


Suffolk Rail Impact Study - Hampton Roads Transportation ...
Upload
khangminh22Category
view
3download
0
Page 1 of 5
The 79th meeting of the CCG Governing Body will take place from 1400 hrs on Tuesday, 7 June 2022 at
Aspen House, Stephenson Road, Colchester, Essex, CO4 9QR Whilst members of the public are welcome to attend to observe the meeting, space is limited due to ongoing social distancing requirements and therefore notification of intended attendance would be appreciated to [email protected], prior to the meeting.
The meeting will also be ‘live streamed’ for members of the public (a link for the live streaming will be available on the CCG website).
Questions relating to agenda items can be submitted via the following means;
1. Prior to the meeting, via email to [email protected] 2. During the live streaming when they will be collated and asked at the appropriate time on the
agenda 3. For those attending in person at the appropriate time on the agenda.
The minutes of the meeting which will include answers to any questions submitted by the public will be published on the CCG website after the meeting.
Members of the Governing Body should inform the Chair of any potential conflicts of interest relating to any item on the agenda as soon as possible, and no later than two working days prior
to the meeting
AGENDA
Time Item No
Subject Director
1400 General Issues
1 Welcome and Introductions
Dr Hasan Chowhan
2. Apologies for Absence
Dr Hasan Chowhan
3. Declaration of Interests
All
4. Minutes of the previous North East Essex CCG Governing Body Meeting To approve as a correct record the Minutes of the North East Essex CCG Governing Body meeting held on 29 March 2022
Dr Hasan Chowhan
5. Matters Arising and Review of Action Log To note and endorse how we have responded to the outstanding issues which arose at the last meeting.
All
Page 2 of 5
6. Chief Executives Update What has been happening in the CCG since the last meeting? To receive a verbal report.
Dr Ed Garratt
7. Health Forum Committee Report To receive and note a report from the Health Forum Committee
Myrna Liles Report No:
NEECCG 22-31
8. Patient and Public Involvement and Experience To receive and note a report from the Director of Nursing
Lisa Nobes Report No:
NEECCG 22-32
1445 Items for Approval
9. Research Strategy for Suffolk and North East Essex Integrated Care System To receive and approve a report from the Director of Nursing
Lisa Nobes Report No:
NEECCG 22-33
10. 2022/23 Plan To receive and approve a report from the Director of Finance
Jane Payling Report No:
NEECCG 22-34
11. Approval of the Suffolk and North East Essex ICB Constitution To receive and endorse a decision by the CCGs Collaborative Group
Amanda Lyes Report No:
NEECCG 22-35
1450 Questions from Members of the Public
1505 Operational Reports
12. Integrated Performance Report To receive and note a report from the Director of Performance Improvement
Paul Gibara Report No:
NEECCG 22-36
13. Remuneration and HR Committee To receive and note a report from the Remuneration and HR Committee Chair
Martyn Hanlon Report No:
NEECCG 22-37
14. Audit Committee To receive and note a report from the Audit Committee Chair
Jerry Wedge Report No:
NEECCG 22-38
15. Quality Committee To receive and note a report from the Director of Nursing
Lisa Nobes Report No:
NEECCG 22-39
16. North East Essex Primary Care Commissioning Committee To receive and note a report from the Chief Operating Officer
Pam Green Report No:
NEECCG 22-40
17. North East Essex (NEE) Alliance Committee Overview Report To receive, note a report from the Chief Operating Officer
Pam Green Report No:
NEECCG 22-41

Page 3 of 5
18. Procurement Update To receive and note a report from the Chief Operating Officer
Pam Green Report No:
NEECCG 22-42
19. Suffolk and North East Essex Area Prescribing Committee (SNEE APC) Meeting- minutes of the meetings February, March and April 2022 To receive and note a report from the Chief Operating Officer.
Pam Green Report No:
NEECCG 22-43
20. Covid-19 Resource Approval Committee (CRAC) To receive and note a report from the Director of Finance
Jane Payling Report No:
NEECCG 22-44
1605 Governance and Corporate Business
21. National Staff Survey Results 2021 To receive and note a report from the Director of Corporate Services and System Infrastructure
Amanda Lyes Report No:
NEECCG 22-45
22. Declaration of Interests To receive and note a report from the Director of Corporate Services and System Infrastructure.
Amanda Lyes Report No:
NEECCG 22-46
23. Governing Body Assurance Framework To receive and note a report from the Director of Corporate Services and System Infrastructure
Amanda Lyes Report No:
NEECCG 22-47
24. Health and Wellbeing Update To receive and note a report from the Director of Corporate Services and System Infrastructure
Amanda Lyes/ Pamela Donnelly
Report No: NEECCG 22-48
1625 25. Any Other Business
1630 26. Date and Time of Next Meeting No further meetings are arranged at present.

Page 4 of 5
GLOSSARY
A&E Accident & Emergency
ACE: Anglian Community Enterprise
AO: Accountable Officer
ARGEM: Arden & Gem CSU – new IT Providers
BCF: Better Care Fund
CAMHS Children and Adolescent Mental Health Service
CC2H Care Closer to Home
CCG: Clinical Commissioning Group
CO: Chief Officer
C.Diff: Clostridium Difficile – An acquired infection often secondary to antibiotic
use
CFO: Chief Financial Officer
CHC: Continuing Health Care Team
CHUFT: Colchester Hospital University Foundation Trust
CQIN: Commissioning for Quality and Innovation
CQC: Care Quality Commission
CRG: Clinical Review Group
CSU: Commissioning Support Unit
D2A: Discharge to Assess
DNLAC: Designated Nurse for Looked After Children
DOL: Refers to Deprivation of Liberties Act requirements
EAU: Emergency Assessment Unit
ECC: Essex County Council
EHCP: Education Health and Care Plan
EIV: Early Intervention Vehicle
EoE: East of England
EoL: End of Life
EPRR: Emergency Preparedness, Resilience and Response
ESNEFT: East Suffolk and North Essex University Foundation Trust
FRG: Financial Recovery Group
GIC: Guaranteed Income Contract
GPwSI: GPs With Special Interests
HSMR: Hospital Standardised Mortality Ratio - An indicator of healthcare quality that
measures whether the death rate at a hospital is higher or lower than you
would expect.
HFC: Health Forum Committee
HOSC: Health Overview and Scrutiny Committee
HWB: Health and Wellbeing Board
IAPT: Improving Access to Psychological Therapies
iBCF: Integrated Better Care Fund
I & ESCCG: Ipswich & East Suffolk Clinical Commissioning Group
IUC: Integrated Urgent Care Service
JCC: Joint Commissioning Committee
JSNA: Joint Strategic Needs Assessment
KPI: Key Performance Indicators
LA: Local Authority
LAT: Local Area Team of NHS England

Page 5 of 5
LD: Learning Disabilities
LMC: Local Medical Council
LSMS: Local Security Management Service
MCP: Multispeciality Community Provider
ME CCG: Mid Essex Clinical Commissioning Group
MH: Mental Health
MOU: Memorandum of Understanding
MRSA: Methicillin Resistant Strep Aureus – An infection often attributed to overuse of
antibiotics
NEE CCG North East Essex Clinical Commissioning Group
NEL CSU: North East London Commission Support Unit
NEPFT: North Essex Partnership Foundation Trust
NHS E NHS England – CCG’s Governing Body
NHS I: NHS Improvement
NICE: National Institute for Clinical Excellence
OEC: Operational Executive Committee
OOH: Out of Hours
PCI: Percutaneous Coronary Intervention
PPCE: Patients, Public and Carers’ Engagement
PPG: Patient Participation Group. Practice Based Patient Groups PropCo: NHS Property Company who will manage NHS estate in future
QIPP: Quality, Innovation, Productivity and Prevention
QISM: Quality Information Sharing Meeting
RAP: Remedial Action Plan
RAS: Rapid Assessment Service
RTT: Referral to treatment time
SCC: Strategic Commissioning Committee
SCCN: Safeguarding Children Clinical Network
Section 75: Statutory agreement between Health and Social Care Section 256:
Statutory agreement between Health and Social Care SETSAF Southend, Essex and
Thurrock Safeguarding Adults Form
SHMI: Summary Hospital-level Mortality Indicator - A hospital-level indicator which reports
mortality at Trust level
SI: Serious Incident
SLA: Service Level Agreement
SNEE: Suffolk and North East Essex
SROG: System Resilience Operations Group SOVA:
Safeguarding of Vulnerable Adults
STP: Sustainability & Transformation Plan
TDC: Transformation & Delivery Committee ToR: Terms of
Reference
UC: Urgent Care
VTE: Venous Thromboembolism
WECCG: West Essex Clinical Commissioning Group
WiC: Colchester Walk in Centre
WSCCG: West Suffolk Clinical Commissioning Group

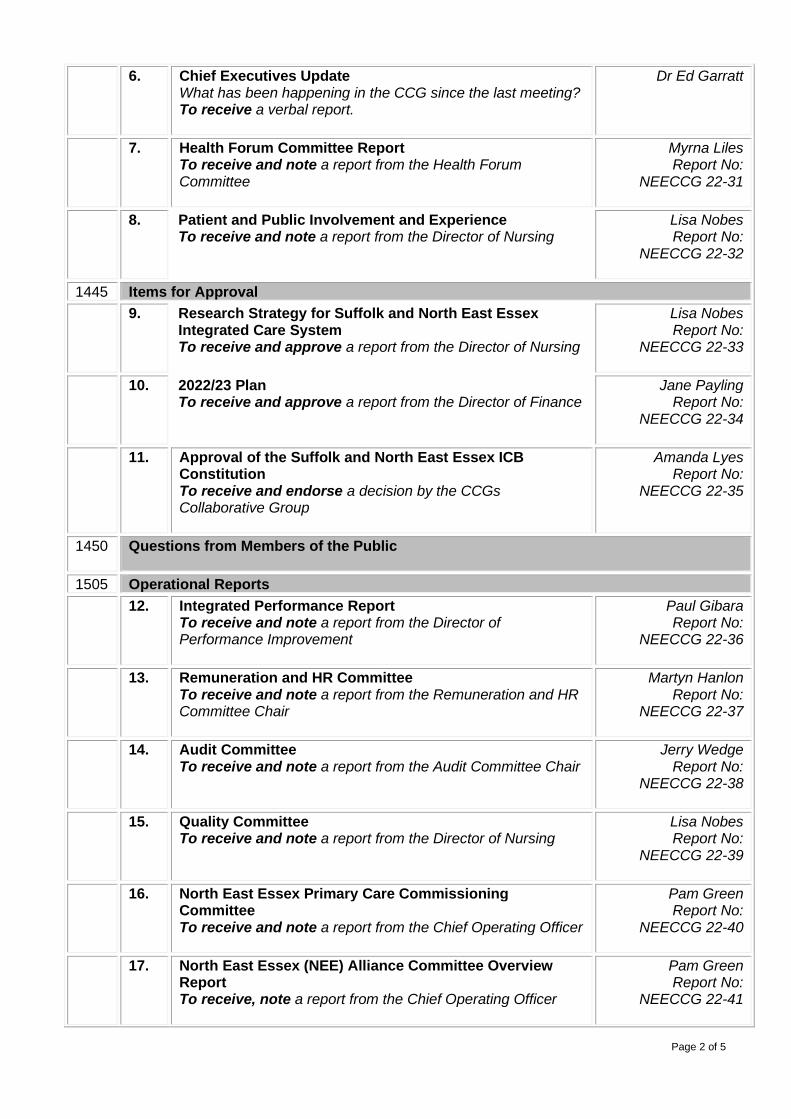
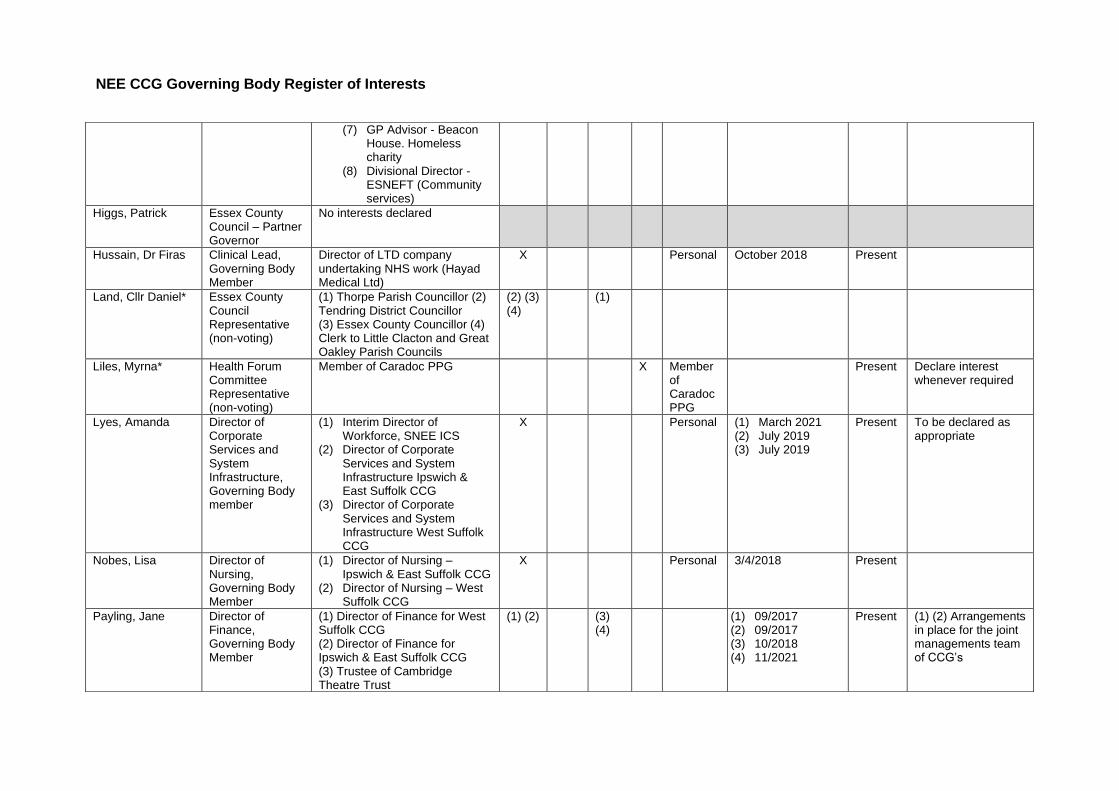
NEE CCG Governing Body Register of Interests
Name Position Declared Interest (Name of the organisation and nature of business)
Type of Interest Nature of Interest
From To Action to mitigate risk
Fin
ancia
l In
tere
st
Non-F
inancia
l
Pro
fessio
na
l In
tere
st
Non-F
inancia
l
Pers
ona
l In
tere
st
Indirect
Inte
rest
Arora, Dr Prashant Elected GP, Governing Body Member
(1) GP Partner at St James Surgery (2) Prashant Arora Ltd (3) St James Surgery part of NEEGPN (4) St James Surgery part of GPPC
X Personal (1) Oct 2016 (2) 2013
Present
Bhatti, Dr Freda Elected GP, Governing Body Member
(1) GP Partner Gt Bentley Practice, Essex (2) Clinical Director Tendring PCN
(3) Local GP LMC Essex (4) Local GP GPPC Federation (5) Husband Local Gastroenterologist at ESNEFT
(1,2, 4)
(3) (5) (1-4) Personal
(5) Husband
Present As per CCG governance
Chowhan, Dr Hasan
Chairman, Governing Body Member
(1) Partner at Creffield Medical Group (2) Director at Colchester Medical Group (3) General Practice Primary Choice LTD- Creffield Medical Group is a member of GP Primary Choice
(1,2, 3,6)
(4,5) Personal (1)2007 (2)2019 (3)2012 (4)2016 (6) 2018
Present

NEE CCG Governing Body Register of Interests
(4) On Panel of Examiners at the Royal College of General Practioners (5) Member of the Royal College of Surgeons (6) Director of North Essex Medical Properties Ltd
Cory, Mark Lay Member, Governing Body Member
(1) Member of Colchester Borough Council. (2) Cabinet Member for Resources Colchester Borough Council (3) Member of Essex County Council. (4) Member of Foster Panel, Eastern Family Services.
X Personal (1) 2007 (2) 2022 (3) 2021 (4) 2022
Present Indicate interests at relevant meetings/decisions
Donnelly, Pam Lay Member, Governing Body Member
Chief Executive - Colchester Borough Council
X Personal Ongoing since start of the CCG
Present
Garratt, Ed Chief Executive, Governing Body Member
(1) Chief Executive Ipswich & East Suffolk CCG (2) Chief Executive West Suffolk CCG (3) Chief Executive – Designate, SNEE ICS (4) Visiting Professor of Integrated Care - University of Suffolk (5) Acting Chief Executive Norfolk & Waveney CCG
(1,2,3 & 5)
(4) Personal (1) March 2016 (2) March 2016 (3) Nov 2021 (4) Apr 2021 (5) 31 March 2022
Present To be declared when appropriate.
Gibara, Paul Director of Performance Improvement, Governing Body Member
(1) Director of Performance Improvement for West Suffolk CCG
(2) Director of Performance Improvement for Ipswich & East Suffolk CCG
X Personal 13/7/2020 Present Arrangements in place for the joint management team of the CCG’s
Green, Pam Chief Operating Officer, Governing Body Member
Governor at Kirby Primary School
X Personal March 2021 Present
Hanlon, Martyn Lay Member, No interests declared.

NEE CCG Governing Body Register of Interests
Governing Body Member
Hickman, Max Elected Member, Governing Body Member
(1) Shareholder in a pharmacy - PrettyGate Limited, Ambrose Avenue Pharmacy, 76 Ambrose Avenue Colchester. In- house 80-hour pharmacy based at the GP surgery.
(2) GP Locum - Work as a self-employed locum in GP practices in North East Essex
(3) GP with special interest (GPSI) - GPSI sessions in cardiology working for North Essex Community Services
(4) Director - Colchester Catalyst Charity. Grant giving charity for the relief of the sick and suffering in North East Essex. Gives grants to health-related charities, community interest companies and NHS and other health- related organisations. Fund’s counselling, respite care, special individual needs.
(5) Locum Director - St Helena Hospice
(6) GP Advisor - Eastern Academic Health and Science Network
Personal (1) 2013 (2) July 2019 (3) July 2019 (4) 2005 (5) February
2020 (6) December
2021 (7) September
2020 (8)
Present Highlight in commissioning decisions if any potential conflict of interest
NEE CCG Governing Body Register of Interests
(7) GP Advisor - Beacon
House. Homeless charity
(8) Divisional Director - ESNEFT (Community services)
Higgs, Patrick Essex County Council – Partner Governor
No interests declared
Hussain, Dr Firas Clinical Lead, Governing Body Member
Director of LTD company undertaking NHS work (Hayad Medical Ltd)
X Personal October 2018 Present
Land, Cllr Daniel* Essex County Council Representative (non-voting)
(1) Thorpe Parish Councillor (2) Tendring District Councillor (3) Essex County Councillor (4) Clerk to Little Clacton and Great Oakley Parish Councils
(2) (3) (4)
(1)
Liles, Myrna* Health Forum Committee Representative (non-voting)
Member of Caradoc PPG X Member of Caradoc PPG
Present Declare interest whenever required
Lyes, Amanda Director of Corporate Services and System Infrastructure, Governing Body member
(1) Interim Director of Workforce, SNEE ICS
(2) Director of Corporate Services and System Infrastructure Ipswich & East Suffolk CCG
(3) Director of Corporate Services and System Infrastructure West Suffolk CCG
X Personal (1) March 2021 (2) July 2019 (3) July 2019
Present To be declared as appropriate
Nobes, Lisa Director of Nursing, Governing Body Member
(1) Director of Nursing – Ipswich & East Suffolk CCG
(2) Director of Nursing – West Suffolk CCG
X Personal 3/4/2018 Present
Payling, Jane Director of Finance, Governing Body Member
(1) Director of Finance for West Suffolk CCG (2) Director of Finance for Ipswich & East Suffolk CCG (3) Trustee of Cambridge Theatre Trust
(1) (2) (3) (4)
(1) 09/2017 (2) 09/2017 (3) 10/2018 (4) 11/2021
Present (1) (2) Arrangements in place for the joint managements team of CCG’s
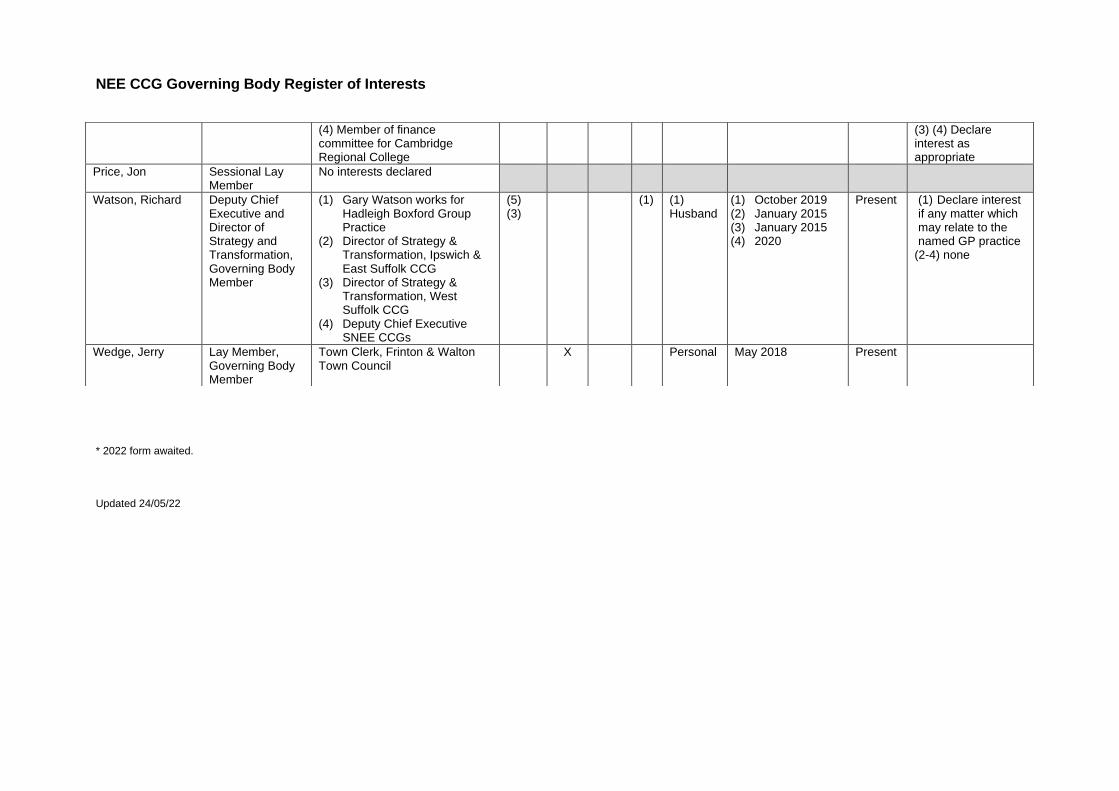
NEE CCG Governing Body Register of Interests
* 2022 form awaited.
Updated 24/05/22
(4) Member of finance committee for Cambridge Regional College
(3) (4) Declare interest as appropriate
Price, Jon Sessional Lay Member
No interests declared
Watson, Richard Deputy Chief Executive and Director of Strategy and Transformation, Governing Body Member
(1) Gary Watson works for Hadleigh Boxford Group Practice
(2) Director of Strategy & Transformation, Ipswich & East Suffolk CCG
(3) Director of Strategy & Transformation, West Suffolk CCG
(4) Deputy Chief Executive SNEE CCGs
(5) (3)
(1) (1) Husband
(1) October 2019 (2) January 2015 (3) January 2015 (4) 2020
Present (1) Declare interest if any matter which may relate to the named GP practice
(2-4) none
Wedge, Jerry Lay Member, Governing Body Member
Town Clerk, Frinton & Walton Town Council
X Personal May 2018 Present

MEETING OF NHS NORTH EAST ESSEX CCG GOVERNING BODY PART ONE
Tuesday 29 March 2022
14.00 hrs
Meeting held via MS Teams and live streamed for members of the public.
Present: Dr Hasan Chowhan HC CCG Chair
Dr Freda Bhatti FB Elected Member
Cllr Mark Cory MC Lay Member (Part)
Dr Ed Garratt EG Chief Executive
Paul Gibara PGi Director of Performance Improvement
Pam Green PG Chief Operating Officer (Part)
Martyn Hanlon MH Lay Member
Dr Max Hickman MHi Elected Member
Dr Firas Hussein FH Elected Member
Cllr Daniel Land DL Essex County Council Observer
Myrna Lilies ML Health Forum Committee Representative
Amanda Lyes AL Director of Corporate Services and System Infrastructure
Lisa Nobes LN Director of Nursing
Jane Payling JP Director of Finance
Richard Watson RW Director of Strategy and Transformation
Jerry Wedge JW Lay Member
In attendance: Jason Joseph JJ Transformation Lead (Item 1314.0 only)
Jo Mael JM Corporate Governance Manager
Simon Morgan SM Communications Lead
Emily Oliver EO Head of Strategic Commissioning and Policy, Essex County Council (Item 1314.0 only)
1305.0 APOLOGIES FOR ABSENCE AND INTRODUCTIONS
The Chair welcomed everyone to the meeting and apologies for absence were noted from; Dr Prashant Arora, Elected Member Pamela Donnelly, Deputy Chair Patrick Higgs, Director of Commissioning, Essex County Council The meeting was noted as quorate.
1306.0 DECLARATION OF INTERESTS
Dr Max Hickman reported that from 1 February 2022 he had taken on the role of Joint Divisional Director for Community Services and therefore declared an interest in items on the agenda that related to ESNEFT as his employer. The Chair congratulated Dr Hickman on his appointment.
1307.0 MINUTES OF THE PREVIOUS NORTH EAST ESSEX CCG GOVERNING BODY MEETING The minutes of the meeting held on 1 February 2022 were approved as a correct record.
1308.0 MATTERS ARISING AND REVIEW OF ACTION LOG There were no matters arising and the action log was reviewed and updated.
1309.0 CHIEF EXECUTIVES UPDATE The Chief Executive reported:
• That thoughts were with all those impacted by the conflict in Ukraine and assurance was provided that the CCG was working with partner agencies to ensure any refugees were welcomed and access to healthcare services provided.
• A Government White Paper had recently been published with an emphasis on place based working.
• A further Government White Paper on levelling up had also been published that had a lot of relevance with communities and County Council focus on deprived communities.
• As set out within the Alliance report on the agenda, Health and Wellbeing work launched by Essex University was highlighted. The work was developing improved health outcomes.
• The Finance Team, and in particular Emily Bosley, had been recognised at Health Care Financial Management Eastern Branch Awards.
• Operational performance was challenging in light of the rise in Covid-19 infections. The increase was also affecting health and sickness rates of staff within providers.
• Planning guidance sought the clearing of 104 week waits by the end of June 2022, there was also emphasis on ambulance delays and response times.
• As seen in the national press there was to be a public inquiry into the deaths of those cared for by the Essex mental health care provider. The CCG would provide support to the inquiry and its thoughts were with all families affected.
The Governing Body noted the update.
1310.0 GOVERNANCE MAPPING AND PUBLIC INVOLVEMENT FOR NORTH EAST ESSEX ALLIANCE – RESPONSE TO ACTION 1290.0 The report sought to present information with regard to governance mapping and public involvement as a response to Action 1290.0 on the Governing Body’s Action Log. In November 2021 the CCG agreed its strategy for Patient and Public involvement. The strategy set out a commitment to work differently with people, in a more collaborative way adopting the principles of partnership and inclusion. Based on the principles of equity, inclusivity, transparency and relationship building the strategy committed to working at place level through Alliances and working with communities to create real impact. The report went on to consider the following questions;
• Why should we be involving citizens in the Alliance?
• Where will involvement and coproduction fit into the Governance structure?
• How will it be different?
• What will the involvement and coproduction look like?
• Who will do this work?
• So where do we start? The report was a helpful example of collaborative working. It was recognised that, at present, people that tended to become involved in engagement were older and it was challenging to get younger people involved. There were however some good examples of specific areas that young people were supporting such as the SEND programme and Ipswich and East Suffolk CCG had recently received a presentation on the Youth Ambassador Programme. ESNEFT also had a good children and young people involvement forum. It was highlighted that digital access to patient and public involvement would be key going forward and there was a need to highlight work and invite feedback. ‘Let’s talk SNEE’ was a key message with an online platform which had facilitated feedback. More work within schools would be beneficial. The Governing Body noted the report
1311.0 HEALTH FORUM COMMITTEE REPORT The Governing Body was in receipt of a report which brought to its attention activities and issues handled by the Health Forum Committee, the co-ordinating body of the North East Essex Health Forum. Key points included: a) Meetings of both the Health Forum Committee and the PPG Liaison bodies for both
Colchester and Tendring resumed over Microsoft Teams in February 2022 through an identified engagement officer working out of West Suffolk.
b) A formal meeting had been held involving Health Forum Committee members, PPG
representatives and some community bodies, for an initial discussion of future patient and public engagement structures within the ICB, Alliance and Primary Care Networks. Follow up meetings had been promised by the ICB engagement team to discuss Terms of Reference.
c) In conjunction with the meeting on future engagement, the existing Health Forum
Committee members met solely to debate which aspects of the current Terms of Reference they wished to be carried forward into the new health structures.
d) The Governing Body was reminded that the Health Forum Committee compiled its
own list of issues, concerns and suggestions raised during the pandemic. Those are currently with CCG and Alliance staff with the hope of constructive reviews being identified before the present structure ceased.
e) A survey, through the engagement team, had taken place to determine the state of
play of PPG activity across North East Essex following the pandemic. The results were eagerly awaited.

The Director of Nursing reported that she had met with the Health Forum Committee representative recently and had agreed some administrative support for the forum and that facilitation of improved communication would be explored. It was recognised that public meetings had been critical to the Health Forum and ways to hold these safely going forward were to be considered. There was concern raised that there had been little engagement with the Health Forum with regard to Clacton Hospital and the Chief Executive agreed to pursue the matter with James Archard, Associate Director at ESNEFT. The Governing Body noted the report. (Cllr Mark Cory left the meeting)
1312.0 2022/23 PLANNING The report updated the Governing Body on the arrangements for finalising the financial plan for 2022/23 and extension of financial arrangements put into place to support Covid-19. The timetable for the 2022/23 plan was as follows:
• Draft plan –17 March 2022
• Final plan –28 April 2022 Work was underway on the draft plan submissions. The timing of the 2022/23 planning deadlines meant that sign-off did not correspond with the schedule of Governing Body meetings. The Governing Body was therefore requested to delegate approval of the various elements of the plans to the following committees
• Financial plan to the Financial Performance Committee
• All other elements of the plan to the Operational Executive Committee The final plan submissions would be brought back to the Governing Body meeting in June 2022. The NHS commissioning elements for 2022/23 were being constructed as a single plan for the Suffolk and North East Essex Integrated Care Board, from which the relevant CCG elements would be extracted for the months prior to the ICB formation. The expenditure made by the CCGs would be matched with allocation from the full year ICB funding such that the CCG element would be shown as a balanced plan; any surplus or deficit would fall into the combined ICB in the latter part of the year. The report went on to seek approval of a roll-over of the 2021/22 budget for the initial period of April until such time as the financial plan was finalised (final deadline currently 28 April 2022. The Governing Body was reminded that it was not only a finance issue as there was ability to put in some structure around programme management and make sure there was sight of health equity. Having emphasized the need to ensure the plans incorporated workforce planning, it was reported that work had taken place with system colleagues to ensure the workforce plan was fit for purpose. The workforce plan had been triangulated with the operational plan. The Governing Body therefore;
1) Noted the planning timetable for 2022/23 2) Delegated approval of the 2022/23 financial plan and budget to the Finance and Performance Committee, with final sign off by the Governing Body in June. 3) Delegated approval of the remaining elements of the 2022/23 plan to Operational
Executive, with final sign off by the Governing Body in June.
1313.0 SAFEGUARDING CHILDREN AND YOUNG PEOPLE AT RISK POLICY The Safeguarding Children at Risk Policy was identified as due for review. Due to the intended move to the Integrated Care Board (ICB) from July 2022, minimal changes had been made to the Policy to ensure it reflected correct terminology and referral processes. A full review would be conducted once the ICB became the statutory body.
Minimal updates have been made to the Policy including: - Updated documents referred to. - Updated terminology in respect of the Safeguarding Partnership and Child Death
Review Processes. - Addition of information and a flow chart for Parental Responsibility. The Policy needed to be updated to ensure assurance could be provided to the auditors and to comply with statutory requirements under Section 11 of The Children Act. The Governing Body approved the Safeguarding Children and Young People at Risk Policy as presented.
1314.0 NEW MODEL FOR MENTAL HEALTH SUPPORTED ACCOMMODATION The Mental Health Accommodation support services sat within the context of a range of support for people experiencing poor mental health in the community. That included supported living, floating support and tenancy sustainment and move on support. Essex County Council, in collaboration with Health, provided accommodation for people with mental health needs. That accommodation was provided when it was necessary to meet people’s assessed needs and was provided as a way of helping people return to independence in the community. Currently it was commissioned in the following format:
• Intensive Enablement Plus (IE+) – for complex needs placements (spot purchased)
• Intensive Enablement – high support, 16+ hours per week
• Support to Independence – low support (7+ hours per week) Following considerable research, engagement and collaborative working with partners and people with lived experience, a new model was proposed which was designed to avoid preventable admissions, improve health and social care outcomes for individuals, provide holistic support and reduce and/ or eliminate out of area placements. The new model was detailed within the report together with key points to note, identified risks, resource implications and engagement. Comments included; It was thought that the new model should have a positive consequence on homelessness by seeking to ensure a sustainable solution for those with mental health challenges. A key area of focus at Alliance level was housing and the utilisation of stock for supported living and for the homeless, together with recognising the impact of poor housing on health and wellbeing.

With the agreement and acknowledgement that there were continued conversations to be had with EPUT around funding of out of area placements and West Essex CCG regarding Individual Placements funding, and; Subject to, an agreement being reached regarding the funding that was currently designated to Individual Placement Team (IPT), that a due diligence process was followed to ensure the funds could be moved within and across the system without a negative impact on other services, the Governing Body subsequently; 1) Approved the proposed service model identified following full review of current
Mental Health Accommodation services via the current S75 Agreement with Essex County Council.
2) Approved additional funding for the full cost of £493,000 for the full procurement of
the new service to start October 2022 (part year effect 22/23 £236,369).
1315.0 QUESTIONS AND COMMENTS FROM MEMBERS OF THE PUBLIC No questions were received.
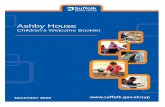
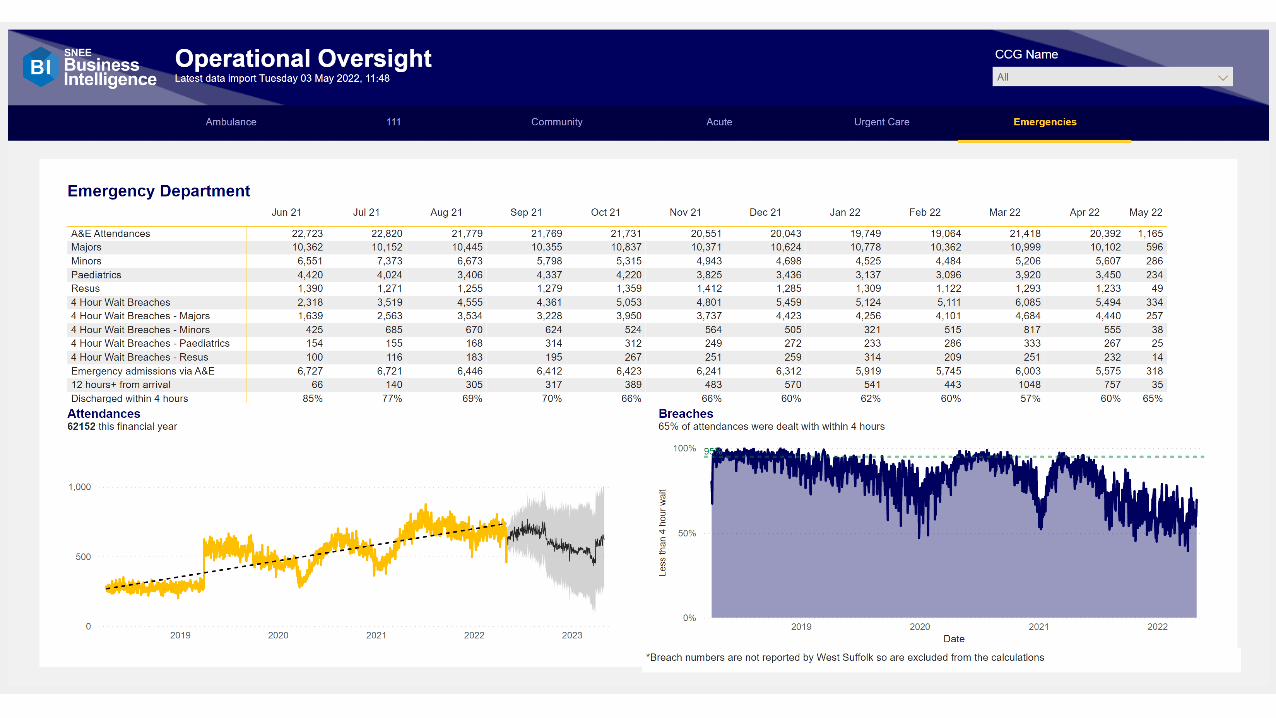
1316.0 INTEGRATED PERFORMANCE REPORT The Integrated Performance Report (IPR) provided an overview of the latest system performance, including the NHS Constitutional Standards. Any significant pressures on performance were also highlighted. The report was taken at a point of time and outlined the published performance for Month 9 and Month 10 (December 2021 and January 2022) where available. The report provided the narrative for those providers where there were key exceptions to report, to support the actions being taken to support improvements in performance. Key performance issues to highlight included;
• The overall waiting list at the end of December stood at 63,959 remaining static from the November position.
• The average routine waiting time was 38 weeks when counting waiting lists from all specialties .
• ESNEFT had seen an increase overall in those patients waiting >52 weeks from November position of 1847 patients to December: 2011
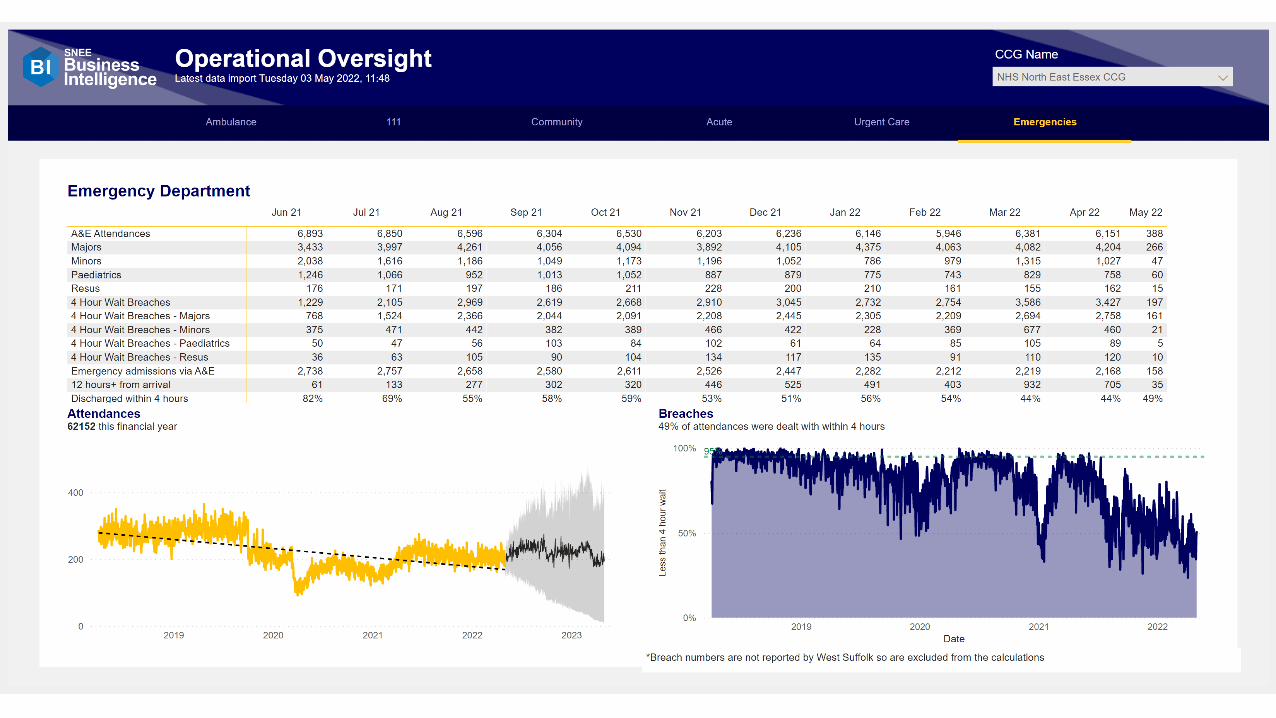
• Cancer: ESNEFT’s 62-day unvalidated performance in December was 76%. The target was subject to a recovery trajectory
• 4-hour A&E performance in January was 76% which showed a small increase in performance however that had remained relatively static for the last few months
• Ambulance response time performance at both a Trust and local level continued to be below the required standard in January, but an improvement was seen on previous months.
The performance highlighted within the report was a barometer of performance at a specific point in time and should be considered in the context of the impact that Covid-19 and urgent care demand had had on routine service delivery. The Director of Performance Improvement reported that although the System had been maintaining Opal Level 3, in the last week or so there had been a significant rise in the number of Covid-19 patients which was causing operational difficulties and affected staff sickness levels. As such the System had recently declared Opal Level 4 and Alliance
partners were working hard to maintain patient safety. Delays in ambulance performance levels were also being seen and the System was working with partners to mitigate any risks. Elective recovery – providers had managed to maintain good activity levels. There were currently 3900 patients waiting in the system with those waiting over one year being given priority. The overall waiting list was growing and being monitored closely. Mutual aid across Trusts was happening to alleviate the situation. There was a requirement to achieve no 104 week waits from the end of June 2022 and, at the last count, there were 36 patients that had waited that long for treatment. Diagnostics continued to remain a challenge and work was taking place with the independent sector to address. Plans recently submitted to the NHSE regional office for 2022/23 committed to the achievement of 110% activity and 120% diagnostics, together with the reduction of 78 week wait patients by the end of March 2023. Although the situation was challenging it was a similar position in other Systems and the message was that the NHS was open for business. The Director of Nursing reported that it was challenging to know how to oversee the quality of care in such times when there was a decrease in the effectiveness of discharge planning, increased complaints, and a workforce focussed on patient safety. Things that added value to the work included the need to talk to patients and families. Tracking the readmission rate could be of benefit in assessing quality outcomes. Cancer services – across the ICS, performance was at 115% of pre pandemic levels of referrals into secondary care, and at 110% of pre pandemic levels of treatment. All Trusts were struggling and a consultation had been launched with regard to proposed changes to cancer waiting time standards. ESNEFT had one of the highest referral rates in the country. Cancer Board meetings were held bi-monthly and the operational group met every month to monitor the situation. Comments included; It was recognised that ESNEFT was doing relatively well compared to other Trusts across the country, although treatments other than cancer were suffering and non- cancer waits were concerning. Whilst noting that it would be beneficial to see a fall in Covid-19 infection rates, other actions were queried. It was reported that publication of new infection control guidance was awaited. In a wider context there was a need to consider delays at the front door and to support providers with regard to public advice and work with local authorities in respect of the discharge of patients. It was highlighted that it was easy to be pessimistic and a number of waiting lists were lower than the average of nine months. The NHS remained open for business and urgent illness waiting times were not much different to pre-pandemic levels. It was suggested that a comparison of other systems might be beneficial. Having noted that MRI activity was growing, it was queried whether the Clacton Diagnostics Centre was increasing capacity. From a regional dataset regarding referral to treatment times, SNEE was top in terms of performance. The Director of Performance Improvement agreed to provide a system to system comparison for waiting list indicators.

Vaccination work was ongoing The CCG’s overall financial position was that it was expecting to breakeven for the year. The Governing Body assured itself that the Finance and Performance Committee was satisfied that where performance was not reaching the required standard, the necessary scrutiny and steps were being undertaken with providers to improve performance.
1317.0 AUDIT COMMITTEE The Audit Committee had met on 15 February 2022 via MS Teams ‘in common’ with the Suffolk CCGs. Key points to note from that meeting were detailed in Section 2 of the report. The Audit Committee was due to meet next week when it would be presented with the draft Head of Internal Audit Opinion. There was a need going forward to look at timings for formation of the ICB to determine if there might be a need for part year accounts. The arrangements for meetings ‘in common’ across the CCGs was working well. The Governing Body noted the report and confirmed it was assured that the Audit Committee was fully carrying out its governance role.
1318.0 REMUNERATION AND HR COMMITTEE The Remuneration and HR Committee was required by its terms of reference to meet on an ‘as and when’ basis, but at least annually. A meeting was held ‘in common’ with the Remuneration and HR Committees of Ipswich and East Suffolk and West Suffolk CCGs on 15 February 2022. Key points to note from that meeting were detailed in Section 2 of the report. The Governing Body noted the report.
1319.0 QUALITY COMMITTEE
The The report sought to bring to the attention of the Governing Body the patient safety and quality exceptions which had been identified in the services commissioned by North East Essex Clinical Commissioning Group (NEECCG).
The Quality Committee received and reviewed quality dashboards with narrative reports about patient experiences relating to all the service providers commissioned by North East Essex Clinical Commissioning Group for: Planned Care; Urgent Care; Primary Care and Mental Health Care. In addition, the March 2022 Quality Committee received and reviewed the following specific clinical service reports:
• Addressing Variations in Health Assessments for Looked After Children
• Continuing Healthcare Update
• Risk Report
• National Safety Standards for Invasive Procedures (NatSSIPs) Report
• Social Prescribing Update
• Mental Health report
• LD and Autism Report Key points to note included;

Safeguarding training compliance for the North East Essex Integrated Community Service (NICS) was significantly below KPI in some areas and was being monitored by the Safeguarding and Quality Teams. The average waiting time for psychology intervention in North East Essex was circa 17 months, which was a significant delay. Essex Partnership University Trust (EPUT) was adding resources to clear the psychology waiting list with expected clearance of 50% by September 2022 and 100% by end of 2022. In NEE, a scoping exercise had been completed for the school nurse provision in Special Schools in NEE to identify gaps. There would be further scoping across Essex of Special School Nursing needs which would be considered at the SEND Joint Commissioning Board during March 2022. The CCG SEND Designated Clinical Officer Team had met with two schools in North East Essex identified as having no school nurse provision. ESNEFT safer staffing data set out the percentage of shift fill against required shift fill. Both were currently RAG rated as amber for qualified staff which was unusual and of concern. Healthcare Assistant numbers had increased to compensate for lower registered nursing numbers. Workforce issues were having an impact on discharge planning, patient experience and harder to measure nursing interventions. Initial health assessments – Essex currently had a low compliance for Looked After Children compliance. Having queried why there had been no mention within the report of the North Clacton Medical Group which was currently being monitored, it was explained that a visit had taken place and a report awaited. The CCG continued to work with the practice and the Care Quality Commission. The Governing Body was reminded that services such as dentists, opticians and pharmacies currently commissioned by NHSE were due to transfer to the ICB by 2023. Investigative work as to how those services might be monitored was currently underway. The Governing Body noted the report and was assured that the Quality Committee was satisfied that where performance was not reaching the required standard that the necessary steps were being undertaken to achieve standards.
1320.0 NORTH EAST ESSEX PRIMARY CARE COMMISSIONING COMMITTEE Primary Care Commissioning – Overview Report An ordinary meeting of the PCCC was held in public via Microsoft Teams on 15 February 2022 chaired by CCG Lay Member, Jon Price. There was no member of the public in attendance, however an elected member was in attendance as an observer. There were no questions received via email from members of the public who were invited to do so prior to the meeting. Healthwatch Essex Representatives reported that access to healthcare in the Harwich area remained a concern. The CCG continued work with the three practices in the Harwich area with temporary list closures to get the lists reopened. Whilst engagement with the Care Quality Commission (CQC) remained, to ensure patient safety and quality of care are at the expected levels. Section 2 of the report detailed discussion at the 15 February 2022 meeting.
There had been a collaborative approach to improve Serious Mental Illness health check performance. Practices had also maintained extended access, with key focus going forward to continue to be GP access and also include opioid dependency and inhaler switches. There had been outstanding results from the diabetic service provided by the Suffolk GP Federation and practices. The service had delivered improved care for patients. The Governing Body; 1) Noted the report.
2) Was assured that the Primary Care Commissioning Committee was satisfied that where primary care services were not reaching the required standard that necessary steps were being undertaken to improve the quality of services.
Primary Care Commissioning Committee – Terms of Reference The Governing Body was asked to approve updated Terms of Reference for the Primary Care Commissioning Committee prior to their submission to NHS England and NHS Improvement (NHS E/I). It was explained that the terms of reference had been subject to annual review with changes made being minor and mainly focussed around current membership and job titles of the participants. The Governing Body approved the terms of reference as presented.
1321.0 NORTH EAST ESSEX (NEE) ALLIANCE COMMITTEE OVERVIEW REPORT The report provided an overview of the Alliance Committee decisions and discussions, but also provided an overview of other NEE Alliance activity and governance including Alliance Partnership Board and System Executive Group (SEG) to provide a rounded picture of progress. Key points to note were detailed in Section 2 of the report and included; Achievements had included the mobilisation of integrated teams for Colchester. The multi-disciplinary team was now taking referrals from the Police, and housing officers etc in order to target complex cases. There was good feedback on the way the team was developing. There was a range of leadership across the teams and good engagement from GP practices. In response to questioning the Governing Body was informed that the Tendring multi-disciplinary team was expected to be operational in South Tendring from the start of May 2022. The Governing Body noted the report.
1322.0 PROCUREMENT UPDATE The report provided ongoing updates for SNEE procurements and reflected:
• Recently Closed or Awarded Projects
• Procurement Pipeline
• Procurement Policies/Workplan
• Proposed Legislative Changes The report went on to detail future procurements and updates to policies and
procedures, together with proposed legislative changes. There was concern at the possible cessation of the Trust Advice and Guidance contract. The Governing Body was informed that work to address the situation was underway with an aim to reinstate some elements. The Governing Body noted the report.
1323.0 SUFFOLK AND NORTH EAST ESSEX AREA PRESCRIBING COMMITTEE (SNEE APC) MEETING- MINUTES OF THE MEETING NOVEMBER 2021 The Governing Body is asked to note the approved guidelines, formulary products, items to improve the medicines governance and the quality of the service delivered to patients across Suffolk and North East Essex Integrated Care System (SNEE ICS). All items were consulted upon by the Clinical Reference group prior to APC approval. The minutes of the meeting were available to reference and demonstrated how the SNEE APC had worked as an integrated care system to support the entry of new medicines into the health economy, review historic decisions and develop guidelines to improve medicines optimisation which included medicines safety. The following were approved at the November 2021 meeting:
• European Antimicrobial Awareness Day and World Health Organisation Antimicrobial Week Social Media Campaign.
• West Suffolk Specialist Infant Formula Policy 2021
• Suffolk Position Statement on the prescribing of Shower Protectors or LimbO® Aids
• EPUT Formulary- Section 22: The Treatment of Hyperprolactinaemia, Section 18: Antimicrobial Prescribing and Section 4: Anticoagulants
The Governing Body noted the report. (Pam Green left the meeting)
1324.0 COVID-19 RESOURCE APPROVAL COMMITTEE (CRAC) The Committee was established in early April as a joint committee working across the three CCGs in Suffolk and North East Essex. It was a sub-committee of the three CCG Governing Bodies which was initially established for the period from April to July 2020, and had been extended in line with the national emergency financial arrangements until the end of September 2021. Oversight of the Committee was via the CCG finance committees. A summary table of the decisions made since the last report was provided in Appendix 1 attached to the report. Whilst many of the emergency measures associated with Covid-19 were coming to an end, the NHS was expecting to receive specific funding for Covid-19 in 2022-23 and was still part of the ongoing Covid vaccination programme funded nationally. It was proposed that the Committee remained in place until the formal commencement of the Integrated Care Board (expected 1 July 2022) to deal with the funding. As previously reported, use of the Committee had reduced significantly with CCG and alliance based decision making routes now being the default. The Governing Body:
1) Noted the report on decisions made by the CRAC committee since the last report 2) Approved the proposed extension of the Committee until the commencement of the
ICB.
1325.0 GOVERNING BODY ASSURANCE FRAMEWORK The Director of Corporate Services and System Infrastructure introduced the Governing Body Assurance Framework which set out the current red risks identified by the CCG and what controls were in place to manage each risk. The report also included a summary of the top risks from the Directorate Risk Register. Amendments and additions to risks were detailed within paragraph 1.1 of the report. The Governing Body was informed that the IT team and IT provider were working to mitigate any risk associated to cyber security which included increased communications to staff and forced patching of the system which had gone well. The Director of Nursing provided an update on the risk with regard to children and young people in acute mental health crisis. The issue had been raised by the Colchester ESNEFT site as a quality concern as it had four individuals with acute admission that required mental health support. One person had remained for 150 days at Colchester awaiting treatment but had now gone to the appropriate place for care and treatment. The children and young peoples’ mental health group was clear about medium and long term actions to support mental health crisis, and was now working on short term measures such as workforce, and the facilitation of mental health practitioners. A system wide summit had been held three weeks ago which brought together representatives from all main partners. A task and finish approach was being taken to look at proposals for consideration by the group, those proposals included working with the voluntary and community sector, and exploring specialist support. ESNEFT had developed costed proposals to support those patients whilst they were in ESNEFT. The Governing Body noted the report.
1326.0 HEALTH AND WELLBEING UPDATE The Governing Body was in receipt of a report which provided an update of work currently underway to support staff Health and Wellbeing across SNEE CCGs’. Key points highlighted included;
• There were now 24 Health and Wellbeing Ambassadors and 13 trained mental health First Aiders.
• The roll out of Health and Wellbeing activity continued and workshops associated to ‘sleep well’ and ‘work well’ had been held.
• Disability networks had been launched and linked into wider sustainability work.
• Staff survey actions from last year had been reviewed and it was expected there would be additional actions from this years staff survey results when presented.
The Governing Body noted the report.
1327.0 ANY OTHER BUSINESS No items of other business were received.
1328.0 DATE AND TIME OF NEXT MEETING

The next meeting was scheduled to take place at 2.00pm on Tuesday, 7 June 2022
NORTH EAST ESSEX CCG Governing Body
ACTION LOG: 29 March 2022 (updated)
MINUTE DETAILS ACTION BY WHOM TIMESCALE/UPDATE
Meeting of 1 February 2022
1301.0 Governing Body
Assurance Framework
With regard to the EEAST risk it was queried whether there
was a forum for issues to be highlighted clinician to
clinician. Whilst issues could retrospectively be fed into
the SNEE meeting with EEAST, it was felt helpful if issues
could be highlighted in real time. The Director of Nursing
agreed to explore options and report back.
Lisa Nobes 29/03/22 – the issue of clinician to clinician
contact had been raised with EEAST and further
info was awaited although they had thought it
was already in place. Ongoing.
Meeting of 29 March 2022
1316.0 Integrated
Performance Report The Director of Performance Improvement agreed
to provide a system to system comparison for
waiting list indicators.
Paul Gibara Information circulated on 13 April 2022 -
Complete

Page 1 of 2
GOVERNING BODY
Agenda Item No. 07
Reference No. NEECCG 22-31
Date. 7 June 2022
Title
Health Forum Committee Report
Lead Director
Pam Green, Chief Operating Officer
Author(s)
Myrna Liles, Health Forum Committee board representative
Purpose
Bringing to the Governing Body’s attention activities and issues handled by the Health Forum Committee, the co-ordinating body of the North East Essex Health Forum.
Applicable CCG Strategic Objectives:
1. To achieve our vision through an inclusive, holistic approach to patient and service user centred commissioning, embedding personalisation of care through integrated health and social care services.
x
2. To transform care and drive continuous improvement in quality and safety. Achieve the best possible outcomes for our service users through high quality care.
x
3. To use commissioning resources effectively and responsibly. To develop our organisation, teams and individual staff to be trusted, competent, well trained, talented, enthusiastic and dedicated.
4 To tackle the biggest health challenges in north east Essex including reducing health inequalities.
x
Recommendation: Contents of the report are for information and should be noted.

Page 2 of 2
1. Summary 1.1 As the Health Forum Committee, the co-ordinating body of the North East Essex Health
Forum, we do our best to ensure that the public, patient, carer and service user voice is genuinely listened to by those taking decisions about or health and social care services. We are predominantly patient, public and carer volunteers but also have representatives from Community Voluntary Services and Healthwatch Essex.
1.2 Engagement and communication are our main functions while equality and diversity are our
watchwords. 1.3 All the matters below that require NEECCG action have already been forwarded to relevant
members of staff. 2. Key Points to Note a) We had hoped that our final report to the board could outline the future pathway for patient,
public and carer engagement in North East Essex. However, as your constituted group, we only have the bare outlines. The general outlook is based on grassroots neighbourhood bodies, feeding into the Quality aspect of the new Alliance and the chair of that group being the link at ICB level.
b) Details and involvement of existing representatives are still to be sorted. Meanwhile, it is
anticipated that at least some of the forum members will continue to represent the community voice until the new systems are established.
c) However, as it passes into history along with the CCG, the forum wishes to thank the board
for the help and assistance provided to this unique engagement body that facilitated so much good work on its behalf across Colchester and Tendring.
d) Over the past decade and a half this has included being provided with Terms of Reference
which allowed us full access to all CCG staff; establishment of our own engagement officer; support of timetables of regular public information meetings; establishing formal links and meetings with GP PPG bodies and finance for a regular newsletter.
e) Efforts have been made to try and ensure as much of that positive liaison and two-way
engagement becomes part of systems going forward. Time will tell how successful we have been.
Page 1 of 2
GOVERNING BODY
Agenda Item No. 08
Reference No. NEECCG 22-32
Date. 7 June 2022
Title Patient and Public Involvement and Experience
Lead Director Lisa Nobes, Director of Nursing
Author(s) Sophie Martin – Head of Patient and Public Involvement
Purpose To provide the Governing Body with a broad overview of patient, public involvement and experience.
Applicable CCG Strategic Objectives:
1. To achieve our vision through an inclusive, holistic approach to patient andservice user centred commissioning, embedding personalisation of carethrough integrated health and social care services.
2. To transform care and drive continuous improvement in quality and safety.Achieve the best possible outcomes for our service users through high qualitycare.
3. To use commissioning resources effectively and responsibly. To develop ourorganisation, teams and individual staff to be trusted, competent, well trained,talented, enthusiastic and dedicated.
4 To tackle the biggest health challenges in north east Essex including reducing health inequalities.
Recommendation:
To note the report.
Page 2 of 2
1. Background
1.1 This is the fourth quarterly report for year 2021/22. All previous reports have been to Governing Body for information.
2. Key Issues
2.1 This report shows the Quarter 4 activity of the Patient and Public Involvement and Experience Team. It records the scope of the activity, number of people involved and impact or outcome achieved.
2.2 The Governing Body is asked to note the activity and impact of coproduction with citizens across the organisation.
3. Patient and Public Engagement
3.1 The breadth and depth of activity across the organisation and within the Alliances demonstrates increased collaboration and coproduction with local citizens.
4. Recommendation
4.1 For note.

Suffolk and North East Essex Patient and Public Involvement and Experience Team Report Quarter 4 2021/2022 – January to March 2022 Patient and Public involvement and Experience is a fundamental pillar in the delivery of quality planning, improvement and control. Either through the work of the governance structures which oversee and assure the CCG of quality in service delivery or, through the work of the Transformation and project teams which seek improvement. The Team provides patient experience data and insight. Our ambition is to build on this work to take a more co-productive and collaborative approach to working with citizens to achieve good health outcomes for the people of Suffolk and north east Essex.
Charter/ Programme Programme Charter/ Programme Programme
Quality Assurance/ monitoring (Lisa Nobes)
• Patient experience data provided in Quality Oversight meetings
• Patients involved in development of Commissioning Specs., service technology testing, governance review processes and transformation programmes.
• Patient experience included in the Quality Newsletter for Vaccines
SNEE Children and Young People 2021/2022 Programme (Jamie Hawkins, Jamie Mills, Kathryn Searle)
• Children’s Emotional Health and Well-being (whole system programme approach)
• Community Services • Special Educational Needs and Disability (SEND) • SEND commissioning
Mental health and learning disabilities SNEE wide (Eugene Staunton)
• Crisis Resolution and Home Treatment Team (CRHTT) including moving First Response Service to 111(2)
• Alternatives to Admission Initiative (i.e., crisis cafes/place of safety to be established in E&WS and evolved in NEE)
• Services Specifications for new Suffolk model with NSFT and SCC.
• Eating disorder Service Specifications for new Suffolk model • VCSE Mental Health Framework- pan SNEE • Suffolk- Suffolk Mind Connect development
Stroke Strategic Programme – SNEE wide (Nerinda Evans)
• Develop plan for the AF feasibility pilot through engagement with clinicians, stroke board and the EAHSN, to implement feasibility pilot with Fibri-Check and Ziopatch.
• Ensure pilot is developed to increased detection of AF in line with national guidance and best evidence.
• Evaluate the pilot to inform the future pathway, develop a model that supports clinicians to effectively review individuals with AF.
Cancer Strategic Programme – SNEE wide (Nerinda Evans)
• Tackling inequalities, including where they may have been further impacted by the COVID-19 pandemic.
• Delivery of supported self-managed pathways, including risk stratified protocols for breast, prostate and colorectal.
• Pre-habilitation /rehabilitation pathway development • Governance pathways across the ICS as RDS integrates
systems • To improve patient representation across SNEE in the
development of cancer services
End of Life Care Board
• Create an app to make a single advance care planning record that is accessible by all authorised users
Covid Vaccination Programme
• To understand and improve the vaccination experience for people across SNEE.
• To understand public intentions regarding vaccinations for 5 – 11-year-olds and how to improve uptake
• To understand why some people are not coming forward to have their covid vaccinations
Maternity and Neonatal Strategic Programme – SNEE wide (Helen Bowles)
• Co-produce a five-year maternity and neonatal strategy. • Support the development and transformation of the three
Maternity Voice Partnerships
Patent Experience (Lisa Nobes)
• PALS and complaints activity is increasing • PALS queries continue to be focused on Covid; in particular,
vaccinations and medicines management. • Complaints are focused predominantly on staff attitude and
behaviour and communication
Additional Items • Let’s Talk SNEE – Engagement Platform • Patient Safety Partners
Suffolk and North East Essex Patient and Public Involvement and Experience Team Report Quarter 4 2021/2022 – January to March 2022
March 2022 Page 2
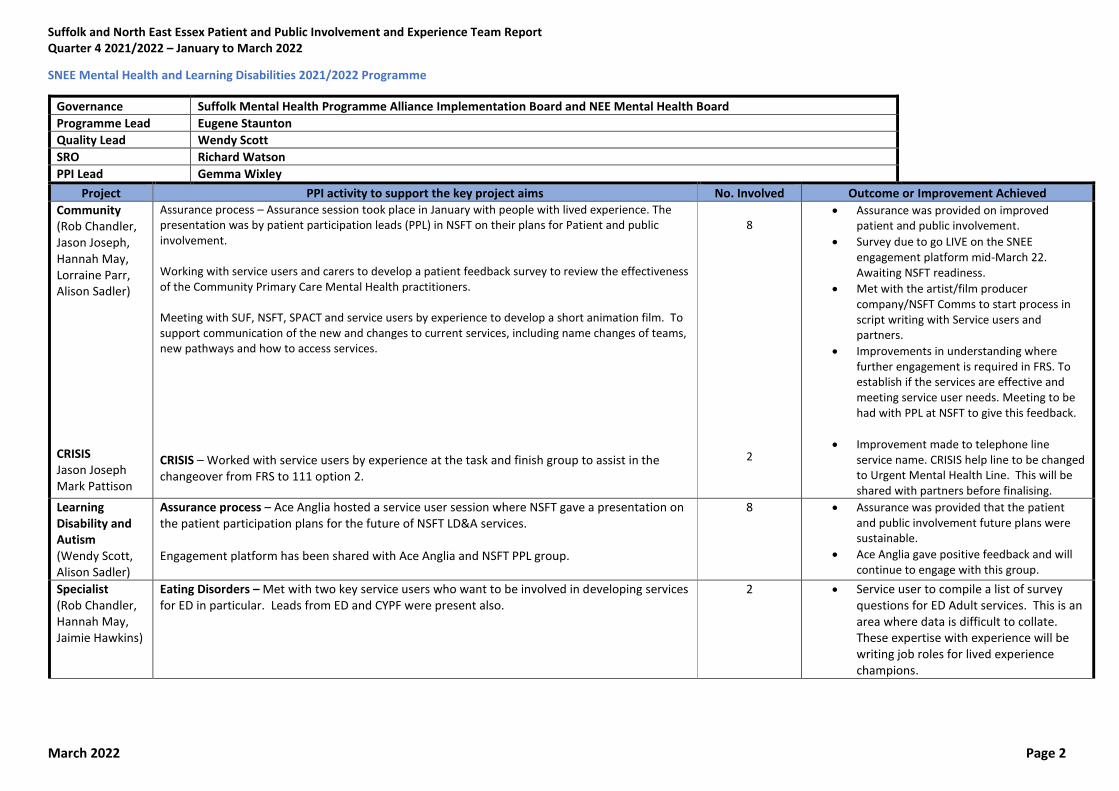
SNEE Mental Health and Learning Disabilities 2021/2022 Programme
Governance Suffolk Mental Health Programme Alliance Implementation Board and NEE Mental Health Board
Programme Lead Eugene Staunton
Quality Lead Wendy Scott
SRO Richard Watson
PPI Lead Gemma Wixley
Project PPI activity to support the key project aims No. Involved Outcome or Improvement Achieved
Community (Rob Chandler, Jason Joseph, Hannah May, Lorraine Parr, Alison Sadler) CRISIS Jason Joseph Mark Pattison
Assurance process – Assurance session took place in January with people with lived experience. The presentation was by patient participation leads (PPL) in NSFT on their plans for Patient and public involvement. Working with service users and carers to develop a patient feedback survey to review the effectiveness of the Community Primary Care Mental Health practitioners. Meeting with SUF, NSFT, SPACT and service users by experience to develop a short animation film. To support communication of the new and changes to current services, including name changes of teams, new pathways and how to access services.
CRISIS – Worked with service users by experience at the task and finish group to assist in the changeover from FRS to 111 option 2.
8
2
• Assurance was provided on improved patient and public involvement.
• Survey due to go LIVE on the SNEE engagement platform mid-March 22. Awaiting NSFT readiness.
• Met with the artist/film producer company/NSFT Comms to start process in script writing with Service users and partners.
• Improvements in understanding where further engagement is required in FRS. To establish if the services are effective and meeting service user needs. Meeting to be had with PPL at NSFT to give this feedback.
• Improvement made to telephone line service name. CRISIS help line to be changed to Urgent Mental Health Line. This will be shared with partners before finalising.
Learning Disability and Autism (Wendy Scott, Alison Sadler)
Assurance process – Ace Anglia hosted a service user session where NSFT gave a presentation on the patient participation plans for the future of NSFT LD&A services. Engagement platform has been shared with Ace Anglia and NSFT PPL group.
8 • Assurance was provided that the patient and public involvement future plans were sustainable.
• Ace Anglia gave positive feedback and will continue to engage with this group.
Specialist (Rob Chandler, Hannah May, Jaimie Hawkins)
Eating Disorders – Met with two key service users who want to be involved in developing services for ED in particular. Leads from ED and CYPF were present also.
2 • Service user to compile a list of survey questions for ED Adult services. This is an area where data is difficult to collate. These expertise with experience will be writing job roles for lived experience champions.
Suffolk and North East Essex Patient and Public Involvement and Experience Team Report Quarter 4 2021/2022 – January to March 2022
March 2022 Page 3
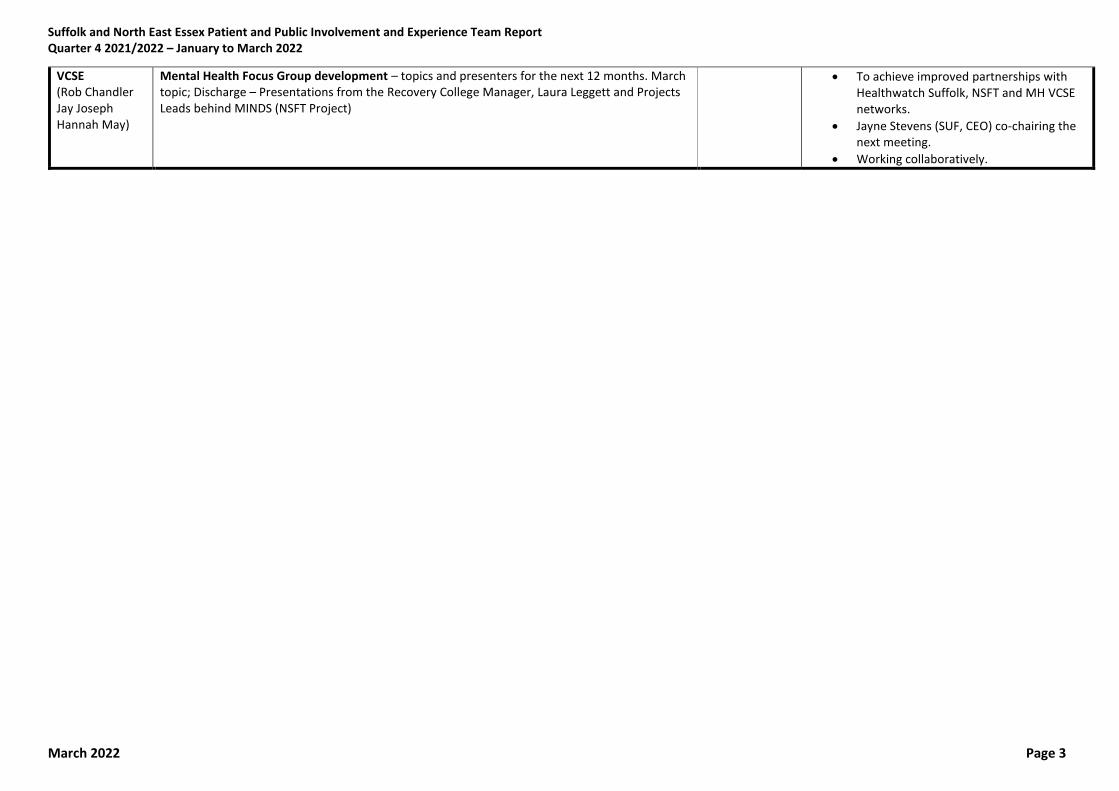
VCSE (Rob Chandler Jay Joseph Hannah May)
Mental Health Focus Group development – topics and presenters for the next 12 months. March topic; Discharge – Presentations from the Recovery College Manager, Laura Leggett and Projects Leads behind MINDS (NSFT Project)
• To achieve improved partnerships with Healthwatch Suffolk, NSFT and MH VCSE networks.
• Jayne Stevens (SUF, CEO) co-chairing the next meeting.
• Working collaboratively.
Suffolk and North East Essex Patient and Public Involvement and Experience Team Report Quarter 4 2021/2022 – January to March 2022
March 2022 Page 4
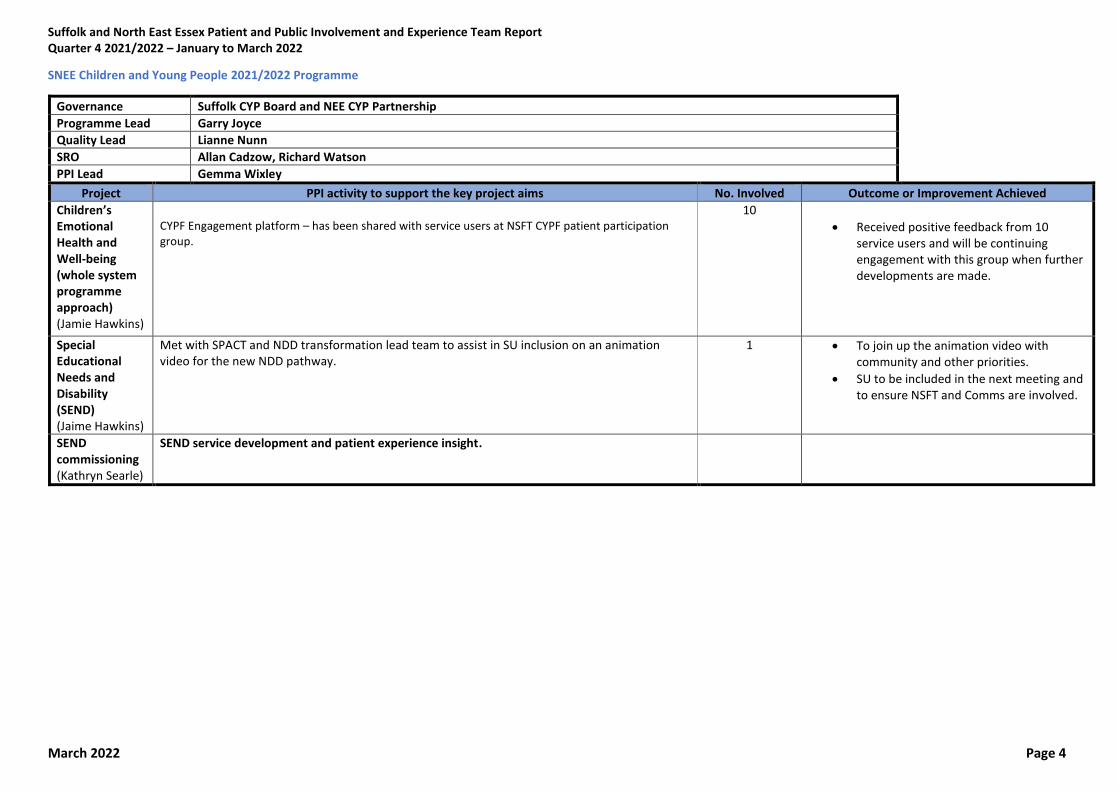
SNEE Children and Young People 2021/2022 Programme
Governance Suffolk CYP Board and NEE CYP Partnership
Programme Lead Garry Joyce
Quality Lead Lianne Nunn
SRO Allan Cadzow, Richard Watson
PPI Lead Gemma Wixley
Project PPI activity to support the key project aims No. Involved Outcome or Improvement Achieved
Children’s Emotional Health and Well-being (whole system programme approach) (Jamie Hawkins)
CYPF Engagement platform – has been shared with service users at NSFT CYPF patient participation group.
10
• Received positive feedback from 10 service users and will be continuing engagement with this group when further developments are made.
Special Educational Needs and Disability (SEND) (Jaime Hawkins)
Met with SPACT and NDD transformation lead team to assist in SU inclusion on an animation video for the new NDD pathway.
1 • To join up the animation video with community and other priorities.
• SU to be included in the next meeting and to ensure NSFT and Comms are involved.
SEND commissioning (Kathryn Searle)
SEND service development and patient experience insight.
Suffolk and North East Essex Patient and Public Involvement and Experience Team Report Quarter 4 2021/2022 – January to March 2022
March 2022 Page 5
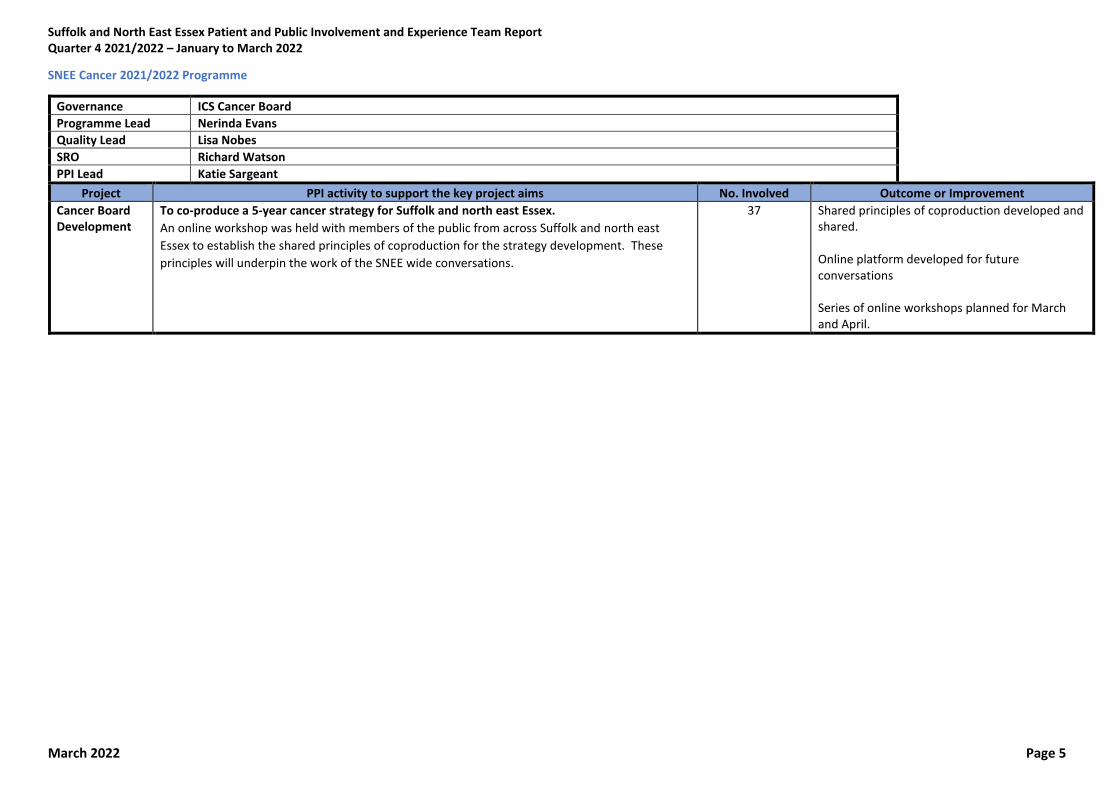
SNEE Cancer 2021/2022 Programme
Governance ICS Cancer Board
Programme Lead Nerinda Evans
Quality Lead Lisa Nobes
SRO Richard Watson
PPI Lead Katie Sargeant
Project PPI activity to support the key project aims No. Involved Outcome or Improvement
Cancer Board Development
To co-produce a 5-year cancer strategy for Suffolk and north east Essex.
An online workshop was held with members of the public from across Suffolk and north east
Essex to establish the shared principles of coproduction for the strategy development. These
principles will underpin the work of the SNEE wide conversations.
37 Shared principles of coproduction developed and shared. Online platform developed for future conversations Series of online workshops planned for March and April.

Suffolk and North East Essex Patient and Public Involvement and Experience Team Report Quarter 4 2021/2022 – January to March 2022
March 2022 Page 6
SNEE Maternity and Neonatal 2021/2022 Programme
Governance Local Maternity Neonatal Services Board
Programme Lead Helen Bowles Quality Lead Lisa Nobes
SRO Lisa Nobes
PPI Lead Katie Sargeant
Project PPI activity to support the key project aims No. involved Outcome or Improvement
Strategic direction of LMNS (Helen Bowles)
Co-produce a five-year maternity and neonatal strategy: Survey asking for peoples experience of maternity services in SNEE. Community conversations with people with learning disability and autism, severe mental illness and substance misuse issues. Forum conversations with members of the public and maternity workforce comments collated and reported to the team Support the development and transformation of thetThree Maternity Voice Partnerships: Working with MVPs on the Maternity and Neonatal Strategy and sharing feedback and insights to support the development of the MVP network across SNEE.
193 survey responses 22 forum discussions 4 community conversations
Report provided to team. All information shared with team for first draft of strategy.
Suffolk and North East Essex Patient and Public Involvement and Experience Team Report Quarter 4 2021/2022 – January to March 2022
March 2022 Page 7
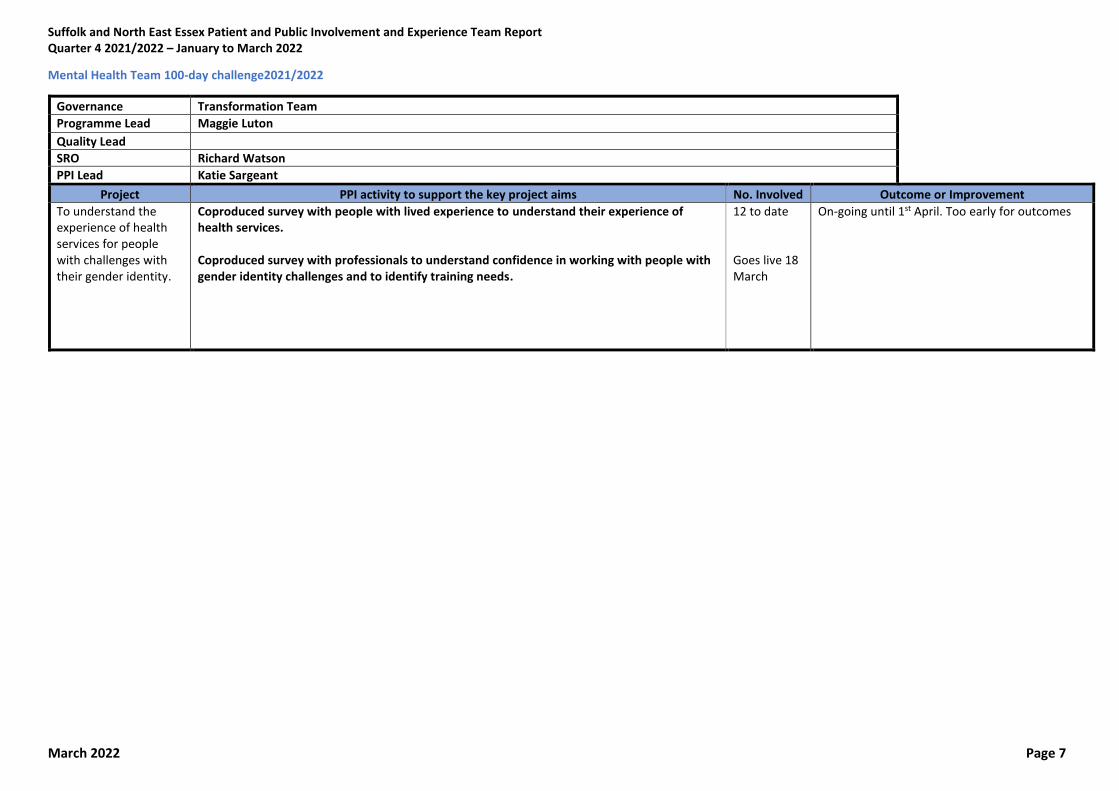
Mental Health Team 100-day challenge2021/2022
Governance Transformation Team
Programme Lead Maggie Luton
Quality Lead
SRO Richard Watson
PPI Lead Katie Sargeant
Project PPI activity to support the key project aims No. Involved Outcome or Improvement
To understand the experience of health services for people with challenges with their gender identity.
Coproduced survey with people with lived experience to understand their experience of health services. Coproduced survey with professionals to understand confidence in working with people with gender identity challenges and to identify training needs.
12 to date Goes live 18 March
On-going until 1st April. Too early for outcomes

Suffolk and North East Essex Patient and Public Involvement and Experience Team Report Quarter 4 2021/2022 – January to March 2022
March 2022 Page 8
SNEE Stroke 2021/2022 Programme
Governance Non-elective/UEC Board
Programme Lead Nerinda Evans
Quality Lead
SRO
PPI Lead Katie Sargeant
Project PPI activity to support the key project aims No. Involved Outcome or Improvement
Development of non-elective/urgent care strategy
To coproduce a non-elective and urgent care strategy for Suffolk and north east Essex. Online engagement platform has been developed to support the public engagement in the development of non-elective/Urgent care strategy. Mapping of existing community groups and organisations who can support the engagement has been carried out. Engagement plan has been developed.
Work ongoing too early for outcomes

Suffolk and North East Essex Patient and Public Involvement and Experience Team Report Quarter 4 2021/2022 – January to March 2022
March 2022 Page 9
SNEE End of Life Programme
Governance End of Life App development - Suffolk Programme Lead Sarah Hedges Quality Lead
SRO Barbara Gale PPI Lead Katie Sargeant
Project PPI activity to support the key project aims No. Involved
Outcome or Improvement
Development of an app that will act as a care record for End of Life patients
Create an app is to make a single advance care planning record that is accessible by all authorised users including professionals, carers and individuals. Members of the public reviewed the functionality of the ROSI app before wider piloting of the service. Recommendations made about the app has resulted in a significant change in the development of the app and further testing is planned for late in March.
12 Feedback and recommendations from coproduction fed into the final design.
Suffolk and North East Essex Patient and Public Involvement and Experience Team Report Quarter 4 2021/2022 – January to March 2022
March 2022 Page 10
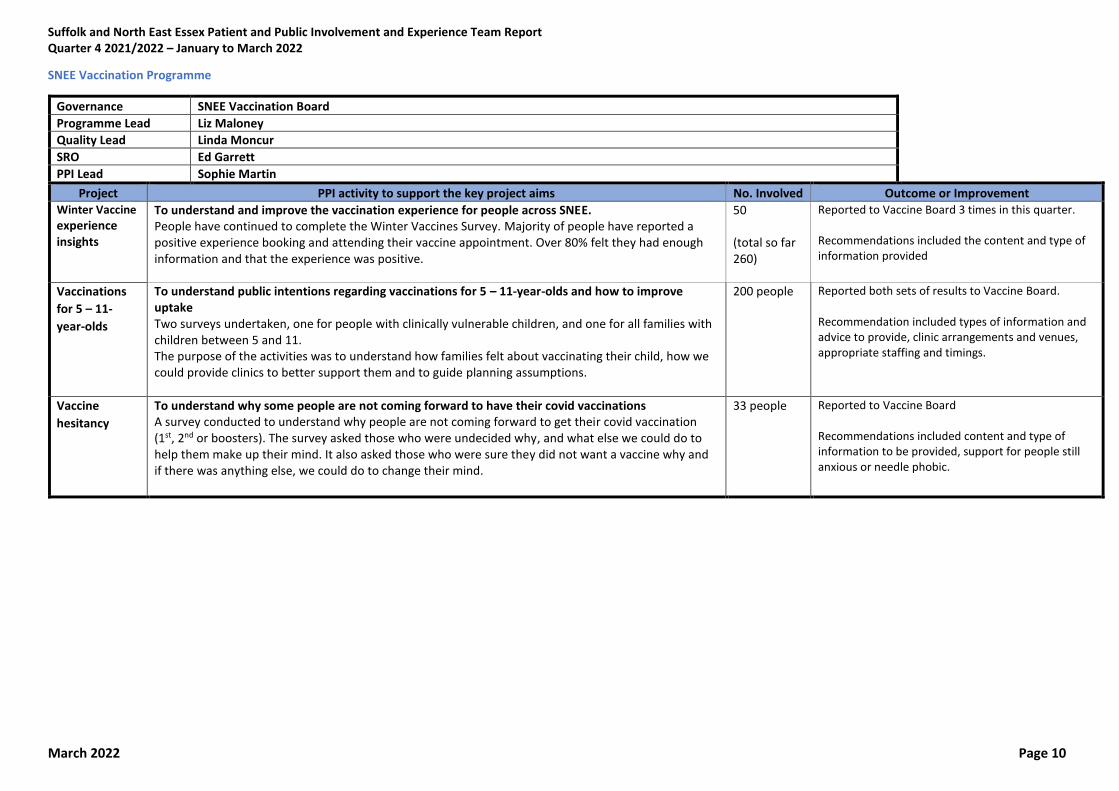
SNEE Vaccination Programme
Governance SNEE Vaccination Board
Programme Lead Liz Maloney
Quality Lead Linda Moncur
SRO Ed Garrett
PPI Lead Sophie Martin
Project PPI activity to support the key project aims No. Involved Outcome or Improvement Winter Vaccine experience insights
To understand and improve the vaccination experience for people across SNEE. People have continued to complete the Winter Vaccines Survey. Majority of people have reported a positive experience booking and attending their vaccine appointment. Over 80% felt they had enough information and that the experience was positive.
50 (total so far 260)
Reported to Vaccine Board 3 times in this quarter. Recommendations included the content and type of information provided
Vaccinations
for 5 – 11-
year-olds
To understand public intentions regarding vaccinations for 5 – 11-year-olds and how to improve uptake Two surveys undertaken, one for people with clinically vulnerable children, and one for all families with children between 5 and 11. The purpose of the activities was to understand how families felt about vaccinating their child, how we could provide clinics to better support them and to guide planning assumptions.
200 people Reported both sets of results to Vaccine Board. Recommendation included types of information and advice to provide, clinic arrangements and venues, appropriate staffing and timings.
Vaccine
hesitancy
To understand why some people are not coming forward to have their covid vaccinations A survey conducted to understand why people are not coming forward to get their covid vaccination (1st, 2nd or boosters). The survey asked those who were undecided why, and what else we could do to help them make up their mind. It also asked those who were sure they did not want a vaccine why and if there was anything else, we could do to change their mind.
33 people Reported to Vaccine Board Recommendations included content and type of information to be provided, support for people still anxious or needle phobic.
Suffolk and North East Essex Patient and Public Involvement and Experience Team Report Quarter 4 2021/2022 – January to March 2022
March 2022 Page 11
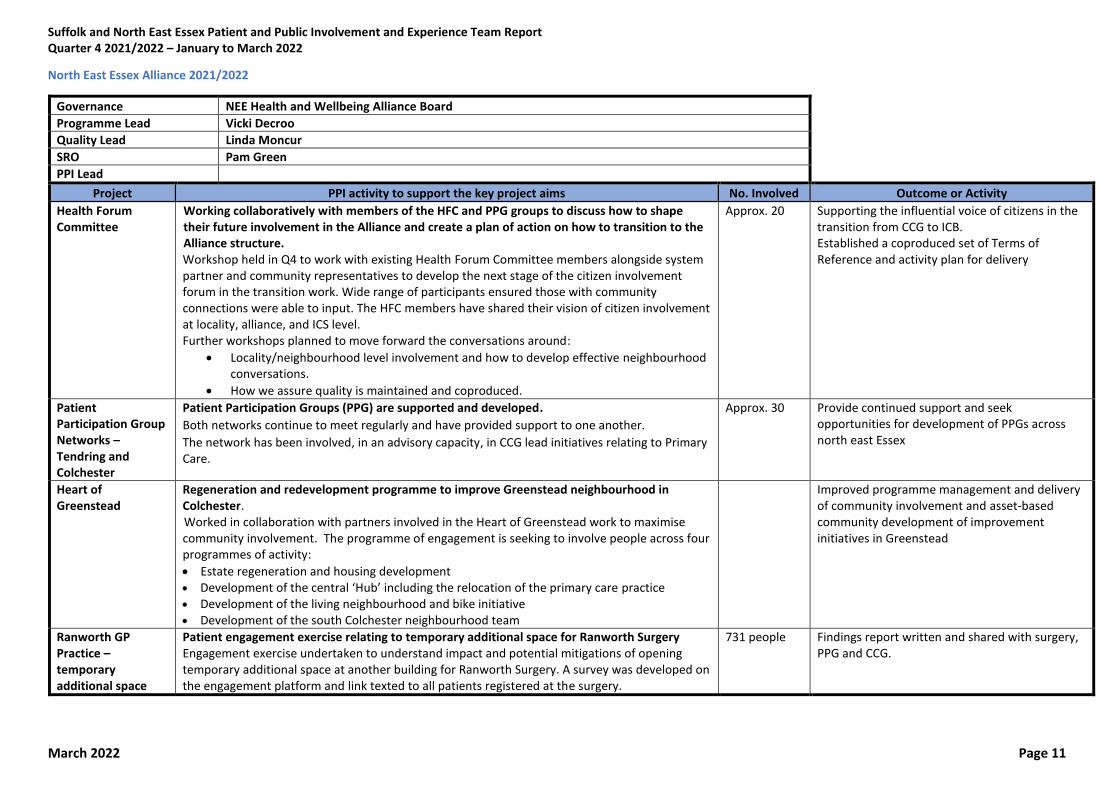
North East Essex Alliance 2021/2022
Governance NEE Health and Wellbeing Alliance Board
Programme Lead Vicki Decroo
Quality Lead Linda Moncur
SRO Pam Green
PPI Lead
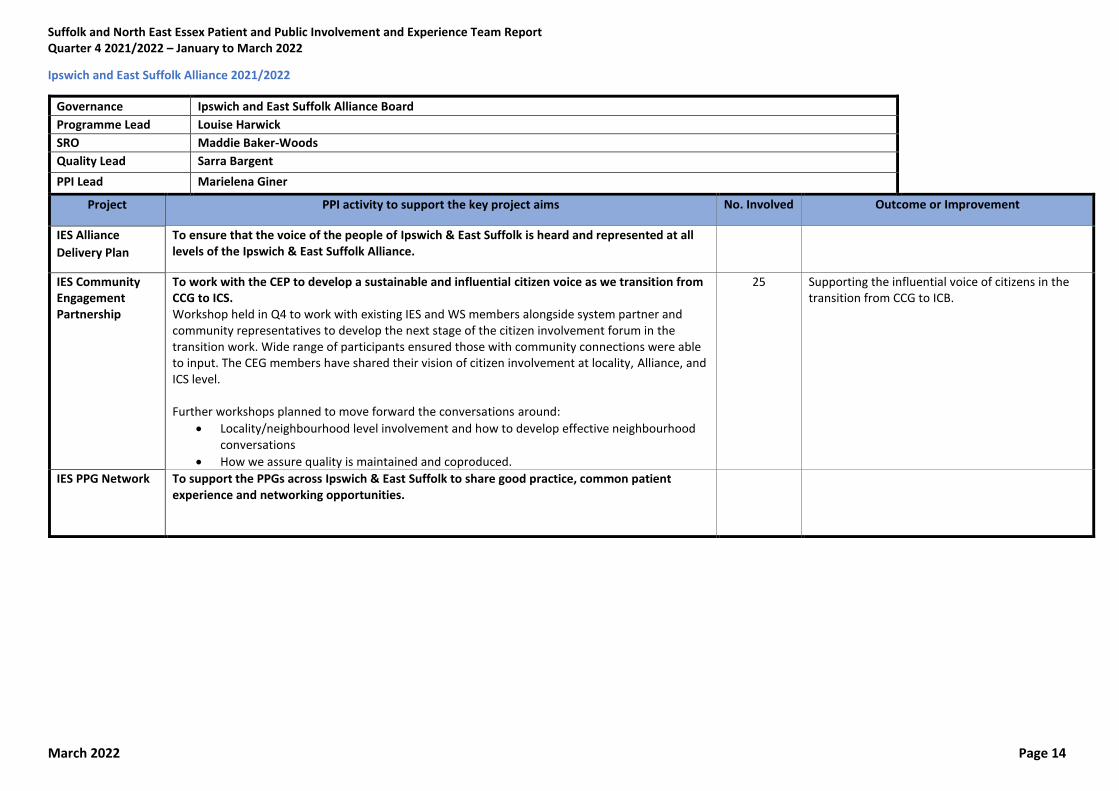
Project PPI activity to support the key project aims No. Involved Outcome or Activity Health Forum Committee
Working collaboratively with members of the HFC and PPG groups to discuss how to shape their future involvement in the Alliance and create a plan of action on how to transition to the Alliance structure. Workshop held in Q4 to work with existing Health Forum Committee members alongside system partner and community representatives to develop the next stage of the citizen involvement forum in the transition work. Wide range of participants ensured those with community connections were able to input. The HFC members have shared their vision of citizen involvement at locality, alliance, and ICS level. Further workshops planned to move forward the conversations around:
• Locality/neighbourhood level involvement and how to develop effective neighbourhood conversations.
• How we assure quality is maintained and coproduced.
Approx. 20 Supporting the influential voice of citizens in the transition from CCG to ICB. Established a coproduced set of Terms of Reference and activity plan for delivery
Patient Participation Group Networks – Tendring and Colchester
Patient Participation Groups (PPG) are supported and developed. Both networks continue to meet regularly and have provided support to one another. The network has been involved, in an advisory capacity, in CCG lead initiatives relating to Primary Care.
Approx. 30 Provide continued support and seek opportunities for development of PPGs across north east Essex
Heart of Greenstead
Regeneration and redevelopment programme to improve Greenstead neighbourhood in Colchester. Worked in collaboration with partners involved in the Heart of Greenstead work to maximise community involvement. The programme of engagement is seeking to involve people across four programmes of activity:
• Estate regeneration and housing development
• Development of the central ‘Hub’ including the relocation of the primary care practice • Development of the living neighbourhood and bike initiative • Development of the south Colchester neighbourhood team
Improved programme management and delivery of community involvement and asset-based community development of improvement initiatives in Greenstead
Ranworth GP Practice – temporary additional space
Patient engagement exercise relating to temporary additional space for Ranworth Surgery Engagement exercise undertaken to understand impact and potential mitigations of opening temporary additional space at another building for Ranworth Surgery. A survey was developed on the engagement platform and link texted to all patients registered at the surgery.
731 people Findings report written and shared with surgery, PPG and CCG.
Suffolk and North East Essex Patient and Public Involvement and Experience Team Report Quarter 4 2021/2022 – January to March 2022
March 2022 Page 12
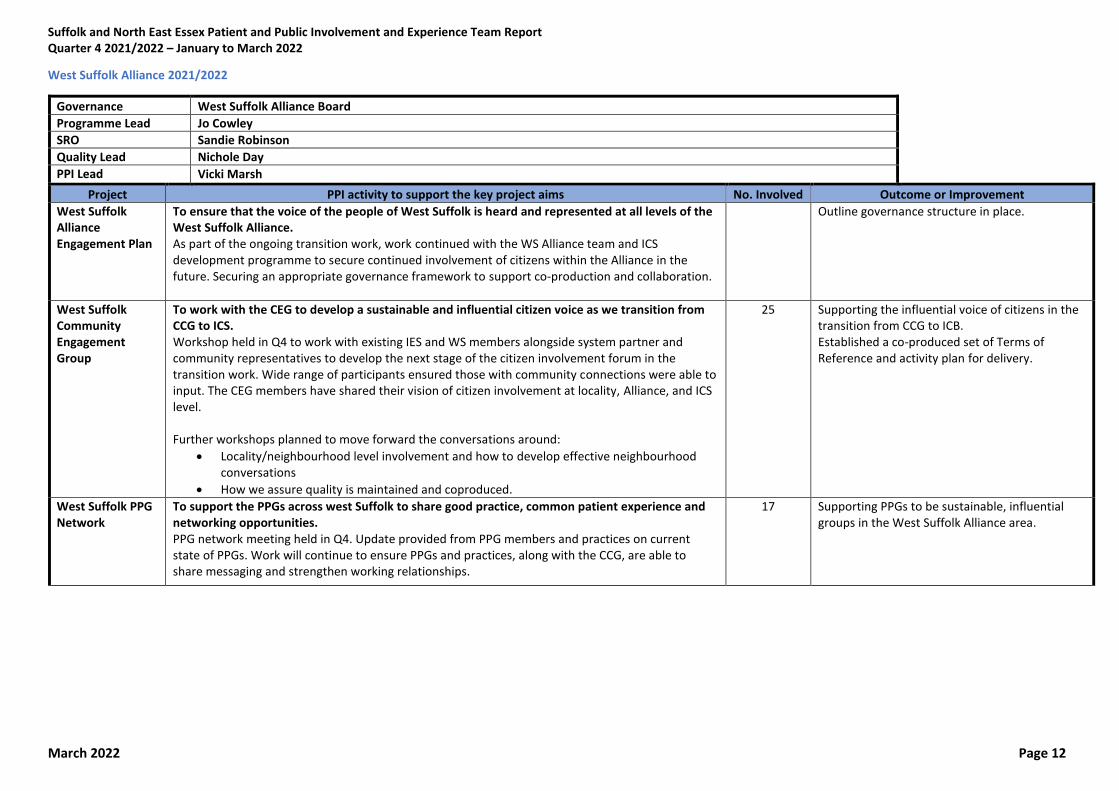
West Suffolk Alliance 2021/2022
Governance West Suffolk Alliance Board
Programme Lead Jo Cowley
SRO Sandie Robinson
Quality Lead Nichole Day
PPI Lead Vicki Marsh
Project PPI activity to support the key project aims No. Involved Outcome or Improvement
West Suffolk Alliance Engagement Plan
To ensure that the voice of the people of West Suffolk is heard and represented at all levels of the West Suffolk Alliance. As part of the ongoing transition work, work continued with the WS Alliance team and ICS development programme to secure continued involvement of citizens within the Alliance in the future. Securing an appropriate governance framework to support co-production and collaboration.
Outline governance structure in place.
West Suffolk Community Engagement Group
To work with the CEG to develop a sustainable and influential citizen voice as we transition from CCG to ICS. Workshop held in Q4 to work with existing IES and WS members alongside system partner and community representatives to develop the next stage of the citizen involvement forum in the transition work. Wide range of participants ensured those with community connections were able to input. The CEG members have shared their vision of citizen involvement at locality, Alliance, and ICS level. Further workshops planned to move forward the conversations around:
• Locality/neighbourhood level involvement and how to develop effective neighbourhood conversations
• How we assure quality is maintained and coproduced.
25 Supporting the influential voice of citizens in the transition from CCG to ICB. Established a co-produced set of Terms of Reference and activity plan for delivery.
West Suffolk PPG Network
To support the PPGs across west Suffolk to share good practice, common patient experience and networking opportunities. PPG network meeting held in Q4. Update provided from PPG members and practices on current state of PPGs. Work will continue to ensure PPGs and practices, along with the CCG, are able to share messaging and strengthen working relationships.
17 Supporting PPGs to be sustainable, influential groups in the West Suffolk Alliance area.
Suffolk and North East Essex Patient and Public Involvement and Experience Team Report Quarter 4 2021/2022 – January to March 2022
March 2022 Page 13
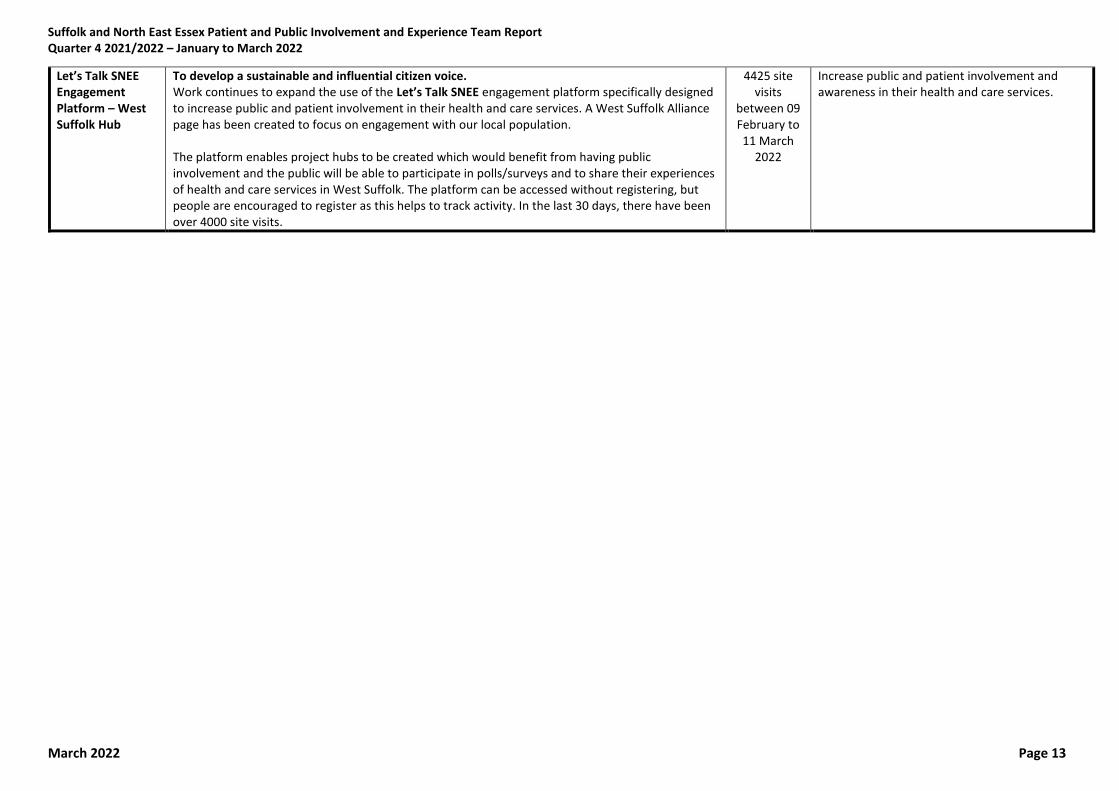
Let’s Talk SNEE Engagement Platform – West Suffolk Hub
To develop a sustainable and influential citizen voice. Work continues to expand the use of the Let’s Talk SNEE engagement platform specifically designed to increase public and patient involvement in their health and care services. A West Suffolk Alliance page has been created to focus on engagement with our local population. The platform enables project hubs to be created which would benefit from having public involvement and the public will be able to participate in polls/surveys and to share their experiences of health and care services in West Suffolk. The platform can be accessed without registering, but people are encouraged to register as this helps to track activity. In the last 30 days, there have been over 4000 site visits.
4425 site visits
between 09 February to 11 March
2022
Increase public and patient involvement and awareness in their health and care services.
Suffolk and North East Essex Patient and Public Involvement and Experience Team Report Quarter 4 2021/2022 – January to March 2022
March 2022 Page 14
Ipswich and East Suffolk Alliance 2021/2022
Governance Ipswich and East Suffolk Alliance Board
Programme Lead Louise Harwick
SRO Maddie Baker-Woods
Quality Lead Sarra Bargent
PPI Lead Marielena Giner
Project PPI activity to support the key project aims No. Involved Outcome or Improvement
IES Alliance
Delivery Plan
To ensure that the voice of the people of Ipswich & East Suffolk is heard and represented at all levels of the Ipswich & East Suffolk Alliance.
IES Community Engagement Partnership
To work with the CEP to develop a sustainable and influential citizen voice as we transition from CCG to ICS. Workshop held in Q4 to work with existing IES and WS members alongside system partner and community representatives to develop the next stage of the citizen involvement forum in the transition work. Wide range of participants ensured those with community connections were able to input. The CEG members have shared their vision of citizen involvement at locality, Alliance, and ICS level. Further workshops planned to move forward the conversations around:
• Locality/neighbourhood level involvement and how to develop effective neighbourhood conversations
• How we assure quality is maintained and coproduced.
25 Supporting the influential voice of citizens in the transition from CCG to ICB.
IES PPG Network To support the PPGs across Ipswich & East Suffolk to share good practice, common patient experience and networking opportunities.

Suffolk and North East Essex Patient and Public Involvement and Experience Team Report Quarter 4 2021/2022 – January to March 2022
March 2022 Page 15
SNEE PPI Team Q3 report additional items
Project PPI involvement to support project aims No. Involved
Outcome or Improvement
Let’s Talk SNEE – Engagement Platform
Digital engagement and interactive platform for SNEE and Alliance based involvement. The Engagement platform has seen a significant increase in the number of people who have been visiting the site. A number of different involvement activities have been hosted:
• 15 Surveys
• 22 forum topics
• 2 quick polls
• 12 news feed items
• 9 stories have been added
• 9 Questions asked and answers
• 8 ideas have been submitted
6,300 visits
A number of reports and recommendations have been shared across the Suffolk and North East Essex footprint.
Patient Safety Partners
Citizens to be involved in governance processes around patient safety and assurance. A more detailed plan for developing these roles has been developed and agreement made to coproduce the locally defined areas.
Plan for delivery being worked up, including opportunities for coproduction.
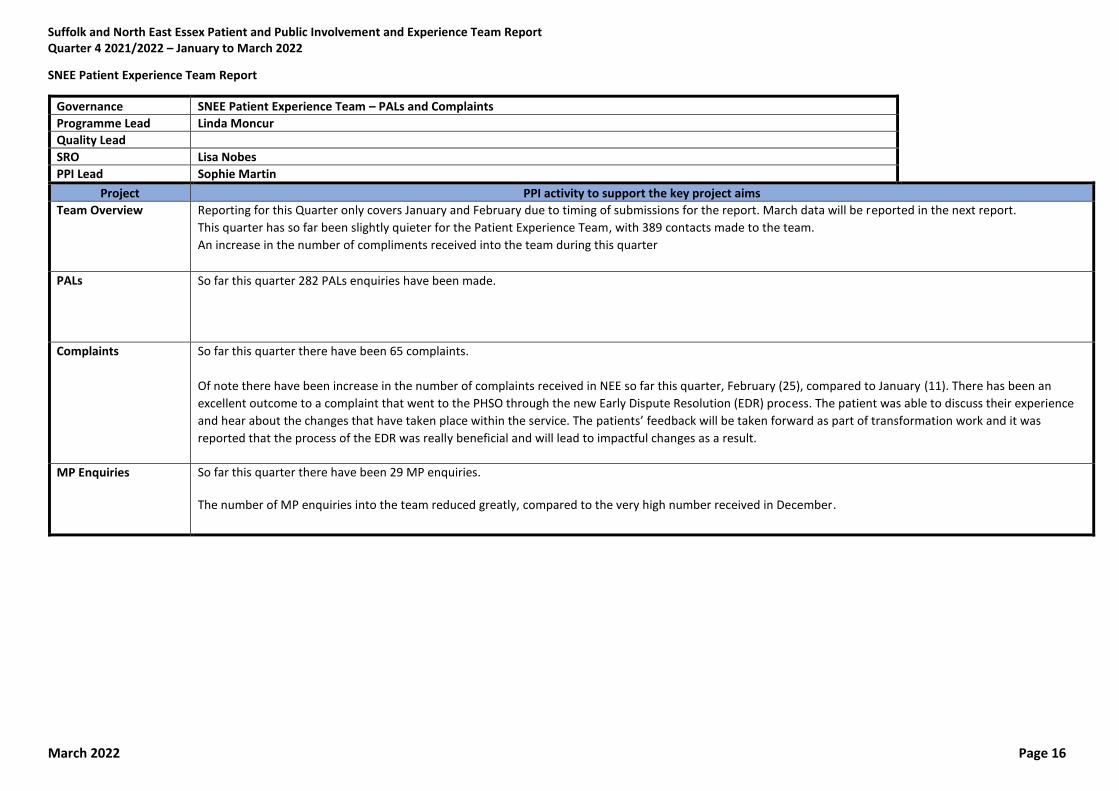
Suffolk and North East Essex Patient and Public Involvement and Experience Team Report Quarter 4 2021/2022 – January to March 2022
March 2022 Page 16
SNEE Patient Experience Team Report
Governance SNEE Patient Experience Team – PALs and Complaints
Programme Lead Linda Moncur
Quality Lead
SRO Lisa Nobes
PPI Lead Sophie Martin
Project PPI activity to support the key project aims
Team Overview Reporting for this Quarter only covers January and February due to timing of submissions for the report. March data will be reported in the next report.
This quarter has so far been slightly quieter for the Patient Experience Team, with 389 contacts made to the team.
An increase in the number of compliments received into the team during this quarter
PALs So far this quarter 282 PALs enquiries have been made.
Complaints So far this quarter there have been 65 complaints.
Of note there have been increase in the number of complaints received in NEE so far this quarter, February (25), compared to January (11). There has been an
excellent outcome to a complaint that went to the PHSO through the new Early Dispute Resolution (EDR) process. The patient was able to discuss their experience
and hear about the changes that have taken place within the service. The patients’ feedback will be taken forward as part of transformation work and it was
reported that the process of the EDR was really beneficial and will lead to impactful changes as a result.
MP Enquiries So far this quarter there have been 29 MP enquiries. The number of MP enquiries into the team reduced greatly, compared to the very high number received in December.

Page 1 of 4
GOVERNING BODY
Agenda Item No. 09
Reference No. NEECCG 22-23
Date. 7 June 2022
Title
Research Strategy for Suffolk and North East Essex Integrated Care System
Lead Director
Lisa Nobes, Director of Nursing
Author(s)
Clare Symms, Head of Research Management, Finance and PPI, Norfolk and Waveney CCG, on behalf of CCGs in Suffolk
Purpose
For approval
Applicable CCG Strategic Objectives:
1. To achieve our vision through an inclusive, holistic approach to patient and service user centred commissioning, embedding personalisation of care through integrated health and social care services.
2. To transform care and drive continuous improvement in quality and safety. Achieve the best possible outcomes for our service users through high quality care.
x
3. To use commissioning resources effectively and responsibly. To develop our organisation, teams and individual staff to be trusted, competent, well trained, talented, enthusiastic and dedicated.
x
4 To tackle the biggest health challenges in north east Essex including reducing health inequalities.
x
Recommendation: For approval with a view to the strategy being adopted as we move from CCGs to an ICB. This strategy is being taken to all 3 SNEE CCG Governing Bodies.

Page 2 of 4
1. Summary 1.1 Following 2 stakeholder workshops in December 2021 a research strategy for SNEE ICS has
been drafted to set out a vision and aims for the ICS over the next 5 years. 1.2 Research is essential in health and social care and is one of the main drivers in providing
evidence-based improved treatment and care options for individuals - evidence demonstrates that hospitals that are research active have better outcomes, and patients and services not directly involved in research still benefit from being in research-active organisations, and CQC includes research activity as one of the characteristics of a ‘Well-Led’ organisation. There is an expectation through the NHS Constitution that users of the NHS will be given opportunities to participate in research relevant to their care
1.3 With the Health and Care Bill shortly to be enacted, ICBs will have duties to promote
research and innovation across their system and support partners to do the same. 1.4 Individual partners within the Suffolk and North East Essex ICS have a good track record of
delivering research and collaborating on studies; working in partnership was key in enabling the delivery of urgent public health research during the COVID-19 pandemic.
1.5 This research strategy, the first for the Suffolk and North East Essex Integrated Care System
(SNEE ICS), sets out a vision to build a culture of research across that is responsive to those in most need in the communities that it serves, building on what has already been achieved. The strategy outlines 5 key aims:
1. To build a flexible, system-wide approach to research across the Suffolk and North East
Essex ICS
2. To build on our academic partnerships to develop research ideas and achieve research
funding
3. To empower research teams, services, service users and carers to work as partners to
help deliver, develop and support high quality research
4. To embed a culture of research, innovation and use of evidence across the ICS
5. For research to be visible, meaningful and accessible
1.6 The strategy also sets out the key outcomes we expect to see if the strategy is delivered and
how this would be measured. 1.7 The strategy also sets out the key outcomes we expect to see if the strategy is delivered as
well as how this would be measured. 1.8 The strategy has been written with a view to being adopted by the CCGs and taken forward
into the ICS and ICB from July. 2. Key Points to Note 2.1 Research brings a number of benefits - It is one of the main drivers in providing evidence-
based improved treatment and care, organisations that are research active have better outcomes for their patients and service users, even within services that are not directly involved, it can help with staff recruitment and retention and professional development.
2.2 ICBs will have specific duties to promote research and innovation across their system and
support partners within the system to do the same. The strategy, the first for SNEE ICS, is expected to provide a framework for delivering the research duties of the ICS and creating a research rich environment that will meet the needs of our population and communities as we move forwards into an ICS.

Page 3 of 4
2.3 Partnership and system wide working, collaboration and co-production are key drivers behind
the aims to build a robust and accessible research system within SNEE. 3. Risks Identified 3.1 Individual organisations within the ICS, may have their individual research strategies and
priorities, however whilst this strategy it may not align directly with individual organisation strategies and priorities it has been developed following workshops with stakeholders and ICS partners with the aim of being flexible and responsive to changing needs as the ICS develops.
3.2 Leadership will be a key aspect in delivering of this strategy and achieving the desired
outcomes across the ICS, alongside a mechanism for overseeing research activity at an ICS level either through existing structures or collaborations or through the establishment of a research specific forum.
4. Resource Implications 4.1 This strategy will need input from the ICB in terms of leadership and supporting partners to
help deliver the strategy. Whilst a Service Level Agreement for Research support exists between the Suffolk CCGs and Norfolk and Waveney CCG via the Research Office and Norfolk and Waveney CCG, ownership of the strategy by the SNEE ICS will be critical if the ambitions within the strategy are to be realised.
4.2 Research infrastructure within the ICS is through research teams within NHS Trusts (the
resources and funding for which varies by organisation), and via the NIHR Clinical Research Network (CRN) East of England. The CRN also provide some funding and infrastructure for research in social care and public health.
4.3 A Service Level Agreement for Research support exists between the Suffolk CCGs and
Norfolk and Waveney CCG via the Research Office at Norfolk and Waveney CCG for support within the CCG and within Primary Care, however ownership of the strategy by the SNEE ICS will be critical if the ambitions within the strategy are to be realised.
4.4 It is hoped that through this strategy and collaborative working further research monies will
be attracted into the region through attracting research studies to the region and achieving research grant funding.
5. Engagement and Communication 5.1 42 attendees (excluding facilitators) took part in the two workshops. A wide range of
stakeholders were represented including representatives from Healthwatch and other patient and public involvement representatives, as well as representatives from the Suffolk and North East Essex CCGs, SuNEE Trusts, GP practices, academic partners, National Institute for Health and Care Research (NIHR) Clinical Research Network (CRN) East of England, and Public Health.
5.2 Across the two workshops, stakeholders explored: where we currently were as a system; our
strengths, weaknesses, opportunities, and challenges; what we would like to see in a successful research system; and what steps we might need to take to get there.
5.3 Individuals who expressed interest in helping to draft the strategy following the workshops
have been given the opportunity to review a draft of this strategy and a number of changes have been made as a result.
Page 4 of 4
6. Equality and Diversity 6.1 Research can help to both identify and address health inequalities at a local level and to
identify those treatments and services that are most effective. 6.2 The key aims of the strategy - to embed a culture of research across the ICS, to empower
individuals to engage with research and to make research meaningful and accessible are specifically designed to broadening the reach of research and working collaboratively with communities, organisations and services to develop and deliver research that works for our region and populations.
1 | P a g e
Research Strategy for Suffolk and North East Essex Integrated Care
System – 2022 - 2027
1 INTRODUCTION
The Suffolk and North East Essex (SNEE) Integrated care system (ICS)1 is one of 42 ICSs
across England, as announced by the Chief Executive of the NHS on April 1, 2021. These
bring together providers and commissioners of NHS services across a geographical area
with local authorities and other local partners to collectively plan health and care services to
meet the needs of their population. ICSs were a key part of the NHS Long Term Plan, and
the Health and Care Bill, which is set to become the Health and Care Act, will put Integrated
Care Systems (ICSs) on a statutory footing from 1st July 2022.
The central aim of each ICSs is to integrate care across different organisations and settings,
joining up hospital and community-based services, physical and mental health, and health
and social care. Research is a core function of health and social care. Thus, development of
a robust research and evidence culture is an essential ingredient to the success of ICSs.
The Suffolk and North East Essex ICS builds on the earlier work of the Suffolk and North
East Essex Sustainability and Transformation Partnership (STP). The full spectrum of
partners engaged in the ICS includes NHS Commissioners, NHS Provider Trusts, Local
government, NHS regulators, primary care – GPs, community pharmacists, optometrists and
dentists, independent sector providers, community and voluntary sector, public, patient and
carer groups, education and research and other sectors including industry, police and
education.
The new Health and Care Bill gives ICSs duties to promote research and innovation, and to
facilitate partners to do the same; the NHS constitution provides a commitment to
“innovation and to the promotion, conduct and use of research to improve the current and
future health and care of the population” and expectation that users of the NHS will be given
opportunities to participate in research relevant to their care. To ensure research that is
aligned with the Suffolk and North East Essex Integrated Care System, this document sets
out our inaugural research strategy over the next 5 years.
2 ACHIEVING OUR AMBITIONS AS AN ICS
Our eight ‘Higher Ambitions’ as an ICS, as set out below, and on our website relate to the
key long standing health and care challenges in our region, and link to the priorities set by
the Health and Wellbeing Boards in Essex and Suffolk in their Joint Health and Wellbeing
Strategies.
• Our Primary Ambition: Reducing Health Inequalities
1 Suffolk & North East Essex Integrated Care System - Suffolk & North East Essex Integrated Care System (sneeics.org.uk)
2 | P a g e
• A healthier life for everyone
• Emotional wellbeing from the start of life
• Zero Suicide
• Earlier diagnosis and treatment for cancer
• An effective treatment pathway for obesity
• The best quality of life as we grow older
• The care and support we need at the end of life
It is the intention that this research strategy will inform the development of a robust
collaborative infrastructure and culture for research across our ICS, enabling the delivery,
development and dissemination of research aligned to these ambitions and the key needs of
our population.
ACADEMIC LINKS Our key academic partners currently include the University of Suffolk (UoS), Anglia Ruskin
University (ARU), University of Essex and University of East Anglia (UEA).
The University of Suffolk (UoS), established in 2016, is the first university in the county, and
fully embraces a culture of research, as demonstrated by its four new research institutes
launched this year; Institute for Social Justice and Crime; Suffolk Sustainability Institute;
Institute of Health and Wellbeing; and the Digital Futures Institute. The Integrated Care
Academy (ICA) at UoS is a unique partnership between SNEE ICS, UoS, Suffolk County
Council and Healthwatch Suffolk; the first in the country to formally bring together the four
pillars of higher education, an integrated care system, local authority, and the voluntary and
community sector. At the ICA co-production is key, with specialised integrated care training
courses offered through its Co-production Hub.
The three priority areas of the ICA purposefully align with SNEE ICS:
• Improving mental health and wellbeing
• Supporting best quality of life as we grow older
• Optimising care and support towards end of life
We have close working relationships through East Suffolk and North Essex NHS Foundation
Trust (ESNEFT) with Anglia Ruskin University (ARU), particularly in relation to AI and the
medical school, and University of Essex. With ARU launching its Wellbeing Research and
Innovation Network in January 2022, with a key goal of improving health and wellbeing
across the Eastern region.
SNEE NHS Trusts and CCGs were also founder partners of the University of East Anglia
(UEA) Health and Social Care Partners (UEAHSCP), which brings together researchers and
academics across health and social care organisations in Norfolk, Suffolk and North East
Essex to conduct collaborative research to address the key health and care challenges for
the region.
Given the infancy of our Integrated Care System, which like the rest of the England, comes
into being on 1st July 2022, this strategy is designed to be flexible to respond to changing
priorities and focus both locally, within SNEE, as well as changes to national strategy and
direction.

