Meta-analysis of the plasminogen activator inhibitor-1 (PAI-1) gene with insertion/deletion 4G/5G...
15
Asian Biomedicine Vol. 6 No. 2 April 2012; 203-217 Original article Meta-analysis of the plasminogen activator inhibitor-1 ( PAI-1) gene with insertion/deletion 4G/5G polymorphism and its susceptibility to ischemic stroke in Thai population Anunchai Assawamakin a , Narin Sriratanaviriyakul b,c , Yupaporn Lalerd b , Wanna Thongnoppakhun b , Oranud Praditsap b , Sissades Tongsima a , Manop Pithukpakorn b,d a Biostatistics and Informatics Laboratory, Genome Institute, National Center for Genetic Engineering and Biotechnology (BIOTEC), Pathumthani 12120, b Division of Molecular Genetics, Department of Research and Development, Faculty of Medicine, Siriraj Hospital, Mahidol University, Bangkok 10700 Thailand, c Internal Medicine Residency Program, University of Hawaii, Hawaii 96822, USA, d Division of Medical Genetics, Department of Medicine, Faculty of Medicine, Siriraj Hospital, Mahidol University, Bangkok 10700, Thailand Backgrounds: Plasminogen activator inhibitor-1 (PAI-1) gene was reported to associate with ischemic stroke, particularly the insertion/deletion 4G/5G promoter polymorphism. However, because of the complexity and multifactorial nature of stroke, many previous studies showed inconsistent results. Objectives: We investigated whether PAI-1 gene polymorphism is associated with ischemic stroke by genetic association and meta-analysis in Thais. Methods: A case-control genetic association study on PAI-1 polymorphism was conducted. It contains 179 patients with ischemic stroke and 229 healthy controls. We also conducted a meta-analysis by combining the results from our work with other published association studies obtained between 1994 and 2010. Results: The genetic association studies on PAI-1 polymorphism on the Thai samples indicate marginal odds ratio between the PAI-1 polymorphisms and the risk of ischemic stroke. Combining our samples with all previously reported PAI-1 association studies, we did not find any genetic model significant by the lambda method. However, the allele-based method showed the recessive genetic model to be significant for the Asian-derived population when analyzed separately from Caucasians. Conclusions: From the meta-analysis on our Thai data combined with other publications, it can be concluded that the homozygous-4G polymorphism is a risk factor for ischemic stroke in Asian, but not Caucasian populations. However, according to marginal odds ratio results, the cryptic genetic contribution, or other missing heritability should be considered for the study of ischemic stroke for Thais. Keywords: Genetic polymorphism, ischemic stroke, meta-analysis, Plasminogen activator inhibitor type 1 (PAI-1), SERPINE DOI: 10.5372/1905-7415.0602.047 Despite the recent advancement in acute stroke therapy, stroke remains the leading cause of severe disability and mortality throughout the world [1, 2]. In the United States alone, the overall prevalence of stroke is about 6.5 million people. Approximately 795,000 individuals suffer from a new or recurrent stroke. Furthermore, there were nearly 140,000 deaths from stroke-related causes in 2005 [2]. Similar large occurrences also appear in less developed countries [3]. One of the most effective measures in combating stroke is deploying a primary prevention program in which identification of risk factors is the most important aspect. Stroke is a heterogeneous disease associated with many known conventional risk factors such as hypertension, diabetes, and dyslipidemia. Ischemic stroke caused by thrombosis is regarded as Correspondence to: Manop Pithukpakorn, Division of Molecular Genetics, Department of Research and Development, Faculty of Medicine, Siriraj Hospital, Mahidol University, Bangkok 10700 Thailand. E-mail: [email protected]
Transcript of Meta-analysis of the plasminogen activator inhibitor-1 (PAI-1) gene with insertion/deletion 4G/5G...

Asian Biomedicine Vol. 6 No. 2 April 2012; 203-217
Original article
Meta-analysis of the plasminogen activator inhibitor-1(PAI-1) gene with insertion/deletion 4G/5G polymorphismand its susceptibility to ischemic stroke in Thaipopulation
Anunchai Assawamakina, Narin Sriratanaviriyakulb,c, Yupaporn Lalerdb, Wanna Thongnoppakhunb,Oranud Praditsapb, Sissades Tongsimaa, Manop Pithukpakornb,d
aBiostatistics and Informatics Laboratory, Genome Institute, National Center for Genetic Engineeringand Biotechnology (BIOTEC), Pathumthani 12120, bDivision of Molecular Genetics, Department ofResearch and Development, Faculty of Medicine, Siriraj Hospital, Mahidol University, Bangkok 10700Thailand, cInternal Medicine Residency Program, University of Hawaii, Hawaii 96822, USA, dDivisionof Medical Genetics, Department of Medicine, Faculty of Medicine, Siriraj Hospital, Mahidol University,Bangkok 10700, Thailand
Backgrounds: Plasminogen activator inhibitor-1 (PAI-1) gene was reported to associate with ischemic stroke,particularly the insertion/deletion 4G/5G promoter polymorphism. However, because of the complexity andmultifactorial nature of stroke, many previous studies showed inconsistent results.Objectives: We investigated whether PAI-1 gene polymorphism is associated with ischemic stroke by geneticassociation and meta-analysis in Thais.Methods: A case-control genetic association study on PAI-1 polymorphism was conducted. It contains 179patients with ischemic stroke and 229 healthy controls. We also conducted a meta-analysis by combining theresults from our work with other published association studies obtained between 1994 and 2010.Results: The genetic association studies on PAI-1 polymorphism on the Thai samples indicate marginal odds ratiobetween the PAI-1 polymorphisms and the risk of ischemic stroke. Combining our samples with all previouslyreported PAI-1 association studies, we did not find any genetic model significant by the lambda method. However,the allele-based method showed the recessive genetic model to be significant for the Asian-derived populationwhen analyzed separately from Caucasians.Conclusions: From the meta-analysis on our Thai data combined with other publications, it can be concluded thatthe homozygous-4G polymorphism is a risk factor for ischemic stroke in Asian, but not Caucasian populations.However, according to marginal odds ratio results, the cryptic genetic contribution, or other missing heritabilityshould be considered for the study of ischemic stroke for Thais.
Keywords: Genetic polymorphism, ischemic stroke, meta-analysis, Plasminogen activator inhibitor type 1 (PAI-1),SERPINE
DOI: 10.5372/1905-7415.0602.047
Despite the recent advancement in acute stroketherapy, stroke remains the leading cause of severedisability and mortality throughout the world [1, 2]. Inthe United States alone, the overall prevalence ofstroke is about 6.5 million people. Approximately795,000 individuals suffer from a new or recurrent
stroke. Furthermore, there were nearly 140,000 deathsfrom stroke-related causes in 2005 [2]. Similar largeoccurrences also appear in less developed countries[3]. One of the most effective measures in combatingstroke is deploying a primary prevention program inwhich identification of risk factors is the most importantaspect.
