
Mid Essex Clinical Commissioning Group Board Meeting
147
Mid Essex Clinical Commissioning Group Board Meeting Part I Agenda Thursday, 30 September 2021 from 1.00 pm to 2.45 pm Members of the Public should use this link to join the meeting Action Papers Lead Time Page No. GENERAL BUSINESS 1. Welcome and apologies for absence To note Verbal Dr Anna Davey 1.00 pm - 2. Declarations of interest and review of Register of Interests To note Attached Dr Anna Davey 2 3. Minutes of the meeting held on 29 July 2021 To approve Attached Dr Anna Davey 1.05 pm 6 4. Action Log and Matters Arising from last meeting (not on Agenda) To note Attached Dr Anna Davey 16 5. Questions from the Public To receive Verbal Dr Anna Davey 1.10 pm - SYSTEM REPORTS 6. Joint Accountable Officer Update To note Verbal Anthony McKeever 1.15 pm - 7. Board Assurance Framework To note Attached Viv Barnes 1.20 pm 17 8. Patient Story To note Presentation Rachel Hearn 1.30 pm - 9. System Performance Report To note Attached Dan Doherty 1.40 pm 29 10. Joint Committee Minutes of 24 June 2021 and 26 August 2021. To note Attached Dr Anna Davey 1.50 pm 39 PLACE REPORTS 11. CCG Chair’s Update Tonote Verbal Dr Anna Davey 1.55 pm - 12. Alliance Director Update To note Verbal Dan Doherty 2.00 pm - 13. Patient Safety & Quality Report To note Attached Viv Barker 2.05 pm 61 14. Month 5 Finance Report To note Attached Mark Barker 2.15 pm 82 15. Mid Essex Place Update To note Attached Kate Butcher 2.20 pm 92 16. Committee Minutes: 16.1 Patient Safety & Quality Committees in Common 16.2 Finance & Performance Committees in Common 16.3 Audit Committees in Common 16.4 Primary Care Commissioning Committee To note To note To note To note Attached Attached Attached Attached Nathalie Wright John Gilham John Gilham Nathalie Wright 2.40 pm 101 103 116 127 139 17. Any Other Business To note Verbal Dr Anna Davey 2.45 pm - FOR INFORMATION 18. Date/time of next Part I Board Meeting: Thursday, 25 November 2021 at 1.00 pm – 3.00 pm. To note Verbal Dr Anna Davey -
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Mid Essex Clinical Commissioning Group Board Meeting
Mid Essex Clinical Commissioning Group Board Meeting
Part I Agenda
Thursday, 30 September 2021 from 1.00 pm to 2.45 pm
Members of the Public should use this link to join the meeting
Action Papers Lead Time Page No.
GENERAL BUSINESS
1. Welcome and apologies for absence
To note Verbal Dr Anna Davey 1.00 pm -
2. Declarations of interest and review of Register of Interests
To note
Attached Dr Anna Davey 2
3. Minutes of the meeting held on 29 July 2021
To approve Attached Dr Anna Davey 1.05 pm
6
4. Action Log and Matters Arising from last meeting (not on Agenda)
To note Attached Dr Anna Davey 16
5. Questions from the Public To receive Verbal Dr Anna Davey 1.10 pm -
SYSTEM REPORTS
6. Joint Accountable Officer Update To note Verbal Anthony McKeever 1.15 pm -
7. Board Assurance Framework To note Attached Viv Barnes 1.20 pm 17
8. Patient Story To note Presentation Rachel Hearn 1.30 pm -
9. System Performance Report To note Attached Dan Doherty 1.40 pm 29
10. Joint Committee Minutes of 24 June 2021 and 26 August 2021.
To note Attached Dr Anna Davey 1.50 pm 39
PLACE REPORTS
11. CCG Chair’s Update Tonote Verbal Dr Anna Davey 1.55 pm -
12. Alliance Director Update To note Verbal Dan Doherty 2.00 pm -
13. Patient Safety & Quality Report To note Attached Viv Barker 2.05 pm 61
14. Month 5 Finance Report To note Attached Mark Barker 2.15 pm 82
15. Mid Essex Place Update To note Attached Kate Butcher 2.20 pm 92
16. Committee Minutes:
16.1 Patient Safety & Quality Committees in Common
16.2 Finance & Performance
Committees in Common
16.3 Audit Committees in Common
16.4 Primary Care
Commissioning Committee
To note To note To note To note
Attached Attached Attached Attached
Nathalie Wright John Gilham John Gilham Nathalie Wright
2.40 pm
101
103
116
127
139
17. Any Other Business
To note Verbal Dr Anna Davey 2.45 pm -
FOR INFORMATION
18. Date/time of next Part I Board Meeting: Thursday, 25 November 2021 at 1.00 pm – 3.00 pm.
To note Verbal Dr Anna Davey -

MID ESSEX CCG BOARD REGISTER OF INTERESTS (SEPTEMBER 2021) AGENDA ITEM 2
First Name Surname Current Position
Declared Interest
(Name of the organisation and nature of
business)
Is the interest
direct or
indirect?
Nature of Interest Actions taken to mitigate risk
Mark Barker Joint Chief Finance Officer Nil N/A
Anna Davey Chair of Mid Essex CCG and Partner at Coggeshall
Surgery
Coggeshall Surgery Provider of General Medical
Services
x Direct Partner in Practice providing
General Medical Services
09/01/17 Ongoing I will not be involved in any discussion, decision
making, procurement or financial authorisation
involving the Coggeshall Surgery or Edgemead
Medical Services Ltd
Anna Davey Chair of Mid Essex CCG and Partner at Coggeshall
Surgery
Colne Valley Primary Care Network x Direct Partner at The Coggeshall
Surgery who are part of the Colne
Valley Primary Care Network - no
formal role within PCN.
01/06/20 Ongoing I will declare my interest if at any time issues
relevant to the organisation are discussed so that
appropriate arrangements can be implemented
and will not participate in any discussion, decision
making, procurement or financial authorisation
involving the Colne Valley PCN.
Daniel Doherty Alliance Director, Mid Essex North East London Foundation Trust x Indirect Spouse is a Community
Physiotherapist at North East
London Foundation Trust
Ongoing There is a potential that this organisation could
bid for work with the CCG, at which point I would
declare my interest so that appropriate
arrangements can be implemented
Daniel Doherty Alliance Director, Mid Essex Provide Community Interest Company x Direct Honorary Clinical Contract Ongoing I am not currently working under this contract, but
it remains in place to perform clinical work if
required. I will declare the interest if necessary
so that appropriate arrangements can be
implemented
Daniel Doherty Alliance Director, Mid Essex All Saints (CoE) Primary School Maldon x Direct Chair of Governors of All Saints
Primary School Maldon
Ongoing Agreed with Line Manager that it is unlikely that
this interest is relevant to my current position, but
I will declare my interest where relevant so that
appropriate action can be taken
Daniel Doherty Alliance Director, Mid Essex Active Essex x Direct Board member 25/03/21 Ongoing Agreed with Line Manager that it is unlikely that
this interest is relevant to my current position, but
I will declare my interest where relevant so that
appropriate action can be taken.
John Gilham Lay Member - Governance The Compass Group x Direct To provide consultancy support
and advice to Compass
Healthcare UK & Ireland
Managing Director and his team
(one day per month management
consultancy contract).
01/07/2018 Ongoing I will declare my interest if at any time issues
relevant to the organisation are discussed so that
appropriate arrangements can be implemented
John Gilham Lay Member - Governance Compass Healthcare UK and Ireland x Direct Consultancy support (organisation
provides hotel cleaning, portering
etc, and commercial shop outlet
services M&S, Costa etc. to NHS
sites).
01/07/2018 Ongoing I will declare my interest if at any time issues
relevant to the organisation are discussed so that
appropriate arrangements can be implemented
John Gilham Lay Member - Governance The North East London NHS Foundation Trust x Indirect Family friend is Chair of The North
East London NHS Foundation
Trust
01/07/2018 Ongoing I will declare my interest if at any time issues
relevant to the organisation are discussed so that
appropriate arrangements can be implemented
John Gilham Lay Member - Governance Barking Havering & Redbridge Hospitals (BHR) NHS
Trust
x Indirect Close family relative works for
Barking Havering & Redbridge
Hospitals.
01/07/2018 Ongoing I will declare my interest if at any time issues
relevant to the organisation are discussed so that
appropriate arrangements can be implemented
John Gilham Lay Member - Governance Essex Partnership University Trust (EPUT) x Indirect Close family members work for
Essex Partnership University Trust
01/07/2018 Ongoing I will declare my interest if at any time issues
relevant to the organisation are discussed so that
appropriate arrangements can be implemented
John Gilham Lay Member - Governance Mid and South Essex Foundation Trust (MSEFT) x Direct Friend is Managing Director of
Basildon site.
03/06/2021 On-going I will declare my interest if at any time issues
relevant to the organisation are discussed so that
appropriate arrangements can be implemented
Fin
an
cia
l
Type of Interest
DeclaredDate of Interest
No
n-F
ina
nc
ial
Pe
rso
na
l In
tere
st From To
No
n-F
ina
nc
ial
Pro
fes
sio
na
l
Inte
res
t
2

MID ESSEX CCG BOARD REGISTER OF INTERESTS (SEPTEMBER 2021) AGENDA ITEM 2
First Name Surname Current Position
Declared Interest
(Name of the organisation and nature of
business)
Is the interest
direct or
indirect?
Nature of Interest Actions taken to mitigate risk
Fin
an
cia
l
Type of Interest
DeclaredDate of Interest
No
n-F
ina
nc
ial
Pe
rso
na
l In
tere
st From To
No
n-F
ina
nc
ial
Pro
fes
sio
na
l
Inte
res
t
John Gilham Lay Member - Governance Dr Kumar, Highwood Surgery, Brentwood x Direct Registered GP surgery On-going I will declare my interest if at any time issues
relevant to the surgery are discussed so that
appropriate arrangements can be implemented
Julia Hale Secondary Care Doctor Member, Basildon &
Brentwood CCG
NHS South East London CCG x Direct Designated Doctor for
Safeguarding
01/11/2018 01/05/21 No immediate action required.
GB / Committee meeting agenda items where the
member is conflicted will be managed on an
individual basis in consultation with the Chair of
the CCG, Chair of the Committee, Conflicts of
Interest Guardian and Head of Corporate
Governance as necessary.
Declarations are requested at the beginning of
every Board and Committee agenda, allowing the
Chair to take appropriate action
Julia Hale Secondary Care Doctor Member, Basildon &
Brentwood CCG
KPMG x Indirect Close family member employed. 2017 On-going No immediate action required.
GB / Committee meeting agenda items where the
member is conflicted will be managed on an
individual basis in consultation with the Chair of
the CCG, Chair of the Committee, Conflicts of
Interest Guardian and Head of Corporate
Governance as necessary.
Declarations are requested at the beginning of
every Board and Committee agenda, allowing the
Chair to take appropriate action
Julia Hale Secondary Care Doctor Member, Basildon &
Brentwood CCG
Provider Trust in West London x Direct Locum Consultant Paediatric work 01/03/2021 On-going No immediate action required.
GB / Committee meeting agenda items where the
member is conflicted will be managed on an
individual basis in consultation with the Chair of
the CCG, Chair of the Committee, Conflicts of
Interest Guardian and Head of Corporate
Governance as necessary.
Declarations are requested at the beginning of
every Board and Committee agenda, allowing the
Chair to take appropriate action
Rachel Hearn Executive Director of Nursing & Quality Nil N/A
Julie McGeachy GP Board member Dengie Medical Partnership (Tillingham &
Maylandsea)
x Direct GP Partner 01/04/18 Ongoing I will declare my interest if at any time issues
relevant to the Surgery are discussed so that
appropriate arrangements can be implemented
Julie McGeachy GP Board member Dengie & South Woodham Primary Care Network x Direct Clinical Director 01/05/18 On-going I will declare my interest if at any time issues
relevant are discussed so that appropriate
arrangements can be implemented
Julie McGeachy GP Board member Provide CIC x Indirect Spouse is employed as Chief
Medical Officer
05/07/21 On-going I will declare my interest if at any time issues
relevant are discussed so that appropriate
arrangements can be implemented
Anthony McKeever Joint Accountable Officer and Executive Lead for Mid
and South Essex ICS
MACS et al Ltd x Direct Director of wholly owned company
through which I contract with the
NHS for interim and other
services.
01/09/00 On-going I will declare my interest if at any time issues
relevant to MACS et al Ltd are discussed so that
appropriate arrangements can be implemented.
Maggie Pacini Consultant in Public Health - Essex County Council Essex County Council. x Direct Employee of local authority
partner to the CCG. Role is to
offer independent professional
advice under mandated offer from
public health in local government
to the NHS.
03/09/15 Ongoing To be clear about distinction when presenting an
independent professional opinion and when the
view of Essex County Council.
3

MID ESSEX CCG BOARD REGISTER OF INTERESTS (SEPTEMBER 2021) AGENDA ITEM 2
First Name Surname Current Position
Declared Interest
(Name of the organisation and nature of
business)
Is the interest
direct or
indirect?
Nature of Interest Actions taken to mitigate risk
Fin
an
cia
l
Type of Interest
DeclaredDate of Interest
No
n-F
ina
nc
ial
Pe
rso
na
l In
tere
st From To
No
n-F
ina
nc
ial
Pro
fes
sio
na
l
Inte
res
t
Maggie Pacini Consultant in Public Health - Essex County Council West Essex CCG x Direct Board member of West Essex
CCG in my capacity as Consultant
in Public Health offering
independent professional advice
under mandated offer from public
health in local government to the
NHS.
03/09/15 Ongoing My role is to provide independent professional
public health advice and therefore independent of
any position of the organisations I work for/with. I
will declare this interest where a decision of Mid
Essex CCG may impact upon West Essex CCG
and maintain confidentiality where appropriate.
Maggie Pacini Consultant in Public Health - Essex County Council Basildon & Brentwood CCG x Direct Non voting Board member of
BBCCG in my capacity as CPH
offering independent professional
advice under mandated offer from
public health in local government
to the NHS
01/05/20 Ongoing My role is to provide independent professional
public health advice and therefore independent of
any position of the organisations I work for/with. I
will declare this interest where a decision of Mid
Essex CCG may impact upon BBCCG and
maintain confidentiality where appropriate.
Fatai Salau GP Board Member EN TUB LTD x Direct Providing Out of Hours GP
Services
01/04/2018 Ongoing I will declare my interest and will not be involved
in any discussion, decision making, procurement
or financial authorisation regarding the provision
of Out of Hours GP services
Fatai Salau GP Board Member Extended Access Hub x Direct Extended Access Hub - Clinic 01/11/2018 Ongoing I will declare my interest and will not be involved
in any discussion, decision making, procurement
of financial authorisation regarding the provision
of the Extended Access Hub.
Fatai Salau GP Board Member Douglas Grove Surgery x Direct Partner 01/04/18 Ongoing I will declare my interest and will not be involved
in any discussion, decision making, procurement
or financial authorisation regarding the provision
of Douglas Grove Surgery
Pauline Stratford Lay Member of the Board for Castle Point &
Rochford, Southend
3rd Lay Member for Mid and Thurrock CCGs
Associate Director of Operations x Direct Married to second cousin. I will declare this interest whenever relevant in
order that this conflict can be managed
appropriately
Pauline Stratford Lay Member of the Board for Castle Point &
Rochford, Southend
3rd Lay Member for Mid and Thurrock CCGs
Greensward Surgery Hockley x Direct Registered GP surgery Ongoing I will declare this interest whenever relevant in
order that this conflict can be managed
appropriately
Mike Steel Councillor at Essex County Council Essex County Council (ECC) x Direct Councillor May 2021 May 2025 Obliged to follow ECC Code of Conduct
Mike Steel Councillor at Essex County Council Chelmsford City Council (CCC) x Direct Councillor May 2019 May 2023 Obliged to follow CCC Code of Conduct
Mike Steel Councillor at Essex County Council Great Waltham Parish Council (GWPC) x Direct Councillor 2001 May 2023 Obliged to follow GWPC Code of Conduct
Mike Steel Councillor at Essex County Council ECC Health & Wellbeing Board x Direct Councillor May 2021 May 2023 Obliged to follow ECC Code of Conduct
Mike Steel Councillor at Essex County Council The Conservative Party x Direct Member 2007 May 2025 Obliged to follow ECC Code of Conduct
Elizabeth Towers GP Board member Whitley House GP Surgery, Chelmsford. x Direct GP Partner 1985 29/03/21 I will declare my interest if at any time issues
relevant to the Surgery are discussed so that
appropriate arrangements can be implemented
Elizabeth Towers GP Board member Clinical Lead for Cancer and End of Life for Mid and
South Essex Sustainability & Transformation
Programme
x Direct Clinical Lead for Cancer and End
of Life for Mid and South Essex
Sustainability & Transformation
Programme
Ongoing Declared at appropriate meetings.
Elizabeth Towers GP Board member Macmillan x Direct Macmillan GP On-going Declared at appropriate meetings.
Elizabeth Towers GP Board member Mid Essex CCG x Indirect I am a close relative of Mid Essex
CCG's Named GP for
Safeguarding
01/04/15 Ongoing Included on the Board Register of Interests and
declared at Board meetings
Elizabeth Towers GP Board member Whitley Urgent Care Limited x N/A No longer relevant - see actions
taken to mitigate risk
N/A N/A This was a consultancy business but ceased
trading in 2014 but is still registed at Companies
House, so declared for audit purposes
4

MID ESSEX CCG BOARD REGISTER OF INTERESTS (SEPTEMBER 2021) AGENDA ITEM 2
First Name Surname Current Position
Declared Interest
(Name of the organisation and nature of
business)
Is the interest
direct or
indirect?
Nature of Interest Actions taken to mitigate risk
Fin
an
cia
l
Type of Interest
DeclaredDate of Interest
No
n-F
ina
nc
ial
Pe
rso
na
l In
tere
st From To
No
n-F
ina
nc
ial
Pro
fes
sio
na
l
Inte
res
t
Elizabeth Towers GP Board member Chelmer City Health x Direct Primary Care Network 01/07/19 On-going I will declare my interest if at any time issues
relevant to the PCN are discussed so that
appropriate arrangements can be implemented. I
hold no formal role within PCN.
Nathalie Wright Lay Member - Patient and Public Participation British Association of Counselling and
Psychotherapy
x Direct Counsellor 01/09/17 Ongoing In the event of me being asked to work in either a
voluntary or paid capacity as a Counsellor for any
of theMid Essex CCG’s providers, I will seek
approval from the Director of Corporate Services
and agree arrangements to be put in place to
mitigate any actual or potential risks.
Nathalie Wright Lay Member - Patient and Public Participation Humber Road and Sunrise Avenue Patient
Participation Groups
x Direct Member 01/04/18 Ongoing I will declare my interest if at any time issues
relevant to the surgery are discussed so that
appropriate arrangements can be implemented
Nathalie Wright Lay Member - Patient and Public Participation Essex Partnership Foundation Trust (EPUT) x Direct Employed on a voluntary and paid
basis.
25/02/21 Ongoing In the event of any of the activities that I am
asked to undertake as part of this role creating
any actual or perceived conflicts of interest, I will
inform the CCG Governance Lead and act upon
the advice provided on how to manage these
conflicts.
Nathalie Wright Lay Member - Patient and Public Participation Mid Essex CCG x Indirect Relative is employed in the CHC
Team.
14/09/21 On-going I will declare my interest if at any time issues
relevant to the surgery are discussed so that
appropriate arrangements can be implemented.
5

PART I BOARD MEETING HELD IN PUBLIC
1.00 pm – 3.30 pm on Thursday, 29 July 2021 Meeting broadcast via ‘MS Teams’
MINUTES
PRESENT: John Gilham (JG) - Deputy Chair and Lay Member (Chair) Anthony McKeever (AMcK) – Interim Joint Accountable Officer (Items 1-11) Mark Barker (MB) – Executive Chief Finance Officer (Items 1–12) Rachel Hearn (RH) – Executive Director of Nursing & Quality Dan Doherty (DD) – Alliance Director for Mid and South Essex Dr Julie McGeachy (JMcG) – Clinical Vice Chair and GP Board member Dr Liz Towers (LT) – GP Board Member Nathalie Wright (NW) – Lay Member (Patient & Public Engagement) APOLOGIES Dr Fatai Salau (FS) – GP Board Member Dr Anna Davey (AD) – Chair IN ATTENDANCE Cllr Mike Steel (MS) – Councillor, Essex County Council Maggie Pacini (MP) – Consultant in Public Health, Essex County Council (Items 1-11) Viv Barnes (VB) - Board Secretary Stephen Mayo (SM) - Interim Director of Nursing and Patient Experience Katherine Raven (KR) – Head of Communications and Engagement Ashley King (AK) – Finance Director of Primary Care and Special Projects Sara O’Connor (SO) - Head of Corporate Governance Charlotte Tannett (CT) – Corporate Governance Support Officer (Minute Taker)
Item No. Item
GENERAL BUSINESS
1. Welcome and Apologies for Absence: Presented by John Gilham JG welcomed all those present and thanked members of the public for joining the meeting and noted apologies listed above. JG explained that in line with Government and NHS guidance on social distancing, the Board would continue to hold its publicly held Part I meetings via MS Teams Live Broadcast.
2. Register of Interests/Declarations of Interest: The Board noted the most recent version of the register of interests. JG reminded members of their obligation to declare any interests they held on any issues arising at Board meetings which might conflict with the business of the CCG at the beginning of the meeting, at the start of each relevant agenda item, or should a relevant interest become apparent during an item under discussion, so that appropriate arrangements could be implemented. Declarations made by Board are listed in the CCG’s Register of Interests available either via the CCG’s Head of Corporate Governance or the CCG website.
AGENDA ITEM 3
6

Item No. Item
Declarations of interest from today’s meeting: JMc declared that her indirect interest in relation to the Joint Commissioning Team had ended on 5 July 2021. JMc also declared a new indirect interest in respect of Provide where her spouse had been appointed as Chief Medical Officer with effect 5 July 2021. MS declared direct interests with Essex County Council, Chelmsford City Council, Great Waltham Parish Council, Essex County Council Health and Wellbeing Board and the Conservative Party. It was noted that the Board Register of Interests had been updated accordingly.
3.
Review of Minutes: Presented by John Gilham Minutes of the Previous Meeting: The minutes were approved with no amendments. Resolved: the minutes of the Part I Board meeting held on 27 May 2021 were approved with no amendments.
4. Review of Action Log and Matters Arising (not on Agenda): Presented by Dr Anna Davey The action log was received and noted and updates were provided. There were no matters arising.
5. Questions and Comments from the Public: Presented by John Gilham and Viv Barnes VB advised that Mr Peter Blackman had submitted a number of questions and requests for information which she summarised as follows:
1. What steps is MECCG taking now to ensure its PCNs engage effectively with their communities? Are their representatives going to attend the next Community Summit Meeting? Are community engagement groups going to be able to present and discuss this with the next meeting of PCNs in Mid Essex?
DD confirmed a Primary Care Network (PCN) meet and greet template had been completed and presented to clinical directors with suggested mechanisms by which PCNs might better communicate with patient representatives. Healthwatch Essex would also look to undertake research into communities to give insight into which mechanisms they would like to be used to engage with them. This would then be used to inform future patient engagement.
2. What is MECCG doing to ensure that all GP Practices maintain a Carers’ Register? What steps are GP Practices in Mid Essex taking to review their patient lists to identify new and existing carers not yet getting carers’ support and refer them to the agencies contracted to provide support to carers in the Mid Essex area?
DD confirmed there were requirements and good practice guides in place for maintaining Carers Registers by NHS England/Improvement (NHSE/I) and the Royal College of General Practitioners which the vast majority of mid Essex practices did follow, however a compliance audit had not been undertaken recently
7

Item No. Item
due to Covid-19 (C-19). An audit would take place as soon as possible to identify any practices where uptake needed to be improved MP noted that some questions from the public were complex and written answers were being provided but not published in the minutes. VB confirmed this issue had been raised before, however each of the Mid and South Essex CCGs had a slightly different approach and so it was hoped a uniform approach would be adopted when the ICS was established.
SYSTEM REPORTS
6. Board Assurance Framework and revised CCG Strategic Objectives: Presented by Viv Barnes VB confirmed the report provided an update on the risks on the Board Assurance Framework (BAF) with a red risk score or rated red in terms of project delivery. The number of Extreme risks on the Risk Register (those with a score of 15 or more) had reduced from 19 to 12 since the last update as a result of 6 of the Finance risks being de-escalated. The risk related to the Ageing Well Beds Programme had also been de-escalated to Amber due to immediate measures having been taken to deal with winter pressures, potential future C-19 waves and agreement to progress a longer-term approach to reconfiguration. The most extreme risk, with a residual risk score of 25, related to achievement of the constitutional standard for Referral to Treatment, in recognition of the referral backlogs that accumulated during the waves of the C-19 pandemic. The current focus was upon ensuring that no patients were waiting longer than 98 weeks by the end of September 2021. Relevant risks were discussed at the Patient Safety & Quality (PSQ) and Finance & Performance (F&P) committees in common. There was a detailed discussion of the Risk Register at the last F&P meeting in relation to whether the rationale for changes in risk ratings was sufficiently clear and this would be followed up directly with the CCG Audit Chairs. VB confirmed the BAF was based upon the strategic objectives for the Mid and South Essex (MSE) CCGs and these had recently been reviewed and amended to ensure that they remained relevant for the current financial year. Minor changes had been made to the strategic objectives and these were set out in Appendix B of the papers. Consultation had taken place with CCG Boards and Executives on these changes and they were now being presented to the CCG Boards for adoption. Resolved: The Board noted the update on the Board Assurance Framework and approved the revised CCG Strategic Objectives.
7. Patient Story: Presented by Rachel Hearn/Stephen Mayo RH welcomed SM, Interim Director of Nursing for Patient Experience, to the Board. SM advised that the Serenity Integrated Mentoring Service (SIMS) and Special High Intensity Focus Team (SHIFT) services had initially been set up to address patients with chaotic lives who were regular users of accident and emergency, ambulance and GP services. The SIMS pilot took place in 2013 and was successful. As a result, in 2018 there was an opportunity for areas to bid to roll out the pilot further and Mid Essex and south east Essex were awarded funding to take the service forward. Mid Essex took the service forward as SIMS and south east
8

Item No. Item
Essex took the service forward as SHIFT. South west Essex did not choose to take a bid forward so there was no similar service in that area. SM highlighted subtle differences between both models, noting that the SIMS model required a diagnosis of personality disorder and mental health teams worked closely with the police. The SHIFT service accepted patients with any mental health problem who were high intensity users of healthcare services and their mental health nurses were based in the community health hubs. All patients registered for these services had to have the capacity to give consent, be known to be at medium/high risk of premature death, have chaotic lifestyles, be in frequent contact with emergency services, have a crisis plan in place and be engaged with the service. There had been some negative feedback received from patients which had prompted a national pause of the service with a local review being carried out by the Essex Partnership Foundation Trust (EPUT). The results of this review would be shared with the Board when completed. The patient story video showed Miranda’s experience of the SHIFT service in south east Essex. SM confirmed he and his team would be looking at how to take Miranda’s positive story forward to inform future commissioning decisions. SM thanked Miranda for sharing her experience with the Board. JMc noted that GPs often experienced high intensity users who put huge demand on services and stated it was very positive to see that the service was improving the quality of patients’ lives. JMc queried how many users of the SIMS service there were at present. SM confirmed he would provide the exact number of service users after the meeting. LT highlighted the positive impact of targeted and personalised care and queried if any physical wellbeing was supported under the service. SM confirmed it had given Miranda the ability to leave the house and be seen in public as she lacked confidence and had a fear of men previous to using the service. Patient stories are available on the CCG’s website Resolved: The Board noted the Patient Story. [Action: SM to provide JMc with the number of patients currently registered with the SIMS service.]
8. Joint Accountable Officer’s Update AM confirmed that ministers had decided that the boundaries for the MSE Integrated Care System (ICS) would be unchanged. Links with colleagues across all MSE local authorities were taking place to ensure all mechanisms for joint working would be streamlined, collaborative and effective. AM went on to advise that Professor Mike Thorne had been confirmed as Chair Designate for the MSE ICS. Professor Thorne was committed to progressing joint working relationships and his appointment marked the first step towards the creation of a new statutory body. Further guidance would be forthcoming which would confirm that a ‘lift and shift’ arrangement would be exercised to ensure continuity of employment for all MSE CCG staff with the exception of the most senior posts. The recruitment process for these senior posts was expected to begin in Autumn 2021.
9

Item No. Item
JG offered his and the Board’s best wishes to Professor Mike Thorne on his appointment.
9. System Performance Report: Presented by Dan Doherty DD advised that the performance report demonstrated how the MSE Foundation Trust (MSE FT) hospitals were coming under increased operational pressure due to a combination of factors including a rise in C-19 case numbers and increased demand for the treatment of Respiratory Syncytial Virus (RSV), flu and other winter viruses. The CCG was in the process of preparing winter plans as usual. JG confirmed a discussion had taken place at a recent F&P committees in common meeting about the advice and guidance service and concerns about response rates. A number of actions had been taken away to address what needed to be done in order to achieve the national target. Resolved: The Board noted the System Performance Report.
10. Joint Committee Update: Presented by Dan Doherty DD confirmed the following reports were considered at the CCG Joint Committee meeting on 24 June 2021:
• Sub-Acute Frailty and Intermediate Care Bed arrangements at Brentwood Community Hospital
• Adult Critical Care Transfer Service
• Neurodevelopmental Pathway
• Autism Spectrum Disorder Diagnostic Backlog
• Mental Health Support Team for Children and Young People
• Update on handling of prior approval requests
• System Finance update
• System Quality report
• Approval of annual Quality Accounts for EPUT, MSEFT, NELFT, Provide, BHRT and Farleigh Hospice
• System Performance report DD highlighted the reported investments in the Mental Health Support Team for Children and Young people, Autism Spectrum Disorder Diagnostic Backlog and Neurodevelopmental Pathway had been well received by GP committee members. Resolved: The Board noted the Joint Committee Update.
PLACE REPORTS
11. Alliance Director Update: Presented by Dan Doherty DD confirmed that his Alliance Director update would comprise a presentation of the Mid Essex Place Plan later on in the agenda. The plan was a joint production with partners, which Simon Froud, Director for Local Delivery for Essex County Council and Lorraine Jarvis, Chief Executive for Chelmsford Community Volunteering Service (CVS), had helped to present to AMc and Mike Thorne. The plan had received positive feedback and DD and his colleagues welcomed the challenge of taking the plan from theory to delivery. Resolved: The Board noted the Alliance Director Update.
10

Item No. Item
12. Patient Safety & Quality Report: Presented by Rachel Hearn RH confirmed the MSE CCGs’ PSQ Committees met in common on a bi-monthly basis and the PSQ report provided a summary of quality highlights for Mid Essex CCG. A historic Serious Incident (SI) from 2019 was being investigated to understand the delay in its completion. RH had requested completion of the SI by the end of July 2021 and would provide the Board with a further update at the next meeting on 30 September 2021. There had been 52 SIs and 3 Never Events reported in Quarter 1 which were all under investigation. The CCG was working closely with the MSE FT to look at immediate improvements to be put in place to address identified themes. A previous outbreak of Methicillin Resistant Staphylococcus Aureus Bacteraemia (MRSAB) in the Burn’s Unit atBroomfield Hospital had now closed with no new cases having been reported since April 2021. Learning was being pulled through for this and all other areas across the MSE system. 26 out of 32 Invasive Group A Streptococcus bacterial infection (iGAS) recommendations had been completed, 2 were not yet due and 4 were presently overdue. The work taking place to support the overdue actions was detailed within the report and it was anticipated that 3 of the actions would be completed by the end of July 2021 and the remaining 1 by November 2021. The MSE system had been allocated £1.9m of Ockenden funding to make improvements to maternity services. Work was underway to ensure the funding would be used proactively to meet all of the immediate requirements from the Ockenden review. The Care Quality Commission (CQC) had begun unannounced inspections of MSE maternity services and their findings would be reported back to the Board once received. 21 Mental Health SIs had been reported to date and any that took place from 1 May 2021 were being progressed through the new Patient Safety Incident Response Framework (PSIRF) which offered a practical risk-based approach. Any SIs reported prior to 1 May 2021 would be investigated via the previous Serious Incident Framework process. On 16 June 2021 EPUT had pleaded guilty to the Health and Safety Executive in relation to its management of an environmental risk associated with fixed ligature points from October 2004 to March 2015 and had received a fine of £1.5m plus costs. EPUT had advised that £10m had been spent to improve safety across the ward estates which had been fully supported by the CCG quality team. Plans were underway for a Parliamentary Independent Investigation into EPUT’s and its predecessor organisations’ patient deaths over a 20-year period from 1 January 2000 to 31 December 2020. The investigation was expected to take 2 years to complete and the investigation’s Terms of Reference would be provided to the Board when available. In Wave 1 of C-19 there had been 24 deaths of patients with Learning Disability (LD) and 57 deaths during Wave 2. Learning Disabilities Mortality Reviews (LeDeR) of these deaths were underway and early learning had identified actions in relation to promoting the overall health of the MSE LD population and the appropriate use of Do Not Attempt to Resuscitate (DNAR) orders.
11

Item No. Item
VB noted the report mentioned the gender disparity in LD patients who were affected by C-19 in Wave 1 which appeared to even out during Wave 2. VB understood that LD was more routinely diagnosed in males and therefore the assumption that infection rates should be the same for men and women was potentially incorrect. RH thanked VB for her helpful insight and confirmed she would feed her comments back into the LeDeR group for consideration. JG highlighted recurrent themes being identified in SIs and Never Events where previous remedial actions had apparently been unsuccessful. JG asked RH to consider what further steps would be needed to reduce the risk of recurrence. Resolved: The Board noted the Patient Safety & Quality Report. [Action: RH to provide an update on the historic SI from 2019 at the next Board meeting.] [Action: RH to report the findings of the unannounced CQC inspections of MSE maternity services at a future meeting.] [Action: RH to feedback VB’s comments in relation to equality monitoring of LD deaths to the LeDeR group.]
13. Month 3 Finance Report: Presented by Mark Barker MB confirmed the report outlined the first in-year presentation of the CCG’s financial performance. Mid Essex CCG acted as the lead CCG for the system, therefore the report highlighted some areas where they were carrying the full cost and responsibility. Adjustments would be made throughout the year as plans were refined. AK highlighted the CCG continued to operate in an abnormal framework and had only been advised of Half 1 financial allocations to date. Key points highlighted from the report were:
• The current overspend of £2.9m year to date and £5.8m forecast overspend (H1) reflected that to date the CCG had not received expected reimbursement for C-19 spend and the Elective Recovery Fund (ERF) – after receipt the net position would be in line with the plan, both year to date and forecast outturn, to breakeven
• Month 3 year to date C-19 costs were £1.6m • Month 3 year to date ERF costs were £1.4m • Overall expenditure pattern/run-rates were comfortable to date • Mid Essex was currently holding the system’s H1 QIPP requirement of
£6.7m. This was expected to be aligned to individual organisations in Months 5/6. Current forecasts showed delivery in full
• Running costs were currently on plan JG referred to the potential risk to delivery of the Mental Health Investment Standard (MHIS) and queried if AK was able to provide the Board with assurances around mitigating actions that might be available to the CCG in the event that the risk materialised. AK confirmed the risk was to budgeting position and not to achieving MHIS. Following the submission of the MHIS a number of additional costs were identified that the CCG was potentially liable for, resulting in a risk of additional cost pressures. The team were working to ascertain if the assumed costs were reasonable or not.
12

Item No. Item
JG noted that additional funding had been allocated to Mid Essex CCG for fully delegated primary care commissioning. Resolved: The Board noted the Month 3 Finance Report.
14. Mid Essex Place Plan: Presented by Dan Doherty: DD summarised the draft Mid Essex Place Plan, which set out how the Mid Essex Alliance, covering the Braintree, Chelmsford and Maldon local authority areas, aimed to meet the following objectives for 2021/22:
• COVID recovery; • Integrated health and social care (including the development of Primary
Care Networks); and • A renewed focus on prevention and reduction of health inequalities.
DD confirmed the plan had received excellent engagement from voluntary sector, district and county council partners. Included in the plan were local health and wellbeing plans which had been co-developed in district areas. These plans offered specialised areas of focus that would prove meaningful for individual communities. The Chelmsford aspects of plan provided a stronger focus on community safety, reduction of drug and alcohol misuse and knife crime. Braintree would focus on health opportunities for children and Maldon had a strong focus on social isolation, loneliness and suicide prevention. The 9 Primary Care Networks (PCNs) offered further hyper-local plans to address the needs of their local population. DD stated a good example of the Mid Essex Alliance coming together to support local communities was through the Cytosponge diagnostic test pilot which was due to launch in September 2021 and had received excellent engagement from the Chelmsford PCN. It was hoped the test would assist the PCN with overall health promotion. DD confirmed his team were working closely with the Central Business Information team to start to create an Alliance Performance Report which would highlight current areas of focus and would be brought to future Board meetings for scrutiny. Resolved: The Board endorsed of the direction, aims and objectives set out in the draft Mid Essex Alliance plan.
15. Communications & Engagement report: Presented by Katherine Raven: KR summarised the report and confirmed it aimed to demonstrate how Mid Essex CCG had informed and engaged local residents and stakeholders during the period 19 March – 18 July 2021 along with plans for the next quarter. KR highlighted the Essex Vax Van which was a visiting vaccination service that was believed to be the first custom built vehicle made for providing C-19 vaccines. This initiative was launched initially with the Chelmsford Muslim Society to provide vaccines to their members and community who were considered hard to reach. Feedback received so far had been very positive with 98% of users having rated the service 10/10 and 100% stating they would recommend the service to others. The initiative had received national media interest and was featured on BBC’s The One Show, BBC Morning Live and ITV News.
13

Item No. Item
A Communications and Engagement Report had been produced to show the breadth of work that had been done to engage with communities, particularly during the C-19 pandemic which had proved challenging. A ‘Cover up sunshine’ campaign had been launched with the support of actor Ray Winston to promote a new technology being rolled out in GP surgeries to help identify skin cancer. Tradespeople had been identified to be particularly at risk of skin cancer and trades companies had been brought on board to help raise awareness. The impact of the campaign was under evaluation. A significant amount of work had been done to engage with staff across the MSE partnership and MSE CCGs in recognition of the huge impact the C-19 pandemic had had on staff since March 2020. A new staff wellbeing campaign, Live Life Connected, had been launched which combined tools for physical and mental health promotion for staff via an online platform. 700 staff from across the MSE system had signed up and were engaged with the platform. A taskforce had been formed to assist in conversations with staff about the upcoming changes related to the formation of the ICS as well as the development of a new MSE CCGs staff intranet. NW thanked members of the public for their attendance at recent patient engagement events and highlighted some positive feedback that had been received with regards to the Essex Vax Van. Members of the African community had stated they felt the van encouraged peer pressure within the community and those who were against having the vaccine were able to ask questions one on one with clinical staff at the van which encouraged uptake further. NW queried if there would be communication provided on the C-19 vaccine booster. KR confirmed the current focus was on encouraging young people to get vaccinated, however phase 3 work was underway to plan a booster campaign and how to reach out to those who were eligible. JG stated it would be encouraging to see evidence of the positive impact of ongoing engagement work in future reports. Resolved: The Board noted the Communications & Engagement report.
16. Emergency Preparedness, Resilience & Response Policies: Presented by Viv Barnes VB confirmed Board approval was being requested to adopt the following amended MSE CCGs policies: • On Call Director policy • Incident Response Plan • Business Continuity Strategy • EPRR Strategy The main changes that had been made to these documents were that they had been streamlined so that they referenced national policies instead of reproducing their content. The full policies had been reviewed by the Audit Committees in Common, who were now recommending them for adoption by CCG Boards. Resolved: The Board approved the Emergency Preparedness, Resilience & Response Policies.
14

Item No. Item
17.
Committee Terms of Reference: Presented by Viv Barnes VB stated that following discussion with the members of the PSQ and F&P committees, it had been agreed that the committees in common model that was originally adopted as part of the CCGs’ business continuity arrangements during C-19, was working well and should be continued. Therefore, harmonised Terms of Reference had been developed so that each CCG’s committee had the same remit and broadly similar membership. The Terms of Reference, as set out in Appendices A and B of the papers, had been approved by both committees in common who now recommended them for adoption by CCG Boards. Resolved: The Board approved the PSQ and F&P Committees Terms of Reference.
18.
Committee Update Reports: Presented by Nathalie Wright/John Gilham The Board received the following committee update reports:
• Patient Safety & Quality Committee meetings held in common on 11 May 2021 and 13 July 2021;
• Finance & Performance Committee meeting held in common on 19 May 2021;
• Audit Committee meetings held in common on 26 May 2021 and 16 July 2021; and
• Primary Care Commissioning Committee meeting held in common on 10 June 2021
Resolved: The Board noted the Committee Update Reports.
19. Part II and Emergency Powers Decisions: Presented by Viv Barnes VB confirmed this part of the agenda was to enable public reporting of any urgent decisions taken between Board meetings or any decisions that were made in the private Part II meetings of the CCG Board. One Emergency Powers decision, relating to approval of the Information Governance Framework Policy and Information Sharing Policy in order that these policies could be amended before submission of the Data Security Protection toolkit, had been taken since the Board meeting held on 27 May 2021. There were no Part II decisions to report. Resolved: The Board noted the Part II and Emergency Powers Decisions.
20. Any Other Business There was no other business discussed.
FOR INFORMATION
21.
Date/time of next Part I Board Meeting: Thursday, 30 September 2021 at 1.00 pm, followed by CCG Annual General Meeting at 3.00 pm.
15

Part I Action Log prepared following Board meeting held on 29 July 2021 No Meeting
Date Agenda
Item Action Lead Deadline for
Completion Outcome/Update
1. 24/09/2020 26/11/2020 25/03/2021 27/05/2021 29/07/2021
9. 4. 4. 4. 4.
Mental Health Transformation Reset Establish whether an Equality and Health Inequalities Impact Assessment (EHIIA) has been undertaken on the reset and transformation of mental health services.
M Tebbs
To be confirmed.
The Alliance Director, Thurrock CCG, advised that an EHIIA will be undertaken for the 2021/22 Mental Health Plan to ensure that any actions identified are up-to-date and relevant. Confirmation of the expected date of completion has been requested by the Governance Team. Further requests for an update have been sent. Response awaited.
2. 29/07/2021 7. Patient Story Advise Dr Julie McGeachy of the number of patients registered with the SIMS service.
S Mayo
ASAP
Completed (13 patients).
3. 29/07/2021 11. Patient Safety & Quality Report RH to provide an update on the historic SI from 2019 at the next Board meeting. RH to report the findings of the unannounced CQC inspections of MSE maternity services at a future meeting. Terms of Reference for the Parliamentary Independent Investigation into patient deaths over a 20-year period to be provided to the Board when available. RH to feedback VBs comments in relation to equality monitoring of LD deaths to the LeDeR group.
R Hearn R Hearn R Hearn R Hearn
30/09/2021 To be confirmed. To be confirmed. 30/09/2021
Rachel Hearn will provide a verbal update at Board, 30 September 2021. Update to be provided to Board when the formal report from the CQC is published Update to be provided to Board when the Terms of reference are published Completed - comments provided to Lorraine Coyle to share with the LeDeR Steering Group.
Agenda Item 4
16

