
Moss, R.A. (1989). New approaches to the assessment and treatment of chronic headaches. Journal...
8
New Approaches in the Assessment and · Treatment of Chronic Headaches Robert A. Moss, Ph.D. E stimates indicate that 10 to 30% of · the population experience chronic headache pain in one form or another. 1 In fact, surveys indicate that headache falls among the top 14 primary complaints io outpatient medical practice. 2 The ramifications of this statistic are widespread and include decreased occupa- tional effectiveness/frequent absence, mal- adaptive social functioning, and family/ interpersonal problems. 3 64 PAIN MANAGEMENT In 1962 the National Institutes of Neuro- logical Diseases and Blindness published a re:. port, based on extensive clinical data, in- tended to differentiate and classify various forms of headache. 4 In this classification sys· tern, four ·types of headache were cited that were not associated with structural changes. These were migraine, muscle contraction, combination migraine/muscle contraction, and conversion headaches. However, conflict- ing results of migraine and tension headache studies have led some. researchers to recom- mend abandoning the. traditional classifica- tion system. 5 In oontrast, some investigators continue to argue that if researchers strictly adhere to the classification system, the differ- entiation of migraines from muscle contrac- tion headaches may be supported. 6 · Recently, my colleagues and I have pub- lished several papers that propose a nontradi- tional view of the etiology and treatment of many chronic headache cases. Specifically, we have proposed that many cases diagnosed as · common migraine may actually result from structural imbalance of the temporomandib- ular joint (TMJ) and from activity of the masticatory muscles. Furthermore, many cases of morning-onset muscle cont:rac-
Transcript of Moss, R.A. (1989). New approaches to the assessment and treatment of chronic headaches. Journal...
New Approaches in the Assessment and · Treatment of Chronic Headaches Robert A. Moss, Ph.D.
E stimates indicate that 10 to 30% of · the population experience chronic headache
pain in one form or another .1 In fact, surveys indicate that headache falls among the top 14 primary complaints io outpatient medical practice. 2 The ramifications of this statistic are widespread and include decreased occupational effectiveness/frequent absence, maladaptive social functioning, and family/ interpersonal problems. 3
64 PAIN MANAGEMENT
In 1962 the National Institutes of Neurological Diseases and Blindness published a re:. port, based on extensive clinical data, intended to differentiate and classify various forms of headache. 4 In this classification sys· tern, four ·types of headache were cited that were not associated with structural changes. These were migraine, muscle contraction, combination migraine/muscle contraction, and conversion headaches. However, conflicting results of migraine and tension headache studies have led some. researchers to recommend abandoning the. traditional classification system. 5 In oontrast, some investigators continue to argue that if researchers strictly adhere to the classification system, the differentiation of migraines from muscle contrac-tion headaches may be supported. 6 ·
Recently, my colleagues and I have published several papers that propose a nontraditional view of the etiology and treatment of many chronic headache cases. Specifically, we have proposed that many cases diagnosed as · common migraine may actually result from structural imbalance of the temporomandibular joint (TMJ) and from ~cessive activity of the masticatory muscles. Furthermore, many cases of morning-onset muscle cont:rac-

tion headaches and classic migraines may well be related to sleep duration.
The role of oral behavioral patterns and TMJ dysfunction in the production of common migraine pain was originally suggested by Ruff, Moss, and Lombardo. 7 These authors reviewed a report indicating that classic migraine patients exhibited vascular changes associated. with headaches, while common migraine subjects exhibited no such changes before, during, or after the headache. 8 In another report, Tfelt-Hansen, Lous, and Olesen9
assessed the presence of muscle tenderness in 18 head, neck, and facial regions during headache attacks in 50 common migraine subjects. In the majority of subjects, muscle tenderness was documented in multiple areas and this tenderness correlated highly with pain site. It was further documented that infiltrating tender areas with either a local anesthetic or saline effectively eliminated migraine symptoms in 28 of the subjects. In a subsequent study, Moss, Ruff,and Sturgis10 found that migraine headache patients reported more frequent oral habits (i.e., teeth clenching, thrusting the jaw forward, cupping the chin in the hand, and resting the hand on the side of the face) than did tension headache arid non-headache subjects. It was suggested that such oral behavioral patterns might lead to excessive ac-
tivity of the anterior temporalis muscle. The muscle later became painful and this pain was interpreted as common migraine pain.
