
Mucorales-specific T cells emerge in the course of invasive mucormycosis and may be used as a...
19
doi:10.1182/blood-2011-07-366526 Prepublished online September 19, 2011; Pecorari, Francesca Cavalleri, Roberto Marasca, Franco Narni and Mario Luppi Ambra Paolini, Monica Maccaferri, Cinzia Del Giovane, Roberto D'Amico, Fabio Rumpianesi, Monica Chiara Quadrelli, Anna Candoni, Johan Maertens, Giulio Rossi, Monica Morselli, Mauro Codeluppi, Leonardo Potenza, Daniela Vallerini, Patrizia Barozzi, Giovanni Riva, Fabio Forghieri, Eleonora Zanetti, and may be used as a surrogate diagnostic marker in high-risk patients -specific T cells emerge in the course of invasive mucormycosis Mucorales (3615 articles) Clinical Trials and Observations (1591 articles) Brief Reports Articles on similar topics can be found in the following Blood collections http://bloodjournal.hematologylibrary.org/site/misc/rights.xhtml#repub_requests Information about reproducing this article in parts or in its entirety may be found online at: http://bloodjournal.hematologylibrary.org/site/misc/rights.xhtml#reprints Information about ordering reprints may be found online at: http://bloodjournal.hematologylibrary.org/site/subscriptions/index.xhtml Information about subscriptions and ASH membership may be found online at: digital object identifier (DOIs) and date of initial publication. the indexed by PubMed from initial publication. Citations to Advance online articles must include final publication). Advance online articles are citable and establish publication priority; they are appeared in the paper journal (edited, typeset versions may be posted when available prior to Advance online articles have been peer reviewed and accepted for publication but have not yet Copyright 2011 by The American Society of Hematology; all rights reserved. 20036. the American Society of Hematology, 2021 L St, NW, Suite 900, Washington DC Blood (print ISSN 0006-4971, online ISSN 1528-0020), is published weekly by For personal use only. by guest on November 9, 2012. bloodjournal.hematologylibrary.org From
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Mucorales-specific T cells emerge in the course of invasive mucormycosis and may be used as a...

doi:10.1182/blood-2011-07-366526Prepublished online September 19, 2011;
Pecorari, Francesca Cavalleri, Roberto Marasca, Franco Narni and Mario LuppiAmbra Paolini, Monica Maccaferri, Cinzia Del Giovane, Roberto D'Amico, Fabio Rumpianesi, MonicaChiara Quadrelli, Anna Candoni, Johan Maertens, Giulio Rossi, Monica Morselli, Mauro Codeluppi, Leonardo Potenza, Daniela Vallerini, Patrizia Barozzi, Giovanni Riva, Fabio Forghieri, Eleonora Zanetti, and may be used as a surrogate diagnostic marker in high-risk patients
-specific T cells emerge in the course of invasive mucormycosisMucorales
(3615 articles)Clinical Trials and Observations � (1591 articles)Brief Reports �
Articles on similar topics can be found in the following Blood collections
http://bloodjournal.hematologylibrary.org/site/misc/rights.xhtml#repub_requestsInformation about reproducing this article in parts or in its entirety may be found online at:
http://bloodjournal.hematologylibrary.org/site/misc/rights.xhtml#reprintsInformation about ordering reprints may be found online at:
http://bloodjournal.hematologylibrary.org/site/subscriptions/index.xhtmlInformation about subscriptions and ASH membership may be found online at:
digital object identifier (DOIs) and date of initial publication. theindexed by PubMed from initial publication. Citations to Advance online articles must include
final publication). Advance online articles are citable and establish publication priority; they areappeared in the paper journal (edited, typeset versions may be posted when available prior to Advance online articles have been peer reviewed and accepted for publication but have not yet
Copyright 2011 by The American Society of Hematology; all rights reserved.20036.the American Society of Hematology, 2021 L St, NW, Suite 900, Washington DC Blood (print ISSN 0006-4971, online ISSN 1528-0020), is published weekly by
For personal use only. by guest on November 9, 2012. bloodjournal.hematologylibrary.orgFrom

