positive symptoms improved following CBTp in the CBTp+SCgroup while negative symptoms tended to deteriorate in the SCcontrol group (Table 7)
NAA concentration tended to increase in the CBTp+SC group frombaseline to follow-up (Table 7)
4 Discussion
The present investigation examined the concentrations of NAACho and Cr in the ACC and their clinical and neuropsychologicalcorrelates in patients with schizophrenia and healthy participants(cross-sectional investigation) The study also explored whetherbaseline metabolite concentration predicted symptom change fol-lowing CBTp+SC and whether a reduction in symptoms followingCBTp+SC was accompanied by higher NAA concentration relative tobaseline (longitudinal investigation)
Table 3ACCmetabolite and greymatter concentrations (mean SD) at baseline at each voxel inpatients and healthy participants
CSI variable(millimolars)
Patient(n=30)
Healthy participants(n=15)
F (p)
NAA 742 126 856 139 7682 (0008)Cho 190 038 199 036 0654 (0423)Cr 703 124 789 102 5345 (0026)Grey matter 5399 1051 6139 858 5549 (0023)
41 Summary of clinical and neuropsychological correlates of metaboliteconcentration (cross-sectional investigation)
The major findings from the cross-sectional analysis were that inpatients (1) NAA concentration was reduced compared to healthyparticipants (2) greaterNAA concentrationwas associatedwith a lowerlevel of positive symptoms general psychopathology and betterworking memory (positive symptoms alone explained 21 of thevariance total variance explained=25) and (3) greater Cho concen-tration was associated with a lower level of positive symptoms andhigher level of antipsychotic medication In healthy participants thefollowing associationswere observed (1) NAA concentration positivelywith working and short-termmemory (2) Cho concentration inverselywith short-term memory and (3) Cr concentration inversely withexecutive function These findings will be discussed in turn
411 Clinical correlates of metabolite concentrationsThe findings of lower ACC NAA concentration in schizophrenia
patients (Deicken et al 1997 Ende et al 2000 Wood et al 2007)and clinical correlates of NAA concentration support previousevidence (Theberge et al 2003 Wood et al 2007 Yamasue et al2002) Our study of a relatively larger sample of patients than mostprevious studies is the first to observe that NAA concentration wasinversely associated with the severity of positive negative andgeneral psychopathology symptoms based on the three-dimensionalmodel of the PANSS (Kay et al 1987) Twenty percent of our patientswere SC treatment responsive giving a wider range to symptomscores than earlier studies Patients who had low symptom severityand were considered to have responded sufficiently to their standard(mostly atypical) antipsychotic treatment tended to show greaterNAA concentration than patients who were symptomatic (baselinecomparisons) suggesting that NAA concentration may vary as afunction of symptom severity and treatment response
NAA concentration being a by-product of neurotransmitter turn-over (Tranberg et al 2004) the symptom severity-metabolite concen-tration associations may reflect the efficiency of neurotransmission Asnoted in Section 1 NAA concentration may be an indicator of NMDA
Table 4Clinical correlates of metabolite concentration at baseline (patients only)
NAA concentration Cho concentration Cr concentration
r or ρ r (P) rp1 (P) r (P) rp
1 (P) r (P) rp1 (P)
Illness duration r minus0059 (0756) 0091 (0640) minus0064 (0735) 0045 (0817) minus0291 (0118) minus0244 (0203)Antipsychotic medication level Rho 0197 (0298) 0442 (0014) 0073 (0700)Symptoms (PANSS)
Positive (P) symptoms r minus0489 (0006) minus0430 (0020) minus0391 (0033) minus0325 (0085) minus0308 (0098) minus0262 (0170)Negative (N) symptoms r minus0297 (0111) minus0418 (0024) minus0287 (0124) minus0366 (0051) minus0211 (0264) minus0262 (0170)General psychopathology (GP) r minus0416 (0022) minus0506 (0005) minus0299 (0109) minus0341 (0070) minus0204 (0281) minus0219 (0254)Total r minus0450 (0013) minus0512 (0004) minus0361 (0050) minus0384 (0040) minus0263 (0160) minus0266 (0163)
Individual symptomsDelusions (P) Rho minus0411 (0024) minus0342 (0064) minus0192 (0309)Disorganisation (P) Rho minus0525 (0003) minus0369 (0045) minus0136 (0475)Persecution (P) Rho minus0390 (0033) minus0193 (0307) minus0068 (0719)Hostility (P) Rho 0062 (0745) 0370 (0044) 0163 (0390)Passive social withdrawal (N) Rho minus0370 (0044) minus0393 (0032) minus0261 (0163)Stereotyped thinking (N) Rho minus0422 (0020) minus0073 (0684) minus0221 (0240)Somatic concern (GP) Rho minus0419 (0021) minus0407 (0026) minus0129 (0496)Preoccupation (GP) Rho minus0528 (0003) minus0201 (0287) minus0264 (0156)
rp1 partial correlation controlling for GM concentration P PANSS positive symptom subscale N PANSS negative symptom subscale GP PANSS general psychopathology subscale
256 P Premkumar et al Psychiatry Research Neuroimaging 182 (2010) 251ndash260
function and neuronal longevity (Tranberg et al 2004) NAA efflux isa delayed response to sudden non-physiological decrease in extracel-lular osmolarity and high K+intra-cellular and NMDA activation(Tranberg et al 2007) Elevated concentration of NAA in the ACC inschizophrenia patients with lower level of symptoms may reflectincreased turnover of neurotransmitters such as dopamine and NMDA
Similarly the association between Cho concentration and total andpositive symptoms may also reflect improved neurotransmitterfunction and neuronal integrity with milder symptoms The Cho peakincludes solublemembranephospholipids includingphosphorylcholine(PCho) glycerophosphocholine (GPCho) and a relatively negligibleamount of free choline (Ross and Sachdev 2004) PCho is involved insynthesis of the insoluble membrane phospholipids while GPCho is aproduct of membrane degradation and free choline is involved insynthesis of the neurotransmitter acetylcholine aswell as inmembranesynthesis (Ross and Sachdev 2004) An increase in the Cho peak isassociated with an increase in membrane breakdown or turnover andmyelination (Ross and Sachdev 2004) The positive associationbetween antipsychotic medication dosage and Cho concentration ameasure of neuronalmembrane turnover (Miller 1991 Ohrmann et al2008) suggests that medication level also influences neuronal activity
412 Neuropsychological correlates of metabolite concentrationIn patients the finding of an association between greater NAA
concentration and better working memory supports evidence for the
Table 5Neuropsychological correlates of metabolite concentration at baseline in patients and healt
Neuropsychological function Group N r or rho NAA concentration
r or rho rp1 (P)
Brixton perseverative errors Patient 30 Rho 0180 (0341)Control 13 Rho 0356 (0232)
WCST perseverative errors Patient 30 r minus0097 (0610) minus013Control 12 r 0271 (0394) 024
Letterndashnumber test number correct Patient 30 r 0303 (0104) 037Control 13 r 0557 (0048) 052
WMS logical memory immediateunit recalled
Patient 29 r 0301 (0112) 033Control 13 r 0330 (0271) 027
Hopkins verbal learning test totalnumber freely recalled
Patient 29 r 0127 (0512) 011Control 13 r 0576 (0039) 055
CPT discriminability Patient 29 r minus0037 (0848) 015Control 12 r 0329 (0297) 027
IGT overall learning Patient 30 r 0179 (0343) 021Control 13 r 0042 (0892) 007
rp1 partial correlation controlling for GM concentration
role of frontal lobe function in working memory using functional MRIand proton MRS in schizophrenia (Bertolino et al 2000 Callicottet al 2000 Ohrmann et al 2007) although this association explainedonly a very small amount (3) of the variance in NAA concentrationthat was additional to that explained by positive symptoms
In the healthy group greater NAA concentration was associatedwith better working and short-term memory The ACC is activatedduring both working and short-term memory (Kim et al 2006Lenartowicz and McIntosh 2005) NAA concentration in the frontallobe white matter was positively associated with working memory inhealthy children which may be related to increased number ofdendritic processes at an early age (Yeo et al 2000) NAA con-centration has a role in neuronal integrity in the form of increasedmyelination and mitochondrial function (Ross and Sachdev 2004)and this may facilitate working and short-term memory
Greater Cho concentration correlated inversely with short-termmemory in the healthy group when controlling for GM concentrationin the ACC A negative association between Cho concentration in theoccipito-parietal white matter and IQ independent of the positiveassociation between NAA concentration and IQ in healthy individualshas been previously reported (Jung et al 1999) Our findings suggestindependentmetabolite concentration-neuropsychological associationsbetween NAA Cho and Cr in healthy individuals Greater Cr concentra-tionwas associatedwith poorer executive function in the present studyA study of elderly males found negative correlations between adjusted
hy participants
Cho concentration Cr concentration
r or rho rp1 (P) r or rho rp
1 (P)
minus0198 (0293) 0331 (0074)0356 (0232) 0579 (0038)
9 (0473) minus0011 (0956) minus0030 (0877) minus0102 (0592) minus0116 (0550)8 (0461) 0390 (0211) 0368 (0265) minus0225 (0483) 0312 (035)9 (0043) minus0163 (0388) minus0160 (0407) minus0130 (0493) minus0124 (0523)9 (0077) 0011 (0971) minus0083 (0797) 0156 (0611) minus0030 (0927)1 (0085) 0054 (0781) 0045 (0822) minus0017 (0932) minus0025 (0898)8 (0382) minus0453 (0120) minus0610 (0035) minus0022 (0946) minus0267 (0401)9 (0564) 0181 (0348) 0177 (0369) 0269 (0159) 0265 (0173)5 (0061) minus0173 (0572) minus0330 (0295) 0277 (036) 0061 (0851)8 (0423) minus0114 (0555) 0016 (0936) 0003 (0986) 0088 (0656)5 (0413) minus0209 (0514) minus0346 (0297) 0207 (0519) 0006 (0986)0 (0273) 0026 (0891) 0029 (0879) 0062 (0747) 0064 (0742)8 (0811) minus0063 (0839) minus0025 (0939) minus0225 (0461) minus0169 (0600)
Table 6Demographic clinical and metabolite concentration characteristics at baseline of CBTp+SC (n=11) SC control (n=13) and SC responsive (n=6) patients
Characteristic CBTp+SC SC control SC responsive χ2 P
Gender malefemale (n) 65 121 60 7185 0028mean SD mean SD
Age in years 3464 862 3746 877 3733 942 0745 0689Years in education 1445 246 1346 176 1377 24 1156 0561Illness duration years 1194 860 1377 970 1317 928 0303 0860Symptoms (PANSS)
Positive 1745 295 1915 264 1117 172 14644 0001Negative 1818 498 1923 386 1433 361 5779 0056General psychopathology 3227 675 340 549 2567 383 6775 0034Total 6791 1287 7239 994 5117 778 9512 0009Medication level 56442 30317 50055 39478 39405 20759 1787 0409
Metabolite concentrationNAA 765 092 685 143 823 091 5313 0070Cho 192 060 186 024 194 018 0493 0781Cr 689 140 687 095 748 160 1047 0592Grey matter 5766 1071 5117 1136 5337 714 1096 0578
257P Premkumar et al Psychiatry Research Neuroimaging 182 (2010) 251ndash260
Cr in the parietal lobe and various cognitive measures including logicalmemory and verbal memory (Ferguson et al 2002) The study did notinclude ameasure of executive function Ferguson et al (2002) believedthat the findings fit with evidence that higher Cr levels are associatedwith cognitive ageing They proposed that poorer neuropsychologicalperformance in healthy ageing is associated with an increase inPhosphocreatine (PCr) due to a reduction in conversion of PCr toAdenosine-tri-phosphate (ATP) for energy Increased Cr concentrationmay be a marker of decreased brain energy metabolism
42 Effect of cognitive behaviour therapy for psychosis on metaboliteconcentration
Our preliminary investigation of change in metabolite concentra-tion in a small number of patients who received CBTp+SC comparedto patients who received SC only revealed a trend for an increase inNAA concentration with CBTp This increase in NAA was concomitantwith improvement in positive symptoms in CBTp+SC patients Thisfinding is consistent with the view that NAA concentration increaseswith alleviation of symptoms as discussed above Recent functionalimaging studies also provide evidence for a role of the ACC inresponsiveness to CBT in psychosis (Kumari et al 2009) as well asmajor depression (Costafreda et al 2009)
43 Limitations and future research
One of the limitations of the study was that the sample sizes ofpatients who received CBTp+SC or SC only and were clinicallyassessed andor scanned at follow-up were small A further limitationwas that gender distribution differed between the patient groupsAlthough there was no gender effect within each patient group in the
Table 7Symptoms metabolite and grey matter concentration (mean SD) at baseline and follow-u
CSI variable Baseline CBTp+SC (n=7) z (P)
FOLLOW-UP
Clinical symptomsPositive symptoms 1814 (234) 1567 (350) minus20Negative symptoms 1857 (571) 1567 (234) minus08General psychopathology 3200 (566) 2733 (497) minus13Total symptoms 6871 (1227) 5867 (1017) minus14
Metabolite concentrationNAA 765 (068) 831 (077) minus18Cho 185 (042) 193 (02) minus05Cr 679 (089) 725 (103) minus08Grey matter 5706 (1155) 5860 (851) minus03
metabolite concentrations in the present study higher ACC glutaminelevel in male compared to female schizophrenia patients has beenpreviously observed (Tayoshi et al 2009) Other effects of gender onACC function have also been reported for example reduced ACCglucose metabolism in male chronic patients relative to healthyparticipants and female patients (Fujimoto et al 2007) Thepredictive value of NAA concentration on symptom change in patientsreceiving psychological treatment or standard care needs to beexamined in a larger sample involving a sufficient number of bothmen and women with schizophrenia Additionally the role of clinicaland neuropsychological variables on ACC NAA levels in patients whoimprove with CBTp needs to be explored
44 Conclusions
Higher NAA and Cho concentrations in the ACC in patients areassociated with lower symptom severity Stronger and moreconsistent associations between metabolite concentrations andsymptom severity than neuropsychological function suggest thatmetabolite concentration and symptoms may co-fluctuate morestrongly Neuropsychological deficits may be more stable (Szokeet al 2008) and not necessarily improve in parallel with symptomimprovement (Hughes et al 2003) NAA concentration may yetreflect symptom changes following CBTp and if replicated in futurestudies has the potential to provide a useful biological marker ofclinical response to psychological treatments
Acknowledgement
The study was supported by funds from the Wellcome Trust UK(067427z02z)
p in CBTp+SC and SC control groups
Baseline SC control (n=4) z (P)
FOLLOW-UP
32 (0042) 1925 (222) 1825 (263) minus0365 (0715)13 (0416) 1875 (499) 2200 (616) minus1841 (0066)82 (0167) 3500 (668) 3275 (591) minus0535 (0593)72 (0141) 7300 (1042) 7300 (1364) minus0001 (1000)
59 (0063) 740 (069) 704 (038) minus1826 (0068)07 (0612) 190 (018) 201 (008) minus0730 (0465)45 (0398) 702 (016) 736 (099) minus0730 (0465)38 (0735) 5353 (549) 5324 (335) minus0365 (0715)
Appendix A Summary of magnetic resonance spectroscopy studies on the anterior cingulate cortex (ACC) in schizophrenia patients
Publication Participants Measures Results
Deicken et al (1997) Schizophrenia patients(n=26 9 on atypical and 17 on typical)Healthy participants (n=16)
NAA Cho and Cr illness durationantipsychotic medication dose
Patients had lower NAA concentrationcompared to healthy participants Nosignificant group differences or lateralizedasymmetries for Cho or Cr No significantcorrelations between NAA and eitherillness duration or antipsychoticmedication dose
Ende et al (2000) Schizophrenia patients(n=19 10 on atypical and 9 on typical)Healthy participants (n=16)
NAA Cho and Cr age illnessduration
Patients had lower NAA concentrationcompared to healthy participantsPatients receiving typical medication(but not atypical) had lower NAAconcentration than healthy participantsNAA concentration was inverselycorrelated with age in patients andhealthy participants and with illnessduration (corrected for age) in patients
Braus et al (2001 2002) Schizophrenia patients(11 on atypical and 10 on typical)
NAA Cho and Cr illness durationduration on atypical antipsychoticmedication WCST
Patients receiving typical antipsychoticshad lower NAA concentration than patientsreceiving atypical antipsychoticsNAA concentration was inverselycorrelated with illness duration andpositively with duration on atypicalantipsychotic medication NAAconcentration was inversely correlatedwith WCST perseverative errors
Goff et al (2002) Schizophrenia patients (n=17of whom 10 switched fromconventional to olanzapine andhad MRS at baseline and 8-week follow-up)
GluCr ratio SANS GluCr ratio was increased by 125(non-significant) following switch toolanzapine Patients who improvedon SANS symptoms had greaterGluCr ratio (458) compared topatients who deteriorated on SANSsymptoms (208) No significantcorrelation between SANS total andchange in GluCr ratio after switch
Yamasue et al (2002) Schizophrenia patients(n=15 all on typical)Healthy participants (n=13)
NAA Cho and Cr grey mattervolume age height body weightsocio-economic status parentalsocio-economic status years ofeducation PANSS onset of illnessillness duration antipsychoticmedication dose
Patients had lower NAACho ratio andgreater ChoCr ratio compared to healthyparticipants after controlling for greymatter volume NAACho ratio waspositively correlated with grey mattervolume in patients not healthy participantsNAACho ratio was inversely correlatedwith PANSS blunted affect score
Theberge et al (2004 2002) First-episode neuroleptic naiumlveschizophrenia patients (n=21)Healthy participants (n=21)
Analysis in Theberge et al 2002NAA Cho Cr Glu Gln mI in leftACC SANS SAPS
From Theberge et al 2002Patients had greater Gln concentrationcompared to healthy participantsMetabolite concentrations were notcorrelated with SANS or SAPS
Analysis in Theberge et al 2004NAA and Cho in left ACC DUPDUI DPS
From Theberge et al 2004NAA concentration was positively correlatedwith DUP and inversely with DPS at trendlevel Cho concentration was positivelycorrelated with DUP
Theberge et al (2003) Schizophrenia patients (n=21atypical n=7 both n=1typical n=13)Healthy participants (n=21)
NAA Cho Cr Glu Gln mI inleft ACC duration of illness
Glu and Gln concentrations were greaterin patients than healthy participants NAAconcentration was inversely correlatedwith duration of positive symptoms
Wood et al (2007) Schizophrenia male patients(n=15 13 atypical 2 medication free)Healthy male participants (n=14)
NAA and Glx in dorsal and rostralregions PANSS five factors illnessduration
Patients had lower NAA concentrationcompared to healthy participantsRight dorsal Glx was inversely correlatedwith illness duration
Ohrmann et al (2008) Schizophrenia patients(n=43 all on atypical)Healthy participants (n=37)
NAA Cho Cr Glx WCST learningpotential
No difference in metabolite concentrationbetween patients and healthy participantsNAA and Glx concentrations were positivelyassociated with WCST learning potential
Sanches et al (2008) Schizophrenia patients (n=37)Healthy participants (n=37)
NAA(Cho+Cr) ratio in left andright anterior middle frontal gyrusACC and perirolandic area (reference)basal skin conductance and skinconductance response to auditorystimuli of 1 s tones of 80 dB Patientsand healthy participants classified intoskin conductance responders (2 SDbelow mean skin conductance in healthyparticipants) and non-responders
NAA(Cho+Cr) ratio was lower in patientsthan healthy participants in the anteriormiddle frontal gyrus and ACC bilaterallyNAA(Cho+Cr) ratio did not differ betweenskin conductance response groups based onskin conductance response to auditory stimuliBasal skin conductance non-responders patientshad lower NAA(Cho+Cr) ratio than healthyparticipants in left and right ACC
258 P Premkumar et al Psychiatry Research Neuroimaging 182 (2010) 251ndash260
Tayoshi et al (2009) Long-term schizophrenia (n=30antipsychotic medication typenot reported)Healthy participants (n=25)
NAA Cho Cr Glu Gln mI Gender PANSStotal and subscales duration of illnessduration of therapy antipsychotic dosagebenzodiazepine dose
Patients had lower Glu and mI concentrationcompared to healthy participants Malepatients had lower NAA Cr Glu and mIconcentration than male healthy participantsMales had greater Gln concentration comparedto females Metabolite concentration wasnot correlated with symptoms or otherclinical variables
Ongur et al (2009) Schizophrenia patients (n=15)Bipolar disorder patients (n=15)Healthy participants (n=22)
Cr in ACC (hypothesized area) andparietal-occipital cortex (reference area)MADRS PANSS YMRS
Patients had lower Cr than healthyparticipants in both ACC andparietal-occipital cortex No significantcorrelations between Cr concentrationand clinical measures
ACC anterior cingulate cortex ChomdashCholine CrmdashCreatinePhosphocreatine DPSmdashduration of psychotic symptoms DUImdashduration of untreated illness DUPmdashduration of untreatedpsychosis GlnmdashGlutamine GlumdashGlutamate GluCr ratio SANSmdashSchedule for the Assessment of Negative Symptoms GlxmdashGlutamate+Glutamine MADRSmdashMontgomery AsbergDepression Rating Scale mImdashmyo-Inositol NAA N-acetyl aspartate PANSSmdashPositive and Negative Syndrome Scale SAPS Schedule for the Assessment of Positive SymptomsWCSTmdashWisconsin Card Sorting test YMRSmdashYoung Mania Rating Scale
Appendix A (continued)
259P Premkumar et al Psychiatry Research Neuroimaging 182 (2010) 251ndash260
Appendix B Supplementary Data
Supplementary data associated with this article can be found inthe online version at doi101016jpscychresns201002008
References
Adler CM Malhotra AK Elman I Goldberg T Egan M Pickar D Breier A 1999Comparison of ketamine-induced thought disorder in healthy volunteers andthought disorder in schizophrenia American Journal of Psychiatry 156 1646ndash1649
Andres RH Ducray AD Schlattner U Wallimann T Widmer HR 2008 Functionsand effects of creatine in the central nervous system Brain Research Bulletin 76329ndash343
Baiano M David A Versace A Churchill R Balestrieri M Brambilla P 2007Anterior cingulate volumes in schizophrenia a systematic review and a meta-analysis of MRI studies Schizophrenia Research 93 1ndash12
Bechara A Damasio AR Damasio H Anderson SW 1994 Insensitivity to futureconsequences following damage to human prefrontal cortex Cognition 50 7ndash15
Behrens TE Woolrich MW Walton ME Rushworth MF 2007 Learning the valueof information in an uncertain world Nature Neuroscience 10 1214ndash1221
Bertolino A Esposito G Callicott JH Mattay VS Van Horn JD Frank JA BermanKF Weinberger DR 2000 Specific relationship between prefrontal neuronal N-acetylaspartate and activation of the working memory cortical network inschizophrenia American Journal of Psychiatry 157 26ndash33
Braus DF Ende G Weber-Fahr W Demirakca T Henn FA 2001 Favorable effecton neuronal viability in the anterior cingulate gyrus due to long-term treatmentwith atypical antipsychotics an MRSI study Pharmacopsychiatry 34 251ndash253
Braus DF Ende G Weber-Fahr W Demirakca T Tost H Henn FA 2002Functioning and neuronal viability of the anterior cingulate neurons followingantipsychotic treatment MR-spectroscopic imaging in chronic schizophreniaEuropean Neuropsychopharmacology 12 145ndash152
Burgess PW Shallice T 1997 The Hayling and Brixton Tests Thames Valley TestCompany Bury St Edmunds
Callicott JH Bertolino A Mattay VS Langheim FJ Duyn J Coppola R Goldberg TEWeinberger DR 2000 Physiological dysfunction of the dorsolateral prefrontal cortexin schizophrenia revisited Cerebral Cortex 10 1078ndash1092
Carter CS van Veen V 2007 Anterior cingulate cortex and conflict detection anupdate of theory and data Cognitive Affective and Behavioral Neuroscience 7367ndash379
Cornblatt BA Risch JJ Faris G Friedman D Erlenmeyer-Kimling L 1988 TheContinuous Performance Test Identical Pairs Version (CPT-IP) I New findingsabout sustained attention in normal families Psychiatry Research 26 223ndash238
Costafreda SG Khanna A Mourao-Miranda J Fu CH 2009 Neural correlates of sadfaces predict clinical remission to cognitive behavioural therapy in depressionNeuroReport 20 637ndash641
Deicken RF Zhou L Schuff N Weiner MW 1997 Proton magnetic resonancespectroscopy of the anterior cingulate region in schizophrenia SchizophreniaResearch 27 65ndash71
Deicken RF Johnson C Pegues M 2000 Proton magnetic resonance spectroscopy ofthe human brain in schizophrenia Reviews in the Neurosciences 11 147ndash158
Ende G Braus DF Walter S Weber-Fahr W Soher B Maudsley AA Henn FA2000 Effects of age medication and illness duration on the N-acetyl aspartatesignal of the anterior cingulate region in schizophrenia Schizophrenia Research 41389ndash395
Fannon D Simmons A Tennakoon L OCeallaigh S Sumich A Doku V Shew CSharma T 2003 Selective deficit of hippocampal N-acetylaspartate in antipsy-chotic-naive patients with schizophrenia Biological Psychiatry 54 587ndash598
Ferguson KJ MacLullich AM Marshall I Deary IJ Starr JM Seckl JR Wardlaw JM2002 Magnetic resonance spectroscopy and cognitive function in healthy elderlymen Brain 125 2743ndash2749
First MB Spitzer RL Gibbon M Williams JBW 2002 Structured Clinical Interviewfor DSM-IV-TR Axis I DisordersmdashPatient Edition (SCID-IP 112002 revision)Biometrics Research Department New York NY
Fornito A Yucel M Dean B Wood SJ Pantelis C 2008 Anatomical abnormalities ofthe anterior cingulate cortex in schizophrenia bridging the gap betweenneuroimaging and neuropathology Schizophrenia Bulletin 35 973ndash993
Fowler D Garety PA Kuipers E 1995 Cognitive Behaviour Therapy for PsychosisTheory and Practice Wiley Chichester
Fujimoto T Takeuch K Matsumoto T Kamimura K Hamada R Nakamura K KatoN 2007 Abnormal glucose metabolism in the anterior cingulate cortex in patientswith schizophrenia Psychiatry Research 154 49ndash58
Goff DC Hennen J Lyoo IK Tsai G Wald LL Evins AE Yurgelun-Todd DARenshaw PF 2002 Modulation of brain and serum glutamatergic concentrationsfollowing a switch from conventional neuroleptics to olanzapine BiologicalPsychiatry 51 493ndash497
Gold JM Carpenter C Randolph C Goldberg TE Weinberger DR 1997 Auditoryworking memory and Wisconsin Card Sorting Test performance in schizophreniaArchives of General Psychiatry 54 159ndash165
Heaton RK Chelune GJ Tally JL Kay GG Curtiss G 1993 Wisconsin Card SortingTest Manual Revised and Expanded Psychological Assessment Resources OdessaFL
Honea R Crow TJ Passingham D Mackay CE 2005 Regional deficits in brainvolume in schizophrenia a meta-analysis of voxel-based morphometry studiesAmerican Journal of Psychiatry 162 2233ndash2245
Hughes C Kumari V Soni W Das M Binneman B Drozd S ONeil S Mathew VSharma T 2003 Longitudinal study of symptoms and cognitive function in chronicschizophrenia Schizophrenia Research 59 137ndash146
Jung RE Brooks WM Yeo RA Chiulli SJ Weers DC Sibbitt Jr WL 1999Biochemical markers of intelligence a proton MR spectroscopy study of normalhuman brain Proceedings Biological Sciences 266 1375ndash1379
Kaneda M Osaka N 2008 Role of anterior cingulate cortex during semantic coding inverbal working memory Neuroscience Letters 436 57ndash61
Kay SR Fiszbein A Opier LA 1987 The Positive and Negative Syndrome Scale(PANSS) for schizophrenia Schizophrenia Bulletin 13 261ndash276
Kennerley SW Dahmubed AF Lara AH Wallis JD 2008 Neurons in the frontallobe encode the value of multiple decision variables Journal of CognitiveNeuroscience 21 1162ndash1178
Kim J Whyte J Wang J Rao H Tang KZ Detre JA 2006 Continuous ASL perfusionfMRI investigation of higher cognition quantification of tonic CBF changes duringsustained attention and working memory tasks Neuroimage 31 376ndash385
Krystal JH Karper LP Seibyl JP Freeman GK Delaney R Bremner JD HeningerGR Bowers Jr MB Charney DS 1994 Subanesthetic effects of the noncom-petitive NMDA antagonist ketamine in humans Psychotomimetic perceptualcognitive and neuroendocrine responses Archives of General Psychiatry 51199ndash214
Kumari V Peters ER Fannon D Antonova E Premkumar P Anilkumar APWilliams SC Kuipers EA 2009 Dorsolateral prefrontal cortex activity predictsresponsiveness to cognitive behaviour therapy in schizophrenia BiologicalPsychiatry 66 594ndash602
Lahti AC Koffel B LaPorte D Tamminga CA 1995 Subanesthetic doses of ketaminestimulate psychosis in schizophrenia Neuropsychopharmacology 13 9ndash19
Lenartowicz A McIntosh AR 2005 The role of anterior cingulate cortex in workingmemory is shaped by functional connectivity Journal of Cognitive Neuroscience 171026ndash1042
Malhotra AK Pinals DA Adler CM Elman I Clifton A Pickar D Breier A 1997Ketamine-induced exacerbation of psychotic symptoms and cognitive impairmentin neuroleptic-free schizophrenics Neuropsychopharmacology 17 141ndash150
260 P Premkumar et al Psychiatry Research Neuroimaging 182 (2010) 251ndash260
McLean MA Woermann FG Barker GJ Duncan JS 2000 Quantitative analysis ofshort echo time (1)H-MRSI of cerebral gray and white matter Magnetic Resonancein Medicine 44 401ndash411
McMorris T Harris RC Swain J Corbett J Collard K Dyson RJ Dye L Hodgson CDraper N 2006 Effect of creatine supplementation and sleep deprivation withmild exercise on cognitive and psychomotor performance mood state and plasmaconcentrations of catecholamines and cortisol Psychopharmacology (Berl) 18593ndash103
McMorris T Harris RC Howard AN Langridge G Hall B Corbett J Dicks MHodgson C 2007 Creatine supplementation sleep deprivation cortisol melatoninand behavior Physiology and Behaviour 90 21ndash28
Miller BL 1991 A review of chemical issues in 1H NMR spectroscopy N-acetyl-L-aspartate creatine and choline NMR in Biomedicine 4 47ndash52
Moghaddam B 2003 Bringing order to the glutamate chaos in schizophrenia Neuron40 881ndash884
Ohrmann P Siegmund A Suslow T Pedersen A Spitzberg K Kersting ARothermundt M Arolt V Heindel W Pfleiderer B 2007 Cognitive impairmentand in vivo metabolites in first-episode neuroleptic-naive and chronic medicatedschizophrenic patients a proton magnetic resonance spectroscopy study Journalof Psychiatric Research 41 625ndash634
Ohrmann P Kugel H Bauer J Siegmund A Kolkebeck K Suslow T Wiedl KHRothermundt M Arolt V Pedersen A 2008 Learning potential on the WCST inschizophrenia is related to the neuronal integrity of the anterior cingulate cortex asmeasured by proton magnetic resonance spectroscopy Schizophrenia Research106 156ndash163
Ongur D Prescot AP Jensen JE Cohen BM Renshaw PF 2009 Creatineabnormalities in schizophrenia and bipolar disorder Psychiatry ResearchNeuroimaging 172 44ndash48
Osaka N Osaka M Kondo H Morishita M Fukuyama H Shibasaki H 2004 Theneural basis of executive function in working memory an fMRI study based onindividual differences Neuroimage 21 623ndash631
Perry G Nunomura A Hirai K Zhu X Perez M Avila J Castellani RJ Atwood CSAliev G Sayre LM Takeda A Smith MA 2002 Is oxidative damage thefundamental pathogenic mechanism of Alzheimers and other neurodegenerativediseases Free Radical Biology and Medicine 33 1475ndash1479
Peterson BS Skudlarski P Gatenby JC Zhang H Anderson AW Gore JC 1999 AnfMRI study of Stroop word-color interference evidence for cingulate subregionssubserving multiple distributed attentional systems Biological Psychiatry 451237ndash1258
Provencher SW 1993 Estimation of metabolite concentrations from localized in vivoproton NMR spectra Magnetic Resonance in Medicine 30 672ndash679
Rae C Digney AL McEwan SR Bates TC 2003 Oral creatine monohydratesupplementation improves brain performance a double-blind placebo-controlledcross-over trial Proceedings Biological Sciences 270 2147ndash2150
Ross AJ Sachdev PS 2004 Magnetic resonance spectroscopy in cognitive researchBrain Research Brain Research Reviews 44 83ndash102
Rushworth MF Walton ME Kennerley SW Bannerman DM 2004 Action sets anddecisions in the medial frontal cortex Trends in Cogntive Sciences 8 410ndash417
Rutten BP Korr H Steinbusch HW Schmitz C 2003 The aging brain less neuronscould be better Mechanisms of Ageing and Development 124 349ndash355
Sanches RF Crippa JA Hallak JE de Sousa JP Araujo D Santos AC Zuardi AW2008 Proton magnetic resonance spectroscopy of the frontal cingulate andperirolandic cortices and its relationship to skin conductance in patients withschizophrenia Brazilian Journal of Medical and Biological Research 41 1132ndash1141
Schlosser RG Koch K Wagner G Nenadic I Roebel M Schachtzabel C Axer MSchultz C Reichenbach JR Sauer H 2008 Inefficient executive cognitive controlin schizophrenia is preceded by altered functional activation during informationencoding an fMRI study Neuropsychologia 46 336ndash347
Shapiro AM Benedict RH Schretlen D Brandt J 1999 Construct and concurrentvalidity of the Hopkins Verbal Learning Test-revised The Clinical Neuropsychol-ogist 13 348ndash358
Smith EE Jonides J 1999 Storage and executive processes in the frontal lobesScience 283 1657ndash1661
Szoke A Trandafir A Dupont ME Meary A Schurhoff F Leboyer M 2008Longitudinal studies of cognition in schizophrenia meta-analysis British Journal ofPsychiatry 192 248ndash257
Tayoshi S Sumitani S Taniguchi K Shibuya-Tayoshi S Numata S Iga JI NakatakiM Ueno SI Harada M Ohmori T 2009 Metabolite changes and genderdifferences in schizophrenia using 3-Tesla proton magnetic resonance spectrosco-py ((1)H-MRS) Schizophrenia Research 108 69ndash77
Theberge J Bartha R Drost DJ Menon RS Malla A Takhar J Neufeld RWRogers J Pavlosky W Schaefer B Densmore M Al-Semaan Y Williamson PC2002 Glutamate and glutamine measured with 40T proton MRS in never-treatedpatients with schizophrenia and healthy volunteers American Journal of Psychiatry159 1944ndash1946
Theberge J Al-Semaan Y Williamson PC Menon RS Neufeld RW Rajakumar NSchaefer B Densmore M Drost DJ 2003 Glutamate and glutamine in theanterior cingulate and thalamus of medicated patients with chronic schizophreniaand healthy comparison subjects measured with 40-T proton MRS AmericanJournal of Psychiatry 160 2231ndash2233
Theberge J Al-Semaan Y Drost DJ Malla AK Neufeld RW Bartha R ManchandaR Menon R Densmore M Schaefer B Williamson PC 2004 Duration ofuntreated psychosis vs N-acetylaspartate and choline in first episode schizophre-nia a 1H magnetic resonance spectroscopy study at 40 Tesla Psychiatry Research131 107ndash114
Tranberg M Stridh MH Guy Y Jilderos B Wigstrom H Weber SG Sandberg M2004 NMDA-receptor mediated efflux of N-acetylaspartate physiological andorpathological importance Neurochemistry International 45 1195ndash1204
Tranberg M Abbas AK Sandberg M 2007 In vitro studies on the putative function ofN-acetylaspartate as an osmoregulator Neurochemical Research 32 1248ndash1255
Walton ME Croxson PL Behrens TE Kennerley SW Rushworth MF 2007Adaptive decision making and value in the anterior cingulate cortex Neuroimage36 (Suppl 2) T142ndashT154
Wechsler D 1987 Wechsler Memory ScalemdashRevised Psychological Corporation NewYork
Weinberger DR Aloia MS Goldberg TE Berman KF 1994 The frontal lobes andschizophrenia Journal of Neuropsychiatry and Clinical Neurosciences 6 419ndash427
Wood SJ Yucel M Wellard RM Harrison BJ Clarke K Fornito A Velakoulis DPantelis C 2007 Evidence for neuronal dysfunction in the anterior cingulate ofpatients with schizophrenia a proton magnetic resonance spectroscopy study at3T Schizophrenia Research 94 328ndash331
Yamasue H Fukui T Fukuda R Yamada H Yamasaki S Kuroki N Abe O Kasai KTsujii K Iwanami A Aoki S Ohtomo K Kato N Kato T 2002 1H-MRspectroscopy and gray matter volume of the anterior cingulate cortex inschizophrenia NeuroReport 13 2133ndash2137
Yeo RA Hill D Campbell R Vigil J Brooks WM 2000 Developmental instabilityand working memory ability in children a magnetic resonance spectroscopyinvestigation Developmental Neuropsychology 17 143ndash159

252 P Premkumar et al Psychiatry Research Neuroimaging 182 (2010) 251ndash260
membrane phospholipids (for review see Ross and Sachdev 2004)while Cr helps maintain the energy homeostasis within the nervecell (Andres et al 2008) The evidence suggests that Cr may alsohave direct effects on neuropsychological function For example oralsupplements of Cr increased intelligence working memory perfor-mance (Rae et al 2003) and executive function (McMorris et al2007 2006)
Previous studies have reported using magnetic resonance spec-troscopy (MRS) lower ACC NAA level in patients with schizophreniaespecially in those treated with typical antipsychotic drugs comparedwith healthy participants (Braus et al 2002 Deicken et al 2000Ende et al 2000 Sanches et al 2008 Tayoshi et al 2009Wood et al2007 Yamasue et al 2002 see Appendix A for detailed information)Within this patient population ACC NAA concentration is reported tobe inversely associated with illness duration in some studies (Brauset al 2002 Ende et al 2000 Theberge et al 2003) but not others(Deicken et al 1997 Tayoshi et al 2009 Theberge et al 2004Woodet al 2007 Yamasue et al 2002) NAA reductions have been reportedin antipsychotic drug-naiumlve first-episode patients and treatment mayincrease NAA levels in both recent-onset cases and patients withchronic illness (Braus et al 2002 Fannon et al 2003) NAAconcentration is positively associated with duration on atypicalantipsychotic medication in long-term patients (Braus et al 2002)and inversely correlated with the duration of positive symptoms infirst-episode neuroleptic-naiumlve patients (Theberge et al 2004) Morerecently Tayoshi et al (2009) observed no association between NAAconcentration and symptoms but reported a positive associationbetween NAA concentration andWisconsin Card Sorting Test (WCST)performance the latter finding was also present in two earlier studies(Braus et al 2002 Ohrmann et al 2008)
Neuropsychologically the ACC is involved in components of thecentral executive that facilitate working memory (Osaka et al 2004Smith and Jonides 1999) including encoding of semantic information(Kaneda and Osaka 2008) and reported to be deactivated inschizophrenia patients compared with healthy participants duringthe stimulus encoding phase of a working memory task (Schlosser etal 2008) A further role of the ACC is in emotional decision-makingwhere there is a relationship between an action and the reinforce-ment value of its outcome (Rushworth et al 2004 Walton et al2007) The ACC is involved in updating and integrating recentinformation to existing information on reward value of outcome interms of predicting future outcome (Behrens et al 2007 Kennerleyet al 2008)
The present study has two parts cross-sectional and longitudinalCross-sectionally the study aimed to compare the ACC NAAconcentrations in patients with schizophrenia and healthy partici-pants and to determine their clinical andor neuropsychologicalcorrelates it also explored these effects in Cho and Cr All except forthree recent studies that examined these metabolites in patients withschizophrenia (Ohrmann et al 2008 Sanches et al 2008 Tayoshiet al 2009) had a smaller sample size than that in our investigationand none undertook a comprehensive examination of metaboliteconcentration relationships with clinical symptoms and neuropsy-chological functions We hypothesized that (1) NAA concentrationwould be reduced in patients compared with healthy participants dueto impaired neuronal function (2) in patients NAA concentrationwould be associated inversely with illness duration (Braus et al 2002Ende et al 2000 Theberge et al 2003) and symptoms on the Positiveand Negative Syndrome Scale (Wood et al 2007) and (3) NAAconcentration would be positively associated with neuropsycholog-ical measures that involve the ACC namely working memory conflictdetection and decision-making (Behrens et al 2007 Carter and vanVeen 2007 Osaka et al 2004 Peterson et al 1999 Smith andJonides 1999 Walton et al 2007) both in healthy participants andpatients though such relationships may be weaker in patientsbecause they as mentioned earlier engage the ACC at a less-than-
normal level during relevant tasks We expected that the clinical orneuropsychological correlates of metabolite concentration would beattenuated or abolished after controlling for ACC grey matter (GM)concentration (Yamasue et al 2002) as GM concentration mayinfluence metabolite availability
Longitudinally the study aimed to determine the effect ofcognitive behavioural therapy for psychosis (CBTp) on metaboliteconcentration A sub-sample of the patients in the present investiga-tion went on to receive CBTp in addition to their standard care Thestudy therefore also examined whether (i) baseline metaboliteconcentration predicted symptom change following CBTp+SC and(ii) there was a change in metabolite concentration in patients whoreceived CBTp in addition to standard care We hypothesized that inthis sub-sample NAA concentration would increase coincident with areduced level of symptoms following CBTp
2 Materials and method