Stroke is a heterogeneous disease associatedwith many known conventional risk factorssuch as hypertension, diabetes, and dyslipidemia.Ischemic stroke caused by thrombosis is regarded as
Correspondence to: Manop Pithukpakorn, Division ofMolecular Genetics, Department of Research and Development,Faculty of Medicine, Siriraj Hospital, Mahidol University,Bangkok 10700 Thailand. E-mail: [email protected]

204 A. Assawamakin, et al.
a multifactorial disease. The thrombosis risk factorscan be generally classified into three groups, strong,moderate and weak based on the number of positiveassociations collected in HUGE Navigator [4]. Thestrong genetic risk factors include PAI-1, antithrombin,protein C and protein S, while the moderate groupcomprises factor V (F5) Leiden, prothrombin 20210A,non-O blood group, and fibrinogen 10034T. The weakgenetic risk factors were reported such as fibrinogen,factor XIII and factor XI variants. Identification ofstroke susceptibility genes and quantification ofassociated risks have been hampered by conflictingresults from underpowered case-control studies.
One leading predisposing factor of ischemicstroke is the plasminogen activator inhibitor-1(PAI-1) gene located on chromosome 7. Due to itsdirect involvement in thrombosis pathway, PAI-1 isan excellent candidate to investigate its role inischemic stroke. The product of PAI-1 acts as amajor inhibitor of tissue plasminogen activator (t-PA)by forming an irreversible one-to-one complex.This process leads to a decrease in fibrinolysis andthrombus degradation [5, 6].
Many polymorphisms have been identified inthis gene, one of which is “4/5” guanosine (4G/5G), asingle-base length polymorphism in the promoter regionof PAI-1. This particular polymorphism affects PAI-1levels [7-12]. Both 4G and 5G alleles have the samebinding site for the transcription activator. The 5G-allele, however, has an additional binding site for arepressor, resulting in lowering of the transcriptionrate and concomitant PAI-1 activity [8, 10]. Hence,homozygous 4G/4G individuals have the highestPAI-1 level, while 5G/5G homozygotes have thelowest.
Several studies have reported that the 4G/4Ggenotype increases the risk of myocardial infarctionand thromboembolism through impairment ofsecondary fibrinolytic function by elevated PAI-1activity [13, 14]. On the other hand, there is discordancebetween published studies regarding the associationof the PAI-1 gene 4G/5G polymorphism and stroke toincrease, neutral, or protective risk [7, 15-20]. Onlyone recent meta-analysis has found PAI-1 4G/5Gassociation with ischemic stroke risk in Han Chinese[3], whereas another meta-analysis [21] failed todemonstrate a significant association with otherpopulations.
The aims of this study were to investigate therole of 4G/5G PAI-1 polymorphism in the susceptibility
of stroke in Thai population and to characterize thedisease risks in different ethnic groups by gatheringall data from case-control studies, including data fromprevious two meta-analysis studies [3].
Materials and methodsStudy subjects and PAI-1 (SERPINE 1)genotypingCases and controls
Thai patients who had been diagnosed with acuteischemic stroke at Siriraj Hospital since October 2008and agreed to participate were invited in the study.Stroke was defined clinically using World HealthOrganization criteria. A diagnosis of ischemic strokewas made only if the patient has a clinical diagnosis ofstroke and if a computed tomography (CT) or magneticresonance imaging (MRI) scan of the brain done afteronset of the symptoms either was normal or showedthe relevant infarction. Patients with hemorrhagictransformation of an infarct were also eligible.Subtyping of the index ischemic stroke was donecentrally on the basis of the abstracted medical recordby a neurologist adjudicator blinded to genotypedata and personal identifiers. Because final subtypediagnosis could vary from initial diagnosis inapproximately one-third of the cases, the adjudicatorused all available and relevant information obtainedafter completion of the stroke work-up. The Trial ofORG10172 in Acute Stroke Treatment (TOAST)classification was mainly used in this study.
The control subjects were recruited from adultmen and women who must be at least 18 years old atthe time of enrollment. They must not have a strokeand must be genetically unrelated to the patients enrolledin this study. The Questionnaire for Verifying Stroke-free Status (QVSS) was used to confirm stroke-freestatus. Patients being treated for coronary or peripheralvascular disease were not included in the controls.This study protocol was reviewed and approved bythe Institutional Review Board (IRB) of the Facultyof Medicine, Siriraj Hospital. All participants signedwritten informed consent prior to the study. Clinicaldata as well as the DNA samples from peripheral bloodwere collected and compared with the control group.
Genotyping of plasminogen activator inhibitor(PAI)-1 promoter polymorphism, -675 ins/del (4G/5G)
Genomic DNAs were extracted from peripheralblood samples by the standard phenol/chloroform

205Vol. 6 No. 2
April 2012PAI-1 gene with insertion/deletion 4G/5G polymorphism
extraction method. For determination of PAI-1promoter polymorphism, -675 ins/del (4G/5G), SNPgenotyping was carried out using the PCR-DHPLCmethod. The 180 bp PCR products were generatedin 25-ml total volumes containing 10 pmoles of eachprimer: sense 5’-GCC AGA CAA GGT TGT TGACA-32 and anti-sense 52 -CAG CCA CGT GATTGT CTA GG-32 , 1.5 mM MgCl
2, 1x detergent-free
HF buffer (518), 200 μM dNTPs, 0.02 U Taq DNApolymerase (Phusion Hot-start High-fidelity DNApolymerase), and 100 ng of genomic DNA. A thermalcycle was performed for 30 seconds at 98°C todenature the DNA template, 40 cycles of 10 secondsat 98°C, 30 seconds at 64°C, and 30 seconds at 72°C,followed by 5 min at 72°C for the final extension.After PCR completion and heteroduplex induction,5-microliters of the amplified products were injectedinto the WAVE® Nucleic Acid Fragment AnalysisSystem (Transgenomic, Inc., Omaha, NE) operatedfor mutation detection in partially denaturing mode.The DNASep® HT column temperature was set at63°C to detect the 675 ins/del (4G/5G) SNP. The linearacetonitrile gradient at a flow rate of 0.9 ml/minutewas formed by mixing buffer A (0.1M TEAA) andbuffer B (0.1M TEAA, 25% acetonitrile) to create agradient of 49.1-59.1% buffer B over two minutes.After each analytical run, the column was cleanedand equilibrated. The eluted DNA fragments wereobserved by an ultraviolet (UV) detector. Thechromatographic elution profile of the polymorphismin a heterozygous state would show a unique peakpattern different from that of the homozygous wildtype, as confirmed by sequencing.
Identification of eligible studies and dataextraction
We examined all association studies betweenPAI-1 4G/5G polymorphisms and ischemic stroke.Articles in which PAI-1 4G/5G polymorphisms weredetermined in ischemic stroke patients and controls,during the years 1994 and 2008 were retrievedusing the PubMed, Embase, and HuGE navigatorsearch engines. The search keywords were “stroke”,“ischemic stroke”, “PAI-1”, “polymorphism”, and“genetic associations”. We also extensively reviewedthe references cited by these selected articles toidentify other publications that might have beenoverlooked by the keyword search. If multiplepublications from the same study group wereidentified, the latest and most complete results would
be used in the analysis. The search results wererestricted to English-language articles. The criteriaused to screen these articles are as follows;
1) The article must be a case-control studyregardless of the study sample size.
2) The article must be an association studybetween PAI-1 4G/5G genotypes and ischemic stroke.
