
Isothermal crystallization kinetics of poly(lactic acid)/synthetic mica nanocomposites
Upload
univ-paris7Category
view
1download
0
doi:10.1182/blood-2009-04-217430Prepublished online September 28, 2009;2009 114: 5216-5224
TamouzaGluckman, Rajagopal Krishnamoorthy, Antoine Toubert, Dominique Charron, Gérard Socié and RyadDjaouida Bengoufa, Nicolas Dulphy, Philippe Haas, Catherine Scieux, Habiba Amroun, Eliane Wahid Boukouaci, Marc Busson, Régis Peffault de Latour, Vanderson Rocha, Caroline Suberbielle, biomarkers of chronic graft-versus-host diseaseMICA-129 genotype, soluble MICA, and anti-MICA antibodies as
http://bloodjournal.hematologylibrary.org/content/114/25/5216.full.htmlUpdated information and services can be found at:
(1877 articles)Transplantation � (1722 articles)Free Research Articles �
Articles on similar topics can be found in the following Blood collections
http://bloodjournal.hematologylibrary.org/site/misc/rights.xhtml#repub_requestsInformation about reproducing this article in parts or in its entirety may be found online at:
http://bloodjournal.hematologylibrary.org/site/misc/rights.xhtml#reprintsInformation about ordering reprints may be found online at:
http://bloodjournal.hematologylibrary.org/site/subscriptions/index.xhtmlInformation about subscriptions and ASH membership may be found online at:
Copyright 2011 by The American Society of Hematology; all rights reserved.Washington DC 20036.by the American Society of Hematology, 2021 L St, NW, Suite 900, Blood (print ISSN 0006-4971, online ISSN 1528-0020), is published weekly
For personal use only. by guest on May 29, 2013. bloodjournal.hematologylibrary.orgFrom

TRANSPLANTATION
MICA-129 genotype, soluble MICA, and anti-MICA antibodies as biomarkers ofchronic graft-versus-host disease*Wahid Boukouaci,1 *Marc Busson,1 Regis Peffault de Latour,2 Vanderson Rocha,2 Caroline Suberbielle,1
Djaouida Bengoufa,1 Nicolas Dulphy,1 Philippe Haas,1 Catherine Scieux,3 Habiba Amroun,1 Eliane Gluckman,2
Rajagopal Krishnamoorthy,4 Antoine Toubert,1 Dominique Charron,1 Gerard Socie,2,5 and Ryad Tamouza1
1Laboratoire d’Immunologie et d’Histocompatibilite, Centre d’Innovations Biomedicales–Hematologie/Oncologie/Greffe (CIB-HOG), AssistancePublique-Hopitaux de Paris/Groupement Hospitalier et Universitaire (AP-HP/GHU)–Nord, Institut Universitaire d’Hematologie (IUH), and Inserm, UMRS, 940,Hopital Saint-Louis, Paris; 2Service d’Hematologie–Greffe de Moelle, Hopital Saint-Louis, Paris; 3Service de Virologie, Hopital Saint-Louis, Paris; 4Inserm, U763,Hopital Robert Debre, Paris; and 5Inserm, U728, Institut Universitaire d’Hematologie, Hopital Saint-Louis, Paris, France
The MHC class I–related chain A (MICA)molecules exist as membrane-bound andsoluble isoforms and are encoded by apolymorphic gene. Their genetic and phe-notype characteristics have been studiedin various pathologic settings but not inthe context of hematopoietic stem celltransplantation (HSCT). Here, we evalu-ated whether MICA-related featuresnamely MICA-129 gene polymorphism, se-rum levels of soluble MICA (sMICA) andanti-MICA antibodies (MICA Abs) before
and after HSCT could influence the inci-dence of chronic graft-versus-host dis-ease (cGVHD) and relapse of their dis-ease in 211 HLA-identical sibling pairsand in a subset of 116 recipients, respec-tively. Although the MICA-129 val/val ge-notype and elevated sMICA serum levelsafter HSCT are independently associatedwith the incidence of cGVHD (P � .002and .001) regardless of history of acuteGVHD, the presence of MICA Abs beforetransplantation confers protection against
cGVHD (P � .04). There is an inverse rela-tionship between MICA Abs and sMICA,suggesting an antibody-based neutraliza-tion of deleterious effects of sMICA. Simi-larly, these genetic and phenotype charac-teristics of MICA influence the incidenceof relapse. Altogether, these data suggestthat the studied MICA genotype and phe-notype specificities could be used asrelevant biomarkers for cGVHD monitor-ing. (Blood. 2009;114:5216-5224)
Introduction
Chronic graft-versus-host disease (cGVHD) is a long-term andoften life-threatening complication affecting 25% to 80% ofpatients surviving 3 months after hematopoietic stem cell transplan-tation (HSCT)1,2 and can occur after the acute form or de novo.3,4
On the basis of its clinical and biologic features, cGVHD is viewedas a disorder of alloimmune and autoimmune systems.5-7 Becausepredictive biomarkers for an impending cGVHD must allow timelyimplementation of effective prophylactic measures, a variety ofgenetic and phenotype markers were explored.8-11 In this regard,the MHC class I–related chain A (MICA) molecules are of par-ticular interest given their participation in non–T cell receptor–mediated immune function.12,13 MICA rather engages NKG2D, aC-type lectin expressed on effector cells, including natural killer(NK), ��- and ��-T cells.14 Such engagement triggers NK cellsand costimulates T lymphocytes to mount adequate immune re-sponse. Further, a soluble isoform of MICA (sMICA), resultingfrom the proteolytic shedding of the membrane-bound molecules,was implicated in the pathogenesis of a variety of cancers,autoimmune, and other organ transplant-related disorders throughNKG2D receptor down-regulation.15-18 The ensuing immune es-cape highlights the functional duality of the membrane-bound andsoluble MICA isoforms. Although MICA expression, induced bycellular stress, was initially considered to be restricted to gastroin-testinal epithelium and epithelial tumors, a more ubiquitousexpression was latter shown, at least at the transcriptional level.19
Functionally relevant polymorphism of the MICA gene (with morethan 60 alleles reported to date)20 may also contribute to interpa-tient variability in alloimmune responses as observed in variousclinical settings, including organ transplantation.21 Interestingly, amethionine (met) to valine (val) change at position 129 of the�2-heavy chain domain categorized the MICA alleles into strong(MICA-129 met) and weak (MICA-129 val) binders of NKG2Dreceptor.22 Recently, we have shown that the MICA-129 dimor-phism could influence the incidence of early onset ankylosingspondylitis (AS)23 and nasopharyngeal cancer (NPC).24
Given the demonstrated importance of MICA in immunepathways, in this study, we explored the MICA-related parametersnamely MICA-129 gene polymorphism, serum levels of sMICAand anti-MICA antibodies (MICA Abs) before and after HSCT in aHLA-matched sibling HSCT setting as potential predictive biomar-kers of cGVHD.