21 Participants and design
The study involved 30 patients with schizophrenia and 15 healthyparticipants all of whom underwent MRS of the ACC at study entryThe patient and control groups were matched on average for age andgender (Table 2) All patients were assessed by a ConsultantPsychiatrist (DF) for clinical diagnosis using the Structured ClinicalInterview for DSM-IV Axis I disorder (First et al 2002) and symptomseverity using the Positive and Negative Syndrome Scale (PANSS Kayet al 1987) All patients were recruited from the South London andMaudsley NHS Foundation Trust as part of a larger project investi-gating the functional neuroimaging correlates and predictors of CBTp(the MRS component was added to the larger project) had been onstable doses of antipsychotic medication for at least 2 years and onthe current antipsychotic drug for at least 3months before taking part
Of the 30 patients at study entry (baseline) 11 patients sub-sequently received CBTp+SC in a specialist clinical service [Psycho-logical Interventions Clinic for Outpatients with Psychosis (PICuP)South London and Maudsley NHS Foundation Trust (SLAM)] inaddition to their standard care and 13 patients continued to receivestandard care only (SC controls) all of these 24 patients (i) received arating of ge60 on the PANSS (ii) reported at least one positivelsquodistressingrsquo symptom of schizophrenia and (iii) wished to receiveCBTp (if available only about 10ndash20 of eligible SLAM patients wereaccepted for CBTp with the existing resources availability was theonly criterion that determined whether or not eligible patientsreceived CBTp) Eight of 11 CBTp+SC patients and 12 of 13 SCcontrol patients were assessed for symptom severity at follow-up ofwhom seven and four patients respectively underwent MRS atfollow-up Six (of 30) patients had low symptom severity at baselinethey were considered to be responsive to antipsychotic treatment bytheir long-term treating clinicians (SC responsive) these patientswere not followed up
The patients in the CBTp+SC and SC control groups wererecruited from the same geographical area were identified by localConsultant Psychiatrists as suitable for CBTp and wished to receiveCBTp in addition to their usual care Allocation to CBTp+SC and SCcontrol groups was not randomised but followed a cohort case-controlled design Patients who were referred to and accepted forCBTp by the Psychological Interventions Clinic for Outpatientswith Psychosis (PICuP) SLAM NHS Foundation Trust went into theCBTp+SC group Others who matched demographically (age andnumber of years in education) and clinically (illness duration andPANSS symptoms) as much as possible those accepted for CBTp bythe PICuP were studied as part of the SC control group over thesame interval as the CBTp+SC group patients SC consisted of casemanagement offered by the case management team for a particulargeographical area Most patients (80) were on a single antipsychotic
253P Premkumar et al Psychiatry Research Neuroimaging 182 (2010) 251ndash260
drug (see Table 2) Of the 12 patients on olanzapine one patient alsotook aripiprazole and a further patient also took trifluoperazine Of thesix patients on clozapine one patient also took quetiapine and afurther patient also took amisulperide Of the two patients onhaloperidol one patient was also on sulperide and the other patienton pipotiazine In addition to antipsychotic drug treatment fourpatients were receiving anti-cholinergics
CBTp followed the procedure developed by Fowler et al (1995)Therapy sessions were conducted on a weekly or fortnightly basis aspreferred by the patient Patients received an average of 16 sessionsAll CBT interventions were formulation-driven and focused on thetherapy goals of the patient The therapists were supervised by one ofthe investigators (EK) who has extensive experience of CBTp
The study procedures were approved by the ethics committee ofthe Institute of Psychiatry and the South London and Maudsley NHSFoundation Trust London All participants provided written informedconsent to their participation and were compensated for their timeand travel
22 Neuropsychological assessments
All patients and 13 healthy participants were assessed onneuropsychological measures (described in Table 1) that areconsidered to recruit the ACC and found to reveal performancedeficits in executive function workingshort-term memory attentionand emotional decision-making in schizophrenia
23 Magnetic resonance spectroscopy data acquisition and processing
Images were acquired using a 15 Tesla GE NVi Signa System(General Electric Milwaukee WI USA) at the Maudsley HospitalSouth London A quadrature birdcage head coil was used for RFtransmission and reception Initially a series of fast gradient echoscout images were acquired in order to orient subsequent imagesrelative to the anterior commissureposterior commissure line andthe interhemispheric fissure Subsequently the whole brain wasscanned with a 3-D inversion recovery prepared fast spoiled GRASST1-weighted dataset Chemical shift images were acquired from aPRESS excited volume in a 15 cm thick slab through the anteriorcommissure correspondingwith the dorsal ACC with a nominal voxelsize of 15 cm3 (24times24 phase-encode steps over a 24 cm FOV) Tominimise relaxation effects a short TE of 35 ms was used and arelatively long TR of 2 s
Only metabolite information with a fitting error (percent standarddeviation) of b20 was included in the final analysis (Ohrmann et al
Table 1Battery of neuropsychological measures
Neuropsychological test Variables used in analysis
Executive functionBrixton Test (Burgess and Shallice 1997) Perseverative errorsWisconsin Card Sorting Test (WCST)(Heaton et al 1993)
Perseverative errors
Workingshort-term memoryLetter number test (Gold et al 1997) Total number of items correctWechsler Memory ScalemdashRevised (WMS-R) LogicalMemory (Wechsler 1987)mdashImmediate recall
Unit recall scaled score
Hopkins Verbal Learning Test(Shapiro et al 1999)
Total number of items freelyrecalled
AttentionContinuous Performance Testmdashidentical pairs(Cornblatt et al 1988)
Discriminability
Emotional decision-makingIowa Gambling Task (Bechara et al 1994) Overall learning
(block 5 minus block 1)
2008) Absolute concentrations of NAA Cho and Cr were measured inmillimolars in all participants using the LCmodel (McLean et al 2000Provencher 1993) For each MRS voxel the proportions of GM whitematter and cerebrospinal fluid (CSF) were calculated by segmentingthe Spoiled Gradient Recalled (SPGR) image (Fig 1) This allowscorrection for CSF contamination within each voxel and extrapolationto concentrations for pure GM (McLean et al 2000) Metaboliteconcentration was calculated as a function of CSF concentrationwithin each voxel using the following formula
Metabolite value=eth1minusCSF concentrationTHORN
100
NAA Cho and Cr absolute concentration estimates in millimolarsare reported rather than metabolite peak ratios such as NAAChoNAACr and ChoCr because absolute concentrations of individualmetabolites are not influenced by fluctuations in the concentration ofthe reference metabolite Metabolite ratios are believed to account foralterations in the Cr reference peak which invalidate its usefulness asan internal reference for the other metabolite peaks of the protonspectrum (Deicken et al 1997)
24 Statistical analysis
241 Cross-sectional analysis
2411 Group comparison of metabolite concentration Differencesbetween patient (across all patients) and healthy participant groupsin metabolite concentration and GM concentration age years ofeducation and clinical and neuropsychological variables wereexamined using analysis of variance (ANOVA) For the neuropsycho-logical variables showing a non-normal distribution (Brixton persev-erative errors) MannndashWhitney U tests were performed A chi-squared test examined group differences in gender distribution
2412 Clinical correlates of metabolite concentration Pearson andpartial correlations controlling for GM concentration or Spearmancorrelations for clinical variables with a non-normal distribution(antipsychotic medication level) were performed between clinicalvariables and metabolite concentrations The clinical variables were
Fig 1 A Spoiled Gradient Recalled (SPGR) brain image in the axial slice in a controlsubject The square indicates the volume of interest (VOI) 15times15times15 cm3 voxel inthe anterior cingulate cortex Within the VOI each tissue (cerebrospinal fluid greymatter and white matter) was segmented
254 P Premkumar et al Psychiatry Research Neuroimaging 182 (2010) 251ndash260
PANSS symptoms illness duration (defined as the difference betweenthe age at onset of psychotic symptoms as reported by the patient andwhere possible confirmed with other sources and age at the time ofbaseline assessments) and antipsychotic medication level (in chlor-promazine equivalents) Spearman correlations were performed toexamine the relationship between metabolite values and individualPANSS items in those subscales that were found to have a significantassociation with metabolite values
2413 Neuropsychological correlates of metabolite concentrationPearson and partial correlations controlling for GM concentration orSpearman correlations for neuropsychological variables with a non-normal distribution (Brixton perseverative errors) were performedbetween neuropsychological performance measures and metaboliteconcentration in patient and healthy participant groups
2414 Multiple regression of clinical andor neuropsychological correlateson metabolite concentration Significant clinical andor neuropsycholog-ical variables that had a normal distribution were entered into themultiple regression model using a stepwise method (to estimate theeffect of individual predictors on variability of criterion variable) andusing a forced-entry method (to explain the combined effect ofpredictors on the variability of the criterion variable)
242 Longitudinal analysis
2421 Group comparison of metabolite concentration Due to the smallsample sizes differences between CBTp+SC SC control and SCresponsive patient groups in age education clinical variables andbaseline metabolite and GM concentrations were examined using non-parametric analyses namely the Kruskal-Wallis test A chi-squared testdetermined group differences in gender distribution
2422 Metabolite concentration as a predictor of symptom changefollowing CBTpSpearman correlationswere performed in the CBTp+SCpatients who were followed up (n=8) between baseline metaboliteconcentrations and residual PANSS symptom change scores frombaseline to follow-up
2423 Change in symptom severity and metabolite concentrationfollowing CBTp Due to the small sample sizes (CBTp+SC n=7 andSC control n=4) changes in symptom severity metabolite and GMconcentrations from baseline to follow-up in the patient groups wereexamined using the Wilcoxon Signed Rank test
All analyses were performed in SPSS windows (version 15) Alphalevel for testing significance of effects was maintained at Pb005 Wechose not to apply the Bonferroni method of adjusting the P valuebecause we expected the size of the relationship between MRS valuesand symptomsneuropsychological functions to be small or at bestmodest given that symptoms in schizophrenia are unlikely to have asingle aetiology and successful task performance on most neuropsy-chological tasks would recruit additional brain regions
3 Results
31 Cross-sectional analysis
311 Group differences in demographic and neuropsychological variablesPatient and healthy participant groups did not differ in gender and
age Patients had fewer years in education and showed deficientperformance on most neuropsychological measures relative tohealthy participants (Table 2)
312 Group differences in metabolite concentration in the ACCNAA Cr and GM concentrations were lower in the patient
compared with the healthy participant group (Table 3)
313 Clinical correlates of metabolite concentrationNAA concentration correlated inversely with positive symptoms
general psychopathology and total symptoms (Table 4) Thesecorrelations remained significant after controlling for GM NAAconcentration correlated inversely with negative symptoms onlyafter controlling for GM PANSS item-wise correlations revealed thatNAA concentration was inversely correlated with delusions disorga-nisation and persecution items of the positive syndrome subscalepassive social withdrawal and stereotyped thinking items of thenegative syndrome subscale and somatic concern and preoccupationitems of the general psychopathology subscale
Cho concentration correlated inversely with positive and totalsymptoms After controlling for GM concentration Cho concentrationcorrelated with total symptoms but not positive symptoms Choconcentration correlated inversely with negative symptoms at a trendlevel only after controlling for GM concentration PANSS item-wisecorrelations revealed that Cho concentration was inversely correlatedwith disorganisation and hostility items of the positive syndromesubscale passive social withdrawal item of the negative syndromesubscale and somatic concern item of the general psychopathologysubscale Cho concentration correlated positively with antipsychoticmedication dosage Cr concentration did not correlate with anyclinical variable
314 Neuropsychological correlates of metabolite concentrationPatients A positive correlation between NAA concentration and
working memory as assessed by the letter number test emerged onlyafter controlling for GM concentration (Table 5)
Healthy participants NAA concentration correlated positively withworking memory as assessed by the letter number test and short-term memory as assessed by the Hopkins verbal learning test thoughthese correlations were reduced to a trend level of significance aftercontrolling for GM concentration (Table 5) Cho concentrationcorrelated inversely with short-term memory as assessed by theWechsler Memory ScalemdashRevised (WMS-R) logical memory imme-diate recall test after controlling for GM concentration Cr concentra-tion correlated inversely with executive function as assessed byBrixton perseverative errors
315 Multiple regression of clinical andor neuropsychologicalcorrelates of metabolite concentration
Patients In the stepwise regression model with NAA concentra-tion as the criterion variable positive symptoms proved to be asignificant predictor (r=minus0489 P=0006) The model explained 21of the variance in NAA concentration In the forced-entry regressionmodel the predictors (positive symptoms general psychopathologyand letter number test) explained 25 of the variance in NAAconcentration
Healthy participants In the stepwise regression model with NAAconcentration as the criterion variable short-term memory asassessed by the Hopkins verbal learning test was a significantpredictor (r=0576 P=0039) The model explained 27 of thevariance in NAA concentration In the forced-entry regression modelthe predictors (Hopkins verbal learning test and letter number test)explained 27 of the model
32 Longitudinal analysis
321 Metabolite concentration differences at baseline between patientsub-groups
NAA concentration tended to differ between patient groups atbaseline mainly due to greater concentration in the low-symptomSC-responsive group (Table 6)
Table 2Demographic clinical and neuropsychological characteristics of patients and healthy participants groups
Characteristic Patients Healthy participants Test χ2 (df) P
Gender malefemale (n) 246 132 Chi-squared 0304 (1) 0581mean SD mean SD F or z (df)
Age in years 3640 864 3540 1334 ANOVA 0092 (143) 0763Years in education 1383 215 1561 323 ANOVA 4555 (141) 0039Illness duration years 1298 894
Symptoms (PANSS)Positive 1693 395Negative 1787 452General psychopathology 3170 639Total 6650 1317Medication level (chlorpromazine equivalents) 50267 32788Medication type (n)
Olanzapine 12Clozapine 6Risperidone 5Aripiprazole 2Flupentixol 2Amisulperide 1Haloperidol 2
Neuropsychological functionBrixton perseverative errors 050 078 031 048 MannndashWhitney U minus0552 (141) 0648WCST perseverative errors 1817 886 1175 751 ANOVA 4870 (140) 0033Letter number test number correct 1380 380 1692 296 ANOVA 6925 (141) 0012WMS logical memory immediate unit recalled 710 258 969 333 ANOVA 7533 (140) 0009Hopkins total freely recalled 2186 538 2692 517 ANOVA 8122 (140) 0007CPT discriminability 029 059 187 100 ANOVA 14257 (139) 0001IGT overall learning 280 1183 892 1473 ANOVA 2092 (141) 0156
255P Premkumar et al Psychiatry Research Neuroimaging 182 (2010) 251ndash260
33 Metabolite concentration correlates of symptom change followingCBTp
In the CBTp+SC group metabolite concentration at baseline wasnot associated with symptom change following CBTp (SupplementaryTable)
34 Symptom severity and metabolite concentration change frombaseline to follow-up in CBTp+SC and SC control groups
Positive symptoms improved following CBTp in the CBTp+SCgroup while negative symptoms tended to deteriorate in the SCcontrol group (Table 7)
NAA concentration tended to increase in the CBTp+SC group frombaseline to follow-up (Table 7)
4 Discussion
The present investigation examined the concentrations of NAACho and Cr in the ACC and their clinical and neuropsychologicalcorrelates in patients with schizophrenia and healthy participants(cross-sectional investigation) The study also explored whetherbaseline metabolite concentration predicted symptom change fol-lowing CBTp+SC and whether a reduction in symptoms followingCBTp+SC was accompanied by higher NAA concentration relative tobaseline (longitudinal investigation)
Table 3ACCmetabolite and greymatter concentrations (mean SD) at baseline at each voxel inpatients and healthy participants
CSI variable(millimolars)
Patient(n=30)
Healthy participants(n=15)
F (p)
NAA 742 126 856 139 7682 (0008)Cho 190 038 199 036 0654 (0423)Cr 703 124 789 102 5345 (0026)Grey matter 5399 1051 6139 858 5549 (0023)
41 Summary of clinical and neuropsychological correlates of metaboliteconcentration (cross-sectional investigation)
The major findings from the cross-sectional analysis were that inpatients (1) NAA concentration was reduced compared to healthyparticipants (2) greaterNAA concentrationwas associatedwith a lowerlevel of positive symptoms general psychopathology and betterworking memory (positive symptoms alone explained 21 of thevariance total variance explained=25) and (3) greater Cho concen-tration was associated with a lower level of positive symptoms andhigher level of antipsychotic medication In healthy participants thefollowing associationswere observed (1) NAA concentration positivelywith working and short-termmemory (2) Cho concentration inverselywith short-term memory and (3) Cr concentration inversely withexecutive function These findings will be discussed in turn
411 Clinical correlates of metabolite concentrationsThe findings of lower ACC NAA concentration in schizophrenia
patients (Deicken et al 1997 Ende et al 2000 Wood et al 2007)and clinical correlates of NAA concentration support previousevidence (Theberge et al 2003 Wood et al 2007 Yamasue et al2002) Our study of a relatively larger sample of patients than mostprevious studies is the first to observe that NAA concentration wasinversely associated with the severity of positive negative andgeneral psychopathology symptoms based on the three-dimensionalmodel of the PANSS (Kay et al 1987) Twenty percent of our patientswere SC treatment responsive giving a wider range to symptomscores than earlier studies Patients who had low symptom severityand were considered to have responded sufficiently to their standard(mostly atypical) antipsychotic treatment tended to show greaterNAA concentration than patients who were symptomatic (baselinecomparisons) suggesting that NAA concentration may vary as afunction of symptom severity and treatment response
NAA concentration being a by-product of neurotransmitter turn-over (Tranberg et al 2004) the symptom severity-metabolite concen-tration associations may reflect the efficiency of neurotransmission Asnoted in Section 1 NAA concentration may be an indicator of NMDA
Table 4Clinical correlates of metabolite concentration at baseline (patients only)
NAA concentration Cho concentration Cr concentration
r or ρ r (P) rp1 (P) r (P) rp
1 (P) r (P) rp1 (P)
Illness duration r minus0059 (0756) 0091 (0640) minus0064 (0735) 0045 (0817) minus0291 (0118) minus0244 (0203)Antipsychotic medication level Rho 0197 (0298) 0442 (0014) 0073 (0700)Symptoms (PANSS)
Positive (P) symptoms r minus0489 (0006) minus0430 (0020) minus0391 (0033) minus0325 (0085) minus0308 (0098) minus0262 (0170)Negative (N) symptoms r minus0297 (0111) minus0418 (0024) minus0287 (0124) minus0366 (0051) minus0211 (0264) minus0262 (0170)General psychopathology (GP) r minus0416 (0022) minus0506 (0005) minus0299 (0109) minus0341 (0070) minus0204 (0281) minus0219 (0254)Total r minus0450 (0013) minus0512 (0004) minus0361 (0050) minus0384 (0040) minus0263 (0160) minus0266 (0163)
Individual symptomsDelusions (P) Rho minus0411 (0024) minus0342 (0064) minus0192 (0309)Disorganisation (P) Rho minus0525 (0003) minus0369 (0045) minus0136 (0475)Persecution (P) Rho minus0390 (0033) minus0193 (0307) minus0068 (0719)Hostility (P) Rho 0062 (0745) 0370 (0044) 0163 (0390)Passive social withdrawal (N) Rho minus0370 (0044) minus0393 (0032) minus0261 (0163)Stereotyped thinking (N) Rho minus0422 (0020) minus0073 (0684) minus0221 (0240)Somatic concern (GP) Rho minus0419 (0021) minus0407 (0026) minus0129 (0496)Preoccupation (GP) Rho minus0528 (0003) minus0201 (0287) minus0264 (0156)
rp1 partial correlation controlling for GM concentration P PANSS positive symptom subscale N PANSS negative symptom subscale GP PANSS general psychopathology subscale
256 P Premkumar et al Psychiatry Research Neuroimaging 182 (2010) 251ndash260
function and neuronal longevity (Tranberg et al 2004) NAA efflux isa delayed response to sudden non-physiological decrease in extracel-lular osmolarity and high K+intra-cellular and NMDA activation(Tranberg et al 2007) Elevated concentration of NAA in the ACC inschizophrenia patients with lower level of symptoms may reflectincreased turnover of neurotransmitters such as dopamine and NMDA
Similarly the association between Cho concentration and total andpositive symptoms may also reflect improved neurotransmitterfunction and neuronal integrity with milder symptoms The Cho peakincludes solublemembranephospholipids includingphosphorylcholine(PCho) glycerophosphocholine (GPCho) and a relatively negligibleamount of free choline (Ross and Sachdev 2004) PCho is involved insynthesis of the insoluble membrane phospholipids while GPCho is aproduct of membrane degradation and free choline is involved insynthesis of the neurotransmitter acetylcholine aswell as inmembranesynthesis (Ross and Sachdev 2004) An increase in the Cho peak isassociated with an increase in membrane breakdown or turnover andmyelination (Ross and Sachdev 2004) The positive associationbetween antipsychotic medication dosage and Cho concentration ameasure of neuronalmembrane turnover (Miller 1991 Ohrmann et al2008) suggests that medication level also influences neuronal activity
412 Neuropsychological correlates of metabolite concentrationIn patients the finding of an association between greater NAA
concentration and better working memory supports evidence for the
Table 5Neuropsychological correlates of metabolite concentration at baseline in patients and healt
Neuropsychological function Group N r or rho NAA concentration
r or rho rp1 (P)
Brixton perseverative errors Patient 30 Rho 0180 (0341)Control 13 Rho 0356 (0232)
WCST perseverative errors Patient 30 r minus0097 (0610) minus013Control 12 r 0271 (0394) 024
Letterndashnumber test number correct Patient 30 r 0303 (0104) 037Control 13 r 0557 (0048) 052
WMS logical memory immediateunit recalled
Patient 29 r 0301 (0112) 033Control 13 r 0330 (0271) 027
Hopkins verbal learning test totalnumber freely recalled
Patient 29 r 0127 (0512) 011Control 13 r 0576 (0039) 055
CPT discriminability Patient 29 r minus0037 (0848) 015Control 12 r 0329 (0297) 027
IGT overall learning Patient 30 r 0179 (0343) 021Control 13 r 0042 (0892) 007
rp1 partial correlation controlling for GM concentration
role of frontal lobe function in working memory using functional MRIand proton MRS in schizophrenia (Bertolino et al 2000 Callicottet al 2000 Ohrmann et al 2007) although this association explainedonly a very small amount (3) of the variance in NAA concentrationthat was additional to that explained by positive symptoms
In the healthy group greater NAA concentration was associatedwith better working and short-term memory The ACC is activatedduring both working and short-term memory (Kim et al 2006Lenartowicz and McIntosh 2005) NAA concentration in the frontallobe white matter was positively associated with working memory inhealthy children which may be related to increased number ofdendritic processes at an early age (Yeo et al 2000) NAA con-centration has a role in neuronal integrity in the form of increasedmyelination and mitochondrial function (Ross and Sachdev 2004)and this may facilitate working and short-term memory
Greater Cho concentration correlated inversely with short-termmemory in the healthy group when controlling for GM concentrationin the ACC A negative association between Cho concentration in theoccipito-parietal white matter and IQ independent of the positiveassociation between NAA concentration and IQ in healthy individualshas been previously reported (Jung et al 1999) Our findings suggestindependentmetabolite concentration-neuropsychological associationsbetween NAA Cho and Cr in healthy individuals Greater Cr concentra-tionwas associatedwith poorer executive function in the present studyA study of elderly males found negative correlations between adjusted
hy participants
Cho concentration Cr concentration
r or rho rp1 (P) r or rho rp
1 (P)
minus0198 (0293) 0331 (0074)0356 (0232) 0579 (0038)
9 (0473) minus0011 (0956) minus0030 (0877) minus0102 (0592) minus0116 (0550)8 (0461) 0390 (0211) 0368 (0265) minus0225 (0483) 0312 (035)9 (0043) minus0163 (0388) minus0160 (0407) minus0130 (0493) minus0124 (0523)9 (0077) 0011 (0971) minus0083 (0797) 0156 (0611) minus0030 (0927)1 (0085) 0054 (0781) 0045 (0822) minus0017 (0932) minus0025 (0898)8 (0382) minus0453 (0120) minus0610 (0035) minus0022 (0946) minus0267 (0401)9 (0564) 0181 (0348) 0177 (0369) 0269 (0159) 0265 (0173)5 (0061) minus0173 (0572) minus0330 (0295) 0277 (036) 0061 (0851)8 (0423) minus0114 (0555) 0016 (0936) 0003 (0986) 0088 (0656)5 (0413) minus0209 (0514) minus0346 (0297) 0207 (0519) 0006 (0986)0 (0273) 0026 (0891) 0029 (0879) 0062 (0747) 0064 (0742)8 (0811) minus0063 (0839) minus0025 (0939) minus0225 (0461) minus0169 (0600)
Table 6Demographic clinical and metabolite concentration characteristics at baseline of CBTp+SC (n=11) SC control (n=13) and SC responsive (n=6) patients
Characteristic CBTp+SC SC control SC responsive χ2 P
Gender malefemale (n) 65 121 60 7185 0028mean SD mean SD
Age in years 3464 862 3746 877 3733 942 0745 0689Years in education 1445 246 1346 176 1377 24 1156 0561Illness duration years 1194 860 1377 970 1317 928 0303 0860Symptoms (PANSS)
Positive 1745 295 1915 264 1117 172 14644 0001Negative 1818 498 1923 386 1433 361 5779 0056General psychopathology 3227 675 340 549 2567 383 6775 0034Total 6791 1287 7239 994 5117 778 9512 0009Medication level 56442 30317 50055 39478 39405 20759 1787 0409
Metabolite concentrationNAA 765 092 685 143 823 091 5313 0070Cho 192 060 186 024 194 018 0493 0781Cr 689 140 687 095 748 160 1047 0592Grey matter 5766 1071 5117 1136 5337 714 1096 0578
257P Premkumar et al Psychiatry Research Neuroimaging 182 (2010) 251ndash260
Cr in the parietal lobe and various cognitive measures including logicalmemory and verbal memory (Ferguson et al 2002) The study did notinclude ameasure of executive function Ferguson et al (2002) believedthat the findings fit with evidence that higher Cr levels are associatedwith cognitive ageing They proposed that poorer neuropsychologicalperformance in healthy ageing is associated with an increase inPhosphocreatine (PCr) due to a reduction in conversion of PCr toAdenosine-tri-phosphate (ATP) for energy Increased Cr concentrationmay be a marker of decreased brain energy metabolism
42 Effect of cognitive behaviour therapy for psychosis on metaboliteconcentration
Our preliminary investigation of change in metabolite concentra-tion in a small number of patients who received CBTp+SC comparedto patients who received SC only revealed a trend for an increase inNAA concentration with CBTp This increase in NAA was concomitantwith improvement in positive symptoms in CBTp+SC patients Thisfinding is consistent with the view that NAA concentration increaseswith alleviation of symptoms as discussed above Recent functionalimaging studies also provide evidence for a role of the ACC inresponsiveness to CBT in psychosis (Kumari et al 2009) as well asmajor depression (Costafreda et al 2009)
43 Limitations and future research
One of the limitations of the study was that the sample sizes ofpatients who received CBTp+SC or SC only and were clinicallyassessed andor scanned at follow-up were small A further limitationwas that gender distribution differed between the patient groupsAlthough there was no gender effect within each patient group in the
Table 7Symptoms metabolite and grey matter concentration (mean SD) at baseline and follow-u
CSI variable Baseline CBTp+SC (n=7) z (P)
FOLLOW-UP
Clinical symptomsPositive symptoms 1814 (234) 1567 (350) minus20Negative symptoms 1857 (571) 1567 (234) minus08General psychopathology 3200 (566) 2733 (497) minus13Total symptoms 6871 (1227) 5867 (1017) minus14
Metabolite concentrationNAA 765 (068) 831 (077) minus18Cho 185 (042) 193 (02) minus05Cr 679 (089) 725 (103) minus08Grey matter 5706 (1155) 5860 (851) minus03
metabolite concentrations in the present study higher ACC glutaminelevel in male compared to female schizophrenia patients has beenpreviously observed (Tayoshi et al 2009) Other effects of gender onACC function have also been reported for example reduced ACCglucose metabolism in male chronic patients relative to healthyparticipants and female patients (Fujimoto et al 2007) Thepredictive value of NAA concentration on symptom change in patientsreceiving psychological treatment or standard care needs to beexamined in a larger sample involving a sufficient number of bothmen and women with schizophrenia Additionally the role of clinicaland neuropsychological variables on ACC NAA levels in patients whoimprove with CBTp needs to be explored
44 Conclusions
Higher NAA and Cho concentrations in the ACC in patients areassociated with lower symptom severity Stronger and moreconsistent associations between metabolite concentrations andsymptom severity than neuropsychological function suggest thatmetabolite concentration and symptoms may co-fluctuate morestrongly Neuropsychological deficits may be more stable (Szokeet al 2008) and not necessarily improve in parallel with symptomimprovement (Hughes et al 2003) NAA concentration may yetreflect symptom changes following CBTp and if replicated in futurestudies has the potential to provide a useful biological marker ofclinical response to psychological treatments
Acknowledgement
The study was supported by funds from the Wellcome Trust UK(067427z02z)
p in CBTp+SC and SC control groups
Baseline SC control (n=4) z (P)
FOLLOW-UP
32 (0042) 1925 (222) 1825 (263) minus0365 (0715)13 (0416) 1875 (499) 2200 (616) minus1841 (0066)82 (0167) 3500 (668) 3275 (591) minus0535 (0593)72 (0141) 7300 (1042) 7300 (1364) minus0001 (1000)
59 (0063) 740 (069) 704 (038) minus1826 (0068)07 (0612) 190 (018) 201 (008) minus0730 (0465)45 (0398) 702 (016) 736 (099) minus0730 (0465)38 (0735) 5353 (549) 5324 (335) minus0365 (0715)
Appendix A Summary of magnetic resonance spectroscopy studies on the anterior cingulate cortex (ACC) in schizophrenia patients
Publication Participants Measures Results
Deicken et al (1997) Schizophrenia patients(n=26 9 on atypical and 17 on typical)Healthy participants (n=16)
NAA Cho and Cr illness durationantipsychotic medication dose
Patients had lower NAA concentrationcompared to healthy participants Nosignificant group differences or lateralizedasymmetries for Cho or Cr No significantcorrelations between NAA and eitherillness duration or antipsychoticmedication dose
Ende et al (2000) Schizophrenia patients(n=19 10 on atypical and 9 on typical)Healthy participants (n=16)
NAA Cho and Cr age illnessduration
Patients had lower NAA concentrationcompared to healthy participantsPatients receiving typical medication(but not atypical) had lower NAAconcentration than healthy participantsNAA concentration was inverselycorrelated with age in patients andhealthy participants and with illnessduration (corrected for age) in patients
Braus et al (2001 2002) Schizophrenia patients(11 on atypical and 10 on typical)
NAA Cho and Cr illness durationduration on atypical antipsychoticmedication WCST
Patients receiving typical antipsychoticshad lower NAA concentration than patientsreceiving atypical antipsychoticsNAA concentration was inverselycorrelated with illness duration andpositively with duration on atypicalantipsychotic medication NAAconcentration was inversely correlatedwith WCST perseverative errors
Goff et al (2002) Schizophrenia patients (n=17of whom 10 switched fromconventional to olanzapine andhad MRS at baseline and 8-week follow-up)
GluCr ratio SANS GluCr ratio was increased by 125(non-significant) following switch toolanzapine Patients who improvedon SANS symptoms had greaterGluCr ratio (458) compared topatients who deteriorated on SANSsymptoms (208) No significantcorrelation between SANS total andchange in GluCr ratio after switch
Yamasue et al (2002) Schizophrenia patients(n=15 all on typical)Healthy participants (n=13)
NAA Cho and Cr grey mattervolume age height body weightsocio-economic status parentalsocio-economic status years ofeducation PANSS onset of illnessillness duration antipsychoticmedication dose
Patients had lower NAACho ratio andgreater ChoCr ratio compared to healthyparticipants after controlling for greymatter volume NAACho ratio waspositively correlated with grey mattervolume in patients not healthy participantsNAACho ratio was inversely correlatedwith PANSS blunted affect score
Theberge et al (2004 2002) First-episode neuroleptic naiumlveschizophrenia patients (n=21)Healthy participants (n=21)
Analysis in Theberge et al 2002NAA Cho Cr Glu Gln mI in leftACC SANS SAPS
From Theberge et al 2002Patients had greater Gln concentrationcompared to healthy participantsMetabolite concentrations were notcorrelated with SANS or SAPS
Analysis in Theberge et al 2004NAA and Cho in left ACC DUPDUI DPS
From Theberge et al 2004NAA concentration was positively correlatedwith DUP and inversely with DPS at trendlevel Cho concentration was positivelycorrelated with DUP
Theberge et al (2003) Schizophrenia patients (n=21atypical n=7 both n=1typical n=13)Healthy participants (n=21)
NAA Cho Cr Glu Gln mI inleft ACC duration of illness
Glu and Gln concentrations were greaterin patients than healthy participants NAAconcentration was inversely correlatedwith duration of positive symptoms
Wood et al (2007) Schizophrenia male patients(n=15 13 atypical 2 medication free)Healthy male participants (n=14)
NAA and Glx in dorsal and rostralregions PANSS five factors illnessduration
Patients had lower NAA concentrationcompared to healthy participantsRight dorsal Glx was inversely correlatedwith illness duration
Ohrmann et al (2008) Schizophrenia patients(n=43 all on atypical)Healthy participants (n=37)
NAA Cho Cr Glx WCST learningpotential
No difference in metabolite concentrationbetween patients and healthy participantsNAA and Glx concentrations were positivelyassociated with WCST learning potential
Sanches et al (2008) Schizophrenia patients (n=37)Healthy participants (n=37)
NAA(Cho+Cr) ratio in left andright anterior middle frontal gyrusACC and perirolandic area (reference)basal skin conductance and skinconductance response to auditorystimuli of 1 s tones of 80 dB Patientsand healthy participants classified intoskin conductance responders (2 SDbelow mean skin conductance in healthyparticipants) and non-responders
NAA(Cho+Cr) ratio was lower in patientsthan healthy participants in the anteriormiddle frontal gyrus and ACC bilaterallyNAA(Cho+Cr) ratio did not differ betweenskin conductance response groups based onskin conductance response to auditory stimuliBasal skin conductance non-responders patientshad lower NAA(Cho+Cr) ratio than healthyparticipants in left and right ACC
258 P Premkumar et al Psychiatry Research Neuroimaging 182 (2010) 251ndash260
Tayoshi et al (2009) Long-term schizophrenia (n=30antipsychotic medication typenot reported)Healthy participants (n=25)
NAA Cho Cr Glu Gln mI Gender PANSStotal and subscales duration of illnessduration of therapy antipsychotic dosagebenzodiazepine dose
Patients had lower Glu and mI concentrationcompared to healthy participants Malepatients had lower NAA Cr Glu and mIconcentration than male healthy participantsMales had greater Gln concentration comparedto females Metabolite concentration wasnot correlated with symptoms or otherclinical variables
Ongur et al (2009) Schizophrenia patients (n=15)Bipolar disorder patients (n=15)Healthy participants (n=22)
Cr in ACC (hypothesized area) andparietal-occipital cortex (reference area)MADRS PANSS YMRS
Patients had lower Cr than healthyparticipants in both ACC andparietal-occipital cortex No significantcorrelations between Cr concentrationand clinical measures
ACC anterior cingulate cortex ChomdashCholine CrmdashCreatinePhosphocreatine DPSmdashduration of psychotic symptoms DUImdashduration of untreated illness DUPmdashduration of untreatedpsychosis GlnmdashGlutamine GlumdashGlutamate GluCr ratio SANSmdashSchedule for the Assessment of Negative Symptoms GlxmdashGlutamate+Glutamine MADRSmdashMontgomery AsbergDepression Rating Scale mImdashmyo-Inositol NAA N-acetyl aspartate PANSSmdashPositive and Negative Syndrome Scale SAPS Schedule for the Assessment of Positive SymptomsWCSTmdashWisconsin Card Sorting test YMRSmdashYoung Mania Rating Scale
Appendix A (continued)
259P Premkumar et al Psychiatry Research Neuroimaging 182 (2010) 251ndash260
Appendix B Supplementary Data
Supplementary data associated with this article can be found inthe online version at doi101016jpscychresns201002008
References
Adler CM Malhotra AK Elman I Goldberg T Egan M Pickar D Breier A 1999Comparison of ketamine-induced thought disorder in healthy volunteers andthought disorder in schizophrenia American Journal of Psychiatry 156 1646ndash1649
Andres RH Ducray AD Schlattner U Wallimann T Widmer HR 2008 Functionsand effects of creatine in the central nervous system Brain Research Bulletin 76329ndash343
Baiano M David A Versace A Churchill R Balestrieri M Brambilla P 2007Anterior cingulate volumes in schizophrenia a systematic review and a meta-analysis of MRI studies Schizophrenia Research 93 1ndash12
Bechara A Damasio AR Damasio H Anderson SW 1994 Insensitivity to futureconsequences following damage to human prefrontal cortex Cognition 50 7ndash15
Behrens TE Woolrich MW Walton ME Rushworth MF 2007 Learning the valueof information in an uncertain world Nature Neuroscience 10 1214ndash1221
Bertolino A Esposito G Callicott JH Mattay VS Van Horn JD Frank JA BermanKF Weinberger DR 2000 Specific relationship between prefrontal neuronal N-acetylaspartate and activation of the working memory cortical network inschizophrenia American Journal of Psychiatry 157 26ndash33
Braus DF Ende G Weber-Fahr W Demirakca T Henn FA 2001 Favorable effecton neuronal viability in the anterior cingulate gyrus due to long-term treatmentwith atypical antipsychotics an MRSI study Pharmacopsychiatry 34 251ndash253
Braus DF Ende G Weber-Fahr W Demirakca T Tost H Henn FA 2002Functioning and neuronal viability of the anterior cingulate neurons followingantipsychotic treatment MR-spectroscopic imaging in chronic schizophreniaEuropean Neuropsychopharmacology 12 145ndash152
Burgess PW Shallice T 1997 The Hayling and Brixton Tests Thames Valley TestCompany Bury St Edmunds
Callicott JH Bertolino A Mattay VS Langheim FJ Duyn J Coppola R Goldberg TEWeinberger DR 2000 Physiological dysfunction of the dorsolateral prefrontal cortexin schizophrenia revisited Cerebral Cortex 10 1078ndash1092
Carter CS van Veen V 2007 Anterior cingulate cortex and conflict detection anupdate of theory and data Cognitive Affective and Behavioral Neuroscience 7367ndash379
Cornblatt BA Risch JJ Faris G Friedman D Erlenmeyer-Kimling L 1988 TheContinuous Performance Test Identical Pairs Version (CPT-IP) I New findingsabout sustained attention in normal families Psychiatry Research 26 223ndash238
