Meeting of the West Suffolk CCG Governing Body
248
Page 1 of 4 Meeting of the West Suffolk CCG Governing Body to be held from 0915–1230 hrs on Wednesday 25 November 2020 In response to the challenges facing the NHS and to reduce the risk of coronavirus transmission, the meeting will be ‘live streamed’ for members of the public (a link for the live streaming will be available on the CCG website). Members of the public are invited to submit questions relating to agenda items either, prior to the meeting, via email to [email protected], or during the live streaming when they will be collated and asked at the appropriate time on the agenda. The minutes of the meeting which will include answers to any questions submitted by the public will be published on the CCG website after the meeting. AGENDA GENERAL BUSINESS 1. Apologies for Absence Dr Christopher Browning 2. Declarations of Interest and any hospitality or gifts. Declarations of interest made by members of the Governing Body are listed in the CCG’s Register of Interests which, along with the CCG’s Hospitality and Gifts Register, is available on the CCG website. All 3. Minutes of the previous West Suffolk CCG Governing Body meeting. To approve as a correct record Minutes of the West Suffolk CCG Governing Body meeting held on 23 September 2020 Dr Christopher Browning 4. Matters Arising and Action Log Dr Christopher Browning 5. General Update To receive a verbal report from the Chief Executive Ed Garratt STRATEGY AND SERVICE DEVELOPMENT 6. Patient Story 7. St Nicholas Hospice for Death literacy To receive and note an update from the Director of Integration Kate Vaughton Report No: WSCCG 20-41 (Verbal Report)
-
Upload
khangminh22 -
Category
Documents
-
view
2 -
download
0
Transcript of Meeting of the West Suffolk CCG Governing Body

Page 1 of 4
Meeting of the West Suffolk CCG Governing Body to be held from 0915–1230 hrs on Wednesday 25 November 2020
In response to the challenges facing the NHS and to reduce the risk of coronavirus transmission, the meeting will be ‘live streamed’ for members of the public (a link for the live streaming will be available on the CCG website).
Members of the public are invited to submit questions relating to agenda items either, prior to the meeting, via email to [email protected], or during the live streaming when they will be collated and asked at the appropriate time on the agenda. The minutes of the meeting which will include answers to any questions submitted by the public will be published on the CCG website after the meeting.
AGENDA
GENERAL BUSINESS 1. Apologies for Absence Dr Christopher Browning 2. Declarations of Interest and any hospitality or gifts.
Declarations of interest made by members of the Governing Body are listed in the CCG’s Register of Interests which, along with the CCG’s Hospitality and Gifts Register, is available on the CCG website.
All
3. Minutes of the previous West Suffolk CCG Governing Body
meeting. To approve as a correct record Minutes of the West Suffolk CCG Governing Body meeting held on 23 September 2020
Dr Christopher Browning
4. Matters Arising and Action Log Dr Christopher Browning 5. General Update
To receive a verbal report from the Chief Executive Ed Garratt
STRATEGY AND SERVICE DEVELOPMENT 6. Patient Story 7. St Nicholas Hospice for Death literacy
To receive and note an update from the Director of Integration
Kate Vaughton Report No:
WSCCG 20-41 (Verbal Report)

Page 2 of 4
8. West Suffolk Alliance Update To receive and note a report from the Director of Integration
Kate Vaughton Report No:
WSCCG 20-42 9. Community Engagement Group and Patient and Public
Involvement To receive and note a report from the Lay Member for Patient and Public Involvement
Lynda Tuck Report No:
WSCCG 20-43
10. Suffolk and North East Essex Clinical Commissioning Groups
Commissioning Intentions 2021-22 To receive and approve a report from the Director for Strategy and Transformation
Richard Watson Report No:
WSCCG 20-44
11. Procurement Update: Summary of Activity 2020/21
To receive and note a report from the Director of Performance Improvement
Paul Gibara Report No:
WSCCG 20-45 12. 2020 Emergency Planning Resilience and Response (EPRR) Core
Standards Audit To receive and note a report from the Director of Performance Improvement
Paul Gibara Report No:
WSCCG 20-46
13. Special Educational Needs and Disability (SEND) Annual Report
2019/20 To receive and note a report from the Director of Nursing
Lisa Nobes Report No:
WSCCG 20-47 14. Covid-19 and Vaccine Update
To receive and note a verbal report from the Director of Nursing Lisa Nobes Report No:
WSCCG 20-48 (Verbal Report)
FINANCE, PERFORMANCE AND SCRUTINY 15. 2020/21 Months 7-12 Budget
To receive and approve a report from the Director of Finance Jane Payling
Report No: WSCCG 20-49
16. Integrated Performance Report - Are the CCGs finances,
performance and quality on track? To receive and note a report from Directors. Order of presentation: 1) Director of Performance Improvement 2) Director of Nursing 3) Director of Strategy and Transformation 4) Director of Integration 5) Director of Finance
Directors Report No:
WSCCG 20-50
17. Governing Body Assurance Framework
To receive and approve a report from the Director of Corporate Services and System Infrastructure
Amanda Lyes Report No:
WSCCG 20-51

Page 3 of 4
GOVERNANCE AND CORPORATE BUSINESS 18. Appointment of External Auditors
To receive and approve a report from the Director of Finance Jane Payling
Report No: WSCCG 20-52
19. Health, Safety and Risk Committee
To receive and note a report from the Director of Corporate Services and System Infrastructure
Amanda Lyes Report No:
WSCCG 20-53 20. Declaration of Interests
To receive and note a report from the Director of Corporate Services and System Infrastructure
Amanda Lyes Report No:
WSCCG 20-54 21. Terms of Reference – Commissioning Governance Committee
To receive and approve the terms of reference for the Commissioning Governance Committee
Amanda Lyes Report No:
WSCCG 20-55 22. Minutes of Meetings:
To receive a report seeking the endorsement of minutes and decisions from the following West Suffolk CCG Sub Committees.
a) Audit Committee
The unconfirmed minutes of a meeting held on 15 September 2020 b) Remuneration and HR Committee
The unconfirmed minutes of a meeting held on 6 October 2020 c) Financial Performance Committee
Minutes from a meeting held on 16 September 2020 d) Covid-19 Resource Approval Committee
Minutes from meetings held on 17 September 2020 and 15 October 2020
e) West Suffolk CCG Primary Care Commissioning Committee
Decision from a virtual meeting held on 20 October 2020 and the unconfirmed minutes of a meeting held on 27 October 2020
f) Commissioning Governance Committee
The minutes from a meeting held on 21 August 2020 and decision from a virtual meeting held on 8 September 2020
g) CCG Collaborative Group
The minutes of a meeting held on 10 September 2020.
h) Suffolk and North East Essex Area Prescribing Committee (SNEE APC) Meeting- minutes of the meeting June-September 2020
Committee Chairs Report No:
WSCCG 20-56
23. Date and Time of future Governing Body meetings
0915 - 1200 Wednesday 27 January 2021
24. Questions from the public – Maximum 15 minutes

Page 4 of 4
Please note questions should relate to the items under discussion and must be a question rather than statement. Where individuals deviate from this requirement they will be asked to stop and will not be invited to take any further part in the meeting.
Exclusion of the Press and Public
The Governing Body is recommended to exclude representatives of the press, and other members of the
public, from the meeting having regard to the confidential nature of the business to be transacted, publicity on which would be prejudicial to the public interest; Section 1(2), Public Bodies (Admission to
Meetings) Act 1960.

Financial Interests
Non Financial Professional
Interests
Non Financial Personal Interests
From To
Governing Body GP Member Zohra Armitage GP and GP Streaming work for Suffolk GP Federation Direct Ongoing 07/10/2020 No further action required YesHusband is a consultant urologist at Cambridge University Hospital Indirect Ongoing 07/10/2020 No further action required YesDirector of company providing urological services to Swan Surgery, BSE Direct Ongoing 07/10/2020 To be declared when appropriate Yes
Lay Member for Governance and Vice Chair CCG Geoff Dobson Former Director of Resource Management with Suffolk County Council Indirect Ongoing 06/10/2020 No further action required YesFamily member attending Healthier You, NHS Diabetes Prevention Programme’' Indirect Apr-20 Ongoing 06/10/2020 No further action required Yes
CCG Chair Christopher Browning PMS Provider, Practice Partner Long Melford Direct 2001 Ongoing 03/04/2020 To be declared at relevant meetings YesOut of Hours doctor for Care UK and Suffolk GP Federation Direct 2010 Ongoing 03/04/2020 To be declared at relevant meetings YesWife is Consultant at West Suffolk Hospital Indirect 2004 Ongoing 03/04/2020 To be declared at relevant meetings YesClinical Director for WGGL PNN" Direct Ongoing 03/04/2020 To be declared at relevant meetings Yes
Lay Member Steve Chicken Owner and MD of Galliform Ltd, consultancy and training company. No NHS activity Direct 2009 Ongoing Leave No further action required YesLay Member for Ipswich and East Suffolk CCG Direct 2016 Ongoing Leave To be declared when appropriate YesWife is President and Director of East of England Co-op Indirect 2018 Ongoing Leave To be declared when appropriate Yes
Chief Officer Ed Garratt Accountable Officer for Ipswich and East Suffolk CCG Direct Mar-16 Ongoing 23/10/2020 To be declared when appropriate YesAccountable Officer for North East Essex CCG Direct Jan-19 Ongoing 23/10/2020 To be declared when appropriate YesExecutive Lead - Suffolk and North East Essex Integrated Care System Direct Apr-19 Ongoing 23/10/2020 To be declared when appropriate Yes
Director of Performance Improvement Paul Gibara Director of Performance Improvement for SNEE CCGs Direct Ongoing 30/10/2020 YesEnhanced Associate GP Andrew Hassan Wife has GDS contract with NHS England Indirect Ongoing 07/10/2020 YesDirector of Corporate Services and System InfrastructureAmanda Lyes Director of Corporate Services and System Infrastructure for Ipswich and East Suffolk and North East Essex CCGs Direct Ongoing 12/10/2020 None YesDirector of Nursing Lisa Nobes Chief Nursing Officer for Ipswich and East Suffolk CCG and North East Essex CCG Direct Ongoing 03/04/2020 None YesDirector of Finance Jane Payling Director of Finance for Ipswich and East Suffolk CCG and North East Essex CCG
Direct 25/09/2017 Ongoing 28/10/2020 Arrangements in place for the joint management team of
the CCGsYes
Trustee of Cambridge Theatre Trust Direct Oct-18 Ongoing 28/10/2020 To declare when appropriate YesGoverning Body GP Member Godfrey Reynolds Member of the Local Medical Committee Direct Ongoing 02/10/2020 None Yes
Chair of Mildenhall Sick and Poor Fund Direct 1989 Ongoing 02/10/2020 None YesConsultant in Public Health Medicine Jep Ronoh Husband is a salaried GP at Hardwicke House Surgery and does locum work for Out of hours provider, Suffolk GP Fed and
other GP Surgeries Direct Ongoing07/11/2019 To declare when appropriate Yes
Governing Body GP Member Bahram Talebpour Medical Director of Sudbury Primary Care Network Direct Ongoing 24/04/2020 No further action required YesGP Partner Direct Ongoing 24/04/2020 No further action required Yes
Chair of Community Engagement Partnership David Taylor Chairman of Hargrave Parish Council Direct Apr-17 Ongoing 23/10/2020 No further action required YesLay Member for Patient and Public Involvement Linda Tuck Nil 05/10/2020 YesChief Operating Officer Kate Vaughton Director of Integration for West Suffolk NHS Foundation Trust, non-voting member of Board Direct Ongoing 03/11/2020 To declare when appropriate YesGoverning Body GP Member Firas Watfeh Local Medical Committee member Direct 01/08/2015 Ongoing 23/10/2020 Yes
Haverhill PCN Director Direct Ongoing 23/10/2020 YesGP Partner at Haverhill Family Practice Direct 04/07/1905 Ongoing 23/10/2020 Yes
Director of Strategy and Transformation Richard Watson Director of Strategy and Transformation for Ipswich and East Suffolk, North East Essex CCGs and West Suffolk CCGs Direct Jan-15 Ongoing 08/10/2020 None YesHusband is employee of Hadleigh Group Practice Direct Oct-19 Ongoing 08/10/2020 None Yes
Governing Body GP Member Victoria Wilson Shares in company for ophthalmology related work Direct Ongoing 16/10/2020 To be declared when appropriateMaternity work for maternity voices partnership, West Suffolk Hospital Direct Ongoing 16/10/2020 No further action required
Governing Body GP Member Andrew Yagar Macmillan GP Direct 2021 Ongoing 31/10/2020 YesGoverning Body GP Member Vacant GP PostGoverning Body PM Member Vacant PostGoverning Body PM Member Vacant PostSecondary Care Doctor Vacant Post
West Suffolk CCG Governing Body and Sub Committee Members
Title First Name Last Name Direct or Indirect
Date of Interest Date of Receipt
Action Taken to Mitigate Consent to Publish
Type of InterestDeclared Interest
Meeting of the West Suffolk CCG Governing Body held in public on Wednesday 23 September 2019 via Microsoft Teams and live streamed for members of the public.
PRESENT: Dr Christopher Browning CCG Chair Dr Zohra Armitage GP Member Geoff Dobson Lay Member for Governance Ed Garratt Chief Executive Paul Gibara Director of Performance Improvement Amanda Lyes Director of Corporate Services and System Infrastructure Lisa Nobes Director of Nursing Jane Payling Director of Finance Dr Godfrey Reynolds GP Member Dr Bahram Talebpour GP Member Lynda Tuck Lay Member: Patient and Public Involvement Kate Vaughton Chief Operating Officer Dr Firas Watfeh GP Member Richard Watson Director of Strategy and Transformation Dr Andrew Yager GP Member IN ATTENDANCE
Sarah Colley Communications Team Dr Andrew Hassan Enhanced Associate GP (Part) Jo Mael Corporate Governance Manager Simon Morgan Head of Communications
20/054 WELCOME AND APOLOGIES FOR ABSENCE
The Chair welcomed everyone to the meeting and apologies for absence were received from; Steve Chicken Lay Member Dr Jep Ronoh Consultant in Public Health Medicine David Taylor Community Engagement Group Chair Dr Victoria Wilson GP Member
20/055 DECLARATIONS OF INTEREST AND HOSPITALITY AND GIFTS
Kate Vaughton declared an interest as Director of Integration and as a non-voting
Board Member of West Suffolk NHS Foundation Trust.
20/056 MINUTES OF PREVIOUS MEETING
The minutes of the meeting held on 29 July 2020 were approved as a correct record.
20/057 MATTERS ARISING AND ACTION LOG

There were no matters arising and the action log was reviewed and updated.
20/058 GENERAL UPDATE
The Chief Executive reported; • There was an excellent paper on the West Alliance on the agenda. • Progress in respect of the ‘What are we missing’ movement had been good and
events were planned in West Suffolk and North East Essex. • Covid-19 – it was likely that the system would move back into a response phase
as well as pursuing recovery. The system recovery plan had been submitted. • Winter plan work was underway together with flu vaccination. • The system People Plan had been submitted and would be presented to a future
Governing Body. Work continued with the University of Suffolk on Integrated Care Academy and a Health and Care Academy had been launched in Colchester and would be rolled into East and West Suffolk in coming months.
• System financial allocations had now been received for the rest of the year. • The Chief Executive was now sitting on a national committee looking at public
health and was specifically involved in health improvement work. An update would be provided to a future Governing Body meeting.
The Governing Body noted the update.
20/059 PATIENT STORY
There was no patient story at today’s meeting.
20/060 WEST SUFFOLK ALLIANCE UPDATE
The report provided a quarterly update for the Governing Body on activity to transform services and outcomes for people within the West Suffolk Alliance area. A number of different teams had contributed to the report, from across the CCG, the hospital and Alliance partners. Alliance partners continued to seek to build on changes made during the past six months where those were in line with the Alliance strategy. The first part of the report outlined some of the key changes in services and ways of working that had taken place during the previous quarter. The next section showed how the Alliance had been working as part of the wider Integrated Care System, (ICS), for example contributing to phase three recovery planning which was co-ordinated ICS wide as well as to other NHS England requirements for example winter planning. The final section of the report updated the Governing Body on Alliance business, governance, leadership and quality improvement. The report demonstrated good understanding and integrated working. It was encouraging to see patient stories incorporated within the report and the need for Carers to be recognised was emphasized. It was highlighted that it might be beneficial for families if they could be given time slots for visits. A business case was in development across Suffolk and North East Essex in relation to a range of initiatives that might encourage the use of 111 and reduce A&E activity. The business case would be presented to the Executive in October 2020. The work was a national initiative with intended implementation from early December 2020.

Having noted that Abbeycroft Leisure had been mentioned within the report, the sustainability of the leisure centre in light of Covid-19 was queried. The Governing Body was informed that the Alliance was working with the leisure centre on how it might introduce new ways of working that would benefit the locality model and support the community. The Governing Body noted the report.
20/061 COMMUNITY ENGAGEMENT GROUP (CEG) AND PATIENT AND PUBLIC
INVOLVEMENT (PPI)
The Governing Body received a report which presented updates from the Community Engagement Group (CEG) meetings and PPI activity between 30 July 2020 – 15 September 2020. Section 2 of the report summarised key issues and themes that had been raised by CEG members between 30 July and 15 September 2020, as well as information shared from the CCG and guest speakers that had attended CEG meetings. Appropriate action had been taken to address all issues raised by members. Points highlighted included; • The CEG had continued to meet monthly on a virtual basis to share experiences
and receive presentations from speakers. • The CEG had raised questions as to how it might help with winter planing and
communications, together with how it might provide feedback to the CCG. • Members of the CEG had participated in interviews, groups and transformation
and delivery opportunities to ensure the patient voice was heard. • There had been concern with regard to the forthcoming flu vaccination
programme and how practices might be supported to deliver and encourage people to have the vaccination.
• Integration was improving and it was felt that the next step was for improved communications between health and social care to ensure continuity of care and advice.
• Virtual appointments had been accepted well by the public. The need to feed ‘what matters to you’ conversations into CCG work was recognised. Although the existence of locality meetings in Newmarket was questioned, the Governing Body was reassured that working groups were in existence and further information should be available in the near future. The Governing Body noted the report.
20/062 PROCUREMENT UPDATE: SUMMARY OF ACTIVITY 2020/21
The Governing Body was provided with an update on procurements completed
since the last update and those currently in progress and planned for 2020/21. Due to the impact of Covid-19 all procurements were stopped in April 2020; some procurements had been restarted, whereas others were now being reviewed in light of the changes due to Covid-19 or the progression of time impacting on the options available. Key points highlighted included;

Work was progressing on the establishment of a Procurement Board; Terms of Reference had been drafted and were out for comment. Once a final draft had been agreed they would be sent to the Executive and Governing Body to ratify the role and responsibilities of the Board. The CCG currently commissioned Pathology Services with NHS West Suffolk CCG and NHS North East Essex CCG through a contract with North Essex & East Suffolk Pathology Services (NEESPS). During December 2019 it was agreed to extend the contract until October 2020, whilst reviews of the service were continued. A further extension was being proposed to enable the procurement to be completed – it was likely to require 12-18 months for a procurement process to be undertaken which would decide the long-term delivery of those services. The Governing Body noted the content of the report and requested that the Executive be provided with updates on the Pathology and Mental Health elements.
20/063 INTEGRATED PERFORMANCE REPORT
The CCG’s Director of Performance Improvement advised that the report had been
produced in the context of Covid-19 and its impact on performance which was likely to carry on into Winter. The report had been scrutinized by the CCG’s Clinical Scrutiny Committee prior to presentation to the Governing Body. Key points included; • Cancer performance performance improved. There was key focus on bringing
cancer capacity back although diagnostics was key to that being possible. Largest risk is endoscopy which is challenging due to Covid-19. 104 waiters have been reduced.
• Referral To Treatment (RTT) times continued to be a cause for concern as
waiting lists were growing. Recovery plans were currently in the early stages. Risk stratification of patients was being considered.
• There was early indication that mental health performance was improving
although the situation was being monitored closely in light of a return to normal activity. Key focus physical health checks and dementia.
• Patient transport activity was expected to increase in Winter. • East of England Ambulance Service NHS Trust (EEAST) – Category two
response times had slightly declined and discussions were taking place regarding a way forward over the Winter months to improve performance.
Having queried what might be required if the system went back into Covid-19 high demand, it was explained that a meeting with West Suffolk NHS Foundation Trust (WSFT) was planned to review its bed and activity plan month by month. Whilst the national team had assumed a 8% contingency for bed capacity, WSFT was putting in additional contingency in light of the possible second wave. There was a need to review the plan and take account of any further data. Winter planning would include support for primary care and Covid-19 testing would be key throughout the winter period. 40% of WSFT outpatient appts were being carried out virtually. Outpatient work was ongoing and a Trust led Clinical Reference Group had been established that CCG GP leads had been invited to attend.

It was queried whether there might be any financial penalty associated to targets mentioned within Simon Stevens recovery letter not being met by hospitals. It was felt that, as it seemed we were heading into a second wave of the pandemic, further communications from the centre were likely. The Director of Nursing reported that a SNEE Flu and Covid-19 Board had been established that reported to the regional board. Workstreams were pulling together all work that primary care and the acutes were doing to increase vaccination of staff and patients. Preparations were being made for roll out of the Covid-19 vaccination when available. Continuing healthcare had restarted with staff currently working through deferred assessments. Suffolk was to be one of the first systems to have a Special Educational Needs and Disability (SEND) visit from Ofsted and the Care Quality Commission in October 2020 to look at how the system had supported children and young people with SEND through Covid-19. Key points highlighted per provider were as follows: West Suffolk NHS Foundation Trust (WSFT) • Oversight of the Care Quality Commission (CQC) improvement plan continued.
Key aspect of the plan was maternity services and a programme of quality visits were planned.
• Quality Improvement Visits were planned in respect of medicines management actions from the CQC inspection and to review the care and treatment of patients with learning disability following incidences of raised concern.
Norfolk and Suffolk NHS Foundation Trust (NSFT) • The waiting list had reduced from 800 to 150 and work was taking place with
the Trust to understand increased acute activity. • Learning Disabilities – one inpatient at present. • There had been low uptake to the early invention psychosis service. • Work had taken place with the Children and Young People leadership team to
review services and identify priorities. • The Emotional Wellbeing Hub had been performing well with 86% of referrals
being responded to within 10 days. East of England Ambulance Service NHS Trust (EEAST) • The Safeguardng team continued its oversight. Safeguarding allegations being
overseen totalled 16 which was a reduction from 85 at the start of the year. • The CQC had carried out an unannounced inspection and the report was
awaited. • The stakeholder group had agreed an action plan to support EEAST with key
issues that might come out of the CQC report. Finance • Finances had been nationally calculated to the end of September 2020 and the
CCG had been required to submit claims for reimbursement. Year to date allocation had been slightly exceeded with top-up of £2m expected.
• Primary care delegated budget continue to be monitored closely. • Variances were, in the main, associated with the way funding was allocated.

Primary Care • Dementia and learning disability health check performance remained
challenging. • Flu vaccination – focus was on encouraging people to come forward for
vaccination. Transformation Recovery Plan – the deadline for submission of the recovery plan had been met. The narrative plan addressed asks from the national team and the second document looked at activity in light of national trajectories regarding pre-Covid-19 demand. Additional information in relation to the Mental Health Investment Standard and a People Plan had also beenn submitted. Integrated and Elective care programme – there had been consultation with regard to community services moving to a seven day service. Strategic programme – stroke early supported discharge work had restarted with the service expected to commence from April 2021. Maternity and cancer service finances were being reprofiled. Early diagnosis of cancer work was taking place. Children and Young Peoples’ programme – childrens mental health pathways were being finalised. The neuro-development pathway had been paused due to Covid-19 and the return of schools. Mental Health – Mental Health Board meeting recently and the outcome of the Crisis assurance process was to be presented to the next Mental Health Board and the November 2020 Governing Body. Having recognised that early cancer diagnosis was also a priority for Primary Care Networks the need to align work was highlighted. The importance of providing community services with an identity to enable them to be more integrated in service provision was also emphasized. (Dr Andrew Hassan joined the meeting) The Governing Body noted the report.
20/064 GOVERNING BODY ASSURANCE FRAMEWORK
The Director of Corporate Services and System Infrastructure presented the current
version of the Governing Body Assurance Framework (GBAF) together with a summary of local risk registers. Amendments and additions to the GBAF were detailed within Section 2 of the report, with key aspects of departmental risk registers being listed in Section 3. Points highlighted included; • The Workforce risk was being progressed by Lisa Llewellyn and her Team. • It was likely that a Brexit risk would return to the GBAF from October 2020. The
Senior Responsible Officer for Brexit would be the Director of Corporate Services and System Infrastructure. The Governing Body was informed that Brexit was a standing agenda item on the Area Prescribing Committee agenda due to the risk to medicine supply.
• It was likely that, following discussion at the Risk Forum, a new Health inequalities risk would appear on the risk register.
The Governing Body was informed of debate in relation to the Stanton surgery extension whereby it was unclear whether the Council would support the planning application. The Chief Operating Officer and Director of Corporate Services and System Infrastructure agreed to discuss issues and concerns outside of the meeting. The Governing Body noted and approved the GBAF as presented.
20/065 2020/21 FINANCIAL REGIME AND FINANCIAL PLANNING
The Director of Finance reported that the financial regime would be changing from
1 October 2020. Whilst, at the time of writing the report, the CCG had not received any information with regard to financial allocations it had since received notification of the way finances would work from October 2020 and system allocations. Work was currently taking place to review the allocations, with key points to report at present being: Emergency arrangements had been in place for the first half of the year and there was now movement back to a ‘business as usual’ situation with CCGs receiving allocations for the rest of the year and central top-up associated with Covid-19 not continuing from 1 October 2020, subject to there being any second wave of the virus. System allocations had been received and were being reviewed. They included allocation for excess Covid-19 costs for the CCG and providers such as ESNEFT, WSFT and EEAST. NSFT was not included as Norfolk was the host commissioner. Some areas remained outside of the new allocations, with the most significant being the hospital discharge programme which would be managed centrally. There was to be a return to marginal payments in relation to activity levels, with marginal increase in payments associated to increased activity. There was concern that the new financial regime might put a cash limit on Covid-19 going forward. It was felt that in the event that Covid-19 re-escalated it would be an issue for the whole system which would need to be addressed. Having queried the effect of a move to system allocations on CCGs, it was explained that the current regime was a hybrid allocation which included detail regarding individual Trusts and CCGs together with some system elements. . Clarification was sought as to whether hospitals continued to have the opportunity to return to payment by results. It was explained that, whilst there was a national move to guaranteed income contracts, in an ordinary year hospitals would have the right to return to payment by results but under current arrangements payments to Trusts were being facilitated by mandatory block payments. The Governing Body: • Approved roll forward of the arrangements currently in place regarding
expenditure until the end of November 2020 (unless a national announcement was received in the meantime)
• Noted that work was underway on a financial plan for the second part of the year.

Confirmed the previous delegation of the development of a financial plan to take effect at the end of the emergency period to the Financial Performance Committee, for final sign off by the Governing Body.
20/066 EXTENSION OF EMERGENCY FINANCIAL ARRANGEMENTS
At its meeting in March 2020, the Governing Body was presented with a paper
setting out potential increases to the sign off limits in the CCG’s scheme of delegation. Whilst the paper suggested permanent increases to deal both with the Covid-19 response period and to continue into business as usual, the Governing Body resolved to implement the increases on a temporary basis with a further review in July 2020. Those temporary changes were provided in Appendix 1 for reference, with changes from the original highlighted in blue shading or red text. In May 2020, the Governing Body approved the establishment of a Covid-19 Resources Approval Committee (CRAC) bringing together the three CCGs in Suffolk and North East Essex to make timely decisions to support our response to the pandemic. That was initially approved until the end of July 2020. In line with the extension of the emergency period, the July 2020 Governing Body approved extension of the temporary limits and CRAC until the end of September 2020. Alongside that, the Governing Body asked the Audit Committee to undertake a review of delegated limits for the longer term. Despite allocations for October 2020 to March 2021 having recently been received to ensure that any decisions relating to Covid-19 follow a rapid and robust approval process, it was proposed that the temporary measures set out above are extended until the end of November 2020. The Audit Committee would commence its review of delegated limits in the longer term which would form part of a wider review of Alliance and CCG governance. The Governing Body; 1) Approved extension of the temporary changes to financial limits until the end
of November 2020 2) Approved the continuation of the Covid-19 Resource Approval Committee
(CRAC) until the end of November 2020
20/067 FINANCIAL PERFORMANCE COMMITTEE ANNUAL REPORT
The Governing Body received the Financial Performance Committee’s Annual Report for 2019/20. The Governing Body noted the report.
20/068 2019-20 SUFFOLK AND NORTH EAST ESSEX AREA PRESCRIBING
COMMITTEE (SNE APC) ANNUAL REPORT
The Governing Body was in receipt of a report which provided an account of the activities undertaken by SNE APC during 2019-20 and outlined progress made, as well as highlighting key areas of concern and the plans going forward for the next year. The functions of the SNE APC Team were multifaceted and covered all aspects of medicines, whether it was commissioning or pathway redesign. It had been recognised that medicine was an enabler for many different work streams across the Integrated Care System.

The Governing Body was informed that the Chairmanship of the Committee was rotated across the three CCGs. Having noted that the documentation stated that the terms of reference required review in respect of patient and public engagement, it was explained that there had been difficulty determining who would provide patient and public involvement across an area committee. Should development of a Patient and Public Involvement policy be felt necessary, the Lay Member for Patient and Public Involvement offered to provide assistance. The Governing Body noted and welcomed the report.
20/069 AUDIT COMMITTEE
Audit Committee Annual Report
The Governing Body received the Audit Committee’s Annual Report for 2019/20. The Governing Body noted the report. Audit Committee Terms of Reference The Governing Body was in receipt of revised Audit Committee Terms of Reference for approval as agreed by the Audit Committee at its meeting held on 15 September 2020. The Governing Body approved the Terms of Reference for the Audit Committee as attached to the report.
20/070 FORMATION OF AUDITOR PANEL AS A COMMITTEE OF THE GOVERNING
BODY
The CCG was currently re-procuring its external audit services, along with the other two CCGs in the Integrated Care System (ICS). As such, the CCG was required to appoint an auditor panel who would make a recommendation to the Governing Body on the choice of external auditor. The auditor panel must be formed in line with a number of regulations, those being; a) The Auditor Panel must consist of at least three members, of which a majority
must be lay members of the Governing Body, and independent. b) The Chair of the Auditor Panel must be both a lay member of the Governing
Body of the organisation and independent. c) Quoracy was a minimum of two of the three members, or 50% of members if
the Committee was larger than that.
The process by which the auditor panel functions was as follows:
a) The Governing Body forms the Auditor Panel and makes appointments to it. b) The Auditor Panel makes a recommendation of an external auditor to be
appointed to the Governing Body. c) The Governing Body may choose to concur or disagree with the
recommendation. Any decision to appoint auditors who were not recommended by the panel must be published on the CCG website.
d) The Governing Body appoints a new external auditor and that is published on the CCG’s website

In order to fulfil the regulations above the panel proposed was as follows: • Geoff Dobson (Audit Chair) • Steve Chicken (Lay Member) • Lynda Tuck (Lay Member) • Jane Payling (Director of Finance) The example terms of reference from the HFMA, adapted for local use, were provided in Appendix I and proposed as the terms of reference to be used for the Auditor Panel. The Governing Body approved the attached terms of reference for the auditor panel, and appointed members to the panel as outlined in this paper.
20/071 MINUTES OF MEETINGS
The Governing Body received the following minutes and decisions from meetings;
a) Clinical Scrutiny Committee
The unconfirmed minutes of a meeting held on 26 August 2020. b) West Suffolk CCG Primary Care Commissioning Committee
The unconfirmed minutes of a meeting held on 26 August 2020. c) Covid-19 Resource Approval Committee
Minutes from meetings held on 9, 23, 30 July 2020, 13 August and 8 September 2020
d) Commissioning Governance Committee Decisions from virtual meetings held on 2 July and 5 August 2020 The Governing Body endorsed the minutes as presented.
20/072 DATE AND TIME OF FUTURE GOVERNING BODY MEETINGS
0915 – 1200 hrs Wednesday, 25 November 2020
20/073 QUESTIONS FROM MEMBERS OF THE PUBLIC
The following questions were received from Cllr Margaret Marks; 1) Question - Think 111 First - is there an additional more detailed paper
identifying exactly how this system will work and will this holistic approach be operating with patients who go via the normal Primary Care system. I note that this is planned to start Dec 1st but with the expected Covid increase, is this realistic?
Response - as explained in the meeting, a business case was to be presented to the CCG’s Executive in October 2020. At present it was unceratin whether the new approach would commence in December although the initiative was seen as something that could assist winter planning. It was probable that the work would move forward and look to learn from early pilot sites. The Director of Strategy and Transformation agreed to link up with the questioner outside of the meeting.
2) Question - the National Agreement with Private providers ended in August – is
there a new National Agreement to support catching up with the vast numbers of patients waiting interventions.

_____________________________ _______________________ Chair (Dr Christopher Browning) Date
Response – the contract with the independent sector was a national contract that was due to end soon. Recovery plans had been submitted without independent sector capacity and no further information had been received in relation to national procurement arrangements.
3) Question - please may I have information on the numbers of patients who have
significant delay in treatment – I have a number of residents waiting orthopaedic interventions who are now suffering with associated problems which will further impact on the NHS and there is currently no visibility when their initial surgery will take place. Are patients being risk rated?
Response – Referral to Treatment times were subject to ongoing discussion and the risk stratification of patients was being explored. The Director of Performance Improvement and Director of Nursing agreed to liaise with Cllr Marks outside of the meeting.

WEST SUFFOLK CCG Governing Body
ACTION LOG: 23 September 2020 (updated) MINUTE DETAILS ACTION BY WHOM TIMESCALE/UPDATE Meeting of 23 September 2020 20/062 Procurement Update:
Summary of Activity 2020/21
The Governing Body noted the content of the report and requested that the Executive be provided with updates on the Pathology and Mental Health elements.
Paul Gibara
20/064 GBAF The Governing Body was informed of debate in relation to the Stanton surgery extension whereby it was unclear whether the Council would support the planning application. The Chief Operating Officer and Director of Corporate Services and System Infrastructure agreed to discuss issues and concerns outside of the meeting.
Kate Vaughton/ Amanda Lyes
20/073 Questions from members of the public
Think 111 First - The Director of Strategy and Transformation agreed to link up with the questioner outside of the meeting. Referral to Treatment times were subject to ongoing discussion and the risk stratification of patients was being explored. The Director of Performance Improvement and Director of Nursing agreed to liaise with Cllr Marks outside of the meeting.
Richard Watson Paul Gibara/ Lisa Nobes
Link made between the questioner and CCG lead for Think 111 First.

Page 1 of 7
GOVERNING BODY Agenda Item No. 08
Reference No. WSCCG 20-42
Date. 25 November 2020 Title
West Suffolk Alliance Update
Lead Director
Kate Vaughton, Director of Integration
Author(s)
Jo Cowley, Senior Alliance Development Lead, WSCCG Sandie Robinson, Associate Director of Transformation, WSCCG Lesley Standring, Head of Operational Improvement, WSFT
Purpose To provide an update to the Governing Body on the West Alliance.
Applicable CCG Priorities 1. Develop clinical leadership x
2. Demonstrate excellence in patient experience & patient engagement x
3. Improve the health & care of older people x
4. Improve access to mental health services x
5. Improve health & wellbeing through partnership working x
6. Deliver financial sustainability through quality improvement x Action required by Governing Body: Note the progress being made on individual initiatives and collaborative working across the system. This paper provides an update on the progress being made with integration in the West Suffolk system including specific transformation projects. This is a combined paper on Alliance development and transformation.

1. Background
1.1. This paper provides a quarterly update for the Governing Body about Alliance activity to
transform services and outcomes for people within the West Suffolk Alliance area. Several different teams contribute to the report, from across the CCG, the hospital and Alliance partners.
2. Winter pressures
2.1. A planning process has been going on to identify risks and preparations for winter. This has involved partner organisations submitting their plans to the CCG for collation.
2.2. Alongside this, the West Suffolk Alliance is running a winter planning forum, using the weekly West Cell meetings which involve all Alliance partners. The forum takes a whole system approach to winter, getting an understanding of the current risks and pressures from different perspectives and ensuring that action is taken to deal with the questions that are being raised.
2.3. This very agile approach to winter demand picks up learning from the pandemic, and focuses on fast resolution of issues, whether this is about data collection, service changes or the sharing of information. Immediate areas of focus include bed use in the community and the services needed to support higher levels of need, resilience in our Integrated Neighbourhood Teams, and how we work with our voluntary and community sector partners more effectively.
3. Alliance business
3.1. #WhatAreWeMissing - West Suffolk - The event was held on 29th September 2020 via MS Teams with over 80 attendees from across alliance partners and local community representatives.
3.2. During the session, two questions were asked. The first question was: What stops people in your community from accessing health and care services? E.g. Going to the doctor. What will help your community stay safe from Covid-19? Below is a word cloud of the key themes:
3.3. The second question asked was: How can we work together now and, in the future, to
support local communities? Below is a word cloud of the key themes:

3.4. A small team are working on the actions from the event. This will include immediate actions and longer-term ones. Links have been made between the clinical leaders from the system and the internal WSFT BAME network and agreement to explore more join up going forward.
3.5. This is the start of the conversation and there are still voices within our communities that we have not heard from that we need to engage with. We are working to set up a community champions group to engage with these voices. The aim of the group will be to explore the key themes from the event so responses will be co-produced from the grass roots and have the lived experience influencing outputs.
4. Community Health Services Development
4.1. Following feedback from the initial listening events, WSFT, CCG and Suffolk County Council (SCC) have committed senior leadership support to ensure our community services are as resilient as possible in preparation for winter and the Covid second wave.
4.2. WSFT have commissioned RETHINK partners to carry out a specific focused piece of
work to help us further understand what staff think our patients need and what they need to support the delivery of the service. This is a 10-week programme due to be completed in mid-December with a full report available.
4.3. To further strengthen the leadership of the community division and develop the visibility of
senior leadership team, a Quadumvirite has been created representing nursing, therapy, operational (health and care) to work very closely as the senior leadership team to support day-to-day decision making.
4.4. To support the divisional leadership team, additional management and transformational
support from Lesley Standring (Head of Operational Improvement West Suffolk Foundation Trust), Sandie Robinson (Deputy Director, Strategy and Transformation NHS West Suffolk Clinical Commissioning Group) and Bernadette Lawrence (Area Director, Adult Community Services SCC) are working with them until March 2021. A programme of work has been developed and updates will be shared at future meetings.
5. Voluntary and Community Sector Funding
5.1. Realising Ambitions Funding update – In 2019 over £450,000 of NHS transformation funding was used to fund 24 projects in the voluntary and community sector with the aim of tackling obesity, loneliness and mental illness. Most grants were under £50,000 with 2 projects receiving grants between £50,000 and £70,000, and decisions were made by a panel of Alliance representatives. Suffolk Community Foundation ran the grants programme and have been working with the projects on their impact assessments, issues raised through the pandemic and their future plans.

5.2. Most projects needed to adapt their delivery model because of Covid, often using on-line
platforms, and one organisation (Age Uk Suffolk) sadly closed. An extension to the time for the projects to complete was given in recognition of current circumstances and 85% of the projects are on track to deliver agreed outcomes by their end dates. Two projects required a small amount of additional funding as a result of adaptations needed, and this has been made available through the Integrated Care System (ICS).
5.3. Full impact reports will be available between April and June 2021. However, Suffolk
Community Foundation has been collecting case studies showing the impact of the projects on people in West Suffolk and the following pages give just some of examples that have been reported.
Epic Dads The need for supporting dads and the benefit of having a centre aimed towards them is more relevant than ever. Many dads have struggled greatly with their mental health during the pandemic and value having a place to meet and talk and receive support. Demand has increased as they receive regular referrals to work with dads supporting them in their parenting and wellbeing as there are few local services which prioritise dads like EPIC Dad. With further funding, they will have the capacity to meet the demand which they expect will only grow. They have created excellent partnerships with Home Start Mid and West Suffolk, Newmarket food bank and Sharing Parenting. In addition, they have just been awarded a Parent and Baby Award for 'Best Father Support Service and Advocacy 2020 - UK' Quotes received as part of the interim evaluation: “Improved relationship with children through learning new ways to engage and communicate. Met local friends through the program as well. Helped in my wellbeing and confidence as a dad.” “The EPIC Dad events give us something to look forward to and to help with in a way that seems to benefit us and the community.” “Allowing children to determine how to play and express themselves gives them a sense of empowerment and purpose Entertainment doesn’t have to be elaborate or expensive to be fun.”
Gatehouse Caring The first Mindfulness for Later Life group was run online, in a response to restrictions put in place due to the COVID-19 pandemic. The content that was intended for the face-to-face group was adapted for the online version, which included adapting presentations for use on a video conferencing platform, programming the pen and paper self-report questionnaire measures and neuro cognitive test measures for online use, and recording practices for the home practice in an online accessible format. Participants talked about the experience of mindfulness, of attending the group online, and the context of COVID-19 during the focus group: “I began to open up my own mind and be less scared about everything.” “… Having been shielding… It’s been relaxing. You know, and I thoroughly enjoyed it and I’m

grateful for it” “I’m beginning to find all kinds of things to be grateful for” Interestingly some participants spoke about preferring attending the group online: “I felt more comfortable being in my own surroundings”
Homestart Mid and West Suffolk Homestart got involved with this family when H, who is a single mum with two young children under 5, was struggling with motivation to keep on top her household chores, or to apply for jobs. She suffers from long standing mental health problems, and her mum who had been supporting her had herself become unwell. At the end of the support from Homestart they looked at how outcomes for H had been achieved. Home visiting has now ended, with reviews showing an improvement in many areas of coping, and both her and the children’s wellbeing increasing. At the end visit, mum had secured a new job and was starting to train the following week. Mum very excited about the job bringing positive change for the family including a new consistent routine and more reassurance they will be financially stable. During many home visits mum completed household chores she would have otherwise not done. Regular home visits increased her motivation to complete chores, while they children were occupied, and she had a listening ear to talk things through. While at the end of home visiting, mum had not completely got on top of her house, she reported that she felt happier that a new routine for work would bring more structure to other areas of their life, helping her to keep on top of the chores in the future. H regularly attended the Home-Start group with one child, which they both thoroughly enjoyed. She enjoyed interacting with the other parents and widening her social network and also took her other child to the group during the holiday. H was very sad she would have to stop going to the group when she started her new job, as she enjoyed going so much. She has said she will pop back to the group if has the time. Outcomes for the children The children now have a more structured and stable lifestyle, with addition of a new consistent routine from mum’s job. They now enjoy more positive time with mum, who is more positive about their future. The children have a more stable future now mum has a consistent job and income. Max gets on very well at school, enjoying playing and interacting with other children. Lily will attend nursery as mum starts her new job.
Artlink Since January 2020, Make, Do & Friends has delivered a total of 52 sessions and consultations, totalling 416 attendances and reaching 280 individuals. 30 of the sessions were in the West, totalling 167 attendances and 94 individuals. Covid has undeniably had a huge impact on this project; from one week to the next, all delivery had to be moved to a remote format with face-to-face connection totally removed from our arsenal. This was massive for a project that’s key stone was to bring people together in their communities.

Make, Do & Friends sessions moved promptly to an online platform in response to lockdown; it became apparent that creatively connecting online was positively impacting people’s wellbeing during an unprecedented period of self-isolation. “This art group [Make, Do & Friends] is absolutely vital to people especially during lockdown. It gives a sense of inspiration, hope and purpose…” Comment from feedback form.
5.4. Community Ambitions Funding – NHS Charities Together have announced a £30 million grants programme aimed at supporting partner organisations across STP/ICSs in England and Health Boards and ICP areas in the devolved nations. The programme recognises that the NHS relies on partnerships in the voluntary, community and care home sectors and aims to encourage and support these partnerships across geographical areas that support communities affected by COVID-19. The expectation is that the funding should be used for projects that benefit the NHS and VCSE sector across each STP/ICS.
5.5. This means that individual organisations are not able to submit applications directly to NHS
Charities Together. Instead a single application for funds must be made for the whole ICS area by the lead NHS Charity who then has responsibility for submitting the application form on behalf of the ICS. That application must be absolutely finalised by 31st March 2021 but submitted before that date. Of the total £30 million available nationally, £445,532.77 has been made available to the Suffolk and North East Essex ICS.
5.6. For the SNEE ICS wide application the three Alliances are working with the ICS team. The
Colchester and Ipswich Hospitals Charity are the lead NHS charity for the bid (required by the fund) and are supporting co-ordination and administration of the engagement, application and reporting.
5.7. The ICS Board agreed to use the opportunity to deploy this funding donated by members
of the public to NHS Charities Together in Suffolk and North East Essex to make a difference to those communities that have been hardest hit by the Covid-19 pandemic – those from BAME and deprived communities.
5.8. A series of events were held across the ICS to help shape the process and to encourage
organisations to submit Expressions of Interest. In all 10 West organisations have sent in expression of interests and 16 groups with pan Suffolk initiatives. The next phase will include an ICS wide workshop to explain the full application process and to talk with organisations about the aims of the programme and how they can remain involved. There will be time within the session for a West Suffolk discussion so we can ensure that our local projects are sited on West Suffolk issues and challenges, as well as looking across the whole of the ICS area.
6. Institute for Healthcare Improvement
6.1. In early October a team from the Institute for Healthcare Improvement (IHI) held a 3-day Foundational Conference in partnership with the Quality Improvement Team hosted at West Suffolk Foundation Trust. As an Alliance we have partnered with IHI to support the implementation of Quality Improvement across our system.
6.2. The purpose of the visit was to work with Alliance partners to learn more about the
challenges we face as a system, and to make recommendations as to how they could support us to improve outcomes for key populations. They spoke with 125 people over a series of 24 meetings, including what they described as a “Building the Will” event - a half day conference on 6th October 2020 with senior leads and managers across the Alliance which included presentation & discussion workshops.

6.3. The full feedback from IHI is due shortly. The initial feedback proposed four populations
where there was system agreement and an opportunity to improve outcomes: - Homelessness - People who are obesity - Older people who are socially isolated - People who are suffering from mental illness
6.4. At the System Executive Group meeting on the 4th November 2020, a decision was made
that homelessness would be initial area of focus. This aligns with the Alliance Delivery Plan, and the IHI involvement will give this a significant boost in terms of partnership action, understanding of measures and change factors and the ability to bring in good practice from other areas who have successfully made a difference for homeless people.
7. Vaccine planning
7.1. At the System Executive Group meeting which took place on the 4th November 2020, a considerable amount of time was spent talking through the plans for delivery of the Covid Vaccine. Partners were able to gain a good understanding of the challenges of the programme and to offer help, including from voluntary sector partners who have people resources that they can mobilise if needed. Specific connections were made between clinical leads which were then taken off- line and it was agreed that system partners would be kept informed in order to mobilised additional support where necessary.
8. Governance review
8.1. The Alliance is working up the details of how it rises to the challenge and opportunities that come out of the CCG governance review. As a first step a small subgroup from the System Executive Group met to discuss the principles for Alliance working. They started off by confirming that we need strong, clear principles which can:
- help us to deliver our ambitions for West Suffolk - hold ourselves to account - build our commitment to Alliance working - use them as a “checklist” to make sure we are working in an Alliance way - be a call to arms – the Alliance should step up a gear and our principles can help
us to take the action we need to do this.
8.2. These will be used to inform further work to be done to evolve our system governance model. This will include make sure we show a golden thread through from the Health and Wellbeing Board outcomes and the ICS higher ambitions.
8.3. Other aspects that will be considered include making sure that the Alliance has the
infrastructure in place to manage subsidiarity from the CCG, along with ensuring that we maintain the strong focus on people’s voice and clinical leadership.
9. Recommendation
9.1. The Governing Body is asked to note the progress being made through the West Suffolk Alliance and the Clinical Commissioning Group’s wider partnership working.

Page 1 of 4
GOVERNING BODY
Agenda Item No. 09
Reference No. WSCCG 20-43
Date. 25 November 2020
Title Community Engagement Group and Patient and Public Involvement
Lead Director Linda Moncur, Deputy Director of Nursing
Author(s) Katie Sargeant, Deputy Head of PPI
Purpose To present the unconfirmed updates from the Community Engagement Group meetings and PPI activity between 24 September 2020 – 29 October 2020
Applicable CCG Priorities 1. Develop clinical leadership2. Demonstrate excellence in patient experience & patient engagement √ 3. Improve the health and care of older people4. Improve access to mental health services5. Improve health and wellbeing through partnership working6. Deliver financial sustainability through quality improvement
Action required by Governing Body:
The Governing Body is asked to comment on and review the CEG and PPI activity.

1. Background 1.1 The Community Engagement Group (CEG) is a public group that represents the patients and
public of west Suffolk. CEG members have been meeting virtually on a monthly basis, which has been well received.
2. Key Issues 2.1 Below is a summary of the key issues and themes that have been raised by CEG members
between 24 September 2020 – 29 October 2020. Issues raised come as a result of members being involved in their local networks, Patient Participation Groups (PPGs), local councils and localities. Appropriate action has been taken to address all issues raised by members.
2.2 Speakers who have attended the virtual CEG during this time have included Alison Sadler,
Transformation Programme Manager for Community Mental Health Services, Emma Reader, Programme Manager for the Suffolk Alliance Mental Health Transformation Team and Sarah Hedges, Integrated Transformation Lead for West Suffolk Community Services.
2.3 The group also welcomes Sophie Martin as the new Head of Patient and Public Involvement
and Experience, who presented an overview of Patient and Public Involvement across the CCGs.
Issue Response
Supporting Locality Working CEG member Lynne Byrne has previously raised concerns about a lack of opportunity for public involvement in the Newmarket Locality conversations. There was an issue raised around increasing obesity levels in Haverhill, notably since lockdown, which may be occurring across other localities. CEG member Margaret Marks wished to make the CCG aware.
Lynne Byrne has been invited to attend the Collaborative Communities group to help develop locality working in Newmarket. CCG to observe and consider comment around increase in obesity.
PPG Update Hardwicke House and Siam surgery are looking to merge, we heard from CEG member Tanya Millar, due to three members recently leaving.
A PPG Network for West Suffolk is being set up virtually, which will be able to support the PPGs and help build relationships and share best practice across the different groups. The first meeting is due to take place on Tuesday 24 November.
Mental Health Transformation and Early Adopter Primary Care sites. Members have raised concerns around drug and alcohol abuse in Haverhill and feel that this should be part of the NHS remit.
Alison Sadler presented to the group and confirmed that Turning Point will be involved in Multidisciplinary team (MDT) meetings in Haverhill.

There was also concern about the workload and resilience of district nursing teams in relation to the community model plans. In response to an update on the SAMHT work, members felt that more clarity was needed around how to access services in the first instance i.e. by GP appointment.
Emma Reader confirmed that her colleague, Rachel Beard, was working on cultural resilience and feeding this in to the Suffolk Alliance Mental Health Transformation (SAMHT) programme. Emma Reader agreed that clearer communication was needed around this for the public.
Communication CEG members, who have attended public CCG meetings, have given feedback over the use of acronyms and expressed concern that they are not understood by the public. A CEG member raised the issue around changes in General Practice and how these were being communicated with patients.
Specific feedback from the Mental Health Transformation Q&A public engagement event has been fed back to the team. The CEG asks the CCG to note and consider the use of acronyms in public meetings and explaining acronyms to the public. Sophie Martin explained that NHSE are making changes daily and any communication sent via letter would be out-of-date very quickly. There is the potential to use text messaging to share information or for GPs to utilise their PPGs in communicating with patients. This will be on the agenda at the PPG Network meeting.
Questions from CEG members 1. Online physiotherapy not working, template exercises can be damaging if patient not properly assessed. 2. Carers notes are being taken from their homes when they must stay in the house.
Issue raised. Issue raised, Lynda Tuck to take forward.
3. Patient and Public Engagement 3.1 The CEG will continue to hold virtual, monthly meetings until such time as national advice
regarding public meetings changes. Meetings will continue to be publicised in the normal way and members of the public are still welcome to attend, via video link.
3.2 CEG member Lynne Byrne was involved in the recruitment of Patient Experience Officer.
Although pleased to be involved, Lynne commented that the process was long winded and there were issues with accessing applications and HR processes. Lynne raised this issue with the hope that future CEG member involvement in recruitment would go more smoothly.
3.3 CEG member Michel Simpkin attended an Integrated Care System (ICS) Rapid Diagnostics
Patient Panel, to provide patient experience. The next panel is due to take place in January 2021.

3.4 CEG member Carol Mansell updated the group about the responsive work churches have been doing throughout the pandemic, supporting food banks with pop-up shops and offering debt counselling and support to young people with mental health issues.
3.5 The Healthwatch representative on the CEG updated the group with their latest surveys and
reports, including patient experiences of using digital health and social care services during the pandemic and end of life care.
4. Recommendation 4.1 The Governing Body is asked to note and consider the issues raised in this report.

Page 1 of 11
GOVERNING BODY Agenda Item No. 10
Reference No. WSCCG 20-44
Date. 25 November 2020 Title
Suffolk and North East Essex Clinical Commissioning Groups Commissioning Intentions 2021-22
Lead Director
Richard Watson, Deputy Chief Executive and Director of Strategy and Transformation
Author(s)
Nerinda Evans, Deputy Director for Strategy and Strategic Programmes
Purpose
To consider and approve the draft commissioning intentions for 2021-22 for publication.
Applicable CCG Priorities 1. Develop clinical leadership X 2. Demonstrate excellence in patient experience & patient engagement X 3. Improve the health and care of older people X 4. Improve access to mental health services X 5. Improve health and wellbeing through partnership working X 6. Deliver financial sustainability through quality improvement X Action required by Governing Body: To consider and approve the draft commissioning intentions for 2021-22 for publication.

1. Background 1.1 2020/21 has been a year of significant change for the NHS both nationally and on a local
level not least with the ongoing COVID 19 pandemic and our response both to managing this and recovery. Major developments over the last year locally include the development of our new mental health model in Suffolk, the development of our new community model in North East Essex, the development across the three Alliance of our End of Like (EOL) models and the development of exciting capital plans for changes at East Suffolk and North Essex Foundation Trust (ESNEFT) and a new build hospital for West Suffolk Foundation Trust (WSFT).
1.2 During this period health, care and wellbeing partners across Suffolk and North East Essex
have continued to work together to set the strategic direction for local services through the ongoing development of our three local Alliances: West Suffolk, North East Essex and Ipswich and East Suffolk as a key part of the wider Integrated Care System (ICS) development.
1.3 The attached letter at appendix one provides a summary of the progress made and our
future plans, providing a summary of key commissioning intentions for the coming years and 2021/22 in particular within each of our system programmes.
1.4 The CCGs recognises that these priorities may change in light of learning from the ongoing
Covid19 recovery phases and in light of any actions needed to be taken as part of the national Covid 19 ongoing response as the national risk level changes.
1.5 The commissioning intentions should be read in conjunction with the ICS Strategy and our
three Alliance Plans which set out more detailed ambitions and priorities for the ICS and Alliances over the next four years.
1.6 In line with the NHS Standard Contract, which requires six months’ notification for any
potential changes to services and counting and coding charging proposals, these intentions will also support the 2020-21 contract negotiations. These commissioning intentions should therefore be considered the CCG’s formal notice letter.
2. Commissioning Intentions 2.1 Our Commissioning Intentions for this year will focus on: Our Integrated Health Care System (ICS)
As key partners in the Suffolk and North East Essex ICS, our three CCGs are working together with local NHS providers, local government and voluntary and community sector organisations around our collective aim to make a difference to the issues that matter to people, and which can only change by working with other partners. Learning from Covid has underlined our commitment to our eight Higher Ambitions and our ICS primary ambition to achieve health quality for the one million population. The challenges of Covid 19 is further embedding our collective learning on 10 key themes: 1. Covid-19 further amplified the many existing inequalities in our communities 2. We underestimated the inherent resilience in our local communities 3. We are more adaptable than we thought – with a collective focus we can move mountains 4. Adopting new technology has potentially brought new opportunities and
challenges 5. The safety, flexibility and resilience of our people and workplaces are vital 6. Knowledge is key - we need the right data and intelligence to deliver better care together 7. We need to be joined up across sectors about funding and investment 8. In recovering our services we need to ‘build back better’ and be prepared to face future challenges 9. We need to plan both for the many and the few 10. Enabling collaboration is even more important now than it ever was. We have continued to come together with other partners through regular ‘Thinking Differently Together’ online events and to further enhance the role of voluntary, community and social enterprise sector in our ICS. We plan to fully realise the further opportunities for integrated care systems set out in the NHS Long Term Plan (2019) by strengthening the way that we work with NHS England and NHS Improvement through NHS ‘System First’. Building on our system capability in key areas including population health management, service redesign, workforce transformation, digital and technology, capital and estates and finance we will develop the way that as an ICS we will undertake the two key roles of leading system transformation and collective management of system performance. We have begun to do this work together with our local partners and with support from the King’s Fund with the aim to upgrade our system governance towards the end of 2020, building on the thinking in our three alliances and ensuring that as system partners our system governance supports collective responsibility, streamlined commissioning and decision making between system partners. In upgrading our system governance we want to further enhance the role of the voluntary, community and social enterprise sector in our ICS, more fully embrace the role of non-executives, governors and lay and elected members, and further embed co-production as ‘business as usual’ in the way that we work.
Achieving Health Equality
We aim to optimise population wellbeing through improving health as an asset and the prevention of illness or illness deterioration. The ICS has a primary ambition of achieving health equality for our whole population. In particular, to address the entrenched problems including leaning from BAME communities highlighted by the pandemic, we have made a start with our Alliance #WhatAreWeMissing events that aim to address health inequalities and access to services, setting up a community champions group and working with community leaders to understand and tackle some of issues. These discussions have shown us that if we are to address racism and inequality in our ICS then we need to listen and learn, change what we do and stand together. Our Covid-19 recovery plans include implementing eight urgent actions identified by NHS England and NHS Improvement: 1.Protect the most vulnerable from COVID-19 2. Restore NHS services inclusively 3. Develop digitally enabled care pathways in ways which increase inclusion 4. Accelerate preventative programmes which proactively engage those at risk of poor health outcomes 5. Particularly support those who suffer mental ill-health 6. Strengthen leadership and accountability 7. Ensure datasets are complete and timely 8. Collaborate locally in planning and delivering action.

