
Monograph on Aspergillus and Aspergillosis in man, animals and birds,Mohamed Refai1, Heidy Abo...
169
1 Monograph on Aspergillus and Aspergillosis in man, animals and birds A guide for classification and identification of aspergilli, diseases caused by them, diagnosis and treatment By Mohamed Refai 1 , Heidy Abo El-Yazid 1 and Atef Hassan 2 1. Department of Microbiology, Faculty of Veterinary Medicine, Cairo University 2. Department of Mycology and Mycotoxins, Animal Health Research Institute, Dokki 2014
Transcript of Monograph on Aspergillus and Aspergillosis in man, animals and birds,Mohamed Refai1, Heidy Abo...
1
Monograph
on
Aspergillus and Aspergillosis in man, animals and birds
A guide for classification and identification of aspergilli, diseases
caused by them, diagnosis and treatment
By
Mohamed Refai1, Heidy Abo El-Yazid
1 and Atef Hassan
2
1. Department of Microbiology, Faculty of Veterinary Medicine, Cairo University
2. Department of Mycology and Mycotoxins, Animal Health Research Institute, Dokki
2014

2
Preface
When Micheli in 1729 discovered the Aspergillus fungus, he had not expected that this fungus would continue
for more than two and half centuries to be a subject of research, economic and medical interest. Species of the
genus Aspergillus, like Aspergillus oryzae, have long been used in the manufacture of citric acid, soy sauce and
other useful products. On the other hand, other species, like Aspergillus flavus, are known to produce highly
toxic and carcinogenic substances in the foodstuffs they infest. Moreover, other species like Aspergillus
fumigatus, cause disease in humans, animals and birds.
By the time Thom and Church published the first major monograph on the genus in 1926, Aspergillus had
become one of the best-known and most studied mould groups. Their prevalence in the natural environment,
their ease of cultivation on laboratory media and the economic importance of several of its species ensured that
many mycologists and industrial microbiologists were attracted to their study. Now we are speaking of a genus,
which is subdivided into sub-genera comprising sections and more than 250 species. The use of molecular
biology in the study of Aspergillus has resulted in the moving of species from one subhenus to the other and
from one section to the other. Some species are considered synonyms and some variants attained the status of a
species. Such changes occur in short periods, so that one needs frequent updating to his knowledge.
Since I came back from Germany in 1965 after finishing my mycology study, I depended on the 3 identification
keys of the Aspergillus species based on colours and micromorphology and we were satisfied to identify the
groups of Aspergillus. Now it becomes difficult, as many species cannot be identified on their morphological
basis, but need molecular biological techniques. This is why my post-graduate students become confused and
asked me to prepare a lecture to simplify the matter. When I started to collect data for the lecture, I was
drowned in a sea of information’s about this fungus. The enormous data which accumulated on my desk during
the last 4 months encouraged me to write a monograph and upload it on my site in the internet to be available to
all students, not only in Egypt, but in other parts of the world as well.
This monograph is dedicated to my supervisors, Prof. Dr.Dr. h.c. Kurt Wagener and Prof. Bisping who
introduced me to the eminent mycologists of Europe, when they allowed me to accompany them, few months
after arriving Germany in April 1962, to Travemuende on the Baltic Sea, to attend a meeting of mycology held
on a ship. There I met Prof. Rieth, who invited me in his laboratory for one year. Prof. Rieth was fond of
photographing fungi and writing teaching materials on all aspects of mycology.
Prof. Wagener Prof. Bisping Prof. Rieth on the ship at Travemuende, 1962

3
Contents item page Item Page
Preface 1 6. Aspergillosis in animals 91
1.Introduction 4 6.1. Aspergillosis in dogs 91
2.Historical 5 6.2. Aspergillosis in cats 94
3. Nomenclature and classification 11 6.3. Aspergillosis in horses 96
4. Description of important aspergilli 17 6.4. Aspergillosis in cattle 98
4.1. Aspergillus Section Restricti 17 6.5. Aspergillosis in Sheep and goats 100
4.2. Aspergillus Section Cervini 18 6.6. Aspergillosis in pigs 104
4.3. Aspergillus section Nigri 19 6.7. Aspergillosis in camels 104
4.4. Aspergillus section Candidi 23 6.8. Aspergillosis in American bisons 105
4.5. Aspergillus section Usti 25 6.9. Aspergillosis in monkeys 106
4.6. Aspergillus section Versicolores 26 6.10. Aspergillosis in deers 106
4.7. Aspergillus section Sparsi 30 6.11. Aspergillosis in rabbits 107
4.8.Aspergillus Section: Aspergillus 31 6.12. Aspergillosis in guinea-pigs 108
4.9. Aspergillus section Terrei 35 4.13. Aspergillosis in lesser blind mole rats 108
4. 10. Aspergillus Section Flavipedes 36 6.14. Aspergillosis in dolphins 109
4. 11. Section: Circumdati 39 7. Aspergillosis in birds 110
4. 12. Aspergillus section Flavi 40 7. 1. Aspergillosis in poultry 110
4.13. Aspergillus Section: Cremei 45 7.2. Aspergillosis in wild birds: 112
4.14. Aspergillus section Fumigati 46 7.2.1. Aspergillosis in penguins 112
4. 15. Aspergillus Section:Clavati 49 7.2.2. Aspergillosis in parrots 114
4. 16. Aspergillus Section:Nidulantes 50 7.2.3. Aspergillosis in quails 115
4. 17. Aspergillus Section:Ornati 52 7.2.4. Aspergillosis in ostrich 116
4. 18. Aspergillus sect. Aeni 52 7.2.5. Aspergillosis in red-tailed hawk 117
5. Aspergillosis in man 7.2.6. Aspergillosis in Red-billed Toucan 117
5.1. Pulmonary aspergillosis 7.2.7. Aspergillosis in Snow Owl 118
5.2. Cerebral aspergillosis 71 7.2.8. Aspergillosis in Goshawk 118
5.3. Cutaneous aspergillosis 73 7.2.9. Aspergillosis in Cormorants 119
5.4. Aspergillus Onychomycosis 75 7.2.10. Aspergillosis in swans 119
5. 5. Ocular aspergillosis 76 7.2.11. Aspergillosis in kiwi 120
5.6. Aspergillus sinusitis 78 8. Laboratory diagnosis of aspergillosis 123
5.7. Paranasal sinuses aspergillosis 79 8.1. Direct microscopic examination 123
5.8. Otoaspergillosis 81 8.2. Isolation and identification 128
5.9. Aspergillus endocarditis 82 8.3.Molecuar identification of aspergilli 132
5.10. Aspergillus thyroiditis 84 8.4. Serological techniques 135
5.11. Hepatic aspergillosis 85 9. Treatment of aspergillosis
140
5.12. Gastrointestinal aspergillosis 86 10. References
143
5.13. Urinary tract aspergillosis 87
5.13. Aspergillus osteomyelitis 88
4
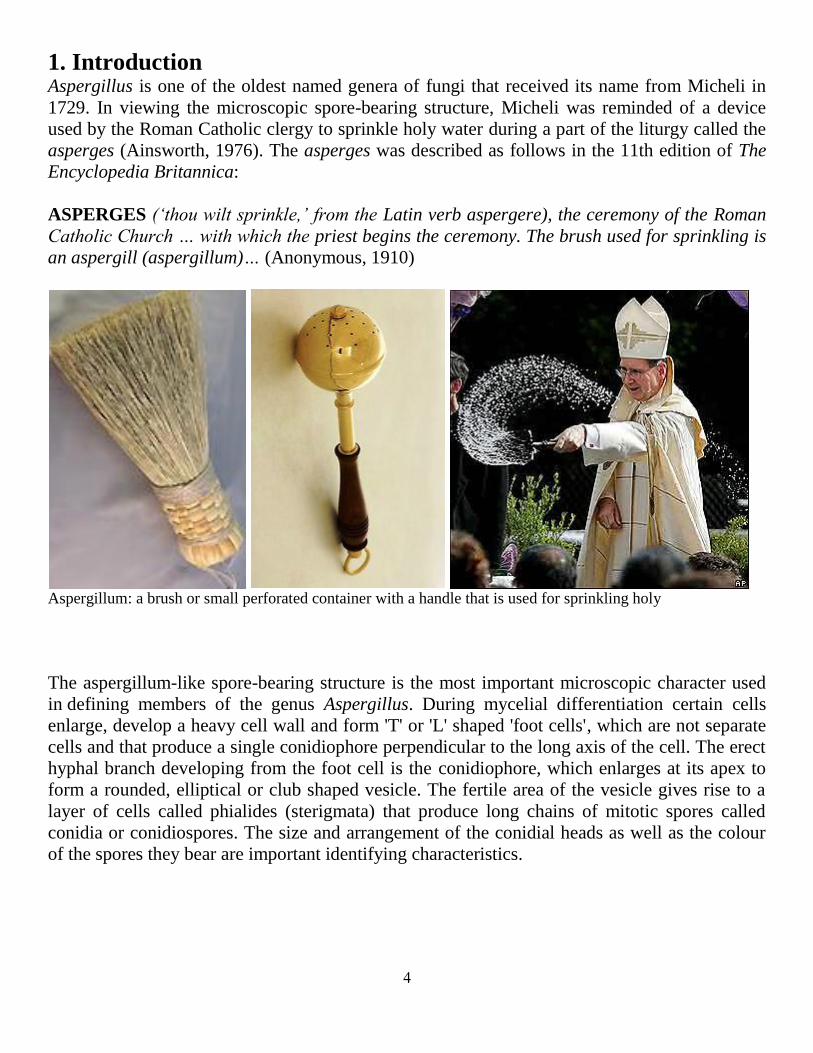
1. Introduction Aspergillus is one of the oldest named genera of fungi that received its name from Micheli in
1729. In viewing the microscopic spore-bearing structure, Micheli was reminded of a device
used by the Roman Catholic clergy to sprinkle holy water during a part of the liturgy called the
asperges (Ainsworth, 1976). The asperges was described as follows in the 11th edition of The
Encyclopedia Britannica:
ASPERGES (‘thou wilt sprinkle,’ from the Latin verb aspergere), the ceremony of the Roman
Catholic Church … with which the priest begins the ceremony. The brush used for sprinkling is
an aspergill (aspergillum)… (Anonymous, 1910)
Aspergillum: a brush or small perforated container with a handle that is used for sprinkling holy
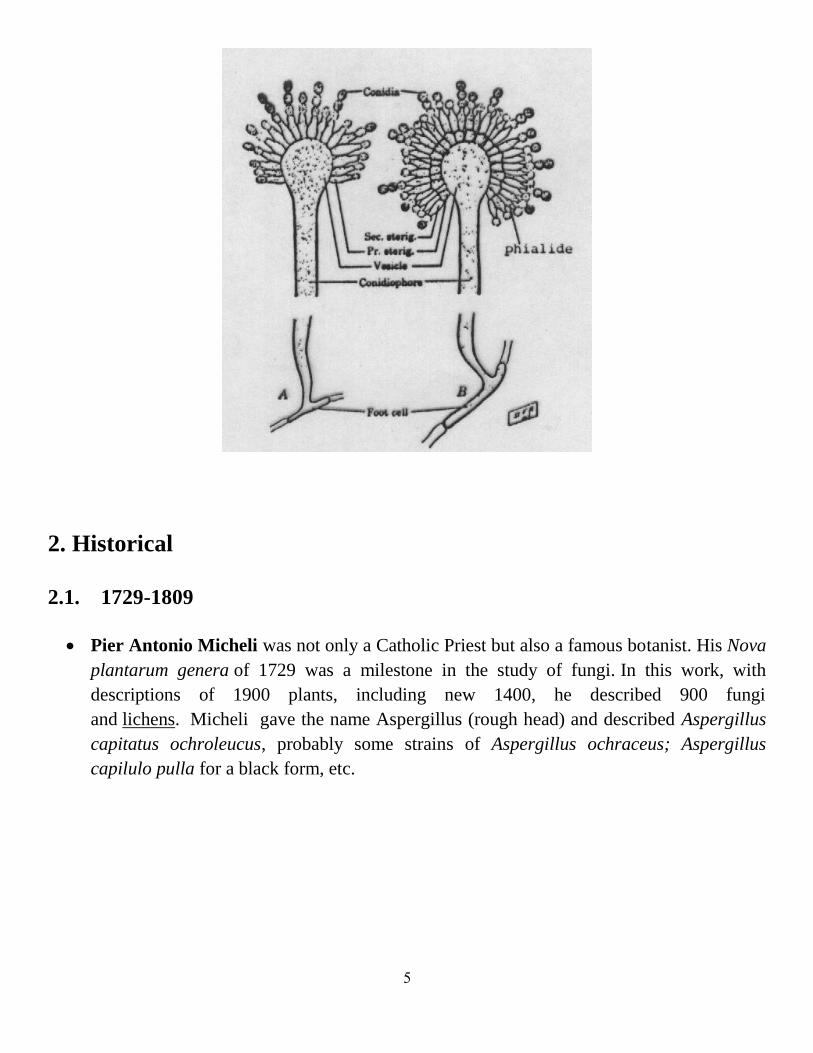
The aspergillum-like spore-bearing structure is the most important microscopic character used
in defining members of the genus Aspergillus. During mycelial differentiation certain cells
enlarge, develop a heavy cell wall and form 'T' or 'L' shaped 'foot cells', which are not separate
cells and that produce a single conidiophore perpendicular to the long axis of the cell. The erect
hyphal branch developing from the foot cell is the conidiophore, which enlarges at its apex to
form a rounded, elliptical or club shaped vesicle. The fertile area of the vesicle gives rise to a
layer of cells called phialides (sterigmata) that produce long chains of mitotic spores called
conidia or conidiospores. The size and arrangement of the conidial heads as well as the colour
of the spores they bear are important identifying characteristics.
5
2. Historical
2.1. 1729-1809
Pier Antonio Micheli was not only a Catholic Priest but also a famous botanist. His Nova
plantarum genera of 1729 was a milestone in the study of fungi. In this work, with
descriptions of 1900 plants, including new 1400, he described 900 fungi
and lichens. Micheli gave the name Aspergillus (rough head) and described Aspergillus
capitatus ochroleucus, probably some strains of Aspergillus ochraceus; Aspergillus
capilulo pulla for a black form, etc.

6
2.2. 1809-1926
Link (1809) described A. glaucus. Aspergillus candidus, Aspergillus
chevalieri, Aspergillus flavus and Eurotium herbariorum
Corda (1828) published his studies of fresh material, as seen under his microscope. He
described several species,e.g. Aspergillus phoenicis, Aspergillus repens
Desmazières (1834) described A. clavatus
DeBary (1854) noticed that an Aspergillus mycelium could produce a cleistothecium as
well as an aspergillum. Cleistothecium-producing mould had been observed before and
given its own name: Eurotium herborarium. DeBary realized that A. glaucum and E.
herborarium were different reproductive phases of the same organism, thus putting the
dual naming of the same fungus in its sexual and asexual stages.
7
Heinrich Anton de Bary Aspergillus glaucus by Anton de Bary (1854) Jean Paul Vuillemin
Fresenius (1863) described Aspergillus fumigatus and Sterigmatocystis sulphurea
Berk. & M. A. Curtis (1868) described Aspergillus erythrocephalis
van Tieghem (1967) described Aspergillus niger
Wilhelm (1877) described Aspergillus ochraceus
Ahlburg (1878) described Eurotium oryzae
Bainier (1880-1913) described A. ustus, A. flavipes, Sterigmatocystis
usta, Sterigmatocystis flavipes, Sterigmatocystis sydowii , Aspergillus gracilis and
Sterigmatocystis carbonaria
Saccardo (1882) described A. repens
Eidam (1883) described Sterigmatocystis nidulans
Winter (1884) described A. nidulans
Cohn (1884) described Aspergillus oryzae
Gasperini (1887) described Aspergillus elegans , Aspergillus violaceofuscus
Delacroix (1893) described Aspergillus brunneus , Eurotium echinulatum
Wehmer (1896-1907) devided the genus Aspergillus in Subgenus Microaspergillus and
Macroaspergillus. He described Aspergillus ostianus , Aspergillus wentii,
Aspergillus fischeri, Aspergillus giganteus, Aspergillus sulphureus , Aspergillus varians,
Aspergillus pulverulentus
Höhn (1902) described Aspergillus citrisporus
Vuillemin (1903-1908) Sterigmatocystis versicolor, Aspergillus versicolor
Saito (1904-1906) described Aspergillus caesiellus, Aspergillus japonicus
Mangin (1909-1910) described Aspergillus chevalieri , Eurotium chevalieri
Yukawa (1911) described Aspergillus melleus
Kita (1913) described Aspergillus tamarii
Blochwitz (1914) described Aspergillus conicus
Massee (1914) described Aspergillus cervinus
Thom and Church (1918) described A. terreus

8
2.3. 1926-1965
Thorn and Church (1926) revised some 350 names, but only 69 species were accepted,
which were more or less arbitrarily considered in 11 groups. Their studies resulted in the
publication in the 1926 of a monograph entitled “The Aspergilli.”
They based their taxonomy of the macroscopic colony charactes and the microscopic
features of the vesicles, conidiophores, the single or double series of the spore-bearing
phialides and the shapes and colours of conidia.
Thom and Raper (1945) used the work of Thorn and Church as a basis for subsequent
taxonomic treatments of the genus in their book entitled “A Manual of the Aspergilli”.
They classified the Aspergillus species into 14 groups and 9 series.
Charles Thom Kenneth Raper
Raper & Fennell (1965) described 150 taxa in their monograph “The Genus
Aspergillus”. They divided the species into 18 informal “groups” based on the authors”
opinions of probable relationships. These groups contained 132 species and 18 varieties.

9
Dorothy Fennell
2.4. 1965-2011
Gams et al (1985) replaced the groups by sections and divided the genus Aspergillus into
18 sections organized in six subgenera.
Pitt et al. (2000), in their the latest compilation of names in current use, listed 182.
Samson (2000) listed another 36 published between 1992 and 1999. More than 40 new
species descriptions have been published since then , bringing the total number to ∼250.
Samson, R.A., and Varga, J.(2007), in their book Aspergillus systematics in the genomic
era, they presented the activities the workshop held on 12-14 April, 2007 at
the CBS, Fungal Biodiversity Centre,Utrecht –The Netherlands covering the following
themes:
o What is the impact of Aspergillus taxonomy in terms of epidemiology, case definitions
and biological understanding of disease?
o What and how many genes should be used to delimit an Aspergillus taxon?
o How does the phylogenetic species concept translate to practical and routine diagnoses?
o What are the roles of Aspergillus databases for species identification?
o What is the value and impact of polyphasic approaches for species identification?
o What genes/methods can be used to design kits for rapid identification?
o How should new species be proposed?

11
Geiser et al. (2008) mentioned that there are approximately 250 named species of
Aspergillus and this number is likely to increase significantly in the near future because of
increasing application of the phylogenetic species concept based on DNA sequence data
rather than on visible morphological characters.
Gustavo H. Goldman and Stephen A. Osmani (2008) published their book “ The
Aspergilli Genomics, Medical Aspects, Biotechnology, and Research Methods”
M. Machida and K. Gomi (2010) published their book “Aspergillus, molecular biology
and genomics” summarized the most important aspects of Aspergillus molecular biology
and genomics. Robert A. Samson, János Varga and Jens C. Frisvad (2011) published in their book “
Taxonomic studies on the genus Aspergillus” new and revisited species in Aspergillus
section Nigri, Aspergillus section Terrei, Aspergillus section Flavi and Aspergillus section
Usti.
W. Gams John Pitt Stephen W. Peterson
Robert A. Samson János Varga Jens C. Frisvad
11
3. Nomenclature and classification
During the 20th century, as mycologists isolated and identified increasing numbers of
isolates, the number of named species of Aspergillus increased. These tended to fall into
morphologically distinct clusters. So in order to facilitate identification, the genus was
divided into intrageneric 'groups'. The Aspergillus glaucus group, for example, was
characterized by abundant, typically green conidial heads, with perithecia generally
present, while the Aspergillus ochraceous group had yellow conidia and abundant cream
to purplish-coloured sclerotia.
The term 'group' does not have nomenclatural status within the formal rules of biological
nomenclature. Therefore, the genus was reorganized into a new subgeneric taxonomic
hierarchy based on 'sections.' In this system, The genus was subdivided into subgenera.
The subgenus 'Aspergillus' consists of xerophilic species. A. glaucus is the type species,
classified in the subgenus Aspergillus and the section Aspergillus.
A new subgenus was introduced called Circumdata that encompassed seven sections, in
which 'section circumdati' was the new rubric for the old 'A. ochraceous group'. The
attempted imposition of subgeneric epithets, only one of which is called 'Aspergillus' is
extremely confusing and has not caught on. On the other hand, most taxonomists now use

12
the term 'section' rather than 'group' for Aspergillus intrageneric classifications and
identifications.
Some Aspergillus species regularly produce both sexual and asexual spores; in other
species the sexual form is rare; for still others, sexual spores have never been seen - and
perhaps never will be seen.
The names used for currently accepted sexual genera with close phylogenetic relationship
or known linkage to Aspergillus species (representative Aspergillus species given in
parenthesis) are:
1. Chaetosartorya (A. wentii);
2. Emericella (A. nidulans);
3. Eurotium (A. glaucus);
4. Fennellia (A. terreus);
5. Hemicarpenteles (A. paradoxus);
6. Neocarpenteles (A. clavatus);
7. Neosartorya (A. fumigatus);
8. Petromyces (A. flavus);
9. Sclerocleista (A. ornatus);
10. Warcupiella (A. spinnulosus).
3.1. Classification according to Thom and Raper (1945)
Thom and Raper (1945) classified the Aspergillus species into 14 groups and 9 series as
follows:
Group 1: THE ASPERGILLUS CLAVATUS GROUP
Group 2: THE ASPERGILLUS GLAUCUS GROUP 1.ASPERGILLUS REPENS SERIES
2.ASPERGILLUS RUBER SERIES
3.ASPERGILLUS CHEVALIERI SERIES
4.ASPERGILLUS AMSTELODAMI SERIES
5.ASPERGILLUS RESTRICTUS SERIES
Group 3: THE ASPERGILLUS FUMIGATUS GROUP 6.ASPERGILLUS FUMIGATUS SERIES
7.ASPERGILLUS FISCHERI SERIES
Group 4: THE ASPERGILLUS NIDULANS GROUP
Group 5: THE ASPERGILLUS USTUS GROUP
Group 6: THE ASPERGILLUS FLAVIPES GROUP
13
Group 7: THE ASPERGILLUS VERSICOLOR GROUP
Group 8: THE ASPERGILLUS TERREUS GROUP
Group 9: THE ASPERGILLUS CANDIDUS GROUP
Group 10:THE ASPERGILLUS NIGER GROUP 8.ASPERGILLUS NIGER SERIES
9.ASPERGILLUS CARBONARIUS SERIES
Group 11:THE ASPERGILLUS WENTII GROUP
Group 12:THE ASPERGILLUS TAMARII GROUP
Group 13:THE ASPERGILLUS FLAVUS-ORYZAE GROUP
Group 14:THE ASPERGILLUS OCHRACEUS GROUP
3.2. Classification according to Raper and Fennel (1965)
Raper and Fennel (1965) divided species into 18 informal “groups” , which contained 132
species and 18 varieties as follows:
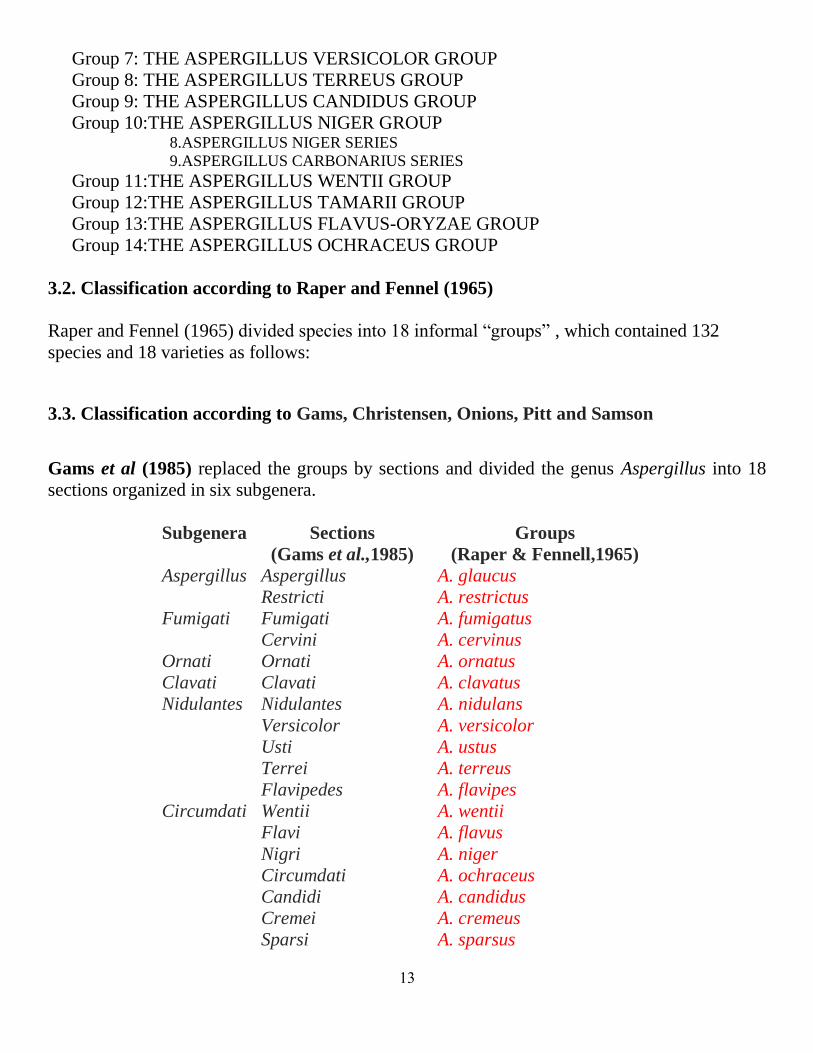
3.3. Classification according to Gams, Christensen, Onions, Pitt and Samson
Gams et al (1985) replaced the groups by sections and divided the genus Aspergillus into 18
sections organized in six subgenera.
Subgenera Sections
(Gams et al.,1985)
Groups
(Raper & Fennell,1965)
Aspergillus
Aspergillus
Restricti
A. glaucus
A. restrictus
Fumigati
Fumigati
Cervini
A. fumigatus
A. cervinus
Ornati Ornati A. ornatus
Clavati Clavati A. clavatus
Nidulantes
Nidulantes
Versicolor
Usti
Terrei
Flavipedes
A. nidulans
A. versicolor
A. ustus
A. terreus
A. flavipes
Circumdati
Wentii
Flavi
Nigri
Circumdati
Candidi
Cremei
Sparsi
A. wentii
A. flavus
A. niger
A. ochraceus
A. candidus
A. cremeus
A. sparsus

14
They then added the teleomorph names as follows:
1. Subgenus Aspergillus
1. Section: Aspergillus (Teleomorph: Eurotium)
2. Section: Restricti
2. Subgenus Circumdati
3. Section: Circumdati (Teleomorph:Neopetromyces)
4. Section: Nigri
5. Section: Flavi (Teleomorph:Petromyces)
6. Section: Cremei (Teleomorph:Chaetosartorya)
7. Section: Candidi
8. Section: Wentii
9. Section: Sparsi
3. Subgenus Clavati
10. Section: Clavati (Teleomorph:Neocarpenteles)
4. Subgenus Fumigati
11. Section: Cervini
12. Section: Fumigati (Teleomorph:Neosartorya)
5. Subgenus Nidulantes
13. Section: Nidulantes (Teleomorph:Emericella)
14. Section: Versicolores
15. Section: Flavipedes (Teleomorph:Fennellia)
16. Section: Usti
17. Section: Terrei (Teleomorph:Fennellia)
6. Subgenus Ornati
18. Section: Ornati (Teleomorph:Sclerocleista)

15
3.4. Classification according Petrson (2000)
Peterson (2000) reported that phylogenetic studies of ribosomal RNA gene sequences led to the
acceptance of 3 subgenera with a total of 16 sections and the so-called »Warcupiella group«, a
treatment currently accepted by most Aspergillus researchers:
Subgenus Aspergillus
1. Section: Aspergillus (Teleomorph: Eurotium)
2. Section: Restricti
3. Section: Cervini
4. Section: Terrei (Teleomorph:Fennellia)
5. Section: Flavipedes (Teleomorph:Fennellia)
6. Section: Nigri
7. Section: Circumdati (Teleomorph:Neopetromyces)
8. Section: Flavi (Teleomorph:Petromyces)
9. Section: Cremei (Teleomorph:Chaetosartorya)
10. Section:Candidi
Subgenus Fumigati
11. Section:Fumigati (Teleomorph:Neosartorya)
12. Section:Clavati (Teleomorph:Neocarpenteles)
Subgenus Nidulantes
13. Section:Nidulantes (Teleomorph:Emericella)
14. Section:Usti
15. Section:Versicolores
16. Section:Ornati (Teleomorph:Hemicarpenteles)
3.5. Molecular classification of Aspergillus and its Teleomorphs
Based on the phylogenetic analysis of multilocus (calmodulin, RNA polymerase 2 and rRNA)
sequence data (Samson and Varga, 2009 and Varga et al. 2010)., Aspergillus can be subdivided
into eight subgenera and 19 sections as follows:
1. Subgenus Aspergillus
1. Sections Aspergillus
2. Sections Restricti;
2. Subgenus Fumigati
3. Sections Fumigati
4. Sections Clavati
5. Sections Cervini
3. Subgenus Circumdati
6. Sections Circumdati

16
7. Sections Nigri
8. Sections Flavi
9. Sections Cremei
10. Aspergillus sect. Aeni sect. nov
4. Subgenus Candidi
11. Section Candidi;
5. Subgenus Terrei
12. Sections Terrei
13. Sections Flavipedes;
6. Subgenus Nidulantes
14. Sections Nidulantes
15. Sections Usti
16. Sections Sparsi;
7. Subgenus Warcupi
17. Sections Warcupi
18. Sections Zonati
8. Subgenus Ornati
19. Sections Ornati.
3.6. Suggested nomenclature and classification of the Genus Aspergillus (Refai, 2014)
It is suggested to divide the Genus Aspergillus into 2 Subgenera:
1. Subgenus I contains 6 Aspergillus sections that have no known teleomorphs yet,
namely Sections Restricti, Cervini, Nigri, Candidi, Usti and Versicolores.
2. Subgenus II contains 10 aspergillus sections that have teleomorphs, namely
Sections Aspergilli, Terrei, Flavipedes, Circumdati, Flavi, Cremei, Fumigati,
Clavati, Nidulantes and Ornati.
3. The name Michelius or Michelia is suggested as the genus name for all
telemorphs, which is devided into the following sections: Euroti, Fennelli,
Neopetromycei, Petromyci, Chaetosartori, Neosartori, Neocarpentelli, Emericelli
and Hemicarpentelli
Consequently, the species that have teleomorphs will be named as follows:
Aspergillus glaucus Link, 1809 Teleomorph: Michelia herbariorum
Synonym: Eurotium herbariorum Link, 1809

17
4. Description of important aspergilli
4.1. Aspergillus Section Restricti
Aspergillus Section Restricti (the Aspergillus restrictus Group) include the following species 1. Aspergillus caesiellus
2. Aspergillus penicillioides
3. Aspergillus restrictus
4. A. conicus
5. A. gracilis
6. A. itaconicus
.
4.1.1. Aspergillus restrictus G. Smith (1931)
Synonym: Penicillium fuscoflavum S. Abe (1956)
Morphology ( http://www.bcrc.firdi.org.tw/fungi/fungal) Colony diameters on Czapek’s Agar 1.3-1.5 cm in 2 weeks at 25°C, dense, rugged, floccose,
with fimbriate margins; mycelium white; conidial heads small, indistinct, covered in slime,
blackish green-gray; reverse uncolored to dark gray green. Colony diameters on M40Y 4.5-5.5
cm in 2 weeks at 25°C, velutinous, tufted or floccose; conidial heads long, narrow, columnar,
sometimes twisted, artemisia green to lily green; reverse colorless to olive brown; vesicles flask
shaped, or pyriform, 5.0-13.0 μm in diameter; stipes thin-walled, smooth or roughened, straight
or sinuous, uncolored, 78-106 × 2.0-6.0 μm. Aspergilla uniseriate, phialides 4.8-10.3 × 2.4-4.4
μm, covering the upper 2/5 of the vesicle. Conidia elongate, doliiform or ellipsoidal to
pyriform, 3.8-9.5 × 3.0-4.4 μm, rough to spinose.
18
S. S. Tzean and J. L. Chen, B Flannigan, R Samson & JD Miller , Joe Akin, Mycobank
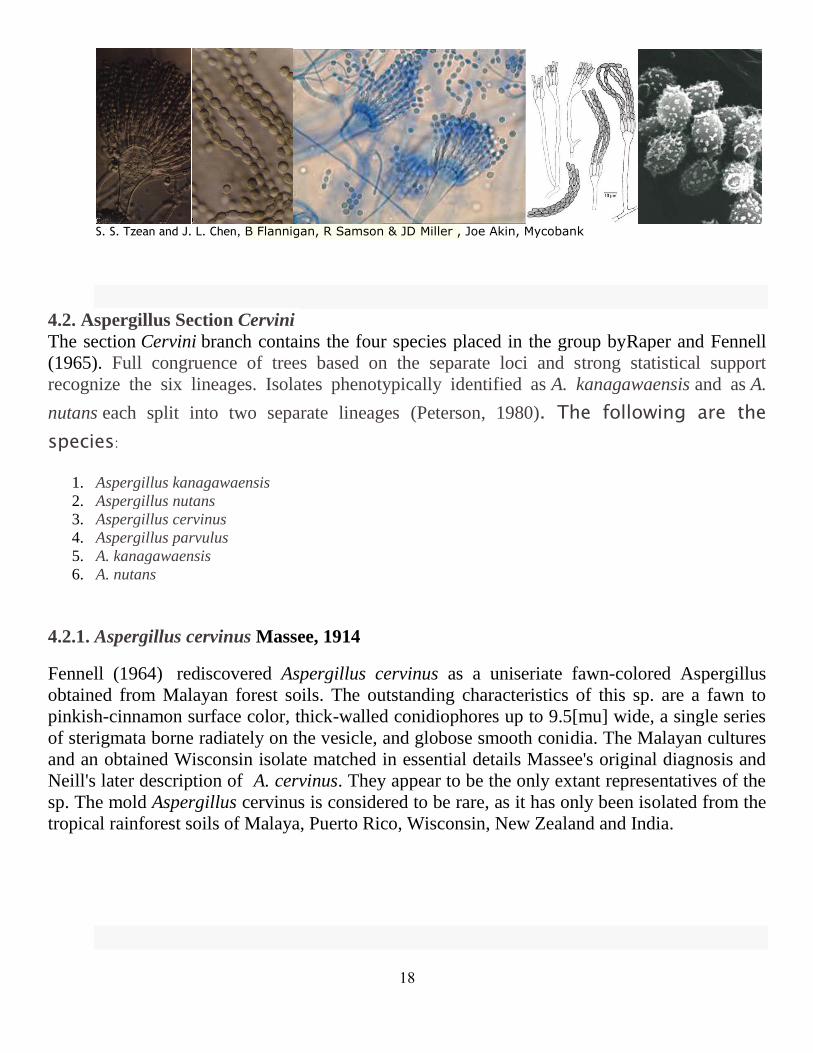
4.2. Aspergillus Section Cervini
The section Cervini branch contains the four species placed in the group byRaper and Fennell
(1965). Full congruence of trees based on the separate loci and strong statistical support
recognize the six lineages. Isolates phenotypically identified as A. kanagawaensis and as A.
nutans each split into two separate lineages (Peterson, 1980). The following are the
species:
1. Aspergillus kanagawaensis
2. Aspergillus nutans
3. Aspergillus cervinus
4. Aspergillus parvulus
5. A. kanagawaensis
6. A. nutans
4.2.1. Aspergillus cervinus Massee, 1914
Fennell (1964) rediscovered Aspergillus cervinus as a uniseriate fawn-colored Aspergillus
obtained from Malayan forest soils. The outstanding characteristics of this sp. are a fawn to
pinkish-cinnamon surface color, thick-walled conidiophores up to 9.5[mu] wide, a single series
of sterigmata borne radiately on the vesicle, and globose smooth conidia. The Malayan cultures
and an obtained Wisconsin isolate matched in essential details Massee's original diagnosis and
Neill's later description of A. cervinus. They appear to be the only extant representatives of the
sp. The mold Aspergillus cervinus is considered to be rare, as it has only been isolated from the
tropical rainforest soils of Malaya, Puerto Rico, Wisconsin, New Zealand and India.

19
4.3. Aspergillus section Nigri
Aspergillus section Nigri are industrially one of the most important taxa of filamentous fungi.
Several strains belonging to this section are used in the fermentation industry for the production
of different organic acids and hydrolytic enzymes.
The observation that black aspergilli including A. niger and A. carbonarius are able to
produce ochratoxins is economically important since A. niger is extensively used in the
food industry.
Taxonomic evaluation of this species complex was carried out using different methods
(Varga et al,. 2011). Among the genotypic approaches, nuclear and mtDNA
polymorphisms and PCR based techniques led to the recognition of four species within
this species complex (A. niger, A. tubingensis, A. brasiliensis, A. foetidus).
Several well known species names such as A. awamorii, A. usamii, A. phoenicis and A.
ficuum have been reduced to synonymy.
Regarding other black Aspergillus species, phylogenetic analysis of ITS sequence data
indicates that at least 9 species belong to this section: 1. Aspergillus heteromorphus,
2. Aspergillus ellipticus,
3. Aspergillus carbonarius,
4. Aspergillus japonicus,
5. Aspergillus aculeatus,
6. Aspergillus. niger,
7. Aspergillus. tubingensis,
8. Aspergillus foetidus and
9. Aspergillus brasiliensis.
Ochratoxin production has been observed only in A. niger and A. carbonarius isolates.
These species are now considered as major sources of ochratoxin contamination in
tropical and subtropical foods including dried vine fruits, wines and coffee
The identification of species of Aspergillus section Nigri depends on:
a. Colony morphology, conidial size and ornamentation of the cultures
b. The temperature range of all species
c. Growth characteristics on creatine agar and boscalid agar.
d. The extrolites produced by each species
e. The response of the Ehrlich reaction
f. Molecular characterization (β-tubulin or calmodulin sequence data)
21
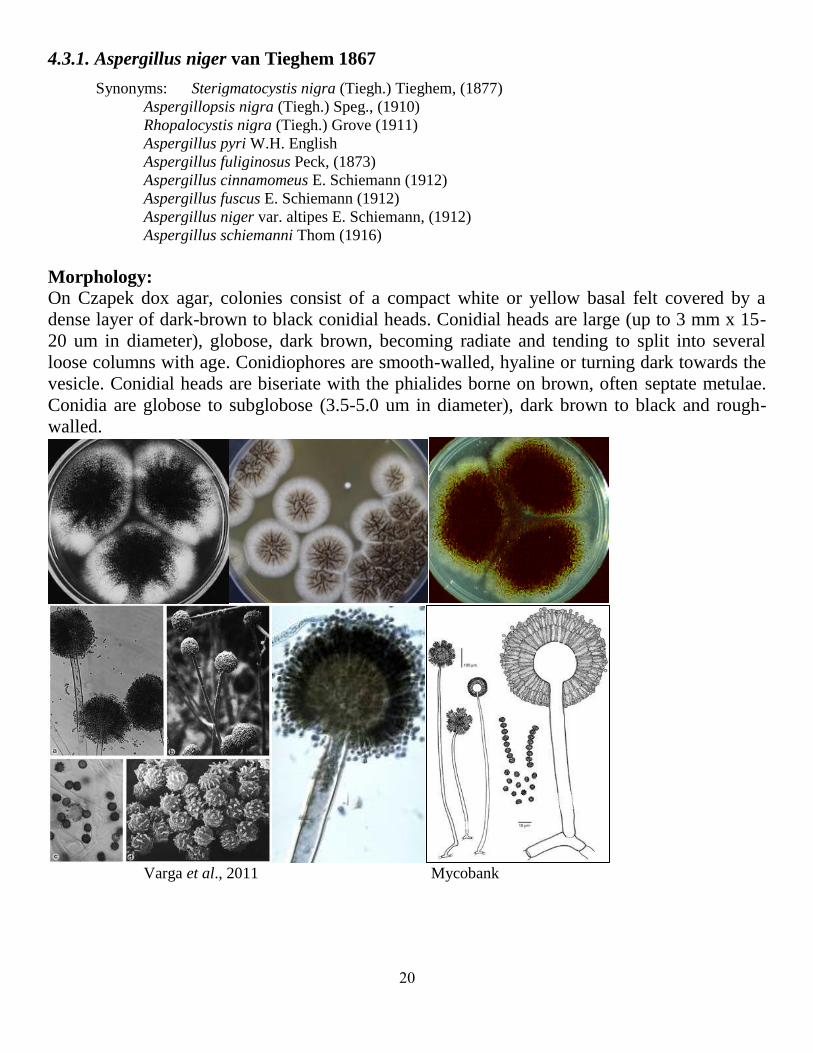
4.3.1. Aspergillus niger van Tieghem 1867
Synonyms: Sterigmatocystis nigra (Tiegh.) Tieghem, (1877)
Aspergillopsis nigra (Tiegh.) Speg., (1910)
Rhopalocystis nigra (Tiegh.) Grove (1911)
Aspergillus pyri W.H. English
Aspergillus fuliginosus Peck, (1873)
Aspergillus cinnamomeus E. Schiemann (1912)
Aspergillus fuscus E. Schiemann (1912)
Aspergillus niger var. altipes E. Schiemann, (1912)
Aspergillus schiemanni Thom (1916)
Morphology:
On Czapek dox agar, colonies consist of a compact white or yellow basal felt covered by a
dense layer of dark-brown to black conidial heads. Conidial heads are large (up to 3 mm x 15-
20 um in diameter), globose, dark brown, becoming radiate and tending to split into several
loose columns with age. Conidiophores are smooth-walled, hyaline or turning dark towards the
vesicle. Conidial heads are biseriate with the phialides borne on brown, often septate metulae.
Conidia are globose to subglobose (3.5-5.0 um in diameter), dark brown to black and rough-
walled.
Varga et al., 2011 Mycobank
21
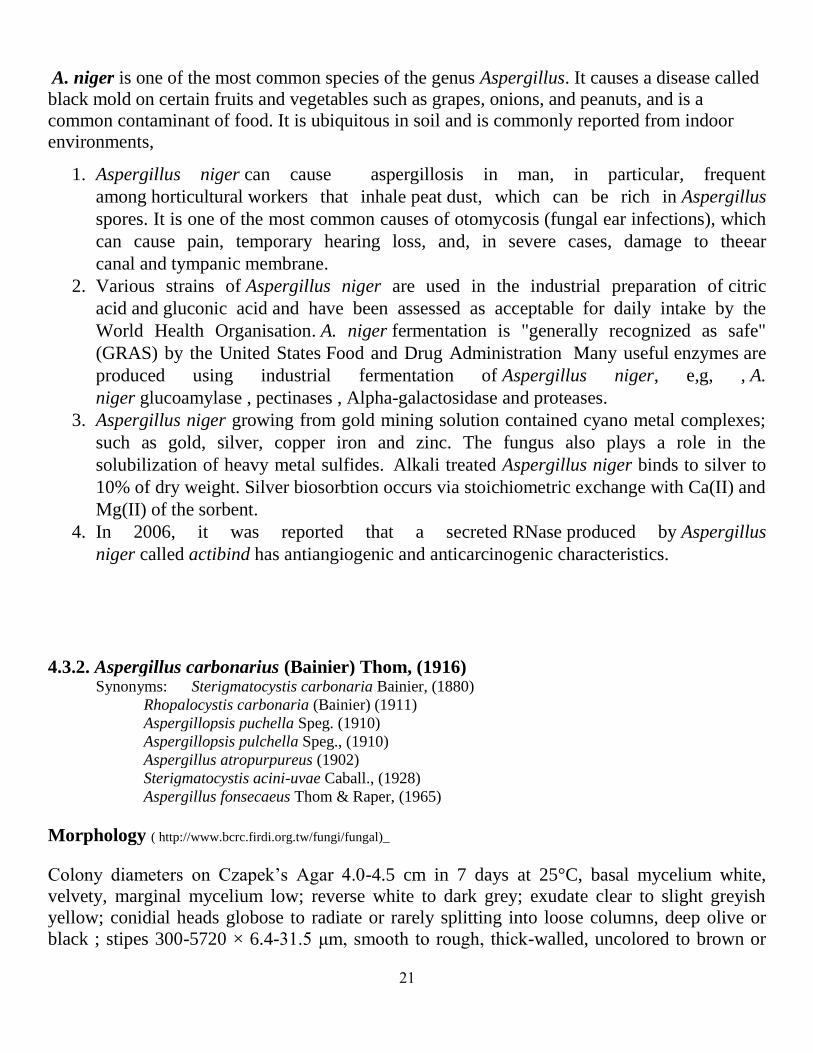
A. niger is one of the most common species of the genus Aspergillus. It causes a disease called
black mold on certain fruits and vegetables such as grapes, onions, and peanuts, and is a
common contaminant of food. It is ubiquitous in soil and is commonly reported from indoor
environments,
1. Aspergillus niger can cause aspergillosis in man, in particular, frequent
among horticultural workers that inhale peat dust, which can be rich in Aspergillus
spores. It is one of the most common causes of otomycosis (fungal ear infections), which
can cause pain, temporary hearing loss, and, in severe cases, damage to theear
canal and tympanic membrane.
2. Various strains of Aspergillus niger are used in the industrial preparation of citric
acid and gluconic acid and have been assessed as acceptable for daily intake by the
World Health Organisation. A. niger fermentation is "generally recognized as safe"
(GRAS) by the United States Food and Drug Administration Many useful enzymes are
produced using industrial fermentation of Aspergillus niger, e,g, , A.
niger glucoamylase , pectinases , Alpha-galactosidase and proteases.
3. Aspergillus niger growing from gold mining solution contained cyano metal complexes;
such as gold, silver, copper iron and zinc. The fungus also plays a role in the
solubilization of heavy metal sulfides. Alkali treated Aspergillus niger binds to silver to
10% of dry weight. Silver biosorbtion occurs via stoichiometric exchange with Ca(II) and
Mg(II) of the sorbent.
4. In 2006, it was reported that a secreted RNase produced by Aspergillus
niger called actibind has antiangiogenic and anticarcinogenic characteristics.
4.3.2. Aspergillus carbonarius (Bainier) Thom, (1916) Synonyms: Sterigmatocystis carbonaria Bainier, (1880)
Rhopalocystis carbonaria (Bainier) (1911)
Aspergillopsis puchella Speg. (1910)
Aspergillopsis pulchella Speg., (1910)
Aspergillus atropurpureus (1902)
Sterigmatocystis acini-uvae Caball., (1928)
Aspergillus fonsecaeus Thom & Raper, (1965)
Morphology ( http://www.bcrc.firdi.org.tw/fungi/fungal)_
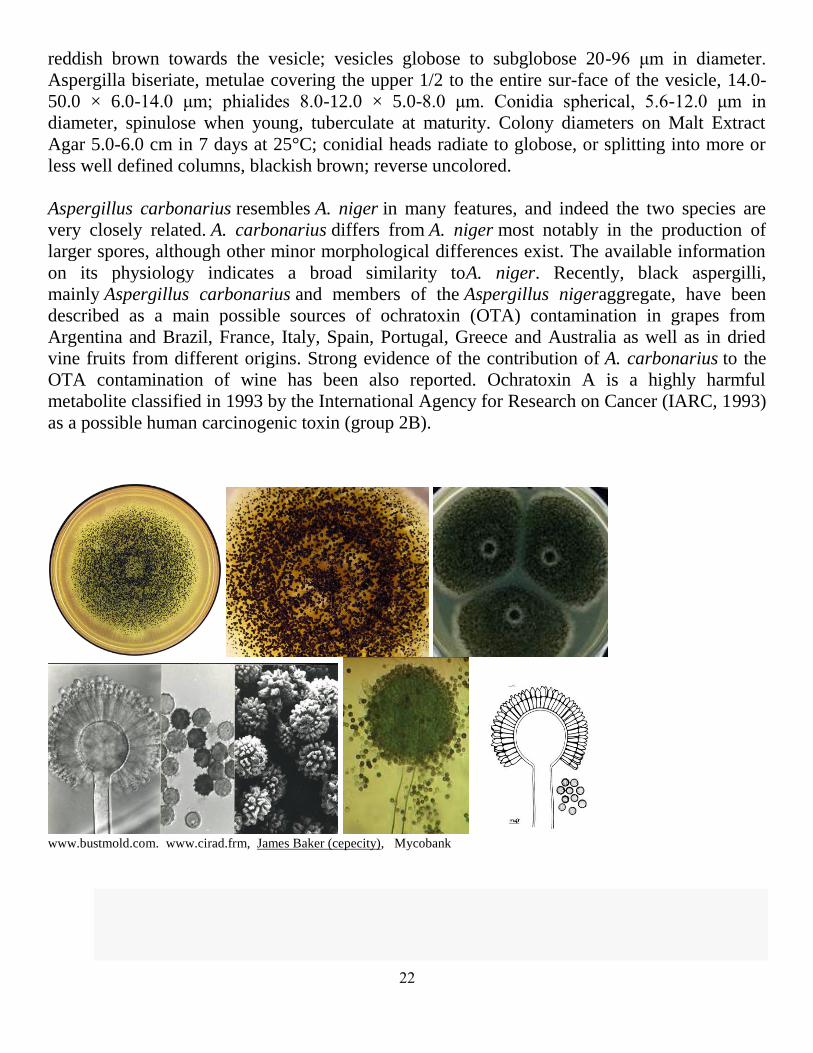
Colony diameters on Czapek’s Agar 4.0-4.5 cm in 7 days at 25°C, basal mycelium white,
velvety, marginal mycelium low; reverse white to dark grey; exudate clear to slight greyish
yellow; conidial heads globose to radiate or rarely splitting into loose columns, deep olive or
black ; stipes 300-5720 × 6.4-31.5 μm, smooth to rough, thick-walled, uncolored to brown or
22
reddish brown towards the vesicle; vesicles globose to subglobose 20-96 μm in diameter.
Aspergilla biseriate, metulae covering the upper 1/2 to the entire sur-face of the vesicle, 14.0-
50.0 × 6.0-14.0 μm; phialides 8.0-12.0 × 5.0-8.0 μm. Conidia spherical, 5.6-12.0 μm in
diameter, spinulose when young, tuberculate at maturity. Colony diameters on Malt Extract
Agar 5.0-6.0 cm in 7 days at 25°C; conidial heads radiate to globose, or splitting into more or
less well defined columns, blackish brown; reverse uncolored.
Aspergillus carbonarius resembles A. niger in many features, and indeed the two species are
very closely related. A. carbonarius differs from A. niger most notably in the production of
larger spores, although other minor morphological differences exist. The available information
on its physiology indicates a broad similarity toA. niger. Recently, black aspergilli,
mainly Aspergillus carbonarius and members of the Aspergillus nigeraggregate, have been
described as a main possible sources of ochratoxin (OTA) contamination in grapes from
Argentina and Brazil, France, Italy, Spain, Portugal, Greece and Australia as well as in dried
vine fruits from different origins. Strong evidence of the contribution of A. carbonarius to the
OTA contamination of wine has been also reported. Ochratoxin A is a highly harmful
metabolite classified in 1993 by the International Agency for Research on Cancer (IARC, 1993)
as a possible human carcinogenic toxin (group 2B).
www.bustmold.com. www.cirad.frm, James Baker (cepecity), Mycobank
23
4.4. Aspergillus section Candidi
Aspergillus section Candidi historically included a single white-spored species, A. candidus.
Later studies clarified that other species may also belong to this section. The revised
sectionCandidi by Varga et al. (2007) includes 4 species: 1. candidus,
2. campestris,
3. taichungensis
4. tritici.
Morphological characteristics of section Candidi:
Slow growing colonies with globose conidial heads having white to yellowish conidia,
Conidiophores smooth, small conidiophores common, metulae present and covering the
entire vesicle,
Some large Aspergillus heads with large metulae,
Presence of diminutive heads in all species,
Conidia smooth or nearly so with a subglobose to ovoid shape,
Presence of sclerotia in three species (A. candidus, A. taichungensis and A. tritici).
All species produce terphenyllins and candidusins and three species (A. candidus, A.
campestris and A. tritici) produce chlorflavonins. Xanthoascins have only been found
in A. candidus.
Each of the species in section Candidi produce several other species specific extrolites,
and none of these have been found in any other Aspergillus species.A. candidus has often
been listed as a human pathogenic species, but this is unlikely as this species cannot grow
at 37 °C.
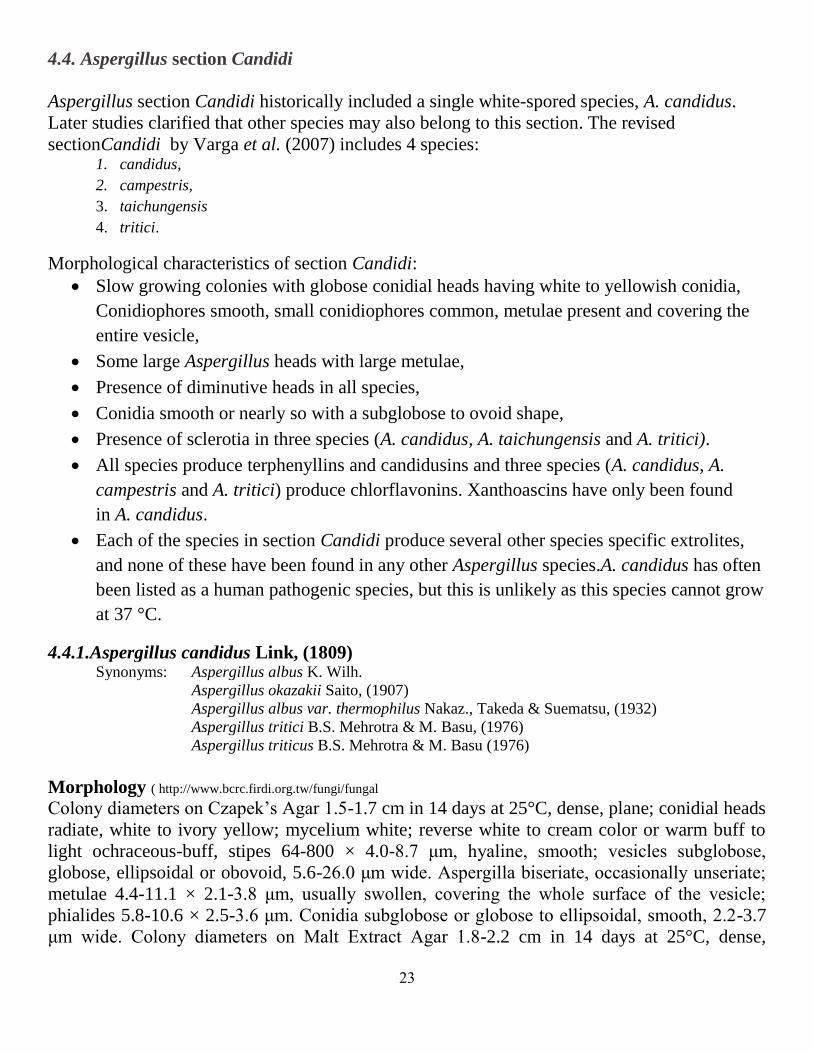
4.4.1.Aspergillus candidus Link, (1809) Synonyms: Aspergillus albus K. Wilh.
Aspergillus okazakii Saito, (1907)
Aspergillus albus var. thermophilus Nakaz., Takeda & Suematsu, (1932)
Aspergillus tritici B.S. Mehrotra & M. Basu, (1976)
Aspergillus triticus B.S. Mehrotra & M. Basu (1976)
Morphology ( http://www.bcrc.firdi.org.tw/fungi/fungal
Colony diameters on Czapek’s Agar 1.5-1.7 cm in 14 days at 25°C, dense, plane; conidial heads
radiate, white to ivory yellow; mycelium white; reverse white to cream color or warm buff to
light ochraceous-buff, stipes 64-800 × 4.0-8.7 μm, hyaline, smooth; vesicles subglobose,
globose, ellipsoidal or obovoid, 5.6-26.0 μm wide. Aspergilla biseriate, occasionally unseriate;
metulae 4.4-11.1 × 2.1-3.8 μm, usually swollen, covering the whole surface of the vesicle;
phialides 5.8-10.6 × 2.5-3.6 μm. Conidia subglobose or globose to ellipsoidal, smooth, 2.2-3.7
μm wide. Colony diameters on Malt Extract Agar 1.8-2.2 cm in 14 days at 25°C, dense,

24
velutinous; conidial heads radiate, white to pale ivory; mycelium white; reverse ivory yellow to
cream color.
Aspergillus candidus. Samson et al., 2011
Aspergillus candidus is a common contaminant of grain dust and which causes
respiratory disease in humans. The species is widely distributed in nature and develops
upon vegetation in the later stages of decay. İt has been reported
from grain, flour, hay, compost and a fur processing facility.
Growth of A. candidus on barley grain occurs at the substrate water content 20-25% and
maximal temperature 30-40°C.
A. candidus may produce citrinin and other mycotoxins. Also this species produces p-
terphenyl metabolites and, which are potent cytotoxic substances.
Some strains of A. candidus produce kojic acid and / or citrinin, molecules that can cause
renal disease in swine.
A. candidus is involved in various human infections: invasive aspergillosis, otomycosis,
onychomycosis.
25
4.5. Aspergillus section Usti
Based on phylogenetic analysis of sequence data (Samson et al.,2011), Aspergillus section
Usti includes the following species: 1. Aspergillu ustus,
2. Aspergillu. puniceus,
3. Aspergillus granulosus,
4. Aspergillu pseudodeflectus,
5. Aspergillu calidoustus,
6. Aspergillus insuetus
7. A. compatibilis (Emericella heterothallica )
8. Aspergillus heterothallicus (Fennellia monodii)
9. A. keveii sp. Nov.
10. Aspergillus germanicus sp. nov. was isolated from indoor air in Germany. This
species is unable to grow at 37 °C, similarly to A. keveii and A. insuetus.
11. Aspergillus carlsbadensis sp. nov. was isolated from the Carlsbad Caverns
National Park in New Mexico. This species is also unable to grow at 37 °C, and
acid production was not observed on CREA.
12. Aspergillus californicus sp. nov. is proposed for an isolate from chamise chaparral
(Adenostoma fasciculatum) in California. This species grew well at 37 °C, and
acid production was not observed on CREA.
13. Aspergillus turkensis sp. nov. was isolated from soil in Turkey. This species grew,
although rather restrictedly at 37 °C, and acid production was not observed on
CREA.
14. Aspergillus pseudoustus sp. nov. was isolated from stored maize, South Africa
15. Aspergillus monodii comb. Nov
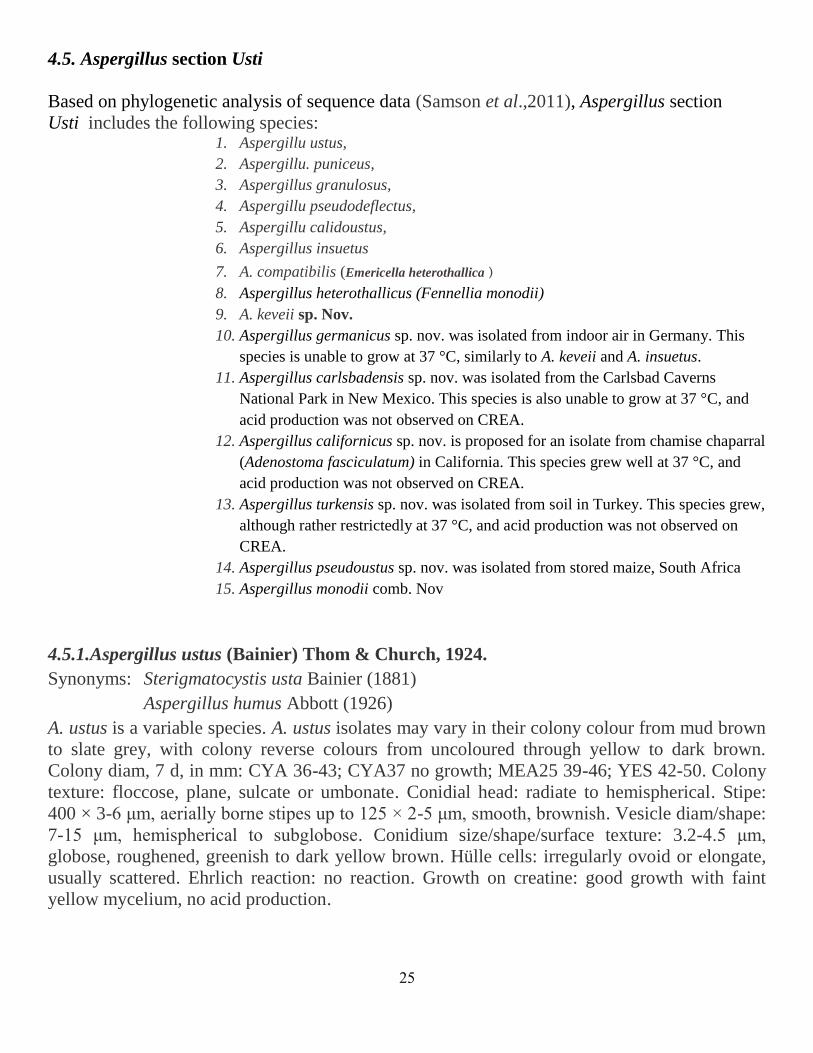
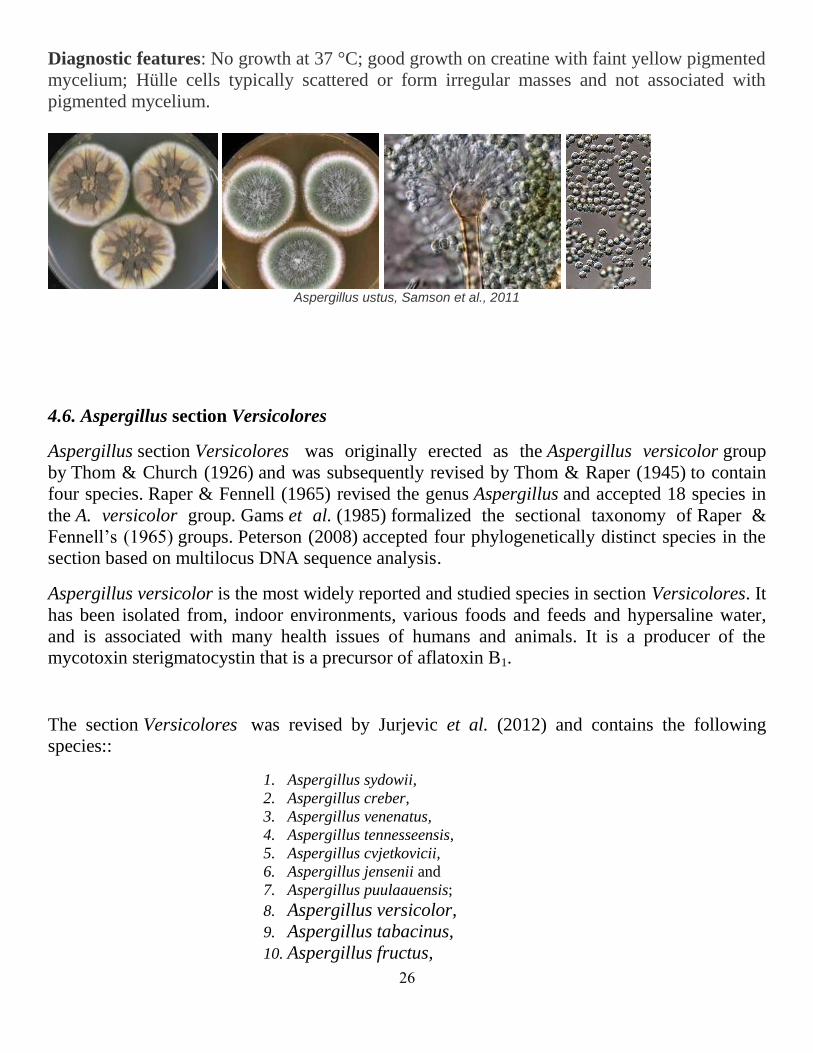
4.5.1.Aspergillus ustus (Bainier) Thom & Church, 1924.
Synonyms: Sterigmatocystis usta Bainier (1881)
Aspergillus humus Abbott (1926)
A. ustus is a variable species. A. ustus isolates may vary in their colony colour from mud brown
to slate grey, with colony reverse colours from uncoloured through yellow to dark brown.
Colony diam, 7 d, in mm: CYA 36-43; CYA37 no growth; MEA25 39-46; YES 42-50. Colony
texture: floccose, plane, sulcate or umbonate. Conidial head: radiate to hemispherical. Stipe:
400 × 3-6 μm, aerially borne stipes up to 125 × 2-5 μm, smooth, brownish. Vesicle diam/shape:
7-15 μm, hemispherical to subglobose. Conidium size/shape/surface texture: 3.2-4.5 μm,
globose, roughened, greenish to dark yellow brown. Hülle cells: irregularly ovoid or elongate,
usually scattered. Ehrlich reaction: no reaction. Growth on creatine: good growth with faint
yellow mycelium, no acid production.
26
Diagnostic features: No growth at 37 °C; good growth on creatine with faint yellow pigmented
mycelium; Hülle cells typically scattered or form irregular masses and not associated with
pigmented mycelium.
Aspergillus ustus, Samson et al., 2011
4.6. Aspergillus section Versicolores
Aspergillus section Versicolores was originally erected as the Aspergillus versicolor group
by Thom & Church (1926) and was subsequently revised by Thom & Raper (1945) to contain
four species. Raper & Fennell (1965) revised the genus Aspergillus and accepted 18 species in
the A. versicolor group. Gams et al. (1985) formalized the sectional taxonomy of Raper &
Fennell’s (1965) groups. Peterson (2008) accepted four phylogenetically distinct species in the
section based on multilocus DNA sequence analysis.
Aspergillus versicolor is the most widely reported and studied species in section Versicolores. It
has been isolated from, indoor environments, various foods and feeds and hypersaline water,
and is associated with many health issues of humans and animals. It is a producer of the
mycotoxin sterigmatocystin that is a precursor of aflatoxin B1.
The section Versicolores was revised by Jurjevic et al. (2012) and contains the following
species::
1. Aspergillus sydowii,
2. Aspergillus creber,
3. Aspergillus venenatus,
4. Aspergillus tennesseensis,
5. Aspergillus cvjetkovicii,
6. Aspergillus jensenii and
7. Aspergillus puulaauensis;
8. Aspergillus versicolor,
9. Aspergillus tabacinus,
10. Aspergillus fructus,

27
11. Aspergillus protuberus,
12. Aspergillus amoenus and
13. Aspergillus. Austroafricanus
14. Aspergillus subversicolor.
4.6.1. Aspergillus sydowii Thom & Church (1926)
Synonyms: Sterigmatocystis tunetana Langeron, (1924)
Aspergillus sydowii var. achlamydosporus Nakaz. et al. (1934)
When grown in pure culture on agar plates, A. sydowii produces blue-green colonies with
reddish-brown shades. Colony on Czapek’s Agar is plane to floccose; conidial heads radiate to
loosely columnar, light grayish olive or green; mycelium white; reverse ivory yellow or maroon
; stipes hyaline to pale brown, smooth; vesicles clavate to subglobose. Aspergilla biseriate,
metulae covering 1/2 to 4/5 of the vesicle; Conidia globose, conspicuously roughened to
spinose. Small aspergilla often present resembling the fruiting structures of Penicillium. Hulle
cells occasionally present, globose to subglobose.