Costafreda SG Khanna A Mourao-Miranda J Fu CH 2009 Neural correlates of sadfaces predict clinical remission to cognitive behavioural therapy in depressionNeuroReport 20 637ndash641
Deicken RF Zhou L Schuff N Weiner MW 1997 Proton magnetic resonancespectroscopy of the anterior cingulate region in schizophrenia SchizophreniaResearch 27 65ndash71
Deicken RF Johnson C Pegues M 2000 Proton magnetic resonance spectroscopy ofthe human brain in schizophrenia Reviews in the Neurosciences 11 147ndash158
Ende G Braus DF Walter S Weber-Fahr W Soher B Maudsley AA Henn FA2000 Effects of age medication and illness duration on the N-acetyl aspartatesignal of the anterior cingulate region in schizophrenia Schizophrenia Research 41389ndash395
Fannon D Simmons A Tennakoon L OCeallaigh S Sumich A Doku V Shew CSharma T 2003 Selective deficit of hippocampal N-acetylaspartate in antipsy-chotic-naive patients with schizophrenia Biological Psychiatry 54 587ndash598
Ferguson KJ MacLullich AM Marshall I Deary IJ Starr JM Seckl JR Wardlaw JM2002 Magnetic resonance spectroscopy and cognitive function in healthy elderlymen Brain 125 2743ndash2749
First MB Spitzer RL Gibbon M Williams JBW 2002 Structured Clinical Interviewfor DSM-IV-TR Axis I DisordersmdashPatient Edition (SCID-IP 112002 revision)Biometrics Research Department New York NY
Fornito A Yucel M Dean B Wood SJ Pantelis C 2008 Anatomical abnormalities ofthe anterior cingulate cortex in schizophrenia bridging the gap betweenneuroimaging and neuropathology Schizophrenia Bulletin 35 973ndash993
Fowler D Garety PA Kuipers E 1995 Cognitive Behaviour Therapy for PsychosisTheory and Practice Wiley Chichester
Fujimoto T Takeuch K Matsumoto T Kamimura K Hamada R Nakamura K KatoN 2007 Abnormal glucose metabolism in the anterior cingulate cortex in patientswith schizophrenia Psychiatry Research 154 49ndash58
Goff DC Hennen J Lyoo IK Tsai G Wald LL Evins AE Yurgelun-Todd DARenshaw PF 2002 Modulation of brain and serum glutamatergic concentrationsfollowing a switch from conventional neuroleptics to olanzapine BiologicalPsychiatry 51 493ndash497
Gold JM Carpenter C Randolph C Goldberg TE Weinberger DR 1997 Auditoryworking memory and Wisconsin Card Sorting Test performance in schizophreniaArchives of General Psychiatry 54 159ndash165
Heaton RK Chelune GJ Tally JL Kay GG Curtiss G 1993 Wisconsin Card SortingTest Manual Revised and Expanded Psychological Assessment Resources OdessaFL
Honea R Crow TJ Passingham D Mackay CE 2005 Regional deficits in brainvolume in schizophrenia a meta-analysis of voxel-based morphometry studiesAmerican Journal of Psychiatry 162 2233ndash2245
Hughes C Kumari V Soni W Das M Binneman B Drozd S ONeil S Mathew VSharma T 2003 Longitudinal study of symptoms and cognitive function in chronicschizophrenia Schizophrenia Research 59 137ndash146
Jung RE Brooks WM Yeo RA Chiulli SJ Weers DC Sibbitt Jr WL 1999Biochemical markers of intelligence a proton MR spectroscopy study of normalhuman brain Proceedings Biological Sciences 266 1375ndash1379
Kaneda M Osaka N 2008 Role of anterior cingulate cortex during semantic coding inverbal working memory Neuroscience Letters 436 57ndash61
Kay SR Fiszbein A Opier LA 1987 The Positive and Negative Syndrome Scale(PANSS) for schizophrenia Schizophrenia Bulletin 13 261ndash276
Kennerley SW Dahmubed AF Lara AH Wallis JD 2008 Neurons in the frontallobe encode the value of multiple decision variables Journal of CognitiveNeuroscience 21 1162ndash1178
Kim J Whyte J Wang J Rao H Tang KZ Detre JA 2006 Continuous ASL perfusionfMRI investigation of higher cognition quantification of tonic CBF changes duringsustained attention and working memory tasks Neuroimage 31 376ndash385
Krystal JH Karper LP Seibyl JP Freeman GK Delaney R Bremner JD HeningerGR Bowers Jr MB Charney DS 1994 Subanesthetic effects of the noncom-petitive NMDA antagonist ketamine in humans Psychotomimetic perceptualcognitive and neuroendocrine responses Archives of General Psychiatry 51199ndash214
Kumari V Peters ER Fannon D Antonova E Premkumar P Anilkumar APWilliams SC Kuipers EA 2009 Dorsolateral prefrontal cortex activity predictsresponsiveness to cognitive behaviour therapy in schizophrenia BiologicalPsychiatry 66 594ndash602
Lahti AC Koffel B LaPorte D Tamminga CA 1995 Subanesthetic doses of ketaminestimulate psychosis in schizophrenia Neuropsychopharmacology 13 9ndash19
Lenartowicz A McIntosh AR 2005 The role of anterior cingulate cortex in workingmemory is shaped by functional connectivity Journal of Cognitive Neuroscience 171026ndash1042
Malhotra AK Pinals DA Adler CM Elman I Clifton A Pickar D Breier A 1997Ketamine-induced exacerbation of psychotic symptoms and cognitive impairmentin neuroleptic-free schizophrenics Neuropsychopharmacology 17 141ndash150
260 P Premkumar et al Psychiatry Research Neuroimaging 182 (2010) 251ndash260
McLean MA Woermann FG Barker GJ Duncan JS 2000 Quantitative analysis ofshort echo time (1)H-MRSI of cerebral gray and white matter Magnetic Resonancein Medicine 44 401ndash411
McMorris T Harris RC Swain J Corbett J Collard K Dyson RJ Dye L Hodgson CDraper N 2006 Effect of creatine supplementation and sleep deprivation withmild exercise on cognitive and psychomotor performance mood state and plasmaconcentrations of catecholamines and cortisol Psychopharmacology (Berl) 18593ndash103
McMorris T Harris RC Howard AN Langridge G Hall B Corbett J Dicks MHodgson C 2007 Creatine supplementation sleep deprivation cortisol melatoninand behavior Physiology and Behaviour 90 21ndash28
Miller BL 1991 A review of chemical issues in 1H NMR spectroscopy N-acetyl-L-aspartate creatine and choline NMR in Biomedicine 4 47ndash52
Moghaddam B 2003 Bringing order to the glutamate chaos in schizophrenia Neuron40 881ndash884
Ohrmann P Siegmund A Suslow T Pedersen A Spitzberg K Kersting ARothermundt M Arolt V Heindel W Pfleiderer B 2007 Cognitive impairmentand in vivo metabolites in first-episode neuroleptic-naive and chronic medicatedschizophrenic patients a proton magnetic resonance spectroscopy study Journalof Psychiatric Research 41 625ndash634
Ohrmann P Kugel H Bauer J Siegmund A Kolkebeck K Suslow T Wiedl KHRothermundt M Arolt V Pedersen A 2008 Learning potential on the WCST inschizophrenia is related to the neuronal integrity of the anterior cingulate cortex asmeasured by proton magnetic resonance spectroscopy Schizophrenia Research106 156ndash163
Ongur D Prescot AP Jensen JE Cohen BM Renshaw PF 2009 Creatineabnormalities in schizophrenia and bipolar disorder Psychiatry ResearchNeuroimaging 172 44ndash48
Osaka N Osaka M Kondo H Morishita M Fukuyama H Shibasaki H 2004 Theneural basis of executive function in working memory an fMRI study based onindividual differences Neuroimage 21 623ndash631
Perry G Nunomura A Hirai K Zhu X Perez M Avila J Castellani RJ Atwood CSAliev G Sayre LM Takeda A Smith MA 2002 Is oxidative damage thefundamental pathogenic mechanism of Alzheimers and other neurodegenerativediseases Free Radical Biology and Medicine 33 1475ndash1479
Peterson BS Skudlarski P Gatenby JC Zhang H Anderson AW Gore JC 1999 AnfMRI study of Stroop word-color interference evidence for cingulate subregionssubserving multiple distributed attentional systems Biological Psychiatry 451237ndash1258
Provencher SW 1993 Estimation of metabolite concentrations from localized in vivoproton NMR spectra Magnetic Resonance in Medicine 30 672ndash679
Rae C Digney AL McEwan SR Bates TC 2003 Oral creatine monohydratesupplementation improves brain performance a double-blind placebo-controlledcross-over trial Proceedings Biological Sciences 270 2147ndash2150
Ross AJ Sachdev PS 2004 Magnetic resonance spectroscopy in cognitive researchBrain Research Brain Research Reviews 44 83ndash102
Rushworth MF Walton ME Kennerley SW Bannerman DM 2004 Action sets anddecisions in the medial frontal cortex Trends in Cogntive Sciences 8 410ndash417
Rutten BP Korr H Steinbusch HW Schmitz C 2003 The aging brain less neuronscould be better Mechanisms of Ageing and Development 124 349ndash355
Sanches RF Crippa JA Hallak JE de Sousa JP Araujo D Santos AC Zuardi AW2008 Proton magnetic resonance spectroscopy of the frontal cingulate andperirolandic cortices and its relationship to skin conductance in patients withschizophrenia Brazilian Journal of Medical and Biological Research 41 1132ndash1141
Schlosser RG Koch K Wagner G Nenadic I Roebel M Schachtzabel C Axer MSchultz C Reichenbach JR Sauer H 2008 Inefficient executive cognitive controlin schizophrenia is preceded by altered functional activation during informationencoding an fMRI study Neuropsychologia 46 336ndash347
Shapiro AM Benedict RH Schretlen D Brandt J 1999 Construct and concurrentvalidity of the Hopkins Verbal Learning Test-revised The Clinical Neuropsychol-ogist 13 348ndash358
Smith EE Jonides J 1999 Storage and executive processes in the frontal lobesScience 283 1657ndash1661
Szoke A Trandafir A Dupont ME Meary A Schurhoff F Leboyer M 2008Longitudinal studies of cognition in schizophrenia meta-analysis British Journal ofPsychiatry 192 248ndash257
Tayoshi S Sumitani S Taniguchi K Shibuya-Tayoshi S Numata S Iga JI NakatakiM Ueno SI Harada M Ohmori T 2009 Metabolite changes and genderdifferences in schizophrenia using 3-Tesla proton magnetic resonance spectrosco-py ((1)H-MRS) Schizophrenia Research 108 69ndash77
Theberge J Bartha R Drost DJ Menon RS Malla A Takhar J Neufeld RWRogers J Pavlosky W Schaefer B Densmore M Al-Semaan Y Williamson PC2002 Glutamate and glutamine measured with 40T proton MRS in never-treatedpatients with schizophrenia and healthy volunteers American Journal of Psychiatry159 1944ndash1946
Theberge J Al-Semaan Y Williamson PC Menon RS Neufeld RW Rajakumar NSchaefer B Densmore M Drost DJ 2003 Glutamate and glutamine in theanterior cingulate and thalamus of medicated patients with chronic schizophreniaand healthy comparison subjects measured with 40-T proton MRS AmericanJournal of Psychiatry 160 2231ndash2233
Theberge J Al-Semaan Y Drost DJ Malla AK Neufeld RW Bartha R ManchandaR Menon R Densmore M Schaefer B Williamson PC 2004 Duration ofuntreated psychosis vs N-acetylaspartate and choline in first episode schizophre-nia a 1H magnetic resonance spectroscopy study at 40 Tesla Psychiatry Research131 107ndash114
Tranberg M Stridh MH Guy Y Jilderos B Wigstrom H Weber SG Sandberg M2004 NMDA-receptor mediated efflux of N-acetylaspartate physiological andorpathological importance Neurochemistry International 45 1195ndash1204
Tranberg M Abbas AK Sandberg M 2007 In vitro studies on the putative function ofN-acetylaspartate as an osmoregulator Neurochemical Research 32 1248ndash1255
Walton ME Croxson PL Behrens TE Kennerley SW Rushworth MF 2007Adaptive decision making and value in the anterior cingulate cortex Neuroimage36 (Suppl 2) T142ndashT154
Wechsler D 1987 Wechsler Memory ScalemdashRevised Psychological Corporation NewYork
Weinberger DR Aloia MS Goldberg TE Berman KF 1994 The frontal lobes andschizophrenia Journal of Neuropsychiatry and Clinical Neurosciences 6 419ndash427
Wood SJ Yucel M Wellard RM Harrison BJ Clarke K Fornito A Velakoulis DPantelis C 2007 Evidence for neuronal dysfunction in the anterior cingulate ofpatients with schizophrenia a proton magnetic resonance spectroscopy study at3T Schizophrenia Research 94 328ndash331
Yamasue H Fukui T Fukuda R Yamada H Yamasaki S Kuroki N Abe O Kasai KTsujii K Iwanami A Aoki S Ohtomo K Kato N Kato T 2002 1H-MRspectroscopy and gray matter volume of the anterior cingulate cortex inschizophrenia NeuroReport 13 2133ndash2137
Yeo RA Hill D Campbell R Vigil J Brooks WM 2000 Developmental instabilityand working memory ability in children a magnetic resonance spectroscopyinvestigation Developmental Neuropsychology 17 143ndash159
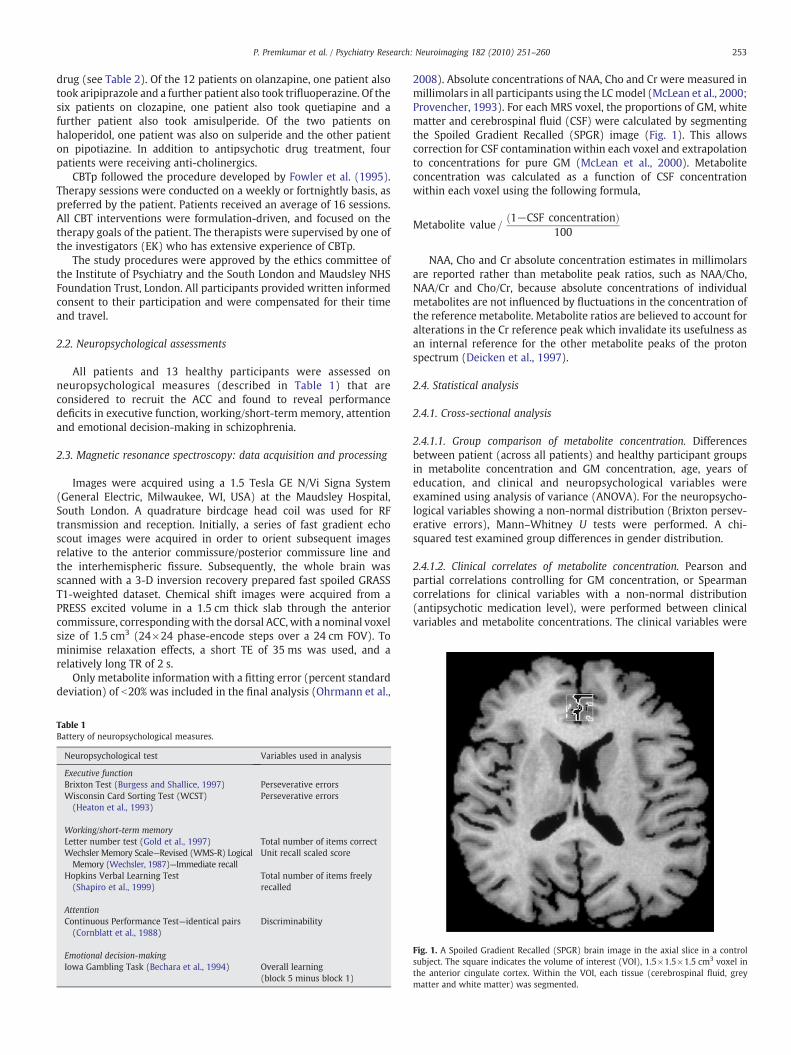
253P Premkumar et al Psychiatry Research Neuroimaging 182 (2010) 251ndash260
drug (see Table 2) Of the 12 patients on olanzapine one patient alsotook aripiprazole and a further patient also took trifluoperazine Of thesix patients on clozapine one patient also took quetiapine and afurther patient also took amisulperide Of the two patients onhaloperidol one patient was also on sulperide and the other patienton pipotiazine In addition to antipsychotic drug treatment fourpatients were receiving anti-cholinergics
CBTp followed the procedure developed by Fowler et al (1995)Therapy sessions were conducted on a weekly or fortnightly basis aspreferred by the patient Patients received an average of 16 sessionsAll CBT interventions were formulation-driven and focused on thetherapy goals of the patient The therapists were supervised by one ofthe investigators (EK) who has extensive experience of CBTp
The study procedures were approved by the ethics committee ofthe Institute of Psychiatry and the South London and Maudsley NHSFoundation Trust London All participants provided written informedconsent to their participation and were compensated for their timeand travel
22 Neuropsychological assessments
All patients and 13 healthy participants were assessed onneuropsychological measures (described in Table 1) that areconsidered to recruit the ACC and found to reveal performancedeficits in executive function workingshort-term memory attentionand emotional decision-making in schizophrenia
23 Magnetic resonance spectroscopy data acquisition and processing
Images were acquired using a 15 Tesla GE NVi Signa System(General Electric Milwaukee WI USA) at the Maudsley HospitalSouth London A quadrature birdcage head coil was used for RFtransmission and reception Initially a series of fast gradient echoscout images were acquired in order to orient subsequent imagesrelative to the anterior commissureposterior commissure line andthe interhemispheric fissure Subsequently the whole brain wasscanned with a 3-D inversion recovery prepared fast spoiled GRASST1-weighted dataset Chemical shift images were acquired from aPRESS excited volume in a 15 cm thick slab through the anteriorcommissure correspondingwith the dorsal ACC with a nominal voxelsize of 15 cm3 (24times24 phase-encode steps over a 24 cm FOV) Tominimise relaxation effects a short TE of 35 ms was used and arelatively long TR of 2 s
Only metabolite information with a fitting error (percent standarddeviation) of b20 was included in the final analysis (Ohrmann et al
Table 1Battery of neuropsychological measures
Neuropsychological test Variables used in analysis
Executive functionBrixton Test (Burgess and Shallice 1997) Perseverative errorsWisconsin Card Sorting Test (WCST)(Heaton et al 1993)
Perseverative errors
Workingshort-term memoryLetter number test (Gold et al 1997) Total number of items correctWechsler Memory ScalemdashRevised (WMS-R) LogicalMemory (Wechsler 1987)mdashImmediate recall
Unit recall scaled score
Hopkins Verbal Learning Test(Shapiro et al 1999)
Total number of items freelyrecalled
AttentionContinuous Performance Testmdashidentical pairs(Cornblatt et al 1988)
Discriminability
Emotional decision-makingIowa Gambling Task (Bechara et al 1994) Overall learning
(block 5 minus block 1)
2008) Absolute concentrations of NAA Cho and Cr were measured inmillimolars in all participants using the LCmodel (McLean et al 2000Provencher 1993) For each MRS voxel the proportions of GM whitematter and cerebrospinal fluid (CSF) were calculated by segmentingthe Spoiled Gradient Recalled (SPGR) image (Fig 1) This allowscorrection for CSF contamination within each voxel and extrapolationto concentrations for pure GM (McLean et al 2000) Metaboliteconcentration was calculated as a function of CSF concentrationwithin each voxel using the following formula
Metabolite value=eth1minusCSF concentrationTHORN
100
NAA Cho and Cr absolute concentration estimates in millimolarsare reported rather than metabolite peak ratios such as NAAChoNAACr and ChoCr because absolute concentrations of individualmetabolites are not influenced by fluctuations in the concentration ofthe reference metabolite Metabolite ratios are believed to account foralterations in the Cr reference peak which invalidate its usefulness asan internal reference for the other metabolite peaks of the protonspectrum (Deicken et al 1997)
24 Statistical analysis
241 Cross-sectional analysis
2411 Group comparison of metabolite concentration Differencesbetween patient (across all patients) and healthy participant groupsin metabolite concentration and GM concentration age years ofeducation and clinical and neuropsychological variables wereexamined using analysis of variance (ANOVA) For the neuropsycho-logical variables showing a non-normal distribution (Brixton persev-erative errors) MannndashWhitney U tests were performed A chi-squared test examined group differences in gender distribution
2412 Clinical correlates of metabolite concentration Pearson andpartial correlations controlling for GM concentration or Spearmancorrelations for clinical variables with a non-normal distribution(antipsychotic medication level) were performed between clinicalvariables and metabolite concentrations The clinical variables were
Fig 1 A Spoiled Gradient Recalled (SPGR) brain image in the axial slice in a controlsubject The square indicates the volume of interest (VOI) 15times15times15 cm3 voxel inthe anterior cingulate cortex Within the VOI each tissue (cerebrospinal fluid greymatter and white matter) was segmented
254 P Premkumar et al Psychiatry Research Neuroimaging 182 (2010) 251ndash260
PANSS symptoms illness duration (defined as the difference betweenthe age at onset of psychotic symptoms as reported by the patient andwhere possible confirmed with other sources and age at the time ofbaseline assessments) and antipsychotic medication level (in chlor-promazine equivalents) Spearman correlations were performed toexamine the relationship between metabolite values and individualPANSS items in those subscales that were found to have a significantassociation with metabolite values
2413 Neuropsychological correlates of metabolite concentrationPearson and partial correlations controlling for GM concentration orSpearman correlations for neuropsychological variables with a non-normal distribution (Brixton perseverative errors) were performedbetween neuropsychological performance measures and metaboliteconcentration in patient and healthy participant groups
2414 Multiple regression of clinical andor neuropsychological correlateson metabolite concentration Significant clinical andor neuropsycholog-ical variables that had a normal distribution were entered into themultiple regression model using a stepwise method (to estimate theeffect of individual predictors on variability of criterion variable) andusing a forced-entry method (to explain the combined effect ofpredictors on the variability of the criterion variable)
242 Longitudinal analysis
2421 Group comparison of metabolite concentration Due to the smallsample sizes differences between CBTp+SC SC control and SCresponsive patient groups in age education clinical variables andbaseline metabolite and GM concentrations were examined using non-parametric analyses namely the Kruskal-Wallis test A chi-squared testdetermined group differences in gender distribution
2422 Metabolite concentration as a predictor of symptom changefollowing CBTpSpearman correlationswere performed in the CBTp+SCpatients who were followed up (n=8) between baseline metaboliteconcentrations and residual PANSS symptom change scores frombaseline to follow-up
2423 Change in symptom severity and metabolite concentrationfollowing CBTp Due to the small sample sizes (CBTp+SC n=7 andSC control n=4) changes in symptom severity metabolite and GMconcentrations from baseline to follow-up in the patient groups wereexamined using the Wilcoxon Signed Rank test
All analyses were performed in SPSS windows (version 15) Alphalevel for testing significance of effects was maintained at Pb005 Wechose not to apply the Bonferroni method of adjusting the P valuebecause we expected the size of the relationship between MRS valuesand symptomsneuropsychological functions to be small or at bestmodest given that symptoms in schizophrenia are unlikely to have asingle aetiology and successful task performance on most neuropsy-chological tasks would recruit additional brain regions
3 Results
31 Cross-sectional analysis
311 Group differences in demographic and neuropsychological variablesPatient and healthy participant groups did not differ in gender and
age Patients had fewer years in education and showed deficientperformance on most neuropsychological measures relative tohealthy participants (Table 2)
312 Group differences in metabolite concentration in the ACCNAA Cr and GM concentrations were lower in the patient
compared with the healthy participant group (Table 3)
313 Clinical correlates of metabolite concentrationNAA concentration correlated inversely with positive symptoms
general psychopathology and total symptoms (Table 4) Thesecorrelations remained significant after controlling for GM NAAconcentration correlated inversely with negative symptoms onlyafter controlling for GM PANSS item-wise correlations revealed thatNAA concentration was inversely correlated with delusions disorga-nisation and persecution items of the positive syndrome subscalepassive social withdrawal and stereotyped thinking items of thenegative syndrome subscale and somatic concern and preoccupationitems of the general psychopathology subscale
Cho concentration correlated inversely with positive and totalsymptoms After controlling for GM concentration Cho concentrationcorrelated with total symptoms but not positive symptoms Choconcentration correlated inversely with negative symptoms at a trendlevel only after controlling for GM concentration PANSS item-wisecorrelations revealed that Cho concentration was inversely correlatedwith disorganisation and hostility items of the positive syndromesubscale passive social withdrawal item of the negative syndromesubscale and somatic concern item of the general psychopathologysubscale Cho concentration correlated positively with antipsychoticmedication dosage Cr concentration did not correlate with anyclinical variable
314 Neuropsychological correlates of metabolite concentrationPatients A positive correlation between NAA concentration and
working memory as assessed by the letter number test emerged onlyafter controlling for GM concentration (Table 5)
Healthy participants NAA concentration correlated positively withworking memory as assessed by the letter number test and short-term memory as assessed by the Hopkins verbal learning test thoughthese correlations were reduced to a trend level of significance aftercontrolling for GM concentration (Table 5) Cho concentrationcorrelated inversely with short-term memory as assessed by theWechsler Memory ScalemdashRevised (WMS-R) logical memory imme-diate recall test after controlling for GM concentration Cr concentra-tion correlated inversely with executive function as assessed byBrixton perseverative errors
315 Multiple regression of clinical andor neuropsychologicalcorrelates of metabolite concentration
Patients In the stepwise regression model with NAA concentra-tion as the criterion variable positive symptoms proved to be asignificant predictor (r=minus0489 P=0006) The model explained 21of the variance in NAA concentration In the forced-entry regressionmodel the predictors (positive symptoms general psychopathologyand letter number test) explained 25 of the variance in NAAconcentration
Healthy participants In the stepwise regression model with NAAconcentration as the criterion variable short-term memory asassessed by the Hopkins verbal learning test was a significantpredictor (r=0576 P=0039) The model explained 27 of thevariance in NAA concentration In the forced-entry regression modelthe predictors (Hopkins verbal learning test and letter number test)explained 27 of the model
32 Longitudinal analysis
321 Metabolite concentration differences at baseline between patientsub-groups
NAA concentration tended to differ between patient groups atbaseline mainly due to greater concentration in the low-symptomSC-responsive group (Table 6)
Table 2Demographic clinical and neuropsychological characteristics of patients and healthy participants groups
Characteristic Patients Healthy participants Test χ2 (df) P
Gender malefemale (n) 246 132 Chi-squared 0304 (1) 0581mean SD mean SD F or z (df)
Age in years 3640 864 3540 1334 ANOVA 0092 (143) 0763Years in education 1383 215 1561 323 ANOVA 4555 (141) 0039Illness duration years 1298 894
Symptoms (PANSS)Positive 1693 395Negative 1787 452General psychopathology 3170 639Total 6650 1317Medication level (chlorpromazine equivalents) 50267 32788Medication type (n)
Olanzapine 12Clozapine 6Risperidone 5Aripiprazole 2Flupentixol 2Amisulperide 1Haloperidol 2
Neuropsychological functionBrixton perseverative errors 050 078 031 048 MannndashWhitney U minus0552 (141) 0648WCST perseverative errors 1817 886 1175 751 ANOVA 4870 (140) 0033Letter number test number correct 1380 380 1692 296 ANOVA 6925 (141) 0012WMS logical memory immediate unit recalled 710 258 969 333 ANOVA 7533 (140) 0009Hopkins total freely recalled 2186 538 2692 517 ANOVA 8122 (140) 0007CPT discriminability 029 059 187 100 ANOVA 14257 (139) 0001IGT overall learning 280 1183 892 1473 ANOVA 2092 (141) 0156
255P Premkumar et al Psychiatry Research Neuroimaging 182 (2010) 251ndash260
33 Metabolite concentration correlates of symptom change followingCBTp
In the CBTp+SC group metabolite concentration at baseline wasnot associated with symptom change following CBTp (SupplementaryTable)
34 Symptom severity and metabolite concentration change frombaseline to follow-up in CBTp+SC and SC control groups
Positive symptoms improved following CBTp in the CBTp+SCgroup while negative symptoms tended to deteriorate in the SCcontrol group (Table 7)
NAA concentration tended to increase in the CBTp+SC group frombaseline to follow-up (Table 7)
4 Discussion
The present investigation examined the concentrations of NAACho and Cr in the ACC and their clinical and neuropsychologicalcorrelates in patients with schizophrenia and healthy participants(cross-sectional investigation) The study also explored whetherbaseline metabolite concentration predicted symptom change fol-lowing CBTp+SC and whether a reduction in symptoms followingCBTp+SC was accompanied by higher NAA concentration relative tobaseline (longitudinal investigation)
Table 3ACCmetabolite and greymatter concentrations (mean SD) at baseline at each voxel inpatients and healthy participants
CSI variable(millimolars)
Patient(n=30)
Healthy participants(n=15)
F (p)
NAA 742 126 856 139 7682 (0008)Cho 190 038 199 036 0654 (0423)Cr 703 124 789 102 5345 (0026)Grey matter 5399 1051 6139 858 5549 (0023)
41 Summary of clinical and neuropsychological correlates of metaboliteconcentration (cross-sectional investigation)
The major findings from the cross-sectional analysis were that inpatients (1) NAA concentration was reduced compared to healthyparticipants (2) greaterNAA concentrationwas associatedwith a lowerlevel of positive symptoms general psychopathology and betterworking memory (positive symptoms alone explained 21 of thevariance total variance explained=25) and (3) greater Cho concen-tration was associated with a lower level of positive symptoms andhigher level of antipsychotic medication In healthy participants thefollowing associationswere observed (1) NAA concentration positivelywith working and short-termmemory (2) Cho concentration inverselywith short-term memory and (3) Cr concentration inversely withexecutive function These findings will be discussed in turn
411 Clinical correlates of metabolite concentrationsThe findings of lower ACC NAA concentration in schizophrenia
patients (Deicken et al 1997 Ende et al 2000 Wood et al 2007)and clinical correlates of NAA concentration support previousevidence (Theberge et al 2003 Wood et al 2007 Yamasue et al2002) Our study of a relatively larger sample of patients than mostprevious studies is the first to observe that NAA concentration wasinversely associated with the severity of positive negative andgeneral psychopathology symptoms based on the three-dimensionalmodel of the PANSS (Kay et al 1987) Twenty percent of our patientswere SC treatment responsive giving a wider range to symptomscores than earlier studies Patients who had low symptom severityand were considered to have responded sufficiently to their standard(mostly atypical) antipsychotic treatment tended to show greaterNAA concentration than patients who were symptomatic (baselinecomparisons) suggesting that NAA concentration may vary as afunction of symptom severity and treatment response
NAA concentration being a by-product of neurotransmitter turn-over (Tranberg et al 2004) the symptom severity-metabolite concen-tration associations may reflect the efficiency of neurotransmission Asnoted in Section 1 NAA concentration may be an indicator of NMDA
Table 4Clinical correlates of metabolite concentration at baseline (patients only)
NAA concentration Cho concentration Cr concentration
r or ρ r (P) rp1 (P) r (P) rp
1 (P) r (P) rp1 (P)
Illness duration r minus0059 (0756) 0091 (0640) minus0064 (0735) 0045 (0817) minus0291 (0118) minus0244 (0203)Antipsychotic medication level Rho 0197 (0298) 0442 (0014) 0073 (0700)Symptoms (PANSS)
Positive (P) symptoms r minus0489 (0006) minus0430 (0020) minus0391 (0033) minus0325 (0085) minus0308 (0098) minus0262 (0170)Negative (N) symptoms r minus0297 (0111) minus0418 (0024) minus0287 (0124) minus0366 (0051) minus0211 (0264) minus0262 (0170)General psychopathology (GP) r minus0416 (0022) minus0506 (0005) minus0299 (0109) minus0341 (0070) minus0204 (0281) minus0219 (0254)Total r minus0450 (0013) minus0512 (0004) minus0361 (0050) minus0384 (0040) minus0263 (0160) minus0266 (0163)
Individual symptomsDelusions (P) Rho minus0411 (0024) minus0342 (0064) minus0192 (0309)Disorganisation (P) Rho minus0525 (0003) minus0369 (0045) minus0136 (0475)Persecution (P) Rho minus0390 (0033) minus0193 (0307) minus0068 (0719)Hostility (P) Rho 0062 (0745) 0370 (0044) 0163 (0390)Passive social withdrawal (N) Rho minus0370 (0044) minus0393 (0032) minus0261 (0163)Stereotyped thinking (N) Rho minus0422 (0020) minus0073 (0684) minus0221 (0240)Somatic concern (GP) Rho minus0419 (0021) minus0407 (0026) minus0129 (0496)Preoccupation (GP) Rho minus0528 (0003) minus0201 (0287) minus0264 (0156)
rp1 partial correlation controlling for GM concentration P PANSS positive symptom subscale N PANSS negative symptom subscale GP PANSS general psychopathology subscale
256 P Premkumar et al Psychiatry Research Neuroimaging 182 (2010) 251ndash260
function and neuronal longevity (Tranberg et al 2004) NAA efflux isa delayed response to sudden non-physiological decrease in extracel-lular osmolarity and high K+intra-cellular and NMDA activation(Tranberg et al 2007) Elevated concentration of NAA in the ACC inschizophrenia patients with lower level of symptoms may reflectincreased turnover of neurotransmitters such as dopamine and NMDA
Similarly the association between Cho concentration and total andpositive symptoms may also reflect improved neurotransmitterfunction and neuronal integrity with milder symptoms The Cho peakincludes solublemembranephospholipids includingphosphorylcholine(PCho) glycerophosphocholine (GPCho) and a relatively negligibleamount of free choline (Ross and Sachdev 2004) PCho is involved insynthesis of the insoluble membrane phospholipids while GPCho is aproduct of membrane degradation and free choline is involved insynthesis of the neurotransmitter acetylcholine aswell as inmembranesynthesis (Ross and Sachdev 2004) An increase in the Cho peak isassociated with an increase in membrane breakdown or turnover andmyelination (Ross and Sachdev 2004) The positive associationbetween antipsychotic medication dosage and Cho concentration ameasure of neuronalmembrane turnover (Miller 1991 Ohrmann et al2008) suggests that medication level also influences neuronal activity
412 Neuropsychological correlates of metabolite concentrationIn patients the finding of an association between greater NAA
concentration and better working memory supports evidence for the
Table 5Neuropsychological correlates of metabolite concentration at baseline in patients and healt
Neuropsychological function Group N r or rho NAA concentration
r or rho rp1 (P)
Brixton perseverative errors Patient 30 Rho 0180 (0341)Control 13 Rho 0356 (0232)
WCST perseverative errors Patient 30 r minus0097 (0610) minus013Control 12 r 0271 (0394) 024
Letterndashnumber test number correct Patient 30 r 0303 (0104) 037Control 13 r 0557 (0048) 052
WMS logical memory immediateunit recalled
Patient 29 r 0301 (0112) 033Control 13 r 0330 (0271) 027
Hopkins verbal learning test totalnumber freely recalled
Patient 29 r 0127 (0512) 011Control 13 r 0576 (0039) 055
CPT discriminability Patient 29 r minus0037 (0848) 015Control 12 r 0329 (0297) 027
IGT overall learning Patient 30 r 0179 (0343) 021Control 13 r 0042 (0892) 007
rp1 partial correlation controlling for GM concentration
role of frontal lobe function in working memory using functional MRIand proton MRS in schizophrenia (Bertolino et al 2000 Callicottet al 2000 Ohrmann et al 2007) although this association explainedonly a very small amount (3) of the variance in NAA concentrationthat was additional to that explained by positive symptoms
In the healthy group greater NAA concentration was associatedwith better working and short-term memory The ACC is activatedduring both working and short-term memory (Kim et al 2006Lenartowicz and McIntosh 2005) NAA concentration in the frontallobe white matter was positively associated with working memory inhealthy children which may be related to increased number ofdendritic processes at an early age (Yeo et al 2000) NAA con-centration has a role in neuronal integrity in the form of increasedmyelination and mitochondrial function (Ross and Sachdev 2004)and this may facilitate working and short-term memory
Greater Cho concentration correlated inversely with short-termmemory in the healthy group when controlling for GM concentrationin the ACC A negative association between Cho concentration in theoccipito-parietal white matter and IQ independent of the positiveassociation between NAA concentration and IQ in healthy individualshas been previously reported (Jung et al 1999) Our findings suggestindependentmetabolite concentration-neuropsychological associationsbetween NAA Cho and Cr in healthy individuals Greater Cr concentra-tionwas associatedwith poorer executive function in the present studyA study of elderly males found negative correlations between adjusted
hy participants
Cho concentration Cr concentration
r or rho rp1 (P) r or rho rp
1 (P)
minus0198 (0293) 0331 (0074)0356 (0232) 0579 (0038)
9 (0473) minus0011 (0956) minus0030 (0877) minus0102 (0592) minus0116 (0550)8 (0461) 0390 (0211) 0368 (0265) minus0225 (0483) 0312 (035)9 (0043) minus0163 (0388) minus0160 (0407) minus0130 (0493) minus0124 (0523)9 (0077) 0011 (0971) minus0083 (0797) 0156 (0611) minus0030 (0927)1 (0085) 0054 (0781) 0045 (0822) minus0017 (0932) minus0025 (0898)8 (0382) minus0453 (0120) minus0610 (0035) minus0022 (0946) minus0267 (0401)9 (0564) 0181 (0348) 0177 (0369) 0269 (0159) 0265 (0173)5 (0061) minus0173 (0572) minus0330 (0295) 0277 (036) 0061 (0851)8 (0423) minus0114 (0555) 0016 (0936) 0003 (0986) 0088 (0656)5 (0413) minus0209 (0514) minus0346 (0297) 0207 (0519) 0006 (0986)0 (0273) 0026 (0891) 0029 (0879) 0062 (0747) 0064 (0742)8 (0811) minus0063 (0839) minus0025 (0939) minus0225 (0461) minus0169 (0600)
Table 6Demographic clinical and metabolite concentration characteristics at baseline of CBTp+SC (n=11) SC control (n=13) and SC responsive (n=6) patients
Characteristic CBTp+SC SC control SC responsive χ2 P
Gender malefemale (n) 65 121 60 7185 0028mean SD mean SD
Age in years 3464 862 3746 877 3733 942 0745 0689Years in education 1445 246 1346 176 1377 24 1156 0561Illness duration years 1194 860 1377 970 1317 928 0303 0860Symptoms (PANSS)
Positive 1745 295 1915 264 1117 172 14644 0001Negative 1818 498 1923 386 1433 361 5779 0056General psychopathology 3227 675 340 549 2567 383 6775 0034Total 6791 1287 7239 994 5117 778 9512 0009Medication level 56442 30317 50055 39478 39405 20759 1787 0409
Metabolite concentrationNAA 765 092 685 143 823 091 5313 0070Cho 192 060 186 024 194 018 0493 0781Cr 689 140 687 095 748 160 1047 0592Grey matter 5766 1071 5117 1136 5337 714 1096 0578
257P Premkumar et al Psychiatry Research Neuroimaging 182 (2010) 251ndash260
Cr in the parietal lobe and various cognitive measures including logicalmemory and verbal memory (Ferguson et al 2002) The study did notinclude ameasure of executive function Ferguson et al (2002) believedthat the findings fit with evidence that higher Cr levels are associatedwith cognitive ageing They proposed that poorer neuropsychologicalperformance in healthy ageing is associated with an increase inPhosphocreatine (PCr) due to a reduction in conversion of PCr toAdenosine-tri-phosphate (ATP) for energy Increased Cr concentrationmay be a marker of decreased brain energy metabolism
42 Effect of cognitive behaviour therapy for psychosis on metaboliteconcentration
Our preliminary investigation of change in metabolite concentra-tion in a small number of patients who received CBTp+SC comparedto patients who received SC only revealed a trend for an increase inNAA concentration with CBTp This increase in NAA was concomitantwith improvement in positive symptoms in CBTp+SC patients Thisfinding is consistent with the view that NAA concentration increaseswith alleviation of symptoms as discussed above Recent functionalimaging studies also provide evidence for a role of the ACC inresponsiveness to CBT in psychosis (Kumari et al 2009) as well asmajor depression (Costafreda et al 2009)
43 Limitations and future research
One of the limitations of the study was that the sample sizes ofpatients who received CBTp+SC or SC only and were clinicallyassessed andor scanned at follow-up were small A further limitationwas that gender distribution differed between the patient groupsAlthough there was no gender effect within each patient group in the
Table 7Symptoms metabolite and grey matter concentration (mean SD) at baseline and follow-u
CSI variable Baseline CBTp+SC (n=7) z (P)
FOLLOW-UP
Clinical symptomsPositive symptoms 1814 (234) 1567 (350) minus20Negative symptoms 1857 (571) 1567 (234) minus08General psychopathology 3200 (566) 2733 (497) minus13Total symptoms 6871 (1227) 5867 (1017) minus14
Metabolite concentrationNAA 765 (068) 831 (077) minus18Cho 185 (042) 193 (02) minus05Cr 679 (089) 725 (103) minus08Grey matter 5706 (1155) 5860 (851) minus03
metabolite concentrations in the present study higher ACC glutaminelevel in male compared to female schizophrenia patients has beenpreviously observed (Tayoshi et al 2009) Other effects of gender onACC function have also been reported for example reduced ACCglucose metabolism in male chronic patients relative to healthyparticipants and female patients (Fujimoto et al 2007) Thepredictive value of NAA concentration on symptom change in patientsreceiving psychological treatment or standard care needs to beexamined in a larger sample involving a sufficient number of bothmen and women with schizophrenia Additionally the role of clinicaland neuropsychological variables on ACC NAA levels in patients whoimprove with CBTp needs to be explored
44 Conclusions
Higher NAA and Cho concentrations in the ACC in patients areassociated with lower symptom severity Stronger and moreconsistent associations between metabolite concentrations andsymptom severity than neuropsychological function suggest thatmetabolite concentration and symptoms may co-fluctuate morestrongly Neuropsychological deficits may be more stable (Szokeet al 2008) and not necessarily improve in parallel with symptomimprovement (Hughes et al 2003) NAA concentration may yetreflect symptom changes following CBTp and if replicated in futurestudies has the potential to provide a useful biological marker ofclinical response to psychological treatments
Acknowledgement
The study was supported by funds from the Wellcome Trust UK(067427z02z)
p in CBTp+SC and SC control groups
Baseline SC control (n=4) z (P)
FOLLOW-UP
32 (0042) 1925 (222) 1825 (263) minus0365 (0715)13 (0416) 1875 (499) 2200 (616) minus1841 (0066)82 (0167) 3500 (668) 3275 (591) minus0535 (0593)72 (0141) 7300 (1042) 7300 (1364) minus0001 (1000)
59 (0063) 740 (069) 704 (038) minus1826 (0068)07 (0612) 190 (018) 201 (008) minus0730 (0465)45 (0398) 702 (016) 736 (099) minus0730 (0465)38 (0735) 5353 (549) 5324 (335) minus0365 (0715)
Appendix A Summary of magnetic resonance spectroscopy studies on the anterior cingulate cortex (ACC) in schizophrenia patients