We will work as partners in the ICS through our three local alliances to implement these actions over the coming months, in close partnership with colleagues in local government, other public services, voluntary and community sector organisations, and local communities.
As CCGs we have made an explicit commitment alongside other local public sector partners by signing our ICS Charter for Anchor Institutions to make a difference in our local communities by:
• purchasing more locally and for social benefit
• using buildings and space to support communities
• working more closely with local partners
• widening access to quality work
• reducing our environmental impact.
We aim to rapidly accelerate the role of social entrepreneurs as a key assets in these deprived local communities. As part of the Public Health England ‘Health Equality Programme’ we want to rapidly identify creative opportunities to deliver local social value by working with social entrepreneurs who we can enable as partners by more fully realising our roles as local anchor institutions e.g. by procuring services for social value. The VCSE sector are key partners in tackling health inequality. Suffolk and North East Essex is blessed by an exceptionally strong and diverse local VCSE sector who continue to face many challenges as a result of the Covid19 pandemic. We will work in partnership with our local VCSE sector through our ICS and Alliances in response to the issues outlined above by: • Developing more agile contracts that offer the additional flexibility and
stability that the sector needs at such a challenging time; • Working in partnership with local government, community funders, VCSE
infrastructure organisations and VCSE leaders to work towards a more sustainable sector;
• Providing infrastructure support alongside other ICS partners with practical issues e.g. safety, HR, estate management, etc.;
• Continuing to maintain good two way communications and strategic working on key issues with VCSE leaders as partners through the ICS VCSE Strategy Group;
• Further enhancing the role in the ICS in our next steps work on ICS governance.
We will also support collaboration between all those supporting volunteers in Suffolk and North East Essex including development of a local volunteer passporting scheme.
Our Alliances Local ‘place-based’ systems of care involve multiple partnerships, including NHS organisations and the local government, working together to provide integrated care across organisational boundaries to improve the health and wellbeing of their populations. In Suffolk and North East Essex ICS there are three ‘place-based’ systems of care called Alliances. Our three Alliances are North East Essex, West Suffolk and Ipswich and East Suffolk, with each defined by the footprint of local health and care partners as well as natural geography, developing differently according to local

circumstances. The Alliances provide the focus for planning and delivering meaningful integrated care and services to the local population with partners working closely with the voluntary and community sector, independent sector organisations and communities. The Alliances will become the default forum for all key commissioning decisions and will work with partners across the SNEE ICS wherever that can add more value for each Alliance population than working alone. This approach will be supported by ensuring the Alliances have oversight of contestability plans to drive from inception the design phase of transformation and future commissioning decisions. It is the expectation that the Alliances will form the basis for the commissioning and management of the Better Care Funds, supporting the ever closer integration between health and local authority services, with the intention to explore opportunities to increase the scope of pooled budgets to include those wider determinants of health such as housing. This will help to fully realise the significant opportunity and benefits associated with integrated place based commissioning with local authority colleagues the support the level of transformational change required. The shift from traditional commissioning models to a population health based approach, supported by outcomes based reporting will continue to be central to the Alliances’ commissioning approach. This will form the basis for targeting our key interventions to support wellbeing in the widest sense for our local population, by recognising the importance of the communities we live and work in and to support the reduction in our health inequalities. We will continue to work with our Alliances to engage in a range of activities to develop solutions for their local populations: Public Involvement
• Work with citizens to understand the wellbeing, social and healthcare needs of the local population
• Create, grow and develop solutions to improve outcomes for the local population
• Co-produce outcomes to reflect the lived experience Continuous Improvement/Innovation
• Review and redesign local services • Work collectively to shape and deliver improvements collectively • Use innovation, including digital solutions, to enable system change
and improve outcomes for the local population Reducing Health and Social Inequalities/Population Health/Planning
• Assess the wellbeing, social and healthcare needs of the local population
• Conduct strategic planning across our local population, identifying opportunities for transformation and improvement
• Develop and implement delivery plans Delivery
• Responsibility for local service provision. Those defined as Specialised Services may be commissioned a system level, but delivery will remain at provider-led alliance level
• Managing risk – finance, quality and performance

• Holding colleagues to account Integration
• Work with system partners to align and integrate service delivery across sectors to create efficiencies in practice and improve outcomes for the local population
• Build and manage relationships across the Alliance network • Work as part of the ICS to inform and deliver systems ambitions
Financial/Contracting
• Shared decision making • Undertake procurement where required, and manage ongoing
contractual arrangements • Local financial management
Each Alliance has their own strategic plan and priorities for 2020/21 which can be found in Appendix One.
Our Localities Localities provide a focus for smaller, identifiable populations based on particular characteristics or needs, agreed within Alliances. Without the need to meet the requirements of a fixed size or model, different areas can find different solutions for different problems. In West Suffolk there are six localities, within Ipswich and East Suffolk there are eight localities and within North East Essex there are six localities. Alliances play a key role in oversight and support of effective locality arrangements that deliver for local populations. These localities are based around GP catchment areas overlaid with local health and social care teams and with the development of Primary Care Networks (PCNs) we will ensure that each locality is clearly defined. At locality level the role of district and borough councils and the voluntary and community sector are also key. The Integrated Neighbourhood/Locality Teams bring together physical, mental health and social care practitioners that work with General Practices within each locality to provide a single coordinated care response for people, underpinned by prevention, self-care, early intervention, reablement and rehabilitation, (including people living in nursing and care homes). There are four main objectives:
• Fewer people need unplanned care and support (reduction in crisis situations).
• Greater numbers of people have access to and are supported by activity outside of statutory services.
• Resources in the delivery of community-based health and care support are used more efficiently.
• The ongoing costs of supporting people are reduced as people’s independence is increased.
In all three of our Alliance there is a focus on the Integrated Neighbourhood/Locality Teams identifying local issues that relate to their specific populations, and developing a joint plan as to how they, as a system, can begin to address these, with support of the CCG.
Our CCGs Our three CCGs have a single accountable officer and a single management team. In 2021/22 they will continue to co-operate with one another and each working increasingly as integrated partners within Alliances with governance to support local decision making. In addition we plan to: establish joint governance across the three CCGs able to support decision making where it is

needed across the whole ICS footprint; explore closer working with local authority commissioning partners, including Public Health; explore the potential of integration of direct commissioning of specialised services at an ICS level; and conclude discussions on the organisational form of the CCGs.
Our PCNs It is increasingly recognised that PCNs play a significant role as an integral building block to support the national and local ambitions. With increased focus on PCNs, it is crucial to support and facilitate the clinical leadership and core teams to enable the capability and leadership to meet that expectation, deliver the national specifications and the local ambition. We are committed to the well-established clinical leadership programmes and intend to expand these further to other clinical and managerial staff. This approach to combined leadership supports the fundamental blocks to integration, and as a means for PCNs to interface with one another. Clinical Directors will be providing leadership, both strategically and clinically to the Alliances at ‘place’ level. PCNs are crucial for the implementation of the NHS Long-Term Plan for effective delivery in primary care in local neighbourhoods delivering against seven new service specifications to cover:
• Plans to help shape primary care services. • Developing an approach to balance increased patient care within
communities whilst also ensuring the development of a more resilient Primary Care system.
• Working across our Alliances to ensure Pharmacists, Opticians, Dentists, GPs and other partners are involved within the PCNs. This will build on our Healthy Living Pharmacy programme in particular.
• Supporting the integration of mental health services into PCNs. • Management of complex patients to localities with PCNs and Integrated
Neighbourhood Teams. • Support existing and new Social Prescribing schemes; ensuring that
learning is shared between localities and completing a full evaluation of impact by March 2021 to enable informed decisions about future models and long-term investment.
Aligning Incentives to Deliver Change
Changes to the financial architecture driven by the emergency response to Covid-19 means that the funding baselines in place during 20/21 have moved away from our previously agreed plans. Our strong system working we have developed in recent years, such as the used of Guaranteed Income Contracts, adoption of system wide control totals and ICS wide financial reporting will provide us with the building blocks to adapt into 21/22. We will consider how to enact the principles of the Social Value Act more consistently when commissioning services. Recognising the added value benefits that organisations can bring to services being delivered or produced, our engagement with social value will allow us to consider and secure the extra benefits which can be delivered by providers.
The CCGs will continue to ensure that Mental Health Services are prioritised in our investments through ensuring that the mental health investment standard is met, maintaining the share of our overall expenditure which is allocated to this area, regardless of the pressures being felt elsewhere in the local system.
We will continue to encourage partnership working to meet our statutory

requirements and to deliver the constitutional standards of the NHS. As such, the priority for any discretionary financial investment remains foremost to deliver constitutional performance with subsequent investment to complement and enhance performance against our system and place-based ambitions and objectives. The CCGs will procure services in accordance with regulations and our schemes of delegation, with reference to our three place-based Alliances, and with regard to the regulations on procurement, competition and choice. The regulations are intended to give commissioners flexibility and adopt a principles-based approach as opposed to providing prescriptive rules on procurement.
Quality Improvement
Quality of care remains at the heart of the commissioning decisions made by our CCGs.Whilst some difficult decisions have to be made, the CCGs will always consider the impact on the effectiveness and safety to ensure that responsible decisions are made. Our intention in 21/22 is to take a supportive approach to quality assurance visits, clinical quality priorities and patient safety issues. Priorities for 20/21 will span across all three Alliances and will include: 1. Infection Prevention & Control 2. Deteriorating Patients 3. Safer Staffing 4. Learning Disability and Autism 5. Falls Prevention 6. End of Life Care 7. Tissue Viability 8. Dementia 9. Hydration & Nutrition 10. Mental health 11.CYP 12. SEND and 13. Safeguarding. SEND programmes of work across the Suffolk and the Essex system continue to be key priorities for us and the progress against the written statements of action for Suffolk and Essex. We intend to ensure that we measure and develop outcome measures for providers and our Suffolk and Essex systems.
Strategic Programmes
Focus areas include: 1. Stroke - transformation and system-wide working on stroke services to
increase the integration of care 2. Neuro-rehabilitation – a new ICS Steering Group with a focus on care
available in appropriate settings dependent on need 3. Diabetes, including support to the ICS Higher Ambition on obesity,
continuation of the national prevention programme and delivery of treatment and care targets
4. Cancer Services – implementation of our agreed delivery plan with a focus on earlier diagnosis
5. Respiratory services (focus on spirometry, pulmonary rehabilitation and remote monitoring of patients)
6. ICS CVD/Cardiology Steering Group to support services Integrated Care (EoL, Urgent and Elective)
Focus areas include: 1. Development of Integrated Neighbourhood /Locality Teams across the ICS; 2. Embed Discharge to Assess (D2A) in each Alliance 3. Year three delivery of the system Managing Demand in Care Home
programme of work with a focus on trusted assessor, responsive in-reach, dementia and tissue viability support and integrating care homes with locality developments
4. Fully embed Trusted Assessment 5. Roll out High Intensity User approach to all providers 6. Implement the Urgent Treatment Service (UTS) model in each Alliance 7. Roll out of Think 111 First 8. Focus on EOL care across all three Alliances will be maintained with

individual workplans to meet the needs of each area while sharing good practice and learning at the ICS EOL Board
9. Support our local trusts in recovering elective activity including inpatients and day case plus diagnostic support including ongoing arrangements with our local Independent Sector (IS) providers
10. Implementation of the adapt and adopt outpatient programme across the ICS
11. Support large scale change such as the new Elective Care Centre at Colchester Hospital.
Mental Health, Learning Disabilities & Autism
Focus areas include: 1. Fully develop and implement the new primary and community care mental
health model (incorporating annual physical health checks, care for people with personality disorder, eating disorders, mental health rehabilitation needs, and complex mental health difficulties)
2. Ongoing focus on dementia including diagnosis rate, annual review and pre and post diagnosis support
3. Evolve further our system wide response to crisis services supporting mental health including mainstreaming crisis telephone lines (111+2), alternatives to crisis admission including crisis cafes, Serenity Intensive Support and joint ventures with Police, Ambulance and VCSE partners.
4. Increased provision of perinatal mental health services expanding access, duration of care and scope of interventions with seamless pathways aligned to maternity services.
5. Commencement of a new IAPT service provision incorporating a strong digital and long-term condition programme whilst integrating access to IAPT services into our core community service model.
6. Investment into early intervention services such as Psychosis and Eating Disorders amongst others, promoting the preventative agenda aligned with raising awareness across primary care and other sectors of the signs and signals of mental health.
7. Expansion of services to effectively support those recovering and wanting to re-engage in the community or return to work. This is in the form of progressing Individual Placement and Support Services, integrating across services lines and utilising the voluntary sector via community hubs or equivalent to enable those to live well in the community.
8. Work to deliver and maintain the aspiration of zero out of area bed placements and reduced lengths of stay, utilising robust community services to manage those appropriate.
9. Further development of LD admission avoidance/early discharge services including pathways and 12-point discharge planning.
Primary Care To continue to implement our primary care strategies and GP Forward View including: 1. Continued development of new models of care – enabling primary care
collaboration and joined up care in our localities – through Integrated Neighbourhood Teams and enable PCNs and INTs to work effectively in unison
2. Specific support for the development of PCNs and their clinical leadership with delivery of the national service specifications of; Structured Medications Review, Enhanced Health in Care Homes, Anticipatory Care, Personalised Care, Supporting Early Cancer Diagnosis, CVD Prevention and Diagnosis and Tackling Neighbourhood Inequalities
3. Workforce recruitment and retention programmes 4. Mental health services – primary care element integrated into INTs, 5. Increased primary care access, digital connectivity, high quality and cost -
effective prescribing 6. Review PMS and GMS LES priorities, reduce inequalities and improve
ethnicity recording

Ambulance 999 Commissioning
Focus areas include: 1. Improving pathways for patients (such as non-injury fallers) and thereby
reducing onward conveyance of these patients to Emergency Departments 2. Ensuring ‘Ageing Well’ and frailty programmes improve patient care to the
elderly 3. Continuing to explore ways of delivering stroke patient testing and
diagnostics on scene 4. Closer integration of our Clinical Assessment Services (111/Out of hours)
with 999 pathways to provide improved responses to lower acuity patients. 5. Developing the Long-Term Plans for mental health services integration into
urgent and emergency care pathways for patients with an underlying mental health condition
Pathology The CCGs intend to develop a specification for GP direct access pathology services that are integrated with local hospital-based testing. The CCGs will work with interested parties to develop plans for how the specification would be best delivered.
Personal Health Budgets (PHBs)
The CCGs will consider procurement options for financial management and control. Providers will be required to design, develop, and implement PHBs in those areas agreed.
Medicines Management and Prescribing
To continue work with primary care and secondary care organisations to optimise medicines management, improving quality, safety and cost-efficiency of medicines and prescribing. For 21-22 examples of schemes will include work on prescribing guidelines, diabetes, appliances – formulary adherence, respiratory, Mental Health, Analgesics and Controlled Drugs (CDs) and dietetics.
Specialised Commissioning
To work with NHSE to review the potential for the integration of specialised services within local health systems, seven areas are under consideration with option appraisals to commence in 2021.
Enablers (IT, Estates and Workforce)
Digital- all providers must meet a minimum level of digital maturity. Our ICS is pursuing a collective investment approach that enables innovation and transformation. This includes adopting a common information governance framework and the My Care Record Information Sharing Approach, shared capability operating models, anchor tenancy model, remote care and enabling shared care records. Our approach and ecosystem will continue to evolve, alongside standards, core architecture principles, capability convergence and cyber security controls. Estates –
• Supporting Primary Care to develop their strategic Primary Care Network Estates Strategies to enable the local challenges, constraints and opportunities to be explored and taken in to account to ensure the delivery of national and ICS priorities.
• Ensure the learning and benefits realised through the Covid-19 pandemic are captured and continue to be integrated to estates development moving forward.
• To work with system partners including NHS Property Services and Community Health Partnership to optimise the use of our estate, reducing unnecessary voids and disposing of surplus land and buildings.
• To continue to develop and implement system wide responses and strategies to mitigate population growth and the impacts this has on the estate and service delivery
• Work to incorporate current and future digital solutions and systems into estates developments to maximise the benefits these offer and ensure patients have the greatest flexibility around how, where and when they interact with health care services.

• Develop and implement an updated Green Plan for the CCG’s to ensure sustainability is put at the centre of all that we do.
Workforce – In September 2020, we developed the SNEE ICS 'Can Do' People Plan –2020-21 which describes the key areas of work to retain and value our people, grow our workforce, attract new people and businesses to work in our system, and build on our ‘'Can Do' Approach’ for Health and care going forward. The following sections detail: the high-level requirements for the 'Can Do' People Plan linking these to the key priorities of the system and Alliances; overview of SNEE ICS as a system in terms of our workforce (paid and unpaid);
• looking after our people; • belonging to SNEE; • new ways of working; and • growing for the future.
3. Patient and Public Engagement 3.1 Patient and public engagement is embedded throughout all our ICS and Alliance
programmes. 4. Recommendation 4.1 To consider and approve the draft commissioning intentions for 2021-22 for publication.

1 | P a g e
Ipswich and East Suffolk Clinical Commissioning Group North East Essex Clinical Commissioning Group West Suffolk Clinical Commissioning Group
Our Ref: 2021/2022 Commissioning Intentions xx November 2020
Email: [email protected] Tel: 01473 770055
Dear Re: Commissioning Intentions 2021/22 1.1. Background
2020/21 has been a year of significant change for the NHS both nationally and on a local level not least with the ongoing COVID 19 pandemic and our response both to managing this and recovery. Major developments over the last year locally include the development of our new mental health model in Suffolk, the development of our new community model in North East Essex, the development across the three Alliance of our End of Like (EOL) models and the development of exciting capital plans for changes at East Suffolk and North Essex Foundation Trust (ESNEFT) and a new build hospital for West Suffolk Foundation Trust (WSFT).
During this period health, care and wellbeing partners across Suffolk and North East Essex have continued to work together to set the strategic direction for local services through the ongoing development of our three local Alliances: West Suffolk, North East Essex and Ipswich and East Suffolk as a key part of the wider Integrated Care System (ICS) development. This letter provides a summary of the progress made and our future plans, providing a summary of key commissioning intentions for the coming years and 2021/22 in particular within each of our system programmes. The CCGs recognises that these priorities may change in light of learning from the ongoing Covid19 recovery phases and in light of any actions needed to be taken as part of the national Covid 19 ongoing response as the national risk level changes.
This should be read in conjunction with the ICS Strategy and our three Alliance Plans which set out more detailed ambitions and priorities for the ICS and Alliances over the next four years. In line with the NHS Standard Contract, which requires six months’ notification for any potential changes to services and counting and coding charging proposals, these intentions will also support the 2020-21 contract negotiations. These commissioning intentions should therefore be considered the CCG’s formal notice letter. The technical changes for 2021-22 can be found in the specific contract and finance intentions in appendix A.

2 | P a g e
2. Our Integrated Care System 2.1 Introduction As key partners in the Suffolk and North East Essex ICS, our three CCGs are working together with local NHS providers, local government and voluntary and community sector organisations around our collective aim to make a difference to the issues that matter to people, and which can only change by working with other partners. Following the unprecedented events of 2020, we have reflected together with other system partners on our collective learning from the challenges of Covid19 drawing out the following ten key themes:
1. Covid-19 further amplified the many existing inequalities in our communities 2. We underestimated the inherent resilience in our local communities 3. We are more adaptable than we thought – with a collective focus we can move mountains 4. Adopting new technology has potentially brought new opportunities and challenges 5. The safety, flexibility and resilience of our people and workplaces are vital 6. Knowledge is key - we need the right data and intelligence to deliver better care together 7. We need to be joined up across sectors about funding and investment 8. In recovering our services we need to ‘build back better’ and be prepared to face future challenges 9. We need to plan both for the many and the few 10. Enabling collaboration is even more important now than it ever was
This learning from Covid19 has further underlined our commitment to our eight ICS Higher Ambitions including, in particular, our ICS Primary Ambition to achieve health quality for the one million people that we serve. We know that the journey to achieving health equality for our population means ‘Thinking Differently’ about health and care in many different ways. We have an established methodology in our ICS for outcome based working and an increasing alumni of literally hundreds of local stakeholders across all sectors who have participated in online training and a community of practice in outcome based approaches, co-production and asset based community development. Despite the current restrictions of Covid19, we have continued to come together with other partners through regular ‘Thinking Differently Together’ online events discussing key issues including the experiences of carers and families through Covid19 and to renew our
commitment to working with partners as local anchor institutions. We will continue to contribute to ‘Thinking Differently Together’ in this way over coming months through collaborative events across a diverse range of themes including:
• Community assets & social prescribing
• Compassionate communities • Population Health Management • Social Entrepreneurship

3 | P a g e
• Innovation in obesity treatment • Financial sustainability • System leadership • Innovation in cancer diagnosis • Connecting Families with Care Homes
We have engaged in active local discussions since June 2020 about the experiences of local BAME communities through a series of #WhatAreWeMissing events in our three alliances and an ICS-wide event about racism and inequality in health and care. These discussions have shown us that if we are to address racism and inequality in our ICS then we need to listen and learn, change what we do and stand together. This means ‘Thinking VERY Differently’ in every part of our system and embracing difficult issues such as privilege, allyship, accountability and trust – which relate to all areas of inequality. Our experiences during Covid19 have also meant that our commitment to collaboration and working together as an ICS is stronger than ever. Building on our initial 2019 ICS governance framework, we have evolved further ways to work flexibly across our sector and organisational boundaries, around a common set of principles and leadership behaviours, creating a way of working for our health and care system as an ‘ecosystem’ with the ability to adapt and flex to meet the needs of the population. Our ICS continues to be a coalition of the willing, through a conscious decision of locality Alliances, neighbourhood working and sovereign organisations to pool resources and efforts to achieve common goals when it makes sense to do so in the interests of the local population. We want this way of working to enable our communities to shape their priorities and release the assets which contribute to their wellbeing, care and health, within a common set of standards which reduce unnecessary variations in performance and outcomes. By working with people in our communities we can develop trust and understanding with stakeholders about what matters. Consequently, they will own and deliver good outcomes. We plan to fully realise the further opportunities for integrated care systems set out in the NHS Long Term Plan (2019) by strengthening the way that we work with NHS England and NHS Improvement through NHS ‘System First’. Building on our system capability in key areas including population health management, service redesign, workforce transformation, digital and technology, capital and estates and finance we will develop the way that as an ICS we will undertake the two key roles of leading system transformation and collective management of system performance. We have begun to do this work together with our local partners and with support from the King’s Fund with the aim to upgrade our system governance towards the end of 2020, building on the thinking in our three alliances and ensuring that as system partners our system governance supports collective responsibility, streamlined commissioning and decision making between system partners. In upgrading our system governance we want to further enhance the role of the voluntary, community and social enterprise sector in our ICS, more fully embrace the role of non-executives, governors and lay and elected members, and further embed co-production as ‘business as usual’ in the way that we work.
2.2 Our Localities Localities provide a focus for smaller, identifiable populations based on particular characteristics or needs, agreed within Alliances. Without the need to meet the requirements of a fixed size or model, different areas can find different solutions for different problems. In West Suffolk there are six localities, within Ipswich and East Suffolk there are eight localities and within North East Essex there are six localities.

4 | P a g e
Alliances play a key role in oversight and support of effective locality arrangements that deliver for local populations. These localities are based around GP catchment areas overlaid with local health and social care teams and with the development of Primary Care Networks (PCNs) we will ensure that each locality is clearly defined. At locality level the role of district and borough councils and the voluntary and community sector are also key. The Integrated Neighbourhood/Locality Teams bring together physical, mental health and social care practitioners that work with General Practices within each locality to provide a single coordinated care response for people, underpinned by prevention, self-care, early intervention, reablement and rehabilitation, (including people living in nursing and care homes). There are four main objectives:
• Fewer people need unplanned care and support (reduction in crisis situations). • Greater numbers of people have access to and are supported by activity outside of
statutory services. • Resources in the delivery of community-based health and care support are used
more efficiently. • The ongoing costs of supporting people are reduced as people’s independence is
increased. In all three of our Alliance there is a focus on the Integrated Neighbourhood/Locality Teams identifying local issues that relate to their specific populations, and developing a joint plan as to how they, as a system, can begin to address these, with support of the CCG. The Integrated Neighbourhood/Locality Teams are supported by the CCG, county and district council teams who provide data analysis, performance information, administrative and other support to help the Core Management Group and Integrated Neighbourhood/Locality Team practitioners focus on delivery. We now have the opportunity to closer align these teams with the PCNs which now cover our whole area and each of which has a Clinical Director. PCNs are crucial to the implementation of the Long-Term Plan, both through more effective delivery of primary care in local neighbourhoods, and the integration of health and care services to better respond to the characteristics and needs of the local population. PCNs are key to addressing the wider ICS ambitions to improve population health and wellbeing, and to building lasting relationships between our partners.

5 | P a g e
It is increasingly recognised that PCNs play a significant role as an integral building block to support the national and local ambitions. With increased focus on PCNs, it is crucial to support and facilitate the clinical leadership and core teams to enable the capability and leadership to meet that expectation, deliver the national specifications and the local ambition. We are committed to the well-established clinical leadership programmes and intend to expand these further to other clinical and managerial staff. This approach to combined leadership supports the fundamental blocks to integration, and as a means for PCNs to interface with one another. Clinical Directors will be providing leadership, both strategically and clinically to the Alliances at ‘place’ level. The focus of Alliances and localities, including PCNs, is to progress against the maturity matrix so that all streams of activity are following the same broad developmental stages. This is totally in line with national policy, moving primary care and community service towards integration and collaboration at locality level. PCNs are delivering against the seven new service specifications that are being introduced to help cement plans to help shape primary care services. These including:
• Developing an approach to balance increased patient care within communities whilst also ensuring the development of a more resilient Primary Care system.
• Working across our Alliances to ensure Pharmacists, Opticians, Dentists, GPs and other partners are involved within the PCNs. This will build on our Healthy Living Pharmacy programme in particular.

6 | P a g e
• Supporting the integration of mental health services into PCNs. • Management of complex patients to localities with PCNs and Integrated
Neighbourhood Teams. • Support existing and new Social Prescribing schemes; ensuring that learning is
shared between localities and completing a full evaluation of impact by March 2021 to enable informed decisions about future models and long-term investment
2.3 Our Alliances
2.3.1 Overview Local ‘place-based’ systems of care involve multiple partnerships, including NHS organisations and the local government, working together to provide integrated care across organisational boundaries to improve the health and wellbeing of their populations. In Suffolk and North East Essex ICS there are three ‘place-based’ systems of care called Alliances. Our three Alliances are North East Essex, West Suffolk and Ipswich and East Suffolk, with each defined by the footprint of local health and care partners as well as natural geography, developing differently according to local circumstances. As in localities, Alliances need to act as a three-dimensional model interpreting need in many ways. The Alliances provide the focus for planning and delivering meaningful integrated care and services to the local population with partners working closely with the voluntary and community sector, independent sector organisations and communities. The Alliances will become the default forum for all key commissioning decisions and will work with partners across the SNEE ICS wherever that can add more value for each Alliance population than working alone. This approach will be supported by ensuring the Alliances have oversight of contestability plans to drive from inception the design phase of transformation and future commissioning decisions. It is the expectation that the Alliances will form the basis for the commissioning and management of the Better Care Funds, supporting the ever closer integration between health and local authority services, with the intention to explore opportunities to increase the scope of pooled budgets to include those wider determinants of health such as housing. This will help to fully realise the significant opportunity and benefits associated with integrated place based commissioning with local authority colleagues the support the level of transformational change required. The shift from traditional commissioning models to a population health based approach, supported by outcomes based reporting will continue to be central to the Alliances’ commissioning approach. This will form the basis for targeting our key interventions to support wellbeing in the widest sense for our local population, by recognising the importance of the communities we live and work in and to support the reduction in our health inequalities. Alliances will provide the focus for:
• System and service transformation across sectors • Securing and delivering integration • Ensuring clinical engagement • Relationship development and management • Ensuring the principles of good system governance are embedded • Reducing health and social inequalities across each Alliance • Producing and resourcing a detailed plan to deliver the overarching strategy

7 | P a g e
• Ensuring public involvement in planning, development, design, priority setting and decision making
• Demonstrating accountability to Alliance members, local people, stakeholders and regulators
• Ensuring continuous improvement and innovation in the quality and delivery of services
• Ensuring the delivery of high quality, safe and caring services • Ensuring good financial management, financial governance and value for money
We will continue to work with our Alliances to engage in a range of activities to develop solutions for their local populations: Public Involvement
• Work with citizens to understand the wellbeing, social and healthcare needs of the local population
• Create, grow and develop solutions to improve outcomes for the local population • Co-produce outcomes to reflect the lived experience
Continuous Improvement/Innovation
• Review and redesign local services • Work collectively to shape and deliver improvements collectively • Use innovation, including digital solutions, to enable system change and improve
outcomes for the local population Reducing Health and Social Inequalities/Population Health/Planning
• Assess the wellbeing, social and healthcare needs of the local population • Conduct strategic planning across our local population, identifying opportunities for
transformation and improvement • Develop and implement delivery plans
Delivery
• Responsibility for local service provision. Those defined as Specialised Services may be commissioned a system level, but delivery will remain at provider-led alliance level
• Managing risk – finance, quality and performance • Holding colleagues to account
Integration
• Work with system partners to align and integrate service delivery across sectors to create efficiencies in practice and improve outcomes for the local population
• Build and manage relationships across the Alliance network • Work as part of the ICS to inform and deliver systems ambitions
Financial/Contracting
• Shared decision making • Undertake procurement where required, and manage ongoing contractual
arrangements • Local financial management
2.3.2 North Essex Health and Well-being Alliance The North East Essex Health and Wellbeing Alliance (the Alliance) is a collaboration of commissioners, providers and other system partners working together to transform the health and wellbeing of the population of North East Essex as an integrated system.

8 | P a g e
The Alliance way of working is a move away from the traditional commissioner and provider ’split’ and has the vision to work together to form locally tailored solution that will improve the health and wellbeing outcomes of the population of North East Essex, by creating the conditions for people to be able to live long, healthy and meaningful lives. NEE HWB Alliance is working as part of the SNEE ICS. The NHS Long Term Plan, published in January 2019 reaffirms the direction of travel for integrated care systems to work at ‘place level’ and to improve population health.1 For NEE this is set in the context of a local health and care economy which is struggling to cope with demand, a fragile primary care base and 13+ years of inequality in life expectancy between the best and worst wards. In order to tackle this, it is recognised that there are a number of determinants wider than health alone that affect people’s health and well-being; so by working together as a system across health, care and by commissioning and delivering services together the Alliance will look to address a number of factors to improve the health of the North East Essex population. These include but are not limited to the following:
• Housing • Poverty • Public health and prevention • Safe, high quality health and social care which is integrated where this improves
outcomes • Strong communities, neighbourhoods and families • Sexual health • Access to high quality primary care • Early Help • Green spaces and community infrastructure • Crime • Creating a vibrant community voluntary sector
The Alliance will continue to embed the “live well” approach building on the existing foundations in place across Essex, to create an all-age approach to tacking health and wellbeing for our communities. The Live Well model, (adapted to reflect NEE priorities), provides a framework for the design, delivery and evaluation of an integrated community model. With its whole population approach, the Live Well model recognises there is a real need to collectively find solutions that contribute towards wellbeing in order to support the shift to a population health system. As highlighted, it is proposed that Live Well will be used as the foundation for the community model in North East Essex and built around six themes: • Start Well – Giving children the best start in life
• Feel Well – Supporting mental wellbeing
• Be Well – Empowering adults to make healthy lifestyle choices
1 The NHS Long Term Plan (2019)

9 | P a g e
• Age Well – Supporting people to live safely and independently as they grow older
• Stay Well – Supporting adults with health or care concerns to access support and maintain healthy, productive and fulfilling lives
• Die Well – Giving individuals nearing end of life choice around their care The Alliance will also continue to build on the development and utilisation of community assets and will actively adopt an Asset Based Community Development (ABCD) approach. A key focus will remain in working with and enhancing voluntary sector capacity, building on existing group, networks and community champions to increasingly concentrate on what is strong rather than what is wrong in our community. This will continue to form a core alliance principle to support how we engage with our local community, particularly with the hard to reach groups to develop the outcomes we will measure our success against and facilitate the sustainability of improvements against our priority areas.
The North East Essex Alliance are focussed around four workstreams for 2021/22:
Prevention and Reducing Inequalities: this workstream has two interrelated purposes:
• Optimise population wellbeing through improving health as an asset and the prevention of illness or illness deterioration.
• Reduce the inequity of health expectancy. To fulfil this purpose, the work stream will take advantage of tactical opportunities that arise whilst also developing approaches to long-term and entrenched problems including leaning from BAME communities following Covid 19.
Integrated Neighbourhood teams: the specific focus of this workstream is to: • lead the further development, mobilisation and delivery of the place-based ‘Live Well’
Integrated Neighbourhood teams (INTS) programme forming a key priority of the NEEH&WB Alliance. This will include the introduction of functioning integrated and multi-disciplinary teams, empowered and supported by all Alliance ‘partners’ to realise the Live Well vision and outcomes based on PCN and neighbourhood boundaries
• In parallel the programme will ensure effective co-ordination and delivery of key transformation activities which further the development of the Live Well model.
• The INTS team will work collaboratively with the System Resilience Group, ensuring short term solutions to system pressures are fully evaluated and embedded as long-term solutions within the Neighbourhood model.
• Development of the Neighbourhood model will be informed by work undertaken within the Prevention & Health Inequalities programme, ensuring that population health is the driver for community resilience.
Acknowledging the NHS Long Term plan requirements for community care; the opportunities through the Alliance for greater flexibility to achieve integration of care and the introduction

10 | P a g e
of Primary Care Networks, the Alliance will continue to have significant involvement in the review of the NICS model development with Alliance partners and key stakeholders to achieve our community care aspirations.
System Resilience: • This group will develop new models of care for key agreed services across the wider
health and care system to ensure urgent and emergency care services are only used when appropriate
• It will support the achievement of key quality and performance standards including achievement of the 95% 4hr ED standard; 3.5% or lower DToC level in both mental health and physical health services, zero ambulance handover delays and reduction in super stranded patient metrics, reduced mental health out of area placements, improved crisis response and a home first philosophy in all care interventions.
• The group will be responsible for embedding ongoing service developments across the Urgent care agenda
• It will have oversight of the initiatives in place to deliver reductions to emergency department conversion rates for non-elective admissions in line with the Alliance Strategy. This will include learning and building on the successes of the reactive emergency assessment community team (REACT) already in place in Ipswich and East Suffolk to provide an UCRS in NEE.
• A key focus will also include ensuring the system can react to system escalations and incidents as they occur, with greater collaboration across the system to support business continuity and provide mutual aid.
System Integration:
• The core purpose of this work stream will be to bring together a selection of enabling activity and programs of work that currently exist in individual organisations in a way that will support other work streams within the Alliance program for 2021/22, and provide structure, oversight and accountability for developing solutions in these areas that supporting the aspirations of the Alliance.
• The enabling activities included in this workstream include: • Communications and Engagement • Digital • Estates • Information Governance • Quality and Safety • Workforce
Whilst the above four priority areas have been identified, these are very much the starting point for the Alliance, with further priorities to be identified during 2021/22 to support the NHS long term plan implementation and this will form part of the development of the Alliance strategy. These will continue to build upon the place level approach to commissioning, working in partnership with the population health management approach adopted by our ICS. The concept of an alliance delivery approach has initially been tested through the development of the Urgent Treatment Service (UTS) which went live in October 2019 and it is proposed that NICS and End of Life care will provide the next areas, building on the lessons learnt from the UTS service for the delivery of an Alliance model of care that is informed by a population health methodology.

11 | P a g e
It is intended that as the Alliance continues to mature, it will increasingly look towards collaborative delivery solutions where appropriate and this will be reflected in the CCGs procurement approach. In response to this, the governance processes of the Alliance continue to be developed to ensure that arrangements support ever closer collaboration, encourage greater pooling of resources including the sharing of risks and benefits and provide assurance that statutory duties are being delivered and are fit for purpose in the context of a rapidly evolving Integrated Care System. The development of a population health management approach will continue to be a central focus across the Alliance in order to inform not only the outcomes of the developing four work streams but the future strategy and long term priorities to ensure we are triangulating data across our system and are creating collective responsibility to support resolution. The Alliance will adopt a patient safety culture to promote patient safety thinking beyond why things go wrong in healthcare (Safety I), to examine why things routinely go right and how that can be maximised (Safety II). Working jointly with the Alliance patient safety partners (patient and public representatives specifically involved in patient safety) as identified in the NHS Patient Safety Strategy a safety programme will be rolled out to address the priority areas and develop Alliance care standards. In line with this safety culture the Alliance will continue to provide oversight to our care home organisations across NEE. The creation of the Local Care Home Hub (LCHH) is a conduit for all parts of local health and social care systems to co-develop strategies and collaboratively plan safe, efficient support to the nursing and residential care home market within NEE. LCHH is the forum where all the partners across the health and social care system will continue to come together to support the system response to the impact the COVID 19 virus (and any other significant outbreaks) is having on our care home population. The group will consider multiple resource plans such as workforce, screening, estate, IPC and business continuity capacity plans to ensure the safety and quality of nursing and residential care. It is anticipated that for future years, the Integrated Care system will issue an overarching set of commissioning intentions with the three Alliances (North East Essex, Ipswich and East Suffolk and West Suffolk) issuing their aligned intentions. 2.3.3 West Suffolk Alliance The West Suffolk Alliance is now operating in its fifth year and has grown in membership from NHS and Suffolk County Council to include district and borough council, voluntary sector, social enterprise and other partners. The Alliance strategy – All About People and Places was agreed in May 2018 and sets out principles for how we work together as partners: • Focus on people and places in West Suffolk integrating services around people’s homes, neighbourhoods and communities. We will give priority to what works for families, individuals and communities and will be bold and ambitious about what can be achieved. • Create a financially sustainable system through managing demand differently and through committing to using the West Suffolk pound in the best way locally, reducing duplication and waste.

12 | P a g e
• Address health inequalities across West Suffolk focusing on prevention, accessibility, integration, effectiveness and sustainability of services to ensure that existing health inequalities in West Suffolk are reduced. • Strive for the best quality services based on the outcomes we have agreed, within the resources available. • Design things together and collaborate working with people, communities and partner organisations in West Suffolk. We will agree collectively how we do things so that we only do them once and support each other through change as our organisations adapt, building trust and having frank and honest discussions when needed. • Be innovative redesigning our services using the experience of people and front-line staff and looking at national and international evidence. We will coproduce our changes designing effective and integrated services which meet people’s needs. We have a shared direction of travel for West Suffolk and articulated this in four Alliance ambitions:
Since its inception the Alliance has worked to develop its six localities, providing integrated services, bringing statutory, voluntary and other services together within the community so that support is co-ordinated around people’s needs. Priorities for change are developed through engagement and though an understanding of local need. Public Health intelligence has been critical in helping us understand where there are poor outcomes for people and where there are opportunities for improvement. Our relationships and past experience of change programmes helped us during the first wave of the pandemic to respond flexibly, sharing resources, intelligence, and together agreeing rapidly on change initiatives. We continue to use this approach to current challenges, such as planning for winter. It is also how we are working together on one of the largest issues in West Suffolk which is the Future Systems programme. Using co-production techniques, we are reviewing how and where services currently delivered in the WSFT site will be delivered in the future. This is a huge opportunity for West Suffolk and will shape the delivery of services over the next decades. The pandemic has also highlighted health inequalities within our communities. We have a programme, #WhatAreWeMissing that aims to address health inequalities and access to services for people from black, Asian and ethnic minority groups. Over the next year we will

13 | P a g e
be setting up a community champions group and working with community leaders to understand and tackle some of issues that impact on people within their communities. The Alliance has adopted a Quality Improvement methodology within our work. This is a systematic approach using specific methods to achieve successful and sustained improvement. The vision of this method is to ensure that everyone has the best care and health possible in West Suffolk. Quality Improvement (QI) is about making a real difference, directly or indirectly, to services for user, their families, staff and stakeholders. Quality improvement is an approach that allows staff to be curious and strive for the excellence, by experimenting with new approaches and seeing if they work. We have partnered with the Institute of Healthcare Improvement who are providing expertise and insight to support us to embed Quality Improvement throughout the Alliance. We are using the QI approach within our Delivery Plan, and for other transformation projects within the West Suffolk system. Our Delivery Plan does not describe all the great work going on in West Suffolk but highlights five areas where making progress will significantly impact on the achievement of our Alliance ambitions. The Alliance Delivery Plan for 20/21 focuses on five themes. Collaborative Communities Understanding and taking action on the wider determinants of health, using an asset-based approach, is core to our way of working within the Alliance. The areas of focus within this theme are:
• All alliance projects to be co-produced and have foundations based on local conversations, local intelligence through appropriate engagement
• Increase volunteering to improve capacity within the INTs and Alliance Localities • More effective management of homeless and complex cases. To improve outcomes
for the individuals and communities and reduce the need for expensive statutory interventions.
• Reduce feelings of loneliness and physical isolation post CV19 Children and Young People Action within this theme will support a partnership approach to the delivery of services for children, young people and families. This is in recognition that the Alliance plan is for all ages, all disabilities – about improving outcomes for all our population. Integrated Neighbourhood Teams This theme is looking to support our front-line health and care teams to provide co-ordinated person-centred care for people within their locality. Integrated Neighbourhood Teams strengthen the support for people to stay well and manage their wellbeing and health in their communities by providing integrated Health and Social Care across West Suffolk, in line with the Alliance Strategy. Integration removes duplication for our patients and customers and provides a holistic approach to addressing an individual's needs or goals. Implicit within this theme is the aim to deliver more services close to where people live. The delivery of this theme will support how we can work better together to use resources flexibly and more effectively. Teams have developed an Integrated Neighbourhood Team Maturity Matrix which describes the steps that they need to go through to become “exemplary” integrated teams. Immediate actions are to introduce more robust multi-disciplinary team approaches to case management, and to move to shared management arrangements for the teams. Responsive Support Getting services right for people when they are experiencing exacerbations in their health and care needs is both good for them, and good for the system. This theme looks to

14 | P a g e
strengthen our response at a local level, providing the right support to ensure people can stay independent and remain at home during a time of changing health or social care needs The three responsive support priorities for winter planning within the next 6 months are: • Discharge to optimise and assess – ensuring more people have the benefit of a holistic approach to planning and support as they come out of hospital to return home • Making sure that we use our community bed base effectively as a transition from hospital home for people who need that extra level of support post hospital • Rolling out the virtual ward model, which provides care and support for people at home, who otherwise would need inpatient hospital care. These actions all require multi-agency input, including from general practice, our voluntary and community sector partners and the private care sector. Collaborative System Working The Alliance is all about collaborative system working, and in common with the other areas listed above not all the actions are contained in the Delivery Plan. The two areas within the plan for this year within this theme are:
• Understanding the impact of our transformation programmes on people in West Suffolk and on our staff. We are testing out whether the introduction of the R-Outcomes approach will support us to deliver improved outcomes for people, as a critical element of our Quality Improvement approach
• The Alliance is reviewing governance arrangements. This will ensure that the Alliance can take advantages of opportunities and changes within the overall system governance structure to strengthen Alliance working, deepen our commitment to collaboration, and ensure that we can articulate this throughout our organisations.
Each theme has a senior level sponsor and lead, who works closely with enabler leads to agree actions. For example we know that our workforce is one of our greatest assets in delivering the changes we have outlined and we are working with workforce, digital and communications leads to ensure we have the expert input, alignment with wider programmes (for instance those run at ICS level) so that our changes are led by our front line staff, as well as by what people in West Suffolk tell us. The enablers to the plan are workforce, digital, estates, finance, communications, engagement and quality improvement. As an Alliance we continue to work as part of the Suffolk and North East Essex Integrated Care System. We benefit from the work that is done across the ICS as a whole, and value the support and experience of our two sister Alliances within the ICS. 2.3.4 Ipswich and East Suffolk Alliance The Ipswich and East Suffolk Alliance (the Alliance) is a collaborative coalition of commissioners, providers and other system partners with a shared vision - “to enable Ipswich and East Suffolk to be a ‘place of strong communities in which everyone is able to stay well, take control over their mental and physical well-being and, when support is needed, receive joined up health and care.” The purpose of the Alliance is to deliver the outcomes of the Suffolk Health and Wellbeing Board:

15 | P a g e
• Every child has the best start in life • People of working age are supported to optimise their health and well-being • Older people in Suffolk have a good quality of life • People in Suffolk have good mental health and well-being
Our shared values are:
• Collaboration – Co-ordination • Compassion – kindness and care • Creativity; innovation • Community-focus • Creating One Team - Combined Clinical and Care Leadership • Cost effectiveness
The Ipswich and East Suffolk (I&ES) Alliance is part of the SNEE ICS. The NHS Long Term Plan, published in January 2019 reaffirms the direction of travel for integrated care systems to work at ‘place level’ and to improve population health.2 For I&ES this is set in the context of a predominantly aging population that is forecast to grow significant over the next twenty years, a combination of lower than average wages and above average house price increases with the consequential impact on health inequalities and demands, and a broad and varied geography. Collectively, these factors present a set of strategic challenges that the alliance will need to overcome through innovation, adaption of services, and even greater collaboration. We recognise that there are several determinants wider than health alone that affect people’s health and well-being, so by working together as a system across health and social care we will continue to:
• engage and involve the people we serve to ensure our care and services are inclusive and meet the greatest needs,
• integrate and simplify the way we work together to improve the public’s experience of services and outcomes.
In addition to ensuring the resilience and integration of our system to manage Covid and ‘regular’ joined up service delivery our work will continue within the following key programmes. Over the next few months we will further develop detailed plans and priorities within each programme of work.
2 The NHS Long Term Plan (2019)

16 | P a g e
The transformation programmes are described in further detail within this letter as most are shared either across Suffolk or with NE Essex or across our whole ICS community. Enabling actions as related to workforce, digital and finance are also described in other sections. Connecting Actions This programme of work focuses on further strengthening the alliance to achieve our shared outcomes. We will continue our work based to: 1. Enable people to stay well – We will continue to promote prevention, self-care and
reablement to help the people living in Ipswich and East Suffolk live well for longer. We will continue to support delivery of the Suffolk Prevention Strategy by focusing our effort on mitigating the eight modifiable risk factors which can have the greatest impact on the six most common preventable diseases. We will continue to evaluate and evolve our local model of social prescribing to ensure it remains at the forefront of meeting local need and national best practice
1. Join up in our communities – We will continue to develop our local community health and care services, working together to care for people in their own home wherever possible enables us to comprehensively understand and support the needs of the whole person and to reduce duplication. We will focus on: • Fewer people needing unplanned care and support (reduction in crisis) • Greater numbers of people having access to and are supported by activity outside of
statutory services • Resources in the delivery of community-based health and care being used more
efficiently • The on-going costs of supporting people being reduced as people’s independence is
increased.
2. Create ‘One Team’ - We will continue to invest in the staff and volunteers who work with the people we serve to retain, develop and attract the best talent and create a supportive, collaborative and innovative environment. We will:
• Continue to embed our shared mission and values • Develop further joint roles and teams across organisational boundaries.

17 | P a g e
• Continue to invest in shared leadership development, providing a variety of opportunities to apply learning in the work we deliver together.
• Maximise opportunities to co-locate and continue to exploit technology to streamline and integrate what we do and how we do it.
3. Reduce inequalities – We will continue to work collaboratively with our communities -
listening to their needs and experiences to ensure our services are inclusive, accessible to all, and outcomes are equal. Our staff and volunteers are the heart of our alliance and we will continue to work in partnership to ensure our workplaces are healthy, inclusive and supportive of all. We will: • Use our role as ‘anchor institutions’ in our community:
o As employers – in our recruitment, training and progression; and in creating healthy workplaces,
o As purchasers – use local supply chains and building our values and expectations into our contracts,
o As land and asset owners and in new developments; and o In how we behave as leaders and partners – upholding our values.
• Review and adapt the way we work and systems that prioritise resources to support
reduction in health inequalities – building on the lessons and innovations arising from the COVID19 pandemic,
• Continue to marry investment to grassroot community designed and delivered initiatives; and
• Harness the knowledge, skills and drive of Integrated Neighbourhood and Connect Teams to reduce inequalities within their areas.
2.4 Our CCGs The CCGs are evolving the way in which they work to enable effective collective commissioning across the ICS within each Alliance area and at a Neighbourhood Team level to make sure that the benefits of integrated care at every level can be fully realised. Commissioning is much more than just the procurement and contracting process. Commissioning for integrated care is about wrapping around all elements of the system in an integrated manner using co-design to work with communities on ways to respond to the needs of a defined population irrespective of size. The needs of our population, national policies and plans require that we take much more decisive action on prevention and population health, investing in new, more integrated, more efficient and more locally applicable models of health and care. Fundamentally, we also need a totally different relationship with our communities to enable them to shape the priorities and release the natural assets which will contribute to their wellbeing, care and health. We are responsible for making the best use of the resources we have in our system and more effective commissioning and grant making has a major part to play in this. Over time, we aim to see a greater emphasis on efficiency coming from wider system improvements. Statutory commissioning bodies responsible for health, care and wellbeing will need to take every opportunity to work with partner organisations/groups/bodies to think outside our current paradigm of what a health and social care system is, to have maximum influence on the causes of causes/wider determinants of health. This must include finding new ways to maximise the added value of voluntary and non-statutory resources that exist in the health, care and wellbeing sectors. Our approach to commissioning must also be driven by the latest evidence, insights and intelligence. To achieve the changes required, all current commissioning and provider organisations in Suffolk and North East Essex are seeking to

18 | P a g e
find a new locally relevant, less hierarchical way of organising and delivering our wellbeing, care and health system. In Suffolk and North East Essex, we are committed to an emphasis on working predominantly at Alliance level and with the CCGs as equal partners in the ICS alongside local government, providers and the voluntary and community sector. The three CCGs have a single Accountable Officer and a single management team, delivering a recurrent 20% running cost saving. The single management team is also playing a significant role in supporting the Chair and Executive Lead of the ICS and in building an effective working relationship with the regional and national teams of the NHS. The management team has five directors with cross-cutting responsibilities across the whole ICS footprint and a locality director aligned to each Alliance. In 2021/22 the CCGs will:
• Continue to co-operate with one another and each working increasingly as integrated partners within Alliances with governance to support local decision making;
• Establish joint governance across the three CCGs able to support decision making where it is needed across the whole ICS footprint;
• Explore closer working with Local Authority commissioning partners, including Public Health;
• Explore the potential of integration of direct commissioning of specialised services at an ICS level;
• Conclude discussions on the organisational form of the CCGs.
2.5 Aligning Incentives to Deliver Change
Changes to the financial architecture driven by the emergency response to Covid-19 mean that the funding baselines in place during 2020/21 have moved away from our previously agreed plans and there have been significant changes to our normal financial mechanisms. As yet, we do not know the extent to which these changes will be permanently adopted or phased out in 2021/22, nor do we know the impact on CCG allocations or the system’s ability to make local decisions regarding contract values and terms. However, the strong system working we have developed in recent years, such as the used of Guaranteed Income Contracts, adoption of system wide control totals and ICS wide financial reporting, provide us with the building blocks to pick up and adapt the new national architecture to our local needs.
We believe that the use of fixed income contracts is one of the key enablers of success in our system; allowing partners to concentrate on developing the most appropriate pattern of services rather than being driven by particular financial incentives, and are pleased to see that the national direction of travel is consistent with our approach. We will consider how to enact the principles of the Social Value Act more consistently when commissioning services. Recognising the added value benefits that organisations can bring to services being delivered or produced, our engagement with social value will allow us to consider and secure the extra benefits which can be delivered by providers.
The CCGs will continue to ensure that Mental Health Services are prioritised in our investments through ensuring that the mental health investment standard is met, maintaining the share of our overall expenditure which is allocated to this area, regardless of the pressures being felt elsewhere in the local system.
We will continue to encourage partnership working to meet our statutory requirements and to deliver the constitutional standards of the NHS. As such, the priority for any discretionary financial investment remains foremost to deliver constitutional performance with subsequent
19 | P a g e
investment to complement and enhance performance against our system and place-based ambitions and objectives.
The CCGs will procure services in accordance with regulations and our schemes of delegation, with reference to our three place-based Alliances, and with regard to the regulations on procurement, competition and choice. The regulations are intended to give commissioners flexibility and adopt a principles-based approach as opposed to providing prescriptive rules on procurement.
2.6 Quality Improvement Quality of care remains at the heart of the commissioning decisions made by our CCGs. . Whilst some difficult decisions have to be made, the CCGs will always consider the impact on the effectiveness and safety to ensure that responsible decisions are made. Our intention is to strengthen the quality improvement framework and to support an outcomes-based approach to integrated health and care. Our focus is on doing the right things and doing the right things well to fully understand the impact and outcome for people who access the services we commission.
It is our intention in 2021, to take a supportive approach to quality assurance visits, clinical quality priorities and patient safety issues. This will be prioritised within a rolling programme and on a more routine basis. Where appropriate we are planning to take a system wide integrated approach to assurance visits.
The CCGs will uphold its statutory responsibilities under the Health and Social Care Act 2012 and later amendments (2014 & 2016) as well as the Five-Year Forward View 2014 to ensure continuous quality improvement in the services it commissions. Suffolk and NEE CCG’s will ensure that it follows and embeds in its practice and its contracts, the national guidance for improving patient care and safety as and when this is published. Priorities for 2021/22 will span across all three Alliances and will include:
1. Safeguarding 2. Infection Prevention& Control 3. Deteriorating Patients 4. Safer Staffing 5. Learning Disability and Autism 6. Falls Prevention 7. End of Life Care 8. Tissue Viability 9. Dementia 10. Hydration & Nutrition 11. Mental health 12. CYP 13. SEND
Within the ICS we will continue to determine the infection prevention and control health contribution to care settings, to ensure that we take a supportive and preventative approach to outbreak management. Our CCGs will only contract with providers that abide by our policies and protocols. These include, but are not limited to, the Clinical Priorities Policy and access criteria including, prior approval thresholds and pathways for BMI and Smoking as determined by the CCG.

20 | P a g e
Referrals should clearly specify when patients meet the criteria for referral and patients should only be treated if they meet the CCG’s criteria for treatment. The Clinical Priorities Policy is the CCGs’ corporate policy which outlines its commissioning approach for treatments and interventions which are considered low clinical priority or have limited evidence to support clinical effectiveness in terms of outcomes. During 2020/21, the CCGs aligned Clinical Priorities/ Service Restriction Polices. This streamlined our commissioning policies, creating a more standardised approach to the funding application process. The CCGs will also look at aligning the agreements in place that support the funding application process; including agreeing a standardised price for medical photography to ensure there is no unwarranted price differential across North East Essex and Ipswich and East Suffolk and West Suffolk CCGs. NEECCG plan to continue to host the Individual Placements Team (IPT) on behalf of Essex CCGs. In so doing, IPT continue to strengthen their contracting function and to develop through robust audit of processes. IPT continue to work collaboratively with Essex commissioning partners, including Local Authorities, to meet the challenges for people needing specialist placements under section 117 and tertiary specialist interventions. Across the ICS, some key priorities in relation to the delivery of mental health, learning disabilities and autism and improvement of wellbeing and mental health for our communities across all three alliance systems are being set. This involves the oversight and assurance regarding the provision and delivery of emotional and mental health services. These include:
• Maintain performance on inpatient trajectory for CCG, CYP and Specialised Commissioning.
• LD admission avoidance/early discharge service to open Oct/Nov 2020. • Admission avoidance pathway and 12-point discharge planning. • C(E)TR compliance remains 100% against NHSE targets. Currently held virtually,
plan to reinstate face to face. • Host commissioner 8 weekly visits completed virtually, plan to reinstate face to face. • LeDeR steering groups/working parties continue to take LeDeR learning into action. • Completing LeDeR trajectory agreed and plans in place to meet target with the use of
experienced bank staff. • Support GP’s to meet ACH target of 67%.
In mental health we will be paying specific attention to:
• Reducing out of area placements from our commissioned Mental health services • Reduction of Seclusion, long term segregation, restraint and rapid tranquilisation
reported by mental health trusts • Ligature compliance on inpatient wards • Si’s and themes for learning, focusing on the implementation of the PSIRF pilot
project • Improved outcomes for children and young people in crisis
We will be addressing the health inequalities for people with learning disabilities and/or autism and measuring providers on the Learning disability improvement standards (2018) for NHS trusts.
SEND programmes of work across the Suffolk and the Essex system continue to be key priorities for us and the progress against the written statements of action for Suffolk and

21 | P a g e
Essex. We intend to ensure that we measure and develop outcome measures for providers and our Suffolk and Essex systems.
2.7 Integrated Care (incl. Urgent Care, End of Life Care and Elective Care)
The following focus areas apply across Ipswich and East Suffolk, North East Essex and West Suffolk CCGs and Alliances:
• Continued roll out and further development of Integrated Neighbourhood /Locality Teams across Suffolk and North East Essex to support delivery of local health and care improvement priorities through localised delivery plans and CCG wide transformation priorities. This includes managing demand at a local level with a particular focus on Long Term Conditions management, Ageing Well and End of Life.
• Fully embed Discharge to Assess (D2A) across the four agreed pathways to continue to support effective patient care and support health and care system demand and capacity; achieving 3.5% or less delayed transfer of care and reduced levels of Stranded and Super Stranded patients and reducing delayed transfers of care at community hospital sites with an aspiration to achieve 3.5% supporting overall system flow.
• Fully embed Trusted Assessment across Suffolk and North East Essex linked to priority integration projects including Integrated Neighbourhood Teams, D2A pathways, Care Homes and admissions avoidance service (responsive home care and support).
• Year three delivery of the system Managing Demand in Care Home programme of work with a focus on trusted assessor, responsive in-reach, dementia and tissue viability support and integrating care homes with locality developments
• Continue to roll out High Intensity User approach to all providers, supporting MDTs and shared care plans. Developing this further with primary care networks/integrated neighbourhood teams to support sustainability across the system.
• System-wide review of diagnostic capacity following the publication of the Sir Mike Richards report to deliver the elective and cancer performance standards via faster access and more pathways straight to test.
• Continue to support our local trusts in recovering elective activity including inpatients and daycase plus diagnostic support including ongoing arrangements with our local Independent Sector (IS) providers.
• Continue to support our local trusts on decreasing waiting lists and waiting times to ensure no long waiters, supporting the 26-week choice process to offer faster treatment elsewhere. Transformation will focus on redesign of outpatients including involvement in the regional adapt and adopt programme and one-stop shops reducing the need for patients to travel for face to face appointments by one third over four years.
• Continue the implementation of large-scale change programmes with local acute trusts and partner organisations, including the new Elective Care Centre on the Colchester Hospital site and the new build hospital programme at WSFT.
• Support the development of additional neuro rehabilitation capacity in Suffolk with partner organisations and continue working with Essex partners to support placing patients into the best care setting to meet their needs using the neuro navigator role.
• Ongoing focus and service improvement related to the front door transformation on

22 | P a g e
all three sites. This will build on the UTS success in NEE to apply the learning to the front door changes at Ipswich and supporting its further development including integration of: GP Streaming and system-wide, urgent and emergency care resources including primary care, paramedic, pharmacist, therapists and developing a Mental Health Crisis element.
• As the UTS Model is developed pathways will be agreed with primary care to support the direction of patients presenting with minor illness to patients registered GP where possible. This will be supported by NHS 111 and the technical ability for NHS 111 to book patient appointments directly with primary care.
• The UTS Collaboration will work with primary care to ensure the standards for GP Extended Hours DES continues to be met and supports the wider demand management plans through improved access to primary care.
• There will be a continued focus on the 111 service in relation to performance against the national standards of the number of calls transferred to 999 as well as attendances at A&E.
• The 111 service may be required to introduce new elements in line with national pilots such as the roll out of NHS Think First which will commence in December 2020.
• Ongoing development of the established 24/7 community based Reactive Emergency Assessment Community Team (REACT) admission prevention service in Ipswich. This will include extending the Frailty Assessment Base; Dementia Intensive Support Team and mental health provision moving to seven days a week service; and the mobilisation and evaluation of urgent community response services in NEE and WS utilising the learning from Ipswich.
• A focus on EOL care across all three Alliances will be maintained with individual workplans to meet the needs of each area while sharing good practice and learning at the ICS EOL board.
3.2 Integrated Care System - Strategic Programmes
The following are strategic programmes across our ICS:
3.2.1 Achieving Health Equality Achieving our primary ambition of achieving health equality for our whole population means that we need to work with partners to tackle the many health inequalities that we know our communities face.
Health inequalities are the preventable, unfair and unjust differences in health status between groups, populations or individuals that arise from the unequal distribution of social, environmental and economic conditions within societies, which determine the risk of people getting ill, their ability to prevent sickness, or opportunities to take action and access
treatment when ill health occurs.
The following diagram summarises the different dimensions of health inequalities:
We know that for some people in Suffolk and North East Essex there

23 | P a g e
are still unfair and avoidable inequalities in their health and in their access to and experiences of NHS services. We also know that there are actions that can be taken on the social determinants of health which can reduce these health inequalities, for example education, employment and housing.
We are therefore committed to addressing health inequalities in a number of ways:
Recovery from Covid-19
One of the key conclusions from our ICS Report ‘Reflections on System Learning from Covid19’ was that Covid19 further amplified the many equalities in our communities in Suffolk and North East Essex. It has become increasingly clear that COVID-19 has had a disproportionate impact on many who already face disadvantage and discrimination. The impact of the virus has been particularly detrimental on people living in areas of high deprivation, on people from Black, Asian and minority ethnic communities (BAME), and on older people, men, those with a learning disability and others with protected characteristics. A central part of our local plans to recover from Covid19 and restore services is to increase the scale and pace of NHS action to tackle health inequalities to protect those at greatest risk. These plans include the following eight urgent actions identified by NHS England and NHS Improvement:
• Protect the most vulnerable from COVID-19 • Restore NHS services inclusively • Develop digitally enabled care pathways in ways which increase inclusion • Accelerate preventative programmes which proactively engage those at risk of poor
health outcomes • Particularly support those who suffer mental ill-health • Strengthen leadership and accountability • Ensure datasets are complete and timely • Collaborate locally in planning and delivering action
We will work as partners in the ICS through our three local alliances to implement these actions over the coming months, in close partnership with colleagues in local government, other public services, voluntary and community sector organisations, and local communities.
Thinking VERY Differently about Health Equality We know that as an ICS if we are to address issues such as racism and inequality in health and care we need to listen and learn, change what we do and stand. What this means is ‘Thinking VERY Differently’ in every part of our system and embracing difficult issues such as privilege, allyship, accountability and trust – which relate to all areas of inequality. We have an established methodology for outcome based working embedded through regular online training to an increasing alumni of literally hundreds of local stakeholders across all sectors and a community of practice in outcome based approaches, co-production and asset based community development. We will build on this work by co-producing with community and VCSE partners as part of the Public Health England ‘Health Equality Programme’ to develop an extended toolkit to this methodology and delivery of online training at scale to inspire local stakeholders from all sectors to be ‘Thinking VERY Differently Together’ about health equality. The key elements to this methodology are likely to comprise: • Thinking about whole population outcomes

24 | P a g e
• Recognising privilege, the way that inequality can arise and it’s impact • The need to engage around inequalities as a novice • The practice of ‘allyship’ in health and care • Enabling health equality through accountability in frontline practice • Enabling health equality through collaboration, co-production and trusted relationships in
local health and care systems. Realising Our Role as Anchor Institutions As CCGs we have made an explicit commitment alongside other local public sector partners by signing our ICS Charter for Anchor Institutions to make a difference in our local communities by:
• purchasing more locally and for social benefit • using buildings and space to support communities • working more closely with local partners • widening access to quality work • reducing our environmental impact.
This is not only a significant vision but an urgent one since our communities include pre-existing areas of significant deprivation who now face an even more considerable threat to their health and well-being arising from the economic consequences of Covid19. This report of our recent ICS event about ‘Our Role as Local Anchor Institutions’ outlines some of the early work across Suffolk and North East Essex which we will continue to develop with partners. We have begun delivery on this agenda as partners through the ICS through our system wide workforce, estates, finance and sustainability programmes. These will each link into an ICS Anchors Board linking in turn into the Essex Partners Board, Suffolk Public Sector Leaders Group, Suffolk Collaborative Communities Board and local economic forums.

25 | P a g e
We aim to rapidly accelerate the role of social entrepreneurs as a key assets in these deprived local communities. As part of the Public Health England ‘Health Equality Programme’ we want to rapidly identify creative opportunities to deliver local social value by working with social entrepreneurs who we can enable as partners by more fully realising our roles as local anchor institutions e.g. by procuring services for social value. We will also continue to support the ambitious work being carried out across Clacton and Jaywick Sands in Essex by a coalition of local partners to improve the health of local people as part of our ambitious programme of levelling up. Jaywick in particular is now at the bottom of the list of most deprived areas in the country. Even as we have seen growth in some areas of the UK recently, Clacton and Jaywick have seen a marked decline in deprivation indicators. Our ICS partners have developed a comprehensive plan for transformation of the local area, using the renewal of sustained employment and economic opportunity as the lynchpin for addressing health inequalities and improving health outcomes. Clacton Place, as we are calling our programme, seeks to take what we know about the links between employment and health and turn the trajectory of a whole community around through collective endeavours. Working in Partnership with the VCSE Sector The VCSE sector are key partners in tackling health inequality. Suffolk and North East Essex is blessed by an exceptionally strong and diverse local VCSE sector who continue to face many challenges as a result of the Covid19 pandemic. Many organisations have experienced a significant loss in their unrestricted core funding as a result of a dramatic reduction in local fundraising. The pandemic has also significantly restricted the delivery of face to face services and projects and many have experienced a significant reduction in support from volunteers. However at the same time the invaluable support offered by the

26 | P a g e
sector to so many vulnerable people in our communities is in more demand than ever as the social and economic consequences of the pandemic continue to deepen. We have undertaken a joint mid-project review of the status and impact of the 80 projects funded through the ICS Realising Ambition programme together with the Suffolk and Essex Community Foundations and found additional funding to enable projects to extend their delivery until 31 March 2021. Our three Alliances will then work with projects and the Community Foundations to plan next steps for the programme in 2021/22. We will work in partnership with our local VCSE sector through our ICS and Alliances in response to the issues outlined above by: • Developing more agile contracts that offer the additional flexibility and stability that the
sector needs at such a challenging time; • Working in partnership with local government, community funders, VCSE infrastructure
organisations and VCSE leaders to work towards a more sustainable sector; • Providing infrastructure support alongside other ICS partners with practical issues e.g.
safety, HR, estate management, etc.; • Continuing to maintain good two way communications and strategic working on key
issues with VCSE leaders as partners through the ICS VCSE Strategy Group; • Further enhancing the role in the ICS in our next steps work on ICS governance.
We will also support collaboration between all those supporting volunteers in Suffolk and North East Essex including development of a local volunteer passporting scheme. Addressing the Health Inequalities Experienced by those Living with Obesity We know that people with obesity experience a broad range of health inequalities and that obesity is also often closely associated with factors such as deprivation, gender and race. We also recognise that the significant stigma experienced by those living with obesity can also contribute to social factors that can drive health inequalities. • We will work with local and national partners including patient groups to make sure that
we fully understand the full range of health and social inequalities affecting people living with obesity in Suffolk and North East Essex, including their experiences of Covid19;
• We will work with people living with obesity to deliver a local stigma campaign both in the community and our local health and care system;
• We will work towards our ICS Higher Ambition of a comprehensive treatment pathway for obesity by working with people living with obesity, clinicians, local NHS providers and national experts to develop plans for an innovative local obesity treatment pathway. This will include consideration of the potential benefits of innovative new digital services, more integrated models of service delivery and the case for the developing local bariatric surgery.
3.2.2 Stroke Services and Neuro Rehabilitation In January 2019 the NHS Long Term Plan (LTP) established stroke as a renewed clinical priority for the NHS. Building on the work of the 2007-17 National Stroke Strategy, the LTP sets out milestones and ambitions for the health and care system to deliver improved prevention, treatment and care for the 85,000 people who have a stroke in England each year.

