
ABO-and-Rh-Incompatibility.-I.-Fetal-and-Neonatal-Mortality ...
Upload
khangminh22Category
view
1download
0
TO STUDY THE PREVALENCE OF ABO INCOMPATIBILITY IN O BLOOD
GROUP MOTHERS AND ASSESSMENT OF IgG SUBCLASSES (IgG1 AND
IgG3) IN THEM AND ITS CORRELATION WITH OCCURRENCE AND
SEVERITY OF ABO HEMOLYTIC DISEASE OF NEWBORN (ABO-HDN) IN
A TERTIARY HEALTH CARE CENTRE IN SOUTH INDIA
A DISSERTATION SUBMITTED IN PART FULFILLMENT OF THE REGULATION
FOR THE AWARD OF THE DEGREE OF M.D. PATHOLOGY BRANCH III
THE TAMIL NADU DR.M.G.R.UNIVERSITY, CHENNAI, TAMIL NADU
MAY - 2020
REGISTRATION NUMBER: 201713358

To study the prevalence of ABO
incompatibility in O blood group mothers
and assessment of IgG subclasses (IgG1 and
IgG3) in them and its correlation with
occurrence and severity of ABO Hemolytic
Disease of Newborn (ABO HDN) in a
tertiary health care centre in South India
A dissertation submitted in part fulfillment of the regulation
for the award of the degree of M.D. Pathology Branch III
CERTIFICATE
This is to certify that the dissertation “To study the prevalence of ABO
incompatibility in O blood group mothers and assessment of IgG subclasses
(IgG1 and IgG3) in them and its correlation with occurrence and severity of ABO
Hemolytic disease of newborn (ABO HDN) in a tertiary health care centre in
south India” is the bonafide work done by Dr. Reshma Kurian, in part fulfillment of
the rules and regulations for the M.D. Branch III (Pathology) Degree Examination of
Tamil Nadu Dr. M.G.R. Medical University, to be held in May 2020.
Dr. Geeta Chacko, MD, PhD.
Professor and Head,
Department of General Pathology,
Christian Medical College,
Vellore.
Dr. Anna B Pulimood, MD, PhD.
Principal,
Christian Medical College,
Vellore.

CERTIFICATE
This is to certify that the dissertation “To study the prevalence of ABO
incompatibility in O blood group mothers and assessment of IgG subclasses
(IgG1 and IgG3) in them and its correlation with occurrence and severity of ABO
Hemolytic disease of newborn (ABO HDN) in a tertiary health care centre in
south India” is the bonafide work done by Dr. Reshma Kurian, in part fulfillment of
the rules and regulations for the M.D. Branch III (Pathology) Degree Examination of
Tamil Nadu Dr. M.G.R. Medical University, to be held in May 2020.
The candidate has independently reviewed the literature, standardized the data
collection methodology and carried out the evaluation towards completion of the
thesis.
Dr. Dolly Daniel, M.B.B.S, MD
Professor, Thesis Guide & Supervisor
Department of Transfusion Medicine and Immunohematology,
Christian Medical College, Vellore.

CERTIFICATE
This is to certify that the dissertation “To study the prevalence of ABO
incompatibility in O blood group mothers and assessment of IgG subclasses
(IgG1 and IgG3) in them and its correlation with occurrence and severity of ABO
Hemolytic disease of newborn (ABO HDN) in a tertiary health care centre in
south India” is the bonafide work done by me, under the guidance of Dr. Dolly
Daniel in part fulfillment of the rules and regulations for the M.D. Branch III
(Pathology) Degree Examination of Tamil Nadu Dr. M.G.R. Medical University, to be
held in May 2020.
.
I have independently reviewed the literature, performed the data collection, analyzed
the data and carried out the evaluation towards completion of the thesis.
Dr. Reshma Kurian,
Postgraduate Registrar,
Department of General Pathology,
Christian Medical College,
Vellore.
ANTI PLAGIARISM CERTIFICATE

CERTIFICATE
This is to certify that this dissertation work titled “To study the prevalence of ABO
incompatibility in O blood group mothers and assessment of IgG subclasses
(IgG1 and IgG3) in them and its correlation with occurrence and severity of ABO
Hemolytic disease of newborn (ABO HDN) in a tertiary health care centre in
south India” of the candidate Reshma Kurian with registration number 201713358 for
the award of Degree of MD Pathology in the branch III. I personally verified the
urkund.com website for the purpose of plagiarism Check. I found that the uploaded
thesis file contains from introduction to conclusion pages and result shows 4% of
plagiarism in the dissertation.
Guide & Supervisor sign with Seal.
ACKNOWLEDGEMENT
First of all I would like to thank God the almighty for me the strength and grace and
for providing me with this opportunity. This journey would have been impossible
without his grace and blessings.
I express my deepest gratitude to my mentor, Dr. Dolly Daniel for being the never
ending support, the encourager and the ever cheering guide who led the way to the
finish line of this dissertation.
I am indebted to my professor Dr. Geeta Chacko for her immense care, concern and
support.
I extend my warmest regards to Dr. Joy Mammen, for his support and encouragement.
I would like to specially thank Mrs. Sheela Kayalvezhi and Mr. Amal Raj,
Department of Transfusion Medicine and Immunohematology for helping me in
executing this project.
I extend my sincere thanks to Dr. Santhanam Sridhar, Dr. Annie Regi, Dr. Manisha
Mathai Beck and Dr. Swathi Rathore for their invaluable help in the clinical aspects of
my study.
I extend my sincere thanks to Miss. Dona Maria, for her patience and input in
statistical analysis.
I wish to thank my spouse Dr. Habie Thomas, for being my pillar of strength and
source of constant motivation and my family, friends and colleagues for their
relentless love, care, help and guidance.

LIST OF ABBREVIATIONS USED
AAP American Academy Of Paediatrics
ADCC Antibody Mediated Cell Dependent Cytotoxicity
AHG Anti Human Globulin
CAT Column Agglutination
CNS Central Nervous System
CH
Constant Heavy chain
CL
Constant Light chain
CLIA
Chemiluminescence Immuno Assay
CMV
Cytomegalo Virus
COHb Carboxy haemoglobin
DAT Direct Antiglobulin Test
DTT
Dithiothreitol
Fab
Fragment, antigen binding
Fc
Fragment, crystallisable
FC
Flow Cytometry
GCT
Gel Centrifugation Test
Hb Haemoglobin
HDN Haemolytic Disease of the Fetus and Newborn
HDFN Haemolytic Disease of the Fetus and Newborn
IgA Immunoglobulin A

IgD Immunoglobulin D
IgE
Immunoglobulin E
IgG Immunoglobulin G
IVIG
Intravenously administered Immunoglobulin
LISS
Low Ionic Strength Saline
LSCS
Lower Segment Caesarian Section
MMA
Monocyte monolayer assay
MTP
Medical Termination of Pregnancy
NICU
Neonatal Intensive Care Unit
NND
Neonatal death
NVD
Normal Vaginal Delivery
PBS
Phosphate buffered saline
RBC
Red Blood Cell
RhD
Rhesus D
RIA
Radio Immuno Assay
TcB
Transcutaneous bilirubinometry
TSB
Total Serum Bilirubin
VH
Variable Heavy chain
VL
Variable Light chain

TABLE OF CONTENTS
INTRODUCTION ................................................................................... 1
AIMS AND OBJECTIVES ........................................................................ 2
MATERIALS AND METHODS ............................................................... 42
DISCUSSION ....................................................................................... 82
CONCLUSIONS ................................................................................... 94
LIMITATIONS ..................................................................................... 96
REFERENCES ...................................................................................... 97
ANNEXURES ..................................................................................... 106

INTRODUCTION

1
INTRODUCTION
ABO Hemolytic disease of the newborn(ABO HDN) is an immune reaction that
occurs most commonly in newborns of A, B or AB blood group born to mothers of O
blood group(1). Following the introduction of Rh immunoprophylaxis, the prevalence
of Rh haemolytic disease has come down drastically and now ABO-HDN is emerging
as the most common cause of HDN in the developed countries (2).
ABO HDN occurs due to transplacental transfer of maternal anti-A and anti-B IgG
antibodies leading to immune haemolysis of fetal erythrocytes. IgG has 4 subtypes –
IgG1, IgG2, IgG3 and IgG4, of which IgG1 and IgG3 are effectively transported
across placenta via an Fc receptor (3).
There is very limited literature on the prevalence and factors that impact on ABO-
HDN from India. Against the background of extremely variable health care facilities in
our country, we thought it is critical to study factors that may predict the severity of
ABO-HDN in mothers with O blood group. Early identification, diagnosis and
intervention can reduce morbidity and mortality due to ABO hemolytic disease of
newborn.

2
AIMS AND OBJECTIVES

3
AIMS
1) To study the prevalence of ABO incompatible pregnancies in O blood group mothers in a
tertiary health care centre in south India.
2) To correlate the maternal IgG1and IgG3 subclasses with occurrence of ABO HDN.
OBJECTIVES
1) To study the prevalence of ABO incompatible pregnancies in O blood group mothers in a
tertiary health care centre in south India.
2) To study the incidence of ABO-HDN.
3) To correlate the maternal IgG anti-A and anti-B titers with occurrence and severity of
ABO HDN.
4) To correlate the maternal IgG1and IgG3 subclasses with occurrence and severity of ABO
HDN.

4
REVIEW OF LITERATURE

5
REVIEW OF LITERATURE
1. History
2. Causes of hyperbilirubinemia in term newborns
3. Spectrum of hemolytic disease of newborn
4. ABO-Haemolytic Disease of Newborn
5. Epidemiology of ABO-HDN
6. Etiology and disease mechanism
7. Pathogenesis of ABO-HDN
8. Factors determining ABO-HDN
9. Grading the severity of ABO-HDN
10. Serological testing in ABO-HDN
11. Hematologic findings in ABO-HDN
12. Prediction of severity of AB0-HDN
13. Therapeutic measures in ABO-HDN
14. Recent advances
15. Conclusion
6
HAEMOLYTIC DISEASE OF NEWBORN
Hemolytic disease of the newborn (HDN) is an immune reaction characterized by the
shortened lifespan of fetal red cells due to transplacental transfer of specific maternal
antibodies that are directed against the paternally derived antigens that are present in
the fetal RBCs. The severe cases manifests as ascites, hydrops, heart failure and even
death in the fetus. The less severe cases present postnatally as neonatal anemia,
hyperbilirubinemia and suppression of erythropoiesis(1,2). The antibodies are
produced in the mother following the previous pregnancy or prior transfusions(3).
ABO hemolytic disease of the newborn (ABO-HDN) more commonly occurs in a
newborn with blood group A, B or AB who are born to O blood group mothers(4).
This is because; the antibodies to A and B formed in individuals with O blood group
are of IgG type while that found in the serum of individuals of blood group A and B is
of IgM type. IgG antibodies cross the placenta effectively.
Following the introduction of anti-D prophylaxis, the incidence of Rh-HDN has
drastically reduced and ABO incompatibility has now emerged as the major cause of
hemolytic disease of the newborn. It is now the largest cause of HDN in the developed
countries. Transfusion services have an imperative role in the timely detection and
providing transfusion support to such cases (5).

7
I.HISTORY:
Hemolytic disease of fetus and newborn as an important cause of fetal loss and death
of newborn was first described by a French midwife named Louis Bourgeois who
worked at the royal court of King Henry IV and Queen Marie de Medicis in 1906. She
noted that while assisting in the delivery of twins, one baby was swollen and died soon
after birth while the other baby developed jaundice and died several days later(5).
The term “erythroblastosis foetalis” was coined by Diamond et al and was identified as
a syndrome in 1932 which encompasses congenital anemia, severe neonatal jaundice
and hydrops foetalis. The pathogenesis of the disease was attributed to a defect in the
erythron (4).
The immunological nature of HDN was described in 1938 by Ruth Darrow and was
proposed that fetal hemoglobin plays a crucial role in the pathogenesis of hemolytic
disease by inducing a maternal antibody response after crossing the placenta. The
Rhesus blood group was discovered by Landsteiner and Wiener in 1940 (6) and
subsequently the Rh(D) antigen was discovered in 1941 by Levine el(7). The RhD
antigen was identified in the D negative mothers following the transplacental transfer
of foetal D positive RBCs. The final clinical event was found to be caused due to the
transfer of maternal anti-D immunoglobulin IgG across the placenta(8). The
contributions of all these scientists have been the stepping stones that have led to our
current knowledge of HDN.
8
II. CAUSES OF HYPERBILIRUBINEMIA IN TERM NEWBORNS:
The common risk factors involved in neonatal hyperbilirubinemia are fetal-maternal
blood group incompatibility, delayed breastfeeding, ethnicity, birth trauma,
prematurity and neonatal infections(9–11).
Neonatal hyperbilirubinemia is classified based on the etiology as follows(12):
1. Increased bilirubin load
A. Hemolytic causes:
Rh incompatibility
ABO and other minor antigen incompatibility
RBC membrane defects
B. Non-hemolytic causes:
Extra vascular sources - Cephalhaematoma, CNS hemorrhage
Delayed cord clamping, twin to twin transfusion
2. Decreased conjugation of bilirubin
Physiologic jaundice
Breast milk jaundice
Crigler Najjar syndrome
Gilbert syndrome
3. Impaired excretion of bilirubin
Biliary obstruction
Dubin Johnson syndrome
Rotor syndrome

9
III. SPECTRUM OF HEMOLYTIC DISEASE OF NEWBORN:
At present, more than fifty different red cell antibodies have been identified which can
lead to hemolytic disease(13). Anti-D is associated with greatest severity of hemolytic
disease. The other frequent alloantibodies are Rh antigens (anti-c, anti-C, anti-e, and
anti-E), Kell antigens, Duffy antigens, Kidd and MNS antigens.
Among the non D (Rh) antibodies, anti-E and anti-c are the most commonly involved
in the pathogenesis of the hemolytic disease(14,15). Absorption of antibodies by fetal
antigen in placenta (17) and lack of the corresponding antigens on fetal red cells (16)
lead to failure of a few antibodies of other blood group systems to cause hemolytic
disease.
Table 1: Alloantibodies reported to cause HDN (1):
Within the Rh system Anti-D, -c, -C – Cw, -Cx, -e, -E, - Ew, -c,
Ce, -Rh32, -Goa ,-Bea, -Evans, -L, W
Outside the Rh system Anti-K, -k, -Ku -Kp8 ,-Kpb ,-Js8, -Jsb, -
Fy8, -Fy3, -Jk8, -Jkb, -M,-N, -S, -s ,-U, -
Vw, -Far, -Mv ,- Mit, -Mta, -M,u r, –Hil, -
Hut, -
Antibodies to high-incidence antigens Anti -At8 ,-J ra, -Lan, -Ge
Antibodies to low incidence antigens - Anti-Bi, -By, -Fr8, -Good, -Rd, -Re8, Zd

10
Rh-HDFN:
Rh alloimmunization leading to HDFN occurs when an Rh- negative mother carries an
Rh- positive fetus(16). Most of the time, the first pregnancy is the sensitizing event,
which goes uneventful and hemolytic disease occurs in subsequent pregnancies.
Following sensitization, re-exposure to the antigen leads to an anamnestic response
increasing the maternal anti-D titers(17). The initial anti-D formed at time of
sensitization is IgM type. In subsequent pregnancies, IgG anti-D is formed which can
be transported across the placenta leading to destruction of fetal RBCs.
As per the studies, Rh hemolytic disease does not occur in primies, but there is
literature to support that it can occur rarely in 1% of first pregnancy(18). Rh
Hemolytic disease is very common in developing countries including which can be
attributed to improper antenatal care and failure to administer Rh IG(19).
Factors influencing Rh (D) HDFN include:(20)
A. Size of feto-maternal hemorrhage: Only a small amount of fetal red cells cross the
placenta into the maternal circulation during the third trimester which is insufficient to
stimulate antibody production in the mother. Transplacental hemorrhage occurs during
delivery which leads to the transfer of fetal red cells into the maternal circulation
leading to sensitization. After the first delivery, mothers form antibodies up to 6
months after delivery. The fetal red cells cross the placenta as early as 24 th week of
gestation in the second pregnancy with Rh (D) positive fetus which further increases
the sensitization and antibody titers leading to HDFN.
11
B. Parity: Parity has been found to correlate significantly with alloimmunization and
risk of HDFN especially associated with second and third pregnancy.
C. Effect of ABO incompatibility between mother and fetus: ABO incompatibility has
been shown to provide some protection from Rh HDFN. It is suggested that an
existing ABO incompatibility between mother and fetus may destroy the Rh (D)
positive fetal red cells as soon as they enter the maternal circulation before they can
initiate any sensitization in mother.
D. Medical termination of pregnancy/abortion: Abortion or any interventional
procedure during pregnancy can also be the sensitizing event leading to
alloimmunization in women.
In cases of ABO incompatible pregnancies, there is reduced risk of sensitization to Rh-
D antigen. This can be attributed to the rapid destruction of fetal cells by anti-A and
anti-B antibodies.
IV. ABO HAEMOLYTIC DISEASE
ABO hemolytic disease is usually considered as a mild form of the disease, with only
less than 1% of affected infants requiring exchange transfusion. It is defined as a
newborn with positive DAT and/ or laboratory evidence of hemolysis of blood group
A, B or AB who are born to O blood group mothers without Rhesus factor
compatibility(21) .
The severe manifestations of ABO HDN are very rare and disease manifests as the
onset of hyperbilirubinemia within 12-48 hours of birth.

12
IV.A. Factors affecting incidence and severity:
Following are the four stages involved in the pathogenesis of hemolytic disease;
1) Alloimmunization of the mother
2) Transplacental transfer of antibodies to the fetus
3) Destruction of the sensitized red cells
4) Secondary clinical manifestations (22)
There are several factors that affect the severity of the disease major ones including the
quantity of maternal antibody(anti-A/ anti-B) that crosses the placenta, antigenic
strength on RBCs of infants, subclasses of immunoglobulins, inhibitory effect of fetal
secretions, absorption capacity of fetal tissues, liver maturity and efficiency of
phagocytosis(23).
ABO HDN usually occurs in A,B or AB blood group infants who are born to mothers
of O group as ABO antibodies occur as high-titer IgG antibodies in individuals with O
blood group than in those with group A or B. The incidence and severity of the disease
is unrelated to the history of prior transfusions or pregnancies in the mother.
Therefore, ABO HDN can occur in the first as well as consequent pregnancies.

