Multi-exposurecancerandnon-cancerriskassessmentoftrihalo- methanes in drinking water supplies – A...
6
Multi-exposure cancer and non-cancer risk assessment of trihalo- methanes in drinking water supplies – A case study of Eastern region of India Minashree Kumari, S.K. Gupta n , B.K. Mishra Department of Environmental Science and Engineering, ISM Dhanbad, 826004 Jharkhand, India article info Article history: Received 8 September 2014 Received in revised form 15 December 2014 Accepted 16 December 2014 Keywords: Trihalomethanes Oral ingestion Dermal absorption Cancer risk Hazard index abstract The lifetime cancer risk and the hazard index of trihalomethanes (THMs) through oral ingestion, dermal absorption, and inhalation exposure from supply water of five WTPs were analysed. THMs concentration varied from plant to plant and was found to be in the range of 274–511 mg/l, which is much higher than the prescribed USEPA standards of 80 mg/l. Chloroform was the most dominant THM followed by bro- modichloromethane (BDCM), and dibromochloromethane (DBCM). Cancer risk analysis through multi- pathways exposure reveals that residents had a higher cancer risk through oral ingestion than other two routes of exposure. The lifetime cancer risks of THMs from supply water were 100 times higher than prescribed USEPA guidelines. The higher cancer risk found for Indian context than those reported for other countries like USA, UK, Japan, Australia, is mainly due to the higher concentration level of THMs, water intake and average body weight. The study also revealed that amongst different THMs, chloroform is the major THMs causing cancer risk through both oral and dermal route of exposure whereas in case of inhalation it was mainly because of BDCM. Average lifetime cancer risk analysis indicated that females are more prone to cancer risk than males. Oral ingestion is a major route indicating the potential impact of non-cancer risk while it was insignificant through dermal exposure. Sensitivity analysis of THMs re- vealed that chloroform is the predominant parameter followed by body weight and exposure duration influencing cancer risk. & 2014 Elsevier Inc. All rights reserved. 1. Introduction Disinfection is the last step in the water treatment processes for the protection of public health. In India, chlorine is used as the primary disinfectant because of its low cost and its convenience for application in water purification. However, the presence of trihalomethanes (THMs) in chlorinated drinking water can pose severe health threat due to its potential carcinogenicity. In recent decades, various epidemiological studies have been conducted to determine the relationship between disinfection by-products (DBPs) and different health outcomes e.g., cancers and re- productive outcomes (Nieuwenhuijsen, 2005; Tardiff et al., 2006; Hrudey, 2009). Many studies suggested that exposure to DBPs increase the risk of bladder, colon, rectum, leukaemia, stomach and rectal cancers (Llopis-González et al., 2011; McGeehin et al., 1993). The results of animal studies have demonstrated that liver, kidney, and intestinal tumorigenesis are associated with chronic ingestion of THMs (Dodds et al., 1999; Yang et al., 2000). In addi- tion, some experimental studies have also demonstrated that ex- posure to DBPs in water is related to spontaneous abortion, and other adverse reproductive outcomes (Waller et al., 1998). Since THMs are the most prevalent and well documented DBP com- pounds in drinking water, they are generally considered as in- dicators of DBP exposure in epidemiological investigations. Recent studies have attempted to improve exposure assess- ment by using individual exposure measures combining routinely collected water system THM measurements with a measure of ingestion, such as number of glasses or water drank per day. However, only a few studies accounted for spatial and temporal fluctuations in THM levels across the distribution system. Fur- thermore, seeking to improve the exposure assessment, studies have begun to incorporate behavioural determinants of different routes of exposure to DBPs such as dermal absorption and in- halation during bathing and showering, and ingestion of drinking water but the contribution of these was unclear (Hoffman et al., 2008; MacLehose et al., 2008). Lee et al. (2004) calculated cancer risks and hazard index of THMs through different exposure routes Contents lists available at ScienceDirect journal homepage: www.elsevier.com/locate/ecoenv Ecotoxicology and Environmental Safety http://dx.doi.org/10.1016/j.ecoenv.2014.12.028 0147-6513/& 2014 Elsevier Inc. All rights reserved. n Corresponding author. Fax: þ91 3262296624. E-mail address: [email protected] (S.K. Gupta). Ecotoxicology and Environmental Safety 113 (2015) 433–438
Transcript of Multi-exposurecancerandnon-cancerriskassessmentoftrihalo- methanes in drinking water supplies – A...

Ecotoxicology and Environmental Safety 113 (2015) 433–438
Contents lists available at ScienceDirect
Ecotoxicology and Environmental Safety
http://d0147-65
n CorrE-m
journal homepage: www.elsevier.com/locate/ecoenv
Multi-exposure cancer and non-cancer risk assessment of trihalo-methanes in drinking water supplies – A case study of Eastern regionof India
Minashree Kumari, S.K. Gupta n, B.K. MishraDepartment of Environmental Science and Engineering, ISM Dhanbad, 826004 Jharkhand, India
a r t i c l e i n f o
Article history:Received 8 September 2014Received in revised form15 December 2014Accepted 16 December 2014
Keywords:TrihalomethanesOral ingestionDermal absorptionCancer riskHazard index
x.doi.org/10.1016/j.ecoenv.2014.12.02813/& 2014 Elsevier Inc. All rights reserved.
esponding author. Fax: þ91 3262296624.ail address: [email protected] (S.K. Gupta).
a b s t r a c t
The lifetime cancer risk and the hazard index of trihalomethanes (THMs) through oral ingestion, dermalabsorption, and inhalation exposure from supply water of five WTPs were analysed. THMs concentrationvaried from plant to plant and was found to be in the range of 274–511 mg/l, which is much higher thanthe prescribed USEPA standards of 80 mg/l. Chloroform was the most dominant THM followed by bro-modichloromethane (BDCM), and dibromochloromethane (DBCM). Cancer risk analysis through multi-pathways exposure reveals that residents had a higher cancer risk through oral ingestion than other tworoutes of exposure. The lifetime cancer risks of THMs from supply water were 100 times higher thanprescribed USEPA guidelines. The higher cancer risk found for Indian context than those reported forother countries like USA, UK, Japan, Australia, is mainly due to the higher concentration level of THMs,water intake and average body weight. The study also revealed that amongst different THMs, chloroformis the major THMs causing cancer risk through both oral and dermal route of exposure whereas in case ofinhalation it was mainly because of BDCM. Average lifetime cancer risk analysis indicated that femalesare more prone to cancer risk than males. Oral ingestion is a major route indicating the potential impactof non-cancer risk while it was insignificant through dermal exposure. Sensitivity analysis of THMs re-vealed that chloroform is the predominant parameter followed by body weight and exposure durationinfluencing cancer risk.
