
Early mobilization and recovery in mechanically ventilated ...
Upload
independentCategory
view
0download
0
Vol. 34 No. 1 July 2007 Journal of Pain and Symptom Management 67
Original Article
Mobilization-Observation-Behavior-Intensity-Dementia Pain Scale (MOBID): Developmentand Validation of a Nurse-Administered PainAssessment Tool for Use in DementiaBettina Sandgathe Husebo, MD, Liv Inger Strand, PhD,Rolf Moe-Nilssen, PhD, Stein Borge Husebo, MD,Andrea Lynn Snow, PhD, and Anne Elisabeth Ljunggren, PhDDepartment of Public Health and Primary Health Care (B.S.H., L.I.S., R.M.-N., A.E.L.), Section for
Physiotherapy Science, University of Bergen, Bergen, Norway; Department of Palliative Care and Ethics
(S.B.H.), Faculty of Interdisciplinary Research and Education, University of Klagenfurt, Vienna,
Austria; and Center for Mental Health and Aging (A.L.S.), Department of Psychology, University of
Alabama, Tuscaloosa, Alabama, USA
AbstractPain assessment in older persons with severe cognitive impairment (SCI) is a challenge due toreduced self-report capacity and lack of movement-related pain assessment instruments. Thepurpose of this article was to describe the development of the Mobilization-Observation-Behaviour-Intensity-Dementia Pain Scale (MOBID) and to investigate aspects of reliabilityand validity. MOBID is a nurse-administered instrument developed for use in patients withSCI, where presence of pain behavior indicators (pain noises, facial expression, and defense)may be observed during standardized active, guided movements, and then inferred torepresent pain intensity. Initially, the MOBID contained seven items (observing at rest,mobilization of the hands, arms, legs, turn over in bed, sitting on bedside, and teeth/mouthcare). This was tested in 26 nursing home patients with SCI. Their primary caregivers, fiveregistered nurses and six licensed practical nurses (LPNs), rated the patients’ pain intensityduring regular morning care, and by MOBID, both at bedside and from video uptakes. Threeexternal raters (LPNs), not knowing the patients, also completed the MOBID by rating thevideos. Internal consistency of the MOBID indicated high Cronbach’s alpha (a¼ 0.90) afterdeleting the items for observation at rest and observation of teeth/mouth care. MOBIDdisclosed significantly more pain than did pain scorings during regular morning care, andvideo observation demonstrated higher pain intensity than bedside scoring. Intertesterreliability for inferred pain intensity was high to excellent (intraclass correlationcoefficient¼ 0.70e0.96), but varied between poor and excellent for pain behavior indicators(k¼ 0.05e0.84). These results suggest that registration of pain behavior indicators duringactive, guided movements, as performed by the MOBID procedure, is useful to disclose reliable
This study was supported by the Norwegian Founda-tion for Health and Rehabilitation (2003/2/0096)and the Kavli’s Research Center for Dementia.
Address reprint requests to: Bettina Husebo, MD,Department of Public Health and Primary Health
� 2007 U.S. Cancer Pain Relief CommitteePublished by Elsevier Inc. All rights reserved.
Care, Section for Physiotherapy Science, Universityof Bergen, Kalfarveien 31, 5018 Bergen, Norway.E-mail: [email protected]
Accepted for publication: October 5, 2006.
0885-3924/07/$esee front matterdoi:10.1016/j.jpainsymman.2006.10.016

68 Vol. 34 No. 1 July 2007Husebo et al.
and valid pain intensity scores in patients with SCI. J Pain Symptom Manage2007;34:67e80. � 2007 U.S. Cancer Pain Relief Committee. Published by Elsevier Inc. Allrights reserved.
Key WordsPain, pain assessment, behavioral assessment, movement-related pain, older adults,dementia, reliability, validity, nursing home
IntroductionAdvancing age is associated with increased
prevalence of pain,1e3 often caused by muscu-loskeletal conditions, previous fractures, andneuropathies.4 Pain is ‘‘an unpleasant sensoryand emotional experience associated withactual or potential tissue damage.’’5 Alwayssubjective, pain depends on the patient’smemory, expectation, and emotion. There-fore, when older adults in pain also have severecognitive impairment (SCI) and reduced com-munication abilities, they are at high risk forbeing underdiagnosed and untreated for theirpain.6
In industrialized countries, 2% of the popu-lation suffer from Alzheimer’s disease andrelated dementias.7 Dementia refers to aclinical syndrome that has many causes, suchas Alzheimer’s disease (50%e60%), vasculardementia (30%e40%), and secondary demen-tia.8 Patients with dementia have memory dis-turbances as well as defects in other mentalabilities, such as abstract thinking, personality,language, and neuropsychological disorders.8
In Norwegian nursing homes (NHs), 72% of pa-tients suffer from dementia, the main reason foradmission.9 The problem of underdiagnosedand untreated pain seems, accordingly, to besubstantial in NHs.1,2,10e14
Although older adults tend to have morepainful acute and chronic illnesses than theiryounger counterparts, they often report lesspain.15,16 Chronic pain may be difficult to de-tect in older adults because they are gettingused to it,15,16 and they might expect pain tobe associated with normal aging.17 The inci-dence of pain, however, differs among studiesof older people, and patients with cognitiveimpairment (CI) are often excluded in thesestudies.18,19 With increasing CI, patients’ abil-ity to report pain decreases,20 and self-reportpain assessment tools cannot be used.21
In response to a strong need to assess painand improve pain management in patientswith SCI, several pain behavioral scales havebeen developed22e36 and reviewed in the liter-ature.37e39 These instruments are based on ob-servation of patients’ behavior and function,involving aspects like sleep, appetite, physicalactivity, mobility, facial/body language, and so-cial indicators, and they intend to provide indi-rect pain measures. There is strong evidencethat pain behavior indicators, such as guarding,bracing, or grimacing, should be used,40,41 butthese indicators may be absent or difficult tointerpret because symptoms attributed todementia may also be indications of pain.42
Furthermore, behavioral indicators are morelikely to be associated with acute pain, which,although important, is less prevalent than per-sistent pain in older adults.43
Movement-related pain behavior seems to beof clinical significance,44 but few attempts havebeen made to investigate the utility of usinga standardized movement protocol.43 A short-coming of existing scales is that pain behaviorin connection with movements is observedonly in daily life activities as they naturally oc-cur.24,26,28,31,35 In a sample of elderly patientswith and without CI, Feldt26 observed high fre-quencies of verbal and nonverbal pain indica-tors during movement and transfer. However,pain tended to change the way activities are per-formed.45 Changes may be subtle and not easilyobserved during daily life activities, as peoplemay simply move less or change the way theymove to avoid pain.46e48 To better capturemovement-related pain behavior, a protocol ofstandardized movements of different body partsmight be used.
The aim of the present study was the devel-opment of an instrument to assess pain in pa-tients with SCI, using a procedure of active,guided movements. The following researchquestions were posed: Is internal consistency

Vol. 34 No. 1 July 2007 69MOBID Pain Scale
and intertester reliability satisfactory regardingpain behavior indicators and inferred pain in-tensity? Is there support that the constructionof the new instrument is appropriate for cap-turing valid data on pain intensity in patientswith SCI?
MethodsInstrument Development
Behavioral terms and pain assessment toolsregarding pain in dementia were reviewedthrough an intensive survey of the literature.Pain behavior indicators observed in connec-tion with movements and inferred to reflectpain intensity were chosen. An initial draft ofthe new pain assessment scale was developedby an expert panel (one registered nurse[RN], one licensed practical nurse [LPN], twophysicians, two physiotherapists, one clinicalpsychologist) experienced in pain assessment,examination of psychometric properties ofassessment tools, and treatment and care ofthe elderly, including patients with SCI. Thepanel consensus was as follows: 1) commonlyused indicators of pain behavior should be in-cluded; 2) active, guided movement itemsshould be included involving joints of all bodyparts (arms, legs, and trunk); 3) the movementsshould be easy to perform by an LPN in connec-tion with morning care; and 4) all items shouldbe obligatory.