13
Table 2: Comparison of ABO v/s Rh HDN (3):
Characteristic feature ABO Rh
First pregnancy
Yes
Rare
IgG antibody Present Present
Severity
DCT
Bilirubin at birth
Mild
Weakly positive/ negative
Normal range
Severe
Strongly positive
Elevated
Anemia at birth No Yes
Phototherapy Yes Yes
Exchange transfusion Rare Sometimes
Intrauterine transfusion None Sometimes
Spherocytosis
Prevention
Yes
Not available
Rare
Rh immunoglobulin
V. EPIDEMIOLOGY:
About 95% cases of the hemolytic disease were caused in the past by maternal
antibodies directed against Rh antigen D. The incidence of hemolytic disease due to
anti D has tremendously decreased since 1968 after the introduction of Rh D
14
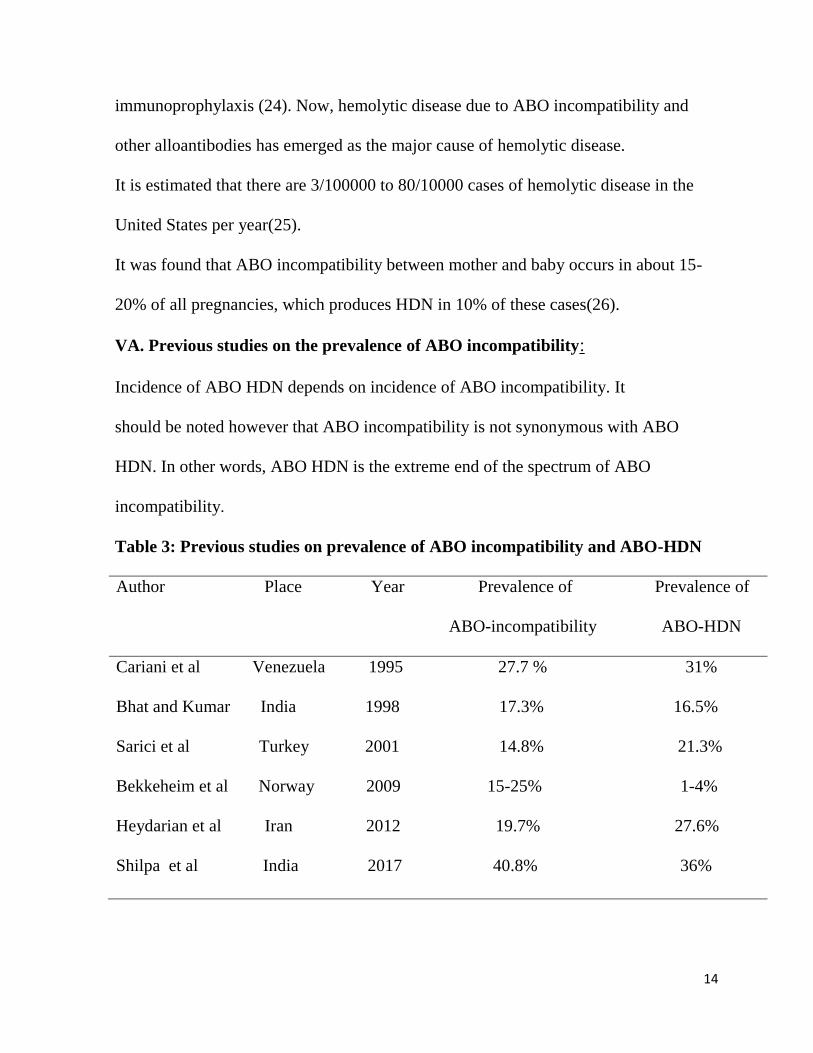
immunoprophylaxis (24). Now, hemolytic disease due to ABO incompatibility and
other alloantibodies has emerged as the major cause of hemolytic disease.
It is estimated that there are 3/100000 to 80/10000 cases of hemolytic disease in the
United States per year(25).
It was found that ABO incompatibility between mother and baby occurs in about 15-
20% of all pregnancies, which produces HDN in 10% of these cases(26).
VA. Previous studies on the prevalence of ABO incompatibility:
Incidence of ABO HDN depends on incidence of ABO incompatibility. It
should be noted however that ABO incompatibility is not synonymous with ABO
HDN. In other words, ABO HDN is the extreme end of the spectrum of ABO
incompatibility.
Table 3: Previous studies on prevalence of ABO incompatibility and ABO-HDN
Author Place Year Prevalence of Prevalence of
ABO-incompatibility ABO-HDN
Cariani et al Venezuela 1995 27.7 % 31%
Bhat and Kumar India 1998 17.3% 16.5%
Sarici et al Turkey 2001 14.8% 21.3%
Bekkeheim et al Norway 2009 15-25% 1-4%
Heydarian et al Iran 2012 19.7% 27.6%
Shilpa et al India 2017 40.8% 36%

15
The low rate of clinically significant severe hemolytic disease due to ABO
incompatibility is due to the following reasons:
1. ABO antigens are expressed by variety of fetal tissue, thereby reducing the
chances of anti-A/B binding to fetal red cells.
2. A and B antigens are not well developed and expressed in the fetal RBCs.
The lower expression of ABH antigens on the fetal RBCs is due to high sialylation,
low 1, 2 a fucosylation, and its unbranched lactosaminyl backbone. This minimizes the
level of feto-maternal incompatibilities following the transplacental transfer of
antibodies(27).
Hemolytic disease due to ABO antibodies can occur in the first pregnancy and can
recur in about 87% cases as maternal ABO antibodies are present without previous
sensitization(25).
3. There is a weaker binding affinity for alloantibodies reacting with A and B
antigens than those reacting with protein antigens.
V B. Racial factors and prevalence of ABO HDN:
There were several studies in the past on race as a vital risk factor in the occurrence of
ABO HDN.
ABO HDN is usually seen in group O mothers with group B infants (African ancestry)
or group A infants (European ancestry)(28). It was proved that as compared to
Caucasians, Asians and black tend to have a higher prevalence of DAT positive ABO
HDN(23).

16
As per studies, ABO incompatibility occurs in one out of every five pregnancies in
Caucasians(29). ABO HDN occurs at a higher rate in blacks as compared to
Caucasians, which is attributed to the higher prevalence of immune anti-A and anti-B
antibody titers in the black population (30).
Neonates with A blood group especially A1 group have a more severe disease as
compared to neonates with B or A2 blood group.
V C. Familial incidence:
An affected infant with severe hemolytic disease is often followed by similar severe
disease in the family; while in families with mild ABO hemolytic disease; affected
infant may be followed by an unaffected infant.
VI . ETIOLOGY AND DISEASE MECHANISM
Hemolytic disease is caused by the destruction of fetal RBCs by maternal allo
antibodies. Transfer of antibodies from mother to fetus takes place only via placenta in
human beings. It is an active process and takes place only in one direction, i.e. from
mother to fetus.
Only small amounts of IgG are transferred in the first 12 weeks of gestation. The mean
IgG concentration is around 1.8 g/dl in 24th week of pregnancy and the concentration
thereafter rises exponentially until term. At term, the IgG level of the fetus is higher
than that of the mother, around 15.12 g/dl in infants and 12.60 g/dl in mothers.
Antibody transfer becomes more significant with the increase in gestational age
leading to more positive DAT and greater incidence of neonatal
hyperbilirubinemia(32). Only immunoglobulin G antibodies are actively transported
17
across the placenta by Fc receptor (FcRn) while IgA and IgM are not. The rate of
transfer is relatively slow at term.
Transfer of IgG antibodies is a physiologic event and is mediated by FcRn which is
similar to class I MHC molecule(1). It is beneficial because it provides passive
immunity to the newborn in the first few months of life as they are targeted against
bacterial, fungal and viral antigens. However, in hemolytic disease, maternal
antibodies are directed against fetal RBC antigens that were inherited from father.
Transport of IgG (IgG1 and IgG3 which causes more effective hemolysis) by the Fc
receptor starts in the second trimester of gestation and continues till the birth of the
baby(32, 36).
FcRn:
The structure of the Fc receptor varies from other receptors. FcRn belongs to MHC
class I protein family and dimerises with beta 2 microglobulin for its function. It is
found in monocytes, dendritic cells and macrophages in humans. The C γ2 and C γ 3
domains of IgG bind with α 2 and β 2 microglobulin domains of FcRn. Following are
the functions of FcRn:
1) Transfer of IgG from mother to fetus thereby providing passive immunity
2) Protection of IgG from normal catabolism.
IgG is transported in vesicles by FcRn which prevents lysosomal degradation. Due to
the above reasons, half-life of IgG is longer than other immunoglobulin classes (22-23
days) in humans(1).

18
VII. PATHOGENESIS OF ABO HDN
VII A. Hemolysis and anemia:
The maternal IgG attaches to fetal red blood cells. The antibody coated red cells are
cleared by the macrophages of the fetal spleen. The antibody titers, specificity as well
as the number of antigenic sites on fetal RBCs determine the rate of destruction of the
fetal RBCs which in turn leads to anemia. Anemia accelerates the RBC production by
the fetal marrow and immature RBCs called erythroblasts are released into the fetal
circulation. This finding is termed as “erythroblastosis foetalis.”
Extramedullary haematopoeisis occurs when the bone marrow fails to keep up the
production of RBCs as compared to the rate of destruction. This leads to enlargement
of the liver and spleen resulting in portal hypertension and hepatocellular damage.
Decreased production of plasma proteins by liver along with severe anemia leads to a
condition termed as hydrops foetalis (24). Hydrops foetalis is characterized by
widespread effusion, high output cardiac failure and death(10).
RBC destruction continues as long as maternal antibodies persist in the fetal
circulation with the rate decreasing after birth as no longer maternal antibodies can
enter the fetal circulation. Antibody binding and hemolysis continue for several weeks
to days after delivery because IgG has a half-life of 25 days and is distributed both in
extra vascular and intravascular compartments.
VII B. Bilirubin:
Hemoglobin which is released following the destruction of RBCs is metabolized into
indirect bilirubin. Indirect bilirubin is conjugated into direct bilirubin in the maternal

19
liver which is then excreted by the mother. In cases of moderate to severe hemolysis,
indirect bilirubin more than 18-20 mg/dl cause kernicterus and permanent damage to
the fetal brain (24).
ABO hemolytic disease leads to early onset of hyperbilirubinemia and may present
with a rapid increase in serum bilirubin values(33).
.VII C. IgG subclasses and allotypes:
There are five classes of immunoglobulins in human beings: IgM, IgD, IgG, IgA and
IgE of which IgG is the most abundant protein (10-20%) plasma. IgG is further sub-
classified in the order of decreasing abundance as IgG1,IgG2,IgG3 and IgG4(33).
Each subclass has a unique property in regards to binding of antigen, activation of
complement, half-life, transplacental transport and immune complex formation(34).
The concentration of IgG subclasses vary depending on the fetal age and are
transported actively across the placenta. IgG1 rises earlier than IgG3 in the gestational
period. There is an acceleration of ratios of IgG1, IgG3 and IgG4 in the third
trimester(35). As per the study conducted by Morell et al in 1971 and Schur eta l in
1973(33,36), there is a relative deficiency of IgG2 in cord serum. This is because Fc
γreceptor in the syncytiotrophoblast cells in the placental tissue binds with IgG1 with a
higher affinity than IgG2(1). IgG4 cannot activate the classic pathway of complement
system and therefore cannot destroy the RBCs.(37)
IgG subclass typing can be done by various methods like Flow Cytometry, ELISA test
or gel test.

20
Table 4: Properties of human IgG subclasses:(38)
Properties IgG1 IgG2 IgG3 IgG4
Abundance (% of total IgG) 70 20 6 4
Half-life in serum (days) 23 23 7 23
Placental passage +++ + +++ +++
Complement fixation + + +++ -
Binding to Fc receptor +++ + ++ -
VII D. Structure of immunoglobulin:
Antibodies are immunoglobulins which belong to the family of proteins and they
combine with antigens and mediate biological effects. The immunoglobulin molecules
are made up of four polypeptide chains - two heavy chains of molecular weight of
50,000-75,000 Daltons and two light chains of molecular weight 22,500 Daltons which
are interconnected by covalent and non-covalent bonds. The covalent bonds are mainly
found in the hinge region. There are five different classes of Ig: IgG, IgM, IgA, IgD
and IgE due to five types of heavy chains termed as γ, α, μ, δ and ε. The light chains
are the same in the five types of Ig, either κ or λ type. It is the heavy chain that varies
for each type. Immunoglobulin has an amino (-NH2) and a carboxyl (-COOH) end.
On treatment with papain enzyme, an immunoglobulin is divided to form one
crystalline Fc fragment and two antigen binding Fab segments. Fc region extends from

21
carboxyl-terminal to the hinge region and is primarily responsible for monocyte
binding and complement fixation, and in IgG subtype, it is the Fc fragment that crosses
the placenta leading to the pathophysiology of hemolytic disease. The Fab fragment
extends from the amino- terminal to the hinge region of the molecule.
The domains of an immunoglobulin molecule are made up of regions of both heavy
and light chains folded into globular structure or loops, and these are made up of
approximately 110-120 amino acids. The domains consist of a variable (V) and
constant (C) regions made up of heavy and light chains. The number of domains
depends upon the immunoglobulin isotype and IgG molecules have three constant
heavy chain regions (CH1, CH2 and CH3). The hinge region of the immunoglobulin
structure exists between CH1 and CH2 domains of the heavy chain. Minor differences
in these hinge regions are used to categorize the four subclasses of IgG.
In IgG molecule, there is a specific constant heavy chain region which allows the
attachment of Fc receptors of monocytes and macrophages. IgG molecules occur as
monomers, IgM as pentamers and IgA as monomers or dimers. IgG is the most
common Ig in plasma with a concentration of 12g/dl.
IgG molecules can be subdivided on the basis of minor differences in the hinge region
of the IgG structure that can be separated by electrophoresis as four subclasses
(IgG1,IgG2,IgG3 and IgG4) in the order of decreasing abundance as follows:
IgG1,6.63; IgG2,3.22; IgG3, 0.58 and IgG4, 0.46(1).
The structures of the four immunoglobulin subclasses are very similar to each other
with over 90% homology in their amino acid sequence and the difference between

22
them affects their ability to bind to receptors and accessory molecules which in turn
affect their function. Most of the variations are found in the hinge region and N-
terminal CH2 domain with few differences in other domains(34).
The number of inter H chain disulfide bonds vary in different subclasses with IgG3
having a much longer hinge region compared to other subclasses.
The IgG immunoglobulin contains four polypeptide chains which are further
composed of two 50kDa heavy chains that are identical to each other and two 25 kDa
light chains.
The light chain consists of kappa and lambda chains which are linked together by
disulfide bonds. The heavy chain comprises of three constant domains (CH1, CH2 and
CH3) and N terminal variable domain (VH). A hinge region is present between CH1
and CH2. The light chain comprises a constant domain (CL) and an N terminal
variable domain (VL). The effector functions of the antibodies are largely due to the
residues in the CH2 domain of Fc part proximal to the hinge region due to the
overlapping in the binding site for C1q complement and IgG-Fc receptor on the
effector cells.

23
Figure 1: Crystal structure of IgG1 molecule viewed from two different
angles
VII E. Structural variation in the hinge region:
The Fab arms and Fc parts are linked together by the hinge region. The hinge exon of
IgG1 encompasses 15 amino acids, IgG2 has 12 amino acids and IgG4 has 14 amino
acids. IgG2 has the shortest hinge of all the IgG subclasses and are rigid and stabilized
by extra interheavy chain disulfide bonds. IgG3 has a much longer hinge region than
all other subtypes containing 62 amino acids. The long hinge region of IgG3 is due to
the duplication of the hinge exon which is encoded by one exon each in IgG1, IgG2
and IgG4 and up to 4 exons in IgG3. The elongated hinge attributes to the high
molecular weight of IgG3. The orientation and movement of the Fab arms and Fc tail
of the IgG antibody is influenced by the difference in the hinge flexibility.
The Fab arms shield the binding site of C1qand/or FcγR which in turn affects the
binding sites of IgG(34). The flexibility of IgG subclasses is in the order:

24
lgG3>lgG1>lgG4>lgG2 which in turn affects their binding to Fc γr and C1q and
antigen binding capacity and immune complex formation(38).
Interchain disulfide bonds:
The IgG subclasses differ from each other with regard to the number of inter heavy
chain disulfide bonds in the hinge region. IgG2 and IgG4 are found as several isomers
due to variations in the interconnections of hinge disulfide bonds.
Hinge isomers in IgG2 and IgG4:
Structural hinge isomers are which are commonly found in IgG2 antibodies with κ
light chains than λ chains. These isomers are formed due to alternative disulfide bond
formation between cysteine in the heavy chain hinge region and those involved in the
formation of disulfide bonds between the heavy and light chains. Two forms of
isomers are described – Classical A form, the most common form, characterized by
four disulfide bridges between the two IgG2 heavy chains and the less common B
form in which disulfide bond is formed between one hinge cysteine and light chain.
The FcRn binding site is common for all the isoforms.
IgG4 Fab arm exchange:
The random combining of half molecules of IgG4 with other half molecules of IgG4 in
vivo, leads to the formation of monovalent bispecific antibodies which prevents
effective cross-linking of the target antigen. In addition to this, non specific
multivalent target binding results in low avidity. IgG4 has low affinity to activate
FcγR and retains high affinity to inhibit FcγIIb.
Allotypes:

25
Allotypes are discovered by serology and are defined as polymorphic immunoglobulin
epitopes that vary between individuals and ethnic groups.
G1m (z, a), G1m (f, a) and G1m (f) are the most common allelic forms of IgG1 of
which G1m (f) is found in Caucasians and G1m (f, a) allele is common in Orientals.
There are no serologically important allotypes for IgG4.
The overall ratio of κ to λ in human IgG is2:1, but the ratio is 1:1 and 8:1 for
individual IgG2 and IgG4 subclasses respectively. The disulfide bonds linking the
heavy chains also act as factors for structural variation among the different subclasses.
While IgG1 and IgG4 have two bonds each, IgG2 and IgG3 have four and five bonds
respectively. The disulfide bonds lend flexibility to the hinge regions of the subclasses
of IgG molecule and the distance the Fab fragment can cover determines the antigen it
can accommodate(39).
Each of the subclass exhibits different properties including placental transfer and
complement fixation. While IgG1 and IgG3 bind to complement C1q molecule more
strongly than IgG2. IgG4 doesn’t bind at all and cannot activate the complement
cascade(1).
Fc region of antibodies is recognized by several membrane-bound receptors. The
lower hinge region of IgG is recognized by FcRI, FcRII and FcRIII. Monomeric IgG1
and IgG3 bind to FcRI, polymeric IgG1 and IgG3 bind to FcRII and FcRIII also. There
are three different types of FcRII- FcRIIa, FcRIIb and FcRIIc. FcRIIa is of two types,
one which binds weakly to IgG2 and other which binds strongly. IgG4 binds to both
forms of FcRIIa
26
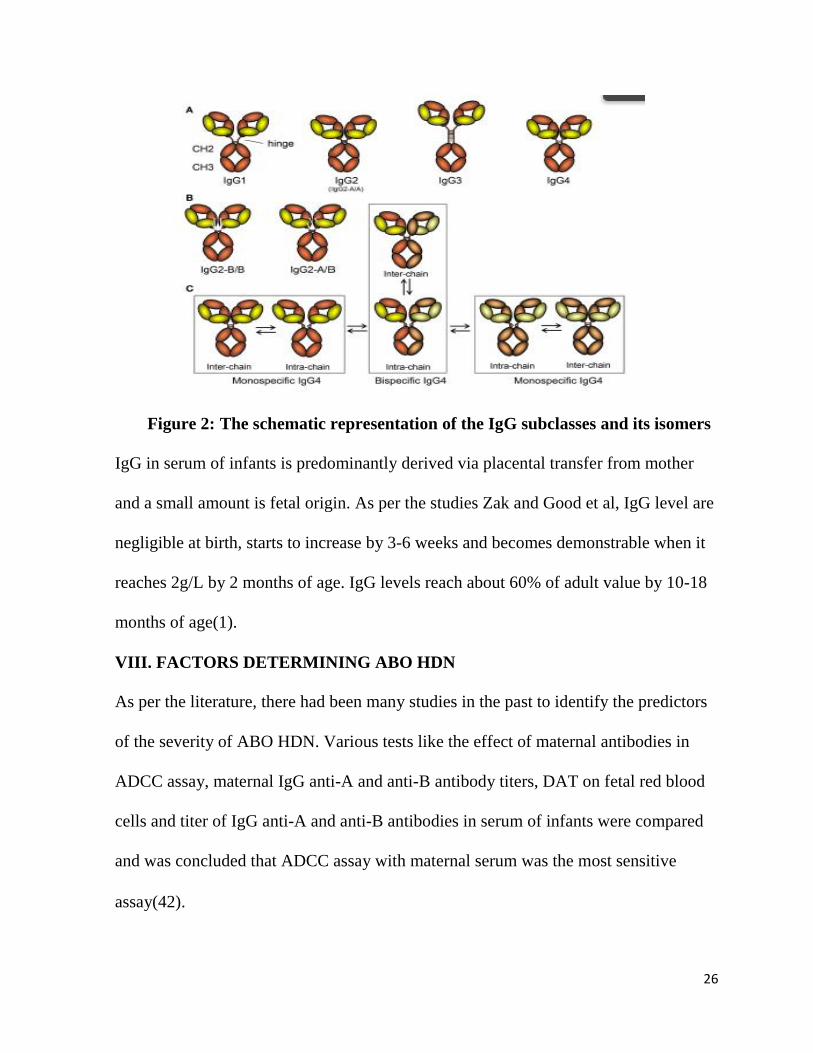
Figure 2: The schematic representation of the IgG subclasses and its isomers
IgG in serum of infants is predominantly derived via placental transfer from mother
and a small amount is fetal origin. As per the studies Zak and Good et al, IgG level are
negligible at birth, starts to increase by 3-6 weeks and becomes demonstrable when it
reaches 2g/L by 2 months of age. IgG levels reach about 60% of adult value by 10-18
months of age(1).
VIII. FACTORS DETERMINING ABO HDN
As per the literature, there had been many studies in the past to identify the predictors
of the severity of ABO HDN. Various tests like the effect of maternal antibodies in
ADCC assay, maternal IgG anti-A and anti-B antibody titers, DAT on fetal red blood
cells and titer of IgG anti-A and anti-B antibodies in serum of infants were compared
and was concluded that ADCC assay with maternal serum was the most sensitive
assay(42).