27 | P a g e
Clinical and operational networks based on patient flows are widely recognised as an effective model for improving standards of health and care outcomes for defined groups of patients. Stroke is no exception, the development of Integrated Stroke Delivery Networks (ISDNs) is essential to lead the delivery of the LTP commitments for stroke. Effective delivery of high-quality stroke services based on a networked approach will reduce overall associated stroke mortality rates and disability, as well as reducing the burden stroke places on families and carers, on the health and care system, and on wider society. The National Stroke Service Model (Draft October 2020) describes a new named configuration for stoke units and service arrangements, including `Comprehensive and Acute Stroke Centres (CSC, ASC) which should be of a sufficient size to ensure expertise, efficiency and a sustainable workforce. Within SNEE ICS the networking and pathway optimisation of stroke services will maximise patient benefit, and ensure pathways are delivered via a 7-day range of services. We will work throughout 2021/22 to embed these new national changes and substantiate our local service plans, already agreed within the ICS 5-year Plan. Key deliverables for ISDNs are:
• Best practice personalised stroke pathways configured and managed from pre-hospital care onward, including ambulance, thrombectomy, Early Supported Discharge (ESD) and six-month reviews within initial implementation, building to include the full pathway from prevention through to life after stroke.
• A flexible, future-proofed competency-based stroke workforce, supported by a skills and capabilities framework and toolkit.
• A comprehensive dataset meeting the needs of clinicians, commissioners and patients describing the quality and outcomes of care provided.
It is anticipated that the SNEE ICS Stroke Board will link to the EoE North ISDN Board which is being established to deliver a programme of work based on joint priorities to improving stroke pathways in line with the ISDN pathway specification. It will utilise expert clinical advice and recommendations from the EoE Stroke Clinical Reference Group and Clinical Advisory Groups to inform the programme of work, including agreeing joint priorities and to provide assurance to the EoE Stroke Board, constituent STP/ICSs partners on delivery of the programme benefits. For the SNEE ICS for 2021/22 the key priorities are:
• to continue delivering services through an integrated arrangement across all three sites within the system to maximise the use of technology
• to embed thrombectomy pathways, in the short-term out with the system but developing plans longer term to establish thrombectomy within the ICS
• to support the delivery of the prevention programme
• complete the successful procurement of an Early Supported Discharge (ESD) service extended into a wider integrated neuro rehab service (by 2022). The development of a stroke recovery service with local delivery and implementation of stroke priorities for IES, NEE and WS alliances with a particular focus on rehabilitation service integration as a post Covid-19 initiative.
These services will help to support the population either suffering from long term neurological conditions or post-acute episodes like stroke or trauma to recover whilst remaining within their own homes. We will work with local providers and our third sector partners to explore the opportunities for establishing increased bed capacity for local access for the differing levels of complexity of care needed for individual patients.
3.2.3 CVD / Cardiology services
Working with colleagues across the ICS and regional and national teams we aim to ensure:
28 | P a g e
• People have the information and support they need to reduce the risk of developing cardiovascular disease
• People with cardiovascular disease have the right treatment and support to manage their condition.
• People have the best possible treatment and care for survival and recovery from cardiovascular disease
We plan to do this by:
• Improving the effectiveness of approaches such as the NHS Health Check to rapidly treat those identified with the high-risk conditions, including atrial fibrillation (AF), high blood pressure and high cholesterol (ABC)
• Increased access to testing in primary care for patient suffering from heart failure and heart valve disease
• Increasing the number of people who know their ABC and provide opportunities for the public to check on their health
• Increased access to cardiac rehabilitation, a programme of exercise and information to help people recover following a heart attack, heart surgery or procedure
• Improving community first response and build defibrillator networks to improve survival from out of hospital cardiac arrest
• Expanding access to genetic testing for Familial Hypercholesterolaemia (FH)
3.2.4 Respiratory services
In alignment with the SNEE 5-year strategic plan, we will work collaboratively with colleagues to ensure better care outcomes for patients experiencing respiratory conditions, including:
• The NHS will do more to detect and diagnose respiratory problems earlier and more accurately
• The NHS will improve quality of life, improve treatment and reduce costs associated with respiratory disease
• The NHS will do more to support those with respiratory disease to receive and use the right medication.
• By working across the Suffolk and North East Essex ICS with a broad range of respiratory based stakeholders, we will work across a range of initiatives to ensure progress towards the overarching outcomes.
• Through early detection and diagnosis, we will support staff to recognise early signs of lung cancer, so that patients can attend screening and testing where needed. Through enhanced population health management, we will be able to identify those who are risk of lung cancer and invite them for screening.
• In the midst of Covid-19 there will need to be a review and future commissioning of spirometry to support the management and diagnose of Chronic Obstructive Pulmonary Disorder and Asthma. Primary care is no longer commissioned to deliver this, so a collective review of how this will support patients in 2021/22 will need to be developed and implemented.
• We will continue to improve awareness and access to Pulmonary Rehabilitation and ensure that patients are appropriately directed to this essential support. Through the impact of Covid-19, this will include the development of virtual sessions and supporting patients who do not have access this technology.
• By working with medicines management colleagues across the ICS, we will adhere to

29 | P a g e
national and local prescribing guidelines to ensure correct inhaler technique used. The development of integrated working will help improve equality of access and health outcomes.
• With significant focus on supporting the reduction of tobacco activity and related consequences, we will support:
- Prevention - creating an environment where people choose not to smoke.
- Protection – protecting people from second-hand smoke and supporting tobacco control interventions
- Cessation – supporting and enabling people to stop smoking
• By supporting the wider regional clinical network and supporting lessons learned from Covid-19, the ICS will be involved in the development of the work and support progress on Non-Invasive Ventilation (NIV). This approach is going to be looking at how to improve the outcomes for people who are admitted with Covid-19 and who require NIV support. This will include access criteria, escalation criteria, standardising pathways around where NIV is initiated and where it is delivered, as well as capacity planning, and management of capacity if there is significant increase in numbers of people on NIV.
• We will support the national expectations and guidance in relation to the emerging condition known as ‘Long Covid’. This will require the development of assessment and management pathways across the footprint of the ICS to support patients who suffer from these long-term effects.
3.2.4 Diabetes
The focus areas for diabetes are:
• We will continue to identify and support people at risk of Type 2 diabetes, in particular those in high risk populations such as Black, Asian and Minority Ethnic (BAME) communities and, have support to prevent individuals from developing the condition. Covid19 has highlighted a significant health inequality given that 1 in 3 Covid deaths were from people with diabetes and BAME groups are up to 4 times more likely to develop diabetes than the general population.
• We will be extending the NHS Diabetes Prevention Programme (NDPP) for a further three years, including a digital option. The extended NDPP (known as NDPP2) will have a much higher referral ceiling and offers the ICS an excellent opportunity to reduce the number of people who could go on to develop type 2 diabetes.
• We will improve information, advice and support on weight management for people who are overweight and obese and their carers. We will increase awareness of our weight management programmes that can improve health and reduce health inequalities. Lifestyle services across the ICS offer an integrated healthy lifestyle service and the ICS is at the forefront of this work having completed a Very Low-Calorie Diet (VLCD) pilot for patients prior to the national initiative due in the near future.
• We will continue, in the Alliances to develop community-based services and support to help people change to healthier living. To support more projects such as community food growing, and cookery classes help promote healthy eating. Local free or low-cost activities such as Couch-to-5K and park runs to help people be more active. We are supporting a community-based Diabetes Prevention service known as the “Shotley” project which supports pre-diabetic and overweight patients in remote parts of the county
30 | P a g e
through highly tailored local interventions. This project provides people with long-term peer group support and the concept was developed by the local people themselves. We will encourage more of such schemes. Healthy meals and cooking skills are support by local restaurants to incentivise people to keep good diet self-management.
• Improving equality of access to diabetes specialist nurse support. Some parts of the ICS have already been developing hospital inpatient support with very positive results, which we intend to roll out to the wider system.
• Improving equality of access and service to high quality multi-disciplinary foot care teams and ensuring that we meet the NICE NG19 footcare standard across the ICS. We are also continuing the roll-out of the diabetes foot care cards.
• The ICS has significantly increased the number of Structured Education (SE) places available for face-to-face (F2F) learning for those with both Type 1 and Type 2 diabetes. This has been possible through the award of transformation funding from NHSEI for the last three years. We will continue to offer newly diagnosed as well as established diabetic patients the chance to do SE. With Covid-19 having stopped all F2F classes and having already trialled digital SE solutions we are well placed to continue our providing digital SE for patients and we will be training the SE trainers to deliver their F2F classes remotely.
• We will be developing support from mentors or buddies. Peer support is an important tool in living well with a long-term condition. A programme of work is underway to support diabetes patients with learning disabilities and services such as Live Well, Living Life to the Full and Wellbeing Suffolk are providing psychological and emotional support for diabetic patients.
• We will enable people with Type 1 diabetes to monitor their condition more effectively and obtain the right support when they need it. This includes making available flash glucose monitors for everyone who meets the appropriate criteria with Type 1 diabetes, including continuous glucose monitoring for all pregnant women with Type 1 diabetes, by March 2021.
• We will work with PCNs ensuring that people with diabetes receive their nine annual care processes and help patients toward achieving their three NICE Treatment Targets. This will help to drive down unwarranted variation in services and minimise the risk of future health complications for people. There will also be a programme of work to ensure that health professionals continue to be educated in the latest diabetes knowledge.
3.2.5 Cancer
We will work to achieve the aims and objectives for Cancer detailed in the NHS long-term plan and we will:
• focus on early diagnosis and increasing the percentage of cancers diagnosed at Stage 1 or 2 from the current 50% to the target of 62% 2023/24 and 75% by 2028
• work towards achieving all national cancer targets, including the new 28-day faster diagnosis target.
• support all national screening programmes and work to identify and correct inequality, and ensure new initiatives are made available promptly to our patients. We will work with our stakeholders across the ICS on prevention and awareness programmes.
• where appropriate, working with colleagues in specialised commissioning, to support technological advances in treatment so they are available to those eligible.

31 | P a g e
• committed to supporting advances in genomic testing, so this is available to all newly diagnosed cancers from 2021.
• introduce initiatives in living with and beyond cancer are vital, and we will provide personalised care based on a holistic need assessment (HNA), care plans and Health and Wellbeing support so individual needs can be identified and addressed at the earliest opportunity. A personalised care plan will include individual self-management plans with rapid self –referral back to secondary care when needed.
• promote access to primary cancer care reviews which will include a holistic needs assessment so that cancer and its consequences are increasingly managed as a long-term condition.
• implement the national pathways in lung, prostate, colo-rectal and upper GI cancers.
• work with and support PCNs in implementing the national cancer Direct Enhanced Service.
• continue to implement and develop the Rapid Diagnostic Service in line with the national specification.
3.3 Children and Young People and Maternity 3.3.1 Children and Young People Working with our colleagues at Suffolk and Essex County Council and wider system partners we will continue to focus on our key work streams and priority areas. The main focus areas are:
• Ensuring the SEND Acton Plans that have developed from the Written Statement of Actions are fully implemented. This should also include Service Delivery and Improvement Plans for each provider to progress the further development of Key Performance Indicators and Outcome measures over the next 12 months.
• Development and implementation of the new model of care for Children’s Speech and Language Therapy, OT and Physio for Essex. This should also be supported by an agreed mobilisation plan and recruitment plan from the service.
• Commence the second stage of the Speech and Language Therapy review for Suffolk to expand the offer up to the age of 25.
• Development and implementation of a new model of care for Neurodevelopmental and Behaviour including new pathways of delivery for both Suffolk and North East Essex which will include the introduction of additional support services to support service users and their families.
• Implementation of a new Mental Health model for Suffolk which will include: o Implementation of the THRIVE model while continuing to achieve the national
access standards as a minimum o Implementation of new Mental Health Crisis Service, including outreach
support o Further development of the Eating Disorders Service including a revised end
to end pathway

32 | P a g e
o Continued implementation of the new Mental Health Support teams in schools o Development of an outcomes framework
• Procurement of a new mental health model and services for Essex • Further development of the Perinatal Service across the SNEE ICS including
additional workforce to meet the goal of 10% of those eligible having access to a service.
• Review of community children’s services and development of a revised model of care for Suffolk, including community nursing teams and community paediatric medical services.
• Recommissioning of community children’s services for North East Essex as part of the wider community recommissioning underway.
3.3.2 Maternity Services The National Maternity Transformation programme clearly defines the way maternity services should be transformed and delivered. The Local Maternity System (LMS) has, to date, been supporting provider trusts to fund and deliver the transformation programme. In 2021/22, the LMS will expect greater leadership from the provider Trusts to fully implement and embed the service pathways in their localities, whilst working with LMNS partners to ensure consistent outcomes for women and babies across the ICS footprint. All deliverables must be achieved and in 2021/22, it will necessitate the Trusts/Alliances to implement the following:
• Saving Babies Lives care bundle version 2 compliant and embedded into practice during 2021/22; to ensure the Trust is progressing to the LTP requirement of 50% reduction in stillbirths, neonatal and maternal deaths (since 2010 baseline) by March 2023.
• Delivery of postnatal care improvement plan including the provision of pregnancy bereavement counselling, pelvic health clinics, UNICEF Baby Friendly status, and seamless pathways into primary care and health visiting services.
• Creation and delivery of a plan to tackle health inequalities, with 75% of women from Black and Minority Ethnic communities and women from deprived communities receiving Continuity of Carer by March 2022.
• To embed the new pathway of Continuous Glucose Monitoring for all pregnant women, liaising directly with the appropriate Diabetes Teams to ensure a seamless and collaborative pathway of care
• To actively participate in the planning and provision of multi-agency mental health systems (formerly known as hubs) within each Alliance area. This will support the co-location and joint working between perinatal mental health care, maternity and sexual health services.
• To have robust business continuity plans to ensure that the quality of maternity care and clinical outcomes are not unduly compromised by any further pandemic lockdown arrangements. This can include the delivery of online 1:1 consultation, education packages and virtual support schemes etc. The recommendations from the MBRRACE report “Saving Lives, Improving Mothers’ Care” 2020 must be incorporated into the pathways of care for pregnant women effected by the Covid-19 pandemic.
• Patient portals in place to enable the roll out of a dynamic maternity electronic record and personalised care plan model. The digital tool should be embedded into practice during 2021/22.
• Each Trust to comprehensively complete the Maternity Services Data Set v2 with high quality information which is compliant with national definitions, to ensure reporting of interventions and outcomes are accurately reported to the CCG’s and NHSE/I. To also provide any other additional reporting schedules as required by the CCG’s/LMNS to monitor performance and transformation.

33 | P a g e
• Delivery of Continuity of Carer roll out plan as per LTP trajectories, to ensure coverage of at least 51% women having received the pathway of care by March 2022, and 100% by March 2023.
• Engagement with Operational Delivery Networks to deliver safe and sustainable models of Neonatal care. The Trust is to ensure that all women who are likely to deliver before 27 weeks of gestation give birth in a maternity unit with an on-site Neonatal Intensive Care Unit, and all neonatal deaths are notified using the standardised Perinatal Mortality Review Tool.
• To be compliant with the Quality Surveillance Framework, be actively involved in system learning from serious incidents and developing clinical governance arrangements across the LMNS.
• All services actively working with their local Maternity Voice Partnership group to embed co-production into service transformation and quality improvement activity.
3.4 Mental Health and Learning Disabilities
3.4.1 Adult Mental Health
The NHS England 10 Year Plan (January 2019) sets out clear expectations of what is required to be delivered from local mental health services. The web link below sets out the national requirements and associated funding flowing through to local integrated care systems.
https://www.longtermplan.nhs.uk/wp-content/uploads/2019/07/nhs-mental-health-implementation-plan-2019-20-2023-24.pdf
The key areas of focus are:
• continued work with system partners to shift the focus of care and resource into community settings with the implementation and embedding of new pathways of care aligned with local placed based needs and heavily integrated with the VCSE.
• roll out of new models of integrated multi-disciplinary primary and community care for adults and older adults with severe mental illnesses, incorporating annual physical health checks, care for people with personality disorder, eating disorders, mental health rehabilitation needs, and complex mental health difficulties. Ongoing focus on dementia including diagnosis rate, annual review and pre and post diagnosis support.
• evolve further our system wide response to crisis services supporting mental health including mainstreaming crisis telephone lines (111+2), alternatives to crisis admission including crisis cafes, Serenity Intensive Support and joint ventures with Police, Ambulance and VCSE partners.
• increased provision of perinatal mental health services expanding access, duration of care and scope of interventions with seamless pathways aligned to maternity services.
• commencement of a new IAPT service provision incorporating a strong digital and long-term condition programme whilst integrating access to IAPT services into our core community service model.
• investment into early intervention services such as Psychosis and Eating Disorders amongst others, promoting the preventative agenda aligned with raising awareness across primary care and other sectors of the signs and signals of mental health.
• expansion of services to effectively support those recovering and wanting to re-

34 | P a g e
engage in the community or return to work. This is in the form of progressing Individual Placement and Support Services, integrating across services lines and utilising the voluntary sector via community hubs or equivalent to enable those to live well in the community.
• work to deliver and maintain the aspiration of zero out of area bed placements and reduced lengths of stay, utilising robust community services to manage those appropriate.
3.4.2 Learning Disability (LD) and Autism
Work with our system partners to continue to improve care for people with learning disabilities, autism or both and behaviour that challenges (learning disabilities) and to raise awareness and support reasonable adjustments.
The key areas of focus are:
• Maintaining performance on inpatient trajectory for CCG, CYP and Specialised Commissioning.
• Further development of LD admission avoidance/early discharge services including pathways and 12-point discharge planning.
• Delivery of Care Education and Treatment Reviews.
• Learning Disability Mortality Review (LeDeR) steering groups/ working parties will continue to take LeDeR learning into action. Complete LeDeR trajectory and deliver plans to meet targets.
• Support GP’s to meet annual health check target of 67%.
3.5 Primary Care
We will continue to implement our Primary Care Strategies and GP Forward View plans including:
• Continued development of new models of care – enabling primary care collaboration and joined up care in our localities – through Integrated Neighbourhood Teams and enable PCNs and INTs to work effectively in unison. This will critically include progressing partnerships with wider primary care partners of opticians, pharmacies and dentists as well as community services, local government and voluntary sector partners in order to improve access to care, experience of care and outcomes
• Specific support for the development of PCNs and their clinical leadership with delivery of the national service specifications of; Structured Medications Review, Enhanced Health in Care Homes, Anticipatory Care, Personalised Care, Supporting Early Cancer Diagnosis, CVD Prevention and Diagnosis and Tackling Neighbourhood Inequalities.
• Reviewing and expanding patient and public involvement in local service development
• Delivery of high-quality Dementia diagnosis services, Learning Disability and SMI Health checks – supporting local practices to enable these patient cohorts to access these services to meet their needs.

35 | P a g e
• Workload - support for the delivery actions to reduce workload and manage patient care.
• Workforce – delivery of GP recruitment and retention programmes as well as support for the integration of new clinical roles in practice especially the new roles that are being rolled out via the PCNs (social prescribers, clinical pharmacists, pharmacy technicians, health & wellbeing coaches, care coordinators, physicians associates, dieticians, podiatrists, occupational therapists, nursing associates , training nurse associates, physiotherapists, mental health nurses and paramedics)
• Mental health – work with local providers of mental health services to implement the prevention, primary community element of the mental health strategy, within our Integrated Neighbourhood Team areas.
• Access – enhancing access to GP-services including in evenings and at weekends and ensuring an efficient and effective transfers of care. We will ensure the smooth transfer of commissioning responsibility for GP+ to local PCNs in line with national requirements
• Infrastructure – creating new physical environments for future care needs utilising the ETTF process and to facilitate the implementation of the NHS Long Term Plan ambitions. This has become even more important due to the increase in staff through the PCN scheme but will also recognise the changing need for space which has been created through remote working and consultation.
• Population health – to support the roll out of a Population Health approach, working closely with local PCNs building on the pilot programme delivered in 2020/21.
• Digital connectivity and digital first – we will work with local partners to continue the transformation journey of access and service delivery, which was accelerated during 2020/21
• Leadership – continuing to invest in clinical and management leadership within primary care and with secondary, community and social care partners in One Clinical Community. We will increasingly look to increase this approach to support the development of PCNs to ensure productive and effective working relationships.
• We will continue to provide leadership, an effective contractual framework and support for safe, high quality and cost-effective prescribing. We will do this by working with local practices, wider clinical partners within our Alliances and across the East of England through the prescribing Priorities Advisory Committee and PRESCQIPP. We will retain particular focus on anti-biotic and Controlled Drug prescribing and management.
• We will also continue our support for practices prior to and subsequent to CQC inspections to ensure shared learning.
• We will continue to review the Primary Medical Services Development Framework and GMS LES to ensure that services respond to national and local priorities.
• We will strive to reduce in-equalities and in particular in-equalities to service access, particularly ensuring that ethnicity is recorded.

36 | P a g e
3.6 Ambulance 999 Commissioning
We will continue to lead on the co-ordination of commissioning the 999 contract across the six STPs and six county footprint of the East of England Ambulance Service (EEAST). We will continue to explore ways of closer integration with urgent and emergency care patient pathways to improve patient outcomes and quality of care.
We are mindful that the 2017/18 Independent Service Review provides a broad contractual framework for the coming year and we will work proactively with our CCG partners and EEAST to ensure that we continue to have a fair and balanced approach that puts our patients first. We intend to ensure that EEAST work on the Carter Report initiatives to become more productive, whilst our commissioning of patient pathways will continue to seek treatment as close to home as possible for patients where appropriate. We will follow national guidance on the emerging sector payment mechanisms for 2021/22, and this may develop the ISR financial framework into new areas as this guidance emerges in the latter half of 2020/21.
Our priorities for 2021/22 are:
• Improving pathways for patients (such as non-injury fallers) and thereby reducing onward conveyance of these patients to Emergency Departments;
• Ensuring ‘Ageing Well’ and frailty programmes improve patient care to the elderly;
• Continuing to explore ways of delivering stroke patient testing and diagnostics on scene;
• Closer integration of our Clinical Assessment Services (111/Out of hours) with 999 pathways to provide improved responses to lower acuity patients. This will be informed by the Herts Urgent Care pilot and subsequent roll outs/testing elsewhere, such as the current C3/C4 validation pilots being tested in Yorkshire and the Midlands;
• Developing the Long-Term Plans for mental health services integration into urgent and emergency care pathways for patients with an underlying mental health condition.
We intend to support EEAST to meet Ambulance Response Standards in 2021/22. In particular we will look at ways of supporting their leadership and workforce strategies to ensure existing front line staff can operate in the best environment possible and to ensure that we can support EEAST’s retention strategies with a focus on developing career pathways for clinical staff within closer, more integrated services for urgent and emergency patient pathways. This will include supporting a rotational skill offer into Primary Care Networks. We also intend to support EEAST in providing key messages to recruit more staff into the ambulance sector, and we welcome the more diversified approach to recruitment that EEAST are taking. 3.7 Pathology The CCGs intend to develop a specification for GP direct access pathology services that are integrated with local hospital-based testing. The specification will outline some must-do features such as: gaining accreditation for the service (if not already in place); networking with others to achieve scale and securing value for money. The CCGs will work with interested parties to develop plans for how the specification would be best delivered. 3.8 Personal Health Budgets

37 | P a g e
The CCGs will be taking all opportunities to review the offer of Personal Health Budgets (PHBs) as part of our transformational approach to redesigning pathways where appropriate. From April 2018 all continuing healthcare adults with a home care package are required to have PHBs as part of package of care. In addition, providers will work with service users in those groups with a legal right to have a PHB to achieve this. The CCGs shall work with all providers to develop PHBs. Providers will be required to design, develop, and implement PHBs in those areas agreed. A. strategic group has already been formed and progress made. The CCGs will consider procurement options for financial management and control. A personal health budget is an amount of money to support a person’s identified health and wellbeing needs, the application of which is planned and agreed between the individual, their representative, or, in the case of children, their families or carers18 and the local NHS team. This is not new money but is money that would normally have been spent by the NHS being spent more flexibly to meet an individual identified care and support needs. The use of personal health budgets is just one way in which the NHS can tailor services and support for people to enable them to have choice, control and flexibility over their care.3 All providers should include support of the personalisation agenda with personal health budgets in their planning and service provision. This could include involving people, their representatives, families and carers in discussions about which elements of care should be included in their personal health budget. Where a PHB is appropriate, providers will support robust care and support planning, and ensure that the 6 key principles of PHBs are met. Providers must publicise and promote the availability of personal health budgets and provide information, and support to those eligible, their representatives, families and carers, to help them decide if a personal health budget is right for them Providers will be required to regularly monitor and review PHBs.
Providers will be required to meet CCG reporting requirements to evidence progress.
3.9 Medicines Management and Prescribing In 2021-22, Suffolk and North East Essex Clinical Commissioning Groups will continue to work with primary care and secondary care organisations to optimise medicines management, improving quality, safety and cost-efficiency of medicines and prescribing. The CCGs will revise their medicines optimisation programmes for primary care. The metrics for these are not available at the time of writing this report but are likely to be aligned to national drivers such as reduction in prescribing of antibiotics, over the counter medication for minor conditions, and items of low clinical value. The CCGs will also retain a strong focus on medicines safety and preventing health inequalities, e.g. highlighting formulations/brands that are suitable for vegans or other communities. Targets will be aligned across the ICS where possible and metrics for 2021-22 are likely to be agreed in quarter 4 of 2020-21. Providers are expected to support the medicines management programmes of work for 2021-22 which will include, but not be limited to the following areas/ schemes:
3 https://www.england.nhs.uk/personal-health-budgets/what-are-personal-health-budgets-phbs/frequently-asked-questions-about-phbs/

38 | P a g e
• Implementation of a joint formulary across the ICS and continued collaborative work
on prescribing guidelines, shared care agreements and other medicines management initiatives.
• Diabetes - Cost effective prescribing of hypoglycaemic agents, blood glucose testing strips, needles and lancets. This includes increasing the uptake of biosimilar insulins and review of new technologies.
• Appliances – Formulary adherence. • Respiratory – Use of ‘greener’ low carbon inhalers and implementation of prescribing
guidelines that promote cost-effective inhaler choices. • Mental Health – Appropriate prescribing of antidepressants, hypnotics and
anxiolytics, and reducing inappropriate prescribing of any Dependence Forming Medicines (DFMs).
• Analgesics and Controlled Drugs (CDs) – Appropriate prescribing and reducing inappropriate prescribing of DFMs such as opioids and gabapentinoids. Safer management of CDs in line with national recommendations, and management of complex patients.
• Dietetics - Formulary adherence and reduction in inappropriate prescribing of dietetic products.
• Simple switches – Practice work supported by Medicines Management Technicians and decision support tools such as Optimise Rx or ScriptSwitch. The aim is to ensure use of cost-effective treatment choices.
• Red (hospital only) drugs: Repatriation to secondary care. • Specials – Avoiding use and switching to cost effective treatment choices in line with
evidence-based guidance documents, e.g. NEWT guidelines. • Low Value Medicines – Reducing use in line with guidance from NHSE/I and NHSCC
(items which should not be routinely prescribed in primary care). • Over the Counter (OTC) Medicines – Reducing use in line with guidance from
NHSE/I and NHSCC (conditions for which OTC medicines should not be routinely prescribed).
• Care homes - Linking with PCN Clinical Pharmacists and Pharmacy Technicians as appropriate to support the uptake of Structured Medication Reviews as outlined in the Network Contract DES.
• Rebates – Working with the pharmaceutical industry as appropriate. • Antimicrobials – Bringing prescribing below or in line with the national targets. • Electronic Repeat Dispensing (eRD) – Increasing uptake of eRD. • Oxygen – Monitoring of the oxygen service and reprocurement of the regional EoE
oxygen contract. • Joint working across the county footprint to support STOMP (Stopping over
medication of people with a learning disability, autism or both) and STAMP (Supporting Treatment and Appropriate Medication in Paediatrics)
• High Cost Drugs – Increasing uptake of biosimilars across all acute providers as per national guidance. Pathway development in line with NICE guidance and local policy.
• Healthy Living Pharmacies (HLPs) - Working with the Local Pharmaceutical Committee to support implementation of HLPs, phase 2. The aim of this programme is to support the delivery of a broad range of high-quality services through community pharmacies to meet local Alliance need, improving the health and wellbeing of the locality population and helping to reduce health inequalities.
• Community Pharmacy Consultation Service - Working with community pharmacy and primary care colleagues to support the implementation of this service, integrating with PCN-identified population health needs where applicable.
• Electronic Medicines Optimisation Pathway (eMOP) also known as Transfers of Care Around Medicines (TCAM) - Working across the primary and secondary care interface to support the development and delivery of this discharge medicines service.

39 | P a g e
• End of Life Medicines - Commissioning a service through–community pharmacies to facilitate the supply of medicines for End of Life patients.
• PrescQIPP – Wide range of tools and resources to support safe, appropriate and cost-effective prescribing. Utilisation of training resources as required.
The CCG Medicines Management Teams will continue to review and monitor prescribing behaviours and spend per practice and PCN and will continue to report these through relevant committees. A joint training post will be offered in 2021/22 for a Pre-Registration Pharmacist, the post will be offered between ESNEFT and a NEE GP practice. As part of this year-long placement the Pre-Registration Pharmacist will spend two weeks with NEE Medicines Management learning how the team works, key priorities and the wider role of pharmacy in primary. 3.10 Specialised Commissioning We will work with NHSE and system partners to help develop a framework for strategic commissioning for the ‘Integration of specialised services with local health and care systems.’ Specialised services require nationally set care standards which all providers should achieve. These provide clarity on the outcomes and appropriate access criteria as well as a minimum level of service quality. The progression of these changes will be through direct engagement between commissioning and clinical teams. Specialised Commissioners will work through regional and system groups to review NHSE Directly Commissioned services to ascertain which could be more aligned to systems, jointly commissioned or have progressively devolved responsibilities. Financial and contracting architecture needs to be developed to enable strategic opportunities to undertake whole pathway redesign and shift towards funding based on population need. There is national recognition that specialised services could be planned across ICS footprints. There are seven areas under consideration for a new delivery model: 1. Specialised Commissioning of complex conditions 2. Health and Justice 3. Public Health 7a 4. GP Medical Services 5. Dental 6. Pharmacy and 7. Optometry. Colleagues across the Region are exploring the opportunities for integrated commissioning and governance with each ICS taking a lead on one of the 7 areas. It is expected by the end of March 2021 clearer recommendations will be developed for each area. 4. Enablers 4.1 Digital and IT Services All providers are expected to play an active part in the work of the East Accord and the ICS Digital Strategy and Innovation Group and their associated local and regional working groups, to progress a real time (or near real-time) digital ecosystem across and beyond the ICS which has the patient at the centre, and so that: 1. People (citizens, patients and carers) and practitioners have easy access to relevant
information 2. People and practitioners are provided useful information 3. Information provides people, our practitioners and the wider public sector value
All providers must meet a minimum level of digital maturity, and share plans for their progress to a more digitally mature position Providers are expected to have:
• Board level leadership for the Digital agenda

40 | P a g e
• A Digital Strategy in line with the ICS Strategy, NHS Long Term Plan and People Plan
• investment plans IRO 4% of turnover on Digital and IT Services. • a plan to further develop their own and support the wider IT services and Digital
workforce • An annual organisational Digital Delivery Plan that is in step with the ICS Digital
Strategy, and partners plans and capabilities • Access and contribution to a Shared Care Record that meets PRSB Core Information
Standards, and available in context no later than September 2021 • A Data Quality Improvement Plan, that considers the accessibility, insight, value and
potential reuse of Data both within and beyond the provider • An accessible digital route to services, including Patient Initiated Follow Up, Advice
and Guidance, Remote Triage and Remote Care All providers will adopt national, regional and ICS agreed standards and best practice, alongside a collective investment approach that enables innovation and transformation. This includes adopting a common information governance framework and the My Care Record Information Sharing Approach, shared capability operating models, anchor tenancy model, remote care and enabling shared care records. Our approach and ecosystem will continue to evolve, alongside standards, core architecture principles, capability convergence and cyber security controls. Minimum standards and expectations include but are not limited to:
• Accessible Information Standard • Access to the Health and Social Care Network, and DSPT Compliance including
meeting Cyber standards • Compliance with Data Guidance issued by NHS England and NHS Digital and with
Data Protection Legislation in relation to protection of patient identifiable data • Compliance with Clinical Safety Standard ISN0160 • Verified NHS Number and Clinical Referral Standard • Access to key clinical information from GP and other provider health and care
records through the ICS Health Information Exchange and supplemented by SCRai • Clinical data meeting the PRSB Core Information Standard, and accessible as
structured information through open interfaces in accordance with Open API Policy and Guidance
• Transfers of Care, Care Connect Standard and Discharge Summary • Personal Health Records • Personalised Care Plans for EoL, Care Home Residents and MH where patient has
Secondary Care MH diagnosis • SCCI 1580 (Palliative Care Coordination: Core Content)
Utilisation data and benefits realised of priority capabilities is provided to (or accessible by) the commissioner either in near real-time, monthly or no less than quarterly. This would include:
• Access to shared care records (HIE, SCRai, CRV / EPR Core) • Utilisation of Video Consultation • Utilisation of Remote Care capabilities • Adoption of RPA and Benefits delivered
All Providers, where updating, developing or procuring any relevant IT system, software, digital capability or service will:
• Ensure the capability is easy, and useful – designed for the user. • Adapt & adopt existing capabilities where appropriate, or build / buy in line with
agreed digital ICS strategy and East Accord Partnership

41 | P a g e
• Adopt HL7/FHIR to support messaging, openEHR to support semantic coherence of structured data, IHE to support management of unstructured records and VNA for data persistence and CDRs
• Have regard to the NHS Internet First Policy and the Code of Conduct for Data Driven Health and Care Technology
Where progress is required on any of the above, the provider will provide a quarterly progress plan. 4.2 Estates Working with system partners are priorities we will continue to focus on the development of fit for purpose estate acting as an enabler to deliver transformed services for the local population. The main focus areas will be:
• Supporting Primary Care to develop their strategic Primary Care Network Estates Strategies to enable the local challenges, constraints and opportunities to be explored and taken in to account to ensure the delivery of national and ICS priorities.
• Ensure the learning and benefits realised through the Covid-19 pandemic are captured and continue to be integrated to estates development moving forward.
• To work with system partners including NHS Property Services and Community Health Partnership to optimise the use of our estate, reducing unnecessary voids and disposing of surplus land and buildings.
• To continue to develop and implement system wide responses and strategies to mitigate population growth and the impacts this has on the estate and service delivery
• Work to incorporate current and future digital solutions and systems into estates developments to maximise the benefits these offer and ensure patients have the greatest flexibility around how, where and when they interact with health care services.
• Develop and implement an updated Green Plan for the CCG’s to ensure sustainability is put at the centre of all that we do.
4.3 Workforce Planning In September 2020, we developed the SNEE ICS 'Can Do' People Plan –2020-21 which describes the key areas of work to retain and value our people, grow our workforce, attract new people and businesses to work in our system, and build on our ‘'Can Do' Approach’ for Health and care going forward. The following sections detail: the high-level requirements for the 'Can Do' People Plan linking these to the key priorities of the system and Alliances; overview of SNEE ICS as a system in terms of our workforce (paid and unpaid);
• looking after our people; • belonging to SNEE; • new ways of working; and • growing for the future.
The 'Can Do' approach for looking after our people will focus on retaining our valuable staff and people working across the three alliances within SNEE ICS. Ensuring they continue to feel valued, identify and belong to our system, and continue to want to work within SNEE.

42 | P a g e
In collaboration with partners, we will support the development of a system level workforce strategy for equality, diversity and inclusion to address the systemic inequality that is experienced by some staff including staff from black and ethnic minorities. The SNEE ICS ambition, through our existing collaborative approach, is to work with our system partners across health, care and voluntary sectors including primary care and higher education, to co-produce and pilot a system level ‘Can Do’ Enhanced Occupational Health (OH) and Wellbeing hub. The aims of the pilot hub will be to test, adapt, and evaluate various strategies and programmes to deliver a sustainable model across the system over the next five years. Alongside the pilot we will introduce a continuing health and wellbeing offer working with local partners including the voluntary sector. The 'Can Do' approach for belonging to SNEE recognises the existing strong collaborative partnerships and relationships within and across alliances and providers. It acknowledges that further work is required to embed and expand these conversations and engagements at scale so staff and people working within and across SNEE are able to identify and understand the benefits to them, and the people they serve and support. Adopting an inclusive approach, 'Can Do' behaviours and celebrating diversity across the providers, alliances and system. The 'Can Do' approach for new ways of working across health and care will include creating new roles, pathways, working with volunteering partners and patient groups, and incorporate digital solutions in how care is delivered. Focusing on ‘seldom heard’ groups for both services being delivered and for attracting new people to work in health and care sectors. Moving away from task oriented to outcome-based care, actively disrupting the status quo and introducing new practices, roles and positive behaviours to deliver person centred care. The 'Can Do' approach for growing for the future. We will invest in our health ambassador and career service and focus on attracting people who have left health and care sectors and are willing and wanting to return with flexible practices and support. Attracting new people, actively encouraging them to apply for existing roles in health and care sector, growing our workforce by exploring the current and future gaps through system-wide workforce planning and actively working with education to encourage younger people to consider working in health and care sectors through the health and care academies. By collaborative working and joint decision-making, we will make the best use of property, people and digital services to meet local health and care needs. Our focus will ensure these areas are fit for purpose, functionally suitable and commercially viable. The CCGs, working with Alliance partners have robust governance arrangements in place for ensuring that decisions about Digital, Estates and Workforce reflect local healthcare priorities and the current and future needs of the local communities. The formation of the relevant ICS Strategy and Delivery Groups has enabled a greater focus on partnership working and enabled all health and social care providers who are members of the group to explore these areas in more depth and work together in line with our transformation plans. We hope this letter helps clarify our current direction of travel and reinforces our commitment to joint working across Suffolk and North East Essex and the wider ICS. Yours sincerely

43 | P a g e
Ed Garratt Chief Executive Ipswich & East Suffolk CCG West Suffolk CCG North East Essex CCG Version Control: Version 1.5 17 November 2020

Page 1 of 4
GOVERNING BODY Agenda Item No. 11
Reference No. WSCCG 20-45
Date. 25 November 2020 Title
Procurement Update: Summary of Activity 2020/21
Lead Director
Paul Gibara, Director of Performance Improvement
Author(s)
Jane Garnett, Procurement Lead
Purpose
To update the Governing Body on the procurements completed since the last procurement update and those currently in progress and planned for 2020/21.
Applicable CCG Priorities 1. Develop clinical leadership 2. Demonstrate excellence in patient experience & patient engagement 3. Improve the health & care of older people 4. Improve access to mental health services 5. Improve health & wellbeing through partnership working 6. Deliver financial sustainability through quality improvement Action required by Governing Body: To note the work undertaken and the evolving procurement work programme for 2020/21.

1. Update 1.1 The table below summarises the current health service procurement activity.
Procurement Name ITT Bidders Awarded to Contract Start
Stroke Early Supported Discharge 1 NHS West Suffolk Foundation Trust
01/04/2021
Vasectomy and Minor Surgery Services tbc tbc tbc
Pathology Services Procurement approach to be decided
Mental Health assurance Portfolio of assurance and procurement
Children’s Neuro Details of approach below Please note table does not include procurements being undertaken exclusively for Ipswich and East Suffolk CCG
Current Procurements 1.2 Stroke Early Supported Discharge
The Stroke Early Supported Discharge tender was re-released on the 3rd July 2020, with a submission return date of the 14th August. This tender has now reached the award stage and assuming there are no issues during the standstill period the mobilisation stage should be underway with West Suffolk NHS Foundation Trust working with East Suffolk and North Essex NHS Foundation Trust and Icanho taking on the provision from Norfolk Community Health and Care.
1.3 Minor Surgery and Vasectomies
The Minor Surgery and Vasectomies procurement was initiated in IESCCG but was paused due to Covid 19. The procurement was not restarted as the progression of time had meant the West Suffolk contracts for these services were nearing their end dates so a review of the options for Minor Surgery and Vasectomy services was undertaken. An options paper is being presented to the West Suffolk Clinical Executive to seek a decision on whether the West Contracts should be included in the procurement process moving forward. For IESCCG it is envisaged that a tender will be released as follows: - Lot 1 - Vasectomy Services delivered as an Any Qualified Provider market - Lot 2 - Minor Surgery held by a single provider If approved as recommended by WSCCG Clinical Executive, it is likely the following approach will be adopted: - Lot 1 - Vasectomy Services delivered as an Any Qualified Provider market across East
and West Suffolk - Lot 2 - East Minor Surgery held by a single provider - Lot 3 - West Minor Surgery held by a single provider
1.4 Pathology Services
The CCG currently commissions Pathology Services with NHS West Suffolk CCG and NHS North East Essex CCG through a contract with North Essex & East Suffolk Pathology Services (NEESPS). This contract has been extended to enable a procurement to be completed and an options paper is progressing through internal governance routes of both CCGs to agree the approach.

1.5 Mental Health Assurance The transformation work continues within mental health services and the first assurance process has been started for the Crisis services, with the first feedback / dialogue session scheduled for the 30th November. The assurance process for crisis is the first in a series of procurement / assurance processes covering the range of mental health services. The assurance for crisis services is due to complete with a report to the Governing Body outlining the evaluation panels assessment in January 2021. The crisis assurance process will consist of a written submission and dialogue with Norfolk and Suffolk Mental Health Trust.
1.6 Support for children, young people with neurodevelopmental conditions and their
families In order to generate innovation around these services it is being proposed that the CCGs approach the market for detailed expressions of interest from any provider interested in supporting these pathways. The expressions of interest will then help to ‘map out’ the offers received to understand how they could work together to deliver a network of services and allow the CCG to refine their requirements and address any gaps in the offers. It is envisaged that the expression of interest stage will progress into an award process to determine how the available funds are allocated. The specification being released is high level and should allow any number of service offers to be returned, from any interested sectors and providers.
Future Procurements
1.7 A number of other services are currently under review and the outcome of these reviews may
fall into the procurement pipeline depending on the need identified, such as Ultrasound services, Mental Health Crisis support and Secure patient transport.
2. Other updates 2.1 Procurement Review
Work continues to progress on the establishment of a Procurement Board; Terms of Reference have been drafted and moving through governance processes across the three CCGs.
2.2 Governance Documentation and Routes Due to the imminent changes to the meetings structure within the three CCGs the current governance flow charts will be reviewed and updated.
2.3 The Commissioning Procurement Policy has been updated and is being presented to the Audit
Committee. A full rewrite will be undertaken once the outcome and impact of Brexit is understood in respect of the regulations governing procurement within the public sector. The Procurement Leads in the Suffolk CCGs and the North East Essex CCG will also start to work together to align processes and policies, working through the Procurement Board and the Audit Committee as appropriate.

3. Key Points 3.1 The following list shows services which are likely to be in the procurement portfolio over the
coming year; the shaded areas denote when it is anticipated that these will be actively tendered and mobilised. Please note some projects do not have a set start date.
Please note this list does not include any Ipswich & East Suffolk CCG only procurements
4. Patient and Public Involvement 4.1 The Procurement Lead will be looking to secure engagement with patient representatives for
the Vasectomy and Minor Surgery procurement and any other procurements as they commence.
4.2 The Mental Health Crisis assurance process has representation from Suffolk User Forum,
Suffolk Family Carers and the Suffolk Parent Carer Network, and will look to use patient and representative panels at the evaluation stage of any procurement process.
4.3 Once the way forward for the pathology procurement is understood the Lead for Procurement
will plan for patient and public involvement within the process. 5. Recommendation 5.1 The Governing Body is asked to note the work undertaken and the evolving procurement work
programme for 2020/21.

Page 1 of 3
GOVERNING BODY Agenda Item No. 12
Reference No. WSCCG 20-46
Date. 25 November 2020 Title
2020 Emergency Planning Resilience and Response (EPRR) Core Standards Audit
Lead Director
Paul Gibara, Director of Performance Improvement
Author(s)
Chris Chapman – EPRR Manager
Purpose
To inform the Governing Body regarding the outcome of the 2020 EPRR Audit
Applicable CCG Priorities 1. Develop clinical leadership 2. Demonstrate excellence in patient experience & patient engagement 3. Improve the health and care of older people 4. Improve access to mental health services 5. Improve health and wellbeing through partnership working 6. Deliver financial sustainability through quality improvement Action required by Governing Body: To note the EPRR Core Standards return for West Suffolk CCG

1. Purpose
1.1 The purpose of this paper is to note the CCGs rating with relation to Emergency Preparedness, Resilience and Response as part of the annual EPRR assurance process.
2. Background
2.1 On 4th September NHS England and Improvement wrote to Accountable Emergency Officers outlining the expectations for the 2020/21 Emergency Preparedness, Resilience and Response [EPRR] assurance process. This is the means by which NHS England obtains assurance that NHS funded organizations are sufficiently able to respond to emergencies.
2.2 This year due to the ongoing COVID19 Pandemic a lighter touch approach was directed where CCGs would review the 20/19 Core Standards submissions and the associated action plans. We were also asked to review both our providers learning from COVID and preparation for this winter and the End of EU Transition.
3. Assurance Audit Rating
3.1 For 2020/21 the CCG has assessed itself as ‘Substantial compliant’ [green] in all the core standard areas. Following the realignment of the CCGs there is still ongoing work to bring all plans and procedures together, upon completion of this process the CCGs will be fully compliant. a) As part of this process the following plans have been re-written.
• Emergency Response Plan • Communicable Disease Plan
b) The following Plans are currently being rewritten: • Business Continuity Plans and Business Impact Assessments are being reviewed
with an updated plan completed in December.
3.2 The assurance audit is peer reviewed and moderated by the EPRR team from NHSE held on the 4th November 2020.
3.3 Overall in our providers returns were positive. The table below summerises the responses from each provider across the ICS.
3.4 This year the Practice Plus Group (previously CareUK) is being reviewed nationally by the NHS England as they are a national provider. The National EPRR team rated the Practice Plus Group as Substantially Compliant which reflects the amount of work in the last 12 months that has been undertaken to improve their rating and ensure their resilience across SuNEE.
Trust Name Compliance level 19-20
Compliance Level 19-20
Work Program in place
Ipswich & East Suffolk CCG Substantial Substantial Yes West Suffolk CCG Substantial Substantial Yes North East Essex CCG Full Substantial Yes West Suffolk FT Substantial Substantial Yes ESNEFT (Ipswich, Colchester and Suffolk Community Care)
Substantial Substantial Yes
Norfolk & Suffolk FT Partial Substantial Yes Practice Plus Group (111) Not Compliant Substantial Yes East of England Ambulance Service Substantial Substantial Yes

Trust Name Compliance level 19-20
Compliance Level 19-20
Work Program in place
E-ZEC (Private Ambulance) Substantial Substantial Yes Anglian Community Partnership (ACE) Partially Compliant Fully Compliant Yes
3.5 As part of the wider system review in relation to winter planning and the end of EU Transition all of our system partners had engaging in planning for both events both at an organizational and system level.
4. Public Engagement
4.1 The outcome of the Core Standards Audit must be published within the CCG Annual Report.
5. Accountable Officers
5.1 Paul Gibara - Director of Performance Improvement and Accountable Emergency Officer
6. Recommendation
6.1 The Governing Body is asked to note the result of the EPRR Core Standards Audit and attached action plan.

Page 1 of 1
GOVERNING BODY Agenda Item No. 13
Reference No. WSCCG 20-47
Date. 25 November 2020 Title
Special Educational Needs and Disabilities (SEND) Annual Progress Report 2019/20
Lead Director
Lisa Nobes, Director of Nursing
Author(s)
Lisa Nobes, Director of Nursing
Purpose
To present the Special Educational Needs and Disabilities (SEND) Annual Progress Report 2019/20.
Applicable CCG Priorities 1. Develop clinical leadership 2. Demonstrate excellence in patient experience & patient engagement x 3. Improve the health and care of older people 4. Improve access to mental health services 5. Improve health and wellbeing through partnership working x 6. Deliver financial sustainability through quality improvement Action required by Governing Body: To note the report.

Special Educational Needs and Disabilities (SEND) Annual Progress Report 2019/20
1. The SEND Transformation Programmes aim is to work together with families and communities to support children and young people with SEND to meet their potential, and live healthy, fulfilling lives in their community.
Our success will be measured by ensuring:
• Our children and young people with SEND make good progress and are successful (through health, education and social care support)
• Our children and young people will have timely access to good quality services (health, education and social care)
• Feedback from our children, young people and families will show they feel supported (health, education and social care)
• Our children, young people and families with trust our SEND system (health, education and social care)
2. Our current SEND Strategy 2017-2020
Suffolk Partners continue to focus on delivering the SEND Strategy 2017-2020 which was co-produced by the partnership following the initial Local Area SEND inspection. The partnership is beginning to plan for the next phase of our Suffolk Strategy for 2021 to 2024, unfortunately this work was put on hold due to Covid 19.


3. Governance and Accountability Arrangements. Please see below a summary of the
governance and accountability the SEND Programme.
Each priority workstream within the programme has an accountable lead and a responsibility to have regular documented project meetings – each month, reports are then provided to the SEND Programme Board and SEND Oversight Board (terms of reference for both attached). All programme information is documented on project sites and has full project governance in place.
A SEND Oversight Board holds the SEND Programme to account. Additional reporting via the CCGs and the Council’s Corporate Leadership Team take place regularly to provide additional assurance on progress and highlight risks. We developed a Self Assessment Event programme. Our most recent ran on the 1st November 2019 the next event is planned for later in 2020. These events give all who access or work in the SEND system an opportunity to provide feedback and learning about the SEND transformation plans and progress we have made in the year. We then take this feedback into our SEND strategy planning process, this is to ensure we are listening to what is important to families and professionals across the system and giving focus on continuing to build on what works well and acting on where improvement is needed.
SEND Oversight Board
CYP Board (of the Alliance)

4. Funding and Commissioning Intentions
Programme wide: The SEND Programme Board has allocated the remaining balance of funding it held from the SEND Reform Grant to support a range of development activities within the revisit action plan. These include:
• Investment in additional capacity to support improved practice in planning for adulthood; improvement and workforce development.
• Developing our young people and children’s ambassador networks to provide an active voice for children of all ages within service development.
• Supporting additional capacity within our Parent Carer Network to increase their reach and capacity to work with us
• Investment in improved search tools for the Local Offer website Council Led Offer: The Council has made the following additional investment:
• Providing dedicated programme manager capacity to strengthen governance and oversight of the programme.
• Increasing our staff capacity to support communications through social media and electronic newsletters
• Commitment of a staff infrastructure team to support the development of new specialist placements for children and young people
• Commitment to the capital investment of up to £45m to create over 800 new special education places within our local offer.
• In 2020/21 this will result in an additional spend within the DSG high needs block of £3.23m in 2020/21 academic year and £10.9m in 2021/22 academic year.
Health Led Offer: • In advance of full re commissioning interim business cases to provide additional
resources to improve mental health services have been agreed. For example; £340K for Emotional Wellbeing Hub
• £2million for all age Crisis, £250K for ADHD. This will further inform commissioning intentions moving forward.
• Following service line reviews, improvement has been noted with improved access times for ADHD. Initial assessments now occur within 8 weeks of referral.The service line reviews identified areas of development and oversight of this improvement has been in place.
• Waveney have undertaken a full review of funding, capacity and demand and planning in place to identify current unmet need.
• The Ipswich & East Suffolk and West Suffolk CCGs have identified their long term commissioning plans for SEND in their commissioning intentions document – here
5. Risk Register and Mitigation Plan. We have an active and updated risk register that is reviewed at each programme board and updated as part of the overall programme governance.

Areas of the priority workstream or action plan that are red or amber will be discussed at project meetings and escalated where necessary to the SEND Programme Board for action.
If there is a new significant risk it will be added to our risk register. The risk register we have in place has mitigation plans and is updated regularly to ensure that mitigation is in appropriate and effective. The risk register is reviewed at the SEND programme board every 8 weeks. More serious risks that cannot be adequately managed via the Programme Board are escalated to SCC Corporate Leadership Team and Health Leadership Teams as appropriate.
6. Evidence of engagement with key partners. We include partners in project meetings,
steering groups, self-assessment events and board meetings as well as specific co-production activities related to specific developments in services and strategy. Targeted e-newsletters provide partners with regular updates on the programme and a new SENCO network has been established for 2019/20 to enhance their links to the programme. The Programme Board holds an annual system wide self- assessment event. The most recent being 1st November 2019. These events give all stakeholders, including parents/carers, children and young people and front-line professionals from across the Suffolk SEND System an opportunity to provide structured evaluative feedback on all aspects of SEND Services and Provision in Suffolk. This helps us to gain a clear understanding from a diverse range of people, identifying good practice and where we need to make improvements. The output from our recent event in November will be used to inform the co-production of the next phase of the SEND Strategy for 2020-2023. Suffolk Parent Carer Network have representatives on SEND decision making meetings across the local authority and health. They also sit on the SEND programme and Oversight board. They have a critical role in co-production and provide valuable feedback via their parent/carer surveys. We work together to publish joint communication messages around key changes and share communication messages across our social media platforms to ensure as much coverage and reach as possible. We work very closely with the Suffolk PCN and support their capacity to engage families and encourage and support the annual parent carer feedback survey and ensure that past surveys inform how we can improve services and outcomes for families. The survey that is due to close in November will be used to inform the SEND Strategy for 2021-2023.
We work within a co-production framework within the SEND Transformation Programme which drives positive change across our services. Our new Speech Language and Communication model design was co-produced and our Neurodevelopmental Model has also been co-produced.

As part of the SEND Programme we have supported the development of a SEND Young People's Network which is now well established and more recently a SEND Children’s network. Both operate across the county in primary and secondary schools and colleges and now extending into alternative provision. Young people can train to be Champions and then they will represent the network at meetings and events. The Champion's training is accredited.
The Champions and the Network have achieved:
• Delivering workshops to parents, carers & professionals - bringing the young person's perspective into the room.
• They have made 2 films, one on accessing health services and about the Network and the other is the recent Hate Crime film.
• Developed guidance for transport providers on supporting young people during their journey to school
• Contributed young people's pages to the Transition Guide • Developing the Local Offer website so that it has an accessible section for young
people. • Developing an access charter for leisure providers to enable young people to feel
more confident in their communities
The difference they make is that they focus on the things that are important to young people and make sure these are listened to and acted on. They make a difference to young people.
7. Performance Dashboard: Our new KPI dashboard provides data and information on
progress and performance across the SEND programme. This covers both quantitative and qualitative information including - parent/carer feedback, educational attainment, exclusions, EHCP timeliness and quality, health referral times and communication impact. The dashboard is regularly reviewed to ensure we are capturing the right data and measures. This will be further complimented with the overarching outcomes framework that is being produced to show the outcome measures from the programmes priorities as a system.

8. What has gone well over the past year:
• The launch of the new online counselling and emotional wellbeing support service for children and young people aged 11-19 years, offering a free and confidential service.
• The full rollout of the multi-agency assessment programme pilot, embedding the learning and positive outcomes already achieved via this programme.
• The full rollout of the moving into adulthood reviews for all children and young people aged 13 years and over.
• The completion of two rounds of commissioning for the establishment of new Specialist Units linked to mainstream schools.
• Our work with the Young Persons Network - The launch of the Stop the Hate Video made by our Young Ambassador Network.
• We have been making good progress on the completion of annual reviews and starting to reduce the number Education Health and Care (EHC) needs assessments going over 20 weeks.
• We have made good progress in the timely completion of EHC plans within 20 weeks, this now exceeds national benchmark levels.
• ‘Time to Listen’ events that were run across the County to allow us to listen to families were well received and immediate feedback and issues acted upon.
• Established a strong governance and partnership structure, which is providing us with the foundations to deliver the changes needed
• Established an annual self-assessment approach that provides representatives from across the SEND system to evaluate progress and identify further action
• Developed an agreed set of KPIs that will be reported to each SEND programme board and used to challenge partners and ensure urgent focus is maintained on improvement across all priorities.
• Established a joint “non-exec” SEND Oversight Board to provide greater direct scrutiny of the work of the programme board and officers across education, health and care.
• Established co-production as a central element to the way we work in Suffolk • Established a young peoples’ ambassador network to support our improvement
journey • Business case for the development of the neuro developmental pathway was
approved by the CCG clinical Executive for the procurement of VCS support. The VCS support procurement will commence by the end of July 2020 with an expected implementation of the support by the end of the year. The coordination function will be established and operational to coincide with the introduction of the VCS offers. The diagnostic pathways will be reviewed and ready for testing by January 2021, the neurodevelopment pathway will run in test form until May 2021 when it will be formally launched alongside the new Mental Health delivery model.
• We will develop more reporting measures as the solutions evolve.

Waveney
• Designated Clinical Officer for Norfolk and Waveney had a Deputy DCO commence in post in May 2019 which has seen an increase in the health presence for Waveney area within SEND programme of work. This has increased the capacity to improve our engagement with contribution to priority areas, support in planning and delivery of training alongside SENDIASS and learning hub, undertaking quality audits with key health providers in the area on health advice and contribute to panels for children and young people with SEND to assist with decision making to inform progress.
• Increased awareness and development of relationships between the CYP team at N&W CCG and the LA specialist Education Services to develop and contribute to key pieces of work that relate to children with medical needs in schools and involvement within the SENCO forums.
• Work to align the children with Continuing care review with their EHCP review has been taking place in Waveney by the CC lead working with the EHCP coordinator.
• School in Waveney to benefit from the recent successful bid for mental health support in schools
• Continual close working with Waveney paediatric service, commissioned from James Paget University Hospital with continual development of multi disciplinary pathways.
• Working with ECCH to support the new service model in Waveney, which aligns to the Norfolk model, ensuring that every child can have the necessary support to develop their speech, language and communication skills. Enabling appropriate assessment and intervention tools and training for early years and primary practitioners/settings
• Implementation of First Response, a 24/7 helpline offering immediate advice, support and signposting for CYP with mental health difficulties
• Funding for three posts secured within NSFT to work across the Norfolk and Waveney system to engage and coproduce with CYP
• Establishment of Norfolk and Waveney Alliance Board made up of key system partners, to oversee and make key decisions to ensure that CYP FLOURISH
• CYP Advisory Group made up of a diverse group of CYP across the system, set up to inform the Alliance Board on health and care services
• In response to the COVID-19 pandemic, both NSFT and Ormiston Families quickly mobilised an advice and signposting service in order to provide support for young people who would otherwise have been unable to access help through routine channels. During this period NSFT supported more than 80 young people from the Great Yarmouth and Waveney area. Over the same period of time Ormiston Families supported over 50 young people. The 2 services are currently piloting the joint triage quality improvement initiative in order to ensure that young people access the appropriate support with minimum disruption. The 2 services are also identifying ways in which they can work together to support the new MHST which will be located in Lowestoft. This will involve joint interview panels, across agency supervision and shared training. Although COVID-19 led to services being delivered

differently in the interim, all work was being overseen by the Norfolk and Waveney CYP Mental Health Transformation Alliance Board.
Inclusion and Specialist Services • Strengthened our early intervention services within specialist education. This
includes the introduction of more early intervention offers including termly inclusion consultations for all schools;
• Completed a sufficiency review for specialist education provision. As a result, a policy development panel was established, which recommended a capital investment programme of 800+ new specialist education places in Suffolk, approved by Cabinet in April 2019;
• Strengthened our panel processes so that children are placed more quickly when they need specialist provision;
• Introduced a new system of high needs funding that is equitable for all children and young people
• Established a joint group with the Regional Schools Commissioner to strengthen inclusive practice in our schools;
• Designed a new integrated model for speech language and communication support, with additional health investment of £1m which is is now implemented.
• Completed all transfers from education statements to education health and care plans
• Strengthened our communication strategy and approach to ensure all stakeholders are informed and communicated to effectively through various channels.
• Completed quality assurance reviews to benchmark our EHC assessment practice and identify improvement targets
• Improved and developed our online training to ensure that all professionals can access and develop their skills to meet our quality and delivery standards.
• Co-produced the re-design of the Neurodevelopment and behaviour pathway to inform the implementation of a single neurodevelopment pathway.
Preparing for Adulthood • Co-produced a new transition guide to support young people and their families with planning
for adulthood this is both online and available in hard copy. This included preparing for adulthood, access to the NHS health system and knowing what to expect.
• Embedded annual reviews in moving into adulthood plans for those aged 13+ • Parental training programme ‘Thinking Ahead’ awarded to a provider and full publication of
offer in progress. • Ensured that the moving into adulthood review and template for their EHCP included
consideration and awareness for the young person to access their yearly annual health check from 14 years onwards.
• Multi agency training has been undertaken by health, education and social care to increase awareness and knowledge on transition to adult services.

Local Offer Website/Communications and Social Media We have improved the quality of information and search functionality on our local offer website and increased the offer via our social media platforms, this includes: • Regular online newsletters for parents/carers, practitioners and strategic leads.
• Landing page views on the Local Offer (running from June 19/20)
66,058 views 15,556 unique 5,954 new users 9,059 returning users
• Highest viewed LO pages (running from June 19/20) Assessment & EHC plans – 6,571 unique views Education – 3,245 Family Services record – 1,443
• Social Media Twitter - 67k impressions Facebook - 158,214 post reach
• Continuous promotion of the Local Offer Website through multi agency and health writing for EHCP training as a resource for health staff to use to aid in directing children/young people and their families/carers to resources available.
• DCO presence at Local Offer meetings and review of health services on Local Offer website.
9. What are the current concerns/issues:
The current level of permanent exclusions for children with SEN or with an EHC plan is high. Work is currently underway to carry out a full review of exclusions and provide recommendations to the SEND board.
To be able to report more outcome measures across the programme – moving away from solely reporting the quantitative measures currently in place.
Listening to our families to ensure we are supporting and resolving issues more effectively – feedback has told us we are not doing this well enough.
Since Covid face to face assessments in schools was suspended, due to social distancing and school closures. This had led to an increasing waiting list for assessments and has had a detrimental impact on the delivery of both Autism and ADHD assessments, effectively stopping them, this is not just an issue in Suffolk but a national issue. When schools reopen in September there will be social bubbles and restrictions to entry to school premises, which will prevent assessments being undertaken in the normal way. In response to this, we are

now working with the services, the SEN teams and parents to look at what support can be put in place for CYP and families whilst alternative solutions are explored. We have been assured by the SEN team that no child will be adversely impacted by not having a diagnosis when applying for an EHCP or school placement.
10. What still needs to happen:
To reinvigorate the work already started to develop the new co-produced SEND Strategy - this will be launched in early 2021
To continue to respond to the SPCN surveys and embed the learning and feedback into the development of the new SEND strategy 2021 – 2024.
To respond to the self-assessment events feedback and embed the feedback and ideas into the new SEND strategy 2021 -2024.
To continue to embed the system wide communications approach and that it is supported by each board member, to ensure that accountability is taken for their role in making the SEND communication as effective as it possibly can be for families in Suffolk. Ensuring that we work with our partners to co-produce comms.
To ensure the KPI dashboard data is reported and areas of new data requirements are being developed and produced in line with the agreed report. This will include new outcome measures across the system.
Continue to engage with families – running our “time to listen… parents/carers and families” sessions virtually.
Continue to improve timeliness and quality of EHCPs, ensuring all parts of the system with responsibility work together with families to improve outcomes.
To embed a co-produced range of outcome measures for key areas of SEND – this will be system wide and sit alongside existing KPI reporting. Leading to a more comprehensive and meaningful view of service provision and the impact on families.
To implement the new mental health strategy for Suffolk
To progress the second phase of the community paediatric review
To implement the neuro developmental pathways for Suffolk
Health input into EHC plan to be reviewed by the member of staff providing the advice or a member of the DCO team to ensure the advice has been translated into the plan correctly.
Improve the capacity and offer in conducting person centred co produced EHc needs assessments, final plans and annual EHCP reviews.

Improve and consider the processes and systems to increase the alignment and join up of agendas with the EHCP reviews, CC reviews, CIN, LAC etc to ensure good information sharing , listening to young people and their parents and only tell their story once.
Improve the system to communicate with any ehcp appeals that is part of the national trial for single route of redress to allow the CCG and social care sufficient time to support and respond in an informed way to have an improve outcome for the child, young person and their family.
11. Progress and Impact
A selection of the KPI areas currently reported for SEND (examples below) – indicating progress and current performance. Outcome data that will sit alongside the quantitative data, is now being developed by our co -production partners – SPCN, SENDIASS and Young Persons Network. Outcome data will incorporate all areas of the SEND system and provide information from families, children and young people in relation to the SEND services/provision they receive. We hope that this data will be ready to include in reporting by the end of the year.
The impact of COVID on the delivery of health services has varied significantly, some services have had to be suspended while others have had to deliver in entirely new ways so the normal reporting of KPIs needs to be redefined. As previously mentioned the impact on Autism and ADHD assessments not being able to be completed has seen the numbers fall to zero in terms of completed assessments and the waiting lists have grown, however, we are working with the services, education and families to look at support for families while the issues around waiting for assessments and potential diagnosis continue. At the same time the Neurodevelopmental pathway is continuing with implementation and as it evolves a new series of KPIs will be developed to demonstrate a child’s journey through the new pathway but more importantly there will be support available for the family while the journey continues.