Pain Behavior IndicatorsBased on clinical experience and survey of
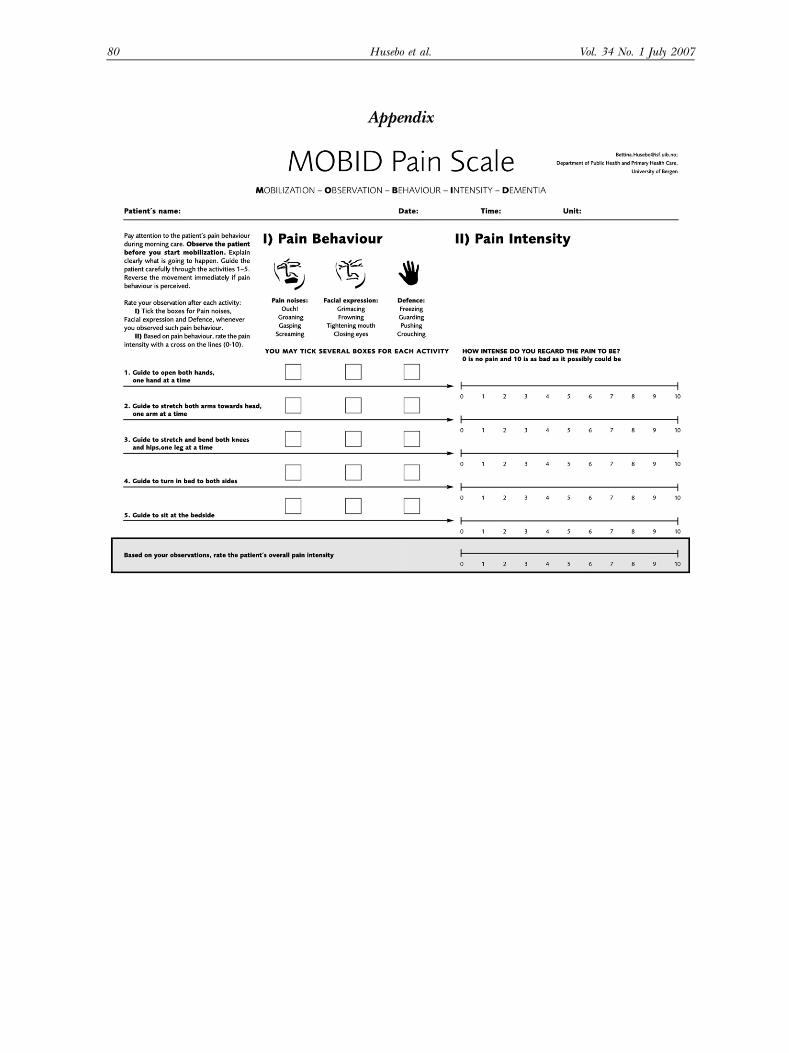
the literature,22,26,28,29,33e35,41,49e55 three indi-cators of pain behavior were selected: ‘‘painnoises,’’ ‘‘facial expression,’’ and ‘‘defense.’’These aspects of pain behavior are all com-monly included in staff-administered instru-ments.38 Verbal expressions of pain, ‘‘painnoises,’’ are often heard in patients experienc-ing pain and are easy to notice by the observer.In the protocol, this indicator was accompa-nied by the explanatory words: ‘‘This hurts!,’’groaning, moaning, gasping, and screaming.‘‘Facial expression’’ is used to denote move-ment caused by pain, expressed by the words:grimacing, frowning, tightening mouth, andclosing eyes. ‘‘Defense’’ is used to register re-luctance to move, or a protective attitude toavoid pain, explained in the test protocol by
the words: stiffening, guarding, pushing, andcrouching. In the instructions, the LPN was en-couraged to tick one or more of the threeboxes for each item when pain behavior indi-cators were observed.
Movements Included in the Protocol. The initialdraft of the Mobilization-Observation-Behavior-Intensity-Dementia Pain Scale (MOBID) con-sisted of one item for observation of painbehavior before movement is started (observethe patient lying in bed for two minutes), fol-lowed by six active, guided movement items:open both hands, one hand at a time; stretchboth arms toward head, one arm at a time;stretch and bend both ankles, knees and hips,one leg at a time; turn over in bed to both sides;sit at the bedside; and brush teeth/do mouthcare.
Pain IntensityAfter the LPN rated the pain behavior indi-
cators, they were encouraged to infer thepain intensity with a cross on a 0e10 pointNumerical Rating Scale (NRS),56 answeringthe question: ‘‘How intense do you regard thepain to be?’’ Finally, after completion of theentire protocol, an overall inferred pain inten-sity rating was completed, again using the NRS.
Instruction to Use the MOBIDNurses were instructed to pay attention to
the patient’s pain behavior during morningcare, observe the patient before starting mobi-lization, clearly explain what was going to hap-pen, mobilize the patient gently through theactivities, reverse the movement immediatelyif pain behavior was demonstrated, rate obser-vation after each activity, tick the boxes for‘‘pain noises,’’ ‘‘facial expression,’’ and ‘‘de-fense’’ whenever observing such pain behavior,and rate pain intensity with a cross on the lines(Appendix).
Face ValidityTo examine face validity, the initial draft of
the MOBID was presented to a focus groupof two RNs, two LPNs, two physiotherapists,one occupational therapist, and two physi-cians, all experienced in evaluation and man-agement of pain in NH patients. Thefollowing questions were discussed: 1) Do thepain behavior indicators and movement items

70 Vol. 34 No. 1 July 2007Husebo et al.
seem adequate and sufficient to disclose painin patients with dementia? 2) Is the test proce-dure easily performed in connection withmorning care?
The focus group maintained that the initialdraft of MOBID seemed well suited to identifypain behavior related to musculoskeletal pain,as well as pain provoked by movements. Theysuggested, however, adding items to capturepain not necessarily provoked by movement,such as visceral and neuropathic pain andheadache syndromes. The focus group consid-ered the test procedure feasible for LPNs toperform in connection with morning care.Some suggestions of change in the layout ofthe instrument were made. The draft ofMOBID pain scale was then pilot tested withthree NH patients with pain and SCI, and mi-nor changes of the written instructions weremade.
NH PatientsThe study site was one of the largest NHs in
Norway, a 174-bed nonprofit facility consistingof 16 units with 8e12 patients in each, situatedin Bergen. Inclusion criteria were age>65years, patients in the long-term wards definedas SCI by the Mini-Mental State Examination(MMSE # 11),57 and having a regular familyvisitor or advocate. Only patients were in-cluded who were suspected to have chronicpain (>three months),58,59 with pain intensitybelieved to be >3 on the NRS. Exclusion crite-ria were delirium, psychosis and receptiveaphasia, severe hearing impairment, acute ill-ness, or acute pain. Thirty patients were notconsidered for inclusion in the study as theywere allocated to rehabilitation and short stayadmissions or palliative care for cancer pa-tients. Among the remaining 144 long-term pa-tients, 26 met the criteria for participation.
Verbal and written informed consent was ob-tained in direct conversation with the patientand his/her legal guardian, usually a regularfamily member or advocate; collateral sourceconsent was required for all patients, given theirlevel of CI. The study was approved by the Re-gional Committee for Medical Research Ethicsof Western Norway (REK-Vest nr: 190.04), theData Inspectorate (nr: 11529). The Departmentfor Health Care, Norway decided that thisresearch project (200502098-/ASD) bore aminimal risk regarding the nature of the
intervention. According to the Council of Eu-rope,60 the investigation would result in a veryslight and temporary negative impact on thehealth of the person concerned.
NH StaffThere were two separate groups of MOBID
raters. The first group consisted of the pa-tients’ primary caregivers (five RNs and sixLPNs) who were familiar with the patients’habits and regular conditions. The secondgroup consisted of external raters A, B, andC (three LPNs), who did not know the pa-tients. Both groups received a one-hour brief-ing in which they learned basic informationabout pain and dementia, pain physiology,pain behavior, and pain assessment. They prac-ticed the use of the MOBID on patients.
