SEROUS LINED EXTRAMURAL ILEAL VALVE: A NEW CONTINENT URINARY OUTLET
Upload
independentCategory
view
3download
0
Molecular Evidence for theIndependent Origin ofExtra-ovarian PapillarySerous Tumors of LowMalignant Potential
Jian Gu, Lawrence M. Roth, CherylYounger, Helen Michael, Fadi W.Abdul-Karim, Shaobo Zhang,Thomas M. Ulbright, John N. Eble,Liang Cheng
Background: Molecular data suggestthat peritoneal tumors in women withadvanced-stage ovarian papillary se-rous adenocarcinoma are monoclonalin origin. Whether the same is true forovarian tumors of low malignant po-tential is not known. We comparedperitoneal and ovarian tumors fromwomen with advanced-stage ovarianpapillary serous tumors of low malig-nant potential to determine whetherthe peritoneal tumors arose from thesame clone as the ovarian tumors.Methods: We studied the clonality of73 peritoneal and ovarian tumors from18 women with advanced-stage ovarianpapillary serous tumors of low malig-nant potential. Formalin-fixed, paraf-fin-embedded tumors and representa-tive normal tissues were sectioned andstained with hematoxylin–eosin, repre-sentative sections from separate tumorswere manually microdissected, geno-mic DNA was extracted from the mi-crodissected tumors, and the polymer-ase chain reaction was used to amplifya CAG polymorphic site in the humanandrogen receptor locus on the X chro-mosome to determine the inactivationpattern of the X chromosome and theclonality of the tumors. Results: Thepattern of X-chromosome inactivationcould be determined from the tumorsof 13 of 18 patients. Of the 13 patients,seven (54%) had nonrandom inactiva-tion of the X chromosome, and six ofthe seven had different inactivationpatterns in the peritoneal and ovariantumors. Three of these patients alsohad different patterns of nonrandomX-chromosome inactivation in tumorsfrom each ovary. The remaining sixpatients had random patterns of X-chromosome inactivation in the perito-neal and ovarian tumors. Conclusions:
Our data suggest that peritoneal andovarian tumors of low malignant po-tential arise independently. [J NatlCancer Inst 2001;93:1147–52]
Epithelial ovarian tumors of low ma-lignant potential, also known as border-line tumors, account for approximately15% of all epithelial ovarian cancers.These tumors, characterized by a prolif-eration of epithelial cells forming papil-lary projections or tufts, lack stromal in-vasion. Patients with ovarian tumors oflow malignant potential may have perito-neal tumors that are morphologicallyidentical to the primary ovarian tumors.However, studies (1–4) have suggestedthat the presence of these peritoneal tu-mors does not imply a poor patient prog-nosis unless the tumors have an invasivegrowth pattern. Indeed, the 5-year sur-vival rate for patients with ovarian tumorsof low malignant potential is greater than90%, compared with approximately 30%for patients with invasive ovarian cancers.
Although ovarian tumors of low ma-lignant potential and the associated peri-toneal tumors are often similar histologi-cally, it is unknown whether the ovarianand peritoneal tumors are of common ori-gin (i.e., arise from the same neoplasticclone). Several studies (5–7) have ad-dressed the clonality of advanced-stageovarian carcinomas and found these tu-mors to be monoclonal at ovarian and ex-tra-ovarian sites. By contrast, papillaryserous carcinomas of the peritoneum havebeen shown to be multifocal in origin (8).Understanding the clonal origin of perito-neal tumors in patients with ovarian tu-mors of low malignant potential may haveimportant biologic and clinical implica-tions for tumor prevention, tumor classi-fication, and treatment.
The clonality of a tumor can be deter-mined by X-chromosome-linked and non-X-chromosome-linked analysis, such asloss of heterozygosity (LOH), gene rear-rangements, and point mutations. Themost consistent informative marker of theclonal composition of neoplastic andpreneoplastic disorders in women is thecellular pattern of X-chromosome inacti-vation. In women, normal somatic cellscontain two X chromosomes, one ofwhich is inactivated during early embryo-genesis. X-chromosome inactivation oc-curs randomly and results in somatic mo-saicism in normal tissues, with an equalmix of cells inactivating the X chromo-some of either maternal or paternal origin.