& 2014 Elsevier Inc. All rights reserved.
1. Introduction
Disinfection is the last step in the water treatment processes forthe protection of public health. In India, chlorine is used as theprimary disinfectant because of its low cost and its conveniencefor application in water purification. However, the presence oftrihalomethanes (THMs) in chlorinated drinking water can posesevere health threat due to its potential carcinogenicity. In recentdecades, various epidemiological studies have been conducted todetermine the relationship between disinfection by-products(DBPs) and different health outcomes e.g., cancers and re-productive outcomes (Nieuwenhuijsen, 2005; Tardiff et al., 2006;Hrudey, 2009). Many studies suggested that exposure to DBPsincrease the risk of bladder, colon, rectum, leukaemia, stomachand rectal cancers (Llopis-González et al., 2011; McGeehin et al.,1993). The results of animal studies have demonstrated that liver,kidney, and intestinal tumorigenesis are associated with chronic
ingestion of THMs (Dodds et al., 1999; Yang et al., 2000). In addi-tion, some experimental studies have also demonstrated that ex-posure to DBPs in water is related to spontaneous abortion, andother adverse reproductive outcomes (Waller et al., 1998). SinceTHMs are the most prevalent and well documented DBP com-pounds in drinking water, they are generally considered as in-dicators of DBP exposure in epidemiological investigations.
Recent studies have attempted to improve exposure assess-ment by using individual exposure measures combining routinelycollected water system THM measurements with a measure ofingestion, such as number of glasses or water drank per day.However, only a few studies accounted for spatial and temporalfluctuations in THM levels across the distribution system. Fur-thermore, seeking to improve the exposure assessment, studieshave begun to incorporate behavioural determinants of differentroutes of exposure to DBPs such as dermal absorption and in-halation during bathing and showering, and ingestion of drinkingwater but the contribution of these was unclear (Hoffman et al.,2008; MacLehose et al., 2008). Lee et al. (2004) calculated cancerrisks and hazard index of THMs through different exposure routes
M. Kumari et al. / Ecotoxicology and Environmental Safety 113 (2015) 433–438434
for tap water in Hong Kong, and reported that exposure throughoral ingestion had higher risk than through dermal absorption andinhalation. A similar result was reported by Tokmak et al. (2004)and Amjad et al. (2013) which concluded that the highest risk wasfrom the exposure to chloroform through oral ingestion. It has alsobeen reported that THMs are generally well absorbed, metabo-lized, and rapidly eliminated by mammals after oral or inhalationexposure (IPCS, 2000). The discrepancy that the importance of thethree exposure pathways ranked differently in the studies may beattributed to different concentration and speciation of THMs pre-sent in the waters.
Traditional risk assessments of water often consider only in-gestion exposure to toxic chemicals, but scientists proposed thatinhalation and dermal absorption be considered in the risk as-sessment of drinking water since 1990 (Jo et al., 1990; Weisel et al.,1999). Therefore, the purpose of this study is to conduct multi-pathway exposure assessment of the drinking water of five watertreatment plants (WTPs) based on the concentrations of THMswithin distribution systems in Jharkhand and West Bengal. In thisstudy, the cancer risks associated with THMs exposure fromdrinking water in Eastern region of India was estimated for eachspecies and each exposure pathway. The THM data in drinkingwater were first collected from WTPs. Furthermore, cancer andnon-cancer risk assessment of THMs for both males and females,respectively were also carried out using different models as nosuch study has been carried out for them in this region.
2. Materials and methods
2.1. Description of WTPs and sampling protocol
For this study, five major WTPs situated in the Eastern region ofIndia namely Indira Gandhi WTP, Kolkata (IGWTP II), Asansol-Durgapur Development Authority WTP, Raniganj (ADDA), Swarn-rekha WTP, Ranchi (SWTP), Maithon WTP, Maithon (MWTP) andMineral Area Development Authority WTP, Dhanbad [MADA (N)]were selected. Two main rivers (i.e. Ganga and Damodar) were thesource of raw waters to these WTPs. The WTPs selected understudy ranged from 5MGD to 260MGD, which shows a wide var-iation in the water supply distribution network. All these watertreatment plants (WTPs) follow the conventional method oftreatment comprising of coagulation-flocculation, sedimentation,filtration, and chlorination or disinfection.
Drinking water samples were collected in triplicates frompublic water supplies between October 2012 and September 2013.A total of 25 samples were collected at each sampling location. Thesamples were collected in 40-mL clean glass vials with poly-propylene cap and PTFE-faced rubber septa and it was added withsodium sulphite (0.010 g) as a dechlorination agent to eliminateany residual chlorine to stop further THM formation. The sampleswere stored in dark at temperature o4 °C for further analysis.
2.2. Analysis of THMs
The samples were subjected to liquid–liquid extraction usingpentane as a solvent. The vials were then shaken vigorously for1 min and allowed to stand for 3 min to facilitate phase separation.The pentane phase was removed and placed in 2 ml auto-samplervials. 1 ml extract was then analysed using nitrogen as the carriergas at a flow rate of 1.2 ml/min. Trihalomethanes were analysed asper USEPA methods 551.1 (USEPA, 1995). A Chemito CERES 800Plus gas chromatograph (Thermo Fischer) equipped with anelectron capture detector (ECD) was used for the determinationand quantification of THMs. The column used for analysis wasfused silica DB-5, 30 m�0.32 mm I.D.�0.30 mm film thicknesses.
Analytical grade calibration standards with a purity of 499.5%were procured from Sigma Aldrich (Germany). The mean recoveryof four THM species ranged between 86.9% and 102.3% for thismethod.
2.3. Quality control/quality assurance procedure (QA/QC)
Laboratory requirements included, initial demonstration of la-boratory capability, determination of method detection limit,analysis of laboratory reagent blanks, field reagent blank, fieldduplicates and calibration check standards (USEPA, 1995).
For the initial demonstration of the laboratory capability, theobserved chromatographic peaks, obtained by running a standardsolution of method analytes were identified by comparing theretention times with those given in the EPA method 551. Then,oven temperature programme was modified according to the re-tention time of the last peak of the method analyte. To obtain asmooth baseline, a non-polar organic solvent (hexane) was runbefore analysis of the each batch of the samples. Before each run,the GC syringe was rinsed three times with hexane.