3 | P a g e
3 THE LOCAL POPULATION
We have a population of around 1 million, with an expected population growth of 10% over
the next 10 years. Our population is aging, the number of older people over 75 living alone
is increasing and the number of residents living in care homes is expected to increase by
40% in the next 10 years2, and the number of older people with dementia to double over the
next 20 years3.
Whilst we have some of the most advantaged neighbourhoods in the country, we also have
some of the most deprived, and our inequalities have deepened. Key health indicators such
as life expectancy, under 75 mortality rates and suicide rate in our areas of highest
deprivation are significantly worse than the national average:
Indicator Period England Colchester Tendring Suffolk
Life expectancy at birth
(Male) 2017 - 19 79.8 80.5 78.2 80.9
Life expectancy at birth
(Female) 2017 - 19 83.4 83.4 81.7 84.3
Under 75 mortality rate from
all causes considered
preventable
2017 - 19 326 122.4 170.5 117.0
Under 75 mortality rate from
all cardiovascular diseases 2017 - 19 70.4 51.1 78.9 60.3
Under 75 mortality rate from
cancer 2017 - 19 129.2 122.0 136.3 117.9
Suicide rate 2017 - 19 10.1 18.5 18.8 10.4
Inequality in life expectancy
at birth (Male) 2017 - 19 9.4 8.0 10.1 7.0
Inequality in life expectancy
at birth (Female) 2017 - 19 7.6 6.2 7.7 5.0
Segment Tool (phe.gov.uk)
Diabetes, mental ill health and obesity are increasing, and our suicide rates, particularly in
North East Essex are significantly higher than the England average4.
Amongst the wider determinants of health, pollution levels (CO2, NOX) are rising, demand for housing outstrips supply, with increases in unemployment, universal credit claimants. Whilst skill levels are rising, educational attainment is relatively weak5. Through systematic gathering of evidence and robust methodologies this research strategy for SNEE can support the drive towards identifying gaps in evidence and priority areas to assist those in greatest need.
2 Our local population - Suffolk & North East Essex Integrated Care System (sneeics.org.uk) 3 Our local population - Suffolk & North East Essex Integrated Care System (sneeics.org.uk) 4 Our local population - Suffolk & North East Essex Integrated Care System (sneeics.org.uk) 5 Presentation from Anna Crisp, Public Health Suffolk at First Strategy Development workshop

4 | P a g e
4 WHY IS RESEARCH IMPORTANT?
Research is essential in health and social care. It is one of the main drivers in providing
evidence-based improved treatment and care options for individuals, helping us to find out
which treatments work better and improving our understanding of individuals experience of
care and what is important to them in managing their health. Research can, and must, help
identify gaps in knowledge and change the way that we work. The research undertaken
during the COVID-19 pandemic not only gave us effective treatments and vaccinations, but it
also led to a greater understanding of how COVID-19 spread, and how the pandemic
affected individuals and society as a whole6.
Co-production in research, working in collaboration with service users and those with whom
the research will have the most impact, to develop and deliver research is recognised as
essential to delivering robust and impactful research. Service users, carers and frontline
staff can not only offer a unique perspective on the questions that are most important, but
also on the deliverability of research and engagement of differing populations and
communities. This is essential if we are to make research accessible to our differing
communities.
There is a growing body of evidence7891011 which demonstrates that hospitals that are
research active have better outcomes, and that patients and services not directly involved in
the trials themselves still benefit from being in research-active organisations. Evidence is
also growing that this also applies to other health and care settings.
The Care Quality Commission (CQC) now includes an assessment of opportunities for
service users to join research projects and clinical trials as one of the characteristics of a
‘Well-Led’ organisation, and research offers learning and development opportunities for staff,
and can help with recruitment and retention, helping organisations to flourish.
This research strategy, the first for SNEE, is key to creating a research rich environment to
identify and generate the reforms necessary as we move into a phase of recovery for a
better future.
5 DEVELOPMENT OF THIS STRATEGY AND VISION
The development of this strategy for research has been informed through two system wide
workshops, held in December 2021 with stakeholders able to comment and shape the
resulting strategy (this strategy) that has emerged.
We would like to express our thanks to all those who attended the workshop and helped to
shape the strategy as it now stands.
6 NIHR Evidence - Browse content - Informative and accessible health and care research 7Patients admitted to more research‐active hospitals have more confidence in staff and are better informed about
their condition and medication: Results from a retrospective cross‐sectional study 8 The correlation between National Health Service trusts' clinical trial activity and both mortality rates and care quality commission ratings: a retrospective cross-sectional study 9 Research activity and the association with mortality; 10 High hospital research participation and improved colorectal cancer survival outcomes: a population-based study 11 Does the engagement of clinicians and organisations in research improve healthcare performance: a three-stage review
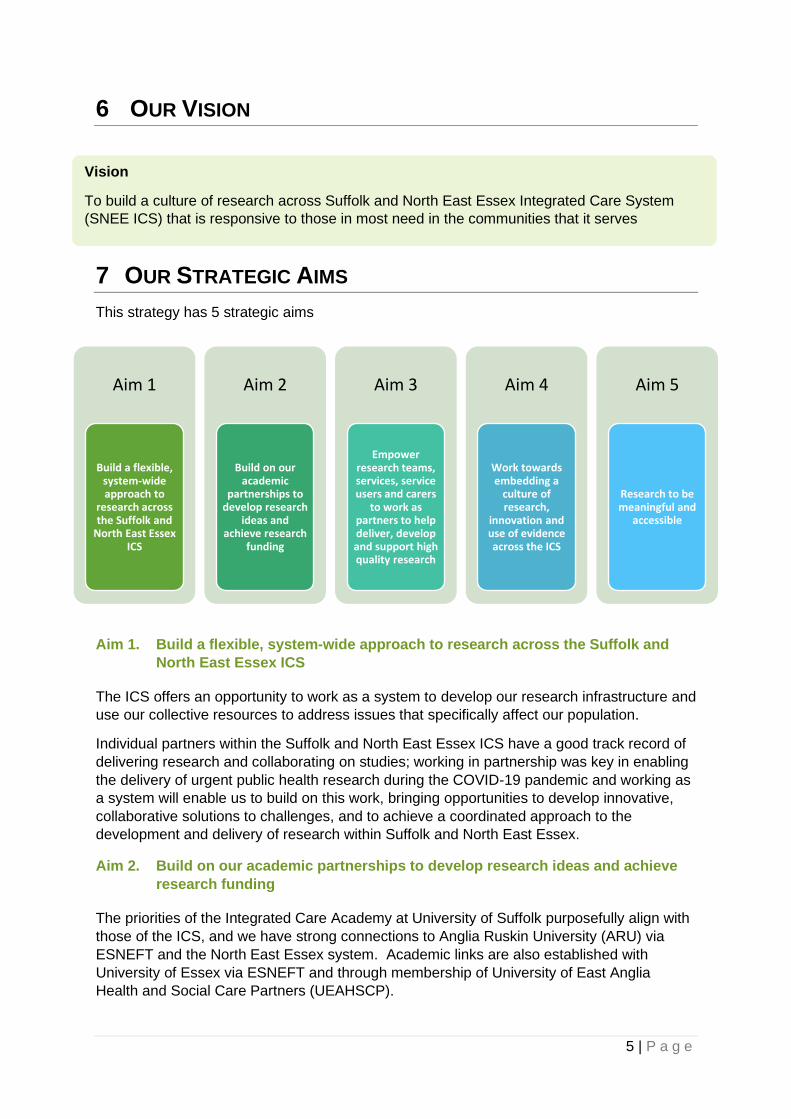
5 | P a g e
6 OUR VISION
7 OUR STRATEGIC AIMS
This strategy has 5 strategic aims
Aim 1. Build a flexible, system-wide approach to research across the Suffolk and
North East Essex ICS
The ICS offers an opportunity to work as a system to develop our research infrastructure and
use our collective resources to address issues that specifically affect our population.
Individual partners within the Suffolk and North East Essex ICS have a good track record of
delivering research and collaborating on studies; working in partnership was key in enabling
the delivery of urgent public health research during the COVID-19 pandemic and working as
a system will enable us to build on this work, bringing opportunities to develop innovative,
collaborative solutions to challenges, and to achieve a coordinated approach to the
development and delivery of research within Suffolk and North East Essex.
Aim 2. Build on our academic partnerships to develop research ideas and achieve
research funding
The priorities of the Integrated Care Academy at University of Suffolk purposefully align with
those of the ICS, and we have strong connections to Anglia Ruskin University (ARU) via
ESNEFT and the North East Essex system. Academic links are also established with
University of Essex via ESNEFT and through membership of University of East Anglia
Health and Social Care Partners (UEAHSCP).
Vision
To build a culture of research across Suffolk and North East Essex Integrated Care System
(SNEE ICS) that is responsive to those in most need in the communities that it serves
Aim 1
Build a flexible, system-wide approach to
research across the Suffolk and
North East Essex ICS
Aim 2
Build on our academic
partnerships to develop research
ideas and achieve research
funding
Aim 3
Empower research teams, services, service users and carers
to work as partners to help deliver, develop and support high quality research
Aim 4
Work towards embedding a
culture of research,
innovation and use of evidence across the ICS
Aim 5
Research to be meaningful and
accessible
6 | P a g e
Building and strengthening these partnerships gives opportunities to identify and develop
ideas at a system wide level and bid for research monies. Bringing together individuals from
across the system to develop truly collaborative projects that are realistic, achievable,
academically sound and meet the needs of our population, to get the best chance of
achieving funding.
Aim 3. Empower research teams, services, service users and carers to work as
partners to help deliver, develop and support high quality research
Involving service users and frontline staff in all aspects of the research pathway helps to
ensure research focuses on what is most important to service users and staff delivering
care; is practical and acceptable to those it is aimed to help; and supports inclusion across
different populations and communities. Co-production is an essential element in addressing
the needs and challenges of the communities the research is designed to serve.
Aim 4. Embedding a culture of research, innovation and use of evidence across the
ICS
As described in section 4, increasing evidence shows that research active organisations
have better outcomes for their patients and services users, providing evidence-based
improved treatment and care options, and offering staff professional developmental
opportunities. Engagement of our services in research also ensures that the findings from
that research are applicable to our population.
Raising awareness and visibility of research, promoting opportunities for staff and service
users and highlighting how staff can get involved, will help to embed research within the
everyday working of the ICS, increasing opportunities for service users and staff to
participate.
Embedding learning from local, national and international research into the commissioning
and delivery of services helps to ensure people receive the most effective services and
provide the best possible outcomes for their health and wellbeing.
Aim 5. Research to be visible, meaningful and accessible
To achieve the best outcomes and engagement, research needs to be accessible to all.
Increasing communication and visibility of research in a format that is accessible and
inclusive will help support the development of a research culture within the ICS, increase
knowledge and engagement of staff and service users and support inclusivity of research.
Consideration is needed around communication of research opportunities, dissemination of
research results and findings, identification of local impact as well as access to, availability
and use of evidence. Much research in health and care is publicly funded, communication
and visibility of research helps demonstrate the benefits of public money invested in
research.

7 | P a g e
8 KEY OUTCOMES
DELIVERY OF THIS STRATEGY IS EXPECTED TO RESULT IN THE FOLLOWING
OUTCOMES.
By 2027 we will have:
1. Built the profile of research within the Suffolk and North East Essex ICS
2. Built a positive reputation for delivery of research within the region
3. Developed locally led collaborative research aligned to local and national priorities
that attracting national funding into the region
4. Established strong networks and partnerships for research across the Suffolk, North
East Essex region – working together across system, place and neighbourhood to
address challenges in research, deliver solutions and champion research
5. Empowered individuals to engage in and champion research
6. Increased dissemination of findings, activities, impact and stories to partners and
service users across our ICS
Measured through:
• An increase in the number and scope of research projects delivered locally
(Outcomes 1,4,5)
• Increased engagement of communities in research, particularly in areas of most need
(Outcomes 1,2,4,5,6)
• Achieving repeat business from external research teams coming back to the SNEE
region to deliver their research (Outcomes 1,2)
• An increase in the number and value of research grants achieving national funding
held by SNEE ICS partners (Outcomes 2,3,4,5).
• An increase in the number of and grant applications developed collaboratively within
SNEE (Outcomes 3,4,5)
• Research champions embedded within ICS partners (Outcome 5)
• An increase in locally led research publications and communications (Outcome 6)
• Research activity featuring more regularly within ICS and partner communications
(Outcome 6)
9 ACKNOWLEDGEMENTS
This strategy was developed following two virtual workshops held in Quarter 3 21/22 which
explored: where we currently were as a system; our strengths, weaknesses, opportunities,
and challenges; what we would like to see in a successful research system; and what steps
we might need to take to get there.
Delegates included: commissioners and practitioners from across the healthcare sector in
Suffolk and North East Essex; representatives from public health, social care, and the public
voice; academic partners and other relevant stakeholders such as the National Institute for
Health and Care Research Clinical Research Network (NIHR CRN) for the Eastern region -
CRN East of England.
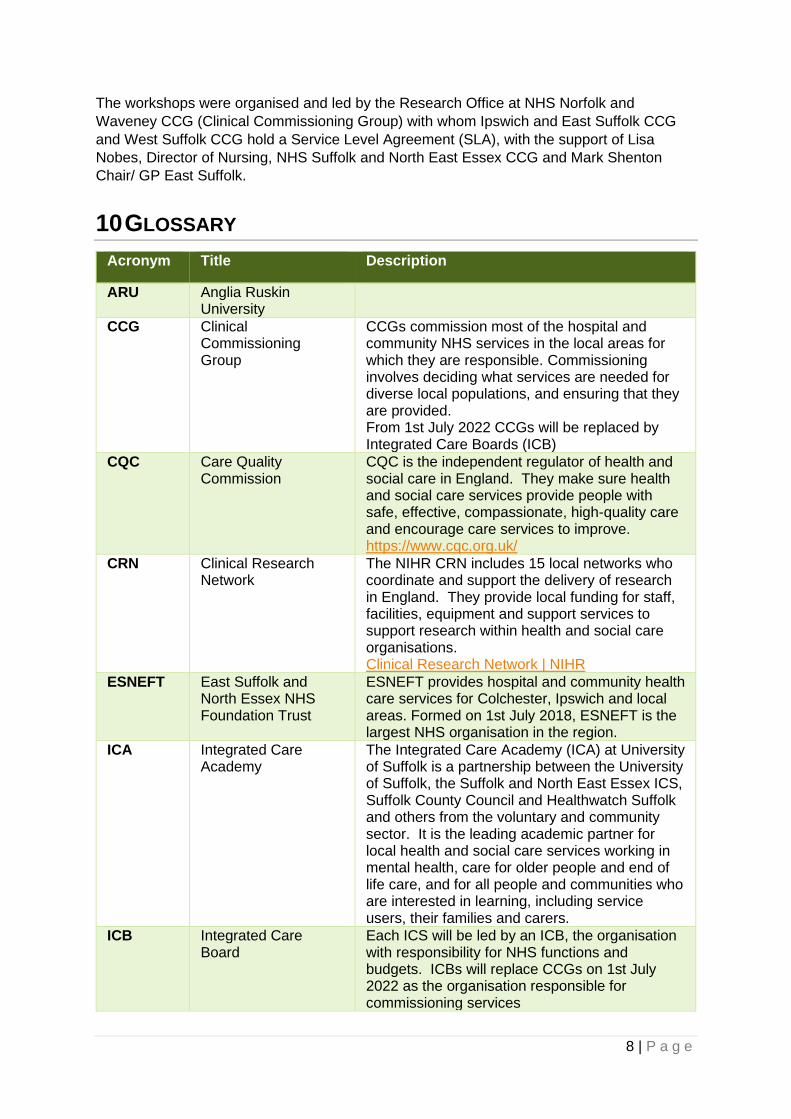
8 | P a g e
The workshops were organised and led by the Research Office at NHS Norfolk and
Waveney CCG (Clinical Commissioning Group) with whom Ipswich and East Suffolk CCG
and West Suffolk CCG hold a Service Level Agreement (SLA), with the support of Lisa
Nobes, Director of Nursing, NHS Suffolk and North East Essex CCG and Mark Shenton
Chair/ GP East Suffolk.
10 GLOSSARY
Acronym Title Description
ARU Anglia Ruskin University
CCG Clinical Commissioning Group
CCGs commission most of the hospital and community NHS services in the local areas for which they are responsible. Commissioning involves deciding what services are needed for diverse local populations, and ensuring that they are provided. From 1st July 2022 CCGs will be replaced by Integrated Care Boards (ICB)
CQC Care Quality Commission
CQC is the independent regulator of health and social care in England. They make sure health and social care services provide people with safe, effective, compassionate, high-quality care and encourage care services to improve. https://www.cqc.org.uk/
CRN Clinical Research Network
The NIHR CRN includes 15 local networks who coordinate and support the delivery of research in England. They provide local funding for staff, facilities, equipment and support services to support research within health and social care organisations. Clinical Research Network | NIHR
ESNEFT East Suffolk and North Essex NHS Foundation Trust
ESNEFT provides hospital and community health care services for Colchester, Ipswich and local areas. Formed on 1st July 2018, ESNEFT is the largest NHS organisation in the region.
ICA Integrated Care Academy
The Integrated Care Academy (ICA) at University of Suffolk is a partnership between the University of Suffolk, the Suffolk and North East Essex ICS, Suffolk County Council and Healthwatch Suffolk and others from the voluntary and community sector. It is the leading academic partner for local health and social care services working in mental health, care for older people and end of life care, and for all people and communities who are interested in learning, including service users, their families and carers.
ICB Integrated Care Board
Each ICS will be led by an ICB, the organisation with responsibility for NHS functions and budgets. ICBs will replace CCGs on 1st July 2022 as the organisation responsible for commissioning services

9 | P a g e
ICS Integrated Care System
ICSs are new partnerships between the organisations that meet health and care needs across an area, to coordinate services and to plan in a way that improves population health and reduces inequalities between different groups
NIHR National Institute for Health and Care Research
The NIHR was established in 2006, and is funded by Department of Health and Social Care. Working in partnership with the NHS, universities, local government, other research funders, patients and the public, the NIHR funds, enables and delivers world-leading health and social care research that improves people's health and wellbeing and promotes economic growth. https://www.nihr.ac.uk/
SLA Service Level Agreement
Agreement between partners to deliver a service – in the case of this document – this is an agreement between Suffolk CCGs and the Norfolk and Waveney CCG to deliver research support
SNEE Suffolk and North East Essex
SNEE is the region this strategy applies to and the region covered by the SNEE ICS
STP Sustainability and Transformation Partnership
Sustainability and transformation partnerships (STPs) were introduced in 2016 to bring together local NHS organisations and local authorities to develop proposals to improve health and the quality of care to provide better services for patients in the areas they serve. These have been replaced by ICSs
UEA University of East Anglia
UEAHSCP UEA Health and Social Care Partners
UEA Health and Social Care Partners (UEAHSCP), brings together world-class researchers and academics across health and social care organisations in Norfolk, Suffolk and North East Essex to conduct collaborative research to address the key health challenges in the region
UoS University of Suffolk

Page 1 of 27
GOVERNING BODY
Agenda Item No. 10
Reference No. NEECCG 22-34
Date. 7 June 2022
Title
2022/23 Plan
Lead Director
Jane Payling, Director of Finance
Author(s)
Paul Gibara, Director of Performance Improvement Richard Watson, Deputy Chief Executive and Director of Strategy and Transformation Amanda Lyes, Director of Corporate Services & System Infrastructure
Purpose
To set out, for approval, the 2022/23 plans on activity, workforce and finance and accompanying narrative. To approve the opening budget for 2022/23 for the CCG.
Applicable CCG Clinical Priorities:
1. To achieve our vision through an inclusive, holistic approach to patient and service user centred commissioning, embedding personalisation of care through integrated health and social care services.
X
2. To transform care and drive continuous improvement in quality and safety. Achieve the best possible outcomes for our service users through high quality care.
X
3. To use commissioning resources effectively and responsibly. To develop our organisation, teams and individual staff to be trusted, competent, well trained, talented, enthusiastic and dedicated.
X
4 To tackle the biggest health challenges in north east Essex including reducing health inequalities.
X
Action required by the Governing Body: To approve the following plans for 2022/23
• Narrative Plan
• Activity and achievement of targets
• Workforce
• Financial To approve the opening budget for 2022/23 for the CCG. To delegate sign off for any changes to the finance committee, with reporting back to the Governing Body.

Page 2 of 27
1. Background 1.1 At its meeting in March the Governing Body was provided with an update on the planning
process for 2022/23. The paper noted the timetable for planning required final submissions to be made on 28 April.
1.2 This paper includes the submissions made in April for sign-off
• Narrative Plan (appendix A)
• Activity & Performance plan (appendix B)
• Workforce Plan (appendix C)
1.3 The planning processes have not formally concluded, due in the main to issues regarding financial balance. The paper explains the progress made to date and the expected next steps. The opening budget for the CCG is presented for approval for audit purposes (appendix D).
2. 2022/23 Planning Guidance Summary 2.1 Planning guidance for 2022/23 was issued on 24 December 2021 and updated on 22
February. The detailed guidance document can be accessed via the following link 2022/23 Priorities and Operational Planning.
2.2 The main priority areas highlighted in the document are similar to those issued in 2021-22, with the introduction to the document explaining:
In 2022/23 we will continue to rise to the challenges of restoring services, meeting the new care demands and reducing the care backlogs that are a direct consequence of the pandemic. While the future pattern of COVID-19 transmission and the resulting demands on the NHS remain uncertain, we know we need to continue to increase our capacity and resilience to deliver safe, high quality services that meet the full range of people’s health and care needs. We will: • accelerate plans to grow the substantive workforce and work differently as we keep our
focus on the health, wellbeing and safety of our staff • use what we have learnt through the pandemic to rapidly and consistently adopt new
models of care that exploit the full potential of digital technologies • work in partnership as systems to make the most effective use of the resources available
to us across acute, community, primary and social care settings, to get above pre-pandemic levels of productivity as the context allows
• use the additional funding government has made available to us to increase our capacity and invest in our buildings and equipment to support staff to deliver safe, effective and efficient care.
2.3 Section 4 of this report introduces the Narrative Plan and sets out the main areas covered. 2.4 The December version of the guidance formally announced the delay in the establishment
of Integrated Care Boards until July, a date which has more recently been confirmed following Royal Assent to the Health and Care Bill. For the purposes of planning, most of the work has been constructed on a Suffolk and North East Essex ICB basis, where the plans differ from this indication has been given in the relevant sections.
3. Process and Timetable 3.1 As discussed at the last meeting, the submission date for the 2022/23 plan was 28 April.
This deadline was achieved by the system.

Page 3 of 27
3.2 At the time of writing the report, we have been made aware by NHSEI that the current financial submissions will not be the final ones, however information on changes which will be required and the timetable for submission have not been confirmed. An update will be provided at the meeting.
4. Suffolk and North East Essex Narrative Plan (Appendx A)
4.1 As part of the 2022/23 Priorities and Operational Planning Guidance submission, a
narrative plan setting out the system approach to achievement was developed. A copy of this document has been included as appendix A, which is a single system level template covering the actions and assumptions that underpin the trajectories within the activity and workforce numerical submission and other critical actions that systems will take to address the priorities set out in the 2022/23 operational planning guidance, including elective recovery.
4.2 The narrative plan sets out priority actions to be taken forward to support delivery of the
planning objectives and by exception, any key areas of concern and emerging risks associated with delivery, including any proposed mitigation to be taken forward. The plan covers the following elements which were requested by NHSE:
• Health Inequalities - Maintain focus on preventing ill-health and tackling health inequalities.
• Invest in our workforce – with more people and new ways of working, and by strengthening the compassionate and inclusive culture needed to deliver outstanding care.
• Maximise elective activity and reduce long waits, taking full advantage of opportunities to transform the delivery of services.
• Complete recovery, to improve performance against cancer waiting times standards.
• Diagnostics to outline the priority actions your system will be taking to increase diagnostic activity to a minimum of 120% of pre-pandemic levels across 2022/23 to support these ambitions and meet local need.
• Urgent and emergency care- keeping patients safe and offering the right care, at the right time, in the right setting. This needs to be supported by creating additional beds, in particular through expansion of virtual ward models, and includes eliminating 12-hour waits in emergency departments (EDs) and minimising ambulance handover delays.
• Transform and build community services capacity to deliver more care at home and improve hospital discharge.
4.3 The Narrative Plan is attached at appendix A. 5. Activity & Performance Plan (Appendix B)
5.1 The planned levels of activity and trajectories for performance for 2022/23 are shown in appendix B. There is an expectation that activity levels, particularly for elective care, will increase to exceed 2019/20 levels and deliver a sustained reduction in the number of patients waiting more than 18 months for treatment.
5.2 The Narrative Plan (appendix A) provides information on the assumptions made for
delivery of the key targets including elective and cancer waiting times, urgent care delivery and mental health services. It also sets out the actions being taken in each area.
6 Workforce Plan (Appendix C) 6.1 The Narrative Plan contains a section which sets out the context and actions planned for
the workforce in 2022/23. The technical workforce plan (appendix C) shows an increase in establishment of 5% with a more 2% increase in total workforce numbers by 03/23.
Page 4 of 27
6.2 The narrative includes information on the ‘One Workforce’ approach which is being adopted
across the system, included supporting the existing workforce, belonging in health and care, new ways of working and growing for the future.
6.3 Triangulation between the activity, workforce and finance numbers has taken place as part
of the process. 7. Financial Plan and Budget (Appendix D) 7.1 The NHS commissioning elements for 22/23 are being constructed as a single plan for the
Suffolk and North East Essex Integrated Care Board, from which the relevant CCG elements will be extracted for the months prior to the ICB formation. The expenditure made by the CCGs will be matched with allocation from the full year ICB funding such that the CCG element will be shown as a balanced plan; any surplus or deficit will fall into the combined ICB in the latter part of the year.
7.2 Appendix D contains a summary of the system financial plan for 2022/23 as it currently
stands and the corresponding CCG budget for the period April-June 2022. The CCG opening budget, which will be balanced by allocation, has been approved by the finance committee (NEE) and Collaborative Committee (IES & WS).
7.3 Full year plans have been produced for the mental health elements of expenditure as
covered by the Mental Health Investment Standard, these demonstrate that the standard will be achieved in 2022/23.
7.4 Further work is expected on financial plans as recognition of the additional costs associated
with increased inflation and Covid-19 patients during April and May is considered at a national level. This is expected to be concluded during June allowing the ICB budget to be signed off by the relevant ICB committees. The Governing Body as asked to delegate final changes to the CCG budget to the finance committees.
8. Recommendation
The Governing Body is requested to 8.1 Approve the following plans subject to final changes
• Narrative Plan (appendix A)
• Activity & Performance plan (appendix B)
• Workforce Plan (appendix C)
• Opening CCG Budget (appendix D) 8.2 Delegate any final changes to the finance committee.
Appendix A
(instruction sheets summarised)
2022-23 priorities and operational planning
Narrative Submission Template SNEE ICS Version 1.1 28 April 2022
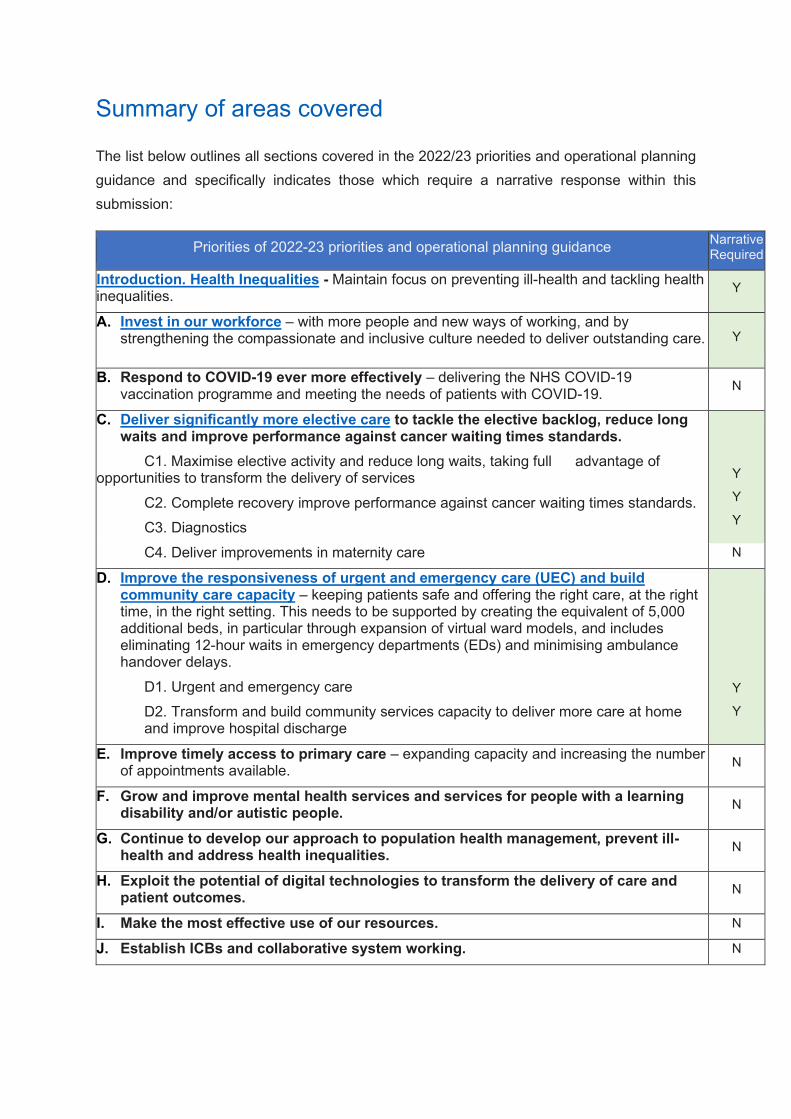
Summary of areas covered
The list below outlines all sections covered in the 2022/23 priorities and operational planning guidance and specifically indicates those which require a narrative response within this submission:
Priorities of 2022-23 priorities and operational planning guidance Narrative Required
Introduction. Health Inequalities - Maintain focus on preventing ill-health and tackling health inequalities. Y
A. Invest in our workforce – with more people and new ways of working, and by strengthening the compassionate and inclusive culture needed to deliver outstanding care. Y
B. Respond to COVID-19 ever more effectively – delivering the NHS COVID-19 vaccination programme and meeting the needs of patients with COVID-19. N
C. Deliver significantly more elective care to tackle the elective backlog, reduce long waits and improve performance against cancer waiting times standards.
C1. Maximise elective activity and reduce long waits, taking full advantage of opportunities to transform the delivery of services
C2. Complete recovery improve performance against cancer waiting times standards. C3. Diagnostics
Y
Y
Y
C4. Deliver improvements in maternity care N
D. Improve the responsiveness of urgent and emergency care (UEC) and build community care capacity – keeping patients safe and offering the right care, at the right time, in the right setting. This needs to be supported by creating the equivalent of 5,000 additional beds, in particular through expansion of virtual ward models, and includes eliminating 12-hour waits in emergency departments (EDs) and minimising ambulance handover delays.
D1. Urgent and emergency care D2. Transform and build community services capacity to deliver more care at home and improve hospital discharge
Y
Y
E. Improve timely access to primary care – expanding capacity and increasing the number of appointments available. N
F. Grow and improve mental health services and services for people with a learning disability and/or autistic people. N
G. Continue to develop our approach to population health management, prevent ill-health and address health inequalities. N
H. Exploit the potential of digital technologies to transform the delivery of care and patient outcomes. N
I. Make the most effective use of our resources. N
J. Establish ICBs and collaborative system working. N

System name: Suffolk and North East Essex ICS
Introduction - Health Inequalities - Maintain focus on preventing ill-health and tackling health inequalities by redoubling efforts on the five priority areas for tackling health inequalities set out in guidance in March 2021. ICSs will take a lead role in tackling health inequalities, building on the Core20PLUS5 approach introduced in 2021/22 to support the reduction of health inequalities experienced by adults, children and young people, at both the national and system level.
Please outline priority actions, assumptions, risks, issues and associated mitigation. Please refer to guidance on the five priority areas and Core20PLUS5 approach to support your response. Actions
Five priority areas Priority 1: Restore NHS services inclusively Health Inequality Improvement funding is supporting the development of comprehensive Equalities and Health Inequalities Impact Assessments (EHIIAs) for all our major programmes. Our first priority area has been elective care recovery, and also, we are developing EHIIAs for maternity, SMI, COPD, cancer and hypertension. These live assessments will inform co-produced action planning to tackle inequalities, and will be live documents, updated as we continue to learn about the impact of the pandemic on groups and communities. The template used includes an action plan with identified mitigations and prioritises these. This approach builds on learning from our Covid19 Vaccination programme. Resources have been shared on our ICS website Covid-19 Vaccine Programme - Suffolk & North East Essex Integrated Care System (sneeics.org.uk) Our Community Ambition programme has invested funding from NHS Charities Together in projects led by grassroots minority ethnic organisations co-producing new solutions to addressing inequalities. Areas include understanding community health needs, culturally competent maternity and mental health services, and healthy lifestyles. Linking these communities to statutory services and strategic forums has enabled these groups’ voices to be heard across our system. A task and finish group, supported by Healthwatch in Suffolk and Essex, will explore improving accessibility to health and care services for people across a wide range of communication needs including language, sensory impairment, and marginalised groups.
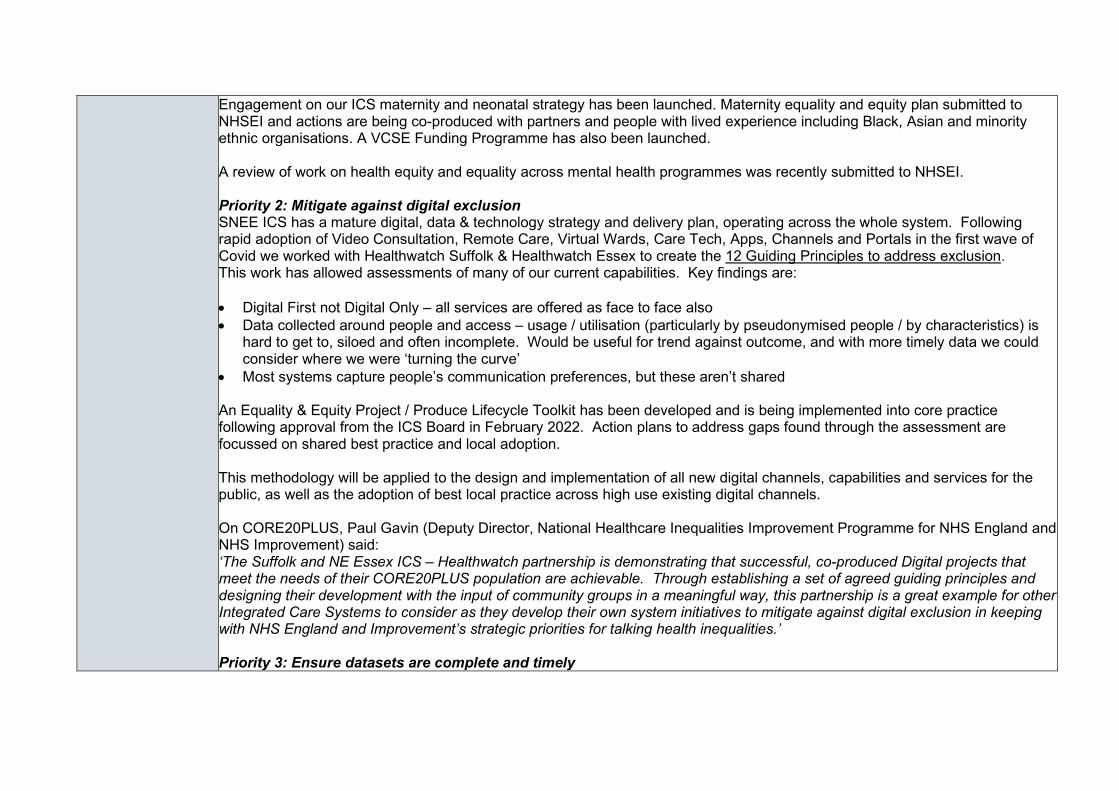
Engagement on our ICS maternity and neonatal strategy has been launched. Maternity equality and equity plan submitted to NHSEI and actions are being co-produced with partners and people with lived experience including Black, Asian and minority ethnic organisations. A VCSE Funding Programme has also been launched. A review of work on health equity and equality across mental health programmes was recently submitted to NHSEI. Priority 2: Mitigate against digital exclusion SNEE ICS has a mature digital, data & technology strategy and delivery plan, operating across the whole system. Following rapid adoption of Video Consultation, Remote Care, Virtual Wards, Care Tech, Apps, Channels and Portals in the first wave of Covid we worked with Healthwatch Suffolk & Healthwatch Essex to create the 12 Guiding Principles to address exclusion. This work has allowed assessments of many of our current capabilities. Key findings are: • Digital First not Digital Only – all services are offered as face to face also • Data collected around people and access – usage / utilisation (particularly by pseudonymised people / by characteristics) is
hard to get to, siloed and often incomplete. Would be useful for trend against outcome, and with more timely data we could consider where we were ‘turning the curve’
• Most systems capture people’s communication preferences, but these aren’t shared An Equality & Equity Project / Produce Lifecycle Toolkit has been developed and is being implemented into core practice following approval from the ICS Board in February 2022. Action plans to address gaps found through the assessment are focussed on shared best practice and local adoption. This methodology will be applied to the design and implementation of all new digital channels, capabilities and services for the public, as well as the adoption of best local practice across high use existing digital channels. On CORE20PLUS, Paul Gavin (Deputy Director, National Healthcare Inequalities Improvement Programme for NHS England and NHS Improvement) said: ‘The Suffolk and NE Essex ICS – Healthwatch partnership is demonstrating that successful, co-produced Digital projects that meet the needs of their CORE20PLUS population are achievable. Through establishing a set of agreed guiding principles and designing their development with the input of community groups in a meaningful way, this partnership is a great example for other Integrated Care Systems to consider as they develop their own system initiatives to mitigate against digital exclusion in keeping with NHS England and Improvement’s strategic priorities for talking health inequalities.’ Priority 3: Ensure datasets are complete and timely
The ICS collects and analyses ethnicity data from a range of national datasets covering secondary care, mental health and community services. We are currently starting a programme to extract a range of data from primary care which includes ethnicity data, as part of our PHM programme. We will be able to regularly review the quality and accuracy of ethnicity and other data recording. There is an ICS elective recovery dashboard that also reviews the current waiting list by Age, Gender, Ethnicity and Deprivation. When a national dashboard is available, we will also link in our local datasets. ICS has adopted Outcome Based Accountability across the ICS training in excess of 700 people. We have linked this methodology to our work around Population Health Management. We are now further developing these approaches to inform the way that we can monitor progress at system and place linked to the development of JSNAs/JHWS in both Essex and Suffolk. We have also been part of a comprehensive review of the role of HWBBs in both Suffolk and Essex and how they will align to the ICP. Priority 4: Accelerate preventative programmes that proactively engage those at greatest risk of poor health outcomes We continue to work to identify and tackle inequalities in the Covid-19 vaccination programme. Our dedicated vaccination website is translatable and includes multi-lingual resources, and we have used diverse community-based resources to inform people about vaccination. Mobile units reach into deprived and marginalised communities, taking the opportunity to offer other health prevention services too. Staff and volunteers have guidance on adjustments, and we monitor vaccine uptake by geography and ethnicity, as well as people’s satisfaction with their experience. More detail is available here. Through our Community Ambition programme, the Bangladeshi Women’s Association of Essex is completing a unique health needs assessment of its community. This will be published in June 2022 and shared locally and regionally to help us tackle health inequalities in South Asian communities. SNEE ICS has a well-established Population Health Management Steering Group, which continues to oversee the ongoing development of our PHM Strategy over time as PHM evolves nationally. We recognise the need to work differently, including the tools and intelligence to utilise prevention. SNEE ICS encompasses complementary work in this field from the Suffolk Office for Data Analytics in linking and sharing data on the wider determinants of health, and the equivalent organisation in Essex (ECDA) also now exploring similar approaches enabling us to take PHM forward in its fullest sense. We have historically explored two different approaches to PHM over recent years. This means we have a unique insight into some of the different ways of approaching PHM. We are working towards planning how we harness and exploit the progress made across the ICS in order to meet the national requirements; agreeing and writing a plan by June 2022 which will put in place the systems, skills and data safeguards that will act as a foundation for PHM; and by April 2023 to have longitudinal linked data available covering the entire

ICS, to enable PHM analytics to be used to redesign care pathways and measure outcomes, with a focus on improving access and health equity for underserved communities. The NHS and both County Councils are collaborating to commission a review of the business case for further development of local weight management resources building on thinking from a recent ICS event on this theme For information on CORE20PLUS5 initiatives, please see below. Priority 5: Strengthen leadership and accountability Our SRO Dr Ed Garratt and the wider ICS Partnership Board has oversight of health inequalities, and each of our programmes has responsibility and accountability for tackling health inequalities within its remit. Data from the Public Health Outcomes Framework has been integrated into our ICS strategy for some time. Our ICS Five Year System Strategic Plan includes these measures throughout and they are included in our ICS strategy on our website. HEPP and Health Inequality Improvement funding has been used to develop our Health Equity workshops, which have been delivered to over 200 people in our system, and encouraging and supporting 100 day challenges. Our Anchor Institutions programme is currently developing a dashboard to evaluate progress against our Charter aims, which include recruiting, commissioning and procuring locally that can directly benefit people who live with discrimination and disadvantage, and deprived communities. Our Social Value and Community Microenterprise project, funded by NIHR, is now operational in North East Essex. Our ICS progress on VCSE development has been identified as an area of good practice. Key developments include plans for a VCSE Assembly and Chair, development of a VCSE Resilience Charter, and a VCSE Workforce review. The Secretary of State for Health held a roundtable with local VCSE leaders on 14 February 2022 to hear about this work. System learning is shared on our ICS website including: • Our film competition sharing lived experiences and two events on the theme of ‘How do we help everyone heal?’ • Our ‘Thinking Differently Together’ events explore a wide range of issues through different perspectives; our publications are
here. Written reports of all events, with recommendations, are considered by our ICS Board and associated action plans taken forward e.g. ICS suicide prevention and trauma informed practice training across the ICS.
Those with lived experience who presented within all these events have continued to influence our strategic approaches.
To support the measuring of our impact, we have adopted Outcome Based Approaches across our ICS, training in excess of 700 people. We are now further developing these approaches to inform the way that we can monitor progress at system and place linked to the development of JSNAs/JHWS in both Essex and Suffolk. CORE20PLUS5 Plans are in place for the five target areas, with accountability through the relevant programme boards and ultimately through the ICS Board. The following approaches will be taken to work towards achieving the five targets:
• Maternity: Continuity of carer plans are being finalised to roll out teams in areas where Black, Asian and Mixed ethnic groups and people living in deprived areas are prioritised. Maternity continuity of carer (MCoC) rollout plans have been submitted to NHSE. All provider plan ambitions are to achieve MCoC for 100% of the population by 2024. Initial teams will focus on areas of need/deprivation. Whilst MCoC is mobilised the LMNS has commissioned voluntary sector partners (including AFiUK) to deliver a maternity focussed community ambassador model within our most diverse communities. Commencing in April 2022 the schemes will empower women by educating them about the maternity pathway, helping to understand terminology used, explaining services, and use advocacy to help them access services and ensure they are personalised to their needs. They will also address wider determinants of health such as housing, domestic abuse, and financial hardship; and also educate our teams to be more culturally aware. We will bring the organisations together every three months to share learning and strengthen the networks between our VCSE organisations and maternity/health visiting colleagues. This will support trust between communities and professionals, support system wide roll-out of learning, and help people to access the right help when they need it and to make our services more inclusive to our communities’ needs. April 2022 May 2022 June 2022 Sept 2022 December 22 Feb 2023
VCSE organisations confirm scope and model of delivery. Training provided to community ambassador on pregnancy pathway, services available, key contacts etc. Schemes commence within communities Network meeting and review of initial learning Coproduction event to bring together learning to date and develop sustainable models of support Network meeting and review of initial learning and forward view to 23/24 Celebration event
Alongside voluntary sector partners the LMNS hosts monthly health inequalities meetings which bring together a wide range of VCSE organisations across the ICS footprint.
• SMI: Increasing health checks and supporting access to post-check interventions that have been identified for people with Severe Mental Illness by collaboration with primary and secondary care and VCSE organisations to remove barriers, and with the Covid vaccine programme to combine health checks and vaccination in the same appointment where appropriate.
Through joint working, outcome measures will be developed and monitored to understand and improve life expectancy. Our target is to increase the numbers of people on GP SMI registers receiving a physical health assessment in the last 12 months from 2,572 in Q1 of 2022/23 to 3,448 in Q4, which will enable us to meet the 60% target by Q4.
• COPD: Plan towards population health management approach to identify groups of patients at risk and areas of deprivation. We have begun a data review of the uptake of vaccinations by people with COPD in areas of deprivation, which will be complete by the end of April 2022. Collaboration with primary care and our key partners will identify actions and areas of improvement to address health inequalities in areas of deprivation by the end of May 2022. The plan will be agreed, and monitoring will be in place through the ICS Respiratory dashboard, and a CORE20PLUS5 pilot will be launched by the end of November 2022. Community spirometry service that is being developed will determine early diagnosis for COPD and treatment.
• Cancer: The SNEE cancer programme will explore a population health management approach to increase the uptake of screening opportunities across our communities. We will support earlier identification of Lung Cancer, Targeted Lung Health Checks will be mobilised in our most deprived ward, the pathway will be co-produced to maximise uptake. We will produce outcome data from the last two years to identify and develop plans to support those specialties and communities whose outcomes have been impacted by the pandemic. We are working with the Cancer Alliance data team on outcomes and have held a workshop in March with our Public Health teams to look at cancer survival and population health data. These plans are currently being finalised and will be launched in Q2. We are developing services closer to home, including in our more deprived areas of Clacton, Ipswich East and Forest Heath, which will commence from Q3 onwards. More detail is available in our Cancer Delivery Plan.
• Hypertension: We are working with the Eastern Academic Health and Science Network (EAHSN) to implement the UCLP Proactive care@HOME framework for Blood Pressure. The risk stratification tools will support our PHM approach to case finding and the overall Blood Pressure Optimisation (BPO) programme, and work will also be undertaken with Pharmacies to case find. The ongoing BP@HOME programme supplies free blood pressure devices to patients to help them to self-care. Data from the online CVD Prevent dashboards can be used to identify those patients who are not engaging with CVD related health services. Digital patient information decks provided by Liberate Pro are being developed to support patients identified with hypertension providing information on the condition and how to manage it in a clear and concise manner. The following milestones are planned for 2022: May/June - Gather CORE20 data – 20% most deprived across SNEE May/June - Gather PLUS data – SNEE specific areas such as LD, SMI, digital excluded who may not be part of the CORE20 numbers June - Set up operational group to analyse the data and decide on course of actions including working with the ICS Health Inequality team August/September - Work with community based “African Families” organisation who are commissioned to support Health Inequalities work across SNEE
We have recently been awarded funding to develop CORE20PLUS Community Connectors. We will work in partnership with African Families in the UK to utilise their established Community Ambassador model to recruit and develop volunteers, initially in Colchester and later rolled out across the ICS. We will develop ways in which Connectors can have their voice heard at PCN, Alliance and system levels of the ICS. The project commenced on 1 April 2022; co-production, recruitment and training of Connectors and a coordinator will take place in the coming months with a view to commencing their full roles by September. Development of the ICP from 1 July 2022 will incorporate ways in which Connectors’ voices can be heard as part of its engagement, and we have started to build relationships with the NEE Alliance and local councils so that we can build on existing local champion roles and link our Connectors to their work. We hope to start exploring rolling out the model to other parts of the ICS footprint in Q4 of 2023. Personalised care Literacy and consumable information are key to My Planned Care and PIFU being successful and as part of our Personalised Care and Health Inequalities programmes we are engaging with our patient representatives, community engagement partnerships and VCSE to ensure that we are co-producing plans with our communities and that they have equity in access through tailored, target consumable information and support. Our ICS Personalised Care Strategy’s inequalities, Patient Choice, Shared Decision Making, Social Prescribing and personalised care and support plans workstreams will have a key role in taking forward this work supported by comms, marketing and workforce enablers. Plans are in place as part of the ICS wide Personal care and support plan workstream to identify unmet need with proactive case-finding and collaboration across acute, primary care and VCSE as part personalised care approaches and partnership working. During 22/23 there will be further roll out of personal care and support plans across care pathways and commissioned services and we are embedding this requirement as part of contract and commissioning approaches with our statutory and VCSE providers. Each Alliance has been accelerating personalised approaches to follow-up care in hospitals for patients on Discharge to Assess pathways 0 and 1. The ‘Welcome Home’ Programme, established over winter 2021/22 will further enhance and support the patient pathway process when people are admitted to Ipswich Hospital’s Emergency Assessment Unit (EAU), Surgical Assessment Unit (SAU) and Trauma & Orthopaedics (T&O). The Welcome Home team follows through the journey of the patient in hospital up to and including discharge and onward referral to the community based Connect for Health Social Prescribing service and our multi-cultural social prescribing service. The 7 day a week service model comprises three WTE social prescribing ‘Advice and Support co-ordinators’ managed by Citizens Advice Bureau who provide additional support and capacity to the existing discharge pathway in place by undertaking personalised care and support planning at ward level with the patient, their family, carers and staff during their hospital stay as
part of an enhanced holistic MDT approach. As part of Welcome Home, one-off Personal Health Budgets (PHBs) will be available to provide people with the support they need to leave the hospital safely and to help meet their health and wellbeing needs and outcomes in line with their personalised care and support plan. For more information on inequalities in elective recovery please see below. Learning Disabilities and Autism Specific actions are being prioritised taking learning from Learning Disability Mortality Reviews (LeDeRs), to tackle the inequalities experienced by people with a learning disability. These are: • Learning Disabilities GP Registers to include people with a learning disability aged 14+ - ongoing review of GP Practice
registers with annual cleanse and update • Develop a practice level Physical health Risk register linked to an overarching Risk Register - this work has been included in
the Learning Disability Register Deep Dive. NSFT have recruited a member of staff to undertake the GP Register Deep Dive. Project working group has been established
• Implementation of RESTORE 2™ Mini tool that will help Carers to identify the early signs of deterioration in people with a learning disability
• Improved Uptake of Annual Health Checks - Peer Educator Network programme funded for a further year (22/23) delivered by ACE Anglia to increase the awareness of LD health checks to people with a learning disability
• Social Prescribing and Personal health Budgets linked to Annual Health Checks Project – development of easy read materials, development of social prescription pathway, Grandpads in use for people with LD, social prescription guide, training for social prescribing link workers in meeting the needs of people with LD
• Quality of Annual health Checks – Development of LD friendly GP practice pilot • Reasonable Adjustment manual and awareness – RA manual been implemented within NSFT. RA plan being developed for
system-wide implementation • Improve awareness of screening and immunisation programmes – identification of people requiring screening and
immunisations, review of decision to cease screening, training and education, communications between services, enabling support for people with LD
Dentistry Our CCG’s have been working closely with NHS England to identify areas of inequality and concern and have agreed a number of actions to support dentistry:
1. Weekend working across Suffolk and North East Essex from February – July 2022. 2. Prioritising Looked After Children for access to dentistry care – Completed in March 2022. 3. NHSE Directly engaging with dental providers for dentistry services in areas that cannot current get easy access to dental
care e.g. Leiston by August 2022.

4. Creating a 10% change in the contract to allow for unknown urgent cases to be seen. A number of other projects are being scoped out and implemented which include:
1. Dental Care education in Care homes 2. Commissioning an Urgent Dental Access Centre 3. Working with HEE and University of Suffolk on training and education. 4. Working with the ICS IT Team on how dental providers can link in with IT. 5. Paediatric dental education.
In addition, an Equalities and Health Inequalities Impact Assessment will be completed in relation to dental issues and barriers to accessing services, during 2022/23. This will place us in a good position to tackle inequalities from the outset of the delegation of dentistry commissioning to ICBs from April 2023.
Assumptions Our aim is not only to tackle historical and emerging inequalities, but also to work towards health equity for all our people and communities. Achieving this depends on: • Strategic leadership to ensure all partners are committed to health equity, and able to provide direction and allocate resources • The gathering and analysis of accurate and complete data, and the use of that data to inform our commissioning and activity • The right knowledge, skills, resources and professional confidence throughout the workforce to contribute individually and
collectively to our aims • Effective oversight and governance to lead and monitor progress, and to manage risks and issues as they arise • The deployment of all appropriate levers to progress our ambitions
Risks, issues and mitigation
Data quality: We know that recording of ethnicity of the people who use our services is not complete, and that population data is derived from the 2011 census, which inevitably impacts on our data quality and analysis. Regular review of recording in our datasets, and our programme to improve data in primary care, will support mitigation of this issue. A framework for accountability will be developed to ensure individual providers (including general practice), PCNs, Alliances and system level ICB can drive improvements in data collection and analysis, using levers as appropriate to ensure the standards we want to achieve are met. Operational pressures: A risk to all our equalities work is the limitations on capacity that arise from the significant operational pressures that we face, in particular the challenges for our providers over winter and the shortages of key skills in certain areas of the workforce. These pressures may impact not only on recovery of services but also data collection and management, and progress on our wider ambitions at PCN, Alliance and system levels. We will continue to monitor closely the impacts on progress across all our programmes including using data and PHM tools. We will also respond in an agile way to develop solutions collaboratively to enable us to minimise impacts as they emerge to continue to move towards our ambition of health equity.

System name: A. Invest in our workforce – with more people and new ways of working, and by strengthening the compassionate and inclusive culture
needed to deliver outstanding care. Please summarise the key assumptions that underpin the numerical workforce plan submissions, highlighting any key risks and issues. Submissions should set out any system actions that are critical to the delivery of the planned workforce levels including recruitment and retention, use of bank and agency, redesign of teams and roles, deployment across sectors and/or organisations and sickness absence. Please ensure the workforce plan underpins the activity levels assumed within the wider planning submission. SCDS for ambulance, acute, community, mental health and specialist trusts including high level detail for primary care. Assumptions System 22/23 forecast
• Although the plan shows an increase in establishment of 5% (970WTE) there is a more modest 2% increase in total workforce numbers by 03/23 (393.3WTE).
• There is a 9% decrease (-129WTE) in bank work, but what appears to be at first a 50% (83.9WTE) increase in agency workers. This increase happens from March 22 to April 22 (80 WTE)
Acute Setting • Nursing shows a 3% increase (168WTE) which is in-line with flow projections of 4.6% for 22/23. • Clinical Support will see a 4% increase (201WTE) of which EEAST accounts for 43% of this due to apprentice
students some of which will eventually convert to Technicians which is below the flow projections of 8.4% and realistic in terms of the high numbers of leavers, although retention is one the key SNEE objectives.
• Medical and Dental will see a projected 6% growth (105wte) from March however the main increase is in April due to converting Bank/Agency into permanent staff. From April onwards there is a 3%(WTE) increase which is in-line with projected supply.
East of England Ambulance Service • An area of concern is the -4%(-100WTE) growth in registered ambulance staff, the gap is to be filled with
overtime while apprentice students are in training, however there will be a 2.2% increase (100WTE) increase in overall EEAST staffing, which if EEAST reduce abstraction rates would facilitate some improvement in operational performance.
• EEAST’s workforce plan is based on the HEE pipeline and a pragmatic long-term solution to the paramedic supply issue, by keeping recruiting to junior levels and for EEAST to grow their own.
Primary Care • In primary care the workforce there are aspirational plans to recruit 85.6 GP’s, but the key is ensuring we retain
and replace leavers, hence the GP workforce numbers remaining stable.

• There has been a decrease in nursing staff in primary care last year and we are working to arrest that decline. In ARRS funded roles we see an increase of 40%, which although is ambitious, this will be partly made up of increasing the hours of the non-ARRS funded staff with ARRS funded hours.
KPI Workforce Turnover • Turnover projections for SNEE at first glance are ambitious, however EEAST and WSFT both have shown low
turnover over the last three year on average below 10%. • ESNFT have a particularly high turnover in comparison at an average of 13%. • EEAST and WSFT should on average be able to achieve their Turnover rate. ESNFT rate is ambitious even
with their retention plans. KPI Sickness Absence
• The projections are an area of concern with an average of 7.5% sickness absence of which the two acutes have a 5% rate. When we look at current data trends non-Covid related sickness absence has remained static however Covid related absence accounts for an extra 40% of sickness absence over the months February, March, and April.
Please see Appendix 1 for supporting data Please see Appendix 2 for EEAST supporting data
Actions Suffolk and North East Essex ICS support providers across health & care with integration and 'one workforce' methodology. We will endeavour to have the right workforce, with the right skills and behaviours, in the right place at the right time within cost, working together in a compassionate and inclusive culture, helping to make the local area a better place to live and work. This will include aligning the transformation of workforce with digital, service, finance, estates and the innovations led by the AHSN and HEIs. The focus will be through the lens of the People Plan and the 10 outcomes-based functions to ensure the workforce are at the centre of the collective ambition. Looking After Our People (See Appendix 3) We believe that our people are our most important asset, they must feel safe, supported and able to maintain a healthy work-life balance. There are a wide range of initiatives at both system and organisational level to ensure staff wellbeing, improve staff retention and to deal with the current cost of living crises. These include:
• The co-production of a Health and Wellbeing Strategy, overseen by the Health and Wellbeing Collaborative Group (chaired by VCSE representative)
• Enhanced Occupational Health including long Covid, Menopause Support and fast-track physiotherapy services as well as procurement of a system-wide OH consultant.
• Enhancing our portfolio of Psychological and Wellbeing Support Services including the launch of My Health My Way and close working with the UoS Institute for Health and Wellbeing.
• Implement a response to the five priorities of the women’s health strategy for staff • To develop a retention plan looking at flexi-working and based on evidence from the learning from the NHS Flex
programme currently being undertaken by ESNEFT • To co-produce and launch the Violence and Aggression Reduction Plan • To continue to work with the ICS Estates colleagues to enhance our system wide Key Worker Housing Project • To support staff with the rising cost of living, by working with Foodbanks for health and social care staff to have
dedicated food bank time slots and finance education and support webinars. Belonging in Health and Care (Appendix 4) It is not enough for any Health and Care system to be non-racist it must be anti-racist. We recognise the need and benefit in championing a racially diverse workforce. Around 5.5% of the SNEE population is minority ethnic, compared to 15% of our workforce. However, at Band 8 and above this drops to just 7%. We know that this is not good enough. We will improve racial equality, diversity, and inclusion so that the system reflects the communities it serves.
• The SNEE ICB have signed Unison’s Anti-Racism Charter and will be encouraging and working with system colleagues to do the same
• An EDI Strategic Lead for workforce has been appointed (jointly with ESNEFT) • An ED&I Strategy will be co-produced in line with the Anti-Racism Charter • Inclusive recruitment training has been rolled out within the ICB during 22/23 • Leadership & Culture Workshop to be organised (Spring’22) – associated strategy/plan to be produced • Expanding Restorative Just and Learning Culture Model (Mersey Care) • Developing a Framework for Clinical and Professional Care Leadership
New Ways of Working and Delivering Care (Appendix 5)
We will continue to positively transform the way in which the community we serve receives it care from a workforce that can meets current and future demands innovatively.
• The Strategic Education Transformation Lead will co-produce a strategic plan with providers including innovations to increase and expand clinical placement capacity and develop a Strategic Education Collaborative Group incl. HEIs to reforming clinical education
• To work in partnership within the SNEE System to develop a “one workforce” integrated plan across health and social care to develop a sustainable workforce that is able to meet the present and future health demands of the Suffolk and North East Essex population.
• The recently established Productivity, Finance and Activity Group will review productivity against workforce and bank/agency spend and then establish productivity interventions in-line with the financial envelope such as better digital rostering, skill mix etc.
• A Dental Working Group (working with HEE Dental Dean) has been established to increase the number of dental staff and practices within the system, which is currently chronically understaffed leading to members of public doing their own dental work. The system is looking at establishing innovative solutions to this.
• The Medical Workforce Collaborative Group (chaired by Associate Post Graduate Dean, HEE) are creating a workforce plan that will focus on a joint approach to International Recruitment, Education Governance, F1 to Consultant career pathway and plans for ‘local’ recruitment
• Working with the Physician Associate Ambassadors to develop a system plan for growing and developing Physician Associates across primary, secondary care and mental health
• The Pharmacy Workforce Collaborative Group (chaired by Chief Pharmacist, ESNEFT) are creating a workforce plan that will focus on cross sector placements, portfolio careers, education support and career development
• The SNEE ICS Reservist Model is being launched in Q1 22/23. The Reservists will work with our system partners (acutes initially) to help services during peak times and emergencies e.g. winter pressures, Covid vaccinations programmes. Year three students will be actively pursued to be part of the programme and then retained when qualified.
• The system is establishing a new roles group to scope and co-ordinate the delivery of several workstreams relating to new roles to avoid duplication across the system (examples include introduction of anaesthetic associates, pathology and cancer.)
Growing for the Future

We believe that the workforce of tomorrow needs to be planned today. We continue to look at attracting local, diverse, and exciting staffing groups to meet the health and social needs of the community we serve.
• The Nursing, Midwifery and AHP Workforce Programme has been established to co-ordinate the delivery of several workstreams relating to the recruitment (including the 50k Nurse Manifesto), retention, and continued professional development of Nurses, Midwives, and Allied Health Professionals across the system footprint. Several pre-existing projects relating to the Clinical Workforce (i.e. Cancer Workforce, CYP Workforce, Pharmacy, Paramedics etc) will feed into these workstreams to avoid duplication across the system.
• The SNEE ICS Health and Care Academy programme will continue to open the eyes of young people to the variety of health and care jobs on offer across the system. The Academies will give young people the opportunity to see what health and care professionals do, to learn some essential life skills, work as a team, solve problems and find out more about what they are interested in.
• The Training Hub – plans to increase student placements, educators, trainers and assessors – working collaboratively on the ARRS to expand workforce
• We will continue to work with system colleagues on the Anchor Programme to show how the local health and care providers can make neighbourhoods healthier, happier and greener. The health and care sector are one of the largest employers in the system, and this programme will enable us to understand better how health and care providers can use their assets and influence to bring about wider positive changes such as local recruitment, apprenticeships, sustainability and helping to address inequality
• Working with providers to increase the numbers of GMTS accessing the scheme • Develop a Leadership and Talent Management Strategy incl. careers coaching service • The implementation of the Medical Applicants Programme which will help young people get the support they
need to apply for Medical School. • Co-ordinate the International Recruitment of workforce across the system • Continue to work with the Integrated Care Academy on Workforce Transformation Training and Development
opportunities and supporting the research and innovation programmes. • We are focusing on an Integrated Care Apprenticeship, which will strengthen the working partnerships between
health and care to support the ‘one workforce’ approach. A system working group is overseeing the progress of this

Risks, issues and mitigation
• Demand on health and care remains high: The back log of activity, continuing pressures on the system and the expectations of both government and public are having an effect on our workforce. This will lead to burnout which will see an increase in sickness absence, turnover and a loss of productivity. To mitigate this we have initiatives as outlined above under “looking after our people”, but our key message is that we are dedicated to ensuring that the system looks at work life balance, creating a flexible working environment that allows staff to truly rest and recuperate.
• The effects of Covid on retention and sickness: Although society and therefore the system needs to “learn to live with Covid” the effects it has had and will continue to have on retention and absence must not be underestimated. Staff can test positive for Covid and be asymptomatic but not test negative for 10 days plus, therefore effecting short term sickness absence, our organisations in the system are looking at how we can address this. There is a great deal of work going into the study of long Covid and its effects, we are currently developing a systemwide approach.
• Turnover: Although turnover has been relatively low in some areas it is seeing a rise within the system at 12.5% (although this is in line with seasonal variations in 2018 & 2019). The areas of concern are that 40% plus of leavers month on month are under the age of 35 and within staff groups in particular care support workers which is at 17.3% turnover and we have 7 FTE less primary care nurses in March 22 compared with the March 21. The system is looking at the work ESNFT has undertaken by recruiting two retention specialists and making the project system wide. The is a co-produced system retention strategy in development and there are also numerous system level projects to look at retention in specific staff groups including CSWs.
• Cost of living impact on the health and care workforce: Inflation is likely to be a minimum of 8% and system cost of living raise is likely to be only 3%, which will lead to retention and sickness absence issues. Although this is a national issue the system has as outlined above looked at what support it can provide to staff. This includes key worker housing, food banks and finance education and support seminars.
• Bank and Agency spend increases: During the planning process it became apparent that in order to mitigate risks and issues such as Bank and Agency spend a Productivity, Finance and Activity Group that can meet to triangulate these issues should be convened. This will allow the system to identify areas of risk and put it place support where necessary.
The actions we propose above will have robust project plans (if not already) including key milestones and mitigations. The People Board will also become more central to the accountability of delivery and therefore holding each other to account
Appendices:
• Clinical Programme • H&WB Programme • Integrated Planning • Demographics • Supporting information for Board Review
System name: Suffolk and North East Essex ICS
C. Deliver significantly more elective care to tackle the elective backlog, reduce long waits and improve performance against cancer waiting times standards.
C1: Maximise elective activity and reduce long waits, taking full advantage of opportunities to transform the delivery of services
Please summarise the key assumptions that underpin the numerical plan submission for elective recovery, highlighting any key risks and issues and mitigation.
Elective Recovery
Activity - National activity plans must deliver in excess of 104% of pre-pandemic value weighted elective activity levels and systems need to agree their (and their constituent providers’) levels of contribution to this ambition, including going further for those that are able to.
Assumptions Our plans demonstrate that we expect to deliver in excess of 104% of pre-pandemic value weighted activity as a system, as individual trusts and in the independent sector. In reaching this assessment we have made the following assumptions:
• The baseline activity is correct and enables a ‘like for like’ comparison with our out-turn

• That mutual aid between trusts and with the independent sector continues, and expands on, the achievements we have realised in 2021/22
• That there is no material withdrawal of independent sector capacity in favour of seeing private patients • That we complete our work in defining a joint access policy and agreeing what a joint PTL across our system means and
that we enact the conclusions of this work • That funding through the revised ERF scheme is sufficient to enable us to put on the additional sessions and capacity
required • That staffing levels are not significantly impacted due to COVID-19, resulting in elective cancellations • That non-elective activity does not impact on elective ward capacity further than outlined below (we are working on further
mitigations against this) • That increased cancer demand does not deplete our resources (beyond our planning assumptions) to deliver 104% • That Reinforced Autoclaved Aerated Concrete (RAAC) plank remedial work at West Suffolk NHS Foundation Trust (WSFT)
will see a reduction in elective activity in January 2023 where we expect the elective ward to be utilised for UEC • That elective activity levels may be impacted by the absence of separate hot and cold elective facilities at WSFT. This will
be addressed in future years, through the development of the Newmarket site, as described in the actions below. • That the visiting surgeon from Cambridge University Hospitals NHS Foundation Trust (CUHFT) remains available to support
East Suffolk and North Essex NHS Foundation Trust (ESNEFT) to clear Oral Maxillo Facial Surgery waiting lists. Actions Modelling methodologies
We have modelled at specialty level what is needed to deliver 104%. We have then discussed with individual specialties what plans they have to increase capacity and assessed the opportunities and risks. Increasing capacity in 2022/23 Building on the approach taken in 2021/22, work will continue with system partners to meet the national thresholds. Mutual aid has been established and inter-trust specialty specific discussions have progressed well in ENT, gynaecology and orthopaedics. Additional capacity has been sourced with the independent sector (orthopaedics, general surgery, urology, gynaecology, ophthalmology diagnostics) and this will continue in 2022/23. Maximising use of existing capacity through weekend working is being progressed. Further work will be taken to explore insourcing opportunities for ophthalmology, urology and general surgery. Capacity options for OMFS are being explored with CUHFT, Norfolk and Norwich University Hospitals NHS Foundation Trust and within Essex. This is to be finalised in March 2022 to ensure no patients are waiting by end of June. Improved productivity: Getting It Right First Time (GIRFT) and High-Volume Low Complexity (HVLC) Actions

Pathway and productivity gains will continue to be taken forward at speciality level within both ESNEFT and WSFT at system level for Eye Care and Musculoskeletal (MSK) pathways. WSFT A high-level review of WSFT’s pathways was undertaken in June 2021 to understand how closely they met the national Get It Right First Time (GIRFT) 29 High Volume Low Capacity (HVLC) procedures. The review of the GIRFT pathways demonstrated that, whilst there is a good degree of compliance, there are opportunities, either at speciality or generic levels, such as advice and guidance (A&G). Recommendations were prioritised at speciality level and form work plans which each speciality is taking forward. The following initiatives are intended to streamline the patient pathway, to enable improved access, shorter lengths of stay and ensuring patients are receiving care in the right place, at the right time. Examples of these initiatives are provided below: ENT:
• Widening the criteria for day case tonsillectomies • Ambulatory care for epistaxis and peri-tonsillar abscess
Eye care: • Looking at expanding community-based pathways for patients • Service review to identify capacity constraints and the potential for new workforce models • Trialling high volume cataract lists and a deep dive into the pathway to identify productivity improvements
MSK: • Engaging with Primary Care/HCP colleagues to redefine pathways • Preparing patients for surgery – patient optimisation • Post -operative care for inpatients • Increase of day case arthroplasty
Urology
• Bladder outflow obstruction – minimally invasive procedure has been launched in DSU • Bladder tumour resection – day case TURBT established • Ureteroscopy/stent management – working to establish a day surgery procedure
ESNEFT Each of the divisional recovery plans are based on three elements:
• Additional capacity • Transformation • Improvements in productivity and efficiency

A detailed evaluation of East Suffolk & North East Essex (ESNEFT) clinical pathways against GIRFT, was undertaken in May 2021. The 29 High Volume Low Complexity (HVLC) procedures were reviewed across all relevant specialties in both Ipswich and Colchester hospitals. The majority of pathways were compliant to best practice, although the review highlighted some variance in practice across the two ESNEFT sites, some of which are being addressed as part of this process. Those specialties requiring improvement were met with, (clinical, operational and nursing leads), and action plans have been created and are being implemented. We are revisiting areas where change has been agreed and implemented, focus areas being reviewed currently for specialties:
– Number of procedures – Follow up appointments – First outpatient appointments – Compliance to best practice
All of the ESNEFT teams are providing continuous updates on their action plans as well as commentary on the additional activity, where services have been impacted by the pandemic. Improved productivity: Digital Aligned to the ‘Delivery plan for tackling the COVID-19 backlog of elective care’ (Feb 2022), digital initiatives are in place and will continue to be developed to support clinical and non-clinical staff in releasing time, for example:
• Implementation of WASP software to speed up referral management time and create a link between Ecare and Advice and Guidance requests
• MMODAL software which improves workflow relating to dictation and transcription. The C2-AI tool has been piloted in Cheshire and Merseyside across three trusts; they have produced a comprehensive toolkit that provides information on how to utilise the C2-Ai system at various stages in the waiting list management process and gives examples of where it has been beneficial for system wide management of waiting lists. ESNEFT began a pilot in February 2022 and this will be reviewed in line with expected benefits of:
• To support HVLC or late notice - the tool will be able to show those patients who fall within a low risk of mortality group and therefore will be more likely to be seen at late notice or within a high-volume low complexity list.
• To be able to give services a comprehensive oversight of their longest waiting patients relating to their risks of mortality, complex co-morbidities and clinical pathways – currently intensive validation is used to manage these patient’s pathways. The tool will allow the patient information to be more accessible and for clinicians to easily review patients who may need to be re-prioritised due to circumstances, i.e. hospital attendances pertaining to their referred condition.
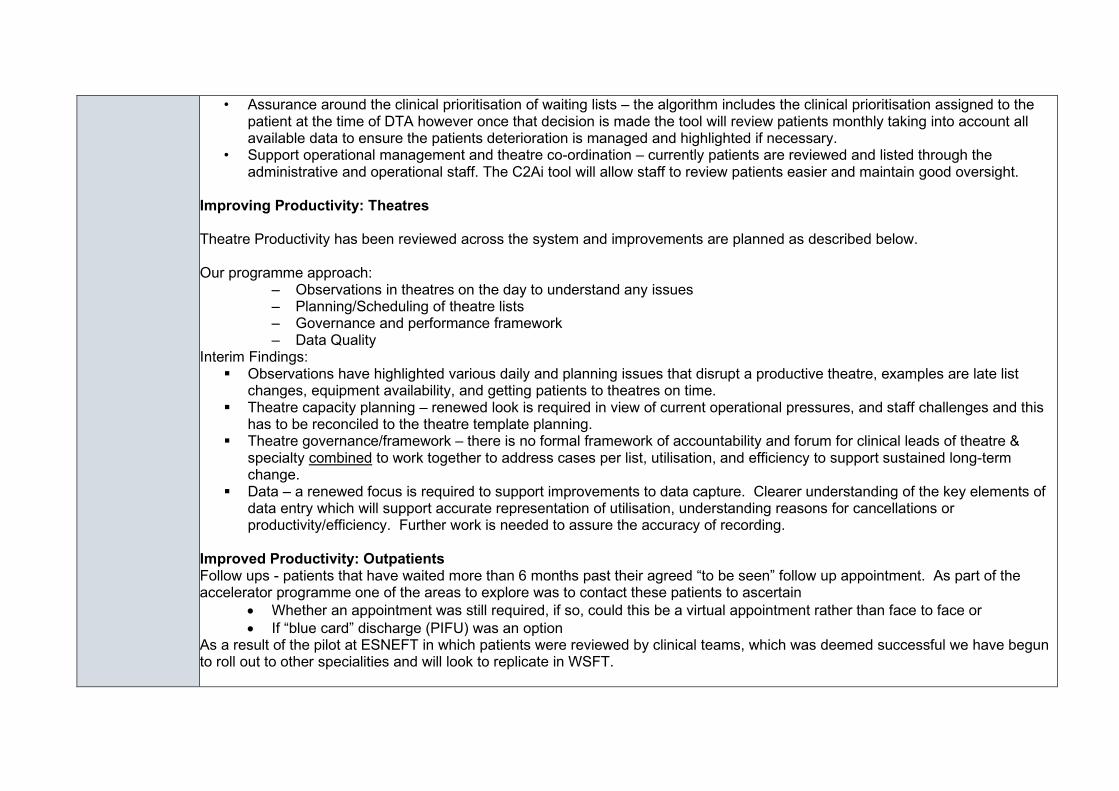
• Assurance around the clinical prioritisation of waiting lists – the algorithm includes the clinical prioritisation assigned to the patient at the time of DTA however once that decision is made the tool will review patients monthly taking into account all available data to ensure the patients deterioration is managed and highlighted if necessary.
• Support operational management and theatre co-ordination – currently patients are reviewed and listed through the administrative and operational staff. The C2Ai tool will allow staff to review patients easier and maintain good oversight.
Improving Productivity: Theatres Theatre Productivity has been reviewed across the system and improvements are planned as described below. Our programme approach:
– Observations in theatres on the day to understand any issues – Planning/Scheduling of theatre lists – Governance and performance framework – Data Quality
Interim Findings: Observations have highlighted various daily and planning issues that disrupt a productive theatre, examples are late list
changes, equipment availability, and getting patients to theatres on time. Theatre capacity planning – renewed look is required in view of current operational pressures, and staff challenges and this
has to be reconciled to the theatre template planning. Theatre governance/framework – there is no formal framework of accountability and forum for clinical leads of theatre &
specialty combined to work together to address cases per list, utilisation, and efficiency to support sustained long-term change.
Data – a renewed focus is required to support improvements to data capture. Clearer understanding of the key elements of data entry which will support accurate representation of utilisation, understanding reasons for cancellations or productivity/efficiency. Further work is needed to assure the accuracy of recording.
Improved Productivity: Outpatients Follow ups - patients that have waited more than 6 months past their agreed “to be seen” follow up appointment. As part of the accelerator programme one of the areas to explore was to contact these patients to ascertain
• Whether an appointment was still required, if so, could this be a virtual appointment rather than face to face or • If “blue card” discharge (PIFU) was an option
As a result of the pilot at ESNEFT in which patients were reviewed by clinical teams, which was deemed successful we have begun to roll out to other specialities and will look to replicate in WSFT.

We will roll out A&G further across the sites to release clinical time further. We will be making changes in speciality use of virtual clinics – During 2021 there were differences across sites and specialities for the use of virtual appointments. We will review this in our work programme for Q1 to assess and review Workforce Our workforce plans detail strategies we are going to employ to improve our recruitment and retention. Initiatives include staff incentives, health and wellbeing support and a reservist model. Better information and support for patients Various initiatives have been established or are being piloted to provide better support to patients and complement the My Planned Care app. These initiatives aim to reduce patient deterioration and optimise health pre-procedure. For example:
• The Waiting Well pilot is a collaboration of WSFT T&O Specialist Care Practitioners with input from Lifelink Suffolk (Social Prescribers), AHPS (Community Physio Team), Forest Health Primary Care Pharmacist and West Suffolk CCG and offers personalised support to patients to reduce the risk of deterioration of their mental and physical health whilst waiting for routine elective surgery. It is expected that the programme will have a positive impact on length of stay and post-operative complications.
• The Surgical School pilot aims to achieve the best possible surgical outcomes by mitigating patient risks thorough preoperative preparation and optimisation. This approach is being trialled in urology and colorectal initially. Outcome measures such as length of stay, post-operative complications and patient satisfaction will be audited through robust data collection. Learning from the pilot project will be shared and acted upon before rolling over the programme to all surgical specialties during autumn 2022. Using apps for patients to be able to access 12-week programmes to “wait well” such as yoga, mindfulness, exercise referred to as CHIP (Complete Health Improvement). This has been piloted in orthopaedics and take up has been good, and there is a plan to rollout across other specialities. A Referral Acknowledgement Letter for patient’s referrals has been initiated, which includes signposting for patients to access helpful tips and hints for them to keep well while waiting. This is an initiative that has also supported primary care and enabled less phone calls to GPs. Continue through 22/23 to monitor this and build on this platform to include other options such as housing, financial support etc.
Medium Term Capacity Developments Medium term, a short form business case has recently been submitted to develop a surgical hub at the Newmarket Community Hospital site. This will comprise 2 laminar-flow operating theatres and a 32-bed inpatient ward together with associated supporting infrastructure. It is assumed that additional activity will be deliverable from Q1 2023/24 as detailed in the business case, subject to approval and consultation timelines.

It is expected that the surgical hub can accommodate an additional 3,300 procedures p.a. which aligns with a requirement for c3,000-3,500 additional procedures per year, in order to make substantial progress to achieve a maximum 18-week wait. ESNEFT are in the process of building an elective orthopaedics centre in Colchester will bring online additional orthopaedic capacity by 2024. In addition, the Trust has applied for other capital schemes which will enable the trust to increase productivity and throughput including additional new laparoscopic theatres at Ipswich. Work is also underway to complete an options appraisal and business case for a community diagnostic hub in West and East Suffolk to support the local community and relieve pressure on the main hospital site for diagnostic testing. We anticipate having additional imaging and endoscopy capacity in these units.
Risks, issues and mitigation
The following are the key risks flagged by our system to the delivery of 104%:
• RAAC plank remedial work at WSFT may impact capacity if deadlines are extended or further work reveals structural findings which requires enhanced or rapid action. Ward work which has commenced and will run through 2022/23, which may impact on ward capacity specifically; an additional decant ward built during 2021 and opened late 2021 for medical Covid capacity, will help to mitigate this risk. RAAC plans will be managed alongside elective delivery plans to pre-empt any likely issues and manage accordingly. Move of the ANC to accommodate RAAC plank remedial work may impact outpatient capacity. Work is underway to develop a virtual consultation pod, which will house a number of specialities and release room capacity for the antenatal service.
• Availability of the independent sector (IS) to support WSFT/ESNEFT, due to capacity, process and workforce issues. Regular meetings and development of standardised processes and SoPs will help to mitigate this risk.
• A general lack of independent sector capacity in and around WSFT and ESNEFT may limit opportunities to outsource. As a system all providers will continue to explore opportunities and will work closely with IS partners.
• Ongoing risk posed by COVID-19 if there continues to be a requirement for patients and staff to self-isolate if positive or sick. This risk can lead to increased cancellations at short notice. We will continue to follow COVID-19 guidance and use a short notice waiting list, to help mitigate this risk.
• Ability to attract staff to specific specialties will impact on capacity to meet waiting list targets. WSFT will work with larger teaching hospitals and explore opportunity to appoint different workforce models such as physician’s assistants, to bridge any foreseen workforce gaps. ESNEFT are proposing to have closer working relationships with HEIs and FE colleges, increasing placement capacity, maximising student/trainee and international recruitment, and widening our participation in apprenticeships. Working differently with New and Advancing roles, training differently (endoscopy and diagnostic capacity, Simulation, multi professional learning), E job planning, e rostering, Leadership development programmes and cultural audits.
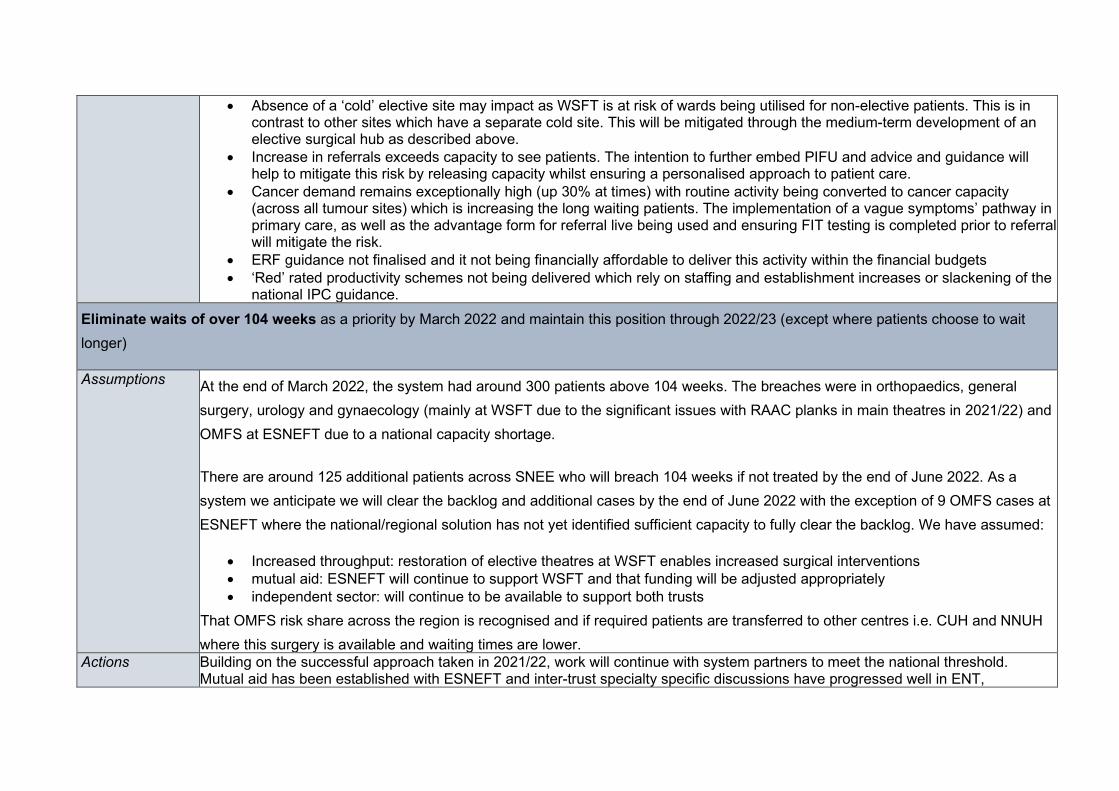
• Absence of a ‘cold’ elective site may impact as WSFT is at risk of wards being utilised for non-elective patients. This is in contrast to other sites which have a separate cold site. This will be mitigated through the medium-term development of an elective surgical hub as described above.
• Increase in referrals exceeds capacity to see patients. The intention to further embed PIFU and advice and guidance will help to mitigate this risk by releasing capacity whilst ensuring a personalised approach to patient care.
• Cancer demand remains exceptionally high (up 30% at times) with routine activity being converted to cancer capacity (across all tumour sites) which is increasing the long waiting patients. The implementation of a vague symptoms’ pathway in primary care, as well as the advantage form for referral live being used and ensuring FIT testing is completed prior to referral will mitigate the risk.
• ERF guidance not finalised and it not being financially affordable to deliver this activity within the financial budgets • ‘Red’ rated productivity schemes not being delivered which rely on staffing and establishment increases or slackening of the
national IPC guidance. Eliminate waits of over 104 weeks as a priority by March 2022 and maintain this position through 2022/23 (except where patients choose to wait longer)
Assumptions At the end of March 2022, the system had around 300 patients above 104 weeks. The breaches were in orthopaedics, general surgery, urology and gynaecology (mainly at WSFT due to the significant issues with RAAC planks in main theatres in 2021/22) and OMFS at ESNEFT due to a national capacity shortage.
There are around 125 additional patients across SNEE who will breach 104 weeks if not treated by the end of June 2022. As a system we anticipate we will clear the backlog and additional cases by the end of June 2022 with the exception of 9 OMFS cases at ESNEFT where the national/regional solution has not yet identified sufficient capacity to fully clear the backlog. We have assumed:
• Increased throughput: restoration of elective theatres at WSFT enables increased surgical interventions • mutual aid: ESNEFT will continue to support WSFT and that funding will be adjusted appropriately • independent sector: will continue to be available to support both trusts
That OMFS risk share across the region is recognised and if required patients are transferred to other centres i.e. CUH and NNUH where this surgery is available and waiting times are lower.
Actions Building on the successful approach taken in 2021/22, work will continue with system partners to meet the national threshold. Mutual aid has been established with ESNEFT and inter-trust specialty specific discussions have progressed well in ENT,

gynaecology and orthopaedics. Additional capacity has been sourced with the independent sector and this will continue in 2022/23, with a specific focus on patients waiting over 104 weeks.
Maximising use of existing capacity through weekend working and enhanced theatre productivity are being progressed, and will continue in 2022/23, together with opportunities to undertake increased day surgery aligned to HVLC/GIRFT recommendations and best practice.
Further work will be taken to explore insourcing opportunities for ophthalmology, urology and general surgery.
A continued shift to undertake cases in a day case setting will be pursued (we have not built this into our figures as the plans are not fully worked up yet). An additional theatre at WSFT is scheduled to be available from May 2022.
Ongoing waiting list validation through the use of the DrDoctor app at WSFT and equivalent at ESNEFT.
Clinical prioritisation will remain a feature of our elective strategy.
Through Q1 to reduce the 104 week waits, we are scoping and planning which patients will be transferred over to ESNEFT from WSH through the already agreed clinical pathways and SOPS. We are currently understanding our OMFS capacity options through the regional conversations – a meeting is being set up with CUH and NNUH, as well as options of capacity in Essex. This is to be finalised in March to enable as much clearance as possible during Q1. At the moment we are forecasting 9 breaches at the end of Q1. Use of IS – Discussions with the Nuffield remain ongoing – they are not able to provide regular staffed capacity, however if they do have capacity, they will offer this to us. Plans are in place for use of Ramsay Oaks capacity and this is also being offered to WSFT. We will continue to use the modular Vanguard unit until July 2022.
We will continue to outsource for endoscopy and insourcing for Pain Management (ESNEFT).
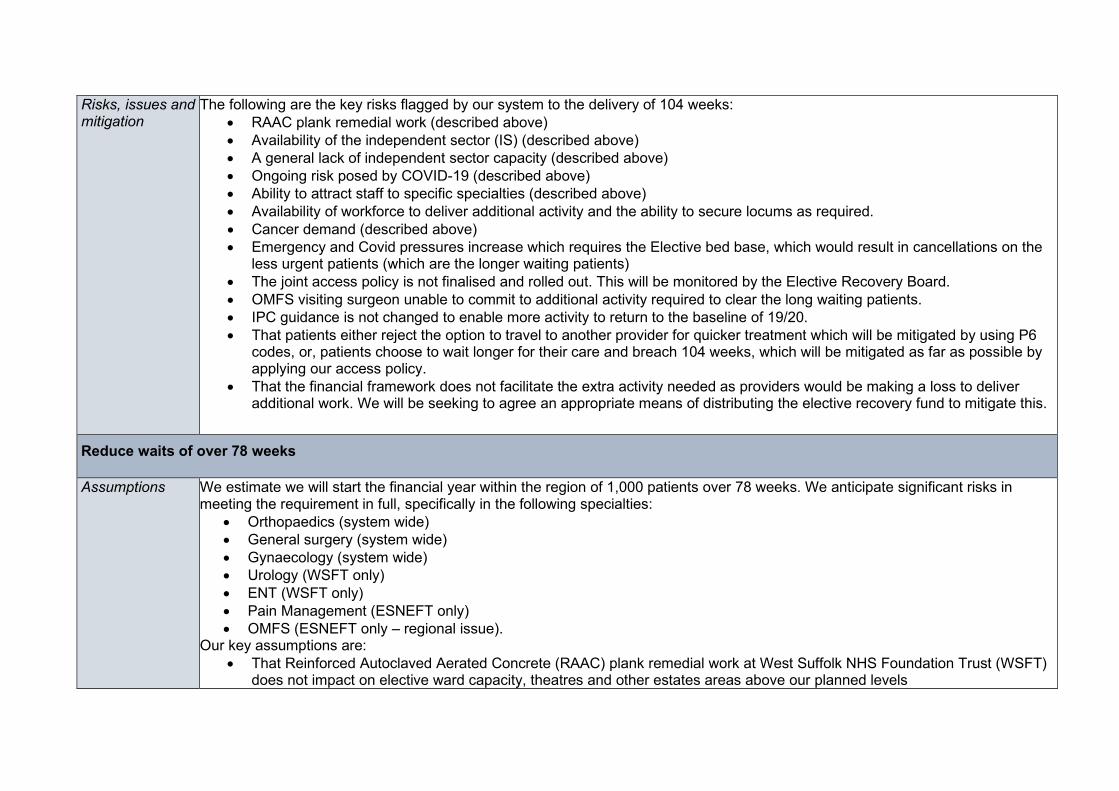
Risks, issues and mitigation
The following are the key risks flagged by our system to the delivery of 104 weeks: • RAAC plank remedial work (described above) • Availability of the independent sector (IS) (described above) • A general lack of independent sector capacity (described above) • Ongoing risk posed by COVID-19 (described above) • Ability to attract staff to specific specialties (described above) • Availability of workforce to deliver additional activity and the ability to secure locums as required. • Cancer demand (described above) • Emergency and Covid pressures increase which requires the Elective bed base, which would result in cancellations on the
less urgent patients (which are the longer waiting patients) • The joint access policy is not finalised and rolled out. This will be monitored by the Elective Recovery Board. • OMFS visiting surgeon unable to commit to additional activity required to clear the long waiting patients. • IPC guidance is not changed to enable more activity to return to the baseline of 19/20. • That patients either reject the option to travel to another provider for quicker treatment which will be mitigated by using P6
codes, or, patients choose to wait longer for their care and breach 104 weeks, which will be mitigated as far as possible by applying our access policy.
• That the financial framework does not facilitate the extra activity needed as providers would be making a loss to deliver additional work. We will be seeking to agree an appropriate means of distributing the elective recovery fund to mitigate this.
Reduce waits of over 78 weeks
Assumptions We estimate we will start the financial year within the region of 1,000 patients over 78 weeks. We anticipate significant risks in meeting the requirement in full, specifically in the following specialties:
• Orthopaedics (system wide) • General surgery (system wide) • Gynaecology (system wide) • Urology (WSFT only) • ENT (WSFT only) • Pain Management (ESNEFT only) • OMFS (ESNEFT only – regional issue).
Our key assumptions are: • That Reinforced Autoclaved Aerated Concrete (RAAC) plank remedial work at West Suffolk NHS Foundation Trust (WSFT)
does not impact on elective ward capacity, theatres and other estates areas above our planned levels

• Elective activity levels may be impacted by the absence of separate hot and cold elective facilities at WSFT. This will be addressed in future years, through the development of the Newmarket site, as described in the actions below.
• That work continues with system partners in relation to the provision of mutual aid. • That there is continued access to the independent sector to provide additional capacity. • That staffing levels are not significantly impacted due to COVID-19, resulting in elective cancellations. • That non-elective activity will not impact on elective ward capacity further than outlined • That it is clinically appropriate to dedicate the required level of non-cancer/urgent capacity to those waiting over 78 weeks
(over other priorities) • That a minimal number of patients with no criteria to reside are delayed to enable length of stay (LOS) to reduce and enable
the non-elective activity to be managed within their bed base. Actions We have set out in the action sections above our plans to increase activity and clear backlogs.
The key actions in relation to the risk specialties listed above are as follows:
• Orthopaedics: maximise independent sector throughput; implement key productivity learning from GIRFT and HVLC through our MSK specific programme; where appropriate, use mutual aid to balance out inequalities in our system.
• General Surgery and Gynaecology: the wait times in each trust are broadly similar so our focus will be on internal productivity and securing capacity for at risk sub-specialties such as Urogynaecology and any are with a significant cancer pressure
• Urology: our trusts will be looking at mutual aid opportunities to close the gap in parity between them. Managing cancer capacity against RTT capacity will be a key focus in this specialty.
• Ear, nose and throat: our trusts will be looking at mutual aid opportunities to close the gap in parity between them. • Pain management: our trusts will be looking at mutual aid opportunities to close the gap in parity between them. • OMFS: we will continue to pursue options with NHSE to secure a regional solution to this very specialised area.
More generally:
• we will have the WSFT theatre capacity back in 21/22 which will increase our throughput. This will give significantly more opportunity to clear surgical backlogs
• mutual aid: there are some specialties where we have significant differences in waits. We have been successful in working together (e.g. ophthalmology had a 52 week wait time differential which is now down to 3 weeks and more recently the orthopaedic difference has dropped by 10 weeks) and will seek to expand this into additional areas (specifically urology and pain management).
• Additional capacity: we have extremely strong working relationships with one of our three major independent sector providers and will be seeking to roll out the learning to the other two. We have also been successful in insourcing support.
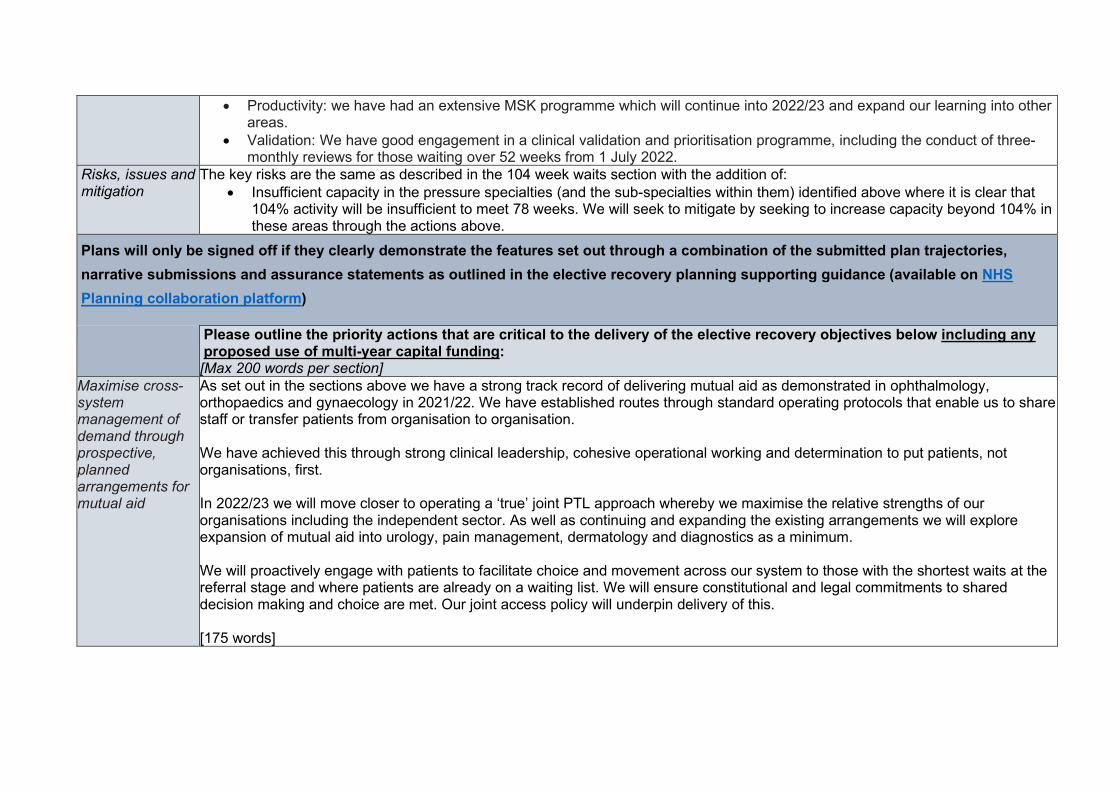
• Productivity: we have had an extensive MSK programme which will continue into 2022/23 and expand our learning into other areas.
• Validation: We have good engagement in a clinical validation and prioritisation programme, including the conduct of three-monthly reviews for those waiting over 52 weeks from 1 July 2022.
Risks, issues and mitigation
The key risks are the same as described in the 104 week waits section with the addition of: • Insufficient capacity in the pressure specialties (and the sub-specialties within them) identified above where it is clear that
104% activity will be insufficient to meet 78 weeks. We will seek to mitigate by seeking to increase capacity beyond 104% in these areas through the actions above.
Plans will only be signed off if they clearly demonstrate the features set out through a combination of the submitted plan trajectories, narrative submissions and assurance statements as outlined in the elective recovery planning supporting guidance (available on NHS Planning collaboration platform)
Please outline the priority actions that are critical to the delivery of the elective recovery objectives below including any proposed use of multi-year capital funding: [Max 200 words per section]
Maximise cross-system management of demand through prospective, planned arrangements for mutual aid
As set out in the sections above we have a strong track record of delivering mutual aid as demonstrated in ophthalmology, orthopaedics and gynaecology in 2021/22. We have established routes through standard operating protocols that enable us to share staff or transfer patients from organisation to organisation. We have achieved this through strong clinical leadership, cohesive operational working and determination to put patients, not organisations, first. In 2022/23 we will move closer to operating a ‘true’ joint PTL approach whereby we maximise the relative strengths of our organisations including the independent sector. As well as continuing and expanding the existing arrangements we will explore expansion of mutual aid into urology, pain management, dermatology and diagnostics as a minimum. We will proactively engage with patients to facilitate choice and movement across our system to those with the shortest waits at the referral stage and where patients are already on a waiting list. We will ensure constitutional and legal commitments to shared decision making and choice are met. Our joint access policy will underpin delivery of this. [175 words]
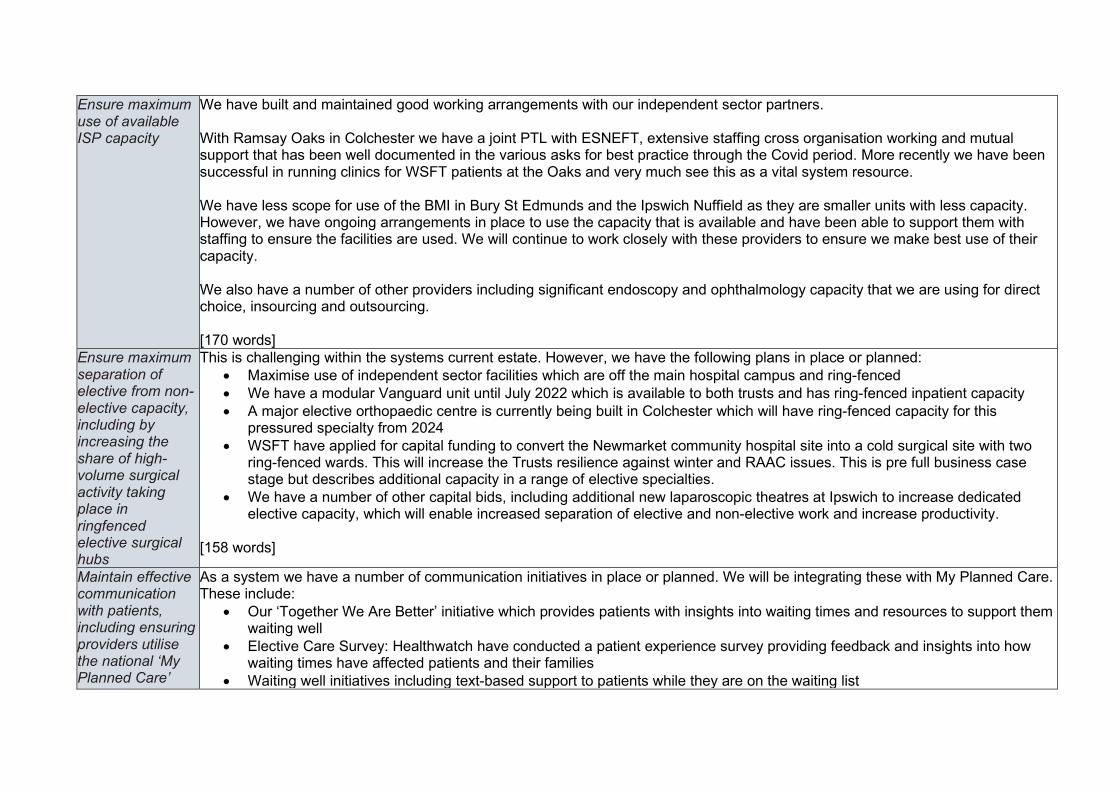
Ensure maximum use of available ISP capacity
We have built and maintained good working arrangements with our independent sector partners. With Ramsay Oaks in Colchester we have a joint PTL with ESNEFT, extensive staffing cross organisation working and mutual support that has been well documented in the various asks for best practice through the Covid period. More recently we have been successful in running clinics for WSFT patients at the Oaks and very much see this as a vital system resource. We have less scope for use of the BMI in Bury St Edmunds and the Ipswich Nuffield as they are smaller units with less capacity. However, we have ongoing arrangements in place to use the capacity that is available and have been able to support them with staffing to ensure the facilities are used. We will continue to work closely with these providers to ensure we make best use of their capacity. We also have a number of other providers including significant endoscopy and ophthalmology capacity that we are using for direct choice, insourcing and outsourcing. [170 words]
Ensure maximum separation of elective from non-elective capacity, including by increasing the share of high-volume surgical activity taking place in ringfenced elective surgical hubs
This is challenging within the systems current estate. However, we have the following plans in place or planned: • Maximise use of independent sector facilities which are off the main hospital campus and ring-fenced • We have a modular Vanguard unit until July 2022 which is available to both trusts and has ring-fenced inpatient capacity • A major elective orthopaedic centre is currently being built in Colchester which will have ring-fenced capacity for this
pressured specialty from 2024 • WSFT have applied for capital funding to convert the Newmarket community hospital site into a cold surgical site with two
ring-fenced wards. This will increase the Trusts resilience against winter and RAAC issues. This is pre full business case stage but describes additional capacity in a range of elective specialties.
• We have a number of other capital bids, including additional new laparoscopic theatres at Ipswich to increase dedicated elective capacity, which will enable increased separation of elective and non-elective work and increase productivity.
[158 words]
Maintain effective communication with patients, including ensuring providers utilise the national ‘My Planned Care’
As a system we have a number of communication initiatives in place or planned. We will be integrating these with My Planned Care. These include:
• Our ‘Together We Are Better’ initiative which provides patients with insights into waiting times and resources to support them waiting well
• Elective Care Survey: Healthwatch have conducted a patient experience survey providing feedback and insights into how waiting times have affected patients and their families
• Waiting well initiatives including text-based support to patients while they are on the waiting list

platform and support development of patient communications via the NHS App
• Surgery School Pilot – to help patients to optimise their health 12 weeks before surgery. • We are acknowledging all referral letters and signposting them to our support website
We will look to align all our communication methods to patients to ensure that there is no duplication including how we utilise the NHS App. [138 words]
Describe the changes that will support moving back to and beyond pre-pandemic levels of elective productivity as soon as the context allows this, consistent with latest UK Health Security Agency (UKHSA) guidance
As described in the 104% section above, each specialty has developed, and risk rated schemes that will bring them back to pre-pandemic levels of productivity and beyond. Some of these are reliant on relaxation of the infection control guidance from the UKHSA and these are currently rated as ‘red’ risk. [50 words]
Ensure the plans enable inclusive recovery and reduce health inequalities where they are identified
We have undertaken detailed reviews of our waiting lists and concluded the following: • There is no statistically significant difference in the waiting time for patients from different ethnicities • At ESNEFT it was observed that patients from the lowest deprivation deciles tend to be treated faster than those from higher
deciles. We hypothesise that this is because patients in that group are presenting later or have more health co-morbidities that result in higher clinical needs and therefore need to be seen faster.
• That NHSE/I data showed no statistically significant difference in waiting time of patients from different deprivation quintiles. We are developing system dashboards to ensure we continually review and act on any issues that prevent non-inclusive recovery, building on our experience of developing automated PowerBI Apps. Our EHIIAs will contribute to addressing entrenched and longstanding inequalities in elective care. As well as a core assessment we will focus on dermatology, ophthalmology and musculoskeletal. Action plans will be agreed by 30 April 2022.
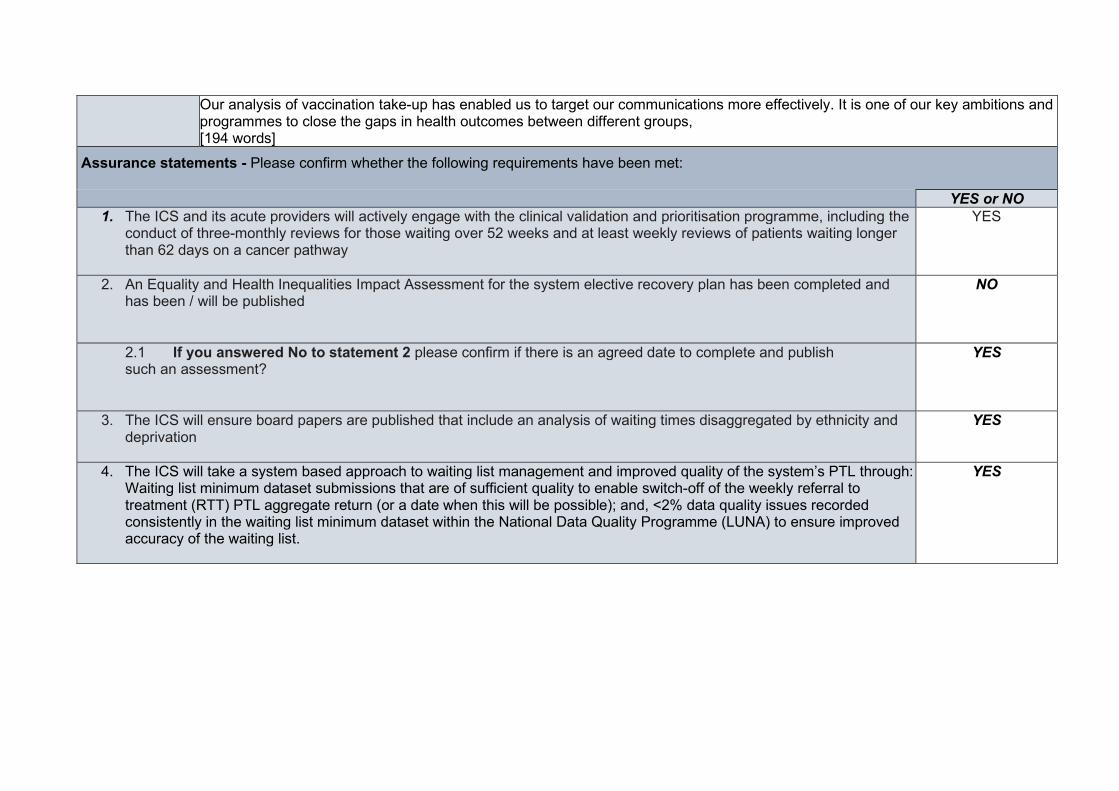
Our analysis of vaccination take-up has enabled us to target our communications more effectively. It is one of our key ambitions and programmes to close the gaps in health outcomes between different groups, [194 words]
Assurance statements - Please confirm whether the following requirements have been met:
YES or NO 1. The ICS and its acute providers will actively engage with the clinical validation and prioritisation programme, including the
conduct of three-monthly reviews for those waiting over 52 weeks and at least weekly reviews of patients waiting longer than 62 days on a cancer pathway
YES
2. An Equality and Health Inequalities Impact Assessment for the system elective recovery plan has been completed and has been / will be published
NO
2.1 If you answered No to statement 2 please confirm if there is an agreed date to complete and publish such an assessment?
YES
3. The ICS will ensure board papers are published that include an analysis of waiting times disaggregated by ethnicity and deprivation
YES
4. The ICS will take a system based approach to waiting list management and improved quality of the system’s PTL through: Waiting list minimum dataset submissions that are of sufficient quality to enable switch-off of the weekly referral to treatment (RTT) PTL aggregate return (or a date when this will be possible); and, <2% data quality issues recorded consistently in the waiting list minimum dataset within the National Data Quality Programme (LUNA) to ensure improved accuracy of the waiting list.
YES
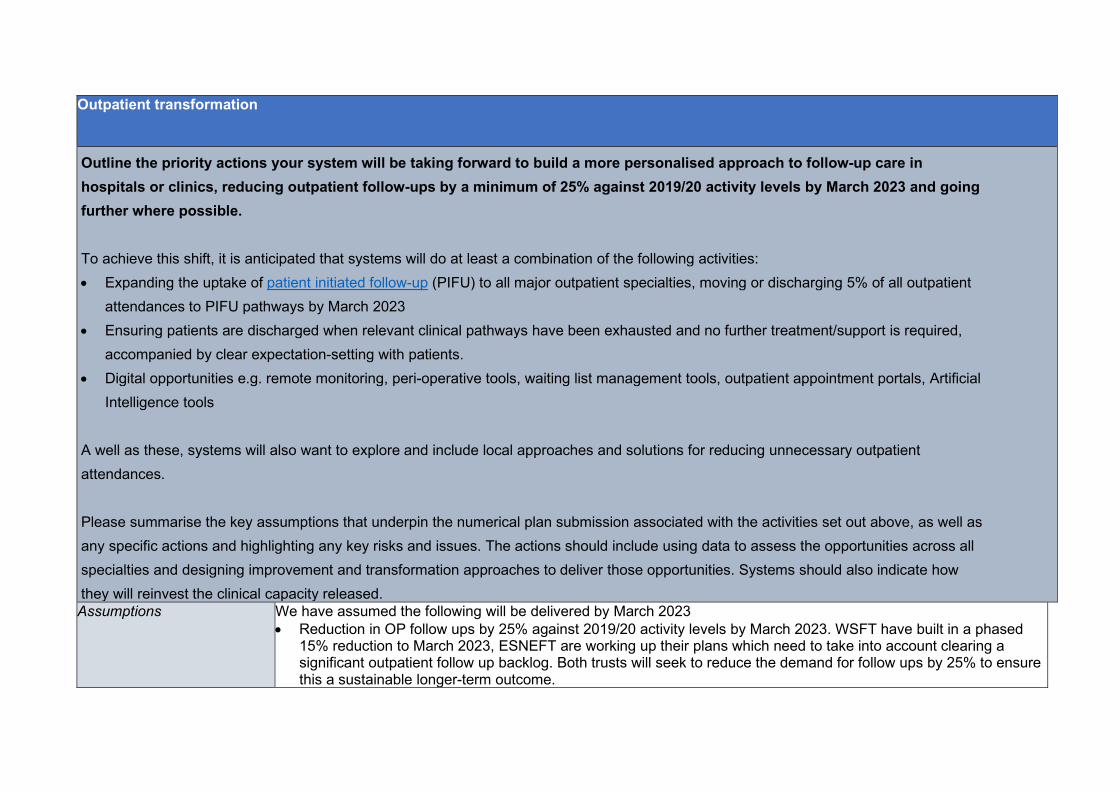
Outpatient transformation Outline the priority actions your system will be taking forward to build a more personalised approach to follow-up care in hospitals or clinics, reducing outpatient follow-ups by a minimum of 25% against 2019/20 activity levels by March 2023 and going further where possible. To achieve this shift, it is anticipated that systems will do at least a combination of the following activities: • Expanding the uptake of patient initiated follow-up (PIFU) to all major outpatient specialties, moving or discharging 5% of all outpatient
attendances to PIFU pathways by March 2023 • Ensuring patients are discharged when relevant clinical pathways have been exhausted and no further treatment/support is required,
accompanied by clear expectation-setting with patients. • Digital opportunities e.g. remote monitoring, peri-operative tools, waiting list management tools, outpatient appointment portals, Artificial
Intelligence tools
A well as these, systems will also want to explore and include local approaches and solutions for reducing unnecessary outpatient attendances. Please summarise the key assumptions that underpin the numerical plan submission associated with the activities set out above, as well as any specific actions and highlighting any key risks and issues. The actions should include using data to assess the opportunities across all specialties and designing improvement and transformation approaches to deliver those opportunities. Systems should also indicate how they will reinvest the clinical capacity released. Assumptions We have assumed the following will be delivered by March 2023
• Reduction in OP follow ups by 25% against 2019/20 activity levels by March 2023. WSFT have built in a phased 15% reduction to March 2023, ESNEFT are working up their plans which need to take into account clearing a significant outpatient follow up backlog. Both trusts will seek to reduce the demand for follow ups by 25% to ensure this a sustainable longer-term outcome.
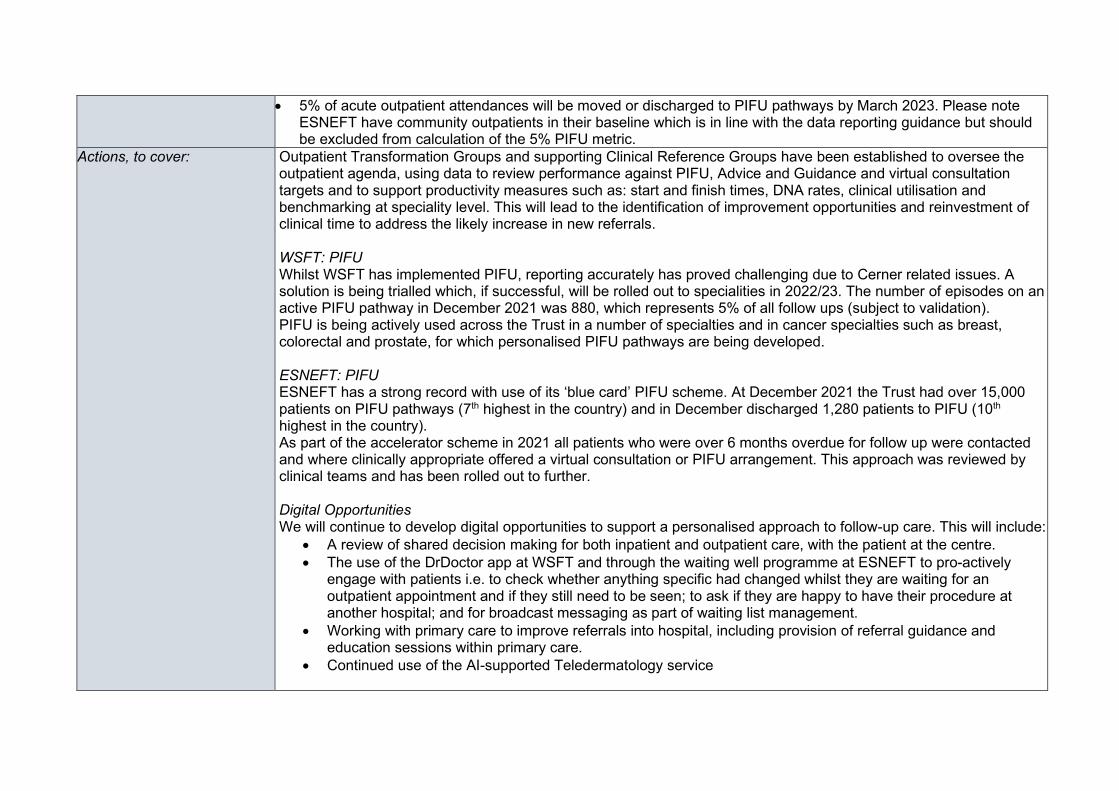
• 5% of acute outpatient attendances will be moved or discharged to PIFU pathways by March 2023. Please note ESNEFT have community outpatients in their baseline which is in line with the data reporting guidance but should be excluded from calculation of the 5% PIFU metric.
Actions, to cover: Outpatient Transformation Groups and supporting Clinical Reference Groups have been established to oversee the outpatient agenda, using data to review performance against PIFU, Advice and Guidance and virtual consultation targets and to support productivity measures such as: start and finish times, DNA rates, clinical utilisation and benchmarking at speciality level. This will lead to the identification of improvement opportunities and reinvestment of clinical time to address the likely increase in new referrals. WSFT: PIFU Whilst WSFT has implemented PIFU, reporting accurately has proved challenging due to Cerner related issues. A solution is being trialled which, if successful, will be rolled out to specialities in 2022/23. The number of episodes on an active PIFU pathway in December 2021 was 880, which represents 5% of all follow ups (subject to validation). PIFU is being actively used across the Trust in a number of specialties and in cancer specialties such as breast, colorectal and prostate, for which personalised PIFU pathways are being developed. ESNEFT: PIFU ESNEFT has a strong record with use of its ‘blue card’ PIFU scheme. At December 2021 the Trust had over 15,000 patients on PIFU pathways (7th highest in the country) and in December discharged 1,280 patients to PIFU (10th highest in the country). As part of the accelerator scheme in 2021 all patients who were over 6 months overdue for follow up were contacted and where clinically appropriate offered a virtual consultation or PIFU arrangement. This approach was reviewed by clinical teams and has been rolled out to further. Digital Opportunities We will continue to develop digital opportunities to support a personalised approach to follow-up care. This will include:
• A review of shared decision making for both inpatient and outpatient care, with the patient at the centre. • The use of the DrDoctor app at WSFT and through the waiting well programme at ESNEFT to pro-actively
engage with patients i.e. to check whether anything specific had changed whilst they are waiting for an outpatient appointment and if they still need to be seen; to ask if they are happy to have their procedure at another hospital; and for broadcast messaging as part of waiting list management.
• Working with primary care to improve referrals into hospital, including provision of referral guidance and education sessions within primary care.
• Continued use of the AI-supported Teledermatology service
Released resources Our trusts will be reviewing job plans in early 2022/23 to ascertain where released capacity can be best redeployed including:
• Additional capacity for advice and guidance • Additional capacity for outpatient first appointments (face to face or virtual) • Other areas to increase clock stops.
Risks, issues and mitigation Our key risks are as follows: • That WSFT continuing issues relating to accurate reporting of PIFU are not quickly resolved. A solution is
currently being tested in a number of cancer specialties and, if successful, will be implemented across all specialties.
• That the increase in referrals exceeds capacity to see patients. The intention to further embed PIFU and advice and guidance will help to mitigate this risk by releasing capacity whilst ensuring a personalised approach to patient care. We will be working with primary care colleagues to ensure referral criteria are adhered to, to mitigate this risk.
• Clinical engagement and leadership of timely job planning to support the delivery – this will be monitored internally to mitigate the risk.
Existing specialities (Patient Initiated Follow Up) Please list the existing specialities within your system that have taken up and are using PIFU.
General Surgery; Urology; T&O; ENT; Ophthalmology; Anaesthetic Service; Gastroenterology; Endocrinology; Cardiology; Dermatology; Medical Oncology; Rheumatology; Paediatric Service, Elderly Medicine; Obstetrics Service; Physiotherapy; Gynaecology; Oral Surgery; Plastic Surgery; General Medicine.
Additional specialities (Patient Initiated Follow Up) Please list any additional specialities within your system that are intending to take up PIFU including an anticipated date of implementation.
The above list shows most specialties are covered in the system.
At WSFT, additional specialties and usage within those specialties will be brought online once we have implemented the solution to record PIFU in EPR. Implementation of this is estimated to be from March 2022 onwards.
Virtual consultations – outline the priority actions your system will be taking to continue offering both video and telephone consultations for outpatient services where clinically appropriate, with a minimum of 25% of consultations taking place via this route, including by raising patient clinician awareness and confidence in virtual consultations.

Assumptions We have assumed that we will meet the requirement that a minimum of 25% of virtual consultations will take place for outpatient services.
Actions As a system we have demonstrated the capacity and capability to meet this standard but on occasions have dipped below 25%. We are reviewing the reasons for this, some of which are clinical, and will be putting in place actions to maximise the appropriate usage of virtual consultations. WSFT WSFT is currently achieving 21% (January 2022) of outpatient appointments through virtual and telephone consultations. Our challenge is to meet the national target and, where possible, go further. The majority of virtual consultations are by telephone and in 2022/23 WSFT will seek to fully embed virtual clinics within the organisation. WSFT is currently looking at a Teams based solution, which is the clinical preference, to increase take up of video consultations. This approach is being worked through with Microsoft and Cerner, with an expected completion date of March 2022. An agreed launch date will be agreed for 2022/23. Further, WSFT is continuing to work with ICS colleagues on a TEAMS based video solution for community. ESNEFT As part of the accelerator programme, ESNEFT reviewed all patients who were overdue for follow up and offered virtual consultations to all who were clinically appropriate. This approach has been clinically reviewed and is being rolled out. We are reviewing changes in speciality use of virtual clinics – during 2021 there were differences across sites and specialities for the use of virtual appointments and this is a priority on our work programme for Q1 to assess and review.

Risks, issues and mitigation The key risks are as follows: • Clinical appropriateness: There is an assumption that 25% is a clinically appropriate proportion of appointments that
could be seen virtually. This is untested over time and the trend shows a reduction in virtual appointments, which is similar to the national pattern and is reflective of a clinical need to see patients face to face post COVID-19. We will continue to review this with our clinicians and drive the move towards virtual consultations wherever this is clinically appropriate.
• Digital access: video/telephone appointments are not accessible to all patients. As part of our work on digital inclusion we will seek to mitigate this.
• Digital: at WSFT there is a risk that the interface between eCare and TEAMS is ineffective, resulting in less clinical engagement.
Digital: That the video consultation system is too difficult and time consuming to use. We are working with Cerner and Microsoft to integrate systems which will make it easier for clinicians to undertake video consultations.
Existing specialities (virtual consultations) Please list the existing specialities within your system that have taken up and are using virtual consultations.
Breast Surgery; Cardiology; Haematology; Colorectal Surgery; Dermatology; Diabetes; Endocrinology; ENT; Gastroenterology; General Medicine; General Surgery; Geriatric Medicine; Gynaecology; Hepatology; Medical Oncology; Nephrology; Neurology; Ophthalmology; Paediatrics; Pain Management; Plastic Surgery; Respiratory; Rheumatology; Stroke & TIA; T&O; Urology; Vascular; A&E; Anaesthetics; Anti-Coagulation; Chemical Pathology
Additional specialities (virtual consultations) Please list any additional specialities within your system that are intending to take up virtual consultations including an anticipated date of implementation.
All specialties using virtual consultations.
Specialist advice, including advice and guidance (A&G) - outline the priority actions your system will be taking to deliver 16 Specialist Advice requests per 100 outpatient first attendances by March 2023, ensuring that primary care is consistently able to access timely, high quality advice; and that high quality, comprehensive data is being collected on all referral optimisation approaches.
Assumptions We expect to deliver 16 specialist advice requests, including A&G, per 100 first attendances by March 2023.
Actions Our two Trusts have had a long history of using advice and guidance and are currently utilising a range of different approaches and platforms to achieve this. WSFT WSFT continues to perform well in relation to the provision of A&G that is undertaken in the trust, however, the Trust will continue to improve on the current rates, in order to release capacity for any increase in referrals in 2022/23. This will be achieved through collaboration with primary care. WSFT is working closely with paediatrics, neurology, nephrology and haematology as initial priority areas and a dashboard is in place to support delivery. In addition, a new referral management system is being rolled out in 2022/23, which will integrate ERS and the electronic patient record, making the processes much simpler for clinicians and support them in achieving higher turnaround times. Building on an audit of referrals undertaken to identify key themes and barriers to A&G use, specialty level plans for A&G improvement will be developed between primary and acute care clinicians. These targeted plans will focus on those specialities which are struggling to increase A&G, such as: T&O. Through this audit, opportunity to develop a ‘surveillance/monitoring’ service to manage MGUS (Monoclonal gammopathy of undetermined significance) and PSA patients (called ‘the third space, monitoring service) has been identified and will be piloted for MGUS patients in 2022/23. WSFT is also exploring national and regional models of A & G and evaluating them for opportunities to improve or transform A&G at WSFT. One such model is the A&G First model, whereby all routine referrals are triaged for the potential to offer A & G as an alternative to an outpatient appointment. ESNEFT- Use of the ALLCAS system in the Ipswich and East Suffolk system is well established and is operating well. Therefore, ESNEFT has primarily been focussing on improving the provision of A&G in North East Essex (NEE), working closely with CCG colleagues in order to improve uptake. The priority has been to work with specialties currently using Consultant Connect for advice and guidance as this service will be switched off on 18th March 2022, These services will migrate to using e-RS advice and guidance, this required pre referral guidance to be in place prior to the switch off. Further measures to improve up take will be to work with the CCG and the specialty clinical leads, to review the current pre referral guidance and agree pathways. Engagement events were scheduled, with consultants being asked to present at GP shutdown events in NEE, which further promoted use of A&G requests in primary care.
These events facilitated better communications between GPs and consultants with the aim of improving the quality of A&G requests. A Standard Operating Protocol (SOP) has been written at system level for provision of A&G across NEE. Greater collaboration will be required across both Ipswich and Colchester to promote use of A&G in primary care. Work is also being undertaken around identifying referrals received that have been cancelled on Lorenzo and Careflow due to advice and guidance being given and going forward how these will be included in the A&G metrics. ESNEFT Business Intelligence team have produced an A&G dashboard, and this will support the programmes engagement plan and identify which services to prioritise. Part of this engagement plan will be to work with specialty clinical leads around the potential use of use of A&G on all non-two-week patients before considering referral. Further opportunities also being explored is to improve the process of how A&G requests are recorded on Evolve by use of robotics process to automatically upload the requests and responses.
Risks, issues and mitigation The following are the key risks with delivering the A&G expectations: Data capture
• There is currently no accurate method of capturing non-eRS data, such as for ophthalmology (e.g. where referrals made by optometrists come through a referrals platform). This will be mitigated by a clearly documented process to be put in place in order to ensure this information is captured.
Clinical Engagement
• There is a risk that clinicians do not use the A&G model and/or do not respond in a timely manner. Roll out of WASP software at WSFT will encourage buy-in, as it simplifies the process for clinicians. In addition, engagement through the Clinical Reference Group will ensure that clinical views are listened to and acted upon, as appropriate.
• The response time to A&G requests within 48 hours has been raised as a risk by CCG colleagues to NHS E/I, and we are waiting for feedback and guidance from the central team.
• Some specialties have paused the A&G service due to operational pressures at ESNEFT. In order to mitigate the risk of GPs not being able to request via e-RS, an interim process has been put in place of how GPs can communicate with consultants. This is being monitored at CRG with plans to resolve this situation by July 2022.
• Consultants not having enough time to provide good quality advice and guidance. This is being addressed by review of the consultant’s job plans.