Throughout the life of the cell, the samematernal or paternal X chromosome willbe inactivated in any subsequent cell di-vision. Because the fidelity of the X-chromosome inactivation is retained, ifthe ovarian and peritoneal tumors arisefrom the same neoplastic clone, theyshould have identical inactive X chromo-somes. Identical patterns of nonrandomX-chromosome inactivation would, there-fore, suggest that the ovarian and perito-neal tumors are monoclonal in origin, im-plying that the peritoneal tumorsmetastasized from the primary ovarian tu-mor. Different patterns of nonrandom X-chromosome inactivation would suggestthat the tumors are independent in origin.
Although there are several methods forassessing X-chromosome inactivation,such as X-linked DNA polymorphism ofhypoxanthine phosphoribosyl transferase(HPRT) or phosphoglycerate kinase, etc.,we took advantage of the polymorphicCAG repeats near the methylation-sensitive sites of the HhaI restriction en-donuclease in exon 1 of the androgen re-ceptor (AR) gene, located in chromosomeXq11–12 (9,10). The frequency of geneticpolymorphism for the human AR gene ismore than 90%, compared with 29% forthat of the HPRT gene. The methylationstatus of the HhaI restriction endonucle-ase site corresponds with the inactivationstatus of the X chromosome and thus al-lows for the distinction between the activeand inactive X chromosomes. In this re-port, we assessed whether ovarian andperitoneal tumors of low malignant poten-tial were of common origin.
PATIENTS AND METHODS
PatientsEighteen women, ranging in age from 18 to 86
years, were diagnosed with advanced-stage ovarianpapillary serous tumors of low malignant potentialand underwent staging laparotomies and resection ofthe ovaries and extra-ovarian tumor sites at IndianaUniversity Hospitals and University Hospitals of
Affiliations of authors: J. Gu, L. M. Roth,C. Younger, H. Michael, S. Zhang, T. M. Ulbright,J. N. Eble, L. Cheng, Department of Pathology andLaboratory Medicine, Indiana University School ofMedicine, Indianapolis; F. W. Abdul-Karim, CaseWestern Reserve University School of Medicine,Cleveland, OH.
Correspondence to: Liang Cheng, M.D., Depart-ment of Pathology and Laboratory Medicine, Indi-ana University Medical Center, University Hospital3465, 550 N. University Blvd., Indianapolis, IN46202 (e-mail: [email protected]).
See “Note” following “References.”
© Oxford University Press
Journal of the National Cancer Institute, Vol. 93, No. 15, August 1, 2001 REPORTS 1147

Cleveland from 1991 to 1999. All samples were pro-cured after obtaining a signed informed consentform in accordance with the Institutional Committeefor the Protection of Human Subjects. All patientshad both ovarian and peritoneal papillary serous tu-mors of low malignant potential. All tumors werestaged according to the criteria of the InternationalFederation of Gynecology and Obstetrics for ovariancarcinoma (11). None of the tumors in our series hada micropapillary pattern (12). Such tumors have alsobeen referred to as micropapillary serous carcinomaby some investigators (13).
Tumor Samples and Microdissection
Histologic sections were prepared from formalin-fixed, paraffin-embedded blocks and stained withhematoxylin–eosin for histopathologic review andthe X-chromosome inactivation analysis. In total,73 separate tumors were obtained from the 18 pa-tients. Tumors were obtained from both ovarian andperitoneal sites for each patient. One control sample(i.e., not involved with the tumor) was obtainedfrom the normal stromal tissue for each patient.
Tumors were microdissected from serial sectionsas described previously (14,15). Briefly, cells of in-terest were selected under direct light microscopicvisualization (Olympus, Tokyo, Japan) and gentlyscraped with the use of a sterile 28-gauge needleuntil the selected cells were detached from the de-paraffinized slides. The cells were then picked up bythe needle and transferred into a single-step extrac-tion buffer (see below). Approximately 400–600cells were microdissected per sample. For examplesof tumor sections before and after microdissection,see Fig. 1.