The field reagent blanks were collected to determine if anyinterference was present in the field environment. Laboratory re-agent blanks were analysed to determine if method analytes orother interferences were present in the laboratory environment,the reagents, or the apparatus. On the other hand, the precision ofthe measurements was estimated using field duplicates (FD). Therelative difference (RPD) between two parallel samples was cal-culated. The method of detection limit was calculated for eachcompound by analysing replicates of standard solution at a con-centration of 0.25 mg/L. Continuing calibration checks were per-formed every 20 samples. If the relative percent difference be-tween the response of the initial calibration and the calibrationcheck standard was 420%, the instrument was considered as outof calibration, and recalibrated.
2.4. Cancer risk estimation
In this study, estimation of lifetime cancer risk of THMs in fiveWTPs is based on the United States Environmental ProtectionAgency (USEPA) guideline (USEPA, 1986, 1999, 2002) and Lee etal.’s (2004) study. However, the guideline values for the para-meters such as water intake, average body weight, exposureduration and frequency were adopted as the Indian conditions(ICMR, 2009). In general, the process of risk assessment includesthe following four components: data collection and evaluation,exposure assessment, toxicity assessment, and risk characteriza-tion (Lee et al., 2004). The exposure source pathways, potentiallyexposed populations, the magnitude, duration, and frequency ofexposure to site contaminants were identified based on the life-style of residents and the behaviour of contaminated chemicals indrinking water. In this study, the cancer risks for exposure throughoral ingestion, dermal absorption, and inhalation exposure wereconsidered. Since, the values of the parameters like average bodyweight, the amount of air breathed, exposure frequency and in-gestion rate of water varies from region to region due to change inclimatic conditions, and standard of living. Therefore, the values ofthese parameters were adopted as per Indian conditions (ICMR,2009). For adults, the exposure rates were converted to a dailydose by assuming 20 m3 aspirated air per day, and average bodyweights of 70 kg for male and 60 kg for female. An entire lifetimeof 70 and 60 years applies to males and females, respectively.
Moreover, the hazard indices of THMs in different exposureroutes are also calculated for non-carcinogenic risk assessment.The calculation of hazard indices for ingestion route and dermalabsorption is described elsewhere (Lee et al., 2004). On the otherhand, calculation of cancer slope factors and unit risk estimates
M. Kumari et al. / Ecotoxicology and Environmental Safety 113 (2015) 433–438 435
were performed to evaluate the carcinogenic effects. The results ofexposure and toxicity assessments were then compared with theintake estimates with appropriate toxicological values to de-termine the likelihood of adverse effects in potentially exposedpopulations.
3. Results and discussion
3.1. Speciation of THMs in drinking water supplies
THM concentrations varied from plant to plant and was foundto be in the range of 274–511 mg/l, which is much higher than theprescribed USEPA standards of 80 mg/l and the concentration re-ported in other countries (Amjad et al., 2013; Karim et al., 2011;Pardakhti et al., 2011; Legay et al., 2011; Chowdhury et al., 2011).Higher values of THMs found in Indian context may be attributedto the variation in the surface water quality and the treatmentsystems adopted. Chloroform was the major contributor to thetotal THMs and its value ranged from 236 to 503 mg/l indicatingmajor contribution (497.2%) to total THMs. BDCM and DBCMmade a trivial contribution of 0.02–2% and 0.03–4%, respectively.Many researchers also reported elevated concentration of thesecompounds in drinking water supplies (Thacker et al., 2002; Hasanet al., 2010; Karim et al., 2011). However, Charrois et al. (2004)reported that bromoform was the major contributor to total THMs,which was due to the presence of bromide in raw water. The ab-sence of bromoform in our study may be due to the absence ofbromide in raw water (Pardakhti et al., 2011; Summerhayes et al.,2011; Uyak and Toroz, 2005). The order of contribution followedby all the THMs was found as chloroform4BDCM4DBCM4bromoform. Similar findings have been reported in the literature(Uyak, 2006; Legay et al., 2011; Karim et al., 2011; Pardakhti et al.,2011).
3.2. Multi-pathway evaluations of lifetime cancer risks for THMs
3.2.1. Ingestion routeFor evaluation of cancer risk, the potency factor of the four
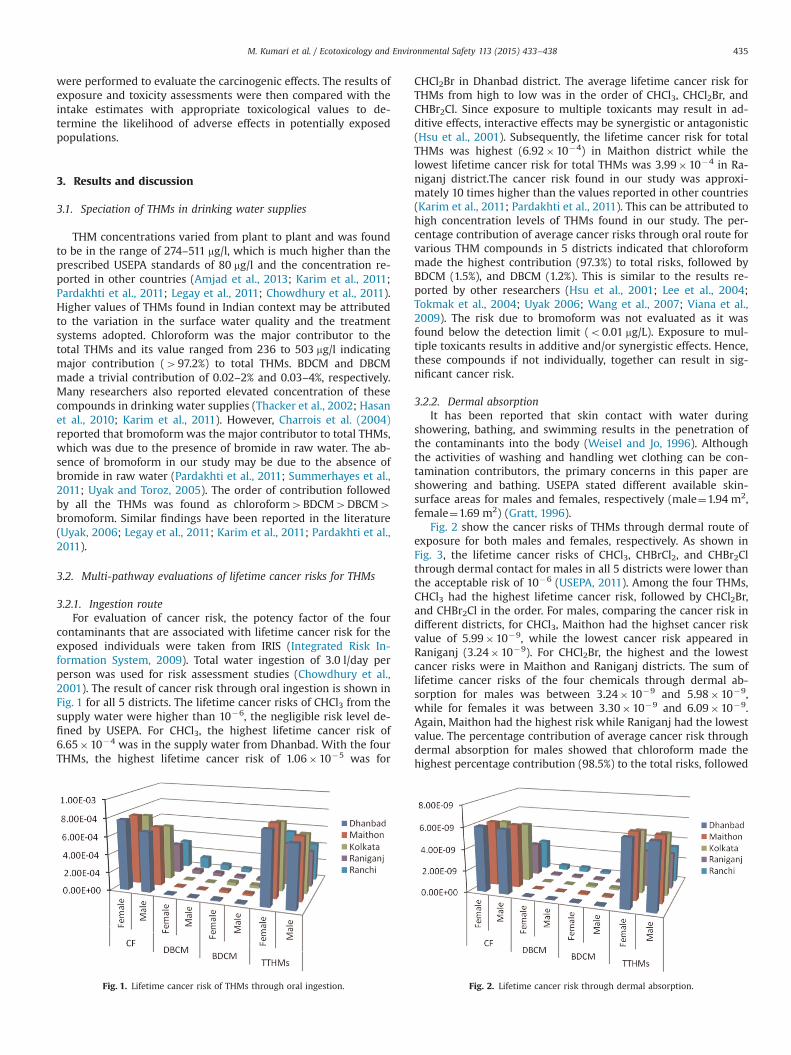
contaminants that are associated with lifetime cancer risk for theexposed individuals were taken from IRIS (Integrated Risk In-formation System, 2009). Total water ingestion of 3.0 l/day perperson was used for risk assessment studies (Chowdhury et al.,2001). The result of cancer risk through oral ingestion is shown inFig. 1 for all 5 districts. The lifetime cancer risks of CHCl3 from thesupply water were higher than 10�6, the negligible risk level de-fined by USEPA. For CHCl3, the highest lifetime cancer risk of6.65�10�4 was in the supply water from Dhanbad. With the fourTHMs, the highest lifetime cancer risk of 1.06�10�5 was for
Fig. 1. Lifetime cancer risk of THMs through oral ingestion.
