
Multisite Experimental Cost Study of Intensive Psychiatric Community Care
12
VOL. 21, NO. 1, 1995 Multisite Experimental Cost Study of Intensive Psychiatric Community Care 129 by Robert Rosenheck, Michael Neale, Philip Leaf, Robert Milstein, and Linda Frisman Abstract A 2-year experimental cost study of 10 Intensive Psychiatric Com- munity Care (IPCC) programs was conducted at Department of Veterans Affairs (VA) medical centers in the Northeast. High hospital users were randomly as- signed to either IPCC (n = 454) or standard VA care (« = 419) at four neuropsychiatric (NP) and six general medical and surgical (GMS) hospitals. National com- puterized data were used to track all VA health care service usage and costs for 2 years fol- lowing program entry. At 9 of the 10 sites, IPCC treatment resulted in reduced inpatient service usage. Overall, for IPCC patients compared with control patients, average inpatient usage was 89 days (33%) less while average cost per patient (for IPCC inpatient, and outpatient services) was $15,556 (20%) less. Additionally, costs for IPCC pa- tients compared with control pa- tients were $33,295 (29%) less at NP sites but were $6,273 (15%) greater at GMS sites. At both NP and GMS sites, costs were lower for IPCC patients in two sub- groups: veterans over age 45 and veterans with high levels of in- patient service use before pro- gram entry. No interaction was noted between the impact of IPCC on costs and other clinical or sociodemographic characteris- tics. Similarly, no linear relation- ship was observed between the intensity of IPCC services and the impact of IPCC on VA costs, although the two sites that did not fully implement the IPCC program had the poorest results. With these sites excluded, the total cost of care for IPCC pa- tients at GMS sites was $579 (3%) more per year than that for the control patients. Schizophrenia Bulletin, 21(1): 129-140, 1995. Over the past 25 years, a central goal of programs for the severely and chronically mentally ill has been the implementation of cost- efficient and clinically effective community-based treatment that reduces hospital usage and clinical symptoms while improving com- munity adjustment and quality of life. A number of experimental studies have shown that assertive community treatment (ACT) and/ or intensive case management pro- grams can achieve these clinical objectives, and that cost savings can be achieved by reductions in other health care expenses and in- creases in vocational productivity (Stein and Test 1980; Weisbrod et al. 1980; Hoult and Reynolds 1984; Mulder 1985; Wasylenki et al. 1985; Kiesler and Sibulkin 1987; Bond et al. 1989). Other studies, however, have found case management to be as- sociated either with no change or with increased service usage and costs (Franklin et al. 1987; Curtis et al. 1992; Rossler et al. 1992). A comprehensive review of published literature on ACT programs re- ports that although such programs often reduce psychiatric inpatient use, they do not always reduce symptoms or improve community adjustment (Olfson 1990). Doubts have also been voiced about the generalizability of previous studies in support of ACT programs because they were well-funded Reprint requests should be sent to Dr. R. Rosenheck, VA Northeast Pro- gram Evaluation Center, 950 Campbell Ave., West Haven, CT 06516. by guest on February 23, 2016 http://schizophreniabulletin.oxfordjournals.org/ Downloaded from
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Multisite Experimental Cost Study of Intensive Psychiatric Community Care
VOL. 21, NO. 1, 1995 Multisite ExperimentalCost Study of IntensivePsychiatric CommunityCare
129
by Robert Rosenheck,Michael Neale, Philip Leaf,Robert Milstein, and LindaFrisman
Abstract
A 2-year experimental cost studyof 10 Intensive Psychiatric Com-munity Care (IPCC) programswas conducted at Department ofVeterans Affairs (VA) medicalcenters in the Northeast. Highhospital users were randomly as-signed to either IPCC (n = 454)or standard VA care (« = 419) atfour neuropsychiatric (NP) andsix general medical and surgical(GMS) hospitals. National com-puterized data were used totrack all VA health care serviceusage and costs for 2 years fol-lowing program entry. At 9 ofthe 10 sites, IPCC treatmentresulted in reduced inpatientservice usage. Overall, for IPCCpatients compared with controlpatients, average inpatient usagewas 89 days (33%) less whileaverage cost per patient (forIPCC inpatient, and outpatientservices) was $15,556 (20%) less.Additionally, costs for IPCC pa-tients compared with control pa-tients were $33,295 (29%) less atNP sites but were $6,273 (15%)greater at GMS sites. At both NPand GMS sites, costs were lowerfor IPCC patients in two sub-groups: veterans over age 45 andveterans with high levels of in-patient service use before pro-gram entry. No interaction wasnoted between the impact ofIPCC on costs and other clinicalor sociodemographic characteris-tics. Similarly, no linear relation-ship was observed between theintensity of IPCC services andthe impact of IPCC on VA costs,although the two sites that didnot fully implement the IPCCprogram had the poorest results.With these sites excluded, thetotal cost of care for IPCC pa-tients at GMS sites was $579
(3%) more per year than thatfor the control patients.
Schizophrenia Bulletin, 21(1):129-140, 1995.
Over the past 25 years, a centralgoal of programs for the severelyand chronically mentally ill hasbeen the implementation of cost-efficient and clinically effectivecommunity-based treatment thatreduces hospital usage and clinicalsymptoms while improving com-munity adjustment and quality oflife. A number of experimentalstudies have shown that assertivecommunity treatment (ACT) and/or intensive case management pro-grams can achieve these clinicalobjectives, and that cost savingscan be achieved by reductions inother health care expenses and in-creases in vocational productivity(Stein and Test 1980; Weisbrod etal. 1980; Hoult and Reynolds 1984;Mulder 1985; Wasylenki et al.1985; Kiesler and Sibulkin 1987;Bond et al. 1989).
Other studies, however, havefound case management to be as-sociated either with no change orwith increased service usage andcosts (Franklin et al. 1987; Curtiset al. 1992; Rossler et al. 1992). Acomprehensive review of publishedliterature on ACT programs re-ports that although such programsoften reduce psychiatric inpatientuse, they do not always reducesymptoms or improve communityadjustment (Olfson 1990). Doubtshave also been voiced about thegeneralizability of previous studiesin support of ACT programsbecause they were well-funded
Reprint requests should be sent toDr. R. Rosenheck, VA Northeast Pro-gram Evaluation Center, 950 CampbellAve., West Haven, CT 06516.
by guest on February 23, 2016http://schizophreniabulletin.oxfordjournals.org/
Dow
nloaded from

130 SCHIZOPHRENIA BULLETIN
research/demonstration projects ex-ecuted by ideologically committedleaders in the field. Althoughthese studies can demonstrate theefficacy of programs under optimalcircumstances, their relevance forthe planning of mental healthservices under more ordinary con-ditions is uncertain (Bachrach1980).
Thus, given the inconsistency inresearch findings, the substantialcost of intensive community careprograms, and the continued pres-sure to disseminate innovative pro-grams throughout public healthcare systems, there is a need toidentify clinical settings and pa-tient subgroups in which intensivecommunity-based mental healthprograms are consistently cost-effective. More specifically, infor-mation is needed to determinewhether these programs should betargeted at a broad range of pa-tients or at specific subgroups,such as the most severely disabledor the highest service users. Suchinformation is especially importantto public mental health systemssuch as the Department of Vet-erans Affairs (VA), which, withlimited and often declining re-sources, treat large numbers ofseverely ill and disabled patients.