Existing specialities (specialist advice, including advice and guidance) Please list the existing specialities within your system that have taken up and are using specialist advice, including advice and guidance.
Breast Surgery; Cardiology; Clinical Haematology; Dermatology; Dietetics; Diabetes; Endocrinology; ENT; Gastroenterology; General Surgery; General Medicine; Geriatric Medicine; Gynaecology; Hepatobiliary and Pancreatic; Nephrology; Neurology; Ophthalmology; Paediatrics; Oral Surgery; Pain; Plastic Surgery; Respiratory; Rheumatology; T&O; Urology; Vascular
Additional specialities (specialist advice, including advice and guidance)
At WSFT, the roll of WASP will make A&G requests via eRS available to all specialties.
At Colchester, the gastroenterology service is currently paused and under review with an anticipated implementation date of July 2022.
C2: Complete recovery, improve performance against cancer waiting times standards
Please summarise the key assumptions that underpin the numerical plan submission associated with the key priorities listed below, highlighting any key risks and issues.
Return the number of people waiting for longer than 62 days to the level in February 2020 (based on the national average in February 2020) and meet the increased level of referrals and treatment required to reduce the shortfall in number of first treatments. Priority actions should centre on ensuring there is sufficient diagnostic and treatment capacity to meet recovering levels of demand, with a particular focus on the three cancers making up two-thirds of the national backlog (lower GI, prostate and skin).
Assumptions Narrative plan should provide details on how diagnostic and treatment capacity will be increased to reduce >62d waiting list. Include details on which pathways, services and providers are most challenged and how actions will be targeted accordingly. Demonstrate alignment between the actions in the plan and the ICS trajectories submitted as part of the operational planning process. Demonstrate how oversight and prioritisation of cancer waiting list management will be increased and maintained. Include description of planned diagnostic activity in the Independent Sector (in and outsourced), linked to wider IS activity plan, and further opportunities being explored.
We have assumed the following will be delivered by March 2023 and built these assumptions into our numerical plan submissions:
• We will ensure there is sufficient diagnostic and treatment capacity in place to meet recovering levels of demand – including use of mutual aid and other system first approaches that make best use of available resources across a whole system. A key increase in available diagnostics will be part of the Clacton Community Diagnostic Centre, additional diagnostic capacity will be available during 22/23 which support the demand and capacity modelling for ESNFTs and the broader diagnostic recovery trajectories. The successful delivery of FD ambition is dependent on this diagnostic capacity.
• We will ensure local providers are maximising use of local Independent Sector (IS) capacity where this would reduce cancer waiting times, actively brokering conversations between IS providers and local trusts where necessary. IS provision for ESNEFT for endoscopy is being supported by the Independent Sector at both the Oaks and InHealth in Ipswich to provide further capacity. The Oaks is also providing routine surgery support which allows for capacity for cancer surgery within the acute provider sites.
• We are focussing on reducing the number of people waiting more than 62 days on the pathways which make up the highest proportion of the backlog (typically lower GI, prostate and skin). The Patient Tracking List (PTL) 62-day backlog comprises 537 patients and is expected to reduce to 263 patients by the end of 2022/23. The 62-day PTL has reduced in size as there was a big push before Christmas to treat and remove patients from the PTL. Providers within Suffolk have ensured that provision for P1 and P2 cancer surgery is prioritised, where clinically appropriate. Impacted by referrals received; diagnostics capacity; PTL workforce; and treatment capacity.
• Increased referrals into the trusts with some specialties now receiving over 135% of usual activity (ESNEFT and WSFT 120%@ 17/3/2022). We are working with the cancer alliance and trusts to understand if this a new ‘new normal’ or Covid recovery. With ESNEFT recently receiving the first 1000 2WW referrals in one week. It should be noted that colorectal treatment numbers for WSFT are significantly higher than average. ESNEFT 2WW Performance – Recovery is showing sustained performance.
• ESNEFT 2WW Performance – Recovery is showing sustained performance improvement. • Increased number of treatments which has supported SNEE to recover their treatment backlog
following the pandemic, for WSFT this was 13% and ESNEFT 10%, current activity is 110% of pre-Covid levels against an England average of 101%. ESNEFT remains one of the trusts, with the highest number of treatments being undertaken, this means that with the high number of referrals this is translating to increased cancer diagnosis’s and therefore treatments including Surgery, Chemotherapy and radiotherapy. ESNEFT 62 Day First - Recovery Trajectory will aim for Trust level compliance by end of December (Q3).
• We will ensure every urgent suspected lower GI FDS referral is accompanied by a faecal immunochemical test (FIT) result; deliver the optimal timed pathway for prostate cancer, including mpMRI prior to biopsy; and ensure tele-dermatology is available as an option for clinicians in all providers receiving FDS referrals. We have incentivised practices with the additional funding from the Cancer Alliance up to end of Qtr.1 2022/23 to undertake FiT and await the result prior to referral and triage following the result and with secondary care to ensure FiT results are informing decisions about onward investigation including maximising Colon capsule endoscopy. Providers are working through demand management on colonoscopies, utilising CT colonoscopies, use of colon capsule endoscopy and FiT test to assist with risk assessment.
• We continue with clinical validation and prioritisation, including a minimum of weekly reviews for patients waiting longer than 62 days on a cancer pathway. As a system we will be commenting on the national consultation which has been launched to review the current cancer waiting time standards (Version 12) which will mean a move to improve performance on cancer standards, with a focus on the 62-day urgent referral to first treatment standard.
• SNEE will continue to work with system partners including providers and the cancer Alliance to review progress against the recovery trajectories developed by the trusts. This will be facilitated by Cancer operational and system oversight meetings utilising system and regional data packs.
• Weekly sit-rep collection will remain ongoing and we will continue to support our systems to support and will analyse the data collected for early trends, including referral numbers, patient tracking list size - including speciality level detail, and breach data in a contemporaneous format which results in us working closely with our system to mitigate new risks as they arise
• The focus for the first quarter will be around the cancer outcome data recently released by the cancer alliance teams, we will use this data to baseline and enable a targeted approach to those pathways that need more support. We are developing a cancer dashboard within SNEE to compliment this approach.
• Using local modelling SNEE recovered their referral volume in December 2021, the assumption is now that current referral levels are projected to continue through 22/23.
• We continue to explore Independent Service Provision (ISP) and mutual aid provision, when available to maximise the opportunities for treatment. Including all routine endoscopy at ESNEFT is currently being undertaken by external providers with Urgent and Cancer pathways at ESNEFT.
• Workforce is a key enabler to restoring cancer services, we will continue to work with our Health Education England colleagues and system workforce leads to identify workforce gaps and develop training. We have recently with the support of Macmillan recruited a Clinical Nurse Specialist workforce lead (ESNEFT) to develop a robust plan to future proof and develop our Clinical Nurse Specialist (CNS) workforce, looking at competencies and succession planning.
• SNEE will continue to work with our tertiary centre providers to ensure we minimise patient delays between centres. Our trackers will continue to support patients being referred in timely way onto tertiary centre pathways. Subsequent treatments however are not tracked which is a risk.
• SNEE will continue to facilitate mutual aid across our providers and endeavour to reduce variation of waiting times across the system. Mutual aid has been utilised mainly on the routine pathway, which supports cancer delivery within the trusts.
Actions
• Independent Sector provision - ESNEFT will continue to utilise the Oaks hospital for RTT which in turns frees up capacity within the trust for cancer pathway deliver. Plans for the use of ISP to support diagnostic delivery both insourcing, and out-sourcing will also continue in conjunction with divisional financial planning agreements. WSFT will continue to use the Oaks and the BMI for Elective recovery, as well as in health for endoscopy and insourcing for endoscopy, all of which ensures cancer is prioritised on the main WSFT. Breast services have now moved back to the main site.
• Within ESNEFT the new T.R.A.C.E system allows for real time tracking within specialties, this means that patients can be identifies at pace within the PTL who require escalating. We will support WSFT to mobilise this system for their PTL by the end of Qtr2.
• We will continue to maximise our ISP provision within the system as long as it remains available. • SNEE will develop a cancer dashboard by the end of Qtr. 1 to compliment regional level cancer data.
The dashboard will enable us to understand where our focus needs to be and highlight our challenged areas in a contemporaneous format. The dashboard will be automated to allow for efficiency within our data collection. The dashboard will include cancer outcomes, processes, case finding and prevention data.
• Evaluate and grow the role of the pre diagnostic nurse within ESNEFT (to assess to be clear on remit as unlikely one CNS can cover all referrals). The nurse supports patients who have complex social and health needs to reduce DNA rates and support access to diagnostics and treatment in a timely and supported way.
• The Cancer programme will continue to link into the development of the Community Diagnostic centres, reviewing pathways available to primary care for pre referral testing and additional opportunities for secondary care in relation to diagnostics.
• SNEE will continue to have workforce as a priority we will work with our system Strategic Health, Wellbeing and Retention Lead and continue to link into Health Education England around training and development opportunities to upskill our staff. This includes upskilling our diagnostic workforce.
• The Clinical Nurse Specialist review has started with an system wide oversight group established, this group will examine current CNS practice, staffing establishment, including the Band 4 role and skill mix
by September 2022, following learning recommendations from the review will be developed, to support a nursing competency framework and the future desired position of the CNS workforce by March 2023.
• SNEE will continue to implement Innovations that support diagnostic capacity including Cytosponge, Colon capsule endoscopy and FIT.
• In quarter one 22/23 SNEE will work with EASHN and the Cancer Alliance to Horizon scan and complete a priority matrix identifying this year’s innovation plan for cancer.
• WSFT are recovering their 28-day skin pathway utilising skin analytics, a delivery group has been established with ESNEFT colleagues to support their recovery and the implementation of the skin best practice pathway, with a new pathway live by Qtr. 4 22/23.
• SNEE will continue to work as a system to support improvements in 62 day and 104 day breaches, by working with our quality teams we have continued to review themes from root cause analysis and implementing transformation following the learning, we currently have a pre diagnosis nurse pilot running following learning relating to complex patients on our PTL and we have recently recruited a Psychological project lead to support the development of a psychological pathway and measuring psychological harm. We will support the development of a psychological support pathway embracing the principles as agreed in the EoE CA ‘Lessons learned and recommendations psychological distress working group’ paper
Risks, issues and mitigation • Over the last year the PTL has continued to grow and out strip capacity - we have linked into the development of the community diagnostic centres to support extra
capacity - we are continuing to work with histopathology to support the development of the digital
histopathology pathways. Digitising the slides will help network delivered care and help with tertiary referrals.
- we will explore innovations as they become available and pilot.
• Oncology nurse vacancies have resulted in pathways delays such that short term and longer vacancies are impacting on systemic therapy timeliness more specifically for subsequent treatments.
- throughout this year we have supported with additional resource for nurses. - IT systems are being reviewed to streamline oncology services - Flexible working patterns have been offered to support further recruitment - Recruitment from abroad is being explored.

• Another COVID variant causing another wave, the impact is reduced capacity within the providers dues to staff shortages and bed capacity. ESNEFT Cancer Recovery assumptions and assurance that the trajectories submitted are deliverable. Tumour site specific detailed recovery plans are available and are the basis of the recovery trajectories themselves. In the same way for WSFT, there are detailed recovery plans that sit underneath the trajectories, whilst the recovery plans will be challenging to all, they are achievable but there are the same risks as highlighted above, which have had a significantly impact throughout Q1.
SNEE will continue to offer flexible workforce options to staff enabled to work to isolation Cancer patients will continue to be prioritised for treatment within the providers.
• Caveats to delivery: Changes to CWT reportable standards (trajectories written before proposed changes were announced), Further impacts of Covid, Unforeseen clinical workforce issues (non-Covid related) i.e. unfilled vacancies
Improve performance against all cancer standards, with a focus on the 62-day urgent referral to first treatment standard, the 28-day faster diagnosis standard and the 31-day decision-to-treat to first treatment standard.
Assumptions Performance against the following cancer waiting times standards: •31-day treatment (First Treatment, Subsequent Surgery, Subsequent Drugs & Subsequent Radiotherapy) • 62-day urgent referral to first treatment (Urgent GP, Urgent Screening and Consultant Upgrade) • Faster Diagnosis Standard (FDS)
• 28-day standard is now being reported as part of cancer wait times, which has supported the system to understand our current position and develop recovery trajectories. We know our challenged pathways and are targeting those pathways with additional support. For ESNEFT - contractual implications/financial incentive as yet unknown however the aim is that trusts should not drop below the 65% CQUIN requirement whilst aiming to meet the national target of 75% by March 2024 (ESNEFT local ambition to deliver 75% from the start of Q2 22/23 and continue to improve /increase delivery to 85% by the end of Q3 22/23.For WSFT performance shows a significant improvement across multiple tumour sites. With the continued focus required within Colorectal, Head and Neck and Urology. Breast has recovered their 28-day position@ end February. ESNEFT - Actual performance to Feb 2022, trajectory April onwards:

WSFT – bottom line is trajectory:
• We will work to develop and implement action plans to improve performance against the existing
Cancer Waiting Times standards, with a focus on pathways which are most adversely affecting overall performance. Breast remains one of the constrained specialities, following a breast workshop to explore options to recover the pathway, a breast pain pathway has been launched within plan to launch later in the year. WSFT has poor 2WW performance on their skin pathway, they have recently gone live with a new Skin AI pathway and have now recovered their 2WW pathway.
• We will support implementation and monitoring of Best Practice Timed Pathways, ensuring that where investment is made this results in expected improvement to performance. We have a SNEE System Charter for the delivery of the Faster Diagnosis Framework with governance and milestones for delivery incorporated. We have non-site-specific pathways established within SNEE for vague symptoms and these are undergoing review in line with the new national FD Framework.
• Operational performance monitoring is a key part of our system Cancer governance structure, ensuring that improvement against the standards is regularly monitored and discussed at the ICS Cancer Programme Board and ICS Cancer Operational Group. A cancer performance improvement dashboard is in development for the ICS, a draft has been reviewed at the ICS Programme Board. The Deputy Director of Performance Improvement is developing the dashboard in conjunction with the Cancer Alliance - Head of Informatics. This supports the requirement to have a nominated performance lead as part of our team to act as the lead and be the key contact point within the system to respond to the Alliance to discuss Operational Performance.
• We will ensure that improvements in operational performance are delivered in an equitable way and use analysis of waiting times disaggregated by ethnicity and deprivation to address any variation. On March 10th we held a system-wide clinical away day, where public heath colleagues from both Suffolk and Essex presented the population health information including prevalence, deprivation, mortality and lifestyle data to the cancer clinical leads within our ICS.
• SNEE have been maximising the ISP provision available across the system and are outsourcing elective work to support cancer as a priority pathway, additional funding has been issued by national teams to support this extra activity, we have planned for this support to be maintained.
• Within SNEE we used our data to target the most challenged pathways, we have held two focused workshops one on Breast and one of dermatology, we now have a live breast pain pathway within our

system with further transformation planned for this year. Following the dermatology workshop, a delivery group has been established within ESNEFT to embed the best practice skin pathway.
• During the last year SNEE has been successful on opening a community diagnostic centres with additional capacity, the plan continues this year with further centres to be agreed and launched. The cancer programme will remain closely linked to this work to additional capacity within the pathway.
• We know a key enabler to achieving the CWTs is the first few days of the cancer pathway with a completed 2WW referral from primary care, we will work with primary care to support improved referrals and empower further triage, we will do this by, evaluating clinical decision support tools, recruiting an early diagnosis co-ordinator and community cancer nurses with a navigator.
Actions • We will implement a clinical decision tool in primary care to support patients to arrive at secondary care with pre referral tests completed, this will ensure there are minimal delays on first days of the 2WW pathway as patients can be appropriately triaged straight to test or to see a specialist first.
• We will improve the feedback loop to primary care to ensure that primary care is aware of the responsibility to ensure all pre referral guidance is completed and encourage uptake in the Non site-specific pathway alongside site specific pathways.
• Within SNEE we have been innovative around our workforce and have had success on the prostate pathway with Nurse Practitioners now undertaking template biopsies and Colposcopy procedures, we will continue to be a leader in staff development with Gynaecology speciality being the initial focus and developing a nurse led surgical triage pathway.
• In Qtr. 1 we will further develop our Straight to test workforce to remove patients who do not have cancer from the PTL, they will be upskilled to review results and support the specialty and patient to reduce waiting time on the pathway.
• SNEE have developed a robotic surgery pathway in many specialties which substantially increases capacity within the pathway, Gynaecology within ESNEFT are now planning to launch a pathway which will reduce patient risk and increase capacity within the specialty, to support the pathway they will recruit an additional CNS to specialise in ensuring the robotic pathway is maximised.
• Oncology is a key enabler in first treatments and has had some delays this year, we will continue working with our system to support oncology capacity. We will continue to work with our providers to ensure capacity within our system. As part of our workforce review, we will look at recruitment and retention of oncology nurses to ensure a sustained workforce. ESNEFT has implemented a cloud-based integrate radiotherapy system and become ‘paper-light’ enabling resilience through cross-cover potential and remote working’.

• WSFT will improve their reporting time for CTs by implementing a Terarecon system in Qtr. one, this will increase capacity for the current radiology team to report, the specialities impacted will be colorectal for their CtCs and the breast pathway.
• Access to diagnostic is a key constraint within the providers, WSFT will increase their diagnostic capacity within their breast one stop shop in the first quarter which will enable an extra clinic in each session.
Risks, issues and mitigation • Over the last two years there has been huge pressures on our workforce and they have continued to work at an exceptional pace and consistently working extra to keep pace with demand and cover unprecedented levels of sickness due to COVID, our workforce is now fatigued, the risk is they will no longer be able to maintain the work required to deliver the required recovery. SNEE are mitigating this by being innovative with our workforce and upskilling where we can. Encouraging and supporting more flexible working across organisations.
• WSFT surgical capacity has been constrained by RAAC plank work, the theatre element of this is due to be completed in Spring, with RAAC work continuing on the wards and other areas of the hospital, with this cancer services will continue to be prioritised during periods of reduced activity. WSFT are currently utilising mutual aid and ISP provision.
• Over the year SNEE have seen a huge increase in referrals into the 2WW pathways, some specialties have seen as much as 130%, with normal seasonal fluctuations not seen this year. Our providers are now modelling their capacity from these new levels, if further increases are seen the levels would out strip capacity available.
• Diagnostic capacity remains a constraint within our system; - CT at WSFT is currently being supported by an additional scanner which will remain in situ,
subject to appropriate funding. CT at ESNEFT Ipswich site is supported by an additional scanner and Clacton now have a CDC supporting their additional CT
- US capacity at WSFT is a continued challenge which is impacting on 28-day performance for Head and Neck, WSFT are in the process of implementing a one stop service.
- Endoscopy remains constrained across the system; it is currently being supported by ISP and CCE. WSFT have recently reviewed their CTC pathway, which has had a positive impact.
- FiT is now going to be incentivised across primary care to support triaging in the early stages of the pathway.
- Demand and Capacity review being supported by NHSE for colorectal being undertaken in the system,
• Within ESNEFT HDU bed capacity is limited which results in cancelled surgical lists. - Staffing being reviewed to support a more sustainable approach to HDU bed capacity.
Extend coverage of non-specific symptom pathways, with at least 75% population coverage by March 2023.
Assumptions Expected volumes should align with the trajectories submitted against this metric by ICSs as part of the operational planning process. The revised NSS projected referral demand tool will help with this. Narrative plans and milestones should focus on how the Cancer Alliance expects pathway implementation to progress across all relevant providers quarter by quarter, as well as key actions the Cancer Alliance proposes to take to support the embedding of the timed pathways and delivery of key milestones. Where possible, Cancer Alliances should seek out and use 'real' data to populate baseline performance and estimates of performance through the year. Where this is not possible, Cancer Alliances should
• We will deliver referral volumes that reflect at least 75% population coverage for NSS pathways by March 2023. For WSFT for the 28-day standard the unvalidated February performance shows a significant improvement across multiple tumour sites. With the continued focus required within Colorectal, Head and Neck and Urology. We can also see that Breast has recovered their 28-day position. At the end of February, the unvalidated position overall was 70.8% For ESNEFT given the improved overall performance in 2WW standard which once sustained will lead to an improvement in 28FDS performance. This is currently 78.6% @ end February.
• We will ensure NSS services will be sustainably commissioned or in commissioning intentions in 2023/24. We have a dedicated Transformation Lead for FDS delivery with a governance structure to support of a Senior Oversight Group and ICS wide delivery group which are accountable to the ICS Cancer Programme Board. A separate Charter for FDS and work programme have been established to meet the national prescribed best practice pathways for the 7-site specific and NSS pathway. We have completed the NSS referral demand tool with 100% population coverage from 1st April as we already had our primary care practices engaged in referrals to vague symptom services.
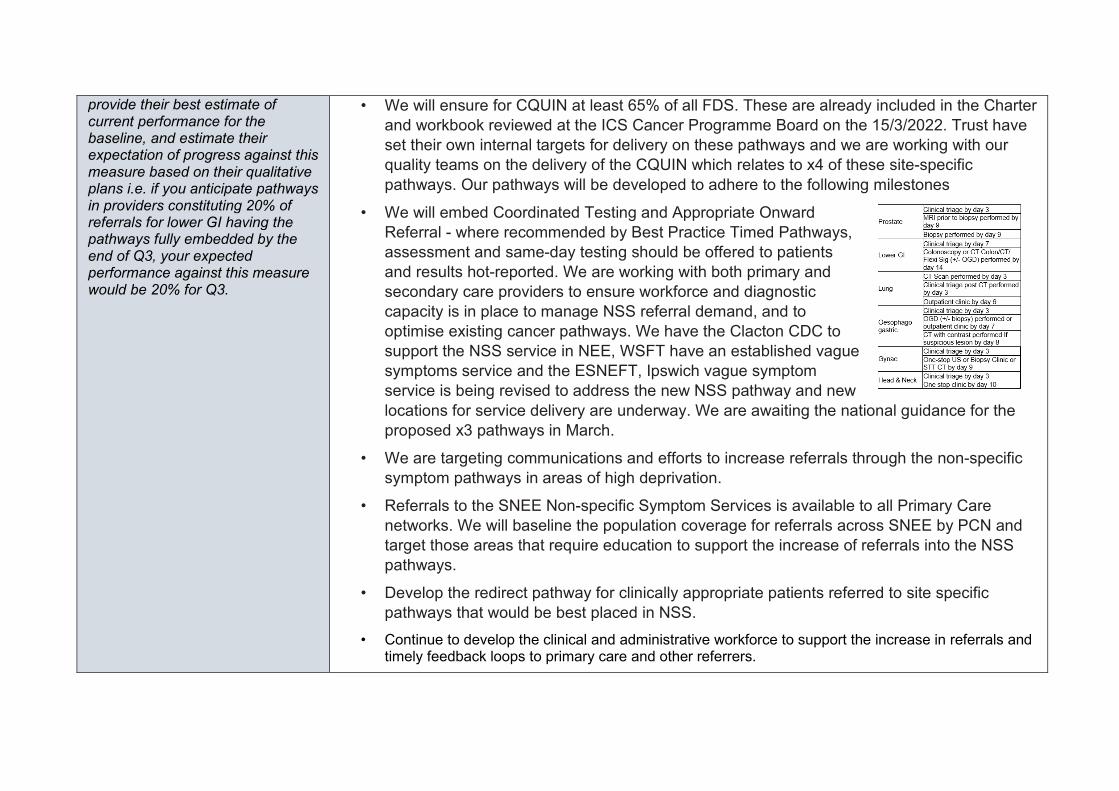
provide their best estimate of current performance for the baseline, and estimate their expectation of progress against this measure based on their qualitative plans i.e. if you anticipate pathways in providers constituting 20% of referrals for lower GI having the pathways fully embedded by the end of Q3, your expected performance against this measure would be 20% for Q3.
• We will ensure for CQUIN at least 65% of all FDS. These are already included in the Charter and workbook reviewed at the ICS Cancer Programme Board on the 15/3/2022. Trust have set their own internal targets for delivery on these pathways and we are working with our quality teams on the delivery of the CQUIN which relates to x4 of these site-specific pathways. Our pathways will be developed to adhere to the following milestones
• We will embed Coordinated Testing and Appropriate Onward Referral - where recommended by Best Practice Timed Pathways, assessment and same-day testing should be offered to patients and results hot-reported. We are working with both primary and secondary care providers to ensure workforce and diagnostic capacity is in place to manage NSS referral demand, and to optimise existing cancer pathways. We have the Clacton CDC to support the NSS service in NEE, WSFT have an established vague symptoms service and the ESNEFT, Ipswich vague symptom service is being revised to address the new NSS pathway and new locations for service delivery are underway. We are awaiting the national guidance for the proposed x3 pathways in March.
• We are targeting communications and efforts to increase referrals through the non-specific symptom pathways in areas of high deprivation.
• Referrals to the SNEE Non-specific Symptom Services is available to all Primary Care networks. We will baseline the population coverage for referrals across SNEE by PCN and target those areas that require education to support the increase of referrals into the NSS pathways.
• Develop the redirect pathway for clinically appropriate patients referred to site specific pathways that would be best placed in NSS.
• Continue to develop the clinical and administrative workforce to support the increase in referrals and timely feedback loops to primary care and other referrers.
• Continue to develop Community Diagnostic Centres (CDC) across SNEE and ensure the NSS is built into this. The CDC at Clacton hospital is operational, resulting in an additional diagnostic capacity within the system which includes CT. Approval for a CDC to be developed on the Newmarket site will commence at end of 22/23, business is in development. A CDC is proposed for IES for 23/24 commencement – venue/location is currently being scoped. As part of the business case development, demand and capacity modelling for cancer referrals are included and colleagues working on FDS are part of the development teams to ensure diagnostics are available to support these pathways. One stop approach for non-site-specific pathways will be part of these new CDCs as spokes with local access.
• Continue to develop and implement innovations that promote earlier identification through screening that will outreach and target existing health inequalities.
Actions • A community (ICE) button has been developed in NEE and IES to facilitate the request for all mandatory first line tests to accompany the NSS referral.
• Implement a communications plan with primary care to advise of any service changes, attend educational sessions and listening events to share experience and practise.
• Monitor and track referral trajectories across PCNs using power BI and pinpoint areas of emerging concern, target communications and educational opportunities. The SNEE Cancer transformation team are working with PCNs to review and improve referral practice: to encourage regular peer review of cancer referrals using templates based on the CRUK NCDA and SEAs; promote the use of clinical decision support tools and use of PCN dashboards they create; use the primary care data pack generated by the EoE CA PCG to identify areas of improvement; and development of electronic referral platforms to ensure completeness of referrals
• Continue the implementation of the Best practice Time Pathways. Ensuring pathways are compliant and developing action plans to support those that require improvement.
• Encourage appropriate access to advice and guidance access across primary and secondary care to promote referring the right patient on the right pathway at the right time.
• Collect high quality patient level data to monitor and improve patient outcomes and experience using the National Minimum data set.
• Analyse and evaluate the SNEE experience of care survey in conjunction with patients, primary and secondary care and third sector stakeholders to drive improvements locally.

Risks, issues and mitigation • Sustaining a workforce with the right skills and experience for the NSS pathway is a key risk in accelerating the referrals to NSS and developing redirect pathways.
- Developing a workforce plan that incorporates timely recruitment, job planning supervision and education will provide an integrated service across primary and secondary care.
• Diagnostic capacity within cancer pathways remain constrained due to demand and diagnostic
workforce. Capital and Revenue funding streams for SNEE are required to develop CDCs and access equipment via the National Procurement Framework in a timely way.
- Strengthen relationships by ensuring early involvement with senior clinicians and diagnostic providers to fully prioritise the demand, capacity and the timeliness required for patients with a suspected cancer.
• Patients presenting to GPs at a late stage. - Actively develop positive patient engagement events. - Deliver targeted early interventions and awareness campaigns. - Incorporate Making Every Contact Count (MECC) to the NSS providing patients with a holistic
assessment that incorporates screening, familial cancer risk and lifestyle support with personalised onward referral and support and affect the working practise and timeliness of patients being reviewed and referred.
Make progress against the ambition in the NHS Long Term Plan to diagnose more people with cancer at an earlier stage, with a particular focus on disadvantaged areas where rates of early diagnosis are lower.
Please outline the priority actions your system and Cancer Alliances will be taking forward that are critical to the delivery of the cancer objectives below: [Max 200 words per section]
Timely presentation and effective primary care pathways (implementation of cancer primary care contract requirements; local awareness campaigns)
Over the last year we have completed cancer champion training with our colleagues in CRUK with our community providers to increase education and awareness in our local communities around the early signs of cancer. We will continue this work over the year by recruiting an Earlier diagnosis and cancer screening transformation lead post in the first quarter of the year. .
SNEE are piloting a community cancer nurse programme, with recruitment planned for June 2022 these nurses with a the support of a cancer co-ordinator will lead on cancer within targeted PCNs, the role of these nurses will be to work with PCNs and their local communities to raise awareness of the early warning signs of cancer and to encourage access. Within PCNs we will ensure complex social and health needs are identified and supported early in the cancer pathway, to maximise clinical outcomes if cancer is diagnosed and subsequent cancer treatment is required. The Social Care role will harmonise with community cancer nurses being developed to ensure that co-morbidity issues are addressed robustly to ensure seamless cancer pathways. Within SNEE we have strong clinical leadership from primary care who continue to work with primary care through GP education to support the implementation of the PCN DES. Supporting PCNs to deliver early diagnosis DES: interrogation of primary care data pack as above; promoting referrals in areas slow to catchup post pandemic (e.g. urology, lung); use of PHM to identify area of lower than expected referral; ensure cancer information is available in multiple languages; and targeted work to increase cancer awareness in underrepresented groups. Co-production is key in developing new services, SNEE are currently developing a patient engagement plan to support improved pathways for cancer patients within primary care. SNEE are part of the GRAIL study, this pilot will run in our system for the next year and support the early identification of cancer patients.
Faster diagnosis (best practice timed pathways and priority pathway improvements including cancer screening) Include information on each provider with teledermatology services in place and the approach to teledermatology being implemented (image taken in primary care, image taken in secondary care, image taken in hub, image taken by patient). Expected activity for each quarter should then be provided as a % of all skin FDS referrals.
• Trusts have set their own internal targets for delivery on these pathways and we are working with our quality teams on the delivery of the CQUIN which relates to x4 of these site-specific pathways. Our pathways will be developed to adhere to the following milestones.
• We will continue to extend the provision of teledermatology services and community spot clinics. We already have well established teledermatology pathways with triage and AI for skin at WSFT which is proving successful for the 28 FDS pathway and consultations reporting that the triage algorithm is very accurate with no clinical assessment changes for onward referral.
• For both trusts SMS reminder systems are in place and being actively utilised. • Targeting communications and efforts to increase referrals to non-specific symptom pathways in areas
of high deprivation. SNEE is working closely with regional diagnostics teams to ensure Community Diagnostic Centres provide required capacity for cancer pathways. Our CDC business case demand and capacity modelling takes into consideration the requirements for increased and faster access to
Narrative milestones should focus on the actions to be taken by the Cancer Alliance to ensure teledermatology is available as an option, and how the Cancer Alliance will encourage both dermatology services and primary care to make appropriate use of the service. Please ensure to provide details of how the Cancer Alliance plans to engage with the local diagnostics team to support and influence the development of plans for Community Diagnostic Centres. Please also set out how the Cancer Alliance plans to assess how planned CDC developments will contribute to the delivery of wider Faster Diagnosis and Operational Performance objectives.
cancer diagnostics as part of the CWTS. The Clacton CDC already incorporates our national Targeted Lung Health Checks service and associated diagnostics.
• In SNEE we have ensured that patients are supported through their pathway. Cancer transformation monies have been utilised to support navigator roles within ESNEFT and WSFT. For ESNEFT more recently via roles in the information centre. We are currently reviewing our options for Navigators within the system following the success of the WSFT navigator project.
• We will work towards the implementation and measurement of the 10 priority Quality Markers which are included in our project plan. We have recruited a Deputy Director Nursing who is supporting the cancer programme and will be leading on these quality markers.
• We will consider other pathway elements within the Faster Diagnosis Framework, such as self-referral. SNEE has implemented a breast cancer symptomatic service – which is a nurse led assessment service in the community. Our next step is to consider self-referrals to this service once is has been operational for a period of time and we have evaluated its performance to ensure the model is sustainable. We are working with Professor Roberts from Nottingham in the implementation of their model and WSFT are starting to look at options for pathway changes to their breast cancer services towards this decoupling of Symptomatic vs 2WW breast lump pathway.
• Active participation in National Faster Diagnosis programme evaluation, including qualitive interviews. Straight to test nurses are now in place on all key tumour sites, over the next year we will review the pathways to and from STT nurses and encourage the feedback loop to primary care for those referrals where pre referral tests have not been completed and support referrals to NSS pathways if clinically indicated.
Further initiatives include:
• SNEE have been working with primary care and secondary care to develop a referral and triage platform, the platform will support primary care to complete required pre referral tests and wait for results prior to referring, the platform will support clinical decision making following the test results and encourage referrals into the Non site specific pathways if clinical indicated.
• Over the next year SNEE will continue to build on the success of this year’s innovative pathways. We will continue to implement Colon Capsule Endoscopy and Cytosponge which increases the diagnostic capacity within the pathway. Following the recovery of the skin pathway at WSFT we will work with ESNEFT to implement the new dermatology timed pathway.

• Histology is a key part of all the best practice pathways; therefore, we will continue to work with the teams to develop digital histopathology pathways across the system,
• Community diagnostic centres are now in development within our system with Clacton Hospital live, the cancer programme will continue to have strong links into the workstream to ensure pathways for cancer patients are considered within the additional diagnostic capacity.
SNEE have had success with the skin analytic pathway within WSFT and this year will expand tele dermatology to ESNEFT.
Targeted case finding and surveillance (Targeted Lung Health Checks, Lynch syndrome, liver surveillance)
SNEE have been awarded targeted lung health checks to be launched in Q2 22/23, a delivery group has been established to support the launch with key stakeholders. Local workstreams are now in development to ensure we have maximum uptake of the offer once it is launched. Within SNEE colorectal lynch testing has been available to service users for some years, we are working with ESNEFT to ensure an endometrial pathway is available to services users on their pathways. WSFT don’t currently see their endometrial patients they all attend CUH where the pathway is established. SNEE will utilise the first quarter of the year to stock take our current Liver surveillance programmes within our systems and to link into our Hep C networks through our system alliance partners in preparation for Expressions of Interest due to be published in Qtr2.
Population screening (restoration of three-year round length for NHS Breast Screening Programme, continued age extension in bowel screening and maximising uptake of breast, bowel and cervical screening)
SNEE have worked with our voluntary sector providers over the last few years to target at risk groups for screening, we will continue to build on the success of this as we move out of COVID and more community groups start to meet up again. We will continue through our SNEE screening group to identify and work with at risk populations. One of our priorities this year is Learning Disability patients and we are currently working with Essex County Council who are auditing LD annual health checks and associated action plans, once this audit is completed we will work with the ECC leads to embed next steps in the screening process. Via this work stream we are developing resources for our LD population to support better uptake of their screening opportunities, Following a recent award of FiT funding we have linked into Bowel Cancer UK; with their support we are going to plan some events in targeted areas promoting bowel screening and sharing best practice on how to take a FiT test. SNEE are currently working with Bowel Cancer awareness, in April we are going to run a series of events across our system promoting early identification of Bowel cancer and improving uptake of screening.

C3: Diagnostics Please summarise the key assumptions that underpin the numerical plan submission associated with the key priorities listed below, highlighting any key risks and issues. Outline the priority actions your system will be taking to increase diagnostic activity to a minimum of 120% of pre-pandemic levels across 2022/23 to support these ambitions and meet local need, including:
• any activity increases associated with the actions planned to improve diagnostic productivity, including utilisation, and the impact of diagnostic digital network and Community Diagnostic Centre implementation
• how your system plans to sustain and increase diagnostic activity levels delivered through acute sites and Community Diagnostic Centres
Assumptions
Subject to completion of the actions and mitigation of the risks below we expect deliver this expectation. Specifically, ESNEFT have identified a risk with achieving 20% in endoscopy (plans currently at 15%) - WSFT have planned on the basis of a 20% increase at this point. We are seeking to close the gaps through our detailed planning and have assumed in our figures we can close the gap to 120% through the independent sector. We have assumed:
• funding will be available to achieve this • RAAC remedial work will not have an impact on diagnostic capacity. • The mobile CT scanner which is currently in use will remain in place and continue to be funded. • A mobile MRI scanner will be sourced and funded to respond to the increased demand. • All insourcing/outsourcing and agency costs for increased activity will be supported and funding remain in place. • That there will be no further activity reductions/restrictions as a result of Covid-19 guidance.
Demand (specifically cancer demand) that might divert capacity away from diagnostics will not increase above the forecast. Actions We will:
• Maximise the use of our current capacity utilising weekend, evening and mobile capacity. Insourcing of staff to support this.
• Continue efforts to source a Mobile MRI scanner in WSFT. Additional MRI in SCC building in Ipswich

• Engage with and expand the cytosponge and colon capsule capacity, with an increase in the volume of patients going through these pathways to free up capacity within endoscopy
• Complete estates work for additional ultrasound resource in trust community settings. • Complete the options appraisal for a Community diagnostic hub in West and East Suffolk. • Implement digital histopathology • Improve productivity by reducing the appointment times by 5 mins for CT and MRI • Completing the Intensive Support Team (IST) review of capacity and demand for endoscopy and implement actions.
Risks, issues and mitigation
The following are our key risks: • Workforce – there is a reliance in many diagnostic areas on agency and locum staff and an inability to permanently
recruit to these posts (nationally). • RAAC – the continuation of the RAAC programme will impact some diagnostic areas, there is mitigation being worked
through in terms of utilising other clinical areas or IS capacity. • Availability of mobile scanners – whilst there is a CT scanner currently on site, the availability of a mobile scanner is a
risk at WSFT. • Age of equipment – many items of capital equipment is significantly aged and is liable to failure. • Finance – any withdrawing of funding to support additional work and mobile units will impact the ability to reach 120%. • Continued increase in inpatient demand therefore impacting capacity on waiting times.
D. Improve the responsiveness of urgent and emergency care (UEC) and build community care capacity – keeping patients safe and offering the right care, at the right time, in the right setting. This needs to be supported by creating the equivalent of 5,000 additional beds, in particular through expansion of virtual ward models, and includes eliminating 12-hour waits in emergency departments (EDs) and minimising ambulance handover delays.
D1: Urgent and emergency care
Please summarise the key assumptions that underpin the numerical plan submission associated with the key priorities listed below, highlighting any key risks and issues.
Reduce 12-hour waits in EDs towards zero and no more than 2%
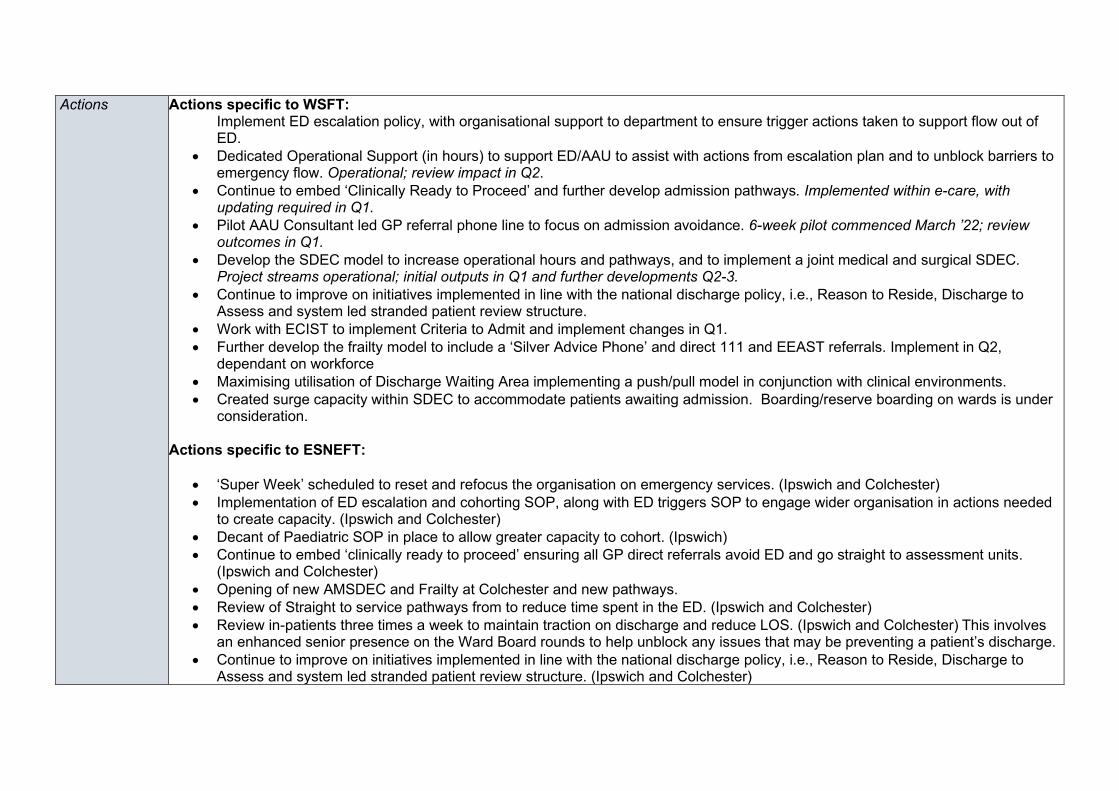
Actions Actions specific to WSFT: Implement ED escalation policy, with organisational support to department to ensure trigger actions taken to support flow out of ED.
• Dedicated Operational Support (in hours) to support ED/AAU to assist with actions from escalation plan and to unblock barriers to emergency flow. Operational; review impact in Q2.
• Continue to embed ‘Clinically Ready to Proceed’ and further develop admission pathways. Implemented within e-care, with updating required in Q1.
• Pilot AAU Consultant led GP referral phone line to focus on admission avoidance. 6-week pilot commenced March ’22; review outcomes in Q1.
• Develop the SDEC model to increase operational hours and pathways, and to implement a joint medical and surgical SDEC. Project streams operational; initial outputs in Q1 and further developments Q2-3.
• Continue to improve on initiatives implemented in line with the national discharge policy, i.e., Reason to Reside, Discharge to Assess and system led stranded patient review structure.
• Work with ECIST to implement Criteria to Admit and implement changes in Q1. • Further develop the frailty model to include a ‘Silver Advice Phone’ and direct 111 and EEAST referrals. Implement in Q2,
dependant on workforce • Maximising utilisation of Discharge Waiting Area implementing a push/pull model in conjunction with clinical environments. • Created surge capacity within SDEC to accommodate patients awaiting admission. Boarding/reserve boarding on wards is under
consideration.
Actions specific to ESNEFT:
• ‘Super Week’ scheduled to reset and refocus the organisation on emergency services. (Ipswich and Colchester) • Implementation of ED escalation and cohorting SOP, along with ED triggers SOP to engage wider organisation in actions needed
to create capacity. (Ipswich and Colchester) • Decant of Paediatric SOP in place to allow greater capacity to cohort. (Ipswich) • Continue to embed ‘clinically ready to proceed’ ensuring all GP direct referrals avoid ED and go straight to assessment units.
(Ipswich and Colchester) • Opening of new AMSDEC and Frailty at Colchester and new pathways. • Review of Straight to service pathways from to reduce time spent in the ED. (Ipswich and Colchester) • Review in-patients three times a week to maintain traction on discharge and reduce LOS. (Ipswich and Colchester) This involves
an enhanced senior presence on the Ward Board rounds to help unblock any issues that may be preventing a patient’s discharge. • Continue to improve on initiatives implemented in line with the national discharge policy, i.e., Reason to Reside, Discharge to
Assess and system led stranded patient review structure. (Ipswich and Colchester)
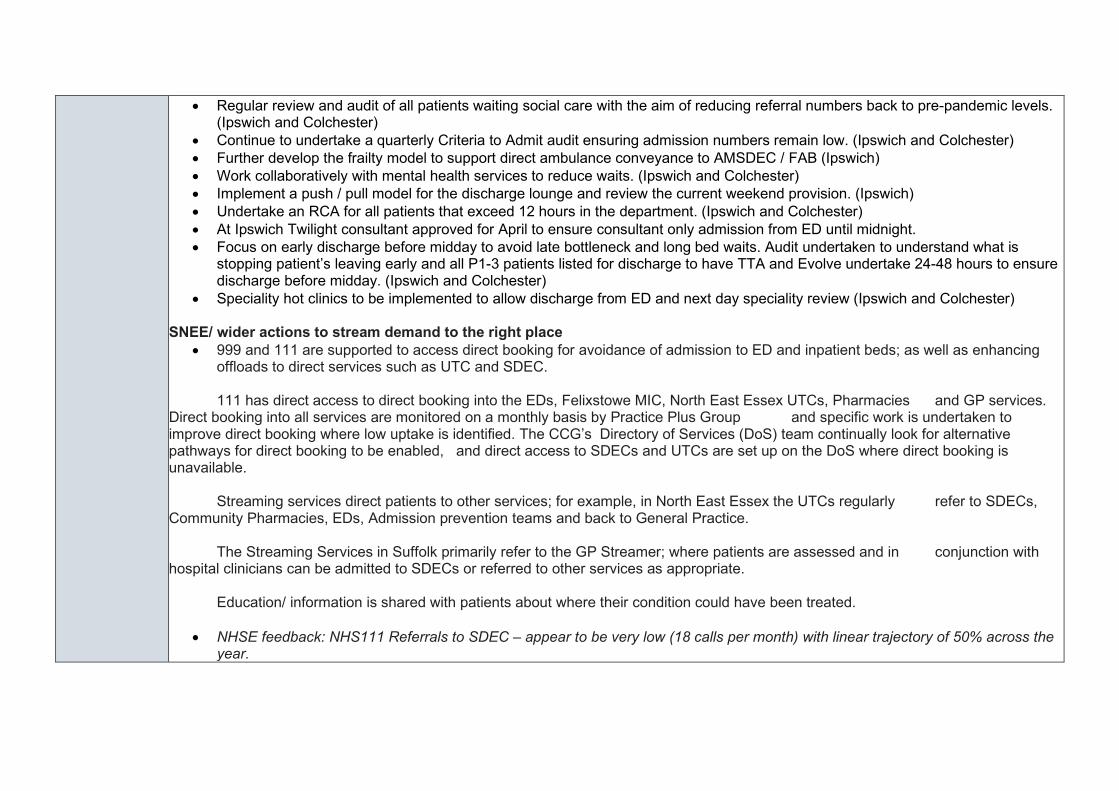
• Regular review and audit of all patients waiting social care with the aim of reducing referral numbers back to pre-pandemic levels. (Ipswich and Colchester)
• Continue to undertake a quarterly Criteria to Admit audit ensuring admission numbers remain low. (Ipswich and Colchester) • Further develop the frailty model to support direct ambulance conveyance to AMSDEC / FAB (Ipswich) • Work collaboratively with mental health services to reduce waits. (Ipswich and Colchester) • Implement a push / pull model for the discharge lounge and review the current weekend provision. (Ipswich) • Undertake an RCA for all patients that exceed 12 hours in the department. (Ipswich and Colchester) • At Ipswich Twilight consultant approved for April to ensure consultant only admission from ED until midnight. • Focus on early discharge before midday to avoid late bottleneck and long bed waits. Audit undertaken to understand what is
stopping patient’s leaving early and all P1-3 patients listed for discharge to have TTA and Evolve undertake 24-48 hours to ensure discharge before midday. (Ipswich and Colchester)
• Speciality hot clinics to be implemented to allow discharge from ED and next day speciality review (Ipswich and Colchester)
SNEE/ wider actions to stream demand to the right place • 999 and 111 are supported to access direct booking for avoidance of admission to ED and inpatient beds; as well as enhancing
offloads to direct services such as UTC and SDEC. 111 has direct access to direct booking into the EDs, Felixstowe MIC, North East Essex UTCs, Pharmacies and GP services. Direct booking into all services are monitored on a monthly basis by Practice Plus Group and specific work is undertaken to improve direct booking where low uptake is identified. The CCG’s Directory of Services (DoS) team continually look for alternative pathways for direct booking to be enabled, and direct access to SDECs and UTCs are set up on the DoS where direct booking is unavailable. Streaming services direct patients to other services; for example, in North East Essex the UTCs regularly refer to SDECs, Community Pharmacies, EDs, Admission prevention teams and back to General Practice. The Streaming Services in Suffolk primarily refer to the GP Streamer; where patients are assessed and in conjunction with hospital clinicians can be admitted to SDECs or referred to other services as appropriate. Education/ information is shared with patients about where their condition could have been treated.
• NHSE feedback: NHS111 Referrals to SDEC – appear to be very low (18 calls per month) with linear trajectory of 50% across the year.
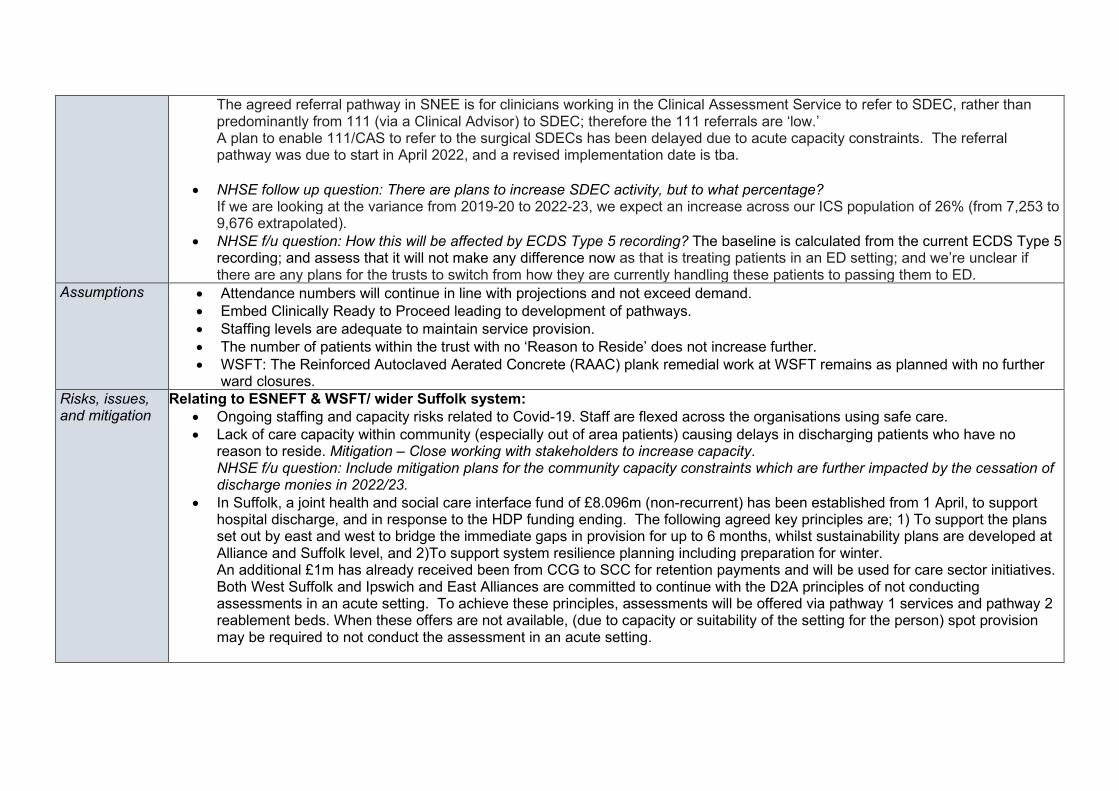
The agreed referral pathway in SNEE is for clinicians working in the Clinical Assessment Service to refer to SDEC, rather than predominantly from 111 (via a Clinical Advisor) to SDEC; therefore the 111 referrals are ‘low.’ A plan to enable 111/CAS to refer to the surgical SDECs has been delayed due to acute capacity constraints. The referral pathway was due to start in April 2022, and a revised implementation date is tba.
• NHSE follow up question: There are plans to increase SDEC activity, but to what percentage? If we are looking at the variance from 2019-20 to 2022-23, we expect an increase across our ICS population of 26% (from 7,253 to 9,676 extrapolated).
• NHSE f/u question: How this will be affected by ECDS Type 5 recording? The baseline is calculated from the current ECDS Type 5 recording; and assess that it will not make any difference now as that is treating patients in an ED setting; and we’re unclear if there are any plans for the trusts to switch from how they are currently handling these patients to passing them to ED.
Assumptions • Attendance numbers will continue in line with projections and not exceed demand. • Embed Clinically Ready to Proceed leading to development of pathways. • Staffing levels are adequate to maintain service provision. • The number of patients within the trust with no ‘Reason to Reside’ does not increase further. • WSFT: The Reinforced Autoclaved Aerated Concrete (RAAC) plank remedial work at WSFT remains as planned with no further
ward closures. Risks, issues, and mitigation
Relating to ESNEFT & WSFT/ wider Suffolk system: • Ongoing staffing and capacity risks related to Covid-19. Staff are flexed across the organisations using safe care. • Lack of care capacity within community (especially out of area patients) causing delays in discharging patients who have no
reason to reside. Mitigation – Close working with stakeholders to increase capacity. NHSE f/u question: Include mitigation plans for the community capacity constraints which are further impacted by the cessation of discharge monies in 2022/23.
• In Suffolk, a joint health and social care interface fund of £8.096m (non-recurrent) has been established from 1 April, to support hospital discharge, and in response to the HDP funding ending. The following agreed key principles are; 1) To support the plans set out by east and west to bridge the immediate gaps in provision for up to 6 months, whilst sustainability plans are developed at Alliance and Suffolk level, and 2)To support system resilience planning including preparation for winter. An additional £1m has already received been from CCG to SCC for retention payments and will be used for care sector initiatives. Both West Suffolk and Ipswich and East Alliances are committed to continue with the D2A principles of not conducting assessments in an acute setting. To achieve these principles, assessments will be offered via pathway 1 services and pathway 2 reablement beds. When these offers are not available, (due to capacity or suitability of the setting for the person) spot provision may be required to not conduct the assessment in an acute setting.

Relating to wider NEE system: ECC have received £760,000 of funding for support to the care market in NEE, and this will be reviewed again as part of ECC planning. ECC use beds currently commissioned to support spot usage, and as such, the pressures for the end of HDF is not as acute. NEE has allocated £1.6m (non-recurrent) for discharge support into next year. Each Alliance has developed detailed plans in response to the capacity constraints. Relating to WSFT:
• RAAC programme leading to reduced bed capacity. Two wards are currently closed with a third to be closed during spring/summer. This reduction creates a challenging context to achieve significant improvement. Mitigation – additional decant ward opened late 2021 for medical Covid capacity.
• Due to outlined capacity issues, WSFT lacks surge capacity, leading to SDEC being used as surge capacity and reducing the ability to operate an effective SDEC model. Mitigation – Limit number of escalation spaces giving four spaces to maintain some SDEC activity.
• Workforce – recruitment, retention, and current vacancy position. The ED footprint expanded over the last eighteen months although not yet recruited into increased establishment. Restarted overseas pipeline although challenged due to global pandemic and lack of available accommodation for overseas nurses. Mitigation – Communications team involved in recruitment campaign, rotational nursing posts available, Estates and Facilities colleagues looking into alternative accommodation.
• If the pilot of a consultant led GP referral phone line for AAU (to focus on admission avoidance) is successful it will require further funding to increase consultant body.
Relating to ESNEFT:
• Mental health capacity for increase in demand for mental health beds – working in close collaboration with mental health service. Minimise handover delays between ambulance and hospital, allowing crews to get back on the road and contribute to achieving the ambulance response standards. Actions SNEE have consistently maintained ambulance handover delays within ISR tolerance zone which is being tracked regionally. However,
focus on this is being maintained given that delays remain significantly higher than pre-pandemic and this continues to be viewed as unacceptable. The system has developed an Operations Hub to support system flow and monitors, taking supportive actions when required in the event of ambulance delays. HALO presence has been funded by the system to support front of door and reduce delays, identifying pinch points and supporting forward planning. Further planned system actions to reduce handover delays include:

1. Learning form ECIST input and agreed organisational plans. 2. Evaluation and forward plan to be developed following triangulation of outcomes from the EEAST Perfect Day on 3 March, and
ESNEFT Perfect Week commencing 28th February. 3. Reviewing and further developing access to the ambulance stack linked with the front door initiative and will continue to work with
EEAST to achieve this. 4. Actions giving ambulance crews direct access to services i.e., SDEC and avoiding the EDs. 5. The system is planning a system review and further actions on Wednesday 2nd March with a view to establishing an Emergency
and urgent care recovery Committee as part of its recovery journey. There will be a key focus on patient safety and outcomes. Actions specific to WSFT:
• Updated ambulance escalation SOP in Feb 22, providing clear escalation procedures within ED, and considering the extended footprint.
• Investigate potential of extending consultant led RAT operating hours. • Working with HALOs to review the handover process to ensure streamlined, safe, and effective handovers. Work streams
established in Feb’22, outputs delivered in Q1. • Departmental refocus on reducing handover delays, working with ED Floor Coordinators, Clinicians, HALOs and dedicated
Operational Support. Workstreams established in Feb’22, outputs delivered in Q1. • Consider relocation of HALO within RAT environment, supporting timely coordination of arriving crews. • Operational support for early consideration of cohorting/off-loading ambulances when inbound demand has increased. Currently
operational and impact to be reviewed in Q2. • Review HALO ED operating hours (included within above work streams). • Embed monthly governance meetings with clinical, operational and HALO teams within ED to undertake RCAs for extended
handover delays, to seek out learning/improvements. Currently operational Actions specific to ESNEFT:
• SGPF conveyance avoidance phone line in place on the Ipswich site. • Re-establish the Frailty Silver phone giving crews direct access to speciality frailty advice. (Ipswich and Colchester) • Ambulance crews to have direct access to AMSDEC and Frailty service avoiding ED. (Ipswich and Colchester) • Updated ambulance escalation and Cohorting SOP as well as a Paediatric decant SOP. (Ipswich) • ‘Super Week’ reset with a focus on creating capacity to reduce ambulance handovers. (Ipswich and Colchester) • ED triggers tool to be reviewed to create a proactive not reactive response. (Ipswich first and then Colchester) • ED huddles to continue with HALO, Floor Coordinator and Site Team identifying key actions required. (Ipswich and Colchester) • Investigate potential of extending consultant led RAT operational hours (Colchester)
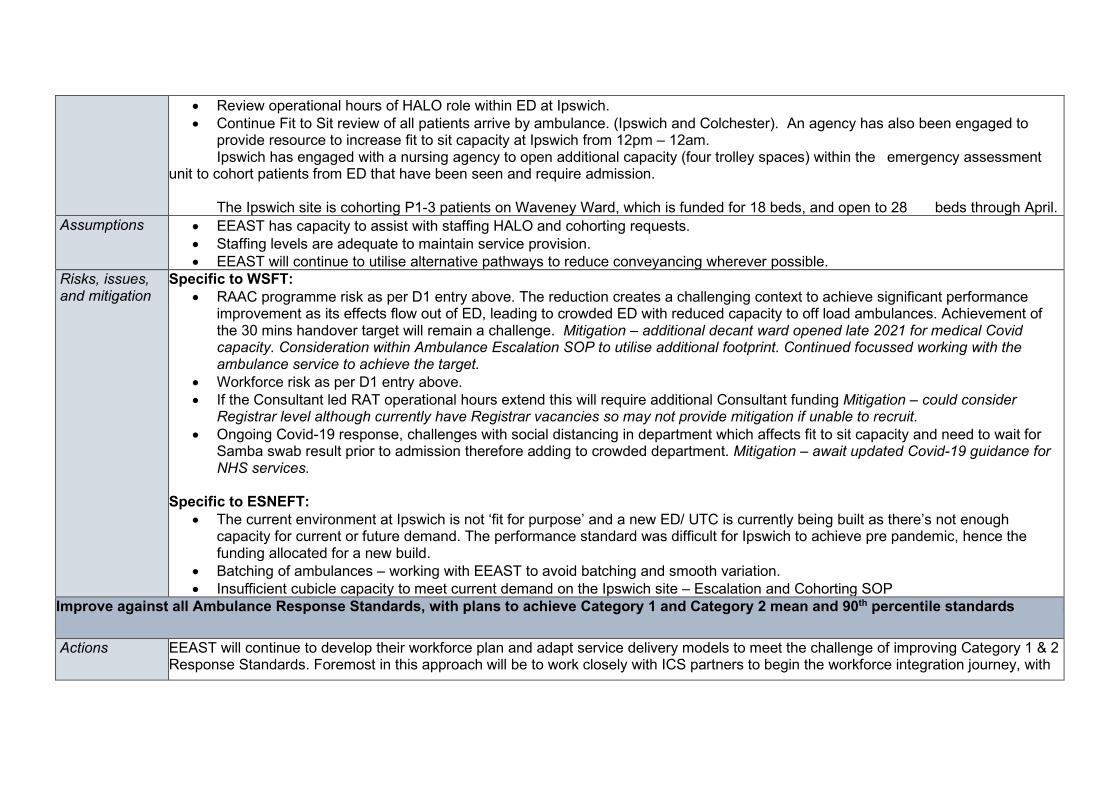
• Review operational hours of HALO role within ED at Ipswich. • Continue Fit to Sit review of all patients arrive by ambulance. (Ipswich and Colchester). An agency has also been engaged to
provide resource to increase fit to sit capacity at Ipswich from 12pm – 12am. Ipswich has engaged with a nursing agency to open additional capacity (four trolley spaces) within the emergency assessment unit to cohort patients from ED that have been seen and require admission. The Ipswich site is cohorting P1-3 patients on Waveney Ward, which is funded for 18 beds, and open to 28 beds through April.
Assumptions • EEAST has capacity to assist with staffing HALO and cohorting requests. • Staffing levels are adequate to maintain service provision. • EEAST will continue to utilise alternative pathways to reduce conveyancing wherever possible.
Risks, issues, and mitigation
Specific to WSFT: • RAAC programme risk as per D1 entry above. The reduction creates a challenging context to achieve significant performance
improvement as its effects flow out of ED, leading to crowded ED with reduced capacity to off load ambulances. Achievement of the 30 mins handover target will remain a challenge. Mitigation – additional decant ward opened late 2021 for medical Covid capacity. Consideration within Ambulance Escalation SOP to utilise additional footprint. Continued focussed working with the ambulance service to achieve the target.
• Workforce risk as per D1 entry above. • If the Consultant led RAT operational hours extend this will require additional Consultant funding Mitigation – could consider
Registrar level although currently have Registrar vacancies so may not provide mitigation if unable to recruit. • Ongoing Covid-19 response, challenges with social distancing in department which affects fit to sit capacity and need to wait for
Samba swab result prior to admission therefore adding to crowded department. Mitigation – await updated Covid-19 guidance for NHS services.
Specific to ESNEFT: • The current environment at Ipswich is not ‘fit for purpose’ and a new ED/ UTC is currently being built as there’s not enough
capacity for current or future demand. The performance standard was difficult for Ipswich to achieve pre pandemic, hence the funding allocated for a new build.
• Batching of ambulances – working with EEAST to avoid batching and smooth variation. • Insufficient cubicle capacity to meet current demand on the Ipswich site – Escalation and Cohorting SOP
Improve against all Ambulance Response Standards, with plans to achieve Category 1 and Category 2 mean and 90th percentile standards
Actions EEAST will continue to develop their workforce plan and adapt service delivery models to meet the challenge of improving Category 1 & 2 Response Standards. Foremost in this approach will be to work closely with ICS partners to begin the workforce integration journey, with

focus on pre-hospital care pathways to ensure patients are referred into the most appropriate care setting, as well conveying alternatives to ED Majors to mitigate ED pressures. EEAST will continue developing their Action Plan to effectively manage abstractions for both the Front Line and the Emergency Operations Centres. NHSE/I and the Lead Commissioner will continue their joint oversight and support to EEAST during 2022/23, and this will include agreeing the recovery trajectory outputs for Cat 1 and Cat 2 to ensure that the standards recover as quickly as reasonably possible. All health systems in the region will continue to address reducing patient handover delays at hospital as a priority action; with extra focus on the seven most challenged ED sites which are all outside our ICS. The new Serious Incident Framework will also ensure that delays in ambulance responses to patients in the community will be reviewed as system delays, and this will allow system leaders the opportunity to collectively assess patient harm and ongoing risks, as well as consider root cause actions to mitigate these risks.
Assumptions • EEAST will deliver all agreed key actions on their workforce and capacity plans. • EEAST will deploy sufficient capacity in Emergency Operations Centres and on the front line to effectively meet patient demand
and to work towards delivery against agreed response time improvement trajectories for C1 and C2 incidents. • Handover delays will reduce in line with agreed, local system trajectories and towards the new 15m/30m/60m arrival to handover
standards. • Referrals into Pre-hospital patient pathways will increase and, therefore, inappropriate patient conveyances to ED sites will reduce.
Risks, issues, and mitigation
• Workforce Capacity – Following completion of the workforce planning analysis being supported externally within the Trust, we will need to ensure there is sufficient capacity to meet training and education obligations in line with national standards and secure a sufficient pipeline of staff.
• Performance improvements – Linked to the above, performance will be affected by available resource within the Trust and ability to meet demand will be impacted by external factors relating to job cycle times e.g., hospital handover delays that the Trust is committed to working in partnership to resolve.
• Handover Delays – Revised HALO service to be deployed at all ED sites (subject to commissioning conversations); Daily system escalation calls across the region, Intelligent Conveyancing; reducing inappropriate ED conveyances, increasing discharge and flow. ‘Rapid release’ protocols to ensure ambulances can respond quickly to acutely unwell patients in the community.
• NHSE f/u question: C1 activity at 101.4% of 2019/20. With a significant reduction in activity predicted for Oct (86.7%) and Nov (87.8%) – what mitigations are in place? For activity, the monthly profiling always differs year on year depending on where the weeks start in any given month of the year (this is particularly noticeable for C1 for the relatively small volumes), and so some months will contain five weeks of activity, and some will have 4 weeks. This approach is consistent with other years in terms of the planning template.
• NHSE f/u question: Increase in C2 activity to 106.1% of 19/20, and C4 activity at 22.8% of 19/20 baseline – is this due to use of UCR? For C2, this is on trend and no further comments to make. C4 has reduced as activity has now switched into C5 due to the national AMPDS coding changes; this activity is therefore contained in a different activity plan line for 2022/23.
Other • NHSE f/u question: Is there broad system appetite of potential involvement in national and regional programme such as rapid
release and call before convey programmes? Yes, there is appetite to be involved in this. The C2 ‘rapid release’ programme is currently being trialled in Norfolk, as well as the initial trial site at The Lister Hospital. The pilot is also planned to roll out to the rest of Herts & West Essex in 2022/23. It has been agreed to initially run the ‘Call Before You Convey’ programme in Cambs and Peterborough which will then be expanded if successful.
• NHSE f/u question: How could 999/111 be supported to access direct booking for avoidance of admission to ED and inpatient beds? This would also enhance offloads to direct services such as UTC and SDEC. This has been extensively discussed with EEAST – very simply put there needs to be single points of call access for crews as they are often displaced away from their usual working location; and this SPOC needs to respond quicker than typical in the area – in line with how the GP Practice Plus Group and Suffolk GP Federation advice lines work in SNEE. If this could be agreed as a standard operating protocol in each STP/ICS, then this would help EEAST significantly; and deliver improved patient outcomes.
• NHSE f/u question. EEAST planning, request expansion with SMART actions throughout planning and clarity on how ambulance crews will maximise alternative pathways See bullet point above– if crews can have a single point of access in each ICS footprint with a guaranteed, ‘swift ‘response time then EEAST managers can fully support See & Treat ACPs. As a system we’re working with EEAST to support demand management and a number of initiatives are in place including; Implemented a C3 & C4 ambulance stack ‘push’ model (with plans to move to a ‘pull’ model) with a MDT process to manage demand in alternate pathways, and improve patient outcomes/ experience; and rapid telephone access to senior clinical advice to support decision making ahead of conveying a patient to hospital. Both models have demonstrated a reduction in people conveyed to ED.
D2: Transform and build community services capacity to deliver more care at home and improve hospital discharge Please summarise the key assumptions that underpin the numerical plan submission associated with the key priorities listed below, highlighting any key risks and issues. Virtual Ward beds - Virtual wards support patients, who would otherwise be in hospital, to receive the acute care, remote monitoring and treatment they need in their own home or usual place of residence, this should be the definition used across your system, for further guidance please see the virtual ward supporting guidance. By December 2023, we expect systems to have completed the comprehensive development of virtual wards (including hospital at home) towards a national ambition of 40–50 virtual beds per 100,000 population. As part of your response explaining how you will achieve this, please provide details on how this will impact positively on bed availability and how you will be supporting compliance with national sitrep and financial reporting for 22/23.
Actions
IES In Ipswich and east Suffolk Alliance (IES) a development group with programme support has been stood up covering both the development of clinical pathways and the identification and procurement digital systems and hardware to enable virtual wards (VW) to be realised in the timescale detailed above. A digital provider has been identified and associated funding sourced to procure both hardware and software. Clinical leads are in place for the development of care pathways and there is a clear focus on cohorts of patients that would otherwise need care in an acute setting for the development and prioritisation of those pathways. A key evaluation metric is the amount of acute bed capacity that will be realised through admission to a virtual ward setting. That in turn will release more capacity for elective recovery and potentially release resources to enable the sustainability of virtual wards into the longer term. The development of clinical pathways will consider both expand capacity to avoid admissions and to discharge people much earlier from acute beds. West Virtual Ward Planning Requirement Status Action Plan 22/23 1. Aim for phased implementation
towards 40 beds being live by early Q4 to support surge capacity with plans to extend incrementally to 100 beds by Dec 2023. Exact ICS
COVID virtual ward in place so infrastructure established.
1. End April: System plan on areas of greatest opportunity with associated business planning signed off by Alliance partners: a. OPAT extension to support admission prevention and supported discharge

Planning ambition targets for VW ward in West Suffolk are to hold 47 VW beds by October 22 rising to 103 by October 23.
b. AKI c. Respiratory d. Frailty and enhanced Integrated Neighbourhood Teams
2. UCR established and aligned to Virtual Ward approach by end Q2
3. 111 offer across SNEE to out of hours support in place by end Q1
4. Point of Care testing in place 2. Compliance with national guidance
on Virtual Ward Two Main areas of focus: - 1.Acute and Tech enabled VW 2.HAH and Tech enabled Frailty
Ward Areas of development and planning: -
- Telehealth expansion, logistics and workforce development
- Medical Model of ward oversight - Workforce modelling for care
provision
Q2 Specification and clinical governance framework for top pathways in place Evaluation framework agreed
NEE Planning in progress with ESNEFT to deliver VW capacity over 8 workstreams – costings still being worked up Sit rep reporting will be via ESNEFT reporting – this is part of the workstream planning We will form a Unified Digital Care Board, and support implementation of multiple projects at an alliance level including adoption of Virtual Wards to meet the requirements above
Assumptions IES
Virtual beds will begin to come online towards the end of Qtr. 1/start Qtr. 2 2022/23; supporting technology (software) will be procured before the end of 2021/22 and hardware procured during Qtr. 1; Clinical pathways will be defined through April and May. Staff support for monitoring and responding to care needs of those in virtual wards will be recruited through Qtr. 1. 22/23 – supported by VW national funding. Any connections with primary care and wider community service can be agreed during Qtr. 1 2022/23. Partnership with HUMA is established and will be developed throughout the set-up of VW and embedded in the governance for the programme with a keen focus on impact, namely the real delivery of acute level care outside of an acute building. Eight draft clinical pathways have been established to be developed. The eight clinical models include the following; • Model A – Inpatient Medical Respiratory – Early Supported Discharge (including ARI & CVW) • Model B - Inpatient Surgical – Early Supported Discharge & Admission Avoidance • Model C - Outpatient services - Admission Avoidance • Model D - Chronic Condition Management - Early Supported Discharge & Admission Avoidance • Model E - Community Outreach: Nursing Homes - Admission Avoidance • Model F - Inpatient Elective Orthopaedics – Early Supported Discharge & Pre-Op • Model G - Frailty – Early Supported Discharge & Admission Avoidance • Model H - Inpatient Medical Cardiac – Early Supported Discharge With those five clinical models, including Frailty, Elective Orthopaedic, Surgical and Medical models are being looked at for as priority roll out. Work is ongoing to evaluate those pathways in the context of the impact we are seeking to achieve. West Investment available to pump prime October 2022 launch and system investment to support reduction in acute LOS UCR plan implemented clinical governance agreed across system partners NEE Eight clinical models have been established by an overarching steering group as models in which the trust will see benefits from the introduction of a VW. The eight clinical models include the following; • Model A – Inpatient Medical Respiratory – Early Supported Discharge (including ARI & CVW) • Model B - Inpatient Surgical – Early Supported Discharge & Admission Avoidance • Model C - Outpatient services - Admission Avoidance • Model D - Chronic Condition Management - Early Supported Discharge & Admission Avoidance • Model E - Community Outreach: Nursing Homes - Admission Avoidance

• Model F - Inpatient Elective Orthopaedics – Early Supported Discharge & Pre-Op • Model G - Frailty – Early Supported Discharge & Admission Avoidance • Model H - Inpatient Medical Cardiac – Early Supported Discharge Five clinical models, including Frailty, Elective Orthopaedic, Surgical and Medical models will be prioritised for FY22/23. The Inpatient Medical Cardiac model will be piloted end of Q1/start of Q2. The following clinical model, to be agreed, will follow at the beginning Q3. The other priority clinical pathways will follow towards the end of financial year. The pilot will enable the trust to test and learn a clinical pathway to provide a proof of concept which subsequent clinical pathways can build on. The clinical model to be lifted as the trailblazer will be the Inpatient Medical Cardiac model. The model will be based around the work that has been successfully embedded and Norfolk & Norwich University Hospital (NNUH). The aim of the model is too safely on-board patients who are awaiting definitive treatment with or without an agreed date to be managed on the VW as appropriate. We have sufficient digital capability & licences exist to enable this (this is part of a wider Unified Digital Care Programme. Application for supporting resources to scale virtual wards will be submitted 11 March – assuming this will be supported, recruitment and programme planning / mobilisation has begun
Risks, issues and mitigation
IES In IES the main risk relates to the ability to recruit staff with sufficient seniority to manage patient risk in virtual wards and to minimise any risks of readmission to acute hospital. Mitigations will include considering support from Physician Associates, ACPs supplemented by support from existing consultant leads to successfully manage risk. West Workforce greatest risk: recruitment plan in development to support new roles Integration of technology solutions across SNEE: SNEE working group on cross cutting themes in development NEE Models still in development with costings still to be reviewed to check they meet the envelop indicated in guidance Risks to not recruiting lead to challenge with mobilising support. Pooled resources at ICS level mitigates this and other associated skills / capacity risks. The risk of widening exclusion will be mitigated by adopting the Equity and Equality approach and through work with Healthwatch and partners
2-hour urgent community response – For 2022/23, systems are asked to explain how they will achieve:
• Achieve full geographic coverage 8am-8pm 7 days a week and cover all 9 clinical conditions or needs of the national 2-hour guidance, if not fully embedded by April 2022;
• Increase the number of 2-hour UCR referrals and contacts and explicitly referrals from 111 and 999/ambulance services; • Increase workforce capacity in line with activity increases and support skill and competency development in line with the 9 clinical conditions. Where
there is no UCR workforce plan in place, please state expected month of achievement; • Improve productivity and reach more patients under 2 hours to exceed the minimum 70% threshold of people seen within 2 hours from the end of
Q3; • Improve data quality and completeness in the community services dataset (CSDS); and • Improve capacity and flow post-2-hour response to other sources of support including reablement, virtual wards, community nursing, VCSE etc.
Actions
Suffolk and North East Essex ICS Transformation Leads are working in partnership to deliver the National Standards for UCR Services and can confirm that services are meeting the criteria set out in the national guidance. Although the UCR teams are delivered through “place” based teams and deliver the service in a slightly different way, joined up working is enabling new system wide approaches to commence that support the whole of the SNEE system. Updates are provided below from each individual alliance placed based team to showcase their position. IES
• In Ipswich and east Suffolk (IES) REACT (Reactive Emergency Assessment Community Team) is well established and already provides a core service 8-8 across 7 days ensuring full geographical coverage across the locality.
• REACT have been working in collaboration with other UCR teams across SNEE (Suffolk and North East Essex) ICS and EEAST (East of England Ambulance Service Trust) to promote an increase in referrals from the ambulance service into UCR teams, including an ambition for UCR clinicians to have direct access to the 999 stack to ‘pull’ appropriate category 3 and 4 referrals. Currently in IES REACT receives an average of 25 from the ambulance service. During 2022/23 we are planning to replicate this collaborative work with our 111 colleagues to increase referrals from 111 into UCR teams. In IES REACT currently receives an average of 33 referrals per month from 111 but these are primarily for the out of hours nursing team and not specifically for the UCR service.
• IES REACT are working closely with TEC and pendant alarm providers to promote referrals into UCR. REACT have completed training with community responders who work as part of HEARS (Ipswich Borough Council’s pendant alarm provider) to increase awareness of UCR and increase referrals from them to reduce numbers of 999 calls as a result of people falling.
• The UCR workforce plan for IES has evolved year on year to build on the existing REACT service since its inception in January 2018. A significant investment has been secured using the 2021/22 Ageing Well monies to bolster the REACT

workforce and ensure the hub and spoke model for UCR is optimised and these posts will be recruited to during 2022/23. There will be a total of 24 WTE posts including nurses, therapists, generic worker & therapy assistant practitioners ensuring a workforce with the competency and skills required for the 9 clinical conditions that present to UCR services: Falls, frailty, reduced function, palliative care, urgent equipment needs, confusion or delirium, urgent catheter care, urgent support for diabetes and carer breakdown. We have also funded additional vehicles (electric cars as art of sustainability plan) to optimise 2-hour response form the three UCR hubs and more community lifting equipment to ensure timely response to non-injured fallers from both UCR and community teams.
• REACT’s current daily admission avoidance target for 21/22 was set at 22 patients referred into the service and this will be stretched to 24 patients per day for 22/23.
• Current indicative data shows REACT historically respond to 68% of crisis referrals within 2 hours. There is a data quality issue that is being resolved to ensure accuracy of CSDS submission. A REACT locality model is in development to optimise numbers of people receiving a 2-hour response. REACT hub and spoke model will see two rural hubs in Woodbridge and Stowmarket mobilised during 2022 which should improve the % to reach 70% or over in line with the national target by the end of Q3 in 2022/23. Advanced plans now moving to implementation for greater flexing of resources between community services to gain more productivity overall.
• From February 2022 the data quality issues with the CSDS submission for SNEE has been addressed. Dedicated data analyst role funded from 2021/22 ageing well monies to work pan-Suffolk to ensure this is maintained and there is data completeness moving forwards.
• REACT’s remit is to provide crisis support for up to 5 days maximum following the initial 2-hour response. Currently the average length of stay (LOS) for a person on the REACT caseload is 2.49 days evidencing good flow out of the service. Delays with transfers of care have historically occurred mainly due to inability to find on-going care. The REACT caseload LOS is regularly monitored, and action plans deployed to address any blockers.
West Suffolk
• Full UCR coverage of 7 day 0800-2000hr provision is in place and established, with an offer of 24/7 to be work through as part of demand and capacity planning by end Q2.
• Source of referral tracked integration with EEAST through pilot at triage in progress. Stretched trajectory to be agreed in Q1 with EEAST and 111 in line with Ageing Well allocation of funding to UCR. Q2 Evaluation of shared triage with EEAST to identify additional workforce and pathways changes relating to high demand 999 calls. Q2 CSDS dashboard in place and DOS review by end Q2
• Workforce mapping in progress and alignment into localities. Trajectory for increase in staffing based on 2021/22 Q4 numbers with a business case for UCR to support service improvement plan approved Q3.
• 70% of 2hr UCR responded within 2 hr by end Q3, with baseline assessment for delivery of response by mid Q1 and improvement trajectory agreed end Q1

• To improve data quality and completeness in CSDS, a digital analyst will be in post to support community compliance with reporting requirements by mid Q1
• To Improve capacity in post urgent community services to support flow and patient outcomes, work is underway to creating capacity in home care market with a review and recovery in progress. WS plan in place by mid Q1
NEE Full geographical coverage is already being delivered across North East Essex, with referrals being accepted between 8am and 8pm 7 days a week for a 2-hour response. The team are able to respond to all 9 clinical conditions in the following ways:
• Direct access to Operation Pendant for non-injured faller pick up - working closely with UCRS in NEE, referrals going both directions to keep patients out of hospital. Work being undertaken to support the service with ECC Adult Social Care Tech services and subsequent referrals through those channels.
• Direct access to Advanced Nurse Practitioners, Community Nursing Teams, the Frailty Unit, and all system admission avoidance partners including Urgent Care Paramedics and Falls vehicles
• Full therapy assessment provided by UCR team in 2-hour response • Working in Partnership with EOL SinglePoint and actively supporting EOL patients with therapy needs • SWAN is the Care / Reablement Provider assigned to the core team who provide ongoing care and support for
the patient, with referrals into core commissioned services • Access to Social Prescribers in the community specifically working with UCR teams to provide non-clinical
community support Increase the number of 2-hour UCR referrals and contacts and explicitly referrals from 111 and 999/ambulance services;
• Work undertaken with EEAST to promote service to all crews with regular review sessions and data sharing on referrals made with EEAST
• Current programme with EEAST to work with UCR teams to take work from the stack which needs further development to continue
• Close working partnership with EEAST Early Intervention Falls and Urgent Paramedic vehicles and referrals being made between services
• 111 – open to DOS and promotion of UCR to clinical leads for referral pathways
Increase workforce capacity in line with activity increases and support skill and competency development in line with the 9 clinical conditions. Where there is no UCR workforce plan in place, please state expected month of achievement;
• Workforce has been developed with ANP offer recently • Additional funding provided for reablement element of the service to provide overflow and meet demand and
capacity issues when referring into Essex County Council
• Current transformation to align other Community Provider and EEAST services to bolster resource in UCR Services
• Currently working in capacity as modelled - model in NEE was always designed to act as a hub and response service, utilising the plethora of admission avoidance services in the system and navigating the referrals into the right service for the right response, whilst responding to those calls appropriate for UCRS directly. The UCRS receive 10 referrals a day on average, however, many more calls through call centre and duty phone line which result in appropriate Admission Avoidance Services being used i.e. Singlepoint EOL, Early Intervention Vehicles, District Nursing etc
• Plans are to integrate the current UCRS with the admission avoidance teams at the front door, OPAT and the urgent response element of community nursing
• The community Nursing element is very much in the planning / funding stage and may need to go out to consultation.
• There will be an additional nurse lead (indicative B7) for the community nurse element of service, with a shared admin across the integrated service and an overarching service lead
•
Improve productivity and reach more patients under 2 hours to exceed the minimum 70% threshold of people seen within 2 hours from the end of Q3;
• Original productivity in 80+%, but seen a dip in Q3 due to change in reporting frameworks and referrals cominginto the team from discharge hub not accurate for a 2-hour response has seen a drop to 61%
Improve data quality and completeness in the community services dataset (CSDS); and
• Data quality is improving, and service is ready to meet CSDS reporting target of March 2022
Improve capacity and flow post-2-hour response to other sources of support including reablement, virtual wards, community nursing, VCSE etc.
• Currently no issues with majority of onward referrals and KPI’s being met, some issues with reablement provision which is a wider issue than North East Essex, being mitigated with regular discussion and system improvement with Newton Europe supporting system flow discussions.
Now receiving CSDS data – next step is to review data to ensure data quality is assured from March 22 Improve response time reporting by March 22 Continue system flow work to enable referrals into reablement in timely fashion
Assumptions ICS wide • Estates will be secured, and capital changes delivered within given timescales and within the providers capital funding
allocation and recurrent budget allocation. • That recruitment is successful and adds capacity in community service delivery rather than moving that capacity about; this is
crucial to picking up extra demand. In the medium/longer term our community integrated neighbourhood teams (INTs) will need to play a greater part in managing crisis demand for their local area.
• Same Day Emergency Care and Virtual Wards aligned and supporting UCR • Ageing Well Funding mapped to delivery of outcomes • Anticipatory Care received from NHSE and model adopted into the ICS • Capacity is within comfort at the moment and no further surges emerge
Risks, issues and mitigation
IES
• 2022/23 Ageing Well funding allocation for SNEE is less than was expected. Majority of investments for UCR in 2021/22 were agreed substantively so considerable proportion of 2022/23 monies is already committed. This leaves minimal amount for further investment into Anticipatory Care (AC) programme. However, this is likely to have minimal impact on UCR performance due to investment already secured. IES system have agreed that remaining ageing well monies for five-year period (e.g., 2023/24) will be focused on AC.
• In IES high vacancy rates across acute and community teams which impact on overall capacity to provide UCR within 2 hours. To mitigate this there are daily capacity meetings to ensure that resources are flexibly deployed to meet areas with most demand.
• Recruitment to new UCR posts (listed above) is challenging and some posts have been recruited to internally which now needs additional recruitment to ensure overall increase in workforce capacity is achieved. Mitigations do relate to the increasing join up in all community services and opportunities thereby in greater flexibility in staff deployment.
• UCR hub and spoke model is dependent upon estates being secured for spoke locations at Woodbridge and Stowmarket.
West
• Home care market capacity and resilience – Action plan in place • Recruitment to the post is challenging
NEE
• As detailed above with reablement, continuing to work with system partners and ECC to support the areas of risk within ECC for Reablement capacity and domiciliary care.
Funding for ANP roles not secured as it stands but will be added into future ageing well funds allocations Community service waiting lists – Please detail how you will develop a plan for and make progress to reduce community service waiting lists and ensure compliance of national sitrep reporting. Actions
IES In IES a Community Services Waiting List group has been established and is undertaking a review of all adult and children community service waiting lists to understand and agree the areas of focus and support that could identify opportunities to improve service resilience and reduced wait times for our population. This review will include both performance data and soft intelligence around the teams delivering the service and will be carried out during Q1 2022/23. An Action Plan will be developed and agreed. West Review of existing baselines across all Integrated Neighbourhood Teams and specialist services by May 2022 Review of triage function and workload scheduling to identify opportunities for improvement and delivery of consistent practice Strengthen pathway with Wellbeing offer with strategic Leisure provider to provide alternative support to people at risk of falls to release capacity in therapy teams NEE Continuing to develop the reporting mechanisms to enable accurate information available. A primary focus for the Community division, with a clear goal in our 2022/23 Business Plan to reduce all waiting times to within 18 weeks (or 6 weeks as appropriate).
Assumptions IES Data provided is accurate and reflects current service provision. West Recruitment to vacancies in Integrated Neighbourhood Teams Access to information to review demand and capacity
NEE Analysis of the Open Pathway data shows that overall we are seeing waiting times at somewhere around those at April 2021 and the reducing waits that we achieved towards the end of the Summer/Autumn, have gradually started to increase over the Winter, as we dealt with the pressures created by the Omicron variant, resulting in service cancelled contacts and patient DNAs. We expect to see this now beginning to turn as we are increasing activity, with less staff absent due to illness/isolation and less patients cancelling their appointments. All services have detailed recovery plans
• Paediatric OT – all children on Motor coordination pathway and majority on PNI pathway waiting over 18 weeks now have a booked appointment
• Community Rehab – additional bank staff have been appointed to offer appointments to the longest waiters • Stroke Rehab – MDTs with the acute wards have been instigated, to improve patient flow • Community Stroke Physio – additional support from the Stroke Association has been secured to release capacity in the
service • Physiotherapy Outpatients – additional estate has been secured for 12 months to increase clinic slots available • Respiratory – COPD patients are being safely discharged with direct SOS access back into the service if required • Podiatry – suitable biomechanics patients are being supported by the Orthotics service to increase capacity and reduce waits
in podiatry and an apprentice has also now been appointed Recovery remains place and actions being taken to mitigate the winter challenges and drive forward recovery.
Risks, issues and mitigation
IES Performance of specific services may be impacted by staff recruitment and retention.
West
Demand in referrals continues to grow exponentially: UCR and anticipatory care planning is progressed at pace Workforce: local workforce plan to be developed to ensure alternative options to recruitment challenges are in place NEE Staff absences - beginning to reduce following COVID surge period – Staff support measures in place Patient DNA’s now also beginning to reduce following vaccination programme and Covid rules being relaxed. Reporting - The BI team are continuing to develop PowerBI reporting for NEECS. This has created some challenges and until such time as waiting time data is able to report the ‘wait to first clinical contact’, which is the most accurate metric for our services, reporting is based on RTT ‘open pathway’ data. This is also impacting on our ability to produce accurate recovery trajectories and we are working this through with BI as we will need to have this available to support the Division’s Business Plan for 2022/23.

Hospital discharge – Please detail the provision and plans you will put in place to ensure timely discharge for all patients, in line with national guidance, and ensure all patients are on the optimum discharge pathway Actions
IES In IES a detailed review of current D2A arrangements has been completed supported by both Attain and ECIST. Several areas of development have been identified and IES Alliance is supporting resource requirements to affect those developments. Both Attain and ECIST will support the implementation of those developments, and this is starting during Qtr. 4 2021/22. Metrics of success primarily focused on the time between patients no longer meeting CTR and point of discharge in pathways 1 – 3 (with a focus on pathways 1 & 2); other relevant signs of success would be impact on acute LOS (connecting to VW work); and overall numbers of patients with no CTR in both acute and community hospitals.
West Post Covid review of Discharge pathways and delivery of transfer of care hub as part of an integrated offer across acute and community Reset community at home model of care Review community Discharge to Assess pathways supported by a demand and capacity review as part of the transition post HDP ceasing System plan in place to strengthen out of hospital capacity to deliver reduction trajectory for no Criteria to Reside delays System oversight group in place to track delivery and outcomes NEE D2A pathways in place with MDT in place with both health and social care senior leadership in place,
• Focussing on and resolving internal delays (UTC/ED/AMSDEC) • Reviewing patients to ensure plans are in place • Ensuring timely escalation of identified issues and agreement of actions, in a similar way to the ‘Red to Green’ process • AMSDEC and frailty service re launch in new environment from early March
Support in place from the Voluntary sector including
• Increased support to the Colchester hospital Discharge Hub including the introduction of Social Prescribers • Early Discharge programme • Pathway light • Discharge PHB
Assumptions IES
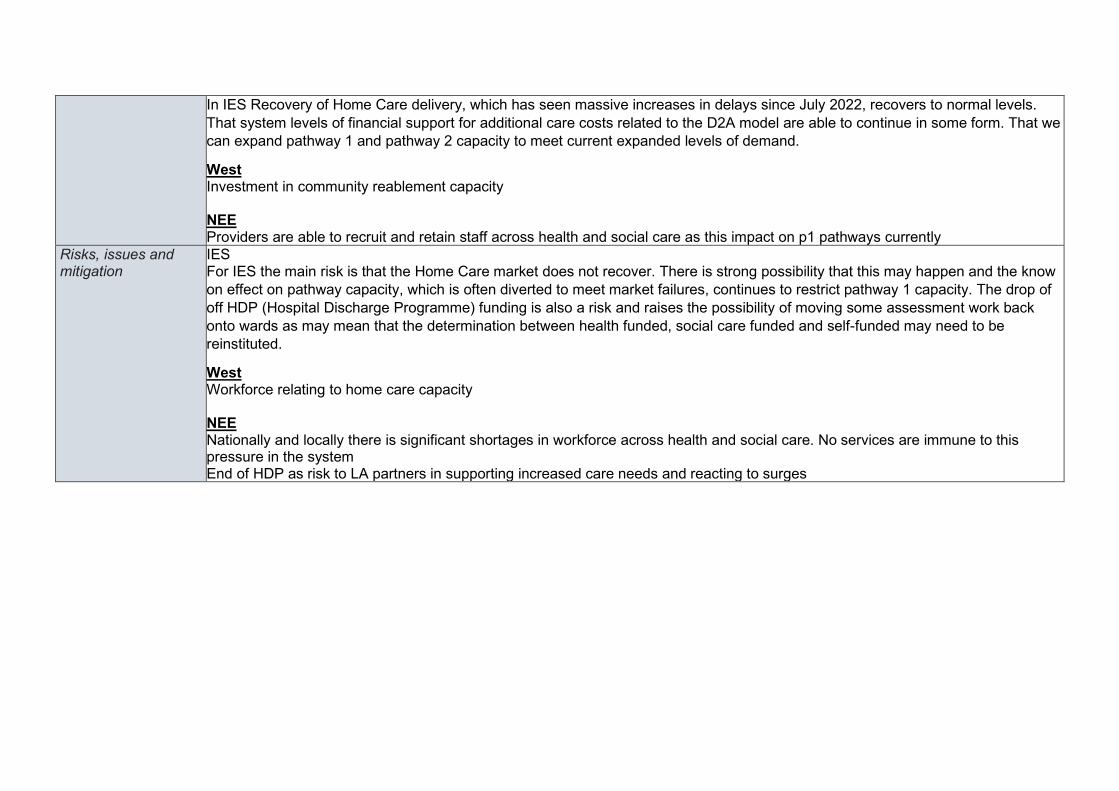
In IES Recovery of Home Care delivery, which has seen massive increases in delays since July 2022, recovers to normal levels. That system levels of financial support for additional care costs related to the D2A model are able to continue in some form. That we can expand pathway 1 and pathway 2 capacity to meet current expanded levels of demand.
West Investment in community reablement capacity NEE Providers are able to recruit and retain staff across health and social care as this impact on p1 pathways currently
Risks, issues and mitigation
IES For IES the main risk is that the Home Care market does not recover. There is strong possibility that this may happen and the know on effect on pathway capacity, which is often diverted to meet market failures, continues to restrict pathway 1 capacity. The drop of off HDP (Hospital Discharge Programme) funding is also a risk and raises the possibility of moving some assessment work back onto wards as may mean that the determination between health funded, social care funded and self-funded may need to be reinstituted.
West Workforce relating to home care capacity NEE Nationally and locally there is significant shortages in workforce across health and social care. No services are immune to this pressure in the system End of HDP as risk to LA partners in supporting increased care needs and reacting to surges
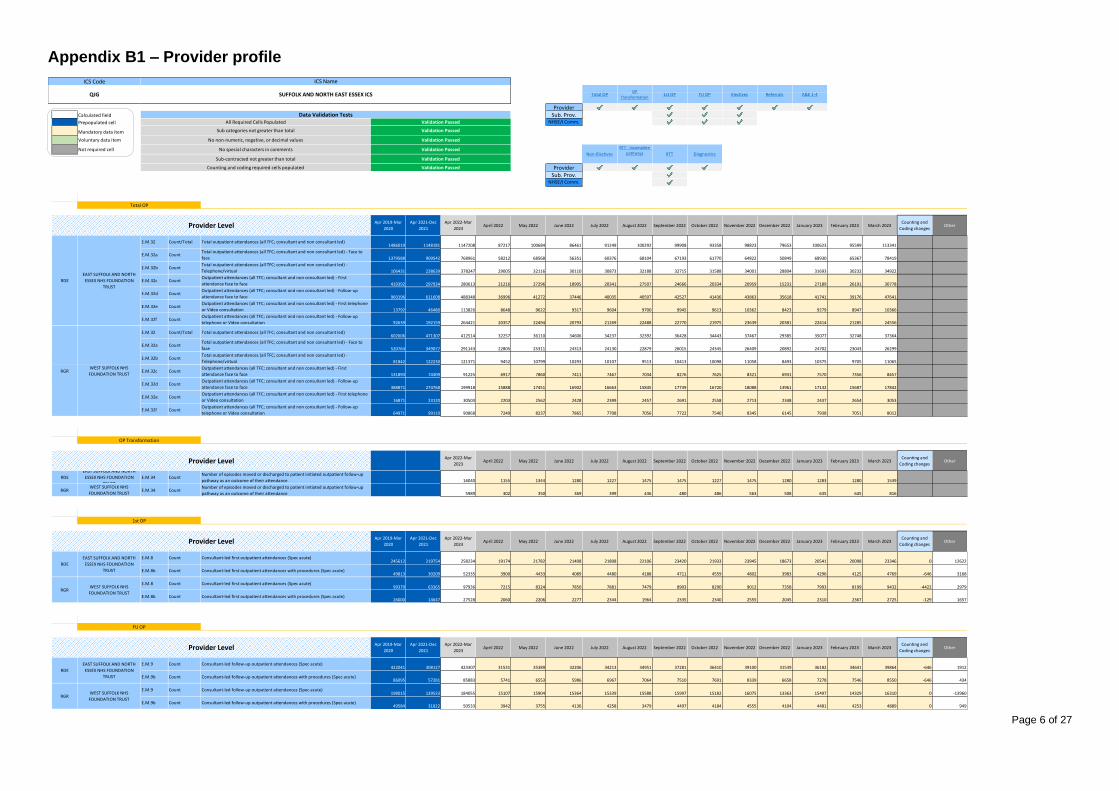
Page 6 of 27
Appendix B1 – Provider profile
$H$19 $H$116 $H$135 $H$167 $H$199 $H$270 $H$315
ProviderCalculated field Sub. Prov.Prepopulated cell NHSE/I Comm.
Mandatory data item Activity7 Activity13 Activity12 Activity9
Voluntary data item $H$360 $H$431 $H$489 $H$534
Not required cell
ProviderSub. Prov.
NHSE/I Comm.
ActivityCategory
TotalActivity10 1 2 3 4 5
Apr 2019-Mar
2020
Apr 2021-Dec
2021
Apr 2022-Mar
2023April 2022 May 2022 June 2022 July 2022 August 2022 September 2022 October 2022 November 2022 December 2022 January 2023 February 2023 March 2023
Counting and
Coding changesOther
Provider1RDEE.M.32 Count/Total Total outpatient attendances (all TFC; consultant and non consultant led)
1486019 1148181 1147208 87217 100684 86461 91249 100292 99908 93358 98823 79653 100623 95599 113341
Provider1RDEE.M.32a Count
Total outpatient attendances (all TFC; consultant and non consultant led) - Face to
face 1379588 909542 768961 58212 68568 56351 60376 68104 67193 61770 64822 50849 68930 65367 78419
Provider1RDEE.M.32b Count
Total outpatient attendances (all TFC; consultant and non consultant led) -
Telephone/virtual 106431 238639 378247 29005 32116 30110 30873 32188 32715 31588 34001 28804 31693 30232 34922
Provider1RDEE.M.32c Count
Outpatient attendances (all TFC; consultant and non consultant led) - First
attendance face to face 419392 297934 280613 21216 27296 18905 20341 27507 24666 20334 20959 15231 27189 26191 30778
Provider1RDEE.M.32d Count
Outpatient attendances (all TFC; consultant and non consultant led) - Follow-up
attendance face to face 960196 611608 488348 36996 41272 37446 40035 40597 42527 41436 43863 35618 41741 39176 47641
Provider1RDEE.M.32e Count
Outpatient attendances (all TFC; consultant and non consultant led) - First telephone
or Video consultation 13792 46480 113826 8648 9622 9317 9604 9700 9945 9613 10362 8423 9279 8947 10366
Provider1RDEE.M.32f Count
Outpatient attendances (all TFC; consultant and non consultant led) - Follow-up
telephone or Video consultation 92639 192159 264421 20357 22494 20793 21269 22488 22770 21975 23639 20381 22414 21285 24556
Provider2RGRE.M.32 Count/Total Total outpatient attendances (all TFC; consultant and non consultant led)
602606 471307 412514 32257 36110 34606 34237 32392 36428 34443 37467 29385 35077 32748 37364
Provider2RGRE.M.32a Count
Total outpatient attendances (all TFC; consultant and non consultant led) - Face to
face 520764 349077 291143 22805 25311 24313 24130 22879 26015 24345 26409 20892 24702 23043 26299
Provider2RGRE.M.32b Count
Total outpatient attendances (all TFC; consultant and non consultant led) -
Telephone/virtual 81842 122230 121371 9452 10799 10293 10107 9513 10413 10098 11058 8493 10375 9705 11065
Provider2RGRE.M.32c Count
Outpatient attendances (all TFC; consultant and non consultant led) - First
attendance face to face 131893 74309 91225 6917 7860 7411 7467 7034 8276 7625 8321 6931 7570 7356 8457
Provider2RGRE.M.32d Count
Outpatient attendances (all TFC; consultant and non consultant led) - Follow-up
attendance face to face 388871 274768 199918 15888 17451 16902 16663 15845 17739 16720 18088 13961 17132 15687 17842
Provider2RGRE.M.32e Count
Outpatient attendances (all TFC; consultant and non consultant led) - First telephone
or Video consultation 16871 23120 30503 2203 2562 2428 2399 2457 2691 2558 2713 2348 2437 2654 3053
Provider2RGRE.M.32f Count
Outpatient attendances (all TFC; consultant and non consultant led) - Follow-up
telephone or Video consultation 64971 99110 90868 7249 8237 7865 7708 7056 7722 7540 8345 6145 7938 7051 8012
ActivityCategory
Activity2
0 1 2 3 4 5 6 7 8 9 10 11
Apr 2022-Mar
2023April 2022 May 2022 June 2022 July 2022 August 2022 September 2022 October 2022 November 2022 December 2022 January 2023 February 2023 March 2023
Counting and
Coding changesOther
Provider1RDERDE E.M.34 Count
Number of episodes moved or discharged to patient initiated outpatient follow-up
pathway as an outcome of their attendance 16040 1155 1344 1280 1227 1475 1475 1227 1475 1280 1283 1280 1539
Provider2RGRRGR E.M.34 Count
Number of episodes moved or discharged to patient initiated outpatient follow-up
pathway as an outcome of their attendance 5989 302 350 369 399 436 480 486 563 508 635 645 816
ActivityCategory
Activity3
0 1 2 3 4 5 6 7 8 9 10 11
Apr 2019-Mar
2020
Apr 2021-Dec
2021
Apr 2022-Mar
2023April 2022 May 2022 June 2022 July 2022 August 2022 September 2022 October 2022 November 2022 December 2022 January 2023 February 2023 March 2023
Counting and
Coding changesOther
Provider1RDEE.M.8 Count Consultant-led first outpatient attendances (Spec acute)
245612 219754 258234 19174 21782 21408 21808 22106 23420 21933 23945 18673 20541 20098 23346 0 12622
Provider1RDEE.M.8b Count Consultant-led first outpatient attendances with procedures (Spec acute)
49813 30209 52335 3900 4433 4089 4480 4188 4711 4559 4802 3983 4296 4125 4769 -646 3168
Provider2RGRE.M.8 Count Consultant-led first outpatient attendances (Spec acute)
99379 63365 97936 7215 8324 7850 7881 7479 8903 8290 9012 7358 7993 8199 9432 -4422 2979
Provider2RGRE.M.8b Count Consultant-led first outpatient attendances with procedures (Spec acute)
26000 14647 27528 2060 2206 2277 2344 1964 2335 2340 2555 2045 2310 2367 2725 -129 1657
ActivityCategory
Activity4
0 1 2 3 4 5 6 7 8 9 10 11
Apr 2019-Mar
2020
Apr 2021-Dec
2021
Apr 2022-Mar
2023April 2022 May 2022 June 2022 July 2022 August 2022 September 2022 October 2022 November 2022 December 2022 January 2023 February 2023 March 2023
Counting and
Coding changesOther
Provider1RDEE.M.9 Count Consultant-led follow-up outpatient attendances (Spec acute)
422041 308127 423307 31531 35389 32206 34213 34951 37281 36410 39100 31539 36182 34641 39864 -646 1912
Provider1RDEE.M.9b Count Consultant-led follow-up outpatient attendances with procedures (Spec acute)
86095 57281 85883 5741 6553 5986 6967 7064 7510 7691 8339 6658 7278 7546 8550 -646 434
Provider2RGRE.M.9 Count Consultant-led follow-up outpatient attendances (Spec acute)
198015 139533 184055 15107 15904 15364 15339 15588 15997 15182 16075 13363 15497 14329 16310 0 -13960
Provider2RGRE.M.9b Count Consultant-led follow-up outpatient attendances with procedures (Spec acute)
49584 31822 50533 3942 3755 4136 4258 3479 4497 4184 4555 4104 4481 4253 4889 0 949
Sub-contracted not greater than total Validation Passed
1st OP
Provider Level
RDE
EAST SUFFOLK AND NORTH
ESSEX NHS FOUNDATION
TRUST
RGRWEST SUFFOLK NHS
FOUNDATION TRUST
Provider Level
RDE
EAST SUFFOLK AND NORTH
ESSEX NHS FOUNDATION
TRUST
RGRWEST SUFFOLK NHS
FOUNDATION TRUST
Provider LevelEAST SUFFOLK AND NORTH
ESSEX NHS FOUNDATION
TRUSTWEST SUFFOLK NHS
FOUNDATION TRUST
OP Transformation
ICS Code ICS Name
Sub categories not greater than total Validation Passed
No non-numeric, negative, or decimal values Validation Passed
QJG SUFFOLK AND NORTH EAST ESSEX ICS
Data Validation TestsAll Required Cells Populated Validation Passed
Total OPOP
Transformation1st OP FU OP Electives Referrals
Validation PassedNo special characters in comments
A&E 1-4
EAST SUFFOLK AND NORTH
ESSEX NHS FOUNDATION
TRUST
RDE
Non-Electives DiagnosticsRTT
RTT - Incomplete
pathways
WEST SUFFOLK NHS
FOUNDATION TRUSTRGR
Provider Level
Total OP
FU OP
Counting and coding required cells populated Validation Passed

Page 7 of 27
Activity5
0 1 2 3 4 5 6 7 8 9 10 11
Apr 2019-Mar
2020
Apr 2021-Dec
2021
Apr 2022-Mar
2023April 2022 May 2022 June 2022 July 2022 August 2022 September 2022 October 2022 November 2022 December 2022 January 2023 February 2023 March 2023
Counting and
Coding changesOther
E.M.10 Count/Total Total number of specific acute elective spells in the period106597 74968 110258 8292 9220 8861 8725 9356 9443 8878 9922 8450 9140 9169 10802 -1698 5359
E.M.10a Count Total number of specific acute elective day case spells in the period94414 66460 97554 7425 8148 7807 7726 8253 8304 7854 8747 7455 8170 8122 9543 -1285 4425
E.M.10b Count Total number of specific acute elective ordinary spells in the period12183 8508 12704 867 1072 1054 999 1103 1139 1024 1175 995 970 1047 1259 -413 934
E.M.10c CountTotal number of specific acute elective day case spells in the period of which children
under 18 years of age 3366 2158 3525 260 293 298 268 307 330 302 336 266 307 260 298
E.M.10d CountTotal number of specific acute elective ordinary spells in the period of which children
under 18 years of age 572 230 613 38 40 70 75 49 59 55 44 43 44 43 53
E.M.10 Count/Total Total number of specific acute elective spells in the period31825 19552 30466 2180 2381 2347 2406 2591 2751 2589 2959 2302 2419 2534 3007 0 -1359
E.M.10a Count Total number of specific acute elective day case spells in the period28155 18059 27717 2009 2212 2084 2193 2327 2507 2330 2669 2088 2300 2311 2687 0 -438
E.M.10b Count Total number of specific acute elective ordinary spells in the period3670 1493 2749 171 169 263 213 264 244 259 290 214 119 223 320 0 -921
E.M.10c CountTotal number of specific acute elective day case spells in the period of which children
under 18 years of age 918 476 905 66 72 68 72 76 82 76 87 68 75 75 88
E.M.10d CountTotal number of specific acute elective ordinary spells in the period of which children
under 18 years of age 193 74 145 9 9 14 11 14 13 14 15 11 6 12 17
ActivityCategory
Activity8
0 1 2 3 4 5 6 7 8 9 10 11
Apr 2019-Mar
2020
Apr 2021-Dec
2021
Apr 2022-Mar
2023April 2022 May 2022 June 2022 July 2022 August 2022 September 2022 October 2022 November 2022 December 2022 January 2023 February 2023 March 2023
Counting and
Coding changesOther
E.M.7 Count/TotalThe total number of GP and other (non-GP) referrals made for first consultant-led
outpatient appointments in specific acute treatment functions (GP + Other)231461 147800 229329 18562 21006 19299 21072 19423 19499 18629 18751 16021 18758 17674 20635
E.M.7a CountThe total number of referrals made from GPs for first consultant-led outpatient
appointments in specific acute treatment functions 140683 80414 139405 10645 13000 12193 12905 11978 12080 11340 11190 9542 11560 10584 12388
E.M.7b CountThe total number of other (non-GP) referral made for first consultant-led outpatient
appointments in specific acute treatment functions 90778 67386 89924 7917 8006 7106 8167 7445 7419 7289 7561 6479 7198 7090 8247
E.M.7 Count/TotalThe total number of GP and other (non-GP) referrals made for first consultant-led
outpatient appointments in specific acute treatment functions (GP + Other) 92950 51038 71554 6234 6099 6488 6025 4945 6190 5985 6639 5003 6182 5688 6076
E.M.7a CountThe total number of referrals made from GPs for first consultant-led outpatient
appointments in specific acute treatment functions 61817 28001 40820 3682 3417 3806 3432 2811 3532 3375 3640 2831 3528 3269 3497
E.M.7b CountThe total number of other (non-GP) referral made for first consultant-led outpatient
appointments in specific acute treatment functions 31133 23037 30734 2552 2682 2682 2593 2134 2658 2610 2999 2172 2654 2419 2579
ActivityCategory
Activity60 1 2 3 4 5 6 7 8 9 10 11
Apr 2019-Mar
2020
Apr 2021-Dec
2021
Apr 2022-Mar
2023April 2022 May 2022 June 2022 July 2022 August 2022 September 2022 October 2022 November 2022 December 2022 January 2023 February 2023 March 2023
Counting and
Coding changesOther
E.M.12 Count/TotalTotal number of attendances at all A&E departments, excluding planned follow-up
attendances (Types 1 & 2 + Types 3 & 4) 217319 187936 232903 19141 19779 19141 19779 19779 19141 19613 19043 20312 19165 17328 20682 16203 -619
E.M.12a CountTotal number of attendances at all Type 1 and Type 2 A&E departments, excluding
planned follow-up attendances 186032 130408 170492 14012 14479 14012 14479 14479 14012 14722 14116 14580 13622 12773 15206 -15084 -456
E.M.12b CountTotal number of attendances at all Type 3 and Type 4 A&E departments, excluding
planned follow-up attendances 31287 57528 62411 5129 5300 5129 5300 5300 5129 4891 4927 5732 5543 4555 5476 31287 -163
E.M.12 Count/TotalTotal number of attendances at all A&E departments, excluding planned follow-up
attendances (Types 1 & 2 + Types 3 & 4) 80821 65378 86499 6949 7529 7277 7698 7260 7133 7454 7026 7086 7068 6531 7488 0 5678
E.M.12a CountTotal number of attendances at all Type 1 and Type 2 A&E departments, excluding
planned follow-up attendances 76414 62020 81784 6570 7119 6880 7278 6864 6744 7048 6643 6700 6683 6175 7080 0 5370
E.M.12b CountTotal number of attendances at all Type 3 and Type 4 A&E departments, excluding
planned follow-up attendances 4407 3358 4715 379 410 397 420 396 389 406 383 386 385 356 408 0 308
ActivityCategory
Activity7
0 1 2 3 4 5 6 7 8 9 10 11
Apr 2019-Mar
2020
Apr 2021-Dec
2021
Apr 2022-Mar
2023April 2022 May 2022 June 2022 July 2022 August 2022 September 2022 October 2022 November 2022 December 2022 January 2023 February 2023 March 2023
Counting and
Coding changesOther
E.M.11 Count/Total Number of specific acute non-elective spells in the period84374 62157 84143 6942 6974 6466 6867 6556 6864 7569 7284 7397 7421 6496 7307 0 -231
E.M.11a CountNumber of specific acute non-elective spells in the period with a length of stay of zero
days 24110 17691 24042 1891 1902 1813 1884 1812 1948 2250 2212 2135 2103 1916 2176 0 -68
E.M.11b Count/TotalNumber of specific acute non-elective spells in the period with a length of stay of one
or more days 60264 44466 60101 5051 5072 4653 4983 4744 4916 5319 5072 5262 5318 4580 5131 0 -163
E.M.11c CountNumber of specific acute non-elective spells in the period with a length of stay of one
or more days (COVID) 83 1250 3094 253 254 233 249 237 246 266 254 263 266 229 344
E.M.11d CountNumber of specific acute non-elective spells in the period with a length of stay of one
or more days (Non-COVID) 60181 43216 57007 4798 4818 4420 4734 4507 4670 5053 4818 4999 5052 4351 4787
E.M.11 Count/Total Number of specific acute non-elective spells in the period28524 21172 28271 2324 2401 2324 2401 2401 2324 2401 2324 2401 2401 2168 2401 0 -253
E.M.11a CountNumber of specific acute non-elective spells in the period with a length of stay of zero
days 6068 5413 6629 545 563 545 563 563 545 563 545 563 563 508 563 0 561
E.M.11b Count/TotalNumber of specific acute non-elective spells in the period with a length of stay of one
or more days 22456 15759 21642 1779 1838 1779 1838 1838 1779 1838 1779 1838 1838 1660 1838 0 -814
E.M.11c CountNumber of specific acute non-elective spells in the period with a length of stay of one
or more days (COVID) 14 409 558 53 74 71 37 18 18 37 53 55 55 50 37
E.M.11d CountNumber of specific acute non-elective spells in the period with a length of stay of one
or more days (Non-COVID) 22442 15350 21084 1726 1764 1708 1801 1820 1761 1801 1726 1783 1783 1610 1801
Referrals
Provider Level
WEST SUFFOLK NHS
FOUNDATION TRUST
Provider Level
RDE
EAST SUFFOLK AND NORTH
ESSEX NHS FOUNDATION
TRUST
RGRWEST SUFFOLK NHS
FOUNDATION TRUST
Non-Electives
RGR
RDE
EAST SUFFOLK AND NORTH
ESSEX NHS FOUNDATION
TRUST
RDE
EAST SUFFOLK AND NORTH
ESSEX NHS FOUNDATION
TRUST
A&E 1-4
WEST SUFFOLK NHS
FOUNDATION TRUST
Provider Level
RGR
EAST SUFFOLK AND NORTH
ESSEX NHS FOUNDATION
TRUST
WEST SUFFOLK NHS
FOUNDATION TRUST
Provider Level
RGR
RDE
Electives
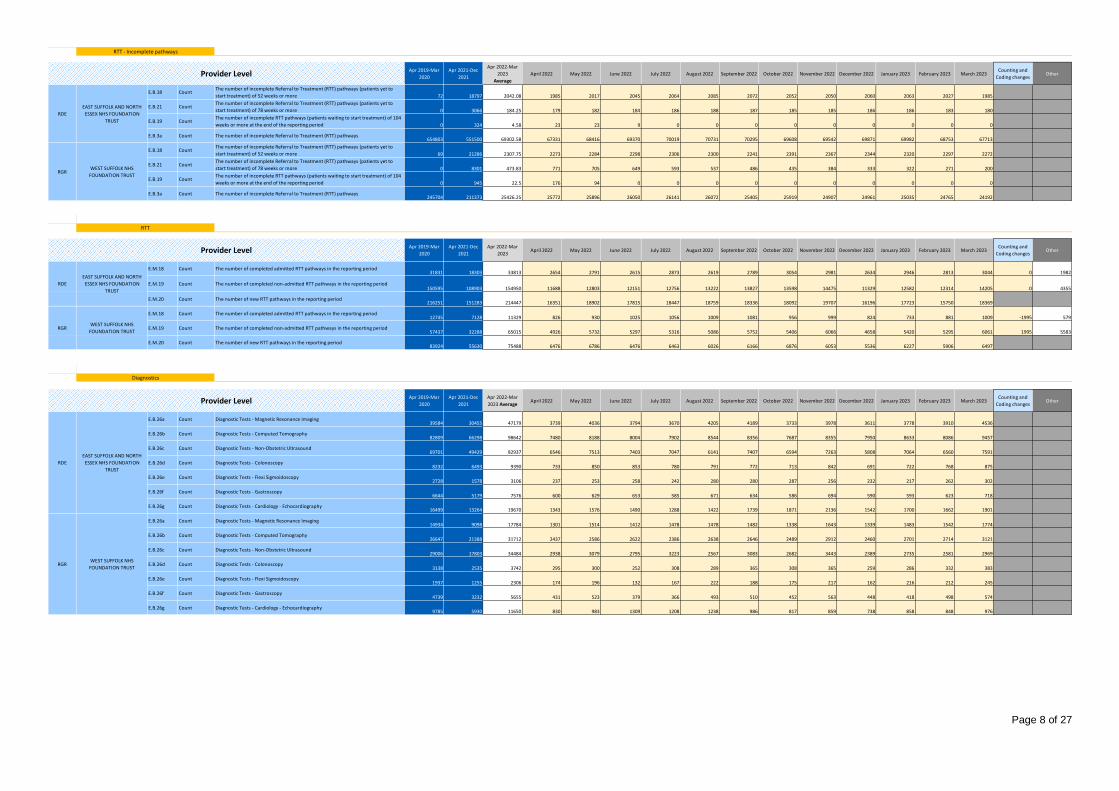
Page 8 of 27
Activity130 1 2 3 4 5 6 7 8 9 10 11
Apr 2019-Mar
2020
Apr 2021-Dec
2021
Apr 2022-Mar
2023
Average
April 2022 May 2022 June 2022 July 2022 August 2022 September 2022 October 2022 November 2022 December 2022 January 2023 February 2023 March 2023Counting and
Coding changesOther
E.B.18 CountThe number of incomplete Referral to Treatment (RTT) pathways (patients yet to
start treatment) of 52 weeks or more 72 18797 2042.08 1985 2017 2045 2064 2085 2072 2052 2050 2060 2063 2027 1985
E.B.21 CountThe number of incomplete Referral to Treatment (RTT) pathways (patients yet to
start treatment) of 78 weeks or more 0 3066 184.25 179 182 184 186 188 187 185 185 186 186 183 180
E.B.19 CountThe number of incomplete RTT pathways (patients waiting to start treatment) of 104
weeks or more at the end of the reporting period 0 324 4.58 23 23 9 0 0 0 0 0 0 0 0 0
E.B.3a Count The number of incomplete Referral to Treatment (RTT) pathways654803 551500 69302.58 67331 68416 69370 70019 70731 70295 69608 69542 69871 69982 68753 67713
E.B.18 CountThe number of incomplete Referral to Treatment (RTT) pathways (patients yet to
start treatment) of 52 weeks or more 69 21286 2307.75 2273 2284 2298 2306 2300 2241 2391 2367 2344 2320 2297 2272
E.B.21 CountThe number of incomplete Referral to Treatment (RTT) pathways (patients yet to
start treatment) of 78 weeks or more 0 8301 473.83 771 705 649 593 537 486 435 384 333 322 271 200
E.B.19 CountThe number of incomplete RTT pathways (patients waiting to start treatment) of 104
weeks or more at the end of the reporting period 0 945 22.5 176 94 0 0 0 0 0 0 0 0 0 0
E.B.3a Count The number of incomplete Referral to Treatment (RTT) pathways245704 211373 25426.25 25772 25896 26050 26141 26072 25405 25919 24907 24961 25035 24765 24192
ActivityCategory
Activity120 1 2 3 4 5 6 7 8 9 10 11
Apr 2019-Mar
2020
Apr 2021-Dec
2021
Apr 2022-Mar
2023April 2022 May 2022 June 2022 July 2022 August 2022 September 2022 October 2022 November 2022 December 2022 January 2023 February 2023 March 2023
Counting and
Coding changesOther
E.M.18 Count The number of completed admitted RTT pathways in the reporting period31831 18303 33813 2654 2791 2615 2873 2619 2789 3054 2981 2634 2946 2813 3044 0 1982
E.M.19 Count The number of completed non-admitted RTT pathways in the reporting period150595 108903 154950 11688 12803 12151 12756 13222 13827 13598 14475 11329 12582 12314 14205 0 4355
E.M.20 Count The number of new RTT pathways in the reporting period216251 151283 214447 16351 18902 17815 18447 18759 18336 18092 19707 16196 17723 15750 18369
E.M.18 Count The number of completed admitted RTT pathways in the reporting period12745 7128 11329 826 930 1025 1056 1009 1081 956 999 824 733 881 1009 -1995 579
E.M.19 Count The number of completed non-admitted RTT pathways in the reporting period57437 32288 65015 4926 5732 5297 5316 5086 5752 5406 6066 4658 5420 5295 6061 1995 5583
E.M.20 Count The number of new RTT pathways in the reporting period83924 55630 75488 6476 6786 6476 6463 6026 6166 6876 6053 5536 6227 5906 6497
ActivityCategory
Activity9
0 1 2 3 4 5 6 7 8 9 10 11
Apr 2019-Mar
2020
Apr 2021-Dec
2021
Apr 2022-Mar
2023 Average April 2022 May 2022 June 2022 July 2022 August 2022 September 2022 October 2022 November 2022 December 2022 January 2023 February 2023 March 2023
Counting and
Coding changesOther
E.B.26a Count Diagnostic Tests - Magnetic Resonance Imaging39584 30455 47179 3739 4036 3794 3670 4205 4189 3733 3978 3611 3778 3910 4536
E.B.26b Count Diagnostic Tests - Computed Tomography82809 66298 98642 7480 8188 8004 7902 8544 8356 7687 8355 7950 8633 8086 9457
E.B.26c Count Diagnostic Tests - Non-Obstetric Ultrasound69701 49429 82937 6546 7513 7403 7047 6141 7407 6594 7263 5808 7064 6560 7591
E.B.26d Count Diagnostic Tests - Colonoscopy8232 6493 9390 733 850 853 780 791 772 713 842 691 722 768 875
E.B.26e Count Diagnostic Tests - Flexi Sigmoidoscopy2728 1578 3106 237 253 258 242 280 280 287 256 232 217 262 302
E.B.26f Count Diagnostic Tests - Gastroscopy6644 5179 7576 600 629 653 585 671 634 586 694 590 593 623 718
E.B.26g Count Diagnostic Tests - Cardiology - Echocardiography16499 13264 19670 1343 1576 1490 1288 1422 1739 1871 2136 1542 1700 1662 1901
E.B.26a Count Diagnostic Tests - Magnetic Resonance Imaging14934 9098 17784 1301 1514 1412 1478 1478 1482 1338 1643 1339 1483 1542 1774
E.B.26b Count Diagnostic Tests - Computed Tomography26647 21388 31712 2437 2586 2622 2386 2638 2646 2489 2912 2460 2701 2714 3121
E.B.26c Count Diagnostic Tests - Non-Obstetric Ultrasound29006 17803 34484 2938 3079 2795 3223 2567 3083 2682 3443 2389 2735 2581 2969
E.B.26d Count Diagnostic Tests - Colonoscopy3138 2535 3742 295 300 252 308 289 365 308 365 259 286 332 383
E.B.26e Count Diagnostic Tests - Flexi Sigmoidoscopy1937 1255 2306 174 196 132 167 222 188 175 217 162 216 212 245
E.B.26f Count Diagnostic Tests - Gastroscopy4739 3232 5655 431 523 379 366 493 510 452 563 448 418 498 574
E.B.26g Count Diagnostic Tests - Cardiology - Echocardiography9785 5930 11650 830 983 1309 1208 1238 986 817 859 738 858 848 976
RDE
EAST SUFFOLK AND NORTH
ESSEX NHS FOUNDATION
TRUST
RGRWEST SUFFOLK NHS
FOUNDATION TRUST
Diagnostics
Provider Level
RTT - Incomplete pathways
Provider Level
RTT
Provider Level
RDE
EAST SUFFOLK AND NORTH
ESSEX NHS FOUNDATION
TRUST
RGRWEST SUFFOLK NHS
FOUNDATION TRUST
RDE
EAST SUFFOLK AND NORTH
ESSEX NHS FOUNDATION
TRUST
RGRWEST SUFFOLK NHS
FOUNDATION TRUST
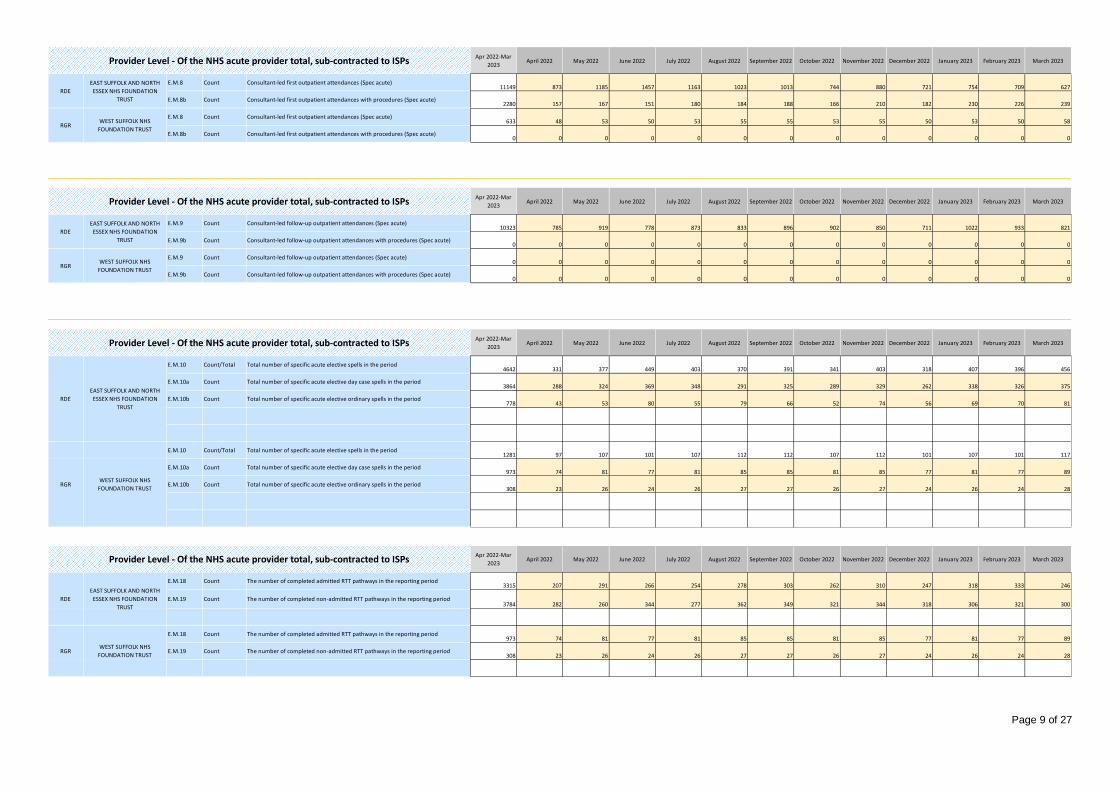
Page 9 of 27
Apr 2022-Mar
2023April 2022 May 2022 June 2022 July 2022 August 2022 September 2022 October 2022 November 2022 December 2022 January 2023 February 2023 March 2023
E.M.8 Count Consultant-led first outpatient attendances (Spec acute)11149 873 1185 1457 1163 1023 1013 744 880 721 754 709 627
E.M.8b Count Consultant-led first outpatient attendances with procedures (Spec acute)2280 157 167 151 180 184 188 166 210 182 230 226 239
E.M.8 Count Consultant-led first outpatient attendances (Spec acute)633 48 53 50 53 55 55 53 55 50 53 50 58
E.M.8b Count Consultant-led first outpatient attendances with procedures (Spec acute)0 0 0 0 0 0 0 0 0 0 0 0 0
Apr 2022-Mar
2023April 2022 May 2022 June 2022 July 2022 August 2022 September 2022 October 2022 November 2022 December 2022 January 2023 February 2023 March 2023
E.M.9 Count Consultant-led follow-up outpatient attendances (Spec acute)10323 785 919 778 873 833 896 902 850 711 1022 933 821
E.M.9b Count Consultant-led follow-up outpatient attendances with procedures (Spec acute)0 0 0 0 0 0 0 0 0 0 0 0 0
E.M.9 Count Consultant-led follow-up outpatient attendances (Spec acute)0 0 0 0 0 0 0 0 0 0 0 0 0
E.M.9b Count Consultant-led follow-up outpatient attendances with procedures (Spec acute)0 0 0 0 0 0 0 0 0 0 0 0 0
Apr 2022-Mar
2023April 2022 May 2022 June 2022 July 2022 August 2022 September 2022 October 2022 November 2022 December 2022 January 2023 February 2023 March 2023
E.M.10 Count/Total Total number of specific acute elective spells in the period4642 331 377 449 403 370 391 341 403 318 407 396 456
E.M.10a Count Total number of specific acute elective day case spells in the period3864 288 324 369 348 291 325 289 329 262 338 326 375
E.M.10b Count Total number of specific acute elective ordinary spells in the period778 43 53 80 55 79 66 52 74 56 69 70 81
E.M.10 Count/Total Total number of specific acute elective spells in the period1281 97 107 101 107 112 112 107 112 101 107 101 117
E.M.10a Count Total number of specific acute elective day case spells in the period973 74 81 77 81 85 85 81 85 77 81 77 89
E.M.10b Count Total number of specific acute elective ordinary spells in the period308 23 26 24 26 27 27 26 27 24 26 24 28
RDE
RGRWEST SUFFOLK NHS
FOUNDATION TRUST
EAST SUFFOLK AND NORTH
ESSEX NHS FOUNDATION
TRUST
RGRWEST SUFFOLK NHS
FOUNDATION TRUST
Provider Level - Of the NHS acute provider total, sub-contracted to ISPs
Provider Level - Of the NHS acute provider total, sub-contracted to ISPs
RDE
EAST SUFFOLK AND NORTH
ESSEX NHS FOUNDATION
TRUST
Provider Level - Of the NHS acute provider total, sub-contracted to ISPs
RDE
EAST SUFFOLK AND NORTH
ESSEX NHS FOUNDATION
TRUST
RGRWEST SUFFOLK NHS
FOUNDATION TRUST
Apr 2022-Mar
2023April 2022 May 2022 June 2022 July 2022 August 2022 September 2022 October 2022 November 2022 December 2022 January 2023 February 2023 March 2023
E.M.18 Count The number of completed admitted RTT pathways in the reporting period3315 207 291 266 254 278 303 262 310 247 318 333 246
E.M.19 Count The number of completed non-admitted RTT pathways in the reporting period3784 282 260 344 277 362 349 321 344 318 306 321 300
E.M.18 Count The number of completed admitted RTT pathways in the reporting period973 74 81 77 81 85 85 81 85 77 81 77 89
E.M.19 Count The number of completed non-admitted RTT pathways in the reporting period308 23 26 24 26 27 27 26 27 24 26 24 28
RGRWEST SUFFOLK NHS
FOUNDATION TRUST
Provider Level - Of the NHS acute provider total, sub-contracted to ISPs
RDE
EAST SUFFOLK AND NORTH
ESSEX NHS FOUNDATION
TRUST