1
MUCORALES-SPECIFIC T CELLS EMERGE IN THE COURSE OF INVASIVE
MUCORMYCOSIS AND MAY BE USED AS A SURROGATE DIAGNOSTIC MARKER IN
HIGH RISK PATIENTS.
Leonardo Potenza1§
, Daniela Vallerini1§
, Patrizia Barozzi1§
, Giovanni Riva1§
, Fabio Forghieri1§
,
Eleonora Zanetti1
, Chiara Quadrelli1
, Anna Candoni2
, Johan Maertens3
, Giulio Rossi4
, Monica
Morselli1
, Mauro Codeluppi5
, Ambra Paolini1
, Monica Maccaferri1
, Cinzia Del Giovane1
, Roberto
D'Amico1
, Fabio Rumpianesi6
, Monica Pecorari6
, Francesca Cavalleri7
, Roberto Marasca1
, Franco
Narni1
, Mario Luppi1*
.
1
Section of Haematology, Department of Oncology, Haematology and Respiratory Diseases;
4
Section of Pathology, Department of Diagnostic and Laboratory Services and Legal Medicine;
5
Clinic of Infectious Diseases, Department of Internal Medicine and Medical Specialties;
6
Microbiology and Virology Unit, Department of Diagnostic and Laboratory Services and Legal
Medicine; 7
Section of Neuroradiology, Department of Neuroscience, all from the University of
Modena and Reggio Emilia, Modena; 2
Hematology and Bone Marrow Transplantation, Udine, all
from Italy.
3
Department of Hematology, Universitaire Ziekenhuizen Leuven, Campus Gasthuisberg, Leuven,
Belgium.
Short Title: Specific T cells to diagnose invasive mucormycosis
§
These authors equally contributed to the study
*Corresponding author:
Mario Luppi M.D., Ph.D.
Blood First Edition Paper, prepublished online September 19, 2011; DOI 10.1182/blood-2011-07-366526
Copyright © 2011 American Society of Hematology
For personal use only. by guest on November 9, 2012. bloodjournal.hematologylibrary.orgFrom

2
Professor of Hematology
Chief, Division of Hematology
Department of Oncology, Hematology and Respiratory Diseases.
University of Modena and Reggio Emilia
Azienda Ospedaliero-Universitaria, Policlinico.
Modena, ITALY
Phone: ++39 059 422.4641 (office)- 5570 (mobile)
Fax: ++39 059 422.4429
e-mail: [email protected]
For personal use only. by guest on November 9, 2012. bloodjournal.hematologylibrary.orgFrom
3
Summary
Mucorales-specific T cells have been investigated in 28 hematologic patients during the course of
their treatment. Three developed proven invasive mucormycosis (IM), 17 infections of known
etiologies but other than IM, and 8 never showed fever upon the period of observation. The
Mucorales-specific T cells may be detected only in patients with IM, at diagnosis and along the
entire course of the IM, but neither before nor long time after the resolution of the infection. Such T
cells produced predominantly interleukin-4, interferon-gamma (IFN-γ), interleukin-10, and to a
lesser extent also interleukin-17, and belonged to either CD4+ or CD8+ subsets. The specific T
cells producing IFN-γ were able to directly induce damage of Mucorales hyphae. None of the 25
patients without IM showed Mucorales-specific T cells. Specific T cells contribute to human
immune responses against fungi of the order Mucorales and could be evaluated as a surrogate
diagnostic marker of IM.
Word count = 150
For personal use only. by guest on November 9, 2012. bloodjournal.hematologylibrary.orgFrom

4
Invasive Mucormycosis (IM), the second-most common cause of invasive mold infections in
hematologic patients, shows mortality rates approaching 70% of affected individuals, because of
difficulties in obtaining an early and undoubted diagnosis1-5. Actually, a definitive diagnosis of IM
relies exclusively on both histopathological demonstration and cultural isolation of the pathogen
from the involved organs6. However, obtaining tissue specimens in hematologic patients is too often
hampered by the presence of several comorbidities, and histologically proven IM may fail to grow
in culture in at least 1/3 of cases7. Furthermore, neither serologic nor antigenic diagnostic methods
exist and the use of polymerase chain reaction (PCR) has almost exclusively been limited to the
identification and the discrimination of fungal species8,9.
Adaptive immunity has been reported to play a crucial role in the defence of the host against
fungi, at least in the case of invasive aspergillosis (IA) and invasive candidiasis10,11, and the
recognition and enumeration of antigen-specific T cells has been demonstrated a useful tool for the
diagnosis of definite infectious diseases, in particular of either active or latent tuberculosis12.
We have explored the possibility that Mucorales-specific T cells are elicited in patients with
IM and that their detection may be of value in the diagnosis of active disease.
For personal use only. by guest on November 9, 2012. bloodjournal.hematologylibrary.orgFrom