Detection of X-ChromosomeInactivation
DNA samples were prepared from distinctly sepa-rate tumors from the same patient. The dissected
cells were placed in 15 �L of buffer (i.e., 10 mMTris–HCl, 1 mM EDTA, 1% Tween 20, and 0.2mg/mL of proteinase K [pH 8.3]) and incubatedovernight at 37 °C (14,15). The solution was boiledfor 10 minutes to inactivate the proteinase K andused directly for subsequent clonal analysis withoutfurther purification. Aliquots (8 �L) of the DNAextract were digested overnight at 37 °C with 1 Uof HhaI restriction endonuclease (New EnglandBiolabs Inc., Beverly, MA) in a total volume of 10�L. Equivalent aliquots of the DNA extracts werealso incubated in the digestion buffer without HhaIendonuclease as control reactions for each sample.After the incubation, 3 �L of digested or nondi-gested DNA was amplified in a 25-�L polymerasechain reaction (PCR) volume containing 0.1 �L32[P]�-labeled deoxyadenosine triphosphate (dATP)(3000 Ci/mmol), 4 �M AR-sense primer (5�
TCCAGAATCTGTTCCAGAGCGTGC3�), 4 �MAR-antisense primer (5�GCTGTGAAGGTTGCT-GTTCCTCAT3�) (9), 4% dimethyl sulfoxide, 2.5mM MgCl2, 300 �M deoxycytidine triphosphate,300 �M deoxythymidine triphosphate, 300 �M de-oxyguanosine triphosphate, 300 �M dATP, and 0.13U Taq DNA polymerase (Perkin-Elmer Corp., Nor-walk, CT). Each PCR amplification had an initialdenaturation step of 95 °C for 8 minutes, followedby 32 cycles at 95 °C for 40 seconds, at 63 °C for40 seconds, and at 72 °C for 60 seconds and thenfollowed by a single final extension step at 72 °Cfor 10 minutes. The PCR products were then dilutedwith 4 �L of loading buffer containing 95% form-amide, 20 mM EDTA, 0.05% bromphenol blue, and0.05% xylene cyanole FF (Sigma Chemical Co.,St. Louis, MO). The samples were heated to 95 °Cfor 5 minutes and then placed on ice. Three micro-liters of the reaction mixture was loaded onto 6.5%polyacrylamide-denaturing gels without formamide,and the PCR products were separated by electropho-resis at 1600 V for 4–7 hours. The bands werevisualized after autoradiography with Kodak X-
OMAT AR film (Eastman Kodak Company, Roch-ester, NY) for 8–16 hours.
Analysis of X-ChromosomeInactivation
The cases were considered to be informative iftwo AR allelic bands were detected after PCR am-plification in normal control samples that had notbeen treated with HhaI. Only informative cases(i.e., those without a skewed pattern of X-chromosome inactivation after being treated withHhaI in normal control samples) were included inthe analysis. In tumor samples, nonrandom X-chromosome inactivation was defined as a completeor a nearly complete absence of an AR allele afterHhaI digestion, which indicated a predominance ofone allele (16–18).
Tumors were considered to be monoclonal if thesame AR allelic inactivation pattern was detected indifferent tumors from the same patient (see Fig. 2,Pattern X). Tumors were considered to be multi-clonal if alternate predominance of AR alleles afterHhaI digestion (different allelic inactivation pat-terns) was detected in different tumors from thesame patient. Tumors with different allelic inactiva-tion patterns were considered to be of independentorigin (see Fig. 2, Pattern Y).
RESULTS
To determine the origin of peritonealand ovarian tumors of low malignant po-tential, we assessed X-chromosome inac-tivation in 73 separate tumor samplesfrom 18 patients. All patients had papil-lary serous ovarian tumors of low malig-nant potential with extra-ovarian site in-volvement (Table 1). Twelve patients hadbilateral ovarian tumors of low malignantpotential; these tumors were morphologi-cally similar. Tumor samples were ob-tained from the ovaries and one or moreperitoneal sites from each patient. Six pa-tients (cases 3, 10, 11, 12, 13, and 17) hadinvasive implants, and two (cases 5 and 6)had noninvasive desmoplastic implants.
