Ascites permagna caused by large mesenteric cyst in 2 years ...
Upload
independentCategory
view
4download
0
Research Article
Midodrine in patients with cirrhosis and refractoryor recurrent ascites: A randomized pilot study
Virendra Singh1,⇑, Sahdeb P. Dhungana2, Baljinder Singh3, Rajesh Vijayverghia4, Chander K. Nain5,Navneet Sharma2, Ashish Bhalla2, Pramod K. Gupta6
1Department of Hepatology, Postgraduate Institute of Medical Education & Research, Chandigarh, India; 2Department of Internal Medicine,Postgraduate Institute of Medical Education & Research, Chandigarh, India; 3Department of Nuclear Medicine, Postgraduate Institute
of Medical Education & Research, Chandigarh, India; 4Department of Cardiology, Postgraduate Institute of Medical Education& Research, Chandigarh, India; 5Department of Gastroenterology, Postgraduate Institute of Medical Education & Research, Chandigarh, India;
6Department of Biostatistics, Postgraduate Institute of Medical Education & Research, Chandigarh, India
Background & Aims: Splanchnic arterial vasodilatation plays an Introduction
important role in cirrhotic ascites. The aim of this study was toevaluate the effects of long term administration of midodrineon systemic hemodynamics, renal function, and control of ascitesin patients with cirrhosis and refractory or recurrent ascites.Methods: Forty cirrhotic patients with refractory or recurrentascites were prospectively studied after long term administrationof midodrine plus standard medical therapy (n = 20) or standardmedical therapy alone (n = 20) in a randomized controlled trial ata tertiary centre.Results: A significant increase in urinary volume, urinary sodiumexcretion, mean arterial pressure, and decrease in plasma reninactivity (p <0.05) was noted after 1 month of midodrine adminis-tration. There was also a significant decrease in cardiac outputand an increase in systemic vascular resistance after midodrinetherapy at 3 months (p <0.05). There was no change in glomeru-lar filtration rate and model for end-stage liver disease (MELD)score. Midodrine plus standard medical therapy was significantlysuperior to standard medical therapy alone in the control of asci-tes (p = 0.013) at 3 months. The mortality rate in the standardmedical therapy group was significantly higher than the mido-drine group (p <0.046). There was no significant difference inthe frequency of various complications at the end of follow-up.Conclusions: The results of this randomized pilot study suggestthat midodrine plus standard medical therapy improves the sys-temic hemodynamics without any renal or hepatic dysfunction inthese patients and is superior to standard medical therapy alonefor the control of ascites.� 2011 European Association for the Study of the Liver. Publishedby Elsevier B.V. All rights reserved.Journal of Hepatology 20
Keywords: Ascites; Cirrhosis; Hemodynamics; Splanchnic vasodilatation;Vasopressors.Received 20 December 2010; received in revised form 6 April 2011; accepted 24 April2011; available online 13 July 2011⇑ Corresponding author. Address: Professor, Department of Hepatology, PGIMER,Chandigarh 160 012, India. Fax: +91 172 2744401.E-mail address: [email protected] (V. Singh).
Ascites is the most common complication of cirrhosis. Refractoryascites develops in approximately 5–10% of all cases of ascitesand 50% of such patients die within 6 months of its development[1]. Portal hypertension and splanchnic vasodilatation are majorfactors in the development of ascites [2,3]. Splanchnic arterialvasodilatation causes more marked arterial underfilling and thesodium retaining mechanisms become permanently activated[4]. The therapeutic options available for patients with refractoryascites are serial therapeutic paracentesis, liver transplantation,transjugular intrahepatic portosystemic shunt (TIPS), and perito-neovenous shunt [5–9]. Several studies have evaluated the effi-cacy of various vasopressors in patients with hepatorenalsyndrome (HRS) [10–13]. Vasopressors have also been used forthe prevention of post-paracentesis circulatory dysfunction withvariable results [14–18]. Recently, various vasoconstrictors havebeen used in nonazotemic cirrhotic patients with ascites andshowed an improvement in circulatory and renal function andsodium excretion [19–21]. Midodrine, an oral a1-adrenergic ago-nist along with octreotide and albumin, has been shown to bettercontrol ascites in a short term pilot study in patients with refrac-tory ascites [22]. There are no reports of long term use of mido-drine in patients with cirrhosis and ascites. Therefore, we planto study the role of long term administration of midodrine inpatients with cirrhosis with refractory or recurrent ascites in apilot study.