Methods
Study population
Two hundred eleven consecutive patients who underwent non–T cell–depleted allogeneic HSCT, between January 1994 and January 2002 in theBone Marrow Transplant Department of Saint Louis Hospital, Paris,France, were included in this study. Among them, 146 received bone
Submitted April 20, 2009; accepted September 2, 2009. Prepublished online asBlood First Edition paper, September 28, 2009; DOI 10.1182/ blood-2009-04-217430.
*W.B. and M.B. contributed equally to this study.
The publication costs of this article were defrayed in part by page chargepayment. Therefore, and solely to indicate this fact, this article is herebymarked ‘‘advertisement’’ in accordance with 18 USC section 1734.
© 2009 by The American Society of Hematology
5216 BLOOD, 10 DECEMBER 2009 � VOLUME 114, NUMBER 25
For personal use only. by guest on May 29, 2013. bloodjournal.hematologylibrary.orgFrom
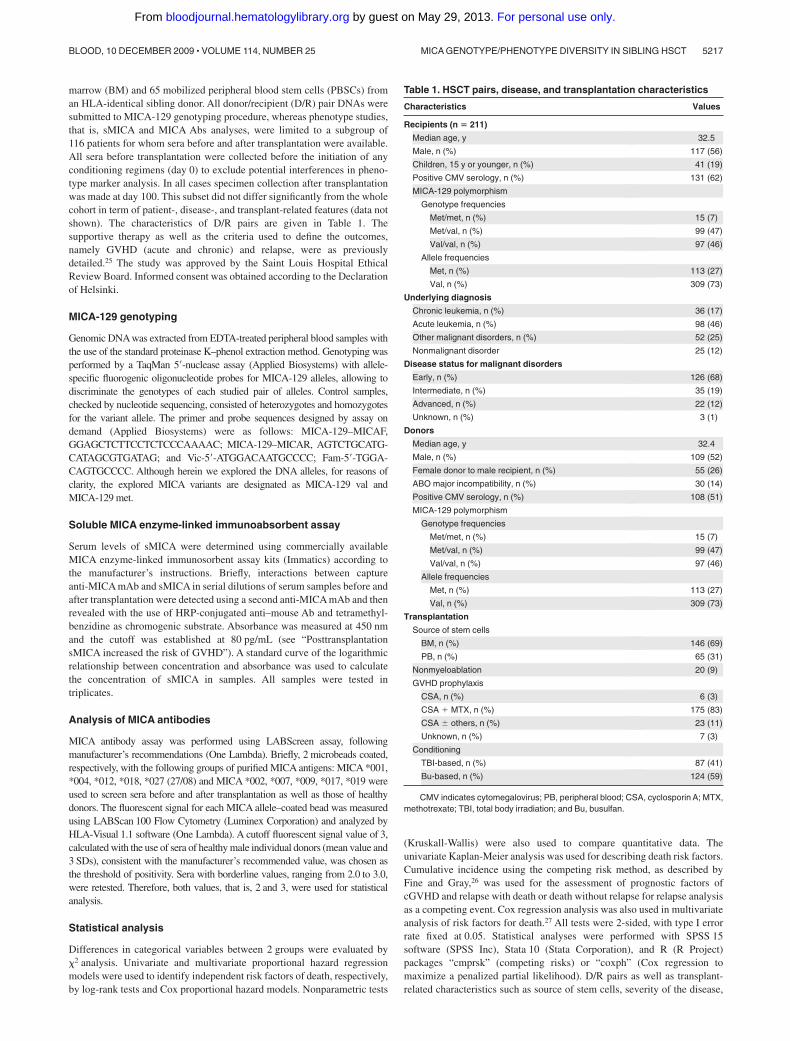
marrow (BM) and 65 mobilized peripheral blood stem cells (PBSCs) froman HLA-identical sibling donor. All donor/recipient (D/R) pair DNAs weresubmitted to MICA-129 genotyping procedure, whereas phenotype studies,that is, sMICA and MICA Abs analyses, were limited to a subgroup of116 patients for whom sera before and after transplantation were available.All sera before transplantation were collected before the initiation of anyconditioning regimens (day 0) to exclude potential interferences in pheno-type marker analysis. In all cases specimen collection after transplantationwas made at day 100. This subset did not differ significantly from the wholecohort in term of patient-, disease-, and transplant-related features (data notshown). The characteristics of D/R pairs are given in Table 1. Thesupportive therapy as well as the criteria used to define the outcomes,namely GVHD (acute and chronic) and relapse, were as previouslydetailed.25 The study was approved by the Saint Louis Hospital EthicalReview Board. Informed consent was obtained according to the Declarationof Helsinki.
MICA-129 genotyping
Genomic DNA was extracted from EDTA-treated peripheral blood samples withthe use of the standard proteinase K–phenol extraction method. Genotyping wasperformed by a TaqMan 5�-nuclease assay (Applied Biosystems) with allele-specific fluorogenic oligonucleotide probes for MICA-129 alleles, allowing todiscriminate the genotypes of each studied pair of alleles. Control samples,checked by nucleotide sequencing, consisted of heterozygotes and homozygotesfor the variant allele. The primer and probe sequences designed by assay ondemand (Applied Biosystems) were as follows: MICA-129–MICAF,GGAGCTCTTCCTCTCCCAAAAC; MICA-129–MICAR, AGTCTGCATG-CATAGCGTGATAG; and Vic-5�-ATGGACAATGCCCC; Fam-5�-TGGA-CAGTGCCCC. Although herein we explored the DNA alleles, for reasons ofclarity, the explored MICA variants are designated as MICA-129 val andMICA-129 met.
Soluble MICA enzyme-linked immunoabsorbent assay
Serum levels of sMICA were determined using commercially availableMICA enzyme-linked immunosorbent assay kits (Immatics) according tothe manufacturer’s instructions. Briefly, interactions between captureanti-MICA mAb and sMICA in serial dilutions of serum samples before andafter transplantation were detected using a second anti-MICA mAb and thenrevealed with the use of HRP-conjugated anti–mouse Ab and tetramethyl-benzidine as chromogenic substrate. Absorbance was measured at 450 nmand the cutoff was established at 80 pg/mL (see “PosttransplantationsMICA increased the risk of GVHD”). A standard curve of the logarithmicrelationship between concentration and absorbance was used to calculatethe concentration of sMICA in samples. All samples were tested intriplicates.