28
Jos A.M.P. Houbraken, Ronald P. de Vries, Robert A. Samson, A. sydowii Mycobank
Aspergillus sydowii is a saprophytic fungus found in soil that can contaminate food and is
occasionally pathogenic to humans. It is the predominant fungus found on wheat Qu, the most
widely used source of raw microorganisms and crude enzymes for Chinese rice
wine brewing.[5]
Since the 1990s it has been found to be present in sea water in the Caribbean
region and has been shown to be the cause of aspergillosis in sea fans
Aspergillus sydowii has been implicated in the pathogenesis of several human diseases,
including aspergillosis, onychomycosis, and keratomycosis.
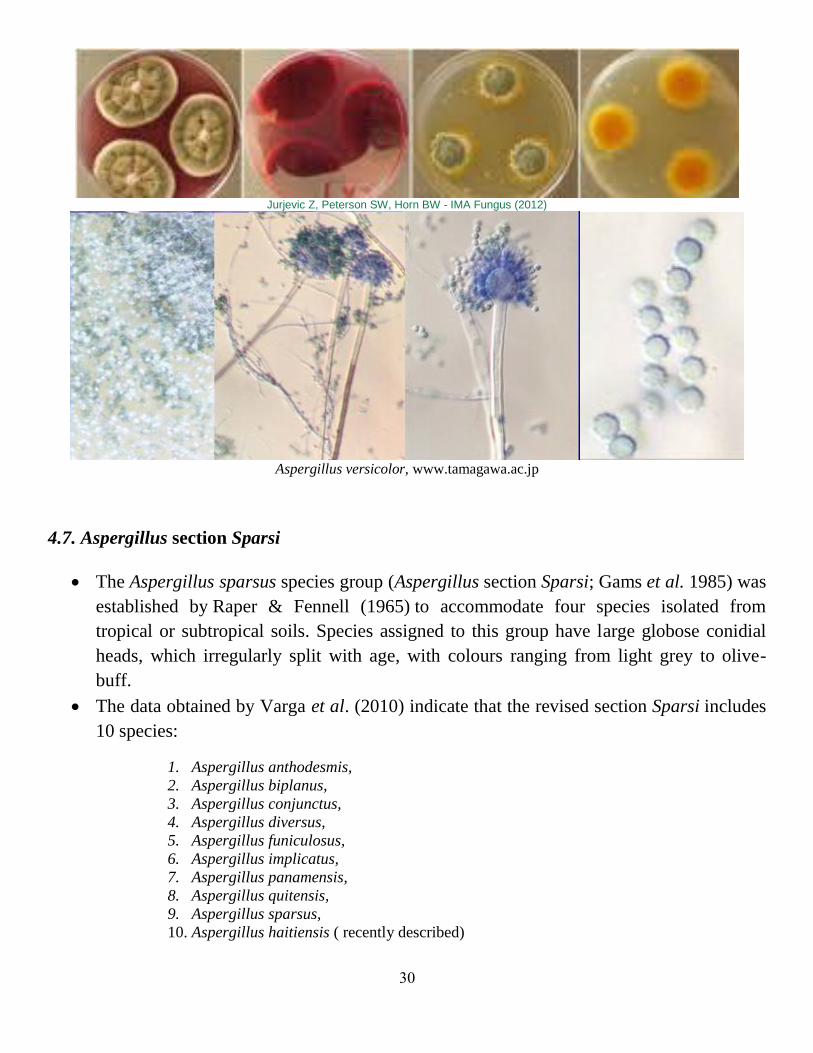
4.6.2. Aspergillus versicolor (Vuill.) Tirab., (1908).
Synonyms:Aspergillus amoenus Roberg, 1931
Aspergillus versicolor var. fulvus Nakaz. et al., 1932
Aspergillus versicolor var. rutilobrunneus J.N. Rai, S.C. Agarwal & J.P. Tewari, 1971
Sterigmatocystis versicolor Vuill., 1903
Morphology
Colonies on CYA 16-25 mm diam, plane or lightly sulcate, low to moderately deep, dense;
mycelium white to buff or orange; conidial heads sparse to quite densely packed, greyish green;
pink to wine red exudate sometimes produced; reverse orange or reddish brown. Colonies on MEA
12-25 mm diam, low, plane, and dense, usually velutinous; mycelium white to buff; conidial heads
numerous, radiate, dull or grey green; reverse yellow brown to orange brown. Colonies on G25N
10-18 mm diam, plane or umbonate, dense, of white, buff or yellow mycelium; reverse pale,

29
yellow brown or orange brown. No growth at 5°C. Usually no growth at 37°C, occasionally
colonies up to 10 mm diam formed.
Conidiophores borne from surface or aerial hyphae, stipes 300-600µm long, with heavy yellow
walls, vesicles variable, the largest nearly spherical, 12-16µm diam, fertile over the upper half to
two-thirds, the smallest scarcely swollen at all and fertile only at the tips, bearing closely packed
metulae and phialides, both 5-8µm long; conidia mostly spherical, very small, 2.0-2.5µm diam,
with walls finely to distinctly roughened or spinose, borne in radiate heads.
Aspergillus versicolor isolates produce the aflatoxin precursor sterigmatocystin, a compound that is
mutagenic and tumorigenic. Animal feed infested with three morphotypes of A. versicolor, all of
which produce sterigmatocystin, have been implicated in dairy animal toxicosis, but it is unknown
whether sterigmatocystin caused the toxicosis.
Aspergillus versicolor has been implicated as the causitive agent of disseminated aspergillosis in
dogs has probably caused aspergillosis in transplant recipients and has been isolated from the
infected eye of a patient suffering from HIV.
A. versicolor, Mycota, Mold-pro.com, fungi myospecies inf.
www.tamagawa.ac.j
31
Jurjevic Z, Peterson SW, Horn BW - IMA Fungus (2012)
Aspergillus versicolor, www.tamagawa.ac.jp
4.7. Aspergillus section Sparsi
The Aspergillus sparsus species group (Aspergillus section Sparsi; Gams et al. 1985) was
established by Raper & Fennell (1965) to accommodate four species isolated from
tropical or subtropical soils. Species assigned to this group have large globose conidial
heads, which irregularly split with age, with colours ranging from light grey to olive-
buff.
The data obtained by Varga et al. (2010) indicate that the revised section Sparsi includes
10 species:
1. Aspergillus anthodesmis,
2. Aspergillus biplanus,
3. Aspergillus conjunctus,
4. Aspergillus diversus,
5. Aspergillus funiculosus,
6. Aspergillus implicatus,
7. Aspergillus panamensis,
8. Aspergillus quitensis,
9. Aspergillus sparsus,
10. Aspergillus haitiensis ( recently described)
31
Aspergillus quitensis and Aspergillus ecuadorensis are synonyms of Aspergillus
amazonicus based on both molecular and physiological data.
The white-spored species A. implicatus has also been found to belong to this section.
Aspergillus haitiensis sp. nov. is characterised by whitish colonies becoming reddish
brown due to the production of conidial heads, and dark coloured smooth stipes.
The taxon produces gregatins, siderin and several unknown but characteristic metabolites.
4.8. Aspergillus Section: Aspergillus (Teleomorph: Eurotium)
Aspergillus section Aspergillus contains economically important, xerophilic fungi that
are widely distributed in nature and the human environment and are known for their
ability to grow on substrates with low water activity.
Eurotium species are the sexual states of Aspergillus species, notably the Aspergillus
glaucus group among others. Eurotium is common and is most closely related to
Emericella, another genus with Aspergillus anamorphs.
Health effects, allergenicity, and toxicity of Eurotium are closely related to the
Aspergillus anamorph and, for the most part, have not been studied apart from that
primary phase. The Aspergillus anamorph is likely to be the identifiable result, at least
with primary growth within one week.
The taxa were revised based on sequence data from four loci, PCR fingerprinting, micro-
and macromorphology, and physiology. The number of taxa was reduced to the following
species:
1. Aspergillus proliferans (The only anamorphic species)
2. Aspergillus niveoglaucus (≡Eurotium niveoglaucum)
3. Aspergillus brunneus [Eurotium echinulatum.].
4. Aspergillus neocarnoyi [Eurotium carnoyi.].
5. Aspergillus glaucus [Eurotium herbariorum].
6. Aspergillus repens (Eurotium repens)
7. Aspergillus rubrobrunneus [Eurotium rubrum]
8. Aspergillus tonophilusi [Eurotium tonophilum].
9. Aspergillus hollandicus (Eurotium amstelodami)
10. Aspergillus chevalieri var. intermedius (≡ Eurotium intermedium)
11. Aspergillus equitis (Eurotium chevalieri)
12. Aspergillus cristatus (≡Eurotium cristatum)
13. Aspergillus xerophilus. [Eurotium xerophilum.].
14. Aspergillus leucocarpus [Eurotium leucocarpum].
32
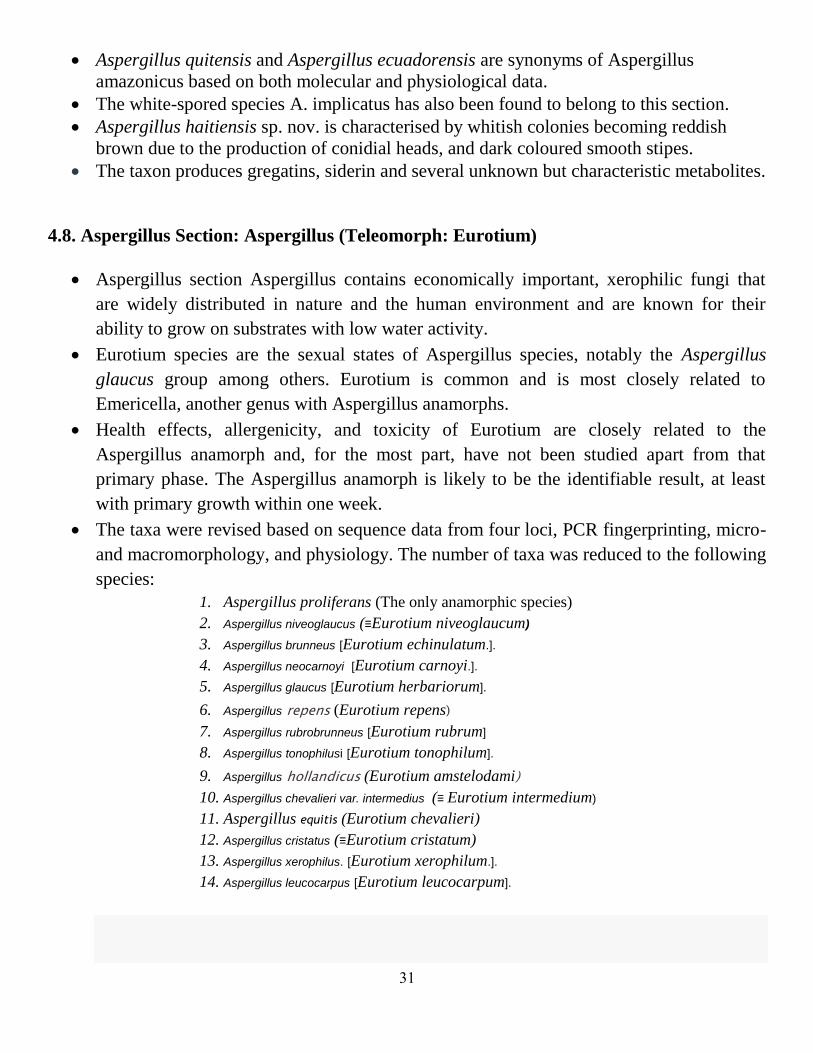
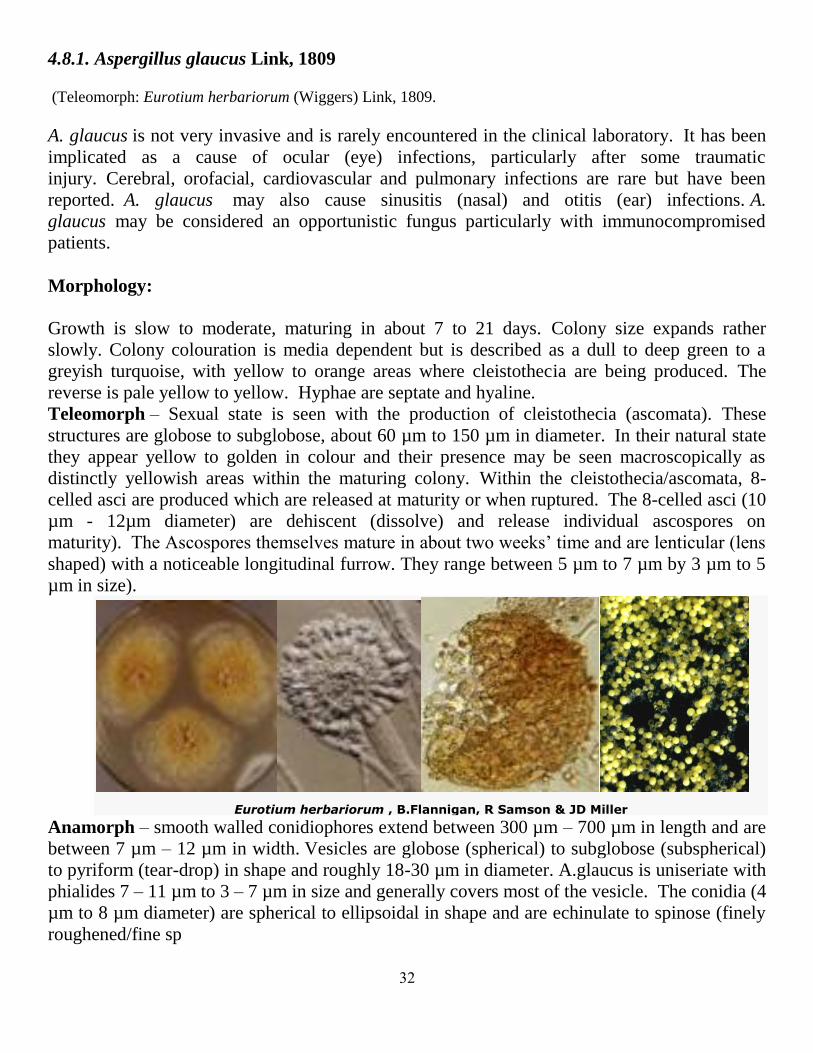
4.8.1. Aspergillus glaucus Link, 1809
(Teleomorph: Eurotium herbariorum (Wiggers) Link, 1809.
A. glaucus is not very invasive and is rarely encountered in the clinical laboratory. It has been
implicated as a cause of ocular (eye) infections, particularly after some traumatic
injury. Cerebral, orofacial, cardiovascular and pulmonary infections are rare but have been
reported. A. glaucus may also cause sinusitis (nasal) and otitis (ear) infections. A.
glaucus may be considered an opportunistic fungus particularly with immunocompromised
patients.
Morphology:
Growth is slow to moderate, maturing in about 7 to 21 days. Colony size expands rather
slowly. Colony colouration is media dependent but is described as a dull to deep green to a
greyish turquoise, with yellow to orange areas where cleistothecia are being produced. The
reverse is pale yellow to yellow. Hyphae are septate and hyaline.
Teleomorph – Sexual state is seen with the production of cleistothecia (ascomata). These
structures are globose to subglobose, about 60 µm to 150 µm in diameter. In their natural state
they appear yellow to golden in colour and their presence may be seen macroscopically as
distinctly yellowish areas within the maturing colony. Within the cleistothecia/ascomata, 8-
celled asci are produced which are released at maturity or when ruptured. The 8-celled asci (10
µm - 12µm diameter) are dehiscent (dissolve) and release individual ascospores on
maturity). The Ascospores themselves mature in about two weeks’ time and are lenticular (lens
shaped) with a noticeable longitudinal furrow. They range between 5 µm to 7 µm by 3 µm to 5
µm in size).
Eurotium herbariorum , B.Flannigan, R Samson & JD Miller Anamorph – smooth walled conidiophores extend between 300 µm – 700 µm in length and are
between 7 µm – 12 µm in width. Vesicles are globose (spherical) to subglobose (subspherical)
to pyriform (tear-drop) in shape and roughly 18-30 µm in diameter. A.glaucus is uniseriate with
phialides 7 – 11 µm to 3 – 7 µm in size and generally covers most of the vesicle. The conidia (4
µm to 8 µm diameter) are spherical to ellipsoidal in shape and are echinulate to spinose (finely
roughened/fine sp

33
GEFOR, Galería de imágenes: Aspergillus Glaucus
4.8.2. Aspergillus equitis Samson & Gams, 1985
Teleomprph: Eurotium chevalieri Mangin, 1909.
Morphology
Colony diameters on Czapek’s Agar 2.8-3.2 cm in 14 days at 25°C; conidial heads radiate, deep greenish glaucous to pistachio green; mycelium yellow. Cleistothecia yellow to buffy citrine, or deep colonial buff to olive; soluble pigment yellow; exudate clear; reverse yellow to Saccardo’s umber. Colony diameters on Czapek’s Agar with 20% added sucrose 6.0-6.5 cm in 14 days at 25°C; conidial heads radiate, gnaphalium green to near dark sage green; mycelium yellow to greyish yellow orange shades; exudate clear; reverse near asphodel green to apricot yellow, or mahogany red to bay; stipes 62-680 × 7.0-20.0 μm, smooth, colorless to pale brown; vesicles obovoid to globose 10.0-46.0 μm wide. Aspergilla uniseriate, phialides covering the entire surface of the vesicle, 4.0-13.1 × 2.8-6.2 μm. Conidia ellipsoidal to doliiform, less commonly subglobose, rough to irregularly roughened, 3.2-7.1 × 2.4-5.0 μm. Cleistothecia greyish yellow, subglobose to globose, up to 178 μm wide, asci 8-spored, spherical to subspherical, ascospores lenticular, with wall smooth to finely roughened, with 2 distinct longitudinal trough flanges, 4.2-5.4 × 3.3-4.0 μm. Colony diameters on M40Y 7.5-8.5 cm in 14 days at 25°C; conidial heads abundant, light hellebore green. Cleistothecia abundant as on C20S enmeshed in or-ange-red hyphae; reverse orange-brown.

34
Conidia Ascospores Mycobank
Aspergillus equitis Samson & W. Gams 1985. , S. S. Tzean and J. L. Chen
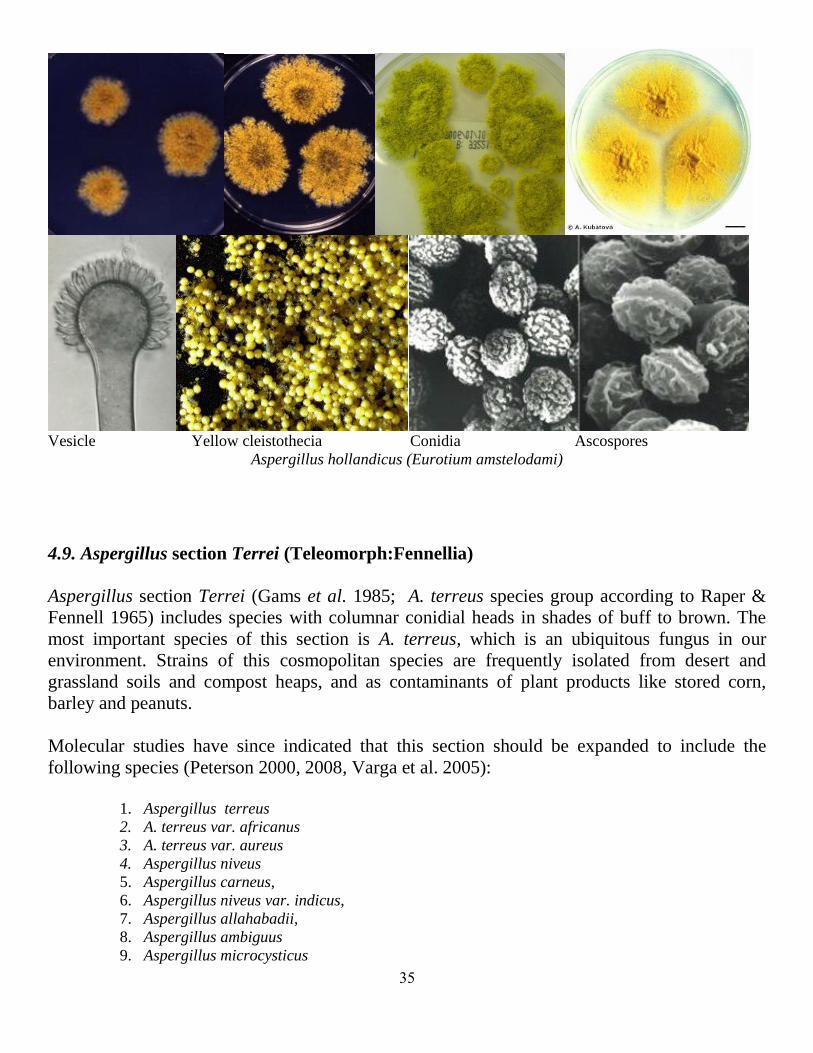
4.8.3. Aspergillus hollandicus Samson & W. Gams 1985. Teleomorph: Eurotium amstelodami Mangin, 1909.
Colony diameters on Czapek’s Agar 2.0-2.5 cm in 14 days at 25°C; conidial heads radiate to
columnar, dark terre verte to dusky green; mycelium white to yellow; reverse uncolored, amber
yellow to olive lake; cleistothecia yellow. Colony diameters on Malt Extract Agar 1.8-2.2 cm in
14 days at 25°C; conidial heads radiate, dark grass green to ivy green; mycelium white to
yellow; reverse colorless or dull wax yellow to dull primuline yellow; cleistothecia yellow.
Colony diameters on Czapek’s Agar with 20% added sucrose 3.5-4.5 cm in 14 days at 25°C;
conidial heads radiate to columnar, ivy green to dark grass green; myce-lium white to yellow;
reverse uncolored, yellow to pale green brown; stipes 60-360 × 4.0-16.0 μm, smooth, colorless,
or pale brown to middle brown; vesicles globose or subglobose to obovoid or pyriform, 6.8-
32.5 μm in diameter. Aspergilla uniseriate, phialides covering 1/2 to 4/5 of the vesicle, 3.2-9.3 ×
3.0-5.3 μm. Conidia globose or subglobose to ovoid, 3.3-6.4 × 3.0-5.2 μm, rough to irregularly
roughened. Cleistothecia globose to subglobose, yellow 60.0-168.0 μm in diameter. Asci 8-
spored, subglobose to globose, 8.7-12.7 × 8.0-10.3 μm. Ascospores lenticular 3.8-5.2 × 3.3-4.8
μm, longitudinal furrow with two irregular ridges, convex surfaces irregularly roughened.
35
Vesicle Yellow cleistothecia Conidia Ascospores
Aspergillus hollandicus (Eurotium amstelodami)
4.9. Aspergillus section Terrei (Teleomorph:Fennellia)
Aspergillus section Terrei (Gams et al. 1985; A. terreus species group according to Raper &
Fennell 1965) includes species with columnar conidial heads in shades of buff to brown. The
most important species of this section is A. terreus, which is an ubiquitous fungus in our
environment. Strains of this cosmopolitan species are frequently isolated from desert and
grassland soils and compost heaps, and as contaminants of plant products like stored corn,
barley and peanuts.
Molecular studies have since indicated that this section should be expanded to include the
following species (Peterson 2000, 2008, Varga et al. 2005):
1. Aspergillus terreus
2. A. terreus var. africanus
3. A. terreus var. aureus
4. Aspergillus niveus
5. Aspergillus carneus,
6. Aspergillus niveus var. indicus,
7. Aspergillus allahabadii,
8. Aspergillus ambiguus
9. Aspergillus microcysticus
36
10. Aspergillus. alabamensis
Aspergillus terreus is an economically important species from a number of aspects. Aspergillus
terreus isolates are used in the fermentation industry for the production of itaconic acid and
itatartaric acid and for enzyme production.
Aspergillus terreus isolates produce a range of secondary metabolites, some of which
have properties valuable for mankind, including lovastatin, a cholesterol lowering drug,
the antitumor metabolites terrein, quadrone and asterriquinone, acetylcholinesterase
inhibitors like territrem B and terreulactone, butyrolactones, and cyclosporine A.
Antiviral compounds such as acetylaranotin has also been reported from Aspergillus
terreus.
Other secondary metabolites reported to be produced by A. terreus isolates are considered
as mycotoxins, including citreoviridin, patulin, citrinin, terretonin, geodin, territrems,
gliotoxin, and cytochalasin E.
Aspergillus terreus is also an important human pathogen, and often causes disseminated
infection with increased lethality compared to other Aspergillus spp.
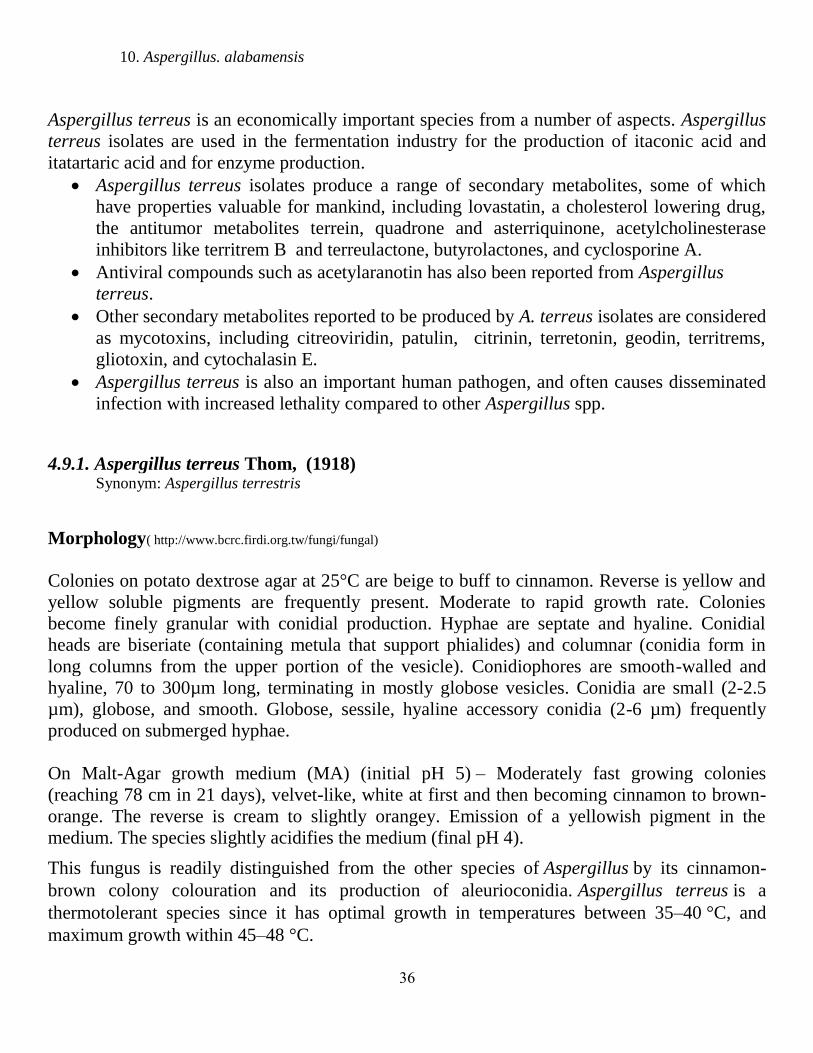
4.9.1. Aspergillus terreus Thom, (1918) Synonym: Aspergillus terrestris
Morphology( http://www.bcrc.firdi.org.tw/fungi/fungal)
Colonies on potato dextrose agar at 25°C are beige to buff to cinnamon. Reverse is yellow and
yellow soluble pigments are frequently present. Moderate to rapid growth rate. Colonies
become finely granular with conidial production. Hyphae are septate and hyaline. Conidial
heads are biseriate (containing metula that support phialides) and columnar (conidia form in
long columns from the upper portion of the vesicle). Conidiophores are smooth-walled and
hyaline, 70 to 300µm long, terminating in mostly globose vesicles. Conidia are small (2-2.5
µm), globose, and smooth. Globose, sessile, hyaline accessory conidia (2-6 µm) frequently
produced on submerged hyphae.
On Malt-Agar growth medium (MA) (initial pH 5) – Moderately fast growing colonies
(reaching 78 cm in 21 days), velvet-like, white at first and then becoming cinnamon to brown-
orange. The reverse is cream to slightly orangey. Emission of a yellowish pigment in the
medium. The species slightly acidifies the medium (final pH 4).
This fungus is readily distinguished from the other species of Aspergillus by its cinnamon-
brown colony colouration and its production of aleurioconidia. Aspergillus terreus is a
thermotolerant species since it has optimal growth in temperatures between 35–40 °C, and
maximum growth within 45–48 °C.

37
mycology.adelaide.edu.au W. New Mexico Univ
Mycobank S. S. Tzean and J. L. Chen
4. 10. Aspergillus Section Flavipedes (Teleomorph:Fennellia) Aspergillus flavipes
Aspergillus niveus
Aspergillus iizukae
Aspergillus carneus
Aspergillus aureofulgens
Aspergillus janus
Aspergillus brevijanus
4.10.1.Aspergillus flavipes (Bain. & Sart.) Thom & Church, 1926.
Colony diameters on Czapek’s Agar 1.3-1.5 cm in 14 days at 25°C, dense, raised; conidial
heads radiate to loosely columnar, white to cartidge buff ; mycelium white to pale capucine
buff; exudate abundant, light yellow; soluble pigment buff-yellow; reverse deep chrome or

38
capucine orange to amber brown; stipes 140-1510 × 2.8-11.1 μm, colorless or light yellow to
pale brown, smooth to slightly roughened; vesicles obovoid, subglobose or pyriform, 6.0-29.4
μm wide. Aspergilla biseriate, metulae covering 1/2 to 4/5 of the vesicle, 4.0-9.4 × 2.5-5.7 μm;
phialides 4.8-8.7 × 2.2-3.0 μm. Conidia globose to subglobose, 2.0-4.0 μm in diameter, smooth
walled. Colony diameters on Malt Extract Agar 3.0-3.5 cm in 14 days at 25°C, plane to
velutinous; conidial heads radiate to columnar, white to light buff; mycelium white to pinkish
buff; soluble pigment red brown; reverse light pinkish cinnamon or vinaceous-cinnamon to
mikado brown.
Gardner, D. E. flavipes, Wiley & Simmons,
4. 11. Section: Circumdati (Teleomorph:Neopetromyces)
Aspergillus section Circumdati historically includes species with biseriate conidial heads in
shades from yellow to ochre. Species of Aspergillus section Circumdati are economically
important as ochratoxin A (OA) producing spoilage organisms.
Aspergillus section Circumdati formed two main clades, which could also be distinguished
based on phenotypic methods. A sexually reproducing ochratoxin producing species and
ochratoxin non-producing. (Frisvad et al., 2004). The section contains the following species:
1. Aspergillus auricomus
2. Aspergillus bridgeri
3. Aspergillus cretensis
4. Aspergillus elegans
5. Aspergillus flocculosus
39
6. Aspergillus insulicola
7. Aspergillus melleus
8. Aspergillus neobridgeri
9. Aspergillus ochraceus
10. Aspergillus ostianus
11. Aspergillus persii
12. Aspergillus petrakii
13. Aspergillus pseudoelegans
14. Aspergillus robustus
15. Aspergillus roseoglobulosus
16. Aspergillus sclerotiorum
17. Aspergillus steynii
18. Aspergillus sulphurous
19. Aspergillus westerdijkiae
20. Neopetromyces muricatus
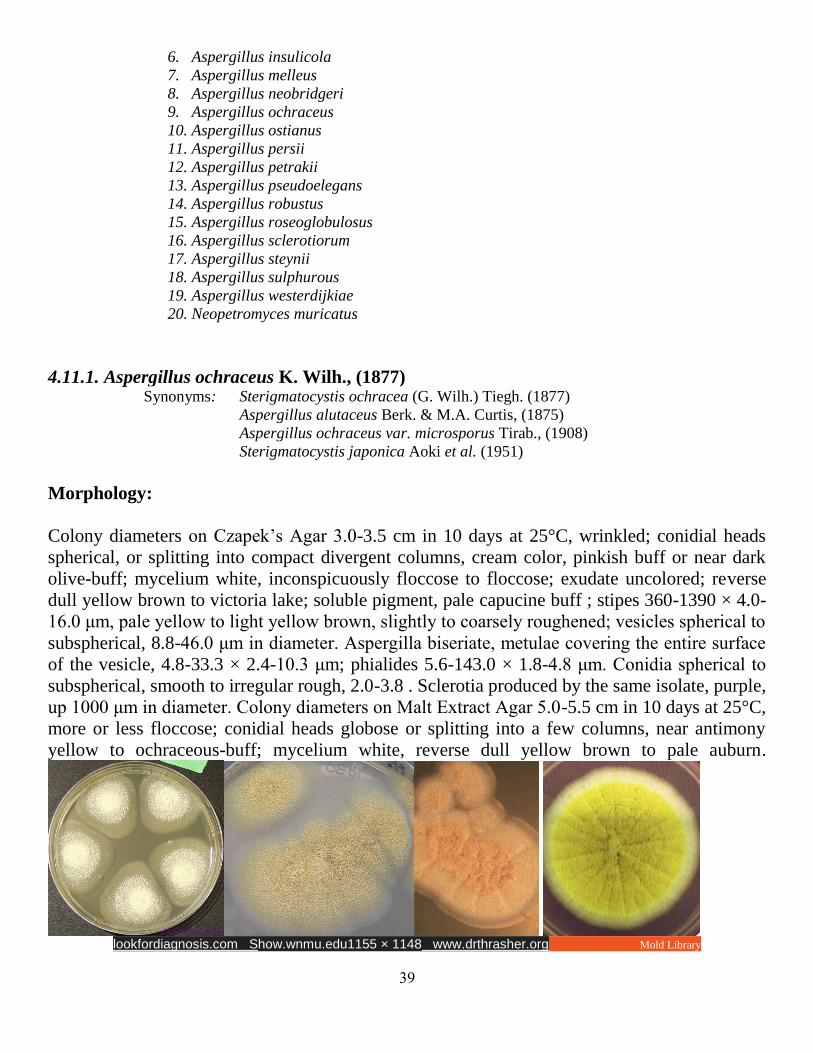
4.11.1. Aspergillus ochraceus K. Wilh., (1877) Synonyms: Sterigmatocystis ochracea (G. Wilh.) Tiegh. (1877)
Aspergillus alutaceus Berk. & M.A. Curtis, (1875)
Aspergillus ochraceus var. microsporus Tirab., (1908)
Sterigmatocystis japonica Aoki et al. (1951)
Morphology:
Colony diameters on Czapek’s Agar 3.0-3.5 cm in 10 days at 25°C, wrinkled; conidial heads
spherical, or splitting into compact divergent columns, cream color, pinkish buff or near dark
olive-buff; mycelium white, inconspicuously floccose to floccose; exudate uncolored; reverse
dull yellow brown to victoria lake; soluble pigment, pale capucine buff ; stipes 360-1390 × 4.0-
16.0 μm, pale yellow to light yellow brown, slightly to coarsely roughened; vesicles spherical to
subspherical, 8.8-46.0 μm in diameter. Aspergilla biseriate, metulae covering the entire surface
of the vesicle, 4.8-33.3 × 2.4-10.3 μm; phialides 5.6-143.0 × 1.8-4.8 μm. Conidia spherical to
subspherical, smooth to irregular rough, 2.0-3.8 . Sclerotia produced by the same isolate, purple,
up 1000 μm in diameter. Colony diameters on Malt Extract Agar 5.0-5.5 cm in 10 days at 25°C,
more or less floccose; conidial heads globose or splitting into a few columns, near antimony
yellow to ochraceous-buff; mycelium white, reverse dull yellow brown to pale auburn.
lookfordiagnosis.com Show.wnmu.edu1155 × 1148 www.drthrasher.org Mold Library

41
S. S. Tzean and J. L. Chen Mycobank
4. 12. Aspergillus section Flavi (Teleomorph:Petromyces)
Aspergillus section Flavi includes species with conidial heads in shades from yellow-
green to brown, and dark sclerotia
Several species assigned to this section are either important mycotoxin producers
including aflatoxins, cyclopiazonic acid, ochratoxins and kojic acid, or are used in
oriental food fermentation processes and as hosts for heterologous gene expression.
The data obtained by Varga et al. (2011) using morphological characters, extrolite
production and partial calmodulin, β-tubulin and ITS sequences indicated that
Aspergillus section Flavi involves 22 species:
1. Aspergillus albertensis
2. Aspergillus alliaceus
3. Aspergillus arachidicola
4. Aspergillus avenaceous
5. Aspergillus bombycis
6. Aspergillus coremiformis
7. Aspergillus caelatus
8. Aspergillus coremiformis
9. Aspergillus flavus
10. Aspergillus lanosus
11. Aspergillus leporis
12. Aspergillus minisclerotium
13. Aspergillus nomius
14. Aspergillus oryzae
15. Aspergillus parasiticus,

41
16. Aspergillus parvisclerotigenus
17. Aspergillus pseudocaelatus
18. Aspergillus pseudonomius
19. Aspergillus pseudotamarii
20. Aspergillus sojae
21. Aspergillus tamari
22. Aspergillus togoensis
The A. flavus« clade includes species characterised with Q-10(H2) as their main
ubiquinone, conidial colours in shades of green and dark sclerotia.
1. Aspergillus flavus Group I includes isolates producing only aflatoxin B and having large
or small sclerotia. This group also includes isolates of A. oryzae, which has previously
been described as having a recombining population species of this clade, P. alliaceus and
P. albertensis, produce high amounts of OA (50–300 mg/mL), and are considered to be
responsible for OA contamination of figs.
2. Aspergillus flavus Group II includes isolates that may produce aflatoxins B or G, and
have large or small sclerotia.
3. Aspergillus Group III includes isolates able to produce both aflatoxins B and G
and have small sclerotia,
4. Aspergillus flavus is the most common species associated with aflatoxin contamination of
agricultural crops.
5. flavus soil populations also contain isolates from two morphologically distinct sclerotial
size variants, termed the L-strain for isolates with average sclerotial size greater than 400
μm and the S-strain for isolates with sclerotial size less that 400 μm. On typical
laboratory growth media S-strain isolates produce higher levels of aflatoxins, more
abundant sclerotia, and generally fewer conidia. Atoxigenic S-strain isolates are very
rarely found in natural environments.

42
4.12.1. Aspergillus flavus Link, 1809 Synonyms: Monilia flava (Link) Pers., (1822)
Sterigmatocystis lutea Tiegh., (1877)
Aspergillus flavus var. proliferans Anguli, Rajam, Thirum., Rangiah & Ramamurthi, (1965)
Morphology
A. flavus is known as a velvety, yellow to green or brown mould with a goldish to red-brown
reverse. On Czapek dox agar, colonies are granular, flat, often with radial grooves, yellow at
first but quickly becoming bright to dark yellow-green with age. Conidial heads are typically
radiate, mostly 300-400 um in diameter, later splitting to form loose columns .The
conidiophores are variable in length, rough, pitted and spiny. They may be either uniseriate or
biseriate. They cover the entire vesicle, and phialides point out in all directions. Conidia are
globose to subglobose, conspicuously echinulate, varying from 3.5 to 4.5 mm in diameter.
Based on the characteristics of the sclerotia produced, A. flavus isolates can be divided into two
phenotypic types. The S strain produces numerous small sclerotia (average diameter ,400 mm).
The L strain produces fewer, larger sclerotia (Cotty, 1989). Within theS strain, some isolates,
termed SB, produce only B aflatoxins, whilst others, named SBG, produce both B and G
aflatoxins.
Aspergillus flavus: human pathogen, allergen and mycotoxin producer
Fungi mycospecies info www.drjacksonkungu.com William McDonald
43
Rahayu WP Mycobank
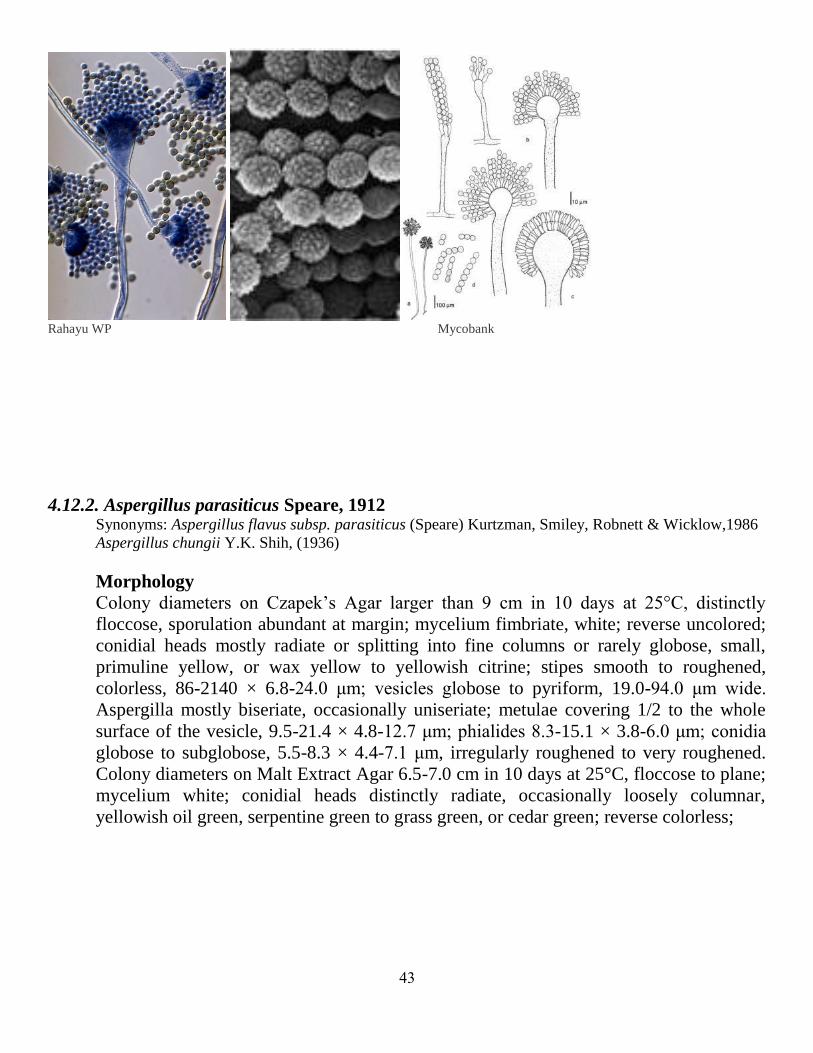
4.12.2. Aspergillus parasiticus Speare, 1912 Synonyms: Aspergillus flavus subsp. parasiticus (Speare) Kurtzman, Smiley, Robnett & Wicklow,1986
Aspergillus chungii Y.K. Shih, (1936)
Morphology
Colony diameters on Czapek’s Agar larger than 9 cm in 10 days at 25°C, distinctly
floccose, sporulation abundant at margin; mycelium fimbriate, white; reverse uncolored;
conidial heads mostly radiate or splitting into fine columns or rarely globose, small,
primuline yellow, or wax yellow to yellowish citrine; stipes smooth to roughened,
colorless, 86-2140 × 6.8-24.0 μm; vesicles globose to pyriform, 19.0-94.0 μm wide.
Aspergilla mostly biseriate, occasionally uniseriate; metulae covering 1/2 to the whole
surface of the vesicle, 9.5-21.4 × 4.8-12.7 μm; phialides 8.3-15.1 × 3.8-6.0 μm; conidia
globose to subglobose, 5.5-8.3 × 4.4-7.1 μm, irregularly roughened to very roughened.
Colony diameters on Malt Extract Agar 6.5-7.0 cm in 10 days at 25°C, floccose to plane;
mycelium white; conidial heads distinctly radiate, occasionally loosely columnar,
yellowish oil green, serpentine green to grass green, or cedar green; reverse colorless;
44
Mycobank S. S. Tzean and J. L. Chen
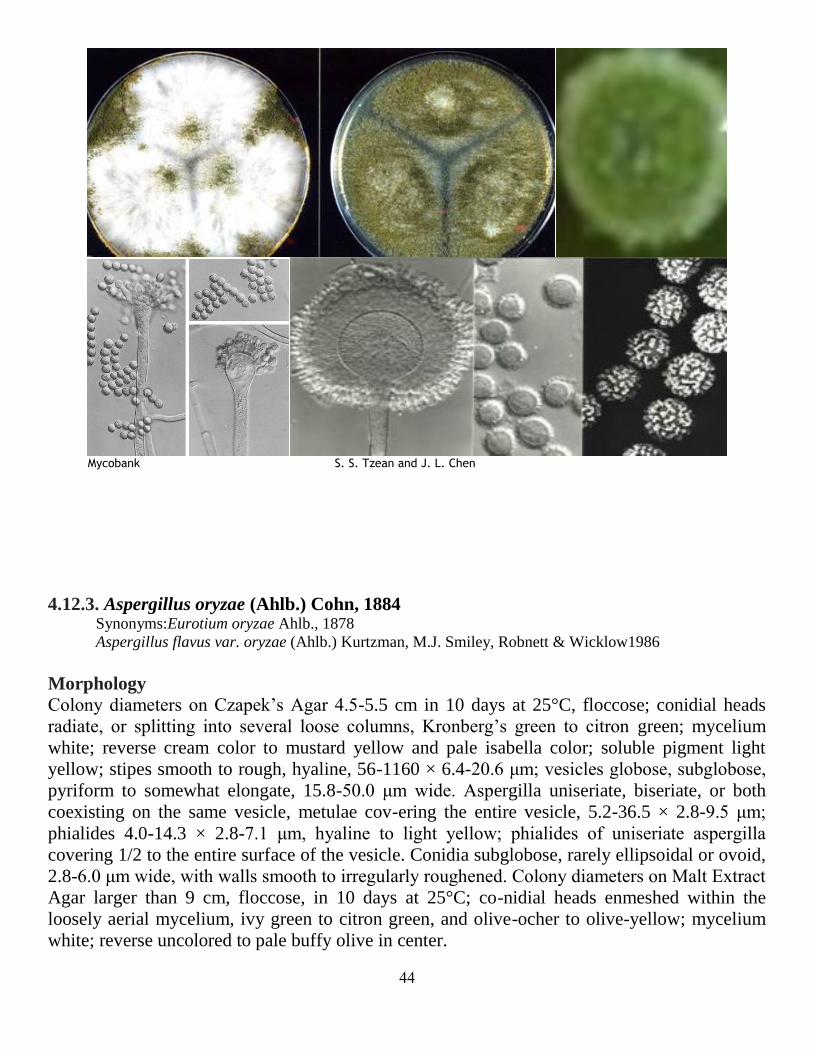
4.12.3. Aspergillus oryzae (Ahlb.) Cohn, 1884 Synonyms:Eurotium oryzae Ahlb., 1878
Aspergillus flavus var. oryzae (Ahlb.) Kurtzman, M.J. Smiley, Robnett & Wicklow1986
Morphology
Colony diameters on Czapek’s Agar 4.5-5.5 cm in 10 days at 25°C, floccose; conidial heads
radiate, or splitting into several loose columns, Kronberg’s green to citron green; mycelium
white; reverse cream color to mustard yellow and pale isabella color; soluble pigment light
yellow; stipes smooth to rough, hyaline, 56-1160 × 6.4-20.6 μm; vesicles globose, subglobose,
pyriform to somewhat elongate, 15.8-50.0 μm wide. Aspergilla uniseriate, biseriate, or both
coexisting on the same vesicle, metulae cov-ering the entire vesicle, 5.2-36.5 × 2.8-9.5 μm;
phialides 4.0-14.3 × 2.8-7.1 μm, hyaline to light yellow; phialides of uniseriate aspergilla
covering 1/2 to the entire surface of the vesicle. Conidia subglobose, rarely ellipsoidal or ovoid,
2.8-6.0 μm wide, with walls smooth to irregularly roughened. Colony diameters on Malt Extract
Agar larger than 9 cm, floccose, in 10 days at 25°C; co-nidial heads enmeshed within the
loosely aerial mycelium, ivy green to citron green, and olive-ocher to olive-yellow; mycelium
white; reverse uncolored to pale buffy olive in center.
45
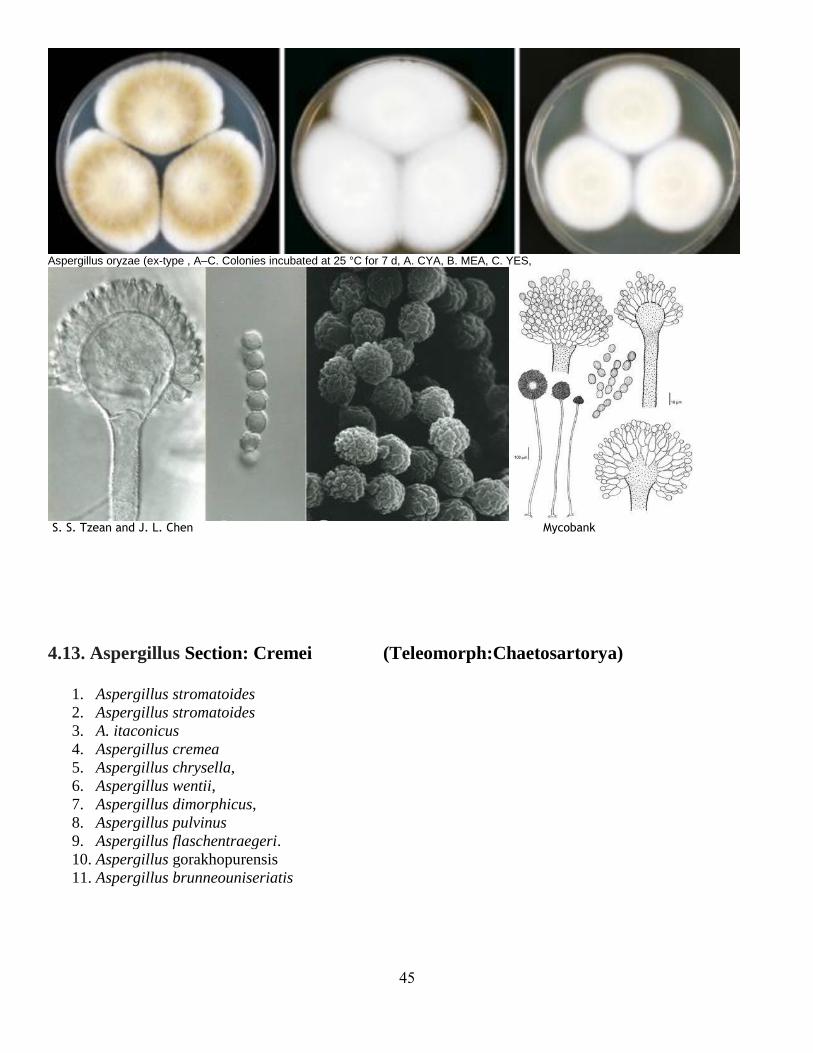
Aspergillus oryzae (ex-type , A–C. Colonies incubated at 25 °C for 7 d, A. CYA, B. MEA, C. YES,
S. S. Tzean and J. L. Chen Mycobank
4.13. Aspergillus Section: Cremei (Teleomorph:Chaetosartorya)
1. Aspergillus stromatoides
2. Aspergillus stromatoides
3. A. itaconicus
4. Aspergillus cremea
5. Aspergillus chrysella,
6. Aspergillus wentii,
7. Aspergillus dimorphicus,
8. Aspergillus pulvinus
9. Aspergillus flaschentraegeri.
10. Aspergillus gorakhopurensis
11. Aspergillus brunneouniseriatis
46
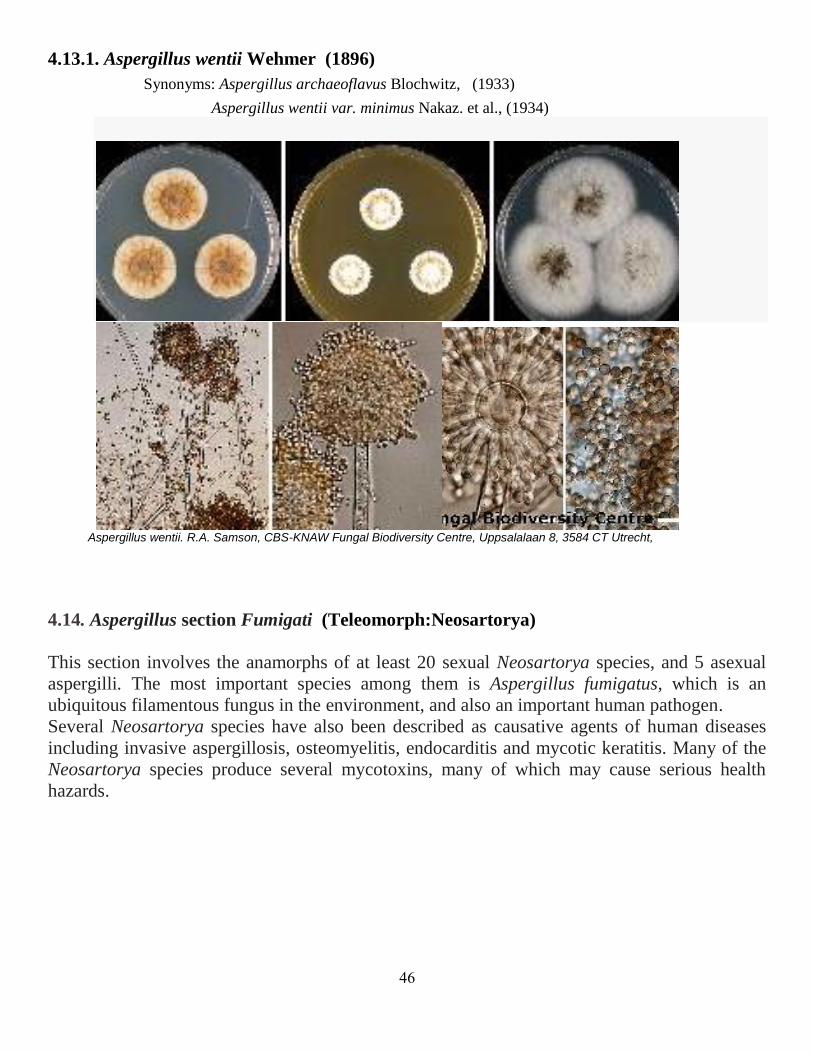
4.13.1. Aspergillus wentii Wehmer (1896)
Synonyms: Aspergillus archaeoflavus Blochwitz, (1933)
Aspergillus wentii var. minimus Nakaz. et al., (1934)
Aspergillus wentii. R.A. Samson, CBS-KNAW Fungal Biodiversity Centre, Uppsalalaan 8, 3584 CT Utrecht,
4.14. Aspergillus section Fumigati (Teleomorph:Neosartorya)
This section involves the anamorphs of at least 20 sexual Neosartorya species, and 5 asexual
aspergilli. The most important species among them is Aspergillus fumigatus, which is an
ubiquitous filamentous fungus in the environment, and also an important human pathogen.
Several Neosartorya species have also been described as causative agents of human diseases
including invasive aspergillosis, osteomyelitis, endocarditis and mycotic keratitis. Many of the
Neosartorya species produce several mycotoxins, many of which may cause serious health
hazards.
47
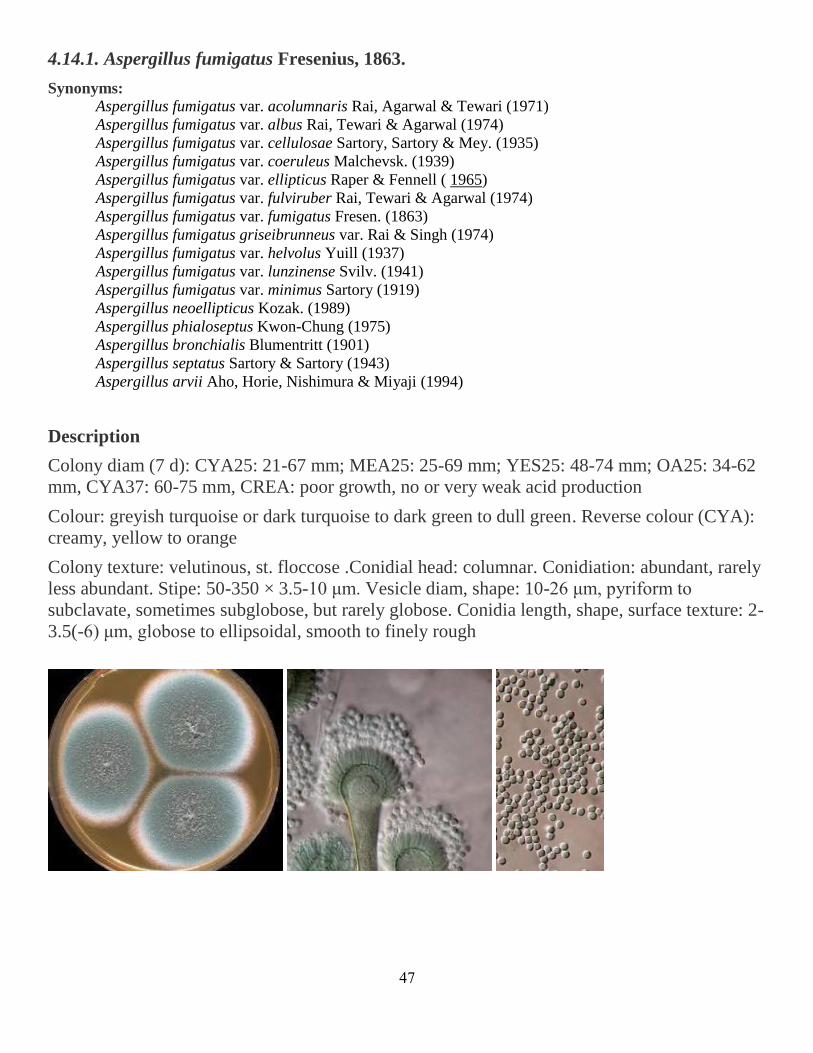
4.14.1. Aspergillus fumigatus Fresenius, 1863.
Synonyms:
Aspergillus fumigatus var. acolumnaris Rai, Agarwal & Tewari (1971)
Aspergillus fumigatus var. albus Rai, Tewari & Agarwal (1974)
Aspergillus fumigatus var. cellulosae Sartory, Sartory & Mey. (1935)
Aspergillus fumigatus var. coeruleus Malchevsk. (1939)
Aspergillus fumigatus var. ellipticus Raper & Fennell ( 1965)
Aspergillus fumigatus var. fulviruber Rai, Tewari & Agarwal (1974)
Aspergillus fumigatus var. fumigatus Fresen. (1863)
Aspergillus fumigatus griseibrunneus var. Rai & Singh (1974)
Aspergillus fumigatus var. helvolus Yuill (1937)
Aspergillus fumigatus var. lunzinense Svilv. (1941)
Aspergillus fumigatus var. minimus Sartory (1919)
Aspergillus neoellipticus Kozak. (1989)
Aspergillus phialoseptus Kwon-Chung (1975)
Aspergillus bronchialis Blumentritt (1901)
Aspergillus septatus Sartory & Sartory (1943)
Aspergillus arvii Aho, Horie, Nishimura & Miyaji (1994)
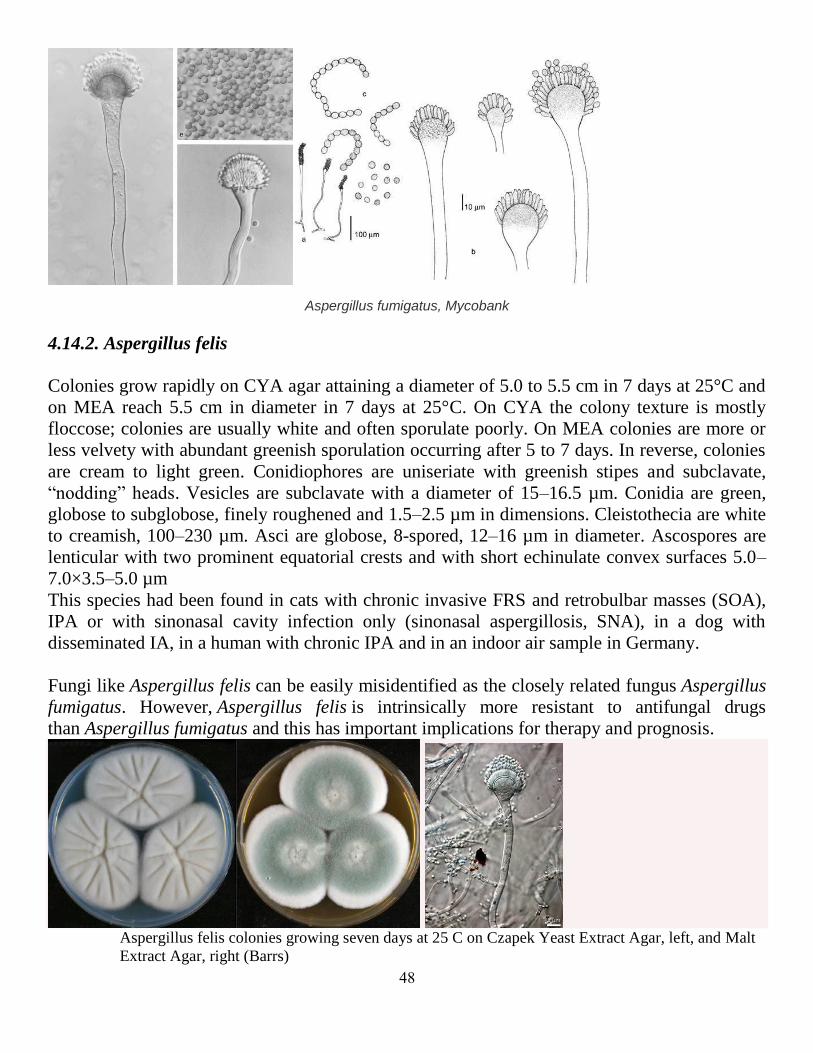
Description
Colony diam (7 d): CYA25: 21-67 mm; MEA25: 25-69 mm; YES25: 48-74 mm; OA25: 34-62
mm, CYA37: 60-75 mm, CREA: poor growth, no or very weak acid production
Colour: greyish turquoise or dark turquoise to dark green to dull green. Reverse colour (CYA):
creamy, yellow to orange
Colony texture: velutinous, st. floccose .Conidial head: columnar. Conidiation: abundant, rarely
less abundant. Stipe: 50-350 × 3.5-10 μm. Vesicle diam, shape: 10-26 μm, pyriform to
subclavate, sometimes subglobose, but rarely globose. Conidia length, shape, surface texture: 2-
3.5(-6) μm, globose to ellipsoidal, smooth to finely rough
48
Aspergillus fumigatus, Mycobank
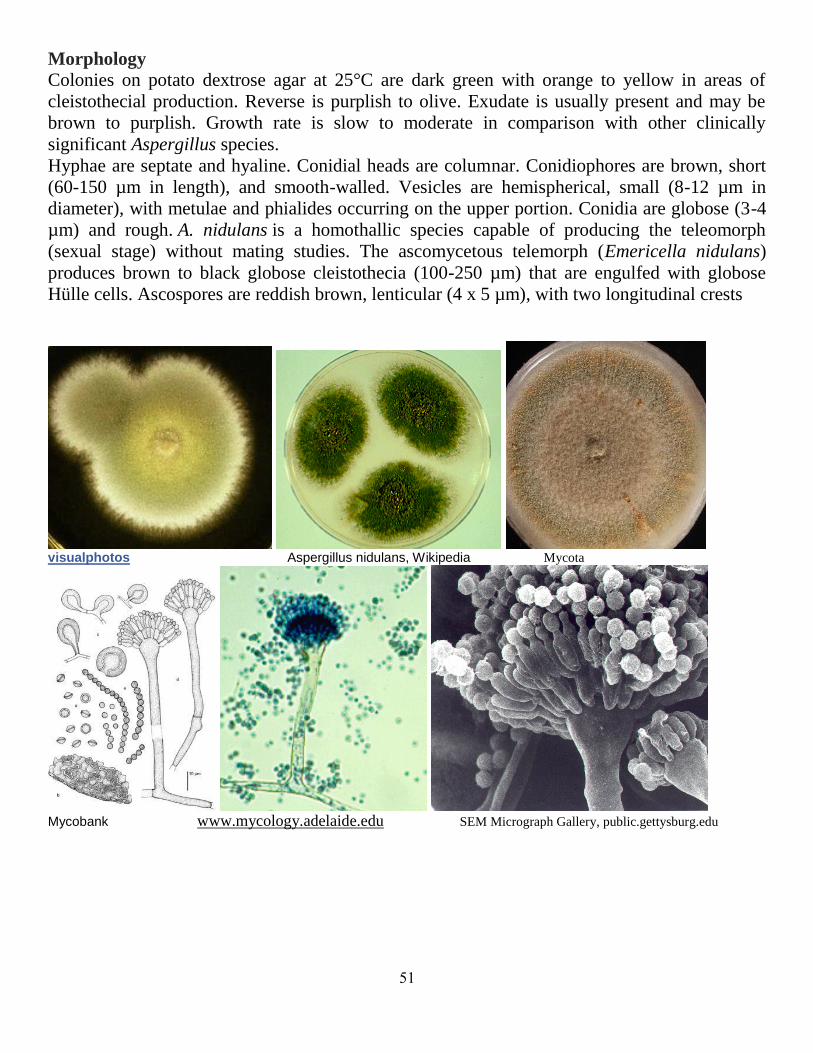
4.14.2. Aspergillus felis
Colonies grow rapidly on CYA agar attaining a diameter of 5.0 to 5.5 cm in 7 days at 25°C and
on MEA reach 5.5 cm in diameter in 7 days at 25°C. On CYA the colony texture is mostly
floccose; colonies are usually white and often sporulate poorly. On MEA colonies are more or
less velvety with abundant greenish sporulation occurring after 5 to 7 days. In reverse, colonies
are cream to light green. Conidiophores are uniseriate with greenish stipes and subclavate,
“nodding” heads. Vesicles are subclavate with a diameter of 15–16.5 µm. Conidia are green,
globose to subglobose, finely roughened and 1.5–2.5 µm in dimensions. Cleistothecia are white
to creamish, 100–230 µm. Asci are globose, 8-spored, 12–16 µm in diameter. Ascospores are
lenticular with two prominent equatorial crests and with short echinulate convex surfaces 5.0–
7.0×3.5–5.0 µm
This species had been found in cats with chronic invasive FRS and retrobulbar masses (SOA),
IPA or with sinonasal cavity infection only (sinonasal aspergillosis, SNA), in a dog with
disseminated IA, in a human with chronic IPA and in an indoor air sample in Germany.
Fungi like Aspergillus felis can be easily misidentified as the closely related fungus Aspergillus
fumigatus. However, Aspergillus felis is intrinsically more resistant to antifungal drugs
than Aspergillus fumigatus and this has important implications for therapy and prognosis.
Aspergillus felis colonies growing seven days at 25 C on Czapek Yeast Extract Agar, left, and Malt
Extract Agar, right (Barrs)