Part I Board Meeting
Board Assurance Framework
Date of Meeting: 30 September 2021 Agenda No
7
Purpose of Report:
‘Check’ (x) relevant box(es).
For Decision (approval/endorsement) ☐ For Assurance (discussion and noting) ☒
For Information Only ☐
Lead Executive Director:
Anthony McKeever, Joint Accountable Officer
Report Author / Presenter:
Sara O’Connor, Head of Corporate Governance, Mid Essex CCG
Executive Summary:
The majority of risks (69) on the BAF are within the remit of the MSE CCG Joint Committee (JC). The remainder (24) are within the remit of CCG Boards, including those relating to primary care. This report provides the Board with an update on:
• The 24 risks currently on the Board Assurance Framework (BAF) which remain within the remit of the Board
• An overview of the 69 risks within the remit of the JC, in particular those currently rated red (risk score between 15 and 25) or rated red in terms of project delivery.
Recommendations and decision/actions required:
The Board is asked to:
• Discuss and note the assurances contained within the report and advise of any further assurances required.
• Advise of any additional risks for inclusion in the Board Assurance Framework.
How does this report link to the CCG’s Strategic Objectives? ‘Check’ (x) relevant
objective(s) Strategic Objective 1 Restore access to services to achieve performance against NHS
Constitutional standards, quality improvement priorities and deliver ongoing COVID-19 requirements.
☒
Strategic Objective 2 Work with partner organisations and our population to address health inequalities, including those derived from Covid-19, and achieve social value.
☒
Strategic Objective 3 Support system transformation and organisational change to ensure the ICS is successfully established and can fulfil its aims and duties.
☒
Strategic Objective 4 Develop and support the creation and wellbeing of a diverse and highly skilled workforce and ensure the safe transition of staff to the new organisation.
☒
Strategic Objective 5 Achieve key statutory financial duties including delivery of the system financial control total, value for money and reduction of the underlying system deficit.
☒
Strategic Objective 6 Build effective Alliances at place to transform and strengthen the ability of Primary and Community Care Services to focus upon prevention and early intervention and improve outcomes in the most appropriate settings.
☒
Strategic Objective 7 Promote digitally delivered services whilst considering the requirements of those who need to access services in other ways.
☒
17

Approval Route:
(List Committees or groups that have reviewed this document).
Group/Committee Date (dd/mm/yy)
Remuneration Committee (HR related risks) 03/09/2021
Joint Committee (risks within remit of JC) 26/08/2021
Patient Safety and Quality Committee (PSQ risks) 14/03/2021
Finance & Performance Committee (F&P risks) 15/09/2021
Please confirm that the Lead Executive Director has signed-off the report prior to submission to the Committee/Board (Committee/sub-committee minutes submitted for information must be signed-off by the relevant Chair/Lead Executive before submission).
Yes
Has the CFO confirmed that any financial implications are within agreed budget and/or within CFO’s limit of delegated authority as per SFIs?
N/A
Have the relevant Impact Assessments been carried out and signed off?
Equality & Health Inequalities: N/A
Quality: N/A Privacy: N/A
Details of Patient & Public Engagement or Consultation:
Not applicable.
Related risks on Board Assurance Framework (BAF) / new risks identified which will be included on the BAF. (please use this link to view the BAF)
Risks within the remit of the Board are set out on Appendix A.
Conflicts of Interest: None identified.
Does the report need to be escalated to Board/Joint Committee or elsewhere?
No (Unless, there are specific issues which need to be brought to the attention of the relevant lead/Committee).
18

BOARD ASSURANCE FRAMEWORK 1. Introduction
The purpose of this report is to ensure that the MSE CCGs comply with their responsibility to regularly monitor and review risks that might impact upon the delivery of the CCGs’ strategic objectives. The report includes an update on:
• Risks on the Board Assurance Framework (BAF) which remain within the remit of the Board (see Section 2 below and Appendix A)
• An overview of risks within the remit of the MSE CCGs Joint Committee (JC), in particular those those currently rated red (risk score between 15 and 25) or rated red in terms of project delivery (see Sections 3 and 4 below).
The majority of risks on the BAF (currently 69) are within the remit of the JC and are reviewed at the JC bi-monthly meetings. The main exception is those risks relating to primary care, plus those within the remit of the Audit and Remuneration Committees for which the Board maintains oversight. Risks are also reviewed by relevant CCG Committees on a bi-monthly basis. All risks were reviewed and updated by Lead Officers during July/August 2021. Those risks within the remit of the Board were updated again in September. The latest review of the BAF included re-mapping risks against new workstreams and the MSE CCGs’ revised Strategic Objectives agreed in July 2021. Committee responsibility for risks has also been updated and discussions are taking place between risk leads and committee members to ensure risks have been allocated appropriately prior to the next round of committee meetings. In addition, at the request of the Audit Committee, a review of risks where the current risk rating score remains the same as the initial score (i.e. as at the date the risk was added to the BAF) is being carried out to understand the reasons for these. The result of this review will be reported to the next Audit Committee meeting in 15 October 2021. 2. Total number of Risks within the remit of CCG Boards As at 23 September 2021, there were 24 risks on the BAF within the remit of the CCG Boards, none of which were rated Red. The table below shows the number of risks by workstream and RAG rating. Workstream
RAG Rating Total No of Risks
Green Amber Red
Digital and Business Intelligence
3 2 0 5
Estates 0 2 0 2
Integrated Care System 1 1 0 2
People 1 3 0 4
Primary Care 4 4 0 8
Urgent Emergency Are 2 0 0 2
Vaccination 0 1 0 1
Total 11 13 0 24
Appendix A sets out these risks in greater detail. Risks are sorted by current risk score in descending order.
19

3. Total number of risks on the BAF within the remit of the Joint Committee
(by Workstream and RAG rating)
The table below set out the 69 risks currently on the BAF within the remit of the Joint Committee.
Workstream
Rating Total No of Risks Green Amber Red
Cancer and End of Life 0 0 2 2
Children and Young People 0 6 2 8
Community 1 3 0 4
Digital and Business Intelligence
2 0 0 2
Estates* 0 0 0 0
Finance 3 8 0 11
Health Inequalities 0 1 0 1
Integrated Care System 2 4 1 7
Maternity 0 2 1 3
Medicines Optimisation 2 1 0 3
Mental Health and Learning Disability
1 8 1 10
People 1 3 0 4
Planned Care 1 4 2 7
Population Health Management
0 0 0 0
Stewardship 0 0 0 0
Urgent Emergency Care 2 4 1 7
Vaccination 0 0 0 0
Total 15 44 10 69
The Joint Committee received a detailed report on these risks at its meeting on 26 August
2021.
4. Red Risks (risk score 15-25 or project delivery rated red) within the remit of the
Joint Committee
At 23 September, there were 9 risks within the remit of the JC rated red as listed in the table below.
Ref Workstream Description Current Score/ RAG rating / Trend
CANC01 Cancer and End of Life
To achieve cancer performance in accordance with Constitutional Standards. Maintaining access to rapid, early diagnostics cancer surgery and other treatments
15 / Red
PLAC01 Planned Care To achieve diagnostic (DM01) performance in accordance with Constitutional Standards. Maintaining access to rapid, early diagnostics ensuring all patients have their diagnostic within 6 weeks of referral
15 / Red
20

Ref Workstream Description Current Score/
RAG rating / Trend
PLAC02 Planned Care To achieve the Constitutional Standard for referral to treatment (RTT). Reduce 98 week waiting patients. Reduce 52week waiting patients. Reduce backlog for patients waiting Initial focus of highly challenged specialties (T&O, Ophthalmology, Urology, Endoscopy, Skin).
25 / Red
AGEW07 Cancer and End of Life
Palliative and End of Life Care. Five Key areas of work identified for Palliative and End of Life Care 24/7 model of care, protocols & clinical guidelines, training and education, bereavement, clinical outcomes.
16 / Red
CYP03 Children and Young People
The CCG will continue to work in partnership with education and care to become fully compliant with the Children and Families Act 2014 in relation to Special Education Needs and Disability (SEND). * Work to rectify areas of significant concern identified by CQC and Ofsted Report. * Transforming care agenda - to deliver the ambitions of and meet national targets for Children and Young People with LD and Autism. *Deliver Care, Education and Treatment Reviews (CETRs) for those CYP at risk of admission and monitor and maintain mechanisms for identification( Risk register) *To ensure CYP age 14+ with LD are on the GP register and receive annual health checks * Implement new neurodevelopmental pathway working with system partners *Reduce the waiting times for CYP Autistic Spectrum Disorder Diagnosis.
16/ Red
UNPC07 Children and Young People
The CCG will continue to work in partnership with education and care to become fully compliant with the Children and Families Act 2014. (Tier 4 Services). To ensure there is sufficient Tier 4 provision for children across MSE and that processes exist to provide wrap around care packages until beds are commissioned by NHSE.
16 / Red
GOSD12 Urgent Emergency Care
Acute / Provider Quality Assurance. Ensuring the care provision for residents is safe, effective, good quality and value for money as defined within the NHS Constitution.
16 / Red
GOSD15 Mental Health and Learning Disability
Mental Health Acute / Provider Quality Assurance. Ensuring the Mental Health care provision for residents is safe, effective, good quality and value for money as defined within the NHS Constitution.
16 / Red
MATS03 (New)
Maternity If the Maternity workforce does not meet the Birthrate Plus and Ockenden staffing requirements, then this will adversely affect delivery of care, resulting in potential adverse outcomes for women and their babies.
15 / Red
21

Of these, 6 risks (Refs PLAC02, AGEW07, CYP03, UNPC07, GOSD12 and GOSD15) are subject to a review to understand why their current risk ratings have remained the same since they were added to the BAF. The outcome of this review will be reported to the Audit Committee on 15 October 2021. The causes of the other 3 red rated risks (Refs CANC01, PLAC01, MATS03) are multi-factorial, including backlogs that have arisen as a result of the pandemic and workforce challenges that are being experienced both locally and nationally. All risks within the remit of the JC will be reviewed by mid October, including their risk ratings, in preparation for the JC meeting on 28 October 2021. Further information on the current performance of services is included within the Performance Report (agenda item 9). 5. Recommendations The Board is asked to • Note the BAF update report; • Seek any further assurances required; • Advise of any additional risks for inclusion on the BAF. 6. Appendices Appendix 1 – Risks within the remit of the CCG Boards. Risks are sorted by current risk score in descending order.
22

Mid and South Essex
Health and Care PartnershipBoard Assurance Framework APPENDIX A
Work
Stream
Description of Risk / Workstream
Objective
Strategic
Objectives
Risk Owner Clinical
Lead
System/
Place Lead
Risks of objective not
being delivered
Init
ial R
isk S
co
re
Update Milestone Deadline Enablers (Gap in Control) Success Measures
(Assurance - 2nd line of
defence)
Current
Performance
Cu
rren
t R
isk R
ati
ng
Targ
et
Ris
k S
co
re /
Ap
peti
te
Pro
ject
Delivery
Tre
nd
Assurance - 3rd line of defence CCG Committee that
will review risk
Primary Care To deliver the key outcomes of the
DES (i.e. Medication Reviews, Ward
rounds, spotting deterioration,
advance care planning etc.) To
ensure that the PCN support to bring
together services (MDT) to support
care better care homes is effective to
manage patients at home and avoid
unnecessary admissions.
1. NHS
Constitutional
Standards and
priorities
2. Address health
inequalities
4. Diverse and
highly skilled
workforce
6. Transform and
strengthen primary
and community
care services
7. Promote digitally
delivered services
William Guy PCN Clinical
Directors
Greer Phillips Service Delivery
Patient Safety & Harm
Acute Hospital Demand
Patient Experience
Inequality
Regulator Penalties
12 20 September 2021:
A session at the Mid Essex 'Time to Learn' Shut Down on 30
September 2021 will focus on WHAZN care home training to
further reinforce this aspect of the EHCH DES requirements.
30 June 2021 Comms & Engagement Performance against DES
measures.
Not sure where this is
reported?
TBA 12 3 A ↔ None Identified. Primary Care
Commissioning
Committee
Primary Care Development of PCNs and Clinical
Directors in line with national
guidance, following the PCN maturity
matrix. Further developing
collaboration and partnership working
linking PCNs with emerging Alliances
at Place and in the wider HCP.
2. Address health
inequalities
4. Diverse and
highly skilled
workforce
5. Achieve
statutory financial
duties
6. Transform and
strengthen primary
and community
care services
7. Promote digitally
delivered services
William Guy Ronan
Fenton
CCG Chairs
Jenni Speller Reputational Damage
Service Delivery
Acute Hospital Demand
Patient Experience
Inequality
12 15 September 2021:
Ongoing work with ICS Medical Director to develop PCN
Clinical Director development plans. The ICS approach to
strategic development of PCNs is being reviewed as part of
the D-LEADER programme.
Population Health Management (PHM) Wave 3 programme
underway and arrangements being established to ensure
knowledge transfer on leadership develoment arrangements
for participating Clinical Directors (CDs). CDs Forum to
include PHM discussion with lead CDs.
Accelerator Programme initiatives in Thurrock, Mid Essex
and South East Essex have commenced and Basildon and
Brentwood initiative is still being scoped.
Progress is being made, however the expectations are
increasing. Consequently the risk rating remains Amber/12
at current time.
30 November 2021
30 September 2021
People Resources
Partnership Working
Comms & Engagement
Annual progress against the
maturity matrix.
Successful completion of
Clinical Directors through the
accelerator programme.
19/20 baseline
undertaken, all at
foundation stage.
Sept 2021: PCNs
have been rated
between
Foundation and
Level 1 across
maturity matrix.
12 6 A ↔ Regular reporting to Primary Care
Commissioning Committee.
Primary Care
Commissioning
Committee
Primary Care Ensuring all PCNs progress to full
utilisation of ARRS offer (full
recruitment).
4. Diverse and
highly skilled
workforce
5. Achieve
statutory financial
duties
6. Transform and
strengthen primary
and community
care services
William Guy CCG Chairs Jenni Speller Acute Hospital Demand
Patient Experience
Service Delivery
12 15 September 2021:
Additional Roles Recovery Action Plan developed and
implemented with weekly monitoring and escalation
arrangements in place. Dedicated Resourcing Advisor
recruited to Workforce Team.
Annual Workforce Planning exercise has commenced with
27 x PCNs.
Revised plans for 2021/22 received from all PCNs and
submitted to NHSE/I.
At August 2021:
• 200 FTE additional roles have been recruited across the
system in total.
Although progress is being made, the risk rating remains
Amber/12 due to ongoing increases in trajectory of number
of roles required.
March 2022
30 November 2021
People Resources
Partnership Working
Human Resources
Estates
Recruitment of additional
staff.
Utilsation of Additional Role
Reimbursement Scheme
annual funding.
Ongoing
To be confirmed in
March 2022.
12 4 A ↔ Regular reporting to Primary Care
Commissioning Committee.
Primary Care
Commissioning
Committee
Primary Care To ensure all 5 CCGs can effectively
discharge their delegated functions
through formal governance
mechanisms.
6. Transform and
strengthen primary
and community
care services
William Guy CCG Chairs Jenni Speller Reputational Damage
Regulator Penalties
Patient Safety & Harm
Patient Experience
12 15 September 2021:
MSE Primary Care Commissioning Committee in Common
estabilished June 2021
Policies and standard operating protocols being developed
Resource requirements under review as part of ICS
Transition Design programme.
Audit of primary care governance being undertaken in Q3.
Risk rating will be reviewed once outcome is known.
31 December 2021 People Resources
Partnership Working
Effective in Common Primary
Care Commissioning
Committee.
PCCC meetings in
common
established.
12 3 A ↔ Regular reporting to Primary Care
Commissioning Committee.
Audit of Primary Care Govenrance
will take place Q3 2021/22.
Primary Care
Commissioning
Committee
23

Mid and South Essex
Health and Care PartnershipBoard Assurance Framework APPENDIX A
Work
Stream
Description of Risk / Workstream
Objective
Strategic
Objectives
Risk Owner Clinical
Lead
System/
Place Lead
Risks of objective not
being delivered
Init
ial R
isk S
co
re
Update Milestone Deadline Enablers (Gap in Control) Success Measures
(Assurance - 2nd line of
defence)
Current
Performance
Cu
rren
t R
isk R
ati
ng
Targ
et
Ris
k S
co
re /
Ap
peti
te
Pro
ject
Delivery
Tre
nd
Assurance - 3rd line of defence CCG Committee that
will review risk
Estates Risk of lack of compliant GP practice
estate to support new models of care,
which might result in inability to
accommodate additional services
within the community.
1. NHS
Constitutional
Standards and
priorities
2. Address health
inequalities
4. Diverse and
highly skilled
workforce
6. Transform and
strengthen primary
and community
care services
7. Promote digitally
delivered services
William Guy PCN Clinical
Directors
Kerry Harding Acute Hospital Demand
Claims & Complaints
Finance
Inequality
Patient Experience
Service Delivery
Reputational Damage
Staffing, HR, OD
12 16 September 2021 update:
Primary Care Network (PCN) Programme Manager recruited
to work with PCNs to develop their individual Estates Plans,
which will be aligned to the HCP Estates Strategy
Template PCN plans to be developed by October 2021.
Risk rating reviewed, but remains the same (Amber/12) at
this time, but is likely to reduce once implementation of plans
commences in early 2022.
31 October 2021
Estates
Finance
IT Infrastructure
Legal
Human Resources
Approval of HCP Estates
Strategy.
Development and approval of
individual PCN Estates Plans.
Sufficient and suitable estate
to accommodate staff to
deliver new models of care.
In final draft.
Not yet
commenced.
Plans in
development.
12 3 A ↔ Reporting to Primary Care Estates
Sub-Group (monthly).
Reporting to HCP Strategic Estates
Group (monthly).
Reporting to Primary Care
Commissioning Committees
meeting in common.
Primary Care
Commissioning
Committee
People If the CCG does not effectively
manage its workforce during a period
of organisational change, then there
is a possibility that the CCG will be
unable to effectively discharge is
responsiblities including 'business as
usual', recovery of services, and
winter pressures, resulting in an
adverse impact on services.
3. Establish
Integrated Care
System
4. Diverse and
highly skilled
workforce
Ruth
Jackson
N/A Vicky
Robertson
Service Delivery 12 23 September 2021:
The CCGs are continuing with engagement with staff and
unions as they move towards consultation during the first
quarter of 2022/23. Recruitment continues to critical posts.
Risk rating has been reviewed but remains the same at
current time. To be reviewed once outcome of all
D-LEADER Workshops has been evaluated.
31 March 2022 People Resources
Comms & Engagement
Human Resources
Turnover of staff.
Engagement levels from staff.
Outcome of Staff Survey (due
February 2022)
TBC 12 4 A ↔ Monthly reporting to ICS Workforce
programme board provide updates.
Remuneration
Committee
People If the MSE CCGs fail to deliver the
equality, diversity and inclusion
elements of the People Promise, then
there could be an adverse impact
upon recruitment, retention and staff
wellbeing, resulting in failiure to
evidence compliance with associated
EDI standards, including the Equality
Delivery System 2 (EDS2), the
Workforce Race Equality Standard
(WRES) and a potential risk of legal
action being taken.
2. Address health
inequalities
4. Diverse and
highly skilled
workforce
Ruth
Jackson
Sunil Gupta Vicky
Robertson
Inequality
Claims & Complaints
Reputational Damage
Staffing, HR, OD
16 23 September 2021:
A Workforce EDI Lead for the system has been appointed
who will develop a system strategy for implementation by
the CCGs.
CCG WRES action plans are being consolidated into an
MSE wide plan. Starting to engage the workforce in terms of
the Equality Diversity and Inclusion Strategy and actions
required.
Risk rating reviewed and remains 12/Amber - to be reviewed
once MSE WRES plan has been finalised.
31 March 2021
People Resources
Finance
Partnership Working
Compliance against WRES.
Compliance with Goal 3 of
EDS2.
Compliant for
2020/21
12 4 A ↔ Review of WRES assessment by
Remuneration Committee.
NHS WRES Data Report on
compares national data from
previous years to assess trends.
Remuneration
Committee
Estates There is a risk that all new Integrated
Medical Centres (IMCs) might be
delayed due to new accounting rules
(International Financial Reporting
Standard 16) which requires all
leases to be capitalised. This might
affect the system's ability to operate
within the allocated system Capital
Departmental Expenditure Limit
(CDEL).
5. Achieve
statutory financial
duties
Dawn
Scrafield
N/A Kerry Harding Finance 16 16 September 2021:
Mitigation for Tilbury and Purfleet has been identified and is
currently being worked through to ensure it is a viable
option. CDEL for Grays may be not be an issue if we can
utilise existing estates or offset by disposals. To be explored
as part of the business case process.
Consequently, risk rating reduced from 16/Red to Amber/12.
30 November 2021 Finance Solution found to enable
agreement for lease to be
completed.
Work ongoing to
agree system
solution.
12 4 A ↓ Regular reporting to Integrated
Medical Centre programme board.
Regular updates with Senior
Responsible Officer.
Primary Care
Commissioning
Committee
24

Mid and South Essex
Health and Care PartnershipBoard Assurance Framework APPENDIX A
Work
Stream
Description of Risk / Workstream
Objective
Strategic
Objectives
Risk Owner Clinical
Lead
System/
Place Lead
Risks of objective not
being delivered
Init
ial R
isk S
co
re
Update Milestone Deadline Enablers (Gap in Control) Success Measures
(Assurance - 2nd line of
defence)
Current
Performance
Cu
rren
t R
isk R
ati
ng
Targ
et
Ris
k S
co
re /
Ap
peti
te
Pro
ject
Delivery
Tre
nd
Assurance - 3rd line of defence CCG Committee that
will review risk
Integrated Care
System
To deliver the national ask of
developing an NHS ICS Body and
Health & Care Partnership in
accordance with legislation and best
practice guidance to commence on
1st April 2022.
3. Establish
Integrated Care
System
Jo Cripps Mike Thompson
/ Phil Reid
Reputational Damage
Staffing, HR, OD
15 22 September 2021:
ICS Transition Programme Board established with seven
work streams (quality and safety; finance; governance and
accountability; digital and data; comms & engagement;
people and organisational development; and system
operating model). Workstreams fully established and
developing/delivering project plans for technical close down
and safe transition of CCG functions into the new statutory
Integrated Care Board (ICB). Creation of the Integrated Care
Partnership (ICP).
National guidance received (final tranche 3 expected end
Sept 21).
The Secretary of State (SoS) confirmed there will be no
boundary changes to the MSE ICS. Due Diligence process
commenced (for regional submission 29/10/21). Q2 System
Development Plan under review (for regional submission
29/10/21) Readiness to Operate Statement (ROS) initial
assessment undertaken (for regional submission 29/10/21.)
On-going discussions in relation to ICB/ICP formation
through the MSE Partnership Board.
Transition programme on track. Consequently risk rating
score reduced from Red/15 to Amber/10.
31 March 2022 People Resources
Partnership Working
Establishment of NHS
Integrated Care Board and
Integrated Partnership by 1
April 2022.
Successful close down of 5 x
CCGs and establishment of
new statutory NHS body in
line with national published
guidance and Health & Care
Bill (subject to the passing of
legislation)
Currently on track
to deliver national
expectation and
delivery timeline.
10 5 A ↓ Oversight by ICS Transition Board.
Programme board chaired by
Accountable Officer with oversight
by regional NHSE partners.
Detailed oversight by Transition
workstream groups (x 7).
Audit Committee
People Acute: Develop plans and policies to
support creation of an effective and
flexible workforce that meets the
needs of patients within the
configuration of the new MSE trust.
Support the merger of the three
former Hospital Trusts into a single
MSE way of working
Improve recruitment procedures,
learning from processes during
COVID 19, so ensuring adequate
staffing
Explore and implement new and
more efficient ways of working.
4. Diverse and
highly skilled
workforce
Ruth
Jackson
Ronan
Fenton
Holly Randall Acute Hospital Demand
Claims & Complaints
Patient Experience
Patient Safety & Harm
Regulator Penalties
Service Delivery
9 23 September 2021:
Director of People and Organisational Development has
advised that this risk should be transferred from the CCG's
BAF to the Sytem Oversight and Assurance Group and once
the ICS People function is established from 1 April 2022, this
should also be monitored by the People Board.
30 September 2021 Comms & Engagement
Estates
Finance
Human Resources
People Resources
Reduction in unfilled
secondary care workforce
vacancies.
Improved attrition and
turnover rates.
Streamlined collaborative
recruitment process.
In initial stages. 9 3 A ↔ Regular review by Recruitment and
Retention Task and Finish sub-
group.
Remuneration
Committee
Digital and
Business
Intelligence
If GP practices decide not to offer on-
line consultations using the range of
free digital solutions provided by the
CCGs (on-line consultation was
implemented by April 2020 and video
consultation by April 2021), then the
requirements of the GMS contract to
offer consultations to patients in this
way might not be met, resulting in
some patients not receiving the same
quality of service/offer across the
ICS.
6. Transform and
strengthen primary
and community
care services
7. Promote digitally
delivered services
Mark Barker Taz Syed Peter King Primary Care Demand
Patient Experience
15 17 September 2021:
Clinical systems review is concluding. Engagement with
primary care was conducted throughout the summer. On-
track to deliver final report to CCG by 30 September 2021.
CCG will then devise action plan by 31 October 2021.
Risk rating has been reviewed, but remains at 9/Amber as
utilisation by practices has remained static. Clinical systems
review should identify root cause of problem to inform
further engagement with practices.
This remains a national issue. There is intense supplier
competition in this market place with unified solutions being
offered covering consultations, call-recall and bulk
messaging. The risks are: [A] GPs remain un-satisfied with
any system. [B] Non-compliance with the GP Operating
Model [based on Practices having the ability to offer online
consultation] [C] Risk of poor patient experience if they are
not aware of the online consultation option due to lack of
promotion by GPs [D] Future financial envelope is not clear
[E] Risk of double-payment during transitions [F] Risk of
patients digitally excluded [F] Risk that new ways of working
are not more efficient. Demand for Video consultations
nationally is only 1-3% of appointments.
31 October 2021 Finance
[A] Practices enabling the
solution
[B] Practices utilising the
solution
At 17/09/21:
[A] 145 out of 149
practices enabled
across M&SE .
[B] 79 out of 149
practices across
MSE actively using
system
9 3 A ↔ Utilisation is monitored via NHS
Digital dashboard.
Updates provided to Alliance
Directors for each place (monthly).
Regular reporting to monthly
Primary Care Digital Board meeting.
Primary Care
Commissioning
Committee
25

Mid and South Essex
Health and Care PartnershipBoard Assurance Framework APPENDIX A
Work
Stream
Description of Risk / Workstream
Objective
Strategic
Objectives
Risk Owner Clinical
Lead
System/
Place Lead
Risks of objective not
being delivered
Init
ial R
isk S
co
re
Update Milestone Deadline Enablers (Gap in Control) Success Measures
(Assurance - 2nd line of
defence)
Current
Performance
Cu
rren
t R
isk R
ati
ng
Targ
et
Ris
k S
co
re /
Ap
peti
te
Pro
ject
Delivery
Tre
nd
Assurance - 3rd line of defence CCG Committee that
will review risk
Digital and
Business
Intelligence
If the ordering of diagnostic tests is
not digitised within Broomfield
hospital, then there is a risk that GPs
in this area will be unable to submit
requests for tests in a timely way,
resulting in a delay in results which
could potentially affect patient safety
and quality.
6. Transform and
strengthen primary
and community
care services
7. Promote digitally
delivered services
Mark Barker Taz Syed Peter King Service Delivery
Patient Safety & Harm
Patient Experience
9 17 September 2021:
The MSE Hospital group have submitted the bid to NHS
Digital for the funding to put the solution in place. The Trust
has received final feedback on their draft letter of agreement
and are expecting a Memorandum of Understanding to
follow pending release for the funding as early as the end of
September 2021.
The Acute Care Portal will allow GP practices to view
phlebotomy results on line. All MSE practices have been
invited to sign-up and this will help to mitigate this risk once
practices have access.
Risk rating reviewed but remains 9/Amber.
NB: MSE Hospitals Project [Mid-Essex Hospital]
MID does not have an ordercoms system in place.
MCCG considering a single phlebotomy solution timescale
18-24 months. ICE roll-out managed by Acute, supported by
IT/Digital.
31 September 2021 People Resources
IT Infrastructure
Finance
% GP Pratices enabling
Order Comms
% Orders received
electronically
% results sent electronically
via MESH
Current zero as no
electronic solution
in place.
9 3 A ↔ None Identified.
Regular reporting to Primary Care
Digital Board (monthly).
Primary Care
Commissioning
Committee
Vaccination To ensure that the plans for COVID-
19 and Flu vaccinations are delivered
within national expectations and any
associated risks are adequately
managed.
1. NHS
Constitutional
Standards and
priorities
William Guy Simon
Williams
Hilary Scott
(EPUT)
Andrew
McLeod
Acute Hospital Demand
Health Inequality
Patient Experience
Patient Safety & Harm
Primary Care Demand
Reputational Damage
Service Delivery
12 15 September 2021:
The CCGs are expecting national announcements and
guidance on the next phase of the vaccination programme
today. Operational planning is underway to deliver.
Recruitment for dedicated team to deliver the programme is
underway, with some posts already appointed - awaiting
start dates.
Programme now expanded to include Flu vaccinations given
level of inter-dependency with COVID-19 vaccination
programme.
New phase 3 of COVID-19 vaccination programme has
commenced to provide booster doses to vulnerable patient
cohorts.
Risk rating reviewed, but remains at 8 / Amber due to
ongoing risk of new variants.
31 March 2022
People Resources
Estates
Information Governance
Partnership Working
Cohorts:
1 - 10 (aged 40+)
11 (aged 30 - 39)
12 (aged 18 - 29)
At 16/09/21:
1st/2nd doses
90% / 88%
71% / 63%
67% / 51%
8 4 A ↔ National and regional NHSE/I
provide close supervision and
direction of all activities (no
significant concerns raised at this
time).
Primary Care
Commissioning
Committee
People Proposed Description:
If MSE system staff do not have
access to enhanced psychological
support and the relevant data is not
regularly monitored to ensure that
appropriate action is taken to address
work-related concerns, then there is a
possibility that there will be an
increase in work-related
absence/presenteeism, and other
associated impacts upon service
delivery.
1. NHS
Constitutional
Standards and
priorities
4. Diverse and
highly skilled
workforce
Ruth
Jackson
Ronan
Fenton
Holly Randall Staffing, HR, OD
Reputational Damage
Acute Hospital Demand
Primary Care Demand
Service Delivery
9 23 September 2021:
Psychological support for staff within the MSE system
remains available through various avenues. Currently being
well utilised through in-reach and out-reach programmes
(e.g. Occupational Health, Here for You Service, Employee
Assistance Programme (EAP). This data is being monitored
via the Health and Wellbeing Sub-Group.
The system is currently awaiting the publication of wellbeing
metric requirements.
Risk rating reviewed and remains 6 / Green. To be
reviewed once up-to-date data for Health and Wellbeing Sub-
Group meeting has been collated.
Ongoing monitoring of
data
None Identified Staff sickness rates,
particularly relating to stress/
anxiety/depression.
Staff survey results on
'burnout morale'.
Engagement data from Here
For You service.
No of Occupational Health
Referrals.
EAP Data.
Data being
collated for Health
and Wellbeing Sub-
Group meeting.
6 3 G ↔ Regular reporting to Health and
Wellbeing Sub-Group.
Remuneration
Committee
Primary Care Ensuring national service
requirements for PCNs are delivered
in accordance with set criteria and
timescales.
6. Transform and
strengthen primary
and community
care services
William Guy CCG Chairs Jenni Speller Reputational Damage
Patient Safety & Harm
Claims & Complaints
Service Delivery
Acute Hospital Demand
Patient Experience
Inequality
9 15 September 2021 Update:
Local Accountabilty Framework being developed as part of
delegated commissioning arrangements.
Resource requirements under review as part of ICS
Transition Design work.
NHS England have published the national requirements up
to March 2023. Consequently, work plans are under review
against these new requirements.
Risk rating reviewed and remains Green/6.
Phased delivery from
1st April 2021.
31 December 2021
Phased delivery from
October 2021.
People Resources
Partnership Working
IT Infrastructure
Delivery of the PCN Impact
Investment Fund metrics
(national definitions are
awaited).
TBC once national
definitions are
received.
6 3 G ↔ Regular reporting to Primary Care
Commissioning Committee.
Primary Care
Commissioning
Committee
26

Mid and South Essex
Health and Care PartnershipBoard Assurance Framework APPENDIX A
Work
Stream
Description of Risk / Workstream
Objective
Strategic
Objectives
Risk Owner Clinical
Lead
System/
Place Lead
Risks of objective not
being delivered
Init
ial R
isk S
co
re
Update Milestone Deadline Enablers (Gap in Control) Success Measures
(Assurance - 2nd line of
defence)
Current
Performance
Cu
rren
t R
isk R
ati
ng
Targ
et
Ris
k S
co
re /
Ap
peti
te
Pro
ject
Delivery
Tre
nd
Assurance - 3rd line of defence CCG Committee that
will review risk
Primary Care Recruitment and retention of roles
within Primary Care
4. Diverse and
highly skilled
workforce
6. Transform and
strengthen primary
and community
care services
William Guy Being
recruited.
Kathryn Perry Service Delivery
Acute Hospital Demand
Patient Experience
9 15 September 2021:
Delivery Programme in place as part of the programme of
work to deliver the Primary Care Strategy.
Infrastructure funding received to support delivery and
recruitment underway to agreed plan.
Governance arrangements currently under review with
support from MSE Partners to ensure allignment with ICS
Governance Model.
Recruitment of clinical lead underway.
Risk rating reviewed and remains the same (Green/6).
31 December 2021
People Resources
Partnership Working
Human Resources
Being reviewed as part of
work with MSE Partners.
All milestones to-
date have been
met.
6 6 A ↔ Regular reporting to Primary Care
Commissioning Committee.
Primary Care
Commissioning
Committee
Digital and
Business
Intelligence
If the MSE CCGs' Digital Team is not
fully resourced, there is a risk that the
CCGs will be unable to deliver the
Digital First Primary Care agenda and
support the formation of the new ICS,
potentially resulting in a number of
projects being delayed.
4. Diverse and
highly skilled
workforce
7. Promote digitally
delivered services
Mark Barker Taz Syed Peter King Service Delivery 15 17 September 2021:
Two new members of the Digital Team commenced
employment 13 September 2021. Further member to
commenced on 1October 2021.
Temporary resource has also been secured until 31 March
2022 to support ICS transition arrangements.
Consequently, current risk rating reviewed and reduced from
9/Amber to 6/Green.
1 October 2021
People Resources Digital Team fully resourced. Team has
increased from 6
to 9. Further
resources still
required and will
be required as part
of transition to ICS.
6 3 G ↓ Not applicable. Primary Care
Commissioning
Committee
Urgent
Emergency
Care
Emergency Preparedness Resilience
and Response (EPRR) Capability
1. NHS
Constitutional
Standards and
priorities
Karen
Wesson
Chris
Patridge
Paula Saunders
/ Jo Martindale
Patient Safety & Harm
Reputational Damage
Service Delivery
20 16 September 2021:
EPRR policies approved by the five CCG governing bodies
(Thurrock, 23 June, Basildon, Mid, CPR and Southend, 29
July 2021).
Evaluation of the on-call pilot was presented to the Audit
Committees meeting in Common and support was granted
for the continuation in its pilot form. To be reviewed in line
with ICS transition.
Staff training on-going to ensure competencies.
EPRR System
assurance summary to
be submited by
31 October 2021
Partnership Working Sufficient resource, training,
experience and planning to
minimise operational impacts
from major incidents.
Compliant 5 5 G BAU
Core standard compliance review
for NHSE completed. All CCGs
were compliant (submitted
31/10/20).
Audit Committee
Urgent
Emergency
Care
To achieve compliance with NHSE
Core Standards for EPRR
1. NHS
Constitutional
Standards and
priorities
Karen
Wesson
Chris
Patridge
Paula Saunders
/ Jo Martindale
Patient Safety & Harm
Reputational Damage
Service Delivery
15 16 September 2021:
EPRR policies approved by the five CCG governing bodies.
2021/22 Core Standards process guidance issued by
NHSE/I. Self-assessment process by CCG and providers
has taken place, with ‘confirm and challenge’ meetings
currently occurring.
EPRR System
assurance summary to
be submited by
31 October 2021
Partnership Working Achievement of EPRR Core
Standards.
Compliant
2020/21.
5 5 G ↔ Local Health Resilience Partnership
meetings will recommence following
pandemic (date TBC).
Audit Committee
Primary Care To ensure that all Primary Care
Providers offer at least the same
capacity as 2019/20. In addition,
recover performance metrics on key
primary care service delivery e.g.
health checks, Immunisations and
Screening and Long Term Conditions
(LTC) management.
2. Address health
inequalities
6. Transform and
strengthen primary
and community
care services
William Guy CCG Chairs Jenni Speller Reputational Damage
Patient Safety & Harm
Service Delivery
Acute Hospital Demand
Patient Experience
Inequality
12 15 September 2021:
Latest figures indicate this metric is currently being
achieved.
Additional funding made available via the Covid Capacity
Expansion Fund to support delivery.
Further work underway with BI Team to strengthen
peformance reports.
Risk rating has been reduced from Amber/8 to Green/4 as
metric is being achieved.
None identified at this
time (metric being
achieved).
People Resources
Estates
Comms & Engagement
Appointments in line with
previous year activity levels
Apr-July 2021
(latest data
available)
B&B: 5.2%
CPR: 9.6%
Mid: - 0.9%
Sthend: 10.8%
Thurrock: - 5.1%
4 3 A ↓ Regular reporting to Primary Care
Commissioning Committee.
Primary Care
Commissioning
Committee
Digital and
Business
Intelligence
If Cyber Security Alerts are not
actioned, there is a risk that the
organisation's systems could be
compromised resulting in service
disruption.
7. Promote digitally
delivered services
Mark Barker Taz Syed Peter King Patient Safety & Harm
Reputational Damage
Service Delivery
16 17 September 2021:
Description has been updated to clarify that it relates to the
risk of cyber attack.
Organisations' duty to protect data, mitigated though security
tools, policies and procedures, including procurement
standards and by following the Care Cert process, with
support from Arden and Gem CSU.
Delivery of Cyber Security action plan 2020/21 achieved.
Annual Cyber audit to take place in September 2021.
Risk rating reduced from 8/Amber to 4/Green as all
outstanding audit recommendations/actions implemented for
20/21. However, this will be reviewed once the outcome of
this year's audit of cyber security is completed.
30 September 2021 None Identified Delivery of 2020/21 Cyber
Security action plan.
Outcome of 2021/22 Cyber
Security audit.
Number of successful cyber
attacks each year.
Achieved.
TBC.
Zero (at 17/09/21)
4 4 G ↓ Annual internal audit of cyber
security.
Audit Committee
27

Mid and South Essex
Health and Care PartnershipBoard Assurance Framework APPENDIX A
Work
Stream
Description of Risk / Workstream
Objective
Strategic
Objectives
Risk Owner Clinical
Lead
System/
Place Lead
Risks of objective not
being delivered
Init
ial R
isk S
co
re
Update Milestone Deadline Enablers (Gap in Control) Success Measures
(Assurance - 2nd line of
defence)
Current
Performance
Cu
rren
t R
isk R
ati
ng
Targ
et
Ris
k S
co
re /
Ap
peti
te
Pro
ject
Delivery
Tre
nd
Assurance - 3rd line of defence CCG Committee that
will review risk
Integrated Care
System
To fulfil the statutory requirement to
engage with the public and patients.
1. NHS
Constitutional
Standards and
priorities
2. Address health
inequalities
3. Establish
Integrated Care
System
6. Transform and
strengthen primary
and community
care services
Claire
Hankey
N/A Claire Hankey Regulator Penalties
Claims & Complaints
Inequality
Patient Experience
Service Delivery
Reputational Damage
12 22 September 2021:
Communications being managed across the MSE CCGs by
the Director of Communications and Engagement for the
ICS.
Co-ordinated approach to all communications where
appropriate.
ICS communications and engagement strategy approved by
ICS Executive, System Leadership Executive and ratified at
Health and Care Partnership board on 16/09/21
30/09/2021 (met)
Partnership Working
Legal
Human Resources
IT Infrastructure
Finance
PPI Assessment status from
NHSE (Good).
Compliant 4 4 G BAU Each CCG completed the Patient
and public involvement assessment
2020/21 for NHSE with satisfactory
outcomes.
Audit Committee
Digital and
Business
Intelligence
To comply with all legislation
associated with the protection of data
for example the Data Protection Act,
General Data Protection Regulations,
Freedom of (Information Act) to
enable the CCG to achieve the
required level of assurance under the
Data Security and Protection Toolkit
(DSPT).
3. Establish
Integrated Care
System
7. Promote digitally
delivered services
Mark Barker Rachel
Hearn
Iain Gear Reputational Damage
Claims & Complaints
Service Delivery
Regulator Penalties
Patient Experience
Patient Safety & Harm
Safeguarding
Staffing, HR, OD
12 22 September 2021:
Standards met and Toolkit achieved for 2020/21. IG Team
involved with various workstreams to ensure that IG
arrangements are implemented for new NHS ICS body.
Action plan for compliance with 21/22 being developed.
Mandatory training compliance met for 20/21 and regularly
monitored. Additional role specific IG training will
recommence during 21/22 - each CCG is in the process of
identifying relevant staff who deal with personal identifiable
information (PID).
IG team currently recruiting to three roles due to staff
resignations.
Risk rating reduced from 8 (Amber) to 4 (Green) as CCGs
have been assessed as compliant with DSPT standards,
new DSPT assertions received with no major changes or
issues identified. Rating to be reviewed at next bi-monthly
update. Internal audit of IG anticipated Q3.
31 March 2022 People Resources
Partnership Working
Standards met DSPT. Compliant for
2020/21
4 4 G ↓ 2020/21 Internal audit of IG
identified 'reasonable' assurance.
Audit Committee
28

Mid Essex Part I CCG Board Meeting 22 September 2021
Performance and Planning Report
Date of Meeting: 30 September 2021 Agenda No
9
Purpose of Report: ‘Check’ (x) relevant box(es).
For Decision (approval/endorsement) ☐
For Assurance (discussion and noting) ☒
For Information Only ☐
Lead Executive Director:
Karen Wesson, Director Commissioning, Performance and EPRR
Report Author / Presenter:
James Buschor, Head of Performance and Planning Dan Doherty, Alliance Director Mid Essex
Executive Summary:
This paper was reviewed by the Finance and Performance Committee meetings in common (F&P CiC) on 15 September 2021 and is intended to:
• provide members with an update and overview of current performance where this is available
• provide members with an update on the dashboard progress
• identify performance risks or breaches
• update on mitigation and plans where known at the time of writing Each Senior Responsible Officer (SRO) for each Programme is working to ensure that their existing governance arrangements are clear of the deliverables they are accountable for. The existing System Delivery Planning and Performance meeting is now established and will be working with each of the SROs to ensure that there is effective reporting, updating, escalation and detail provided in the System Performance & Planning Oversight dashboard to enable the System Oversight and Assurance Group (SOAG) and the F&P CiC to have confidence, oversight and assurance that actions are in place. In terms of progress developing the System Performance & Planning Oversight Dashboard, this is detailed for each work programme in Table 1 below. In summary:
• an update summary of performance is provided within this paper for the following programmes: Elective; Mental Health; Urgent and Emergency Care; Children and Young People and Learning Disabilities.
• For Place programmes, South East reporting is being developed aligned to the signed off Place plan and reported at the weekly SEE Engine Room for oversight. Once complete this can be replicated for the other Place programmes. All Place plans have been shared to facilitate this work.
• Community, Maternity, Workforce, BI & Data programmes are in development to be reported within this paper at the next SOAG.
The System Oversight Framework (SOF) and Terms of Reference review will support this model for oversight and assurance. This is being discussed at the 8 September 2021 SOAG meeting.
29