CHCl2Br in Dhanbad district. The average lifetime cancer risk forTHMs from high to low was in the order of CHCl3, CHCl2Br, andCHBr2Cl. Since exposure to multiple toxicants may result in ad-ditive effects, interactive effects may be synergistic or antagonistic(Hsu et al., 2001). Subsequently, the lifetime cancer risk for totalTHMs was highest (6.92�10�4) in Maithon district while thelowest lifetime cancer risk for total THMs was 3.99�10�4 in Ra-niganj district.The cancer risk found in our study was approxi-mately 10 times higher than the values reported in other countries(Karim et al., 2011; Pardakhti et al., 2011). This can be attributed tohigh concentration levels of THMs found in our study. The per-centage contribution of average cancer risks through oral route forvarious THM compounds in 5 districts indicated that chloroformmade the highest contribution (97.3%) to total risks, followed byBDCM (1.5%), and DBCM (1.2%). This is similar to the results re-ported by other researchers (Hsu et al., 2001; Lee et al., 2004;Tokmak et al., 2004; Uyak 2006; Wang et al., 2007; Viana et al.,2009). The risk due to bromoform was not evaluated as it wasfound below the detection limit (o0.01 mg/L). Exposure to mul-tiple toxicants results in additive and/or synergistic effects. Hence,these compounds if not individually, together can result in sig-nificant cancer risk.
3.2.2. Dermal absorptionIt has been reported that skin contact with water during
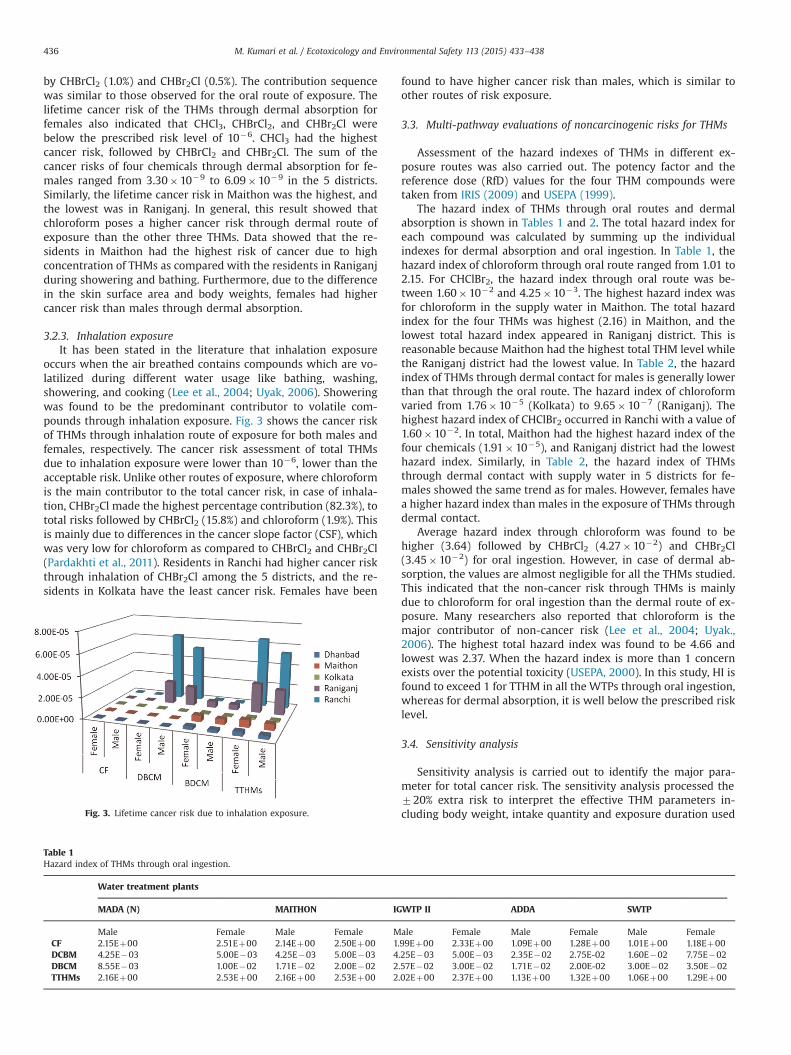
showering, bathing, and swimming results in the penetration ofthe contaminants into the body (Weisel and Jo, 1996). Althoughthe activities of washing and handling wet clothing can be con-tamination contributors, the primary concerns in this paper areshowering and bathing. USEPA stated different available skin-surface areas for males and females, respectively (male¼1.94 m2,female¼1.69 m2) (Gratt, 1996).
Fig. 2 show the cancer risks of THMs through dermal route ofexposure for both males and females, respectively. As shown inFig. 3, the lifetime cancer risks of CHCl3, CHBrCl2, and CHBr2Clthrough dermal contact for males in all 5 districts were lower thanthe acceptable risk of 10�6 (USEPA, 2011). Among the four THMs,CHCl3 had the highest lifetime cancer risk, followed by CHCl2Br,and CHBr2Cl in the order. For males, comparing the cancer risk indifferent districts, for CHCl3, Maithon had the highset cancer riskvalue of 5.99�10�9, while the lowest cancer risk appeared inRaniganj (3.24�10�9). For CHCl2Br, the highest and the lowestcancer risks were in Maithon and Raniganj districts. The sum oflifetime cancer risks of the four chemicals through dermal ab-sorption for males was between 3.24�10�9 and 5.98�10�9,while for females it was between 3.30�10�9 and 6.09�10�9.Again, Maithon had the highest risk while Raniganj had the lowestvalue. The percentage contribution of average cancer risk throughdermal absorption for males showed that chloroform made thehighest percentage contribution (98.5%) to the total risks, followed
Fig. 2. Lifetime cancer risk through dermal absorption.