In 1987, on the basis of pub-lished research and consultationwith national leaders concerningthe care of the severely mentallyill, the regional director for theNortheast region of the VA initi-ated a clinical demonstration proj-ect of Intensive Psychiatric Com-munity Care (IPCC). It appearedthen that impending Gramm-Rudman Federal deficit reductionlegislation would substantiallydecrease the VA's health carebudget. As a result, there was ad-ministrative interest in determiningwhether intensive case manage-
ment teams, given responsibilityfor the care of a limited numberof the most severely recidivist VApatients, could (1) significantly re-duce these patients' reliance on in-patient treatment, thereby shiftingtheir care to community locations;and (2) justify the transfer of cur-rent inpatient resources to fund in-tensive community care teams.
This article presents data from a2-year experimental design evalua-tion that assessed the impact ofIPCC on VA health service useand related VA health care costs.Although public policymakersmust use full social cost analysesto guide their decisionmaking,analyses of costs to specific agen-cies are also useful. Indeed, mostdecisions about implementing high-intensity programs are made byadministrators whose principalconcern is the impact of such pro-grams on their own institution ororganization. Data on this aspectof the program are comprehensiveand complete. The specific impactof IPCC on VA costs is thus anarea of special interest.
This study focused particular at-tention on (1) monitoring programimplementation at each site; (2)comparing treatment available tothe control patients across sites;and (3) assessing differences in theeffectiveness of IPCC with patientshospitalized at the time of pro-gram entry at two different typesof VA medical centers: neuropsy-chiatric hospitals (NP sites) andgeneral medical and surgical hos-pitals (GMS sites). Typically lo-cated in suburban or rural settings,NP sites are large facilities thattraditionally provide long-term careto severely disabled patients; assuch, they are similar in back-ground and recent history to Statemental hospitals. GMS sites are lo-cated in urban centers and are
closely affiliated with medicalschools. They provide shorter term,crisis-oriented inpatient care akinto that offered in academic andcommunity general hospitals. Thedifferential impact of IPCC withage and diagnostic subgroups wasalso examined, along with differ-ences in the impact of IPCC pro-grams providing services at differ-ent levels of intensity.
This study is unique among ex-perimentally designed evaluationsof community-based psychiatriccare in that it involves (1) multiplesites of two distinct types; (2)treatment within a single publichealth care system in which simi-lar administrative procedures areused at all sites; (3) a complete ac-counting of within-system costs forall study participants; (4) an em-pirical comparison of both experi-mental and control treatmentsacross sites; (5) implementationunder routine circumstances, aswould be the case in dissemina-tion across a large public healthcare system; and (6) a sufficientlylarge sample to consider the im-pact of the intervention on ageand diagnostic subgroups.
Methods
Program Planning. Conceptual-ization of the IPCC program wasbased on a comprehensive reviewof the literature and on consulta-tion with an expert in the Wiscon-sin ACT model. Ten IPCC pro-grams were selected for studyafter competitive review of pro-posals from 22 VA hospitals in theNortheast. Proposals were first re-viewed by a panel of VA profes-sionals. The final selections werethen reviewed, modified, and ap-proved by a panel of three na-tional experts in community-basedmental health treatment. Consulta-
by guest on February 23, 2016http://schizophreniabulletin.oxfordjournals.org/
Dow
nloaded from
VOL 21, NO. 1, 1995 131
tion, including several site visitsand attendance at programwidestaff meetings, was obtained froma second expert in the PACT ap-proach. Responsibility for overallprogram design and implementa-tion rested with the first author,while responsibility for clinical careprovided at each site rested withthe chiefs of psychiatry, psychol-ogy, nursing, social work, and, inone case, recreation service. Activeefforts were made (with varyingdegrees of success) to improveprogram implementation at siteswhere the model did not appearto be fully implemented.
Clinical Programs. Proposals se-lected were for programs designedto operate under four coreprinciples:
1. Intensity. Patients were to beseen as often as clinically indi-cated, and caseloads were to below (7-15 patients per clinician) tofacilitate frequent contact.
2. Flexibility and community ori-entation. Clinicians were urged tosee patients wherever maximalclinical leverage could be obtainedand were encouraged to providemost of the contacts in communitysettings. Special emphasis wasplaced on involving natural sup-port systems in treatment (familymembers, landlords, employers,etc.).
3. Rehabilitation focus. Clinicalcontacts were to emphasize abroad range of rehabilitation serv-ices, including training in practicalproblem solving, crisis resolution,and adaptive skill building in nat-ural settings. The focus of the in-terventions was to be on linkagewith—and optimal usage of—bothcommunity and clinical resources,emphasizing in situ development
of community living skills.4. Continuity of care. IPCC teams
were to be a "fixed point of con-tinuing responsibility" (Test 1979,p. 18), assertively maintaining con-tact with even the most reluctantpatients. If a patient moved away,for example, contact was to bemaintained, even over long dis-tances, by telephone.
The IPCC programs were inte-grated interdisciplinary teams im-plemented under the direction ofsocial workers and nurses, and op-erating under the joint supervisionof the chief of psychiatry and thechiefs of selected other professionalservices at the sponsoring VAmedical center. Most of the teammembers were master' s-level socialworkers and nurses, and eachteam was staffed with a part-timepsychiatrist. Teams met to reviewcases at least weekly (in some in-stances daily) and were availableby phone after hours and onweekends to other VA clinicians(i.e., emergency room and inpa-tient staff members) and, throughthem, to patients, when necessary.
Program implementation wasmonitored using both weekly logs,on which all clinical contacts wererecorded, and semiannual struc-tured clinical process summaries,which were completed on eachcase. These data allowed programimplementation to be evaluated ateach site with respect to (1) thefrequency and intensity of clinicalcontacts (number of weeks withany contact, contacts per week,and minutes per contact); (2) thelocation of contacts (percentage ofclinical time taking place in com-munity settings); (3) the types ofservices provided to each patient(percentage of patients receivingone or more of several types ofrehabilitation service listed on the
semiannual summaries); and (4)the duration of involvement (per-centage of patients who terminatedbefore completing 2 years oftreatment).
To maximize consistency andquality in implementing IPCCtreatment at all sites, monthly tel-ephone conference calls involvingall program clinicians; two pro-gramwide training conferences; 30site visits by the central manage-ment/evaluation team; and fre-quent telephone contact with pro-gram managers were used.
Eligibility and Program Entry.Veterans were eligible for the ex-periment if they (1) were currentlyhospitalized on a VA psychiatricinpatient unit, (2) had a primarypsychiatric diagnosis other thansubstance abuse or organic braindisorder, and (3) met site-specificcriteria for high recent psychiatricinpatient utilization. Althoughsome patients had been hospital-ized at both NP and GMS hospi-tals, site-type assignment for ana-lytic purposes was based on thehospital to which they were admit-ted when they consented to par-ticipate in this study. Utilizationcriteria from program entry had tobe site specific because patterns ofusage differed considerably be-tween NP and GMS sites. At NPsites in this study, for example,the average number of bed daysof care per year for nonsubstanceabuse psychiatric patients dis-charged in 1988 (n = 2,942) was82 days, and 16 percent of pa-tients were hospitalized for 150 ormore days (an average of 105 pa-tients per facility). In contrast, theaverage number of bed days ofcare per year for patients at GMSsites (n = 3,753) was 25 days, andonly 4 percent of patients were
by guest on February 23, 2016http://schizophreniabulletin.oxfordjournals.org/
Dow
nloaded from

132 SCHIZOPHRENIA BULLETIN
hospitalized for 150 or more daysduring the year (an average of 14patients per facility).
Therefore, entry criteria werestricter at NP facilities. Patientshad to have 180 days of hospital-ization during the previous year,or four or more admissions (ex-cluding the current episode) dur-ing the previous year. At GMSsites, on the other hand, entry cri-teria were either 40 or more daysof psychiatric hospitalization ortwo previous admissions. Afterproviding written informed consentand completing a standardizedbaseline assessment interview, sub-jects were randomly assigned, bythe coin flip of an independentrandomizer, to either IPCC orstandard VA treatment (STD-VA).After assignment to treatment con-dition, those receiving IPCC wereintroduced to their clinicians, whowere encouraged to begin workingon plans for community reentry asquickly as possible.