49
4. 15. Aspergillus Section:Clavati (Teleomorph:Neocarpenteles)
Aspergillus section Clavati has been revised by Varga et al. (2007) using morphology,
secondary metabolites, physiological characters and DNA sequences. Phylogenetic analysis of
beta-tubulin, ITS and calmodulin sequence data indicated that Aspergillus section Clavati
includes 6 species:
1. Aspergillus clavatus
1. giganteus
2. longavesica
3. clavatonanicus
4. rhizopodus
5. Neocarpenteles acanthosporus
4. 15. 1. Aspergillus clavatus Desmazières (1834)
Synonyms: A. apicalis Mehrotra & Basu,1976
A. pallidus Kamyschko,1963
Colony diameters on Czapek’s Agar 4.7-5.0 cm in 14 days at 25°C, zonation conspicuous to
inconspicuous; conidial heads radiate or splitting into well defined columns in age, niagara
green to bice green, or artemisia green to slate-olive (R., Plate XVII, XXXIII, XLVII); my-
celium white; exudate clear; reverse colorless, or ivory yellow to cartridge buff (R., Plate
XXX); stipes 250-2300 × 4.8-40.0 μm, uncolored, smooth; vesicles clavate, 8.7-80.0 μm wide.
Aspergilla uniseriate, phialides covering the entire surface of the vesicle, 5.3-21.4 × 2.4-5.6 μm.
Conidia subspherical, ellipsoidal, occasionally cylindrical, 3.3-7.1 × 2.4-4.4 μm, smooth.
Colony diameters on Malt Extract Agar 5.0-5.5 cm in 14 days at 25°C, zonation conspicuous;
conidial heads radiate or splitting into well defined columns, bluish gray-green to artemisia
green (R., Plate XLII, XLVII); mycelium white; reverse uncolored.

51
labmed.ucsf.edu Varga, Frisvad , Samson RA S. S. Tzean and J. L. Chen Mycobank
4. 16. Aspergillus Section:Nidulantes (Teleomorph:Emericella)
1. A. nidulans
2. A. quadrilineata
3. E. rugulosa
4. E. nidulans var. echinulata
4.16.1. Aspergillus nidulans (Eidam) G. Winter (1884) Teleomorphic state: Emericella nidulans
Synonyms: Sterigmatocystis nidulans Eidam (1883)
Diplostephanus nidulans (Eidam) Neveu-Lem. (1921)
Sterigmatocystis nidulans var. nicollei Pinoy,(1906)
Aspergillus nidulans var. cesarii Pinoy (1915)
Aspergillus nidulellus Samson & W. Gams (1986)
51
Morphology Colonies on potato dextrose agar at 25°C are dark green with orange to yellow in areas of
cleistothecial production. Reverse is purplish to olive. Exudate is usually present and may be
brown to purplish. Growth rate is slow to moderate in comparison with other clinically
significant Aspergillus species.
Hyphae are septate and hyaline. Conidial heads are columnar. Conidiophores are brown, short
(60-150 µm in length), and smooth-walled. Vesicles are hemispherical, small (8-12 µm in
diameter), with metulae and phialides occurring on the upper portion. Conidia are globose (3-4
µm) and rough. A. nidulans is a homothallic species capable of producing the teleomorph
(sexual stage) without mating studies. The ascomycetous telemorph (Emericella nidulans)
produces brown to black globose cleistothecia (100-250 µm) that are engulfed with globose
Hülle cells. Ascospores are reddish brown, lenticular (4 x 5 µm), with two longitudinal crests
visualphotos Aspergillus nidulans, Wikipedia Mycota
Mycobank www.mycology.adelaide.edu SEM Micrograph Gallery, public.gettysburg.edu

52
4. 17. Aspergillus Section:Ornati (Teleomorph:Hemicarpenteles)
4.17.1. Aspergillus ornatus Raper, Fennell & Tresner (1953) Synonyms: Sclerocleista ornata (Raper, Fennell & Tresner) Subram., (1972)
Neosartorya ornata (Raper, Fennell & Tresner) Malloch & Cain, (1973)
Hemicarpenteles ornatus (Raper, Fennell & Tresner) Arx, (1974)
Hemicarpenteles ornata (Subram.) Arx (1974)
Chaetosartorya ornata (Raper, Fennell & Tresner) Bilai & Koval, (1988) [
4. 18. Aspergillus sect. Aeni
Aspergillus sect. Aeni is a new section that includes the following species 1. Aspergillus karnatakaensis
2. Aspergillus aeneus,
3. Aspergillus crustosus,
4. Aspergillus eburneocremeus,
5. Aspergillus heyangensis,
6. Emericella bicolor,
7. Emericella discophora,
8. Emericella spectabilis,
9. E. foeniculicola.
Aspergillus karnatakaensis isolates were found to produce karnatakafurans A and B, terrein,
gregatins, asteltoxin and the partially characterised metabolite NIDU. Both gregatins and NIDU
are also produced by A. granulosus, while karnatakafurans are produced in common with A.
aeneus and A. multicolor. Emericella bicolor produces sterigmatocystin, versicolorins, some
anthraquinones, and a polar extrolite with end-absorption; E. foeniculicola produces
sterigmatocystin (and many other sterigmatocystin and versicolorin-related compounds),
xanthocillin derivatives, and the partially characterized (but common) metabolite DRI; E.
spectabilis produces two members of the shamixanthone biosynthetic family (both more polar
than shamixanthone itself) and a member of the sterigmatocystin biosynthetic family; A.
heyangensis produces a decaturin in common with A. aeneus and A. karnatakaensis and NIDU,
while E. discophora produces sterigmatocystin and versicolorins (Varga et al., 2010)

53
4.18.1. Aspergillus granulosus Raper and Thom (1944)
Morphology
Colonies are cream to white and floccose at the periphery and buff to yellowish tan centrally,
with a very slight clear exudate. Colonies on CZA are mostly cream, more irregularly furrowed,
and exhibited reduced conidiation. The central granular areas on PFA consisted of colorless
masses of thick-walled (6 to 8 μm), predominately globose but also oval to elongate to
irregularly shaped Hülle cells with individual, mature cells ranging from 20 to 40 μm.
Robust Aspergillus fruiting heads are sparse and are borne on long (200 to 480 μm), subhyaline
to brown, smooth, thick-walled conidiophores terminating in small (12 to 18 μm wide by 15 to
25 μm long), oval to elliptical vesicles. Metulae and bottle-shaped phialides of almost equal
length (3.5 to 5.5 μm) covered most of the surface of the vesicle. Conidia pale green in mass,
globose, and finely echinulate, measuring 3.5 to 5.5 μm in diameter. More commonly, fruiting
structures are reduced in size with small, Penicillium-like vesicles or single chains of conidia
are borne from solitary phialides
A. granulosus, Sutton et al., J. Clin. Microbiol. October 2009vol. 47 no. 10 3386-3390
A. granulosus, Houbraken J, Due M, Varga J, Meijer M, Frisvad JC, Samson RA - Stud. Mycol. (2007), Mycobank

54
5. Aspergillosis in man
5.1. Pulmonary aspergillosis
5.1.1. Aspergilloma (Saprophytic aspergillosis, fungus ball)
Aspergilloma is an Aspergillus infection without tissue invasion.
The aspergilloma is a mass composed of fungal hyphae, inflammatory cells, fibrin,
mucus and tissue debris that develops in a pre-existing cavity in the lung, without invade
the surrounding lung parenchyma or blood vessels.
The most common underlying causes are tuberculosis and sarcoidosis. Other conditions
that occasionally may be associated with aspergilloma include bronchogenic cyst,
pulmonary sequestration, and pneumatoceles secondary to Pneumocystis
carinii pneumonia in patients with acquired immunodeficiency syndrome (AIDS).
At radiography, aspergilloma is characterized by the presence of a solid, round or oval
mass with soft-tissue opacity within a lung cavity. Typically, the mass is separated from
the wall of the cavity by an airspace of variable size and shape, resulting in the “air
crescent” sign. A change in the position of the fungus ball after moving the patient,
demonstrating that this mass is mobile because does not usually invade the surrounding
lung parenchyma.
Aspergillomas are often associated with thickening of the cavity wall and adjacent pleura.
In such cases, pleural thickening may be the earliest radiographic sign before any visible
changes are seen within the cavity. Approximately 10% of mycetomas resolve
spontaneously. Reversibility of the pleural thickening corresponding to the resolution of
intracavitary fungal material has been demonstrated at follow-up radiography
Surgical resection of the cavity and removal of the fungus ball is usually indicated in
patients with recurrent haemoptysis, if their pulmonary function is sufficient to allow
surgery or bronchial artery embolization in patients with poor lung function.

55
Aspergilloma www.brown.edu radiopaedia.org pathhsw5m54.ucsf.edu
Aspergilloma - “Chest x-ray of a man with extensive bullous lung
pathologyimages.wordpress.com, de.wikipedia.org Aspergilloma,
www.histopathology-india.net www.flickriver.com
56
Recently reported cases: 1. Aspergilloma and massive haemoptysis.
45
2. A rare case of calcified pulmonary aspergilloma46
.
3. Adjuvant antifungal therapy after pulmonary surgery foraspergilloma: is it useful?47
4. Aspergilloma and the surgeon.48
5. Pulmonary Diseases with Imaging Findings MimickingAspergilloma. Lung.49
6. Is video-assisted thoracic surgery a versatile treatment for both simple and
complex pulmonary aspergilloma? 50
7. Pulmonary Aspergilloma: An Unexpected Complication of Radiofrequency Ablation in the Management
of Targeted Therapy for a Patient With Metastatic Renal Cell Carcinoma.51
8. Treatment of pulmonary aspergilloma in Srinagarind Hospital52
.
9. Surgical therapy of pulmonary aspergillomas: a 30-year North American experience.53
10. Intrapulmonary aspergilloma in an old tuberculous cavity with access to the bronchial system.54
11. . Case 3: aspergilloma. 55
12. Pulmonary aspergilloma: a treatment challenge in sub-Saharan Africa. 56
13. [Gougerot-Sjögren syndrome complicated by pulmonaryaspergilloma].57
14. A case of pulmonary aspergilloma treated with radiofrequency ablation.58
15. [Surgical treatment of pulmomary tuberculosis complicated withaspergilloma].59
16. Always expect the unexpected: lung abscess due to pseudomonas aeruginosa
mimicking pulmonary aspergillomain acute B-cell leukemia.60
17. Video-assisted thoracic surgery for pulmonary aspergilloma: a safe and effective procedure. 61
18. 'Monod' and 'air crescent' sign in aspergilloma.62
19. Calcium oxalate crystal deposition in a patient withAspergilloma due to Aspergillus niger. 63
20. Surgical treatment of aspergilloma grafted in hydatid cyst cavity.64
21. Haemoptysis after four years of lobectomy for aspergilloma.65
22. Aspergilloma coexisting with idiopathic pulmonary fibrosis: a rare occurrence. 66
23. Aspergilloma mimicking a lung cancer. 67
24. A Case of Endobronchial Aspergilloma Associated with Foreign Body in Immunocompetent Patient
without Underlying LungDisease.68
25. Pulmonary aspergilloma in a cavity formed after percutaneous radiofrequency ablation.69
26. Co-existence of HIV, active tuberculosis and aspergilloma in a single individual--a case report.70
.
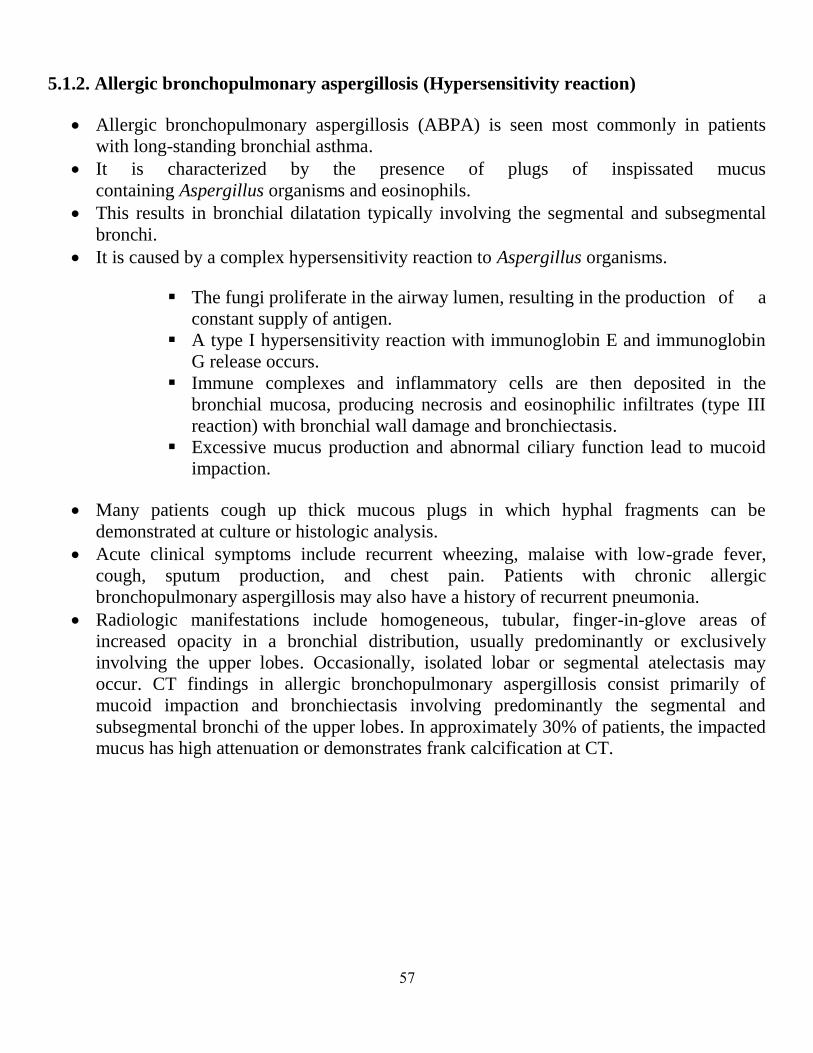
57
5.1.2. Allergic bronchopulmonary aspergillosis (Hypersensitivity reaction)
Allergic bronchopulmonary aspergillosis (ABPA) is seen most commonly in patients
with long-standing bronchial asthma.
It is characterized by the presence of plugs of inspissated mucus
containing Aspergillus organisms and eosinophils.
This results in bronchial dilatation typically involving the segmental and subsegmental
bronchi.
It is caused by a complex hypersensitivity reaction to Aspergillus organisms.
The fungi proliferate in the airway lumen, resulting in the production of a
constant supply of antigen.
A type I hypersensitivity reaction with immunoglobin E and immunoglobin
G release occurs.
Immune complexes and inflammatory cells are then deposited in the
bronchial mucosa, producing necrosis and eosinophilic infiltrates (type III
reaction) with bronchial wall damage and bronchiectasis.
Excessive mucus production and abnormal ciliary function lead to mucoid
impaction.
Many patients cough up thick mucous plugs in which hyphal fragments can be
demonstrated at culture or histologic analysis.
Acute clinical symptoms include recurrent wheezing, malaise with low-grade fever,
cough, sputum production, and chest pain. Patients with chronic allergic
bronchopulmonary aspergillosis may also have a history of recurrent pneumonia.
Radiologic manifestations include homogeneous, tubular, finger-in-glove areas of
increased opacity in a bronchial distribution, usually predominantly or exclusively
involving the upper lobes. Occasionally, isolated lobar or segmental atelectasis may
occur. CT findings in allergic bronchopulmonary aspergillosis consist primarily of
mucoid impaction and bronchiectasis involving predominantly the segmental and
subsegmental bronchi of the upper lobes. In approximately 30% of patients, the impacted
mucus has high attenuation or demonstrates frank calcification at CT.

58
Areas of tubular (Panel A, arrows) and cystic (Panel A, arrowhead) bronchiectasis, predominantly in the upper lobes, and bilateral mucous plugging (Panel B, arrows)
101
The CXR shows bronchial wall thickening and impressive central bronchiectasis.101
Recently reported cases 1. Antifungal treatment in allergic bronchopulmonary aspergillosis with and without cystic fibrosis: a
systematic review. Clin Exp Allergy. 71
2. Omalizumab therapy for allergic bronchopulmonary aspergillosis in children with cystic fibrosis: a
synthesis of published evidence72
.
3. Fungal allergy in asthma-state of the art and research needs.73
4. Excellent outcome of Aspergillous endophthalmitis in a case ofallergic bronchopulmonary aspergillosis. 74
5. A retrospective study of patients with a delayed diagnosis ofallergic bronchopulmonary
aspergillosis/allergicbronchopulmonary mycosis. 75
6. Allergic bronchopulmonary aspergillosis coexists with hereditary bisalbuminemia. 76
7. Role of inhaled amphotericin in allergic bronchopulmonary aspergillosis. 77
8. Pulse methylprednisolone in allergic bronchopulmonary aspergillosis exacerbations. 78
.
9. Unexpected decrease in total IgE in a patient with allergic bronchopulmonary aspergillosis treated with
omalizumab. 79
59
10. ABPA Concomitantly Occurring with Invasive SinusAspergillosis: A Short Report on Two Patients. 80
11. Atypical Presentation of Allergic Bronchopulmonary Aspergillosis: An Unusual Cause of Difficult-to-
Treat Asthma. 81
12. [Allergic bronchopulmonary aspergillosis in patients with chronic obstructive pulmonary disease: report
of 3 cases].82
13. Evaluation of serum levels of carcinoembryonic antigen inallergic bronchopulmonary aspergillosis. 83
14. Allergic bronchopulmonary aspergillosis mimicking relapsing chronic eosinophilic pneumonia in non-
asthma patient. 84
15. Treatment options in severe fungal asthma and allergic bronchopulmonary aspergillosis.85
16. Anti-IgE therapy for allergic bronchopulmonary aspergillosis. 86
17. [Analysis of clinical features and allergic status of asthmatic patients with positive serum mycosis-
specific IgE]. 87
18. Allergic bronchopulmonary aspergillosis in asthma: epidemiological, clinical and therapeutic issues.88
19. Bronchial asthma with ABPA presenting as PTE. 89
20. Anti-IgE therapy for allergic bronchopulmonary aspergillosisin people with cystic fibrosis. 90
21. . Development of allergic bronchopulmonary aspergillosiswith central bronchiectasis over a 10-year
period: the need to recheck allergen sensitization. 91
22. Dissociation between sensitizing and colonizing fungi in patients with allergic bronchopulmonary
aspergillosis.92
23. . Allergic bronchopulmonary aspergillosis in garden waste (compost) collectors--occupational
implications.93
24. Allergic bronchopulmonary aspergillosis with repeated isolation of nontuberculous mycobacteria.94
25. Allergic bronchopulmonary aspergillosis: review of literature and proposal of new diagnostic and
classification criteria. ABPA complicating asthma ISHAM working group. 95
26. Uncertain areas in the diagnosis of allergic bronchopulmonary aspergillosis in patients with asthma.96
27. When to suspect and work up allergic bronchopulmonary aspergillosis.97
28. Allergic bronchopulmonary aspergillosis: a clinico-serological correlation with radiologic profile.98
29. Allergic bronchopulmonary aspergillosis presenting as chronic cough in an elderly woman without
previously documented asthma.99
30. Coexistence of allergic bronchopulmonary aspergillosis andallergic aspergillus sinusitis in a patient
without clinical asthma.100
31. Ting-hsu Chen,., and Helen Hollingsworth, Allergic Bronchopulmonary Aspergillosis.101

61
5.1.3. Chronic necrotizing aspergillosis (Semi-invasive aspergillosis)
Semi-invasive aspergillosis, also known as chronic necrotizing aspergillosis, is an
indolent, destructive process of the lung due to local invasion by Aspergillus species,
with tissue necrosis and granulomatous inflammation.
Factors associated with the development of this form of aspergillosis include chronic
debilitating illness, diabetes mellitus, malnutrition, alcoholism, advanced age, prolonged
corticosteroid therapy, and chronic obstructive pulmonary disease.
Clinical symptoms include chronic cough, sputum production, fever, and constitutional
symptoms. In patients with chronic obstructive pulmonary disease, semi-invasive
aspergillosis may manifest with a variety of nonspecific clinical symptoms such as
cough, sputum production, and fever lasting more than 6 months. Hemoptysis has been
reported in 15% of affected patients.
Radiologic manifestations of semi-invasive aspergillosis include unilateral or bilateral
segmental areas of consolidation with or without cavitation or adjacent pleural
thickening, and multiple nodular areas of increased opacity. Aspergillus necrotizing
bronchitis may be seen at CT as an endobronchial mass, obstructive pneumonitis or
collapse, or a hilar mass. Only a few reports have described CT findings
in Aspergillus necrotizing bronchitis involving the central airways; reported
abnormalities include circumferential bronchial wall thickening and bronchial
obstruction.
In clinical practice, the diagnosis of Aspergillus necrotizing bronchitis is usually based on
the presence of abnormal findings at chest radiography and bronchoscopic biopsy, which
are consistent with tissue invasion.
Aspergilloma/chronic necrotising pulmonary aspergillosis
122

61
Recently reported cases:
1. Chronic necrotizing pulmonary aspergillosis in a renal transplant recipient.122
2. Prognostic factors in 194 patients with chronic necrotizingpulmonary aspergillosis. 123
3. [Three autopsy cases of chronic necrotizing pulmonaryaspergillosis]. 124
4. Systemic dissemination of chronic necrotizing pulmonaryaspergillosis in an elderly woman without
comorbidity: a case report.125
5. Systemic biomarkers of inflammation and haemostasis in patients with
chronic necrotizing pulmonary aspergillosis.126
6. Efficacy and safety of short- and long-term treatment of itraconazole
on chronic necrotizing pulmonary aspergillosisin multicenter study.127
7. [Chronic necrotizing pulmonary aspergillosis following an infection by Mycobacterium malmoense].128
8. [Retrospective analysis of the safety of four hours administration of liposomal amphotericin B in
patients with chronicnecrotizing pulmonary aspergillosis]. 129
9. A surgically treated case of chronic necrotizing aspergillosiswith pleural invasion. 130
10. Chronic necrotizing pulmonary aspergillosis presenting as bilateral pleural effusion: a case report.131
11. Chronic necrotizing pulmonary aspergillosis. 132
12. Resolution of galactomannan antigenemia in a patient receiving oral voriconazole
for chronic necrotizing pulmonaryaspergillosis. 133
13. [Chronic necrotizing pulmonary aspergillosis as a complication of silicosis].134
14. [Case of chronic necrotizing pulmonary aspergillosiscomplicated by elevated eosinophils and serum
IgE].135
15. Chronic necrotizing pulmonary aspergillosis in a patient treated with a tumor necrosis factor-alpha
inhibitor. 136
16. [Lethal case of chronic necrotizing pulmonary aspergillosis(CNPA)].137
17. Progressive increase in cavitation with the evolution of fungus ball: A clue to the diagnosis
of chronic necrotizing pulmonaryaspergillosis.138
18. [A case of pulmonary actinomycosis mimicking chronicnecrotizing pulmonary aspergillosis].139
19. Clinical characteristics and treatment outcomes of chronicnecrotizing pulmonary aspergillosis: a review
of 43 cases.140
20. Chronic necrotizing pulmonary aspergillosis or invasive pulmonary aspergillosis. 141
62
5.1.4. Invasive pulmonary aspergillosis
Invasive pulmonary aspergillosis occurs almost exclusively in immunocompromised
patients with severe neutropenia.
The reasons of the substantial increase in the number of patients at risk for developing
invasive aspergillosis include the development of new intensive chemotherapy regimens
for solid tumors, difficult-to-treat lymphoma, myeloma, and resistant leukemia as well as
an increase in the number of solid organ transplantations and increased use of
immunosuppressive regimens for other autoimmune diseases.
Invasive pulmonary aspergillosis is characterized by the presence of Aspergillus
organisms deep to basement membrane of bronchi or bronchioles, usually with a
neutrophil reaction and presence of hyphae in the involved airway. Surrounding the
airway is often found a variably sized zone of hemorrhage and/or organizing pneumonia.
Invasive pulmonary aspergillosis is characterized at histologic analysis by the invasion
and occlusion of small to medium-sized pulmonary arteries by fungal hyphae, which
leads to the formation of necrotic hemorrhagic nodules or pleura-based, wedge-shaped.
Characteristic CT findings consist of nodules surrounded by a halo of ground-glass
attenuation (“halo sign”) or pleura-based, wedge-shaped areas of consolidation. These
findings correspond to hemorrhagic infarcts. In severely neutropenic patients, the halo
sign is highly suggestive of invasive pulmonary aspergillosis.
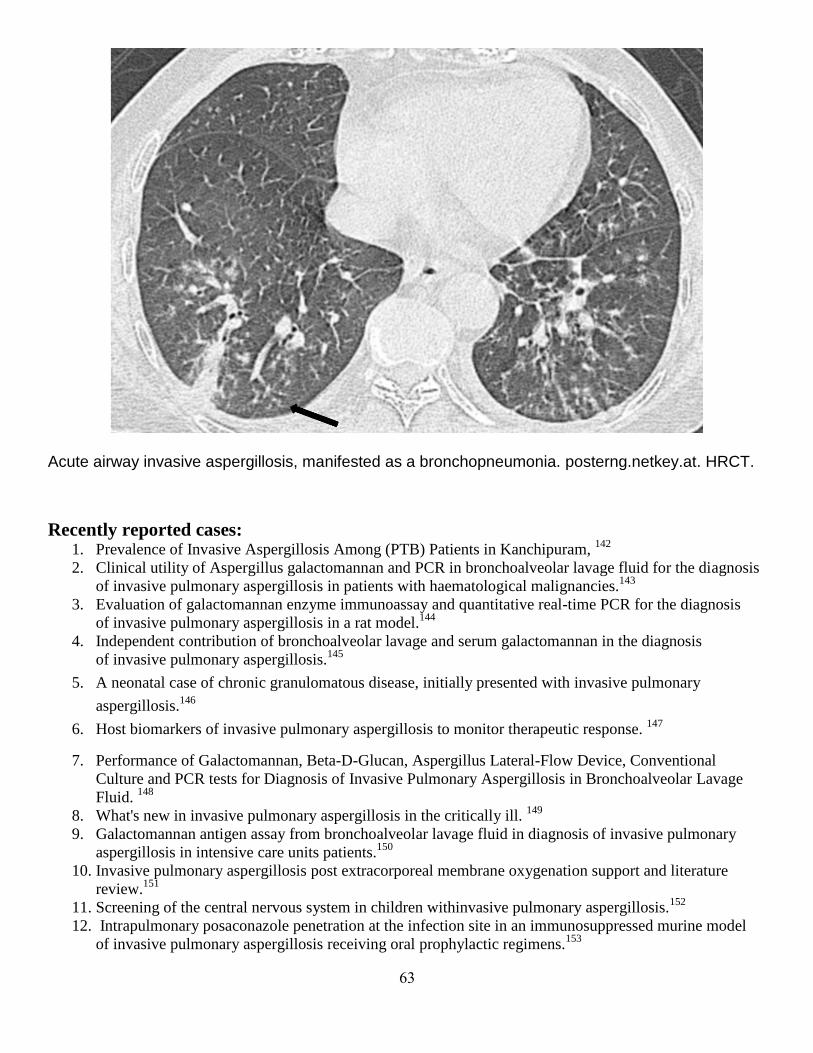
63
Acute airway invasive aspergillosis, manifested as a bronchopneumonia. posterng.netkey.at. HRCT.
Recently reported cases: 1. Prevalence of Invasive Aspergillosis Among (PTB) Patients in Kanchipuram,
142
2. Clinical utility of Aspergillus galactomannan and PCR in bronchoalveolar lavage fluid for the diagnosis
of invasive pulmonary aspergillosis in patients with haematological malignancies.143
3. Evaluation of galactomannan enzyme immunoassay and quantitative real-time PCR for the diagnosis
of invasive pulmonary aspergillosis in a rat model.144
4. Independent contribution of bronchoalveolar lavage and serum galactomannan in the diagnosis
of invasive pulmonary aspergillosis.145
5. A neonatal case of chronic granulomatous disease, initially presented with invasive pulmonary
aspergillosis.146
6. Host biomarkers of invasive pulmonary aspergillosis to monitor therapeutic response. 147
7. Performance of Galactomannan, Beta-D-Glucan, Aspergillus Lateral-Flow Device, Conventional
Culture and PCR tests for Diagnosis of Invasive Pulmonary Aspergillosis in Bronchoalveolar Lavage
Fluid. 148
8. What's new in invasive pulmonary aspergillosis in the critically ill. 149
9. Galactomannan antigen assay from bronchoalveolar lavage fluid in diagnosis of invasive pulmonary
aspergillosis in intensive care units patients.150
10. Invasive pulmonary aspergillosis post extracorporeal membrane oxygenation support and literature
review.151
11. Screening of the central nervous system in children withinvasive pulmonary aspergillosis.152
12. Intrapulmonary posaconazole penetration at the infection site in an immunosuppressed murine model
of invasive pulmonary aspergillosis receiving oral prophylactic regimens.153
64
13. Diagnosis of invasive pulmonary aspergillosis: updates and recommendations. 154
14. Approach to invasive pulmonary aspergillosis in critically ill patients.155
15. Invasive pulmonary aspergillosis after influenza a infection in an immunocompetent patient.156
.
16. Clinical findings in 19 cases of invasive pulmonary aspergillosis with liver cirrhosis. 157
17. Altered CD8(+) T-cell counts as an early predictor of prognosis in critically ill immunocompromised
patients with invasive pulmonary aspergillosis. 158
18. Prognostic value of serum galactomannan index in critically ill patients with chronic
obstructive pulmonary disease at risk ofinvasive pulmonary aspergillosis. 159
19. Real-life diagnosis of invasive pulmonary aspergillosis in a non neutropenic critically ill patient. 160
20. Hypothermic endpoint for an intranasal invasive pulmonary aspergillosis mouse model. 161
21. Early diagnosis and treatment of invasive pulmonary aspergillosis in a patient with cystic fibrosis.162
22. Early diagnosis of invasive pulmonary aspergillosis in hematologic patients: an opportunity to improve
the outcome. 163
23. Risk factors for invasive pulmonary aspergillosis and hospital mortality in acute-on-chronic liver failure
patients: a retrospective-cohort study. 164
24. Invasive pulmonary aspergillosis in patients with chronic obstructive pulmonary disease. 165
25. Coinfection of Pneumocystis jirovecii and invasive pulmonary aspergillosis in an immunocompromised
patient: a diagnostic challenge. 166
26. Isavuconazole (BAL4815) pharmacodynamic target determination in an in vivo murine model
of invasive pulmonary aspergillosis against wild-type and cyp51 mutant isolates of Aspergillus
fumigatus. 167
27. Diagnosis of airway-invasive pulmonary aspergillosis by tree-in-bud sign in an immunocompetent
patient: case report and literature review.168
28. The strategy for the diagnosis of invasive pulmonary aspergillosis should depend on both the underlying
condition and the leukocyte count of patients with hematologic malignancies. 169
29. Invasive pulmonary aspergillosis: prediction at thin-section CT in patients with neutropenia--a
prospective study.170
30. Invasive aspergillosis in the immunocompromised host: utility of computed tomography and
bronchoalveolar lavage. 171

65
5.1.5. Angioinvasive aspergillosis
Angioinvasive aspergillosis is most aggressive form of aspergillosis, with a mortality rate
that may exceed 50%.
It occurs when the hyphae invade bronchial wall and subsequently the accompanying
arterioles, with consequent thrombosis and the formation of necrotic hemorrhagic
nodules or subpleural wedge-shaped hemorrhagic infarcts.
It is seen almost exclusively in severely immunocompromised. Neutropenia is the most
important risk factor, following by prolonged Corticosteroid therapy, transplantation,
hematologic malignancy, Cytotoxic therapy and AIDS.
Aspergillus may disseminate to another organs, most commonly to the brain (seizures,
ring-enhancing lesions, cerebral infarctions, intracranial haemorrhage, meningitis and
epidural abscess), skin, kidneys, heart, esophagus and liver.
Radiographic abnormalities include single or multiple nodular infiltrates; segmental or
subsegmental consolidation; diffuse ground-glass pattern (often progressing to
consolidation) and cavitation (air-crescent sign); pleural effusions are uncommon.
Chest CT scan may shows multiple nodules surrounded by areas of ground-glass
attenuation known as halo sign and areas of segmental and non-segmental consolidation,
which are often bilateral, with or without a halo.“The halo sign” represents haemorrhage
around a pulmonary nodule and is highly suggestive of angioinvasive aspergillosis.
Another finding are wedge-shaped areas of consolidation with a broad base abutting a
peripheral pleural surface by hemorrhagic infarcts.
The cavitation and “air crescent sign" are viewed when area of necrotic tissue is
reabsorbed from the periphery, which causing retraction of the infarct from viable lung
parenchyma and leaves a space of air surrounding. This air-space doesn´t change with
position of patient and it´s different to monod sign of aspergilloma.
A typical image of Angioinvasive aspergillosis in a 45 year-old neutropenic patient after hematopoietic stem cell transplantation
(HSCT) , Tomas Franquet Casas, Hospital de Sant Pau in Barcelona

66
Angioinvasive aspergillosis ww.flickr.com
5.1.6. Aspergillus bronchitis and tracheobronchitis
Aspergillus tracheobronchitis is defined as an Aspergillus infection which is limited
entirely or predominantly confined to the tracheobronchial tree. In addition, Denning
suggested the term be applied to patients in whom there is evidence of bronchial and/or
tracheal inflammation, excess mucus production, with Aspergillus as the only pathogen
and without invasion of bronchial mucosa on biopsy, but full criteria for this diagnosis
have not been validated.
Aspergillus infection of the large airways has several manifestations. Many authors try to
propose a classification to describe the disease, but to date; there is still no ideal
classification. Overlapping clinical features can make cases difficult to classify.
Interestingly Young et al. described a non-invasive form of infection, with the bronchial
mucosa is usually preserved, but this contrasts with many reported invasive cases in
patients with immunosuppression and poor immunological host responses
Aspergillus fumigatus is the most common species being isolated (74-84%), followed
withAspergillus flavus (8-21%). Other Aspergillus species (3-5%) have also been
isolated, such as Aspergillus niger, Aspergillus terreus, Aspergillus
nidulans and Aspergillus versicolor
Wu et al.(2009) proposed a classification based on bronchoscopic morphology of the
intraluminal lesions into four types: superficial infiltration type (Type I), full-layer
involvement type (Type II), occlusion type (Type III) and mixed type (Type IV), then a
mixed type which an overlapping bronchoscopic features seen in all morphological types.
1. Superficial infiltration type: Inflammatory infiltration, mucosa
hyperaemia, mucosa oedematous and superficial ulcer which is confined to
the mucosa and submucosa; mild plaques of pseudomembrane formation
without obvious airway obstruction or deeper tissue invasion
2. Full-layer involvement type: Tracheobronchial lesions infiltrating through
the matrix layer of bronchi, often with substantial and deep ulceration,
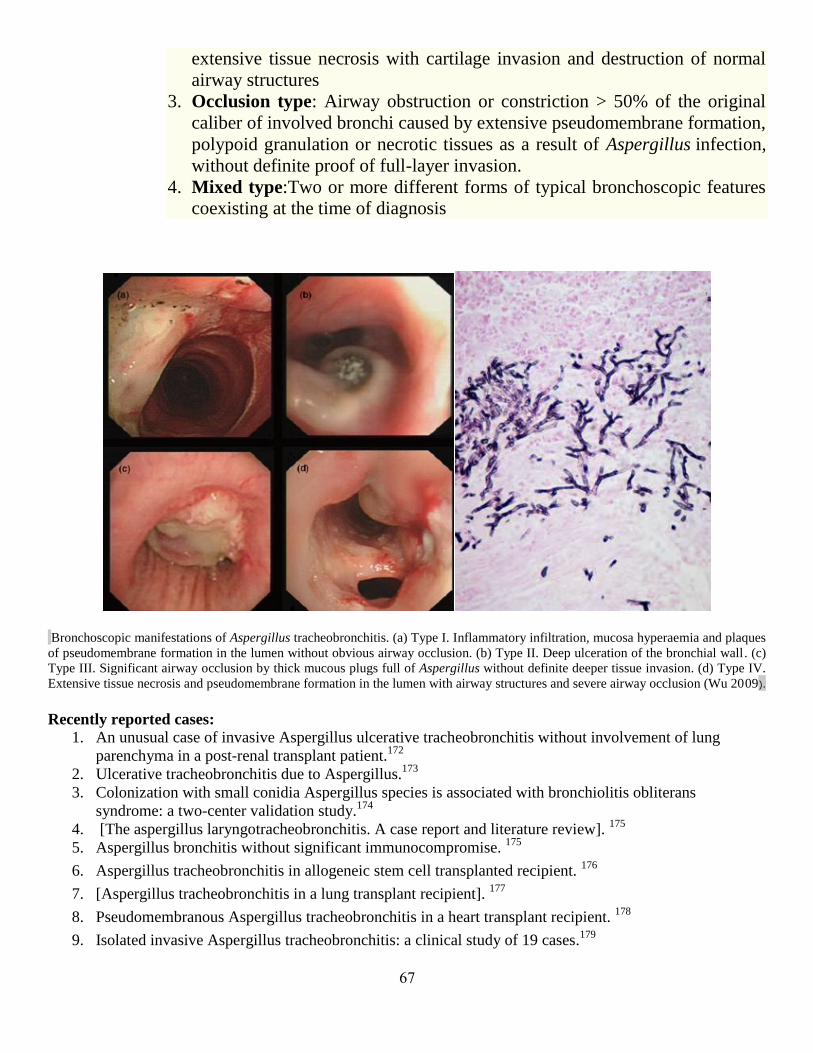
67
extensive tissue necrosis with cartilage invasion and destruction of normal
airway structures
3. Occlusion type: Airway obstruction or constriction > 50% of the original
caliber of involved bronchi caused by extensive pseudomembrane formation,
polypoid granulation or necrotic tissues as a result of Aspergillus infection,
without definite proof of full-layer invasion.
4. Mixed type:Two or more different forms of typical bronchoscopic features
coexisting at the time of diagnosis
Bronchoscopic manifestations of Aspergillus tracheobronchitis. (a) Type I. Inflammatory infiltration, mucosa hyperaemia and plaques
of pseudomembrane formation in the lumen without obvious airway occlusion. (b) Type II. Deep ulceration of the bronchial wall. (c)
Type III. Significant airway occlusion by thick mucous plugs full of Aspergillus without definite deeper tissue invasion. (d) Type IV.
Extensive tissue necrosis and pseudomembrane formation in the lumen with airway structures and severe airway occlusion (Wu 2009).
Recently reported cases:
1. An unusual case of invasive Aspergillus ulcerative tracheobronchitis without involvement of lung
parenchyma in a post-renal transplant patient.172
2. Ulcerative tracheobronchitis due to Aspergillus.173
3. Colonization with small conidia Aspergillus species is associated with bronchiolitis obliterans
syndrome: a two-center validation study.174
4. [The aspergillus laryngotracheobronchitis. A case report and literature review]. 175
5. Aspergillus bronchitis without significant immunocompromise. 175
6. Aspergillus tracheobronchitis in allogeneic stem cell transplanted recipient. 176
7. [Aspergillus tracheobronchitis in a lung transplant recipient]. 177
8. Pseudomembranous Aspergillus tracheobronchitis in a heart transplant recipient. 178
9. Isolated invasive Aspergillus tracheobronchitis: a clinical study of 19 cases.179

68
10. Ulcerative and pseudomembranous Aspergillus tracheobronchitis in a patient with acute myeloid
leukemia. 180
11. Aspergillus niger causing tracheobronchitis and invasive pulmonary aspergillosis in a lung transplant
recipient: case report. 181
12. Ulcerative tracheobronchitis due to Aspergillus.199
13. Tracheal oxalosis associated with Aspergillus niger tracheobronchitis. 200
14. Colonization with small conidia Aspergillus species is associated with bronchiolitis obliterans
syndrome: a two-center validation study. 201
15. [The aspergillus laryngotracheobronchitis. A case report and literature review].202
16. Aspergillus bronchitis without significant immunocompromise.203
17. Tracheobronchial Manifestations of Aspergillus Infections 204
.
18. Pseudomembranous Aspergillus tracheobronchitis in a heart transplant recipient.205
19. Isolated invasive Aspergillus tracheobronchitis: a clinical study of 19 cases. 206
5.1.7. Chronic cavitary pulmonary aspergillosis (CCPA)
The commonest symptom complex consists of weight loss, chronic cough, hemoptysis,
fatigue and shortness of breath.
While the clinical signs and symptoms of CCPA are non-specific, their presence and
severity is an important point of distinction from simple aspergilloma.
Radiological examination usually reveals one or more cavities, typically within the upper
lobes which may or may not contain fungus balls. New cavity formation or expansion of
one or more existing cavities over time is highly characteristic.
Peri-cavitary infiltrates and adjacent pleural thickening are frequently observed and
appear to be indicative of disease activity; these radiological abnormalities may remit
with effective antifungal therapy leaving residual thin-walled empty cavities.
Severe bilateral chronic pulmonary aspergillosis with the left upper lobe replaced by one large and several smaller
cavities. w ww.life-worldwide.org
69
Chronic cavitary pulmonary aspergillosis is a multicavitary disease in immunocompetent patients and progresses over time. Previous mycobacterium infection w ww.life-worldwide.org
Recently reported cases:
1. A prominent role for the IL1 pathway and IL15 in susceptibility tochronic cavitary pulmonary
aspergillosis. 182
2. Pulmonary aspergillosis in an immunocompetent patient. 183
3. Itraconazole in chronic cavitary pulmonary aspergillosis: a randomised controlled trial and systematic
review of literature.184
4. Cavitary pulmonary lesion associated with Aspergillus fumigatus infection in a German shepherd dog. 185
5. Distinct alleles of mannose-binding lectin (MBL) and surfactant proteins A (SP-A) in patients
with chronic cavitary pulmonary aspergillosis and allergic bronchopulmonary aspergillosis. 186
6. The efficacy and tolerability of voriconazole in the treatment ofchronic cavitary pulmonary
aspergillosis. 187
5.1.8. Disseminated aspergillosis (Invasive aspergillosis)
Invasive aspergillosis is generally seen in severely immunocompromised individuals and
carries a high mortality rate.
Risk factors for invasive aspergillosis include neutropenia, immunosuppressive therapy,
high-dose systemic corticosteroids, AIDS, solid organtransplant and haematopoietic stem
cell transplant.
The lungs are the most common site of primary invasive disease. The CNS is the most
common secondary site of invasive disease.
Invasive infections due to Aspergillus fumigatus are increasing, and despite new
therapies, are associated with greater than 50% mortality.
Invasion of blood vessels is a hallmark pathologic feature of invasive aspergillosis and
plays a critical role in the development of local and disseminated disease.
This process of angioinvasion and subsequent dissemination is unique to A. fumigatus
and a handful of other pathogenic molds, and its mechanism is not well understood.
Histopathologic studies suggest that there are several key steps by which the organism
gains entry to and subsequently exits from the vascular system.
Hyphae from an infectious focus must invade the abluminal surface of the blood vessel,
and penetrate endothelial cells to gain access to the blood vessel lumen.
Hyphal fragments are borne by the bloodstream to distal sites where they adhere to and
penetrate the luminal surface of the endothelial cells lining the blood vessel and
thereby invade the deep organs.
It is hypothesed that the interactions of A. fumigatus with the vascular endothelium are
critical to the pathogenesis of invasive aspergillosis.
71
Recently reported cases:
1. Primary gut aspergillosis in a patient with acute myeloid leukaemia: the importance of
early suspicion and definitive treatment.188
2. Disseminated aspergillosis as the herald manifestation of chronic granulomatous disease
in an adult patient. 189
3. Immune reconstitution syndrome-like entity in lung transplant recipients with
invasive aspergillosis.190
4. Aspergillus felis sp. nov., an emerging agent of invasiveas pergillosis in humans, cats,
and dogs. 191
5. [Mixed invasive fungal infection due to Rhizomucor pusillus and Aspergillus niger in an
immunocompetent patient.]192
6. [An autopsy case of ulcerative colitis with disseminated aspergillosis, complicated by
brain hemorrhage]. 193
7. Invasive aspergillosis masquerading as catastrophic antiphospholipid syndrome.194
8. Disseminated Aspergillosis due to Aspergillus niger in Immunocompetent Patient: A
Case Report. 195
9. Clinical experience in invasive fungal infections: multiple fungal infection as the first
presentation of HIV.196
10. Pharmacodynamics and dose-response relationships of liposomal amphotericin B against
different azole-resistant Aspergillus fumigatus isolates in a murine model of
disseminated aspergillosis. 197
11. Systemic dissemination of chronic necrotizing pulmonary aspergillosis in an elderly
woman without comorbidity: a case report. 198
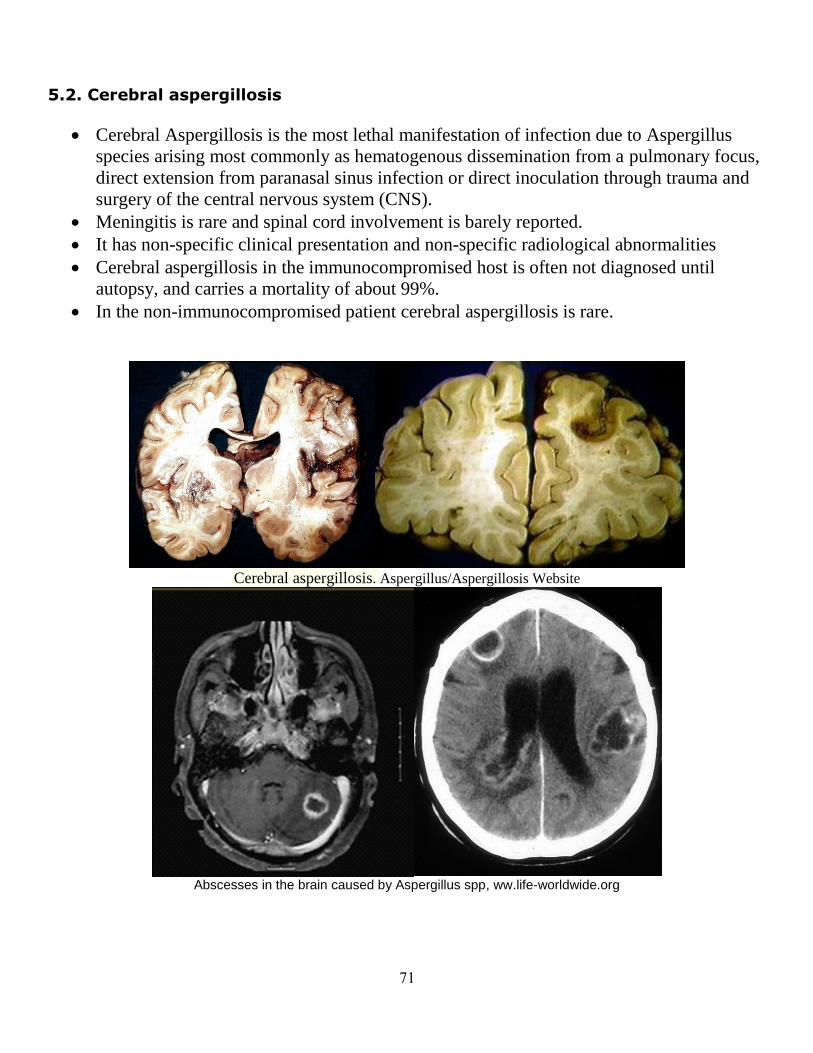
71
5.2. Cerebral aspergillosis
Cerebral Aspergillosis is the most lethal manifestation of infection due to Aspergillus
species arising most commonly as hematogenous dissemination from a pulmonary focus,
direct extension from paranasal sinus infection or direct inoculation through trauma and
surgery of the central nervous system (CNS).
Meningitis is rare and spinal cord involvement is barely reported.
It has non-specific clinical presentation and non-specific radiological abnormalities
Cerebral aspergillosis in the immunocompromised host is often not diagnosed until
autopsy, and carries a mortality of about 99%.
In the non-immunocompromised patient cerebral aspergillosis is rare.
Cerebral aspergillosis. Aspergillus/Aspergillosis Website
Abscesses in the brain caused by Aspergillus spp, ww.life-worldwide.org