M. Kumari et al. / Ecotoxicology and Environmental Safety 113 (2015) 433–438436
by CHBrCl2 (1.0%) and CHBr2Cl (0.5%). The contribution sequencewas similar to those observed for the oral route of exposure. Thelifetime cancer risk of the THMs through dermal absorption forfemales also indicated that CHCl3, CHBrCl2, and CHBr2Cl werebelow the prescribed risk level of 10�6. CHCl3 had the highestcancer risk, followed by CHBrCl2 and CHBr2Cl. The sum of thecancer risks of four chemicals through dermal absorption for fe-males ranged from 3.30�10�9 to 6.09�10�9 in the 5 districts.Similarly, the lifetime cancer risk in Maithon was the highest, andthe lowest was in Raniganj. In general, this result showed thatchloroform poses a higher cancer risk through dermal route ofexposure than the other three THMs. Data showed that the re-sidents in Maithon had the highest risk of cancer due to highconcentration of THMs as compared with the residents in Raniganjduring showering and bathing. Furthermore, due to the differencein the skin surface area and body weights, females had highercancer risk than males through dermal absorption.
3.2.3. Inhalation exposureIt has been stated in the literature that inhalation exposure
occurs when the air breathed contains compounds which are vo-latilized during different water usage like bathing, washing,showering, and cooking (Lee et al., 2004; Uyak, 2006). Showeringwas found to be the predominant contributor to volatile com-pounds through inhalation exposure. Fig. 3 shows the cancer riskof THMs through inhalation route of exposure for both males andfemales, respectively. The cancer risk assessment of total THMsdue to inhalation exposure were lower than 10�6, lower than theacceptable risk. Unlike other routes of exposure, where chloroformis the main contributor to the total cancer risk, in case of inhala-tion, CHBr2Cl made the highest percentage contribution (82.3%), tototal risks followed by CHBrCl2 (15.8%) and chloroform (1.9%). Thisis mainly due to differences in the cancer slope factor (CSF), whichwas very low for chloroform as compared to CHBrCl2 and CHBr2Cl(Pardakhti et al., 2011). Residents in Ranchi had higher cancer riskthrough inhalation of CHBr2Cl among the 5 districts, and the re-sidents in Kolkata have the least cancer risk. Females have been
Fig. 3. Lifetime cancer risk due to inhalation exposure.
Table 1Hazard index of THMs through oral ingestion.
Water treatment plants
MADA (N) MAITHON IG
Male Female Male Female MCF 2.15Eþ00 2.51Eþ00 2.14Eþ00 2.50Eþ00 1.DCBM 4.25E�03 5.00E�03 4.25E�03 5.00E�03 4DBCM 8.55E�03 1.00E�02 1.71E�02 2.00E�02 2TTHMs 2.16Eþ00 2.53Eþ00 2.16Eþ00 2.53Eþ00 2
found to have higher cancer risk than males, which is similar toother routes of risk exposure.
3.3. Multi-pathway evaluations of noncarcinogenic risks for THMs
Assessment of the hazard indexes of THMs in different ex-posure routes was also carried out. The potency factor and thereference dose (RfD) values for the four THM compounds weretaken from IRIS (2009) and USEPA (1999).
The hazard index of THMs through oral routes and dermalabsorption is shown in Tables 1 and 2. The total hazard index foreach compound was calculated by summing up the individualindexes for dermal absorption and oral ingestion. In Table 1, thehazard index of chloroform through oral route ranged from 1.01 to2.15. For CHClBr2, the hazard index through oral route was be-tween 1.60�10�2 and 4.25�10�3. The highest hazard index wasfor chloroform in the supply water in Maithon. The total hazardindex for the four THMs was highest (2.16) in Maithon, and thelowest total hazard index appeared in Raniganj district. This isreasonable because Maithon had the highest total THM level whilethe Raniganj district had the lowest value. In Table 2, the hazardindex of THMs through dermal contact for males is generally lowerthan that through the oral route. The hazard index of chloroformvaried from 1.76�10�5 (Kolkata) to 9.65�10�7 (Raniganj). Thehighest hazard index of CHClBr2 occurred in Ranchi with a value of1.60�10�2. In total, Maithon had the highest hazard index of thefour chemicals (1.91�10�5), and Raniganj district had the lowesthazard index. Similarly, in Table 2, the hazard index of THMsthrough dermal contact with supply water in 5 districts for fe-males showed the same trend as for males. However, females havea higher hazard index than males in the exposure of THMs throughdermal contact.
Average hazard index through chloroform was found to behigher (3.64) followed by CHBrCl2 (4.27�10�2) and CHBr2Cl(3.45�10�2) for oral ingestion. However, in case of dermal ab-sorption, the values are almost negligible for all the THMs studied.This indicated that the non-cancer risk through THMs is mainlydue to chloroform for oral ingestion than the dermal route of ex-posure. Many researchers also reported that chloroform is themajor contributor of non-cancer risk (Lee et al., 2004; Uyak.,2006). The highest total hazard index was found to be 4.66 andlowest was 2.37. When the hazard index is more than 1 concernexists over the potential toxicity (USEPA, 2000). In this study, HI isfound to exceed 1 for TTHM in all the WTPs through oral ingestion,whereas for dermal absorption, it is well below the prescribed risklevel.