Analysis of MICA antibodies
MICA antibody assay was performed using LABScreen assay, followingmanufacturer’s recommendations (One Lambda). Briefly, 2 microbeads coated,respectively, with the following groups of purified MICA antigens: MICA *001,*004, *012, *018, *027 (27/08) and MICA *002, *007, *009, *017, *019 wereused to screen sera before and after transplantation as well as those of healthydonors. The fluorescent signal for each MICA allele–coated bead was measuredusing LABScan 100 Flow Cytometry (Luminex Corporation) and analyzed byHLA-Visual 1.1 software (One Lambda). A cutoff fluorescent signal value of 3,calculated with the use of sera of healthy male individual donors (mean value and3 SDs), consistent with the manufacturer’s recommended value, was chosen asthe threshold of positivity. Sera with borderline values, ranging from 2.0 to 3.0,were retested. Therefore, both values, that is, 2 and 3, were used for statisticalanalysis.
Statistical analysis
Differences in categorical variables between 2 groups were evaluated by�2 analysis. Univariate and multivariate proportional hazard regressionmodels were used to identify independent risk factors of death, respectively,by log-rank tests and Cox proportional hazard models. Nonparametric tests
(Kruskall-Wallis) were also used to compare quantitative data. Theunivariate Kaplan-Meier analysis was used for describing death risk factors.Cumulative incidence using the competing risk method, as described byFine and Gray,26 was used for the assessment of prognostic factors ofcGVHD and relapse with death or death without relapse for relapse analysisas a competing event. Cox regression analysis was also used in multivariateanalysis of risk factors for death.27 All tests were 2-sided, with type I errorrate fixed at 0.05. Statistical analyses were performed with SPSS 15software (SPSS Inc), Stata 10 (Stata Corporation), and R (R Project)packages “cmprsk” (competing risks) or “coxph” (Cox regression tomaximize a penalized partial likelihood). D/R pairs as well as transplant-related characteristics such as source of stem cells, severity of the disease,
Table 1. HSCT pairs, disease, and transplantation characteristics
Characteristics Values
Recipients (n � 211)
Median age, y 32.5
Male, n (%) 117 (56)
Children, 15 y or younger, n (%) 41 (19)
Positive CMV serology, n (%) 131 (62)
MICA-129 polymorphism
Genotype frequencies
Met/met, n (%) 15 (7)
Met/val, n (%) 99 (47)
Val/val, n (%) 97 (46)
Allele frequencies
Met, n (%) 113 (27)
Val, n (%) 309 (73)
Underlying diagnosis
Chronic leukemia, n (%) 36 (17)
Acute leukemia, n (%) 98 (46)
Other malignant disorders, n (%) 52 (25)
Nonmalignant disorder 25 (12)
Disease status for malignant disorders
Early, n (%) 126 (68)
Intermediate, n (%) 35 (19)
Advanced, n (%) 22 (12)
Unknown, n (%) 3 (1)
Donors
Median age, y 32.4
Male, n (%) 109 (52)
Female donor to male recipient, n (%) 55 (26)
ABO major incompatibility, n (%) 30 (14)
Positive CMV serology, n (%) 108 (51)
MICA-129 polymorphism
Genotype frequencies
Met/met, n (%) 15 (7)
Met/val, n (%) 99 (47)
Val/val, n (%) 97 (46)
Allele frequencies
Met, n (%) 113 (27)
Val, n (%) 309 (73)
Transplantation
Source of stem cells
BM, n (%) 146 (69)
PB, n (%) 65 (31)
Nonmyeloablation 20 (9)
GVHD prophylaxis
CSA, n (%) 6 (3)
CSA � MTX, n (%) 175 (83)
CSA � others, n (%) 23 (11)
Unknown, n (%) 7 (3)
Conditioning
TBI-based, n (%) 87 (41)
Bu-based, n (%) 124 (59)
CMV indicates cytomegalovirus; PB, peripheral blood; CSA, cyclosporin A; MTX,methotrexate; TBI, total body irradiation; and Bu, busulfan.
MICA GENOTYPE/PHENOTYPE DIVERSITY IN SIBLING HSCT 5217BLOOD, 10 DECEMBER 2009 � VOLUME 114, NUMBER 25
For personal use only. by guest on May 29, 2013. bloodjournal.hematologylibrary.orgFrom

conditioning regimen, D/R age and sex, and CMV serology that couldpotentially influence the outcomes after HSCT were evaluated in all pairs.Those that were found significantly associated with cGVHD or relapse byunivariate analysis (P .05) were further included in the multivariateanalysis involving MICA-related variables.
Results
Chronic graft-versus-host disease
Recipient MICA-129 val/val genotype is a risk factor for cGVHD.A total of 211 patient and donor pairs were typed for MICA-129alleles. As expected, the sibling pairs fully matched for MICA-129 alleles and genotypes. The observed overall frequencieswere as follows: MICA-129 val, 308 (73%) of 422; MICA-129met, 113 (27%) of 422; MICA-129 met/met, 15 (7%) of 211;MICA-129 met/val, 99 (47%) of 211; MICA-129 val/val,97 (46%) of 211.
In our study group, 100 patients experienced cGVHD (47%)with a cumulative incidence of 53% at 3 years. Sixty-two of themdeveloped an extensive form. The onset of cGVHD was within thefirst year in 86% of cases ( 6 months, 48%; 6-11 months, 38%)and latter in 14% (12-17 months, 5%; 18-23 months, 4%; and 23 months, 5%). These patients were categorized as follows:early onset (3-8 months after HSCT; 80%) and late onset( 9 months; 20%).
Univariate analysis using competing risk showed that MICA-129 val/val genotype is more frequent in patients who experiencedcGVHD without reaching significance. Because the susceptibilitystatus seemed to be dose dependent (Figure 1A), we analyzed thepredictive effect of the MICA-129 val/val genotype versus othersand found that patients bearing the MICA-129 val/val genotypewere at a higher risk of developing cGVHD (63% vs 45% at3 years; P � .03; Figure 1B). These data were further confirmed inmultivariate analysis adjusted for confounding variables. Three fac-tors reached significance: recipient MICA-129 val/val genotype(HR, 1.52; 95% confidence interval [CI] 95%, 1.02-2.24; P � .04),older recipient age (� 15 years; HR, 3.36; 95% CI, 1.65-6.84;P � .001), and source of stem cells (PBSCs vs BM; HR, 1.67; 95%CI, 1.10-2.53; P � .017). Because acute GVHD (aGVHD) is amajor risk factor for subsequent cGVHD, we then introducedaGVHD as a time-dependent covariate in the multivariate analysismodel. This analysis confirmed that the risk conferred by theMICA-129 val/val genotype is independent from aGVHD [thefactors found to increase independently the risk of cGVHD were:aGVHD (HR, 1.96; 95% CI, 1.34-2.87; P � .001); MICA-129val/val genotype (HR, 1.61; 95% CI, 1.08-2.40; P � .019), olderage (� 15 years; HR, 2.97; 95% CI, 1.45-6.07; P � .003), and thesource of stem cells (PBSCs vs BM; HR, 1.66; 95% CI, 1.09-2.52;P � .018)].