Publication Participants Measures Results
Deicken et al (1997) Schizophrenia patients(n=26 9 on atypical and 17 on typical)Healthy participants (n=16)
NAA Cho and Cr illness durationantipsychotic medication dose
Patients had lower NAA concentrationcompared to healthy participants Nosignificant group differences or lateralizedasymmetries for Cho or Cr No significantcorrelations between NAA and eitherillness duration or antipsychoticmedication dose
Ende et al (2000) Schizophrenia patients(n=19 10 on atypical and 9 on typical)Healthy participants (n=16)
NAA Cho and Cr age illnessduration
Patients had lower NAA concentrationcompared to healthy participantsPatients receiving typical medication(but not atypical) had lower NAAconcentration than healthy participantsNAA concentration was inverselycorrelated with age in patients andhealthy participants and with illnessduration (corrected for age) in patients
Braus et al (2001 2002) Schizophrenia patients(11 on atypical and 10 on typical)
NAA Cho and Cr illness durationduration on atypical antipsychoticmedication WCST
Patients receiving typical antipsychoticshad lower NAA concentration than patientsreceiving atypical antipsychoticsNAA concentration was inverselycorrelated with illness duration andpositively with duration on atypicalantipsychotic medication NAAconcentration was inversely correlatedwith WCST perseverative errors
Goff et al (2002) Schizophrenia patients (n=17of whom 10 switched fromconventional to olanzapine andhad MRS at baseline and 8-week follow-up)
GluCr ratio SANS GluCr ratio was increased by 125(non-significant) following switch toolanzapine Patients who improvedon SANS symptoms had greaterGluCr ratio (458) compared topatients who deteriorated on SANSsymptoms (208) No significantcorrelation between SANS total andchange in GluCr ratio after switch
Yamasue et al (2002) Schizophrenia patients(n=15 all on typical)Healthy participants (n=13)
NAA Cho and Cr grey mattervolume age height body weightsocio-economic status parentalsocio-economic status years ofeducation PANSS onset of illnessillness duration antipsychoticmedication dose
Patients had lower NAACho ratio andgreater ChoCr ratio compared to healthyparticipants after controlling for greymatter volume NAACho ratio waspositively correlated with grey mattervolume in patients not healthy participantsNAACho ratio was inversely correlatedwith PANSS blunted affect score
Theberge et al (2004 2002) First-episode neuroleptic naiumlveschizophrenia patients (n=21)Healthy participants (n=21)
Analysis in Theberge et al 2002NAA Cho Cr Glu Gln mI in leftACC SANS SAPS
From Theberge et al 2002Patients had greater Gln concentrationcompared to healthy participantsMetabolite concentrations were notcorrelated with SANS or SAPS
Analysis in Theberge et al 2004NAA and Cho in left ACC DUPDUI DPS
From Theberge et al 2004NAA concentration was positively correlatedwith DUP and inversely with DPS at trendlevel Cho concentration was positivelycorrelated with DUP
Theberge et al (2003) Schizophrenia patients (n=21atypical n=7 both n=1typical n=13)Healthy participants (n=21)
NAA Cho Cr Glu Gln mI inleft ACC duration of illness
Glu and Gln concentrations were greaterin patients than healthy participants NAAconcentration was inversely correlatedwith duration of positive symptoms
Wood et al (2007) Schizophrenia male patients(n=15 13 atypical 2 medication free)Healthy male participants (n=14)
NAA and Glx in dorsal and rostralregions PANSS five factors illnessduration
Patients had lower NAA concentrationcompared to healthy participantsRight dorsal Glx was inversely correlatedwith illness duration
Ohrmann et al (2008) Schizophrenia patients(n=43 all on atypical)Healthy participants (n=37)
NAA Cho Cr Glx WCST learningpotential
No difference in metabolite concentrationbetween patients and healthy participantsNAA and Glx concentrations were positivelyassociated with WCST learning potential
Sanches et al (2008) Schizophrenia patients (n=37)Healthy participants (n=37)
NAA(Cho+Cr) ratio in left andright anterior middle frontal gyrusACC and perirolandic area (reference)basal skin conductance and skinconductance response to auditorystimuli of 1 s tones of 80 dB Patientsand healthy participants classified intoskin conductance responders (2 SDbelow mean skin conductance in healthyparticipants) and non-responders
NAA(Cho+Cr) ratio was lower in patientsthan healthy participants in the anteriormiddle frontal gyrus and ACC bilaterallyNAA(Cho+Cr) ratio did not differ betweenskin conductance response groups based onskin conductance response to auditory stimuliBasal skin conductance non-responders patientshad lower NAA(Cho+Cr) ratio than healthyparticipants in left and right ACC
258 P Premkumar et al Psychiatry Research Neuroimaging 182 (2010) 251ndash260
Tayoshi et al (2009) Long-term schizophrenia (n=30antipsychotic medication typenot reported)Healthy participants (n=25)
NAA Cho Cr Glu Gln mI Gender PANSStotal and subscales duration of illnessduration of therapy antipsychotic dosagebenzodiazepine dose
Patients had lower Glu and mI concentrationcompared to healthy participants Malepatients had lower NAA Cr Glu and mIconcentration than male healthy participantsMales had greater Gln concentration comparedto females Metabolite concentration wasnot correlated with symptoms or otherclinical variables
Ongur et al (2009) Schizophrenia patients (n=15)Bipolar disorder patients (n=15)Healthy participants (n=22)
Cr in ACC (hypothesized area) andparietal-occipital cortex (reference area)MADRS PANSS YMRS
Patients had lower Cr than healthyparticipants in both ACC andparietal-occipital cortex No significantcorrelations between Cr concentrationand clinical measures
ACC anterior cingulate cortex ChomdashCholine CrmdashCreatinePhosphocreatine DPSmdashduration of psychotic symptoms DUImdashduration of untreated illness DUPmdashduration of untreatedpsychosis GlnmdashGlutamine GlumdashGlutamate GluCr ratio SANSmdashSchedule for the Assessment of Negative Symptoms GlxmdashGlutamate+Glutamine MADRSmdashMontgomery AsbergDepression Rating Scale mImdashmyo-Inositol NAA N-acetyl aspartate PANSSmdashPositive and Negative Syndrome Scale SAPS Schedule for the Assessment of Positive SymptomsWCSTmdashWisconsin Card Sorting test YMRSmdashYoung Mania Rating Scale
Appendix A (continued)
259P Premkumar et al Psychiatry Research Neuroimaging 182 (2010) 251ndash260
Appendix B Supplementary Data
Supplementary data associated with this article can be found inthe online version at doi101016jpscychresns201002008
References
Adler CM Malhotra AK Elman I Goldberg T Egan M Pickar D Breier A 1999Comparison of ketamine-induced thought disorder in healthy volunteers andthought disorder in schizophrenia American Journal of Psychiatry 156 1646ndash1649
Andres RH Ducray AD Schlattner U Wallimann T Widmer HR 2008 Functionsand effects of creatine in the central nervous system Brain Research Bulletin 76329ndash343
Baiano M David A Versace A Churchill R Balestrieri M Brambilla P 2007Anterior cingulate volumes in schizophrenia a systematic review and a meta-analysis of MRI studies Schizophrenia Research 93 1ndash12
Bechara A Damasio AR Damasio H Anderson SW 1994 Insensitivity to futureconsequences following damage to human prefrontal cortex Cognition 50 7ndash15
Behrens TE Woolrich MW Walton ME Rushworth MF 2007 Learning the valueof information in an uncertain world Nature Neuroscience 10 1214ndash1221
Bertolino A Esposito G Callicott JH Mattay VS Van Horn JD Frank JA BermanKF Weinberger DR 2000 Specific relationship between prefrontal neuronal N-acetylaspartate and activation of the working memory cortical network inschizophrenia American Journal of Psychiatry 157 26ndash33
Braus DF Ende G Weber-Fahr W Demirakca T Henn FA 2001 Favorable effecton neuronal viability in the anterior cingulate gyrus due to long-term treatmentwith atypical antipsychotics an MRSI study Pharmacopsychiatry 34 251ndash253
Braus DF Ende G Weber-Fahr W Demirakca T Tost H Henn FA 2002Functioning and neuronal viability of the anterior cingulate neurons followingantipsychotic treatment MR-spectroscopic imaging in chronic schizophreniaEuropean Neuropsychopharmacology 12 145ndash152
Burgess PW Shallice T 1997 The Hayling and Brixton Tests Thames Valley TestCompany Bury St Edmunds
Callicott JH Bertolino A Mattay VS Langheim FJ Duyn J Coppola R Goldberg TEWeinberger DR 2000 Physiological dysfunction of the dorsolateral prefrontal cortexin schizophrenia revisited Cerebral Cortex 10 1078ndash1092
Carter CS van Veen V 2007 Anterior cingulate cortex and conflict detection anupdate of theory and data Cognitive Affective and Behavioral Neuroscience 7367ndash379
Cornblatt BA Risch JJ Faris G Friedman D Erlenmeyer-Kimling L 1988 TheContinuous Performance Test Identical Pairs Version (CPT-IP) I New findingsabout sustained attention in normal families Psychiatry Research 26 223ndash238
Costafreda SG Khanna A Mourao-Miranda J Fu CH 2009 Neural correlates of sadfaces predict clinical remission to cognitive behavioural therapy in depressionNeuroReport 20 637ndash641
Deicken RF Zhou L Schuff N Weiner MW 1997 Proton magnetic resonancespectroscopy of the anterior cingulate region in schizophrenia SchizophreniaResearch 27 65ndash71
Deicken RF Johnson C Pegues M 2000 Proton magnetic resonance spectroscopy ofthe human brain in schizophrenia Reviews in the Neurosciences 11 147ndash158
Ende G Braus DF Walter S Weber-Fahr W Soher B Maudsley AA Henn FA2000 Effects of age medication and illness duration on the N-acetyl aspartatesignal of the anterior cingulate region in schizophrenia Schizophrenia Research 41389ndash395
Fannon D Simmons A Tennakoon L OCeallaigh S Sumich A Doku V Shew CSharma T 2003 Selective deficit of hippocampal N-acetylaspartate in antipsy-chotic-naive patients with schizophrenia Biological Psychiatry 54 587ndash598
Ferguson KJ MacLullich AM Marshall I Deary IJ Starr JM Seckl JR Wardlaw JM2002 Magnetic resonance spectroscopy and cognitive function in healthy elderlymen Brain 125 2743ndash2749
First MB Spitzer RL Gibbon M Williams JBW 2002 Structured Clinical Interviewfor DSM-IV-TR Axis I DisordersmdashPatient Edition (SCID-IP 112002 revision)Biometrics Research Department New York NY
Fornito A Yucel M Dean B Wood SJ Pantelis C 2008 Anatomical abnormalities ofthe anterior cingulate cortex in schizophrenia bridging the gap betweenneuroimaging and neuropathology Schizophrenia Bulletin 35 973ndash993
Fowler D Garety PA Kuipers E 1995 Cognitive Behaviour Therapy for PsychosisTheory and Practice Wiley Chichester
Fujimoto T Takeuch K Matsumoto T Kamimura K Hamada R Nakamura K KatoN 2007 Abnormal glucose metabolism in the anterior cingulate cortex in patientswith schizophrenia Psychiatry Research 154 49ndash58
Goff DC Hennen J Lyoo IK Tsai G Wald LL Evins AE Yurgelun-Todd DARenshaw PF 2002 Modulation of brain and serum glutamatergic concentrationsfollowing a switch from conventional neuroleptics to olanzapine BiologicalPsychiatry 51 493ndash497
Gold JM Carpenter C Randolph C Goldberg TE Weinberger DR 1997 Auditoryworking memory and Wisconsin Card Sorting Test performance in schizophreniaArchives of General Psychiatry 54 159ndash165
Heaton RK Chelune GJ Tally JL Kay GG Curtiss G 1993 Wisconsin Card SortingTest Manual Revised and Expanded Psychological Assessment Resources OdessaFL
Honea R Crow TJ Passingham D Mackay CE 2005 Regional deficits in brainvolume in schizophrenia a meta-analysis of voxel-based morphometry studiesAmerican Journal of Psychiatry 162 2233ndash2245
Hughes C Kumari V Soni W Das M Binneman B Drozd S ONeil S Mathew VSharma T 2003 Longitudinal study of symptoms and cognitive function in chronicschizophrenia Schizophrenia Research 59 137ndash146
Jung RE Brooks WM Yeo RA Chiulli SJ Weers DC Sibbitt Jr WL 1999Biochemical markers of intelligence a proton MR spectroscopy study of normalhuman brain Proceedings Biological Sciences 266 1375ndash1379
Kaneda M Osaka N 2008 Role of anterior cingulate cortex during semantic coding inverbal working memory Neuroscience Letters 436 57ndash61
Kay SR Fiszbein A Opier LA 1987 The Positive and Negative Syndrome Scale(PANSS) for schizophrenia Schizophrenia Bulletin 13 261ndash276
Kennerley SW Dahmubed AF Lara AH Wallis JD 2008 Neurons in the frontallobe encode the value of multiple decision variables Journal of CognitiveNeuroscience 21 1162ndash1178
Kim J Whyte J Wang J Rao H Tang KZ Detre JA 2006 Continuous ASL perfusionfMRI investigation of higher cognition quantification of tonic CBF changes duringsustained attention and working memory tasks Neuroimage 31 376ndash385
Krystal JH Karper LP Seibyl JP Freeman GK Delaney R Bremner JD HeningerGR Bowers Jr MB Charney DS 1994 Subanesthetic effects of the noncom-petitive NMDA antagonist ketamine in humans Psychotomimetic perceptualcognitive and neuroendocrine responses Archives of General Psychiatry 51199ndash214
Kumari V Peters ER Fannon D Antonova E Premkumar P Anilkumar APWilliams SC Kuipers EA 2009 Dorsolateral prefrontal cortex activity predictsresponsiveness to cognitive behaviour therapy in schizophrenia BiologicalPsychiatry 66 594ndash602
Lahti AC Koffel B LaPorte D Tamminga CA 1995 Subanesthetic doses of ketaminestimulate psychosis in schizophrenia Neuropsychopharmacology 13 9ndash19
Lenartowicz A McIntosh AR 2005 The role of anterior cingulate cortex in workingmemory is shaped by functional connectivity Journal of Cognitive Neuroscience 171026ndash1042
Malhotra AK Pinals DA Adler CM Elman I Clifton A Pickar D Breier A 1997Ketamine-induced exacerbation of psychotic symptoms and cognitive impairmentin neuroleptic-free schizophrenics Neuropsychopharmacology 17 141ndash150
260 P Premkumar et al Psychiatry Research Neuroimaging 182 (2010) 251ndash260
McLean MA Woermann FG Barker GJ Duncan JS 2000 Quantitative analysis ofshort echo time (1)H-MRSI of cerebral gray and white matter Magnetic Resonancein Medicine 44 401ndash411
McMorris T Harris RC Swain J Corbett J Collard K Dyson RJ Dye L Hodgson CDraper N 2006 Effect of creatine supplementation and sleep deprivation withmild exercise on cognitive and psychomotor performance mood state and plasmaconcentrations of catecholamines and cortisol Psychopharmacology (Berl) 18593ndash103
McMorris T Harris RC Howard AN Langridge G Hall B Corbett J Dicks MHodgson C 2007 Creatine supplementation sleep deprivation cortisol melatoninand behavior Physiology and Behaviour 90 21ndash28
Miller BL 1991 A review of chemical issues in 1H NMR spectroscopy N-acetyl-L-aspartate creatine and choline NMR in Biomedicine 4 47ndash52
Moghaddam B 2003 Bringing order to the glutamate chaos in schizophrenia Neuron40 881ndash884
Ohrmann P Siegmund A Suslow T Pedersen A Spitzberg K Kersting ARothermundt M Arolt V Heindel W Pfleiderer B 2007 Cognitive impairmentand in vivo metabolites in first-episode neuroleptic-naive and chronic medicatedschizophrenic patients a proton magnetic resonance spectroscopy study Journalof Psychiatric Research 41 625ndash634
Ohrmann P Kugel H Bauer J Siegmund A Kolkebeck K Suslow T Wiedl KHRothermundt M Arolt V Pedersen A 2008 Learning potential on the WCST inschizophrenia is related to the neuronal integrity of the anterior cingulate cortex asmeasured by proton magnetic resonance spectroscopy Schizophrenia Research106 156ndash163
Ongur D Prescot AP Jensen JE Cohen BM Renshaw PF 2009 Creatineabnormalities in schizophrenia and bipolar disorder Psychiatry ResearchNeuroimaging 172 44ndash48
Osaka N Osaka M Kondo H Morishita M Fukuyama H Shibasaki H 2004 Theneural basis of executive function in working memory an fMRI study based onindividual differences Neuroimage 21 623ndash631
Perry G Nunomura A Hirai K Zhu X Perez M Avila J Castellani RJ Atwood CSAliev G Sayre LM Takeda A Smith MA 2002 Is oxidative damage thefundamental pathogenic mechanism of Alzheimers and other neurodegenerativediseases Free Radical Biology and Medicine 33 1475ndash1479
Peterson BS Skudlarski P Gatenby JC Zhang H Anderson AW Gore JC 1999 AnfMRI study of Stroop word-color interference evidence for cingulate subregionssubserving multiple distributed attentional systems Biological Psychiatry 451237ndash1258
Provencher SW 1993 Estimation of metabolite concentrations from localized in vivoproton NMR spectra Magnetic Resonance in Medicine 30 672ndash679
Rae C Digney AL McEwan SR Bates TC 2003 Oral creatine monohydratesupplementation improves brain performance a double-blind placebo-controlledcross-over trial Proceedings Biological Sciences 270 2147ndash2150
Ross AJ Sachdev PS 2004 Magnetic resonance spectroscopy in cognitive researchBrain Research Brain Research Reviews 44 83ndash102
Rushworth MF Walton ME Kennerley SW Bannerman DM 2004 Action sets anddecisions in the medial frontal cortex Trends in Cogntive Sciences 8 410ndash417
Rutten BP Korr H Steinbusch HW Schmitz C 2003 The aging brain less neuronscould be better Mechanisms of Ageing and Development 124 349ndash355
Sanches RF Crippa JA Hallak JE de Sousa JP Araujo D Santos AC Zuardi AW2008 Proton magnetic resonance spectroscopy of the frontal cingulate andperirolandic cortices and its relationship to skin conductance in patients withschizophrenia Brazilian Journal of Medical and Biological Research 41 1132ndash1141
Schlosser RG Koch K Wagner G Nenadic I Roebel M Schachtzabel C Axer MSchultz C Reichenbach JR Sauer H 2008 Inefficient executive cognitive controlin schizophrenia is preceded by altered functional activation during informationencoding an fMRI study Neuropsychologia 46 336ndash347
Shapiro AM Benedict RH Schretlen D Brandt J 1999 Construct and concurrentvalidity of the Hopkins Verbal Learning Test-revised The Clinical Neuropsychol-ogist 13 348ndash358
Smith EE Jonides J 1999 Storage and executive processes in the frontal lobesScience 283 1657ndash1661
Szoke A Trandafir A Dupont ME Meary A Schurhoff F Leboyer M 2008Longitudinal studies of cognition in schizophrenia meta-analysis British Journal ofPsychiatry 192 248ndash257
Tayoshi S Sumitani S Taniguchi K Shibuya-Tayoshi S Numata S Iga JI NakatakiM Ueno SI Harada M Ohmori T 2009 Metabolite changes and genderdifferences in schizophrenia using 3-Tesla proton magnetic resonance spectrosco-py ((1)H-MRS) Schizophrenia Research 108 69ndash77
Theberge J Bartha R Drost DJ Menon RS Malla A Takhar J Neufeld RWRogers J Pavlosky W Schaefer B Densmore M Al-Semaan Y Williamson PC2002 Glutamate and glutamine measured with 40T proton MRS in never-treatedpatients with schizophrenia and healthy volunteers American Journal of Psychiatry159 1944ndash1946
Theberge J Al-Semaan Y Williamson PC Menon RS Neufeld RW Rajakumar NSchaefer B Densmore M Drost DJ 2003 Glutamate and glutamine in theanterior cingulate and thalamus of medicated patients with chronic schizophreniaand healthy comparison subjects measured with 40-T proton MRS AmericanJournal of Psychiatry 160 2231ndash2233
Theberge J Al-Semaan Y Drost DJ Malla AK Neufeld RW Bartha R ManchandaR Menon R Densmore M Schaefer B Williamson PC 2004 Duration ofuntreated psychosis vs N-acetylaspartate and choline in first episode schizophre-nia a 1H magnetic resonance spectroscopy study at 40 Tesla Psychiatry Research131 107ndash114
Tranberg M Stridh MH Guy Y Jilderos B Wigstrom H Weber SG Sandberg M2004 NMDA-receptor mediated efflux of N-acetylaspartate physiological andorpathological importance Neurochemistry International 45 1195ndash1204
Tranberg M Abbas AK Sandberg M 2007 In vitro studies on the putative function ofN-acetylaspartate as an osmoregulator Neurochemical Research 32 1248ndash1255
Walton ME Croxson PL Behrens TE Kennerley SW Rushworth MF 2007Adaptive decision making and value in the anterior cingulate cortex Neuroimage36 (Suppl 2) T142ndashT154
Wechsler D 1987 Wechsler Memory ScalemdashRevised Psychological Corporation NewYork
Weinberger DR Aloia MS Goldberg TE Berman KF 1994 The frontal lobes andschizophrenia Journal of Neuropsychiatry and Clinical Neurosciences 6 419ndash427
Wood SJ Yucel M Wellard RM Harrison BJ Clarke K Fornito A Velakoulis DPantelis C 2007 Evidence for neuronal dysfunction in the anterior cingulate ofpatients with schizophrenia a proton magnetic resonance spectroscopy study at3T Schizophrenia Research 94 328ndash331
Yamasue H Fukui T Fukuda R Yamada H Yamasaki S Kuroki N Abe O Kasai KTsujii K Iwanami A Aoki S Ohtomo K Kato N Kato T 2002 1H-MRspectroscopy and gray matter volume of the anterior cingulate cortex inschizophrenia NeuroReport 13 2133ndash2137
Yeo RA Hill D Campbell R Vigil J Brooks WM 2000 Developmental instabilityand working memory ability in children a magnetic resonance spectroscopyinvestigation Developmental Neuropsychology 17 143ndash159

254 P Premkumar et al Psychiatry Research Neuroimaging 182 (2010) 251ndash260
PANSS symptoms illness duration (defined as the difference betweenthe age at onset of psychotic symptoms as reported by the patient andwhere possible confirmed with other sources and age at the time ofbaseline assessments) and antipsychotic medication level (in chlor-promazine equivalents) Spearman correlations were performed toexamine the relationship between metabolite values and individualPANSS items in those subscales that were found to have a significantassociation with metabolite values
2413 Neuropsychological correlates of metabolite concentrationPearson and partial correlations controlling for GM concentration orSpearman correlations for neuropsychological variables with a non-normal distribution (Brixton perseverative errors) were performedbetween neuropsychological performance measures and metaboliteconcentration in patient and healthy participant groups
2414 Multiple regression of clinical andor neuropsychological correlateson metabolite concentration Significant clinical andor neuropsycholog-ical variables that had a normal distribution were entered into themultiple regression model using a stepwise method (to estimate theeffect of individual predictors on variability of criterion variable) andusing a forced-entry method (to explain the combined effect ofpredictors on the variability of the criterion variable)
242 Longitudinal analysis
2421 Group comparison of metabolite concentration Due to the smallsample sizes differences between CBTp+SC SC control and SCresponsive patient groups in age education clinical variables andbaseline metabolite and GM concentrations were examined using non-parametric analyses namely the Kruskal-Wallis test A chi-squared testdetermined group differences in gender distribution
2422 Metabolite concentration as a predictor of symptom changefollowing CBTpSpearman correlationswere performed in the CBTp+SCpatients who were followed up (n=8) between baseline metaboliteconcentrations and residual PANSS symptom change scores frombaseline to follow-up
2423 Change in symptom severity and metabolite concentrationfollowing CBTp Due to the small sample sizes (CBTp+SC n=7 andSC control n=4) changes in symptom severity metabolite and GMconcentrations from baseline to follow-up in the patient groups wereexamined using the Wilcoxon Signed Rank test
All analyses were performed in SPSS windows (version 15) Alphalevel for testing significance of effects was maintained at Pb005 Wechose not to apply the Bonferroni method of adjusting the P valuebecause we expected the size of the relationship between MRS valuesand symptomsneuropsychological functions to be small or at bestmodest given that symptoms in schizophrenia are unlikely to have asingle aetiology and successful task performance on most neuropsy-chological tasks would recruit additional brain regions
3 Results
31 Cross-sectional analysis
311 Group differences in demographic and neuropsychological variablesPatient and healthy participant groups did not differ in gender and
age Patients had fewer years in education and showed deficientperformance on most neuropsychological measures relative tohealthy participants (Table 2)
312 Group differences in metabolite concentration in the ACCNAA Cr and GM concentrations were lower in the patient
compared with the healthy participant group (Table 3)
313 Clinical correlates of metabolite concentrationNAA concentration correlated inversely with positive symptoms
general psychopathology and total symptoms (Table 4) Thesecorrelations remained significant after controlling for GM NAAconcentration correlated inversely with negative symptoms onlyafter controlling for GM PANSS item-wise correlations revealed thatNAA concentration was inversely correlated with delusions disorga-nisation and persecution items of the positive syndrome subscalepassive social withdrawal and stereotyped thinking items of thenegative syndrome subscale and somatic concern and preoccupationitems of the general psychopathology subscale
Cho concentration correlated inversely with positive and totalsymptoms After controlling for GM concentration Cho concentrationcorrelated with total symptoms but not positive symptoms Choconcentration correlated inversely with negative symptoms at a trendlevel only after controlling for GM concentration PANSS item-wisecorrelations revealed that Cho concentration was inversely correlatedwith disorganisation and hostility items of the positive syndromesubscale passive social withdrawal item of the negative syndromesubscale and somatic concern item of the general psychopathologysubscale Cho concentration correlated positively with antipsychoticmedication dosage Cr concentration did not correlate with anyclinical variable
314 Neuropsychological correlates of metabolite concentrationPatients A positive correlation between NAA concentration and
working memory as assessed by the letter number test emerged onlyafter controlling for GM concentration (Table 5)
Healthy participants NAA concentration correlated positively withworking memory as assessed by the letter number test and short-term memory as assessed by the Hopkins verbal learning test thoughthese correlations were reduced to a trend level of significance aftercontrolling for GM concentration (Table 5) Cho concentrationcorrelated inversely with short-term memory as assessed by theWechsler Memory ScalemdashRevised (WMS-R) logical memory imme-diate recall test after controlling for GM concentration Cr concentra-tion correlated inversely with executive function as assessed byBrixton perseverative errors
315 Multiple regression of clinical andor neuropsychologicalcorrelates of metabolite concentration
Patients In the stepwise regression model with NAA concentra-tion as the criterion variable positive symptoms proved to be asignificant predictor (r=minus0489 P=0006) The model explained 21of the variance in NAA concentration In the forced-entry regressionmodel the predictors (positive symptoms general psychopathologyand letter number test) explained 25 of the variance in NAAconcentration
Healthy participants In the stepwise regression model with NAAconcentration as the criterion variable short-term memory asassessed by the Hopkins verbal learning test was a significantpredictor (r=0576 P=0039) The model explained 27 of thevariance in NAA concentration In the forced-entry regression modelthe predictors (Hopkins verbal learning test and letter number test)explained 27 of the model
32 Longitudinal analysis
321 Metabolite concentration differences at baseline between patientsub-groups
NAA concentration tended to differ between patient groups atbaseline mainly due to greater concentration in the low-symptomSC-responsive group (Table 6)
Table 2Demographic clinical and neuropsychological characteristics of patients and healthy participants groups
Characteristic Patients Healthy participants Test χ2 (df) P
Gender malefemale (n) 246 132 Chi-squared 0304 (1) 0581mean SD mean SD F or z (df)
Age in years 3640 864 3540 1334 ANOVA 0092 (143) 0763Years in education 1383 215 1561 323 ANOVA 4555 (141) 0039Illness duration years 1298 894
Symptoms (PANSS)Positive 1693 395Negative 1787 452General psychopathology 3170 639Total 6650 1317Medication level (chlorpromazine equivalents) 50267 32788Medication type (n)
Olanzapine 12Clozapine 6Risperidone 5Aripiprazole 2Flupentixol 2Amisulperide 1Haloperidol 2
Neuropsychological functionBrixton perseverative errors 050 078 031 048 MannndashWhitney U minus0552 (141) 0648WCST perseverative errors 1817 886 1175 751 ANOVA 4870 (140) 0033Letter number test number correct 1380 380 1692 296 ANOVA 6925 (141) 0012WMS logical memory immediate unit recalled 710 258 969 333 ANOVA 7533 (140) 0009Hopkins total freely recalled 2186 538 2692 517 ANOVA 8122 (140) 0007CPT discriminability 029 059 187 100 ANOVA 14257 (139) 0001IGT overall learning 280 1183 892 1473 ANOVA 2092 (141) 0156
255P Premkumar et al Psychiatry Research Neuroimaging 182 (2010) 251ndash260
33 Metabolite concentration correlates of symptom change followingCBTp
In the CBTp+SC group metabolite concentration at baseline wasnot associated with symptom change following CBTp (SupplementaryTable)
34 Symptom severity and metabolite concentration change frombaseline to follow-up in CBTp+SC and SC control groups
Positive symptoms improved following CBTp in the CBTp+SCgroup while negative symptoms tended to deteriorate in the SCcontrol group (Table 7)
NAA concentration tended to increase in the CBTp+SC group frombaseline to follow-up (Table 7)
4 Discussion
The present investigation examined the concentrations of NAACho and Cr in the ACC and their clinical and neuropsychologicalcorrelates in patients with schizophrenia and healthy participants(cross-sectional investigation) The study also explored whetherbaseline metabolite concentration predicted symptom change fol-lowing CBTp+SC and whether a reduction in symptoms followingCBTp+SC was accompanied by higher NAA concentration relative tobaseline (longitudinal investigation)
Table 3ACCmetabolite and greymatter concentrations (mean SD) at baseline at each voxel inpatients and healthy participants
CSI variable(millimolars)
Patient(n=30)
Healthy participants(n=15)
F (p)
NAA 742 126 856 139 7682 (0008)Cho 190 038 199 036 0654 (0423)Cr 703 124 789 102 5345 (0026)Grey matter 5399 1051 6139 858 5549 (0023)
41 Summary of clinical and neuropsychological correlates of metaboliteconcentration (cross-sectional investigation)
The major findings from the cross-sectional analysis were that inpatients (1) NAA concentration was reduced compared to healthyparticipants (2) greaterNAA concentrationwas associatedwith a lowerlevel of positive symptoms general psychopathology and betterworking memory (positive symptoms alone explained 21 of thevariance total variance explained=25) and (3) greater Cho concen-tration was associated with a lower level of positive symptoms andhigher level of antipsychotic medication In healthy participants thefollowing associationswere observed (1) NAA concentration positivelywith working and short-termmemory (2) Cho concentration inverselywith short-term memory and (3) Cr concentration inversely withexecutive function These findings will be discussed in turn
411 Clinical correlates of metabolite concentrationsThe findings of lower ACC NAA concentration in schizophrenia
patients (Deicken et al 1997 Ende et al 2000 Wood et al 2007)and clinical correlates of NAA concentration support previousevidence (Theberge et al 2003 Wood et al 2007 Yamasue et al2002) Our study of a relatively larger sample of patients than mostprevious studies is the first to observe that NAA concentration wasinversely associated with the severity of positive negative andgeneral psychopathology symptoms based on the three-dimensionalmodel of the PANSS (Kay et al 1987) Twenty percent of our patientswere SC treatment responsive giving a wider range to symptomscores than earlier studies Patients who had low symptom severityand were considered to have responded sufficiently to their standard(mostly atypical) antipsychotic treatment tended to show greaterNAA concentration than patients who were symptomatic (baselinecomparisons) suggesting that NAA concentration may vary as afunction of symptom severity and treatment response
NAA concentration being a by-product of neurotransmitter turn-over (Tranberg et al 2004) the symptom severity-metabolite concen-tration associations may reflect the efficiency of neurotransmission Asnoted in Section 1 NAA concentration may be an indicator of NMDA
Table 4Clinical correlates of metabolite concentration at baseline (patients only)
NAA concentration Cho concentration Cr concentration
r or ρ r (P) rp1 (P) r (P) rp
1 (P) r (P) rp1 (P)
Illness duration r minus0059 (0756) 0091 (0640) minus0064 (0735) 0045 (0817) minus0291 (0118) minus0244 (0203)Antipsychotic medication level Rho 0197 (0298) 0442 (0014) 0073 (0700)Symptoms (PANSS)
Positive (P) symptoms r minus0489 (0006) minus0430 (0020) minus0391 (0033) minus0325 (0085) minus0308 (0098) minus0262 (0170)Negative (N) symptoms r minus0297 (0111) minus0418 (0024) minus0287 (0124) minus0366 (0051) minus0211 (0264) minus0262 (0170)General psychopathology (GP) r minus0416 (0022) minus0506 (0005) minus0299 (0109) minus0341 (0070) minus0204 (0281) minus0219 (0254)Total r minus0450 (0013) minus0512 (0004) minus0361 (0050) minus0384 (0040) minus0263 (0160) minus0266 (0163)
Individual symptomsDelusions (P) Rho minus0411 (0024) minus0342 (0064) minus0192 (0309)Disorganisation (P) Rho minus0525 (0003) minus0369 (0045) minus0136 (0475)Persecution (P) Rho minus0390 (0033) minus0193 (0307) minus0068 (0719)Hostility (P) Rho 0062 (0745) 0370 (0044) 0163 (0390)Passive social withdrawal (N) Rho minus0370 (0044) minus0393 (0032) minus0261 (0163)Stereotyped thinking (N) Rho minus0422 (0020) minus0073 (0684) minus0221 (0240)Somatic concern (GP) Rho minus0419 (0021) minus0407 (0026) minus0129 (0496)Preoccupation (GP) Rho minus0528 (0003) minus0201 (0287) minus0264 (0156)
rp1 partial correlation controlling for GM concentration P PANSS positive symptom subscale N PANSS negative symptom subscale GP PANSS general psychopathology subscale
256 P Premkumar et al Psychiatry Research Neuroimaging 182 (2010) 251ndash260
function and neuronal longevity (Tranberg et al 2004) NAA efflux isa delayed response to sudden non-physiological decrease in extracel-lular osmolarity and high K+intra-cellular and NMDA activation(Tranberg et al 2007) Elevated concentration of NAA in the ACC inschizophrenia patients with lower level of symptoms may reflectincreased turnover of neurotransmitters such as dopamine and NMDA
Similarly the association between Cho concentration and total andpositive symptoms may also reflect improved neurotransmitterfunction and neuronal integrity with milder symptoms The Cho peakincludes solublemembranephospholipids includingphosphorylcholine(PCho) glycerophosphocholine (GPCho) and a relatively negligibleamount of free choline (Ross and Sachdev 2004) PCho is involved insynthesis of the insoluble membrane phospholipids while GPCho is aproduct of membrane degradation and free choline is involved insynthesis of the neurotransmitter acetylcholine aswell as inmembranesynthesis (Ross and Sachdev 2004) An increase in the Cho peak isassociated with an increase in membrane breakdown or turnover andmyelination (Ross and Sachdev 2004) The positive associationbetween antipsychotic medication dosage and Cho concentration ameasure of neuronalmembrane turnover (Miller 1991 Ohrmann et al2008) suggests that medication level also influences neuronal activity
412 Neuropsychological correlates of metabolite concentrationIn patients the finding of an association between greater NAA
concentration and better working memory supports evidence for the
Table 5Neuropsychological correlates of metabolite concentration at baseline in patients and healt
Neuropsychological function Group N r or rho NAA concentration
r or rho rp1 (P)
Brixton perseverative errors Patient 30 Rho 0180 (0341)Control 13 Rho 0356 (0232)
WCST perseverative errors Patient 30 r minus0097 (0610) minus013Control 12 r 0271 (0394) 024
Letterndashnumber test number correct Patient 30 r 0303 (0104) 037Control 13 r 0557 (0048) 052
WMS logical memory immediateunit recalled
Patient 29 r 0301 (0112) 033Control 13 r 0330 (0271) 027
Hopkins verbal learning test totalnumber freely recalled
Patient 29 r 0127 (0512) 011Control 13 r 0576 (0039) 055
CPT discriminability Patient 29 r minus0037 (0848) 015Control 12 r 0329 (0297) 027
IGT overall learning Patient 30 r 0179 (0343) 021Control 13 r 0042 (0892) 007
rp1 partial correlation controlling for GM concentration
role of frontal lobe function in working memory using functional MRIand proton MRS in schizophrenia (Bertolino et al 2000 Callicottet al 2000 Ohrmann et al 2007) although this association explainedonly a very small amount (3) of the variance in NAA concentrationthat was additional to that explained by positive symptoms
In the healthy group greater NAA concentration was associatedwith better working and short-term memory The ACC is activatedduring both working and short-term memory (Kim et al 2006Lenartowicz and McIntosh 2005) NAA concentration in the frontallobe white matter was positively associated with working memory inhealthy children which may be related to increased number ofdendritic processes at an early age (Yeo et al 2000) NAA con-centration has a role in neuronal integrity in the form of increasedmyelination and mitochondrial function (Ross and Sachdev 2004)and this may facilitate working and short-term memory
Greater Cho concentration correlated inversely with short-termmemory in the healthy group when controlling for GM concentrationin the ACC A negative association between Cho concentration in theoccipito-parietal white matter and IQ independent of the positiveassociation between NAA concentration and IQ in healthy individualshas been previously reported (Jung et al 1999) Our findings suggestindependentmetabolite concentration-neuropsychological associationsbetween NAA Cho and Cr in healthy individuals Greater Cr concentra-tionwas associatedwith poorer executive function in the present studyA study of elderly males found negative correlations between adjusted
hy participants
Cho concentration Cr concentration
r or rho rp1 (P) r or rho rp
1 (P)
minus0198 (0293) 0331 (0074)0356 (0232) 0579 (0038)
9 (0473) minus0011 (0956) minus0030 (0877) minus0102 (0592) minus0116 (0550)8 (0461) 0390 (0211) 0368 (0265) minus0225 (0483) 0312 (035)9 (0043) minus0163 (0388) minus0160 (0407) minus0130 (0493) minus0124 (0523)9 (0077) 0011 (0971) minus0083 (0797) 0156 (0611) minus0030 (0927)1 (0085) 0054 (0781) 0045 (0822) minus0017 (0932) minus0025 (0898)8 (0382) minus0453 (0120) minus0610 (0035) minus0022 (0946) minus0267 (0401)9 (0564) 0181 (0348) 0177 (0369) 0269 (0159) 0265 (0173)5 (0061) minus0173 (0572) minus0330 (0295) 0277 (036) 0061 (0851)8 (0423) minus0114 (0555) 0016 (0936) 0003 (0986) 0088 (0656)5 (0413) minus0209 (0514) minus0346 (0297) 0207 (0519) 0006 (0986)0 (0273) 0026 (0891) 0029 (0879) 0062 (0747) 0064 (0742)8 (0811) minus0063 (0839) minus0025 (0939) minus0225 (0461) minus0169 (0600)
Table 6Demographic clinical and metabolite concentration characteristics at baseline of CBTp+SC (n=11) SC control (n=13) and SC responsive (n=6) patients
Characteristic CBTp+SC SC control SC responsive χ2 P
Gender malefemale (n) 65 121 60 7185 0028mean SD mean SD
Age in years 3464 862 3746 877 3733 942 0745 0689Years in education 1445 246 1346 176 1377 24 1156 0561Illness duration years 1194 860 1377 970 1317 928 0303 0860Symptoms (PANSS)
Positive 1745 295 1915 264 1117 172 14644 0001Negative 1818 498 1923 386 1433 361 5779 0056General psychopathology 3227 675 340 549 2567 383 6775 0034Total 6791 1287 7239 994 5117 778 9512 0009Medication level 56442 30317 50055 39478 39405 20759 1787 0409
Metabolite concentrationNAA 765 092 685 143 823 091 5313 0070Cho 192 060 186 024 194 018 0493 0781Cr 689 140 687 095 748 160 1047 0592Grey matter 5766 1071 5117 1136 5337 714 1096 0578
257P Premkumar et al Psychiatry Research Neuroimaging 182 (2010) 251ndash260
Cr in the parietal lobe and various cognitive measures including logicalmemory and verbal memory (Ferguson et al 2002) The study did notinclude ameasure of executive function Ferguson et al (2002) believedthat the findings fit with evidence that higher Cr levels are associatedwith cognitive ageing They proposed that poorer neuropsychologicalperformance in healthy ageing is associated with an increase inPhosphocreatine (PCr) due to a reduction in conversion of PCr toAdenosine-tri-phosphate (ATP) for energy Increased Cr concentrationmay be a marker of decreased brain energy metabolism
42 Effect of cognitive behaviour therapy for psychosis on metaboliteconcentration