Recommendations and decision/actions required:
The Board is asked to:
• Discuss and note the assurances contained within the report and advise of any further assurances required.
How does this report link to the CCG’s Strategic Objectives? ‘Check’ (x) relevant
objective(s)
Strategic Objective 1 Restore access to services to achieve performance against NHS Constitutional standards, quality improvement priorities and deliver ongoing COVID-19 requirements.
☒
Strategic Objective 2 Work with partner organisations and our population to address health inequalities, including those derived from Covid-19, and achieve social value.
☐
Strategic Objective 3 Support system transformation and organisational change to ensure the ICS is successfully established and can fulfil its aims and duties.
☒
Strategic Objective 4 Develop and support the creation and wellbeing of a diverse and highly skilled workforce and ensure the safe transition of staff to the new organisation.
☐
Strategic Objective 5 Achieve key statutory financial duties including delivery of the system financial control total, value for money and reduction of the underlying system deficit.
☐
Strategic Objective 6 Build effective Alliances at place to transform and strengthen the ability of Primary and Community Care Services to focus upon prevention and early intervention and improve outcomes in the most appropriate settings.
☐
Strategic Objective 7 Promote digitally delivered services whilst considering the requirements of those who need to access services in other ways.
☐
Approval Route: (List Committees or groups that have reviewed this document).
Group/Committee Date (dd/mm/yy)
SOAG 08/092021
F&P CiC 15/09/2021
Please confirm that the Lead Executive Director has signed-off the report prior to submission to the Committee/Board (Committee/sub-committee minutes submitted for information must be signed-off by the relevant Chair/Lead Executive before submission).
Yes
Has the CFO confirmed that any financial implications are within agreed budget and/or within CFO’s limit of delegated authority as per SFIs?
N/A
Have the relevant Impact Assessments been carried out and signed off?
Equality & Health Inequalities: N/A
Quality: N/A Privacy: N/A
Details of Patient & Public Engagement or Consultation:
N/A
Related risks on Board Assurance Framework (BAF) / new risks identified which will be included on the BAF. (please use this link to view the BAF)
No new risks identified
Conflicts of Interest: None identified.
Does the report need to be escalated to Board/Joint Committee or elsewhere?
No
30

Performance and Planning Report – September 2021
Table 1. Progress summary against completing each system programme reporting
within the System Performance & Planning Oversight Dashboard, in terms of both the
Deliverables and Performance sections.
31

Elective
Key issues for the Elective programme outlined below include:
• Performance being below standards for Cancer, RTT and Diagnostic waiting times.
• Recovery of Advice and Guidance service and utilisation.
• Introduction and implementation of Patient Initiated Follow Up (PIFU) pathways.
Key Issue 1 Cancer waiting time standards not being achieved.
Note: current position outlined below is for MSEFT as at July 2021.
• Two week wait (Standard: >= 93%): Below standard consecutive months year to date with current position at 81.7%.
• Two week wait breast symptomatic (Standard: >= 93%): Below standard consecutive months year to date with current position at 73.5%.
• 31-day first treatment (Standard = >=96%): Below standard consecutive months year to date with current position at 88.2%.
• 31-day subsequent treatment – surgery (Standard: >=94%): Below standard consecutive months year to date with current position at 75%.
• 62 day (Standard = >=85%): Below standard consecutive months year to date with current position at 56.9%.
o Standard is based on treatments therefore dependent on reducing the backlog to a sustainable position. For the trust this has been calculated at 118 patients. Plan submitted during 2021/22 planning round was to reduce backlog to 163 by end of H1 (September 2021). This is not possible to achieve as backlog has increased to 381 as at week ending 29/08.
• 62-day standard - screening (Standard: >=90%): Below standard consecutive months year to date with current position at 71.3%.
Mitigating actions:
• Oversight and detail picked up at: o Weekly Operational Recovery and System Oversight
Group (SSROG). o Monthly Cancer Programme Delivery Group with
Trust/Commissioner/NHSEI/Cancer Alliance attendance. o System oversight at monthly cancer board.
Key Issue 2 RTT 18 week standard.
Note: Position outlined below is for MSEFT as at week ending 29/08.
• Waiting list size is increasing: Has increased by circa 24k patients since start of financial year to 113,788.
o This “bulge” in the waiting list profile is a risk to the 52+ week position with potential impact this time next year for the start of 2022/23 on top of the following highlighted risks.
• Large number of patients waiting 52+ weeks. Current position is 4,550 patients.
o Position has been decreasing positively due to the impact of the decreased demand over a year ago during the initial Covid-19 pandemic peak period. Risk as recently seeing position stabilising rather than continuing to decrease. Predicted to increase as demand increased last summer after the initial Covid-19 pandemic peak, together with the
32

potential upcoming winter pressures impact.
• Large number of patients waiting 78+ weeks. Current position is 1,898 patients.
• Number of patients waiting 98+ weeks. Current position is 305 patients. Commitment and recovery plan/trajectory agreed to ensure no patients waiting 98+ weeks as at end of September (backstop). This is not possible to achieve.
Mitigating actions:
• Detailed model developed jointly between trust/commissioning colleagues.
o Outlines weekly requirement in terms of treatments to eliminate 98+ week waits; reduce to exception reporting position 90+ week waits (to sustain a zero 98+ week wait position); and reducing 78+ and 52+ week waits.
o Monitors treatments vs plan and resulting trajectories at specialty level on a weekly basis.
• The capacity in terms of treatment volumes and additional recovery capacity/efficiencies agreed with specialties. Reworking week commencing 06/09 as not achieving 98+ week backstop for end of September.
• Monitored through the fortnightly MSEFT Planning and Delivery - Planned Care meeting with Trust/commissioners/NHSEI regulator exec attendance.
• Patient level detail by specialty picked up at trust weekly PTL meeting.
• Audit commenced 23/08/21 to understand the detail behind the PTL management processes e.g. triaging of patients.
Key Issue 3 Diagnostics waiting time standard not being achieved.
Note: Position outlined below is for MSEFT as at June 2021.
• Six-week Standard (Standard: >=99%): Below standard consecutive months year to date with current position at 68.2%.
• Large number of patients waiting 13+ weeks. Backlog decreasing with current position at 3,383 patients.
Mitigating actions:
• The system oversight governance is being developed in partnership with MSEFT and NHSE/I colleagues.
Key Issue 4 Advice and Guidance response times and utilisation.
A good, highly utilised Advice and Guidance (A&G) service with quick response turnaround times is key to support demand management. Demand management is a key requirement to tackle the demand and capacity gap outlined in the elective waiting list issues and risks highlighted above.
• Over the last six months ending May 2021 the 95th percentile response time at MSEFT for MSE CCG requests made is averaging 56 days (Range between 44 and 84 days). The service aims for responses to be within 2 days.
Note: August data is available but unable to calculate more recent response times due to number of requests raised not having a response yet by the end of the month and therefore subject to being refreshed.
33

• Utilisation has increased reaching a year to date monthly average of circa 1,700 requests across MSE. Requirement to work with each specialty to understand the potential full utilisation possibilities.
Mitigating actions:
• Oversight at MSEFT Outpatient Programme Board.
• Recovery plan focusing on both responding to backlog of outstanding requests and reducing turnaround times of new requests.
• Carving out dedicated time and resource in job plans for responding to Advice and Guidance requests.
Key Issue 5 Patient Initiated Follow Up (PIFU) pathways implementation.
Introducing PIFU pathways during 2021/22 is a key to potentially free up the capacity required to work through the elective waiting list backlogs outlined above.
• Elective Recovery Fund (ERF) requirement to introduce PIFU in at least three major outpatient specialties.
o MSEFT went live in Therapies and Cardiology in June 2021
o Third specialty still to go live.
• MSEFT challenge in recording of PIFU data to evidence.
Mitigating actions:
• Implementation and oversight led by MSEFT Outpatient Programme Board.
• Recording of PIFU challenge being resolved locally.
Time scale for benefits to be realised
Ongoing throughout 2021/22 and beyond.
Risks • Key Issues one and two are growing risks as outlined above.
Mental Health
Key issues for the Mental Health programme outlined below include
performance being below standard for:
o Out of Area Placements (OAP) o Improving Access to Psychological Therapies (IAPT) o IAPT in treatment pathway waits o Dementia diagnosis rate o Annual physical health checks for people with serious mental
illness (SMI)
Key Issue 1
Number of Inappropriate Out of Area Placements (OAP).
• There are a total of 605 inappropriate out of area placements across MSE as at April 2021.
Mitigating actions:
• Oversight at the monthly Mid and South Essex Mental Health Partnership Board.
34

Key Issue 2
IAPT – patients entering psychological therapies.
• The position year to date is 306 patients below plan as at June 2021. South East Essex Place is meeting the plan number of patients, whilst other Place areas are below plan.
Mitigating actions:
• Oversight at the monthly Mid and South Essex Mental Health Partnership Board and at local Place level.
Key Issue 3
IAPT - In-treatment pathway waits over 90 days between first and second appointment.
• The number of patients waiting for a second appointment over 90 days is below standard at 18.5% as at May 2021. The standard is not being met for Basildon and Brentwood, Thurrock and South East Essex places.
Mitigating actions:
• Oversight at the monthly Mid and South Essex Mental Health Partnership Board and at local Place level.
Key Issue 4
Dementia diagnosis rate.
• Dementia diagnosis rate is below standard across MSE at 59.6% of the estimated number of people with dementia which is a shortfall of 1,078 people to meet the 66.7% standard as at June 2021.
Mitigating actions:
• Oversight at the monthly Mid and South Essex Mental Health Partnership Board and at local Place level.
Key Issue 5
Annual physical health
check for people with
serious mental illness.
• The number of people with serious mental illness receiving their annual physical health checks is significantly below standard across MSE. There is a gap of 2,455 patients across MSE as at July 2021 to reach the 60% standard.
Mitigating actions:
• Oversight at the monthly Mid and South Essex Mental Health Partnership Board.
Time scale for benefits to be realised
Ongoing throughout 2021/22 and beyond.
Risks • Performance below standard across a number of Mental Health constitutional standards.
Urgent and Emergency Care (UEC)
Key issues for the UEC programme outlined below include:
• performance being below standard for: o Emergency Department – four-hour standard. o 111 calls answered in 60 seconds. o Ambulance Response Times o Ambulance Handover Times
Key Issue 1 • Performance below the 95% standard for MSEFT for
35

Emergency Department – four-hour standard.
consecutive months year to date to July 2021 ranging between 82.8% and 89.5%.
Mitigating actions:
• Oversight at the UEC Strategic Board.
• Daily operational calls held with system partners.
Key Issue 2
111 calls answered in 60 seconds.
• Performance below the 95% standard for consecutive months year to date to June 2021 ranging between 54.4% and 74.1%.
Mitigating actions:
• Oversight at contract meeting with provider and at UEC strategic board.
Key Issue 3
Ambulance Response Times
Note: position outlined below is for EEAST for MSE CCGs as at June 2021.
• Category 1 Calls - Total (Standard: Mean <= 7min): With the exception of Southend CCG, mean response times below standard.
• Category 1 Calls - Total (Standard: 90th centile <= 15min): Below standard consecutive months year to date for Mid Essex CCG and in June 2021 for Thurrock CCG.
• Category 2 calls (Standard: Mean <= 18min; 90th Centile <= 40min): Both mean and 90th centile below standard consecutive months year to date for all CCGs.
• Category 3 calls (Standard: 90th Centile <= 120min (02:00:00)): Below standard consecutive months year to date for all CCGs.
• Category 4 calls (Standard: 90th Centile <= 180min (03:00:00)): Below standard consecutive months year to date for all CCGs.
Mitigating actions:
• Oversight at the UEC Strategic Board.
• Daily operational calls held with system partners.
• Via commissioner provider meetings.
Key Issue 4
Ambulance Handover Times
• Percentage of Arrival to Handovers within 15min (Standard: None
set): Year to date monthly range by site as follows: o Basildon: 55.5% – 68% o Broomfield: 41.7% - 67.2% o Southend: 21% - 22.3%
• Number of Arrival Handovers >= 30min (Standard: Zero): Year to date monthly range by site as follows:
o Basildon: 67 - 164 o Broomfield: 25 - 72 o Southend: 265 – 320
• Number of Arrival Handovers >= 60min (Standard: Zero): Year to date monthly range by site as follows:
o Basildon: 8 - 20 o Broomfield: 1 - 10 o Southend: 23 - 63
36

Mitigating actions:
• Oversight at the UEC Strategic Board.
• Daily operational calls held with system partners.
• Via commissioner provider meetings.
Time scale for benefits to be realised
Ongoing throughout 2021/22.
Risks • Performance below standard across a number of areas and approaching winter pressures.
Community Key issues for the Community programme outlined below include:
• Currently being worked through with programme leads.
Maternity Key issues for the Maternity programme outlined below include:
• Currently being worked through with Chief Nurse and MSEFT maternity lead.
Children and Young People (CYP)
No performance or planning risks to highlight.
Learning Disabilities (LD)
No performance or planning risks to highlight.
Workforce Key issues for the Workforce programme outlined below include:
• Currently being worked thorough with the programme leads and BI Team.
BI & Data Key issues for the BI & Data programme outlined below include:
• Currently being worked through with the programme leads.
37

Place Basildon and Brentwood
Key issues for the Basildon and Brentwood Place programme outlined below include:
• Currently being worked through with the programme leads.
Place Thurrock Key issues for the Thurrock Place programme outlined below include:
• Currently being worked through with the programme leads.
Place South East Essex
Key issues for the South East Place programme outlined below include:
• Currently working through with Place team to develop. Reporting into weekly South East Essex Place Engine Room Meeting for assurance and oversight.
Place Mid Essex Key issues for the Mid Essex Place programme outlined below include:
• Currently being worked through with the programme leads.
38

Mid Essex CCG Part I Board Meeting
Minutes of Mid and South Essex CCGs’ Joint Committee Meetings
Date of Meeting: 30 September 2021 Agenda No
10
Purpose of Report: ‘Check’ (x) relevant box(es).
For Decision (approval/endorsement) ☐
For Assurance (discussion and noting) ☒
For Information Only ☐
Lead Executive Director:
Anthony McKeever, Joint Accountable Officer
Report Author /Presenter:
Sara O’Connor, Head of Corporate Governance
Executive Summary:
The approved minutes of the MSE CCGs’ Joint Committee (JC) Part I meeting held on 24 June 2021 and the draft minutes of the JC Part I meeting held on 26 August 2021 are attached for the information of the Board. The Joint Committee is chaired by the M&SE CCG Chairs on a rotational basis, with Dr Anna Davey, Chair of Mid Essex CCG, currently performing this role.
Recommendations and decision/actions required:
The Board is asked to note the minutes of the MSE CCGs’ Joint Committee meetings held on 24 June 2021 (draft) and 26 August 2021 (approved) and seek any further assurances required.
How does this report link to the CCG’s Strategic Objectives? ‘Check’ (x) relevant
objective(s)
Strategic Objective 1 Restore access to services to achieve performance against NHS Constitutional standards, quality improvement priorities and deliver ongoing COVID-19 requirements.
☒
Strategic Objective 2 Work with partner organisations and our population to address health inequalities, including those derived from Covid-19, and achieve social value.
☒
Strategic Objective 3 Support system transformation and organisational change to ensure the ICS is successfully established and can fulfil its aims and duties.
☒
Strategic Objective 4 Develop and support the creation and wellbeing of a diverse and highly skilled workforce and ensure the safe transition of staff to the new organisation.
☒
Strategic Objective 5 Achieve key statutory financial duties including delivery of the system financial control total, value for money and reduction of the underlying system deficit.
☒
Strategic Objective 6 Build effective Alliances at place to transform and strengthen the ability of Primary and Community Care Services to focus upon prevention and early intervention and improve outcomes in the most appropriate settings.
☒
Strategic Objective 7 Promote digitally delivered services whilst considering the requirements of those who need to access services in other ways.
☒
Approval Route: (List Committees or groups that have reviewed this document).
Group/Committee Date (dd/mm/yy)
39

Please confirm that the Lead Executive Director has signed-off the report prior to submission to the Committee/Board (Committee/sub-committee minutes submitted for information must be signed-off by the relevant Chair/Lead Executive before submission).
Yes
Has the CFO confirmed that any financial implications are within agreed budget and/or within CFO’s limit of delegated authority as per SFIs?
N/A
Have the relevant Impact Assessments been carried out and signed off?
Equality & Health Inequalities: N/A
Quality: N/A Privacy: N/A
Details of Patient & Public Engagement or Consultation:
N/A
Related risks on Board Assurance Framework (BAF) / new risks identified which will be included on the BAF. (please use this link to view the BAF)
The BAF report under agenda item 7 highlights the red rated risks under the remit of the JC.
Conflicts of Interest: None identified.
Does the report need to be escalated to Board/Joint Committee or elsewhere?
No
40

MID AND SOUTH ESSEX (M&SE) CCG JOINT COMMITTEE MEETING
HELD IN PUBLIC
Held on Thursday, 24 June 2021 from 12.30 pm – 2.30 pm Meeting broadcast via ‘MS Teams’
PART I MINUTES
PRESENT
Representative Name Job Title / Position Organisation
Dr Anna Davey (AD) CCG Chair and Chair of M&SE CCGs Joint Committee
Mid Essex CCG
Dr Boye Tayo (BT) CCG Chair Basildon and Brentwood CCG
Dr Sunil Gupta (SG) CCG Chair Castle Point and Rochford CCG
Dr Jose Garcia (JG) CCG Chair Southend CCG
Dr Anil Kallil (AK) CCG Chair Thurrock CCG
William Guy (WG) NHS Alliance Director Basildon and Brentwood CCG
Dan Doherty (DD) NHS Alliance Director Mid Essex CCG
Patricia D’Orsi (PD) NHS Alliance Director South East Essex CCGs
Mark Tebbs (MT) NHS Alliance Director Thurrock CCG
Tracey Freeman (TF) Lay Member (Governance) and Audit Committee Chair
South East Essex CCGs
Mark Barker (MB) Chief Finance Officer Mid and South Essex CCGs
Rachel Hearn (RH) Director of Nursing & Quality Mid and South Essex CCGs
APOLOGIES
Anthony McKeever (AMcK)
Joint Accountable Officer Mid and South Essex CCGs
IN ATTENDANCE
Viv Barnes (VB) Joint Committee Secretary Mid Essex CCG
Karen Wesson (KW) Director of Commissioning, Performance and Emergency Planning
Mid and South Essex CCGs
Helen Farmer Interim Director of Children and Young People and Learning Disability.
Mid and South Essex CCGs
Paula Saunders (PS) Associate Director, Involvement and Governance
Basildon and Brentwood CCG
Gerdalize Du Toi (GDT) (items 1 – 6)
Programme Director for Ageing Well Mid and South Essex Health and Care Partnership
Jo Cripps (JC) Programme Director Mid and South Essex Integrated Care System
Sara O’Connor (SO) Head of Corporate Governance (minute taker)
Mid Essex CCG
AGENDA ITEM 3
41

Item No. Item
GENERAL BUSINESS
1. Welcome and Apologies for Absence: Presented by Dr Anna Davey AD welcomed committee members and members of the public to the meeting and advised that, in line with Government and NHS guidance on social distancing, the Mid and South Essex CCG Joint Committee (JC) continued to hold its Part I meetings via MS Teams Live Broadcast. AD explained that the JC acted collectively on behalf of the five mid and south Essex (M&SE) CCGs to commission services to meet the needs of their combined population, including acute, mental health and community services, as well as emergency care services including NHS 111 and the Ambulance service. AD noted that apologies had been received from AMcK and invited the other members of the JC to introduce themselves.
2. Register of Interests/Declarations of Interest: The JC noted the most recent version of the register of interests. AD reminded members of their obligation to declare any interests they held on any issues arising at JC meetings which might conflict with the business of the CCGs at the beginning of the meeting, at the start of each relevant agenda item, or should a relevant interest become apparent during an item under discussion, so that appropriate arrangements could be implemented. Declarations made by CCG Board members are also listed in the Register of Interests available on the M&SE CCG websites. Declarations of interest from today’s meeting SG declared an indirect financial interest in relation to agenda item 8 (Neuro-developmental pathways) on the basis that his wife worked as a paediatrician.
3. Minutes of the CCG Joint Committee meeting of 20 May 2021 and Action Log: Presented by Dr Anna Davey AD asked if members had any suggested amendments to the minutes of the JC meeting held on 20 May 2021. No amendments were received and the minutes were therefore approved. The Action Log was reviewed. In relation to actions 1 and 2, VB confirmed that the JC agenda for 26 August 2021 would include updates on the Mid and South Essex NHS Foundation Trust legal undertakings and the Adult Mental Health Transformation Plan 2021/22. With regard to action 3, VB advised it had been clarified that the Mid and South Essex Medicines Optimisation Committee (MSEMOC) was established in October 2020, but this was not via a Central Incident Management Team (CIMT) or CCG decision as reported at the previous JC meeting. However, approval of all the MSEMOC recommendations was sought from the JC and subsequently reported to CCG Boards. VB advised that she hoped that this information satisfactorily answered the queries raised by Lesley Buckland, Audit Committee Chair from Thurrock CCG. Resolved: The Joint Committee:
• Approved the minutes of the Part I JC meeting held on 20 May 2021 without amendment.
• Noted the Action Log.
42

Item No. Item
4. Questions and Comments from the Public: Presented by Dr Anna Davey and Viv Barnes VB advised that questions had been received from Mr Peter Blackman, firstly expressing concern regarding the administration of the Ophthalmology service at MSEFT. VB confirmed that information was being sought and a response would be provided to Mr Blackman as soon as possible. Mr Blackman had also sought an update on the procurement of Level 2B Rehabilitation services. KW advised that the five M&SE CCGs were reviewing the stroke service provision model and rehabilitation services and explained that there were a number of inter-dependencies between these. There was currently no plan to go back out to procurement for the Level 2B service. Brentwood Community Hospital continued to be used for intermediate care and sub-acute intermediate care services to support patient flow. However, the current service provision would continue for the time being. VB advised that no further questions from members of the public had been submitted via the ‘Q&A’ function, but she would monitor this throughout the meeting and advise AD if any were received. [Action: VB to arrange for a response to be provided to Mr Blackman’s query regarding the administration of the Ophthalmology service at MSEFT.]
SYSTEM REPORTS
5. Board Assurance Framework: Presented by Viv Barnes VB explained that the majority of the risks on the Board Assurance Framework (BAF) fell within the responsibility of the JC and the BAF would therefore be a regular item on the JC agenda. There were currently 19 risks rated red, either because the risk rating score was 15 or above or because the associated project delivery was rated red. The red risks had been reviewed prior to the JC meeting, with the exception of the finance risks which it had not been possible to update due to the Finance Team’s need to focus on the end of year accounts. VB explained that the format and content of the BAF was being reviewed by SO as set out in the report. VB also advised that during the last review, three previously red-rated risks (Refs DITR01, DITR03 and PLAC06) had been reduced to amber. VB outlined the reasons for this as set out in the report and asked if JC members had any concerns that the reduction in the re-rating was not justified at the current time. No concerns were raised. Resolved: The Joint Committee noted the Board Assurance Framework report and agreed that three risks (DITR01, DITR03 and PLAC06) should remain rated as amber.
6. Sub-Acute Frailty and Intermediate Care Bed arrangements at Brentwood Community Hospital: Presented by Gerdalize Du Toit GD advised that the executive summary of her report outlined the ongoing arrangements for sub-acute frailty and explained that bed-based service delivery during the pandemic had been consolidated at Brentwood Community Hospital (BCH). This arrangement was initially until 30 June 2021 but had been extended until March 2022 in response to ongoing COVID-19 secure measures and to support appropriate flow of patients. In addition, the Intermediate Care (IMC) provision had been enhanced on the BCH site and the JC were being asked to note that the Chief Finance Officer had agreed a short extension of this arrangement during July and August 2021.
43

Item No. Item
GD explained that a proposal was being developed between MSEFT and the community collaborative to consider the model of care to support system flow and surge requirements during September 2021 to Spring 2022. Approval of the proposals would be taken through the appropriate governance route. WG commented that when this development was discussed at Basildon and Brentwood CCG there was general support for it, with an offer from primary care colleagues from B&B to work with the Trust to develop step-up arrangements. AD advised that step-up arrangements had a fundamental impact upon how patients were cared for within the community and she was confident that her primary care colleagues would be keen to become involved where necessary. In response to a query from MT, GDT confirmed that evaluation and audit of the above services would continue during the extension periods. In addition, it was hoped that a set of both process and patient outcomes would be developed and applied across all IMC pathways to enable comparison across these services to be undertaken. MB noted that the extension of sub-acute frailty at BCH from July 2021 to March 2022 was cost neutral and the second short-term extension for enhanced IMC provision between July and August was covered within planned assumptions. Consequently, there were no additional cost pressures to the system. Resolved: The Joint Committee noted:
• The extension of the current Sub-Acute Frailty arrangements at BCH from July 2021 – March 2022.
• That the Chief Finance Officer (CFO) had agreed a short extension of the current community hospital ward provision at BCH for July and August 2021.
• That a proposal to expand the model of care was under development, which would cover the time frame September 2021– Spring 2022. Approval of any proposals to this effect would be undertaken via the appropriate governance route.
7. Adult Critical Care Transfer Service: Presented by Karen Wesson KW advised that the report set out a request from Specialised Commissioning for approval of the Adult Critical Care Transfer Service (ACCTS), with the Full Business Case (FBC) outlined within the paper. The JC was being asked to approve the commissioning of this service in addition to ambulance provision. KW advised that the ACCTS would support transfers from local hospitals in dedicated ambulances over a 12-hour shirt period. Clinical colleagues who were supporting the project had confirmed that this would be of benefit to the system. KW confirmed that critical care services had financial support until the end of the financial year. Thereafter, partners would need to identify funding if they wished to continue supporting this model. The basis of CCG funding would be decided by the Chief Finance Officer. Members were also asked to approve the process undertaken by Specialised Commissioning and the award of the contract to Cambridge University Hospitals NHS Foundation Trust. MB reassured members that an investment reserve had been set aside to help support this proposal and whilst it was not quite the value initially expected, it was very close. The expectation was that there would be no financial pressures to the system that could not be managed within existing funding for 2021/22. For future years, there would be an opportunity to build funding into planning assumptions and ultimately to fund from growth allocations. Consequently, he supported the proposals being put forward to members.
44

Item No. Item
In response to a query from BT regarding the cost of the proposals, KW advised that East of England Ambulance Service Trust (EEAST) could not provide the Critical Care transfer service within existing provision as it took them away from responding to 999 calls for a significant period of time to facilitate these transfers. The arrangements also avoided taking staff from critical care or other acute hospital services to support the transfer, thus avoiding depletion of local services whilst facilitating safe transfer of acutely unwell patients to critical care units across the region. The financial arrangements were referred to within the business case and would be dealt with as part of ongoing work. In response to queries raised by JG, KW advised that the proposals were different to the inter-hospital transfers approved by the JC in July 2018 and were influenced by the transfers that occurred during the pandemic as well as the consistent numbers of transfers that occurred at other times across the region. MB advised AK it was recognised that although the proposals created a small pressure to the system, it was manageable within existing finances. A number of Finance & Performance Committee members had also queried whether efficiencies could be identified through the ambulance contract to offset additional costs. MB confirmed this work would be undertaken, but if further efficiencies were not possible, a decision on whether to extend the service would be taken on the basis of clinical effectiveness and benefit to patients. AW advised that cardio-thoracic transfers were part of the existing East of England transfer model, however, if someone was in the critical care cardio-thoracic unit and required a transfer to another critical care bed unit, the new service model would be used. This would also be the case for critical care neurology patients. RH advised that the assumption was that the new model would improve quality, safety and patient outcomes and the service would therefore be closely monitored to identify whether these objectives were being met. Resolved: The Joint Committee:
• Approved the commissioning case for the regional Adult Critical Care Transfer Service.
• Noted that the final decision regarding the basis of CCG funding will be taken by the Chief Finance Officer.
• Approved the process undertaken by Specialised Commissioning, the outcome of which was award of contract to Cambridge University Hospitals NHS Foundation Trust.
8. Neurodevelopmental Pathway: Presented by Patricia D’Orsi and Helen Farmer PD informed members that the committee had received three reports (agenda items 8, 9 and 10) outlining the current areas of focus for services for children and young people, which would ensure greater compliance with the Written Statement of Action (WSOA) for Special Educational Needs and Disabilities (SEND). HF advised that Autism services were a priority area due to growing demand both locally and nationally and consequently there was a greater focus on neurodevelopmental pathways. This group of patients were at greater risk of health inequalities and often required additional support, sometimes through youth offending / criminality pathways, or through children’s mental health services. They also experienced poorer outcomes with regard to education and employment. There were currently variations in service provision across the mid and south Essex footprint, which meant some patients and families did not receive the level of support the CCGs would wish for them. Following recent Care Quality Commission (CQC) and
45

Item No. Item
OFSTED inspections, all three local authority areas had received WSOAs indicating significant areas of concern, including a need to improve neurodevelopmental pathways. A series of workshops were facilitated during 2018/19 to develop a cohesive model, co-designed by health and social care partners, children and their families/carers. However, the pandemic had delayed its implementation. There were 12 programmes of work in progress to improve the service offer, including developing pre-diagnostic support to ensure that children were identified and diagnosed at the right time within the right pathway. Work was also being undertaken to reduce the division between mental health and physical health pathways. In addition, the post-diagnostic offer of support would be made more responsive to include an immediate post-diagnostic offer plus long term support, recognising a need to move away from episodic interventions. HF advised there were a number of funding opportunities available from NHSE/I, but noted that the investment outlined within the report was mostly non-recurrent, which allowed new models to be piloted in collaboration with community providers, children and their families to design future models of care. HF confirmed that business cases for future proposals would go through appropriate governance processes. MB confirmed that the vast majority of the proposals were already accounted for within existing budgets and plans and therefore did not pose a material pressure to the system. However, there were a number of further proposals currently being scoped and the cost of these would be considered. JG confirmed that he welcomed the proposals and highlighted the importance of service providers regularly communicating with patients and their families regarding the diagnostic process and available support. MT noted that the waiting list size appeared to be smallest in south east Essex despite it having the lowest level of investment and asked how equality of waiting times and provision would be made consistent across M&SE. HF confirmed that although there appeared to be significant variation in waiting times, the way data was collected differed across Essex. Work was being undertaken to implement consistent reporting to provide a true picture of need to enable future investment to be targeted appropriately. In addition, some areas had received local funding enabling them to move forward with projects in advance of others, but the aspiration was to address these inconsistencies. In response to a query from AK, HF advised that community providers were working to identify opportunities to deliver services at both system and place and in an integrated way with social care and education colleagues. In response to queries from BT and MT, PD advised that although it was clear that there was a significant amount of good work being undertaken by individual CCGs, there were differences in the level of oversight maintained by the governing bodies, historical investment and the pace of change. Going forward, the JC would have oversight of these areas and, in collaboration with local authority partners, would work to ensure that patients and families did not have to wait a significant amount of time for diagnosis and support. Six priorities had been established for children and young people, which would be overseen by the Growing Well Programme Board, chaired by Dr Sooraj Natarajan, with progress already having been made. Resolved: The Joint Committee:
• Noted the contents of the Neurodevelopmental Pathway report; and
• Approved the proposal to continue to focus on coordinating the approach across the Mid and South Essex.
46

Item No. Item
9. Autism Spectrum Disorder (ASD) Diagnostic Backlog: Presented by Helen Farmer HF advised that addressing the backlog of ASD assessments for children and young people was a local and national priority, with significant assurances being sought by NHSE/I regarding progress. Commissioners had liaised with community providers to agree how funding could be invested in the most appropriate way. However, community providers had advised they were not currently in a position to respond, mainly because of workforce issues and the specialist skills required to perform ASD diagnosis. Consequently, a contract was awarded to Provide Wellbeing - a subsidiary of Provide Community Interest Company - to provide additional assessments for all five CCG areas. An assurance group had been established to monitor progress against negotiated trajectories, with a target of delivering at least 1,100 additional assessments in a phased approach over 9 – 10 months. Significant progress had already been made. Approval was being sought from the committee to continue this arrangement. Resolved: The Joint Committee:
• Noted the contents of the report; and
• Approved the proposal to reduce the backlog of Autism Spectrum Disorder Diagnostic Assessments for children & young people in Mid & South Essex.
10. Mental Health Support Teams for Children and Young People: Presented by Helen Farmer HF advised that the purpose of the report was to provide the committee with assurance regarding the provision of Mental Health Support Teams (MHST) for children and young people (CYP) following a significant investment by the NHS. The provision of MHSTs was a collaboration between the Department of Education and the NHS to deliver services for children at the earliest opportunity. The NHS Long Term Plan initially included an ambition of 25% coverage of schools by 2024. This had since been increased to 35% by 2024 due to the impact of the pandemic. Although CYP were not at the greatest direct risk from COVID-19, the indirect consequences were undoubtedly impacting upon them. The programme was being developed and delivered in partnership with Essex County Council, Southend Council and Thurrock Council, with funding for six MHSTs already having been awarded via an ‘expressions of interest’ process, although a slightly different stance to funding was now being taken. A further seven MHSTs would be rolled out next across MSE. The contract for provision of the service had been directly awarded to North East London NHS Foundation Trust (NELFT), which was currently performing very well against tight timescales. The service was currently funded via transformation monies on a phased basis, however it was envisaged that by 2024 it would be included within CCG baselines. The primary role for the MHSTs was to provide direct intervention, secondly to provide a whole school approach to improving mental health within the school environment, and thirdly to provide a link between CYP mental health and wider community services. AD noted that although the current MHST target was set nationally, the need for these services was very high. HF advised that the pace of roll out was largely determined by the requirement to train new staff associated with the MHST workforce, including educational health practitioners who were required to undertake a year-long course, but the local aspiration was to have 100% coverage as soon as possible. AD and PD both thanked HF for the updates provided and welcomed the current focus on CYP mental health. Resolved: The Joint Committee noted the report on Mental Health Support Teams for Children and Young People.
47

Item No. Item
11. Implementation of Service Restriction Policy: Presented by Paula Saunders PS explained that the Service Restriction Policy (SRP), which was used as a clinical prioritisation tool, had been reviewed as part of work to address the backlog of elective procedures. PS advised that in normal circumstances a prior approval agreement for a procedure lasted for twelve months, but a number of people had been waiting longer than this due to the pandemic. The CCGs had no desire to require providers to go through the prior approval process again, especially as the SRP had not been changed, apart from a minor amendment relating to specialist fertility treatment in Thurrock. PS also confirmed that equity of offer would be maintained across MSE. In response to a query from AK, PS advised that patients should be advised at the point of referral that they have been listed subject to funding approval. The reason for doing this was to facilitate the prioritisation of patients with higher clinical priority. Resolved: The Joint Committee approved the following recommendations:
• Prior approvals (group and individual) to be extended for a further 12 months from the date the CCG approved the request, with the exception of specialist fertility treatment in Thurrock.
• Prior approvals to be obtained for all procedures for patients already on a waiting list and, where the criteria is not met, the patient will be removed from the waiting list.
• Prior approvals, where necessary, to be obtained before new patients are added to a waiting list for a procedure.
12. Finance Report: Presented by Mark Barker MB confirmed that the external audit for 2020/21 had been completed by KPMG for all five MSE CCGs. The audit comprised of a review of the annual accounts, annual report, a value for money (VFM) review and controls review and scrutiny. All CCGs had been issued with a clean audit report and a value for money statement was due to be received which demonstrated that the services commissioned were VFM and were subject to appropriate scrutiny and governance. There were no audit adjustments to the bottom line reported position. As a consequence, all of the CCGs reported either break-even or a slight surplus financial position of up to £400k. The relevant reports and accounts would be published on the CCGs’ websites in line with the national timetable. MB advised that in respect of 2021/22, all MSE CCGs were currently reporting they were on plan, with no slippages. There were also no concerns regarding efficiency shortfalls or productivity improvements that had not been recognised or achieved in accordance with the financial plan. Budgeted expenditure was also on track for all service areas, although there were a number of minor underspends, including continuing healthcare, which was partly due to the ongoing pandemic and the reluctance of some elderly patients to move into placements. The CCGs continued to review finances via the Senior Finance Leaders Group, which comprised of system-wide Chief Finance Officers and their deputies. In addition, efficiencies and productivity improvements were being monitored via the System Efficiency Programme Board. To date, it appeared likely that expenditure would be contained within the system envelope. Work was ongoing to address backlogs caused by the pandemic. Resolved: The Joint Committee noted the Finance update report.
13. Patient Safety and Quality Report, including approval of CCG Responses to Provider Quality Accounts: Presented by Rachel Hearn
48

Item No. Item
RH explained that the report provided a summary of the considerable amount of work considered by the Patient Safety and Quality Committee on 11 May 2021. The committee had considered infection prevention and control priorities for 2021/22 and noted that there had been 8 Never Events reported the previous year. RH confirmed that the CCGs were providing support to providers to enable them to implement learning from these types of events, which mainly occurred within surgical settings. Harm reviews continued to ensure that patients were reviewed while they awaited procedures. The committee had also received an update on progress against the Maternity Improvement Plan which focused upon Basildon Hospital, but also included Southend and Broomfield Hospitals. Each committee agenda included a ‘deep dive’ into a particular service area, which included an associated patient story, with cancer services having been considered during the May meeting. RH advised that CCG responses to provider quality accounts were also appended to the report and explained that it had not been possible for the PSQ Committee to consider these responses at its May meeting due to tight national timescales. Consequently, it had been necessary to seek virtual support for the responses from committee members prior to submission to providers. Resolved: The Joint Committee:
• Noted the Patient Safety and Quality report; and
• Approved CCG responses to the 2020/21 Quality Accounts of: Essex Partnership University Foundation Trust Mid & South Essex Foundation Trust North East London Foundation Trust Provide Community Interest Company Barking, Havering and Redbridge University Hospital Trust Farleigh Hospice
14. Performance Report: Presented by Karen Wesson KW advised that significant support had been provided by Macmillan GPs and other colleagues to recover against the two-week wait cancer standard. Additional Cancer Alliance funding had also been received to support recovery against the 62 day cancer standard. However, challenges remained within gynaecology, breast, urology and skin, with the latter being due to a significant increase in the volume of referrals received. Work was ongoing to review the skin referral pathway, which would be supported by increased use of Skin Analytics. There was a national requirement to have no patients waiting longer than 98 weeks by the end of September 2021, which was currently on-plan to deliver. Although clinical prioritisation would occur, the length of time patients had waited would also be taken into consideration. KW confirmed that challenges remained regarding diagnostic capacity. New clinical prioritisation guidance had been published which would be implemented by the hospitals. Performance against the 95% emergency department standard was currently 89.2%, with significant pressures having been experienced at all three hospital sites over the past few weeks, particularly in relation to children’s services. A new Urgent and Emergency Care Board would review all relevant pathways. A recovery plan had been developed to improve performance against the Improving Access to Psychological Therapies (IAPT) standard and work was ongoing to improve
49

Item No. Item
the performance of children and young people’s mental health services. The dementia diagnosis pilot would be evaluated at the end of July, with the results being submitted to the JC at a later date. In response to a query from AK, KW advised that the graph on page 159 referred to the increase in the number of referrals which had resulted in a decrease in performance. KW also confirmed that clinical leads were being identified to assist with the review of pathways and recovery of services. Resolved: The Joint Committee noted the Performance Report.
15. 15.1
Committee Summary Reports: Presented by Mark Barker Finance and Performance Committees in Common (F&P CiC) MB confirmed that the F&P CiC continued to focus upon the mitigation of current financial and performance risks to bring them within acceptable levels. However, circumstances often changed very quickly and it was therefore important to ensure that timely action was taken when required. Dawn Scrafield, Chief Finance Officer for MSEFT, had provided the CiC with an update on progress on system financial sustainability and Price Waterhouse Coopers were at the closing stages of undertaking a ‘peer comparison’ of services, the outcome of which would be shared with the committee and Boards. MB explained that there remained a system pressure of circa £200 million and some clear decisions would therefore need to be taken to improve upon this position and achieve financial stability. A business plan and budget had been set for the first half of the financial year (H1) which took account of ongoing COVID-19 requirements, but it was envisaged that the second half (H2) would focus upon implementation of ‘business as usual’, taking account of learning from the pandemic. AK asked how MSE’s financial position compared with other systems. MB advised that MSE was not a significant outlier and the underlying deficit had remained fairly consistent for the past 10 years. The whole NHS was experiencing significant pressures, mainly as a consequence of the pandemic, but it was acknowledged that greater focus was required to ensure robust financial discipline. Resolved: The Joint Committee noted the Finance and Performance Committees in Common update report relating to the meeting held on 19 May 2021.
16.
Any Other Business: Presented by Dr Anna Davey There was no other business discussed.
17. Date and Time of Next Joint Committee Meeting: Presented by Dr Anna Davey AD confirmed that the next JC meeting would take place on Thursday, 26 August 2021, at 10.30 am to 12.30 pm, via MS Teams. VB mentioned that it might be necessary to amend the date or time of some meetings to facilitate AMcK’s attendance and JC members would be notified if this proved necessary.
50

MID AND SOUTH ESSEX (M&SE) CCG JOINT COMMITTEE MEETING
Held on Thursday, 26 August 2021 from 10.30 am – 12.30 pm Meeting broadcast via ‘MS Teams’
PART I MINUTES
PRESENT
Representative Name Job Title / Position Organisation
Dr Anna Davey (AD) CCG Chair and Chair of M&SE CCGs Joint Committee
Mid Essex CCG
Anthony McKeever (AMcK)
Joint Accountable Officer Mid and South Essex CCGs
Dr Boye Tayo (BT) CCG Chair Basildon and Brentwood CCG
Dr Sunil Gupta (SG) CCG Chair Castle Point and Rochford CCG
Dr Jose Garcia (JG) CCG Chair Southend CCG
Dr Anil Kallil (AK) CCG Chair Thurrock CCG
Dan Doherty (DD) NHS Alliance Director Mid Essex CCG
Patricia D’Orsi (PD) NHS Alliance Director South East Essex CCGs
Emma Timpson (ET) (on behalf of William Guy)
Director of Planning and Performance
Basildon and Brentwood CCG
APOLOGIES
Mark Tebbs (MT) NHS Alliance Director Thurrock CCG
William Guy (WG) NHS Alliance Director Basildon and Brentwood CCG
IN ATTENDANCE
Mark Barker (MB) Chief Finance Officer Mid and South Essex CCGs Rachel Hearn (RH) Director of Nursing & Quality Mid and South Essex CCGs
John Gilham (JGil) Lay Member (Governance) and Audit Committee Chair
Mid Essex CCG
Viv Barnes (VB) Joint Committee Secretary Mid Essex CCG
Karen Wesson (KW) Director of Commissioning, Performance and Emergency Planning
Mid and South Essex CCGs
Emily Hughes (EH) Associate Director of Commissioning Acute Commissioning Team, Mid and South Essex CCGs
Jo Cripps (JC) Programme Director Mid and South Essex Integrated Care System
Sara O’Connor (SO) Head of Corporate Governance (minute taker)
Mid Essex CCG
Item No. Item
GENERAL BUSINESS
1. Welcome and Apologies for Absence: Presented by Dr Anna Davey AD welcomed committee members and members of the public to the meeting. AD explained that the Joint Committee (JC) acted collectively on behalf of the five mid and south Essex (MSE) Clinical Commissioning Groups (CCGs) to commission services to meet the needs of their combined population, including acute, mental health and
AGENDA ITEM #
51