Materials and methods
A total of 59 patients with cirrhosis and refractory or recurrent ascites were eval-uated for inclusion in the study between December 2007 and June 2009. Nineteenof 59 screened patients were excluded during the screening period for variousreasons (spontaneous bacterial peritonitis in 6, encephalopathy in 6, acute renalfailure in 3, hepatorenal syndrome in 1, and gastrointestinal bleeding in 3patients). Therefore, 40 patients with cirrhosis and refractory or recurrent ascites[23] with stable renal function (creatinine level <1.5 for at least 7 days) attendingthe Hepatology Department of a tertiary centre were prospectively included inthis study. The study was approved by the Institute Ethics Committee. Writteninformed consent was taken. Diagnosis of cirrhosis was based on clinical, labora-tory, and ultrasonographic findings with or without liver biopsy [24]. Inclusion
12 vol. 56 j 348–354

JOURNAL OF HEPATOLOGY
criteria were presence of refractory or recurrent ascites; patients less than70 years of age; absence of gastrointestinal bleeding, hepatorenal syndrome,hepatic encephalopathy of grade 2 or higher or infection within 1 month preced-ing the study or during the study, presence of diabetes, intrinsic renal or cardio-vascular disease or arterial hypertension on history and physical examination,abnormal urine analysis, chest radiograph, or electrocardiogram, presence ofhepatocellular carcinoma or portal vein thrombosis, no treatment with drugswith known effects on systemic and renal hemodynamics within 7 days beforeinclusion. These patients were randomized to either the standard medical therapyarm or standard medical therapy with midodrine arm. A computer made the ran-domization code with 40 envelopes, with half for standard medical therapy andhalf for standard medical therapy with midodrine. Patients and investigatorswere blinded to the treatment assignments. These patients were on low sodiumdiet (2 g/day) for at least 7 days before inclusion in the study. A combination ofloop diuretic (furosemide 40–160 mg/day) and a distal acting diuretic (spirono-lactone 100–400 mg/day) was given with dose escalation by one step at a time.Large volume paracentesis (LVP) was performed along with intravenous albumin(8 g/L ascites removed) using standard clinical methodology wherever required.Subjects randomized to midodrine were prescribed oral midodrine 7.5 mg every8 h and was stopped whenever the end points were achieved.Refractory ascites was defined as ascites that cannot be mobilized or the earlyrecurrence of which cannot be satisfactorily prevented by lack of response tosodium – restricted diet and high-dose diuretic treatment (400 mg/day of spiro-nolactone and 160 mg/day furosamide) or development of diuretic-induced com-plications that preclude the use of an effective diuretic dosage [23,25]. Recurrent
Table 1. Baseline clinical, biochemical and hormonal variables of patients in two st
Variables Standard medical therap(n = 20)
Age (years) 47.6 ± 11.033Sex
Male 20 (100%)Female 0
Etiology1. Alcoholic 12 (60%)2. Others 8
HCV related 3 (15%)HBV related 5 (25%)Autoimmune 0
Recurrent ascites 14 (70%)Refractory ascites 6 (30%)Weight (kg) 64.43 ± 12.15Mean arterial pressure (mmHg) 83.59 ± 11.44MELD score 14.85 ± 4.68Cardiac output (L/min) 5.81 ± 1.8Systemic vascular resistance (dynes/s/cm5) 1247.0 ± 390.5GFR (ml/min) 92.22 ± 25.324 hr urine output (ml/24 hr) 1381.2 ± 636.8Serum bilirubin (mg/dl) 2.73 ± 1.40Serum albumin (g/dl) 2.71 ± 0.57Prothrombin time (INR) 1.25 ± 0.46Serum sodium (meq/L) 134.15 ± 5.5Serum creatinine (mg/dl) 1.03 ± 0.31Urinary sodium excretion (meq/24 hr) 70.47 ± 30.24Plasma renin activity (ng/ml/h) 13.12 ± 3.88Plasma aldosterone concentration (pg/ml) 1545.3 ± 630.9
Data are mean ± SD or number (%) of patients; MELD, model for end-stage liver disease
Journal of Hepatology 201
ascites was defined as tense ascites that recurred on at least at three occasionswithin a 12-month period despite standard treatment [23]. The standard medicaltreatment was defined by restriction of sodium, treatment with diuretics andrepeated LVP as needed. A combination of a loop-acting diuretic (furosemide,40–160 mg/day) and a distal-acting diuretic (spironolactone, 100–400 mg/day)was given with dose escalation by one step at a time permitted for a >10 lbweight gain. Repeat LVP with infusion of albumin was performed in both armsfor tense, symptomatic ascites with weight gain >10 lb from immediately previ-ous nadir weight despite maximal diuretic therapy or inability to use an effectivedose of diuretics due to diuretic-related side effects. On day of admission, baselineworkup, including body weight, blood pressure, heart rate, electrocardiogram,systemic vascular resistance (SVR), liver function tests, and renal function tests,was obtained. Glomerular filtration rate (GFR) was estimated by using Cock-croft–Gault equation [26]. SVR was measured as mean arterial pressure/cardiacoutput (MAP/CO) [20]. CO was evaluated by recording the diastolic mitral flow[27] with duplex-Doppler apparatus (Vivid Five, Vingmed Technology, Japan).These clinical and biochemical parameters were assessed in all patients at base-line and at 1, 3, and 6 month interval. Along with that, arterial blood sample wascollected after overnight fast and bed rest at least for 8 h in supine position forplasma renin activity and plasma aldosterone concentration. Blood samples weretaken from the radial artery, put into chilled ethylenediaminetetraacetic acidtubes, centrifuged at 2500 rpm for 10 min at �3 �C and stored at �80 �C. Patientswere followed up at weekly interval for 1 month, then at monthly interval tilldeath or termination of the study. All patients were instructed to come for para-centesis when become symptomatic.