Posttransplantation sMICA increased the risk of cGVHD. Wethen investigated sMICA levels in sera of a subset of 116 patients
A
0 10 20 30 40
0.0
0.2
0.4
0.6
0.8
1.0
Months
Cu
mu
lati
ve in
cid
ence val/val
met/val
met/met
63%
46%
40%
P = .12
B
0 10 20 30 40
0.0
0.2
0.4
0.6
0.8
1.0
Months
Cu
mu
lati
ve in
cid
ence
met/met or met/val
val/val
P = .03
63%
45%
Figure 1. Cumulative incidence for cGVHD based on MICA-129genotype. (A) MICA-129 val allele increased the risk of chronic graft-versus-host disease (cGVHD) in a dose-dependent manner (univariateanalysis). (B) MICA-129 val/val genotype is more represented in patientswho developed cGVHD (univariate analysis).
5218 BOUKOUACI et al BLOOD, 10 DECEMBER 2009 � VOLUME 114, NUMBER 25
For personal use only. by guest on May 29, 2013. bloodjournal.hematologylibrary.orgFrom

for whom serum aliquots before and after transplantation (atday 100) were available as well in 35 healthy donors. The analysisof sMICA serum level in healthy donors showed an overall absenceof sMICA, whereas in patients before and after transplantation themean values were, respectively, 52.95 pg/mL (95% CI, 42.77-63.13 pg/mL) and 71.82 pg/mL (95% CI, 60.58-83.05 pg/mL).From the distribution profile, a cutoff value for sMICA at the 70thpercentile was noted (Figure 2A). Subsequent univariate analysisshowed a highly significant association between posttransplanta-tion sMICA higher than 80 pg/mL and the incidence of cGVHD(82% vs 46%, at 3 years; P .00111; Figure 2B). Multivariateanalysis using similar methods as described earlier found anincreased risk of cGVHD associated with the following factors:aGVHD (HR, 1.74; 95% CI, 1.07-2.84; P � .03), MICA-129val/val genotype (HR, 2.60; 95% CI, 1.48-4.56; P � .001), sMICA(HR, 2.75; 95% CI, 1.59-4.76; P .001), and older age (� 15 years;HR, 2.89; 95% CI, 0.99-8.37; P � .05). Moreover, comparisonbetween sMICA levels before and after HSCT did not show anystatistically significant correlation (data not shown).
MICA-129 and sMICA exert an independent but additiveeffect on cGVHD incidence. Given that both MICA-129 geno-type and sMICA serum levels are associated with a high incidenceof cGVHD, we questioned if MICA-129 genotype could influencesMICA levels, but nonparametric testing failed to show anyrelationship (Figure 3A). However, the cumulative incidence ofcGVHD accounting for the different combinations of MICA-129genotypes (val/val, met/val, or met/met) and serum levels ofsMICA ( 80 pg/mL and 80 pg/mL) showed that each of these
risk factors raised the risk of cGVHD in an additive manner.Patients bearing the val/val genotype together with serum sMICAlevel greater than 80 pg/mL was at highest risk of developingcGVHD (93% at 20 months), whereas the lower risk was observedfor those with MICA-129 met/met or met/val in combination withsMICA level below 80 pg/mL (23% at 20 months; P .001;Figure 3B).
Pretransplantation anti-MICA antibodies protect againstcGVHD. We stratified, as recommended by the manufacturer, thethreshold of MICA antibodies as either 0 to 2 (negative), 2 to 3(borderline), and greater than 3 (positive) or less than 2 (negative)and greater than 2 (positive). In univariate analysis, patientspositive for pretransplantation MICA Abs had a lower incidence ofcGVHD whatever the stratification schedule used in the analysis(P � .04 and .01; Figure 4A-B). This was further confirmed inmultivariate analysis without affecting the status of previouslyidentified risk factors [aGVHD (HR, 1.88; 95% CI, 1.12-3.13;P � .01), MICA-129 val/val genotype (HR, 2.45; 95% CI, 1.39-4.33; P � .002), sMICA (HR, 2.55; 95% CI, 1.47-4.41; P � .001),MICA Abs (HR, 1.80; 95% CI, 1.01-3.20; P � .04)]. These dataprompted us to analyze if there was any relationship betweenMICA Abs and sMICA level on the one hand and the incidence ofcGVHD on the other hand. We found an inverse relationshipbetween pretransplantation MICAAbs and sMICA level at day 100(values 3 correlate with serum levels 80 pg/mL; Figure 4C),potentially reflecting a neutralizing effect of such isoforms byMICA antibodies with a subsequent decrease on cGVHD incidence.Indeed, the lower risk of cGVHD was noted in patients with MICA
A
cases
70th percentile80
B
0 10 20 30 40
0.0
0.2
0.4
0.6
0.8
1.0
Months
Cu
mu
lati
ve in
cid
ence
sMICA > 80
sMICA < 80
P = .00003
82%
45%
100
200
300
0
Aft
er t
ran
spla
nt
sMIC
A
Figure 2. sMICA distribution profile among patients and cumulativeincidence for cGVHD based on sMICA serum levels after transplanta-tion. (A) The analysis of the distribution profile of post-HSCT sMICAallowed us to pinpoint a cutoff at the 70th percentile. (B) Patients havingsMICA serum level greater than 80 pg/mL after transplantation are thoseat high risk of developing cGVHD (univariate analysis).
MICA GENOTYPE/PHENOTYPE DIVERSITY IN SIBLING HSCT 5219BLOOD, 10 DECEMBER 2009 � VOLUME 114, NUMBER 25
For personal use only. by guest on May 29, 2013. bloodjournal.hematologylibrary.orgFrom

Abs greater than 3 and sMICA less than 80 pg/mL, whereas thehighest in those having MICA Abs less than 3 with sMICA greaterthan 80 pg/mL (35% vs 81%; Figure 4D). Note that a sex-basedcomparison of patients immunized against MICA did not showsignificant differences between males and females albeit a slightincrease among females older than 15 years (data not shown).