27
VIII A. The role of IgG subclasses in ABO HDN:
The role of anti-Rh (D) IgG subclasses on the severity of hemolytic disease was
studied in the past and was proved that IgG subclasses have a significant correlation
with hemolytic disease, of which IgG1 or the combination of IgG1and IgG3 was
significantly associated with the severity of the hemolytic disease. The onset of
hydrops was earliest with a combination of IgG1+IgG3 than with IgG1 alone(43–45).
But there is very limited literature on the correlation of IgG subclasses and ABO
hemolytic disease. As per the study conducted in 2011, by Yi-qiang et al in China, it
was concluded that IgG1 and IgG3 titer levels, especially that of IgG1, had a
significant correlation with ABO hemolytic disease(46). This was contradicting the
findings of the study by Kaplan et al in 2009 in umbilical cord blood samples, that IgG
subclass 1, was not predictive of ABO HDN(47).
VIII B. The role of maternal titers in predicting ABO HDN:
In addition to blood grouping and direct antiglobulin testing, maternal anti-A/-B titers
contribute to the prediction of risk of severe hyperbilirubinemia in neonates. They can
be used as a guide in the management of maternal-fetal ABO incompatibility(1).
Owa J A et al, in their study conducted on 50 mothers with O blood group, suggested
treatment and exchange transfusion is indicated when the maternal anti-A and anti-B
titer was 1:64 and more(48). As per the study conducted by Yi-qiang et al in China, it
was suggested that neonates with maternal IgG titers more than 64 were prone to
develop ABO-HDN(46). As per some other studies, 1:512 was the cut off for initiation
of phototherapy, immunoglobulin treatment and exchange transfusion(49–51). A

28
study by Kadri et al, with the titer > 256, the risk of neonatal jaundice becomes 18
times higher than those with low antibody titers <256(52).On the other hand, a few
trials proved that there was no association between maternal anti-A and anti-B titers
with ABO-HDN(29).
Therefore, the role of maternal anti-A and anti-B titers and IgG subclasses on
predicting the risk of ABO-HDN remains controversial.
VIII C. OA and OB incompatibility:
In the western population, hemolysis due to anti-A is more common than anti-B(49).
As per a few studies, ABO incompatibility due to anti-B is more severe(53). and there
are reported cases of hydrops foetalis due to the same(54).
As per a few reports, there is an increase in trend of exchange transfusion in first 24
hours of life in cases of O-B incompatibility as compared to O- A incompatibility(55–
57) while a few studies established that there is no relationship between the clinical
course and infant’s blood group(58). As per the study by Bekkeheim et al and a few
others, there is a considerably increased rate of invasive treatments in O-B infants than
O-A(50). As per the studies by Sisson and Kaplan, there is no significant difference in
response to therapy in O-B neonates compared to O-A(59).
As per the studies, OA and OB incompatibility between mother and fetus renders 90%
and 50% protection respectively to immunization to D antigen. The theory proposed
behind this is the protective ability of anti-A and anti-B to destroy fetal RBCs in the
maternal circulation.(22)

29
IX. GRADING THE SEVERITY OF ABO-HDN:
ABO-HDN is usually considered as a sub clinical condition and less severe than Rh-HDN.
Nonetheless, there are reported cases from the Indian subcontinent on unusually severe cases
of ABO-HDN necessitating multiple exchange transfusions(60,61).
It is described in literature that the severity of HDN is determined by the severity of
haemolysis. Mild haemolytic disease of newborn presents as mild jaundice and can be
managed with phototherapy alone and severe HDN causes kernicterus and brain damage.
Following are the different guidelines used worldwide available till date to classify HDN.
The major grading system used to grade the disease severity in HDN was put forward by
Walker in 1971(62):
1. Mild HDN : DAT positive cases requiring no transfusion
2. Moderate HDN: DAT positive cases with cord blood Hb >11 g/dL and requiring
transfusion
3. Severe HDN: DAT-positive cases with cord blood Hb <11 g/dL and requiring
transfusion;
4. Very severe HDN: DAT-positive cases with cord blood Hb <7.5 g/dL, or hydropic.
Another grading system proposed by Andrew et al is as follows(63):
1. Mild - Grade 0; Hb > 12.5 g/dL, no transfusions
2. Moderate - Grade 1: Hb > 12.5 g/dL + top-up or exchange transfusion

30
3. Severe- Grade 2: Hb < 12.5 g/dL + exchange transfusion
4. Very Severe- Grade 3: intrauterine transfusions and/or Hb < 10.0 g/dL ± exchange
transfusions or foetal death.
Choudhuri et al has proposed the following way of classifying Rh-HDN(45):
1. Mild: Positive DAT alongside some evidence of haemolysis but requiring no
intervention.
2. Moderate: Cases with evidence of haemolysis and intervention was limited to
phototherapy
3. Severe: When the baby was hydropic or intrauterine/ exchange or top up transfusion
was required.
In spite of a few grading systems offered, there is no consensus on grading of HDN. In our
study, a combination of DAT positivity, hyperbilirubinemia, anemia and intervention required
defined the HDN secondary to ABO incompatibility and also in grading its severity.
X. SEROLOGICAL TESTING IN NEWBORN:
Investigation of a newborn suspected of ABO HDN broadly includes the following:
1. ABO grouping
2. Rh typing
3. DAT
4. Hemoglobin estimation
5. Serum bilirubin

31
6. Hematological parameters
CO-oximeters can be used to measure COHb which can confirm hemolysis in infants
with ABO incompatibility(64).
X A. Direct Antiglobulin Testing:
DAT is an important screening tool for ABO hemolytic disease. It can detect
immunoglobulin or complement bound to the RBCs using anti-human reagents.
There are different platforms for performing DAT like tube method, micro column or
gel method and solid phase. The gel and solid phase are automated methods with
greater sensitivity than conventional tube testing(65).
A positive DAT indicates that there is a sensitization of fetal red cells. DAT can be
negative in ABO hemolytic disease. This is because A and B antigenic sites are
weak(66) and there is very little anti-A or anti-B antibody in the newborn RBC
membrane, as a result of which cord blood DAT can be weakly positive or often
reported as negative unless a sensitive platform like gel test is used(67). A positive
DAT indicated that at least 150 molecules of the maternal antibody are adsorbed into
the fetal red cell(68). Using more sensitive platforms like autoanalyzer with low ionic
strength solution with enhancer, anti-A and anti-B can be demonstrated in all ABO
incompatible cases.
As compared to Rh hemolytic disease, DAT tends to be weakly positive or negative in
ABO incompatibility.

32
The infant’s red cells do not react with anti-C3d owing to low levels of complement in
the serum of newborns and weak expression A and B antigens on the fetal red cell
surface.
X B. Elution of antibody from infant’s red cells:
In the newborn with positive DAT and clinical features of HDN, red cell eluate
confirms the antibody specificity and the diagnosis of HDN can be confirmed by the
presence of the corresponding antigen on the red cells(19). Eluates from infant’s red
cells give stronger IAT even in cases of weak positive or negative DAT due to a
considerable increase in antibody concentration through elution procedure.
X C. Spontaneous agglutination of red cells:
Red cells taken from ABO incompatible infants tend to clump more spontaneously;
also washed red cells from ABO incompatible infants tend to sediment more rapidly in
PVP when compared to similarly treated red cells which prove that there is some
alteration in charges on those red cells.
X D. Secretor status of infant:
It is proved that there is no role of secretor status in protecting against ABO hemolytic
disease(1).
XI. HAEMATOLOGICAL FINDINGS:
There is no single diagnostic test for ABO-HDN.

33
ABO-HDN is one among the causes to be investigated in a newborn infant developing
jaundice. As compared to the Rh hemolytic disease, immunological findings of ABO
HDN do not correlate well with the severity of the clinical manifestations.
Following are the diagnostic criteria:
a) Varying degrees of jaundice and anemia
b) Microspherocytosis
c) Polychromasia and reticulocytosis (> 4.6%)
d) Positive DAT(69)
Positive DAT with a family history of neonatal jaundice and high reticulocyte count
are considered as the strong predictors of hyperbilirubinemia in ABO
incompatibility(70).
Anemia is usually mild and rarely occurs in ABO incompatibility. In cases of the
severe hemolytic disease, the cord blood hemoglobin may be low but it is very rare to
have persistent anemia beyond two weeks as compared to Rh hemolytic disease. The
normal range of reticulin in term neonate is between 1.8-4.6% and reticulocytosis is to
compensate for the hemolysis.
Microspherocytes is one of the most common peripheral smear finding in ABO
incompatibility. It occurs due to the reduction in erythrocyte surface area due to
phagocytosis of the RBC membrane by macrophages(69). Similarly, red cells osmotic
fragility is mostly above the normal limits as compared to Rh hemolytic disease.

34
Neonates with blood group B tend to receive higher invasive treatment than those with
blood group A(53) and reports indicate that ABO-HDN due to anti-B is more severe
and there are reported cases of antenatal hydrops due to IgG anti-B(54).
In contrast to Rh HDN, there are no preventable measures for ABO-HDN. Hence
ABO incompatibility is the single most common cause of neonatal jaundice(58).
XII. PREDICTION OF SEVERITY OF HDN
The management of HDN relies on screening and detection of the antibody and
predicting its significance in the development of hemolytic disease. Several methods
are used for predicting the severity of hemolytic disease including serological,
quantitative and cellular assays.
XII A. Serological assay
Indirect Antiglobulin Test: Titration studies facilitate in detecting the critical titer
which plays a vital role in fetal monitoring(71). It is a semi-quantitative technique of
measuring an antibody in the serum employing a serial double dilution of the serum
against selected red cells. Titer is the reciprocal of the highest serum dilution at which
macroscopic agglutination occurs after the addition of antiglobulin reagent (68).
XII B. Quantitative assay: Enzyme Linked Immunosorbent Assay (73), Flow
cytometry and RIA (74)have been developed to accurately measure the level of red
cell binding IgG anti-D in maternal serum. Auto analyzers can process a large number
of samples with a greater reproducibility than manual antibody titration method by
IAT (75).
XII C. Cellular assay
35
K cell antibody-dependent cell-mediated cytotoxicity Assay: In addition to antibody
concentration, variations in functional and biological activities of antibodies in
different individuals help in predicting the severity of the hemolytic disease. Monocyte
mediated and K cell mediated assays are based on the differences in their interaction
with IgG sensitized red cells.
K cell mediated ADCC assay was the first cellular assay that was developed to predict
the severity of the hemolytic disease. As per the study conducted by Urbaniak et al,
this assay was able to predict the babies with mild HDN from moderate HDN(76)
while the study by Hadley et al failed to prove the correlation between KADCC and
the severity of HDN(77).
The monocyte-mediated ADCC assay: MADCC assay is a better predictor of disease
severity when compared with the Indirect Antiglobulin Test. It is similar to KADCC
except that peripheral blood mononuclear cells are used as effector cells(78).
Monocyte monolayer assay: MMA aims at microscopic evaluation of adherence and
phagocytosis of red cells by adherent monolayers of macrophages. It has been
ha proved to have a significant correlation with severity of HDN when compared with
manual titration(79).
Chemiluminescence test: CLIA has a better correlation with the fetal outcome when
compared to other auto analyzers. It is based on the principle of incubation of
monocytes and the sensitized red cells in the presence of luminol. Luminol helps in the
conversion of metabolic byproducts into light which is then measured by a
luminometer(63).

36
Cellular assays have a greater additive value when used in conjunction with serologic
and quantitative assays.
XIII. THERAPEUTIC MEASURES IN ABO-HDN:
The spectrum of hemolytic disease of the newborn has changed over time and was
almost synonymous with Rh-D allo-immunization around forty years back. In the past,
it led to overt hemolysis, marked hyperbilirubinemia and severe anemia in neonates
which led to their mortality and morbidity. Early diagnosis and adequate care are
necessary to prevent complications such as kernicterus. With the advancements in the
field of transfusion and neonatology services, the clinical burden of HDN has
drastically reduced over the years.
The spectrum of hemolytic disease also got altered following the introduction of new
treatment modalities like phototherapy, intravenous immunoglobulin and exchange
transfusion(80). The earliest and timely intervention helps to prevent bilirubin
encephalopathy and kernicterus with subsequent development of neurological sequelae
and death(81).
Guidelines for the management of neonatal hyperbilirubinemia in newborns > 35
weeks of gestation has been published by the American Academy Of Paediatrics
(AAP)(82) and also in guidelines of other counties like Canada, Israel, Norway, South
Africa, the Netherlands and the United Kingdom(83–88). In view of no similar
guidelines for the treatment of infants < 35 weeks of gestation, NICU s have
37
established their own criteria based on birth weight and gestational age for the use of
phototherapy and exchange transfusion(89).
XIII A. Phototherapy:
Phototherapy aims to convert unconjugated bilirubin into biliverdin. It can prevent the
need for exchange transfusion in cases of mild to moderate hemolysis(24). The gold
standard treatment for severe hyperbilirubinemia is Exchange transfusion(90).
As per the AAP guidelines, the four important risk factors for severe
hyperbilirubinemia are: blood group incompatibility with positive DAT, high-risk zone
TSB values predischarge, preterm babies and jaundice in the first 24 hours of life(91).
There were many studies in the past regarding the level of bilirubin and the risk of
kernicterus. As per the study conducted by Hsia et al in 1952, it was concluded that
risk of kernicterus increased significantly when serum bilirubin exceeded 340 pmol/L
and the risk rose to 50% when the serum bilirubin levels were above 510 pmol/L.
The use of phototherapy was well established by 1979. Cockinton et al developed
different thresholds as per the birth weight and age in hours for the initiation of
exchange transfusion in addition to phototherapy(92). Bhutani et al further modified
the approach to jaundiced near term and term infants based on the age in hours(93).
Based on the various intensities of light, phototherapy can be classified as close
phototherapy, double conventional and triple therapy. The conventional phototherapy
exposes the newborn to 7-10Uw/CM2/nm which helps in decline in serum bilirubin to
6-20% in the initial 24 hours(45). Double conventional phototherapy is more effective
than single phototherapy in reducing the serum bilirubin levels and duration of

38
treatment in term infants of birth weight over 2500g. But the role of double surface
phototherapy in abating the role of exchange transfusion is not well studied(90).
Efficacy of prophylactic phototherapy in preventing neonatal hyperbilirubinemia in
newborns with ABO incompatibility and positive DAT were studied in the past with
inconclusive results(94,95). A few studies concluded that prophylactic phototherapy
administered on the first day of life leads to a significant reduction in TSB in first 48
hours but not later on(70).
XIII B. Exchange transfusion:
Exchange transfusion is employed in conditions wherever there is a significant threat
of kernicterus being caused by hyperbilirubinemia or when phototherapy has not been
effective. It contributes to get rid of the maternal antibodies in the circulation in
addition to removing excess bilirubin, thereby reducing the further probabilities of
ongoing hemolysis.
It is performed with double volume irradiated (160 ml/kg), leukocyte depleted,
compatible blood, negative for CMV via an intravenous catheter inserted in the
umbilical vein. This procedure has its own independent risk hazards and is associated
with a high risk of procedure related morbidity(92, 92, 93).
Intravenous immunoglobulin has become an alternative therapy to exchange
transfusion. Even though, multiple doses of IVIG may be required to prevent the
ongoing hemolysis, even a single dose of IVIG has been well tried to be very
effective(94, 95).

39
Large evidence based studies have been limited due to the low prevalence of disease
which has led to the dearth of literature to compare the transfusion needs and outcome
measures. It is not possible to avert the incompatibility reaction. Prenatal counseling
is not a practical solution as ABO incompatibility neither leads t o significant mortality
nor lifelong morbidity. There have been significant changes made in the antenatal and
postnatal management strategies. New diagnostic techniques, monitoring tools and
management options are constantly under investigation and can go a long way to
reduce the factors that increase the severity and morbidity of hyperbilirubinemia of
newborn.
XIII C. Alternative to exchange transfusion:
Treatment with oral D pencillamine and A or B trisaccharides were also described in
ABO incompatible infants in the literature(1).
XIV. RECENT ADVANCES:
There is emerging literature on the use of Flow cytometry (FC) to estimate the number
of soluble or RBC bound IgG as it has a higher exactitude and reliability when
compared to standard serological procedures. It can be used to study the IgG subclass
and amount on the red cells. The downside of FC is that it is cost and unavailability in
most of the laboratories(100).
A Gel Centrifugation Test (GCT) has been recently developed for the quantification of
the RBC bound antibodies and IgG1 and IgG3 subclasses. It has been proved to be

40
extra sensitive in the demonstration of RBC allo-antibodies and conjointly the
determination of IgG subclasses and was found to be in agreement with the Flow
Cytometry results(101).
The degree of RBC destruction is determined not only by the IgG subclasses and
density of red cell bound antibodies but also conjointly by numerous other factors like
the effector cell type and its Fc receptor, complement activation, factors affecting the
actions of the monocyte-macrophage system and the type of hemolytic disease(78).
There were a few studies in the past, which concluded that severe forms of Rh-HDN
were associated with IgG1 carrying G1M (3) allotypes as compared to G1M (1)
allotypes. GM allotypes are located on the heavy chains of Ig. GM typing can be done
on slides or microtiter plates or by using gel test(102).
A few studies were conducted to investigate the polymorphism of FcγRIIa (CD32) in
cases of ABO-HDN. FcγRIIa is a member of FcRn which mediates the placental
transfer of IgG by binding to the subclasses(35). Polymorphism within the gene can
affect the binding of IgG subclass and was concluded that HR131 genotype was
associated with susceptibility to ABO-HDN.
XV. CONCLUSION:
ABO incompatibility is now emerging as the main cause of hemolytic disease. Early
blood grouping and DAT-testing in neonates with early jaundice are recognized as risk
appraisals. The current study aims to assess the prevalence of ABO incompatible
pregnancies and to see if high maternal IgG anti-A or anti-B titers and IgG subclasses

41
are consistent with increased risk of developing ABO hemolytic disease of newborn.
Against the backdrop of a country such as ours, where neonatal assessment and care
may be limited in large areas, it may be prudent to utilize these tools to guide mothers
at high risk to centers where appropriate care is available. Timely diagnosis and
interventions can reduce the incidence of ABO haemolytic disease of newborn and
improve the population quality.
This study was performed to determine the prevalence of IgG subclasses in ABO
hemolytic disease of the newborn using DAT IgG1/IgG3 card test on the column
agglutination platform to see if it helps in the prognostication of HDN. It is a simple
and low cost technique using small quantity of serum. This might allow early
intervention and proactive management of the newborn. If this is found to be clinically
relevant, it can be enforced within the routine prenatal investigation.

42
MATERIALS AND METHODS
43
MATERIALS AND METHODS
SETTING:
This study was conducted in Christian Medical College, Vellore, Tamil Nadu. It is a
teaching hospital providing tertiary medical care to residents of Vellore and
surrounding districts of Tamil Nadu, Andhra Pradesh and Kerala. It also serves as a
referral centre for patients from rest of India and South East Asia. This observational
cohort study was carried out in Department of Transfusion Medicine and
Immunohematology (Blood Bank) in coordination with departments of Obstetrics and
Neonatology.
The study was approved by Institutional Review Board of Institute. Informed consent
was obtained from the mothers who were recruited for study and venous samples were
collected from them.
BIAS:
All efforts were made to eliminate any bias in selection of patients. Despite this the
prevalence of ABO incompatible pregnancies may show a skewed result since CMC is
a tertiary hospital and cases at risk are often referred here. Instrumental bias was likely
to be negligible as variables were measured using calibrated and automated analyzers
in the clinical pathology department and blood bank and all serological tests done in
blood bank were run in duplicates. Investigator bias in interpretation of severity of
HDN was avoided as the investigator was not involved in the treatment directly.

44
SAMPLE SIZE:
Sample size was estimated to be approximately 575.
According to the study conducted by Heydarian F et al in 355 cases of ABO
incompatibility, the prevalence of ABO-HDN was detected to be 27%. This
prevalence was taken into consideration and the following formula was used for
statistical analysis.
N=4xpq/d2= 4x27x73/49 =161
p=percentage of ABO incompatibility; q=1-p; d=precision=7%
Using the precision of 75 and 95% confidence interval, at least 161 cases of ABO
incompatible pregnancies were to be considered to obtain 27% prevalence of ABO-
HDN.
The prevalence of ABO incompatible pregnancies among O blood group mothers was
28% as per the study by Cernadas et al. Therefore to detect 161 cases of ABO
incompatible pregnancies, 575 mothers with O blood group were recruited for the
study.
Screening number=161/0.28=575
Note: There was no proper literature available for prevalence of IgG subtypes among
ABOHDN. So the prevalence of hemolytic disease among ABO incompatibility was
used for sample size calculation.

45
References for calculation of sample size:
1. Farhad Heydarian, Seyedeh Fatemeh Khatami, Pouya Parvaresh, Masumeh
Reanjad et al. ABO Hemolytic Disease Leading to Hyperbilirubinemia in term
Newborns: Value of Immuno hematological Tests. Iranian Journal of
Neonatology Vol.3, No.2, 2012
2. JM ceriani Cernadas, C Fustinana, M Bujas et al. 23 Epidemiology of the ABO
incompatibility. Pediatric Research Volume 15,February 1981
PARTICIPANTS:
Inclusion criteria: : All O blood group mothers who were negative for alloantibodies
on a red cell antibody screen, and who gave birth to babies with A, B or AB blood
group were included in this study.
Exclusion criteria: Neonates with other known causes of jaundice and hemolysis other
than ABO incompatibility.
STUDY IMPLEMENTATION:
All antenatal women during their antenatal visit had a blood grouping and typing and
antibody screen performed as per the routine protocol. Mothers with O blood group
with a negative antibody screen and who delivered at term (after 37 weeks of
gestation) were recruited for our study. The proforma was explained to the mothers or
care givers and informed consent regarding participation in the study was obtained in
the regional language. 8 ml venous samples were collected from those mothers who

46
fulfilled the above inclusion criteria. The plasma was separated and frozen for
maternal IgG anti-A /anti-B titer analysis and IgG1/ IgG3 subclass typing.
The babies were then followed up with help of Department of Neonatology and
medical records. Clinical details and relevant laboratory investigations were accessed
from the clinical workstation of the hospital, both for the mother and subsequently for
the baby. Data was collected as per the pre-structured clinical research form designed
at the beginning of the study.
The newborn was evaluated for the presence or absence of HDN. Unlike Rh-HDN,
there were no clear guidelines to grade the severity of ABO-HDN.
SAMPLE PROCESSING:
8ml venous samples were collected from the mothers using EDTA vaccutainers. The
samples were centrifuged at 3000 rpm for 10 minutes, plasma was separated and
stored in eppendorf tubes at -70 degree C. IgG anti-A and anti-B titer analysis was
done using tube method and double dilution technique. IgG1 and IgG3 subclass typing
was done by column agglutination technique using ID card DAT IgG1/IgG3 DiaMed
GmbH 1785Cressier FR Switzerland (BIO-RAD).