3) The article must provide sufficient informationto calculate odds ratio (OR) and hence, the followingtypes of article must be excluded;
a. The article containing redundant dataoriginally from the same source(s)
b. The article that the number of wild-type/mutant genotypes cannot be ascertained
c. Linkage analysis and family-based studiesTwo investigators independently extracted the
following information: first author, a journal nameand year of publication, ethnicity of the studiedpopulation(s), the number of cases and controls, andthe genotype and allele frequency from the PAI-1 4G/5G polymorphisms. The same investigators alsoindependently assessed the quality of each study.Qualities of scoring criteria were modified from theprevious meta-analyses of the observational studies.Each paper was assigned with a score in the rangeof 0 (worst) to 12 (best). The third investigator wasappointed for adjudicating any disagreement betweenthe first two investigators.
Statistical analysisFor each eligible study, allele frequencies of
PAI-1 4G/5G from the control group were used tocompute Hardy–Weinberg equilibrium (HWE)using Fisher’s exact test. The studies that do notsatisfy HWE were removed from the analysis. Weexamined the different allelic effects of PAI-1 4G/5Gpolymorphism. For each study, the Odds Ratio (OR)and the corresponding 95% confidence interval (CI)were determined. We assessed the variation fromwithin the same study and among different studiesusing Cochran’s Q-statistic to evaluate the nullhypothesis that all studies should report the sameeffect resulting from PAI-1 4G/5G polymorphism.A significant Q-statistic value (p <0.10) indicatesheterogeneity of association results across the selectedstudies. Overall gene effect from the three groups ofgenotyping, namely 4G/4G, 4G/5G and 5G/5G, was thenanalyzed using logistic regression. When the calculationof gene effect is positive, the genetic model would beevaluated using lambda value (λ), which is the ratio

206 A. Assawamakin, et al.
of log OR4G/5G
to log OR4G/4G
. The genetic model isevaluated as recessive, dominant and co-dominant ifλ = 0, 1, and 0.5 respectively. Pooled ORs wereestimated using both random and fixed effect models.Under the random effect model, weighting individualORs were carried out using the reciprocal of theirvariances. In addition, we also performed a subgroupanalysis to eliminate other factors such as ethnicityand age groups. Egger’s linear regression test andthe funnel plot were used to assess publication bias.All analyzed data were performed using the softwareMIX version 1.7. A p-value less than 0.05 is consideredstatistically significant, except for the test ofheterogeneity in which p <0.10 was used.
ResultsPatients and genotyping
One hundred and seventy nine patients with acuteischemic stroke and 229 healthy controls wererecruited to genotype 4G/5G PAI-1 polymorphism.No deviation from HWE was found (Exact tests;p = 0.596920). The PAI-1 4G-allele, which is themutant form, is more prevalent than the 5G-allele fromboth group (0.56 in cases and 0.53 in controls). Thegenotype frequencies of control group were 29.26%of 4G/4G, 48.03% of 4G/5G, and 22.70% of 5G/5G.Similar to control group, the genotype frequencies ofcases were 28.50% of 4G/4G, 54.19% of 4G/5G, and17.31% of 5G/5G. The 4G/5G genotype is the mostcommon in both groups followed by 4G/4G, and 5G/5G. Either genotype frequency or allele frequency wasnot significantly different between two groups,although a trend towards a higher prevalence ofthe heterozygous 4G/5G in the cases was observed[odds ratio (OR) 1.279; 95% confidence interval [CI]= 0.8638, 1.896]. In a regression analysis, the oddsratio (OR) for 4G/4G versus 4G/5G+5G/5G was1.038 (95% confidence interval [CI] = 0.674-1.598)(de Finetti); that is no clear association between4G/5G PAI-1 polymorphism and the acute ischemicstroke phenotype.
Meta-Analysis of PAI-1 4G/5GTwenty-seven studies were obtained using
keyword search from online publication databases.Three of these articles were the meta-analysis[3, 22]. Forty-nine case-control studies were reviewed[1, 3, 5-7, 9, 15-19, 22-50]. Twenty-five studies wereineligible, which can be characterized as 1) two studiesinvestigated stroke in the young 2) five studies were
irrelevant 3) seven studies had no genotypic data, and4) fourteen studies were duplicates [5, 7, 15-18, 28,31, 32, 36, 44, 46, 51]. Therefore, 26 studies includingpresent data from our study were considered inthis meta-analysis. There was, however, a diversityof ethnic groups studied from a wide geographicalrange. Thirteen studies were among Caucasians andthirteen studies were performed among Asians. Themeta-analysis experiments were performed on allstudies combined with no regard to ethnicity, andseparately for Caucasian and Asian populations(subgroup analysis). All individuals with stroke wererecruited only if an association exists between geneticsusceptibility and ischemic stroke in the studies. Thequality of these studies was determined by our meta-analysis ranged from 3 to 11.
The genotype frequencies of PAI-1 polymorphismwere classified as stroke and control. After addingthe results by combining with previous studies, meta-analysis was performed. The genotype distribution ofthe control group was in Hardy-Weinberg equilibrium(HWE). Heterogeneity between the studies wasobserved according to the calculation of bothI2 = 75.51% and Q statistic value <0.0001 respectively.Subgroup analysis was performed in order to handleethnic stratification. The heterogeneity factors weredescribed by I2 = 75.7 % and Q statistic value <0.0001in Asians and I2 = 69.08% and Q-statistic value<0.0004 in Caucasians. Therefore, the cause of theunderlying heterogeneity should be explored by furthersensitivity analysis.
A quality assessment scoring system was adoptedto review individual study bias so that the heterogeneitycan be re-calculated after excluding some studies.Similar heterogeneity results were obtained. We theninvestigated the most proper genetic model using thelambda method as described in the methodologysection. A non-significant genetic model was derivedfrom all analyses overall (λ = −1.65), and for Asian(λ = −0.53) and Caucasian (λ = −0.37) subgroupanalyses. Nonetheless, we could not find anappropriate genetic model for this polymorphism.Evidences from previous studies showed that therisk alleles of stroke affected only Asian population,while Caucasian results were inconclusive [3]. Thesubgroup analysis should be seriously considered. Weconducted the meta-analysis in all models to comparethe allele-based method (4G versus 5G), and thegenotype-based method (4G/4G vs. 5G/5G, 4G/4G vs.the remainders, and the remainders vs. 5G/5G).