ExaminationParticipant information on demographics
was taken from the patients’ medical charts.The two physicians responsible for the pa-tients’ diagnostic and treatment in the NHcollected the information about medical con-ditions including the international classifica-tion of diagnoses (ICD-10), dementia type,and pain etiology. They also rated eachpatient’s cognitive function by the MMSE,57
Clinical Dementia Rating (CDR),61 and SevereImpairment Rating Scale (SIRS).62 Measure-ments of daily functioning included the CornellScale for Depression in Dementia,63 the Neuro-psychiatric Inventory,64 and Activities of DailyLiving (ADL)65 collected by a geriatric studynurse and the patients’ primary caregivers.
Two responsible physicians performed clini-cal examinations of the patients focusing onpain, following a standard procedure used atthe NH. This included observation of pain be-havior in connection with the consultation, pal-pation for trigger points, and active and/orpassive movements of the limbs. After comple-tion of the examination, an overall painintensity was suggested, using the NRS. Exami-nations by the physicians were performed thesame day, shortly before the MOBID assess-ments by the patients’ primary caregivers.
Test ProceduresThe patients’ primary caregivers carefully ob-
served two to three patients each during regularmorning care procedure (washing and

Vol. 34 No. 1 July 2007 71MOBID Pain Scale
dressing) and rated an overall pain intensity us-ing an NRS after care completion. Shortly afterregular morning care, the patients were as-sessed by their caregivers using the MOBID pro-cedure at the bedside (MOBID-b). For at leasttwo minutes, each patient was observed while ly-ing in bed (item 1). A clear explanation aboutwhat was going to happen was given to the pa-tients before starting each movement, e.g.,‘‘Mrs., can you please open and close your lefthand? I will help you!’’ Then each item (2e7)was performed by gentle, standardized move-ments. Registration of pain behavior indicatorsand inferred pain intensity for each item wascompleted. At completion of this bedside exam-ination, an overall assessment of pain intensitywas made.
Video UptakesThe patient’s behavior during the standard-
ized movements of the MOBID was recordedby continuous video uptakes with a stationary(3.80 m distance) and a mobile camera. Voicesand noises by the patient and staff were docu-mented by a sensitive microphone. The opera-tor processed the video uptakes (n¼ 26) bya visual dictionary66 regarding film frame, mo-tion time, and noises. In the final presentation,each MOBID item was announced by a shorttitle. The film sequence for each patient lastedfor six to eight minutes, resulting in threehours of film material.
Pain Assessment by MOBID from VideosEach primary caregiver assessed her own
video uptakes and repeated the scoring byMOBID-video (MOBID-v) four to six days afterthe bedside assessment (MOBID-b). Addition-ally, three external raters assessed the 26 videosconcurrently and independently. They wereblinded from each other’s scorings and fromthe results of the primary caregivers and physi-cians. The ratings were performed in the courseof one working day, with regular breaks after rat-ing four to six videos to maintain attention.
Statistical Analyses
ReliabilityInternal Consistency. An estimate of the sevenMOBID pain intensity items was computedfor the external raters watching video uptakes
(n¼ 26) using Cronbach’s a formula, an indi-cator of reliability. Ideally, the Cronbach’s a co-efficient of a scale should be >0.7.67 Internalconsistency refers to the degree to which theitems that make up the scale are measuringthe same underlying construct, and careshould be taken not to include items that as-sess a different construct.68 Corrected item-to-tal correlations and a scores also werecalculated if each item was deleted from theMOBID. Corrected item-total correlation givesan indication of the degree to which each itemcorrelates with the total score. The term ‘‘ifitem deleted’’ compares these values with thefinal a-value obtained.67
Inter-Rater Reliability of Pain Behavior Indicatorsand Pain Intensity. Overall interobserveragreement was assessed pair-wise (AeB, AeC,and BeC) by the external raters watchingthe video uptakes for each MOBID item. Inter-observer agreement for pain behavior indica-tors was analyzed by kappa (k) statistics. Thistest provides a measure of concordance be-tween the raters and is chance-corrected. In-terpretation of k was as follows: #0.20(poor), 0.21e0.40 (fair), 0.41e0.60 (moder-ate), 0.61e0.80 (good), and $0.81 (very goodagreement).69,70 Interobserver agreement forpain intensity was analyzed by intraclass corre-lation coefficient (ICC) model 1.1.71 Thewithin-subject standard deviation (sw) was alsocalculated, which includes both random andsystematic components of measurement errorand is expressed in the same metric unit asthe measurement tool.72
Construct Validity. The nonparametric Wil-coxon Signed Rank Test67 was used to examinethe following questions: 1) Is less overall painintensity captured during regular care activi-ties than during standardized, guided move-ments by MOBID? 2) Are pain intensityscores of MOBID items obtained in a bedsidesituation different from those obtained fromvideo watching? 3) Is the ability to observepain behavior by MOBID dependent on know-ing the patient? Spearman correlation wasused to examine the association between thescores. Spearman correlation was finally usedto examine the association between the maxi-mum and the mean pain intensity scores ofeach test item and the overall pain intensity.

72 Vol. 34 No. 1 July 2007Husebo et al.
The number of pain behavior indicators, andthe mean and standard deviation (SD) of painintensities for each of the five items were calcu-lated. The research question whether the num-ber (0e3) of observed pain behavior indicatorsrelated to the staff’s interpretation of painintensity was calculated by one-way between-groups ANOVA with linear trend. ANOVA com-pares one independent variable (pain behaviorindicators) and one dependent continuousvariable (pain intensity scale).67,73
The data were analyzed using SPSS forWindows 13.0.
ResultsParticipants
Patients. Mean age of the 26 patients was 87.0(SD¼ 6.1) years; the majority were female(89%) and widowed (81%). They had lived inthe NH for a mean of 34 months (SD¼ 23).The patients’ SCI was demonstrated by MMSE(mean¼ 4.3, SD¼ 4.3), CDR (mean¼ 16.7,SD¼ 2.0), and SIRS (mean¼ 7.0, SD¼ 7.0).Daily functioning was characterized by ADLscore (mean¼ 5.9, SD¼ 5.9). They were neitherdepressed nor demonstrated psychiatric disor-ders. Negative correlations between MOBID-band depression (r¼�0.009) and neuropsychi-atric disorders (r¼�0.110) could be shown.They had multiple ICD-10 diagnoses (mean¼5.1, SD¼ 1.4), as well as pain diagnoses(mean¼ 2.9, SD¼ 1.2) distributed betweenshoulder, knee, back, hip, and elbow. Meannumber of medications was 4.0 (SD¼ 1.6),including pain medication (mean¼ 1.2,SD¼ 0.7). All patients except one received oneor more analgesic; 19.2% received an opioid.
Raters. Mean age of the patients’ primary care-givers and the external raters was 37.9 years(SD¼ 11.4). Both the groups had long workingexperience (mean¼ 11.2 years, SD¼ 10.2) andworked at the NH for years (mean¼ 7.7 years,SD¼ 6.8). In this period, they all received paineducation (mean¼ 7.7 hours, SD¼ 7.6).