Measurement of Service Use.The major clinical outcome of in-terest in this report is hospital andnursing home service use. VAhealth service utilization data werederived from the VA's nationalcomputerized workload monitoringsystems: the patient treatment filefor completed episodes of inpatienttreatment, the extended file forcompleted episodes of nursinghome and domiciliary treatment,and the outpatient file for outpa-tient treatment. The VA census fileand a supplementary survey con-ducted for this study were usedto identify usage among veteranswho were hospitalized but not dis-charged at the end of the study.These data bases are carefullycompiled since they are used bythe VA for resource allocation, andtogether they document health care
services delivered at all VA medi-cal centers nationwide. Data onVA medical care usage are there-fore available on all participants.Although coding errors and fail-ures to input data are likely tooccur to some (unfortunately un-known) degree, errors are assumedto occur at the same rate for IPCCand control subjects.
The patient treatment file classi-fies all VA beds into 20-bed sec-tions, which we collapsed intofour categories (psychiatric, med-ical, surgical, and intermediatemedical). Outpatient VA servicesare classified in the outpatient fileby 119 unique "stop codes," whichhave been collapsed into four psy-chiatric categories (individual psy-chiatric treatment, group psychiat-ric treatment, day hospital, andsubstance abuse treatment) andfour nonpsychiatric categories(medical-surgical clinic, admissions-emergency room, laboratory serv-ices, and ancillary medical serv-ices) for this analysis. Psychiatricoutpatient treatment includes treat-ment provided by other profes-sionals (e.g., psychologists, nurses,and social workers) in mentalhealth clinics. Unfortunately, pre-scribed medications are not codedin the outpatient file.
Measurement of VA Health CareCosts. Total VA health care costsfor each patient were determinedby multiplying the units of serviceconsumed by the site-specific aver-age cost per unit of service. Unitcosts for each of the four types ofinpatient care, for domiciliary andnursing home care, and for eachof the eight types of non-IPCCoutpatient care were estimated foreach medical center using theVA's standardized national CostDistribution Report (CDR). TheCDR is a facility-by-facility ac-
counting record that identifies totalexpenditures and unit costs associ-ated with VA inpatient and out-patient health care services. Usingaccounting procedures standardizedacross the entire VA system, theCDR identifies and distributes toeach major type of health careservice both direct health carecosts (for personnel services andsupplies) and indirect costs (foradministration, building mainte-nance, engineering service, equip-ment depreciation, etc.). However,data on the duration of visits, thenumber of clinicians involved ineach outpatient visit, and the in-tensity of inpatient services are notavailable from VA data bases, sothe precision of these cost esti-mates is limited.
Because it was a demonstrationprogram, site-specific expendituresfor the IPCC program itself werenot uniformly recorded on theCDR. IPCC costs were thereforeestimated through separate proce-dures specifically designed to en-sure that methods for measuringIPCC costs were the same as thoseused to measure standard costs.Included were all direct costs forprogram personnel, supplies, andequipment, and the proportion ofindirect costs for services used forIPCC (administration, buildingmanagement, engineering, etc.) thatwere provided by the sponsoringmedical center. IPCC workloaddata from the final 18 months ofthe trial were used to compute theaverage cost of program care perpatient and per visit at each site.Methods used to estimate IPCCcosts are described in detail else-where (Rosenheck et al., in press).
Two methods, also detailed else-where (Rosenheck et al. 1994)were used to estimate the oppor-tunity cost of capital. One methodused local medical office rents,
by guest on February 23, 2016http://schizophreniabulletin.oxfordjournals.org/
Dow
nloaded from
VOL 21, NO. 1, 1995 133
and the other was based on esti-mates of the replacement cost ofhospital buildings and land. Over-all, the two methods for measur-ing capital cost yielded similaraverage values across facilities.
Analyses. Analysis of covariance(ANCOVA) was used to compareutilization and costs for IPCC andSTD-VA groups, for each type ofservice for the entire 2-year periodafter program entry, for each ofthe two facility types. Data fromGMS and NP sites were analyzedseparately because different entrycriteria were used for each sitetype. In each analysis, unmeasuredsite differences were statisticallycontrolled using N-l dummy-codedsite indicators.
Factorial ANCOVA was thenused to examine the differentialimpact of IPCC on various patientsubgroups. These analyses testedthe statistical significance of theinteraction of treatment condition(IPCC vs. STD-VA) with six otherfactors in relation to VA healthcare costs. The six factors are (1)age (45 years old or less vs. allothers); (2) psychotic clinical diag-nosis (schizophrenia, schizoaffec-tive, and manic-depressive vs. allothers); (3) comorbid substanceabuse (also determined by clinicaldiagnosis); (4) marital status (evermarried vs. never married); (5)preentry days above the medianfor that site type (88 days at GMSsites, 412 days at NP sites); and(6) receipt of VA compensationpayments. Because cost and usagedata were highly skewed, all sta-tistical analyses were conducted onlogarithmically transformed varia-bles.
Comparison of Non-IPCC Treat-ment Across Sites. In a multisitestudy, differences across sites or
site types in the quality of careavailable to "control" patients mayinfluence the relative effectivenessof IPCC treatment. For example,in a facility that offers outpatienttreatment characterized by high in-tensity and continuity, the additionof IPCC treatment might not resultin substantial additional cost re-duction or clinical improvement.To assess differences in the gen-eral level of psychiatric care of-fered at the sites participating inthe study, measures were obtainedfor (1) the intensity and continuityof outpatient psychiatric care, (2)readmission rates after discharge,and (3) staffing levels in inpatientprograms. Fiscal year 1988 outpa-tient files were used, first, to de-termine the intensity of outpatientservices delivered at each facility,as measured by the average num-ber of contacts per psychiatric out-patient. Next, continuity of carewas assessed by determining thenumber of psychiatric outpatientservices received by schizophreniapatients during the year followinga discharge from inpatient care.Readmission rates during the 15days after discharge, another in-dicator of successful transition tothe community, were also com-pared. Finally, the staff-to-patientratio on general psychiatric inpa-tient units in each facility was ex-amined using administrative datagathered through a special survey.