KPI 4. Education health and care needs assessments are completed within statutory timescales. (20 weeks)
KPI 7. Annual reviews are well managed and impactful.
KPI 9. All young people aged 16 – 25 with an EHC plan are in education, employment or training
Rational: This is a statutory measurement of timeliness that is reported nationally by all LAs. The whole process, from the point an assessment is requested, to the issue of a finalised plan, must be completed within 20 weeks. A local authority has six weeks in which to respond to a request for an EHC assessment with a decision. If the LA carries out an assessment but decides that an EHC plan is not needed, then the LA must notify the parents/young person of the decision within 16 weeks from the request for assessment
Rational: An annual review is a statutory requirement to review the EHC plan to ensure a child/young person is making progress toward their outcomes and receiving the provision in order to meet these.
EHC plans must be reviewed every 12 months (if a child is under five years old, reviews must be six monthly).
Rational: The LA wants to ensure that all YP (16-25) with an EHC plan are in Education, employment or training (EET). Working with the FE sector, businesses etc to create opportunities. This KPI allows us to monitor the progress in achieving this and being able to identify any gaps to address.
Indicator baseline: EHCP timeliness data – proportion of EHCP issued within 20 weeks (exc. exceptions)
2019/20 2020/21
Indicator baseline: % of LA responses to annual review reports within 2 weeks of receipt
Current Perf Target
Indicator baseline: Percentage of young people 16-25 years old that are EET
Current Perf Target April 20 Sept 19 Jan 20 May 20

Q2 Q3 Q4 Q1 Jun-20
Total issued 271 261 200 231 87 Total issued within 20 weeks 90 92 133 199 82 % issued within 20 weeks
33%
35% 67% 86% 94%
Current Perf Target June 20 Sept 19 Jan 20 May 20
94 % June 2020
41 % average for
the first quarter of 2019/20 50% 65% 70%
May 20 Sept 19 Jan 20 May 20 72.7% June 2020
17.4% Dec 2018 50% 70% 90%
% of draft amended plans issued within a further 6 weeks
Current Perf Target May 20 Sept 19 Jan 20 May 20
85% May 2020
44.0% Dec 2018 50% 60% 70%
50.2% 80.1% 90% 90% 90% Dec 19
Story behind the baseline and current performance: This KPI has been developed to allow closer scrutiny of the timeliness of EHC plan completion. This is also reported on a
Story behind the baseline and current performance: This KPI has been developed to allow closer scrutiny of the timeliness of the annual review process for EHC
Story behind the baseline and current performance: This KPI has been developed to allow closer scrutiny of the EET figures in Suffolk to ensure we can monitor
weekly and monthly basis to support visibility within teams to improve performance. The baseline that has been set is in line with the current national average. Commentary for Qtr 1: Performance has been maintained with a YTD average for all new plans issued within 20 weeks of 77% (Jan-June), exceeding the May 2020 target set by the Programme Board and the national benchmark of 60.4% published in May 2020 with 2 assessments exceeding 20 weeks. The number of new assessment requests has remained lower when compared to the same period in 2019 and the potential increased demand is being modelled for the Autumn.
plans. The baseline has been set to encourage high level of completion and in recognition of the importance of annual reviews to ensure children and YPs plans are demonstrating progress and meeting potential and outcomes. This data demonstrates the increase in performance since 2018 - there has been an increase in total reviews completed and in the % completed within 6 weeks. Commentary for Qtr 1: The rate of processing annual reviews within the two week target has improved by 5% to 67% YTD (6 months to end of June). However, we strive to further improve practice in this area and are working with specific teams regarding local systems and practice whilst the EHC Needs assessment demand is reduced. This is data for up to May, due to being collated 6 weekly. June data is not ready at this point of collection. The YTD performance for issuing of draft amended plans has risen by 5% to 73% Jan to June. We are keen to improve this performance further and have a particular focus on this with our teams during the current period.
achievement but to also recognise any gaps or dips to address. review process for EHC plans. The data demonstrates that although the cohort numbers have increased from 2018- 2019 the % in EET has not. Commentary for Qtr 1: This data is a concern and is an area of focus. There have been issues in tracking data returns due to schools/colleges being in lockdown. There has also been an impact on YP who have been furloughed.
12. Action Plans and other strategy plan in place:
SEND strategy priority action plans:
I. The Local Offer II. The SEND Journey

III. Developing Services and provision IV. Moving into Adulthood
• DfE/NHSE Review Action plan
• SEND KPIs
• Children’s Alliance project action plans
Current Partners: CCGs, Schools and FE, SPCN, SENDIASS, Voluntary Partner Organisations

Page 1 of 8
GOVERNING BODY Agenda Item No. 15
Reference No. WSCCG 20-49
Date. 25 November 2020 Title
2020/21 Months 7-12 Budget
Lead Director
Jane Payling, Director of Finance
Author(s)
Chris Armitt, Deputy Director of Finance Ameeta Bhagwat, Head of Financial Management and Planning
Purpose
To set out the financial budget and arrangements for the remainder of the financial year.
Applicable CCG Clinical Priorities: 1. Develop clinical leadership 2. Demonstrate excellence in patient experience & patient engagement 3. Improve the health & care of older people 4. Improve access to mental health services 5. Improve health & wellbeing through partnership working 6. Deliver financial sustainability through quality improvement Action required by the Governing Body: The Governing Body is requested to:
• Approve the M7-12 budget, noting the further actions planned to achieve financial balance.
Extend the arrangements put in place to support CCGs financial decision making during the covid response period namely:
• Extend the Covid Approval Response Committee (CRAC) until the end of March • Extend the changes to the scheme of delegation until the end of March

Page 2 of 8
1. Background 1.1 The Governing Body has been kept informed of the changing financial landscape which the
NHS has faced during 2020-21. 1.2 As updated previously, NHS finances have been running very differently to normal during
2020-21 due to the coronavirus pandemic. National emergency financial arrangements had originally been put into place between April and July 2020 and subsequently extended to the end of September. These arrangements included additional funding for NHS organisations to offset specific additional costs associated with responding to the pandemic, suspension of planning and contracting and an emergency block payment system for providers which has been calculated and mandated centrally.
1.2 CCG allocations for the first half of the year were notified to allow CCGs to put in place systems to facilitate the emergency arrangements set out above. The CCG has submitted monthly returns based on the revised allocations as shown in the finance report. Top up funding to enable the CCG to break even is being allocated retrospectively based on these returns, compensating the CCG for any costs, including those which are directly related to Covid-19, which cannot be covered within the revised allocation.
1.3 Allocations for month 7-12 were received in late September. The ‘Financial Architecture’ for
the second part of the year has the following features as previously reported:
• Return to an allocation based system • Funding for C-19 costs will not be subject to additional claims but included within
allocations on a fair shares basis • Continuation of block payments for providers, following some recalibration • Expectation that local systems will determine the distribution of the remaining funds,
once nationally determined elements are removed - a small element of ‘growth’ funding was allocated to CCGs for local determination for determination - see appendix 1
• Expectation that long term plan commitments, and particularly the mental health investment standard, will be achieved
1.4 Guidance which would enable the implementation of final expected feature of the
architecture for M7-12 has not yet been received and therefore has not yet been implemented
• marginal cost increases and reductions relating to elective and outpatient activity (now
referred to as the elective incentive scheme) 1.5 Each organisation has submitted a draft financial plan to cover the period from October to
March (months 7-12) which is presented for approval. Section 2 sets out the basis of allocations within the system and section 3 presents the plan.
1.6 A draft budget was reviewed by the Financial Performance Committee at its meeting on the
11 November. This draft showed a ‘gap’ between allocation and expenditure of £3.9m. The committee requested a series of actions to be undertaken with the aim of closing the gap. Progress has been made such that a revised plan with a gap of £2.9m was submitted on 18 November.
2 CCG allocations for M7-12 2.1 Appendix 1 shows the build up of the allocation for the CCG for the remaining 6 months.
This is made up of a number of elements: • CCG allocation which is received in the usual three elements: programme allocation,
primary care delegated budget and running costs

Page 3 of 8
• Share of system Covid-19 funding • Weighted capitation share of system growth funding for distribution • National Service Development Funding (SDF, formerly known as Long Term Plan
funding) for the CCG relating to the second half of 2020-21.
West Suffolk CCG
M7-12 allocations
Programme Allocation 162,583Primary Care Delegated Commissioning 18,498Running Costs 2,439
183,520System COVID allocation 1,099System growth allocation 4,193Recurrent Allocation 188,812
Non recurrent allocations (incl SDF) 2,605WSFT System COVID allocation (via WSCCG) 6,871WSFT top up funding (via WSCCG) 22,428
220,716 2.2 The system growth allocation has been passed to CCGs based on a weighted capitation
formula. The three CCGs have worked with their local alliances to determine distribution. Priority has been given to continuation of additional services which have been implemented in the early part of the year to support service delivery during the Covid-19 response, dealing with national must-do areas, and supporting the delivery of the Winter plan. The proposed allocation of the growth funding is given in appendix 1. The unallocated element will be retained by the CCG and distributed to support any pressures occurring in M7-12.
3 CCG Expenditure plans for M7-12 3.1 The table below provides a high-level summary of the expenditure plans for month 7-12.
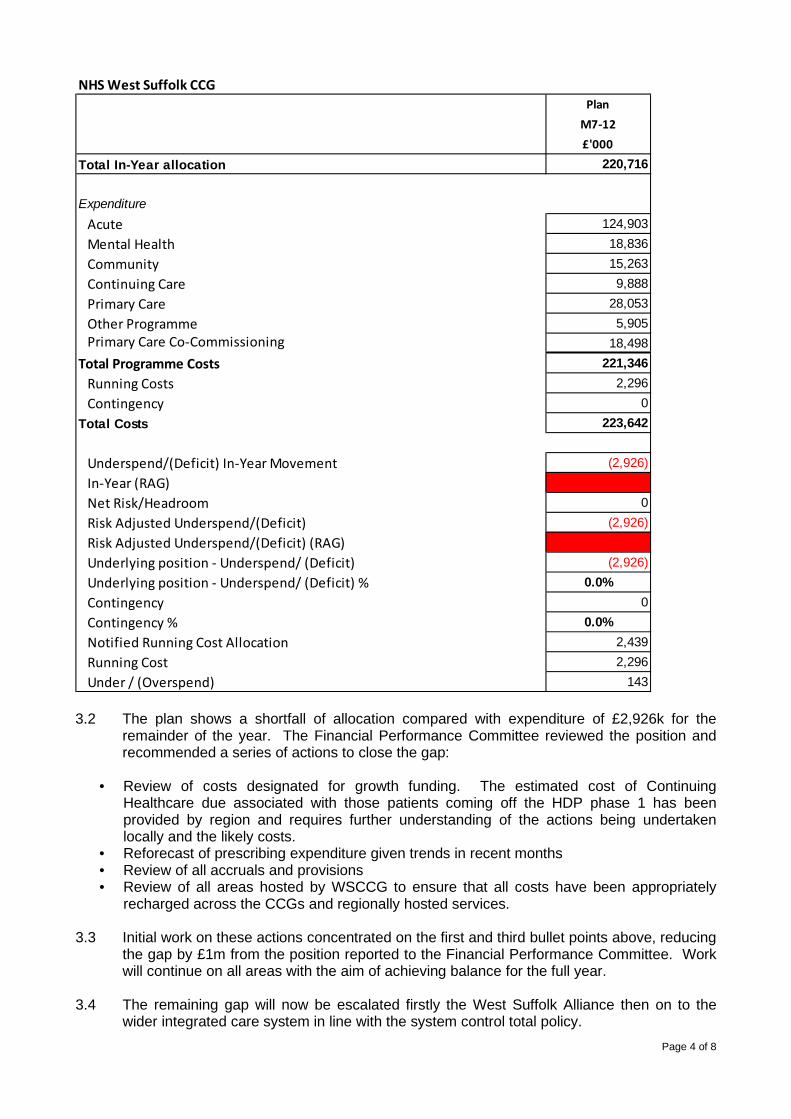
Page 4 of 8
NHS West Suffolk CCGPlan
M7-12£'000
Total In-Year allocation 220,716
ExpenditureAcute 124,903Mental Health 18,836Community 15,263Continuing Care 9,888Primary Care 28,053Other Programme 5,905Primary Care Co-Commissioning 18,498
Total Programme Costs 221,346Running Costs 2,296Contingency 0
Total Costs 223,642
Underspend/(Deficit) In-Year Movement (2,926)In-Year (RAG) 3Net Risk/Headroom 0Risk Adjusted Underspend/(Deficit) (2,926)Risk Adjusted Underspend/(Deficit) (RAG) 3Underlying position - Underspend/ (Deficit) (2,926)Underlying position - Underspend/ (Deficit) % 0.0%Contingency 0Contingency % 0.0%Notified Running Cost Allocation 2,439Running Cost 2,296Under / (Overspend) 143
3.2 The plan shows a shortfall of allocation compared with expenditure of £2,926k for the
remainder of the year. The Financial Performance Committee reviewed the position and recommended a series of actions to close the gap:
• Review of costs designated for growth funding. The estimated cost of Continuing
Healthcare due associated with those patients coming off the HDP phase 1 has been provided by region and requires further understanding of the actions being undertaken locally and the likely costs.
• Reforecast of prescribing expenditure given trends in recent months • Review of all accruals and provisions • Review of all areas hosted by WSCCG to ensure that all costs have been appropriately
recharged across the CCGs and regionally hosted services. 3.3 Initial work on these actions concentrated on the first and third bullet points above, reducing
the gap by £1m from the position reported to the Financial Performance Committee. Work will continue on all areas with the aim of achieving balance for the full year.
3.4 The remaining gap will now be escalated firstly the West Suffolk Alliance then on to the
wider integrated care system in line with the system control total policy.
Page 5 of 8
3.5 In line the methodology used to create CCG allocations for M7-12 the CCG is not able or
expected to hold the usual 0.5% contingency which means there is reduced ability to absorb any further pressures.
3.6 It should be noted that the costs of mass vaccination and any significant additional costs
associated with a second wave of covid-19 are not included within the plan. The mass vaccination programme is subject to a separate costing exercise which is currently underway.
4 Extension of emergency financial arrangements until the end of March 4.1 To facilitate the fast moving operational delivery agenda, and support the implementation of
mass vaccination during the busy winter period it is proposed that the processes put in place by the CCG to put in place robust and expedient financial decision making are continued until the end of March.
4.2 The specific measures which the Governing Body is asked to extend are set out below. A Continuation of the Covid Resource Allocation Committee 4.3 This committee which works across the 3 CCGs in Suffolk and North East Essex has
worked effectively from 1 April. Whilst it is the aim of the committee to ensure decision making is made at alliance level where appropriate, there are times when the added flexibility and speed of the joint committee mean that decisions can be taken in a more timely manner.
4.4 It is proposed that the covid-19 resource allocation for the 3 CCGs will be overseen by this
committee and that it will be required to make decisions relating to the mass vaccination programme which is being undertaken at pace. Oversight for decisions made by the committee will be via the Financial Performance Committee with the minutes being reported to the Governing Body.
B Continuation of the Changes to Delegated Authorisation Levels 4.5 The delegated limits for directors and senior officers have been increased during the year to
facilitate decision making (attached in appendix 3). It is proposed that this change is extended until the end of March. In reality, the increased limits have been used on a limited number of occasions, with decisions being overseen by the Covid Resource Allocation Committee.
4.6 A piece of work is underway to look at the scheme of delegation in the light of the
developing alliance governance structure. The financial elements of this work are being overseen by the Audit Committee. The changes outlined above represent an interim measure to cover the immediate period,
5. Recommendation
The Governing Body is requested to: 5.1 Approve the M7-12 budget, noting the further actions planned to achieve financial balance.
Extend the arrangements put in place to support CCGs financial decision making during the covid response period namely:
5.2 Extend the Covid Approval Response Committee (CRAC) until the end of March 5.3 Extend the changes to the scheme of delegation until the end of March

Appendix 1 Growth Allocation Funding M7-12
WEST SUFFOLK £K £K
(4,193)CHC pressure expected due to cessation of HDP 1,544 Under continued review CCG Pressure. Figure notified by region
Think 111 First (net) 141 CCG Pressure iro difference between cost pressure and allocation
Enhanced End of Life / Virtual Ward 350 As agreed via CRAC cttee for continuation of Enhanced EOL Services
RAAC support (attain) 500 CCG funding additional non-recurrent work in this area
EIT support to care homes 23 From WS winter plan
Virtual Ward WSFT 296 From WS winter plan
Bed Capacity as per winter plan 584 From WS winter plan
Homefirst capacity (joint with SCC) 95 From WS winter plan
Prescribing pressure 650 Under continued review cost pressure.
Total Earmarked 4,183
Not yet committed/contingency (10)
Growth Allocation

Page 7 of 8
Appendix 2 Current and Proposed Limits of Financial Authority:
Relevant DETAILED FINANCIAL POLICIES
Section
Delegated to
Financial Limit (Current)
Financial Limit (Proposed)
Operational Responsibility
Authorisation of waiver of Formal tendering procedures
Authorisation of Tenders and Competitive Quotations
Commissioning
Non-Pay Expenditure
Capital Investment
* Senior Officers include:
Chief Executive Director of Finance Director of Performance Improvement Director of Nursing Chief Operating Officer
Budget holders
Financial limit as delegated to each Budget holder as agreed and set by the Chief Executive and Director of Finance and reviewed from time to time (for the avoidance of doubt such financial limit shall not exceed £37,999).
Financial limit as delegated to each Budget holder as agreed and set by the Chief Executive and Director of Finance and reviewed from time to time (for the avoidance of doubt such financial limit shall not exceed £37,999).
Budget holder
Senior Officers *
Up to £38,000
Up to £500,000
Senior Officer
Chief Executive following consultation with the Director of Finance and with the Chair on all significant proposals, where possible.
Up to £250,000
Up to £1,000,000
(Up to £3,000,000 in exceptional circumstances, on consultation with the chair only) (N1)
Chief Executive and Director of Finance following consultation with the Chair on all significant proposals
CCG Governing Body
Over £250,000
Over £1,000,000
Senior Officer
The Senior Officers named above may be substituted for their nominated deputy in the instance that the Senior Officer is unavailable. N1 – where the exceptional circumstances limit is used, this expenditure is to be brought to the next available Governing Body for review.

Page 8 of 8
Appendix 3 Proposed Limits for CHC Approval Packages or equipment costs of £700/week or under:
• Nurse Co-ordinators or; • Director of Nursing (or nominated deputy) or; • Head of CHC, Clinical Lead or; • Head of CHC, Operational Lead; or • Clinical Commissioning Manager/Locality Manager; or • CHC PHB Clinical Lead
Packages or equipment costs of £1500/week or under:
• Director of Nursing (or nominated deputy) or; • Head of CHC, Clinical Lead or; • Head of CHC, Operational Lead; or • Clinical Commissioning Manager/Locality Manager; or • CHC PHB Clinical Lead
Packages or equipment costs of £4000/week or under:
• Director of Nursing (or nominated deputy) or; • Head of CHC, Clinical Lead or; • Head of CHC, Operational Lead
Packages or equipment costs of over £4000/week:
• Director of Nursing (or nominated deputy) and;
One of the following:
• Head of CHC, Clinical Lead or; • Head of CHC, Operational Lead

1
GOVERNING BODY
Agenda Item No. 16
Reference No. WSCCG 20-50
Date. 25 November 2020
Title Integrated Performance Report
Lead Director Joint Leadership Team
Author(s) Joint Leadership Team
Purpose To present to the Governing Body the latest Integrated Performance Report.
Applicable CCG Priorities 1. Develop clinical leadership 2. Demonstrate excellence in patient experience & patient engagement 3. Improve the health & care of older people 4. Improve access to mental health services 5. Improve health & wellbeing through partnership working 6. Deliver financial sustainability through quality improvement
Action required by Governing Body:
To note the report.

1
West Suffolk CCG Performance Pack
November 2020 (reporting on September 2020 unless stated)

2
Contents (Ctrl + Click on Provider to follow the link)
• Summary & Key Issues
• West Suffolk Foundation NHS Trust
• Cambridge University NHS Foundation Trust
• Norfolk and Suffolk FT (NSFT)
• Practice Plus Group (Integrated Urgent Care Service)
• E-Zec Medical – Non-Emergency Patient Transport (Suffolk)
• EEAST
• WS Primary Care
• WS Finance
• CCG Metrics

Summary – July 2020 (1 of 2)
3
Provider Service Quality Performance Demand vs 19/20
Productivity vs 19/20
Workforce Transformation Contract Finance
Provider finance
Key changes in month
West Suffolk NHS FT
Acute CQC: Requires ImprovementLocal: Level 3
Key metrics missed
Referrals downED attends down
Throughput down
Work in progress
Work in progress
Work in progress
Work in progress
Demand and throughput down
Community (West Alliance)
Mixed performance
Mixed data Mixed data Work in progress
Mix of projects on and off track
Work in progress
Work in progress
No key changes
Cambridge University Hospitals NHS FT
Acute CQC: GoodNot locally reviewed (CPCCG)
Key metrics missed
Referrals downED attends down
Throughput down
Not locally reviewed (CPCCG)
See WSFT Work in progress
Work in progress
Demand and throughput down

Summary – July 2020 (2 of 2)
4
Provider Service Quality Performance Demand vs 19/20
Productivity vs 19/20
Workforce Transformation Contract Finance
Provider finance
Key changes in month
Norfolk and Suffolk NHS FT
Mental Health CQC: Requires ImprovementLocal: Level 3
Key metrics missed
Demand down Mixed metrics All metrics missed
Work in progress
Work in progress
Work in progress
Access performance deterioratingVacancy rate falling
Care UK Integrated Urgent Care Service
CQC: GoodLocal: Level 2
Key metrics not met
Calls up on 19/20, down on plan
On line throughput up
Work in progress
Work in progress
Work in progress
Work in progress
Not reviewed
E-Zec Patient Transport
CQC: Not rated yetLocal: Level 2
Mixed metrics Referrals down See demand Work in progress
Not applicable Under plan Not reported Quality rating improved
East of England Ambulance Service NHS FT
Patient Transport
CQC: Requires ImprovementLocal: Level 2
No reporting in M2
No reporting in M2
No reporting in M2
No reporting in M2
No reporting in M2
No reporting in M2
No reporting in M2
Emergency No reporting in M2
No reporting in M2
No reporting in M2
No reporting in M2
No reporting in M2
No reporting in M2
No reporting in M2

Key Issues – September 2020
Pan Suffolk1. Issue 12. Issue 23. Issue 3
Integrated Care system1. Issue 12. Issue 23. Issue 3
Pan ESNEFT issues1. Issue 12. Issue 23. Issue 3
West Suffolk Alliance1. Securing longer term capacity and
integration:• Development of Primary Care
Networks;• Embedding Integrated
Neighbourhood Teams• WSFT new build.
2. Covid19 recovery to BAU and new normal
3. Addressing inequalities such as eliminating rough sleeping
North East Essex Alliance
1. Covid19 wave 2 response alongside ongoing service delivery for elective services.
2. Mental Health presentations increase in both older adults and young people in Crisis both the ED and MH Crisis services.
3. Discharge flow across the system
Pan Suffolk1. Mental Health Transformation2. Joint working with Suffolk County
Council3. Children’s services integration/
development
Integrated Care system1. ICS strategic priorities such as
cancer, stroke care etc.2. Reducing health inequalities3. Improving sustainability
Pan ESNEFT issues1. RTT elective recovery- maintaining
safety of patients with long waits; maximising independent sector capacity to clear waiting lists
2. Diagnostic testing capacity 3. Cancer performance
Ipswich and East Suffolk Alliance1. Covid19 recovery to BAU and
new normal 2. Preparation for winter and flu
vaccinations3. Reducing health inequalities
5

Wes
t Suf
folk
Fou
ndat
ion
Trus
t (W
SFT)
CCG Quality Assurance
Rating: Level 3 (→ from last month) CQC Rating: 2020: Requires improvement
Month updated: Nov-20 (Sep-20 data) QSG surveillance Rating: Enhanced
Issues / Concerns / Comments Actions / Progress Hospital
1. The Jan 2020 CQC report rated WSFT as ‘requires improvement’.
2. Quality assurance visits have been undertaken to ensure Safe storage of Medication (20 October) as this was an area of concern raised by the CQC.
3. The Cancer sitrep for week ending 11th Oct 2020 indicates there were 275 new 2ww referrals. There are 136 (122)
patients on 63+ days and 26 (26) patients waiting above 104+ days. (source: EoE Cancer Alliance).
4. The NRLS report cites WSFT’s incident reporting rate as 54.81/1000 bed day for Oct 2019- Mar 2020. This is an increase from Oct 2018-Mar 2019 when it was 49.11 /1000 days. The report states this is not a significant change. The timeliness of reporting shows that 50% of incidents were reported after 47 (59) days. The report states that they should be reported as quickly as possible and at least every month.
5. WSFT are an early adopter for the Patient Safety Incident Response Framework (PSIRF), which will replace the Serious Incident Framework 2015.
6. Falls at WSFT (August data): 7.12 per 1000 bed days. There were 69 (58) in-patient falls, none of which resulted in
moderate or severe harm. The Trusts are recruiting a Falls Lead; have developed Champions for each ward and there is a champions event on 11 November 2020.
7. There was a total of 6 Trust attributed C.diff cases in September (4 HOHA ,2 COHA)There were 3 Trust apportioned E.coli bacteraemia’s identified in September 2020. There were 4 Trust apportioned MSSA bacteraemia’s identified in
September 2020.
8. Patient First: Project reset in emergency medicine, (CQC, Oct. 2020). This tool has actions for departmental, trust and wider system level, to maximise capacity, maintain effective patient flow, and keep staff and patients safe.
9. The hospital has noted an increase of presentations in ED and admissions where the patient has complexities of needs which require a multi-agency acute and community response in managing care and treatment. A number of factors including resource, expertise and lack of multi-agency partnership working have contributed to four of these individuals remaining in a hospital bed despite being medically optimised and where there has been a need for the CCG MCA/DOLS Lead and Safeguarding expertise support to become involved.
Community
10. 13 (8) in-patient falls occurred with a falls per 1000 bed days of 11.89 (7.31).
11. There were 1 (0) in-patient pressure ulcer. There were 40 (32) pressure ulcers reported in the community: 26 (19) cateogory-2; 6 (3) category-3; 0 (1) category-4 and 14 (9) were unstageable.
Hospital
1. WSFT has a robust Trust Improvement Plan, with a BBRAG status for 32 ‘must do’ CQC findings. The Trust have established an Improvement Programme Board (a sub-committee of the Board) led by the Chief Exec. It has three work-streams: CQC improvement; COVID-19 recovery and a QI methods programme. The CCG attends the meetings.
2. Assurance was provided that medication is stored safely and that effective risk assessment is in place. Further quality assurance visits are planned around the care of patients with a learning disability and care of patients with sepsis.
3. The East of England (EOE) Cancer Quality Task and Finish Group have created guidance and quality indicators
regarding potential paint harms in terms of the patient pathways. Providers are required to bench mark their cancer harm review policy and SOP to meet the standards by the end of October.
4. The CCG Patient Safety and Clinical Effectiveness Lead meets regularly with the Patient Safety Team at WSFT for assurance and oversight regarding patient safety. The Clinical Quality Lead meets fortnightly with the Compliance Manager to discuss key issues and concerns.
5. WSFT are meeting with the CCG and NHS-E to discuss the Patient Response Incident Response Plan (PSIRP). It is anticipated that this will commence in Jan. 2021.
6. The Trust is recruiting a Falls Lead and has identified Falls Champions for each ward.
7. WSFT has been unable to appoint to the IPC lead role which has been vacant since the end of August. This leaves a potential IPC risk for the Trust going into the winter period as the current team covers the hospital and community services. The team has been offered support from SNEE IPC team and from ESNEFT IPC team.
8. The CCG has advised the Trust to benchmark their current position and advocated local Trusts peer review for further assurance.
9. CCG MCA/DOLS Lead is coordinating a task and finish group to look at complexities of needs and what we can learn and improve across health in capacity assessing, DOLS and Self Neglect pathways for these patients.
Community
10. Monthly meetings have resumed between the Head of Nursing for Community and the Clinical Quality Team. This allows in-depth discussion about concern and progress and enables the CCG to be more involved with the clinical quality initiatives taking place.
11. Clinical Quality Lead will attend the Trust’s Pressure Ulcer and Complex Wound Meeting to gain assurance around work
being undertaken to reduce pressure ulcers. The previous Category 4 pressure ulcer serious incident report will be reviewed at SI panel for learning and actions taken.
West Suffolk FT - Month 6 YTD – Quality Plan on a Page

7
West Suffolk FT – Month 6 – Top 10 Performance Items
Elective StandardThis
Month
Last
MonthAssurance SPC Trend
18 wk RTT Incomplete(N) 92.0% 55.1% 49.0%Consistently
failed
Special cause
variation: Low
RTT 52 Week Waiters(N) 0 1,484 1,242Both met and
failed
Special cause
variation: High
18 wk RTT Incomplete(N) 19,817 19,082 TBD - Trend or CCV
Diagnostic test waiting times(N) 1.0% 46.0% 54.1%Both met and
failed
Special cause
variation: High
Cancer StandardThis
Month
Last
MonthAssurance SPC Trend
All Cancer 2 week wait(N) 93.0% 65.3% 71.2%Both met and
failed
Special cause
variation: Low
Two week wait for breast symptoms(N) 93.0% 93.1% 91.7%Both met and
failedTBD - Trend or CCV
Cancer 31 day wait: Percentage receiving 1st
treatment within one month of cancer diagnosis
(N)
96.0% 100.0% 100.0% Consistently met TBD - Trend or CCV
Cancer 62 day wait: urgent GP referral for
suspected cancer(N)85.0% 75.0% 80.6%
Both met and
failedTBD - Trend or CCV
A&E StandardThis
Month
Last
MonthAssurance SPC Trend
A&E 4 Hour Standard-Nat'l 95.0% No Data No DataNo Data
CollectedPart of A&E Pilot
ISSUES:1. 18 weeks: throughput plateauing at between 70 and 90% of
2019/20 rate. Demand was at around 75% of 2019/20. The waiting list increased by 735 patients in September with long waits up 242.
2. Concerns at decline in bed based throughput seen through increasing length of stay and delayed transfers of care.
3. 2 week and 62 day wait cancer access standards continue to be an issue. A lack of endoscopy capacity is one of the key causes.
4. Diagnostic long waits reduced but the waiting list grew to over 7,000 patients.
ACTIONS:1. Trust is continuing to seek to increase throughput with outsourcing,
but there is concern this may not have sufficient to achiever recovery.
2. CCG and Trust are implementing high impact changes to outpatients. A dashboard will be complete this month.
3. National discharge guidance needs to be embedded4. Trust unable to produce a recovery plan for cancer at this point.5. CCG and Trust are implementing outsourcing/ insourcing options to
address diagnostic waits.

DRAFT8
West Suffolk Community – Month 6 Key Performance Items
Issues:• Most Key Performance Indicators achieved the
threshold.• Children in care – initial health assessments
completed within 15 days was 72.73% (8/11). Performance is planned to improve from October when additional GP capacity is in place.
• Lymphoedema service performance was impacted by COVID. The service restoration plan has been shared / reviewed and the service can sustain current demand for new and follow ups.
• Exploring the reasons for a general reduction in the timeliness of community hospital discharge summaries being shared with GP practices.
• There continue to be 18 wk. RTT breaches for consultant paediatrics. Recovery options have been reviewed and there is support to change the service skill mix. WSFT is developing a recovery proposal which will be reviewed next month.
Adult Standard This Month Last Month Assurance SPC Trend
% of patients seen following triage within 72 hrs. 95.0% 100.0% 99.7% Consistently met TBD - Trend or CCV
% of patients seen following triage within 4 hrs. 95.0% 98.4% 100.0% Consistently met TBD - Trend or CCV
% of patients seen following triage – emergency within 2 hrs.
(Referrals to REACT and EIT Teams)95.0%
No data
available this
month
No data
available this
month
Both met and
failed
Special cause
variation: High
Improving discharges and maintaining delayed transfers of
care at a minimum level3.5% 10.5% 8.8%
Consistently
failedTBD - Trend or CCV
Children and Yound People Standard This Month Last Month Assurance SPC Trend
CYP-SALT % of children started treatment within 12 weeks of
initial assessment-Commiunity Clinics95.0% 31.6% 52.9%
Both met and
failedTBD - Trend or CCV
CYP-SALT % of children started treatment within 12 weeks of
initial assessment-Mainstream schools95.0% 14.3%
No data
available this
month
Consistently
failedTBD - Trend or CCV
CIC % of initial health assessments completed within 15 WD
of receiving all relevant paperwork.95.0% 61.5% 72.7%
Both met and
failedTBD - Trend or CCV
% of responses submitted to the Local Authority (LA) within 6
weeks of receipt of the request90.0% 93.8% 94.6% Consistently met
Special cause
variation: Low
18 week RTT for Paediatric Consultant led services 95.0% 57.6% 62.9%Consistently
failedTBD - Trend or CCV
18 week RTT for Paediatric non-Consultant led services 95.0% 96.4% 95.8%Both met and
failedTBD - Trend or CCV
Specialist Standard This Month Last Month Assurance SPC Trend
Standard equipment delivered on Time 96.7% 99.7% 99.8% Consistently met TBD - Trend or CCV
18 week RTT for non-Consultant led services - (West
Community - 10 services)95.0% 97.8% 98.1%
Both met and
failedTBD - Trend or CCV
Care Coordination Centre
% of calls answered within 60 seconds90.0% 84.3% 90.4%
Both met and
failed
Special cause
variation: Low
CYP % of Service Users where equipment was delivered in 18
weeks of being referred to the service92.0% 93.8% 100.0% Consistently met
Special cause
variation: Low
Lymphoedema service (west only) % of palliative referrals
seen within 2 weeks of referral95.0% 100.0% 100.0%
Both met and
failedTBD - Trend or CCV
Lymphoedema service (west only) % of urgent referrals seen
within 4 weeks of referral95.0% 100.0% 100.0% Consistently met TBD - Trend or CCV
Lymphoedema service (west only) % of routine referrals seen
within 14 weeks of referral95.0% 92.9% 50.0%
Both met and
failedTBD - Trend or CCV

West Alliance Programme DashboardOverall Programme
RAG
Apr-20 May-20 Jun-20 Jul-20 Aug-20 Sep-20 Oct-20 Nov-20 Dec-20 Jan-21 Feb-21 Mar-21
At risk At Risk At Risk At Risk At risk
Programme Status: Many areas have progressed well and exceeded original timescales including some elements of the programme that were postponed (outpatients in particular).
Project RAG Update/Action Required in Red or AmberProject
ProjectRAG Update/Action Required in Red or Amber
WS 20-01 Urgent and Emergency
Care At Risk
Think 111 progressing as planned with deadline for implementation by 1 December across SNEE on track. National team have approved SNEE gorgo live and ED SOPs and evaluation approach in development. Sustainable options for RICV continuing beyond 2021 being scoped for consideration by Alliance partners. High Intensity Users (HIU) case finding and MDTs have commenced in Newmarket although unlikely to extend further throughout winter and lockdown as capacity is aligned to maintain business as usual services.
WS 20-03 Outpatients Transformation
AtRisk
Project Plan developed and workstream leads identified. Interim reporting tool will be available at the end of Nov which will enable us to set the baseline data. Agreed to use number of patients on the waiting list as at 31 October 2020 as the baseline for the Clinical Validation workstream.Where applicable, workstream leads are on track to map existing provision, develop plans, SOPs and engage services to start discussions. Visionable video consultation tool to be re-launched mid- November and the patient portal being promoted to increase take up.Full operational model for MSK in place across Suffolk commissioned through AHPS directly with PCNs. Potential of WSFT Clinical Photography App and its integration with S1 & EMIS being explored. Clinical review of LPPs across SNEE to be agreed through SNEE Elective Care Board. Validation work is in progress with each specialty having developed its recovery plan.
WS 20-02 Out of Hospital and
Community CareOn track
Key work this month has focussed on building resilience within the community ahead of winter including:• Supporting Abbeycroft Leisure to work with the Integrated Neighbourhood Teams to pick up people at risk of falls who have been referred and waiting - due to start 9th Nov• Increasing pulmonary rehab capacity to work through backlog of people waiting for their support programme - the Abbeycroft class has been rebranded to enable more respiratory patient inclusions • Virtual ward business case has been completed and going to CRAC for winter funding request• Securing agreement to change use of Newmarket beds to support national discharge Annex A guidance. Mapping of Annex A to identify potential patient cohorts who could be suitable has commenced and aims to be
completed by the end of November.• Finalising the out of hospital bed model to support winter including optimising use of Marham House care home beds. The funding model for these beds is based on the national discharge guidance which has now been agreed
with Suffolk County Council. • The Early Intensive Support Team (EIT) to support care homes proposal to go to CRAC Committee for winter plans.• Commissioning additional community nursing capacity through Homelink. • Telehealth extension opportunities are being scoped at an ICS level with West Suffolk Alliance opting for pulse oximetry, remote vital signs monitoring in care homes and out in the community.
Ageing Well ProgrammeBid in development to secure three additional months of funding for the dedicated EIT support to care homes from end December.Support from providers secured to use nhs.net in communication with care homes to encourage care home uptake of portal.
Integrated Neighbourhood TeamsBaseline assessment of maturity matrix completed across all six teams and action plans now being developed. Work has commenced to align dementia and mental health support into each INT to ensure MDT working is more robust over winter. This includes ensuring Wellbeing Service support is aligned to specific pathways.
Community modelWork continues to progress to inform out of hospital model as part of the Future System Programme. ReTHINK partners commissioned to undertake listening exercise with community health and social care staff to identify opportunities.

SNEE Strategic Programme DashboardOverall Programme
RAG
Apr-20 May-20 Jun-20 Jul-20 Aug-20 Sep-20 Oct-20 Nov-20 Dec-20 Jan-21 Feb-21 Mar-21
On Track On Track On Track On Track On Track
Programme Status: Although some of the projects are at risk the programme of work is largely on track.
Project RAG Update/Action Required in Red or Amber Project RAG Update/Action Required in Red or Amber
SNEE CVD On Track
Delays due to COVID 19. Inaugural CVD board meeting has now taken place and meeting has representation from across ICS. Members will work on priorities in line with the strategic plans. Work has started to map existing services across the ICS. From this mapping priorities will become clear as to which pathways will need to be a priority. We have been approached to take part in a pilot study for Familial hypercholesterolemia, expressions of interests have been requested from across the ICS, several practices have returned expressions of interest in relation to this project.
SNEE StrokeOn Track
ESD procurement is currently in stand still period post award and closed on the 13/11, decision will be made public on the 16th November. A new timeline was issued with the new service to start in April 2021.Work on co-production with patients and carers, TIA pathways and service integration across the ICS are the key priorities to pick up now post Covid-19.SNEE ICS Stroke Board endorsed at their meeting on the 29th October support for participation in the Integrated Stroke Delivery Board (ISDN) – North. Approval was recommended to support the contribution required from our system to support the establishment of a dedicated team, hosted by Queen Elizabeth Hospital at King’s Lynn via an agreed MOU. New national stroke guidance issued on the 7th October which describes the new named configuration and integrated arrangements for stroke services which the Stroke Board will now focus on implementing.
SNEE Maternity At Risk
National deliverables were finally published on 30/09/2020 that included additional deliverables associated with reducing inequalities through the rollout of Continuity of Carer (CoC) which will be challenging for SNEE LMNS due to demographics, but mitigated as far as possible through rollout phasing. Progress made with ESNEFT regarding moving to safe levels as defined by Birth-rate+ workforce tool, awaiting date for fulfilment from ESNEFT. This will enable CoC rollout to commence. Staff CoC consultation due to commence 19/10/20. WSFT staff consultation completed with formal rollout commencing 23/11/20. Significant campaign completed to engage with BAME communities and ensure clinical outcomes optimised through threshold changes and public communications. Neonatal and Postnatal workstreams established and had inaugural meetings and work plans agreed. Financial allocation formally confirmed but finance colleagues establishing whether this has been passed directly to providers or within CCG funds, therefore spending plan paused until confirmation received. Data quality remains a risk as NHSE now using as measure of assurance for target delivery. MSDS not 100% completed by providers, ESNEFT Ipswich site and WSFT are not on IT platform which enable automatic uplift to MSDS. Manual spreadsheet adopted by midwives to enable MSDS to be checked for accuracy if targets not achieved as a mitigation for now.
SNEE Neuro Rehab
On Track
An inaugural Neuro-Rehabilitation Board meeting has now taken place and meeting has representation from ICS. Dr Andy Graham, Consultant Neurologist at ESNEFT has agreed to the Chair. Board members will work on priorities in line with the strategic plans. Work has started to map existing services across the ICS to identify priority pathways. As above (Stroke) ESD procurement has been completed and mobilisation is due to start in November - the ICS Neuro rehab Board will help develop this service in the months. Review of Level 2b bed commissioning and provision, integration of rehabilitation services within the community and support to the long Covid agenda are key priorities.

SNEE Strategic Programme DashboardProject RAG Update/Action Required in Red or Amber Project RAG Update/Action Required in Red or Amber
SNEE Respiratory
On Track
• Governance - well attended and populated respiratory operational groups across each Alliance.
• Spirometry - This has been an issue since Covid commenced. Primary care not likely to reengage this assessment before the Spring, so looking to run some specific training and education events for clinical staff across the ICS.
• Long Covid - In the latter part of this month, the ICS has received instruction to embed support for patients presenting with Long Covid. Much of the service requirements for this cohort of patients is already developed across the three Alliances, but now working to establish how they can be linked into a single integrated pathway.
• Remote monitoring - A short term opportunity to scope, develop and implement remote monitoring for our most vulnerable has been identified in early November. This is now under development with a well formed small task and finish group to establish options for each Alliance, with potential to support patients with long term conditions to support their discharge from hospital and avoid hospital admissions.
• Pulmonary rehabilitation (PR) - although PR was suspended during Covid, each Alliance is working to increase face to face session where possible and drive down any outstanding waiting lists. There will be coordinated efforts through November to share learning.
SNEECancer
At Risk
2WW referrals - SNEE ICS have recovered in most tumour sites to pre-covid level of referrals, with some sites exceeding expected levels. Following a successful 'Help us to Help you Campaign' and the second lockdown in progress, a task and finish group has been developed to rerun the campaign and minimise any reduction in 2WW referrals. Patient Engagement - Initial patient engagement events have been held for the faster diagnosis pathway, Rapid Diagnostic Service and the personalised care pathways. Screening - Breast and bowel screening has restarted across the ICS, the current focus is high risk patients and those who have missed screening while the services were paused, these services plan to continue during the second C19 lockdown. Suffolk GP Federation has been held as an exemplar for the work it has started to support an increase in cancer screening across Suffolk, Cancer Research UK have produced a paper sharing their best practice. Faster diagnosis pathways - Best practice pathway stocktakes have been completed and shared with the regional teams. Endoscopy remains an issue within the ICS, WSFT plan to open their third room in November to add additional resource for their lists. A mobile CT scanner has been procured at WSFT to support additional capacity. ESNEFT have been awarded additional funding for Colon Endoscopy Capsule. Rapid Diagnostic Services - the non site specific pathway (Vague Symptoms) clinicians have been appointed at ESNEFT. Ipswich Cancer hub have recruited to the required posts and plan to start receiving referrals in phased tumour sites from Dec2020. Personalised self-managed pathways - Stocktake completed across the ICS. Breast business case has been signed off at ESNEFT for PCFU across both sites. Somerset training taking place at Ipswich site across all tumour sites to support RMS. WSFT to pilot Holistic Needs assessment (HNAs) in PCFU for breast via the patient portal. MacMillan Navigators - evaluation parameters agreed for the ICS navigator programme. ESNEFT Navigators have now launched their pathway. Telederm - Launched in Ipswich and I&ES, phase two at Ipswich site underway following success of phase one, end to end testing underway for 2WW, planned launch in line with the new Ipswich Cancer hub. WSFT pathway agreed and 1.4 wte band 4s have been recruited to support telederm pathway. NEE task and finish group has been established and are currently developing Advice and guidance pathway. Cancer Innovation - Prioritisation framework reviewed and innovations priorities agreed, paper to be presented at ICS Cancer Programme Board November 2020.
SNEE Diabetes At Risk
The National Diabetes Prevention Programme (NDPP) communications plan is being worked up though a presentation to North East Essex (NEE) has already been completed. A presentation to West Suffolk (WS) is planned and Ipswich and East Suffolk (IES) will happen on 2/12 via the virtual Trinity Park event. Options for NDPP2 referral generation are still being worked through with several good ideas about how to resolve this. The NDPP self referral pathway is now being advertised by OneLife Suffolk as part of a Public Health campaign. The Diabetes Inpatient Specialist Nursing (DISN) project is currently having the contract worked up which will allow the interested trusts to go out to advertisement in order to get their full complement of DISNs. Transformation funding has been secured for the next two years to cover this with the expectation that the trusts would then maintain these roles.Multi Disciplinary Footcare Teams (MDFT) - All in year priorities/actions now have a named person who will be responsible for completing tasks identified as gaps in service. A rough calculation of the number of podiatrists needed to reach a full complement has been calculated at 3 whole time equivalents. This is based on Nice Guidance 19.In order to support the more vulnerable groups with Diabetes such as the Black, Asian and Minority Ethnic (BAME) community we are planning a meeting this month with various community leaders to explore some existing ideas and seek their views on how we might go about thisWe completed an Eclipse software walk through at virtual Trinity Park for primary care colleagues and have created a system wide diabetes performance report to help with identifying and levelling up diabetes service variation across the systemSupporting the roll out of Continuous Glucose Monitoring (CGM) for type 1 women who become pregnant. This cohort should each have up to a years access to CGM devices to help them control their Diabetes from April 2021.Use of digital Structured Education (SE) is ongoing while patients cannot access face to face classes. We are monitoring the numbers of patients on waiting lists closely.

Children and Young People’s Programme DashboardOverall
Programme RAG
Apr-20 May-20 Jun-20 Jul-20 Aug-20 Sep-20 Oct-20 Nov-20 Dec-20 Jan-21 Feb-21 Mar-21
GREEN GREEN AMBER AMBER AMBER
Programme Status: The SaLT work is delayed due to a pause during the ongoing COVID 19 pandemic. Work has now recommenced. All other projects either on track or risks to delivery being managed.
Project RAG Update/Action Required in Red or Amber Project RAG Update/Action Required in Red or Amber
CYP 20-01 NEE CAMHS
On Track
Public engagement now complete and feedback included in the service specification which is now finalised. Costings for the revised specification being worked on to determine affordability - finance decision to be made on 17th November. Market engagement events concluded.
CYP 20-05 NEE Neuro
DevelopmentalOn Track
Three Task and Finish Groups have been established to focus on outcomes, integrated single pathway and the desired future model. A business case is being developed for Feb 2021 covering all of these three areas. The key areas of unmet need and focus have been identified which include:• -Identification of need• -Information & Communication• -Coordination function• -Early Support Family offer • -TransitionA Memorandum of Understanding will be developed to underpin the implementation of any pathway changes, improved ways of working.Presentation made to the November meeting of the NEE Alliance Cttee with support gained for the proposed approach detailed above. CYP 20-03 NEE
SaLT Late
Essex wide review of SaLT underway led by West Essex CCG. Project group setup supported by Better Communication CIC , an external consultancy company.
The current pan Essex timelines are for implementation are July 2022. This does not fit with need for local implementation to be July 2021 in line with, and driven by community services (CC2H) re-procurement. As such, outline model will be included in the CC2H procurement and signal Essex wide work underway.
A proposal has been put forward for mapping all three therapies concurrently (OT and physio alongside SaLT) – workshop due to be held in Dec with Essex partners to make a decision on this.
Working with local NEE providers to keep them informed and to identify project leads within their organisations.
CYP 20-07 Suffolk Community Paediatrics
At risk
Phase 2 review underway focussed on three areas: nursing, medical and therapies. Nursing is the first area being looked as to develop a future model and options for provision with a deadline of end of Dec 21 for this to be set out. Currently on track to meet this deadline. Future milestones for medical and therapies being scoped.
CYP 20-04 Suffolk SLT
Late
Steering group re-established to update on progress after a pause due to COVID 19 pandemic. Language link and speechlink training and sign up from schools almost completed - only 6 schools in Waveney have failed to sign up. Recruitment is completed for the expanded service and overall the service currently has only six vacancies predominately down to maternity leave. Service specification should be ready for sign off and varied in to the main contract by the end of the calendar year.

Children and Young People’s Programme DashboardProject RAG Update/Action Required in Red or Amber Project RAG
Update/Action Required in Red or Amber
CYP 20-02 Suffolk CAMHS
On Track
1. CYP Transformation – SuffolkCYP model development on track. Feedback from the public and workforce engagement, clinical reference group (8 Dec), clinical senate (11 Nov), and the work in the Early Adopter Areas (Haverhill, Ipswich and Coastal) will continue to inform development of the model. However, further work is also needed and a number of sub-task & finish groups including demand & capacity have been established that will deliver additional work to meet the deadline of full development of the CYPF pathway by the end of December 2020.
2. CrisisThe CYP Crisis Task & Finish Group has been established to oversee and support the delivery of the following:• The delivery of the CYP elements of the all age crisis business case – First Response/111 option 2, Assessment and brief intervention, Core 24
psychiatric liaison at both West Suffolk and ESNEFT hospitals. • The mobilisation of the new CYP Self Harm Pilot which provides an NSFT clinical assessment and then therapeutic interventions delivered by
Suffolk County Council and 4YP - pilot began on 5 October 2020 to complete in June 2021• The mobilisation of the new multi-agency CYP Crisis Outreach/Home Treatment service.
3. Current servicesBusiness case development is ongoing for CYP Eating Disorders and Personality Disorders due to be available for decision Dec/Jan including elements of support that VCS organisations can provide.
Discussion about how the current MIND step down service might be extended to support CYP as part of the all age community approach.
Additional family support capacity commissioned to March 2021 with Barnardos, Annie Clements, Suffolk Family Carers and Homestart
4. CYP Coproduction Network
We have created a new CYP Coproduction Network, that brings together a range of partners who will support the creation, development and delivery of all CYP mental health involvement work. Recent work includes explaining how children and young people’s mental health services are being transformed through a LIVE engagement event with young people and the co-produced film. Young people, from our CAT Network and Young Adult Carers, designed the video to look like a board game. It has lots of doors to highlight the ‘no wrong door’ philosophy and their avatars change into real people at the end to demonstrate how you can feel much more yourself once you’ve had support with your mental health.
CYP 20-06 Suffolk Neuro Developmental On Track
The project is broken down into three key areas of work:
1.Support offer
Procurement of support offer due out to EOI in W/C 9 November 2020. Aim for service start on 01/04/21 to allow for procurement process to conclude.
2. Coordination function
Confirmed that EWB Hub is preferred option to host the Coordination Function (CF). No alternatives identified by members but further work underway to set out how this would operate.
3. Clinical pathway
Task and finish group set up with clinical leads. 0-18 service to start but planning for 18-25 to begin at go live. But support offer will be 0-25
Triage Panel set up to look at that particular part of pathway, main points agreed:• Pathway to be front loaded, senior
clinicians at triage panel, to include CAMHS, Paed Consultant, Ed Psych, Social care, all with requisite experience
• To include all suspected NDD or behaviour that challenges
• Referral form drafted
Next meeting to look at process from triage to assessment and discharge

14
Cambridge UHFT – Month 6 – Top 10 Performance Items
1. Endoscopy rooms reopened w/c 2nd November and increased insourcing and Saturday working
2. CUH guide prioritisation of cases to stratify patients on both clinical risk and vulnerability via EPIC amendments
3. All outpatients departments have opened with some capacity. CUH exploring ways to maximise use of the estate and room allocations has been centralised.
1. Covid has had a significant impact on RTT with a continual increase of patients currently breaching 52 weeks. An additional 419 in September
2. >6wk diagnostic wait times total 811 for Suffolk patients (2.4% of total at CUH)
3. As the data for CUH is obtained from a different source this is currently being validated
4. CUH are a trial site for A&E, hence no data
ISSUES:
ACTIONS:
(*) CUHFT figures for Elective are based on all Suffolk patients attending CUHFT until national figures are published on Thursday, after which we shall attempt to get these revised figures out ASAP after this time.
Elective StandardThis
Month
Last
MonthAssurance SPC Trend
18 wk RTT Incomplete(N) 92.0% 59.9% 53.0%Consistently
failed
Special cause
variation: Low
RTT 52 Week Waiters(N) 0 1,193 774Both met and
failed
Special cause
variation: High
18 wk RTT Incomplete(N) 34,769 33,312 TBD - Trend or CCV
Diagnostic test waiting times(N) 1.0% 56.7% 59.6%Both met and
failed
Special cause
variation: High
Cancer StandardThis
Month
Last
MonthAssurance SPC Trend
All Cancer 2 week wait(N) 93.0% 93.6% 92.7%Both met and
failedTBD - Trend or CCV
Two week wait for breast symptoms(N) 93.0% 93.0% 97.4%Both met and
failedTBD - Trend or CCV
Cancer 31 day wait: Percentage receiving 1st
treatment within one month of cancer diagnosis
(N)
96.0% 84.5% 87.6%Both met and
failedTBD - Trend or CCV
Cancer 62 day wait: urgent GP referral for
suspected cancer(N)85.0% 76.5% 80.2%
Both met and
failedTBD - Trend or CCV
A&E StandardThis
Month
Last
MonthAssurance SPC Trend
A&E 4 Hour Standard(N) 95.0% 0 0No Data
CollectedPart of A&E Pilot

Norfo
lk an
d Suff
olk Fo
unda
tion T
rust
(NSF
T) (S
uffolk
servi
ces)
CCG Quality Assurance Rating: Level 3 (→ from last month) CQC Rating: 2020: Requires improvement
Month updated: Nov-20 (Sep-20 data) QSG surveillance Rating: Enhanced
Issues / Concerns / Comments Actions / Progress
1. CCGs have sought assurance around eating disorder service performance and improvement.
2. Waiting times and patients on caseload with no recorded activity for 9 months identified as a concern across all services within NSFT.
3. Ensuring quality oversight of NSFT as a provider in special measures.
4. The CCGs have noted the continuation of positive outcomes in relation to LD inpatient numbers for Suffolk – there
has been no LD admissions since before Christmas 2019, an achievement recognised by both the regional system and nationally by NHSE/I.
5. SEND written statement of action progress and update in relation to mental health services
6. CCGs have sought assurance around training compliance, specifically around Basic Life Support, Immediate Life Support and PMA Physical Intervention - the CCGs have continued to see low levels of compliance reported in each of these areas across East and West care groups.
7. Concerns have been raised over NSFT progression of outstanding section 42 enquiries where the organisation had been delegated the lead role for the enquiries by MASH. Through CCG, NSFT and ACS and Police Safeguarding Leads working together, this list has been brought down to a more manageable number of enquiries the trust can continue to progress. There has been an increase in numbers of children and young people requiring use of 136 suites. This is impacting on adults who cannot access 136 suites as they are full. This brings risks for adults whereby police are having to keep them safe in police cells.
8. NSFT are an early adopter of the Patient Safety Incident Response Framework (PSIRF), which will replace the NHS Serious Incident Framework 2015.
9. Current vaccination rate is 44.08% (80% expected by March 2021)
1. There is now an all age improvement board in place with NSFT and key stakeholders. The CCGs are awaiting the
identified staffing needs to deliver the service and are expecting to receive request for further investment. The reconciliation of national data to local data KPI reporting remains an issue. This is because national data is a 12-month rolling position versus locally a 3-month rolling position. Work is underway with contracting colleagues to understand data reconciliation and to provide one complete picture of performance. The service director from NSFT is now the project lead for ensuring progress is made.
2. The CCG has sought clarity regarding the range and extent of services affected and a deep dive was requested at the
October QCPM. The deep dive has provided assurance regarding who these patients are and the reasons for this. This s picked up by the care groups as part of their service user tracking process (SUTL) so there is also assurance around the clinical governance.
3. The QA process was due to take place during October and November. This process will involve a colleague from HPFT
in an agreed collaboration of peer review as agreed with NHSE quality leads. This will build upon the outcomes from the CCGs 2019 QA programme of work and aim to monitor level of improvement made, helping to identify areas of concern/further focus. CQC are currently inspecting NSFT so QA reviews will be delayed until December/ January 20/21.
4. Discussions have begun to explore how inpatient funding can be converted into increased community provision to build resilience. This is being picked up as part of the priority 4 workstream.
5. NSFT have now allocated their lead nurse as their designated SEND lead and the CCGs are starting to see improvements, particularly in terms of better engagement with the SEND programme of work. The CCGs have committed to review all of their SEND KPI’s with providers to ensure the right outcomes are being measured. Stakeholder feedback
continues to be reviewed and monitored to ensure MH services are delivered in a timely and safe way as part of the SEND programme of work.
6. This is being monitored through QCPM and will continue to be an area of increased focus via the QA revisits.
7. Senior CCG, NSFT and ACS Leads joined Designate/Safeguarding Leads monthly meetings. Weekly meetings ACS/NSFT/CCG to address risks to patients in outstanding enquiries. Safeguarding Partnership Board stepped into chair multi agency meetings to develop a Standard Operational Policy to ensure, moving forward, NSFT are allocated section 42 enquiries the trust can appropriately lead and progress. Joint working with police to establish joined up approaches whereby police will work in partnership with NSFT on section 42 enquiries. Monthly Meetings set up with CCG/MASH/NSFT to continue monitoring allocation of section 42 enquiries to the trust. CCG Transformation Role to commence October. The purpose of this role is to improve working relationships between MASH health and NHS provider Safeguarding teams that will lead to improved partnership working. Meeting planned to look at and understand why there has been an increase in children and young people referrals.
8. As part of the new framework all providers have to develop a Patient Safety Incident Response Plan (PSIRP). This explains how the organisation will respond to its incidents in order to maintain safety. NSFT will be taking their PSIRP to their Board in November 2020. The PSIRP will then come to the CCG for sign off, with an anticipated start date 1 December 2020 for the new framework.
9. NSFT demonstrates good IPC assurance and reporting processes are in place. Each service presents their compliance with the annual plan at the IPAC committee. The Board Assurance Framework (BAF) reflects latest guidance and gives assurance with very few identified gaps.
NSFT – Month 6 YTD – Quality Plan on a Page

16
Suffolk CCGs at NSFT – Month 6 Year to Date – Top 10 Performance Items
1. NSFT proactively contacting all service users, under harm review protocols: weekly SUTL in place:. Resuming F2F contact wherever possible,: covid restrictions have meant reduced opportunity for baseline physical health checks (BP monitoring) prior to medication initiation: Shared care protocols under development
2. Development of age inclusive business case ongoing3. Benchmarking shows CCGs perform well - no long staged waits
1. RTT/RTA rates static or improving: however long waits on incomplete pathways ,and active caseload with no contact for 9 months, predominantly in ADHD/Adult autism services:
2. Urgent ED at 55% for last three months: Routine ED has improved over the last year compared to historic, but remains non compliant and waiting lists are beginning to grow across the board
3. Recovery rates remain good in IAPT service
ISSUES:
ACTIONS:

SNEE Mental Health and Learning Disabilities Programme DashboardOverall
Programme RAG
Apr-20 May-20 Jun-20 Jul-20 Aug-20 Sep-20 Oct-20 Nov-20 Dec-20 Jan-21 Feb-21 Mar-21
On Track On Track At Risk At Risk At Risk
Programme Status: At risk due to slippage on some of the projects within the programme.
Project RAG Update/Action Required in Red or Amber Project RAG Update/Action Required in Red or Amber
SMI Physical Health -
At Risk
20/21 Q2 data for physical health checks for people with SMI (60% target: NEECCG: 19%; WSCCG: 21.5%; I&ESCCG: 39.5%.)
Suffolk:Proposal in development between NSFT SMI Physical Health Team and Suffolk User Forum to incorporate VCS peer support offer into SMI pathway.SMI leads now identified in all GP practices in West Suffolk.Review and cleanse of SMI registers underway across E&W Suffolk.
North East Essex:Action plan in place for NEE to address performance. Review of registers planned in Q3 in line with Suffolk's approach.
GPPC will focus on all surgeries under 30% completion for the core six checks to resolve mass data validity issue. Working with surgeries to clarify the parameters of the core checks with clinicians, what can be done remotely, and taking advantage of when patients come in for routine meds reviews etc.
IAPT Wellbeing At Risk
Suffolk IAPT:Suffolk Wellbeing IAPT expansion business case to commission activity up to 30% due to be presented by NSFT at the Suffolk Mental Health Alliance Board 14/12/20.
Risk identified of not achieving 25% access rate by March 2021 due to impact on referrals of Covid-19. Following recent CCG deep dive session, a number of actions were agreed including benchmarking of local performance to help support achievement.
Gynae Oncology and MSK wellbeing pathways in development in line with Long Term Conditions (LTC) plan. Conversations underway with ESNEFT and WSFT to develop wellbeing offer to elective long waiters as part of NHSE Phase 3 Recovery. Gastro and Cancer are the final pathways in development in year two of the planned LTC work.
NEE IAPT:Planning for mobilisation of new service with EPUT has commenced for going live on 1/4/21. Plans in progress for end of November to provide modelling to achieve the increased access targets of up to 30% intervention rate and supporting business case. As part of the new specification, further LTC pathways to be implemented as specified in the contract. Living Life to the Full (LLTTF) has stopped as agreed to proceed with 'Theory for You' EPUT model. Continued engagement with incumbent provider on reducing backlogs and aspiring to achieve national access targets et al. FYE access forecast to be c18-20% with backlogs slightly increasing and contracts team looking at mitigation.
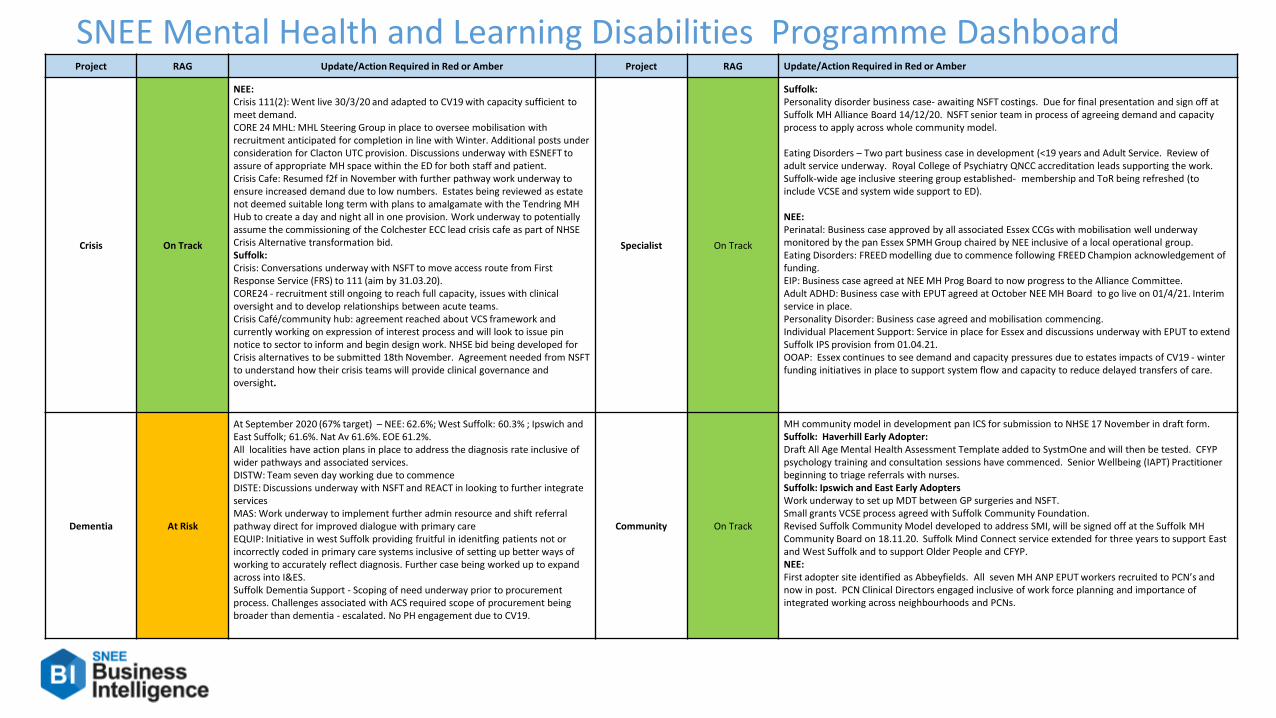
SNEE Mental Health and Learning Disabilities Programme DashboardProject RAG Update/Action Required in Red or Amber Project RAG Update/Action Required in Red or Amber
Crisis On Track
NEE:Crisis 111(2): Went live 30/3/20 and adapted to CV19 with capacity sufficient to meet demand.CORE 24 MHL: MHL Steering Group in place to oversee mobilisation with recruitment anticipated for completion in line with Winter. Additional posts under consideration for Clacton UTC provision. Discussions underway with ESNEFT to assure of appropriate MH space within the ED for both staff and patient.Crisis Cafe: Resumed f2f in November with further pathway work underway to ensure increased demand due to low numbers. Estates being reviewed as estate not deemed suitable long term with plans to amalgamate with the Tendring MH Hub to create a day and night all in one provision. Work underway to potentially assume the commissioning of the Colchester ECC lead crisis cafe as part of NHSE Crisis Alternative transformation bid. Suffolk:Crisis: Conversations underway with NSFT to move access route from First Response Service (FRS) to 111 (aim by 31.03.20). CORE24 - recruitment still ongoing to reach full capacity, issues with clinical oversight and to develop relationships between acute teams.Crisis Café/community hub: agreement reached about VCS framework and currently working on expression of interest process and will look to issue pin notice to sector to inform and begin design work. NHSE bid being developed for Crisis alternatives to be submitted 18th November. Agreement needed from NSFT to understand how their crisis teams will provide clinical governance and oversight.
Specialist On Track
Suffolk:Personality disorder business case- awaiting NSFT costings. Due for final presentation and sign off at Suffolk MH Alliance Board 14/12/20. NSFT senior team in process of agreeing demand and capacity process to apply across whole community model.
Eating Disorders – Two part business case in development (<19 years and Adult Service. Review of adult service underway. Royal College of Psychiatry QNCC accreditation leads supporting the work. Suffolk-wide age inclusive steering group established- membership and ToR being refreshed (to include VCSE and system wide support to ED).
NEE: Perinatal: Business case approved by all associated Essex CCGs with mobilisation well underway monitored by the pan Essex SPMH Group chaired by NEE inclusive of a local operational group. Eating Disorders: FREED modelling due to commence following FREED Champion acknowledgement of funding.EIP: Business case agreed at NEE MH Prog Board to now progress to the Alliance Committee. Adult ADHD: Business case with EPUT agreed at October NEE MH Board to go live on 01/4/21. Interim service in place.Personality Disorder: Business case agreed and mobilisation commencing. Individual Placement Support: Service in place for Essex and discussions underway with EPUT to extend Suffolk IPS provision from 01.04.21.OOAP: Essex continues to see demand and capacity pressures due to estates impacts of CV19 - winter funding initiatives in place to support system flow and capacity to reduce delayed transfers of care.
Dementia At Risk
At September 2020 (67% target) – NEE: 62.6%; West Suffolk: 60.3% ; Ipswich and East Suffolk; 61.6%. Nat Av 61.6%. EOE 61.2%.All localities have action plans in place to address the diagnosis rate inclusive of wider pathways and associated services.DISTW: Team seven day working due to commenceDISTE: Discussions underway with NSFT and REACT in looking to further integrate servicesMAS: Work underway to implement further admin resource and shift referral pathway direct for improved dialogue with primary careEQUIP: Initiative in west Suffolk providing fruitful in idenitfing patients not or incorrectly coded in primary care systems inclusive of setting up better ways of working to accurately reflect diagnosis. Further case being worked up to expand across into I&ES.Suffolk Dementia Support - Scoping of need underway prior to procurement process. Challenges associated with ACS required scope of procurement being broader than dementia - escalated. No PH engagement due to CV19.
Community On Track
MH community model in development pan ICS for submission to NHSE 17 November in draft form. Suffolk: Haverhill Early Adopter:Draft All Age Mental Health Assessment Template added to SystmOne and will then be tested. CFYP psychology training and consultation sessions have commenced. Senior Wellbeing (IAPT) Practitioner beginning to triage referrals with nurses. Suffolk: Ipswich and East Early AdoptersWork underway to set up MDT between GP surgeries and NSFT.Small grants VCSE process agreed with Suffolk Community Foundation. Revised Suffolk Community Model developed to address SMI, will be signed off at the Suffolk MH Community Board on 18.11.20. Suffolk Mind Connect service extended for three years to support East and West Suffolk and to support Older People and CFYP. NEE: First adopter site identified as Abbeyfields. All seven MH ANP EPUT workers recruited to PCN’s and now in post. PCN Clinical Directors engaged inclusive of work force planning and importance of integrated working across neighbourhoods and PCNs.