Pain
Pain Behavior and Pain Intensity of Each MOBIDItem. Highest number of pain behavior
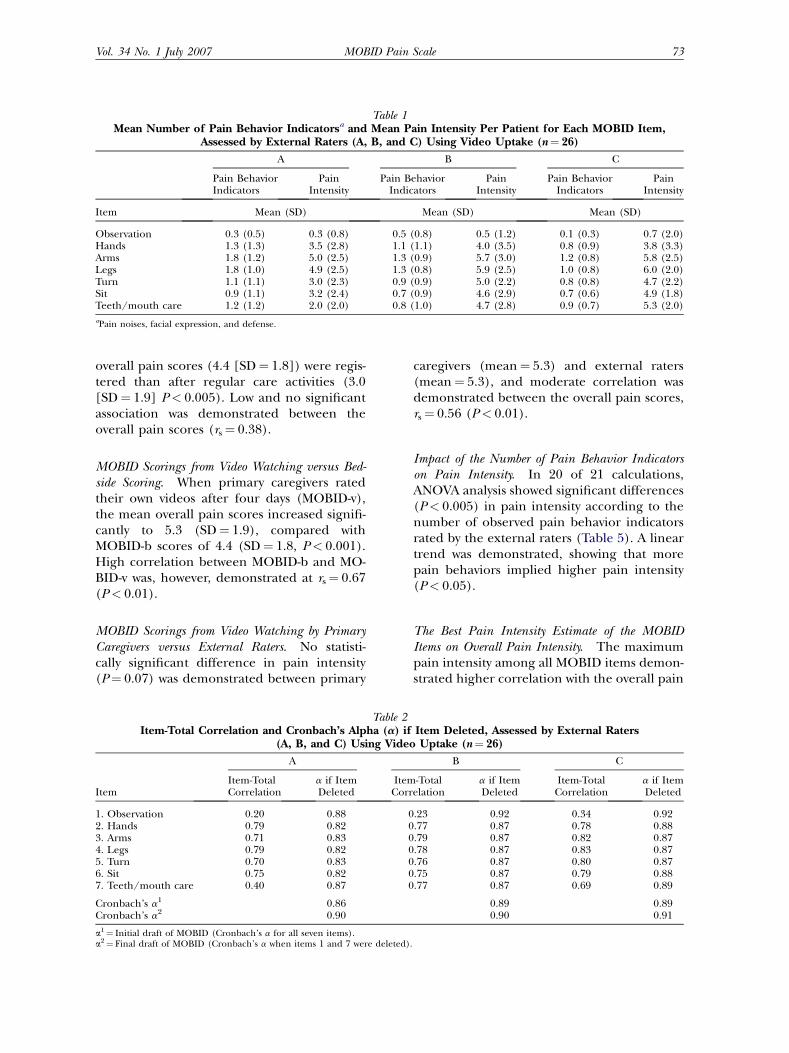
indicators per patient assessed by the externalraters was observed for mobilizing the arms(mean range 1.2e1.8) and legs (mean range1.0e1.8) (Table 1). Little pain behavior was as-sessed for observation of the patients lying inbed (mean range 0.1e0.5). Facial expressionwas the most demonstrated pain behavior indi-cator (mean range 2.2e3.2), followed by painnoises (mean range 1.9e2.3) and defense(mean range 0.4e1.5). The most painfulmovements were mobilizing the arms (meanrange 5.0e5.8) and mobilizing the legs(mean range 4.9e6.0). Less pain intensitywas referred for the observation item (meanrange 0.3e0.7). The intensity scores of theteeth/mouth care item were shown to differbetween the raters (mean range 2.0e5.3).
Reliability
Internal Consistency. Cronbach’s a1 of theseven MOBID items rated by the three exter-nal raters ranged from 0.86 to 0.89. Items forobservation during rest and teeth/mouthcare demonstrated low correlation with the to-tal score for all raters (Table 2). When theseitems were deleted, Cronbach’s alpha (a2) in-creased, ranging from 0.90 to 0.91. As a conse-quence, the items for observation and teeth/mouth care were removed from the initial MO-BID draft.
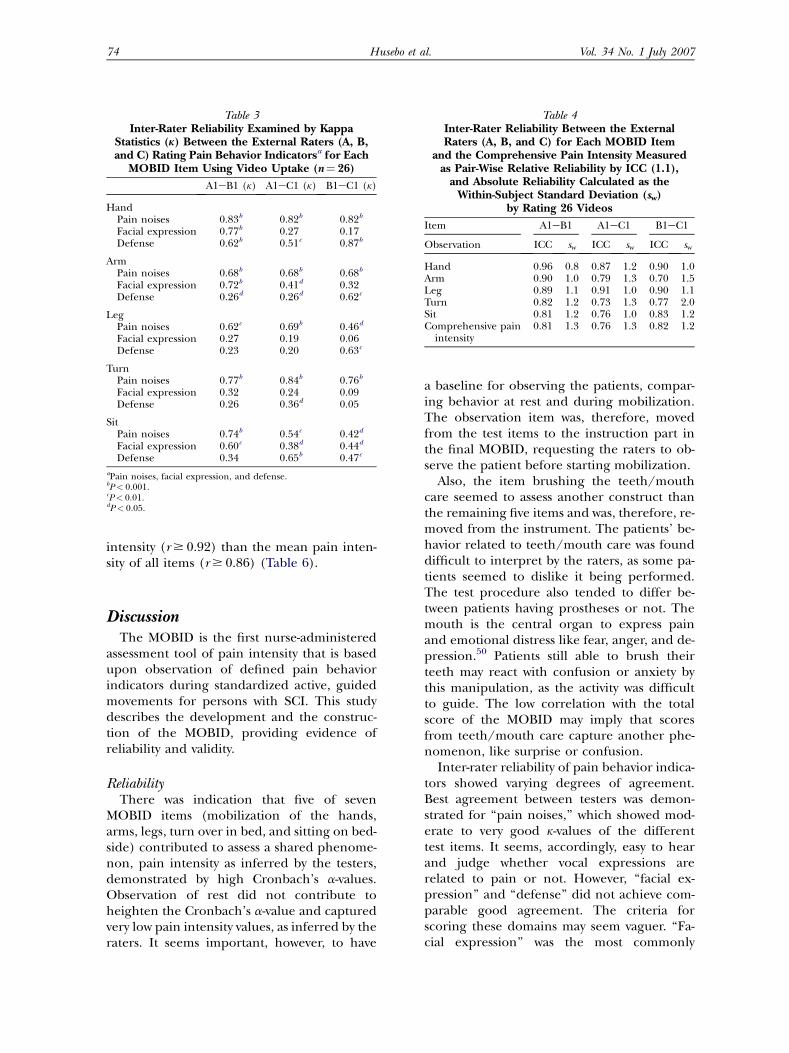
Inter-Rater Reliability of Pain Behavior Indicators ofPain Intensity. Moderate to very good k-valueswere demonstrated for ‘‘pain noises’’(k¼ 0.42e0.84). Low to good agreement wasshown for ‘‘facial expression’’ (k¼ 0.06e0.77)and low to very good agreement for ‘‘defense’’(k¼ 0.05e0.87) (Table 3). Good to excellentinter-rater reliability of inferred pain intensitywas demonstrated for each MOBID item,ICC¼ 0.70e0.96, sw # 1.5, and for the compre-hensive pain intensity score, ICC¼ 0.76e0.82,sw # 1.3 (Table 4). Inter-rater reliability esti-mated between the three raters (AeBeC)was high (ICC¼ 0.86, sw # 1.3).
Construct Validity
Pain Intensity Based on Regular Care Activitiesversus the MOBID Procedure. When primarycaregivers used the MOBID procedure duringbedside examination (MOBID-b), higher
Vol. 34 No. 1 July 2007 73MOBID Pain Scale
Table 1Mean Number of Pain Behavior Indicatorsa and Mean Pain Intensity Per Patient for Each MOBID Item,
Assessed by External Raters (A, B, and C) Using Video Uptake (n¼ 26)
A B C
Pain BehaviorIndicators
PainIntensity
Pain BehaviorIndicators
PainIntensity
Pain BehaviorIndicators
PainIntensity
Item Mean (SD) Mean (SD) Mean (SD)
Observation 0.3 (0.5) 0.3 (0.8) 0.5 (0.8) 0.5 (1.2) 0.1 (0.3) 0.7 (2.0)Hands 1.3 (1.3) 3.5 (2.8) 1.1 (1.1) 4.0 (3.5) 0.8 (0.9) 3.8 (3.3)Arms 1.8 (1.2) 5.0 (2.5) 1.3 (0.9) 5.7 (3.0) 1.2 (0.8) 5.8 (2.5)Legs 1.8 (1.0) 4.9 (2.5) 1.3 (0.8) 5.9 (2.5) 1.0 (0.8) 6.0 (2.0)Turn 1.1 (1.1) 3.0 (2.3) 0.9 (0.9) 5.0 (2.2) 0.8 (0.8) 4.7 (2.2)Sit 0.9 (1.1) 3.2 (2.4) 0.7 (0.9) 4.6 (2.9) 0.7 (0.6) 4.9 (1.8)Teeth/mouth care 1.2 (1.2) 2.0 (2.0) 0.8 (1.0) 4.7 (2.8) 0.9 (0.7) 5.3 (2.0)
aPain noises, facial expression, and defense.
overall pain scores (4.4 [SD¼ 1.8]) were regis-tered than after regular care activities (3.0[SD¼ 1.9] P< 0.005). Low and no significantassociation was demonstrated between theoverall pain scores (rs¼ 0.38).