Page 10 of 27
Appendix B2 – Commissioner profile
$H$16 $H$29 $H$49 $H$70 $H$82 $H$103 $H$160 $H$169 $H$118 $H$139
System
Calculated field AlignMeasure7 AlignMeasure8 AlignMeasure9 AlignMeasure10AlignMeasure11AlignMeasure12AlignMeasure13
Prepopulated cell $H$177 $H$188 $H$199 $H$210 $H$221 $H$232 $H$243
Mandatory data item
Voluntary data item
Not required cell System
ActivityCategory
TotalActivity10 1 2 3 4 5 6 7 8 9 10 5
April 2019-Mar
2020 (CCG
aggregated)
Apr 2021-Dec 2021
(CCG aggregated)
Apr 2022-Mar
2023April 2022 May 2022 June 2022 July 2022 August 2022 September 2022 October 2022 November 2022 December 2022 January 2023 February 2023 March 2023
ICSQJGE.M.32 Count/Total
2078433 1602008 2004891 155967 178800 159806 162740 164801 170209 164355 177242 147420 165840 156342 201369
ICSQJG
E.M.32a Count
1896651 1252973 1499319 116618 133728 119543 121683 123259 127303 122904 132529 110261 123980 116916 150595
ICSQJGE.M.32b Count
181782 349035 505572 39349 45072 40263 41057 41542 42906 41451 44713 37159 41860 39426 50774
ICSQJG
E.M.32c Count
554502 373097 432066 33557 38768 35095 36012 35525 37182 35746 38554 31238 34716 33110 42563
ICSQJG
E.M.32d Count
1342149 879876 1067253 83061 94960 84448 85671 87734 90121 87158 93975 79023 89264 83806 108032
ICSQJG
E.M.32e Count
29744 68162 136717 10577 12259 11105 11452 11271 11779 11355 12218 9870 10947 10443 13441
ICSQJG
E.M.32f Count
152038 280873 368855 28772 32813 29158 29605 30271 31127 30096 32495 27289 30913 28983 37333
ActivityCategory
TotalActivity110 1 2 3 4 5 6 7 8 9 10 5
Apr 2022-Mar
2023April 2022 May 2022 June 2022 July 2022 August 2022 September 2022 October 2022 November 2022 December 2022 January 2023 February 2023 March 2023
ICSQJG
E.M.33 Count/Total
96803 7362 8541 7764 8010 7925 8317 8034 8690 7061 7870 7536 9693
ICSQJG
E.M.33a Count
89199 6674 7766 7043 7397 7272 7679 7497 8045 6512 7292 7008 9014
ICSQJG
E.M.33b Count
7604 688 775 721 613 653 638 537 645 549 578 528 679
ActivityCategory
Activity2
0 1 2 3 4 5 6 7 8 9 10 5
Apr 2022-Mar
2023April 2022 May 2022 June 2022 July 2022 August 2022 September 2022 October 2022 November 2022 December 2022 January 2023 February 2023 March 2023
ICSQJG
E.M.34 Count
18493 486 757 862 1069 1235 1482 1611 1937 1732 2107 2186 3029
Ordinary
Non-Obs Ultra
Counting and coding required cells populated
Outpatient attendances (all TFC; consultant and non consultant led) - Follow-up
telephone or Video consultation
OP Transformation (ICS)
ICS-commissioned
SUFFOLK AND NORTH EAST ESSEX ICS
SUFFOLK AND NORTH EAST ESSEX ICS
OP Transformation
ICS-commissioned
Number of requests for post referral specialist advice (including referral triage
models)
MRI
Outpatient attendances (all TFC; consultant and non consultant led) - First telephone
or Video consultation
No special characters in comments
Validation Passed
Validation Passed
Total outpatient attendances (all TFC; consultant and non consultant led)
Number of requests for specialist advice, including advice and guidance (A&G) or
equivalent via other triage approaches
Number of requests for pre referral specialist advice (including Advice & Guidance
models)
All Required Cells Populated
Sub categories not greater than total
Validation Passed
Validation Passed
SUFFOLK AND NORTH EAST ESSEX ICS
Data Validation Tests
No non-numeric, negative, or decimal valuesCT
Number of episodes moved or discharged to patient initiated outpatient follow-up
pathway as an outcome of their attendance
ICS Code ICS Name
QJG SUFFOLK AND NORTH EAST ESSEX ICS Total OP 1st OP 1st OP - Proc FU OPOP Transformation
(ICS)FU OP - Proc Referrals RTT Day Case
Echocardio
Total outpatient attendances (all TFC; consultant and non consultant led) -
Telephone/virtual
Outpatient attendances (all TFC; consultant and non consultant led) - First
attendance face to face
Outpatient attendances (all TFC; consultant and non consultant led) - Follow-up
attendance face to face
Total OP
ICS-commissioned
GastroscopyFlexi Sig
Total outpatient attendances (all TFC; consultant and non consultant led) - Face to
face
Colonoscopy
Validation Passed

Page 11 of 27
AlignMeasure1
1095 1096 1097 1098 1099 1100 1101 1102 1103 1104 1105 1106
% of System Total Total
91.3% 446484 33511 39484 36081 37292 36701 38980 37351 40709 32446 36104 35001 42824
6.8% 33388 2399 2826 2629 2696 2726 2914 2658 3037 2599 2929 2734 3241
0.0% 24 0 3 2 0 4 1 2 6 1 2 1 2
336744 274548 98.1% 479896 35910 42313 38712 39988 39431 41895 40011 43752 35046 39035 37736 46067 0 143152
0.0% 7 1 0 2 1 0 0 2 0 0 0 0 1
0.2% 960 58 49 62 61 60 83 75 98 68 101 103 142
0.0% 0 0 0 0 0 0 0 0 0 0 0 0 0
0.0% 14 1 1 0 0 4 2 1 3 0 0 1 1
0.3% 1251 54 304 367 99 136 65 33 50 23 38 29 53
0.1% 482 0 0 1 0 22 37 72 67 66 81 81 55
0.0% 36 2 0 1 6 3 4 1 7 3 3 2 4
1.3% 6528 1114 768 480 399 371 508 449 468 387 432 509 643
8728 6645 1.9% 9278 1230 1122 913 566 596 699 633 693 547 655 725 899 0 550
345471 281387 100.0% 489174 37140 43435 39625 40554 40027 42594 40644 44445 35593 39690 38461 46966 0 143703
E.M.8b MeasureName
AlignMeasure2
1095 1096 1097 1098 1099 1100 1101 1102 1103 1104 1105 1106
% of System Total Total
88.1% 87299 6561 7541 6912 7376 6683 7597 7486 8000 6317 7177 7026 8623
6.5% 6412 484 594 530 493 549 504 515 543 491 592 532 585
0.0% 21 0 3 1 0 4 1 2 6 0 2 0 2
74807 43982 94.6% 93732 7045 8138 7443 7869 7236 8102 8003 8549 6808 7771 7558 9210 0 18925
5187 2547 5.4% 5356 445 451 418 352 339 472 423 473 359 422 500 702 0 169
79993 46657 100.0% 99088 7490 8589 7861 8221 7575 8574 8426 9022 7167 8193 8058 9912 0 19095
E.M.9 MeasureName
AlignMeasure3
1095 1096 1097 1098 1099 1100 1101 1102 1103 1104 1105 1106
% of System Total Total
91.4% 1056604 80695 92778 82799 84196 88942 90128 87550 94495 81417 89831 86207 97566
7.6% 88036 6834 7540 7018 7175 7130 7311 7270 7957 6323 7677 6959 8842
0.0% 35 0 0 1 0 0 0 0 0 19 14 1 0
579602 418748 99.0% 1144675 87529 100318 89818 91371 96072 97439 94820 102452 87759 97522 93167 106408 0 565073
0.0% 12 0 0 0 1 2 1 0 2 0 4 1 1
0.1% 1326 99 154 95 106 79 105 95 117 87 149 107 133
0.0% 0 0 0 0 0 0 0 0 0 0 0 0 0
0.0% 51 4 2 4 5 6 4 7 7 3 6 2 1
0.2% 2127 182 201 167 154 164 172 163 183 144 179 188 230
0.0% 371 0 0 0 0 0 12 10 40 64 67 80 98
0.0% 139 4 10 7 9 7 12 11 14 10 11 16 28
0.6% 7321 1349 924 406 521 346 574 458 629 302 481 515 816
9678 3675 1.0% 11347 1638 1291 679 796 604 880 744 992 610 897 909 1307 0 1669
589279 422655 100.0% 1156022 89167 101609 90497 92167 96676 98319 95564 103444 88369 98419 94076 107715 0 566743
Total ISP
System Total Activity
Other
Total ISP
System Total Activity
Ramsay
Spamedica
Spire
QJG - SUFFOLK AND NORTH EAST ESSEX ICS
Total ISP
ICS-commissionedApril 2019-Mar
2020 (CCG
aggregated)
System Total Activity
Consultant-led follow-up outpatient attendances (Spec acute)
QJG - SUFFOLK AND NORTH EAST ESSEX ICS
Within System NHS Acute Providers
Counting and
Coding changes
November 2022 December 2022 January 2023 February 2023 March 2023
Other
Total
October 2022Counting and
Coding changesOther
Counting and
Coding changesOther
Consultant-led first outpatient attendances (Spec acute)
QJG - SUFFOLK AND NORTH EAST ESSEX ICS
Within System NHS Acute Providers
Ind
epen
den
t Se
cto
r Pr
ovi
der
s
Aspen
BMI
Nuffield
Practice Plus Group
Total NHS
Practice Plus Group
Ramsay
Spamedica
Spire
Other
BMI
Nuffield
NHS Acute Provider outside system
Ind
epen
den
t Se
cto
r Pr
ovi
der
s
Consultant-led first outpatient attendances with procedures (Spec acute)
Within System NHS Acute Providers
NHS Acute Provider outside system
Other non-Acute NHS Providers and other
Apr 2021-Dec 2021
(CCG aggregated)
Other non-Acute NHS Providers and other
Total NHS
NHS Acute Provider outside system
Other non-Acute NHS Providers and other
Total NHS
July 2022 August 2022
Aspen
April 2022 May 2022 June 2022 November 2022 December 2022ICS-commissionedApril 2019-Mar
2020 (CCG
aggregated)
September 2022 October 2022 January 2023 February 2023 March 2023
September 2022ICS-commissionedApril 2019-Mar
2020 (CCG
aggregated)
Apr 2021-Dec 2021
(CCG aggregated)
Total
April 2022 May 2022 June 2022 July 2022 August 2022
Apr 2021-Dec 2021
(CCG aggregated)
Total
April 2022 May 2022 June 2022 July 2022 August 2022 September 2022 October 2022 November 2022 December 2022 January 2023 February 2023 March 2023
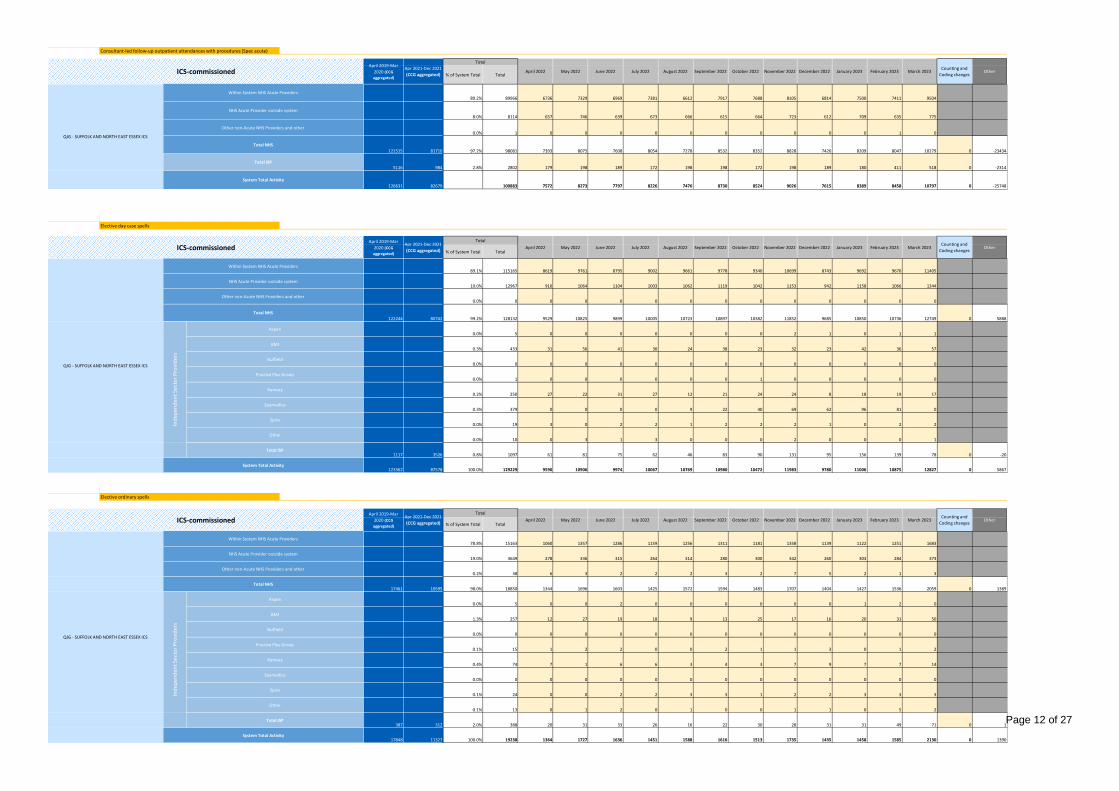
Page 12 of 27
AlignMeasure41095 1096 1097 1098 1099 1100 1101 1102 1103 1104 1105 1106
% of System Total Total
89.2% 89966 6736 7329 6969 7381 6612 7917 7688 8105 6814 7500 7411 9504
8.0% 8114 657 746 639 673 666 615 664 723 612 709 635 775
0.0% 1 0 0 0 0 0 0 0 0 0 0 1 0
121515 81710 97.2% 98081 7393 8075 7608 8054 7278 8532 8352 8828 7426 8209 8047 10279 0 -23434
5116 984 2.8% 2802 179 198 189 172 198 198 172 198 189 180 411 518 0 -2314
126631 82679 100883 7572 8273 7797 8226 7476 8730 8524 9026 7615 8389 8458 10797 0 -25748
E.M.10a MeasureName
AlignMeasure5
1095 1096 1097 1098 1099 1100 1101 1102 1103 1104 1105 1106
% of System Total Total
89.1% 115165 8619 9761 8795 9002 9661 9778 9340 10699 8743 9692 9670 11405
10.0% 12967 910 1064 1104 1003 1062 1119 1042 1153 942 1158 1066 1344
0.0% 0 0 0 0 0 0 0 0 0 0 0 0 0
122244 80742 99.2% 128132 9529 10825 9899 10005 10723 10897 10382 11852 9685 10850 10736 12749 0 5888
0.0% 5 0 0 0 0 0 0 0 2 1 0 1 1
0.3% 433 31 56 41 30 24 38 23 32 23 42 36 57
0.0% 0 0 0 0 0 0 0 0 0 0 0 0 0
0.0% 1 0 0 0 0 0 0 1 0 0 0 0 0
0.2% 250 27 22 31 27 12 21 24 24 8 18 19 17
0.3% 379 0 0 0 0 9 22 40 69 62 96 81 0
0.0% 19 3 0 2 2 1 2 2 2 1 0 2 2
0.0% 10 0 3 1 3 0 0 0 2 0 0 0 1
1117 3526 0.8% 1097 61 81 75 62 46 83 90 131 95 156 139 78 0 -20
123362 87578 100.0% 129229 9590 10906 9974 10067 10769 10980 10472 11983 9780 11006 10875 12827 0 5867
E.M.10b MeasureName
AlignMeasure6
1095 1096 1097 1098 1099 1100 1101 1102 1103 1104 1105 1106
% of System Total Total
78.8% 15163 1060 1357 1286 1159 1256 1311 1181 1358 1139 1122 1251 1683
19.0% 3649 278 336 315 264 314 280 300 342 260 303 284 373
0.2% 38 6 3 2 2 2 3 2 7 5 2 1 3
17461 10595 98.0% 18850 1344 1696 1603 1425 1572 1594 1483 1707 1404 1427 1536 2059 0 1389
0.0% 5 0 0 2 0 0 0 0 0 0 1 2 0
1.3% 257 12 27 19 18 9 13 25 17 16 20 31 50
0.0% 0 0 0 0 0 0 0 0 0 0 0 0 0
0.1% 15 1 2 2 0 0 2 1 1 3 0 1 2
0.4% 74 7 1 6 6 3 4 3 7 9 7 7 14
0.0% 0 0 0 0 0 0 0 0 0 0 0 0 0
0.1% 24 0 0 2 2 3 3 1 2 2 3 3 3
0.1% 13 0 1 2 0 1 0 0 1 1 0 5 2
387 312 2.0% 388 20 31 33 26 16 22 30 28 31 31 49 71 0 1
17848 11327 100.0% 19238 1364 1727 1636 1451 1588 1616 1513 1735 1435 1458 1585 2130 0 1390
April 2019-Mar
2020 (CCG
aggregated)
Other non-Acute NHS Providers and other
Consultant-led follow-up outpatient attendances with procedures (Spec acute)
ICS-commissioned July 2022 August 2022 September 2022
Counting and
Coding changesOther
Counting and
Coding changesOther
Counting and
Coding changesOther
October 2022 February 2023 March 2023
October 2022 November 2022
ICS-commissionedApril 2019-Mar
2020 (CCG
aggregated)
Other
Total ISP
System Total Activity
ICS-commissionedApril 2019-Mar
2020 (CCG
aggregated)
Total
Spire
Other
Total ISP
QJG - SUFFOLK AND NORTH EAST ESSEX ICS
Total NHS
Ind
epen
den
t Se
cto
r Pr
ovi
der
s
Aspen
BMI
Nuffield
Ramsay
Spamedica
Spire
Total
Elective day case spells
System Total Activity
Total NHS
Ind
epen
den
t Se
cto
r Pr
ovi
der
s
Aspen
BMI
Nuffield
Practice Plus Group
Ramsay
Spamedica
Practice Plus Group
Within System NHS Acute Providers
Total ISP
Apr 2021-Dec 2021
(CCG aggregated)
Total
April 2022
Elective ordinary spells
May 2022
NHS Acute Provider outside system
Other non-Acute NHS Providers and other
Within System NHS Acute Providers
NHS Acute Provider outside system
QJG - SUFFOLK AND NORTH EAST ESSEX ICS
Total NHS
System Total Activity
October 2022 November 2022 December 2022 January 2023 February 2023 March 2023
QJG - SUFFOLK AND NORTH EAST ESSEX ICS
Within System NHS Acute Providers
NHS Acute Provider outside system
Other non-Acute NHS Providers and other
Apr 2021-Dec 2021
(CCG aggregated)April 2022 May 2022 June 2022 July 2022 August 2022 September 2022
August 2022 September 2022Apr 2021-Dec 2021
(CCG aggregated)April 2022 May 2022 June 2022 July 2022
December 2022 January 2023 February 2023 March 2023
November 2022 December 2022 January 2023
June 2022

Page 13 of 27
Activity80 1 2 3 4 5 6 7 8 9 10 5
April 2019-Mar
2020 (CCG
aggregated)
Apr 2021-Dec 2021
(CCG aggregated)
Apr 2022-Mar
2023April 2022 May 2022 June 2022 July 2022 August 2022 September 2022 October 2022 November 2022 December 2022 January 2023 February 2023 March 2023
Counting and
Coding changesOther
E.M.7 Count/Total
348062 216274 302757 26441 28399 26306 30347 25019 25273 27990 24333 22242 25934 23467 17006
E.M.7a Count203987 113396 163677 13927 15858 14892 16865 13958 14011 15104 12677 11534 14082 12457 8312
E.M.7b Count144075 102878 139080 12514 12541 11414 13482 11061 11262 12886 11656 10708 11852 11010 8694
ActivityCategory
Activity12
0 1 2 3 4 5 6 7 8 9 10 5
April 2019-Mar
2020 (CCG
aggregated)
Apr 2021-Dec 2021
(CCG aggregated)
Apr 2022-Mar
2023April 2022 May 2022 June 2022 July 2022 August 2022 September 2022 October 2022 November 2022 December 2022 January 2023 February 2023 March 2023
Counting and
Coding changesOther
E.M.18 Count51480.94741 32873 45142 3480 3721 3640 3929 3628 3870 4010 3980 3458 3679 3694 4053 -1995 -4343.947411
E.M.19 Count220817.2771 145980 219965 16614 18535 17448 18072 18308 19579 19004 20541 15987 18002 17609 20266 1995 -2847.277094
E.B.26a MeasureName
AlignMeasure71095 1096 1097 1098 1099 1100 1101 1102 1103 1104 1105 1106
58910 43056 70671 5815 5873 5636 6047 5747 5822 6097 5772 5359 6021 5926 6556
0 0 0 0 0 0 0 0 0 0 0 0 0
4794 3671 5817 459 526 584 419 467 509 518 389 502 382 494 568
0 0 0 0 0 0 0 0 0 0 0 0 0
E.B.26b MeasureName
AlignMeasure81095 1096 1097 1098 1099 1100 1101 1102 1103 1104 1105 1106
113058 91817 135804 10759 11168 10984 11611 11016 10927 11639 11042 10707 12284 11171 12496
0 0 0 0 0 0 0 0 0 0 0 0 0
28 26 33 5 4 0 5 8 4 1 1 0 1 2 2
0 0 0 0 0 0 0 0 0 0 0 0 0
E.B.26c MeasureName
AlignMeasure9
1095 1096 1097 1098 1099 1100 1101 1102 1103 1104 1105 1106
97188 67692 124820 10345 11046 10736 11850 8660 10306 10932 10577 8618 11077 9836 10837
0 0 0 0 0 0 0 0 0 0 0 0 0
19742 11048 15603 1348 1195 1143 1304 1632 1233 1394 1483 1209 1196 1147 1319
0 0 0 0 0 0 0 0 0 0 0 0 0
Counting and
Coding changes
Counting and
Coding changesOther
Counting and
Coding changesOther
February 2023 March 2023
Of which Community Diagnostic Centres
Total NHS
ICS-commissioned
Of which Community Diagnostic Centres
Total ISP
Of which Community Diagnostic Centres
Diagnostic Tests - Computed Tomography
QJG - SUFFOLK AND NORTH EAST ESSEX ICS
Total NHS
Of which Community Diagnostic Centres
Total ISP
Referrals
Apr 2021-Dec 2021
(CCG aggregated)
April 2019-Mar
2020 (CCG
aggregated)
Apr 2022-Mar
2023
ICS-commissioned
SUFFOLK AND NORTH EAST ESSEX ICS
The number of completed admitted RTT pathways in the reporting period
The number of completed non-admitted RTT pathways in the reporting period
RTT
QJG - SUFFOLK AND NORTH EAST ESSEX ICS
Diagnostic Tests - Magnetic Resonance Imaging
ICS-commissioned
ICS-commissioned
SUFFOLK AND NORTH EAST ESSEX ICS
The total number of GP and other (non-GP) referrals made for first consultant-led
outpatient appointments in specific acute treatment functions (GP + Other)
The total number of referrals made from GPs for first consultant-led outpatient
appointments in specific acute treatment functions
The total number of other (non-GP) referral made for first consultant-led outpatient
appointments in specific acute treatment functions
August 2022 December 2022 January 2023 OtherSeptember 2022 October 2022
March 2023
April 2019-Mar
2020 (CCG
aggregated)
Apr 2021-Dec 2021
(CCG aggregated)
Apr 2022-Mar
2023April 2022 May 2022 June 2022 July 2022 August 2022 September 2022
April 2022 May 2022 June 2022 July 2022 November 2022
ICS-commissionedApril 2019-Mar
2020 (CCG
aggregated)
Apr 2021-Dec 2021
(CCG aggregated)
Apr 2022-Mar
2023April 2022 May 2022 June 2022 July 2022 August 2022
Diagnostic Tests - Non-Obstetric Ultrasound
QJG - SUFFOLK AND NORTH EAST ESSEX ICS
Total NHS
Of which Community Diagnostic Centres
Total ISP
Of which Community Diagnostic Centres
September 2022 October 2022 November 2022 December 2022 January 2023 February 2023 March 2023
October 2022 November 2022 December 2022 January 2023 February 2023

Page 14 of 27
AlignMeasure10
1095 1096 1097 1098 1099 1100 1101 1102 1103 1104 1105 1106
QJG 11063 8684 12637 1020 1032 1032 1119 968 1021 1110 1097 916 1062 1081 1179
QJG 0 0 0 0 0 0 0 0 0 0 0 0 0
QJG 2116 970 3191 216 333 261 274 217 369 335 178 247 258 234 269
QJG 0 0 0 0 0 0 0 0 0 0 0 0 0
E.B.26e MeasureName
AlignMeasure11
1095 1096 1097 1098 1099 1100 1101 1102 1103 1104 1105 1106
QJG 4467 2778 5278 410 423 378 425 470 438 495 429 370 449 449 542
QJG 0 0 0 0 0 0 0 0 0 0 0 0 0
QJG 390 206 585 36 28 36 31 54 35 60 49 49 62 74 71
QJG 0 0 0 0 0 0 0 0 0 0 0 0 0
E.B.26f MeasureName
AlignMeasure121095 1096 1097 1098 1099 1100 1101 1102 1103 1104 1105 1106
QJG 11880 8716 13279 1062 1076 1023 1060 1135 1106 1169 1161 1058 1122 1099 1208
QJG 0 0 0 0 0 0 0 0 0 0 0 0 0
QJG 3004 1795 4591 472 407 396 301 294 328 297 465 282 267 503 579
QJG 0 0 0 0 0 0 0 0 0 0 0 0 0
E.B.26g MeasureName
AlignMeasure131095 1096 1097 1098 1099 1100 1101 1102 1103 1104 1105 1106
QJG 28122 21248 33772 2456 2825 2952 2924 2742 2777 3119 3027 2414 2884 2699 2953
QJG 0 0 0 0 0 0 0 0 0 0 0 0 0
QJG 3 2 5 0 0 0 0 0 0 0 4 1 0 0 0
QJG 0 0 0 0 0 0 0 0 0 0 0 0 0
Counting and
Coding changesOther
Diagnostic Tests - Gastroscopy
QJG - SUFFOLK AND NORTH EAST ESSEX ICS
Total NHS
Of which Community Diagnostic Centres
Total ISP
Of which Community Diagnostic Centres
QJG - SUFFOLK AND NORTH EAST ESSEX ICS
Of which Community Diagnostic Centres
Of which Community Diagnostic Centres
ICS-commissioned
ICS-commissioned
Diagnostic Tests - Flexi Sigmoidoscopy
Of which Community Diagnostic Centres
QJG - SUFFOLK AND NORTH EAST ESSEX ICS
Total NHS
Of which Community Diagnostic Centres
Total ISP
QJG - SUFFOLK AND NORTH EAST ESSEX ICS
Diagnostic Tests - Colonoscopy
ICS-commissionedApril 2019-Mar
2020 (CCG
aggregated)
Apr 2021-Dec 2021
(CCG aggregated)
Diagnostic Tests - Cardiology - Echocardiography
Total NHS
Total ISP
May 2022 July 2022 August 2022 November 2022 December 2022 January 2023June 2022Apr 2022-Mar
2023April 2022 September 2022 October 2022
March 2023
April 2019-Mar
2020 (CCG
aggregated)
Apr 2021-Dec 2021
(CCG aggregated)
Apr 2022-Mar
2023April 2022 May 2022 June 2022 July 2022 August 2022
April 2019-Mar
2020 (CCG
aggregated)
Apr 2021-Dec 2021
(CCG aggregated)
Apr 2022-Mar
2023April 2022 May 2022 June 2022 July 2022 August 2022 December 2022September 2022 October 2022 November 2022
Counting and
Coding changesOther
December 2022 January 2023 February 2023 March 2023Counting and
Coding changesSeptember 2022 October 2022 OtherNovember 2022
January 2023 February 2023
Of which Community Diagnostic Centres
Total ISP
Of which Community Diagnostic Centres
Counting and
Coding changesOther
Total NHS
ICS-commissionedApril 2019-Mar
2020 (CCG
aggregated)
Apr 2021-Dec 2021
(CCG aggregated)
Apr 2022-Mar
2023April 2022 May 2022 June 2022 July 2022 August 2022 September 2022 October 2022 November 2022 December 2022 January 2023 February 2023 March 2023
February 2023 March 2023
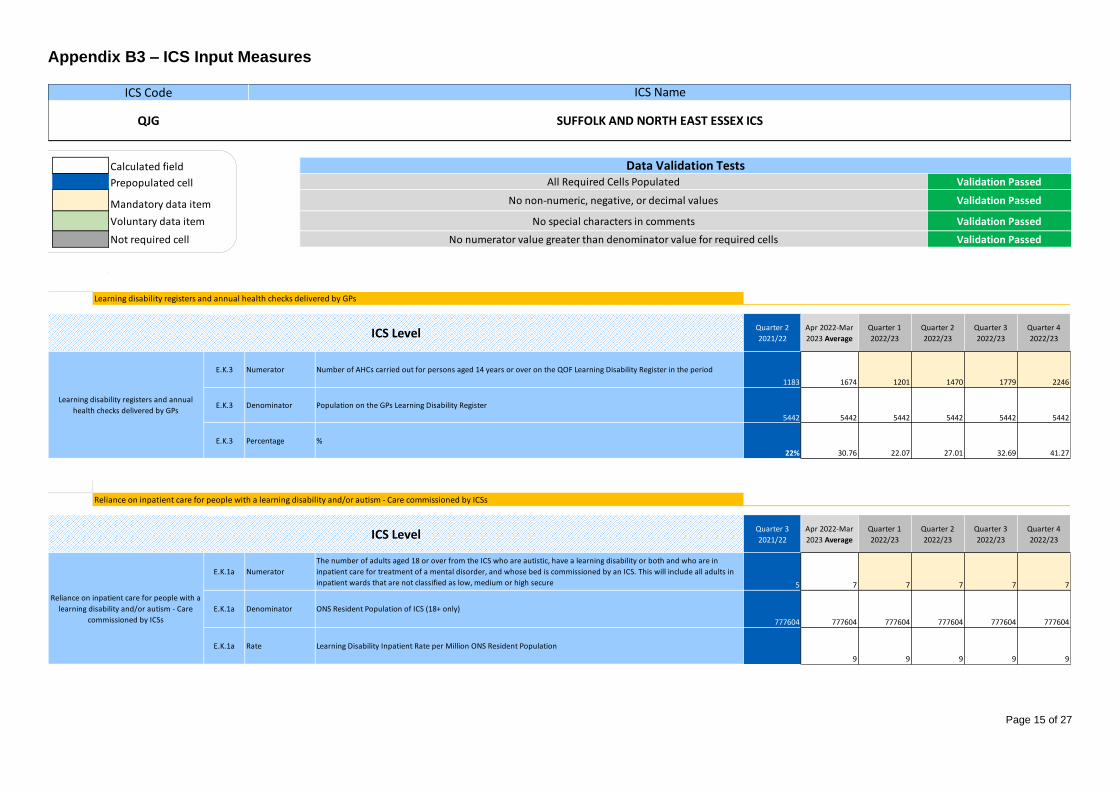
Page 15 of 27
Appendix B3 – ICS Input Measures
Calculated field
Prepopulated cell
Mandatory data item
Voluntary data item
Not required cell
Validation Passed
Validation Passed
No non-numeric, negative, or decimal values Validation Passed
All Required Cells Populated
Data Validation Tests
ICS Code ICS Name
QJG SUFFOLK AND NORTH EAST ESSEX ICS
No special characters in comments
No numerator value greater than denominator value for required cells Validation Passed
ICSMeasure1
PlanningRef 0 1 2 3
Quarter 2
2021/22
Apr 2022-Mar
2023 Average
Quarter 1
2022/23
Quarter 2
2022/23
Quarter 3
2022/23
Quarter 4
2022/23
E.K.3 Numerator Number of AHCs carried out for persons aged 14 years or over on the QOF Learning Disability Register in the period
1183 1674 1201 1470 1779 2246
E.K.3 Denominator Population on the GPs Learning Disability Register
5442 5442 5442 5442 5442 5442
E.K.3 Percentage %
22% 30.76 22.07 27.01 32.69 41.27
MeasureName
ICSMeasure2PlanningRef 0 1 2 3
Quarter 3
2021/22
Apr 2022-Mar
2023 Average
Quarter 1
2022/23
Quarter 2
2022/23
Quarter 3
2022/23
Quarter 4
2022/23
E.K.1a Numerator
The number of adults aged 18 or over from the ICS who are autistic, have a learning disability or both and who are in
inpatient care for treatment of a mental disorder, and whose bed is commissioned by an ICS. This will include all adults in
inpatient wards that are not classified as low, medium or high secure 5 7 7 7 7 7
E.K.1a Denominator ONS Resident Population of ICS (18+ only)
777604 777604 777604 777604 777604 777604
E.K.1a Rate Learning Disability Inpatient Rate per Million ONS Resident Population
9 9 9 9 9
Reliance on inpatient care for people with a learning disability and/or autism - Care commissioned by ICSs
ICS Level
Reliance on inpatient care for people with a
learning disability and/or autism - Care
commissioned by ICSs
Learning disability registers and annual
health checks delivered by GPs
ICS Level
Learning disability registers and annual health checks delivered by GPs

Page 16 of 27
ICSMeasure3
PlanningRef 0 1 2 3
Quarter 3
2021/22
Apr 2022-Mar
2023 Average
Quarter 1
2022/23
Quarter 2
2022/23
Quarter 3
2022/23
Quarter 4
2022/23
E.K.1b Numerator
The number of adults aged 18 or over from the ICS who are autistic, have a learning disability or both and who are in
inpatient care for the treatment of a mental disorder, and whose bed is commissioned by NHS England or via a provider
collaborative. This will include all adults in inpatient wards that are classified as low, medium or high-secure10 7 7 7 7 7
E.K.1b Denominator ONS Resident Population of ICS (18+ only)
777604 777604 777604 777604 777604 777604
E.K.1b Rate Learning Disability Inpatient Rate per Million ONS Resident Population
9 9 9 9 9
MeasureName
ICSMeasure4PlanningRef 0 1 2 3
Quarter 3
2021/22
Apr 2022-Mar
2023 Average
Quarter 1
2022/23
Quarter 2
2022/23
Quarter 3
2022/23
Quarter 4
2022/23
E.K.1c Numerator
The number of children aged under 18 years from the ICS who are autistic, have a learning disability or both and are in
inpatient care for the treatment of a mental disorder and whose bed is commissioned by NHS England or via a provider
collaborative * 2 2 2 2 2
E.K.1c Denominator ONS Resident Population of ICS (Under 18)
196280 196280 196280 196280 196280 196280
E.K.1c Rate Learning Disability Inpatient Rate per Million ONS Resident Population
10.19 10.19 10.19 10.19 10.19
MeasureName
ICSMeasure5PlanningRef 0 1 2 3
Quarter 2
2021/22
Apr 2022-Mar
2023 Average
Quarter 1
2022/23
Quarter 2
2022/23
Quarter 3
2022/23
Quarter 4
2022/23
E.N.1 Count Number of personal health budgets that have been in place, at any point during the financial year to date, per ICS
762 1718.5 687 1375 2062 2750
MeasureName
ICSMeasure6PlanningRef 0 1 2 3
Quarter 2
2021/22
Apr 2022-Mar
2023 Average
Quarter 1
2022/23
Quarter 2
2022/23
Quarter 3
2022/23
Quarter 4
2022/23
E.N.2 Count Total number of FTE PCN Network Contract DES funded social prescribing link workers employed in year
4.88 25 25 25 25 25
E.N.2 Count Total number of social prescribing referrals in year into social prescribing link workers
9969 1070.25 409 845 1282 1745
Social Prescribing Referrals
Personal Health Budgets
Social Prescribing Referrals
ICS Level
Personal Health Budgets
ICS Level
Reliance on inpatient care for people with a
learning disability and/or autism - Care for
children
ICS Level
ICS Level
Reliance on inpatient care for people with a
learning disability and/or autism - Care
commissioned by NHS England or via a
Provider Collaborative
Reliance on inpatient care for people with a learning disability and/or autism - Care for children
Reliance on inpatient care for people with a learning disability and/or autism - Care commissioned by NHS England or via a Provider Collaborative
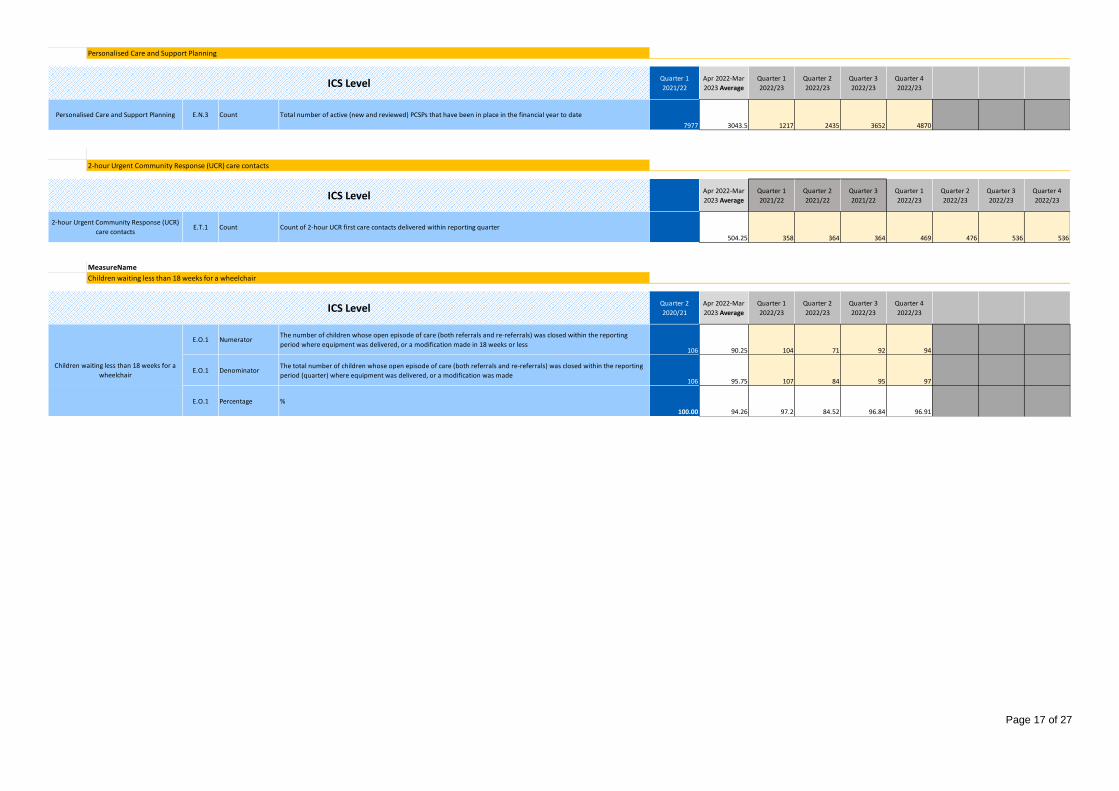
Page 17 of 27
ICSMeasure7
PlanningRef 0 1 2 3
Quarter 1
2021/22
Apr 2022-Mar
2023 Average
Quarter 1
2022/23
Quarter 2
2022/23
Quarter 3
2022/23
Quarter 4
2022/23
E.N.3 Count Total number of active (new and reviewed) PCSPs that have been in place in the financial year to date
7977 3043.5 1217 2435 3652 4870
MeasureName
ICSMeasure9
PlanningRef 0 1 2 3 4 5 6
Apr 2022-Mar
2023 Average
Quarter 1
2021/22
Quarter 2
2021/22
Quarter 3
2021/22
Quarter 1
2022/23
Quarter 2
2022/23
Quarter 3
2022/23
Quarter 4
2022/23
E.T.1 Count Count of 2-hour UCR first care contacts delivered within reporting quarter
504.25 358 364 364 469 476 536 536
MeasureName
ICSMeasure8
PlanningRef 0 1 2 3
Quarter 2
2020/21
Apr 2022-Mar
2023 Average
Quarter 1
2022/23
Quarter 2
2022/23
Quarter 3
2022/23
Quarter 4
2022/23
E.O.1 NumeratorThe number of children whose open episode of care (both referrals and re-referrals) was closed within the reporting
period where equipment was delivered, or a modification made in 18 weeks or less106 90.25 104 71 92 94
E.O.1 DenominatorThe total number of children whose open episode of care (both referrals and re-referrals) was closed within the reporting
period (quarter) where equipment was delivered, or a modification was made106 95.75 107 84 95 97
E.O.1 Percentage %
100.00 94.26 97.2 84.52 96.84 96.91
2-hour Urgent Community Response (UCR)
care contacts
Children waiting less than 18 weeks for a wheelchair
ICS Level
Children waiting less than 18 weeks for a
wheelchair
Personalised Care and Support Planning
2-hour Urgent Community Response (UCR) care contacts
ICS Level
Personalised Care and Support Planning
ICS Level
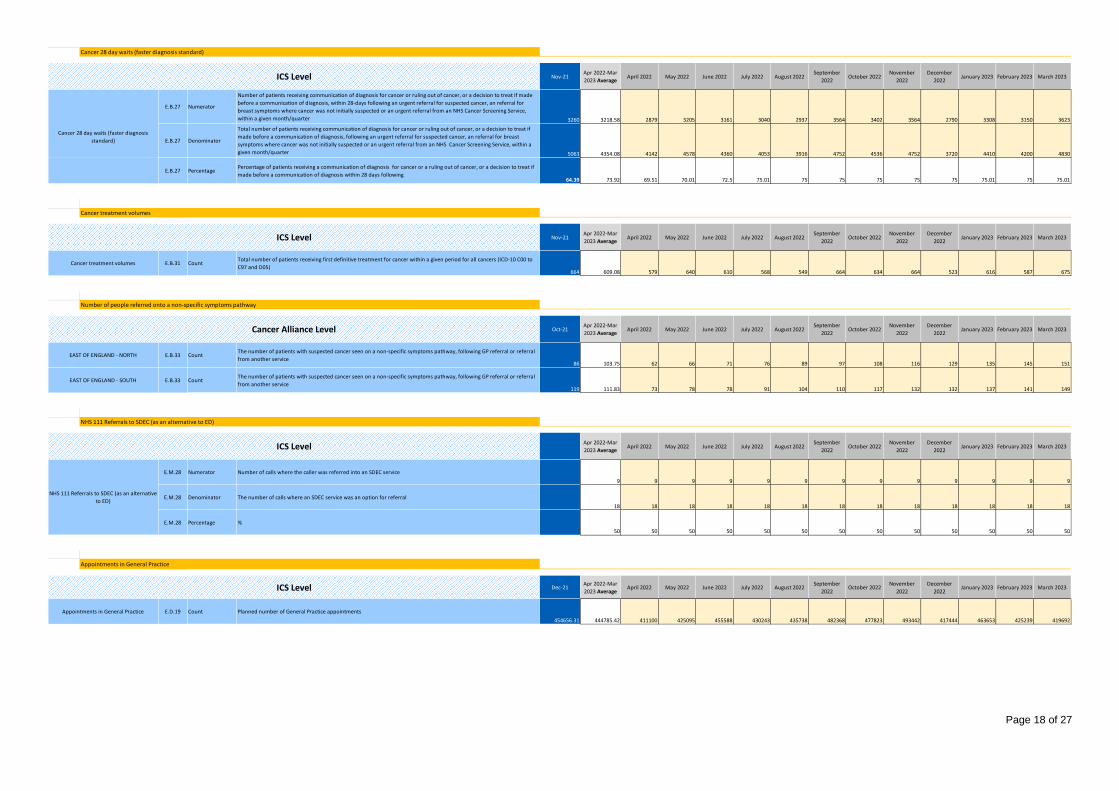
Page 18 of 27
ICSMeasure10
PlanningRef 0 1 2 3 4 5 6 7 8 9 10 11
Nov-21Apr 2022-Mar
2023 Average April 2022 May 2022 June 2022 July 2022 August 2022
September
2022October 2022
November
2022
December
2022January 2023 February 2023 March 2023
E.B.27 Numerator
Number of patients receiving communication of diagnosis for cancer or ruling out of cancer, or a decision to treat if made
before a communication of diagnosis, within 28-days following an urgent referral for suspected cancer, an referral for
breast symptoms where cancer was not initially suspected or an urgent referral from an NHS Cancer Screening Service,
within a given month/quarter 3260 3218.58 2879 3205 3161 3040 2937 3564 3402 3564 2790 3308 3150 3623
E.B.27 Denominator
Total number of patients receiving communication of diagnosis for cancer or ruling out of cancer, or a decision to treat if
made before a communication of diagnosis, following an urgent referral for suspected cancer, an referral for breast
symptoms where cancer was not initially suspected or an urgent referral from an NHS Cancer Screening Service, within a
given month/quarter 5063 4354.08 4142 4578 4360 4053 3916 4752 4536 4752 3720 4410 4200 4830
E.B.27 PercentagePercentage of patients receiving a communication of diagnosis for cancer or a ruling out of cancer, or a decision to treat if
made before a communication of diagnosis within 28 days following64.39 73.92 69.51 70.01 72.5 75.01 75 75 75 75 75 75.01 75 75.01
MeasureName
ICSMeasure11PlanningRef 0 1 2 3 4 5 6 7 8 9 10 11
Nov-21Apr 2022-Mar
2023 Average April 2022 May 2022 June 2022 July 2022 August 2022
September
2022October 2022
November
2022
December
2022January 2023 February 2023 March 2023
E.B.31 CountTotal number of patients receiving first definitive treatment for cancer within a given period for all cancers (ICD-10 C00 to
C97 and D05)664 609.08 579 640 610 568 549 664 634 664 523 616 587 675
MeasureName
ICSMeasure15PlanningRef 0 1 2 3 4 5 6 7 8 9 10 11
Oct-21Apr 2022-Mar
2023 Average April 2022 May 2022 June 2022 July 2022 August 2022
September
2022October 2022
November
2022
December
2022January 2023 February 2023 March 2023
E.B.33 CountThe number of patients with suspected cancer seen on a non-specific symptoms pathway, following GP referral or referral
from another service86 103.75 62 66 71 76 89 97 108 116 129 135 145 151
E.B.33 CountThe number of patients with suspected cancer seen on a non-specific symptoms pathway, following GP referral or referral
from another service119 111.83 73 78 78 91 104 110 117 132 132 137 141 149
MeasureName
ICSMeasure12
PlanningRef 0 1 2 3 4 5
Apr 2022-Mar
2023 Average April 2022 May 2022 June 2022 July 2022 August 2022
September
2022October 2022
November
2022
December
2022January 2023 February 2023 March 2023
E.M.28 Numerator Number of calls where the caller was referred into an SDEC service
9 9 9 9 9 9 9 9 9 9 9 9 9
E.M.28 Denominator The number of calls where an SDEC service was an option for referral
18 18 18 18 18 18 18 18 18 18 18 18 18
E.M.28 Percentage %
50 50 50 50 50 50 50 50 50 50 50 50 50
MeasureName
ICSMeasure14
PlanningRef 0 1 2 3 4 5 6 7 8 9 10 11
Dec-21Apr 2022-Mar
2023 Average April 2022 May 2022 June 2022 July 2022 August 2022
September
2022October 2022
November
2022
December
2022January 2023 February 2023 March 2023
E.D.19 Count Planned number of General Practice appointments
454656.31 444785.42 411100 425095 455588 430243 435738 482368 477823 493442 417444 463653 425239 419692
Appointments in General Practice
Appointments in General Practice
ICS Level
Cancer treatment volumes
Cancer 28 day waits (faster diagnosis
standard)
Cancer treatment volumes
NHS 111 Referrals to SDEC (as an alternative
to ED)
ICS Level
Cancer 28 day waits (faster diagnosis standard)
NHS 111 Referrals to SDEC (as an alternative to ED)
ICS Level
ICS Level
EAST OF ENGLAND - NORTH
EAST OF ENGLAND - SOUTH
Number of people referred onto a non-specific symptoms pathway
Cancer Alliance Level

Page 19 of 27
ICSMeasure13
PlanningRef 0 1
Apr 2022-Mar
2023 Average
Quarter 1
2022/23
Quarter 2
2022/23
E.D.17 Count The number of extended access appointments booked excluding did not attends
37713 37713 37713
ActivityCategory
Activity140 1 2 3 4 5 6 7 8
Apr 2022-Mar
2023 Average April 2022 May 2022 June 2022 July 2022 August 2022
September
2022October 2022
November
2022
December
2022January 2023 February 2023 March 2023
E.T.3 Count/Total The number of people discharged by location and discharge pathway per month
74542 6032 6326 6501 6423 5969 5931 5972 6305 6481 6067 6019 6516
E.T.3a Count Hospital discharge pathway activity - pathway 0
65534 5303 5561 5715 5647 5248 5214 5251 5543 5698 5334 5291 5729
E.T.3b Count Hospital discharge pathway activity - pathway 1
3426 277 291 299 295 274 273 274 290 298 279 277 299
E.T.3c Count Hospital discharge pathway activity - pathway 2
4095 331 348 357 353 328 326 328 346 356 333 331 358
E.T.3d Count Hospital discharge pathway activity - pathway 3
1487 121 126 130 128 119 118 119 126 129 121 120 130
MeasureName
ICSMeasure16
PlanningRef 0 1 2 3
Apr 2022-Mar
2023 Average
Quarter 1
2022/23
Quarter 2
2022/23
Quarter 3
2022/23
Quarter 4
2022/23
E.T.5 Count The number of patients that the virtual ward is able to simultaneously manage
92.5 0 0 185 185
ActivityCategory
Activity150 1 2 3 4
Apr 2022-Mar
2023 Average
Quarter 3
2021/22
Quarter 1
2022/23
Quarter 2
2022/23
Quarter 3
2022/23
Quarter 4
2022/23
E.T.2 Count Number of patients waiting at a point in time aggregated for a, in scope CYP and b, in scope Adult services
54246 9878 11261 11148 11036 10923
E.T.2a Count Number of CYP (0-17 years) on community waiting lists per system
16546 3013 3435 3400 3366 3332
E.T.2b Count Number of Adults (18+ years) on community waiting lists per system
37700 6865 7826 7748 7670 7591
Community services waiting list
ICS Level
Community services waiting list
Virtual ward capacity
ICS Level
Virtual ward capacity
Hospital discharge pathway activity
Hospital discharge pathway activity
ICS Level
Extended Access Appointment Utilisation
Extended Access Appointment Utilisation
ICS Level

Page 20 of 27
MeasureName
CCGMeasure5
PlanningRef
Quarter 1
2021/22
Oct 2021-Mar
2022 Average
Quarter 3
2021/22
Quarter 4
2021/22
The number of adults aged 18 or over from the CCG who are autistic, have a learning disability or both and who are in inpatient care for the treatment of a mental disorder, and whose bed is commissioned by NHS England or via a Provider CollaborativeCCG1E.K.1bCCG106L
E.K.1b Numerator
The number of adults aged 18 or over from the CCG who are autistic, have a learning disability or both and who are in
inpatient care for the treatment of a mental disorder, and whose bed is commissioned by NHS England or via a Provider
Collaborative 5 5 5 5
ONS Resident Population of CCG (18+ only)CCG1E.K.1bCCG106L
E.K.1b Denominator ONS Resident Population of CCG (18+ only)
325389 325389 325389 325389
Learning Disability Inpatient Rate per Million ONS Resident Population CCG1E.K.1bCCG106L
E.K.1b Rate Learning Disability Inpatient Rate per Million ONS Resident Population
15.37 15.37 15.37
The number of adults aged 18 or over from the CCG who are autistic, have a learning disability or both and who are in inpatient care for the treatment of a mental disorder, and whose bed is commissioned by NHS England or via a Provider CollaborativeCCG2E.K.1bCCG206T
E.K.1b Numerator
The number of adults aged 18 or over from the CCG who are autistic, have a learning disability or both and who are in
inpatient care for the treatment of a mental disorder, and whose bed is commissioned by NHS England or via a Provider
Collaborative 5 7 7 7
ONS Resident Population of CCG (18+ only)CCG2E.K.1bCCG206T
E.K.1b Denominator ONS Resident Population of CCG (18+ only)
268670 268670 268670 268670
Learning Disability Inpatient Rate per Million ONS Resident Population CCG2E.K.1bCCG206T
E.K.1b Rate Learning Disability Inpatient Rate per Million ONS Resident Population
26.05 26.05 26.05
The number of adults aged 18 or over from the CCG who are autistic, have a learning disability or both and who are in inpatient care for the treatment of a mental disorder, and whose bed is commissioned by NHS England or via a Provider CollaborativeCCG3E.K.1bCCG307K
E.K.1b Numerator
The number of adults aged 18 or over from the CCG who are autistic, have a learning disability or both and who are in
inpatient care for the treatment of a mental disorder, and whose bed is commissioned by NHS England or via a Provider
Collaborative * 2 2 2
ONS Resident Population of CCG (18+ only)CCG3E.K.1bCCG307K
E.K.1b Denominator ONS Resident Population of CCG (18+ only)
183545 183545 183545 183545
Learning Disability Inpatient Rate per Million ONS Resident Population CCG3E.K.1bCCG307K
E.K.1b Rate Learning Disability Inpatient Rate per Million ONS Resident Population
10.9 10.9 10.9
CCG7CCG7
CCG8CCG8
CCG8CCG8
CCG9CCG9
CCG9CCG9
MeasureName
CCGMeasure6
PlanningRef
Quarter 1
2021/22
Oct 2021-Mar
2022 Average
Quarter 3
2021/22
Quarter 4
2021/22
The number of adults aged 18 or over from the CCG who are autistic, have a learning disability or both and who are in inpatient care for treatment of a mental disorder, and whose bed is commissioned by a CCGCCG1E.K.1aCCG106LE.K.1a Numerator
The number of adults aged 18 or over from the CCG who are autistic, have a learning disability or both and who are in
inpatient care for treatment of a mental disorder, and whose bed is commissioned by a CCG * 5 5 5
ONS Resident Population of CCG (18+ only)CCG1E.K.1aCCG106LE.K.1a Denominator ONS Resident Population of CCG (18+ only)
325389 325389 325389 325389
Learning Disability Inpatient Rate per Million ONS Resident Population CCG1E.K.1aCCG106LE.K.1a Rate Learning Disability Inpatient Rate per Million ONS Resident Population
15.37 15.37 15.37
The number of adults aged 18 or over from the CCG who are autistic, have a learning disability or both and who are in inpatient care for treatment of a mental disorder, and whose bed is commissioned by a CCGCCG2E.K.1aCCG206TE.K.1a Numerator
The number of adults aged 18 or over from the CCG who are autistic, have a learning disability or both and who are in
inpatient care for treatment of a mental disorder, and whose bed is commissioned by a CCG 5 6 6 6
ONS Resident Population of CCG (18+ only)CCG2E.K.1aCCG206TE.K.1a Denominator ONS Resident Population of CCG (18+ only)
268670 268670 268670 268670
Learning Disability Inpatient Rate per Million ONS Resident Population CCG2E.K.1aCCG206TE.K.1a Rate Learning Disability Inpatient Rate per Million ONS Resident Population
22.33 22.33 22.33
The number of adults aged 18 or over from the CCG who are autistic, have a learning disability or both and who are in inpatient care for treatment of a mental disorder, and whose bed is commissioned by a CCGCCG3E.K.1aCCG307KE.K.1a Numerator
The number of adults aged 18 or over from the CCG who are autistic, have a learning disability or both and who are in
inpatient care for treatment of a mental disorder, and whose bed is commissioned by a CCG * 2 2 2
ONS Resident Population of CCG (18+ only)CCG3E.K.1aCCG307KE.K.1a Denominator ONS Resident Population of CCG (18+ only)
183545 183545 183545 183545
Learning Disability Inpatient Rate per Million ONS Resident Population CCG3E.K.1aCCG307KE.K.1a Rate Learning Disability Inpatient Rate per Million ONS Resident Population
10.9 10.9 10.9
MeasureName
CCGMeasure8
PlanningRef
Apr 2021-Sep
2021
Oct 2021-Mar
2022October 2021 November 2021 December 2021 January 2022 February 2022 March 2022
Number of calls where the caller was referred into an SDEC serviceCCG1E.M.28CCG106LE.M.28 Numerator Number of calls where the caller was referred into an SDEC service
18 54 9 9 9 9 9 9
The number of calls where an SDEC service was an option for referralCCG1E.M.28CCG106LE.M.28 Denominator The number of calls where an SDEC service was an option for referral
42 108 18 18 18 18 18 18
%CCG1E.M.28CCG106LE.M.28 Percentage %
42.86 50 50 50 50 50 50 50
Number of calls where the caller was referred into an SDEC serviceCCG2E.M.28CCG206TE.M.28 Numerator Number of calls where the caller was referred into an SDEC service
15 12 2 2 2 2 2 2
The number of calls where an SDEC service was an option for referralCCG2E.M.28CCG206TE.M.28 Denominator The number of calls where an SDEC service was an option for referral
36 24 4 4 4 4 4 4
%CCG2E.M.28CCG206TE.M.28 Percentage %
41.67 50 50 50 50 50 50 50
Number of calls where the caller was referred into an SDEC serviceCCG3E.M.28CCG307KE.M.28 Numerator Number of calls where the caller was referred into an SDEC service
12 60 10 10 10 10 10 10
The number of calls where an SDEC service was an option for referralCCG3E.M.28CCG307KE.M.28 Denominator The number of calls where an SDEC service was an option for referral
36 120 20 20 20 20 20 20
%CCG3E.M.28CCG307KE.M.28 Percentage %
33.33 50 50 50 50 50 50 50
06L NHS IPSWICH AND EAST SUFFOLK CCG
06T NHS NORTH EAST ESSEX CCG
07K NHS WEST SUFFOLK CCG
Reliance on inpatient care for people with a learning disability and/or autism - Care commissioned by CCGs
CCG Level
Reliance on inpatient care for people with a learning disability and/or autism - Care commissioned by NHS England
07K NHS WEST SUFFOLK CCG
CCG Level
06L NHS IPSWICH AND EAST SUFFOLK CCG
06T NHS NORTH EAST ESSEX CCG
NHS 111 Referrals to SDEC (as an alternative to ED)
CCG Level
06L NHS IPSWICH AND EAST SUFFOLK CCG
06T NHS NORTH EAST ESSEX CCG
07K NHS WEST SUFFOLK CCG
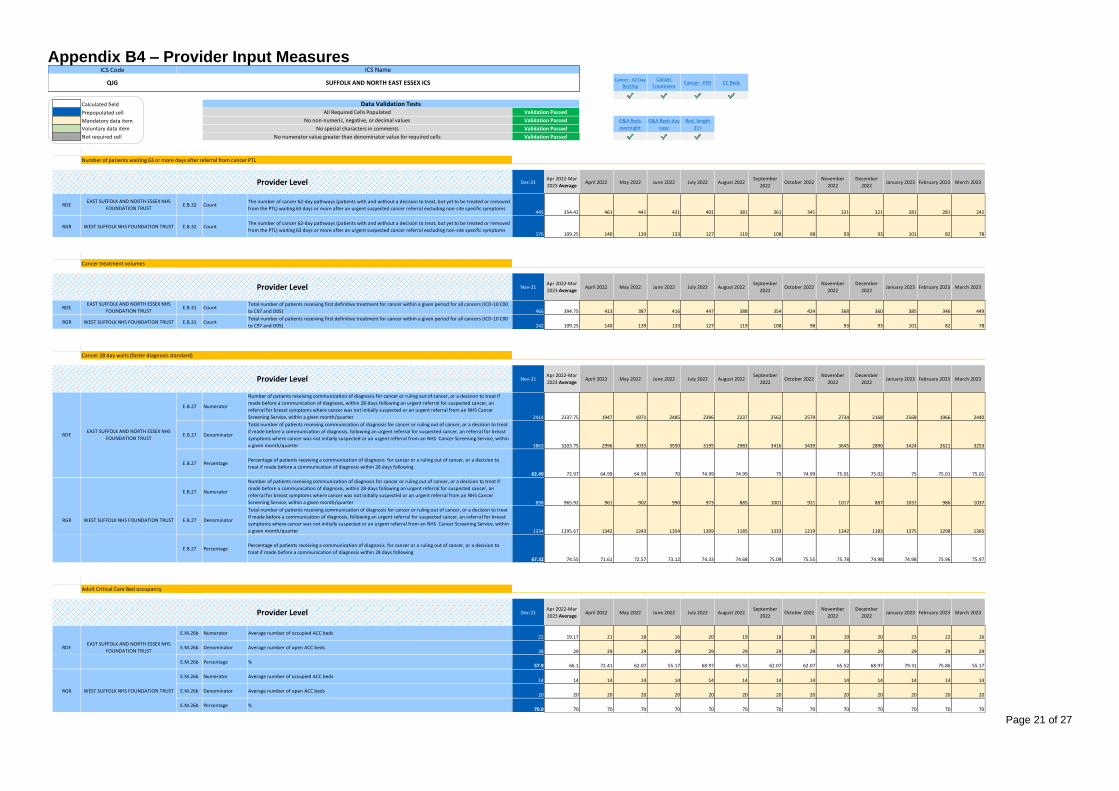
Page 21 of 27
Appendix B4 – Provider Input Measures $H$15 $H$34 $H$53 $H$98
Calculated field ProvMeasure5ProvMeasure6ProvMeasure8
Prepopulated cell $H$143 $H$201 $H$233
Mandatory data item
Voluntary data item
Not required cell
MeasureName
ProvMeasure1PlanningRef
Dec-21Apr 2022-Mar
2023 Average April 2022 May 2022 June 2022 July 2022 August 2022
September
2022October 2022
November
2022
December
2022January 2023 February 2023 March 2023
Provider1RDE
RDE E.B.32 CountThe number of cancer 62-day pathways (patients with and without a decision to treat, but yet to be treated or removed
from the PTL) waiting 63 days or more after an urgent suspected cancer referral excluding non-site specific symptoms445 354.42 461 441 421 401 381 361 341 321 321 281 281 242
Provider2RGR
RGR E.B.32 CountThe number of cancer 62-day pathways (patients with and without a decision to treat, but yet to be treated or removed
from the PTL) waiting 63 days or more after an urgent suspected cancer referral excluding non-site specific symptoms176 109.25 140 139 133 127 119 108 98 93 93 101 82 78
MeasureName
ProvMeasure2
PlanningRef
Nov-21Apr 2022-Mar
2023 Average April 2022 May 2022 June 2022 July 2022 August 2022
September
2022October 2022
November
2022
December
2022January 2023 February 2023 March 2023
Provider1RDERDE E.B.31 Count
Total number of patients receiving first definitive treatment for cancer within a given period for all cancers (ICD-10 C00
to C97 and D05) 466 394.75 413 387 416 447 388 354 424 368 360 385 346 449
Provider2RGRRGR E.B.31 Count
Total number of patients receiving first definitive treatment for cancer within a given period for all cancers (ICD-10 C00
to C97 and D05) 142 109.25 140 139 133 127 119 108 98 93 93 101 82 78
MeasureName
ProvMeasure7PlanningRef
Nov-21Apr 2022-Mar
2023 Average April 2022 May 2022 June 2022 July 2022 August 2022
September
2022October 2022
November
2022
December
2022January 2023 February 2023 March 2023
Provider1RDE
E.B.27 Numerator
Number of patients receiving communication of diagnosis for cancer or ruling out of cancer, or a decision to treat if
made before a communication of diagnosis, within 28-days following an urgent referral for suspected cancer, an
referral for breast symptoms where cancer was not initially suspected or an urgent referral from an NHS Cancer
Screening Service, within a given month/quarter 2414 2337.75 1947 1971 2485 2396 2237 2562 2579 2734 2168 2568 1966 2440
Provider1RDE
E.B.27 Denominator
Total number of patients receiving communication of diagnosis for cancer or ruling out of cancer, or a decision to treat
if made before a communication of diagnosis, following an urgent referral for suspected cancer, an referral for breast
symptoms where cancer was not initially suspected or an urgent referral from an NHS Cancer Screening Service, within
a given month/quarter 3863 3203.75 2996 3033 3550 3195 2983 3416 3439 3645 2890 3424 2621 3253
Provider1RDE
E.B.27 PercentagePercentage of patients receiving a communication of diagnosis for cancer or a ruling out of cancer, or a decision to
treat if made before a communication of diagnosis within 28 days following
62.49 72.97 64.99 64.99 70 74.99 74.99 75 74.99 75.01 75.02 75 75.01 75.01
Provider2RGR
E.B.27 Numerator
Number of patients receiving communication of diagnosis for cancer or ruling out of cancer, or a decision to treat if
made before a communication of diagnosis, within 28-days following an urgent referral for suspected cancer, an
referral for breast symptoms where cancer was not initially suspected or an urgent referral from an NHS Cancer
Screening Service, within a given month/quarter 898 965.92 961 902 990 973 885 1001 921 1017 887 1031 986 1037
Provider2RGR
E.B.27 Denominator
Total number of patients receiving communication of diagnosis for cancer or ruling out of cancer, or a decision to treat
if made before a communication of diagnosis, following an urgent referral for suspected cancer, an referral for breast
symptoms where cancer was not initially suspected or an urgent referral from an NHS Cancer Screening Service, within
a given month/quarter 1334 1295.67 1342 1243 1354 1309 1185 1333 1219 1342 1183 1375 1298 1365
Provider2RGR
E.B.27 PercentagePercentage of patients receiving a communication of diagnosis for cancer or a ruling out of cancer, or a decision to
treat if made before a communication of diagnosis within 28 days following
67.32 74.55 71.61 72.57 73.12 74.33 74.68 75.09 75.55 75.78 74.98 74.98 75.96 75.97
MeasureName
ProvMeasure4PlanningRef
Dec-21Apr 2022-Mar
2023 Average April 2022 May 2022 June 2022 July 2022 August 2022
September
2022October 2022
November
2022
December
2022January 2023 February 2023 March 2023
Provider1RDEE.M.26b Numerator Average number of occupied ACC beds
22 19.17 21 18 16 20 19 18 18 19 20 23 22 16
Provider1RDEE.M.26b Denominator Average number of open ACC beds
38 29 29 29 29 29 29 29 29 29 29 29 29 29
Provider1RDEE.M.26b Percentage %
57.9 66.1 72.41 62.07 55.17 68.97 65.52 62.07 62.07 65.52 68.97 79.31 75.86 55.17
Provider2RGRE.M.26b Numerator Average number of occupied ACC beds
14 14 14 14 14 14 14 14 14 14 14 14 14 14
Provider2RGRE.M.26b Denominator Average number of open ACC beds
20 20 20 20 20 20 20 20 20 20 20 20 20 20
Provider2RGRE.M.26b Percentage %
70.0 70 70 70 70 70 70 70 70 70 70 70 70 70
Provider Level
Cancer 28 day waits (faster diagnosis standard)
RDEEAST SUFFOLK AND NORTH ESSEX NHS
FOUNDATION TRUST
RGR WEST SUFFOLK NHS FOUNDATION TRUST
Provider Level
EAST SUFFOLK AND NORTH ESSEX NHS
FOUNDATION TRUST
WEST SUFFOLK NHS FOUNDATION TRUST
Cancer treatment volumes
Provider Level
EAST SUFFOLK AND NORTH ESSEX NHS
FOUNDATION TRUST
Validation Passed
No numerator value greater than denominator value for required cells Validation Passed
WEST SUFFOLK NHS FOUNDATION TRUST
G&A Beds
overnight
G&A Beds day
case
Red. length
21+
ICS Code ICS Name
QJG SUFFOLK AND NORTH EAST ESSEX ICS
Data Validation Tests
Cancer - 62 Day
Backlog
All Required Cells Populated Validation Passed
No non-numeric, negative, or decimal values Validation Passed
Number of patients waiting 63 or more days after referral from cancer PTL
No special characters in comments
Cancer
TreatmentCancer - FDS CC Beds
Adult Critical Care Bed occupancy
Provider Level
RDEEAST SUFFOLK AND NORTH ESSEX NHS
FOUNDATION TRUST
RGR WEST SUFFOLK NHS FOUNDATION TRUST

Page 22 of 27
ProvMeasure5
PlanningRef
Dec-21Apr 2022-Mar
2023 Average April 2022 May 2022 June 2022 July 2022 August 2022
September
2022October 2022
November
2022
December
2022January 2023 February 2023 March 2023
E.M.26a Numerator Average number of overnight G&A beds occupied1034 1029.5 1028 1028 1028 1028 1028 1028 1031 1031 1031 1031 1031 1031
E.M.26a Denominator Average number of overnight G&A beds available1154 1119 1117 1117 1117 1117 1117 1117 1121 1121 1121 1121 1121 1121
E.M.26a Percentage %89.6 92 92.03 92.03 92.03 92.03 92.03 92.03 91.97 91.97 91.97 91.97 91.97 91.97
E.M.26a Count Average number of overnight G&A beds available which are operationally separate for elective patients only105 105 105 105 105 105 105 105 105 105 105 105 105
E.M.26a Numerator Average number of overnight G&A beds occupied394 350.17 335 335 335 335 335 335 342 370 370 370 370 370
E.M.26a Denominator Average number of overnight G&A beds available463 380.5 364 364 364 364 364 364 372 402 402 402 402 402
E.M.26a Percentage %85.1 92.03 92.03 92.03 92.03 92.03 92.03 92.03 91.94 92.04 92.04 92.04 92.04 92.04
E.M.26a Count Average number of overnight G&A beds available which are operationally separate for elective patients only16 16 16 16 16 16 16 16 16 16 16 16 16
MeasureName
ProvMeasure6
PlanningRef
Sep-21Apr 2022-Mar
2023 Average April 2022 May 2022 June 2022 July 2022 August 2022
September
2022October 2022
November
2022
December
2022January 2023 February 2023 March 2023
E.M.26c Count Average number of day case G&A beds available146 146 146 146 146 146 146 146 146 146 146 146 146 146
E.M.26c Count Average number of day case G&A beds available which are operationally separate for elective patients only46 46 46 46 46 46 46 46 46 46 46 46 46
E.M.26c Count Average number of day case G&A beds available0 16 16 16 16 16 16 16 16 16 16 16 16 16
E.M.26c Count Average number of day case G&A beds available which are operationally separate for elective patients only16 16 16 16 16 16 16 16 16 16 16 16 16
MeasureName
ProvMeasure8PlanningRef
Dec-21Apr 2022-Mar
2023 Average April 2022 May 2022 June 2022 July 2022 August 2022
September
2022October 2022
November
2022
December
2022January 2023 February 2023 March 2023
RDE E.M.25 Count Average number of adult patients in an acute hospital bed for 21 days and over129 114.5 114 114 114 114 114 114 115 115 115 115 115 115
RGR E.M.25 Count Average number of adult patients in an acute hospital bed for 21 days and over65 59.33 64 62 60 58 56 56 58 58 60 60 60 60
Provider Level
EAST SUFFOLK AND NORTH ESSEX NHS
FOUNDATION TRUST
WEST SUFFOLK NHS FOUNDATION TRUST
Reducing length of stay for patients in hospital for 21 days and over
Provider Level
General and Acute overnight bed occupancy
General and Acute day bed available
Provider Level
RDEEAST SUFFOLK AND NORTH ESSEX NHS
FOUNDATION TRUST
RGR WEST SUFFOLK NHS FOUNDATION TRUST
RDEEAST SUFFOLK AND NORTH ESSEX NHS
FOUNDATION TRUST
RGR WEST SUFFOLK NHS FOUNDATION TRUST
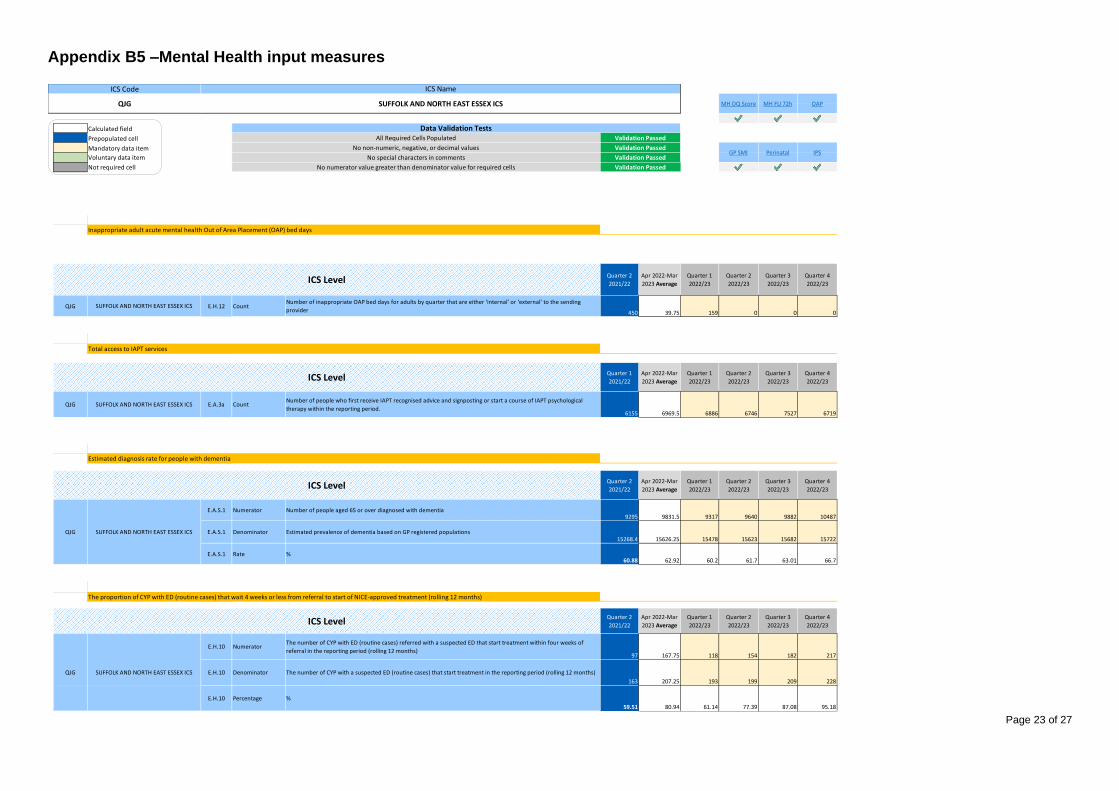
Page 23 of 27
Appendix B5 –Mental Health input measures
$H$17 $H$27 $H$45
Calculated field MeasureMH6MeasureMH7MeasureMH8
Prepopulated cell $H$93 $H$100 $H$107
Mandatory data item
Voluntary data item
Not required cell
MeasureName
MeasureMH5
PlanningRef
PlanningRef
Quarter 2
2021/22
Apr 2022-Mar
2023 Average
Quarter 1
2022/23
Quarter 2
2022/23
Quarter 3
2022/23
Quarter 4
2022/23
ICSQJGQJG E.H.12 Count
Number of inappropriate OAP bed days for adults by quarter that are either ‘internal’ or ‘external’ to the sending
provider 450 39.75 159 0 0 0
MeasureName
MeasureMH1
PlanningRef
Quarter 1
2021/22
Apr 2022-Mar
2023 Average
Quarter 1
2022/23
Quarter 2
2022/23
Quarter 3
2022/23
Quarter 4
2022/23
ICSQJG
QJG E.A.3a CountNumber of people who first receive IAPT recognised advice and signposting or start a course of IAPT psychological
therapy within the reporting period.6155 6969.5 6886 6746 7527 6719
MeasureName
MeasureMH2
PlanningRef
Quarter 2
2021/22
Apr 2022-Mar
2023 Average
Quarter 1
2022/23
Quarter 2
2022/23
Quarter 3
2022/23
Quarter 4
2022/23
ICSQJGE.A.S.1 Numerator Number of people aged 65 or over diagnosed with dementia
9295 9831.5 9317 9640 9882 10487
ICSQJGE.A.S.1 Denominator Estimated prevalence of dementia based on GP registered populations
15268.4 15626.25 15478 15623 15682 15722
ICSQJGE.A.S.1 Rate %
60.88 62.92 60.2 61.7 63.01 66.7
MeasureName
MeasureMH3
PlanningRef
Quarter 2
2021/22
Apr 2022-Mar
2023 Average
Quarter 1
2022/23
Quarter 2
2022/23
Quarter 3
2022/23
Quarter 4
2022/23
ICSQJG
E.H.10 NumeratorThe number of CYP with ED (routine cases) referred with a suspected ED that start treatment within four weeks of
referral in the reporting period (rolling 12 months)97 167.75 118 154 182 217
ICSQJG
E.H.10 Denominator The number of CYP with a suspected ED (routine cases) that start treatment in the reporting period (rolling 12 months)
163 207.25 193 199 209 228
ICSQJG
E.H.10 Percentage %
59.51 80.94 61.14 77.39 87.08 95.18
Perinatal IPSNo special characters in comments Validation Passed
Data Validation TestsAll Required Cells Populated Validation Passed
No non-numeric, negative, or decimal values Validation PassedGP SMI
The proportion of CYP with ED (routine cases) that wait 4 weeks or less from referral to start of NICE-approved treatment (rolling 12 months)
QJG SUFFOLK AND NORTH EAST ESSEX ICS
ICS Level
QJG SUFFOLK AND NORTH EAST ESSEX ICS
ICS Level
ICS Level
Estimated diagnosis rate for people with dementia
Inappropriate adult acute mental health Out of Area Placement (OAP) bed days
SUFFOLK AND NORTH EAST ESSEX ICS
SUFFOLK AND NORTH EAST ESSEX ICS
ICS Level
Total access to IAPT services
No numerator value greater than denominator value for required cells Validation Passed
ICS Code ICS Name
QJG SUFFOLK AND NORTH EAST ESSEX ICS MH DQ Score MH FU 72h OAP

Page 24 of 27
MeasureMH4
PlanningRef
Quarter 2
2021/22
Apr 2022-Mar
2023 Average
Quarter 1
2022/23
Quarter 2
2022/23
Quarter 3
2022/23
Quarter 4
2022/23
E.H.11 NumeratorThe number of CYP with ED (urgent cases) referred with a suspected ED that start treatment within one week of
referral in the reporting period (rolling 12 months)15 33 27 31 33 41
E.H.11 Denominator The number of CYP with a suspected ED (urgent cases) that start treatment in the reporting period (rolling 12 months)
33 40.5 39 41 39 43
E.H.11 Percentage %
45.45 81.48 69.23 75.61 84.62 95.35
MeasureName
MeasureMH6
PlanningRef
Quarter 2
2021/22
Apr 2022-Mar
2023 Average
Quarter 1
2022/23
Quarter 2
2022/23
Quarter 3
2022/23
Quarter 4
2022/23
QJG E.H.13 CountThe number of people on the General Practice SMI registers who have received a physical health assessment in the 12
months to the end of the period2551 4962.25 4072 4826 5387 5564
MeasureName
MeasureMH7
PlanningRef
Quarter 2
2021/22
Apr 2022-Mar
2023 Average
Quarter 1
2022/23
Quarter 2
2022/23
Quarter 3
2022/23
Quarter 4
2022/23
QJG E.H.15 Count Number of women accessing specialist community PMH and MMHS services in the reporting period
700 660.5 305 542 779 1016
MeasureName
MeasureMH8
PlanningRef
Quarter 1
2021/22
Apr 2022-Mar
2023 Average
Quarter 1
2022/23
Quarter 2
2022/23
Quarter 3
2022/23
Quarter 4
2022/23
QJG E.H.17 Count Number of people accessing IPS services as a rolling total each quarter
185 482.5 193 386 579 772
People with severe mental illness receiving a full annual physical health check and follow up interventions
ICS Level
QJG SUFFOLK AND NORTH EAST ESSEX ICS
Women Accessing Specialist Community Perinatal Mental Health Services
Access to Individual Placement and Support Services
SUFFOLK AND NORTH EAST ESSEX ICS
SUFFOLK AND NORTH EAST ESSEX ICS
ICS Level
ICS Level
The proportion of CYP with ED (urgent cases) that wait one week or less from referral to start of NICE-approved treatment (rolling 12 months)
ICS Level
SUFFOLK AND NORTH EAST ESSEX ICS
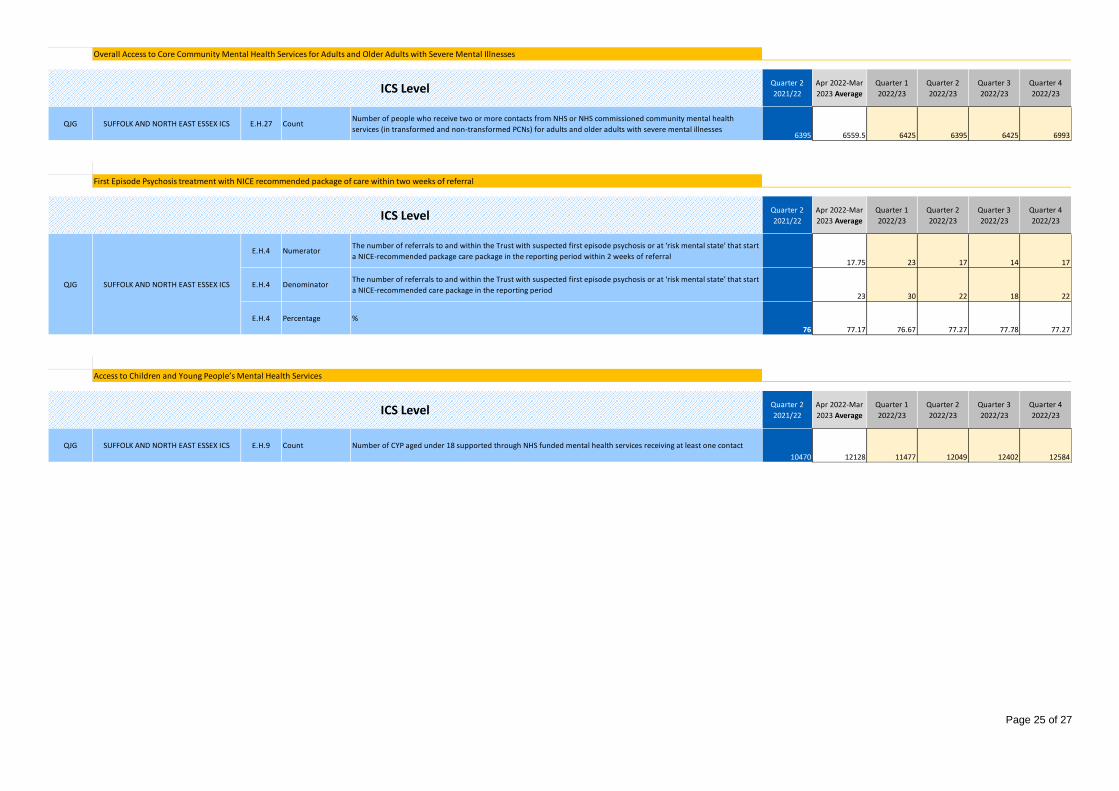
Page 25 of 27
MeasureMH10
PlanningRef
Quarter 2
2021/22
Apr 2022-Mar
2023 Average
Quarter 1
2022/23
Quarter 2
2022/23
Quarter 3
2022/23
Quarter 4
2022/23
QJG E.H.27 CountNumber of people who receive two or more contacts from NHS or NHS commissioned community mental health
services (in transformed and non-transformed PCNs) for adults and older adults with severe mental illnesses6395 6559.5 6425 6395 6425 6993
MeasureName
MeasureMH12
PlanningRef
Quarter 2
2021/22
Apr 2022-Mar
2023 Average
Quarter 1
2022/23
Quarter 2
2022/23
Quarter 3
2022/23
Quarter 4
2022/23
E.H.4 NumeratorThe number of referrals to and within the Trust with suspected first episode psychosis or at ‘risk mental state’ that start
a NICE-recommended package care package in the reporting period within 2 weeks of referral17.75 23 17 14 17
E.H.4 DenominatorThe number of referrals to and within the Trust with suspected first episode psychosis or at ‘risk mental state’ that start
a NICE-recommended care package in the reporting period23 30 22 18 22
E.H.4 Percentage %
76 77.17 76.67 77.27 77.78 77.27
MeasureName
MeasureMH13
PlanningRef
Quarter 2
2021/22
Apr 2022-Mar
2023 Average
Quarter 1
2022/23
Quarter 2
2022/23
Quarter 3
2022/23
Quarter 4
2022/23
QJG E.H.9 Count Number of CYP aged under 18 supported through NHS funded mental health services receiving at least one contact
10470 12128 11477 12049 12402 12584
Overall Access to Core Community Mental Health Services for Adults and Older Adults with Severe Mental Illnesses
ICS Level
SUFFOLK AND NORTH EAST ESSEX ICS
QJG SUFFOLK AND NORTH EAST ESSEX ICS
First Episode Psychosis treatment with NICE recommended package of care within two weeks of referral
ICS Level
SUFFOLK AND NORTH EAST ESSEX ICS
Access to Children and Young People’s Mental Health Services
ICS Level
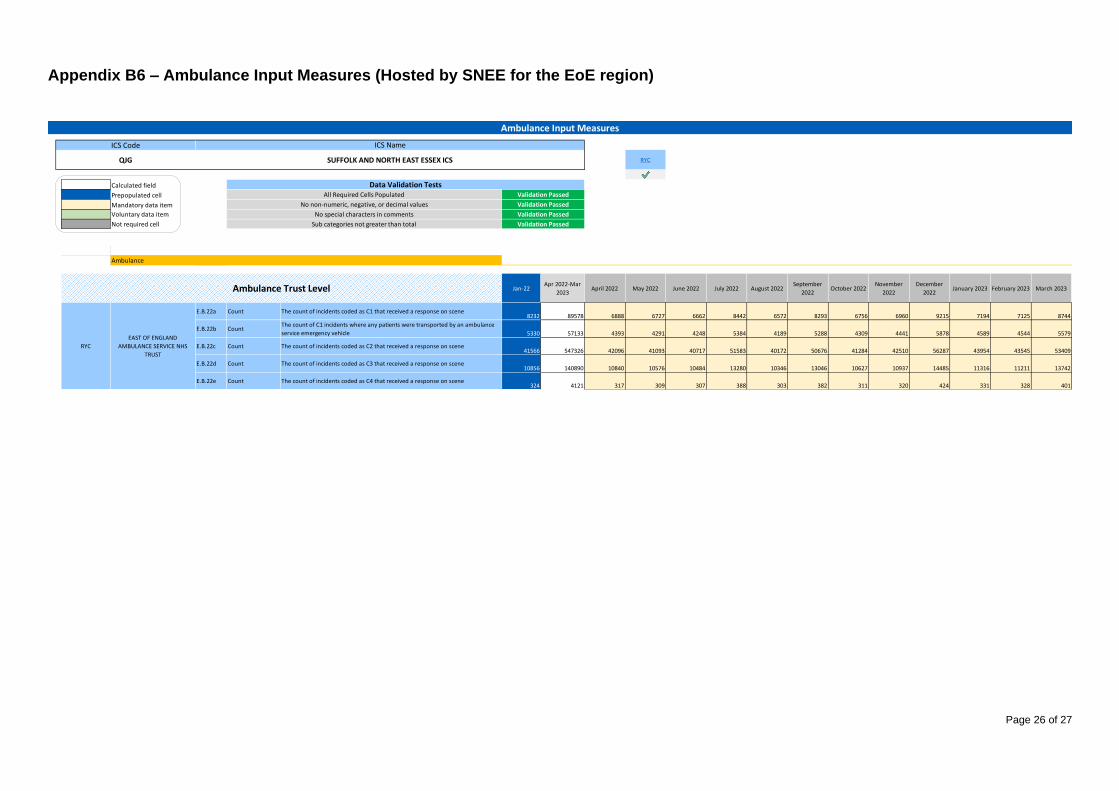
Page 26 of 27
Appendix B6 – Ambulance Input Measures (Hosted by SNEE for the EoE region)
RYC
$G$18 #N/A
Calculated field
Prepopulated cell
Mandatory data item
Voluntary data item
Not required cell
Ambulance trust PlanningRef 0 1 2 3 4 5
Jan-22Apr 2022-Mar
2023April 2022 May 2022 June 2022 July 2022 August 2022
September
2022October 2022
November
2022
December
2022January 2023 February 2023 March 2023
Ambulance - C1 Incidents (A8)Ambulance1E.B.22aAmbulance1RYCE.B.22a Count The count of incidents coded as C1 that received a response on scene
8232 89578 6888 6727 6662 8442 6572 8293 6756 6960 9215 7194 7125 8744
Ambulance - C1T Incidents (A9)Ambulance1E.B.22bAmbulance1RYCE.B.22b Count
The count of C1 incidents where any patients were transported by an ambulance
service emergency vehicle 5330 57133 4393 4291 4248 5384 4189 5288 4309 4441 5878 4589 4544 5579
Ambulance - C2 Incidents (A10)Ambulance1E.B.22cAmbulance1RYCE.B.22c Count The count of incidents coded as C2 that received a response on scene
41566 547326 42096 41093 40717 51583 40172 50676 41284 42510 56287 43954 43545 53409
Ambulance - C3 incidents (A11)Ambulance1E.B.22dAmbulance1RYCE.B.22d Count The count of incidents coded as C3 that received a response on scene
10856 140890 10840 10576 10484 13280 10346 13046 10627 10937 14485 11316 11211 13742
Ambulance - C4 incidents (A12)Ambulance1E.B.22eAmbulance1RYCE.B.22e Count The count of incidents coded as C4 that received a response on scene
324 4121 317 309 307 388 303 382 311 320 424 331 328 401
Ambulance
Ambulance Trust Level
RYC
EAST OF ENGLAND
AMBULANCE SERVICE NHS
TRUST
No special characters in comments Validation Passed
Ambulance Input Measures
ICS Code ICS Name
QJG SUFFOLK AND NORTH EAST ESSEX ICS RYC
No non-numeric, negative, or decimal values Validation Passed
Data Validation TestsValidation PassedAll Required Cells Populated
Sub categories not greater than total Validation Passed

Page 27 of 27
Appendix C – Workforce Plan
Establishme
ntBaseline Plan Plan Plan Plan Plan Plan Plan Plan Plan Plan Plan Plan
Establishme
nt
System Input Summary2021/2022
Staff in post
outturn
22-23 (End
of Year Mar-
23)
Suffolk And North East Essex STP Year End
(31-Mar-22)
Year End
(31-Mar-22)Whole Year
Workforce (WTE) Total WTE Total WTE Total WTE Total WTE Total WTE Total WTE Total WTE Total WTE Total WTE Total WTE Total WTE Total WTE Total WTE Total WTE Total WTE
Total Workforce (WTE) 19,883.57 21,122.29 20,852.68 20,891.11 20,959.06 20,797.86 20,826.93 21,311.68 21,352.72 21,566.31 21,554.65 21,587.17 21,585.20 21,599.55 20,989.57
Registered nursing, midwifery and health visiting staff (substantive total) 4,329.23 4,903.93 4,778.91 4,788.12 4,805.88 4,802.98 4,798.71 4,977.75 4,968.54 5,001.33 4,992.82 4,997.45 5,009.49 5,007.68 4,624.05
Registered scientific, therapeutic and technical staff 1,832.45 1,895.61 1,854.75 1,859.07 1,869.19 1,880.07 1,888.09 1,927.22 1,935.83 1,938.16 1,944.80 1,953.98 1,954.29 1,965.60 1,955.99
Registered ambulance service staff 2,833.00 2,556.70 2,537.94 2,519.29 2,507.94 2,492.01 2,476.28 2,474.79 2,482.52 2,476.04 2,485.46 2,468.90 2,472.41 2,455.88 2,902.61
Support to clinical staff 4,624.12 5,097.85 5,145.89 5,176.19 5,238.53 5,090.50 5,105.05 5,348.28 5,379.04 5,560.90 5,550.74 5,573.86 5,566.31 5,577.29 4,867.56
Total NHS infrastructure support 4,519.66 4,864.59 4,731.30 4,730.58 4,714.80 4,715.62 4,712.84 4,736.96 4,734.82 4,737.66 4,728.93 4,734.03 4,725.62 4,731.54 4,880.69
Medical and dental 1,738.11 1,801.48 1,801.75 1,815.72 1,820.59 1,814.55 1,843.84 1,844.56 1,849.84 1,850.09 1,849.77 1,856.82 1,854.95 1,859.42 1,751.67
Any other staff 7.00 2.13 2.13 2.13 2.13 2.13 2.13 2.13 2.13 2.13 2.13 2.13 2.13 2.13 7.00
Substantive WTE 19,883.57 19,503.68 19,540.93 19,558.89 19,609.84 19,628.39 19,640.85 20,085.15 20,126.47 20,153.14 20,155.46 20,171.43 20,186.79 20,171.74 20,989.57
Registered nursing, midwifery and health visiting staff (substantive total) 4,329.23 4,335.54 4,346.75 4,351.32 4,348.69 4,383.81 4,381.22 4,542.36 4,533.82 4,525.71 4,522.41 4,524.51 4,540.10 4,533.76 4,624.05
Registered scientific, therapeutic and technical staff (substantive total) 1,832.45 1,783.23 1,796.02 1,798.86 1,809.70 1,819.33 1,827.29 1,865.45 1,873.95 1,875.65 1,883.35 1,891.15 1,892.84 1,901.64 1,955.99
Registered ambulance service staff (substantive total) 2,833.00 2,556.70 2,537.94 2,519.29 2,507.94 2,492.01 2,476.28 2,474.79 2,482.52 2,476.04 2,485.46 2,468.90 2,472.41 2,455.88 2,902.61
Support to clinical staff (substantive total) 4,624.12 4,677.33 4,699.58 4,724.01 4,788.20 4,773.79 4,787.93 5,011.66 5,041.99 5,075.70 5,066.84 5,083.82 5,080.93 5,080.93 4,867.56
Total NHS infrastructure support (substantive total) 4,519.66 4,539.63 4,537.51 4,532.21 4,519.54 4,518.64 4,516.33 4,538.28 4,536.69 4,537.65 4,533.34 4,534.33 4,531.15 4,529.51 4,880.69
Medical and dental (substantive total) 1,738.11 1,609.12 1,621.00 1,631.06 1,633.63 1,638.68 1,649.66 1,650.47 1,655.38 1,660.26 1,661.93 1,666.59 1,667.22 1,667.88 1,751.67
Any other staff (substantive total) 7.00 2.13 2.13 2.13 2.13 2.13 2.13 2.13 2.13 2.13 2.13 2.13 2.13 2.13 7.00
Bank 1,450.48 1,132.98 1,150.65 1,163.40 993.93 1,009.72 1,045.18 1,044.52 1,218.62 1,205.95 1,220.21 1,204.78 1,230.76
Registered nursing, midwifery and health visiting staff (Bank Total) 537.49 396.71 400.66 419.87 381.58 380.04 396.48 395.84 436.65 432.10 434.16 431.20 434.86
Registered scientific, therapeutic and technical staff (Bank Total) 60.46 33.42 34.40 33.86 34.62 34.62 35.07 35.13 35.56 34.80 35.69 34.75 36.40
Registered ambulance service staff (Bank Total) - - - - - - - - - - - - -
Support to clinical staff (Bank Total) 408.22 401.65 407.32 405.18 271.24 271.37 288.11 288.50 436.51 434.95 440.74 436.10 446.67
Total NHS infrastructure support (Bank Total) 313.77 187.54 191.73 188.88 190.43 189.99 192.06 191.48 193.21 189.12 192.89 188.06 194.98
Medical and dental (Bank Total) 130.54 113.66 116.54 115.61 116.06 133.70 133.47 133.56 116.69 114.98 116.73 114.66 117.85
Any other staff (Bank Total) - - - - - - - - - - - - -
Agency 168.13 178.77 181.57 185.82 175.53 176.37 181.35 181.72 194.54 193.24 195.54 193.64 197.05
Registered nursing, midwifery and health visiting staff (Agency Total) 30.90 35.46 36.14 37.31 37.60 37.45 38.91 38.88 38.97 38.31 38.79 38.19 39.06
Registered scientific, therapeutic and technical staff (Agency Total) 51.92 25.31 25.81 25.62 26.11 26.18 26.70 26.75 26.96 26.65 27.14 26.69 27.56
Registered ambulance service staff (Agency Total) - - - - - - - - - - - - -
Support to clinical staff (Agency Total) 12.30 44.65 44.87 45.15 45.47 45.75 48.51 48.56 48.69 48.96 49.29 49.28 49.69
Total NHS infrastructure support (Agency Total) 11.19 6.25 6.63 6.37 6.54 6.51 6.62 6.64 6.80 6.47 6.81 6.41 7.04
Medical and dental (Agency Total) 61.82 67.10 68.12 71.35 59.81 60.48 60.61 60.90 73.14 72.86 73.50 73.06 73.70
Any other staff (Agency Total) - - - - - - - - - - - - -
As at the
end of Oct-
22
As at the
end of Nov-
22
As at the
end of Dec-
22
As at the
end of Jan-
23
As at the
end of Feb-
23
As at the
end of Mar-
23
As at the
end of Apr-
22
As at the
end of May-
22
As at the
end of Jun-
22
As at the
end of Jul-
22
As at the
end of Aug-
22
As at the
end of Sep-
22

Financial Plan & Budgets 2022-23 Governing Body May 2022
1
Appendix D

Updated Guidance from NHSEI£
2
• NHSE/I have formally acknowledged the 2022/23 guidance sets out levels of inflation and COVID-19 which are significantly below current levels.
• For the submission on 28 April they required plans to reflect the reality of current cost pressures – specifically price inflation and the current COVID-19 wave.
• Items which were allowed for the submission as ‘acceptable drivers of deficit’ agreed by EoE NHSE/I included:• Price inflation at current (rather than prospective) levels.• Existing high rates until the end of April, tailing off during May to a ‘low-level’ of COVID-19 for the rest of the year.
• Items to be included were ‘unmitigated risks’: • Any estimate of further non-pay inflation (in expectation of further increases in CPI/energy costs for example);• The impact of COVID-19, greater than low-level, extending beyond May 22: either the current wave or any possible
future wave.
• It is anticipated that NHSE/I will issue further allocations to systems to support (not fully mitigate) inflationary costs and there will be another planning submission in mid June.

Background£
3
• ICB and its partner trusts must ensure both capital and revenue resources do not exceed the limit set by NHSEI.• ICBs have a duty to at least break even individually and collectively with partner Trusts.• CCG expenditure will be matched with allocation such that the CCGs will break even; any surplus or deficit for
the year will fall into the combined ICB in the latter part of the year.
• Rollover of system envelopes from (H2) 2021/22 adjusted to remove back pay and provider income support.• Convergence adjustment applied to all systems to move towards underlying funding. Value for SNEE is -0.45%
which is the second lowest in the region.• Growth included to reflect 1.7% net tariff increase and other price/activity increases. • Covid funding reduced by 57%.• Hospital Discharge Programme (HDP) no longer available.• Elective Recovery Fund (ERF) indicative value £32m but dependent on delivery of 104% of 19/20 levels.• Delegated Primary Care Allocation increased by 6.6% to reflect national contractual commitments.• ICB Running Cost Allowance uplifted only for impact of employer NI increases due to Health & Social Care levy.

Core System Allocation£
4
Values, £000sAdjusted System
envelope fundingx 2
21/22 H1 envelope funding
CCG allocations - programme 681,104 1,362,208
Growth funding (H2 20/21) 17,390 34,779
System top-up 70,444 140,888
CNST inflation funding 986 1,971
Funding for free car parking for patient and staff groups 371 742
Funding adjustments for 21/22 H2 (includes H2 pay uplift)
CCG programme allocations growth 8,934 17,867
Pay uplift on Growth funding (H2 20/21) 243 487
Pay uplift on System top-up 817 1,634
Contribution to provider other income pay uplift 703 1,405
Capacity funding 5,006 10,013
System top-up efficiency reflecting distance to FIT target (7,101) (14,202)
H2 Adjusted system envelope funding 778,897 1,557,794
Technical Adjustments
Offset for baseline increases to SpecComm blocks (14,438)
Removal of funding for LVA from provider system (inc. ODC) (7,564)
Add back funding for NCA/LVA to ICB commissioner system 13,817
Add back funding for community non-demographic growth 3,496
Removal of mental health SDF from baseline (1,149)
Baseline post technical adjustments 1,551,955
Base Growth 4.23% - 65,691
"Adjusted convergence adjustment" -0.45% - (7,115)
Recurrent allocation after convergence - 1,610,531
Additional allocations
Health inequalities distribution 2,723
Transfer in - maternity 1,378
Covid Funding 39,742
ERF 34,205
22/23 system envelope funding 1,688,579
The total core system envelope for 2022/23 is £1.688m as shown in the tables to the right.
Core growth net of convergence reduction is 3.7% but after reduction in HDP and covid funding there is actually a reduction in the envelope of 0.3% compared to H2 2021/22 assuming we achieve the full ERF available as shown in the table below.
Values, £000sSystem
Envelope
Adjusted H2 envelope x 2 1,557,794
Movement exc technical adjustments
Base Growth 4.23% 65,691
Adjusted convergence adjustment -0.45% (7,115)
Health inequalities distribution 2,723
Support for NHS provider other income loss (3,081)
Subtotal Movement exc technical adjustments 58,218
Net Change % 3.7%
Covid reduction (52,612)
HDP reduction (17,000)
ERF Increase v 21/22 6,103
Subtotal Movement inc Covid /HDP (5,292)
Net Change % -0.3%

National Assumptions£
5
The table below shows the national assumptions which underpin the funding adjustments.Further funding is only available for specific national priorities funded via Service Development Funding.
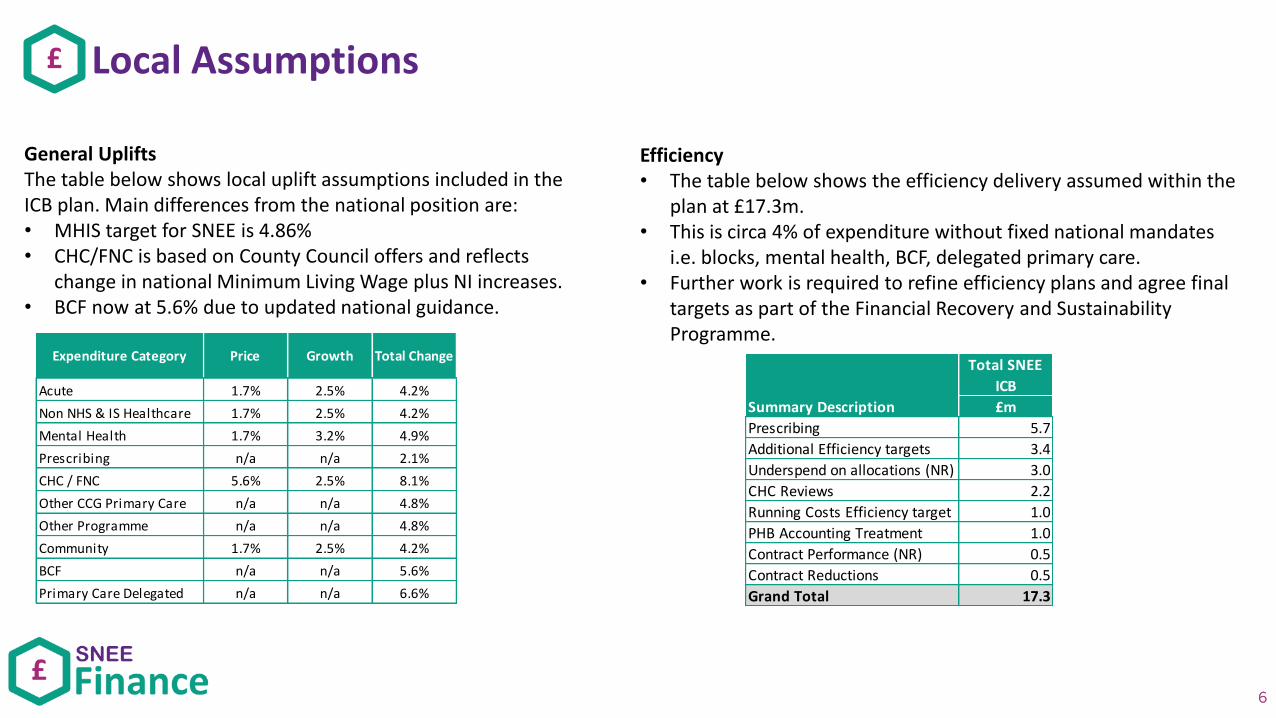
Local Assumptions£
6
General UpliftsThe table below shows local uplift assumptions included in the ICB plan. Main differences from the national position are:• MHIS target for SNEE is 4.86%• CHC/FNC is based on County Council offers and reflects
change in national Minimum Living Wage plus NI increases.• BCF now at 5.6% due to updated national guidance.
Efficiency• The table below shows the efficiency delivery assumed within the
plan at £17.3m. • This is circa 4% of expenditure without fixed national mandates
i.e. blocks, mental health, BCF, delegated primary care.• Further work is required to refine efficiency plans and agree final
targets as part of the Financial Recovery and Sustainability Programme.
Expenditure Category Price Growth Total Change
Acute 1.7% 2.5% 4.2%
Non NHS & IS Healthcare 1.7% 2.5% 4.2%
Mental Health 1.7% 3.2% 4.9%
Prescribing n/a n/a 2.1%
CHC / FNC 5.6% 2.5% 8.1%
Other CCG Primary Care n/a n/a 4.8%
Other Programme n/a n/a 4.8%
Community 1.7% 2.5% 4.2%
BCF n/a n/a 5.6%
Primary Care Delegated n/a n/a 6.6%
Total SNEE
ICB
£m
Prescribing 5.7
Additional Efficiency targets 3.4
Underspend on allocations (NR) 3.0
CHC Reviews 2.2
Running Costs Efficiency target 1.0
PHB Accounting Treatment 1.0
Contract Performance (NR) 0.5
Contract Reductions 0.5
Grand Total 17.3
Summary Description

Changes from the draft submission£
7
• Following the draft submission of a £11.1m ICB deficit further work on efficiency targets reduced this to £6.9m.
• The additional direction to reflect the current situation has increased estimated costs by £1.4m (covid) and £10.2m (inflation).
• This has resulted in an updated draft deficit of £18.5m.• Initial indications are that this is comparable to other systems
planned submissions following the guidance from NHSEI.
• The previous plan already included costs within CHC which would fall into both these categories due to the recurrent impact of the discharge policy during covid and increased market costs not reflected in the national assumptions.
• Reflecting this results in being able to present a deficit plan driven by “allowable” cost drivers.
Bridge from draft submission
2022/23
£'m
Draft Surplus/(deficit) at 17/03/22 (11.1)
Additional Efficiency 5.7
Additional costs (1.5)
Subtotal (6.9)
Further "allowable" pressures per NHSEI
Current Covid wave (1.4)
Additional non pay inflation (10.2)
Draft Surplus/(deficit) at 22/04/22 (18.5)
Driven by
2022/23
£'m
Revised covid-19 profile (5.5)
Non-pay inflation higher than national guidance (13.0)
Total "allowable" deficit (18.5)
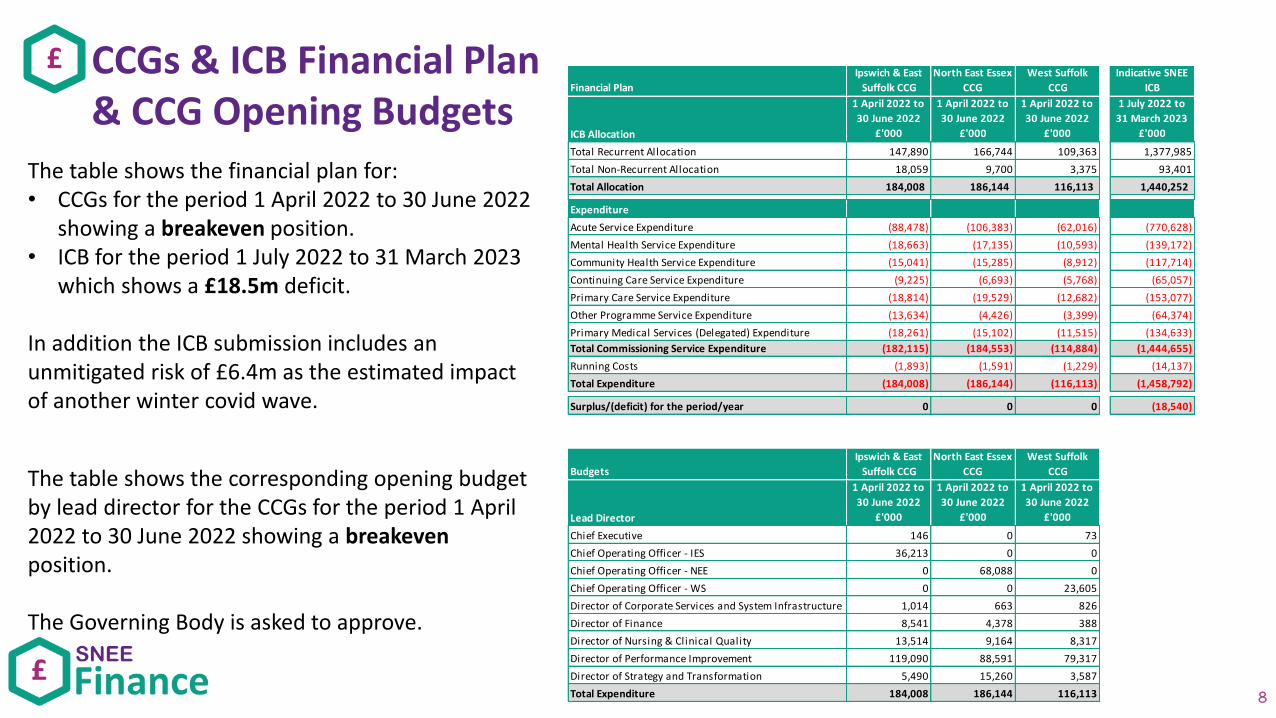
CCGs & ICB Financial Plan& CCG Opening Budgets
£
8
The table shows the financial plan for:• CCGs for the period 1 April 2022 to 30 June 2022
showing a breakeven position.• ICB for the period 1 July 2022 to 31 March 2023
which shows a £18.5m deficit.
In addition the ICB submission includes an unmitigated risk of £6.4m as the estimated impact of another winter covid wave.
Financial Plan
Ipswich & East
Suffolk CCG
North East Essex
CCG
West Suffolk
CCG
Indicative SNEE
ICB
ICB Allocation
1 April 2022 to
30 June 2022
£'000
1 April 2022 to
30 June 2022
£'000
1 April 2022 to
30 June 2022
£'000
1 July 2022 to
31 March 2023
£'000
Total Recurrent Allocation 147,890 166,744 109,363 1,377,985
Total Non-Recurrent Allocation 18,059 9,700 3,375 93,401
Total Allocation 184,008 186,144 116,113 1,440,252
Expenditure
Acute Service Expenditure (88,478) (106,383) (62,016) (770,628)
Mental Health Service Expenditure (18,663) (17,135) (10,593) (139,172)
Community Health Service Expenditure (15,041) (15,285) (8,912) (117,714)
Continuing Care Service Expenditure (9,225) (6,693) (5,768) (65,057)
Primary Care Service Expenditure (18,814) (19,529) (12,682) (153,077)
Other Programme Service Expenditure (13,634) (4,426) (3,399) (64,374)
Primary Medical Services (Delegated) Expenditure (18,261) (15,102) (11,515) (134,633)
Total Commissioning Service Expenditure (182,115) (184,553) (114,884) (1,444,655)
Running Costs (1,893) (1,591) (1,229) (14,137)
Total Expenditure (184,008) (186,144) (116,113) (1,458,792)
Surplus/(deficit) for the period/year 0 0 0 (18,540)
Budgets
Ipswich & East
Suffolk CCG
North East Essex
CCG
West Suffolk
CCG
Lead Director
1 April 2022 to
30 June 2022
£'000
1 April 2022 to
30 June 2022
£'000
1 April 2022 to
30 June 2022
£'000
Chief Executive 146 0 73
Chief Operating Officer - IES 36,213 0 0
Chief Operating Officer - NEE 0 68,088 0
Chief Operating Officer - WS 0 0 23,605
Director of Corporate Services and System Infrastructure 1,014 663 826
Director of Finance 8,541 4,378 388
Director of Nursing & Clinical Quality 13,514 9,164 8,317
Director of Performance Improvement 119,090 88,591 79,317
Director of Strategy and Transformation 5,490 15,260 3,587
Total Expenditure 184,008 186,144 116,113
The table shows the corresponding opening budget by lead director for the CCGs for the period 1 April 2022 to 30 June 2022 showing a breakevenposition.
The Governing Body is asked to approve.
Page 1 of 3
GOVERNING BODY
Agenda Item No. 11
Reference No. NEECCG 22-35
Date. 7 June 2022
Title
Approval of the Suffolk and North East Essex ICB Constitution
Lead Director
Amanda Lyes – Director of Corporate Services & System Infrastructure
Author(s)
Colin Boakes – Independent Governance Advisor, Suffolk CCGs
Purpose
Endorsement of a decision by the CCG Collaborative Group to propose approval of the Suffolk & North East Essex ICB draft Constitution to NHS England
Applicable CCG Clinical Priorities:
1. To achieve our vision through an inclusive, holistic approach to patient and service user centred commissioning, embedding personalisation of care through integrated health and social care services.
x
2. To transform care and drive continuous improvement in quality and safety. Achieve the best possible outcomes for our service users through high quality care.
x
3. To use commissioning resources effectively and responsibly. To develop our organisation, teams and individual staff to be trusted, competent, well trained, talented, enthusiastic and dedicated.
x
4 To tackle the biggest health challenges in north east Essex including reducing health inequalities.
x
Action required by Governing Body: Endorsement of the Collaborative Groups Decision

Page 2 of 3
1. BACKGROUND
1.1 The Health and Care Act 2022 states that Clinical Commissioning Groups (CCGs) must propose the Constitution for the first Integrated Care Board (ICB) to be established for the ICB area of Suffolk and North East Essex.
1.2 This paper presents the final draft of the Suffolk and North East Essex ICB Constitution which was submitted to NHS England for final approval on 20 May 2022. This is attached at Appendix 1.
1.3 In view of the constricted timescales for the approvals process, the CCGs Collaborative Group met on 18 May 2022 and agreed under the Urgent Decisions provision of their Standing Orders to make the proposal to NHS England (NHSE) for approval of the draft ICB Constitution on behalf of the CCG Governing Bodies.
2. KEY POINTS 2.1 In line with NHS England guidance, the CCG has developed the ICB Constitution in
consultation with system partners and key stakeholders. We have used the ICB model Constitution produced by NHSE which includes significant mandated elements comprising legal or policy requirements and some elements which have been modified locally, but broadly based on example wording in order to ensure compliance with the model.
2.2 Consultation on the Constitution content was achieved through a series of ICS Board
workshops, ICS Board meetings and discussions with individual partners and stakeholders. 2.3 To ensure that the CCG complies with the Health and Care Act 2022, in addition to the
consultation process there have been discussions and reviews of the various drafts of the Constitution with NHSE, we are required to confirm that we have concluded this element of the process. A summary of the substantive consultation feedback and how responses have been considered is recorded in a ‘You Said - We Did’ report which is attached at Appendix 2.
3. SUBSEQUENT STEPS 3.1 The decision to propose the Constitution made by the Collaborative Group on behalf of the
CCG Governing Body has been followed by the CCG Chief Executive, as Accountable
Officer, formally communicating this decision and the proposed Suffolk and North East Essex
ICB Constitution to the NHSE East of England Regional Director.
3.2 The NHSE Regional Director will recommend to the NHSE Chief Executive whether the proposed Constitution should be approved. It should also be noted that the model Constitution allows for NHSE to attach conditions to its approval, for example where it is recognised that proposals may be appropriate initially but will need to be revisited as the ICB develops.
3.3 The Health and Care Act 2022, provides, if necessary, for NHSE to impose a Constitution if
the proposal has deviated significantly from the model or CCGs have not carried out appropriate consultation.
3.4 Once approved, NHSE will bring the proposed ICB Constitution into effect from 1 July 2022
through the ICB Establishment Order.
Page 3 of 3
3.5 There is no requirement for the first meeting of the ICB Board, scheduled for Friday 1 July 2022, to approve the Constitution. However, it will be important to ensure that all Board members are familiar with the Constitution and the provisions within it.
4. RECOMMENDATION 4.1 The Governing Body is asked to endorse the decision taken by the CCG Collaborative Group,
under the Urgent Decisions provision, to propose the Suffolk and North East Essex ICB Constitution attached at Appendix 1 for approval by NHS England, in accordance with their requirements.

Suffolk and North East Essex
Integrated Care Board
CONSTITUTION

CONTENTS
1. Introduction ..................................................................................................................................... 5
1.1 Background/ Foreword ..................................................................................................................... 5
1.2 Name ................................................................................................................................................. 6
1.3 Area Covered by the Integrated Care Board ..................................................................................... 6
1.4 Statutory Framework ........................................................................................................................ 6
1.5 Status of this Constitution ................................................................................................................. 7
1.6 Variation of this Constitution ............................................................................................................ 8
1.7 Related Documents ........................................................................................................................... 8
2 Composition of The Board of the ICB ............................................................................................. 10
2.1 Background…………………………………………………………………………………………………………………………………..9
2.2 Board Membership………………………………………………………………………………………………………………………10
2.3 Regular Participants and Observers at Board Meetings ................................................................. 11
3 Appointments Process for the Board ............................................................................................. 12
3.1 Eligibility Criteria for Board Membership……………………………………………………………………………………12
3.2 Disqualification Criteria for Board Membership .............................................................................. 12
3.3 Chair ................................................................................................................................................ 14
3.4 Chief Executive ................................................................................................................................ 15
3.5 Partner Members – NHS Trusts and Foundation Trusts .................................................................. 15
3.6 Partner Members - Providers of Primary Medical Services. ............................................................ 17
3.7 Partner Members - Local Authorities .............................................................................................. 18
3.8 Medical Director .............................................................................................................................. 20
3.9 Director of Nursing .......................................................................................................................... 20
3.10 Director of Finance .......................................................................................................................... 20
3.11 Independent Non-Executive Members ............................................................................................ 21
3.12 Other Board Members - Member for Voluntary, Community and Social Enterprise (VCSE)……..….21
3.13 Board Members: Removal from Office. ........................................................................................... 22
3.14 Terms of Appointment of Board Members ...................................................................................... 23
3.15 Specific arrangements for appointment of ordinary members made at establishment………………..23
4 Arrangements for the Exercise of our Functions. ........................................................................... 25
4.1 Good Governance ............................................................................................................................ 25
4.2 General ............................................................................................................................................ 25
4.3 Authority to Act ............................................................................................................................... 25
4.4 Scheme of Reservation and Delegation ........................................................................................... 26
4.5 Functions and Decision Map ........................................................................................................... 26

4.6 Committees and Sub-Committees ................................................................................................... 27
4.7 Delegations made under section 65Z5 of the 2006 Act ................................................................... 28
5 Procedures for Making Decisions ................................................................................................... 29
5.1 Standing Orders ............................................................................................................................... 29
5.2 Standing Financial Instructions (SFIs) .............................................................................................. 29
6 Arrangements for Conflicts of Interest Management and Standards of Business Conduct ............. 29
6.1 Conflicts of Interest ......................................................................................................................... 29
6.2 Principles ......................................................................................................................................... 30
6.3 Declaring and Registering Interests ................................................................................................ 31
6.4 Standards of Business Conduct ....................................................................................................... 31
7 Arrangements for ensuring Accountability and Transparency ........................................................ 32
7.2 Principles ......................................................................................................................................... 32
7.3 Meetings and publications .............................................................................................................. 32
7.4 Scrutiny and Decision Making ......................................................................................................... 33
7.5 Annual Report ................................................................................................................................. 34
8 Arrangements for Determining the Terms and Conditions of Employees. ...................................... 34
9 Arrangements for Public Involvement ........................................................................................... 35
Appendix 1: Definitions of Terms Used in This Constitution ........................................................................ 37
Appendix 2: Standing Orders ....................................................................................................................... 40
1. Introduction ................................................................................................................................... 40
2. Amendment and review ................................................................................................................ 40
3. Interpretation, application and compliance ................................................................................... 40
4. Meetings of the Integrated Care Board .......................................................................................... 41
4.1. Calling Board Meetings .................................................................................................................. 41
4.2 Chair of a meeting.......................................................................................................................... 41
4.3 Agenda, supporting papers and business to be transacted ............................................................ 42
4.4 Petitions ........................................................................................................................................ 42
4.5 Nominated Deputies ...................................................................................................................... 42
4.6 Virtual attendance at meetings ...................................................................................................... 43
4.7 Quorum ......................................................................................................................................... 43
4.8 Vacancies and Defects in Appointment .......................................................................................... 43
4.9 Decision making ............................................................................................................................. 43
4.10 Minutes ......................................................................................................................................... 45
4.11 Admission of public and the press ................................................................................................. 45
5 Suspension of Standing Orders ...................................................................................................... 45
VERSION CONTROL
Version Date Approved by the ICB
Effective Date
V1.0 1 July 2022
1. Introduction
1.1 Background/ Foreword
1.1.1 NHS England has set out the following as the four core purposes of ICSs:
a) improve outcomes in population health and healthcare b) tackle inequalities in outcomes, experience and access c) enhance productivity and value for money d) help the NHS support broader social and economic development.
1.1.2 The ICB will use its resources and powers to achieve demonstrable progress
on these aims, collaborating to tackle complex challenges, including:
a) improving the health of children and young people b) supporting people to stay well and independent c) acting sooner to help those with preventable conditions d) supporting those with long-term conditions or mental health issues e) caring for those with multiple needs as populations age f) getting the best from collective resources so people get care as quickly
as possible.
1.1.3 Suffolk and North East Essex Integrated Care Board (the ICB) brings together partners responsible for planning and delivering health and care across Suffolk and North East Essex to ensure shared leadership and joint action to improve the health and wellbeing of the one million people who live locally.
1.1.4 ICBs are central to the NHS Long Term Plan and have a key role in ensuring joint working across the NHS and Local Authorities to make shared commissioning decisions together with providers on how to use resources, design services and improve population health.
1.1.5 The ICB will enable communities to continue to shape priorities and release the assets which contribute to their wellbeing, care and health, within a common set of standards which reduce unnecessary variations in performance and outcomes. By working with people in our communities the ICB will develop trust and understanding with stakeholders about what matters.
1.1.6 Integrated care systems are partnerships of health and care organisations,
local government and the voluntary sector. They exist to improve population
health, tackle health inequalities, enhance productivity and help the NHS
support broader social and economic development. Each ICS is comprised of
an Integrated Care Board working with an Integrated Care Partnership
committee formed jointly with local authority partners.
1.1.7 The ICP is required to produce an integrated care strategy and the ICB and local authorities are required by law to have regard to the ICPs strategy when making decisions, commissioning and delivering services.
1.2 Name
1.2.1 The name of this Integrated Care Board is NHS Suffolk and North East Essex
Integrated Care Board (“the ICB”).
1.3 Area Covered by the Integrated Care Board
The area covered by the ICB includes the District of Babergh, Borough of
Colchester, Borough of Ipswich, District of Mid Suffolk, District of Tendring and
the District of West Suffolk Statutory Framework. The area also includes part
of the District of East Suffolk (LSOAs: E01030201, E01030219, E01030222,
E01030154, E01030172, E01030173, E01030174, E01030176, E01030186,
E01030208, E01030209, E01030210, E01030212, E01030152, E01030153,
E01030187, E01030188, E01030189, E01030193, E01030194, E01030195,
E01030220, E01030175, E01030200, E01030221, E01030199, E01033443,
E01033445, E01033446, E01033448, E01033449, E01030155, E01030185,
E01030203, E01030211, E01030179, E01030180, E01030183, E01030184,
E01030207, E01030181, E01030190, E01030191, E01030192, E01030198,
E01033442, E01033444, E01033447, E01030196, E01030197, E01030204,
E01030205, E01030206, E01030171, E01030214, E01030215, E01030216,
E01030217, E01030218, E01030158, E01030159, E01030164, E01030166,
E01033450, E01030160, E01030161, E01030168, E01030169, E01030170,
E01030162, E01030163, E01030165, E01030167)
1.3.1 The ICB is established by order made by NHS England under powers in the
2006 Act.
1.3.2 The ICB is a statutory body with the general function of arranging for the
provision of services for the purposes of the health service in England and is
an NHS body for the purposes of the 2006 Act.
1.3.3 The main powers and duties of the ICB to commission certain health services
are set out in sections 3 and 3A of the 2006 Act. These provisions are
supplemented by other statutory powers and duties that apply to ICBs, as well
as by regulations and directions (including, but not limited to, those made
under the 2006 Act).
1.3.4 In accordance with section 14Z25(5) of, and paragraph 1 of Schedule 1B to, the 2006 Act the ICB must have a constitution, which must comply with the requirements set out in that Schedule. The ICB is required to publish its constitution (section 14Z29). This constitution is published at www.suffolkandnortheastessex.icb.nhs.uk
1.3.5 The ICB must act in a way that is consistent with its statutory functions, both
powers and duties. Many of these statutory functions are set out in the 2006 Act but there are also other specific pieces of legislation that apply to ICBs. Examples include, but are not limited to, the Equality Act 2010 and the Children Acts. Some of the statutory functions that apply to ICBs take the form
of general statutory duties, which the ICB must comply with when exercising its functions. These duties include but are not limited to:
a) Having regard to and acting in a way that promotes the NHS
Constitution (section 2 of the Health Act 2009 and section 14Z32 of
the 2006 Act);
b) Exercising its functions effectively, efficiently and economically
(section 14Z33 of the 2006 Act);
c) Duties in relation children including safeguarding, promoting welfare
etc (including the Children Acts 1989 and 2004, and the Children and
Families Act 2014)
d) Adult safeguarding and carers (the Care Act 2014)
e) Equality, including the public-sector equality duty (under the Equality
Act 2010) and the duty as to health inequalities (section 14Z35); and
f) Information law, (for instance, data protection laws, such as the UK
General Data Protection Regulation 2016/679 and Data Protection Act
2018, and the Freedom of Information Act 2000).
g) Provisions of the Civil Contingencies Act 2004
1.3.6 The ICB is subject to an annual assessment of its performance by NHS
England which is also required to publish a report containing a summary of the
results of its assessment.
1.3.7 The performance assessment will assess how well the ICB has discharged its
functions during that year and will, in particular, include an assessment of how
well it has discharged its duties under—
a) section 14Z34 (improvement in quality of services),
b) section 14Z35 (reducing inequalities),
c) section 14Z38 (obtaining appropriate advice),
d) section 14Z43 (duty to have regard to effect of decisions)
e) section 14Z44 (public involvement and consultation),
f) sections 223GB to 223N (financial duties), and
g) section 116B(1) of the Local Government and Public Involvement in
Health Act 2007 (duty to have regard to assessments and strategies).
1.3.8 NHS England has powers to obtain information from the ICB (section 14Z58
of the 2006 Act) and to intervene where it is satisfied that the ICB is failing, or
has failed, to discharge any of its functions or that there is a significant risk
that it will fail to do so (section 14Z59).
1.4 Status of this Constitution
1.4.1 The ICB was established on 1 July 2022 by [name and reference of
establishment order], which made provision for its constitution by reference to
this document.