72
Cerebral aspergillosis, brain biopsy, Braz J Infect Dis vol.12 no.4 Salvador Aug. 2008
Recently freported cases:
1. Improving Outcomes in Cerebral Aspergillosis. World Neurosurg. 207
2. High weekly doses of liposomal amphotericin B as secondary prophylaxis
after cerebral aspergillosis in a paediatric patient. 208
3. Striated enhancement sign in invasive cerebral fungal granuloma by Aspergillus: a case
report. 209
4. Cerebral aspergillosis in adult critically ill patients: a descriptive report of 10 patients
from the AspICU cohort. 210
5. A Case of Acute Cerebral Aspergillosis Complicating Influenza A/H1N1pdm 2009. 211
6. Cerebral aspergillosis and acute myeloid leukemia.212
7. Pituitary aspergillosis in a kidney transplant recipient and review of the literature. 213
8. Isolated Cerebral Aspergillosis in Immunocompetent Patients.214
9. Aspergillus brain abscess. 215
10. Cerebral aspergillosis with multiple enhancing nodules in the right cerebral hemisphere
in the immune-competent patient. 216
11. Unusual case of cerebral aspergillosis with clinical and imaging findings mimicking
lymphoma. 217
73
12. Early diagnosis of cerebral aspergillosis with various methods: a case report.218
13. Cerebral aspergillus infection in pediatric acute lymphoblastic leukemia induction
therapy. 219
14. Aspergillus galactomannan antigen for diagnosis and treatment monitoring
in cerebral aspergillosis.229
15. Cranial aspergilloma masquerading as meningioma.221
16. Antifungal therapy of aspergillosis of the central nervous system and aspergillus
endophthalmitis.222
17. Fatal case of cerebral aspergillosis : a case report and literature review. 223
18. Central nervous system aspergillosis: a series of 14 cases from a general hospital and
review of 123 cases from the literature.224
19. Relapsing cerebral aspergilloma associated with pregnancy.225
20. Treatment of refractory cerebral aspergillosis in a liver transplant recipient with
voriconazole: case report and review of the literature. 226
5.3. Cutaneous aspergillosis
Cutaneous aspergillosis has been described as primary or secondary to haematogenous
dissemination.
Primary cutaneous aspergillosis usually follows local trauma and appears as a purplish
oedematous lesion at the site of inoculation. Primary cutaneous aspergillosis is a rare
disease usually caused by Aspergillus fumigatus, Aspergillus flavus, Aspergillus terreus
and Aspergillus ustus.
It is usually seen in immunocompromised hosts, though some cases are also reported in
immunocompetent hosts.
It usually develops in relation to local trauma (intravenous injection site, injury or burns).
Clinically, it is characterized by the presence of violaceous macules, papules,
haemorrhagic bullae, ulcerations with central necrosis, and pustules or subcutaneous
abscess.
The occurrence of varying clinical manifestations of fungal diseases has been
demonstrated in patients with altered host defences. Immunocompromised patients with
primary cutaneous aspergillosis occasionally present with solitary non-ulcerated nodules.
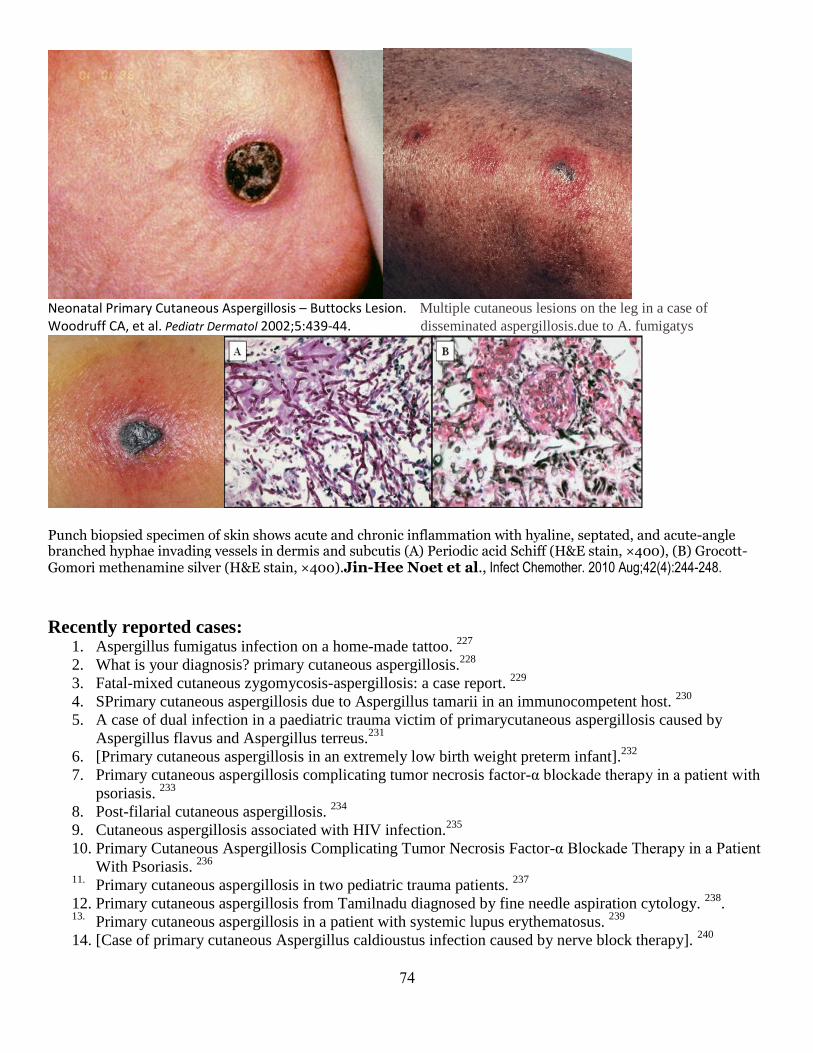
74
Neonatal Primary Cutaneous Aspergillosis – Buttocks Lesion. Multiple cutaneous lesions on the leg in a case of
Woodruff CA, et al. Pediatr Dermatol 2002;5:439-44. disseminated aspergillosis.due to A. fumigatys
Punch biopsied specimen of skin shows acute and chronic inflammation with hyaline, septated, and acute-angle branched hyphae invading vessels in dermis and subcutis (A) Periodic acid Schiff (H&E stain, ×400), (B) Grocott-Gomori methenamine silver (H&E stain, ×400).Jin-Hee Noet et al., Infect Chemother. 2010 Aug;42(4):244-248.
Recently reported cases: 1. Aspergillus fumigatus infection on a home-made tattoo.
227
2. What is your diagnosis? primary cutaneous aspergillosis.228
3. Fatal-mixed cutaneous zygomycosis-aspergillosis: a case report. 229
4. SPrimary cutaneous aspergillosis due to Aspergillus tamarii in an immunocompetent host. 230
5. A case of dual infection in a paediatric trauma victim of primarycutaneous aspergillosis caused by
Aspergillus flavus and Aspergillus terreus.231
6. [Primary cutaneous aspergillosis in an extremely low birth weight preterm infant].232
7. Primary cutaneous aspergillosis complicating tumor necrosis factor-α blockade therapy in a patient with
psoriasis. 233
8. Post-filarial cutaneous aspergillosis. 234
9. Cutaneous aspergillosis associated with HIV infection.235
10. Primary Cutaneous Aspergillosis Complicating Tumor Necrosis Factor-α Blockade Therapy in a Patient
With Psoriasis. 236
11. Primary cutaneous aspergillosis in two pediatric trauma patients.
237
12. Primary cutaneous aspergillosis from Tamilnadu diagnosed by fine needle aspiration cytology. 238
. 13. Primary cutaneous aspergillosis in a patient with systemic lupus erythematosus.
239
14. [Case of primary cutaneous Aspergillus caldioustus infection caused by nerve block therapy]. 240
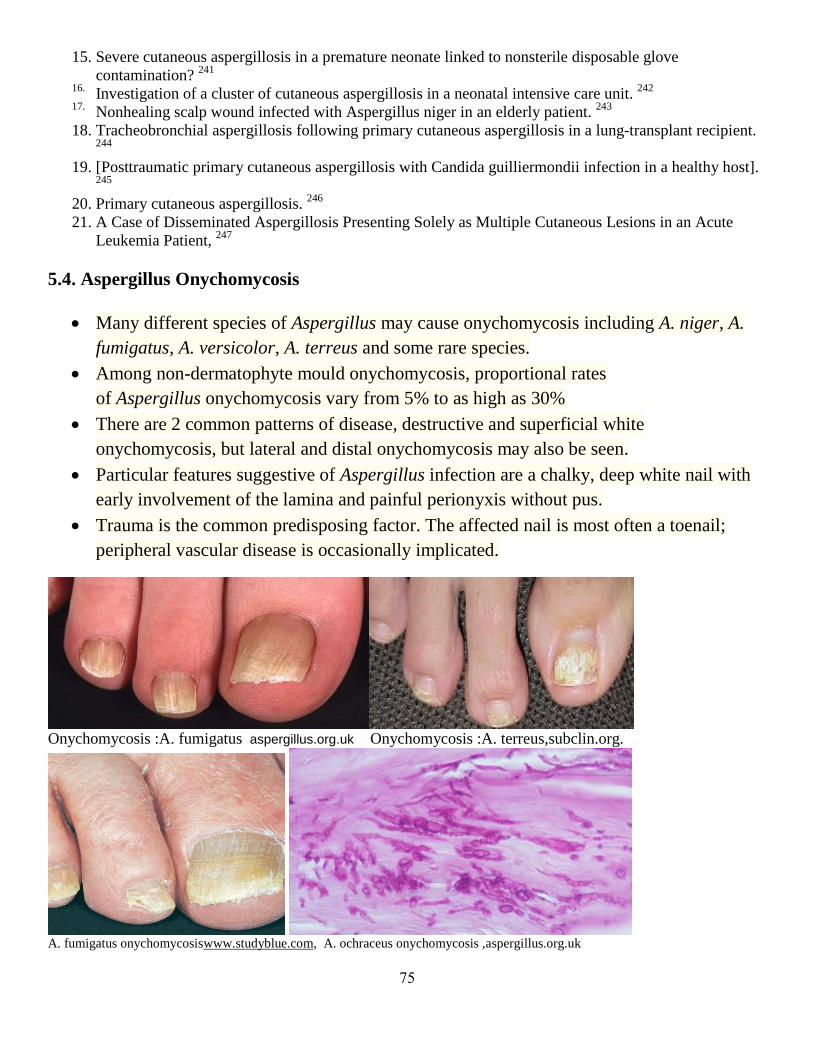
75
15. Severe cutaneous aspergillosis in a premature neonate linked to nonsterile disposable glove
contamination? 241
16. Investigation of a cluster of cutaneous aspergillosis in a neonatal intensive care unit.
242
17. Nonhealing scalp wound infected with Aspergillus niger in an elderly patient. 243
18. Tracheobronchial aspergillosis following primary cutaneous aspergillosis in a lung-transplant recipient. 244
19. [Posttraumatic primary cutaneous aspergillosis with Candida guilliermondii infection in a healthy host]. 245
20. Primary cutaneous aspergillosis. 246
21. A Case of Disseminated Aspergillosis Presenting Solely as Multiple Cutaneous Lesions in an Acute
Leukemia Patient, 247
5.4. Aspergillus Onychomycosis
Many different species of Aspergillus may cause onychomycosis including A. niger, A.
fumigatus, A. versicolor, A. terreus and some rare species.
Among non-dermatophyte mould onychomycosis, proportional rates
of Aspergillus onychomycosis vary from 5% to as high as 30%
There are 2 common patterns of disease, destructive and superficial white
onychomycosis, but lateral and distal onychomycosis may also be seen.
Particular features suggestive of Aspergillus infection are a chalky, deep white nail with
early involvement of the lamina and painful perionyxis without pus.
Trauma is the common predisposing factor. The affected nail is most often a toenail;
peripheral vascular disease is occasionally implicated.
Onychomycosis :A. fumigatus aspergillus.org.uk Onychomycosis :A. terreus,subclin.org.
A. fumigatus onychomycosiswww.studyblue.com, A. ochraceus onychomycosis ,aspergillus.org.uk
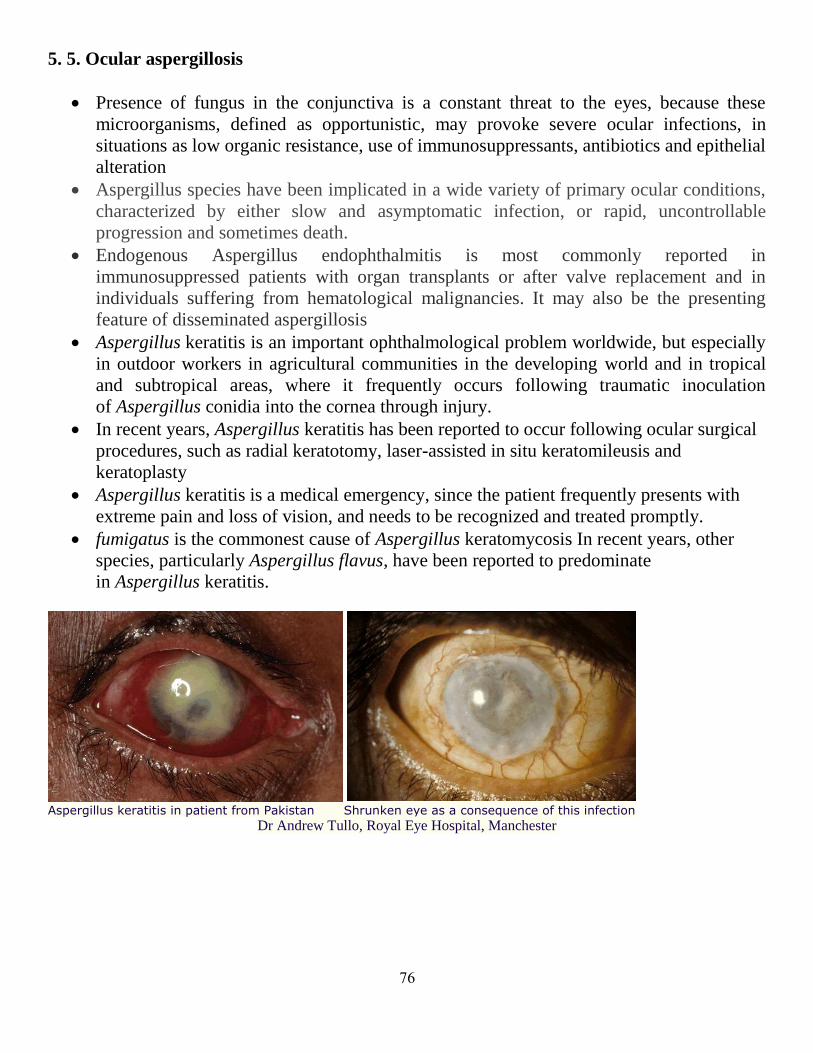
76
5. 5. Ocular aspergillosis
Presence of fungus in the conjunctiva is a constant threat to the eyes, because these
microorganisms, defined as opportunistic, may provoke severe ocular infections, in
situations as low organic resistance, use of immunosuppressants, antibiotics and epithelial
alteration
Aspergillus species have been implicated in a wide variety of primary ocular conditions,
characterized by either slow and asymptomatic infection, or rapid, uncontrollable
progression and sometimes death.
Endogenous Aspergillus endophthalmitis is most commonly reported in
immunosuppressed patients with organ transplants or after valve replacement and in
individuals suffering from hematological malignancies. It may also be the presenting
feature of disseminated aspergillosis
Aspergillus keratitis is an important ophthalmological problem worldwide, but especially
in outdoor workers in agricultural communities in the developing world and in tropical
and subtropical areas, where it frequently occurs following traumatic inoculation
of Aspergillus conidia into the cornea through injury.
In recent years, Aspergillus keratitis has been reported to occur following ocular surgical
procedures, such as radial keratotomy, laser-assisted in situ keratomileusis and
keratoplasty
Aspergillus keratitis is a medical emergency, since the patient frequently presents with
extreme pain and loss of vision, and needs to be recognized and treated promptly.
fumigatus is the commonest cause of Aspergillus keratomycosis In recent years, other
species, particularly Aspergillus flavus, have been reported to predominate
in Aspergillus keratitis.
Aspergillus keratitis in patient from Pakistan Shrunken eye as a consequence of this infection
Dr Andrew Tullo, Royal Eye Hospital, Manchester
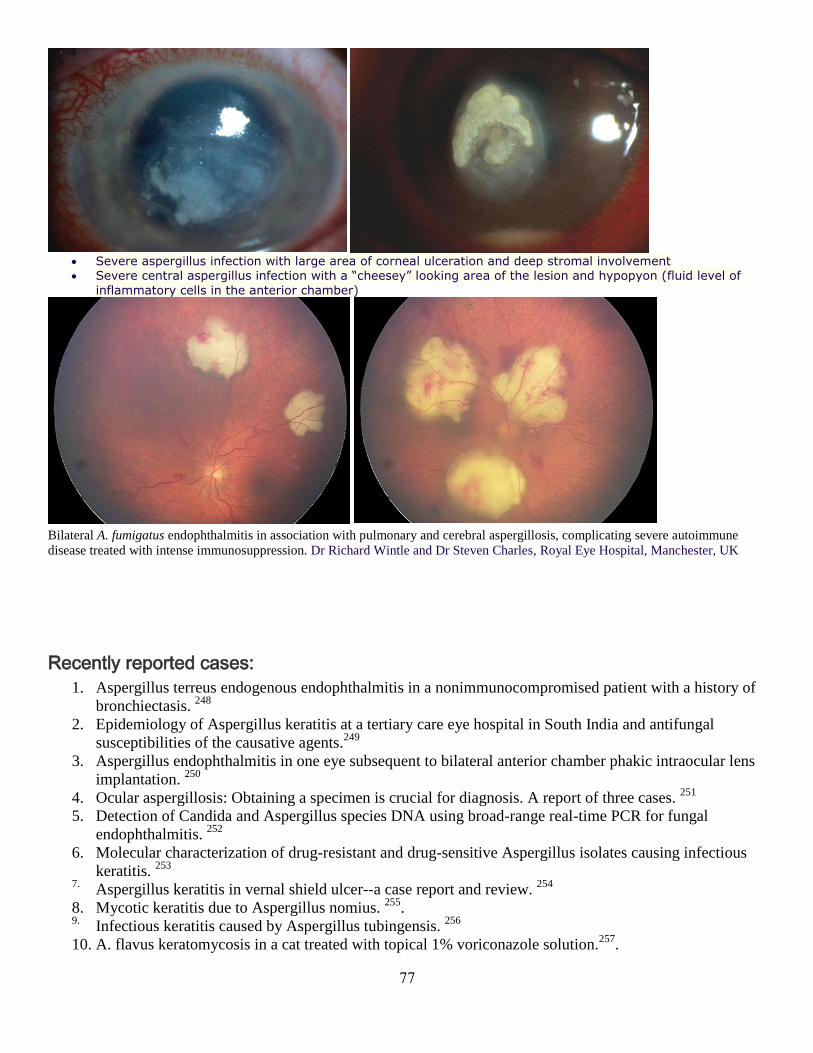
77
Severe aspergillus infection with large area of corneal ulceration and deep stromal involvement Severe central aspergillus infection with a “cheesey” looking area of the lesion and hypopyon (fluid level of
inflammatory cells in the anterior chamber)
Bilateral A. fumigatus endophthalmitis in association with pulmonary and cerebral aspergillosis, complicating severe autoimmune
disease treated with intense immunosuppression. Dr Richard Wintle and Dr Steven Charles, Royal Eye Hospital, Manchester, UK
Recently reported cases:
1. Aspergillus terreus endogenous endophthalmitis in a nonimmunocompromised patient with a history of
bronchiectasis. 248
2. Epidemiology of Aspergillus keratitis at a tertiary care eye hospital in South India and antifungal
susceptibilities of the causative agents.249
3. Aspergillus endophthalmitis in one eye subsequent to bilateral anterior chamber phakic intraocular lens
implantation. 250
4. Ocular aspergillosis: Obtaining a specimen is crucial for diagnosis. A report of three cases. 251
5. Detection of Candida and Aspergillus species DNA using broad-range real-time PCR for fungal
endophthalmitis. 252
6. Molecular characterization of drug-resistant and drug-sensitive Aspergillus isolates causing infectious
keratitis. 253
7. Aspergillus keratitis in vernal shield ulcer--a case report and review.
254
8. Mycotic keratitis due to Aspergillus nomius. 255
. 9. Infectious keratitis caused by Aspergillus tubingensis.
256
10. A. flavus keratomycosis in a cat treated with topical 1% voriconazole solution.257
.

78
5.6. Aspergillus sinusitis
Aspergillus disease can happen in the sinuses leading to Aspergillus sinusitis. Just as in
the lungs, Aspergillus can cause the three diseases - allergic sinusitis, a fungal ball or
invasive aspergillosis.
Allergic disease is associated with long standing symptoms of a runny blocked up nose,
and may lead to nasal polyps.
The fungal ball caused by Aspergillus happens in a similar way to an aspergilloma. In
those with normal immune systems, stuffiness of the nose, chronic headache or
discomfort in the face is common.
When patients have damaged immune systems - if, for example they have had leukaemia
or have had a bone marrow transplant - Aspergillus sinusitis is more serious. In these
cases the sinusitis is a form of invasive aspergillosis. The symptoms include fever, facial
pain, nasal discharge and headaches.
Base of skull at autopsy showing pus in the sphenoid sinus and destruction of the lateral wall of the sinus, as demonstrated on the CT
scan. Cultures from the sinus and brain abscess grew Aspergillus fumigatus, ww.njmoldinspection.com
Recently reported cases:
1. [Allergic fungal sinusitis--new aspects of clinical features, laboratory diagnosis and therapy]. 258
.
2. Aspergillosis sinusitis with cranio-orbital spread in an apparently immunocompetent patient. 259
3. Mycotic aneurysm due to Aspergillus sinusitis.
260
4. Coexistence of allergic bronchopulmonary aspergillosis and allergic aspergillus sinusitis in a patient
without clinical asthma. 261
5. [Clinicopathologic study of invasive fungal rhinosinusitis caused by Aspergillus and Mucorales] 262
6. [Cellular and tissue reactions of the mucous membrane of the maxillary sinus in the patients presenting
with odontogenic aspergillous maxillary sinusitis]. 263
7. [Application of PCR combined with reverse line blot assay in detection and identification of common
pathogenic Aspergillusin fungal sinusitis]. 264

79
5.7. Paranasal sinuses aspergillosis
Paranasal sinus Aspergillosis is now classified into invasive (acute fulminant, chronic
invasive, granulomatous invasive) and non-invasive (fungus ball and allergic fungal
rhinosinusitis) forms with their own pathophysiology and clinical presentation.
Any type of paranasal Aspergillosis may progress to more aggressive disease illustrating
the importance of early recognition of this increasingly encountered disease.
Prerequisites for diagnosis are sinonasal polyps, infiltrative or non-infiltrative fungal
hyphae on microscopy with Potassium Hydroxide (KOH) and histopathological
examination of the resected polyps and positive fungal culture of the tissue following
surgery.
Intracranial spread of the infection occurs due to close proximity of the sinuses with
cranial cavity. It is a dreaded complication, as it is usually fatal if not treated promptly.
Orbital involvement occurs by contiguous spread of the disease from paranasal sinuses,
by expansion or bone erosion due to pressure effect of the polyps or fungal tissue
invasion.
It is considered to worsen the prognosis of sinonasal aspergillosis. Moreover, the superior
orbital fissure and optic canal directly open into the middle cranial fossa, and are ready
pathways for further intracranial spread of the infection.
Acute inflammatory polyp obstructing the sinuses in an operational patient Allergic polyps with fungal infection, Vijay K. Andad
Left:Double density sign (white arrows) of non-invasive aspergillus infection of paranasal sinuses on coronal
contrast enhanced CT scan.Right:Extensive sino-nasal polyposis (white arrow) involving all sinus cavities and
nose on coronal contrast enhanced CT scan.

81
Sections of the maxillary sinus show (a) Aspergillus in necrotic background (H and E, ×250), (b) fungal hyphae
in giant cell (H and E, ×400), (c) many eosinophils and hyphae (H and E, ×250), special stains highlighting the
fungal morphology (d; PAS, ×250) and (e; silver methanamine, ×250). Divya Sharma, Nidhi Mahajan, Seema Rao, Nita
Khurana, Shyama Jain, Department of Pathology, Maulana Azad Medical College, New Delhi, India
Recently reported cases 1. Diagnosis and treatment of paranasal sinus fungus ball of odontogenic origin: case report.
265
2. Computed tomographic features of feline sino-nasal and sino-orbital aspergillosis. 266
3. Granulomatous invasive aspergillosis of paranasal sinusesmasquerading as actinomycosis and review of
published literature. 267
4. ABPA Concomitantly Occurring with Invasive SinusAspergillosis: A Short Report on Two Patients. 268
5. [Allergic fungal sinusitis--new aspects of clinical features, laboratory diagnosis and therapy]. 269
6. [Invasive aspergillosis of sphenoidal sinus in a patient in Djibouti, revealed by palsy of cranial nerves: a
case report]. 270
7. Invasive fungal rhinosinusitis.271
8. [Unilateral frontal sinus aspergillosis: the combined endoscopic and mini-trephination approach]. 272
9. Isolated primary frontal sinus aspergillosis: role of endonasal endoscopic approach.
273
10. Chronic invasive aspergillosis of paranasal sinuses: A case report with review of literature. 274
11. Highly effective unconventional management of aspergillosis of the left maxillary sinus in an 11-year-
old girl with rhabdomyosarcoma embryonale of the frontal sinus. 275
12. [Chronic diseases of the nose and nasal sinuses in cats: a retrospective study]. 276
13. Simultaneous actinomycosis with aspergillosis in maxillary sinus. 277
14. Clotrimazole and enilconazole distribution within the frontalsinuses and nasal cavity of nine dogs with
sinonasalaspergillosis. 278
81
15. [Invasive aspergillosis of the maxillary sinus in an immunocompetent patient].279
16. Aspergillus Infection of Paranasal Sinuses.
280
5.8. Otoaspergillosis (Otomycosis)
Otomycosis is subacute or chronic superficial fungal infection of the external auditory
canal and auricle. It is the most frequently encountered fungal infection in ear, nose and
throat clinics. The fungi are usually secondary invaders of tissue already rendered
susceptible by bacterial infections, physical injury or excessive accumulation of cerumen
in the external auditory canal. Sometimes it is merely non-pathogenic fungal colonization
of the external auditory canal.
The disease is worldwide in distribution. Otomycosis is more prevalent in warm, humid
climates, particularly in the rainy season as compared to arid or cold climates. It is more
frequent in individuals of lower socio-economic status with poor hygienic conditions.
There are many local predisposing factors of otomycosis such as chronic infection of the
ear, use of oils, ear-drops, steroids, swimming and evidence of fungal infection
elsewhere. Local lesions observed in bacterial otitis create favourable conditions for the
growth of fungi in the external and middle ear, as well as in post-operative cavities,
especially in cases of open-type surgery. Persistent wetness of the external auditory canal
predisposes to fungal
In about 75-92% cases of otomycosis, Aspergillus genus alone is the causative
agent. A. niger is the most common cause, with occasional cases caused by A.
flavus and A. fumigatus .
Otomycosis usually presents with a history of itching, irritation, discomfort, pain and
scanty discharge from the affected ear. There is also a feeling of blockage in the ear due
to collection of debris material in external auditory canal. Irritation is more marked in
fungal as compared to bacterial otitis externa. Pruritus and discharge are the most
common symptoms, with reddened epidermis and lining of the tympanic cavity being
common.
Otoscopic examination reveals infection confined to the ear canal. There is greenish or
black fuzzy growth on cerumen or debris resembling wet ‘blotting paper’, which may fill
up the entire meatus. There may be slight conduction deafness also due to mechanical
obstruction of the external auditory canal. The local area may be hyperemic and
sometimes bleeding may be observed. In immunocompromised patients especially
diabetics, Aspergillus may invade locally to adjacent anatomical sites like mastoid bone
or even brain.
Aspergillus may cause invasive external otitis (necrotizing or malignant otitis externa)
with local spread to bone and cartilage, which is a severe and potentially life-threatening
disease. This may be associated with underlying immunocompromised situation, diabetes
mellitus or patient receiving haemodialysis entailing high mortality. Invasive otitis
externa is more frequently caused by A. fumigatus than A. niger . In addition,

82
invasive Aspergillus tympanomastoiditis may be encountered in immunocompetent
patients as well.
Otomycosis (Aspergillus niger) , Dr. T. Balasubramanian
Recently reported cases
1. Otomycosis in the north of Iran: common pathogens and resistance to antifungal agents. Eur Arch
Otorhinolaryngol. 281
2. Prevalence of otomycosis in Khouzestan Province, south-west Iran.
282
3. Otomycosis in central iran: a clinical and mycological study. 283
4. Otomycosis in immunocompetent and immunocompromised patients: comparative study and literature
review. 284
5. Molecular identification and antifungal susceptibilities of blackAspergillus isolates
from otomycosis cases in Hungary. 285
6. Species assignment and antifungal susceptibilities of black aspergilli recovered from otomycosis cases
in Iran. 286
7. Otomycosis due to filamentous fungi. 287
8. Prevalence of otomycosis in Ibadan: a review of laboratory reports.
288
9. Otomycosis: Diagnosis and treatment. 289
5.9. Aspergillus endocarditis
Most cases of Aspergillus endocarditis (AE) involve adults.
Pre-requisites for developing AE. are valvular anatomic abnormalities, rheumatic heart
disease, previous bacterial endocarditis. previous surgery.
Conditions that predispose to invasive fungal infections (eg malignancy, antimicrobial
use, neutropenia, injecting drug use and immunosuppressive states and therapy) are also
commonly found in AE.

83
Diagnosis of AE is difficult and frequently delayed: the diagnosis is made post-mortem.
Blood cultures are almost always negative. Mycological examination of vegetations or
emboli is the most common means of diagnosis.
Crude mortality from FE in general is around 72% although in recent years this has
dropped to around 59%. For AE the mortality rate was 68% (McCormack, 2010). The
cause of death is directly attributable to Aspergillus in 90% of cases and is usually due to
catastrophic valvular failure or complications secondary to major embolic phenomena:
usually cerebral.
Aspergillus endocarditis, www.aspergillus.org.uk Aspergillus pericarditis
Recently reported cases:
1. Aspergillus endocarditis in a paediatric patient after a cardiac surgery, associated with septic pulmonary
embolism and pulmonary hypertension. 290
2. Isolated aspergillosis myocardial abscesses in a liver-transplant patient. 291
3. Acute myocardial infarction caused by coronary embolism from Aspergillus endocarditis.292
4. Aspergillus pacemaker lead endocarditis. 293
5. Fungal endocarditis. 294
6. Successful surgical intervention in an unusual case of Aspergillus endocarditis with acute myeloid
leukemia. 295
7. . [Aspergillus prosthetic aortic valve endocarditis; report of a case]. 296
8. Aspergillus endocarditis in lung transplant recipient: successful surgical treatment. 297
9. The tell-tale heart: Aspergillus fumigatus endocarditis in an immunocompetent patient. 298
10. Aspergillus endocarditis in the era of new antifungals: major role for antigen detection. 299
11. A Report of 2 Cases of Disseminated Invasive Aspergillosis with Myocarditis in Immunocompromised
Patients . 300
12. Aspergillus endocarditis in a native valve without prior cardiac surgery. 301
13. Aspergillus endocarditis: a case of near complete left ventricular outflow obstruction.302
14. NikoTwo cases of aspergillus endocarditis in non neutropenic children on chemotherapy for acute
lymphoblastic leukaemia. 303
15. Infective endocarditis due to Aspergillus following kidney transplantation. 304
16. Molecular diagnosis of Aspergillus fumigatus endocarditis. 305
17. . Cardiac aspergillosis: endocardial or endomyocardial? 306
18. [Cardiac invasive aspergillosis in a heart transplant recipient]. 307
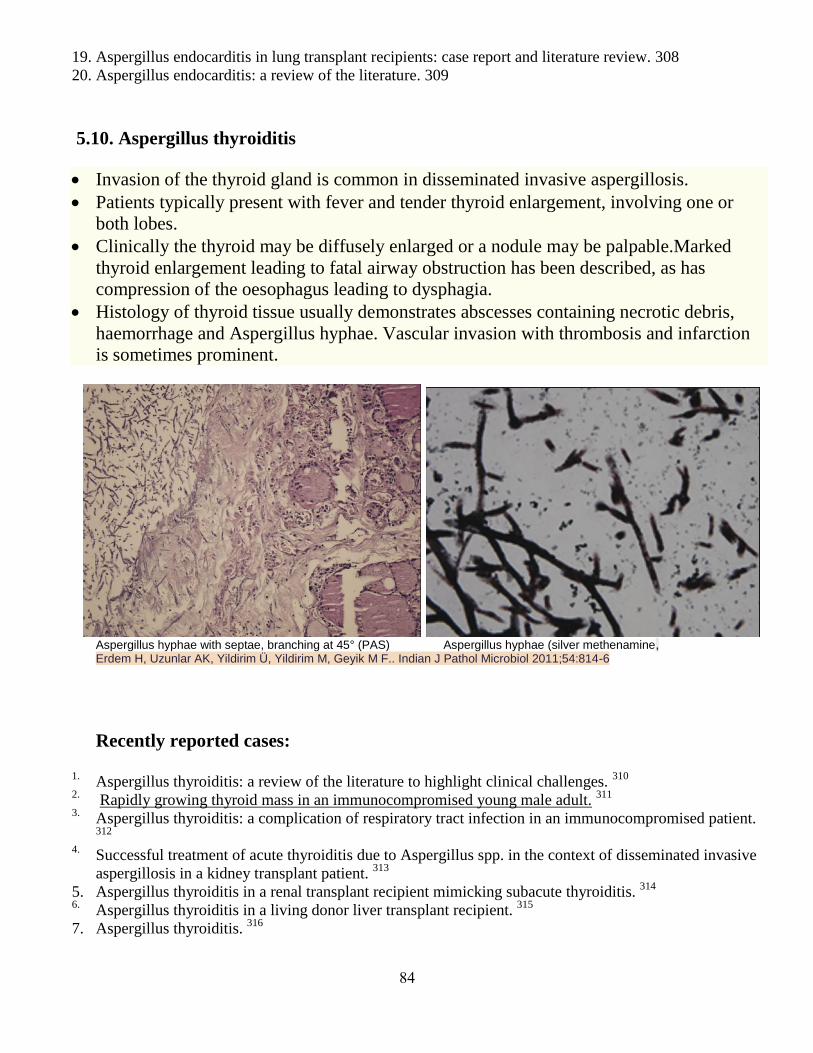
84
19. Aspergillus endocarditis in lung transplant recipients: case report and literature review. 308
20. Aspergillus endocarditis: a review of the literature. 309
5.10. Aspergillus thyroiditis
Invasion of the thyroid gland is common in disseminated invasive aspergillosis.
Patients typically present with fever and tender thyroid enlargement, involving one or
both lobes.
Clinically the thyroid may be diffusely enlarged or a nodule may be palpable.Marked
thyroid enlargement leading to fatal airway obstruction has been described, as has
compression of the oesophagus leading to dysphagia.
Histology of thyroid tissue usually demonstrates abscesses containing necrotic debris,
haemorrhage and Aspergillus hyphae. Vascular invasion with thrombosis and infarction
is sometimes prominent.
Aspergillus hyphae with septae, branching at 45° (PAS) Aspergillus hyphae (silver methenamine, Erdem H, Uzunlar AK, Yildirim Ü, Yildirim M, Geyik M F.. Indian J Pathol Microbiol 2011;54:814-6
Recently reported cases:
1. Aspergillus thyroiditis: a review of the literature to highlight clinical challenges.
310
2. Rapidly growing thyroid mass in an immunocompromised young male adult. 311
3. Aspergillus thyroiditis: a complication of respiratory tract infection in an immunocompromised patient. 312
4. Successful treatment of acute thyroiditis due to Aspergillus spp. in the context of disseminated invasive
aspergillosis in a kidney transplant patient. 313
5. Aspergillus thyroiditis in a renal transplant recipient mimicking subacute thyroiditis. 314
6. Aspergillus thyroiditis in a living donor liver transplant recipient.
315
7. Aspergillus thyroiditis. 316
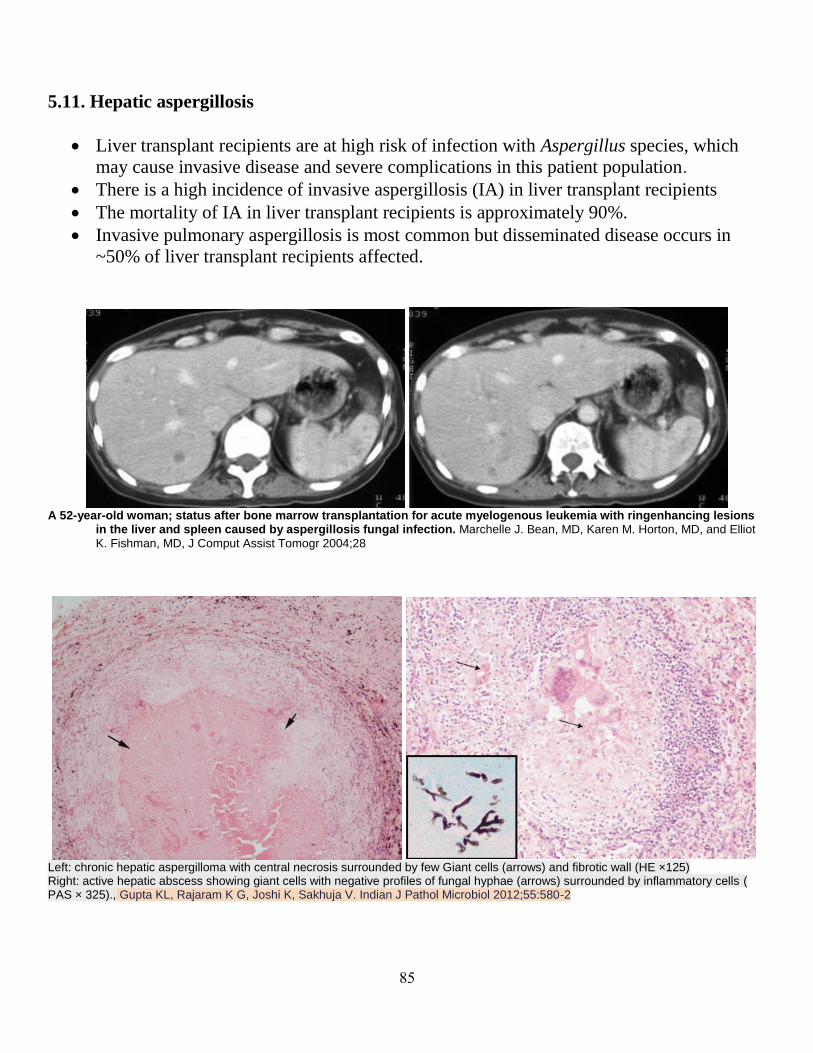
85
5.11. Hepatic aspergillosis
Liver transplant recipients are at high risk of infection with Aspergillus species, which
may cause invasive disease and severe complications in this patient population.
There is a high incidence of invasive aspergillosis (IA) in liver transplant recipients
The mortality of IA in liver transplant recipients is approximately 90%.
Invasive pulmonary aspergillosis is most common but disseminated disease occurs in
~50% of liver transplant recipients affected.
A 52-year-old woman; status after bone marrow transplantation for acute myelogenous leukemia with ringenhancing lesions
in the liver and spleen caused by aspergillosis fungal infection. Marchelle J. Bean, MD, Karen M. Horton, MD, and Elliot
K. Fishman, MD, J Comput Assist Tomogr 2004;28
Left: chronic hepatic aspergilloma with central necrosis surrounded by few Giant cells (arrows) and fibrotic wall (HE ×125) Right: active hepatic abscess showing giant cells with negative profiles of fungal hyphae (arrows) surrounded by inflammatory cells ( PAS × 325)., Gupta KL, Rajaram K G, Joshi K, Sakhuja V. Indian J Pathol Microbiol 2012;55:580-2
86
Recently reported cases:
1. Primary hepatic aspergillosis following induction chemotherapy for acute leukemia. 317
2. Progression of hepatic aspergillosis following second renal transplantation in a patient with recurrent
glomerulonephritis. 318
3. Invasive aspergillosis in patients with severe alcoholic hepatitis. 319
4. Aspergillosis after liver transplantation in the context of common variable immunodeficiency: case
report. 320
5.12. Gastrointestinal aspergillosis
There are few reports in the literature of gastrointestinal aspergillosis without
pulmonary involvement as the initial presentation of disseminated disease.
Tumour-like masses (aspergillomas) in the gastrointestinal tract have been very rarely
reported.
The port of entry is usually the lungs and wide dissemination is possible after vascular
invasion.
The gastrointestinal tract may be involved via oesophageal or bowel ulceration,
especially in the immunocompromised host.
Necrotizing enterocolitis may precede aspergillosis and disruption of mucosal barriers
may provide a port of entry for germinating spores.
The features of gastrointestinal tract involvement are mild anaemia, weight loss,
diarrhoea with malabsorption, in the absence of any other cause for the diarrhoea,
gastrointestinal haemorrhage and a swinging fever not responding to antibiotics.
Occasionally, there may by signs of peritonitis, especially if there is bowel perforation
or infarction.
Gastrointestinal haemorrhage is a known complication of aspergillus infection of the gut.
This may be due to gut infarction, colonic or duodenal ulceration.
Uncontrollable upper gastrointestinal bleeding due to erosion into the descending aorta,
resulting in a rapidly fatal outcome, has been reported in oesophageal aspergilloma.
Recently reported cases:
1. Primary gastrointestinal aspergillosis 6 months after allogeneic hematopoietic cell transplantation: a case
report.321
2. Invasive Aspergillus infection localized to the gastric wall: report of a case. 322
3. A retrospective series of gut aspergillosis in haematology patients.323
4. A case of isolated invasive Aspergillus colitis presenting with hematochezia in a nonneutropenic patient
with colon cancer. 324
5. Necrotizing colitis caused by systemic aspergillosis in a burn patient.325
6. Successful treatment of acute thyroiditis due to Aspergillus spp. in the context
of disseminated invasive aspergillosis in a kidney transplant patient. 326
87
5.13. Urinary tract aspergillosis
Aspergillosis limited to the urinary tract is a rare disease, often occurring in
immunocompromised patients.
Three different patterns of renal Aspergillus infection have been: disseminated
aspergillosis with hematogenous renal involvement, aspergillosis of the renal pelvis with
bezoars formation, and ascending panurothelial aspergillosis. Extrarenal aspergillosis of
the urinary tract is sparse, with few cases of testicular and adrenal involvement being
described.
The kidney is the most frequently involved part of the urinary tract in invasive
aspergillosis.
Both bladder and prostate aspergillosis are also described.
Outflow obstructive symptoms, similar to those due to benign prostate hypertrophy
(BPH) are predominant. Other related symptoms could be dysuria, perineal or suprapubic
discomfort and hematuria.
The prostate fungal infection is indistinguishable from BPH, bacterial and tuberculus
prostatitis or malignancy of the gland. Prolonged courses of antibiotics, steroid intake and
an indwelling bladder catheter have been identified as presumed predisposing factors in
these cases.
Renal involvement is usually silent if the disease is localised to the cortex of the kidney
and is a relatively frequent finding at autopsy in the context of disseminated disease.
Despite the increased incidence of invasive aspergillosis in transplant recipients, urinary
tract infections caused by Aspergillus species are uncommon and usually as a
consequence of a systemic haematogenous dissemination, characterized by multiple
parenchymal microabscesses.
More common, although still rare, is renal pelvis involvement. Involvement may be
unilateral or bilateral. Typical host groups include diabetics and intravenous drug
abusers. Fungal masses (bezoars) fill the pelvis of the kidney causing hydronephrosis.
These masses may be passed in the urine as `balls' and may cause renal colic.
Anuria due to bilateral ureteral obstruction with mycelial clumps, although rare, has been
recently reported. Aspergillus is usually cultured from the urine and can be cultured and
visualised in the fungal balls.
Recently reported cases:
1. An unusual case of non-disseminated bladder aspergillosis in a setting of transitional cell carcinoma. 327
2. Nosocomial urinary tract aspergilloma in an immunocompetent host: an unusual occurrence. 328
3. Localized primary renal aspergillosis in a diabetic patient following lithotripsy--a case report. 329
4. An unusual cause of ureteral obstruction in a renal transplant recipient: ureteric aspergilloma. 330
5. Aspergillus in a cervico-vaginal smear of an adult postmenopausal female: An unusual case. 331
.
6. Isolated bladder aspergillosis as the primary presentation of non-oliguric acute renal failure. 332
88
7. Aspergillus "fungus ball" of the bladder after hematopoietic transplantation in a pediatric patient:
successful treatment with intravesical voriconazole and surgery. 333
8. Emphysematous renal tract disease due to Aspergillusfumigatus. 334
9. Renal aspergillosis secondary to renal intrumentation in immunocompetent patient.
335
10. Aspergillosis prostatitis post-renal transplantation. 336
11. Prostatitis and epididymo-orchitis due to Aspergillus fumigatus in a patient with AIDS. 337
12. [Aspergillus prostatitis and prolonged corticotherapy. Apropos of a case report].
338
13. [Renal aspergilloma: first manifestation of an occult sarcomatoid carcinoma]. 339
14. Aspergillus vertebral osteomyelitis and ureteral obstruction after liver transplantation. 340
5.13. Aspergillus osteomyelitis
Aspergillus osteomyelitis is an uncommon manifestation of invasive aspergillosis. It may
involve bones of the axial or appendicular skeleton.
Aspergillus osteomyelitis is a particularly important cause of morbidity and mortality in
immunocompromised hosts, especially in patients with chronic granulomatous disease,
solid organ transplantation (SOT) and hematopoietic stem cell transplantation (HSCT),
diabetes mellitus, and chronic corticosteroid use. Furthermore, Aspergillus osteomyelitis
also is reported in alcoholics and illicit intravenous drug
use.Notably, Aspergillus osteomyelitis is reported in patients without apparent
immunodeficiency.
Symptoms and signs of Aspergillus osteomyelitis tend to be non-specific.
Histopathology and microbiologic examination of bone tissue biopsy are the gold
standards for identification of Aspergillus spp.
Vertebral osteomyelitis with or without discitis is the most common osteoarticular
manifestation of Aspergillus. It may be caused by hematogenous dissemination from a
distant site, by traumatic or surgical inoculation, or more rarely, from adjacent tissues,
usually lungs. Host factors associated with Aspergillus vertebral osteomyelitis include
chronic granulomatous disease, primary monocyte killing deficiency, chronic obstructive
pulmonary disease treated with inhaled or systemic corticosteroids, intravenous
corticosteroid treatment, solid organ transplantation, HSCT, diabetes mellitus,
hematological malignancies, illicit intravenous drug use, pulmonary aspergillosis, and
prior back surgery.
Sternal aspergillosis is strongly associated with thoracic surgery. The route of infection
is likely through direct inoculation of the wound through surgery, post-operative wound
care or airborne transmission of conidia. Aspergillus sternal osteomyelitis may present in
the immediate post-operative period, or later in the ensuing weeks, months, or even years
after the operation
Osteomyelitis of the Ribs and Long Bones is common in patients with chronic
granulomatous disease, immunosuppressed recipients of solid organ transplants and
individuals who have experienced traumatic or surgical inoculation of affected bones.

89
Primary rib and long bone aspergillosis in immunocompetent individuals may rarely
occur.
Invasive Aspergillus mastoiditis may develop as an extension of infection from the
middle ear into the mastoid process, petrous and temporal bones. It is characterized by
otalgia, otorrhea, hearing loss and cranial nerve deficits, Aspergillus mastoiditis may be
indolent or rapidly progressive. Chronic fungal otitis media and regional surgical
procedures may progress to invade the petrous bone, transverse venous sinus, and
the cranial nerves, resulting in sinus thrombosis, cranial nerve palsies, and high mortality.
Aspergillus osteomyelitis of the cranium and mandible may occur as a sequela of other
infectious processes, e.g., invasive Aspergillus otitis or sinusitis. There are different
routes via which Aspergillus may invade the temporal bone and lateral skull base, such as
the external ear or the tympanic cavity during the process of acute or chronic otitis media.
Aspergillosis of the skull may also develop secondary to traumatic or surgical
inoculation.
Joint space infection caused by Aspergillus spp. (Septic arthritis) is uncommon.
Septic arthritis may be subsequent to hematogenous dissemination of pulmonary
aspergillosis, dissemination fromadjacent bone tissue infection, or associated with
traumatic or surgical manipulation. Aspergillus septic arthritis is commonly associated
with intra-articular corticosteroid injections and orthopedic hardware. Other host factors
that may exist simultaneously, with or independent of iatrogenic inoculation
of Aspergillus into the joint, include malignancy and its management, neutropenia, solid
organ or HSCT receipt, GVHD, alcoholic cirrhosis, and chronic granulomatous
disease. Aspergillus septic arthritis rarely occurs in an otherwise healthy host,
independent of any potential iatrogenic inoculation. Aspergillosis of the joint space also
may occur in the context of disseminated aspergillosis.
Axial high-resolution computed tomography scan of temporal bone demonstrating R (right) - soft tissue lesion (*) involving the tympanic membrane (TM) and external auditory canal (EAC) L (left) - soft tissue lesion (a) involving the TM and EAC with
erosion of posterior canal wall and facial canal near 2nd
genu (b). Bradoo RA, Shah KD, Gayathri H, Kapadia MA. Invasive
aspergillosis of the temporal bone. Indian J Otol 2012;18:30-3
91
Recently reported cases:
1. A rare case of spontaneous Aspergillus spondylodiscitis with epidural abscess in a 45-year-old
immunocompetent female.341
2. Does surgery influence the outcome of Aspergillusosteomyelitis? 342
3. Osteomyelitis caused by Aspergillusspecies. 343
4. Sternal osteomyelitis caused by Aspergillus fumigatus following cardiac surgery: Case and review. 344
5. Aspergillosis of bones and joints - a review from 2002 until today.345
6. Aspergillus osteomyelitis: epidemiology, clinical manifestations, management, and outcome. 346
7. Costochondritis caused by Aspergillus flavus following cardiac surgery.347
8. Osteomyelitis caused by Aspergillus species: a review of 310 reported cases.348
9. Case report of Aspergillus osteomyelitis of the ribs in an immunocompetent patient.349
10. A case-based discussion on a patient with non-otogenic fungal skull base osteomyelitis: pitfalls in
diagnosis.350
11. Vertebral osteomyelitis and epidural abscess due toAspergillus nidulans resulting in spinal cord
compression: case report and literature review. 351
12. Involvement of the opportunistic pathogen Aspergillustubingensis in osteomyelitis of the maxillary
bone: a case report. 352
13. Aspergillus osteomyelitis of the proximal humerus: a case report.353
14. Aspergillus vertebral osteomyelitis in immunocompetent patients. 354
15. Skull base osteomyelitis and potential cerebrovascular complications in children.355
16. Aspergillus osteomyelitis of the lumbar spine complicated with orbital apex syndrome: A potential role
of the Batson's plexus in disease propagation.356
17. Successful treatment of Aspergillus flavus spondylodiscitis with epidural abscess in a patient with
chronic granulomatous disease.357
18. Aspergillus fumigatus spondylodiskitis in renal transplant patient: voriconazole experience. 358
19. Osteomyelitis due to Aspergillus species in chronic granulomatous disease: an update of the literature. 359
20. Aspergillus vertebral osteomyelitis and ureteral obstruction after liver transplantation. 360
21. Aspergillus fumigatus osteomyelitis in a patient receiving alemtuzumab for B-cell chronic lymphocytic
leukaemia. 361
22. Aspergillus vertebral osteomyelitis in immunocompetent hosts: role of triazole antifungal therapy. 362
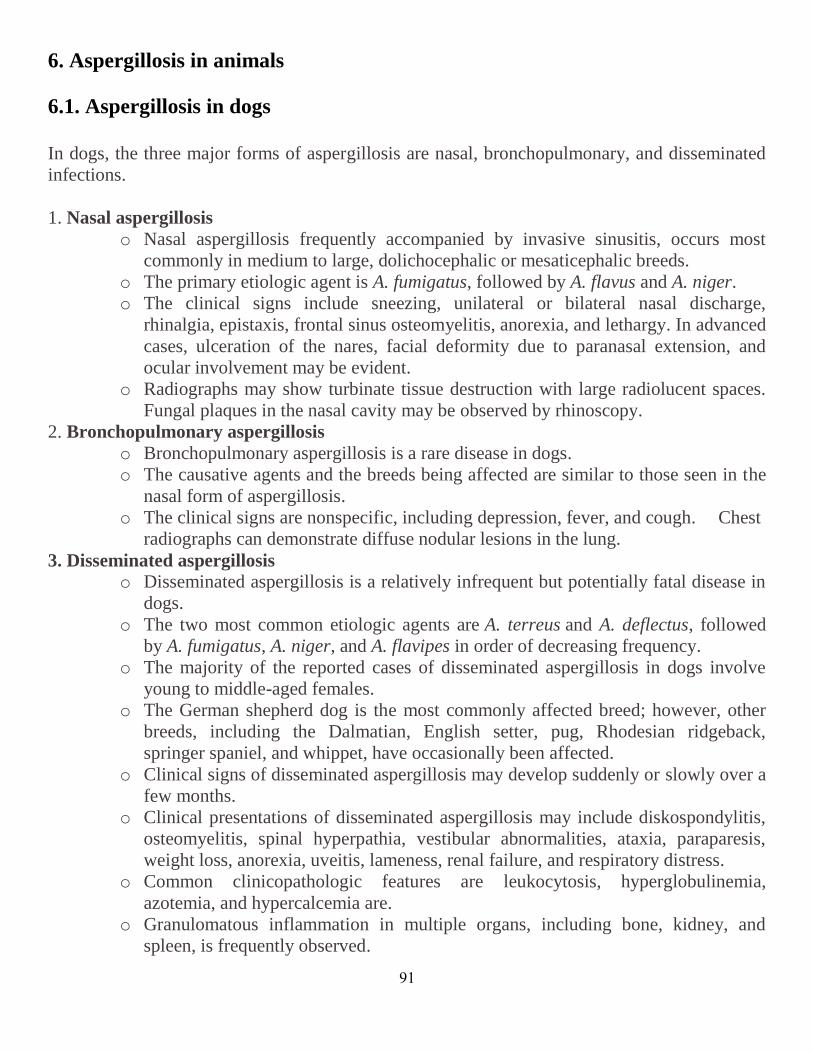
91
6. Aspergillosis in animals
6.1. Aspergillosis in dogs
In dogs, the three major forms of aspergillosis are nasal, bronchopulmonary, and disseminated
infections.
1. Nasal aspergillosis
o Nasal aspergillosis frequently accompanied by invasive sinusitis, occurs most
commonly in medium to large, dolichocephalic or mesaticephalic breeds.
o The primary etiologic agent is A. fumigatus, followed by A. flavus and A. niger.
o The clinical signs include sneezing, unilateral or bilateral nasal discharge,
rhinalgia, epistaxis, frontal sinus osteomyelitis, anorexia, and lethargy. In advanced
cases, ulceration of the nares, facial deformity due to paranasal extension, and
ocular involvement may be evident.
o Radiographs may show turbinate tissue destruction with large radiolucent spaces.
Fungal plaques in the nasal cavity may be observed by rhinoscopy.
2. Bronchopulmonary aspergillosis
o Bronchopulmonary aspergillosis is a rare disease in dogs.
o The causative agents and the breeds being affected are similar to those seen in the
nasal form of aspergillosis.
o The clinical signs are nonspecific, including depression, fever, and cough. Chest
radiographs can demonstrate diffuse nodular lesions in the lung.
3. Disseminated aspergillosis
o Disseminated aspergillosis is a relatively infrequent but potentially fatal disease in
dogs.
o The two most common etiologic agents are A. terreus and A. deflectus, followed
by A. fumigatus, A. niger, and A. flavipes in order of decreasing frequency.
o The majority of the reported cases of disseminated aspergillosis in dogs involve
young to middle-aged females.
o The German shepherd dog is the most commonly affected breed; however, other
breeds, including the Dalmatian, English setter, pug, Rhodesian ridgeback,
springer spaniel, and whippet, have occasionally been affected.
o Clinical signs of disseminated aspergillosis may develop suddenly or slowly over a
few months.
o Clinical presentations of disseminated aspergillosis may include diskospondylitis,
osteomyelitis, spinal hyperpathia, vestibular abnormalities, ataxia, paraparesis,
weight loss, anorexia, uveitis, lameness, renal failure, and respiratory distress.
o Common clinicopathologic features are leukocytosis, hyperglobulinemia,
azotemia, and hypercalcemia are.
o Granulomatous inflammation in multiple organs, including bone, kidney, and
spleen, is frequently observed.
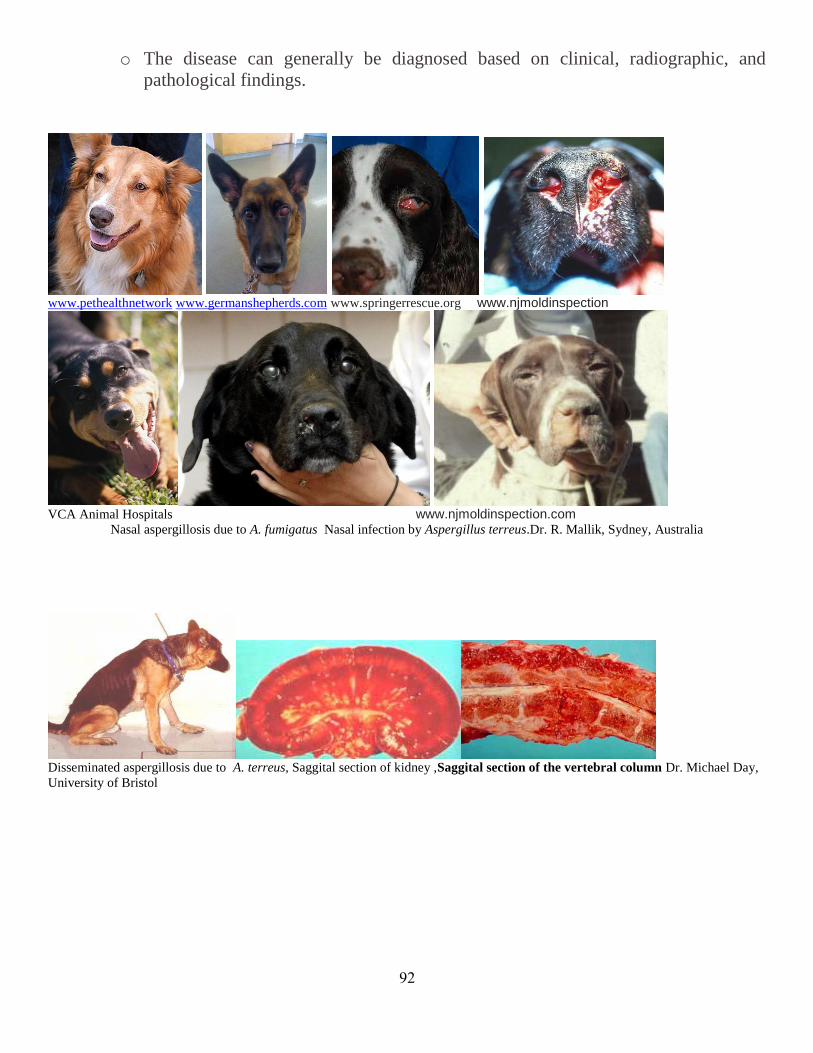
92
o The disease can generally be diagnosed based on clinical, radiographic, and
pathological findings.
www.pethealthnetwork www.germanshepherds.com www.springerrescue.org www.njmoldinspection
VCA Animal Hospitals www.njmoldinspection.com
Nasal aspergillosis due to A. fumigatus Nasal infection by Aspergillus terreus.Dr. R. Mallik, Sydney, Australia
Disseminated aspergillosis due to A. terreus, Saggital section of kidney ,Saggital section of the vertebral column Dr. Michael Day,
University of Bristol

93
Higher magnification showing marked granulomatous inflammation with giant cell formation (arrowhead) surrounding septate fungal
hyphae and bulbous spore-like structures (arrow)m Grocott's methenamine silver-stained section demonstrating prominent fungal
hyphae and terminal conidiophores (arrows).. Dr. Michael Day, Bristol Univ
Cases recently reported:
1. Diagnostic value of MRI in dogs with inflammatory nasal disease.
363
2. What causes canine sino-nasal aspergillosis? A molecular approach to species identification. 364
3. Spontaneous pneumothorax associated with Aspergillus bronchopneumonia in a dog. 365
4. Cytokine and transcription factor expression by Aspergillus fumigatus-stimulated peripheral blood
mononuclear cells in dogs with sino-nasal aspergillosis. 366
5. A novel case of canine disseminated aspergillosis following mating. 367
6. Sinonasal aspergillosis in dogs: a review. 368
7. Toll- and NOD-like receptor mRNA expression in canine sino-nasal aspergillosis and idiopathic
lymphoplasmacytic rhinitis.369
8. Clotrimazole and enilconazole distribution within the frontal sinuses and nasal cavity of nine dogs with
sinonasalaspergillosis. 370
9. Analysis of gene expression in canine sino-nasal aspergillosisand idiopathic lymphoplasmacytic rhinitis:
a transcriptomic analysis. 371
10. Disseminated aspergillosis in a dog due to Aspergillus alabamensis. 372
11. Sensitivity and specificity of a blood and urine galactomannan antigen assay for diagnosis of
systemic aspergillosis in dogs. 373
12. A novel case of canine disseminated aspergillosis following mating. 374
13. Aspergillus fumigatus bronchopneumonia in a Hellenic shepherd dog. 375
14. Cavitating pulmonary lesions in German shepherd dogs. 376
15. Clinical resolution of nasal aspergillosis following therapy with a homeopathic remedy in a dog. 377
16. Aspergillus versicolor, a new causative agent of canine disseminated aspergillosis.
378
17. Frontal sinus depth at four landmarks in breeds of dog typically affected by sinonasal aspergillosis. 379
18. Aspergillus fumigatus Bronchopneumonia in a Hellenic Shepherd Dog.
380
19. Acute phase protein concentrations in dogs with nasal disease. 381
20. Long term survival in two German shepherd dogs with Aspergillus-associated cavitary pulmonary
lesions. 382
21. Otomycosis due to Aspergillus spp. in a dog: case report and literature review.
383
22. Efficacy of intrasinusal administration of bifonazole cream alone or in combination with enilconazole
irrigation in canine sino-nasal aspergillosis: 17 cases. 384
23. Chronic monolateral otomycosis in a dog caused by Aspergillus ochraceus. 385
24. Repeated rhinoscopic and serologic assessment of the effectiveness of intranasally administered
clotrimazole for the treatment of nasal aspergillosis in dogs. 386

94
25. Roland Kozdrowsk, Aspergillosis of a dog genital tract—Case report, 387
26. Aspergillosis of a dog genital tract-Case report. 388
6.2. Aspergillosis in cats
Feline aspergillosis includes
o Sinonasal aspergillosis (SNA) can be invasive or noninvasive and is most
commonly caused by Aspergillus fumigatus and Aspergillus niger. SNA has a
favorable prognosis with treatment
o Sino orbital aspergillosis (SOA) is an invasive mycosis that is being increasingly
recognized, and is most commonly caused by a recently discovered pathogen
Aspergillus felis. The prognosis for SOA remains poor.
Veterinary images, Nasal, sinus and orbital aspergillosis in a cat.