MOBID Scorings from Video Watching versus Bed-side Scoring. When primary caregivers ratedtheir own videos after four days (MOBID-v),the mean overall pain scores increased signifi-cantly to 5.3 (SD¼ 1.9), compared withMOBID-b scores of 4.4 (SD¼ 1.8, P< 0.001).High correlation between MOBID-b and MO-BID-v was, however, demonstrated at rs¼ 0.67(P< 0.01).
MOBID Scorings from Video Watching by PrimaryCaregivers versus External Raters. No statisti-cally significant difference in pain intensity(P¼ 0.07) was demonstrated between primary
caregivers (mean¼ 5.3) and external raters(mean¼ 5.3), and moderate correlation wasdemonstrated between the overall pain scores,rs¼ 0.56 (P< 0.01).
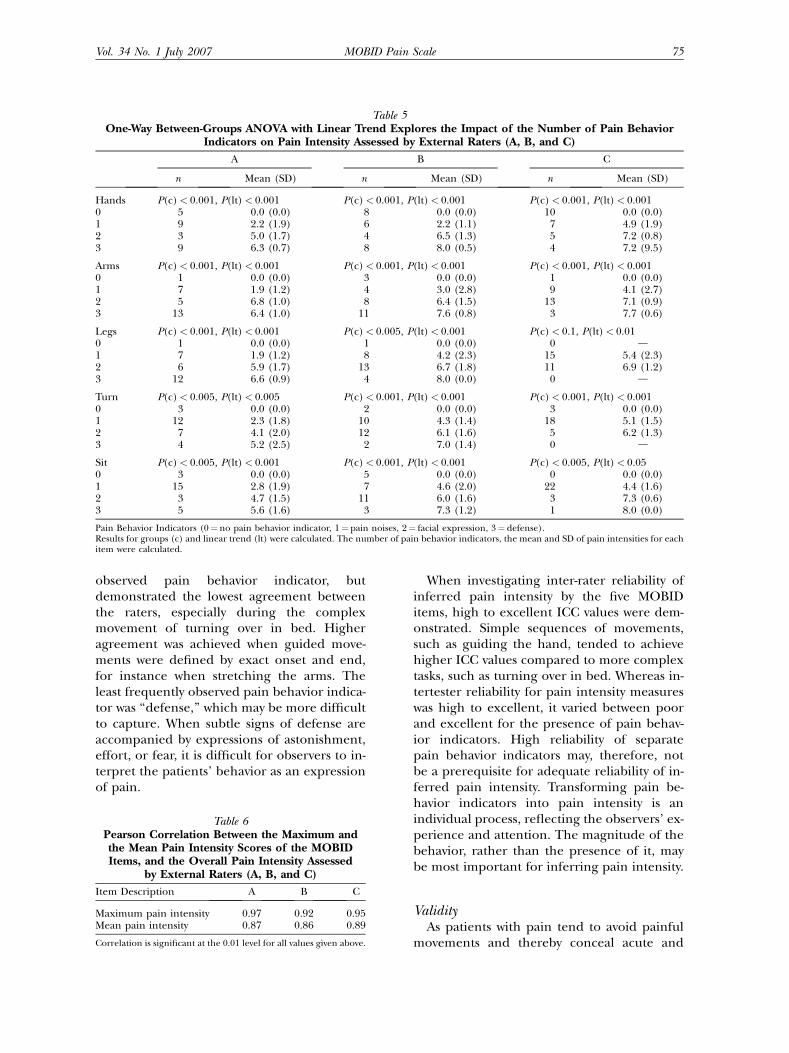
Impact of the Number of Pain Behavior Indicatorson Pain Intensity. In 20 of 21 calculations,ANOVA analysis showed significant differences(P< 0.005) in pain intensity according to thenumber of observed pain behavior indicatorsrated by the external raters (Table 5). A lineartrend was demonstrated, showing that morepain behaviors implied higher pain intensity(P< 0.05).
The Best Pain Intensity Estimate of the MOBIDItems on Overall Pain Intensity. The maximumpain intensity among all MOBID items demon-strated higher correlation with the overall pain
Table 2Item-Total Correlation and Cronbach’s Alpha (a) if Item Deleted, Assessed by External Raters
(A, B, and C) Using Video Uptake (n¼ 26)
Item
A B C
Item-TotalCorrelation
a if ItemDeleted
Item-TotalCorrelation
a if ItemDeleted
Item-TotalCorrelation
a if ItemDeleted
1. Observation 0.20 0.88 0.23 0.92 0.34 0.922. Hands 0.79 0.82 0.77 0.87 0.78 0.883. Arms 0.71 0.83 0.79 0.87 0.82 0.874. Legs 0.79 0.82 0.78 0.87 0.83 0.875. Turn 0.70 0.83 0.76 0.87 0.80 0.876. Sit 0.75 0.82 0.75 0.87 0.79 0.887. Teeth/mouth care 0.40 0.87 0.77 0.87 0.69 0.89
Cronbach’s a1 0.86 0.89 0.89Cronbach’s a2 0.90 0.90 0.91
a1¼ Initial draft of MOBID (Cronbach’s a for all seven items).a2¼ Final draft of MOBID (Cronbach’s a when items 1 and 7 were deleted).
74 Vol. 34 No. 1 July 2007Husebo et al.
intensity (r $ 0.92) than the mean pain inten-sity of all items (r $ 0.86) (Table 6).
DiscussionThe MOBID is the first nurse-administered
assessment tool of pain intensity that is basedupon observation of defined pain behaviorindicators during standardized active, guidedmovements for persons with SCI. This studydescribes the development and the construc-tion of the MOBID, providing evidence ofreliability and validity.
ReliabilityThere was indication that five of seven
MOBID items (mobilization of the hands,arms, legs, turn over in bed, and sitting on bed-side) contributed to assess a shared phenome-non, pain intensity as inferred by the testers,demonstrated by high Cronbach’s a-values.Observation of rest did not contribute toheighten the Cronbach’s a-value and capturedvery low pain intensity values, as inferred by theraters. It seems important, however, to have
Table 3Inter-Rater Reliability Examined by Kappa
Statistics (k) Between the External Raters (A, B,and C) Rating Pain Behavior Indicatorsa for Each
MOBID Item Using Video Uptake (n¼ 26)
A1eB1 (k) A1eC1 (k) B1eC1 (k)
HandPain noises 0.83b 0.82b 0.82b
Facial expression 0.77b 0.27 0.17Defense 0.62b 0.51c 0.87b
ArmPain noises 0.68b 0.68b 0.68b
Facial expression 0.72b 0.41d 0.32Defense 0.26d 0.26d 0.62c
LegPain noises 0.62c 0.69b 0.46d
Facial expression 0.27 0.19 0.06Defense 0.23 0.20 0.63c
TurnPain noises 0.77b 0.84b 0.76b
Facial expression 0.32 0.24 0.09Defense 0.26 0.36d 0.05
SitPain noises 0.74b 0.54c 0.42d
Facial expression 0.60c 0.38d 0.44d
Defense 0.34 0.65b 0.47c
aPain noises, facial expression, and defense.bP< 0.001.cP< 0.01.dP< 0.05.
a baseline for observing the patients, compar-ing behavior at rest and during mobilization.The observation item was, therefore, movedfrom the test items to the instruction part inthe final MOBID, requesting the raters to ob-serve the patient before starting mobilization.
Also, the item brushing the teeth/mouthcare seemed to assess another construct thanthe remaining five items and was, therefore, re-moved from the instrument. The patients’ be-havior related to teeth/mouth care was founddifficult to interpret by the raters, as some pa-tients seemed to dislike it being performed.The test procedure also tended to differ be-tween patients having prostheses or not. Themouth is the central organ to express painand emotional distress like fear, anger, and de-pression.50 Patients still able to brush theirteeth may react with confusion or anxiety bythis manipulation, as the activity was difficultto guide. The low correlation with the totalscore of the MOBID may imply that scoresfrom teeth/mouth care capture another phe-nomenon, like surprise or confusion.