In the tumors from five of 18 patients(cases 6, 7, 11, 14, and 16), the patterns ofX-chromosome inactivation for all siteswere noninformative. Of the remaining 13informative cases, six (cases 2, 3, 5, 10,13, and 18) showed random inactivationof the X chromosome, with two allelicbands present after digestion with HhaI;six (cases 1, 8, 9, 12, 15, and 17) haddifferent nonrandom X-chromosome-inactivation patterns in the ovarian andperitoneal tumors (Fig. 3), and one (case4) had the same pattern of nonrandomX-chromosome inactivation in both theovarian and peritoneal tumors (Table 1).In cases 8 (Fig. 3, A), 15, and 17, thetumor samples from the left and rightovary had different patterns of nonran-dom X-chromosome inactivation. In case
Fig. 1. Sequential microdissection of ovarian serous borderline tumors (case 8). Panel A: tumor from rightovary before microdissection. Panel B: tumor from right ovary after microdissection. Panel C: tumor fromthe left ovary before microdissection. Panel D: tumor from the left ovary after microdissection. Originalmagnification ×400.
1148 REPORTS Journal of the National Cancer Institute, Vol. 93, No. 15, August 1, 2001

9, each tumor from the left and rightovary and the right fallopian tube had adifferent pattern of X-chromosome inac-tivation. In case 12, the tumor sampledfrom the peritoneal nodule had a differentpattern of nonrandom X-chromosome in-activation than the tumors sampled fromthe omentum and small bowel mucosa. Ofthe six cases (cases 3, 10, 11, 12, 13, and17) with invasive implants, two (cases 12and 17) had nonrandom X-chromosomeinactivation. The tumors that were mono-clonal were histologically indistinguish-able from those that had a randomX-chromosome-inactivation pattern.
DISCUSSION
The monoclonal origin of advancedepithelial ovarian carcinomas and theirconcurrent metastatic tumors is welldocumented (5–7,19). Jacobs et al. (20)analyzed LOH, p53 mutations, and X-chromosome inactivation status andfound that tumors from multiple sites inpatients with advanced serous ovariancarcinoma were monoclonal in origin.However, whether the peritoneal tumorsin cases of ovarian papillary serous tumor
of low malignant potential arise as mul-tiple primary tumors or through the meta-static spread from primary ovarian tumorsis unknown. We used exon 1 of the ARgene in chromosome Xq11–12 for the de-tection of nonrandom X-chromosome in-activation. This particular exon was cho-sen because of a highly polymorphicmarker, the CAG–nucleotide repeat,and the methylation-sensitive restrictionendonuclease HhaI sites close to theCAG repeat (9). We detected nonrandomX-chromosome inactivation in seven(54%) of 13 informative cases, indicatingthat these tumors were derived clonally.We detected different patterns of nonran-dom X-chromosome inactivation in theovarian and peritoneal tumors in sixcases, suggesting that these tumors werederived independently. Furthermore,three cases had different patterns of non-random X-chromosome inactivation intumors derived from contralateral ovaries.These data indicate that the multiple ovar-ian tumors of low malignant potentialfrom different sites arise independentlyin some patients, supporting the “fieldeffect” hypothesis of ovarian tumorigen-esis (21).
There are several striking differencesbetween ovarian tumors of low malignantpotential and ovarian carcinomas. For ex-ample, in contrast to ovarian carcinomas,ovarian tumors of low malignant potentiallack destructive stromal invasion (7,22,23). LOH or microsatellite instability(24,25) and p53 mutations are uncommonin ovarian tumors of low malignant po-tential (26). In addition, K-ras mutationsare more common in ovarian tumors oflow malignant potential than in ovariancarcinomas (26,27). Although these char-acteristics may, in part, be responsible forthe better prognosis and 5-year survivalrate for women diagnosed with ovariantumors of low malignant potential (1,28–33), they suggest that ovarian carcinomasand ovarian tumors of low malignant po-tential might arise through differentmechanisms of carcinogenesis (24,25).