3.4. Sensitivity analysis
Sensitivity analysis is carried out to identify the major para-meter for total cancer risk. The sensitivity analysis processed the720% extra risk to interpret the effective THM parameters in-cluding body weight, intake quantity and exposure duration used
WTP II ADDA SWTP
ale Female Male Female Male Female99Eþ00 2.33Eþ00 1.09Eþ00 1.28Eþ00 1.01Eþ00 1.18Eþ00.25E�03 5.00E�03 2.35E�02 2.75E-02 1.60E�02 7.75E�02.57E�02 3.00E�02 1.71E�02 2.00E-02 3.00E�02 3.50E�02.02Eþ00 2.37Eþ00 1.13Eþ00 1.32Eþ00 1.06Eþ00 1.29Eþ00
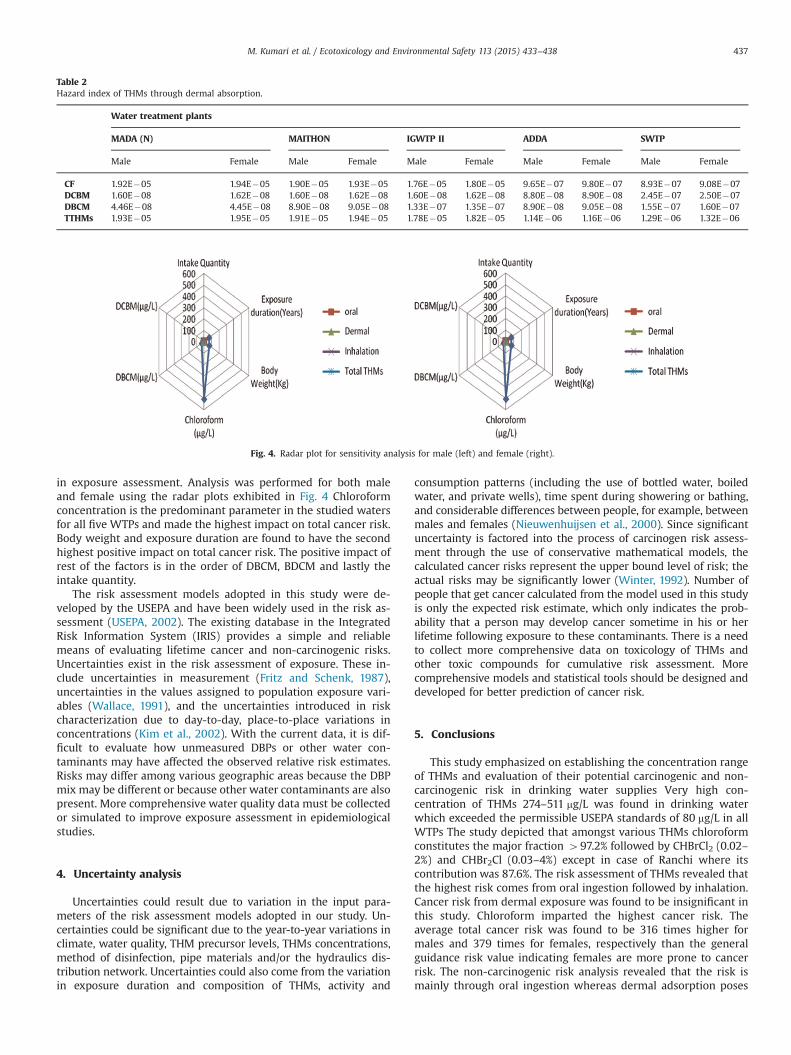
Table 2Hazard index of THMs through dermal absorption.
Water treatment plants
MADA (N) MAITHON IGWTP II ADDA SWTP
Male Female Male Female Male Female Male Female Male Female
CF 1.92E�05 1.94E�05 1.90E�05 1.93E�05 1.76E�05 1.80E�05 9.65E�07 9.80E�07 8.93E�07 9.08E�07DCBM 1.60E�08 1.62E�08 1.60E�08 1.62E�08 1.60E�08 1.62E�08 8.80E�08 8.90E�08 2.45E�07 2.50E�07DBCM 4.46E�08 4.45E�08 8.90E�08 9.05E�08 1.33E�07 1.35E�07 8.90E�08 9.05E�08 1.55E�07 1.60E�07TTHMs 1.93E�05 1.95E�05 1.91E�05 1.94E�05 1.78E�05 1.82E�05 1.14E�06 1.16E�06 1.29E�06 1.32E�06
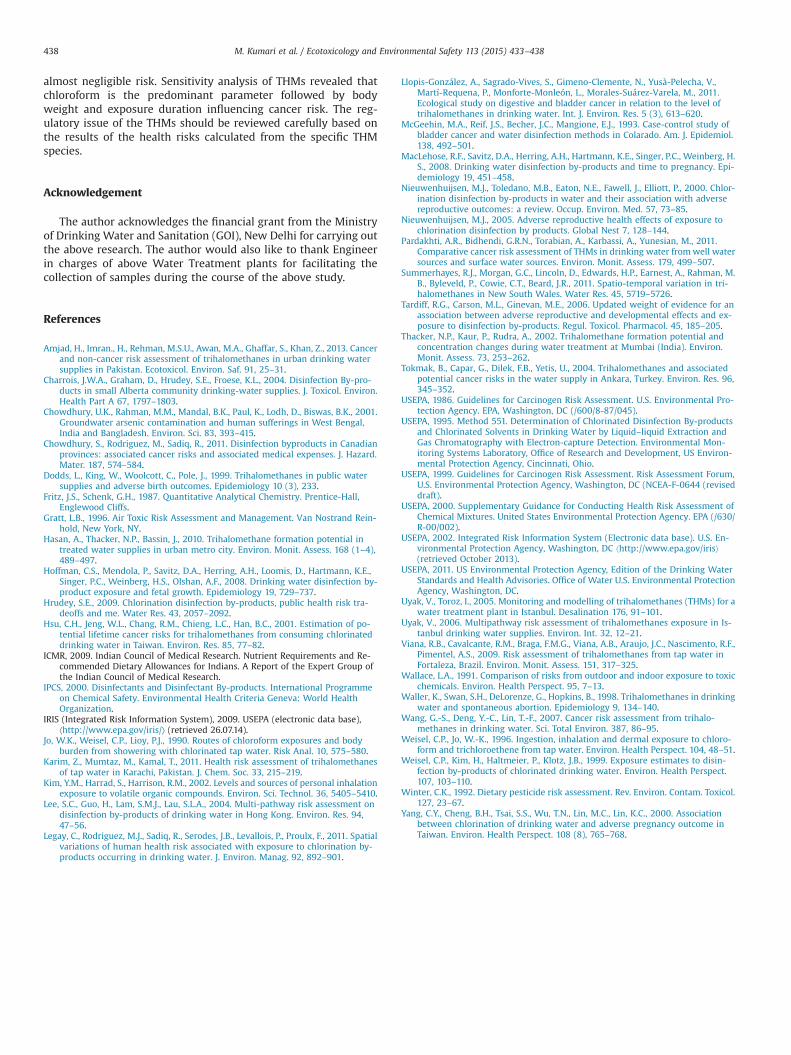
Fig. 4. Radar plot for sensitivity analysis for male (left) and female (right).
M. Kumari et al. / Ecotoxicology and Environmental Safety 113 (2015) 433–438 437
in exposure assessment. Analysis was performed for both maleand female using the radar plots exhibited in Fig. 4 Chloroformconcentration is the predominant parameter in the studied watersfor all five WTPs and made the highest impact on total cancer risk.Body weight and exposure duration are found to have the secondhighest positive impact on total cancer risk. The positive impact ofrest of the factors is in the order of DBCM, BDCM and lastly theintake quantity.