udy groups.
y group Midodrine group (n = 20)
p value
45.6 ± 10.049 0.5530.231
17 (85%)3 (15%)
0.30717 (85%)31 (5%)1 (5%)1 (5%)14 (70%) 0.6346 (30%)68.45 ± 18.70 0.65885.6 ± 10.7 0.70412.9 ± 3.13 0.1405.68 ± 1.66 0.6501297.5 ± 377.4 0.820115.5 ± 57.06 0.2391235 ± 665.1 0.6802.5 ± 1.0 0.5562.84 ± 0.79 0.4711.328 ± 0.2 0.084134.6 ± 10.57 0.8670.86 ± 0.27 0.07473.14 ± 35.63 0.67113.73 ± 4.41 0.6451601.5 ± 789.7 0.805
; GFR, glomerular filtration rate.
2 vol. 56 j 348–354 349

Research Article
Blood sample was also collected for plasma renin activity and plasma aldoste-rone concentration at 1 month. Plasma renin activity was measured by radioim-munoassay using Gamma Coat 125I RIA plasma renin activity kit (Immunotech SA,France). Plasma aldosterone concentration was measured by radioimmunoassayusing RIA aldosterone kit (Immunotech SA, France).
Outcome measures
The primary end point of the study was control of ascites. Secondary end pointsinclude frequency of worsening encephalopathy, liver and renal function, and fre-quency of other complications of cirrhosis (e.g. variceal hemorrhage or develop-ment of hepatorenal syndrome) and 3 months of midodrine therapy. Complete
Table 2. Clinical and laboratory parameters before and after 1, 3, and 6 months of t
Variables Standard medical therapy group
Base-line
Month p valueB vs.
1 3 6 1 3 6
Weight(kg)
64.43 ± 12.15
65.5 ± 10.79
69.12 ± 9.84
67.7 ± 10.74
0.142 0.185 0.973
Mean arterial pressure (mmHg)
83.59 ± 11.44
83.01 ± 8.50
82.61 ± 8.63
79.24 ± 7.52
0.710 0.997 0.570
MELDscore
14.8± 4.6
16.1± 5.6
17.3± 4.3
19.5± 5.1
0.003 0.002 0.001
Cardiac output (L/min)
5.81± 1.82
5.69± 1.55
5.53± 0.54
5.43± 0.76
0.632 0.590 0.108
Systemic vascular resistance (dynes/s/cm5)
1247.0 ± 390.5
1232.8 ± 302.9
1196.3 ± 119.2
1171.7 ± 103.8
0.819 0.976 0.098
Heart rate(beat/min)
89.87± 11.75
94.56± 12.67
104.57 ± 16.39
101.8± 9.28
0.246 0.198 0.263
Serum sodium (meq/L)
134.15 ± 5.5
131.93 ± 5.421
127.62 ± 4.62
131.25 ± 3.4
0.030 0.001 0.611
Serum creatinine (mg/dl)
1.03± 0.310
1.01± 0.227
1.3 ± 0.54
1.08± 0.25
0.952 0.123 0.163
Glomerular
rate (ml/min)
92.22 ± 25.3
88.36 ± 23.64
99.15 ± 39.97
103.4± 32.9
0.648 0.825 0.941
Urineoutput(ml/day)
1381.2 ± 636.8
1496.8 ± 549.6
1531± 497.8
1340± 378.15
0.343 0.297 0.852
Urinarysodium excretion (meq/24 hr)
70.47 ± 30.24
68.75 ± 18.93
71.0 ± 15.67
57.0 ± 18.02
0.798 0.638 0.216
Plasma renin activity (ng/ml/hr)
13.12± 3.88
14.75± 3.48
0.079
Plasma aldosterone(pg/ml)
1545.3 ± 630.9
1440.59 ± 497.3
0.776
Data are mean ± SD; B, baseline.
350 Journal of Hepatology 201
response was defined as the elimination of ascites; a partial response as the pres-ence of ascites not requiring paracentesis and absence of a response was definedas the persistence of ascites requiring paracentesis [28].
Statistical analysis
Data were analyzed using SPSS for MS-Windows (version 13.0, SPSS Inc., Chicago,IL, USA). The baseline patient characteristics (clinical as well as biochemical) werecompared between two groups by using unpaired t test or ‘Chi-square test’. Intra-group comparisons were done using paired t test. Two-factor repeated-measuresANOVA was used for analysis. The first factor analyzed the nature of treatment(midodrine or standard medical therapy) and the second factor analyzed the rep-
herapy.
Midodrine group
Base-line
Month p valueB vs.