Several theories have been put forth toexplain the clonality of ovarian cancers.In the monoclonal theory of carcinogene-sis, a single malignant cell expandsclonally to form a primary malignancyand its metastases. However, the mono-clonal model of carcinogenesis cannoteasily explain the clinical observations ofmultifocal, synchronous, or metachronoustumors in the ovaries. Therefore, othermodels that consider field effect haveevolved. During ovarian carcinogenesis, afield effect may promote the independenttransformation of epithelial cells at differ-ent locations. Indeed, Buller et al. (21)proposed that multiple recurrent tumorsarose de novo and were different clonallyfrom primary ovarian tumors. An alterna-tive theory, suggested by Segal and Hart(34), was based on the observation thatmost patients with advanced serous bor-derline tumors had ovarian cortical sur-face involvement. Segal and Hart (34)proposed that neoplastic epithelial cellsbecome detached from the papillary ex-crescences growing on the external sur-faces of the ovary and subsequently im-plant on the peritoneum, omentum, andserosal surfaces of other visceral organs,resulting in multifocal disease (34). How-ever, earlier, Russell (23) argued thatperitoneal tumors are not truly metastaticin nature but arise independently (in situ)in response to the same tumorigenicagents that are responsible for the ovariantumors.
Approximately 30%–40% of patientswith serous ovarian tumors of low malig-nant potential have bilateral or multifocallesions at the time of diagnosis (28,29,
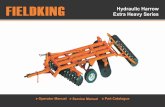
Fig. 2. Schematic of de-termining X-chromosome-inactivation patterns. Non-random methylation of Xchromosomes may occur inwomen by the hypermethyl-ation of exon 1 of the andro-gen receptor (AR) gene onthe X chromosome. Thesegenetic alterations (both thehypermethylation and theX-chromosome inactiva-tion) will be maintained insubsequent cell doublings.Clonal analysis was per-formed by a polymerasechain reaction-based endo-nuclease restriction enzyme-dependent method (9,16),which took advantage of anX-chromosome-linkedpolymorphic marker, aCAG–nucleotide repeat ofthe AR gene (HUMARA),and several methylation-sensitive HhaI (GCGC) en-donuclease sites, to detectthe nonrandom inactivationof X chromosomes. Tumorswith identical allelic losspatterns (Pattern X) are ofmonoclonal origin. Tumorswith different allelic inacti-vation patterns (Pattern Y)are of independent origin.
Journal of the National Cancer Institute, Vol. 93, No. 15, August 1, 2001 REPORTS 1149

31,32,35). Determining the clonal originof peritoneal and bilateral ovarian tumorsof low malignant potential may have im-portant biologic and clinical implications.Multiple tumors that originate from asingle tumor clone through metastasismay indicate an aggressive clinical courseand thus warrant the designation of ahigher tumor stage. On the other hand,tumors arising independently in the peri-toneum would not necessarily have thesame clinical relevance. In this study, wefound that tumor samples from the leftand right ovaries showed different pat-terns of nonrandom X-chromosome inac-tivation, suggesting that bilateral ovariantumors of low malignant potential ariseindependently from different clones. Insome cases, tumor samples from the ova-ries and peritoneum showed different pat-terns of nonrandom X-chromosome inac-tivation. These results suggest that theperitoneal tumors in patients with multi-focal ovarian tumors of low malignant po-tential are of independent origin. Lu et al.(16) hypothesized that peritoneal tumorsin patients with ovarian tumors of lowmalignant potential may be independentearly papillary serous tumors of the peri-toneum, which have been shown to have amulticlonal origin (8). Because data sug-gest that some peritoneal tumors in ad-vanced-stage ovarian serous tumors oflow malignant potential are derived fromdifferent clones than those that give riseto the ovarian tumors, the designation ofperitoneal tumors as “implants” may notbe appropriate. So-called invasive im-plants may actually represent primaryperitoneal carcinomas. It is of interest tonote that, in case 17, the invasive implantsin the peritoneal tumors had a differentnonrandom pattern of X-chromosome in-activation than that of the ovarian tumors,indicating the polyclonal origin of thesetumors. Furthermore, the different patternof nonrandom X-chromosome inactiva-tion observed in different peritoneal tu-mors, as in case 12, strongly suggests thatthese peritoneal tumors arise indepen-dently as a result of a field effect.