5
PATIENTS AND METHODS
Twenty-eight hematologic patients have been studied. Patients 1-3 had disseminated (pulmonary
and splenic), tracheo-bronchial and cerebral proven IM, respectively (Figures S1,S2).
The antifungal treatments of the three patients with proven IM have been described in details in
supplemental data.
The remaining 25 cases included 17 patients presenting infectious complications of proven etiology
on the basis of cultural and/or histologic examinations, but other than IM, and 8 who have not
developed infectious complications during the course of their induction chemotherapy. Patients'
clinical characteristics have been reported in Table S1. Informed consent was obtained in
accordance with the Declaration of Helsinki, and the study was approved by the University of
Modena and Reggio Emilia Ethical Committee.
The enzyme linked immunospot (ELISpot) assay has been performed to detect either Mucorales- or
Aspergillus-specific T cell, as reported13 and described in details in supplemental data, on 80
peripheral blood samples (range 2 to 6 per patients). Time points analysed were: in patient 1, the
beginning of induction chemotherapy, 20 days before the pulmonary biopsy, at the histological and
cultural identification of Rhizomucor pusillus infection, the beginning of consolidation
chemotherapy, and 16 weeks after the resolution of the infection; in patient 2, the day of cultural
and histologic demonstration of Rhizopus oryzae infection, and until death in four further occasions
during the course of IM; in patient 3, the day of histologic and molecular demonstration of Absydia
corymbifera infection, three occasions during the course of IM, and at the complete resolution of
the infection. All the other patients were analysed at least twice during the course of their either
infections or chemotherapeutic treatments (Table S1).
The phenotypic and functional characterization of Mucorales-specific T cells has been performed
with the cytokine secretion assay (CSA) as already reported14 and described in details in
supplemental data. Molecular studies, micromanipulation and single-cell PCR to identify Mucorales
species (Figure S2) were performed as previously reported15 and described in details in
For personal use only. by guest on November 9, 2012. bloodjournal.hematologylibrary.orgFrom
6
supplemental data. Anti-Mucorales activity of specific T cells was performed as reported in
supplemental data.
For personal use only. by guest on November 9, 2012. bloodjournal.hematologylibrary.orgFrom