207Vol. 6 No. 2
April 2012PAI-1 gene with insertion/deletion 4G/5G polymorphism
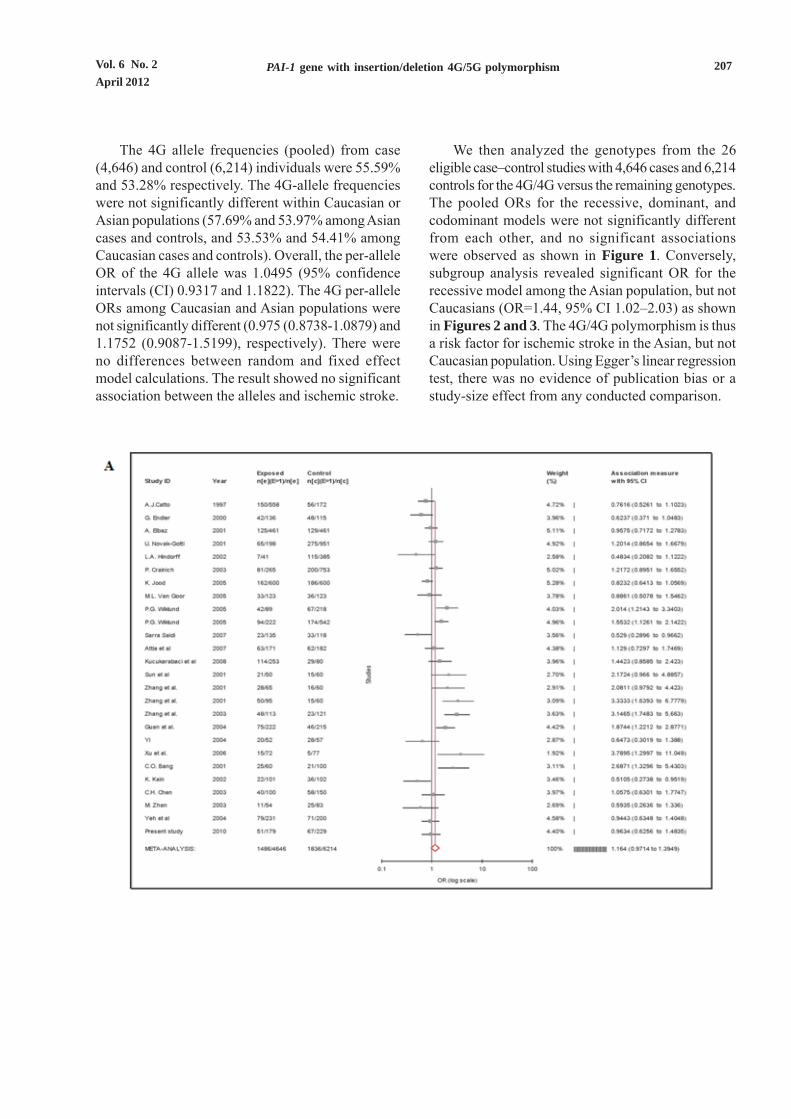
The 4G allele frequencies (pooled) from case(4,646) and control (6,214) individuals were 55.59%and 53.28% respectively. The 4G-allele frequencieswere not significantly different within Caucasian orAsian populations (57.69% and 53.97% among Asiancases and controls, and 53.53% and 54.41% amongCaucasian cases and controls). Overall, the per-alleleOR of the 4G allele was 1.0495 (95% confidenceintervals (CI) 0.9317 and 1.1822). The 4G per-alleleORs among Caucasian and Asian populations werenot significantly different (0.975 (0.8738-1.0879) and1.1752 (0.9087-1.5199), respectively). There wereno differences between random and fixed effectmodel calculations. The result showed no significantassociation between the alleles and ischemic stroke.
We then analyzed the genotypes from the 26eligible case–control studies with 4,646 cases and 6,214controls for the 4G/4G versus the remaining genotypes.The pooled ORs for the recessive, dominant, andcodominant models were not significantly differentfrom each other, and no significant associationswere observed as shown in Figure 1. Conversely,subgroup analysis revealed significant OR for therecessive model among the Asian population, but notCaucasians (OR=1.44, 95% CI 1.02–2.03) as shownin Figures 2 and 3. The 4G/4G polymorphism is thusa risk factor for ischemic stroke in the Asian, but notCaucasian population. Using Egger’s linear regressiontest, there was no evidence of publication bias or astudy-size effect from any conducted comparison.

208 A. Assawamakin, et al.
Figure 1. Forest plots from meta-analysis of all 26 eligible case-control association studies (Caucasian and Asiancombined). The effect size of each study is represented by a closed square point (the size of each pointcorresponds inversely to its variance) where the horizontal rule shows the 95% confidence interval of eachpoint. The red diamond at the bottom of the plot indicates the summary of effect sizes from the meta-analysis.A: recessive model (4G/4G versus the remainder) B: codominant model (4G/4G versus 5G/5G) C: dominantmodel (5G/5G versus the remainder)
209Vol. 6 No. 2
April 2012PAI-1 gene with insertion/deletion 4G/5G polymorphism

210 A. Assawamakin, et al.
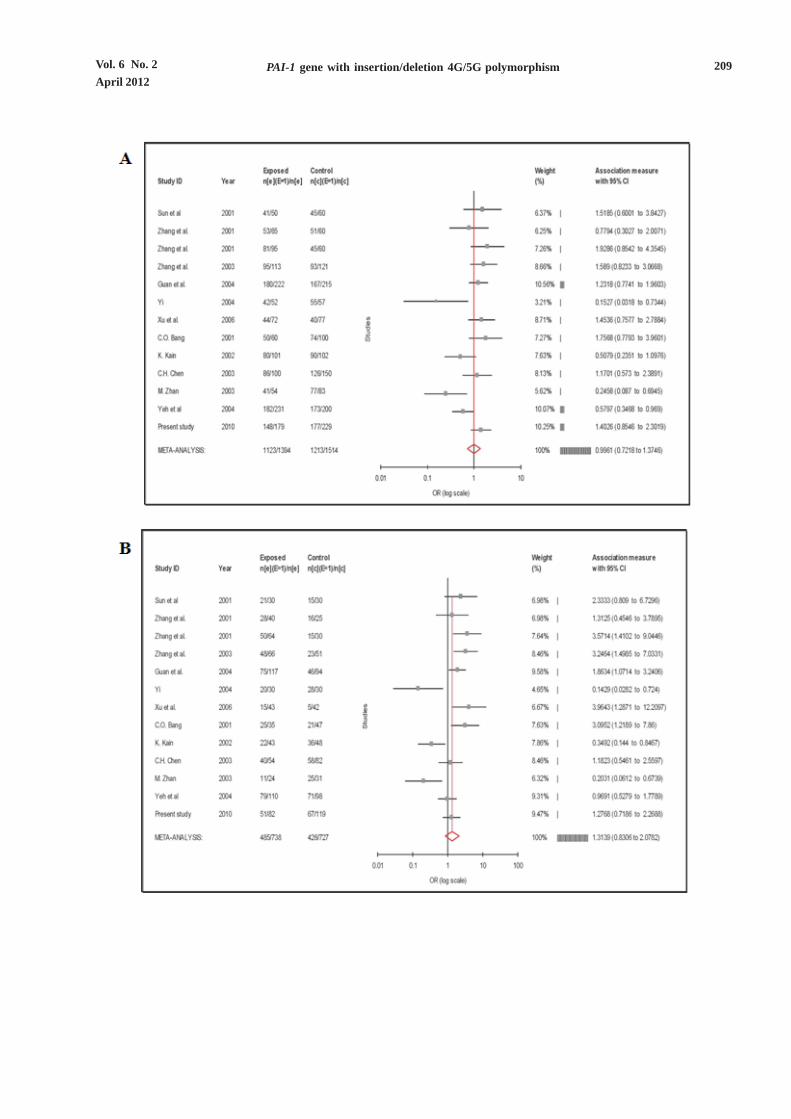
Figure 2. Forest plots from meta-analysis of 13 Asian-derived case-control association studies. The effect size of eachstudy is represented by a closed square point (the size of each point corresponds inversely to its variance)whereas the horizontal rule shows the 95% confidence interval of each point. The red diamond at the bottom ofthe plot indicates the summary of effect sizes from the meta-analysis. A: recessive model (4G/4G versus theremainder) B: codominant model (4G/4G versus 5G/5G) C: dominant model (5G/5G versus the remainder)

211Vol. 6 No. 2
April 2012PAI-1 gene with insertion/deletion 4G/5G polymorphism
Figure 3. Forest plots from meta-analysis of 13 Caucasian case-control association studies. The effect size of each studyis represented by a closed square point (the size of each point corresponds inversely to its variance) where thehorizontal rule shows the 95% confidence interval of each point. The red diamond at the bottom of the plotindicates the summary of effect sizes from the meta-analysis. A: recessive model (4G/4G versus the remainder)B: codominant model (4G/4G versus 5G/5G) C: dominant model (5G/5G versus the remainder)