In support of this proposition, Christensen, 11 Scott and Lundeen, 12 and Villarosa and Moss13 each reported the ability of spe-, cific oral habits to produce pain in the temporal region in analog subjects. Moss14 later reported the role of such oral habits in the production of characteristic headache pain in several subjects diagnosed as having common migraine. Interestingly, habit reversal procedures designed to decrease the frequency with which these four headache patients performed oral habits decreased the headache pain in each subject. Finally; in a theoretical paper based upon clinical cases and· prior research, Moss 15 suggested that the production of many forms of facial pain and common migraine symptoms could result from an interaction of anterior displacement of the articular disk in the TMJ and engaging in a high frequency of oral habits.' In this regard, it was proposed that the internal derangement of the TMJ results in an imbalance that creates unequal activation of the masticatory muscula-' ture during oral habits. This imbalance itself would not necessarily cause pain. Rather, when the patient performs a high rate of oral habits, the unequal distribution of pressures would lead to unequal activation of the muscles, and the muscles being most activated would become tender and painful.
In relation to the effects of sleep duration on classic migraine headaches and early morning-onset headaches, Moss, Lombardo, Cooley, Villarosa, and Gramling16 reviewed the research literature and found that the neurophysiological systems for both sleep and pain share many common characteristics •. It was concluded that excessive sleep could lead to decreased serotonin levels, which . would correlate with a reduction in the pain threshold. In this paper, two cases of classic mi-
MARCH/APRIL 1988 65

graine and one of early morning-onset tension headaches were discussed. All demonstrated a history in which the individuals experienced increased headache pain with increased sleep duration and all eliminated their headaches with. a reduction of total sleep time. It was concluded that excessive sleep could create headache pain in certain individuals and it was further speculated that such effects might -interact with other physiological mechanisms to exacerbate pam in other areas of the body (e.g., back pain).
· Although each ·of these new areas of research are in the early stages of development, ongoing research continues to support these contentions~ It has been found that, in clinical practice, the use of this formulation is proving valuable and is benefitting many patients. · Therefore, the remainder of this paper is directed toward giving the reader the ability to assess the involvement of these factors in specific headache cases and to suggest treatment approaches for each of these problems~
Assessment Issues
History. For patients experiencing a TMJ/ masticatory muscle invQlvement in the· production of their headaches, several originating factors may be involved. Blows to the ~, resulting from being struck or falls, often precede the ·development of headache pain. Additionally, whiplash injuries can also create TMJ derangement and can eventually lead to headache pain of. the temporal region. Nontraumatic events can also be associated with TMJ derangement and include activities such as cheerleading, playing musical instruments requiring specific chin positions (e.g., violin, flute), and dental procedures requiring excessive mouth opening (e.g., root canals, wisdom teeth removal). Although headache pain may not begin immediately afterwards, it will usually be seen within several months of the TMJ
66 PAIN MANAGEMENT
internal derangement and is probably the result of a hyperactivity and/or hypertrophying of specific muscles that occurs gradually as a result of the TMJ imbalance and masticatory muscle activity. In these cases, most individuals will recall a popping or clicking from the TMJ upon opening the mouth. This may have resolved over time but, importandy, does not indicate that the articular disk has repositioned itself over the head of the condyle.· Instead, it more .likely indicates that the articular disk is remaining anteriorly displaced throughout mouth opening. Over time, osteoarthritic processes are likely and a characteristic grating in the TMJ may be heard or felt upon palpation.