1 3 6 1 3 6
68.45 ± 18.70
67.15± 19.78
68.06 ± 19.47
60.6± 25.06
0.330 0.091 0.001
85.60 ± 10.70
92.88± 7.91
85.75 ± 9.167
79.92 ± 9.01
0.001 0.989 0.336
12.9± 3.13
13.9± 4.1
13.5± 3.3
14.5± 3.7
0.10 0.065 0.06
5.68± 1.66
5.33 ± 1.37
5.25 ± 1.62
6.03 ± 0.40
0.210 0.012 0.066
1297.5 ± 377.4
1329.9 ± 274.9
1443.7 ± 498.0
1028.8 ± 69.0
0.647 0.026 0.680
94.2± 15.01
92.4± 13.3
93.86± 12.59
90.4± 8.98
0.601 0.864 0.465
134.6 ± 10.57
132.75 ± 4.435
133.2± 4.056
134.57 ± 6.29
0.432 0.355 0.897
0.85± 0.272
0.84± 0.205
0.91± 0.241
0.90± 0.524
0.952 0.115 0.717
115.5 ± 57.06
113.08 ± 48.8
100.2± 42.97
69.67 ± 30.06
0.755 0.161 0.376
1235± 665.12
1830± 564.84
1933± 599.6
1775± 650.0
0.001 0.001 0.649
73.14± 35.63
93.21 ± 32.19
96.07 ± 33.03
72.4 ± 15.38
0.003 0.019 0.464
13.73± 4.41
9.66 ± 2.51
0.002
1601.5± 789.7
921.5± 547.8
0.008
2 vol. 56 j 348–354

Plas
ma
reni
n ac
tivity
(ng/
ml/h
)BeforeAfter
1-20: midodrine group 21-40: SMT group
25
20
15
10
5
1 5 9 13 17 21 25 29 33 37 41
Fig. 1. Individual changes in plasma renin activity before and after 1 monthof therapy (1–20: midodrine group, 21–40: standard medical therapy group).
JOURNAL OF HEPATOLOGY
etition of measures (i.e. at baseline and on 1/3/6 months). The results werereported as mean values ± SD. p <0.05 was taken as significant. Since we con-ducted a pilot study, no power calculation was performed.
Results
The demographic profile, clinical and laboratory parameters weresimilar between standard medical therapy and midodrine groups(Table 1). Twenty-eight patients had recurrent and 12 refractoryascites. Four patients did not respond to sodium-restricted dietand high-dose diuretic treatment. Eight patients stopped thesemedications due to side-effects. Baseline body weight did not dif-fer significantly between two groups (p = 0.658). In both treat-ment groups, no significant difference in weight was noted at 1and 3 months (Table 2). Body weight significantly decreased in
Plas
ma
ald
oste
rone
(pg/
ml)
BeforeAfter
1-20: midodrine group 21-40: SMT group
4000
3000
2000
1000
0
1 5 9 13 17 21 25 29 33 37 41
Fig. 2. Individual changes in plasma aldosterone concentration before andafter 1 month of therapy (1–20: midodrine group, 21–40: standard medicaltherapy group).
Journal of Hepatology 201
the midodrine group at 6 months (p = 0.001; Table 2) but not inthe standard medical therapy group (p = 0.973).
Baseline mean arterial pressure did not differ between stan-dard medical therapy and midodrine groups (p = 0.704). Signifi-cant increase in mean arterial pressure was noted in themidodrine group at 1 month (p = 0.001) but it did not change sig-nificantly in the standard medical therapy group (p = 0.710). Thechanges in values after treatment at 3 and 6 months were not sig-nificant in both groups.
Baseline cardiac output did not differ between standard med-ical therapy and midodrine groups (p = 0.65). It significantlydecreased in the midodrine group at 3 months after treatment(p = 0.012) but no significant change was noted in either groupat 1 month and 6 months after therapy. The systemic vascularresistance increased significantly at 3 months after therapy inthe midodrine group (p = 0.026); however, it did not change sig-nificantly in the standard medical therapy group at 3 months andin either group at 1 months and 6 months after therapy (Table 2).
Baseline urine output did not differ between standard medicaltherapy and midodrine groups (p = 0.680). The urine output wassignificantly higher in the midodrine group after treatment(p = 0.001) but not in the standard medical therapy group(Table 2). Baseline urinary sodium excretion was comparable inboth standard medical therapy and midodrine groups(p = 0.671). Urinary sodium excretion significantly increased inthe midodrine group after treatment at 1 month (p = 0.003) and3 months (p = 0.019) but not so in the standard medical therapygroup.
Baseline serum sodium values were similar in both groups(p = 0.867). They decreased significantly in the standard medicaltherapy group after treatment at 1 month (p = 0.03) and3 months (p = 0.001, Table 2). However, no significant change inserum sodium values was noted in the midodrine group aftertreatment.
Baseline values for serum creatinine and glomerular filtrationrate between standard medical therapy and midodrine groupswere similar. There was no significant change in these variablesin either group after treatment.