1.4.2 This constitution must be reviewed and maintained in line with any agreements
with, and requirements of, NHS England set out in writing at establishment
1.4.3 Changes to this constitution will not be implemented until, and are only effective from, the date of approval by NHS England.
1.5 Variation of this Constitution
1.5.1 In accordance with paragraph 15 of Schedule 1B to the 2006 Act this
constitution may be varied in accordance with the procedure set out in this
paragraph. The constitution can only be varied in two circumstances:
a) where the ICB applies to NHS England in accordance with NHS
England’s published procedure and that application is approved; and
b) where NHS England varies the constitution of its own initiative, (other
than on application by the ICB).
1.5.2 The procedure for proposal and agreement of variations to the constitution is
as follows:
a) The Chief Executive may periodically propose amendments to the Constitution which shall be considered and approved by the ICB prior to making an application to vary the Constitution to NHS England.
b) Proposed amendments to this Constitution will not be implemented until an application to NHS for variation has been approved
1.5.3 Before any amendments can be approved under Clause 1.6.2, above, the
proposed amendments must be provided to all relevant respondents with a
period of twenty-one days from the date the amendments are sent in which
they can respond with any comments on the amendments. Any comments
provided must be submitted to the Board in writing before the meeting at
which the amendments proposed are to be considered.
1.6 Related Documents
1.6.1 This Constitution is also supported by a number of documents which provide
further details on how governance arrangements in the ICB will operate.
1.6.2 The following are appended to the constitution and form part of it for the
purpose of clause 1.6 and the ICB’s legal duty to have a constitution:
a) Standing orders– which set out the arrangements and procedures
to be used for meetings and the selection and the processes to
appoint the ICB committees.
1.6.3 The following do not form part of the constitution but are required to be
published.
a) The Scheme of Reservation and Delegation (SoRD) sets out those
decisions that are reserved to the Board of the ICB and those decisions
that have been delegated in accordance with the powers of the ICB and
which must be agreed in accordance with and be consistent with the
constitution. The SoRD identifies where, or to to whom functions and
decisions have been delegated to.
b) Functions and Decision map: a high-level structural chart that sets
out which key decisions are delegated and taken by which part or parts
of the system. The Functions and Decision map also includes decision
making responsibilities that are delegated to the ICB (for example, from
NHS England).
c) Standing Financial Instructions – which set out the arrangements for
managing the ICB’s financial affairs.
d) The ICB Governance Handbook – This brings together all the ICBs
governance documents so it is easy for interested people to navigate.
It includes:
• The above documents a) to c)
• Terms of reference for all committees and sub-committees of the
Board that exercise ICB functions.
• Delegation arrangements for all instances where ICB functions
are delegated, in accordance with section 65Z5 of the 2006 Act,
to another ICB, NHS England, an NHS trust, NHS foundation trust,
local authority, combined authority or any other prescribed body;
or to a joint committee of the ICB and one or those organisations
in accordance with section 65Z6 of the 2006 Act.
• Terms of reference of any joint committee of the ICB and another
ICB, NHS England, an NHS trust, NHS foundation trust, local
authority, combined authority or any other prescribed body; or to
a joint committee of the ICB and one or those organisations in
accordance with section 65Z6 of the 2006 Act.
• The up to date list of eligible providers of primary medical services
under clause 3.6.2
e) Key policy documents - including:
• Standards of Business Conduct Policy
• Conflicts of interest policy and procedures
• Policy for public involvement and engagement

2 Composition of The Board of the ICB
2.1 Background
2.1.1 This part of the constitution describes the membership of the Integrated Care
Board. Further information about the criteria for the roles and how they are
appointed is in section 3.
2.1.2 Further information about the individuals who fulfil these roles can be found
on our website www.suffolkandnortheastessex.icb.nhs.uk
2.1.3 In accordance with paragraph 3 of Schedule 1B to the 2006 Act, the
membership of the ICB (referred to in this constitution as “the Board” and
members of the ICB are referred to as “Board Members”) consists of:
a) a Chair
b) a Chief Executive
c) at least three Ordinary members.
2.1.4 The Membership of the ICB (the Board) shall meet as a unitary board and shall
be collectively accountable for the performance of the ICBs function
2.1.5 NHS England Policy requires the ICB to appoint the following additional Ordinary Members: a) three executive members, namely:
• Director of Finance
• Medical Director
• Director of Nursing b) At least two independent non-executive members
2.1.6 The Ordinary Members include at least three members who will bring
knowledge and a perspective from their sectors. These members (known as
Partner Members) are nominated by the following and appointed in
accordance with the procedures set out in Section 3 below:
• NHS trusts and foundation trusts who provide services within the ICB’s
area and are of a prescribed description
• the primary medical services (general practice) providers within the
area of the ICB and are of a prescribed description
• the local authorities which are responsible for providing social care
and whose area coincides with or includes the whole or any part of the
ICB’s area.
While the Partner Members will bring knowledge and experience from their
sector and will contribute the perspective of their sector to the decisions of
the board, they are not to act as delegates of those sectors.
2.2 Board Membership
2.2.1 The ICB has seven Partner Members, as follows:

a) Two members who bring the perspective of the acute and community sector
b) One member who brings the perspective of the mental health sector c) Two members who bring the perspective of the primary care sector d) Two members from the upper tier local authorities whose area coincides
with or includes the whole or any part of the ICB’s area
2.2.2 The ICB has appointed the following further Ordinary Members to the Board:
a) Non-Executive Member
b) Member representing the VCSE sector
2.2.3 The Board is therefore composed of the following members:
a) Chair
b) Chief Executive
c) Three Partner Members NHS and Foundation Trusts
d) Two Partner Members Primary Medical Services
e) Two Partner Members Local Authorities
f) One Member for the VCSE sector
g) Three Non-Executive Members
h) Director of Finance
i) Medical Director
j) Director of Nursing
2.2.4 The Chair will exercise their function to approve the appointment of the
Ordinary Members with a view to ensuring that at least one of the Ordinary
Board Members will have knowledge and experience in connection with
services relating to the prevention, diagnosis and treatment of mental illness.
2.2.5 The Board will keep under review the skills, knowledge and experience that it
considers necessary for Members of the Board to possess (when taken
together) in order for the Board effectively to carry out its functions and will
take such steps as it considers necessary to address or mitigate any
shortcoming.
2.3 Regular Participants and Observers at Board Meetings
2.3.1 The Board may invite specified individuals to be Participants or Observers at its meetings to inform its decision-making and the discharge of its functions as it sees fit.
2.3.2 Participants will receive advanced copies of the notice, agenda and papers for Board meetings. They may be invited to attend any or all of the Board meetings, or part(s) of a meeting by the Chair. Any such person may be invited, at the discretion of the Chair to ask questions and address the meeting but may not vote.
2.3.3 The Board will regularly invite the following individuals to attend any or all of its
meetings as regular participants:

a) Director: North East Essex Alliance
b) Director: Ipswich and East Suffolk Alliance
c) Director: West Suffolk Alliance
d) Director of People and Workforce
e) Director of Strategy and Transformation
f) Director of Performance and Improvement
2.3.4 Observers will receive advanced copies of the notice, agenda and papers for
Board meetings. They may be invited to attend any or all of the Board
meetings, or part(s) of a meeting by the Chair. Any such person may not
address the meeting and may not vote.
2.3.5 The Board will regularly invite a number of observers to attend any or all of its
meetings to include Healthwatch Suffolk and Healthwatch Essex together with
Lay Member representatives from the North East Essex, Ipswich and East
Suffolk and West Suffolk Alliances.
2.3.6 Participants and/or observers may be asked to leave the meeting by the Chair
in the event that the board passes a resolution to exclude the public as per the
Standing Orders.
3 Appointments Process for the Board
3.1 Eligibility Criteria for Board Membership:
3.1.1 Each member of the ICB must:
a) Comply with the criteria of the “fit and proper person test”
b) Be willing to uphold the Seven Principles of Public Life (known as the Nolan
Principles)
c) Fulfil the requirements relating to relevant experience, knowledge, skills
and attributes set out in a role specification
d) Familiarise themselves with the eligibility and ineligibility requirements,
confirming their eligibility prior to appointment and immediately notifying
the Chair of the ICB of a change of circumstances that may render them
no longer eligible
3.2 Disqualification Criteria for Board Membership
3.2.1 A Member of Parliament.
3.2.2 A person whose appointment as a Board Member (‘’the candidate’) is
considered by the person making the appointment as one which could
reasonably be regarded as undermining the independence of the health
service because of the candidate’s involvement in the private healthcare
sector or otherwise
3.2.3 A person who, within the period of five years immediately preceding the date of the proposed appointment, has been convicted: a) in the United Kingdom of any offence, or b) outside the United Kingdom of an offence which, if committed in any part
of the United Kingdom, would constitute a criminal offence in that part, and,
in either case, the final outcome of the proceedings was a sentence of
imprisonment (whether suspended or not) for a period of not less than
three months without the option of a fine.
3.2.4 A person who is subject to a bankruptcy restrictions order or an interim
bankruptcy restrictions order under Schedule 4A to the Insolvency Act 1986,
sections 56A to 56K of the Bankruptcy (Scotland) Act 1985 or Schedule 2A to
the Insolvency (Northern Ireland) Order 1989 (which relate to bankruptcy
restrictions orders and undertakings).
3.2.5 A person who, has been dismissed within the period of five years immediately
preceding the date of the proposed appointment, otherwise than because of
redundancy, from paid employment by any Health Service Body.
3.2.6 A person whose term of appointment as the chair, a member, a director or a governor of a health service body, has been terminated on the grounds:
a) that it was not in the interests of, or conducive to the good management of,
the health service body or of the health service that the person should continue to hold that office
b) that the person failed, without reasonable cause, to attend any meeting of
that health service body for three successive meetings,
c) that the person failed to declare a pecuniary interest or withdraw from
consideration of any matter in respect of which that person had a pecuniary
interest, or
d) of misbehaviour, misconduct or failure to carry out the person’s duties;
3.2.7 A health care professional (within the meaning of section 14N of the 2006 Act) or other professional person who has at any time been subject to an investigation or proceedings, by any body which regulates or licenses the profession concerned (“the regulatory body”), in connection with the person’s fitness to practise or any alleged fraud, the final outcome of which was: a) the person’s suspension from a register held by the regulatory body, where
that suspension has not been terminated
b) the person’s erasure from such a register, where the person has not been
restored to the register
c) a decision by the regulatory body which had the effect of preventing the
person from practising the profession in question, where that decision has
not been superseded, or

d) a decision by the regulatory body which had the effect of imposing
conditions on the person’s practice of the profession in question, where
those conditions have not been lifted.
3.2.8 A person who is subject to: a) a disqualification order or disqualification undertaking under the Company
Directors Disqualification Act 1986 or the Company Directors
Disqualification (Northern Ireland) Order 2002, or
b) an order made under section 429(2) of the Insolvency Act 1986 (disabilities
on revocation of administration order against an individual).
3.2.9 A person who has at any time been removed from the office of charity trustee
or trustee for a charity by an order made by the Charity Commissioners for
England and Wales, the Charity Commission, the Charity Commission for
Northern Ireland or the High Court, on the grounds of misconduct or
mismanagement in the administration of the charity for which the person was
responsible, to which the person was privy, or which the person by their
conduct contributed to or facilitated.
3.2.10 A person who has at any time been removed, or is suspended, from the management or control of a body under:
a) section 7 of the Law Reform (Miscellaneous Provisions) (Scotland) Act
1990(f) (powers of the Court of Session to deal with the management of charities), or
b) section 34(5) or of the Charities and Trustee Investment (Scotland) Act
2005 (powers of the Court of Session to deal with the management of
charities).
3.3 Chair
3.3.1 The ICB Chair is to be appointed by NHS England, with the approval of the
Secretary of State for Health and Social Care.
3.3.2 In addition to criteria specified at 3.1, this member must fulfil the following
additional eligibility criteria
a) The Chair will be independent.
3.3.3 Individuals will not be eligible if:
a) They hold a role in another health and care organisation within the ICB
area.
b) Any of the disqualification criteria set out in 3.2 apply
3.3.4 The term of office for the Chair will be 3 years and the total number of terms a
Chair may serve is 3 terms. The maximum term of 9 years is in place to ensure
ongoing independence.

3.4 Chief Executive
3.4.1 The Chief Executive will be appointed by the Chair of the ICB in accordance
with any guidance issued by NHS England.
3.4.2 The appointment will be subject to approval of NHS England in accordance
with any procedure published by NHS England
3.4.3 The Chief Executive must fulfil the following additional eligibility criteria
a) Be an employee of the ICB or a person seconded to the ICB who is
employed in the civil service of the State or by a body referred to in
paragraph 18(4)(b) of Schedule 1B to the 2006 Act
b) Meets the ICB leadership competency domains
c) Meets the requirements of the role function and specification that the Board
shall approve and including:
(i) Executive health care experience
(ii) Substantial experience of operating at board level and as a
CEO leading across complex, regulated environment. A track
record of navigating the media and political stakeholders
(iii) Extensive knowledge of the health, care and local government
landscape and an understanding of the social determinants of
public health
(iv) Sound understanding of strategic financial planning, oversight
and control of significant public funds
(v) Communication skills which engender community confidence,
strong collaborations and partnerships
(vi) Strong critical thinking and strategic problem-solving skills
3.4.4 Individuals will not be eligible if
a) Any of the disqualification criteria set out in 3.2 apply
b) Subject to clause 3.4.3(a), they hold any other employment or executive
role
3.5 Partner Members – NHS Trusts and Foundation Trusts
3.5.1 These Partner Members are jointly nominated by the Partners which provide
services within the area and meet the forward plan condition or the level of
services provided condition
a) East Suffolk and North Essex NHS Foundation Trust
b) West Suffolk NHS Foundation Trust
c) Norfolk and Suffolk NHS Foundation Trust
d) Essex Partnership University NHS Foundation Trust
e) East of England Ambulance Service NHS Trust
3.5.2 This/these members must fulfil the eligibility criteria set out at 3.1 and also the following additional eligibility criteria:
a) Be the Chief Executive Officer or another Executive Director of one of the
NHS Trusts or FTs within the ICB’s area
b) Meet any other criteria set out in NHS England guidance or supporting
legislation
c) Meets the requirements of the role specification for the post
d) One member shall have specific knowledge, skills and experience of the
provision of acute services
e) One member shall have specific knowledge, skills and experience of the
provision of community services
f) One member shall have specific knowledge, skills and experience of the
provision of mental health services
3.5.3 Individuals will not be eligible if:
a) Any of the disqualification criteria set out in 3.2 apply b) Any other disqualification criteria prescribed through NHS England
guidance or supporting legislation apply c) A conflict of interest is evident, as determined by the Chair or the ICB
Board appointment panel, which results in the individual being unable to fulfil the role
3.5.4 These members will be appointed by the Chief Executive subject to the
approval of the Chair in accordance with the process set out at 3.5.5 below.
3.5.5 The appointment process will be as follows:
a) Joint Nomination:
• When a vacancy arises, each eligible organisation listed at 3.5.1 a) to e) will be invited to make up to two nominations each per role (one Partner Member role for acute, one Partner Member role for community and one Partner Member role for mental health)
• The nomination of an individual must be seconded by one other eligible organisation outside the nominated individual’s own eligible organisation
• Eligible organisations may nominate individuals from their own organisation or another organisation
• All eligible organisations will be requested to confirm whether they jointly agree to nominate the whole list of nominated individuals with a failure to confirm within five working days being deemed to constitute agreement. This will be determined by a simple majority being in favour with nil responses taken as assent. If they do agree, the list will be put forward to step b) below. If they do not agree the list, the nomination process will be re-run until a majority acceptance is reached on the nominations put forward.
b) Assessment, Selection and Appointment Subject to Approval of the Chair under c):
• The full list of nominees will be considered by a panel convened by the Chief Executive
• The panel will assess the suitability of the nominees against the requirements of the role (published before the nomination process is initiated) and will confirm that nominees meet the requirements set out in clause 3.5.2 and 3.5.3
• In the event that there is more than one suitable nominee, the panel will select the most suitable for appointment
c) Chair’s Approval:
• The Chair will determine whether to approve the appointment of the most suitable nominee as identified under b)
3.5.6 The term of office for these Partner Members will be 3 years and the total
number of terms they may serve is 3 terms.
3.6 Partner Members - Providers of Primary Medical Services.
3.6.1 These Partner Members are jointly nominated by providers of primary
medical services for the purposes of the health service within the
integrated care board’s area, and that are primary medical services
contract holders responsible for the provision of essential services, within
core hours to a list of registered persons for whom the ICB has core
responsibility.
3.6.2 The list of identified eligible providers of primary medical services for this
purpose is published as part of the Governance Handbook. The list will
be kept up to date but does not form part of the Constitution.
3.6.3 These members must fulfil the eligibility criteria set out at 3.1 and also the
following additional eligibility criteria
a) Is a partner or salaried GP working in a GP practice within the ICB
geographical area and included on the Medical Performer List
b) Is a Practice Manager or Healthcare Professional working within the
ICB geographical area
c) Is actively engaged in the work of the ICS at place
d) As a commitment to the ICB, this member shall work for a minimum one
session per week
e) Meets the requirements of the role specification for the post f) Collectively provide different perspectives of the Suffolk and North East
Essex populations
3.6.4 Individuals will not be eligible if:
a) Any of the disqualification criteria set out in 3.2 apply
b) They are a GP working predominantly in the out-of-hours service
c) A conflict of interest is evident, as determined by the Chair or the ICB
Board appointments panel, which results in the individual being unable
to fulfil the role
3.6.5 These member(s) will be appointed by the Chief Executive subject to the
approval of the Chair in accordance with the process set out at 3.6.6 below.
3.6.6 The appointment process will be as follows:
a) Joint Nomination:
• When a vacancy arises, each eligible organisation described at 3.6.1 and listed in the Governance Handbook will be invited to make up to two nominations each per role
• The nomination of an individual must be seconded by one other eligible organisation outside the nominated individual’s own eligible organisation
• Eligible organisations may nominate individuals from their own organisation or another organisation
• All eligible organisations will be requested to confirm whether they jointly agree to nominate the whole list of nominated individuals with a failure to confirm within five working days being deemed to constitute agreement. This will be determined by a simple majority being in favour with nil responses taken as assent. If they do agree, the list will be put forward to step b) below. If they do not agree the list, the nomination process will be re-run until a majority acceptance is reached on the nominations put forward.
b) Assessment, Selection and Appointment Subject to Approval of the Chair under c):
• The full list of nominees will be considered by a panel convened by the Chief Executive
• The panel will assess the suitability of the nominees against the requirements of the role (published before the nomination process is initiated) and will confirm that nominees meet the requirements set out in clause 3.6.3 and 3.6.4
• In the event that there is more than one suitable nominee, the panel will select the most suitable for appointment
c) Chair’s Approval:
• The Chair will determine whether to approve the appointment of the most suitable nominee as identified under b)
3.6.7 The term of office for this Partner Member(s) will be 3 years and the total
number of terms they may serve is 3 terms.
3.7 Partner Members - Local Authorities
3.7.1 These Partner Members are jointly nominated by the local authorities whose
areas coincide with, or include the whole or any part of, the ICB’s area. Those
local authorities are:
a) Suffolk County Council
b) Essex County Council
3.7.2 These members will fulfil the eligibility criteria set out at 3.1 and also the
following additional eligibility criteria

a) Be the Chief Executive or hold a relevant Executive level role of one of the bodies listed at 3.7.1
b) Meets the requirements of the role specification for the post c) Collectively provide different perspectives of the Suffolk and Essex
populations
3.7.3 Individuals will not be eligible if
a) Any of the disqualification criteria set out in 3.2 apply
b) Any other disqualification criteria prescribed through NHS England
guidance or supporting legislation apply
c) A conflict of interest is evident, as determined by the Chair or the ICB Board
appointment panel, which results in the individual being unable to fulfil the
role
3.7.4 These members will be appointed by the Chief Executive subject to the
approval of the Chair in accordance with the process set out at 3.7.5 below.
3.7.5 The appointment process will be as follows:
a) Joint Nomination:
• When a vacancy arises, each eligible organisation listed at 3.7.1 will be invited to make up to one nomination each per role
• Eligible organisations may nominate individuals from their own organisation or another organisation
• All eligible organisations will be requested to confirm whether they jointly agree to nominate the whole list of nominated individuals with a failure to confirm within five working days being deemed to constitute agreement. This will be determined by a simple majority being in favour with nil responses taken as assent. If they do agree, the list will be put forward to step b) below. If they do not agree the list, the nomination process will be re-run until a majority acceptance is reached on the nominations put forward.
b) Assessment, Selection and Appointment Subject to Approval of the Chair under c):
• The full list of nominees will be considered by a panel convened by the Chief Executive
• The panel will assess the suitability of the nominees against the requirements of the role (published before the nomination process is initiated) and will confirm that nominees meet the requirements set out in clause 3.7.2 and 3.7.3
• In the event that there is more than one suitable nominee, the panel will select the most suitable for appointment
c) Chair’s Approval:
• The Chair will determine whether to approve the appointment of the most suitable nominee as identified under b)
3.7.6 The term of office for this Partner Member will be 3 years and the total number
of terms they may serve is 3 terms.
3.8 Medical Director
3.8.1 This member will fulfil the eligibility criteria set out at 3.1 and also the following
additional eligibility criteria
a) Be an employee of the ICB or a person seconded to the ICB who is
employed in the civil service of the State or by a body referred to in
paragraph 18(4)(b) of Schedule 1B to the 2006 Act
b) Be a registered Medical Practitioner
c) Meets the ICB leadership competency domains
d) Meets the requirements of the role specification for the post
3.8.2 Individuals will not be eligible if:
a) Any of the disqualification criteria set out in 3.2 apply
3.8.3 This member will be appointed by the Chief Executive subject to the approval
of the Chair
3.9 Director of Nursing
3.9.1 This member will fulfil the eligibility criteria set out at 3.1 and also the following
additional eligibility criteria:
a) Be an employee of the ICB or a person seconded to the ICB who is
employed in the civil service of the State or by a body referred to in
paragraph 18(4)(b) of Schedule 1B to the 2006 Act
b) Be a Registered Nurse
c) Meets the ICB leadership competency domains
d) Meets the requirements of the role specification for the post
3.9.2 Individuals will not be eligible if:
a) Any of the disqualification criteria set out in 3.2 apply
b) They do not maintain a current Nursing and Midwifery Council (NMC)
registration
3.9.3 This member will be appointed by the Chief Executive subject to the approval
of the Chair
3.10 Director of Finance
3.10.1 This member will fulfil the eligibility criteria set out at 3.1 and also the following
additional eligibility criteria:
a) Be an employee of the ICB or a person seconded to the ICB who is
employed in the civil service of the State or by a body referred to in
paragraph 18(4)(b) of Schedule 1B to the 2006 Act
b) Is a qualified accountant with full membership
c) Meets the ICB leadership competency domains
d) Meets the requirements of the role specification for the post
3.10.2 Individuals will not be eligible if:
a) Any of the disqualification criteria set out in 3.2 apply
b) They do not maintain the necessary professional qualification
requirements
3.10.3 This member will be appointed by the Chief Executive subject to the approval
of the Chair
3.11 Three Independent Non-Executive Members
3.11.1 The ICB will appoint three independent Non-Executive Members
3.11.2 The appointment process for these members will include local advertising via
established channels. Interviews will be conducted by a panel comprising
members of the Board and appointments will be subject to the approval of the
Chair.
3.11.3 These members will fulfil the eligibility criteria set out at 3.1 and also the
following additional eligibility criteria
a) Not be an employee of the ICB or a person seconded to the ICB
b) Not hold a role in another health and care organisation in the ICS area
c) One shall have specific knowledge, skills and experience that makes them
suitable for appointment to the Chair of the Audit Committee
d) One should have specific knowledge, skills and experience that makes
them suitable for appointment to the Chair of the Remuneration and
Human Resources Committee
e) One should have general knowledge, skills and experience in quality and
safety that makes them suitable for the role
f) Must live or work within the area of the ICB
3.11.4 Individuals will not be eligible if
a) Any of the disqualification criteria set out in 3.2 apply
b) They hold a role in another health and care organisation within the ICB
area
3.11.5 The term of office for an independent non-executive member will be 3 years
and the total number of terms an individual may serve is 3 terms after which
they will no longer be eligible for re-appointment.
3.11.6 Initial appointments may be for a shorter period in order to avoid all non-
executive members retiring at once. Thereafter, new appointees will ordinarily
retire on the date that the individual they replaced was due to retire in order to
provide continuity.
3.11.7 Subject to satisfactory appraisal the Chair may approve the re-appointment of
an independent non-executive member up to the maximum number of terms
permitted for their role.
3.12 Other Board Members – Member for Voluntary, Community and Social
Enterprise (VCSE)
3.12.1 This Member represents the VCSE Assembly
3.12.2 This member must fulfil the eligibility criteria set out at 3.1 and also the
following additional eligibility criteria:
a) Be the Chief Executive Officer or another Executive Director/Officer of one
of the VCSE organisations within the ICB’s area
3.12.3 Individuals will not be eligible if: a) Any of the disqualification criteria set out in 3.2 apply
3.12.4 The appointment process will be as follows:
a) The nomination will be received from the VCSE Assembly
3.12.5 This member will be appointed by the ICB Chief Executive subject to the
approval of the Chair
3.12.6 The term of office for this Member will be 3 years and the total number of terms
they may serve is 3 terms.
3.13 Board Members: Removal from Office.
3.13.1 Arrangements for the removal from office of Board members is subject to the
term of appointment, and application of the relevant ICB policies and
procedures.
3.13.2 With the exception of the Chair, Board Members shall be removed from office
if any of the following occurs:
a) If they no longer fulfil the requirements of their role or become ineligible
for their role as set out in this constitution, regulations or guidance
b) If they fail to attend a minimum of 75% of the meetings to which they are
invited unless agreed with the Chair in extenuating circumstances
c) If they are deemed to not meet the expected standards of performance at
their annual appraisal
d) If they have behaved in a manner or exhibited conduct which has or is
likely to be detrimental to the honour and interest of the ICB and is likely
to bring the ICB into disrepute. This includes but it is not limited to
dishonesty; misrepresentation (either knowingly or fraudulently);
defamation of any member of the ICB (being slander or libel); abuse of
position; non-declaration of a known conflict of interest; seeking to
manipulate a decision of the ICB in a manner that would ultimately be in
favour of that member whether financially or otherwise
e) Are deemed to have failed to uphold the Nolan Principles of Public Life
f) Are subject to disciplinary proceedings by a regulator or professional body
3.13.3 Members may be suspended pending the outcome of an investigation into
whether any of the matters in 3.13.3 apply.
3.13.4 Executive Directors (including the Chief Executive) will cease to be Board
members if their employment in their specified role ceases, regardless of the
reason for termination of the employment.
3.13.5 The Chair of the ICB may be removed by NHS England, subject to the
approval of the Secretary of State.
3.13.6 If NHS England is satisfied that the ICB is failing or has failed to discharge any
of its functions or that there is a significant risk that the ICB will fail to do so, it
may:
a) 3.13.7.1 terminate the appointment of the ICB’s Chief Executive; and
b) 3.13.7.2 direct the Chair of the ICB as to which individual to appoint as
a replacement and on what terms.
3.14 Terms of Appointment of Board Members
3.14.1 With the exception of the Chair and Non-Executive members, arrangements
for remuneration and any allowances will be agreed by the Remuneration and
Human Resources Committee in line with the ICB remuneration policy and
any other relevant policies or any guidance issued by NHS England or other
relevant body. Remuneration for Chairs will be set by NHS England.
Remuneration for Non-Executive members will be set by a Non-Executive
Member Remuneration Panel.
3.14.2 Other terms of appointment will be determined by the Remuneration and
Human Resources Committee.
3.14.3 Terms of appointment of the Chair will be determined by NHS England.
3.15 Specific Arrangements for Appointment of Ordinary Members made at
Establishment
3.15.1 Individuals may be identified as “designate ordinary members” prior to the
ICB being established.

3.15.2 Relevant nomination procedures for partner members in advance of
establishment are deemed to be valid so long as they are undertaken in full
and in accordance with the provisions of 3.5-3.7.
3.15.3 Any appointment and assessment processes undertaken in advance of
establishment to identify designate ordinary members should follow, as far
as possible, the processes set out in section 3.5-3.12 of this constitution.
However, a modified process, agreed by the Chair, will be considered valid.
3.15.4 On the day of establishment, a committee consisting of the Chair, Chief
Executive and an HR representative will appoint the ordinary members who
are expected to be all individuals who have been identified as designate
appointees pre ICB establishment and the Chair will approve those
appointments.
3.15.5 For the avoidance of doubt, this clause is valid only in relation to the
appointments of the initial ordinary members and all appointments post
establishment will be made in accordance with clauses 3.5 to 3.12

4 Arrangements for the Exercise of our Functions.
4.1 Good Governance
4.1.1 The ICB will, at all times, observe generally accepted principles of good
governance. This includes the Nolan Principles of Public Life and any
governance guidance issued by NHS England. These include but are not
limited to:
a) The highest standards of propriety involving impartiality, integrity
and objectivity in relation to the stewardship of public funds, the management of the organisation and the conduct of its business
b) The Good Governance Standard for Public Services c) The seven key principles of the NHS Constitution d) The Equality Act 2010 e) The Standards for Members of NHS Boards and Governing
Bodies in England
4.1.2 The ICB has agreed a code of conduct and behaviours which sets out the
expected behaviours that members of the Board and its committees will uphold
whilst undertaking ICB business. It also includes a set of principles that will
guide decision making in the ICB. The ICB code of conduct and behaviours is
published in the governance handbook
4.2 General
4.2.1 The ICB will:
a) comply with all relevant laws including but not limited to the 2006 Act and the
duties prescribed within it and any relevant regulations
b) comply with directions issued by the Secretary of State for Health and Social
Care
c) comply with directions issued by NHS England
d) have regard to statutory guidance including that issued by NHS England
e) take account, as appropriate, of other documents, advice and guidance issued
by relevant authorities, including that issued by NHS England
f) respond to reports and recommendations made by local Healthwatch
organisations within the ICB area
4.2.2 The ICB will develop and implement the necessary systems and processes to
comply with (a)-(e) above, documenting them as necessary in this constitution,
its governance handbook and other relevant policies and procedures as
appropriate.
4.3 Authority to Act
4.3.1 The ICB is accountable for exercising its statutory functions and may grant
authority to act on its behalf to:

a) any of its members or employees
b) a committee or sub-committee of the ICB
4.3.2 Under section 65Z5 of the 2006 Act, the ICB may arrange with another ICB,
an NHS Trust, NHS Foundation Trust, NHS England, a local authority,
combined authority or any other body prescribed in Regulations, for the ICB’s
functions to be exercised by or jointly with that other body or for the functions
of that other body to be exercised by or jointly with the ICB. Where the ICB
and other body enters such arrangements, they may also arrange for the
functions in question to be exercised by a joint committee of theirs and/or for
the establishment of a pooled fund to fund those functions (section 65Z6). In
addition, under section 75 of the 2006 Act, the ICB may enter partnership
arrangements with a local authority under which the local authority exercises
specified ICB functions or the ICB exercises specified local authority functions,
or the ICB and local authority establish a pooled fund.
4.3.3 Where arrangements are made under section 65Z5 or section 75 of the 2006
Act the board must authorise the arrangement, which must be described as
appropriate in the SoRD.
4.4 Scheme of Reservation and Delegation
4.4.1 The ICB has agreed a scheme of reservation and delegation (SoRD) which is
published in full in the ICB Governance Handbook
4.4.2 Only the Board may agree the SoRD and amendments to the SoRD may
only be approved by the Board
4.4.3 The SoRD sets out:
4.4.3.1 those functions that are reserved to the Board;
4.4.3.2 those functions that have been delegated to an individual or to committees
and sub-committees;
4.4.3.3 those functions delegated to another body or to be exercised jointly with
another body, under section 65Z5 and 65Z6 of the 2006 Act
4.4.4 The ICB remains accountable for all of its functions, including those that it has
delegated. All those with delegated authority are accountable to the Board for
the exercise of their delegated functions.
4.5 Functions and Decision Map
4.5.1 The ICB has prepared a Functions and Decision Map which sets out at a high
level its key functions and how it exercises them in accordance with the SoRD.
4.5.2 The Functions and Decision Map is published at
www.suffolkandnortheastessex.icb.nhs.uk

4.5.3 The map includes:
a) Key functions reserved to the Board of the ICB
b) Commissioning functions delegated to committees and individuals.
c) Commissioning functions delegated under section 65Z5 and 65Z6 of the
2006 Act to be exercised by, or with, another ICB, an NHS trust, NHS
foundation trust, local authority, combined authority or any other
prescribed body;
d) functions delegated to the ICB (for example, from NHS England).
4.6 Committees and Sub-Committees
4.6.1 The ICB may appoint committees and arrange for its functions to be exercised
by such committees. Each committee may appoint sub-committees and
arrange for the functions exercisable by the committee to be exercised by
those sub-committees.
4.6.2 All committees and sub-committees are listed in the SoRD.
4.6.3 Each committee and sub-committee established by the ICB operates under
terms of reference agreed by the Board. All terms of reference are published
in the Governance Handbook.
4.6.4 The Board remains accountable for all functions, including those that it has
delegated to committees and subcommittees and therefore, appropriate
reporting and assurance arrangements are in place and documented in terms
of reference. All committees and sub committees that fulfil delegated functions
of the ICB, will be required to:
a) Submit regular decision and assurance reports to the Board
b) Submit minutes of committee meetings to the Board
c) Ensure that the committee Chair or designated deputy attends meetings
of the Board as necessary
d) Comply with internal audit findings and committee effectiveness reviews
4.6.5 Any committee or sub-committee established in accordance with clause 4.6
may consist of or include persons who are not ICB Members or employees.
4.6.6 All members of committees and sub-committees that exercise the ICB
commissioning functions will be approved by the Chair. The Chair will not
approve an individual to such a committee or sub-committee if they consider
that the appointment could reasonably be regarded as undermining the
independence of the health service because of the candidate’s involvement
with the private healthcare sector or otherwise.
4.6.7 The following committees will be maintained:
a) Audit Committee: This committee is accountable to the Board and provides an independent and objective view of the ICB’s compliance with its statutory responsibilities. The committee is responsible for arranging appropriate internal and external audit.
The Audit Committee will be chaired by an independent non-executive
member (other than the Chair of the ICB) who has the qualifications,
expertise or experience to enable them to express credible opinions on
finance and audit matters.
b) Remuneration and Human Resources Committee: This committee is
accountable to the Board for matters relating to remuneration, fees and
other allowances (including pension schemes) for employees and other
individuals who provide services to the ICB.
The Remuneration and Human Resources Committee will be chaired by
an independent Non-Executive member other than the Chair or the Chair
of Audit Committee.
4.6.8 The terms of reference for each of the above committees are published in the
governance handbook.
4.6.9 The Board has also established a number of other committees to assist it with
the discharge of its functions. These committees are set out in the SoRD and
further information about these committees, including terms of reference, are
published in the Governance Handbook.
4.7 Delegations made under section 65Z5 of the 2006 Act
4.7.1 As per 4.3.2 The ICB may arrange for any functions exercisable by it to be
exercised by or jointly with any one or more other relevant bodies (another
ICB, NHS England, an NHS trust, NHS foundation trust, local authority,
combined authority or any other prescribed body).
4.7.2 All delegations made under these arrangements are set out in the ICB Scheme
of Reservation and Delegation and included in the Functions and Decision
Map.
4.7.3 Each delegation made under section 65Z5 of the Act will be set out in a
delegation arrangement which sets out the terms of the delegation. This may,
for joint arrangements, include establishing and maintaining a pooled fund.
The power to approve delegation arrangements made under this provision will
be reserved to the Board.
4.7.4 The Board remains accountable for all the ICB’s functions, including those that
it has delegated and therefore, appropriate reporting and assurance
mechanisms are in place as part of agreeing terms of a delegation and these
are detailed in the delegation arrangements, summaries of which will be
published in the ICBs Governance Handbook.
4.7.5 In addition to any formal joint working mechanisms, the ICB may enter into
strategic or other transformation discussions with its partner organisations on
an informal basis.
5 Procedures for Making Decisions
5.1 Standing Orders
5.1.1 The ICB has agreed a set of standing orders which describe the processes
that are employed to undertake its business. They include procedures for:
• conducting the business of the ICB
• the procedures to be followed during meetings; and
• the process to delegate functions.
5.1.2 The Standing Orders apply to all committees and sub-committees of the ICB
unless specified otherwise in terms of reference which have been agreed by
the Board.
5.1.3 A full copy of the Standing Orders is included in Appendix 2 and form part of
this constitution.
5.2 Standing Financial Instructions (SFIs)
5.2.1 The ICB has agreed a set of SFIs which include the delegated limits of financial
authority set out in the SoRD.
5.2.2 A copy of the SFIs are published in the ICB Governance Handbook.
6 Arrangements for Conflicts of Interest Management
and Standards of Business Conduct
6.1 Conflicts of Interest
6.1.1 As required by section 14Z30 of the 2006 Act, the ICB has made
arrangements to manage any actual and potential conflicts of interest to
ensure that decisions made by the ICB will be taken and seen to be taken
without being unduly influenced by external or private interest and do not, (and
do not risk appearing to) affect the integrity of the ICB’s decision-making
processes.
6.1.2 The ICB has agreed policies and procedures for the identification and
management of conflicts of interest, including registers of interest which are
published on the ICBs website
6.1.3 All Board, committee and sub-committee members, and employees of the ICB,
will comply with the ICB policy on conflicts of interest in line with their terms of
office and/ or employment. This will include but not be limited to declaring all
interests on a register that will be maintained by the ICB.
6.1.4 All delegation arrangements made by the ICB under Section 65Z5 of the 2006
Act will include a requirement for transparent identification and management
of interests and any potential conflicts in accordance with suitable policies and
procedures comparable with those of the ICB.
6.1.5 Where an individual, including any individual directly involved with the
business or decision-making of the ICB and not otherwise covered by one of
the categories above, has an interest, or becomes aware of an interest which
could lead to a conflict of interests in the event of the ICB considering an action
or decision in relation to that interest, that must be considered as a potential
conflict, and is subject to the provisions of this Constitution and the Standards
of Business Conduct and Conflicts of Interest Policy.
6.1.6 The ICB has appointed the Audit Chair to be the Conflicts of Interest Guardian.
In collaboration with the ICB’s governance lead, their role is to:
a) Act as a conduit for members of the public and members of the partnership
who have any concerns with regards to conflicts of interest
b) Be a safe point of contact for employees or workers to raise any concerns
in relation to conflicts of interest
c) Support the rigorous application of conflicts of interest principles and
policies
d) Provide independent advice and judgment to staff and members where
there is any doubt about how to apply conflicts of interest policies and
principles in an individual situation
e) Provide advice on minimising the risks of conflicts of interest.
6.2 Principles
6.2.1 In discharging its functions, the ICB will abide by the following principles:
a) acting in good faith and in the interests of the ICB b) following the Seven Principles of Public Life; set out by the
Committee on Standards in Public Life (the Nolan
Principles);
c) compliance with the standards set out in the Professional
Standards Authority guidance - Standards for Members of
NHS Boards and Governing Bodies in England; and
d) comply with the ICB’s Standards of Business Conduct and
Conflicts of Interest Policy, including the requirements set out
in the policy for managing conflicts of interest which is
available on the ICB’s website and will be made available on
request.
6.3 Declaring and Registering Interests
6.3.1 The ICB maintains registers of the interests of:
a) Members of the ICB
b) Members of the Board’s committees and sub-committees
c) Its employees
6.3.2 In accordance with section 14Z30(2) of the 2006 Act registers of interest are
published on the ICB website www.suffolkandnortheastessex.icb.nhs.uk
6.3.3 All relevant persons as per 6.1.3 and 6.1.5 must declare any conflict or
potential conflict of interest relating to decisions to be made in the exercise of
the ICB’s commissioning functions.
6.3.4 Declarations should be made as soon as reasonably practicable after the
person becomes aware of the conflict or potential conflict and in any event
within 28 days. This could include interests an individual is pursuing. Interests
will also be declared on appointment and during relevant discussion in
meetings.
6.3.5 All declarations will be entered in the registers as per 6.3.1
6.3.6 The ICB will ensure that, as a matter of course, declarations of interest are
made and confirmed, or updated at least annually.
6.3.7 Interests (including gifts and hospitality) of decision-making staff will remain
on the public register for a minimum of six months. In addition, the ICB will
retain a record of historic interests and offers/receipt of gifts and hospitality for
a minimum of six years after the date on which it expired. The ICB’s published
register of interests states that historic interests are retained by the ICB for the
specified timeframe and details of whom to contact to submit a request for this
information.
6.3.8 Activities funded in whole or in part by third parties who may have an interest
in ICB business such as sponsored events, posts and research will be
managed in accordance with the ICB policy to ensure transparency and that
any potential for conflicts of interest are well-managed.
6.4 Standards of Business Conduct
6.4.1 Board members, employees, committee and sub-committee members of the
ICB will at all times comply with this Constitution and be aware of their
responsibilities as outlined in it. They should:
a) act in good faith and in the interests of the ICB
b) follow the Seven Principles of Public Life; set out by the Committee on
Standards in Public Life (the Nolan Principles)
c) comply with the ICB Standards of Business Conduct and Conflicts of
Interest Policy, and any requirements set out in the policy for managing
conflicts of interest.
6.4.2 Individuals contracted to work on behalf of the ICB or otherwise providing
services or facilities to the ICB will be made aware of their obligation to declare
conflicts or potential conflicts of interest. This requirement will be written into
their contract for services and is also outlined in the ICB’s Standards of
Business Conduct and Conflicts of Interest Policy.
7 Arrangements for ensuring Accountability and
Transparency
7.1.1 The ICB will demonstrate its accountability to local people, stakeholders and
NHS England in a number of ways, including by upholding the requirement for
transparency in accordance with paragraph 11(2) of Schedule 1B to the 2006
Act.
7.2 Principles
7.2.1 The ICB will demonstrate its accountability to its Members, local people,
stakeholders and NHS England in a number of ways, including by being open
and transparent.
7.2.2 In addition to statutory requirements, the CCG will demonstrate its
accountability by publishing a range of documents and information on its
website at www.suffolkandnortheastessex.icb.nhs.uk
7.3 Meetings and publications
7.3.1 Board meetings, and committees composed entirely of board members or
which include all board members will be held in public except where a
resolution is agreed to exclude the public on the grounds that it is believed to
not be in the public interest.
7.3.2 Papers and minutes of all meetings held in public will be published.
7.3.3 Annual accounts will be externally audited and published.
7.3.4 A clear complaints process will be published.
7.3.5 The ICB will comply with the Freedom of Information Act 2000 and with the
Information Commissioner Office requirements regarding the publication of
information relating to the ICB.
7.3.6 information will be provided to NHS England as required.
7.3.7 The constitution and governance handbook will be published as well as other
key documents including but not limited to:
a) Standards of Business Conduct and Conflicts of Interest Policy and
procedures
b) Registers of interests
c) Key policies
7.3.8 The ICB will publish, with our partner NHS trusts and NHS foundation trusts,
a plan at the start of each financial year that sets out how the ICB proposes to
exercise its functions during the next five years. The plan will explain how the
ICB proposes to discharge its duties under:
• section 14Z34 (improvement in quality of services),
• section 14Z35 (reducing inequalities),
• section 14Z43 (have regard to effect of decisions)
• section 14Z44 (public involvement and consultation), and
• sections 223H and 223J (financial duties).
And
a) proposed steps to implement the Suffolk and North East Essex joint local
health and wellbeing strategy
7.4 Scrutiny and Decision Making
7.4.1 At least three independent non-executive members will be appointed to the
board including the Chair; and all of the board and committee members will
comply with the Nolan Principles of Public Life and meet the criteria described
in the Fit and Proper Person Test.
7.4.2 Healthcare services will be arranged in a transparent way, and decisions
around who provides services will be made in the best interests of patients,
taxpayers and the population, in line with the rules set out in the NHS Provider
Selection Regime.
7.4.3 The ICB will comply with the requirements of the NHS Provider Selection
Regime including:
a) Ensuring appropriate governance structures and arrangements are in
place to deal with any provider selection challenges which may arise.
b) Retaining evidence to underpin the proper exercise of the ICBs
responsibilities for arranging healthcare
c) Publishing intentions for arranging relevant healthcare services in
advance
d) Publishing contracts awarded and retaining records of decision making
e) Ensuring audit arrangements are capable of examining the decisions
made

7.4.4 The ICB will comply with local authority health overview and scrutiny
requirements.
7.5 Annual Report
7.5.1 The ICB will publish an annual report in accordance with any guidance
published by NHS England and which sets out how it has discharged its
functions and fulfilled its duties in the previous financial year and in particular
how it has discharged its duties under sections
a) 14Z34 (improvement in quality of services),
b) 14Z35 (reducing inequalities),
c) 14z43 (have regard to the effect of decisions)
d) 14Z44 (public involvement and consultation), and
7.5.2 The annual report will also review the extent to which the ICB has exercised
its functions in accordance with the plans published under section
a) 14Z50 (Integrated Care System plan), and
b) 14Z54 (capital resource use plan), and
7.5.3 Review any steps the board has taken to implement any joint health and
wellbeing strategy to which it was required to have regard under section
116B(1) of the Local Government and Public Involvement in Health Act 2007.
8 Arrangements for Determining the Terms and
Conditions of Employees.
8.1.1 The ICB may appoint employees, pay them remuneration and allowances as
it determines and appoint staff on such terms and conditions as it determines.
8.1.2 The Board has established a Remuneration and Human Resources
Committee which is chaired by a Non-Executive member other than the Chair
or Audit Chair.
8.1.3 The membership of the Remuneration and Human Resources Committee is
determined by the Board. No employees may be a member of the
Remuneration Committee, but the Board ensures that the Remuneration
Committee has access to appropriate advice by:
a) A senior representative for HR and the Chief Executive attending in an
advisory capacity. It is acknowledged that HR advice should be sought to
assist the Committee in reaching decisions and it would be expected for
the HR representative to be present throughout the meeting, unless the
majority of the Committee and the Chair considered otherwise.
b) Other Directors or Senior Managers invited to attend as appropriate.
8.1.4 The Board may appoint independent members or advisers to the
Remuneration Committee who are not members of the board.
8.1.5 The main purpose of the Remuneration and Human Resources Committee is
to exercise the functions of the ICB regarding remuneration included in
paragraphs 18 to 20 of Schedule 1B to the 2006 Act.
8.1.6 The duties of the Remuneration and Human Resources Committee are set out
in detail in its terms of reference which in summary are to confirm the ICB Pay
Policy including adoption of any pay frameworks for all employees including
senior managers/directors (including board members) and non-executive
directors. The full terms of reference are included in the ICB Governance
Handbook.
8.1.7 The ICB may make arrangements for a person to be seconded to serve as a
member of the ICB’s staff.
9 Arrangements for Public Involvement
9.1.1 In line with section 14Z44(2) of the 2006 Act the ICB has made arrangements
to secure that individuals to whom services which are, or are to be, provided
pursuant to arrangements made by the ICB in the exercise of its functions,
and their carers and representatives, are involved (whether by being consulted
or provided with information or in other ways) in:
a) the planning of the commissioning arrangements by the Integrated Care Board
b) the development and consideration of proposals by the ICB
c) for changes in the commissioning arrangements where the
implementation of the proposals would have an impact on the manner in
which the services are delivered to the individuals (at the point when the
service is received by them), or the range of health services available to
them, and d) decisions of the ICB affecting the operation of the commissioning
arrangements where the implementation of the decisions would (if made) have such an impact.
9.1.2 In line with section 14Z52 of the 2006 Act the ICB will ensure
arrangements are made to consult the local population on its system plan
following best practice for the conduct of public consultations published by
HM Government.
9.1.3 The ICB has adopted the ten principles set out by NHS England for
working with people and communities:
a) Put the voices of people and communities at the centre of decision-making and governance, at every level of the ICB.
b) Start engagement early when developing plans and feed back to people and communities how it has influenced activities and decisions.
c) Understand your community’s needs, experience and aspirations for health and care, using engagement to find out if change is working.
d) Build relationships with excluded groups – especially those affected by inequalities.
e) Work with Healthwatch and the voluntary, community and social enterprise sector as key partners.
f) Provide clear and accessible public information about vision, plans and progress to build understanding and trust.
g) Use community development approaches that empower people and communities, making connections to social action.
h) Use co-production, insight and engagement to achieve accountable health and care services.
i) Co-produce and redesign services and tackle system priorities in partnership with people and communities.
j) Learn from what works and build on the assets of all partners in the ICS – networks, relationships, activity in local places.
9.1.4 These principles will be used when developing and maintaining arrangements
for engaging with people and communities.
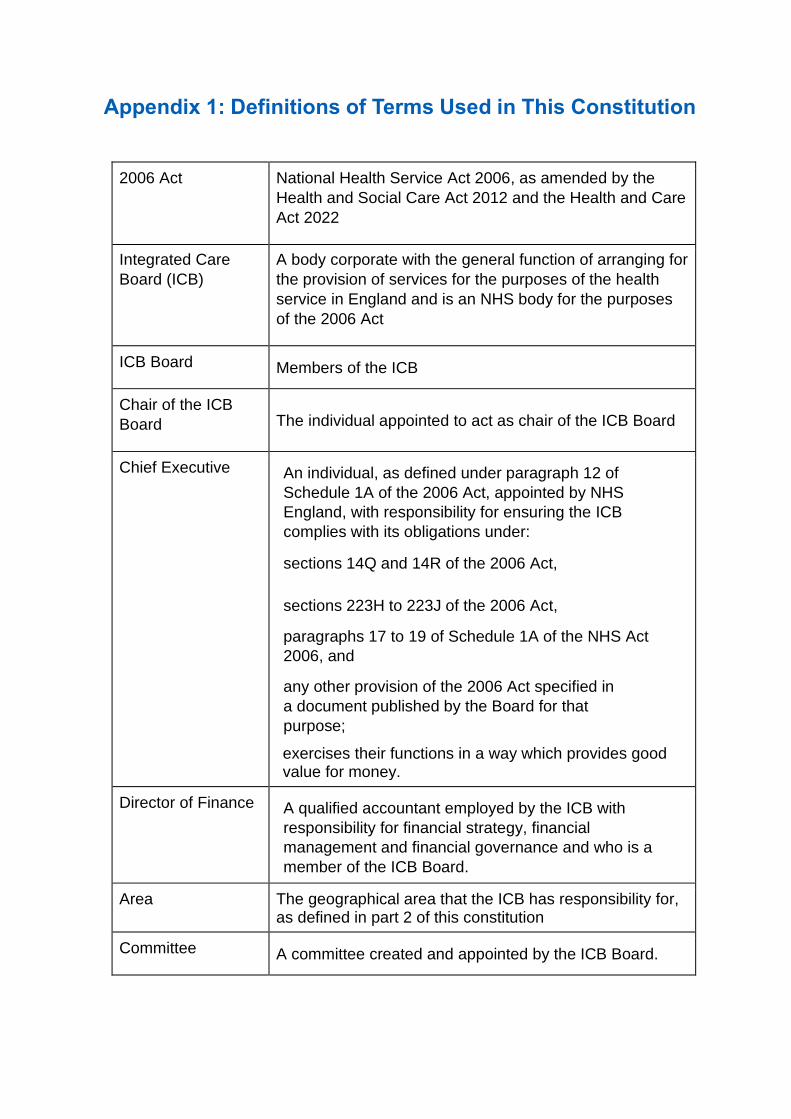
Appendix 1: Definitions of Terms Used in This Constitution
2006 Act National Health Service Act 2006, as amended by the
Health and Social Care Act 2012 and the Health and Care
Act 2022
Integrated Care
Board (ICB)
A body corporate with the general function of arranging for
the provision of services for the purposes of the health
service in England and is an NHS body for the purposes
of the 2006 Act
ICB Board Members of the ICB
Chair of the ICB
Board The individual appointed to act as chair of the ICB Board
Chief Executive An individual, as defined under paragraph 12 of
Schedule 1A of the 2006 Act, appointed by NHS
England, with responsibility for ensuring the ICB
complies with its obligations under:
sections 14Q and 14R of the 2006 Act,
sections 223H to 223J of the 2006 Act,
paragraphs 17 to 19 of Schedule 1A of the NHS Act
2006, and
any other provision of the 2006 Act specified in
a document published by the Board for that
purpose;
exercises their functions in a way which provides good value for money.
Director of Finance A qualified accountant employed by the ICB with
responsibility for financial strategy, financial
management and financial governance and who is a
member of the ICB Board.
Area The geographical area that the ICB has responsibility for, as defined in part 2 of this constitution
Committee A committee created and appointed by the ICB Board.
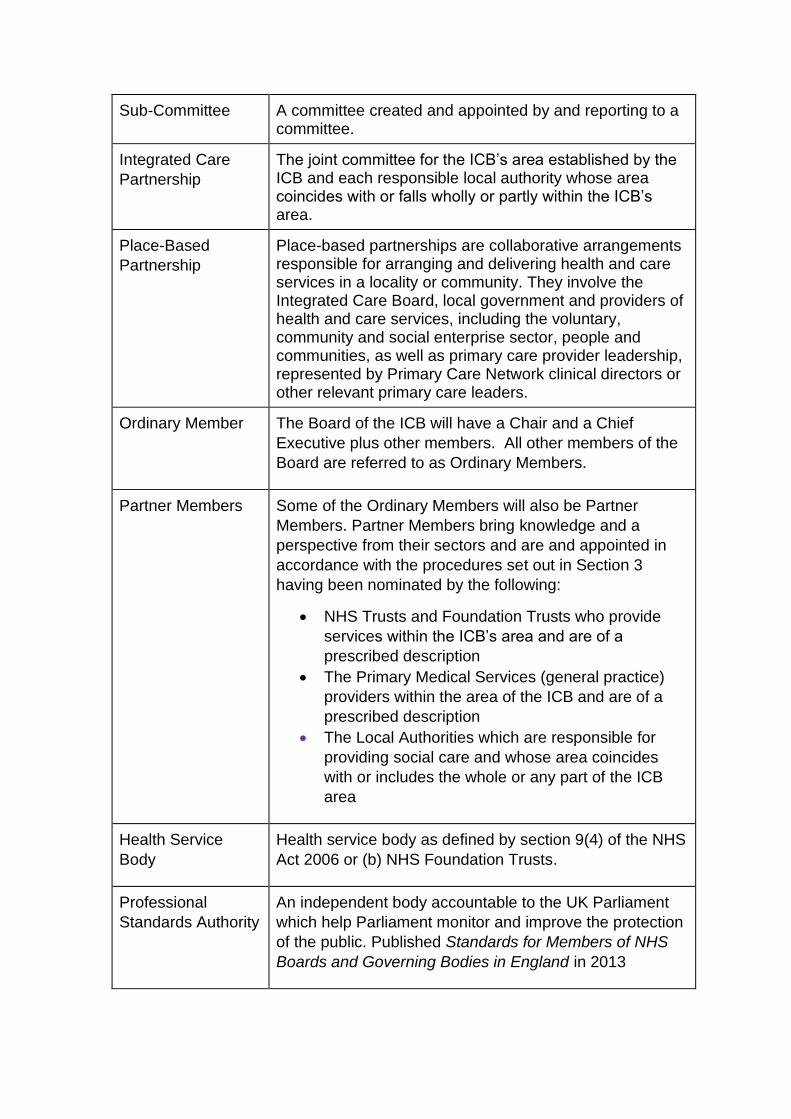
Sub-Committee A committee created and appointed by and reporting to a committee.
Integrated Care
Partnership
The joint committee for the ICB’s area established by the ICB and each responsible local authority whose area coincides with or falls wholly or partly within the ICB’s area.
Place-Based
Partnership
Place-based partnerships are collaborative arrangements responsible for arranging and delivering health and care services in a locality or community. They involve the Integrated Care Board, local government and providers of health and care services, including the voluntary, community and social enterprise sector, people and communities, as well as primary care provider leadership, represented by Primary Care Network clinical directors or other relevant primary care leaders.
Ordinary Member The Board of the ICB will have a Chair and a Chief
Executive plus other members. All other members of the
Board are referred to as Ordinary Members.
Partner Members Some of the Ordinary Members will also be Partner
Members. Partner Members bring knowledge and a
perspective from their sectors and are and appointed in
accordance with the procedures set out in Section 3
having been nominated by the following:
• NHS Trusts and Foundation Trusts who provide
services within the ICB’s area and are of a
prescribed description
• The Primary Medical Services (general practice)
providers within the area of the ICB and are of a
prescribed description
• The Local Authorities which are responsible for
providing social care and whose area coincides
with or includes the whole or any part of the ICB
area
Health Service
Body
Health service body as defined by section 9(4) of the NHS
Act 2006 or (b) NHS Foundation Trusts.
Professional
Standards Authority
An independent body accountable to the UK Parliament
which help Parliament monitor and improve the protection
of the public. Published Standards for Members of NHS
Boards and Governing Bodies in England in 2013

NHS England The body which leads the NHS in England
Appendix 2: Standing Orders
1. Introduction
1.1. These Standing Orders have been drawn up to regulate the proceedings of
the Suffolk and North East Essex Integrated Care Board so that the ICB can
fulfil its obligations as set out largely in the 2006 Act (as amended). They form
part of the ICB’s Constitution.
2. Amendment and review
2.1. The Standing Orders are effective from 1 July 2022
2.2. Standing Orders will be reviewed on an annual basis or sooner if required.
2.3. Amendments to these Standing Orders will be made as per clause number
1.6 in the constitution which sets out the procedure for making amendments
to the Constitution and its constituent parts
2.4. All changes to these Standing Orders will require an application to NHS
England for variation to the ICB Constitution and will not be implemented until
the constitution has been approved.
3. Interpretation, application and compliance
3.1. Except as otherwise provided, words and expressions used in these Standing
Orders shall have the same meaning as those in the main body of the ICB
Constitution and as per the definitions in Appendix 1.
3.2. These standing orders apply to all meetings of the Board, including its
committees and sub-committees unless otherwise stated. All references to
Board are inclusive of committees and sub-committees unless otherwise
stated.
3.3. All members of the Board, members of committees and sub-committees and
all employees, should be aware of the Standing Orders and comply with them.
Failure to comply may be regarded as a disciplinary matter.
3.4. In the case of conflicting interpretation of the Standing Orders, the Chair,
supported with advice from the Independent Governance Adviser will provide
a settled view which shall be final.
3.5. All members of the Board, its committees and sub-committees and all
employees have a duty to disclose any non-compliance with these Standing
Orders to the Chief Executive as soon as possible.
3.6. If, for any reason, these Standing Orders are not complied with, full details of
the non-compliance and any justification for non-compliance and the

circumstances around the non-compliance, shall be reported to the next
formal meeting of the Board for action or ratification and the Audit Committee
for review.
4. Meetings of the Integrated Care Board
4.1. Calling Board Meetings
4.1.1 Meetings of the Board of the ICB shall be held at regular intervals at
such times and places as the ICB may determine.
4.1.2 In normal circumstances, each member of the Board will be given not
less than one month’s notice in writing of any meeting to be held.
However:
a) The Chair may call a meeting at any time by giving not less than
14 calendar days notice in writing.
b) One third of the members of the Board may request the Chair to
convene a meeting by notice in writing, specifying the matters
which they wish to be considered at the meeting. If the Chair
refuses, or fails, to call a meeting within seven calendar days of
such a request being presented, the Board members signing the
requisition may call a meeting by giving not less than 14 calendar
days notice in writing to all members of the Board specifying the
matters to be considered at the meeting.
c) In emergency situations the Chair may call a meeting with two
days notice by setting out the reason for the urgency and the
decision to be taken.
4.1.3 A public notice of the time and place of meetings to be held in public
and how to access the meeting shall be given by posting it at the offices
of the ICB body and electronically at least three clear days before the
meeting or, if the meeting is convened at shorter notice, then at the time
it is convened.
4.1.4 The agenda and papers for meetings to be held in public will be
published electronically in advance of the meeting excluding, if thought
fit, any item likely to be addressed in part of a meeting is not likely to be
open to the public.
4.2 Chair of a meeting
4.2.1 The Chair of the ICB shall preside over meetings of the Board.
4.2.2 If the Chair is absent or is disqualified from participating by a conflict of
interest the Deputy Chair, if present, shall preside.

4.2.3 If both the Chair and Deputy Chair are absent, or are disqualified from
participating, then a member of the Board shall be chosen by the
members present, or by a majority of them, and shall preside
4.2.4 The Board shall appoint a Chair to all committees and sub-committees
that it has established. The appointed committee or sub-committee
Chair will preside over the relevant meeting. Terms of reference for
committees and sub-committees will specify arrangements for
occasions when the appointed Chair is absent.
4.3 Agenda, supporting papers and business to be
transacted
4.3.1 The agenda for each meeting will be drawn up and agreed by the Chair
of the meeting.
4.3.2 Except where the emergency provisions apply, supporting papers for
all items must be submitted at least seven calendar days before the
meeting takes place. The agenda and supporting papers will be
circulated to all members of the Board at least five calendar days before
the meeting.
4.3.3 Agendas and papers for meetings open to the public, including details
about meeting dates, times and venues, will be published on the ICB’s
website at www.suffolkandnortheastessex.icb.nhs.uk
4.4 Petitions
4.4.1 Where a valid petition has been received by the ICB it shall be included
as an item for the agenda of the next meeting of the Board in
accordance with the ICB policy as published in the Governance
Handbook.
4.5 Nominated Deputies
4.5.1 With the permission of the person presiding over the meeting, the
Executive Directors and the Partner Members of the Board may
nominate a deputy to attend a meeting of the Board that they are
unable to attend. The deputy may speak and vote on their behalf if
authorised to do so in advance.
4.5.2 The decision of person presiding over the meeting regarding
authorisation of nominated deputies is final.
4.5.3 If a member of the ICB is unable to attend two consecutive meetings,
other than as the result of illness or other exceptional circumstance,
the member will be asked to meet with the Chair

4.6 Virtual attendance at meetings
4.6.1 The Board of the ICB and its committees and sub-committees may
meet virtually using telephone, video and other electronic means when
necessary, unless the terms of reference prohibit this.
4.7 Quorum
4.7.1 The quorum for meetings of the Board will be 50% of its members,
including:
a) The Chair or nominated deputy
b) Either the Chief Executive or the Director of Finance
c) Either the Medical Director or the Director of Nursing
d) At least one independent Non-Executive Member
e) At least two Partner Members
4.7.2 For the sake of clarity:
a) No person can act in more than one capacity when determining
the quorum.
b) An individual who has been disqualified from participating in a
discussion on any matter and/or from voting on any motion by
reason of a declaration of a conflict of interest, shall no longer
count towards the quorum.
4.7.3 For all committees and sub-committees, the details of the quorum for
these meetings and status of deputies are set out in the appropriate
terms of reference.
4.8 Vacancies and Defects in Appointment
4.8.1 The validity of any act of the ICB is not affected by any vacancy among
members or by any defect in the appointment of any member.
4.8.2 In the event of vacancy or defect in appointment the following temporary
arrangement for quorum will apply:
a) Vacant roles will not be included in the total number.
4.9 Decision making
4.9.1 The ICB has agreed to use a collective model of decision-making that
seeks to find consensus between system partners and make
decisions based on unanimity as the norm, including working though
difficult issues where appropriate.
4.9.2 Generally, it is expected that decisions of the ICB will be reached by
consensus. Should this not be possible then a vote will be required.
The process for voting, which should be considered a last resort, is
set out below:
a) All members of the Board who are present at the meeting will be
eligible to cast one vote each.
b) Under no circumstances may an absent member vote by proxy.
Absence is defined as being absent at the time of the vote, but this
does not preclude anyone attending by teleconference or other
virtual mechanism from participating in the meeting, including
exercising their right to vote if eligible to do so.
c) For the sake of clarity, any additional participants and observers (as
detailed within Section 2.1 of the Constitution) will not have voting
rights.
d) A resolution will be passed if more votes are cast for the resolution
than against it.
e) If an equal number of votes are cast for and against a resolution,
then the Chair (or in their absence, the person presiding over the
meeting) will have a second and casting vote.
f) Should a vote be taken, the outcome of the vote, and any dissenting
views, must be recorded in the minutes of the meeting.
Disputes
4.9.3 Where helpful the board may draw on third party support to assist
them in resolving any disputes, such as peer review or support from
NHS England.
Urgent decisions
4.9.4 In the case urgent decisions and extraordinary circumstances, every
attempt will be made for the Board to meet virtually. Where this is not
possible the following will apply.
4.9.5 The powers which are reserved or delegated to the Board, may for an
urgent decision be exercised by the Chair and Chief Executive (or
relevant lead director in the case of committees) subject to every effort
having made to consult with as many members as possible in the
given circumstances.
4.9.6 The exercise of such powers shall be reported to the next formal
meeting of the Board for formal ratification and the Audit Committee
for oversight.
4.10 Minutes
4.10.1 The names and roles of all members present shall be recorded in the
minutes of the meetings.
4.10.2 The minutes of a meeting shall be drawn up and submitted for
agreement at the next meeting where they shall be signed by the
person presiding at it.
4.10.3 No discussion shall take place upon the minutes except upon their
accuracy or where the person presiding over the meeting considers
discussion appropriate.
4.10.4 Where providing a record of a meeting held in public, the minutes shall
be made available to the public.
4.11 Admission of public and the press
4.11.1 In accordance with Public Bodies (Admission to Meetings) Act 1960 All
meetings of the Board and all meetings of committees which are
comprised of entirely board members or all board members, at which
public functions are exercised will be open to the public.
4.11.2 The Board may resolve to exclude the public from a meeting or part of
a meeting where it would be prejudicial to the public interest by reason
of the confidential nature of the business to be transacted or for other
special reasons stated in the resolution and arising from the nature of
that business or of the proceedings or for any other reason permitted
by the Public Bodies (Admission to Meetings) Act 1960 as amended or
succeeded from time to time.
4.11.3 The person presiding over the meeting shall give such directions as
he/she thinks fit with regard to the arrangements for meetings and
accommodation of the public and representatives of the press such as
to ensure that the Governing Body’s business shall be conducted
without interruption and disruption.
4.11.4 As permitted by Section 1(8) Public Bodies (Admissions to Meetings)
Act 1960 as amended from time to time) the public may be excluded
from a meeting suppress or prevent disorderly conduct or behaviour.
4.11.5 Matters to be dealt with by a meeting following the exclusion of
representatives of the press, and other members of the public shall be
confidential to the members of the Board.
5 Suspension of Standing Orders
5.1 In exceptional circumstances, except where it would contravene any
statutory provision or any direction made by the Secretary of State for
Health and Social Care or NHS England, any part of these Standing
Orders may be suspended by the Chair in discussion with at least 2
other members,
5.2 A decision to suspend Standing Orders together with the reasons for
doing so shall be recorded in the minutes of the meeting.
5.3 A separate record of matters discussed during the suspension shall be
kept. These records shall be made available to the Audit Committee for
review of the reasonableness of the decision to suspend Standing
Orders.

SUFFOLK AND NORTH EAST ESSEX INTEGRATED CARE BOARD
DRAFT CONSTITUTION – SUMMARY OF CONSULTATION
The Suffolk and North East Essex system is a genuinely ‘can do’ organisation characterised in the way that we work together as a local health and care system. We are committed to improving health and wellbeing outcomes for the population that we serve and we are ambitious about what we can achieve together. At its heart, our ICS is an equal partnership across the NHS, Local Government and Voluntary, Community and Social Enterprise Sector (VCSE) increasingly characterised by positive relationships between local health and care leaders, joint action to address problems and a genuine attitude that enables meaningful partnership and integrated thinking and working at every level. In view of this we have engaged partners and key stakeholders throughout the process of transition and specifically around approval of the ICB draft Constitution. This has largely been achieved by consultation through the ICS Partnership Board whose wide membership includes circa 45 members together with additional attendees drawn from and representing commissioners, NHS Trusts and Foundation Trusts, primary care, local authorities, the voluntary and community sector and other partners. Those who have had an opportunity to comment on the draft Constitution therefore includes:
• ICS Chair and ICB Chair (Designate)
• ICS Lead and ICB Chief Executive (Designate)
• ICS Programme Director
• Director of Nursing – Suffolk and North East Essex CCGs
• Director of Transformation and Deputy Chief Executive – Suffolk and North East Essex CCGs
• ICS Clinical Lead and Chair – Ipswich and East Suffolk CCG
• Chair – North East Essex CCG
• Chair – West Suffolk CCG
• Acting Chief Executive – East Suffolk and North Essex NHS Foundation Trust
• Director of Strategy, Research and Innovation - East Suffolk and North Essex NHS Foundation Trust
• Interim Chief Executive – West Suffolk Hospital NHS Foundation Trust
• Chief Executive – Essex Partnership University NHS Foundation Trust
• Chief Executive – Norfolk and Suffolk NHS Foundation Trust
• Head of Operations – East of England Ambulance NHS Trust
• Executive Director: People Services – Suffolk County Council
• Director for Health and Social Care Integration – Essex County Council
• Executive Director: Adult Social Care Services – Essex County Council
• Director of Public Health – Suffolk County Council
• Director of Public Health – Essex County Council
• Strategic Director of Customer Relationships – Colchester Borough Council
• Representative – Tendring District Council
• Representative – Suffolk District and Borough Councils
• Representative – North East Essex District and Borough Councils
• Representative – Suffolk LMC
• Representative – North Essex LMC
• Chief Executive – GP Primary Care

• Medical Director – Suffolk GP Federation
• Chair – Essex and Anglia Local Pharmaceutical Network
• Chief Executive – Healthwatch Suffolk
• Chief Executive – Healthwatch Essex
• Chief Executive – Suffolk Community Foundation
• Chief Executive – CVS Tendring
• Chief Executive – Community Action Suffolk
• Chief Executive – Age Concern Colchester
• Chief Executive – Survivors in Transition
• Chief Executive – Suffolk MIND
• Chief Executive – St. Helena Hospice
• Chief Executive – St. Elizabeth Hospice
• Director – West Suffolk Alliance
• Director – Ipswich and East Suffolk Alliance
• Director – North East Essex Alliance
• ICS Interim Director of Workforce and Director of Corporate Services and System Infrastructure – Suffolk and North East Essex CCGs
• Director of Finance – Suffolk and North East Essex CCGs
• Chair – ICS Chairs Group
• Representative – NHS England
• Voluntary Sector Representatives A system workshop took place in November 2021 to discuss the draft Constitution and to finalise the ICB Board profile. There was over 80 attendees from across Suffolk North East Essex from a range of partners, including statutory health and care organisations, VCSE organisations and charitable foundations. This was followed by further discussion at the ICS Partnership Board in December 2021 and in addition to ongoing individual conversations and communications since publication of the first draft of the Constitution and its subsequent updates, the consultation culminated in a discussion at the ICS Partnership Board on 13 May 2022, following which this ‘You Said – We Did’ report has been produced outlining the key issues raised and our responses to them. Notwithstanding that the majority of the draft Constitution had to be written in accordance with the NHS England model, the following comments and issues have been received and addressed:
CONSTITUTION REFERENCE
ACUTE, COMMUNITY & MENTAL HEALTH 2.3.3 Naming specific officers in the
observer section might inhibit the ability to be flexible in the future
It is only regular participants which are listed in the Constitution and it is they, who at the discretion of the Chair may ask questions and address the meeting. Observers, who may not address the meeting are not listed and therefore this will not inhibit future flexibility about who may be invited to observe
3.1.1 a) We wonder if including “fit and proper person” test as an eligibility criteria is sufficient. We would
We noted this comment and whilst Regulation 5 is not specifically referred to in the NHS England model
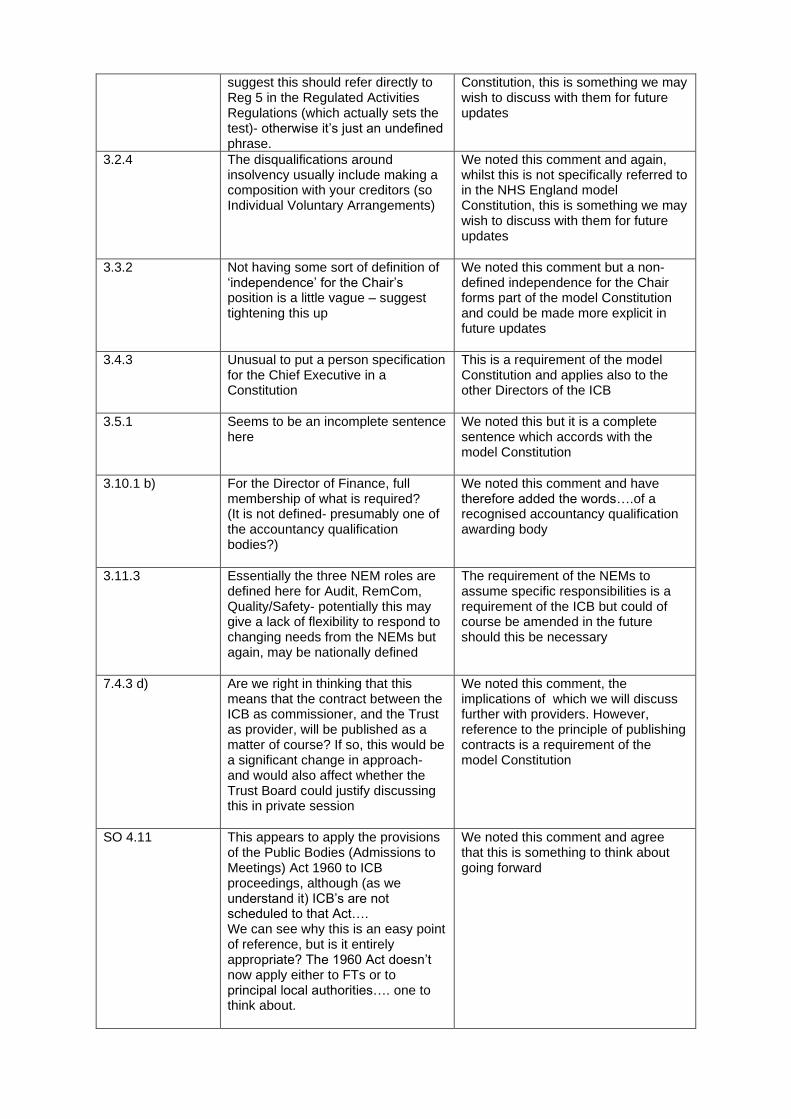
suggest this should refer directly to Reg 5 in the Regulated Activities Regulations (which actually sets the test)- otherwise it’s just an undefined phrase.
Constitution, this is something we may wish to discuss with them for future updates
3.2.4 The disqualifications around insolvency usually include making a composition with your creditors (so Individual Voluntary Arrangements)
We noted this comment and again, whilst this is not specifically referred to in the NHS England model Constitution, this is something we may wish to discuss with them for future updates
3.3.2 Not having some sort of definition of ‘independence’ for the Chair’s position is a little vague – suggest tightening this up
We noted this comment but a non-defined independence for the Chair forms part of the model Constitution and could be made more explicit in future updates
3.4.3 Unusual to put a person specification for the Chief Executive in a Constitution
This is a requirement of the model Constitution and applies also to the other Directors of the ICB
3.5.1 Seems to be an incomplete sentence here
We noted this but it is a complete sentence which accords with the model Constitution
3.10.1 b) For the Director of Finance, full membership of what is required? (It is not defined- presumably one of the accountancy qualification bodies?)
We noted this comment and have therefore added the words….of a recognised accountancy qualification awarding body
3.11.3 Essentially the three NEM roles are defined here for Audit, RemCom, Quality/Safety- potentially this may give a lack of flexibility to respond to changing needs from the NEMs but again, may be nationally defined
The requirement of the NEMs to assume specific responsibilities is a requirement of the ICB but could of course be amended in the future should this be necessary
7.4.3 d) Are we right in thinking that this means that the contract between the ICB as commissioner, and the Trust as provider, will be published as a matter of course? If so, this would be a significant change in approach- and would also affect whether the Trust Board could justify discussing this in private session
We noted this comment, the implications of which we will discuss further with providers. However, reference to the principle of publishing contracts is a requirement of the model Constitution
SO 4.11 This appears to apply the provisions of the Public Bodies (Admissions to Meetings) Act 1960 to ICB proceedings, although (as we understand it) ICB’s are not scheduled to that Act…. We can see why this is an easy point of reference, but is it entirely appropriate? The 1960 Act doesn’t now apply either to FTs or to principal local authorities…. one to think about.
We noted this comment and agree that this is something to think about going forward
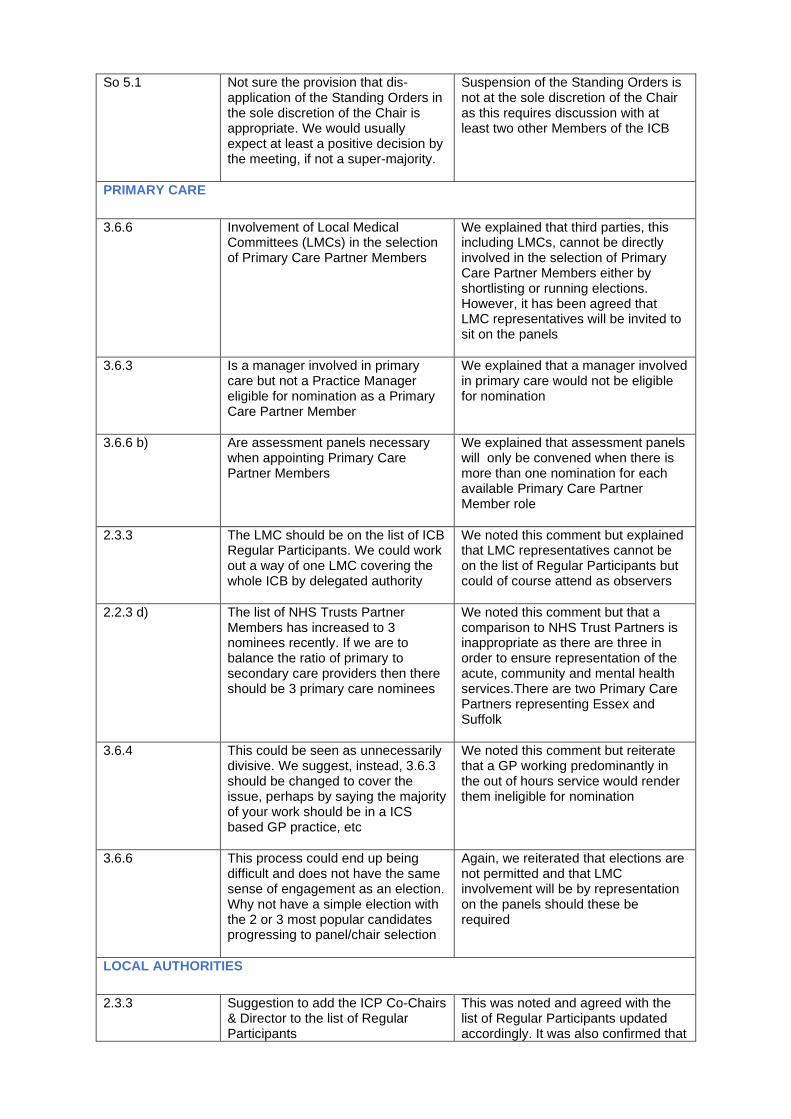
So 5.1 Not sure the provision that dis-application of the Standing Orders in the sole discretion of the Chair is appropriate. We would usually expect at least a positive decision by the meeting, if not a super-majority.
Suspension of the Standing Orders is not at the sole discretion of the Chair as this requires discussion with at least two other Members of the ICB
PRIMARY CARE
3.6.6 Involvement of Local Medical Committees (LMCs) in the selection of Primary Care Partner Members
We explained that third parties, this including LMCs, cannot be directly involved in the selection of Primary Care Partner Members either by shortlisting or running elections. However, it has been agreed that LMC representatives will be invited to sit on the panels
3.6.3 Is a manager involved in primary care but not a Practice Manager eligible for nomination as a Primary Care Partner Member
We explained that a manager involved in primary care would not be eligible for nomination
3.6.6 b) Are assessment panels necessary when appointing Primary Care Partner Members
We explained that assessment panels will only be convened when there is more than one nomination for each available Primary Care Partner Member role
2.3.3 The LMC should be on the list of ICB Regular Participants. We could work out a way of one LMC covering the whole ICB by delegated authority
We noted this comment but explained that LMC representatives cannot be on the list of Regular Participants but could of course attend as observers
2.2.3 d) The list of NHS Trusts Partner Members has increased to 3 nominees recently. If we are to balance the ratio of primary to secondary care providers then there should be 3 primary care nominees
We noted this comment but that a comparison to NHS Trust Partners is inappropriate as there are three in order to ensure representation of the acute, community and mental health services.There are two Primary Care Partners representing Essex and Suffolk
3.6.4 This could be seen as unnecessarily divisive. We suggest, instead, 3.6.3 should be changed to cover the issue, perhaps by saying the majority of your work should be in a ICS based GP practice, etc
We noted this comment but reiterate that a GP working predominantly in the out of hours service would render them ineligible for nomination
3.6.6 This process could end up being difficult and does not have the same sense of engagement as an election. Why not have a simple election with the 2 or 3 most popular candidates progressing to panel/chair selection
Again, we reiterated that elections are not permitted and that LMC involvement will be by representation on the panels should these be required
LOCAL AUTHORITIES
2.3.3 Suggestion to add the ICP Co-Chairs & Director to the list of Regular Participants
This was noted and agreed with the list of Regular Participants updated accordingly. It was also confirmed that
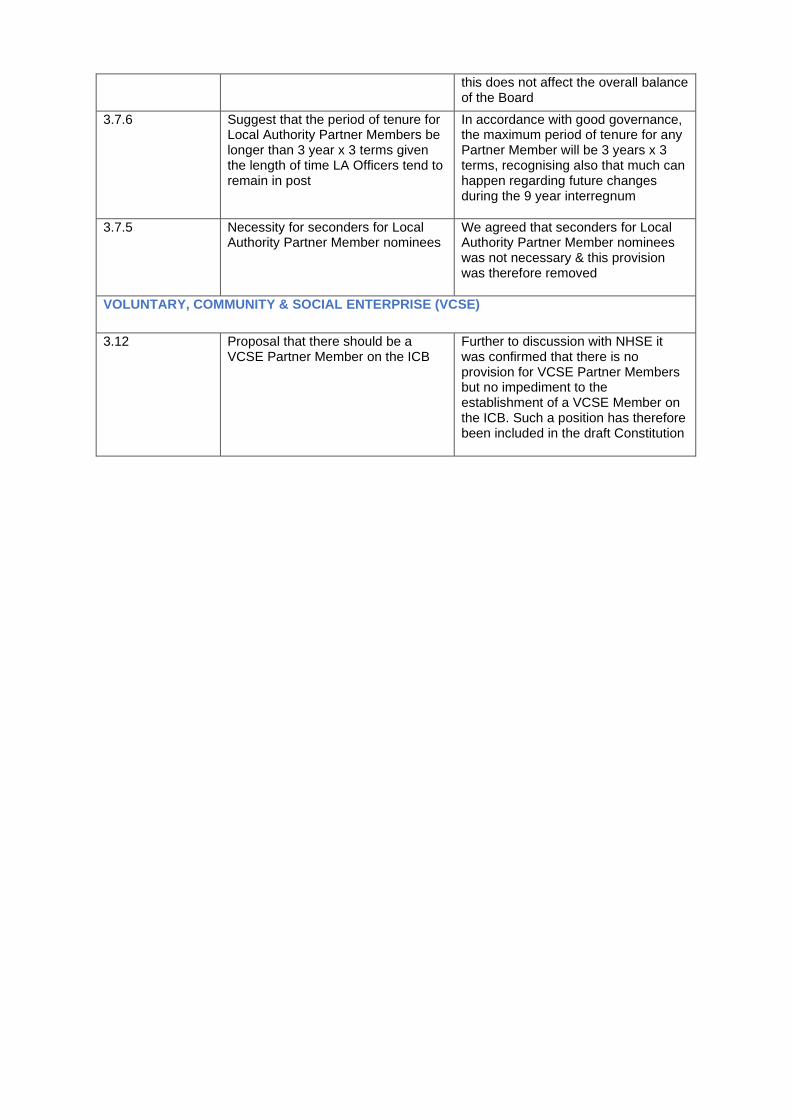
this does not affect the overall balance of the Board
3.7.6 Suggest that the period of tenure for Local Authority Partner Members be longer than 3 year x 3 terms given the length of time LA Officers tend to remain in post
In accordance with good governance, the maximum period of tenure for any Partner Member will be 3 years x 3 terms, recognising also that much can happen regarding future changes during the 9 year interregnum
3.7.5 Necessity for seconders for Local Authority Partner Member nominees
We agreed that seconders for Local Authority Partner Member nominees was not necessary & this provision was therefore removed
VOLUNTARY, COMMUNITY & SOCIAL ENTERPRISE (VCSE)
3.12 Proposal that there should be a VCSE Partner Member on the ICB
Further to discussion with NHSE it was confirmed that there is no provision for VCSE Partner Members but no impediment to the establishment of a VCSE Member on the ICB. Such a position has therefore been included in the draft Constitution

GOVERNING BODY
Agenda Item No. 12
Reference No. NEECCG 22-36
Date. 7 June 2022
Title
Integrated Performance Report
Lead Director
Paul Gibara- Director of Performance Improvement and Martyn Hanlon, Chair of the Finance & Performance Committee
Author(s)
Vicky Sawtell – Deputy Director of Performance & Contracts and Lizzie Amodio- Head of Alliance Development & Outcomes
Purpose
To provide the Governing Body with an update on Constitutional and wider system performance and the actions being taken to mitigate the risks to performance delivery.
Applicable CCG Strategic Objectives:
1. To achieve our vision through an inclusive, holistic approach to patient and service user centred commissioning, embedding personalisation of care through integrated health and social care services.
✓
2. To transform care and drive continuous improvement in quality and safety. Achieve the best possible outcomes for our service users through high quality care.
✓
3. To use commissioning resources effectively and responsibly. To develop our organisation, teams and individual staff to be trusted, competent, well trained, talented, enthusiastic and dedicated.
✓
4 To tackle the biggest health challenges in north east Essex including reducing health inequalities.
Recommendation: The Governing Body is asked to assure itself that the Finance and Performance Committee is satisfied that where performance is not reaching the required standard, the necessary scrutiny and steps are being undertaken with providers to improve performance.
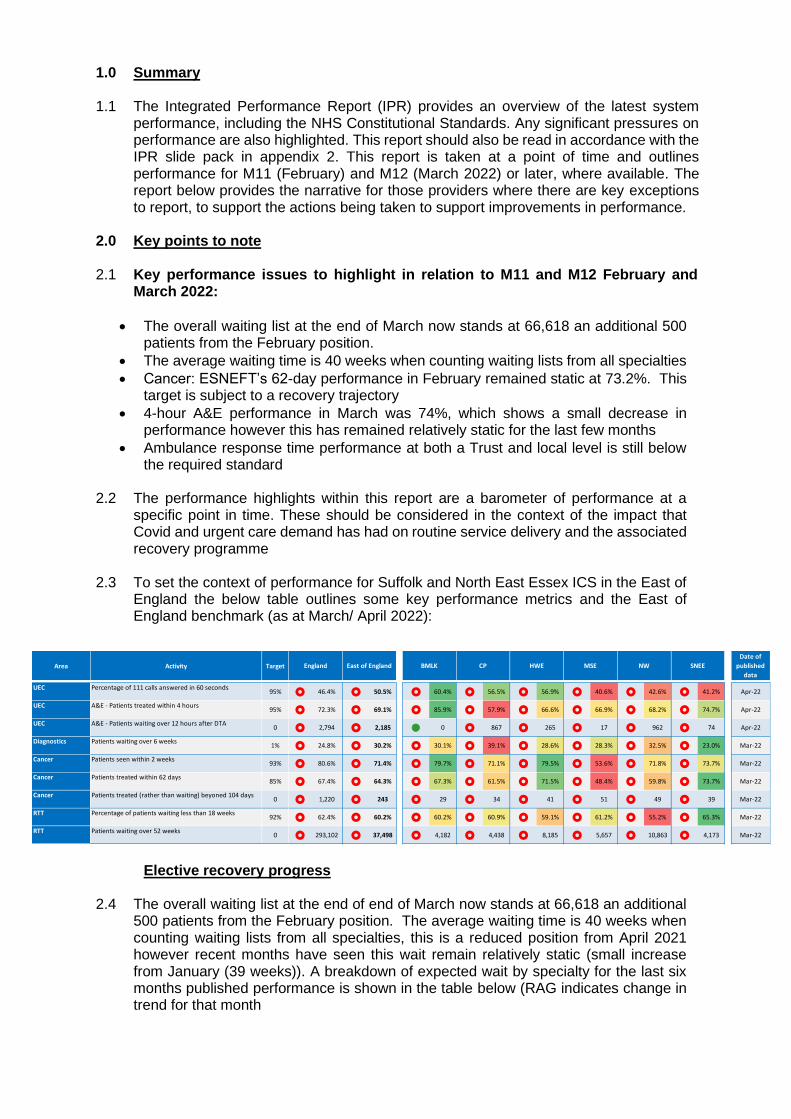
1.0 Summary 1.1 The Integrated Performance Report (IPR) provides an overview of the latest system
performance, including the NHS Constitutional Standards. Any significant pressures on performance are also highlighted. This report should also be read in accordance with the IPR slide pack in appendix 2. This report is taken at a point of time and outlines performance for M11 (February) and M12 (March 2022) or later, where available. The report below provides the narrative for those providers where there are key exceptions to report, to support the actions being taken to support improvements in performance.
2.0 Key points to note 2.1 Key performance issues to highlight in relation to M11 and M12 February and
March 2022:
• The overall waiting list at the end of March now stands at 66,618 an additional 500 patients from the February position.
• The average waiting time is 40 weeks when counting waiting lists from all specialties
• Cancer: ESNEFT’s 62-day performance in February remained static at 73.2%. This target is subject to a recovery trajectory
• 4-hour A&E performance in March was 74%, which shows a small decrease in performance however this has remained relatively static for the last few months
• Ambulance response time performance at both a Trust and local level is still below the required standard
2.2 The performance highlights within this report are a barometer of performance at a
specific point in time. These should be considered in the context of the impact that Covid and urgent care demand has had on routine service delivery and the associated recovery programme
2.3 To set the context of performance for Suffolk and North East Essex ICS in the East of
England the below table outlines some key performance metrics and the East of England benchmark (as at March/ April 2022):
Elective recovery progress
2.4 The overall waiting list at the end of end of March now stands at 66,618 an additional 500 patients from the February position. The average waiting time is 40 weeks when counting waiting lists from all specialties, this is a reduced position from April 2021 however recent months have seen this wait remain relatively static (small increase from January (39 weeks)). A breakdown of expected wait by specialty for the last six months published performance is shown in the table below (RAG indicates change in trend for that month
Area Activity Target
UEC Percentage of 111 calls answered in 60 seconds95% 46.4% 50.5% 60.4% 56.5% 56.9% 40.6% 42.6% 41.2% Apr-22
UEC A&E - Patients treated within 4 hours95% 72.3% 69.1% 85.9% 57.9% 66.6% 66.9% 68.2% 74.7% Apr-22
UEC A&E - Patients waiting over 12 hours after DTA0 2,794 2,185 l 0 867 265 17 962 74 Apr-22
Diagnostics Patients waiting over 6 weeks1% 24.8% 30.2% 30.1% 39.1% 28.6% 28.3% 32.5% 23.0% Mar-22
Cancer Patients seen within 2 weeks93% 80.6% 71.4% 79.7% 71.1% 79.5% 53.6% 71.8% 73.7% Mar-22
Cancer Patients treated within 62 days85% 67.4% 64.3% 67.3% 61.5% 71.5% 48.4% 59.8% 73.7% Mar-22
Cancer Patients treated (rather than waiting) beyoned 104 days0 1,220 243 29 34 41 51 49 39 Mar-22
RTT Percentage of patients waiting less than 18 weeks92% 62.4% 60.2% 60.2% 60.9% 59.1% 61.2% 55.2% 65.3% Mar-22
RTT Patients waiting over 52 weeks0 293,102 37,498 4,182 4,438 8,185 5,657 10,863 4,173 Mar-22
NWEast of England BMLK CP HWE SNEEMSEEngland
Date of
published
data

2.5 ESNEFT saw an increase overall in the number of patients waiting >52weeks from February position of 1938 to March 2097 patients. This is a reduction of approximately 2500 since April 2021. Weekly specialty PTLs run by ESNEFT focus on performance, prioritisation, >52 weeks, >40 weeks, patients awaiting results, open referral number, cases requiring administration action (partial booking, duplicates, patients not on pathway). As mutual aid between the WSFT and ESNEFT increases it is expected that long waiters and overall average wait are going to increase within ESNEFT over coming months
2.6 ESNEFT RTT performance in February against 18ww target was 66% (January also
66%), this has remained relatively static since April however recent months are showing a downward trend in overall performance.
2.7 In recognition of the challenges facing elective treatment the 2022/23 Operational
Planning and Priorities Guidance NHS England’s expectations regarding elective performance recovery is primarily focussed on reducing long waits; recognising that the 18 weeks standard has been severely impacted by the Covid pandemic. Priorities for local systems are as below and have been factored into activity planning assumptions:
• waits of over 104 weeks as a priority and maintain this position through 2022/23 (except where patients choose to wait longer)
• reduce waits of over 78 weeks and conduct three-monthly reviews for this cohort of patients, extending the three-monthly reviews to patients waiting over 52 weeks from 1 July 2022
• develop plans that support an overall reduction in 52-week waits where possible
Cancer Overall performance
2.8 The Trusts performance for February/March has remained consistent in almost every
standard (although March data was still unvalidated at the point of writing this report).
General Surgery 50 weeks 51 weeks 52 weeks 50 weeks 50 weeks 51 weeks
Urology 32 weeks 30 weeks 31 weeks 30 weeks 31 weeks 33 weeks
Trauma & Orthopaedics 46 weeks 45 weeks 45 weeks 44 weeks 43 weeks 44 weeks
Ear, Nose & Throat (ENT) 33 weeks 32 weeks 33 weeks 33 weeks 32 weeks 34 weeks
Ophthalmology 27 weeks 27 weeks 28 weeks 29 weeks 31 weeks 32 weeks
Oral Surgery 31 weeks 31 weeks 32 weeks 32 weeks 30 weeks 28 weeks
Plastic Surgery 22 weeks 24 weeks 24 weeks 27 weeks 30 weeks 32 weeks
General Medicine 18 weeks 19 weeks 21 weeks 23 weeks 24 weeks 25 weeks
Gastroenterology 39 weeks 38 weeks 40 weeks 41 weeks 43 weeks 43 weeks
Cardiology 17 weeks 18 weeks 19 weeks 18 weeks 17 weeks 18 weeks
Dermatology 34 weeks 37 weeks 39 weeks 42 weeks 45 weeks 48 weeks
Thoracic Medicine 38 weeks 39 weeks 39 weeks 37 weeks 35 weeks 32 weeks
Neurology 23 weeks 23 weeks 25 weeks 25 weeks 23 weeks 23 weeks
Rheumatology 33 weeks 26 weeks 26 weeks 27 weeks 21 weeks 22 weeks
Geriatric Medicine 11 weeks 13 weeks 16 weeks 14 weeks 12 weeks 10 weeks
Gynaecology 43 weeks 42 weeks 43 weeks 44 weeks 44 weeks 45 weeks
January
92%ile wait
(weeks)
December
92%ile wait
(weeks)
November
92%ile wait
(weeks)
February
92%ile
wait
(weeks)
March
92%ile
wait
(weeks)
October
92%ile wait
(weeks)
Treatment function

2.9 The February data below shows a further breakdown at specialty level which
demonstrates clearly the more challenged tumour sites. 2ww 28 FDS
2.10 31-day recovery - Whilst a number of breaches are due to complex pathways, many are delayed because other patients have been identified as a higher clinical priority. There has also been a number of delays due to further diagnostics being required as well as administrative delays. These are mainly due to the sheer volume of patients the admin staff have to manage on a daily basis. The Trust plan to recover the standard in Q1, 22-23. 31 day first
2.11 62-day recovery – The Trust’s recovery trajectory, submitted at the end of March,
shows their ambition to recover within Q3 2022/23. This is heavily reliant on a number of factors however and this may well be superseded by changes to national cancer waiting times and the merging of 9 standards into just 3.
Delivery in Q3 assumes
• no further Covid outbreaks that would potentially impact overall trust performance i.e., ED/Patient flow, Inpatient bed capacity, diagnostic capacity, ITU/HDU capacity
• Referral numbers do not continue to increase from current levels
• That clinical work force numbers stay the same or improve
• Staff sickness absence improves
• Tertiary centers recover at the same pace or sooner 62- day first treatment standard

Referrals
2.12 Colorectal and skin referrals remain high, with a decrease in breast, which may be attributed to the new breast pain pathway and GPs thinking about referrals differently now there are 2 pathways in place.
2.13 There has been some increased awareness around colorectal cancer following the
media highlighting the Deborah James blog, which may have influenced patients to see their GP. April was also the national bowel cancer awareness month. There is currently a piece of ongoing work being undertaken reviewing the whole colorectal pathway.
2.14 May is skin awareness month and an increase in referrals is expected following
promotional activities and increased awareness. 2.15 As part of improving early access to cancer services a screening bus is being used.
This was at Ipswich for a month but only received 8-9 referrals. The smaller bus in Clacton has only been on site for a week and there are already 16 referrals. Ipswich had 4 urology referrals and 4 prostate all confirmed cancer.
Diagnostics (Cancer impacts)
2.16 Vacancies are significantly impacting on the Trusts ability to report in timely way.
Currently the Trust are reporting primary cancer pathways within a turnaround times of around75/80% of the time; the impact is what that is doing to RTT (DMO1 figures below).
Organisation Value Sep-21 Oct-21 Nov-21 Dec-21 Jan-22 Feb-22Actual Progress April 2021 to latest
month
2021/22 TargetApril 2021 to March
2022
Actual 5,035 4,650 5,024 3,926 4,378 4,284
Trajectory 4,500 4,865 4,760 4,510 4,457 4,398
Actual 4,951 4,567 4,972 3,854 4,256 4,190
Trajectory 4,620 4,137 4,334 4,137 3,900 3,900
CWT - 2WW Referrals Seen
ICS (Trust-Based) 48,621 49,256
ICS (CCG-Based) 47,630 49,271
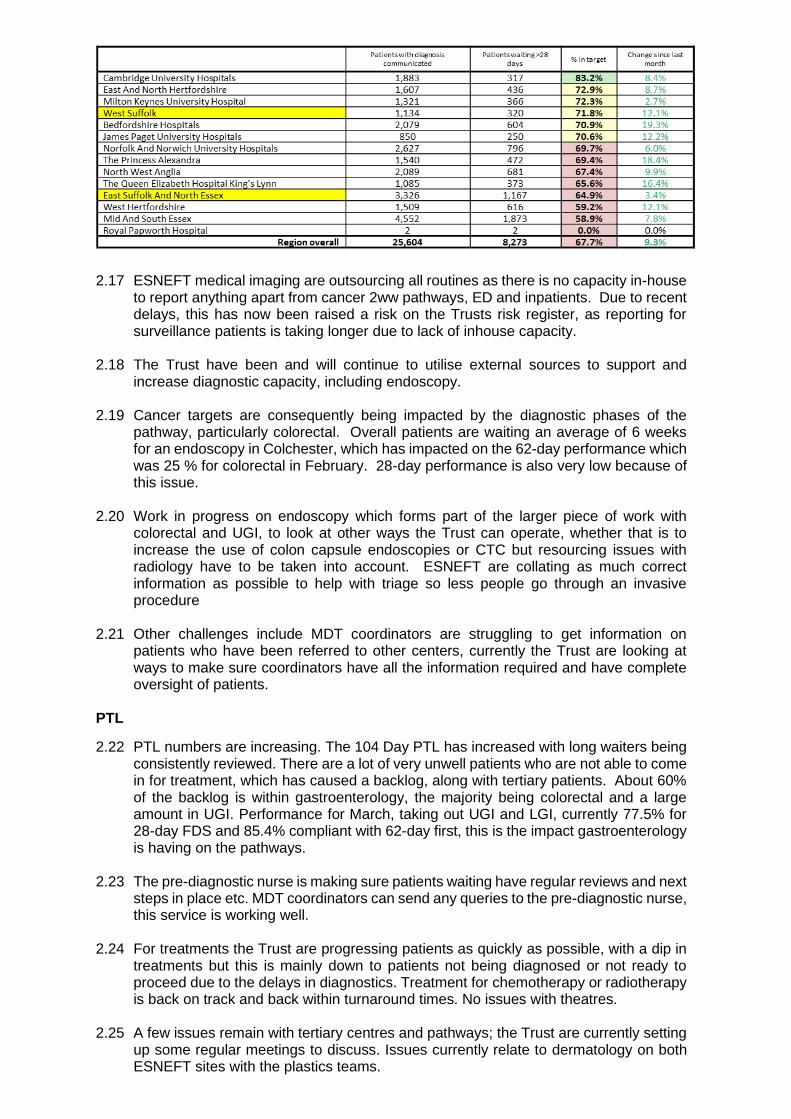
2.17 ESNEFT medical imaging are outsourcing all routines as there is no capacity in-house to report anything apart from cancer 2ww pathways, ED and inpatients. Due to recent delays, this has now been raised a risk on the Trusts risk register, as reporting for surveillance patients is taking longer due to lack of inhouse capacity.
2.18 The Trust have been and will continue to utilise external sources to support and
increase diagnostic capacity, including endoscopy. 2.19 Cancer targets are consequently being impacted by the diagnostic phases of the
pathway, particularly colorectal. Overall patients are waiting an average of 6 weeks for an endoscopy in Colchester, which has impacted on the 62-day performance which was 25 % for colorectal in February. 28-day performance is also very low because of this issue.
2.20 Work in progress on endoscopy which forms part of the larger piece of work with
colorectal and UGI, to look at other ways the Trust can operate, whether that is to increase the use of colon capsule endoscopies or CTC but resourcing issues with radiology have to be taken into account. ESNEFT are collating as much correct information as possible to help with triage so less people go through an invasive procedure
2.21 Other challenges include MDT coordinators are struggling to get information on
patients who have been referred to other centers, currently the Trust are looking at ways to make sure coordinators have all the information required and have complete oversight of patients.
PTL
2.22 PTL numbers are increasing. The 104 Day PTL has increased with long waiters being consistently reviewed. There are a lot of very unwell patients who are not able to come in for treatment, which has caused a backlog, along with tertiary patients. About 60% of the backlog is within gastroenterology, the majority being colorectal and a large amount in UGI. Performance for March, taking out UGI and LGI, currently 77.5% for 28-day FDS and 85.4% compliant with 62-day first, this is the impact gastroenterology is having on the pathways.
2.23 The pre-diagnostic nurse is making sure patients waiting have regular reviews and next steps in place etc. MDT coordinators can send any queries to the pre-diagnostic nurse, this service is working well.
2.24 For treatments the Trust are progressing patients as quickly as possible, with a dip in
treatments but this is mainly down to patients not being diagnosed or not ready to proceed due to the delays in diagnostics. Treatment for chemotherapy or radiotherapy is back on track and back within turnaround times. No issues with theatres.
2.25 A few issues remain with tertiary centres and pathways; the Trust are currently setting
up some regular meetings to discuss. Issues currently relate to dermatology on both ESNEFT sites with the plastics teams.

Diagnostics
2.26 ESNEFT diagnostic activity in March increased to 25,264 completed; this is the highest volume over the last 24 months and above average of just over 20,000 average tests per month of 20,000 between April-June 2021.
2.27 The overall waiting list has also fallen to 12,497 at the end of March from 12,891 patients wating at the end of February. This has also seen the number of patients waiting >10 weeks fall to 898 in March from 1462 in February and 1911 in January. Those waiting >13 weeks also reducing from 724 in January to 598 in February and 370 at the end of March.
2.28 The biggest areas making up the waits over >10weeks remain Endoscopy,
Echocardiology and Ultrasound. MRI has seen a big decrease in waiters supported by mobile facility, those left waiting are not suitable for this resource and so it cannot be used to support all of the backlog. 7 day working consultation has started. CT have also started a 7-day working consultation.
2.29 There are site specific areas of focus with Ipswich site struggling mainly with MRI,
Ultrasound and Echocardiology and Colchester site Endoscopy. 2.30 The previously long patient list within CT has completely disappeared over the last 2
months and is now compliant against standards due to the impact of actions that were put in place 2 months ago. 7 day working and increasing efficiency with shorter appointment times allocation expected to maintain this position now.
2.31 Other actions: -
MRI – MRI mobile scanner in place until June, improved capacity is showing decreasing long waiters. Long term planning includes adopting 7 day working.
Ultrasound – Additional machine in Felixstowe has allowed consultant room to be freed up at the hospital. Current capacity is meeting demand but is keeping position stable currently and not improving.
Endoscopy – Available capacity at community provider is being utilised although further work on maximising this is still ongoing.
A&E
2.32 4-hour A&E performance in March was 74% which shows a small decrease in
performance however this has remained relatively static for the last few months. There has continued to be significant pressures in urgent and emergency care demand over the last few months, which is discussed regularly at system wide meetings to determine options to alleviate this pressure. The East of England region has also experienced severe urgent care pressures in March and April, with the region moving to a Level 4 Incident in early April. Additional schemes in SNEE utilising winter funding remain in place and have been extended where possible.
2.33 Activity through A&E both walk-in and via ambulances remains very high. This continues to have a big impact on the speed of ambulance handovers which have
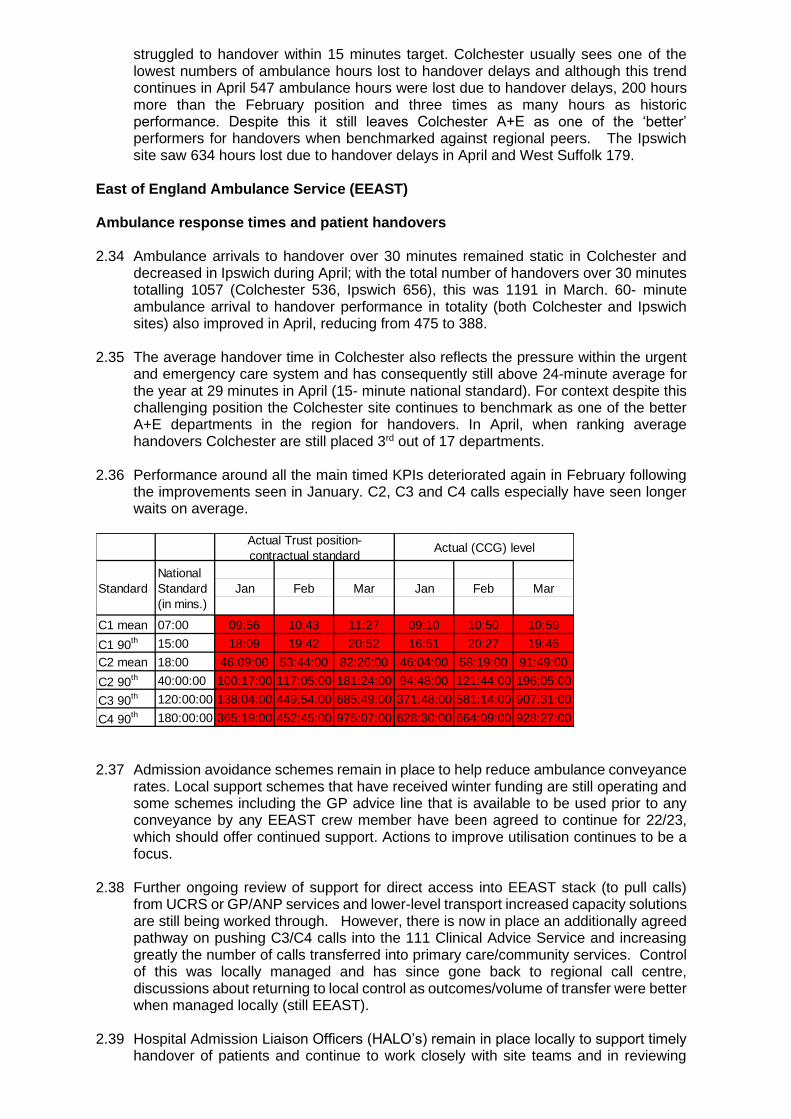
struggled to handover within 15 minutes target. Colchester usually sees one of the lowest numbers of ambulance hours lost to handover delays and although this trend continues in April 547 ambulance hours were lost due to handover delays, 200 hours more than the February position and three times as many hours as historic performance. Despite this it still leaves Colchester A+E as one of the ‘better’ performers for handovers when benchmarked against regional peers. The Ipswich site saw 634 hours lost due to handover delays in April and West Suffolk 179.
East of England Ambulance Service (EEAST) Ambulance response times and patient handovers 2.34 Ambulance arrivals to handover over 30 minutes remained static in Colchester and
decreased in Ipswich during April; with the total number of handovers over 30 minutes totalling 1057 (Colchester 536, Ipswich 656), this was 1191 in March. 60- minute ambulance arrival to handover performance in totality (both Colchester and Ipswich sites) also improved in April, reducing from 475 to 388.
2.35 The average handover time in Colchester also reflects the pressure within the urgent and emergency care system and has consequently still above 24-minute average for the year at 29 minutes in April (15- minute national standard). For context despite this challenging position the Colchester site continues to benchmark as one of the better A+E departments in the region for handovers. In April, when ranking average handovers Colchester are still placed 3rd out of 17 departments.
2.36 Performance around all the main timed KPIs deteriorated again in February following
the improvements seen in January. C2, C3 and C4 calls especially have seen longer waits on average.
2.37 Admission avoidance schemes remain in place to help reduce ambulance conveyance
rates. Local support schemes that have received winter funding are still operating and some schemes including the GP advice line that is available to be used prior to any conveyance by any EEAST crew member have been agreed to continue for 22/23, which should offer continued support. Actions to improve utilisation continues to be a focus.
2.38 Further ongoing review of support for direct access into EEAST stack (to pull calls) from UCRS or GP/ANP services and lower-level transport increased capacity solutions are still being worked through. However, there is now in place an additionally agreed pathway on pushing C3/C4 calls into the 111 Clinical Advice Service and increasing greatly the number of calls transferred into primary care/community services. Control of this was locally managed and has since gone back to regional call centre, discussions about returning to local control as outcomes/volume of transfer were better when managed locally (still EEAST).
2.39 Hospital Admission Liaison Officers (HALO’s) remain in place locally to support timely
handover of patients and continue to work closely with site teams and in reviewing
Jan Feb Mar Jan Feb Mar
C1 mean 07:00 09:56 10:43 11:27 09:10 10:50 10:59
C1 90th 15:00 18:09 19:42 20:52 16:51 20:27 19:46
C2 mean 18:00 46:09:00 53:44:00 82:26:00 46:04:00 58:19:00 91:49:00
C2 90th 40:00:00 100:17:00 117:05:00 181:24:00 94:48:00 121:44:00 196:05:00
C3 90th 120:00:00 138:04:00 449:54:00 685:49:00 371:48:00 581:14:00 907:31:00
C4 90th 180:00:00 365:19:00 452:45:00 975:07:00 628:30:00 664:09:00 928:27:00
Actual Trust position-
contractual standardActual (CCG) level
Standard
National
Standard
(in mins.)

whether the admissions are appropriate. It has now been agreed that HALO will form part of the EEAST core contract moving forward and be a recurrent investment.
EEAST- Non-urgent Patient Transport (PTS)
2.40 In recent months PTS has seen some of the highest number of journeys undertaken during March since June last year which has impacted upon performance for some KPIs, though the overall number of journeys fell slightly in the month of April. The total number of journeys in April (5816) decreased from March (6278). EEAST is continuing to utilise additional PAS vehicles, private taxis, to manage activity where necessary. The number of cancelled journeys for the month of April was 772, down from 863 in March though still above the 12% threshold at 13%. This was discussed at QCPM as to what this would look like if exceptions were included and EEAST agreed to review i.e. outpatient appointment cancellations by ESNEFT, booking errors and EEAST capacity due to staff sickness. Assurance has been provided from EEAST that there was no impact to patient safety as any cancellations were clinically assessed. This continues to be monitored monthly via the QCPM.
2.41 Due to increasing pressures in the month of March and April, EEAST requested that the Contract revert to Essential services only for the month of April. Discussions were had around what other services should remain and conversations took place to ensure all resources had been exhausted and mutual aid options were discussed. In light of the imminent IPC guidance changes EEAST felt they were able to manage their journeys without reverting to essential services only and this continues to be monitored. In view of these ongoing pressures at the time of the diarised QCPM it was agreed by all parties that the April QCPM would be stood down and any imminent risks or concerns were agreed to be discussed as they occurred. The IPC guidance has now been released which confirms social distancing measures can be relaxed.
2.42 Collection time – Same Day A&E Post Treats – it is noted that despite previously seen
improved performance that March has seen a deterioration in April to 85%, short of the 90% target. This may have been due to the impact of both TCOs having COVID and will continue to be monitored through the QCPM meetings.
2.43 Collection time – Same Day Renal KPI performance remains compliant at 92% for the
month of April. 2.44 Arrival time at hospital (Same Day) Renal - performance has deteriorated despite
some improvement during January and February and continues to be an of concern, despite improved communication between PTS staff and the renal unit colleagues. EEAST have refreshed patient communication leaflets and posters to inform patients of the importance of being “ready” on time as some factors influencing compliance remain out of EEASTs control. EEAST and ESNEFT colleagues continue to plan and manage any potential service changes efficiently so that any impacts within their control are proactively managed. Year to date performance at the end of the reporting year was at 63% and month of April was at 53%, this continues to be monitored.
2.45 Collection time at hospital (ALL) – Compliance is met this month at 91%. This KPI is
split into 3 separate elements to enable analysis and to determine where performance is causing areas of concern. Discharge collection times deteriorated further to 75% in the month of April, compared with March at 82%. This is an area which is continuously monitored and discussed within the QCPM to resolve.
2.46 Arrival time at hospital same day bookings has been an area of recent concern due to
patients providing insufficient notice to PTS staff to enable the planning and co-ordination of same day journey requests to be met. There is no cut off time for a patient being able to request a journey to their appointment with PTS always doing what they can to accommodate these short notice requests. Performance continues to be reviewed and discussed each month with the provider and it is recognised that some issues continue to remain outside of EEAST’s control i.e. traffic delays and delays at

patient’s/nursing home. However notably in the month of May performance against this target increased to 88% which meant they achieved compliance, the first month since December 2021.
Practice Plus Group - Integrated Urgent Care (111 & OOH)
2.47 PPG reported that February was again a challenging month with staff
absence/isolation. There continued to be high demand and challenged rota fill across all areas of IUC. This reflects both the experience of all SNEE System Partners and the national picture for 111. PPG report Demand profile continues to reflect significant increase in low acuity daytime activity and cases presented from failed access to GP in-hour services.
2.48 111 locally is doing comparable to Regional and National services, with the average time to answer in February of 356 seconds, this is against a KPI of 20 seconds, however this is still considered good, with the National service having average waits of 396 seconds. Clinical response times for Practice Plus Group are also some of the best in the region and well above the current national level. The local call abandonment rate increased significantly to 10.4% this is against a national picture of 16.8% In support of the wider system requests of us, PPG have put over 200 staff through a 4-hour Probing workshop, which is aimed to refresh their skills and assist in reducing Ambulance dispatch rates. Initial information on this training has shown a circa 10% drop in Cat 2 ambulance out of the overall ambulance sent, but an increase in Cat 3, however this will support the ambulance service getting to Cat 2 ambulance faster.
2.49 The service has also seen a 2.3% drop-in ED rates in two months, this is a result of
validation and less severity patients calling 111. 2.50 There have been over 1,000 consultations using the GoodSam (A video consultation
service) and it has been reported that there have been a number of excellent outcomes where the patient management has been changed as a direct result. An evaluation report is being produced.
2.51 Towards the end of 2022 the CCG’s will no longer be measuring KPI’s relating to 111
Health Advisors. NHE England have directed that all regions should move towards a regionalised operational model, which from an IT perspective has technically been implemented. The full model of the SVCC and agreement on how it will work needs to be agreed by 1st October 2022. The model directed has a single commissioner taking responsibility for the ‘front end’ of the Integrated Urgent Care Services and this is likely to be Herts and West Essex.
2.52 NHS England are also working with all providers and commissioners across the East
of England to implement EEAST C3/C4/C5 stack reviews. This will involve cases being shared between 999 and the IUC Clinical Assessment Service and is aiming to go live in April 2022 however this has been delayed due to operational pressures in EEAST.
2.53 The IUC Support continues to be delivered to EEAST to reduce conveyances. Which
include a Dedicated support line for On Scene Crews with a 10-minute call back target, the transfer of low acuity cases from Control Room to CAS and Twice daily reviews of ‘Stack’
2.54 Rota fill across all IUC Services is an ongoing challenge, reasons for this are variable
and include: IR35, which continues to impact the CAS and OOH rotas for SEMP GPs. The Central Recruitment and Local Teams continue to focus on the attraction of Clinicians for these Services including a current drive for GP Registrars completing their training.
2.55 The number of ambulance and ED validations decreased this month with the service
able to validate 1384 Category 3&4 Ambulances in 111 with 74% being downgraded along with 2342 ED outcomes calls of which 50% were downgraded.