7
RESULTS
Identification of Mucorales-specific T cells
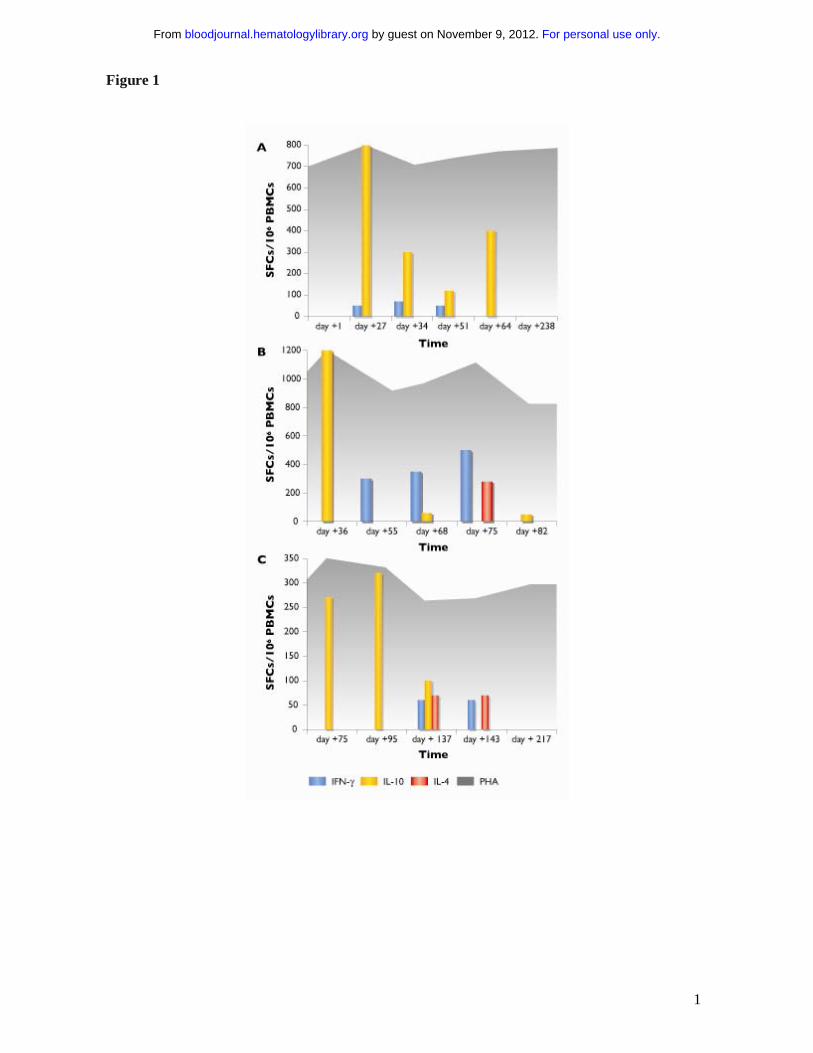
In patient 1, the ELISpot resulted positive for the presence of Mucorales-specific T cells producing
interleukin (IL)-10 in the second, third, fourth and fifth samples, and Mucorales-specific T cells
producing interferon gamma (IFN-γ) in the second, third and fourth samples. In contrast, no
Mucorales-specific T cells could be detected before the occurrence of the infection (at day +1 of
induction chemotherapy) and long time after its resolution (day +238) (Figure 1A).
In patient 2 and 3, the ELISpot showed the sole presence of Mucorales-specific T cells producing
IL-10 in the first sample (on the day of cultural and histologic demonstration of IM) in both
patients; increasing numbers of Mucorales-specific T cells producing IFN-γ in the second, third
and fourth samples in patient 2, and in the third and fourth samples in patient 3; the occurrence of
Mucorales-specific T cells producing IL-4 in the fourth sample in patient 2 and in the third and
fourth samples in patient 3. The last examination demonstrated the sole presence of Mucorales-
specific T cells producing IL-10 in patient 2, close to death, and the absence of specific responses in
patient 3, at the time of complete resolution of the infection (Figure 1B,C).
The differences between the median frequencies of Mucorales-specific T cells producing IL-10,
IFN-γ and IL-4 did not result statistically significant in all the three patients (p = .3), not even when
the results of the first two patients with more disseminated diseases were compared with those of
the third patient, with a more limited infection (p = .5).
In the 25 control patients, the ELISpot never showed the presence of Mucorales-specific T cells.
None of the analysed patients demonstrated the occurrence of Aspergillus-specific T cell at any
time point (Table S1).
Phenotypic and Functional Characterization of Mucorales-specific T cells
In patients 1-3, Mucorales-specific T cells resulted: 1) predominantly CD8 + T cells (mean
CD8+/CD4+ frequencies 3.62%/0.57%) of CM phenotype, producing IFN-γ; 2) predominantly
CD8+ T cells (mean CD8+/CD4+ frequencies 4.35%/2.60%) of EM phenotype producing IL-4; 3)
For personal use only. by guest on November 9, 2012. bloodjournal.hematologylibrary.orgFrom

8
either CD4+ or CD8+ T cells (mean CD4+/CD8+ frequencies 0.32%/0.26%), the former of either
CM or EM phenotype, the latter mainly of CM, producing IL-10. Mucorales-specific T cells
producing IL-17 were also detectable, being either CD4+ or CD8+ (mean frequency 0.44% and
0.56%, respectively), and exhibiting, predominantly, the CM phenotype (Figure 2A,B).
Lytic Activity of Mucorales-specific T cells
Mucorales-specific T cells from patients 1-3 were capable to induce direct damage to the hyphae of
the two clinical isolates, similar to that of either PMNs or APCs. Only the combination of all the
three cell types resulted in a significantly higher hyphal damage (p<0.05) (Figure 2C,D).
For personal use only. by guest on November 9, 2012. bloodjournal.hematologylibrary.orgFrom