The incidence of nonrandom X-chromosome inactivation (54%) in thecurrent study is higher than reported pre-viously (36). This difference may be ex-plained by the methods of sample collec-tion and the different types of malignancystudied. For example, we used tissue mi-crodissection for the procurement of theDNA samples, and none of our patientshad invasive ovarian cancer.
Table 1. Summary of patient data and X-chromosome inactivation pattern*
Case No. Age, y Tumor location Tumor implants X-chromosome status
1 54 Left ovary �Left ovary �Right ovary �Peritoneum NII �
2 54 Left ovaryRight ovaryDiaphragm NIISigmoid NIIOmentum NII
3 28 Left ovaryRight ovaryPeritoneum NIIPeritoneum NIIPeritoneum NIIOmentum IIOmentum IIFallopian tube NII
4 48 Left ovary �Right ovary �Peritoneum NII �Peritoneum NII �
5 35 Left ovaryRight ovaryPeritoneum NII-D
6 18 Right ovary NIRectosigmoid serosa NII-D NIColonic serosa NII NIRight pelvic lymph node NILeft pelvic lymph node NIAnterior cul de sac NII-D NI
7 26 Left ovary NIRight ovary NILeft fallopian NII NIRight fallopian NII NI
8 68 Left ovary �Right ovary �Uterine serosa NII �
9 60 Left ovaryRight ovary �Right fallopian tube NII �
10 35 Left ovaryLeft fallopian tube IIOmentum IIColonic serosa II
11 37 Right ovary NICul de sac II NILeft pelvic lymph node II NI
12 46 Left ovary �Omentum NII �Small bowel serosa II �Peritoneal nodule NII �
13 37 Left ovaryRight ovaryLeft pelvic lymph node II
14 51 Left ovary NIEpiploicae NII NIBladder serosa NII NI
15 33 Left ovary �Right ovary �Cul de sac NII �
16 32 Left ovary NILeft fallopian tube NII NIUterine serosa NII NIParametrium NII NIOmentum NII NI
(Table continues)
1150 REPORTS Journal of the National Cancer Institute, Vol. 93, No. 15, August 1, 2001

In summary, we used X-chromosomeinactivation to determine the clonality ofadvanced-stage papillary serous ovariantumors of low malignant potential. Some
patients with bilateral ovarian tumors oflow malignant potential had two primarytumors instead of one ovarian tumor withmetastases to the other ovary. Our results
indicate that the peritoneal tumors associ-ated with ovarian tumors of low malig-nant potential may arise independentlyfrom their own primary tumor clones.
REFERENCES
(1) Kennedy AW, Hart WR. Ovarian papillary se-rous tumors of low malignant potential (serousborderline tumors). A long-term follow-upstudy, including patient with microinvasion,lymph node metastasis, and transformation toinvasive serous carcinoma. Cancer 1996;78:278–86.
(2) Bostwick DG, Tazelaar HD, Ballon SC,Hendrickson MR, Kempson RL. Ovarian epi-thelial tumors of borderline malignancy. Aclinical and pathologic study of 109 cases.Cancer 1986;58:2052–65.
(3) Michael H, Roth LM. Invasive and noninva-sive implants in ovarian serous tumors of lowmalignant potential. Cancer 1986;57:1240–7.
(4) Bell DA, Weinstock MA, Scully RE. Peritone-al implants of ovarian serous borderline tu-mors. Histologic features and prognosis. Can-cer 1988;62:2212–22.
(5) Tsao SW, Mok CH, Knapp RC, Oike K, MutoMG, Welch WR, et al. Molecular genetic evi-dence of a unifocal origin for human serousovarian carcinomas. Gynecol Oncol 1993;48:5–10.
(6) Mok CH, Tsao SW, Knapp RC, FishbaughPM, Lau CC. Unifocal origin of advanced hu-man epithelial ovarian cancers. Cancer Res1992;52:5119–22.
(7) Kupryjanczyk J, Thor AD, Beauchamp R,Poremba C, Scully RE, Yandell DW. Ovarian,peritoneal, and endometrial serous carcinoma:clonal origin of multifocal disease. Mod Pathol1996;9:166–73.