47
575 antenatal women with O blood group
and negative antibody screen who
presented to the labour room at term were
recruited for the study
Pregnancies were followed up. 8 ml
venous samples were collected from
mothers who delivered babies with non
O group
DAT was performed in all newborns and
they were monitored as per the
guidelines of neonatology department
Plasma was
separated and
frozen
Cases were classified based on the
presence or absence of ABO HDN.
Maternal IgG1/IgG3 subtypes and IgG
anti-A and anti- B titers were correlated
with the occurrence of ABO-HDN

48
DATA COLLECTION AND SOURCE OF DATA:
Data of mother
1. Demographic
2. Personal
3. Blood group and Rh typing
4. Period of gestation
5. Obstetric history
6. Indirect antiglobulin test
7. Outcome of pregnancy
Baby’s data
1. Live/ still birth/intrauterine death
2. Preterm/term/post-term
3. Gender
4. Birth weight
5. Blood group
6. Direct Antiglobulin test
7. Haemoglobin (monitored over hospital stay; lowest level documented)
8. Total serum bilirubin (monitored over hospital stay; highest level documented)
9. Direct serum bilirubin
10. Transcutaneous bilirubin (if done)
11. Reticulocyte count (monitored over hospital stay; highest level documented)

49
12. Peripheral smear
13. Treatment required – including admission to Neonatal intensive care unit
14. Treatment details:
15. Phototherapy – single/ double surface
16. Exchange transfusion
17. Intra- uterine transfusion
18. None
Tests done in the blood bank:
On mother’s sample:
1. Blood grouping and Rh typing
2. Antibody screen
3. Maternal IgG anti-A and anti-B titer
4. IgG subclass typing (IgG1 and IgG3) using Column agglutination technique,
finding high(1:100) and low titers(1:1) for each respectively
On newborns’ sample:
1. Blood grouping and Rh typing
2. Direct Antiglobulin Test

50
COLUMN AGGUTINATION TECHNOLOGY:
It is a commonly used platform in blood banks presently, and it uses gel or glass beads
to trap agglutinated red cells following an antigen antibody reaction. Test can be
performed on this platform manually or by automated means, which allow for
processing multiple samples at the same time. CAT as it is commonly known as, can
be used for tests like blood grouping, antibody screening, DAT, IAT and cross-
matching. Antigens expressed on the red cells interact with antibodies in the chambers
at the top of a column, and after proper incubation and centrifugation as recommended
by the manufacturer, the test can be interpreted. The agglutinated red cells remain at
the top, and are read as a positive reaction, while the free red cells are forced through
the column to the bottom and read as negative. This forms the principle of many tests
carried out via this platform in our blood bank.
STATISTICAL ANALYSIS:
Categorical variables were summarized using counts and percentages. Quantitative
variables were summarized using mean and standard deviation or median and IQR.
The expression of IgG subclasses were presented as numbers and frequencies. Pearson
and Fischer’s exact chi square was used for comparison of categorical data. Univariate
and binary logistic regression analysis was used for comparing the categorical data and
to calculate the odds ratio. P value <0.05 was considered significant. SPSS 16.0 was
used for statistical analysis.

51
RESULTS AND ANALYSES
52
RESULTS AND ANALYSIS
A total of 575 mothers with O blood group and negative antibody screen who
delivered during the period June 2018 to August 2019 were considered for our study.
I.PREVALENCE OF ABO INCOMPATIBLE PREGNANCIES:
Out of the 575 mothers, 203 mothers delivered babies of A or B blood group.
Therefore the prevalence of ABO incompatible pregnancies was found to be 35.30 %
in O blood group mothers.
II. DEMOGRAPHIC DETAILS:
II 1. Geographic distribution:
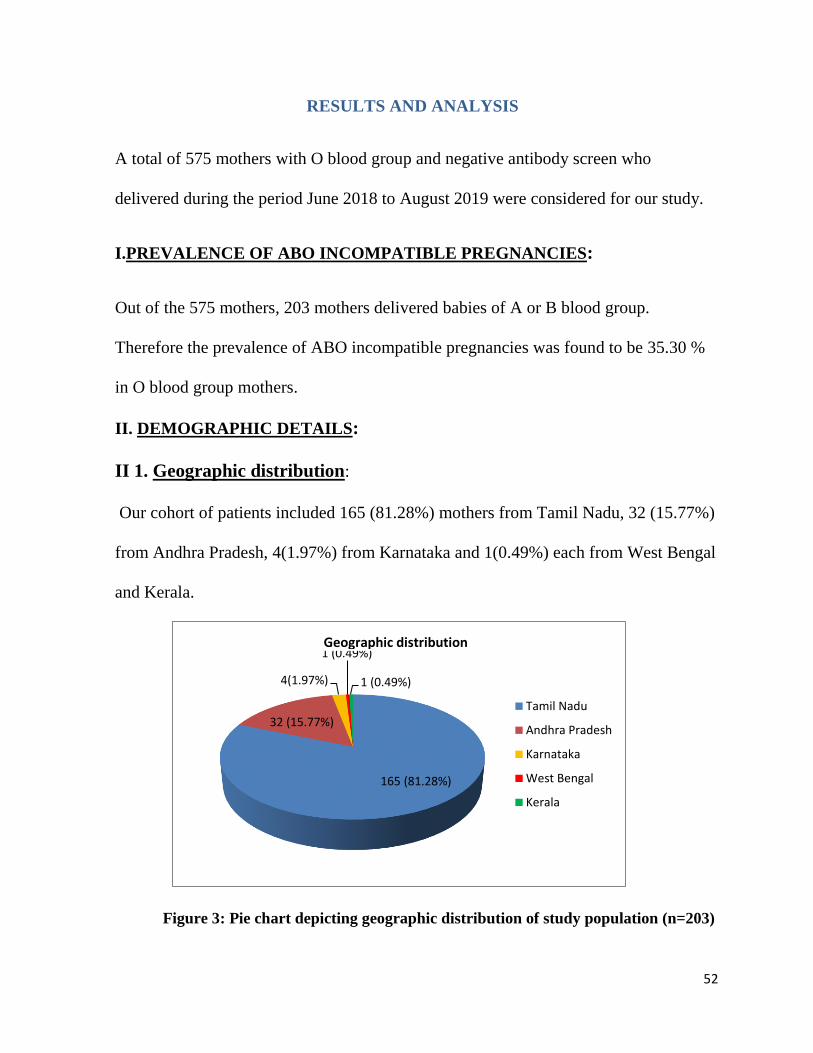
Our cohort of patients included 165 (81.28%) mothers from Tamil Nadu, 32 (15.77%)
from Andhra Pradesh, 4(1.97%) from Karnataka and 1(0.49%) each from West Bengal
and Kerala.
Figure 3: Pie chart depicting geographic distribution of study population (n=203)
165 (81.28%)
32 (15.77%)
4(1.97%)
1 (0.49%)
1 (0.49%)
Tamil Nadu
Andhra Pradesh
Karnataka
West Bengal
Kerala
Geographic distribution

53
I.2 Age of mothers:
The mean age of the study population was 28 years (Maximum 37 years and minimum
19 years).
I.3 Parity of mothers:
With regards to parity, 102 (50.25 %) of these patients were primiparous and
101(49.76 %) were multiparous.
Among the multiparous mothers, 63 (31.04%), 25(12.31%), 11(5.42%), 1(0.49%) and
1(0.49%) belonged to gravida G2, G3, G4, G5 and G7 respectively.
Figure 4: Pie chart depicting parity of mothers in study population (n=203)
I.4 Previous obstetric history:
Among the multiparous mothers, 54 out of 101 (53.46 %) mothers had an uneventful
obstetric history. However a bad obstetric history (BOH) defined by events such as
101 (49.76%)
63(31.04%)
25 (12.31%)11(5.42%)
1 (0.49%)
1(0.49%)G1
G2
G3
G4
G5
G7
G= Gravida
Parity of mothers

54
previous 1st or 2nd trimester loss, still birth, neonatal death or medical termination of
pregnancy were recorded for 47(46.54 %) mothers among the multiparous group. 36
mothers had a previous history of abortion, 5 had history of neonatal death, 4 abortion
and 2 medical termination of pregnancy.
* NND: Neonatal death, MTP: Medical Termination of Pregnancy
Figure 5: Bar graph depicting BOH among multiparous mothers (n=101)
I.5 Mode of delivery:
Analysis of the 203 mothers under consideration, showed that 95(46.79%) delivered
by normal vaginal delivery, 56(27.59%) by LSCS and rest 52(25.62%) by instrumental
delivery.
0
5
10
15
20
25
30
35
40
Abortion NND Still birth MTP
36
5 42
Nu
mb
er
of
case
s
Bad obstetric history
Bad obstetric history in multiparous mothers

55
*NVD: Normal Vaginal Delivery, LSCS: Lower Segment Caesarian Section
Figure 6: Pie chart illustrating mode of delivery of the study population (n=203)
I.6. Gender of the newborn:
Among the 203 babies delivered, 110(54.19%) were males and 93(45.82%) were
females.
Figure 7: Pie chart depicting gender distribution of newborns (n=203)
95( 46.79%)
56(27.59%)
52(25.62%)
NVD
LSCS
Instrumentaldelivery
Mode of delivery
110 (54.19%)
93 (45.81%) Male
Female
Gender distribution of newborn

56
I.7. Birth weight of the newborn:
Among the 203 babies, 23 (11.33%) were found to be of low birth weight (birth
weight <2.5 kg) and the rest 180 (88.67%) were of normal weight.
Figure 8: Pie chart illustrating birth weight of newborns (n=203)
II. BLOOD GROUP DISTRIBUTION IN BABIES:
81(39.90 %) out of the 203 newborns were A blood group and 122 (60.10%) were of B
blood group.
Figure 9: Pie chart showing prevalence of blood groups in newborns (n=203)
23 (11.33%)
180 (88.67%)
Low birth weight
Normal birth weight
Birth weight of newborns
81( 39.90%)
122( 60.10%)A group
B group
Distribution of blood groups in newborns

57
III. IMMUNO-HAEMATOLOGY PARAMETERS:
III.1 Antibody titration: Antibody titration was performed using tube method and
double dilution technique in the 203 plasma samples.
Table 5. Distribution of titers in mothers included in study:
Titer level Number of cases (n=203) Percentage of cases
2 10 4.93 %
4 8 3.94 %
8 34 16.75%
16 33. 16.26%
32 49 24.13%
64 44 21.68 %
128 22 10.83 %
256 3 1.48 %
The most frequently observed titer was 32 (24.13 % cases) followed by 64 in 44 cases
(21.68%). The least frequently observed titer was 256 in 3 cases (1.48%)
III.2 IgG subclasses identified (IgG1 and IgG3):
IgG subclass typing was performed using a DAT IgG1/IgG3 ID-Card from DiaMed
GmbH, using CAT in total 203 samples.

58
Our study showed the overall prevalence for IgG1 and /or IgG3 subclasses in our
population of antenatal women to be 46.79 %.
Table 6. Prevalence of IgG1/IgG3 subclasses in mothers (n=203)
IgG1/IgG3 results in mothers(n=203):
IgG1/IgG3 positive IgG1/IgG3 negative
95 (46.79%) 108(53.20%)
Analyzing it within subclasses showed the prevalence of IgG1/IgG3 as follows:
Table 7. Distribution of IgG1/IgG3 subclasses in mothers (n=203)
IgG subclasses No. of cases Percentage
Only IgG1(1:1) 34 16.75 %
Only IgG1 (1:100) 13 6.40 %
Both IgG1(1:100) and IgG3(1:100) 42 20.69 %
Both IgG1(1:100) and IgG3(1:1) 6 2.96 %
Negative for both 108 53.20 %
On analysis, we concluded that 108 cases( 53.20) % of our study group did not have
either IgG1 or IgG3, while in 42 cases (20.69%), both these subclasses co-existed in
high titers. It was interesting to note that all patients who had IgG3, also had IgG1 in
high titers i.e, IgG3 was not detected in isolation.

59
IV. LABORATORY PARAMETERS OF THE NEWBORNS:
IV 1. Anaemia:
Anaemia is defined as serum Hb levels below 14.6 g/dl in a term neonate. Clinical
assessment formed the initial mode of assessment. In suspected cases of haemolysis, in
which newborns presented with jaundice; haemoglobin and total bilirubin levels were
estimated. Haemoglobin levels were available for 170 out of the total 203 newborns,
of which 49(28.82%) newborns had anemia.
Figure 10: Pie chart depicting prevalence of anemia in ABO incompatible cases
1V. 2 Hyperbilirubinemia
Neonatal hyperbilirubinemia is defined as any PTB values above ≥ 95th percentile on
the hour of life specific normogram. In our study, serum bilirubin levels or
transcutaneous bilirubin (TcB) levels were estimated. Majority of neonates developed
jaundice on second day (46%) followed by third day (24%). The mean age of
49(28.82%)
121( 71.17%)
<14.6 g/dl
≥14.6 g/dl
Anaemia in newborn

60
presentation of jaundice was 2.35± 1.15 days, earliest cases of hyperbilirubinemia
reported within 24 hours. The mean initial indirect bilirubin was 14.64 ± 3.92 mg%
with the range from 7.46 mg% to 27.51 mg%.
1V. 3. Reticulocytosis
Reticulocytosis in newborn is defined as reticulocyte count >4.6%. Reticulocyte count
was available for 106 newborns and a high reticulocyte count was found in
51(48.11%) cases.
Figure 11: Pie chart showing prevalence of reticulocytosis in ABO incompatible cases
V. MODE OF TREATMENT:
Treatment details were available for all cases of ABO incompatibility. Single Light
Phototherapy (SLPT) was the most common treatment administered in around 65%
cases followed by Double Surface Phototherapy (DSPT) in 6.3% cases and Exchange
Transfusion (ET) in 1 case. In 7 cases, DSPT was administered following SLPT.
51( 48.11%)55( 51.89%)
≥4.6%
<4.6%
Reticulocyte count in study population

61
Table 8: Mode and average duration of treatment administered (n=203)
VI. Follow up of pregnancy and diagnosis of ABO-HDN
ABO-HDN is defined as a newborn with blood group A, B or AB with positive DCT
and laboratory evidence of haemolysis, born to a mother with blood group O.
Among the 203 cases of ABO incompatibility analyzed, 76 newborns were found to
have early onset jaundice, positive DCT and evidence of haemolysis, and therefore,
the prevalence of ABO-HDN was estimated to be 37.43%.
Figure 12: Pie chart illustrating the prevalence of ABO-HDN (n=203)
76(37.43%)
127(62.57%)ABO HDN
No HDN
Prevalence of ABO-Haemolytic disease of newborn
Mode of treatment Number of cases(n=203) Average duration
Single phototherapy (hrs) 133 32.5 hours
Double phototherapy (hrs) 13 46 hours
Exchange Transfusion 1 Once

62
Figure 13: Flow chart to illustrate patient follow up and results
Mothers who delivered babies of either A, B or
AB blood group (n=203). 8 ml maternal
venous samples were collected. Plasma was
separated and frozen.
Cases with ABO-HDN
(N=76).
IgG anti-A and anti-B
titers and IgG1/IgG3
subtyping was done on
maternal samples.
Cases without HDN
(N=127).
Maternal titers and subclasses were correlated with occurrence of ABO-HDN
Newborns were monitored with the help of
neonatology department to see if they
developed ABO-HDN.
Total number of antenatal mothers with O
blood group and negative antibody screen who
were recruited for the study (N=575)

63
VII. DEMOGRAPHIC DETAILS IN ABO- HDN:
VII. 1 Geographic distribution:
Among the 76 cases of ABO-HDN, 59 (77.64%) of their mothers were from Tamil
Nadu, 16 (21.05%) from Andhra Pradesh and 1(1.31%) from Karnataka.
Figure 14: Pie chart depicting geographic distribution of mothers of ABO-HDN
VII. 2. Age of the mother:
The mean age of the study population of mothers was 28 years (Maximum 38 years
and minimum 19 years).
VII. 3. Parity of mother:
Among 76 cases of ABO-HDN, 39(51.31%) of the mothers were primiparous and
37(48.69%) were multiparous.
59(77.64%)
16(21.05%)
1( 1.31%)
Tamil Nadu
Andhra Pradesh
Karnataka
Geographic distribution of mothers of ABO-HDN group

64
Figure 15: Pie chart illustrating the parity of mothers of ABO-HDN (n=76)
Among the multiparous mothers, 22 (28.95 %), 9 (11.84 %), 5 (6.58%) and 1(1.32%)
were G2, G3, G4 and G5 gravida respectively.
Figure 16: Pie chart illustrating overall distribution of parity among mothers
39( 51.31%)
37( 48.69%) Primiparous
Multiparous
Parity of mothers in ABO-HDN group
39(51.31%)
22(28.95%)
9(11.84)%)
5(6.58%) 1(1.32%)
G1
G2
G3
G4
G5
Distribution of parity in mothers in ABO-HDN group

65
Table 9. Correlation between parity of mother and occurrence of ABO-HDN
Parity ABO-HDN No HDN p value
Primiparous 39 63 0.885
Multiparous 37 64
Occurrence of ABO haemolytic disease of newborn was independent of the parity of
mother.
VII. 4. Mode of delivery:
Out of the total 76 cases of ABO HDN, 38(50%), 18 (23.68%) and 20(26.32%) were
by normal vaginal delivery, LSCS and instrumental delivery respectively.
*NVD: Normal vaginal delivery, LSCS: Lower Segment Caesarian Section
Figure 15: Pie chart showing mode of delivery of mothers in cases with ABO-HDN
38 (50%)
18 (23.68%)
20 (26.32%)
NVD
LSCS
Instrumental
Mode of delivery in mothers of ABO-HDN group

66
Table 10: Correlation between mode of delivery and occurrence of ABO-HDN
ABO-HDN Vaginal delivery LSCS Instrumental p value
Present 38 18 20 0.61
Absent 57 38 32
There was no association between occurrence of ABO-HDN and mode of delivery.
VII. 5. Gender of the newborn:
39(51.31%) out of 76 newborns were males and 37(48.69%) were females.
Figure 16: Pie chart depicting gender distribution in cases of ABO-HDN
Table 11: Correlation between gender of newborn and occurrence of ABO-HDN
Gender of
newborn
ABO-HDN No HDN p value
Males 39 71 0.56
Females 37 56
39 (51.31%) 37 (48.69%)
Males
Females
Gender distribution of newborns in ABO-HDN group

67
There was no association between gender of the newborn and occurrence of ABO-
HDN.
VII. 6. Birth weight of the newborns:
Among the 76 cases of ABO-HDN analyzed, 8(10.52%) babies were of low birth
weight (<2.5kg) and rest 68 (88.48%) were of normal birth weight.
Figure 17: Prevalence of low birth weight in ABO-HDN group (n=76)
Table:12: Correlation between birth weight and occurrence of ABO-HDN
Birth weight ABO-HDN No HDN p value
< 2.5 kg 68 112 0.823
≥ 2.5 kg 8 15
There was no association between birth weight of newborn and occurrence of ABO-
HDN.
8(10.52%)
68 (88.48%)
Low birth weight
Normal weight
Prevalence of low birth weight in ABO-HDN cases

68
VII.7. Blood group distribution in ABO HDN cases:
33 out of 76 newborns (43.42%) were A blood group and 43 (56.58%) were B blood
group
Figure 18: Blood group distribution in ABO-HDN (n=76)
Table 13 : Correlation between blood group and occurrence of ABO-HDN
Blood group ABO-HDN No HDN p value
A group 33 48 0.428
B group 43 79
Occurrence of ABO-HDN was independent of the blood group of the newborn.
VII. IMMUNO-HAEMATOLOGY PARAMETERS IN ABO-HDN GROUP
VII 1. Antibody titration: Antibody titration was performed using tube method and
double dilution technique.
33( 43.42%)
43( 56.58%) A group
B group
Blood group distribution in newborns

69
Table 14: Comparison of titer levels in ABO-HDN and no HDN group:
Titer level ABO-HDN (n=76) No HDN (n=127)
Number Percentage Number Percentage
2 0 0 % 10 4.93 %
4 0 0 % 8 3.94 %
8 0 0 % 34 16.75 %
16 2 0.99 % 31 15.27 %
32 12 5.91 % 37 18.23 %
64 37 18.23 % 7 3.44 %
128 22 10.83 % 0 0 %
256 3 1.48 % 0 0 %
It was observed that the study group without ABO-HDN had a lower titer levels
ranging from 2 to a maximum of 64 when compared to the ABO-HDN group. The
latter group had a higher range of titers ranging from 16 to a maximum of 256. The
most frequently observed titer level in ABO-HDN group was 64 (48.68%) and in no
ABO-HDN group was 32 (15.79%). It was observed that, with increase in the maternal
IgG titer levels >64, there was an increase in trend of newborns developing ABO-
HDN.