Prac
tice P
lus G
roup
CCG Quality Assurance
Rating: Level 2 (→ from last month) CQC Rating: Care UK 2017: Good
Month updated: Nov-20 (Sep-20 data) QSG surveillance Rating: Routine
Key Issues / Concerns / Comments Actions / Progress
1. Performance for KPIs specific to call handler response time has
dropped to 66.54 % for September. A deteriorating position from 85.47% in August and 92.6% in July (target 95%).
2. 999 category 3 and 4 ambulance validations are at 59.41% for September. A deteriorating position from 66.06% in August and 72.17% in July (target 80%).
3. Full staff audits have resumed with some backlog following reduced auditing in CV-19 emergency.
4. Improved reporting, specifically in relation to the OOH service in Suffolk (this element of the service is subcontracted).
5. Work in relation to the star (*) line, used to fast track health care professional callers to a clinician in the CAS has progressed. A pilot for 25 care homes in Suffolk 1 will go live Oct 2020. The aim is to roll this out into NEE following an evaluation period.
6. Patient experience data remains good quality. Complaints have been investigated within the required timeframe and evidence learning and appropriate actions where indicated. There have been no SI for this reporting period. Mechanisms in place regarding the health and wellbeing of staff, with focus on resilience given response required to manage COVID.
1. Scrutiny remains in place for assurance regarding performance. Tail
breach narrative reports are requested where the service has not responded to the patient in the allocated disposition time. Tail breaches for September have been reviewed.
2. Assurance sought at QCPMs. CCG colleagues also joined 111/EEAST call review meetings. A very positive forum with a multi-provider approach to QI.
3. New starters and those with previous alerts were maintained throughout the period. Backlog is anticipated to be completed by October 2020.
4. August & Sept. data evidences a significant improvement in
subcontractors reporting with evidence of improved mandatory training and HR compliance. Ongoing monitoring via QCPM performance pack.
5. Patient safety quality metrics will be monitored through the contract
reporting requirements. Outcome measures developed and will be monitored and reviewed by the Project Group.
6. Scrutiny remains in place via QCPMs. Quality data shared at NHSE Regional Clinical Quality Assurance Group. A local Clinical Quality Assurance Group (CQAG) has been introduced to provide further opportunity for clinical quality oversight, assurance and quality improvement.
Practice Plus Group – Month 6 YTD – Quality Plan on a Page

20
Project RAG Update/Action Required
111 Online – CPCS Emergency Prescription Completed Completed.
MIC Direct Booking Completed Completed.
GP+ Direct Booking On Track Planned go live - 1st December 2020
GP Connect - Records Viewers Completed Completed.
ED ITK Messages On Track This has been activated for WSH. We are awaiting Endpoints for ESNEFT hospitals. This is on track for 1st December 2020
111 Online – CPCS Minor Injuries Completed. Completed.
GP OOH Direct Booking On Track Currently aiming to implement for April 2021
Non-Clinical Care Homes Line to the CAS Completed Completed.
Option 2 Mental Health Crisis Line Changes to 111.
At Risk Implementation delayed due to COVID – Planned to go live in December 2020
Beautiful Information Project Completed. Completed.
Border re-alignment within Suffolk At Risk Currently trying to engage with Norfolk and Waveney CCG to realign borders with Suffolk, currently Suffolk take 1,000 calls a months of Waveney patients and N&W take 250 SNEE calls.
Multimedia capability within the IUC. Completed. Practice Plus Group and SGPF now have access to remote consultation software.
Practice Plus Group Urgent Care - Transformation Summary

Non-
Emer
genc
y Pati
ent T
rans
port – (
E-Ze
c Med
ical)
CCG Quality Assurance Rating: Level 2 (→ from last month) CQC Rating: Report Pending
Month updated: Nov-20 (Sep-20 data) QSG surveillance Rating: Routine
Issues / Concerns / Comments Actions / Progress
1. September data shows KPIs for inbound out-patient journeys at: 65.92%
(70.5) and outbound (outpatient) journeys at 85.87% (92.6) Outbound discharge and transfer journeys at 73.64% (77.45)
2. A recruitment strategy is ongoing and has been effective through NHS jobs website. The current recruitment strategy aims to reduce reliance on bank roles. There are currently 11.75 wte. Ambulance Care Assistant (ACA)posts vacant. There is an induction training w/c 2nd November, with 10 ACAs enrolled.
3. 41 (21) staff appraisals are outstanding. E-Zec Medical have an appraisal
action plan in place to address this, which states they will be completed by 9th November 2020.
4. There were 6 (7) direct complaints during September and 12 (3) incidents
raised via the 2 acute trusts. E-Zec reported a further 18 (8) incidents, but no serious incidents. The CCG is aware of a serious incident which occurred in October and has received the 3-day report.
5. The CCG is working with E-Zec medical to support the collection/analysis of more patient feedback. E-Zec Medical currently survey 40 patients per month.
1. The figures show a slight deterioration for the third consecutive month. The
requisite social distancing has reduced the passenger capacity for each vehicle.
2. The CCGs have requested a more comprehensive workforce report and data.
There have been some improvements already. The CCGs Contracts and Clinical Quality Teams will resume work with E-Zec to improve the reporting requirements, especially in relation to workforce data.
3. The CCG have asked for more detail regarding the recovery plan for staff appraisals and this will be discussed at the November contract meeting.
4. The CCG continues to support E-Zec Medical to ensure there is assurance of appropriate learning from complaints, incidents and serious incidents.
5. The CCG would like more data collected and collated for analysis regarding patient experience and engagement.
E-Zec Medical – Month 6 YTD – Quality Plan on a Page

22
E-Zec PTS – Month 6 – Top Performance ItemsISSUES:1. Patients arriving between 5 and 60 minutes for planned
outpatient appointments continues to be below the target set. Patients arriving between 0 and 60 minutes (on time) is currently sitting at 77.6%, a drop of 5% from last month.
2. Outbound discharge performance has declined this month which is the dedicated vehicles supported by E-zec and the acutes. 93.1% of patients were collected within 2 hours.
3. Covid-19 restrictions around social distancing etc. remains, impacting available resources.
ACTIONS:1. Recruitment is ongoing to reach establishment and enhance
resilience for winter and Covid-19 impact. A further 9 road based staff have joined w/c 9/11 and 3rd party is being utilised to support.
2. Any capacity issues for discharges and outpatients continue to be worked through with the acute trusts to achieve the best outcomes for patients.
3. SuNEE PTS meetings are happening fortnightly recognising the revised national guidance and increase in Covid activity.
KPI Description StandardThis
Month
Last
MonthAssurance SPC Trend
In-bound - % Service Users arriving between 5
and 60 mins prior to their booked appointment
time.
95% 65.9% 70.5%Consistently
failedTBD - Trend or CCV
Journey Times - % Service Users on the vehicle
between 0 and 90 minutes.90.0% 95.6% 95.7%
Both met and
failedTBD - Trend or CCV
Journey Times - % Service Users in the IESCCG &
WSCCG footprint on vehicle between 0 and 60
min.
85.0% 88.1% 89.3%Consistently
failed
Special cause
variation: High
Outbound OP Journeys - % Service Users waiting
no more than 60 mins after booked collection
time.
95.0% 85.9% 92.7%Consistently
failedTBD - Trend or CCV
Outbound Discharge - % Service Users waiting
less than 60 mins after their booked collection
time.
95.0% 73.6% 77.5%Consistently
failedTBD - Trend or CCV
Unplanned short notice booking - % patients
collected in a 4 hr timeframe from initial request.90.0% 98.4% 99.6% Consistently met TBD - Trend or CCV
Unplanned short notice booking in hours service -
% Short Notice Journeys Honoured by the
Provider.
100.0% 99.4% 99.9%Both met and
failedTBD - Trend or CCV
End of Life Trfs from hospital to choice of
placement - % met in 2 hours of the original
request.
95.0% 100.0% 94.1%Both met and
failedTBD - Trend or CCV
Front Door and Assessment Area -% Service
Users collected less than 60 minutes after init
contact
90.0% 71.7% 76.9%Consistently
failedTBD - Trend or CCV
Call Handling - % Calls received by the patient line
answered within 3 minutes95.0% 99.7% 99.1%
Both met and
failedTBD - Trend or CCV

East
of E
ngla
nd A
mbu
lanc
e Se
rvic
e Tr
ust (
EEAS
T) (R
egio
nal)
CCG Quality Assurance Rating: Level 2 (→ last month) CQC Rating: 2019: Requires Improvement
Month updated: Nov-20 (Sep-20 Data) QSG surveillance Rating: Routine
Key Issues / Concerns / Comments Actions / Progress
1. CQC action plan, CQC oversight and system responses.
2. CCG IPC assurance and COVID-19: The BAF reflects the latest national guidance. The Trust’s Track and Trace system
is robust. The Flu campaign is operational and current vaccination rate is 55.72% (80% expected by March 2021)
3. The CCG received whistleblowing concerns regarding safety and quality at EEAST.
1. On the 30 September the CQC published their report following a well led inspection undertaken in June. On the basis of this inspection CQC have recommended the Trust be placed in special measures. The CQC issued an urgent notice, under Section 31 of the Health and Social Care Act 2008, on the 29 July 2020, to impose conditions on the trust registration as a service provider in respect of the regulated activities: Treatment of disease, disorder or injury and Transport services, triage and medical advice provided remotely. Some concerns raised relate to health and well-being of staff, leadership and culture and fundamental issues with the quality of HR function. The CQC undertook further enforcement and issued a warning notice, on the 28 August 2020. This identified specific areas that the trust must improve and set a date for compliance as 28 November 2020. A risk summit took place during September and a ten-point plan for sustained improvement has been completed. In order to track progress a monthly Oversight and Assurance Group has been established.
Weekly senior leader meetings with EEAST Executive Lead for Safeguarding. Designate pre meets with EEAST Safeguarding Leads to agree agendas and actions for EEAST Safeguarding Committee meetings and allow CCG Safeguarding leads to read and digest information and reports provided by the Trust. Monthly attendance of Suffolk CCG Designates at EEAST Safeguarding Committee Meetings. Engagement in EEAST recruitment processes and interview panel for new EEAST Safeguarding Lead. Regular meetings between regional designate safeguarding leads, led by Suffolk. Regular meetings with EEAST to provide support in developing robust safeguarding and HR policies. These meetings are supported by regional CCG safeguarding colleagues and NHSE/. DBS Action Plan is discussed as agenda item with EEAST within their CCG QCPM Meetings.
The Suffolk CCGs, as lead commissioner for EEAST, are working on commissioning improvements to promote a ‘system
first’ approach. This is seeking, amongst other things, a unified oversight and support for EEAST between commissioners,
NHSE/I and CQC to facilitate a system wide approach to identifying problems, joint ownership and delivery of the solutions.
2. Flu uptake and provision of PPE supplies is included within the EEAST Winter Plan. An update on Flu vaccination was
provided at October PQRM; there are no concerns with EEAST in relation to Flu Uptake at present. An update on EEAST preparedness for COVID-19 vaccine has been request for December PQRM. The most recent Infection Prevention and Control Group meeting was held on 29.09.20. The Board Assurance Framework reflects latest guidance and give assurance. All audit types achieved an average of above 90%. The cleaning schedules have been maintained with high compliance. The infection control knowledge audits achieved 99%.
3. In response, the CCG quality team arranged a round table meeting with EEAST which included the EEAST Medical Director, HR lead and quality lead. The CCG Director of Corporate Services also attended. The CCG was assured EEAST were making necessary improvements in relation to the Serious Incident (SI) process and their HR policies. EEAST agreed to share evidence of further improvements they are currently undertaking to address the issues raised.
EEAST Emergency Ambulance – Month 6 YTD – Quality Page

East
of En
gland
Amb
ulanc
e Serv
ice Tr
ust (E
EAST
) (S
uffolk
and N
orth
East
Esse
x STP
area
) CCG Quality Assurance
Rating: Level 2 (→ from last month) CQC Rating: 2019: Requires improvement
Month updated: Nov-20 (Sep-20 data) QSG surveillance Rating: Routine
Issues / Concerns / Comments Actions / Progress
Headlines for EEAST as of 03-09-2020
• Staff in post numbers are much closer to target in SNEE compared to 2019/20. • C1 Driving Licence Training programme has been prioritised to ensure all new staff in front line roles can be deployed as required. • Category 1 response times have improved in July, with main challenge being improving Category 2 further. • Rapid Response Vehicle locations remain under review to optimise response times for higher acuity calls.
STP SNEE
C1M C1 90th C2M C2 90th C3 90th C4 90th
Standard 7 Mins 15 Mins 18 Mins 40 Mins 2 Hrs 3 hrs
Aug - 20 00.07.48 00.15.11 00.24.36 00.51.22 02.38.35 03.10.19
Year to Date 00.08.00 00.15.18 00.23.30 00.48.48 02.16.17 03.16.48
EEAST Emergency Ambulance – Month 6 YTD – Quality Page

25
EEAST Ambulance - WSCCG - Month 6 - Key Performance ItemsISSUES:1. Workforce - Local area skill mix inbalance. 2. Conveyance rates to A+E beginning to increase and are returning to
normal levels of conveyances, pressure being added to A+E departments.
3. Hand over delays becoming an issue.
1. Workforce recruitment plan is in place and this continues to be monitored on bi-weekly ICS calls with EEAST. Recruitment is currently good at technician level.
2. 111 enhanced clinical validation of C3/4 calls. Currently validating 60% of calls and redirecting 75%. CCG have set up programme with 111 for ambulance validation to improve this position.
3. HALOs have been agreed at hospital site 12/7 until end of October.
ACTIONS:
Elective StandardThis
Month
Last
MonthAssurance SPC Trend
Category 1 - 7 min mean response time(L) 00:07:00 00:08:34 00:07:48Consistently
failedTBD - Trend or CCV
Category 1T - mean response time(L) 00:11:07 00:10:56 TBD - Trend or CCV
Category 2 - 18 min mean response time(L) 00:18:00 00:21:31 00:18:35Both met and
failedTBD - Trend or CCV
Category 3 - 120 min 90th centile response
time(L)02:00:00 02:18:26 01:27:20
Both met and
failedTBD - Trend or CCV
Hear & Treat Rate 7.9% 7.1% No Data
Conveyed to ED % 52.3% 54.8% No Data
LQR8 Time to Answer (99th Centile secs)(L) 60 39 28Both met and
failedTBD - Trend or CCV
LQR3 - 90th centile - Stroke for Ambulance
Patients (Time from call to hospital arrival)01:57 01:42 No Data
LQR1 - ROSC at time of arrival at Hospital 30.0% 25.6% 29.3%Both met and
failedTBD - Trend or CCV
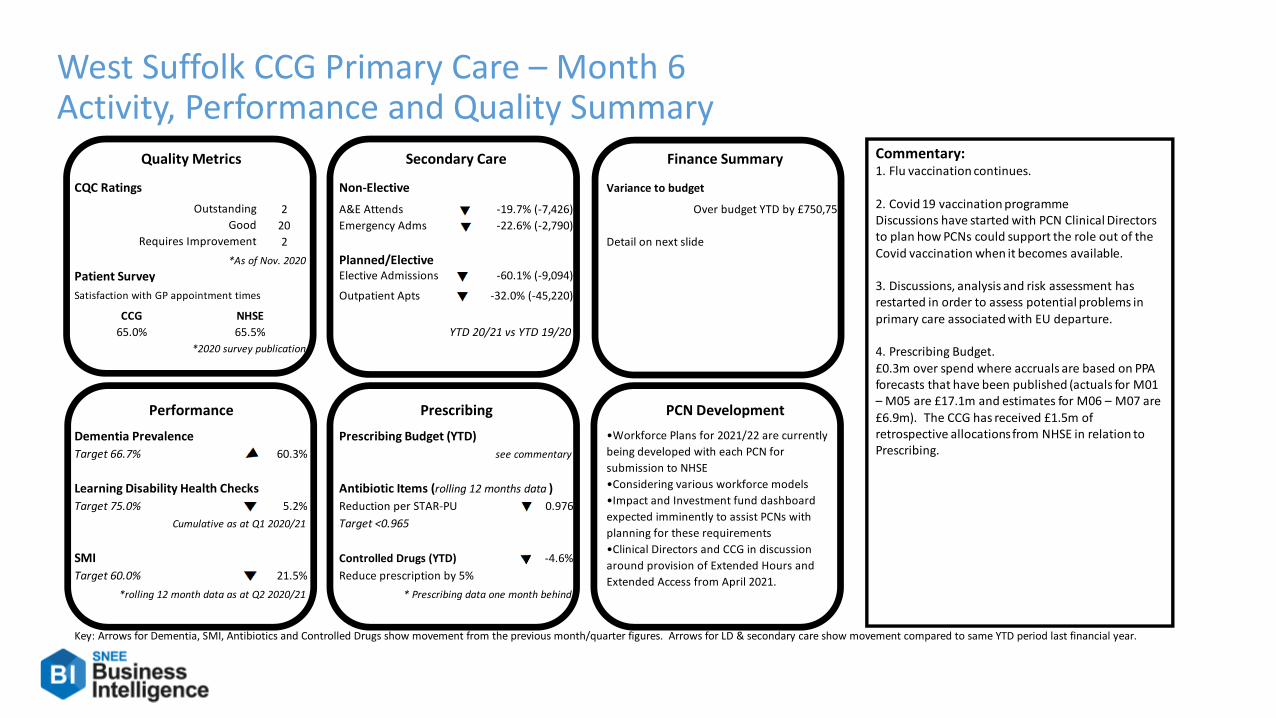
DRAFT26
West Suffolk CCG Primary Care – Month 6Activity, Performance and Quality Summary
CQC Ratings Non-Elective Variance to budget
2 A&E Attends -19.7% (-7,426) Over budget YTD by £750,752
20 Emergency Adms -22.6% (-2,790)
2 Detail on next slide
*As of Nov. 2020 Planned/ElectivePatient Survey Elective Admissions -60.1% (-9,094)
Satisfaction with GP appointment times Outpatient Apts -32.0% (-45,220)
CCG
65.0%
*2020 survey publication
Dementia Prevalence Prescribing Budget (YTD)
Target 66.7% 60.3% see commentary
Learning Disability Health Checks Antibiotic Items (rolling 12 months data )
Target 75.0% 5.2% Reduction per STAR-PU 0.976
Cumulative as at Q1 2020/21 Target <0.965
SMI Controlled Drugs (YTD) -4.6%
Target 60.0% 21.5% Reduce prescription by 5%
*rolling 12 month data as at Q2 2020/21 * Prescribing data one month behind
Key: Arrows for Dementia, SMI, Antibiotics and Controlled Drugs show movement from the previous month/quarter figures. Arrows for LD & secondary care show movement compared to same YTD period last financial year.
•Workforce Plans for 2021/22 are currently
being developed with each PCN for
submission to NHSE
•Considering various workforce models
•Impact and Investment fund dashboard
expected imminently to assist PCNs with
planning for these requirements
•Clinical Directors and CCG in discussion
around provision of Extended Hours and
Extended Access from April 2021.
Quality Metrics
Outstanding
Good
Requires Improvement
NHSE
65.5%
Secondary Care
YTD 20/21 vs YTD 19/20
Performance Prescribing
Finance Summary
PCN Development
Commentary:1. Flu vaccination continues.
2. Covid 19 vaccination programmeDiscussions have started with PCN Clinical Directors to plan how PCNs could support the role out of the Covid vaccination when it becomes available.
3. Discussions, analysis and risk assessment hasrestarted in order to assess potential problems in
primary care associated with EU departure.
4. Prescribing Budget.£0.3m over spend where accruals are based on PPA forecasts that have been published (actuals for M01 – M05 are £17.1m and estimates for M06 – M07 are £6.9m). The CCG has received £1.5m of retrospective allocations from NHSE in relation to Prescribing.

27
West Suffolk CCG Finance Report M7 October 2020

28
West Suffolk CCG Finance Report M07 Forecast – October 2020

29
West Suffolk CCG Finance Commentary M07 – October 2020The CCG has reported a deficit position for M07 in line with the latest M07-12 plan submission.
The CCG anticipates receiving the retrospective allocation of £2.6m for M06 costs in M08 – this will fully cover both the COVID and non-COVID pressures as at M06. The expectation is that, following the assurance process of the M06 retrospective adjustment, CCGs will breakeven across all areas of programme categories of reporting (e.g. Acute, Mental Health etc) up to M06.
In addition to the above, the CCG anticipates £0.5m for the Hospital Discharge Programme (HDP) and a small amount for Flu costs for M07.
The year to date COVID and HDP costs at M07 are £7.4m. See breakdown on next page.
The forecast is in line with the M07-12 plan once the above retrospective top-ups have been received.
Key variances for M07 are:
Continuing Healthcare shows an over spend due to costs associated with HDP.
Mental Health shows a slight increase in SCC Shared costs.
Acute increase in spend on insulin pumps and payments to independent providers.
Primary Care Delegated Commissioning over spend against plan as inflation on contracts with PMS practices within the CCG exceeds the inflationary uplift included in the allocation.
Primary Care Includes release of contingency budget to offset the Delegated Commissioning pressure above. Overspend on Prescribing of £0.3m for the year to date – it is anticipated that this will be offset by the M06 retrospective allocation.

30
West Suffolk CCG Finance COVID-19 Analysis M07 - October 2020
COVID SPEND YTDBank
Holidays
Hospital
Discharge
Programme
Other
Covid-19
Remote
Managemen
t of Patients
NHS 111
Additional
Capacity
National
Procuremen
t Areas
Enhanced PTS
After Care
and
Support
Costs
Support for
Stay at
Home
Models
GP SMS
Additional
Costs
Flu Vaccine NHS Block Total
£'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000
Acute 0 0 10 0 0 0 0 0 0 0 0 1,145 1,155
Mental Health 0 0 0 106 0 0 0 0 155 0 0 0 260
Community 0 1,627 0 169 0 1 0 0 11 0 0 0 1,808
Continuing Care 0 2,229 18 0 0 0 0 0 0 0 0 0 2,248
Primary Care 501 0 26 626 47 40 0 5 0 41 1 0 1,287
Other Programme 0 0 61 229 122 72 195 0 0 0 0 0 678
Total 501 3,856 115 1,130 168 113 195 5 166 41 1 1,145 7,436

31
West Suffolk CCG – Month 6 – Key Performance ItemsElective Standard
This
Month
Last
MonthAssurance SPC Trend
18 wk RTT Incomplete(N) 92.0% 56.6% 49.8%Consistently
failed
Special cause
variation: Low
RTT 52 Week Waiters(N) 0 1,262 1,046Both met and
failed
Special cause
variation: High
Diagnostic test waiting times(N) 1.0% 48.5% 52.2%Both met and
failed
Special cause
variation: High
Cancer StandardThis
Month
Last
MonthAssurance SPC Trend
All Cancer 2 week wait(N) 93.0% 70.0% 72.6%Both met and
failed
Special cause
variation: Low
Two week wait for breast symptoms(N) 93.0% 92.6% 93.4%Both met and
failedTBD - Trend or CCV
Cancer 31 day wait: Percentage receiving 1st
treatment within one month of cancer diagnosis
(N)
96.0% 95.6% 99.0% Consistently metSpecial cause
variation: Low
Cancer 31 day wait: for cancer treatments-
surgery(N)94.0% 68.8% 92.9%
Both met and
failed
Special cause
variation: Low
Cancer 31 day wait: for cancer treatments-anti
cancer drug regimens(N)98.0% 100.0% 100.0% Consistently met TBD - Trend or CCV
Cancer 31 day wait: for cancer treatments-
radiotherapy(N)94.0% 95.3% 100.0% Consistently met TBD - Trend or CCV
Cancer 62 day wait: urgent GP referral for
suspected cancer(N)85.0% 73.9% 76.5%
Both met and
failedTBD - Trend or CCV
Other StandardThis
Month
Last
MonthAssurance SPC Trend
Estimated diagnosis rate for people with
dementia(N)66.7% 60.3% 59.9%
Consistently
failed
Special cause
variation: Low

Page 1 of 4
GOVERNING BODY
Agenda Item No. 17
Reference No. WSCCG 20-51
Date. 25 November 2020
Title Governing Body Assurance Framework and Chief Officers Risk Registers
Lead Director Amanda Lyes, Director of Corporate Services and System Infrastructure
Author(s) Tony Buckle, Risk Manager
Purpose To provide the Governing Body with the updated CCG Governing Body Assurance Framework (GBAF) document for November 2020.
Applicable CCG Priorities 1. Develop clinical leadership 2. Demonstrate excellence in patient experience & patient engagement 3. Improve the health & care of older people 4. Improve access to mental health services 5. Improve health & wellbeing through partnership working 6. Deliver financial sustainability through quality improvement
Action required by the Governing Body:
The Governing Body is requested to review and approve the updated West Suffolk CCG GBAF for November 2020.

1. Background 1.1 Content of the GBAF is reviewed by the Joint Leadership Team every month and by the Governing Body, Clinical Scrutiny and Audit Committees at each of their meetings. 2. GBAF - Key Issues
2.1 The following amendments have been agreed by the JLT at their regular review meeting, and are included in a separate table for West Suffolk CCG. The wording in the GBAFs has been revised to reflect the new leadership team structure.
2.2 The following amendments have been agreed by the JLT at their regular review meeting:
Risk No and
Owner Risk description and actions update
WSFT RTT 33
Paul Gibara
WSFT is failing in their 18-week RTT performance on both an aggregate level and individual specialty level. Action 4 update - Achievement of 92% RTT target. Target: To be reviewed in light of Covid 19. Update: October 2020 - Demand in September was at approximately 75% of 2019/20. Activity in October continues to increase and as a result we are starting to see the rate of deterioration of the waiting list slowing.
WSFT A&E 37
Paul Gibara
A&E failing to deliver timely care presenting a potential risk to patient safety and experience. 1. Actions update - Complete actions from A&E Delivery Board Action Plans: a. Improve streaming options in A&E. b. Improve NHS111 call triage and streaming to clinicians. c. Improve ambulance triage and streaming to alternative responses. d. Improved patient flow within the hospital. e. Improved discharge from hospital. f. Actions monitored monthly by the Assurance Group. g. Revised remedial action plan agreed with WSFT. h. Winter Surge.
Target date: not set as there is no metric to measure this - see below. Oct 2020 update; WSFT part of the trial of alternative A&E metrics and not reporting on 4-hour standard as per NHSE instruction. Target will be revisited once clarity on standard received. In the meantime, quality reviews will continue.
WSFT Cancer
Targets 45
Paul Gibara
WSFT is failing in the nationally mandated quality requirement requiring that Service Users wait no more than 62 days from urgent GP referral to first definitive treatment for cancer. Action 1 update; Trajectory had been agreed pre Covid-19. Updated October 2020. Latest data shows WSFT did not meet this standard in August 2020 at 81%. However, improvements in the long waits position continue and patient risk is monitored continually.
WSFT Finance 52
Jane Payling
Financial pressures at WSFT present a risk to service delivery and create knock on financial pressures across the WS Alliance. Granular operational risks amended. 2020/21 initial financial plan submitted by trust did not achieve target despite significant support from CCG. 20/21 plan for M7-12 shows continued financial pressures in both WSFT and WSCCG. Key control established amended. 3rd finance deputy post established which will specifically support the WS system to understand the pressures and build recovery plans. Assurance of controls amended. M7-12 financial plan drawn up which shows more clearly where the in-year pressures lie. Action 1 update; Work with trust to understand the drivers of the increasing overspend. Target date now January 2021
WSFT CQC Inspection
53
Lisa Nobes
January 2020 CQC inspections of WSFT rated the Trust as requires improvement overall. Actions update - October 2020 update: Feedback has been provided to Trust Improvement Programme Board, following Sept. QA visit. Full report pending.
WSFT Maternity 54
Lisa Nobes
CCG and Provider Trust failure to meet national maternity standards / targets and contract obligations. Action 1 update - Discussion between CCG CFO and Provider Trust DoF’s to ascertain if there is a solution to financial pressure. November 2020 update: Meeting held with regional chief midwife and ESNEFT DON. ESNEFT have accepted assistance from maternity transformation team to produce business case to ESNEFT Board for funding.
NSFT CQC Inspection
27a
Lisa Nobes
CQC and CCG inspections of NSFT services in Suffolk demonstrate that the service ‘requires improvement’ leading to a risk of patient harm and poor experience. Action 1 update - Implementation of Suffolk emotional wellbeing and mental health strategy to be commissioned through most capable provider process. Oct 2020 Update: QCPM meetings have fully resumed in Sep. Oversight of quality concerns continue to be

overseen through OAG. QCPM and the planned QA visits. NSFT
Performance 27b
Paul Gibara
Poor performance of mental health services. Actions updated below.
1. Early intervention in psychosis. Target (60% (3-month average)): To be agreed with NSFT as BAU restarts. Update (September 2020): Aug validated: 73% Sept unvalidated: 50%
2. Eating Disorders (urgent). Target (95% (3-month average)): To be agreed with NSFT as BAU restarts. Update (September 2020): Aug validated: 100% Sept unvalidated: 100%
3. Eating Disorders (routine). Target (95% (3-month average)): To be agreed with NSFT as BAU restarts. Update (September 2020): Aug validated: 92% Sept unvalidated:871%
4. Emergency referrals. Target (95% (3-month average)): To be agreed with NSFT as BAU restarts. Update (September 2020): Aug validated: Adult 91% Children 95% Sept unvalidated: Adult 92%; Children 96%
5. Routine referrals. Target (95%): To be agreed with NSFT as BAU restarts. Update (September 2020): Aug validated: Adult 90% Children 74%. Sept unvalidated: Adult 90%; Children 73%
6. Referral to Treatment. Target (95%): To be agreed with NSFT as BAU restarts. Update (September 2020): Aug validated: Adult 95%; Children 65% Sept unvalidated: Adult 98%; Children 82%
7. Children’s emotional wellbeing hub. Target (95%): To be agreed with NSFT as BAU restarts Update (September 2020): Aug validated: 94% Sept unvalidated: 87%
EEAST Performance
39
Ed Garratt
EEAST is failing performance targets against ambulance response categories, particular concern are delays in the higher acuity Category 1 and 2 calls. Action 1 update - EEAST have target workforce/capacity gap taking longer to fill than expected. November 2020 Update. Response times improvements largely sustained, some pressure on C1/ C2 although long waits/tails remain steady. Front-line workforce gap has continued to reduce and has a deficit of 56 WTEs at end of September 2020. Hospital handover delays are elevated in a number of sites outside of SNEE (regional average handover times is 22 minutes in mid-October). Winter planning oversight meeting has been set up as joint meeting with NHS E/I and is due to meet in first week of November and this will establish onwards monitoring routine.
Covid-19 Outbreak 56
Lisa Nobes
Level 4 National Emergency. Current UK Alert Level: 4. The Alert level has been raised in light in increased case numbers. The Incident level currently remains at Level 3. Granular operational risks update. As of 4th November, 1,099,059 people have tested positive. Of those tested positive for coronavirus in the England (within 28 days), across all settings, 47,742 have died. The UK ‘R Number’ is between 1.1 – 1.3. Action update - Monitoring of proliferation of virus will remain on-going. CCG will implement national guidance as required. Oct 2020 Update: ICC operations remain in place to support coordination of information from National/ Region teams to providers. Service provision has been maintained to meet demand of COVID19 patients. Continue local engagement in local resilience forums. Service recovery groups established. Winter planning being finalised, and stress tested with providers.
Covid-19 Resource
and Finance 57
Jane Payling
Expenditure to support the Covid-19 response may result in financial risks for the CCGs and wider system leaving a requirement to restrict future services or fail financial targets. Granular operational risk amended. Funding from M7-12 notified and being worked through. Initial assessment shows that funding is insufficient to cover costs in second half of the year. Assurance of controls amended. Positive Audit opinion on 2019/20 accounts. Positive Internal audit assurance received on financial governance arrangements. Action update - Adjusted financial plan in place for 2020/21. Update: adjusted financial plan developed to be approved at the November Governing Body.
2020 Flu Campaign
58
COO Chairs
The 2020 flu campaign will be suboptimal due to several factors and targets will not be met. Action 1 update – In close communication with NHSE following regional and national level guidance regarding most of the granular risks. Target date: Dec 2020.
EU Exit 43
Amanda Lyes
Brexit and the possibility of a ‘no deal’ exit from the European Union. Additional key control established. CCGs linking with Local Resilience Forums. Action 3 new action - National assurance exercise to be published end Nov 2020. Action 4 new action - SNEE Meds Mgmt. group to be established. Action 5 new action - Regional meeting on 12 Nov 2020 to seek assurance for the end of the EU Transition Period. Action 6 new action - Roche learning event debrief to be used to inform Brexit transition planning. All actions have target date of 31 December 2020.

3. Chief Officers Risk Registers
3.1 As previously agreed, a brief highlight report on current risks which may cause concern to the CCGs from local Risk Registers is included in a summary table document with this report. These are reviewed on a regular basis by the JLT and by the Risk Forum.
3.2 The Risk Forum reviews all the departmental risk registers each month and they are all
up to date. The accompanying risk register summary table has been updated.

Board / Governing Body Assurance
Framework
2020 - 2021
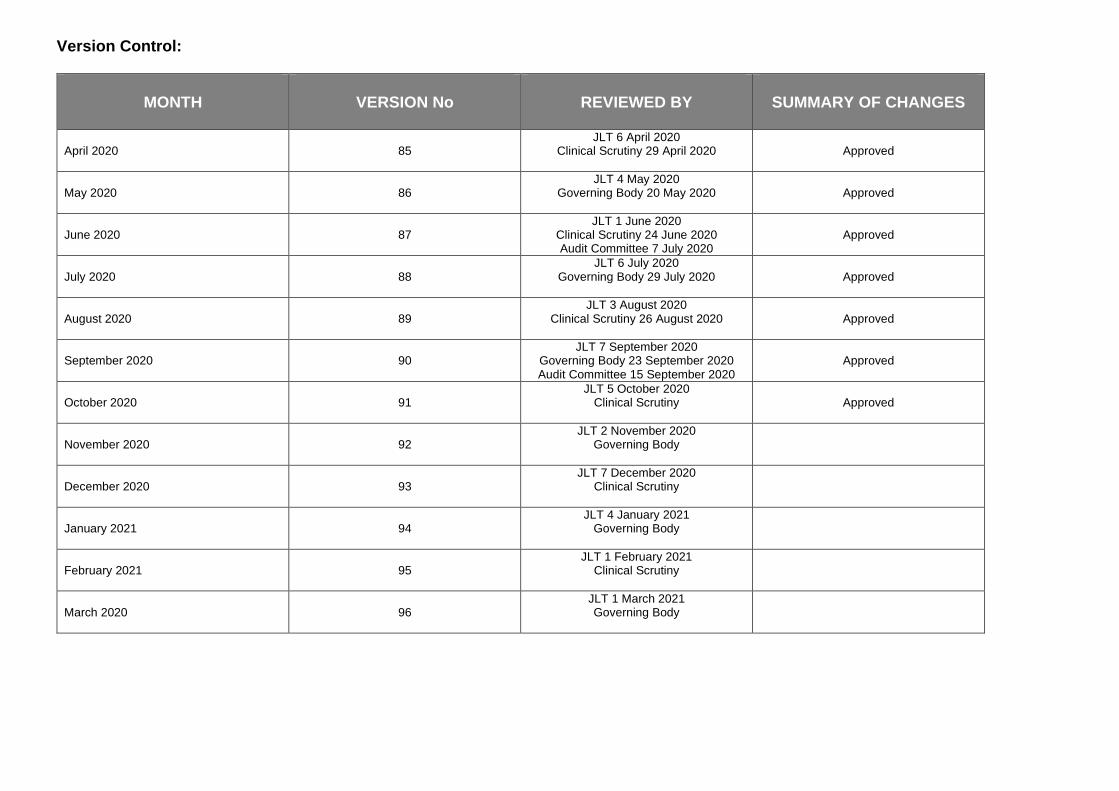
Version Control:
MONTH
VERSION No
REVIEWED BY
SUMMARY OF CHANGES
April 2020
85
JLT 6 April 2020 Clinical Scrutiny 29 April 2020
Approved
May 2020
86
JLT 4 May 2020 Governing Body 20 May 2020
Approved
June 2020
87
JLT 1 June 2020 Clinical Scrutiny 24 June 2020 Audit Committee 7 July 2020
Approved
July 2020
88
JLT 6 July 2020 Governing Body 29 July 2020
Approved
August 2020
89
JLT 3 August 2020 Clinical Scrutiny 26 August 2020
Approved
September 2020
90
JLT 7 September 2020 Governing Body 23 September 2020 Audit Committee 15 September 2020
Approved
October 2020
91
JLT 5 October 2020 Clinical Scrutiny
Approved
November 2020
92
JLT 2 November 2020 Governing Body
December 2020
93
JLT 7 December 2020 Clinical Scrutiny
January 2021
94
JLT 4 January 2021 Governing Body
February 2021
95
JLT 1 February 2021 Clinical Scrutiny
March 2020
96
JLT 1 March 2021 Governing Body

Board / Governing Body Assurance Framework
Overview
The Board / Governing Body Assurance Framework (B/GBAF hereafter) provides the NHS West Suffolk Clinical Commissioning Group (CCG) with a simple but comprehensive method for the effective and focused management of risk. Through the B/GBAF the CCG Board / Governing Body gains assurance that risks are being appropriately managed throughout the organisation. The B/GBAF identifies which of the organisation’s strategic objectives may be at risk because of inadequacies in the operation of controls, or where the CCG has insufficient assurance. At the same time it encompasses the control of risk, provides structured assurances about where risks are being managed and ensures that objectives are being delivered. This allows the Board / Governing Body to determine how to make the most efficient use of resources and address the issues identified in order to improve the quality and safety of care. The B/GBAF also brings together all of the evidence required to support the Annual Governance Statement. The B/GBAF should be seen as a working document and will be updated regularly by the Joint Leadership Team, monitored by the Audit Committee, Clinical Scrutiny and reported to the Board / Governing Body at each of its meetings. The B/GBAF is linked to the Directorate’s Risk Register, the content of which is also provided for review by the Joint Leadership Team. A flow chart setting out how risks are identified and managed is set out overleaf. In order to ensure consistency in the risk assessment process, the likelihood and consequences of all risks on the Risk Register are assessed against the former National Patient Safety Agency (NPSA) 5X5 risk matrix and those scoring 15 and above and are of strategic concern migrate to the B/GBAF and thereby inform the Board / Governing Body agenda. Once added to the B/GBAF, a risk should remain in place until its RAG rating has been mitigated to a score of 1-6 when it is considered manageable and therefore no longer a strategic concern. The 5X5 risk matrix and subsequent red, amber, green (RAG) score identify the level at which identified risks will be managed within the organisation. It also assigns priorities for remedial action, and determines whether risks are to be accepted on the basis of the colour bandings and risk ratings. In terms of evaluation of effectiveness, the RAG rating system is also used to present how well the agreed controls are operating.

RISKS IDENTIFIED THROUGH:
External Assessment & Audit + Guidance & Alerts
Serious Incidents, Complaints, Public Health &
Quality Issues
Public & Stakeholder Engagement
Business & Service Delivery Plans
CCG Board / Governing Body Own & Manage
Risks & the Joint Leadership Team
Reviews the Directorate Risk
Registers and the B/GBAF
Board/Governing Body Assurance Framework
Overview & Scrutiny by the Audit Committee
Assurance to the Board/Governing Body
Individual Risks Jointly Managed by Designated
Directors & Clinical Leads
Work Stream Risk Assessments
Review by Clinical Scrutiny Committee
Review by Local Risk Forum

RAG Score Framework
Likelihood score → 1: Rare 2: Unlikely 3: Possible 4: Likely 5: Almost Certain
Consequence score ↓
5: Catastrophic 5 10 15 20 25
4: Major 4 8 12 16 20
3: Moderate 3 6 9 12 15
2: Minor 2 4 6 8 10
1: Negligible 1 2 3 4 5
The subsequent red, amber, green (RAG) scores identify the level at which identified risks will be managed within the organisation. It also assigns priorities for remedial action, and determines whether risks are to be accepted on the basis of the colour bandings and risk ratings. In terms of evaluation of effectiveness, the RAG rating system is also used to present how well the agreed controls are operating within the following classifications:
Risk Appetite For all risks that have been agreed and then assessed and rated, an action plan should be drawn up containing the actions that will be taken, with timescales, in order to either totally eliminate the risk or to reduce its consequences to a level that the CCG is prepared to accept. It is useful to consider the ‘Four T’s’ when considering the management of risks:
TOLERATE
Where the CCG accepts the risk and lives with it
TREAT
Where the CCG takes action to reduce the risk
TRANSFER
Where the CCG lets someone else carry the risk such as by passing the responsibility for the risk to a contractor
TERMINATE
Where the CCG feels that the risk is too great and does not continue with the activity giving rise to it
In order to determine the likely consequence arising from an identified risk and using the 5X5 matrix:
• Define the risk explicitly in terms of the adverse consequence or consequences that might arise
• Use the table below for examples, by risk domains, to determine the consequence score relevant to the risk identified

Consequence score (severity levels) and example of descriptions
1 2 3 4 5
Risk Domains Negligible Minor Moderate Major Catastrophic 1. Impact on the safety of patients, staff or public (physical/psychological harm)
Minimal injury requiring no/minimal intervention or treatment. No time off work
Minor injury or illness, requiring minor intervention Requiring time off work for >3 days Increase in length of hospital stay by 1-3 days
Moderate injury requiring professional intervention Requiring time off work for 4-14 days Increase in length of hospital stay by 4-15 days RIDDOR/agency reportable incident An event which impacts on a small number of patients
Major injury leading to long-term incapacity/disability Requiring time off work for >14 days Increase in length of hospital stay by >15 days Mismanagement of patient care with long-term effects
Incident leading to death Multiple permanent injuries or irreversible health effects An event which impacts on a large number of patients
2. Quality / complaints / audit
Peripheral element of treatment or service suboptimal Informal complaint/inquiry
Overall treatment or service suboptimal Formal complaint (stage 1) Local resolution Single failure to meet internal standards Minor implications for patient safety if unresolved Reduced performance rating if unresolved
Treatment or service has significantly reduced effectiveness Formal complaint (stage 2) complaint Local resolution (with potential to go to independent review) Repeated failure to meet internal standards Major patient safety implications if findings are not acted on
Non-compliance with national standards with significant risk to patients if unresolved Multiple complaints/ independent review Low performance rating Critical report
Totally unacceptable level or quality of treatment/service Gross failure of patient safety if findings not acted on Inquest/ombudsman inquiry Gross failure to meet national standards
3. Human resources / organisational development/staffing / competence
Short-term low staffing level that temporarily reduces service quality (< 1 day)
Low staffing level that reduces the service quality
Late delivery of key objective/ service due to lack of staff Unsafe staffing level or competence (>1 day) Low staff morale Poor staff attendance for mandatory/key training
Uncertain delivery of key objective/service due to lack of staff Unsafe staffing level or competence (>5 days) Loss of key staff Very low staff morale No staff attending mandatory/ key training
Non-delivery of key objective/service due to lack of staff Ongoing unsafe staffing levels or competence Loss of several key staff No staff attending mandatory training /key training on an ongoing basis

4. Statutory duty/ inspections
No or minimal impact or breech of guidance/ statutory duty
Breech of statutory legislation Reduced performance rating if unresolved
Single breech in statutory duty Challenging external recommendations/ improvement notice
Enforcement action Multiple breeches in statutory duty Improvement notices Low performance rating Critical report
Multiple breeches in statutory duty Prosecution Complete systems change required Zero performance rating Severely critical report
5. Adverse publicity / reputation
Rumours
Potential for public concern
Local media coverage – short-term reduction in public confidence Elements of public expectation not being met
Local media coverage – long-term reduction in public confidence
National media coverage with <3 days service well below reasonable public expectation
National media coverage with >3 days service well below reasonable public expectation. MP concerned (questions in the House) Total loss of public confidence
6. Business objectives / projects
Insignificant cost increase/ schedule slippage
<5 per cent over project budget Schedule slippage
5–10 per cent over project budget Schedule slippage
Non-compliance with national 10–25 per cent over project budget Schedule slippage Key objectives not met
Incident leading >25 per cent over project budget Schedule slippage Key objectives not met
7. Finance including claims
Small loss Risk of claim remote
Loss of 0.1–0.25 per cent of budget Claim less than £10,000
Loss of 0.25–0.5 per cent of budget Claim(s) between £10,000 and £100,000
Uncertain delivery of key objective/Loss of 0.5–1.0 per cent of budget Claim(s) between £100,000 and £1 million Purchasers failing to pay on time
Non-delivery of key objective/ Loss of >1 per cent of budget Failure to meet specification/ slippage Loss of contract / payment by results Claim(s) >£1 million
8. Service/business interruption
Loss/interruption of >1 hour
Loss/interruption of >8 hours
Loss/interruption of >1 day
Loss/interruption of >1 week
Permanent loss of service or facility
9. Environmental impact
Minimal or no impact on the environment
Minor impact on environment
Moderate impact on environment
Major impact on environment
Catastrophic impact on environment

WSFT – RTT. Risk 33 added February 2017
AC
CO
UN
TAB
LE O
FFIC
ER
& G
P O
WN
ER
DESCRIPTION OF STRATEGIC RISK
GRANULAR OPERATIONAL RISKS
IN
ITIA
L R
AG
RA
TIN
G
(LIK
ELIH
OO
D x
CO
NSE
QU
ENC
E)
KEY CONTROLS ESTABLISHED
ASSURANCE OF CONTROLS
RISK APPETITE
(Treat, Tolerate, Transfer,
Terminate)
R
AG
RA
TIN
G L
AST
MO
NTH
R
EVIS
ED R
AG
RA
TIN
G
TAR
GET
RIS
K
ACTION POINTS & TARGET DATES FOR
COMPLETION
PG
WSFT is failing in their 18-week RTT performance on both an aggregate level and individual specialty level. Risk to CCG If WSFT fail to meet the 18-week RTT standard then the CCG will fail to meet its constitutional performance requirements as stipulated by the Department of Health.
Specialities with the greatest need for improvement are orthopaedics, ophthalmology, general surgery and gynaecology. 52wk breaches are increasing due to capacity restrictions. The delay may have an impact on service user’s quality of life and potentially on outcomes. Phase 3 plans confirm the need for additional theatre and diagnostic capacity.
4 x 4
16
Elective assurance Group will meet at least monthly.
Contractual performance review at each contract meeting as well as;
o Weekly access meeting
o Validation of waiting lists
o Demand and capacity planning ongoing
o Additional internal activity in place
o Additional external activity outsourced and insourced
• Demand management projects.
Monthly review of waiting times and backlog clearance plan going forward CCG Priority Demonstrate excellence in patient experience
Treat
4 x 4
16
4 x 4
16
2 x 4 8
4. Achievement of 92% RTT target
Target: To be reviewed in light of Covid 19 Update: October 2020 Demand in September was at approximately 75% of 2019/20. Activity in October continues to increase and as a result we are starting to see the rate of deterioration of the waiting list slowing. Patient safety reviews of long waiters continue.

WSFT – A&E. Risk 37 added December 2017
AC
CO
UN
TAB
LE O
FFIC
ER
& G
P O
WN
ER
DESCRIPTION OF STRATEGIC RISK
GRANULAR OPERATIONAL RISKS
IN
ITIA
L R
AG
RA
TIN
G
(LIK
ELIH
OO
D x
CO
NSE
QU
ENC
E)
KEY CONTROLS ESTABLISHED
ASSURANCE OF CONTROLS
RISK APPETITE
(Treat, Tolerate, Transfer,
Terminate)
R
AG
RA
TIN
G L
AST
MO
NTH
R
EVIS
ED R
AG
RA
TIN
G
TAR
GET
RIS
K
ACTION POINTS & TARGET DATES FOR
COMPLETION
PG/F
W
A&E failing to deliver timely care presenting a potential risk to patient safety and experience. Risk to CCG If WSFT fail to deliver timely care then the CCG would have failed to meet its constitutional performance requirements as stipulated by the Department of Health Please note WSFT are part of the trial of new A&E standards and are not currently required to report on the 4-hour standard.
Clinical risk of patients not being seen in appropriate timescales or insufficient beds to accommodate appropriate environments. Risk of patient experience deterioration due to long waits. Risk of breaching constitutional obligations. Risk of no agreed plan to manage increase in winter demand for services During the Covid-19 escalation period the ED has changed its processes to operate a red route for suspected Covid-19 patients (through the old CDU) and green route for non Covid-19 patients. Overall demand has reduced but is beginning to return. The risk remains challenging as the underlying issues pre-Covid-19 have not been resolved.
4 x 4
16
• Daily reporting of performance.
• Escalation of health Dtoc daily for CCG and system support.
• OOH cover and 111 support continually reviewed to ensure rotas are in place to manage surges.
• Admission avoidance schemes fully operational and a rolling reminder in place to primary care and OOH.
• GP streaming in place.
• 111 targets to reduce inappropriate referrals to A+E.
• A&E Board in place. • Assess and address
staff shortages in medical and nursing rotas 10 days in advance.
• CCG escalation team working with WSFT to improve flow
Monthly system wide urgent care meeting to be established post Covid 19.
Daily performance information supplied and monitored, regular discussions and monthly formal contract meetings. Formal contract notification to WSFT for joint working and review of performance in A+E requirement. Remedial Action Plan established by A+E delivery board. Assurance being reviewed and A&EDB to be replaced.
CCG Priority Improve health and wellbeing through partnership working. Integrated performance report area. Contractual Performance
Treat
3 x 4
12
3 x 4
12
2 x 4 8
1. Complete actions from A&E Delivery Board Action Plans:
a. Improve streaming options in A&E
b. Improve NHS111 call triage and streaming to clinicians
c. Improve ambulance triage and streaming to alternative responses
d. Improved patient flow within the hospital
e. Improved discharge from hospital
f. Actions monitored monthly by the Assurance Group
g. Revised remedial action plan agreed with WSFT
h. Winter Surge Target date: not set as there is no metric to measure this - see below. Oct 2020 update; WSFT part of the trial of alternative A&E metrics and not reporting on 4-hour standard as per NHSE instruction. Target will be revisited once clarity on standard received. In the meantime, quality reviews will continue.

WSFT – Cancer targets. Risk 45 added January 2019
AC
CO
UN
TAB
LE O
FFIC
ER
& G
P O
WN
ER
DESCRIPTION OF STRATEGIC RISK
GRANULAR OPERATIONAL RISKS
IN
ITIA
L R
AG
RA
TIN
G
(LIK
ELIH
OO
D x
C
ON
SEQ
UEN
CE)
KEY CONTROLS ESTABLISHED
ASSURANCE OF CONTROLS
RISK APPETITE
(Treat, Tolerate, Transfer,
Terminate)
R
AG
RA
TIN
G L
AST
MO
NTH
R
EVIS
ED R
AG
RA
TIN
G
TAR
GET
RIS
K
ACTION POINTS & TARGET DATES FOR
COMPLETION
PG
WSFT is failing in the nationally mandated quality requirement requiring that Service Users wait no more than 62 days from urgent GP referral to first definitive treatment for cancer. Risk to the CCGs If WSFT fail to meet the 62-day cancer standard then the CCG will fail to meet its constitutional performance requirements as stipulated by the Department of Health.
• Standard has been consistently missed. This is due to capacity and complex pathway issues in a number of specialties most notably Gynae, Skin, Head and Neck, Urology, and Lower GI.
• Clinical risk of patients not being seen in appropriate timescales.
• Risk of deteriorating patient outcomes and experience due to long waits.
• Risk of breaching constitutional obligations.
Risk of increasing patient harm both physically and mentally due to being on Cancer pathway for extended period of time. During the Covid-19 escalation period cancer work continues and the risks remain critical. In addition to the above there is a new risk emerging relating to patients not attending cancer appointments.
4 x 4
16
WSFT weekly review the priority waiting list to identify risks/mitigations.
Cancer board working across the system to improve performance by systematically identifying and mitigating bottlenecks.
Remedial Action Plan had been drafted; needs to be revisited post Covid 19.
Capacity bottlenecks in diagnostics/theatres exacerbated by Covid 19; WSFT working on plans to insource/outsource additional capacity.
Progress reviewed monthly at Contract meeting; an additional performance improvement meeting instigated to review all areas of elective performance (cancer/ RTT /diagnostics).
Monthly breach reports show pseudonymised patient level details for days waiting with breach reason reviewed at monthly QCPM.
Full RCAs undertaken for patients waiting >104 days for any harm caused; reviewed at monthly Quality meeting.
Provider has reviewed attendance, process and governance for PTL meeting ensuring it works more efficiently.
Progress is reviewed at: • Contract meetings • Quality meetings • Cancer Board • Clinical Scrutiny • Clinical Executive • Governing Body.
Treat
4 x 4
16
4 x 4
16
2 x 4 8
1. Trajectory had been agreed pre Covid. Updated October 2020. Latest data shows WSFT did not meet this standard in August 2020 at 81%. However, improvements in the long waits position continue and patient risk is monitored continually. Revised Target: To be agreed. Target will be revisited post Covid-19.

WSFT – Finance Risk 52 added September 2019
AC
CO
UN
TAB
LE O
FFIC
ER
& G
P O
WN
ER
DESCRIPTION OF STRATEGIC RISK
GRANULAR OPERATIONAL RISKS
IN
ITIA
L R
AG
RAT
ING
(L
IKEL
IHO
OD
x C
ON
SEQ
UEN
CE)
KEY CONTROLS ESTABLISHED
ASSURANCE OF CONTROLS
RISK APPETITE
(Treat, Tolerate, Transfer,
Terminate)
R
AG
RA
TIN
G L
AST
MO
NTH
R
EVIS
ED R
AG
RA
TIN
G
TAR
GET
RIS
K
ACTION POINTS & TARGET DATES FOR
COMPLETION
JP
Financial pressures at WSFT present a risk to service delivery and create knock on financial pressures across the WS Alliance. Emergency funding measures during Covid-19 mean that trust and CCGs should be funded to make necessary investments, deliver BAU and achieve FIT. However, underlying issues will re-emerge at the end of the current crisis period.
19/20 financial performance at WSFT was off plan indicating non achievement of control total. 2020/21 initial financial plan submitted by trust did not achieve target despite significant support from CCG. 20/21 plan for M7-12 shows continued financial pressures in both WSFT and WSCCG. Suffolk and North East Essex ICS has elected to manage financial control totals at alliance level within the overall ICS control total– therefore financial risks at WSFT will put the achievement of the alliance and system control total at risk.
4 x 5
20
West Alliance Financial Strategy Group (FSG) now in place to monitor achievement of West Suffolk control total and discuss financial performance across the Alliance. Pressures that cannot be dealt with within the alliance are escalated to ICS.
3rd finance deputy post established which will specifically support the WS system to understand the pressures and build recovery plans.
Reporting back discussions at Alliance FSG to CCG Executive and CCG FPC. ICS financial reporting. M7-12 financial plan drawn up which shows more clearly where the in year pressures lie.
Treat
3 x 5
15
3 x 5
15
2 x 5 10
1. Work with trust to understand the drivers of the increasing overspend
Target date: December 2020 West Suffolk Alliance and wider ICS partners to determine actions and service changes to be made to enable the WS system to live within resources for 20/21 and return to FIT for 21/22. Target date: January 2021
Completion date:

WSFT – CQC Inspection. Risk 53 added February 2020.
AC
CO
UN
TAB
LE O
FFIC
ER
& G
P O
WN
ER
DESCRIPTION OF STRATEGIC RISK
GRANULAR OPERATIONAL RISKS
IN
ITIA
L R
AG
RAT
ING
(L
IKEL
IHO
OD
x C
ON
SEQ
UEN
CE)
KEY CONTROLS ESTABLISHED
ASSURANCE OF CONTROLS
RISK APPETITE
(Treat, Tolerate, Transfer,
Terminate)
R
AG
RA
TIN
G L
AST
MO
NTH
R
EVIS
ED R
AG
RA
TIN
G
TAR
GET
RIS
K
ACTION POINTS & TARGET DATES FOR
COMPLETION
LN
January 2020 CQC inspections of WSFT rated the Trust as requires improvement overall. Following the well-led inspection, the CQC undertook enforcement action in respect of the Maternity and Midwifery Service to enable the improvement of patient safety within the service. They issued a warning notice under Section 29A of the Health and Social Care Act 2008 on the 14th Nov 2019 and informed the Trust it must improve by the 31st January 2020. Risk to the CCGs Statutory Duty to ensure patient safety within commissioned services.
There are 22 operational risks, mainly maternity, including
- Drug room ambient temp monitoring
- Monitoring of women’s records
- Carbon monoxide monitoring assessments
- Domestic violence screening - Triage of vital signs
monitoring for women and new babies
- Resus equipment checks - Ensuring up to date clinical
guidelines - Ensure labour suite
coordinator is supernumerary - Mandatory training
compliance - Team meeting information
sharing - Effective audit of WHO 5 steps
to safer surgery checklist - Incident reporting and closure - Creation of action plans
following national and local audits
Staff appraisal rates - Processes for midwife
supervision Friend and family data
collection in all areas - Consumable equipment use - Evidence based bereavement
care pathway - Women’s pain scores
completion
4 x 5
20
Partnership working with WSFT to provide scrutiny, challenge and assurance on the CQC actions. CCG integrated into WSFT quality governance including internal meetings, quality walks. Monthly contract meeting with WSFT
CQC action outcomes and evidence of change. Design and implementation of new quality assurance framework. CCG Priority
Treat
3 x 5
15
3 x 5
15
3 x 2 6
1. Review maternity service action plans against all must and should dos.
Target date: Dec 2020 Completion date: 23/06/2020 update Maternity action plan has been shared with CCG. 2. Complete evidence
check and ongoing improvements in maternity service.
Target date: Dec 2020 Completion date: October 2020 update: Feedback has been provided to Trust Improvement Programme Board, following Sept. QA visit. Full report pending.

WSFT – Maternity Risk 54 added March 2020
AC
CO
UN
TAB
LE O
FFIC
ER
& G
P O
WN
ER
DESCRIPTION OF STRATEGIC RISK
GRANULAR OPERATIONAL RISKS
IN
ITIA
L R
AG
RAT
ING
(L
IKEL
IHO
OD
x C
ON
SEQ
UEN
CE)
KEY CONTROLS ESTABLISHED
ASSURANCE OF CONTROLS
RISK APPETITE
(Treat, Tolerate, Transfer,
Terminate)
R
AG
RA
TIN
G L
AST
MO
NTH
R
EVIS
ED R
AG
RA
TIN
G
TAR
GET
RIS
K
ACTION POINTS & TARGET DATES FOR
COMPLETION
LN
CCG and Provider Trust failure to meet national maternity standards / targets and contract obligations. This is due to provider trusts unable to fund Birthrate+ recommended staffing levels, and also the increased workforce required to implement the continuity of care model
• CCG Assurance Framework noncompliance
• Trust not compliant with NHSE standard contract or national transformation programme targets and will experience regulatory scrutiny/penalties
• Trust not compliant with CNST therefore creating income risk (circa £1m) and reputational risk
• Inability to maintain staffing levels and service delivery
• Inequitable clinical outcomes for women and babies across the ICS
4 x 5
20
LMS funded evidence-based workforce planning tool to enable accurate workforce plans to be developed. National lead for CoC advised on staffing model. Attempting to calculate longer-term savings to the system. ICS Board made aware of programme costs and potential system savings. Evaluation from wave 1 teams showed rolling caseload of 1:36 manageable compared to 1:36 pa therefore reducing cost pressure. CCG commissioning intentions stated CoC must be implemented as per national targets and NHS standard contract requires target delivery.
• All Heads of Midwifery aware of recommended safe staffing levels
• Full roll out plans received from providers to demonstrate how the CoC model can be rolled out when funding available
• All options explored as to implementation at minimal cost
Tolerate
4 x 5
20
4 x 5
20
2 x 2 4
1. Discussion between CCG CFO and Provider Trust DoF’s to ascertain if there is a solution to financial pressure.
Target date: Dec 2020 Completion date:
November 2020 update: Meeting held with regional chief midwife and ESNEFT DON. ESNEFT have accepted assistance from maternity transformation team to produce business case to ESNEFT Board for funding.