Relapse
Because it is well admitted that cGVHD is closely related todecreased relapse rate28 and because MICA has been associatedwith malignancies, we examined the relapse rate in this patientpopulation along with incidence of cGVHD despite the absence ofa relationship between the 2 complications in our study group (datanot shown). The cumulative incidence of relapse at 3 years was21%. Forty-one patients (22% of 186 who received a transplant formalignant diseases) had relapsed or progressed with their disease.MICA-129 met/met genotype, sMICA, and posttransplantationMICA Abs less than 3 were all associated with increased risk ofrelapse, albeit for the 2 latter the statistical significance wasborderline (ie, MICA-129 met/met vs MICA-129 met/val orMICA-129 val/val, 51% vs 19%, P � .007; Figure 5; sMICA 80,37% vs 17%, P � .05; and MICA Abs 3, 26% vs 6%, P � .05).In multivariate analysis, only MICA-129 met/met genotype (HR,2.69; 95% CI, 1.12-6.43; P � .02) remained significant togetherwith relapse risk of the underlying malignant disease (high orintermediate vs low; HR, 1.91; 95% CI, 1.02-3.58; P � .04).
Discussion
The underlying immune mechanisms involved in cGVHD pathogen-esis remain elusive. Nevertheless, there is consensus that immunedysfunction involves alloreactive T- and B-cell compartments aswell as autoimmune responses.29-31 In such context, MICA mol-ecules, proven to play prominent roles in immune processes,attracted our attention by their potential implication in the develop-ment of cGVHD and prompted us to analyze whether their geneticand phenotypic diversity could serve as potent biomarkers.
In particular, we focused our attention on functionally relevantcharacteristics of MICA, namely MICA-129 genetic polymor-phism and propensity to elaborate sMICA formation and MICAAbs. We found that the MICA-129 val in an allele dose-dependentmanner increased the risk of cGVHD, suggesting that the effect isrecessive. Because such MICA-associated risk was independent ofaGVHD occurrence, the pathogenesis of cGVHD could be consid-ered as a de novo event in our study group. These findings andinterpretations are in line with other pathologic contexts, namelyAS and NPC. Indeed, we found that the MICA-129 met/metgenotype was a risk factor for the early onset of AS independent ofHLA-B27 antigen, whereas the homozygous state for MICA-129val allele increased the risk of developing NPC.23,24 The functionalrelevance of this variant in NK and T-cell activation, led us tohypothesize that NKG2D and MICA interaction either with high-affinity (MICA-129 met) or low-affinity (MICA-129 val) alleles
A
Recipient genotype MICA 129
val/valmet/valmet/met
Aft
er t
ran
spla
nt
sMIC
A
400
300
200
100
0
P = .52
B
0 10 20 30 40
0.0
0.2
0.4
0.6
0.8
1.0
Months
Cu
mu
lati
ve in
cid
ence
sMICA > 80 val/val
sMICA > 80 met/val or met/met
sMICA < 80 val/val
sMICA < 80 met/val or met/met
93%
74%
51%
23%
P = .00005
Figure 3. Relationship between MICA-129 genotypes and sMICAserum levels and cumulative incidence for cGVHD based on theircombinations. (A) Kruskall-Wallis nonparametric testing did not showany association between MICA-129 genotypes and sMICA serum levels.(B) Patients bearing the val/val genotype together with sMICA serumlevel greater than 80 pg/mL are at high risk of developing cGVHD,whereas the lowest risk was observed for those with MICA-129 met/metor met/val in combination with sMICA level below 80 pg/mL (univariateanalysis).
5220 BOUKOUACI et al BLOOD, 10 DECEMBER 2009 � VOLUME 114, NUMBER 25
For personal use only. by guest on May 29, 2013. bloodjournal.hematologylibrary.orgFrom

favor, respectively, chronic inflammation or tumor escape inpersons otherwise genetically predisposed to these immune disor-ders. Similarly, in the context of cGVHD, the weak engagement ofNKG2D receptors by the weak binder MICA-129 val allele may
impair NK/cytotoxic T lymphocyte cell activation/costimulation,possibly skewing the TH1 pathway toward TH2 with consequent B-cellactivation and Ab production (2 hallmarks of cGVHD pathogenesis),albeit such possibility was challenged in a recent report implying both
A
0 10 20 30 40
0.0
0.2
0.4
0.6
0.8
1.0
Months
Cu
mu
lati
ve in
cid
ence
> 3
2 - 3
0 - 266%
48%
41%
P = .04
P = .02
B
0 10 20 30 40
0.0
0.2
0.4
0.6
0.8
1.0
Months
Cu
mu
lati
ve in
cid
ence < 2
> 2
66%
45%
P = .012
C
Co
un
t
60
50
40
30
20
10
0
>= 3 (Positive)0 <3 (Negative)
> 80< 80
P = .022
57
32
22
3
D
0 10 20 30 40
0.0
0.2
0.4
0.6
0.8
1.0
Months
Cu
mu
lati
ve in
cid
ence
MICA Abs < 3 and sMICA < 80
MICA Abs < 3 and sMICA > 80
MICA Abs > 3 and sMICA < 80
81%
53%
35%
P = .0003
P = .0026
P = .17
P = .0004
Before transplant MICA Abs
After transplant sMICA
Figure 4. Cumulative incidence for cGVHD based on pretransplantation MICA Abs using different cutoffs. Relationship between pretransplantation MICA Abs, sMICAserum level, and cGVHD. (A-B) Patients having the lower titer of pretransplantation MICAAbs are those at high risk of cGVHD whatever the cutoff values, ie, 2 or 3 (univariateanalysis). (C) Nonparametric testing showed an inverse relationship between MICAAbs and sMICA levels (values 3 correlates with serum levels 80 pg/mL). (D) The lowerrisk for cGVHD was noted in patients with MICAAbs greater than 3 and sMICA less than 80 pg/mL, whereas the highest was in those having MICAAbs less than 3 with sMICAgreater than 80 pg/mL (univariate analysis). Of note, the patient group with MICAAbs greater than 3 and sMICA greater than 80 pg/mL is not represented in the figure becauseof the low number of patients (n � 3).