Results
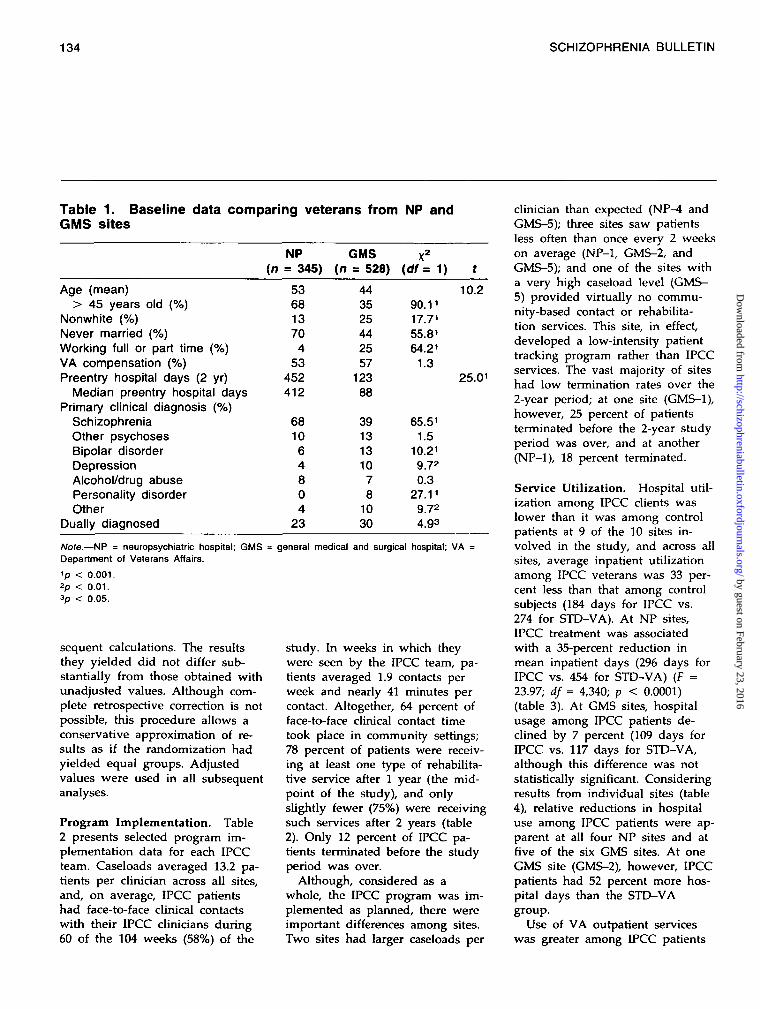
Sample Characteristics. Table 1presents baseline data for patientsfrom NP and GMS sites. Com-pared with patients from GMSsites (n = 528), those from NPsites (« = 345) were older andmore likely to be white, hadpoorer social-vocational adjustment,
and had greater hospital utiliza-tion. Patients at NP sites were alsomore likely to carry a clinical di-agnosis of schizophrenia or otherpsychoses, and were less likely tohave comorbid substance abuse di-agnoses (i.e., to be dually diag-nosed). Veterans at both site typeswere severely ill and highly serv-ice dependent.
After being pooled by site type,IPCC and control groups werecompared, to test the success ofthe randomization procedure. Al-though no significant differenceswere noted between IPCC andcontrol groups for demographic(age, race, sex) or clinical-diagnos-tic features, a significant differencein inpatient days before programentry was found among NP sites.This difference was attributableto one NP site (NP-3 on tables 4and 5) at which the experimentalgroup had fewer inpatient hospitaldays than the control group. Tocompensate for the imbalance atthis site, a conservative three-stepadjustment was made.1 The ad-justed values were used in all sub-
'First, a regression coefficient was cal-culated for the control patients, re-flecting the relationship between num-ber of inpatient days before programentry ("before days") and number ofhospital days after program entry("after days"). Second, the number of"deficit before days" was determinedfor each experimental patient at thatparticular site by subtracting that pa-tients's actual "before" days from themean "before" days of the controlgroup at that site. Finally, the numberof deficit days was multiplied by theregression coefficient, and the productwas added to the number of "afterprogram entry" days for that patient.This adjustment was made separatelyfor each type of inpatient care (psy-chiatric, medical, etc.) and for inpa-tient costs at the site involved.
by guest on February 23, 2016http://schizophreniabulletin.oxfordjournals.org/
Dow
nloaded from
134 SCHIZOPHRENIA BULLETIN
Table 1. Baseline data comparing veterans from NP andGMS sites
NP GMS x2
(/? = 345) (n = 528) (df = 1)
Age (mean)> 45 years old (%)
Nonwhite (%)Never married (%)Working full or part time (%)VA compensation (%)Preentry hospital days (2 yr)
Median preentry hospital daysPrimary clinical diagnosis (%)
SchizophreniaOther psychosesBipolar disorderDepressionAlcohol/drug abusePersonality disorderOther
Dually diagnosed
53681370
453
452412
681064804
23
443525442557
12388
3913131078
1030
90.1117.7155.81
64.21
1.3
65.511.5
10.219.720.3
27.119.724.93
10.2
25.01
Note.—NP = neuropsychiatric hospital; GMS = general medical and surgical hospital; VADepartment of Veterans Affairs.1p < 0.001.2p < 0.01.ap < 0.05.
sequent calculations. The resultsthey yielded did not differ sub-stantially from those obtained withunadjusted values. Although com-plete retrospective correction is notpossible, this procedure allows aconservative approximation of re-sults as if the randomization hadyielded equal groups. Adjustedvalues were used in all subsequentanalyses.
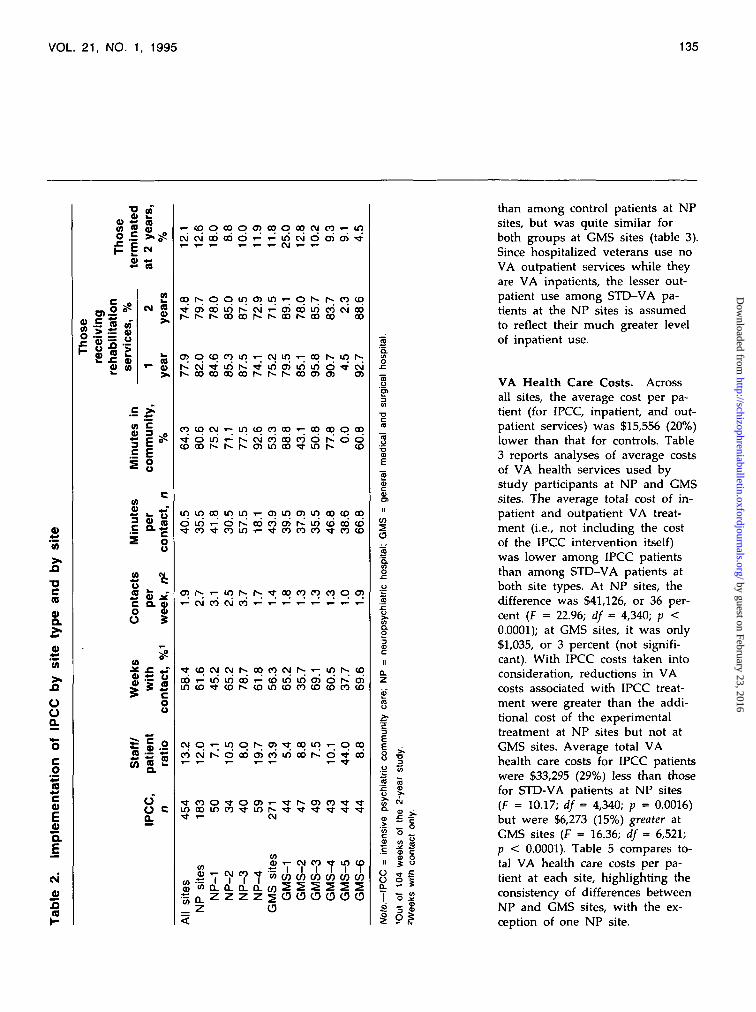
Program Implementation. Table2 presents selected program im-plementation data for each IPCCteam. Caseloads averaged 13.2 pa-tients per clinician across all sites,and, on average, IPCC patientshad face-to-face clinical contactswith their IPCC clinicians during60 of the 104 weeks (58%) of the
study. In weeks in which theywere seen by the IPCC team, pa-tients averaged 1.9 contacts perweek and nearly 41 minutes percontact. Altogether, 64 percent offace-to-face clinical contact timetook place in community settings;78 percent of patients were receiv-ing at least one type of rehabilita-tive service after 1 year (the mid-point of the study), and onlyslightly fewer (75%) were receivingsuch services after 2 years (table2). Only 12 percent of IPCC pa-tients terminated before the studyperiod was over.