NSFT – CQC Inspection. Risk 27a added July 2015 (Renumbered January 2016)
AC
CO
UN
TAB
LE O
FFIC
ER
& G
P O
WN
ER
DESCRIPTION OF STRATEGIC RISK
GRANULAR OPERATIONAL RISKS
IN
ITIA
L R
AG
RA
TIN
G
(LIK
ELIH
OO
D x
CO
NSE
QU
ENC
E)
KEY CONTROLS ESTABLISHED
ASSURANCE OF CONTROLS
RISK APPETITE
(Treat, Tolerate, Transfer,
Terminate)
R
AG
RA
TIN
G L
AST
MO
NTH
R
EVIS
ED R
AG
RA
TIN
G
TAR
GET
RIS
K
ACTION POINTS & TARGET DATES FOR
COMPLETION
LN
CQC and CCG inspections of NSFT services in Suffolk demonstrate that the service ‘requires improvement’ leading to a risk of patient harm and poor experience. Risk to the CCGs Statutory Duty to ensure patient safety within commissioned services: The Trust inability to demonstrate appropriate safety standards throughout it services present significant patient safety risks to the population of Suffolk.
• Inability to meet performance and clinical quality targets in access to service, care in service and discharge arrangements
• Inability to maintain safer staffing levels in accordance with NICE and National Quality Board guidance
• Lack of confidence in performance data
• Lack of patient safety culture throughout organisation impacting clinical risk assessment, care planning.
• Lack of clinical leadership structure throughout organisation
4 x 4
16
Quality assurance process initiated jointly with NSFT to review every service line in NSFT. Monthly meetings to review / challenge quality performance. Quality dashboard. Attendance at monthly stakeholder assurance meetings led by NHS Improvement / CQC. Oversight of quality improvement plans (trust / local) and monthly monitoring of progress. Monitor primary care contract issues and Trust response. New Chair appointed and partnership arrangement agreed with East London Foundation Trust (ELFT). Quality Improvement methodology introduced by Trust and training rolled out. Weekly CCG: NSFT Director meeting to check progress against actions and escalate concerns. Escalation through joint NHSI: CCG oversight meeting. Service user tracker list commenced, and patient harm review process commenced.
Improvements to patient safety and experience noted through QA process.
Demonstrated improvement against identified contractual key performance indicators evidenced through quality dashboard escalation of issues via Contract Quality Performance Review (CQPR) meetings.
Confidence that NSFT have capability and capacity to deliver the required quality improvements.
Assurance that actions detailed in the quality improvement plan have been implemented. CCG Priority To improve access to mental health services
Tolerate
4 x 5
20
4 x 5
20
3 x 2 6
1. Implementation of Suffolk emotional wellbeing and mental health strategy to be commissioned through most capable provider process Timescales for completion have been revised due to Covid-19. CCG currently unable to visit but maintaining two weekly care group lead meetings to oversee progress and maintain oversight under present conditions. CCG Associate Director of Nursing- CYP, MH, LD and Autism is liaising with Trust as part of this. NSFT have implemented a first response service, open 24/7 to manage patient need under the Covid-19 outbreak. Oct 2020 Update: QCPM meetings have fully resumed in Sep. Oversight of quality concerns continue to be overseen through OAG. QCPM and the planned QA visits.

NSFT – Performance. Risk 27b added January 2016
AC
CO
UN
TAB
LE O
FFIC
ER
& G
P O
WN
ER
DESCRIPTION OF STRATEGIC RISK
GRANULAR OPERATIONAL RISKS
IN
ITIA
L RA
G R
ATIN
G
(LIK
ELIH
OO
D x
CO
NSE
QU
ENC
E)
KEY CONTROLS ESTABLISHED
ASSURANCE OF CONTROLS
RISK APPETITE
(Treat, Tolerate, Transfer,
Terminate)
R
AG
RA
TIN
G L
AST
MO
NTH
R
EVIS
ED R
AG
RA
TIN
G
TAR
GET
RIS
K
ACTION POINTS & TARGET DATES FOR
COMPLETION

PG/J
H
Poor performance of mental health services Risk to CCG If performance does not improve to the contractual agreed standard then service users will continue to receive an inadequate service and the CCG would have failed in its duty to commission quality safe services
Poor performance against a number of performance indicators. National standards: 1. Early intervention in
psychosis (14 days referral to treatment)
2. Eating disorder (1-week urgent referral to treatment)
3. Eating disorder (4-week routine referral to treatment)
Local standards: 4. Emergency referrals (4
hours referral to assessment)
5. Routine referrals (28 days referral to assessment)
6. Referral to treatment (15 weeks)
7. Children’s emotional wellbeing hub (10 days referral to discharge)
4 x 4
16
National standards subject to scrutiny from NHS E/ I. CCG teams (transformation, quality performance, finance and improvement,) working closely with NSFT counterparts to identify root causes of problems: • Demand over plan • Throughout under plan • Workforce gaps • System gaps • Underinvestment. Monthly MDT meetings in place, to review issues and actions. Monthly joint quality/ performance meetings with NSFT operational/ clinical/contract leads. Regular joint meetings of CCG and NSFT boards. During Covid 19: • CCG teams have
maintained close contact with NSFT colleagues
• NSFT have expanded their virtual and telephone offering
The CCGs have invested in additional voluntary sector capacity to manage lower risk patients.
Reported to the multi-disciplinary team, clinical scrutiny, Clinical Executive and Governing Body as appropriate. CAHMS issues also overseen by EWB Hub Board Progress routinely monitored at monthly Quality Contracts & Performance (QCPM) meeting. CCG Priority To improve access to mental health services
Treat
4 x 5
20
4 x 5
20
2 x 5 10
1. Early intervention in psychosis
Target (60% (3-month average)): To be agreed with NSFT as BAU restarts Update (September 2020): Aug validated: 73%Sept unvalidated: 50%
2. Eating Disorders (urgent) Target (95% (3-month average)): To be agreed with NSFT as BAU restarts Update (September 2020): Aug validated: 100% Sept unvalidated: 100%
3. Eating Disorders (routine) Target (95% (3-month average)): To be agreed with NSFT as BAU restarts Update (September 2020): Aug validated: 92% Sept unvalidated:871%
4. Emergency referrals Target (95% (3-month average)): To be agreed with NSFT as BAU restarts Update (September 2020): Aug validated: Adult 91% Children 95% Sept unvalidated: Adult 92%; Children 96%
5. Routine referrals Target (95%): To be agreed with NSFT as BAU restarts Update (September 2020): Aug validated: Adult 90% Children 74% Sept unvalidated: Adult 90%; Children 73%
6. Referral to Treatment Target (95%): To be agreed with NSFT as BAU restarts Update (September 2020): Aug validated: Adult 95%; Children 65% Sept unvalidated: Adult 98%; Children 82%
7. Children’s emotional wellbeing hub
Target (95%): To be agreed with NSFT as BAU restarts Update (September 2020): Aug validated: 94% Sept unvalidated: 87%
EEAST – Performance. Risk 39 added February 2018 – risk is owned by Ipswich and East Suffolk CCG. For note on West Suffolk CCG GBAF
AC
CO
UN
TAB
LE O
FFIC
ER
& G
P O
WN
ER
DESCRIPTION OF STRATEGIC RISK
GRANULAR OPERATIONAL RISKS
IN
ITIA
L RA
G R
ATIN
G
(LIK
ELIH
OO
D x
CO
NSE
QU
ENC
E)
KEY CONTROLS ESTABLISHED
ASSURANCE OF CONTROLS
RISK APPETITE
(Treat, Tolerate, Transfer,
Terminate)
R
AG
RA
TIN
G L
AST
MO
NTH
R
EVIS
ED R
AG
RA
TIN
G
TAR
GET
RIS
K
ACTION POINTS & TARGET DATES FOR
COMPLETION

IQ/E
G
EEAST is failing performance targets against ambulance response categories, particular concern are delays in the higher acuity Category 1 and 2 calls.
Leadership Interim COO recently appointed. Workforce EEAST underperforming on recruitment against ISR plan impacting on the level of PFSH available to deploy on the road.
Handover delays Arrival of ambulance to handover at ED delays and handover at ED to clear, ready for next call delays. COVID 19 During Covid the volume of lower end ambulance calls has reduced dramatically this has allowed improved performance. This however is not sustainable and call volumes are beginning to increase.
5 x 3
15
Monthly quality and performance meetings held locally to be restarted post Covid. Monthly quality and performance meetings held regionally to be restarted post Covid. Commissioner attendance at EEAST internal Strategic Efficiency and Capacity review meetings. Review of delay serious incidents. Joint commissioner, EEAST and ESNEFT handover meetings held monthly. NHS 111/IUC enhanced clinical validation of C2, C3 and C4 ambulance dispositions.
N.B. Covid-19 Pandemic: • Ambulance Quality
Indicators will continue to be collected and monitored
Distribution of minutes and actions from sector and regional meetings. Weekly review of performance and handovers. Monthly review of NHS 111/IUC clinical validation performance. Clinical review of serious incidents through newly established SI panel. C1 and C2 performance improvements have been seen but not consistent CCG Priorities To ensure high quality local services where possible. To improve the health of those most in need.
Tolerate
4 x 4
16
4 x 4
16
2 x 3 6
1. Action – EEAST have target workforce/capacity gap taking longer to fill than expected – overall Staff in Post is 2894 vs ISR target of 3146 SIP, patient facing staff hours below funded levels. Actions/mitigations for safe service are:
a. Incidents monitored monthly through lead team/PQRM
b. Overtime/Private Ambulance Capacity targeted to peak demand shifts.
c. Productivity/rota redesign work accelerated, and revised strategic winter action plan agreed with NHSI/E
d. Local demand management schemes in place, these contribute to activity being 6% under agreed plan at month 8
e. Handover delays managed /monitored weekly
November 2020 Update. Response times improvements largely sustained, some pressure on C1/ C2 although long waits/tails remain steady. Front-line workforce gap has continued to reduce and has a deficit of 56 WTEs at end of September 2020. Hospital handover delays are elevated in a number of sites outside of SNEE (regional average handover times is 22 minutes in mid-October). Winter planning oversight meeting has been set up as joint meeting with NHS E/I and is due to meet in first week of November and this will establish onwards monitoring routine.

Cyber Security. Risk 42 added September 2018
AC
CO
UN
TAB
LE O
FFIC
ER
& G
P O
WN
ER
DESCRIPTION OF STRATEGIC RISK
GRANULAR OPERATIONAL RISKS
IN
ITIA
L RA
G R
ATIN
G
(LIK
ELIH
OO
D x
CO
NSE
QU
ENC
E)
KEY CONTROLS ESTABLISHED
ASSURANCE OF CONTROLS
RISK APPETITE
(Treat, Tolerate, Transfer,
Terminate)
R
AG
RA
TIN
G L
AST
MO
NTH
R
EVIS
ED R
AG
RA
TIN
G
TAR
GET
RIS
K
ACTION POINTS & TARGET DATES FOR
COMPLETION

AL/J
J
Potential impact of cyber security incident could lead to wide scale IT system outages, meaning no access to patient records, e-dispensing services etc Risk to the CCGs The CCGs would suffer significant service disruption and potential patient harm and financial loss
National requirements have increased, in respect of the need to achieve cyber essentials + accreditation.
No national funding has been identified specifically for cyber security work to mitigate against the increased risk, and the increased requirements.
No access to systems – would require frontline services to fully enact Business Continuity and Disaster Recovery procedures.
Potential for lack of access to relevant IT skills and insight to develop a recovery plan (dependent on type of attack).
Restoration of services complex, would involve multiple vendors and take a significant period of time
4 x 5
20
Note - eliminating risk of cyber-attack completely is not possible. Following external cyber assessment (post-Wannacry cyber-attack local review); a number of areas to be addressed to reduce risk of an attack and any potential impacts (see actions). In progress: Service provider (NEL) undergoing wide scale review of cyber assurance, have achieved cyber essentials accreditation March 2019, and working toward cyber essentials + accreditation. CCG has own domain (green) under NEL is working towards achieving cyber essentials accreditation for the CCG. TIAA reviewed cyber controls. Assurance received. ETTF (GP IT Capital) funding successful to implement security product (DarkTrace) to improve network monitoring. Additional ETTF (GP Capital) funds have been successful to implement a NAC solution, details being worked up with NEL. Board level training to IESCCG and WSCCG Board and Lay Members. W10 rollout 99.95% complete. Handful of remaining W10 PCs will be decommissioned in Oct/Nov when works to enable them to be decommissioned are complete – they remain under support.
External Audit. Internal audit complete Monthly SLA provider meetings. Monthly service review provider meetings. Bi-monthly Joint Digital and IT Services Board. Audit Committee review. Scrutiny Committee review Governing Body
Treat
4 x 5
20
4 x 5
20
3 x 4
12
1. Regular communications to users re phishing threats.
Target date: 31 March 2021 Completion: 2. Wide scale review of
patching processes and application.
Target date: 31 March 2021 Completion: Proposed further actions as implementation plans progress: Procure and rollout new network switching system with NAC (stage 1). Implement new licencing using new national licencing model. Access to Teams available for all CCG and GP staff. Security licencing and continued 365 licencing for GP applied for. Procure and rollout identity management system. Implement end user training programme. Rollout DarkTrace

Provider Workforce Risk 49 added July 2019
AC
CO
UN
TAB
LE O
FFIC
ER
& G
P O
WN
ER
DESCRIPTION OF STRATEGIC RISK
GRANULAR OPERATIONAL RISKS
IN
ITIA
L R
AG
RA
TIN
G
(LIK
ELIH
OO
D x
CO
NSE
QU
ENC
E)
KEY CONTROLS ESTABLISHED
ASSURANCE OF CONTROLS
RISK APPETITE
(Treat, Tolerate, Transfer,
Terminate)
R
AG
RA
TIN
G L
AST
MO
NTH
R
EVIS
ED R
AG
RA
TIN
G
TAR
GET
RIS
K
ACTION POINTS & TARGET DATES FOR
COMPLETION
AL
Lack of sufficient workforce across the system leading to risks to patient safety, care and services
The system has ageing clinical workforce with insufficient younger workforce to replace, leading to clinical risk of patients not being seen in appropriate timescales and inability to meet clinical and performance quality targets.
Brexit instability affecting overseas workforce.
Inability to maintain safer staffing levels in accordance with NICE and National Quality Board guidance.
Higher sickness absence of staff due to workload further impact on patient safety, care and services impact on staff retention, losing staff due to increased workload. Risk of patient experience deterioration due to long waits.
Risk of breaching constitutional obligations.
Primary care risk of some practices not being able to function and list closures.
EEAST underperforming on recruitment against ISR plan impacting on the level of PFSH available to deploy
3 x 5
15
At system level, a workforce strategy is in place.
• Collaborative working across providers to deliver.
• Joint recruitment initiatives,
• Career development, portfolio careers,
• Joint training (clinical and non-clinical)
Interim NHS People Plan released. Local Workforce Assurance Boards established. System wide Primary Care Training Hub established.
GP Support Hub providing support for the recruitment and retention of GPs. Regular monthly data showing progress.
IESCCG and WSCCG LWAGs (Local Workforce Assurance Group) reporting to Local Workforce Assurance Board (LWAB). IESCCG and WSCCG Training Hub Advisory Groups (THAG) reporting to the Training Hub Governance Group. The THAG’s continue to meet bi-monthly
3 x 4
12
3 x 4
12
2 x 3 6
1. Established nursing programme. Meeting target to raise student nurse placements by 15%. Fundamentals programme available for new nurses.
Target date: March 2021 Completion date:
2. Next Generation Project established for careers advice and joint recruitments events across Suffolk/NEE. Working with schools and colleges.
Target date: March 2021 Completion date:

Covid-19 Outbreak – Risk 56 added March 2020
AC
CO
UN
TAB
LE O
FFIC
ER
& G
P O
WN
ER
DESCRIPTION OF STRATEGIC RISK
GRANULAR OPERATIONAL RISKS
IN
ITIA
L R
AG
RA
TIN
G
(LIK
ELIH
OO
D x
CO
NSE
QU
ENC
E)
KEY CONTROLS ESTABLISHED
ASSURANCE OF CONTROLS
RISK APPETITE
(Treat, Tolerate, Transfer,
Terminate)
R
AG
RA
TIN
G L
AST
MO
NTH
R
EVIS
ED R
AG
RA
TIN
G
TAR
GET
RIS
K
ACTION POINTS & TARGET DATES FOR
COMPLETION
LN
Level 4 National Emergency. Current UK Alert Level: 4 The Alert level has been raised in light in increased case numbers. The Incident level currently remains at Level 3. The impact of a widespread Epidemic on the CCG will see an increase in demand on all commissioned services. The CCG could see significant changes to establish ways of working. The CCG may have absenteeism as staff self-isolate / ill over the period of the outbreak.
Current Situation in the UK. As of 4th November, 1,099,059 people have tested positive. Of those tested positive for coronavirus in the England (within 28 days), across all settings, 47,742 have died. The UK ‘R Number’ is between 1.1 – 1.3. Increased risk of fraud from Covid-19 related claims.
4 x 5
20
Business continuity plan in use. SuNEE incident room 0800-1800 Mon-Fri and 1000-1600 weekends with on-call cover outside these hours. Daily SuNEE operational and tactical meetings. Tactical resource supporting the Suffolk Outbreak Management Centre Local Outbreak Management Plan released 30/06/2020 Daily tracking of case numbers in place. Local Resilience Forum have stood up both TCG & SCG meetings.
CCG staff working virtually where possible and strict controls in place at office locations to support social distancing LCFS distributed warnings re Covid related fraud and passed to relevant finance staff. Invoice checking remains in place, where there are changes to these they do not relate to new suppliers and all items will be reconciled as required.
SuNEE Covid-19 Incident room staffed on rota basis Virtual support from Primary Care/ Care homes/ Communications and IPC teams. Business continuity plans in full operational use.
Treat
4 x 5
20
4 x 5
20
2 x 2 4
2. Monitoring of proliferation of virus will remain on-going. CCG will implement national guidance as required.
Target date: 31 March 2021 Completion date: Oct 2020 Update: ICC operations remain in place to support coordination of information from National/ Region teams to providers. Service provision has been maintained to meet demand of COVID19 patients. Continue local engagement in local resilience forums Service recovery groups established Winter planning being finalised, and stress tested with providers.
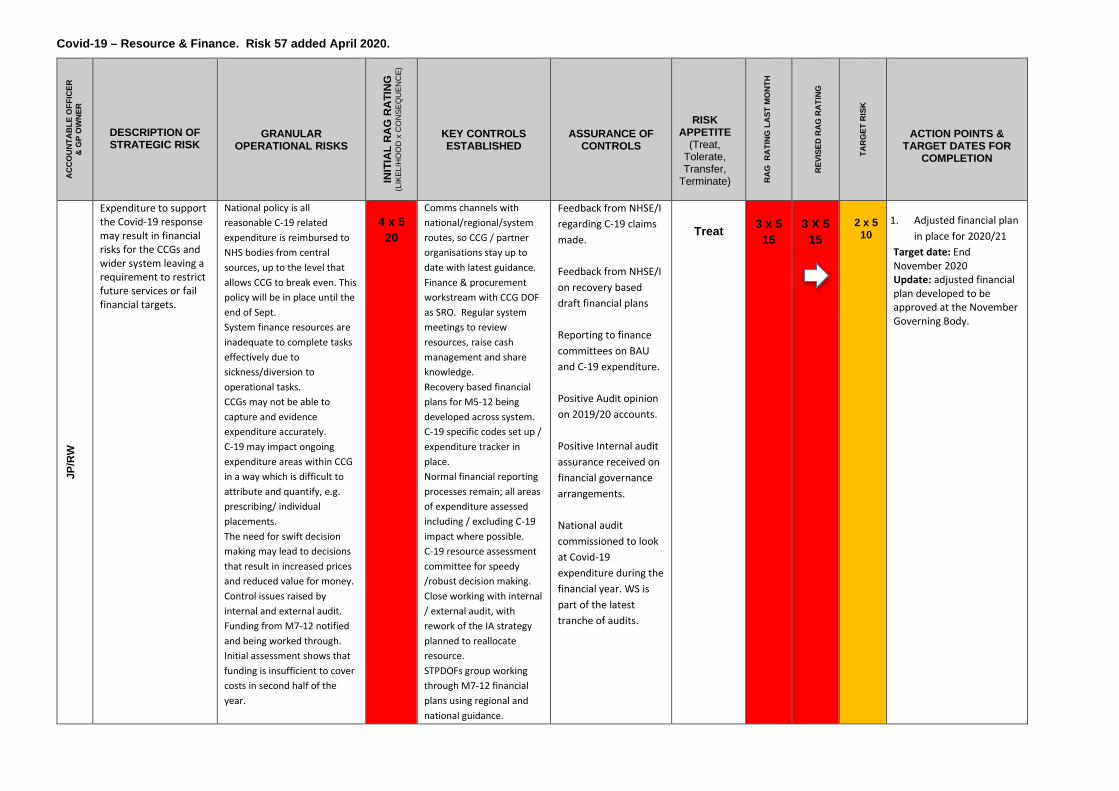
Covid-19 – Resource & Finance. Risk 57 added April 2020.
AC
CO
UN
TAB
LE O
FFIC
ER
& G
P O
WN
ER
DESCRIPTION OF STRATEGIC RISK
GRANULAR OPERATIONAL RISKS
IN
ITIA
L R
AG
RA
TIN
G
(LIK
ELIH
OO
D x
CO
NSE
QU
ENC
E)
KEY CONTROLS ESTABLISHED
ASSURANCE OF CONTROLS
RISK APPETITE
(Treat, Tolerate, Transfer,
Terminate)
R
AG
RA
TIN
G L
AST
MO
NTH
R
EVIS
ED R
AG
RA
TIN
G
TAR
GET
RIS
K
ACTION POINTS & TARGET DATES FOR
COMPLETION
JP/R
W
Expenditure to support the Covid-19 response may result in financial risks for the CCGs and wider system leaving a requirement to restrict future services or fail financial targets.
National policy is all reasonable C-19 related expenditure is reimbursed to NHS bodies from central sources, up to the level that allows CCG to break even. This policy will be in place until the end of Sept. System finance resources are inadequate to complete tasks effectively due to sickness/diversion to operational tasks. CCGs may not be able to capture and evidence expenditure accurately. C-19 may impact ongoing expenditure areas within CCG in a way which is difficult to attribute and quantify, e.g. prescribing/ individual placements. The need for swift decision making may lead to decisions that result in increased prices and reduced value for money. Control issues raised by internal and external audit. Funding from M7-12 notified and being worked through. Initial assessment shows that funding is insufficient to cover costs in second half of the year.
4 x 5
20
Comms channels with national/regional/system routes, so CCG / partner organisations stay up to date with latest guidance. Finance & procurement workstream with CCG DOF as SRO. Regular system meetings to review resources, raise cash management and share knowledge. Recovery based financial plans for M5-12 being developed across system. C-19 specific codes set up / expenditure tracker in place. Normal financial reporting processes remain; all areas of expenditure assessed including / excluding C-19 impact where possible. C-19 resource assessment committee for speedy /robust decision making. Close working with internal / external audit, with rework of the IA strategy planned to reallocate resource. STPDOFs group working through M7-12 financial plans using regional and national guidance.
Feedback from NHSE/I regarding C-19 claims made. Feedback from NHSE/I on recovery based draft financial plans Reporting to finance committees on BAU and C-19 expenditure. Positive Audit opinion on 2019/20 accounts. Positive Internal audit assurance received on financial governance arrangements. National audit commissioned to look at Covid-19 expenditure during the financial year. WS is part of the latest tranche of audits.
Treat
3 x 5
15
3 X 5
15
2 x 5 10
1. Adjusted financial plan
in place for 2020/21 Target date: End November 2020 Update: adjusted financial plan developed to be approved at the November Governing Body.

2020 Flu Campaign – Risk 58 *Risk added July 2020*
AC
CO
UN
TAB
LE O
FFIC
ER
& G
P O
WN
ER
DESCRIPTION OF STRATEGIC RISK
GRANULAR OPERATIONAL RISKS
IN
ITIA
L R
AG
RA
TIN
G
(LIK
ELIH
OO
D x
CO
NSE
QU
ENC
E)
KEY CONTROLS ESTABLISHED
ASSURANCE OF CONTROLS
RISK APPETITE
(Treat, Tolerate, Transfer,
Terminate)
R
AG
RA
TIN
G L
AST
MO
NTH
R
EVIS
ED R
AG
RA
TIN
G
TAR
GET
RIS
K
ACTION POINTS & TARGET DATES FOR
COMPLETION
CO
O
Chai
rs
That the 2020 flu campaign will be suboptimal due to several factors and targets will not be met
1. Lack of PPE 2. Lack of capacity given
that the injections will take 3 /4 times longer due to social distancing/ donning & doffing PPE
3. Delays and phased deliveries making flu messaging difficult
4. Availability of sufficient vaccine
5. Storage capacity 6. Many practices unable to
run clinics that support social distancing
7. Logistics of running clinics in non-practice settings – CQC reg, IT/data issues, cold chain
8. Increased cost of process 9. Ability to encourage risk
averse patients to attend 10. Absence of national
SOP 11. How to ensure the
most vulnerable pts receive the first vaccines
12. The addition of the 50- 64 year old cohort will amplify the existing risks on capacity/ PPE / vaccine stock etc
The capacity taken from PC to do this work could result in significant loss of LTC checks (Qof) which means practices will prioritise work that protects their income / business
4 x 4
16
1. NHSE has issued guidance that removes the requirement for changing between each patient
2. Practices are building workforce capacity with immunization training where possible
3. CCG supporting practices to use drive through options, village halls and larger spaces
The CCG will monitor vaccination rate via system reporting and feedback from practices. Regular updates to NHSE will be required
Tolerate
4 x 4
16
4 x 4
16
3 x 3
12
1. In close communication with NHSE following regional and national level guidance regarding most of the granular risks.
Target date: Dec 2020 Completion date:
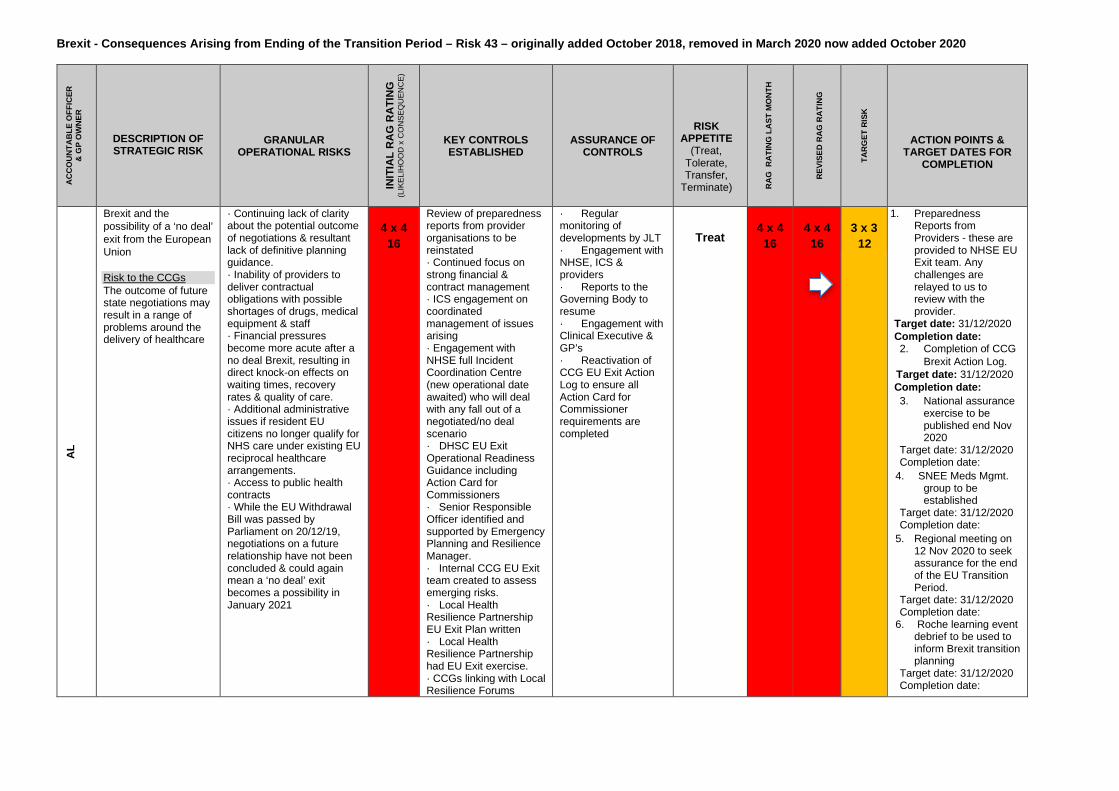
Brexit - Consequences Arising from Ending of the Transition Period – Risk 43 – originally added October 2018, removed in March 2020 now added October 2020
AC
CO
UN
TAB
LE O
FFIC
ER
& G
P O
WN
ER
DESCRIPTION OF STRATEGIC RISK
GRANULAR OPERATIONAL RISKS
IN
ITIA
L R
AG
RAT
ING
(L
IKEL
IHO
OD
x C
ON
SEQ
UEN
CE)
KEY CONTROLS ESTABLISHED
ASSURANCE OF CONTROLS
RISK APPETITE
(Treat, Tolerate, Transfer,
Terminate)
R
AG
RA
TIN
G L
AST
MO
NTH
R
EVIS
ED R
AG
RA
TIN
G
TAR
GET
RIS
K
ACTION POINTS & TARGET DATES FOR
COMPLETION
AL
Brexit and the possibility of a ‘no deal’ exit from the European Union Risk to the CCGs The outcome of future state negotiations may result in a range of problems around the delivery of healthcare
· Continuing lack of clarity about the potential outcome of negotiations & resultant lack of definitive planning guidance. · Inability of providers to deliver contractual obligations with possible shortages of drugs, medical equipment & staff · Financial pressures become more acute after a no deal Brexit, resulting in direct knock-on effects on waiting times, recovery rates & quality of care. · Additional administrative issues if resident EU citizens no longer qualify for NHS care under existing EU reciprocal healthcare arrangements. · Access to public health contracts · While the EU Withdrawal Bill was passed by Parliament on 20/12/19, negotiations on a future relationship have not been concluded & could again mean a ‘no deal’ exit becomes a possibility in January 2021
4 x 4
16
Review of preparedness reports from provider organisations to be reinstated · Continued focus on strong financial & contract management · ICS engagement on coordinated management of issues arising · Engagement with NHSE full Incident Coordination Centre (new operational date awaited) who will deal with any fall out of a negotiated/no deal scenario · DHSC EU Exit Operational Readiness Guidance including Action Card for Commissioners · Senior Responsible Officer identified and supported by Emergency Planning and Resilience Manager. · Internal CCG EU Exit team created to assess emerging risks. · Local Health Resilience Partnership EU Exit Plan written · Local Health Resilience Partnership had EU Exit exercise. · CCGs linking with Local Resilience Forums
· Regular monitoring of developments by JLT · Engagement with NHSE, ICS & providers · Reports to the Governing Body to resume · Engagement with Clinical Executive & GP’s · Reactivation of CCG EU Exit Action Log to ensure all Action Card for Commissioner requirements are completed
Treat
4 x 4
16
4 x 4
16
3 x 3
12
1. Preparedness Reports from Providers - these are provided to NHSE EU Exit team. Any challenges are relayed to us to review with the provider.
Target date: 31/12/2020 Completion date: 2. Completion of CCG
Brexit Action Log. Target date: 31/12/2020 Completion date:
3. National assurance exercise to be published end Nov 2020
Target date: 31/12/2020 Completion date:
4. SNEE Meds Mgmt. group to be established
Target date: 31/12/2020 Completion date:
5. Regional meeting on 12 Nov 2020 to seek assurance for the end of the EU Transition Period.
Target date: 31/12/2020 Completion date:
6. Roche learning event debrief to be used to inform Brexit transition planning
Target date: 31/12/2020 Completion date:

Directorate Risk Register summary of top risks
Date: November 2020
Department Risk Description / consequences
Current controls / assurance RAG Actions with status Completion date
Responsible person
1. Corporate Services
Hawthorn Drive Surgery are 100% over capacity in current premises; housing developments in the area will add further pressure to the patient list
Feasibility study being conducted to identify all public assets in the area and the potential for the surgery relocation to co-located premises / new build health and care hub (first proposal due Dec 19). Final draft of feasibility study report awaited; expected June/July delivery of this was delayed due to Covid-19 Short-term plan being developed whilst the long-term plan is underway to place a portacabin on site to offer 2 additional clinical rooms and admin space. Confirmation awaited on asset transfer to enable this to move to delivery phase, this is expected in next couple of months.
4
1. The Feasibility Study for the long-term concluded, SCC have agreed in principle to develop a Health and Care Hub at the Chantry Site. Business case being developed and to be presented to informal cabinet in Dec 20 to see if funding of £14m will be approved subject to FBC.
2. Ipswich Borough now signing contracts for purchase of Head Lease for the surgery premises. Once complete portacabin will be ordered/implemented for short-term capacity needs whilst long-term plan is developed.
Short-term portacabin
implemented by March 2021
Long-term plan
funding decision
December 2020
Julia Hiley
2. Corporate Services
Sizewell C proposal approved with no system mitigation agreed to support the impact on the health infrastructure
Joint health workstream established led by SCC – all communication with EDF is jointly reviewed and agreed
9 Escalation to ICS board for wider health input. Escalation to NHSI for national support and expertise.
Decision by planning
inspector due December
2021
Amanda Lyes
Risk Description / consequences
Current controls / assurance RAG Actions with status Completion date
Responsible person
1. COO Ipswich & East and West
A practice in IES have encountered significant GP staffing issues which may impact on their ability to see patients in a timely manner
CCG is working with local practices and the current provider to develop a plan to deal with this issue.
16
Initial scoping discussions with practice. Work on the way with the practice in respect of building project.
December 2020
David Brown

Risk Description / consequences
Current controls / assurance RAG Actions with status Completion date
Responsible person
1. Performance Improvement
Covid-19 Recovery Many of our commissioned providers have had to withdraw or re-provide services in a different way. In some cases, there are risks to the stability of organisations (e.g. charities whose non-NHS income has dropped). If those organisations fail or are unable to restart some services in a timely way there may be an impact on the health and wellbeing of patients.
All providers have been contacted and supplied an analysis of their risks and concerns. Contract managers and colleagues have been in contact with all providers expressing concern. Periodically the CCG will seek updates from all providers on their risks and concerns.
9
Where possible the CCG have put in place measures to ensure financial security during the Covid-19 escalation period. The CCG has begun recovery planning and is contacting organisations about their plans and concerns relating to restoring their services. The CCG are working closely with the hospices in particular to support their financial situations as far as possible. The CCG will be working with ICS partners to review our strategic approach to the VCSE sector.
31 March 2021 Jon Reynolds Nicola Brunning
Vicky Sawtell
2. Performance Improvement
Roche Reagent Supply Roche supply chain issues have led to a shortage of reagents needed to process tests in NHS laboratories. This is now impacting on a number of trusts’ ability to offer routine blood tests and they are having to prioritise which tests are carried out and processed
Trusts have put in place plans to ensure that they preserve their stocks and focus on the most urgent tests being analysed. Where appropriate, mutual aid arrangements have been put in place.
12
Further stocks have been delivered but the situation is being closely monitored by the CCGs and Trusts until the situation is fully resolved.
31 December 2020
Paul Gibara
Risk Description / consequences
Current controls / assurance RAG Actions with status Completion date
Responsible person
1. Finance There is a risk that NHS Pension Scheme regulations (which are laid down in law) have not been complied with in relation to GP Governing Body/Board Members and Clinical Leads.
GP Board Members are treated as employees, this may not be correct. For some GP Clinical Leads, the correct processes has been applied from 19/20. GP Solo Pension contributions are deducted at source and paid to the correct body in accordance with the declarations
12
Current controls do not remove retrospective risks. The CCG must make a decision confirming the employment status of GP Board Members /Clinical Leads so correct pension processes can be implemented, being cognisant
December 2020
Jane Payling

made about their pension circumstances on joining the CCG. This means different processes exist depending on the GP.
of the consequences of either decision. Action to minimise retrospective risks required: either action to quantify the risks of claims from people classed as employees but not treated as them, or action to quantify possible consequences of failure to have treated GP SOLO payments correctly (and therefore potentially failure to pay over at the correct rate).
2. Finance Failure to achieve in year financial balance, secure financial sustainability and deliver optimum service from financial resources available.
Guaranteed Income Contracts in place with key providers. Clinical Executive and Governing Body review expenditure and significant investments. Project management approach to delivery of QIPP through PMO
10
Regular executive level dialogue between CCG and providers. Regular FPC reporting. Note that payments have been altered due to Covid-19 and the extent and length of these changes is as yet uncertain: the Covid-19 GBAF risk covers this.
March 2021 Jane Payling
Risk Description / consequences
Current controls / assurance RAG Actions with status Completion date
Responsible person
1. Nursing The capacity of the team to achieve annual ICS objectives restricted by the unfilled hours to support IPC in NEECCG. This is exacerbated by new CDI reporting process, increase in workload for the team.
1. 2nd staff member appointed to SNEE. 2. Temp support for IPC in ICC room from transformation lead. Full support from care homes teams in Suffolk and NEE. Support from quality teams members to provide IPC train trainer programme to all care homes. Following posts are supporting - Band 8b 3x days week NEE. Band 8b 3x days per week agency Suffolk CCG. Band 7 4 days week to support SNEE IPC post.
16
Care Sector IPC Strategy and recruitment posts out to advert. Current risks relate to actual potential start dates. To mitigate this risk in Suffolk SNEE IPC band 7 covering Care sector, SNEE IPC -X1 nurse under capacity. Resource challenges continue. October 2020: No further update available.
April 2021 Julia Shields

2. Nursing Lack of recent validated data makes it difficult to measure the success of saving babies lives implementation, and the required 20% reduction of neonatal and maternal deaths and brain injuries. This creates a risk that the system is not on track to deliver the required reduction.
1. Providers to submit local data to LMS clinical lead/PM to enable crude analysis of compliance 2. Clinical leadership to SBL action group to ensure the bundle is implemented and therefore outcomes will positively impact our reduction
15
1. Keep monitoring locally, until data is published at the end of 2020. 2. October 2020 – no update.
Sept 2021 Helen Bowles
Risk Description / consequences
Current controls / assurance RAG Actions with status Completion date
Responsible person
1. Transformation Failure to achieve national Dementia diagnosis target for WSCCG of 67% in line with the Prime Minister's Challenge on Dementia 2020. WSCCG at March 61.4% April 60.6% - 6.1% below the target (Covid19 impact regionally all diagnosis declined).
Full Programme of work underway as agreed with NHSE. Highlights include meds management focus on “at risk” register; Care Homes Liaison Nurse working closely with care home and practices; West Suffolk Dementia Operational Group established; Community Dementia Together Navigator working well engaging with localities and the local community.
12
SEP 20 Transformation programme active. Work underway to improve the MAS pathway, 7-day service DIST pilot due to commence and work underway across primary care to enhance engagement and coding practices. In both August and September, the dementia diagnosis rate went up, now standing at 60.3%. East of England is 61%. As well as Post Diagnostic support. Immediate focus will be data integrity, communication throughout the pathway and raising awareness across the locality in the importance of a dementia diagnosis.
Dec 2020 Gail Cardy / Rob Chandler

Page 1 of 2
GOVERNING BODY
Agenda Item No. 18
Reference No. WSCCG 20-52
Date. 25 November 2020
Title Appointment of External Auditors
Lead Director Jane Payling, Director of Finance
Author(s) Emily Bosley, Financial Governance Accountant
Purpose Approve the appointment of new external auditors.
Applicable CCG Priorities:
1. Develop clinical leadership2. Demonstrate excellence in patient experience & patient engagement3. Improve the health & care of older people4. Improve access to mental health services5. Improve health & wellbeing through partnership working6. Deliver financial sustainability through quality improvement X
Action required by Governing Body:
Approve the appointment of new external auditors, BDO, on an initial three year term with the option to extend up to five years, in line with the recommendation of the auditor panel.

1. Background 1.1 The CCG was able to tender for new auditors this year, facilitating synergies by looking to
appoint a single auditor across the three CCGs. A procurement exercise by further competition under a framework agreement has been completed. The Auditor Panel appointed by the Governing Body at its last meeting has reviewed the procurement process and recommends the appointment of BDO.
2. Key Issues 2.1 The key issues considered while completing this procurement included how to ensure the best
value for money for the CCGs, and to this end a series of detailed questions were asked to applicants such that their evidence in relation to various key audit questions were addressed.
2.2 Audit Committee Chairs from each of the three CCGs, along with the Director of Finance and
Deputy Director of Finance (Financial Reporting and Governance) scored the applicants, taking all three initial applicants (EY, KPMG, BDO) forward as the quality of all answers were high. The bidders were then invited to present to a panel consisting of the above individuals, where follow up questions were answered. The highest score went to BDO, due to a combination of a high quality answers with a lower price.
2.3 The Governing Body should note that the market for External Audit services to the NHS is
known to be difficult due to the competing forces of downward pressure on price and increases in costs and quality requirements. We were fortunate to receive three high quality, credible bids in this exercise but it should be noted that all bids showed an increase in cost compared to the combined costs paid by the CCGs in 19/20. Bidders were asked to provide costings for the scenario of 3 CCGs alongside that of a merged CCG (including the costs of audit requirements to support the merger). The different bidders anticipated significantly different costing changes relating to the pre and post merger scenarios.
2.4 The contract is for a minimum of three and a maximum of five years, although the CCG has
the right to withdraw prior to three if necessary. The bidder is entitled to an annual RPI based inflationary uplift.
3. Resource Implications 3.1 If the CCGs remain as separate statutory organisations the cost per CCG will be £57,333 per
annum + VAT, with annual increases in line with RPI. If the organisations merge, the cost for the merged CCG would be £110k per annum + VAT, again with annual increases in line with RPI.
4. Patient and Public Engagement 4.1 Applicants for the position of external auditor were asked to explain how they ensured their
communications with patients and members of the public were accessible and useable while maintaining audit rigor. BDO received the joint top score for this question which was asked alongside others.
5. Recommendation 5.1 The auditor panel has reviewed the scoring from the procurement and recommends that the
Governing Body approves the appointment of BDO as our new external auditor, for financial year 20/21 inclusive and onwards.

Page 1 of 2
GOVERNING BODY Agenda Item No. 19
Reference No. WSCCG 20-53
Date. 25 November 2020 Title
Health, Safety and Risk Committee
Lead Director
Amanda Lyes, Director of Corporate Services and System Infrastructure
Author(s)
Tony Buckle, Risk Manager
Purpose
To update the Governing Body on current health and safety issues
Applicable CCG Clinical Priorities: 1. Develop clinical leadership 2. Demonstrate excellence in patient experience & patient engagement 3. Improve the health & care of older people 4. Improve access to mental health services 5. Improve health & wellbeing through partnership working 6. Deliver financial sustainability through quality improvement Action required by Governing Body: To note the report.

1. Purpose
To advise the Governing Body of work currently being undertaken in relation to Health & Safety.
2. Background
The Health, Safety and Risk Committee, chaired by the Director of Corporate Services and System Infrastructure, continues to meet twice per year. The committee review the H&S annual plan at these meetings to ensure that the CCGs remain compliant with current H&S legislation.
3. Key Points
The last meeting of the committee was on 29 October 2020. Issues reviewed included the following items.
• Covid-19 workplace risk assessments have been completed for all CCG buildings and are available on the intranet. Current position is to work from home unless this is not possible or if there is a business need.
• An update was given in relation to the CCG staff flu vaccinations. Up to 29 October a total of 68 vaccinations had been given to staff. Supplies had run out, but more available w/c 2 November. CCGs can order more vaccines if necessary, the current order is for 200 but this can be increased to 450 to cover all staff. The vaccinations are available at all main hospital sites.
• The 2020 / 2021 was presented, and it was agreed to include a section on
homeworking and the risk assessment process for that.
• The Terms of Reference for the committee were reviewed. A few changes were highlighted which will be made.
• There have been no health and safety related incidents since the last meeting. It
was agreed that the committee would look at staff Covid-19 positive cases.
• The latest sickness absence figures were discussed. The figures have been low since the start of lockdown. The nursing directorate has the highest and contributes to over half of the sickness absence costs. Stress and depression are the main cause of days lost and cost.

Page 1 of 2
GOVERNING BODY
Agenda Item No. 20
Reference No. WSCCG 20-54
Date. 25 November 2020
Title Declaration of Interests
Lead Director Amanda Lyes, Chief Corporate Services Officer
Author(s) Colin Boakes, Independent Governance Advisor
Purpose The report provides a public record of relevant and material interests declared by members of the Ipswich and East Suffolk CCG Governing Body, its sub-committees, staff and member practices.
Applicable CCG Clinical Priorities: 1. Develop clinical leadership2. Demonstrate excellence in patient experience & patient engagement3. Improve the health & care of older people4. Improve access to mental health services5. Improve health & wellbeing through partnership working6. Deliver financial sustainability through quality improvement X
Action required by Governing Body:
The Governing Body is asked to review the current register and consider whether any action in relation to non-responders might be required.

Page 2 of 2
1. Background 1.1 Clinical commissioning groups (CCGs) manage conflicts of interest as part of their day-
to-day activities. Effective handling of conflicts of interest is crucial to give confidence to patients, tax payers, healthcare providers and Parliament that CCG commissioning decisions are robust, fair and transparent and offer value for money. It is essential in order to protect healthcare professionals and maintain public trust in the NHS. Failure to manage conflicts of interest could lead to legal challenge and even criminal action in the event of fraud, bribery and corruption.
1.2 Conflicts of interest are inevitable in commissioning. It is how we manage them that
matters. Section 14O of the National Health Service Act 2006 (as amended by the Health and Social Care Act 2012) (“the Act”) sets out the minimum requirements of what both NHS England and CCGs must do in terms of managing conflicts of interest.
1.3 As a minimum, CCGs must have robust systems in place to identify and manage
conflicts of interest. This should involve creating an environment in which CCG staff, Governing Body and sub-committee members, and member practices feel able, encouraged and obliged to be open, honest and upfront about actual or potential conflicts. Transparency in this regard is expected to lead to effective identification and management of conflicts. The effect should be to make everyone aware of what to do if they suspect a conflict and ensure decision-making is efficient, transparent and fair.
1.4 CCGs are required to have systems in place to satisfy themselves that their registers of
interest are accurate and up-to-date. 2. Key Points 2.1 As regards declarations and registers of interest, guidance requires that all CCG
Officers, Governing Body members, GPs, all staff, including students, agency and seconded staff, together with practice staff with involvement in CCG business complete declarations. However, only those staff classed as ‘decision makers’ will be included in the register published on the CCG’s web site.
2.2 Declarations are sought by the CCG on a six-monthly basis – in October by submission
of a signed declaration and in April by exception should there have been changes. The decision makers declarations constitute the register published on the CCG’s website. The current register is attached to the report at Appendix 1. (Dates highlighted in ‘Red’ denote where there has been no response to the request for declarations in October 2020)
2.3 In view of the Covid19 pandemic, we have managed the collection of declarations of
interest slightly differently this year. For example, where it has not been possible for staff members to send in signed hard copy declarations, we have accepted e-mailed copies with electronic signatures. Similarly, where there has been no change to an individual’s declaration or where there is a nil return, these have been signed off by the Corporate Governance Manager on my behalf.
3. Recommendation 3.1 The Governing Body is asked to review the current register and consider whether any
action in relation to non-responders might be required.

Interests of:
Governing Body and Sub-Committee MembersDecision Making Staff
Member Practices
Register of Interests
October 2020
West Suffolk CCG

Financial Interests
Non Financial Professional
Interests
Non Financial Personal Interests
From To
Governing Body GP Member Zohra Armitage GP and GP Streaming work for Suffolk GP Federation Direct Ongoing 07/10/2020 No further action required YesHusband is a consultant urologist at Cambridge University Hospital Indirect Ongoing 07/10/2020 No further action required YesDirector of company providing urological services to Swan Surgery, BSE Direct Ongoing 07/10/2020 To be declared when appropriate Yes
Lay Member for Governance and Vice Chair CCG Geoff Dobson Former Director of Resource Management with Suffolk County Council Indirect Ongoing 06/10/2020 No further action required YesFamily member attending Healthier You, NHS Diabetes Prevention Programme’' Indirect Apr-20 Ongoing 06/10/2020 No further action required Yes
CCG Chair Christopher Browning PMS Provider, Practice Partner Long Melford Direct 2001 Ongoing 03/04/2020 To be declared at relevant meetings YesOut of Hours doctor for Care UK and Suffolk GP Federation Direct 2010 Ongoing 03/04/2020 To be declared at relevant meetings YesWife is Consultant at West Suffolk Hospital Indirect 2004 Ongoing 03/04/2020 To be declared at relevant meetings YesClinical Director for WGGL PNN" Direct Ongoing 03/04/2020 To be declared at relevant meetings Yes
Lay Member Steve Chicken Owner and MD of Galliform Ltd, consultancy and training company. No NHS activity Direct 2009 Ongoing Leave No further action required YesLay Member for Ipswich and East Suffolk CCG Direct 2016 Ongoing Leave To be declared when appropriate YesWife is President and Director of East of England Co-op Indirect 2018 Ongoing Leave To be declared when appropriate Yes
Chief Officer Ed Garratt Accountable Officer for Ipswich and East Suffolk CCG Direct Mar-16 Ongoing 23/10/2020 To be declared when appropriate YesAccountable Officer for North East Essex CCG Direct Jan-19 Ongoing 23/10/2020 To be declared when appropriate YesExecutive Lead - Suffolk and North East Essex Integrated Care System Direct Apr-19 Ongoing 23/10/2020 To be declared when appropriate Yes
Director of Performance Improvement Paul Gibara Director of Performance Improvement for SNEE CCGs Direct Ongoing 30/10/2020 YesEnhanced Associate GP Andrew Hassan Wife has GDS contract with NHS England Indirect Ongoing 07/10/2020 YesDirector of Corporate Services and System InfrastructureAmanda Lyes Director of Corporate Services and System Infrastructure for Ipswich and East Suffolk and North East Essex CCGs Direct Ongoing 12/10/2020 None YesDirector of Nursing Lisa Nobes Chief Nursing Officer for Ipswich and East Suffolk CCG and North East Essex CCG Direct Ongoing 03/04/2020 None YesDirector of Finance Jane Payling Director of Finance for Ipswich and East Suffolk CCG and North East Essex CCG
Direct 25/09/2017 Ongoing 28/10/2020 Arrangements in place for the joint management team of
the CCGsYes
Trustee of Cambridge Theatre Trust Direct Oct-18 Ongoing 28/10/2020 To declare when appropriate YesGoverning Body GP Member Godfrey Reynolds Member of the Local Medical Committee Direct Ongoing 02/10/2020 None Yes
Chair of Mildenhall Sick and Poor Fund Direct 1989 Ongoing 02/10/2020 None YesConsultant in Public Health Medicine Jep Ronoh Husband is a salaried GP at Hardwicke House Surgery and does locum work for Out of hours provider, Suffolk GP Fed and
other GP Surgeries Direct Ongoing07/11/2019 To declare when appropriate Yes
Governing Body GP Member Bahram Talebpour Medical Director of Sudbury Primary Care Network Direct Ongoing 24/04/2020 No further action required YesGP Partner Direct Ongoing 24/04/2020 No further action required Yes
Chair of Community Engagement Partnership David Taylor Chairman of Hargrave Parish Council Direct Apr-17 Ongoing 23/10/2020 No further action required YesLay Member for Patient and Public Involvement Linda Tuck Nil 05/10/2020 YesChief Operating Officer Kate Vaughton Director of Integration for West Suffolk NHS Foundation Trust, non-voting member of Board Direct Ongoing 03/11/2020 To declare when appropriate YesGoverning Body GP Member Firas Watfeh Local Medical Committee member Direct 01/08/2015 Ongoing 23/10/2020 Yes
Haverhill PCN Director Direct Ongoing 23/10/2020 YesGP Partner at Haverhill Family Practice Direct 04/07/1905 Ongoing 23/10/2020 Yes
Director of Strategy and Transformation Richard Watson Director of Strategy and Transformation for Ipswich and East Suffolk, North East Essex CCGs and West Suffolk CCGs Direct Jan-15 Ongoing 08/10/2020 None YesHusband is employee of Hadleigh Group Practice Direct Oct-19 Ongoing 08/10/2020 None Yes
Governing Body GP Member Victoria Wilson Shares in company for ophthalmology related work Direct Ongoing 16/10/2020 To be declared when appropriateMaternity work for maternity voices partnership, West Suffolk Hospital Direct Ongoing 16/10/2020 No further action required
Governing Body GP Member Andrew Yagar Macmillan GP Direct 2021 Ongoing 31/10/2020 YesGoverning Body GP Member Vacant GP PostGoverning Body PM Member Vacant PostGoverning Body PM Member Vacant PostSecondary Care Doctor Vacant Post
West Suffolk CCG Governing Body and Sub Committee Members
Title First Name Last Name Direct or Indirect
Date of Interest Date of Receipt
Action Taken to Mitigate Consent to Publish
Type of InterestDeclared Interest

Declared Interest
Financial Interests
Non Financial
Professional Interests
Non Financial Personal Interests
From To
yes Mrs Helen Abel Senior Contracts Manager Nil 05/10/2020 Yes
yes Mr. Adewale Abimbola Senior Pharmacist Nil 26/10/2020 Yes
yes Miss Carrie Bacchus Contract Manager Nil 06/10/2020 Yes
yes Mrs Clare Banyard Asso Director of Transformation Not for publication Direct 2019 Ongoing 02/10/2019 No further action required No
Not for publication Direct Ongoing 02/10/2019 No further action required No
yes Miss Julie Baran Int GP Recruitment Manager Nil 12/10/2020 Yes
yes Mrs Amanda Bennett GP Nurse Education Lead Secondary role as Freedom to Speak Up Guardian at West Suffolk Hospital Direct Ongoing 01/10/2020 Yes
yes Mrs. Ameeta Bhagwat Finance Manager Nil 05/10/2020 Yes
yes Mr Peter Broughton Contracts Manager Nil 02/10/2020 Yes
yes Mr. David Brown Deputy Chief Operating Officer Nil 23/10/2020 Yes
yes Mr Gregory Brown Contracts Manager Autism - family members have autism Indirect Ongoing 23/10/2020 No further action required Yes
yes Mrs. Nicola Brunning Lead Contracts Manager - Community Sister is nurse at East Suffolk and North Essex NHS Foundation Trust Indirect Ongoing 15/10/2020 No further action required Yes
yes Mrs. Valerie Butcher Acute Commissioning Finance Specialist Nil 01/10/2020 Yes
yes Miss Catherine Butler Head of GP Prescribing Partner works as a CQC registration inspector in Midlands and East Region Indirect Oct-15 Ongoing Leave None Yes
Partner is starting a private slimming clinic business and will be a Director Indirect Oct-19 Ongoing 04/10/2019 None Yes
yes Mrs. Joanne Bye Senior Medicines Management Technician NVQ Assessor and Internal Verifier in Pharmacy Services for West Suffolk College, Bury St Edmunds. Casual paid contract
Direct Sep-04 Ongoing 21/11/2019 No further action required Yes
Revalidation CPD Reviewer and Return to Practice Reviewer for General Pharmaceutical Council (GPhC). Casual paid contract.
Direct Jul-05 Ongoing 21/11/2019 No further action required Yes
Active committee member of Barton Mills Parish Council Direct Nov-19 Ongoing 21/11/2019 No further action required Yes
yes Ms. Sonia Carnegie Int GP Recruitment Coordinator Nil 24/10/2019 Yes
yes Mrs. Sandra Chambers Business Support Manager Nil 23/10/2020 Yes
yes Mr Christopher Chapman Emergency Planning & Resilience Officer Volunteer for St John Ambulance as Area Manager Direct 01/09/2018 Ongoing 23/10/2020 No further action required Yes
yes Mr Rifat Choudhury Advanced Practice Support Pharmacist Wife working as a locum community pharmacist Indirect Ongoing 02/10/2020 Yes
Wife works at EPUT as a mental health pharmacist Indirect 2018 Ongoing 04/04/2018 No further action required Yes
yes Mr Mark Clinton Snr Mangement Accountant Wife works for Stroke Early Supported Discharge Team provided by Norfolk Communty Health and Care
Indirect Ongoing 14/10/2020 No further action required Yes
yes Ms Anna Cochrane Head of ICT & Informatics Not for publication Indirect Ongoing 02/10/2020 None No
yes Mr. Richard Cracknell Head of Operations Family members work for Care UK and East Suffolk and North Essex Foundation Trust
Indirect Ongoing 04/10/2019 - To declare when appropriate Yes
Trustee of charity funding care in Romania Direct Ongoing 04/10/2019 To declare when appropriate Yes
Family Members work for Suffolk GP Federation Direct Ongoing 04/10/2019 To declare when appropriate Yes
yes Mrs Nichole Day Deputy Chief Nursing Officer Nil 09/11/2020 Yes
yes Mrs. Cindie Dunkling Designated Nurse Safeguarding Children Nil 23/10/2020 Yes
yes Ms. Amanda Estall Redesign Project Manager Daughter is an Emergency Nurse Practitioner at Addenbrookes A&E Indirect 31/10/2016 Ongoing 01/10/2020 None Yes
Stepfather has multiple LTCs and is a service user of WSFT services. (Diabetes, Respiratory, Oncology/Haematology
Indirect Ongoing 01/10/2020 None Yes
yes Ms. Nerinda Evans Associate Director of Redesign Nil 09/10/2020 Yes
yes Mrs. Helen Farrow Senior Executive Assistant Nil 02/10/2020 Yes
yes Mrs. Lucy Game Operational Manager, NHS Continuing Healthcare Husband is Deputy Director of Finance Accounting and Control for Ipswich and East, North East Essex and West Suffolk CCGs
Indirect Ongoing 19/10/2020 No further action required Yes
yes Mr. Mark Game Head of Accounting and Control Wife is Continuing Healthcare Operational Mgr for both CCGs Indirect Ongoing 09/05/2019 No further action required Yes
yes Ms. Gabrielle Gilhooly PALS Manager Nil 01/10/2020 Yes
yes Mrs. Elizabeth Hallworth Clinical Executive & Chief Operating Office Operation ManaFather and brother owners of Optometric Practices in Suffolk Indirect Nov-13 Ongoing 02/10/2020 None Yes
yes Mrs. Louise Hardwick Head of Primary Care Partnerships Nil 07/10/2020 Yes
yes Mr James Hayward Information Analyst Nil 07/10/2020 Yes
yes Mr. Roger Holt Financial Accounts Manager Nil 03/11/2020 Yes
yes Ms. Suzanne Hoy Contract Manager Nil 02/10/2020 Yes
yes Mr. Matthew Hunt Enterprise Architect Not for publication 02/10/2020 No
yes Mrs. Julie Irving Information Sharing Programme Manager Nil 01/10/2020 Yes
yes Mrs. Jo John Transformation Lead Nil 12/10/2020 Yes
yes Mrs. Julie Kerridge Senior Management Accountant Nil 19/10/2020 Yes
yes Mrs. Linda Lord Chief Pharmacist Nil 01/10/2020 Yes
yes Mr Darren Maguire Escalation Coordinator Nil 01/10/2020 Yes
yes Mrs. Hannah Morgan Assistant Management Accountant Nil 23/10/2020 Yes
yes Ms. Jacqueline Morris Business Support Officer Nil 08/10/2020 Yes
yes Mrs. Gillian Mountague Redesign Project Manager Nil 01/10/2020 Yes
Direct or Indirect
Decision Making Staff ListBudget
Signatory £5k+
Consent to PublishDate of Receipt
Action Taken to MitigateTitle First Name Last Name Type of Interest Date of InterestPosition Title

yes Miss Sheila Murnion Head of High Cost Drugs Management Nil 01/10/2020 Yes
yes Ms. Lianne Nunn Clinical Quality Contract Lead School Governor for Holbrook Academy, Ipswich Direct Ongoing 04/11/2020 Yes
yes Mr. Dean Onno Transformation Lead Nil 05/10/2020 Yes
yes Mrs Amy Osborne Contracts Manager Nil 22/10/2020 Yes
yes Mrs. Lorraine Parr Transformation Lead Nil 06/10/2020 Yes
yes Miss Claire Pemberton Commissisoning Implementation Manager Nil 02/10/2019 Yes
yes Mr Scott Pomroy Commissioning Support Officer Member of Suffolk Parent Carers Network Direct Jul-18 Ongoing 02/10/2020 None Yes
yes Mrs Hannah Pont Transformation Lead Nil 04/04/2018 Yes
yes Mrs. Caroline Procter Co-Commissioning Manager Nil 22/10/2020 Yes
yes Mrs. Jemma Redfern Senior Co-ordinator Continuing Healthcare Nil 05/10/2020 Yes
yes Mr. Jonathan Reynolds Deputy Chief Contracts Officer Volunteer for Christians Against Poverty/Hope Church, Ipswich Direct Nov-18 Ongoing 02/10/2020 Yes
Volunteer for the Ipswich Soup Kitchen Direct Ongoing 02/10/2020 Yes
yes Mrs. Sandie Robinson Head of Planning and Delivery Nil 02/10/2020 Yes
yes Mrs. Alison Sadler Redesign Project Manager Nil 12/10/2020 Yes
yes Mrs. Wendy Scott Children's Paediatric Continuing/Shared Care Reviewer Nil 01/10/2020 Yes
yes Mrs. Rachel Seago Practice Support Manager Husband is a consultant for Fellowship on non-digital branding projects. Direct Ongoing 02/10/2020 No further action required Yes
yes Ms Nicole Smith Transformation Lead Husband works for East of England Procurement Hub (employed by West Suffolk Hospital
Indirect Ongoing 20/10/2020 To be declared when appropriate Yes
yes Mr. Eugene Staunton Head of Planning and Delivery Not for publication Direct 2012 Ongoing 01/10/2020 No further action required No
yes Ms. Fiona Sutton Contracts Manager Nil 23/10/2020 Yes
yes Mrs. Anita Taylor Contract Manager Nil 12/10/2020 Yes
yes Mrs. Jessica Taylor-Allum Information Analyst Nil 03/10/2019 Yes
yes Mr James Thompson Financial Accounts Manager My partner is a social worker and works at the Sudbury office covering that i
Indirect Ongoing 23/10/2020 Yes
yes Mr John Troup Communications Manager Nil 02/10/2020 Yes
yes Mr. Giles Turner HR Business Partner Nil 03/11/2020 Yes
yes Mrs. Rebecca Turner Transformation Project Officer Nil 02/10/2020 Yes
yes Mr. James Waites Account Manager (contracts) Nil 02/10/2020 Yes
yes Miss Eleanor Ward International GP Recruitment Co-ordinator Father is Leader of Babergh District Council Indirect Ongoing 02/10/2020 No further action required Yes
yes Mrs. Melanie Webster Senior Co-ordinator Continuing Healthcare Volunteer Representative for Cardiac Risk in the Young Direct Ongoing 29/10/2020 No further action required Yes
yes Ms. Caroline Wells Referral Pathways Support Manager Husband is physio at Colchester Hospital Indirect Ongoing 07/10/2020 No further action required Yes
yes Mr. Michael Wigg Clinical Quality Contracts Manager Nil 16/04/2019 Yes
yes Mrs. Lois Wreathall Head of Practice Support Trustee of Abbeycroft Direct Mar-16 Ongoing 01/10/2020 To declare when appropriate Yes