212 A. Assawamakin, et al.
DiscussionOur findings reported no association between
the PAI-1 polymorphism and the risk of stroke inThai population. Due to the limitation of the samplesizes of our study, we then add our findings to previouspublished similar studies and performed meta-analysis.The meta-analysis of published studies demonstrateda significant association between the 4G/5Gpolymorphism in the promoter region of the PAI-1 geneand ischemic stroke in the Asian population. Theobserved association in Asians was robust underthe recessive model, which was consistent with theassumed role of this gene in the disease. On the otherhand, the 4G/5G polymorphism has no ischemicstroke association in Caucasians, which masks theassociation in Asians in the combined analysis.
Previous studies assumed that this polymorphismis likely to affect ischemic stroke in a recessive geneticmodel as the genotype reflects the expression of aprotein directly implicated in the disease. Surprisingly,the corresponding genetic model across all populationscould not be clearly established from these studies,which we showed using the lambda method.Nonetheless, comprehensive testing of all recessive,dominant and codominant models separately amongCaucasians and Asians did reveal that only therecessive model explains the association of 4G/4G inthe Asian population, which is in agreement with anearlier meta-analysis of the Han Chinese population[3]. Since stroke is regarded as a complex disease, itpotentially associates with many risk factors, bothenvironmental and genetic. Therefore, we might notbe able to unequivocally determine a genetic modelof the 4G/5G polymorphism among some populations,i.e. Caucasian.
Apart from the known effect of 4G/5Gpolymorphism on the expression of PAI-1 [7-12], otherfactors exist which control PAI-1 levels, such as verylow density lipoprotein [52], insulin and glucose [13].Moreover, these polymorphisms act as an acute-phasereactant [5, 8, 53], which means that difference inPAI-1 levels between 4G and 5G is more apparent inthe presence of stimulating factors [54]. It is worthnoting that although the 4G allele has been reportedto affect ischemic stroke, it is not yet establishedwhether it has a protective, neutral or harmful effect[13]. Therefore, all information pertaining to the 4Gallele and ischemic stroke was collated. The followingfindings might reveal the involvement of thispolymorphism in both being a risk and protective factor.
4G/4G genotype as a risk factor for ischemicstroke
1. 4G/4G polymorphism is related to higherPAI-1 levels in the circulation [7-12] and PAI-1 servesas a major physiological inhibitor of tissue plasminogenactivator (t-PA), thus impairing the fibrinolysis process[5, 6].
2. 4G/4G increases genetic susceptibility toelevated PAI-1 responses after an inflammatoryprocess. PAI-1 is considered as an acute-phasereactant which is regulated by inflammatory factorssuch as interleukin-1, TNF-α and TGF-β [5, 8, 53].It is believed that high levels of PAI-1 after a life-threatening condition impair fibrinolysis and increasesthe risk for ischemic stroke [39, 55].
3. Since ischemic stroke is one of the conditionsthat are caused by impaired circulation from thethromboembolic phenomenon, similar to coronaryartery disease and venous thromboembolism, theimpact of PAI-1 levels on the fibrinolysis pathway[5, 6] should be considered as a risk factor for thesediseases. For myocardial infarction, two meta-analysesshowed association of the 4G/4G genotype withincreased risk of myocardial infarction [14, 56]. Fordeep vein thrombosis, another meta-analysis partiallysupported the association of the 4G allele with therisk of venous thromboembolism [13, 21].
4. PAI-1 is associated with obesity, cholesteroland insulin resistance [27, 28, 57, 58], which areconsidered as risk factors for coronary artery diseaseand ischemic stroke. These might account for analternative hypothesis that this polymorphism alsoincreases the risk of myocardial infarction [59] as wellas ischemic stroke.
4G/4G genotype as a protective factor for ischemicstroke
Despite the impact of PAI-1 protein on thefibrinolysis pathway, many studies showed that the4G/4G genotype is associated with a decline in strokeincidence [16-20, 36, 38]. The current hypotheses areas follows:
1. Although tissue plasminogen activator (t-PA)has a major role in the fibrinolysis pathway, whichhelps clear clots, it also has a deleterious neurotoxiceffect. Neuronal death induced by t-PA can berescued by astrocytes and serpins, such as type-1plasminogen-activator inhibitor (PAI-1) andneuroserpin (NSP) [60].

213Vol. 6 No. 2
April 2012PAI-1 gene with insertion/deletion 4G/5G polymorphism
2. t-PA could also exacerbate the extracellularmatrix (ECM) degradation, which causesdestabilization of atherosclerotic plaques [61]. PAI-1serves as a protective role possibly involvingsuppression of matrix-degrading enzymes in theplaque, resulting in limited plaque growth andprevention of abnormal matrix remodeling [20, 62].
3. Animal studies have demonstrated that localcellular production of PAI-1 and t-PA might beinvolved in localized inflammatory processes, therebyplaying a major role in the process of atherosclerosisand plaque rupture [63, 64]. We hypothesize that atthe inflammatory sites, the putative elevation ofPAI-1 level is stronger for the 4G allele. This may, forinstance, result in plaque stabilization and increasedneutralization of t-PA, which is potentially neurotoxic[19].
4. 4G/4G polymorphism showed association withlower serum triglyceride levels in one study [38].
An alternative hypothesis is that the relationshipbetween elevated PAI-1 levels and myocardialinfarction is more straightforward than that of ischemicstroke. This hypothesis might explain the differencesin pathophysiological mechanisms betweenmyocardial infarction and stroke. In myocardialinfarction, rupture of atherosclerotic plaque is the mainmechanism and the plaques are associated withelevated PAI-1 level [65]. On the other hand, inthe case of ischemic stroke, small vessel diseaseand thromboembolism are more common causes ofcerebral ischemia than carotid and aortic archatherosclerosis [66].