Our preliminary investigation of change in metabolite concentra-tion in a small number of patients who received CBTp+SC comparedto patients who received SC only revealed a trend for an increase inNAA concentration with CBTp This increase in NAA was concomitantwith improvement in positive symptoms in CBTp+SC patients Thisfinding is consistent with the view that NAA concentration increaseswith alleviation of symptoms as discussed above Recent functionalimaging studies also provide evidence for a role of the ACC inresponsiveness to CBT in psychosis (Kumari et al 2009) as well asmajor depression (Costafreda et al 2009)
43 Limitations and future research
One of the limitations of the study was that the sample sizes ofpatients who received CBTp+SC or SC only and were clinicallyassessed andor scanned at follow-up were small A further limitationwas that gender distribution differed between the patient groupsAlthough there was no gender effect within each patient group in the
Table 7Symptoms metabolite and grey matter concentration (mean SD) at baseline and follow-u
CSI variable Baseline CBTp+SC (n=7) z (P)
FOLLOW-UP
Clinical symptomsPositive symptoms 1814 (234) 1567 (350) minus20Negative symptoms 1857 (571) 1567 (234) minus08General psychopathology 3200 (566) 2733 (497) minus13Total symptoms 6871 (1227) 5867 (1017) minus14
Metabolite concentrationNAA 765 (068) 831 (077) minus18Cho 185 (042) 193 (02) minus05Cr 679 (089) 725 (103) minus08Grey matter 5706 (1155) 5860 (851) minus03
metabolite concentrations in the present study higher ACC glutaminelevel in male compared to female schizophrenia patients has beenpreviously observed (Tayoshi et al 2009) Other effects of gender onACC function have also been reported for example reduced ACCglucose metabolism in male chronic patients relative to healthyparticipants and female patients (Fujimoto et al 2007) Thepredictive value of NAA concentration on symptom change in patientsreceiving psychological treatment or standard care needs to beexamined in a larger sample involving a sufficient number of bothmen and women with schizophrenia Additionally the role of clinicaland neuropsychological variables on ACC NAA levels in patients whoimprove with CBTp needs to be explored
44 Conclusions
Higher NAA and Cho concentrations in the ACC in patients areassociated with lower symptom severity Stronger and moreconsistent associations between metabolite concentrations andsymptom severity than neuropsychological function suggest thatmetabolite concentration and symptoms may co-fluctuate morestrongly Neuropsychological deficits may be more stable (Szokeet al 2008) and not necessarily improve in parallel with symptomimprovement (Hughes et al 2003) NAA concentration may yetreflect symptom changes following CBTp and if replicated in futurestudies has the potential to provide a useful biological marker ofclinical response to psychological treatments
Acknowledgement
The study was supported by funds from the Wellcome Trust UK(067427z02z)
p in CBTp+SC and SC control groups
Baseline SC control (n=4) z (P)
FOLLOW-UP
32 (0042) 1925 (222) 1825 (263) minus0365 (0715)13 (0416) 1875 (499) 2200 (616) minus1841 (0066)82 (0167) 3500 (668) 3275 (591) minus0535 (0593)72 (0141) 7300 (1042) 7300 (1364) minus0001 (1000)
59 (0063) 740 (069) 704 (038) minus1826 (0068)07 (0612) 190 (018) 201 (008) minus0730 (0465)45 (0398) 702 (016) 736 (099) minus0730 (0465)38 (0735) 5353 (549) 5324 (335) minus0365 (0715)
Appendix A Summary of magnetic resonance spectroscopy studies on the anterior cingulate cortex (ACC) in schizophrenia patients
Publication Participants Measures Results
Deicken et al (1997) Schizophrenia patients(n=26 9 on atypical and 17 on typical)Healthy participants (n=16)
NAA Cho and Cr illness durationantipsychotic medication dose
Patients had lower NAA concentrationcompared to healthy participants Nosignificant group differences or lateralizedasymmetries for Cho or Cr No significantcorrelations between NAA and eitherillness duration or antipsychoticmedication dose
Ende et al (2000) Schizophrenia patients(n=19 10 on atypical and 9 on typical)Healthy participants (n=16)
NAA Cho and Cr age illnessduration
Patients had lower NAA concentrationcompared to healthy participantsPatients receiving typical medication(but not atypical) had lower NAAconcentration than healthy participantsNAA concentration was inverselycorrelated with age in patients andhealthy participants and with illnessduration (corrected for age) in patients
Braus et al (2001 2002) Schizophrenia patients(11 on atypical and 10 on typical)
NAA Cho and Cr illness durationduration on atypical antipsychoticmedication WCST
Patients receiving typical antipsychoticshad lower NAA concentration than patientsreceiving atypical antipsychoticsNAA concentration was inverselycorrelated with illness duration andpositively with duration on atypicalantipsychotic medication NAAconcentration was inversely correlatedwith WCST perseverative errors
Goff et al (2002) Schizophrenia patients (n=17of whom 10 switched fromconventional to olanzapine andhad MRS at baseline and 8-week follow-up)
GluCr ratio SANS GluCr ratio was increased by 125(non-significant) following switch toolanzapine Patients who improvedon SANS symptoms had greaterGluCr ratio (458) compared topatients who deteriorated on SANSsymptoms (208) No significantcorrelation between SANS total andchange in GluCr ratio after switch
Yamasue et al (2002) Schizophrenia patients(n=15 all on typical)Healthy participants (n=13)
NAA Cho and Cr grey mattervolume age height body weightsocio-economic status parentalsocio-economic status years ofeducation PANSS onset of illnessillness duration antipsychoticmedication dose
Patients had lower NAACho ratio andgreater ChoCr ratio compared to healthyparticipants after controlling for greymatter volume NAACho ratio waspositively correlated with grey mattervolume in patients not healthy participantsNAACho ratio was inversely correlatedwith PANSS blunted affect score
Theberge et al (2004 2002) First-episode neuroleptic naiumlveschizophrenia patients (n=21)Healthy participants (n=21)
Analysis in Theberge et al 2002NAA Cho Cr Glu Gln mI in leftACC SANS SAPS
From Theberge et al 2002Patients had greater Gln concentrationcompared to healthy participantsMetabolite concentrations were notcorrelated with SANS or SAPS
Analysis in Theberge et al 2004NAA and Cho in left ACC DUPDUI DPS
From Theberge et al 2004NAA concentration was positively correlatedwith DUP and inversely with DPS at trendlevel Cho concentration was positivelycorrelated with DUP
Theberge et al (2003) Schizophrenia patients (n=21atypical n=7 both n=1typical n=13)Healthy participants (n=21)
NAA Cho Cr Glu Gln mI inleft ACC duration of illness
Glu and Gln concentrations were greaterin patients than healthy participants NAAconcentration was inversely correlatedwith duration of positive symptoms
Wood et al (2007) Schizophrenia male patients(n=15 13 atypical 2 medication free)Healthy male participants (n=14)
NAA and Glx in dorsal and rostralregions PANSS five factors illnessduration
Patients had lower NAA concentrationcompared to healthy participantsRight dorsal Glx was inversely correlatedwith illness duration
Ohrmann et al (2008) Schizophrenia patients(n=43 all on atypical)Healthy participants (n=37)
NAA Cho Cr Glx WCST learningpotential
No difference in metabolite concentrationbetween patients and healthy participantsNAA and Glx concentrations were positivelyassociated with WCST learning potential
Sanches et al (2008) Schizophrenia patients (n=37)Healthy participants (n=37)
NAA(Cho+Cr) ratio in left andright anterior middle frontal gyrusACC and perirolandic area (reference)basal skin conductance and skinconductance response to auditorystimuli of 1 s tones of 80 dB Patientsand healthy participants classified intoskin conductance responders (2 SDbelow mean skin conductance in healthyparticipants) and non-responders
NAA(Cho+Cr) ratio was lower in patientsthan healthy participants in the anteriormiddle frontal gyrus and ACC bilaterallyNAA(Cho+Cr) ratio did not differ betweenskin conductance response groups based onskin conductance response to auditory stimuliBasal skin conductance non-responders patientshad lower NAA(Cho+Cr) ratio than healthyparticipants in left and right ACC
258 P Premkumar et al Psychiatry Research Neuroimaging 182 (2010) 251ndash260
Tayoshi et al (2009) Long-term schizophrenia (n=30antipsychotic medication typenot reported)Healthy participants (n=25)
NAA Cho Cr Glu Gln mI Gender PANSStotal and subscales duration of illnessduration of therapy antipsychotic dosagebenzodiazepine dose
Patients had lower Glu and mI concentrationcompared to healthy participants Malepatients had lower NAA Cr Glu and mIconcentration than male healthy participantsMales had greater Gln concentration comparedto females Metabolite concentration wasnot correlated with symptoms or otherclinical variables
Ongur et al (2009) Schizophrenia patients (n=15)Bipolar disorder patients (n=15)Healthy participants (n=22)
Cr in ACC (hypothesized area) andparietal-occipital cortex (reference area)MADRS PANSS YMRS
Patients had lower Cr than healthyparticipants in both ACC andparietal-occipital cortex No significantcorrelations between Cr concentrationand clinical measures
ACC anterior cingulate cortex ChomdashCholine CrmdashCreatinePhosphocreatine DPSmdashduration of psychotic symptoms DUImdashduration of untreated illness DUPmdashduration of untreatedpsychosis GlnmdashGlutamine GlumdashGlutamate GluCr ratio SANSmdashSchedule for the Assessment of Negative Symptoms GlxmdashGlutamate+Glutamine MADRSmdashMontgomery AsbergDepression Rating Scale mImdashmyo-Inositol NAA N-acetyl aspartate PANSSmdashPositive and Negative Syndrome Scale SAPS Schedule for the Assessment of Positive SymptomsWCSTmdashWisconsin Card Sorting test YMRSmdashYoung Mania Rating Scale
Appendix A (continued)
259P Premkumar et al Psychiatry Research Neuroimaging 182 (2010) 251ndash260
Appendix B Supplementary Data
Supplementary data associated with this article can be found inthe online version at doi101016jpscychresns201002008
References
Adler CM Malhotra AK Elman I Goldberg T Egan M Pickar D Breier A 1999Comparison of ketamine-induced thought disorder in healthy volunteers andthought disorder in schizophrenia American Journal of Psychiatry 156 1646ndash1649
Andres RH Ducray AD Schlattner U Wallimann T Widmer HR 2008 Functionsand effects of creatine in the central nervous system Brain Research Bulletin 76329ndash343
Baiano M David A Versace A Churchill R Balestrieri M Brambilla P 2007Anterior cingulate volumes in schizophrenia a systematic review and a meta-analysis of MRI studies Schizophrenia Research 93 1ndash12
Bechara A Damasio AR Damasio H Anderson SW 1994 Insensitivity to futureconsequences following damage to human prefrontal cortex Cognition 50 7ndash15
Behrens TE Woolrich MW Walton ME Rushworth MF 2007 Learning the valueof information in an uncertain world Nature Neuroscience 10 1214ndash1221
Bertolino A Esposito G Callicott JH Mattay VS Van Horn JD Frank JA BermanKF Weinberger DR 2000 Specific relationship between prefrontal neuronal N-acetylaspartate and activation of the working memory cortical network inschizophrenia American Journal of Psychiatry 157 26ndash33
Braus DF Ende G Weber-Fahr W Demirakca T Henn FA 2001 Favorable effecton neuronal viability in the anterior cingulate gyrus due to long-term treatmentwith atypical antipsychotics an MRSI study Pharmacopsychiatry 34 251ndash253
Braus DF Ende G Weber-Fahr W Demirakca T Tost H Henn FA 2002Functioning and neuronal viability of the anterior cingulate neurons followingantipsychotic treatment MR-spectroscopic imaging in chronic schizophreniaEuropean Neuropsychopharmacology 12 145ndash152
Burgess PW Shallice T 1997 The Hayling and Brixton Tests Thames Valley TestCompany Bury St Edmunds
Callicott JH Bertolino A Mattay VS Langheim FJ Duyn J Coppola R Goldberg TEWeinberger DR 2000 Physiological dysfunction of the dorsolateral prefrontal cortexin schizophrenia revisited Cerebral Cortex 10 1078ndash1092
Carter CS van Veen V 2007 Anterior cingulate cortex and conflict detection anupdate of theory and data Cognitive Affective and Behavioral Neuroscience 7367ndash379
Cornblatt BA Risch JJ Faris G Friedman D Erlenmeyer-Kimling L 1988 TheContinuous Performance Test Identical Pairs Version (CPT-IP) I New findingsabout sustained attention in normal families Psychiatry Research 26 223ndash238
Costafreda SG Khanna A Mourao-Miranda J Fu CH 2009 Neural correlates of sadfaces predict clinical remission to cognitive behavioural therapy in depressionNeuroReport 20 637ndash641
Deicken RF Zhou L Schuff N Weiner MW 1997 Proton magnetic resonancespectroscopy of the anterior cingulate region in schizophrenia SchizophreniaResearch 27 65ndash71
Deicken RF Johnson C Pegues M 2000 Proton magnetic resonance spectroscopy ofthe human brain in schizophrenia Reviews in the Neurosciences 11 147ndash158
Ende G Braus DF Walter S Weber-Fahr W Soher B Maudsley AA Henn FA2000 Effects of age medication and illness duration on the N-acetyl aspartatesignal of the anterior cingulate region in schizophrenia Schizophrenia Research 41389ndash395
Fannon D Simmons A Tennakoon L OCeallaigh S Sumich A Doku V Shew CSharma T 2003 Selective deficit of hippocampal N-acetylaspartate in antipsy-chotic-naive patients with schizophrenia Biological Psychiatry 54 587ndash598
Ferguson KJ MacLullich AM Marshall I Deary IJ Starr JM Seckl JR Wardlaw JM2002 Magnetic resonance spectroscopy and cognitive function in healthy elderlymen Brain 125 2743ndash2749
First MB Spitzer RL Gibbon M Williams JBW 2002 Structured Clinical Interviewfor DSM-IV-TR Axis I DisordersmdashPatient Edition (SCID-IP 112002 revision)Biometrics Research Department New York NY
Fornito A Yucel M Dean B Wood SJ Pantelis C 2008 Anatomical abnormalities ofthe anterior cingulate cortex in schizophrenia bridging the gap betweenneuroimaging and neuropathology Schizophrenia Bulletin 35 973ndash993
Fowler D Garety PA Kuipers E 1995 Cognitive Behaviour Therapy for PsychosisTheory and Practice Wiley Chichester
Fujimoto T Takeuch K Matsumoto T Kamimura K Hamada R Nakamura K KatoN 2007 Abnormal glucose metabolism in the anterior cingulate cortex in patientswith schizophrenia Psychiatry Research 154 49ndash58
Goff DC Hennen J Lyoo IK Tsai G Wald LL Evins AE Yurgelun-Todd DARenshaw PF 2002 Modulation of brain and serum glutamatergic concentrationsfollowing a switch from conventional neuroleptics to olanzapine BiologicalPsychiatry 51 493ndash497
Gold JM Carpenter C Randolph C Goldberg TE Weinberger DR 1997 Auditoryworking memory and Wisconsin Card Sorting Test performance in schizophreniaArchives of General Psychiatry 54 159ndash165
Heaton RK Chelune GJ Tally JL Kay GG Curtiss G 1993 Wisconsin Card SortingTest Manual Revised and Expanded Psychological Assessment Resources OdessaFL
Honea R Crow TJ Passingham D Mackay CE 2005 Regional deficits in brainvolume in schizophrenia a meta-analysis of voxel-based morphometry studiesAmerican Journal of Psychiatry 162 2233ndash2245
Hughes C Kumari V Soni W Das M Binneman B Drozd S ONeil S Mathew VSharma T 2003 Longitudinal study of symptoms and cognitive function in chronicschizophrenia Schizophrenia Research 59 137ndash146
Jung RE Brooks WM Yeo RA Chiulli SJ Weers DC Sibbitt Jr WL 1999Biochemical markers of intelligence a proton MR spectroscopy study of normalhuman brain Proceedings Biological Sciences 266 1375ndash1379
Kaneda M Osaka N 2008 Role of anterior cingulate cortex during semantic coding inverbal working memory Neuroscience Letters 436 57ndash61
Kay SR Fiszbein A Opier LA 1987 The Positive and Negative Syndrome Scale(PANSS) for schizophrenia Schizophrenia Bulletin 13 261ndash276
Kennerley SW Dahmubed AF Lara AH Wallis JD 2008 Neurons in the frontallobe encode the value of multiple decision variables Journal of CognitiveNeuroscience 21 1162ndash1178
Kim J Whyte J Wang J Rao H Tang KZ Detre JA 2006 Continuous ASL perfusionfMRI investigation of higher cognition quantification of tonic CBF changes duringsustained attention and working memory tasks Neuroimage 31 376ndash385
Krystal JH Karper LP Seibyl JP Freeman GK Delaney R Bremner JD HeningerGR Bowers Jr MB Charney DS 1994 Subanesthetic effects of the noncom-petitive NMDA antagonist ketamine in humans Psychotomimetic perceptualcognitive and neuroendocrine responses Archives of General Psychiatry 51199ndash214
Kumari V Peters ER Fannon D Antonova E Premkumar P Anilkumar APWilliams SC Kuipers EA 2009 Dorsolateral prefrontal cortex activity predictsresponsiveness to cognitive behaviour therapy in schizophrenia BiologicalPsychiatry 66 594ndash602
Lahti AC Koffel B LaPorte D Tamminga CA 1995 Subanesthetic doses of ketaminestimulate psychosis in schizophrenia Neuropsychopharmacology 13 9ndash19
Lenartowicz A McIntosh AR 2005 The role of anterior cingulate cortex in workingmemory is shaped by functional connectivity Journal of Cognitive Neuroscience 171026ndash1042
Malhotra AK Pinals DA Adler CM Elman I Clifton A Pickar D Breier A 1997Ketamine-induced exacerbation of psychotic symptoms and cognitive impairmentin neuroleptic-free schizophrenics Neuropsychopharmacology 17 141ndash150
260 P Premkumar et al Psychiatry Research Neuroimaging 182 (2010) 251ndash260
McLean MA Woermann FG Barker GJ Duncan JS 2000 Quantitative analysis ofshort echo time (1)H-MRSI of cerebral gray and white matter Magnetic Resonancein Medicine 44 401ndash411
McMorris T Harris RC Swain J Corbett J Collard K Dyson RJ Dye L Hodgson CDraper N 2006 Effect of creatine supplementation and sleep deprivation withmild exercise on cognitive and psychomotor performance mood state and plasmaconcentrations of catecholamines and cortisol Psychopharmacology (Berl) 18593ndash103
McMorris T Harris RC Howard AN Langridge G Hall B Corbett J Dicks MHodgson C 2007 Creatine supplementation sleep deprivation cortisol melatoninand behavior Physiology and Behaviour 90 21ndash28
Miller BL 1991 A review of chemical issues in 1H NMR spectroscopy N-acetyl-L-aspartate creatine and choline NMR in Biomedicine 4 47ndash52
Moghaddam B 2003 Bringing order to the glutamate chaos in schizophrenia Neuron40 881ndash884
Ohrmann P Siegmund A Suslow T Pedersen A Spitzberg K Kersting ARothermundt M Arolt V Heindel W Pfleiderer B 2007 Cognitive impairmentand in vivo metabolites in first-episode neuroleptic-naive and chronic medicatedschizophrenic patients a proton magnetic resonance spectroscopy study Journalof Psychiatric Research 41 625ndash634
Ohrmann P Kugel H Bauer J Siegmund A Kolkebeck K Suslow T Wiedl KHRothermundt M Arolt V Pedersen A 2008 Learning potential on the WCST inschizophrenia is related to the neuronal integrity of the anterior cingulate cortex asmeasured by proton magnetic resonance spectroscopy Schizophrenia Research106 156ndash163
Ongur D Prescot AP Jensen JE Cohen BM Renshaw PF 2009 Creatineabnormalities in schizophrenia and bipolar disorder Psychiatry ResearchNeuroimaging 172 44ndash48
Osaka N Osaka M Kondo H Morishita M Fukuyama H Shibasaki H 2004 Theneural basis of executive function in working memory an fMRI study based onindividual differences Neuroimage 21 623ndash631
Perry G Nunomura A Hirai K Zhu X Perez M Avila J Castellani RJ Atwood CSAliev G Sayre LM Takeda A Smith MA 2002 Is oxidative damage thefundamental pathogenic mechanism of Alzheimers and other neurodegenerativediseases Free Radical Biology and Medicine 33 1475ndash1479
Peterson BS Skudlarski P Gatenby JC Zhang H Anderson AW Gore JC 1999 AnfMRI study of Stroop word-color interference evidence for cingulate subregionssubserving multiple distributed attentional systems Biological Psychiatry 451237ndash1258
Provencher SW 1993 Estimation of metabolite concentrations from localized in vivoproton NMR spectra Magnetic Resonance in Medicine 30 672ndash679
Rae C Digney AL McEwan SR Bates TC 2003 Oral creatine monohydratesupplementation improves brain performance a double-blind placebo-controlledcross-over trial Proceedings Biological Sciences 270 2147ndash2150
Ross AJ Sachdev PS 2004 Magnetic resonance spectroscopy in cognitive researchBrain Research Brain Research Reviews 44 83ndash102
Rushworth MF Walton ME Kennerley SW Bannerman DM 2004 Action sets anddecisions in the medial frontal cortex Trends in Cogntive Sciences 8 410ndash417
Rutten BP Korr H Steinbusch HW Schmitz C 2003 The aging brain less neuronscould be better Mechanisms of Ageing and Development 124 349ndash355
Sanches RF Crippa JA Hallak JE de Sousa JP Araujo D Santos AC Zuardi AW2008 Proton magnetic resonance spectroscopy of the frontal cingulate andperirolandic cortices and its relationship to skin conductance in patients withschizophrenia Brazilian Journal of Medical and Biological Research 41 1132ndash1141
Schlosser RG Koch K Wagner G Nenadic I Roebel M Schachtzabel C Axer MSchultz C Reichenbach JR Sauer H 2008 Inefficient executive cognitive controlin schizophrenia is preceded by altered functional activation during informationencoding an fMRI study Neuropsychologia 46 336ndash347
Shapiro AM Benedict RH Schretlen D Brandt J 1999 Construct and concurrentvalidity of the Hopkins Verbal Learning Test-revised The Clinical Neuropsychol-ogist 13 348ndash358
Smith EE Jonides J 1999 Storage and executive processes in the frontal lobesScience 283 1657ndash1661
Szoke A Trandafir A Dupont ME Meary A Schurhoff F Leboyer M 2008Longitudinal studies of cognition in schizophrenia meta-analysis British Journal ofPsychiatry 192 248ndash257
Tayoshi S Sumitani S Taniguchi K Shibuya-Tayoshi S Numata S Iga JI NakatakiM Ueno SI Harada M Ohmori T 2009 Metabolite changes and genderdifferences in schizophrenia using 3-Tesla proton magnetic resonance spectrosco-py ((1)H-MRS) Schizophrenia Research 108 69ndash77
Theberge J Bartha R Drost DJ Menon RS Malla A Takhar J Neufeld RWRogers J Pavlosky W Schaefer B Densmore M Al-Semaan Y Williamson PC2002 Glutamate and glutamine measured with 40T proton MRS in never-treatedpatients with schizophrenia and healthy volunteers American Journal of Psychiatry159 1944ndash1946
Theberge J Al-Semaan Y Williamson PC Menon RS Neufeld RW Rajakumar NSchaefer B Densmore M Drost DJ 2003 Glutamate and glutamine in theanterior cingulate and thalamus of medicated patients with chronic schizophreniaand healthy comparison subjects measured with 40-T proton MRS AmericanJournal of Psychiatry 160 2231ndash2233
Theberge J Al-Semaan Y Drost DJ Malla AK Neufeld RW Bartha R ManchandaR Menon R Densmore M Schaefer B Williamson PC 2004 Duration ofuntreated psychosis vs N-acetylaspartate and choline in first episode schizophre-nia a 1H magnetic resonance spectroscopy study at 40 Tesla Psychiatry Research131 107ndash114
Tranberg M Stridh MH Guy Y Jilderos B Wigstrom H Weber SG Sandberg M2004 NMDA-receptor mediated efflux of N-acetylaspartate physiological andorpathological importance Neurochemistry International 45 1195ndash1204
Tranberg M Abbas AK Sandberg M 2007 In vitro studies on the putative function ofN-acetylaspartate as an osmoregulator Neurochemical Research 32 1248ndash1255
Walton ME Croxson PL Behrens TE Kennerley SW Rushworth MF 2007Adaptive decision making and value in the anterior cingulate cortex Neuroimage36 (Suppl 2) T142ndashT154
Wechsler D 1987 Wechsler Memory ScalemdashRevised Psychological Corporation NewYork
Weinberger DR Aloia MS Goldberg TE Berman KF 1994 The frontal lobes andschizophrenia Journal of Neuropsychiatry and Clinical Neurosciences 6 419ndash427
Wood SJ Yucel M Wellard RM Harrison BJ Clarke K Fornito A Velakoulis DPantelis C 2007 Evidence for neuronal dysfunction in the anterior cingulate ofpatients with schizophrenia a proton magnetic resonance spectroscopy study at3T Schizophrenia Research 94 328ndash331
Yamasue H Fukui T Fukuda R Yamada H Yamasaki S Kuroki N Abe O Kasai KTsujii K Iwanami A Aoki S Ohtomo K Kato N Kato T 2002 1H-MRspectroscopy and gray matter volume of the anterior cingulate cortex inschizophrenia NeuroReport 13 2133ndash2137
Yeo RA Hill D Campbell R Vigil J Brooks WM 2000 Developmental instabilityand working memory ability in children a magnetic resonance spectroscopyinvestigation Developmental Neuropsychology 17 143ndash159
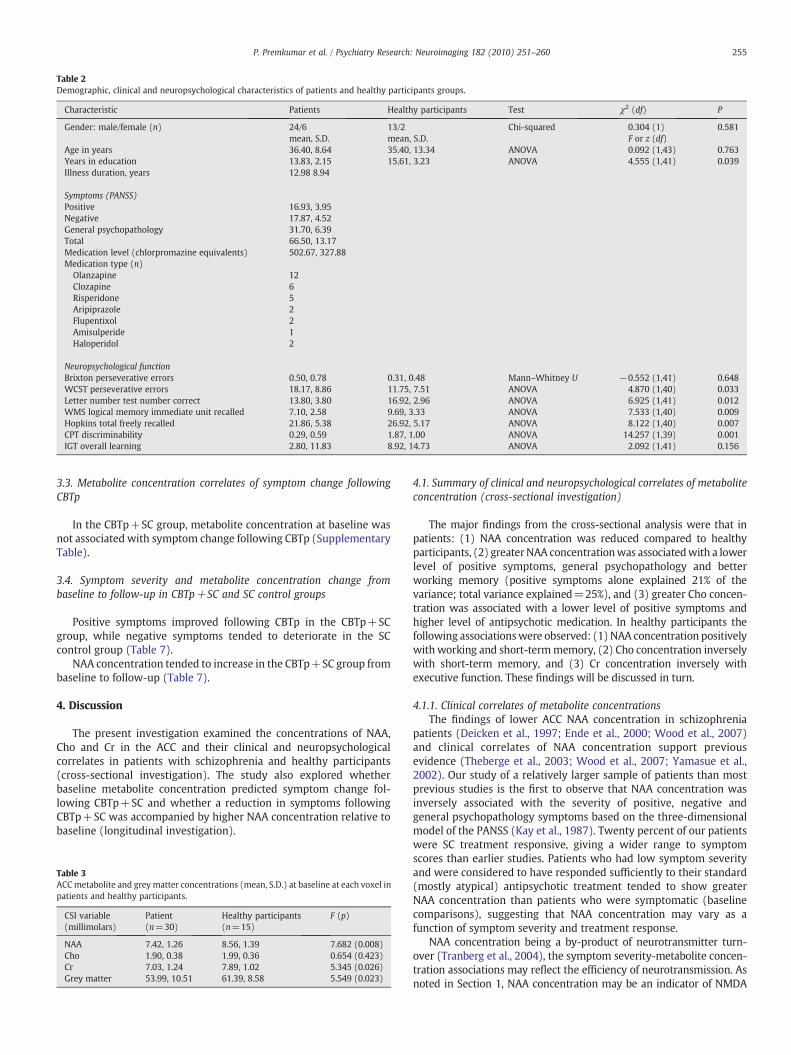
Table 2Demographic clinical and neuropsychological characteristics of patients and healthy participants groups
Characteristic Patients Healthy participants Test χ2 (df) P
Gender malefemale (n) 246 132 Chi-squared 0304 (1) 0581mean SD mean SD F or z (df)
Age in years 3640 864 3540 1334 ANOVA 0092 (143) 0763Years in education 1383 215 1561 323 ANOVA 4555 (141) 0039Illness duration years 1298 894
Symptoms (PANSS)Positive 1693 395Negative 1787 452General psychopathology 3170 639Total 6650 1317Medication level (chlorpromazine equivalents) 50267 32788Medication type (n)
Olanzapine 12Clozapine 6Risperidone 5Aripiprazole 2Flupentixol 2Amisulperide 1Haloperidol 2
Neuropsychological functionBrixton perseverative errors 050 078 031 048 MannndashWhitney U minus0552 (141) 0648WCST perseverative errors 1817 886 1175 751 ANOVA 4870 (140) 0033Letter number test number correct 1380 380 1692 296 ANOVA 6925 (141) 0012WMS logical memory immediate unit recalled 710 258 969 333 ANOVA 7533 (140) 0009Hopkins total freely recalled 2186 538 2692 517 ANOVA 8122 (140) 0007CPT discriminability 029 059 187 100 ANOVA 14257 (139) 0001IGT overall learning 280 1183 892 1473 ANOVA 2092 (141) 0156
255P Premkumar et al Psychiatry Research Neuroimaging 182 (2010) 251ndash260
33 Metabolite concentration correlates of symptom change followingCBTp
In the CBTp+SC group metabolite concentration at baseline wasnot associated with symptom change following CBTp (SupplementaryTable)
34 Symptom severity and metabolite concentration change frombaseline to follow-up in CBTp+SC and SC control groups
Positive symptoms improved following CBTp in the CBTp+SCgroup while negative symptoms tended to deteriorate in the SCcontrol group (Table 7)
NAA concentration tended to increase in the CBTp+SC group frombaseline to follow-up (Table 7)
4 Discussion
The present investigation examined the concentrations of NAACho and Cr in the ACC and their clinical and neuropsychologicalcorrelates in patients with schizophrenia and healthy participants(cross-sectional investigation) The study also explored whetherbaseline metabolite concentration predicted symptom change fol-lowing CBTp+SC and whether a reduction in symptoms followingCBTp+SC was accompanied by higher NAA concentration relative tobaseline (longitudinal investigation)
Table 3ACCmetabolite and greymatter concentrations (mean SD) at baseline at each voxel inpatients and healthy participants
CSI variable(millimolars)
Patient(n=30)
Healthy participants(n=15)
F (p)
NAA 742 126 856 139 7682 (0008)Cho 190 038 199 036 0654 (0423)Cr 703 124 789 102 5345 (0026)Grey matter 5399 1051 6139 858 5549 (0023)
41 Summary of clinical and neuropsychological correlates of metaboliteconcentration (cross-sectional investigation)
The major findings from the cross-sectional analysis were that inpatients (1) NAA concentration was reduced compared to healthyparticipants (2) greaterNAA concentrationwas associatedwith a lowerlevel of positive symptoms general psychopathology and betterworking memory (positive symptoms alone explained 21 of thevariance total variance explained=25) and (3) greater Cho concen-tration was associated with a lower level of positive symptoms andhigher level of antipsychotic medication In healthy participants thefollowing associationswere observed (1) NAA concentration positivelywith working and short-termmemory (2) Cho concentration inverselywith short-term memory and (3) Cr concentration inversely withexecutive function These findings will be discussed in turn
411 Clinical correlates of metabolite concentrationsThe findings of lower ACC NAA concentration in schizophrenia
patients (Deicken et al 1997 Ende et al 2000 Wood et al 2007)and clinical correlates of NAA concentration support previousevidence (Theberge et al 2003 Wood et al 2007 Yamasue et al2002) Our study of a relatively larger sample of patients than mostprevious studies is the first to observe that NAA concentration wasinversely associated with the severity of positive negative andgeneral psychopathology symptoms based on the three-dimensionalmodel of the PANSS (Kay et al 1987) Twenty percent of our patientswere SC treatment responsive giving a wider range to symptomscores than earlier studies Patients who had low symptom severityand were considered to have responded sufficiently to their standard(mostly atypical) antipsychotic treatment tended to show greaterNAA concentration than patients who were symptomatic (baselinecomparisons) suggesting that NAA concentration may vary as afunction of symptom severity and treatment response
NAA concentration being a by-product of neurotransmitter turn-over (Tranberg et al 2004) the symptom severity-metabolite concen-tration associations may reflect the efficiency of neurotransmission Asnoted in Section 1 NAA concentration may be an indicator of NMDA
Table 4Clinical correlates of metabolite concentration at baseline (patients only)
NAA concentration Cho concentration Cr concentration
r or ρ r (P) rp1 (P) r (P) rp
1 (P) r (P) rp1 (P)
Illness duration r minus0059 (0756) 0091 (0640) minus0064 (0735) 0045 (0817) minus0291 (0118) minus0244 (0203)Antipsychotic medication level Rho 0197 (0298) 0442 (0014) 0073 (0700)Symptoms (PANSS)
Positive (P) symptoms r minus0489 (0006) minus0430 (0020) minus0391 (0033) minus0325 (0085) minus0308 (0098) minus0262 (0170)Negative (N) symptoms r minus0297 (0111) minus0418 (0024) minus0287 (0124) minus0366 (0051) minus0211 (0264) minus0262 (0170)General psychopathology (GP) r minus0416 (0022) minus0506 (0005) minus0299 (0109) minus0341 (0070) minus0204 (0281) minus0219 (0254)Total r minus0450 (0013) minus0512 (0004) minus0361 (0050) minus0384 (0040) minus0263 (0160) minus0266 (0163)
Individual symptomsDelusions (P) Rho minus0411 (0024) minus0342 (0064) minus0192 (0309)Disorganisation (P) Rho minus0525 (0003) minus0369 (0045) minus0136 (0475)Persecution (P) Rho minus0390 (0033) minus0193 (0307) minus0068 (0719)Hostility (P) Rho 0062 (0745) 0370 (0044) 0163 (0390)Passive social withdrawal (N) Rho minus0370 (0044) minus0393 (0032) minus0261 (0163)Stereotyped thinking (N) Rho minus0422 (0020) minus0073 (0684) minus0221 (0240)Somatic concern (GP) Rho minus0419 (0021) minus0407 (0026) minus0129 (0496)Preoccupation (GP) Rho minus0528 (0003) minus0201 (0287) minus0264 (0156)
rp1 partial correlation controlling for GM concentration P PANSS positive symptom subscale N PANSS negative symptom subscale GP PANSS general psychopathology subscale
256 P Premkumar et al Psychiatry Research Neuroimaging 182 (2010) 251ndash260
function and neuronal longevity (Tranberg et al 2004) NAA efflux isa delayed response to sudden non-physiological decrease in extracel-lular osmolarity and high K+intra-cellular and NMDA activation(Tranberg et al 2007) Elevated concentration of NAA in the ACC inschizophrenia patients with lower level of symptoms may reflectincreased turnover of neurotransmitters such as dopamine and NMDA
Similarly the association between Cho concentration and total andpositive symptoms may also reflect improved neurotransmitterfunction and neuronal integrity with milder symptoms The Cho peakincludes solublemembranephospholipids includingphosphorylcholine(PCho) glycerophosphocholine (GPCho) and a relatively negligibleamount of free choline (Ross and Sachdev 2004) PCho is involved insynthesis of the insoluble membrane phospholipids while GPCho is aproduct of membrane degradation and free choline is involved insynthesis of the neurotransmitter acetylcholine aswell as inmembranesynthesis (Ross and Sachdev 2004) An increase in the Cho peak isassociated with an increase in membrane breakdown or turnover andmyelination (Ross and Sachdev 2004) The positive associationbetween antipsychotic medication dosage and Cho concentration ameasure of neuronalmembrane turnover (Miller 1991 Ohrmann et al2008) suggests that medication level also influences neuronal activity
412 Neuropsychological correlates of metabolite concentrationIn patients the finding of an association between greater NAA
concentration and better working memory supports evidence for the
Table 5Neuropsychological correlates of metabolite concentration at baseline in patients and healt
Neuropsychological function Group N r or rho NAA concentration
r or rho rp1 (P)
Brixton perseverative errors Patient 30 Rho 0180 (0341)Control 13 Rho 0356 (0232)
WCST perseverative errors Patient 30 r minus0097 (0610) minus013Control 12 r 0271 (0394) 024
Letterndashnumber test number correct Patient 30 r 0303 (0104) 037Control 13 r 0557 (0048) 052
WMS logical memory immediateunit recalled
Patient 29 r 0301 (0112) 033Control 13 r 0330 (0271) 027
Hopkins verbal learning test totalnumber freely recalled
Patient 29 r 0127 (0512) 011Control 13 r 0576 (0039) 055
CPT discriminability Patient 29 r minus0037 (0848) 015Control 12 r 0329 (0297) 027
IGT overall learning Patient 30 r 0179 (0343) 021Control 13 r 0042 (0892) 007
rp1 partial correlation controlling for GM concentration
role of frontal lobe function in working memory using functional MRIand proton MRS in schizophrenia (Bertolino et al 2000 Callicottet al 2000 Ohrmann et al 2007) although this association explainedonly a very small amount (3) of the variance in NAA concentrationthat was additional to that explained by positive symptoms
In the healthy group greater NAA concentration was associatedwith better working and short-term memory The ACC is activatedduring both working and short-term memory (Kim et al 2006Lenartowicz and McIntosh 2005) NAA concentration in the frontallobe white matter was positively associated with working memory inhealthy children which may be related to increased number ofdendritic processes at an early age (Yeo et al 2000) NAA con-centration has a role in neuronal integrity in the form of increasedmyelination and mitochondrial function (Ross and Sachdev 2004)and this may facilitate working and short-term memory
Greater Cho concentration correlated inversely with short-termmemory in the healthy group when controlling for GM concentrationin the ACC A negative association between Cho concentration in theoccipito-parietal white matter and IQ independent of the positiveassociation between NAA concentration and IQ in healthy individualshas been previously reported (Jung et al 1999) Our findings suggestindependentmetabolite concentration-neuropsychological associationsbetween NAA Cho and Cr in healthy individuals Greater Cr concentra-tionwas associatedwith poorer executive function in the present studyA study of elderly males found negative correlations between adjusted
hy participants
Cho concentration Cr concentration
r or rho rp1 (P) r or rho rp
1 (P)
minus0198 (0293) 0331 (0074)0356 (0232) 0579 (0038)
9 (0473) minus0011 (0956) minus0030 (0877) minus0102 (0592) minus0116 (0550)8 (0461) 0390 (0211) 0368 (0265) minus0225 (0483) 0312 (035)9 (0043) minus0163 (0388) minus0160 (0407) minus0130 (0493) minus0124 (0523)9 (0077) 0011 (0971) minus0083 (0797) 0156 (0611) minus0030 (0927)1 (0085) 0054 (0781) 0045 (0822) minus0017 (0932) minus0025 (0898)8 (0382) minus0453 (0120) minus0610 (0035) minus0022 (0946) minus0267 (0401)9 (0564) 0181 (0348) 0177 (0369) 0269 (0159) 0265 (0173)5 (0061) minus0173 (0572) minus0330 (0295) 0277 (036) 0061 (0851)8 (0423) minus0114 (0555) 0016 (0936) 0003 (0986) 0088 (0656)5 (0413) minus0209 (0514) minus0346 (0297) 0207 (0519) 0006 (0986)0 (0273) 0026 (0891) 0029 (0879) 0062 (0747) 0064 (0742)8 (0811) minus0063 (0839) minus0025 (0939) minus0225 (0461) minus0169 (0600)
Table 6Demographic clinical and metabolite concentration characteristics at baseline of CBTp+SC (n=11) SC control (n=13) and SC responsive (n=6) patients
Characteristic CBTp+SC SC control SC responsive χ2 P
Gender malefemale (n) 65 121 60 7185 0028mean SD mean SD
Age in years 3464 862 3746 877 3733 942 0745 0689Years in education 1445 246 1346 176 1377 24 1156 0561Illness duration years 1194 860 1377 970 1317 928 0303 0860Symptoms (PANSS)
Positive 1745 295 1915 264 1117 172 14644 0001Negative 1818 498 1923 386 1433 361 5779 0056General psychopathology 3227 675 340 549 2567 383 6775 0034Total 6791 1287 7239 994 5117 778 9512 0009Medication level 56442 30317 50055 39478 39405 20759 1787 0409
Metabolite concentrationNAA 765 092 685 143 823 091 5313 0070Cho 192 060 186 024 194 018 0493 0781Cr 689 140 687 095 748 160 1047 0592Grey matter 5766 1071 5117 1136 5337 714 1096 0578
257P Premkumar et al Psychiatry Research Neuroimaging 182 (2010) 251ndash260
Cr in the parietal lobe and various cognitive measures including logicalmemory and verbal memory (Ferguson et al 2002) The study did notinclude ameasure of executive function Ferguson et al (2002) believedthat the findings fit with evidence that higher Cr levels are associatedwith cognitive ageing They proposed that poorer neuropsychologicalperformance in healthy ageing is associated with an increase inPhosphocreatine (PCr) due to a reduction in conversion of PCr toAdenosine-tri-phosphate (ATP) for energy Increased Cr concentrationmay be a marker of decreased brain energy metabolism
42 Effect of cognitive behaviour therapy for psychosis on metaboliteconcentration
Our preliminary investigation of change in metabolite concentra-tion in a small number of patients who received CBTp+SC comparedto patients who received SC only revealed a trend for an increase inNAA concentration with CBTp This increase in NAA was concomitantwith improvement in positive symptoms in CBTp+SC patients Thisfinding is consistent with the view that NAA concentration increaseswith alleviation of symptoms as discussed above Recent functionalimaging studies also provide evidence for a role of the ACC inresponsiveness to CBT in psychosis (Kumari et al 2009) as well asmajor depression (Costafreda et al 2009)
43 Limitations and future research
One of the limitations of the study was that the sample sizes ofpatients who received CBTp+SC or SC only and were clinicallyassessed andor scanned at follow-up were small A further limitationwas that gender distribution differed between the patient groupsAlthough there was no gender effect within each patient group in the
Table 7Symptoms metabolite and grey matter concentration (mean SD) at baseline and follow-u
CSI variable Baseline CBTp+SC (n=7) z (P)
FOLLOW-UP
Clinical symptomsPositive symptoms 1814 (234) 1567 (350) minus20Negative symptoms 1857 (571) 1567 (234) minus08General psychopathology 3200 (566) 2733 (497) minus13Total symptoms 6871 (1227) 5867 (1017) minus14
Metabolite concentrationNAA 765 (068) 831 (077) minus18Cho 185 (042) 193 (02) minus05Cr 679 (089) 725 (103) minus08Grey matter 5706 (1155) 5860 (851) minus03
metabolite concentrations in the present study higher ACC glutaminelevel in male compared to female schizophrenia patients has beenpreviously observed (Tayoshi et al 2009) Other effects of gender onACC function have also been reported for example reduced ACCglucose metabolism in male chronic patients relative to healthyparticipants and female patients (Fujimoto et al 2007) Thepredictive value of NAA concentration on symptom change in patientsreceiving psychological treatment or standard care needs to beexamined in a larger sample involving a sufficient number of bothmen and women with schizophrenia Additionally the role of clinicaland neuropsychological variables on ACC NAA levels in patients whoimprove with CBTp needs to be explored
44 Conclusions
Higher NAA and Cho concentrations in the ACC in patients areassociated with lower symptom severity Stronger and moreconsistent associations between metabolite concentrations andsymptom severity than neuropsychological function suggest thatmetabolite concentration and symptoms may co-fluctuate morestrongly Neuropsychological deficits may be more stable (Szokeet al 2008) and not necessarily improve in parallel with symptomimprovement (Hughes et al 2003) NAA concentration may yetreflect symptom changes following CBTp and if replicated in futurestudies has the potential to provide a useful biological marker ofclinical response to psychological treatments
Acknowledgement
The study was supported by funds from the Wellcome Trust UK(067427z02z)
p in CBTp+SC and SC control groups
Baseline SC control (n=4) z (P)
FOLLOW-UP
32 (0042) 1925 (222) 1825 (263) minus0365 (0715)13 (0416) 1875 (499) 2200 (616) minus1841 (0066)82 (0167) 3500 (668) 3275 (591) minus0535 (0593)72 (0141) 7300 (1042) 7300 (1364) minus0001 (1000)
59 (0063) 740 (069) 704 (038) minus1826 (0068)07 (0612) 190 (018) 201 (008) minus0730 (0465)45 (0398) 702 (016) 736 (099) minus0730 (0465)38 (0735) 5353 (549) 5324 (335) minus0365 (0715)
Appendix A Summary of magnetic resonance spectroscopy studies on the anterior cingulate cortex (ACC) in schizophrenia patients
Publication Participants Measures Results
Deicken et al (1997) Schizophrenia patients(n=26 9 on atypical and 17 on typical)Healthy participants (n=16)
NAA Cho and Cr illness durationantipsychotic medication dose