Financial Interests
Non Financial
Professional Interests
Non Financial Personal Interests
From To
Angel Hill GP Sara Garrod Nil 09/11/2020 YesGP Paul Harrison Nil 09/11/2020 YesGP Laura Leach Nil 06/10/2020 YesGP Elizabeth Polli Husband is partner at Mount Farm Surgery, Bury St Edmunds Indirect Ongoing 10/11/2020 No further action required YesGP Helen Spring Nil 08/10/2020 YesGP Sujata Surti Nil 02/10/2020 YesGP William Tasker Nil 12/10/2020 Yes
Botesdale Health Centre GP Lauren Bate Shares Suffolk GP Federation Direct Ongoing 06/10/2020 YesGP Jude Chapman Not for publication Direct Ongoing 03/11/2020 No
Blackbourne Rural PCN Clinical Director Direct Ongoing 03/11/2020 NoWife is consultant at NNUH Indirect Ongoing 03/11/2020 No
GP Lisa Fennelow Shares Suffolk GP Federation Direct Ongoing 06/10/2020 YesGP Donald MacFachern Shares Suffolk GP Federation Direct Ongoing 04/11/2020 Yes
Brandon Medical Practice GP Emmanuel Obiabo Nil 06/10/2020 YesGP Jacquelyn Rae Nil 06/10/2020 Yes
Clements Christmas MaltingsGlemsford Surgery GP Matthew Piccaver Not for publication Direct Oct-15 Ongoing 15/10/2020 To be declared when appropriate NoGuildhall Surgery GP Simon Whitehead Nil 13/10/2020 Yes
GP Jane O'Donnell Nil 13/10/2020 YesGP Jonathan Huck Nil 13/10/2020 YesGP Adam Bone Nil 13/10/2020 Yes
Guildhall and Barrow Surgery GP Heather Griffin Director of G&B Med Services Ltd providing pharmacy services Direct 2013 Ongoing 18/10/2018 To declare at all relevant committees when in attendance YesGP Mark Hunter Director of G&B Med Services Ltd providing pharmacy services Direct 2013 Ongoing 10/10/2018 To declare at all relevant committees when in attendance YesGP Michael Jones Director of G&B Med Services Ltd providing pharmacy services Direct 2013 Ongoing 05/10/2018 To declare at all relevant committees when in attendance YesGP Peter Smye Director of G&B Med Services Ltd providing pharmacy services Direct 2013 Ongoing 10/10/2018 To declare at all relevant committees when in attendance YesGP Kate Wallace Director of G&B Med Services Ltd providing pharmacy services Direct 2013 Ongoing 18/10/2018 To declare at all relevant committees when in attendance Yes
Hardwicke House Surgery GP Alison Cook Nil 04/11/2019 YesGP Jamie Gilmour Nil 31/10/2019 YesGP Bassam Morgan Nil 31/10/2019 YesGP Susmitha Pavulvi Nil 04/11/2019 YesGP Rakesh Raja GP Partner in PMS dispensing Practice Direct Ongoing 31/10/2019 To declare at all relevant committees when in attendance Yes
Provides cover for rehab beds at Hazell Court Direct Ongoing 31/10/2019 To declare at all relevant committees when in attendance YesWife works for same practice Indirect Ongoing 31/10/2019 No further action required Yes
GP Bahram Talebpour Medical Director of Sudbury Primary Care Network Direct Ongoing 01/10/2019 No further action required YesGP Partner Direct Ongoing 01/10/2019 No further action required Yes
GP Amanda Woods Nil 17/05/2019 YesHaverhill Family Practice GP Firas Watfeh Local Medical Committee member Direct 01/08/2015 Ongoing 23/10/2020 Yes
Haverhill PCN Director Direct Ongoing 23/10/2020 YesGP Partner at Haverhill Family Practice Direct 04/07/1905 Ongoing 23/10/2020 Yes
GP Emma Hern Nil 02/10/2020 YesLakenheath GP E Bower Nil 03/10/2018 Yes
GP Judith Roberts Nil 02/10/2019 YesGP Sarah Hutchinson Nil 15/10/2018 Yes
Long Melford Practice GP Christopher Browning PMS Provider, Practice Partner Long Melford Direct 2001 Ongoing 03/04/2020 To be declared at relevant meetings YesOut of Hours doctor for Care UK and Suffolk GP Federation Direct 2010 Ongoing 03/04/2020 To be declared at relevant meetings YesWife is Consultant at West Suffolk Hospital Indirect 2004 Ongoing 03/04/2020 To be declared at relevant meetings YesClinical Director for WGGL PNN" Direct Ongoing 03/04/2020 To be declared at relevant meetings Yes
GP Elizabeth Hornung GP Partner of Dr Browning WSCCG Chair Indirect Ongoing 09/04/2019 None YesMarket Cross Surgery GP A Mabourukoje
GP Godfrey Reynolds Member of the Local Medical Committee Direct Ongoing 29/10/2019 None YesChair of Mildenhall Sick and Poor Fund Direct 1989 Ongoing 29/10/2019 None Yes
GP J SatishMount Farm Surgery GP Jennifer Allen Nil 20/10/2020 Yes
GP Senior Partner Claire Giles CSA - SOX Facilitator Direct 2018 Ongoing 07/10/2020 None YesExaminer for RCGP Direct Ongoing 07/10/2020 None YesGP appraiser Direct Ongoing 07/10/2020 None Yes
GP Brian Ainsworth Nil 06/10/2020 YesGP Bethan Hughes Nil 06/10/2020 YesGP Deepa Parthasarathy Nil 13/10/2020 YesGP Martin Polli Wife is a partner at Angel Hill Surgery Indirect Ongoing 15/10/2020 To be declared at relevant meetings Yes
Orchard House Surgery GP Emma Holland Partner of Surgery Direct Ongoing 01/10/2018 No further action required YesGP Sarah Ladner Nil 30/10/2019 YesGP Judith Lomas Member of Orchard House Health Ltd and shares in Pharmacy Direct Ongoing 13/10/2020 To be declared when appropriate YesGP Tom McGonigle Shareholder in Orchard House Health Ltd with shares in pharmacy Direct 01/02/2017 Ongoing 04/11/2020 To be declared at relevant meetings YesGP Helen Pullan Member of Orchard House Health Ltd and shares in Pharmacy Direct Ongoing 13/10/2020 To be declared when appropriate YesGP Rupert Wace Not for publication Direct Ongoing 04/11/2020 To be declared when appropriate No
Oakfield Surgery, Newmarket GP Andrea Barkley Suffolk Primary Care participates in research ethics approved GSK clinical trail to recruit 10 COPD patients to a triple therapy medication
Direct Ongoing 14/10/2019 To be declared when appropriate Yes
Partners have working collaboration with Orbital Media Ltd to develop digital patient information AI self care tool Virt Turi
Direct Ongoing 14/10/2019 To be declared when appropriate Yes
West Suffolk Member Practices
Practice First Name Last Name Declared Interest Type of Interest Direct or Indirect
Date of Interest Date of Receipt
Action Taken to Mitigate Consent to Publish
Title
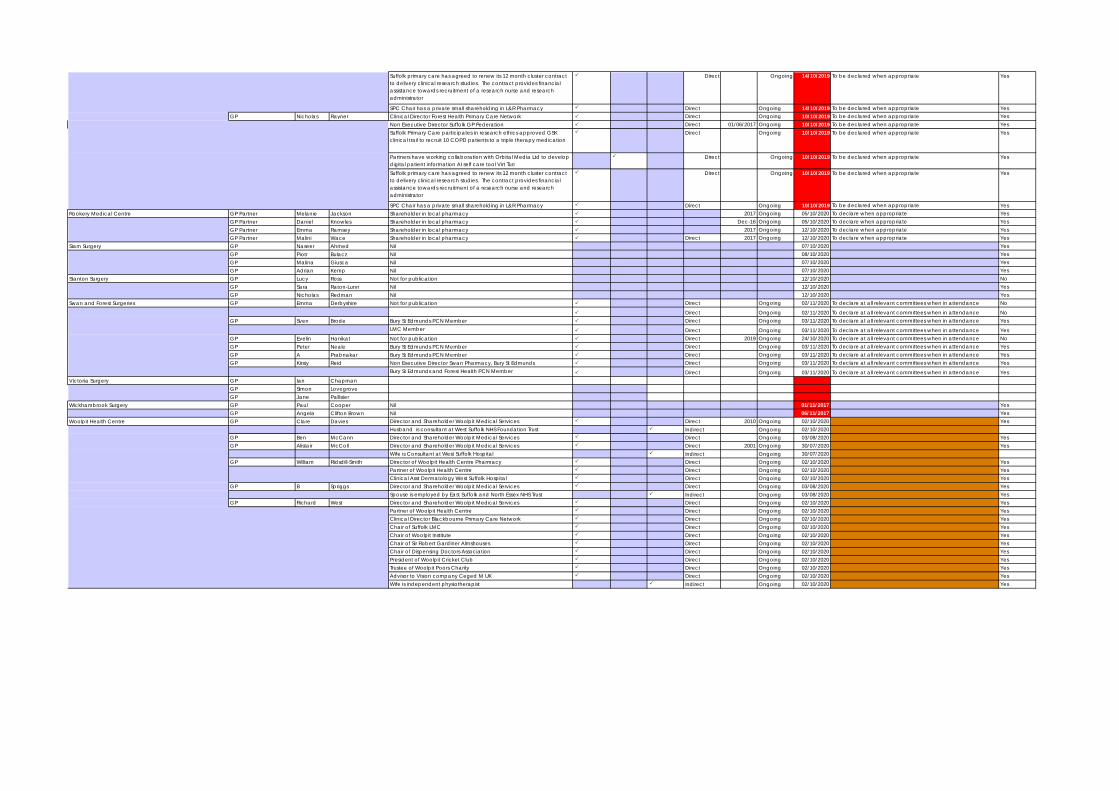
Suffolk primary care has agreed to renew its 12 month cluster contract to delivery clinical research studies. The contract provides financial assistance towards recruitment of a research nurse and research administrator
Direct Ongoing 14/10/2019 To be declared when appropriate Yes
SPC Chair has a private small shareholding in L&R Pharmacy Direct Ongoing 14/10/2019 To be declared when appropriate YesGP Nicholas Rayner Clinical Director Forest Health Primary Care Network Direct Ongoing 10/10/2019 To be declared when appropriate Yes
Non Executive Director Suffolk GP Federation Direct 01/06/2017 Ongoing 10/10/2019 To be declared when appropriate YesSuffolk Primary Care participates in research ethics approved GSK clinical trail to recruit 10 COPD patients to a triple therapy medication
Direct Ongoing 10/10/2019 To be declared when appropriate Yes
Partners have working collaboration with Orbital Media Ltd to develop digital patient information AI self care tool Virt Turi
Direct Ongoing 10/10/2019 To be declared when appropriate Yes
Suffolk primary care has agreed to renew its 12 month cluster contract to delivery clinical research studies. The contract provides financial assistance towards recruitment of a research nurse and research administrator
Direct Ongoing 10/10/2019 To be declared when appropriate Yes
SPC Chair has a private small shareholding in L&R Pharmacy Direct Ongoing 10/10/2019 To be declared when appropriate YesRookery Medical Centre GP Partner Melanie Jackson Shareholder in local pharmacy 2017 Ongoing 05/10/2020 To declare when appropriate Yes
GP Partner Daniel Knowles Shareholder in local pharmacy Dec-16 Ongoing 05/10/2020 To declare when appropriate YesGP Partner Emma Ramsey Shareholder in local pharmacy 2017 Ongoing 12/10/2020 To declare when appropriate YesGP Partner Malini Wace Shareholder in local pharmacy Direct 2017 Ongoing 12/10/2020 To declare when appropriate Yes
Siam Surgery GP Naseer Ahmed Nil 07/10/2020 YesGP Piotr Bulacz Nil 08/10/2020 YesGP Malina Giusca Nil 07/10/2020 YesGP Adrian Kemp Nil 07/10/2020 Yes
Stanton Surgery GP Lucy Ross Not for publication 12/10/2020 NoGP Sara Raton-Lunn Nil 12/10/2020 YesGP Nicholas Redman Nil 12/10/2020 Yes
Swan and Forest Surgeries GP Emma Derbyshire Not for publication Direct Ongoing 02/11/2020 To declare at all relevant committees when in attendance No
Direct Ongoing 02/11/2020 To declare at all relevant committees when in attendance NoGP Sven Brode Bury St Edmunds PCN Member Direct Ongoing 03/11/2020 To declare at all relevant committees when in attendance Yes
LMC Member Direct Ongoing 03/11/2020 To declare at all relevant committees when in attendance YesGP Evelin Hanikat Not for publication Direct 2019 Ongoing 24/10/2020 To declare at all relevant committees when in attendance NoGP Peter Neale Bury St Edmunds PCN Member Direct Ongoing 03/11/2020 To declare at all relevant committees when in attendance YesGP A Prabnakar Bury St Edmunds PCN Member Direct Ongoing 03/11/2020 To declare at all relevant committees when in attendance YesGP Kirsty Reid Non Executive Director Swan Pharmacy, Bury St Edmunds Direct Ongoing 03/11/2020 To declare at all relevant committees when in attendance Yes
Bury St Edmunds and Forest Health PCN Member Direct Ongoing 03/11/2020 To declare at all relevant committees when in attendance YesVictoria Surgery GP Ian Chapman
GP Simon LovegroveGP Jane Pallister
Wickhambrook Surgery GP Paul Cooper Nil 01/11/2017 YesGP Angela Clifton Brown Nil 06/11/2017 Yes
Woolpit Health Centre GP Clare Davies Director and Shareholder Woolpit Medical Services Direct 2010 Ongoing 02/10/2020 YesHusband is consultant at West Suffolk NHS Foundation Trust Indirect Ongoing 02/10/2020
GP Ben McCann Director and Shareholder Woolpit Medical Services Direct Ongoing 03/08/2020 YesGP Alistair McColl Director and Shareholder Woolpit Medical Services Direct 2001 Ongoing 30/07/2020 Yes
Wife is Consultant at West Suffolk Hospital Indirect Ongoing 30/07/2020GP William Ridsdill-Smith Director of Woolpit Health Centre Pharmacy Direct Ongoing 02/10/2020 Yes
Partner of Woolpit Health Centre Direct Ongoing 02/10/2020 YesClinical Asst Dermatology West Suffolk Hospital Direct Ongoing 02/10/2020 Yes
GP B Spriggs Director and Shareholder Woolpit Medical Services Direct Ongoing 03/08/2020 YesSpouse is employed by East Suffolk and North Essex NHS Trust Indirect Ongoing 03/08/2020 Yes
GP Richard West Director and Shareholder Woolpit Medical Services Direct Ongoing 02/10/2020 YesPartner of Woolpit Health Centre Direct Ongoing 02/10/2020 YesClinical Director Blackbourne Primary Care Network Direct Ongoing 02/10/2020 YesChair of Suffolk LMC Direct Ongoing 02/10/2020 YesChair of Woolpit Institute Direct Ongoing 02/10/2020 YesChair of Sir Robert Gardiner Almshouses Direct Ongoing 02/10/2020 YesChair of Dispensing Doctors Association Direct Ongoing 02/10/2020 YesPresident of Woolpit Cricket Club Direct Ongoing 02/10/2020 YesTrustee of Woolpit Poors Charity Direct Ongoing 02/10/2020 YesAdvisor to Vision company Ceged M UK Direct Ongoing 02/10/2020 YesWife is independent physiotherapist Indirect Ongoing 02/10/2020 Yes

Meeting Date Committee/Body Individual Declaration Made Attendance Capacity27/04/2016 Joint Commissioning Committee Dr Christopher Browning As a GP within the West Suffolk area Remained in meeting
21-Feb-17 Remuneration and HR Committee Colin Boakes Item 8 (IR35 - New HMRC Off Payroll Rules) Colin Boakes declared interest as he was affected Remained in meeting - no decision taken
18/04/2017 Remuneration and HR Committee Amanda Lyes Amanda Lyes declared an interest in agenda item 09 (Remuneration of GP Governing Body Members and Chief Officers) and left the room when that item was discussed.
Left the room when item discussed
13-Jun-17 Audit Committee Kevin Bernard Item 13 - Waivers - as the practice manager for Botesdale Health Centre provider of ultrasound services
Remained in meeting as no decision required
25-Oct-17 Governing Body 'Private' Dr Christopher Browning As an employee of the out of hours service Remained in the meeting29/11/2017 Primary Care Commissioning Committee Dr Christopher Browning As a GP within the West Suffolk area Remained in meeting29/11/2017 Governing Body Dr Christopher Browning and Dr
Firas WatfehDr Christopher Browning and Dr Firas Watfeh declared an interest in agenda item 13 (Emergency Department Streaming Update) as they were both employed to carry out sessions as part of the streaming service. They both remained in the meeting whilst the item, which was for note, was discussed.
Remained in meeting
24/01/2018 Primary Care Commissioning Committee Dr Christopher Browning Dr Christopher Browning declared an interest as a GP within the CCG area. Remained in meeting28/02/2018 Primary Care Commissioning Committee Dr Christopher Browning Dr Christopher Browning declared an interest as a GP within the CCG area Remained in meeting28/02/2018 Commissioning Governance Committee Dr Christopher Browning No declarations of interests, other than those already published, were received. (Dr Christopher
Browning had previously declared as a GP contract holder at Long Melford and PMS contract holder)
Remained in meeting
27/03/2018 Primary Care Commissioning Committee Dr Christopher Browning Dr Christopher Browning declared an interest as a Personal Medical Services (PMS) provider. Remained in meeting28/03/2018 WSCCG Governing Body Ed Garratt
Jane PaylingRichard WatsonChris Hooper
On behalf of all Chief Officers present, the Chief Officer declared an interest in agenda item 11 (Aligning Clinical Commissioning Groups to support development of the Integrated Care System).
Remained in meeting
25/04/2018 WSCCG Executive Dr Zohra ArmitageDr Christopher BrowningDr Andrew HassanDr Bahram TalebpourDr Firas Watfeh
Drs Armitage, Browning, Hassan, Talebpour and Watfeh all declared an interest in agenda item 4 (Subcutaneous Methotrexate Injection Options Paper) insofar as it might relate to primary care, they remained in the meeting.
Remained in meeting
25/04/2018 WSCCG Clinical Scrutiny Committee Dr Firas Watfeh As a GP in Haverhill, Dr Firas Watfeh declared an interest in item 6 (Governing Body Assurance Framework) insofar as it related to Haverhill Practices.
Remained in meeting
16/05/2018 WSCCG Clinical Scrutiny Committee Dr Zohra ArmitageDr Christopher BrowningDr Firas Watfeh
Drs Armitage, Browning, and Watfeh declared an interest in agenda items 9 (GP Practice Resilience) and 10 ( West Suffolk Dementia LES)
Remained in meeting
23/05/2018 Primary Care Commissioning Committee Dr Christopher Browning Dr Christopher Browning declared an interest as a Personal Medical Services (PMS) provider. Remained in meeting23/05/2018 Governing Body - Part Two Dr Zohra Armitage
Dr Christopher BrowningDr Firas Watfeh
The following declarations were made in respect of agenda item 06 (Integrated Urgent Care Services Procurement);1) Dr Zohra Armitage insofar as the item related to GP streaming.2) Dr Christopher Browning insofar as the item related to the Out of Hours service and GP streaming.3) Dr Firas Watfeh insofar as the item related to the Suffolk GP Federation and the Out of Hours service.
Remained in meeting
12/06/2018 Remuneration and HR Committee Dr Christopher BrowningAmanda Lyes
Dr Mike McCullagh, GP, declared an interest in agenda item 05 (Remuneration of GP Governing Body Members and Chief Officers) and left the meeting when that item was discussed.
Amanda Lyes, Chief Corporate Services Officer, declared an interest in agenda item 05 (Remuneration of GP Governing Body Members and Chief Officers) and, following presentation of the report left the meeting when the decision was being made
Left the meeting for the item.
Left the meeting for the decision
25/07/2018 Governing Body - Part Two Dr Firas Watfeh Dr Firas Watfeh declared an interest as his practice was a member of the Suffolk GP Federation. Remained in the meeting25/07/2018 Primary Care Commissioning Committee -Part One Dr Christopher Browning
Dr Christopher Browning declared an interest in items on the agenda as a Personal Medical Services (PMS) provider and specifically in Agenda item 12 (Closure of Hartest Branch Surgery) as the Chair of Hartest Parish Council. It was agreed that Dr Browning remain in the meeting during the discussion.
Remained in the meeting
25/07/2018 Primary Care Commissioning Committee - Part Two Dr Christopher Browning Dr Christopher Browning declared an interest in items on the agenda as a Personal Medical Services (PMS) provider
Remained in the meeting
WEST SUFFOLK CCG - LOG OF DECLARATIONS

31/07/2018 Audit Committee Mark Game Mark Game declared an interest as his wife, who also worked for the CCG, would be presenting agen Remained in the meeting31/07/2018 Audit Committee Internal Audit and TIAA It was agreed that those affected by agenda item 18 (Internal Audit and Local Counter Fraud
Services Market Testing), would leave the room when the item was discussed.Left the meeting
28/11/2018 Primary Care Commissioning Committee - Parts One and Two Dr Christopher Browning Dr Christopher Browning declared an interest in items on the agenda as a Personal Medical Services (PMS) provider
Remained in the meeting
23/01/2019 WSCCG Private Governing Body Jon ReynoldsKate VaughtonAll GPs
Jon Reynolds, Deputy Chief Contracts Officer and Kate Vaughton, Chief Operating Officer declared an interest in agenda item 07 (Integrated Pain Management Services Procurement) as they were both currently carrying out work on behalf of West Suffolk NHS Foundation Trust on a part-time basis. Both remained in the meeting.
All GPs declared an interest in agenda item 08 (Report of Decision by Commissioning Governance Committee on 21 November 2018 re GP Pension Payments) and the Chair advised that the report would be taken as written.
Remained in meeting
Report taken as written with no discussion.
23/01/2019 WSCCG Commissioning Governance Committee Jon ReynoldsKate Vaughton
Jon Reynolds, Deputy Chief Contracts Officer and Kate Vaughton, Chief Operating Officer declared an interest in agenda item 07 (Integrated Pain Management Services Procurement) as they were both currently carrying out work on behalf of West Suffolk NHS Foundation Trust on a part-time basis. Both remained in the meeting.
Remained in meeting
06/03/2019 WSCCG 'Private' Governing Body (Virtual) Kate VaughtonLisa NobesJane PaylingAmanda LyesRichard WatsonJane Webster
Declarations of interest were noted from all Chief Officers. As they would be conflicted in any established CCG forum, a quorum was not possible and, as such, approval on this occasion was on the basis of a simple majority as the approval was for a process and not a definitive decision.
Given the subject matter and that the Accountable Officer and all Chief Officers are conflicted and would be so in any established CCG forum, a quorum was not possible and, as such, approval on this occasion is on the basis of a simple majority as the approval is for a process and not a definitive decision.
27/03/2019 WSCCG 'Private' Governing Body Amanda LyesLisa NobesJane PaylingKate VaughtonRichard WatsonJane Webster
All Chief Officers declared an interest in agenda item 11 (Appointment of a single Accountable Officer for Ipswich and East Suffolk, West Suffolk and North East Essex Clinical Commissioning Groups), as the item required endorsement of a previous decision they remained in the meeting when the item was discussed.
Remained in the meeting
27/03/2019 WSCCG 'Private' Governing Body Ed Garratt Ed Garratt declared an interest in agenda item 11 (Appointment of a single Accountable Officer for Ipswich and East Suffolk, West Suffolk and North East Essex Clinical Commissioning Groups), and left the meeting when the item was discussed.
Left the meeting
27/03/2019 WSCCG Primary Care Commissioning Committee (Part One and Two)
Dr Christopher Browning Dr Christopher Browning declared an interest in the agenda as holder of a Personal Medical Services (PMS) contract, and a specific interest in agenda item 7 (PMS Development Framework/Local Enhanced Services) of the public meeting, as a non-voting member the Committee agreed that he could remain in the meeting when the item was discussed.
Remained in the meeting
24/04/2019 WSCCG Primary Care Commissioning Committee (Part Two) Dr Christopher Browning Dr Christopher Browning declared an interest in the agenda as a GP and holder of a Personal Medical Services (PMS) contract.
Remained in the meeting
24/04/2019 WSCCG 'Private' Governing Body Dr Christopher BrowningDr Godfrey ReynoldsDr Zohra ArmitageDr Firas Watfeh
All GPs declared an interest in agenda item 09 (Rookery Medical Centre) and remained in the meeting, in particular, Dr Godfrey Reynolds declared an interest in respect of the development of primary care networks.
Remained in the meeting
24/04/2019 WSCCG 'Private' Governing Body Kate Vaughton Kate Vaughton declared an interest in the agenda insofar as it related to West Suffolk NHS Foundation Trust, as a non-voting Board member of the Trust.
Remained in the meeting
24/04/2019 WSCCG Clinical Scrutiny Committee Kate Vaughton Kate Vaughton declared an interest in the agenda insofar as it related to West Suffolk NHS Foundation Trust, as a non-voting Board member of the Trust.
Remained in the meeting
22/05/2019 WSCCG Primary Care Commissioning Committee (Part One and Two)
Dr Christopher Browning Dr Christopher Browning declared an interest in the agenda as holder of a Personal Medical Services (PMS) contract.
Remained in the meeting
26/06/2019 WSCCG Clinical Scrutiny Committee Kate Vaughton Kate Vaughton declared an interest in the agenda insofar as it related to West Suffolk NHS Foundation Trust, as a non-voting Board member of the Trust.
Remained in the meeting
24/07/2019 WSCCG Primary Care Commissioning Committee (Part One and Dr Christopher BrowningKate Vaughton
Dr Christopher Browning declared an interest in the agenda as holder of a Personal Medical Services (PMS) contract.Kate Vaughton declared an interest in the agenda insofar as it related to West Suffolk NHS Foundation Trust, as a non-voting Board member of the Trust.
Remained in the meeting
24/07/2019 WSCCG Governing Body (Part One and Two) Kate Vaughton Kate Vaughton declared an interest in the agenda insofar as it related to West Suffolk NHS Foundation Trust, as a non-voting Board member of the Trust.
Remained in the meeting

24/07/2019 WSCCG Governing Body Kate Vaughton Kate Vaughton declared an interest in the agenda insofar as it related to West Suffolk NHS Foundation Trust, as a non-voting Board member of the Trust.
Steve Chicken declared an interest in agenda item 8 (East and West Suffolk Mental Health Update) insofar as it related to the Citizens Advice Bureau as his daughter was an employee.
Dr Christopher Browning declared an interest in agenda item 10 (Integrated Performance Report) insofar as it related to discharge summaries at West Suffolk NHS Foundation Trust being a reviewer of such performance.
Remained in the meeting
09/10/2019 Remuneration and HR Committee Jo MaelJo Mael declared an interest in agenda item 3 (NHS West Suffolk, Ipswich and East Suffolk and North East Essex CCG Change Programme 2019) as CCG employees.
Remained in meeting
22/10/2019 WSCCG Primary Care Commissioning Committee (Part One and Two)
Kate Vaughton Kate Vaughton declared an interest as Director of Integration and as a non-voting Board Member of West Suffolk NHS Foundation Trust.
Remained in meeting
30/10/2019 WSCCG Private Governing Body
Amanda LyesLisa NobesJane PaylingRichard Watson
As Directors of the CCG, Amanda Lyes, Lisa Nobes, Jane Payling and Richard Watson all declared an interest in Agenda item 7 (Endorsement of Remuneration and HR Committee Decision re Director Salaries), and left the room when that item was discussed.
Left the meeting
27/11/2019 WSCCG Governing Body Dr Zohra ArmitageDr Christopher BrowningDr Bahram TalebpourDr Firas Watfeh
Declared an interest in agenda item 10 (Integrated Front Door Model at West Suffolk NHS Foundation Trust) insofar as it related to the Suffolk GP Federation and the GP Streaming service, but remained in the meeting for the discussion.
Remained in meeting
11/02/2020 Remuneration and HR Committee Geoff Dobson Geoff Dobson declared an interest in agenda item 5 (Dr Padmanabhan Badrinath – Salary Thresholds) insofar as he had been a previous colleague.
Remained in the meeting
26/02/2020 WSCCG Primary Care Commissioning Committee (Part Two) Dr Christopher Browning Dr Christopher Browning declared an interest in agenda item 13 (Primary Care Funding) as CCG Chair and a member of one of the practices.
Remained in the meeting
23/04/2020 Covid-19 Resource Approval Committee Dr Christopher BrowningKate Vaughton
Dr Christopher Browning made a declaration of interest as an employee of the Suffolk GP Federation in a clinical role, and Kate Vaughton made a declaration of interest as a West Suffolk NHS Foundation Trust Board Member.
Remained in the meeting
04/06/2020 CRAC Dr Christopher Browning Dr Christopher Browning declared an interest in agenda items 05a (East Accord – Digital Investments) and 05b (Learning Disabilities Care Home Support Offer from General Practice), as primary care contract holders.
Remained in meeting
10/06/2020 CRAC Dr Christopher Browning Dr Christopher Browning declared an interest in agenda item 5 (Signage Joint Purchase) as a member of a practice within the CCG area and remained in the meeting.
Remained in the meeting
24/06/2020 Covid-19 Resource Approval Committee Dr Christopher Browning Dr Christopher Browning delcared an interest as a GP insofar as the agend related to the home visiting Remained in meeting02/07/2020 WSCCG Commissioning Governance Committee Geoff Dobson Family members was part of diabetes prevention programme Remained in meeting23/09/2020 West Suffolk CCG Governing Body Kate Vaughton Kate Vaughton declared an interest as Director of Integration and as a non-voting Board Member of
West Suffolk NHS Foundation Trust.Remained in meeting

Page 1 of 5
GOVERNING BODY Agenda Item No. 21
Reference No. WSCCG 20-55
Date. 25 November 2020 Title
Terms of Reference – Commissioning Governance Committee
Lead Director
Amanda Lyes, Director of Corporate Services and System Infrastructure
Author(s)
Jo Mael, Corporate Governance Manager
Purpose
To present for approval the terms of reference for the Commissioning Governance Committee.
Applicable CCG Clinical Priorities: 1. Develop clinical leadership 2. Demonstrate excellence in patient experience & patient engagement 3. Improve the health & care of older people 4. Improve access to mental health services 5. Improve health & wellbeing through partnership working 6. Deliver financial sustainability through quality improvement X Action required by Governing Body: To consider approval of terms of reference for the Commissioning Governance Committee.

Page 2 of 5
WEST SUFFOLK CLINICAL COMMISSIONING GROUP
COMMISSIONING GOVERNANCE COMMITTEE
TERMS OF REFERENCE
1. OVERVIEW
Managing potential conflicts of interest appropriately is needed to protect the integrity of the NHS commissioning system and Clinical Commissioning Groups (CCGs) and GP practices from any perceptions of wrong-doing.
An essential feature of the new commissioning arrangements is that CCGs should be able to procure a range of community based services, including primary care services, to improve quality and outcome for patients. In accordance with devolved commissioning arrangements, the CCG has also established a Primary Care Commissioning Committee with NHS England whereby the CCG has authority to exercise primary care commissioning functions in accordance with section 13Z of the NHS Act and as set out in the terms of reference for that committee.
The Commissioning Governance Committee therefore provides an additional safeguard for the CCG when commissioning services for which GP practices are the recommended providers. Where the Governing Body would not be quorate for approving commissioning intentions, due to the withdrawal of GP members because of conflict of interest, the Commissioning Governance Committee assumes delegated responsibility, reporting its decisions to the Governing Body in public.
2. PURPOSE OF THE COMMITTEE
As a formal committee of the CCG Governing Body, the purpose of the Commissioning Governance Committee is to:
(i) Provide a forum, with delegated decision-making powers, for approval of
commissioning intentions where the recommended providers are GP practices.
(ii) Provide assurance to the Governing Body, Audit Committee, NHS England and general public that the CCG has the necessary governance arrangements in place

Page 3 of 5
to manage conflict of interest in regard to the procurement of services provided by GP practices.
(iii) Facilitate a culture of openness and probity around the local commissioning of GP
services. (iv) Demonstrate that the CCG and member practices are acting fairly and transparently
and that final commissioning decisions are made in ways that preserve the integrity of the decision making process.
3. ROLE OF THE COMMITTEE
On behalf of the Governing Body, the role of the Commissioning Governance Committee will scrutinise and approve proposals ensuring that where the recommended provider of services is to be a GP practice, there is evidence that they:
(i) Clearly meet local health needs and have been planned appropriately
(ii) Go beyond the scope of the GP contract
(iii) Have been procured using the appropriate methodology
(iv) Promote improvements in the quality of primary medical care
(v) Demonstrate the achievement of improved outcomes and value for money
(vi) Cannot be delivered by another provider to the same level of quality, specification and/or price
(vii) Include details for monitoring the quality of service provision
(viii) Include the details of any actual or potential conflict of interest having been
appropriately declared and entered in the register which is publicly available
(ix) Maintain confidence and trust between patients and GP’s
(x) Have been clearly detailed within the agreed proforma 4. AUTHORITY
The Committee is accountable to the CCG Governing Body and operates within agreed delegated powers.
5. MEETINGS
The Committee will not meet routinely but on an as required basis.
Meetings may be conducted on a ‘virtual’ basis through the use of e-mail communication, video or teleconferencing facilities if necessary.

Page 4 of 5
Minutes will be recorded for both actual and virtual meetings and these will be presented to the next available meeting of the CCG Governing Body in public.
Agendas and any papers for Committee meetings will be circulated to members at least five days in advance. Where the Committee meets in person, a Committee and Governance Officer will attend to formally minute the proceedings. Where the meetings are held on a virtual basis, the Committee and Governance Officer will provide minutes from the e-mail or verbal comments received from members.
6. MEMBERSHIP
Membership of the Committee comprises the CCG Chief Officer, Chief Finance Officer, Chief Contracts Officer, the Secondary Care Doctor and Governing Body Lay Members. When the Committee meets in person: When the Committee meets in person or by video or teleconferencing:
The Lay Member for Governance will chair the committee.
A quorum shall comprise at least four members, one of whom shall be the Lay Member Chair and three other members.
In the absence of the Chair, the Lay Member for Patient and Public Engagement shall chair the meeting. When the Committee is convened to make decisions by e-mail: A physical quorum is not necessary but responses must be received from the Lay Member Chair and at least three other members for a decision to be carried.
In both circumstances, where a vote is required and in the event of an equality of votes, the Chair shall have a casting vote.
When the Committee meets on a virtual basis: The Lay Member for Governance as chair must be one of the participants/correspondents A quorum of participants/correspondents will still be required and shall comprise at least four members, one of whom shall be a Lay Member and three other members. In the absence of the Chairman, the Lay Member for Patient and Public Engagement must be one of the participants/correspondents.
Where voting is required and in the event of an equality of votes, the Chairman shall have a casting vote.
7. REVIEW
The Committee shall review its own performance and terms of reference on a bi-annual basis.

Page 5 of 5
8. AUTHOR
Colin Boakes – Independent Governance Advisor
Date Approved: March 2014 Review Date: September 2020 Next Review Date: September 2021

GOVERNING BODY
Agenda Item No. 22
Reference No. WSCCG 20-56
Date. 25 November 2020
Title Minutes of Meetings
Lead Director Amanda Lyes, Director of Corporate Services and System Infrastructure
Author(s) Jo Mael, Corporate Governance Officer
Purpose To receive a report from the Lay Member for Governance seeking the endorsement of minutes and decisions from West Suffolk CCG Sub Committees,
a) Audit CommitteeThe unconfirmed minutes of a meeting held on 15 September 2020
b) Remuneration and HR CommitteeThe unconfirmed minutes of a meeting held on 6 October 2020
c) Financial Performance CommitteeMinutes from a meeting held on 16 September 2020
d) Covid-19 Resource Approval CommitteeMinutes from meetings held on 17 September 2020 and 15 October 2020
e) West Suffolk CCG Primary Care Commissioning CommitteeDecision from a virtual meeting held on 20 October 2020 and theunconfirmed minutes of a meeting held on 27 October 2020
f) Commissioning Governance CommitteeThe minutes from a meeting held on 21 August 2020 and decision from avirtual meeting held on 8 September 2020
g) CCG Collaborative GroupThe minutes of a meeting held on 10 September 2020.
h) Suffolk and North East Essex Area Prescribing Committee (SNEEAPC) Meeting- minutes of the meeting June-September 2020
Applicable CCG Priorities 1. Develop clinical leadership 2. Demonstrate excellence in patient experience & patient engagement 3. Improve the health & care of older people 4. Improve access to mental health services

5. Improve health & wellbeing through partnership working 6. Deliver financial sustainability through quality improvement Action required by Governing Body: To endorse the minutes and decisions as attached to the report whilst noting that ‘unconfirmed’ minutes remain subject to change by the relevant Committee/Group.

Unconfirmed Minutes of a Meeting of the West Suffolk Clinical Commissioning Group Audit Committee held on 15 September 2020
PRESENT Geoff Dobson - Lay Member for Governance (Chair) Lynda Tuck - Lay Member for Patient and Public Involvement IN ATTENDANCE Colin Boakes - Governance Advisor Emily Bosley - Financial Governance Accountant Mark Game - Deputy Director of Finance Mark Kidd - RSM UK, Local Counter Fraud Specialist Amanda Lyes - Director of Corporate Services and System Infrastructure Jo Mael - Corporate Governance Manager Jane Payling - Director of Finance Liz Wright - RSM UK, Internal Audit 20/041 WELCOME AND APOLOGIES FOR ABSENCE
The Chair welcomed everyone to the meeting and apologies for absence were noted from; Steve Chicken - Lay Member
20/042 DECLARATIONS OF INTEREST AND HOSPITALITY AND GIFTS
No declarations of interest or hospitality or gifts were received.
20/043 MINUTES OF PREVIOUS MEETING
The minutes of an Audit Committee meeting held on 7 April 2020 and
Extraordinary meeting held on 17 June 2020 were approved as correct records. 20/044 MATTERS ARISING AND REVIEW OF ACTION LOG
There were no matters arising and the action log was reviewed and updated. 20/045 REVIEW OF UPDATED AUDIT COMMITTEE TERMS OF REFERENCE
The Committee was in receipt of a report which provided an update on changes
made to the Audit Committee Terms of Reference and their alignment to the HFMA NHS Audit Committee Handbook recommended terms of reference. A full review and update of all three CCGs’ Audit Committee Terms of Reference had been completed. The Terms of Reference had been sent to the three Audit Chairs prior to the meeting for advance review and their comments had been incorporated into the Terms of Reference as presented. The Terms of Reference had been aligned across the three CCGs to ensure that

the remit of the Audit Committees was equivalent.
The Committee approved the attached terms of reference for presentation to the Governing Body for final approval.
20/046 INTERNAL AUDIT PROGRESS REPORT
The Committee was in receipt of the current internal audit progress report and the
Healthcare Benchmarking report. Key points highlighted during discussion included; • The CCG had received ‘substantial’ assurance for its audit of Governance
associated to the pandemic. • Open actions were currently of a low level and there was nothing of concern. • The internal audit plan had been reviewed in relation to the impact of Covid-19
and dates for audits were all agreed and scopes finalised. The Committee was reassured that relevant personnel associated with planned audits were all aware and it was anticipated that all audits could be completed before year end. Healthcare Benchmarking Report The CCG had performed higher than the average and was in a good position going forward.
The Committee noted the reports and approved the audit plan as presented.
20/047 LOCAL COUNTER FRAUD SPECIALIST ANNUAL REPORT
The Committee was in receipt of the Local Counter Fraud Specialist’s (LCFS)
annual report with key points highlighted being; • The annual report summarised work undertaken in 2019/20. • The CCG had received an ‘amber’ rating in respect of ‘hold to account’ due to
not having any sanctions. The amber rating had not affected the overall green score.
Audit Committee Chairs and Counter Fraud were thanked for their support in meeting the sign off deadlines. Having queried how much of the work carried out overlapped with that undertaken by internal audit, it was explained that there had been joint work on financial governance with further joint work planned on conflicts of interest. The Committee noted the report.
20/048 a) Review of Updated and Combined Counter-Fraud, Anti-Corruption and
Anti-Bribery Policy b) Whistleblowing Policy
The Committee was in receipt of a revised Counter Fraud, Anti-Corruption and Anti-Bribery Policy, and a Whistleblowing Policy for review and approval. Counter Fraud, Anti-Corruption and Anti-Bribery Policy The CCG currently had a Counter-Fraud and Anti-Corruption Policy, and an Anti-Bribery Policy. NEECCG had a single Counter-Fraud, Anti-Corruption and Anti-Bribery Policy. The policy was due for review, and the opportunity had been taken to align the policies across the three CCGs. The policy had been reviewed by the Local Counter Fraud Specialist (LCFS) prior

to sharing with the Committee. The Committee approved the policy as presented. Whistleblowing Policy Whilst the CCGs already had whistleblowing policies in place, a national policy, which could be adapted for local use had been developed and the CCGs were adopting that, whilst maintaining and including key features from previous whistleblowing policies. The policy was also aligned with the new counter-fraud, anti-corruption and anti-bribery policy. The national policy was designed to be clear, easy to read and brief. The appendices were longer but included additional information for those reading the policy. The national policy required the nomination of a lay member with responsibility for whistleblowing – it was felt appropriate to have one lay member from each organisation, and the Audit Committee was being asked to nominate one person from each Committee as that lay member.
The Committee approved the policy as presented and nominated Chair of Audit Committee as the lay member with responsibility for whistleblowing. The Committee approved the policies as presented.
20/049 GOVERNING BODY ASSURANCE FRAMEWORK (GBAF)
The Committee was in receipt of the latest Governing Body Assurance Framework
(GBAF) and risk registers in order to satisfy itself that appropriate risk management processes were in place. The Audit Committee was reassured that the Joint Leadership Team and the CCG’s Risk Forum regularly reviewed the GBAF and risk registers. The need to review risks in light of Covid-19 and Brexit was recognised. It was explained that whilst Brexit was currently on the Corporate Services Risk Register it was likely to return to the GBAF in the near future. The Director of Corporate Services agreed to discuss the review of risks with the Joint Leadership Team. The Director of Corporate Services also agreed to ensure all risk updates were up to date prior to presentation to the Governing Body next week The Committee noted the GBAF as presented.
20/050 RISK MANAGEMENT STRATEGY
The Risk Management Strategy had been revised as part of the regular review
cycle and in light of internal audit findings and alignment with NEECCG risk management. The revisions had been left in red text otherwise the information remained the same. • Risk Appetite was introduced to use the four T’s when considering the
management of risk. • Target Risk was introduced to establish a score at which the CCG would
accept the risk. • A description of the purpose of the risk register summary table was explained. A point raised prior to the meeting was in relation to ensuring responsibility passed to contractors when risks were transferred and that was to be incorporated into the table on transferring risks by the Director of Corporate Services and System Infrastructure’. Also, it was proposed that, in order to bring the Strategy in line with that of North East Essex, that the Strategy be revised to include two

additional paragraphs in respect of;
• A request that the wording and assurances of risks are reviewed. • That risks include a specific target date.
Subject to the minor amendments highlighted, the Audit Committee approved the Risk Management Strategy.
20/051 REVIEW OF DELEGATED LIMITS OF EXPENDITURE AND ROUTES OF
EXPENDITURE APPROVAL
The purpose of the report was to inform the Committee of the different choices made in relation to delegated limits of expenditure by other regional CCGs, discuss some of the options available and invite the Committee to comment on potential changes to limits in future. The review of the scheme of delegation was one element of a much wider piece of work looking at Alliance governance. The Audit Committee’s view was being sought so that the wider discussion could proceed without becoming overly concerned regarding the impact of changing limits on the role of the Committees and ensuring there was appropriate decision making. The draft proposal being brought to the Committee for its view and comment was: • To retain the increased levels of delegation put into place for Covid-19 on a
permanent basis. • Decisions relating to running costs to be made within the delegated limits with
the input of the CCG executive Joint Leadership Team (for running costs) • Decisions relating to Primary Care Delegated budgets to continue as before
via the Primary Care Commissioning Committee within the new framework. • All decisions which relate to programme budgets and concern commissioning
of new clinical services or non-technical (e.g. inflationary) changes to clinical services to be reviewed by the Clinical Executive (or appropriate committee in alliance structure). Clinical Executive to make recommendations to the executive team or Governing Body as required by the new delegated limits.
• Decisions where there was a direct conflict of interest for the Clinical Executive/Governing Body are referred to the Commissioning Governance Committee as before.
Comments included;
• The need to clearly identify clinical input was emphasized. • Having queried how often the £3m limit had been breached, the Committee
was informed that to date it had not been breached. All decisions re Covid-19 were currently going through the Covid-19 Resource Approval Committee which operated across the three CCGs.
• The Committee was informed that the timeline for a move to the new
Constitution was to be presented to a forthcoming Executive meeting and a paper on future Governance was being prepared for the next Collaborative Group.
The Committee was supportive of the direction of travel and welcomed a further report in November incorporating Alliance information.
20/052 BRIEFING ON ASSURANCE ENGAGEMENT ON THE MENTAL HEALTH
INVESTMENT STANDARD (MHIS)
The Committee was in receipt of a report which provided an update on the progress of the MHIS audit and included a copy of the final reports.

The Mental Health Investment Standard (MHIS) required the CCG to increase its spending on specified areas of mental health (i.e. excluding dementia and learning difficulties) at a faster rate than its general spending increases. NHS England had mandated that CCGs must publish a statement on their websites stating whether or not they met the standard and that the statement must be audited. NHS England required the audit of the amounts spent on mental health in both 2018/19 (the Current Year for the purposes of the engagement) and 2017/18 (the comparative year). In future years, only the year just completed would need to be audited, as the comparative year would have been previously audited. NHS England had mandated that the procedure must be completed as a reasonable assurance engagement, rather than a limited assurance engagement. The audit was to be completed by 30 September 2019. Across the country, significant delays were experienced with audit completion, and NHS England only permitted publication of the reports in July 2020. The CCG had finalised its report from Grant Thornton, which gave a clean opinion on the CCG’s mental health investment standard spend. There was one “Other Matter” noted on the report, which noted that the CCG’s compliance statement was based on expenditure amounts which complied with the 2018/19 MHIS requirements, but that those amounts differed slightly from the amounts submitted in the original NHS England submissions, which were in line with older guidance The report had been signed and published on the CCG website. In response to questioning the Committee noted that a new procurement exercise would be required to appoint future auditors for the MHIS. The Committee noted the content of the report.
20/053 POLICIES FOR APPROVAL
The Committee was in receipt of the following policies for approval:
a) Petitions Policy
A new policy based on best practice that had been created as a result of the Elective Orthopaedic Care Centre work.
b) Incident Reporting and Information Security Policy
Amalgamation of policies across three CCGs. The Committee was informed that the paragraph highlighted in yellow should have been deleted prior to presentation.
The Committee approved the policies subject to removal of the highlighted paragraph within the Incident Reporting and Information Security Policy.
20/054 ADDITIONAL WORDING TO THE INFORMATION GOVERNANCE POLICIES
Following a recent internal GDPR audit, recommendations were made to add
additional information to Information Governance policies for best practice. That additional information was detailed in Appendix 1 of the report. The Audit Committee approved the additional information in respect of Information Governance policies as detailed in Appendix 1 of the report.
20/055 APPROVAL OF INFORMATION GOVERNANCE STEERING GROUP TERMS
OF REFERENCE

The Committee was informed that the Information Governance Team had reviewed the IG Steering Group’s Terms or Reference (TOR) and were presenting them to the Audit Committee for approval. Having queried whether the membership included representation from West Sufoflk CCG, the Committee was informed that the CCG’s Head of Primary Care had attended the Group and some posts operated across the three CCGs. The Committee approved the Information Governance Steering Group terms of reference as presented.
20/056 CYBER SECURITY UPDATE
The report provided an update on progress in each of the seven key principles
relating to cyber security which were identified in the well led-framework, based around the role of audit chairs in respect of cyber security. Between March and August 2020, there had been necessary focus on the Covid-19 response work, which had extended the implementation period of some areas of the cyber security improvements, however, it should be noted that the business as usual cyber security activities during that period had been in place, and under regular review due to the potential for an increase in cyber security attacks during a period of instability within the country. While we had not seen an increase in attacks to date, monitoring remained in a higher state of vigilance. Comments included; • Having queried why iPads had not been mentioned within the report, it was
explained that as they were still being used by staff they should be included and the Director of Corporate Services and System Infrastructure agreed to discuss with the Head of ICT and Informatics.
• The Committee was informed that future funding had been identified as a
concern at the recent IT Board. • Having queried whether mandatory training information from practices would
be easy to collect, the Committee was reassured that the IT team would work closely with the primary care team to acquire the data.
The Committee noted the report and recommended; 1) That the report be shared with the Joint Digital and IT Services Board for
information. 2) That an audit be undertaken on mandatory staff training across all Suffolk
Practices, and Providers – that should be requested within contract meetings, and for GP Practices as part of the new GP IT Operating model and Practice Agreement.
20/057 COVID-19 UPDATE
The Director of Finance reported that emergency funding arrangements remained
in place at present with allocations awaited. It was anticipated that the Covid-19 Resource Approval Committee would continue for the foreseeable future and the CCG’s Financial Performance Committee had been updated on the current situation with regard to allocations. The Committee was informed that the recovery estate workstream was focussing on Covid-19 vaccination planning for when a vaccination might become available. It was thought that the central depository for Suffolk and North East Essex would be ESNEFT. Flu vaccinations for staff were being rolled-out through ESNEFT’s Occupational

Health provider at end of September 2020, with the option to attend clinics at CCG sites, other sites in Ipswich and Colchester or to seek reimbursement following vaccination at a pharmacy. Ipswich and East Suffolk CCG had been selected in the second round of those to be audited in relation to Covid-19 returns. The Committee noted the report.
20/058 DRAFT AUDIT COMMITTEE ANNUAL REPORT
The Annual Report was intended to provide assurance that the Audit Committee
had satisfied its Terms of Reference during 2019/2020 in relation to its establishment and ways of working by ensuring appropriate attendance at meetings, reviewing the schedule of meetings and the annual calendar of agenda items, regular reporting to the Governing Body, and by carrying out and responding to an annual self-assessment. In carrying out its work the Committee continued to develop its ways of working to increase its efficiency and improve the quality of reporting on internal controls. The attached draft Annual Report had been developed for approval prior to its presentation to the Governing Body in September 2020. In response to questioning the Director of Corporate Services agreed to clarify whether all meetings had been quorate prior to presentation of the report to the Governing Body. The Audit Committee approved its Annual Report as presented for presentation to the Governing Body in September 2020.
20/059 AUDIT COMMITTEE SELF-ASSESSMENT
The Audit Committee was asked to approve the carrying out of an annual self-
assessment with the results to be reported back to the next meeting. Having been informed that there were other examples of self-assessments that were less lengthy, the Director of Corporate Services and System Infrastructure agreed to liaise with Internal Audit prior to circulation of a newly formatted assessment.
20/060 GOVERNANCE LOGS
Waivers
No waivers of competitive tendering were received. Hospitality and Gifts Register The Committee received the current hospitality and gifts register for review. The Committee noted the hospitality and gifts register as presented.
20/061 REVISED TERMS OF REFERENCE FOR THE COMMISSIONING
GOVERNANCE COMMITTEE
The Committee was in receipt of revised terms of reference for the Commissioning Governance Committee for approval. The Committee approved the terms of reference subject to their further revision in order to clarify the role of the Chair in virtual meetings.
20/062 ANY OTHER BUSINESS AND REFLECTION

No items of other business were received. 20/063 DATE OF NEXT MEETING
The next meeting was agreed as that of 8 December 2020 – 2.00pm-4.00pm,

Unconfirmed Minutes of a meeting of the West Suffolk Clinical Commissioning Group Remuneration and Human Resources Committee Meeting held on
Tuesday, 6 October 2020
PRESENT: Geoff Dobson Lay Member for Governance (Chair) Lynda Tuck Lay Member for Patient and Public Involvement IN ATTENDANCE: Dr Hasan Chowhan Chair. North East Essex CCG (Part) Cllr Mark Cory Lay Member, North East Essex CCG (Part) Martyn Hanlon Lay Member, North East Essex CCG Julie Kerridge Senior Management Accountant Graham Leaf Lay Member, Ipswich and East Suffolk CCC Judith Low HR Advisor, North East Essex CCG Amanda Lyes Director of Corporate Services and System Infrastructure Dr Mike McCullagh GP Clinical Executive Member, Ipswich and East Suffolk CCG Jo Mael Corporate and Governance Officer Victoria Robertson Deputy Director of People and Culture Jerry Wedge Lay Member, North East Essex CCG 20/038 WELCOME AND APOLOGIES FOR ABSENCE
The Chair welcomed everyone to the meeting and no apologies for absence
were received. 20/039 DECLARATIONS OF INTEREST
No declarations of interest were received. Members were reminded of the
need to declare any hospitality or gifts via completion of the relevant documentation.
20/040 MINUTES OF THE PREVIOUS MEETING
The minutes of the West Suffolk CCG Remuneration and Human Resources
Committee meeting held on 9 June 2020 were reviewed and confirmed as a correct record.
20/041 MATTERS ARISING AND REVIEW OF THE ACTION LOG
There were no matters arising and the action log was reviewed and updated. 20/042 MANAGEMENT RUNNING COSTS UPDATE - AUGUST 2020
The Committee was provided with an overview of the year to date
management running costs at the end of August 2020.
Part One

The appendix to the report set out the management running costs expenditure against budget for the five months ending 31 August 2020. The Suffolk and North East Essex running cost allocation for 2020/21 for the first six months was £9,071k. The allocation for months 7-12 was £9,448k, bringing a total of £18,519k for the full year. Based on the six-month forecast, calculated spend per head for the full year was expected to be £17.78 Appendix 2 outlined Covid-19 management running costs expenditure for the first five months and the expected retrospective top up from NHS England. The Committee was informed that going forward no Covid-19 would be included. The reduction in management costs was highlighted which, it was felt, demonstrated how well the CCG had driven costs down by the facilitation of one management team across the three CCGs. Having queried the reduction of spend on operations management, it was explained that the figures related to the Chief Operating Offices’ of the CCGs. Any underspend achieved was accrued on a monthly basis to ensure adequate funding for the rest of the year. The CCGs were currently on plan although the filling of vacancies would reduce the accrual. In response to questioning it was reported that sickness/absence levels had declined during the pandemic and work was taking place to better understand the reasons behind the change. The organisational development group was to introduce an etiquette for the use of MS Teams which would be circulated to staff in the near future. Having queried the disproportionate number of female leavers, it was explained that many were associated to the continuing healthcare teams that had a large amount of female employees. The Committee noted the content of the report
20/043 WORKFORCE REPORT – SUFFOLK AND NORTH EAST ESSEX
The Committee was in receipt of a report from the Director of Corporate
Services and System Infrastructure which provided information on a wide range of workforce performance indicators. Points highlighted during discussion included; The CCGs currently had a good grip on the reasons for staff leaving and sickness/absence levels. Although concern was raised with regard to the narrative surrounding staff in post, it was explained that the confusion was due to a mis-spelling within the report. It was also reported that increased requests for flexible working was likely to have affected the figures. With regard to mandatory training figures, there was a need to ensure that staff were provided with the time to complete mandatory training online and to refocus them on the need for its completion. Having queried what a reasonable rate of staff turnover might be for the NHS, the Committee was advised that anything under 10% should be reasonable. The Committee requested that it receive further information to a future meeting on the reasons given by leavers for their departure at exit interviews.

Having queried whether female workers might leave due to consideration that male workers were more likely to be promoted, the Committee was reassured that there was no evidence that was a concern. The need to ensure that flexible working remained a high priority of the people plan and that senior staff were provided with the same opportunity as other staff was highlighted. The Committee noted the content of the report.
20/044 WORKFORCE RACE EQUALITY STANDARD (WRES) AND EQUALITY,
DIVERSITY AND INCLUSION
The report and presentation were designed to provide the Remuneration Committee with an overview of the work taking place across the three CCGs with regard to the equality, diversity and inclusion agenda. The work comprised of three main themes – Workforce Race Equality Standard (WRES) data and action planning, Diversity and Inclusion Partners Programme and the NHS People Plan 20/21. Section 2 of the report detailed key areas of work and points highlighted during discussion included; The Committee was informed that data had been submitted and the plan was being developed for publication by the end of the month. The Committee was pleased that the work demonstrated good co-production of the action plan. The importance of emphasizing its co-production when publishing the plan was recognised. It was noted that the final action plan would provide more detail and would credit all its contributors. The Committee noted the content of the report.
(Cllr Mark Cory joined the meeting)
20/045 CONFLICTS OF INTEREST TRAINING UPDATE
The Director of Corporate Services and System Infrastructure reported that the current position of Suffolk CCGs with regard to the completion of conflict of interest training was 93% with three members of staff having been identified as outstanding and it brought to their attention. North East Essex CCG’s position was 48%. The CCG had identified a way of improving performance via facilitation of the use of online training to improve the response rate. The Committee noted the update.
20/046 INTEGRATED CARE SYSTEM (ICS) UPDATE
The Director of Corporate Services and System Infrastructure reported;
That work continued to strengthen governance across the ICS and build it into Alliance governance. Governance workshops had been scheduled across the system with the objective to take stock as a system and determine how to move forward to system by default and align with current governance. The Director of Corporate Services and System Infrastructure agreed to circulate workshop documentation to members outside of the meeting. Discussions had taken place as to how the role of elected members, lay members and non-executives might be brought more into the work of the ICS. Work to ensure that sub-groups reporting into the ICS Board had lay member or elected member chairs had been paused during the pandemic but was to be reinstated.

The Committee noted the update. 20/047 SNEE INTEGRATED CARE SYSTEM PEOPLE PLAN
The Committee was in receipt of the Suffolk and North East Essex Integrated
Care System People Plan. Points highlighted during discussion included; • Boundaries of the plan were not in line with County Councils which was
challenging. • There was a challenge for the Remuneration and HR Committee as to how
the system workforce plan might be incorporated into the CCG workforce people plan.
• Feedback from NHSE/I was that the system had good sickness rates and low vacancy rates. There was a need to explore what else might be required to support staff and to set out a broad context as to how to deliver the plan.
• A Mutual Aid Agreement had been signed to allow movement of staff across areas.
• Rapid upskilling of staff had taken place and it was envisaged that would be maintained going forward.
• There was good engagement for the five year people plan and delivery would also be at Alliance and Primary Care Network level.
• The full five year plan was expected to be developed by March 2021. • The work carried out had been shared with Trade Unions who were keen
to support going forward. Having identified that there was no reference to costing within the proposals, the Committee was informed that it was difficult to evidence how the work might affect costs. Whilst some of the areas would require investment the team was good at seeking out funding streams. The need to be careful when considering any expenditure alongside other priorities was highlighted. It was suggested that value for money might be demonstrated from improved outcomes for patients. When considering system versus local, it was felt there was a need to ensure that local aspects were known in respect of the common themes. The Committee noted the report.
(Dr Hasan Chowhan and Cllr Mark Cory left the meeting)
20/048 NATIONAL STAFF SURVEY
The Director of Corporate Services and System Infrastructure reported that staff were currently being asked to participate in the National Staff Survey, the outcome of which would be reported to a future meeting. The Committee noted the update.
20/049 HEALTH AND SAFETY
The Director of Corporate Services and System Infrastructure reported;
• Work had taken place over recent months to ensure work bases and
places of work were ready for reoccupation following the pandemic. Work had taken place to ensure safety and that appropriate things were in place.
• Communication to staff continued to be that working from home was the default position although where staff needed to be brought back the CCGs were able to support those staff.
• Home working – additional IT kit had been purchased for staff to use at

home if required. The Committee noted the update.
20/050 REVIEW OF TERMS OF REFERENCE (NORTH EAST ESSEX ONLY)
The Committees of the Governing Board were required to review their terms of
reference at least annually in the autumn of each year and to submit their terms of reference to the Governing Body for approval. The key proposed changes to the terms of reference of the Remuneration and HR Committee were detailed in Section 2 of the report. As the Committee now meets in common with the Remuneration and HR Committees of the West Suffolk and Ipswich and East Suffolk CCGs, most of the changes proposed were to align the work of the three Committees. The Committee was informed that the Chair of North East Essex CCG would be making a decision about membership in the near future. The Committee agreed the proposed changes to the terms of reference for the Remuneration & HR Committee and recommended they be presented to the Governing Body for approval.
20/051 INVESTORS IN PEOPLE (SUFFOLK ONLY)
The Committee was in receipt of the Investors in People 12-month review
following the Suffolk CCG’s having achieved the platinum Investors in People award last year. The Committee was informed that it was intended the work also be taken forward within North East Essex CCG. The Director of Corporate Services and System Infrastructure agreed to discuss further with North East Essex CCG members outside of the meeting. The Committee noted the report.
20/052 JOINT STAFF PARTNERSHIP COMMITTEE (SUFFOLK ONLY)
The Joint Staff Partnership Committee had met on 12 June 2020 with key
points discussed being; • The Committee felt that the membership should be extended to include
representation from NEE colleagues. • RIDDOR reporting – it was confirmed that four RIDDOR reports had been
submitted. • Office reoccupation - Risk Assessments on reoccupation of all CCG office
bases had been completed. Staff were under no pressure to return to the office. Suffolk County Council was bringing some staff back working on a priority basis. • (in accordance with government advice staff have been since been
asked to remain working from home where possible)
• It was highlighted that Suffolk staff were fully supported to work flexibly around home and work life balance, particularly parents that had children at home.
• Health and Wellbeing - weekly messages had been circulated to all
colleagues across the three CCGs, which included information on such issues as; Bereavement, Mindfulness, keeping well, Mental Health First Aiders, and lots of resources and signposting.

• Preparations were underway for the 2020 Staff Survey.
Having queried the RIDDOR reports, it was explained that they all related to the possible exposure of staff to Covid-19 as a result of redeployment. The Committee was informed that although North East Essex CCG currently had few employees that were part of a Union, it was intended that a joint report be presented in future.
The Committee noted the report.
20/053 POLICIES FOR APPROVAL
No policies were received for approval. 20/054 ANNUAL PLAN OF WORK
The Committee noted its current annual plan of work and that it would be
revised in line with actions agreed at today’s meeting. It was agreed that an annual review of training and development be included.
20/055 ANY OTHER BUSINESS
The Committee was informed that Attain, management consultancy was
supporting the CCGs with regard to organisational development work which would be launched early November 2020. The Committee was informed that North East Essex CCG members might require instruction as to how to access agenda and papers via MS Teams. The Director of Corporate Services and System Infrastructure agreed to investigate.
20/056
DATE AND TIME OF NEXT MEETING
The next meeting was scheduled to take place on 9 February 2021 at 10.30am.