With all the present information regarding theassociation between PAI-1 4G/5G polymorphism andrisk of ischemic stroke, it remains uncertain whethersuch a polymorphism has protective or harmful effect.Nevertheless, our meta-analysis revealed that ethnicitymight be an important factor in determining the effectof this polymorphism. Furthermore, there could bemany inherent variations across different studies thatinfluence the association result. First, ischemic strokeis a complex disease and genetic heterogeneity mayexist among different populations. Second, linkagedisequilibrium (LD) of the genetic markers fromdifferent studies may also contribute to the associationdiscrepancy. In other words, because differentpopulations sometimes have different LD patterns, thesame polymorphism could play a different role indisease susceptibility in different populations. Thisimplicates that the polymorphism might not be a causal
variant, i.e., it may be in the same LD block with anearby causal mutation in one population but not inanother [18, 67]. Third, the association differencesmight happen by chance, such as type I/II statisticalerrors, or due to lacking of multiple testing correctionwhich inflates the type I error [67]. Finally, theprevalence of the 4G allele varies among differentpopulations.
According to our comprehensive review results,the contribution of the 4G/5G polymorphism to ischemicstroke remains inconclusive. This may be because:
1. Stroke itself is a complex disease and hasmultiple risk factors.
2. PAI-1 protein may have variable influencesin different tissues, organs, conditions, or populationsas previously discussed in this paper.
3. The limitation from the individual studies’ biasincluding our meta-analysis, which exhibited highheterogeneity even in the subgroup analysis. Theheterogeneity could contribute to various factors, e.g.,ethnicity, particular sub-type of stroke, etc.
Meta-analysis, hence, should be interpreted verycarefully even when the meta-analysis was correctlycarried out.
ConclusionsAdding Thai samples to the pool of previously
published Asian data supports 4G/4G genotype as asignificant risk factor for Asians. Including data fromall populations resulted in non-significant association,which entails that PAI-1polymorphisms could be usedto predispose the risk of the disease only for specificpopulation. However, the low log OR
4G/4G from this
meta-analysis indicates that PAI-1 is not the only factorfor ischemic stroke, even though PAI-1 serves as amajor physiological inhibitor of tissue plasminogenactivator. Hence, the meta-analysis results from thisstudy support that the risk of ischemic stroke shouldnot be identified by only one major candidate PAI-1gene.
AcknowledgementsThe authors would like to thank Dr. Philip J. Shaw
for constructively commenting on the manuscript.Oranud Praditsap is supported by the ThailandResearch Fund (TRF) through the Royal GoldenJubilee Ph.D. Program (Grant No. PHD/4.I.MU.49/C.1). Sissades Tongsima is supported in part bythe National Center for Genetic Engineeringand Biotechnology (BIOTEC) and Anunchai

214 A. Assawamakin, et al.
Assawamakin (BIOTEC Post-doctoral FellowshipsProgram). Finally, Manop Pithukpakorn and SissadesTongsima acknowledge Thailand Research Fund(TRF) and the National Research Council of Thailand(NRCT) for partially supporting this work.
The authors declare no conflict of interest inconducting this study. Anunchai Assawamakin andNarin Sriratanaviriyakul equally contributed to thework.
References1. Yamada Y. Identification of genetic factors and
development of genetic risk diagnosis systems for
cardiovascular diseases and stroke. Circ. 2006; 70:
1240-8.
2. Lloyd-Jones D, Adams R, Carnethon M, De Simone G,
Ferguson TB, Flegal K, et al. Heart disease and stroke
statistics--2009 update: a report from the American
Heart Association Statistics Committee and Stroke
Statistics Subcommittee. Circulation. 2009; 119:e21-81.
3. Xu X, Li J, Sheng W, Liu L. Meta-analysis of genetic
studies from journals published in China of ischemic
stroke in the Han Chinese population. Cerebrovasc
Dis. 2008; 26:48-62.
4. Yu W, Gwinn M, Clyne M, Yesupriya A, Khoury MJ. A
navigator for human genome epidemiology. Nat Genet.
2008; 40:124-5.
5. Van Goor ML, Garcia EG, Leebeek F, Brouwers GJ,
Koudstaal P, Dippel D. The plasminogen activator
inhibitor (PAI-1) 4G/5G promoter polymorphism and
PAI-1 levels in ischemic stroke. A case-control study.
Thromb Haemost. 2005; 93:92-6.
6. Tsantes AE, Nikolopoulos GK, Bagos PG, Tsiara CG,
Kapsimali V, Travlou A, et al. Plasminogen activator
inhibitor-1 4G/5G polymorphism and risk of ischemic
stroke: a meta-analysis. Blood Coagul Fibrinolysis.
2007; 18:497-504.
7. Bang CO, Park HK, Ahn MY, Shin HK, Hwang KY,
Hong SY. 4G/5G polymorphism of the plasminogen
activator inhibitor-1 gene and insertion/deletion
polymorphism of the tissue-type plasminogen
activator gene in atherothrombotic stroke. Cerebrovasc
Dis. 2001; 11:294-9.
8. Dawson SJ, Wiman B, Hamsten A, Green F, Humphries
S, Henney AM. The two allele sequences of a common
polymorphism in the promoter of the plasminogen
activator inhibitor-1 (PAI-1) gene respond differently
to interleukin-1 in HepG2 cells. J Biol Chem. 1993; 268:
10739-45.
9. Ding J, Nicklas BJ, Fallin MD, de Rekeneire N,
Kritchevsky SB, Pahor M, et al. Plasminogen activator
inhibitor type 1 gene polymorphisms and haplotypes
are associated with plasma plasminogen activator
inhibitor type 1 levels but not with myocardial
infarction or stroke. Am Heart J. 2006; 152:1109-15.
10. Eriksson P, Kallin B, van ‘t Hooft FM, Bavenholm P,
Hamsten A. Allele-specific increase in basal
transcription of the plasminogen-activator inhibitor 1
gene is associated with myocardial infarction. Proc Natl
Acad Sci USA. 1995; 92:1851-5.
11. Stegnar M, Uhrin P, Peternel P, Mavri A, Salobir-Pajnic
B, Stare J, et al. The 4G/5G sequence polymorphism in
the promoter of plasminogen activator inhibitor-
1 (PAI-1) gene: relationship to plasma PAI-1 level in
venous thromboembolism. Thromb Haemost. 1998; 79:
975-9.
12. Zoller B, Garcia de Frutos P, Dahlback B. A common
4G allele in the promoter of the plasminogen activator
inhibitor-1 (PAI-1) gene as a risk factor for pulmonary
embolism and arterial thrombosis in hereditary protein
S deficiency. Thromb Haemost. 1998; 79:802-7.
13. Tsantes AE, Nikolopoulos GK, Bagos PG, Bonovas S,
Kopterides P, Vaiopoulos G. The effect of the
plasminogen activator inhibitor-1 4G/5G polymorphism
on the thrombotic risk. Thrombosis Research. 2008;
122:736-42.
14. Boekholdt SM, Bijsterveld NR, Moons AH, Levi M,
Buller HR, Peters RJ. Genetic variation in coagulation
and fibrinolytic proteins and their relation with acute
myocardial infarction: a systematic review. Circulation.
2001; 104:3063-8.
15. Wiklund PG, Nilsson L, Ardnor SN, Eriksson P,
Johansson L, Stegmayr B, et al. Plasminogen activator
inhibitor-1 4G/5G polymorphism and risk of stroke:
replicated findings in two nested case-control studies
based on independent cohorts. Stroke. 2005; 36:
1661-5.