TMJ derangernent and subsequent TMJ/masticatory ·muscle headache may result from such ~raumatic . events as blows to the chin or
. whiplash, or from nontraumatic ones, such as cheerleadirig, playing the violin or flute, or from dental procedures requiring prolonged mouth opening. -
·For those patients experiencing a sleeprelated headache pattern, it is commonly observed that one of two circumstances . exist historically. First, there may have been a time that the patient compressed his/her sleep time . as a result of situational. demands. For exam .. ple, one of our- patients reported th:;J.t after leaving home to ·attend school, she typically · acquired 4 to 5 hours of sleep each evening, as compared to 7 or 8 hours prior to :that time. Upon completing her college degree, she returned to what she considered ~~normal" sleep time of 7 to 8 hours and her headaches began. The second, and perhaps more frequent, observation is that patients will have worked.on a swing shift or night shift preceding· the de-

velopment of the headaches. Some continue to have inconsistent sleep, while others have returned to more "normal" sleep patterns, although this may exceed their bodies' sleep need ..
In these patients, the headaches typically begin upon awakening and reflect a dull, deep, diffuse pattern that is interpreted as tension headaches. dassic migraineurs may be awakened from sleep with a severe, throbbing, unilateral headache. For those classic migraineurs who report headaches developing laterin·the day, the headaches are immediately preceded by visual symptoms. Many of these patients will report spontaneous remission of headache problems which, if investigated, correlate highly with periods of reduced sleep, often due to situationat changes. Obviously, the headaches should be worse during times that extended sleep is possible, such as on weekends, holidays, and vacations.
Sleep-related headaches are observed commonly when a patient compresses his sleep time due to situational demands or, more frequently, when a patient has worked on a swing or night shift. The important factor is that the patient's sleep time is exceeding his body's need for sleep.
Initial Examination. In the evaluation of a . TMJ/masticatory muscle involvement in the headache pattern,. a brief evaluation of the mandibular region is warranted. First, the patient should open and shut the mouth slowly while the clinician either listens with a stethoscope to the TMJ or palpates the region. If the mandible deviates to one side during opening and. returns to a central relationship when the click or pop is heard or felt, this indicates that the articular disk is anteriorly displaced while
the mouth is closed. Additionally, any grating sounds or feelings should be rioted, as these could indicate an osteoarthritic process. If no click or pop is noted during mouth opening, the clinician should watch carefully to deter.; mine if the mandible deviates to one side upon mouth opening. In many eases, this would indicate that the articular disk is displaced anteriorly although. it. might be associated with some other physiological process (e.g., muscle spasm). A measurement of incisal opening distance should be made and can be done with a standard ruler measuring from the top of the front lower teeth to the top of the front upper teeth. If the mouth opening distance is less than 40 millimeters, the clinician should suspect that one or both of the articular disks is remaining displaced anteriorly {this is called a "dosed lock"). If the mouth opening distance is less than 20 millimeters, however, the clinician should suspect a more acute muscular involvement. This information is based upon the noteworthy work of Farrar and McCarty.t7
Additional symptoms often seen with TMJrelated headaches are tinnitus, facial pain, dizziness, and abnormal sensations of the ear and its canal {e.g., itchiness, wetness or dripping sensation, pain, fullness). Importantly,· the headaches tend to be in the same location in all attacks and, may involve not only the temple region, but the whole side ofthe·head and neck. Most of the cases exhibiting such headaches tend to report retro-orbital pain. If
. the masticatory muscles are palpated, mariy tend to be very tender. .
If TMJ derangement is suspected, the only way to make a definitive diagnosis is through radiographic techniques. To develop a better understanding. of accepted American Dental Association {ADA) diagnostic and. treatn'lent procedures for temporomandibular disqrders,
· the reader is referred to Griffiths. :ts · · One additional factor that should be as-,
MARcHtAPRIL 1988 67
sessed in suspected TMJ headache cases is the existence of oral habits. To facilitate this, the clinician can use the Oral Habits Survey (Appendix 1), which assesses a wide range of these behaviors. In patients with TMJ-related headaches, it will usually be observed that one or more of the oral habits is rated at a level of 5 to 10 ( 10 = almost always performing the behavior). To provide a definitive cause and effect relationship between oral habits and headaches, the patient may be requested to clench his/her teeth for two to· three minutes, or less if the pain becomes extreme. The ensuing pain should be identical in location and character to that normally experienced during headache episodes.