Item No. Item
community services and emergency care services including NHS 111 and the ambulance service. AD noted that apologies had been received from WG and MT and invited the other members of the JC to introduce themselves. AD also advised that members of the public were welcome to raise questions via the ‘Q&A’ function on MS Teams.
2. Register of Interests/Declarations of Interest: The JC noted the most recent version of the register of interests. AD reminded members of their obligation to declare any interests they held on any issues arising at JC meetings that might conflict with the business of the CCGs at the beginning of the meeting, at the start of each relevant agenda item, or should a relevant interest become apparent during an item under discussion, so that appropriate arrangements could be implemented. Declarations made by CCG Board members are also listed in the Register of Interests available on the MSE CCG websites. Declarations of interest from today’s meeting There were no additional declarations of interest made by JC members.
3. Minutes of the CCG Joint Committee meeting of 24 June 2021 and Action Log: Presented by Dr Anna Davey AD asked if members had any suggested amendments to the minutes of the JC meeting held on 24 June 2021. KW requested the following amendment to the minute for Item 7 - Adult Critical Care Transfer service - to ensure factual accuracy:
• ‘the service would be funded out of existing East of England Ambulance provisions due to the fact ambulances would not be required to respond to 999 calls for a significant period of time to facilitate these transfers’ to be amended to: ‘East of England Ambulance Service Trust (EEAST) cannot provide the Critical Care transfer service within existing provision as it takes them away from responding to 999 calls for a significant period of time to facilitate these transfers’.
Resolved: The Joint Committee approved the minutes of the Part I JC meeting held on 24 June 2021 subject to the amendment detailed above.
4. Review of Action Log: Presented by Dr Anna Davey The Action Log was reviewed. It was noted that action 1, Mid and South Essex NHS Foundation Trust (MSEFT) Undertakings, was included on the agenda and action 2 (Adult Mental Health Transformation Plan 2021/22) had been deferred until the JC meeting on 28 October 2021. With regard to action 3, VB confirmed a response to questions raised by Mr Peter Blackman regarding the administration of the Ophthalmology service at MSEFT had been provided. Resolved: The Joint Committee noted the Action Log.
52

Item No. Item
5. Questions and Comments from the Public: Presented by Dr Anna Davey and Viv Barnes VB confirmed that no questions had been received from members of the public prior to the meeting, nor had any been submitted via the Teams ‘Q&A’ function, although this would be monitored during the meeting.
SYSTEM REPORTS
6. Board Assurance Framework: Presented by Viv Barnes VB advised that a review of all risks on the MSE CCGs’ Board Assurance Framework (BAF) was undertaken during July and August 2021, which included aligning risks to revised Strategic Objectives approved by the CCG Boards in July 2021. There were currently ten risks within the remit of the JC rated red, as set out on pages 20 to 21 of the report. Six new risks had been added and the committee was being asked to endorse the closure of nine risks. VB highlighted that there were nine risks where assurances were yet to be identified and confirmed this would be an area of focus during the next round of updates. BT noted that there were no Estates risks included on the JC register. VB advised that she would check if any such risks needed to be added to the MSE BAF. JGil referred to risk ref FIN14, relating to a risk of a lack of demand and capacity analysis and alignment, and asked whether the risk rating was representative of the current position as he believed the current score of 12 should be higher. AMcK explained that, with support from JGil, the CCGs were focused on improving modelling to enable waiting lists to be forecast at least a month ahead, which would take account of the timeframe within which patients were booked. MSEFT’s bed model looked at emergency and non-emergency pressures, particularly whilst beds were configured to deal with COVID-19 which affected the Trust’s ability to undertake elective care and deal with emergencies as they arose. Work was ongoing to take all variables into consideration to increase the accuracy of forecasting, which had improved since this time last year, enabling the degree of risk to be calibrated much better than before and the current score reflected this. MB added that significant work was being undertaken by the provider collaborative to understand future needs to prevent risks materialising into a financial pressure. MB advised that the finance report would provide further information and context. JGil also advised that the CCGs’ internal capacity and ability to deliver efficiency savings had been discussed at the Finance and Performance Committees in common (F&P CiC) and he was not sure whether that risk was articulated in the BAF. MB advised that the CCG was recruiting additional staff to enhance its IT/digital capacity and to the Programme Management Office (PMO) to enable the delivery of efficiency savings. Recruitment to ensure that the transformation process could gather pace was also in progress. MB confirmed this risk would be considered during the next round of BAF updates. AMcK welcomed the support provide by JGil regarding the risk management process and explained that it was an ongoing process which was constantly reviewed and monitored and helped him to escalate appropriate responses. AMcK also advised that efficiencies were often made as a result of stopping services that had been delivered for a long time which were not necessarily value for money and sometimes these decisions were controversial, especially when trying to save considerable amounts of money to address disparities across parts of the health service and in that respect, organisations might need to take further difficult decisions to achieve this.
53

Item No. Item
Resolved: The Joint Committee:
• Noted the Board Assurance Framework update report
• Endorsed closure of risks as set out in the report (Refs FIN05, FIN07, GOSD05, MENH07, MENH08, PLAC08, PLAC10, PRCC13, UNPC04).
[Action: VB to ascertain whether there are any Estates risks on the MSE CCG Board Assurance Framework and advise BT accordingly].
7. Non-Emergency Patient Transport Service Procurement: Presented by Karen Wesson and Emily Hughes EH advised that prior to the pandemic, the JC approved a project to undertake redesign and engagement followed by a formal procurement process for non-emergency Patient Transport Services (NEPTS), which had now been completed. The Patient Transport Service Project Board was making a recommendation to the JC to note the outcome of the process and approve the award of the contract to the highest scoring bidder. EH explained that due to commercial confidentiality, the names of the bidders were not included within the paper presented and must remain confidential. Consequently, there might be questions that she would be unable to answer in a public forum. EH outlined the process that had been undertaken, as outlined within the report, and confirmed that although a number of questions were received from potential bidders, there was nothing to suggest that the specification was not robust or what was being asked was not deliverable. Five bidders submitted bids, although one did not proceed through the initial qualification stage based on financial standing. Four bids were taken through the full technical and qualitative evaluation and moderation process. This process was weighted towards quality (80%) with the remaining 20% focusing on price, because it was expected that bids would be close to the CCGs’ financial envelope and, therefore, scoring based on price would not be as significant. The qualitative evaluation included questions relating to financial and commercial elements, for example, delivery of efficiencies during the life of the contract. Of the four bidders who went through the technical evaluation process, one did not exceed the quality threshold set and therefore their price was not considered when comparing the financial elements of the evaluation. Three bidders completed the entire process, with Bidder D achieving the highest overall score. Subject to approval by the JC, the next step would be to write to bidders to inform them of the outcome of the procurement process, following which there would be a 10-day standstill period before the contract was formally awarded. During that period, bidders had the opportunity to challenge the outcome of the process. Following contract award, the Project Board would move into the mobilisation stage in partnership with the preferred bidder. The project risk register, a summary of which was included within the report, would be updated accordingly in due course. EH noted that the outcome would become public at the end of the standstill period. BT noted the significant amount of work, scrutiny and engagement undertaken to progress the procurement process. AD also thanked those involved. Resolved: The Joint Committee unanimously approved the outcome of the procurement process and the recommendation to award the contract for Non-Emergency Patient Transport Services to Bidder D.
54

Item No. Item
8. Community Beds: Presented by Mark Baker MB explained that there had been significant changes to community bed provision as a result of the pandemic. Four wards were within Brentwood Community Hospital (BCH), two of which were managed by MSEFT and the other two by North East London NHS Foundation Trust (NELFT). There was also a ward at Mayfield, facilities at St Peter’s Hospital and the Cumberlege Intermediate Care Centre to support stroke provision. There was also a recovery at home facility (20 beds equivalent) supported and maintained by the provider collaborative and acute colleagues. Mountnessing was currently closed. A contract extension for the two additional NELFT wards at BCH had been approved, which would expire on 31 August 2021. A considerable amount of work had been undertaken by the provider collaborative to look at the ongoing cost of that service. Retaining the beds was critical to maintain patient flows. Costings had recently been completed that identified a net cost to the system of £1.1 million, which sat within the delegated authority of Executive leads. Consequently, they approved the extension of the two temporary wards (Tower and Gibson) under NELFT to 31 March 2022. This would enable existing facilities to remain open and maintain patient flows to avoid beds being blocked within acute settings. MB advised that the current position comprised of the continuation of 104 intermediate care beds across the system plus 26 stroke and 20 recovery at home beds, which was slightly more than pre-COVID. A business case would be progressed, led by community provider colleagues, to consider the future provision of community beds to achieve a long term solution. The business case would be reviewed and scrutinised by the System Finance Leaders Group (SFLG). Finance colleagues would complete their review prior to the 2022/23 planning round so that the JC could consider proposals for long term arrangements, which MB anticipated would be submitted to the December JC meeting. In response to a query from ET, MB advised that Gerdalize Du Toit and James Wilson were leading on workforce modelling and the suitability of facilities, with the re-opening of Mountnessing remaining an option if demand increased. PD advised that community bed provision had shown how the community providers could work collaboratively to find effective solutions during the pandemic and noted the positive impact this was having on services and patients. PD mentioned that services for patients with acquired brain injuries who had not had a stroke were good but could be strengthened further by using a similar approach and asked that this was considered during 2022. AK asked if the provision for ‘step-up’ beds would remain. KW advised that as part of the discussions held, the ability of primary care or community services to step-up patients into community beds existed and there were open criteria and no limit on the number available for this purpose. The model for this was being reviewed and ideally more people would come straight from the community rather than having to go into acute hospital and then out again. AD and KW advised that these beds were accessible via the Urgent Care Response Team (UCRT). JG commented that he had not seen or had experience of these beds being used. KW explained that because of the need to maintain flow within the acute hospital, the community hospital beds were regularly full which unfortunately meant that there were not many beds for the UCRT to use, but she would ask for the pathway to be re-promoted. KW also advised that in response to PD’s comments, prior to the pandemic the JC had considered neuro-rehabilitation services. A newly constituted group was reviewing the
55

Item No. Item
stroke and wider neuro-rehabilitation pathway and details on progress would be provided to the JC in due course. AD highlighted the importance of ensuring that step-up beds were available and asked that this was considered further. KW advised that she would ascertain the demand / unmet need from primary care and provide details to a future meeting. AMcK highlighted that difficulties being experienced within social care often affected the ability to discharge patients. Workforce challenges could also hinder the ability to increase the number of community beds, as doing this might require staff to be diverted away from other services. AMcK advised that he had written to local authority Directors of Social Care to ask what mitigation they could offer. AMcK also asked whether the JC would wish other services to be depleted of staff to increase step-up community beds. AD advised that this was not necessary, but suggested that some patients who were ultimately admitted to hospital could have their needs met adequately in a care home if that provision was available and she trusted that managers would make the right decisions to balance patient and service needs. MB confirmed that community bed provision would be regularly and closely monitored and it was possible that additional bed capacity would be required. AD asked for an update to be provided at a future CCG Chairs update meeting in approximately four weeks’ time. Resolved: The Joint Committee noted the verbal update on Community Beds. [Action: KW to ask for the community beds pathway accessible by primary care and community colleagues via the Urgent Care Response Team to be re-promoted and to request information on the demand / unmet need from primary care to be provided to a future meeting]. [Action: MB to provide a further update on community beds at CCG Chairs’ update meeting in late September].
9. Acute Performance Report: Presented by Karen Wesson KW advised that the two-week, 62 day and 104 day cancer wait standards were currently not being achieved and were off-trajectory. This was in part due to an increase in the number of COVID patients resulting in some surgery being cancelled. Cancer Alliance colleagues were drawing upon mutual aid to progress delayed surgery. Local pathways were also being reviewed and recovery work was being undertaken using cancer transformation funding, which included recruiting additional staff to ensure patients were on the correct pathway and received the right support. The rapid diagnostic centre had helped considerably. The skin pathway had benefitted as a result of Skin Analytics tele-dermatology which helped to identify whether patients needed to be put on a two-week pathway. A few GP practices had not yet signed up to use Skin Analytics and KW’s team were working with relevant practices to increase uptake. KW also highlighted other work being undertaken to improve performance against cancer standards, including for the lower gastro-intestinal cancer pathway, plus action being taken to ensure theatre slots were available for cancer surgery. KW advised that although significant work was being undertaken to improve referral to treatment (RTT) performance, the ambition of zero 98+ week waits by 30 September 2021 was at risk. Service Restriction Policies had been reviewed and should help to support recovery. Patients waiting for diagnostic tests were being reviewed to ensure that those with an urgent clinical need were prioritised.
56

Item No. Item
KW advised that the report also articulated ambulance and NHS 111 performance. Challenges were being experienced regarding advice and guidance (A&G) and turnaround times. In response to a question from AK, KW confirmed that evaluation of the first phase of the Skin Analytics pilot could be shared with members of the committee. KW advised that the programme was being supported by feedback from JC members and other users and the software had been updated as a result of this. There remained technical issues regarding the time it took to upload photographs and the project team was liaising with IT colleagues to resolve this. In response to a query from JGil regarding ‘clock stops’, KW advised that workforce challenges remained and there had been an increase in the unplanned trauma list which had affected theatre capacity. Work was ongoing regarding theatre capacity and utilisation, with support being provided by regional colleagues. JGil also referred to the A&G target of 2 days, whereas current performance was circa 22 days, and asked what action was being taken to address this. KW explained that A&G had not yet been factored into the job plans of Consultants who would be undertaking the review of this service. The CCGs had therefore queried whether the A&G service should be temporarily stopped to enable the review to be completed and then relaunched. The key point was to ensure that primary care, as users of A&G, were involved in discussions to ensure new arrangements were appropriate and effective. AMcK advised that a considerable amount of support had been provided by colleagues from MSEFT, including Andrew Pike, but there remained gaps in the plans built centrally by Andrew and his team and what occurred within each specialty. AMcK explained that currently only half of admitted patients had a clinical priority assigned to them, whereas it had been made clear that procedures should be based on this. Trust staff had been reminded of this requirement and a specialist had been engaged to check that this was being adhered to within all specialties. AMcK advised that it might be necessary to take a number of tough decisions to ensure that performance was improved. AMcK also highlighted a 70,000 gap in the number of calls made to NHS 111 and the availability of slots within primary care and outlined the challenges involved to address this. BT highlighted that pent-up demand was high due to the pandemic and this would affect diagnostic capacity. KW confirmed that work was underway to identify ‘missing’ cancer diagnoses as a result of the pandemic and confirmed that the only pathway that had remained relatively the same for the number of diagnoses was lung cancer which had often been picked up as a result of tests or treatment for COVID-19. AD advised that routine blood tests for routine chronic disease monitoring, such as diabetes, had also reduced during the pandemic which meant that other conditions that could be identified through this route had not been picked up. Resolved: The Joint Committee noted the Acute Performance Report. [Action: KW to share evaluation of the first phase of the Skin Analytics pilot with JC members].
10. Finance Report: Presented by Mark Barker MB advised that the report provided a summary of the month 4 financial position for the five MSE CCGs and the system position for month 3. MB explained that system reporting was a month behind due to the timing of submissions by provider organisations. The CCGs were showing a £3.3 million net deficit, but this was prior to receiving any top-up funding expected from the hospital discharge programme and elective recovery
57
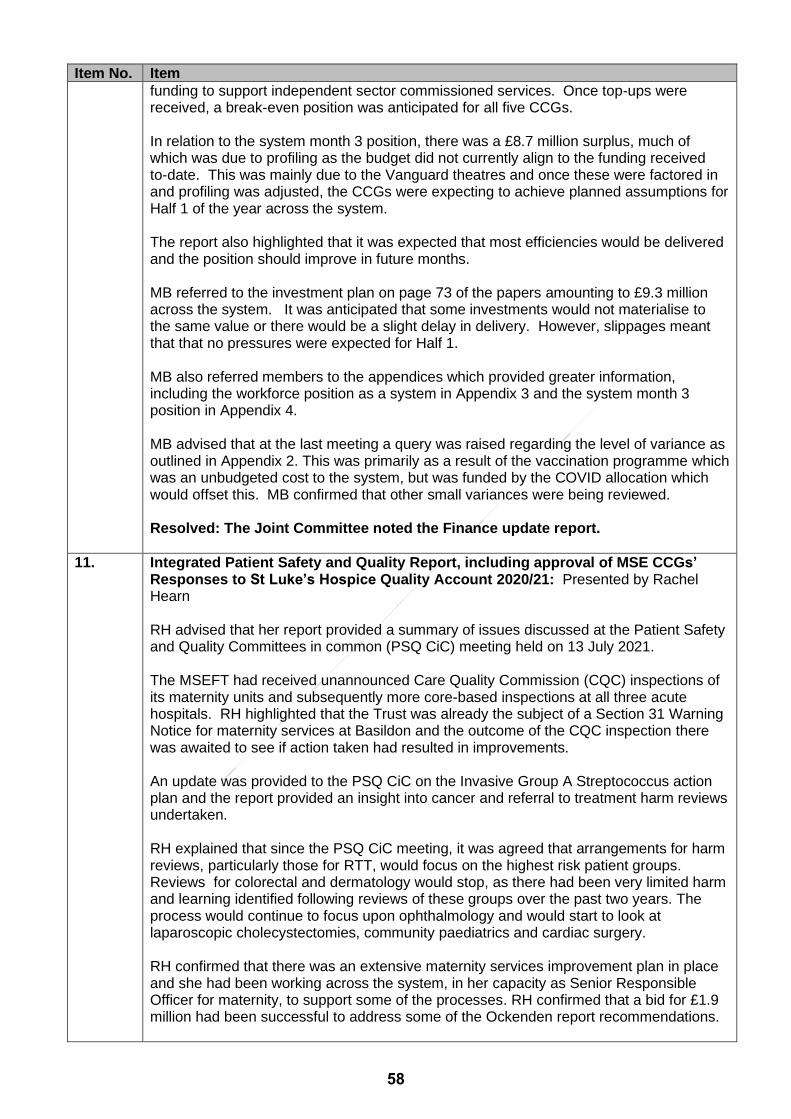
Item No. Item
funding to support independent sector commissioned services. Once top-ups were received, a break-even position was anticipated for all five CCGs. In relation to the system month 3 position, there was a £8.7 million surplus, much of which was due to profiling as the budget did not currently align to the funding received to-date. This was mainly due to the Vanguard theatres and once these were factored in and profiling was adjusted, the CCGs were expecting to achieve planned assumptions for Half 1 of the year across the system. The report also highlighted that it was expected that most efficiencies would be delivered and the position should improve in future months. MB referred to the investment plan on page 73 of the papers amounting to £9.3 million across the system. It was anticipated that some investments would not materialise to the same value or there would be a slight delay in delivery. However, slippages meant that that no pressures were expected for Half 1. MB also referred members to the appendices which provided greater information, including the workforce position as a system in Appendix 3 and the system month 3 position in Appendix 4. MB advised that at the last meeting a query was raised regarding the level of variance as outlined in Appendix 2. This was primarily as a result of the vaccination programme which was an unbudgeted cost to the system, but was funded by the COVID allocation which would offset this. MB confirmed that other small variances were being reviewed. Resolved: The Joint Committee noted the Finance update report.
11. Integrated Patient Safety and Quality Report, including approval of MSE CCGs’ Responses to St Luke’s Hospice Quality Account 2020/21: Presented by Rachel Hearn RH advised that her report provided a summary of issues discussed at the Patient Safety and Quality Committees in common (PSQ CiC) meeting held on 13 July 2021. The MSEFT had received unannounced Care Quality Commission (CQC) inspections of its maternity units and subsequently more core-based inspections at all three acute hospitals. RH highlighted that the Trust was already the subject of a Section 31 Warning Notice for maternity services at Basildon and the outcome of the CQC inspection there was awaited to see if action taken had resulted in improvements. An update was provided to the PSQ CiC on the Invasive Group A Streptococcus action plan and the report provided an insight into cancer and referral to treatment harm reviews undertaken. RH explained that since the PSQ CiC meeting, it was agreed that arrangements for harm reviews, particularly those for RTT, would focus on the highest risk patient groups. Reviews for colorectal and dermatology would stop, as there had been very limited harm and learning identified following reviews of these groups over the past two years. The process would continue to focus upon ophthalmology and would start to look at laparoscopic cholecystectomies, community paediatrics and cardiac surgery. RH confirmed that there was an extensive maternity services improvement plan in place and she had been working across the system, in her capacity as Senior Responsible Officer for maternity, to support some of the processes. RH confirmed that a bid for £1.9 million had been successful to address some of the Ockenden report recommendations.
58

Item No. Item
RH highlighted that her report also outlined progress being made on the new Patient Safety Incident Response Framework, Mental Health Taskforce work, the Parliamentary Independent Investigation and the outcome of the Health and Safety Executive hearing on 16 June 2021. RH advised that the report contained an error on page 91 which referred to 571 LeDeR deaths, which should have been 57. Of these, 24 reviews had been completed, the outcomes of which were included within the report. RH advised that the PSQ CiC had started to undertake reviews of areas including the care sector, primary care, safeguarding, complaints and medicines optimisation. RH asked members to approve the MSE CCG’s response to the 2020/21 Quality Account for St Luke’s Hospice, as supported by Basildon and Brentwood and Thurrock CCGs’ PSQ Committees which covered the areas served by the hospice. RH commented that St Luke’s provided a highly regarded and valued service. PD thanked RH for the information contained in the report and noted the considerable amount of work being undertaken to improve patient safety and quality. PD advised that she was aware there had been an increase in patients with sepsis and asked what action was being taken to prevent this. RH confirmed that Greer Phillips, Care Sector Lead, was ensuring that care homes were using the tools available to identify deteriorating patients. Workforce challenges within the community sector were believed to have contributed to this trend. RH confirmed that this issue would be focused upon in the next quality report to JC. JGil referred to previous discussions regarding plans versus delivery and asked RH if she was confident that plans were being delivered and whether she had any specific concerns that improvements were not being embedded. RH advised that the methodology of constant review and audit provided evidence and assurance, but although she had confidence in the plans, every provider organisation was currently experiencing workforce challenges and this was a notable factor when reviewing investigation reports. Resolved: The Joint Committee:
• Noted the Patient Safety and Quality report and
• Approved the MSE CCGs’ responses to St Luke’s Hospice 2020/21 Quality Accounts.
[Action: RH to provide an update on action being taken to improve the early identification of deteriorating patients to prevent sepsis within the next JC Patient Safety report].
12. Mid and South Essex Hospitals NHS Foundation Trust – Legal Undertakings: Presented by Jo Cripps JC reminded members that MSEFT had been found in breach of its licence and had subsequently agreed to a set of legal undertakings across five categories, namely governance, maternity services, harm reviews, diagnosis and treatment of cancer and elective care. Discharge of the undertakings was being overseen internally by the Trust’s Audit Committee and on behalf of the ICS by the System Oversight Assurance Group (SOAG) which was co-chaired by AMcK and a regional director from NHS England/Improvement. JC advised that despite the pandemic and ongoing workforce challenges, MSEFT had made good progress and was keen to ensure this process was not a ‘tick-box’ exercise, but would result in sustainable and embedded improvements.
59

Item No. Item
JC drew members’ attention to progress against each of the five categories as set out in the report. There were plans in place to exit some of the undertaking categories which would need to be agreed through SOAG and the regional support group. In response to a query from BT, JC advised that notwithstanding the ongoing challenges experienced by the Trust, the undertakings were very specifically worded and therefore the RAG ratings accurately reflected progress against the improvements required. Resolved: The Joint Committee noted the content of the update report on MSEFT Legal Undertakings.
13. 13.1 13.2
Committee Summary Reports: Presented by Rachel Hearn and Mark Barker Patient Safety and Quality Committees in Common (PSQ CiC) AD asked if members had any questions to ask regarding the content of the minutes of the last Patient Safety and Quality Committee meeting in common. No queries were raised. Resolved: The Joint Committee noted the draft minutes of the Patient Safety and Quality Committees meeting in common of 13 July 2021. Finance and Performance Committees in Common (F&P CiC) AD asked if members had any questions to ask regarding the content of the minutes of the last two Finance and Performance Committee meeting in common. It was noted that Dr Anand Deshpande’s title should be amended to make it clear that he was Chair of Thurrock CCG’s F&P Committee, as opposed to being CCG Chair. Resolved: The Joint Committee noted the:
• Approved minutes of the Finance and Performance Committees meeting in common of 16 June 2021 and
• Draft minutes of the Finance and Performance Committees meeting in common of 21 July 2021.
[Action: MB to ensure that Dr Anand Deshpande’s role is accurately recorded within future F&P CiC minutes].
14.
Any Other Business: Presented by Dr Anna Davey There was no other business discussed.
15. Date and Time of Next Joint Committee Meeting: Presented by Dr Anna Davey AD confirmed that the next JC meeting would take place on Thursday, 28 October 2021, at 10.30 am to 12.30 pm, via MS Teams.
60

Part I Board Meeting
Quality and Patient Safety Report
Date of Meeting: 30 September 2021 Agenda No
13
Purpose of Report: ‘Check’ (x) relevant box(es).
For Decision (approval/endorsement) ☐
For Assurance (discussion and noting) ☒
For Information Only ☐
Lead Executive Director:
Rachel Hearn Executive Director of Nursing Mid & South Essex Clinical Commissioning Groups
Report Author / Presenter:
Rachel Hearn Executive Director of Nursing Mid & South Essex Clinical Commissioning Groups
Executive Summary:
This report provides a high-level summary of the main quality and patient safety issues reviewed by the PSQ CiC. The Committees in Common receive a much more detailed report covering all services commissioned by the Mid and South Essex CCGs, as a result of which only issues requiring escalation are reported.
Recommendations and decision/actions required:
The Board/Committee is asked to: Note the Quality and Patient Safety report and seek further assurance as necessary.
How does this report link to the CCG’s Strategic Objectives? ‘Check’ (x) relevant
objective(s)
Strategic Objective 1 Restore access to services to achieve performance against NHS Constitutional standards, quality improvement priorities and deliver ongoing COVID-19 requirements.
☒
Strategic Objective 2 Work with partner organisations and our population to address health inequalities, including those derived from Covid-19, and achieve social value.
☒
Strategic Objective 3 Support system transformation and organisational change to ensure the ICS is successfully established and can fulfil its aims and duties.
☒
Strategic Objective 4 Develop and support the creation and wellbeing of a diverse and highly skilled workforce and ensure the safe transition of staff to the new organisation.
☐
Strategic Objective 5 Achieve key statutory financial duties including delivery of the system financial control total, value for money and reduction of the underlying system deficit.
☐
Strategic Objective 6 Build effective Alliances at place to transform and strengthen the ability of Primary and Community Care Services to focus upon prevention and early intervention and improve outcomes in the most appropriate settings.
☐
Strategic Objective 7 Promote digitally delivered services whilst considering the requirements of those who need to access services in other ways.
☐
Approval Route: (List Committees or groups that have reviewed this document).
Group/Committee Date (dd/mm/yy)
PSQ Committees in Common 14/09/21
61

Please confirm that the Lead Executive Director has signed-off the report prior to submission to the Committee/Board (Committee/sub-committee minutes submitted for
information must be signed-off by the relevant Chair/Lead Executive before submission).
Yes
Has the CFO confirmed that any financial implications are within agreed budget and/or within CFO’s limit of delegated authority as per SFIs?
N/A
Have the relevant Impact Assessments been carried out and signed off?
Equality & Health Inequalities: N/A
Quality: N/A Privacy: N/A
Details of Patient & Public Engagement or Consultation:
N/A this report relates to the quality performance of already commissioned services
Related risks on Board Assurance Framework (BAF) / new risks identified which will be included on the BAF. (please use this link to view the BAF)
Risk alignment is identified at the commencement of each section within this report
Conflicts of Interest: None identified
Does the report need to be escalated to Board/Joint Committee or elsewhere?
No
62

Quality and Patient Safety Report
1. Infection Prevention and Control (IPC)
National/Local standard or objective
Health and Social Care (Safety and Quality) Act 2015 – Reducing Harm in Care.
Key Issue 1 Rising Healthcare Associated Infections, Methicillin Resistant Staphylococcus Aureus Bacteraemia (MRSAB) and Clostridioides difficile infection (CDI) against Zero tolerance/set objective ceiling expectations respectively.
Key Issue 2 SARS-CoV-2 (Covid-19) cases per 100,000 are reducing. However, with lockdown measures easing there is a public health concern raised by the UK Health Security Agency (UKHSA) that cases may rise. Emerging Covid-19 variants continue to cause concern.
Time scale for benefits to be realised
Ongoing annual work plan in place to reduce Healthcare Associated Infections (HCAI).
Risks GOSD11: Infection Prevention and Control Our patients are protected from avoidable infections by robust implementation of published Infection Prevention & Control guidelines by all involved in delivering patient care. Infections may include, but are not limited to MRSA, CDI, SARS-CoV-2 (Covid-19) iGAS
MRSAB – All CCG Cases (Acute and Community) There is zero tolerance to MRSA and all cases are considered as a breach in policy.
MRSAB – All CCG Cases (Acute and Community)
Two new community cases have been reported (CPRCCG and TCCG).
Post 48 hours - Acute cases
Clostridioides difficile infection (CDI) Annual objectives have been published for 2021/2022 (NHS Standard Contract 2021/22) ‘Minimising Clostridioides difficile and Gram-negative Bloodstream Infections’ V1 July 2021. The threshold for MSEFT is 177. We await advice from the Director of Infection Prevention & Control as to how these thresholds will be divided across the three sites. The management of Gram-negative thresholds is to be discussed.
All Cases Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar YTD
BBCCG 1 0 0 1 0 2
CPRCCG 0 0 0 2 0 2
MECCG 2 2 2 1 0 7
SCCG 0 0 2 0 0 2
TCCG 1 0 0 1 0 2
MSEFT Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar YTD
Basildon 0 0 0 0 0 0
Broomfield 0 0 1 0 0 1
Southend 0 0 0 1 0 1
Total 0 0 1 1 0 2
63

All CCG Cases (Acute and Community)
Acute Cases
NB: It is important to note that the data tables may vary due to late notification or identification of a case found on the DCS where notification from an Acute Trust has not been received.
Learning From Infection As outlined in previous reports learning remains unchanged with no new emerging themes. Cross organisational work will aim to address common themes identified from Root Cause Analysis (RCA) and Post Infection Reviews (PIR). In light of the increased number of Southend hospital attributed cases, a CDI reduction plan for the Southend site has been developed. A question was raised at the Thurrock Board meeting regarding the PIR process for CDI and monitoring of antibiotic prescribing in emergency departments (ED). Assurance was given that prescribing issues are escalated to the Infection Control Doctor, Microbiologist and Antimicrobial Pharmacist during the process. Additionally, such issues are raised and discussed at Infection Prevention and Control Committee meetings. Outbreaks and Periods of Increased Incidence (PII)
None in this reporting period
Nosocomial SARS-CoV-2 (Covid-19) outbreaks:
➢ Broomfield hospital: Reported an outbreak in June on one ward involving two patients and one member of staff. All staff and patients had PCR tests, no further cases were identified and the outbreak was closed after 28 days.
➢ EPUT Mental Health Services: Reported two wards at Basildon Mental Health Unit with
Covid 19 outbreaks. The first outbreak identified on 15 July involved two patients and no staff, immediate outbreak management was instigated. One further positive patient was identified on 19 July (total three patients, no staff) following which there were no further cases and the outbreak was closed after 28 days.
The second outbreak was identified on 12 August involving three patients and no staff, a further three positive patients and three staff were reported (total six patients and three staff). Outbreak management ongoing with the ward closed to admissions at the time of the writing the report.
➢ Marillac Neurological Rehabilitation Centre (Brentwood): Reported an outbreak on
1 August involving seven patients and six staff. The outbreak was managed with support from PHE and the CCG.
➢ Basildon Hospital: A ward at Brentwood Community Hospital (BCH) reported an
outbreak on 14 August initially involving five patients and no staff, three of these patients
All Cases Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar YTD Ceiling
BBCCG 3 1 10 6 3 0 0 0 0 0 0 0 23 94
CPRCCG 7 5 5 7 3 0 0 0 0 0 0 0 27 48
MECCG 6 6 5 9 3 0 0 0 0 0 0 0 29 123
SCCG 4 3 7 6 3 0 0 0 0 0 0 0 23 48
TCCG 1 5 6 1 2 0 0 0 0 0 0 0 15 44
MSEFT Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar YTD Ceiling
Basildon 3 4 10 5 2 0 0 0 0 0 0 0 24
Broomfield 6 2 3 5 1 0 0 0 0 0 0 0 17
Southend 10 4 8 8 4 0 0 0 0 0 0 0 34
Total 19 10 21 17 7 0 0 0 0 0 0 0 74 177
64

were transferred from a ward at Basildon hospital, both wards were closed to admissions at the time of writing this report.
2. Acute Serious Incidents and Never Events
National/Local Standard or objective
The Serious Incident Framework (published 27/03/2015) sets out that Provider focussed internal investigations should be completed within 60 days of the incident being reported.
Key Issue 1 The number of outstanding serious incident investigations across Mid and South Essex Foundation Trust (MSEFT).
Key Issue 2 Timeliness of investigation during Covid-19 pandemic.
Time scale for benefits to be realised
Trajectory for Stop the Clocks to be confirmed
Risks GOSD13: Management of Serious Incidents
Oversight of hospital serious incidents to ensure they are managed appropriately. Review of all serious incidents and working closely with providers to determine their closure and implement required actions. Ensuring that learning from serious incidents is disseminated across the Health Care Partnership (HCP) system.
There were a total of 38 Serious Incidents (SIs) reported in June and July 2021. The StEIS categories for these incidents and the location are as follows:
No Never Events were reported in this period. It is noted there are 3 declared year to date from MSEFT relating to wrong site surgery (2 ophthalmology and 1 in orthopaedics). This is in line
Acute Commissioning SI's raised June 2021 - by StEIS Category and OrganisationBasildon
Hospital
Broomfield
Hospital
Southend
Hospital
Spire
HealthcareTotal
Diagnosis Incident Including Delay Meeting SI Criteria 0 1 2 0 3
Healthcare/Infection Control Incident Meeting SI Criteria 1 0 0 0 1
Maternity/Obstetrics Incident Meeting SI Criteria - Baby Only 0 1 0 0 1
Maternity/Obstetrics Incident Meeting SI Criteria - Mother & Baby 1 0 0 0 1
Pending Review 0 0 0 0 0
Pressure Ulcer Meeting SI Criteria 0 2 0 0 2
Slips/Trips/Falls Meeting SI Criteria 1 0 0 0 1
Sub-Optimal Care of Deteriorating Patient Meeting SI Criteria 1 0 0 0 1
Surgical/Invasive Procedure 1 2 0 1 4
Treatment Delay Meeting SI Criteria 1 1 3 0 5
VTE Meeting SI Criteria 1 1 0 0 2
Total 7 8 5 1 21
Acute Commissioning SI's raised July 2021 - by StEIS Category and OrganisationBasildon
Hospital
Broomfield
Hospital
Southend
HospitalTotal
Apparent/Actual/Suspected Self Inflicted Harm Meeting SI Criteria 0 1 0 1
Diagnosis Incident Including Delay Meeting SI Criteria 0 2 3 5
Maternity/Obstetrics Incident Meeting SI Criteria - Baby Only 0 0 1 1
Maternity/Obstetrics Incident Meeting SI Criteria - Mother & Baby 0 1 0 1
Pressure Ulcer Meeting SI Criteria 0 1 0 1
Slips/Trips/Falls Meeting SI Criteria 2 0 0 2
Sub-Optimal Care of Deteriorating Patient Meeting SI Criteria 4 0 0 4
Treatment Delay Meeting SI Criteria 1 0 1 2
Total 7 5 5 17
65

with the national picture for Never Events, with 364 declared in total during 2020/21 of which wrong site surgery was the dominant category with 226 cases.
3. Cancer Quality
National/Local Standard or objective
100% of patients waiting longer than 104/63 days from urgent referral for suspected cancer to their first definitive treatment receive a root cause analysis (RCA) of the delay and a clinical harm review.
Key Issue 1 Undertakings in relation to Cancer Harm Review Ensure that the Cancer harm review process is sustained on all three hospital sites as a business as usual model for completion within 90 days.
Key Issue 2 To establish a coordinated approach to oversee the quality issues affecting cancer services and seek assurance that plans are in place to address these.
Time scale for benefits to be realised
Ongoing
Risks CANC02: Harm Review for Cancer Working to reduce those patients waiting for their cancer treatment over 62 days (to 181 Pre-COVID19 by March 2021) and over 104 days (zero by March 2021).
Harm Review data (as of 16th August 2021). Cancer harm review performance for 2020/2021 is now 100%. MSEFT Figures for 2021/2022 to date as at 16th August 2021: There are 74 harm reviews outstanding, 11 are overdue, 63 are not required to be completed until the end of August as there is a 3-month period before a cancer harm review becomes overdue – this period is classed as ‘business as usual’. A breakdown by month is given below:
2020/2021 MSE
Cancer Harm Reviews
Ap
ril
May
Jun
e
July
Au
gust
Sep
tem
ber
Oct
ob
er
No
vem
ber
Dec
emb
er
Jan
uar
y
Feb
ruar
y
Mar
ch
2020/2021 Performance
to Date
63-103 days
% undertaken 91% 60% 72%
Total number due
68 98 166
No. Undertaken 62 59 121
Outstanding 6 39 45
104 Days
+
% undertaken 88% 40% 59%
Total number due
43 40 83
No. Undertaken 38 16 54
Outstanding 5 24 29
66

Themes and Learning Report MSEFT released its quarterly report detailing themes and learning on 1 June 2021. The level of harm deemed through the Harm Review Process is recorded for each case. A brief summary is detailed below for those cases where harm has been identified: MSE Harm Review Outcomes – April 2019 to 31 May 2021:
There have been 2622 cases of no harm identified which is equivalent to 99% of the total number of completed cases. The breakdown of tumour sites where harm has been determined are:
Low Harm There have been 19 cases of low harm identified (0.7% of the total completed cases). The learning from these and improvements put in place include:
• Referrals made from Primary Care need to identify patients with disabilities and learning difficulties from the outset.
• Delayed referral, appointment/s or diagnostic tests.
• Some evidence of psychological harm but not on a prolonged basis as evidenced by the patients received counselling and/or CNS support in their pathway
• Cancellation of operations and services due to Covid-19 but ultimately the delay did not change the course of treatment.
Moderate Harm
67

There have been 6 cases of moderate harm identified (0.2% of the total completed cases) – 3 within Haematology, 1 Breast case (relating to Pathology), 1 Skin and 1 Lung case. A Serious Incident (SI) has been declared for each of the 3 cases where moderate harm was established, the other 3 have been investigated following local incident processes. A brief summary of the findings is as follows:
• All diagnostic core biopsies are to be reviewed prior to discussion at the MDT.
• Consultant Histopathologists that report breast pathology must be registered and participate in the breast External Quality Assessment (EQA) scheme and meet the minimum required Continuing Professional Development (CPD) activities in breast pathology to meet the Breast Screening Programme’s requirements.
• Implementation of a departmental process to enable double reporting of breast biopsies so more complex cases can be reviewed by a second Histopathologist.
• Ensuring all reporting Consultants Breast pathology report the minimum case load (50/year)
• Synoptic template is to be used in all reporting of screening and symptomatic breast cancers.
Severe Harm There has been 1 case of severe harm identified:
• Radiology capacity needs to better match demand. This has already been achieved with a combination of out-sourcing of reports and consultants within the department increasing workload.
• Use of electronic referrals to avoid the potential for lost documents in the post and to provide a clearer audit trail to ensure timely action which has already been implemented in the Department.
• Greater use of the multidisciplinary lung cancer pre-diagnostic meeting to grade urgent referrals to the respiratory department.
4. Referral to Treatment (RTT) Harm reviews
National/Local Standard or objective
NHS England established an operational standard to ensure that no-one waits more than 52 weeks from referral to treatment (RTT) and that 52-week breaches should trigger a review process.
Key Issue 1 Ensure that the RTT review process is sustained on all three hospital sites as a business as usual model for completion within 60 days (no harm review more than 2 months old from treatment/discharge month)
Time scale for benefits to be realised
End of Quarter 2 2021/22
Risks GOSD12: Acute/Provider Quality Assurance Ensuring the care provision for residents is safe, effective, good quality and value for money as defined within the NHS Constitution. PLAC02: To achieve the Constitutional Standard for RTT. Reduce 52week waiting patients Reduce backlog for patients waiting Initial focus of highly challenged specialties (T&O, Ophthalmology, Urology, Endoscopy, Skin).
Harm Review data (as of 31 July 2021) NHSE/I Undertakings were served against MSEFT that required them to complete all 52-week breach harm reviews in the risk stratified areas from April 2019-January 2021 by 31 March 2021. All reviews were completed within the undertakings period resulting in the Trust then moving to
68

operate under Business as Usual (BAU) model as of 1 April 2021 (no harm review more than 2 months old from treatment/discharge month). Total MSE completion rate of harm reviews for 2020/21 Figure 1 is almost at 99.9% (9 outstanding). A breakdown by month is given below:
Figure 1 - MSE Figures from April 2020 to March 2021 as on 31/07/2021:
2020/2021
Ap
ril
May
Jun
e
July
Au
gust
Sep
tem
ber
Oct
ob
er
No
vem
ber
Dec
emb
er
Jan
uar
y
Feb
ruar
y
Mar
ch
2020/2021 Performance
to Date MSE RTT Harm
Review Performance
% undertaken 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% 96% 99.90%
Total number due 5 20 76 206 149 600 335 322 441 235 120 216 2725
a) colorectal 1 2 13 23 20 27 38 43 26 17 21 42 273
b) ophthalmology 3 10 22 67 66 495 271 260 406 215 94 168 2077
c) dermatology 1 8 41 116 63 78 26 19 9 3 5 6 375
No. Undertaken 5 20 76 206 149 601 334 322 441 235 54 207 2716
Number Outstanding 0 0 0 0 0 0 0 0 0 0 0 9 9
Total MSE completion rate of harm reviews for 2021/22 Figure 2 is at 42% (253 outstanding).
Figure 2 - MSE Figures from April 2021 to March 2022 as on 31/07/2021:
2021/2022
Ap
ril
Ma
y
Ju
ne
Ju
ly
Au
gu
st
Se
pte
mb
e
r
Octo
ber
No
vem
ber
De
cem
ber
Ja
nu
ary
Feb
rua
ry
Ma
rch
2021/2022 Performance
to Date MSE RTT
Harm Review Performance
% undertaken 64% 66% 19% 52.00%
Total number due 190 117 122 429
a) colorectal 32 18 27 77
b) ophthalmology 157 95 94 346
c) dermatology 1 4 1 6
No. Undertaken 121 77 23 221
Number Outstanding
69 40 99 208
Harm reviews for June 2021 are not due for completion until the end of August 2021 as there is a 60-day period before a harm review becomes overdue – this period is classed as BAU. There are 253 harm reviews outstanding of which 142 cases are overdue and classed as a backlog (March-May). A total of 139 of the 142 backlog are within the ophthalmology speciality on the Broomfield site (see figure 3 below). This service has not been able to achieve BAU since the national undertakings in February 2021 and has been severely impacted by staff shielding, clinical capacity and annual leave. This has been escalated within the Trust and to the Systems Oversight Assurance Group (SOAG). There is a trajectory to clear the ophthalmology cases by 27 August 2021 with additional harm review sessions scheduled to ensure delivery. Risk Stratification A presentation was made to the System Oversight and Assurance Group in July 2021 to review the current risk stratification for completion of RTT harm reviews. Below is a summary of the current position:
69