(8) Muto MG, Welch WR, Mok SC, Bandera CA,Fishbaugh PM, Tsao S, et al. Evidence for amultifocal origin of papillary serous carcinomaof the peritoneum. Cancer Res 1995;55:490–2.
(9) Allen RC, Zoghbi HY, Moseley AB, Rosen-blatt HM, Belmont JW. Methylation of HpaIIand HhaI sites near the polymorphic CAGrepeat in the human androgen-receptor genecorrelates with X chromosome inactivation.Am J Hum Genet 1992;51:1229–39.
(10) Tilley WD, Marcelli M, Wilson JD, McPhaulMJ. Characterization and expression of acDNA encoding the human androgen receptor.Proc Natl Acad Sci U S A 1989;86:327–31.
(11) International Federation of Gynecology andObstetrics. Classification and staging of malig-nant tumours in the female pelvis. Acta ObstetGynecol Scand 1971;50:1–7.
(12) Eichhorn JH, Bell DA, Young RH, Scully RE.Ovarian serous borderline tumors with micro-papillary and cribriform patterns: a study of 40cases and comparison with 44 cases withoutthese patterns. Am J Surg Pathol 1999;23:397–409.
(13) Burks RT, Sherman ME, Kurman RJ. Micro-papillary serous carcinoma of the ovary. A dis-tinctive low-grade carcinoma related to serousborderline tumors. Am J Surg Pathol 1996;20:1319–30.
Fig. 3. Representative results of inactivation of X-chromosome analysis. Panel A: Tumors (case 8) from theleft and right ovary showed different patterns of X-chromosome inactivation (Pattern Y), consistent withindependent origin. Panel B: Case 1 shows that the peritoneal tumor is of independent origin and that theovarian tumors are of monoclonal origin. Panel C: Case 12 shows that the left ovarian tumor and two of theperitoneal implants (OM and SBS) are of monoclonal origin, and one peritoneal nodule (PN) is of inde-pendent origin. DNA was prepared from tumor and normal tissues, digested with (+) or without (−) the HhaImethylation-specific restriction enzyme, and amplified by polymerase chain reaction. Arrows point to theallelic bands. N � normal tissue (control); LO � left ovary; LO1 � left ovary, sample 1; LO2 � left ovary,sample 2; RO � right ovary; P � peritoneum (case 1); OM � omentum; SBS � small bowel serosa; andPN � peritoneal nodule (case 12).
Table 1 (continued). Summary of patient data and X-chromosome inactivation pattern*
Case No. Age, y Tumor location Tumor implants X-chromosome status
17 30 Left ovary �Right ovary �Peritoneum �Left fallopian tube NII �
18 64 Left ovaryRight ovaryOmentum NIIRight pelvic sidewall nodes NII
*NII � noninvasive (nondesmoplastic) implant; II � invasive implant; NII-D � noninvasive desmo-plastic implant; NI � noninformative; � � lower allele inactivated; � � upper allele inactivated; and �
heterozygous.
Journal of the National Cancer Institute, Vol. 93, No. 15, August 1, 2001 REPORTS 1151

(14) Zhuang Z, Bertheau P, Emmert-Buck MR,Liotta LA, Gnarra J, Linehan WM, et al. Amicrodissection technique for archival DNAanalysis of specific cell population in le-sions <1 mm in size. Am J Pathol 1995;146:620–5.
(15) Zhuang Z, Merino MJ, Chuaqui R, Liotta LA,Emmert-Buck MR. Identical allelic loss onchromosome 11q13 in microdissected in situand invasive human breast cancer. Cancer Res1995;55:467–71.
(16) Lu KH, Bell DA, Welch WR, Berkowitz RS,Mok SC. Evidence for the multifocal origin ofbilateral and advanced human serous border-line ovarian tumors. Cancer Res 1998;58:2328–30.
(17) Cheng L, Song SY, Pretlow TG, Abdul-KarimFW, Kung HJ, Dawson DV, et al. Evidenceof independent origin of multiple tumors frompatients with prostate cancer. J Natl CancerInst 1998;90:233–7.
(18) Cheng L, Shan A, Cheville JC, Qian J,Bostwick DG. Atypical adenomatous hyper-plasia of the prostate: a premalignant lesion?Cancer Res 1998;58:389–91.