95
Severe bone erosion rostrally through the nasal bone.
Martin L. Whitehead, & Peter W. Kettlewell,. Chipping Norton Veterinary Hospital, Chipping Norton,Oxon
Cases recently reported:
1. Aspergillosis in cats: ABCD guidelines on prevention and management. 389
2. Aspergillus felis sp. nov., an emerging agent of invasiveaspergillosis in humans, cats, and dogs. 390
.
3. Feline aspergillosis. 391
4. Otomycosis due to Aspergillus spp. in a dog: case report and literature review. 392
5. Chronic monolateral otomycosis in a dog caused by Aspergillus ochraceus. 393
6. Invasive mould infections of the naso-orbital region of cats: a case involving Aspergillus fumigatus and
an aetiological review. 394
7. Intranasal infusion of clotrimazole for the treatment of nasalaspergillosis in two cats. 395
8. Bilateral orbital and nasal aspergillosis in a cat. 396.
9. Computed tomographic findings of fungal rhinitis and sinusitis in cats. 397
10. Aspergillus flavus keratomycosis in a cat treated with topical 1% voriconazole solution. 398
11. Isolation of Aspergillus udagawae from a fatal case of feline orbitalaspergillosis. 399
12. Feline sino-orbital aspergillosis:an emerging clinical syndrome. 400
13. Use of posaconazole in the management of invasive orbitalaspergillosis in a cat. 401

96
6.3. Aspergillosis in horses
Aspergillosis in horses is a fungal disease caused by Aspergillus spp Aspergillus spp are very
common in the environment, especially in moldy feed and bedding. They are opportunistic
pathogens and often cause disease in horses that are immunosuppressed from debilitating
conditions (e.g., enterocolitis, septicemia, neoplasia, Cushing's disease, equine protozoal
myeloencephalitis) or major surgery or that have been treated with immunosuppressive drugs.
They can infect internal organs, most commonly affects the guttural pouches but infection may also lead to abortion, keratomycosis, rhinitis and rarely pulmonary aspergillosis.
1. Equine Aspergillus Rhinitis, , Pulmonary Aspergillosis
Historical
Rivolta (1856) recorded the first case of aspergillosis in horses, but was frequently restricted to infection of the nasal sinuses and the guttural pouches. In a case described
Thary and Lucet (1895) described a rapidly developed rapidly disease that showed generalized interstitial
haemorrhage with caseous nodules in the kidneys in a four-year-old mare.
Foulerton (1899) described the lung of a horse with typical aspergillotic nodules
Noller & Krause in 1924, and Tscherniak (1928) gave details of several more cases Romanov (1928) reported meningeal involvement.
Infection is by inhalation of an overwhelming number of spores or by translocation of
organisms across an inflamed gastrointestinal tract. Aspergillus pneumonia is almost uniformly
fatal, often with no or mild respiratory signs. The two forms of Aspergillus pneumonia probably
reflect the two portals of entry, with fungal proliferation and invasion of the small airways
occurring secondary to inhalation, and angioinvasive aspergillosis with lesions centered around
large blood vessels likely due to hematogenous infection originating from the gastrointestinal
tract. In two retrospective studies of invasive pulmonary aspergillosis, 41 of 49 cases were
associated with enterocolitis.
Pulmonary aspergillosis is characterized grossly by multiple nodules throughout the lungs. On
histologic examination, there is often necrosis and purulent inflammation. Necrosis is due to
toxin and enzyme production as well as vascular obstruction. Fungal invasion of blood vessels
is common and results in vasculitis, thrombosis, infarction, and necrosis. Chronic lesions are
granulomatous, with macrophages, neutrophils, and multinucleated giant cells predominating.
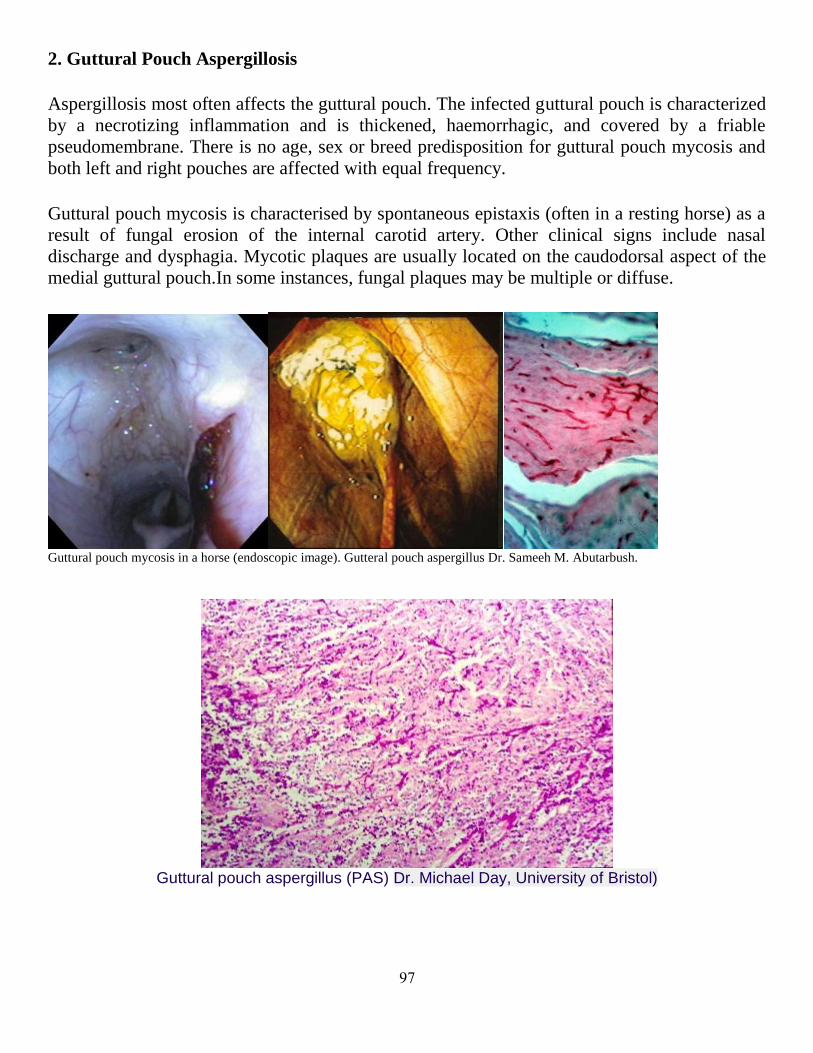
97
2. Guttural Pouch Aspergillosis
Aspergillosis most often affects the guttural pouch. The infected guttural pouch is characterized
by a necrotizing inflammation and is thickened, haemorrhagic, and covered by a friable
pseudomembrane. There is no age, sex or breed predisposition for guttural pouch mycosis and
both left and right pouches are affected with equal frequency.
Guttural pouch mycosis is characterised by spontaneous epistaxis (often in a resting horse) as a
result of fungal erosion of the internal carotid artery. Other clinical signs include nasal
discharge and dysphagia. Mycotic plaques are usually located on the caudodorsal aspect of the
medial guttural pouch.In some instances, fungal plaques may be multiple or diffuse.
Guttural pouch mycosis in a horse (endoscopic image). Gutteral pouch aspergillus Dr. Sameeh M. Abutarbush.
Guttural pouch aspergillus (PAS) Dr. Michael Day, University of Bristol)
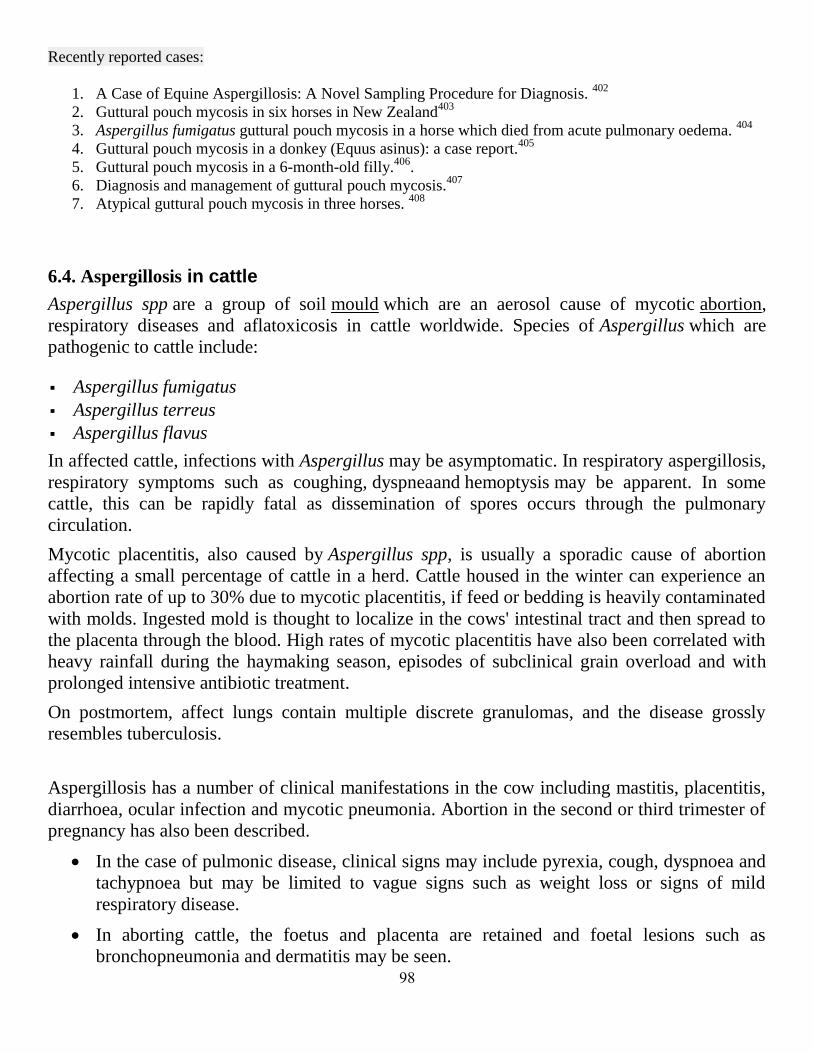
98
Recently reported cases:
1. A Case of Equine Aspergillosis: A Novel Sampling Procedure for Diagnosis. 402
2. Guttural pouch mycosis in six horses in New Zealand403
3. Aspergillus fumigatus guttural pouch mycosis in a horse which died from acute pulmonary oedema. 404
4. Guttural pouch mycosis in a donkey (Equus asinus): a case report.405
5. Guttural pouch mycosis in a 6-month-old filly.406
.
6. Diagnosis and management of guttural pouch mycosis.407
7. Atypical guttural pouch mycosis in three horses. 408
6.4. Aspergillosis in cattle
Aspergillus spp are a group of soil mould which are an aerosol cause of mycotic abortion,
respiratory diseases and aflatoxicosis in cattle worldwide. Species of Aspergillus which are
pathogenic to cattle include:
Aspergillus fumigatus
Aspergillus terreus
Aspergillus flavus
In affected cattle, infections with Aspergillus may be asymptomatic. In respiratory aspergillosis,
respiratory symptoms such as coughing, dyspneaand hemoptysis may be apparent. In some
cattle, this can be rapidly fatal as dissemination of spores occurs through the pulmonary
circulation.
Mycotic placentitis, also caused by Aspergillus spp, is usually a sporadic cause of abortion
affecting a small percentage of cattle in a herd. Cattle housed in the winter can experience an
abortion rate of up to 30% due to mycotic placentitis, if feed or bedding is heavily contaminated
with molds. Ingested mold is thought to localize in the cows' intestinal tract and then spread to
the placenta through the blood. High rates of mycotic placentitis have also been correlated with
heavy rainfall during the haymaking season, episodes of subclinical grain overload and with
prolonged intensive antibiotic treatment.
On postmortem, affect lungs contain multiple discrete granulomas, and the disease grossly
resembles tuberculosis.
Aspergillosis has a number of clinical manifestations in the cow including mastitis, placentitis,
diarrhoea, ocular infection and mycotic pneumonia. Abortion in the second or third trimester of
pregnancy has also been described.
In the case of pulmonic disease, clinical signs may include pyrexia, cough, dyspnoea and
tachypnoea but may be limited to vague signs such as weight loss or signs of mild
respiratory disease.
In aborting cattle, the foetus and placenta are retained and foetal lesions such as
bronchopneumonia and dermatitis may be seen.
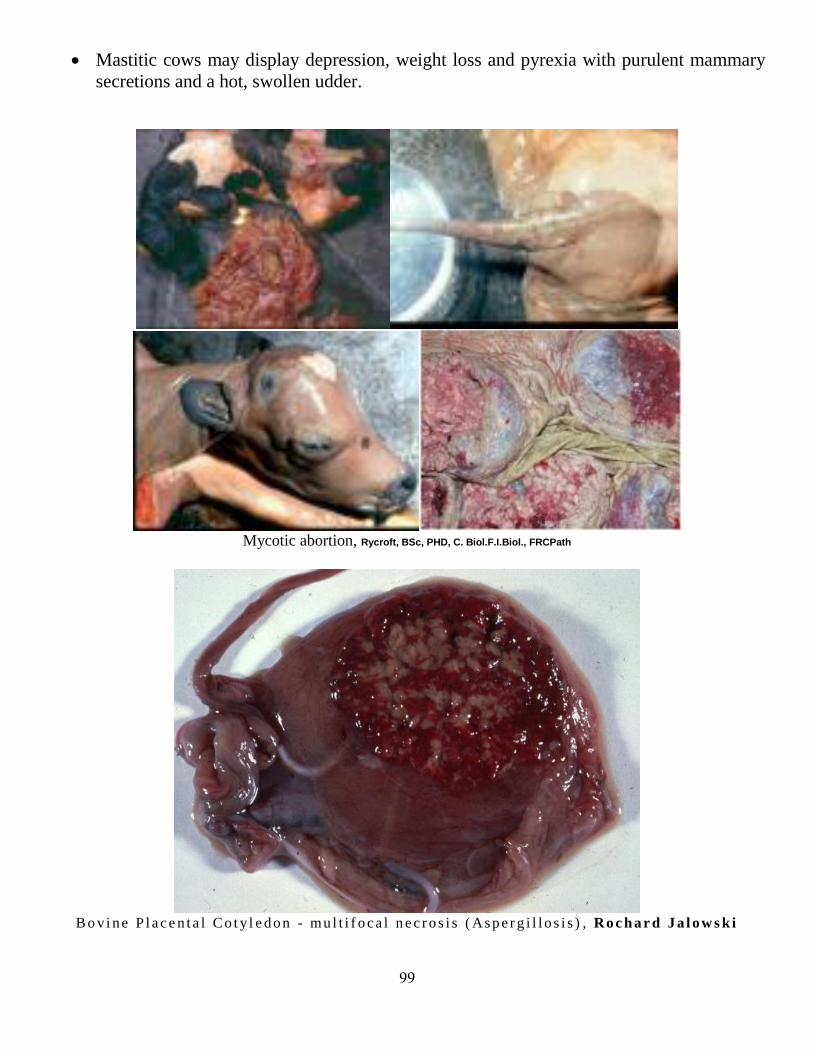
99
Mastitic cows may display depression, weight loss and pyrexia with purulent mammary
secretions and a hot, swollen udder.
Mycotic abortion, Rycroft, BSc, PHD, C. Biol.F.I.Biol., FRCPath
B o vi n e P l a c e n t a l Co t y l e d o n - mu l t i f o c a l n e c r o s i s ( As p e r g i l l o s i s ) , Ro c h a r d J a l o w s k i
111
Recently reported cases:
1. Involvement of fungal species in bovine mastitis in and around .
409
2. Application of real-time PCR for detection of Aspergillus species in aborted ruminant foetuses. 410
3. Mycotic abortion in cattle .411
4. Abortus by Aspergillus fumigatus and A. nigerin cattle in southern Brazil. 412
5. Mastitis by Aspergillus fumigatusin sheep. 413
6. [Mycotic placentitis in cattle]. 414
7. Pathogenesis of experimental bovine mycotic placentitis produced by Aspergillus fumigatus. 415
8. Aspergillus nidulans and Aspergillus fumigatus as causal agents of bovine mastitis. 416
9. Cases of Aspergillus mastitis in cattle].417
10. Caprine mastitis due to aspergillosis and zygomycosis: a pathological and immunohistochemical
study418
6.5. Aspergillosis in Sheep and goats
There have been only five reports of aspergillosis in sheep. The lesions in lambs consist of
small (2-3 mm. Diam.) bluish-grey nodules surrounded by a narrow haemorrhagic zone, and
closely resemble those caused by the lungworm Muellerius capillaris (Andersen 1927). The
most recent report of the disease is in the Annual Report of the New Zealand Department of
Agriculture for 1955.
Van Hellens (1902-03) investigated in Finland one of the few epidemics of aspergillosis on
record among sheep. The animals were adult and showed chronic bronchitis and catarrhal
pneumonia closely resembling the symptoms of tuberculosis.
Death occurred up to one year after the appearance of symptoms. Conidiophores
of A.fumigatus were found in the sputum of affected sheep and numerous discrete and
sometimes well calcified nodules 1-7 mm. in diam. were present in the lungs. Nobel & Shamir
(1956) described a rather different condition in which granulomatous lesions containing the
hyphae of A.fumigatus were found in the lungs of a day-old lamb, and they considered the
infection had taken place in utero.
Recently, two cases of systemic aspergillosis were described by Pérez, 1999, in dairy sheep
from a flock in which fungal mastitis appeared subsequent to the antibiotic treatment of animals
before parturition. Lesions characterized by necrosis and a pyogranulomatous exudate were
observed in the mammary glands, supramammary and mediastinal lymph nodes, kidneys, lung,
liver, heart, forestomachs and brain. The intense vasculitis with thrombosis observed in various
organs, but especially in the mammary glands, suggested a haematogenous dissemination of the
infection from this organ. The aetiological diagnosis was accomplished by the
immunohistochemical staining of the fungal structures seen in the histological sections by the
specific Aspergillus monoclonal antibody Mab-WF-AF-1 together with the isolation of
Aspergillus fumigatus in pure culture from affected tissues.
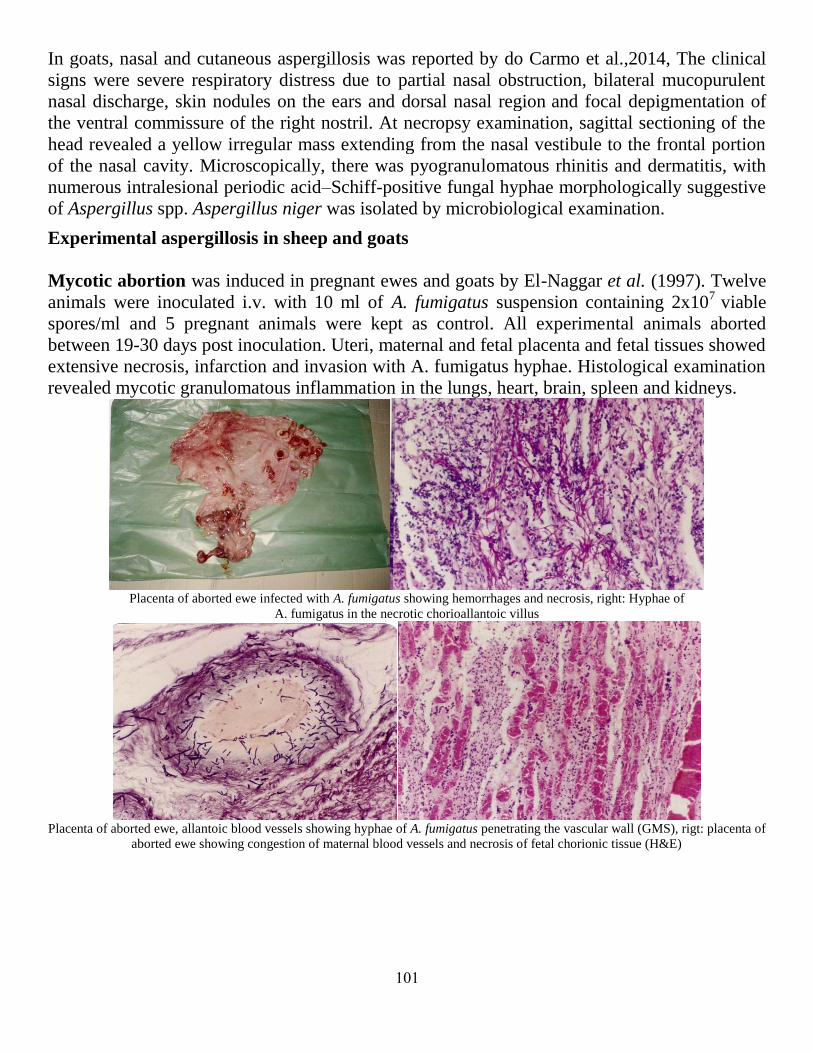
111
In goats, nasal and cutaneous aspergillosis was reported by do Carmo et al.,2014, The clinical
signs were severe respiratory distress due to partial nasal obstruction, bilateral mucopurulent
nasal discharge, skin nodules on the ears and dorsal nasal region and focal depigmentation of
the ventral commissure of the right nostril. At necropsy examination, sagittal sectioning of the
head revealed a yellow irregular mass extending from the nasal vestibule to the frontal portion
of the nasal cavity. Microscopically, there was pyogranulomatous rhinitis and dermatitis, with
numerous intralesional periodic acid–Schiff-positive fungal hyphae morphologically suggestive
of Aspergillus spp. Aspergillus niger was isolated by microbiological examination.
Experimental aspergillosis in sheep and goats
Mycotic abortion was induced in pregnant ewes and goats by El-Naggar et al. (1997). Twelve
animals were inoculated i.v. with 10 ml of A. fumigatus suspension containing 2x107
viable
spores/ml and 5 pregnant animals were kept as control. All experimental animals aborted
between 19-30 days post inoculation. Uteri, maternal and fetal placenta and fetal tissues showed
extensive necrosis, infarction and invasion with A. fumigatus hyphae. Histological examination
revealed mycotic granulomatous inflammation in the lungs, heart, brain, spleen and kidneys.
Placenta of aborted ewe infected with A. fumigatus showing hemorrhages and necrosis, right: Hyphae of
A. fumigatus in the necrotic chorioallantoic villus
Placenta of aborted ewe, allantoic blood vessels showing hyphae of A. fumigatus penetrating the vascular wall (GMS), rigt: placenta of
aborted ewe showing congestion of maternal blood vessels and necrosis of fetal chorionic tissue (H&E)
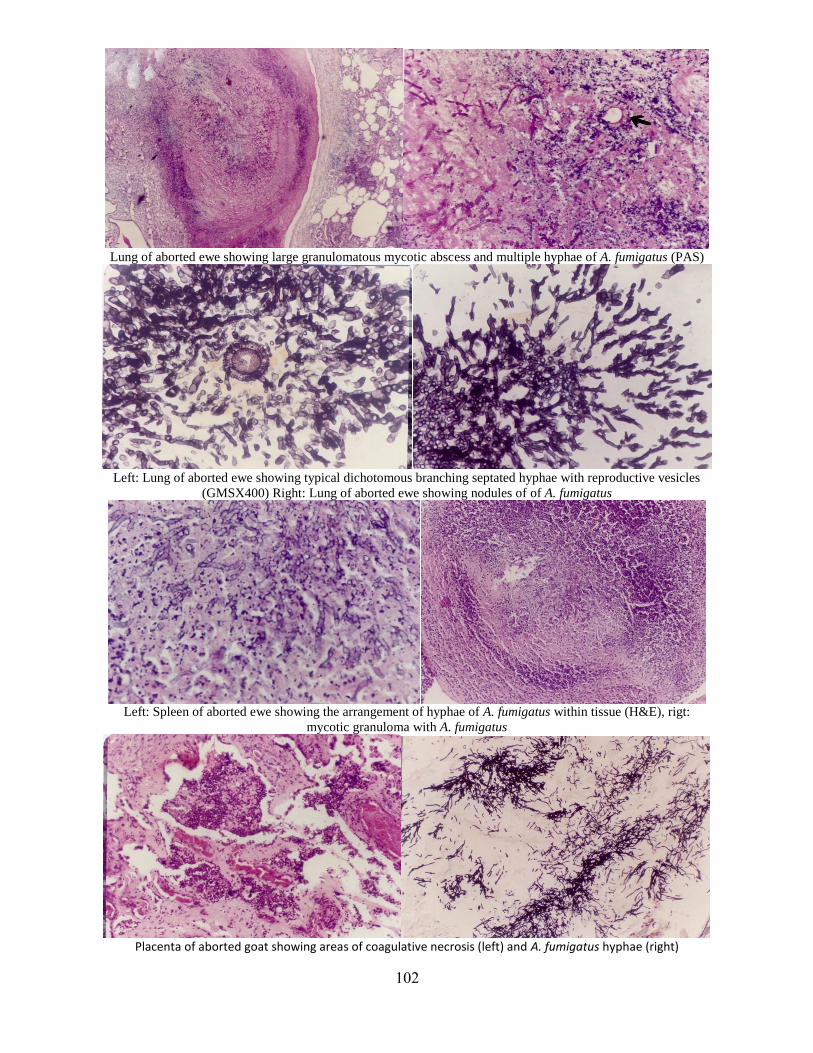
112
Lung of aborted ewe showing large granulomatous mycotic abscess and multiple hyphae of A. fumigatus (PAS)
Left: Lung of aborted ewe showing typical dichotomous branching septated hyphae with reproductive vesicles
(GMSX400) Right: Lung of aborted ewe showing nodules of of A. fumigatus
Left: Spleen of aborted ewe showing the arrangement of hyphae of A. fumigatus within tissue (H&E), rigt:
mycotic granuloma with A. fumigatus
Placenta of aborted goat showing areas of coagulative necrosis (left) and A. fumigatus hyphae (right)
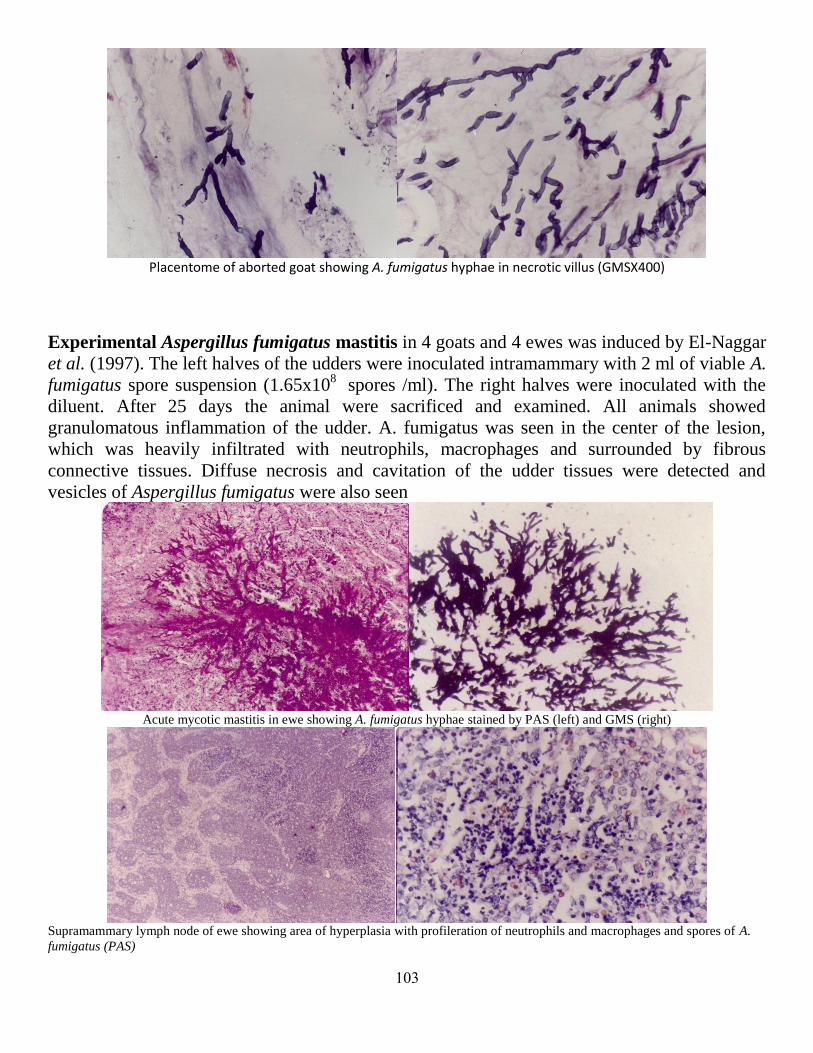
113
Placentome of aborted goat showing A. fumigatus hyphae in necrotic villus (GMSX400)
Experimental Aspergillus fumigatus mastitis in 4 goats and 4 ewes was induced by El-Naggar
et al. (1997). The left halves of the udders were inoculated intramammary with 2 ml of viable A.
fumigatus spore suspension (1.65x108
spores /ml). The right halves were inoculated with the
diluent. After 25 days the animal were sacrificed and examined. All animals showed
granulomatous inflammation of the udder. A. fumigatus was seen in the center of the lesion,
which was heavily infiltrated with neutrophils, macrophages and surrounded by fibrous
connective tissues. Diffuse necrosis and cavitation of the udder tissues were detected and
vesicles of Aspergillus fumigatus were also seen
Acute mycotic mastitis in ewe showing A. fumigatus hyphae stained by PAS (left) and GMS (right)
Supramammary lymph node of ewe showing area of hyperplasia with profileration of neutrophils and macrophages and spores of A.
fumigatus (PAS)
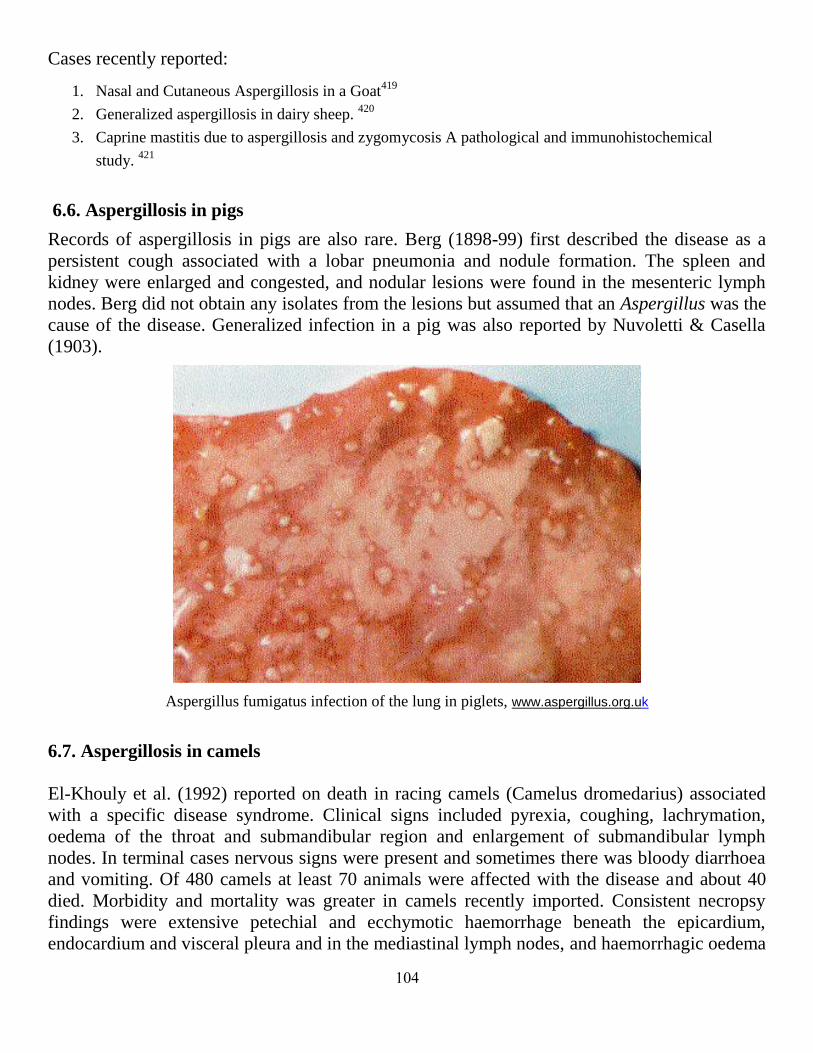
114
Cases recently reported:
1. Nasal and Cutaneous Aspergillosis in a Goat419
2. Generalized aspergillosis in dairy sheep. 420
3. Caprine mastitis due to aspergillosis and zygomycosis A pathological and immunohistochemical
study. 421
6.6. Aspergillosis in pigs
Records of aspergillosis in pigs are also rare. Berg (1898-99) first described the disease as a
persistent cough associated with a lobar pneumonia and nodule formation. The spleen and
kidney were enlarged and congested, and nodular lesions were found in the mesenteric lymph
nodes. Berg did not obtain any isolates from the lesions but assumed that an Aspergillus was the
cause of the disease. Generalized infection in a pig was also reported by Nuvoletti & Casella
(1903).
Aspergillus fumigatus infection of the lung in piglets, www.aspergillus.org.uk
6.7. Aspergillosis in camels
El-Khouly et al. (1992) reported on death in racing camels (Camelus dromedarius) associated
with a specific disease syndrome. Clinical signs included pyrexia, coughing, lachrymation,
oedema of the throat and submandibular region and enlargement of submandibular lymph
nodes. In terminal cases nervous signs were present and sometimes there was bloody diarrhoea
and vomiting. Of 480 camels at least 70 animals were affected with the disease and about 40
died. Morbidity and mortality was greater in camels recently imported. Consistent necropsy
findings were extensive petechial and ecchymotic haemorrhage beneath the epicardium,
endocardium and visceral pleura and in the mediastinal lymph nodes, and haemorrhagic oedema

115
of the pharyngeal and laryngeal areas. Haemorrhages occurred more variably in abdominal
organs and on the omasal and abomasal mucosa. Bronchopneumonia, omasitis and abomasitis
were observed on microscopic examination, together with liver and kidney lesions of presumed
toxic origin. Fungal hyphae and, occasionally, the characteristic conidial morphology of
Aspergillus fumigatus were seen in sections and direct smears from lesions in the respiratory
and alimentary tracts. A fumigatus was cultured from trachea, bronchi, bronchioles, lung tissue,
heart blood, omasum, abomasum, ileum and submandibular lymph nodes. Whether the role of
Aspergillus in the overall syndrome is primary or secondary has not been established; no other
potential aetiological agent has been identified.
Dehkordi et al. (2012) performed research for detection of Aspergillus species (A. fumigatus, A.
flavus, A. niger and A. terreus) in aborted bovine, ovine, caprine and camel foetuses by real-
time PCR in Iran. After modification of real-time PCR on abomasal contents, from the total
number of 970 samples, 141 (14.53%) gave positive results for Aspergillus species. Of them, 62
(17.71%), 33 (14.04%), 27 (12.05%) and 19 (11.8%) positive specimens were detected in
bovine, ovine, caprine and camel foetuses respectively. Statistical analysis showed significant
differences (P<0.05) between bovine and camel and bovine and caprine aborted foetuses.
Aspergillus abortion was the most prevalent in cattle whereas camels tended to be the most
resistant.
An invasive form of aspergillosis in an alpaca (Lama pacos) was described, with dissemination
causing small abscesses and multifocal areas of necrosis in the lung, heart, spleen and kidneys.
Histological sections showed hyphae morphologically compatible with an Aspergillus species.
Direct immunofluorescent testing confirmed the diagnosis of aspergillosis.( Severo et al., 1989).
6.8. Aspergillosis in American bisons
Rewell & Ainsworth (1947) showed how the respiratory passages of an American bison at the
London zoo were found on post-mortem examination to be lined with a greenish felt
of A.fumigatus with absence of severe lung lesions.
de los Monteros et al. (1999) reported on concomitant nasal zygomycosis and pulmonary
aspergillosis in a 3-mo-old female American bison calf (Bison bison) in Pennsylvania (USA).
Etiologic diagnosis was made by immunohistochemistry using a panel of monoclonal
antibodies and heterologously absorbed polyclonal antibodies. In the lungs fungal infection was
accompanied by hemorrhage, fibrin exudation, and infiltration with neutrophils. Fungi were
observed to penetrate apparently normal epithelial lining of the nasal turbinates, and there was
hemorrhage, edema, and invasion of blood vessels in the submucosa. In vessels fungi were
typically associated with thrombosis. The calf may have been infected due to a high level of
exposure to mouldy feed and litter in the environment in combination with a collapse of it's
natural defence mechanisms.

116
6.9. Aspergillosis in monkeys
Scott (1930) gave details of nine cases of mycosis (aspergillosis?) and a further nine associated
with tuberculosis in captive monkeys encountered at the London zoo. The lungs were the chief
organs involved but miliary nodules were occasionally found throughout the viscera.
Jurczynski (2012) reported on invasive aspergillosis in a putty-nosed monkey (Cercopithecus
nictitans) with adrenocortical Cushing's syndrome. An 18-year-old captive female putty-nosed-
monkey (Cercopithecus nictitans) with a history of long-term infertility and
hyperglucocorticism was euthanized because of perforating thoracic trauma induced by group
members and subsequent development of neurological signs.
Complete necropsy and histopathological examination of formalin-fixed tissue samples was
carried out. The monkey showed invasive pulmonary and cerebral infection with Aspergillus
fumigatus together with adrenocortical neoplasia and signs of Cushing’s syndrome, such as
alopecia with atrophic skin changes, evidence for diabetes mellitus and marked
immunosuppression.
6.10. Aspergillosis in deers
Outbreaks of pulmonary aspergillosis have been reported in hares in Sweden (Thjostta, 1933;
Hölphers & Lilleengen, 1947) and also in roe-deer in that country and Switzerland, in which the
conchal and ethmoid bones as well as the lungs and other organs became affected by tumour-
like growths containing hyphae (Krembs, 1937; Burgisser, 1955). When specific determination
had been carried out, A.fumigatus was the most frequent isolate but Burgeon (1929)
reported A.niger from nodular lesions in the lungs of a bull, a heifer and a stag in Indo-China.
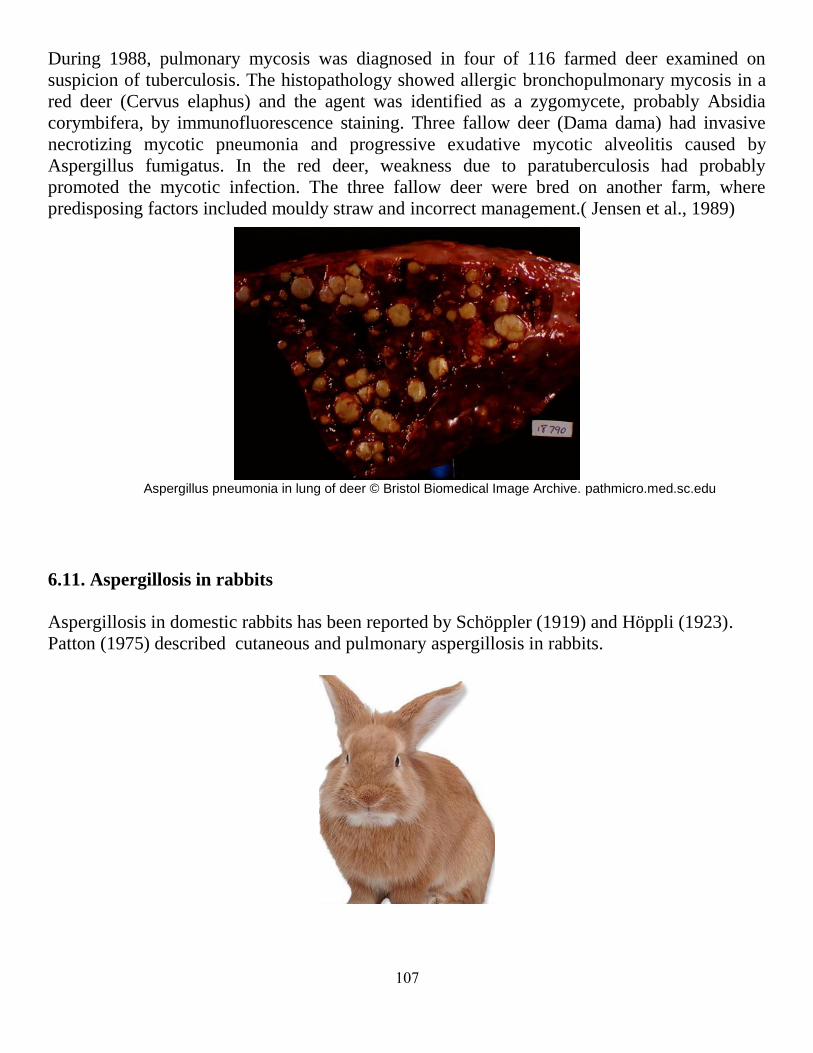
117
During 1988, pulmonary mycosis was diagnosed in four of 116 farmed deer examined on
suspicion of tuberculosis. The histopathology showed allergic bronchopulmonary mycosis in a
red deer (Cervus elaphus) and the agent was identified as a zygomycete, probably Absidia
corymbifera, by immunofluorescence staining. Three fallow deer (Dama dama) had invasive
necrotizing mycotic pneumonia and progressive exudative mycotic alveolitis caused by
Aspergillus fumigatus. In the red deer, weakness due to paratuberculosis had probably
promoted the mycotic infection. The three fallow deer were bred on another farm, where
predisposing factors included mouldy straw and incorrect management.( Jensen et al., 1989)
Aspergillus pneumonia in lung of deer © Bristol Biomedical Image Archive. pathmicro.med.sc.edu
6.11. Aspergillosis in rabbits
Aspergillosis in domestic rabbits has been reported by Schöppler (1919) and Höppli (1923).
Patton (1975) described cutaneous and pulmonary aspergillosis in rabbits.

118
6.12. Aspergillosis in guinea-pigs
Ainsworth & Austwick (1955a) have recorded the disease in guinea-pigs. Recently, guinea-pigs
are used for assessment of Aspergillus fumigatus burden in pulmonary tissue of antimycotics.
Histological examination of guinea pig lungs exposed to and infected with aerosolized A. fumigatus aac.asm.org
4.13. Aspergillosis in lesser blind mole rats
Tamam and Refai (2013) reported on seven wild Egyptian lesser blind mole rat (Spalax
leucodon Egyptiacus) that died naturally in the wild. All the animals had large pulmonary
lesions that on microscopic, microbiological, and ultrastructural analysis were shown to contain
mixed infections with Alternaria alternata and Aspergillus candidus. Some of the lesions were
circumscribed with fibroblastic proliferation and inflammatory response. The lungs had
haemorrhage and chronic inflammatory response to the organisms, which is likely to have been
the cause of death.
(A) Thoracic cavity of Spalax leucodon showing large, tumour-like lesions replacing the apical left lung lobe and large, firm brown
lesions in the caudal and right lobes (yellow arrows). (B) Thoracic cavity containing brown, consolidating focal lesions in the centre of
the left lung lobe, emphysematous change (red arrows), and red hepatisation of the lower right lobe (violet arrow).

119
6.14. Aspergillosis in dolphins.
Reidarson et al. (1998) reported on a 4-yr-old male bottlenose dolphin (Tursiops truncatus) that
developed an Aspergillus fumigatus pneumonia. Fungal elements were identified by cytology
and microbiology from endoscopic bronchoalveolar lavage and brushings of a raised yellow
endobronchial lesion. The results of qualitative immunodiffusion serology, a technique that
identifies specific circulating antibodies to Aspergillus fumigatus, were suggestive of an active
infection. The dolphin was treated with itraconazole for over 2 yr, which resulted in remission
of clinical signs. Pneumonia caused by Aspergillus sp. accounts for the large majority of
pulmonary mycoses in marine mammals
The clinical history, laboratory data, and gross and histological findings are described and
discussed by Brian et al. (2005) for three cases of fatal pulmonary aspergillosis in three species
of dolphins.
Reorted cases
1. Invasive aspergillosis in a Putty-nosed monkey (Cercopithecus nictitans) with adrenocortical
Cushing’s syndrome. 422
2. Aspergillosis in camels affected with a specific respiratory and enteric syndrome. 423
3. Pulmonary mycosis in farmed deer: allergic zygomycosis and invasive aspergillosis424
4. Application of real-time PCR for detection of Aspergillus species in aborted ruminant foetuses. 425
5. Efficacy of voriconazole against invasive pulmonary aspergillosis in a guinea-pig model. 426
6. Experimental aspergillosis in guinea pigs: influence of itraconazole on fungaemia and invasive fungal
growth. 427
7. Occurrence of Aspergillus fumigatus Fresen. in the Lung of an American Bison. 428
8. Nasal zygomycosis and pulmonary aspergillosis in an American bison.429
9. Bronchoscopic and serologic diagnosis of Aspergillus fumigatus pulmonary infection in a bottlenose
dolphin (Tursiops truncatus). 430
10. Invasive aspergillosis in an alpaca (Lama pacos). 431
11. Pulmonary aspergillosis in three species of dolphin. 432
12. Cutaneous and pulmonary aspergillosis in rabbits.433
13. Dual mycotic pulmonary granulomas caused by Alternaria alternata and Aspergillus candidus in the
wild egyptian mole rat (spalax leucodon egyptiacus). 434
111
7. Aspergillosis in birds
Aspergillosis was first described in a wild duck in 1833 and in turkeys as early as 1898.
All species of birds probably are susceptible.
Aspergillus fumigatus is a common cause of the disease. However, other species like A.
flavus, A. niger, A. nidulans, andA. terreus may also be isolated from avian cases of
aspergillosis (sometimes in mixed infections) but much less frequently than A. fumigatus
The bird comes in contact with the organisms through contaminated feed, litter or
premises. The disease is not contagious and does not spread from one bird to another.
Most healthy birds can withstand repeated exposure to these organisms. Inhalation of
large amounts of the infectious form of the mould or reduced resistance of the bird
apparently results in infection.
7. 1. Aspergillosis in poultry
Infection by Aspergillus sp. has been reported in almost all domesticated avian species and
production types: layer cockerels, pullets in cages, broiler breeders, and growers of chicken or
turkey poults, duck breeders and goslings. Aspergillosis is a disease, usually of the respiratory
system, of chickens, turkeys, and less frequently ducklings, pigeons and geese, In chickens and
turkeys, the disease may be endemic on some farms.
Aspergillus fumigatus can penetrate egg shells under ideal growth conditions and thus
infect the embryos. Such eggs will often appear green when candled (the embryo will be
dead). Infected embryos may hatch with well- developed lesions.
If infected eggs break in the hatchery, large numbers of spores are released which
contaminate the hatchery environment and air systems can lead to severe outbreaks in
very young birds (less than 3 weeks of age). Eggs punctured for in-ovo injection are
particularly susceptible to contamination. Even low-level contamination of hatchers or air
systems can result in mortalities of 50% or greater when in-ovo injection is used.
High mortality rates are seen in newly hatched chicks and poults that inhale large
numbers of spores during hatching in contaminated incubators. The diseased is called
brooder pneumonia. In older birds, infection is caused primarily by inhalation of spore
laden dust from contaminated litter or feed or dusty range areas.
Dyspnea, hyperpnea, somnolence and other signs of nervous system involvement,
inappetence, emaciation, and increased thirst may be seen. In chicks or poults up to 6
weeks, the lungs are most frequently involved.
Airsacculitis in young mature turkeys is a leading cause of postmortem condemnation.
Pulmonary lesions are characterized by cream-coloured plaques a few mm to several cm
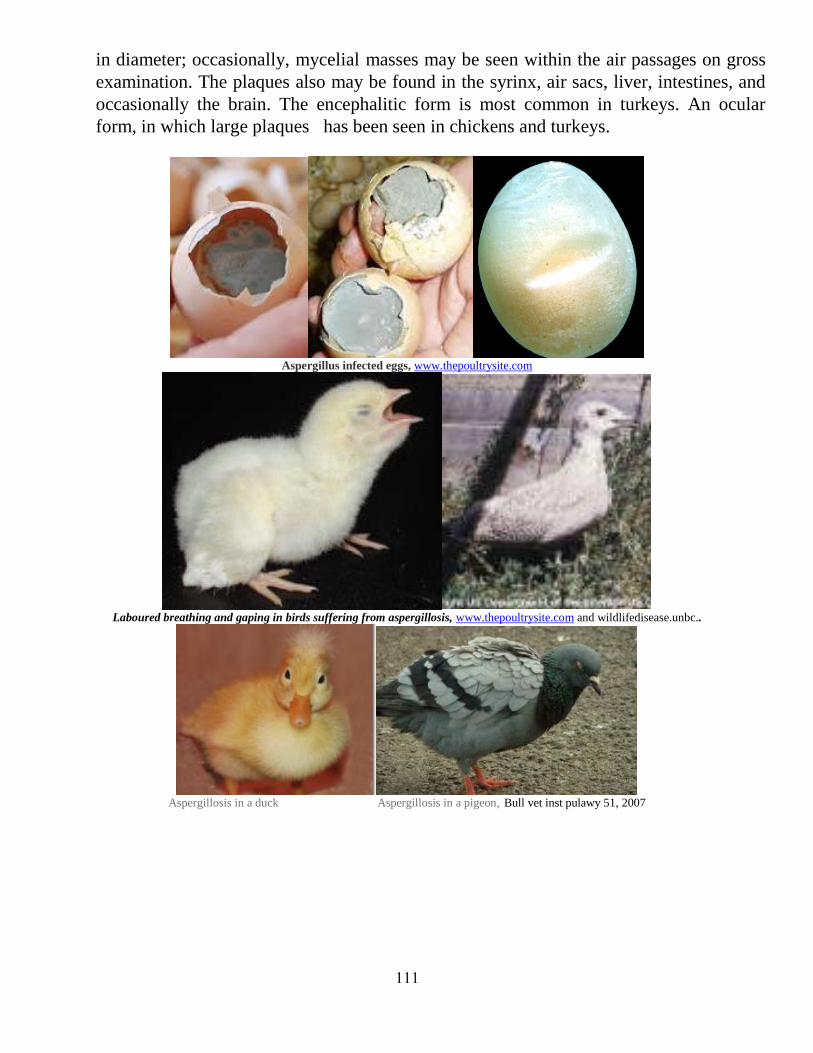
111
in diameter; occasionally, mycelial masses may be seen within the air passages on gross
examination. The plaques also may be found in the syrinx, air sacs, liver, intestines, and
occasionally the brain. The encephalitic form is most common in turkeys. An ocular
form, in which large plaques has been seen in chickens and turkeys.
Aspergillus infected eggs, www.thepoultrysite.com
Laboured breathing and gaping in birds suffering from aspergillosis, www.thepoultrysite.com and wildlifedisease.unbc..
Aspergillosis in a duck Aspergillosis in a pigeon, Bull vet inst pulawy 51, 2007

112
Left: Aspergillosis in the air sacs of a chick, www.sandhillvet.co.uk
Right: Multiple nudules in the liver of 3 weeks old poult, due to aspergillosis., www.poultrymed.com
Aspergillus granulomas of the serous coats:www.thepoultrysite.com
Lung nodules =aspergillosis, OldVe T.com Multiple nodular lesions in the lung of a duck. Parasitology-Mycology, ENVA
7.2. Aspergillosis in wild birds:
A. fumigatus has been isolated from lesions in wild birds since the early 1800s. Major die-offs
of free-ranging wild birds have been reported from waterfowl, gulls, and corvids following
dumping of mouldy waste grains in areas where birds feed.. Aspergillosis has also been
reported in penguins, raptors, migratory , waterfowl, psittacines and zoologic specimens, such
as flamingos.
7.2.1. Aspergillosis in penguins
On Sunday, November 10th,2013, staff at the Calgary Zoo made the difficult decision to
euthanize a 14-year-old male Gentoo penguin Houdini. He had been sick for almost a month.
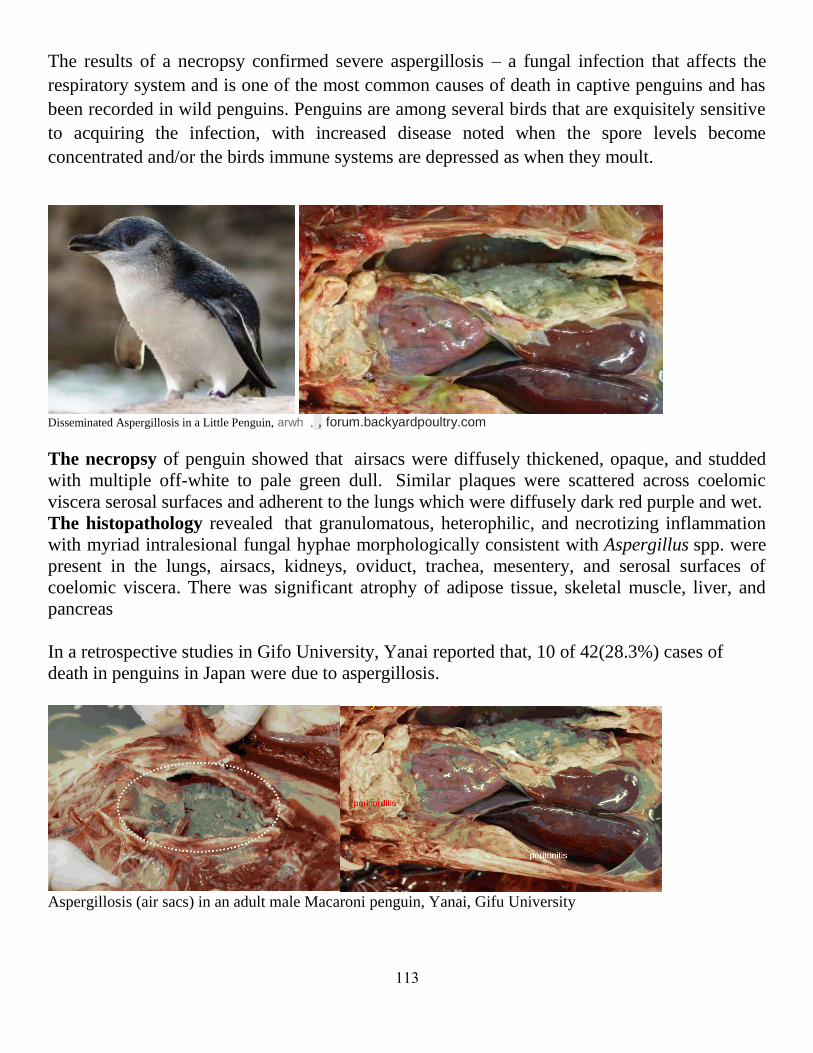
113
The results of a necropsy confirmed severe aspergillosis – a fungal infection that affects the
respiratory system and is one of the most common causes of death in captive penguins and has
been recorded in wild penguins. Penguins are among several birds that are exquisitely sensitive
to acquiring the infection, with increased disease noted when the spore levels become
concentrated and/or the birds immune systems are depressed as when they moult.
Disseminated Aspergillosis in a Little Penguin, arwh , , forum.backyardpoultry.com
The necropsy of penguin showed that airsacs were diffusely thickened, opaque, and studded
with multiple off-white to pale green dull. Similar plaques were scattered across coelomic
viscera serosal surfaces and adherent to the lungs which were diffusely dark red purple and wet.
The histopathology revealed that granulomatous, heterophilic, and necrotizing inflammation
with myriad intralesional fungal hyphae morphologically consistent with Aspergillus spp. were
present in the lungs, airsacs, kidneys, oviduct, trachea, mesentery, and serosal surfaces of
coelomic viscera. There was significant atrophy of adipose tissue, skeletal muscle, liver, and
pancreas
In a retrospective studies in Gifo University, Yanai reported that, 10 of 42(28.3%) cases of
death in penguins in Japan were due to aspergillosis.
Aspergillosis (air sacs) in an adult male Macaroni penguin, Yanai, Gifu University
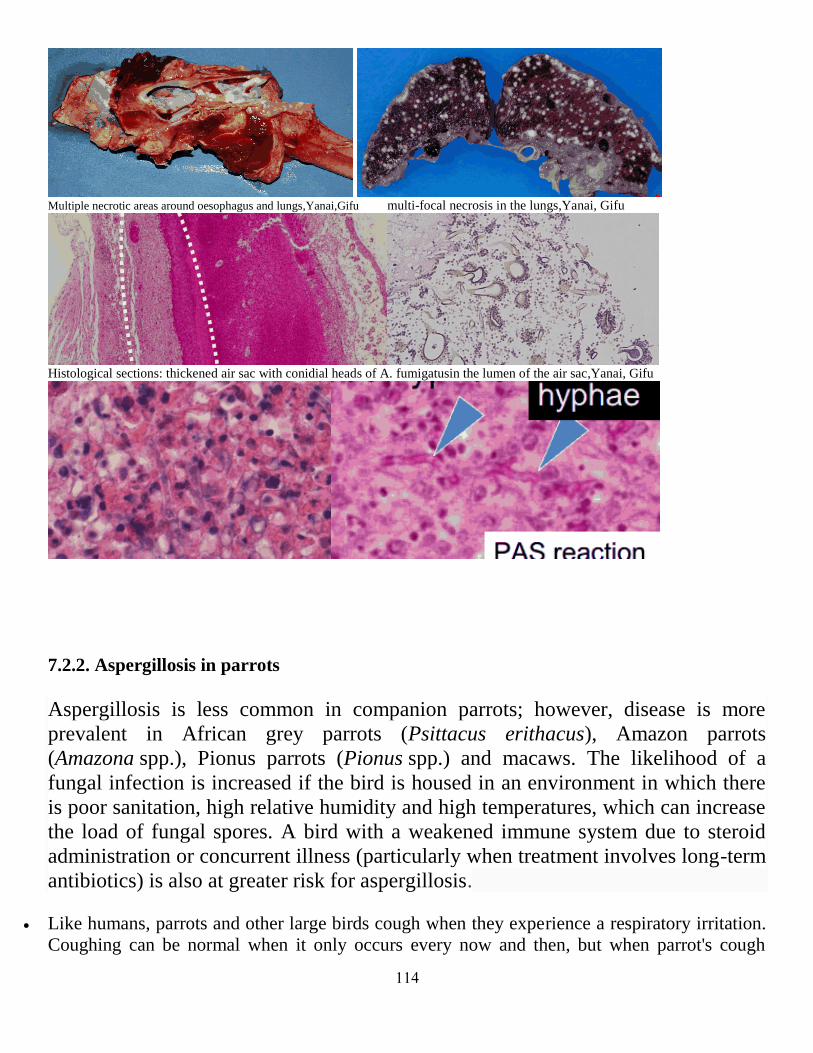
114
Multiple necrotic areas around oesophagus and lungs,Yanai,Gifu multi-focal necrosis in the lungs,Yanai, Gifu
Histological sections: thickened air sac with conidial heads of A. fumigatusin the lumen of the air sac,Yanai, Gifu
7.2.2. Aspergillosis in parrots
Aspergillosis is less common in companion parrots; however, disease is more
prevalent in African grey parrots (Psittacus erithacus), Amazon parrots
(Amazona spp.), Pionus parrots (Pionus spp.) and macaws. The likelihood of a
fungal infection is increased if the bird is housed in an environment in which there
is poor sanitation, high relative humidity and high temperatures, which can increase
the load of fungal spores. A bird with a weakened immune system due to steroid
administration or concurrent illness (particularly when treatment involves long-term
antibiotics) is also at greater risk for aspergillosis.
Like humans, parrots and other large birds cough when they experience a respiratory irritation.
Coughing can be normal when it only occurs every now and then, but when parrot's cough

115
becomes chronic, it could be a sign of aspergillosis. Spores released by the aspergillus can get
trapped in the bird's respiratory system, causing the cough.
In addition to coughing, when aspergillus spores get into parrot's throat and lungs its voice may
change and it may refuse to talk entirely.
Spores released by aspergillus affect different parts of the respiratory system in different ways.
Such symptoms include labored breathing or sudden fits of suffocation. Your bird's neck may
turn blue as it tries to talk or cough. This is indicative of choking, but the bird could also be
suffocating on an aspergillus spore. In some instances, parrots are known to suddenly drop dead
after inhaling an aspergillus spore.
African Grey parrot Amazon parrots Pionus parrots Blue Yellow Macaw
7.2.3. Aspergillosis in quails
Aspergillosis in quail is charachterized by the formation of yellowish white nodular growth in
lungs and intercostal areas with thickened air sacs. Histopathologically, lungs show severe
congestion with focal haemorrhages, multiple granulomatous inflammation with caesative
necrotic areas in centre. Various fungal elements like conidia, long septate hyphae with
mononuclear and heterophilic infiltration are seen in these areas. Microbiological study reveals
velvety bluish green colony of Aspergillus fumigatus.
Nodules in the air sacs and on the peritoneal serosa in a case of aspergillosis in a common quail. www.fmv.utl.
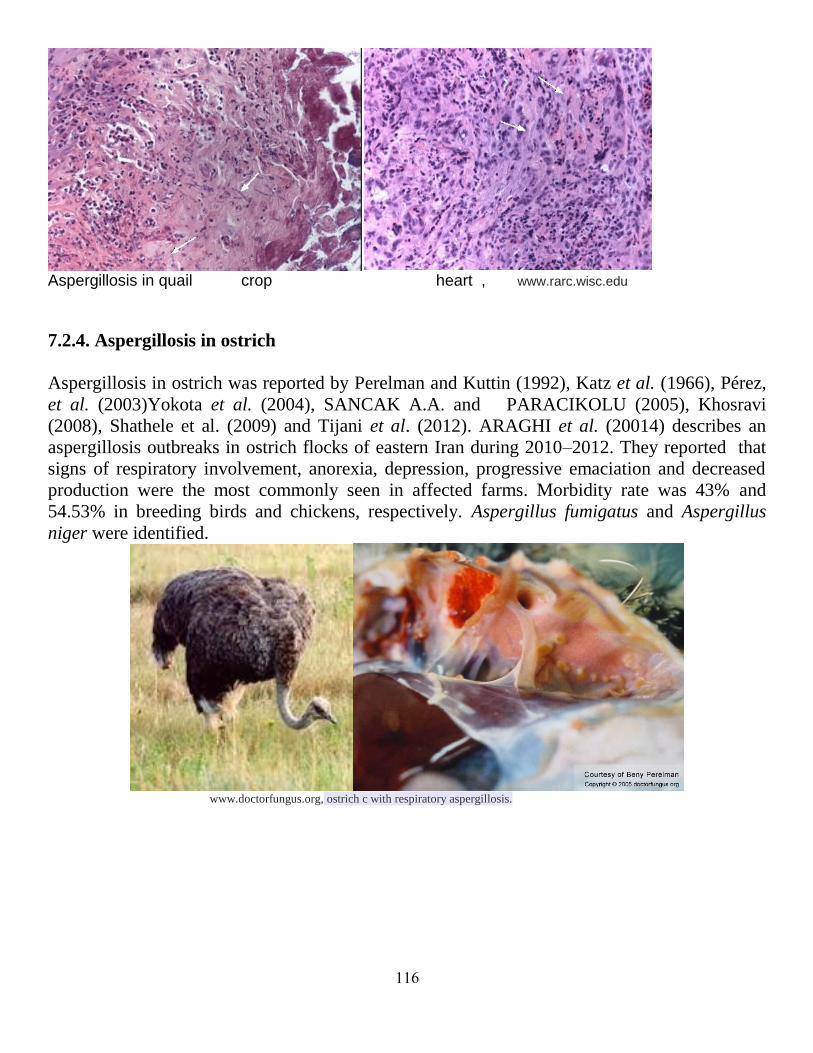
116
Aspergillosis in quail crop heart , www.rarc.wisc.edu
7.2.4. Aspergillosis in ostrich
Aspergillosis in ostrich was reported by Perelman and Kuttin (1992), Katz et al. (1966), Pérez,
et al. (2003)Yokota et al. (2004), SANCAK A.A. and PARACIKOLU (2005), Khosravi
(2008), Shathele et al. (2009) and Tijani et al. (2012). ARAGHI et al. (20014) describes an
aspergillosis outbreaks in ostrich flocks of eastern Iran during 2010–2012. They reported that
signs of respiratory involvement, anorexia, depression, progressive emaciation and decreased
production were the most commonly seen in affected farms. Morbidity rate was 43% and
54.53% in breeding birds and chickens, respectively. Aspergillus fumigatus and Aspergillus
niger were identified.
www.doctorfungus.org, ostrich c with respiratory aspergillosis.