• Colorectal and dermatology harm reviews identified only small numbers of harm, all at low level, there has been little learning from these reviews.
• Ophthalmology harm reviews identified some harms at moderate and high level, though low in number, recognition of useful learning.
• There are some high-volume procedures (e.g. cataracts) where there is low risk of harm from delay but in which harm reviews take up considerable clinical time. Clinicians are anxious to prioritise use of clinical time for the greatest benefit.
• There are some conditions outside of the prioritised specialties where delays may result in harm and in which harm reviews are not currently undertaken.
It was agreed to have a rolling programme identifying the highest risk patient groups, reviewed on an annual basis and results shared through the Quality Improvement Board and the Mid and South Essex NHS Foundation Trust Quality Committee. 2021/2022 Agreed RTT Harm Review risk stratification:
• Colorectal and Dermatology harm reviews to cease.
• Ophthalmology RTT harm reviews to continue (but exclude cataracts, ptosis, epiphora, cysts)
• Additional risk groups to be added:
1. Laparoscopic cholecystectomy patients
2. Community paediatrics
3. Cardiac surgery patients with delays > 6 months
5. Maternity
National/Local Standard or objective
To reduce the number of Maternal deaths, Stillbirths, Neonatal deaths and brain injuries by 50% by 2025. The Maternity ambition has extended to include reducing preterm births from 8% to 6%.
Key Issue 1 The Maternity Services Support Programme report by NHSE/I is under review by MSEFT and its findings are awaited.
Key Issue 2 A Section 31 notice must take and should take actions remains in place for the MSEFT.
Time scale for benefits to be realised
30th November 2021- submit an equity and equality analysis and a coproduction plan. 28th February 2021- coproduce equity and equality action plans
Risks MATS01: Delivery of Maternity Transformation Programme MATS02: Acute Maternity Trust Performance and Section 31 Warning Notice)
The National Priorities and Operational Planning Narrative template was submitted to Region on 6 May 2021. Following a successful bid, £1.948,672 has been awarded to MSEFT to support the national and regional assurance, to deliver improvements in Maternity care. The funding is for additional staff to meet the recommendations of the Ockenden review. A Section 31 notice ‘must take’ and ‘should take’ actions remains in place for tMSEFT. Evidence is currently been reviewed with regards to requesting exit of the section 31. The Regional Maternity Quality Lead has now completed sixty supportive quality safety steps on all three Maternity sites within MSEFT. The findings are awaited and will be summarised in
70

the next report. The CQC have additionally undertaken maternity focused inspections during August 2021 with the outcomes expected to be published in late October.
The national ambition to have the majority of pregnant women on a Continuity of Carer (CofC) pathway remains a challenge for MSEFT. This is due to workforce deficits and competing priorities. A CofC roadmap was submitted to Region on 30 July 2021 which details the planning timeline for implementation of further CofC team rollout across MSEFT. Work continues to map the process with Suffolk and North East Essex LMNS as our LMNS ‘critical buddy’. The remaining work requires Obstetric & Neonatal commitment to be aligned within their current job plans. On the 5 August 2021 the national team published draft guidance for Equity and Equality: safe personalised care for all. There five priorities aligned to the 2021/22 planning guidance are: -
• Priority 1: Restore NHS service inclusively. Continue to implement the COVID 19 four actions.
• Priority 2: Mitigate against digital exclusion. Personalised care plans in various languages & formats.
• Priority 3: Ensure datasets are complete and timely. Improve data quality of ethnic coding and the mother’s postcode.
• Priority 4: Accelerate preventative programmes that proactively engage those at greatest risk of poor health outcomes.
a) Understand your population and co-produce interventions b) Action on maternal mortality, morbidity and experience c) Action on maternal mortality, morbidity d) Support for maternity and neonatal staff (Cultural Competency & Workforce Race Equality Standards WRES)
• Priority 5: Strengthen leadership & accountability. 30th September 2021- submit an equity and equality analysis and a coproduction plan.31st December 2021- coproduce equity and equality action plans.
Care Quality Commission (CQC) – Maternity Inspection Basildon Hospital Maternity Services: A Section 29A was issued on 26 June 2020 and a Section 31 issued on 24 June 2020. The CQC undertook an unannounced visit on 12 June 2020 where they found serious concerns in relation to 6 serious incidents involving babies born in poor condition. The CQC report confirmed the maternity service rating of ‘Inadequate’ overall with the safe, effective and well-led domains all individually rated as inadequate. The CQC made a further announced visit to Basildon Maternity Unit on 18 September 2020 with some areas of improvement noted around storage of records and completion of WHO checklist, however there were concerns raised about culture, handovers, adherence to Personal Preventative Equipment guidance and incomplete prescription charts. Core services inspections were published in March 2020 for Broomfield and Southend (both rated Requires Improvement) and Basildon (rated Good) in 2019, leading to a combined rating of ‘Requires Improvement’. The latest maternity rating does not alter the overall rating for MSEFT. Additionally, focused reports have been issued in respect of maternity services at Basildon Hospital on 19 August 2020 and 19 November 2020, an IPC focused inspection on 8 April 2021 and an IR(ME)R focused inspection at Broomfield Hospital on 6 May 2021. The CQC have also undertaken unannounced visits to all MSEFT maternity sites during the week commencing 26 July 2021 and to Southend - ED, Basildon – Medicine, Surgery; theatres and ophthalmology across all sites during the week commencing 2 August 2021. Reports on
71
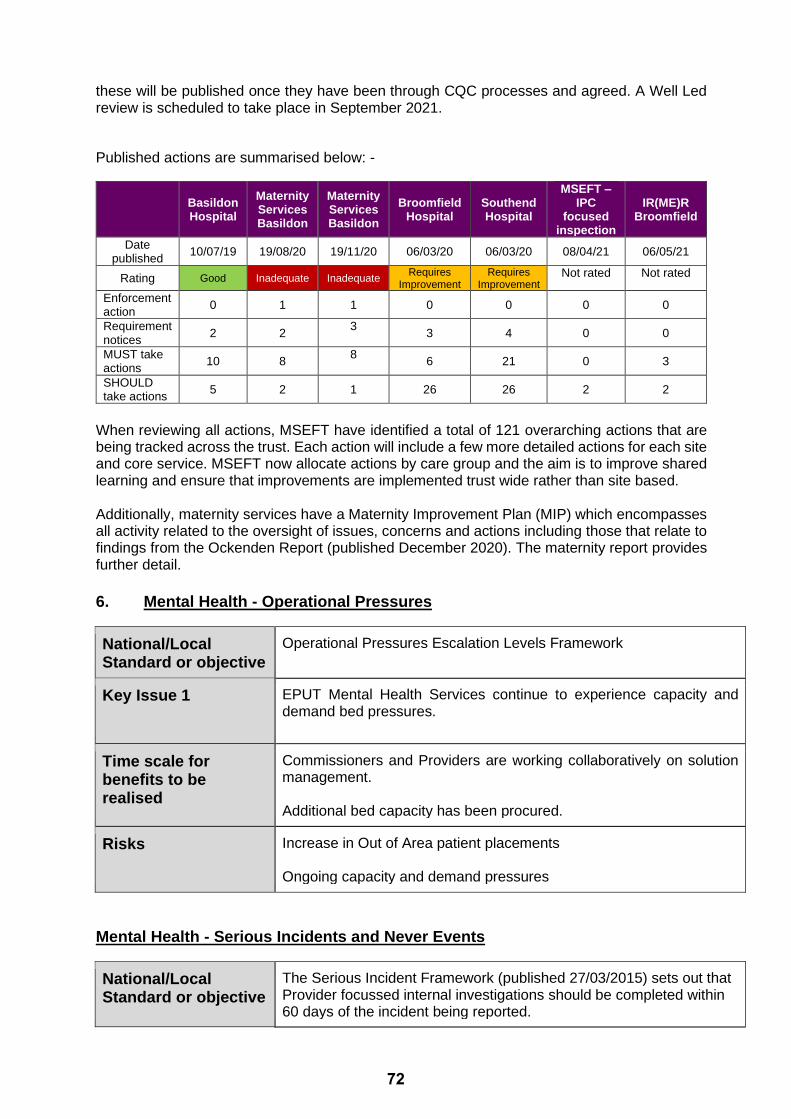
these will be published once they have been through CQC processes and agreed. A Well Led review is scheduled to take place in September 2021.
Published actions are summarised below: -
Basildon Hospital
Maternity Services Basildon
Maternity Services Basildon
Broomfield Hospital
Southend Hospital
MSEFT – IPC
focused inspection
IR(ME)R Broomfield
Date published
10/07/19 19/08/20 19/11/20 06/03/20 06/03/20 08/04/21 06/05/21
Rating Good Inadequate Inadequate Requires
Improvement Requires
Improvement Not rated Not rated
Enforcement action
0 1 1 0 0 0 0
Requirement notices
2 2 3
3 4 0 0
MUST take actions
10 8 8
6 21 0 3
SHOULD take actions
5 2 1 26 26 2 2
When reviewing all actions, MSEFT have identified a total of 121 overarching actions that are being tracked across the trust. Each action will include a few more detailed actions for each site and core service. MSEFT now allocate actions by care group and the aim is to improve shared learning and ensure that improvements are implemented trust wide rather than site based. Additionally, maternity services have a Maternity Improvement Plan (MIP) which encompasses all activity related to the oversight of issues, concerns and actions including those that relate to findings from the Ockenden Report (published December 2020). The maternity report provides further detail.
6. Mental Health - Operational Pressures
National/Local Standard or objective
Operational Pressures Escalation Levels Framework
Key Issue 1 EPUT Mental Health Services continue to experience capacity and demand bed pressures.
Time scale for benefits to be realised
Commissioners and Providers are working collaboratively on solution management. Additional bed capacity has been procured.
Risks Increase in Out of Area patient placements Ongoing capacity and demand pressures
Mental Health - Serious Incidents and Never Events
National/Local Standard or objective
The Serious Incident Framework (published 27/03/2015) sets out that Provider focussed internal investigations should be completed within 60 days of the incident being reported.
72

Key Issue 1 There are a number of outstanding queries with EPUT which are being managed through regular meetings with EPUT’s Head of Patient Safety.
Key Issue 2 A number of high-level Serious Incidents and Level 3 independent investigations and external reports with potential for adverse impact on EPUT
Time scale for benefits to be realised
Positive progress and benefits are being realised due to the collaborative management and reduction in numbers of any outstanding reports a number of closures have been achieved. A variation letter as detailed below has been sent to EPUT
Risks The CCG might lose sight of Serious incident information due to adoption of PSIRF.
There are currently 9 active serious incidents reported by EPUT Mid & South Essex Mental Health Services being managed by Thurrock CCG. The table below shows the number of incidents by STEIS reporting category:
STEIS Reporting Category Number of incidents Inpatient setting (mental health/acute)
Number of Incidents Community Setting
Unexpected/potentially death 0 7
Unexpected / potentially avoidable injury causing serious harm
0 1
Apparent/actual/suspected homicide 0 1
Update on Patient Safety Incident Response Framework (PSIRF) EPUT adopted the PSIRF from 1 May 2021. Incidents reported prior to this date continue to be investigated in accordance with the Serious Incident Framework 2015. The MSECCGs and EPUT will continue with twice monthly Serious Incident update meetings to review existing Serious Incidents. The MSECCG Quality and Patient Safety Team, along with colleagues from North East Essex (NEE) CCG and West Essex (WE) CCG, will be meeting with EPUT on a monthly basis as a pan Essex group to ensure continued PSIRF assurance and to identify any trends enabling an Essex wide approach to sharing learning. Level 3 Independent Investigation – Legacy Case A legacy case from 2016 was transferred to Thurrock CCG as the coordinating commissioner in October 2019. The Level 3 Independent Investigation has been completed. The final report has now been finalised, which was published on 24 August 2021 and can be found at Niche-EPUT-Mr-Z-FINAL-report-1-July-2021.pdf (england.nhs.uk) The inquest into the death of the victim concluded on 20 August 2021. Her Majesty’s Coroner concluded that Mrs X died as a result of complications arising from inhalation of air fumes, which was a fatal consequence of a fire that started at her front door. This was noted as an ‘unlawful killing’. A narrative conclusion was provided, which in summary stated that, on the balance of probability, had Mr Z’s depot medication been reintroduced, provided either by primary or secondary care services at any point prior to the end of April 2016, it was considered unlikely the fire would have been set and Mrs X would not have died.
73

HM Coroner has advised that EPUT will be issued with a Prevention of Future Deaths report (PFDR), which may also be addressed to the five CCGs involved in the Mid and South Essex implementation of the primary care mental health nurse team. This is in relation to the wider need for a shared protocol with regards to implementation and administration of depot medication within primary and secondary care. Quality Assurance Visits
• Danbury Ward at the Priory Hospital Chelmsford was visited on 9 July 2021
• Ruby ward at The Crystal Centre was visited on 22 July 2021
• The First Response, Recovery & Wellbeing and Assertive Outreach Teams based at Grays Hall were visited on 4 August 2021.
A series of visits were undertaken in June 2021 to a number of inpatient wards across the EPUT estate to review areas including ligature risks and their mitigations. Themes and trends identified:
➢ Environmental issues e.g. social distancing impacting on ward occupancy ➢ Staff reported a lack of interoperability of IT systems ➢ Workforce issues ➢ Infection Prevention and Control issues
The CCGs are supporting EPUT with their action plans and developing a joint Evidence Assurance group to ensure robust oversight of sustained improvement. The MSE CCGs are working closely with colleagues in NEECCG and WECCG to ensure robustness across the pan Essex footprint, harmonising visits across the footprint, especially where geographical locations overlap, attending other CCG’s quality assurance visits and sharing information across the footprint. Care Quality Commission (CQC) There have been no notifications of CQC visits to adult services within EPUT. There have been CQC unannounced visits to the St Aubyn’s Centre CAMHS inpatient unit and Poplar Ward CAMHS inpatient unit. Following these visits a Section 31 Notice was served to EPUT. The CQC reports for these visits have not been officially published at the time of this report. MSE CCG Mental Health Task Force. The Taskforce was formed in December 2020. To date there have been five reviews covering:
• Perinatal Services
• Personality Disorder Services
• Eating Disorder Services
• Discharge Follow up and Care Planning
• Estates and ligature points The final review focusing on partnership working and IT interoperability was presented on 16 August 2021, following which a final summary report will be developed. Running alongside the last 3 reviews we have had a focused Significant Incident review linked to the subject of each of the focused reviews. The Taskforce has agreed robust recommendations after each review and there is a pan-Essex structure in place to take the recommendations forward and develop action plans to achieve the agreed recommendations. Good progress is being made system wide against the actions.
74

It has been agreed that there will be 3 monthly touch points with the Independent Chair and Task Force lead to assess and maintain oversight of the delivery of the action plan. Cross cutting themes from the reviews are:
➢ To create stronger, more cohesive links between CCG departments. ➢ To create stronger, more cohesive links and information processes between CCGs and
Adult Social Care. ➢ To create more joined up learning, surveillance and information sharing pan-Essex. ➢ To incorporate all partners in co-production, including users of services and families/carers. ➢ Work needs to be undertaken immediately to improve monitoring of incident action plans
and dissemination of learning at both System and Place. Mental Health Options appraisal of pan Essex Mental Health commissioning teams. In response to the themes and recommendations of the Mental Health Task Force, the three pan Essex Accountable Officers have tasked the mental health commissioning teams to develop an options appraisal with a focus on how the commissioning system can work in greater collaboration and more effectively. Parliamentary Independent investigation As previously reported, Dr Geraldine Strathdee was appointed as the Independent Chair for the Essex Mental Health Independent Inquiry (EMHII), a non-statutory review of quality and safety issues within EPUT Mental Health services and predecessor organisations (SEPT/NEPT). This review commenced on 1 April 2021 and will investigate patient deaths over a twenty-year period – 1 January 2000 to 31 December 2020. It is anticipated that the Inquiry will take two years to complete. Following publication of a press release by the EMHII on 26 May 2021, an initial six-week consultation period began, the families and others affected were urged to give their views on the issues to be considered by the Inquiry. Following the end of the six-week initial consultation period, the Inquiry published its draft terms of reference and opened a two-week consultation for further opportunity for families and the public to comment on the draft terms of reference. The draft Terms of Reference that were published and the issues the inquiry will consider included:
• Key factors that led to the deaths of mental health in-patients who were under the care of the Trust(s) including care and treatment pathways;
• The role, involvement and communication with the patient and their families, carers, and other trusted individuals in their care;
• The culture, leadership, and governance that may have impacted on the ability of the Trust(s) to improve inpatient safety, treatment, and care and reduce inpatient deaths;
• The quality of previous investigations into mental health inpatient deaths, the conclusions and recommendations of those investigations, and the response by the Trust(s) and the wider system;
• Recommendations for the Trust(s) to ensure action is taken so that current and future mental health inpatients receive appropriate and safe treatment and care; and
• Further recommendations for the Trust(s), mental health services, the NHS, and the wider system.
The full Draft Terms of Reference and further information can be found at https://emhii.org.uk/. The Inquiry’s findings are expected to be published in spring 2023.
7. Learning Disability
75

National/Local Standard or objective
Health and Social Care Act 2008 (Regulated Activities) Regulations 2014. Care Act 2014. Mental Capacity (Amendment) Act 2019. Children Act 1989. Children Act 2004.
Key Issue 1 Assurance of the achieved trajectory of 75% of completed annual health checks as set by NHS England/Improvement
Key Issue 2 Assurance that the correct services are being received regardless of post code and provided as part of the ELDP contract.
Key Issue 3 Assurance that the learning from LeDeR reviews are being implemented in a timely fashion and that the new LeDeR process adheres to the recent national changes implemented.
Time scale for benefits to be realised
Progress report at next Quality and Patient Safety Committees in Common related to above issues
Risks • The CCGs will not be able to meet their objective to safeguard and protect people in vulnerable groups within their area of responsibility • Failure to protect vulnerable people from harm. • Loss of reputation.
The trajectory has increased and been reset to 75% trajectory for 2021/2022. The table below identifies that 2 out of the 5 CCGs are performing above monthly trajectory with overall completion rate across the system of 5% (275). Due to movement of posts there are currently gaps within LD commissioning at Place. The system post for LD commissioning across MSE CCG is currently being reviewed. Monthly performance data at Primary Care Networks (PCN) and at practice level is now available and due to be shared with primary care to cascade. Social care prescribing continues to support. Discussions between system leads, NHSE and Primary Care Commissioners continue to consider whether different ways to support GPs using QOF money can be implemented. Table 1. Current Cumulative data of completed Annual Health Checks up to July 2021
Apr May Jun Jul
LD Checks - 20/21 21 27 69 105
20/21 Checks as a % of Register 2% 2% 6% 9%
LD Checks - 21/22 33 57 107 150
21/22 Checks as a % of Register 3% 5% 9% 12%
LD Checks - 20/21 0 6 31 53
20/21 Checks as a % of Register 0% 1% 4% 7%
LD Checks - 21/22 22 43 64 86
21/22 Checks as a % of Register 3% 6% 9% 12%
CCG
Cumulative Number of Checks Completed
MonthlyPatients on
LD Register -
Current
Register
Size (from
Phase 3
Plans)
722 699
NHS
Basildon &
Brentwood
CCG
1,180 1,258
NHS Castle
Point &
Rochford
CCG
76

8. Care Sector Review
National/Local Standard or objective
National Enhanced Care in Care Homes (EHCH) objectives Care Quality Commission Statutory requirements Local initiatives and support offer Due to the breadth and scope of the Care Sector remit, this report focuses mainly on the EHCH work being undertaken in nursing and residential homes; it also considers the impact on the wider care sector work.
Key Issue 1 Homes with current significant safeguarding / quality concerns, poor compliance and interaction interventions
Key Issue 2 Covid and Respiratory Outbreaks and exposure
Key Issue 3 Resilience of the care Market
Time scale for benefits to be realised
Continuous monitoring and interventions managed via CSTOG and Collaborative Care Sector Hubs
Risks • Sub optimum care of individuals • Sub optimal health and wellbeing of individuals and reduced capacity in the Care Sector impaction on Acute flow. • Reduction in capacity of Care Home beds
During the Covid pandemic the health and wellbeing of our population with care and support needs was very much brought to the fore. It became imperative that there was consistency of support and intervention across the CCGs in MSE. The formation of multi-agency support Hubs at place quickly engaged with Care Providers and were able to give almost immediate response to emerging issues and support with rapidly changing government guidance. To bring together identified emerging issues and risks the Hub Leads would escalate to the newly formed Care Sector Tactical Meeting. From here system wide issues were highlighted to the Covid Incident Management Team. Further system work was escalated to the Care Sector Strategic Group for oversight and to deliver our NHSE commitment to improve the health and well-being outcomes for residents within MSE by promoting improved support to care providers through the EHCH framework and other community based best practice by 2022/23;
LD Checks - 20/21 6 14 30 44
20/21 Checks as a % of Register 0% 1% 2% 3%
LD Checks - 21/22 17 64 132 203
21/22 Checks as a % of Register 1% 4% 9% 13%
LD Checks - 20/21 0 5 8 32
20/21 Checks as a % of Register 0% 0% 1% 3%
LD Checks - 21/22 35 91 166 225
21/22 Checks as a % of Register 3% 8% 15% 20%
LD Checks - 20/21 0 0 5 13
20/21 Checks as a % of Register 0% 0% 1% 3%
LD Checks - 21/22 17 20 38 78
21/22 Checks as a % of Register 3% 4% 7% 15%
LD Checks - 20/21 27 52 143 247
20/21 Checks as a % of Register 1% 1% 3% 5%
LD Checks - 21/22 124 275 507 742
21/22 Checks as a % of Register 2% 5% 10% 14%
5,057 5,132
NHS
Thurrock
CCG
Total - Mid
& South
Essex
CCG's
1,525 1,536
1,100 1,102
530 537
NHS Mid
Essex CCG
NHS
Southend
CCG
77

implementing all elements of the framework across the HCP footprint through local place level teams. Outbreaks and Exposures The number of overall reported care home outbreaks of COVID infection across the MSE system has reduced from nine to six at the time of this report and the total number of exposures reported has also decreased from eleven to nine. Training needs survey Following a survey of care homes and their training needs, 18 care homes have advised what they would prefer to receive in terms of support. This information was mainly collected via a series of ‘phone calls. The online surveys only received 3 answers each. The following summarises the training requested:
• All homes mentioned GULP, Significant 7, End of Life and Swallowing support. There were a number requiring support with continence and constipation.
• Most wanted to face to face training (if COVID safe) and the majority of homes said they had accessed training over the last year.
• Of the 9 that answered the Infection Prevention and Control (IPC) survey, most had accessed the IPC webinars and found them either ‘extremely’ or ‘somewhat’ useful.
A meeting is planned with partners across the system to facilitate a joined up approach to training needs. This will ensure consistency with a view to improving the quality of care provided to individuals within the care homes. Whzan roll out, training and competencies continue, with increasing compliance. This work has shown a tentative impact on reduction of A&E attendances and non-elective admissions. The scope of the Whzan equipment continues to be explored in improving the quality of care and impact on the areas covered within the EHCH requirements. Aligning PCNs to care homes All CQC registered care homes are aligned to each PCN across the system. In South East Essex two care homes are aligned to two different PCNs and have separate local enhanced contracts with individual GPs, as well as an integrated care bed contract in place in one of the homes. This is currently being reviewed with the commissioners, PCNs and individual GP surgeries as to the ongoing service provision in October/November. Home Rounds To support virtual home rounds during the COVID incident response, 100% of care homes were provided with a Samsung tablet which includes MS Teams to support practices to undertake virtual consultations. Seymour John has been commissioned to further support care homes to set parameters and sharing arrangements with practices to access Whzan data – 50 practices are now ready to go live. Additional ECG and digital stethoscopes are being provided to care homes across MSE to expand on the initial pilot and support virtual consultations. PCN level MDTs are still in various stages of formation across the system. Structured Medication Reviews (SMR) The Medicines Optimisation Team are just finalising updated SMR support pack for the CCGs. The Team are offering support to PCNs and practice pharmacists via the MMT and by purchasing training packs through PresQipp, they can also send complex queries to [email protected].
78

Primary Care support to care home (DES) leaflet A leaflet has been developed to inform residents and Care Home Staff what care to expect if they are under a GP whose primary care network (PCN) supports the care home. A small number of the PCN leaflets are being printed over the next few weeks which will be delivered to homes via health and care providers that provide care and support. Copies have also been provided electronically for the homes to print as required. These leaflets can also help care home managers and staff to guide residents through their personal care / wellbeing plans. This will assist in supporting residents to achieve the care they want/works for them, and how this can be supported by their local primary care team with their wishes made available on SystmOne as a Wellbeing plan and guide to refer back to.
9. Safeguarding The Patient Safety & Quality Committee in Common receive a full Safeguarding report that looks at the plethora of adult and children’s safeguarding areas., including insight of case reviews in progress – Safeguarding Adult Reviews, Domestic Homicide Reviews, Child Safeguarding Practice Reviews and Safeguarding Children’s Reviews. A few pertinent subjects are highlighted within this report.
Primary care safeguarding reports In July 2019, NHS England and NHS Improvement directed CCGs to make arrangements to support effective safeguarding arrangements in general practice. The sharing of information by general practice on request from local authorities is not resourced under national NHS contracts. Individual GPs have a statutory and professional duty to share information in a timely fashion, but GP practices are entitled to seek payment for local authority requested work. Arrangements for payments for safeguarding activity are currently being implemented across MSE CCGs. Safeguarding support and advice, including potential issues such as setting precedents through this process, has been provided. A working group is currently looking at processes for payment, robust monitoring and quality assurance processes and standardisation of templates.
Failure to learn from, or positively respond to statutory safeguarding reviews/serious incidents There are a number of statutory reviews that require input from health:
i. Child Safeguarding Practice Reviews (CSPRs) ii. Safeguarding Adult Reviews (SARs) iii. Domestic Homicide Reviews (DHRS) iv. Serious Incidents (SIs) v. Child Death Reviews (CDRs)
Responsibility for oversight and governance of case reviews and subsequent recommendations sit with the commissioning body e.g. safeguarding partnerships. However, as CCGs transition to an ICS, effective systems need to be developed in the rapidly changing NHS landscape so that evidence active learning is an integrated component of every aspect of healthcare commissioning and delivery. The Safeguarding Clinical Network have formed a working group to:
• Review the current status of all case review action plans
• Identify themes that indicate lessons are embedded into an organisational culture
• Work with partners to develop efficient, robust and timely processes for learning Liberty Protection Safeguards The Mental Capacity (Amendment) Bill (2018) was passed into law in May 2019 thereby becoming the Mental Capacity (Amendment) Act 2019. This replaced the Deprivation of Liberty Safeguards (DoLS) with a scheme known as LPS, which is now planned to be implemented by
79

April 2022. The publication of a Code of Practice and Regulations for consultation is anticipated sometime during the summer. There will be a suite of training cascaded centrally for LPS, including the facility for current Best Interest Assessors (BIAs) to transfer to AMCPs. There will also be a development and cascade of national centrally agreed datasets. A number of LPS implementation regional leads are also being established on a 2-year secondment basis by NHS England. Steering Group and workstreams (3) are in place and continue to actively engage in system wide planning and implementation of LPS. Next steps:
➢ NHS England funding has been identified to deliver training specifically in relation to MCA in preparedness for LPS. Legal providers are currently being sourced to deliver training. Consistent messaging is being developed to present at GP Shutdowns/ Forums/Time to Learn Events
➢ Active engagement of adult Continuing Health Care (CHC) representatives ➢ Continued dialogue is required throughout all workstreams to establish current levels of
resource and workforce planning. A scoping tool will aid in outlining requirements ➢ Implementation of ICSs and LPS will occur concurrently. Consistent revaluation needs
to occur across workstreams as to the potential impact in relation to a more collaborative working approach moving forward
➢ Continued dialogue needs to be maintained with Local Authorities ➢ Consideration for a Southend, Essex and Thurrock (SET) wide secondment post to
focus and drive the leadership of MCA/LPS implementation forward in conjunction with NHSE Regional Leads
10. Primary Care Quality
National/Local Standard or objective
CCGs have a statutory duty to secure continuous improvement in the quality of primary medical services, as described in Section 14S of the NHS Act 2006.
Key Issue 1 Harmonised/new processes for monitoring Primary Care quality need to be implemented now that all M&SE CCGs are fully delegated for Primary Care commissioning
Key Issue 2 Harmonised/ new processes in place to ensure that PLACE is also aware of any potential quality/ patient safety concerns within Primary Care
Time scale for benefits to be realised
Ongoing
Risks A failure to monitor the quality of services could result in poor patient experience, risks to patient safety and a lack of practice sustainability leading to regulatory/contractual action and potential practice closures.
Across Mid and South Essex there are 150 GP practices. There are 27 Primary Care Networks (PCNs). 8 of the 150 GP practices are rated as either requires improvement or inadequate by the Care Quality Commission (CQC). The smallest list size of any MSE GP practice is 1,884 patients and the largest list size is 27,739 patients. The average list size is 8,283 patients. The table below highlights current CQC ratings across Mid and South Essex.
80

PLACE Number of Practices Rating
Basildon & Brentwood CCG
1 Inadequate
1 Requires Improvement
32 Good
1 To be inspected
CPR & Southend CCG’s 1 Inadequate
1 Requires Improvement
45 Good
1 To be inspected
Mid Essex CCG 0 Inadequate
1 Requires Improvement
31 Good
4 Outstanding
4 To be inspected
Thurrock CCG 2 Inadequate
0 Requires Improvement
24 Good
1 To be inspected
For the month of May 2021 452,835 appointments were offered within Primary Care, 271,000 of which were face to face appointments. Online/ Video appointments and home visit appointments are also included within that total. The national uptake of face to face appointments for May currently accounts for 56% of appointments offered. The Mid and South Essex comparison shows that primary care are offering 60% of appointments as face to face.
12. Recommendation The CCG Board is asked to note the report and discuss as required.
81

Mid Essex CCG Part I Board Meeting
Finance Report Month 5
Date of Meeting: 30 September 2021 Agenda No
14
Purpose of Report: ‘Check’ (x) relevant box(es).
For Decision (approval/endorsement) ☐
For Assurance (discussion and noting) ☒
For Information Only ☐
Lead Executive Director:
Mark Barker, Joint Chief Finance Officer
Report Author / Presenter:
Jennifer Kearton, Deputy Chief Finance Officer
Executive Summary:
Key points to note from the financial position to-date:
• Current overspend of £1.143m year to date and £3.054m forecast overspend (H1). As directed, the CCG overspend is reported before central reimbursements. The net position is forecast to breakeven.
• Year-to-date Covid expenditure £4.6m
• Year-to-date Elective Recovery Fund (ERF) costs £1.9m
• Overall expenditure pattern/run-rates are on trajectory
• Running costs are currently on plan.
Recommendations and decision/actions required:
The Board is asked to note the reported financial position and the content of this report.
How does this report link to the CCG’s Strategic Objectives? ‘Check’ (x) relevant
objective(s)
Strategic Objective 1 Restore access to services to achieve performance against NHS Constitutional standards, quality improvement priorities and deliver ongoing COVID-19 requirements.
☐
Strategic Objective 2 Work with partner organisations and our population to address health inequalities, including those derived from Covid-19, and achieve social value.
☐
Strategic Objective 3 Support system transformation and organisational change to ensure the ICS is successfully established and can fulfil its aims and duties.
☐
Strategic Objective 4 Develop and support the creation and wellbeing of a diverse and highly skilled workforce and ensure the safe transition of staff to the new organisation.
☐
Strategic Objective 5 Achieve key statutory financial duties including delivery of the system financial control total, value for money and reduction of the underlying system deficit.
☒
Strategic Objective 6 Build effective Alliances at place to transform and strengthen the ability of Primary and Community Care Services to focus upon prevention and early intervention and improve outcomes in the most appropriate settings.
☐
Strategic Objective 7 Promote digitally delivered services whilst considering the requirements of those who need to access services in other ways.
☐
Approval Route: (List Committees or groups that have reviewed this document).
Group/Committee Date (dd/mm/yy)
Finance and Performance Committees in Common 15/09/21
82

Please confirm that the Lead Executive Director has signed-off the report prior to submission to the Committee/Board (Committee/sub-committee minutes submitted for
information must be signed-off by the relevant Chair/Lead Executive before submission).
Yes
Has the CFO confirmed that any financial implications are within agreed budget and/or within CFO’s limit of delegated authority as per SFIs?
Yes
Have the relevant Impact Assessments been carried out and signed off?
Equality & Health Inequalities: N/A
Quality: N/A Privacy: N/A
Details of Patient & Public Engagement or Consultation:
N/A
Related risks on Board Assurance Framework (BAF) / new risks identified which will be included on the BAF.
Financial Risks are summarised within the Board Assurance Framework, Refs FIN01, 02, 03, 06, 08, 09, 10, 11, 12, 13 & 14.
Conflicts of Interest: None identified.
Does the report need to be escalated to Board/Joint Committee or elsewhere?
No
83

Finance Report Month 5
National Standard Key statutory financial duties include delivery of the system financial control total, value for money and reduction of the underlying system deficit
Key Issue 1 N/A
Key Issue 2 N/A
Time scale for benefits to be realised N/A
Risks Financial Risks are set out in the Board Assurance Framework.
1. Purpose & Background
The purpose of this report is to inform the CCG Governing Body of the financial position as at Month 5. In line with national guidance, the CCG and System plans are currently for M1-6 (H1) only. At the time of writing, guidance for the second half of the financial year (H2) is imminent. It is anticipated that the current arrangements will continue to H2, however we have been advised to expect an efficiency target in the region of 3%. The CCGs have worked together to be consistent in their use of planning assumptions on inflation etc. Local CCG plans are based upon ongoing commitments. Mid Essex continues to hold the system investment resource and the H1 efficiency gap. Progress has been made to redistribute investments as shown in Appendix A. Allocation of the efficiency target has been made and transactions are due to completed over the second half of the financial year. NHSE currently hold several funding streams that the CCG can access to cover specific costs – these include the Hospital Discharge Programme and Elective Recovery Fund. The CCG is required to report its position gross including these figures although we anticipate reimbursement in future months, the costs remain a risk until fully reimbursed. Please see Appendix B for a summary of the month 5 position. 2. Key Points
2.1. Overview
i. Current overspend of £1.143m year to date and £3.054m forecast overspend (H1) reflects the fact that the CCG has not received reimbursement for Covid spend considered to be outside the CCGs core allocations. The net position is in line with the plan, both year to date and forecast outturn, to breakeven
ii. Month 5 year to date Covid costs £4.6m iii. Month 5 year to date ERF costs £1.9m iv. Overall expenditure pattern/run-rates are on trajectory.
84

v. Running costs are currently on plan.
2.2. Local issues
Delivery of the Mental Health Investment Standard (MHIS)
i. The CCG is currently forecasting a slight over delivery against the MHIS. This is due to two key issues; increasing spend in the Individual Placements budget and the cost of the new IAPT contract.
ii. In respect of Individual Placements, Mid Essex is working with colleagues from North East Essex and West Essex CCGs to understand the difference in spending patterns across the north and the south of the county. Meetings have been set with the Lead for the Hosted team and data is currently being gathered and reviewed.
iii. The IAPT contract has been agreed and the CCG is now working to mitigate the budget pressure this financial year and moving forward. The CCG will continue to work with the provider to ensure delivery of outcomes and the best use of resources.
Delivery of System Efficiencies
iv. Mid Essex is currently holding the system’s H1 efficiency requirement of £6.7m. This has been aligned to organisations within the system. Organisations are currently agreeing the appropriate actions internally ahead of finalising the necessary transactions to Mid Essex. This remains a risk until completely transacted, either in month 6 or with an even profile over H2. It is important to note that whilst the target is held within the CCG’s ledger, it will continue to be considered a system wide risk, which will necessitate a system wide solution.
Full Delegation of Primary Care
v. Mid Essex CCG received full delegation of its Primary Care budget at the beginning of 2021/22. All new budgets present new risks and opportunities and the CCG continues to work closely with NHSE in order to support its Primary Care partners. The delegated budget is performing in line with expectations at month 5 and is forecast to breakeven.
3. Next steps
i. Interpret impact of H2 guidance when distributed nationally. ii. Finalise arrangements to transact balances to clear system efficiency
gap. iii. Progress discussions and understanding in respect of IPT pressures
4. Recommendation
The Governing Body is asked to note the reported financial position and the content of this report.
85

5. Appendices
Appendix A – 2021/22 Resource Limit Funding
Appendix B - 2021/22 Financial Performance as at 31/8/2021
Appendix C – Statement of Financial Position
Appendix D – Aged Debtors and Creditors
Appendix E – Cashflow Statement as at 31/8/2021
86

87
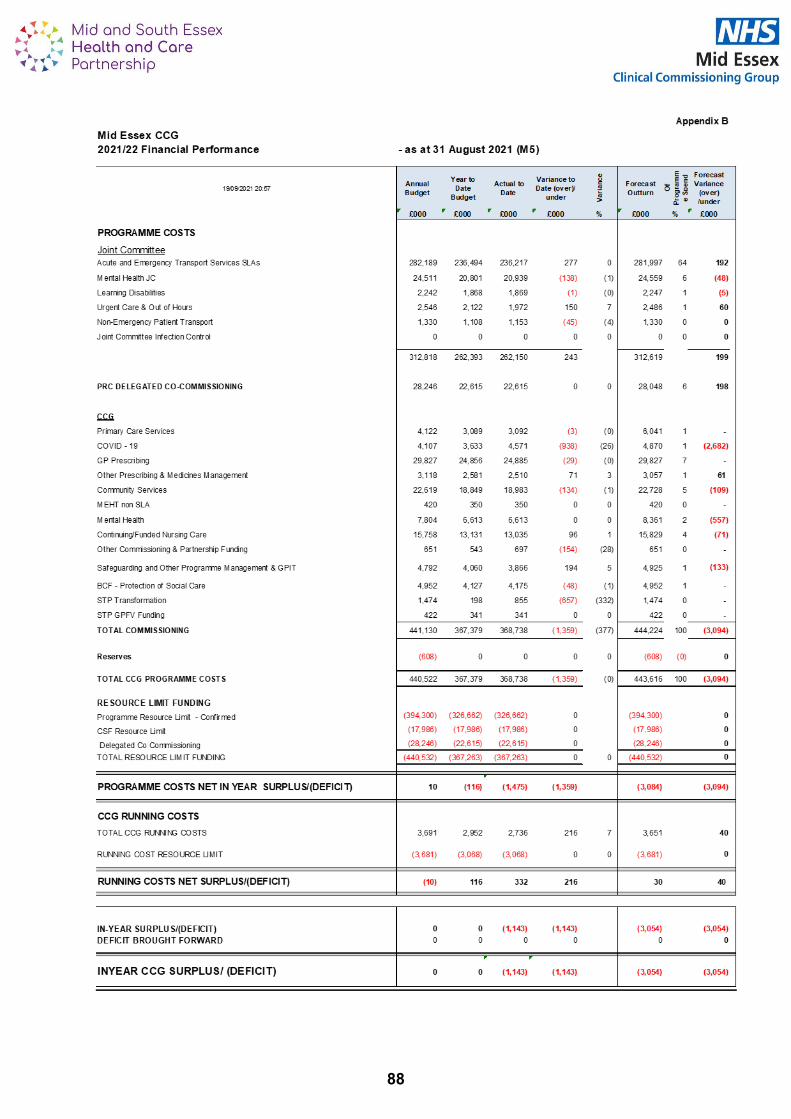
88

Appendix C
NHS Mid Essex CCG
Statement of Financial Position
31 March 2021
31 August
2021
£000 £000
Non-current assets:
Property, plant and equipment 0 0
Intangible assets 0 0
Other financial assets 0 0
Total non-current assets 0 0
Current assets:
Trade and other receivables 8,724 2,333
Cash and cash equivalents 0 1,116
Total current assets 8,724 3,449
Total assets 8,724 3,449
Current liabilities
Trade and other payables (43,998) (54,922)
Borrowings 0 0
Provisions (705) (645)
Total current liabilities (44,703) (55,567)
Non-Current Assets less Net Current Assets/Liabilities (35,979) (52,118)
Non-current liabilities
Trade and other payables 0 0
Provisions (2,549) (2,549)
Total non-current liabilities (2,549) (2,549)
Assets less Liabilities (38,528) (54,667)
Financed by Taxpayers’ Equity
General fund (38,528) (54,667)
Other reserves 0 0
Total taxpayers' equity: (38,528) (54,667)
The CCG makes a payment run early in the month funded from the new cash drawdown received on the 1st of
the month. The payments are accrued into the national financial system in the last few days of the previous
month. For national cash flow purposes and for monitoring against the CCG's requirement not to overspend
against the cash available - the payment has not left the CCG's bank account until the new month when the
new cash drawdown is available. But the system (and the accounts at the year end) may depict that the CCG
is overdrawn on the last day of the previous month - reported in the Statement of Financial Position here as
"borrowings".
89
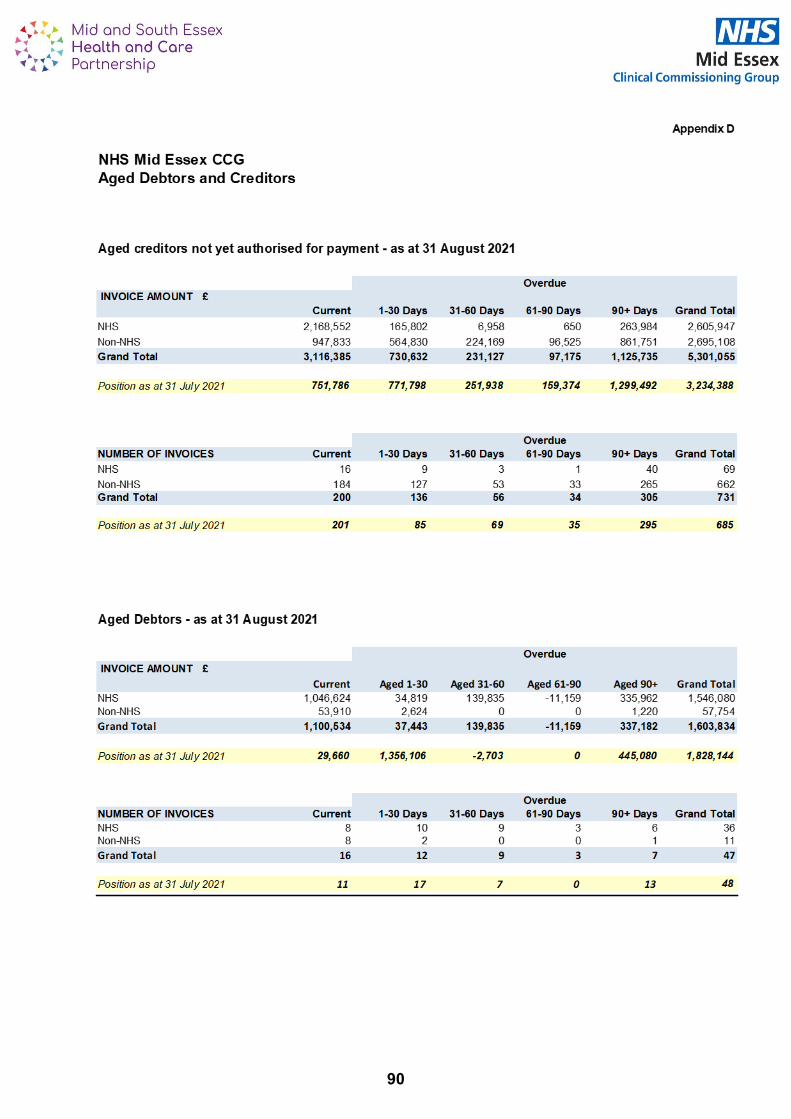
90