Inter-rater reliability of pain behavior indica-tors showed varying degrees of agreement.Best agreement between testers was demon-strated for ‘‘pain noises,’’ which showed mod-erate to very good k-values of the differenttest items. It seems, accordingly, easy to hearand judge whether vocal expressions arerelated to pain or not. However, ‘‘facial ex-pression’’ and ‘‘defense’’ did not achieve com-parable good agreement. The criteria forscoring these domains may seem vaguer. ‘‘Fa-cial expression’’ was the most commonly
Table 4Inter-Rater Reliability Between the ExternalRaters (A, B, and C) for Each MOBID Item
and the Comprehensive Pain Intensity Measuredas Pair-Wise Relative Reliability by ICC (1.1),
and Absolute Reliability Calculated as theWithin-Subject Standard Deviation (sw)
by Rating 26 Videos
Item A1eB1 A1eC1 B1eC1
Observation ICC sw ICC sw ICC sw
Hand 0.96 0.8 0.87 1.2 0.90 1.0Arm 0.90 1.0 0.79 1.3 0.70 1.5Leg 0.89 1.1 0.91 1.0 0.90 1.1Turn 0.82 1.2 0.73 1.3 0.77 2.0Sit 0.81 1.2 0.76 1.0 0.83 1.2Comprehensive pain
intensity0.81 1.3 0.76 1.3 0.82 1.2
Vol. 34 No. 1 July 2007 75MOBID Pain Scale
Table 5One-Way Between-Groups ANOVA with Linear Trend Explores the Impact of the Number of Pain Behavior
Indicators on Pain Intensity Assessed by External Raters (A, B, and C)
A B C
n Mean (SD) n Mean (SD) n Mean (SD)
Hands P(c)< 0.001, P(lt)< 0.001 P(c)< 0.001, P(lt)< 0.001 P(c)< 0.001, P(lt)< 0.0010 5 0.0 (0.0) 8 0.0 (0.0) 10 0.0 (0.0)1 9 2.2 (1.9) 6 2.2 (1.1) 7 4.9 (1.9)2 3 5.0 (1.7) 4 6.5 (1.3) 5 7.2 (0.8)3 9 6.3 (0.7) 8 8.0 (0.5) 4 7.2 (9.5)
Arms P(c)< 0.001, P(lt)< 0.001 P(c)< 0.001, P(lt)< 0.001 P(c)< 0.001, P(lt)< 0.0010 1 0.0 (0.0) 3 0.0 (0.0) 1 0.0 (0.0)1 7 1.9 (1.2) 4 3.0 (2.8) 9 4.1 (2.7)2 5 6.8 (1.0) 8 6.4 (1.5) 13 7.1 (0.9)3 13 6.4 (1.0) 11 7.6 (0.8) 3 7.7 (0.6)
Legs P(c)< 0.001, P(lt)< 0.001 P(c)< 0.005, P(lt)< 0.001 P(c)< 0.1, P(lt)< 0.010 1 0.0 (0.0) 1 0.0 (0.0) 0 d1 7 1.9 (1.2) 8 4.2 (2.3) 15 5.4 (2.3)2 6 5.9 (1.7) 13 6.7 (1.8) 11 6.9 (1.2)3 12 6.6 (0.9) 4 8.0 (0.0) 0 d
Turn P(c)< 0.005, P(lt)< 0.005 P(c)< 0.001, P(lt)< 0.001 P(c)< 0.001, P(lt)< 0.0010 3 0.0 (0.0) 2 0.0 (0.0) 3 0.0 (0.0)1 12 2.3 (1.8) 10 4.3 (1.4) 18 5.1 (1.5)2 7 4.1 (2.0) 12 6.1 (1.6) 5 6.2 (1.3)3 4 5.2 (2.5) 2 7.0 (1.4) 0 d
Sit P(c)< 0.005, P(lt)< 0.001 P(c)< 0.001, P(lt)< 0.001 P(c)< 0.005, P(lt)< 0.050 3 0.0 (0.0) 5 0.0 (0.0) 0 0.0 (0.0)1 15 2.8 (1.9) 7 4.6 (2.0) 22 4.4 (1.6)2 3 4.7 (1.5) 11 6.0 (1.6) 3 7.3 (0.6)3 5 5.6 (1.6) 3 7.3 (1.2) 1 8.0 (0.0)
Pain Behavior Indicators (0¼ no pain behavior indicator, 1¼ pain noises, 2¼ facial expression, 3¼ defense).Results for groups (c) and linear trend (lt) were calculated. The number of pain behavior indicators, the mean and SD of pain intensities for eachitem were calculated.
observed pain behavior indicator, butdemonstrated the lowest agreement betweenthe raters, especially during the complexmovement of turning over in bed. Higheragreement was achieved when guided move-ments were defined by exact onset and end,for instance when stretching the arms. Theleast frequently observed pain behavior indica-tor was ‘‘defense,’’ which may be more difficultto capture. When subtle signs of defense areaccompanied by expressions of astonishment,effort, or fear, it is difficult for observers to in-terpret the patients’ behavior as an expressionof pain.
Table 6Pearson Correlation Between the Maximum andthe Mean Pain Intensity Scores of the MOBIDItems, and the Overall Pain Intensity Assessed
by External Raters (A, B, and C)
Item Description A B C
Maximum pain intensity 0.97 0.92 0.95Mean pain intensity 0.87 0.86 0.89
Correlation is significant at the 0.01 level for all values given above.
When investigating inter-rater reliability ofinferred pain intensity by the five MOBIDitems, high to excellent ICC values were dem-onstrated. Simple sequences of movements,such as guiding the hand, tended to achievehigher ICC values compared to more complextasks, such as turning over in bed. Whereas in-tertester reliability for pain intensity measureswas high to excellent, it varied between poorand excellent for the presence of pain behav-ior indicators. High reliability of separatepain behavior indicators may, therefore, notbe a prerequisite for adequate reliability of in-ferred pain intensity. Transforming pain be-havior indicators into pain intensity is anindividual process, reflecting the observers’ ex-perience and attention. The magnitude of thebehavior, rather than the presence of it, maybe most important for inferring pain intensity.
ValidityAs patients with pain tend to avoid painful
movements and thereby conceal acute and

76 Vol. 34 No. 1 July 2007Husebo et al.
chronic pain, standardized movements wereincluded in MOBID to unmask pain. Our find-ings showed that overall observed pain inten-sity was substantially higher following theMOBID procedure than after regular care ac-tivities. There seems, accordingly, to be sup-port for using this movement procedure tocapture pain in patients with SCI.
Overall pain intensity scores by the MOBIDwere shown to be higher when scoring fromvideo rating than from bedside observation, al-though the scores were highly correlated. Thisfinding indicates that important pain indica-tors may be overlooked during bedside obser-vation. To move the patient and observe himwhile interpreting pain behavior is demand-ing. A primary caregiver commented on herexperience: ‘‘Pain is more visible when watch-ing the video. You have better time to studythe patient’s face and defense, and you betterhear his voice. I am concerned that I did notrecognize the entire patient’s pain reactionduring regular care.’’ Video seems, accordingly,to be a valuable tool to mediate pain in patientswith SCI.74 However, video filming is not practi-cal to use in everyday practice. The high corre-lation between bedside and video scoringssupports the use of bedside scores, but it shouldbe taken into consideration that pain behaviorand inferred pain intensity probably are evenmore pronounced than what is observed andscored in a bedside situation.
The number of pain behavior indicators wasshown to influence the raters’ interpretationof pain intensity. When no pain behavior was ob-served, no pain intensity was registered, whereasan increasing number of pain behavior indica-tors caused increased pain intensity scores,with linear trend. Transforming pain behaviorindicators into pain intensity is an individualprocess, reflecting the observers’ experienceand attention. High reliability of pain intensityseems, however, to be based on the overall con-cept of the behavior indicators, rather than thepresence of it. Facial expression alone may notbe suitable to measure pain in patients withSCI, whereas body reactions are suitable.75 Lit-tle is known about the validity and reliability ofproxy pain report for patients with SCI, butagreement between patient and proxy reportsregarding pain assessment underlines that thenurses’ perception and observation may be animportant source.27,76
Scoring procedures of an assessment toolmay not be straightforward. To get an overallimpression of a problem, the mean or sumscores of test items are commonly calculated.It was an unexpected finding that the highestintensity score of all MOBID items was a betterdeterminant of overall pain intensity than themean score of all items. This makes sense, asit is probably less important for a patient tobe pain-free, in his knees, for example, whenhe struggles with serious back pain, becauseback pain will dominate his overall painexperience.