The risk assessment models adopted in this study were de-veloped by the USEPA and have been widely used in the risk as-sessment (USEPA, 2002). The existing database in the IntegratedRisk Information System (IRIS) provides a simple and reliablemeans of evaluating lifetime cancer and non-carcinogenic risks.Uncertainties exist in the risk assessment of exposure. These in-clude uncertainties in measurement (Fritz and Schenk, 1987),uncertainties in the values assigned to population exposure vari-ables (Wallace, 1991), and the uncertainties introduced in riskcharacterization due to day-to-day, place-to-place variations inconcentrations (Kim et al., 2002). With the current data, it is dif-ficult to evaluate how unmeasured DBPs or other water con-taminants may have affected the observed relative risk estimates.Risks may differ among various geographic areas because the DBPmix may be different or because other water contaminants are alsopresent. More comprehensive water quality data must be collectedor simulated to improve exposure assessment in epidemiologicalstudies.
4. Uncertainty analysis
Uncertainties could result due to variation in the input para-meters of the risk assessment models adopted in our study. Un-certainties could be significant due to the year-to-year variations inclimate, water quality, THM precursor levels, THMs concentrations,method of disinfection, pipe materials and/or the hydraulics dis-tribution network. Uncertainties could also come from the variationin exposure duration and composition of THMs, activity and
consumption patterns (including the use of bottled water, boiledwater, and private wells), time spent during showering or bathing,and considerable differences between people, for example, betweenmales and females (Nieuwenhuijsen et al., 2000). Since significantuncertainty is factored into the process of carcinogen risk assess-ment through the use of conservative mathematical models, thecalculated cancer risks represent the upper bound level of risk; theactual risks may be significantly lower (Winter, 1992). Number ofpeople that get cancer calculated from the model used in this studyis only the expected risk estimate, which only indicates the prob-ability that a person may develop cancer sometime in his or herlifetime following exposure to these contaminants. There is a needto collect more comprehensive data on toxicology of THMs andother toxic compounds for cumulative risk assessment. Morecomprehensive models and statistical tools should be designed anddeveloped for better prediction of cancer risk.
5. Conclusions
This study emphasized on establishing the concentration rangeof THMs and evaluation of their potential carcinogenic and non-carcinogenic risk in drinking water supplies Very high con-centration of THMs 274–511 mg/L was found in drinking waterwhich exceeded the permissible USEPA standards of 80 mg/L in allWTPs The study depicted that amongst various THMs chloroformconstitutes the major fraction 497.2% followed by CHBrCl2 (0.02–2%) and CHBr2Cl (0.03–4%) except in case of Ranchi where itscontribution was 87.6%. The risk assessment of THMs revealed thatthe highest risk comes from oral ingestion followed by inhalation.Cancer risk from dermal exposure was found to be insignificant inthis study. Chloroform imparted the highest cancer risk. Theaverage total cancer risk was found to be 316 times higher formales and 379 times for females, respectively than the generalguidance risk value indicating females are more prone to cancerrisk. The non-carcinogenic risk analysis revealed that the risk ismainly through oral ingestion whereas dermal adsorption poses
M. Kumari et al. / Ecotoxicology and Environmental Safety 113 (2015) 433–438438
almost negligible risk. Sensitivity analysis of THMs revealed thatchloroform is the predominant parameter followed by bodyweight and exposure duration influencing cancer risk. The reg-ulatory issue of the THMs should be reviewed carefully based onthe results of the health risks calculated from the specific THMspecies.
Acknowledgement
The author acknowledges the financial grant from the Ministryof Drinking Water and Sanitation (GOI), New Delhi for carrying outthe above research. The author would also like to thank Engineerin charges of above Water Treatment plants for facilitating thecollection of samples during the course of the above study.
References
Amjad, H., Imran., H., Rehman, M.S.U., Awan, M.A., Ghaffar, S., Khan, Z., 2013. Cancerand non-cancer risk assessment of trihalomethanes in urban drinking watersupplies in Pakistan. Ecotoxicol. Environ. Saf. 91, 25–31.
Charrois, J.W.A., Graham, D., Hrudey, S.E., Froese, K.L., 2004. Disinfection By-pro-ducts in small Alberta community drinking-water supplies. J. Toxicol. Environ.Health Part A 67, 1797–1803.
Chowdhury, U.K., Rahman, M.M., Mandal, B.K., Paul, K., Lodh, D., Biswas, B.K., 2001.Groundwater arsenic contamination and human sufferings in West Bengal,India and Bangladesh. Environ. Sci. 83, 393–415.
Chowdhury, S., Rodriguez, M., Sadiq, R., 2011. Disinfection byproducts in Canadianprovinces: associated cancer risks and associated medical expenses. J. Hazard.Mater. 187, 574–584.
Dodds, L., King, W., Woolcott, C., Pole, J., 1999. Trihalomethanes in public watersupplies and adverse birth outcomes. Epidemiology 10 (3), 233.
Fritz, J.S., Schenk, G.H., 1987. Quantitative Analytical Chemistry. Prentice-Hall,Englewood Cliffs.
Gratt, L.B., 1996. Air Toxic Risk Assessment and Management. Van Nostrand Rein-hold, New York, NY.
Hasan, A., Thacker, N.P., Bassin, J., 2010. Trihalomethane formation potential intreated water supplies in urban metro city. Environ. Monit. Assess. 168 (1–4),489–497.
Hoffman, C.S., Mendola, P., Savitz, D.A., Herring, A.H., Loomis, D., Hartmann, K.E.,Singer, P.C., Weinberg, H.S., Olshan, A.F., 2008. Drinking water disinfection by-product exposure and fetal growth. Epidemiology 19, 729–737.
Hrudey, S.E., 2009. Chlorination disinfection by-products, public health risk tra-deoffs and me. Water Res. 43, 2057–2092.
Hsu, C.H., Jeng, W.L., Chang, R.M., Chieng, L.C., Han, B.C., 2001. Estimation of po-tential lifetime cancer risks for trihalomethanes from consuming chlorinateddrinking water in Taiwan. Environ. Res. 85, 77–82.
ICMR, 2009. Indian Council of Medical Research. Nutrient Requirements and Re-commended Dietary Allowances for Indians. A Report of the Expert Group ofthe Indian Council of Medical Research.
IPCS, 2000. Disinfectants and Disinfectant By-products. International Programmeon Chemical Safety. Environmental Health Criteria Geneva: World HealthOrganization.
IRIS (Integrated Risk Information System), 2009. USEPA (electronic data base),⟨http://www.epa.gov/iris/⟩ (retrieved 26.07.14).
Jo, W.K., Weisel, C.P., Lioy, P.J., 1990. Routes of chloroform exposures and bodyburden from showering with chlorinated tap water. Risk Anal. 10, 575–580.