16. Catto AJ, Carter AM, Stickland M, Bamford JM, Davies
JA, Grant PJ. Plasminogen activator inhibitor-1 (PAI-
1) 4G/5G promoter polymorphism and levels in subjects
with cerebrovascular disease. Thromb Haemost. 1997;
77:730-4.
17. Endler G, Lalouschek W, Exner M, Mitterbauer G, Haring
D, Mannhalter C. The 4G/4G genotype at nucleotide
position -675 in the promotor region of the
plasminogen activator inhibitor 1 (PAI-1) gene is less
frequent in young patients with minor stroke than in
controls. Br J Haematol. 2000; 110:469-71.
18. Hindorff LA, Schwartz SM, Siscovick DS, Psaty BM,
Longstreth WT, Reiner AP. The association of PAI-1

215Vol. 6 No. 2
April 2012PAI-1 gene with insertion/deletion 4G/5G polymorphism
promoter 4G/5G insertion/deletion polymorphism with
myocardial infarction and stroke in young women. J
Cardiovasc Risk 2002; 9:131-7.
19. Hoekstra T, Geleijnse JM, Kluft C, Giltay EJ, Kok FJ,
Schouten EG. 4G/4G genotype of PAI-1 gene is
associated with reduced risk of stroke in elderly. Stroke.
2003; 34:2822-8.
20. Roest M, van der Schouw YT, Banga JD, Tempelman
MJ, de Groot PG, Sixma JJ, et al. Plasminogen activator
inhibitor 4G polymorphism is associated with
decreased risk of cerebrovascular mortality in older
women. Circulation. 2000; 101:67-70.
21. Tsantes AE, Nikolopoulos GK, Bagos PG, Rapti E,
Mantzios G, Kapsimali V, et al. Association between
the plasminogen activator inhibitor-1 4G/5G
polymorphism and venous thrombosis. A meta-
analysis. Thromb Haemost. 2007; 97:907-13.
22. Attia J, Thakkinstian A, Wang Y, Lincz L, Parsons M,
Sturm J, et al. The PAI-1 4G/5G gene polymorphism
and ischemic stroke: an association study and meta-
analysis. J Stroke Cerebrovasc Dis. 2007; 16:173-9.
23. Akar N, Akar E, Yilmaz E, Deda G. Plasminogen activator
inhibitor-1 4G/5G polymorphism in Turkish children
with cerebral infarct and effect on factor V 1691 A
mutation. J Child Neurol. 2001; 16:294-5.
24. Ando R, Doi M, Yamauchi K, Chida Y, Ida T, Endo K,
Yanagi H, Tomura S. Association of beta-fibrinogen
and factor VII polymorphism with plasma fibrinogen
and factor VII levels, and no association of PAI-1
polymorphism with plasma PAI-1 levels in hemodialysis
patients. Clin Nephrol. 2002; 58:25-32.
25. Arlestig L, Wallberg Jonsson S, Stegmayr B, Rantapaa-
Dahlqvist S. Polymorphism of genes related to
cardiovascular disease in patients with rheumatoid
arthritis. Clin Exp Rheumatol. 2007; 25:866-71.
26. Austin H, Chimowitz MI, Hill HA, Chaturvedi S,
Wechsler LR, Wityk RJ, et al. Cryptogenic stroke in
relation to genetic variation in clotting factors and
other genetic polymorphisms among young men and
women. Stroke. 2002; 33:2762-8.
27. Boncoraglio GB, Bodini A, Brambilla C, Carriero MR,
Ciusani E, Parati EA. An effect of the PAI-1 4G/5G
polymorphism on cholesterol levels may explain
conflicting associations with myocardial infarction
and stroke. Cerebrovasc Dis. 2006; 22:191-5.
28. Chen CH, Eng HL, Chang CJ, Tsai TT, Lai ML,
Chen HY, et al. 4G/5G promoter polymorphism of
plasminogen activator inhibitor-1, lipid profiles, and
ischemic stroke. J Lab Clin Med. 2003; 142:100-5.
29. Elbaz A, Cambien F, Amarenco P. Plasminogen
activator inhibitor genotype and brain infarction.
Circulation. 2001; 103, e13-14; author reply e13-14.
30. Guan WJ, Wang JX. Effect of gene polymorphism of
the PAI-1 gene promoter region on patients with
essential hypertension complicated by cerebral
infarction. Zhong Hua Lao Nian Yi Xue Za Zhi. 2004;
10:765-8.
31. Jood K, Ladenvall P, Tjarnlund-Wolf A, Ladenvall C,
Andersson M, Nilsson S, et al. Fibrinolytic gene
polymorphism and ischemic stroke. Stroke. 2005; 36:
2077-81.
32. Kain K, Young J, Bamford J, Bavington J, Grant PJ,
Catto AJ. Determinants of plasminogen activator
inhibitor-1 in South Asians with ischaemic stroke.
Cerebrovasc Dis. 2002; 14:77-83.
33. Komitopoulou A, Platokouki H, Kapsimali Z,
Pergantou H, Adamtziki E, Aronis S. Mutations and
polymorphisms in genes affecting hemostasis proteins
and homocysteine metabolism in children with arterial
ischemic stroke. Cerebrovasc Dis. 2006; 22:13-20.
34. Lee C, Kong M. An interactive association of common
sequence variants in the neuropeptide Y gene with
susceptibility to ischemic stroke. Stroke. 2007; 38:
2663-9.
35. Nowak-G�ttl U, Str�ter R, Kosch A, von Eckardstein
A, Schobess R, Luigs P, et al. The plasminogen
activator inhibitor (PAI)-1 promoter 4G/4G genotype
is not associated with ischemic stroke in a population
of Germanchildren. Eur J Hematol. 2001; 66:57-62.
36. Petrovic D, Milanez T, Kobal J, Bregar D, Potisk KP,
Peterlin B. Prothrombotic gene polymorphisms and
atherothrombotic cerebral infarction. Acta Neurol
Scand. 2003; 108:109-13.
37. Reiner AP, Schwartz SM, Frank MB, Longstreth WT,
Hindorff LA, Teramura G, et al. Polymorphisms of
coagulation factor XIII subunit A and risk of nonfatal
hemorrhagic stroke in young white women. Stroke.
2001; 32:2580-6.
38. Saidi S, Slamia LB, Mahjoub T, Ammou SB, Almawi
WY. Association of PAI-1 4G/5G and -844G/A gene
polymorphism and changes in PAI-1/tPA levels in
stroke: a case-control study. J Stroke Cerebrovasc Dis.
2007; 16:153-9.
39. Sirgo G, Perez-Vela JL, Morales P, Del Rey M, Vendrell
J, Gutierrez C, et al. Association between 4G/5G
polymorphism of the plasminogen activator inhibitor
1 gene with stroke or encephalopathy after cardiac
surgery. Intensive Care Med. 2006; 32:668-75.
40. Sun Q, Zhang YD, Liu Y. The study of plasma PAI-1
activity and its gene polymorphism in cerebral

216 A. Assawamakin, et al.
infarction. Nao Yu ShenJing Ji Bing Za Zhi. 2001; 9:
323-6.
41. Xu BZC, Xian BX. A study of the plasma plasminogen
activator inhibitor-1 activity and its promoter region
4G/5G gene polymorphism in acute cerebral infarction,
Zhong Guo Yi Shi Jin Xiu Za Zhi. 2006; 29:26-8.