Patients had lower NAA concentrationcompared to healthy participants Nosignificant group differences or lateralizedasymmetries for Cho or Cr No significantcorrelations between NAA and eitherillness duration or antipsychoticmedication dose
Ende et al (2000) Schizophrenia patients(n=19 10 on atypical and 9 on typical)Healthy participants (n=16)
NAA Cho and Cr age illnessduration
Patients had lower NAA concentrationcompared to healthy participantsPatients receiving typical medication(but not atypical) had lower NAAconcentration than healthy participantsNAA concentration was inverselycorrelated with age in patients andhealthy participants and with illnessduration (corrected for age) in patients
Braus et al (2001 2002) Schizophrenia patients(11 on atypical and 10 on typical)
NAA Cho and Cr illness durationduration on atypical antipsychoticmedication WCST
Patients receiving typical antipsychoticshad lower NAA concentration than patientsreceiving atypical antipsychoticsNAA concentration was inverselycorrelated with illness duration andpositively with duration on atypicalantipsychotic medication NAAconcentration was inversely correlatedwith WCST perseverative errors
Goff et al (2002) Schizophrenia patients (n=17of whom 10 switched fromconventional to olanzapine andhad MRS at baseline and 8-week follow-up)
GluCr ratio SANS GluCr ratio was increased by 125(non-significant) following switch toolanzapine Patients who improvedon SANS symptoms had greaterGluCr ratio (458) compared topatients who deteriorated on SANSsymptoms (208) No significantcorrelation between SANS total andchange in GluCr ratio after switch
Yamasue et al (2002) Schizophrenia patients(n=15 all on typical)Healthy participants (n=13)
NAA Cho and Cr grey mattervolume age height body weightsocio-economic status parentalsocio-economic status years ofeducation PANSS onset of illnessillness duration antipsychoticmedication dose
Patients had lower NAACho ratio andgreater ChoCr ratio compared to healthyparticipants after controlling for greymatter volume NAACho ratio waspositively correlated with grey mattervolume in patients not healthy participantsNAACho ratio was inversely correlatedwith PANSS blunted affect score
Theberge et al (2004 2002) First-episode neuroleptic naiumlveschizophrenia patients (n=21)Healthy participants (n=21)
Analysis in Theberge et al 2002NAA Cho Cr Glu Gln mI in leftACC SANS SAPS
From Theberge et al 2002Patients had greater Gln concentrationcompared to healthy participantsMetabolite concentrations were notcorrelated with SANS or SAPS
Analysis in Theberge et al 2004NAA and Cho in left ACC DUPDUI DPS
From Theberge et al 2004NAA concentration was positively correlatedwith DUP and inversely with DPS at trendlevel Cho concentration was positivelycorrelated with DUP
Theberge et al (2003) Schizophrenia patients (n=21atypical n=7 both n=1typical n=13)Healthy participants (n=21)
NAA Cho Cr Glu Gln mI inleft ACC duration of illness
Glu and Gln concentrations were greaterin patients than healthy participants NAAconcentration was inversely correlatedwith duration of positive symptoms
Wood et al (2007) Schizophrenia male patients(n=15 13 atypical 2 medication free)Healthy male participants (n=14)
NAA and Glx in dorsal and rostralregions PANSS five factors illnessduration
Patients had lower NAA concentrationcompared to healthy participantsRight dorsal Glx was inversely correlatedwith illness duration
Ohrmann et al (2008) Schizophrenia patients(n=43 all on atypical)Healthy participants (n=37)
NAA Cho Cr Glx WCST learningpotential
No difference in metabolite concentrationbetween patients and healthy participantsNAA and Glx concentrations were positivelyassociated with WCST learning potential
Sanches et al (2008) Schizophrenia patients (n=37)Healthy participants (n=37)
NAA(Cho+Cr) ratio in left andright anterior middle frontal gyrusACC and perirolandic area (reference)basal skin conductance and skinconductance response to auditorystimuli of 1 s tones of 80 dB Patientsand healthy participants classified intoskin conductance responders (2 SDbelow mean skin conductance in healthyparticipants) and non-responders
NAA(Cho+Cr) ratio was lower in patientsthan healthy participants in the anteriormiddle frontal gyrus and ACC bilaterallyNAA(Cho+Cr) ratio did not differ betweenskin conductance response groups based onskin conductance response to auditory stimuliBasal skin conductance non-responders patientshad lower NAA(Cho+Cr) ratio than healthyparticipants in left and right ACC
258 P Premkumar et al Psychiatry Research Neuroimaging 182 (2010) 251ndash260
Tayoshi et al (2009) Long-term schizophrenia (n=30antipsychotic medication typenot reported)Healthy participants (n=25)
NAA Cho Cr Glu Gln mI Gender PANSStotal and subscales duration of illnessduration of therapy antipsychotic dosagebenzodiazepine dose
Patients had lower Glu and mI concentrationcompared to healthy participants Malepatients had lower NAA Cr Glu and mIconcentration than male healthy participantsMales had greater Gln concentration comparedto females Metabolite concentration wasnot correlated with symptoms or otherclinical variables
Ongur et al (2009) Schizophrenia patients (n=15)Bipolar disorder patients (n=15)Healthy participants (n=22)
Cr in ACC (hypothesized area) andparietal-occipital cortex (reference area)MADRS PANSS YMRS
Patients had lower Cr than healthyparticipants in both ACC andparietal-occipital cortex No significantcorrelations between Cr concentrationand clinical measures
ACC anterior cingulate cortex ChomdashCholine CrmdashCreatinePhosphocreatine DPSmdashduration of psychotic symptoms DUImdashduration of untreated illness DUPmdashduration of untreatedpsychosis GlnmdashGlutamine GlumdashGlutamate GluCr ratio SANSmdashSchedule for the Assessment of Negative Symptoms GlxmdashGlutamate+Glutamine MADRSmdashMontgomery AsbergDepression Rating Scale mImdashmyo-Inositol NAA N-acetyl aspartate PANSSmdashPositive and Negative Syndrome Scale SAPS Schedule for the Assessment of Positive SymptomsWCSTmdashWisconsin Card Sorting test YMRSmdashYoung Mania Rating Scale
Appendix A (continued)
259P Premkumar et al Psychiatry Research Neuroimaging 182 (2010) 251ndash260
Appendix B Supplementary Data
Supplementary data associated with this article can be found inthe online version at doi101016jpscychresns201002008
References
Adler CM Malhotra AK Elman I Goldberg T Egan M Pickar D Breier A 1999Comparison of ketamine-induced thought disorder in healthy volunteers andthought disorder in schizophrenia American Journal of Psychiatry 156 1646ndash1649
Andres RH Ducray AD Schlattner U Wallimann T Widmer HR 2008 Functionsand effects of creatine in the central nervous system Brain Research Bulletin 76329ndash343
Baiano M David A Versace A Churchill R Balestrieri M Brambilla P 2007Anterior cingulate volumes in schizophrenia a systematic review and a meta-analysis of MRI studies Schizophrenia Research 93 1ndash12
Bechara A Damasio AR Damasio H Anderson SW 1994 Insensitivity to futureconsequences following damage to human prefrontal cortex Cognition 50 7ndash15
Behrens TE Woolrich MW Walton ME Rushworth MF 2007 Learning the valueof information in an uncertain world Nature Neuroscience 10 1214ndash1221
Bertolino A Esposito G Callicott JH Mattay VS Van Horn JD Frank JA BermanKF Weinberger DR 2000 Specific relationship between prefrontal neuronal N-acetylaspartate and activation of the working memory cortical network inschizophrenia American Journal of Psychiatry 157 26ndash33
Braus DF Ende G Weber-Fahr W Demirakca T Henn FA 2001 Favorable effecton neuronal viability in the anterior cingulate gyrus due to long-term treatmentwith atypical antipsychotics an MRSI study Pharmacopsychiatry 34 251ndash253
Braus DF Ende G Weber-Fahr W Demirakca T Tost H Henn FA 2002Functioning and neuronal viability of the anterior cingulate neurons followingantipsychotic treatment MR-spectroscopic imaging in chronic schizophreniaEuropean Neuropsychopharmacology 12 145ndash152
Burgess PW Shallice T 1997 The Hayling and Brixton Tests Thames Valley TestCompany Bury St Edmunds
Callicott JH Bertolino A Mattay VS Langheim FJ Duyn J Coppola R Goldberg TEWeinberger DR 2000 Physiological dysfunction of the dorsolateral prefrontal cortexin schizophrenia revisited Cerebral Cortex 10 1078ndash1092
Carter CS van Veen V 2007 Anterior cingulate cortex and conflict detection anupdate of theory and data Cognitive Affective and Behavioral Neuroscience 7367ndash379
Cornblatt BA Risch JJ Faris G Friedman D Erlenmeyer-Kimling L 1988 TheContinuous Performance Test Identical Pairs Version (CPT-IP) I New findingsabout sustained attention in normal families Psychiatry Research 26 223ndash238
Costafreda SG Khanna A Mourao-Miranda J Fu CH 2009 Neural correlates of sadfaces predict clinical remission to cognitive behavioural therapy in depressionNeuroReport 20 637ndash641
Deicken RF Zhou L Schuff N Weiner MW 1997 Proton magnetic resonancespectroscopy of the anterior cingulate region in schizophrenia SchizophreniaResearch 27 65ndash71
Deicken RF Johnson C Pegues M 2000 Proton magnetic resonance spectroscopy ofthe human brain in schizophrenia Reviews in the Neurosciences 11 147ndash158
Ende G Braus DF Walter S Weber-Fahr W Soher B Maudsley AA Henn FA2000 Effects of age medication and illness duration on the N-acetyl aspartatesignal of the anterior cingulate region in schizophrenia Schizophrenia Research 41389ndash395
Fannon D Simmons A Tennakoon L OCeallaigh S Sumich A Doku V Shew CSharma T 2003 Selective deficit of hippocampal N-acetylaspartate in antipsy-chotic-naive patients with schizophrenia Biological Psychiatry 54 587ndash598
Ferguson KJ MacLullich AM Marshall I Deary IJ Starr JM Seckl JR Wardlaw JM2002 Magnetic resonance spectroscopy and cognitive function in healthy elderlymen Brain 125 2743ndash2749
First MB Spitzer RL Gibbon M Williams JBW 2002 Structured Clinical Interviewfor DSM-IV-TR Axis I DisordersmdashPatient Edition (SCID-IP 112002 revision)Biometrics Research Department New York NY
Fornito A Yucel M Dean B Wood SJ Pantelis C 2008 Anatomical abnormalities ofthe anterior cingulate cortex in schizophrenia bridging the gap betweenneuroimaging and neuropathology Schizophrenia Bulletin 35 973ndash993
Fowler D Garety PA Kuipers E 1995 Cognitive Behaviour Therapy for PsychosisTheory and Practice Wiley Chichester
Fujimoto T Takeuch K Matsumoto T Kamimura K Hamada R Nakamura K KatoN 2007 Abnormal glucose metabolism in the anterior cingulate cortex in patientswith schizophrenia Psychiatry Research 154 49ndash58
Goff DC Hennen J Lyoo IK Tsai G Wald LL Evins AE Yurgelun-Todd DARenshaw PF 2002 Modulation of brain and serum glutamatergic concentrationsfollowing a switch from conventional neuroleptics to olanzapine BiologicalPsychiatry 51 493ndash497
Gold JM Carpenter C Randolph C Goldberg TE Weinberger DR 1997 Auditoryworking memory and Wisconsin Card Sorting Test performance in schizophreniaArchives of General Psychiatry 54 159ndash165
Heaton RK Chelune GJ Tally JL Kay GG Curtiss G 1993 Wisconsin Card SortingTest Manual Revised and Expanded Psychological Assessment Resources OdessaFL
Honea R Crow TJ Passingham D Mackay CE 2005 Regional deficits in brainvolume in schizophrenia a meta-analysis of voxel-based morphometry studiesAmerican Journal of Psychiatry 162 2233ndash2245
Hughes C Kumari V Soni W Das M Binneman B Drozd S ONeil S Mathew VSharma T 2003 Longitudinal study of symptoms and cognitive function in chronicschizophrenia Schizophrenia Research 59 137ndash146
Jung RE Brooks WM Yeo RA Chiulli SJ Weers DC Sibbitt Jr WL 1999Biochemical markers of intelligence a proton MR spectroscopy study of normalhuman brain Proceedings Biological Sciences 266 1375ndash1379
Kaneda M Osaka N 2008 Role of anterior cingulate cortex during semantic coding inverbal working memory Neuroscience Letters 436 57ndash61
Kay SR Fiszbein A Opier LA 1987 The Positive and Negative Syndrome Scale(PANSS) for schizophrenia Schizophrenia Bulletin 13 261ndash276
Kennerley SW Dahmubed AF Lara AH Wallis JD 2008 Neurons in the frontallobe encode the value of multiple decision variables Journal of CognitiveNeuroscience 21 1162ndash1178
Kim J Whyte J Wang J Rao H Tang KZ Detre JA 2006 Continuous ASL perfusionfMRI investigation of higher cognition quantification of tonic CBF changes duringsustained attention and working memory tasks Neuroimage 31 376ndash385
Krystal JH Karper LP Seibyl JP Freeman GK Delaney R Bremner JD HeningerGR Bowers Jr MB Charney DS 1994 Subanesthetic effects of the noncom-petitive NMDA antagonist ketamine in humans Psychotomimetic perceptualcognitive and neuroendocrine responses Archives of General Psychiatry 51199ndash214
Kumari V Peters ER Fannon D Antonova E Premkumar P Anilkumar APWilliams SC Kuipers EA 2009 Dorsolateral prefrontal cortex activity predictsresponsiveness to cognitive behaviour therapy in schizophrenia BiologicalPsychiatry 66 594ndash602
Lahti AC Koffel B LaPorte D Tamminga CA 1995 Subanesthetic doses of ketaminestimulate psychosis in schizophrenia Neuropsychopharmacology 13 9ndash19
Lenartowicz A McIntosh AR 2005 The role of anterior cingulate cortex in workingmemory is shaped by functional connectivity Journal of Cognitive Neuroscience 171026ndash1042
Malhotra AK Pinals DA Adler CM Elman I Clifton A Pickar D Breier A 1997Ketamine-induced exacerbation of psychotic symptoms and cognitive impairmentin neuroleptic-free schizophrenics Neuropsychopharmacology 17 141ndash150
260 P Premkumar et al Psychiatry Research Neuroimaging 182 (2010) 251ndash260
McLean MA Woermann FG Barker GJ Duncan JS 2000 Quantitative analysis ofshort echo time (1)H-MRSI of cerebral gray and white matter Magnetic Resonancein Medicine 44 401ndash411
McMorris T Harris RC Swain J Corbett J Collard K Dyson RJ Dye L Hodgson CDraper N 2006 Effect of creatine supplementation and sleep deprivation withmild exercise on cognitive and psychomotor performance mood state and plasmaconcentrations of catecholamines and cortisol Psychopharmacology (Berl) 18593ndash103
McMorris T Harris RC Howard AN Langridge G Hall B Corbett J Dicks MHodgson C 2007 Creatine supplementation sleep deprivation cortisol melatoninand behavior Physiology and Behaviour 90 21ndash28
Miller BL 1991 A review of chemical issues in 1H NMR spectroscopy N-acetyl-L-aspartate creatine and choline NMR in Biomedicine 4 47ndash52
Moghaddam B 2003 Bringing order to the glutamate chaos in schizophrenia Neuron40 881ndash884
Ohrmann P Siegmund A Suslow T Pedersen A Spitzberg K Kersting ARothermundt M Arolt V Heindel W Pfleiderer B 2007 Cognitive impairmentand in vivo metabolites in first-episode neuroleptic-naive and chronic medicatedschizophrenic patients a proton magnetic resonance spectroscopy study Journalof Psychiatric Research 41 625ndash634
Ohrmann P Kugel H Bauer J Siegmund A Kolkebeck K Suslow T Wiedl KHRothermundt M Arolt V Pedersen A 2008 Learning potential on the WCST inschizophrenia is related to the neuronal integrity of the anterior cingulate cortex asmeasured by proton magnetic resonance spectroscopy Schizophrenia Research106 156ndash163
Ongur D Prescot AP Jensen JE Cohen BM Renshaw PF 2009 Creatineabnormalities in schizophrenia and bipolar disorder Psychiatry ResearchNeuroimaging 172 44ndash48
Osaka N Osaka M Kondo H Morishita M Fukuyama H Shibasaki H 2004 Theneural basis of executive function in working memory an fMRI study based onindividual differences Neuroimage 21 623ndash631
Perry G Nunomura A Hirai K Zhu X Perez M Avila J Castellani RJ Atwood CSAliev G Sayre LM Takeda A Smith MA 2002 Is oxidative damage thefundamental pathogenic mechanism of Alzheimers and other neurodegenerativediseases Free Radical Biology and Medicine 33 1475ndash1479
Peterson BS Skudlarski P Gatenby JC Zhang H Anderson AW Gore JC 1999 AnfMRI study of Stroop word-color interference evidence for cingulate subregionssubserving multiple distributed attentional systems Biological Psychiatry 451237ndash1258
Provencher SW 1993 Estimation of metabolite concentrations from localized in vivoproton NMR spectra Magnetic Resonance in Medicine 30 672ndash679
Rae C Digney AL McEwan SR Bates TC 2003 Oral creatine monohydratesupplementation improves brain performance a double-blind placebo-controlledcross-over trial Proceedings Biological Sciences 270 2147ndash2150
Ross AJ Sachdev PS 2004 Magnetic resonance spectroscopy in cognitive researchBrain Research Brain Research Reviews 44 83ndash102
Rushworth MF Walton ME Kennerley SW Bannerman DM 2004 Action sets anddecisions in the medial frontal cortex Trends in Cogntive Sciences 8 410ndash417
Rutten BP Korr H Steinbusch HW Schmitz C 2003 The aging brain less neuronscould be better Mechanisms of Ageing and Development 124 349ndash355
Sanches RF Crippa JA Hallak JE de Sousa JP Araujo D Santos AC Zuardi AW2008 Proton magnetic resonance spectroscopy of the frontal cingulate andperirolandic cortices and its relationship to skin conductance in patients withschizophrenia Brazilian Journal of Medical and Biological Research 41 1132ndash1141
Schlosser RG Koch K Wagner G Nenadic I Roebel M Schachtzabel C Axer MSchultz C Reichenbach JR Sauer H 2008 Inefficient executive cognitive controlin schizophrenia is preceded by altered functional activation during informationencoding an fMRI study Neuropsychologia 46 336ndash347
Shapiro AM Benedict RH Schretlen D Brandt J 1999 Construct and concurrentvalidity of the Hopkins Verbal Learning Test-revised The Clinical Neuropsychol-ogist 13 348ndash358
Smith EE Jonides J 1999 Storage and executive processes in the frontal lobesScience 283 1657ndash1661
Szoke A Trandafir A Dupont ME Meary A Schurhoff F Leboyer M 2008Longitudinal studies of cognition in schizophrenia meta-analysis British Journal ofPsychiatry 192 248ndash257
Tayoshi S Sumitani S Taniguchi K Shibuya-Tayoshi S Numata S Iga JI NakatakiM Ueno SI Harada M Ohmori T 2009 Metabolite changes and genderdifferences in schizophrenia using 3-Tesla proton magnetic resonance spectrosco-py ((1)H-MRS) Schizophrenia Research 108 69ndash77
Theberge J Bartha R Drost DJ Menon RS Malla A Takhar J Neufeld RWRogers J Pavlosky W Schaefer B Densmore M Al-Semaan Y Williamson PC2002 Glutamate and glutamine measured with 40T proton MRS in never-treatedpatients with schizophrenia and healthy volunteers American Journal of Psychiatry159 1944ndash1946
Theberge J Al-Semaan Y Williamson PC Menon RS Neufeld RW Rajakumar NSchaefer B Densmore M Drost DJ 2003 Glutamate and glutamine in theanterior cingulate and thalamus of medicated patients with chronic schizophreniaand healthy comparison subjects measured with 40-T proton MRS AmericanJournal of Psychiatry 160 2231ndash2233
Theberge J Al-Semaan Y Drost DJ Malla AK Neufeld RW Bartha R ManchandaR Menon R Densmore M Schaefer B Williamson PC 2004 Duration ofuntreated psychosis vs N-acetylaspartate and choline in first episode schizophre-nia a 1H magnetic resonance spectroscopy study at 40 Tesla Psychiatry Research131 107ndash114
Tranberg M Stridh MH Guy Y Jilderos B Wigstrom H Weber SG Sandberg M2004 NMDA-receptor mediated efflux of N-acetylaspartate physiological andorpathological importance Neurochemistry International 45 1195ndash1204
Tranberg M Abbas AK Sandberg M 2007 In vitro studies on the putative function ofN-acetylaspartate as an osmoregulator Neurochemical Research 32 1248ndash1255
Walton ME Croxson PL Behrens TE Kennerley SW Rushworth MF 2007Adaptive decision making and value in the anterior cingulate cortex Neuroimage36 (Suppl 2) T142ndashT154
Wechsler D 1987 Wechsler Memory ScalemdashRevised Psychological Corporation NewYork
Weinberger DR Aloia MS Goldberg TE Berman KF 1994 The frontal lobes andschizophrenia Journal of Neuropsychiatry and Clinical Neurosciences 6 419ndash427
Wood SJ Yucel M Wellard RM Harrison BJ Clarke K Fornito A Velakoulis DPantelis C 2007 Evidence for neuronal dysfunction in the anterior cingulate ofpatients with schizophrenia a proton magnetic resonance spectroscopy study at3T Schizophrenia Research 94 328ndash331
Yamasue H Fukui T Fukuda R Yamada H Yamasaki S Kuroki N Abe O Kasai KTsujii K Iwanami A Aoki S Ohtomo K Kato N Kato T 2002 1H-MRspectroscopy and gray matter volume of the anterior cingulate cortex inschizophrenia NeuroReport 13 2133ndash2137
Yeo RA Hill D Campbell R Vigil J Brooks WM 2000 Developmental instabilityand working memory ability in children a magnetic resonance spectroscopyinvestigation Developmental Neuropsychology 17 143ndash159
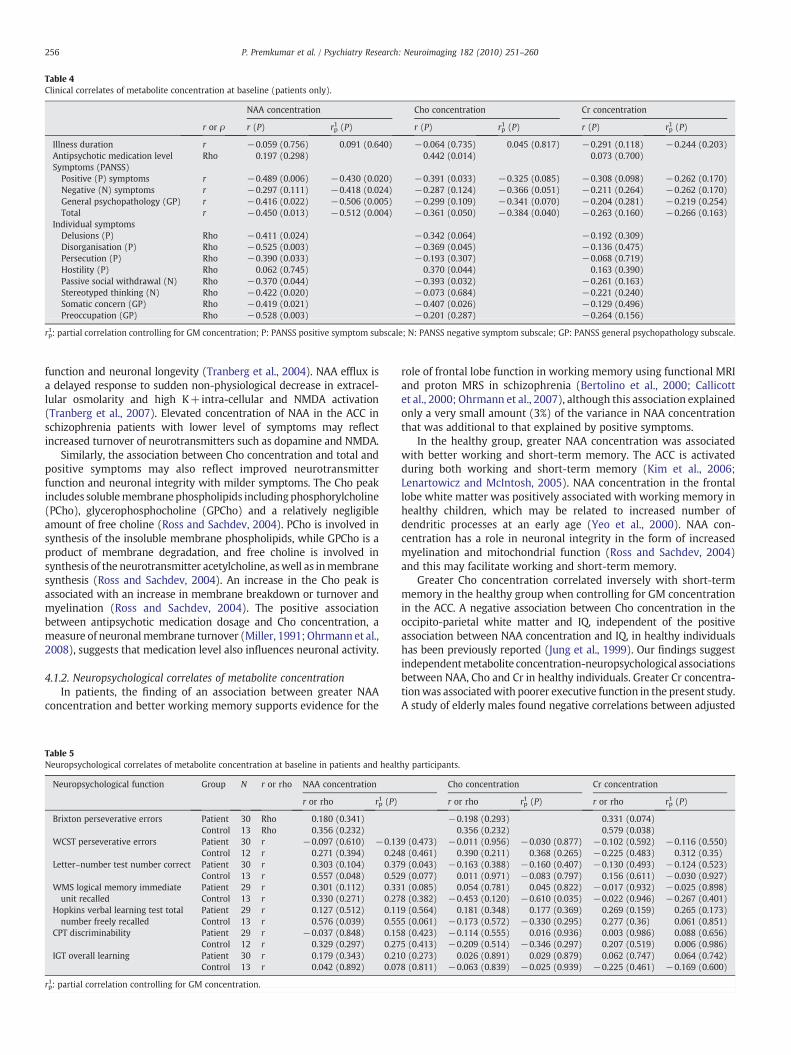
Table 4Clinical correlates of metabolite concentration at baseline (patients only)
NAA concentration Cho concentration Cr concentration
r or ρ r (P) rp1 (P) r (P) rp
1 (P) r (P) rp1 (P)
Illness duration r minus0059 (0756) 0091 (0640) minus0064 (0735) 0045 (0817) minus0291 (0118) minus0244 (0203)Antipsychotic medication level Rho 0197 (0298) 0442 (0014) 0073 (0700)Symptoms (PANSS)
Positive (P) symptoms r minus0489 (0006) minus0430 (0020) minus0391 (0033) minus0325 (0085) minus0308 (0098) minus0262 (0170)Negative (N) symptoms r minus0297 (0111) minus0418 (0024) minus0287 (0124) minus0366 (0051) minus0211 (0264) minus0262 (0170)General psychopathology (GP) r minus0416 (0022) minus0506 (0005) minus0299 (0109) minus0341 (0070) minus0204 (0281) minus0219 (0254)Total r minus0450 (0013) minus0512 (0004) minus0361 (0050) minus0384 (0040) minus0263 (0160) minus0266 (0163)
Individual symptomsDelusions (P) Rho minus0411 (0024) minus0342 (0064) minus0192 (0309)Disorganisation (P) Rho minus0525 (0003) minus0369 (0045) minus0136 (0475)Persecution (P) Rho minus0390 (0033) minus0193 (0307) minus0068 (0719)Hostility (P) Rho 0062 (0745) 0370 (0044) 0163 (0390)Passive social withdrawal (N) Rho minus0370 (0044) minus0393 (0032) minus0261 (0163)Stereotyped thinking (N) Rho minus0422 (0020) minus0073 (0684) minus0221 (0240)Somatic concern (GP) Rho minus0419 (0021) minus0407 (0026) minus0129 (0496)Preoccupation (GP) Rho minus0528 (0003) minus0201 (0287) minus0264 (0156)
rp1 partial correlation controlling for GM concentration P PANSS positive symptom subscale N PANSS negative symptom subscale GP PANSS general psychopathology subscale
256 P Premkumar et al Psychiatry Research Neuroimaging 182 (2010) 251ndash260
function and neuronal longevity (Tranberg et al 2004) NAA efflux isa delayed response to sudden non-physiological decrease in extracel-lular osmolarity and high K+intra-cellular and NMDA activation(Tranberg et al 2007) Elevated concentration of NAA in the ACC inschizophrenia patients with lower level of symptoms may reflectincreased turnover of neurotransmitters such as dopamine and NMDA
Similarly the association between Cho concentration and total andpositive symptoms may also reflect improved neurotransmitterfunction and neuronal integrity with milder symptoms The Cho peakincludes solublemembranephospholipids includingphosphorylcholine(PCho) glycerophosphocholine (GPCho) and a relatively negligibleamount of free choline (Ross and Sachdev 2004) PCho is involved insynthesis of the insoluble membrane phospholipids while GPCho is aproduct of membrane degradation and free choline is involved insynthesis of the neurotransmitter acetylcholine aswell as inmembranesynthesis (Ross and Sachdev 2004) An increase in the Cho peak isassociated with an increase in membrane breakdown or turnover andmyelination (Ross and Sachdev 2004) The positive associationbetween antipsychotic medication dosage and Cho concentration ameasure of neuronalmembrane turnover (Miller 1991 Ohrmann et al2008) suggests that medication level also influences neuronal activity
412 Neuropsychological correlates of metabolite concentrationIn patients the finding of an association between greater NAA
concentration and better working memory supports evidence for the
Table 5Neuropsychological correlates of metabolite concentration at baseline in patients and healt
Neuropsychological function Group N r or rho NAA concentration
r or rho rp1 (P)
Brixton perseverative errors Patient 30 Rho 0180 (0341)Control 13 Rho 0356 (0232)
WCST perseverative errors Patient 30 r minus0097 (0610) minus013Control 12 r 0271 (0394) 024
Letterndashnumber test number correct Patient 30 r 0303 (0104) 037Control 13 r 0557 (0048) 052
WMS logical memory immediateunit recalled
Patient 29 r 0301 (0112) 033Control 13 r 0330 (0271) 027
Hopkins verbal learning test totalnumber freely recalled
Patient 29 r 0127 (0512) 011Control 13 r 0576 (0039) 055
CPT discriminability Patient 29 r minus0037 (0848) 015Control 12 r 0329 (0297) 027
IGT overall learning Patient 30 r 0179 (0343) 021Control 13 r 0042 (0892) 007
rp1 partial correlation controlling for GM concentration
role of frontal lobe function in working memory using functional MRIand proton MRS in schizophrenia (Bertolino et al 2000 Callicottet al 2000 Ohrmann et al 2007) although this association explainedonly a very small amount (3) of the variance in NAA concentrationthat was additional to that explained by positive symptoms
In the healthy group greater NAA concentration was associatedwith better working and short-term memory The ACC is activatedduring both working and short-term memory (Kim et al 2006Lenartowicz and McIntosh 2005) NAA concentration in the frontallobe white matter was positively associated with working memory inhealthy children which may be related to increased number ofdendritic processes at an early age (Yeo et al 2000) NAA con-centration has a role in neuronal integrity in the form of increasedmyelination and mitochondrial function (Ross and Sachdev 2004)and this may facilitate working and short-term memory
Greater Cho concentration correlated inversely with short-termmemory in the healthy group when controlling for GM concentrationin the ACC A negative association between Cho concentration in theoccipito-parietal white matter and IQ independent of the positiveassociation between NAA concentration and IQ in healthy individualshas been previously reported (Jung et al 1999) Our findings suggestindependentmetabolite concentration-neuropsychological associationsbetween NAA Cho and Cr in healthy individuals Greater Cr concentra-tionwas associatedwith poorer executive function in the present studyA study of elderly males found negative correlations between adjusted
hy participants
Cho concentration Cr concentration
r or rho rp1 (P) r or rho rp
1 (P)
minus0198 (0293) 0331 (0074)0356 (0232) 0579 (0038)
9 (0473) minus0011 (0956) minus0030 (0877) minus0102 (0592) minus0116 (0550)8 (0461) 0390 (0211) 0368 (0265) minus0225 (0483) 0312 (035)9 (0043) minus0163 (0388) minus0160 (0407) minus0130 (0493) minus0124 (0523)9 (0077) 0011 (0971) minus0083 (0797) 0156 (0611) minus0030 (0927)1 (0085) 0054 (0781) 0045 (0822) minus0017 (0932) minus0025 (0898)8 (0382) minus0453 (0120) minus0610 (0035) minus0022 (0946) minus0267 (0401)9 (0564) 0181 (0348) 0177 (0369) 0269 (0159) 0265 (0173)5 (0061) minus0173 (0572) minus0330 (0295) 0277 (036) 0061 (0851)8 (0423) minus0114 (0555) 0016 (0936) 0003 (0986) 0088 (0656)5 (0413) minus0209 (0514) minus0346 (0297) 0207 (0519) 0006 (0986)0 (0273) 0026 (0891) 0029 (0879) 0062 (0747) 0064 (0742)8 (0811) minus0063 (0839) minus0025 (0939) minus0225 (0461) minus0169 (0600)
Table 6Demographic clinical and metabolite concentration characteristics at baseline of CBTp+SC (n=11) SC control (n=13) and SC responsive (n=6) patients
Characteristic CBTp+SC SC control SC responsive χ2 P
Gender malefemale (n) 65 121 60 7185 0028mean SD mean SD
Age in years 3464 862 3746 877 3733 942 0745 0689Years in education 1445 246 1346 176 1377 24 1156 0561Illness duration years 1194 860 1377 970 1317 928 0303 0860Symptoms (PANSS)
Positive 1745 295 1915 264 1117 172 14644 0001Negative 1818 498 1923 386 1433 361 5779 0056General psychopathology 3227 675 340 549 2567 383 6775 0034Total 6791 1287 7239 994 5117 778 9512 0009Medication level 56442 30317 50055 39478 39405 20759 1787 0409
Metabolite concentrationNAA 765 092 685 143 823 091 5313 0070Cho 192 060 186 024 194 018 0493 0781Cr 689 140 687 095 748 160 1047 0592Grey matter 5766 1071 5117 1136 5337 714 1096 0578
257P Premkumar et al Psychiatry Research Neuroimaging 182 (2010) 251ndash260
Cr in the parietal lobe and various cognitive measures including logicalmemory and verbal memory (Ferguson et al 2002) The study did notinclude ameasure of executive function Ferguson et al (2002) believedthat the findings fit with evidence that higher Cr levels are associatedwith cognitive ageing They proposed that poorer neuropsychologicalperformance in healthy ageing is associated with an increase inPhosphocreatine (PCr) due to a reduction in conversion of PCr toAdenosine-tri-phosphate (ATP) for energy Increased Cr concentrationmay be a marker of decreased brain energy metabolism
42 Effect of cognitive behaviour therapy for psychosis on metaboliteconcentration
Our preliminary investigation of change in metabolite concentra-tion in a small number of patients who received CBTp+SC comparedto patients who received SC only revealed a trend for an increase inNAA concentration with CBTp This increase in NAA was concomitantwith improvement in positive symptoms in CBTp+SC patients Thisfinding is consistent with the view that NAA concentration increaseswith alleviation of symptoms as discussed above Recent functionalimaging studies also provide evidence for a role of the ACC inresponsiveness to CBT in psychosis (Kumari et al 2009) as well asmajor depression (Costafreda et al 2009)
43 Limitations and future research
One of the limitations of the study was that the sample sizes ofpatients who received CBTp+SC or SC only and were clinicallyassessed andor scanned at follow-up were small A further limitationwas that gender distribution differed between the patient groupsAlthough there was no gender effect within each patient group in the
Table 7Symptoms metabolite and grey matter concentration (mean SD) at baseline and follow-u
CSI variable Baseline CBTp+SC (n=7) z (P)
FOLLOW-UP
Clinical symptomsPositive symptoms 1814 (234) 1567 (350) minus20Negative symptoms 1857 (571) 1567 (234) minus08General psychopathology 3200 (566) 2733 (497) minus13Total symptoms 6871 (1227) 5867 (1017) minus14
Metabolite concentrationNAA 765 (068) 831 (077) minus18Cho 185 (042) 193 (02) minus05Cr 679 (089) 725 (103) minus08Grey matter 5706 (1155) 5860 (851) minus03
metabolite concentrations in the present study higher ACC glutaminelevel in male compared to female schizophrenia patients has beenpreviously observed (Tayoshi et al 2009) Other effects of gender onACC function have also been reported for example reduced ACCglucose metabolism in male chronic patients relative to healthyparticipants and female patients (Fujimoto et al 2007) Thepredictive value of NAA concentration on symptom change in patientsreceiving psychological treatment or standard care needs to beexamined in a larger sample involving a sufficient number of bothmen and women with schizophrenia Additionally the role of clinicaland neuropsychological variables on ACC NAA levels in patients whoimprove with CBTp needs to be explored
44 Conclusions
Higher NAA and Cho concentrations in the ACC in patients areassociated with lower symptom severity Stronger and moreconsistent associations between metabolite concentrations andsymptom severity than neuropsychological function suggest thatmetabolite concentration and symptoms may co-fluctuate morestrongly Neuropsychological deficits may be more stable (Szokeet al 2008) and not necessarily improve in parallel with symptomimprovement (Hughes et al 2003) NAA concentration may yetreflect symptom changes following CBTp and if replicated in futurestudies has the potential to provide a useful biological marker ofclinical response to psychological treatments
Acknowledgement
The study was supported by funds from the Wellcome Trust UK(067427z02z)
p in CBTp+SC and SC control groups
Baseline SC control (n=4) z (P)
FOLLOW-UP
32 (0042) 1925 (222) 1825 (263) minus0365 (0715)13 (0416) 1875 (499) 2200 (616) minus1841 (0066)82 (0167) 3500 (668) 3275 (591) minus0535 (0593)72 (0141) 7300 (1042) 7300 (1364) minus0001 (1000)
59 (0063) 740 (069) 704 (038) minus1826 (0068)07 (0612) 190 (018) 201 (008) minus0730 (0465)45 (0398) 702 (016) 736 (099) minus0730 (0465)38 (0735) 5353 (549) 5324 (335) minus0365 (0715)
Appendix A Summary of magnetic resonance spectroscopy studies on the anterior cingulate cortex (ACC) in schizophrenia patients
Publication Participants Measures Results
Deicken et al (1997) Schizophrenia patients(n=26 9 on atypical and 17 on typical)Healthy participants (n=16)
NAA Cho and Cr illness durationantipsychotic medication dose
Patients had lower NAA concentrationcompared to healthy participants Nosignificant group differences or lateralizedasymmetries for Cho or Cr No significantcorrelations between NAA and eitherillness duration or antipsychoticmedication dose
Ende et al (2000) Schizophrenia patients(n=19 10 on atypical and 9 on typical)Healthy participants (n=16)
NAA Cho and Cr age illnessduration
Patients had lower NAA concentrationcompared to healthy participantsPatients receiving typical medication(but not atypical) had lower NAAconcentration than healthy participantsNAA concentration was inverselycorrelated with age in patients andhealthy participants and with illnessduration (corrected for age) in patients
Braus et al (2001 2002) Schizophrenia patients(11 on atypical and 10 on typical)
NAA Cho and Cr illness durationduration on atypical antipsychoticmedication WCST
Patients receiving typical antipsychoticshad lower NAA concentration than patientsreceiving atypical antipsychoticsNAA concentration was inverselycorrelated with illness duration andpositively with duration on atypicalantipsychotic medication NAAconcentration was inversely correlatedwith WCST perseverative errors
Goff et al (2002) Schizophrenia patients (n=17of whom 10 switched fromconventional to olanzapine andhad MRS at baseline and 8-week follow-up)
GluCr ratio SANS GluCr ratio was increased by 125(non-significant) following switch toolanzapine Patients who improvedon SANS symptoms had greaterGluCr ratio (458) compared topatients who deteriorated on SANSsymptoms (208) No significantcorrelation between SANS total andchange in GluCr ratio after switch
Yamasue et al (2002) Schizophrenia patients(n=15 all on typical)Healthy participants (n=13)
NAA Cho and Cr grey mattervolume age height body weightsocio-economic status parentalsocio-economic status years ofeducation PANSS onset of illnessillness duration antipsychoticmedication dose
Patients had lower NAACho ratio andgreater ChoCr ratio compared to healthyparticipants after controlling for greymatter volume NAACho ratio waspositively correlated with grey mattervolume in patients not healthy participantsNAACho ratio was inversely correlatedwith PANSS blunted affect score
Theberge et al (2004 2002) First-episode neuroleptic naiumlveschizophrenia patients (n=21)Healthy participants (n=21)
Analysis in Theberge et al 2002NAA Cho Cr Glu Gln mI in leftACC SANS SAPS
From Theberge et al 2002Patients had greater Gln concentrationcompared to healthy participantsMetabolite concentrations were notcorrelated with SANS or SAPS
Analysis in Theberge et al 2004NAA and Cho in left ACC DUPDUI DPS
From Theberge et al 2004NAA concentration was positively correlatedwith DUP and inversely with DPS at trendlevel Cho concentration was positivelycorrelated with DUP
Theberge et al (2003) Schizophrenia patients (n=21atypical n=7 both n=1typical n=13)Healthy participants (n=21)
NAA Cho Cr Glu Gln mI inleft ACC duration of illness
Glu and Gln concentrations were greaterin patients than healthy participants NAAconcentration was inversely correlatedwith duration of positive symptoms
Wood et al (2007) Schizophrenia male patients(n=15 13 atypical 2 medication free)Healthy male participants (n=14)
NAA and Glx in dorsal and rostralregions PANSS five factors illnessduration
Patients had lower NAA concentrationcompared to healthy participantsRight dorsal Glx was inversely correlatedwith illness duration
Ohrmann et al (2008) Schizophrenia patients(n=43 all on atypical)Healthy participants (n=37)
NAA Cho Cr Glx WCST learningpotential
No difference in metabolite concentrationbetween patients and healthy participantsNAA and Glx concentrations were positivelyassociated with WCST learning potential
Sanches et al (2008) Schizophrenia patients (n=37)Healthy participants (n=37)
NAA(Cho+Cr) ratio in left andright anterior middle frontal gyrusACC and perirolandic area (reference)basal skin conductance and skinconductance response to auditorystimuli of 1 s tones of 80 dB Patientsand healthy participants classified intoskin conductance responders (2 SDbelow mean skin conductance in healthyparticipants) and non-responders
NAA(Cho+Cr) ratio was lower in patientsthan healthy participants in the anteriormiddle frontal gyrus and ACC bilaterallyNAA(Cho+Cr) ratio did not differ betweenskin conductance response groups based onskin conductance response to auditory stimuliBasal skin conductance non-responders patientshad lower NAA(Cho+Cr) ratio than healthyparticipants in left and right ACC
258 P Premkumar et al Psychiatry Research Neuroimaging 182 (2010) 251ndash260
Tayoshi et al (2009) Long-term schizophrenia (n=30antipsychotic medication typenot reported)Healthy participants (n=25)
NAA Cho Cr Glu Gln mI Gender PANSStotal and subscales duration of illnessduration of therapy antipsychotic dosagebenzodiazepine dose
Patients had lower Glu and mI concentrationcompared to healthy participants Malepatients had lower NAA Cr Glu and mIconcentration than male healthy participantsMales had greater Gln concentration comparedto females Metabolite concentration wasnot correlated with symptoms or otherclinical variables
Ongur et al (2009) Schizophrenia patients (n=15)Bipolar disorder patients (n=15)Healthy participants (n=22)
Cr in ACC (hypothesized area) andparietal-occipital cortex (reference area)MADRS PANSS YMRS
Patients had lower Cr than healthyparticipants in both ACC andparietal-occipital cortex No significantcorrelations between Cr concentrationand clinical measures
ACC anterior cingulate cortex ChomdashCholine CrmdashCreatinePhosphocreatine DPSmdashduration of psychotic symptoms DUImdashduration of untreated illness DUPmdashduration of untreatedpsychosis GlnmdashGlutamine GlumdashGlutamate GluCr ratio SANSmdashSchedule for the Assessment of Negative Symptoms GlxmdashGlutamate+Glutamine MADRSmdashMontgomery AsbergDepression Rating Scale mImdashmyo-Inositol NAA N-acetyl aspartate PANSSmdashPositive and Negative Syndrome Scale SAPS Schedule for the Assessment of Positive SymptomsWCSTmdashWisconsin Card Sorting test YMRSmdashYoung Mania Rating Scale
Appendix A (continued)
259P Premkumar et al Psychiatry Research Neuroimaging 182 (2010) 251ndash260
Appendix B Supplementary Data
Supplementary data associated with this article can be found inthe online version at doi101016jpscychresns201002008
References
Adler CM Malhotra AK Elman I Goldberg T Egan M Pickar D Breier A 1999Comparison of ketamine-induced thought disorder in healthy volunteers andthought disorder in schizophrenia American Journal of Psychiatry 156 1646ndash1649
Andres RH Ducray AD Schlattner U Wallimann T Widmer HR 2008 Functionsand effects of creatine in the central nervous system Brain Research Bulletin 76329ndash343
Baiano M David A Versace A Churchill R Balestrieri M Brambilla P 2007Anterior cingulate volumes in schizophrenia a systematic review and a meta-analysis of MRI studies Schizophrenia Research 93 1ndash12
Bechara A Damasio AR Damasio H Anderson SW 1994 Insensitivity to futureconsequences following damage to human prefrontal cortex Cognition 50 7ndash15
Behrens TE Woolrich MW Walton ME Rushworth MF 2007 Learning the valueof information in an uncertain world Nature Neuroscience 10 1214ndash1221
Bertolino A Esposito G Callicott JH Mattay VS Van Horn JD Frank JA BermanKF Weinberger DR 2000 Specific relationship between prefrontal neuronal N-acetylaspartate and activation of the working memory cortical network inschizophrenia American Journal of Psychiatry 157 26ndash33
Braus DF Ende G Weber-Fahr W Demirakca T Henn FA 2001 Favorable effecton neuronal viability in the anterior cingulate gyrus due to long-term treatmentwith atypical antipsychotics an MRSI study Pharmacopsychiatry 34 251ndash253
Braus DF Ende G Weber-Fahr W Demirakca T Tost H Henn FA 2002Functioning and neuronal viability of the anterior cingulate neurons followingantipsychotic treatment MR-spectroscopic imaging in chronic schizophreniaEuropean Neuropsychopharmacology 12 145ndash152
Burgess PW Shallice T 1997 The Hayling and Brixton Tests Thames Valley TestCompany Bury St Edmunds
Callicott JH Bertolino A Mattay VS Langheim FJ Duyn J Coppola R Goldberg TEWeinberger DR 2000 Physiological dysfunction of the dorsolateral prefrontal cortexin schizophrenia revisited Cerebral Cortex 10 1078ndash1092