Baseline values for plasma renin activity were similar in bothtreatment groups (p = 0.645). Plasma renin activity significantlydecreased at 1 month (p = 0.002, Table 2 and Fig. 1) in the mido-drine group but did not differ significantly in the standard med-ical therapy group (p = 0.079, Table 2 and Fig. 1). Baseline plasmaaldosterone concentrations did not differ between the midodrinegroup and the standard medical therapy group (p = 0.805).Plasma aldosterone concentrations decreased significantly at1 month from baseline value in the midodrine group (p = 0.008;Table 2 and Fig. 2) but there was no significant change in thestandard medical therapy group (p = 0.776; Table 2 and Fig. 2).
There was significant change in rate of response to treatmentin the midodrine group at 3 months (p = 0.013) although nochange was noted at 1 month and 6 months after therapy(Table 3). There was no significant change in rate of response totreatment in the standard medical therapy group at anytime.
Baseline MELD scores were similar in both treatment groups(p = 0.140). MELD score significantly increased at 1, 3, and6 months from baseline in the standard medical therapy groupbut did not differ significantly from baseline in the midodrinegroup (Table 2). Pain abdomen was noted in 6 patients in themidodrine group and 4 patients in the standard medical therapygroup which was mild and subsided on its own.
2 vol. 56 j 348–354 351
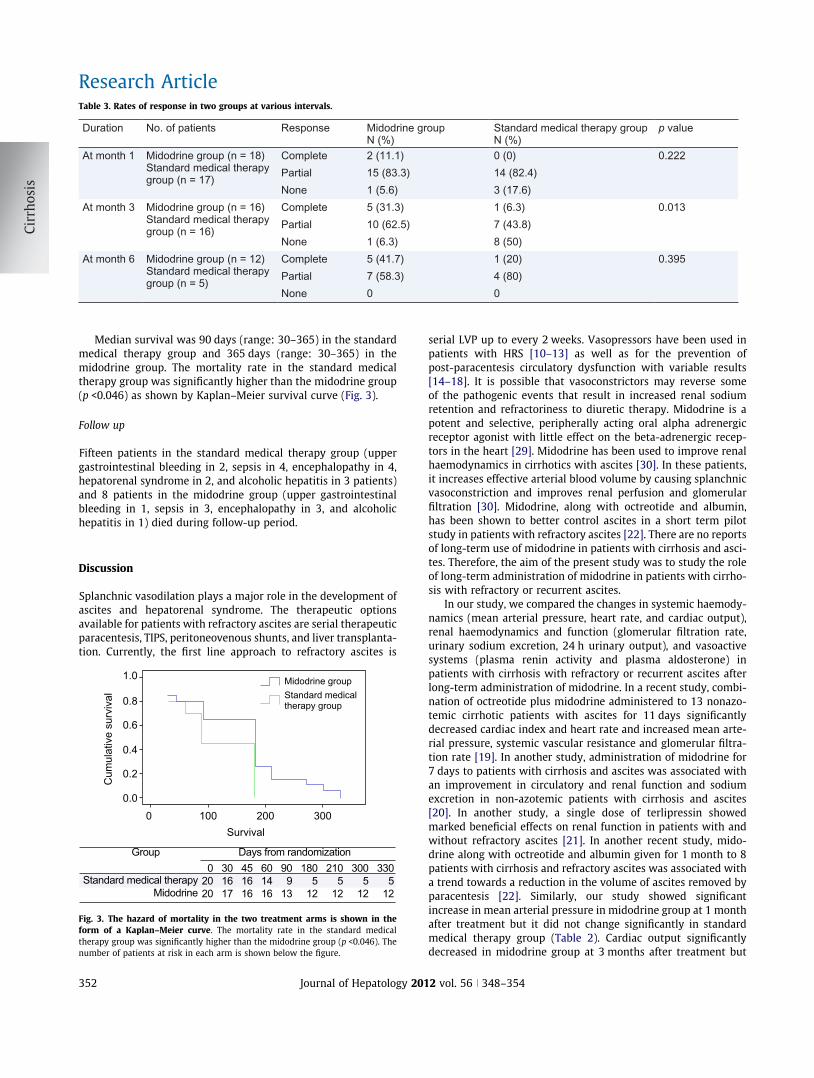
Table 3. Rates of response in two groups at various intervals.
Duration No. of patients Response Midodrine groupN (%)
Standard medical therapy group N (%)
p value
At month 1 Midodrine group (n = 18)Standard medical therapy group (n = 17)
Complete 2 (11.1) 0 (0) 0.222Partial 15 (83.3) 14 (82.4)None 1 (5.6) 3 (17.6)
At month 3 Midodrine group (n = 16)Standard medical therapy group (n = 16)
Complete 5 (31.3) 1 (6.3) 0.013Partial 10 (62.5) 7 (43.8)None 1 (6.3) 8 (50)
At month 6 Midodrine group (n = 12)Standard medical therapy group (n = 5)
Complete 5 (41.7) 1 (20) 0.395Partial 7 (58.3) 4 (80)None 0 0
Research Article
Median survival was 90 days (range: 30–365) in the standardmedical therapy group and 365 days (range: 30–365) in themidodrine group. The mortality rate in the standard medicaltherapy group was significantly higher than the midodrine group(p <0.046) as shown by Kaplan–Meier survival curve (Fig. 3).