9
DISCUSSION
We have shown, for the first time, that Mucorales-specific T cells may occur during the infection
course in patients with IM and exhibit direct antifungal activity, comparable, at least in vitro, to that
of either PMNs or APCs. The contribution of T cells to host defences against these moulds could
only be suspected, based on the enhanced fungicidal activity against Mucorales of
polymorphonuclear leukocytes exposed to IFN-γ16, but it has not yet been formally demonstrated.
The presence of Mucorales-specific T cells only during the course of IM, but neither before nor
after the resolution of the infection in patients 1-3, and their absence in patients without infections
or with infections other than IM, suggest that they are closely related to the occurrence of IM and
may result a marker of overt disease. Of note, the presence of Mucorales-specific T cells has been
demonstrated the only proof of IM in patient 1, largely before the obtainment of the biopsy. The
lower frequencies of specific T cells in patient 3 seem to suggest that a more confined IM could be
associated with responses of inferior magnitude. However, no statistically significant differences
were observed between the median numbers of Mucorales-specific T cells in our three patients.
Unfortunately, as all the samples were collected either when the patients were undergoing
antifungal treatment or after the drug withdrawal, no interaction between antifungal therapy and the
occurrence of Mucorales-specific T cells could be determined in our study.
The cytokine production profile of Mucorales-specific T cells, in our study, is partially in line with
what observed either in mice affected by IA or in human T cell clones stimulated with different
Aspergillus antigens in vitro17-19. The demonstration that CD8+ Mucorales-specific T cells may
produce either IL-4 or IL-10, predominantly in the late phase of the infection, is reminiscent of the
type 2 cytokine shift of CD8+ lymphocytes, so far reported only in patients with the cavitary phase
of tuberculosis and the late phase of human immunodeficiency virus infection20-21.
In conclusion, Mucorales-specific T cells emerge in the course of IM and contribute to the human
immune responses against Mucorales. The detection of Mucorales-specific T cells may be
evaluated as a surrogate diagnostic marker of IM.
For personal use only. by guest on November 9, 2012. bloodjournal.hematologylibrary.orgFrom