MICA GENOTYPE/PHENOTYPE DIVERSITY IN SIBLING HSCT 5221BLOOD, 10 DECEMBER 2009 � VOLUME 114, NUMBER 25
For personal use only. by guest on May 29, 2013. bloodjournal.hematologylibrary.orgFrom

pathways.32 The inability of MICA-129 val allele to activate NK cellscorroborate with the finding that the NK-cell dose inversely correlateswith the incidence of cGVHD.33 Indeed, we have reported that the riskof cGVHD was high in patients receiving low-donor NK-cell load.34
These data corroborate our findings in D/R sibling pairs fully matchedfor the MICA-129 polymorphism, wherein donor cell compartmentpossesses relatively low MICA-mediated capacity of NK-cell activationthrough the MICA-129 val allele. The ultimate consequence of suchweak interaction could lead to overexpression of NKG2D receptors aspreviously shown in autoimmune settings such as rheumatoid arthritis,17
celiac disease,35 and type 1 diabetes,36 events believed to mediateautoimmunity,37 and much more recently in early the post-HSCTsetting.38 This situation could favor the binding of other ligands such asUL16 binding proteins.13 Thus, in a highly IL-15–enriched microenvi-ronment, repeated T and NK stimulation favors an autoimmune-likesituation breaking down the self-tolerance with consequent auto-Abproduction. Interestingly, a recent study has shown that CD4� autoreac-tive donor T cells emerge during cGVHD. It was also shown that,although the host antigen-presenting cells are important for the initiationof aGVHD, donor antigen-presenting cells are involved in the develop-ment of cGVHD.39
We also found that the homozygous state for the strong NKG2Dbinder MICA-129 met allele was associated with a high incidenceof relapse (it is important to highlight that among 15 patientsbearing the MICA-129 met/met genotype, 12 (80%) relapsed fortheir initial disease). Because this variant protects against cGVHD,it could favor in turn a diminished graft-versus-leukemia effect.Indeed, in murine allo–BM transplantation model, alloreactive NKcells had been successfully used to protect against GVHD and toenhance graft-versus-leukemia effect.40 Similarly, in human trans-plantation, alloreactive NK cells protected patients against rejec-tion, GVHD, and relapse in KIR ligand-mismatched transplanta-tions.41 From our data obtained in MICA-matched context, theactivated NK cells (by the met/met genotype), albeit protectiveagainst cGVHD, seem inefficient to mediate antitumor activityagainst self-targets. This observation generates a model that needs adistinct study design for further exploration of the above possibili-ties. It is however of note that MICA polymorphism was found tobe associated with relapse rate independently of the disease-riskstatus. Nevertheless, we cannot exclude the possibility that theMICA-129 dimorphism behaves as a closely linked geneticmarker to a yet-to-be-defined causative locus or as an SNP tagaccounting for some functionally relevant variations lyingwithin or outside the MICA gene. Because recent studieshighlight the particular functional characteristics of the common
MICA*008 variant allele, including raised levels of sMICAsecretion,42 we tested the potential relationship between theHLA-B and MICA-129 genotypes in patients having or nothaving experienced cGVHD. Focused analysis of HLA-B*07,-B*08, and -B*44 (all linked to MICA*008 with MICA-129 valand with MICA A5.1 STR variation)43 failed to show anyassociation with cGVHD, rendering MICA*008 unlikely to bethe marker for susceptibility to cGVHD. The question howevermerits in its own right a detailed study of MICA polymorphismin its entirety in the context of HSCT.
Concerning sMICA, the sera of patients before transplantation(86% of them with malignant disorders) had higher levels ofsMICA than sera of healthy donors, consistent with the reportedelevated levels in a variety of cancers, including leukemia.44,45
Further increase of sMICA in posttransplantation conditions in ourpatients is associated with a higher incidence of cGVHD indepen-dent of preexisting history of aGVHD as well as MICA-129genotype. Albeit several works analyzed the relationship betweensMICA and diseases, in settings such as cancer, autoimmunity,infection, or organ transplantation, there is a paucity of informationin HSCT. Overall, MICA shedding by means of cellular isomerasesand proteinase enzymes46,47 with consequent release of the solubleforms result both in the reduction of MICA cell-surface density andsystemic NKG2D down-regulation on NK and T cells, 2 mecha-nisms thought to subvert NKG2D-mediated immune surveillance.This broadly admitted mechanism seems to have different func-tional consequences, depending on the underlying pathology.Although the above-mentioned pathway promotes tumor evasion/progression, premalignancy transformation,48 immune deficiencyin end-stage renal dysfunction,49 and acute bacterial infections,50 inheart transplantation settings, a recent study showed that patientshaving a high amount of sMICA molecules are protected from graftrejection.18 The investigators hypothesized that the impairment ofNK/T -cell activation through NKG2D inactivation by sMICAcould provoke a tolerogenic situation favoring graft maintenance.Similarly to MICA-129 genotype, the association between sMICAand cGVHD could be discussed under the conceptual frame-work based on the ability of such isoforms to mediate NK-cellinactivation, through NKG2D down-regulation. Impaired effectorcell activation could lead here again to a TH1/TH2 imbalance andan autoimmune-like situation. Because we did not find significantcorrelation between levels of sMICA before and after transplanta-tion, it is likely that the observed increase could be related to thetransplantation event per se. Nevertheless, we cannot exclude fullythat the observed raised levels of sMICA may merely reflect theinflammatory status common in clinical situations such as cGVHDand thus may behave as a generic marker of inflammation (notstrictly specific to these complication).
Because MICA molecules may act as an alloantigen capableof eliciting alloantibody response, we checked the presence ofMICAAbs before and after HSCT and found significant levels inboth periods. Interestingly, we found also that the presence ofAbs before transplantation correlates with low levels of sMICAafter transplantation and consequently with a low incidence ofcGVHD, strongly suggesting a neutralizing effect of MICA Abson sMICA. Our data are consistent with a study showing thatpatients with monoclonal gammopathy of undetermined signifi-cance with high MICA Abs were those with the lower level ofsMICA as well as with a relatively low tendency to evolvetoward multiple myeloma.51 It has also been shown that patientswith melanoma who respond to antibody blockade of cytotoxic
0 10 20 30 40 50 60
0.0
0.2
0.4
0.6
0.8
1.0
Months
Cu
mu
lati
ve in
cid
ence
met/met
val/val or met/val
51%
19%
P = 0.007
Figure 5. Cumulative incidence for relapse, based on MICA-129 genotype.MICA-129 met/met genotype is associated with high risk of relapse (univariateanalysis).
5222 BOUKOUACI et al BLOOD, 10 DECEMBER 2009 � VOLUME 114, NUMBER 25
For personal use only. by guest on May 29, 2013. bloodjournal.hematologylibrary.orgFrom

T lymphocyte-associated antigen 4 or to vaccination with autolo-gous irradiated tumor cells produced high amounts of MICAAbs and had low circulating sMICA accompanied by an increasein NK and CD8� T cell–mediated cytotoxicity. The same studyshowed the capacity of MICA Abs to opsonize efficiently thecancer cells and to participate in the complement-mediatedlysis.52 These data perfectly fit with the trend we observed inthat MICA Abs confers protection against relapse.
To our knowledge, this study provides the first observationabout MICA-related features in human HSCT and highlights theirpotential use as predictive biomarkers for cGVHD. If confirmed ina larger patient cohort, our data may open up prophylacticimmunotherapeutic strategies against cGVHD.