Follow up
Fifteen patients in the standard medical therapy group (uppergastrointestinal bleeding in 2, sepsis in 4, encephalopathy in 4,hepatorenal syndrome in 2, and alcoholic hepatitis in 3 patients)and 8 patients in the midodrine group (upper gastrointestinalbleeding in 1, sepsis in 3, encephalopathy in 3, and alcoholichepatitis in 1) died during follow-up period.
Discussion
Splanchnic vasodilation plays a major role in the development ofascites and hepatorenal syndrome. The therapeutic optionsavailable for patients with refractory ascites are serial therapeuticparacentesis, TIPS, peritoneovenous shunts, and liver transplanta-tion. Currently, the first line approach to refractory ascites is
Cum
ulat
ive
surv
ival
Standard medical therapyMidodrine
Survival
1.0
02020
301617
451616
601416
909
13
1805
12
2105
12
3005
12
3305
12
0 100 200 300
Group Days from randomization
Standard medicaltherapy group
Midodrine group
0.8
0.6
0.4
0.2
0.0
Fig. 3. The hazard of mortality in the two treatment arms is shown in theform of a Kaplan–Meier curve. The mortality rate in the standard medicaltherapy group was significantly higher than the midodrine group (p <0.046). Thenumber of patients at risk in each arm is shown below the figure.
352 Journal of Hepatology 201
serial LVP up to every 2 weeks. Vasopressors have been used inpatients with HRS [10–13] as well as for the prevention ofpost-paracentesis circulatory dysfunction with variable results[14–18]. It is possible that vasoconstrictors may reverse someof the pathogenic events that result in increased renal sodiumretention and refractoriness to diuretic therapy. Midodrine is apotent and selective, peripherally acting oral alpha adrenergicreceptor agonist with little effect on the beta-adrenergic recep-tors in the heart [29]. Midodrine has been used to improve renalhaemodynamics in cirrhotics with ascites [30]. In these patients,it increases effective arterial blood volume by causing splanchnicvasoconstriction and improves renal perfusion and glomerularfiltration [30]. Midodrine, along with octreotide and albumin,has been shown to better control ascites in a short term pilotstudy in patients with refractory ascites [22]. There are no reportsof long-term use of midodrine in patients with cirrhosis and asci-tes. Therefore, the aim of the present study was to study the roleof long-term administration of midodrine in patients with cirrho-sis with refractory or recurrent ascites.
In our study, we compared the changes in systemic haemody-namics (mean arterial pressure, heart rate, and cardiac output),renal haemodynamics and function (glomerular filtration rate,urinary sodium excretion, 24 h urinary output), and vasoactivesystems (plasma renin activity and plasma aldosterone) inpatients with cirrhosis with refractory or recurrent ascites afterlong-term administration of midodrine. In a recent study, combi-nation of octreotide plus midodrine administered to 13 nonazo-temic cirrhotic patients with ascites for 11 days significantlydecreased cardiac index and heart rate and increased mean arte-rial pressure, systemic vascular resistance and glomerular filtra-tion rate [19]. In another study, administration of midodrine for7 days to patients with cirrhosis and ascites was associated withan improvement in circulatory and renal function and sodiumexcretion in non-azotemic patients with cirrhosis and ascites[20]. In another study, a single dose of terlipressin showedmarked beneficial effects on renal function in patients with andwithout refractory ascites [21]. In another recent study, mido-drine along with octreotide and albumin given for 1 month to 8patients with cirrhosis and refractory ascites was associated witha trend towards a reduction in the volume of ascites removed byparacentesis [22]. Similarly, our study showed significantincrease in mean arterial pressure in midodrine group at 1 monthafter treatment but it did not change significantly in standardmedical therapy group (Table 2). Cardiac output significantlydecreased in midodrine group at 3 months after treatment but
2 vol. 56 j 348–354

JOURNAL OF HEPATOLOGY
no significant change was noted in either group at 1 month and6 months after therapy (Table 2). Systemic vascular resistanceincreased significantly at 3 months after therapy in midodrinegroup (Table 2). The urine output was significantly higher inthe midodrine group after treatment (Table 2). In a previousstudy by our group [17] midodrine resulted in significantly more24 h urine output and sodium excretion. In the present study, uri-nary sodium significantly increased in the midodrine group aftertreatment at 1 month and 3 months but not in the standard med-ical therapy group (Table 2).Serum sodium decreased significantly in the standard medicaltherapy group after treatment at 1 month and 3 months (Table 2).However, no significant changes in serum sodium values werenoted in the midodrine group after treatment. Hyponatremia is afrequent complication of diuretic therapy in these patients [23,31].
Midodrine therapy was effective in suppressing the renin–angiotensin–aldosterone axis as evidenced by significant decreasein plasma renin activity and plasma aldosterone concentrationnoted after 1 month of therapy which was not observed in thestandard medical therapy group (Table 2). Previous studies alsoshowed suppression of activity of the renin–angiotensin systemin patients with ascites after use of vasoconstrictors [20–22].