Although, considered as awhole, the IPCC program was im-plemented as planned, there wereimportant differences among sites.Two sites had larger caseloads per
clinician than expected (NP^4 andGMS-5); three sites saw patientsless often than once every 2 weekson average (NP-1, GMS-2, andGMS-5); and one of the sites witha very high caseload level (GMS-5) provided virtually no commu-nity-based contact or rehabilita-tion services. This site, in effect,developed a low-intensity patienttracking program rather than IPCCservices. The vast majority of siteshad low termination rates over the2-year period; at one site (GMS-1),however, 25 percent of patientsterminated before the 2-year studyperiod was over, and at another(NP-1), 18 percent terminated.
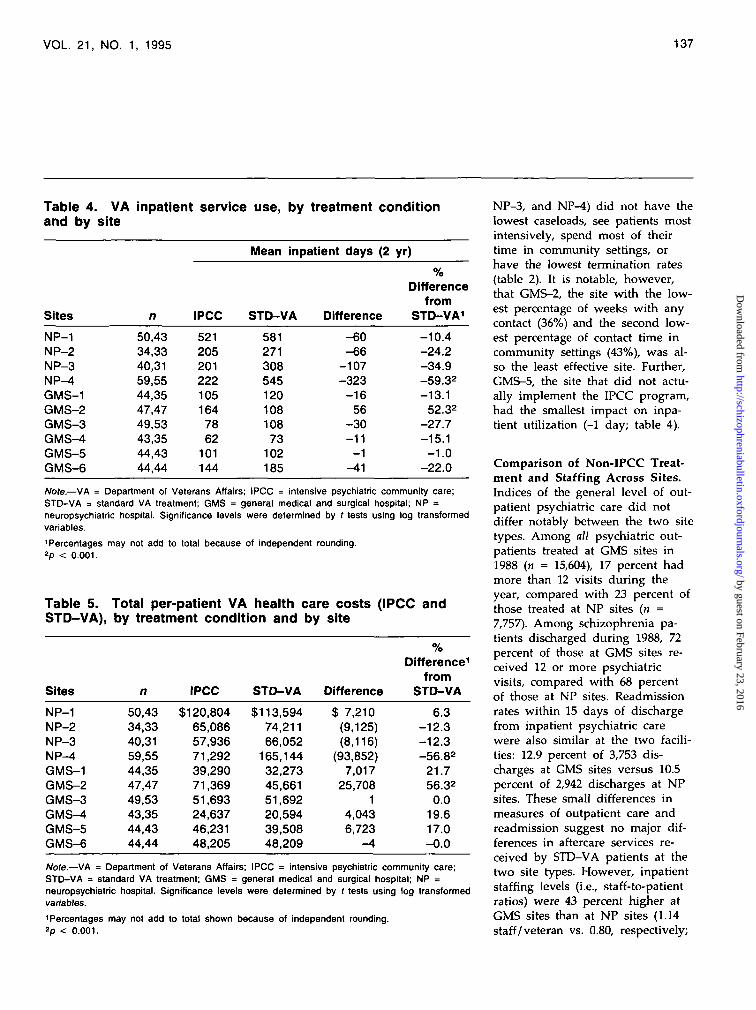
Service Utilization. Hospital util-ization among IPCC clients waslower than it was among controlpatients at 9 of the 10 sites in-volved in the study, and across allsites, average inpatient utilizationamong IPCC veterans was 33 per-cent less than that among controlsubjects (184 days for IPCC vs.274 for STD-VA). At NP sites,IPCC treatment was associatedwith a 35-percent reduction inmean inpatient days (296 days forIPCC vs. 454 for STD-VA) (F =23.97; df = 4,340; p < 0.0001)(table 3). At GMS sites, hospitalusage among IPCC patients de-clined by 7 percent (109 days forIPCC vs. 117 days for STD-VA,although this difference was notstatistically significant. Consideringresults from individual sites (table4), relative reductions in hospitaluse among IPCC patients were ap-parent at all four NP sites and atfive of the six GMS sites. At oneGMS site (GMS-2), however, IPCCpatients had 52 percent more hos-pital days than the STD-VAgroup.
Use of VA outpatient serviceswas greater among IPCC patients
by guest on February 23, 2016http://schizophreniabulletin.oxfordjournals.org/
Dow
nloaded from
VOL. 21, NO. 1, 1995 135
•o
0)
OOQ.
co
0)
oa.
CM
•O <«a> -S to« « «2 •£=»$?
•S CO
• J *1.2 88 s -s
0. «,
.£ >>v> c
II*H °2 o
(0
ii ou
I/I fi
a « *c Q. a>o vO 3
• * £ *T4) .*" O0) > a
5 s
S g.22 = T3« g.2
uOQ.
(pqtooo)oqqffl(\in i n
iri i c i o d h c oGO
o cq
CM
( 0, . <0 y- C M C O( A -«—• 1 1 1
• ^ Q ^ Z Z Z Z ^ O O O O O O
* in (D
WWW
•ffl
•5.
I! o
of
o i23 891
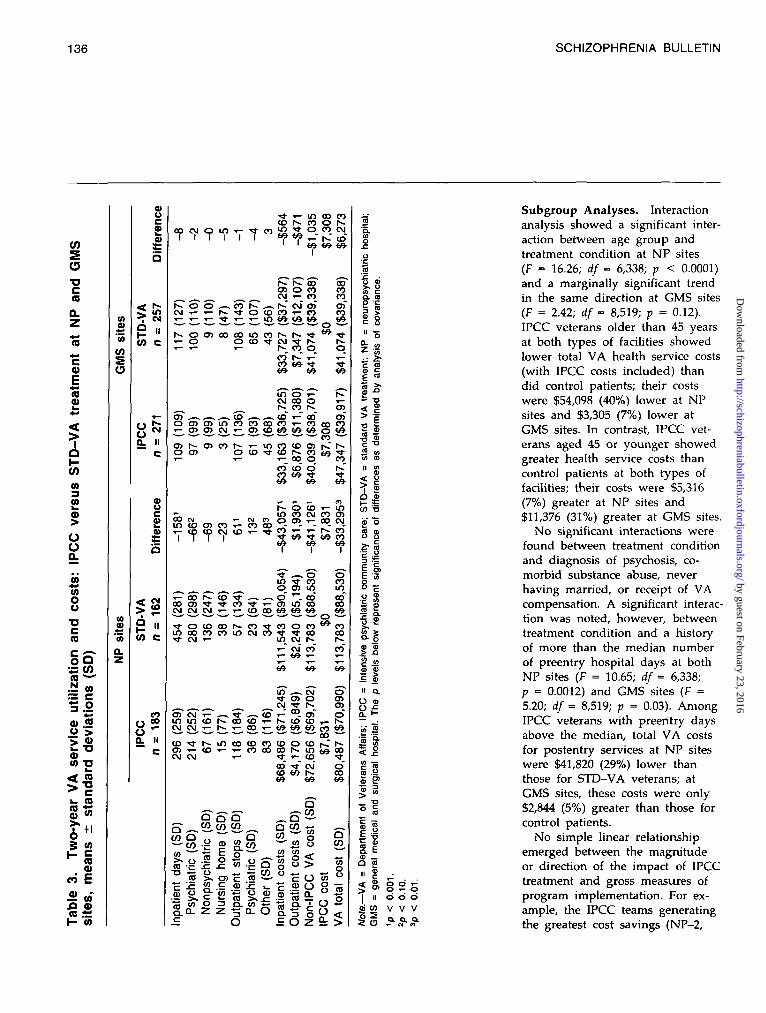
than among control patients at NPsites, but was quite similar forboth groups at GMS sites (table 3).Since hospitalized veterans use noVA outpatient services while theyare VA inpatients, the lesser out-patient use among STD-VA pa-tients at the NP sites is assumedto reflect their much greater levelof inpatient use.