In assessing the role of sleep duration in headache production, there are currently no proposed clinical examination procedures other than the exclusion of other possible causes. Therefore, the clinician must rely upon the patient's history and self-monitoring data to demonstrate a sleep duration cause for the headaches. Patients who fail to experience daily headaches may be requested to selfmonitor the time they go to bed and awaken, as well as the presence of headaches on each of these days.
After two weeks, the clinician can compare the headache versus nonheadache days in relation to time of awakening and sleep duration. If a positive sleep effect is present, the patient should experience many more headaches on those days that he/she slept later and · for longer periods. For patients experiencing daily headaches, it is recommended that the clinician institute a sleep reduction program immediately and monitor its effects on the headache. Self-monitoring during baseline cannot demonstrate any specific sleep effects because nonheadache days do not exist. In such cases, the sleep duration treatment recommendations outlined in the next section should be followed and, if a relationship ex-
68 PAIN MANAGEMENT
ists, reduced sleep duration should lead to reduction or elimination of the headaches. It a reduction is seen in the headaches, the patient can be convinced of the association between sleep duration and pain simply by having them increase their sleep· duration on certain days and observing the fact that headaches occur on those days only.
Treatmentlssues. As has been suggested for migraine and tension headache treatment, relaxation training represents the first step in the treatment of TMJ/masticatory muscle headaches. Although many other forJDs of relaxation are available, the form currently used by the author involves tension and relaxation
exercises* for all the masticatory muscles.1
Additionally, specific treatment is indicated to reduce the frequency of oral habits.
Although these procedures appear very simple at first, the clinician will find that many patients fail to comply with treatment. Therefore, in patients who appear to have TMJ/masticatory muscle headaches and who do not improve as a result of these procedures, the clinician should immediately suspect noncompliance and again emphasize to the patient the need to practice relaxation at least twice a day and to carefully monitor oral habits.
Some patients with morning-onset headaches-those who are "sleep drunk" upon awakening and who snore loudly and those who say they are insomniacs who do not snore-may have sleep apnea syndrome and should be referred to a sleep disorders clinic.
A number of dental procedures have been employed in the treatment of TMJ derangement in facial and head pain. Many of these have proven effective in reducing headaches, although the ADA's position is that reversible procedures should be attempted first. 18 The first line of treatment typically involves the use of occlusal appliances or splints that tend to move the condyle forward. The splints prevent full mouth closure and, as a result, would be expected to greatly reduce the frequency of oral habits. If the splint is being used in an attempt to reposition the articular disk, it must be worn continually for approximately six weeks.17 The rationale for this is that if the
* Audiotaped relaxation exercises are available from the author.
mouth is allowed to close fully while the splint is not worn, then the disk may once again reposition itself anterior to the condyle. Therefore, the patient is instructed to leave the splint in place both day and night, during all activities, except for brushing the teeth, during which time the mouth is not closed.
Although restorative and equilibration procedures are performed frequently in the treatment of facial and headache pain, they should · be done only if internal derangement of the TMJ has been evaluated and corrected. Such treatment is considered irreversible and the position of the ADA is that such procedures should not be used routinely and especially not during the acute stage of TMJ disorders.18
TMJ surgery is not the initial treatment of choice for disk displacement, but after the failure of currently acceptable non-surgical treatments it may be considered.18 However, failure of such conservative treatments alone should not be considered the only criterion for surgery, as surgical intervention must be based on dearly defined criteria of intracapsular pathologic conditions or anatomic derangement.
A final form of treatment that may prove beneficial to patients with TMJ/masticatory muscle headaches is physical therapy. Specifically, exercises designed to increase the strength of the shoulder and neck muscles may assist in correcting postural difficulties that can contribute to such pain ·problems. Although there is not a great deal of evidence supporting the utility of physical therapy procedures for facial and head pain related to TMJ derangement, this is a reversible form of treatment and subjective evaluations by many pain patients indicate that it may be very useful in individual cases.