2.56 There remain some challenges with home visits within 2 hours which have been affected by Covid 19. All patients with COVID-19 symptoms are triaged by a clinician before being requested to come into base or a home visit is arranged. This means that patients require 2 contact points within this disposition timeframe to allow the NQR target to be met.
Quality Standards Target Jan Feb Mar
% urgents consulted within 2 hours 95% 87% 95% 90%
% routines consulted within 6 hours 95% 98% 99% 91%
% routines consulted within 12 hours 95% 99% 100% 98%
% routines consulted within 24 hours 95% 100% 100% 100%
% urgents visited within 2 hours 95% 75% 86% 69%
% urgents visited within 6 hours 95% 83% 92% 79%
% urgents visited within 12 hours 95% 100% 89% 100%
% urgents visited within 24 hours 95% 100% 100% 100%
% Home visiting 37% 32% 39%
2.57 For the 2-hour home visits, if the time was taken from the clinical triaged, then
performance would be 91% rather than the 69% shown and for 6-hour home visits, performance would be 93% rather than the 79% shown.
Urgent Treatment Service (UTS) 2.58 April attendance levels reduced following March’s peak, with 7,662 patients using the
service. This is still below the expected ‘normal’ activity levels overall however the service has had high staff sickness rates which has caused additional challenges in meeting demand.
2.59 The 4 hour wait target has been consistently met across all sites all year and was met at 98.80% in April.
2.60 Walk-ins clinically assessed within 15 minutes is consistently above 98% in Colchester,
Clacton performance continued to not achieve the target, but did see an improvement in April achieving 93.23% bringing overall performance to 97.23%. Clacton site have continued to see a high demand of patients during April.
2.61 The 98% target for walk-in patients to be seen within 2 hours of arrival declined in April
(achieving 90.56%) and remains below target, which has not been met since April 2021. Colchester site continues to share 30% of their space with ED overflow patients, which impacts on efficiency, but has improved working relationships between ED and UTS staff. Work is ongoing to separate the space however until Covid requirements reduce this will continue to be a challenge.
2.62 Further work to evaluate the UTS model at all sites is planned as part of the service
development plan, to ensure the service develops to meet changing patient and system needs. Members from the collaborative met this month to commence this work.
NICS Collaborative (Community Services)
2.63 Focus on all services recovering longer waits following Covid delays remains a priority
for community services. ESNEFT have confirmed there are considerable waits within the services after the data cleanse, however they have stated that there are still some services that required some manual cleansing to ensure they are correct, this will include some administration as to how the data is recorded within SystemOne. Waits continue to be high within children’s therapies, podiatry and pulmonary rehab. Some long waits have been identified within the GP 24-hour tape service and this is currently being investigated by the team and further information will be supplied.
2.64 In relation to the recovery of community services, particular focus has been provided on children’s therapy services. Regular reporting on paediatric therapy waiting times is now being shared and discussions on supporting ESNEFT with specific recovery
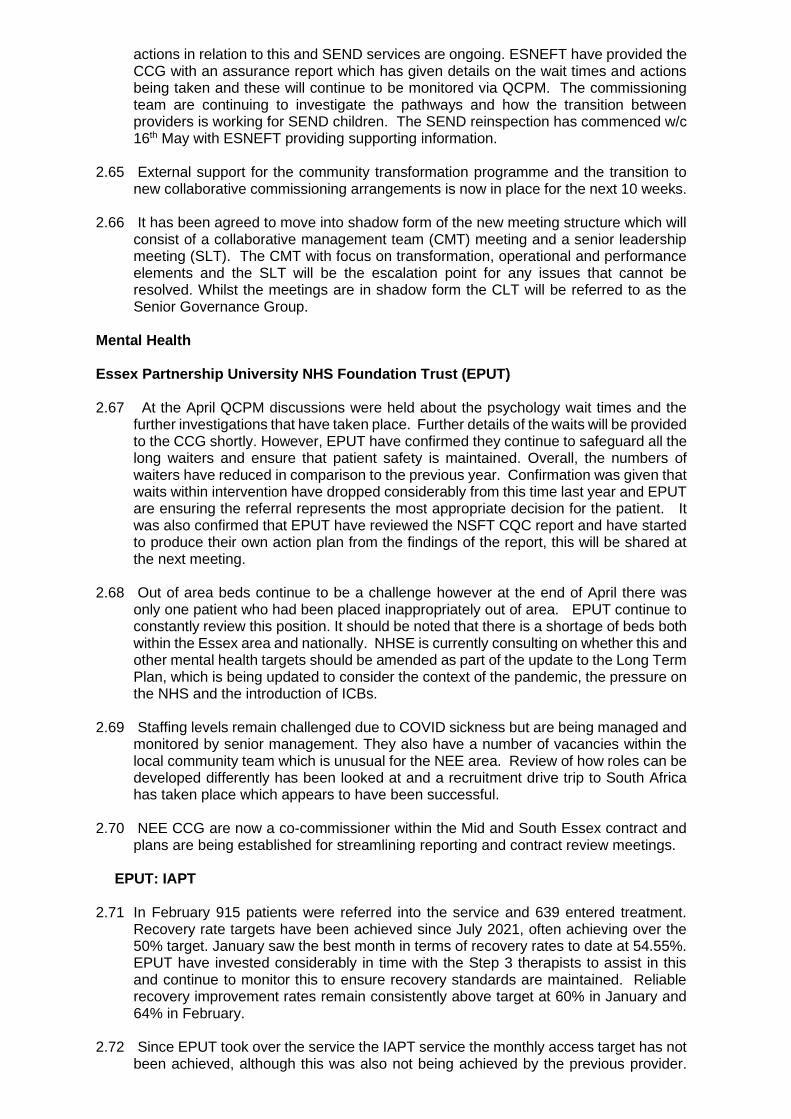
actions in relation to this and SEND services are ongoing. ESNEFT have provided the CCG with an assurance report which has given details on the wait times and actions being taken and these will continue to be monitored via QCPM. The commissioning team are continuing to investigate the pathways and how the transition between providers is working for SEND children. The SEND reinspection has commenced w/c 16th May with ESNEFT providing supporting information.
2.65 External support for the community transformation programme and the transition to
new collaborative commissioning arrangements is now in place for the next 10 weeks. 2.66 It has been agreed to move into shadow form of the new meeting structure which will
consist of a collaborative management team (CMT) meeting and a senior leadership meeting (SLT). The CMT with focus on transformation, operational and performance elements and the SLT will be the escalation point for any issues that cannot be resolved. Whilst the meetings are in shadow form the CLT will be referred to as the Senior Governance Group.
Mental Health Essex Partnership University NHS Foundation Trust (EPUT)
2.67 At the April QCPM discussions were held about the psychology wait times and the
further investigations that have taken place. Further details of the waits will be provided to the CCG shortly. However, EPUT have confirmed they continue to safeguard all the long waiters and ensure that patient safety is maintained. Overall, the numbers of waiters have reduced in comparison to the previous year. Confirmation was given that waits within intervention have dropped considerably from this time last year and EPUT are ensuring the referral represents the most appropriate decision for the patient. It was also confirmed that EPUT have reviewed the NSFT CQC report and have started to produce their own action plan from the findings of the report, this will be shared at the next meeting.
2.68 Out of area beds continue to be a challenge however at the end of April there was only one patient who had been placed inappropriately out of area. EPUT continue to constantly review this position. It should be noted that there is a shortage of beds both within the Essex area and nationally. NHSE is currently consulting on whether this and other mental health targets should be amended as part of the update to the Long Term Plan, which is being updated to consider the context of the pandemic, the pressure on the NHS and the introduction of ICBs.
2.69 Staffing levels remain challenged due to COVID sickness but are being managed and
monitored by senior management. They also have a number of vacancies within the local community team which is unusual for the NEE area. Review of how roles can be developed differently has been looked at and a recruitment drive trip to South Africa has taken place which appears to have been successful.
2.70 NEE CCG are now a co-commissioner within the Mid and South Essex contract and
plans are being established for streamlining reporting and contract review meetings.
EPUT: IAPT
2.71 In February 915 patients were referred into the service and 639 entered treatment. Recovery rate targets have been achieved since July 2021, often achieving over the 50% target. January saw the best month in terms of recovery rates to date at 54.55%. EPUT have invested considerably in time with the Step 3 therapists to assist in this and continue to monitor this to ensure recovery standards are maintained. Reliable recovery improvement rates remain consistently above target at 60% in January and 64% in February.
2.72 Since EPUT took over the service the IAPT service the monthly access target has not been achieved, although this was also not being achieved by the previous provider.
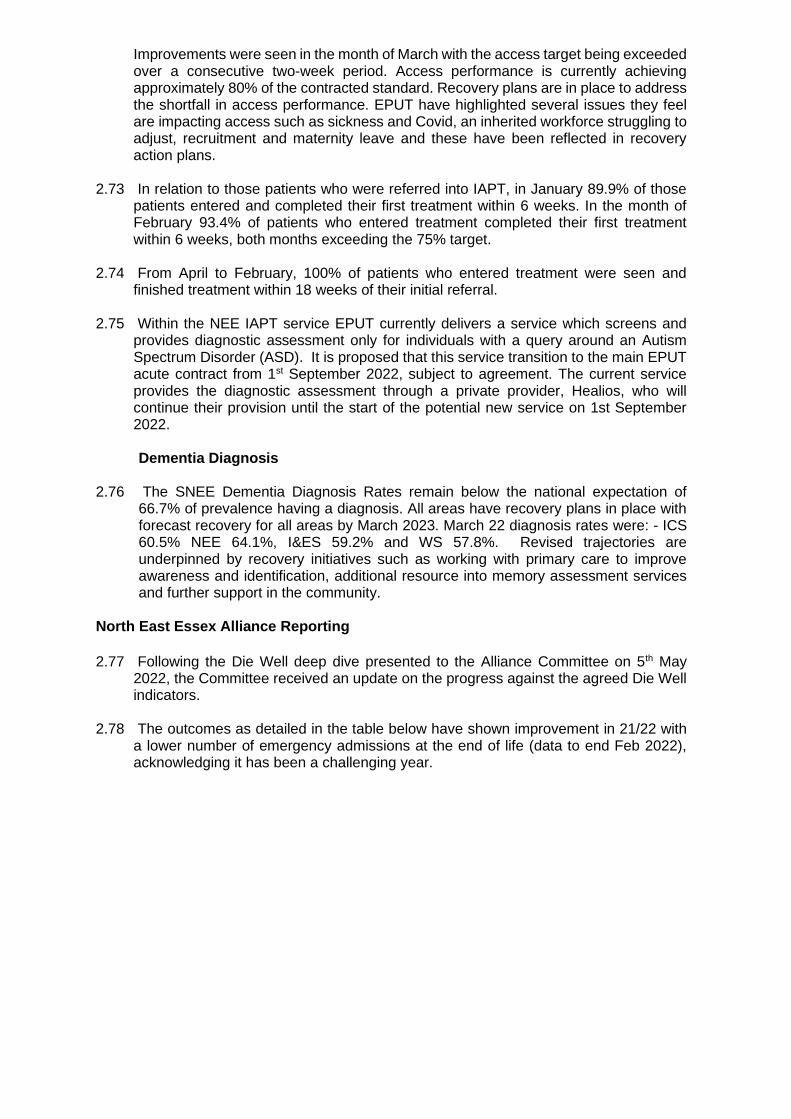
Improvements were seen in the month of March with the access target being exceeded over a consecutive two-week period. Access performance is currently achieving approximately 80% of the contracted standard. Recovery plans are in place to address the shortfall in access performance. EPUT have highlighted several issues they feel are impacting access such as sickness and Covid, an inherited workforce struggling to adjust, recruitment and maternity leave and these have been reflected in recovery action plans.
2.73 In relation to those patients who were referred into IAPT, in January 89.9% of those
patients entered and completed their first treatment within 6 weeks. In the month of February 93.4% of patients who entered treatment completed their first treatment within 6 weeks, both months exceeding the 75% target.
2.74 From April to February, 100% of patients who entered treatment were seen and
finished treatment within 18 weeks of their initial referral. 2.75 Within the NEE IAPT service EPUT currently delivers a service which screens and
provides diagnostic assessment only for individuals with a query around an Autism Spectrum Disorder (ASD). It is proposed that this service transition to the main EPUT acute contract from 1st September 2022, subject to agreement. The current service provides the diagnostic assessment through a private provider, Healios, who will continue their provision until the start of the potential new service on 1st September 2022. Dementia Diagnosis
2.76 The SNEE Dementia Diagnosis Rates remain below the national expectation of 66.7% of prevalence having a diagnosis. All areas have recovery plans in place with forecast recovery for all areas by March 2023. March 22 diagnosis rates were: - ICS 60.5% NEE 64.1%, I&ES 59.2% and WS 57.8%. Revised trajectories are underpinned by recovery initiatives such as working with primary care to improve awareness and identification, additional resource into memory assessment services and further support in the community.
North East Essex Alliance Reporting
2.77 Following the Die Well deep dive presented to the Alliance Committee on 5th May
2022, the Committee received an update on the progress against the agreed Die Well indicators.
2.78 The outcomes as detailed in the table below have shown improvement in 21/22 with a lower number of emergency admissions at the end of life (data to end Feb 2022), acknowledging it has been a challenging year.
2.79 It should also be noted that ethnicity data now flows into the dashboard and initial results suggest no inequalities in end-of-life outcomes.
From 21/22 plan We said we would Position
Deliver access to care homes for MCCR
Partially achieved – impacted by NHS Toolkit requirement
Teach social prescribers on MCCT
Completed
Continue the primary care network community palliative care teams
Business as Usual
Support EPUT dementia wards to accredit in gold standard framework (GSF).
Completed
Recruit primary care network end of life champions
Seven recruited
Relaunch GSF training in care homes
Two cycles completed
Recruit three new palliative care roles
One started, two others recruited.
Development of the domain reporting dashboard
2.80 As updated to the Board within the last Alliance reporting update, the Die Well domain
is currently the only domain where we have an established dashboard

2.81 Recruitment within the business intelligence team has now concluded, with those leads attending the domain leads meeting on 12/05/22 to discuss outlines plans to create dashboards across all the domains.
2.82 All domain leads have been assigned the task to review their current list of indicators
with their steering groups and confirm these remain the correct list of indicators in order to inform the developing plans. Further detail on the developing dashboard schedule will be provided to the Board within the next report.
3 Risks Identified
3.1 The main risk to the delivery of Constitutional targets remains the residual impact of
COVID-19 and urgent care demand system pressures. Covid impacts both staff sickness and the operational delivery of services. The risk to patients is the increased waiting times for elective procedures and the absence of staff due to Covid infection or isolation. Infection Control (IPC) guidance has recently been updated by NHS England however and following local risk assessment may provide greater flexibility to providers.
3.2 The formal recovery plans from the major acute trusts in the ICS continue to be monitored by the Elective Recovery Groups.
3.3 The associated areas of the CCG Risk Register that correspond with the risks to
Constitution are CCG 006-009.
4 Resource implications
4.1 Performance recovery for elective services and the Constitutional Standards is part of the COVID 19 elective recovery programme and plans and these require oversight from several teams across the ICS organisations and not just the CCG, including performance improvement, transformation, and quality teams.
5 Engagement and Communication
5.1 No additional actions for engagement and communication this month.
6 Equality and Diversity
6.1 No additional impact on equality and diversity because of the content of this paper.

Appendix 1 Constitutional and other key performance standards – M11 and M12 February and March 2022

1
NEECCG Performance Pack May 2022
*** Please note all slides in this pack show data for March M12 unless otherwise stated ***

2
Contents (Ctrl + Click on Heading to follow the link)
• Elective Care, RTT & Diagnostics
• Urgent Emergency Care
• Cancer
• COVID Vaccination
• CYP & Mental Health
• Quality
• Transformation
• CCG Finance

Elective Care RTT & Diagnostics
Elective Care (March 2022)ContextMarch was a productive month in our hospitals and independent sector partners. Significant activity was undertaken and our longest waiter numbers reduced. WSFT had access to additional theatres and were able to increase the numbers of patients treated in this month.
System workingESNEFT supported WSFT by providing support in the form of enabling orthopaedic and gynaecology patients to transfer and receive their care earlier.
Independent SectorOur independent sector partners have continued to support our elective recovery by providing additional capacity to the system.
Waiting timesAs detailed on the following pages overall waiting times were relatively stable, but the number of patients waiting longer than 2 years for treatment fell. In April, we have seen further reductions in the very long waiters and aim to have eliminated all 2 year waiters by July 2022.
With the exception of CT waits at ESNEFT diagnostic waiting times were either stable or grew in March and we are seeking to source additional capacity to address this issue.
Outpatient TransformationBoth Trusts continue to focus on the following initiatives:• Advice and Guidance is being made more available to GPs and
patients who wish to discuss care with a consultant and may not need to come to hospital for an appointment
• Patient Initiated Follow Ups (PIFU): where clinically appropriate, patients are being offered the opportunity to have a patient initiated follow up such that they only need come back into the hospital if they are worried or are experiencing symptoms that have been discussed with the team on discharge from the hospital
• Virtual consultations: where clinically appropriate, patients are being offered telephone or video consultations as an alternative to them having to attend the hospital.
Other transformationOur trusts are focussing on the following initiatives to increase productivity:• Theatre productivity: reviews are taking place to understand the
potential for increasing theatre throughput• High Volume, Low Complexity (HVLC) pathways: reviews of routine
elective pathways are ongoing to identify and realise greater efficiencies
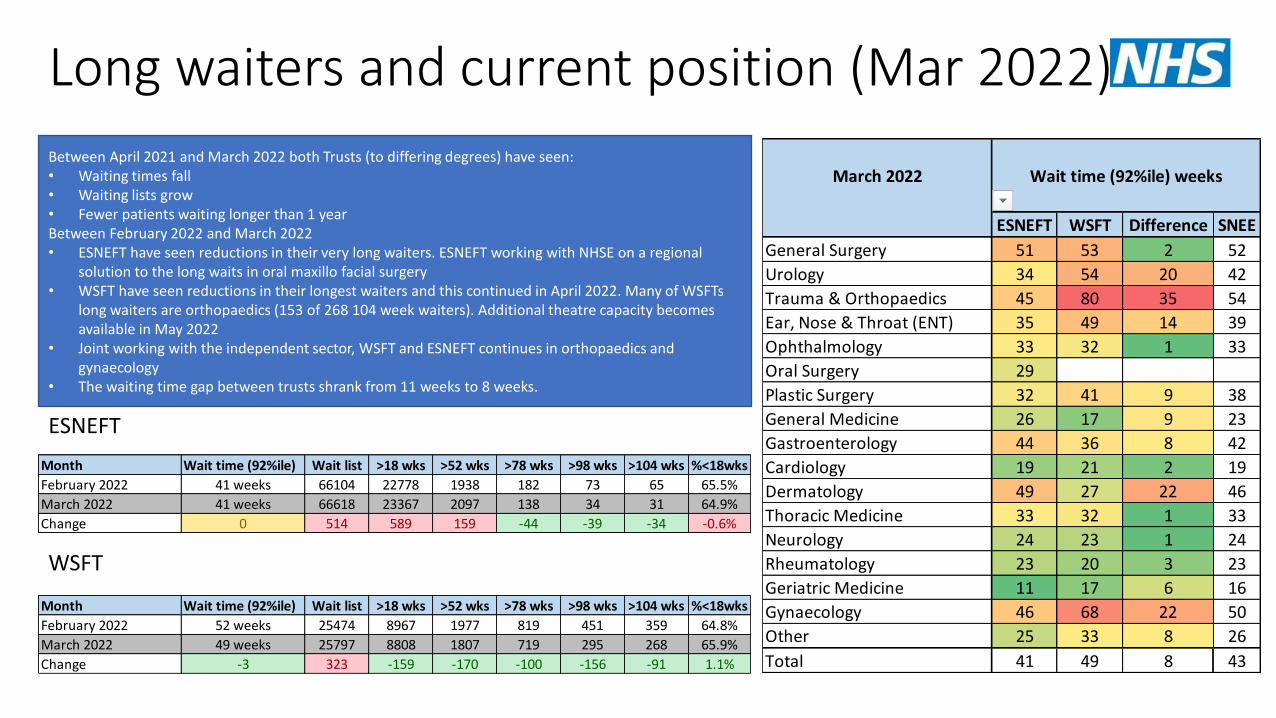
Long waiters and current position (Mar 2022)
ESNEFT
WSFT
Between April 2021 and March 2022 both Trusts (to differing degrees) have seen:• Waiting times fall• Waiting lists grow• Fewer patients waiting longer than 1 yearBetween February 2022 and March 2022• ESNEFT have seen reductions in their very long waiters. ESNEFT working with NHSE on a regional
solution to the long waits in oral maxillo facial surgery• WSFT have seen reductions in their longest waiters and this continued in April 2022. Many of WSFTs
long waiters are orthopaedics (153 of 268 104 week waiters). Additional theatre capacity becomes available in May 2022
• Joint working with the independent sector, WSFT and ESNEFT continues in orthopaedics and gynaecology
• The waiting time gap between trusts shrank from 11 weeks to 8 weeks.
Month Wait time (92%ile) Wait list >18 wks >52 wks >78 wks >98 wks >104 wks %<18wks
February 2022 41 weeks 66104 22778 1938 182 73 65 65.5%
March 2022 41 weeks 66618 23367 2097 138 34 31 64.9%
Change 0 514 589 159 -44 -39 -34 -0.6%
Month Wait time (92%ile) Wait list >18 wks >52 wks >78 wks >98 wks >104 wks %<18wks
February 2022 52 weeks 25474 8967 1977 819 451 359 64.8%
March 2022 49 weeks 25797 8808 1807 719 295 268 65.9%
Change -3 323 -159 -170 -100 -156 -91 1.1%
March 2022
ESNEFT WSFT Difference SNEE
General Surgery 51 53 2 52
Urology 34 54 20 42
Trauma & Orthopaedics 45 80 35 54
Ear, Nose & Throat (ENT) 35 49 14 39
Ophthalmology 33 32 1 33
Oral Surgery 29
Plastic Surgery 32 41 9 38
General Medicine 26 17 9 23
Gastroenterology 44 36 8 42
Cardiology 19 21 2 19
Dermatology 49 27 22 46
Thoracic Medicine 33 32 1 33
Neurology 24 23 1 24
Rheumatology 23 20 3 23
Geriatric Medicine 11 17 6 16
Gynaecology 46 68 22 50
Other 25 33 8 26
Total 41 49 8 43
Wait time (92%ile) weeks

Diagnostics update (Mar 2022 - validated)ESNEFT: Demand growth has been an issue in most areas – specifically the growth in cancer demand and sub specialisation. Additional capacity is being explored and sourced. An IST review of capacity and demand has taken place – actions are being planned which will increase capacity. Significant progress was made in CT and MRI in February.
WSFT: Waits grew in most areas this month. A recovery plan is in place for ultrasound. Additional capacity for endoscopy is being explored.
Modality ESNEFT WSFT
Waiting time99%ile
WL Trend Narrative Waiting time99%ile
WL Trend Narrative
MRI 13+ weeks (-) Falling Activity increased 11 weeks (-) Stable Activity increased
CT 6 weeks (-1) Stable Activity stable 12 weeks (+4) Growing Activity stable
Non obs ultrasound 13+ weeks (-) Stable Activity stable 13+ weeks (-) Falling Activity stable
Echocardiography 13+ weeks (-) Growing Activity stable 8 weeks (-) Growing Activity fell
Colonoscopy 13+ weeks (-) Stable Activity stable 13+ weeks (-) Growing Activity stable
Flexible Sigmoidoscopy 13+ weeks (-) Stable Activity stable 13+ weeks (-) Growing Activity stable
Cystoscopy 13 weeks (+1) Stable Activity stable 13+ weeks (-) Stable Activity stable
Gastroscopy 13+ weeks (-) Stable Activity stable 13+ weeks (-) Growing Activity stable

Urgent Emergency Care
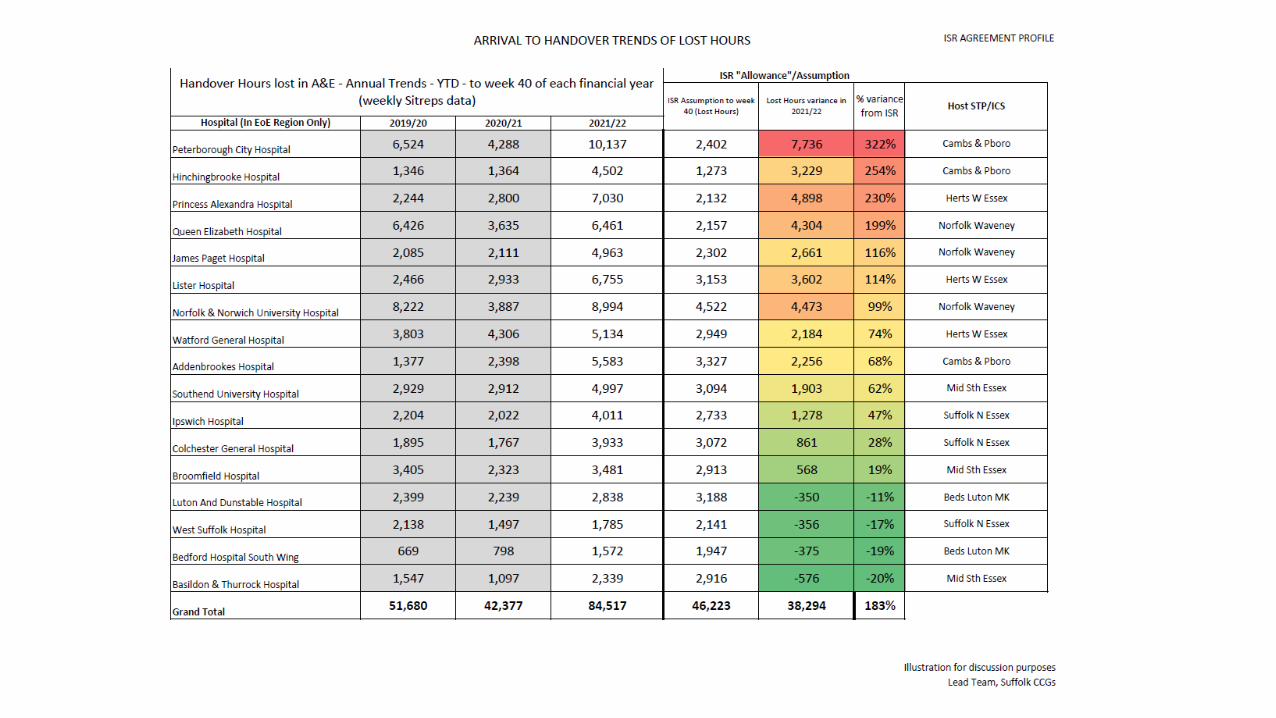

Urgent and emergency care summary
• The National Incident Level remains at Level 4 and the SNEE Command, Control and Coordination structures continue to support 0800-1800 seven days a week.
• Our Operating Pressure Escalation Level (OPEL) reduced to OPEL 3 on the 8th April and this has further reduced to OPEL 2 on the 28th April (we are one of a handful of systems nationally at this stable level). EEAST remain at REAP level 4, although we have seen more frequent de-escalation of Surge levels during the end of April/ beginning of May.
• Workforce absence has improved across all providers with the Acute sites now showing 27.8% of sickness Covid related which is reduced from 44.8% mid April.
• Covid patients occupying hospital beds has also reduced to 158 patients as of 4/5/22. Overall occupancy in hospitals remains high (>95%).
• ED 4 hour performance at ESNEFT has continued to be below national standards, but generally one of the highest in the EoE region. We have seen a slight improvement over April. WSFT average journey time for April was 278 minutes.
• Discharges have continued to be challenging, partly because of care availability (impacted by workforce and holidays – both of which are improving) and differences in national guidance on Covid for health and care. This is also now improving with teams supporting to improve understanding and confidence across the care sector. Pathway 2 (Carehome) patients with no criteria to reside remain high in Ipswich & east.
Overall, the system continues to be challenged due to high demand at ED, impacts of bank holidays on flow and recovery activities. The focus for the system remains on flow, reducing occupancy and planning for the Jubilee weekend.
▪ EEAST activity reduced on 20/21 levels, achieving required patient facing staff hours on day to day basis remains the focus and issue.
▪ Performance in March showing stable or worsening response times. Expected this will show small improvements in April however still not achieving national standards.
▪ Additional support and process now formalised for c3/c4 ambulance stacked patients to transfer to IUC CAS. Also conveyance reduction support lines (paramedic on scene to GP access) remain in place.
▪ Handover delays, West Suffolk remain below allowance planned into EEAST models for handover performance. Colchester and Ipswich are above allowance however benchmark well against other hospital sites. HALO continuation has been agreed for Ipswich and West Suffolk and NEE going through final governance sign off. HALO will now become part of ESNEFT core contract moving forwards.
Urgent and emergency care summary
• As a system we’re working with EEAST to support demand management and a number of initiatives are now in place including; Implemented a C3 & C4 ambulance stack ‘push’ model (with plans to move to an electronic solution directly transferring cases to the IUC for validation being advanced with NHS England); and rapid telephone access to senior clinical advice to support decision making ahead of conveying a patient to hospital. Both models have demonstrated a reduction in the number of people conveyed to ED.
• The IUC Service have implemented additional training for advisors to look to reduce Cat 2 ambulance, this has broadly been very successful with a 8% drop in C2 ambulances, however this has resulted in more C3 ambulance so ambulances sent remains the same. The implementation of DoS Validation has also resulted in a 2% drop in ED outcomes to around 7% of triaged calls, both of these initiatives have been extremely positive for helping reduce demand on the Urgent and Emergency Care Services.

Cancer

ICS • The 22/23 Cancer delivery plan has been submitted, the priority areas are;
• Faster diagnosis and operational performance
• Earlier Diagnosis
• Treatments and personalised care.
• Histopathology remains constrained across the system. A digital histopathology programme is in development.
• Regional cancer performance teams have developed KLOEs to support 62 day recovery.
• System oversight meetings remain ongoing monthly to facilitate recovery discussions.
ESNEFT• ESNEFT continue to report high levels of referrals into the trust with some weeks now exceeding 1000 2WW referrals, specifically in
the surgical division, which includes, Colorectal, UGI and Prostate.
• Endoscopy currently has a delay which is impacting on cancer performance, all routine endoscopy is being seen in independent providers, resulting in only urgent and cancer in the trusts to support recovery. Additional funding has been awarded to support super Saturdays and a Vanguard is now in place at Ipswich to support additional activity.
• ESNEFT remains the 3rd highest provider in England in terms of the number of primary 62 day treatments that have been delivered and they have recovered their backlog following the pandemic.
• Breast pain pathway is now live at ESNEFT, a clinic a week is now being seen on each site, this means these patients will be seen at a community appointment first by a Breast burse specialist.
• The Gynaecology surgical pathway now have a robot, the result is they have been able to increase surgery capacity, with a newnurse role planned for April 2022 who will enable further triage.
• Radiotherapy – despite all the pressures we have implemented a paperless system across the sites. It is not yet fully embedded but it’s working very well
• Spike of referrals noted following the Easter break, referrals have now levelled out.
• Skin referrals are now being booked at day 21 - Dermatology delivery group established to support recovery of the pathway.

WSFT
• WSFT continue to see high levels of referrals into the trust with Breast, colorectal and UGI being the most challenged pathways.
• New CTC pathway has resulted in reduce delays at the front end of the colorectal pathway, also endoscopies remain constrained, they do have the same level of independent sector provision available so remains in house.
• Due to RAAC plank work theatres have been closed in WSFT, this work is due to conclude at the end of June.
• Chemotherapy patients are being seen between 7- 10 days managing to maintain.
• Oncology – no change COVID issues with nursing staff better. Mobile Unit continues to go out 4 days a week and is well utilised.
• A new terarecon service has been implemented in the radiology department, this new system will increase the radiology capacity to read reports, this will have a positive impact on the breast and colorectal pathways.
• CTC service paused due to a CT scanner not available, which has resulted in delays in the pathway – Mutual aid being explored. Patients in the pathway has been reviewed by the lead consultant and patients reallocated.
• WSFT recovery trajectory is constrained due to the CTC issue.
• 2WW referrals into the trusts have continued to raise with March seeing the highest number of referrals.
• COVID related sickness has impacted some pathways, Head and Neck and Gynaecology teams are small and therefore sickness has had an impact.
• Capacity remains constrained in the diagnostic end of the pathway, once diagnosed treatment capacity is good.
• Skin 2WW pathway recovered ahead of trajectory due to Skin Analytics being launched on the pathway.
Covid Vaccination

Children and Young People/Mental
Health
26
North East Essex Commentary
EPUT• EIP standard has been consistently apart from one month in October 2021
IAPT• Recovery standards have been consistently met since July 2021, achieving over the 50% target. January saw the
best month in terms of recovery rates to date at 54.55%. Access performance is currently achieving approximately 80% of the contracted standard. Recovery plans are in place to address the shortfall in access performance. EPUT have highlighted a number of issues they feel are impacting access; such as sickness and Covid, an inherited workforce struggling to adjust, recruitment and maternity leave and these have been reflected in their recovery action plans.

Quality Assurance Updates
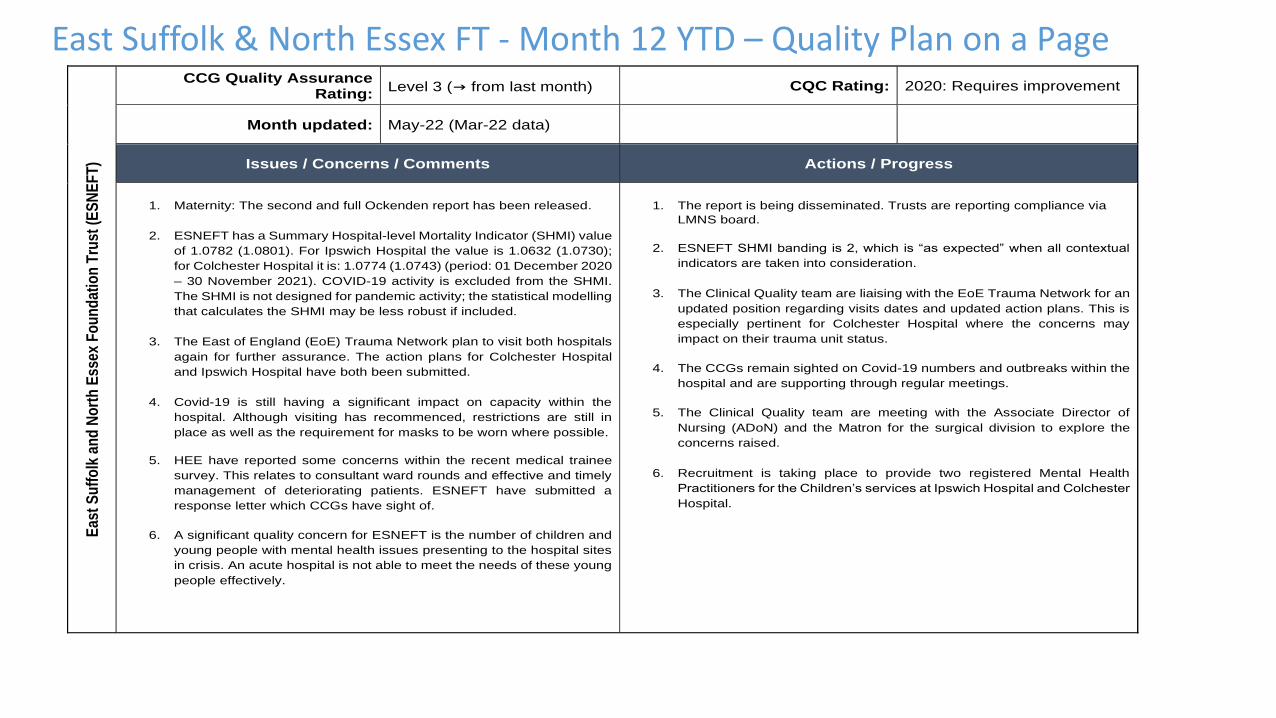
East Suffolk & North Essex FT - Month 12 YTD – Quality Plan on a Page
Eas
t S
uff
olk
an
d N
ort
h E
ssex
Fo
un
dat
ion
Tru
st (
ES
NE
FT
) CCG Quality Assurance
Rating: Level 3 (→ from last month) CQC Rating: 2020: Requires improvement
Month updated: May-22 (Mar-22 data)
Issues / Concerns / Comments Actions / Progress
1. Maternity: The second and full Ockenden report has been released.
2. ESNEFT has a Summary Hospital-level Mortality Indicator (SHMI) value
of 1.0782 (1.0801). For Ipswich Hospital the value is 1.0632 (1.0730);
for Colchester Hospital it is: 1.0774 (1.0743) (period: 01 December 2020
– 30 November 2021). COVID-19 activity is excluded from the SHMI.
The SHMI is not designed for pandemic activity; the statistical modelling
that calculates the SHMI may be less robust if included.
3. The East of England (EoE) Trauma Network plan to visit both hospitals
again for further assurance. The action plans for Colchester Hospital
and Ipswich Hospital have both been submitted.
4. Covid-19 is still having a significant impact on capacity within the
hospital. Although visiting has recommenced, restrictions are still in
place as well as the requirement for masks to be worn where possible.
5. HEE have reported some concerns within the recent medical trainee
survey. This relates to consultant ward rounds and effective and timely
management of deteriorating patients. ESNEFT have submitted a
response letter which CCGs have sight of.
6. A significant quality concern for ESNEFT is the number of children and
young people with mental health issues presenting to the hospital sites
in crisis. An acute hospital is not able to meet the needs of these young
people effectively.
1. The report is being disseminated. Trusts are reporting compliance via
LMNS board.
2. ESNEFT SHMI banding is 2, which is “as expected” when all contextual
indicators are taken into consideration.
3. The Clinical Quality team are liaising with the EoE Trauma Network for an
updated position regarding visits dates and updated action plans. This is
especially pertinent for Colchester Hospital where the concerns may
impact on their trauma unit status.
4. The CCGs remain sighted on Covid-19 numbers and outbreaks within the
hospital and are supporting through regular meetings.
5. The Clinical Quality team are meeting with the Associate Director of
Nursing (ADoN) and the Matron for the surgical division to explore the
concerns raised.
6. Recruitment is taking place to provide two registered Mental Health
Practitioners for the Children’s services at Ipswich Hospital and Colchester
Hospital.

EPUT – Month 12 YTD – Quality Plan on a PageE
ss
ex
Pa
rtn
ers
hip
Un
ive
rsit
y T
rus
t (E
PU
T)
CCG Quality Assurance Rating:
Level 2 (→ from last month) CQC Rating: Good
Month updated: May-22 (Mar-22 data)
Issues / Concerns / Comments Actions / Progress
1. Capacity and demand continue to challenge the Suffolk and North
East Essex (NEE) system. There is a national shortage of beds
(especially female) within the acute mental health services. This
has resulted in breaches as patients have longer waits in the
Emergency Department.
2. Improving Access to Psychological Therapies (IAPT) – Confidence
in Data; some improvements.
3. Transition to new assurance processes.
4. Psychology waiting lists in NEE Community (around 18 months for
some cohorts)
1. EPUT/ SNEE Exec to Exec meetings taking place to address this.
EPUT Director of Urgent Care Pathway intervention.
2. Contract meetings now feature comprehensive recovery plan, reviewed
every month.
3. Mental Health Task Force paper now published and single Mental Health
contract in place plus collaborative agreement with Mid and South Essex
and Herts and West Essex. Joint quality working in progress.
4. Plan to half waiting lists by summer and then clear by Christmas 2022; to
be overseen through contract monitoring meetings. Have requested this to
be a reporting requirement in the joint contract. Now added to the SNEE
GBAF and on EPUT Risk Register. Trajectories still on target but waiting
list cohorts represent vulnerable groups.

Practice Plus Group – Month 12 YTD – Quality Plan on a PageP
ract
ice
Plu
s G
rou
p (
PP
G)
CCG Quality Assurance Rating:
Level 2 (→ from last month) CQC Rating: Latest review 5 August 2021: No evidence to reassess rating
Month updated: May-22 (Mar-22 data)
Key Issues / Concerns / Comments Actions / Progress
1. QCPMs to recommence.
2. PPG continue to support admission avoidance – 63.97% of calls with an
initial category 3 and 4 were revalidated. 74.37% ED dispositions were
revalidated. Support for EEAST On Scene Crews and Control Room
remains in place.
3. IPC –risk assessments for all staff remain in place.
4. Staffing/workforce – rota fill discussed in updates. Continue to see new
recruits. Rolling out mental health first aider training and mental health
training for managers. Exploring apprenticeships in 111 with local
colleague.
5. Patient experience data remains good quality. Proportion of survey
respondents satisfied or very satisfied 76%. Complaints and Incidents
have been investigated within the required timeframe and evidence
learning and appropriate actions where indicated. Those requiring
further assurance are discussed in more detail in quality focus forums.
6. LCQAG – focused conversation on end-to-end review completed for
end of life patient.
7. LCQAG - discussed recent patient journey for patient with urgent
mental health needs.
8. I x SI for Suffolk OOH progressing through SI process. Expected to be
completed by next reporting period.
1. Scrutiny in place for assurance regarding 111, OOH and CAS KPIs. Monthly performance packs shared and reviewed.
2. Outside 80% target however indicating improved patient pathway.
3. Infection Prevention Control plan in place. PPG able to activate BCP if required as mitigation.
4. Rota fill continues to be monitored via QCPMs. In the event of any staffing issues these are escalated in real time.
5. Local Clinical Quality Assurance Group (LCQAG) providing the opportunity for more focussed conversations and actions at a system level.
6. Case to be shared with End of Life Programme for wider learning.
7. End-to-end review to be arranged with system partners.
8. Any immediate risks mitigated. SI is following due process through
patient safety team.

EEAST PTS – Month 12 YTD – Quality Plan on a PageN
on
-Em
erg
ency
Pat
ien
t T
ran
spo
rt S
ervi
ce (
NE
PT
S)
(EE
AS
T)
CCG Quality Assurance Rating:
Level 1 (→ from last month) CQC Rating: Sept 2020: Requires Improvement
Month updated: May-22 (Mar-22 data)
Issues / Concerns / Comments Actions / Progress
1. The February data shows the KPIs for inbound outpatient
journeys at 88% (89%) and outbound (outpatient) journeys at
94% (93%). The outbound discharge and transfer journeys are at
86% (79%).
2. Friends and Family Test (Feb. 22 data, NHS-England) shows that
there were 61 (51) surveys undertaken, from a possible 44,283
(45,429). Of the 61, 97% were positive and 2% were
negative. The feedback is positive, albeit from a small number of
patients.
1. The data shows there has been a consistent performance, with the in-
patient discharges showing improvement in February.
2. The response rate is 0.11% (0.13); it will be important that EEAST
identify how to promote the survey to access more feedback. The CCG
Clinical Quality and Patient Engagement teams are working with
EEAST to further develop this. Work is also taking place to enhance the
quality reporting provided for improved assurance and oversight of
quality initiatives.
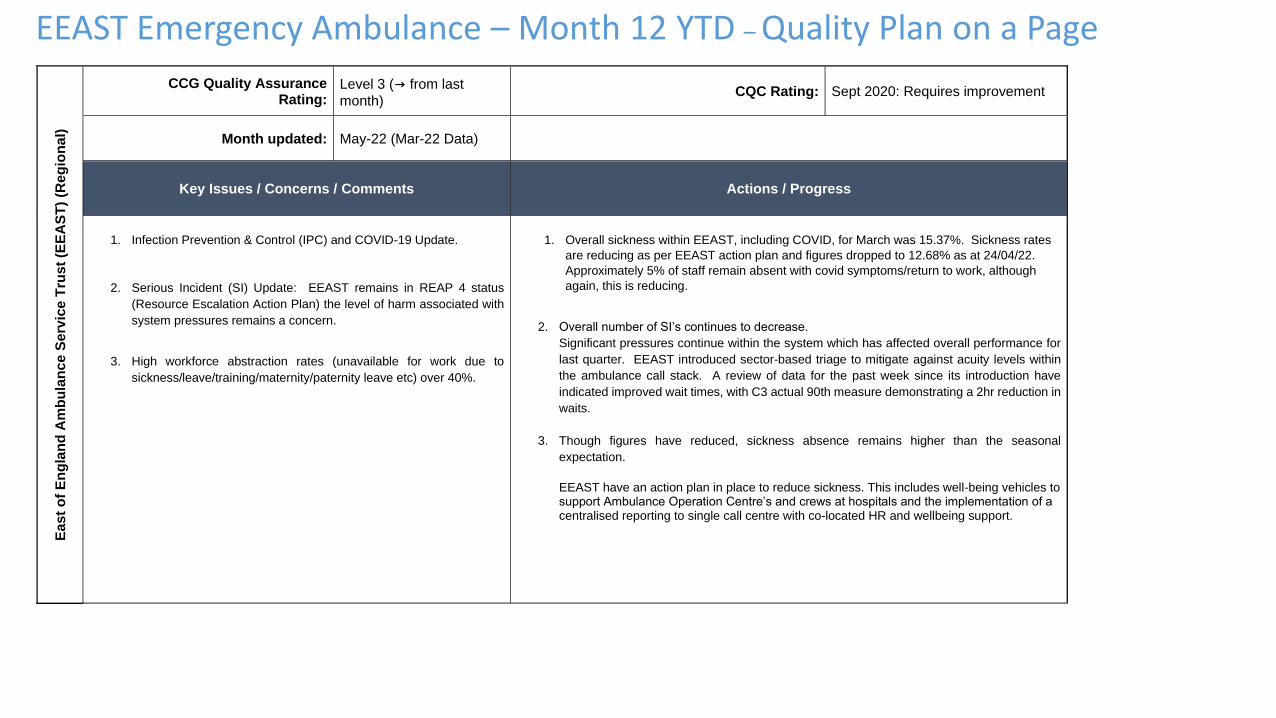
EEAST Emergency Ambulance – Month 12 YTD – Quality Plan on a PageE
as
t o
f E
ng
lan
d A
mb
ula
nc
e S
erv
ice
Tru
st
(EE
AS
T)
(Re
gio
na
l)
CCG Quality Assurance Rating:
Level 3 (→ from last
month) CQC Rating: Sept 2020: Requires improvement
Month updated: May-22 (Mar-22 Data)
Key Issues / Concerns / Comments Actions / Progress
1. Infection Prevention & Control (IPC) and COVID-19 Update.
2. Serious Incident (SI) Update: EEAST remains in REAP 4 status
(Resource Escalation Action Plan) the level of harm associated with
system pressures remains a concern.
3. High workforce abstraction rates (unavailable for work due to
sickness/leave/training/maternity/paternity leave etc) over 40%.
1. Overall sickness within EEAST, including COVID, for March was 15.37%. Sickness rates
are reducing as per EEAST action plan and figures dropped to 12.68% as at 24/04/22.
Approximately 5% of staff remain absent with covid symptoms/return to work, although
again, this is reducing.
2. Overall number of SI’s continues to decrease.
Significant pressures continue within the system which has affected overall performance for
last quarter. EEAST introduced sector-based triage to mitigate against acuity levels within
the ambulance call stack. A review of data for the past week since its introduction have
indicated improved wait times, with C3 actual 90th measure demonstrating a 2hr reduction in
waits.
3. Though figures have reduced, sickness absence remains higher than the seasonal
expectation.
EEAST have an action plan in place to reduce sickness. This includes well-being vehicles to support Ambulance Operation Centre’s and crews at hospitals and the implementation of a centralised reporting to single call centre with co-located HR and wellbeing support.
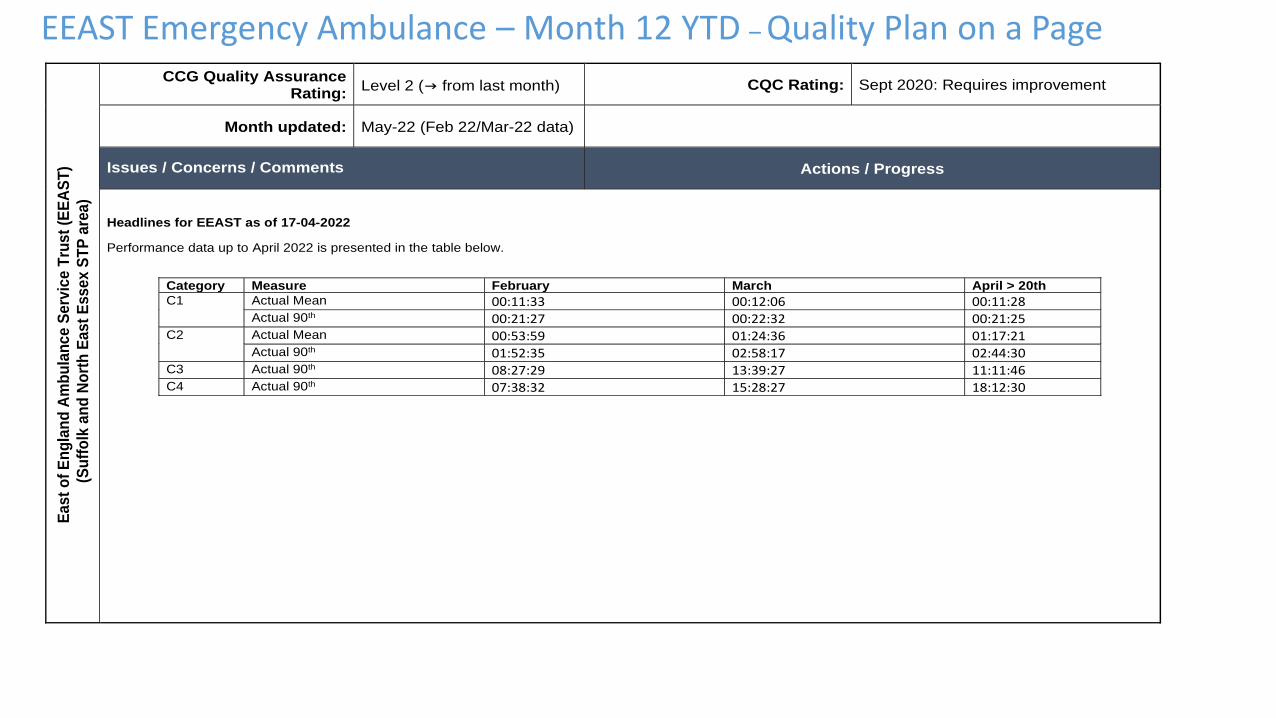
EEAST Emergency Ambulance – Month 12 YTD – Quality Plan on a Page
E
as
t o
f E
ng
lan
d A
mb
ula
nc
e S
erv
ice
Tru
st
(EE
AS
T)
(S
uff
olk
an
d N
ort
h E
as
t E
ss
ex S
TP
are
a)
CCG Quality Assurance Rating:
Level 2 (→ from last month) CQC Rating: Sept 2020: Requires improvement
Month updated: May-22 (Feb 22/Mar-22 data)
Issues / Concerns / Comments Actions / Progress
Headlines for EEAST as of 17-04-2022
Performance data up to April 2022 is presented in the table below.
Category Measure February March April > 20th
C1 Actual Mean 00:11:33 00:12:06 00:11:28
Actual 90th 00:21:27 00:22:32 00:21:25
C2 Actual Mean 00:53:59 01:24:36 01:17:21
Actual 90th 01:52:35 02:58:17 02:44:30
C3 Actual 90th 08:27:29 13:39:27 11:11:46
C4 Actual 90th 07:38:32 15:28:27 18:12:30
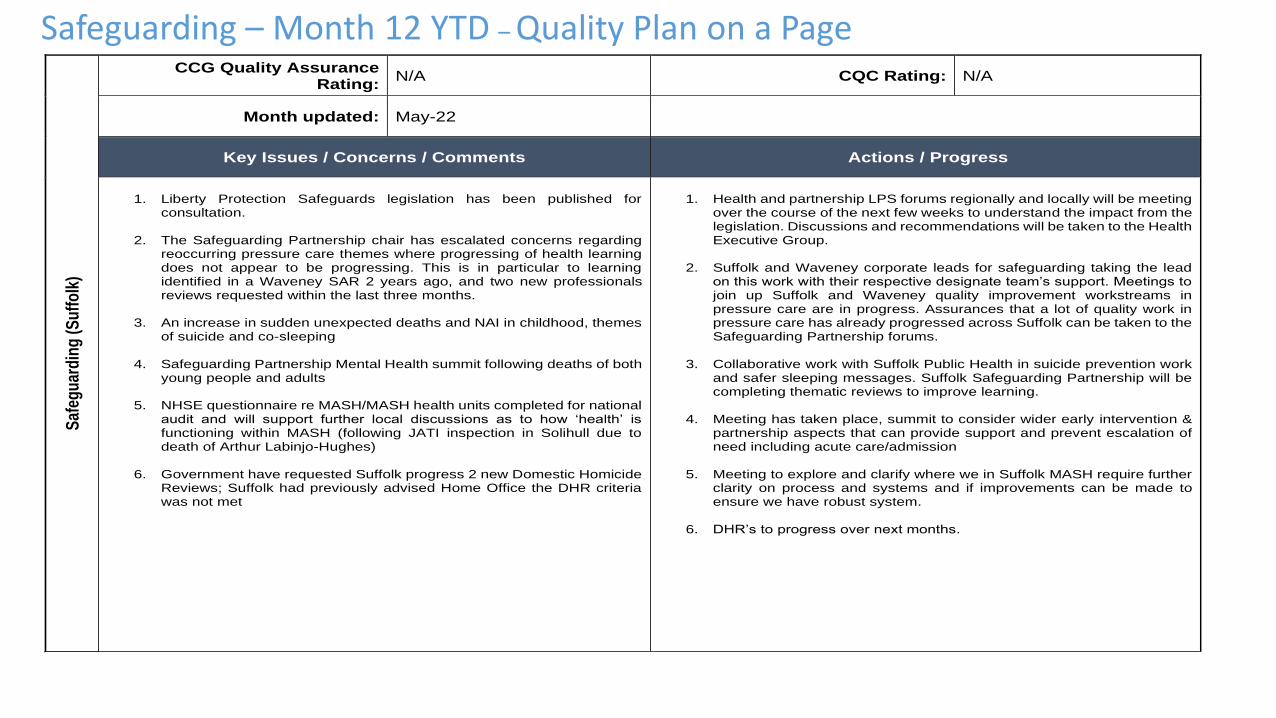
Safeguarding – Month 12 YTD – Quality Plan on a PageS
afeg
uar
din
g (
Su
ffo
lk)
CCG Quality Assurance Rating:
N/A CQC Rating: N/A
Month updated: May-22
Key Issues / Concerns / Comments Actions / Progress
1. Liberty Protection Safeguards legislation has been published for
consultation.
2. The Safeguarding Partnership chair has escalated concerns regarding reoccurring pressure care themes where progressing of health learning does not appear to be progressing. This is in particular to learning identified in a Waveney SAR 2 years ago, and two new professionals reviews requested within the last three months.
3. An increase in sudden unexpected deaths and NAI in childhood, themes
of suicide and co-sleeping
4. Safeguarding Partnership Mental Health summit following deaths of both young people and adults
5. NHSE questionnaire re MASH/MASH health units completed for national
audit and will support further local discussions as to how ‘health’ is functioning within MASH (following JATI inspection in Solihull due to death of Arthur Labinjo-Hughes)
6. Government have requested Suffolk progress 2 new Domestic Homicide
Reviews; Suffolk had previously advised Home Office the DHR criteria was not met
1. Health and partnership LPS forums regionally and locally will be meeting
over the course of the next few weeks to understand the impact from the legislation. Discussions and recommendations will be taken to the Health Executive Group.
2. Suffolk and Waveney corporate leads for safeguarding taking the lead
on this work with their respective designate team’s support. Meetings to join up Suffolk and Waveney quality improvement workstreams in pressure care are in progress. Assurances that a lot of quality work in pressure care has already progressed across Suffolk can be taken to the Safeguarding Partnership forums.
3. Collaborative work with Suffolk Public Health in suicide prevention work
and safer sleeping messages. Suffolk Safeguarding Partnership will be completing thematic reviews to improve learning.
4. Meeting has taken place, summit to consider wider early intervention &
partnership aspects that can provide support and prevent escalation of need including acute care/admission
5. Meeting to explore and clarify where we in Suffolk MASH require further
clarity on process and systems and if improvements can be made to ensure we have robust system.
6. DHR’s to progress over next months.

Su
ffo
lk a
nd
No
rth
Eas
t E
ssex
Car
e H
om
es
CCG Quality Assurance Rating:
CQC Rating:
Month updated: May-22
Issues / Concerns / Comments Actions / Progress
Suffolk Outbreaks are now managed with a system response and are categorised as follows:
Situation = staff/resident potential contact with COVID.
Incident = confirmed or suspected case within the setting, not understood to have originated in the setting.
Outbreak = two or more confirmed or suspected cases among staff/residents.
• Care Home data as at 27 April 2022
• Supporting Housing data as at 27 April 2022
North East Essex
As at 02 May 2022 there were 23 COVID19 outbreaks and 2 exposures in North East Essex Care Homes.
Suffolk Outbreak
Care Home
IES 24
WS 16
Supported Housing
IES/WS Total 28
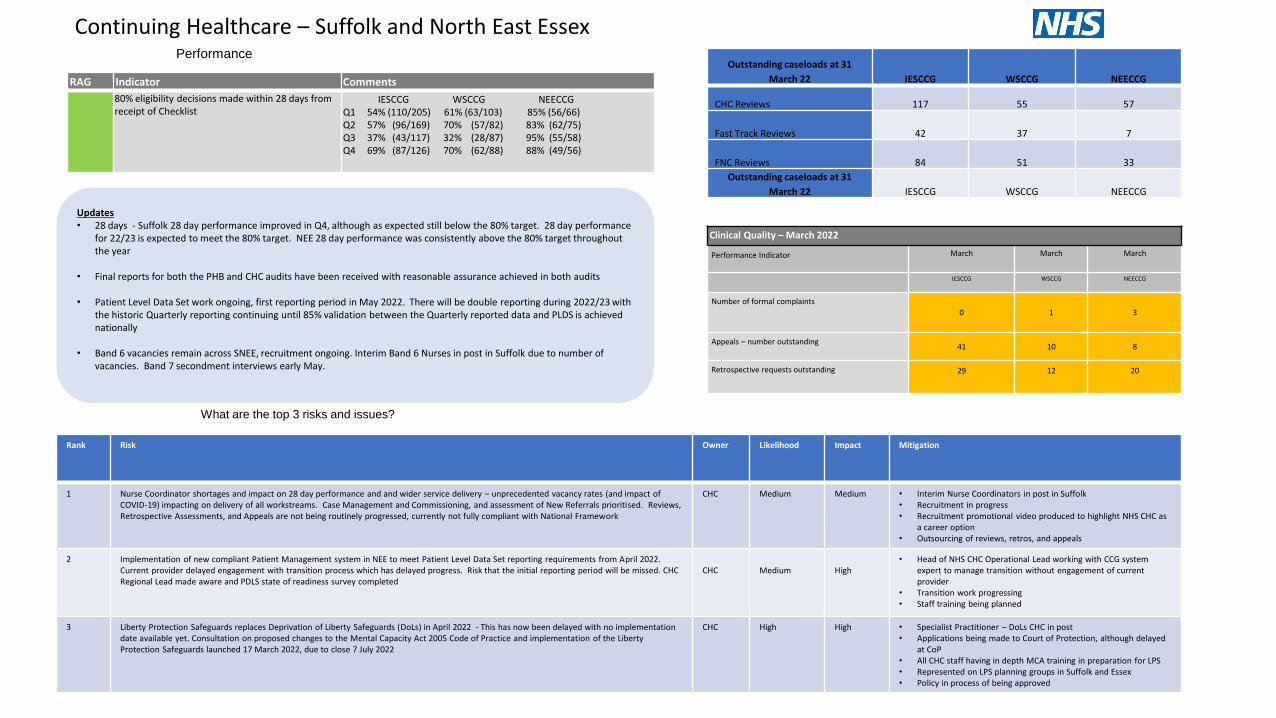
What are the top 3 risks and issues?
Continuing Healthcare – Suffolk and North East EssexPerformance
Outstanding caseloads at 31
March 22 IESCCG WSCCG NEECCG
CHC Reviews 117 55 57
Fast Track Reviews 42 37 7
FNC Reviews 84 51 33
Outstanding caseloads at 31
March 22 IESCCG WSCCG NEECCG
Updates• 28 days - Suffolk 28 day performance improved in Q4, although as expected still below the 80% target. 28 day performance
for 22/23 is expected to meet the 80% target. NEE 28 day performance was consistently above the 80% target throughout the year
• Final reports for both the PHB and CHC audits have been received with reasonable assurance achieved in both audits
• Patient Level Data Set work ongoing, first reporting period in May 2022. There will be double reporting during 2022/23 with the historic Quarterly reporting continuing until 85% validation between the Quarterly reported data and PLDS is achieved nationally
• Band 6 vacancies remain across SNEE, recruitment ongoing. Interim Band 6 Nurses in post in Suffolk due to number of vacancies. Band 7 secondment interviews early May.
Clinical Quality – March 2022
Performance Indicator March March March
IESCCG WSCCG NEECCG
Number of formal complaints
0 1 3
Appeals – number outstanding41 10 8
Retrospective requests outstanding 29 12 20
Rank Risk Owner Likelihood Impact Mitigation
1 Nurse Coordinator shortages and impact on 28 day performance and and wider service delivery – unprecedented vacancy rates (and impact of COVID-19) impacting on delivery of all workstreams. Case Management and Commissioning, and assessment of New Referrals prioritised. Reviews, Retrospective Assessments, and Appeals are not being routinely progressed, currently not fully compliant with National Framework
CHC Medium Medium • Interim Nurse Coordinators in post in Suffolk• Recruitment in progress• Recruitment promotional video produced to highlight NHS CHC as
a career option• Outsourcing of reviews, retros, and appeals
2 Implementation of new compliant Patient Management system in NEE to meet Patient Level Data Set reporting requirements from April 2022. Current provider delayed engagement with transition process which has delayed progress. Risk that the initial reporting period will be missed. CHC Regional Lead made aware and PDLS state of readiness survey completed
CHC Medium High• Head of NHS CHC Operational Lead working with CCG system
expert to manage transition without engagement of current provider
• Transition work progressing• Staff training being planned
3 Liberty Protection Safeguards replaces Deprivation of Liberty Safeguards (DoLs) in April 2022 - This has now been delayed with no implementation date available yet. Consultation on proposed changes to the Mental Capacity Act 2005 Code of Practice and implementation of the Liberty Protection Safeguards launched 17 March 2022, due to close 7 July 2022
CHC High High • Specialist Practitioner – DoLs CHC in post• Applications being made to Court of Protection, although delayed
at CoP• All CHC staff having in depth MCA training in preparation for LPS• Represented on LPS planning groups in Suffolk and Essex• Policy in process of being approved
RAG Indicator Comments
80% eligibility decisions made within 28 days from receipt of Checklist
IESCCG WSCCG NEECCGQ1 54% (110/205) 61% (63/103) 85% (56/66)Q2 57% (96/169) 70% (57/82) 83% (62/75) Q3 37% (43/117) 32% (28/87) 95% (55/58)Q4 69% (87/126) 70% (62/88) 88% (49/56)
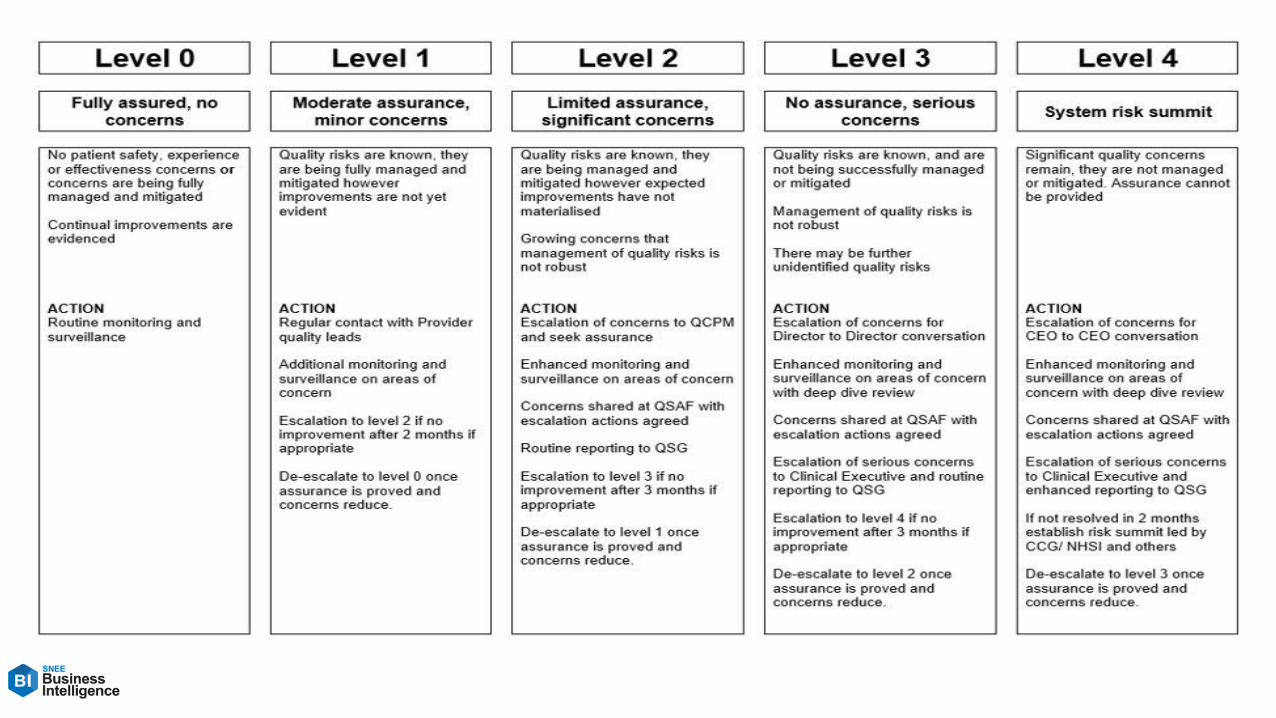

Transformation Programmes 21-22
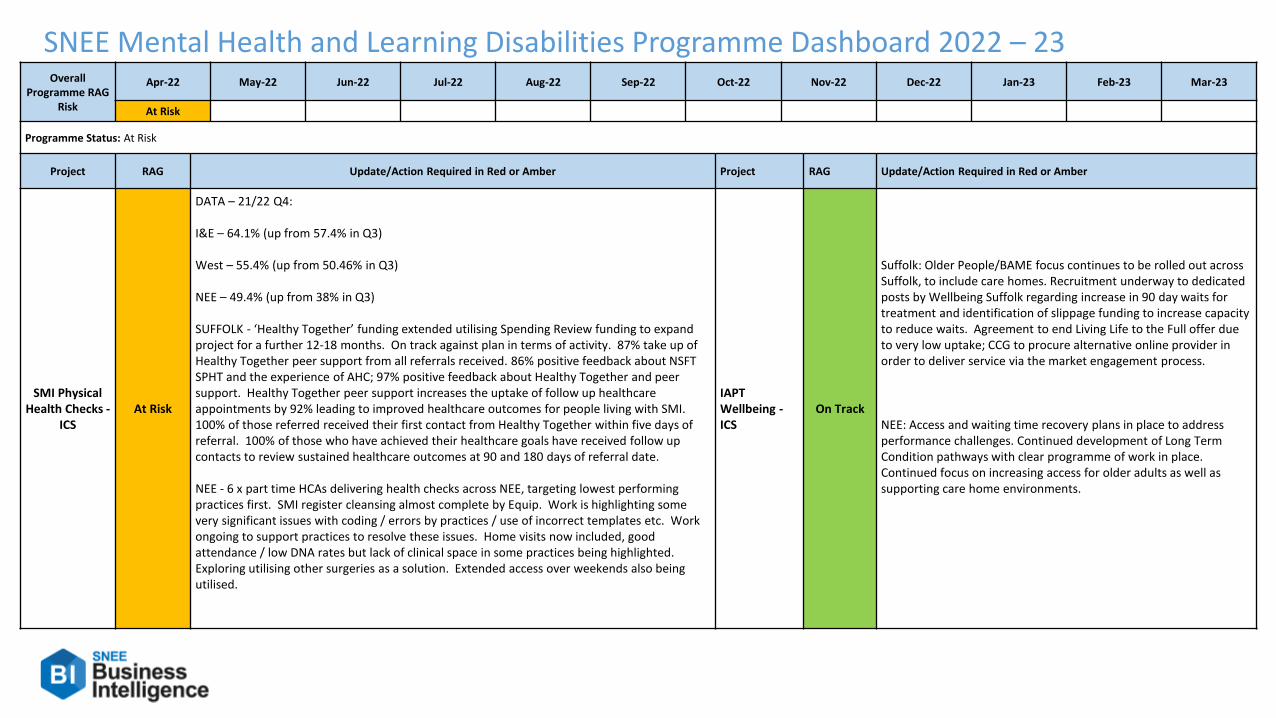
SNEE Mental Health and Learning Disabilities Programme Dashboard 2022 – 23Overall
Programme RAG Risk
Apr-22 May-22 Jun-22 Jul-22 Aug-22 Sep-22 Oct-22 Nov-22 Dec-22 Jan-23 Feb-23 Mar-23
At Risk
Programme Status: At Risk
Project RAG Update/Action Required in Red or Amber Project RAG Update/Action Required in Red or Amber
SMI Physical Health Checks -
ICSAt Risk
DATA – 21/22 Q4:
I&E – 64.1% (up from 57.4% in Q3)
West – 55.4% (up from 50.46% in Q3)
NEE – 49.4% (up from 38% in Q3)
SUFFOLK - ‘Healthy Together’ funding extended utilising Spending Review funding to expand project for a further 12-18 months. On track against plan in terms of activity. 87% take up of Healthy Together peer support from all referrals received. 86% positive feedback about NSFT SPHT and the experience of AHC; 97% positive feedback about Healthy Together and peer support. Healthy Together peer support increases the uptake of follow up healthcare appointments by 92% leading to improved healthcare outcomes for people living with SMI. 100% of those referred received their first contact from Healthy Together within five days of referral. 100% of those who have achieved their healthcare goals have received follow up contacts to review sustained healthcare outcomes at 90 and 180 days of referral date.
NEE - 6 x part time HCAs delivering health checks across NEE, targeting lowest performing practices first. SMI register cleansing almost complete by Equip. Work is highlighting some very significant issues with coding / errors by practices / use of incorrect templates etc. Work ongoing to support practices to resolve these issues. Home visits now included, good attendance / low DNA rates but lack of clinical space in some practices being highlighted. Exploring utilising other surgeries as a solution. Extended access over weekends also being utilised.
IAPT Wellbeing -ICS
On Track
Suffolk: Older People/BAME focus continues to be rolled out across Suffolk, to include care homes. Recruitment underway to dedicated posts by Wellbeing Suffolk regarding increase in 90 day waits for treatment and identification of slippage funding to increase capacity to reduce waits. Agreement to end Living Life to the Full offer due to very low uptake; CCG to procure alternative online provider in order to deliver service via the market engagement process.
NEE: Access and waiting time recovery plans in place to address performance challenges. Continued development of Long Term Condition pathways with clear programme of work in place. Continued focus on increasing access for older adults as well as supporting care home environments.
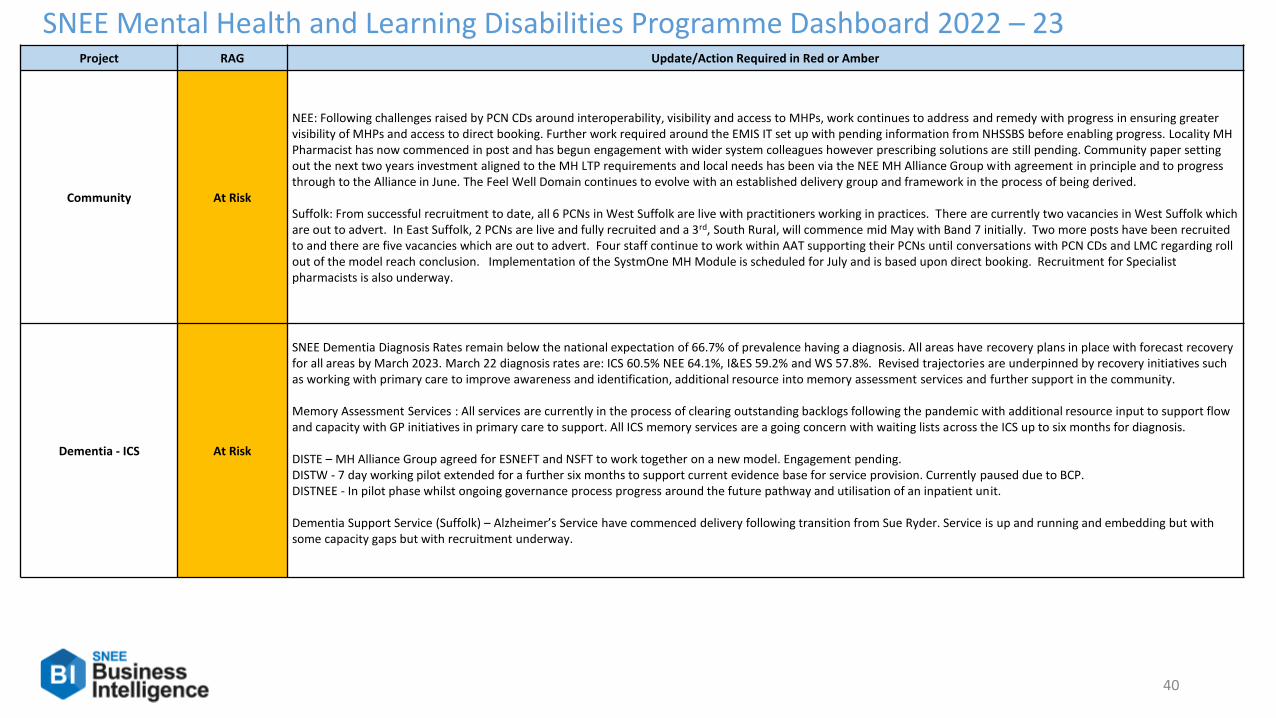
40
SNEE Mental Health and Learning Disabilities Programme Dashboard 2022 – 23Project RAG Update/Action Required in Red or Amber
Community At Risk
NEE: Following challenges raised by PCN CDs around interoperability, visibility and access to MHPs, work continues to address and remedy with progress in ensuring greater visibility of MHPs and access to direct booking. Further work required around the EMIS IT set up with pending information from NHSSBS before enabling progress. Locality MH Pharmacist has now commenced in post and has begun engagement with wider system colleagues however prescribing solutions are still pending. Community paper setting out the next two years investment aligned to the MH LTP requirements and local needs has been via the NEE MH Alliance Group with agreement in principle and to progress through to the Alliance in June. The Feel Well Domain continues to evolve with an established delivery group and framework in the process of being derived.
Suffolk: From successful recruitment to date, all 6 PCNs in West Suffolk are live with practitioners working in practices. There are currently two vacancies in West Suffolk which are out to advert. In East Suffolk, 2 PCNs are live and fully recruited and a 3rd, South Rural, will commence mid May with Band 7 initially. Two more posts have been recruited to and there are five vacancies which are out to advert. Four staff continue to work within AAT supporting their PCNs until conversations with PCN CDs and LMC regarding roll out of the model reach conclusion. Implementation of the SystmOne MH Module is scheduled for July and is based upon direct booking. Recruitment for Specialist pharmacists is also underway.
Dementia - ICS At Risk
SNEE Dementia Diagnosis Rates remain below the national expectation of 66.7% of prevalence having a diagnosis. All areas have recovery plans in place with forecast recovery for all areas by March 2023. March 22 diagnosis rates are: ICS 60.5% NEE 64.1%, I&ES 59.2% and WS 57.8%. Revised trajectories are underpinned by recovery initiatives such as working with primary care to improve awareness and identification, additional resource into memory assessment services and further support in the community.
Memory Assessment Services : All services are currently in the process of clearing outstanding backlogs following the pandemic with additional resource input to support flow and capacity with GP initiatives in primary care to support. All ICS memory services are a going concern with waiting lists across the ICS up to six months for diagnosis.
DISTE – MH Alliance Group agreed for ESNEFT and NSFT to work together on a new model. Engagement pending. DISTW - 7 day working pilot extended for a further six months to support current evidence base for service provision. Currently paused due to BCP.DISTNEE - In pilot phase whilst ongoing governance process progress around the future pathway and utilisation of an inpatient unit.
Dementia Support Service (Suffolk) – Alzheimer’s Service have commenced delivery following transition from Sue Ryder. Service is up and running and embedding but with some capacity gaps but with recruitment underway.

41
SNEE Mental Health and Learning Disabilities Programme Dashboard 2022 – 23
Project RAG Update/Action Required in Red or Amber
Specialist –ICS
On Track
PERSONALITY DISORDERS & COMPLEX NEEDS PATHWAY:NORTH EAST ESSEX: Business Case approved in 20/21 with recruitment completed. Essex wide system Steering Group commenced on the 29th September 2021 with scope and approach to be agreed in terms of objectives andoutcomes. Inpatient model proposed and conversation ongoing to develop connectivity with community models of care.
SUFFOLK: Recruitment on track, including B6 post in West that was providing difficult to recruit to, and Peer Support Worker. Funding identified as part of community transformation allocation to deliver bitesize training tostaff working with older people. Needs typing workshops: 23 delivered, 2 scheduled; PDCN Bitesize: 4 delivered, more in development; Knowledge and Understanding Framework: KUF lead in post, additional lived and learnedexperience trainers being recruited. 4 courses scheduled to be delivered to end March 22, then 3 per month for 22/23. DBT Essential Skills: 8 courses delivered (136 people) in different formats to accommodate differentworking patterns; 7 courses scheduled from Feb onwards (210 places). DBT Intensive Systemic: 9 people trained to date; Further course to be scheduled to coincide with when new recruits are in post. Service users acrossSuffolk can access Dialectical Behaviour Therapy programmes of which there are currently 4 in progress. Emotional Regulation groups in progress. Additional provision is needed in all areas and will be rolled out once newrecruits are in position and fully trained. Brief interventions: Workbooks are in development and will be rolled out during 22/22.KUF: Advanced Lived Experience KUF Lead in post since September (the start date was scheduled to coincide with the national training programme start); 0.6 WTE Band 5 Lived Experience trainer appointed and in post. 0.5WTE Band 6 Learned Experience trainer (50% funded from N&W/Suffolk) in post. Train the trainer: 4 people have attended the national hub TTT course; KUF 3 day: 8 people have attended; KUF 1 day: 2 people have attended;4 further courses scheduled to end March, and more will follow from April.
PERINATALNORTH EAST ESSEX: SPMH business case to meet LTP requirements agreed and continues it’s roll out – slightly behind plan in delivery of some quality standards however access in excess of ambition at 13%. MMHS scopingand engagement is due to conclude moving to design and business case phase with the ambition of service Go Live later this year.
SUFFOLK: No update from Trust regarding a permanent base for the team which is impacting on wellbeing and morale and recently recruited PSW has now resigned from post due to impact of this. Referral rates remain atexpected level. MMHS scoping/mapping exercise underway, survey developed and distributed early May and outcomes to be reviewed and fed into business case.
EIPSUFFOLK: Continue with estates challenges which have persisted for a number a years now with no permanent solution or estates strategy available. Service operates at L2 and is in the process of reviewing business casedelivery and deriving a case for a local ARMS offer.
NORTH EAST ESSEX: business case inclusive of ARMS element agreed in 20/21. ARMS pathway in the process of completion alongside recruitment.
IPSNORTH EAST ESSEX: Integration with other EPUT services underway such as EIP and community models. Fidelity review audit has been paused due to unforeseen circumstances and will resume later this year.
SUFFOLK: EPUT fidelity review undertaken via IPS Grow with positive result and identified improvements identified to action such as furthering integration with NSFT services inclusive of community models to enhancereferrals. Identified underspend identified and reallocated to support service delivery. Access remains below plan and in recovery following covid with an upward trend.
ADULT EATING DISORDERS:SUFFOLK: Beat contract in place and teams working together to establish clear referral pathway and MDT conversations about appropriate referrals. Delay in contract sign off for Suffolk Mind Recovery Service due to NSFTcontracts capacity. Meeting scheduled 12/5 for final review and sign off. Dedicated project manager in post overseeing development of all clinical pathways and support VCSE integration. Difficulties recruiting Band 6 Nursingposts to specialist team, impacting on service's ability to implement FREED model and commence transformation focus on Medical Monitoring and ARFID pathways. Fortnightly reviews of performance and risks/issues withNSFT/CCG now include NHSE regional ED lead(s) and primary care input. ARFID pathway conversations have commenced with clinical lead in CYP team.
NORTH EAST ESSEX: Essex-wide T&F group overseeing development of staffing model and costings. Agreement that NEE will have a local focus in terms of developing FREED model and medical monitoring as these are two keypriorities in the national LTP. Initial discussion with GPPC to explore potential for SMI Physical Health Checks team to deliver Medical Monitoring in primary care, using C&P model as a template.

SNEE Mental Health and Learning Disabilities Programme Dashboard 2022 – 23Project RAG Update/Action Required in Red or Amber Project RAG Update/Action Required in Red or Amber
Crisis - ICSOn Track
NEECORE 24 – Agreement for capital investment to address environmental issues and ensure compliance with standards. Work should commence in coming months111(2) & CRHT – No further updates Crisis alternatives – Both Clacton and Colchester venues fully functional with ongoing work to address environments to make more therapeutic
Suffolk Crisis 111(2) & FRS – Service switched from First Response Service to NHS111 option 2 on 5th April. No major issued with switch and numbers of calls have already dropped dramatically. Total calls for April were 2190, abandoned 776 (35%) average answering waiting time 16:52 min, average call handling time 11:13 min.Further work with Norfolk to relocate staff from Wedgewood to Norwich, staff in Wedgewood are currently split S/N. High intensity User project is beginning to have an impact on call trajectory for repeat callers.Core MHL – Additional SDF template completed looking to add peer support workers to Mental Health liaison service, East team have requested non-medical prescriber to assist pathway. Recruitment about to begin and further exploration in capital funding.Crisis Alternatives – Procurement process ended Access Community Trust successful and mobilisation underway with soft launch in July 2022 and formal launch in October 2022.
Learning Disability and
AutismOn Track
SUFFOLKLD&A Transformation (Priority 4) - This is now moving into mobilisation phase for the specialist community team and IST. Business cases are now being approved and recruitment can then start for the Health Facilitators in the community team and the further workforce that will be required for the Intensive Support Team.
NEEASD Business Case agreed in principle by NEE Alliance Committee but only to fund for 6 months of 22/23. This is due to the cost pressure from 23/24 associated with the new service. Alliance Cttee requested this to be included as part of the wider prioritisation. EPUT expressed concerns around trying to recruit to a service for a period of 6 months primarily due to recruitment issues and risks associated with continuity of care. Operational Executive Cttee signed off the waiver and discussed next steps post Alliance Cttee outcome on future service delivery given the response from EPUT and the additional risks arising. OEC requested that further work needed to take place on understanding how the current activity is being paid for and future liabilities. This work is now underway and will be discussed at an Extraordinary OEC on 12th May.

SNEE Mental Health and Learning Disabilities Programme KPIs 2021 – 22
Metric Standard Date IES CCG WS CCG NEE CCG Notes
IAPT Access NationalMonthly
n/a Jan-221,130 625 650
Source is IAPT monthly report (NHS Digital)Rolling Quarter 3,245 1,775 2,035
IAPT Access LocalMonthly n/a
Mar-22924 553 881
Data from local contract reports; note later month than national reporting
Rolling Quarter n/a 2,959 1,682 2,196
IAPT Access YTDNational
n/aJan-22
9,815 5,265 6,400 Source is IAPT monthly report (NHS Digital)
Local Mar-2215,788 8,591 10,396
Local contract report (later month than NHSD)
IAPT Access 65+ National Quarterly n/a Dec-21 275 165 135 Source is IAPT quarterly report (NHS Digital)
IAPT Recovery RateMonthly National
50%Jan-22 53% 52% 54% Source is IAPT monthly report (NHS Digital) - rate as published
Monthly Local Mar-22 52% 52% 56% Local contract report (later month than NHSD)
IAPT 6 Week WaitMonthly National
75%Jan-22 96% 98% 90% Source is IAPT monthly report (NHS Digital) - rate as published
Monthly Local Mar-22 95% 96% 94% Local contract report (later month than NHSD)
IAPT 18 Week WaitMonthly National
95%Jan-22 100% 100% 100% Source is IAPT monthly report (NHS Digital) - rate as published
Monthly Local Mar-22 100% 100% 100% Local contract report (later month than NHSD)
IAPT in treatment pathway waits of 90+ days Monthly National 10% Jan-22 8.0% 12.0% 25.0%
Source is IAPT monthly report (NHS Digital)
Monthly national data for numerator and denominator is rounded and the rate is
calculated (rate is not published within NHSD data)
Dementia 66.70% Mar-22 59.20% 58.00% 64.10% Reported as NHSD Recorded Dementia Diagnosis Summary
SMI Physical Health Checks
Activity n/a Dec-21 1406 687 1226Source is NHS England - activity published as Future NHS Mental Health Core
Data Pack
n/a Q4 64.1% 55.4% 49.4%Percentage of people with severe mental illness (SMI) to receive the complete list
of physical health checks in the preceding 12 months.
Perinatal Activity n/a Dec-21 335 155 405
Source is NHS England - activity published as Future NHS Mental Health Core
Data Pack
Focus is now on YTD activity. Number of women with at least one attended
contact with a specialist community perinatal mental health service in the financial
year
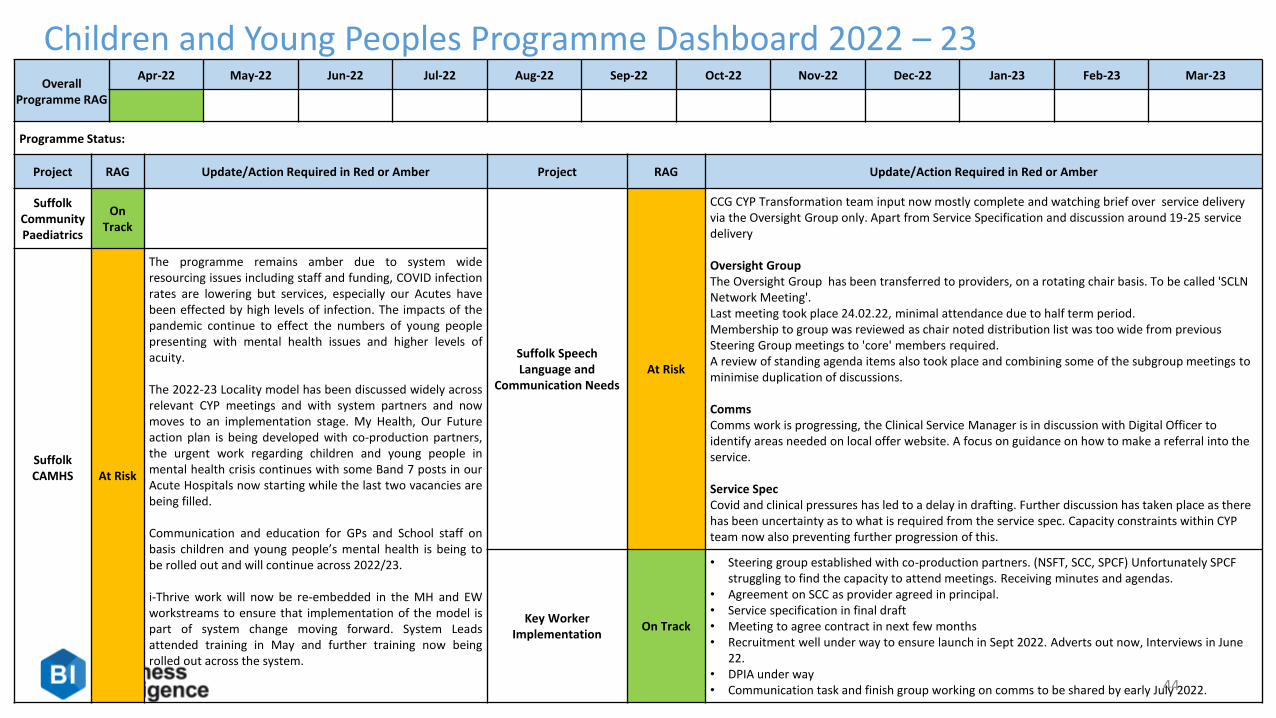
44
Children and Young Peoples Programme Dashboard 2022 – 23Overall
Programme RAG
Apr-22 May-22 Jun-22 Jul-22 Aug-22 Sep-22 Oct-22 Nov-22 Dec-22 Jan-23 Feb-23 Mar-23
Programme Status:
Project RAG Update/Action Required in Red or Amber Project RAG Update/Action Required in Red or Amber
Suffolk Community Paediatrics
OnTrack
Suffolk Speech Language and
Communication NeedsAt Risk
CCG CYP Transformation team input now mostly complete and watching brief over service delivery via the Oversight Group only. Apart from Service Specification and discussion around 19-25 service delivery
Oversight GroupThe Oversight Group has been transferred to providers, on a rotating chair basis. To be called 'SCLN Network Meeting'.Last meeting took place 24.02.22, minimal attendance due to half term period. Membership to group was reviewed as chair noted distribution list was too wide from previous Steering Group meetings to 'core' members required. A review of standing agenda items also took place and combining some of the subgroup meetings to minimise duplication of discussions.
CommsComms work is progressing, the Clinical Service Manager is in discussion with Digital Officer to identify areas needed on local offer website. A focus on guidance on how to make a referral into the service.
Service SpecCovid and clinical pressures has led to a delay in drafting. Further discussion has taken place as there has been uncertainty as to what is required from the service spec. Capacity constraints within CYP team now also preventing further progression of this.
Suffolk CAMHS At Risk
The programme remains amber due to system wideresourcing issues including staff and funding, COVID infectionrates are lowering but services, especially our Acutes havebeen effected by high levels of infection. The impacts of thepandemic continue to effect the numbers of young peoplepresenting with mental health issues and higher levels ofacuity.
The 2022-23 Locality model has been discussed widely acrossrelevant CYP meetings and with system partners and nowmoves to an implementation stage. My Health, Our Futureaction plan is being developed with co-production partners,the urgent work regarding children and young people inmental health crisis continues with some Band 7 posts in ourAcute Hospitals now starting while the last two vacancies arebeing filled.
Communication and education for GPs and School staff onbasis children and young people’s mental health is being tobe rolled out and will continue across 2022/23.
i-Thrive work will now be re-embedded in the MH and EWworkstreams to ensure that implementation of the model ispart of system change moving forward. System Leadsattended training in May and further training now beingrolled out across the system.
Key Worker Implementation
On Track
• Steering group established with co-production partners. (NSFT, SCC, SPCF) Unfortunately SPCF struggling to find the capacity to attend meetings. Receiving minutes and agendas.
• Agreement on SCC as provider agreed in principal. • Service specification in final draft• Meeting to agree contract in next few months• Recruitment well under way to ensure launch in Sept 2022. Adverts out now, Interviews in June
22.• DPIA under way• Communication task and finish group working on comms to be shared by early July 2022.
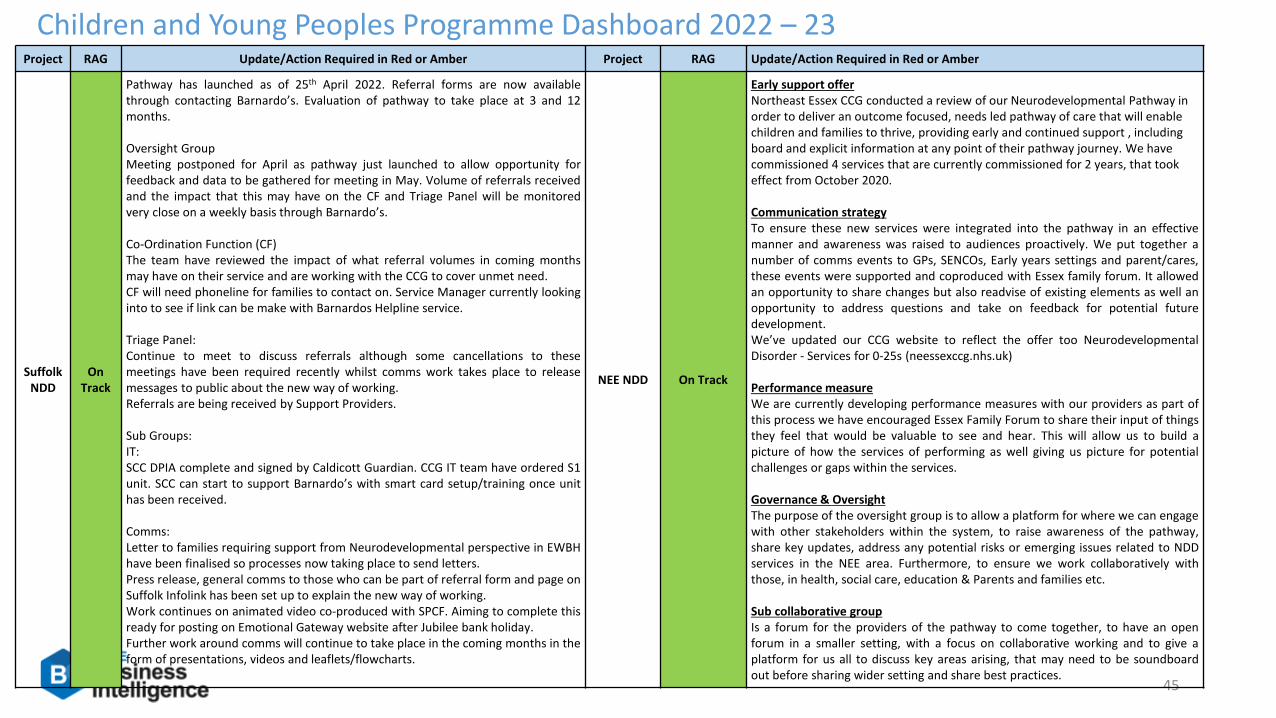
45
Children and Young Peoples Programme Dashboard 2022 – 23Project RAG Update/Action Required in Red or Amber Project RAG Update/Action Required in Red or Amber
Suffolk NDD
On Track
Pathway has launched as of 25th April 2022. Referral forms are now availablethrough contacting Barnardo’s. Evaluation of pathway to take place at 3 and 12months.
Oversight GroupMeeting postponed for April as pathway just launched to allow opportunity forfeedback and data to be gathered for meeting in May. Volume of referrals receivedand the impact that this may have on the CF and Triage Panel will be monitoredvery close on a weekly basis through Barnardo’s.
Co-Ordination Function (CF)The team have reviewed the impact of what referral volumes in coming monthsmay have on their service and are working with the CCG to cover unmet need.CF will need phoneline for families to contact on. Service Manager currently lookinginto to see if link can be make with Barnardos Helpline service.
Triage Panel:Continue to meet to discuss referrals although some cancellations to thesemeetings have been required recently whilst comms work takes place to releasemessages to public about the new way of working.Referrals are being received by Support Providers.
Sub Groups:IT:SCC DPIA complete and signed by Caldicott Guardian. CCG IT team have ordered S1unit. SCC can start to support Barnardo’s with smart card setup/training once unithas been received.
Comms:Letter to families requiring support from Neurodevelopmental perspective in EWBHhave been finalised so processes now taking place to send letters.Press release, general comms to those who can be part of referral form and page onSuffolk Infolink has been set up to explain the new way of working.Work continues on animated video co-produced with SPCF. Aiming to complete thisready for posting on Emotional Gateway website after Jubilee bank holiday.Further work around comms will continue to take place in the coming months in theform of presentations, videos and leaflets/flowcharts.
NEE NDD On Track
Early support offer Northeast Essex CCG conducted a review of our Neurodevelopmental Pathway in order to deliver an outcome focused, needs led pathway of care that will enable children and families to thrive, providing early and continued support , including board and explicit information at any point of their pathway journey. We have commissioned 4 services that are currently commissioned for 2 years, that took effect from October 2020.
Communication strategyTo ensure these new services were integrated into the pathway in an effectivemanner and awareness was raised to audiences proactively. We put together anumber of comms events to GPs, SENCOs, Early years settings and parent/cares,these events were supported and coproduced with Essex family forum. It allowedan opportunity to share changes but also readvise of existing elements as well anopportunity to address questions and take on feedback for potential futuredevelopment.We’ve updated our CCG website to reflect the offer too NeurodevelopmentalDisorder - Services for 0-25s (neessexccg.nhs.uk)
Performance measureWe are currently developing performance measures with our providers as part ofthis process we have encouraged Essex Family Forum to share their input of thingsthey feel that would be valuable to see and hear. This will allow us to build apicture of how the services of performing as well giving us picture for potentialchallenges or gaps within the services.
Governance & OversightThe purpose of the oversight group is to allow a platform for where we can engagewith other stakeholders within the system, to raise awareness of the pathway,share key updates, address any potential risks or emerging issues related to NDDservices in the NEE area. Furthermore, to ensure we work collaboratively withthose, in health, social care, education & Parents and families etc.
Sub collaborative groupIs a forum for the providers of the pathway to come together, to have an openforum in a smaller setting, with a focus on collaborative working and to give aplatform for us all to discuss key areas arising, that may need to be soundboardout before sharing wider setting and share best practices.

Project RAG Update/Action Required in Red or Amber
NEE CAMHS On Track
Mobilisation of the new SET CAMH service model effective from 1st April 2022 with NELFT in partnership with HCRG, formerly Virgin Health Care, is underway; working to the principles of the Thrive framework for service delivery.
The SET CAMHS NHS Standard contract 2022/23 is complete and signed by NELFT, and now with SET commissioning partners for sign off.
Additional investment in NOW is the time for change across Essex 2022/23; providing therapeutic health-based coaching to all familieswith a separate programme for parents who have children- with ASD.
PCN workers- initial meeting with PCN’s at Clinical Directors was positively received with several expressing an interest in taking forward. Working towards developing the role with these partners initially.
The limited availability of CAMHS Tier 4 beds nationally continues, resulting in delays in access to inpatient admissions for young people. Due to the pressures on access to Tier 4 beds, the acute providers and NELFT remain challenged by the numbers of CYP having to becontained in the community or acute setting
46
Children and Young Peoples Programme Dashboard 2022 – 23

47
Children and Young Peoples Programme KPIs 2021 – 22
Metric Standard Date IES CCG WS CCG NEE CCG Notes
CYP Access (1+ contacts)Number of CYP under 18 with
at least one contactn/a Jan-22 5,455 2,765 3,845 Source is MHSDS- 12 month rolling
CYP Eating Disorder Waiting Time
UrgentUrgent 95% Dec-21 25.00% 94.40% 25.00% 12 month rolling
CYP Eating Disorder Waiting Time
RoutineRoutine 95% Dec-21 36.10% 69.80% 94.10% 12 month rolling
Paediatric Consultant led services 18 week RTT 95% Mar-22 30.38% Data not collected in NEE
Key Worker Function
% of CYP ragged amber or red
on the DSR allocated a Key
Worker
Q3 50%
Q4 90%
Function does not cover NEE. Launch date
01/09/2022

48
SNEE Strategic Programme Dashboard 2022 – 23Overall
Programme RAG
Apr-22 May-22 Jun-22 Jul-22 Aug-22 Sep-22 Oct-22 Nov-22 Dec-22 Jan-23 Feb-23 Mar-23
On Track
Programme Status:
Project RAG Update/Action Required in Red or Amber Project RAG Update/Action Required in Red or Amber
CVD - ICS At Risk
• The 22/23 Cardio Vascular Disease (CVD) charter has been written and was positively received at the last CVD committee meeting. The plan focusses on prevention via blood pressure control and Lipid management (which overlaps with Diabetes), removing Health Inequalities, treatment and care, innovation and using good data to drive improvement.
• The final Liberate Pro cardiac rehab demo was successfully completed and we are imminently soft launching these patients education slide decks across the area.
Stroke - ICS On Track
10% of Stoke patients are eligible and require a Mechanical Thrombectomy Service for Acute Ischaemic Stroke - The East of England (EoE) Stroke Network in collaboration with NHSE Specialised Commissioning Team have been working with Cambridge University Hospitals NHS Trust (CUHFT) to expand both the population coverage for the existing service and the operational times which the service will be available. This service development has been awaited, so the first stepped change is welcomed for an 8am-4pm service operating 5 days a week. By April 2023 this will become an 8am to 8pm service 7 days a week and ultimately a 24/7 service. Patients are to be repatriated in a timely fashion post intervention within 24-72 hours for local rehabilitation or ongoing inpatient care. This requires responsive patient transport which is being negotiated.
The focus across the ICS has been to develop stroke services with a focus on the national priorities as agreed by the Regional Stroke Integrated Service Delivery Network (North), we are part of support structure to develop services across regional and local geography. We have been working with our hospitals to develop a ‘pre-alert of stroke’ pathway, reviewing our ‘mimic’ pathways and evaluating the pathway of reduced call to door times and optimised cannulation rates.
We have introduced some pilots for increased detection of people with AF and to improve patient experience through at home monitoring. We are working with clinicians, stroke board and the EAHSN, to implement a pilot with two approaches.We continue to engage with secondary care clinicians to understand metrics relating to thrombolysis rates and the scoping of the thrombolysis pathways to identify processes that can be streamlined for greater efficiency.
Undertake mapping of ICSS model vs current services provided and identify aspects for development to achieve the targets set by ISDN such as 6/52 and 6/12 reviews SNAPP data – there have been changes to the data collection timescales with a renewed focus from the ISDN for provider compliance and improvement on these service standards.

49
SNEE Strategic Programme Dashboard 2022 – 23Project RAG Update/Action Required in Red or Amber Project RAG Update/Action Required in Red or Amber
Diabetes -ICS
On Track
• Our Care Processes (CP) and Treatment Target (TT) performance continues to be monitored via our monthly dashboard with end of year figures showing the following:
North east Essex (end 21/22)CP 68% (pre-Covid 80%) TT 19.4% (pre-Covid 27%)
Ipswich and east Suffolk (end 21/22)CP 50% (Pre-Covid 71%)TT 16.2% (pre-Covid 22.9%)
West Suffolk (end 21/22)CP 36% (pre-Covid 57%)TT 10.4% (pre-Covid 17.6%)
• The first draft of the 22/23 Diabetes plan and charter has been written and submitted to NHS England. The plan will be refined further with the intentions to ratify at the next Diabetes committee meeting on 20th
May. The plan centres on recovery of the Care Processes and Treatment targets to pre-Covid levels whilst getting the National Diabetes Prevention Programme (NDPP) back on its pre-Covid trajectory. It also shows (as previously agreed) we will fund the second year of two podiatrists to support footcare and seven diabetes inpatient specialist nurses (DISNs) along with a second year of the Diabetes technology lead.
• Xyla Health & Wellbeing who run the National Diabetes Prevention Programme on our behalf have appointed a new Engagement Officer to support referral generation across our Integrated Care System. The latest performance figures (March 22) show an increase in monthly referrals and the number of patients attending their first lesson (known as Milestone 1). Work continues to transfer patients from remote to face to face learning. Working with the Comm’s team we have secured a package of communications via digital and radio for national diabetes week (13–19 June) to promote referrals and awareness of the programme.
Maternity -ICS
On Track
• Ockenden final report gap analysis underway, with reporting to LMNS Board 23rd May.• Safe staffing levels, Trusts have requested Birthrate+ safe staffing review as need to be repeated every 3
years. This will be based on acuity of care provided and therefore may require an increasedestablishment.
• Inequalities 5 year plan under development, informed by active inequalities workstream. Filming tocommence May/June of series of films to increase inequalities awareness.
• VCSE projects commenced to work with diverse, deprived and lived experience communities to improvetheir service user experience, address wider determinants of health, and support through pregnancyand postnatal journey.
• LMNS strategy been socialised with NHSE, system partners, CYP Board, clinical executives and due to goto CCG Governing Bodies and ICS Board in May 2022
• Training and Development programme under development to include cultural awareness, motivational interviewing, LGBTQI+ awareness and sexual abuse awareness training for teams.
• Scoping LMNS wide recruitment and retention strategy, leadership pathways, culture and reverse mentoring
• Spending plan to be approved by LMNSB in May 2022, funding confirmation for glucose monitoring still awaited from NHSE
• Digital lead appointed, commencing in June 22 to scope LMNS digital strategy and support providers to move at pace with personalised care plans and ECR
• Working with MVP to establish best ways of communicating information about their pregnancy and parenting, to promoted selfcare, informed decisions making, and signposting to services.
• Joint work with health visiting to establish presence in family hubs and how to expand model to wider MDT
• Maternal Mental Health service joint working with MH team to develop bereavement pathway ready for 23/24 commencement
• Continuity of Carer plans reviewed in light of Ockenden recommendations and will be approved by Trust Boards and LMNS Board prior to submission to NHSE in mid June 22
• Smokefree pregnancy enhanced pathway designed, awaiting funding transfer but should commence in early summer 22
• Perinatal Quality surveillance and safety forum processes embedded in LMNS and enabling risks and outlier positions to be easily detected and acted upon, with escalation to LMNS Board where necessary
• Preconception plan under development to provide universal information and targeted interventions. Joint working with Public Health and Health Visiting colleagues to optimise impact. Workshop planned for early summer to confirm preconception and prevention agenda
• Neonatal critical care review gap analysis completed. QI nurse to be advertised to address any gaps in compliance but to move QI programme forward across the system.
• Preterm birth workstream approved to drive all transformation and QI work forward at pace, as SNEE a regional outlier.
• Post Partum Haemorrhage also risk and exploring whether population health management system can assist in identifying themes/risk factors common in women to enable targeted action.
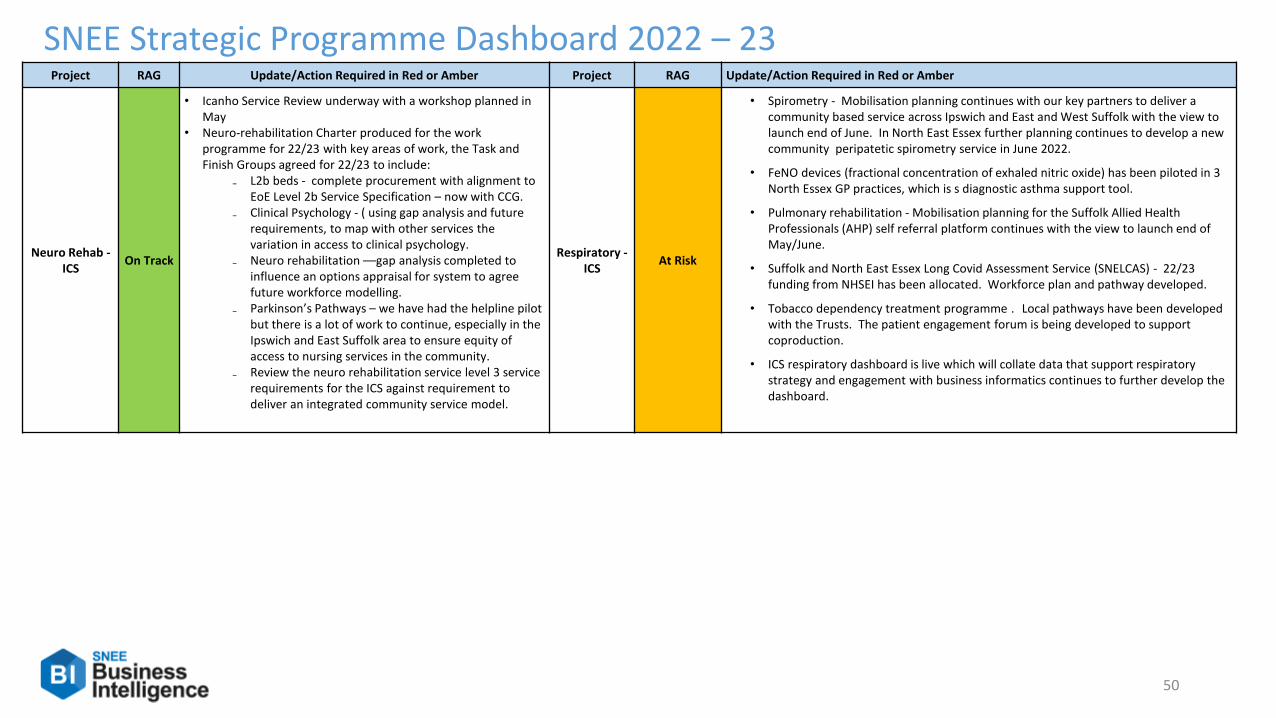
50
SNEE Strategic Programme Dashboard 2022 – 23Project RAG Update/Action Required in Red or Amber Project RAG Update/Action Required in Red or Amber
Neuro Rehab -ICS
On Track
• Icanho Service Review underway with a workshop planned in May
• Neuro-rehabilitation Charter produced for the work programme for 22/23 with key areas of work, the Task and Finish Groups agreed for 22/23 to include:
₋ L2b beds - complete procurement with alignment to EoE Level 2b Service Specification – now with CCG.
₋ Clinical Psychology - ( using gap analysis and future requirements, to map with other services the variation in access to clinical psychology.
₋ Neuro rehabilitation ––gap analysis completed to influence an options appraisal for system to agree future workforce modelling.
₋ Parkinson’s Pathways – we have had the helpline pilot but there is a lot of work to continue, especially in the Ipswich and East Suffolk area to ensure equity of access to nursing services in the community.
₋ Review the neuro rehabilitation service level 3 service requirements for the ICS against requirement to deliver an integrated community service model.
Respiratory -ICS
At Risk
• Spirometry - Mobilisation planning continues with our key partners to deliver a community based service across Ipswich and East and West Suffolk with the view to launch end of June. In North East Essex further planning continues to develop a new community peripatetic spirometry service in June 2022.
• FeNO devices (fractional concentration of exhaled nitric oxide) has been piloted in 3 North Essex GP practices, which is s diagnostic asthma support tool.
• Pulmonary rehabilitation - Mobilisation planning for the Suffolk Allied Health Professionals (AHP) self referral platform continues with the view to launch end of May/June.
• Suffolk and North East Essex Long Covid Assessment Service (SNELCAS) - 22/23 funding from NHSEI has been allocated. Workforce plan and pathway developed.
• Tobacco dependency treatment programme . Local pathways have been developed with the Trusts. The patient engagement forum is being developed to support coproduction.
• ICS respiratory dashboard is live which will collate data that support respiratory strategy and engagement with business informatics continues to further develop the dashboard.
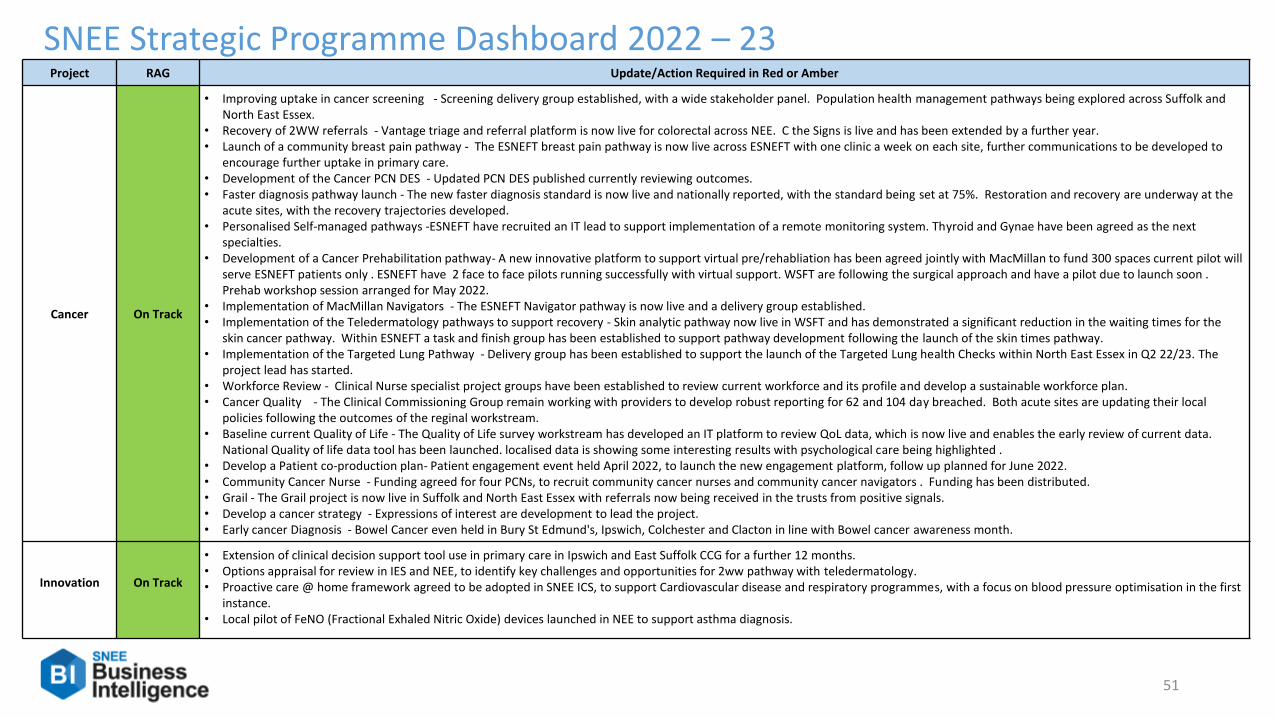
51
SNEE Strategic Programme Dashboard 2022 – 23Project RAG Update/Action Required in Red or Amber
Cancer On Track
• Improving uptake in cancer screening - Screening delivery group established, with a wide stakeholder panel. Population health management pathways being explored across Suffolk and North East Essex.
• Recovery of 2WW referrals - Vantage triage and referral platform is now live for colorectal across NEE. C the Signs is live and has been extended by a further year. • Launch of a community breast pain pathway - The ESNEFT breast pain pathway is now live across ESNEFT with one clinic a week on each site, further communications to be developed to
encourage further uptake in primary care. • Development of the Cancer PCN DES - Updated PCN DES published currently reviewing outcomes. • Faster diagnosis pathway launch - The new faster diagnosis standard is now live and nationally reported, with the standard being set at 75%. Restoration and recovery are underway at the
acute sites, with the recovery trajectories developed. • Personalised Self-managed pathways -ESNEFT have recruited an IT lead to support implementation of a remote monitoring system. Thyroid and Gynae have been agreed as the next
specialties. • Development of a Cancer Prehabilitation pathway- A new innovative platform to support virtual pre/rehabliation has been agreed jointly with MacMillan to fund 300 spaces current pilot will
serve ESNEFT patients only . ESNEFT have 2 face to face pilots running successfully with virtual support. WSFT are following the surgical approach and have a pilot due to launch soon . Prehab workshop session arranged for May 2022.
• Implementation of MacMillan Navigators - The ESNEFT Navigator pathway is now live and a delivery group established. • Implementation of the Teledermatology pathways to support recovery - Skin analytic pathway now live in WSFT and has demonstrated a significant reduction in the waiting times for the
skin cancer pathway. Within ESNEFT a task and finish group has been established to support pathway development following the launch of the skin times pathway. • Implementation of the Targeted Lung Pathway - Delivery group has been established to support the launch of the Targeted Lung health Checks within North East Essex in Q2 22/23. The
project lead has started. • Workforce Review - Clinical Nurse specialist project groups have been established to review current workforce and its profile and develop a sustainable workforce plan. • Cancer Quality - The Clinical Commissioning Group remain working with providers to develop robust reporting for 62 and 104 day breached. Both acute sites are updating their local
policies following the outcomes of the reginal workstream. • Baseline current Quality of Life - The Quality of Life survey workstream has developed an IT platform to review QoL data, which is now live and enables the early review of current data.
National Quality of life data tool has been launched. localised data is showing some interesting results with psychological care being highlighted .• Develop a Patient co-production plan- Patient engagement event held April 2022, to launch the new engagement platform, follow up planned for June 2022.• Community Cancer Nurse - Funding agreed for four PCNs, to recruit community cancer nurses and community cancer navigators . Funding has been distributed. • Grail - The Grail project is now live in Suffolk and North East Essex with referrals now being received in the trusts from positive signals. • Develop a cancer strategy - Expressions of interest are development to lead the project. • Early cancer Diagnosis - Bowel Cancer even held in Bury St Edmund's, Ipswich, Colchester and Clacton in line with Bowel cancer awareness month.
Innovation On Track
• Extension of clinical decision support tool use in primary care in Ipswich and East Suffolk CCG for a further 12 months.• Options appraisal for review in IES and NEE, to identify key challenges and opportunities for 2ww pathway with teledermatology.• Proactive care @ home framework agreed to be adopted in SNEE ICS, to support Cardiovascular disease and respiratory programmes, with a focus on blood pressure optimisation in the first
instance.• Local pilot of FeNO (Fractional Exhaled Nitric Oxide) devices launched in NEE to support asthma diagnosis.

52
Elective Care IES/NEE Transformation Programmes 2022 – 23
Overall Programme RAG
Apr-22 May-22 Jun-22 Jul-22 Aug-22 Sep-22 Oct-22 Nov-22 Dec-22 Jan-23 Feb-23 Mar-23
On Track
Project RAG Update/Action Required in Red or Amber Project RAG Update/Action Required in Red or Amber
National Pathway Improvement Programme
On Track
Implementation of National Pathway Improvement Programme (MSK)• SNEE Physio Partnership meeting held and reviewed combined Strengths, Weaknesses,
Opportunities & Threats (SWOT) analysis, agreeing four key areas of initial focus• SNEE Dashboard - reviewed current dashboard with a few minor amendments and requested
inclusion of the BestMSK Health Pathway Improvement Key Outcome Metrics• SNEE MSK Equality & Health Inequalities Impact Assessment (EHIIA) - begun review of
findings and begun development of action plan• ESNEFT MSK Pathways meeting held focussing on shared decision making• Begun review of Transfer of Patients Standard Operating Procedure (SOP) based on learnings• Non-Elective Back Pain - Supported sign-off of Back Pain Assessment Tool (BPAT), reviewed
the current Acute Back Pain leaflet as well as identified opportunities for education to support this work
National Pathway Improvement Programme (Ophthalmology)• SNEE Dashboard first draft finalised for Ophthalmology capturing Referral to Treatment
(RTT); Wait times; referrals by condition, source; cataract conversion rates; triage outcomes; A&G metrics; On-call activity and outcomes and more. Acute data now being reported by place. Community data from Evolutio still being sought. NICS data from ESNEFT - some basic data may be reported but nothing likely until ERS platform procured and in place for NEE
• SNEE Ophthalmology Equality & Health Inequalities Impact Assessment (EHIIA) - begun review of findings and begun development of action plan
• Pathway Review Group (PRG) met for the first time to discuss: 1. Community Glaucoma Pathway - IES and NEE - review successful consultant-led service in WS and take lessons learned from recent NEE Pilot to form new community glaucoma pathway covering rest of ICS. 2. Urgent eye Care Pathway - WS - understand issues and possible resolutions. Scope current pathway, review activity, agree improvements needed and support implementation, 3. Cataract Pathway - 1 year on - review pathway work and compare across ICS, 4. AMD and Retina
Waiting well On Track
• Project plan drafted and approved via ESNEFT• Review of quantitive data from Primary Care
reviewed across IES & NEE to ascertain improvement in quality of experience when awaiting surgery completed
• Review Phase 1 activities against initial scoping document completed
• Draft Phase 1 summary report completed for review by project team

53
Elective Care IES/NEE Transformation Programmes 2022 – 23
Project RAG Update/Action Required in Red or Amber
Health Inequalities & Armed Forces
On Track
ARMED FORCES • Health profiling on Military Veterans sourced confirming national data • Draft of current commissioning arrangements completed• Recommendations of Healthwatch Essex with regards to Veterans lived experienced reviewed• Initial Veterans Working Group (MDT) scheduled for 19th May 2022
HEALTH INEQUALITIES• Established key intervention and project team via National Association of Primary Care• Confirmation via NEE PC team to incorporate alongside Population Health Management Workstream• Confirmation via ATTAIN procurement team proposed project solution may be granted via Direct Award
Oral & Eye Health Prevention Programme
On Track
• Initial engagement completed with Public Health Essex and Suffolk to understand existing oral and eye health campaigns. • Attended Suffolk Oral Health Group and North East Essex Oral Healthcare Group which both took place on 5/04/22.• Introductory meetings held with other colleagues in Suffolk County Council and CCG who are involved in dental health. • Meeting held with public health lead and OneLife Suffolk on 25/04/22 - agreed potential opportunities to explore for improving connections with primary
care to support oral health in children.
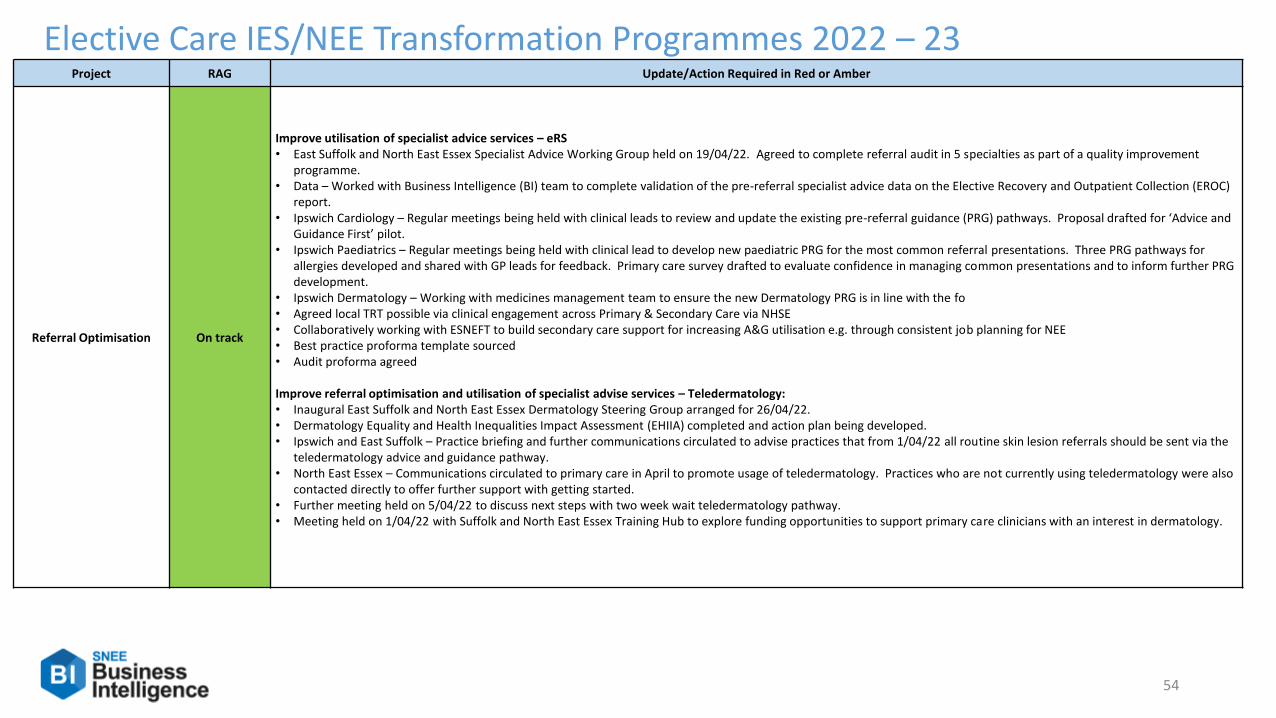
54
Elective Care IES/NEE Transformation Programmes 2022 – 23Project RAG Update/Action Required in Red or Amber
Referral Optimisation On track
Improve utilisation of specialist advice services – eRS• East Suffolk and North East Essex Specialist Advice Working Group held on 19/04/22. Agreed to complete referral audit in 5 specialties as part of a quality improvement
programme. • Data – Worked with Business Intelligence (BI) team to complete validation of the pre-referral specialist advice data on the Elective Recovery and Outpatient Collection (EROC)
report. • Ipswich Cardiology – Regular meetings being held with clinical leads to review and update the existing pre-referral guidance (PRG) pathways. Proposal drafted for ‘Advice and
Guidance First’ pilot. • Ipswich Paediatrics – Regular meetings being held with clinical lead to develop new paediatric PRG for the most common referral presentations. Three PRG pathways for
allergies developed and shared with GP leads for feedback. Primary care survey drafted to evaluate confidence in managing common presentations and to inform further PRG development.
• Ipswich Dermatology – Working with medicines management team to ensure the new Dermatology PRG is in line with the fo• Agreed local TRT possible via clinical engagement across Primary & Secondary Care via NHSE• Collaboratively working with ESNEFT to build secondary care support for increasing A&G utilisation e.g. through consistent job planning for NEE• Best practice proforma template sourced • Audit proforma agreed
Improve referral optimisation and utilisation of specialist advise services – Teledermatology:• Inaugural East Suffolk and North East Essex Dermatology Steering Group arranged for 26/04/22. • Dermatology Equality and Health Inequalities Impact Assessment (EHIIA) completed and action plan being developed. • Ipswich and East Suffolk – Practice briefing and further communications circulated to advise practices that from 1/04/22 all routine skin lesion referrals should be sent via the
teledermatology advice and guidance pathway. • North East Essex – Communications circulated to primary care in April to promote usage of teledermatology. Practices who are not currently using teledermatology were also
contacted directly to offer further support with getting started. • Further meeting held on 5/04/22 to discuss next steps with two week wait teledermatology pathway. • Meeting held on 1/04/22 with Suffolk and North East Essex Training Hub to explore funding opportunities to support primary care clinicians with an interest in dermatology.

55
Elective Care IES/NEE Transformation Headlines 2021 – 22
Activity is significantly effected due to the Covid-19 outbreak.
• IESCCG at ESNEFT Outpatients is 23.6% higher YTD 21/22 than the same period last year. Activity levels are higher than 20/21 however still remain slightly lower than 18/19 and 19/20.
•
• First face to face are significantly higher 83.3%, first telephones are lower 30.9% compared to the same period last year.
• Follow ups face to face are significantly higher 70.9%, follow up telephones are lower 32.0% YTD.
• Outpatients procedures are 13.0% higher compared to the same period last year.
• IESCCG at ESNEFT planned admissions are significantly higher 36.5% YTD 21/22 compared to the same period last year. Split, daycases are 35.2% higher and electives are 50.5% higher.
• Total 18 week patient waiting list for February-22 28,003. April-21 patient waiting list was 26,506. (Length of RTT period for patients whose 18 week clock is still running)
* Outpatients TFC 560 Maternity under reported for this month, this is due to be rectified next month.
Comparison against 19/20.
• IESCCG at ESNEFT Outpatients is 6.5% lower YTD 21/22 compared to the same period in 19/20.
• First face to face are (4,705) 3.9% higher, first telephones are higher (13,924) 267.1% compared to the same period in 19/20.
• Follow ups face to face are (-57,410) -24.2% lower, follow up telephones are higher (57,895) 240.4% compared to the same period in 19/20.
• Outpatients procedures are (-53,523) -38.0% lower compared to the same period in 19/20.
*Given the impact of covid and the resulting change to telephone consultations, these numbers appear realistic.
• IESCCG at ESNEFT planned admissions are (-2,163) -4.7% lower compared to same period in 19/20. Split, daycases are (-1,543) -3.8% lower and electives are (-620) -13.2% lower compared to 19/20.
• Total 18 week patient waiting list for February-22 28,003 comparing to 26,606 in January-19. (Length of RTT period for patients whose 18 week clock is still running)
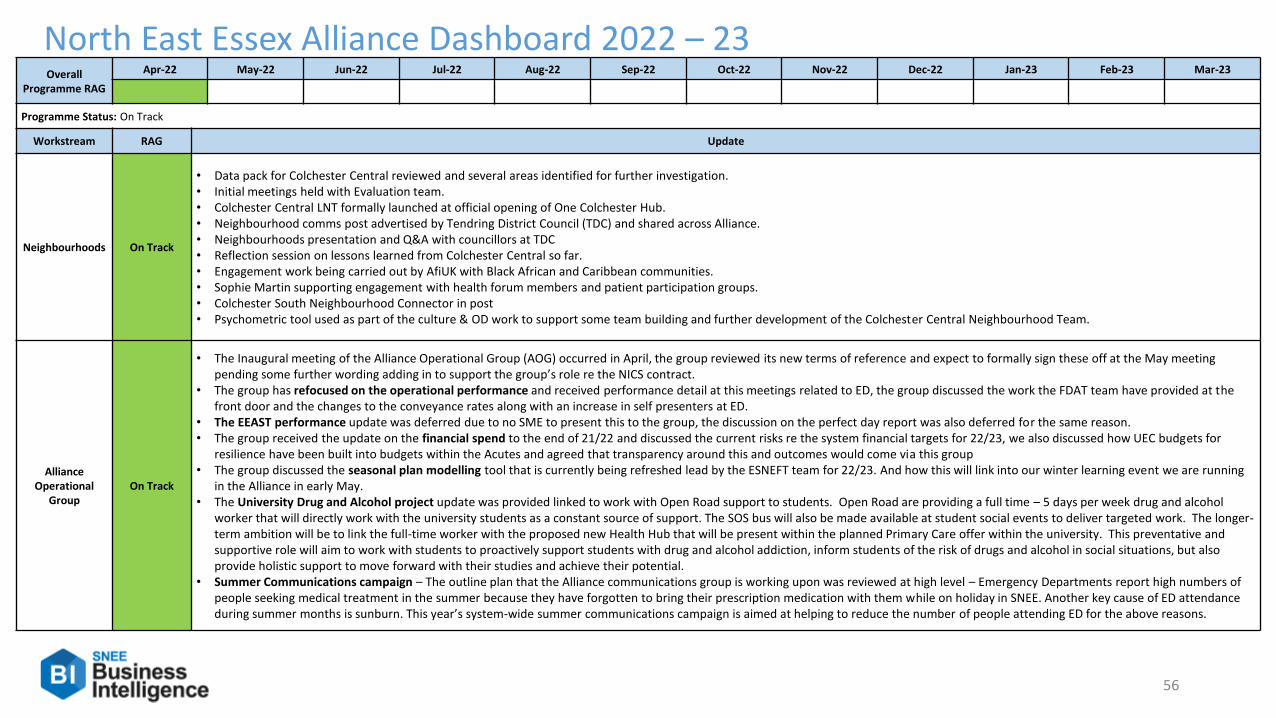
56
North East Essex Alliance Dashboard 2022 – 23Overall
Programme RAG
Apr-22 May-22 Jun-22 Jul-22 Aug-22 Sep-22 Oct-22 Nov-22 Dec-22 Jan-23 Feb-23 Mar-23
Programme Status: On Track
Workstream RAG Update
Neighbourhoods On Track
• Data pack for Colchester Central reviewed and several areas identified for further investigation.• Initial meetings held with Evaluation team.• Colchester Central LNT formally launched at official opening of One Colchester Hub. • Neighbourhood comms post advertised by Tendring District Council (TDC) and shared across Alliance.• Neighbourhoods presentation and Q&A with councillors at TDC• Reflection session on lessons learned from Colchester Central so far.• Engagement work being carried out by AfiUK with Black African and Caribbean communities.• Sophie Martin supporting engagement with health forum members and patient participation groups.• Colchester South Neighbourhood Connector in post• Psychometric tool used as part of the culture & OD work to support some team building and further development of the Colchester Central Neighbourhood Team.
Alliance Operational
GroupOn Track
• The Inaugural meeting of the Alliance Operational Group (AOG) occurred in April, the group reviewed its new terms of reference and expect to formally sign these off at the May meeting pending some further wording adding in to support the group’s role re the NICS contract.
• The group has refocused on the operational performance and received performance detail at this meetings related to ED, the group discussed the work the FDAT team have provided at the front door and the changes to the conveyance rates along with an increase in self presenters at ED.
• The EEAST performance update was deferred due to no SME to present this to the group, the discussion on the perfect day report was also deferred for the same reason.• The group received the update on the financial spend to the end of 21/22 and discussed the current risks re the system financial targets for 22/23, we also discussed how UEC budgets for
resilience have been built into budgets within the Acutes and agreed that transparency around this and outcomes would come via this group• The group discussed the seasonal plan modelling tool that is currently being refreshed lead by the ESNEFT team for 22/23. And how this will link into our winter learning event we are running
in the Alliance in early May. • The University Drug and Alcohol project update was provided linked to work with Open Road support to students. Open Road are providing a full time – 5 days per week drug and alcohol
worker that will directly work with the university students as a constant source of support. The SOS bus will also be made available at student social events to deliver targeted work. The longer-term ambition will be to link the full-time worker with the proposed new Health Hub that will be present within the planned Primary Care offer within the university. This preventative and supportive role will aim to work with students to proactively support students with drug and alcohol addiction, inform students of the risk of drugs and alcohol in social situations, but also provide holistic support to move forward with their studies and achieve their potential.
• Summer Communications campaign – The outline plan that the Alliance communications group is working upon was reviewed at high level – Emergency Departments report high numbers of people seeking medical treatment in the summer because they have forgotten to bring their prescription medication with them while on holiday in SNEE. Another key cause of ED attendance during summer months is sunburn. This year’s system-wide summer communications campaign is aimed at helping to reduce the number of people attending ED for the above reasons.