70
Table 15: Association of maternal titer levels with occurrence of ABO-HDN:
Titer levels ABO HDN No ABO-HDN Odds ratio CI for odds ratio
< 64 14 120
64-128 37 7 45.306 17.01, 0.63
≥ 128 25 0
The odds of developing HDN at a titer of 64-128 is 45.31(95% CI 17.01-0.63) times as
compared to cases with titers < 64.
Table 16: Correlation between maternal titer levels and occurrence of ABO-HDN:
Titer levels ABO HDN No ABO-HDN p value
< 64 14 120 < 0.001
≥ 64 62 7
VII.2 IgG subclasses identified (IgG1 and IgG3):
IgG1 and / or IgG3 subclasses were present in all the cases of ABO-HDN i.e. the
prevalence of IgG1 and / or IgG3 subclasses was 100% in the ABO-HDN group

71
Table 17: Analyzing within IgG subclass:
IgG subclasses No. of cases Percentage
Only IgG1(1:1) 18 23.68 %
Only IgG1 (1:100) 11 14.47 %
Both IgG1(1:100) and IgG3(1:100) 45 52.27 %
Both IgG1(1:100) and IgG3(1:1) 5 6.58 %
Table 18: Correlation between presence of IgG1/ IgG3 and occurrence of HDN:
ABO - HDN
IgG1 and / or IgG3
present
IgG1 and / or IgG3
absent
p value
HDN present
76 0 <0.001
HDN absent
19 108
Presence of IgG1/IgG3 subclasses was significantly associated with occurrence of
ABO-HDN. This was independent of the maternal IgG anti-A or anti-B titers.

72
Comparison of distribution of IgG1/G3 subclasses in ABO-HDN and no HDN
groups:
Figure 19: Bar graph showing distribution of IgG1/IgG3 subclasses
Table 19: Presence of IgG1/IgG3 subclass at various titers and occurrence of
ABO-HDN:
Titer ABO-HDN IgG1/IgG3
present
IgG1/IgG3
absent
2
HDN Present 0 0
HDN Absent 0 10
4
HDN Present 0 0
HDN Absent 0 8
8
HDN Present 0 0
HDN Absent 6 28
16
HDN Present 2 0
HDN Absent 3 28
0
5
10
15
20
25
30
35
40
45
IgG1 low titeronly
IgG1 high titeronly
Both IgG1 andIgG3 high
IgG1 high andIgG3 low
18
11
42
5
16
20 1
ABO-HDN
No HDN

73
32
HDN Present 12 0
HDN Absent 8 29
64
HDN Present 37 0
HDN Absent 2 5
128
HDN Present 22 0
HDN Absent 0 0
256
HDN Present 3 0
HDN Absent 0 0
It was observed that, ABO-HDN was not present at lower maternal titers. With the
gradual increase in maternal IgG titers, there was a gradual increase in the incidence of
ABO-HDN also, with a maximum of 37 cases at a titer of 64. At titers > 64, all the
cases developed ABO-HDN.
Correlation between presence IgG subclasses with occurrence of ABO-HDN at
various titers:
Correlation between the presence of IgG1/IgG3 subclasses with occurrence of ABO-
HDN were analyzed at various titers ranging from ≥ 16 to ≤ 64. Titers < 16 and > 64
were excluded for this comparison, as there were no cases of HDN reported at titer <
16 and at a titer of > 64, all the cases had HDN.

74
Table 20: Correlation between presence IgG subclasses with occurrence of ABO-
HDN at titer 16 (n=33)
ABO-HDN
IgG1 and / or IgG3
present
IgG1 and / or IgG3
absent
p value
HDN present
2 0 0.040
HDN absent
3 28
At a titer of 16, presence of IgG1/IgG3 subclasses is significantly associated with the
occurrence of ABO-HDN.
Table 21: Correlation between presence IgG subclasses with occurrence of ABO-
HDN at titer 32 (n=49)
ABO-HDN
IgG1 and / or IgG3
present
IgG1 and / or IgG3
absent
p value
HDN present
12 0 < 0.001
HDN absent
8 29
At a titer of 32, presence of IgG1/IgG3 subclasses is significantly associated with the
occurrence of ABO-HDN.
Table 22: Correlation between presence IgG subclasses with occurrence of ABO-
HDN at titer 64 (n=44)
ABO-HDN
IgG1 and / or IgG3
present
IgG1 and / or IgG3
absent
p value
HDN present
37 0 < 0.001
HDN absent
2 5
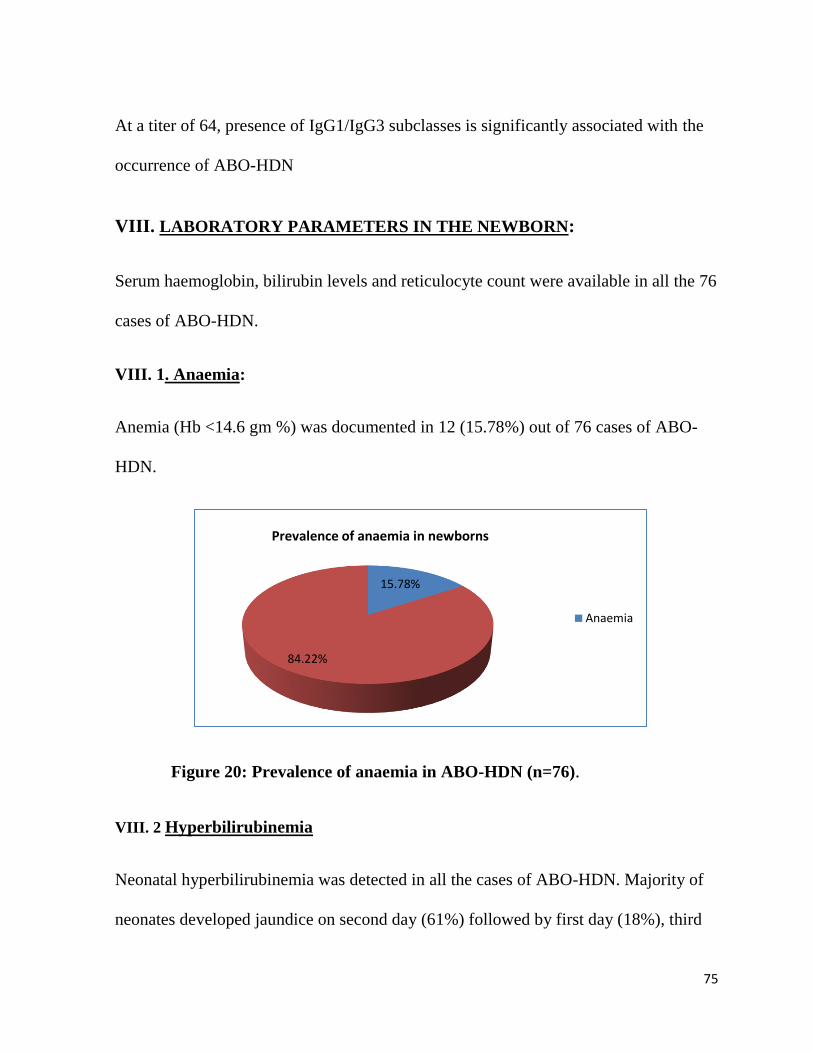
75
At a titer of 64, presence of IgG1/IgG3 subclasses is significantly associated with the
occurrence of ABO-HDN
VIII. LABORATORY PARAMETERS IN THE NEWBORN:
Serum haemoglobin, bilirubin levels and reticulocyte count were available in all the 76
cases of ABO-HDN.
VIII. 1. Anaemia:
Anemia (Hb <14.6 gm %) was documented in 12 (15.78%) out of 76 cases of ABO-
HDN.
Figure 20: Prevalence of anaemia in ABO-HDN (n=76).
VIII. 2 Hyperbilirubinemia
Neonatal hyperbilirubinemia was detected in all the cases of ABO-HDN. Majority of
neonates developed jaundice on second day (61%) followed by first day (18%), third
15.78%
84.22%
Anaemia
Prevalence of anaemia in newborns

76
day (16%) and fourth day (5%). The mean initial indirect bilirubin was 16.24 ± 4.04
mg% ranging from 7.46 mg% to 27.51 mg%.
VIII. 3. Reticulocytosis:
Reticulocyte count was documented in all cases of ABO-HDN. Reticulocytosis
(reticulocyte count >4.6%) was observed in 42(55.26%) out of 76 cases of ABO-HDN.
Figure 21: Pie chart depicting prevalence of reticulocytosis in ABO-HDN.
42(55.26%)
34(44.74%)
Reticulocytosis
Reticulocyte count

77
Table 23: Comparison of parameters of newborns in ABO-HDN and without
ABO-HDN
Parameters ABO-HDN No HDN
Male/ Female 42/34 68/59
Birth weight(kg) 3.06 ± 0.60 2.99 ± 0.50
A blood group 33 48
B blood group 43 79
Haemoglobin (gm %)
Total bilirubin (mg %)
Retic count (%)
Polychromasia and
microspherocytes
16.68 ± 1.8
16.24 ± 4.04
5.63 ± 3.05
37%
15.38 ± 3.32
13.30 ± 3.30
3.74 ± 1.68
4%
DCT negativ

78
Table 24: Comparison of parameters of newborns in OA-HDN and OB-HDN.
Characteristic Total OA HDN (n=33) OB HDN (n=43)
Gender:
Male 42 20 22
Female 34 13 21
Birth weight:
< 2.5 kg 8 5 3
≥ 2.5 kg 68 28 40
Mode of delivery:
Normal vaginal 38 17 21
Instrumental 20 5 15
LSCS 18 11 7
Parity:
Primigravida 39 15 24
Multigravida 37 18 19
Titer level
< 64 14 5 9
≥ 64 62 28 34

79
IX. TREATMENT DETAILS IN ABO-HDN:
Treatment details were available for all 76 cases of ABO-HDN. Single Light
phototherapy (SLPT) was initiated in 93.4% cases. Double Surface Phototherapy was
administered in 15.7% cases of which 5 of the cases were given both SLPT and DSPT.
Exchange Transfusion was performed in one case.
Table 25: Mode and average duration of treatment in ABO-HDN
Treatment modality Number of cases Average duration
Single phototherapy 64 (84.21%) 40.50 hrs
Double phototherapy 12 (15.78%) 8.84 hrs
ExchangeTransfusion 1 (1.31%) Once
X. GRADING OF ABO-HDN:
We used the grading system proposed by Choudhuri et al classification of Rh-HDN to
grade the severity of cases in our study, which was as follows:
1. Mild: Positive DAT alongside some evidence of haemolysis but requiring no
intervention.
2. Moderate: Cases with evidence of haemolysis and intervention was limited to
phototherapy
3. Severe: When the baby was hydropic or intrauterine/ exchange or top up transfusion
was required.

80
Using the above guidelines of grading ABO-HDN, there were 75 cases of mild/
moderate ABO-HDN and one case of severe ABO-HDN in our study.
XI. FAMILIAL INCIDENCE OF ABO-HDN:
Among the 203 cases of ABO incompatible cases, 33 (16.2%) had a prior family
history of the same. 9 (11.84%) out of 76 ABO-HDN cases and 5 (3.9%) out of 127
non HDN cases had history of ABO-HDN in their siblings.
Table 26: Correlation between family history and occurrence of ABO-HDN
ABO-HDN
Family history of ABO- HDN
p value Present Absent
Present 9 68 0.043
Absent 5 122
Family history of ABO-HDN was significantly associated with occurrence of ABO-
HDN. Newborns with siblings who had history of ABO-HDN were at higher risk of
developing ABO-HDN when compared to newborns with a negative family history.

81
DISCUSSION

82
DISCUSSION
ABO haemolytic disease of newborn (ABO-HDN) is emerging as the most common
cause of haemolytic disease of newborn in the developed countries. There have been
constant attempts to develop tests which can predict the onset of HDN in Rh-HDN,
and also to assess its severity, in order to put therapeutic interventions in place on
time. But there is a dearth of literature on the prevalence and factors that impact ABO-
HDN from overseas and India. Against the background of extremely variable health
care facilities in our country, we thought it is critical to study factors that may predict
the severity of ABO-HDN in mothers with O blood group. At present, there are no
satisfactory methods to predict the occurrence of ABO-HDN.
Early blood grouping and DAT in newborns with jaundice are a well recognized risk
appraisal in ABO incompatible newborns. Our study aimed to find the prevalence of
ABO incompatible pregnancies in O blood group mothers and investigated the role of
maternal IgG anti-A and anti-B titers and IgG1/IgG3 subclasses as a powerful
predictor of occurrence of ABO-HDN. Various maternal and fetal parameters and their
association with ABO-HDN were also analyzed.
The study included 575 O blood group mothers who were recruited during the study
period July 2018 to September 2019.

83
Geographical distribution:
According to previous studies, race was a risk factor in ABO-HDN and the incidence
of ABO HDN was higher in black population than caucasians. This could be attributed
to the higher prevalence of anti-A and anti-B titers in the black population(103).
Our cohort of patients included more than 80% mothers from Tamil Nadu, around
15% from Andhra Pradesh and rest from Karnataka, West Bengal and Kerala.
Age of mother:
The median age of the study population of mothers was 28 years and ranged from 19
years to 37 years. There were no studies available till date which proved the effect of
maternal age on occurrence of ABO-HDN.
Prevalence of ABO incompatible pregnancies:
Among the total 575 mothers, 203 mothers delivered babies of either A or B blood
group (non-O group) and the prevalence of ABO incompatibility was thus estimated to
be 35.3% i.e, one third of the pregnancies in O blood group mothers were found to be
ABO incompatible. None of the babies had AB blood group. All previous literature
has reported a varying range of prevalence of ABO incompatibility, which differed
from geographical area and population. The prevalence in our study was similar to that
observed in the studies done by Christensen et al in which a prevalence 32.4 % was
reported in a cohort of 42,529 neonates (104) and 40.8% as reported by Shilpa et al in
a cohort of 250 O blood group mothers (105). But this was higher than the prevalence
of 28 % as reported in the studies by Cernadas et al(106) , 17.3 % by Bhat and Kumar
(21)and 14.8% by Sarici et al(107).

84
ABO-Haemolytic Disease of Newborn:
ABO-HDN is defined in the literature as a condition which occurs in newborns with
blood group A, B or AB having positive DAT and laboratory evidence of haemolysis,
born to a mother with blood group O (22). Evidence of haemolysis included
reticulocytosis and spherocytes in the peripheral smear (108). In our study, 76 out of
the 203 newborns with ABO incompatibility developed ABO haemolytic disease as
per these criteria. Therefore, the prevalence of ABO-HDN was estimated to 37.4%.
That is one out of 3 newborns were affected by ABO-HDN. This was similar to the
observations of Cariani et al (29)who reported 31% prevalence of ABO HDN in 68
ABO incompatible pregnancies and Heydarian et al (Iran), who reported 27.6%
prevalence of ABO-HDN in ABO incompatible pregnancies(109). There are only a
few studies from India which has looked into the prevalence of hyperbilirubinemia and
haemolysis in ABO incompatible newborns. As per the study by Bhat and Kumar, in
which they studied 151 cases of ABO incompatible pregnancies, 30.4% had significant
hyperbilirubinemia and 16.5% had laboratory evidence of hemolysis which was much
lower prevalence when compared to our study. Studies by Bekkeheim et al and Alani
et al concluded that the prevalence of ABO-HDN was 1-4% and 4.3% respectively in
ABO incompatible pregnancies. The prevalence of ABO-HDN as estimated in our
study was much higher than that observed in studies from India and overseas. This
could be attributed to the lesser awareness of ABO incompatibility compared to Rh
incompatibility, ineffective neonatal screening and absence of well developed hospital
protocols in the management of ABO-HDN worldwide.

85
Parity of mother
The number of primiparous and multiparous mothers were almost equal in the total
study population as well as in cases of ABO-HDN. As per our study, there was no
association between occurrence of ABO-HDN and parity of mother (p value= 0.88).
This was similar to the observation made in studies by Kattimani et al, Shah A et al
and Kalakheti et al, that parity had no effect on ABO-HDN(81,110,111). Our study
also concluded that ABO-HDN can occur in first pregnancy unlike in Rh-HDN and
can recur in about 87% cases as maternal ABO antibodies are present without previous
sensitization.
Mode of delivery:
The mode of delivery in all 203 cases were analyzed. About half of the mothers
delivered by normal vaginal delivery (46.7%) and the rest by LSCS (27 %) and
instrumental delivery (26.5%). In our study, occurrence of ABO haemolytic disease
was independent of the mode of delivery. This was similar to the observations made in
the study by Kattimani VS et al(81).
Gender of newborn:
Among the total 203 babies delivered, the number of male babies (54.1%) were
slightly higher than females(45.9%). But, there was a uniform sex wise distribution in
the HDN group (48.7% males and 51.3% females). In our study there was no
significant association between the gender of newborn and occurrence of ABO-HDN

86
(p value=0.56). This observation was comparable with that of the studies by Kattimani
et al, Kumar A et al, Akgul Set al(81,112,113). A few studies in the past postulated
that male newborns had an increased risk of developing jaundice(114,115).
Birth weight of newborn:
Low birth weight is defined as < 2.5 kg at birth in India. In our study, 23 (11.3%) out
of 203 babies were found to be of low birth weight. Among the 76 cases with ABO
HDN, 10.5 % were of low birth weight. There was no correlation with birth weight
and occurrence of ABO-HDN (p value=0.82).
OA and OB HDN:
In our study, though OB incompatibility was found to be more common (56.6%) than
OA incompatibility, there was no significant difference in occurrence of ABO-HDN in
both groups (p value=0.42). This was similar to the observations made in study by
Bhat and Kumar et al(21). As per the western literature, there is conflicting evidence
regarding occurrence of ABO-HDN and blood group of newborn. In a few studies, it
was observed that greater hemolytic activity was seen associated with anti-B
antibodies with an increase in trend of transfusion in first 24 hours of life in O-B
incompatibility as compared to O- A incompatibility(55–57) while a few studies
established that there was no relationship between the clinical course and infant’s
blood group (58).
Family history:

87
In our study, presence of a sibling with ABO haemolytic disease was found to be
significantly associated with occurrence of ABO-HDN in current pregnancy. Similar
trend was also observed in studies by Heydarian et al and Sarici et al (109,107).
Laboratory parameters:
Anaemia:
Anaemia is defined as Hb levels below 14.6 g/dl in term neonates(116). Clinical
assessment of newborns was done and in suspected cases of haemolysis, haemoglobin,
bilirubin levels and reticulocyte counts were estimated. Haemoglobin levels were
available for 170 out of the total 203 newborns, of which 50 (29.4%) newborns had
anemia. In the 76 cases of ABO-HDN, anaemia was documented in 13 cases (17.1%).
The lowest level of haemoglobin documented in our study was 10 gm/dl.
Hyperbilirubinemia:
Neonatal hyperbilirubinemia is defined as any PTB values above ≥ 95th percentile on
the hour of life specific normogram. In our study it was estimated by serum bilirubin
levels or by measuring transcutaneous serum bilirubin (TSB). Neonatal
hyperbilirubinemia was detected in all the cases of ABO-HDN. Majority of neonates
developed jaundice after 24 hours (61% cases) followed by those within 24 hours of
birth (18% cases). The mean initial indirect bilirubin was 16.24 ± 4.04 mg%.
Reticulocytosis:
88
Reticulocytosis in newborn is defined as reticulocyte count >4.6%. Reticulocyte count
was available for 106 newborns and a high reticulocyte count was found in 51(48.1%)
cases. Reticulocyte count was documented in all cases of ABO-HDN and was
observed in 42(55%) out of 76 cases of ABO-HDN.
Treatment of ABO-HDN:
Treatment details were available for all cases of ABO incompatibility. Single Light
Phototherapy (SLPT) was the most common treatment modality in about 65% cases,
followed by Double Surface Phototherapy (DSPT) in about 6.5% cases. In cases with
ABO-HDN, Single Light phototherapy (SLPT) was initiated in 93.4% cases. Double
Surface Phototherapy was administered in 15.7% cases of which 5 of the cases were
given both SLPT and DSPT. Exchange Transfusion was performed in one case, in
which the blood group of the newborn was group B. The initial haemoglobin level was
12.8 g%, indirect serum bilirubin was as high as 26.91 mg% and a reticulocyte count
was 10.65%. Both IgG1 and IgG3 were detected to be in high titers and maternal IgG
anti-B titer was recorded to be 256. Following exchange transfusion, the newborn’s
clinical and laboratory conditions improved significantly.
Maternal IgG anti-A and anti-B titers:
The maternal IgG anti-A and anti-B titers have been studied by many groups
worldwide as they tend to impact the occurrence of ABO-HDN. It was concluded in
our study that titer level > 64 was significantly associated with occurrence of ABO-