In the treatment of suspected sleep-related headaches, the actual sleep manipulation procedures are simple. There are no apparent associated risks of slightly reduced sleep, other
MARCH/APRIL 1988 69
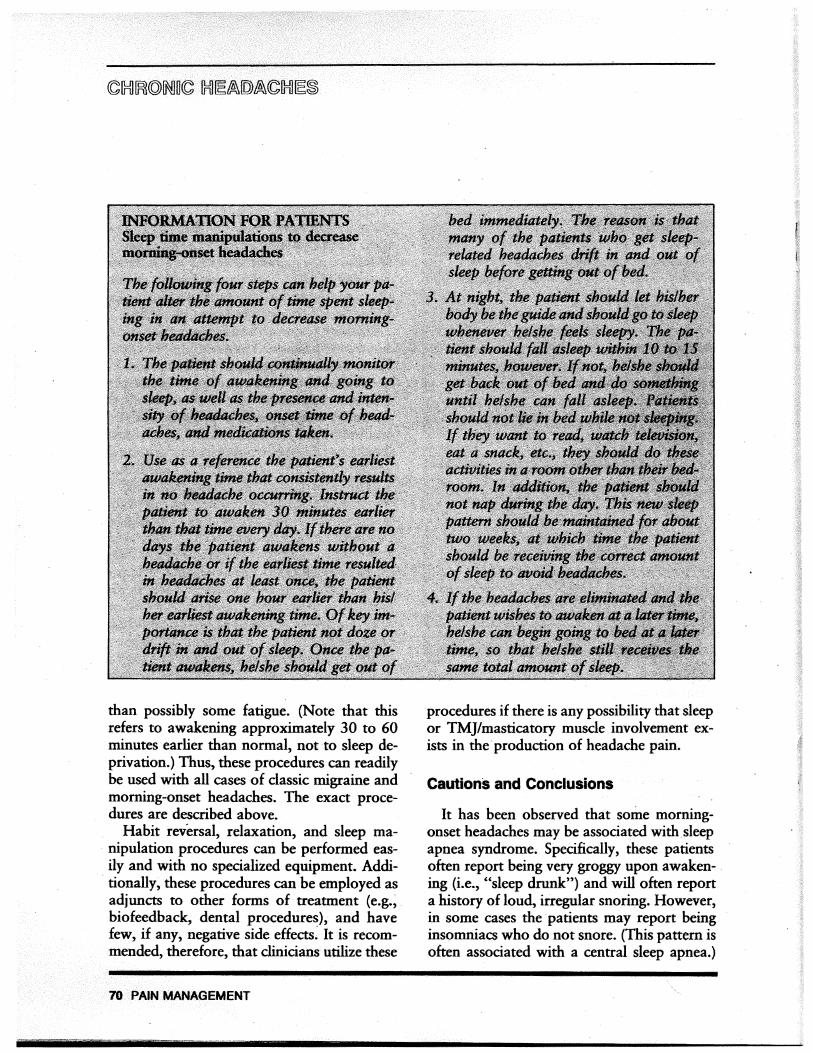
than possibly some fatigue. (Note that this refers to awakening approximately 30 to 60 minutes earlier than normal, not to sleep deprivation.) Thus, these procedures can readily be used with all cases of classic migraine and morning...:onset headaches. The exact procedures are described above.
Habit reversal, relaxation, and sleep manipulation procedures can be performed easily and with no specialized equipment. Additionally, these procedures can be employed as adjuncts to other forms of treatment (e.g., biofeedback, dental procedures), and have few, if any, negative side effects~ It is recommended, therefore, that clinicians utilize these
70 PAIN MANAGEMENT
procedures if there is any possibility that sleep or TMJ/masticatory muscle involvement exists in the· production of headache pain.
Cautions and Conclusions
It has been observed that some morningonset headaches may be associated with sleep apnea syndrome. Specifically, these patients often report being very groggy upon awaken- . ing (i.e., "sleep drunk"} and will often report a history of loud, irregular snoring. However, in some cases the patients may report being insomniacs who do not snore. (This pattern is often associated with a central sleep apnea.)