1
ACKNOWLEDGEMENTS
This study was supported by the Associazione Italiana per la Ricerca sul Cancro (AIRC), Milan,
Italy (M.L.); the European Commission’s FP6 Life-Science-Health Programme (INCA project;
LSHC-CT-2005-018704) (M.L.); the Associazione Italiana Lotta alle Leucemie, Linfoma e
Mieloma (AIL)-Sezione “Luciano Pavarotti”-Modena-ONLUS (L.P.; F.F.), the Programma di
ricerca Regione-Universita` 2007–2009, Regione Emilia Romagna (M.L., F.N.), and the Societa`
Italiana di Ematologia Sperimentale (SIES; “Piero Martino” award to L.P.).
For personal use only. by guest on November 9, 2012. bloodjournal.hematologylibrary.orgFrom
11
AUTHORSHIP CONTRIBUTIONS
LP and ML conceived, designed the study and wrote the manuscript; DV, PB, GiRi, GiRo, FR and
MP made the ELISpot analysis, the CSA analysis, the XTT assays, histological examination,
performed the molecular characterization of fungi and interpreted the data; AC, JM, FF, MoMo,
MC, AP, MoMa, RM, FN provided well-characterized patient samples and critically revised the
manuscript; CDG and RDA made the statistical analysis and interpreted the data; FC made the
radiological studies and critically revised the manuscript.
For personal use only. by guest on November 9, 2012. bloodjournal.hematologylibrary.orgFrom
1
DISCLOSURE OF CONFLICTS OF INTEREST
ML received research funds by Merck Sharp & Dohme and Gilead Sciences. ML serves in Advisory
Boards for Merck Sharp & Dohme and Gilead Sciences, and received honoraria from these two
pharmaceutical industries and from Pfizer and Nanogen. LP serves in an Advisory Board for Merck
Sharp & Dohme. AC serves in Advisory Board for Merck Sharp & Dohme and received funds by
Merck Sharp & Dohme, Gilead Sciences and Pfizer.
ML, LP and PB have applied for a European patent regarding clinical applications of the ELISpot
assay for the diagnosis of Aspergillus infection [PCT: WO2008/075395A3, EP2094295,
IT2007/000867]. ML, LP, DV, PB and FF have applied for an Italian patent regarding clinical
applications of the ELISpot assay for the diagnosis of Mucorales infection (No. MI2010A002224).
All the other authors have no conflicts of interest to declare. In particular they have neither
employment, nor consultancy, including stock options in a start-up company, nor ownership interest
in a publicly traded company, nor research funding. They received neither honoraria nor paid expert
testimony. They have neither other potential financial relationship (e.g., holding a patent or
receiving royalties), nor membership on another entity’s Board of Directors or its advisory
committees.
For personal use only. by guest on November 9, 2012. bloodjournal.hematologylibrary.orgFrom
1
REFERENCES
1. Hibbett DS, Binder M, Bischoff JF, et al. A higher-level phylogenetic classification of the
Fungi. Mycol Res. 2007;111(Pt 5):509-547.
2. Kontoyiannis DP, Marr KA, Park BJ, et al. Prospective surveillance for invasive fungal
infections in hematopoietic stem cell transplant recipients, 2001-2006: overview of the
Transplant-Associated Infection Surveillance Network (TRANSNET) Database. Clin Infect
Dis. 2010;50(8):1091-1100.
3. Pagano L, Caira M, Candoni A, et al. The epidemiology of fungal infections in patients with
hematologic malignancies: the SEIFEM-2004 study. Haematologica/the hematology journal
2006;91(8):1068-1075.
4. Chamilos G, Luna M, Lewis RE, et al. Invasive fungal infections in patients with
hematologic malignancies in a tertiary care cancer center: an autopsy study over a 15-year
period (1989-2003). Haematologica/the hematology journal. 2006;91(7):986-989.
5. Chamilos G, Lewis RE, Kontoyiannis DP. Delaying amphotericin B-based frontline therapy
significantly increases mortality among patients with hematologic malignancy who have
zygomycosis. Clin Infect Dis 2008;47:503-509.
6. De Pauw B, Walsh TJ, Donnelly JP, et al. Revised definitions of invasive fungal disease
from the European Organization for Research and Treatment of Cancer/Invasive Fungal
Infections Cooperative Group and the National Institute of Allergy and Infectious Diseases
Mycoses Study Group (EORTC/MSG) Consensus Group. Clin Infect Dis.
2008;46(12):1813-1821.
7. Roden MM, Zaoutis TE, Buchanan WL, et al. Epidemiology and outcome of zygomycosis: a
review of 929 reported cases. Clin Infect Dis. 2005;41(5):634-653.
8. Bialek R, Konrad F, Kern J et al. PCR based identification and discrimination of agents of
mucormycosis and aspergillosis in paraffin wax embedded tissue. J Clin Pathol.
2005;58(11):1180-1184.
For personal use only. by guest on November 9, 2012. bloodjournal.hematologylibrary.orgFrom

1
9. Dannaoui E, Schwarz P, Slany M, et al. Molecular detection and identification of
zygomycetes species from paraffin-embedded tissues in a murine model of disseminated
zygomycosis: a collaborative European Society of Clinical Microbiology and Infectious
Diseases (ESCMID) Fungal Infection Study Group (EFISG) evaluation. J Clin Microbiol.
2010;48(6):2043-2046.
10. Romani L. Immunity to fungal infections. Nat Rev Immunol 2004;4(1):1-23.
11. Hebart H, Bollinger C, Fisch P, et al. Analysis of T-cell responses to Aspergillus fumigatus
antigens in healthy individuals and patients with hematologic malignancies. Blood.
2002;100(13):4521-4528.
12. Lalvani A, Pathan AA, Durkan H, et al. Enhanced contact tracing and spatial tracking of
Mycobacterium tuberculosis infection by enumeration of antigen-specific T cells. Lancet.
2001;357(9273):2017-2021.
13. Potenza L, Barozzi P, Vallerini D, et al. Diagnosis of invasive aspergillosis by tracking
Aspergillus-specific T cells in hematologic patients with pulmonary infiltrates. Leukemia.
2007;21(10):578-581.
14. Riva G, Luppi M, Barozzi P, et al. Emergence of BCR-ABL-specific cytotoxic T cells in the
bone marrow of patients with Ph+ acute lymphoblastic leukemia during long-term imatinib
mesylate treatment. Blood. 2010;115(8):1512-1518.
15. Potenza L, Luppi M, Barozzi P, et al. HHV-6A in syncytial giant-cell hepatitis. N Engl J
Med. 2008; 359(6):593-602.
16. Gil-Lamaignere C, Simitsopoulou M, Roilides E, Maloukou A, Winn RM, Walsh TJ.
Interferon- gamma and granulocyte-macrophage colony-stimulating factor augment the
activity of polymorphonuclear leukocytes against medically important zygomycetes. J Infect
Dis. 2005;191(7):1180-1187.
17. Bozza S, Clavaud C, Giovannini G, et al. Immune sensing of Aspergillus fumigatus proteins,
glycolipids, and polysaccharides and the impact on Th immunity and vaccination. J
For personal use only. by guest on November 9, 2012. bloodjournal.hematologylibrary.orgFrom