42. Yeh PS, Lin HJ, Li YH, Lin KC, Cheng, TJ, Chang CY,
Ke DS. Prognosis of young ischemic stroke in Taiwan:
impact of prothrombotic genetic polymorphisms.
Thromb Haemost. 2004; 92:583-9.
43. Zee RY, Cook NR, Cheng S, Reynolds R, Erlich HA,
Lindpaintner K, Ridker PM. Polymorphism in the
P-selectin and interleukin-4 genes as determinants of
stroke: a population-based, prospective genetic
analysis. Hum Mol Genet. 2004; 13:389-96.
44. Zhan M, Zhou Y, Han Z. Plasminogen activator
inhibitor-1 4G/5G gene polymorphism in patients with
myocardial or cerebrovascular infarction in Tianjin,
China. Chin Med J. 2003; 116:1707-10.
45. Zhang SB, Wang JX. The associationof PAI-1 4G/5G
polymorphismwith cerebral infarction. Shan Dong
Yi Yao. 2003; 43:42-3.
46. Zhang C, Li J, Li L, Luo B. The study of PAI-1
promotor region gene polymorphism in
cerebrovascular disease. Zhonghua Yi Xue Yi Chuan
Xue Za Zhi. 2001; 18:383-7.
47. Zhang YDSQ, Liu Y. The association of PAI-1 gene
polymorphism with cerebral infarction and recurrent
cerebral infarction. Lin Chuang Shen Jing Bing Xue
Za Zhi. 2001; 14:262-5.
48. Yi G. A study of the plasma plasminogenactivator
inhibitor-1 activity and its promoterregion gene
polymorphism in acute cerebralinfarction., Qing Dao
Da Xue Yi XueYuan Xue Bao. 2004; 40:229-31.
49. Crainich PJN, Tang Z, Arnold AM, Kuller LH,
Manolio T. Lack of association of the plasminogen
activator inhibitor-1 4G/5G promoter polymorphism
with cardiovascular disease in the elderly. J Thromb
Haemost. 2003;1 :1799-804.
50. Kucukarabaci B, Gunes HV, Ozdemir G, Cosan D,
Ozbabalik D, Dikmen M, Degirmenci I. Investigation
of association between plasminogen activator
inhibitor type-1 (PAI-1) gene 4G/5G polymorphism
frequency and plasma PAI-1 enzyme activity in
patients with acute stroke. Genet Test12.2008; xxx:
443-51.
51. Crainich P, Jenny NS, Tang, Z, Arnold AM, Kuller LH,
Manolio T, et al. Lack of association of the plasminogen
activator inhibitor-1 4G/5G promoter polymorphism
with cardiovascular disease in the elderly. J Thromb
Haemost1. 2003;1799-1804.
52. Nilsson L, Gafvels M, Musakka L, Ensler K, Strickland
DK, Angelin B, et al. VLDL activation of plasminogen
activator inhibitor-1 (PAI-1) expression: involvement
of the VLDL receptor. J Lipid Res. 1999; 40:913-9.
53. Van Hinsbergh VW, Kooistra T, Van den Berg EA,
Princen HM, Fiers W, Emeis, JJ. Tumor necrosis
factor increases the production of plasminogen
activator inhibitor in human endothelial cells in vitro
and in rats in vivo. Blood. 1988; 72:1467-73.
54. Hoekstra T, Geleijnse JM, Schouten EG, Kluft C.
Plasminogen activator inhibitor-type 1: its plasma
determinants and relation with cardiovascular risk.
Thromb Haemost. 2004; 91:861-72.
55. Vergouwen MD, Frijns CJ, Roos YB, Rinkel GJ, Baas
F, Vermeulen M. Plasminogen activator inhibitor-1 4G
allele in the 4G/5G promoter polymorphism increases
the occurrence of cerebral ischemia after aneurysmal
subarachnoid hemorrhage. Stroke. 2004; 35:1280-3.
56. Ye Z, Liu EH, Higgins JP, Keavney BD, Lowe GD,
Collins R, Danesh J. Seven haemostatic gene
polymorphisms in coronary disease: meta-analysis
of 66,155 cases and 91,307 controls. Lancet. 2006; 367:
651-8.
57. Bastard JP, Pieroni L, Hainque B. Relationship between
plasma plasminogen activator inhibitor 1 and insulin
resistance. Diabetes Metab Res Rev. 2008; 16:192-201.
58. Sartori MT, Vettor R, De Pergola G, De Mitrio V,
Saggiorato G, Della Mea P, et al. Role of the 4G/5G
polymorphism of PaI-1 gene promoter on PaI-1 levels
in obese patients: influence of fat distribution and
insulin-resistance. Thromb Haemost. 2001; 86:1161-9.
59. Iacoviello L, Burzotta F, Di Castelnuovo A, Zito F,
Marchioli R, Donati MB. The 4G/5G polymorphism of
PAI-1 promoter gene and the risk of myocardial
infarction: a meta-analysis. Thromb Haemost. 1998; 80:
1029-30.
60. Benchenane K, Lopez-Atalaya JP, Fernandez-
Monreal M, Touzani O, Vivien D. Equivocal roles of
tissue-type plasminogen activator in stroke-induced
injury. Trends Neurosci. 2004; 27:155-60.
61. Underwood MJ, De Bono DP. Increased fibrinolytic
activity in the intima of atheromatous coronary arteries:
protection at a price. Cardiovasc Res. 1993; 27:882-5.
62. Heymans S, Luttun A, Nuyens D, Theilmeier G,
Creemers E, Moons L, et al. Inhibition of plasminogen
activators or matrix metalloproteinases prevents
cardiac rupture but impairs therapeutic angiogenesis
and causes cardiac failure. Nat Med. 1999; 5:1135-42.
63. Carmeliet P, Moons L, Dewerchin M, Mackman N,

217Vol. 6 No. 2
April 2012PAI-1 gene with insertion/deletion 4G/5G polymorphism
Luther T, Breier G, et al. Insights in vessel development
and vascular disorders using targeted inactivation
and transfer of vascular endothelial growth factor,
the tissue factor receptor, and the plasminogen
system. Ann N Y Acad Sci. 1997; 811:191-206.
64. Nagai N, De Mol M, Lijnen HR, Carmeliet P, Collen D.
Role of plasminogen system components in focal
cerebral ischemic infarction: a gene targeting and
gene transfer study in mice. Circulation. 1999; 99:
2440-4.
65. Kohler HP, Grant PJ. Plasminogen-activator inhibitor
type 1 and coronary artery disease. N Engl J Med.
2000; 342:1792-801.
66. Adams HP, Bendixen BH, Kappelle LJ, Biller J, Love
BB, Gordon DL, et al. Classification of subtype of
acute ischemic stroke. Definitions for use in a
multicenter clinical trial. TOAST. Trial of Org 10172 in
Acute Stroke Treatment. Stroke. 1993; 24:35-41.
67. Han S, Li Y, Mao Y, Xie Y. Meta-analysis of the
association of CTLA-4 exon-1 +49A/G polymorphism
with rheumatoid arthritis. Hum Genet. 2005; 118:
123-32.