Another common observation is that the patients will have hypertension, which o&en began in roughly the same time period as the headaches. In such cases, any attempts at performing sleep reduction will simply exacerbate the patient's feeling of fatigue and the headaches will not resolve. If such a problem is suspected, it is mandatory that the patient be evaluated at a qualified sleep disorders clinic.
Although the present paper has suggested several new approaches in the assessment and management of chronic headaches, it is importantto state once again that the research is only in the early stages of development. Therefore, it is not possible to know how many cases of diagnosed common migraine actually fit the patterns for TMJ/masticatory muscle headaches and it is also not possible to know whether all cases of classic migraines and early morning-onset "tension" headaches will actually respond to sleep manipulation. · However, because these do represent conservative and reversible therapies, they should be among the first treatments employed in the . clinical management of chronic headache pain. In conclusion, it is hoped that the foregoing discussion has served the intended purpose of allowing the reader to begin using these new approaches because they may prove to be quite beneficial to a significant number of patients.
References
1. Feuerstein M, Gainer J: Chronic Headache. In Doleys DM, Meredith RL. Ciminero AR (Eds.): Behavioral Medicine: Assessment and Treatment Strategies. New York, Plenum, 1982. 2. DeLozier JE, Gagnon RO: National Ambulatory
Medical Care Survey: 1973 Summary, United States,
May, 1973-April, 1974 (DHEW publication number HRA79-1772). Washington, D.C., U.S. Government Printing Office, 1975.
3. Clarke GJR, Waters WE: Headache and migraine in a London general practice. In Cumings JN (Ed.): The Epidemiology of Migraines. Bracknell, Boehringer In-gelheim, 1974. ·
4. Ad Hoc Committee on Classification of Headache. Neurology 12:378-380, 1962. 5. Bakal DA: Headache. In Woody RH (Ed.): Ency
clopedia of Clinical Assessment. San Francisco, JosseyBass, 1980. 6. Thompson JK: Diagnosis of head . pain: An idio
graphic approach to assessment and classification. Headache 22:221-232, 1982. 7. Ruff GA, Moss RA, Lombarto TW: Common mi
graine: A review and proposal for a nonvascular etiology. 1 Oral Rehabi/1986.
8. Olesen J, Lauritzen M, Tfelt-Hansen P, et al: Spreading cerebral oligemia in classic migraine and normal cerebral blood flow and common migraine. Headache 22:242-248, 1982.
9. Tfelt-Hansen P, Lous I, Olesen J: Prevalence and significance of muscle tenderness 'during common migraine attacks. Headache 21:49-54, 1981. 10. Moss RA, Ruff MH, Sturgis ET: Oral behavioral patterns in facial pain, headache, and non-headache populations. Behav Res Ther 22:683-687, 1984. 11. Christensen LV: Facial pains in the jaw muscles: A review. 1 Oral Rehabil 8:193-201, 1981. 12. Scott DS, Lundeen TF: Myofascial pain involving the masticatory muscles: An experimental model. Pain 8:207-215, 1980. 13. Villarosa GA, Moss RA: Oral behavioral patterns as factors contributing to the development of head and
. facial pain. 1 Prosthet Dent 54:427-430, 1985. 14. Moss RA: Oral behavioral habits in common migraine.] Craniomandib Prac (in press). 15. Moss RA: A structural imbalance/muscular hyperactivity interactional theory of common migraine pain. 1 Craniomandib Prac (in press). 16. Moss RA, Lombardo TW, Cooley JE, et al: Effects of sleep duration on classic migraine and depression headache pain: Case reports. 1 Craniomandib Prac (in press). 17. Farrar WB, McCarty WL: A Oinical Outline of Temporomandibular Joint Diagnosis and Treatment. Montgomery, AL: Walker Printing Company, 1983. 18. Griffiths RH: Report of the president's eonference on the examination, diagnosis, and management of temporomandibular disorders. 1 Am Dent Assoc 106:75-77, 1983.
MARCH/APRil 1988 71




