VA Health Care Costs. Acrossall sites, the average cost per pa-tient (for IPCC, inpatient, and out-patient services) was $15,556 (20%)lower than that for controls. Table3 reports analyses of average costsof VA health services used bystudy participants at NP and GMSsites. The average total cost of in-patient and outpatient VA treat-ment (i.e., not including the costof the IPCC intervention itself)was lower among IPCC patientsthan among STD-VA patients atboth site types. At NP sites, thedifference was $41,126, or 36 per-cent (F = 22.96; df = 4,340; p <0.0001); at GMS sites, it was only$1,035, or 3 percent (not signifi-cant). With IPCC costs taken intoconsideration, reductions in VAcosts associated with IPCC treat-ment were greater than the addi-tional cost of the experimentaltreatment at NP sites but not atGMS sites. Average total VAhealth care costs for IPCC patientswere $33,295 (29%) less than thosefor STD-VA patients at NP sites(F = 10.17; df = 4,340; p = 0.0016)but were $6,273 (15%) greater atGMS sites (F = 16.36; df = 6,521;p < 0.0001). Table 5 compares to-tal VA health care costs per pa-tient at each site, highlighting theconsistency of differences betweenNP and GMS sites, with the ex-ception of one NP site.
by guest on February 23, 2016http://schizophreniabulletin.oxfordjournals.org/
Dow
nloaded from
136 SCHIZOPHRENIA BULLETIN
COso•DcraQ.Zre
0)
racu
CO<O
CO
>
OoQ.
sts:
ou•ocracora£{
uti
0)o'>L .
OJ(0
>
ra0)
63
CO
i i
CO
c_ora"5cu
• o
•D
ra•ocra(0
COcraa>Eof
ra2(0
P II
cy>
o N
a. IIc
< w> *
CO C
7 i n TS •*- in oo co_ r*- co o h-
co S .t o « w•>- r~- c o
r>- O OCM i - T -
cn o co^ —. 'H *°.
. CO h* .—. I— CM O>•«t O CO CO i - COr- y- in Vi Vi V>
en co i n co r» r>- • *co t CM • * r>-soo
co" r~" i-"CO Vi r)-
in o T-CM 00 Or - co r^
. co" T^ co"o o i o i i n n n o o t O i - . .>- O) O) N T- O> ( O ( 6 W « 5o> r** 05 co r -o o) o
' coco co en i C
$°Eo8fe
» o
t-~
CO
int>» o co f- _.rv in co CM co cnOOcvj -- « n O O) T- COCM
-CNJCO^^-W^^^CO
" *f «f
S ^T- (O S00 O> *?CM CM CM
•* o co co r- co TJ-in co co co in CM co• * CM f-
cn CM T - ~~.(D T-ini i n co f-- co co •>—
^ ^ CM
o> o
CDTt(-~inoocococoO > t — C O T — i— C O C O O OCM CM T- -f
O COf- inT-_ CO_
•^•" CM"
ocncn
Q - ^ ^ JO CO CO. ^ ^
•fi & c e « §2.2
a coco ~
o
QCO
QCO
tnV>
?Ia. 3£ O
co<
ii12it >
Q.
Iu
•c
.2
a oc 8
" ~o
c «
is
<p o
O o
eg,I5
1%.11II a
> ™
I!
II
| it o d dqj c/) V V V
Subgroup Analyses. Interactionanalysis showed a significant inter-action between age group andtreatment condition at NP sites(F = 16.26; df = 6,338; p < 0.0001)and a marginally significant trendin the same direction at GMS sites(F = 2.42; df = 8,519; p = 0.12).IPCC veterans older than 45 yearsat both types of facilities showedlower total VA health service costs(with IPCC costs included) thandid control patients; their costswere $54,098 (40%) lower at NPsites and $3,305 (7%) lower atGMS sites. In contrast, IPCC vet-erans aged 45 or younger showedgreater health service costs thancontrol patients at both types offacilities; their costs were $5,316(7%) greater at NP sites and$11,376 (31%) greater at GMS sites.
No significant interactions werefound between treatment conditionand diagnosis of psychosis, co-morbid substance abuse, neverhaving married, or receipt of VAcompensation. A significant interac-tion was noted, however, betweentreatment condition and a historyof more than the median numberof preentry hospital days at bothNP sites (F = 10.65; df = 6,338;p = 0.0012) and GMS sites (F =5.20; df = 8,519; p = 0.03). AmongIPCC veterans with preentry daysabove the median, total VA costsfor postentry services at NP siteswere $41,820 (29%) lower thanthose for STD-VA veterans; atGMS sites, these costs were only$2,844 (5%) greater than those forcontrol patients.
No simple linear relationshipemerged between the magnitudeor direction of the impact of IPCCtreatment and gross measures ofprogram implementation. For ex-ample, the IPCC teams generatingthe greatest cost savings (NP-2,
by guest on February 23, 2016http://schizophreniabulletin.oxfordjournals.org/
Dow
nloaded from
VOL 21, NO. 1, 1995 137
Table 4. VA inpatient service use, by treatment conditionand by site
Sites
NP-1NP-2NP-3NP-4GMS-1GMS-2GMS-3GMS-4GMS-5GMS-6
n
50,4334,3340,3159,5544,3547,4749,5343,3544,4344,44
IPCC
5212052012221051647862
101144
Mean inpatient days
STD-VA
58127130854512010810873
102185
(2yr)
Differencefrom
Difference STD-VA1
-60-66
-107-323
-1656
-30-11
-1-41
-10.4-24.2-34.9-59.32
-13.152.32
-27.7-15.1-1.0
-22.0
Note.—VA = Department of Veterans Affairs; IPCC = intensive psychiatric community care;STD-VA = standard VA treatment; GMS = general medical and surgical hospital; NP =neuropsychiatric hospital. Significance levels were determined by f tests using log transformedvariables.
'Percentages may not add to total because of independent rounding.2p < 0.001.
Table 5. Total per-patient VA health care costs (IPCC andSTD-VA), by treatment condition and by site
Sites
NP-1NP-2NP-3NP-4GMS-1GMS-2GMS-3GMS-4GMS-5GMS-6
n
50,4334,3340,3159,5544,3547,4749,5343,3544,4344,44
IPCC
$120,80465,08657,93671,29239,29071,36951,69324,63746,23148,205
STD-VA
$113,59474,21166,052
165,14432,27345,66151,69220,59439,50848,209
Difference
$ 7,210(9,125)(8,116)
(93,852)7,017
25,7081
4,0436,723
-4
Difference1
fromSTD-VA
6.3-12.3-12.3-56.82
21.756.32
0.019.617.0-0.0
Note.—VA = Department of Veterans Affairs; IPCC = intensive psychiatric community care;STD-VA = standard VA treatment; GMS = general medical and surgical hospital; NP =neuropsychiatric hospital. Significance levels were determined by ( tests using log transformedvariables.
'Percentages may not add to total shown because of independent rounding.2p < 0.001.
NP-3, and NP-4) did not have thelowest caseloads, see patients mostintensively, spend most of theirtime in community settings, orhave the lowest termination rates(table 2). It is notable, however,that GMS-2, the site with the low-est percentage of weeks with anycontact (36%) and the second low-est percentage of contact time incommunity settings (43%), was al-so the least effective site. Further,GMS-5, the site that did not actu-ally implement the IPCC program,had the smallest impact on inpa-tient utilization (-1 day; table 4).