117
7.2.5. Aspergillosis in red-tailed hawk (Buteo jamaicensis).
Aspergillosis in red-tailed hawk Multiple granulomas in the lungs A. fumigatus colony with spores in air sacs,MVS
7.2.6. Aspergillosis in Red-billed Toucan (Yanai, Gifu Univ)
Aspergillosis in Red-billed Toucan, Yanai, Gifu Univ.: multifocal lesions in the lung and liver
Hyphae radiating from a central necrotic nodule Conidia heads of Aspergillus in a pulmonary cavity
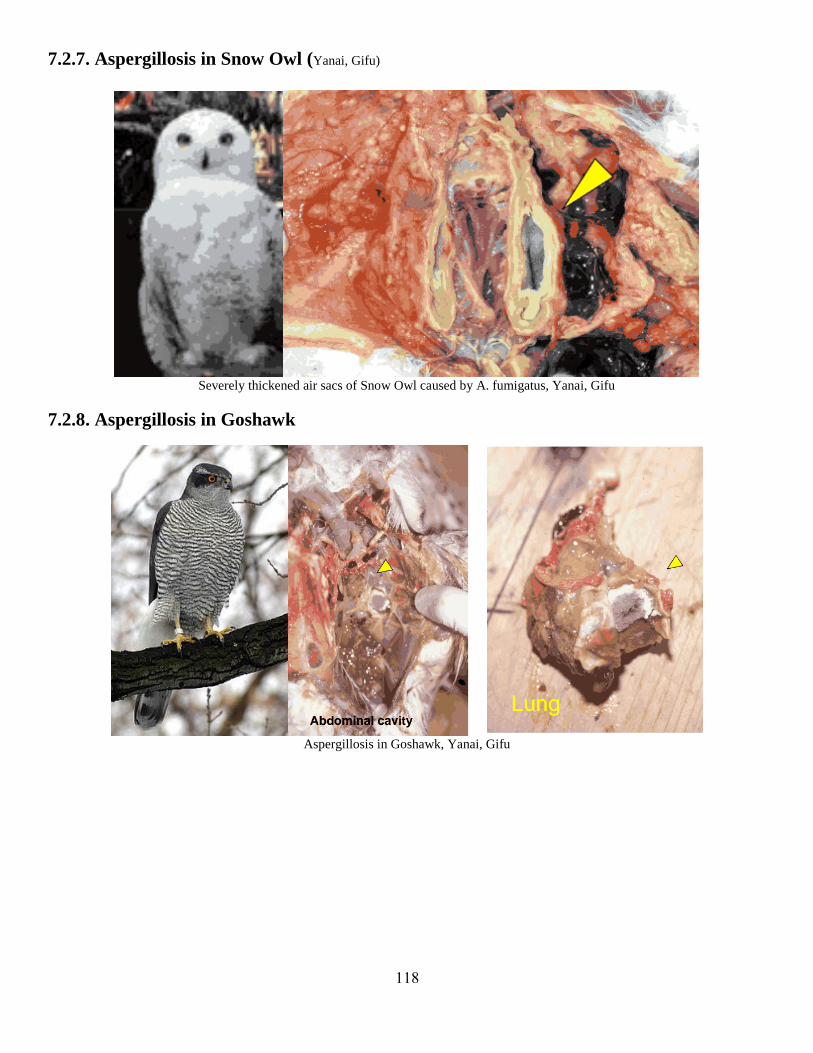
118
7.2.7. Aspergillosis in Snow Owl (Yanai, Gifu)
Severely thickened air sacs of Snow Owl caused by A. fumigatus, Yanai, Gifu
7.2.8. Aspergillosis in Goshawk
Aspergillosis in Goshawk, Yanai, Gifu

119
7.2.9. Aspergillosis in Cormorants
Aspergillosis in Cormorants, multifocal necrosis with Aspergillus hyphae in the lung
7.2.10. Aspergillosis in swans
Souza et al. (2005) reported on mortality in wild swans inNorthwest Washington State due to
aspergillosis.
Abou-Rawash et al. (2008) reported on disseminated aspergillosis in a Whooper Swan (Cygnus
Cygnus) in Japan. A Whooper Swan which usually migrates from Siberia to the north of Japan
in the winter season was found in Kume Island at the south of Japan in a state of pronounced
illness. Blood and serum analysis revealed hypoalbuminaemia elevated serum level of uric acid
(UA) and creatinin phosphokinase (CPK). The bird succumbed after unsuccessful attempts for
treatment. At necropsy, the bird had multiple focal and coalescent caseated granulomatous
nodules of whitish greenish color on the thoracic and abdominal air sacs, the lungs, and the
serosal surfaces of the spleen, liver and kidneys. At the inner side of the air sacs hyphal growth
with dark greenish color were scattered on most of the surface. Histopathologically, the present
case had a sever degree of chronic disseminated aspergillosis. The granulomas had a central
necrotic areas consisted of necrotic cell debris and hyphae with the microscopical features of
Aspergillus. A. fimigatus was identified in tissues by PAS, GMS, and immunohistochemically.
PCR was very successful to identify the causative fungus like other infectious agent.
On Jan. 27, 2014, 149 dead swans have been found in Whatcom County. The death was
attributed also here to aspergillosis. a disease which is being blamed for the deaths of trumpeter
swans spending the winter on Whatcom County's Wiser Lake.

121
Whooper swan, multifocal white nodules in the air sacs with frequent fungi, Yanai, Gifu
Multiple mycotic lesions in the lungs and larynx of a whooper swan, Yanai, Gifu
7.2.11. Aspergillosis in kiwi
The Wellington Zoo reported on 30 September 2013 that, eight young rowi—the rarest
species of kiwi—have died from respiratory tract infections. The kiwi were being treated for
nematodes (a type of worm) in Wellington Zoo when they started to show signs of respiratory
problems.The respiratory tract infection was caused by the fungus Aspergillus spp. which is
commonly found in the environment. It is thought that the birds’ weakened immunity from the
nematodes made them susceptible to this.
Travis et al. (2014) reported on Isolation and Identification of Aspergillus spp. from Brown
Kiwi (Apteryx mantelli) Nocturnal Houses in New Zealand.

121
A Rowi kiwi chick. Photo / File Eight Kiwi chicks have died from respiratory tract infections at Wellington Zoo.
Recently reported cases:
1. Secondary Aspergillus fumigatus infection associated with coloidal goiter in a black-masked lovebird
(Agapornis personata). 435
2. Drug resistance of Aspergillus fumigatus strains isolated from flocks of domestic geese in Poland. 436
3. Isolation and identification of Aspergillus spp. from brown kiwi (Apteryx mantelli) nocturnal houses in
New Zealand. 437
4. Monitoring of fungal loads in seabird rehabilitation centers with comparisons to natural seabird
environments in northern California.438
5. Mutations in the Cyp51A gene and susceptibility to itraconazole in Aspergillus fumigatus isolated from
avian farms in France and China.439
6. Environmental contamination by Aspergillus spp. in laying hen farms and associated health risks for
farm workers. 440
7. Isolation and identification of Aspergillus spp. from brown kiwi (Apteryx mantelli) nocturnal houses in
New Zealand. 441
8. [Radiographic findings in raptors affected with a mycosis of the respiratory tract].442
9. A model for treating avian aspergillosis: serum and lung tissue kinetics for Japanese quail (Coturnix
japonica) following single and multiple aerosol exposures of a nanoparticulate itraconazole suspension. 443
10. Inflammatory marker profiles in an avian experimental model of aspergillosis.444
11. Opportunistic infection of Aspergillus and bacteria in captive Cape vultures (Gyps coprotheres). 445
12. Emerging and reemerging diseases of avian wildlife.446
13. Assessment of Aspergillus fumigatus pathogenicity in aerosol-challenged chickens (Gallus gallus)
belonging to two lineages. 447
14. Aspergillosis in Japanese quail (Coturnix coturnix japonica). 448
15. . The occurrence of aspergillosis in flock of turkey poults.449
16. Serum protein electrophoresis by using high-resolution agarose gel in clinically healthy and Aspergillus
species-infected falcons. 450
17. Innate Immunity and the Role of Epithelial Barrier During Aspergillus fumigatus Infection.451
18. A longitudinal study on the incidence of mortality of infectious diseases of commercial layer birds in
Bangladesh.452
.
19. Aspergillus fumigatus and other thermophilic fungi in nests of wetland birds. 453

122
20. Microsatellite typing of Aspergillus flavus from clinical and environmental avian isolates.454
.
21. Genetic structure of Aspergillus flavus populations in human and avian isolates.455
22. Aspergillus fumigatus from normal and condemned carcasses with airsacculitis in commercial poultry.456
23. Retrospective study of aspergillosis and other fungi in poultry (1980-2008).457
24. Serologic testing for aspergillosis in commercial broiler chickens and turkeys.458
25. Aspergillosis in gamebirds and ducks. 459
26. Macroscopic and Microscopic Diagnosis of Aspergillosis in Poultry. 460
27. Aspergillosis in gamebirds and ducks. 461
28. Spinal aspergillosis in pheasants. 462
29. Aspergillus fumigatus in Poultry. 463
30. Aspergillus fumigatus in Poultry. 464
31. Diagnosis and Treatment of Aspergillosis in An Ostrich Flock.465
32. Microsatellite typing of avian clinical and environmental isolates of Aspergillus fumigatus. 466
33. Articular Aspergillosis of Hip Joints in Turkeys. 467
34. Molecular epidemiology and virulence assessment of Aspergillus fumigatus isolates from white stork
chicks and their environment. 468
35. Aspergillus infections in birds: a review. 469
36. Embryonated eggs as an alternative infection model to investigate Aspergillus fumigatusvirulence. 470
37. Pyogranulomatous Aspergillosis in An Endemic Formosan Blue Magpie. 471
38. Aspergillosis in turkey poults.472
39. Clinical, mycological and pathological findings in turkeys experimentally infected by Aspergillus
fumigatus. 473
40. Efficacy of voriconazole in Japanese quail (Coturnix japonica) experimentally infected withAspergillus
fumigatus. 474
41. Development of a method for the identification using the polymerase chainre action of Aspergillus
fumigatus isolated from ostriches. 475
42. Aspergillosis in ostriches. 476
43. Aspergillosis and gastric impaction in an ostrich. 477
44. Aspergillus fumigatus infection in an ostrich (Struthio camelus). 478
45. Outbreak of severe disseminated aspergillosis in a flock of ostrich (Struthio camelus).479
46. Fatal Aspergillosis in an Ostrich (Struthio camelus) Predisposed by Pulmonary Haemangioma in the
Kingdom of Saudi Arabia.480
47. Aspergillosis outbreaks in ostrich flocks of eastern iran during 2010–2012 . 481
48. Outbreak of aspergillosis in a flock of adult ostriches (Struthio camelus)482
49. Pulmonary Aspergillosis in an Adult Male Ostrich (Struthio camelus): A Case Report.483
50. Disseminated aspergillosis in a Whooper Swan (Cygnus Cygnus). 484
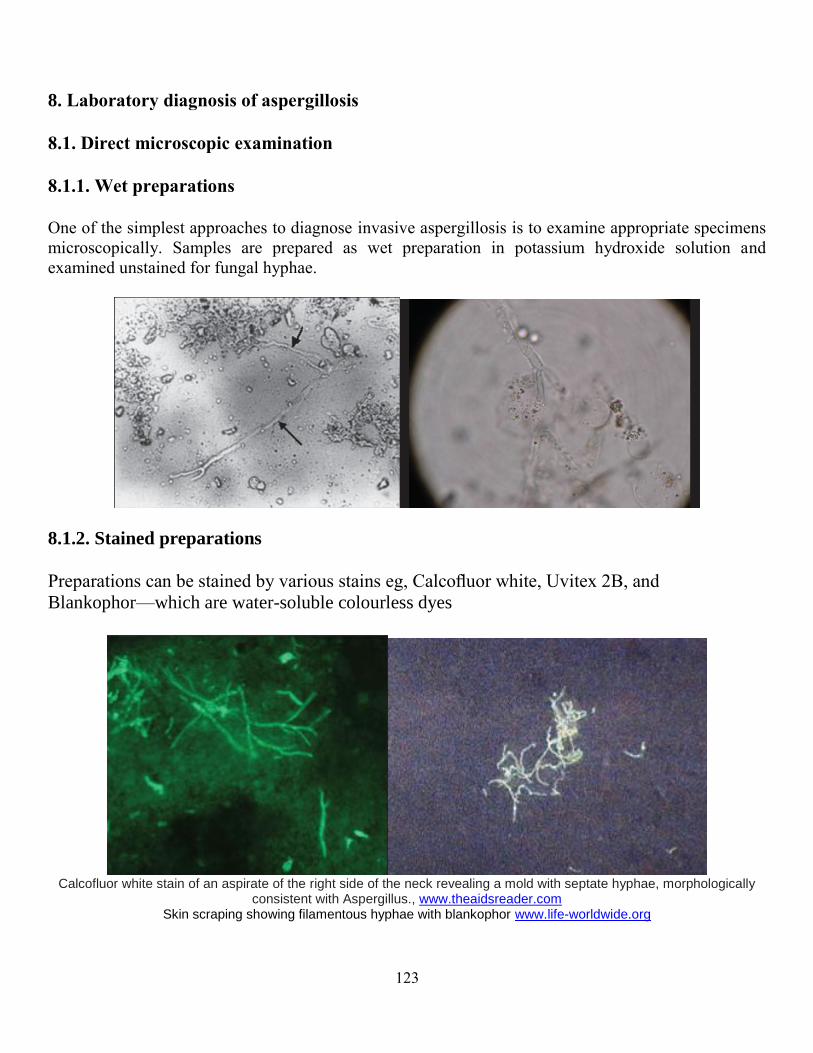
123
8. Laboratory diagnosis of aspergillosis
8.1. Direct microscopic examination
8.1.1. Wet preparations
One of the simplest approaches to diagnose invasive aspergillosis is to examine appropriate specimens
microscopically. Samples are prepared as wet preparation in potassium hydroxide solution and
examined unstained for fungal hyphae.
8.1.2. Stained preparations
Preparations can be stained by various stains eg, Calcofluor white, Uvitex 2B, and
Blankophor—which are water-soluble colourless dyes
Calcofluor white stain of an aspirate of the right side of the neck revealing a mold with septate hyphae, morphologically
consistent with Aspergillus., www.theaidsreader.com Skin scraping showing filamentous hyphae with blankophor www.life-worldwide.org

124
8.1.3. Histopathological examination
Histopathological examination of biopsy or autopsy material provides a diagnosis of proven
invasive fungal infection (IFI). Tissue sections are stained by standard haematoxylin and eosin
staining should reveal the presence of Aspergillus hyphae but stains such as period acid Schiff
and Grocott’s silver should be carried out whenever a fungal infection is suspected.
Aspergillus hyphae seen in tissue sections tend to be narrow (1–3 um in diameter) and septate
a Septate, branching hypha (arrow) of Aspergillus flavus in corneal scrape material from a patient with keratitis (Gram stain; 1,000×). Leema G,
Kaliamurthy J, Geraldine P, Thomas PA - Mol. Vis. (2010), b.Direct microscopic examination of corneal material by the method of Gram staining revealed the presence of fungal hyphae.b.Aspergillus keratitis:
Histopathology of the biopsied mass showed a giant cell granuloma with surrounding numerous branching, septate hyphae. (H and E, x 40)
Akhtar K, Mehdi G, Shahid M, Alam A. Tropical India. Ann Trop Med Public Health 2012;5:357-9
a.Angioinvasion – Aspergillus hyphae invading a blood vessel, GMS stain, www.stritch.luc.edu
b. Bronchoscopic biopsy demonstrated septate hyphae with branching at 45o (methenamine silver stain). www.aspergillus.org.uk
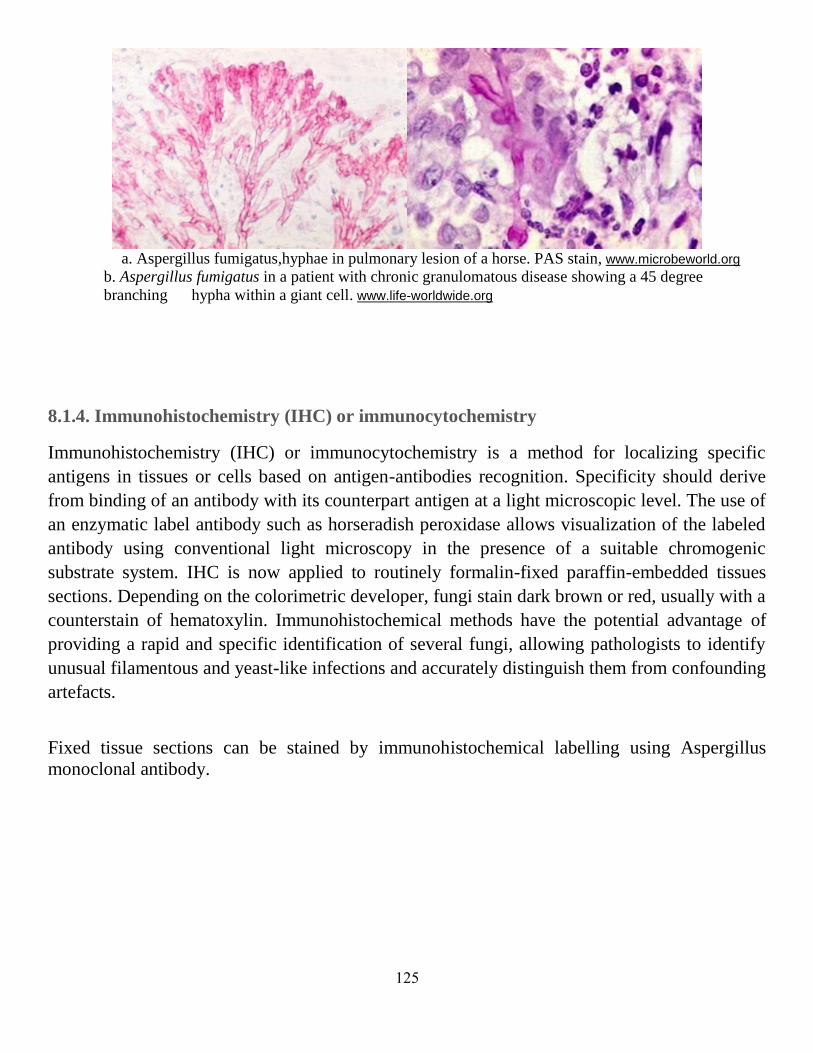
125
a. Aspergillus fumigatus,hyphae in pulmonary lesion of a horse. PAS stain, www.microbeworld.org
b. Aspergillus fumigatus in a patient with chronic granulomatous disease showing a 45 degree
branching hypha within a giant cell. www.life-worldwide.org
8.1.4. Immunohistochemistry (IHC) or immunocytochemistry
Immunohistochemistry (IHC) or immunocytochemistry is a method for localizing specific
antigens in tissues or cells based on antigen-antibodies recognition. Specificity should derive
from binding of an antibody with its counterpart antigen at a light microscopic level. The use of
an enzymatic label antibody such as horseradish peroxidase allows visualization of the labeled
antibody using conventional light microscopy in the presence of a suitable chromogenic
substrate system. IHC is now applied to routinely formalin-fixed paraffin-embedded tissues
sections. Depending on the colorimetric developer, fungi stain dark brown or red, usually with a
counterstain of hematoxylin. Immunohistochemical methods have the potential advantage of
providing a rapid and specific identification of several fungi, allowing pathologists to identify
unusual filamentous and yeast-like infections and accurately distinguish them from confounding
artefacts.
Fixed tissue sections can be stained by immunohistochemical labelling using Aspergillus
monoclonal antibody.

126
Aspergillus Polyclonal Antibody. Immunohistochemistry with anti-NY-BR-1 Monoclonal Anti, www.pierce-antibodies.com
Anti-Aspergillus antibody , www.abcam.com, Immunohistochemistry (Frozen sections) - Anti-Aspergillus antibody (ab20419)Image from Grahl N
et al., PLoS Pathog. 2011 Jul;7(7):e1002145
. Anti-Aspergillus antibody. ab20419, staining Aspergillus (green) in lung tissue from a murine model of corticosteroid-induced invasive pulmonary
aspergillosis, by Immunohistochemistry www.abcam.com.
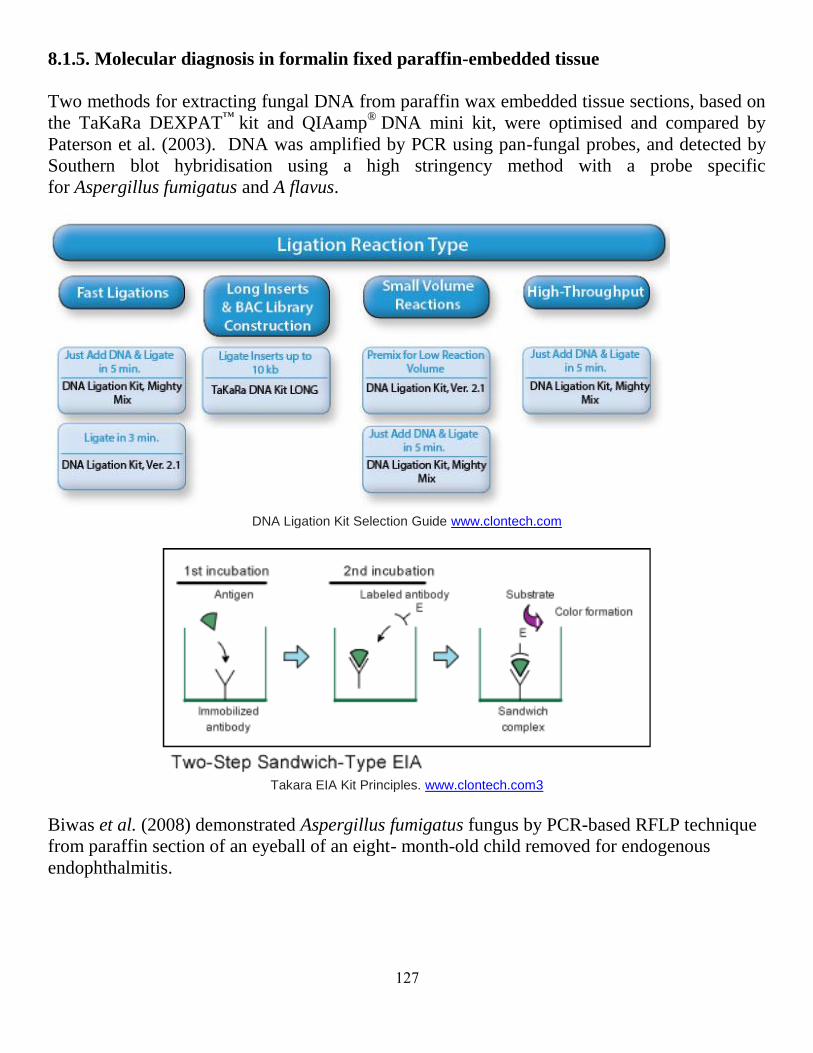
127
8.1.5. Molecular diagnosis in formalin fixed paraffin-embedded tissue
Two methods for extracting fungal DNA from paraffin wax embedded tissue sections, based on
the TaKaRa DEXPAT™
kit and QIAamp® DNA mini kit, were optimised and compared by
Paterson et al. (2003). DNA was amplified by PCR using pan-fungal probes, and detected by
Southern blot hybridisation using a high stringency method with a probe specific
for Aspergillus fumigatus and A flavus.
DNA Ligation Kit Selection Guide www.clontech.com
Takara EIA Kit Principles. www.clontech.com3
Biwas et al. (2008) demonstrated Aspergillus fumigatus fungus by PCR-based RFLP technique
from paraffin section of an eyeball of an eight- month-old child removed for endogenous
endophthalmitis.

128
Diagnosis of Aspergillus fumigatus endophthalmitis from formalin fixed tissue. Biwas et al. (2008) www.scienceopen.com...
Sometimes a fungus is seen in a specimen or tissue and not cultured. It is important to identify
such fungi to genus and preferably species level. Fresh non-embedded tissues have shown that
sensitivity for PCR detection of fungi exceeds 95%, while the sensitivity of paraffin-embedded
samples is currently ~60%. If fungal infection is strongly suspected prior to biopsy or resection,
retention of some of the sample fresh (ie not placed in formalin) may facilitate aetiological
diagnosis. Only for Aspergillus spp. is a commercially available technique to determine the
genus of fungi found in tissue sections published, but this method does not separate species
of Aspergillus. The majority of the published assays target specific rRNA genes (18S or D1-2
of 28S) or the intervening internal transcribed spacer (ITS1 and ITS2).
8.2. Isolation and identification
Most Aspergillus sp. grow relatively rapidly (typically within 48 hr) and on most microbiology
media including both mycological media such as Sabouraud’s agar and blood agars used for
general bacteriological culture.Identification of cultures of most species Aspergillus is generally
straightforward by colony and microscopic morphology.
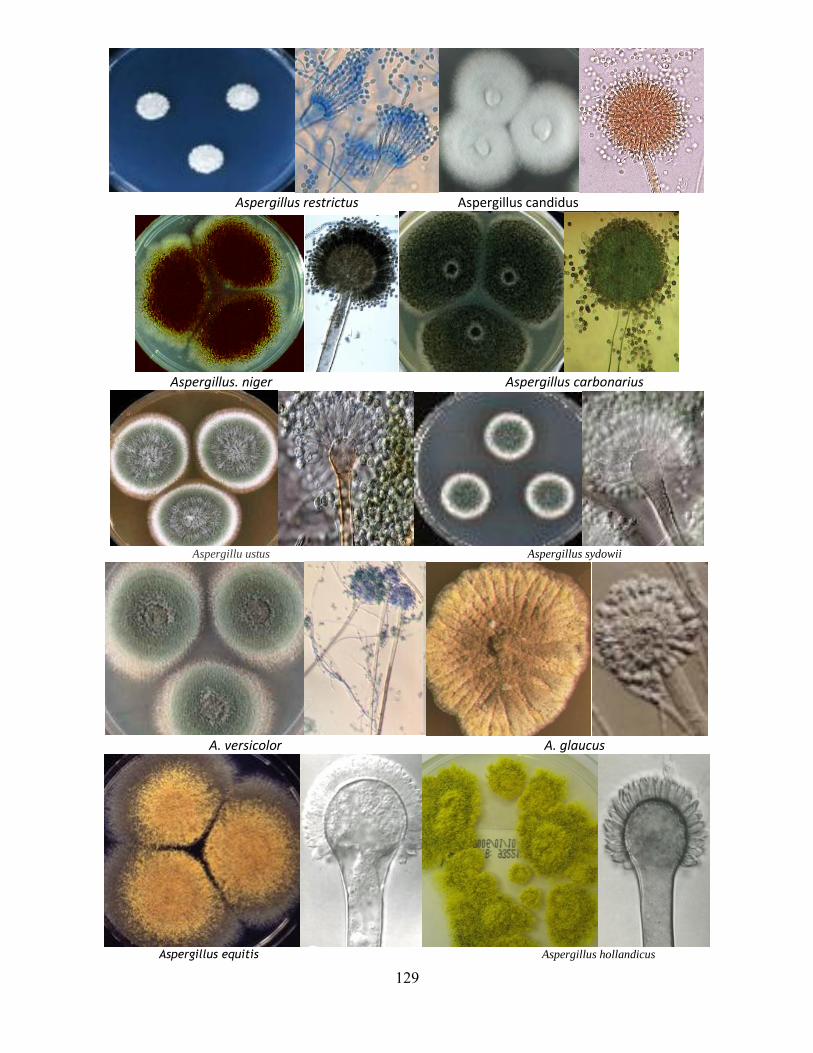
129
Aspergillus restrictus Aspergillus candidus
Aspergillus. niger Aspergillus carbonarius
Aspergillu ustus Aspergillus sydowii
A. versicolor A. glaucus
Aspergillus equitis Aspergillus hollandicus

131
Aspergillus terreus Aspergillus flavipes
Aspergillus ochraceus Aspergillus flavus
Aspergillus parasiticus Aspergillus oryzae
Aspergillus wentii Aspergillus fumigatus

131
Aspergillus felis Aspergillus clavatus
Aspergillus nidulans Aspeergillus avenaceous
Aspergillus carneus, Aspergillus giganteus
Aspergillus indologenus Aspergillus deflectus

132
8.3.Molecuar identification of aspergilli
Sequencing of genes, such as actin, calmodulin, ITS, rodlet A (rodA) and/or β-tubulin (βtub),
has been used to distinguish A. fumigatus from related species. Multilocus sequence typing can
alternatively be used for the identification of those related species, which is a strategy that also
involves sequencing of several gene fragments. A few other techniques, such as random
amplified polymorphic DNA, restriction fragment length polymorphisms and a new proposed
microsphere-based Luminex assay, may enable molecular identification of A. fumigatus without
sequencing. However, these methodologies are quite time consuming and labour demanding
and are thus impractical in most clinical labs. In addition, they can be very expensive when
employed to study collections of large numbers of isolates (Serrano et al., 2011).
Electrophoretic profile of several species of sectionFumigati. F1 - Aspergillus fumigatiaffinis, F2 - Aspergillus lentulus, F3 -Aspergillus
novofumigatus, F4 - Aspergillus unilateralis, F5 - Neosartorya hiratsukae, F6 - Neosartorya pseudofischeri, F7 - Neosartorya udagawae; AF1, AF2
and AF3 -Aspergillus fumigatus strains.
Alignment of β-tubulin sequences from species of section Fumigati. Serrano et al. BMC Microbiology 2011 11:82 doi:10.1186/1471-2180-11-82

133
Alignment of rodlet A sequences from species of section Fumigati.
Serrano et al. BMC Microbiology 2011 11:82
As reported by Balajee et al. (2009) the molecular identification scheme was as follows:
Genomic DNA was extracted from aspergilli grown for 48 h on Sabouraud dextrose agar plates
by using a DNeasy tissue kit (Qiagen, Valencia, CA). Universal fungal primers directed to the
ITS1-5.8S-ITS2 and the β-tubulin regions were employed to amplify DNA from
all Aspergillus isolates, as described previously. The resultant PCR amplicons were purified by
using an ExoSAP-IT enzyme system (USB Corporation, Cleveland, OH), according to the
manufacturer's instructions. Sequencing of both strands (with the same primers used for PCR
amplification) was performed with a BigDye Terminator (version 1.1) cycle sequencing kit
(Applied Biosystems). All cycle sequencing reactions were performed on a GeneAmp PCR
system 9700 thermocycler (Applied Biosystems) by using an initial denaturation at 96°C for 5
s, followed by 30 cycles of 96°C for 10 s, 50°C for 5 s, and 60°C for 4 min. The products were
purified with an Agencount CleanSEQ system (Beckman Coulter, Beverly, MA), dried,
resuspended in 0.1 mM EDTA, and run on a 3730 DNA analyzer (Applied Biosystems) using
of the protocols supplied by the manufacturer. The resultant nucleotide sequences were edited
by using the Sequencher program (Gene Codes Corporation, Ann Arbor, MI) and aligned by
using the program CLUSTAL W. Gene sequences derived from the ITS1-5.8S-ITS2 and the β-
tubulin regions of all the Aspergillus isolates were compared with sequences in the GenBank
database to identify isolates to the species complex level and to the species level within the
complex.
134
Rapid detection of Aspergillus spp. DNA from respiratory and serum samples using Real-Time PCR
Effective extraction of fungal DNA from respiratory samples
Aspergillus niger PCR Detection Kit [32900] : Norgen Biotek Aspergillus niger PCR Primer Set and Controls
Aspergillus fumigatus PCR Detection Kit New rtPCR kit to detect Aspergillus infection,
135
8.4. Serological techniques
8.4.1. Antigen detection in the diagnosis of invasive aspergillosis
In his excellent review on the diagnosis of invasive aspergillosis, Verweij (2005) mentioned
that Aspergillus species are known to release exo-antigens during growth in vitro and in vivo.
Low levels of antigens may be present in body fluids of patients with
invasive Aspergillus infection such as serum, urine and CSF. A number of methods have been
developed and evaluated which employ antibodies directed against antigens produced by
Aspergillus. These methods include:
1. latex agglutination: Detection limit 15 ng/ml
2. radioimmunoassay: Detection limit 10 ng/ml
3. ELISA inhibition : Detection limit 5 ng/ml
4. sandwich ELISA : Detection limit 1 ng/ml
8.4.1.1. Detection of Aspergillus galactomannan
Two antigen detection kits are commercially available and have been evaluated in several
institutes.
The latex agglutination (LA) test (Pastorex Aspergillus, Sanofi Diagnostics Pasteur, Marnes-La-
Coquette, France) employs the rat monoclonal antibody EB-A2 to
detect Aspergillus galactomannan.
Recently, a sandwich enzyme-linked immunosorbent assay (ELISA) was developed
(Platelia® Aspergillus, Sanofi Diagnostics Pasteur) which employs the same monoclonal
antibody as the latex agglutination test. The detection limit of the sandwich ELISA was lowered
10-fold by employing the monoclonal antibody as a captor and detector, thus allowing 0.5 to 1.0
ng/ml of galactomannan to be detected. Several investigations have shown that the sensitivity of
the sandwich ELISA was higher that that of the LA-test.
Detection of Aspergillus galactomannan antigen Aspergillus Galactomannan detection kits

136
The assay was originally designed for serum, but has also been used on bronchoalveolar lavage
fluid (BAL), sputum, CSF, pleural fluid, pericardial fluid and tissue. The generally accepted
cutoff in serum for positives is 0.5.
The higher the OD the greater the likelihood of invasive aspergillosis. No cutoff has been
defined for any other specimen type, but in BAL fluids different authors have recommended
cutoffs from 1.0 to 2.0. This variation partly reflects different patient populations and different
dilution factors during bronchoalveolar lavage.
Overall specificity of Aspergillus antigen detection using the galactomannan EIA is
approximately 80%. Several antibiotics and other patient factors may yield false positives.
Several beta-lactam antibiotics are manufactured using fungal fermentation as s first step. This
often results in carryover of galactomannan into the antibiotic preparation and ‘false positive’
galactomannan results that can persist for some days. The most common antibiotics to be
implicated are piperacillin/tazobactam (Tazocin) False positive reactivity of the ELISA was
found in up to 8% of serum samples and occurred especially with samples obtained within 30
days of BMT or cytotoxic chemotherapy, and in premature infants. False positive reactivity in a
single serum sample can be overcome by performing ELISA with additional serum samples
and most investigators now define positive as two separate positive samples. If positive, other
tests and procedures are required to localise and confirm the presence of infection.
8.4.1.2. Detection of 1,3 β-D-Glucan (BDG)
As mentioned by Barton (2013), the cell walls of Aspergillus contain relatively large amounts
of glucan of which 1,3 -D-glucan forms a large part. In vitro analysis of growing A.
fumigatus showed that, like GM, BDG is released during logarithmic growth, though slightly
later.
BDG can be detected through a pathway in the Limulus amoebocyte lysate (LAL) coagulation
cascade that has traditionally be used for the detection of bacterial endotoxin. Whilst endotoxin
interacts with LAL via factors B and C, factor G in the LAL interacts with BDG activating a
proclotting enzyme which can then cleave a chromogenic substrate to generate a product
detectable by spectrophotometry down to 10 pg/mL
There are four different commercial assays for the detection of BDG in clinical specimens. The
Associates of Cape Cod Fungitell kit uses amoebocyte lysates from Limulus polyphemus while
the Seikagaku Fungitec-G test uses reagents from Tachypleus tridentarius as does the Wako β-
Glucan test. Recommended cutoffs for reporting positive results vary between assays.
Manufacturers of the Fungitell assay requires >80 pg/mL to be detected for a positive with 60–
79 pg/mL Cutoffs for the T. tridentatus based assays are lower at 20 pg/mL and even lower
137
cutoffs of 11 pg/mL or two sera at 7 pg/mL have been proposed. A fourth assay, GKT-25-M has
been reported in the Chinese literature.
Fungitell® Assay, www.bioresearchonline.com Fungitech G-test, Seikagaku Co, www.pfdb.net
8.4.2. Aspergillus antibody detection
There are multiple marketed IgG antibody tests to detect A. fumigatus antibodies. A smaller
number of less well used and often usually incompletely validated tests are available for other
species of Aspergillus including A. flavus, A. terreus, A. niger, A. versicolor and A. clavatus. All
testing is on serum.There are multiple marketed IgG antibody tests to detect A.
fumigatus antibodies, including Immy,Serion/Virion, Bioenche, BioRad, Thermofisher, Elitech,
and Microgen.
8.4.2.1. Aspergillus Immunodiffusion test
The ID test is very helpful in the diagnosis of ABPA and aspergilloma, the two forms of
aspergillosis observed in immunocompetent individuals where infection can be correlated
with a rise in specific antibodies. Precipitins can be found in >90% of patients with
aspergilloma and in 70% of patients with ABPA.
In contrast to immunocompetent hosts, growth of Aspergillus in the tissues of an
immunosuppressed host does not correlate with an increase in anti-Aspergillus antibody
titers. The parallel use of ID and CF tests and clinical data is an effective means for
specific diagnosis of Aspergillosis Precipitins can be found in >90% of patients with
aspergillomas and in 70% of patients with ABPA.
The greatest number of Aspergillosis cases may be detected by the use of A. fumigatus,
A. flavus, A. niger, and A. terreus antigens in separate ID tests performed at the same
time. Precipitins are less frequent in patients with invasive Aspergillosis.
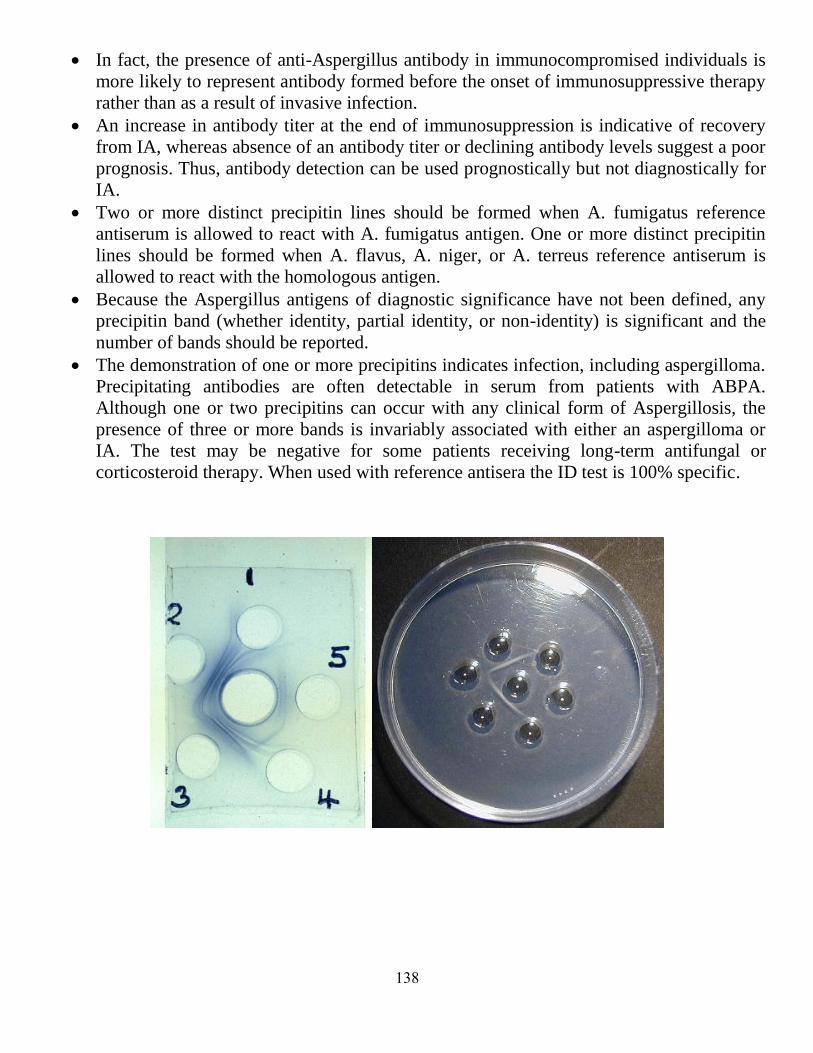
138
In fact, the presence of anti-Aspergillus antibody in immunocompromised individuals is
more likely to represent antibody formed before the onset of immunosuppressive therapy
rather than as a result of invasive infection.
An increase in antibody titer at the end of immunosuppression is indicative of recovery
from IA, whereas absence of an antibody titer or declining antibody levels suggest a poor
prognosis. Thus, antibody detection can be used prognostically but not diagnostically for
IA.
Two or more distinct precipitin lines should be formed when A. fumigatus reference
antiserum is allowed to react with A. fumigatus antigen. One or more distinct precipitin
lines should be formed when A. flavus, A. niger, or A. terreus reference antiserum is
allowed to react with the homologous antigen.
Because the Aspergillus antigens of diagnostic significance have not been defined, any
precipitin band (whether identity, partial identity, or non-identity) is significant and the
number of bands should be reported.
The demonstration of one or more precipitins indicates infection, including aspergilloma.
Precipitating antibodies are often detectable in serum from patients with ABPA.
Although one or two precipitins can occur with any clinical form of Aspergillosis, the
presence of three or more bands is invariably associated with either an aspergilloma or
IA. The test may be negative for some patients receiving long-term antifungal or
corticosteroid therapy. When used with reference antisera the ID test is 100% specific.

139
8.4.2.2. Aspergillus Antibody, Complement Fixation test
Single titers >=1:32 are indicative of recent infection. Titers of 1:8 or 1:16 may be indicative
of either past or recent infection, since CF antibody levels persist for only a few months. A
four-fold or greater increase in titer between acute and convalescent specimens confirms the
diagnosis. Sensitivity of the CF test for aspergillosis is lower than that of the immunodiffusion
test. Crossreactions may occur in patients with histoplasmosis and coccidioidomycosis. This test
is approved for New York patient testing.
Comments of Richard C. Barton (2013) on methods of laboratory diagnosis of aspergillosis
Of the wide variety of methods reviewed of diagnosing invasive aspergillosis, direct
microscopy and histopathology are undoubtedly the most subjective, skilled, and labour
intensive.
Though histopathological detection of Aspergillus of tissue will remain an essential
capacity and help define the highest level of certainty in diagnostic criteria, less invasive
and more rapid methods have already overtaken this approach in most settings. Some will
also consider that traditional culture-based methods may also be superceded by DNA and
antigen detection methods.
However, in the recent US PATH registry update culture of Aspergillus for the diagnosis
of IA was still the most frequent laboratory approach. Furthermore, cultures
of Aspergillus allow further analysis such as susceptibility to testing, recent
developments in direct molecular detection of resistance notwithstanding, and the
possibility of molecular typing in epidemiological investigations. Furthermore, new
species of Aspergillus causing invasive disease continue to be uncovered by culture
whose applicability to serological and molecular detection cannot be assumed. Culture of
respiratory specimens in clinical laboratories is unlikely to be abandoned in the near
future and culture of Aspergillus will remain an important if generally insensitive
approach to the diagnosis of IA.
The detection of galactomannan in clinical specimens is firmly established as the test of
choice for any laboratory providing diagnostic services for patients at risk of IA. Serum
detection remains a key approach and amenable to serial measurements whilst BAL
material appears to have a higher sensitivity but is often harder to obtain. False positives
are less of an issue than is often claimed with antibiotic sources of GM now rarely seen
and neonatal samples likely to account for a tiny fraction of samples analysed. Sensitivity
is clearly affected by antifungal treatment, though the biological basis for this is unclear,
this remains the main limitation to the use of the assay particularly in patients undergoing
antifungal prophylaxis. A plethora of meta-analyses have confirmed the clinical value of
GM testing and at least some analyses of GM serum kinetics point to the potential for this

141
assay to guide therapy beyond diagnosis. The BDG assay has yet to be widely adopted as
a diagnostic tool, perhaps suffering from the need to also require more specific diagnostic
methods to target therapy in positive patients. Meta-analysis suggests that problems with
specificity were probably overestimated in initial studies and sensitivity is comparable
with GM. The BDG assay will probably find its place in some centres in carefully
designed care pathways where the negative predictive value can be used to reduce
empiric therapy. The PCR assay to detect Aspergillus DNA held a large amount of
promise but has been limited up until recently by a lack of standardisation. The scientists
of EAPCRI have nobly met the challenge of technical diversity in PCR assays and
provided meticulously researched standard methods for extraction of DNA from whole
blood and serum.
9. Treatment of aspergillosis
As mentioned by Mayo Clinic Staff, the following guidelines are recommended:
1. Observation. Aspergillomas often don't need treatment, and medications aren't usually
effective in treating these fungal masses. Instead, aspergillomas that don't cause
symptoms may simply be closely monitored by chest X-ray.
2. Oral corticosteroids. The goal in treating allergic bronchopulmonary aspergillosis is to
prevent existing asthma or cystic fibrosis from becoming worse. The best way to do this
is with oral corticosteroids. Antifungal medications by themselves aren't helpful for
allergic bronchopulmonary aspergillosis, but they may be used in combination with
corticosteroids to reduce the dose of steroids and improve lung function.
3. Antifungal medications. These drugs are the standard treatment for invasive pulmonary
aspergillosis. Historically, the drug of choice has been amphotericin B, but the newer
medication voriconazole (Vfend) is now preferred because it appears more effective and
may have fewer side effects. All antifungals can cause serious problems, however,
including kidney and liver damage, and they frequently interact with other medications
given to people who have weakened immune systems.
4. Surgery. Because antifungal medications don't penetrate aspergillomas very well,
surgery to remove the fungal mass is the first-choice treatment when bleeding from the
mass in the lungs occurs. But the surgery is risky, and your doctor may instead suggest
embolization. In this procedure, your doctor, usually a radiologist, threads a small
catheter into the artery that supplies blood to the cavity containing the fungus ball, and
injects a special material that clogs the artery. Though this procedure can stop massive
bleeding, it doesn't prevent it from recurring, so it's generally considered a temporary
treatment.
141
Therapeutically Important Antifungal Agents (Khan, 2013)
1. Polyene Antibiotic (Amphotericin B):
Amphotericin B (AmB) is a polyene (containing multiple double bonds) macrolide
antibiotic originally isolated from a Streptomyces species. It binds to ergosterol, a
component of the fungal cell membrane. Binding to ergosterol destroys fungal
membrane integrity, resulting in leakage of cellular content and then cell death.
Being highly insoluble in water and in its original formulation, AmB was
complexed with deoxycholate.
AmB is poorly absorbed orally and requires parenteral administration. Following
IV administration, the drug is released slowly and is highly bound to protein
(>90%). AmB accumulates significantly in the liver and spleen, and it is present in
synovial, pleural, and peritoneal fluid. Central nervous system (CNS) penetration is
minimal. AmB has a half-life of 15 days and is excreted very slowly from the
kidney.
AmB adverse effects (AEs):
1. Infusion reactions include fever, shaking, chills, hypotension, and
tachypnea.
2. Renal toxicity is characterized by renal ischemia, hypokalemia, and
tubular acidosis.
3. Reduction of the production of erythropoietin (a glycoprotein that
stimulates bone marrow to produce RBCs) in the kidney.
AmB should not be administered concurrently with other nephrotoxic agents
(aminoglycosides, nonsteroidal anti-inflammatory drugs).
Serious AEs have prompted the development of lipid formulations of AmB. Lipid
formulations that minimize the renal toxicity of AmB are AmB colloidal dispersion
(ABCD), liposomal AmB (L-AmB), and AmB lipid complex (ABLC). These
formulations have largely replaced AmB.
2. Azoles (Voriconazole, Posaconazole, Itraconazole):
Chemically, azoles are triazole derivatives. These agents act by inhibiting fungal sterol-14-
alpha-demethylase, a cytochrome-dependent enzyme associated with ergosterol synthesis.
Inhibition of this enzyme enables the accumulation of methylsterol, thus impairing other
cellular functions. The main azoles are:
1. Voriconazole is formulated for oral and parenteral administration. Minimally bound to
plasma proteins, it is metabolized in the liver by CYP enzymes (CYP3A4, CYP2C9,
CYP2C19) and also inhibits these enzymes. Voriconazole is excreted renally. Transient

142
visual disturbances (blurred vision, changes in color vision or brightness) are associated
with this drug.
2. Posaconazole is administered orally as a suspension. Its absorption is increased with
food. Posaconazole is metabolized by glucuronidation and is excreted in the feces. The
drug inhibits CYP3A4 and is a substrate of P-glycoprotein (PgP). AEs include headache
and GI distress.
3. Itraconazole i. Itraconazole is available in oral and parenteral formulations. It is absorbed
well orally in the presence of food and low pH and is excreted fecally.
ii. Itraconazole is significantly bound to plasma proteins and is metabolized by
CYP3A4. Hydroxyitraconazole is an active metabolite of the parent drug.
iii. Itraconazole inhibits CYP enzymes and PgP, and it results in liver toxicity.
iv. Itraconazole has a negative inotropic effect on the heart and should not be
used in patients with ventricular dysfunction or congestive heart failure.
4. Echinocandins (Caspofungin, Micafungin):
These agents inhibit 1,3-beta-glucan synthase, an enzyme responsible for
fungal cell wall synthesis.
i. Echinocandins have selective toxicity against fungi because mammalian
cells do not possess a cell wall.
ii. Echinocandins are semisynthetic lipopeptides and are administered IV only.
These agents are significantly bound to plasma proteins (>95%), and CNS
penetration is inadequate.
iii. Echinocandins are excreted predominantly via the feces. Echinocandins do
not induce or inhibit CYP enzymes, nor do they interact with PgP. As a
result, the potential for drug interactions with other therapeutic agents is
negligible.
iv. Echinocandins are usually well tolerated, and the most common AEs are
elevated liver enzymes and creatinine (Cr), histamine-mediated effects (rash,
pruritus, facial swelling), GI distress, headache, and pyrexia.
143
10. References
1. Micheli , Pier Antonio (1729). Nova plantarum genera juxta Tournefortii methodum disposita .
Florentiae : Bernardi Paperini
2. Link, H.F. 1809. Observationes in ordines plantarum naturales. Dissertatio I. Magazin der Gesellschaft
Naturforschenden Freunde Berlin. 3:3-42
3. Desmazières, J.B.H.J. 1834. Descriptions et figures de six hyphomycètes inédites à ajouter à la flore
Française. Annales des Sciences Naturelles Botanique. 2:69-73
4. de Bary, A. (1854). Ueber die Entwickelung und den Zusammenhang von Aspergillus
glaucus undEurotium. Botanische Zeitung 12:425.
5. Fresenius, G. (1863). Aspergillus fumigatus Beiträge zur Mykologie. 3 81 (1863)
6. Tieghem, P. van. 1867. Description d'une nouvelle espèce d'Aspergillus: A. niger. Annales des Sciences
Naturelles Botanique
7. Wilhelm, K. (1877). Beiträge zur Kenntnis der Pilzgattung Aspergillus. In Dissertation, Strassburg. 66,
1-70
8. Saccardo, P.A. (1882). Fungi boreali-americani. Michelia. 2(8):564-582
9. Winter, G. 1884. Rabenhorst's Kryptogamen-Flora, Pilze - Ascomyceten. 1(2):1-192
10. Cohn, F. (1884). Über Schimmelpilze aIs Gährungserreger. Jahresbericht der Schlesischen Gesellschaft
für Vaterländische Kultur. 61:226
11. Gasperini, G. (1887). Sopra un nuovo morbo, che attacca i limoni e sopra alcuni ifomiceti. Atti della
Societa Toscana di Scienze Naturali. 8(2):328-332
12. Wehmer (1896),Aspergillus wentii Centralbl. Bakteriol.: 150
13. Wehmer (1899),Aspergillus ostianus Wehmer, Bot. Centralbl.: 461
14. Saito, K. (1906), Aspergillus japonicus. Bot. Mag. Tokyo 20: 61
15. Yukawa, M. (1911, Aspergillus melleus J. Coll. Agric. Imp. Univ. Tokyo 1: 358
16. Kita, G. (1913), Aspergillus tamarii Kita, Centralbl. Bakteriol., Abt. 2 37: 433
17. Blochwitz, in Dale, E. (1914) On the fungi of the soil. Part II. Fungi from chalky soil, uncultivated
mountain peat, and the "black earth" of the reclaimed fenland. Annales Mycologici. 12(1):33-62
18. Thom, C.; Church, M.B. (1918). Aspergillus fumigatus, A. nidulans, A. terreus n. sp. and their allies.
American Journal of Botany. 5(2):84-104
19. Thom, C., and Church, M. (1926). The Aspergilli (Baltimore: Williams & Wilkins)
20. Vuillemin, P. 1927. Sartorya, nouveau genre de Plectascinées angiocarpes. Comptes Rendues des
Séances Hebdomadaires de l'Académie des Sciences Paris. 184:136-137
21. Thom, C., and Raper, K.B. (1945) A Manual of the Aspergilli (Baltimore: Williams & Wilkins)
22. Raper, K.B., and Fennell, D.I. (1965) The Genus Aspergillus (Baltimore: Williams & Wilkins)
23. Samson, R.A., and Pitt, J.I. (1985) Advances in Penicillium and Aspergillus Systematics (New
York:Plenum)
24. W. Gams, M. Christensen, A. H. S. Onions, J. I. Pitt, R. A.Samson: Infrageneric taxa of Aspergillus. In:
Advances in Penicillium and Aspergillus Systematics, R. A. Samson, J. I. Pitt (Eds.), Plenum Press, New
York (1985) pp. 55–61.
144
25. Geiser, D.M., Timberlake, W.E., and Arnold, M.L. (1996). Loss of meiosis in Aspergillus. Mol. Biol.
Evol. 13: 809–817.
26. Samson, R.A, and J. I. Pitt, eds.( 2000 ). Integration of Modern Taxonomic Methods for Penicillium and
Aspergillus classification (Amsterdam: Harwood Academic Publications)
27. Peterson, S. W.: Phylogenetic relationships in Aspergillus based on rDNA sequence analysis. In:
Integration of Modern Taxonomic Methods for Penicillium and Aspergillus Classification, R. A. Samson,
J. I. Pitt (Eds.), Harwood Acad. Publ.,Amsterdam (2000) pp. 323–355.
28. Klich, M.A. (2002) Identification of Common Aspergillus Species (Utrecht: Centraalbureau voor
Schimmelcultures).
29. Frisvad, Jens C. J. Mick Frank, Jos A.M.P. Houbraken, Angelina F.A. Kuijpers3 and Robert A. Samson.
New ochratoxin A producing species of Aspergillus section Circumdati. STUDIES IN MYCOLOGY 50:
23–43. 2004.
30. Flannigan, B., R Samson & JD Miller (From Microorganisms in home and indoor work environments,
Published by Taylor and Francis)
31. Geiser, D.M. (2008). Sexual structures in Aspergillus: morphology, importance and genomics. Med.
Mycol. 46 (suppl. 1), S1-S6.
32. Geiser, D.M., Gueidan, C., Miadlikowska, J., Lutzoni, F., Kauff, F., Hofstetter, V., Fraker, E., Schoch,
C.L., Tibell, L., Untereiner, W.A., et al. (2006). Eurotiomycetes: Eurotiomycetidae and
Chaetothyriomycetidae. Mycologia 98, 1053–1065. Geiser, D.M., Klich, M.A., Frisvad, J.C., Peterson,
S.W.,
33. Varga, J., and Samson, R.A. (2007). The current status of species recognition and identification in
Aspergillus. Stud. Mycol. 59, 1–10.
34. Varga, J., J.C. Frisvad,
and R.A. Samson. Polyphasic taxonomy of Aspergillus section Candidi based on
molecular, morphological and physiological data. Stud Mycol. 2007; 59: 75–88.
35. Varga J, Due M, Frisvad JC, Samson RA - Taxonomic revision of Aspergillus section Clavati based on
molecular, morphological and physiological data. Stud. Mycol. (2007)
36. Varga,J Jens C. Frisvad and Robert A. Samson. Aspergillus sect. Aeni sect. nov., a new section of the
genus for A. karnatakaensis sp. nov. and some allied fungi. IMA FuNguS · voLuME 1 · No 2: 197–
205,2010
37. Varga, J., J.C. Frisvad, S. Kocsubé, B. Brankovics, B. Tóth, G. Szigeti and R.A. Samson. New and
revisited species in Aspergillus section Nigri. SIM June 30, 2011, 69,1, 1-17
38. Varga, J., Jens C. Frisvad and Robert A. Samson1. Polyphasic taxonomy of Aspergillus section Sparsi.
IMA FuNgus · voluMe 1 · No 2: 187–195, 2010
39. Varga J, Frisvad JC, Samson RA - Stud. Mycol. (2011). Two new aflatoxin producing species, and an
overview of Aspergillus section Flavi. Stud Mycol. Jun 30, 2011; 69(1): 57–80.
40. Samson, R.A. and Varga, J. (2009). Molecular Systematics of Aspergillus and its Teleomorphs. In:
Aspergillus: molecular biology and genomics., (pp. 19-40).
41. Geiser, D.M., Samson, R.A., Varga, J., Rokas, A., and Witiak, S.M. (2008). A review of molecular
phylogenetics in Aspergillus, and prospects for a robust genus-wide phylogeny. In: Aspergillus in the
Genomic Era, Varga, J., and Samson, R.A., eds. (Netherlands:Wageningen Academic Pubs), pp. 17–32.
42. Samson , R.A. , S.W. Peterson, J.C. Frisvad and J. Varga. New species in Aspergillus section Terrei.
Studies in Mycology 69: 39–55. 2011.,4
43. Samson , R.A. , J. Varga , M. Meijer and J.C. Frisvad . New taxa in Aspergillus section Usti. Studies in
Mycology 69: 81–97. 2011.