Limitations of the StudyIn this paper, the development and con-
struction of MOBID has been described, andaspects of validity and reliability have beenexamined. However, this is only an initialexamination of measurement properties ofthe instrument, and further investigation isneeded. Suggestions were made in our focusgroup that the instrument should also includeitems that were not necessarily provoked bymovement, such as visceral and neuropathicpain. Such items will be included in a secondpart of the instrument and are not within thescope of this paper.
The procedure of using standardized active,guided movements may be debated, as thesemay be more pain provoking than naturally oc-curring movements. Observation of, and carefor, a patient in pain, however, represents a psy-chological burden for the staff. They may try toavoid the pain problem during daily care, asexpressed by one of the primary caregivers:‘‘It’s usual to see pain during morning care,but knowing the localization of pain, I try toavoid this area. I do not move a painful arm!To defend myself, I try not to acknowledgethe pain problem when I hurt the patient.It’s like forbidden. I hurry to get ready andsay: ‘Oh, does it hurt? I apologize. I am soonready.’’’ Presence of pain contributes to lessmobilization of the patient, causing less mus-cle volume, contractures, and often morepain. The ethics of ignoring pain by the pri-mary caregivers may, accordingly, be ques-tioned. The aim of the MOBID procedure isnot to provoke unnecessary pain, but to dis-close the problem and to give the staff a painassessment instrument as a prerequisite forpain management.

Vol. 34 No. 1 July 2007 77MOBID Pain Scale
It is a challenge to distinguish pain behaviorfrom psychological distress, such as fear, de-pression, or restlessness caused by dementia.The explicit instruction for raters to observebehavior of the person simply lying in bed isthe basis for observing pain behavior duringthe movement items. Common behavior re-lated to dementia, such as rocking, yelling, ora sad look, was not considered expressions ofpain in MOBID. However, the issue of discrim-ination between behavior caused by dementia,and caused by dementia and pain, is difficultto handle and was a major concern in the pres-ent study of MOBID development.
ConclusionMOBID is a nurse-administered assessment
tool to assess pain intensity, which is basedupon observation of defined pain behavior in-dicators during standardized active, guidedmovements for persons with SCI. Internal con-sistency of the final version and inter-rater reli-ability of pain intensity scores were high,although pain behavior indicators demon-strated varying degrees of intertester reliability.Indications were provided that the guidedmovements can be used to disclose pain behav-ior in a bedside situation, although videowatching seemed to yield higher pain intensityscores.
AcknowledgmentsThe authors wish to thank Trond Bentsen,
Odontological Faculty, Audiovisual Section, atthe University of Bergen, who produced thevideo uptakes, and Aase Huus, who designedthe MOBID questionnaire. In addition, the au-thors would like to thank the patients, rela-tives, and the multidisciplinary team of theRed Cross Nursing Home, Bergen, for theirwillingness and motivation that made thisstudy possible.
References1. AGS Panel on Chronic Pain in Older Persons.
The management of chronic pain in older persons.J Am Geriatr Soc 1998;46:635e651.
2. Ferrell BA, Ferrell BR, Osterweil D. Pain in thenursing-home. J Am Geriatr Soc 1990;38(4):409e414.
3. Teno JM, Kabumoto G, Wetle T, Roy J, Mor V.Daily pain that was excruciating at some time inthe previous week: prevalence, characteristics, andoutcomes in nursing home residents. J Am GeriatrSoc 2004;52(5):762e767.
4. Feldt KS, Ryden MB, Miles S. Treatment of painin cognitively impaired compared with cognitivelyintact older patients with hip-fracture. J Am GeriatrSoc 1998;46(9):1079e1085.
5. Lindblom U, Merskey H, Mumford JM, et al.Pain termsda current list with definitions and noteson usage. Pain 1986;3:215e221.
6. Krulewitch H, London MR, Skakel VJ, et al.Assessment of pain in cognitively impaired olderadults: a comparison of pain assessment tools andtheir use by nonprofessional caregivers. J AmGeriatr Soc 2000;48(12):1607e1611.
7. Ferri CP, Prince M, Brayne C, et al. Global prev-alence of dementia: a Delphi consensus study. Lan-cet 2005;366(9503):2112e2117.
8. Friedland RP, Wilcock GK. Dementia. In:Evans JG, Williams TF, Beattie BL, Michel J-P,Wilcock GK, eds. Oxford textbook of geriatricmedicine. Oxford: Oxford University Press, 2000:922e932.
9. Engedal K, Haugen PK. The prevalence of de-mentia in a sample of elderly Norwegians. J GeriatrPsychiatr 1993;8(7):565e570.
10. Cohen-Mansfield J. Relatives’ assessment ofpain in cognitively impaired nursing home resi-dents. J Pain Symptom Manage 2002;24(6):562e571.
11. Frampton M. Experience assessment and man-agement of pain in people with dementia. Age Age-ing 2003;32(3):248e251.
12. Weiner D, Peterson B, Keefe F. Chronic pain-associated behaviors in the nursing home: residentversus caregiver perceptions. Pain 1999;80(3):577e588.
13. Weiner D, Peterson B, Ladd K, McConnell E,Keefe F. Pain in nursing home residents: an explora-tion of prevalence, staff perspectives, and practicalaspects of measurement. Clin J Pain 1999;15(2):92e101.
14. Weiner DK. Pain in nursing home residents:what does it really mean, and how can we help? JAm Geriatr Soc 2004;52(6):1020e1022.
15. Brattberg G, Parker MG, Thorslund M. A longi-tudinal study of pain: reported pain from middleage to old age. Clin J Pain 1997;13(2):144e149.
16. Sengstaken EA, King SA. The problems of painand its detection among geriatric nursing-home res-idents. J Am Geriatr Soc 1993;41(5):541e544.
78 Vol. 34 No. 1 July 2007Husebo et al.
17. Ferrell BA. Pain management in elderly people.J Am Geriatr Soc 1991;39(1):64e73.
18. Gagliese L, Melzack R. Chronic pain in elderlypeople. Pain 1997;70(1):3e14.
19. Helme RD, Gibson SJ. The epidemiology ofpain in elderly people. Clin Geriatr Med 2001;17(3):417e431.
20. Huffman JC, Kunik ME. Assessment and under-standing of pain in patients with dementia. Geron-tologist 2000;40(5):574e581.
21. Closs SJ, Barr B, Briggs M, Cash K, Seers K. Acomparison of five pain assessment scales for nurs-ing home residents with varying degrees of cognitiveimpairment. J Pain Symptom Manage 2004;27(3):196e205.
22. Abbey J. The Abbey Pain Scale: a 1-minute nu-merical indicator for people with end-stage demen-tia. Int J Palliat Nurs 2004;10:6e13.
23. Baulon A, Alix M, Ammar A, et al. Pain and pal-liative care. Standards and quality criteria. GerontolGeriatr 1999;32(2):50.
24. Davies E, Male M, Reimer V, Turner M, Wylie K.Pain assessment and cognitive impairment: Part 1.Nurs Stand 2004;19(12):39e42.
25. Desson JF, Morello R, Alix M. Pain assessmentin non-communicating elderly patientsddescriptionof the first validated behavioural seals (EPCA).Gerontol Geriatr 1999;32(2):245.
26. Feldt K. The checklist of nonverbal pain indica-tors (CNPI). Pain Manage Nurs 2000;1:13e21.
27. Fisher SE, Burgio LD, Thorn BE, et al. Pain as-sessment and management in cognitively impairednursing home residents: association of certifiednursing assistant pain report, Minimum Data Setpain report, and analgesic medication use. J AmGeriatr Soc 2002;50(1):152e156.
28. Fuchs-Lacelle S. Development and preliminaryvalidation of the pain assessment checklist for se-niors with limited ability to communicate (PAC-SLAC). Pain Manage Nurs 2004;5:37e49.
29. Hurley AC, Volicer BJ, Hanrahan PA, Houde S,Volicer L. Assessment of discomfort in advancedAlzheimer patients. Res Nurs Health 1992;15(5):369e377.