Comparison of Non-IPCC Treat-ment and Staffing Across Sites.Indices of the general level of out-patient psychiatric care did notdiffer notably between the two sitetypes. Among all psychiatric out-patients treated at GMS sites in1988 (« = 15,604), 17 percent hadmore than 12 visits during theyear, compared with 23 percent ofthose treated at NP sites (n =7,757). Among schizophrenia pa-tients discharged during 1988, 72percent of those at GMS sites re-ceived 12 or more psychiatricvisits, compared with 68 percentof those at NP sites. Readmissionrates within 15 days of dischargefrom inpatient psychiatric carewere also similar at the two facili-ties: 12.9 percent of 3,753 dis-charges at GMS sites versus 10.5percent of 2,942 discharges at NPsites. These small differences inmeasures of outpatient care andreadmission suggest no major dif-ferences in aftercare services re-ceived by STD-VA patients at thetwo site types. However, inpatientstaffing levels (i.e., staff-to-patientratios) were 43 percent higher atGMS sites than at NP sites (1.14staff/veteran vs. 0.80, respectively;
by guest on February 23, 2016http://schizophreniabulletin.oxfordjournals.org/
Dow
nloaded from

138 SCHIZOPHRENIA BULLETIN
F = 11.82; df = 5,3; p = 0.07). Thericher staffing at GMS sites maymean that inparient units at thosehospitals may have routinely hadmore staff time to devote to dis-charge planning.
Discussion
This clinical demonstration showsthat intensive community-basedpsychiatric care, implemented atmultiple sites, reduces hospital andnursing home usage at most sitesand can be cost-efficient for theagency sponsoring the initiative.The impact of the IPCC interven-tion was greatest at long-term hos-pitals, with older patients, andwith patients with higher levelsof preintervention inpatient serviceusage. There did not appear to beany significant difference in serviceusage or cost impact among dif-ferent diagnostic subgroups.
At three of the four long-termcare sites, cost savings by IPCCpatients were greater than the costof IPCC treatment by more than$8,000 per patient over the 2years, or by $4,000 per year. Atacute care sites, in contrast, al-though hospital usage declinedsomewhat, savings in inpatientpsychiatric costs fell short of IPCCcosts by an average of about$6,000 per patient over the 2 yearsof the study, or by $3,000 peryear. Patients at NP sites had fargreater average inpatient use thanpatients at GMS facilities to beginwith, and almost twice the averagehealth care costs. In an earlier,conceptual paper, we showed thatsavings potentials are far greateramong patients with the highesthealth care costs (Rosenheck et al.1993); this simple fact may wellexplain the difference in total costefficiency of IPCC at the twotypes of medical centers. The fact
that IPCC had significantly greaterimpact on veterans whose preentrydays were above the median atboth types of sites lends supportto this interpretation.
Other systematic differences be-tween site types might also ac-count for the divergence in pro-gram impact on VA costs. Forexample, there may have beengreater continuity between inpa-tient treatment and STD-VA out-patient care at urban GMS facili-ties than at rural or suburban NPsites. The absence of substantialdifferences in intensity and con-tinuity of outpatient care and inreadmission rates between sitetypes, however, suggests that dif-ferences in the intensity of stand-ard outpatient care do not accountfor the observed results. Looked atfrom another perspective, the dif-ferential effect of the programacross site types might be under-stood as reflecting more limitedresources devoted to communityplacement at NP sites. Althoughall the NP sites maintain commu-nity residential care programs thatsupport veterans in the communityafter discharge (Linn 1981), theirsubstantially lower inpatient staff-ing levels may result in less inten-sive efforts at community place-ment for current inpatients. It ispossible that IPCC makes up forthis resource shortage.
While it is noteworthy that IPCCwas most effective with older pa-tients and that NP facilities hadtwice as many patients over age45 as GMS hospitals (68% vs.32%), the greater efficiency ofIPCC with older veterans accountsfor only part of its differential im-pact across site types. Even amongthe older veterans, savings at NPfacilities were 16 times greaterthan those at GMS facilities. Thedifferential effectiveness of IPCC
by age group is, however, of in-trinsic interest and is perhaps ex-plained by a greater amenability ofolder veterans to clinical directivesor a greater responsiveness to sup-port. Older patients may be lesssensitive to the restrictions on theirpersonal autonomy that accompanyparticipation in intensive commu-nity treatment. A study of deinsti-tutionalization at NorthamptonState Hospital in Massachusettsalso found older patients (thoseover age 60) to be least vulnerablefor rehospitalization after commu-nity placement (Geller et al. 1990).
Of particular note in this studywere the lack of cost savings asso-ciated with IPCC at GMS sites andthe considerable variation in theimpact of IPCC at those sites. Al-though IPCC patients used moretotal health care resources thancontrol patients at GMS facilities,at two sites this difference wasvirtually zero while at another siteit exceeded $27,000 (GMS-2). It isimportant to note that when datafrom the two facilities that did notfully implement the IPCC modelare excluded, the additional annualhealth care associated with IPCCtreatment drops to $1,158 over 2years, or only $579 per veteranper year—3 percent more than forthe controls.
Linear relationships were not ob-served between the frequency, du-ration, or type of IPCC servicesdelivered at each site and theirimpact on hospital usage or VAhealth care costs. However, resultsat the two GMS sites that showedleast conformity to the IPCC clini-cal model were among the poor-est. The one site that providedintensive services, but did not pro-vide them in community settings(GMS-2) actually increased bothinpatient usage and cost by morethan 50 percent, while the site that
by guest on February 23, 2016http://schizophreniabulletin.oxfordjournals.org/
Dow
nloaded from

VOL. 21, NO. 1, 1995 139
implemented a low-intensity model(GMS-5) had little impact at all oninpatient service usage and alsoshowed a substantial increase incosts. Thus, while no simple dose-response relationship was observedbetween IPCC and cost reduction(perhaps because of the smallnumber of sites), incomplete imple-mentation of the program was as-sociated with poor results.
One factor that probably limitedthe impact of the intervention atGMS sites overall was that IPCCteams did not have final decision-making authority to admit or dis-charge veterans from inpatientcare. Although they had substan-tial clinical input into dischargedecisions, their capacity to functionas gatekeepers was somewhat lim-ited even before their patientswere discharged to the community.Our impression, in addition, isthat critical factors outside of theprogram design significantly influ-enced program effectiveness atsome sites. The IPCC team atGMS-2, for example, was givenoffice space 20 miles away fromwhere most of the patients lived,was located in a large city with avery tight housing market, andwas unsuccessful in its efforts tohire a nurse clinical specialist.Such implementation barriers ap-peared to hamper severely theeffectiveness of that particularIPCC program.
Three limitations of the presentcost analysis must be noted. First,this study only concerns costs tothe VA; data on non-VA serviceuse and costs (and on VA phar-maceutical costs) were not in-cluded. In Weisbrod's well-knownstudy of the original ACT program(1980), a comprehensive view ofall social costs yielded quite dif-ferent conclusions from those gen-erated by the cost data from the
sponsoring facility alone. The VA,however, is a far more comprehen-sive health care system than themental health facilities studied byWeisbrod in Wisconsin, and sup-plementary data on non-VA healthservice use and costs (and onoverall pharmaceutical use andcosts) gathered from a subsampleof patients in this study indicatethat study participants obtainedthe vast majority of their healthcare from the VA, and that thecentral findings reported are notaltered by inclusion of non-VAcosts. These data will be reportedin the future in a presentation ofthe full social costs of thisinitiative.
Second, data on symptom status,social adjustment, and quality oflife are needed to estimate theclinical effectiveness of this treat-ment across facility types. Suchdata are available for only 70 per-cent of IPCC participants but willbe essential to the final evaluationof the benefit of IPCC treatment.