No significant differences between standard medical therapyand midodrine groups were observed between values for serumcreatinine and glomerular filtration rates after treatment. Thereare variable reports of renal function abnormalities after vaso-pressor therapy in these patients [19–21].
There was a significant deterioration in the MELD score duringtreatment as well as on follow-up in the standard medical ther-apy group and not in the midodrine group. Earlier studies evalu-ating midodrine [20] or midodrine plus octreotide [19] in non-azotemic cirrhotics did not show a significant change in hepaticfunction. However, in a recent pilot study, there was a significantdeterioration in the MELD score during treatment with mido-drine [22].
Rates of response to treatment (measured as need for large vol-ume paracentesis and reduction of ascites) with standard medicaltherapy or midodrine therapy were measured. There was a signif-icant change in the rate of response to treatment in the midodrinegroup at 3 months although no change was observed at 1 monthand 6 months after therapy (Table 3). There was a higher survivalin the midodrine group at the end of follow-up. There are no stud-ies in literature on the long-term use of midodrine in patients withcirrhosis with refractory or recurrent ascites.
During treatment with midodrine, pain abdomen was presentin 6 patients. However, all episodes were mild and did not requirediscontinuation of therapy. Other studies have demonstrated noserious side effects with midodrine [20,32].
In conclusion, the results of this randomized pilot study sug-gest that long-term midodrine plus standard medical therapyimproves systemic hemodynamics and better controls asciteswithout any renal or hepatic dysfunction in nonazotemic patientswith refractory or recurrent ascites with cirrhosis as compared tostandard medical therapy alone.
Conflict of interest
The authors who have taken part in this study declared that theydo not have anything to disclose regarding funding or conflict ofinterest with respect to this manuscript.
Journal of Hepatology 201
References
[1] Bories P, Garcia-Compean D, Michel H, Bourel M, Capron JP, Gauthier A, et al.The treatment of refractory ascites by the LeVeen shunt: a multi centrecontrolled trial (57 patients). J Hepatol 1986;3:212–218.
[2] Schrier RW, Arroyo V, Bernardi M, Epstein M, Henriksen JH, Rodes J.Peripheral arterial vasodilation hypothesis: a proposal for the initiation ofrenal sodium and water retention in cirrhosis. Hepatology1988;8:1151–1157.
[3] Gines P, Cardeenas A, Arroyo V, Rodes J. Management of cirrhosis and ascites.N Engl Med 2004;350:1646–1654.
[4] Cardenas A, Arroyo V. Mechanism of water and sodium retention in cirrhosisand the pathogenesis of ascites. Best Pract Res Clin Endocrinal Metab2003;17:607–622.
[5] Runyon BA. Management of adult patients with ascites caused by cirrhosis.Hepatology 1998;27:264–272.
[6] Runyon BA. Ascites and spontaneous bacterial peritonitis. In: Feldman M,Friedman LS, Sleisenger MH, editors. Sleinger and Fordtrans’s gastrointes-tinal and liver disease. Philadelphia: Saunders; 2002. p. 1517–1542.
[7] Stanley MM, Ochi S, Lee KK, Nemchausky BA, Greenlee HB, Allen JI, et al.Peritoneovenous shunting as compared with medical treatment in patientswith alcoholic cirrhosis and massive ascites. N Engl J Med1989;321:1632–1638.
[8] Rossle M, Ochs A, Gulberg V, Siegerstetter V, Holl J, Deibert P, et al. Acomparison of paracentesis and transjugular intrahepatic portosystemicshunting in patients with ascites. N Engl J Med 2000;342:1701–1707.
[9] Gines P, Uriz J, Calahorra B, Garcia-Tsao G, Kamath PS, Ruiz del Arbol L, et al.Transjugular intrahepatic portosystemic shunting versus paracentesis andalbumin for refractory ascites in cirrhosis. Gastroenterology2002;123:1839–1847.
[10] Moreau R, Durand F, Poynard T, Duhamel C, Jean P, Ichai P, et al. Terlipressinin patients with cirrhosis and type 1 hepatorenal syndrome: a retrospectivemulticentre study. Gastroenterology 2002;122:923–930.
[11] Ortega R, Gines P, Uriz J, Cardenas A, Calahorra B, De Las HD, et al.Terlipressin therapy with and without albumin for patients with hepatore-nal syndrome: results of a prospective, nonrandomized study. Hepatology2002;36:941–948.
[12] Uriz J, Gines P, Cardenas A, Sort P, Jimenez W, Salmeron JM, et al. Terlipressinplus albumin infusion: an effective and safe therapy of hepatorenalsyndrome. J Hepatol 2000;33:43–48.
[13] Duvoux C, Zanditenas D, Hezode C, Chauvat A, Monin JL, Roudot Thoraval F,et al. Effects of noradrenaline and albumin in patients with type 1hepatorenal syndrome: a pilot study. Hepatology 2002;36:374–380.