89
HDN (p value <0.001). The odds of developing HDN at a titer of 64-128 is 45.31(95%
CI 17.01-0.63) times as compared to cases with titers < 64. This was independent of
the presence of IgG subclasses. This range of titer levels were also in concordance
with the studies conducted by Owa J et al(48) on 50 ABO incompatible pregnancies
in Nigeria and Yi-qiang et al (46)on 625 ABO incompatible pregnancies in China.
According to the study conducted by Usha and Sulochana in India, an IgG titer levels
between 32 and 1024 were found to be critical(26).
Other studies by Li et al in China on 5246 mothers (51) and by Kadri et al (52) in
Indonesia on 268 mothers observed significantly high titers than our study. Li et al, in
their study concluded that antibody titers ≥ 512 was significantly associated with
neonatal jaundice. Kadri el al suggested that titer ≥ 256 had a significant risk
associated with neonatal hyperbilirubinemia. Our study differed from a few studies in
the past which opined that there was no correlation between maternal IgG titers and
occurrence of HDN(29,108).
Maternal IgG titers tend to rise rapidly in the third trimester. Therefore, antenatal
monitoring of maternal IgG anti-A and anti-B titers can significantly predict the
occurrence of ABO-HDN(52), though it was also dependent on factors like placenta
density, red cell surface antigen and IgG antibody subclass(117).
IgG subclasses:
The predictive diagnosis of ABO-HDN was further improved by studying the IgG
subclasses. In our study, it was IgG1 and IgG3 which were looked at to prognosticate
ABO-HDN, in view of all previous literature, which stated that these were the

90
predominant subclasses involved in the causation of Haemolytic Disease of Newborn.
In contrast, IgG2 was the least efficient among all the IgG subclasses in crossing the
placenta, and also the contribution of IgG2 and IgG4 in HDN is limited due to absence
of receptors for these on the monocytes. The effect of IgG subclasses on Rh-HDN is
quite clear but their role in ABO-HDN is uncertain. There was no major study from
India which explored the prognostic value of IgG subclasses on ABO-HDN. We
initiated our study in this background.
IgG subclass typing was performed using a DAT IgG1/IgG3 ID-Card from DiaMed
GmbH, using CAT in total 203 samples. This test contains dilutions of IgG1 and IgG3
in 1:1 and 1:100 strengths alongside a positive and negative control. The strength of
each of the subclass IgG1 and IgG3 could therefore be interpreted according to
positivity recorded on the relevant micro tubes representing strengths of either 1:1(low
titre) or 1:100(high titre). This is a relatively easy test and can be used for rapid
identification of IgG1 and IgG3 subclasses.
We found that the overall prevalence of IgG1/IgG3 subclasses in the study group to be
46.7%. IgG1/IgG3 subclasses were detected in all the cases with ABO-HDN. In our
study, IgG3 subclass was never detected in isolation, but always in association with
high titer of IgG1. The most frequently observed subclass was a combination of high
titer IgG1and low titer IgG3 in 42 cases (20.6%). In our study, the presence of IgG1
and IgG3 subclasses was significantly associated with the occurrence of ABO-HDN
and was independent of the maternal IgG anti-A and anti-B titer levels. It was

91
interesting to compare our results to those published by Zhou Yi-qiang et al in their
study from China. They found that maternal titer more than 64 and maternal
concentration of IgG1 and IgG3 subclasses, especially IgG1 subclass were
significantly associated with ABO-HDN.
This result was very similar to that observed in our study. Our study differed from the
findings by Kaplan et al in a study conducted in California in umbilical cord blood
samples which postulated that identification of IgG subclass in umbilical cord blood
was not predictive of hemolysis in ABO-incompatible neonates(47).
We also studied the correlation between the presence of IgG1/IgG3 subclasses at
various maternal IgG anti-A/ anti-B titers. It was concluded that at titer of 16, presence
of IgG1 and/ or IgG3 subclasses were significantly associated with occurrence of
ABO-HDN ( p value= 0.040). Titers higher than or equal to 32 along with presence of
IgG1 and/ or IgG3 subclasses had a highly significant association with occurrence of
ABO-HDN (p value <0.01).
Our results helped us identify, that 35.3% in O blood group mothers can be ABO
incompatible and among them, almost 37.4% of ABO can develop ABO-Haemolytic
disease of newborn. Occurrence of ABO-HDN was independent of the factors like
parity of mother, birth weight and blood group of newborn.
We could conclude that presence of IgG1 and /or IgG3 subclasses in maternal plasma
was significantly associated with the occurrence of ABO-HDN, and this was
independent of the maternal IgG anti-A and anti-B titer levels. We also inferred that
the odds of developing HDN progressively increased when the maternal IgG anti-A/B
92
titer ≥64. Presence of either of these subclasses at maternal IgG titers ≥16 had highly
significant association with occurrence of ABO-HDN.
The spectrum of heamolytic disease of newborn has changed over the last few
decades. The incidence of Rh D alloimmunization in pregnancy has decreased
drastically and now ABO HDN has emerged as the major cause of HDN in the
developed countries. Early blood grouping and DAT testing in newborns are already
recognized as risk appraisals in ABO-HDN, but our study clearly indicates that high
maternal IgG anti-A/B titers and presence of IgG1/G3 subclasses are consistent with
an increased risk of developing ABO-HDN. Therefore, it will be prudent to use these
parameters in the prediction of occurrence of ABO-HDN and take active preventive
and treatment measures which is critical in preventing the long-term sequelae. Against
the backdrop of a country such as ours, where neonatal assessment and care may be
limited in large areas, it may be prudent to utilize these tools to guide mothers at high
risk to centers where appropriate timely management can be initiated. This high-risk
approach should be adopted if there is a history of ABO-HDN in previous pregnancies
or if there is ABO incompatibility between the partners. Early identification, diagnosis
and intervention can reduce morbidity and mortality due to HDN due to ABO
Incompatibility.

93
CONCLUSIONS

94
CONCLUSIONS
1. The prevalence of ABO incompatible pregnancies in O blood group mothers was
35.30% and among them 37.4% cases developed ABO-HDN.
2. The overall prevalence of IgG1 and / or IgG3 subclasses in O blood group mothers
was 46.79%.
3. IgG1/ IgG3 subclasses was present in all mothers whose newborns developed ABO-
HDN.
4. There was an independent and strong association between occurrence of ABO-HDN
and presence of IgG1/IgG3 subclasses (p< 0.001).
5. There was an independent and strong association between occurrence of ABO-HDN
and IgG anti-A/B titers ≥ 64 when comparing mothers with titers < 64 (p< 0.001).
6. Presence of IgG1/IgG3 subclasses at titers ≥16 , was significantly associated with
occurrence of ABO-HDN.
7. IgG1/IgG3 subclass typing using the CAT is a simple test, which if implemented
can contribute significantly to clinical decision making algorithms and appropriate
timely interventions in the context of ABO-HDN.

95
LIMITATIONS

96
LIMITATIONS
1. Most of our patients (81.6%) are from Tamil Nadu, and hence it may not be able to
extrapolate our findings regarding IgG sub class as representative of the South Indian
population, as we had hoped it to be.
2. Laboratory investigations were not available for a few of the newborns in no ABO –
HDN group. Therefore, it was difficult to assess the degree of haemolysis, if present in
them

IgG1 and IgG3 subclass typing
Figure 22: IgG1 low titer (1:1) positive n=34
Figure 23: IgG1 high titer (1:100) positive n=13

Figure 24: IgG1 high titer and IgG3 low titer positive n=6
Figure 25: Both IgG1 and IgG3 high titer positive n=42

Figure 26: Both IgG1 and IgG3 negative n=127
97
REFERENCES
1. G. Klein H, J. Anstee D. Mollison’s Blood Transfusion in Clinical Medicine. 12th ed. U.K: WILEY
2. Delaney M, Matthews DC. Hemolytic disease of the fetus and newborn: managing the
mother, fetus, and newborn. Hematol Am Soc Hematol Educ Program. 2015;2015:146–51.
3. M. Harmening D. Modern Blood Banking and Transfusion Practices. 5th ed. Philadelphia: F.A
Davis company
4. Ozolek JA, Watchko JF, Mimouni F. Prevalence and lack of clinical significance of blood group
incompatibility in mothers with blood type A or B. J Pediatr. 1994 Jul;125(1):87–91.
5. Reali G. Forty years of anti-D immunoprophylaxis. Blood Trasfus Sangue. 2007 Jan;5(1):3–6.
6. Landsteiner K, Wiener AS. An Agglutinable Factor in Human Blood Recognized by Immune
Sera for Rhesus Blood. Proc Soc Exp Biol Med. 1940 Jan 1;43(1):223–223.
7. Rh Antibodies in the Maternal Circulation Without Clinical Manifestations of Erythroblastosis
in the Child | The Journal of Immunology [Internet]. [cited 2019 Jun 8]. Available from:
http://www.jimmunol.org/content/48/4/241
8. Liumbruno GM, D’Alessandro A, Rea F, Piccinini V, Catalano L, Calizzani G, et al. The role of
antenatal immunoprophylaxis in the prevention of maternal-foetal anti-Rh(D) alloimmunisation.
Blood Transfus Trasfus Sangue. 2010 Jan;8(1):8–16.
9. Nelson Textbook of Pediatrics 21st Edition 2019 (2 Volume Set) [Internet]. [cited 2019 Jun
19]. Available from: https://www.atithibooks.com/product/nelson-textbook-of-pediatrics-21st-
edition-2019-2-volume-set
10. Dennery PA, Seidman DS, Stevenson DK. Neonatal Hyperbilirubinemia. N Engl J Med. 2001
Feb 22;344(8):581–90.
11. ISSUES IN NEWBORN CARE - Primary Care: Clinics in Office Practice [Internet]. [cited 2019 Jun
19]. Available from: https://www.primarycare.theclinics.com/article/S0095-4543(05)70159-7/pdf
12. The Harriet Lane Handbook - 21st Edition [Internet]. [cited 2019 Jun 19]. Available from:
https://www.elsevier.com/books/the-harriet-lane-handbook/unknown/978-0-323-39955-5
13. Moise KJ. Red blood cell alloimmunization in pregnancy. Semin Hematol. 2005 Jul;42(3):169–
78.
14. Hackney DN, Knudtson EJ, Rossi KQ, Krugh D, O’Shaughnessy RW. Management of
pregnancies complicated by anti-c isoimmunization. Obstet Gynecol. 2004 Jan;103(1):24–30.

98
15. Joy SD, Rossi KQ, Krugh D, O’Shaughnessy RW. Management of pregnancies complicated by
anti-E alloimmunization. Obstet Gynecol. 2005 Jan;105(1):24–8.
16. Avent ND, Reid ME. The Rh blood group system: a review. Blood. 2000 Jan 15;95(2):375–87.
17. Avery’s Diseases of the Newborn 10th Edition Pdf Free Download | Medical e-Books | Books,
Pdf, Free books [Internet]. [cited 2019 Jun 19]. Available from:
https://in.pinterest.com/pin/636485359816832979/
18. Drabik-Clary K, Reddy VVB, Benjamin WH, Boctor FN. Severe Hemolytic Disease of the
Newborn in a Group B African-American Infant Delivered by a Group O Mother. Ann Clin Lab Sci.
2006 Mar 20;36(2):205–7.
19. Basu S, Kaur R, Kaur G. Hemolytic disease of the fetus and newborn: Current trends and
perspectives. Asian J Transfus Sci. 2011 Jan;5(1):3–7.
20. Saran RK, India, Directorate General of Health Services, World Health Organization.
Transfusion medicine: technical manual. New Delhi: Directorate General of Health Services, Ministry
of Health and Family Welfare, Govt. of India; 2003.
21. Bhat YR, Kumar CGP. Morbidity of ABO haemolytic disease in the newborn. Paediatr Int Child
Health. 2012 May;32(2):93–6.
22. Laboratory assays for predicting the severity of haemolytic disease of the fetus and newborn.
- PubMed - NCBI [Internet]. [cited 2019 Jul 28]. Available from:
https://www.ncbi.nlm.nih.gov/pubmed/12216949
23. Toy PT, Reid ME, Papenfus L, Yeap HH, Black D. Prevalence of ABO maternal-infant
incompatibility in Asians, Blacks, Hispanics and Caucasians. Vox Sang. 1988;54(3):181–3.
24. Pancreatic Cancer Stages [Internet]. [cited 2019 May 5]. Available from:
https://www.cancer.org/cancer/pancreatic-cancer/detection-diagnosis-staging/staging.html
25. Geaghan SM. Diagnostic laboratory technologies for the fetus and neonate with
isoimmunization. Semin Perinatol. 2011 Jun;35(3):148–54.
26. Usha KK, Sulochana PV. Detection of high risk pregnancies with relation to ABO haemolytic
disease of newborn. Indian J Pediatr. 1998 Dec;65(6):863–5.
27. Fukuda M. Cell surface glycoconjugates as onco-differentiation markers in hematopoietic
cells. Biochim Biophys Acta. 1985;780(2):119–50.
28. Firan M, Bawdon R, Radu C, Ober RJ, Eaken D, Antohe F, et al. The MHC class I-related
receptor, FcRn, plays an essential role in the maternofetal transfer of gamma-globulin in humans. Int
Immunol. 2001 Aug;13(8):993–1002.

99
29. ABO-haemolytic disease of the newborn (ABO-HDN): factors influencing its severity and
incidence in Venezuela. - PubMed - NCBI [Internet]. [cited 2019 May 26]. Available from:
https://www.ncbi.nlm.nih.gov/pubmed/7723123
30. Kulkarni AG, Ibazebe R, Fleming AF. High frequency of anti-A and anti-B haemolysins in
certain ethnic groups of Nigeria. Vox Sang. 1985;48(1):39–41.
31. Goraya J, Basu S, Sodhi P, Mehta S. Unusually severe ABO hemolytic disease of newborn.
Indian J Pediatr. 2001 Mar;68(3):285–6.
32. Indication of Mild Hemolytic Reaction Among Preterm Infants With ABO Incompatibility. -
PubMed - NCBI [Internet]. [cited 2019 Jun 19]. Available from:
https://www.ncbi.nlm.nih.gov/pubmed/26841084
33. Schur PH. IgG subclasses. A historical perspective. Monogr Allergy. 1988;23:1–11.
34. Vidarsson G, Dekkers G, Rispens T. IgG subclasses and allotypes: from structure to effector
functions. Front Immunol. 2014;5:520.
35. Wu Q, Zhang Y, Liu M, Wang B, Liu S, He C. Correlation of Fc(gamma)RIIa (CD32)
Polymorphism and IgG Antibody Subclasses in Hemolytic Disease of Newborn. Neonatology.
2009;96(1):1–5.
36. Human IgG Subclasses in Maternal and Fetal Serum - Morell - 1971 - Vox Sanguinis - Wiley
Online Library [Internet]. [cited 2019 Sep 26]. Available from:
https://onlinelibrary.wiley.com/doi/pdf/10.1111/j.1423-0410.1971.tb04808.x
37. Leger RM. In vitro cellular assays and other approaches used to predict the clinical
significance of red cell alloantibodies: a review. Immunohematology. 2002;18(3):65–70.
38. Roux KH, Strelets L, Michaelsen TE. Flexibility of human IgG subclasses. J Immunol Baltim Md
1950. 1997 Oct 1;159(7):3372–82.
39. ihc staining methods guidebook 5th edition - Google Search [Internet]. [cited 2019 Jun 19].
Available from https://www.google.com/search?q=ihc+staining+methods+guidebook+
5th+edition&oq=IHC+staining+methods+guidebook+5th+ed&aqs=chrome.1.69i57j33.22806j0j4&sou
rceid=chrome&ie=UTF-8
40. Brouwers HA, Overbeeke MA, van Ertbruggen I, Schaasberg W, Alsbach GP, van der Heiden C,
et al. What is the best predictor of the severity of ABO-haemolytic disease of the newborn? Lancet
Lond Engl. 1988 Sep 17;2(8612):641–4.
41. Frankowska K, Górska B. IgG subclasses of anti-Rh antibodies in pregnant women. Arch
Immunol Ther Exp (Warsz). 1978;26(1–6):1095–100.

100
42. Pollock JM, Bowman JM. Anti-Rh(D) IgG subclasses and severity of Rh hemolytic disease of
the newborn. Vox Sang. 1990;59(3):176–9.
43. Choudhuri J, Chacko MP, Kuruvilla AK, Jose R, Mathews J, Regi A, et al. Clinical impact and
prevalence of IgG1 and IgG3 subclasses in antenatal alloimmunized women: experience from a
tertiary medical centre in South India. ISBT Sci Ser. 2016;11(1):58–61.
44. Correlation study between IgG subclasses and neonatal ABO hemolytic disease--
《Guangdong Medical Journal》2011年02期 [Internet]. [cited 2019 May 15]. Available from:
http://en.cnki.com.cn/Article_en/CJFDTOTAL-GAYX201102022.htm
45. Kaplan M, Na’amad M, Kenan A, Rudensky B, Hammerman C, Vreman HJ, et al. Failure to
predict hemolysis and hyperbilirubinemia by IgG subclass in blood group A or B infants born to group
O mothers. Pediatrics. 2009 Jan;123(1):e132-137.
46. Owa JA, Durosinmi MA, Alabi AO. Determinants of severity of neonatal hyperbilirubinaemia
in ABO incompatibility in Nigeria. Trop Doct. 1991 Jan;21(1):19–22.
47. Chen JY, Ling UP. Prediction of the development of neonatal hyperbilirubinemia in ABO
incompatibility. Zhonghua Yi Xue Za Zhi Chin Med J Free China Ed. 1994 Jan;53(1):13–8.
48. Bakkeheim E, Bergerud U, Schmidt-Melbye A-C, Akkök CA, Liestøl K, Fugelseth D, et al.
Maternal IgG anti-A and anti-B titres predict outcome in ABO-incompatibility in the neonate. Acta
Paediatr Oslo Nor 1992. 2009 Dec;98(12):1896–901.
49. Li P, Pang L-H, Liang H-F, Chen H-Y, Fan X-J. Maternal IgG Anti-A and Anti-B Titer Levels
Screening in Predicting ABO Hemolytic Disease of the Newborn: A Meta-Analysis. Fetal Pediatr
Pathol. 2015;34(6):341–50.
50. Kadri N. The role of maternal anti-A and anti-B antibody titers in predicting ABO hemolytic
disease of the newborn. Med J Indones. 1998 Apr 1;7(2):79–83.
51. Waldron P, de Alarcon P. ABO hemolytic disease of the newborn: a unique constellation of
findings in siblings and review of protective mechanisms in the fetal-maternal system. Am J Perinatol.
1999;16(8):391–8.
52. Ziprin JH, Payne E, Hamidi L, Roberts I, Regan F. ABO incompatibility due to immunoglobulin
G anti-B antibodies presenting with severe fetal anaemia. Transfus Med Oxf Engl. 2005 Feb;15(1):57–
60.
53. Kanto WP, Marino B, Godwin AS, Bunyapen C. ABO hemolytic disease: a comparative study
of clinical severity and delayed anemia. Pediatrics. 1978 Sep;62(3):365–9.
54. Peevy KJ, Wiseman HJ. ABO hemolytic disease of the newborn: evaluation of management
and identification of racial and antigenic factors. Pediatrics. 1978 Mar;61(3):475–8.
101
55. Brink S. A laboratory survey of A-B-O blood-group incompatibility and neonatal jaundice.
South Afr Med J Suid-Afr Tydskr Vir Geneeskd. 1969 Aug 23;43(34):1047–50.
56. Dufour DR, Monoghan WP. ABO hemolytic disease of the newborn. A retrospective analysis
of 254 cases. Am J Clin Pathol. 1980 Mar;73(3):369–73.
57. Pildes RS, Sisson TR, Kaplan E. Phototherapy in ABO incompatibility. J Pediatr. 1972
Jun;80(6):1063–4.
58. Haque KM, Rahman M. An unusual case of ABO-haemolytic disease of the newborn.
Bangladesh Med Res Counc Bull. 2000 Aug;26(2):61–4.
59. Lucas GN. Neonatal jaundice due to ABO incompatibility in Sri Lankan. Indian J Pediatr. 1996
Jun;63(3):381–4.
60. W W, D G, D H. Recent Advances in Paediatrics. London; 1971. 119–170 p.
61. The ability of the chemiluminescence test to predict clinical outcome and the necessity for
amniocenteses in pregnancies at risk of haemolytic dise... - PubMed - NCBI [Internet]. [cited 2019 Jun
11]. Available from: https://www.ncbi.nlm.nih.gov/pubmed/9501793
62. The role of carboxyhemoglobin measured with CO-oximetry in the detection of hemolysis in
newborns with ABO alloimmunization. - PubMed - NCBI [Internet]. [cited 2019 Jun 19]. Available
from: https://www.ncbi.nlm.nih.gov/pubmed/25604086
63. The Direct Antiglobulin Test: Indications, Interpretation, and Pitfalls | Archives of Pathology
& Laboratory Medicine [Internet]. [cited 2019 May 28]. Available from:
https://www.archivesofpathology.org/doi/full/10.5858/arpa.2015-0444-RS
64. Romans DG, Tilley CA, Dorrington KJ. Monogamous bivalency of IgG antibodies. I. Deficiency
of branched ABHI-active oligosaccharide chains on red cells of infants causes the weak antiglobulin
reactions in hemolytic disease of the newborn due to ABO incompatibility. J Immunol Baltim Md
1950. 1980 Jun;124(6):2807–11.
65. Lapierre Y, Rigal D, Adam J, Josef D, Meyer F, Greber S, et al. The gel test: a new way to
detect red cell antigen-antibody reactions. Transfusion (Paris). 1990 Feb;30(2):109–13.
66. Whyte J, Graham H. Prediction of the severity of ABO haemolytic disease of the newborn by
cord blood tests. Acta Paediatr Scand. 1981 Mar;70(2):217–22.
67. Dharmayani D, Gatot D, Rohsiswatmo R, Tridjaja B. Serological profile and hemolytic disease
in term neonates with ABO incompatibility. Paediatr Indones. 2009 Aug 31;49(4):219–23.
68. Does Prophylactic Phototherapy Prevent Hyperbilirubinemia in Neonates with ABO
Incompatibility and Positive Coombs’ Test? | Journal of Perinatology [Internet]. [cited 2019 May 28].
Available from: https://www.nature.com/articles/7211356