Finally, an important feature, al-though not necessarily a weakness,of this study is that treatment wasnot standardized at all sites. Aswe have seen in this study, wecannot easily separate the impactof program design from the influ-ence of idiosyncratic implementa-tion conditions at each site. Animportant distinction has beendrawn in recent years between theroles of "studies of efficacy" and"studies of effectiveness" inevaluating medical technologies(Salive et al. 1990). The centralcharacteristic of efficacy studies isthat they allow the impact of in-terventions to be evaluated underoptimal conditions—that is, whenthey are implemented by highlyskilled clinicians using comprehen-sive treatment protocols under ex-pert supervision. In contrast, effec-
tiveness studies, such as this one,are designed to further the evalua-tion of the impact of interventionswhose potential value has alreadybeen demonstrated through effi-cacy studies; this is accomplishedby assessing their impact undermore routine clinical circumstances.This study, therefore, moves be-yond efficacy studies and supportsthe conclusion that, under ordinaryimplementation conditions, hospitalusage is reduced and savings asso-ciated with IPCC programs canequal the additional costs of suchprograms. This result is most like-ly at long-term psychiatric facili-ties, with high inpatient serviceusers, with older patients, andwhen the program receives admin-istrative support that ensures itsfull implementation. It will be im-portant in the future to developmethods that ensure full imple-mentation of the IPCC model,especially at GMS sites.
References
Bachrach, L.L. Overview: Modelprograms for chronic mental pa-tients. American Journal of Psychia-try, 137:1023-1031, 1980.
Bond, G.R.; Miller, L.D.; Krum-wied, R.D.; and Ward, R.S. Asser-tive case management in threeCMHCs: A controlled study. Hos-pital and Community Psychiatry,39:411-418, 1989.
Curtis, J.L.; Millman, E.J.; Streu-ning, E.; and D'Ercole, A. Effect ofcase management on rehospitaliza-tion and utilization of ambulatorycare services. Hospital and Com-munity Psychiatry, 43:895-899, 1992.
Franklin, J.; Solovitz, B.; Mason,M.; demons, J.R.; and Miller, G.E.An evaluation of case manage-ment. American Journal of PublicHealth, 77:674-678, 1987.
by guest on February 23, 2016http://schizophreniabulletin.oxfordjournals.org/
Dow
nloaded from
140 SCHIZOPHRENIA BULLETIN
Geller, J.L.; Fisher, W.H.; Simon,L.J.; and Wirth-Cauchon, J.L.Second-generation deinstitutionali-zation: II. The impact of Brewsterv. DuKakis on correlates of com-munity and hospital utilization.American Journal of Psychiatry,147:988-993, 1990.Hoult, }., and Reynolds, I. Schizo-phrenia: A comparative trial ofcommunity oriented and hospitaloriented psychiatric care. Ada Psy-chiatrica Scandinavica, 69:359-372,1984.Kiesler, C.A., and Sibulkin, A.E.Mental Hospitalization: Myths andFacts About a National Crisis. New-bury Park, CA: Sage, 1987.Linn, M.W. Can foster care sur-vive? New Directions for MentalHealth Services, 11:35-47, 1981.Mulder, R. Evaluation of the Har-binger Program, 1982-1985. Lansing,MI: Michigan Department of Men-tal Health, 1985.
Olfson, M. Assertive communitytreatment: An evaluation of the ex-perimental evidence. Hospital andCommunity Psychiatry, 41:634-641,1990.Rosenheck, R.A.; Frisman, L.K.;and Neale, M.S. Estimating thecapital component of health carecosts in the public sector. Admin-istration and Policy in MentalHealth, 21:493-509, 1994.Rosenheck, R.A.; Massari, L.A.;and Frisman, L.K. Who should re-ceive high-cost mental health treat-ment and for how long? Schizo-phrenia Bulletin, 19(4):843-852, 1993.Rosenheck, R.A.; Neale, M.S.; andFrisman, L.K. Program costs of in-tensive case management: Estimat-ing costs and accounting for inter-site variation. Psychiatric Quarterly,in press.Rossler, W.; Loffler, W.; Fatken-heuer, B.; and Reicher-Rossler, A.
Does case management reduce therehospitalization rate? Ada Psychi-atrica Scandinavica, 86:445-449,1992.Salive, M.E.; Mayfield, J.A.; andWeissman, N.W. Patient outcomesresearch teams and the Agency forHealth Care Policy Research.Health Services Research, 25:697-708,1990.Stein, L.I., and Test, M.A. Alterna-tive to mental hospital treatment:I. Conceptual model, treatmentprogram, and clinical evaluation.Archives of General Psychiatry,37:392-397, 1980.Test, M.A. Continuity of care incommunity treatment. New Direc-tions for Mental Health Services,2:15-23, 1979.
Wasylenki, D.A.; Goering, P.N.;Lancee, W.J.; Ballantyne, R.; andFarkas, M. Impact of a case man-ager program on psychiatric after-care. Journal of Nervous and MentalDisease, 173:303-308, 1985.Weisbrod, B.; Test, M.A.; andStein, L.I. Alternative to mentalhospital treatment: II. Economiccost benefit analysis. Archives ofGeneral Psychiatry, 37:400-405,1980.
Acknowledgments
The authors thank Paul Errera,M.D. (Veterans Affairs MedicalCenter [VAMC], West Haven, CT),and Al Washko (Deaconness Hos-pital, Boston, MA), who initiatedthis project, and the followingclinical staff at 10 Departments ofthe VAMC for their assistanceover the last several years in thepreparation of this study: MarkHahn, A.C.S.W., M.P.A., and NickPazienza, Ph.D. (VAMC, Albany,NY); Nan Denton, LIC.S.W.,M.S.W., and Douglas Bitman,Ph.D. (VAMC, Boston, MA); Ming
T. Tsuang, M.D., Ph.D., JohnSimpson, Ph.D., and Greg Lock-wood, LIC.S.W. (VAMC, BrocktonWest Roxbury, MA); DanielHeimowitz, M.S.W., Debbie HarrisCobbinah, C.N.S., and SylviaRochester, C.N.S. (VAMC, Bronx,NY); Sudha Krishnaswamy, M.D.,Pauline Marsh, M.S.N., and LynnMarie Smith, M.S.W. (VAMC, Buf-falo, NY); Brad Lewis, R.N., Pa-tricia Courtwright, R.N., and FrankWilliams, C.S.W. (VAMC, Canan-daigua, NY); Arthur Russo,M.S.W., and Elizabeth Garrett, R.N.(Franklin Delano Roosevelt VAHospital, Montrose, NY); LawrenceLantinga, Ph.D., Gary Kline, M.A.,and Marilyn Baker, B.A. (VAMC,Syracuse, NY); Laurie Harkness,Ph.D., Debbie Deegan, M.S.W.,Barbara Johnson, M.S.N., andCarolyn Sweeney, R.N. (VAMC,West Haven, CT).
The Authors
Robert Rosenheck, M.D., is Direc-tor, Veterans Administration (VA)Northeast Program Evaluation Cen-ter and Clinical Professor of Psy-chiatry, Yale University, NewHaven, CT. Michael Neale, Ph.D.,is VA Intensive Psychiatric Com-munity Care Project Director, VANortheast Program Evaluation Cen-ter, West Haven, CT. Philip Leaf,Ph.D., is Professor of PublicHealth, The Johns Hopkins Univer-sity, Baltimore, MD. Robert Mil-stein, M.D., Ph.D., is AssistantClinical Professor of Psychiatry,Yale University, New Haven, CT.Linda K. Frisman, Ph.D., is ProjectDirector, Evaluation of VA HealthCare for Homeless Veterans Pro-gram, VA Northeast Program Eval-uation Center, West Haven, CT,and Associate Research Scientist,Yale University, New Haven, CT.
by guest on February 23, 2016http://schizophreniabulletin.oxfordjournals.org/
Dow
nloaded from




