[14] Moreau R, Asselah T, Caudat B, De Kerguenec C, Pessione F, Bernard B, et al.Comparison of the effect of terlipressin and albumin on arterial bloodvolume in patients with cirrhosis and tense ascites treated by paracentesis:a randomized pilot study. Gut 2002;50:90–94.
[15] Singh V, Kumar R, Nain CK, Singh B, Sharma N, Bhalla A, et al. Noradrenalineand albumin in paracentesis-induced circulatory dysfunction in cirrhosis: arandomized pilot study. J Intern Med 2006;260:62–68.
[16] Singh V, Kumar R, Nain CK, Singh B, Sharma AK. Terlipressin versus albuminin paracentesis-induced circulatory dysfunction in cirrhosis: a randomizedcontrolled trial. J Gastroenterol Hepatol 2006;21:303–307.
[17] Singh V, Dheerendra PC, Singh B, Nain CK, Chawla D, Sharma N, et al.Midodrine versus albumin in the prevention of paracentesis-inducedcirculatory dysfunction in cirrhotics: a randomized pilot study. Am JGastroenterol 2008;103:1399–1405.
[18] Appenrodt B, Wolf A, Grunhage F, Trebicka J, Schepke M, Rabe C, et al.Prevention of paracentesis-induced circulatory dysfunction: midodrine vs.albumin. A randomized pilot study. Liver Int 2008;28:1019–1025.
[19] Kalambokis G, Economou M, Fotopoulos A, Bokharhii JA, Pappas C, KatsarakiA, et al. The effects of chronic treatment with octreotide versus octreotideplus midodrine on systemic hemodynamics and renal hemodynamics andfunction in nonazotemic cirrhotic patients with ascites. Am J Gastroenterol2005;100:879–885.
[20] Kalambokis G, Fotopoulos A, Economou M, Pappas K, Tsinos EV. Effects of a 7day treatment with midodrine in nonazotemic cirrhotic patients with andwithout ascites. J Hepatol 2007;46:213–221.
[21] Krag A, Moller S, Henriksen JH, Niels-Henrik HR, Finn L. Terlipressinimproves renal function in patients with cirrhosis and ascites withouthepatorenal syndrome. Hepatology 2007;46:1863–1871.
[22] Tandon P, Tsuyuki RT, Mitchell L, Hoskinson M, Ma MM, Wong WW, et al.The effect of 1 month of therapy with midodrine, octreotide-LAR andalbumin in refractory ascites: a pilot study. Liver Int 2009;29:169–174.
2 vol. 56 j 348–354 353

Research Article
[23] Arroyo V, Gines P, Gerbes AL, Dudley FJ, Gentilini P, Laffi G, et al. Definitionand diagnostic criteria of refractory ascites and hepatorenal syndrome incirrhosis. Hepatology 1996;23:164–176.
[24] Ruiz-Del-Arbol L, Monescillo A, Jimenez W, Garcia-Plaza A, Arroyo V, Rodes J.Paracentesis induced circulatory dysfunction: mechanism and effect onhepatic hemodynamics in cirrhosis. Gastroenterology 1997;113:579–586.
[25] Moore KP, Wong F, Gines P, Bernardi M, Ochs A, Salerno F, et al. Themanagement of ascites in cirrhosis: report on the consensus conference ofthe International Ascites Club. Hepatology 2003;38:258–266.
[26] Cockcroft DW, Gault MH. Prediction of creatinine clearance from serumcreatinine. Nephron 1976;16:31–41.
[27] Kupari M, Koskinen P. Systolic flow velocity profile in the left ventricularoutflow tract in persons free of heart disease. Am J Cardiol 1993;72:1172–1178.
[28] Cardenas A, Gines P. Management of hyponatremia in cirrhosis. Ascites andrenal dysfunction in liver disease. 2nd ed. Oxford: Blackwell Publishing;2005, p. 315–340.
354 Journal of Hepatology 201
[29] McTavish D, Goa KL. Midodrine: a review of its pharmacological propertiesand therapeutic use in orthostatic hypotension and secondary hypotensivedisorders. Drugs 1989;38:757–777.
[30] Angeli P, Volpin R, Piovan D, Bortoluzzi A, Craighero R, Bottaro S, et al. Acuteeffects of the oral administration of midodrine, an alpha-adrenergic agonist,on renal hemodynamics and renal function in cirrhotic patients with ascites.Hepatology 1998;28:937–943.
[31] Gines P, Tito LI, Arroyo V, Planas R, Panes J, Viver J, et al. Randomisedcomparative study of therapeutic paracentesis with and without intrave-nous albumin in cirrhosis. Gastroenterology 1988;94:1493–1502.
[32] Angeli P, Volpin R, Gerunda G, Craighero R, Roner P, Merenda R, et al.Reversal of type 1 hepatorenal syndrome with the administration ofmidodrine and octreotide. Hepatology 1999;29:1690–1697.
2 vol. 56 j 348–354
Copyright © 2022 FDOKUMEN