102
69. Judd WJ, Luban NL, Ness PM, Silberstein LE, Stroup M, Widmann FK. Prenatal and perinatal
immunohematology: recommendations for serologic management of the fetus, newborn infant, and
obstetric patient. Transfusion (Paris). 1990 Feb;30(2):175–83.
70. Full text of “AABB Technical Manual 18th Ed 2014” [Internet]. [cited 2019 Jun 11]. Available
from: https://archive.org/stream/AABBTechnicalManual18thEd2014
/AABB+Technical+Manual+18th+Ed+2014_djvu.txt
71. ADCC and other cellular bioassays for predicting the clinical significance of red cell
alloantibodies. - PubMed - NCBI [Internet]. [cited 2019 Jun 19]. Available from:
https://www.ncbi.nlm.nih.gov/pubmed/2224152
72. Kumpel BM, Hadley AG. Functional interactions of red cells sensitized by IgG1 and IgG3
human monoclonal anti-D with enzyme-modified human monocytes and FcR-bearing cell lines. Mol
Immunol. 1990 Mar 1;27(3):247–56.
73. Morley G, Gibson M, Eltringham D. Use of discriminant analysis in relating maternal anti-D
levels to the severity of haemolytic disease of the Newborn. Vox Sang. 1977;32(2):90–8.
74. Urbaniak S j., Greiss MA, Crawford R j., Fergusson M j. c. Prediction of the Outcome of Rhesus
Haemolytic Disease of the Newborn: Additional Information Using an ADCC Assay. Vox Sang. 1984
May 1;46(5):323–9.
75. Hadley AG, Kumpel BM, Leader KA, Poole GD, Fraser ID. Correlation of serological,
quantitative and cell-mediated functional assays of maternal alloantibodies with the severity of
haemolytic disease of the newborn. Br J Haematol. 1991 Feb;77(2):221–8.
76. Engelfriet CP, Overbeeke MA, Dooren MC, Ouwehand WH, von dem Borne AE. Bioassays to
determine the clinical significance of red cell alloantibodies based on Fc receptor-induced destruction
of red cells sensitized by IgG. Transfusion (Paris). 1994 Jul;34(7):617–26.
77. Nance SJ, Nelson JM, Horenstein J, Arndt PA, Platt LD, Garratty G. Monocyte monolayer
assay: an efficient noninvasive technique for predicting the severity of hemolytic disease of the
newborn. Am J Clin Pathol. 1989 Jul;92(1):89–92.
78. Murray NA, Roberts IAG. Haemolytic disease of the newborn. Arch Dis Child - Fetal Neonatal
Ed. 2007 Mar 1;92(2):F83–8.
79. Kattimani VS, B UC. Hemolytic disease of the new-born due to ABO incompatibility. Int J
Contemp Pediatr. 2018 Feb 22;5(2):605–11.
80. Hyperbilirubinemia S on. Management of Hyperbilirubinemia in the Newborn Infant 35 or
More Weeks of Gestation. Pediatrics. 2004 Jul 1;114(1):297–316.

103
81. van Imhoff DE, Dijk PH, Hulzebos CV, BARTrial study group, Netherlands Neonatal Research
Network. Uniform treatment thresholds for hyperbilirubinemia in preterm infants: background and
synopsis of a national guideline. Early Hum Dev. 2011 Aug;87(8):521–5.
82. Kaplan M, Merlob P, Regev R. Israel guidelines for the management of neonatal
hyperbilirubinemia and prevention of kernicterus. J Perinatol Off J Calif Perinat Assoc. 2008
Jun;28(6):389–97.
83. Rennie J, Burman-Roy S, Murphy MS, Guideline Development Group. Neonatal jaundice:
summary of NICE guidance. BMJ. 2010 May 19;340:c2409.
84. National guidelines for treatment of jaundice in the newborn. - PubMed - NCBI [Internet].
[cited 2019 May 25]. Available from: https://www.ncbi.nlm.nih.gov/pubmed/21114525
85. Guidelines for detection, management and prevention of hyperbilirubinemia in term and late
preterm nGuidelines for detection, management and prevention of hyperbilirubinemia in term and
late preterm newborn infants | Canadian Paediatric Society [Internet]. [cited 2019 May 25]. Available
from: https://www.cps.ca/en/documents/position/hyperbilirubinemia-newborn
86. Horn AR, Kirsten GF, Kroon SM, Henning PA, Möller G, Pieper C, et al. Phototherapy and
exchange transfusion for neonatal hyperbilirubinaemia: neonatal academic hospitals’ consensus
guidelines for South African hospitals and primary care facilities. South Afr Med J Suid-Afr Tydskr Vir
Geneeskd. 2006 Sep;96(9):819–24.
87. Maisels MJ, Watchko JF, Bhutani VK, Stevenson DK. An approach to the management of
hyperbilirubinemia in the preterm infant less than 35 weeks of gestation. J Perinatol Off J Calif
Perinat Assoc. 2012 Sep;32(9):660–4.
88. Woodgate P, Jardine LA. Neonatal jaundice: phototherapy. BMJ Clin Evid [Internet]. 2015
May 22 [cited 2019 May 25];2015. Available from:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4440981/
89. Management of Hyperbilirubinemia in the Newborn Infant 35 or More Weeks of Gestation |
AMERICAN ACADEMY OF PEDIATRICS | Pediatrics [Internet]. [cited 2019 Jun 19]. Available from:
https://pediatrics.aappublications.org/content/114/1/297
90. Cockington RA. A guide to the use of phototherapy in the management of neonatal
hyperbilirubinemia. J Pediatr. 1979 Aug;95(2):281–5.
91. Bhutani VK, Johnson L, Sivieri EM. Predictive ability of a predischarge hour-specific serum
bilirubin for subsequent significant hyperbilirubinemia in healthy term and near-term newborns.
Pediatrics. 1999 Jan;103(1):6–14.

104
92. Efficacy of phototherapy in prevention and management of neonatal hyperbilirubinemia. -
PubMed - NCBI [Internet]. [cited 2019 May 28]. Available from:
https://www.ncbi.nlm.nih.gov/pubmed/3881731
93. Phototherapy for Hyperbilirubinemia of Hemolytic Disease of the Newborn | Articles |
Pediatrics [Internet]. [cited 2019 May 28]. Available from:
https://pediatrics.aappublications.org/content/75/2/407
94. Birchenall KA, Illanes SE, Lopez F, Overton T, Liebling R, Soothill PW, et al. Neonatal outcomes
of pregnancies affected by haemolytic disease of the foetus and newborn and managed with
intrauterine transfusion: a service evaluation. Blood Transfus. 2013 Oct;11(4):548.
95. Lopriore E, Rath MEA, Liley H, Smits-Wintjens VEHJ. Improving the management and
outcome in haemolytic disease of the foetus and newborn. Blood Transfus. 2013 Oct;11(4):484–6.
96. Gottstein R, Cooke R. Systematic review of intravenous immunoglobulin in haemolytic
disease of the newborn. Arch Dis Child Fetal Neonatal Ed. 2003 Jan;88(1):F6–10.
97. Tanyer G, Siklar Z, Dallar Y, Yildirmak Y, Tiraş U. Multiple dose IVIG treatment in neonatal
immune hemolytic jaundice. J Trop Pediatr. 2001;47(1):50–3.
98. Correlation between in vivo hemolysis and the amount of red cell-bound IgG measured by
flow cytometry. - PubMed - NCBI [Internet]. [cited 2019 Jun 11]. Available from:
https://www.ncbi.nlm.nih.gov/pubmed/2402775
99. Lynen R, Krone O, Legler TJ, Köhler M, Mayr WR. A newly developed gel centrifugation test
for quantification of RBC-bound IgG antibodies and their subclasses IgG1 and IgG3: comparison with
flow cytometry. Transfusion (Paris). 2002 May;42(5):612–8.
100. Alié-Daram SJ, Fournié A, Dugoujon JM. Gel test assay for IgG subclass detection by GM
typing: application to hemolytic disease of the newborn. J Clin Lab Anal. 2000;14(1):1–4.
101. Akanmu. Estimating the risk of ABO Hemolytic Disease of the Newborn in Lagos. (A).
102. Christensen RD, Baer VL, MacQueen BC, O’Brien EA, Ilstrup SJ. ABO hemolytic disease of the
fetus and newborn: thirteen years of data after implementing a universal bilirubin screening and
management program. J Perinatol Off J Calif Perinat Assoc. 2018 May;38(5):517–25.
103. Assistant Professor, Government Medical College Trivandrum, Nair DS. ABO Incompatibility
and Neonatal Outcome with Reference to Hemolytic Disease of Newborn. J Med Sci Clin Res. 2017
Jan 26;05(01):16065–8.
104. Cernadas JMC, Fustiñana C, Bujas M. 23 EPIDEMIOLOGY OF THE ABO BLOOD
INCOMPATIBILITY [Internet]. Nature Publishing Group; 1981 Feb [cited 2019 Jun 9] p. 179. Available
from: https://www.nature.com/articles/pr1981169

105
105. An early (sixth-hour) serum bilirubin measurement is useful in predicting the development of
significant hyperbilirubinemia and severe ABO hemolyti... - PubMed - NCBI [Internet]. [cited 2019 Sep
7]. Available from: https://www.ncbi.nlm.nih.gov/pubmed/11927726
106. Chen M, Zeng Y, Chen X. Effects of maternal serum IgG anti-A (B) and neonatal direct anti
globulin red blood cell antibody expression on the occurrence and development of neonatal ABO
haemolysis. Biomed Res [Internet]. 2017 [cited 2019 Sep 15];28(4). Available from:
http://www.alliedacademies.org/abstract/effects-of-maternal-serum-igg-antia-b-and-neonatal-
direct-anti-globulin-red-blood-cell-antibody-expression-on-the-occurrence-and-d-6627.html
107. Heydarian F, Khatami SF, Parvaresh P, Rezanejad M. ABO Hemolytic Disease Leading to
Hyperbilirubinemia in Term Newborns: Value of Immunohematological Tests. :5.
108. prediction-of-the-development-of-neonatal-hyperbilirubinemia-by-increased-umbilical-cord-
blood-bilirubin.pdf [Internet]. [cited 2019 Sep 15]. Available from:
http://www.alliedacademies.org/articles/prediction-of-the-development-of-neonatal-
hyperbilirubinemia-by-increased-umbilical-cord-blood-bilirubin.pdf
109. Kalakheti BK, Singh R, Bhatta NK, Karki A, Baral N. Risk of neonatal hyperbilirubinemia in
babies born to “O” positive mothers: a prospective cohort study. Kathmandu Univ Med J KUMJ. 2009
Mar;7(25):11–5.
110. Akgül S, Korkmaz A, Yiğit S, Yurdakök M. Neonatal hyperbilirubinemia due to ABO
incompatibility: does blood group matter? Turk J Pediatr. 2013 Oct;55(5):506–9.
111. Kumar et al. - 2013 - Hemolytic Disease of the Newborn A study of 50 ca.pdf [Internet]. [cited
2019 Sep 15]. Available from: https://www.ijss-
sn.com/uploads/2/0/1/5/20153321/original_article_13.pdf
112. Mamtani M, Patel A, Renge R, Kulkarni H. Prognostic value of direct bilirubin in neonatal
hyperbilirubinemia. Indian J Pediatr. 2007 Sep;74(9):819–22.
113. Maisels MJ, Kring E. Length of stay, jaundice, and hospital readmission. Pediatrics. 1998
Jun;101(6):995–8.
114. Greenburg AG. Pathophysiology of anemia. Am J Med. 1996 Aug 26;101(2A):7S-11S.
115. Taylor E, Vu D, Legare C, Keene D. Intravenous immune globulin-related hemolysis:
comparing two different methods for case assessment. Transfusion (Paris). 2015 Jul;55 Suppl 2:S23-
27.
106
ANNEXURES

107
STANDARD OPERATING PROCEDURE:
A. IgG1 and IgG3 subtyping:
The risk of hemolysis in HDN depends upon the amount of IgG coated on the red cells
as well as the class of IgG involved. To induce phagocytosis, it is suggested that
approximately 1000-4000 IgG1 molecules or 135-500 IgG3 molecules must coat the
red cells. Therefore, it is important to identify the presence of these subclasses.
Principle: The ID-card “DAT IgG1/IgG3” has two dilutions (1:1 and 1:100) of both
the subclasses and works on the principle of CAT.
Materials: ID card with 6 columns as in fig (having four micro tubes for IgG1 and
IgG3 in two dilutions each, a negative control well, a positive control well), ID-Dia
cell (0.8%) suspension, pipettes, tips, incubator and centrifuge.
Procedure:
1. Previously stored serum or plasma at -70 degree C is thawed to room
temperature and centrifuged at 1500 g for 10 minutes to avoid fibrin residues
which can interfere with reaction pattern
2. Label the ID card with appropriate patient hospital number.
3. Remove the aluminium foil, holding the card in upright position.
4. Pipette 50 μl of ID-Dia cell into each microtube.
5. Add 25 μl of patient’s plasma to each microtube
6. Incubate the card for 15 minutes at 37 degrees C in the incubator.

108
7. Centrifuge the card at 910 rpm for ten minutes.
8. Interpret and record the agglutination reaction
If the positive or negative controls failed, the test was considered un-interpretable.
Interpretation:
A. Positive: Agglutinated cells form a red line on the surface of the gel (strong
reaction) or the agglutinates tend to disperse in gel in a weaker reaction.
B. Negative: Compact button of cells at the bottom of microtube.
A positive reaction with 1:1 dilution has a sensitivity of approximately 1000 Ig1
molecules and 125 anti- Ig3 molecules respectively. A positive reaction in
1:100 dilution is indicative of a higher strength of antibodies in the plasma.
Figure: The DAT IgG1/IgG3 card
DAT IgG1/IgG3 card consists of six micro tubes as depicted in the figure.
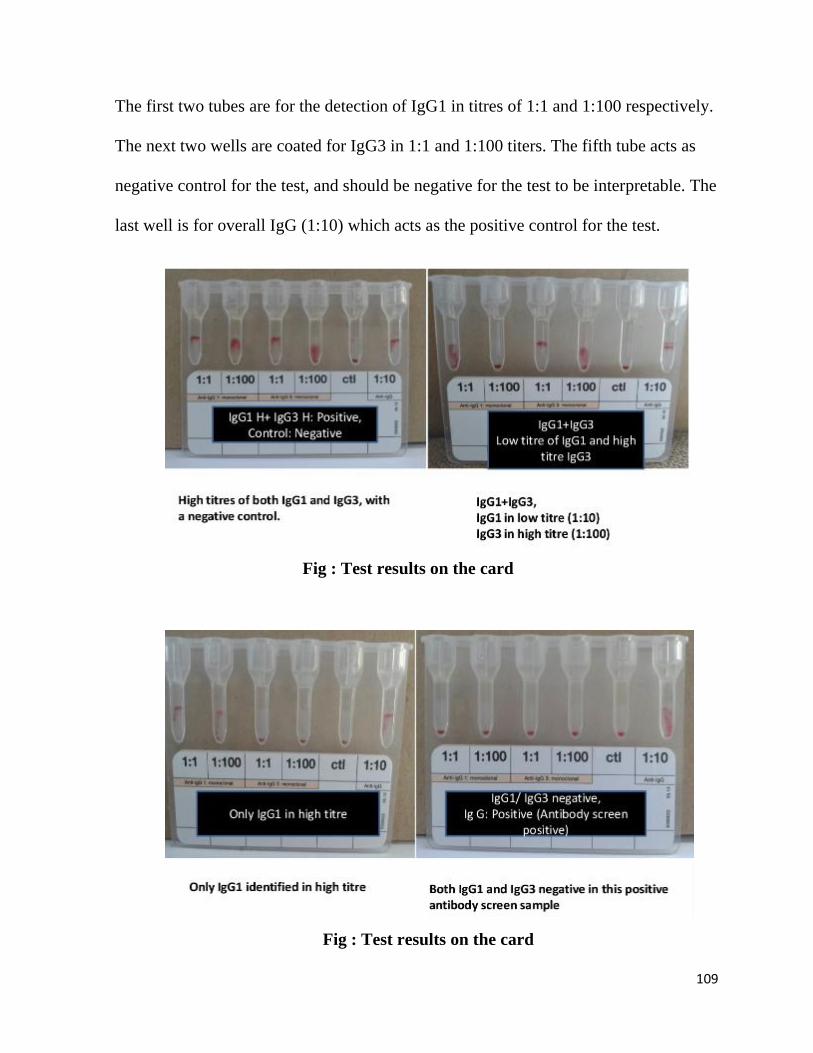
109
The first two tubes are for the detection of IgG1 in titres of 1:1 and 1:100 respectively.
The next two wells are coated for IgG3 in 1:1 and 1:100 titers. The fifth tube acts as
negative control for the test, and should be negative for the test to be interpretable. The
last well is for overall IgG (1:10) which acts as the positive control for the test.
Fig : Test results on the card
Fig : Test results on the card

110
Table 2: Result interpretation on the DAT IgG1/IgG3 card
IgG1
IgG3 Control IgG
1:1 1:100 1:1 1:100 1:10
Reaction 2+ - - - - 3+
Interpretation Moderate risk of hemolysis (Subclass IgG1; low concentration)
Reaction 3+ 2+ - - - 3+
Interpretation High risk of hemolysis ( Subclass IgG1; high concentration)
Reaction 3+ 2+ 2+ - - 3+
Interpretation High risk of hemolysis ( IgG1 high concentration; low concentration
IgG3)
Reaction - - 3+ 2+ - 3+
Interpretation High risk of hemolysis (Subclass IgG3; high concentration)
Reaction - - 2+ - - 3+
Interpretation Moderate risk of hemolysis (Subclass IgG3; low concentration)
Reaction 2+ - 3+ 2+ - 3+
Interpretation High risk of hemolysis (IgG1, low concentration, IgG3 in high
concentration)
Reaction 2+ 2+ - - - 3+
Interpretation Moderate risk of hemolysis (Subclasses IgG1 and IgG3, low
concentration)
Reaction 3+ 2+ 3+ 3+ 2+ - 3+
Interpretation High risk of hemolysis (Subclasses IgG1 and IgG3, high
concentration)

111
Note: The first two micro tubes contain Anti-IgG1 (cell line M345/795) in two
dilutions and third and fourth micro tubes contains Anti-IgG3 (cell line M346/805) in
two dilutions
respectively.
Reference: DAT IgG1/IgG3 ID-card, (Diamed GmbH 1785 Cressier FR Switzerland)
BIO-RAD manual
STANDARD OPERATING PROCEDURE FOR ALL OTHER TESTS:
A. ANTIBODY SCREENING:
Antibody screening is routinely done in blood bank for all donor and patient’s samples
to detect irregular antibodies. It is based on the indirect antiglobulin test. This test uses
patient’s plasma/ serum against red cells to detect unexpected antibodies.
Screen cells used for this test are commercially prepared 2-5% suspension of group O
cells obtained from individual donors and phenotyped for the most commonly
encountered and clinically important red blood cell antigens, which is in contrast to
IAT which utilizes inhouse preparation of O pooled cells from three phenotyped
donors. Screen cells require the expression of the antigens as per the BCSH guidelines
for antibody screening in antenatal women: D,C,E, c,e,M,N,S,s,Lea ,K,k,Jka, JKb,
Fya, Fy b. Group O red cells are preferred since it does not contain A and B antigens
on the red cell membrane, minimizing the chances of reacting anti-A and anti-B
antibodies, and making it insensitive to the “regular or expected antibodies”
Material required:
112
1. Coombs cassette
2. Biorad system centrifuge
3. Micropipette and tips
4. Low ionic strength solution(LISS)
5. Dia Cel –I-II-III Asia cells(Three panel reagent cells)
6. Incubator
Procedure:
Antibody screening is done using commercial 3 cell panel DiaCel –I-II-III Asia.
Antibody screening is done using a Coombs cassette
1. Label the coombs cassette with patient/donor ID
2. Label three columns D1, D2 and D3
3. Pipette 50 μl of reagent cells into columns labelled as D1, D2 and D3.
4. Pipette 25 μl of patient’s plasma into the 3 wells.
5. Incubate for 15 minutes at 37 degrees.
6. Centrifuge the card in Diamed card centrifuge for 10 minutes at 910 rpm.
7. Read the cassette from both sides.
8. Read and record the results.
Interpretation of column agglutination testing:
Negative - All cells settle at the bottom

113
1+ reaction -A button of cells at the bottom with most aggregates remaining at the
lower half of the beaded column.
2+ reaction- A small button of cells may also be visible at the bottom while
aggregates are observed throughout the length of the beaded column.
3+ reaction -Most aggregates remain in the upper half of beaded column.
+/- reaction – Indeterminate
Weak reaction-Granular suspension
MF reaction-Mixed field agglutination/double population
Reporting of results:
Antibody screen-positive or negative–mentioning which screen cells are positive and
strength of positivity. Entry of results to be made on the patient card filed in blood
bank.
Quality control:
To check the proficiency of screen cells and the coombs card, antibody screening is
done with diluted anti –D IgG (1 in 10 dilution) as positive control and LISS as
negative control.
COOMBS TEST (DIRECT ANTIGLOBULIN TEST)
Aim: To detect the presence of incomplete antibodies and complement binding
antibodies in serum /plasma or those coated on patients red cells.