(19) Pejovic T, Heim S, Mandahl N, Elmfors B,Furgyik S, Floderus UM, et al. Bilateral ovar-ian carcinoma: cytogenetic evidence of unicen-tric origin. Int J Cancer 1991;47:358–61.
(20) Jacobs IJ, Kohler MF, Wiseman RW, MarksJR, Whitaker R, Kerns BA, et al. Clonal originof epithelial ovarian carcinoma: analysis byloss of heterozygosity, p53 mutation, and X-chromosome inactivation. J Natl Cancer Inst1992;84:1793–8.
(21) Buller RE, Skilling JS, Sood AK, Plaxe S,Baergen RN, Lager DJ. Field cancerization:why late “recurrent” ovarian cancer is not re-current. Am J Obstet Gynecol 1998;178:641–9.
(22) Scully RE. Ovarian tumors: a review. AmJ Pathol 1977;87:686–720.
(23) Russell P. The pathological assessment ofovarian neoplasms. I: Introduction to the com-mon “epithelial” tumours and analysis of be-nign epithelial tumours. Pathology 1979;11:5–26.
(24) Cheng PC, Gosewehr JA, Kim TM, VelicescuM, Wan M, Zheng J, et al. Potential role of theinactivated X chromosome in ovarian epithelialtumor development. J Natl Cancer Inst 1996;88:510–8.
(25) Shih YC, Kerr J, Hurst TG, Khoo SK, WardBG, Chenevix-Trench G. No evidence for mi-crosatellite instability from allelotype analysisof benign and low malignant potential ovarianneoplasms. Gynecol Oncol 1998;69:210–3.
(26) Teneriello MG, Ebina M, Linnoila RI, HenryM, Nash JD, Park RC, et al. p53 and Ki-rasgene mutations in epithelial ovarian neo-plasms. Cancer Res 1993;53:3103–8.
(27) Mok SC, Bell DA, Knapp RC, Fishbaugh PM,Welch WR, Muto MG, et al. Mutation of K-rasprotooncogene in human ovarian epithelial tu-mors of borderline malignancy. Cancer Res1993;53:1489–92.
(28) Rice LW, Berkowitz RS, Mark SD, YavnerDL, Lage JM. Epithelial ovarian tumors of bor-derline malignancy. Gynecol Oncol 1990;39:195–8.
(29) Link CJ Jr, Reed E, Sarosy G, Kohn EC. Bor-
derline ovarian tumors. Am J Med 1996;101:217–25.
(30) Nikrui N. Survey of clinical behavior of pa-tients with borderline epithelial tumors of theovary. Gynecol Oncol 1981;12:107–19.
(31) Massad LS Jr, Hunter VJ, Szpak CA, Clarke-Pearson DL, Creasman WT. Epithelial ovariantumors of low malignant potential. ObstetGynecol 1991;78:1027–32.
(32) Leake JF, Currie JL, Rosenshein NB, Wood-ruff JD. Long-term follow-up of serous ovariantumors of low malignant potential. GynecolOncol 1992;47:150–8.
(33) Kurman RJ, Trimble CL. The behavior of se-rous tumors of low malignant potential: arethey ever malignant? Int J Gynecol Pathol1993;12:120–7.
(34) Segal GH, Hart WR. Ovarian serous tumors oflow malignant potential (serous borderline tu-mors). The relationship of exophytic surfacetumor to peritoneal “implants.” Am J SurgPathol 1992;16:577–83.
(35) Chambers JT, Merino MJ, Kohorn EI, SchwartzPE. Borderline ovarian carcinoma. Am J Ob-stet Gynecol 1988;159:1088–94.
(36) Buller RE, Sood AK, Lallas T, Buekers T,Skilling JS. Association between nonrandomX-chromosome inactivation and BRCA1 mu-tation in germline DNA of patients withovarian cancer. J Natl Cancer Inst 1999;91:339–46.
NOTE
Manuscript received February 9, 2001; revisedMay 28, 2001; accepted June 4, 2001.
1152 REPORTS Journal of the National Cancer Institute, Vol. 93, No. 15, August 1, 2001
Copyright © 2022 FDOKUMEN