Appendix E
Mid Essex CCG
Cashflow Statement
£000
H1 CCG Cash Limit as at 31 August 443,910
Anticipated Adjustments H2 277,925
Income and Opening Cash 12,067
Capital Cash 0
Forecast Maximum Cash Available 733,901
Forecast Cash Used 733,378
Balance of Cash Limit not utilised 0
Forecast Cash Balance in Bank as at 31st March 2022 523 0
Apr to June July to Aug Sept Oct to Dec Jan to Feb
Actual Actual Forecast Forecast Forecast TOTALS
£000 £000 £000 £000 £000 £000
BALANCE BROUGHT FORWARD 303 3,172 2,548 2,391 609 303
CASH IN
Cash Limit - Main Funds 160,000 174,000 68,500 133,000 137,000 672,500
- Prescribing Income 12,808 8,527 4,000 12,000 12,000 49,335
VAT Refund 416 104 49 300 300 1,169
Other Income 3,198 2,138 877 3,354 1,027 10,594
Total Cash Income 176,422 184,768 73,426 148,654 150,327 733,598
CASH OUT
Service Level Agreements/Contracts 146,845 167,833 63,108 121,164 121,739 620,690
PPA Topslice 12,808 8,527 4,000 12,000 12,000 49,335
Salaries, Tax, NI & Pensions 3,314 2,213 1,185 3,555 3,555 13,822
BACS 10,156 6,362 5,183 13,400 12,800 47,901
Capital Expenditure 0 0 0 0 0 0
Other 430 458 106 318 318 1,630
Total Cash Expenditure 173,553 185,393 73,582 150,437 150,413 733,378
BALANCE CARRIED FORWARD 3,172 2,548 2,391 609 523 523
- as at 31 August 2021 (M5)
91

Mid Essex CCG Part I Board Meeting
Mid Essex Place Update
Date of Meeting: 30 September 2021 Agenda No
15
Purpose of Report: ‘Check’ (x) relevant box(es).
For Decision (approval/endorsement) ☐
For Assurance (discussion and noting) ☐
For Information Only ☒
Lead Executive Director:
Dan Doherty- Alliance Director for Mid Essex
Report Author / Presenter:
Kate Butcher- Deputy Alliance Director for Mid Essex (Interim)
Executive Summary:
In spring 2021 the mid Essex Alliance were asked to develop a Mid Essex Place Plan for the year 2021/22. The plan set out 3 high level ambitions for 2021-22:
• COVID recovery,
• Integrated health and social care (including the development of Primary Care Networks) and
• A renewed focus on prevention and reduction of health inequalities. The plan was presented to the Board meeting in July and this report aims to update on progress against the 3 priority areas and the workstreams within them and next steps.
Recommendations and decision/actions required:
The Board is asked to note the information contained within the report.
How does this report link to the CCG’s Strategic Objectives? ‘Check’ (x) relevant
objective(s)
Strategic Objective 1 Restore access to services to achieve performance against NHS Constitutional standards, quality improvement priorities and deliver ongoing COVID-19 requirements.
☒
Strategic Objective 2 Work with partner organisations and our population to address health inequalities, including those derived from Covid-19, and achieve social value.
☒
Strategic Objective 3 Support system transformation and organisational change to ensure the ICS is successfully established and can fulfil its aims and duties.
☒
Strategic Objective 4 Develop and support the creation and wellbeing of a diverse and highly skilled workforce and ensure the safe transition of staff to the new organisation.
☐
Strategic Objective 5 Achieve key statutory financial duties including delivery of the system financial control total, value for money and reduction of the underlying system deficit.
☒
Strategic Objective 6 Build effective Alliances at place to transform and strengthen the ability of Primary and Community Care Services to focus upon prevention and early intervention and improve outcomes in the most appropriate settings.
☒
Strategic Objective 7 Promote digitally delivered services whilst considering the requirements of those who need to access services in other ways.
☐
Approval Route: (List Committees or groups that have reviewed this document).
Group/Committee Date (dd/mm/yy)
n/a
92

Please confirm that the Lead Executive Director has signed-off the report prior to submission to the Committee/Board (Committee/sub-committee minutes submitted for information must be signed-off by the relevant Chair/Lead Executive before submission).
Yes
Has the CFO confirmed that any financial implications are within agreed budget and/or within CFO’s limit of delegated authority as per SFIs?
N/A
Have the relevant Impact Assessments been carried out and signed off?
Equality & Health Inequalities: N/A
Quality: N/A Privacy: N/A
Details of Patient & Public Engagement or Consultation:
N/A
Related risks on Board Assurance Framework (BAF) / new risks identified which will be included on the BAF. (please use this link to view the BAF)
N/A
Conflicts of Interest: None identified
Does the report need to be escalated to Board/Joint Committee or elsewhere?
No
93

Mid Essex Place Update In spring 2021 the mid Essex Alliance were asked to develop a Mid Essex Place Plan for the year 2021/22. The plan set out 3 high level ambitions for 2021-22:
• COVID recovery,
• Integrated health and social care (including the development of Primary Care Networks) and
• A renewed focus on prevention and reduction of health inequalities. The plan was presented to the Board meeting in July and this report aims to update on progress against the 3 priority areas and workstreams within them and next steps. Priority 1- COVID-19 Recovery Vaccination Programmes Primary Care COVID-19 Vaccination Programme There has been good uptake of the COVID-19 vaccination across Mid Essex as can be seen in the table below. All 9 Primary Care Networks (PCNs) in Mid Essex signed up to deliver at least part of the vaccination programme.
As of 20 September, 58.4% of 16-17 year olds have been vaccinated. At risk 12-15 year olds have been identified and invited for vaccination and the EPUT Schools Immunisation Team has started going into schools to vaccinate healthy 12-15 year olds. As we merge into the Phase 3 booster campaign, people can still come forward to access their primary course - the Evergreen Offer. We continue to work across Mid and South Essex (MSE) to identify cohorts of the population who have not come forward for vaccination and offer support in helping them make an informed decision about whether they wish to have the vaccine.
Data Source: NIMS and SystmOne Mid and South Essex CCG Reporting Units
Cohort 1-4 Cohort 6 - Aged 16-64
CCG Age 70+ %
1st dose
Age 70+
Number not
vaccinated
Age 70+ %
2nd dose
Housebound
% 1st dose
Housebound
Number not
vaccinated
Housebound
% 2nd dose
CEV % 1st
dose
CEV
Number not
vaccinated
CEV % 2nd
dose
Cohort 6
Excluding
Carers % 1st
dose
Cohort 6
Excluding
Carers
Number not
vaccinated
Cohort 6
Excluding
Carers % 2nd
dose
Cohort 6 -
Carers % 1st
dose
Cohort 6 -
Carers
Number not
vaccinated
Cohort 6 -
Carers % 2nd
dose
NHS Mid Essex CCG 97.0% 1,805 96.4% 95.3% 94 94.2% 95.6% 988 94.0% 87.3% 3,787 84.1% 92.8% 195 90.3%
Covid Vaccinations - LVS Performance as at 20/09/2021 17:08 Note - CEV patients aged 70+ are double counted in the Cohort 1-4 & 6 Total as they are also counted in the
Age Cohort 70+. Housebound are not added into the Total, as they are a subset of the Age Cohort 70+.
Covid Vaccinations - LVS Performance as at 20/09/2021 17:08Data Source: NIMS and SystmOne Mid and South Essex CCG Reporting Units
Cohort 1-4 & 6 TotalCohort 7 - Aged 60 and Over (60-69)
Excludng CEV and Cohort 6
Cohort 8 - Aged 55-59 Excludng CEV and
Cohort 6
Cohort 9 - Aged 50-54 Excludng CEV and
Cohort 6
Cohort 10 - Aged 40-49 Excludng CEV and
Cohort 6
CCG Total Number Not
Vaccinated
CEV 70+
Number Not
Vaccinated
Total Number
Not Vaccinated
(CEV 70+
duplicates
removed)
Cohort 7
(Excluding
CEV and
Cohort 6 )
% 1st Dose
Cohort 7
(Excluding
CEV and
Cohort 6)
Number not
vaccinated
Cohort 7
(Excluding
CEV and
Cohort 6 )
% 2nd Dose
Cohort 8
(Excluding
CEV and
Cohort 6 )
% 1st Dose
Cohort 8
(Excluding
CEV and
Cohort 6)
Number not
vaccinated
Cohort 8
(Excluding
CEV and
Cohort 6 )
% 2nd Dose
Cohort 9
(Excluding
CEV and
Cohort 6 )
% 1st Dose
Cohort 9
(Excluding CEV
and Cohort 6)
Number not
vaccinated
Cohort 9
(Excluding CEV
and Cohort 6 )
% 2nd Dose
Cohort 10
(Excluding
CEV and
Cohort 6 )
% 1st Dose
Cohort 10
(Excluding CEV
and Cohort 6)
Number not
vaccinated
Cohort 10
(Excluding CEV
and Cohort 6 )
% 2nd Dose
NHS Mid Essex CCG 6,775 222 6,553 95.1% 1,727 94.3% 93.4% 1,355 92.1% 91.8% 1,903 90.3% 86.3% 6,053 82.8%
Total Excluding CEV 70+
Covid Vaccinations - LVS Performance as at 20/09/2021 17:08Data Source: NIMS and SystmOne Mid and South Essex CCG Reporting Units
Cohort 11 - Aged 30-39 Excludng CEV and
Cohort 6
Cohort 12 - Aged 18-29 Excludng CEV and
Cohort 6
Cohorts 7 to 12 Total
Excluding CEV and
Cohort 6
GRAND TOTAL
Excluding double
counting
Cohorts 1 to 9
Total
CCG Cohort 11
(Excluding
CEV and
Cohort 6 )
% 1st Dose
Cohort 11
(Excluding CEV
and Cohort 6)
Number not
vaccinated
Cohort 11
(Excluding CEV
and Cohort 6 )
% 2nd Dose
Cohort 12
(Excluding
CEV and
Cohort 6 )
% 1st Dose
Cohort 12
(Excluding CEV
and Cohort 6)
Number not
vaccinated
Cohort 12
(Excluding CEV
and Cohort 6 )
% 2nd Dose
Total Number Not
Vaccinated
Total Number Not
Vaccinated
Cohorts 1 to 9
Not Vaccinated
NHS Mid Essex CCG 76.0% 11,203 69.2% 72.5% 13,211 59.0% 35,452 42,005 11,538
94

Flu Vaccination Programme The Flu vaccination programme has now commenced. It has been impacted by logistical issues and some practices have yet to receive their vaccine, but all GP practices are expected to start delivering flu vaccines in the next two weeks. People can also access their vaccine through community pharmacies. Seasonal Planning An all-partner Mid Essex Alliance approach is underway to identify opportunities for proactive management of issues that may impact on winter wellbeing in mid Essex. This has a focus on the wider determinants of health that would prevent deterioration and reduce further demand on health and care services.
• Groups who may be more at risk are being identified, with the resulting approach seeking to maximise the value of every contact wherever that occurs. The focus is upon the needs of the individual rather than being limited to the primary expertise of the service the person is seeing.
• Whilst ‘winter’ resilience is the immediate priority, the nature of increased demand from COVID-19 and lockdown means that this work will set the tone for a new way of genuine partnership working, promoting joint planning and integrated delivery with a focus on early intervention.
Winter planning is also underway across MSE to look at anticipated demand and capacity across the health and care system and what additional schemes and support is needed to manage demand. Supporting Improved Cancer Performance As part of the PCN enhanced service, PCNs must deliver a service specification on ‘Improved Early Cancer Diagnosis’. Mid Essex CCG are committed to supporting PCNs to achieve their requirements of this specification and to ultimately increase survival rates through early detection of cancer at stages 1 and 2. Several initiatives commenced this year across the MSE Health and Care Partnership to support with this work, as detailed below:
• The successful rollout of the Cervical Screening Programme to help PCNs achieve the 80% national standard. All screening inequalities and dashboards are shared with PCNs on a monthly basis. All PCNs are working to achieve the higher threshold in all 3 cancer screening programmes.
• A new programme of work is underway to look at how we can enhance Breast Pain Clinics into the Community and support self-referral.
• To help meet the requirements on engaging with local system partners, the Macmillan GPs have been arranging GP Cancer education sessions. There have been 6 well engaged sessions so far that have raised topics including Gynaecology, Skin, Head and Neck.
• Commissioners have been working closely with the system’s Macmillan GPs, who have met with individual PCNs to discuss implementation of the specification and outcomes from audits of cancer referrals.
• Introduction of Faecal Immunochemical Testing (FIT) in primary care for lower GI 2 week wait referrals. A revised pathway was created in June asking for referrals to be accompanied by FIT results: the number of FIT requests in Mid Essex rose by 125% between May and August from 280 to 630.
• A tele-dermatology pilot delivered by Skin Analytics was launched in May, which supports early cancer diagnosis. 33 of 39 GP practices are now live. The feedback from practices was used to refine and update the Skin Analytics' commissioned service in September 2021.
• A pilot is due to commence later in the year which will support the early detection of abnormal cells in the oesophagus which can lead to cancer. There will be a mobile unit in
95

place in Melbourne, Chelmsford, which will initially serve the population of Chelmsford West PCN.
Improved Access to Primary Care Since the start of the pandemic, Mid Essex GP practices have remained open (apart from some short-term closures for deep cleaning and infection control purposes) offering face to face, telephone and online consultations, providing choice of consultation to their patients. The total number of appointments available continues to be higher now than it was pre pandemic. In August 2021, an average 61% of GP appointments were delivered face to face. Of 39 GP practices in Essex, there is currently one practice whose list is closed to new registrations following approval of this closure by the Mid and South Essex Primary Care Commissioning Committees in Common in July 2021. One other practice is currently operating a temporary restriction to patient registrations. The CCG is working with these GP practices and their neighbouring practices to minimise the impact on residents and to enable them to reopen their lists as soon as possible. The CCG’s extended access service was launched in 2018 to offer appointments during evenings and weekends when local GP surgeries are traditionally closed. Prior to the COVID-19 lockdown, the CCG extended access service was offering at least 738 additional appointments per week (3,200 appointments a month) to patients in Mid Essex across a range of sites in Chelmsford, Halstead, and Maldon with peripheral hubs in Witham and South Woodham Ferrers. The service has continued to operate during the pandemic, albeit that in common with practically all other health care services, an initial telephone triage is undertaken with any patients deemed to need a face to face appointment being asked to attend the main site in Chelmsford. More recently, the other hubs in Halstead and Maldon have reopened and the other sites are being kept under review for potential reopening in future weeks. Utilisation of the service has consistently been above the 75% national target since January 2021, with August utilisation being over 90%. A National Patient Survey is undertaken on behalf of NHS England and NHS Improvement on an annual basis. This is an England-wide annual survey, providing practice-level data about patients’ experiences of their GP practices. In 2021, 44% of survey questionnaires issued were completed and returned by Mid-Essex patients. Out of 5,175 responses, 78% of patients indicated that their overall experience of their GP practice was good, an increase of 2% compared to last year’s results. 10% of patients indicated their experience of accessing GP practice was poor. 53% of patients found it easy to access their GP practice by telephone, compared to only 48% in 2020. While recognising the efforts made by most practices to improve access for their patients, Mid Essex CCG is aware that work needs to be done to further improve the position, bringing the lower performing GP practices up to the CCG average and improving the overall CCG position. The CCG is working with practices to identify issues and areas of concern to support them in finding solutions and putting in quality markers to improve patient access. This will also ensure a more equitable standard of care is provided to all Mid Essex patients. The table below shows the CCG’s performance and trend against some of the key indicators from the national patient survey and comparison with national average.
POSITIVE SATISFACTION
CHANGE SINCE 2020
Question CCG result (%)
National result
(%)
CCG result (%)
National result (%)
Overall experience of GP practice (likely IAF indicator
78 83 +2 +1
Ease of access to practice via phone
53 68 +5 +3
96

POSITIVE SATISFACTION
CHANGE SINCE 2020
Question CCG result (%)
National result
(%)
CCG result (%)
National result (%)
Helpfulness of practice receptionist
86 89 +2 0
Ease of use of online services
74 75 -1 -1
Satisfaction with appointment times available
60 67 +4 +4
Choice of appointment when last booked
60 69 +7 +9
Satisfaction with type of appointment offered
80 82 +9 +9
Overall experience of making an appointment
63 71 +6 +6
Mental health needs recognised and understood
85 86 +2 +1
Priority 2- Integrated Health and Care Mid Essex Alliance Development The Mid Essex Alliance has been meeting monthly since March 2021. The group has now agreed its priorities and plan for the remainder of 2021/22. The group have continued to build relationships and are focusing upon this, over form, for the time being. However, the next steps for the development of the Alliance are to create a governance structure that sits around it to ensure we are delivering against our plan. Also, to develop the Alliance through some externally facilitated organisational development to ensure we work in the most collaborative and integrated way possible to improve the overall health and wellbeing of our population. The Alliance has recently agreed to commission the three Councils for Voluntary Services (CVS) across mid Essex to undertake a piece of work on Asset Based Community Development to understand the assets we have across mid Essex, including the 3 district areas and the 9 PCN areas, to identify where the gaps are. This will help us to start to develop our communities and support the overall ethos of the Alliance to help our population to live well. Alongside this work Healthwatch have also been commissioned to undertake a piece of work to support the Alliance in how we engage with our communities’ seldom heard groups. Development of Primary Care Networks There were no changes to the configuration of PCNs in mid Essex for 2021/22. We continue to have 9 PCNs across the 3 district areas. NHS England & NHS Improvement have recently published additional contractual requirements for PCNs, including revisions to the Investment and Impact Fund and two further specifications for introduction from October 2021: ‘Cardiovascular Disease Prevention’ and ‘Diagnosis and Tackling Neighbourhood Health Inequalities’. The CCG’s transformation team are outlining support available to PCNs to meet delivery of the requirements. The CCG has commissioned external support for PCNs to help in their development following requests from PCNs and Clinical Directors for additional support, recognising the pressures on primary care currently. External facilitators are supporting teams to help ensure wider general practice teams understand PCNs and the opportunities they present, help understand PCNs individual development areas and to deliver activity to address those needs and support PCNs in developing their visions and priorities. Work has commenced to translate the requirements of the PCN Maturity Matrix into a local context, with the intention that doing so will enable clearer planning for achieving progress across all Alliance 97

partners. One fundamental aspect of the maturity matrix is partnership, joint planning and integrated care. To progress this, workshops are being planned to promote collaboration between primary care PCN leads and wider system partners. Initially taking place in Chelmsford, a dedicated workshop in October will set out to develop relationships between key partners, emphasise the benefit to all of collaboration and identify specific opportunities/deliverables. This will also directly support delivery of the new PCN DES specifications where there is a clear emphasis on delivery through collaboration. Chelmsford West PCN has now started as an accelerator site, with dedicated senior support from the CCG to expedite development opportunities. Colne Valley PCN has initiated a ‘Low Carb Diet’ programme. This is a GP led healthy weight management programme that supports people to adopt a low carb lifestyle and achieve their health goals. This programme was developed and rolled-out due to growing concern around the rise in the incidence of Type 2 diabetes in the last few years, alongside the widely reported rapid increase in obesity in the UK population. It is a 12 week programme and equips patients with information, skills, tips and support to help them to adopt a low carb approach and achieve their health goals. As well as health benefits, the project is also helping to support the development of communities as people are coming together to support each other in achieving their goals for the programme. Priority 3- Prevention and Health Inequalities Population Health Management There are currently two key parts to the Population Health Management Programme. One is a national programme run by NHS England which is working with Colne Valley PCN. The other is working with the MSE population health analysis team which is currently focusing on Chelmsford West PCN. Colne Valley PCN alongside numerous stakeholders have run 3 Action Learning Sets which have led to the identification of a cohort of 70 people. The cohort consists of people under the age of 40 who have alcohol or substance misuse recorded. The next step is to develop a project that addresses their needs to improve their quality of life. Segmentation data is being developed to support Chelmsford West in identifying cohorts to focus on. A meeting will take place on 29 September to develop the next steps and the process will become a blueprint in supporting other PCNs with population health management. Learning from these two projects will be used to support the roll out of population health management across all PCNs. Diabetes There are 8 care process identified by NICE, to be delivered through a series of annual checks, to monitor and improve the health of people with diabetes. For the past 6 months the CCG has shown continued recovery for achievement of care processes within the context of the pandemic. According to Eclipse data, the CCG’s rolling 12-month care process completion rate has risen from 18% in March 21 to 28% in September 21. Mid Essex is currently the only CCG in Mid and South Essex that hasn’t been escalated to the Regional team for concerns regarding continued care process deterioration during the pandemic. The CCG is in the process of continued consultation with GPs and practice nurses to export local models of excellence across Mid Essex practices in order to sustain the increase in performance. There are instances of Mid Essex practices that, after having taken up the CCG diabetes HCA offer in 2019, are now benchmarking nearly twice as high as the national average. Workshops and training events are being scheduled throughout Autumn. NICE recommended 3 specific treatment targets (HbA1c (blood sugar), cholesterol and blood pressure) for the management of diabetes. The past 6 months has shown continued recovery for CCG compliance with 3 treatment targets. Eclipse data shows the CCG average has risen from 19%
98

in March 21 to 22% in September 21. Local clinical consensus is that the continued improvement in care processes should have a subsequent positive impact on treatment targets. Discussions are underway to hold educational discussions targeted at practice clinical pharmacists to improve knowledge of diabetes and managing treatment targets as part of the diabetes annual review process. Mid Essex CCG continues to be on course with the national target for referral rates into the National Diabetes Prevention Programme with 980 referrals sent to the provider since April 2021. Provide Community Interest Company (CIC) Diabetes Team are responsible for delivering structured education to our patients in Mid Essex. They offer a range of options to referred patients with either a Type 2 Diabetes UK information brochure, access to the MyDiabetes app and/or a call with one of their clinicians. Provide CIC and their digital coordinator have helped give access and support to nearly 600 patients with the MyDiabetes app. A self-referral pathway has been established for any diabetic patients across Mid Essex who may be interested in using the app, with details being included in the new PCN websites. Respiratory The Mid Essex Respiratory Oversight Group, comprised of primary, secondary and community care, pharmacy and commissioning representatives, continue to meet on a monthly basis to discuss and consult on respiratory care in Mid Essex and for general oversight of respiratory transformation. An interim spirometry service has been commissioned by MECCG and is delivered by the COPD respiratory team in Provide CIC until 4 November 2021. The service aims to support early and accurate detection and diagnosis of respiratory disease e.g. asthma / COPD, compliant with NICE and QOF guidance and the NHS LTP. The service has been well utilised by primary care, since first commissioned in December 2020, and has provided the support and resilience requested by practices following COVID. Commissioners are currently seeking approval to extend the service until March 2022 to work towards the longer-term vision of an integrated diagnostic hub service, currently being developed by the MSE Respiratory Transformation Board and MSE Community Collaborative. Respiratory Virtual Clinics are being planned for roll out across each Mid Essex PCN to commence from November with the offer to the 9 Mid Essex PCNs to join a virtual MDT with a secondary care consultant and representation from the COPD respiratory team three times a year. Funding has been obtained from an MSE demand management bid and the project replicates the successful pilot programme previously implemented prior to the pandemic in Witham and Maldon PCN and Chelmsford City Health PCN. The programme aims to improve the knowledge and confidence of primary care regarding respiratory disease and hence improve respiratory care for patients such as by earlier detection and diagnosis, optimised medication and improved access to pulmonary rehabilitation – all key deliverables of the NHS Long Term Plan. In addition, with recognition of the impact of the pandemic on respiratory health, the Mid Essex Oversight Group have delivered a dedicated ‘Time to Learn’ (TTL) session on Long COVID and plan to deliver another general ‘Respiratory’ session at the October TTL to support GP practices with this long term condition. Mental Health Integrated Primary Care Community (IPCC) The IPCC programme is funded through mental health transformation funding and the overall aim is to integrate primary, secondary and voluntary sector organisations to deliver mental health services more holistically without organisational barriers. Within the IPCC programme a Physical Healthcare Team pilot has launched with a nursing team working directly with PCNs to deliver health checks. The key measure and target we aim to improve is the Serious Mental Illness health check which is currently at 23% against a target of 60%. Next steps in the programme are to launch a recovery
99

college which aims to provide a range of online educational courses and resources to people struggling with mental health issues. Serious Mental Illness Physical Health checks (SMI) Mid Essex are adopting a triple pronged approach to achieving the SMI health check target of 60%: i) EPUT are responsible for 30% delivery of the target ii) Primary care deliver 70% of the target and iii) the IPCC pilot bolsters the existing SMI arrangements to ensure the health check is complete as well as ensuring that other quality screening and care coordination is offered to all SMI patients. The next steps are to continue with expanding the physical healthcare team to wrap around all PCNs in Mid. EPUT are working to improve the digital interoperability to ensure data is correct. EPUT are also reviewing premises to deliver SMI health checks and refine the blood collection routes to improve efficiency. Early Intervention in Psychosis (EIP) The relaunch of Mid Essex EIP services occurred under EPUT’s restructure of all of its community services. Since the relaunch and focus on quality the service has completed the annual National Clinical Audit of Psychosis (NCAP) and have achieved level 3, a vast improvement from their original outcome of level 1. The next steps include recruiting a medical consultant and additional psychology as a permanent fixture in the workforce and service. Improved Access to Psychological Therapies (IAPT) IAPT continue to deliver psychological therapies in new ways since the pandemic e.g. virtual group therapy. The service has recently achieved accreditation status again with the Accreditation Programme for Psychological Therapies Services (APPTS) – the only IAPT service in our region (1 of 6 nationally). The accreditation alongside the high-quality service delivery model have meant waiting times are at an all-time low (98% of people treated within 28 days) and recovery is consistently achieved above the 50% recovery target. Hertfordshire Partnership Foundation Trust, which delivers the Mid Essex IAPT service, is integral to the IPCC programme and next steps include developing the service to include advanced psychological therapies in primary care. Dementia There have been early diagnosis of dementia in primary care pilots running in Mid Essex since February 2021. This model has been cited as best practice. The current national target for diagnosis remains at 67%. In Mid Essex the national data is showing current performance of 55%. Historically we know that we have a high number of people with dementia who will not be shown on the national data set. There have been ongoing issues with accurate reporting data from EPUT and an improvement plan is being developed to address this. Recommendation The Board is asked to note the information contained within the report.
100

Mid Essex CCG Part I Board Meeting
Committee Minutes
Date of Meeting: 30 September 2021 Agenda No
16
Purpose of Report: ‘Check’ (x) relevant box(es).
For Decision (approval/endorsement) ☐
For Assurance (discussion and noting) ☒
For Information Only ☐
Lead Executive Director:
Mark Barker, Chief Finance Officer Rachel Hearn, Executive Director of Nursing and Quality Dan Doherty, Alliance Director (Mid Essex)
Report Author / Presenter:
Sara O’Connor, Head of Corporate Governance
Executive Summary:
The most recently available minutes of Committee meetings are provided to the Board for information and assurance purposes, as follows: 16.1 Patient Safety & Quality Committees in Common (draft) - 14/09/2021 16.2 Finance & Performance Committees in Common (final) - 21/07/2021 16.3 Audit Committees in Common (draft) - 16/07/2021 16.4 Primary Care Commissioning Committee (draft) - 12/08/2021 Draft minutes will be formally approved at the next relevant committee meeting.
Recommendations and decision/actions required:
The Board/Committee is asked to note the minutes of the above mentioned committees.
How does this report link to the CCG’s Strategic Objectives? ‘Check’ (x) relevant
objective(s)
Strategic Objective 1 Restore access to services to achieve performance against NHS Constitutional standards, quality improvement priorities and deliver ongoing COVID-19 requirements.
☒
Strategic Objective 2 Work with partner organisations and our population to address health inequalities, including those derived from Covid-19, and achieve social value.
☒
Strategic Objective 3 Support system transformation and organisational change to ensure the ICS is successfully established and can fulfil its aims and duties.
☒
Strategic Objective 4 Develop and support the creation and wellbeing of a diverse and highly skilled workforce and ensure the safe transition of staff to the new organisation.
☒
Strategic Objective 5 Achieve key statutory financial duties including delivery of the system financial control total, value for money and reduction of the underlying system deficit.
☒
Strategic Objective 6 Build effective Alliances at place to transform and strengthen the ability of Primary and Community Care Services to focus upon prevention and early intervention and improve outcomes in the most appropriate settings.
☒
Strategic Objective 7 Promote digitally delivered services whilst considering the requirements of those who need to access services in other ways.
☒
101

Approval Route: (List Committees or groups that have reviewed this document).
Group/Committee Date (dd/mm/yy)
Finance & Performance CiC (approval of minutes) 15/09/21
Please confirm that the Lead Executive Director has signed-off the report prior to submission to the Committee/Board (Committee/sub-committee minutes submitted for information must be signed-off by the relevant Chair/Lead Executive before submission).
Yes
Has the CFO confirmed that any financial implications are within agreed budget and/or within CFO’s limit of delegated authority as per SFIs?
N/A
Have the relevant Impact Assessments been carried out and signed off?
Equality & Health Inequalities: N/A
Quality: N/A Privacy: N/A
Details of Patient & Public Engagement or Consultation:
N/A
Related risks on Board Assurance Framework (BAF) / new risks identified which will be included on the BAF. (please use this link to view the BAF)
Each committee reviews risks within its remit. Please refer to relevant section.
Conflicts of Interest: None identified
Does the report need to be escalated to Board/Joint Committee or elsewhere?
No
102

MINUTES OF PART I PATIENT SAFETY & QUALITY COMMITTEES IN
COMMON MEETING OF BASILDON & BRENTWOOD, CASTLE POINT
& ROCHFORD, MID ESSEX, THURROCK AND SOUTHEND CCGs
Held via MS Teams on 14 September 2021 at 11.00 am – 1.00 pm
Member Job Title/Position
Committee Quorate?
Dr Sunil Gupta (SG) (Items 8-20)
Chair of CPR CCG and Lead Chair for CiC
Patient Safety & Quality, CP&R CCG
YES (3 members)
Rachel Hearn (RH)
Executive Director of Nursing & Quality
Patient Safety & Quality, CP&R CCG
Janis Gibson (JG)
Lay Member Patient Safety & Quality, CP&R CCG
Tracey Freeman (TF)
Lay Member Patient Safety & Quality, Southend CCG
Rachel Hearn As above Patient Safety & Quality, Southend CCG
YES (3 members)
Dr Taz Syed (TS) GP member Patient Safety & Quality, Southend CCG
Tracey Freeman (TF)
As above Patient Safety & Quality, Southend CCGs
Janis Gibson (JG)
As above Patient Safety & Quality, Southend CCGs
Dr Sooraj Natarajan (SN)
PSQ Chair Patient Safety & Quality, Basildon and Brentwood CCG
YES (3 members)
Dr Julie Hale (JH) Secondary Care Consultant
Patient Safety & Quality, Basildon and Brentwood CCG
Rachel Hearn As above Patient Safety & Quality, Basildon and Brentwood CCG
Gill Jones (GJ) (Items 1-12)
Lay Member Patient Safety & Quality Basildon and Brentwood CCG
Rachel Hearn As above As above
YES (3 members)
Henry Okoi (HO) GP Member Quality & Patient Safety, Thurrock CCG
Lesley Buckland (LB)
Lay Member Quality & Patient Safety, Thurrock CCG
Alan Hudson (AH)
Lay Member Quality & Patient Safety, Thurrock CCG
Dr Anna Davey GP Member Quality & Patient Safety, Mid Essex CCG
YES (3 members)
Rachel Hearn As above Quality & Patient Safety, Mid Essex CCG
Nathalie Wright (NW)
Lay Member Quality & Patient Safety Mid Essex CCG
In Attendance Job Title/Position
Committee/Organisation
Charlotte Tannett (note taker)
Governance Support Officer
Mid Essex CCG N/A
103

Member Job Title/Position
Committee Quorate?
Sara O’Connor (SO) (Items 1-9)
Head of Corporate Governance
Mid Essex CCG N/A
Viv Barnes Director of Governance & Performance
Mid Essex CCG N/A
Viv Barker Deputy Chief Nurse
Mid Essex CCG N/A
Lorraine Coyle (LC)
Deputy Chief Nurse
CP&R and Southend CCGs N/A
Matt Gillam (MG) Head of Nursing CP&R and Southend CCGs
Stephen Mayo (SM)
Deputy Chief Nurse
Thurrock CCG N/A
Simon Williams (SW)
Deputy Alliance Director
Mid and South Essex CCGs N/A
Vicky Cline (VC) Lead Nurse, Primary Care
South East Essex CCGs N/A
Jackie Barrett (JB)
Designate Nurse for Safeguarding Adults
Mid Essex CCG N/A
Leila Francis (LF) (Items 12-20)
Designate Nurse for Safeguarding Children
Mid Essex CCG N/A
Ahmed Yasin (AY)
GP Member Thurrock CCG N/A
Marie McEntee Children and Young People’s Commissioning Manager
Mid and South Essex HCP N/A
Carolyn Lowe (CL)
Head of Children’s Continuing Care Commissioning
Mid Essex CCG N/A
Apologies
Pauline Stratford (PS)
Lay Member Patient Safety & Quality, CP&R and Southend CCGs
N/A
Dan Doherty (DO)
Alliance Director Mid Essex CCG N/A
Patricia D’Orsi Alliance Director South East Essex CCGs N/A
Nic Spenceley (NS)
Lay Member Basildon & Brentwood CCG N/A
Dr Anita Pereira (AP)
GP Member Basildon & Brentwood CCG N/A
Dr Olugbenga Odutola (OO)
GP Member Basildon & Brentwood CCG N/A
Eleanor Sherwen Interim Head of Nursing
Basildon & Brentwood CCG N/A
William Guy (WG)
Alliance Director Basildon & Brentwood CCG N/A
Sanjeev Maskara (SM)
GP Member Thurrock CCG N/A
Mark Tebbs (MT) Alliance Director Thurrock CCG N/A
Jose Garcia (JG) GP Member South East Essex CCGs N/A
104

Member Job Title/Position
Committee Quorate?
Mark Metcalfe (MM)
GP Member South East Essex CCGs N/A
Greer Philips (GP)
Patient Safety & Quality Manager
Basildon & Brentwood CCG N/A
ITEM SUBJECT
OPENING BUSINESS
1.
2.
3.
4.
5.
Roll Call and Quoracy Check VB performed a roll call of those in attendance. Apologies were noted. VB confirmed that any members who had been unable to attend the meeting would be contacted after the meeting and asked to endorse any items where quoracy was needed for a decision. Declarations of Interest No interests were declared. Minutes of previous Patient Safety and Quality Committees meeting held in common (PSQ CiC) on 13 July 2021 The committee reviewed the minutes of the PSQ CIC meeting held on 13 July 2021. LB highlighted that her apologies were not noted at the previous meeting. Resolved: The minutes of the PSQ CiC meeting held on 13 July 2021 were approved subject to the above minor amendment. Matters Arising None. Review of Action Log The committee reviewed the Action Log, updates were provided and all completed actions were closed. Resolved: The PSQ Committees in Common noted the Action Log and updates provided.
FOCUSED DISCUSSION
6.
Patient Story RH explained that due to technical difficulties the patient story was unavailable to present to the committee. A final edited version would be provided to the committee for review when available. LC advised that the patient story featured Anne, a patient with learning difficulties (LD) who had had a traumatic experience during an inpatient event. Anne had found the confidence to tell her story following her then positive experiences with health facilitation and LD nurse support. LC confirmed Anne’s experiences would be shared with Essex Learning Disability Partnership (ELDP) and the Mid and South Essex (MSE) Group partners.
105

ITEM SUBJECT
7.
RH asked the committee for feedback on the patient stories overall and whether they were having a benefical impact. JGib stated she welcomed the patient stories which had been powerful and brought the work undertaken by the CCGs and their system partners to life. JGib added she also welcomed hearing both the positive and negative experiences of patients to promote discussion of these issues at the committee meeting. HO stated he felt the patient stories were an innovative idea and would support them continuing. LB agreed with HO’s comments. SN also agreed with HO’s comments and noted the time and care that had been taken by the team to provide a balanced view. Resolved: The PSQ Committees in Common noted the Patient Story update. [Action: RH/LC to cascade the final version of Anne’s Patient Story when available.] Deep Dive – Learning Disability LC summarised the Provider Collaboration Review (PCR) and LD Progress presentation which had been jointly developed with PD and Phil Brown, Clinical Advisor. She advised that the Care Quality Commission (CQC) had undertaken a review to identify how providers had worked collaboratively as a system in response to the COVID-19 (C-19) pandemic and the experience of people with LD living independently in the community during the C-19 pandemic, including those who lived with families and those living in supported accommodation. The objective was to support providers by sharing learning. The review took place during the weeks of 15 and 22 March 2021 and included the following:
• 26 interviews with health and social care staff, senior managers and executive leaders
• Three focus groups including social care providers and support groups for people with a LD and their families
• Case-tracking patient journeys of five individuals with LD to determine how effectively their needs were met across a range of services
• How effectively the person's needs were met, how quickly needs were met and whether services responded appropriately to meet the person's needs during the pandemic
• A webinar held with voluntary and community sector organisations which included Mencap and Healthwatch to share headline themes/findings and check if findings resonated with what they had heard
The review focused on the geographical footprint of MSE Integrated Care System (ICS). The review did not assess the role that commissioning played within the system. Examples of identified good practice included:
• MSE decision to vaccinate LD patients earlier than the government recommendation • Good arrangements in place to support carers to have vaccines • Needle Phobia service • Learning Disability Mortality (death) Review (LeDer) programme and shared learning • Good partnership working between Primary Care Networks (PCNs) and Community
Services • Voluntary organisations and Healthwatch provided additional support and signposting to
people about who to contact for support • Examples of timely support from all partners within the system
LC asked the committee for feedback on any areas of potential future development.
106

ITEM SUBJECT
8.
MG noted there had been some instances during the pandemic where LD day centres were closed and individuals had accessed other community groups which had resulted in positive integration into the community. MG queried if commissioners had explored alternative options such as this. JGib queried how the MSE system might further explore relationship management with LD patients and carers and how communities might be developed to offer further non-clinical support which could include Annual Health Check (AHC) reminders. GJ highlighted her experience as Governor of a local school that specialised in special needs where parents had expressed concerns about the lack of effective links between schools and GPs. They had requested that AHCs take place in schools to allow input from teachers and staff. LC stated she would explore how Initial Health Assessments (IHAs) Education Health and Care Plans and AHCs might be combined in collaboration with schools in the future. SN supported GJ’s comments and stated he had experienced difficulties contacting LD patients and their carers via digital means and so felt schools would be good way to engage with them. Resolved: The PSQ Committees in Common noted the Learning Disability Deep Dive. [Action: LC to explore how Initial Health Assessments (IHAs) Education Health and Care Plans and Annual Health Checks might be combined in collaboration with schools in the future.] Patient Safety & Quality (PSQ) Risks RH summarised the Patient Safety & Quality Risks and highlighted that all risks on the MSE CCG Board Assurance Framework (BAF) had been reviewed prior to the Joint Committee (JC) meeting on 26 August 2021. As part of this review, risk leads were asked which committee each risk should be allocated to, with 33 risks being allocated to PSQ CiC as set out in Appendix A of the report. A further review by RH had resulted in her suggesting that 20 of these risks should be reallocated to the Finance & Performance (F&P) Committee. The views of relevant colleagues had been sought. RH highlighted 3 new risks had been added to the BAF, 2 in relation to CYP and Health Inequalities which were rated as amber and one for maternity workforce which was rated as red. There were 6 red rated risks in relation to Special Educational Needs and Disability (SEND) for Children and Young People (CYP), Tier 4 beds for CYP, general quality in the Mid and South Essex Foundation Trust (MSEFT), general quality in the Essex Partnership University Foundation Trust (EPUT), ICS delivery of the national ask and maternity workforce. All risks had been reviewed by the respective leads during July and August 2021 and a robust oversight process was in place. SM confirmed there was a general workforce risk across the system and that all providers had been sent a written request to review their risks and share them with the CCGs to ensure they could be reflected in the BAF. SO advised that the extensive use of agency staff would be explored during the next BAF update. HO added that more work with community paediatricians might be necessary to decide if children with LD aged 14+ had learning disability or learning difficulty as this required further clarification in some cases. TF noted a reluctance to reduce a risk rating when awaiting feedback and asked if risk leads were confident feedback would reduce the risk and this was a timing issue or if a new action
107

ITEM SUBJECT
9.
10.
might need to be explored to achieve the required result. TF asked if this could be articulated in future reports. RH noted TFs challenge and stated some instances of delaying the reduction of a risk rating were due to awaiting CQC reports on quality which would provide a fuller picture of whether the risk might be reduced. Resolved: The PSQ Committees in Common noted the Patient Safety & Quality Risks. [Action: SO/RH to include details of any feedback being awaited in relation to PSQ risks in future risk reports.] [Action: LC to explore potential links with community paediatricians to determine whether children aged 14+ had learning difficulty or learning disability.] Patient Safety Framework update MG summarised the report and highlighted the National Patient Safety Strategy, launched in 2019 and more recently updated in June 2021, set out goals for NHS organisations to ensure the continuous patient safety improvement journey. It was suggested that the achievement of the identified goals by 2023/24 could save up to 1,000 extra lives per year. There was also the opportunity to safely reduce care and litigation costs by £100 million and £750million respectively by 2025 by achieving better outcomes for people. NHS England/Improvement (NHSE/I) received feedback from consultation around the strategy which strongly supported the development of a network of Patient Safety Specialists (PSS) in local systems. The network was launched on October 2020 and required each of the 5 CCGs within the MSE ICS to identify at least one person as their designated PSS.
The Patient Safety Syllabus was subsequently launched on 13 May 2021 and outlined a new approach to patient safety, emphasising an organisational culture shift as well as a more proactive approach to identifying risks to safe care while also including improved understanding around how systems can enhance, but also hinder patient safety.
It was planned that PSSs would be fully trained to level 5 in the syllabus by April 2023. However, it was intended that all staff working for NHS organisations, including non-clinical and senior management to Board level, would be required to complete a level 1 foundation course. In June 2021, NHSE/I launched the final version of the Framework which included how to involve patients in patient safety. The committee were asked to note that the request from NHSE/I to nominate individuals to be PSS came during the second C-19 lockdown, whilst the local system was experiencing significant numbers of staff redeployments and intense system pressure. The intention to implement the ambitious strategy also came at a time of significant organisational change as the MSE CCGs commenced the transition into an ICS. RH stated her team would be highlighting the work that needed to be carried out around the framework and PSSs and would develop a business case for finance colleague’s consideration. Resolved: The PSQ Committees in Common noted the Patient Safety Framework update. NHS Patient Safety Updates: 27 July 2021 & 31 August 2021 MG summarised the report and highlighted risks around the capacity for blood testing and Field Safety Notices for Philips ventilators and CPAP machines. Resolved: The PSQ Committees in Common noted the NHS Patient Safety Updates.
108