114
Principle: Washed red cells which are coated with immune antibodies (commonly
IgG) and complement components (generally C3) will show agglutination with broad
spectrum AHG reagent. The coating (sensitization) of red cells can occur in vivo or in
vitro following incubation at 37 deg C with serum containing antibody.
Methodology:
Coombs test can be done by the following techniques:
A) Tube technique
B) CAT
Sample: Properly labeled 4 ml EDTA samples/ 6 ml clotted serum samples are
required. Hemolysed samples are not acceptable.
Materials required for Tube method for DAT:
Test tube 10x75 mm
Test tube rack
Marker
Centrifuge
Pasteur pipette
Slide
Normal saline
Microscope
Water bath at 37 degree C

115
Reagents for DAT:
1. Coombs serum
2. Negative control for DAT- 3-5% suspension of saline washed pooled O group cells.
3. Positive control for DAT- Sensitized O pooled cells – (made by adding 0.5 ml of
IAT positive control to 1 ml of washed and packed O pooled cells and incubating at 37
degree for half an hour )
Procedure for DAT:
Tube technique:
1. Take 3 tubes and label as patient ID, positive control and negative control.
2. Add one drop of patient cells, positive control, negative control to the respective
tubes.
3. Wash 3 times with normal saline.
4. After a final wash, decant the supernatant completely.
5. Add one drop of coombs serum to all the 3 tubes, mix and centrifuge at 3000 rpm
for 15 seconds.
6. The dissolve the button gently and read both macroscopically and microscopically
and grade the reactions.

116
GRADING OF THE REACTIONS FOR ALL TESTS DONE BY TUBE
TECHNIQUE: (Reference AABB Manual)
No agglutination Negative
Small aggregation 1+ Positive
Medium size aggregation 2+ Positive
Several large aggregates 3+ Positive
One solid aggregate 4+ Positive
The presence of haemolysis in the supernatant also indicates a positive reaction.
Column Agglutination Technique:
Material required: Coombs card
ID centrifuge
Normal saline
Micropipette and tips
Biovue system work rack/ID holder
LISS
Heat block(Incubator)/ID card Incubator

117
Procedure for DAT using Bio-Rad card
1. Ensure that the cassette is at room temperature before use.
2. Label the cassette appropriately with patient ID and control ID.
3. Add 50μl of 0.8% suspension of patient, positive and negative control cells
respectively to all the 3 wells.
4. Centrifuge the card in ID card centrifuge for 10 minutes at 910 rpm.
5. Read and record the reactions (read the card from both sides)
Grading of results by CAT as mentioned previously.
Precautions:
1. Adequate washing of sensitized cells is the critical part of the test. A trace
amount of residual globulin, due to improper washing causes neutralization of
the AHG serum
2. A false negative reaction can occur if testing is interrupted or delayed. Washing
of sensitized cells, addition of AHG serum and centrifugation must be quick
and uninterrupted to avoid elution of antibodies attached to red cells and
neutralization of AHG serum.
3. Inappropriate serum to cell ratio.
4. Failure to add AHG reagent may give false negative results.
5. Under centrifugation may not provide optimal conditions for agglutination.
6. Failure to check the negative reaction microscopically.

118
7. Over centrifugation packs red cells tightly that they cannot be dispersed
completely.
8. Red cells may be agglutinated before washing and this may persist through the
washing phase i.e. adsorption of complement during storage. In such cases, a
positive antiglobulin test may be incorrectly interpreted as a result of the IgG or
complement coating.
Documentation and Result entry: All reactions to be entered in the grouping
worksheet. All results to be entered with strength of reactivity on patient grouping
card.
ANTIBODY TITRATION (Coombs with DTT):
Principle: Titration is a semi quantitative technique of measuring the concentration of
an antibody in a serum. The titer of an antibody is usually determined by testing the
serial two fold dilution of the serum against selected red cells. Dithiothreitol (DTT) is
used to abolish IgM antibody activity to permit detection of coexisting IgG antibodies.
Specimen required: Properly labeled 4 ml EDTA sample/ 6ml clotted serum sample
is required. Haemolysed samples are not accepted.
Materials:
1. 100 μl automatic pipette and pipette tips
2. Test red blood cells 3-5%
3. Sterile 12x75 ml test tubes

119
4. Sterile saline 0.9%
5. Serofuge
6. Glass slides
7. Water bath
8. Microscope
Reagents Required:
0.01M Dithiothreitol (DTT)
Phosphate buffered saline (PBS) at pH 7.3
Procedure:
DTT treated plasma/serum is used for coombs antibody titration
To prepare DTT treated serum:
1. Dispense 200μl of serum or plasma into each of two test tubes
2. To one tube (labeled dilution control), add 200μl of PBS
3. To the other tube (labeled test), add 200μl of 0.01M DTT
4. Mix and incubate at 37degC for 30 to 60 minutes
5. One set label as Serum+DTT and another set as Serum+PBS
Coombs (AHG) Titre:
1. Label the tubes according to the serial dilution using 1:2 through 1:1024
2. Deliver one volume of saline(100 μl) of saline into all tubes
120
3. Add one volume (100 μl) of the DTT treated serum/plasma to tube 1:2
4. Mix the contents of the tube several times and transfer one volume (100 μl) of
the mixture from 1:2 to 1:4 and continue through the remaining tubes.
5. Discard 100 μl from the tenth tube i.e. 1:1024
6. Add on volume of (100 μl) of 3-5% saline cell suspension of appropriate red
cells to each tube.
7. Mix well and incubate the serum mixture at 37 deg C for one hour.
8. After one hour, wash three times with normal saline.
9. After the third wash, decant the supernatant and add AHG serum
10. Spin at 3000rpm for 15 seconds
11. Gently dislodge the button. Examine the test result macroscopically and grade
the reaction
12. If there is agglutination in the tube containing the most diluted serum, an end
point has not been reached. Prepare and test additional dilutions.
Grading of the Reaction: As for all test done by tube technique.
Interpretation:
1. The titre is the reciprocal of the highest serum dilution at which macroscopic
agglutination is observed.
2. Reactivity in the dilution control serum and no reactivity in the DTT treated
indicate an IgM antibody.
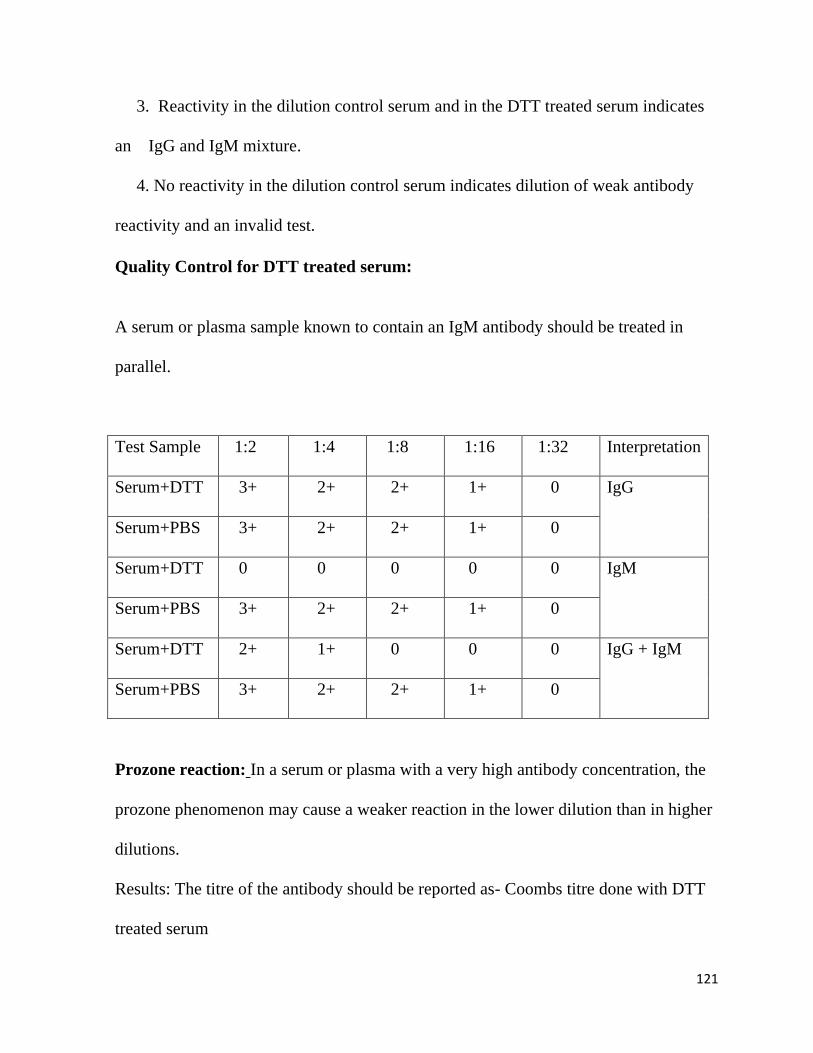
121
3. Reactivity in the dilution control serum and in the DTT treated serum indicates
an IgG and IgM mixture.
4. No reactivity in the dilution control serum indicates dilution of weak antibody
reactivity and an invalid test.
Quality Control for DTT treated serum:
A serum or plasma sample known to contain an IgM antibody should be treated in
parallel.
Test Sample 1:2 1:4 1:8 1:16 1:32 Interpretation
Serum+DTT 3+ 2+ 2+ 1+ 0 IgG
Serum+PBS 3+ 2+ 2+ 1+ 0
Serum+DTT 0 0 0 0 0 IgM
Serum+PBS 3+ 2+ 2+ 1+ 0
Serum+DTT 2+ 1+ 0 0 0 IgG + IgM
Serum+PBS 3+ 2+ 2+ 1+ 0
Prozone reaction: In a serum or plasma with a very high antibody concentration, the
prozone phenomenon may cause a weaker reaction in the lower dilution than in higher
dilutions.
Results: The titre of the antibody should be reported as- Coombs titre done with DTT
treated serum

122
BLOOD GROUPING BY COLUMN AGGLUTINATION TECHNIQUE:
Using the ABD card:
1. Label the ABD card with patient/ donor ID.
2. Insert the liner
3. Pipette 10 μl of 3% cell suspension of patient/ donor cells to the wells labelled
Anti-A, Anti-B and Anti-D (3% saline suspension)
4. Centrifuge the card in Bio-Vue centrifuge for 5 minutes which will spin at 800
rpm for the first 2 minutes followed by 1500 rpm for the next 3 minutes
(biphasic centrifugation)
5. Read and record the reactions
Using the ABD reverse card:
1. Label the ABD reverse column agglutination card with patient/ donor ID.
2. Insert the liner
3. Pipette 10 μl of 3% cell suspension of patient/ donor cells to the wells labelled
Anti-A, Anti-B and Anti-D (3% saline suspension)
4. To the wells labelled as O,A and B cells add 40 μl of patient/ donor serum
5. Pipette 10 μl of reverse typing A,B and O cells into the respective columns
6. Centrifuge the card in Bio-Vue centrifuge for 5 minutes which has a
programme 800 rpm for the first 2 minutes followed by 1500 rpm for the next 3
minutes (biphasic centrifugation)
7. Read and record the reactions
Blood grouping by Column Agglutination Technique

123
Using the ABD card: Two types of ABD cards are used-Donor grouping is done
using DVI+ cards and patient grouping is done using DVI- cards
1. Label the ABD card with patient ID/ donor ID
2. Pipette 12.5 μl of 5% cell suspension of patient/ donor cells to the wells labelled
Anti-A, Anti-B and Anti-D (5% cell suspension)
3. Centrifuge the card in Diamed centrifuge for 10 minutes at 910 rpm
4. Read and record the reactions
Interpretation:
Group FRONT TYPING BACK TYPING
Anti-A Anti-B Anti AB A cell B cell O cell
A + - + - + -
B - + + + - -
AB + + + - - -
O - - - + + -
Bombay - - - + + +
Quality control:
1. Before starting the technical procedure everyday, every shift, known AB
positive and O negative group samples have to be processed to check the
working proficiency of both reverse typing cells and the card
2. If QC fails, a new batch of cards need to be obtained and the tests repeated

124
3. If it clears, then the failed batch of cards to be discarded, reported to the
supplier
4. Every new group is performed by 2 different technologists on 2 different
platforms

125
Proforma
To study the prevalence of ABO incompatibility in O blood group mothers and assessment of IgG
subclasses (IgG1 and IgG3) in them and its correlation with occurrence and severity of ABO
Hemolytic disease of the newborn (ABO HDN) in a tertiary health care centre in south India.
Name of mother Study number
Hospital number Telephone number
Age/ DOB Address
Husband’s name
Mother’s information
Blood group and Rh typing
IgG anti A and anti B titer
Period of gestation
IgG subclass:
IgG1 1:1 1:100 IgG3 1:1 1:100
Obstetric formula
Antibody screen
Newborn’s information
Hospital number Hemoglobin Live/still born/IUD Total Bilirubin Pre/Term/Post Direct Bilirubin Normal/Instrumental/LSCS Retic count Gender Peripheral smear Birth weight Treatment required Yes/ No
Blood grouping and Rh typing
Single phototherapy
DCT Double phototherapy Exchange transfusion

126
Informed Consent form to participate in a research study
Study Title:
To study the prevalence of ABO incompatibility in O blood group mothers and assessment of
IgG subclasses (IgG1 and IgG3) in them and its correlation with occurrence and severity of
ABO Hemolytic disease of Newborn (ABO HDN) in a tertiary health care centre in south
India.
Study Number: ____________
Subject’s Initials: __________________
Subject’s Name: _________________________________________
Date of Birth / Age: ___________________________
(Subject)
(i) I confirm that I have read and understood the information sheet dated
____________ for the above study and have had the opportunity to ask
questions. [ ]
(ii) I understand that my participation in the study is voluntary and that I am free to
withdraw at any time, without giving any reason, without my medical care or
legal rights being affected. [ ]
(iii) I understand that the Sponsor of the clinical trial, others working on the
Sponsor’s behalf, the Ethics Committee and the regulatory authorities will not
need my permission to look at my health records both in respect of the current

127
study and any further research that may be conducted in relation to it, even if I
withdraw from the trial. I agree to this access. However, I understand that my
identity will not be revealed in any information released to third parties or
published. [ ]
(iv) I agree not to restrict the use of any data or results that arise from this study
provided such a use is only for scientific purpose(s). [ ]
(v) I agree to take part in the above study. [ ]
Signature (or Thumb impression) of the Subject/Legally Acceptable
Date: _____/_____/______
Signatory’s Name: _________________________________ Signature:
Or
Representative: _________________
Date: _____/_____/______
Signatory’s Name: _________________________________
Signature of the Investigator: ________________________
Date: _____/_____/______

128
Study Investigator’s Name: _________________________
Signature (or) thumb impression of the Witness: ___________________________
Date: _____/_____/_______
Name and Address of the Witness: ______________________________
129
Information sheet
What is this study about? ABO Hemolytic Disease Of Newborn (ABO HDN) is the
most common materno-fetal blood group incompatibility. It is seen in group A, B or
AB babies born to O blood group mothers. It is caused by maternal immunoglobulin
IgG, mostly by IgG1 and IgG3 as they can cross the. Through this study, we aim to
assess the prevalence of ABO incompatible pregnancies in O blood group mothers and
correlation of IgG1 and IgG3with occurrence and severity of ABO Hemolytic Disease
Of Newborn.
What do you need to do if you decide to participate? You will be asked to fill the
informed consent sheet. 8 ml venous sample will be collected from you for the study
purpose and frozen. We will proceed as per our set protocol and will not incur any
extra expense from you.
What are the drawbacks of participation? There are no major drawbacks other than
having to undergo extra blood collection. If you have other blood tests that need to be
done, blood for these can be drawn at the same time. You will also have to spend a few
minutes of your time to fill out the questionnaire.
What are the benefits of participation? There are no direct benefits in the study.
Do you need to pay for participation in the study? No.
Can you refuse to participate in the study? Yes. Participation in the study is entirely
a matter of your choice. The tests ordered by your doctor will be done even if you do
not want to participate in the study. This choice will not affect how you are are looked
after in our hospital.

130

131
132
133
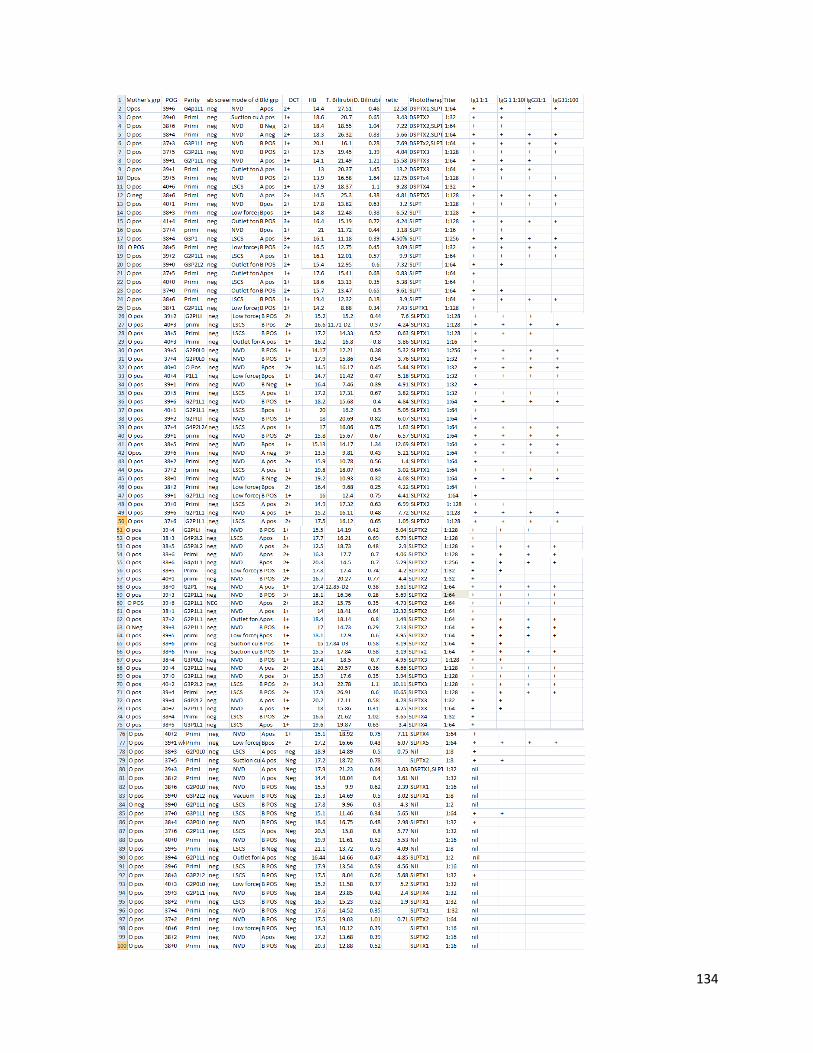
134

135
Copyright © 2022 FDOKUMEN




