145
44. Jurjevic, Zeljko, Stephen W. Peterson, and Bruce W. Horn. Aspergillus section Versicolores: nine new
species and multilocus DNA sequence based phylogeny. IMA Fungus. Jun 2012; 3(1): 59–79.
45. Ding WY, Chan T, Yadavilli RK, McWilliams R. Aspergilloma and massive haemoptysis. BMJ Case
Rep. 2014 Apr 16;2014.
46. Vishak KA, Yogitha AP, Preetam AP, Anand R, Naik UB. A rare case of
calcified pulmonary aspergilloma. Lung India. 2014 Jan;31(1):79-81.
47. Benhamed L, Woelffle D. Adjuvant antifungal therapy after pulmonary surgery foraspergilloma: is it
useful? Interact Cardiovasc Thorac Surg. 2014 Mar 18. [Epub ahead of print]
48. Moodley L, Pillay J, Dheda K. Aspergilloma and the surgeon.
J Thorac Dis. 2014 Mar;6(3):202-209. Review.
49. Gazzoni FF, Severo LC, Marchiori E, Guimarães MD, Garcia TS, Irion KL, Camargo JJ, Felicetti JC, de
Mattos Oliveira F, Hochhegger B. Pulmonary Diseases with Imaging Findings MimickingAspergilloma.
Lung. 2014 Mar 11. [Epub ahead of print]
50. Yuan P, Wang Z, Bao F, Yang Y, Hu J. Is video-assisted thoracic surgery a versatile treatment for both
simple and complex pulmonary aspergilloma? J Thorac Dis. 2014 Feb;6(2):86-90.
51. Daste A, Gross-Goupil M, Ravaud A. Pulmonary Aspergilloma: An Unexpected Complication of
Radiofrequency Ablation in the Management of Targeted Therapy for a Patient With Metastatic Renal
Cell Carcinoma. Clin Genitourin Cancer. 2014 Jan 15. pii: S1558-7673(14)00004-4.
52. Kuptarnond C, Prathanee S. Treatment of pulmonary aspergilloma in Srinagarind Hospital. J Med Assoc
Thai. 2013 Sep;96 Suppl 4:S142-8.
53. Muniappan A, Tapias LF, Butala P, Wain JC, Wright CD, Donahue DM, Gaissert HA, Lanuti M,
Mathisen DJ. Surgical therapy of pulmonary aspergillomas: a 30-year North American experience. Ann
Thorac Surg. 2014 Feb;97(2):432-8.
54. Lopez-Pastorini A, Plönes T, Ludwig C, Stoelben E. Intrapulmonary aspergilloma in an old tuberculous
cavity with access to the bronchial system. Eur J Cardiothorac Surg. 2013 Dec 8. [Epub ahead of print]
55. Murphy D, Murphy D, Murray J, Gaine S. Case 3: aspergilloma. Ir Med J. 2013 Sep;106(8):247.
56. Pohl C, Jugheli L, Haraka F, Mfinanga E, Said K, Reither K. Pulmonary aspergilloma: a treatment
challenge in sub-Saharan Africa. PLoS Negl Trop Dis. Oct 2013; 7(10): e2352.
57. Ajili F, Boussetta N . [Gougerot-Sjögren syndrome complicated by pulmonaryaspergilloma].. Pan Afr
Med J. 2013 Jun 25;15:71.
58. Hiraki T, Gobara H, Kato K, Fujiwara H, Iguchi T, Matsui Y, Kanazawa S. A case
of pulmonary aspergilloma treated with radiofrequency ablation. Cardiovasc Intervent Radiol. 2014
Apr;37(2):554-7.
59. Ruan JZ, Zhang TH, Duan Y, Wang ZT. [Surgical treatment of pulmomary tuberculosis complicated
withaspergilloma]. Zhonghua Yi Xue Za Zhi. 2013 Jul 2;93(25):1975-7.
60. Ruan JZ, Zhang TH, Duan Y, Wang ZT. Always expect the unexpected: lung abscess due to
pseudomonas aeruginosa mimicking pulmonary aspergillomain acute B-cell leukemia.
Klin Padiatr. 2013 Nov;225(6):347-9.
61. Chen QK, Chen C, Chen XF, Jiang GN. Video-assisted thoracic surgery for pulmonary aspergilloma: a
safe and effective procedure. Ann Thorac Surg. 2014 Jan;97(1):218-23.
62. Sharma S, Dubey SK, Kumar N, Sundriyal D. 'Monod' and 'air crescent' sign in aspergilloma. BMJ Case
Rep. 2013 Sep 13;2013. pii: bcr2013200936.
63. Oda M, Saraya T, Wakayama M, Shibuya K, Ogawa Y, Inui T, Yokoyama E, Inoue M, Shimoyamada H,
Fujiwara M, Ota T, Takizawa H, Goto H.Calcium oxalate crystal deposition in a patient
withAspergilloma due to Aspergillus niger. J Thorac Dis. 2013 Aug;5(4):E174-8.
64. El Hammoumi M, Traibi A, El Oueriachi F, Arsalane A, Kabiri EH. Surgical treatment
of aspergilloma grafted in hydatid cyst cavity.
Rev Port Pneumol. 2013 Nov-Dec;19(6):281-3.
146
65. Sindhwani G, Rawat J, Kesarwani V.Haemoptysis after four years of lobectomy for aspergilloma. Indian
J Chest Dis Allied Sci. 2013 Jan-Mar;55(1):43-4.
66. Kumar N, Mishra M, Singhal A, Kaur J, Tripathi V. Aspergilloma coexisting with
idiopathic pulmonary fibrosis: a rare occurrence. J Postgrad Med. 2013 Apr-Jun;59(2):145-8.
67. Yasuda M, Nagashima A, Haro A, Saitoh G. Aspergilloma mimicking a lung cancer. Int J Surg Case
Rep. 2013;4(8):690-2.
68. Jung SW, Kim MW, Cho SK, Kim HU, Lee DC, Yoon BK, Jeong JP, Ko YC. A Case of
Endobronchial Aspergilloma Associated with Foreign Body in Immunocompetent Patient without
Underlying LungDisease.
Tuberc Respir Dis (Seoul). 2013 May;74(5):231-4.
69. Alberti N, Frulio N, Trillaud H, Jougon J, Jullie ML, Palussiere J. Pulmonary aspergilloma in a cavity
formed after percutaneous radiofrequency ablation. Cardiovasc Intervent Radiol. 2014 Apr;37(2):537-
40.
70. Singh UP, Aneja P, Aditi, Patel K. Co-existence of HIV, active tuberculosis and aspergilloma in a single
individual--a case report. Indian J Tuberc. 2013 Jan;60(1):55-8.
71. Moreira AS, Silva D, Ferreira AR, Delgado L. Antifungal treatment in allergic bronchopulmonary
aspergillosis with and without cystic fibrosis: a systematic review. Clin Exp Allergy. 2014 May 8. doi:
10.1111/cea.12333.
72. Tanou K, Zintzaras E, Kaditis AG. Omalizumab therapy for allergic bronchopulmonary aspergillosis in
children with cystic fibrosis: a synthesis of published evidence.
Pediatr Pulmonol. 2014 May;49(5):503-7.
73. Denning DW, Pashley C, Hartl D, Wardlaw A, Godet C, Del Giacco S, Delhaes L, Sergejeva S. Fungal
allergy in asthma-state of the art and research needs.
Clin Transl Allergy. 2014 Apr 15;4(1):14.
74. Khan B, Vohra R, Kaur R, Singh S; Ashapritpal; Vartika. Excellent outcome of Aspergillous
endophthalmitis in a case ofallergic bronchopulmonary aspergillosis. Indian J Ophthalmol. 2014
Mar;62(3):352-4.
75. Mou Y, Ye L, Ye M, Yang D, Jin M. A retrospective study of patients with a delayed diagnosis
ofallergic bronchopulmonary aspergillosis/allergicbronchopulmonary mycosis. Allergy Asthma Proc.
2014 Mar;35(2):21-6.
76. Chen X, Li J, Zhao X. Allergic bronchopulmonary aspergillosis coexists with hereditary bisalbuminemia.
Chin Med J (Engl). 2014;127(7):1391-3.
77. Sehgal IS, Agarwal R. Role of inhaled amphotericin in allergic bronchopulmonary aspergillosis. J
Postgrad Med. 2014 Jan-Mar;60(1):41-5.
78. Singh Sehgal I, Agarwal R. Pulse methylprednisolone in allergic bronchopulmonary
aspergillosis exacerbations. Eur Respir Rev. 2014 Mar 1;23(131):149-52.
79. Wolf BL, Johnson A. Unexpected decrease in total IgE in a patient with allergic bronchopulmonary
aspergillosis treated with omalizumab. J Allergy Clin Immunol Pract. 2014 Jan-Feb;2(1):111-3.
80. Mohindra S, Mehta R, Bal A. ABPA Concomitantly Occurring with Invasive SinusAspergillosis: A
Short Report on Two Patients. Indian J Otolaryngol Head Neck Surg. 2014 Jan;66(Suppl 1):329-33.
81. Pandit S, Choudhury S, Das A, Datta S, Das SK. Atypical Presentation of Allergic Bronchopulmonary
Aspergillosis: An Unusual Cause of Difficult-to-Treat Asthma. J Family Med Prim Care. 2013
Jan;2(1):98-100.
82. Liu XF, Sun YC, Jin JM, Li R, Liu Y. [Allergic bronchopulmonary aspergillosis in patients with chronic
obstructive pulmonary disease: report of 3 cases]. Zhonghua Jie He He Hu Xi Za Zhi. 2013
Oct;36(10):741-5.
83. Noguchi T, Yamamoto K, Moriyama G, Saito Y, Kyoyama H, Mikami S, Ono R, Kobayashi T, Yamana
K, Uematsu K. Evaluation of serum levels of carcinoembryonic antigen inallergic bronchopulmonary
aspergillosis. J Nippon Med Sch. 2013;80(6):404-9.
147
84. Lee JY, Choi H, Chon GR. Allergic bronchopulmonary aspergillosis mimicking relapsing chronic
eosinophilic pneumonia in non-asthma patient. Allergol Int. 2014 Mar;63(1):133-5.
85. Moss RB. Treatment options in severe fungal asthma and allergic bronchopulmonary aspergillosis. Eur
Respir J. 2014 May;43(5):1487-500.
86. Homma T, Kurokawa M, Matsukura S, Yamaguchi M, Adachi M. Anti-IgE therapy for allergic
bronchopulmonary aspergillosis. J Microbiol Immunol Infect. 2013 Nov 28. pii: S1684-1182(13)00197-
7.
87. Mou Y, Ye L, Gong Y, Zhang ZF, Jin ML. [Analysis of clinical features and allergic status of asthmatic
patients with positive serum mycosis-specific IgE]. Zhonghua Jie He He Hu Xi Za Zhi. 2013
Aug;36(8):563-6.
88. Agarwal R, Chakrabarti A. Allergic bronchopulmonary aspergillosis in asthma: epidemiological, clinical
and therapeutic issues. Future Microbiol. 2013 Nov;8(11):1463-74.
89. Azad C, Jat KR, Aggarwal P. Bronchial asthma with ABPA presenting as PTE. Indian J Crit Care Med.
2013 May;17(3):188-9.
90. Jat KR, Walia DK, Khairwa A. Anti-IgE therapy for allergic bronchopulmonary aspergillosisin people
with cystic fibrosis. Cochrane Database Syst Rev. 2013 Sep 17;9:CD010288.
91. Yoshida Y, Shirai T, Mikamo M, Shishido Y, Akita T, Morita S, Asada K, Fujii M, Suda T.
Development of allergic bronchopulmonary aspergillosiswith central bronchiectasis over a 10-year
period: the need to recheck allergen sensitization. Intern Med. 2013;52(18):2135-8.
92. Matsuse H, Tsuchida T, Fukahori S, Kawano T, Nishino T, Fukushima C, Kohno S. Dissociation
between sensitizing and colonizing fungi in patients with allergic bronchopulmonary aspergillosis. Ann
Allergy Asthma Immunol. 2013 Sep;111(3):190-3.
93. Poole CJ, Wong M. Allergic bronchopulmonary aspergillosis in garden waste (compost) collectors--
occupational implications. Occup Med (Lond). 2013 Oct;63(7):517-9.
94. Ishiguro T, Takayanagi N, Takaku Y, Kagiyama N, Shimizu Y, Yanagisawa T, Kawabata Y, Sugita Y.
Allergic bronchopulmonary aspergillosis with repeated isolation of nontuberculous mycobacteria. Intern
Med. 2013;52(15):1721-6.
95. Agarwal R, Chakrabarti A, Shah A, Gupta D, Meis JF, Guleria R, Moss R, Denning DW; Allergic
bronchopulmonary aspergillosis: review of literature and proposal of new diagnostic and classification
criteria.
ABPA complicating asthma ISHAM working group. Clin Exp Allergy. 2013 Aug;43(8):850-73.
96. Park MR, Nam YH, Lee SK, Kim KH, Roh MS, Lee HW, Jeong IH, Um SJ, Son CH. Uncertain areas in
the diagnosis of allergic bronchopulmonary aspergillosis in patients with asthma. Allergol Immunopathol
(Madr). 2013 Jul 1. pii: S0301-0546(13)00151-1.
97. Greenberger PA. When to suspect and work up allergic bronchopulmonary aspergillosis. Ann Allergy
Asthma Immunol. 2013 Jul;111(1):1-4.
98. Kumar R, Goel N. Allergic bronchopulmonary aspergillosis: a clinico-serological correlation with
radiologic profile. J Asthma. 2013 Sep;50(7):759-63.
99. Roth R, Schatz M. Allergic bronchopulmonary aspergillosis presenting as chronic cough in an elderly
woman without previously documented asthma. Perm J. 2013 Spring;17(2):e103-8.
100. Ghosh G, Sharma B, Chauhan A, Chawla MP. Coexistence of allergic bronchopulmonary
aspergillosis andallergic aspergillus sinusitis in a patient without clinical asthma. BMJ Case Rep. 2013
May 2;2013. pii: bcr2013008683.
101. Ting-hsu Chen,., and Helen Hollingsworth, Allergic Bronchopulmonary Aspergillosis. N Engl J Med
2008; 359:e7August 7, 2008DOI: 10.1056/NEJMicm055764
102. Nakamoto K, Takayanagi N, Kanauchi T, Ishiguro T, Yanagisawa T, Sugita Y. Prognostic factors in 194
patients with chronic necrotizingpulmonary aspergillosis. Intern Med. 2013;52(7):727-34.
103. Namesaya N, Tomioka H, Kaneda T, Kida Y, Kaneko M, Fuji H, Katsuyama E. [Three autopsy cases
of chronic necrotizing pulmonaryaspergillosis]. Kansenshogaku Zasshi. 2012 Sep;86(5):597-603.
148
104. Tokui K, Kawagishi Y, Inomata M, Taka C, Okazawa S, Yamada T, Miwa T, Hayashi R, Matsui S,
Takano Y, Tobe K. Systemic dissemination of chronic necrotizing pulmonaryaspergillosis in an elderly
woman without comorbidity: a case report. J Med Case Rep. 2012 Aug 31;6(1):270.
105. Rødland EK, Ueland T, Bjørnsen S, Sagen EL, Dahl CP, Naalsund A, Mollnes TE, Brosstad FR, Müller
F,Aukrust P, Frøland SS. Systemic biomarkers of inflammation and haemostasis in patients with
chronic necrotizing pulmonary aspergillosis. BMC Infect Dis. 2012 Jun 25;12:144.
106. Yoshida K, Kurashima A, Kamei K, Oritsu M, Ando T, Yamamoto T, Niki Y. Efficacy and safety of
short- and long-term treatment of itraconazole on chronic necrotizing pulmonary aspergillosisin
multicenter study. J Infect Chemother. 2012 Jun;18(3):378-85.
107. Gomez-Abreo D, Prost C, Couraud S, Parmeland L, Carret G, Boibieux A, Gagnieu MC, Gérinière L,
Avrillon V, Souquet PJ. [Chronic necrotizing pulmonary aspergillosis following an infection by
Mycobacterium malmoense]. Rev Mal Respir. 2012 Mar;29(3):435-9.
108. Yatera K, Yamasaki K, Kozaki M, Shimauchi M, Kawanami T, Nagata S, Suzuki Y, Tokuyama S, Inoue
N, Nishida C, Ishimoto H, Kawajiri T, Awaya Y, Tsuda T, Mukae H.
[Retrospective analysis of the safety of four hours administration of liposomal amphotericin B in
patients with chronicnecrotizing pulmonary aspergillosis]. Jpn J Antibiot. 2011 Oct;64(5):311-8.
109. Lee KH, Ryu SM, Park SM, Park HS, Lee KH, Cho SJ. A surgically treated case
of chronic necrotizing aspergillosiswith pleural invasion. Korean J Thorac Cardiovasc Surg. 2012
Feb;45(1):56-9.
110. Nasim A, Baqi S, Zeeshan SM, Aziz T. Chronic necrotizing pulmonary aspergillosis in a renal
transplant recipient. J Pak Med Assoc. 2011 Dec;61(12):1242-4.
111. Rajalingham S, Anshar FM. Chronic necrotizing pulmonary aspergillosis presenting as bilateral pleural
effusion: a case report. J Med Case Rep. 2012 Feb 14;6(1):62.
112. Lovrenski A, Panjković M, Eri Z, Klem I, Povazan D, Ilincić D, Milić M.
Chronic necrotizing pulmonary aspergillosis. Vojnosanit Pregl. 2011 Nov;68(11):988-91.
113. Wu CJ, Lee HC, Lo HJ, Ko WC. Resolution of galactomannan antigenemia in a patient receiving oral
voriconazole for chronic necrotizing pulmonaryaspergillosis. Diagn Microbiol Infect Dis. 2011
Aug;70(4):528-30.
114. Blanco JJ, Barcala FJ, Moure MA, Mao MC. [Chronic necrotizing pulmonary aspergillosis as a
complication of silicosis]. An Sist Sanit Navar. 2011 Jan-Apr;34(1):109-14.
115. Morita H, Oguri T, Uemura T, Iwashima Y, Nakamura A, Sato S. [Case
of chronic necrotizing pulmonary aspergillosiscomplicated by elevated eosinophils and serum IgE].
Nihon Kokyuki Gakkai Zasshi. 2010 Nov;48(11):842-6.
116. Lee EJ, Song R, Park JN, Lee YA, Son JS, Hong SJ, Yang HI, Lee SH.
Chronic necrotizing pulmonary aspergillosis in a patient treated with a tumor necrosis factor-alpha
inhibitor. Int J Rheum Dis. 2010 Aug;13(3):e16-9.
117. Rüchel R. [Lethal case of chronic necrotizing pulmonary aspergillosis(CNPA)]. Mycoses. 2010 May;53
Suppl 1:3-4.
118. Prasad R, Garg SR. Progressive increase in cavitation with the evolution of fungus ball: A clue to the
diagnosis of chronic necrotizing pulmonaryaspergillosis. Lung India. 2009 Jul;26(3):95-7.
119. Kitasato Y, Takata S, Tao Y, Koga T, Takita A, Okabayashi K, Kawasaki M, Aizawa H. [A case of
pulmonary actinomycosis mimicking chronicnecrotizing pulmonary aspergillosis]. Nihon Kokyuki
Gakkai Zasshi. 2010 Feb;48(2):140-4.
120. Nam HS, Jeon K, Um SW, Suh GY, Chung MP, Kim H, Kwon OJ, Koh WJ. Clinical characteristics and
treatment outcomes of chronicnecrotizing pulmonary aspergillosis: a review of 43 cases.
Int J Infect Dis. 2010 Jun;14(6):e479-82.
121. Du H, Huang W. Chronic necrotizing pulmonary aspergillosis or invasive pulmonary aspergillosis.
Chest. 2009 Oct;136(4):1189-90.
149
122. Asma Nasim, Shehla Baqi, Syed Mohammed Zeeshan, Tahir Aziz Chronic necrotizing pulmonary
aspergillosis in a renal transplant recipient. JPMA, 61, 12, 2011
123. Nakamoto K, Takayanagi N, Kanauchi T, Ishiguro T, Yanagisawa T, Sugita Y. Prognostic factors in 194
patients with chronic necrotizingpulmonary aspergillosis. Intern Med. 2013;52(7):727-34.
124. Namesaya N, Tomioka H, Kaneda T, Kida Y, Kaneko M, Fuji H, Katsuyama E. [Three autopsy cases
of chronic necrotizing pulmonaryaspergillosis]. Kansenshogaku Zasshi. 2012 Sep;86(5):597-603.
125. Tokui K, Kawagishi Y, Inomata M, Taka C, Okazawa S, Yamada T, Miwa T, Hayashi R, Matsui S,
Takano Y, Tobe K. Systemic dissemination of chronic necrotizing pulmonaryaspergillosis in an elderly
woman without comorbidity: a case report. J Med Case Rep. 2012 Aug 31;6(1):270.
126. Rødland EK , Ueland T, Bjørnsen S, Sagen EL, Dahl CP, Naalsund A, Mollnes TE, Brosstad FR, Müller
F,Aukrust P, Frøland SS. Systemic biomarkers of inflammation and haemostasis in patients with
chronic necrotizing pulmonary aspergillosis. BMC Infect Dis. 2012 Jun 25;12:144.
127. Yoshida K, Kurashima A, Kamei K, Oritsu M, Ando T, Yamamoto T, Niki Y. Efficacy and safety of
short- and long-term treatment of itraconazole on chronic necrotizing pulmonary aspergillosisin
multicenter study. J Infect Chemother. 2012 Jun;18(3):378-85.
128. Gomez-Abreo D, Prost C, Couraud S, Parmeland L, Carret G, Boibieux A, Gagnieu MC, Gérinière L,
Avrillon V, Souquet PJ. [Chronic necrotizing pulmonary aspergillosis following an infection by
Mycobacterium malmoense]. Rev Mal Respir. 2012 Mar;29(3):435-9.
129. Yatera K, Yamasaki K, Kozaki M, Shimauchi M, Kawanami T, Nagata S, Suzuki Y, Tokuyama S, Inoue
N, Nishida C, Ishimoto H, Kawajiri T, Awaya Y, Tsuda T, Mukae H.[Retrospective analysis of the safety
of four hours administration of liposomal amphotericin B in patients
with chronicnecrotizing pulmonary aspergillosis]. Jpn J Antibiot. 2011 Oct;64(5):311-8.
130. Lee KH, Ryu SM, Park SM, Park HS, Lee KH, Cho SJ. A surgically treated case
of chronic necrotizing aspergillosiswith pleural invasion. Korean J Thorac Cardiovasc Surg. 2012
Feb;45(1):56-9.
131. Rajalingham S, Anshar FM. Chronic necrotizing pulmonary aspergillosis presenting as bilateral pleural
effusion: a case report. J Med Case Rep. 2012 Feb 14;6(1):62.
132. Lovrenski A, Panjković M, Eri Z, Klem I, Povazan D, Ilincić D, Milić M.
Chronic necrotizing pulmonary aspergillosis. Vojnosanit Pregl. 2011 Nov;68(11):988-91.
133. Wu CJ, Lee HC, Lo HJ, Ko WC. Resolution of galactomannan antigenemia in a patient receiving oral
voriconazole for chronic necrotizing pulmonaryaspergillosis. Diagn Microbiol Infect Dis. 2011
Aug;70(4):528-30.
134. Blanco JJ, Barcala FJ, Moure MA, Mao MC. [Chronic necrotizing pulmonary aspergillosis as a
complication of silicosis]. An Sist Sanit Navar. 2011 Jan-Apr;34(1):109-14.
135. Morita H, Oguri T, Uemura T, Iwashima Y, Nakamura A, Sato S. [Case
of chronic necrotizing pulmonary aspergillosiscomplicated by elevated eosinophils and serum IgE].
Nihon Kokyuki Gakkai Zasshi. 2010 Nov;48(11):842-6.
136. Lee EJ, Song R, Park JN, Lee YA, Son JS, Hong SJ, Yang HI, Lee SH.
Chronic necrotizing pulmonary aspergillosis in a patient treated with a tumor necrosis factor-alpha
inhibitor. Int J Rheum Dis. 2010 Aug;13(3):e16-9.
137. Rüchel R. [Lethal case of chronic necrotizing pulmonary aspergillosis(CNPA)]. Mycoses. 2010 May;53
Suppl 1:3-4.
138. Prasad R, Garg SR. Progressive increase in cavitation with the evolution of fungus ball: A clue to the
diagnosis of chronic necrotizing pulmonaryaspergillosis. Lung India. 2009 Jul;26(3):95-7.
139. Kitasato Y, Takata S, Tao Y, Koga T, Takita A, Okabayashi K, Kawasaki M, Aizawa H. [A case of
pulmonary actinomycosis mimicking chronicnecrotizing pulmonary aspergillosis]. Nihon Kokyuki
Gakkai Zasshi. 2010 Feb;48(2):140-4.
140. Nam HS, Jeon K, Um SW, Suh GY, Chung MP, Kim H, Kwon OJ, Koh WJ. Clinical characteristics and
treatment outcomes of chronicnecrotizing pulmonary aspergillosis: a review of 43 cases. Int J Infect Dis.
2010 Jun;14(6):e479-82.

151
141. Du H, Huang W. Chronic necrotizing pulmonary aspergillosis or invasive pulmonary aspergillosis.
Chest. 2009 Oct;136(4):1189-90.
142. Sivasankari S,1 Senthamarai S,
2 Anitha C,
3 Apurba Sankar Sastry,
4 Sandhya Bhatt,
5Kumudhavathi
M.S,6 and Amshavathani S.K. Prevalence of Invasive Aspergillosis Among (PTB) Patients in
Kanchipuram, India. J Clin Diagn Res. 2014 Mar;8(3):22-3.
143. Heng SC, Chen SC, Morrissey CO, Thursky K, Manser RL, De Silva HD, Halliday CL, Seymour JF,
Nation RL, Kong DC, Slavin MA. Clinical utility of Aspergillus galactomannan and PCR in
bronchoalveolar lavage fluid for the diagnosis of invasive pulmonary aspergillosis in patients with
haematological malignancies. Diagn Microbiol Infect Dis. 2014 Mar 29. pii: S0732-8893(14)00131-X.
144. Lin JC, Xu WM, Zhang CR, Li M, Xin YL, Bo P, Niu YY. Evaluation of galactomannan enzyme
immunoassay and quantitative real-time PCR for the diagnosis of invasive pulmonary aspergillosis in a
rat model.
J Microbiol Biotechnol. 2014 Apr 18.
145. Fisher CE, Stevens AM, Leisenring W, Pergam SA, Boeckh M, Hohl TM. Independent contribution of
bronchoalveolar lavage and serum galactomannan in the diagnosis of invasive pulmonary
aspergillosis.Transpl Infect Dis. 2014 Apr 12. doi: 10.1111/tid.12211.
146. Saito S Oda A, Kasai M, Minami K, Nagumo H, Shiohara M, Ogiso Y, Kawakami Y. A neonatal case
of chronic granulomatous disease, initially presented with invasive pulmonary aspergillosis. J Infect
Chemother. 2014 Mar;20(3):220-3.
147. Krel M, Petraitis V, Petraitiene R, Jain MR, Zhao Y, Li H, Walsh TJ, Perlin DS. Host Biomarkers
of Invasive Pulmonary Aspergillosis to Monitor Therapeutic Response. Antimicrob Agents Chemother.
2014 Mar 31.
148. Hoenigl M, Prattes J, Spiess B, Wagner J, Prueller F, Raggam RB, Posch V, Duettmann W, Hoenigl K,
Wölfler A, Koidl C, Buzina W, Reinwald M, Thornton CR, Krause R, Buchheidt D. Performance of
Galactomannan, Beta-D-Glucan, Aspergillus Lateral-Flow Device, Conventional Culture and PCR tests
for Diagnosis of Invasive Pulmonary Aspergillosis in Bronchoalveolar Lavage Fluid. J Clin Microbiol.
2014 Mar 26.
149. Koulenti D, Vogelaers D, Blot S. What's new in invasive pulmonary aspergillosis in the critically ill.
Intensive Care Med. 2014 May;40(5):723-6.
150. Khorvash F, Meidani M, Babaei L, Abbasi S, Ataei B, Yaran M. Galactomannan antigen assay from
bronchoalveolar lavage fluid in diagnosis of invasive pulmonary aspergillosis in intensive care units
patients. Adv Biomed Res. 2014 Jan 27;3:68.
151. Parcell BJ, B C Raju PK, Johnson EM, Fardon TC, Olver WJ. Invasive pulmonary aspergillosis post
extracorporeal membrane oxygenation support and literature review. Med Mycol Case Rep. 2014 Feb
10;4:12-5.
152. Broenen E, Mavinkurve-Groothuis A, Kamphuis-van Ulzen K, Brüggemann R, Verweij P, Warris A.
Screening of the central nervous system in children withinvasive pulmonary aspergillosis. Med Mycol
Case Rep. 2014 Feb 20;4:8-11.
153. Seyedmousavi S, Brüggemann RJ, Melchers WJ, Verweij PE, Mouton JW. Intrapulmonary
posaconazole penetration at the infection site in an immunosuppressed murine model of invasive
pulmonary aspergillosis receiving oral prophylactic regimens. Antimicrob Agents Chemother. 2014
May;58(5):2964-7.
154. Desoubeaux G, Bailly É, Chandenier J. Diagnosis of invasive pulmonary aspergillosis: updates and
recommendations. Med Mal Infect. 2014 Mar;44(3):89-101.
155. Koulenti D, Garnacho-Montero J, Blot S. Approach to invasive pulmonary aspergillosis in critically ill
patients. Curr Opin Infect Dis. 2014 Apr;27(2):174-83.
156. Kwon OK, Lee MG, Kim HS, Park MS, Kwak KM, Park SY. Invasive pulmonary aspergillosis after
influenza a infection in an immunocompetent patient. Tuberc Respir Dis (Seoul). 2013 Dec;75(6):260-3.
151
157. Chen J, Yang Q, Huang J, Li L. Clinical findings in 19 cases of invasive pulmonary aspergillosis with
liver cirrhosis. Multidiscip Respir Med. 2014 Jan 8;9(1):1.
158. Cui N, Wang H, Long Y, Liu D. Altered CD8(+) T-cell counts as an early predictor of prognosis in
critically ill immunocompromised patients with invasive pulmonary aspergillosis. Chin Med J
(Engl). 2014;127(1):36-42.
159. He H, Li Q, Chang S, Ding L, Sun B, Li F, Zhan Q. Prognostic value of serum galactomannan index in
critically ill patients with chronic obstructive pulmonary disease at risk ofinvasive pulmonary
aspergillosis. Chin Med J (Engl). 2014;127(1):23-8.
160. Jean T, Antoine L, Thierry V, Frédéric C, Christophe L, Eric D, Olivier B. Real-life diagnosis
of invasive pulmonary aspergillosis in a non neutropenic critically ill patient. Respir Care. 2013 Dec 10.
161. Adamson TW, Diaz-Arevalo D, Gonzalez TM, Liu X, Kalkum M. Hypothermic endpoint for an
intranasal invasive pulmonary aspergillosis mouse model. Comp Med. 2013;63(6):477-81.
162. Mosquera RA, Estrada L, Clements RM, Jon CK. Early diagnosis and treatment of invasive pulmonary
aspergillosis in a patient with cystic fibrosis.
BMJ Case Rep. 2013 Nov 18;2013.
163. Nucci M, Nouér SA, Cappone D, Anaissie E. Early diagnosis of invasive pulmonary aspergillosis in
hematologic patients: an opportunity to improve the outcome. Haematologica. 2013 Nov;98(11):1657-
60.
164. Chen J, Yang Q, Huang J, Li L. Risk factors for invasive pulmonary aspergillosis and hospital mortality
in acute-on-chronic liver failure patients: a retrospective-cohort study. Int J Med Sci. 2013 Sep
18;10(12):1625-31.
165. Tutar N, Metan G, Koç A, Yilmaz I, Bozkurt I, Simsek ZO, Buyukoglan H, Kanbay A, Oymak F,
Gulmez I, Demir R. Invasive pulmonary aspergillosis in patients with chronic
obstructive pulmonary disease. Multidiscip Respir Med. 2013 Sep 4;8(1):59.
166. Baumann S, Reinwald M, Haghi D, Hofmann WK, Buchheidt D. Coinfection of Pneumocystis jirovecii
and invasive pulmonary aspergillosis in an immunocompromised patient: a diagnostic challenge.
Onkologie. 2013;36(10):582-4.
167. Lepak AJ, Marchillo K, Vanhecker J, Andes DR. Isavuconazole (BAL4815) pharmacodynamic target
determination in an in vivo murine model of invasive pulmonary aspergillosis against wild-type and
cyp51 mutant isolates of Aspergillus fumigatus. Antimicrob Agents Chemother. 2013 Dec;57(12):6284-
9.
168. Xu XY, Sun HM, Zhao BL, Shi Y. Diagnosis of airway-invasive pulmonary aspergillosis by tree-in-bud
sign in an immunocompetent patient: case report and literature review. J Mycol Med. 2013
Mar;23(1):64-9.
169. Bergeron A, Porcher R, Sulahian A, de Bazelaire C, Chagnon K, Raffoux E, Vekhoff A, Cornet M,
Isnard F, Brethon B, Lacroix C, Poirot JL, Bouges C, Derouin F, Tazi A, Ribaud P. The strategy for the
diagnosis of invasive pulmonary aspergillosis should depend on both the underlying condition and the
leukocyte count of patients with hematologic malignancies. Blood. 2012 Feb 23;119(8):1831-7
170. Won HJ, Lee KS, Cheon JE, Hwang JH, Kim TS, Lee HG, Han J. Invasive pulmonary aspergillosis:
prediction at thin-section CT in patients with neutropenia--a prospective study. Radiology. 1998
Sep;208(3):777-82.
171. Brown MJ, Worthy SA, Flint JD, Müller NL. Invasive aspergillosis in the immunocompromised host:
utility of computed tomography and bronchoalveolar lavage. Clin Radiol. 1998 Apr;53(4):255-7.
172. Schulze M, Vogel W, Spira D, Sauter A, Hetzel J, Horger M. Reduced perfusion in pulmonary infiltrates
of high-risk hematologic patients is a possible discriminator of pulmonary angioinvasive mycosis: a pilot
volume perfusion computed tomography (VPCT) study. Acad Radiol. 2012 J;19(7):842-50.

152
173. Michels G, Bovenschulte H, Cornely OA, Kochanek M. [62-year-old patient with chronic lymphatic
leukaemia and persistent fever in chemotherapy induced bone marrow
aplasia.Angioinvasive aspergillosis].Dtsch Med Wochenschr. 2011;136(28-29):1477-8.
174. Sebastianes PM, Fortes M, Meirelles GS. Angioinvasive aspergillosis with halo sign on computed
tomography of the lungs. Rev Soc Bras Med Trop. 2008 ;41(2):219-20.
175. Gasparetto EL, Souza CA, Tazoniero P, Davaus T, Escuissato DL, Marchiori E.
Angioinvasive pulmonary aspergillosis after allogeneic bone marrow transplantation: clinical and high-
resolution computed tomography findings in 12 cases. Braz J Infect Dis. 2007 Feb;11(1):110-3.
176. Kami M, Murashige N, Nannya Y, Kusumi E, Sakai M, Tanaka Y, Kanda Y, Mori S, Chiba S,
Kusumoto M, Miyakoshi S, Hirai H, Taniguchi S, Sakamaki H, Takaue Y. Chest computed tomography
of late invasive aspergillosis after allogeneic hematopoietic stem cell transplantation. Kojima R, Tateishi
U, Biol Blood Marrow Transplant. 2005 Jul;11(7):506-11.Mycoses. 2014 May;57(5):257-70.
177. Sonnet S, Buitrago-Téllez CH, Tamm M, Christen S, Steinbrich W. Direct detection
of angioinvasive pulmonary aspergillosis in immunosuppressed patients: preliminary results with high-
resolution 16-MDCT angiography.
AJR Am J Roentgenol. 2005 Mar;184(3):746-51.
178. Nootigattu VK, Sundaram J, Shabbani A, Playfor SD. Angioinvasive aspergillosis. Arch Dis Child.
2004 Aug;89(8):784.
179. McKerlie I, Bloom C, Kreisman H. Staphylococcus aureus septic pulmonary emboli presenting
asangioinvasive aspergillosis: case report. Can Assoc Radiol J. 2001 Dec;52(6):395-8.
180. Arbona GA, Tarver RD, Conces DJ Jr. Angioinvasive pulmonary aspergillosis. Semin Respir Infect.
2000 Jun;15(2):178-82.
181. Ramos Fernández V, Prieto Rodríguez M, Paradís Alós A, López Chulía F, Salom Fúster JV, Vera-
Sempere FJ. [Angio-invasive disseminated aspergillosis: autopsy diagnosis in leukemic patients]. An
Med Interna. 1993 Jul;10(7):337-40.
182. Smith NL, Hankinson J, Simpson A, Bowyer P, Denning DW. A prominent role for the IL1 pathway
and IL15 in susceptibility tochronic cavitary pulmonary aspergillosis. Clin Microbiol Infect. 2013 Nov
26. doi: 10.1111/1469-0691.12473.
183. Wei-Lun Chien; Jeng-Sen Tseng. Pulmonary aspergillosis in an immunocompetent patient. Braz J Infect
Dis vol.17 no.3 Salvador May/June 2013
184. Agarwal R, Vishwanath G, Aggarwal AN, Garg M, Gupta D, Chakrabarti A. Itraconazole
in chronic cavitary pulmonary aspergillosis: a randomised controlled trial and systematic review of
literature. Mycoses. 2013 Sep;56(5):559-70.
185. Kulendra E, Halfacree Z, Goggs R, Dennis S, Summers B, Lamb CR, Brockman D.
Cavitary pulmonary lesion associated with Aspergillus fumigatus infection in a German shepherd dog. J
Small Anim Pract. 2010 May;51(5):271-4.
186. Vaid M, Kaur S, Sambatakou H, Madan T, Denning DW, Sarma PU. Distinct alleles of mannose-
binding lectin (MBL) and surfactant proteins A (SP-A) in patients with chronic cavitary pulmonary
aspergillosis and allergic bronchopulmonary aspergillosis. Clin Chem Lab Med. 2007;45(2):183-6.
187. Jain LR, Denning DW. The efficacy and tolerability of voriconazole in the treatment
ofchronic cavitary pulmonary aspergillosis. J Infect. 2006 May;52(5):e133-7.
188. Li E, Hussein H, Todiwala A, Kirby R. Primary gut aspergillosis in a patient with acute myeloid
leukaemia: the importance of early suspicion and definitive treatment. BMJ Case Rep. 2014 Mar
18;2014.
189. Alavi Darazam I, Akhavan Zanjani H, Sanaee D, Tabarsi P, Alavi Moghaddam M, Mansouri D.
Disseminated aspergillosis as the herald manifestation of chronic granulomatous disease in an adult
patient. Iran J Allergy Asthma Immunol. 2014 Feb;13(1):66-70.
190. Singh N, Suarez JF, Avery R, Lass-Flörl C, Geltner C, Pasqualotto AC, Lyon GM, Barron M, Husain S,
Wagener MM, Montoya JG. Immune reconstitution syndrome-like entity in lung transplant recipients
153
with invasive aspergillosis. Transpl Immunol. 2013 Dec;29(1-4):109-13. doi:
10.1016/j.trim.2013.09.007. Epub 2013 Sep 25.
191. Barrs VR, van Doorn TM, Houbraken J, Kidd SE, Martin P, Pinheiro MD, Richardson M, Varga J,
Samson RA. Aspergillus felis sp. nov., an emerging agent of invasiveas pergillosis in humans, cats, and
dogs. PLoS One. 2013 Jun 14;8(6):e64871
192. Pozo-Laderas JC, Pontes-Moreno A, Robles-Arista JC, Bautista-Rodriguez MD, Candau-Alvarez A,
Caro-Cuenca MT, Linares-Sicilia MJ. [Mixed invasive fungal infection due to Rhizomucor pusillus and
Aspergillus niger in an immunocompetent patient.] Rev Iberoam Micol. 2013 Apr 11. pii: S1130-
1406(13)00024-7.
193. Hizawa K, Hatada T, Morinaga S, Kudo T, Nakamori M, Matsumoto T, Iida M. [An autopsy case of
ulcerative colitis with disseminated aspergillosis, complicated by brain hemorrhage]. Nihon Shokakibyo
Gakkai Zasshi. 2013 Apr;110(4):648-54.
194. Robinett KS, Weiler B, Verceles AC. Invasive aspergillosis masquerading as catastrophic
antiphospholipid syndrome. Am J Crit Care. 2013 Sep;22(5):448-51.
195. Ergene U, Akcali Z, Ozbalci D, Nese N, Senol S. Disseminated Aspergillosis due to Aspergillus niger in
Immunocompetent Patient: A Case Report. Case Rep Infect Dis. 2013;2013:385190
196. Mihon C, Alexandre T, Pereira A. Clinical experience in invasive fungal infections: multiple fungal
infection as the first presentation of HIV. Clin Drug Investig. 2013 Feb;33 Suppl
197. Seyedmousavi S, Melchers WJ, Mouton JW, Verweij PE. Pharmacodynamics and dose-response
relationships of liposomal amphotericin B against different azole-resistant Aspergillus fumigatus isolates
in a murine model of disseminated aspergillosis. Antimicrob Agents Chemother. 2013 Apr;57(4):1866-
71.
198. Tokui K, Kawagishi Y, Inomata M, Taka C, Okazawa S, Yamada T, Miwa T, Hayashi R, Matsui S,
Takano Y, Tobe K. Systemic dissemination of chronic necrotizing pulmonary aspergillosis in an elderly
woman without comorbidity: a case report. J Med Case Rep. 2012 Aug 31;6(1):270.
199. Dominelli GS, Shaipanich T.Ulcerative tracheobronchitis due to Aspergillus. J Bronchology Interv
Pulmonol. 2013 Oct;20(4):326-9.
200. Gómez F, Tarín V, Cuadrado M, Vecilla F, Blanquer D, Costa-Bauzá A, Grases F, Bachiller D. Tracheal
oxalosis associated with Aspergillus niger tracheobronchitis. Eur Respir J. 2013 Apr;41(4):995-7.
201. Weigt SS, Copeland CA, Derhovanessian A, Shino MY, Davis WA, Snyder LD, Gregson AL, Saggar R,
Lynch JP 3rd, Ross DJ, Ardehali A, Elashoff RM, Palmer SM, Belperio JA. Colonization with small
conidia Aspergillus species is associated with bronchiolitis obliterans syndrome: a two-center validation
study. Am J Transplant. 2013 Apr;13(4):919-27.
202. Hu B, He G, Hu X. [The aspergillus laryngotracheobronchitis. A case report and literature review]. Lin
Chung Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2012 Oct;26(20):953-5.
203. Chrdle A, Mustakim S, Bright-Thomas RJ, Baxter CG, Felton T, Denning DW.
Aspergillus bronchitis without significant immunocompromise. Ann N Y Acad Sci. 2012 Dec;1272:73-
85.
204. Krenke, Rafal and Grabczak, Elzbieta M. Tracheobronchial Manifestations of Aspergillus
Infections .TheScientificWorldJournal 2011;11:2310-2329.
205. Ramos A, Segovia J, Gómez-Bueno M, Salas C, Lázaro MT, Sanchez I, Pulpón L.
Pseudomembranous Aspergillus tracheobronchitis in a heart transplant recipient. Transpl Infect Dis. 2010
Feb;12(1):60-3.
206. Wu N, Huang Y, Li Q, Bai C, Huang HD, Yao XP. Isolated invasive Aspergillus tracheobronchitis: a
clinical study of 19 cases. Clin Microbiol Infect. 2010 Jun;16(6):689-95.
207. Hall WA. Improving Outcomes in Cerebral Aspergillosis. World Neurosurg. 2014 Mar 5. pii: S1878-
8750(14)00220-4
208. Brazzola P, Rossi MR. High weekly doses of liposomal amphotericin B as secondary prophylaxis
after cerebral aspergillosis in a paediatric patient. Med Mycol Case Rep. 2013 Nov 6;3:1-3.

154
209. Chen ZY, Li JF, Ma L. Striated enhancement sign in invasive cerebral fungal granuloma by Aspergillus:
a case report. Chin Med Sci J. 2013 Dec;28(4):237-8.
210. Spapen H, Spapen J, Taccone FS, Meersseman W, Rello J, Dimopoulos G, Charles PE, Rao R, Pérez M,
Martin C, Vogelaers D, Blot SI; Cerebral aspergillosis in adult critically ill patients: a descriptive report
of 10 patients from the AspICU cohort. Int J Antimicrob Agents. 2014 Feb;43(2):165-9.
211. Kim MJ, Kim MK, Kang CK, Jun KI, Bang JH, Park SW, Oh MD. A Case of
Acute Cerebral Aspergillosis Complicating Influenza A/H1N1pdm 2009. Infect Chemother. 2013
Jun;45(2):225-9.
212. Matis GK, Voultsinou D, Chrysou O, Birbilis T, Geroukis T. Cerebral aspergillosis and acute myeloid
leukemia. J Neurosci Rural Pract. 2013 Aug;4(Suppl 1):S134-5.
213. Vijayvargiya P, Javed I, Moreno J, Mynt MA, Kotapka M, Zaki R, Ortiz J. Pituitary aspergillosis in a
kidney transplant recipient and review of the literature. Transpl Infect Dis. 2013 Oct;15(5):E196-200.
214. Bokhari R, Baeesa S, Al-Maghrabi J, Madani T.Isolated Cerebral Aspergillosis in Immunocompetent
Patients.World Neurosurg. 2013 Sep 25. pii: S1878-8750(13)01225-4.
215. Bhaskar N, Mohammad K, Kaur V. Aspergillus brain abscess. J Ark Med Soc. 2013 Aug;110(2):41-2.
216. Lee GJ, Jung TY, Choi SM, Jung MY. Cerebral aspergillosis with multiple enhancing nodules in the
right cerebral hemisphere in the immune-competent patient. J Korean Neurosurg Soc. 2013
May;53(5):312-5.
217. Sidani C, Freiser ME, Saigal G, Sklar E. Unusual case of cerebral aspergillosis with clinical and imaging
findings mimicking lymphoma. Neuroradiol J. 2013 Jun;26(3):290-6.
218. Sav H, Atalay MA, Demir G, Akif Ozdemir M, Nedret Koc A. Early diagnosis
of cerebral aspergillosis with various methods: a case report. Infez Med. 2013 Jun;21(2):134-8.
219. Prakash G, Thulkar S, Arava SK, Bakhshi S. Cerebral aspergillus infection in pediatric acute
lymphoblastic leukemia induction therapy. Indian J Med Paediatr Oncol. 2012 Oct;33(4):236-8.
220. Soeffker G, Wichmann D, Loderstaedt U, Sobottka I, Deuse T, Kluge S. Aspergillus galactomannan
antigen for diagnosis and treatment monitoring in cerebral aspergillosis. Prog Transplant. 2013
Mar;23(1):71-4.
221. Verma R, Singh P, Kumar A, Paliwal VK. Cranial aspergilloma masquerading as meningioma. BMJ
Case Rep. 2013 Jan 9;2013. pii: bcr2012008118.
222. Hoenigl M, Krause R. Antifungal therapy of aspergillosis of the central nervous system and aspergillus
endophthalmitis. Curr Pharm Des. 2013;19(20):3648-68. Review.
223. Lee JC, Lim DJ, Ha SK, Kim SD, Kim SH. Fatal case of cerebral aspergillosis : a case report and
literature review. J Korean Neurosurg Soc. 2012 Oct;52(4):420-2.
224. Kourkoumpetis TK, Desalermos A, Muhammed M, Mylonakis E. Central nervous system aspergillosis:
a series of 14 cases from a general hospital and review of 123 cases from the literature. Medicine
(Baltimore). 2012 Nov;91(6):328-36.
225. Kruetzelmann A, Sobottka I, Fiehler J, Tolosa E, Gerloff C, Rosenkranz M.
Relapsing cerebral aspergilloma associated with pregnancy. Clin Neurol Neurosurg. 2013
Jul;115(7):1154-6.
226. Cherian T, Giakoustidis A, Yokoyama S, Heneghan M, O'Grady J, Rela M, Wendon J, Heaton DN,
Verma A. Treatment of refractory cerebral aspergillosis in a liver transplant recipient with voriconazole:
case report and review of the literature. Exp Clin Transplant. 2012 Oct;10(5):482-6. Review.
227. Kluger N, Saarinen K.. Aspergillus fumigatus infection on a home-made tattoo. Br J Dermatol. 2014 Feb
3. doi: 10.1111/bjd.12859. [Epub ahead of print]
228. Trotter SC, Sammons DL. What is your diagnosis? primary cutaneous aspergillosis. Cutis. 2013
Nov;92(5):219, 223, 224.
229. Cateau E, Randriamalala E, Elsendoorn A, Giot JP, du Sorbier CM, Rodier MH.Fatal-
mixed cutaneous zygomycosis-aspergillosis: a case report. Mycopathologia. 2013 Dec;176(5-6):423-7.

155
230. Sharma S, Yenigalla BM, Naidu SK, Pidakala P. Primary cutaneous aspergillosis due to Aspergillus
tamarii in an immunocompetent host. BMJ Case Rep. 2013 Aug 22;2013:010128.
231. Tak V, Mathur P, Xess I, Kale P, Sagar S, Misra MC. A case of dual infection in a paediatric trauma
victim of primarycutaneous aspergillosis caused by Aspergillus flavus and Aspergillus terreus. Indian J
Med Microbiol. 2013 Apr-Jun;31(2):193-6.
232. Klotz D, Kneitz H, Wirbelauer J. [Primary cutaneous aspergillosis in an extremely low birth weight
preterm infant]. Hautarzt. 2013 Sep;64(9):664-5.
233. Osório F, Magina S, Azevedo F. Primary cutaneous aspergillosis complicating tumor necrosis factor-α
blockade therapy in a patient with psoriasis. Actas Dermosifiliogr. 2012 Dec;103(10):939-41.
234. Dhotre SV, Hiremath SL. Post-filarial cutaneous aspergillosis. Int J Dermatol. 2012 Dec;51(12):1485-6.
235. Gedela K, Nelson M, Francis N, Mohabeer M, Jones R. Cutaneous aspergillosis associated with HIV
infection. Int J STD AIDS. 2012 Sep;23(9):679-80.
236. Osório F, Magina S, Azevedo F. Primary Cutaneous Aspergillosis Complicating Tumor Necrosis
Factor-α Blockade Therapy in a Patient With Psoriasis. Actas Dermosifiliogr. 2012 Dec;103(10):939-
941.
237. Martin EB, Gastañaduy PA, Camacho-Gonzalez AF, Ross AC, Hebbar K.
Primary cutaneous aspergillosis in two pediatric trauma patients. Pediatr Infect Dis J. 2012
Apr;31(4):427-8.
238. Venugopal TV, Venugopal PV. Primary cutaneous aspergillosis from Tamilnadu diagnosed by fine
needle aspiration cytology. Med Mycol Case Rep. 2012 Sep 29;1(1):103-6.
239. Chen Y, Liao W, Wen H, Chen J, Gu J. Primary cutaneous aspergillosis in a patient with systemic lupus
erythematosus. Mycoses. 2012 Mar;55(2):e42-4.
240. Sato Y, Suzino K, Suzuki A, Fukasawa N, Ouchi Y, Yaguchi T, Sato T. [Case
of primary cutaneous Aspergillus caldioustus infection caused by nerve block therapy]. Med Mycol J.
2011;52(3):239-44.
241. Stock C, Veyrier M, Raberin H, Fascia P, Rayet I, Lavocat MP, Teyssier G, Berthelot P.
Severe cutaneous aspergillosis in a premature neonate linked to nonsterile disposable glove
contamination? Am J Infect Control. 2012;40(5):465-7.
242. Etienne KA, Subudhi CP, Chadwick PR, Settle P, Moise J, Magill SS, Chiller T, Balajee SA.
Investigation of a cluster of cutaneous aspergillosis in a neonatal intensive care unit. J Hosp Infect. 2011
Dec;79(4):344-8.
243. Robinson A, Fien S, Grassi MA. Nonhealing scalp wound infected with Aspergillus niger in an elderly
patient. Cutis. 2011 Apr;87(4):197-200.
244. Cho WH, Kim JE, Jeon DS, Kim YS, Chin HW, Shin DH.
Tracheobronchial aspergillosis following primary cutaneous aspergillosis in a lung-transplant recipient.
Intern Med. 2011;50(2):131-4.
245. Türkşen Z, Yağcı S, Karadağ AS, Tezer A, Taner OF, Tekin F, Arıkan Akdağlı S.
[Posttraumatic primary cutaneous aspergillosis with Candida guilliermondii infection in a healthy host].
Mikrobiyol Bul. 2010 Oct;44(4):665-70.
246. Nakashima K, Yamada N, Yoshida Y, Yamamoto O. Primary cutaneous aspergillosis. Acta Derm
Venereol. 2010 Sep;90(5):519-20.

156
247. Jin-Hee No, Jin-Sok Yu, Eun-Ok Kim, Hyun-Ho Choi, Si-Hyun Kim, Jae-Cheol Kwon, Dong-Gun Lee,
Su-Mi Choi, Sun-Hee Park, Jung-Hyun Choi, Jin-Hong Yoo, Hee-Je Kim and Woo-Sung Min. A Case
of Disseminated Aspergillosis Presenting Solely as Multiple Cutaneous Lesions in an Acute Leukemia
Patient, Infect Chemother. 2010 Aug;42(4):244-248.
248. Ho S, Krishnan P, Teoh SC. Aspergillus terreus endogenous endophthalmitis in a
nonimmunocompromised patient with a history of bronchiectasis. Ng J, Ocul Immunol Inflamm. 2013
Jun;21(3):231-3.
249. Manikandan P, Varga J, Kocsubé S, Anita R, Revathi R, Németh TM, Narendran V, Vágvölgyi C,
Panneer Selvam K, Shobana CS, Babu Singh YR, Kredics L.
Epidemiology of Aspergillus keratitis at a tertiary care eye hospital in South India and antifungal
susceptibilities of the causative agents.
Mycoses. 2013 Jan;56(1):26-33.
250. Jalili M, Hashemi H, Jabarvand M, Tabatabai SA. Aspergillus endophthalmitis in one eye subsequent to
bilateral anterior chamber phakic intraocular lens implantation. J Refract Surg. 2012 May;28(5):363-5.
251. Comez AT, Komur B, Akcali A, Otkun MT. Ocular aspergillosis: Obtaining a specimen is crucial for
diagnosis. A report of three cases. Med Mycol Case Rep. 2012 Jun 16;1(1):39-41.
252. Sugita S, Kamoi K, Ogawa M, Watanabe K, Shimizu N, Mochizuki M. Detection of Candida and
Aspergillus species DNA using broad-range real-time PCR for fungal endophthalmitis. Graefes Arch
Clin Exp Ophthalmol. 2012 Mar;250(3):391-8.
253. Nayak N, Satpathy G, Prasad S, Titiyal JS, Pandey RM, Vajpayee RB. Molecular characterization of
drug-resistant and drug-sensitive Aspergillus isolates causing infectious keratitis. Indian J Ophthalmol.
2011 Sep-Oct;59(5):373-7.
254. Jain V, Mhatre K, Nair AG, Shome D, Natarajan S. Aspergillus keratitis in vernal shield ulcer--a case
report and review. Int Ophthalmol. 2010 Dec;30(6):641-4.
255. Manikandan P, Varga J, Kocsubé S, Samson RA, Anita R, Revathi R, Dóczi I, Németh TM, Narendran
V, Vágvölgyi C, Manoharan C, Kredics L. Mycotic keratitis due to Aspergillus nomius. J Clin Microbiol.
2009 Oct;47(10):3382-5.
256. Kredics L, Varga J, Kocsubé S, Rajaraman R, Raghavan A, Dóczi I, Bhaskar M, Németh TM, Antal Z,
Venkatapathy N, Vágvölgyi C, Samson RA, Chockaiya M, Palanisamy M. Infectious keratitis caused by
Aspergillus tubingensis. Cornea. 2009 Sep;28(8):951-4.
257. Labelle AL, Hamor RE, Barger AM, Maddox CW, Breaux CB. Aspergillus flavus keratomycosis in a
cat treated with topical 1% voriconazole solution. Vet Ophthalmol. 2009 Jan-Feb;12(1):48-52.
258. Arsenijević VA, Barać A, Pekmezović M, Stosović R, Pender I. [Allergic fungal sinusitis--new aspects
of clinical features, laboratory diagnosis and therapy]. Srp Arh Celok Lek. 2013 Sep-Oct;141(9-10):698-
704.
259. Singh N, Nadig A, Pal P, Subudhi CP, Gnanalingham K. Aspergillosis sinusitis with cranio-orbital
spread in an apparently immunocompetent patient. J Neurol Surg A Cent Eur Neurosurg. 2013 Dec;74
Suppl 1:e237-8.
260. Negoro E, Morinaga K, Taga M, Kaizaki Y, Kawai Y.Mycotic aneurysm due to Aspergillus sinusitis. Int
J Hematol. 2013 Jul;98(1):4-5.
261. Ghosh G, Sharma B, Chauhan A, Chawla MP. Coexistence of allergic bronchopulmonary aspergillosis
and allergic aspergillus sinusitis in a patient without clinical asthma. BMJ Case Rep. 2013 May 2;2013.
pii: bcr2013008683.
262. He CY, Piao YS, Tian C, Li LL, Liu HG. by Aspergillus and Mucorales].[Clinicopathologic study of
invasive fungal rhinosinusitis caused Zhonghua Bing Li Xue Za Zhi. 2012 Oct;41(10):662-6.
263. [Cellular and tissue reactions of the mucous membrane of the maxillary sinus in the patients presenting
with odontogenic aspergillous maxillary sinusitis]. [No authors listed] Vestn Otorinolaringol.
2012;(1):17-9.