1
Immunol. 2009;183(4):2407-2414.
18. Ramadan G, Davies B, Kurup VP, Keever-Taylor CA. Generation of cytotoxic T cell
responses directed to human leucocyte antigen Class I restricted epitopes from the
Aspergillus f16 allergen. Clin Exp Immunol. 2005;140(1):81-91.
19. Chai LY, van de Veerdonk F, Marijnissen RJ, et al. Anti-Aspergillus human host defence
relies on type 1 T helper (Th1), rather than type 17 T helper (Th17), cellular immunity.
Immunology. 2010;130(1):46-54.
20. van Crevel R, Karyadi E, Preyers F, et al. Increased production of interleukin 4 by CD4+
and CD8+ T cells from patients with tuberculosis is related to the presence of pulmonary
cavities. J Infect Dis. 2000;181(3):1194-1197.
21. Elrefaei M, Burke CM, Baker CA, et al. TGF-beta and IL-10 production by HIV-specific
CD8+ T cells is regulated by CTLA-4 signaling on CD4+ T cells. PLoS One.
2009;4(12):e8194.
For personal use only. by guest on November 9, 2012. bloodjournal.hematologylibrary.orgFrom

1
FIGURE LEGEND
Figure 1 A-C. Kinetics of Mucorales-specific T-cell responses, by IFN-γ, IL-10 and IL-4
ELISpot assay, in the three patients with invasive mucormycosis. A. Patient 1. B. Patient 2. C.
Patient 3. Yellow columns represent the number of Mucorales-specific T cells producing interleukin
10 (IL-10). Blue columns represent the number of Mucorales-specific T cells producing interferon
gamma (IFN-γ). Red columns represent the number of Mucorales-specific T cells producing
interleukin 4 (IL-4). The dark grey background represents the T-cell responses in wells with
phytohemagglutinin (PHA). Vertical axis shows the number of spot forming cells (SFCs) per
million of peripheral blood mononuclear cells (PBMCs). Horizontal axis indicates the time in days
from the beginning of induction chemotherapy.
Figure 2 A-D. Cytokine production profile and lytic activities of Mucorales-specific T cells.
A,B. The frequencies of Mucorales specific T cells producing IFNγ, IL-10, IL-4 or IL-17, either as
EM (light grey) or CM (dark grey), are shown as mean % positive cells, computed over the three
patients with IM. Results are expressed as percentages of either CD4+ T cells (A) or of CD8+ T cells
(B). Mean frequencies of specific cytokine-producing T cells for individual patients are reported on
each column, either as EM (�) or CM (O). EM = effector memory. CM = central memory.
C,D. Hyphal damage at 2 (C) and 22 (D) hours to Rhizomucor pusillus and Rhizopus oryzae
induced by anti-Mucorales T cells (T), polymorphonuclear leukocytes (PMNs), and antigen-
presenting cells (APCs), alone or in combination, deriving from patient 1 and patient 2 during the
course of IM. E:T = effector/target cells ratios.
For personal use only. by guest on November 9, 2012. bloodjournal.hematologylibrary.orgFrom
1
Figure 1
For personal use only. by guest on November 9, 2012. bloodjournal.hematologylibrary.orgFrom

1
Figure 2
For personal use only. by guest on November 9, 2012. bloodjournal.hematologylibrary.orgFrom




