Minutes of a meeting of the West Suffolk CCG Financial Performance Committee held on 16 September 2020
PRESENT: Geoff Dobson Lay Member for Governance (Chair) Dr Zohra Armitage GP Governing Body Member Dr Christopher Browning CCG Chair Paul Gibara Director of Performance Improvement Amanda Lyes Director of Corporate Services and System Infrastructure Jane Payling Director of Finance
Dr Bahram Talebpour GP Governing Body Member Lynda Tuck Lay Member for Patient and Public Involvement Kate Vaughton Director of Integration Dr Victoria Wilson GP Governing Body Member IN ATTENDANCE: Mark Game Deputy Director of Finance (Part) Dr Andrew Hassan Enhanced Associate GP Jo Mael Corporate Governance Manager
20/025 WELCOME AND APOLOGIES FOR ABSENCE
The Chair welcomed everyone to the meeting and apologies for absence were received from;
Steve Chicken Lay Member Ed Garratt Chief Executive Dr Godfrey Reynolds GP Governing Body Member Dr Firas Watfeh GP Governing Body Member Dr Andrew Yager GP Governing Body Member
20/026 DECLARATIONS OF INTEREST HOSPITALITY AND GIFTS
No declarations of interest were received.
20/027 MINUTES OF PREVIOUS MEETING
The minutes of the meeting held on 17 June 2020 were agreed as a correct record.
20/028 MATTERS ARISING AND REVIEW OF ACTION LOG
There were no matters arising and the action log was reviewed and updated.
20/029 FINANCIAL PERFORMANCE COMMITTEE ANNUAL REPORT
The Committee was in receipt of its Annual Report for review and approval prior to its presentation to the Governing Body on 22 September 2020 The Committee approved the Financial Performance Committee Annual Report as presented.

20/030 UPDATE ON FINANCIAL REGIME
The Director of Finance reported that allocations had been received overnight and work was underway to review them. The Committee was reminded that a number of agreements were due to expire at the end of September 2020 and as it would take time to run thorough the allocations it was expected that some items would continue to be presented to the Covid-19 Resource Approval Committee in the short term. It was expected that, rather than the reimbursement process associated to the first half of the year, that the second half would move to allocations per CCG. There was a need to understand the system allocation for Covid-19 and for the system to work to determine distribution going forward. Work carried out by Region suggested there was a shortfall at a regional and national level and work continued to clarify the position. The Committee noted the update and welcomed further information in due course.
(Agenda item 8 was taken before agenda item 7)
20/031 PHASE 3 FINANCE PLANNING UPDATE
On 3 September 2020, at the request of East of England regional office, Suffolk and North East Essex submitted a high level financial forecast to the end of March 2021. The forecast was intended to accompany the national submissions required for Phase 3 planning which included information requirements in respect of activity, performance, workforce and mental health. Submissions were supported by a comprehensive narrative. For financial reporting purposes only, the Suffolk and North East Essex ICS was considered to consist of, Ipswich and East CCG, West Suffolk CCG, North East Essex CCG, East Suffolk and North Essex Foundation Trust, West Suffolk Foundation Trust and the East of England Ambulance Service. The system’s mental health partners, Norfolk and Suffolk Foundation Trust and Essex Partnership University Trust, report via Norfolk STP and Essex STP respectively. The report went on to set out the financial gap reported to the region at draft stage. Work continued to triangulate the assumptions between commissioners and providers and also across workforce and activity assumptions. The Committee was informed that further work was required to understand Covid-19 claims from West Suffolk NHS Foundation Trust (WSFT) and it was likely that the west Suffolk system would be under pressure during the second half of the year. There was a national expectation to have a balanced financial position at year-end. In light of the expected pressure on the west Suffolk system more dedicated finance support was being sought. Since circulation of the report allocations had now been received and the system was now expected to resubmit a final plan on, or after the 5 October 2020. Having queried why West Suffolk’s allocation was disproportionate, it was explained that allocations for months 1-6 had been centrally calculated and, across the three CCGs was slightly less in West Suffolk which might be due to West Suffolk’s higher spend in the independent sector. There was concern at the financial position of WSFT. Whilst there had been good engagement throughout the planning process there was a need to offer support in order to gain assurance going forward and to be clear about actions to address the situation. The Committee noted the report and welcomed further updates.
(Mark Game joined the meeting)
20/032 MONTH FIVE EXPENDITURE

The CCG received a retrospective allocation of £1.7m for M04 costs - this fully covered both
the Covid-19 and non-Covid-19 year to date pressures as at M04. The year to date Covid-19 costs at M05 were £5.1m. Primary Care Delegated Commissioning was £0.6m overspent due in part to underfunding of inflation in the NHSE Covid-19 budget model, this adds to the ongoing pressure existing within the delegated budget primarily relating to the proportion of PMS practices within the CCG exceeding the national average. Continuing Care was £0.4m overspent due to costs incurred in relation to Covid-19. Other Programme was £0.4m overspent primarily due to a shortfall in the NHSE Covid-19 budget. The budget model was based on the month 11 2019/20 year to date actual spend which included non-recurrent benefits. The recurrent spend was higher than the budget. £0.1m of the overspend was due to costs incurred in relation to Covid-19. Mental Health was £0.3m overspent primarily because variances after the removal of Covid-19 expenditure were impacted by the instruction from NHSE to ensure the budget lines were as per their model (devised from M11 actual spend). Having queried action to take in light of discrepancy associated with inflation on PMS practices, it was explained that although the number of PMS practices in Suffolk was high, the issue had been exacerbated by the Covid-19 central model which had been given standard inflation. The CCG continued to try to create flexibility and offset any overspend within the programme budget. Having queried the continuing healthcare (CHC) underspend, the Committee was informed that much of the underspend was due to a discrepancy between the CHC team and Finance as to what was Covid-19 funding which had been addressed in month 5. The prescribing overspend was due to a price increase associated to one specific drug and, as indicated in the action log, a more detailed prescribing report was to be presented to a future meeting. The Committee noted the content of the report.
(Mark Game left the meeting)
20/033 COVID-19 RESOURCE APPROVAL COMMITTEE – REPORT ON EXPENDITURE
The Covid-19 Resources Approval Committee was initially set up to cover the period April to
July 2020, which was subsequently extended to the end of September to match the emergency response period. The report set out the approvals made from the inception of the Committee up to 8 September 2020. As requested by Ipswich and East Suffolk CCG the approvals had been broken down in terms of approximate value per CCG. Please note that those values had in some cases been apportioned using usual CCG splits and therefore might not match the final values. Approvals for West Suffolk had amounted to just below £3.5m. The Committee was informed that all CCGs would be subject to audit with regard to Covid-19 claims and Ipswich and East Suffolk CCG had been selected for audit in the second round. It was anticipated that the auditors would review Covid-19 claims from Months 1 and 2. Having queried the future of the Covid-19 Resource Approval Committee (CRAC) should there be a second wave of the pandemic, the Director of Finance reported that it would be beneficial to keep CRAC going for the remainder of year in case there was increased demand. At its meeting to be held on 23 September 2020, the Governing Body would be asked to extend the availability of the CRAC to the end of November 2020.

The Committee noted the content of the report. 20/034 INTEGRATED CARE SYSTEM FINANCE REPORT
The Committee was in receipt of a report that set out financial information on the health and
care organisations within the Suffolk and North East Essex ICS, combining where possible, to show the position for each of the three local alliances. Key headlines included; • Month 4 marked the end of the first ‘NHS planning and reporting period’ in 2020/21; it
appeared that there would be two further reporting periods (two months to 30 September 2020, and six months to 31 March 2021). In the latter of those periods significant changes were expected to the finance regime.
• As the first period end had been reached, the report did not include a forecast. There had been further changes to the NHS reporting templates, more significantly on the commissioner side, providing greater detail on Covid-19 costs. That had required changes to the dashboard, which had limited the time available for the development of a summary dashboard or infographic.
• Information from the County Councils had been added to the dashboard for Month 4. • At the end of July 2020 all NHS organisations were reporting break-even or better, subject
to the receipt (commissioners) of the additional costs associated with Covid-19, and the audit (providers) of Covid-19 costs that had been reimbursed.
• Financial risks related primarily to uncertainty regarding the recovery of Covid-19 costs, and the details of financial regime which had yet to be announced for months 7-12.
• Limited activity reporting was available. Figures did not compare with plan but rather activity levels compared with the prior year however comparison could be made with Regional and National activity performance figures.
There was concern that the risk element of the report for WSFT flagged the audit of covid expenditure. The committee noted that WSFT claims are relatively high as a total of expenditure. Having queried detail behind the capital planning amount reported by WSFT, the Director of Finance agreed to liaise with the Chief Operating Officer outside of the meeting. The Committee noted the content of the report.
20/035 ANY OTHER BUSINESS AND REFLECTION
Continuing Healthcare (CHC)
The Director of Finance shared a document regarding CHC which highlighted comparisons with other CCGs such as Ipswich and East Suffolk and North East Essex CCGs. When compared to the other CCGs West Suffolk CHC spend to M5 was at the higher end slightly below that of Ipswich and East Suffolk CCG. Funding Nursing Care expenditure was in line with the others although Covid-19 expenditure was slightly higher than the other two. Whilst there was a known cost pressure in west Suffolk it was not an outlier compared with its peers. Having compared activity levels on the previous year, both West Suffolk and Ipswich and East Suffolk CCGS had experienced reduced activity in February 2020. North East Essex CCG had seen an increase which could be due to alignment of working practices across the three CCGs. There had been a sharp decrease in fast track patients which might be a result of some having fallen into Covid-19 expenditure. The Director of Finance agreed to circulate the CHC paper to members outside of the meeting.
20/036 DATE OF NEXT MEETING
The next meeting was scheduled to take place on 16 December 2020 0900-1030hrs

Ipswich & East Suffolk Clinical Commissioning Group West Suffolk Clinical Commissioning Group
North East Essex Clinical Commissioning Group
Minutes of the CCG Covid-19 Resource Approval Committee meeting held on 17 September 2020
PRESENT Dr Mark Shenton Chair, Ipswich and East Suffolk CCG (Chair) Dr Christopher Browning Chair, West Suffolk CCG Dr Hasan Chowhan Chair, North East Essex CCG Ed Garratt Chief Executive Jane Payling Director of Finance Richard Watson Director of Strategy and Transformation IN ATTENDANCE Paul Gibara Director of Performance Improvement Pam Green Chief Operating Officer, NEECCG Paul Little Director of Community Services, ESNEFT and SCC. Jo Mael Corporate Governance Manager William Pope Chair, Integrated Care System Minute
20/140 Welcome and apologies The Chair welcomed everyone to the meeting. Apologies for absence were received from; Amanda Lyes Director of Corporate Services and System Infrastructure
20/141 Declarations of Interest, Hospitality and Gifts
No declarations of interest, hospitality or gifts were received.
20/142 Minutes of the previous meeting
The minutes of the previous meeting held on 08 September 2020 were approved as a correct record.
20/143 Matters Arising and Review of Action Log
There were no matters arising and the action log was reviewed and updated.
20/144 Requests for Covid-19 related investment
Revised D2A pathways - Commissioned Community Bed Space The commissioning of short term bed based facilities outside of an hospital environment, that promote a reablement focus and provide the ability to assess people’s needs for the longer term outside of an acute setting helps us move more people into their communities, more quickly and with better long term results. The approach had a proven positive impact in enabling people to regain greater levels of independence, reducing dependency on long term care and demands on the system as a whole. The request was to utilise the recently announced post discharge six week funding commitment from the NHS to fund an additional 35 commissioned beds enabling greater numbers of people to be discharged without the need for any care assessment within an acute setting. That would bolster the current model of bed based reablement through the

established pathway two route to community hospitals, giving extra capacity for more patients that needed a bed-based model of care to be discharged without delay. Thus far the additional cost of that work had been funded from short term funding provided to cover additional expenditure related to coping with the demands of the pandemic, however the proposal sought to firm up the arrangements in line with recent discharge policy announcements and associated funding for the remainder of the financial year. The extra 35 beds would supplement 15 beds commissioned and funded by SCC as part of the revised discharge pathway with the same provider, giving a total capacity of 50. Financial implications were detailed in Section 3 of the report and key issues in Section 4. The Committee was informed that the number of extra beds had been decreased from 75 to 35. It was suggested that should more capacity be required there might be a need to consider block purchase. There was confidence that the 35 beds would be utilised and the scheme fitted the requirements for post six weeks discharge funding, discharge to assess and was integral to ESNEFT’s winter plan. Having queried whether Better Care Fund monies might be available, it was explained that those monies were already utilized within community services. A similar schemes had already been approved for West Suffolk and discussions were taking place in North East Essex re discharge planning. The Committee was informed that although the CCG had now received its allocation for months 7-12, the Hospital Discharge Programme (HDP) sat outside of that funding. Discharges after 31 August 2020 would be subject to separate funding as HDP phase 2 the detail of which was unclear at present. The Director of Finance raised concern at the financial risk of void costs should the additional capacity not be utilised. The Committee was informed that lack of use should not be a problem as it was unlikely that discharges would decrease as they were currently averaging at 60 per month. Subject to clarification on the availability of funding, the Committee approved the provision of the funding as proposed within the report. Extension of Covid-19 Enhanced End of Life Services The Committee is asked to consider and approve the extension of the current arrangements for Hospice (CCGs) into month seven. Models are being developed within the three alliances and it was planned to take those through alliance governance routes where sufficiently progressed. However, the timing of Committees means that decisions cannot be made effectively to start on 1 October 2020. Based on original approvals, extension for a further month would cost (maximum) as follows; St Helena = £104k St Nicholas = £113k* (Note that Community costs for St Nicholas Hospice have been claimed via WSFT Covid-19 top-up. Full budget unlikely to be required). St Elizabeth = £114k Note that all reimbursements are made on an open book, actual cost basis. The Committee approved extension of the current arrangements for end of life provision led by our three hospices for a further month until the end of October 2020. Noted that a paper on utilisation, actual costs claimed and evaluation would be prepared for CRAC and alliance committees as soon as possible. Anglia Community Enterprise (ACE) extension of current arrangements CRAC had previously received two specific papers on ACE – the first outlining the overall arrangements and the second extending those arrangements to the end of September 2020, including some further support for IT and temporary staffing expenditure relating to the D2A

service. For the first six months of 2020/21 a system had been in place to reimburse ACE’s Covid-19 expenditure on the basis of actual costs incurred. Those costs included the addition of 23 Community Hospital Beds. At its meeting on 23 July 2020, CRAC received the second paper which extended the arrangements and acknowledged additional costs relating to the D2A service. That related to the need to use locum/agency staff to deliver the D2A service at approximately £100,000 per month. Allocations for months 7-12 had just been received, but it was unlikely that those could be processed through appropriate alliance governance routes in order to give certainty to the provider for the 1 October 2020. CRAC was therefore being asked to extend the current arrangements for a further month to allow work on the M7-12 financial allocations to be progressed. The Committee was informed that following review it was thought that the figures set out in the report could be capped at a maximum of £500k. The Committee was reassured that there was robust review and audit of costs for affordability and value. With an expectation that the action cost would be lower, the Committee approved the following estimated reimbursement costs for ACE: The continuation of reimbursement of Covid-19 costs for October 2020 at a maximum of £500k, based on actual spend, pending further review via the NEE alliance.
Healthwatch Survey of Peoples Experiences of Dying, Death, Grief and Bereavement during Covid-19 The ICS End Of Life (EOL) Board had expressed a desire to learn from and understand how Covid-19 had affected and impacted on people’s experiences of EOL care and services. The work would complement existing EOL pre-Covid-19 work and planning and would be closely aligned to the public engagement work designed to develop resilient and compassionate communities for EOL. The survey would provide a unique opportunity to capture user experiences of services that had been delivered in different ways, valuable insight into how our original planning/thinking for EOL services might need to be revised, and assist with our planning to respond to a second wave/further spike. The steering group was cognisant that we needed to capture experiences from a wide range of people; feedback from our recent BAME workshops highlighted the need for us to engage better and work more closely with our BAME communities and groups. Funding was already secured for Healthwatch to conduct the survey, and the relevant project structure was in place. Funding was also already secured for publicity/launching the survey and associated materials. In total the amount requested is set out below. Healthwatch Suffolk had advised that costs could either be paid direct to the relevant organisations, without VAT added, or if desired, could be passed through Healthwatch with VAT added, therefore both prices were included in the paper • Healthwatch Suffolk had advised that the cost of engagement for a community group was
£300 per day per group, for five groups, three days of engagement with each community = £4,500, or £5,400 inc VAT.
• 20 interviews were to be undertaken (included in original costs) with at least five of the
interviews being with people from a BAME background. Cost per interview was £50. Total costs for five interviews would be either £250, or £320 inc VAT.
The need to link the work with patient insight work commissioned by NEECCG through ARU

was recognised. There was lack of clarity as to the purpose of the paper and funding amounts being requested. As a result of the lack of clarity the Committee DID NOT approve the proposal and asked that the Director of Finance request further information form Healthwatch with regard to the total cost being requested, and the level of BAME engagement and representation across the community. Once further information was obtained, it was agreed that it be circulated to Members for decision via email.
20/145 Update on Finance Regime M7-12
The Director of Finance reported that the CCGs had recently received allocations for months 7-12. The allocations did not contain specific recovery funding and whilst there had been recognition of higher costs due to Covid-19 the amount of funding provided was half of what had been spent during months 1-6. Work continued to review the detail. Papers were to be presented to the Governing Body meetings at the end of September requesting that the Covid-19 Resource Approval Committee continue for the time being in light of the possibility of a second wave.
20/146 Forward Planner
End of Life, new models. S75 Agreement to support the changed Hospital Discharge Programme Clarify role of Committee going forward.
20/147 Any Other Business
No items of other business were received 20/148 Date of Next Meeting
Week commencing 28 September 2020 or early October 2020.

Ipswich & East Suffolk Clinical Commissioning Group
West Suffolk Clinical Commissioning Group North East Essex Clinical Commissioning Group
Unconfirmed Minutes of the CCG Covid-19 Resource Approval Committee meeting held on
15 October 2020
PRESENT Dr Hasan Chowhan Chair, North East Essex CCG (Chair) Dr Mark Shenton Chair, Ipswich and East Suffolk CCG Dr Christopher Browning Chair, West Suffolk CCG Ed Garratt Chief Executive Jane Payling Director of Finance Richard Watson Director of Strategy and Transformation (Part) IN ATTENDANCE Jane Garnett Procurement Lead (Part) Paul Gibara Director of Performance Improvement Jennifer Kearton Deputy Director of Finance (Part) Jo Mael Corporate Governance Manager Sheila Murnion Lead Contract Manager (Part) Minute
20/149 Welcome and apologies The Chair welcomed everyone to the meeting. Apologies for absence were received from; Amanda Lyes Director of Corporate Services and System Infrastructure William Pope Chair, Integrated Care System
20/150 Declarations of Interest, Hospitality and Gifts
No declarations of interest, hospitality or gifts were received.
20/151 Minutes of the previous meeting
The minutes of the previous meeting held on 17 September 2020 were approved as a correct record.
20/152 Matters Arising and Review of Action Log
There were no matters arising and the action log was reviewed and updated. The Committee endorsed its approval, via email circulated on 30 September 2020, of CRAC 20-76, support for BAME groups to widen participation in the End of Life Survey.
(It was agreed that agenda item 06 (NHS Financial Architecture to March 2021) would be taken first).
20/153 Other issues for discussion and agreement or information NHS Financial architecture to March 2021 Key elements of financial architecture to March 2021 included; • Move to System First - allocations had been made at system level, with additional
envelopes being devolved to CCGs to distribute or pass through to organisations where appropriate. Block contracts remained in place with a process to adjust if required.
• An allocation for Covid-19 top up in months 7-12 had been provided to replace

retrospective top-ups. • CCGs were in receipt of growth funding for the system and the top up funding which had
previously gone directly to NHS providers. • National solutions were in place for PPE, ongoing funding for testing and an element of
the Hospital Discharge Programme. • An Elective Incentive Scheme had been introduced attracting additional payments for
performance above target and penalties for those below. The report went on to outline the approach, key elements of which included; • The System Finance Group (ICS DOFS) had agreed an approach to the distribution of
the Covid-19 top up for months 7-12. • In recognition that the Covid-19 Allocation was available to support the ongoing costs of
Covid-19, the allocation was split firstly on the spend experienced by sector in months 3-5 (to reduce the impact of setup costs in the early months). That provided a sector allocation shown in the top section of the table aside.
• The sector allocation was then proportioned based on weighted capitation. Weighted capitation was used to recognise that there was a premium on treating on all patients in Covid-19 safe environments.
The Committee was informed that there was a need to review the Covid-19 tracker and take out elements that could no longer be claimed for. The remaining elements would then be presented to the Committee for agreement to them being entered into CCG budget positions. Growth funding was intended to cover new services introduced by the system since 1 April 2020, with it being distributed to reflect growth in expenditure. Funding should be aligned to new pressures within the system and should provide support to ESNEFT and WSFT (acute and community) and areas such as End of Life. Work to identify priorities was underway. The need to recognise that, whilst routed via the CCG, the funding was system funding and its use defined via a system approach, was emphasized. Risks associated to the elected incentive scheme were questioned. It was explained that the acute Trusts were currently prioritising what was required. The Committee noted the report and endorsed the approach.
(Richard Watson and Jennifer Kearton left the meeting)
20/154 Requests for Covid-19 related investment
Update on CCG spend on Personal Protective Equipment (PPE) and other Covid-19 equipment
The Covid-19 response required providers to use the most appropriate PPE to reduce the risk of spreading the virus. As a direct result the demand for PPE increased exponentially which left some providers including primary care struggling to source sufficient and /or appropriate stock that met the guidelines. The CCGs’ utilised staff with procurement and logistical skills and knowledge to provide an emergency stock from Aspen House. Through NHS Supply Chain and other suppliers they had sourced a range of stock that had proved critical for some of our front line services as detailed in paragraph 2.1 of the report. Due to the potential gravity of the second wave it was not proposed to ‘shut down’ the SNEE-PPE inbox yet as there were still supply issues with some critical items, and it was felt prudent to retain a volume of the key items, as listed within the report, for our own staff and any emergency situations moving forward. Although the risk of FFP3 equipment going to waste was raised, the Committee was reassured that. in date, stock was redistributed where appropriate. Support could be provided to voluntary sector organisations upon request.

The re-sterilisation of equipment was questioned and it was explained that whilst some equipment had been retested and found to be okay following re-sterilisation that did not apply to all equipment. Although it was queried whether all the PPE equipment should continue to be stored at Aspen House, the Committee was informed that whilst it could be divided up there was not that much equipment currently stored. The Committee noted and approved spend commitments to date and agreed principles for the future of PPE support from the CCGs. (Jane Garnett left the meeting) Application to extend the block contract arrangements with Sue Ryder - Specialist Neurological Care Centre. Historically we have had a contract with Sue Ryder on a cost and volume arrangement for 12-week packages of care. In response to the pandemic, a block contract for six months for six beds at Sue Ryder was agreed and approved by the Committee on 28 April 2020 (ref CRAC 20-05) which secured exclusive access to the six beds available. The beds supported discharge from hospital for level two neuro rehab patients. When the contract was on a cost and volume basis, the CCG often had to make out of area placements which was difficult for patients and their families. During the first six months of 2021 there had been increased patient throughput with improved patient experiences. Care was being tailored to the individual needs of each patient often resulting in earlier discharges, with no detriment to outcomes. The overall cost of the service had been contained within the original rehab budget with more patients being able to access care. Approval of an extension of the block contract for a further six months to March 2021 was being sought. The block contract value was £18K per week, for six beds i.e. £468K for six months (within existing budget) The Committee was informed that Sue Ryder had been informed that increased reporting would be required to demonstrate cost effectiveness going forward. The Committee felt that the paper was positive and it was good to see that block contracts could provide innovation and improve outcomes. Further work was to be carried out to explore whether any elements were claimable in respect of the hospital discharge programme. The Committee approved the extension of the block arrangement from 1 October 2020 to 31 March 2021. (Sheila Murnion left the meeting) Enhanced End of Life Services until March 2021 During the emergency period the three Hospices within the SNEE system had developed offers of support in line with the Enhanced Discharge Guidance published on the 19 March 2020. The Committee agreed to support the hospices financially in order to deliver, extended virtual and physical capacity, single point services and bereavement support. The report reflected on the financial envelopes agreed and provided an overview of the ongoing Enhanced End of Life Services the Hospices were able to provide until March 2021. The Committee was asked to set a financial envelope in which the local alliances could work to refine the operational parameters of each service, in a way that best supported the delivery of plans for winter and phase 3 recovery in each of the Alliances. The CCG would pay for the services agreed, based on actual costs incurred up to the agreed

funding level. It was felt that the acute Trusts should gain benefit from the proposal via the different way of working. Handing the funding back to the Alliances, with appropriate scrutiny, was the right thing to do and should provide opportunity to compare and contrast and share learning. The Committee approved the expenditure as proposed in the report subject to a process for scrutiny and evaluation being in place. Month 5 and 6 (August/September) Covid-19 Expenditure Return NHS England had confirmed that the financial arrangements for Covid-19 for 2020-21 were not based on a direct reimbursement of expenditure incurred. The CCGs had received reduced financial allocations for the emergency period from April to September 2020 and were told that their financial position would be adjusted to break-even on a monthly basis. Allocation adjustments had been issued monthly in arrears since month three to fully reimburse the CCGs for Covid-19 costs where the total year to date overspend exceeded the value of those costs. The month five and six Covid-19 expenditure returns were submitted to NHS England as part of the CCGs monthly finance return submission and were summarised in appendix 1. The Covid-19 expenditure returns included some items of recurring spend where the CCGs reimbursed actual costs incurred and the values changed on a monthly basis. Although those areas of spend had previously been approved by the Committee, only the value of the month one to four spend had been approved to date, therefore the Committee was asked to approve the month five and six costs for the spend areas as specified within the report. The Committee noted the total expenditure returns submitted by the CCGs for months five and six and approved the month five and six elements of previously approved expenditure areas included in those returns as detailed in sections 2.3 to 2.7 of the report. ACE provision of a safer UTC service at Clacton by offering a dedicated red area in response to National COVID-19 IPC directions Following National Covid-19 IPC advice to segregate patients that were symptomatic or met isolation criteria, the UTC at Clacton required alterations to support the capability to maintain a safe environment for both visiting patients and staff. A previous proposal put forward in July 2020 was denied, offering to fully relocate the UTC service on site, giving access to isolation areas, extending the UTC output capabilities and support future site investment, seeking to obtain financial support from NHSE/I Covid-19 funding. That scheme was understandably denied with excess of £1.5M cost and not deliverable until March 2021. The current funding request sought to resolve the necessity which would provide a more limited but effective solution with dedicated Red entrance, waiting facility, consulting rooms as well as WC and storage. The site enhancements would seek to satisfy the expected numbers for the ongoing period of Covid-19 and isolation requirements thereafter. Construction bids had been received and no more than £47,520+VAT (including an 8% contingency) was required. Having questioned why other community hospitals had not felt the need to seek similar funding, it was explained that any such claims should they have been made would have come via ESNEFT or WSFT and not via the Committee. Having queried whether the proposal was aligned with the plans in place for Clacton Hospital, it was felt that there was a need to investigate further and obtain further information prior to making a decision. The Committee therefore DID NOT approve the expenditure and requested additional

information be sought and circulated prior to the Committee being asked to make a ‘virtual’ decision.
20/155 Other issues for discussion and agreement or information
Activity based contracts – proposed approach for remainder of the year The Director of Finance advised that the intended approach in respect of activity based contracts was if that contracts were PAYG providers would be expected to reestablish activity and attempt to return to normal levels. Proposals from providers would be reviewed on a case by case basis but needed to be within the original budget. Information was currently being collated and would be presented to a future meeting. The Committee supported the approach. ACE discharge hub and community beds – reversion to alliance decision Approvals were being reviewed to ascertain what was outstanding. ACE was the largest one outstanding and it was intended that it be passed on to the NEE Alliance for review as part of its growth funding. The Committee supported the approach.
20/156 Forward Planner
S75 for phase 2 hospital discharge programmes.
20/157 Any Other Business
No items of other business were received 20/158 Date of Next Meeting
To be confirmed.

WEST SUFFOLK CCG
PRIMARY CARE COMMISSIONING COMMITTEE
20 October 2020 (Virtual Meeting)
Decision Record
QOF funding 2020/21 To receive and approve a report from the Deputy Director of Primary Care
Lois Wreathall Report No:
WSCCG/CGC 20-20P Primary Care Commissioning Committee Members: Lynda Tuck (Chair), Lay Member for Patient and Public Involvement Geoff Dobson, Governing Body Lay Member for Governance Ed Garratt, Chief Executive Paul Gibara, Director of Performance Improvement Jane Payling, Director of Finance Kate Vaughton, Director of Integration Declarations of Interest
No declarations of interest were received.
Decision
The Committee approved the principle on the points contained within the report together with the associated monetary award.

Unconfirmed minutes of a Meeting of the West Suffolk CCG Primary Care Commissioning Committee held ‘in common’ with the Primary Care Commissioning Committee of Ipswich and
East Suffolk CCG and GP Commissioning Committee of North East Essex CCG, on
Tuesday 27 October 2020, via Microsoft Teams Members of the public were invited to email questions prior to the meeting.
PRESENT: Lynda Tuck Lay Member, Patient and Public Involvement (Chair) Geoff Dobson Lay Member for Governance Paul Gibara Director of Performance Improvement Jane Payling Director of Finance Lois Wreathall Deputy Director of Primary Care Dr Christopher Browning West Suffolk CCG Chair Simon Jones Suffolk, Local Medical Committee Charlotte Mackenzie NHS England Stuart Quinton Primary Care Contracts Manager, NHS England IN ATTENDANCE: Sarra Bargent Head of Clinical Quality – Primary Care, North East Essex CCG Ameeta Bhagwat Head of Financial Planning and Management Accounts David Brown Deputy Chief Operating Officer, Ipswich and East Suffolk CCG Dr John Flather GPCC Member, North East Essex CCG Pam Green Chief Operating Officer, North East Essex CCG (Part) Dr Max Hickman Elected Member, North East Essex CCG Dr Firas Hussein Elected Member, North East Essex CCG Dr Lorna Kerr Secondary Care Doctor Graham Leaf Lay Member for Governance Lisa Llewellyn Director of Workforce Jo Mael Corporate Governance Manager Charlotte Mackenzie Head of Finance, North East Essex CCG Claire Pemberton Head of Primary Care, Ipswich and East Suffolk CCG Jon Price Chair, GPCC, North East Essex CCG Dr V Raja Essex Local Medical Committee Carol Sampson Head of Medicines Management, North East Essex CCG Vicky Sawtell Deputy Director of Performance and Contracts Anthony West Head of Transformation (Planned Care), North East Essex CCG
20/44 APOLOGIES FOR ABSENCE
Apologies for absence were noted from; Steve Chicken Lay Member Ed Garratt Chief Executive Cllr James Reeder Health and Wellbeing Board Kate Vaughton Director of Integration

Andy Yacoub Chair, Healthwatch The meeting was confirmed as quorate.
20/45 DECLARATIONS OF INTEREST AND HOSPITALITY AND GIFTS
No declarations of interest, hospitality or gifts were received.
20/46 THE RESTORATION OF PRIMARY CARE SERVICES POST COVID-19
The Committee was in receipt of a report which provided information about the issues facing General Practice as services were re-started following the first wave of Covid-19. The report also set out the key points of the current NHS England guidance on the subject. At the time of the Covid-19 pandemic starting to have a significant impact on the safe delivery of services delivered by general practice, NHS England had issued several pieces of guidance. In summary that guidance had asked practices to ensure that all patients were triaged by telephone and to only see patients face to face if clinically necessary. It also asked practices to stop a significant amount of non-urgent activity such as routine checks, to minimise infection risks. The net effect was that a significant amount of routine care was either stopped altogether or delivered remotely. As the peak of the first wave passed, local practices and the CCGs started to have conversations about how services should be restored in a way that was safe for patients and staff and provided effective care. Appendix B to the report provided a description of the key issues in respect of service restoration and how primary care was responding in each case. Appendix C identified the position of the three CCGs against a range of metrics which had been set out by NHS England, with key areas to be addressed set out in paragraph 3.3 of the report. Learning from Wave 1 that might be applied to Wave 2 was outlined in Section 4 of the report. Whilst it was queried whether practices would be able to facilitate virtual ward rounds for care homes during the second wave of Covid-19, the importance of highlighting such suggestions for consideration was recognised. The Committee noted the content of the report.
20/47 PRIMARY CARE STRATEGY REFRESH
The Committee was provided with an opportunity to review the draft STP primary medical
service strategy; to provide assurance as to how primary care would meet the objectives of the NHS Long Term Plan and continue to deliver the commitments of the General Practice Forward View (GPFV) whilst remaining consistent with local Alliance and primary medical care strategies. General practice played a pivotal role in delivering localised, high quality, safe and effective services to its population. There had been an increased focus on the role of primary care, how it was structured and how services were delivered. More recently as described in the document, Investment and evolution; a five-year framework for GP contract reform, to support the implementation of the NHS Long Term Plan. The patients of Suffolk and North East Essex are generally served by high quality practices with care delivered by experienced and qualified professionals. There was some variation in access and performance. In 2019 NHS England wrote to the STP/ICSs requesting that joint primary care strategies were refreshed or developed in the context of the NHS Long Term plan and the new GP Contract which saw the formation of Primary Care Networks. A strategy was produced and signed off by the ICS Sustainability and Transformation Partnership Board using existing primary care strategies that were locally co-produced between 2015-2017 by GPs, practice managers, patients and partner organisations. Those documents remained relevant and aligned with current priorities.

In 2017, the STP collectively submitted a GPFV submission which was rated ‘good’ by NHS England. Content from that, the three Alliance strategies and the ICS Operational plan also remained central to the development of the new joint strategy. With the introduction of Primary Care Networks, the strategy went further in supporting a ‘bottom up approach’ that strengthened the role at neighbourhood level. The strategy as presented, focused on existing, agreed local plans and fulfilled the requirements requested by NHS England for submission, and set out current programmes of action. It was recognised that action plans needed go further to respond both to new national requirements and local need, and to articulate: • further local demand management measures including alignment of Alliance prevention
and self-care strategies; • local support for Primary Care Networks, specifically including their Clinical Directors; • workload management measures beyond national measures; • further workforce plans (specifically but not limited to recruitment and retention issues); • estates and digital integration; • a local funding strategy for primary care.
The strategy was now being reviewed for 2020, to include the challenges that we are currently facing and to update the strategy in general. The CCGs would continue to refine the document (Appendix 1), working with wider partners to ensure it was a strategy that reflected the wider ambitions of the system. The need to make distinction between primary and community services was emphasized. It was noted that community services within Suffolk were linked with secondary care providers. It was felt that more clarity was required with regard to primary care team links with community and integrated neighbourhood teams. Primary Care leads within the CCGs agreed to review the document to ensure clarity prior to the final draft. It was explained that the primary care strategy was based on population health needs with different delivery across the ICS. The need to consider services based on the needs of the population and ensure the integration of teams to deliver those services was emphasized. The Committee noted the Strategy and commitment to the next steps.
(Pam Green joined the meeting)
20/48 SUFFOLK AND NORTH EAST ESSEX FLU UPDATE
The Flu vaccination was one of the most effective interventions that could reduce pressure on the health and social care system during winter. 2020/21 had the potential to be one of the most challenging in the administration of the flu vaccine because of the impact of Covid-19 on health and social care services, so it was important that there were plans in place to increase the effort to deliver the Flu vaccine (NHSE, 2020) as those most at risk from flu were also vulnerable to Covid-19.
Groups to be offered the vaccine were identified paragraph 1.3 of the report with key elements of the Suffolk and North East Essex Flu and Covid-19 Plan detailed in Section 2 of the report and governance in Section 3. Progress to date and next steps included;
Six workstreams had been identified with clear delivery objectives, a job advert was currently live to fulfil a lead for Covid-19 workstreams One and Two (Delivery Model and Logistics).
The CCGs had been working closely with GP practices to ensure maximum preparedness in primary care leading to the achievement of maximum vaccine uptake in eligible groups. GP Practices, community pharmacies and providers had ordered vaccine for the 2020/21 as per national guidance in the 1st annual flu letter (to deliver 2019/20 ambitions). National vaccine

manufacturers had closed to additional orders from primary care. Additional vaccine would now only be available via DHSC.
To ensure the primary care patient record was reflective of status, a data and technology workstream had been established. That workstream was able to monitor uptake and delivery of the Flu vaccine and had mapped data flows from acute, school and pharmacy records.
The Flu communications went live on 21 September (in line with national communications) and would continue through October and November 2020.
As of 6 October 2020:
• Suffolk and North East Essex are in the top six CCGs for achievement to date compared to East of England (out of 21 CCGs).
• Vaccinations for high risk groups were progressing well with 75% of care home residents and 73% of pregnant women already completed. The over 65 group was 35% completed, which was our biggest cohort, Suffolk and North East Essex were on track for completion within the deadline of 15 December 2020.
• School immunisations were on track and there had been no impact on vaccinations due to school closures or bubble closures, the school immunisations team business continuity plan was robust and tied into the primary care business continuity plan in the case of full local lockdowns.
• Community pharmacy had delivered double the amount of flu vaccinations in comparison to the same time last year.
The Committee was informed that, since circulation of the report, practices could now order additional vaccines although flu stock remained for ‘at risk’ cohorts at present. It was explained that Suffolk figures within the report were based on actual figures and that North East Essex figures were based on informed data. In response to questioning, the Committee was advised that pharmacies, along with schools, sent practices notifications of those patients that had received vaccinations in order that all information might be collated by the CCG. Having queried the reported maternity vaccination numbers, it was explained that maternity departments had been issued with vaccine and were directly providing vaccinations to pregnant women. The Committee noted the content of the report.
20/49 PRIMARY CARE PERFORMANCE REPORT FOR SUFFOLK AND NORTH EAST ESSEX
The Committee was in receipt of a report which provided an update on performance related
matters in respect of GP Practices and actions taken; seeking further recommendations and areas for consideration for the Primary Care teams. The report provided information and outlined ongoing actions in respect of the following areas; • Prescribing and medicines management • Severe mental illness and physical health checks • Learning Disabilities (LD) health checks • Dementia diagnosis rates • Care Quality Commission practice ratings The following points were highlighted during discussion; • Prescribing – each CCG’s overspend was similar to that of last year. Practices were
aware of the need to review processes such as polypharmacy. • Performance targets – Severe Mental Illness health checks, Learning Disability health

checks and Dementia diagnosis performance had all been adversely affected by the pandemic. Norfolk and Suffolk NHS Foundation Trust had been working with Suffolk practices to assist with data cleanse of patient lists. The Local Enhanced Service had been re-issued to allow for work to be carried out virtually. A review of learning disability health check data in quarter one had identified performance was low which might be a result of the pandemic and the reluctance of individuals to attend appointments. Learning Disability nurses were providing reassurance and considering other ways of working.
• Care Quality Inspections had mainly paused during March- September 2020 and were now beginning to recommence. The CCGs continued to support practices where appropriate.
North East Essex CCG figures within the report associated to STAR PU antibiotics were queried and the Head of Medicines Management agreed to clarify the position outside of the meeting. The Committee noted the report and that North East Essex CCG had previously agreed a ‘deep dive’ into medicines management.
20/50 CONTRACTUAL UPDATE
The report served to update the Committee on the contractual changes relating to GP
practices within the Suffolk and North East Essex STP over the last quarter (July-September 2020). Key issues were as follows; Branch closures - the White House Surgery (D83078) had removed its branch site ‘White House Surgery’ from the contract following approval at the last West Suffolk Primary Care Commissioning Committee (26/08/2020). A report which sought approval to operate out of the Mildenhall Hub would be presented at the relevant PCCC if the estates business case was approved. (West Suffolk CCG) Practice name changes: • Christmas Maltings and Clements Practice (D83012) had formally changed its name to
Unity Healthcare. (West Suffolk CCG)
• The White House Surgery (D83078) had formally changed its name to The Reynard Surgery. (West Suffolk CCG)
List closures: • Mayflower Medical Centre (F81019), Harewood Surgery (F81606) and Fronks Road
Family Surgery (F81221) continued to communicate to the public that they were not accepting new patients. That was also displayed on the NHS Choices page for each practice. (North East Essex CCG)
• The Barham and Claydon Surgery (D83615) had formally applied to close its list to new patients for 12 months. That would be presented for decision in November following the current stakeholder engagement exercise. (Ipswich and East Suffolk CCG)
Super Partnerships: • Suffolk Primary Care Super Partnership variation agreement was near completion. The
partnership had been sent a formal contract letter to recognise the partnership formation in 2017, but the variation agreement would be effective from 01/01/2020. (Ipswich and East Suffolk CCG & West Suffolk CCG)
• The Colte Partnership Super Partnership variation agreement was near completion. The partnership had been sent a formal comfort letter to recognise the partnership formation in 2017, but the variation agreement would be effective from 01/10/2020. (North East Essex CCG)
The Committee noted the content of the report.

20/51 INTEGRATED CARE SYSTEM (ICS) WIDE FINANCE REPORT – SEPTEMBER 2020
(MONTH 6)
The Committee was provided with an overview of the month six Primary Care Delegated Commissioning budget and other associated Primary Care budgets for the three CCGs which made up the Suffolk and North East Essex Integrated Care System (ICS). Due to the Covid-19 situation, allocations for NHS finance were initially released for the first six months of the year, and included the Delegated Primary Care (DPC) budget. For months 1-6 a combined DPC allocation £74,503k was received, against which a cumulative overspend had been made of £1,887k broken down by CCG as set out in paragraph 2.1. Although the CCGs had recently received confirmation of their full year allocations, to date there had only been a release of budget to month six and there was only a requirement to report a financial position for months 1-6. The budgets and forecast would be amended to reflect the full year position from October (m7) reporting. Allocations for months 7-12 remained largely unchanged from those in months 1-6. The current overspend for the two Suffolk CCGs was driven predominantly by the PMS Premiums, List Size increases up to Q2 and Locum cover allowance. The issue had been raised consistently at recent primary care committees with the current overspend reflecting the balance of the allocation received compared with the payments made to practices, for which the higher than average level of PMS in Suffolk results, inter alia, in a cost pressure. North East Essex was managing to meet its financial requirements within budget, the position would be reviewed in line with months 7-12 allocation. As the CCGs had reported the financial position for months 1-6 only, risks in relation to that period had been included in the forecast. Across three CCGs those included pending rent reviews, practice support, forecast list size adjustments and locum allowance. That would continue to apply going forward. The budget for Primary Care Delegated Commissioning was received as a specific allocation whilst budget for Other Primary Care was received as part of the CCG programme allocation. based on the Covid-19 budget model. Other Primary Care Services included Local Enhanced Services and GPFV. To date the position across the ICS was an overspend of £635k against a budget of £7,016k. In response to questioning the Director of Finance reported that a key issue for the second part of the year would be the impact of the Covid-19 second wave on budgets issued in line with the expected recovery of services. All CCGs were to be subject to audit in respect of Covid-19 expenditure and Ipswich and East Suffolk CCG had been notified it would be audited in the first round of audits. The Committee noted the content of the report.
20/52 PRIMARY CARE NETWORK (PCN) – SUMMARY UPDATE
The Committee was updated on the latest developments and requirements for Primary Care
Networks (PCNs) and provided with assurance of progress against the primary care contract. There were five main elements to the PCN network contract for 2020/21; Additional Roles Reimbursement Scheme, Impact and Investment Fund and the introduction of three service specifications. The report went on to detail progress in respect of each of those areas. Key points highlighted during discussion included; • West Suffolk Primary Care Networks (PCNs) continued to grow with development tracked
across a number of issues. • All North East Essex CCG practices were now in a PCN and less change was anticipated

in year two. • North East Essex CCG received regular reports against the maturity matrix, and it was
anticipated that Suffolk CCGs would receive similar reports going forward. • The maturity matrix tracked PCN development and system progress. Some elements,
such as the sharing of records, were outside the responsibility of the PCN. • NHS England had added another two roles to the list of additional roles for reimbursement.
There was concern by NHSE that recruitment had not yet been as envisaged and it was likely that the reason was that practices were being cautious and seeking evidence of benefit and support prior to recruiting.
• Investment and impact fund – PCNs would need to achieve certain elements in order to access future funding. The requirements of the fund were similar to those of the Quality Outcomes Framework and there would be a need for practices to share information within their respective PCNs.
• Care homes – equipment had been provided to care homes to facilitate virtual ward rounds. North East Essex CCG had 175 care homes within its area and all had been allocated to a PCN.
• Dedicated workforce leads within the ICS had resulted in a huge improvement for practices.
It was quered whether as a result of increased GP contact with care home residents there had been any increase in referrals to dentistry, dietitians, therapists to be proactive in preventing illness or speeding up recovery. It was explained the community services were evolving around PCNs, INTs and care homes. Care home forums had been established and provided a link with primary care and available support. Having noted that GP trainees were only due to spend a year in hospital, it was highlighted that training had been disruptive during 2020 due to the change of roles and limited learning opportunities as a result of the pandemic. It was suggested that the trainees might require additional support. The Committee was informed that the Deanery was taking the matter forward and putting systems in place to make transitional change. The benefit of being able to work at scale in respect of recruitment was emphasized.
The Committee noted the content of the report.
20/53 PATIENT PARTICIPATION GROUP (PPG) UPDATE
NHS England had mandated that all practices must have a PPG as set out in paragraph 5.2
(Patient Participation) of the GMS contract detailed within the report. Engagement by the CCG with its PPGs was detailed in Appendix 1 to the report and the Ipswich and East Suffolk PPG network was seen as an exemplar nationally. Presentations, learning and support was made available to Regional and National Teams. The PPGs had supported the introduction of Care Navigators into practice through communication of their role to the local population and PPG members provided support to the vulnerable during Covid-19 via befriending schemes, help with shopping and medicines collection. SNEE PPGS were active and not isolated forums. PPG networks were being established where learning could be shared, and messages and communication cascaded. There had been transformation in the way practices engaged with PPGs via technology which had been welcomed. Future challenges included how PPGs might become embedded in PCNs going forward. The benefit of PPGs being moved to a locality footprint was highlighted. Some PPG chairs are already active members of their locality meetings. The Committee noted the report and welcomed future combined progress updates.
20/54 WORKFORCE UPDATE

The Committee was in receipt of a report which summarised key project areas underway
within workforce which included; recruitment; pipeline of workforce; workforce planning; quality assurance and supply; retention; apprenticeships; and wellbeing support. Key points highlighted included; • Workforce remained challenging across the ICS and primary care. The mutual aid
agreement which enabled the movement of staff across the system during the pandemic had been extended into winter, although it was recognised that it might prove more challenging in light of the recovery of services alongside the second wave.
• The health and wellbeing of staff was paramount and support had been provided in a
number of ways which included occupational therapy, and mental health support. • The need to work together and collaboratively, making the best use of resources, to
develop services had been recognised. • At the Colchester Health and Care Academy the primary care team had described how it
had developed roles within practices. • The range of available placements and integration work was encouraging. • It was recognised that the recruitment of additional roles was not just about workforce but
also the willingness of practices to accept those roles and often it was different roles that were required.
• The ability for primary care to have the capacity and capability to train staff within work
was critical to future sustainability. The need to continue to attract funding to facilitate such work was highlighted.
The Committee noted the report.
20/55 DATE OF NEXT MEETING
The next meeting was scheduled to take place on Wednesday, 23 December 2020.
20/56 QUESTIONS FROM THE PUBLIC
No questions had been received.

Unconfirmed Minutes of a meeting of the West Suffolk CCG Commissioning Governance Committee held on 21 August 2020
COMMITTEE: Geoff Dobson Lay Member: Governance (Chair) Ed Garratt Chief Officer Paul Gibara Director of Performance Improvement Jane Payling Chief Finance Officer Lynda Tuck Lay Member: Patient and Public Involvement PRESENT: Jo Mael Corporate Governance Officer Linda Lord Chief Pharmacist
20/007 APOLOGIES FOR ABSENCE
The Chair welcomed everyone to the meeting and apologies for absence were noted from; Steve Chicken Lay Member Kate Vaughton Chief Operating Officer
20/008 DECLARATIONS OF INTEREST
No declarations of interest were received.
20/009 MINUTES OF THE PREVIOUS MEETING
The minutes of the meeting held on 26 February 2020 were approved as a correct record.
20/010 MATTERS ARISING AND ACTION LOG
There were no matters arising from the previous meeting and the action log was reviewed and updated.
20/011 ENHANCED SERVICES: POLYPHARMACY, RHEUMATOLOGY AND SHARED
CARE
The Committee was in receipt of a report which sought review of the following Enhanced Services (ESs): • Current Polypharmacy ES • Current Rheumatology ES • Proposed new Shared Care ES • Proposed adjusted Polypharmacy ES

The report also sought review of the Network Contract DES, Section 7.2 Structured Medication Review and Medicines Optimisation Determination if (and how) the Network Contract DES should impact on the Polypharmacy ES To find an affordable way to update the current Rheumatology ES to a new Shared Care ES. This would fund practices to prescribe and monitor drugs that are currently rated amber (shared care) on the WSCCG traffic light system, and require significant monitoring. This paper is not about introducing new amber drugs or new shared care agreements. The report went on to detail each of the mentioned Enhanced Services and its associated issues. It was explained that four options had been presented to the WSCCG Executive via a virtual meeting from 24/7/20 – 4/8/20, and also discussed further at the Executive meeting on 5/8/20. Options one and three had not been supported and therefore only options two and four were being presented to the Commissioning Governance Committee today for consideration, those being; Option Two:
Advantages
– Full benefits (financial and safety) of Polypharmacy ES maintained – Fairer payment system for GPs to prescribe and monitor shared care
drugs that require significant monitoring – Fewer problems with GPs refusing to prescribe shared care drugs that
require significant monitoring – Practice payments from these ESs increased by £73,535 p.a.
Disadvantages – Practices paid twice for similar medication review activity – Cost pressure for CCG of £73,535 p.a.
Option Four:
Cost p.a. for WSCCG
Stop Rheumatology ES
Introduce new Shared Care ES £176,310
Adjust Polypharmacy ES to complement (not duplicate) the structured medication reviews described in the Network Contract DES
Estimated £80,000 based on reducing the current payments by 50%

TOTAL Estimated £256,310
Advantages
– Benefits (financial and safety) of targeted polypharmacy medication reviews maintained
– Fairer payment system for GPs to prescribe and monitor shared care drugs that require significant monitoring, so fewer problems with GPs refusing to prescribe shared care drugs with that require significant monitoring
– Practices not paid twice for similar medication review activity – Estimate no/little changes regarding current costs to CCG and practice
payments
Disadvantages – Full benefits of Polypharmacy ES lost. However, the structured
medication reviews included in the Network Contract DES should compensate for this.
– Cost pressure for CCG if Polypharmacy ES payments > £89k. However, polypharmacy medication reviews do pay for themselves so this is not an overall cost pressure.
The options were reviewed by the WSCCG Executive (virtual meeting 24/7/20 – 4/8/20) and the following recommendations were made: Option Two
– 6/19 (32%) of Executive members voted for this option. All supporters of this option were GPs.
– Key points raised by voters to explain why not Option 4: • PCNs have not yet recruited sufficient clinical pharmacists to
enable the SMRs described in the Network Contract DES to be completed
• PCNs are having trouble recruiting, with few candidates applying and the ones who do apply are asking for higher salaries. NHSE are only reimbursing PCNs for clinical pharmacist salaries at band 7-8a, which is low for the role. Also there are shortages of pharmacists in general.
• Even if PCNs did manage to recruit, the clinical pharmacists would have a broad portfolio and would not be able to focus solely on SMRs
• The existing Polypharmacy ES does seem to be a good enabler for containing prescribing costs, and improving safety. Removing it may cause prescribing costs to rise and other pressures on the healthcare system to increase, e.g. hospital admissions from adverse drug reactions. Adjusting the Polypharmacy ES as described in Option 4 may be ‘throwing out the baby with the bath water’
– A further review is recommended, with a potential move to Option 4 after 1 year
– Including hydroxycarbamide for myeloproliferative disorders and sickle cell disease in the new Shared Care ES is accepted.
Option Four – 10/19 (52%) of Executive members voted for this option. All supporters of
this option were non-GPs All Executive comments are recorded in Appendix 6 A middle ground between options two and four may be the solution, and hence an option 5 is now proposed Option Five:

Cost p.a. for WSCCG
Stop Rheumatology ES
Introduce new Shared Care ES £176,310
Adjust the Polypharmacy ES further to draft v2 to mitigate concerns raised by the Executive GPs, whilst containing costs for the CCG
Estimated £80,000 based on reducing the current payments by 50%
TOTAL Estimated £256,310
Details
– Middle ground between options 2 and 4 – No cost pressure for CCG (current cost approximately £266k p.a.) – Polypharmacy ES now adjusted further to draft v2. Comparison with draft v1:
• Removed: Requirement that must be for patients with 6 – 9 medicines on their repeat. This mitigates concerns that patients with 10 or more medicines on their repeat may not yet be reviewed by PCN pharmacists via the Network Contract DES.
• Retained: Requirement to focus on DFMs, aiming to reduce doses or stop treatment if possible, for safety. This means that the ES funding is now only for medication reviews that are more challenging to implement and encompasses all patients on DFMs, regardless of how many medicines they have on repeat. This spans wider than the Network Contract DES which only funds SMRs for patients on ≥10 medicines. By removing non-DFM, the overall costs will be lower. Stopping the funding for non-DFM reviews does not mean these reviews should stop; they should continue as ‘business as usual’ following 5 years of the Polypharmacy ES being in place. Reviews of non-DFMs are generally easier to implement than reviews of DFMs.
• Retained: Specifies that the reviews can be done by a PCN pharmacist, and remotely. It therefore encourages newly recruited PCN pharmacists to focus on SMRs rather than other priorities, and to become proficient at doing them for DFMs.
• Added: Promotion of an e-learning course on DFMs. This is in addition to the guidelines and resources on DFMs that are already included in the ES and on the WSCCG website. This will upskill PCN pharmacists (and others) for longer term benefits.
• Added: Duration extended from 6 months to 1 year, so now 1/10/20 – 30/9/21, and for review in June 2021. This will allow time for recruitment of further PCN pharmacists, in line with Exec GP requests.
Points highlighted during discussion included; In response to questioning the Committee was informed that reviews could be carried out by both Pharmacists and GPs and should involve a two way discussion with the patient. It was recognised that the Polypharmacy ES had been good for patients and there was concern that straightforward medication reviews might not continue if the ES was stopped. Payment for reviews was currently £50.

Although it was queried whether retention of the Polypharmacy ES might offset cost pressures associated to Option two, the Committee was advised that such confirmation could not be given at the current time. It was noted that the Polypharmacy ES was unique to West Suffolk CCG as whilst, the principle behind the ES was common across the country, no other CCGs were funding it and work was carried out within normal practice. The need to encourage patients and nurses to question medications was emphasized. Having queried whether the Polypharmacy ES payments were capped, it was explained that whilst they were not capped a Senior Pharmacy Technician reviewed the polypharmacy reports from practices each month and challenged practices where savings were low. It was suggested that, in light of the potential duplication of work associated to Option two, that the payment of £50 for reviews be reduced to £25. After careful consideration, the Committee recommended that the CCG’s Executive be asked to consider both Option 5 as detailed within the report and Option two with a reduced review payment of £25. The outcome of that discussion to be presented back to the Committee for final approval.
20/012 DATE OF NEXT MEETING
Meetings of the Commissioning Governance Committee are arranged as and when
required.

West Suffolk CCG
Commissioning Governance Committee (via email) 08 September 2020
Decision Record
Commissioning Governance Committee Members: Geoff Dobson (Chair), Governing Body Lay Member for Governance Ed Garratt, Chief Executive Jane Payling, Director of Finance Lynda Tuck, Lay Member for Patient and Public Involvement Declarations of Interest No declarations of interest were received. 1 Enhanced Services:
Polypharmacy, Rheumatology and Shared Care – A further Review To receive and approve a report from the Chief Pharmacist
Linda Lord Report No:
WSCCG/CGC 20-17 Decision The Commissioning Governance Committee Approved
The updated Shared Care ES is formally accepted for implementation from 1/10/20 Option C is supported for the Polypharmacy ES from 1/10/20

Ipswich & East Suffolk Clinical Commissioning Group West Suffolk Clinical Commissioning Group
North East Essex Clinical Commissioning Group
Minutes of the CCG Collaborative Group meeting held on 10 September 2020
PRESENT Graham Leaf (GL) Lay Member (Governance) Ipswich & East Suffolk CCG (Chair) Dr Christopher Browning (CB) Chair, West Suffolk CCG Governing Body Dr Hasan Chowhan (HC) Chair, North East Essex CCG Governing Body Dr Mark Shenton (MS) Chair, Ipswich and East Suffolk CCG Governing Body Jon Price (JP) Lay Member (Governance) North East Essex CCG Ed Garratt (EG) Chief Executive, Ipswich & East Suffolk, North East Essex and West Suffolk CCGs IN ATTENDANCE Jo Mael (JM) Corporate Governance Manager Amanda Lyes (JP) Director of Corporate Services and System Infrastructure (Part) Minute
Action
20/016 Welcome and apologies The Chair welcomed all to the meeting. Apologies had been received from: Steve Chicken and it was agreed that Graham Leaf act as Chair. Geoff Dobson Lay Member (Governance) West Suffolk CCG
20/017 Declarations of Interest
No declarations of interest were received.
20/018 Minutes of meeting held on 8 October 2019 and 7 February 2020
The minutes of meetings held on 8 October 2019 and 7 February 2020 were approved as correct records.
20/019 Matters arising and review of action log
The action log was reviewed and updated and it was reported that the NEECCG Constitution was now with NHSEI for sign off.
20/020 Transition to the NHSEI Model Constitution for CCGs and developing
our Governance NHS England had published a model Constitution for CCGs in September 2018, the first update since the original version was published upon the creation of CCGs back in 2012. The new template was a welcome update as it was more flexible and concise, making it much easier for CCGs to make changes and tailor their Constitutions to reflect local practices. Key changes were set out in Section 1 of the report. Amendments for both Suffolk CCG Constitutions were submitted to NHSEI for approval some months ago. Those were purely administrative amendments to reflect the joint working arrangements with North East Essex CCG. NHSEI had suggested many other amendments, in addition to those submitted for approval, and have advised that when any amendments to old
style Constitutions are submitted, they are now obliged to review the entire document and not just the amendments requested. That was not the case for the new model Constitution which NHSEI were very keen to see all CCGs adopt as soon as possible. As a result, it was suggested that the CCGs now adopt the model Constitution with three separate but probably almost identical documents for each CCG with the aim of having them approved and published by 1 April 2021. On the basis of moving to the model Constitution, NHSEI requested that we produce an agreed timeline for getting us to approval by 1 April 2021. The Senior System Governance and Assurance Lead for the East of England at NHSEI had undertaken to review the drafts in November and December 2020 meaning that we could get Governing Body approval in January or March 2021. Comments included; • The need to ensure wider membership sign up was questioned and it was
explained that the current guidance was that whilst non-material changes did not require sign up by membership, material changes did. It would be important to evidence consultation with membership.
• The new model constitution was more concise with one element being the
development of a handbook which contained those documents that required regular update.
• It was felt that the in light of the need to consult with membership the
timetable might require review.
The Director of Corporate Services and System Infrastructure agreed to produce a short bullet pointed document highlighting the main changes in the new and old models, together with reviewing the timetable in light of the need to consult membership.
The CCG Collaborative Group approved transition to the NHSEI Model Constitution for CCGs from 1 April 2021 and the proposed timeline as set out within the report. The Group went on to have a discussion in respect of Governance. It was reported that discussions had taken place with individual CCGs with regard to Alliance governance and further Director discussions were to take place. There was a desire from staff to make governance arrangements less complicated and remove duplication. The need to move work from the CCG to the Alliance space was recognised although the challenge associated to ‘letting go’ was recognised. The need to move to holding Committees ‘in common’ where appropriate was highlighted. Having noted that CCG elections were on the horizon the need to be mindful of future vision when carrying out elections or extensions to service was emphasized. The Chief Executive and Director of Corporate Services and System Infrastructure agreed to draft governance proposals for presentation to the Collaborative Group at a later date.
(Amanda Lyes left the meeting)

20/021 Accountable Officer Update The Collaborative Group was in receipt of a paper from the Chief Executive, which set out key objects for the Suffolk and North East Essex Integrated Care System going forward. Points highlighted included: • The first two slides covered inequalities and recovery. Work on health
inequalities was very strong and extra work was being carried out in respect of the BAME agenda and disproportionate effect of Covid-19.
• There was a plan to meet national recovery requirements of 90% pre Covid-19 levels.
• ESNEFT was performing well with non-elective and discharge processes. • There had been a lot of focus on cancer services and it was anticipated
that the backlog would be cleared by October 2020. Two week wait referrals were back to pre Covid-19 levels.
• There was a strong plan in place for mental health which had received good feedback from NHSEI, although there was concern at the demand on GPs going forward.
• Workforce - a health and care academy had been launched in Colchester to assist 16-18 year olds enter into care jobs. Work with the University of Suffolk continued.
• The East of England Ambulance Service NHS Trust (EEAST) continued to give cause for concern in respect of its culture and a risk summit was due to take place on 11 September 2020.
The Chief Executive agreed to provide recovery detail in respect of specialties and provide feedback to individual CCGs following the EEAST risk summit. The Group noted the content of the report.
20/022 CCG Mergers
Discussed under item 20/020.
20/023 Integrated Care System
Discussed under item 20/020.
20/024 Deputies Feedback
The Group was in receipt of a presentation which detailed feedback from Chief Executive 1:1 interviews held with deputies. Views expressed were anonymised and would inform the external organisational design facilitation and staff recognition event. Attain had been asked to provide organisational development support. The Group noted the report and welcomed an update on the organisational development plan to a future meeting.
20/025 Any Other Business
The Group was provided with an update from a recent Chairs Group meeting.
20/026 Date of Next Meeting
The next meeting is scheduled to take place on 10 November 2020, at 2.00pm.

Page 1 of 2
Title
Suffolk and North East Essex Area Prescribing Committee (SNEE APC) Meeting- minutes of the meeting June-September 2020
Lead Director
Pam Green- Chief Operating Officer
Author(s)
Emily Rutherford- Medicines Management Support Officer, NHS Ipswich and East Suffolk Clinical Commissioning Group Anisha Sharma, Senior Interface Pharmacist, ESNEFT, NHS Ipswich and East Suffolk CCG and NHS North East Essex CCG
Purpose
The purpose for submitting SNEE APC outcomes to the Governing Body is to provide assurance of the activities undertaken by the Committee. The Governing Body is asked to note the approved guidelines, formulary products, items to improve the medicines governance and the quality of the service delivered to patients across Suffolk and North East Essex Integrated Care System (SNEE ICS).
Recommendation: The SNEE APC decisions have been submitted to the Governing Body for information. . The minutes of the meeting are available to reference and demonstrates how the SNEE APC have worked as an integrated care system to support the entry of new medicines into the health economy, review historic decisions and develop guidelines to improve medicines optimisation which includes medicines safety. The following are key points to note for each of the meetings: June 2020 The Committee focused on the Terms of Reference of the SNEE APC to help establish this Committee as decision making. The SNEE APC agreed the following SNEE ICS documents:
• Shared care agreements for leflunomide and sulfasalazine were agreed (approved for NHS North East Essex CCG).
July 2020 The SNEE APC agreed the following documents for the SNEE ICS:
• The medicines reuse scheme documents for the COVID-19 panedemic response, • SNEE APC annual report • East of England Priorities Advisory Committee (PAC) statement for sodium oxybate,
electronic cigarettes and unlicensed cannabis based medicinal preparations • Alogliptin switch protocol
September 2020 The SNEE APC agreed the following documents for the SNEE ICS:
• Mesalazine GP Factsheet • Antimicrobial newsletter • Acute contracting business cases for biologic pathways, tacroliumus for GN and
Infliximab for ICPI for the SNEE ICS The following were approved for NEECCG:
• EPUT formulary chapter 10 • Switch Agreement adhesive removers

Page 2 of 2
• Switch agreement barrier products, • Antimicrobial dressing wound infection pathway • Tapentadol GP information sheet • Infant formulae stopping protocol and appropriate prescribing protocol
October 2020 The following documents were approved for the SNEE ICS:
• Antimicrobial newsletter • Formulary Traffic light definition • SCA for Mycophenolate (non-transplant) and hydroxycarbamide
The following were approved for NEECCG:
• The NEECCG Pain website documents • EPUT formulary section 1 and 12