Carter CS van Veen V 2007 Anterior cingulate cortex and conflict detection anupdate of theory and data Cognitive Affective and Behavioral Neuroscience 7367ndash379
Cornblatt BA Risch JJ Faris G Friedman D Erlenmeyer-Kimling L 1988 TheContinuous Performance Test Identical Pairs Version (CPT-IP) I New findingsabout sustained attention in normal families Psychiatry Research 26 223ndash238
Costafreda SG Khanna A Mourao-Miranda J Fu CH 2009 Neural correlates of sadfaces predict clinical remission to cognitive behavioural therapy in depressionNeuroReport 20 637ndash641
Deicken RF Zhou L Schuff N Weiner MW 1997 Proton magnetic resonancespectroscopy of the anterior cingulate region in schizophrenia SchizophreniaResearch 27 65ndash71
Deicken RF Johnson C Pegues M 2000 Proton magnetic resonance spectroscopy ofthe human brain in schizophrenia Reviews in the Neurosciences 11 147ndash158
Ende G Braus DF Walter S Weber-Fahr W Soher B Maudsley AA Henn FA2000 Effects of age medication and illness duration on the N-acetyl aspartatesignal of the anterior cingulate region in schizophrenia Schizophrenia Research 41389ndash395
Fannon D Simmons A Tennakoon L OCeallaigh S Sumich A Doku V Shew CSharma T 2003 Selective deficit of hippocampal N-acetylaspartate in antipsy-chotic-naive patients with schizophrenia Biological Psychiatry 54 587ndash598
Ferguson KJ MacLullich AM Marshall I Deary IJ Starr JM Seckl JR Wardlaw JM2002 Magnetic resonance spectroscopy and cognitive function in healthy elderlymen Brain 125 2743ndash2749
First MB Spitzer RL Gibbon M Williams JBW 2002 Structured Clinical Interviewfor DSM-IV-TR Axis I DisordersmdashPatient Edition (SCID-IP 112002 revision)Biometrics Research Department New York NY
Fornito A Yucel M Dean B Wood SJ Pantelis C 2008 Anatomical abnormalities ofthe anterior cingulate cortex in schizophrenia bridging the gap betweenneuroimaging and neuropathology Schizophrenia Bulletin 35 973ndash993
Fowler D Garety PA Kuipers E 1995 Cognitive Behaviour Therapy for PsychosisTheory and Practice Wiley Chichester
Fujimoto T Takeuch K Matsumoto T Kamimura K Hamada R Nakamura K KatoN 2007 Abnormal glucose metabolism in the anterior cingulate cortex in patientswith schizophrenia Psychiatry Research 154 49ndash58
Goff DC Hennen J Lyoo IK Tsai G Wald LL Evins AE Yurgelun-Todd DARenshaw PF 2002 Modulation of brain and serum glutamatergic concentrationsfollowing a switch from conventional neuroleptics to olanzapine BiologicalPsychiatry 51 493ndash497
Gold JM Carpenter C Randolph C Goldberg TE Weinberger DR 1997 Auditoryworking memory and Wisconsin Card Sorting Test performance in schizophreniaArchives of General Psychiatry 54 159ndash165
Heaton RK Chelune GJ Tally JL Kay GG Curtiss G 1993 Wisconsin Card SortingTest Manual Revised and Expanded Psychological Assessment Resources OdessaFL
Honea R Crow TJ Passingham D Mackay CE 2005 Regional deficits in brainvolume in schizophrenia a meta-analysis of voxel-based morphometry studiesAmerican Journal of Psychiatry 162 2233ndash2245
Hughes C Kumari V Soni W Das M Binneman B Drozd S ONeil S Mathew VSharma T 2003 Longitudinal study of symptoms and cognitive function in chronicschizophrenia Schizophrenia Research 59 137ndash146
Jung RE Brooks WM Yeo RA Chiulli SJ Weers DC Sibbitt Jr WL 1999Biochemical markers of intelligence a proton MR spectroscopy study of normalhuman brain Proceedings Biological Sciences 266 1375ndash1379
Kaneda M Osaka N 2008 Role of anterior cingulate cortex during semantic coding inverbal working memory Neuroscience Letters 436 57ndash61
Kay SR Fiszbein A Opier LA 1987 The Positive and Negative Syndrome Scale(PANSS) for schizophrenia Schizophrenia Bulletin 13 261ndash276
Kennerley SW Dahmubed AF Lara AH Wallis JD 2008 Neurons in the frontallobe encode the value of multiple decision variables Journal of CognitiveNeuroscience 21 1162ndash1178
Kim J Whyte J Wang J Rao H Tang KZ Detre JA 2006 Continuous ASL perfusionfMRI investigation of higher cognition quantification of tonic CBF changes duringsustained attention and working memory tasks Neuroimage 31 376ndash385
Krystal JH Karper LP Seibyl JP Freeman GK Delaney R Bremner JD HeningerGR Bowers Jr MB Charney DS 1994 Subanesthetic effects of the noncom-petitive NMDA antagonist ketamine in humans Psychotomimetic perceptualcognitive and neuroendocrine responses Archives of General Psychiatry 51199ndash214
Kumari V Peters ER Fannon D Antonova E Premkumar P Anilkumar APWilliams SC Kuipers EA 2009 Dorsolateral prefrontal cortex activity predictsresponsiveness to cognitive behaviour therapy in schizophrenia BiologicalPsychiatry 66 594ndash602
Lahti AC Koffel B LaPorte D Tamminga CA 1995 Subanesthetic doses of ketaminestimulate psychosis in schizophrenia Neuropsychopharmacology 13 9ndash19
Lenartowicz A McIntosh AR 2005 The role of anterior cingulate cortex in workingmemory is shaped by functional connectivity Journal of Cognitive Neuroscience 171026ndash1042
Malhotra AK Pinals DA Adler CM Elman I Clifton A Pickar D Breier A 1997Ketamine-induced exacerbation of psychotic symptoms and cognitive impairmentin neuroleptic-free schizophrenics Neuropsychopharmacology 17 141ndash150
260 P Premkumar et al Psychiatry Research Neuroimaging 182 (2010) 251ndash260
McLean MA Woermann FG Barker GJ Duncan JS 2000 Quantitative analysis ofshort echo time (1)H-MRSI of cerebral gray and white matter Magnetic Resonancein Medicine 44 401ndash411
McMorris T Harris RC Swain J Corbett J Collard K Dyson RJ Dye L Hodgson CDraper N 2006 Effect of creatine supplementation and sleep deprivation withmild exercise on cognitive and psychomotor performance mood state and plasmaconcentrations of catecholamines and cortisol Psychopharmacology (Berl) 18593ndash103
McMorris T Harris RC Howard AN Langridge G Hall B Corbett J Dicks MHodgson C 2007 Creatine supplementation sleep deprivation cortisol melatoninand behavior Physiology and Behaviour 90 21ndash28
Miller BL 1991 A review of chemical issues in 1H NMR spectroscopy N-acetyl-L-aspartate creatine and choline NMR in Biomedicine 4 47ndash52
Moghaddam B 2003 Bringing order to the glutamate chaos in schizophrenia Neuron40 881ndash884
Ohrmann P Siegmund A Suslow T Pedersen A Spitzberg K Kersting ARothermundt M Arolt V Heindel W Pfleiderer B 2007 Cognitive impairmentand in vivo metabolites in first-episode neuroleptic-naive and chronic medicatedschizophrenic patients a proton magnetic resonance spectroscopy study Journalof Psychiatric Research 41 625ndash634
Ohrmann P Kugel H Bauer J Siegmund A Kolkebeck K Suslow T Wiedl KHRothermundt M Arolt V Pedersen A 2008 Learning potential on the WCST inschizophrenia is related to the neuronal integrity of the anterior cingulate cortex asmeasured by proton magnetic resonance spectroscopy Schizophrenia Research106 156ndash163
Ongur D Prescot AP Jensen JE Cohen BM Renshaw PF 2009 Creatineabnormalities in schizophrenia and bipolar disorder Psychiatry ResearchNeuroimaging 172 44ndash48
Osaka N Osaka M Kondo H Morishita M Fukuyama H Shibasaki H 2004 Theneural basis of executive function in working memory an fMRI study based onindividual differences Neuroimage 21 623ndash631
Perry G Nunomura A Hirai K Zhu X Perez M Avila J Castellani RJ Atwood CSAliev G Sayre LM Takeda A Smith MA 2002 Is oxidative damage thefundamental pathogenic mechanism of Alzheimers and other neurodegenerativediseases Free Radical Biology and Medicine 33 1475ndash1479
Peterson BS Skudlarski P Gatenby JC Zhang H Anderson AW Gore JC 1999 AnfMRI study of Stroop word-color interference evidence for cingulate subregionssubserving multiple distributed attentional systems Biological Psychiatry 451237ndash1258
Provencher SW 1993 Estimation of metabolite concentrations from localized in vivoproton NMR spectra Magnetic Resonance in Medicine 30 672ndash679
Rae C Digney AL McEwan SR Bates TC 2003 Oral creatine monohydratesupplementation improves brain performance a double-blind placebo-controlledcross-over trial Proceedings Biological Sciences 270 2147ndash2150
Ross AJ Sachdev PS 2004 Magnetic resonance spectroscopy in cognitive researchBrain Research Brain Research Reviews 44 83ndash102
Rushworth MF Walton ME Kennerley SW Bannerman DM 2004 Action sets anddecisions in the medial frontal cortex Trends in Cogntive Sciences 8 410ndash417
Rutten BP Korr H Steinbusch HW Schmitz C 2003 The aging brain less neuronscould be better Mechanisms of Ageing and Development 124 349ndash355
Sanches RF Crippa JA Hallak JE de Sousa JP Araujo D Santos AC Zuardi AW2008 Proton magnetic resonance spectroscopy of the frontal cingulate andperirolandic cortices and its relationship to skin conductance in patients withschizophrenia Brazilian Journal of Medical and Biological Research 41 1132ndash1141
Schlosser RG Koch K Wagner G Nenadic I Roebel M Schachtzabel C Axer MSchultz C Reichenbach JR Sauer H 2008 Inefficient executive cognitive controlin schizophrenia is preceded by altered functional activation during informationencoding an fMRI study Neuropsychologia 46 336ndash347
Shapiro AM Benedict RH Schretlen D Brandt J 1999 Construct and concurrentvalidity of the Hopkins Verbal Learning Test-revised The Clinical Neuropsychol-ogist 13 348ndash358
Smith EE Jonides J 1999 Storage and executive processes in the frontal lobesScience 283 1657ndash1661
Szoke A Trandafir A Dupont ME Meary A Schurhoff F Leboyer M 2008Longitudinal studies of cognition in schizophrenia meta-analysis British Journal ofPsychiatry 192 248ndash257
Tayoshi S Sumitani S Taniguchi K Shibuya-Tayoshi S Numata S Iga JI NakatakiM Ueno SI Harada M Ohmori T 2009 Metabolite changes and genderdifferences in schizophrenia using 3-Tesla proton magnetic resonance spectrosco-py ((1)H-MRS) Schizophrenia Research 108 69ndash77
Theberge J Bartha R Drost DJ Menon RS Malla A Takhar J Neufeld RWRogers J Pavlosky W Schaefer B Densmore M Al-Semaan Y Williamson PC2002 Glutamate and glutamine measured with 40T proton MRS in never-treatedpatients with schizophrenia and healthy volunteers American Journal of Psychiatry159 1944ndash1946
Theberge J Al-Semaan Y Williamson PC Menon RS Neufeld RW Rajakumar NSchaefer B Densmore M Drost DJ 2003 Glutamate and glutamine in theanterior cingulate and thalamus of medicated patients with chronic schizophreniaand healthy comparison subjects measured with 40-T proton MRS AmericanJournal of Psychiatry 160 2231ndash2233
Theberge J Al-Semaan Y Drost DJ Malla AK Neufeld RW Bartha R ManchandaR Menon R Densmore M Schaefer B Williamson PC 2004 Duration ofuntreated psychosis vs N-acetylaspartate and choline in first episode schizophre-nia a 1H magnetic resonance spectroscopy study at 40 Tesla Psychiatry Research131 107ndash114
Tranberg M Stridh MH Guy Y Jilderos B Wigstrom H Weber SG Sandberg M2004 NMDA-receptor mediated efflux of N-acetylaspartate physiological andorpathological importance Neurochemistry International 45 1195ndash1204
Tranberg M Abbas AK Sandberg M 2007 In vitro studies on the putative function ofN-acetylaspartate as an osmoregulator Neurochemical Research 32 1248ndash1255
Walton ME Croxson PL Behrens TE Kennerley SW Rushworth MF 2007Adaptive decision making and value in the anterior cingulate cortex Neuroimage36 (Suppl 2) T142ndashT154
Wechsler D 1987 Wechsler Memory ScalemdashRevised Psychological Corporation NewYork
Weinberger DR Aloia MS Goldberg TE Berman KF 1994 The frontal lobes andschizophrenia Journal of Neuropsychiatry and Clinical Neurosciences 6 419ndash427
Wood SJ Yucel M Wellard RM Harrison BJ Clarke K Fornito A Velakoulis DPantelis C 2007 Evidence for neuronal dysfunction in the anterior cingulate ofpatients with schizophrenia a proton magnetic resonance spectroscopy study at3T Schizophrenia Research 94 328ndash331
Yamasue H Fukui T Fukuda R Yamada H Yamasaki S Kuroki N Abe O Kasai KTsujii K Iwanami A Aoki S Ohtomo K Kato N Kato T 2002 1H-MRspectroscopy and gray matter volume of the anterior cingulate cortex inschizophrenia NeuroReport 13 2133ndash2137
Yeo RA Hill D Campbell R Vigil J Brooks WM 2000 Developmental instabilityand working memory ability in children a magnetic resonance spectroscopyinvestigation Developmental Neuropsychology 17 143ndash159
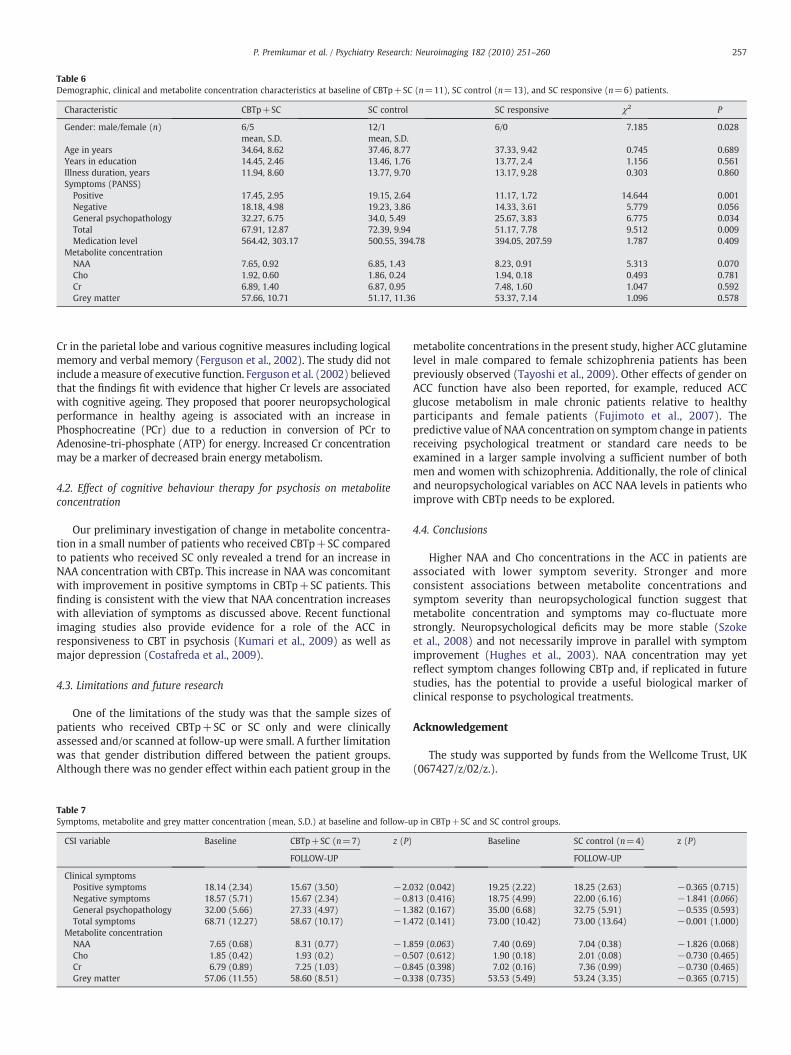
Table 6Demographic clinical and metabolite concentration characteristics at baseline of CBTp+SC (n=11) SC control (n=13) and SC responsive (n=6) patients
Characteristic CBTp+SC SC control SC responsive χ2 P
Gender malefemale (n) 65 121 60 7185 0028mean SD mean SD
Age in years 3464 862 3746 877 3733 942 0745 0689Years in education 1445 246 1346 176 1377 24 1156 0561Illness duration years 1194 860 1377 970 1317 928 0303 0860Symptoms (PANSS)
Positive 1745 295 1915 264 1117 172 14644 0001Negative 1818 498 1923 386 1433 361 5779 0056General psychopathology 3227 675 340 549 2567 383 6775 0034Total 6791 1287 7239 994 5117 778 9512 0009Medication level 56442 30317 50055 39478 39405 20759 1787 0409
Metabolite concentrationNAA 765 092 685 143 823 091 5313 0070Cho 192 060 186 024 194 018 0493 0781Cr 689 140 687 095 748 160 1047 0592Grey matter 5766 1071 5117 1136 5337 714 1096 0578
257P Premkumar et al Psychiatry Research Neuroimaging 182 (2010) 251ndash260
Cr in the parietal lobe and various cognitive measures including logicalmemory and verbal memory (Ferguson et al 2002) The study did notinclude ameasure of executive function Ferguson et al (2002) believedthat the findings fit with evidence that higher Cr levels are associatedwith cognitive ageing They proposed that poorer neuropsychologicalperformance in healthy ageing is associated with an increase inPhosphocreatine (PCr) due to a reduction in conversion of PCr toAdenosine-tri-phosphate (ATP) for energy Increased Cr concentrationmay be a marker of decreased brain energy metabolism
42 Effect of cognitive behaviour therapy for psychosis on metaboliteconcentration
Our preliminary investigation of change in metabolite concentra-tion in a small number of patients who received CBTp+SC comparedto patients who received SC only revealed a trend for an increase inNAA concentration with CBTp This increase in NAA was concomitantwith improvement in positive symptoms in CBTp+SC patients Thisfinding is consistent with the view that NAA concentration increaseswith alleviation of symptoms as discussed above Recent functionalimaging studies also provide evidence for a role of the ACC inresponsiveness to CBT in psychosis (Kumari et al 2009) as well asmajor depression (Costafreda et al 2009)
43 Limitations and future research
One of the limitations of the study was that the sample sizes ofpatients who received CBTp+SC or SC only and were clinicallyassessed andor scanned at follow-up were small A further limitationwas that gender distribution differed between the patient groupsAlthough there was no gender effect within each patient group in the
Table 7Symptoms metabolite and grey matter concentration (mean SD) at baseline and follow-u
CSI variable Baseline CBTp+SC (n=7) z (P)
FOLLOW-UP
Clinical symptomsPositive symptoms 1814 (234) 1567 (350) minus20Negative symptoms 1857 (571) 1567 (234) minus08General psychopathology 3200 (566) 2733 (497) minus13Total symptoms 6871 (1227) 5867 (1017) minus14
Metabolite concentrationNAA 765 (068) 831 (077) minus18Cho 185 (042) 193 (02) minus05Cr 679 (089) 725 (103) minus08Grey matter 5706 (1155) 5860 (851) minus03
metabolite concentrations in the present study higher ACC glutaminelevel in male compared to female schizophrenia patients has beenpreviously observed (Tayoshi et al 2009) Other effects of gender onACC function have also been reported for example reduced ACCglucose metabolism in male chronic patients relative to healthyparticipants and female patients (Fujimoto et al 2007) Thepredictive value of NAA concentration on symptom change in patientsreceiving psychological treatment or standard care needs to beexamined in a larger sample involving a sufficient number of bothmen and women with schizophrenia Additionally the role of clinicaland neuropsychological variables on ACC NAA levels in patients whoimprove with CBTp needs to be explored
44 Conclusions
Higher NAA and Cho concentrations in the ACC in patients areassociated with lower symptom severity Stronger and moreconsistent associations between metabolite concentrations andsymptom severity than neuropsychological function suggest thatmetabolite concentration and symptoms may co-fluctuate morestrongly Neuropsychological deficits may be more stable (Szokeet al 2008) and not necessarily improve in parallel with symptomimprovement (Hughes et al 2003) NAA concentration may yetreflect symptom changes following CBTp and if replicated in futurestudies has the potential to provide a useful biological marker ofclinical response to psychological treatments
Acknowledgement
The study was supported by funds from the Wellcome Trust UK(067427z02z)
p in CBTp+SC and SC control groups
Baseline SC control (n=4) z (P)
FOLLOW-UP
32 (0042) 1925 (222) 1825 (263) minus0365 (0715)13 (0416) 1875 (499) 2200 (616) minus1841 (0066)82 (0167) 3500 (668) 3275 (591) minus0535 (0593)72 (0141) 7300 (1042) 7300 (1364) minus0001 (1000)
59 (0063) 740 (069) 704 (038) minus1826 (0068)07 (0612) 190 (018) 201 (008) minus0730 (0465)45 (0398) 702 (016) 736 (099) minus0730 (0465)38 (0735) 5353 (549) 5324 (335) minus0365 (0715)
Appendix A Summary of magnetic resonance spectroscopy studies on the anterior cingulate cortex (ACC) in schizophrenia patients
Publication Participants Measures Results
Deicken et al (1997) Schizophrenia patients(n=26 9 on atypical and 17 on typical)Healthy participants (n=16)
NAA Cho and Cr illness durationantipsychotic medication dose
Patients had lower NAA concentrationcompared to healthy participants Nosignificant group differences or lateralizedasymmetries for Cho or Cr No significantcorrelations between NAA and eitherillness duration or antipsychoticmedication dose
Ende et al (2000) Schizophrenia patients(n=19 10 on atypical and 9 on typical)Healthy participants (n=16)
NAA Cho and Cr age illnessduration
Patients had lower NAA concentrationcompared to healthy participantsPatients receiving typical medication(but not atypical) had lower NAAconcentration than healthy participantsNAA concentration was inverselycorrelated with age in patients andhealthy participants and with illnessduration (corrected for age) in patients
Braus et al (2001 2002) Schizophrenia patients(11 on atypical and 10 on typical)
NAA Cho and Cr illness durationduration on atypical antipsychoticmedication WCST
Patients receiving typical antipsychoticshad lower NAA concentration than patientsreceiving atypical antipsychoticsNAA concentration was inverselycorrelated with illness duration andpositively with duration on atypicalantipsychotic medication NAAconcentration was inversely correlatedwith WCST perseverative errors
Goff et al (2002) Schizophrenia patients (n=17of whom 10 switched fromconventional to olanzapine andhad MRS at baseline and 8-week follow-up)
GluCr ratio SANS GluCr ratio was increased by 125(non-significant) following switch toolanzapine Patients who improvedon SANS symptoms had greaterGluCr ratio (458) compared topatients who deteriorated on SANSsymptoms (208) No significantcorrelation between SANS total andchange in GluCr ratio after switch
Yamasue et al (2002) Schizophrenia patients(n=15 all on typical)Healthy participants (n=13)
NAA Cho and Cr grey mattervolume age height body weightsocio-economic status parentalsocio-economic status years ofeducation PANSS onset of illnessillness duration antipsychoticmedication dose
Patients had lower NAACho ratio andgreater ChoCr ratio compared to healthyparticipants after controlling for greymatter volume NAACho ratio waspositively correlated with grey mattervolume in patients not healthy participantsNAACho ratio was inversely correlatedwith PANSS blunted affect score
Theberge et al (2004 2002) First-episode neuroleptic naiumlveschizophrenia patients (n=21)Healthy participants (n=21)
Analysis in Theberge et al 2002NAA Cho Cr Glu Gln mI in leftACC SANS SAPS
From Theberge et al 2002Patients had greater Gln concentrationcompared to healthy participantsMetabolite concentrations were notcorrelated with SANS or SAPS
Analysis in Theberge et al 2004NAA and Cho in left ACC DUPDUI DPS
From Theberge et al 2004NAA concentration was positively correlatedwith DUP and inversely with DPS at trendlevel Cho concentration was positivelycorrelated with DUP
Theberge et al (2003) Schizophrenia patients (n=21atypical n=7 both n=1typical n=13)Healthy participants (n=21)
NAA Cho Cr Glu Gln mI inleft ACC duration of illness
Glu and Gln concentrations were greaterin patients than healthy participants NAAconcentration was inversely correlatedwith duration of positive symptoms
Wood et al (2007) Schizophrenia male patients(n=15 13 atypical 2 medication free)Healthy male participants (n=14)
NAA and Glx in dorsal and rostralregions PANSS five factors illnessduration
Patients had lower NAA concentrationcompared to healthy participantsRight dorsal Glx was inversely correlatedwith illness duration
Ohrmann et al (2008) Schizophrenia patients(n=43 all on atypical)Healthy participants (n=37)
NAA Cho Cr Glx WCST learningpotential
No difference in metabolite concentrationbetween patients and healthy participantsNAA and Glx concentrations were positivelyassociated with WCST learning potential
Sanches et al (2008) Schizophrenia patients (n=37)Healthy participants (n=37)
NAA(Cho+Cr) ratio in left andright anterior middle frontal gyrusACC and perirolandic area (reference)basal skin conductance and skinconductance response to auditorystimuli of 1 s tones of 80 dB Patientsand healthy participants classified intoskin conductance responders (2 SDbelow mean skin conductance in healthyparticipants) and non-responders
NAA(Cho+Cr) ratio was lower in patientsthan healthy participants in the anteriormiddle frontal gyrus and ACC bilaterallyNAA(Cho+Cr) ratio did not differ betweenskin conductance response groups based onskin conductance response to auditory stimuliBasal skin conductance non-responders patientshad lower NAA(Cho+Cr) ratio than healthyparticipants in left and right ACC
258 P Premkumar et al Psychiatry Research Neuroimaging 182 (2010) 251ndash260
Tayoshi et al (2009) Long-term schizophrenia (n=30antipsychotic medication typenot reported)Healthy participants (n=25)
NAA Cho Cr Glu Gln mI Gender PANSStotal and subscales duration of illnessduration of therapy antipsychotic dosagebenzodiazepine dose
Patients had lower Glu and mI concentrationcompared to healthy participants Malepatients had lower NAA Cr Glu and mIconcentration than male healthy participantsMales had greater Gln concentration comparedto females Metabolite concentration wasnot correlated with symptoms or otherclinical variables
Ongur et al (2009) Schizophrenia patients (n=15)Bipolar disorder patients (n=15)Healthy participants (n=22)
Cr in ACC (hypothesized area) andparietal-occipital cortex (reference area)MADRS PANSS YMRS
Patients had lower Cr than healthyparticipants in both ACC andparietal-occipital cortex No significantcorrelations between Cr concentrationand clinical measures
ACC anterior cingulate cortex ChomdashCholine CrmdashCreatinePhosphocreatine DPSmdashduration of psychotic symptoms DUImdashduration of untreated illness DUPmdashduration of untreatedpsychosis GlnmdashGlutamine GlumdashGlutamate GluCr ratio SANSmdashSchedule for the Assessment of Negative Symptoms GlxmdashGlutamate+Glutamine MADRSmdashMontgomery AsbergDepression Rating Scale mImdashmyo-Inositol NAA N-acetyl aspartate PANSSmdashPositive and Negative Syndrome Scale SAPS Schedule for the Assessment of Positive SymptomsWCSTmdashWisconsin Card Sorting test YMRSmdashYoung Mania Rating Scale
Appendix A (continued)
259P Premkumar et al Psychiatry Research Neuroimaging 182 (2010) 251ndash260
Appendix B Supplementary Data
Supplementary data associated with this article can be found inthe online version at doi101016jpscychresns201002008
References
Adler CM Malhotra AK Elman I Goldberg T Egan M Pickar D Breier A 1999Comparison of ketamine-induced thought disorder in healthy volunteers andthought disorder in schizophrenia American Journal of Psychiatry 156 1646ndash1649
Andres RH Ducray AD Schlattner U Wallimann T Widmer HR 2008 Functionsand effects of creatine in the central nervous system Brain Research Bulletin 76329ndash343
Baiano M David A Versace A Churchill R Balestrieri M Brambilla P 2007Anterior cingulate volumes in schizophrenia a systematic review and a meta-analysis of MRI studies Schizophrenia Research 93 1ndash12
Bechara A Damasio AR Damasio H Anderson SW 1994 Insensitivity to futureconsequences following damage to human prefrontal cortex Cognition 50 7ndash15
Behrens TE Woolrich MW Walton ME Rushworth MF 2007 Learning the valueof information in an uncertain world Nature Neuroscience 10 1214ndash1221
Bertolino A Esposito G Callicott JH Mattay VS Van Horn JD Frank JA BermanKF Weinberger DR 2000 Specific relationship between prefrontal neuronal N-acetylaspartate and activation of the working memory cortical network inschizophrenia American Journal of Psychiatry 157 26ndash33
Braus DF Ende G Weber-Fahr W Demirakca T Henn FA 2001 Favorable effecton neuronal viability in the anterior cingulate gyrus due to long-term treatmentwith atypical antipsychotics an MRSI study Pharmacopsychiatry 34 251ndash253
Braus DF Ende G Weber-Fahr W Demirakca T Tost H Henn FA 2002Functioning and neuronal viability of the anterior cingulate neurons followingantipsychotic treatment MR-spectroscopic imaging in chronic schizophreniaEuropean Neuropsychopharmacology 12 145ndash152
Burgess PW Shallice T 1997 The Hayling and Brixton Tests Thames Valley TestCompany Bury St Edmunds
Callicott JH Bertolino A Mattay VS Langheim FJ Duyn J Coppola R Goldberg TEWeinberger DR 2000 Physiological dysfunction of the dorsolateral prefrontal cortexin schizophrenia revisited Cerebral Cortex 10 1078ndash1092
Carter CS van Veen V 2007 Anterior cingulate cortex and conflict detection anupdate of theory and data Cognitive Affective and Behavioral Neuroscience 7367ndash379
Cornblatt BA Risch JJ Faris G Friedman D Erlenmeyer-Kimling L 1988 TheContinuous Performance Test Identical Pairs Version (CPT-IP) I New findingsabout sustained attention in normal families Psychiatry Research 26 223ndash238
Costafreda SG Khanna A Mourao-Miranda J Fu CH 2009 Neural correlates of sadfaces predict clinical remission to cognitive behavioural therapy in depressionNeuroReport 20 637ndash641
Deicken RF Zhou L Schuff N Weiner MW 1997 Proton magnetic resonancespectroscopy of the anterior cingulate region in schizophrenia SchizophreniaResearch 27 65ndash71
Deicken RF Johnson C Pegues M 2000 Proton magnetic resonance spectroscopy ofthe human brain in schizophrenia Reviews in the Neurosciences 11 147ndash158
Ende G Braus DF Walter S Weber-Fahr W Soher B Maudsley AA Henn FA2000 Effects of age medication and illness duration on the N-acetyl aspartatesignal of the anterior cingulate region in schizophrenia Schizophrenia Research 41389ndash395
Fannon D Simmons A Tennakoon L OCeallaigh S Sumich A Doku V Shew CSharma T 2003 Selective deficit of hippocampal N-acetylaspartate in antipsy-chotic-naive patients with schizophrenia Biological Psychiatry 54 587ndash598
Ferguson KJ MacLullich AM Marshall I Deary IJ Starr JM Seckl JR Wardlaw JM2002 Magnetic resonance spectroscopy and cognitive function in healthy elderlymen Brain 125 2743ndash2749
First MB Spitzer RL Gibbon M Williams JBW 2002 Structured Clinical Interviewfor DSM-IV-TR Axis I DisordersmdashPatient Edition (SCID-IP 112002 revision)Biometrics Research Department New York NY
Fornito A Yucel M Dean B Wood SJ Pantelis C 2008 Anatomical abnormalities ofthe anterior cingulate cortex in schizophrenia bridging the gap betweenneuroimaging and neuropathology Schizophrenia Bulletin 35 973ndash993
Fowler D Garety PA Kuipers E 1995 Cognitive Behaviour Therapy for PsychosisTheory and Practice Wiley Chichester
Fujimoto T Takeuch K Matsumoto T Kamimura K Hamada R Nakamura K KatoN 2007 Abnormal glucose metabolism in the anterior cingulate cortex in patientswith schizophrenia Psychiatry Research 154 49ndash58
Goff DC Hennen J Lyoo IK Tsai G Wald LL Evins AE Yurgelun-Todd DARenshaw PF 2002 Modulation of brain and serum glutamatergic concentrationsfollowing a switch from conventional neuroleptics to olanzapine BiologicalPsychiatry 51 493ndash497
Gold JM Carpenter C Randolph C Goldberg TE Weinberger DR 1997 Auditoryworking memory and Wisconsin Card Sorting Test performance in schizophreniaArchives of General Psychiatry 54 159ndash165
Heaton RK Chelune GJ Tally JL Kay GG Curtiss G 1993 Wisconsin Card SortingTest Manual Revised and Expanded Psychological Assessment Resources OdessaFL
Honea R Crow TJ Passingham D Mackay CE 2005 Regional deficits in brainvolume in schizophrenia a meta-analysis of voxel-based morphometry studiesAmerican Journal of Psychiatry 162 2233ndash2245
Hughes C Kumari V Soni W Das M Binneman B Drozd S ONeil S Mathew VSharma T 2003 Longitudinal study of symptoms and cognitive function in chronicschizophrenia Schizophrenia Research 59 137ndash146
Jung RE Brooks WM Yeo RA Chiulli SJ Weers DC Sibbitt Jr WL 1999Biochemical markers of intelligence a proton MR spectroscopy study of normalhuman brain Proceedings Biological Sciences 266 1375ndash1379
Kaneda M Osaka N 2008 Role of anterior cingulate cortex during semantic coding inverbal working memory Neuroscience Letters 436 57ndash61
Kay SR Fiszbein A Opier LA 1987 The Positive and Negative Syndrome Scale(PANSS) for schizophrenia Schizophrenia Bulletin 13 261ndash276
Kennerley SW Dahmubed AF Lara AH Wallis JD 2008 Neurons in the frontallobe encode the value of multiple decision variables Journal of CognitiveNeuroscience 21 1162ndash1178
Kim J Whyte J Wang J Rao H Tang KZ Detre JA 2006 Continuous ASL perfusionfMRI investigation of higher cognition quantification of tonic CBF changes duringsustained attention and working memory tasks Neuroimage 31 376ndash385
Krystal JH Karper LP Seibyl JP Freeman GK Delaney R Bremner JD HeningerGR Bowers Jr MB Charney DS 1994 Subanesthetic effects of the noncom-petitive NMDA antagonist ketamine in humans Psychotomimetic perceptualcognitive and neuroendocrine responses Archives of General Psychiatry 51199ndash214
Kumari V Peters ER Fannon D Antonova E Premkumar P Anilkumar APWilliams SC Kuipers EA 2009 Dorsolateral prefrontal cortex activity predictsresponsiveness to cognitive behaviour therapy in schizophrenia BiologicalPsychiatry 66 594ndash602
Lahti AC Koffel B LaPorte D Tamminga CA 1995 Subanesthetic doses of ketaminestimulate psychosis in schizophrenia Neuropsychopharmacology 13 9ndash19
Lenartowicz A McIntosh AR 2005 The role of anterior cingulate cortex in workingmemory is shaped by functional connectivity Journal of Cognitive Neuroscience 171026ndash1042
Malhotra AK Pinals DA Adler CM Elman I Clifton A Pickar D Breier A 1997Ketamine-induced exacerbation of psychotic symptoms and cognitive impairmentin neuroleptic-free schizophrenics Neuropsychopharmacology 17 141ndash150
260 P Premkumar et al Psychiatry Research Neuroimaging 182 (2010) 251ndash260
McLean MA Woermann FG Barker GJ Duncan JS 2000 Quantitative analysis ofshort echo time (1)H-MRSI of cerebral gray and white matter Magnetic Resonancein Medicine 44 401ndash411
McMorris T Harris RC Swain J Corbett J Collard K Dyson RJ Dye L Hodgson CDraper N 2006 Effect of creatine supplementation and sleep deprivation withmild exercise on cognitive and psychomotor performance mood state and plasmaconcentrations of catecholamines and cortisol Psychopharmacology (Berl) 18593ndash103
McMorris T Harris RC Howard AN Langridge G Hall B Corbett J Dicks MHodgson C 2007 Creatine supplementation sleep deprivation cortisol melatoninand behavior Physiology and Behaviour 90 21ndash28
Miller BL 1991 A review of chemical issues in 1H NMR spectroscopy N-acetyl-L-aspartate creatine and choline NMR in Biomedicine 4 47ndash52
Moghaddam B 2003 Bringing order to the glutamate chaos in schizophrenia Neuron40 881ndash884
Ohrmann P Siegmund A Suslow T Pedersen A Spitzberg K Kersting ARothermundt M Arolt V Heindel W Pfleiderer B 2007 Cognitive impairmentand in vivo metabolites in first-episode neuroleptic-naive and chronic medicatedschizophrenic patients a proton magnetic resonance spectroscopy study Journalof Psychiatric Research 41 625ndash634
Ohrmann P Kugel H Bauer J Siegmund A Kolkebeck K Suslow T Wiedl KHRothermundt M Arolt V Pedersen A 2008 Learning potential on the WCST inschizophrenia is related to the neuronal integrity of the anterior cingulate cortex asmeasured by proton magnetic resonance spectroscopy Schizophrenia Research106 156ndash163
Ongur D Prescot AP Jensen JE Cohen BM Renshaw PF 2009 Creatineabnormalities in schizophrenia and bipolar disorder Psychiatry ResearchNeuroimaging 172 44ndash48
Osaka N Osaka M Kondo H Morishita M Fukuyama H Shibasaki H 2004 Theneural basis of executive function in working memory an fMRI study based onindividual differences Neuroimage 21 623ndash631
Perry G Nunomura A Hirai K Zhu X Perez M Avila J Castellani RJ Atwood CSAliev G Sayre LM Takeda A Smith MA 2002 Is oxidative damage thefundamental pathogenic mechanism of Alzheimers and other neurodegenerativediseases Free Radical Biology and Medicine 33 1475ndash1479
Peterson BS Skudlarski P Gatenby JC Zhang H Anderson AW Gore JC 1999 AnfMRI study of Stroop word-color interference evidence for cingulate subregionssubserving multiple distributed attentional systems Biological Psychiatry 451237ndash1258
Provencher SW 1993 Estimation of metabolite concentrations from localized in vivoproton NMR spectra Magnetic Resonance in Medicine 30 672ndash679
Rae C Digney AL McEwan SR Bates TC 2003 Oral creatine monohydratesupplementation improves brain performance a double-blind placebo-controlledcross-over trial Proceedings Biological Sciences 270 2147ndash2150
Ross AJ Sachdev PS 2004 Magnetic resonance spectroscopy in cognitive researchBrain Research Brain Research Reviews 44 83ndash102
Rushworth MF Walton ME Kennerley SW Bannerman DM 2004 Action sets anddecisions in the medial frontal cortex Trends in Cogntive Sciences 8 410ndash417
Rutten BP Korr H Steinbusch HW Schmitz C 2003 The aging brain less neuronscould be better Mechanisms of Ageing and Development 124 349ndash355
Sanches RF Crippa JA Hallak JE de Sousa JP Araujo D Santos AC Zuardi AW2008 Proton magnetic resonance spectroscopy of the frontal cingulate andperirolandic cortices and its relationship to skin conductance in patients withschizophrenia Brazilian Journal of Medical and Biological Research 41 1132ndash1141
Schlosser RG Koch K Wagner G Nenadic I Roebel M Schachtzabel C Axer MSchultz C Reichenbach JR Sauer H 2008 Inefficient executive cognitive controlin schizophrenia is preceded by altered functional activation during informationencoding an fMRI study Neuropsychologia 46 336ndash347
Shapiro AM Benedict RH Schretlen D Brandt J 1999 Construct and concurrentvalidity of the Hopkins Verbal Learning Test-revised The Clinical Neuropsychol-ogist 13 348ndash358
Smith EE Jonides J 1999 Storage and executive processes in the frontal lobesScience 283 1657ndash1661
Szoke A Trandafir A Dupont ME Meary A Schurhoff F Leboyer M 2008Longitudinal studies of cognition in schizophrenia meta-analysis British Journal ofPsychiatry 192 248ndash257
Tayoshi S Sumitani S Taniguchi K Shibuya-Tayoshi S Numata S Iga JI NakatakiM Ueno SI Harada M Ohmori T 2009 Metabolite changes and genderdifferences in schizophrenia using 3-Tesla proton magnetic resonance spectrosco-py ((1)H-MRS) Schizophrenia Research 108 69ndash77
Theberge J Bartha R Drost DJ Menon RS Malla A Takhar J Neufeld RWRogers J Pavlosky W Schaefer B Densmore M Al-Semaan Y Williamson PC2002 Glutamate and glutamine measured with 40T proton MRS in never-treatedpatients with schizophrenia and healthy volunteers American Journal of Psychiatry159 1944ndash1946
Theberge J Al-Semaan Y Williamson PC Menon RS Neufeld RW Rajakumar NSchaefer B Densmore M Drost DJ 2003 Glutamate and glutamine in theanterior cingulate and thalamus of medicated patients with chronic schizophreniaand healthy comparison subjects measured with 40-T proton MRS AmericanJournal of Psychiatry 160 2231ndash2233
Theberge J Al-Semaan Y Drost DJ Malla AK Neufeld RW Bartha R ManchandaR Menon R Densmore M Schaefer B Williamson PC 2004 Duration ofuntreated psychosis vs N-acetylaspartate and choline in first episode schizophre-nia a 1H magnetic resonance spectroscopy study at 40 Tesla Psychiatry Research131 107ndash114
Tranberg M Stridh MH Guy Y Jilderos B Wigstrom H Weber SG Sandberg M2004 NMDA-receptor mediated efflux of N-acetylaspartate physiological andorpathological importance Neurochemistry International 45 1195ndash1204
Tranberg M Abbas AK Sandberg M 2007 In vitro studies on the putative function ofN-acetylaspartate as an osmoregulator Neurochemical Research 32 1248ndash1255
Walton ME Croxson PL Behrens TE Kennerley SW Rushworth MF 2007Adaptive decision making and value in the anterior cingulate cortex Neuroimage36 (Suppl 2) T142ndashT154
Wechsler D 1987 Wechsler Memory ScalemdashRevised Psychological Corporation NewYork
Weinberger DR Aloia MS Goldberg TE Berman KF 1994 The frontal lobes andschizophrenia Journal of Neuropsychiatry and Clinical Neurosciences 6 419ndash427
Wood SJ Yucel M Wellard RM Harrison BJ Clarke K Fornito A Velakoulis DPantelis C 2007 Evidence for neuronal dysfunction in the anterior cingulate ofpatients with schizophrenia a proton magnetic resonance spectroscopy study at3T Schizophrenia Research 94 328ndash331
Yamasue H Fukui T Fukuda R Yamada H Yamasaki S Kuroki N Abe O Kasai KTsujii K Iwanami A Aoki S Ohtomo K Kato N Kato T 2002 1H-MRspectroscopy and gray matter volume of the anterior cingulate cortex inschizophrenia NeuroReport 13 2133ndash2137
Yeo RA Hill D Campbell R Vigil J Brooks WM 2000 Developmental instabilityand working memory ability in children a magnetic resonance spectroscopyinvestigation Developmental Neuropsychology 17 143ndash159
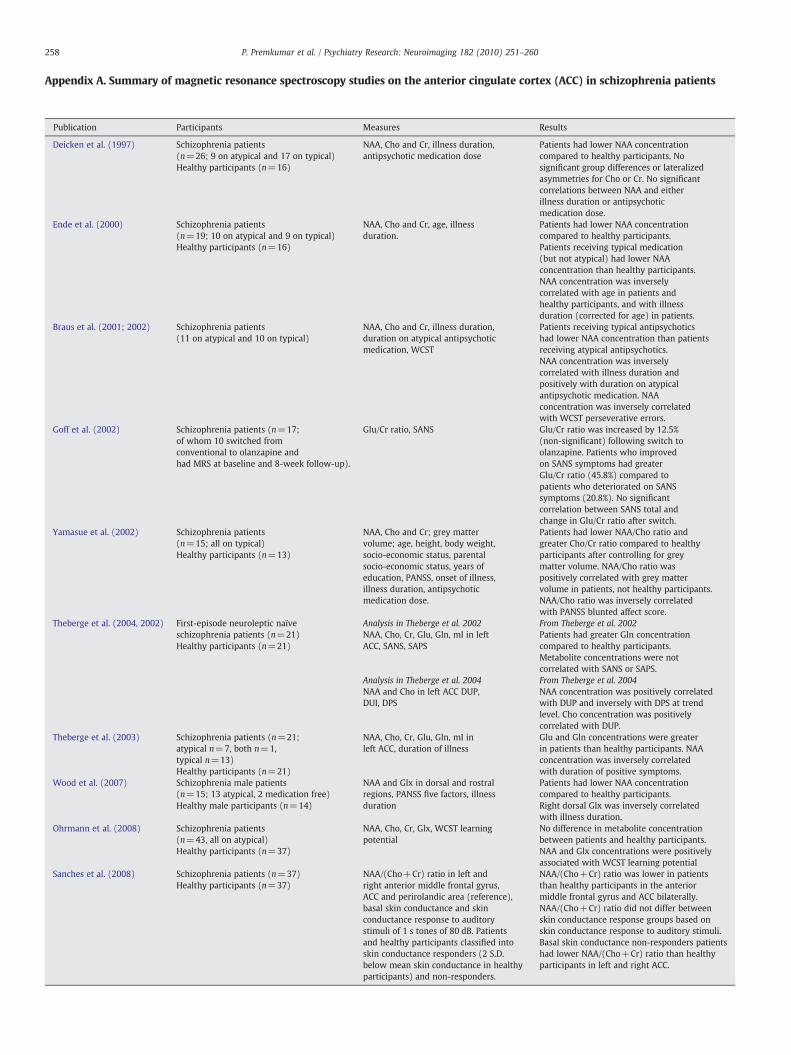
Appendix A Summary of magnetic resonance spectroscopy studies on the anterior cingulate cortex (ACC) in schizophrenia patients
Publication Participants Measures Results
Deicken et al (1997) Schizophrenia patients(n=26 9 on atypical and 17 on typical)Healthy participants (n=16)
NAA Cho and Cr illness durationantipsychotic medication dose
Patients had lower NAA concentrationcompared to healthy participants Nosignificant group differences or lateralizedasymmetries for Cho or Cr No significantcorrelations between NAA and eitherillness duration or antipsychoticmedication dose
Ende et al (2000) Schizophrenia patients(n=19 10 on atypical and 9 on typical)Healthy participants (n=16)
NAA Cho and Cr age illnessduration
Patients had lower NAA concentrationcompared to healthy participantsPatients receiving typical medication(but not atypical) had lower NAAconcentration than healthy participantsNAA concentration was inverselycorrelated with age in patients andhealthy participants and with illnessduration (corrected for age) in patients
Braus et al (2001 2002) Schizophrenia patients(11 on atypical and 10 on typical)
NAA Cho and Cr illness durationduration on atypical antipsychoticmedication WCST
Patients receiving typical antipsychoticshad lower NAA concentration than patientsreceiving atypical antipsychoticsNAA concentration was inverselycorrelated with illness duration andpositively with duration on atypicalantipsychotic medication NAAconcentration was inversely correlatedwith WCST perseverative errors
Goff et al (2002) Schizophrenia patients (n=17of whom 10 switched fromconventional to olanzapine andhad MRS at baseline and 8-week follow-up)
GluCr ratio SANS GluCr ratio was increased by 125(non-significant) following switch toolanzapine Patients who improvedon SANS symptoms had greaterGluCr ratio (458) compared topatients who deteriorated on SANSsymptoms (208) No significantcorrelation between SANS total andchange in GluCr ratio after switch
Yamasue et al (2002) Schizophrenia patients(n=15 all on typical)Healthy participants (n=13)
NAA Cho and Cr grey mattervolume age height body weightsocio-economic status parentalsocio-economic status years ofeducation PANSS onset of illnessillness duration antipsychoticmedication dose
Patients had lower NAACho ratio andgreater ChoCr ratio compared to healthyparticipants after controlling for greymatter volume NAACho ratio waspositively correlated with grey mattervolume in patients not healthy participantsNAACho ratio was inversely correlatedwith PANSS blunted affect score
Theberge et al (2004 2002) First-episode neuroleptic naiumlveschizophrenia patients (n=21)Healthy participants (n=21)
Analysis in Theberge et al 2002NAA Cho Cr Glu Gln mI in leftACC SANS SAPS