57
North East Essex Alliance Dashboard 2022 – 23
Domain RAG Update
Start Well On Track
• Feel well sub group agreed TOR and meetings established to drive forward the action plan. • Completion of 12 month evaluation of Tendring MDT and submitted Change Control Notice to successfully extend the pilot for 10 months. • Strengthened the Children's Partnership Start Well TOR and governance to reflect the funding and resourcing responsibilities that are delegated to Start Well from the Alliance. Established
a funding panel to provide oversight in the spending of the £700k allocated from the CCG.• Drafted reporting templates for each Start well sub group , to be completed by the sponsor to ensure progress is being met on the agreed outcomes.
Feel Well On Track
Recurrent theme throughout work streams is Reasonable Adjustments for all to enable access to services and support.
• Adult MH Programmes - Development of new models of care to ensure right care, right place, right time. Includes mental health practitioners in PCNs and closer working with voluntary sector through projects such as Together We Grow, Haven Supported Discharge, Age Well East Older Adult Mental Health Support etc. Participation of MHPs in neighbourhood MDTs
• Suicide prevention - EPUT suicide prevention plan linking in with Quality Improvement Initiatives Zero Tolerance training available to all staff across the ICS. STORM training/train the trainer
recommencing in EPUT
• Connected communities/Reducing Loneliness - Asset mapping report to be published, this will inform themes for the Feel Well Domain for the coming year Established monthly Steering group and identify Key Stakeholders for the Feel Well Domain
• Continued monitoring of Realising Ambitions projects. One Colchester Hub launch & market place event. Participation in NEE Commitment to Carers Group and Pledge. Analyse current provision under RA budget in line with community asset mapping to identify gaps
• Community Microenterprise project progressing – posters promoting the work are being planned for distribution

58
North East Essex Alliance Dashboard 2022 – 23
Domain RAG Update
Be Well On Track
Local Delivery Pilot:• Essex Pedal Power in Tendring recently hosted an away day at Jaywick Martello Tower, bringing together colleagues and stakeholders from across Essex as well as Birmingham to share
learnings so far and begin to put together plans for future delivery.• Colchester and Tendring have appointed for a new joint physical activity post employed by CBC but embedded in the CCG to begin in late April.• Continue to attend various system meetings to present plans for the inequalities programme over NEE that covers aspects of the Be Well indices. Inequalities spending plans are being drawn
up in more detail to cover additional funding.• Work across both authorities continues around the Ukraine refugee response. We are ensuring that Be Well indices such as physical wellbeing, mental health and housing are a part of the
wider solution.• Cycle parking around Clacton and Jaywick has recently been installed by Essex County Council.
Clacton place:• March Tendring Jobs and Careers Roadshow held 20th April at Morrisons in Harwich, well attended by partners and good feedback received. McDonalds and Rose Builders joined us for the
first time: New partners are continued to be sort, and venues are currently being agreed for the next few months including sites in Colchester. • The work continues with the Breaking Barriers team on the NHSEI project. No issues or concerns reported by either partner.• Conversations continue taking place with several Secondary schools across Tendring to identify key actions on planning future Heath and Care Academies. The idea of having a careers
roadshow style events have been agreed with the plans well underway for the first roadshow to be delivered to Clacton Coastal Academy in the coming weeks. • Conversations continue with the construction and green energy sectors and introductions to schools to identify these providers can deliver careers information to students. Discussion taking
place with ECC on how this work can be better coordinated, response from ECC has been positive. • Levelling Up roundtable planned for the beginning of May to look at what projects, partners and funding is involved across Tendring. Participants from strategic partners are expected to
attend. • Social Micro Enterprise team were unable to join us at the April Roadshow. However, a number of conversations took place with members of the public at the March event but as yet there
have been no outcomes from these interactions. There have been 10 micro-enterprises enrolled in the CME development programme at the time of the second change group meeting in February 2022. The number of micro-enterprises enrolled in the CME development programme has increased to 17: they worked with a total of 19 CMEs, including 2 that left the programme recently (they already had sufficient clients and chose not to complete the CME required training).
• Primary Care:• Evaluation of PCN Development projects • Estates Strategy Funding on track for all PCNs. Once complete over coming months this will also be aggregated to support Alliance integrational plans• PCNs preparing for 2022/23 Investment and Impact Fund (IIF). Indicators align with all Live Well Domains• NEE Spirometry diagnostic service in process of procurement• Working with PCNs on 22/23 workforce plans. C. 75 WTE 21/22 additional. Increase to occur 22/23 including but not limited to roles to support Be well• Children and Young Persons PCN Mental Health Practitioner in development for PCNs

59
North East Essex Alliance 2022 – 23Domain RAG Update
Stay Well On Track
UTS:• Refresh of Service Development Improvement Plan to be completed in May 22 with priority to continuation of service model review with aim to continue to support the increase in demand
and pressures of flow within the system. Milestones for 22/23 will then be agreed via the UTS CMT.• Establishment of friends and family test at Colchester site in April has demonstrated improvement in volume of feedback with positive outcome.• To link SDIP work with the outputs from the system workshops to be held in may regarding Seasonal demand and longer term UEC strategy
Planned Care:• A big push on promotion of the wait well messages has occurred SNEE wide, supporting messaging for those waiting for hospital treatments due to the covid backlogs.
Integrated Immediate Care• ECC team have progressed work in the service specifications for the ILLOR and reablement services a market event has been planned for the end of April to update on timescales and the vision
for the services going forward • Bridging & ILOR contracts are ending in the Summer of 2022• ECL contract is let until May 2024 but has scope to flex to meet needs• Evaluation of the Tendring housing pilot has been undertaken, future planning regarding this is taking pace within Alliance Team
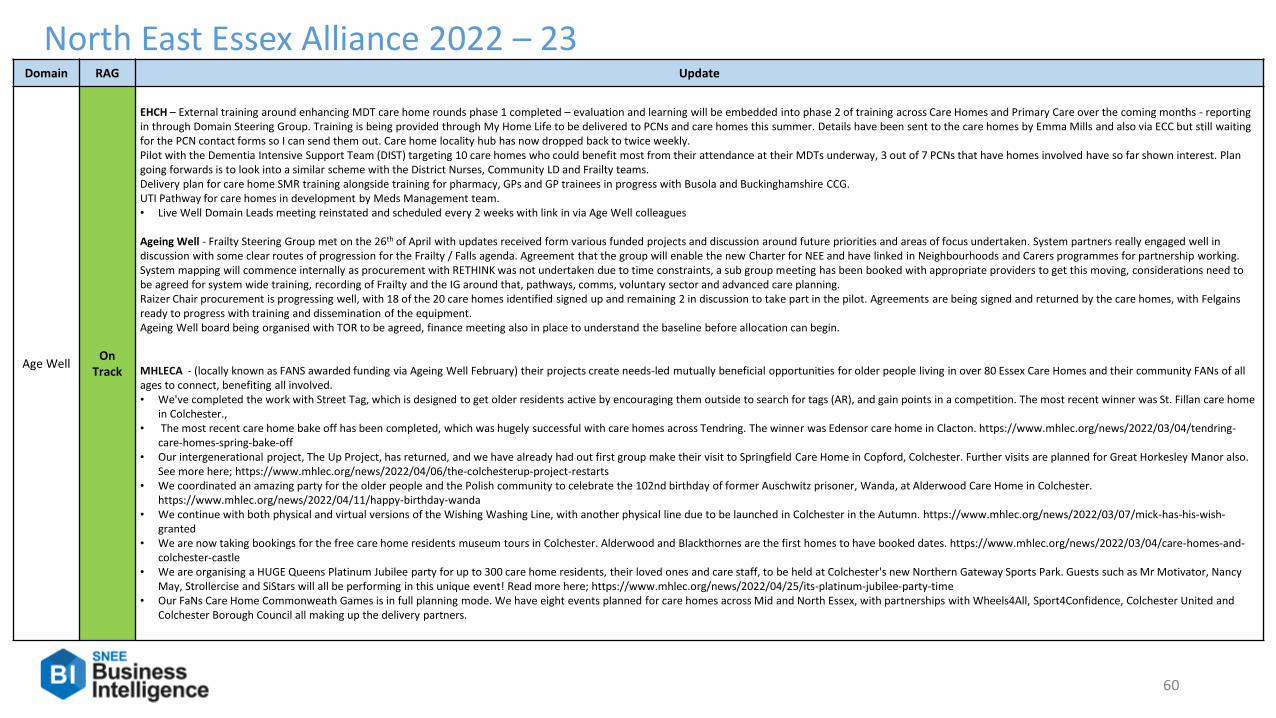
60
North East Essex Alliance 2022 – 23Domain RAG Update
Age WellOn
Track
EHCH – External training around enhancing MDT care home rounds phase 1 completed – evaluation and learning will be embedded into phase 2 of training across Care Homes and Primary Care over the coming months - reporting in through Domain Steering Group. Training is being provided through My Home Life to be delivered to PCNs and care homes this summer. Details have been sent to the care homes by Emma Mills and also via ECC but still waiting for the PCN contact forms so I can send them out. Care home locality hub has now dropped back to twice weekly. Pilot with the Dementia Intensive Support Team (DIST) targeting 10 care homes who could benefit most from their attendance at their MDTs underway, 3 out of 7 PCNs that have homes involved have so far shown interest. Plan going forwards is to look into a similar scheme with the District Nurses, Community LD and Frailty teams. Delivery plan for care home SMR training alongside training for pharmacy, GPs and GP trainees in progress with Busola and Buckinghamshire CCG.UTI Pathway for care homes in development by Meds Management team.• Live Well Domain Leads meeting reinstated and scheduled every 2 weeks with link in via Age Well colleagues
Ageing Well - Frailty Steering Group met on the 26th of April with updates received form various funded projects and discussion around future priorities and areas of focus undertaken. System partners really engaged well in discussion with some clear routes of progression for the Frailty / Falls agenda. Agreement that the group will enable the new Charter for NEE and have linked in Neighbourhoods and Carers programmes for partnership working. System mapping will commence internally as procurement with RETHINK was not undertaken due to time constraints, a sub group meeting has been booked with appropriate providers to get this moving, considerations need to be agreed for system wide training, recording of Frailty and the IG around that, pathways, comms, voluntary sector and advanced care planning. Raizer Chair procurement is progressing well, with 18 of the 20 care homes identified signed up and remaining 2 in discussion to take part in the pilot. Agreements are being signed and returned by the care homes, with Felgainsready to progress with training and dissemination of the equipment. Ageing Well board being organised with TOR to be agreed, finance meeting also in place to understand the baseline before allocation can begin.
MHLECA - (locally known as FANS awarded funding via Ageing Well February) their projects create needs-led mutually beneficial opportunities for older people living in over 80 Essex Care Homes and their community FANs of all ages to connect, benefiting all involved.• We've completed the work with Street Tag, which is designed to get older residents active by encouraging them outside to search for tags (AR), and gain points in a competition. The most recent winner was St. Fillan care home
in Colchester.,• The most recent care home bake off has been completed, which was hugely successful with care homes across Tendring. The winner was Edensor care home in Clacton. https://www.mhlec.org/news/2022/03/04/tendring-
care-homes-spring-bake-off• Our intergenerational project, The Up Project, has returned, and we have already had out first group make their visit to Springfield Care Home in Copford, Colchester. Further visits are planned for Great Horkesley Manor also.
See more here; https://www.mhlec.org/news/2022/04/06/the-colchesterup-project-restarts• We coordinated an amazing party for the older people and the Polish community to celebrate the 102nd birthday of former Auschwitz prisoner, Wanda, at Alderwood Care Home in Colchester.
https://www.mhlec.org/news/2022/04/11/happy-birthday-wanda• We continue with both physical and virtual versions of the Wishing Washing Line, with another physical line due to be launched in Colchester in the Autumn. https://www.mhlec.org/news/2022/03/07/mick-has-his-wish-
granted• We are now taking bookings for the free care home residents museum tours in Colchester. Alderwood and Blackthornes are the first homes to have booked dates. https://www.mhlec.org/news/2022/03/04/care-homes-and-
colchester-castle• We are organising a HUGE Queens Platinum Jubilee party for up to 300 care home residents, their loved ones and care staff, to be held at Colchester's new Northern Gateway Sports Park. Guests such as Mr Motivator, Nancy
May, Strollercise and SiStars will all be performing in this unique event! Read more here; https://www.mhlec.org/news/2022/04/25/its-platinum-jubilee-party-time• Our FaNs Care Home Commonweath Games is in full planning mode. We have eight events planned for care homes across Mid and North Essex, with partnerships with Wheels4All, Sport4Confidence, Colchester United and
Colchester Borough Council all making up the delivery partners.

61
North East Essex Alliance 2022 – 23Domain RAG Update
Age Well On Track
NICS: • Governance Group agreed CLT and CMT will be established in shadow form by June 22• Workshop to be held in June 22 to develop transition and transformation plans including prioritisation exercise – Priority to schedule date of workshop• Proposal for Children’s therapy service model under consideration – for agreement in June 22.• Diabetes Service sub-contract now in place from 1st May, with Suffolk GP Fed continuing to deliver the service.
Carers:• Action for Family Carers progressing to mobilise their Young Carers proposal to improve outcomes for Young Carers - vulnerable children and young people - in North East Essex through
the development of a coherent and locally responsive model of best practice. Recruitment of two (Colchester/Tendring) District Young Carer Leads progresses, and the opening of a Young Carers Club in Tendring has been prioritised. Timeline to be agreed.
• The Commitment to Carers Network Group continues to meet and is currently reviewing the Commitment to Carers Pledge which, once finalised, will be recommended to Alliance Partners for approval and sign up.
• Numerous events, forums and activities are being organised across North East Essex for National Carers Week (7-12 June 22) and as many of these would be shared via the various Organisations’ social media and comms channels. Raising awareness amongst existing carers, as well as engaging with those who do not currently identify as a family/unpaid carer.
UCRS – service is seeking to redesign alongside other community teams such as nursing, OPAT and IRAS to provide a wider arching service across the community in NEE. UCRS now meeting twice daily with EEAST control room to take live jobs from the stack and increase community referrals. April has seen the biggest jump in EEAST referrals into UCRS since they began delivery in December 2020, with 45 referrals and 30 of those remaining the clinical responsibility of UCRS, so the project is achieving great outcomes for the system pressures.
Anticipatory Care – ICS project worked up around Primary Care and PCN -SNEE scheme commissioned to EASHN to provide the baseline review of Primary Care Integration across SNEE in relation to Anticipatory Care. The initial meeting with EASHN was productive, GP lead established for NEE and Project support in place to assist EASHN with delivery. Work to commence soon with stakeholder engagement.
Die Well On Track
• Ethnicity data now flows into the dashboard and initial results suggest no inequalities in end of life outcomes.• The 21/22 final report is in the last stages of being written due to be completed end of April 2022.• The outcomes have shown improvement in 21/22 with a lower number of emergency admissions at the end of life (data to end Feb 2022)• The 22/23 plan is in the final stages of preparation and is due for sign off at the April EoL board.• Business plan for End of Life champions in the community wards have been approved.• 3 Palliative community nurses have been appointed for Tendring to support the addressing of inequalities.• Advance care planning training is being delivered across the Alliance.• The End of Life board approved funding for 10 nurses to join a national community of practice. These have been selected and are due to start
Financial Position Updates 21-22
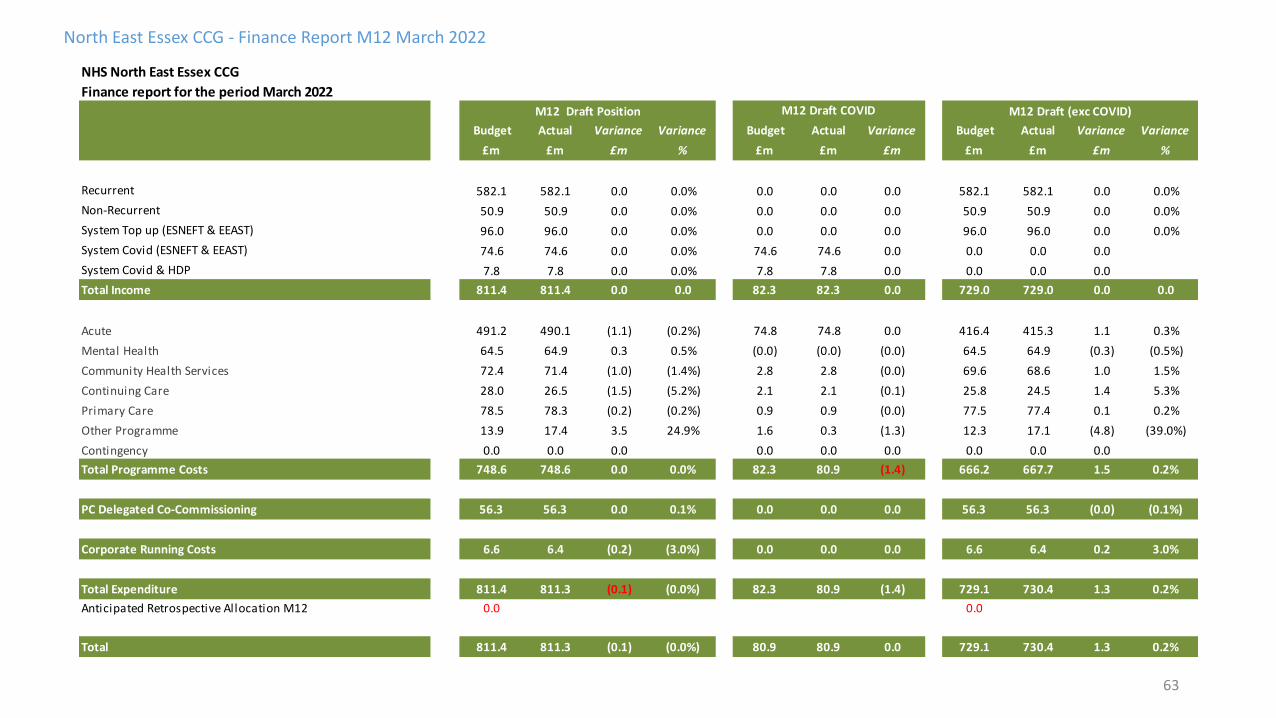
63
North East Essex CCG - Finance Report M12 March 2022
NHS North East Essex CCG
Finance report for the period March 2022
Budget Actual Variance Variance Budget Actual Variance Budget Actual Variance Variance
£m £m £m % £m £m £m £m £m £m %
Recurrent 582.1 582.1 0.0 0.0% 0.0 0.0 0.0 582.1 582.1 0.0 0.0%
Non-Recurrent 50.9 50.9 0.0 0.0% 0.0 0.0 0.0 50.9 50.9 0.0 0.0%
System Top up (ESNEFT & EEAST) 96.0 96.0 0.0 0.0% 0.0 0.0 0.0 96.0 96.0 0.0 0.0%
System Covid (ESNEFT & EEAST) 74.6 74.6 0.0 0.0% 74.6 74.6 0.0 0.0 0.0 0.0
System Covid & HDP 7.8 7.8 0.0 0.0% 7.8 7.8 0.0 0.0 0.0 0.0
Total Income 811.4 811.4 0.0 0.0 82.3 82.3 0.0 729.0 729.0 0.0 0.0
Acute 491.2 490.1 (1.1) (0.2%) 74.8 74.8 0.0 416.4 415.3 1.1 0.3%
Mental Health 64.5 64.9 0.3 0.5% (0.0) (0.0) (0.0) 64.5 64.9 (0.3) (0.5%)
Community Health Services 72.4 71.4 (1.0) (1.4%) 2.8 2.8 (0.0) 69.6 68.6 1.0 1.5%
Continuing Care 28.0 26.5 (1.5) (5.2%) 2.1 2.1 (0.1) 25.8 24.5 1.4 5.3%
Primary Care 78.5 78.3 (0.2) (0.2%) 0.9 0.9 (0.0) 77.5 77.4 0.1 0.2%
Other Programme 13.9 17.4 3.5 24.9% 1.6 0.3 (1.3) 12.3 17.1 (4.8) (39.0%)
Contingency 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0
Total Programme Costs 748.6 748.6 0.0 0.0% 82.3 80.9 (1.4) 666.2 667.7 1.5 0.2%
PC Delegated Co-Commissioning 56.3 56.3 0.0 0.1% 0.0 0.0 0.0 56.3 56.3 (0.0) (0.1%)
Corporate Running Costs 6.6 6.4 (0.2) (3.0%) 0.0 0.0 0.0 6.6 6.4 0.2 3.0%
Total Expenditure 811.4 811.3 (0.1) (0.0%) 82.3 80.9 (1.4) 729.1 730.4 1.3 0.2%
Anticipated Retrospective Allocation M12 0.0 (1.4) 0.0
Total 811.4 811.3 (0.1) (0.0%) 80.9 80.9 0.0 729.1 730.4 1.3 0.2%
M12 Draft (exc COVID)M12 Draft Position M12 Draft COVID
64
North East Essex CCG - Finance Report M12 March Commentary
1. Commentary
NHS North East Essex CCG
Finance report for the period March 2022
CCG received its historic surplus of £14.023m in M6.
Detailed report with Key variances will be presented to next the committee meeting.
The CCG is reporting £0.106m Surplus position for Month 12. The CCG has submitted Draft Accounts on 26th April 22 to NHS England and External Auditor are in a process
of carrying out an audit. The Final Audited Accounts are due to be submitted by end of May 22.
The CCG has received Full year recurrent allocations of £582.1m and non recurrent allocations of £229.227m, the non recurrent allocations include ESNEFT
& EEAST system top ups , system COVID and HDP totalling £178.302m and ERF allocations of £14.632m.
The year to date COVID and HDP costs at M12 are £6.338m, of this £1.339m of the CCG's COVID allocations were unspent which is included in the CCG's overall
position.
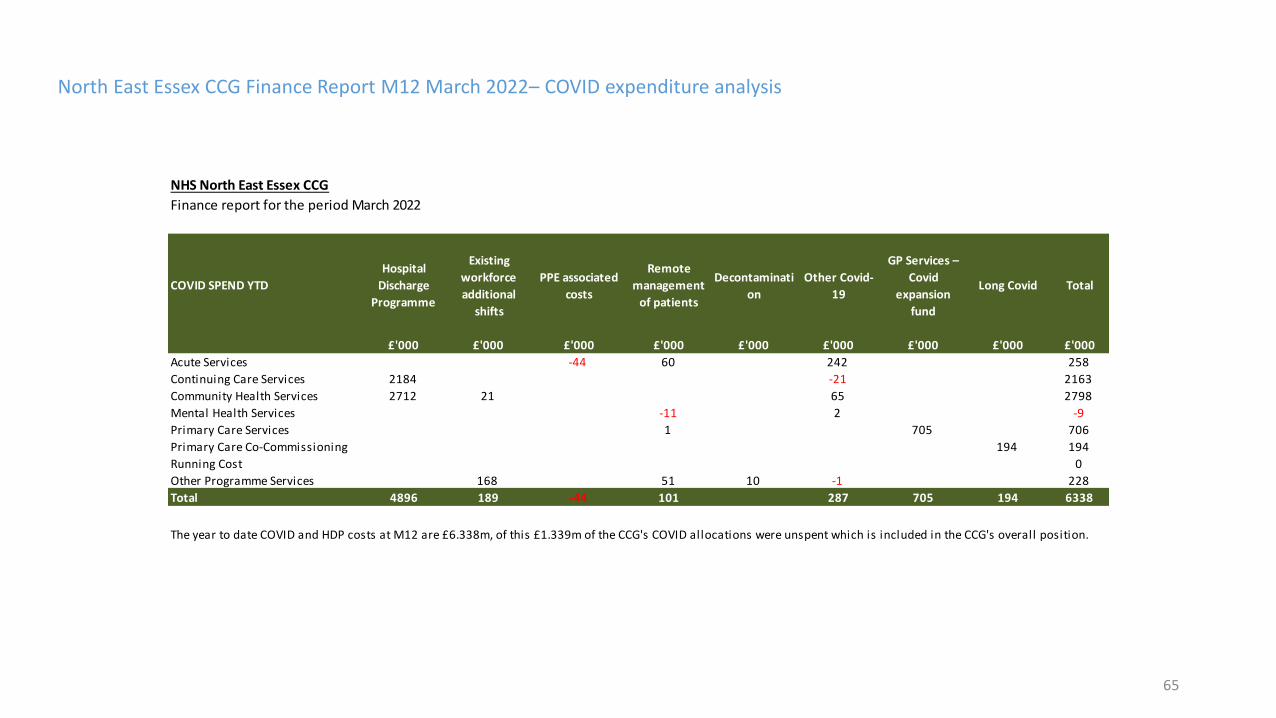
65
North East Essex CCG Finance Report M12 March 2022– COVID expenditure analysis
NHS North East Essex CCG
Finance report for the period March 2022
COVID SPEND YTD
Hospital
Discharge
Programme
Existing
workforce
additional
shifts
PPE associated
costs
Remote
management
of patients
Decontaminati
on
Other Covid-
19
GP Services –
Covid
expansion
fund
Long Covid Total
£'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000
Acute Services -44 60 242 258
Continuing Care Services 2184 -21 2163
Community Health Services 2712 21 65 2798
Mental Health Services -11 2 -9
Primary Care Services 1 705 706
Primary Care Co-Commissioning 194 194
Running Cost 0
Other Programme Services 168 51 10 -1 228
Total 4896 189 -44 101 287 705 194 6338
Total 748 0 0 2 532 1303
The year to date COVID and HDP costs at M12 are £6.338m, of this £1.339m of the CCG's COVID allocations were unspent which is included in the CCG's overall position.
Page 1 of 3
GOVERNING BODY
Agenda Item No. 13
Reference No. NEECCG 22-37
Date. 7 June 2022
Title
Remuneration and HR Committee Report
Lead Director
Martyn Hanlon, Chair Remuneration and HR Committee Amanda Lyes, Director of Corporate Services and System Infrastructure
Author(s)
Jo Mael, Corporate Governance Manager
Purpose
To present an update on the work of the CCG’s Remuneration and HR Committee.
Applicable CCG Strategic Objectives:
1. To achieve our vision through an inclusive, holistic approach to patient and service user centred commissioning, embedding personalisation of care through integrated health and social care services.
2. To transform care and drive continuous improvement in quality and safety. Achieve the best possible outcomes for our service users through high quality care.
3. To use commissioning resources effectively and responsibly. To develop our organisation, teams and individual staff to be trusted, competent, well trained, talented, enthusiastic and dedicated.
√
4 To tackle the biggest health challenges in north east Essex including reducing health inequalities.
Recommendation: The Governing Body is asked to note the report.

Page 2 of 3
1. Summary The Remuneration and HR Committee is required by its terms of reference to meet on an ‘as and when’ basis, but at least annually. A meeting was held ‘in common’ with the Remuneration and HR Committees of Ipswich and East Suffolk and West Suffolk CCGs on 5 April 2022.
2. Key Points to Note
At the meeting held on 5 April 2022 the following items were discussed:
2.1 The Committee reviewed its terms of reference. 2.2 Susannah Howard, Integrated Care Partnership Programme Director was welcomed to the
meeting and proceeded to provide a presentation on progress in respect of transition to the ICS.
2.3 The Committee was presented with the latest workforce report with key highlights being;
• Staff Headcount and FTE had increased slowly for three months and was now remaining stable.
• The number of female and male staff members had both increased by 8% and 9% respectively.
• Staff turnover numbers had remained stable. There had been 118 starters and 75 leavers and work was taking place to better understand the reasons that people left.
• Sickness absence duration and cost was showing a slight increase year on year, which could be mainly attributed to absence reasons likely indicating Covid-19 infections.
2.4 Management running costs were reviewed. 2.5 The Committee was presented with a report which detailed feedback from the recent
National Staff Survey and set out an action plan going forward. Further information on the staff survey is to be presented to the Governing Body later on today’s agenda.
2.6 Under the Equality Act 2010 (Gender Pay Gap Information) Regulations 2017, all employers
with 250 or more staff were required to report, on an annual basis, their gender pay gap. The report presented to the Committee:
• Provided information on the requirements.
• Set out the gender pay gap and provided some analysis.
• Proposed next steps. 2.7 The Committee was also provided with an updates on the most recent meeting of the Joint
Staff Partnership Committee. 3. Risks Identified
None 4. Resource Implications
None 5. Engagement and Communication

Page 3 of 3
N/A
6. Equality and Diversity
No negative or positive equality and diversity implications assessed at this time.

Page 1 of 3
GOVERNING BODY
Agenda Item No. 14
Reference No. NEECCG 22-38
Date. 7 June 2022
Title
Audit Committee Report
Lead
Jerry Wedge, Lay Member and Chair of the Audit Committee
Author(s)
Corporate Governance Officer
Purpose
To assure the Governing Body the Audit Committee is fully carrying out its governance role.
Applicable CCG Strategic Objectives:
1. To achieve our vision through an inclusive, holistic approach to patient and service user centred commissioning, embedding personalisation of care through integrated health and social care services.
2. To transform care and drive continuous improvement in quality and safety. Achieve the best possible outcomes for our service users through high quality care.
3. To use commissioning resources effectively and responsibly. To develop our organisation, teams and individual staff to be trusted, competent, well trained, talented, enthusiastic and dedicated.
x
4 To tackle the biggest health challenges in north east Essex including reducing health inequalities.
Recommendation: The Governing Body is asked to note this report and confirm it is assured that the Audit Committee is fully carrying out its governance role.

Page 2 of 3
1. Summary
The Audit Committee met on 5th April 2022 via teleconferencing, this was a meeting in common with the Suffolk CCGs. Full minutes are available on the Extranet under the Board Member section.
2. Key Points to Note 2.1 2.2 2.3 2.4 2.5 2.6 2.7 2.8 2.9
The Committee received the Auditor Sector Update report from the External Auditors The External Audit Progress Report was presented providing an update on the progress of the audit for the year ending 31st March 2021. The Draft Head of Internal Audit For the 12 months ending 31 March 2022 was received and is as follows: ‘The organisation has an adequate and effective framework for risk management, governance and internal control. However, our work has identified further enhancements to the framework of risk management, governance and internal control to ensure that it remains adequate and effective’.
The Committee discussed the Internal Audit Progress Report and noted the subsequent reports:
a) Safeguarding Children - Substantial Assurance b) Personal Health Budgets - Reasonable Assurance c) Continuing Healthcare - Reasonable Assurance d) Conflict of Interest - Reasonable Assurance e) Patient and Public Involvement - Reasonable Assurance
The Committee approved the Local Counter Fraud Workplan for 2022/23. The Committee were presented with a timetable of key dates in relation to the production of the Annual Report and Accounts. The Committee discussed and noted the Governing Body Assurance Framework and Directorate Risk Registers.
The Committee noted the list of waivers presented. The Committee:
• Recommended approval of the Standing Financial Instructions and the Scheme of Delegation (SoRD) noting further work is required around the procurement element
• Approved the principles of working as set out within the Suffolk and NEE ICB Emergency Preparedness, Resilience, Response and Business Continuity Policy
3. Risks Identified
This report does not highlight any specific risks.
4. Resource Implications

Page 3 of 3
This report does not have any direct resource implications 5. Engagement and Communications
None 6. Equality and Diversity
This report does not have an equality and diversity assessment undertaken as produced as a performance review of the Audit Committee.
Page 1 of 9
GOVERNING BODY
Agenda Item No. 15
Reference No. NEECCG 22-39
Date. 7 June 2022
Title
Quality Committee Overview Report
Lead Director
Lisa Nobes, Director of Nursing
Author(s)
Joe Allen, Head of Patient Safety
Purpose
To provide assurance of quality scrutiny
Applicable CCG Strategic Objectives:
1. To achieve our vision through an inclusive, holistic approach to patient and service user centred commissioning, embedding personalisation of care through integrated health and social care services.
√
2. To transform care and drive continuous improvement in quality and safety. Achieve the best possible outcomes for our service users through high quality care.
√
3. To use commissioning resources effectively and responsibly. To develop our organisation, teams and individual staff to be trusted, competent, well trained, talented, enthusiastic and dedicated.
√
4 To tackle the biggest health challenges in north east Essex including reducing health inequalities.
√
Recommendation:
The Governing Body is asked to note the content of this report and raise any concerns or questions in relation to the assurance of quality in provider organisations, commissioned for north east Essex patients.
The Governing Body is asked to assure itself that the Quality Committee is satisfied that
where performance is not reaching the required standard that the necessary steps are being undertaken to achieve standards.
Page 2 of 9
1. Summary 1.1 The aim of this report is to bring to the attention of the Board the patient safety and
quality exceptions which have been identified in the services commissioned by North East Essex Clinical Commissioning Group (NEECCG).
1.2 The May 2022 Quality Committee was the final meeting; from July 2022 the Suffolk and
North East Essex Integrated Care Board and the North East Essex Alliance assume the Quality and Safety oversight for services in North East Essex. Given this was the closing meeting, the Committee received and reviewed the following specific clinical service reports to establish position and key risks for transfer over to the requisite Alliance or Integrated Care System (ICS) quality and safety forum.
• Closure of NEE Quality Committee
• Risk Report
• Pan Essex Section 117 Protocol
• Children and Young People’s Continuing Care Annual Report
• Patient & Public Involvement and Experience Q4 Report
• Serious Incident Position
• IPT Summary Report
• LD and Autism hospital numbers and reviews update
• Outcome of Inquest into the death of Bethany Lilley
• ESNEFT Quality Report
• ESNEFT Pathology Quality Report
• NICS Quality Report
• Marie Stopes Quality Report
• EEAST PTS Quality Report
• Tollgate Centre Quality Report 1.3 Clinical service reports are triangulated to seek assurance that patients receive safe,
quality care. Where concerns have been identified, the CCG will take the appropriate measures to bring this to the attention of the provider(s).
1.4 This provides assurance of how the CCG continues to monitor and review progress with
commissioned services; on maintaining and enhancing the quality of services; and that improvements in patient safety, patient experience and clinical effectiveness, are being implemented.
2. Key Points to Note 2.1 At East Suffolk and North East Essex Foundation Trust, the total nursing staffing fill rate
for March 2022 saw a drop in staffing numbers for this reporting period. This will continue to be monitored throughout transition to the ICS.
2.2 This is was the final Quality Committee meeting for North East Essex CCG. Reports
were received giving a position of issues and risks for each Provider in order to support a safe transition to an Integrated Care System.
2.3 In respect of Children and Young Persons Continuing Care (CYPCC) Any Qualified
Providers (AQP) are experiencing difficulties with recruitment of nursing and care staff, which is impacting on commissioned care. This is identified as a national and system wide problem. Currently, across Essex, this has led to commissioning with providers not on the AQP framework.
Page 3 of 9
2.4 The CCG have met with ESNEFT to discuss the planned response to findings by Health Education England (HEE) and await further information on progress regarding an action plan to address the findings.
3. Risks Identified 3.1 In March 2022, there was an inquest hearing at Essex Coroner’s Court following the
death of Bethany Lilley, a patient under the care of EPUT, who died by ligature on the 16 January 2019 at Thorpe Ward, Basildon Mental Health Unit. The inquest found, on the balance of probability, there were failings which amounted to a gross failure to provide basic medical care. The CCG, as part of a collaborative arrangement, continues to work with all Essex CCG’s in order to strengthen oversight of EPUT services.
3.2 East of England Ambulance Service Trust continue to remain in REAP 4 (Resource
Escalation Action Plan) status since July 2021. This was implemented following system pressures and ambulance response delays. This means the Trust undertake a series of measures to maximise ambulance response times. Serious Incidents continue to be reported and monitored where patients experience treatment delays. In Suffolk and North East Essex, we have launched the Urgent and Emergency Care Framework to review system incidents where patients have been harmed.
4. Resource Implications
None Identified
5. Engagement and Communication 5.1 The CCG will need to manage any potential enquiries from stakeholders about
performance or quality concerns, in order to provide assurance of the steps the CCG are taking to ensure services are safe and of high quality.
6. Equality and Diversity 6.1 Seeking assurance that our commissioned services are providing safe and quality
services, should not adversely impact on any particular group and general improvement in quality should address areas of inequality.
Page 4 of 9
QUALITY COMMITTEE OVERVIEW REPORT 1. PRIMARY CARE 1.1 North East Essex Integrated Community Service (NICS)
The CCG continues to monitor quality and safety for the NICS service. Key issues for this reporting period are: The CCG is still awaiting data in order to understand how compliance for Safeguarding Adult training will be improved for ESNEFT community staff. Training remains below KPI. This follows problems with competency alignment between the previous provider, Anglia Community Enterprise and ESNEFT. In addition, ESNEFT are seeking support for funding from the Alliance Committee to continue seven days services for respiratory and the leg ulcer service. Following concerns regarding a number of wait times over 18 weeks for some services, ESNEFT have demonstrated that these services have detailed recovery plans. NHSE/I funds for service recovery have been secured by ESNEFT, who are currently looking at how this will be utilised. Finally, Commissioning for Quality and Innovation (CQUINs) for 2022/23 continue to be discussed. The aim is to agree and finalise reporting arrangements for these in the coming weeks.
2. URGENT CARE
2.1 East Suffolk and North East Essex Foundation Trust (ESNEFT) 2.1.1 Serious Incidents (SI) The CCG is working closely with ESNEFT to facilitate closure of the outstanding SIs. All 60-day reports have now been received and reviewed and the last pre-merger action plan was completed in April 2022; all pre-merger investigations and action plans are now fully closed. Currently 9 SIs have queries outstanding, 3 are with the CCG to review/gain additional assurance. The Trust is in the process of reviewing all outstanding action plans to provide an update to the CCG. 2.1.2 Patient Safety Incident Response Framework (PSIRF)
PSIRF assurance meetings are held monthly with ENSEFT, who provide an overview and update on: recent incidents; themes; significant events and areas of concern. In respect of maternity services, assurance is received at a joint meeting with West Suffolk Foundation Trust; the inaugural meeting was held in March 2022 with limited attendance by ESNEFT. Terms of Reference have been agreed. ESNEFT are now in the process of reviewing their patient safety data in order to refresh their Patient Safety Incident Response Plan (PSIRP) priorities. An updated version of their PSRIP will be published on the Trust website and shared with the CCG. 2.1.2 Safer Staffing

Page 5 of 9
The total nursing staffing levels fill rate for March 2022 as reported on the ESNEFT Website, reflects staffing levels as follows:
• Qualified day: 98.16%
• Qualified Night: 80.742 % (Amber)
• Unqualified Day: 70.346.2 % (Red)
• Unqualified Night: 41.188 % (Red) With the exception of Qualified day staffing, this is a reduction in the previous data reported from January 2022:
• Qualified day: 87.3% (Amber)
• Qualified Night: 88.6 % (Amber)
• Unqualified Day: 75.2 % (Red)
• Unqualified Night: 101.40% (Green) The quality team will continue to monitor ESNEFT staffing levels as part of oversight work when the Integrated Care System is formally established on 1 July 2022. 2.1.3 ESNEFT mortality data The Hospital Standardised Mortality Ratio (HSMR) measures whether the number of deaths in hospital is higher or lower than you would expect. A score of 100 means that the number of deaths is similar to what you would expect. A higher score means more deaths; a lower score, fewer. For ESNEFT the January 2022 12-month HSMR (which excludes Covid-19 on admission) is 106.6 (incomplete data). The Summary Hospital-level Mortality Indicator (SHMI) is the ratio between the actual number of patients who die following hospitalisation at the trust and the number that would be expected to die on the basis of average England figures, given the characteristics of the patients treated there. It includes deaths which occurred in hospital and deaths which occurred outside of hospital within 30 days (inclusive) of discharge. SHMI in the 12 months to November 2022 was 1.0782 ‘as expected’.
• Ipswich acute – 1.0632 ‘as expected’.
• Colchester – 1.0774 ‘as expected’. Specific mortality data for April 2022:
Site Apr 22 No. of Deaths
Apr 21 No. deaths
Rolling 12 months
Ipswich acute IP
116 (103)
102 114
Colchester acute IP
148 (136)
125 126
Ipswich ED 8 (8) 8 7
Colchester ED 18 (12) 6 11

Page 6 of 9
Figures in parenthesis refer to the previous months data. 2.1.4 Health Education England (HEE) As previously reported, HEE wrote to the Trust during February 2022 following a Foundation Trainee engagement meeting. HEE highlighted positive feedback from trainers and trainees; however, there were areas for improvement and one specific patient safety concern highlighted to the Trust. ESNEFT are addressing concerns and have been asked to provide a response to HEE. The CCG have met with ESNEFT to discuss the planned response and await further information on progress regarding an action plan to address the findings. 2.2 East England Ambulance Service NHS Trust (EEAST) 2.2.1 Urgent and Emergency Care Draft Incident Framework As previously reported, the CCG, working with EEAST, have written a draft Urgent and Emergency Care Framework, which changes the management of system incidents. System incidents are where there is learning for the system and comprise of: Delays in the community; conveyancing delays (including call handling delays); and delays in offload of ambulances due to handover delays at hospitals. The Framework transfers these incidents away from substantive investigation by EEAST and into each system in either tactical, multidisciplinary or operational meetings to stimulate a collective system-based response within each ICS. The aim is to create actions at system level to reduce treatment delays in urgent care as described in the NHSE/I letter dated 26 October 2021. This letter asks each system to address ambulance handover delays collectively. The established practice of fully investigating each incident and producing an action plan is not reducing harm; system delay incidents continue to be raised weekly. Across Suffolk and North East Essex, CCG have now held the introductory meeting and will begin processing incidents according to the Framework in regular system meetings. 2.2.3 Serious Incidents (SI) There is a total of 23 SIs open on Strategic Executive Information System (StEIS) for the Trust, relating to incidents occurring in Suffolk and North East Essex. The CCG will continue to work with EEAST to ensure these investigations are closed and learning is identified. The CCG have also begun conversations with EEAST in preparation for the national publication of the Patient Safety Incident Response Framework, which EEAST will begin implementing later this year. 2.2.4 EEAST Patient Transport Services The patient transport service has been affected by workforce during this reporting period. This was mainly due to the impact of high levels of Covid-19 circulating in the community. Very high staff sickness rates, and adherence to strict social distancing guidance on transport (reducing the number of patients transported in a vehicle) led the service to request they only convey ‘essential services’ (as defined in the contract). In response, Regular contact was maintained, and support given by CCG to the service. Fortunately, EEAST did not ultimately

Page 7 of 9
impose any restrictions on their service. Social distancing guidance has since changed and sickness rates in the service have improved. Overall, the service has been providing the expectations set out within the Contract and in accordance with relevant national guidelines. There have been additional contract/quality meetings to provide oversight of renal journeys. EEAST utilise the FFT (Friends and Family Test), but the number of surveys completed is low (<16%) so support is in place from the CCG Patient Engagement Team to help rectify this. Risks and ongoing quality assurance of the patient transport service will be monitored at the ICB Quality Committee going forward. 2.2 Marie Stopes International (MSI) MSI have been commissioned to provide the service for Termination of Pregnancy within North East Essex. The current contract commenced in September 2016. Comprehensive reports covering the service locally, regionally and nationally have provided the requisite assurance on quality. A range of service improvements have been undertaken, especially during the pandemic, to ensure the service is safe, effective and responsive. Patient feedback has been very positive and new ways to access appointments and support have been made available which has been extremely beneficial to patients. There are no key risks in relation to this service. Moving forward, quality assurance and any associated risks of this service will be monitored at the NEE Alliance Quality Committee.
3. MENTAL HEALTH CARE 3.1 Essex Partnership University Foundation Trust (EPUT) 3.1.1 Serious Incidents (SI) The CCG is working closely with EPUT to facilitate closure of the remaining 5 SIs open on StEIS and submission of the completed action plans. 3 SIs are awaiting a response to CCG feedback, but a recent update from the Trust has indicated these are in progress. The last 60-day report has now been received and is with the CCG for review. 3.1.2 Patient Safety Incident Response Framework (PSIRF) The Essex commissioners are working collaboratively and hold monthly joint PSIRF meetings with EPUT. The CCG attends EPUT Clinical Review Panel, where incidents are reviewed and methods of investigation are agreed. This is providing additional assurance. EPUT are currently in the process of completing thematic reviews for some of the completed Patient Safety Incident Investigation (PSIIs) in order to develop system improvement plans (SIP). SIPs are being developed regarding: Care delivery; Communication; Electronic patient records; Falls; Handover and MDT; Medication; Family engagement; Physical health; Record keeping and Safeguarding. The CCG have undertaken an annual review since implementation of the new Framework last year. This will be shared later this year. EPUT will also begin refreshing their incident response plan after one year of working with the new Framework. 2.3.1 Inquest Into the death of Bethany Lilley

Page 8 of 9
In March 2022, there was an inquest hearing at Essex Coroner’s Court following the death of Bethany Lilley. Bethany was a patient from North East Essex under the care of EPUT who died by ligature on the 16 January 2019 at Thorpe Ward, Basildon Mental Health Unit. The inquest found, on the balance of probability, the following failings were sufficiently serious to amount to a gross failure to provide basic medical care: Inadequate care plan; unsatisfactory discharge summaries lacking relevant information; failure to complete risk assessments as and when required; incomplete Level 1 observation sheet on the 16th January 2019; insufficient monitoring of leave from the ward on the 16th January 2019; and the inability of clinical staff to access all patient record systems. ICB oversight of EPUT arrangements are developing including a collaborative arrangement with all Essex Clinical Commissioning Groups, to oversee contracting and quality of the EPUT MH services across Essex. The Collaborative are in active and continuous dialogue with EPUT senior colleagues and have developed processes for shared intelligence and information with identified quality leads from across Essex including a draft Terms of Reference. In addition, North East Essex wards have been audited by the EPUT internal compliance team and an action plan with deadlines is in place. 3 Children & Young Peoples’ Continuing Care (CYPCC) Service CCG Annual Report – 2021/22 The CCG has 23 children /young people on the CYPCC caseload (there 25 active children in total during 2021/22). 15 of these cases are Joint funded with social care and 4 cases are tri part funded with social care and education. There are 4 Young people who will transition to adult services during 2022/23. Personal Health Budgets are in place for 16 children. In terms of risks, CYPCC Any Qualified Providers (AQP) are experiencing difficulties with recruitment of nursing and care staff, which is impacting on commissioned care. This is identified as a national and system wide problem with limited understanding of the risk long term. Currently, there is a limited response from AQP Providers to deliver new care packages leading to the need to commission with providers not on the AQP framework. It is expected this risk will be transferred for monitoring at North East Essex Alliance Committee for how workforce challenges affect new care packages. 4 Patient Experience Report Quarter Four1 Across Suffolk and North East Essex, 282 PALS enquiries have been made and 65 complaints have been received. There has been an increase in the number of complaints received in NEE so far this quarter, February (25), compared to January (11). In relation to MP enquiries, there have been 29 received. This is a reduction on the numbers received in December 2021. The patient experience team have been contributing to a Regeneration and redevelopment programme to improve the Greenstead neighbourhood in Colchester. The team have worked in collaboration with partners involved in the heart of the area to maximise community involvement. The programme of engagement is seeking to involve people across four programmes of activity: Estate regeneration and housing development; Development of the central ‘Hub’ including the relocation of the primary care practice; Development of the living neighbourhood and bike initiative; and development of the south Colchester neighbourhood team.
1 Team overview reporting for this quarter does not include date for March 2020, which will be reported in the subsequent papers to this.

Page 9 of 9
5 Pan Essex Section 117 Protocol
Section 117 of the Mental Health Act 1983 requires Clinical Commissioning Groups and local authorities, in co-operation with voluntary agencies, to provide or arrange for the provision of after-care to particular patients detained in hospital for treatment who then cease to be detained. The Pan Essex Section 117 Protocol has been reviewed and amended. The review has taken place in the context of the Pan Essex Section 117 Steering Group and has been reviewed on behalf of the Essex CCGs and Essex County Council by Essex Legal Services. There are minor changes made to processes and some funding protocols have been clarified, but no major changes overall. The financial implication of the clarifications to funding protocols are minimal. EPUT, Hertfordshire Partnership Foundation Trust (HPFT) and North East London Foundation Trust (NELFT) require an up-to-date protocol upon which to base training of their staff. There are formatting changes to follow but the substance of the document is now ready for approval.
- Report Ends -
GOVERNING BODY
Agenda Item No. 16
Reference No. NEECCG 22-40
Date. 7 June 2022
Title
North East Essex (NEE) Primary Care Commissioning Committee
Lead Director
Pam Green, Chief Operating Officer NHS NEECCG
Author(s)
Oge Chesa, Deputy Director of Primary Care and Medicines Management
Purpose
To present an update on the work of the CCG’s Primary Care Commissioning Committee.
Applicable CCG Strategic Objectives:
1. To achieve our vision through an inclusive, holistic approach to patient and service user centred commissioning, embedding personalisation of care through integrated health and social care services.
x
2. To transform care and drive continuous improvement in quality and safety. Achieve the best possible outcomes for our service users through high quality care.
x
3. To use commissioning resources effectively and responsibly. To develop our organisation, teams and individual staff to be trusted, competent, well trained, talented, enthusiastic and dedicated.
x
4 To tackle the biggest health challenges in north east Essex including reducing health inequalities.
x
Recommendation:
The Governing Body is asked to note the content of this report and raise any concerns or questions in relation to the assurance of primary care services commissioned for NEE residents.
The Governing Body is asked to assure itself that the Primary Care Commissioning Committee (PCCC) is satisfied that where primary care services are not reaching the required standard that necessary steps are being undertaken to improve the quality of services.
1. Summary
1.1 An ordinary meeting of the PCCC was held in public via Microsoft Teams on 12th April 2022 chaired by CCG Lay Member, Jon Price.
1.2 There was no member of the public in attendance.
1.3 There were no questions received via email from members of the public who were
invited to do so prior to the meeting.
2. Key Points to Note
The Committee at its meeting: 2.1 Noted contents of the Primary Care Integrated Performance Report (excerpt in Appendix
1 using data from April 21 to March 22 reported monthly, quarterly or annually where applicable and associated RAG rating). Some are cited below:
- Extended access: 1) Appointments; continues to achieve above the 75% target for extended access utilised. 2) GP utilisation: remains above 75% target at 87%
- Diabetes (improvement of 3 clinical treatment targets): above the national average of 24.1% at around 32%.
- Additional Roles Reimbursement Scheme (ARRS): the ARRS budget utilisation in 2022/23 has seen an increase close to 60% with 75 out of 135 (55%) expected roles in PCNs.
2.2 Noted Severe Mental Illness (SMI) Deep Dive by Chief Officer, GP Primary Choice Ltd:
- Percentages increased from 26.9% in Q2 to 38% in Q3 & 49.4% in Q4 showing just under a 30% increase from Q1 21/22 19.9% baseline.
- Two phlebotomy courses held to upskill EPUT staff to enable them to take blood whilst carrying out health checks.
- The team size increased from 2 to 4 at the end of Q3, running 1 clinic per week each – averaging 11 patients per clinic.
2.3 Approved the implementation of an Essex wide report proposal focusing on the
prevalence of racism and discrimination faced by staff and patients from Black and Ethnic Minority backgrounds in general practice. Funded by SNEE Training Hub, Essex Local Medical Committee (LMC) will undertake a similar process carried out by the Humberside LMC.
2.4 Noted the Primary Care update:
- Primary Care Network Direct Enhanced Service (PCN DES): • 2022/23 contract and associated service specifications including, the
Investment and Impact Fund (IIF) a financial incentive for PCNs, was published 31st March 2022. A number the IIF indicators are mirrored in QoF and the Community Pharmacy contractual Framework for overall population benefit.
• Enhanced Health in Care Homes DES; the CCG is supporting production of a Urinary Tract Infection management pathway to enable care home staff identify symptoms that will inform efficient prescribing of antibiotics
- List closures: 3 practices remain with temporary list closures. Mayflower Medical Centre business case is now approved to provide greater capacity to the practice and data on the impact of closed lists is being reviewed to help with discussions on reopening the lists.
Refugees: Afghan refugees continue to be supported in the contingency hotel. Home Office has ceased funding for transport. Alternative provision via Voluntary sector partners is being sought; Ukraine refugees coming into NEE are also being supported.
The Committee noted that NHSE/I had approved the Committee’s revised terms of reference agreed by the Governing Body at its meeting on 29 March.
3. Risks Identified
No new risks were identified. 4. Resource Implications
No additional resources were identified at this Committee. 5. Implications for engagement and communication
There is a continued need to engage with the public to ensure awareness that primary care is open for business.
6. Equality & Diversity
No negative or positive equality and diversity implications assessed at this time.
North East Essex Primary Care Integrated
Performance Report
Summary to the North East Essex Board
June 2022
(April data)
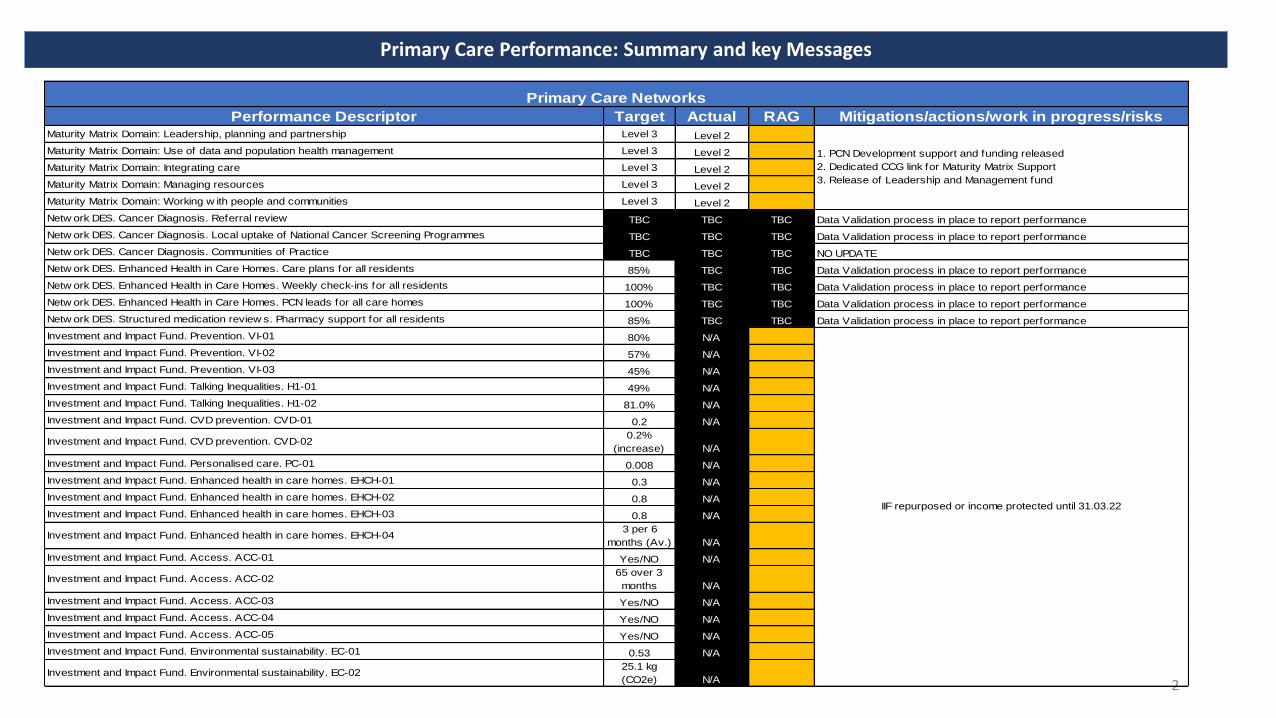
Primary Care Performance: Summary and key Messages
2
Performance Descriptor Target Actual RAG Mitigations/actions/work in progress/risksMaturity Matrix Domain: Leadership, planning and partnership Level 3 Level 2
Maturity Matrix Domain: Use of data and population health management Level 3 Level 2
Maturity Matrix Domain: Integrating care Level 3 Level 2
Maturity Matrix Domain: Managing resources Level 3 Level 2
Maturity Matrix Domain: Working w ith people and communities Level 3 Level 2
Netw ork DES. Cancer Diagnosis. Referral review TBC TBC TBC Data Validation process in place to report performance
Netw ork DES. Cancer Diagnosis. Local uptake of National Cancer Screening Programmes TBC TBC TBC Data Validation process in place to report performance
Netw ork DES. Cancer Diagnosis. Communities of Practice TBC TBC TBC NO UPDATE
Netw ork DES. Enhanced Health in Care Homes. Care plans for all residents 85% TBC TBC Data Validation process in place to report performance
Netw ork DES. Enhanced Health in Care Homes. Weekly check-ins for all residents 100% TBC TBC Data Validation process in place to report performance
Netw ork DES. Enhanced Health in Care Homes. PCN leads for all care homes 100% TBC TBC Data Validation process in place to report performance
Netw ork DES. Structured medication review s. Pharmacy support for all residents 85% TBC TBC Data Validation process in place to report performance
Investment and Impact Fund. Prevention. VI-01 80% N/A
Investment and Impact Fund. Prevention. VI-02 57% N/A
Investment and Impact Fund. Prevention. VI-03 45% N/A
Investment and Impact Fund. Talking Inequalities. H1-01 49% N/A
Investment and Impact Fund. Talking Inequalities. H1-02 81.0% N/A
Investment and Impact Fund. CVD prevention. CVD-01 0.2 N/A
Investment and Impact Fund. CVD prevention. CVD-020.2%
(increase) N/A
Investment and Impact Fund. Personalised care. PC-01 0.008 N/A
Investment and Impact Fund. Enhanced health in care homes. EHCH-01 0.3 N/A
Investment and Impact Fund. Enhanced health in care homes. EHCH-02 0.8 N/A
Investment and Impact Fund. Enhanced health in care homes. EHCH-03 0.8 N/A
Investment and Impact Fund. Enhanced health in care homes. EHCH-043 per 6
months (Av.) N/A
Investment and Impact Fund. Access. ACC-01 Yes/NO N/A
Investment and Impact Fund. Access. ACC-0265 over 3
months N/A
Investment and Impact Fund. Access. ACC-03 Yes/NO N/A
Investment and Impact Fund. Access. ACC-04 Yes/NO N/A
Investment and Impact Fund. Access. ACC-05 Yes/NO N/A
Investment and Impact Fund. Environmental sustainability. EC-01 0.53 N/A
Investment and Impact Fund. Environmental sustainability. EC-0225.1 kg
(CO2e) N/A
Primary Care Networks
1. PCN Development support and funding released
2. Dedicated CCG link for Maturity Matrix Support
3. Release of Leadership and Management fund
IIF repurposed or income protected until 31.03.22
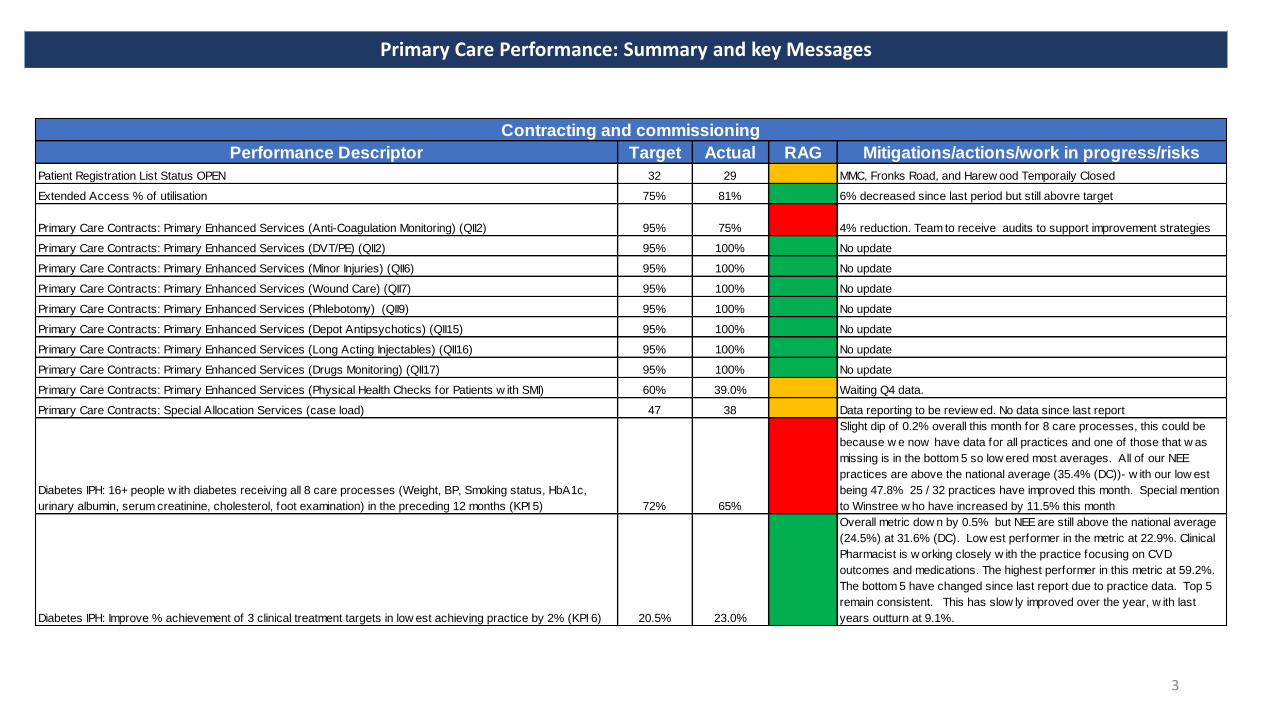
Primary Care Performance: Summary and key Messages
3
Performance Descriptor Target Actual RAG Mitigations/actions/work in progress/risks
Patient Registration List Status OPEN 32 29 MMC, Fronks Road, and Harew ood Temporaily Closed
Extended Access % of utilisation 75% 81% 6% decreased since last period but still abovre target
Primary Care Contracts: Primary Enhanced Services (Anti-Coagulation Monitoring) (QII2) 95% 75% 4% reduction. Team to receive audits to support improvement strategies
Primary Care Contracts: Primary Enhanced Services (DVT/PE) (QII2) 95% 100% No update
Primary Care Contracts: Primary Enhanced Services (Minor Injuries) (QII6) 95% 100% No update
Primary Care Contracts: Primary Enhanced Services (Wound Care) (QII7) 95% 100% No update
Primary Care Contracts: Primary Enhanced Services (Phlebotomy) (QII9) 95% 100% No update
Primary Care Contracts: Primary Enhanced Services (Depot Antipsychotics) (QII15) 95% 100% No update
Primary Care Contracts: Primary Enhanced Services (Long Acting Injectables) (QII16) 95% 100% No update
Primary Care Contracts: Primary Enhanced Services (Drugs Monitoring) (QII17) 95% 100% No update
Primary Care Contracts: Primary Enhanced Services (Physical Health Checks for Patients w ith SMI) 60% 39.0% Waiting Q4 data.
Primary Care Contracts: Special Allocation Services (case load) 47 38 Data reporting to be review ed. No data since last report
Diabetes IPH: 16+ people w ith diabetes receiving all 8 care processes (Weight, BP, Smoking status, HbA1c,
urinary albumin, serum creatinine, cholesterol, foot examination) in the preceding 12 months (KPI 5) 72% 65%
Slight dip of 0.2% overall this month for 8 care processes, this could be
because w e now have data for all practices and one of those that w as
missing is in the bottom 5 so low ered most averages. All of our NEE
practices are above the national average (35.4% (DC))- w ith our low est
being 47.8% 25 / 32 practices have improved this month. Special mention
to Winstree w ho have increased by 11.5% this month
Diabetes IPH: Improve % achievement of 3 clinical treatment targets in low est achieving practice by 2% (KPI 6) 20.5% 23.0%
Overall metric dow n by 0.5% but NEE are still above the national average
(24.5%) at 31.6% (DC). Low est performer in the metric at 22.9%. Clinical
Pharmacist is w orking closely w ith the practice focusing on CVD
outcomes and medications. The highest performer in this metric at 59.2%.
The bottom 5 have changed since last report due to practice data. Top 5
remain consistent. This has slow ly improved over the year, w ith last
years outturn at 9.1%.
Contracting and commissioning

Primary Care Performance: Summary and key Messages
4
Performance Descriptor Target Actual RAG Mitigations/actions/work in progress/risksCQC Rating - Overall N/A N/A A Outstanding - 0, Good - 29, Requires Improvement -3 , Inadequate - 2.
Number of PALS (YTD) 0 143 A
Number of complaints (YTD) 0 63 A
QOF Achievement N/A N/A N/A QOF to be reported in future report
"FFT: % likely to recommend GP service to friends & family N/A N/A N/A Indicator currently paused due to Pandemic
Overall experience of GP Practice (National Average 83%) 83% 79%
Overall experience percentage has moved up by 2% compared to
previous year
Children's Safeguarding Training Level 1 95% 94% 4 % increase
Children's Safeguarding Training Level 2 95% 83% 8 % increase
Children's Safeguarding Training Level 3 95% 80% 3 % increase
Looked after Children Training 95% 75% 4 % reduction
Adults Safeguarding Training Level One 95% 92% 2% increase
Adults Safeguarding Training Level Tw o 95% 96% No Change
Quality and Experience
Performance Descriptor Target Actual RAG Mitigations/actions/work in progress/risksARRS budget (Variance) 0% -35% Workforce plans in place.
Workforce roles in Primary Care Netw orks (WTE) - - Admin/Non-Clinical N/A 458 N/A Reduction by 2 since last report
Workforce roles in Primary Care Netw orks (WTE) - - Direct Patient Care N/A 101 N/A Reduction by 2 since last report
Workforce roles in Primary Care Netw orks (WTE) - - GP N/A 173 N/A Reduction by 5 since last report
Workforce roles in Primary Care Netw orks (WTE) - - Nurses N/A 137 N/A No change
Workforce roles in Primary Care Netw orks (Headcount) - - Admin/Non-Clinical N/A 655 N/A increase by 4 since last report
Workforce roles in Primary Care Netw orks (Headcount) - - Direct Patient Care N/A 146 N/A Reduction by 4 since last report
Workforce roles in Primary Care Netw orks (Headcount) - - GP N/A 206 N/A Reduction by 4 since last report
Workforce roles in Primary Care Netw orks (Headcount) - - Nurses N/A 181 N/A Reduction by 1 since last report
Workforce

Primary Care Performance: Summary and key Messages
5
Performance Descriptor Target Actual RAG Mitigations/actions/work in progress/risks
GP Connect - Total Records View edN/A 7778 N/A
Variance of + 2197 from previous month (July). Highest f igure since Sept
2020
GP Connect - Total Search for Free Slots N/A 2950 N/A
Variance of -969 from previous month (June). Low est f igure since
November 2020. Second highest period since March 2020
GP Connect - Total Appointments Booked N/A 506 N/A
Variance of -161 from previous month (June). Low est f igure since June
2021.
NHS App - Registrations N/A 11765 N/A Reduction since last period
NHS App logins N/A 171360 N/A Stable trajectory
NHS App - bookings N/A 687 N/A Reduction since last period
NHS App - Cancellations N/A 256 N/A Reduction since last period
NHS App - Prescription requests N/A 8280 N/A Highest recorded figure since May 2020
NHS App - medical record accesses N/A 15664 N/A Second Highest recorded figure since May 2020
Digitalisation
Performance Descriptor Target Actual RAG Mitigations/actions/work in progress/risks
Delegated Budgets - YTD Variance - Contractual £0.00 -£ 4.05 Plans in place. Overall Delegated budget balanced
Delegated Budgets - YTD Variance - QOF £0.00 -£ 54.82 Plans in place. Overall Delegated budget balanced
Delegated Budgets - YTD Variance - Enhanced Services £0.00 -£ 1,502.08 Plans in place. Overall Delegated budget balanced
Delegated Budgets - YTD Variance - Premises Cost £0.00 -£ 53,775.18 Plans in place. Overall Delegated budget balanced
Delegated Budgets - YTD Variance - Professional Fees - Disp \ Prescr £0.00 -£ 38,183.76 Plans in place. Overall Delegated budget balanced
Delegated Budgets - YTD Variance - Locum Allowance \ GP Retainers £0.00 -£ 1.03 Plans in place. Overall Delegated budget balanced
Delegated Budgets - YTD Variance - Primary Care Networks £0.00 -£ 10,105.78 Plans in place. Overall Delegated budget balanced
Delegated Budgets - YTD Variance - Other - GP Services £0.00 £ 516,161.30 Plans in place. Overall Delegated budget balanced
Delegated Budgets - YTD Variance - Other - Reserves £0.00 -£ 412,234.00 Plans in place. Overall Delegated budget balanced
Finance

Workforce (1)
6
Data source: 11
Additional Role
In Post and
Val idated
Planned or
unval idated
In Post and
Val idated
Planned or
unval idated
In Post and
Val idated
Planned or
unval idated
In Post and
Val idated
Planned or
unval idated
In Post and
Val idated
Planned or
unval idated
In Post and
Val idated
Planned or
unval idated
In Post and
Val idated
Planned or
unval idated
In Post and
Val idated
Planned or
unval idated
In Post and
Val idated
Planned or
unval idated
In Post and
Val idated
Planned or
unval idated
In Post and
Val idated
Planned or
unval idated
Social Prescribing Link Worker 1.0 0.0 1.0 0.0 1.0 0.0 1.0 0.0 1.0 0.0 1.0 0.0 1.0 0.0 1.0 0.0 1.0 0.0 1.0 0.0 10 0
Clinical Pharmacist 5.0 0.0 4.8 0.0 0.0 0.0 2.0 0.0 1.4 0.0 2.0 0.0 0.0 2.6 1.8 0.0 2.2 0.0 2.0 0.0 21 3
First Contact Physiotherapist 0.0 0.0 1.0 0.0 2.0 0.0 1.0 0.0 1.0 0.0 1.0 0.0 0.0 1.0 0.4 0.0 1.0 0.0 0.9 0.0 8 1
Physician Associate 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0 0
Paramedic 2.0 0.0 0.0 0.0 1.0 0.0 0.0 0.0 1.0 0.0 0.0 0.0 0.0 4.0 0.9 0.0 2.0 0.0 0.0 0.0 7 4
Pharmacy Technician 1.0 0.0 0.0 0.0 1.0 0.0 1.8 0.0 0.0 0.0 1.0 0.0 0.0 1.0 0.0 0.0 1.0 0.0 0.0 0.0 6 1
Care Coordinator 0.0 0.0 1.6 0.0 2.0 0.0 0.0 0.0 0.0 0.0 1.0 0.0 0.0 2.0 4.4 0.0 0.0 0.0 2.0 0.0 11 2
Health and Wellbeing Coach 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 1.0 0.0 0.0 0.0 1 0
Dietician 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0 0
Podiartrist 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0 0
Occupational Therapist 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 1.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 1 0
Nursing Associates 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0 0
Trainee Nursing Associates 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0 0
Mental Health Pratitioner 1.0 0.0 1.0 0.0 1.0 0.0 1.0 0.0 1.0 0.0 1.0 0.0 1.0 0.0 1.0 0.0 1.0 0.0 1.0 0.0 10 0
Advanced Practitioner 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0 0
Total 10 0 9 0 8 0 7 0 5 0 8 0 2 11 10 0 9 0 7 0 75.3 11
Table 4a: Primary Care Network Additional Roles Reimbursement Scheme - Roles by PCN
PC
N C
lact
on
Ran
wo
rth
PC
N
CM
P
CO
LTE
Par
tner
ship
(RM
T)
CO
LTE
Par
tner
ship
(WC
W)
CO
LTE
Par
tner
ship
(AR
A)
Cre
ffie
ld M
edic
al
Gro
up
East
Hill
&
Ab
bey
fiel
d
No
rth
Co
lch
este
r
Ten
dri
ng
CC
G
Additional Role Apr-21 May-21 Jun-21 Jul-21 Aug-21 Sep-21 Oct-21 Nov-21 Dec-21 Jan-22 Feb-22 Mar-22 TREND
Social Prescribing Link Worker 10 10 10 10 10 10 10 10 10 10 10
Clinical Pharmacist 10 11 14 17 15 19 18 21 21 22 21
First Contact Physiotherapist 7 10 10 10 10 10 9 10 9 8 8
Physician Associate 2 2 2 2 2 2 2 2 1 0 0
Paramedic 3 3 4 4 7 6 10 11 11 7 7
Pharmacy Technician 4 5 5 4 4 4 5 5 5 6 6
Care Coordinator 2 2 3 2 9 9 10 9 10 10 11
Health and Wellbeing Coach 2 2 2 1 1 1 1 1 1 1 1
Dietician 0 0 0 0 0 0 0 0 0 0 0
Podiartrist 0 0 0 0 0 0 0 0 0 0 0
Occupational Therapist 0 0 0 1 1 1 1 1 1 1 1
Nursing Associates 0 0 0 0 0 0 0 0 0 0 0
Trainee Nursing Associates 0 0 0 0 0 0 0 0 0 0 0
Mental Health Pratitioner 0 0 0 10 10 10 10 10 10 10 10
Advanced Practitioner 0 0 0 0 0 0 0 0 0 0 0
Total 40 45 51 61 69 73 77 81 79 75 75
Table 4b: Primary Care Network Additional Roles Reimbursement Scheme - Roles by CCG - Last 12 months

Workforce (2)
7
Additional Role Apr-21 May-21 Jun-21 Jul-21 Aug-21 Sep-21 Oct-21 Nov-21 Dec-21 Jan-22 Feb-22 Mar-22 TREND
PCN Clacton 4 3 3 3 4 8 9 9 9 10 10 0.0
Ranworth PCN 9 9 9 9 9 10 10 10 9 9 9 0.0
CMP 6 6 6 5 7 7 7 7 7 8 8 0.0
COLTE Partnership (RMT) 7 6 6 5 7 7 3 5 5 7 7 0.0
COLTE Partnership (WCW) 2 2 3 5 6 5 5 5 5 5 5 0.0
COLTE Partnership (ARA) 4 4 5 6 7 7 8 8 8 8 8 0.0
Creffield Medical Group 1 7 8 8 9 7 10 11 10 2 2 0.0
East Hill & Abbeyfield 2 2 2 2 8 8 10 10 10 10 10 0.0
North Colchester 5 5 5 5 7 7 8 8 9 10 9 0.0
Tendring 1 2 4 4 6 6 7 7 8 7 7 0.0
Total 41 46 52 52 69 73 77 81 79 75 75 0
Table 4c: Primary Care Network Additional Roles Reimbursement Scheme - Roles by PCN - Last 12 months
Note
There is currently a validation process in progress
as Follows:
1) Creffield Medical Group > January 2022
Page 1 of 8
GOVERNING BODY
Agenda Item No. 17
Reference No. NEECCG 22-41
Date. 7 June 2022
Title
North East Essex (NEE) Alliance Overview Report
Lead Director
Pam Green, Chief Operating Officer NHS NEECCG, Exec lead for NEEHWB (North East Essex Health and Wellbeing) Alliance on behalf of the chair of the Alliance Committee
Author(s)
Elizabeth Amodio – Head of Alliance Development and Outcomes
Purpose
To provide an overview of:
• discussions and decisions taken by the NEE Alliance Committee;
• recent NEE Alliance activity and progress
•
Applicable CCG Strategic Objectives:
1. To achieve our vision through an inclusive, holistic approach to patient and service user centred commissioning, embedding personalisation of care through integrated health and social care services.
x
2. To transform care and drive continuous improvement in quality and safety. Achieve the best possible outcomes for our service users through high quality care.
x
3. To use commissioning resources effectively and responsibly. To develop our organisation, teams and individual staff to be trusted, competent, well trained, talented, enthusiastic and dedicated.
x
4 To tackle the biggest health challenges in north east Essex including reducing health inequalities.
x
Recommendation: The Governing Body is asked to note the content of this report.
Page 2 of 8
1. Summary 1.1. This report provides an overview of the Alliance Committee decisions and discussions, but
also provides an overview of other NEE Alliance activity and governance linked to the updated Alliance functions and Decisions map as agree at Alliance Committee to provide a rounded picture of progress.
1.2. Please note the title of the sections below have been updated to reflect the revised Alliance
governance structure as shared in the last Governing Body update. 2. Key Points to Note 2.1 This report aligns updates from all Live Well Domains and Alliance programme workstreams
to provide greater visibility and opportunity for learning across the Alliance. This months report also includes an overview of the revised Governance structure.
The following table provides a summary of key recent activity and plans for the coming months:
Alliance Executive Group (AEG)
The AEG, previously known as System Executive Group (SEG) has continued to meet on a fortnightly basis and has received some key updates since the last Board update. Most recently it has:
• Received a detailed overview of the North East Essex Primary Care Network Estates Strategy, with the recommendation to use the Local Estates Forum to try and help solve some of the identified issues.
• An overview of the Neighbourhoods programme update was provided with a particular need to increase primary care engagement, with the plan to focus on engagement with primary care networks and use an engagement event to increase awareness.
• A brief overview of the Alliance Communication Group for NEE was provided, with focus on Ukrainian support packs and planning communications to support the summer tourist visitors.
• Revised terms of reference agreed with the recommendation to include a standing agenda item at the end of these meetings to reflect on learnings and ensure a difference has been made.
• Essex County Council provided overview of the Research Collaboration Bid for North East Essex; the purpose being to improve the evidence base that is available when it comes to the wider determinants of health. Agreed further links to the voluntary sector to be supported.
• Approved the name change of the Inequalities group to Widening Equity of Local Lives to align with our Alliance brand was requested. The group was broadly supportive with agreement for this to be further circulated and to be shared with the Local Workforce Action Group.
• ICB digital leads gave a detailed overview of the digital enabler updates for all three Alliances. Agreed actions include, working with the vol sector to create Digital workshops to increase general awareness and understanding.
• Received the spot light report for the Die Well domain, with modest improvements being seen in what has been a challenging year. Commitment maintained to deliver the

Page 3 of 8
predicted trajectory for EOL admissions to free resources and improve community services.
• Received the update that the EOL Board had approved funding for 10 nurses (across EPUT, the community and the Hospice) to join a national community of practice and a pilot agreed for 4 collaborative roles to be operational between single point and EEAST.
• Approved the End of Life Programme Group terms of reference (which will now be known as a group rather than board) to align to the revised Alliance governance structure.
• Recommended the action for Die Well and Start Well domains to link further to ensure we have an all age approach to the die well strategy.
• Received an overview of the care tech hub outline business case by the University of Essex, commissioned by DragonGate market intelligence to support the care sector with innovation and stimulate economic growth, confirmation that £50k had been secured from ECC to support this work. Recommendations made by the group included recognising the patient voice and the need to reflect on previous experiences and capturing behaviours, challenges from the care sector.
• Received an update on the Feel Well domain spotlight report, priority areas included a focus on 18-25 year olds, drug and alcohol services and LD and autism. The group were to feed in the recommendations and outcomes from the recent Feel Well asset mapping report which focused on three key areas (social isolation, complex needs and suicide prevention).
• Approved a three month extension at a cost of £6,468 via IBCF funding to continue the service past the current end date of 16th May whilst discussion are taking place regarding longer term funding provision.
Alliance Operational Group
• The Inaugural meeting of the Alliance Operational Group (AOG) occurred in April, the group reviewed its new terms of reference and expect to formally sign these off at the May meeting pending some further wording adding in to support the group’s role re the NICS contract.
• The group has refocused on the operational performance and received performance detail at this meeting related to ED.
• The group received the update on the financial spend to the end of 21/22 and discussed the current risks re the system financial targets for 22/23, we also discussed how UEC budgets for resilience have been built into budgets within the Acutes and agreed that transparency around this and outcomes would come via this group
• The University Drug and Alcohol project update was provided linked to work with Open Road support to students.
• Open Road are providing a full time – 5 days per week drug and alcohol worker that will directly work with the university students as a constant source of support. The SOS bus will also be made available at student social events to deliver targeted work.
• Reviewed the outline plan for the Alliance summer communications campaign.
Widening Equity • Membership, terms of reference and new name change agreed.

Page 4 of 8
for Local Lives Group (formally known as Inequalities Group)
• Kate Crofts, the Alliance Inequalities lead was welcomed to assist the development of the group.
• New forward workplan developed including an updated timetable for the domains to present their work to the inequalities group.
• Recruitment underway to appoint inequalities co-ordinators to both Colchester Borough Council and Tendring District Council
• Presentations to be received from Everyone’s Essex strategy and ECC equality objective updates to be received at the next meeting.
Neighbourhoods • Multi-disciplinary team (MDT) meetings for Colchester Central continue with positive actions being achieved for those cases discussed with police partners now engaged.
• Agreement received from the Neighbourhoods steering group in response to capacity across the system to hold one MDT across Colchester and one across Tendring.
• Data pack for Colchester Central reviewed and several areas identified for further investigation with the team on 24/05/22.
• Initial meetings held with Evaluation team to commence their scoping phase.
• Colchester Central Live Well Neighbourhood Team formally launched at official opening of One Colchester Hub on 22/04/22.
• Neighbourhood communications post now agreed to be hosted by Essex Partnership University Foundation Trust (EPUT), with updated job descriptions following previous unsuccessful recruitment attempts.
• Number of engagements held including, Tendring District Council, Colchester borough councillors (both ward councillors and assistant directors) and system partner team meetings.
• Engagement work being carried out by African Families in the UK with Black African and Caribbean communities.
• Reflection sessions held on lessons learned from Colchester Central to date.
• Colchester South Neighbourhood Connector in post • Psychometric tool used as part of the culture & OD work to
support some team building and further development of the Colchester Central Neighbourhood Team.
• GP education event scheduled for 26/05/22. • Initial face to face meet of Colchester South Live Well
Neighbourhood Team to be held at Greenstead community centre – 24th May.
Clacton Place - Tendring Jobs and Careers Roadshow held 20th April at Morrisons in Harwich, well attended by partners including McDonalds and Rose Builders, with positive feedback received. New partners continue to be sought, and venues are currently being agreed for the next few months including expanding sites to Colchester.
- Conversations continue to take place with several Secondary schools across Tendring to identify key actions on planning future Heath and Care Academies. The idea of having a careers roadshow style events have been agreed with the plans well underway for the first roadshow to be delivered to Clacton Coastal Academy in the coming weeks.
- Continuing to facilitate links between the construction and green energy sectors and introductions to schools to identify these providers can deliver careers information to students. Further
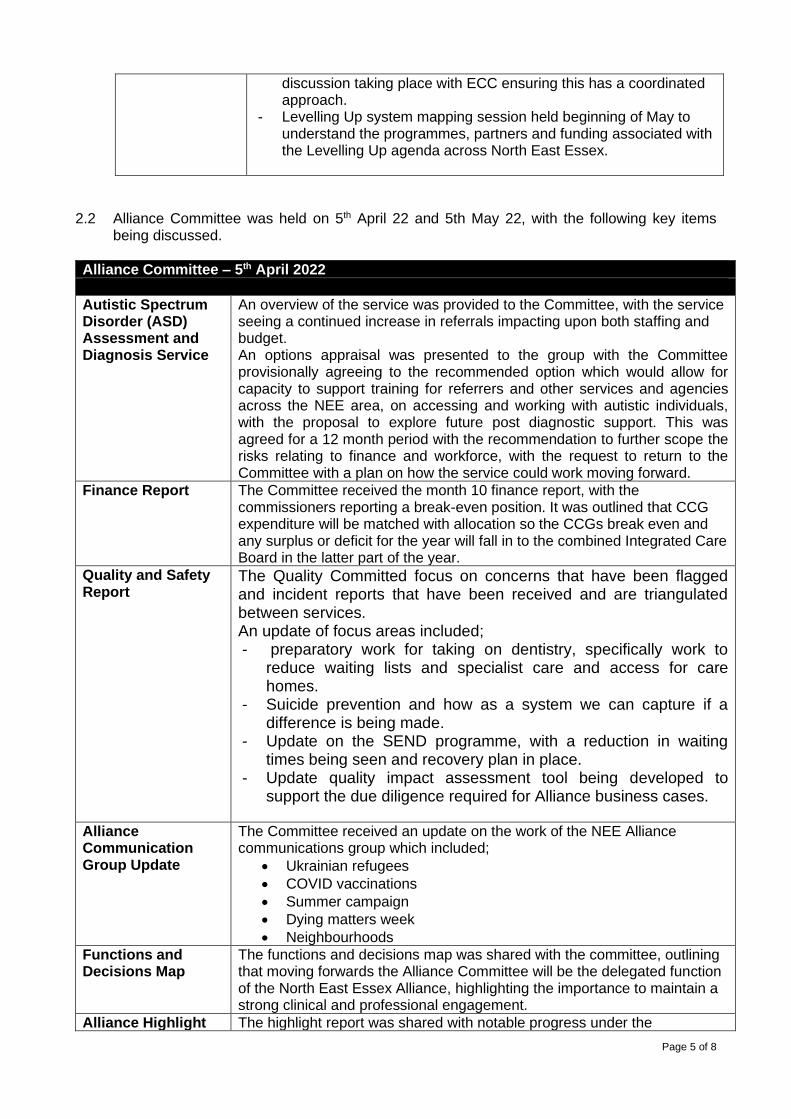
Page 5 of 8
discussion taking place with ECC ensuring this has a coordinated approach.
- Levelling Up system mapping session held beginning of May to understand the programmes, partners and funding associated with the Levelling Up agenda across North East Essex.
2.2 Alliance Committee was held on 5th April 22 and 5th May 22, with the following key items being discussed.
Alliance Committee – 5th April 2022
Autistic Spectrum Disorder (ASD) Assessment and Diagnosis Service
An overview of the service was provided to the Committee, with the service seeing a continued increase in referrals impacting upon both staffing and budget. An options appraisal was presented to the group with the Committee provisionally agreeing to the recommended option which would allow for capacity to support training for referrers and other services and agencies across the NEE area, on accessing and working with autistic individuals, with the proposal to explore future post diagnostic support. This was agreed for a 12 month period with the recommendation to further scope the risks relating to finance and workforce, with the request to return to the Committee with a plan on how the service could work moving forward.
Finance Report The Committee received the month 10 finance report, with the commissioners reporting a break-even position. It was outlined that CCG expenditure will be matched with allocation so the CCGs break even and any surplus or deficit for the year will fall in to the combined Integrated Care Board in the latter part of the year.
Quality and Safety Report
The Quality Committed focus on concerns that have been flagged and incident reports that have been received and are triangulated between services. An update of focus areas included; - preparatory work for taking on dentistry, specifically work to
reduce waiting lists and specialist care and access for care homes.
- Suicide prevention and how as a system we can capture if a difference is being made.
- Update on the SEND programme, with a reduction in waiting times being seen and recovery plan in place.
- Update quality impact assessment tool being developed to support the due diligence required for Alliance business cases.
Alliance Communication Group Update
The Committee received an update on the work of the NEE Alliance communications group which included;
• Ukrainian refugees
• COVID vaccinations
• Summer campaign
• Dying matters week
• Neighbourhoods
Functions and Decisions Map
The functions and decisions map was shared with the committee, outlining that moving forwards the Alliance Committee will be the delegated function of the North East Essex Alliance, highlighting the importance to maintain a strong clinical and professional engagement.
Alliance Highlight The highlight report was shared with notable progress under the
Page 6 of 8
Report neighbourhoods workstream discussed by the group.
Alliance Committee – 05th May 2022
Die Well Spotlight Report
The Committee received a presentation on the die well domain with the following highlights:
• Modest improvements made in End of Life (EoL) outcomes in what was a challenged year
• The end of year report highlights for 21/22 – outcomes around identification of EoL have improved - Achievement of preferred place of care remains good. - Hospital deaths (as proportion of total deaths) remain lower
than expected - Financial modelling shows better outcomes are being delivered
for better value as more care is being delivered in peoples own homes
The Committee commented this as a real exemplar of how to work across the domains and the benefits of shared ownership.
Civic University Agreement
• An overview was provided on this is a national initiative following work commissioned by the UPP Foundation led by Lord Kerslake to look at engagement between universities and their local areas.
• Principles that came from the work include collaborative working, benefitting place, creating social benefits; the priorities were discussed in further detail, with opportunities noted around Freeport East and Greenstead.
• The committee noted and supported the creation of a Civic University Agreement between the University of Essex and the partners listed in the report.
Quality Update The Committee were presented with the following highlights;
Engagement Forum underway; governance has been agreed and a programme of work developed Child Death Review (CDR) - The Ockenden Report is a focus Quality Impact Assessment (QIA) tool in development to provide the Committee with tangible account of clinical, quality, financial and contractual assurance on any business proposal of the Live Well Strategy; the tool will provide a gap analysis of where further assurance is required Work taking place for COVID-19 boosters for the over 75’s and for young children
Finance Update The Committee were presented with an update on Month 11 and
informed of key changes from last month:
• ESNEFT reported a £7.4m surplus.
• NEE reported a small surplus of £108k for year end
• IBCF tracker - £1.1m to be carried forward into 2022/23
• System resilience funding reported a £249k underspend in Month 11; the position has since increased by a further £300k for Month 12
• Financial Plans have been revised according to NHSEI guidance; the mitigated risk of £6.9m has been increased to £18.5m across the ICB which takes into account COVID-19 cost pressures and reflects an additional £10m of non-pay inflation rates (region deficit noted as £275m)

Page 7 of 8
• The initial proposal is that all directorates are issued with an annual recurrent efficiency target equating 5% of budget/spend.
• Financial Recovery and sustainability group formed; future business cases for new services will be reviewed by this group initially
Feel Well Community Asset Deep Dive Report
The Committee were presented with the following highlights from the Community asset report in relation to the Feel Well domain:
• Focus on Berechurch and Pier wards due to the different
demographics and high levels of demand
• Prevalence and depth of mental ill-health in NEE demonstrates the impact on wider determinants of health; written exclusion from services comes from a range of factors such as communication difficulties, stigmas and assumptions about living circumstances
• Limited scope and spread of information about local assets
• There has been a shift in advice sought from Citizens Advice Tendring post COVID-19
Widening Equity for Local Lives Update
The Committee received the following updates;
• Terms of reference now in place and membership reviewed
• New Forward Workplan developed
• Upcoming presentation on Everyone’s Essex Strategy and ECC Equality Objective updates
• One Colchester funding panel up and running
• Challenges include domains being in different levels of maturity, capacity within the system and the data and information available is vast, therefore looking to use what is readily available
NEE Alliance Supporting Domain Development and Achievements
It was reported two of the three Alliance Delivery Leads are now in post to support alliance SROs; interviews for the final two posts took place on 11/05/22. Funding has been allocated to domains to support the delivery of ambitions. Work is taking place to embed this within the realising ambitions money and embed work into the domains. All 6 domains will work in a similar way to Die Well with its own budget to agree how funding links to the delivery of the domain work programme which will link into the alliance delivery plan. For Start Well, a funding panel is being established that sits under the current Children’s Partnership Board which will include commissioners and local authority.
Essex SEND Strategy
Formal notification has been received of the SEND reinspection for Essex due to take place between 17th-19th May 2022. The SEND Strategy sets out the 5 priorities for Essex which focus on equity, inclusion and ambition. The strategy aims to address the areas of improvement noted within the Written Statement of Action issued in 2019. The Committee approved the SEND strategy.
Patient and Public Involvement and Experience Team Report
The Committee were presented with a report that covers activity of the Patient and Public Involvement and Experience Team that work within the CCG. The paper reports on activity for Quarter 4 2021/2022 – January to March 2022.
Page 8 of 8
The report highlighted activities within the CCG, future reports will reflect wider work that takes place across the whole of the alliance.
3. Risks Identified 3.1 No risk identified at this stage 4. Resource Implications 4.1 The infrastructure of the Alliance itself operates on a partnership contribution model but
where specific change management resources are required transformation funds can be requested from this committee from non-recurrent sources when available, some funding is allocated in the iBCF to support ongoing Alliance development in this financial year.
5. Engagement and Communication 5.1 There is a continued need to engage with the public to ensure awareness of the NEEHWB
approach integrated commissioning and delivery of services in NEE. 6. Equality and Diversity 6.1 No negative or positive equality and diversity implications assessed at this time.

Page 1 of 2
GOVERNING BODY
Agenda Item No. 18
Reference No. NEECCG 22-42
Date. 7 June 2022
Title
Procurement Update
Lead Director
Pam Green - NEE CCG Chief Operating Officer; Paul Gibara, Director of Performance Improvement
Author(s)
Maninder Singh Dulku - Associate Director for Attain – supporting NEE CCG as Commercial & Procurement Lead
Purpose
Update
Applicable CCG Strategic Objectives:
1. To achieve our vision through an inclusive, holistic approach to patient and service user centred commissioning, embedding personalisation of care through integrated health and social care services.
X
2. To transform care and drive continuous improvement in quality and safety. Achieve the best possible outcomes for our service users through high quality care.
X
3. To use commissioning resources effectively and responsibly. To develop our organisation, teams and individual staff to be trusted, competent, well trained, talented, enthusiastic and dedicated.
X
4 To tackle the biggest health challenges in north east Essex including reducing health inequalities.
Recommendation:
The Governing Body is asked to acknowledge the procurement updates provided in the attached
report.
Page 2 of 2
1. Summary
The report provides ongoing updates for SNEE procurements and reflects:
• Recently Closed or Awarded Projects
• Procurement Pipeline
• Procurement Policies/Workplan
• Proposed Legislative Changes 2. Key Points to Note
Future procurement pipeline. Future updates to policies and procedures, and proposed legislative changes.
3. Risks Identified
Ensure future procurements, processes, documentation are fully legally compliant, to mitigate any risk of legal challenge.
4. Resource Implications
N/A
5. Engagement and Communication
Continue to engage with Cabinet Office, NHS England and NHS Improvement, and seek external legal input.
6. Equality and Diversity Consider as part of procurement strategy.
June 2022
Procurement Update

2
The report provides ongoing updates for North East Essex (NEE) Clinical Commissioning Group (CCG) procurements and reflects:
1. Recently Awarded Contracts2. Procurement Pipeline3. Procurement Policy/Strategy/Workplan4. Proposed Legislative Changes
Contents

3
1. Recently Awarded Contracts
Project Value Lead Comments & Update
Primary Care Careers (PCC), new branding and website redesign
£49,160 (excl. VAT), and £58,992 (incl. VAT).
Head of Primary Care Careers
The requirements incorporate for the new branding, website design, build, testing, launch, training and hand over. The aim of the new website is to help generate awareness of PCC services, showcase achievements, highlight the latest career opportunities and educate the potential and current workforce on the different roles and career paths available. A competitive quotation process has been undertaken. Contract awarded to Vibe Agency. Period of agreement will be from 04/04/2022 to 03/10/2022.
Community Spirometry Diagnostic Service
£230,000 Transformation Programme Manager (Respiratory/M
E&CFS)
The service provider will work with the GP practices to deliver spirometry testing to enable the accurate diagnosis of Chronic Obstructive Pulmonary Disease (COPD) and asthma in patients. Spirometry is an essential investigation for diagnosis and severity assessment in people with COPD and asthma. Failure to diagnose matters because decline in lung function is faster in the earlier stages of COPD and undiagnosed patients do not receive the treatment that is known to make a big difference to outcomes. Contract awarded to GP Primary Choice Ltd following an invitation to quote process. Period of agreement will be from 28 June 2022 to 27 June 2023 (with option to extend for a further 12 months).
North East Essex Alliance Cultural Development Support
£108,500 Head of Alliance Development & Outcomes
The project will deliver on three elements of an organisational development programme i.e. *organisational and cultural development within the Live Well Neighbourhood Teams; *1-1 Coaching support to the neighbourhood manager and the Domain Leads; and *Individual coaching to CCG leads (from 8B above).

4
1. Recently Awarded Contracts (cont.)(2)
Project Value Lead Comments & Update
Variation of the Mid & South Essex Contract with Essex Partnership University NHS Foundation Trust (EPUT) for acute inpatient and Mental Health Services, to add North East Essex CCG, Ipswich and East Suffolk CCG, and West Suffolk CCG as Associate Commissioners
Annual value of NEE EPUT
contract approx.
£43.5m, I&ES is £912k, WS is £573k. The aggregated
contract value based on a 2 year term is
approx. £90m.The value of
the MSE contract is
£125.9m per annum
MSE will be the lead
commissioner, and NEE CCG, I&ES CCG, and WS CCG will be
added as associates to the
contract
A direct award has been made to EPUT via a Contract Variation to the MSE contract to ensure continuity of care for the delivery of acute inpatient and community mental health services. Traditionally mental health services, like acute NHS hospital contracts have not been subject to contestability which is why the EPUT contract has been “rolled over” with EPUT as the main Essex provider of mental health services. By joining the commissioning approach for mental health via one contract with EPUT will create economies of scale for improving quality and performance; with joined up approaches for quality, commissioning and contract management being advocated.
The MSE EPUT contract expires on 31 Match 2024.
The contract variation took place from 1st April 2022.

5
1. Recently Awarded Contracts (cont.)(3)
Project Value Lead Comments & Update
Integrated activities to improve health and wellbeing and reduce inequalities in North East Essex
£624,000 Deputy Chief Operating Officer
The direct award has been made to University of Essex, due to its position both as a significant anchor organisation situated in the middle of the community in which this work with both directed and aims to support but also as their place as a community within that neighbourhood due to the student and staff populations living in and being part of the community, this work is aimed at supporting. The university brings a number of skills that are directly linked to the work and have work ongoing with schools and the community as part of other research and outreach in the local community. Period of agreement will be from 20/03/22 to 19/09/22, with the option to extend by a further 6 months.
Community Based Cardiovascular Disease Support (Lipid Clinic)
£161,000 Head of Innovation
Recognising that CVD is a key strategic priority nationally and local priorities for CVD in Suffolk and North East Essex (SNEE); (1) People should have the information and support they need to reduce the risk of developing cardiovascular disease and (2) People with cardiovascular disease should have the right treatment and support to manage their condition. The recommendation is to support the implementation of a new NEECCG community-based lipid clinic. Contract awarded to GP Primary Choice Ltd. After the 12 month pilot an evaluation will be conducted to assess success, which could then result in procurement to secure a longer-term arrangement.
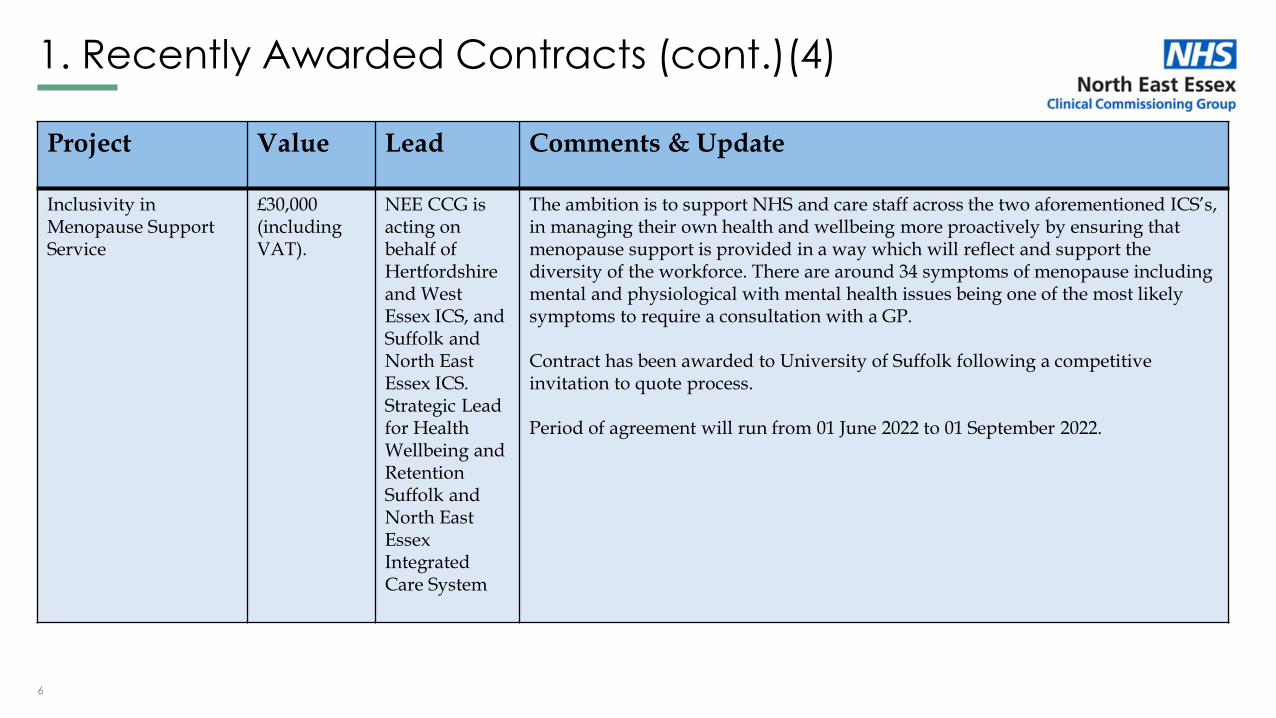
6
1. Recently Awarded Contracts (cont.)(4)
Project Value Lead Comments & Update
Inclusivity in Menopause Support Service
£30,000 (including VAT).
NEE CCG is acting on behalf of Hertfordshire and West Essex ICS, and Suffolk and North East Essex ICS. Strategic Lead for Health Wellbeing and RetentionSuffolk and North East Essex Integrated Care System
The ambition is to support NHS and care staff across the two aforementioned ICS’s, in managing their own health and wellbeing more proactively by ensuring that menopause support is provided in a way which will reflect and support the diversity of the workforce. There are around 34 symptoms of menopause including mental and physiological with mental health issues being one of the most likely symptoms to require a consultation with a GP.
Contract has been awarded to University of Suffolk following a competitive invitation to quote process.
Period of agreement will run from 01 June 2022 to 01 September 2022.
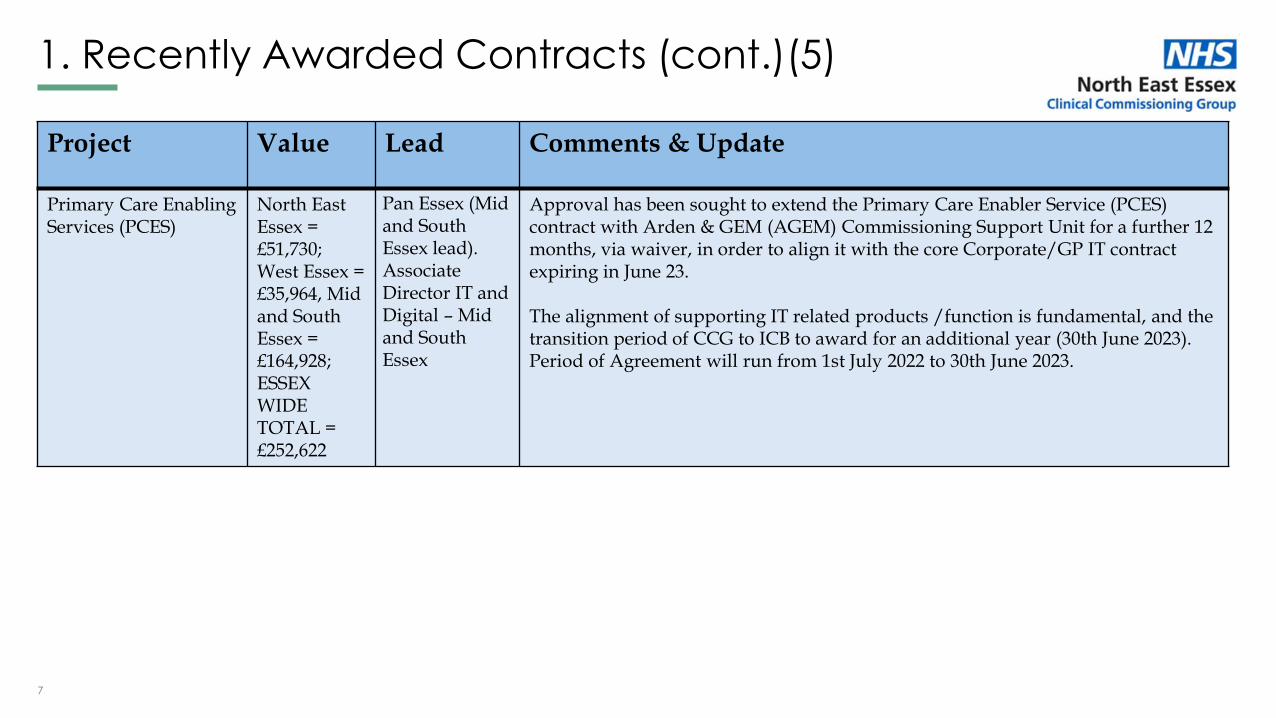
7
1. Recently Awarded Contracts (cont.)(5)
Project Value Lead Comments & Update
Primary Care Enabling Services (PCES)
North East Essex = £51,730; West Essex = £35,964, Mid and South Essex = £164,928; ESSEX WIDE TOTAL = £252,622
Pan Essex (Mid and South Essex lead). Associate Director IT and Digital – Mid and South Essex
Approval has been sought to extend the Primary Care Enabler Service (PCES) contract with Arden & GEM (AGEM) Commissioning Support Unit for a further 12 months, via waiver, in order to align it with the core Corporate/GP IT contract expiring in June 23.
The alignment of supporting IT related products /function is fundamental, and the transition period of CCG to ICB to award for an additional year (30th June 2023). Period of Agreement will run from 1st July 2022 to 30th June 2023.
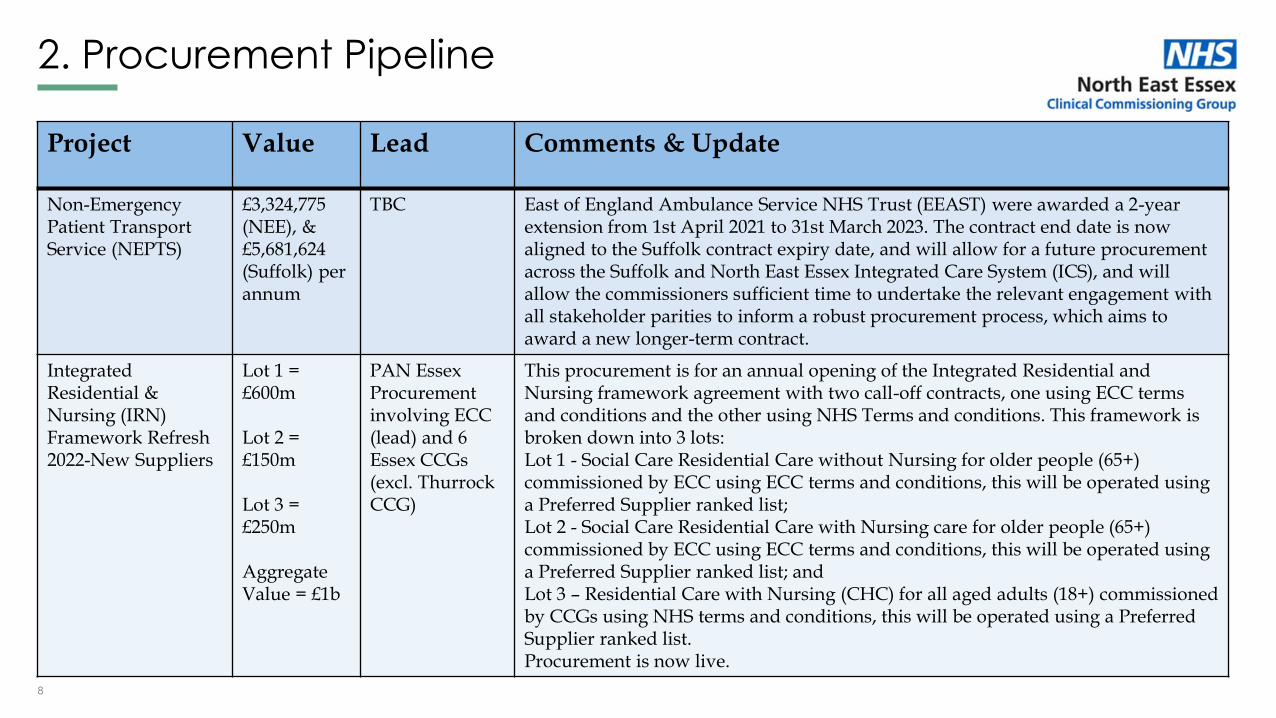
8
2. Procurement Pipeline
Project Value Lead Comments & Update
Non-Emergency Patient Transport Service (NEPTS)
£3,324,775 (NEE), & £5,681,624 (Suffolk) per annum
TBC East of England Ambulance Service NHS Trust (EEAST) were awarded a 2-year extension from 1st April 2021 to 31st March 2023. The contract end date is now aligned to the Suffolk contract expiry date, and will allow for a future procurement across the Suffolk and North East Essex Integrated Care System (ICS), and will allow the commissioners sufficient time to undertake the relevant engagement with all stakeholder parities to inform a robust procurement process, which aims to award a new longer-term contract.
Integrated Residential & Nursing (IRN) Framework Refresh 2022-New Suppliers
Lot 1 = £600m
Lot 2 = £150m
Lot 3 = £250m
Aggregate Value = £1b
PAN Essex Procurement involving ECC (lead) and 6 Essex CCGs (excl. Thurrock CCG)
This procurement is for an annual opening of the Integrated Residential and Nursing framework agreement with two call-off contracts, one using ECC terms and conditions and the other using NHS Terms and conditions. This framework is broken down into 3 lots:Lot 1 - Social Care Residential Care without Nursing for older people (65+) commissioned by ECC using ECC terms and conditions, this will be operated using a Preferred Supplier ranked list;Lot 2 - Social Care Residential Care with Nursing care for older people (65+) commissioned by ECC using ECC terms and conditions, this will be operated using a Preferred Supplier ranked list; andLot 3 – Residential Care with Nursing (CHC) for all aged adults (18+) commissioned by CCGs using NHS terms and conditions, this will be operated using a Preferred Supplier ranked list.Procurement is now live.

9
2. Procurement Pipeline (cont.)(2)
Project Value Lead Comments & Update
Home Oxygen Service (HOS)
TBC Collaborative
procurement
across the East
of England
region
The BOC contract is currently managed by West Essex CCG on behalf of the 19CCGs in the East of England. The current contract was due to expire on 28th September 2021. The impact of Covid-19 meant that capacity to deliver a robust procurement process prior to the end of the contract was not likely. Short term extension was enacted to 31st March 2022. The total value of the 6-month extension across all EoE CCGs was £4,100,000. A procurement process was launched on 7th June 2021. The procurement process has now concluded, and a recommendation has been put forward to respective organisations to award the new contract. The proposed contract was due to go live on 1st April 2022 and will be in place for 7 years with the option to extend for a further 3 years. However, the contract award has been paused.
Children's Bereavement Services
TBC Alliance
Transformation
Lead
Options appraisal has been completed and a recommendation will be presented to the Operational Executive Committee for approval.

10
Project Value Lead Comments & Update
Applicant Tracking System for Primary Care Careers
TBC Head of Primary Care Careers
TBC
Population Health Management
TBC TBC TBC
End of Life Virtual Ward Service
£822,000 Alliance Transformation Lead
In the shorth term the CCG will continue to support with contribution via grant funding. For the longer term the CCG is assessing all other commercial options.
Urgent Primary Care (Parachute) -round 2 – Pan Essex
Aggregate value over term is £57.5m
Head of Primary Care and Alliance Transformation
The Pseudo Dynamic Purchasing System (PDPS) is a framework of pre-approved Providers from which the Essex CCGs can quickly ‘call-off’ contracts for Urgent Primary Medical Care Services. Providers can apply to join the PDPS at any point during the PDPS cycle. The PDPS opened up again on 1st April 2022 to enable new providers to apply and joining the PDPS. All suitable applicants, who meet the selection criteria and avoid exclusion, will be admitted onto the PDPS.
2. Procurement Pipeline (cont.)(3)
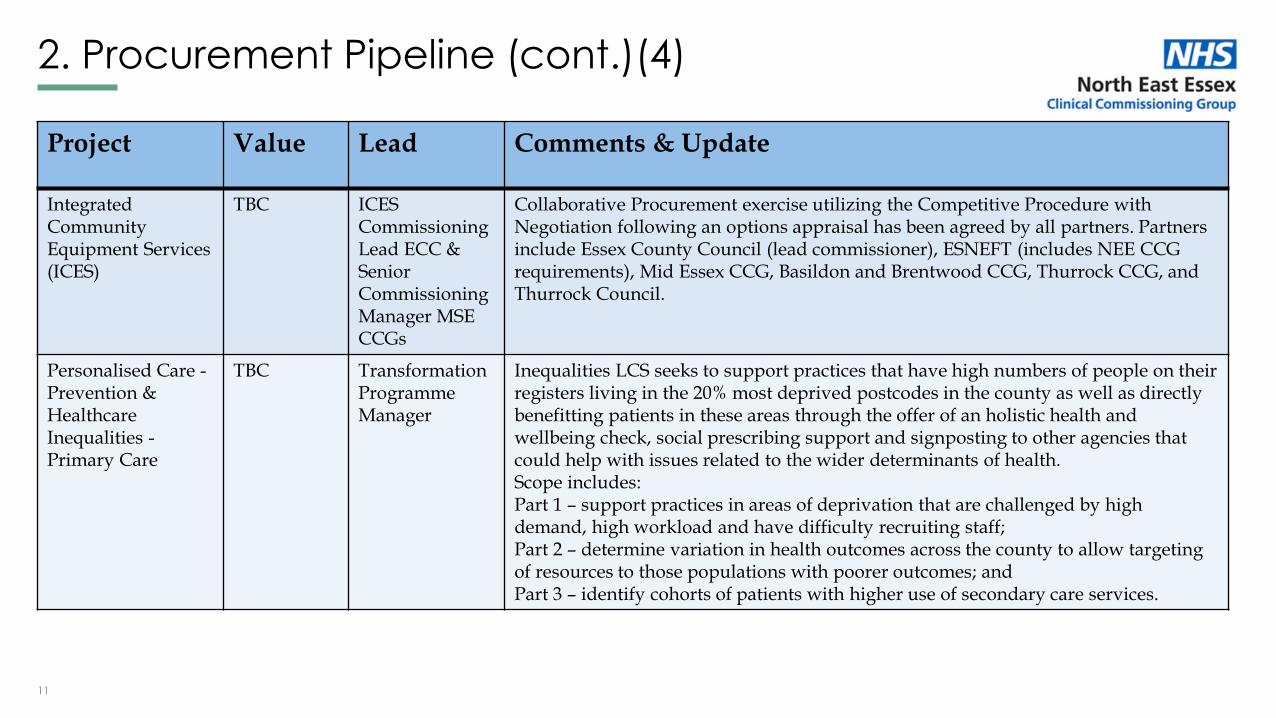
11
Project Value Lead Comments & Update
Integrated Community Equipment Services (ICES)
TBC ICES Commissioning Lead ECC & Senior Commissioning Manager MSE CCGs
Collaborative Procurement exercise utilizing the Competitive Procedure with Negotiation following an options appraisal has been agreed by all partners. Partners include Essex County Council (lead commissioner), ESNEFT (includes NEE CCG requirements), Mid Essex CCG, Basildon and Brentwood CCG, Thurrock CCG, and Thurrock Council.
Personalised Care -Prevention & Healthcare Inequalities -Primary Care
TBC Transformation Programme Manager
Inequalities LCS seeks to support practices that have high numbers of people on their registers living in the 20% most deprived postcodes in the county as well as directly benefitting patients in these areas through the offer of an holistic health and wellbeing check, social prescribing support and signposting to other agencies that could help with issues related to the wider determinants of health.Scope includes:Part 1 – support practices in areas of deprivation that are challenged by high demand, high workload and have difficulty recruiting staff;Part 2 – determine variation in health outcomes across the county to allow targeting of resources to those populations with poorer outcomes; andPart 3 – identify cohorts of patients with higher use of secondary care services.
2. Procurement Pipeline (cont.)(4)

12
Project Value Lead Comments & Update
Keyworker Service for Children & Young Persons with Learning Disabilities and Autism across Essex
Cumulative contract value over 3 years is £2.5m
Associate Director, Specialist Learning Disability Health CommissioningWorking on behalf of the CCGs and Local Authorities of Southend, Essex and Thurrock
The pan Essex Integrated LD Commissioning Team have been successful in its bid for NHSE Funding to implement the Keyworker Service on behalf of the Southend, Essex and Thurrock (SET) Transforming Care Partnership (TCP). The outcome of consultation with Attain identified that an Open / Accelerated Procurement Process under the “Light Touch Regime” is preferred in order to satisfy ambitious NHSE timescales for mobilisation and delivery. National learning also suggests that a formal procurement process has delivered the best results. The Operational Executive Committee has confirmed that it supports this recommendation, noting the options and risks and approve the CCGs to proceed to engage the market and undertake the procurement process.
Castle Point and Rochford CCG will be the lead commissioner for this project.
2. Procurement Pipeline (cont.)(5)
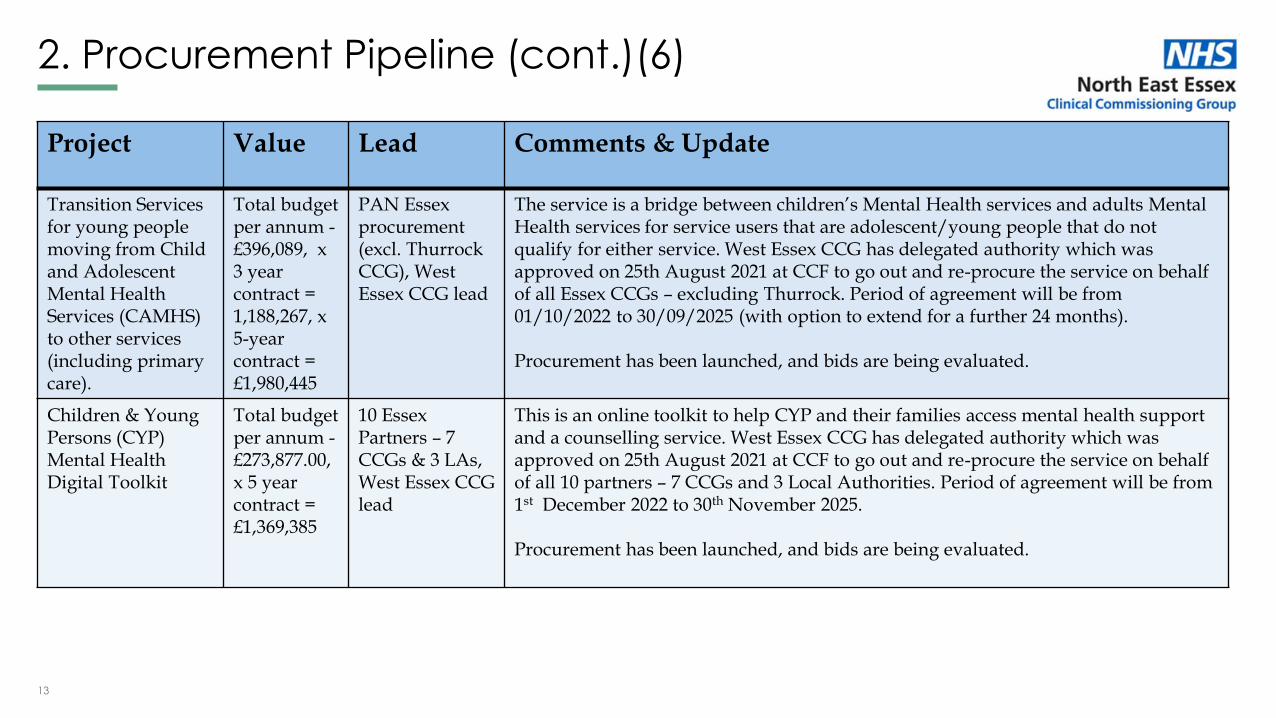
13
Project Value Lead Comments & Update
Transition Services for young people moving from Child and Adolescent Mental Health Services (CAMHS) to other services (including primary care).
Total budget per annum -£396,089, x 3 year contract = 1,188,267, x 5-year contract = £1,980,445
PAN Essex procurement (excl. Thurrock CCG), West Essex CCG lead
The service is a bridge between children’s Mental Health services and adults Mental Health services for service users that are adolescent/young people that do not qualify for either service. West Essex CCG has delegated authority which was approved on 25th August 2021 at CCF to go out and re-procure the service on behalf of all Essex CCGs – excluding Thurrock. Period of agreement will be from 01/10/2022 to 30/09/2025 (with option to extend for a further 24 months).
Procurement has been launched, and bids are being evaluated.
Children & Young Persons (CYP) Mental Health Digital Toolkit
Total budget per annum -£273,877.00, x 5 year contract = £1,369,385
10 Essex Partners – 7 CCGs & 3 LAs, West Essex CCG lead
This is an online toolkit to help CYP and their families access mental health support and a counselling service. West Essex CCG has delegated authority which was approved on 25th August 2021 at CCF to go out and re-procure the service on behalf of all 10 partners – 7 CCGs and 3 Local Authorities. Period of agreement will be from 1st December 2022 to 30th November 2025.
Procurement has been launched, and bids are being evaluated.
2. Procurement Pipeline (cont.)(6)

14
Project Value Lead Comments & Update
Frailty Mapping TBC TBC TBC
Autism Spectrum Disorder (ASD) Diagnostic Service
TBC TBC TBC
TB Screening TBC TBC TBC
2. Procurement Pipeline (cont.)(7)
15
• Procurement policies, processes, documentation, governance arrangements will be aligned across the Suffolk and North East Essex (SNEE) Integrated Care Board (ICB), to ensure best practice and audit is maintained, whilst ensuring compliance with the procurement regulations.
• The procurement workplans for Suffolk and North East Essex are in the process of being updated. The intention is to create one consolidated workplan which covers the SNEE ICB, but will also include projects that are part of other collaborative arrangements e.g. PAN Essex procurements, and services jointly commissioned with Councils.
• A transition checklist has been developed and an ICB Procurement Committee is being formed, who will be responsible for providing oversight and challenge to ensure procurement policy and processes are delivered appropriately to secure quality value for money services through procedures which are transparent, proportionate, fair and non-discriminatory.
3. Procurement Policy/Strategy/Workplan

16
• Further to the Queens speech recently, a Procurement Bill has been published in the House of Lords.
• The ambition is to create a new regulatory framework that delivers the best commercial outcomes with the least burden on providers and contracting authorities. Clinical healthcare services and non-clinical services will be covered by separate rules.
• Furthermore, the intention is to embed transparency throughout the commercial lifecycle so that public spending can be properly scrutinised.
• The Procumbent Bill comprises of 122 pages, and can be accessed by clicking onto the enclosed link
• There will be a minimum of 6 months transition period, before the regime goes live.
• Existing procurement legislation will continue to apply until the new rules come into force.
4. Proposed Legislative Changes

17
Thank you

Suffolk and North East Essex Area Prescribing Committee (SNE APC) NHS Ipswich and East Suffolk CCG (IESCCG), NHS North East Essex CCG (NEECCG), NHS West Suffolk CCG (WSCCG)
East Suffolk and North Essex NHS Foundation Trust (ESNEFT), Norfolk and Suffolk NHS Foundation Trust (NSFT), West Suffolk NHS Foundation Trust (WSFT), Anglian Community Enterprise (ACE), Essex Partnership University Trust (EPUT)
GOVERNING BODY
Agenda Item No. 19
Reference No. NEECCG 22043
Date. 7 June 2022
Title
Suffolk and North East Essex Area Prescribing Committee (SNEE APC) Meeting- minutes of the meetings February, March and April 2022
Lead Director
Pam Green- Chief Operating Officer
Author(s)
Emily Rutherford- Medicines Management Support Officer, NHS Ipswich and East Suffolk Clinical Commissioning Group (February 2022 Meeting) Anisha Sharma, Senior Interface Pharmacist, ESNEFT, NHS Ipswich and East Suffolk CCG and NHS North East Essex CCG
Purpose
The SNEE APC decisions have been submitted to the Governing Body for information to provide assurance of the activities undertaken by the Committee.
Applicable CCG Strategic Objectives:
1. To achieve our vision through an inclusive, holistic approach to patient and service user centred commissioning, embedding personalisation of care through integrated health and social care services.
2. To transform care and drive continuous improvement in quality and safety. Achieve the best possible outcomes for our service users through high quality care.
x
3. To use commissioning resources effectively and responsibly. To develop our organisation, teams and individual staff to be trusted, competent, well trained, talented, enthusiastic and dedicated.
x
4 To tackle the biggest health challenges in north east Essex including reducing health inequalities.