Acknowledgments
This work was supported by research grants from the ATC InsermMedicament et Vectorization (A04166HS) and institutional fund-ing to AP-HP and Inserm UMRS 940.
Authorship
Contribution: W.B. designed the research, analyzed and interpreteddata, and wrote the manuscript; M.B. collected data, performedstatistical analysis, and analyzed and interpreted data; R.P.d.L. andV.R. collected clinical data; C. Suberbielle, D.B., N.D., P.H., and C.Scieux were involved in phenotype analysis; H.A. performed theresearch; E.G. critically reviewed the manuscript; R.K. designedthe research and critically reviewed the manuscript; A.T. partici-pated in the research design and critically reviewed the manuscript;D.C. critically reviewed the manuscript; G.S. analyzed and inter-preted data and critically reviewed the manuscript; and R.T.designed the research, analyzed and interpreted data, and wrote themanuscript.
Conflict-of-interest disclosure: The authors declare no compet-ing financial interests.
Correspondence: Ryad Tamouza, Laboratoire d’Immunologie etd’Histocompabilite. Centre Hayem 3eme etage, Hopital SaintLouis, 1 avenue Claude Vellefaux, 75010, Paris, France; e-mail:[email protected].
References
1. Fraser CJ, Bhatia S, Ness K, et al. Impact ofchronic graft-versus-host disease on the healthstatus of hematopoietic cell transplantation survi-vors: a report from the Bone Marrow TransplantSurvivor Study. Blood. 2006;108(8):2867-2873.
2. Santos GW, Hess AD, Vogelsang GB. Graft-versus-host reactions and disease. Immunol Rev.1985;88:169-192.
3. Ferrara JLM, Antin JH. The pathophysiology ofgraft-versus-host disease. In: Blume KG, FormanSJ, Appelbaum SJ, Malden MA, eds. Thomas’Hematopoietic Cell Transplantation. Malden, MA:Blackwell Science; 1999:305-368.
4. Cutler C, Antin JH. Chronic graft-versus-host dis-ease. Curr Opin Oncol. 2006;18(2):126-131.
5. Tyndall A, Dazzi F. Chronic GVHD as an autoim-mune disease. Best Pract Res Clin Haematol.2008;21(2):281-289.
6. Schultz KR, Miklos DB, Fowler D, et al. Towardbiomarkers for chronic graft-versus-host disease:National Institutes of Health consensus develop-ment project on criteria for clinical trials in chronicgraft-versus-host disease, III: Biomarker WorkingGroup Report. Biol Blood Marrow Transplant.2006;12(2):126-137.
7. Shimada M, Onizuka M, Machida S, et al. Asso-ciation of autoimmune disease-related gene poly-morphisms with chronic graft-versus-host dis-ease. Br J Haematol. 2007;139(3):458-463.
8. Bogunia-Kubik K, Wysoczanska B, Lange A.Non-HLA gene polymorphisms and the outcomeof allogeneic hematopoietic stem cell transplanta-tion. Curr Stem Cell Res Ther. 2006;1(2):239-253.
9. Fujii H, Cuvelier G, She K, et al. Biomarkers innewly diagnosed pediatric-extensive chronicgraft-versus-host disease: a report from the Chil-dren’s Oncology Group. Blood. 2008;111(6):3276-3285.
10. She K, Gilman AL, Aslanian S, et al. Altered Toll-like receptor 9 responses in circulating B cells atthe onset of extensive chronic graft-versus-hostdisease. Biol Blood Marrow Transplant. 2007;13(4):386-397.
11. Imamura M, Hashino S, Kobayashi H, et al. Se-rum cytokine levels in bone marrow transplanta-tion: synergistic interaction of interleukin-6,interferon-gamma, and tumor necrosis factor-alpha in graft-versus-host disease. Bone MarrowTransplant. 1994;13(6):745-751.
12. Bahram S. MIC genes: from genetics to biology.Adv Immunol. 2000;76:1-60.
13. Bahram S, Inoko H, Shiina T, Radosavljevic M.MIC and other NKG2D ligands: from none to toomany. Curr Opin Immunol. 2005;17(5):505-509.
14. Eagle RA, Trowsdale J. Promiscuity and thesingle receptor: NKG2D. Nat Rev Immunol. 2007;7(9):737-744.
15. Groh V, Wu J, Yee C, Spies T. Tumour-derivedsoluble MIC ligands impair expression of NKG2Dand T-cell activation. Nature. 2002;419(6908):734-738.
16. Salih HR, Rammensee HG, Steinle A. Cuttingedge: down-regulation of MICA on human tumorsby proteolytic shedding. J Immunol. 2002;169(8):4098-4102.
17. Groh V, Bruhl A, El-Gabalawy H, Nelson JL,Spies T. Stimulation of T cell autoreactivity byanomalous expression of NKG2D and its MICligands in rheumatoid arthritis. Proc Natl Acad SciU S A. 2003;100(16):9452-9457.
18. Suarez-Alvarez B, Lopez-Vazquez A, Díaz-Molina B, et al. The predictive value of solublemajor histocompatibility complex class I chain-related molecule A (MICA) levels on heart allo-graft rejection. Transplantation. 2006;82(3):354-361.
19. Schrambach S, Ardizzone M, Leymarie V, SibiliaJ, Bahram S. In vivo expression pattern of MICAand MICB and its relevance to auto-immunity andcancer. PLoS ONE. 2007;2(6):e518; 1-10.
20. European Bioinformatics Institute. IMGT/HLA(ImMunoGeneTics/histocompatibility complex)Sequence Database. http://www.ebi.ac.uk/imgt/hla/. Accessed August 16, 2009.
21. Stastny P, Zou Y, Fan Y, Qin Z, Lavingia B. Theemerging issue of MICA antibodies: antibodies toMICA and other antigens of endothelial cells.Contrib Nephrol. 2009;162:99-106.
22. Steinle A, Li P, Morris DL, et al. Interactions ofhuman NKG2D with its ligands MICA, MICB, andhomologs of the mouse RAE-1 protein family. Im-munogenetics. 2001;53(4):279-287.
23. Amroun H, Djoudi H, Busson M, et al. Early-onsetankylosing spondylitis is associated with a func-tional MICA polymorphism. Hum Immunol. 2005;66(10):1057-1061.
24. Douik H, Chaaben AB, Romdhane NA, et al. As-sociation of MICA-129 polymorphism with naso-
pharyngeal cancer risk in a Tunisian population.Hum Immunol. 2009;70(1):45-48.
25. Rocha V, Franco RF, Porcher R, et al. Host de-fense and inflammatory gene polymorphisms areassociated with outcomes after HLA-identical sib-ling bone marrow transplantation. Blood. 2002;100(12):3908-3918.