From Theberge et al 2002Patients had greater Gln concentrationcompared to healthy participantsMetabolite concentrations were notcorrelated with SANS or SAPS
Analysis in Theberge et al 2004NAA and Cho in left ACC DUPDUI DPS
From Theberge et al 2004NAA concentration was positively correlatedwith DUP and inversely with DPS at trendlevel Cho concentration was positivelycorrelated with DUP
Theberge et al (2003) Schizophrenia patients (n=21atypical n=7 both n=1typical n=13)Healthy participants (n=21)
NAA Cho Cr Glu Gln mI inleft ACC duration of illness
Glu and Gln concentrations were greaterin patients than healthy participants NAAconcentration was inversely correlatedwith duration of positive symptoms
Wood et al (2007) Schizophrenia male patients(n=15 13 atypical 2 medication free)Healthy male participants (n=14)
NAA and Glx in dorsal and rostralregions PANSS five factors illnessduration
Patients had lower NAA concentrationcompared to healthy participantsRight dorsal Glx was inversely correlatedwith illness duration
Ohrmann et al (2008) Schizophrenia patients(n=43 all on atypical)Healthy participants (n=37)
NAA Cho Cr Glx WCST learningpotential
No difference in metabolite concentrationbetween patients and healthy participantsNAA and Glx concentrations were positivelyassociated with WCST learning potential
Sanches et al (2008) Schizophrenia patients (n=37)Healthy participants (n=37)
NAA(Cho+Cr) ratio in left andright anterior middle frontal gyrusACC and perirolandic area (reference)basal skin conductance and skinconductance response to auditorystimuli of 1 s tones of 80 dB Patientsand healthy participants classified intoskin conductance responders (2 SDbelow mean skin conductance in healthyparticipants) and non-responders
NAA(Cho+Cr) ratio was lower in patientsthan healthy participants in the anteriormiddle frontal gyrus and ACC bilaterallyNAA(Cho+Cr) ratio did not differ betweenskin conductance response groups based onskin conductance response to auditory stimuliBasal skin conductance non-responders patientshad lower NAA(Cho+Cr) ratio than healthyparticipants in left and right ACC
258 P Premkumar et al Psychiatry Research Neuroimaging 182 (2010) 251ndash260
Tayoshi et al (2009) Long-term schizophrenia (n=30antipsychotic medication typenot reported)Healthy participants (n=25)
NAA Cho Cr Glu Gln mI Gender PANSStotal and subscales duration of illnessduration of therapy antipsychotic dosagebenzodiazepine dose
Patients had lower Glu and mI concentrationcompared to healthy participants Malepatients had lower NAA Cr Glu and mIconcentration than male healthy participantsMales had greater Gln concentration comparedto females Metabolite concentration wasnot correlated with symptoms or otherclinical variables
Ongur et al (2009) Schizophrenia patients (n=15)Bipolar disorder patients (n=15)Healthy participants (n=22)
Cr in ACC (hypothesized area) andparietal-occipital cortex (reference area)MADRS PANSS YMRS
Patients had lower Cr than healthyparticipants in both ACC andparietal-occipital cortex No significantcorrelations between Cr concentrationand clinical measures
ACC anterior cingulate cortex ChomdashCholine CrmdashCreatinePhosphocreatine DPSmdashduration of psychotic symptoms DUImdashduration of untreated illness DUPmdashduration of untreatedpsychosis GlnmdashGlutamine GlumdashGlutamate GluCr ratio SANSmdashSchedule for the Assessment of Negative Symptoms GlxmdashGlutamate+Glutamine MADRSmdashMontgomery AsbergDepression Rating Scale mImdashmyo-Inositol NAA N-acetyl aspartate PANSSmdashPositive and Negative Syndrome Scale SAPS Schedule for the Assessment of Positive SymptomsWCSTmdashWisconsin Card Sorting test YMRSmdashYoung Mania Rating Scale
Appendix A (continued)
259P Premkumar et al Psychiatry Research Neuroimaging 182 (2010) 251ndash260
Appendix B Supplementary Data
Supplementary data associated with this article can be found inthe online version at doi101016jpscychresns201002008
References
Adler CM Malhotra AK Elman I Goldberg T Egan M Pickar D Breier A 1999Comparison of ketamine-induced thought disorder in healthy volunteers andthought disorder in schizophrenia American Journal of Psychiatry 156 1646ndash1649
Andres RH Ducray AD Schlattner U Wallimann T Widmer HR 2008 Functionsand effects of creatine in the central nervous system Brain Research Bulletin 76329ndash343
Baiano M David A Versace A Churchill R Balestrieri M Brambilla P 2007Anterior cingulate volumes in schizophrenia a systematic review and a meta-analysis of MRI studies Schizophrenia Research 93 1ndash12
Bechara A Damasio AR Damasio H Anderson SW 1994 Insensitivity to futureconsequences following damage to human prefrontal cortex Cognition 50 7ndash15
Behrens TE Woolrich MW Walton ME Rushworth MF 2007 Learning the valueof information in an uncertain world Nature Neuroscience 10 1214ndash1221
Bertolino A Esposito G Callicott JH Mattay VS Van Horn JD Frank JA BermanKF Weinberger DR 2000 Specific relationship between prefrontal neuronal N-acetylaspartate and activation of the working memory cortical network inschizophrenia American Journal of Psychiatry 157 26ndash33
Braus DF Ende G Weber-Fahr W Demirakca T Henn FA 2001 Favorable effecton neuronal viability in the anterior cingulate gyrus due to long-term treatmentwith atypical antipsychotics an MRSI study Pharmacopsychiatry 34 251ndash253
Braus DF Ende G Weber-Fahr W Demirakca T Tost H Henn FA 2002Functioning and neuronal viability of the anterior cingulate neurons followingantipsychotic treatment MR-spectroscopic imaging in chronic schizophreniaEuropean Neuropsychopharmacology 12 145ndash152
Burgess PW Shallice T 1997 The Hayling and Brixton Tests Thames Valley TestCompany Bury St Edmunds
Callicott JH Bertolino A Mattay VS Langheim FJ Duyn J Coppola R Goldberg TEWeinberger DR 2000 Physiological dysfunction of the dorsolateral prefrontal cortexin schizophrenia revisited Cerebral Cortex 10 1078ndash1092
Carter CS van Veen V 2007 Anterior cingulate cortex and conflict detection anupdate of theory and data Cognitive Affective and Behavioral Neuroscience 7367ndash379
Cornblatt BA Risch JJ Faris G Friedman D Erlenmeyer-Kimling L 1988 TheContinuous Performance Test Identical Pairs Version (CPT-IP) I New findingsabout sustained attention in normal families Psychiatry Research 26 223ndash238
Costafreda SG Khanna A Mourao-Miranda J Fu CH 2009 Neural correlates of sadfaces predict clinical remission to cognitive behavioural therapy in depressionNeuroReport 20 637ndash641
Deicken RF Zhou L Schuff N Weiner MW 1997 Proton magnetic resonancespectroscopy of the anterior cingulate region in schizophrenia SchizophreniaResearch 27 65ndash71
Deicken RF Johnson C Pegues M 2000 Proton magnetic resonance spectroscopy ofthe human brain in schizophrenia Reviews in the Neurosciences 11 147ndash158
Ende G Braus DF Walter S Weber-Fahr W Soher B Maudsley AA Henn FA2000 Effects of age medication and illness duration on the N-acetyl aspartatesignal of the anterior cingulate region in schizophrenia Schizophrenia Research 41389ndash395
Fannon D Simmons A Tennakoon L OCeallaigh S Sumich A Doku V Shew CSharma T 2003 Selective deficit of hippocampal N-acetylaspartate in antipsy-chotic-naive patients with schizophrenia Biological Psychiatry 54 587ndash598
Ferguson KJ MacLullich AM Marshall I Deary IJ Starr JM Seckl JR Wardlaw JM2002 Magnetic resonance spectroscopy and cognitive function in healthy elderlymen Brain 125 2743ndash2749
First MB Spitzer RL Gibbon M Williams JBW 2002 Structured Clinical Interviewfor DSM-IV-TR Axis I DisordersmdashPatient Edition (SCID-IP 112002 revision)Biometrics Research Department New York NY
Fornito A Yucel M Dean B Wood SJ Pantelis C 2008 Anatomical abnormalities ofthe anterior cingulate cortex in schizophrenia bridging the gap betweenneuroimaging and neuropathology Schizophrenia Bulletin 35 973ndash993
Fowler D Garety PA Kuipers E 1995 Cognitive Behaviour Therapy for PsychosisTheory and Practice Wiley Chichester
Fujimoto T Takeuch K Matsumoto T Kamimura K Hamada R Nakamura K KatoN 2007 Abnormal glucose metabolism in the anterior cingulate cortex in patientswith schizophrenia Psychiatry Research 154 49ndash58
Goff DC Hennen J Lyoo IK Tsai G Wald LL Evins AE Yurgelun-Todd DARenshaw PF 2002 Modulation of brain and serum glutamatergic concentrationsfollowing a switch from conventional neuroleptics to olanzapine BiologicalPsychiatry 51 493ndash497
Gold JM Carpenter C Randolph C Goldberg TE Weinberger DR 1997 Auditoryworking memory and Wisconsin Card Sorting Test performance in schizophreniaArchives of General Psychiatry 54 159ndash165
Heaton RK Chelune GJ Tally JL Kay GG Curtiss G 1993 Wisconsin Card SortingTest Manual Revised and Expanded Psychological Assessment Resources OdessaFL
Honea R Crow TJ Passingham D Mackay CE 2005 Regional deficits in brainvolume in schizophrenia a meta-analysis of voxel-based morphometry studiesAmerican Journal of Psychiatry 162 2233ndash2245
Hughes C Kumari V Soni W Das M Binneman B Drozd S ONeil S Mathew VSharma T 2003 Longitudinal study of symptoms and cognitive function in chronicschizophrenia Schizophrenia Research 59 137ndash146
Jung RE Brooks WM Yeo RA Chiulli SJ Weers DC Sibbitt Jr WL 1999Biochemical markers of intelligence a proton MR spectroscopy study of normalhuman brain Proceedings Biological Sciences 266 1375ndash1379
Kaneda M Osaka N 2008 Role of anterior cingulate cortex during semantic coding inverbal working memory Neuroscience Letters 436 57ndash61
Kay SR Fiszbein A Opier LA 1987 The Positive and Negative Syndrome Scale(PANSS) for schizophrenia Schizophrenia Bulletin 13 261ndash276
Kennerley SW Dahmubed AF Lara AH Wallis JD 2008 Neurons in the frontallobe encode the value of multiple decision variables Journal of CognitiveNeuroscience 21 1162ndash1178
Kim J Whyte J Wang J Rao H Tang KZ Detre JA 2006 Continuous ASL perfusionfMRI investigation of higher cognition quantification of tonic CBF changes duringsustained attention and working memory tasks Neuroimage 31 376ndash385
Krystal JH Karper LP Seibyl JP Freeman GK Delaney R Bremner JD HeningerGR Bowers Jr MB Charney DS 1994 Subanesthetic effects of the noncom-petitive NMDA antagonist ketamine in humans Psychotomimetic perceptualcognitive and neuroendocrine responses Archives of General Psychiatry 51199ndash214
Kumari V Peters ER Fannon D Antonova E Premkumar P Anilkumar APWilliams SC Kuipers EA 2009 Dorsolateral prefrontal cortex activity predictsresponsiveness to cognitive behaviour therapy in schizophrenia BiologicalPsychiatry 66 594ndash602
Lahti AC Koffel B LaPorte D Tamminga CA 1995 Subanesthetic doses of ketaminestimulate psychosis in schizophrenia Neuropsychopharmacology 13 9ndash19
Lenartowicz A McIntosh AR 2005 The role of anterior cingulate cortex in workingmemory is shaped by functional connectivity Journal of Cognitive Neuroscience 171026ndash1042
Malhotra AK Pinals DA Adler CM Elman I Clifton A Pickar D Breier A 1997Ketamine-induced exacerbation of psychotic symptoms and cognitive impairmentin neuroleptic-free schizophrenics Neuropsychopharmacology 17 141ndash150
260 P Premkumar et al Psychiatry Research Neuroimaging 182 (2010) 251ndash260
McLean MA Woermann FG Barker GJ Duncan JS 2000 Quantitative analysis ofshort echo time (1)H-MRSI of cerebral gray and white matter Magnetic Resonancein Medicine 44 401ndash411
McMorris T Harris RC Swain J Corbett J Collard K Dyson RJ Dye L Hodgson CDraper N 2006 Effect of creatine supplementation and sleep deprivation withmild exercise on cognitive and psychomotor performance mood state and plasmaconcentrations of catecholamines and cortisol Psychopharmacology (Berl) 18593ndash103
McMorris T Harris RC Howard AN Langridge G Hall B Corbett J Dicks MHodgson C 2007 Creatine supplementation sleep deprivation cortisol melatoninand behavior Physiology and Behaviour 90 21ndash28
Miller BL 1991 A review of chemical issues in 1H NMR spectroscopy N-acetyl-L-aspartate creatine and choline NMR in Biomedicine 4 47ndash52
Moghaddam B 2003 Bringing order to the glutamate chaos in schizophrenia Neuron40 881ndash884
Ohrmann P Siegmund A Suslow T Pedersen A Spitzberg K Kersting ARothermundt M Arolt V Heindel W Pfleiderer B 2007 Cognitive impairmentand in vivo metabolites in first-episode neuroleptic-naive and chronic medicatedschizophrenic patients a proton magnetic resonance spectroscopy study Journalof Psychiatric Research 41 625ndash634
Ohrmann P Kugel H Bauer J Siegmund A Kolkebeck K Suslow T Wiedl KHRothermundt M Arolt V Pedersen A 2008 Learning potential on the WCST inschizophrenia is related to the neuronal integrity of the anterior cingulate cortex asmeasured by proton magnetic resonance spectroscopy Schizophrenia Research106 156ndash163
Ongur D Prescot AP Jensen JE Cohen BM Renshaw PF 2009 Creatineabnormalities in schizophrenia and bipolar disorder Psychiatry ResearchNeuroimaging 172 44ndash48
Osaka N Osaka M Kondo H Morishita M Fukuyama H Shibasaki H 2004 Theneural basis of executive function in working memory an fMRI study based onindividual differences Neuroimage 21 623ndash631
Perry G Nunomura A Hirai K Zhu X Perez M Avila J Castellani RJ Atwood CSAliev G Sayre LM Takeda A Smith MA 2002 Is oxidative damage thefundamental pathogenic mechanism of Alzheimers and other neurodegenerativediseases Free Radical Biology and Medicine 33 1475ndash1479
Peterson BS Skudlarski P Gatenby JC Zhang H Anderson AW Gore JC 1999 AnfMRI study of Stroop word-color interference evidence for cingulate subregionssubserving multiple distributed attentional systems Biological Psychiatry 451237ndash1258
Provencher SW 1993 Estimation of metabolite concentrations from localized in vivoproton NMR spectra Magnetic Resonance in Medicine 30 672ndash679
Rae C Digney AL McEwan SR Bates TC 2003 Oral creatine monohydratesupplementation improves brain performance a double-blind placebo-controlledcross-over trial Proceedings Biological Sciences 270 2147ndash2150
Ross AJ Sachdev PS 2004 Magnetic resonance spectroscopy in cognitive researchBrain Research Brain Research Reviews 44 83ndash102
Rushworth MF Walton ME Kennerley SW Bannerman DM 2004 Action sets anddecisions in the medial frontal cortex Trends in Cogntive Sciences 8 410ndash417
Rutten BP Korr H Steinbusch HW Schmitz C 2003 The aging brain less neuronscould be better Mechanisms of Ageing and Development 124 349ndash355
Sanches RF Crippa JA Hallak JE de Sousa JP Araujo D Santos AC Zuardi AW2008 Proton magnetic resonance spectroscopy of the frontal cingulate andperirolandic cortices and its relationship to skin conductance in patients withschizophrenia Brazilian Journal of Medical and Biological Research 41 1132ndash1141
Schlosser RG Koch K Wagner G Nenadic I Roebel M Schachtzabel C Axer MSchultz C Reichenbach JR Sauer H 2008 Inefficient executive cognitive controlin schizophrenia is preceded by altered functional activation during informationencoding an fMRI study Neuropsychologia 46 336ndash347
Shapiro AM Benedict RH Schretlen D Brandt J 1999 Construct and concurrentvalidity of the Hopkins Verbal Learning Test-revised The Clinical Neuropsychol-ogist 13 348ndash358
Smith EE Jonides J 1999 Storage and executive processes in the frontal lobesScience 283 1657ndash1661
Szoke A Trandafir A Dupont ME Meary A Schurhoff F Leboyer M 2008Longitudinal studies of cognition in schizophrenia meta-analysis British Journal ofPsychiatry 192 248ndash257
Tayoshi S Sumitani S Taniguchi K Shibuya-Tayoshi S Numata S Iga JI NakatakiM Ueno SI Harada M Ohmori T 2009 Metabolite changes and genderdifferences in schizophrenia using 3-Tesla proton magnetic resonance spectrosco-py ((1)H-MRS) Schizophrenia Research 108 69ndash77
Theberge J Bartha R Drost DJ Menon RS Malla A Takhar J Neufeld RWRogers J Pavlosky W Schaefer B Densmore M Al-Semaan Y Williamson PC2002 Glutamate and glutamine measured with 40T proton MRS in never-treatedpatients with schizophrenia and healthy volunteers American Journal of Psychiatry159 1944ndash1946
Theberge J Al-Semaan Y Williamson PC Menon RS Neufeld RW Rajakumar NSchaefer B Densmore M Drost DJ 2003 Glutamate and glutamine in theanterior cingulate and thalamus of medicated patients with chronic schizophreniaand healthy comparison subjects measured with 40-T proton MRS AmericanJournal of Psychiatry 160 2231ndash2233
Theberge J Al-Semaan Y Drost DJ Malla AK Neufeld RW Bartha R ManchandaR Menon R Densmore M Schaefer B Williamson PC 2004 Duration ofuntreated psychosis vs N-acetylaspartate and choline in first episode schizophre-nia a 1H magnetic resonance spectroscopy study at 40 Tesla Psychiatry Research131 107ndash114
Tranberg M Stridh MH Guy Y Jilderos B Wigstrom H Weber SG Sandberg M2004 NMDA-receptor mediated efflux of N-acetylaspartate physiological andorpathological importance Neurochemistry International 45 1195ndash1204
Tranberg M Abbas AK Sandberg M 2007 In vitro studies on the putative function ofN-acetylaspartate as an osmoregulator Neurochemical Research 32 1248ndash1255
Walton ME Croxson PL Behrens TE Kennerley SW Rushworth MF 2007Adaptive decision making and value in the anterior cingulate cortex Neuroimage36 (Suppl 2) T142ndashT154
Wechsler D 1987 Wechsler Memory ScalemdashRevised Psychological Corporation NewYork
Weinberger DR Aloia MS Goldberg TE Berman KF 1994 The frontal lobes andschizophrenia Journal of Neuropsychiatry and Clinical Neurosciences 6 419ndash427
Wood SJ Yucel M Wellard RM Harrison BJ Clarke K Fornito A Velakoulis DPantelis C 2007 Evidence for neuronal dysfunction in the anterior cingulate ofpatients with schizophrenia a proton magnetic resonance spectroscopy study at3T Schizophrenia Research 94 328ndash331
Yamasue H Fukui T Fukuda R Yamada H Yamasaki S Kuroki N Abe O Kasai KTsujii K Iwanami A Aoki S Ohtomo K Kato N Kato T 2002 1H-MRspectroscopy and gray matter volume of the anterior cingulate cortex inschizophrenia NeuroReport 13 2133ndash2137
Yeo RA Hill D Campbell R Vigil J Brooks WM 2000 Developmental instabilityand working memory ability in children a magnetic resonance spectroscopyinvestigation Developmental Neuropsychology 17 143ndash159

Tayoshi et al (2009) Long-term schizophrenia (n=30antipsychotic medication typenot reported)Healthy participants (n=25)
NAA Cho Cr Glu Gln mI Gender PANSStotal and subscales duration of illnessduration of therapy antipsychotic dosagebenzodiazepine dose
Patients had lower Glu and mI concentrationcompared to healthy participants Malepatients had lower NAA Cr Glu and mIconcentration than male healthy participantsMales had greater Gln concentration comparedto females Metabolite concentration wasnot correlated with symptoms or otherclinical variables
Ongur et al (2009) Schizophrenia patients (n=15)Bipolar disorder patients (n=15)Healthy participants (n=22)
Cr in ACC (hypothesized area) andparietal-occipital cortex (reference area)MADRS PANSS YMRS
Patients had lower Cr than healthyparticipants in both ACC andparietal-occipital cortex No significantcorrelations between Cr concentrationand clinical measures
ACC anterior cingulate cortex ChomdashCholine CrmdashCreatinePhosphocreatine DPSmdashduration of psychotic symptoms DUImdashduration of untreated illness DUPmdashduration of untreatedpsychosis GlnmdashGlutamine GlumdashGlutamate GluCr ratio SANSmdashSchedule for the Assessment of Negative Symptoms GlxmdashGlutamate+Glutamine MADRSmdashMontgomery AsbergDepression Rating Scale mImdashmyo-Inositol NAA N-acetyl aspartate PANSSmdashPositive and Negative Syndrome Scale SAPS Schedule for the Assessment of Positive SymptomsWCSTmdashWisconsin Card Sorting test YMRSmdashYoung Mania Rating Scale
Appendix A (continued)
259P Premkumar et al Psychiatry Research Neuroimaging 182 (2010) 251ndash260
Appendix B Supplementary Data
Supplementary data associated with this article can be found inthe online version at doi101016jpscychresns201002008
References
Adler CM Malhotra AK Elman I Goldberg T Egan M Pickar D Breier A 1999Comparison of ketamine-induced thought disorder in healthy volunteers andthought disorder in schizophrenia American Journal of Psychiatry 156 1646ndash1649
Andres RH Ducray AD Schlattner U Wallimann T Widmer HR 2008 Functionsand effects of creatine in the central nervous system Brain Research Bulletin 76329ndash343
Baiano M David A Versace A Churchill R Balestrieri M Brambilla P 2007Anterior cingulate volumes in schizophrenia a systematic review and a meta-analysis of MRI studies Schizophrenia Research 93 1ndash12
Bechara A Damasio AR Damasio H Anderson SW 1994 Insensitivity to futureconsequences following damage to human prefrontal cortex Cognition 50 7ndash15
Behrens TE Woolrich MW Walton ME Rushworth MF 2007 Learning the valueof information in an uncertain world Nature Neuroscience 10 1214ndash1221
Bertolino A Esposito G Callicott JH Mattay VS Van Horn JD Frank JA BermanKF Weinberger DR 2000 Specific relationship between prefrontal neuronal N-acetylaspartate and activation of the working memory cortical network inschizophrenia American Journal of Psychiatry 157 26ndash33
Braus DF Ende G Weber-Fahr W Demirakca T Henn FA 2001 Favorable effecton neuronal viability in the anterior cingulate gyrus due to long-term treatmentwith atypical antipsychotics an MRSI study Pharmacopsychiatry 34 251ndash253
Braus DF Ende G Weber-Fahr W Demirakca T Tost H Henn FA 2002Functioning and neuronal viability of the anterior cingulate neurons followingantipsychotic treatment MR-spectroscopic imaging in chronic schizophreniaEuropean Neuropsychopharmacology 12 145ndash152
Burgess PW Shallice T 1997 The Hayling and Brixton Tests Thames Valley TestCompany Bury St Edmunds
Callicott JH Bertolino A Mattay VS Langheim FJ Duyn J Coppola R Goldberg TEWeinberger DR 2000 Physiological dysfunction of the dorsolateral prefrontal cortexin schizophrenia revisited Cerebral Cortex 10 1078ndash1092
Carter CS van Veen V 2007 Anterior cingulate cortex and conflict detection anupdate of theory and data Cognitive Affective and Behavioral Neuroscience 7367ndash379
Cornblatt BA Risch JJ Faris G Friedman D Erlenmeyer-Kimling L 1988 TheContinuous Performance Test Identical Pairs Version (CPT-IP) I New findingsabout sustained attention in normal families Psychiatry Research 26 223ndash238
Costafreda SG Khanna A Mourao-Miranda J Fu CH 2009 Neural correlates of sadfaces predict clinical remission to cognitive behavioural therapy in depressionNeuroReport 20 637ndash641
Deicken RF Zhou L Schuff N Weiner MW 1997 Proton magnetic resonancespectroscopy of the anterior cingulate region in schizophrenia SchizophreniaResearch 27 65ndash71
Deicken RF Johnson C Pegues M 2000 Proton magnetic resonance spectroscopy ofthe human brain in schizophrenia Reviews in the Neurosciences 11 147ndash158
Ende G Braus DF Walter S Weber-Fahr W Soher B Maudsley AA Henn FA2000 Effects of age medication and illness duration on the N-acetyl aspartatesignal of the anterior cingulate region in schizophrenia Schizophrenia Research 41389ndash395
Fannon D Simmons A Tennakoon L OCeallaigh S Sumich A Doku V Shew CSharma T 2003 Selective deficit of hippocampal N-acetylaspartate in antipsy-chotic-naive patients with schizophrenia Biological Psychiatry 54 587ndash598
Ferguson KJ MacLullich AM Marshall I Deary IJ Starr JM Seckl JR Wardlaw JM2002 Magnetic resonance spectroscopy and cognitive function in healthy elderlymen Brain 125 2743ndash2749
First MB Spitzer RL Gibbon M Williams JBW 2002 Structured Clinical Interviewfor DSM-IV-TR Axis I DisordersmdashPatient Edition (SCID-IP 112002 revision)Biometrics Research Department New York NY
Fornito A Yucel M Dean B Wood SJ Pantelis C 2008 Anatomical abnormalities ofthe anterior cingulate cortex in schizophrenia bridging the gap betweenneuroimaging and neuropathology Schizophrenia Bulletin 35 973ndash993
Fowler D Garety PA Kuipers E 1995 Cognitive Behaviour Therapy for PsychosisTheory and Practice Wiley Chichester
Fujimoto T Takeuch K Matsumoto T Kamimura K Hamada R Nakamura K KatoN 2007 Abnormal glucose metabolism in the anterior cingulate cortex in patientswith schizophrenia Psychiatry Research 154 49ndash58
Goff DC Hennen J Lyoo IK Tsai G Wald LL Evins AE Yurgelun-Todd DARenshaw PF 2002 Modulation of brain and serum glutamatergic concentrationsfollowing a switch from conventional neuroleptics to olanzapine BiologicalPsychiatry 51 493ndash497
Gold JM Carpenter C Randolph C Goldberg TE Weinberger DR 1997 Auditoryworking memory and Wisconsin Card Sorting Test performance in schizophreniaArchives of General Psychiatry 54 159ndash165
Heaton RK Chelune GJ Tally JL Kay GG Curtiss G 1993 Wisconsin Card SortingTest Manual Revised and Expanded Psychological Assessment Resources OdessaFL
Honea R Crow TJ Passingham D Mackay CE 2005 Regional deficits in brainvolume in schizophrenia a meta-analysis of voxel-based morphometry studiesAmerican Journal of Psychiatry 162 2233ndash2245
Hughes C Kumari V Soni W Das M Binneman B Drozd S ONeil S Mathew VSharma T 2003 Longitudinal study of symptoms and cognitive function in chronicschizophrenia Schizophrenia Research 59 137ndash146
Jung RE Brooks WM Yeo RA Chiulli SJ Weers DC Sibbitt Jr WL 1999Biochemical markers of intelligence a proton MR spectroscopy study of normalhuman brain Proceedings Biological Sciences 266 1375ndash1379
Kaneda M Osaka N 2008 Role of anterior cingulate cortex during semantic coding inverbal working memory Neuroscience Letters 436 57ndash61
Kay SR Fiszbein A Opier LA 1987 The Positive and Negative Syndrome Scale(PANSS) for schizophrenia Schizophrenia Bulletin 13 261ndash276
Kennerley SW Dahmubed AF Lara AH Wallis JD 2008 Neurons in the frontallobe encode the value of multiple decision variables Journal of CognitiveNeuroscience 21 1162ndash1178
Kim J Whyte J Wang J Rao H Tang KZ Detre JA 2006 Continuous ASL perfusionfMRI investigation of higher cognition quantification of tonic CBF changes duringsustained attention and working memory tasks Neuroimage 31 376ndash385
Krystal JH Karper LP Seibyl JP Freeman GK Delaney R Bremner JD HeningerGR Bowers Jr MB Charney DS 1994 Subanesthetic effects of the noncom-petitive NMDA antagonist ketamine in humans Psychotomimetic perceptualcognitive and neuroendocrine responses Archives of General Psychiatry 51199ndash214
Kumari V Peters ER Fannon D Antonova E Premkumar P Anilkumar APWilliams SC Kuipers EA 2009 Dorsolateral prefrontal cortex activity predictsresponsiveness to cognitive behaviour therapy in schizophrenia BiologicalPsychiatry 66 594ndash602
Lahti AC Koffel B LaPorte D Tamminga CA 1995 Subanesthetic doses of ketaminestimulate psychosis in schizophrenia Neuropsychopharmacology 13 9ndash19
Lenartowicz A McIntosh AR 2005 The role of anterior cingulate cortex in workingmemory is shaped by functional connectivity Journal of Cognitive Neuroscience 171026ndash1042
Malhotra AK Pinals DA Adler CM Elman I Clifton A Pickar D Breier A 1997Ketamine-induced exacerbation of psychotic symptoms and cognitive impairmentin neuroleptic-free schizophrenics Neuropsychopharmacology 17 141ndash150
260 P Premkumar et al Psychiatry Research Neuroimaging 182 (2010) 251ndash260
McLean MA Woermann FG Barker GJ Duncan JS 2000 Quantitative analysis ofshort echo time (1)H-MRSI of cerebral gray and white matter Magnetic Resonancein Medicine 44 401ndash411
McMorris T Harris RC Swain J Corbett J Collard K Dyson RJ Dye L Hodgson CDraper N 2006 Effect of creatine supplementation and sleep deprivation withmild exercise on cognitive and psychomotor performance mood state and plasmaconcentrations of catecholamines and cortisol Psychopharmacology (Berl) 18593ndash103
McMorris T Harris RC Howard AN Langridge G Hall B Corbett J Dicks MHodgson C 2007 Creatine supplementation sleep deprivation cortisol melatoninand behavior Physiology and Behaviour 90 21ndash28
Miller BL 1991 A review of chemical issues in 1H NMR spectroscopy N-acetyl-L-aspartate creatine and choline NMR in Biomedicine 4 47ndash52
Moghaddam B 2003 Bringing order to the glutamate chaos in schizophrenia Neuron40 881ndash884
Ohrmann P Siegmund A Suslow T Pedersen A Spitzberg K Kersting ARothermundt M Arolt V Heindel W Pfleiderer B 2007 Cognitive impairmentand in vivo metabolites in first-episode neuroleptic-naive and chronic medicatedschizophrenic patients a proton magnetic resonance spectroscopy study Journalof Psychiatric Research 41 625ndash634
Ohrmann P Kugel H Bauer J Siegmund A Kolkebeck K Suslow T Wiedl KHRothermundt M Arolt V Pedersen A 2008 Learning potential on the WCST inschizophrenia is related to the neuronal integrity of the anterior cingulate cortex asmeasured by proton magnetic resonance spectroscopy Schizophrenia Research106 156ndash163
Ongur D Prescot AP Jensen JE Cohen BM Renshaw PF 2009 Creatineabnormalities in schizophrenia and bipolar disorder Psychiatry ResearchNeuroimaging 172 44ndash48
Osaka N Osaka M Kondo H Morishita M Fukuyama H Shibasaki H 2004 Theneural basis of executive function in working memory an fMRI study based onindividual differences Neuroimage 21 623ndash631
Perry G Nunomura A Hirai K Zhu X Perez M Avila J Castellani RJ Atwood CSAliev G Sayre LM Takeda A Smith MA 2002 Is oxidative damage thefundamental pathogenic mechanism of Alzheimers and other neurodegenerativediseases Free Radical Biology and Medicine 33 1475ndash1479
Peterson BS Skudlarski P Gatenby JC Zhang H Anderson AW Gore JC 1999 AnfMRI study of Stroop word-color interference evidence for cingulate subregionssubserving multiple distributed attentional systems Biological Psychiatry 451237ndash1258
Provencher SW 1993 Estimation of metabolite concentrations from localized in vivoproton NMR spectra Magnetic Resonance in Medicine 30 672ndash679
Rae C Digney AL McEwan SR Bates TC 2003 Oral creatine monohydratesupplementation improves brain performance a double-blind placebo-controlledcross-over trial Proceedings Biological Sciences 270 2147ndash2150
Ross AJ Sachdev PS 2004 Magnetic resonance spectroscopy in cognitive researchBrain Research Brain Research Reviews 44 83ndash102
Rushworth MF Walton ME Kennerley SW Bannerman DM 2004 Action sets anddecisions in the medial frontal cortex Trends in Cogntive Sciences 8 410ndash417
Rutten BP Korr H Steinbusch HW Schmitz C 2003 The aging brain less neuronscould be better Mechanisms of Ageing and Development 124 349ndash355
Sanches RF Crippa JA Hallak JE de Sousa JP Araujo D Santos AC Zuardi AW2008 Proton magnetic resonance spectroscopy of the frontal cingulate andperirolandic cortices and its relationship to skin conductance in patients withschizophrenia Brazilian Journal of Medical and Biological Research 41 1132ndash1141
Schlosser RG Koch K Wagner G Nenadic I Roebel M Schachtzabel C Axer MSchultz C Reichenbach JR Sauer H 2008 Inefficient executive cognitive controlin schizophrenia is preceded by altered functional activation during informationencoding an fMRI study Neuropsychologia 46 336ndash347
Shapiro AM Benedict RH Schretlen D Brandt J 1999 Construct and concurrentvalidity of the Hopkins Verbal Learning Test-revised The Clinical Neuropsychol-ogist 13 348ndash358
Smith EE Jonides J 1999 Storage and executive processes in the frontal lobesScience 283 1657ndash1661
Szoke A Trandafir A Dupont ME Meary A Schurhoff F Leboyer M 2008Longitudinal studies of cognition in schizophrenia meta-analysis British Journal ofPsychiatry 192 248ndash257
Tayoshi S Sumitani S Taniguchi K Shibuya-Tayoshi S Numata S Iga JI NakatakiM Ueno SI Harada M Ohmori T 2009 Metabolite changes and genderdifferences in schizophrenia using 3-Tesla proton magnetic resonance spectrosco-py ((1)H-MRS) Schizophrenia Research 108 69ndash77
Theberge J Bartha R Drost DJ Menon RS Malla A Takhar J Neufeld RWRogers J Pavlosky W Schaefer B Densmore M Al-Semaan Y Williamson PC2002 Glutamate and glutamine measured with 40T proton MRS in never-treatedpatients with schizophrenia and healthy volunteers American Journal of Psychiatry159 1944ndash1946
Theberge J Al-Semaan Y Williamson PC Menon RS Neufeld RW Rajakumar NSchaefer B Densmore M Drost DJ 2003 Glutamate and glutamine in theanterior cingulate and thalamus of medicated patients with chronic schizophreniaand healthy comparison subjects measured with 40-T proton MRS AmericanJournal of Psychiatry 160 2231ndash2233
Theberge J Al-Semaan Y Drost DJ Malla AK Neufeld RW Bartha R ManchandaR Menon R Densmore M Schaefer B Williamson PC 2004 Duration ofuntreated psychosis vs N-acetylaspartate and choline in first episode schizophre-nia a 1H magnetic resonance spectroscopy study at 40 Tesla Psychiatry Research131 107ndash114
Tranberg M Stridh MH Guy Y Jilderos B Wigstrom H Weber SG Sandberg M2004 NMDA-receptor mediated efflux of N-acetylaspartate physiological andorpathological importance Neurochemistry International 45 1195ndash1204
Tranberg M Abbas AK Sandberg M 2007 In vitro studies on the putative function ofN-acetylaspartate as an osmoregulator Neurochemical Research 32 1248ndash1255
Walton ME Croxson PL Behrens TE Kennerley SW Rushworth MF 2007Adaptive decision making and value in the anterior cingulate cortex Neuroimage36 (Suppl 2) T142ndashT154
Wechsler D 1987 Wechsler Memory ScalemdashRevised Psychological Corporation NewYork
Weinberger DR Aloia MS Goldberg TE Berman KF 1994 The frontal lobes andschizophrenia Journal of Neuropsychiatry and Clinical Neurosciences 6 419ndash427
Wood SJ Yucel M Wellard RM Harrison BJ Clarke K Fornito A Velakoulis DPantelis C 2007 Evidence for neuronal dysfunction in the anterior cingulate ofpatients with schizophrenia a proton magnetic resonance spectroscopy study at3T Schizophrenia Research 94 328ndash331
Yamasue H Fukui T Fukuda R Yamada H Yamasaki S Kuroki N Abe O Kasai KTsujii K Iwanami A Aoki S Ohtomo K Kato N Kato T 2002 1H-MRspectroscopy and gray matter volume of the anterior cingulate cortex inschizophrenia NeuroReport 13 2133ndash2137
Yeo RA Hill D Campbell R Vigil J Brooks WM 2000 Developmental instabilityand working memory ability in children a magnetic resonance spectroscopyinvestigation Developmental Neuropsychology 17 143ndash159
260 P Premkumar et al Psychiatry Research Neuroimaging 182 (2010) 251ndash260
McLean MA Woermann FG Barker GJ Duncan JS 2000 Quantitative analysis ofshort echo time (1)H-MRSI of cerebral gray and white matter Magnetic Resonancein Medicine 44 401ndash411
McMorris T Harris RC Swain J Corbett J Collard K Dyson RJ Dye L Hodgson CDraper N 2006 Effect of creatine supplementation and sleep deprivation withmild exercise on cognitive and psychomotor performance mood state and plasmaconcentrations of catecholamines and cortisol Psychopharmacology (Berl) 18593ndash103
McMorris T Harris RC Howard AN Langridge G Hall B Corbett J Dicks MHodgson C 2007 Creatine supplementation sleep deprivation cortisol melatoninand behavior Physiology and Behaviour 90 21ndash28
Miller BL 1991 A review of chemical issues in 1H NMR spectroscopy N-acetyl-L-aspartate creatine and choline NMR in Biomedicine 4 47ndash52
Moghaddam B 2003 Bringing order to the glutamate chaos in schizophrenia Neuron40 881ndash884
Ohrmann P Siegmund A Suslow T Pedersen A Spitzberg K Kersting ARothermundt M Arolt V Heindel W Pfleiderer B 2007 Cognitive impairmentand in vivo metabolites in first-episode neuroleptic-naive and chronic medicatedschizophrenic patients a proton magnetic resonance spectroscopy study Journalof Psychiatric Research 41 625ndash634
Ohrmann P Kugel H Bauer J Siegmund A Kolkebeck K Suslow T Wiedl KHRothermundt M Arolt V Pedersen A 2008 Learning potential on the WCST inschizophrenia is related to the neuronal integrity of the anterior cingulate cortex asmeasured by proton magnetic resonance spectroscopy Schizophrenia Research106 156ndash163
Ongur D Prescot AP Jensen JE Cohen BM Renshaw PF 2009 Creatineabnormalities in schizophrenia and bipolar disorder Psychiatry ResearchNeuroimaging 172 44ndash48
Osaka N Osaka M Kondo H Morishita M Fukuyama H Shibasaki H 2004 Theneural basis of executive function in working memory an fMRI study based onindividual differences Neuroimage 21 623ndash631
Perry G Nunomura A Hirai K Zhu X Perez M Avila J Castellani RJ Atwood CSAliev G Sayre LM Takeda A Smith MA 2002 Is oxidative damage thefundamental pathogenic mechanism of Alzheimers and other neurodegenerativediseases Free Radical Biology and Medicine 33 1475ndash1479
Peterson BS Skudlarski P Gatenby JC Zhang H Anderson AW Gore JC 1999 AnfMRI study of Stroop word-color interference evidence for cingulate subregionssubserving multiple distributed attentional systems Biological Psychiatry 451237ndash1258
Provencher SW 1993 Estimation of metabolite concentrations from localized in vivoproton NMR spectra Magnetic Resonance in Medicine 30 672ndash679
Rae C Digney AL McEwan SR Bates TC 2003 Oral creatine monohydratesupplementation improves brain performance a double-blind placebo-controlledcross-over trial Proceedings Biological Sciences 270 2147ndash2150
Ross AJ Sachdev PS 2004 Magnetic resonance spectroscopy in cognitive researchBrain Research Brain Research Reviews 44 83ndash102
Rushworth MF Walton ME Kennerley SW Bannerman DM 2004 Action sets anddecisions in the medial frontal cortex Trends in Cogntive Sciences 8 410ndash417
Rutten BP Korr H Steinbusch HW Schmitz C 2003 The aging brain less neuronscould be better Mechanisms of Ageing and Development 124 349ndash355
Sanches RF Crippa JA Hallak JE de Sousa JP Araujo D Santos AC Zuardi AW2008 Proton magnetic resonance spectroscopy of the frontal cingulate andperirolandic cortices and its relationship to skin conductance in patients withschizophrenia Brazilian Journal of Medical and Biological Research 41 1132ndash1141
Schlosser RG Koch K Wagner G Nenadic I Roebel M Schachtzabel C Axer MSchultz C Reichenbach JR Sauer H 2008 Inefficient executive cognitive controlin schizophrenia is preceded by altered functional activation during informationencoding an fMRI study Neuropsychologia 46 336ndash347
Shapiro AM Benedict RH Schretlen D Brandt J 1999 Construct and concurrentvalidity of the Hopkins Verbal Learning Test-revised The Clinical Neuropsychol-ogist 13 348ndash358
Smith EE Jonides J 1999 Storage and executive processes in the frontal lobesScience 283 1657ndash1661
Szoke A Trandafir A Dupont ME Meary A Schurhoff F Leboyer M 2008Longitudinal studies of cognition in schizophrenia meta-analysis British Journal ofPsychiatry 192 248ndash257
Tayoshi S Sumitani S Taniguchi K Shibuya-Tayoshi S Numata S Iga JI NakatakiM Ueno SI Harada M Ohmori T 2009 Metabolite changes and genderdifferences in schizophrenia using 3-Tesla proton magnetic resonance spectrosco-py ((1)H-MRS) Schizophrenia Research 108 69ndash77
Theberge J Bartha R Drost DJ Menon RS Malla A Takhar J Neufeld RWRogers J Pavlosky W Schaefer B Densmore M Al-Semaan Y Williamson PC2002 Glutamate and glutamine measured with 40T proton MRS in never-treatedpatients with schizophrenia and healthy volunteers American Journal of Psychiatry159 1944ndash1946
Theberge J Al-Semaan Y Williamson PC Menon RS Neufeld RW Rajakumar NSchaefer B Densmore M Drost DJ 2003 Glutamate and glutamine in theanterior cingulate and thalamus of medicated patients with chronic schizophreniaand healthy comparison subjects measured with 40-T proton MRS AmericanJournal of Psychiatry 160 2231ndash2233
Theberge J Al-Semaan Y Drost DJ Malla AK Neufeld RW Bartha R ManchandaR Menon R Densmore M Schaefer B Williamson PC 2004 Duration ofuntreated psychosis vs N-acetylaspartate and choline in first episode schizophre-nia a 1H magnetic resonance spectroscopy study at 40 Tesla Psychiatry Research131 107ndash114
Tranberg M Stridh MH Guy Y Jilderos B Wigstrom H Weber SG Sandberg M2004 NMDA-receptor mediated efflux of N-acetylaspartate physiological andorpathological importance Neurochemistry International 45 1195ndash1204
Tranberg M Abbas AK Sandberg M 2007 In vitro studies on the putative function ofN-acetylaspartate as an osmoregulator Neurochemical Research 32 1248ndash1255
Walton ME Croxson PL Behrens TE Kennerley SW Rushworth MF 2007Adaptive decision making and value in the anterior cingulate cortex Neuroimage36 (Suppl 2) T142ndashT154
Wechsler D 1987 Wechsler Memory ScalemdashRevised Psychological Corporation NewYork
Weinberger DR Aloia MS Goldberg TE Berman KF 1994 The frontal lobes andschizophrenia Journal of Neuropsychiatry and Clinical Neurosciences 6 419ndash427
Wood SJ Yucel M Wellard RM Harrison BJ Clarke K Fornito A Velakoulis DPantelis C 2007 Evidence for neuronal dysfunction in the anterior cingulate ofpatients with schizophrenia a proton magnetic resonance spectroscopy study at3T Schizophrenia Research 94 328ndash331
Yamasue H Fukui T Fukuda R Yamada H Yamasaki S Kuroki N Abe O Kasai KTsujii K Iwanami A Aoki S Ohtomo K Kato N Kato T 2002 1H-MRspectroscopy and gray matter volume of the anterior cingulate cortex inschizophrenia NeuroReport 13 2133ndash2137
Yeo RA Hill D Campbell R Vigil J Brooks WM 2000 Developmental instabilityand working memory ability in children a magnetic resonance spectroscopyinvestigation Developmental Neuropsychology 17 143ndash159