ITEM SUBJECT
11.
11.1
Joint Committee (JC) / Acute Commissioning Team (ACT) Updates Acute (including Patient Safety, Maternity, EEAST, IC24) RH highlighted a number of key issues within the report. Infection Prevention & Control (IP&C) There had been 15 cases of Meticillin Resistant Staphylococcus Aureus Bacteraemia (MRSAB) during the year to date, mainly in the mid Essex area. The IPC team were exploring all cases and learning would be circulated back to the committee. There had been 117 Clostridioides difficile infections (CDI) year to date against a threshold of 357, which was positive, however the Autumn/Winter period was expected to bring challenges with overall nosocomial infections expected to rise. Due to an increase in infections at the Southend Hospital site, a reduction plan was in development. There continued to be nosocomial outbreaks at the MSEFT Broomfield site, EPUT and the Marillac which were being overseen by the IP&C team. Serious Incidents (SIs) There were 38 new SIs during the reporting period with no new Never Events. There had been 3 Never Events year to date, 2 in Ophthalmology where the same patient was injected in the wrong eye on two occasions and 1 wrong-site surgery case in Orthopaedics. A large piece of work was underway with MSEFT around their use of the World Health Organisation (WHO) checklist and initial learning had been shared with the CCGs and CQC at the Quality System Group. Harm Reviews Data had showed a downward trend in outstanding cancer cases with only 52 outstanding at the time of reporting. All 2020/2021 Harm Reviews were fully completed. There were 74 reviews outstanding for 2021/22, 63 of which were completed at the end of August 2021. Referral to Treatment (RTT) Harm Reviews A new RTT Harm Review process had been agreed with system partners through the System Oversight and Assurance Group (SOAG) which would see the end of RTT Harm Reviews on Colorectal and Dermatology patients. Reviews would continue with Ophthalmology patients and Laparoscopic Cholecystectomy patients, Community Paediatrics and Cardiac Surgery patients with delays of more than 6 months would also be reviewed. Maternity The CCGs had been awarded £1.9m of Ockendon funding from NHSE/I which would go towards the maternity workforce. MSEFT continued to experience issues with recruiting to vacant roles in the Midwifery, Consultant and Doctor workforce and the CCG was working with the Trust to help drive recruitment. MSEFT had appointed a new Director of Midwifery who was due to start in October 2021. A new MSE system Consultant Midwife had also been appointed who would be working alongside system partners to champion maternity services. The CQC had carried out a maternity review at all three MSEFT hospital sites along with a core review of services focusing on emergency departments, medicine and surgery and a well-led review. Initial feedback indicated that no new warning notices had been issued. JGib raised a concern around the patient who had been injected in the wrong eye twice and queried what measures would be put in place to avoid this recurring. VRB stated a full investigation report had been received which showed the cause to be due to a mistake having been made at an initial outpatient appointment which was then not checked thoroughly at the time of treatment. The error took place for a second time when the clinician only checked the last set of patient notes which were incorrect. There had been a vast amount of learning from the
109

ITEM SUBJECT
11.2
incident in terms of process and understanding around how patient notes needed to follow patients through the complexities of an Ophthalmology appointment. HO queried if the committee might receive a quarterly or half-year comparison of SIs against previous years to ascertain whether improvements had been made. TF requested that the breakdown of the 11 overdue Harm Reviews by tumour site be circulated to committee members as soon as it was available. Resolved: The PSQ Committees in Common noted the Joint Committee (JC) / Acute Commissioning Team (ACT) Updates. [Action: Quarterly or half-year comparisons to previous years of Serious Incidents to be provided in future Joint Committee Acute reports to provide assurance improvements were being made.] [Action: RH to circulate the breakdown of the 11 overdue Harm Reviews by tumour site to committee members when available.] EPUT Mental Health SM summarised the report and highlighted that as EPUT moved from their previous SI Framework into the new Patient Safety Incident Response Framework (PSIRF) they were working through their historical SIs with the oldest one from 2016 having now been closed. There had been several high-level SIs, Level 3 independent investigations and external reports with the potential for adverse impact on EPUT and for attracting adverse public scrutiny and media attention. The committee were asked to note a legacy case from 2016 that had transferred to Thurrock CCG as the coordinating commissioner in October 2019. NHSE/I had commissioned a Level 3 Independent Investigation of this incident, the final report of which was published on 24 August 2021. The Coroner’s Court would be issuing EPUT with a Prevention of Future Deaths report in relation to this case and it was possible that the report would also be addressed to the five CCGs involved in the MSE implementation of the primary care mental health nurse team. There had been some staffing challenges in the CCGs’ Mental Health Quality team, however several quality visits had still taken place within EPUT. Environmental issues, C-19 and social distancing, workforce, IP&C and lack of operability of IT systems had been identified as quality concerns. The CCGs were supporting EPUT with their action plans and developing a joint Evidence Assurance Group to ensure robust oversight of sustained improvement. There had been unannounced CQC visits to the St Aubyn’s Centre Children and Young People's Mental Health Services (CAMHS) inpatient unit and Poplar Ward CAMHS inpatient unit. Following these visits a Section 31 Notice was served to EPUT. The CQC reports for these visits had not been officially published at the time of reporting. The Mental Health Task Force had now completed its review on all planned areas of focus which covered:
• Perinatal Services
• Personality Disorder Services
• Eating Disorder Services
• Discharge Follow up and Care Planning
• Estates and ligature points
110

ITEM SUBJECT
11.3
The final Task Force review, focusing on partnership working and IT interoperability, was due to be presented on 16 August 2021 following which a final report would be developed. The Task Force had agreed robust recommendations and there was a pan-Essex structure in place to take the recommendations forward and develop action plans to achieve the agreed recommendations. Good progress was being made system wide against the actions. It had been agreed that there would be 3 monthly touch points with the Independent Chair and Taskforce lead to assess and maintain oversight of the delivery of the action plan. HO queried whether workforce issues in the eating disorder service would impact upon the service accepting referrals from GPs. SM confirmed temporary staff were in place so usual referral processes should remain in place, but asked that any specific issues be reported to him in order that he could follow them up. Resolved: The PSQ Committees in Common noted the EPUT Mental Health Update. Learning Disability (LD) LC summarised the report and highlighted that only 2 of the 5 MSE CCGs had hit the monthly trajectory for AHCs. Due to staff movement internally, some gaps had been identified in local place LD commissioning roles which were key in championing the AHCs. These concerns had been raised with the Alliance Directors and LC had sought advice on any interim contingency plans to manage the staffing gaps. The LD team were working on better communication with PCNs in relation to their AHC position with the aim of changing the culture about when the assessments were undertaken. The CCGs LD team had met with the Essex Learning Disability Partnership (ELDP). Staffing had been identified as a key issue with a shortage of staff in some inpatient wards, however the LD team were satisfied with the contingency plans the ELDP had in place. LB queried if the ELDP covered Thurrock. LC confirmed the ELDP covered all 7 Essex CCGs including Thurrock. SM suggested that the need to identify and register those who required AHCs was also an issue. LC confirmed this would be looked at by the Allied Health Care Group that she now chaired. TS highlighted there was now a needs-based assessment tool published by NHSE/I available to primary care practitioners to identify those patients in need of an LD AHC without the need for a formal IQ test. The ELDP were rolling out a training programme which would be standardised across the MSE CCGs. LC asked the committee to recognise that TS had been heavily involved in this work. HO queried if the assessment tool might be made available on System One. LC confirmed she would explore this. Norfolk and Waverley had commissioned a 2019 Safeguarding Adult Review (SAR) on 3 registered LD patients with particularly challenging behaviour who were admitted to Cawston Park after family crisis. Although they were not MSE patients, LC noted the importance of bringing this case to the committee’s attention. T The SAR looked at the experiences of patients and carers in the unit, care management, support services, commissioning arrangements and the impact of recent CQC reviews which had highlighted that patients’ length of stay was 17/18 months longer than necessary. The SAR had identified a number of failings and the unit was subsequently closed and 57 patients were repatriated. The Transforming Care Lead had been consulted who found that between 2016 and 2020, 7 MSE patients had been admitted to Cawston Park. All individuals were reviewed, and their discharges were planned with 6 going into community placements and 1 into secure forensic inpatient care. The Transforming Care Lead and their team had reviewed
111

ITEM SUBJECT
12.
13.
commissioning arrangements for all independent hospital settings. There were 10 MSE patients in such settings for whom 8 weekly reviews, face to face patient assessments and regular 6 monthly Care and Treatment Reviews were taking place. A written briefing would be provided at next meeting. Resolved: The PSQ Committees in Common noted the Learning Disability Report. [Action: LC/TS to explore uploading the LD AHC self-assessment tool onto System One.] Primary Care Quality Report VC summarised the report and highlighted the table on page 116 of the papers which detailed which MSE CCG GP practices were in receipt of additional support from the Quality team. NHS Digital had published appointment data for May 2021 demonstrating that 56% of GP appointments were taking place face to face, with an even higher rate for MSE practices of 60%. VC highlighted that a CQC report had been published for a Basildon and Brentwood practice and its rating revised from ‘Inadequate’ to ‘Good’. A CQC report had also been produced for a Thurrock practice which was currently being challenged for factual accuracy by the practice. A CCG support offer had since been taken up by the practice and an action plan was in progress. LB suggested the CCGs should be seeking to communicate more positive outcomes, such as the percentage of face to face GP appointments being undertaken, with members of the public. VC confirmed she would liaise with the Communications and Engagement team about this. Resolved: The PSQ Committees in Common noted the Primary Care Quality Report. [Action: VC to liaise with the Communications team with regards to communicating the percentage of face to face appointments being offered within MSE.] Local Escalations (as required): Basildon & Brentwood CCG VRB confirmed there were no local escalations from Basildon & Brentwood CCG. Castle Point & Rochford / Southend CCG MG noted there had been 80+ Afghan refugees placed in a Southend hotel. Communications were ongoing with Southend Borough Council to ensure there were no safeguarding issues. The other MSE CCGs were asked to be prepared for potential last-minute placements of refugees in their areas. Mid Essex CCG VRB confirmed Public Health England (PHE) had published a report on Invasive Group A Streptococcal Disease (iGAS) on 10 September 2021. There had been no specific reference to the outbreak in Mid Essex within the report, however the Communications and Engagement team and relevant providers had been advised. The report detailed an additional recommendation for CCGs that was not in the MECCG iGAS action plan in relation to provider’ s occupational health services and their ability to be responsive and support outbreak management and investigation. The IP&C team had been asked to explore potential system solutions for this moving forward. The report was sent to committee members for their information. Thurrock CCG SM raised an escalation around insufficient resources for Court of Protection cases which would be discussed under Item 14 of the agenda.
112

ITEM SUBJECT
14.
15.
16.
Resolved: The PSQ Committees in Common noted the Local Escalations. Adults and Children Safeguarding System Report JB summarised the report and highlighted the risks around Liberty Protection Safeguards (LPS) that were being managed by the LPS Steering Group. A risk had been identified in Thurrock around insufficient resources for Court of Protection cases and the pressures this had caused in respect of applications to the Court of Protection for C-19 vaccinations. A number of safeguarding concerns in relation to care homes had been raised which were being managed by the Care Sector Hubs. LF confirmed work continued around Initial Health Assessments for children and plans were in place to mitigate this risk. Work was ongoing around primary care safeguarding reports with associated quality assurance and how learning from statutory case reviews and SIs might be embedded. Resolved: The PSQ Committees in Common noted the Adults and Children Safeguarding System Report. Medicines Management/Controlled Drugs SW apologised for the lack of a written paper to present to the committee due to absences in the team. He advised that there were no escalations in relation to controlled drugs and work was progressing as planned. The MSE system had been working together to investigate alternate pain pathways. SW noted that a risk around D-MARS/anti-coagulation drugs had been added to the BAF due to concerns about the ongoing provision of these medicines. Interim arrangements via community pharmacy and Southend Hospital had been put in a place while a broader system approach was explored. Resolved: The PSQ Committees in Common noted the Medicines Management/Controlled Drugs update. Care Sector Report VRB summarised the report and highlighted that a regular focus had been put onto the quality and safeguarding of the care market. Any elements of concern had been highlighted on page 139 of the report and she reassured the committee that the Continuing Health Care (CHC), Quality teams and the local authority had work collaboratively to provide the appropriate level of support and oversight to maintain confidence in patient services. Some care homes had given notice of closure in the Southend area and the relevant teams were working together to support those individuals who were affected. Support had been provided to care home providers in relation to the requirement for all care home staff to have received the C-19 vaccination by November 2021. This included improved access to vaccines and understanding care home’s business continuity plans in the event of an interruption to service provision. LB noted that the chart on page 140 of the papers relating to care home outbreaks and exposures did not include data for Thurrock CCG. VRB confirmed she would feed this back to
113

ITEM SUBJECT
17.
18.
the report authors. Resolved: The PSQ Committees in Common noted the Care Sector Report. [Action: VRB to highlight the omission of data for Thurrock CCG within the outbreaks and exposures section of the Care Sector report.] Little Havens CL summarised the report and highlighted the main provider for End of Life (EOL) hospice care for CYP was Little Havens who were currently experiencing some challenges. Their EOL inpatient facility was currently closed due to unsafe staffing levels however the building was being utilised for day activities to support health and wellbeing and for 2/3 nights of respite for CYP with life limiting conditions. Key actions being led by the CYP Commissioning team in partnership with stakeholders were:
• Support the hospice’s recruitment campaign, including linking in with the CCGs’ Communications team
• Monthly monitoring meetings with hospice’s senior management team to support implementation plans and development.
• Facilitating discussions between the hospice and the Children’s Community Nursing Teams in EPUT, NELFT and Provide to ensure joint working protocols and pathways were established.
Little Havens also delivered ‘The J’s’ service for 16-40-year olds and it had been recognised that this service was not delivering against its original service specification. Work was being undertaken to review the caseload and to consider what the service would look like from 1 April 2022 onwards. This had been covered within the CYP portfolio but was now being jointly carried out with adults given the impact on the adult patient cohort. Work to identify the care and intervention required by the cohort of complex young people over the age of 25 would be led by the Director of Commissioning, Performance and Emergency Preparedness Resilience and Response who was also the Senior Responsible Officer for End of Life and Palliative Care. People on the service’s caseload would be kept informed and involved with any service changes and it had been agreed that the service would continue to accept referrals against agreed criteria until a solution and proposal for service change had been approved. MG queried if there were any unmet needs as a result of the closure of Little Havens’ inpatient facility. CL confirmed all patients needs were being met on a bespoke basis. Resolved: The PSQ Committees in Common noted the Little Havens report. Virtual Decisions taken since last meeting The committee were advised of the virtual decisions taken since the date of the last PSQ CiC meeting held on 13 July 2021, as set out below: Approval of CCGs’ Response to St Luke’s Hospice Quality Account 2020/21 The MSE CCGs’ response to St Luke’s Hospice Quality Account 2020/21 was reviewed by the PSQ Committees of Basildon & Brentwood and Thurrock CCG (the areas served by the hospice) via email on 9 August 2021. The draft response was supported by relevant PSQ CiC members and approved by the MSE CCGs Joint Committee at its Part I meeting on 26 August 2021
114

ITEM SUBJECT
19.
20.
Resolved: The PSQ Committees in Common noted the Virtual Decisions taken since last meeting. Any Other Business / Reporting to CCG Boards The following items were identified for highlighting to CCG Boards:
• PHE iGAS report
• Cawston Park and escalation to NHSE/I of local learning Resolved: The PSQ Committees in Common noted the reporting to CCG Boards. Date and time of Next Meeting Wednesday 10 November 2021 at 11.00am – 1.00pm via MS Teams
115

MINUTES OF FINANCE AND PERFORMANCE COMMITTEES IN
COMMON MEETING OF BASILDON & BRENTWOOD, CASTLE POINT
& ROCHFORD, MID ESSEX, THURROCK AND SOUTHEND CCGs
Held via MS Teams on 21 July 2021 at 3.00 pm – 5.00 pm
Representative Job Title/Position Committee/Organisation Quorate?
Lesley Buckland (Chair) (LBuc)
Lay Member Governance & Audit Chair
Finance & Performance, Thurrock CCG
YES (4 members
including a clinician)
Mark Barker (MB) Joint Chief Finance Officer
Finance & Performance, Thurrock CCG
Dr Luis Leighton (LL) GP Member Finance & Performance, Thurrock CCG
Alan Hudson (AH) Lay Member Finance & Performance, Thurrock CCG
Dr Anand Deshpande (AD)
CCG Board Member Finance & Performance, Thurrock CCG
Mark Barker (MB) Joint Chief Finance Officer
Quality, Finance & Performance, SE Essex CCGs
YES (AO/CFO/ DoN, 2 x clinicians,
2 x lay members)
Pauline Stratford (PS) Lay Member Quality, Finance & Performance, SE Essex CCGs
Tracey Freeman (TF) Lay Member Quality, Finance & Performance, SE Essex CCGs
Janis Gibson (JGib) Lay Member Quality, Finance & Performance, SE Essex CCGs
Dr Sunil Gupta (SG) GP Board Member Quality, Finance & Performance, SE Essex CCGs
Dr Ken Wrixon (KWr) GP Board Member Finance & Performance, B&B CCG
YES (2 x GP
members, 2 x Exec members)
Dr Femi Salako (FS)
GP Board Member Finance & Performance, B&B CCG
William Guy (WG)
Alliance Director, Basildon & Brentwood
Finance & Performance, B&B CCG
Mark Barker (MB) Joint Chief Finance Officer
Finance & Performance, B&B CCG
John Gilham (JGil) Lay Member, Governance and Audit Chair
Finance & Performance, Mid Essex CCG
YES (Chair/Deputy
Chair, 2 other members, one of which must
be a clinician)
Dan Doherty (DDo) Alliance Director, Mid Essex
Finance & Performance, Mid Essex CCG
Rachel Hearn (RH) Director of Nursing, M&SE CCGs
Finance & Performance, Mid Essex CCG
Mark Barker (MB) Joint Chief Finance Officer
Finance & Performance, Mid Essex CCG
In Attendance
Viv Barnes (VB) Director of Governance & Performance
Mid Essex CCG N/A
Andy Ray (AR)
Chief Finance Officer, Acute Commissioning Team N/A
James Buschor (JB)
Head of Performance Acute Commissioning Team N/A
Dawn Scrafield (DS) Chief Finance Officer Mid & South Essex NHS Foundation Trust (MSEFT)
N/A
116

Representative Job Title/Position Committee/Organisation Quorate?
Nick Jones (NJ) Director for Health Analytics
PwC
N/A
David Triggs (DT)
Head of Corporate Governance
B&B CCG N/A
Deborah Jeffery Executive Assistant to Joint Chief Finance Officer
Finance & Performance, Mid Essex CCG
N/A
Mike Thompson (MT) Interim Programme Director
Mid and South Essex Health and Care Partnership
N/A
Emma Timpson (ET) Executive Member Finance & Performance, B&B CCG
N/A
Apologies
Anthony McKeever (Mac)
Joint Accountable Officer
MSE CCGs
Karen Wesson (KWe) Director of Commissioning, Performance and EPRR
Acute Commissioning Team
Tricia D’orsi (TD) Alliance Director Quality, Finance & Performance, SE Essex CCGs
Dr Taz Syed (TS) GP Board Member Quality, Finance & Performance, SE Essex CCGs
Nimit Dabas (ND) GP Board Member Finance & Performance, B&B CCG
ITEM SUBJECT
OPENING BUSINESS
1. Welcome and Apologies The Chair welcomed members to the meeting and noted that all members of the CCGs F&P Committees had been invited to attend. Apologies were recorded as listed above. The Chair welcomed Deborah Jeffery to the meeting to take the minutes and support the committee administration. Members were asked to refer to DT or DJ if any queries or concerns. The Chair noted concerns regarding the timing of previous meetings and thanked all for their comments following the last meeting. These will be addressed at the end of the meeting and Chair agreed to share her thoughts around the things that could be put into place to support meetings keeping to time. The Chair advised that she planned to change the order of the agenda to accommodate guests Dawn Scrafield and Nick Jones who cannot attend until after 4:00 p.m. With support from the members the Chair aimed to tackle the full agenda with the exception of item 8 by 4:00 p.m. and allow the second half of the meeting for item 8. DT asked through the Chair if there was no objection, he wished to record the meeting for the purpose of supporting preparation of the draft minutes. The record would be deleted after 30 days.
2.
Declarations of Interest There were no additional declarations of interest to those already recorded by members.
3.
Minutes of previous meeting and Action Log The Action Log was discussed and amended.
117

ITEM SUBJECT
Chair referred to Minutes of last meeting from page 13 in the meeting papers pack. AD noted a correction to his title as a GP Board Member but not Chair. AD asked for clarification on the rule of quoracy and it was confirmed that each CCG committee needed to be quorate. Where a CCG was not quorate the required attendees would be approached to give their support to the decision after the meeting. As a matter arising the Chair drew members attention to the post meeting note on Item 9.- Adult Critical Care Transfer Service Business Case. The note explained the discussions that followed the meeting and that it had been referred to the Joint Committee. Subject to the correction highlighted above the minutes were accepted as an accurate record. RESOLVED: that the minutes of the meeting of the F&P CiC meeting held on 16 June 2021 be approved as a correct record subject to the amendment highlighted above.
SHARED BUSINESS
Items for Decision
None
Items for Assurance
4. Financial and Performance Risks The Chair invited AR to present the report noting that Sara O’Connor, Mid Essex Head of Corporate Governance had taken on the role for coordinating the Board Assurance framework (BAF) including the finance and performance risks. She thanked Nicola Adams who had been coordinating the BAF previously and who had guided the CCGs through the changes approved by the CCG Boards last year. AR introduced the executive summary including the 11 key finance risks of which 8 are medium and 3 low risk. A review of the financial risks had been completed and were listed in appendix 1. The system performance risks were listed in appendix 2. He updated the Committee on the following: - early indications from discussions with the Department of Health and NHSE/I are H2 (2nd half
year) financial allocations will be tougher than H1 (1st half year). Therefore, H2 efficiency targets will be significantly higher than the targets for H1.
- An issue, to be covered in second paper concerns the fact that is the National thresholds for the Elective Recovery Framework had been unexpectedly changed. The element of activity thresholds has been increased placing a cost-pressure on the system.
- Changes from last month’s paper were highlight in the risk tables. - Following comments raised last month around the risk mitigations and actions an additional
item had been included and the intention will be that in next month’s report it will highlight areas needed to achieve the forecast risk target.
During discussion the following comments were made: AD questioned which of the higher risks had moved to moderate and the assurances that were behind these changes? AR advised the two risks predominately moved were those around achieving the financial target, for H1 on plan, system on plan and slightly over-achieving on plan. Assessments needed to be made following Senior Finance Leaders’ Group (SFLG) discussion. He explained that as part of a later report the Committee would receive an update of the high-level savings schemes. Of the two or three major schemes, the biggest scheme is CHC which is quite advanced in delivering but the risks of this are yet to be fully evaluated.
118

ITEM SUBJECT
JGil raised concern that when reading the paper he was not able to identify if the controls in place are delivering and if not, what actions are being taken to mitigate those controls; and what confidence do Executives have that the controls will deliver the target outcomes? He went on to refer to the Performance report which he felt did not provide assurance, an explanation as to why the risks had been adjusted and whether in the mind of the author they are logical or appropriate adjustments. MB thanked JGil for the challenge and accepted the points made. He explained that experience over the past few weeks showed that matters had changed frequently providing a challenging environment in which to ensure risks and mitigations are up to date. There would be additional updates as part of the Finance paper later in agenda. He and finance colleagues would work with Sara O’Connor to ensure the BAF is as up to date and accurate at the time of publishing the papers as possible and provide a verbal update at the meeting. JGil asked that the reports indicate in the report the level of assurance, how confident the Executives are that based on actions in place the target risk score can be achieved? The Chair proposed that Audit Chairs meet with MB, SO’C and MT to collectively move this forward. ACTION : a) AR to discuss with MB the presentation and the need to provide the committee more assurance regarding actions taken in H2. b) MB, to liaise with SO’C, MT and Audit Chairs as described above. JB presented a summary of the performance risks including: - Cancer diagnostic - RTT (Referral to Treatment) particularly 98 weeks The Committee discussed the performance risks. KWr challenged why some risks have got a high current risk score with what appeared to be an acceptable target risk score but a milestone deadline of two months giving the example of RTT with current risk 25; acceptable risk 5 and target date 30th September. Was this achievable? JB explained this was not referring to the 18 weeks RTT constitutional standard, but the RTT target to remove any 98 week waits. A clear commitment had been made to the NHSE Eastern Region that no patients are waiting 98+ weeks after end September. There had been an escalation to ensure additional mitigating measures to complete this by the end-September but confidence was low that this could be delivered on time. KWr asked a similar question with respect to other risks i.e. the Cancer Constitutional target? JB advised that to achieve the Cancer constitutional target the key is to reduce the back log. This seems achievable with new recovery actions into the Cancer Programme Board, they are sharing smart sheet recovery action plan from the Trust that feeds directly into that. ACTION : JB to look at acceptable Cancer target risk score and revisit for next meeting. JGil referred to the KWr point raised above and some reports received as part evidence of whether risk is being delivered or not. Looking at the data he considered there is a high risk in the ability to deliver current performance.
119

ITEM SUBJECT
TF supported the comments from colleagues around the need to receive assurance that we are able to mitigate the risks with the proposed actions. The Chair thanked JB for his report and members for the constructive discussion and it was agreed that a follow up meeting be arranged to respond to the points raised concerning the need to provide robust assurance. RESOLVED: That the report outlining the financial risk register be received and noted. ACTION: MB to lead on further discussions.
5. JCT Finance Report (Independent Sector and Elective Recovery Framework) AR introduced Angela Reynolds who works in AR’s team with JJ and the Independent Sector Providers (ISP). AR acknowledged the work that ARen and her team has undertaken in developing ISP relationships. AR went on to give an overview of the report and highlighted key issues. Positive figures had been received based on the latest internal estimates income for independent sector based on activity provided on final freeze and suss data activity. The Committee noted the following highlights based on the latest estimates: - Positive - system elective activity is above the national threshold set, exceeding considerably
in the first three months of the year. - Activity not as high as the system stretch target. The plans submitted were based on setting
a high stretch target. - The thresholds to achieve each month were set at the start of the year had been changed at
short notice across the country and thresholds increased. This has had a negative impact across the system and within MSE CCGs there is expected to be a loss of £1.2m with MSEFT expecting a deficit of around. £3.7m.
- Based on activity projections and revised thresholds the risk of achieving additional income to cover the cost of mobile theatres etc. is not meeting the full costs.
- the MSEFT activity in the first two months was higher than expected and the Trust was working though potential additional income to see if it can mitigate the income loss.
TF thanked AR for the update and questioned how the stretch target had been set. AR responded that regular discussions were held with the ISP’s to understand the position prior to submitting a return to NHSE. Feedback from NHSE was that the system is doing well in addressing the RTT backlog, although it remains extremely large and an ongoing challenge. The Committee noted that NHSE had confirmed that full payment would be received for additional activity completed by the MSEFT by way of a correction. ACTION: AR to circulate additional papers and provide a post note for the minutes. JGil raised a question as to whether Tier 2 activity was or was not included. AR agreed to clarify that all like for like activity would qualify for ERF. He gave assurance that his team are working closely with Tier 2 Providers to ensure that allowable activity is included. RESOLVED: that the report on the ERF key issues and next steps be noted.
120

ITEM SUBJECT
6. Performance Report
a) Acute JB presented highlights of the Acute performance report. It was noted that there was no report on non-acute performance pending a new system assurance report. JB referred to the first part on page 57 and highlighted the following: - Cancer standards in the risk register and the backlog trajectory of 163 by the end September.
To provide assurance, the Cancer Board and Cancer Delivery Group are receiving actions/progress by each tumour site and the detail is further broken down by each tumour site. It was noted that the Trust share data with partners including the Cancer Alliance, so commissioners are aware when the agreed trajectories are off track.
- RTT 98 weeks graph shows the trend in patients waiting 98 weeks – in the week prior to the Committee it was 369 patients. The trajectory needed to improve.
- A diagnostic working group has been established with Clinical Leads to monitor recovery of the diagnostics standard with oversight NHSE Eastern Region and SOAG.
The Chair thanked JB for the comprehensive update and highlighting the assurances. PS raised a query on the ambulance arrival handover and emergency care information reported to F&P meetings previously and how the Committee should receive assurances that these are on target? Also, with reference to NHS 111 Performance this shows 65% against a target of 95% is there a recovery plan? JB agreed to report back regarding the questions around ambulance and NHS 111 Performance. ACTION: JB to liaise with Karen Wesson regarding UEC and Ambulance performance reporting to F&P. ACTION: JB to collate information from Emily Hughes team regards performance reporting for NHS 111 and update at next meeting. TF raised a concern that projections are based on dates a long way into the future. Following the recent release of COVID restrictions it would be useful to see if there had been any impact on the trajectories that had been set. JB agreed to bring this information to the Committee as soon as it is available. JGil raised concern on advice and guidance as there is nothing regarding trajectory or actions to address despite information, he had picked up indicating that there were issues to be addressed. As an example, he referenced 6000 referrals that had been returned to Mid-Essex recently. It would be useful to have data to show how many had been returned without action. DD clarified that GPs in all CCGs had raised issues that they had been inundated with advice and guidance referrals that had been returned and not actioned. The Chair noted that this issue was being picked up elsewhere. Action: JB to follow up JGil’s concern on trajectory and the 6000 referrals risk and update progress at next meeting. RESOLVED: that the Performance report be noted.
121

ITEM SUBJECT
7.
M3 Finance report MB introduce the report and provided a brief overview of his paper. - the M3 year to date position showed that CCGs remain on plan to hit the half year target
subject to receiving the top-up funding for both the Hospital Discharge Programme (HDP) costs and Independent Sector (IS) ERF funding.
- The MSE System report for M2 YTD, is showing £9m surplus which relates to the Elected Recovery Funding predicted within MSEFT.
- Note that the target of £16m of efficiencies and £9m of investments is slightly behind expected trajectory as at M3.
The Committee noted the following emerging Risks and Issues: - Pressures including the Elective Recovery funding. - COVID pressures as the next wave develops. - A significant increase in infection rates but at the current time this was not translating into
hospitalisations. - Efficiencies and investment plan slower than anticipated – only with these can we plan to
make the transformational changes needed for H2. - Domiciliary care pressures are emerging from partner local authorities not helped by a
shortage of carers. - Pressures on staffing from the NHS COVID App ‘pingdemic’. - IMCs for planned development in Thurrock which will, when in place, allow the closure of
Orsett Hospital. - Additional costs arising from National guidance to ensure the UK meets its target to achieve
‘Net 0 Carbon emissions’. The CFO highlighted mitigations in place including; - Additional £55m nationally awarded to support Ambulance services - impact for MSE is
£5.5m additional funding granted to East of England Ambulance Service Trust (EEAST) on behalf of the system. To receive proposals from EEAST as to how they wish to utilise to ensure services improve.
- Long COVID funding awarded £1.75m. Paul Taylor is working on how we can service and support long COVID patients.
- HDP funding set aside by Region over £11m for our system. - Additional IBCF funding carried forward from last year to allow flexibility for care for the
elderly and allow opportunity for additional resources to manage capacity pressures. - Work to understand the H2 pressures. - COVID funding expected to fall away but the timing for this is unknown. - Additional efficiency asks have been made of the system with an expectation of 3.5% (i.e.
around £47m) for the second half year target. JGil raised a question concerning Appendix 2 which showed 3 negative forecast variances for Admin & Cler £9m, Med & Dental £8.5m and Other £10.7m. He asked for additional clarity to understand the reasons for these. Action: MB to follow up with JGil outside of meeting. RESOLVED: that the M3 report be received and noted.
122

ITEM SUBJECT
8. System Financial Sustainability Plan The Chair welcomed DS and NJ and clarified that the additional background information provided was supporting and there was no expectation to analyse prior to the meeting. DS introduced the presentation and provided some context to the paper and the work being undertaken by PwC. She explained that the System has been working to develop a financial sustainability plan which will underpin the efficiency delivery across the system. Simultaneously, work has been carried out on validating the underlying deficit of the System, as well as diagnosing the drivers of this deficit. This started with the most complex cost drivers at Mid and South Essex NHS Foundation Trust and was then expanded into the System. The financial challenge across the system has been reviewed by PwC and the interim assessment concluded an underlying deficit for the system of £201m excluding Provider Sustainability Funding (PSF)/Financial Recovery Fund (FRF) and Marginal Rate Elective threshold (MRET) funding. Nick Jones from PwC shared the MSE Financial Sustainability presentation explaining that work had focused on identifying key areas of high cost across the Trust and System. Five overarching intervention themes have been identified that address the underlying building blocks of these high costs. For each of the five overarching interventions there are a number of tactical interventions that help to set the foundations for delivering long term sustainability. Each intervention has been designed to support the Trust and the System to address the financial challenges identified. Across all of the interventions it was estimated that there was around £141m of releasable costs. The phasing of interventions has been assessed over a three-year period with the ambition of driving system work programmes to realise the benefits from interventions as a means to address the underlying system deficit. In the first instance the priority areas are outpatients which identifies a significant opportunity (system referral and provider productivity), workforce (reducing temporary staff costs) and Continuing Healthcare. Even with the full delivery of the interventions identified the Mid and South Essex System has an ongoing reliance on the £10m MRET and £89m FRF (as valued in 2019/20). It was noted that at this stage the continuance of these funding sources had not been confirmed. It was explained that in parallel work had been ongoing to discuss a financial strategy whereby a full or partial freeze of allocation and use of future growth funding is necessary to manage the deterioration in deficit. DS thanked NJ and outlined the next steps;
• The transformation work that needs to happen to address underlying system deficit.
• The benefits if achieved 100% of transformation opportunities is around £112m against the system underlying deficit of £201m.
• She explained that to address the underlying position we need, as a system, to continue to receive the financial recovery fund, to lobby for additional funding.
• The challenge would be for the system to reach the underlying financial position within a 3-year period.
Questions were raised by the Committee including; Are the proposed savings realistic or do they rely on heroic assumptions about being able to recruitment sufficient permanent staff?
DS accepted the challenge but argued that there had been positive examples re pipeline recruitment into critical care with international nurses. Discussions were underway with the Head of Workforce, Ruth Jackson as to how the system could look at vacancies collectively rather than as individual organisations.
123

ITEM SUBJECT
AH raised a point that he had heard from Ian Wake (Corporate Director for Adults, Housing and Health) that money is in the system but in the wrong places. Was it realistic to ask people to give up their share of funding? DS reflected it is often easier not to spend money. She agreed with Ian Wakes’ reflection, but one of the problems is around population health and the fact that we are spending into the wrong place because we are a deficit system. We are spending £201m in wrong place every year unless we do something about it. Creating a programme to allow us to shift the resource and have a framework that allows us to achieve that. ET referred to the Connect Programme of work undertaken and asked if the pathway reviews and benefits that we are hoping to deliver through productivity were separate to this analysis or included? DS confirmed they are included. In response to a question around the medicines optimisation and prescribing QIPP targets DS asked that NJ shares the approach taken around prescribing and medicines optimisation at a headline level. NJ advised a colleague would look into this The Chair suggested that it would be useful if there was another meeting outside as she has touched on an area of significant potential. ACTION: To arrange a further meeting to discuss BAU and accountability. JGil welcomed the logical focused presentation providing a positive way forward. He raised the following points and questions;
- How do we connect the whole system, Place, GP, Primary Care etc, to see what the opportunities identified translate into something deliverable, how can we establish what can be delivered financially and at what place? We need to focus on care pathways and processes rather than pounds.
- Re population health and lower cost services; how can we engage the public in more about self-care to minimise demand. The issue of demand and growth isn’t pulled out enough. How the focus around population health and wider ways of doing things at place can contribute with small amounts of money to make a difference and financially drive or allocate budgets, bringing these things together to make happen,
NJ responded good points raised re the wellness agenda as well as care delivery agenda. This was mentioned in the detail of report in population health intervention, there are elements related to self-management of conditions and more general wellness of population. How to build into the pathway budgets managing is a challenge to then operationalise some of the savings. DS referred to JGil’ s point regarding engaging the public. As part of the key re-fresh of the SEPB one of the tasks and recommendations is as a system we prioritise the best way to achieve the £112m. A task is to get the profile right and focus on the next 3 years. Also mapping what resources we already have aligned to some Programmes (i.e. Connect, CHC, Outpatients Programme). Some National and Regional forums looking to map how we should get the information and intel to help drive the information. There can be an element within those programmes about public engagement and depending on the programme of activity will depend on what the extent the public engagement needs to be. Potential to be managed through the programmes of work and a key reflection within that structure. A question was asked about the need to reflect the financial performance of difference CCGs.
124

ITEM SUBJECT
NJ advised in Chapter 3 of the system report, there is a section dedicated to CCGs by CCG so when describing system challenge is in aggregate terms and built up from the individual positions and the report does reflect the varying initial report historically from the varying CCGS. MB summarised that through the work that PwC have supported several opportunities have been identified that will impact upon our deficit. We could not be expected to do them all at the same time but to identify and target those with the greatest impact and improvement to quality standardisation and performance, as well as delivering the financial savings desired to achieve. Work to be undertaken with operational buy-in to ensure this can happen as won’t be finance driven but operationally owned. Chaired echoed MBs thoughts and thanked DS and NJ for the work put into the report, and positive moving forward. We will need the assurance of it happening and the targets to be met. The Chair suggested it would be helpful to have a regular agenda item to pick up the progress and have further discussion moving forward. DS suggested the best way for F&P CiC to get assurance is for reports to come from the SEPB setting out how this work is progressing and what the priorities are. ACTION: An update report is provided to the Committee at its next meeting. The Chair thanks DS and NJ for their presentation.
Items for Information 9. The Committee received and noted the following on page 98 in pack:
9a) ACT Finance Report 9b) System Finance Leaders Group Minutes – June Approved 9c) No virtual decisions to report
10. Any Other Business: Chair asked members if there were any further items for AOB. None raised.
11. Items for escalation to other committees / future agenda items: - The Chair thanked those who wrote in about timings - Following discussions with Audit Chairs and a proposed review the content of cover sheets to
provide greater assurance with the view to highlighting assurances she was confident that meetings could be managed within the two-hour time frame.
ACTION : LBuc and MT to look at cover sheets for all CiCs to ensure they are suitable to gain assurances immediately and challenge questions appropriately.
12. a). Frequency of Meetings: - A proposal was put forward to move to bi-monthly meetings. MB explained that the timetable
of September, November, January and March would fit with the financial and performance timetable. However, there would be an opportunity to manage urgent business between meetings. MB agreed to advise mid-month if there is anything that the Committee needed to be made aware of.
RESOLVED: That the move to bi-monthly be agreed subject to no urgent issues arising and that the CFO would update Committee members if any urgent issues arise in intervening months.
125

ITEM SUBJECT
TF thanked Chair for comments on meetings and papers etc. and would like to raise a comment on note 9b. Minutes for SFLG, relevant to what has been discussed so far but the impact of a statement included in the Minutes around the beds, COVID and waiting lists. TF referred to JGil’ s point and that it is alarming that we must know what’s going on as we can’t mitigate something we don’t know about. Can that be followed up and would like further understanding of the discussion? ACTION : MB to follow up a discussion with TF Chair advised of the plans to go forward and asked if any issues to raise, to email Chair, MB or MT to moving forward bi-monthly recognising the exceptions and pick up but meeting on bi-monthly basis going forward. b). Date of next meeting: 15th September 2021, 3.00-5.00 p.m. via MS Teams. The Chair thanked all for tolerance and referring to the work undertaken regarding cover sheets moving forward, getting smarter and meeting bi-monthly will enhance that. All will be informed on items if needed, between meetings. The Chair thanked DS and NJ again and all members for coming to the meeting. Meeting closed at 5:10 p.m.
126

Minutes of Meetings in Common of the Audit Committees of
Basildon & Brentwood, Castle Point & Rochford, Mid Essex, Thurrock and Southend CCGs
9.30 am, Friday, 16TH July 2021 (Via Microsoft Teams Meeting)
Representative Job Title/Position Committee/Organisation Quorate?
Present:
Mr N Spenceley (NS) Audit Chair Basildon Brentwood CCG YES
2 x Members Dr J Hale (JH) Secondary Care Consultant Basildon Brentwood CCG
Ms T Freeman (TF) Lay Member (Governance), Audit Chair (Chair on Rotation)
CP&R and Southend CCGs CP&R:
YES: 2 x Members
Southend
YES: 2 x Members
Dr R Liebmann (RL) Secondary Care Consultant CP&R CCG
Ms J Gibson (JGib) Lay Member (PPI) CP&R and Southend CCGs
Ms P Stratford (PS) Lay Member (Primary Care) CP&R and Southend CCGs
Ms L Buckland (LB) Deputy Chair & Lay Member (Governance), Audit Chair Thurrock CCG
NO *(See item 1)
2 x Members
Mr J Gilham (JGil) Deputy Chair & Lay Member (Governance), Audit Chair
Mid Essex CCG
YES
2 x Members Dr E Towers (ET) GP Board Member Mid Essex CCG
Ms N Wright (NW) Lay Member (Patient Public Engagement)
Mid Essex CCG
Mr M Barker (MB) Chief Finance Officer Mid & South Essex CCGs
Representative Job Title/Position Organisation
In Attendance:
Ms N Adams (NA) Governance Lead Thurrock CCG
Ms T Mnangagwa (TM) Deputy Chief Finance Officer Thurrock CCG
Ms J King (JK) (Minutes) Governance Officer Thurrock CCG
Ms V Barnes (VB) Governance Lead Mid Essex CCG
Mr D Triggs (DT) Governance Lead Basildon Brentwood CCG
Ms N Brodie (NB) Deputy Chief Finance Officer Basildon Brentwood CCG
Ms S O’Connor (SOC) Head of Corporate Governance Mid Essex CCG
Ms D Smith-Shaw (DS-S) (Item 5e only)
Information Governance Mid & South Essex CCGs
127

Ms J Martindale (JM) (Item 5d only)
Business Continuity & EPRR Officer
Mid & South Essex CCGs
Mr S Williams (SW) (Item 8 only)
Director of Partnerships and Integration
NHS Castle Point and Rochford CCG
Mr P King (PK) (Item 8 only)
Associate Director – IT / Digital Mid & South Essex CCGs
Mr C Larby (CL) Deputy Head of Audit Assurance West Midlands Ambulance Service NHS Foundation Trust (WMAS)
Mr A Woodhead (AW) Audit Manager West Midlands Ambulance Service NHS Foundation Trust (WMAS)
Ms E Larcombe (EL) Director KPMG
Ms M Seager Manager KPMG
Apologies
Ms G Jones Lay Member Basildon Brentwood CCG
Mr A Hudson Lay Member (PPI) Thurrock CCG
Dr K Barusya GP Board Member Southend CCG
Dr M Metcalfe GP Board Member CP&R CCG
Mr M Thompson Interim Programme Director Mid & South Essex CCGs
Mr L Bushell Deputy Chief Finance Officer CP&R and Southend CCGs
Ms F Niebour Engagement Partner KPMG
Ms E Gill Lead Counter Fraud Manager West Midlands Ambulance Service NHS Foundation Trust (WMAS)
Mr I Gear Information Governance Lead Mid & South Essex CCGs
Item Subject
1. Welcome & Apologies
NS welcomed everyone to the Audit Committees in Common (ACiC) meeting. Apologies were noted as above. NA explained the Committees in Common etiquette and stated that there was no place specific confidential business therefore, breakout sessions following core meeting were not required. NA therefore proposed that individual CCG minutes would be approved under Item 3.
* It was noted the meeting was quorate for all CCGs except Thurrock, however AH, Lay Member for Thurrock, had reviewed the agenda and virtually approved the Thurrock CCG minutes in advance of the meeting to ensure that decisions were quorate. There were no other items on the Agenda for approval.
128