26. Fine JP, Gray RJ. A proportional hazards modelfor the sub distribution of a competing risk. J AmStat Assoc. 1999;94:496.
27. Cox DR. Regression models and life tables (withdiscussion). J R Stat Soc Series B Stat Methodol.1972;34:187-220.
28. Fraser CJ, Scott Baker K. The management andoutcome of chronic graft-versus-host disease.Br J Haematol. 2007;138(2):131-145.
29. Pavletic SZ, Carter SL, Kernan NA, et al. Influ-ence of T-cell depletion on chronic graft-versus-host disease: results of a multicenter randomizedtrial in unrelated marrow donor transplantation.Blood. 2005;106(9):3308-3313.
30. Schultz KR, Paquet J, Bader S, HayGlass KT.Requirement for B cells in T cell priming to minorhistocompatibility antigens and development ofgraft-versus-host disease. Bone Marrow Trans-plant. 1995;16(2):289-295.
31. Zhang C, Todorov I, Zhang Z, et al. Donor CD4 Tand B cells in transplants induce chronic graftversus- host disease with autoimmune manifesta-tions. Blood. 2006;107(7):2993-3001.
32. Imanguli MM, Swaim WD, League SC, Gress RE,Pavletic SZ, Hakim FT. Increased T-bet� cyto-toxic effectors and type I interferon-mediated pro-cesses in chronic graft versus host disease of theoral mucosa. Blood. 2009;113(15):3620-3630.
33. Kim DH, Sohn SK, Lee NY, et al. Transplantationwith higher dose of natural killer cells associatedwith better outcomes in terms of non-relapse mor-tality and infectious events after allogeneic pe-ripheral blood stem cell transplantation from HLA-matched sibling donors. Eur J Haematol. 2005;75(4):299-308.
34. Larghero J, Rocha V, Porcher R, et al. Associa-tion of bone marrow natural killer cell dose withneutrophil recovery and chronic graft-versus-hostdisease after HLA identical sibling bone marrowtransplants. Br J Haematol. 2007;138(1):101-9.
35. Hue S, Mention JJ, Monteiro RC, et al. A directrole for NKG2D/MICA interaction in villous atro-phy during celiac disease. Immunity. 2004;21(3):367-377.
MICA GENOTYPE/PHENOTYPE DIVERSITY IN SIBLING HSCT 5223BLOOD, 10 DECEMBER 2009 � VOLUME 114, NUMBER 25
For personal use only. by guest on May 29, 2013. bloodjournal.hematologylibrary.orgFrom

36. Ogasawara K, Hamerman JA, Ehrlich LR, et al.NKG2D blockade prevents autoimmune diabetesin NOD mice. Immunity. 2004;20(6):757-767.
37. Caillat-Zucman S. How NKG2D ligands triggerautoimmunity? Hum Immunol. 2006;67(3):204-207.
38. Dulphy N, Haas P, Busson M, et al. An unusualCD56(bright) CD16(low) NK cell subset domi-nates the early posttransplant period followingHLA-matched hematopoietic stem cell transplan-tation. J Immunol. 2008;181(3):2227-2237.
39. Tivol E, Komorowski R, Drobyski WR. Emergentautoimmunity in graft-versus-host disease. Blood.2005;105(12):4885-4891.
40. Asai O, Longo DL, Tian ZG, et al. Suppression ofgraft-versus-host disease and amplification ofgraft-versus-tumor effects by activated naturalkiller cells after allogeneic bone marrow trans-plantation. J Clin Invest. 1998;101(9):1835-1842.
41. Ruggeri L, Capanni M, Urbani E, et al. Effective-ness of donor natural killer cell alloreactivity inmismatched hematopoietic transplants. Science.2002;295(5562):2097-2100.
42. Lu M, Xia B, Ge L, et al. Role of major histocom-
patibility complex class I-related moleculesA*A5.1 allele in ulcerative colitis in Chinese pa-tients. Immunology. 2008;128:e230-e236.
43. Gao X, Single RM, Karacki P, Marti D, O’Brien SJ,Carrington M. Diversity of MICA and linkage dis-equilibrium with HLA-B in two North Americanpopulations. Hum Immunol. 2006;67(3):152-158.
44. Holdenrieder S, Stieber P, Peterfi A, Nagel D,Steinle A, Salih HR. Soluble MICA in malignantdiseases. Int J Cancer. 2006;118(3):684-687.
45. Salih HR, Antropius H, Gieseke F, et al. Func-tional expression and release of ligands for theactivating immunoreceptor NKG2D in leukemia.Blood. 2003;102(4):1389-1396.
46. Kaiser BK, Yim D, Chow IT, et al. Disulphide-isomerase-enabled shedding of tumour-associated NKG2D ligands. Nature. 2007;447(7143):482-486.
47. Waldhauer I, Goehlsdorf D, Gieseke F, et al.Tumor-associated MICA is shed by ADAM pro-teases. Cancer Res. 2008;68(15):6368-6376.
48. Arreygue-Garcia NA, Daneri-Navarro A, delToro-Arreola A, et al. Augmented serum level ofmajor histocompatibility complex class I-related
chain A (MICA) protein and reduced NKG2Dexpression on NK and T cells in patients withcervical cancer and precursor lesions. BMCCancer. 2008;8:16.
49. Peraldi MN, Berrou J, Dulphy N, et al. Oxidativestress mediates a reduced expression of the acti-vating receptor NKG2D in NK cells from end-stage renal disease patients. J Immunol. 2009;182(3):1696-1705.
50. Holdenrieder S, Eichhorn P, Beuers U, et al.Soluble NKG2D ligands in hepatic autoimmunediseases and in benign diseases involved inmarker metabolism. Anticancer Res. 2007;27(4A):2041-2045.
51. Jinushi M, Vanneman M, Munshi NC, et al. MHCclass I chain-related protein A antibodies andshedding are associated with the progression ofmultiple myeloma. Proc Natl Acad Sci U S A.2008;105(4):1285-1290.
52. Jinushi M, Hodi FS, Dranoff G. Therapy-inducedantibodies to MHC class I chain-related protein Aantagonize immune suppression and stimulateantitumor cytotoxicity. Proc Natl Acad Sci U S A.2006;103(24):9190-915.
5224 BOUKOUACI et al BLOOD, 10 DECEMBER 2009 � VOLUME 114, NUMBER 25
For personal use only. by guest on May 29, 2013. bloodjournal.hematologylibrary.orgFrom
Copyright © 2022 FDOKUMEN






![Topic 11 Revision [129 marks] - IB Questionbank](https://static.fdokumen.com/doc/165x107/6315a7f3b1e0e0053b0f274d/topic-11-revision-129-marks-ib-questionbank.jpg)