Karim, Z., Mumtaz, M., Kamal, T., 2011. Health risk assessment of trihalomethanesof tap water in Karachi, Pakistan. J. Chem. Soc. 33, 215–219.
Kim, Y.M., Harrad, S., Harrison, R.M., 2002. Levels and sources of personal inhalationexposure to volatile organic compounds. Environ. Sci. Technol. 36, 5405–5410.
Lee, S.C., Guo, H., Lam, S.M.J., Lau, S.L.A., 2004. Multi-pathway risk assessment ondisinfection by-products of drinking water in Hong Kong. Environ. Res. 94,47–56.
Legay, C., Rodriguez, M.J., Sadiq, R., Serodes, J.B., Levallois, P., Proulx, F., 2011. Spatialvariations of human health risk associated with exposure to chlorination by-products occurring in drinking water. J. Environ. Manag. 92, 892–901.
Llopis-González, A., Sagrado-Vives, S., Gimeno-Clemente, N., Yusà-Pelecha, V.,Martí-Requena, P., Monforte-Monleón, L., Morales-Suárez-Varela, M., 2011.Ecological study on digestive and bladder cancer in relation to the level oftrihalomethanes in drinking water. Int. J. Environ. Res. 5 (3), 613–620.
McGeehin, M.A., Reif, J.S., Becher, J.C., Mangione, E.J., 1993. Case-control study ofbladder cancer and water disinfection methods in Colarado. Am. J. Epidemiol.138, 492–501.
MacLehose, R.F., Savitz, D.A., Herring, A.H., Hartmann, K.E., Singer, P.C., Weinberg, H.S., 2008. Drinking water disinfection by-products and time to pregnancy. Epi-demiology 19, 451–458.
Nieuwenhuijsen, M.J., Toledano, M.B., Eaton, N.E., Fawell, J., Elliott, P., 2000. Chlor-ination disinfection by-products in water and their association with adversereproductive outcomes: a review. Occup. Environ. Med. 57, 73–85.
Nieuwenhuijsen, M.J., 2005. Adverse reproductive health effects of exposure tochlorination disinfection by products. Global Nest 7, 128–144.
Pardakhti, A.R., Bidhendi, G.R.N., Torabian, A., Karbassi, A., Yunesian, M., 2011.Comparative cancer risk assessment of THMs in drinking water fromwell watersources and surface water sources. Environ. Monit. Assess. 179, 499–507.
Summerhayes, R.J., Morgan, G.C., Lincoln, D., Edwards, H.P., Earnest, A., Rahman, M.B., Byleveld, P., Cowie, C.T., Beard, J.R., 2011. Spatio-temporal variation in tri-halomethanes in New South Wales. Water Res. 45, 5719–5726.
Tardiff, R.G., Carson, M.L., Ginevan, M.E., 2006. Updated weight of evidence for anassociation between adverse reproductive and developmental effects and ex-posure to disinfection by-products. Regul. Toxicol. Pharmacol. 45, 185–205.
Thacker, N.P., Kaur, P., Rudra, A., 2002. Trihalomethane formation potential andconcentration changes during water treatment at Mumbai (India). Environ.Monit. Assess. 73, 253–262.
Tokmak, B., Capar, G., Dilek, F.B., Yetis, U., 2004. Trihalomethanes and associatedpotential cancer risks in the water supply in Ankara, Turkey. Environ. Res. 96,345–352.
USEPA, 1986. Guidelines for Carcinogen Risk Assessment. U.S. Environmental Pro-tection Agency. EPA, Washington, DC (/600/8-87/045).
USEPA, 1995. Method 551. Determination of Chlorinated Disinfection By-productsand Chlorinated Solvents in Drinking Water by Liquid–liquid Extraction andGas Chromatography with Electron-capture Detection. Environmental Mon-itoring Systems Laboratory, Office of Research and Development, US Environ-mental Protection Agency, Cincinnati, Ohio.
USEPA, 1999. Guidelines for Carcinogen Risk Assessment. Risk Assessment Forum,U.S. Environmental Protection Agency, Washington, DC (NCEA-F-0644 (reviseddraft).
USEPA, 2000. Supplementary Guidance for Conducting Health Risk Assessment ofChemical Mixtures. United States Environmental Protection Agency. EPA (/630/R-00/002).
USEPA, 2002. Integrated Risk Information System (Electronic data base). U.S. En-vironmental Protection Agency, Washington, DC ⟨http://www.epa.gov/iris⟩(retrieved October 2013).
USEPA, 2011. US Environmental Protection Agency, Edition of the Drinking WaterStandards and Health Advisories. Office of Water U.S. Environmental ProtectionAgency, Washington, DC.
Uyak, V., Toroz, I., 2005. Monitoring and modelling of trihalomethanes (THMs) for awater treatment plant in Istanbul. Desalination 176, 91–101.
Uyak, V., 2006. Multipathway risk assessment of trihalomethanes exposure in Is-tanbul drinking water supplies. Environ. Int. 32, 12–21.
Viana, R.B., Cavalcante, R.M., Braga, F.M.G., Viana, A.B., Araujo, J.C., Nascimento, R.F.,Pimentel, A.S., 2009. Risk assessment of trihalomethanes from tap water inFortaleza, Brazil. Environ. Monit. Assess. 151, 317–325.
Wallace, L.A., 1991. Comparison of risks from outdoor and indoor exposure to toxicchemicals. Environ. Health Perspect. 95, 7–13.
Waller, K., Swan, S.H., DeLorenze, G., Hopkins, B., 1998. Trihalomethanes in drinkingwater and spontaneous abortion. Epidemiology 9, 134–140.
Wang, G.-S., Deng, Y.-C., Lin, T.-F., 2007. Cancer risk assessment from trihalo-methanes in drinking water. Sci. Total Environ. 387, 86–95.
Weisel, C.P., Jo, W.-K., 1996. Ingestion, inhalation and dermal exposure to chloro-form and trichloroethene from tap water. Environ. Health Perspect. 104, 48–51.
Weisel, C.P., Kim, H., Haltmeier, P., Klotz, J.B., 1999. Exposure estimates to disin-fection by-products of chlorinated drinking water. Environ. Health Perspect.107, 103–110.
Winter, C.K., 1992. Dietary pesticide risk assessment. Rev. Environ. Contam. Toxicol.127, 23–67.
Yang, C.Y., Cheng, B.H., Tsai, S.S., Wu, T.N., Lin, M.C., Lin, K.C., 2000. Associationbetween chlorination of drinking water and adverse pregnancy outcome inTaiwan. Environ. Health Perspect. 108 (8), 765–768.