2. Declaration of Interest
“In accordance with Section 14O of the National Health Service Act 2006 (as amended by the Health and Social Care Act 2012 (and subsequent statutory guidance) the CCG must ensure that it manages any and all conflicts of interest that may arise. All members (and those attending the meeting) have a duty to declare any interest they may have on any issues arising at committee meetings which might conflict with the business of the MSE CCGs. Can I therefore ask anyone in this meeting to declare now any conflicts (real or potential) that they may have, declared or otherwise, in relation to the planned agenda for today’s meeting. Should any unforeseen conflicts arising during the meeting, please ensure that you stop the proceedings to declare it accordingly. All declared interests are recorded in respective MSE CCG’s register of interests and any conflicts arising during any MSE CCG meeting will be recorded within the ‘Recorded Conflicts of Interest Register’, which are available on the respective MSE CCG’s website”
The Chair asked Members to be mindful of the statement on declaring interests and reiterated the importance of following good governance and CCG Policy in declaring interests. The Chair requested any declaration of interest that was not already on the register or any interests that had a specific impact on intended agenda items, none were declared. [The meeting began recording in agreement with all present. It was noted that Committee meeting recordings would be kept for 30 days and subsequently deleted.]
3. Minutes
The Minutes of the following Audit Committees were approved by the respective CCG Audit Committee Members:
• MSE Audit Committees in Common - 25th May 2021 - Approved
• BBCCG – 25th May 2021 and 10th June 2021 - Approved
• MCCG – 25th May 2021 and 9th June 2021 – approved with minor amendment, that the final outturn position stated within the finance report was stated as £482k, but should be £411k.
• SECCGs – 25th May 2021 and 10th June 2021 - Approved
• TCCG – 25th May 2021 and 10th June 2021- Approved
4. Action Log
The Committee noted that all ACiC actions had been completed and closed.
5. Corporate Business/Risk
MSE BAF & CRR NS welcomed SOC to the meeting to present the latest mid and south Essex CCGs Board Assurance Framework (BAF) and Corporate Risk Register (CRR). It was noted most risks on the BAF were within the remit of the Joint Committee which, from June 2021, would meet on a bi-monthly basis and the BAF would be updated in the intervening months, commencing July 2021. All risks on the BAF were reviewed in April 2021 in preparation for the CCG Board and Joint Committee (JC) meetings held in May 2021. With the exception of financial risks (that were in the process of being updated in preparation for Finance and Performance (F&P) Committee 21 July 2021), red-rated risks (either in terms of impact x likelihood, or because ‘project delivery’ is rated red) were updated prior to the JC meeting held on 24 June 2021. As a result of the latest review the ratings for the following three red rated risks were amended to amber, it was noted the risk leads had been invited to provide an update to the Committee under Item 8.
1. Digital Transformation (DITR01) 2. Digital First Primary Care (DITR03) 3. Service Provision of high-risk medicines (PLAC06)
129

Members of the JC, held on 24th June 2021, confirmed they had no objection to the risk ratings for the above three risks being reduced to Amber. SOC explained that work was underway to re-start the BAF process which included a new process for adding and closing risks, links to relevant committees, improved consistency of risk rating and scoring and risks to be mapped against new 2021/22 strategic objectives. The main Provider BAFs were also reviewed to compare to that of the CCG identify any gaps, the findings were shared with the JC Team. SOC advised that specific workstream BAFs would be provided on a regular basis to teams for risks to be fully embedded and to enable regular updates and monitoring. The development of a revised Risk Management Policy was underway, as well as how the process can be integrated with the System Oversight and Assurance Group (SOAG). JG thanked SOC for the update and commented that it would be useful to receive assurance that the BAF is being used appropriately in future reports. JG also commented that where risks hadn’t changed over a period of three iterations of the BAF, assurance should be provided that the sub-committees or groups had reviewed the risk in detail to ensure all actions possible were being taken. SOC felt that once the BAF was embedded within working groups she would like to see a review of risks at these meetings and for risks that hadn’t decreased or risks on the increase, leads would be asked to meet with executives. TF noted that some inherent risk ratings were the same as residual ratings. SOC commented that the inherent risk was the initial risk rating and the current rating would be the residual rating and at times this would appear the same, depending on the movement of the risks. In its current format the spreadsheet does not track the movement of risk, once there is more certainty around structures and ICSs boundaries etc. consideration will be given to an appropriate risk management system which would track risk movement. TF also commented that for those risks whose inherent risk rating remained the same as the residual rating, risk leads should consider that the actions taken aren’t mitigating the risk and therefore should be escalated in order to change the outcome. SOC advised there were a number of risks that had not been updated for some time and following an update, their status may have changed. ACTION: Undertake a review of risks whose residual rating has remained the same as the inherent risk rating and escalate those risks to the lead to seek advice on the action being taken to reduce risk. MB extended thanks for work undertaken on the Risk Register. MB made Committee Members aware that, in relation to the ERF Finance Risk, NHSE had advised that changes had been made in respect of reimbursement rates which would make it a growing risk. MB did not think it was a significant risk, but Committee members would need to be sighted on the emerging funding arrangements. LB commented that Audit Committee risk discussions should not be around designing the process and suggested the Audit Chairs met with SOC separately to discuss process and the information required by the Audit Chairs to provide appropriate assurance. SOC took on board the comments made and would be happy to meet with the Audit Chairs but suggested discussion follow after the new process had been implemented and she had had an opportunity to meet with risk leads and it was hoped this would show an improvement in reporting. CL offered his assistance or advice around the BAF development and process to SOC if required and enquired whether the Q3 timing of the Governance and Risk Management Internal Audit review was still appropriate given there would be changes to the BAF and process. SOC agreed that the Audit could be undertaken in Q3.
130

NS highlighted the high level of appreciation across the Committee for the hard work undertaken on the BAF. 10:04 SOC left the meeting. The Audit Committees NOTED the updated Board Assurance Framework. Conflicts of Interest Quarterly Declaration The requirement for CCGs to submit quarterly Conflict of Interest returns remained paused as part of the move to reduce some of the burden on CCGs in order to support the pandemic response and NHS England were yet to formally reinstate the submission of COI data. NA reported that the Audit Committee would normally receive assurance through the quarterly return process regarding the management of conflicts of interest and in lieu of this return the governance leads across mid and south Essex provided the following assurances to the audit committees: There have been no conflicts of interest breaches or incidents to report in the 2020/21 period to date in any of the MSE CCGs. The Internal Auditors reviewed processes for the management of conflicts of interest that was reported separately to the audit committees and confirmed that robust processes are in place and operating effectively. The Audit Committee NOTED the update on the Conflicts of Interest Quarterly Declaration. Procurement Register NA explained there was a mandatory requirement for CCGs to publish a procurement register on a quarterly basis for purchases over £25,000. Historically, Attain (CCG procurement advisors) managed the updating of the procurement register and provided a quarterly update to be published on the CCG websites. The contracting arrangements with Attain changed and consequently the procurement register process was no longer managed by Attain. CCGs have struggled to update the register more recently, as there was no one ‘owner of the process’. A single point of reference was therefore required to strengthen the process going forward. The Committee noted that from July 2021, the joint contracting team would take over the responsibility for the management of the register of procurement decisions and liaise with the relevant CCG departments in order to update the procurement registers. Additionally, a new standardised process would be embedded to manage the capture and collation of procurement decisions across the CCG (either by Executive Approval, Finance & Performance Committee in Common, or Joint Committee), and a standardised register in place across the five CCGs, which would be a necessary requirement as the system transitions into the NHS ICS Statutory Body. The process would be aligned with the Contract Award and Extension form process (which includes waivers where contracts are being extended or awarded outside of approved procurement processes). The new process would also have due regard to the recent consultation on NHS Provider Selection Regime, ensuring that appropriate information is captured to support the proposed new regime. Decision making bodies must be able to justify their decisions for arranging services in relation to key criteria (Quality and Innovation, Value, Integration and Collaboration, Access, Inequalities and Choice, and Service sustainability and social value) as set out in the proposed regime, and records must be kept of the considerations and decisions made under the regime. Once the process is developed, the joint Contracting team would provide regular extracts of the registers for Audit Committee in Common, and quarterly for publication on CCG websites. For reference, the existing procurement registers for the mid and south Essex CCGs were provided for noting and would be
131

uploaded onto the CCG websites with a note that the registers were currently being updated. Full, updated registers would be provided to the next Audit Committee meeting in October 2021, with the quarter 2 registers. ACTION: Existing procurement registers for the mid and south Essex CCGs to be uploaded onto the CCG websites with a note that the registers were currently being updated. TF extended thanks to MB and NA for progressing the work on the Procurement Registers and to the Commissioning team for taking this workstream on. The Audit Committee NOTED the Procurement Registers for the mid and south Essex CCGs and update. Emergency Preparedness Resilience and Response (EPRR) NS welcomed JM to the Committee to give a summary of the EPRR work undertaken during Q1 which included ongoing support to the Pandemic response function, EU Exit transition, a review of EPRR plans and policies in line with the CCGs schedule and various EPRR training sessions. A specific piece of work undertaken by the Emergency Planning Team (EPT) included a roll out of a six-month pilot to align the on-call workforce currently operating across the 5 CCGs to a single rota via the implementation of a two-tier on-call model. The interim approach was to ensure that the mid and south Essex CCGs could fulfil their function as a Category Two responder under the Civil Contingencies Act, whilst having enough staff to populate the rota. JM advised that an evaluation exercise would take place during July/August 2021 to obtain feedback and inform a future model, with feedback provided to the Remuneration committee in August 2021 which will inform the paper to the Executive Team for support to continue or change the approach. TF asked if any initial feedback had been received. JM explained that early informal staff feedback was positive. JG thanked JM for the update and enquired whether she felt assured that everything that could be done is being done in line with requirements, whether there were any gaps that required work and whether the CCGs were carrying any risks. JM commented that there were no major issues with EPRR planning, the Pandemic response showed there were plans in place to cope in an emergency and the CCGs have a solid base to work from. JG also enquired how teams work together on Cyber Security. JM commented that as Cyber threats and security are ever evolving, it is something that will be continued to work on collaboratively. JG suggested it would be helpful for Cyber Security to be included in the next EPRR report. CL confirmed Cyber Security arrangements were currently under internal audit review and hoped to bring a report to the next ACIC meeting which would help inform discussions. The Audit Committee NOTED the Q1 EPRR update. Information Governance (IG) The Information Governance Team (IGT), hosted by NHS Basildon and Brentwood CCG on behalf of all CCGs in Essex, is made up of staff with expertise in Data Protection, Confidentiality, Records Management, Information Security and Freedom of Information. NS welcomed DSS to the Committee meeting who was standing in for the Information Governance Lead who had sent apologies. The Committee noted that all mid and south Essex CCGs had submitted their DSPT toolkits for 2020/21 on time and standards were met. NA extended thanks to the IG team for their support in completing to deadline.
132

VB enquired whether there is still a moratorium to respond to FOI requests within statutory time limits. NA clarified that following a recent discussion with the Information Governance lead, FOI requests should be treated as business as usual and that breaches were not acceptable to which MB and LB concurred. NA suggested that communications should be sent to all staff to ensure FOI requests are treated as business as usual and that breaches are not acceptable. IG Champions would work with the FOI Team and CCG staff to enforce this message. ACTION: Communications to be sent to all staff to remind that FOI requests are treated as business as usual and that breaches are not acceptable. JG asked for an update on the progress of GP and PCN Information Governance. DSS understood that all GP toolkits across the mid and south Essex area, except for two (in Mid Essex) were completed which was a great achievement and improvement on the previous year. The IG Team were working closely with PCNs and GPs to ensure GPs were compliant and processes in place. The Audit Committees NOTED the IG Quarter 4 2020/21 Report. 10:19 ET left the meeting. Mid Essex CCG remained quorate although there were no further decisions to make.
6. Internal Audit
Internal Audit Progress Report CL presented the Internal Audit Progress Report for the mid and south Essex CCGs. It was highlighted that the finalised Data Security and Protection Toolkit (DSPT) report had been issued to each of the CCGs and that work had commenced on Personal Health Budgets (PHB) reviews across all five CCGS, with draft reports issued to the Essex CCGs. It was expected that Mid would receive their report imminently and audit work continued in Thurrock. The final combined PHB report would be reported at the next ACiC meeting. The Cyber Security review was under way and the outcome of the review was expected to be reported at the next Audit CiC meeting in October 2021. For Q2, CL advised that Terms of Reference had been issued for the Adult Safeguarding Review and meetings had taken place with the Safeguarding Leads and Executive Director of Nursing. Terms of Reference had also been issued for the Equality and Diversity review, with the Thurrock NHS Alliance Director identified as lead. VB commented that the lead for the Primary Care Governance review should be noted as Jennifer Speller and that the lead for the Violence Prevention and Reduction Standards review should be with Governance rather than HR. CL noted this and confirmed that some initial governance conversations had taken place. CL presented the finalised DSPT report for the mid and south Essex CCGs, highlighting that all five CCGs had successfully completed the required declaration of compliance by the deadline of 30th June 2021. Overall, the outcome was a reasonable level of assurance with detailed findings and recommendations set out in the report. 10:34 RL left the meeting. CPR CCG remained quorate although there were no further decisions to make. CL advised there had been good engagement across the CCGs in providing status updates on the outstanding internal audit recommendations. DT confirmed that the outstanding recommendation for BB CCG had now been resolved and could be removed. The Committee noted there were no other overdue recommendations for the CCGs, however some had received revised implementation dates at the request of the CCGs.
133

The Audit Committees NOTED the Internal Audit Progress Report. LCFS and LSMS Progress Report CL presented the LCFS Report which outlined the counter fraud and security management work carried out since the last meeting. The report noted there had been two new referrals, one for Thurrock CCG and one for Southend CCG. Investigation found both cases related to GP surgeries and there was nothing further for Counter Fraud to investigate. TF enquired whether GP colleagues were supported in progressing the investigations. CL confirmed that the Counter Fraud Specialist had provided advice to the Practices and, for these cases, it was appropriate for the Practices to refer the matter to the authorities, e.g. the Police. CL reported that the findings of the significant Mid Essex CCG investigation had been discussed with the CFO and the case had been closed as new evidence had suggested there was no case to answer. Although not present at the meeting, CL advised that the Counter Fraud Specialist would be happy to discuss the investigation outcome further with members of the Mid Essex CCG Audit Committee at a separate meeting, if required. JG noted that a significant amount of time and effort had been involved on the investigation and asked whether there was any learning that had emerged. CL confirmed that, following an internal review, one of the key issues was to make sure all evidence streams were identified as soon as possible. In this case, records logged on the provider’s clinical system were the initial source of evidence, however issues with the quality of system data was an issue, therefore it was necessary to identify and refer to the primary source of evidence which in this case was written evidence. In respect of the Violence Prevention and Reduction Standards, CL advised there had been initial conversations around security management and how internal audit can support the implementation process. The plan was to undertake an audit later in the year to monitor compliance. VB reiterated that the response should be proportionate to the number of referrals received for the CCGs which was very low. NA confirmed she had met with the WMAS Security Management Specialist who confirmed that a pragmatic approach to the audit would be taken. PS highlighted the need to ensure that once staff begin to return to offices, they are aware of security procedures and must be up to date as there had recently been a security incident at the offices of CPR. NS extended thanks and appreciation to CL and his team for their continued hard work. The Audit Committees NOTED the LCFS and LSMS Progress Report
6. External Audit
EL confirmed that since the last Audit Committee annual accounts had been finalised and submitted for all mid and south Essex CCGs. EL apologised to the Committee for the delay in submitting finalised accounts due to unforeseen circumstances. EL explained that it was necessary for KPMG to install priority updates to its IT systems and infrastructure which caused some delay to the completion of the audit file documentation ahead of the original submission deadline. Consequently, additional time was required to complete work prior to the signing of audit opinions. KPMG kept NHSE/I and the mid and south Essex CFO informed of the delay and advised it was due to IT system updates and there were no issues with the audit process. In response, NHSE/I extended the submission deadline for CCGs to 18th June 2021. All MSE CCGs accounts were filed ahead of the revised deadline.
134

NS was grateful for the explanation to the Audit Committee for the delay in the annual report submission process. The Audit Committees NOTED the Combined mid and south Essex External Audit Progress update.
8. Risk Assurance
High Risk Medications NS welcomed SW to the meeting to provide assurance that the high-risk medications risk was being appropriately managed. SW advised Warfarin and disease-modifying anti-rheumatic drugs (DMARDS) no longer formed part of the GPs statutory remit and some GPs had given notice not to prescribe, therefore this had been identified as a red risk. As interim measures to address the issue, in Thurrock, a number of pharmacies signed up to a service to enable access to these drugs in a safe way until at least the end of this financial year and, in Southend, a number patients were being treated directly by Southend Hospital. SW advised that the Medicines Optimisations Team were working on a longer-term solution with clinical teams and commissioners across the system to provide a single specification provision at PCN level. TF commented that, given the complexity of the risk, the committee would like assurance that everything within the CCGs control is being done and outcomes were being achieved, whether there was anything to escalate, change or advise the Audit Committee. SW stated the aim was to identify a ‘one fit’ solution and to have a plan place by end of September 2021 which was the challenge. LB requested assurance from SW as to whether the risk reflected the whole area of high-risk medications or was just warfarin. SW commented that there would always be risk around high-risk medications that are not used often. SW explained that shared care was discussed at the last MSE Medicines Optimisation Committee where high-risk drugs are initiated within the hospital setting but can be continued in primary care. There are appropriate systems in place in primary care and pharmacies when prescribing specific drugs, warnings are displayed on systems flagging up high-risk medications. LB felt that more assurance was required in the area of medicines management as the Audit Committee received less information since the commencement of Medicine Optimisation meetings. SW agreed that place reporting was important to have and a key aspect of budgeting and would be discussed with Alliance Directors. LB felt assured that this was a work in progress. TF asked for assurance that, should SW be met with resistance in implementing any actions necessary to mitigate risks, that SW is aware of appropriate forums to escalate any issues. SW confirmed the Alliance Directors would be his point of escalation and understand the issues faced by the CCGs. NS thanked SW for providing the extra assurances to the Audit Committee around high-risk medications. The Audit Committees NOTED the assurance update around high-risk medications. Digital Transformation NS welcomed PK to the meeting. PK explained that when online consultations were introduced at the beginning the Pandemic, a one size fits all approach was used. It had become clear, however, that the system in use had limitations. PK advised that a review of all clinical systems was currently under way to ensure digital requirements were identified ahead of the imminent IT procurement process to ensure the right products are purchased for the right people. PK explained that online consultations were likely to be a risk for many NHS organisations.
135
Digital First Primary Care PK explained that the Digital First Primary Care risk was predominantly around resourcing. PK advised that, whilst funding was in place to recruit to the digital team and the recruitment process was underway, there was a limited resource pool which had impacted on the ability to recruit to the roles. Following the development of the Primary Care Strategy, a Digital Board had been established who had oversight of the digital risks. Additionally, there was a clinical subgroup plus links into the Primary Care Commissioning Committee which provided a wide range of visibility into the digital risks and mitigating actions across multiple groups and committees. MB enquired whether the level of risk could be quantified and, should there be problems recruiting, would there be an option to enlist the services of a recruitment agency who may have a wider pool of candidates. PK explained that job adverts were now closed with interviews scheduled for the following week, it was hoped successful candidates would commence posts in September. If recruitment was unsuccessful, the alternative plan was either to use a recruitment agency or re-evaluate the structure. PK acknowledged the current team was fairly small but very dynamic and recruitment was intended to enhance the primary care offer. JG enquired whether a test of patient experience of online services would be part of the team’s long-term strategy. PK confirmed it was and that although patient feedback so far had been positive, some GPs had raised concerns which confirmed the need for robust user engagement. TF enquired whether, should there be difficulties with recruitment to posts, this would have an impact on the risk around Digital First Primary Care. PK confirmed the risks were interlinked as part of the reason to expand the team was to enable a greater visibility on the ground in order to support the business change model. TF asked what Plan B would be should the mitigating actions for the Digital Transformation risk fail. PK explained there was a need to re-procure the online business solution because the contract was due to end. 11:17 NW left the meeting. It was noted that Mid Essex CCG was no longer quorate however there were no further decisions to make. TF and PK agreed to discuss what actions would be required to reduce the digital risks to green outside of the meeting. ACTION: Meeting to be arranged for TF and PK to discuss what actions would be required to reduce the digital risks to green. JG commented that as digitalisation is key to moving forward, was the organisation working effectively to assess how IT can help deliver its business agenda and whether this would be considered a risk. PK responded that the Pandemic response had highlighted how much IT and digital technology had been an enabler and agreed it should be flagged as a risk, however by way of assurance PK explained there was a huge amount of interaction with the CCGs keen to discuss digital transformation and digital technology, during organisation change it is important to recognise the options digital technology presents. PK advised the IT team were working with the audit team to conduct a second Cyber Security audit which will include home working.
9. Finance Assurance / Escalation (including Losses Waivers & Special Payments)
136

MB provided a verbal summary of Month 3 to the Audit CiC. Full Month 3 reports would be presented to the Finance & Performance Committees in Common on 21st July 2021. MB highlighted to the Committee that there had been some improvement on the system position performance for Month 3 which was mostly due to an accelerated elective recovery programme in earlier months which has helped secure a positive variance within MSEFT, however as there would be changes this may present some difficulties in the future. MB explained the investments and efficiencies programme was progressing at a slower pace than had been anticipated. MB also advised it may be difficult to deliver efficiencies at speed during the second half of the year if a further wave of Covid occurs. It is expected that 2022/23 would be a very tough year financially for the organisation. LB sought assurance that any potential financial bailouts across regions would be avoided by the organisation. LB advised that she intended to also raise this issue at the Finance and Performance Committee. MB said there had not been any discussions to indicate potential ‘bailouts’ however, if the situation did arise he would strongly resist. The Audit Committees NOTED the verbal Finance summary Waiver Report Following the last Audit Committee in Common there was discussion between the Audit Chairs and DCOs regarding the format and method of reporting waivers. There was agreement that, in liaison with both senior finance representatives and Audit Chairs, the report would be refined and developed to provide sufficient detail and assurance to members over the processes followed, both in individual CCGs, and across the STP patch. In total, there were 4 waivers approved since those reported to last Audit Committee in Common, for a total value of £2,858k. The Audit Committees NOTED the Waiver Paper. Losses and Special Payments MB advised there were no losses or special payments for any of the CCGs to report to the Audit Committees. The Audit Committees NOTED the update on losses and special payments.
8. For Information:
The following approved minutes of committee meetings were NOTED by the Audit Committees:
• Joint Committee – 20th May 2021
• Finance & Performance Committees in Common – 19th May 2021
9. Items to Escalate
There were no items to the BAF, Board or other Committees.
12. Any other Business
Urgent Decision taken by MECCG A decision was taken by the MECCG Audit Committee Members to increase the maximum sign off limit of the Joint CFO from £19.5m to £25m for two months only to enable urgent financial transfers to be made to MSEFT. The decision will be taken to the Mid Essex CCG Board for noting. Risk Management Policy
137

Audit Committee members agreed that the Risk Management Policy could be circulated virtually for approval. ACTION: Circulate the Risk Management Policy for virtual consideration and approval. Strategic Objectives The Audit chairs, NHS Alliance Directors and the wider Executive Team were engaged in drafting the strategic objectives which will go to July Boards for approval. New Appointments NA confirmed the following new appointments (commencing 3rd August 2021) that will affect the Audit Committee.
• Thurrock CCG and Mid Essex CCG appointed Pauline Stratford as the new Third Lay Member
• Thurrock CCG have appointed Dr Rachel Liebmann as Secondary Care Consultant
• Mid Essex CCG have appointed Julia Hale as Secondary Care Consultant (but she will not be a member of the Audit Committee).
The meeting finished at 12:00
Date of Next Meeting
15th October 2021
138

MINUTES OF THE PART I PRIMARY CARE COMMISSIONING
COMMITTEES OF BASILDON & BRENTWOOD, CASTLE POINT &
ROCHFORD, MID ESSEX, THURROCK AND SOUTHEND CCGs
MEETING IN COMMON
Held via MS Teams on 12 August 2021 at 2.00 pm – 3.30 pm
Members
Name Job Title/Position PCC Committee Quorate?
Pauline Stratford (PS) Lay Member and Lead PCCC Chair
CP&R and Southend CCGs
YES (4 members, including 1
Lay Member and 1 clinically qualified
member)
Vicky Cline (VC) – deputy for Rachel Hearn
Lead Nurse, Primary Care
CP&R and Southend CCGs
William Guy (WG) NHS Alliance Director, B&B CCG and SRO for Primary Care
CP&R and Southend CCGs
Mark Barker (MB) Joint Chief Finance Officer
CP&R and Southend CCGs
Patricia D’Orsi Alliance Director, SE Essex CCGs
CP&R and Southend CCGs
Janis Gibson (JGib) Lay Member CP&R and Southend CCGs
John Weir (JW) Independent GP CP&R and Southend CCGs
Nick Spenceley (NS) Lay Member Basildon & Brentwood CCG YES
(4 members, including 1 Lay Member and 1 clinically qualified
member)
Vicky Cline As above Basildon & Brentwood CCG
Mark Barker As above Basildon & Brentwood CCG
William Guy (WG) As above Basildon & Brentwood CCG
Julie Hale (JH) Secondary Care Consultant
Basildon & Brentwood CCG
Alan Hudson (AH) Lay Member and PCCC Chair
Thurrock CCG YES
4 members, including 1 Lay Member and 1 clinically qualified
member)
Lesley Buckland (LB) Lay Member Thurrock CCG
Rahul Chaudhuri (RC) Interim Deputy Alliance Director
Thurrock CCG
William Guy (WG) As above Thurrock CCG
Vicky Cline As above Thurrock CCG
Mark Barker As above
Nathalie Wright (NW) Lay Member and PCCC Chair
Mid Essex CCG YES
(4 members, one of which must be
Chair/Deputy Chair)
John Gilham (JGil) Lay member Mid Essex CCG
Vicky Cline As above Mid Essex CCG
Mark Barker As above Mid Essex CCG
William Guy (WG) As above Mid Essex CCG
In Attendance
Name Job Title/Position Organisation Quorate?
Jenni Speller (JS) Deputy Director, Primary Care
MSE CCGs N/A
Viv Barnes (VB) Governance Lead Mid Essex CCG N/A
Charlotte Tannett (CT) Minute Taker Mid Essex CCG N/A
Ashley King NHS Alliance Finance Director
M&SE CCGs N/A
139

Adam Townsend (AT) Head of Contracts Mid Essex CCG N/A
Elaine Roe (ER) Contract Manager, Mid & South Essex
NHSE England/Improvement N/A
Sarah Cansell (SC) Contracting Support Manager
NHS England/Improvement N/A
Robert Evans (RE) Head of Operational Primary Care
Mid Essex CCG N/A
Boye Tayo (BT) CCG Chair B&B CCG N/A
Julie McGeachy (JM) GP Board Member Mid Essex CCG N/A
Rajan Mohlie (RM) GP Board Member Thurrock CCG N/A
Anil Kallil (AKil) CCG Chair Thurrock CCG N/A
Romi Bose (RB) Head of Primary Care
Thurrock CCG N/A
Peter King Associate Director, IT / Digital
MSE CCGs N/A
Kerry Harding Estates Director MSE CCGs N/A
Owen Richards (OR) Observer Southend Healthwatch N/A
Mariam Zbadi Member of the Public
Yext Public Sector Team N/A
Apologies from members
Rachel Hearn (RH) Executive Director of Nursing & Quality
MSE CCGs N/A
Gill Jones (GJ) Lay Member Basildon & Brentwood CCGs N/A
Katherine Kirk (KK) Lay member and PCC Chair
Basildon & Brentwood CCGs N/A
Dan Doherty (DD) NHS Alliance Director, Mid Essex
MSE CCGs N/A
Mark Tebbs (MT) NHS Alliance Director, Thurrock
MSE CCGs N/A
ITEM SUBJECT
Committee Administration
1.
2.
3.
Roll Call and Quoracy Check VB performed a roll call of those in attendance. Apologies were noted. VB confirmed that any members who had been unable to attend the meeting would be contacted after the meeting and asked to endorse any items where quoracy was needed for a decision. Declarations of Interest
• RM declared he was registered with Orsett Surgery.
• NS declared he was registered at Blackwater Medical Centre.
• BT declared he was registered at Southend Medical Centre. Minutes of Primary Care Commissioning Committees in Common held on 10 June 2021 The minutes of the meeting held on 10 June 2021 were approved with no amendments.
140

ITEM SUBJECT
4.
The Action log was reviewed and updates were provided. Resolved: The PCC Committees meeting in common:
• Approved the minutes of Primary Care Commissioning Committees in Common held on 10 June 2021; and
• Noted the Action Log Questions from the Public Mariam Zbadi from the Yext Public Sector Team submitted a written question asking to be put in touch with the relevant CCG team to discuss the services that Yext could provide to improve online user experience. VB agreed to follow this up with colleagues outside of the meeting. [Action: VB to forward request to IT/Digital team.}
Items for Decision/Discussion
5.
Primary Care Contracts Update JS summarised the report and highlighted that since 1 April 2021 several applications for variations to contracts had been received relating to partnership changes. Where applications had resulted in no change to contract status, they had been approved by CCG officers and were being reported to the committee for noting. Two applications received relating to Island Surgery (Canvey) and the Southend Road Surgery (Stanford-le-Hope) had resulted in a change of contract status and approval had been received via the relevant committee in each case. A signed variation of contract was yet to be returned from Purfleet Care Centre to confirm an extension to their APMS contract from 01/07/21 to 30/06/22 with an option to extend for a further 12 months. This had been requested from Virgin Care Services with a deadline of 6 August 2021. A new 12-month contract had been awarded for North Shoebury Surgery following the death of the previous contract holder. Arrangements were in place for use of the premises for this period and work was underway to support providers. In addition to the above local contract updates, Jenni provided a briefing covering the following issues:
• All practices had now submitted their Annual eDeclaration for 2020. Work was underway to analyse the results and determine next steps.
• All but one Mid and South Essex (MSE) practices had declared achievement with the Quality and Outcomes Framework (QOF).
• All 149 MSE practices were now signed up to the Primary Care Network (PCN) Network Direct Enhanced Services (DES).
• Weight Management and Long COVID Enhanced Services had been established with all MSE practices having been invited to sign up with a deadline of 30 July 2021. 17 practices had yet to respond as at 4 August 2021 and were being followed up by the CCG.
• Locally Commissioned Services (including Multiple Community Services) contractual arrangements across MSE had been extended for current financial year and work had commenced to determine commissioning intentions post April 2022.
141

ITEM SUBJECT
• A recovery action plan had been put in place to support increased performance of the PCN recruitment programme. The annual workforce planning exercise was underway with PCNs to review their intentions for this financial year and their proposals for following years.
• The COVID-19 (C-19) pandemic continued to have a significant impact on demand for Primary Medical Services across the country. Locally work was underway to confirm sign up to Phase 3 of the Covid-19 Vaccination Programme which was due to commence from 1 September 2021.
• A new contract had been awarded to Commisceo PCS Ltd for the MSE Special Allocation Service (SAS) from 1 April 2021 with 80 MSE patients on the scheme as at 4 August 2021.
• A contract award following the regional procurement for Translation and Interpreting services was expected shortly.
PD queried if 100% of practices had signed up to the Learning Disability (LD) Annual Health Check DES. SC confirmed she would confirm the position outside of the meeting. JGib noted that some community groups had funding to support vaccination and resident and patient care during Phase 3 of the vaccination programme. JS stated she was aware of this funding and work was underway to connect the funding within the system. LB noted that the lack of PCN recruitment was disappointing and asked for further information on the MSE SAS. JS advised that the SAS was a scheme for patients who had been excluded from general practice, usually due to violent behaviour. The scheme allowed for primary care services to be delivered in a secure setting for a period while work was done with individuals to enable them to re-join a GP patient list. JGil queried how the supply and demand on PCN recruitment was being calculated. JS confirmed practices received an allocation of funding based upon their population and the contract holder would then determine the staff and skill mix required. This resulted in a significant amount of variation between practices in terms of their identified recruitment needs. BT highlighted there might be a lack of awareness of the MSE SAS within practices. BT added that the committee should be clear about the difficulties being experienced with PCN recruitment and that the funding available did not always cover the cost of the required posts. JS confirmed if it was felt there was a lack of awareness amongst practices of the SAS, details of the service could be redistributed to ensure its existence was well known. JS stated that the issues impacting upon PCN recruitment were not purely financial and practices had flagged many other contributing factors. OR queried if there was a way for Healthwatch and the CCGs to work together to better deliver the message to the public that over 60% of all GP appointments were face to face. JS stated communication around primary care continued to be challenging and welcomed the support of Healthwatch in getting the correct message out to the public. JS stated she would ensure the CCGs’ communications team continued to link with Healthwatch on the matter. AKil highlighted the difficulty for PCNs to accommodate extra staff into their current premises. JS confirmed that premises were one of issues reported by PCNs as inhibiting recruitment and a role had been created to work with the estates and primary care teams and PCNs to develop plans to tackle the issue. Unfortunately recruitment to this role had so far been unsuccessful. AH queried if the ability to book forward appointments might alleviate some of the concerns about appointment availability. PD explained that this would increase the risk of ‘Did Not Attends’ which would heighten the pressures on the system.
142

ITEM SUBJECT
6.
RC highlighted GP premises were physically unable to accommodate additional bodies, even on a shared rotational basis, therefore it was important for commissioners to work with PCNs and Clinical Directors to find a solution. Resolved: The Primary Care Commissioning Committee noted the Primary Care Contracts update. [Action: SC to provide data to PD on how many MSE practices have signed up to the LD Annual Health Check DES]. Primary Care Quality and Safety Report VC summarised the report and highlighted that 7 practices in mid and south Essex had been rated by the Care Quality Commission (CQC) as either inadequate or requiring improvement. However, the inspection report for the Carnarvon Medical Centre (Southend) had recently been published and its rating revised from Inadequate to Good. For the month of May 2021 452,835 appointments were offered within primary care, 271,000 of which were face to face appointments. Online/Video appointments and home visits were also included within this total. Face to face appointments currently accounted for 56% of all appointments offered nationally, whereas this figure across MSE was 60%. The Practice Risk Review Group meetings were ongoing, at which 11 practices had been rated as Red, 19 as Amber and 120 as Green. Practices rated at Red had been identified as requiring support from the Primary Care quality team. A meeting had been held with the quality and safety teams of the CCGs and NHSE/I Heads of Nursing at which it was agreed to develop a plan to ensure that primary care incidents were being logged appropriately and themes and trends would be shared through the GP bulletin. The Primary Care quality team also continued to work with the governance teams to ensure that responses to complaints and concerns were available for patients. All formal Primary Care complaints continued to be monitored by NHSE/I. Links to the CQC reports for the Rigg Milner surgery in East Tilbury (rated Inadequate) and Dr M Aslam’s practice in Basildon (rated Good) were provided on page 48 of the papers. PD thanked VC for her report and congratulated her on Carnarvon Medical Centre’s improved CQC rating. PD highlighted that according to the access data on page 47 of the report, Castle Point & Rochford CCG (CPR CCG) appeared to have carried out zero home visits for the month of May 2021. JS stated that NHS Digital had published the access data with a caveat around data quality due to the various ways that practices coded their appointment data. Practices had recently all completed a national data mapping exercise designed to improve consistency of how appointments were reported and to improve data quality. This would allow for better benchmarking to inform service planning and improvement. JGib noted that the access data did not support practices in their messaging to the public about the availability of appointments. JS confirmed there was a publicly available description from NHS Digital about the caveats to the data quality. LB noted the importance of including the patient population size for each CCG when providing future reports on appointment availability.
143

ITEM SUBJECT
7.
BT highlighted that the access data from Basildon & Brentwood also appeared to be incorrect and queried how the practices rated as Outstanding by the CQC might be better celebrated to encourage other practices to aspire to a higher rating. Resolved: The PCC Committees meeting in common noted the Primary Care Quality report. Primary Care Finance Report MB summarised the report and highlighted the Month 3 position and assumptions. The MSE CCGs had only been advised of allocations for the first half of the year. Whilst this could be reconciled back to previously published primary care allocations, there was a risk that Half 2 allocations received would be lower than anticipated. The financial forecasting included in report and used to set the budgets assumed a Half 2 allocation equal to Half 1 and an even profile of expenditure across the year. CCG allocations did not include the full funding requirement for the entitlements PCNs had under the Additional Roles Reimbursement Scheme with 45% of this allocation retained by NHSE/I. Should a CCG see their PCN claims collectively exceed the 55% included in the baselines, they could claim the balance from NHSE/I. Budgets had been set in accordance with the contractual entitlements of practices and PCNs and historic spend levels for other financial entitlements, including locally utilised transformation funding. Adjustments had been made where contractual changes had come into force from 1 April 2021. Where there was a balance between the assumed Full Year allocation and budgets, this had been placed in a general reserve. For Mid Essex CCG where budgets exceeded anticipated allocations this was represented as a negative impact on reserve that would need to be addressed as a system in line with the financial framework that CCGs were currently operating under. The CCGs were currently reporting minor variations in the year to date position whilst forecasting a Half 1 breakeven position for each organisation. The CCGs were reliant on the NHSE/I finance team for financial support for the delegated budgets and with three of the five CCGs only taking on full delegation from April 2021, local knowledge was limited. Capacity issues including staff turnover within the NHSE/I team had been identified as a risk and discussions are underway as to how this would be mitigated. JGib queried the variance in ‘Other’ expenditure for CPR CCG in the data shown on page 58 of the report. MB stated there was no project or transformation scheme that would pinpoint the additional expenditure in comparison to the other CCGs, however he would investigate this further outside of the meeting. LB stated she would like assurances around the financial risk to Thurrock CCG detailed within the report. MB confirmed he was happy to discuss this further outside of the meeting. BT queried asked what the purpose was of the ‘Care Homes Premium’ referenced in page 52 of the papers. MB believed it related to the Network DES payments but advised that he would explore this further and report back. PS queried if the risks highlighted within the report were recorded on the Board Assurance Framework (BAF) and being managed through this route. MB confirmed he would look into this
144

ITEM SUBJECT
8.
9.
outside of the meeting but noted the risk to whether planning was being made on the correct set of assumptions should be noted and recognised by the committee. Resolved: The PCC Committees meeting in common noted the Primary Care Finance Report. [Action: MB to advise JGib of the reasons for the variance in ‘Other’ expenditure in Month 3 data for CPR CCG.] [Action: MB and LB to discuss the Thurrock CCG financial risk.] [Action: MB to explain the purpose of the ‘Care Homes Premium’.] [Action: MB to explore if the current financial risks relating to primary care are recorded on the BAF]. Primary Care IT and Digital Report PK summarised the report and highlighted that offers had been made against three vacant roles with the IT/Digital team following a challenging recruitment process. The Clinical System Review had been signed off by the Joint Procurement Committee and work had commenced on engagement with primary care. A final report was due to be submitted on 30 September 2021. LB asked for clarification where the Joint Procurement Committee fitted into the MSE CCGs’ governance arrangements. VB confirmed she would explore this outside of the meeting. JGil queried how Artificial Intelligence (AI) would be used to maximise IT to enable better access to services. PK confirmed one of the online consultation systems made use of AI for triage, however nationally and regionally the uptake of online consultations was low. Resolved: The PCC Committees meeting in common noted the Primary Care IT and Digital Report. [Action: VB to seek clarification of the role of the Joint Procurement Committee within the MSE CCGs’ governance arrangements.] Primary Care Estates Report KH summarised the report and highlighted that the Gore Surgery premises had been handed back and the practice was now operating from the George Hurd Centre. The project had since been de-commissioned. The team had met with the Beaulieu Park developers where some positive discussions had taken place regarding the progress of the project. A timeline from developers for completion of the project was expected imminently. KH highlighted that the report contained only those projects where progress had recently been made and asked for the committee’s feedback on the content of future reports. PS stated it would be helpful to see progress against all ongoing projects within future reports as this would link into ongoing discussions around premises within primary care.
145

ITEM SUBJECT
10.
PS asked about the membership of the Health and Care Partnership (HCP) Primary Care Estates Sub Group and the HCP Strategic Estates Group and if there was appropriate lay member and GP representation. KH confirmed she would share the Terms of Reference for both groups with the committee. OR confirmed he would find it useful to have a full list of projects to assist with queries received from the public. NS confirmed he was in support of a longer report referencing all projects. KH confirmed she would develop a report together with a notes section to provide updates on each project. KH added that the HCP Estates Strategy was now in final draft and offered more information on the work being undertaken as well as strategic work moving forward which should provide additional assurance. JS stated she had queried with governance teams if a map of the various groups and sub-groups related to primary care might be developed to help the committee better understand how they were linked. JGib highlighted that she had attended several HCP Estates Group meetings and the estates team had been extremely helpful in resolving any issues raised. Resolved: The Primary Care Commissioning Committee noted the Primary Care Estates Report. [Action: KH to share the Terms of Reference of the HCP Primary Care Estates Sub Group and the HCP Strategic Estates Group with the committee.] [Action: KH to expand report to include all ongoing estates projects for future committee meetings.] Part II / Virtual Decisions VB confirmed that at the last Part II confidential meeting the relevant CCG Primary Care Commissioning Committees made the following decisions which could now be reported in public:
• The Mid Essex Primary Care Commissioning Committee upheld an appeal from the Blandford Medical Practice and approved the practice’s request to temporarily close its patient list for a period of 6 months, with an option to seek an extension beyond this time if required.
• The Mid Essex Primary Care Commissioning Committee approved a request from Dr Chandralingam of the Collingwood Road practice to form a partnership with Dr Reshma Rasheed and Dr Alyn Williams with effect from 1 October 2021.
• The Southend Primary Care Commissioning Committee approved the issue of a short-term GMS contract to North Shoebury Surgery to allow time for full consideration of the long-term options for the area following the sad death in service of Dr Paul Moss.
These decisions had been communicated to the practices for onward dissemination to their patients as appropriate. The following urgent decisions had been taken by the relevant CCG Primary Care Commissioning Committees since the last meeting:
146

ITEM SUBJECT
11.
12.
13.
• The Castlepoint & Rochford Primary Care Commissioning Committee approved a request from Dr Linacero-Gracia of the Island Surgery, Central Canvey Primary Care Centre, to form a partnership with the practice and business manager, Jackie Brown, as a non GP partner with effect from 1 August 2021.
• The Thurrock Primary Care Commissioning Committee approved a request from Dr Deshpande of the Southend Road Surgery, Stanford-le-Hope, to form a partnership with Dr Esi Folson with effect from 1 July 2021.
Resolved: The Primary Care Commissioning Committee noted the Part II/Virtual Decisions. Any Other Business There was no other business. Items for Escalation/Future Agenda Items None. Date and time of Next Meeting 14 October 2021, 2.00 – 3.30 pm, via MS Teams.
147




