30. Keefe FJ, Block AR. Development of an observa-tion method for assessing pain behavior in chroniclow-back-pain patients. Behav Ther 1982;13(4):363e375.
31. Lefebvre-Chapiro S. The Doloplus 2 scalerdevaluating pain in the elderly. Eur J Palliat Care2001;8:191e194.
32. Morris JN, Fries BE, Mehr DR, et al. Mds Cogni-tive Performance Scale(C). J Gerontol 1994;49(4):M174eM182.
33. Simons W, Malabar R. Assessing pain in elderlypatients who cannot respond verbally. J Adv Nurs1995;22(4):663e669.
34. Snow AL, Weber JB, O’Malley KJ, et al. NOP-PAIN: a nursing assistant-administered pain assess-ment instrument for use in dementia. DementGeriatr Cogn Disord 2004;17(3):240e246.
35. Villanueva MR. Pain assessment for the dement-ing elderly (PADE): reliability and validity of a newmeasure. J Am Med Dir Assoc 2003;4:1e8.
36. Warden V, Volicer L, Hurley AC, Rogers EN.Pain assessment in advanced dementia. Gerontolo-gist 2001;41:146.
37. Herr KA, Mobily PR, Kohout FJ, Wagenaar D.Evaluation of the Faces Pain Scale for use with theelderly. Clin J Pain 1998;14(1):29e38.
38. Stolee P, Hillier LM, Esbaugh J, et al. Instru-ments for the assessment of pain in older personswith cognitive impairment. J Am Geriatr Soc 2005;53(2):319e326.
39. Zwakhalen SM, Hamers JP, Abu-Saad HH,Berger MP. Pain in elderly people with severe de-mentia: a systematic review of behavioural pain as-sessment tools. BMC Geriatr 2006;6:3.
40. Hadjistavropoulos T, LaChapelle D, Hale C,MacLeod FK. Age- and appearance-related stereo-types about patients undergoing a painful medicalprocedure. Pain Clinic 2000;12(1):25e33.
41. Keefe FJ, Williams DA, Smith SJ. Assessment ofpain behaviors. In: Turk DC, Melzack R, eds. Hand-book of pain assessment, 2nd ed. New York: TheGuilford Press, 2001: 170e187.
42. Herr K. Pain assessment in cognitively impairedolder adults. Am J Nurs 2002;102(12):65e67.
43. Gibson SJ. Older people’s pain. Pain: Clin Up-dates 2006;XIV(3):1e4.
44. Mercadante S, Arcuri E. Breakthrough pain incancer patients. Pain: Clin Updates 2006;XIV(1):1e4.
45. Magnussen L, Strand LI, Lygren H. Reliabilityand validity of the back performance scale: observ-ing activity limitation in patients with back pain.Spine 2004;29(8):903e907.
46. Hasenbring M, Hallner D, Klasen B. Psycholog-ical mechanisms in the transition from acute tochronic pain: over- or underrated? Schmerz 2001;15(6):442e447.
47. Lethem J, Slade PD, Troup JDG, Bentley G. Out-line of a fear-avoidance model of exaggerated painperceptiondI. Behav Res Ther 1983;21(4):401e408.
48. Vlaeyen JWS, Kolesnijders AMJ, Boeren RGB,vanEek H. Fear of movement (re)injury in chroniclow-back-pain and its relation to behavioral perfor-mance. Pain 1995;62(3):363e372.
Vol. 34 No. 1 July 2007 79MOBID Pain Scale
49. Craig KD, Hyde SA, Patrick CJ. Genuine, sup-pressed and faked facial behavior during exacerba-tion of chronic low-back-pain. Pain 1991;46(2):161e171.
50. Craig KD. Emotions and psychobiology. In:McMahon SB, Koltzenburg M, eds. Textbook ofpain, 5th ed. Edinburgh: Churchill Livingstone,2006: 231e239.
51. Ekman P. Facial expression and emotion. AmPsychologist 1993;48(4):384e392.
52. Hadjistavropoulos T, LaChapelle D,MacLeod FK. Measuring movement-exacerbatedpain in cognitively impaired frail elderly. Clin JPain 2000;16:54e56.
53. Hadjistavropoulos T, LaChapelle DL,Hadjistavropoulos HD, Green S, Asmundson GJG.Using facial expressions to assess musculoskeletalpain in older persons. Eur J Pain 2002;6(3):179e187.
54. Prkachin KM. Dissociating spontaneous and de-liberate expressions of paindsignal-detection analy-ses. Pain 1992;51(1):57e65.
55. Prkachin KM, Berzins S, Mercer SR. Encodingand decoding of pain expressionsda judgmentstudy. Pain 1994;58(2):253e259.
56. Jensen MP, Turner JA, Romano JM, Fisher LD.Comparative reliability and validity of chronic painintensity measures. Pain 1999;83(2):157e162.
57. Folstein MF, Folstein SE, Mchugh PR. Mini--Mental Statedpractical method for grading cogni-tive state of patients for the clinician. J PsychiatrRes 1975;12(3):189e198.
58. Merskey H. Introduction: the need of taxon-omy. Pain Suppl 1986;3:3e9.
59. Merskey H, Bogduk N, eds. Classification ofchronic pain: Descriptions of chronic pain syn-dromes and definitions of pain terms. Seattle:IASP Press, 1994.
60. Council of Europe. Additional protocol to theConvention on Human Rights and Biomedicine,concerning Biomedical Research, Article 17. Stras-bourgh: Convent Human Rights Biomed, 2005.
61. Hughes CP, Berg L, Danziger WL, Coben LA,Martin RL. A new clinical scale for the staging of de-mentia. Br J Psychiatry 1982;140:566e572.
62. Rabins PV, Steele CD. A scale to measure im-pairment in severe dementia and similar conditions.Am J Geriatr Psychiatry 1996;4(3):247e251.
63. Alexopoulos GS, Abrams RC, Young RC,Shamoian CA. Cornell Scale for Depression in De-mentia. Biol Psychiatry 1988;23(3):271e284.
64. Cummings JL, Mega M, Gray K. The Neuropsy-chiatry Inventory. Neurology 1994;44:2308e2314.
65. Sheikh K, Smith DS, Meade TW, et al. Repeati-bility and validity of a modified actvities of daily liv-ing (ADL) index in studies of chronic disability. IntRehabil Med 1979;1:51e58.
66. Ekman P, Friesen WV. A tool for the analyses ofmotion picture film or video tape. Am Psychol 1969;24:240e243.
67. Pallant J. SPSS survival manual. Berkshire, UK:Open University Press, 2005.
68. Streiner DL, Norman GR. Selecting the items.In: Streiner DL, Norman GR, eds. Health measure-ment scales: A practical guide to their developmentand use, 2nd ed. Oxford: Oxford Medical Publica-tions, 2001: 54e68.
69. Altman DG. Practical statistics for medical re-search. London: Chapman & Hall, 1995. 396e439.
70. Daly LE, Bourke GJ. Interpretation and use ofmedical statistics, 5th ed. Oxford: Blackwell Science,2000.
71. Shrout PE, Fleiss JL. Intraclass correlationsduses in assessing rater reliability. Psychol Bullet1979;86(2):420e428.
72. Bland JM, Altman DG. Measurement error. BMJ1996;312:1654.
73. Domholdt E. Rehabilitation research: Principlesand applications, 3rd ed. Philadelphia: WB Saun-ders, 2005.
74. Manfredi PL, Breuer B, Meier DE, Libow L.Pain assessment in elderly patients with severe de-mentia. J Pain Symptom Manage 2003;25(1):48e52.
75. Defrin R, Lofan M, Meier DE, Pick CG. Theevaluation of acute pain in individuals with cogni-tive impairment: a differential effect of the level ofimpairment. Pain 2006;124(3):312e320.
76. Boyer F, Novella JL, Morrone I, Jolly D,Blanchard F. Agreement between dementia patientreport and proxy reports using the NottinghamHealth Profile. J Geriatr Psychiatr 2004;19(11):1026e1034.
80 Vol. 34 No. 1 July 2007Husebo et al.
Appendix
Copyright © 2022 FDOKUMEN




