157
264. Li LL, Zhao ZT, Wan Z, Li RY, Liu HG. [Application of PCR combined with reverse line blot assay in
detection and identification of common pathogenic Aspergillusin fungal sinusitis]. Zhonghua Bing Li
Xue Za Zhi. 2012 Jan;41(1):6-10.
265. Fanucci E, Nezzo M, Neroni L, Montesani L Jr, Ottria L, Gargari M. Diagnosis and treatment
of paranasal sinus fungus ball of odontogenic origin: case report. Oral Implantol (Rome). 2014 Apr
4;6(3):63-6.
266. Barrs VR, Beatty JA, Dhand NK, Talbot JJ, Bell E, Abraham LA, Chapman P, Bennett S, van Doorn T,
Makara M. Computed tomographic features of feline sino-nasal and sino-orbital aspergillosis. Vet J.
2014 Feb 28. pii: S1090-0233(14)00074-4.
267. Vinay K, Khullar G, Yadav S, Kanwar AJ, Saikia UN, Shivaprakash MR, Chakrabarti A, Dogra S.
Granulomatous invasive aspergillosis of paranasal sinusesmasquerading as actinomycosis and review of
published literature. Mycopathologia. 2014 Apr;177(3-4):179-85.
268. Mohindra S, Mehta R, Bal A. ABPA Concomitantly Occurring with Invasive SinusAspergillosis: A
Short Report on Two Patients. Indian J Otolaryngol Head Neck Surg. 2014 Jan;66(Suppl 1):329-33.
269. Arsenijević VA, Barać A, Pekmezović M, Stosović R, Pender I. [Allergic fungal sinusitis--new aspects
of clinical features, laboratory diagnosis and therapy]. Srp Arh Celok Lek. 2013 Sep-Oct;141(9-10):698-
704.
270. Crambert A, Gauthier J, Vignal R, Conessa C, Lombard B. [Invasive aspergillosis of sphenoidal sinus in
a patient in Djibouti, revealed by palsy of cranial nerves: a case report]. Med Sante Trop. 2013 May
1;23(2):217-20.
271. Duggal P, Wise SK. Chapter 8: Invasive fungal rhinosinusitis.
Am J Rhinol Allergy. 2013 May-Jun;27 Suppl 1:S28-30. doi: 10.2500/ajra.2013.27.3892. Review.
272. Rinaldi V, Portmann D, Boudard P. [Unilateral frontal sinus aspergillosis: the combined endoscopic and
mini-trephination approach]. Rev Laryngol Otol Rhinol (Bord). 2012;133(2):97-9.
273. Gupta R, Gupta AK. Isolated primary frontal sinus aspergillosis: role of endonasal endoscopic approach.
J Laryngol Otol. 2013 Mar;127(3):274-8.
274. Tamgadge AP, Mengi R, Tamgadge S, Bhalerao SS. Chronic invasive aspergillosis of paranasal sinuses:
A case report with review of literature. J Oral Maxillofac Pathol. 2012 Sep;16(3):460-4.
275. Peregud-Pogorzelski J, Wawrykow P, Wozniak S, Zakowska A, Brodkiewicz A. Highly effective
unconventional management of aspergillosis of the left maxillary sinus in an 11-year-old girl with
rhabdomyosarcoma embryonale of the frontal sinus. J Med Microbiol. 2013 Apr;62(Pt 4):652-4.
276. Galler A, Shibly S, Bilek A, Hirt R. [Chronic diseases of the nose and nasal sinuses in cats: a
retrospective study]. Schweiz Arch Tierheilkd. 2012 May;154(5):209-16.
277. Won HR, Park JH, Kim KS. Simultaneous actinomycosis with aspergillosis in maxillary sinus. Br J Oral
Maxillofac Surg. 2013 Jun;51(4):e51-3.
278. Sharman M, Lenard Z, Hosgood G, Mansfield C. Clotrimazole and enilconazole distribution within the
frontalsinuses and nasal cavity of nine dogs with sinonasalaspergillosis. J Small Anim Pract. 2012
Mar;53(3):161-7.
279. Abir B, Abouchadi A, Hamama J, Oukabli M, Nassih M, Rzin A. [Invasive aspergillosis of the
maxillary sinus in an immunocompetent patient]. Rev Stomatol Chir Maxillofac. 2012 Apr;113(2):127-
30.
280. Maroof Aziz Khan, Abid Rasheed, Muhammad Rashid Awan, Azhar Hameed, Aspergillus Infection of
Paranasal Sinuses. Journal of Taibah University Medical Sciences. Volume 5, Issue 2, 2010, Pages 60–65
281. Nemati S, Hassanzadeh R, Khajeh Jahromi S, Delkhosh Nasrollah Abadi A. Otomycosis in the north of
Iran: common pathogens and resistance to antifungal agents. Eur Arch Otorhinolaryngol. 2014
May;271(5):953-7.
282. Saki N, Rafiei A, Nikakhlagh S, Amirrajab N, Saki S. Prevalence of otomycosis in Khouzestan
Province, south-west Iran. J Laryngol Otol. 2013 Jan;127(1):25-7.
283. Barati B, Okhovvat SA, Goljanian A, Omrani MR. Otomycosis in central iran: a clinical and
mycological study. Iran Red Crescent Med J. 2011 Dec;13(12):873-6.
158
284. Viswanatha B, Sumatha D, Vijayashree MS. Otomycosis in immunocompetent and
immunocompromised patients: comparative study and literature review. Ear Nose Throat J. 2012
Mar;91(3):114-21. Review.
285. Szigeti G, Kocsubé S, Dóczi I, Bereczki L, Vágvölgyi C, Varga J. Molecular identification and
antifungal susceptibilities of blackAspergillus isolates from otomycosis cases in Hungary.
Mycopathologia. 2012 Aug;174(2):143-7.
286. Szigeti G, Sedaghati E, Mahmoudabadi AZ, Naseri A, Kocsubé S, Vágvölgyi C, Varga J. Species
assignment and antifungal susceptibilities of black aspergilli recovered from otomycosis cases in Iran.
Mycoses. 2012 Jul;55(4):333-8.
287. García-Agudo L, Aznar-Marín P, Galán-Sánchez F, García-Martos P, Marín-Casanova P, Rodríguez-
Iglesias M. Otomycosis due to filamentous fungi. Mycopathologia. 2011 Oct;172(4):307-10.
288. Fayemiwo SA, Ogunleye VO, Adeosun AA, Bakare RA. Prevalence of otomycosis in Ibadan: a review
of laboratory reports. Afr J Med Med Sci. 2010 Dec;39 Suppl:219-22.
289. Vennewald I, Klemm E. Otomycosis: Diagnosis and treatment. Clin Dermatol. 2010 Mar 4;28(2):202-
11.
290. Miranda JO, de Sousa AR, Monterroso J. Aspergillus endocarditis in a paediatric patient after a cardiac
surgery, associated with septic pulmonary embolism and pulmonary hypertension. Cardiol Young. 2014
Apr 4:1-3.
291. Dang-Tran KD1, Chabbert V
1, Esposito L
2, Guilbeau-Frugier C
3, Dédouit F
4, Rostaing L
5, Rousseau
H6,Otal P
6, Kamar N
5. Isolated aspergillosis myocardial abscesses in a liver-transplant patient. Case Rep
Transplant. 2014;2014:418357.
292. Seo GW, Seol SH, No TH, Jeong HJ, Kim TJ, Kim JK, Song PS, Kim DK, Kim KH, Kim DI. Acute
myocardial infarction caused by coronary embolism from Aspergillus endocarditis. Intern Med.
2014;53(7):713-6.
293. Pillai J, Mubeen M, Chaudhari A, Dalmia B. Aspergillus pacemaker lead endocarditis. Asian Cardiovasc
Thorac Ann. 2013 Apr;21(2):211-4.
294. Tacke D, Koehler P, Cornely OA. Fungal endocarditis. Curr Opin Infect Dis. 2013 Dec;26(6):501-7.
295. Ansari Aval Z, Mirhosseini SM, Fakhri M, Mozaffary A, Adimi Naghan P, Behzadnia N, Ahmadi ZH.
Successful surgical intervention in an unusual case of Aspergillus endocarditis with acute myeloid
leukemia. Acta Med Iran. 2013 Aug 7;51(7):506-8.
296. Fujita A, Kamota T, Sato M, Okada H. [Aspergillus prosthetic aortic valve endocarditis; report of a
case]. Kyobu Geka. 2013 Jul;66(7):593-7.
297. Regueiro F, Gutiérrez F, Mons R, Riancho G, Revuelta JM. Aspergillus endocarditis in lung transplant
recipient: successful surgical treatment. Ann Thorac Surg. 2013 Jul;96(1):321-3.
298. Vohra S, Taylor R, Aronowitz P. The tell-tale heart: Aspergillus fumigatus endocarditis in an
immunocompetent patient. Hosp Pract (1995). 2013 Feb;41(1):117-21
299. Rivière S, Lortholary O, Michon J, Bougnoux ME, Mainardi JL, Sendid B, Bretagne S, Lefort A.
Aspergillus endocarditis in the era of new antifungals: major role for antigen detection. J Infect. 2013
Jul;67(1):85-8..
300. Tetsuhiro Yoshino, Hiroko Nishida, Takashi Takita, Masanori Nemoto, Michihiro Sakauchi, Mami
Hatano, Kazuyuki Koyama, Masao Hori, Katsuyuki Obara. A Report of 2 Cases of Disseminated
Invasive Aspergillosis with Myocarditis in Immunocompromised Patients . Open Journal of Pathology,
2013, 3, 166-169
301. Kuroki K, Murakami T. Aspergillus endocarditis in a native valve without prior cardiac surgery. Gen
Thorac Cardiovasc Surg. 2012; 60(11):771-3.
302. Attia RQ, Nowell JL, Roxburgh JC. Aspergillus endocarditis: a case of near complete left ventricular
outflow obstruction. Interact Cardiovasc Thorac Surg. 2012 Jun;14(6):894-6.

159
303. Nikolousis E, Velangi M. Two cases of aspergillus endocarditis in non neutropenic children on
chemotherapy for acute lymphoblastic leukaemia. Hematol Rep. 2011 Jan 13;3(1):e7.
304. Nose K, Nishioka T, Hayashi T. Infective endocarditis due to Aspergillus following kidney
transplantation. Int J Urol. 2011 Nov;18(11):801-2
305. Palomares JC, Bernal S, Marín M, Holgado VP, Castro C, Morales WP, Martin E. Molecular diagnosis
of Aspergillus fumigatus endocarditis. Diagn Microbiol Infect Dis. 2011 Aug;70(4):534-7.
306. Davutoglu V, Ercan S, Tekbaş E. Cardiac aspergillosis: endocardial or endomyocardial? Int J Infect Dis.
2011 Sep;15(9):e653.
307. Eworo A, Muñoz P, Yáñez JF, Palomo J, Guembe P, Roda J, Valerio M, Guinea J, Bouza E. [Cardiac
invasive aspergillosis in a heart transplant recipient]. Rev Iberoam Micol. 2011 Jul-Sep;28(3):134-8.
308. Lázaro M, Ramos A, Ussetti P, Asensio A, Laporta R, Muñez E, Sánchez-Romero I, Tejerina E, Burgos
R, Moñivas V, Varela A. Aspergillus endocarditis in lung transplant recipients: case report and literature
review. Transpl Infect Dis. 2011 Apr;13(2):186-91.
309. Kalokhe AS, Rouphael N, El Chami MF, Workowski KA, Ganesh G, Jacob JT.
Aspergillus endocarditis: a review of the literature. Int J Infect Dis. 2010 Dec;14(12):e1040-7.
310. Nguyen J, Manera R, Minutti C. Aspergillus thyroiditis: a review of the literature to highlight clinical
challenges. Eur J Clin Microbiol Infect Dis. 2012 Dec;31(12):3259-64.
311. Santiago M, Martinez JH, Palermo C, Figueroa C, Torres O, Trinidad R, Gonzalez E, Miranda Mde L,
Garcia M, Villamarzo G. Rapidly growing thyroid mass in an immunocompromised young male adult.
Case Rep Endocrinol. 2013;2013:290843.
312. Alvi MM, Meyer DS, Hardin NJ, Dekay JG, Marney AM, Gilbert MP. Aspergillus thyroiditis: a
complication of respiratory tract infection in an immunocompromised patient. Case Rep Endocrinol.
2013;2013:741041
313. Cicora F, Mos F, Paz M, Roberti J. Successful treatment of acute thyroiditis due to Aspergillus spp. in
the context of disseminated invasive aspergillosis in a kidney transplant patient. Nefrologia.
2013;33(4):618-9.
314. Solak Y, Atalay H, Nar A, Ozbek O, Turkmen K, Erekul S, Turk S. Aspergillus thyroiditis in a renal
transplant recipient mimicking subacute thyroiditis. Transpl Infect Dis. 2011 Apr;13(2):178-81.
315. Matsui Y, Sugawara Y, Tsukada K, Kishi Y, Shibahara J, Makuuchi M. Aspergillus thyroiditis in a
living donor liver transplant recipient. J Infect. 2006;53(6):e231-3.
316. Ayala AR, Basaria S, Roberts KE, Cooper DS. Aspergillus thyroiditis. Postgrad Med J. 2001
May;77(907):336.
317. Chasan R, Patel G, Malone A, Finn M, Huprikar S. Primary hepatic aspergillosis following induction
chemotherapy for acute leukemia. Transpl Infect Dis. 2013 Oct;15(5):E201-5.
318. Gupta KL, Rajaram KG, Joshi K, Sakhuja V. Progression of hepatic aspergillosis following second renal
transplantation in a patient with recurrent glomerulonephritis. Indian J Pathol Microbiol. 2012 Oct-
Dec;55(4):580-2.
319. Gustot T, Maillart E, Bocci M, Surin R, Trépo E, Degré D, Lucidi V, Taccone FS, Delforge ML,
Vincent JL, Donckier V, Jacobs F, Moreno C. Invasive aspergillosis in patients with severe alcoholic
hepatitis. J Hepatol. 2014 Feb;60(2):267-74.
320. Chen Y, Cameron A. Aspergillosis after liver transplantation in the context of common variable
immunodeficiency: case report. Transpl Infect Dis. 2013 Oct;15(5):540-4.
321. Mora D, Barba P, Ruiz I, Castillo N, Aizpurua M, Roselló E, Bosch F, Valcárcel D. Primary
gastrointestinal aspergillosis 6 months after allogeneic hematopoietic cell transplantation: a case report.
Transpl Infect Dis. 2013 Jun;15(3):E107-10.
322. Karaman I, Karaman A, Boduroğlu EC, Erdoğan D, Tanır G. nvasive Aspergillus infection localized to
the gastric wall: report of a case. Surg Today. 2013 Jun;43(6):682-4.
323. Kazan E, Maertens J, Herbrecht R, Weisser M, Gachot B, Vekhoff A, Caillot D, Raffoux E, Fagot A
retrospective series of gut aspergillosis in haematology patients.

161
324. Choi SH, Chung JW, Cho SY, Kim BJ, Kwon GY. A case of isolated
invasive Aspergillus colitis presenting with hematochezia in a nonneutropenic patient with colon cancer.
Gut Liver. 2010 Jun;4(2):274-7
325. Andres LA, Ford RD, Wilcox RM. Necrotizing colitis caused by systemic aspergillosis in a burn patient.
J Burn Care Res. 2007 Nov-Dec;28(6):918-21.
326. Cicora F, Mos F, Paz M, Roberti J. Successful treatment of acute thyroiditis due to Aspergillus spp. in
the context of disseminated invasive aspergillosis in a kidney transplant patient. Nefrologia.
2013;33(4):618-9.
327. Siddappa S, Mythri KM, Kowsalya R, Shivalingaiah M. An unusual case of non-disseminated bladder
aspergillosis in a setting of transitional cell carcinoma. Indian J Med Microbiol. 2012 Jan-Mar;30(1):106-
8.
328. Singal A, Grover C, Pandhi D, Das S, Jain BK. Nosocomial urinary tract aspergilloma in an
immunocompetent host: an unusual occurrence. Indian J Dermatol. 2013 Sep;58(5):408.
329. Haq JA, Khan MA, Afroze N, Haq T. Localized primary renal aspergillosis in a diabetic patient
following lithotripsy--a case report. BMC Infect Dis. 2007 Jun 14;7:58.
330. Vuruskan H, Ersoy A, Girgin NK, Ozturk M, Filiz G, Yavascaoglu I, Oktay B. An unusual cause of
ureteral obstruction in a renal transplant recipient: ureteric aspergilloma. Transplant Proc. 2005
Jun;37(5):2115-7.
331. Deb P, Srivastava A. Aspergillus in a cervico-vaginal smear of an adult postmenopausal female: An
unusual case. J Cytol. 2009 Jul;26(3):123-4.
332. Dervisoglu E, Dikmen E, Filinte D, Yilmaz A. Isolated bladder aspergillosis as the primary presentation
of non-oliguric acute renal failure. Scand J Urol Nephrol. 2008;42(2):189-91.
333. González-Vicent M, Lassaletta A, López-Pino MA, Romero-Tejada JC, de la Fuente-Trabado M, Díaz
MA. Aspergillus "fungus ball" of the bladder after hematopoietic transplantation in a pediatric patient:
successful treatment with intravesical voriconazole and surgery. Pediatr Transplant. 2008 Mar;12(2):242-
5.
334. Ahmad M, Dakshinamurty KV. Emphysematous renal tract disease due to Aspergillusfumigatus. J
Assoc Physicians India. 2004 Jun;52:495-7.
335. Paul S, Singh V, Sankhwar S, Garg M. Renal aspergillosis secondary to renal intrumentation in
immunocompetent patient. BMJ Case Rep. 2013 Sep 11;2013.
336. Banks FC, Kelkar A, Harvey CJ, Williams G. Aspergillosis prostatitis post-renal transplantation.
Nephrol Dial Transplant. 2005 Dec;20(12):2865-6.
337. Hood SV, Bell D, McVey R, Wilson G, Wilkins EG. Prostatitis and epididymo-orchitis due
to Aspergillus fumigatus in a patient with AIDS. Clin Infect Dis. 1998 ;26(1):229-31.
338. Cherasse A, Herin M, Oana M, Marievoet C. [Aspergillus prostatitis and prolonged corticotherapy.
Apropos of a case report]. Acta Urol Belg. 1997 Mar;65(1):43-8.
339. Sobel C, Franzaring I, Pullwitt J, Melchior S. [Renal aspergilloma: first manifestation of an occult
sarcomatoid carcinoma]. Urologe A. 2012 Oct;51(10):1444-6.
340. Zhu LP, Chen XS, Wu JQ, Yang FF, Weng XH. Aspergillus vertebral osteomyelitis and ureteral
obstruction after liver transplantation. Transpl Infect Dis. 2011 Apr;13(2):192-9.
341. Raj KA, Srinivasamurthy BC, Nagarajan K, Sinduja MG. A rare case of
spontaneous Aspergillus spondylodiscitis with epidural abscess in a 45-year-old immunocompetent
female. J Craniovertebr Junction Spine. 2013 4(2):82-4.
342. Ma H, Lv G, Wang B. Does surgery influence the outcome of Aspergillusosteomyelitis? Clin Microbiol
Infect. 2014 Mar 26. doi: 10.1111/1469-0691.12588.
343. Gabrielli E, Fothergill AW, Brescini L, Sutton DA, Marchionni E, Orsetti E, Staffolani S, Castelli P,
Gesuita R, Barchiesi F. Reply to Ma et al.: Osteomyelitis caused by Aspergillusspecies. Clin Microbiol
Infect. 2014 Mar 4. doi: 10.1111/1469-0691.12613.

161
344. Asare KA, Jahng M, Pincus JL, Massie L, Lee SA. Sternal osteomyelitis caused
by Aspergillus fumigatus following cardiac surgery: Case and review. Med Mycol Case Rep. 2012 Dec
7;2:4-6.
345. Koehler P, Tacke D, Cornely OA. Aspergillosis of bones and joints - a review from 2002 until today.
Mycoses. 2014 Jun;57(6):323-35.
346. Gamaletsou MN, Rammaert B, Bueno MA, Moriyama B, Sipsas NV, Kontoyiannis DP, Roilides E,
Zeller V, Prinapori R, Taj-Aldeen SJ, Brause B, Lortholary O, Walsh TJ. Aspergillus osteomyelitis:
epidemiology, clinical manifestations, management, and outcome. J Infect. 2014 May;68(5):478-93.
347. Mirhosseini SJ, Salehi M, Ali-Hassan-Sayegh S, Forouzannia K, Karimi-Bondarabadi AA.
Costochondritis caused by Aspergillus flavus following cardiac surgery. Acta Med Iran. 2013
Oct;51(10):733-5.
348. Gabrielli E, Fothergill AW, Brescini L, Sutton DA, Marchionni E, Orsetti E, Staffolani S, Castelli P,
Gesuita R, Barchiesi F. Osteomyelitis caused by Aspergillus species: a review of 310 reported cases. Clin
Microbiol Infect. 2013 Sep 5. doi: 10.1111/1469-0691.12389.
349. D'sa SR, Singh S, Satyendra S, Mathews P.Case report of Aspergillus osteomyelitis of the ribs in an
immunocompetent patient. J Glob Infect Dis. 2013 Jul;5(3):118-20.
350. Asimakopoulos P, Supriya M, Kealey S, Vernham GA. A case-based discussion on a patient with non-
otogenic fungal skull base osteomyelitis: pitfalls in diagnosis. J Laryngol Otol. 2013 Aug;127(8):817-21.
351. Jiang Z, Wang Y, Jiang Y, Xu Y, Meng B. Vertebral osteomyelitis and epidural abscess due
toAspergillus nidulans resulting in spinal cord compression: case report and literature review. J Int Med
Res. 2013;41(2):502-10.
352. Bathoorn E, Escobar Salazar N, Sepehrkhouy S, Meijer M, de Cock H, Haas PJ. Involvement of the
opportunistic pathogen Aspergillustubingensis in osteomyelitis of the maxillary bone: a case report.
BMC Infect Dis. 2013 Feb 1;13:59.
353. Hall GL, Villanueva-Siles E, Borzykowski RM, Gruson KI, Dorfman HD, Geller DS.
Aspergillus osteomyelitis of the proximal humerus: a case report. Skeletal Radiol. 2012 Aug;41(8):1021-
5.
354. Sethi S, Siraj F, Kalra K, Chopra P. Aspergillus vertebral osteomyelitis in immunocompetent patients.
Indian J Orthop. 2012 Mar;46(2):246-50.
355. Severino M, Liyanage S, Novelli V, Cheesborough B, Saunders D, Gunny R, Rossi A. Skull
base osteomyelitis and potential cerebrovascular complications in children. Pediatr Radiol. 2012
Jul;42(7):867-74.
356. Camargo JF, Seriburi V, Tenner M, El Khoury MY. Aspergillus osteomyelitis of the lumbar spine
complicated with orbital apex syndrome: A potential role of the Batson's plexus in disease propagation.
Med Mycol Case Rep. 2012 Mar 15;1(1):9-12.
357. Chang HM, Yu HH, Yang YH, Lee WI, Lee JH, Wang LC, Lin YT, Chiang BL. Successful treatment
of Aspergillus flavus spondylodiscitis with epidural abscess in a patient with chronic granulomatous
disease. Pediatr Infect Dis J. 2012 Jan;31(1):100-1
358. Ersoy A, Dizdar OS, Koc AO, Akalin H, Ener B. Aspergillus fumigatus spondylodiskitis in renal
transplant patient: voriconazole experience. Exp Clin Transplant. 2011 Aug;9(4):265-9.
359. Dotis J, Roilides E. Osteomyelitis due to Aspergillus species in chronic granulomatous disease: an
update of the literature. Mycoses. 2011 Nov;54(6):e686-96.
360. Zhu LP, Chen XS, Wu JQ, Yang FF, Weng XH. Aspergillus vertebral osteomyelitis and ureteral
obstruction after liver transplantation. Transpl Infect Dis. 2011 Apr;13(2):192-9.
361. Karia S, Jeyapalan K, Kennedy B. Aspergillus fumigatus osteomyelitis in a patient receiving
alemtuzumab for B-cell chronic lymphocytic leukaemia. Br J Haematol. 2011 Apr;153(2):147.
362. Studemeister A, Stevens DA. Aspergillus vertebral osteomyelitis in immunocompetent hosts: role of
triazole antifungal therapy. Clin Infect Dis. 2011 Jan 1;52(1):e1-6.
363. Furtado AR, Caine A, Herrtage ME. Diagnostic value of MRI in dogs with inflammatory nasal disease. J
Small Anim Pract. 2014 Apr 23. doi: 10.1111/jsap.12223.
162
364. Talbot JJ, Johnson LR, Martin P, Beatty JA, Sutton DA, Billen F, Halliday CL, Gibson JS, Kidd S,
Steiner JM, Ujvari B, Barrs VR. What causes canine sino-nasal aspergillosis? A molecular approach to
species identification. Vet J. 2014 Apr;200(1):17-21.
365. Trempala CL, Herold LV. Spontaneous pneumothorax associated with Aspergillus bronchopneumonia
in a dog. J Vet Emerg Crit Care (San Antonio). 2013 Nov-Dec;23(6):624-30.
366. Vanherberghen M, Bureau F, Peters IR, Day MJ, Lynch A, Fievez L, Billen F, Clercx C, Peeters D.
Cytokine and transcription factor expression by Aspergillus fumigatus-stimulated peripheral blood
mononuclear cells in dogs with sino-nasal aspergillosis. Vet Immunol Immunopathol. 2013 Aug
15;154(3-4):111-20.
367. Walker JT, Frazho JK, Randell SC. A novel case of canine disseminated aspergillosis following mating.
Can Vet J. 2012 Feb;53(2):190-2.
368. Sharman MJ, Mansfield CS. Sinonasal aspergillosis in dogs: a review. J Small Anim Pract. 2012
Aug;53(8):434-44.
369. Mercier E, Peters IR, Day MJ, Clercx C, Peeters D. Toll- and NOD-like receptor mRNA expression in
canine sino-nasal aspergillosis and idiopathic lymphoplasmacytic rhinitis.Vet Immunol Immunopathol.
2012 Feb 15;145(3-4):618-24
370. Sharman M, Lenard Z, Hosgood G, Mansfield C. Clotrimazole and enilconazole distribution within the
frontal sinuses and nasal cavity of nine dogs with sinonasalaspergillosis. J Small Anim Pract. 2012
Mar;53(3):161-7.
371. Vanherberghen M, Bureau F, Peters IR, Day MJ, Clercx C, Peeters D. Analysis of gene expression in
canine sino-nasal aspergillosisand idiopathic lymphoplasmacytic rhinitis: a transcriptomic analysis. Vet
Microbiol. 2012 May 25;157(1-2):143-51.
372. Burrough E, Deitz K, Kinyon J, Andreasen C, Frana T, Sutton D, Thompson E, Fu J, Wickes B,
Hostetter J. Disseminated aspergillosis in a dog due to Aspergillus alabamensis. Med Mycol Case Rep.
2012 Mar 1;1(1):1-4.
373. Garcia RS, Wheat LJ, Cook AK, Kirsch EJ, Sykes JE. Sensitivity and specificity of a blood and urine
galactomannan antigen assay for diagnosis of systemic aspergillosis in dogs. J Vet Intern Med. 2012 Jul-
Aug;26(4):911-9.
374. Walker JT, Frazho JK, Randell SC. A novel case of canine disseminated aspergillosis following mating.
Can Vet J. 2012 Feb;53(2):190-2.
375. Adamama-Moraitou KK, et al. 2011. Aspergillus fumigatus bronchopneumonia in a Hellenic shepherd
dog. J. Am. Anim. Hosp. Assoc.47:e13–e18.
376. Kelly DF. Cavitating pulmonary lesions in German shepherd dogs. J Small Anim Pract. 2011
Dec;52(12):665.
377. Epstein S, Hardy R. Clinical resolution of nasal aspergillosis following therapy with a homeopathic
remedy in a dog. J Am Anim Hosp Assoc. 2011 Nov-Dec;47(6):e110-5
378. Zhang S, Corapi W, Quist E, Griffin S, Zhang M. Aspergillus versicolor, a new causative agent of
canine disseminated aspergillosis. J Clin Microbiol. 2012 Jan;50(1):187-91.
379. Burrow R, McCarroll D, Baker M, Darby P, McConnell F, Cripps P. Frontal sinus depth at four
landmarks in breeds of dog typically affected by sinonasal aspergillosis. Vet Rec. 2012 Jan 7;170(1):20.
380. Adamama-Moraitou KK, Pardali D, Day MJ, Denning DW, Papazoglou L, Papastefanou A, Rallis TS.
Aspergillus fumigatus Bronchopneumonia in a Hellenic Shepherd Dog. J Am Anim Hosp Assoc. 2011
Mar-Apr;47(2):13-8.
381. Sheahan D, Bell R, Mellanby RJ, Gow AG, Friend E, Heller J, Bence LM, Eckersall PD. Acute phase
protein concentrations in dogs with nasal disease. Vet Rec. 2010 Dec 4;167(23):895-9.
382. Whitley NT, Cauvin A, Burton C, Bray J, Van Dongen P, Littlewood J. Long term survival in two
German shepherd dogs with Aspergillus-associated cavitary pulmonary lesions. J Small Anim Pract.
2010 Oct;51(10):561.
383. Coyner K. Otomycosis due to Aspergillus spp. in a dog: case report and literature review. Vet Dermatol.
2010 Dec;21(6):613-8.
163
384. Billen F, Guieu LV, Bernaerts F, Mercier E, Lavoué R, Tual C, Peeters D, Clercx C. Efficacy of
intrasinusal administration of bifonazole cream alone or in combination with enilconazole irrigation in
canine sino-nasal aspergillosis: 17 cases. Can Vet J. 2010 Feb;51(2):164-8.
385. Ghibaudo G, Peano A. Chronic monolateral otomycosis in a dog caused by Aspergillus ochraceus. Vet
Dermatol. 2010 Oct;21(5):522-6.
386. Pomrantz JS, Johnson LR. Repeated rhinoscopic and serologic assessment of the effectiveness of
intranasally administered clotrimazole for the treatment of nasal aspergillosis in dogs. J Am Vet Med
Assoc. 2010 Apr 1;236(7):757-62
387. Marta J. Siemieniucha,
Dariusz J. Skarzynskia, Roland Kozdrowsk, Aspergillosis of a dog genital tract—
Case report, Animal Reproduction Science. 112, 1–2, May 2009, 164–171
388. Siemieniuch MJ, Skarzynski DJ, Kozdrowski R. Aspergillosis of a dog genital tract-Case report. Anim
Reprod Sci. 2009 May;112(1-2):164-71.
389. Hartmann K, Lloret A, Pennisi MG, Ferrer L, Addie D, Belák S, Boucraut-Baralon C, Egberink H,
Frymus T, Gruffydd-Jones T, Hosie MJ, Lutz H, Marsilio F, Möstl K, Radford AD, Thiry E, Truyen U,
Horzinek MC. Aspergillosis in cats: ABCD guidelines on prevention and management. J Feline Med
Surg. 2013 Jul;15(7):605-10.
390. Barrs VR, van Doorn TM, Houbraken J, Kidd SE, Martin P, Pinheiro MD, Richardson M, Varga J,
Samson RA. Aspergillus felis sp. nov., an emerging agent of invasiveaspergillosis in humans, cats, and
dogs. PLoS One. 2013 Jun 14;8(6):e64871.
391. Barrs VR, Talbot JJ. Feline aspergillosis. Vet Clin North Am Small Anim Pract. 2014 Jan;44(1):51-73.
doi: 10.1016/j.cvsm.2013.08.001. Epub 2013 Sep 17.
392. Coyner K. Otomycosis due to Aspergillus spp. in a dog: case report and literature review. Vet Dermatol.
2010 Dec;21(6):613-8. doi: 10.1111/j.1365-3164.2010.00903.x. Review.
393. Ghibaudo G, Peano A. Chronic monolateral otomycosis in a dog caused by Aspergillus ochraceus. Vet
Dermatol. 2010 Oct;21(5):522-6.
394. Giordano C, Gianella P, Bo S, Vercelli A, Giudice C, Della Santa D, Tortorano AM, Peruccio C, Peano
A. Invasive mould infections of the naso-orbital region of cats: a case involving Aspergillus fumigatus
and an aetiological review. J Feline Med Surg. 2010 Sep;12(9):714-23.
395. Furrow E, Groman RP. Intranasal infusion of clotrimazole for the treatment of nasalaspergillosis in two
cats. J Am Vet Med Assoc. 2009 Nov 15;235(10):1188-93.
396. Barachetti L, Mortellaro CM, Di Giancamillo M, Giudice C, Martino P, Travetti O, Miller PE. Bilateral
orbital and nasal aspergillosis in a cat. Vet Ophthalmol. 2009;12(3):176-82.
397. Karnik K, Reichle JK, Fischetti AJ, Goggin JM. Computed tomographic findings of fungal rhinitis and
sinusitis in cats. Vet Radiol Ultrasound. 2009 Jan-Feb;50(1):65-8.
398. Labelle AL, Hamor RE, Barger AM, Maddox CW, Breaux CB. Aspergillus flavus keratomycosis in
a cat treated with topical 1% voriconazole solution. Vet Ophthalmol. 2009 Jan-Feb;12(1):48-52.
399. Kano R, Itamoto K, Okuda M, Inokuma H, Hasegawa A, Balajee SA. Isolation of Aspergillus udagawae
from a fatal case of feline orbitalaspergillosis. Mycoses. 2008 Jul;51(4):360-1.
400. Barrs VR, Beatty JA, Lingard AE, Malik R, Krockenberger MB, Martin P, O'Brien C, Angles JM,
Dowden M, Halliday C. Feline sino-orbital aspergillosis:an emerging clinical syndrome. Aust Vet J.
2007 Mar;85(3):N23. No abstract available.
401. McLellan GJ, Aquino SM, Mason DR, Kinyon JM, Myers RK. Use of posaconazole in the management
of invasive orbitalaspergillosis in a cat. J Am Anim Hosp Assoc. 2006 Jul-Aug;42(4):302-.
402. Claudia Cafarchia Romina Paradies Luciana A. Figueredo Barbara Padalino Maria Fiorella
Greco Grazia Greco Domenico Otranto. A Case of Equine Aspergillosis: A Novel Sampling Procedure
for Diagnosis. Journal of Equine Veterinary Science, 2012 | 32 | 10 | 634-637
164
403. RM Archera*
, CG Knighta & WJ Bishop
. Guttural pouch mycosis in six horses in New Zealand. New
Zealand Veterinary Journal. 60, 3, 2012
404. Moretta, I.; Veronesi, F.; Lepri, E.; Secco, I.; Rossodivita, M. E.; Moretti, A.. Aspergillus
fumigatus guttural pouch mycosis in a horse which died from acute pulmonary oedema. Journal
Ippologia 2010 Vol. 21 No. 2 pp. 11-17
405. F. Laus, E. Paggi, M. Cerquetella, D. Spaziante, A. Spaterna, B. Tesei. Guttural pouch mycosis in a
donkey (Equus asinus): a case report. Veterinarni Medicina, 55, 2010 (11): 561–565 Case Report
406. Hugh Millar. Guttural pouch mycosis in a 6-month-old filly. Can Vet J. Mar 2006; 47(3): 259–261.
407. P. J. Pollock. Diagnosis and management of guttural pouch mycosis. Equine Veterinary Education,
Volume 19, Issue 10, pages 522–527, November 2007
408. James L Carmalt1and Keith E. Baptiste. Atypical guttural pouch
mycosis in three horses. Pferdeheilkunde 20 (2004)
409. Pachauri S, Varshney P, Dash SK and Gupta MK (2013) Involvement of fungal species in bovine
mastitis in and around . Mathura, India, Vet World 6(7):393-395,
410. Dehkordi, F. Safarpoor, H. Momtaz & A. Doosti, 2012. Application of real-time PCR for detection of
Aspergillus species in aborted ruminant foetuses. Bulg. J. Vet. Med., 15, No 1, 30−36.
411. R. Ali and i. H. Khan1. Mycotic abortion in cattle . Pakistan Vet. J., 2006, 26(1): 44-46
412. Corbellini, Luís G. et al. Abortus by Aspergillus fumigatus and A. nigerin cattle in southern Brazil. Pesq.
Vet. Bras. [online]. 2003, 23, 2, 82-86.
413. Máximo Fernández Díez. Mastitis by Aspergillus fumigatusin sheep. Rev Iberoam Micol 2000; 17: S13-
S17
414. Vos JH, Fontijne P, Elsinghorst TA [Mycotic placentitis in cattle]. Tijdschr Diergeneeskd. 1986 Jan
1;111(1):14-9.
415. Hill, MW, C E Whiteman, M M Benjamin, L Ball. Pathogenesis of experimental bovine mycotic
placentitis produced by Aspergillus fumigatus. Veterinary Pathology (Impact Factor: 1.93). 02/1971;
8(2):175-92.
416. Schällibaum, M, J Nicolet, H König. Aspergillus nidulans and Aspergillus fumigatus as causal agents of
bovine mastitis. Sabouraudia 04/1980; 18(1):33-8.
417. Walser K, Kleinschroth E. Cases of Aspergillus mastitis in cattle].Berliner und Münchener tierärztliche
Wochenschrift. 92:7 1979, 1, 129-3.
418. Jensen HE, Espinosa de los Monteros A, Carrasco L. Caprine mastitis due to aspergillosis and
zygomycosis: a pathological and immunohistochemical study. Journal of comparative pathology 114:2
1996 Feb pg 183-91
419. do Carmo, P.M.S. , R.A. Portela, J.C. de Oliveira-Filho, A.F.M. Dantas, S.V.D. Simões, F. Garino, F.
Riet-Correa, Nasal and Cutaneous Aspergillosis in a Goat, Journal of Comparative Pathology ,2014
150, 1, 4-7
420. Pérez V, Corpa JM, Garćia Marín JF, Adúriz JJ, Jensen HE, Generalized aspergillosis in dairy sheep.
Zentralbl Veterinarmed B. 1999 Nov;46(9):613-21.

165
421. Jensen, H. E.; Espinosa De Los Monteros, A.; Carrasco, L., 1996: Caprine mastitis due to aspergillosis
and zygomycosis A pathological and immunohistochemical study. Journal Of Comparative Pathology.
114(2): 183-191
422. Jurczynski, K., E. Gruber-Dujardin2,†
, D. Widmer1, F.-J. Kaup
2 and K. Mätz-Rensing. Invasive
aspergillosis in a Putty-nosed monkey (Cercopithecus nictitans) with adrenocortical Cushing’s
syndrome. Journal of Medical Primatology, Volume 41, Issue 3, pages 172–175, June 2012
423. El-Khouly AB, Gadir FA, Cluer DD, Manefield GW. Aspergillosis in camels affected with a specific
respiratory and enteric syndrome. Aust Vet J. 1992 Aug;69(8):182-6.
424. Jensen HE1, Jørgensen JB, Schønheyder H. Pulmonary mycosis in farmed deer: allergic zygomycosis
and invasive aspergillosis. J Med Vet Mycol. 1989;27(5):329-34.
425. Dehkordi, F. Safarpoor, H. Momtaz & A. Doosti, 2012. Application of real-time PCR for detection of
Aspergillus species in aborted ruminant foetuses. Bulg. J. Vet. Med., 15, No 1, 30−36.
426. Chandrasekar, P. H.Jessica Cutright and Elias Manavathu. Efficacy of voriconazole against invasive
pulmonary aspergillosis in a guinea-pig model. J. Antimicrob. Chemother. (2000)45 (5): 673-
676.doi: 10.1093/jac/45.5.673
427. Arrese, J. E., P. Delvenne , J. van Cutsem, C. Piérard-Franchimont andG. E. Piérard. Experimental
aspergillosis in guinea pigs: influence of itraconazole on fungaemia and invasive fungal growth.
Mycoses. Volume 37, Issue 3-4, pages 117–122, March 1994
428. REWELL , R. E. & G. C. AINSWORTH. Occurrence of Aspergillus fumigatus Fresen. in the Lung of
an American Bison. Nature 160, 362-363 (13 September 1947)
429. de los Monteros AE1, Carrasco L, King JM, Jensen HE.Nasal zygomycosis and pulmonary aspergillosis
in an American bison. J Wildl Dis. 1999 Oct;35(4):790-5.
430. Reidarson TH1, Harrell JH, Rinaldi MG, McBain J. Bronchoscopic and serologic diagnosis of
Aspergillus fumigatus pulmonary infection in a bottlenose dolphin (Tursiops truncatus). J Zoo Wildl
Med. 1998 Dec;29(4):451-5.
431. Severo, L.C. ,J.C. Bohrer, G.R. Geyer and L. Ferreiro. Invasive aspergillosis in an alpaca (Lama pacos).
1989, Vol. 27, No. 3 , Pages 193-195
432. Brian E. Joseph1,*
, Lanny H. Cornell1,John G. Simpson
2, George Migaki
3andLynn Griner
1 Pulmonary
aspergillosis in three species of dolphin. Zoo Biology. Volume 5, Issue 3, pages 301–308, 1986
433. Patton NM. Cutaneous and pulmonary aspergillosis in rabbits. Lab Anim Sci. 1975 Jun;25(3):347-50
434. Tamam, Omar and Mohamed Refai. Dual mycotic pulmonary granulomas caused by Alternaria
alternata and Aspergillus candidus in the wild egyptian mole rat (spalax leucodon egyptiacus). Assiut
Vet. Med. J. Vol. 59 No. 139 October 2013
435. Guilherme Augusto Marietto-Gonçalves, Fabrizio Grandi, Noeme Sousa Rocha, Raphael Lucio ,
Andreatti Filho. SECONDARY Aspergillus fumigatus infection associated with coloidal goiter in a
black-masked lovebird (Agapornis personata). Acta Veterinaria Brasilica, v.8, n.1, p.68-73, 2014
436. Ziołkowska G, Tokarzewski S, Nowakiewicz A. Drug resistance of Aspergillus fumigatus strains
isolated from flocks of domestic geese in Poland. Poult Sci. 2014 May;93(5):1106-12
437. Glare TR, Gartrell BD, Brookes JJ, Perrott JK. Isolation and identification of Aspergillus spp. from
brown kiwi (Apteryx mantelli) nocturnal houses in New Zealand. Avian Dis. 2014 Mar;58(1):16-24.
438. Burco JD, Massey JG, Byrne BA, Tell L, Clemons KV, Ziccardi MH. Monitoring of fungal loads in
seabird rehabilitation centers with comparisons to natural seabird environments in northern California.J
Zoo Wildl Med. 2014 Mar;45(1):29-40.
439. Wang DY, Gricourt M, Arné P, Thierry S, Seguin D, Chermette R, Huang WY, Dannaoui E, Botterel F,
Guillot J. Mutations in the Cyp51A gene and susceptibility to itraconazole in Aspergillus fumigatus
isolated from avian farms in France and China.Poult Sci. 2014 Jan;93(1):12-5.

166
440. Cafarchia C, Camarda A, Iatta R, Danesi P, Favuzzi V, Di Paola G, Pugliese N, Caroli A, Montagna
MT, Otranto D. Environmental contamination by Aspergillus spp. in laying hen farms and associated
health risks for farm workers. J Med Microbiol. 2014 Mar;63(Pt 3):464-70.
441. Glare TR, Gartrell BD, Brookes JJ, Perrott JK.Isolation and identification of Aspergillus spp. from
brown kiwi (Apteryx mantelli) nocturnal houses in New Zealand. Avian Dis. 2014, Mar;58(1):16-24.
442. Vorbrüggen S, Bailey T, Krautwald-Junghanns ME. [Radiographic findings in raptors affected with a
mycosis of the respiratory tract].Tierarztl Prax Ausg K Kleintiere Heimtiere. 2013;41(5):311-8.
443. Rundfeldt C, Wyska E, Steckel H, Witkowski A, Jeżewska-Witkowska G, Wlaź P. A model for treating
avian aspergillosis: serum and lung tissue kinetics for Japanese quail (Coturnix japonica) following
single and multiple aerosol exposures of a nanoparticulate itraconazole suspension. Med Mycol. 2013
Nov;51(8):800-10.
444. Goetting V, Lee KA, Woods L, Clemons KV, Stevens DA, Tell LA. Inflammatory marker profiles in an
avian experimental model of aspergillosis. Med Mycol. 2013 Oct;51(7):696-703
445. Chege S, Howlett J, Al Qassimi M, Toosy A, Kinne J, Obanda V, Muller MG. Opportunistic infection of
Aspergillus and bacteria in captive Cape vultures (Gyps coprotheres). Asian Pac J Trop Biomed. 2013
;3(5):401-6.
446. Pello SJ, Olsen GH. Emerging and reemerging diseases of avian wildlife. Vet Clin North Am Exot
Anim Pract. 2013 May;16(2):357-81.
447. Thierry S, Durand B, Melloul E, Tafani JP, Wang DY, Deville M, Cordonnier N, Chermette R, Guillot
J, Arné P. Assessment of Aspergillus fumigatus pathogenicity in aerosol-challenged chickens (Gallus
gallus) belonging to two lineages. Comp Immunol Microbiol Infect Dis. 2013 Jul;36(4):379-85.
448. Borah M.K.*, Jangir Babu Lal, Raut S.S., Gogoi R.1, Sharma G.D.. Aspergillosis in Japanese quail
(Coturnix coturnix japonica). Indian Journal of Veterinary Pathology,34.203-204,2010
449. Kureljušić B., Radanović O., Kureljušić J., Jezdimirović N., Maslić-Strižak D., Prodanović R., Ivetić V.
The occurrence of aspergillosis in flock of turkey poults, Biotechnology in Animal Husbandry, 2012
28(1):129-136
450. Kummrow M, Silvanose C, Di Somma A, Bailey TA, Vorbrüggen S. Serum protein electrophoresis by
using high-resolution agarose gel in clinically healthy and Aspergillus species-infected falcons. J Avian
Med Surg. 2012 Dec;26(4):213-20.
451. Svirshchevskaya E, Zubkov D, Mouyna I, Berkova N. Innate Immunity and the Role of Epithelial
Barrier During Aspergillus fumigatus Infection. Curr Immunol Rev. 2012 Aug;8(3):254-261.
452. Rashid MH, Xue C, Islam MR, Islam MT, Cao Y. A longitudinal study on the incidence of mortality of
infectious diseases of commercial layer birds in Bangladesh. Prev Vet Med. 2013 May 1;109(3-4):354-8.
453. Korniłłowicz-Kowalska T, Kitowski I. Aspergillus fumigatus and other thermophilic fungi in nests of
wetland birds. Mycopathologia. 2013 Feb;175(1-2):43-56.
454. Hadrich I, Drira I, Neji S, Mahfoud N, Ranque S, Makni F, Ayadi A. Microsatellite typing of
Aspergillus flavus from clinical and environmental avian isolates. J Med Microbiol. 2013 Jan;62(Pt
1):121-5.
455. Hadrich I, Amouri I, Neji S, Mahfoud N, Ranque S, Makni F, Ayadi A. Genetic structure of Aspergillus
flavus populations in human and avian isolates.Eur J Clin Microbiol Infect Dis. 2013 Feb;32(2):277-82.
456. Spanamberg A Gustavo Machado
; Renata Assis Casagrande
I ; Gabriela Miller Sales
, Cibele Floriano
Fraga; Luís Gustavo Corbellini]; David Driemeier
]; Laerte Ferreiro
. Aspergillus fumigatus from normal
and condemned carcasses with airsacculitis in commercial poultry, Pesq. Vet. Bras. 33,9. Rio de
Janeiro Sept. 2013
457. Clara N Kwanashie, Paul A Abdu, Jarlath U Umoh, Haruna M. Kazeem. Retrospective study of
aspergillosis and other fungi in poultry (1980-2008), Int. J. Livest. Res.. 2012; 2(3): 84-88
458. França M, Cray C, Shivaprasad HL. Serologic testing for aspergillosis in commercial broiler chickens
and turkeys.Avian Dis. 2012 Mar;56(1):160-4.
459. Walker AK. Aspergillosis in gamebirds and ducks. Vet Rec. 2012 Jan 21;170(3):84

167
460. Ceolin L.V., Flores F., Oliveira I.M.C., Lovato M., Galiza G.J.N., Kommers G.D., Risso N. & Santurio
J.M. 2012. Macroscopic and Microscopic Diagnosis of Aspergillosis in Poultry. Acta Scient. Vet.
40(3):1061.
461. Parker CD. Aspergillosis in gamebirds and ducks. Vet Rec. 2011 Dec 3;169(23):613-
462. Simpson V. Spinal aspergillosis in pheasants. Vet Rec. 2011 Nov 19;169(21):562.
463. Arné P, Thierry S, Wang D, Deville M, Le Loc'h G, Desoutter A, Féménia F, Nieguitsila A, Huang W,
Chermette R, Guillot J. Aspergillus fumigatus in Poultry. Int J Microbiol. 2011;2011:746356.
464. Arné, P ,*
Simon Thierry, 2
Dongying Wang, 1, 3
Manjula Deville, 1, 4
Guillaume Le Loc'h, 1, 5
Anaïs
Desoutter, 1
Françoise Féménia, 6
Adélaïde Nieguitsila, 1
Weiyi Huang, 3
René Chermette, 1, 4
and Jacques
Guillot . Aspergillus fumigatus in Poultry. Int J Microbiol. 2011; 2011: 746356.
465. Hasan İÇEN, Nuretin IŞIK, Simten YEŞİLMEN, Mehmet TUZCU, Servet SEKİN. Diagnosis and
Treatment of Aspergillosis in An Ostrich Flock. Kafkas Univ Vet Fak Derg. 17 (4): 671-674, 2011
466. VanWaeyenberghe L., Pasmans F., Beernaert L.A., Haesebrouck F.,Vercammen F., Verstappen F., Dorr
estein G. M., Klaassen C. H., Martel A. (2011). Microsatellite typing of avian clinical and environmental
isolates of Aspergillus fumigatus. Avian Pathol 40, 73–77.
467. Olias P, Rüdiger Hauck , Heinrich Windhaus , Elisabeth van der Grinten
, Achim D. Gruber
, and
Hafez M. Hafez . Articular Aspergillosis of Hip Joints in Turkeys. Avian Diseases 54(3):1098-1101.
2010
468. Olias P., Gruber A. D., Hafez H. M., Lierz M., Slesiona S., Brock M., Jacobsen I. D. (2011). Molecular
epidemiology and virulence assessment of Aspergillus fumigatus isolates from white stork chicks and
their environment. Vet Microbiol 148, 348–355.
469. Beernaert LA, Pasmans F, Van Waeyenberghe L, Haesebrouck F, Martel A. Aspergillus infections in
birds: a review. Avian Pathology. 2010;39(5):325–331.
470. Jacobsen ID, Große K, Slesiona S, Hube B, Berndt A, Brock M. Embryonated eggs as an alternative
infection model to investigate Aspergillus fumigatusvirulence. Infection and Immunity. 2010;78(7):2995–
3006.
471. Po-Hsuan CHIU, Fang-Tse CHAN, Lee-Jen CHEN, Ching-Lin SHYU, Pet-T LIN,Ling-Min
WANG, Kun-Cho CHEN, Cheng-Chung LIN, Woon-Fa CHANG, , Jiunn-Wang LIAO. Case report:
Pyogranulomatous Aspergillosis in An Endemic Formosan Blue Magpie ( ). Taiwan Vet J 36 (1): 18-22,
2010
472. Singh S., Borah M. K., Sharma D. K., Joshi G. D., Gogoi R. Aspergillosis in turkey poults, Indian
Journal of Veterinary Pathology, 2009, 33, 2, 220 – 221
473. Femenia F1, Fontaine JJ, Lair-Fulleringer S, Berkova N, Huet D, Towanou N, Rakotovao F, Granet
OI, Le Loc'h G, Arné P, Guillot J. Clinical, mycological and pathological findings in turkeys
experimentally infected by Aspergillus fumigatus. J Avian Pathol. 213-9 36 2007
474. Lisa A. Tell, Karl V. Clemons
†, Yvonne Kline
*, Leslie Woods
+, Philip H. Kass
#,Marife
Martinez† and David A. Stevens
†. Efficacy of voriconazole in Japanese quail (Coturnix japonica)
experimentally infected withAspergillus fumigatus. Med Mycol (2010) 48 (2): 234-244.
475. Katz, M.E., S.C. Love, H.S. Gill and B.F. Cheetham, 1996. Development of a method for the
identification using the polymerase chainre action of Aspergillus fumigatus isolated from ostriches. Aust.
Vet. J., 74: 50-54.
476. Perelman, B. and E.S. Kuttin, 1992. Aspergillosis in ostriches. Avian Pathol., 21: 159-163.
477. Sancak, A.A. and J. Paracikoglu, 2005. Aspergillosis and gastric impaction in an ostrich. Turk. J. Vet.
Anim. Sci., 29: 933-935.
478. Yokota, T., T. Shibahara, Y. Wada, R. Hiraki, Y. Ishikawa and K. Kadota, 2004. Aspergillus
fumigatus infection in an ostrich (Struthio camelus). J. Vet. Med. Sci., 66: 201-204.
479. Khosravi AR, Shokri H, Ziglari T, Naeini AR, Mousavi Z, Hashemi H. Outbreak of severe disseminated
aspergillosis in a flock of ostrich (Struthio camelus). Mycoses. 2008 Nov;51(6):557-9
168
480. Shathele, M.S. , A. Fadlelmula, F.A. Al-Hizab and M.M. Zaki, 2009. Fatal Aspergillosis in an Ostrich
(Struthio camelus) Predisposed by Pulmonary Haemangioma in the Kingdom of Saudi
Arabia. International Journal of Zoological Research, 5: 80-85.
481. ARAGHI, M., A. GHANIEI & T. HEIDARI. ASPERGILLOSIS OUTBREAKS IN OSTRICH
FLOCKS OF EASTERN IRAN DURING 2010–2012 . Bulgarian Journal of Veterinary Medicine, 2014
482. Pérez, J. , P. M. García, A. Méndez,, R. Astorga, I. Luque, C. Tarradas. Outbreak of aspergillosis in a
flock of adult ostriches (Struthio camelus), Veterinary Record 2003;153:4 124-
125doi:10.1136/vr.153.4.124
483. Tijani, MO, OO Alaka, AO Ogunleye, OO Esan. Pulmonary Aspergillosis in an Adult Male Ostrich
(Struthio camelus): A Case Report. Tropical Veterinarian. 30, 3 (2012)
484. Abou-Rawash, A. A., Yanai, T.; Kano R.; Murakami, M.; Masegi, T.; Fukushi, H.; Nagamine, T. and
Hasegawa, A. Disseminated aspergillosis in a Whooper Swan (Cygnus Cygnus). Egypt. J. Comp. Path.
& Clinic. Path. Vol. 21 No. 2 (April) 2008; 161- 174
485. El-Naggar, A., Ahmed, Y., Ibrahim, F. and Refai, M. : Some pathological studies in the udder of small
ruminants intramammarily infected with Aspergillus fumigatus and Candida albicans. J. Comp. Pathol. &
Clinc. Pathol. 10, 93-104 (1997)
486. El-Naggar, A., Ahmed, Y., Ibrahim, F. and Refai, M:Mycotic abortion in small ruminants induced by
Aspergillus fumigatus. J. Comp. Pathol. & Clinc. Pathol. 10, 59-76 (1997)
487. Verweij PE. Advances in diagnostic testing. Med Mycol. 2005 May;43 Suppl 1:S121-4. Review.
488. Biwas, Jyotirmay, R Bagyalakshmi, , Lily K Therese, Diagnosis of Aspergillus fumigatus
endophthalmitis from formalin fixed paraffin-embedded tissue by polymerase chain reaction-based
restriction fragment length polymorphism. Indian Journal of Ophthalmology. Jan-Feb 2008
489. Paterson, P J, P J S Seaton,1 J McLaughlin,
2 and C C Kibbler. Development of molecular methods for
the identification of aspergillus and emerging moulds in paraffin wax embedded tissue sections. Mol
Pathol. Dec 2003; 56(6): 368–370.
490. Barton, Richard C. “Laboratory Diagnosis of Invasive Aspergillosis: From Diagnosis to Prediction of
Outcome,” Scientifica, vol. 2013, Article ID 459405, 29 pages, 2013. doi:10.1155/2013/459405
491. Serrano, Rita, Leonor Gusmão, António Amorim and Ricardo Araujo. Rapid identification
of Aspergillus fumigatus within the section Fumigati. BMC Microbiology 2011, 11:82
492. Balajee, S. Arunmozhi , Rui Kano, John W. Baddley, Stephen A. Moser, Kieren A. Marr, Barbara D
Alexander, David Andes, Dimitrios P. Kontoyiannis, Giancarlo Perrone, Stephen Peterson, Mary E.
Brandt, Peter G. Pappas and Tom Chiller. Molecular Identification of Aspergillus Species Collected for
the Transplant-Associated Infection Surveillance Network▿ J. Clin. Microbiol. October 2009vol. 47 no.
10 3138-3141
493. Seher A. Khan. Antifungal Therapy for Invasive Aspergillosis, US Pharm. 2013;38(4):HS2-HS5.
494. Refai, M. and Abbasi, K. : A preliminary investigation on an outbreak of aspergillosis in turkey chicks.
Vet. Med. J. Giza 12, 377-378 (1966)
495. Youssef, H., Saad, I., Sefein, S, Abdel-Salam, H., Taha, M. and Refai, M. : Fungus precipitins in
workers of Quose sugar factory. Egypt. J.Chest Dis.&Tub. 23, 49-60 (1980)
496. Youssef, H. H., Youssef, Y. A., Abogamra, M., Hammad, H. and Refai, M. : Mycological and
serological studies on grain workers in mill factories in Cairo. Egypt. J. Chest Dis.&Tub. 23, 33-48
(1980)
497. Youssef, H. H., El-Sarangawy, A., Youssef, Y. A., Hassan, M. N., Taha, M., Hammad, H. and Refai, M.
: Preliminary study of mycoflora in sputum of poultry workers and screening of their sera for antifungal
precipitins. Egypt. J. Chest Dis.&Tub. 23, 61-70 (1980)

169
498. Abdalla, M., El-Mowafy, N. and Refai, M. : Mycological studies of the conjunctival sac of healthy and
diseased eyes. 16th Scientific Meeting of the German Mycological Association, Erlangen (1981)
499. Bassiyoni, A., Saad, F., Refai, M. and El Batrawi, A. : Efficacy of serological and allergic diagnosis of
A. fumigatus infection in chickens. J. Egypt. Vet. Med. Ass. 41, 161-171 (1981)
500. Refai, M., Hammad, H., Salem, N., Abdel-Aziz, A., El-Shater, S., Azzam, A. and Edris, G. :Mycotic
infections in birds and rabbits and their control. Vet. Med. J. 38, 129-143 (1990)
501. Refai, M,, S..A Attttiia,, R..M.. Sallem and E..M.. All--Dahshan ((2004)):: Studies on the pathogenicity
and enzymatic activities of Aspergillus fumigatus, A. flavus and A. niger isoated from chickens and their
environment. Egypt. G. Comp. Path.&Clin.Path. 17 (2) 193-205.




