Suffolk and North East Essex Area Prescribing Committee (SNE APC) NHS Ipswich and East Suffolk CCG (IESCCG), NHS North East Essex CCG (NEECCG), NHS West Suffolk CCG (WSCCG)
East Suffolk and North Essex NHS Foundation Trust (ESNEFT), Norfolk and Suffolk NHS Foundation Trust (NSFT), West Suffolk NHS Foundation Trust (WSFT), Anglian Community Enterprise (ACE), Essex Partnership University Trust (EPUT)
Recommendation: The Governing Body are asked to note the approved guidelines, formulary products, items to improve the medicines governance and the quality of the service delivered to patients across Suffolk and North East Essex Integrated Care System (SNEE ICS) for the period up to April 2022. All items were consulted upon by the Clinical Reference group prior to APC approval. Summary: The minutes of the meeting are available to reference and demonstrates how the SNEE APC have worked as an integrated care system to support the entry of new medicines into the health economy, review historic decisions and develop guidelines to improve medicines optimisation which includes medicines safety. The following were approved at the February 2022 meeting (Appendix 1):
• SNEE APC Terms of Reference Update
• Suffolk Lymphoedema Venous Compression Garments Formulary
• SNEE Asthma Quick Reference Guide
• SNEE COPD Quick Reference Guide
• West Suffolk GP Advance Authorisation Form: Medication reviews conducted by WSCCG Medicines Management Pharmacy Technicians
• NEE Woundcare formulary
• NEE Continence formulary
• NEE Urinary catheter passport
• East Suffolk and North Essex New Medicines Request Prednisolone Suppositories and Proctitis treatment pathway
• Ipswich and East Suffolk Hyperhydrosis pathway
• SNEE Position Statement for Inclisiran
• SNEE Sativex® Oromucosal spray for Multiple sclerosis in adults The following were approved at the March 2022 meeting (Appendix 2):
• SNEE Policy For The Prescribing Of Home Oxygen To Patients Who Are Known To Smoke
• Suffolk Continence Formulary (Appliances)
• Suffolk Position Statement on the Prescribing of Orthotics
• SNEE ICS Inhaler carbon footprint guide
• North East Essex Skin Care Aid Memoir
• North East Essex lymphoedema garments formulary
• North East Essex Guidelines for Home Glucose Monitoring for Adults with Type 1 & 2 Diabetes
• NEECCG Historic formulary position for degarlix The following were approved at the April 2022 meeting (Appendix 3):
• COPD Plus project- NHS North East Essex CCG
• North East Essex Continence formulary
• North East Essex- Roflumilast formulary positon
• Prescribing Commissioning Policy for Biosimilar Insulin
• NEE/NEEDS Insulin use in Type 1 and Type 2 diabetes update
• SNEE Edoxaban Switching Position Statement
• SNEE Diabetes Guidance- response to NICE NG28
• Interim Rheumatoid Arthritis pathway
• Prescribing policy for Wegovy ® (Simaglutide)

Suffolk and North East Essex Area Prescribing Committee (SNE APC) NHS Ipswich and East Suffolk CCG (IESCCG), NHS North East Essex CCG (NEECCG), NHS West Suffolk CCG (WSCCG)
East Suffolk and North Essex NHS Foundation Trust (ESNEFT), Norfolk and Suffolk NHS Foundation Trust (NSFT), West Suffolk NHS Foundation Trust (WSFT), Anglian Community Enterprise (ACE), Essex Partnership University Trust (EPUT)
Appendix 1: February 2022 SNEE APC Minutes Final Version 1
Minutes of the Meeting
Meeting: Suffolk and North East Essex Area Prescribing Committee (SNEE APC)
Date and Time: Tuesday 8th February 2022 15:00-17:00
Venue: Virtually via Microsoft Teams
Chair: Dr David Egan
Attendees:
Name Title and organisation
Dr David Egan DE NHS Ipswich and East Suffolk CCG Clinical Lead for Prescribing
Dr Prashant Arora PA Tendring GP Elect Member, NHS North East Essex CCG
Dr Andrew Hassan AH NHS West Suffolk CCG Clinical Lead for Prescribing
Dr Jon Tuppen JP Suffolk LMC representative
Catherine Butler CB
NHS Ipswich and East Suffolk CCG Chief Pharmacist and NHS West Suffolk CCG Interim Chief Pharmacist
Rifat Choudhury RC NHS Ipswich and East Suffolk CCG Deputy Chief Pharmacist (15:34 onwards)
Sarah Spink SS Deputy Chief Pharmacist, NHS West Suffolk CCG
Ben Leung BL Deputy Chief Pharmacist, NHS West Suffolk CCG (until 16:36)
Sheila Murnion SM Suffolk CCGs Lead Contracts Manager, High Cost Drugs
Oge Chesa OC
NHS North East Essex CCG Deputy Director of Primary Care and Medicines Management
Olubusola (Busola) Daramola
OD Head of Medicines Management, NHS North East Essex CCG Pharmacist
Vicki Saliba VS Deputy Chief Pharmacist, NHS North East Essex CCG Lead
Rosie Thomson RT Lead Pharmacist, The Oaks Hospital
Hilary Scott HS
Essex Partnership University NHS Foundation Trust – Chief Pharmacist (from 15.52)
Oweikumo Eradiri OE
East Suffolk and North Essex NHS Foundation Trust, Joint Interim Chief Pharmacist
Judith Esterhuizen JE West Suffolk Hospital NHS Foundation Trust Formulary Pharmacist
Tania Farrow TF Suffolk Local Pharmaceutical Committee (LPC) Chief Officer
Emily Rutherford ER NHS Ipswich and East Suffolk CCG Support Officer
Anisha Sharma AS Senior Interface Pharmacist, East Suffolk and North Essex NHS Foundation Trust and NHS Ipswich and East Suffolk CCG
Apologies
Name Title
Dr James Broadway JB East Suffolk and North Essex NHS Foundation Trust Medicines Optimisation Committee Chair and Consultant Anaesthetist
Liz Buxton LB Anglia Community Enterprise (CIC) Assistant Director of Quality
Simon Whitworth SW West Suffolk Hospital NHS Foundation Trust Chief Pharmacist
Rachel Belton RB
Deputy Chief Pharmacist, NHS Ipswich and East Suffolk CCG Medicines Management Pharmacist
Anam Baksh AB Medicines Management Pharmacist, NHS Ipswich and East Suffolk CCG
Lisa Stephenson LS Deputy Chief Pharmacist, NHS North East Essex CCG Pharmacist
Esther Johnston EJ Chief Pharmacist , Norfolk and Suffolk NHS Foundation Trust
Emma Travers ET East Suffolk and North Essex NHS Foundation Trust, Joint Interim Chief Pharmacist
Paul Mills PM East Suffolk and North Essex NHS Foundation Trust- Assistant Chief Pharmacist
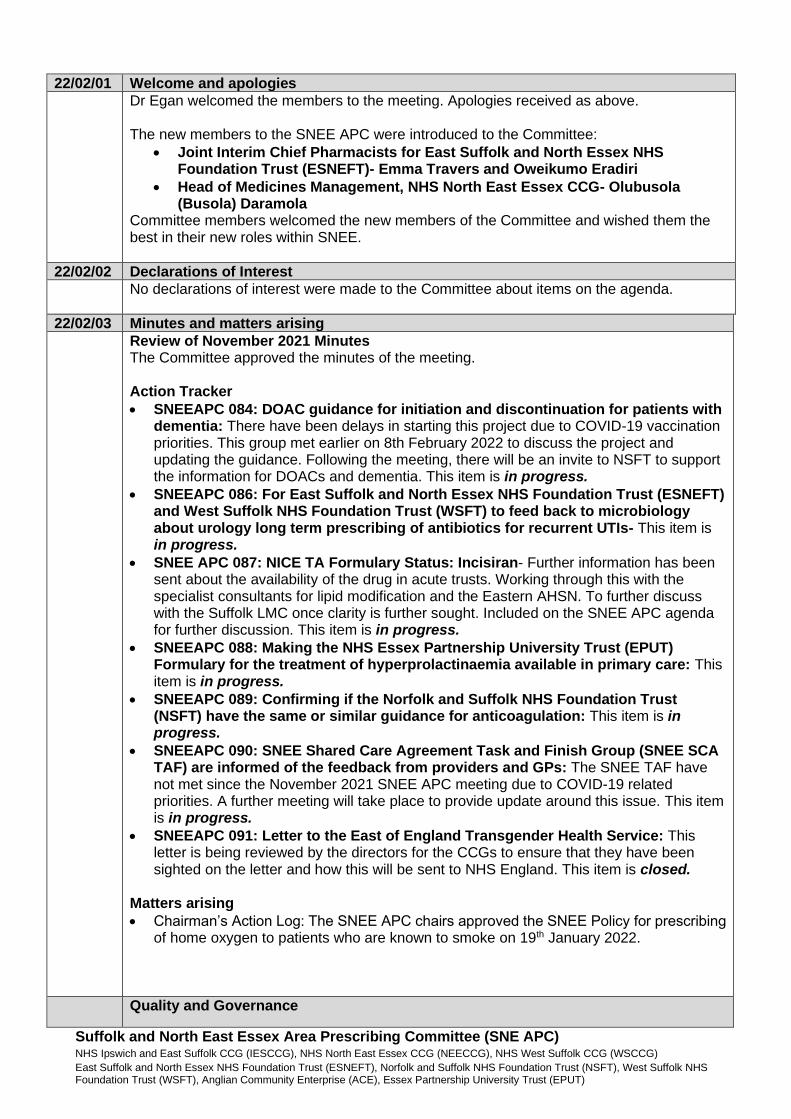
Suffolk and North East Essex Area Prescribing Committee (SNE APC) NHS Ipswich and East Suffolk CCG (IESCCG), NHS North East Essex CCG (NEECCG), NHS West Suffolk CCG (WSCCG)
East Suffolk and North Essex NHS Foundation Trust (ESNEFT), Norfolk and Suffolk NHS Foundation Trust (NSFT), West Suffolk NHS Foundation Trust (WSFT), Anglian Community Enterprise (ACE), Essex Partnership University Trust (EPUT)
22/02/01 Welcome and apologies
Dr Egan welcomed the members to the meeting. Apologies received as above. The new members to the SNEE APC were introduced to the Committee:
• Joint Interim Chief Pharmacists for East Suffolk and North Essex NHS Foundation Trust (ESNEFT)- Emma Travers and Oweikumo Eradiri
• Head of Medicines Management, NHS North East Essex CCG- Olubusola (Busola) Daramola
Committee members welcomed the new members of the Committee and wished them the best in their new roles within SNEE.
22/02/02 Declarations of Interest
No declarations of interest were made to the Committee about items on the agenda.
22/02/03 Minutes and matters arising
Review of November 2021 Minutes The Committee approved the minutes of the meeting. Action Tracker
• SNEEAPC 084: DOAC guidance for initiation and discontinuation for patients with dementia: There have been delays in starting this project due to COVID-19 vaccination priorities. This group met earlier on 8th February 2022 to discuss the project and updating the guidance. Following the meeting, there will be an invite to NSFT to support the information for DOACs and dementia. This item is in progress.
• SNEEAPC 086: For East Suffolk and North Essex NHS Foundation Trust (ESNEFT) and West Suffolk NHS Foundation Trust (WSFT) to feed back to microbiology about urology long term prescribing of antibiotics for recurrent UTIs- This item is in progress.
• SNEE APC 087: NICE TA Formulary Status: Incisiran- Further information has been sent about the availability of the drug in acute trusts. Working through this with the specialist consultants for lipid modification and the Eastern AHSN. To further discuss with the Suffolk LMC once clarity is further sought. Included on the SNEE APC agenda for further discussion. This item is in progress.
• SNEEAPC 088: Making the NHS Essex Partnership University Trust (EPUT) Formulary for the treatment of hyperprolactinaemia available in primary care: This item is in progress.
• SNEEAPC 089: Confirming if the Norfolk and Suffolk NHS Foundation Trust (NSFT) have the same or similar guidance for anticoagulation: This item is in progress.
• SNEEAPC 090: SNEE Shared Care Agreement Task and Finish Group (SNEE SCA TAF) are informed of the feedback from providers and GPs: The SNEE TAF have not met since the November 2021 SNEE APC meeting due to COVID-19 related priorities. A further meeting will take place to provide update around this issue. This item is in progress.
• SNEEAPC 091: Letter to the East of England Transgender Health Service: This letter is being reviewed by the directors for the CCGs to ensure that they have been sighted on the letter and how this will be sent to NHS England. This item is closed.
Matters arising
• Chairman’s Action Log: The SNEE APC chairs approved the SNEE Policy for prescribing of home oxygen to patients who are known to smoke on 19th January 2022.
Quality and Governance

Suffolk and North East Essex Area Prescribing Committee (SNE APC) NHS Ipswich and East Suffolk CCG (IESCCG), NHS North East Essex CCG (NEECCG), NHS West Suffolk CCG (WSCCG)
East Suffolk and North Essex NHS Foundation Trust (ESNEFT), Norfolk and Suffolk NHS Foundation Trust (NSFT), West Suffolk NHS Foundation Trust (WSFT), Anglian Community Enterprise (ACE), Essex Partnership University Trust (EPUT)
22/02/04 COVID-19 No items were discussed for this standing agenda item.
22/02/05 SNEE APC Terms of Reference Update The SNEE APC Terms of Reference (ToR) have been updated to allow for the SNEE APC to have oversight and provide the governance structure to implement the NHS Integration of Pharmacy and Medicines Optimisation (IPMO) within the SNEE Integrated Care System (SNEE ICS). A line has been added to allow for the SNEE APC to manage the requirements for the SNEE IPMO process. DECISION: The Committee approved the update to the SNEE APC Terms of Reference which will now go to the SNEE CCGs Governing Bodies for approval.
22/02/06 SNEE ICS MI enquiries Q1 2021-22 The SNEE APC were informed of the types of enquires that the Midlands and East Medicines Advice Service (MEMAS) receive from primary care within SNEE. The report summarises the types of enquiries from primary care and the enquirer with the objective to identify further areas of support that may be required in primary care. This is the first report and the Committee were encouraged to provide feedback on if they would like any changes to be made or if there are other opportunities to consider going forward. The Quarter 1 report for 2021-22 showed that there were a number of enquiries from community pharmacies and practice based pharmacists. The theme was mostly related to the reconciliation of medicines on discharge letters. Committee members discussed the following with regards to enquiries received by the MEMAS service:
• Some primary care clinicians report issues such as those with discharge letters directly to the specialist teams and not through the MEMAS service and queried whether this was appropriate or if it affects the data. Although this does affect the information available, the Committee were informed not to change the current process but the report may help inform of next steps in terms of education and training needs for primary care staff.
• Although there have been some enquiries from practice staff to the MEMAS team, a member requested for some communications to be sent out to Primary Care Network (PCN) staff in SNEE about the MEMAS service. It was agreed that this will be looked into. ACTION SNEEAPC 091: AS to confirm with MEMAS team if communications on the service could be sent to PCNs in SNEE.
• The members of the Committee agreed that the medicines reconciliation process is a major workload pressure within primary care particularly with outpatient letters requesting for medicines particularly from ophthalmology. Some solutions explored by SNEE APC include ensuring there is sessions available on the hospital induction for doctors and other prescribers.
• It was agreed that where there are significant issues, to use the provider concern form to ensure it is escalated up correctly to be investigated and solutions within the provider organisation are found.
DECISION: The SNEE APC noted the report for SNEE ICS MI enquiries Q1 2021-22.
22/02/07 NICE Adherence- Technology appraisals and guidelines This item was included for information on the new Technology Appraisals (TA) released in October 2021. The following NICE Technology appraisals relate to pathways commissioned by CCGs or prescribed in primary care:
• Sodium zirconium cyclosilicate for treating hyperkalaemia
Suffolk and North East Essex Area Prescribing Committee (SNE APC) NHS Ipswich and East Suffolk CCG (IESCCG), NHS North East Essex CCG (NEECCG), NHS West Suffolk CCG (WSCCG)
East Suffolk and North Essex NHS Foundation Trust (ESNEFT), Norfolk and Suffolk NHS Foundation Trust (NSFT), West Suffolk NHS Foundation Trust (WSFT), Anglian Community Enterprise (ACE), Essex Partnership University Trust (EPUT)
• Solriamfetol for treating excessive daytime sleepiness caused by narcolepsy- the Respiratory Support and Sleep Centre (RSSC) at Royal Papworth Hospital NHS Foundation Trust will be the only provider organisation to provide this drug. Clinicians in East Suffolk and North Essex NHS Foundation Trust (ESNEFT) and West Suffolk NHS Foundation Trust (WSFT) will not initiate solriamfetol.
• Cenobamate for treating focal onset seizures in epilepsy- the pathway for this drug is currently being reviewed. It was noted that it should be initiated in a tertiary referral centre but can be continued in primary care. It is not a high cost drug and is within tariff.
• Upadacitinib for treating moderate rheumatoid arthritis- This drug will be incorporated into the Rheumatoid Arthritis pathway and remain as a hospital only drug.
• Tofacitinib for treating juvenile idiopathic arthritis- This is an NHS England commissioned indication but once the paediatric patient transitions to adult services, this will be a CCG commissioned drug.
DECISION: The Committee noted the Technology Appraisals released for October, November, December 2021 and January 2022.
22/02/08 Medicines Safety
• National Patient Safety Alerts in General Practice- it was clarified that for this section provider and commissioner organisations will report back on how a national patient safety alert was implemented.
• Specialist Pharmacy Service (SPS) Medicines Safety Officer (MSO) Observatory January 2022: The Committee noted that the SPS MSO Observatory is a comprehensive summary outlining key notifications within the NHS including supply notifications and for the document to continue to be included in the SNEE APC agenda as a regular standing item. The January 2022 SPS MSO Observatory contains information from November and December 2021 and January 2022.
o Medicines Supply Shortage Notification: These were noted by the committee and agreed that none were related to primary care. The SPS webpage now has a Medicines Supply Tool to support the NHS in managing shortages.
o MHRA Drug Safety Update: Key points that were highlighted are haloperidol risk for elderly patients and dapagliflozin is no longer authorised for type 1 diabetes.
o MHRA Drug Shortages: None related to primary care within the SPS MSO Observatory document. However, the Committee were made aware of a shortage of 3mg and 4mg Trulicity shortage via the diabetes team at NEEDs and ESNEFT. Information has not been released about this shortage via CAS alerts or the SPS Medicines Shortage Tracker. The diabetes team at ESNEFT-Ipswich and NEEDs in NEE have developed a position statement and further information is required to support and manage this shortage.
o MHRA Drug recalls and notifications: These were noted by the Committee
Members of the Committee requested a summary of items which impact primary care to be included going forward which will be a part of the SNEE APC coversheet. In addition the Specialist Pharmacy Service (SPS) Medicines Safety Officer (MSO) Observatory will be highlighted to PCNs as part of regular updates to help support medicines safety discussions. DECISION: The Committee agreed in using the SPS MSO Observatory documents going forward as a standing agenda item with the summary of information included.
GUIDELINES AND FORMULARY
22/02/09 Suffolk Lymphoedema Venous Compression Garments Formulary This document has been developed alongside specialists across Suffolk and NEE to support the prescribing of Lymphoedema and Venous Compression Garments for the lower limbs. It includes pathways and guidance for clinicians on assessment and treatment.
Suffolk and North East Essex Area Prescribing Committee (SNE APC) NHS Ipswich and East Suffolk CCG (IESCCG), NHS North East Essex CCG (NEECCG), NHS West Suffolk CCG (WSCCG)
East Suffolk and North Essex NHS Foundation Trust (ESNEFT), Norfolk and Suffolk NHS Foundation Trust (NSFT), West Suffolk NHS Foundation Trust (WSFT), Anglian Community Enterprise (ACE), Essex Partnership University Trust (EPUT)
This is a comprehensive formulary to support primary care in an area where a number of prescribers are unfamiliar with. DECISION: The Committee approved the SNEE Lymphoedema and Venous Compression Garments Formulary.
22/02/10 Suffolk Homely Remedies and self care tool This is an update to the existing toolkit which includes a table related to loperamide which was omitted from the current document. DECISION: SNEE APC approved the Suffolk Homely Remedies and self-care tool for NHS Ipswich and East Suffolk CCG (IESCCG) and NHS North East Essex CCG (NEECCG)
22/02/11 Asthma Quick Reference Guide This is an updated to the existing joint asthma guidelines available between East Suffolk and North Essex NHS Foundation Trust (ESNEFT), IESCCG and NEECCG. This update includes access to greener inhalers and outlines options and opportunities to embed the green agenda locally for inhalers. There is also an update related to Short-A Beta-Agonist (SABA) monotherapy, spacers and secondary care referrals. There will be an SNEE ICS wide guidance to be developed in the near future which will include NHS West Suffolk CCG (WSCCG) and West Suffolk NHS Foundation Trust (WSFT). The Committee agreed that it was the relevant group to support and endorse items related to medicines for the NHS sustainability agenda. This work facilitates the Primary Care Network (PCN) Investment and Impact Fund (IIF) deliverables and can be monitored on the PCN dashboard. PrescQIPP will also provide monitoring tools which can be shared with SNEE APC and PCNs. The Committee requested for a comprehensive communication plan to be in place and include why there is a need to switch to dry powder inhalers (DPI) or soft mist inhalers (SMI) over traditional Metered Dose Inhaler (MDI) which were the focus for many years. This will support primary care clinicians in understanding the rationale around the NHS carbon reduction strategy. SNEE APC were assured that a communications plan has been developed to support the introduction of the updated guidance which will be released following the approval. A training session with PCN pharmacists has occurred and a session will be held for practice nurses in March 2022. The SNEE APC GP members were in agreement that the document is very supportive, easy to read and manage and welcome the sustainability initiative. DECISION: The Committee approved the Asthma Quick Reference Guide jointly used between ESNEFT, IESCCG and NEECCG.
22/02/12 COPD Quick Reference Guide This is an updated to the existing joint COPD guidelines available between East Suffolk and North Essex NHS Foundation Trust (ESNEFT), IESCCG and NEECCG. This update includes access to greener inhalers including the RAG coding for inhalers and information on disposal. Trimbow ® has been added to support the green agenda for inhalers. Patients have been encourage to return used inhalers to their community pharmacy to ensure that they do not ‘end up in’ landfill. There will be an SNEE ICS wide guidance to be developed in the near future which will include NHS West Suffolk CCG (WSCCG) and West Suffolk NHS Foundation Trust (WSFT).

Suffolk and North East Essex Area Prescribing Committee (SNE APC) NHS Ipswich and East Suffolk CCG (IESCCG), NHS North East Essex CCG (NEECCG), NHS West Suffolk CCG (WSCCG)
East Suffolk and North Essex NHS Foundation Trust (ESNEFT), Norfolk and Suffolk NHS Foundation Trust (NSFT), West Suffolk NHS Foundation Trust (WSFT), Anglian Community Enterprise (ACE), Essex Partnership University Trust (EPUT)
DECISION: The Committee approved the COPD Quick Reference Guide jointly used between ESNEFT, IESCCG and NEECCG.
22/02/13 GP Advance Authorisation Form: Medication reviews conducted by WSCCG Medicines Management Pharmacy Technicians This document has been developed to support Medicines Management Pharmacy Technicians in WSCCG to undertake work in practices through advanced authorisation for work. This is a similar document to those developed for work by the WSCCG MOCH team and WSCCG Appliance Nurses. DECISION: The Committee approved the use of the document in WSCCG.
22/02/14 NEE Directory of prescribing policies- update The NEECCG Directory of prescribing policies has been updated to include mild to moderate dry eyes includes for moderate as per the NHS England guidance to CCG for prescribing of over the counter medicines in primary care. The “do not prescribe” sections have been clarified. Implementation of the mild to moderate dry eyes will take place with the ophthalmology specialists in due course. There have also been some amendments to support clarity around the ‘Do not prescribe’ DECISION: SNEE APC approved the updated document to use in NEECCG
22/02/15 Logo and structural changes The following three existing documents have been updated with new logos and a change to the title page to reflect the SNEE ICS templates for documents.
• NEE Woundcare formulary
• NEE Continence formulary
• NEE Urinary catheter passport It was agreed by the SNEE APC to only request a summary or list of document that have been updated with new logos or minor amendments in the visual layout of the document going forward and the full document does not need to be submitted. There may be more documents in the future following the move to an SNEE Integrated Care System (ICS) website. DECISION: The SNEE APC approved the update to the documents.
22/02/16 New Medicines Request Prednisolone Suppositories and Proctitis treatment pathway Following a request from the Inflammatory Bowel Disease (IBD) team in ESNEFT- Ipswich site, it was noted that prednisolone suppositories have not been agreed on the formulary. A formal application has been made as a result to include prednisolone suppositories on the joint formulary for ESNEFT, IESCCG and NEECCG. As part of the application a Treatment of proctitis in patients with Inflammatory bowel disease was developed to support the appropriate prescribing of prednisolone in primary care. There is a clear place for prednisolone suppositories in the treatment of proctitis for patients with IBD as it provides topical steroid treatment in a localised area. Other rectal preparations such as rectal enema are not effective as they do not work on the required site and work further to the ascending colon and foam enemas only reach as far as the descending colon. WSCCG and WSFT were informed of the application and if they wished to be included in the application. DECISION: The Committee approved both the formulary application and the treatment of proctitis in patients with IBD pathway for ESNEFT, IESCCG and NEECCG. It was confirmed that prednisolone suppositories are available for this indication in West Suffolk.
22/02/17 Ipswich and East Suffolk Hyperhydrosis pathway This is the hyperhidrosis pathway for Ipswich and East Suffolk (IES) only. There is an established pathway in North East Essex in line with the East of England Priorities Advisory Committee which the IES pathway was adapted from.
Suffolk and North East Essex Area Prescribing Committee (SNE APC) NHS Ipswich and East Suffolk CCG (IESCCG), NHS North East Essex CCG (NEECCG), NHS West Suffolk CCG (WSCCG)
East Suffolk and North Essex NHS Foundation Trust (ESNEFT), Norfolk and Suffolk NHS Foundation Trust (NSFT), West Suffolk NHS Foundation Trust (WSFT), Anglian Community Enterprise (ACE), Essex Partnership University Trust (EPUT)
The following documents were developed:
• Practice Briefing Hyperhidrosis- explaining why we are trying to implement the local pathway.
• Treatment pathway for hyperhidrosis in Primary Care v0.5- This pathway has been developed based on the East of England Priorities Advisory Committee
• Information leaflet - Self management of excessive sweating v0.3 DRAFT- This patient information will be made available to clinicians in primary care to help patients understand the options available for treatment, what is available for self-care and what is available on the NHS. The only NHS option is oral anticholinergics as they are all a prescription only medication.
• Referral form for Iontophoresis- this is an existing form to help support the referral to trial iontophoresis.
• Information leaflet - Iontophoresis for hyperhydrosis DRAFT 1.2- this leaflet provides information to the patient on what to expect and how to trial the iontophoresis. It is expected that the patient will purchase if successful and this is the position across the NHS as iontophoresis is not available on the NHS throughout England.
• Hyperhidrosisuk.org leaflet A majority of the pathway is supported in primary care and self-care from the patient. A patient information leaflet has been developed to support patients in understanding where in the pathway GPs will support the prescribing. However, a majority of the pathway is managing via self-care. This only applies to IES and ESNEFT (Ipswich) as North East Essex and ESNEFT (Colchester) have an established pathway in line with the East of England Priorities Advisory Committee before the merger. The difference in the two pathways is that Botulinum toxin is available on the NEE pathway but not on the IES pathway. This is because patient numbers who require Botulinum toxin are unknown as historically the hyperhidrosis pathway was not available in IES. This coupled with capacity concerns in the dermatology department in ESNEFT-Ipswich site does not allow for patients to be managed with Botulinum toxin. It is not a drug which is NICE Technology Appraised and evidence is limited. The ESNEFT Medicines Governance Group have requested that the position for Botulinum toxin be reviewed in 18 months to align the place for this therapy across ESNEFT. The Committee noted that the ESNEFT-Ipswich Dermatology team does not have sufficient capacity within its service to include Botulinum toxin within the pathway. Botulinum toxin is not a ‘in tariff’ drug currently but may be a drug included within the tariff going forward. SNEE APC were informed that the Individual Funding Request (IFR) panel should not be overburdened with requests for Botulinum toxin for hyperhidrosis which was agreed an in most cases the requests do not show exceptionality therefore are declined. It was agreed that there needs to be a review point to consider the alignment of the guidance with NHS North East Essex CCG going forward which should be within 18 months to 2 years. ACTION SNEEAPC092: To request the ESNEFT-Ipswich Dermatology to work with the dermatology team in North East Essex to agree the pathway going forward. DECISION: SNEE APC approved the hyperhidrosis guidelines and supporting information for IES.
22/02/18 Lipid Modification Guidance: Inclisiran Inclisiran received a positive NICE Technology appraisal in October 2021: (Inclisiran for treating primary hypercholesterolaemia or mixed dyslipidaemia Technology appraisal guidance [TA733]Published: 06 October 2021). Following it’s agreement, NHS England produced information on the medicines optimisation for incilisiran and have commissioned the Academic Health Science Networks (AHSN)

Suffolk and North East Essex Area Prescribing Committee (SNE APC) NHS Ipswich and East Suffolk CCG (IESCCG), NHS North East Essex CCG (NEECCG), NHS West Suffolk CCG (WSCCG)
East Suffolk and North Essex NHS Foundation Trust (ESNEFT), Norfolk and Suffolk NHS Foundation Trust (NSFT), West Suffolk NHS Foundation Trust (WSFT), Anglian Community Enterprise (ACE), Essex Partnership University Trust (EPUT)
across the country to provide training, education and support the implementation of inclisiran in the local health economy. The Eastern AHSN are the local AHSN for SNEE. SNEE has an interim position about the inclisiran which makes it available on formulary but not assigned a formulary status (please click here) which was agreed via Chairman’s action in November 2021, which expired in January 2022. The request is for this position statement to be extended by one month for the following reasons:
• The local lipidologists are working with the Eastern AHSN to support the NHSE process for inclisiran. They have not been involved in the beginning and they did not have the opportunity to gain experience in the use of inclisiran. As of 24th January 2022, NHSE has made inclisiran a drug available to NHS Hospitals and we are currently scoping the pathway with this new information in mind.
• Inclisiran was discussed at the NEE Clinical Reference Group (CRG) on 25th January 2022 and there was support to introduce inclisiran in the primary care pathway by the group of GPs.
• The Suffolk LMC have written to the SNEE APC about their view on inclisiran which is in line with the RCGP and BMA position (please click here).
• There is an opportunity to use inclisiran as a ‘Green’ drug as per our definition in SNEE (Specialist in any setting to advise/initiate, primary care to continue).
• We do need to also inform the SNEE CVD ICS Board of the implementation of the lipid modification pathway.
In order to address and clarify the pathway, the ask is to extend the current position statement by one month until 8th March 2022 so we can support the discussions with our specialists in hospital, the Suffolk LMC and have the pathway agreed at the prescribing workstreams as well as NEE CRG. DECISION: The Committee approved the extension of the position statement until 8th March 2022 where it will be discussed at the next SNEE APC.
22/02/19 SPS: New Medicines News October 2021, November 2021 and December 2021 The Specialist Pharmacy Services (SPS) New medicines news November 2021, December 2021 and January 2022 was included for information to inform the committee of newly licensed medicines which may be considered as part of the treatment pathway in the future. DECISIONS: The Committee noted the New Medicines News for November 2021, December 2021 and January 2022.
COMMISSIONING
22/02/20 Sativex® Oromucosal spray for Multiple sclerosis in adults
Sativex® Oromucosal spray is commissioned for patients with MS in line with NICE Guideline NG144, Cannabis-based medicinal Products and CG186; Multiple sclerosis in adults: management for patients who meet the criteria detailed in the business case. Sativex® Oromucosal spray is not commissioned to manage chronic pain in adults, in line with NICE Guideline NG144, Cannabis-based medicinal products.
Sativex ® oromucosal spray would be available to a cohort of patients who have gone through the pathway and have no other options for treatment. The application for funding will be made before the responders scheme is applied for. The vast majority of patients are found to not tolerate or respond to this drug so the likely numbers are lower than that on the NICE guidance. However, there have been patients who have significantly responded and benefited from treatment which significantly improves their quality of life. However, there is a point of disease progression where the patient no longer responds.
Treatment costs are offset by the problems the patient develops such as hospital admissions, sepsis risk and impact on carers or resources needed for support.

Suffolk and North East Essex Area Prescribing Committee (SNE APC) NHS Ipswich and East Suffolk CCG (IESCCG), NHS North East Essex CCG (NEECCG), NHS West Suffolk CCG (WSCCG)
East Suffolk and North Essex NHS Foundation Trust (ESNEFT), Norfolk and Suffolk NHS Foundation Trust (NSFT), West Suffolk NHS Foundation Trust (WSFT), Anglian Community Enterprise (ACE), Essex Partnership University Trust (EPUT)
The annual review process is available in the Blueteq form which will be reviewed at a 12-monthly date. If the patient fails to meet the criteria, the treatment will be stopped.
DECISION: SNEE APC approved the use of Sativex ® Oromucosal spray for patients with Multiple Sclerosis patients in line with the NICE Guidelines 144. This will remain a RED hospital drug.
22/02/21 Pharmacy Integration
• GP CPCS: The NHS Community Pharmacist Consultation Service (CPCS) was launched by NHS England and NHS Improvement on the 29 October 2019, to progress the integration of community pharmacy into local NHS urgent care services, providing more convenient treatment closer to patients’ homes. This has now been developed to allow GP practices to refer patients into the service for pharmacy support. In addition it support the NHS England guidance for CCGs: Prescribing over the counter medicines in primary care position. The SNEE ICS is the highest performing area for the uptake of this service and the Committee applauded the work from our primary care practices.
DECISION: SNEE APC noted the pharmacy integration activity for the GP CPCS across the ICS.
• Pharmacy technician pre-registration training (PTPT): As per the NHS Long Term Plan, it has been identified that there is a workforce requirement to support the development and availability of pharmacy technicians across the NHS. Pharmacy Technician roles have been included as part of the NHS Additional Roles Reimbursement Scheme (ARRS) with funding allocated through Health Education England (HEE). There are placements available in SNEE via GP and Community pharmacies as well as hospital joint posts with GP practices. From September 2022, there will be three pharmacy technicians rotating through different sectors across SNEE over two years. DECISION: SNEE APC noted the pharmacy integration activity for the Pharmacy technician pre-registration training (PTPT)
• Pilots: applications and start-ups - PILOT 1 - Oral Contraception Management Service in Community
Pharmacy- this pilot went live on 30th November 2021 allowing for the North East Ipswich Primary Care Network (PCN) together with community pharmacies within that PCN.
- Pilot 2 - Community Pharmacy GP SystmOne Clinical Record Read/Write and Task Access: this is to support the QoF delivery and this pilot was supported across Suffolk supported by the Suffolk LPC to allow community pharmacists to enable and facilitate read/write activities to support the PCN DES deliverables. This would support primary care for integration of community pharmacy. This pilot is to test the impact for the providers.
DECISION: SNEE APC noted the pilots related to the application and start-ups.
22/02/22 OTHER ITEMS
Any other business
• Trulicity Shortage: There is currently a shortage of the 3mg and 4.5mg until April 2022. The ESNEFT- Ipswich Diabetes team and the North East Essex Diabetes Service

Suffolk and North East Essex Area Prescribing Committee (SNE APC) NHS Ipswich and East Suffolk CCG (IESCCG), NHS North East Essex CCG (NEECCG), NHS West Suffolk CCG (WSCCG)
East Suffolk and North Essex NHS Foundation Trust (ESNEFT), Norfolk and Suffolk NHS Foundation Trust (NSFT), West Suffolk NHS Foundation Trust (WSFT), Anglian Community Enterprise (ACE), Essex Partnership University Trust (EPUT)
(NEEDS) have requested that patients are switched over to the 1.5mg strength until stocks of 3mg and 4.5mg resume and not to meet the patient’s existing dose. There is minimum impact on the patients HbA1c at lower doses. The communications will be sent to practices to switch patients over to the lower strength one. Once stocks of 3mg and 4.5mg doses have returned, the patient will return to their normal dose.
• SM is retiring in February 2022 and this was her last SNEE APC meeting. The Committee thanked SM for her support and help over the years and wish her a happy and successful retirement.
• ER will be on maternity leave from 14th February 2022 and the SNEE APC wished her well during this time.
• Following the SNEE APC meeting, the Joint Co-Chairs met with SS and AS to finalise and sign-off the East of England Gender Service Pilot letter from SNEE APC to NHS England.
Suffolk and North East Essex Area Prescribing Committee (SNE APC) NHS Ipswich and East Suffolk CCG (IESCCG), NHS North East Essex CCG (NEECCG), NHS West Suffolk CCG (WSCCG)
East Suffolk and North Essex NHS Foundation Trust (ESNEFT), Norfolk and Suffolk NHS Foundation Trust (NSFT), West Suffolk NHS Foundation Trust (WSFT), Anglian Community Enterprise (ACE), Essex Partnership University Trust (EPUT)
Appendix 2: March 2022 SNEE APC Minutes Final Version 1
Minutes of the Meeting
Meeting: Suffolk and North East Essex Area Prescribing Committee (SNEE APC)
Date and Time: Tuesday 8th March 2022 15:00-17:00
Venue: Virtually via Microsoft Teams
Chair: Dr Andrew Hassan
Attendees:
Name Title and organisation
Dr David Egan DE NHS Ipswich and East Suffolk CCG Clinical Lead for Prescribing
Dr Prashant Arora PA Tendring GP Elect Member, NHS North East Essex CCG
Dr Andrew Hassan AH NHS West Suffolk CCG Clinical Lead for Prescribing
Dr Jon Tuppen JP Suffolk LMC representative
Catherine Butler CB
NHS Ipswich and East Suffolk CCG Chief Pharmacist and NHS West Suffolk CCG Interim Chief Pharmacist
Rachel Belton RB
Deputy Chief Pharmacist, NHS Ipswich and East Suffolk CCG Medicines Management Pharmacist
Anam Baksh AB Medicines Management Pharmacist, NHS Ipswich and East Suffolk CCG
Sarah Spink SS Deputy Chief Pharmacist, NHS West Suffolk CCG
Ben Leung BL Deputy Chief Pharmacist, NHS West Suffolk CCG
Oge Chesa OC
NHS North East Essex CCG Deputy Director of Primary Care and Medicines Management
Vicki Saliba VS Deputy Chief Pharmacist, NHS North East Essex CCG Lead
Rosie Thomson RT Lead Pharmacist, The Oaks Hospital
Oweikumo Eradiri OE
East Suffolk and North Essex NHS Foundation Trust, Joint Interim Chief Pharmacist (until 16.00)
Anisha Sharma AS Senior Interface Pharmacist, East Suffolk and North Essex NHS Foundation Trust and NHS Ipswich and East Suffolk CCG
Simon Whitworth SW West Suffolk Hospital NHS Foundation Trust Chief Pharmacist
Lisa Stephenson LS Deputy Chief Pharmacist, NHS North East Essex CCG Pharmacist
Esther Johnston EJ Chief Pharmacist , Norfolk and Suffolk NHS Foundation Trust
Gemma Shanks GS NHS West Suffolk CCG, Medicines Management Pharmacy Technician
Debra Lovering DL
NHS North East Essex, Prescribing Support Pharmacy Technician for item 22/03/07
Donna Briggs DB
NHS North East Essex, Prescribing Support Pharmacy Technician for item 22/03/07
Apologies
Name Title
Dr James Broadway JB East Suffolk and North Essex NHS Foundation Trust Medicines Optimisation Committee Chair and Consultant Anaesthetist
Liz Buxton LB Anglia Community Enterprise (CIC) Assistant Director of Quality
Hilary Scott HS Essex Partnership University NHS Foundation Trust – Chief Pharmacist
Emma Travers ET East Suffolk and North Essex NHS Foundation Trust, Joint Interim Chief Pharmacist
Paul Mills PM East Suffolk and North Essex NHS Foundation Trust- Assistant Chief Pharmacist
Rifat Choudhury RC NHS Ipswich and East Suffolk CCG Deputy Chief Pharmacist
Olubusola (Busola) Daramola
OD Head of Medicines Management, NHS North East Essex CCG Pharmacist
Judith Esterhuizen JE West Suffolk Hospital NHS Foundation Trust Formulary Pharmacist
Suffolk and North East Essex Area Prescribing Committee (SNE APC) NHS Ipswich and East Suffolk CCG (IESCCG), NHS North East Essex CCG (NEECCG), NHS West Suffolk CCG (WSCCG)
East Suffolk and North Essex NHS Foundation Trust (ESNEFT), Norfolk and Suffolk NHS Foundation Trust (NSFT), West Suffolk NHS Foundation Trust (WSFT), Anglian Community Enterprise (ACE), Essex Partnership University Trust (EPUT)
Tania Farrow TF Suffolk Local Pharmaceutical Committee (LPC) Chief Officer
22/02/23 Welcome and apologies
Dr Hassan welcomed the members to the meeting. Apologies received as above.
22/03/01 Declarations of Interest
No declarations of interest were made to the Committee about items on the agenda.
22/03/02 Minutes and matters arising
Review of February 2022 Minutes The Committee approved the minutes of the meeting pending the following changes:
• To remove the highlighted text on the apologies section.
• To remove the section 22/02/21 notes for the secretary “There was a general agreement that these pilots and pharmacy integration projects is positive for the local area. The GP practices were selected considering the very tight turn-around after considering which practices will be willing to support this. There will be a call for Foundation Trainee Pharmacists which is due for 14th February 2022. There needs to be an advertisement going out across SNEE GP practices. This has been sent out to PCNs, clinical directors and prescribing leads, but the communications strategy will be reviewed. Lucy Beer would be happy to be involved in matching GP practices and community pharmacies. Very exciting times to integrate community pharmacy to primary care and make every contact count. Interesting to deal with long term conditions. Partnerships developed after deadline the contact with HEE will be able to help possibly. Added to orial after 31st March 2022. In terms of information governance for the pilot 2 there has been DPO signoff with NHSE. SNEE Digital team were not involved but the ICS strategic digital team have been involved. This is being piloted with SystmOne but the interoperability is questionable. Post april, the system number will increase but we are unsure of how this will happen. Trying to make this work for primary care.”
Approved pending changes. Action Tracker
• SNEEAPC 084: DOAC guidance for initiation and discontinuation for patients with dementia: BL leading this guidance and position statement ICS wide to include this for comments. This item is in progress.
• SNEEAPC 086: For East Suffolk and North Essex NHS Foundation Trust (ESNEFT) and West Suffolk NHS Foundation Trust (WSFT) to feed back to microbiology about urology long term prescribing of antibiotics for recurrent UTIs- . This was discussed with the antimicrobial pharmacist who has changed. Has been picked up again with the new antimicrobial pharmacist and will bring a further update in April 2022. This item is in progress.
• SNEE APC 087: NICE TA Formulary Status: Incisiran- Agenda item 22/03/14. This item is in progress.
• SNEEAPC 088: Making the NHS Essex Partnership University Trust (EPUT) Formulary for the treatment of hyperprolactinaemia available in primary care: EPUT are happy for this document to be shared pending agreement with endocrinology. The outcome will be brought to the April 2022 SNEE APC.This item is in progress.
• SNEEAPC 089: Confirming if the Norfolk and Suffolk NHS Foundation Trust (NSFT) have the same or similar guidance for anticoagulation: To confirm with EJ the context of this action. This item is in progress.
• SNEEAPC 090: SNEE Shared Care Agreement Task and Finish Group (SNEE SCA TAF) are informed of the feedback from providers and GPs: Finalised the draft versions with comments from specialists for the outstanding local shared care agreement. Arranging a SNEE SCA TAF for March/April 2022. This item is in progress.

Suffolk and North East Essex Area Prescribing Committee (SNE APC) NHS Ipswich and East Suffolk CCG (IESCCG), NHS North East Essex CCG (NEECCG), NHS West Suffolk CCG (WSCCG)
East Suffolk and North Essex NHS Foundation Trust (ESNEFT), Norfolk and Suffolk NHS Foundation Trust (NSFT), West Suffolk NHS Foundation Trust (WSFT), Anglian Community Enterprise (ACE), Essex Partnership University Trust (EPUT)
• SNEEAPC 091: Letter to the East of England Transgender Health Service: The letter has been sent to NHS England. This item is closed.
• SNEEAPC 092: Inform ESNEFT dermatology to align the hyperhidrosis pathway in 18 months- the dermatology teams have been informed and will meet to discuss next steps. This item is closed.
Matters arising – Nil noted.
Quality and Governance
22/03/03 COVID-19 No items were discussed for this standing agenda item.
22/03/04 NICE Adherence- Technology appraisals and guidelines This item was included for information on the new Technology Appraisals (TA) released in February 2022. The following NICE Technology appraisals relate to pathways commissioned by CCGs or prescribed in primary care:
• Upadacitinib for treating active psoriatic arthritis after inadequate response to DMARDs: No significant resource impact is anticipated
• Palforzia for treating peanut allergy in children and young people: Expected to be provided via allergy clinics within the NHS and will be a hospital only drug.
• Fremanezumab for preventing migraine- No significant resource impact is anticipated as a RED hospital only drug.
DECISION: The Committee noted the Technology Appraisals released for February 2022.
22/03/05 Medicines Safety
• National Patient Safety Alerts (NPSA) in General Practice- There were no NPSAs in February 2022. In March 2022 the following alerts were to note:
o Potential contamination of Alimentum and Elecare infant formula food products- this alert has been cascaded to practices and paediatric teams within the hospitals.
DECISION: The Committee noted NPSA for Potential contamination of Alimentum and Elecare infant formula food products
• MHRA Drug Safety Update- February 2022 - COVID-19 antivirals: reporting to the UK COVID-19 Antivirals Pregnancy
Registry- can report an exposure to a COVID-19 antiviral during pregnancy or
around the time of conception, or of partners on a COVID-19 antiviral around
the time of conception. Can encourage self-reporting
- Hydroxychloroquine, chloroquine: increased risk of cardiovascular events when
used with macrolide antibiotics; reminder of psychiatric reactions- routinely used
for Rheumatoid Arthritis and not to use macrolides (Azithromycin, erythromycin
and clarithromycin) concurrently. hydroxychloroquine and chloroquine has
existing cardiac warning.
- Ivacaftor, tezacaftor, elexacaftor (Kaftrio▼) in combination with ivacaftor
(Kalydeco): risk of serious liver injury; updated advice on liver function testing-
used for CF by specialists.
DECISION: The Committee noted the MHRA Drug Safety Update.
• Medicines Supply Shortages The following supply issues were discussed: - Levomepromazine 25mg/1ml solution for injection ampoules- palliative care teams
aware. Pharmacies commissioned in SNEE have small supplies where absolutely needed.
- Ciprofloxacin 0.3% / Dexamethasone 0.1% ear drops - Dulaglutide (Tulicity) 3mg and 4.5mg- information available - Mesalazine (Asacol®) MR gastro-resistant tablets- Mesalazine switch protocol in
place in IESCCG and NEECCG
Suffolk and North East Essex Area Prescribing Committee (SNE APC) NHS Ipswich and East Suffolk CCG (IESCCG), NHS North East Essex CCG (NEECCG), NHS West Suffolk CCG (WSCCG)
East Suffolk and North Essex NHS Foundation Trust (ESNEFT), Norfolk and Suffolk NHS Foundation Trust (NSFT), West Suffolk NHS Foundation Trust (WSFT), Anglian Community Enterprise (ACE), Essex Partnership University Trust (EPUT)
- Estradiol (FemSeven) 100micrograms/24hours transdermal patches The Committee noted that there may be a distribution or supply issues following the conflict in Ukraine. This may include supplies of drugs from the region. There is currently no intelligence on the impact and medium to long term effectives. In addition, to note, there are continued supply issues with Metformin Liquid. This has an impact on Norfolk and Suffolk NHS Foundation Trust (NSFT). The Committee suggested alternatives from crushing tablets such as metformin sachets.
DECISION: The SNEE APC noted the supply issues and discussed further support required.
GUIDELINES AND FORMULARY
22/03/06 SNEE Policy For The Prescribing Of Home Oxygen To Patients Who Are Known To Smoke This is an update to the existing document for SNEE Policy For The Prescribing Of Home Oxygen To Patients Who Are Known To Smoke. The following changes were requested for the SNEE APC approval:
• Appendix 1 and Appendix 2 previously indicated that patients should be non-smokers or smoke free for six weeks but this is now aligned to the policy to state that the patient must be offered and accepted smoking cessation support.
• In addition there is an additional point for the patient to be responsible to inform their home insurance companies.
The Committee noted that there is a review of the smoking status every six months If the smoking cessation changes and continue to smoke what would happen- this is included as part of the policy and there is compliance reviews every 6 months by BOC. DECISION: The SNEE APC approved the SNEE Policy For The Prescribing Of Home Oxygen To Patients Who Are Known To Smoke with the updates.
22/03/07 Suffolk Continence Formulary (Appliances) This document has been updated with the following changes:
• Updated prices
• Continence order for inserted as clinicians requested page 7.
• New cost effective open tipped catheter added as per urology request. Page 3. This is a Suffolk only document. This document has undergone a review with the clinical review panel and they have also agreed this document. DECISION: The Committee approved the update to the existing Suffolk Continence Formulary (Appliances) document for Suffolk.
22/03/08 Suffolk Position Statement on the Prescribing of Orthotics The position statement has been developed to support prescribers in Suffolk for orthotic devices and detailing the referral criteria for patients to have an assessment across Suffolk. Orthotic devices must be assessed, measured, and fitted by the appropriate clinician and should only be prescribed in primary care on exceptional circumstances. DECISION: The SNEE APC approved the Suffolk Position Statement on the Prescribing of Orthotics
22/03/09 SNEE ICS Inhaler carbon footprint guide A SNEE ICS Inhaler carbon footprint guide aims to support prescribers in considering low carbon options in respiratory conditions. It provides examples to identify ways to optimise therapy based on the patients ability to use the inhaler as well as recommendations for switching for suitable patients.
Suffolk and North East Essex Area Prescribing Committee (SNE APC) NHS Ipswich and East Suffolk CCG (IESCCG), NHS North East Essex CCG (NEECCG), NHS West Suffolk CCG (WSCCG)
East Suffolk and North Essex NHS Foundation Trust (ESNEFT), Norfolk and Suffolk NHS Foundation Trust (NSFT), West Suffolk NHS Foundation Trust (WSFT), Anglian Community Enterprise (ACE), Essex Partnership University Trust (EPUT)
DECISION: The SNEE APC approved the SNEE ICS Inhaler carbon footprint guide pending agreement with the NHS West Suffolk CCG Prescribing Workstream.
22/03/10 North East Essex Skin Care Aid Memoir The existing document has been update to include Epimax ointment and Epimax Oatmeal as diprobase ointment has been discontinued. This will be used by CCG technicians and practice staff. There is in addition a request to add these to the NEE and ESNEFT formulary (both are already formulary in the Suffolk). DECISION: The Committee approved the update to the Skin Care Memoir for North East Essex.
22/03/11 North East Essex lymphoedema garments formulary The document has been developed to support prescribers in the prescribing and management of lymphoedema garments in NHS North East Essex. The commissioning arrangements differ from Suffolk therefore have to have a separate formulary. The document includes a list of garments to support practices and specialists that prescribe or request prescriptions for patients that require Lymphoedema and Venous compression treatment. DECISION: The Committee approved the update to the lymphoedema garments formulary for North East Essex.
22/03/12 North East Essex Guidelines for Home Glucose Monitoring for Adults with Type 1 & 2 Diabetes The document has been updated to include the following
• Review points for blood glucose levels
• Decreasing quantities of test strips when on Flash Glucose Technology
• Consideration of oral therapy or insulin and have There is an ambition to develop this guidance across the Suffolk and North East Essex Integrated Care Service (SNEE ICS). DECISION: The SNEE approved the update to the Home Glucose Monitoring for Adults with Type 1 & 2 Diabetes for North East Essex.
22/03/13 Lipid Modification
Following a clinical consultation with the Lipid Consultants in SNEE the following were developed:
• SNEE Lipid Modification for primary and secondary prevention- this is a document adapted from the AAC guidance endorsed by NICE with local amendments to support the system in order to safely prescribe for lipid modification
• SNEE Statin Intolerance Pathway- this was adapted from the AAC guidance to support prescribers to appropriately manage statin intolerance in primary care. There will be some review of the LDL-C reduction of 40% instead of 50% as it currently states.
• SNEE Inclisiran prescribing information sheet- this supports all prescribers who are not specialists to manage patients appropriate for inclisiran.
• Inclisiran formulary position- the formulary position has been proposed as a green drug. To be either initiated or recommended by a specialist in primary care or secondary care. This includes GPs with Specialist Interest, specialist nurses etc.
• Funding arrangements- Inclisiran will be centrally funded in both primary and secondary care. In primary care practices or pharmacies will be able to purchase through the wholesaler at £45 and will be reimbursed at £55. This will be through the personally administered route (FP34D) for practices and FP10 prescriptions for community pharmacies. Hospitals will be able to access inclisiran via BlueTeq paid completely by NHS England. Feedback from the East of England region has shown that no additional

Suffolk and North East Essex Area Prescribing Committee (SNE APC) NHS Ipswich and East Suffolk CCG (IESCCG), NHS North East Essex CCG (NEECCG), NHS West Suffolk CCG (WSCCG)
East Suffolk and North Essex NHS Foundation Trust (ESNEFT), Norfolk and Suffolk NHS Foundation Trust (NSFT), West Suffolk NHS Foundation Trust (WSFT), Anglian Community Enterprise (ACE), Essex Partnership University Trust (EPUT)
funding has been proposed by any Integrated Care System or Clinical Commissioning Group.
We are currently trying to finalise the documents with the following:
• Suffolk Local Medicines Committee (Suffolk LMC) who raised concerns about the introductions of this drug to the health economy
• NHS Ipswich and East Suffolk CCG Prescribing Workstreams
• NHS West Suffolk CCG Prescribing Workstreams
• West Suffolk NHS Foundation Trust Drugs and Therapeutics Group
• East Suffolk and North Essex NHS Foundation Trust (ESNEFT) Medicines Governance Group
Once agreed the request may be brought to the SNEE APC for chairmans action to approve across SNEE. However, it was noted that there is still significant work required to be completed for this piece of work including consultation with the stakeholders. Committee members raised the following:
• If the pathway was agreed with the care of the elderly specialists? As lipid management and modification requires a tailored approach for the patients, considering the risk versus benefit. However, when developing the pathways we did consider the age outlined by the AAC guidance and understood that the age of 80 and below should be considered.
• Was there modelling on the patient numbers for the Suffolk and North East Essex (SNEE) Area? There has been patient numbers modelled across the country for different areas. In SNEE it’s expected to be numbers around 8000 patients. However, the proposal is to gain experience in using the drug across the SNEE system as there a patients who are in the specialist clinics who do not meet the NICE TA criteria for PCSK-9 inhibitors and therefore unable to use any form of lipid modification but do meet the requirements for inclisiran but are unable to access it.
• Is this the most appropriate commissioning route for inclisiran, as appropriate funding needs to be agreed for the activity if it were to be agreed for primary care prescribing? There are capacity issues within general practice as with secondary care which need to be considered: Funding has been made available centrally but the points raised have been submitted to the Eastern Academic Health Science Networks (AHSN). There is also a disparity in SNEE as there is support from the NHS North East Essex CCG Clinical Reference Group (NEECCG CRG) to make this drug available in primary care to support their patient cohorts.
• The SNEE Integrated Care System (SNEE ICS) should be informed of the issues related to the implementation of inclisiran and the lipid modification pathway.
• There is a premature discussion as there needs to be further consultation and there has been issues identified by other organisations which also needs to be shared with the SNEE APC as well as the system, which OC has shared with AS.
ACTION SNEEAPC 087: To workup a document outlining the way in which inclisiran has been agreed and implemented in other systems, to carry out the stakeholder engagement including the commissioning impact and arrangements. DECISION: The Committee agreed there needs to be further work-up and implementation process adopted by others.
22/03/14 Shared Care Guidelines
• NEECCG Historic formulary position for degarlix: NEECCG had a historic position for the prescribing of degralix in primary care which is not reflected on the current formulary platform, NetFormulary. NEECCG asked to include the holding position for NEE. Degralix is an Amber (Shared Care) drug in NEECCG and a holding position was
Suffolk and North East Essex Area Prescribing Committee (SNE APC) NHS Ipswich and East Suffolk CCG (IESCCG), NHS North East Essex CCG (NEECCG), NHS West Suffolk CCG (WSCCG)
East Suffolk and North Essex NHS Foundation Trust (ESNEFT), Norfolk and Suffolk NHS Foundation Trust (NSFT), West Suffolk NHS Foundation Trust (WSFT), Anglian Community Enterprise (ACE), Essex Partnership University Trust (EPUT)
agreed by SNEE APC for six months until the formulary position is aligned across the SNEE ICS.
22/03/15 SPS: New Medicines News January 2022 The Specialist Pharmacy Services (SPS) New medicines news for January 2022 was included for information to inform the committee of newly licensed medicines which may be considered as part of the treatment pathway in the future. Key drugs to note are:
• Licensing updates for Nirmatrelvir + ritonavir (Paxlovid), Remdesivir (Veklury), Sotrovimab (Xevudy) (reflected in the national guidance)
• Insulin lispro (Admelog)- Humalog equivalent- highlight to all prescribers and dispensing teams.
DECISIONS: The Committee noted the New Medicines News for January 2022.
COMMISSIONING
22/03/16 Pharmacy Integration
• GP Community Pharmacist Consultation Service (CPCS): This update includes the note that the national procurement of IT support for the CPCS service, currently PharmOutcomes, is due to stop at the end of March 2022. Contractors that wish to continue providing CPCS must confirm their choice of CPCS IT system. The referrals into community pharmacy will continue but there is further questions around the referral back to the GP practice.
DECISION: SNEE APC noted the pharmacy integration activity for the GP CPCS across the ICS.
• Community pharmacy GP SystmOne Clinical Record Read/Write and Task Access Following the successful agreement for practices and community pharmacies, there is approval to have pilot sites represent urban areas where the community pharmacies involved have a share of the prescription activity. Therefore, for the remaining spaces we are moving away from the PCN approach and are looking to identify more rural sited GP practices that have a close working relationship with one community pharmacy, with that pharmacy dispensing a high volume of their prescriptions. We have nominated 2 practices and community pharmacies meeting the new criteria; o Creffield Medical Centre and Cavalry and West Bergholt pharmacies o Eye Pharmacy and Practice and Needham Market Pharmacy
DECISION: SNEE APC noted the update to the Community pharmacy GP SystmONe Clinical Record Read/Write and Task Access
• Pharmacy technician pre-registration training (PTPT): Placements across SNEE are as follows: - Creffield medical centre and Cavalry pharmacy in North East Essex have recruited two technicians. The new recruits are current employees of Cavalry pharmacy. The existing staff will begin in the new role from 21st March 2022 - West Suffolk hospital has recruited the third placement to partner with Two Rivers medical centre. Staff in post from 28th Feb 2022.
DECISION: SNEE APC noted the pharmacy integration activity for the Pharmacy technician pre-registration training (PTPT)
22/03/17 OTHER ITEMS
Any other business
• Formulary status of Lurasidone: The Committee noted that there is a difference in the formulary positon for lurasidone and it was requested that the SNEE ICS notes this.
Suffolk and North East Essex Area Prescribing Committee (SNE APC) NHS Ipswich and East Suffolk CCG (IESCCG), NHS North East Essex CCG (NEECCG), NHS West Suffolk CCG (WSCCG)
East Suffolk and North Essex NHS Foundation Trust (ESNEFT), Norfolk and Suffolk NHS Foundation Trust (NSFT), West Suffolk NHS Foundation Trust (WSFT), Anglian Community Enterprise (ACE), Essex Partnership University Trust (EPUT)
West Suffolk have a different formulary status of “Red” for Lurasidone whereas the other systems for which NSFT is a partner support the prescribing in primary care. The rationale as to why there is a difference was discussed particularly the very small numbers of patients. There has been some development in primary care with integrated roles for specialist mental health nurses and pharmacists in primary care. This is an evolving area of work as is the development and formation of the SNEE ICS. These integrated roles and ICS structure may be able to support the review of the formulary position of lurasidone, but currently it is too early to review this position.
• Freestyle Libre 3 – this device will soon be available but to note that it is a Continuous Glucose Monitoring (CGM) device not a flash product like FreeStyle Libre and FreeStyle Libre 2. The SNEE APC agree with the request to ensure that patients are not switched to FreeStyle Libre 3 unless advised and in line with the local commissioning arrangements for CMG. FreeStyle Libre 3 is not currently available on prescribing systems therefore we cannot currently add a message on OptimiseRx or ScriptSwich. ACTION SNEEAPC 093: To flag the difference between FreeStyle Libre 3 as it's a CGM device to paedatrics and diabetes teams. Patients should not be switched to FreeStyle Libre 3 as it's has a different commissioning arrangement.
• ICS website to include SNEE APC: This work has begun with the three pharmacy technicians in each CCG. The SNEE APC section will include the following sections: About us, SNEE APC Terms of Reference, Contact info, Dates of meeting, Annual Report, Minutes, Templates
• Community pharmacy strategy webinar on 15th March at 12.30 to 2pm: Committee members were informed of the webinar and information provided.

Suffolk and North East Essex Area Prescribing Committee (SNE APC) NHS Ipswich and East Suffolk CCG (IESCCG), NHS North East Essex CCG (NEECCG), NHS West Suffolk CCG (WSCCG)
East Suffolk and North Essex NHS Foundation Trust (ESNEFT), Norfolk and Suffolk NHS Foundation Trust (NSFT), West Suffolk NHS Foundation Trust (WSFT), Anglian Community Enterprise (ACE), Essex Partnership University Trust (EPUT)
Appendix 3: April 2022 SNEE APC Minutes Final Version 1
Minutes of the Meeting Meeting: Suffolk and North East Essex Area Prescribing Committee (SNEE APC)
Date and Time: Tuesday 12th April 2022 15:00-17:00
Venue: Virtually via Microsoft Teams
Chair: Dr Andrew Hassan
Attendees:
Name Title and organisation
Dr David Egan DE NHS Ipswich and East Suffolk CCG Clinical Lead for Prescribing
Dr Prashant Arora PA Tendring GP Elect Member, NHS North East Essex CCG
Dr Andrew Hassan AH NHS West Suffolk CCG Clinical Lead for Prescribing
Dr Jon Tuppen JP Suffolk LMC representative
Catherine Butler CB
NHS Ipswich and East Suffolk CCG Chief Pharmacist and NHS West Suffolk CCG Interim Chief Pharmacist
Anam Baksh AB Medicines Management Pharmacist, NHS Ipswich and East Suffolk CCG
Ben Leung BL Deputy Chief Pharmacist, NHS West Suffolk CCG
Oge Chesa OC
NHS North East Essex CCG Deputy Director of Primary Care and Medicines Management(from 15.30)
Oweikumo Eradiri OE
East Suffolk and North Essex NHS Foundation Trust, Joint Interim Chief Pharmacist (from 15.30)
Anisha Sharma AS Senior Interface Pharmacist, East Suffolk and North Essex NHS Foundation Trust and NHS Ipswich and East Suffolk CCG
Simon Whitworth SW
West Suffolk Hospital NHS Foundation Trust Chief Pharmacist (until 16.00)
Lisa Stephenson LS Deputy Chief Pharmacist, NHS North East Essex CCG Pharmacist
Esther Johnston EJ Chief Pharmacist , Norfolk and Suffolk NHS Foundation Trust
Gemma Shanks GS NHS West Suffolk CCG, Medicines Management Pharmacy Technician
Abbie Holden AH
NHS West Suffolk CCG, Administrative Support Officer, Medicines Management
Paul Mills PM East Suffolk and North Essex NHS Foundation Trust- Assistant Chief Pharmacist
Rifat Choudhury RC NHS Ipswich and East Suffolk CCG Deputy Chief Pharmacist
Olubusola (Busola) Daramola
OD Head of Medicines Management, NHS North East Essex CCG Pharmacist
Hilary Scott HS
Essex Partnership University NHS Foundation Trust – Chief Pharmacist (from 15.30)
Apologies
Name Title
Dr James Broadway JB East Suffolk and North Essex NHS Foundation Trust Medicines Optimisation Committee Chair and Consultant Anaesthetist
Liz Buxton LB Anglia Community Enterprise (CIC) Assistant Director of Quality
Rachel Belton RB
Deputy Chief Pharmacist, NHS Ipswich and East Suffolk CCG Medicines Management Pharmacist
Sarah Spink SS Deputy Chief Pharmacist, NHS West Suffolk CCG
Vicki Saliba VS Deputy Chief Pharmacist, NHS North East Essex CCG Lead
Rosie Thomson RT Lead Pharmacist, The Oaks Hospital
Emma Travers ET East Suffolk and North Essex NHS Foundation Trust, Joint Interim Chief Pharmacist
Judith Esterhuizen JE West Suffolk Hospital NHS Foundation Trust Formulary Pharmacist

Suffolk and North East Essex Area Prescribing Committee (SNE APC) NHS Ipswich and East Suffolk CCG (IESCCG), NHS North East Essex CCG (NEECCG), NHS West Suffolk CCG (WSCCG)
East Suffolk and North Essex NHS Foundation Trust (ESNEFT), Norfolk and Suffolk NHS Foundation Trust (NSFT), West Suffolk NHS Foundation Trust (WSFT), Anglian Community Enterprise (ACE), Essex Partnership University Trust (EPUT)
Tania Farrow TF Suffolk Local Pharmaceutical Committee (LPC) Chief Officer
22/04/01 Welcome and apologies
Dr Hassan welcomed the members to the meeting. Apologies received as above.
22/04/02 Declarations of Interest
No declarations of interest were made to the Committee about items on the agenda.
22/04/03 Minutes and matters arising
Review of March 2022 Minutes The Committee approved the minutes of the meeting. Action Tracker
• SNEEAPC 084: DOAC guidance for initiation and discontinuation for patients with dementia: See agenda item 22/04/14 for update. This item is in progress.
• SNEEAPC 086: For East Suffolk and North Essex NHS Foundation Trust (ESNEFT) and West Suffolk NHS Foundation Trust (WSFT) to feed back to microbiology about urology long term prescribing of antibiotics for recurrent UTIs- The microbiologists have spoken with the urologists about this and have requested for examples in any further issues raised. This item is closed.
• SNEE APC 087: NICE TA Formulary Status: Inclisiran- See agenda item 22/04/16 for update. This item is in progress.
• SNEEAPC 088: Making the NHS Essex Partnership University Trust (EPUT) Formulary for the treatment of hyperprolactinaemia available in primary care: EPUT did not obtain feedback from the endocrinologists but used The Maudsley Prescribing Guidelines in Psychiatry as the reference source for this section. The SNEE APC wish to continue to ask the local endocrinologists to confirm the support. This item is in progress.
• SNEEAPC 090: SNEE Shared Care Agreement Task and Finish Group (SNEE SCA TAF) are informed of the feedback from providers and GPs: See item 22/04/15 for update. This item is in progress.
• SNEEAPC 093: AOB FreeStyle Libre 3: The message has been developed by NEE on 28th March 2022 and shared with the Ipswich diabetes team as well as the West Suffolk Pharmacy team to implement across SNEE. This item is in progress.
Matters arising
• Chair’s action: The SNEE APC Joint Chairs were asked to approve the updated inclisiran position statement for the SNEE ICS after identifying an issue around the funding. The position statement has been extended to 31st May 2022. Further information provided in item 22/04/16.
• Nitrofurantoin- SNEE APC noted that GPs in SNEE are concerned about the long term adverse effects of nitrofurantoin particularly with the recent article in the Drug and Therapeutics Bulletin (April 2022 Volume 60 no 4 page 59). This information will be shared with the microbiologists and urologists following a review of the NICE guidance. ACTION SNEEAPC 094: AS and RC to share this with the ESNEFT microbiology team and urology teams.
Quality and Governance
22/04/04 COVID-19 West Suffolk NHS Foundation Trust (WSFT) and East Suffolk and North Essex Foundation Trust (ESNEFT) informed the SNEE APC that the numbers of patients with COVID-19 are increasing in hospital, adding to the pressure within the hospital.
22/04/05 COPD Plus project- NHS North East Essex CCG SNEE APC were informed that NHS North East Essex CCG (NEECCG) are supporting the offer made by the national Services for Health Improvement Ltd (NSHI) who are an
Suffolk and North East Essex Area Prescribing Committee (SNE APC) NHS Ipswich and East Suffolk CCG (IESCCG), NHS North East Essex CCG (NEECCG), NHS West Suffolk CCG (WSCCG)
East Suffolk and North Essex NHS Foundation Trust (ESNEFT), Norfolk and Suffolk NHS Foundation Trust (NSFT), West Suffolk NHS Foundation Trust (WSFT), Anglian Community Enterprise (ACE), Essex Partnership University Trust (EPUT)
independent provider to support practices with availability of Respiratory Specialist nurses to deliver care related to respiratory diseases. NSHI not associated any one pharmaceutical companies but does work in collaboration with a number of different companies. NEE note that this is during a time of pressures within primary care and backlog of work. There is also the added pressure of the NHS targets for low carbon options for inhalers. NEECCG Clinical Reference Group (CRG) and the Primary Care Board have also approved this project. The process will involve those practices identified as requiring support will contact NSHI to arrange the review within their practice and sign up to the service. This project is linked to the spirometry work within NEECCG. NEECCG are endorsing the service from NSHI after a critical appraisal of the options available. The Committee noted that NHS Ipswich and East Suffolk CCG (IESCCG) do not endorse the use of third party providers such as NSHI and this is a historic position following previous issues identified with the service. IESCCG therefore requires practices to review the appropriateness of these services on an individual practice level within the practice governance process. This position is different to NEECC and NHS West Suffolk CCG (WSCCG). SNEE APC agreed that there will need to be direction from the SNEE Integrated Care Board (ICB) once the Integrated Care System (ICS) is established. The Committee agreed that this should be discussed with the ICB at the earliest opportunity to try and align the practice across the SNEE system. This request will be added to the SNEE APC action tracker in a separate section called “ICB questions” DECISION: SNEE APC support the COPD Plus project for NEECCG.
22/04/06 NICE Adherence- Technology appraisals and guidelines This item was included for information on the new Technology Appraisals (TA) released in March 2022. The following NICE Technology appraisals relate to pathways commissioned by CCGs or prescribed in primary care:
• Empagliflozin for treating chronic heart failure with reduced ejection fraction: This is likely to be prescribed in primary care in line with the dapagliflozin for heart failure and be supported with the Heart Failure pathway and a prescribing information sheet.
• Dapagliflozin for treating chronic kidney disease: This is likely to be prescribed in primary care in line with the dapagliflozin for heart failure and be supported with the CKD pathway from the Eastern Academic Health Sciences Network (AHSN) and a prescribing information sheet.
DECISION: The Committee noted the Technology Appraisals released for March 2022.
22/04/07 Medicines Safety
• National Patient Safety Alerts (NPSA) in General Practice The SNEE APC noted the NaPSA - Inadvertent oral administration of potassium permanganate released in April 2022 and requires action across Suffolk and North East Essex by October 2022 which follows on from the Patient Safety Alert raised in 2014. The issue of patients ingesting potassium permanganate tables continues. In November 2019, a Datix was raised in ESNEFT with a similar issue. Potassium permanganate is routinely used in the NHS as a dilute solution to treat weeping and blistering skin conditions, such as acute weeping/ infected eczema and leg ulcers. It is not licensed as a medicine. This alert is requesting for all organisations to:
1. Review the use of potassium permanganate 2. Ensure that all BAD recommendations are implemented
Suffolk and North East Essex Area Prescribing Committee (SNE APC) NHS Ipswich and East Suffolk CCG (IESCCG), NHS North East Essex CCG (NEECCG), NHS West Suffolk CCG (WSCCG)
East Suffolk and North Essex NHS Foundation Trust (ESNEFT), Norfolk and Suffolk NHS Foundation Trust (NSFT), West Suffolk NHS Foundation Trust (WSFT), Anglian Community Enterprise (ACE), Essex Partnership University Trust (EPUT)
A number of the actions have already been implemented within ESNEFT as outlined in the document submitted to the SNEE APC. The Committee noted that the use of potassium permanganate in NHS Ipswich and East Suffolk CCG is minimal and is an agenda item on the Medicines Safety Working Group in ESNEFT. The use within the hospital setting is minimal but there are requests from dermatology and the Tissue Viability Nurses (TVNs). The Committee agreed to submit individual organisations plans on implementation. DECISION: The Committee noted NPSA for potassium permanganate.
• MHRA Drug Safety Update- March 2022 The March 2022 MHRA Drug Safety Update provided the following to note: - Cladribine (Mavenclad): new advice to minimise risk of serious liver injury: This
is a hospital only drug very rarely used in at the hospital. Neurology teams in ESNEFT have been informed.
- Amiodarone (Cordarone X): reminder of risks of treatment and need for patient monitoring and supervision: This alert has already been raised as part of the shared care development. Further updates to be given in due course.
- Metformin in pregnancy: study shows no safety concerns it has been noted that metformin has been used for diabetes type 2 and polycystic ovarian syndrome (PCOS).
- DECISION: The Committee noted the MHRA Drug Safety Update.
• Medicines Supply Shortages The following supply issues were discussed: - Adrenaline (base) 1mg/1ml (1 in 1,000) solution for injection pre-filled syringes- this is
not the EpiPen or Emerade pens. - Ciprofloxacin 0.3% / Dexamethasone 0.1% ear drops- do not initiate new patients,
consider Cetraxal Plus® (ciprofloxacin 0.3%, fluocinolone acetonide 0.025%) ear drops or Cetraxal® (ciprofloxacin 0.2%) ear drops as alternative options where ciprofloxacin +/- steroid is needed
- Oxybutynin 3.9mg/24hours transdermal patches- very small patient numbers but bigger impact to note. Alternatives are available on the SPS Medicines Supply Tracker.
- Trulicity ® 3mg and 4.5mg stock issues have been resolved and availability started 11th April 2022.
DECISION: The SNEE APC noted the supply issues and discussed further support required.
GUIDELINES AND FORMULARY
22/04/08 North East Essex Continence formulary This is an update to an existing document to include the changes related to the contacts for the service provider, update to the prices for the continence products and change to the 1st line product. DECISIONS: The Committee approve the update to the NEE Continence formulary.
22/04/09 North East Essex- Roflumilast formulary positon It was noted that the NetFormulary does not reflect the NEECCG and Colchester position for Roflumilast which is “Green”. Therefore, it is requested that the position of this drug revert back to Green for NEE in the interim until the Respiratory Group are able to align the formulary position across SNEE. DECISIONS: The SNEE APC have agreed a holding position for six months until the formulary position is aligned across the SNEE ICS.
22/04/10 Microguide Application and guide
Suffolk and North East Essex Area Prescribing Committee (SNE APC) NHS Ipswich and East Suffolk CCG (IESCCG), NHS North East Essex CCG (NEECCG), NHS West Suffolk CCG (WSCCG)
East Suffolk and North Essex NHS Foundation Trust (ESNEFT), Norfolk and Suffolk NHS Foundation Trust (NSFT), West Suffolk NHS Foundation Trust (WSFT), Anglian Community Enterprise (ACE), Essex Partnership University Trust (EPUT)
The Microguide App is a programme currently being used within ESNEFT as the platform to support the antimicrobial guidelines. It currently also contains the antibiotic guidelines for primary care and A&E. The tool is free to download on a smartphone and tablet device. The Committee noted that the Microguide app will only be used in ESNEFT, IESCCG and NEECCG but WSFT and WSCCG will not be using this. It was agreed that there may be merit in aligning the digital opportunities and solutions across the SNEE ICS. DECISIONS: The Committee noted the use of Microguide for ESNEFT.
22/04/11 Prescribing Commissioning Policy for Biosimilar Insulin The NEECCG and North East Essex Diabetes Service (NEEDS) have update the Commissioning Policy for Biosimilar Insulin to include the differences between the biosimilar insulin and the originator product. This is to support practices in understanding the difference. Feedback was given that the information provided was very useful and commended for primary care use. DECISIONS: The SNEE APC approved the Prescribing Commissioning Policy for Biosimilar Insulin for NEECCG and NEEDS.
22/04/12 NEE/NEEDS Insulin use in Type 1 and Type 2 diabetes update This is an update to the current guidance in NEECCG. The update includes information from the new NICE Guidance and management of the interventions. This documents supports the selection of the insulin. The committee commented on the usefulness and support of the documents. DECISIONS: The Committee approved the NEE/NEEDS Insulin use in Type 1 and Type 2 diabetes guidance for NEECCG.
22/04/13 SNEE Edoxaban Switching Position Statement Following a national procurement exercise by NHS England, edoxaban was identified as the most cost effective option with the aim to increase the use of DOACs to support the identification of patients with atrial fibrillation (AF). A positon statement has been devised for SNEE to support prescribers in initiation edoxaban but to refrain from switching patients to edoxaban until guidance is agreed to safely switch appropriate patients. The next steps will be to involve stakeholders in the development and agreement of the edoxaban switching guidance. The guidance for Atrial Fibrillation (AF) will also be developed and supported across SNEE. DECISIONS: The SNEE APC approved the SNEE Edoxaban Switching Position Statement for SNEE.
22/04/14 SNEE Diabetes Guidance- response to NICE NG28 This document summarises the SNEE ICS position for the management of diabetes following the NICE Clinical Guidance release. The diabetes team across the ICS have supported the document. The document is in line with the NICE NG28 with adaption from the American Diabetes Association’s (ADA’s) Standards of Medical Care in Diabetes and the European Society of Cardiology and European Association for the Study of Diabetes (EASD) 2019 Guidelines on Diabetes, Pre-Diabetes and Cardiovascular Diseases. The Committee agreed that the document was clear, supportive and provided information in a concise and efficient manner and would like to ensure it is cascaded to all relevant diabetes specialists within primary care and that this would be a useful education and training session. The Committee noted that the Sodium-glucose Cotransporter-2 (SGLT-2) inhibitors are adopted earlier than advised in the NICE guidance (NG) 28: Type 2 diabetes in adults: Management because as a system the ADA and EASD were adopted for a number of years and has been effective for our local population. The document provides evidence base and rationale to support the use of SGLT-2 inhibitors at this stage and the guidance allows it to
Suffolk and North East Essex Area Prescribing Committee (SNE APC) NHS Ipswich and East Suffolk CCG (IESCCG), NHS North East Essex CCG (NEECCG), NHS West Suffolk CCG (WSCCG)
East Suffolk and North Essex NHS Foundation Trust (ESNEFT), Norfolk and Suffolk NHS Foundation Trust (NSFT), West Suffolk NHS Foundation Trust (WSFT), Anglian Community Enterprise (ACE), Essex Partnership University Trust (EPUT)
be more bespoke for the cardiovascular risk of individual patients and aims to ensure to improve the outcomes for diabetes in a larger population. DECISIONS: The Committee approved SNEE Diabetes Guidance- response to NICE NG28 for SNEE pending approval by the ESNEFT Medicines Governance Group (MGG), West Suffolk NHS Foundation Trust (WSFT) Drugs and Therapeutics Group (D&T), NEECCG CRG and West Suffolk CCG (WSCCG) Prescribing Workstreams.
22/04/15 RMOC Shared Care Working Group- update The SNEE APC were informed that the national RMOC Shared Care Working Group have developed a number of shared care guidelines to support the NHS across England. These documents are currently in their final versions following national consultations wait for NHS England to publish. There is now further delay due to discussions between NHS England, the relevant national leads and comments from the British Medical Association (BMA), General Practitioners Committee (GPC) and the Consultant’s Committee, which are pending. Like a number of system, the SNEE APC were awaiting publication of these shared care guidelines for local implementation and on a few occasions continued with extending the review dates of some of these shared care guidelines. It was noted that there are a number of shared care guidelines currently out of date, which are on the national list as well as local shared care such as denosumab. The SNEE APC were presented with three options to consider and were recommended option 1- to extend the shared care guidelines for 6 months. The Committee and the LMC agree that all the options are agreeable and would like to support the option recommended in the paper. DECISIONS: The SNEE APC noted the issues from the national consultation and supported option 1 for SNEE.
22/04/16 Lipid Modification and Inclisiran The SNEE APC were informed of the current issues with the implementation of Inclisiran for treating primary hypercholesterolaemia or mixed dyslipidaemia NICE Technology appraisal guidance [TA733] Published: 06 October 2021:
• As inclisiran requires a healthcare professional to administer, there are capacity issues within practices to deliver this.
• The Royal Collage of General Practitioners (RCGP) and British Medical Association (BMA) joint statement for inclisiran in primary care setting has not been addressed by NHS England. It raises concerns on the rollout of inclisiran in primary care.
• The hospital lipidology services are unable to manage the capacity of 8000 patients for SNEE to support the implementation.
• The Suffolk Local Medical Committee (LMC) have raised concerns around the central funding provided for inclisiran. They have been quoted that there will be a loss for every administration as the NHS England document Summary information on the funding and supply of inclisiran (Leqvio ®) in February 2022 calculations for personally administered drug does not take into account that practices do pay for VAT and clawback.
• Although some areas in the East of England have implemented inclisiran in their health economy, most have not. Nationally, most have a position statement outlining that they are awaiting further information to support the implementation.
These points have been raised to the NHS England team via the Eastern Academic Health Science Networks (AHSN) and SNEE are still awaiting the outcomes of these discussions. As a result, the SNEE APC have updated the position statement of inclisiran to reflect the issues related to the funding in primary care. The Committee noted that the WSFT Lipidology service wishes for this to be available at the earliest opportunity especially as inclisiran is a more cost effective option than other proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitors. There is frustration from the

Suffolk and North East Essex Area Prescribing Committee (SNE APC) NHS Ipswich and East Suffolk CCG (IESCCG), NHS North East Essex CCG (NEECCG), NHS West Suffolk CCG (WSCCG)
East Suffolk and North Essex NHS Foundation Trust (ESNEFT), Norfolk and Suffolk NHS Foundation Trust (NSFT), West Suffolk NHS Foundation Trust (WSFT), Anglian Community Enterprise (ACE), Essex Partnership University Trust (EPUT)
WSFT lipidology service on the timelines for implementation. The ongoing issues in primary care were acknowledged and it was agreed that a clear pathway is what would benefit the patient. DECISIONS: The SNEE APC noted the issues raised on the implementation of inclisiran.
22/04/17 SPS: New Medicines News February 2022 The Specialist Pharmacy Services (SPS) New medicines news for February 2022 was included for information to inform the committee of newly licensed medicines which may be considered as part of the treatment pathway in the future. Key drugs to note are:
• Insulin aspart biphasic biosimilar (Truvelog ®) The Committee discussed the implementation of Palforzia ®. It is now a NICE Technology Appraisal drug (NICE TA 769) Palforzia for treating peanut allergy in children and young people. This is a CCG commissioned drug that is available to prescribe in hospital via the allergy service only. DECISIONS: The Committee noted the New Medicines News for February 2022.
COMMISSIONING
22/04/18 Pharmacy Integration
• GP Community Pharmacist Consultation Service (CPCS): The update for this includes binary indicators for the Network Contract Directed Enhanced Service (DES) Contract Specification 2020/2 which was paused but it is included in the Investment and Impact Fund (IIF) 2022-23. Their current contract runs from April to September 2022 with room to extend. They will be supported with practices for referral pathways for Community Pharmacy Consultation Service (CPCS). It was noted that from April 2022, the software will not be paid for by NHS England and community pharmacy contractors will be expected to pay for the software. The SNEE ACP agreed that this would be a cost pressure for community pharmacy going forward.
DECISION: SNEE APC noted the pharmacy integration activity for the GP CPCS across the ICS.
• Pharmacy technician pre-registration training (PTPT): There are two forms of funding that SNEE have benefited from which includes regional and national funding. The rotation has been delayed until May 2022 following the holidays. There has been further regional funding for six posts across SNEE but the staff are required to be deployed by 31st March 2022. DECISION: SNEE APC noted the pharmacy integration activity for the Pharmacy technician pre-registration training (PTPT)
• Community pharmacy GP SystmOne Clinical Record Read/Write and Task Access This pilot now covers community pharmacies and rural practices. The digital teams and information governance teams are involved for a smooth rollout. The aim is to improve the referral processes within primary care between community pharmacy and GP practices. The system will need to ensure that there is a process for tasks preventing issues. The tasking process will be informed and appropriate. DECISION: SNEE APC noted the update to the Community pharmacy GP SystmOne Clinical Record Read/Write and Task Access
• Oral Contraceptive Management service (OCMS)

Suffolk and North East Essex Area Prescribing Committee (SNE APC) NHS Ipswich and East Suffolk CCG (IESCCG), NHS North East Essex CCG (NEECCG), NHS West Suffolk CCG (WSCCG)
East Suffolk and North Essex NHS Foundation Trust (ESNEFT), Norfolk and Suffolk NHS Foundation Trust (NSFT), West Suffolk NHS Foundation Trust (WSFT), Anglian Community Enterprise (ACE), Essex Partnership University Trust (EPUT)
Eight community pharmacies in Suffolk have agreed to deliver the Oral Contraceptive Management service (OCMS) pilot from April 2022 supported with one practice. DECISION: SNEE APC noted the pharmacy integration activity for the Oral Contraceptive Management service (OCMS)
In terms of SNEE pharmacy workforce, there is support for the acute band 7 provision via
the MOU to support the discharge medicines service.
22/04/19 Interim Rheumatoid Arthritis pathway The SNEE APC were requested to extend the interim rheumatoid arthritis pathway by six months to enable clinicians to bypass 2nd line rituximab especially as COVID-19 numbers continue to increase. DECISION: The Committee extended the Interim Rheumatoid Arthritis pathway by six months for SNEE.
22/04/20 Prescribing policy for Wegovy ® (Simaglutide) Wegovy ® (Simaglutide) is a newly licensed product for weight management and a NICE technology appraisal is in development due to be released 25th May 2022. The draft guidance highlights that the responsibility will remain in a specialist weight management service such as a tier 3 or 4 service. This position statement has been developed to ensure primary care do not prescribe Wegovy ® in line with the commissioning arrangements. ESNEFT and WSFT do not have a tier 3 or 4 weight management service. DECISION: SNEE APC approved the position statement for NEECCG and recommended it be extended to the rest of the ICS.
22/04/21 OTHER ITEMS
Any other business
• SNEE APC August and December meetings: The SNEE APC were informed that as per the terms of reference of the Committee, August and December meetings do not take place due to a number of members being on annual leave. However, the last two years have seen an unprecedented number of chairman’s action and requests. It was advised to hold the August and December meetings and review attendance closer to the time.
• Log of queries for the ICB- the Committee agreed to hold a log of queries for the ICB to consider. This will be added to the current SNEE APC Action Tracker.
Page 1 of 3
GOVERNING BODY
Agenda Item No. 20
Reference No. NEECCG 22-44
Date. 7 June 2022
Title
Covid-19 Resource Approval Committee
Lead Director
Jane Payling, Director of Finance
Author(s)
Jane Payling, Director of Finance
Purpose
To update the Governing Body on the decisions made at the CRAC and to approve the extension of the committee until the formal commencement of the Integrated Care Board.
Applicable CCG Strategic Objectives:
1. To achieve our vision through an inclusive, holistic approach to patient and service user centred commissioning, embedding personalisation of care through integrated health and social care services.
2. To transform care and drive continuous improvement in quality and safety. Achieve the best possible outcomes for our service users through high quality care.
3. To use commissioning resources effectively and responsibly. To develop our organisation, teams and individual staff to be trusted, competent, well trained, talented, enthusiastic and dedicated.
x
4 To tackle the biggest health challenges in north east Essex including reducing health inequalities.
Recommendation: The Governing Body is asked to
• note the report on decisions made by the CRAC committee

Page 2 of 3
1. Summary 1.1 The committee was established in early April as a joint committee working across the three
CCGs in Suffolk and North East Essex. It is a sub-committee of the three CCG Governing Bodies which was initially established for the period from April to July 2020, and has been extended until the formation of the ICB on 1 July. Oversight of the committee is via the CCG finance committees.
1.2 The purpose of the Committee is to:
(i) Make funding decisions outside of normal budgets in response to the current
pandemic situation
(ii) On behalf of the Governing Bodies/Board, exercise the necessary oversight and
scrutiny of funding requests and/or decisions related to the current pandemic
situation
(iii) Review requests for expenditure over £10k and up to £3m
(iv) Ensure that any expenditure requested meets the criteria of being a necessary
exceptional spend
(v) Ensure that any expenditure approved is effective and represents value for money
(vi) Ensure that any expenditure approved is reclaimable wherever this is possible
(vii) Hold to account the relevant Directors and managers for any agreed exceptional
expenditure
(viii) Refer any primary care funding requests to the relevant Commissioning Governance
Committees in Suffolk and to the Chair of the Primary Care Committee in North East
Essex in the normal way
(ix) Be mindful of the increasing incidence of fraud related to the Covid-19 pandemic
when approving expenditure
1.3 The committee met initially on 23 April 2020 and since that time has met on 34 further occasions, one of which was in March 2022 and included in this report. At recent meetings the committee has also reviewed costs associated with the Covid-19 vaccination programme which are subject to a separate central reimbursement process.
2. Summary of Decisions 2.1 A summary table of the decisions made since the last report to date is given in appendix 1. 3. Recommendation 3.1 The Governing Body is asked to note the report on decisions made by the CRAC
committee since the last report

Page 3 of 3
Appendix 1 – CRAC Papers/Decision log from 10 March 2022 to 17 May 2022
Date Short title for Board reporting Approved Y/N 21/22 £ IES WS NEE
15/03/2022 CHC review support y y 370,000 y y
15/03/2022 Post covid demand and capacity model y y 250,000 y y y
15/03/2022 Covid Vaccination costs (programme staffing costs via WSCCG) y y 199,083 y y
15/03/2022 Retrospective approvals (M9-11)
Hospital discharge programme (CCG Dec-Feb) y y 1,265,000 y y y
Hospital discharge programme (social care Dec-Jan) y y 2,010,000 y y y
Hospital discharge programme (Social care - February) y y 1,350,000 y y y
Page 1 of 5
GOVERNING BODY
Agenda Item No. 21
Reference No. NEECCG 22-45
Date. 7 June 2022
Title
National Staff Survey Results 2021
Lead Director
Amanda Lyes, Interim Director of Workforce, Suffolk and North East Essex Integrated Care System & Director of Corporate Services and System Infrastructure
Author(s)
Ben Askew, Head of People and Culture
Purpose
For Information
Applicable CCG Strategic Objectives:
1. To achieve our vision through an inclusive, holistic approach to patient and service user centred commissioning, embedding personalisation of care through integrated health and social care services.
2. To transform care and drive continuous improvement in quality and safety. Achieve the best possible outcomes for our service users through high quality care.
3. To use commissioning resources effectively and responsibly. To develop our organisation, teams and individual staff to be trusted, competent, well trained, talented, enthusiastic and dedicated.
*
4 To tackle the biggest health challenges in north east Essex including reducing health inequalities.
Recommendation: For information only
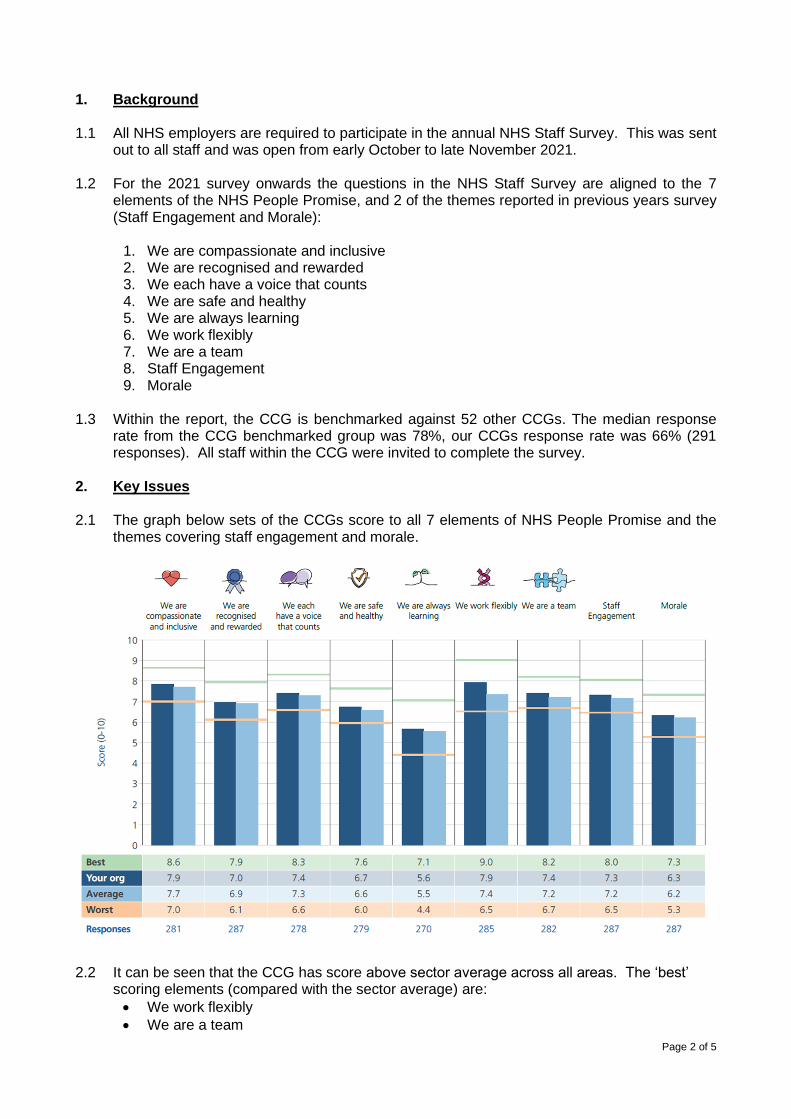
Page 2 of 5
1. Background 1.1 All NHS employers are required to participate in the annual NHS Staff Survey. This was sent
out to all staff and was open from early October to late November 2021. 1.2 For the 2021 survey onwards the questions in the NHS Staff Survey are aligned to the 7
elements of the NHS People Promise, and 2 of the themes reported in previous years survey (Staff Engagement and Morale):
1. We are compassionate and inclusive 2. We are recognised and rewarded 3. We each have a voice that counts 4. We are safe and healthy 5. We are always learning 6. We work flexibly 7. We are a team 8. Staff Engagement 9. Morale
1.3 Within the report, the CCG is benchmarked against 52 other CCGs. The median response
rate from the CCG benchmarked group was 78%, our CCGs response rate was 66% (291 responses). All staff within the CCG were invited to complete the survey.
2. Key Issues 2.1 The graph below sets of the CCGs score to all 7 elements of NHS People Promise and the
themes covering staff engagement and morale.
2.2 It can be seen that the CCG has score above sector average across all areas. The ‘best’
scoring elements (compared with the sector average) are:
• We work flexibly
• We are a team
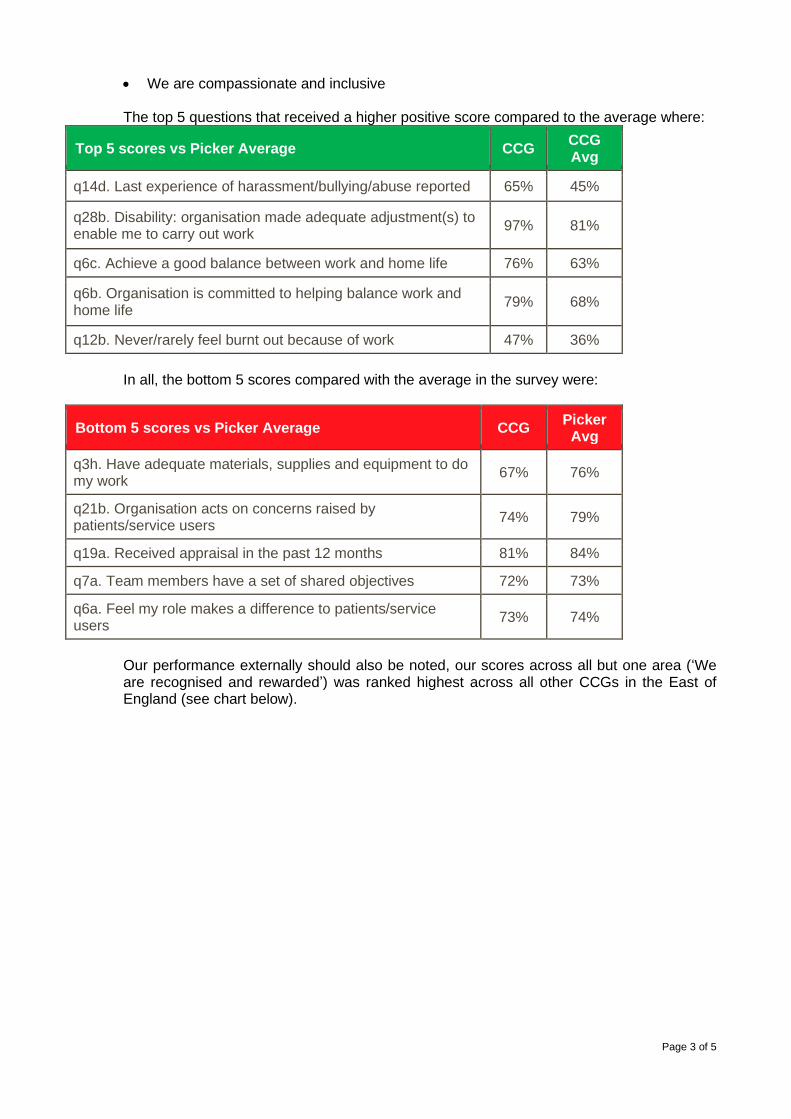
Page 3 of 5
• We are compassionate and inclusive
The top 5 questions that received a higher positive score compared to the average where:
Top 5 scores vs Picker Average CCG CCG Avg
q14d. Last experience of harassment/bullying/abuse reported 65% 45%
q28b. Disability: organisation made adequate adjustment(s) to enable me to carry out work
97% 81%
q6c. Achieve a good balance between work and home life 76% 63%
q6b. Organisation is committed to helping balance work and home life
79% 68%
q12b. Never/rarely feel burnt out because of work 47% 36%
In all, the bottom 5 scores compared with the average in the survey were:
Bottom 5 scores vs Picker Average CCG Picker
Avg
q3h. Have adequate materials, supplies and equipment to do my work
67% 76%
q21b. Organisation acts on concerns raised by patients/service users
74% 79%
q19a. Received appraisal in the past 12 months 81% 84%
q7a. Team members have a set of shared objectives 72% 73%
q6a. Feel my role makes a difference to patients/service users
73% 74%
Our performance externally should also be noted, our scores across all but one area (‘We are recognised and rewarded’) was ranked highest across all other CCGs in the East of England (see chart below).
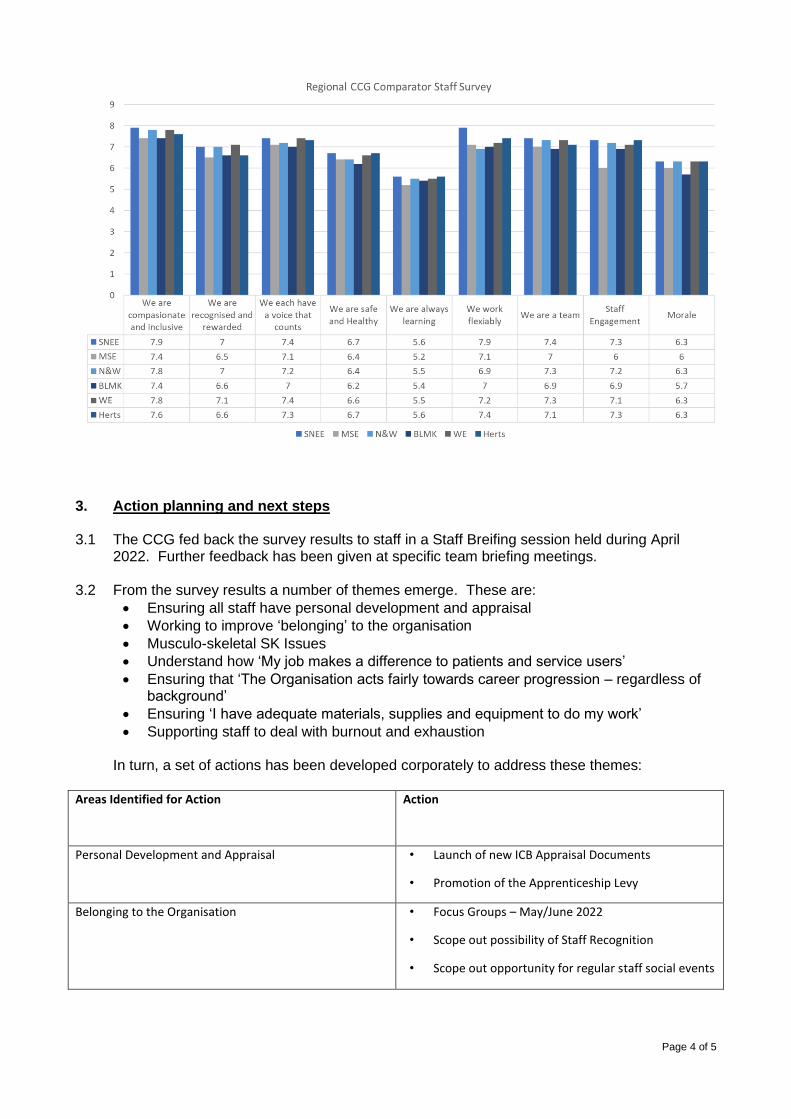
Page 4 of 5
3. Action planning and next steps 3.1 The CCG fed back the survey results to staff in a Staff Breifing session held during April
2022. Further feedback has been given at specific team briefing meetings. 3.2 From the survey results a number of themes emerge. These are:
• Ensuring all staff have personal development and appraisal
• Working to improve ‘belonging’ to the organisation
• Musculo-skeletal SK Issues
• Understand how ‘My job makes a difference to patients and service users’
• Ensuring that ‘The Organisation acts fairly towards career progression – regardless of background’
• Ensuring ‘I have adequate materials, supplies and equipment to do my work’
• Supporting staff to deal with burnout and exhaustion
In turn, a set of actions has been developed corporately to address these themes: Areas Identified for Action Action
Personal Development and Appraisal • Launch of new ICB Appraisal Documents
• Promotion of the Apprenticeship Levy
Belonging to the Organisation • Focus Groups – May/June 2022
• Scope out possibility of Staff Recognition
• Scope out opportunity for regular staff social events
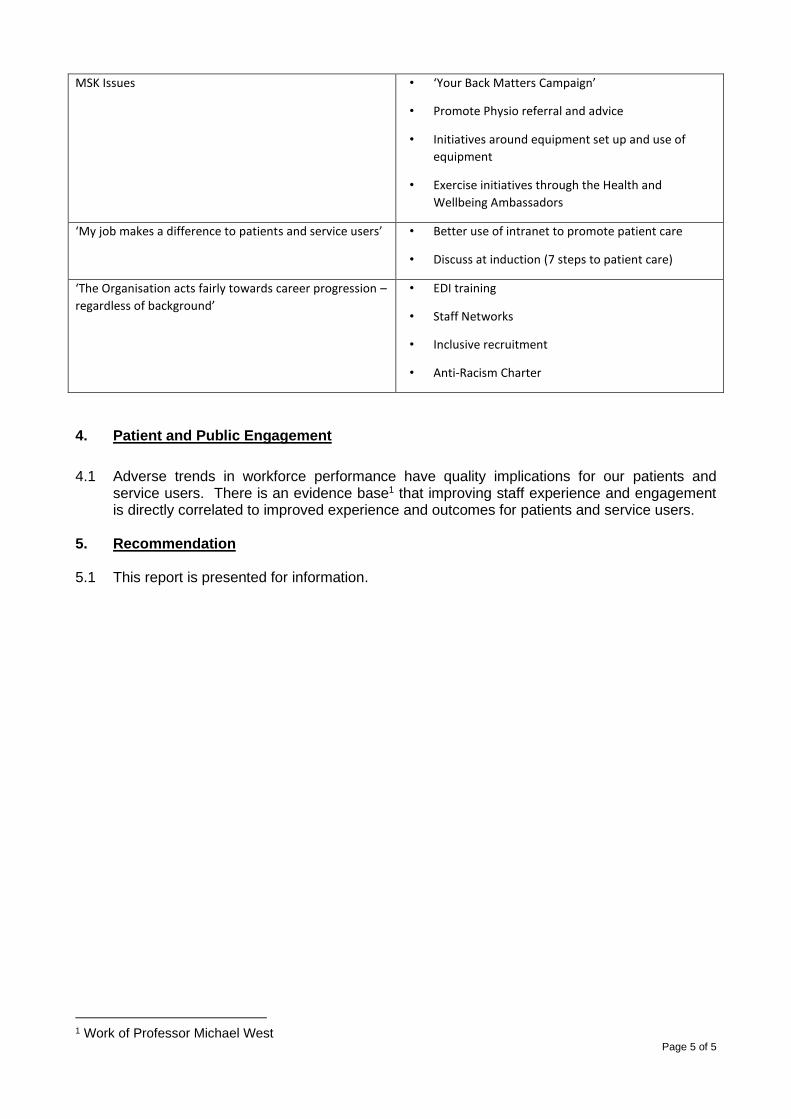
Page 5 of 5
MSK Issues • ‘Your Back Matters Campaign’
• Promote Physio referral and advice
• Initiatives around equipment set up and use of
equipment
• Exercise initiatives through the Health and
Wellbeing Ambassadors
‘My job makes a difference to patients and service users’ • Better use of intranet to promote patient care
• Discuss at induction (7 steps to patient care)
‘The Organisation acts fairly towards career progression –
regardless of background’
• EDI training
• Staff Networks
• Inclusive recruitment
• Anti-Racism Charter
4. Patient and Public Engagement
4.1 Adverse trends in workforce performance have quality implications for our patients and service users. There is an evidence base1 that improving staff experience and engagement is directly correlated to improved experience and outcomes for patients and service users.
5. Recommendation
5.1 This report is presented for information.
1 Work of Professor Michael West
Page 1 of 2
GOVERNING BODY
Agenda Item No. 22
Reference No. NEECCG 22-46
Date. 7 June 2022
Title
Declaration of Interests
Lead Director
Amanda Lyes, Chief Corporate Services Officer
Author(s)
Jo Mael, Corporate Governance Manager
Purpose
The report provides a record of relevant and material interests declared by members of the North East Essex CCG Governing Body, and decision making staff.
Applicable CCG Clinical Priorities:
1. To achieve our vision through an inclusive, holistic approach to patient and service user centred commissioning, embedding personalisation of care through integrated health and social care services.
2. To transform care and drive continuous improvement in quality and safety. Achieve the best possible outcomes for our service users through high quality care.
3. To use commissioning resources effectively and responsibly. To develop our organisation, teams and individual staff to be trusted, competent, well trained, talented, enthusiastic and dedicated.
x
4 To tackle the biggest health challenges in north east Essex including reducing health inequalities.
Action required by Governing Body: The Governing Body is asked to review the current register and consider whether any action in relation to non-responders might be required.
Page 2 of 2
1. Background 1.1 Clinical commissioning groups (CCGs) manage conflicts of interest as part of their day-
to-day activities. Effective handling of conflicts of interest is crucial to give confidence to patients, tax payers, healthcare providers and Parliament that CCG commissioning decisions are robust, fair and transparent and offer value for money. It is essential in order to protect healthcare professionals and maintain public trust in the NHS. Failure to manage conflicts of interest could lead to legal challenge and even criminal action in the event of fraud, bribery and corruption.
1.2 Conflicts of interest are inevitable in commissioning. It is how we manage them that
matters. Section 14O of the National Health Service Act 2006 (as amended by the Health and Social Care Act 2012) (“the Act”) sets out the minimum requirements of what both NHS England and CCGs must do in terms of managing conflicts of interest.
1.3 As a minimum, CCGs must have robust systems in place to identify and manage
conflicts of interest. This should involve creating an environment in which CCG staff, and Governing Body and sub-committee members, feel able, encouraged and obliged to be open, honest and upfront about actual or potential conflicts. Transparency in this regard is expected to lead to effective identification and management of conflicts. The effect should be to make everyone aware of what to do if they suspect a conflict and ensure decision-making is efficient, transparent and fair.
1.4 CCGs are required to have systems in place to satisfy themselves that their registers of
interest are accurate and up-to-date.
2. Key Points 2.1 Declarations are sought by the CCG on a six monthly basis and the decision makers
declarations constitute the register published on the CCG’s website. The current register is attached to the report at Appendix 1.
3. Recommendation 3.1 The Governing Body is asked to review the current register and consider whether any
action in relation to non-responders might be required.
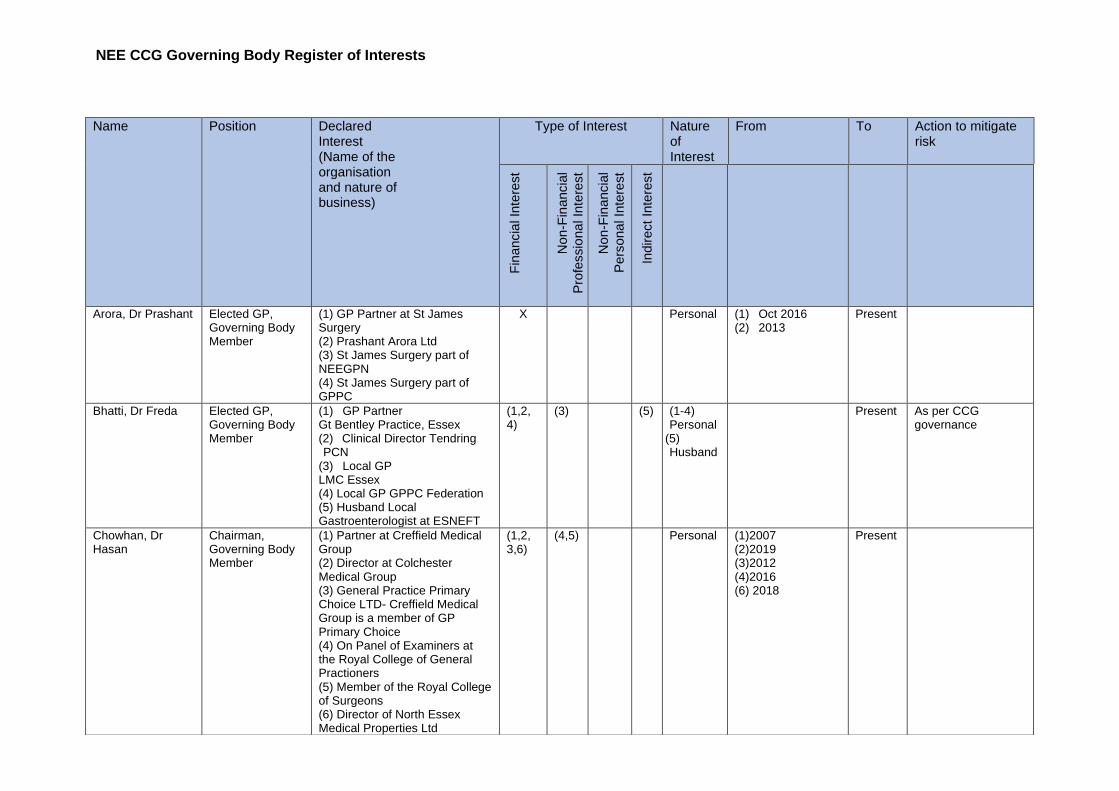
NEE CCG Governing Body Register of Interests
Name Position Declared Interest (Name of the organisation and nature of business)
Type of Interest Nature of Interest
From To Action to mitigate risk
Fin
ancia
l In
tere
st
Non-F
inancia
l
Pro
fessio
na
l In
tere
st
Non-F
inancia
l
Pers
ona
l In
tere
st
Indirect
Inte
rest
Arora, Dr Prashant Elected GP, Governing Body Member
(1) GP Partner at St James Surgery (2) Prashant Arora Ltd (3) St James Surgery part of NEEGPN (4) St James Surgery part of GPPC
X Personal (1) Oct 2016 (2) 2013
Present
Bhatti, Dr Freda Elected GP, Governing Body Member
(1) GP Partner Gt Bentley Practice, Essex (2) Clinical Director Tendring PCN
(3) Local GP LMC Essex (4) Local GP GPPC Federation (5) Husband Local Gastroenterologist at ESNEFT
(1,2, 4)
(3) (5) (1-4) Personal
(5) Husband
Present As per CCG governance
Chowhan, Dr Hasan
Chairman, Governing Body Member
(1) Partner at Creffield Medical Group (2) Director at Colchester Medical Group (3) General Practice Primary Choice LTD- Creffield Medical Group is a member of GP Primary Choice (4) On Panel of Examiners at the Royal College of General Practioners (5) Member of the Royal College of Surgeons (6) Director of North Essex Medical Properties Ltd
(1,2, 3,6)
(4,5) Personal (1)2007 (2)2019 (3)2012 (4)2016 (6) 2018
Present

Cory, Mark Lay Member, Governing Body Member
(1) Member of Colchester Borough Council. (2) Cabinet Member for Resources Colchester Borough Council (3) Member of Essex County Council. (4) Member of Foster Panel, Eastern Family Services.
X Personal (1) 2007 (2) 2022 (3) 2021 (4) 2022
Present Indicate interests at relevant meetings/decisions
Donnelly, Pam Lay Member, Governing Body Member
Chief Executive - Colchester Borough Council
X Personal Ongoing since start of the CCG
Present
Garratt, Ed Chief Executive, Governing Body Member
(1) Chief Executive Ipswich & East Suffolk CCG (2) Chief Executive West Suffolk CCG (3) Chief Executive – Designate, SNEE ICS (4) Visiting Professor of Integrated Care - University of Suffolk (5) Acting Chief Executive Norfolk & Waveney CCG
(1,2,3 & 5)
(4) Personal (1) March 2016 (2) March 2016 (3) Nov 2021 (4) Apr 2021 (5) 31 March 2022
Present To be declared when appropriate.
Gibara, Paul Director of Performance Improvement, Governing Body Member
(1) Director of Performance Improvement for West Suffolk CCG
(2) Director of Performance Improvement for Ipswich & East Suffolk CCG
X Personal 13/7/2020 Present Arrangements in place for the joint management team of the CCG’s
Green, Pam Chief Operating Officer, Governing Body Member
Governor at Kirby Primary School
X Personal March 2021 Present
Hanlon, Martyn Lay Member, Governing Body Member
No interests declared.
Hickman, Max Elected Member, Governing Body Member
(1) Shareholder in a pharmacy - PrettyGate Limited, Ambrose Avenue Pharmacy, 76 Ambrose Avenue Colchester. In- house 80-hour pharmacy based at the GP surgery.
(2) GP Locum - Work as a self-employed locum in
Personal (1) 2013 (2) July 2019 (3) July 2019 (4) 2005 (5) February
2020 (6) December
2021 (7) September
2020 (8)
Present Highlight in commissioning decisions if any potential conflict of interest
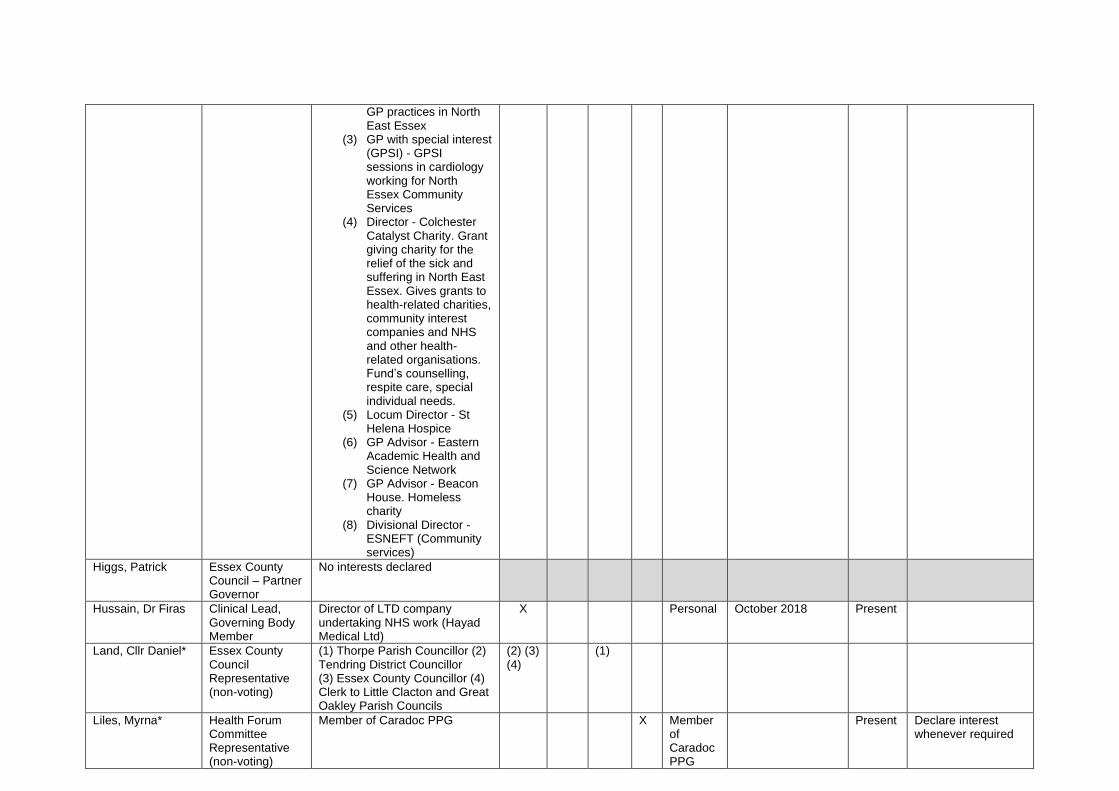
GP practices in North East Essex
(3) GP with special interest (GPSI) - GPSI sessions in cardiology working for North Essex Community Services
(4) Director - Colchester Catalyst Charity. Grant giving charity for the relief of the sick and suffering in North East Essex. Gives grants to health-related charities, community interest companies and NHS and other health- related organisations. Fund’s counselling, respite care, special individual needs.
(5) Locum Director - St Helena Hospice
(6) GP Advisor - Eastern Academic Health and Science Network
(7) GP Advisor - Beacon House. Homeless charity
(8) Divisional Director - ESNEFT (Community services)
Higgs, Patrick Essex County Council – Partner Governor
No interests declared
Hussain, Dr Firas Clinical Lead, Governing Body Member
Director of LTD company undertaking NHS work (Hayad Medical Ltd)
X Personal October 2018 Present
Land, Cllr Daniel* Essex County Council Representative (non-voting)
(1) Thorpe Parish Councillor (2) Tendring District Councillor (3) Essex County Councillor (4) Clerk to Little Clacton and Great Oakley Parish Councils
(2) (3) (4)
(1)
Liles, Myrna* Health Forum Committee Representative (non-voting)
Member of Caradoc PPG X Member of Caradoc PPG
Present Declare interest whenever required
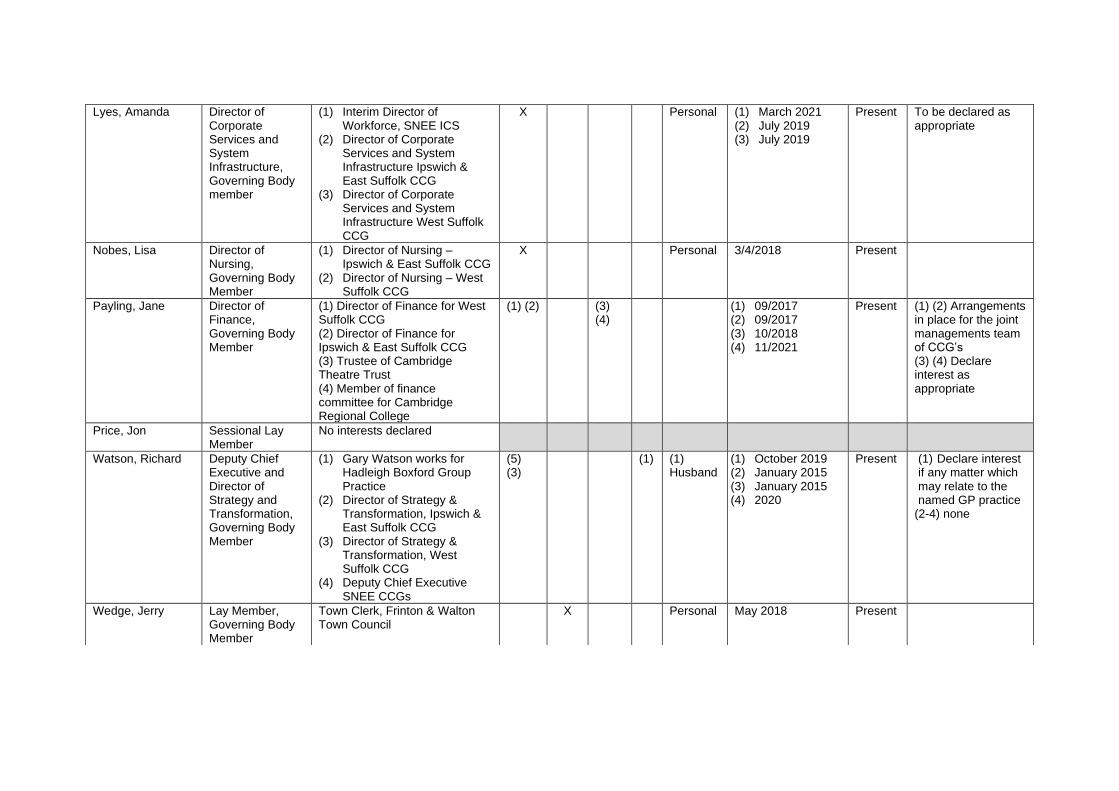
Lyes, Amanda Director of Corporate Services and System Infrastructure, Governing Body member
(1) Interim Director of Workforce, SNEE ICS
(2) Director of Corporate Services and System Infrastructure Ipswich & East Suffolk CCG
(3) Director of Corporate Services and System Infrastructure West Suffolk CCG
X Personal (1) March 2021 (2) July 2019 (3) July 2019
Present To be declared as appropriate
Nobes, Lisa Director of Nursing, Governing Body Member
(1) Director of Nursing – Ipswich & East Suffolk CCG
(2) Director of Nursing – West Suffolk CCG
X Personal 3/4/2018 Present
Payling, Jane Director of Finance, Governing Body Member
(1) Director of Finance for West Suffolk CCG (2) Director of Finance for Ipswich & East Suffolk CCG (3) Trustee of Cambridge Theatre Trust (4) Member of finance committee for Cambridge Regional College
(1) (2) (3) (4)
(1) 09/2017 (2) 09/2017 (3) 10/2018 (4) 11/2021
Present (1) (2) Arrangements in place for the joint managements team of CCG’s (3) (4) Declare interest as appropriate
Price, Jon Sessional Lay Member
No interests declared
Watson, Richard Deputy Chief Executive and Director of Strategy and Transformation, Governing Body Member
(1) Gary Watson works for Hadleigh Boxford Group Practice
(2) Director of Strategy & Transformation, Ipswich & East Suffolk CCG
(3) Director of Strategy & Transformation, West Suffolk CCG
(4) Deputy Chief Executive SNEE CCGs
(5) (3)
(1) (1) Husband
(1) October 2019 (2) January 2015 (3) January 2015 (4) 2020
Present (1) Declare interest if any matter which may relate to the named GP practice
(2-4) none
Wedge, Jerry Lay Member, Governing Body Member
Town Clerk, Frinton & Walton Town Council
X Personal May 2018 Present

NEE CCG Decision Making Staff Register of Interests
Name Position Declared Interest (Name of the organisation and nature of business)
Type of Interest Nature of Interest
From To Action to mitigate risk
Fin
ancia
l In
tere
st
Non
-Fin
ancia
l
Pro
fessio
na
l In
tere
st
Non
-Fin
ancia
l
Pers
ona
l In
tere
st
Indirect
Inte
rest
Jackie Bland Acting Head of IPT
No interest declared
Briggs, Victoria Deputy Director of Nursing
No interest declared
Bryant, Andrew* IT Programme Manager
No interest declared
Chambers, Sandy CHC Business Manager
No interest declared
Chandler, Robert Senior Transformation Lead
No interest declared
Chesa, Oge Deputy Director of Primary Care and Medicines Management
(1) NICE Medicines and Prescribing Associate (2) NICE Adoption and Impact Programme Reference Panel Member (3) Ad hoc Training Adviser (Medicines Management) with Opus Pharmacy Services
(3) (1) (2)
Personal (1)04/2014 (2)12/2015 (3)04/2006
Present (3)Declare at relevant meetings
Colley, Sarah Digital Marketing Manager
No interest declared
Daramola, Olubusola Head of Medicines Management
No interest declared
Decroo, Vicki Deputy Chief Operating Officer
(1) Husband is an employee of ESNEFT – working as a technician on the Children’s ward (2) Uncle in law and cousin are a director’s of Wiremek a company that bids for NHS electrical contracts
X (1) Spouse (2) Close
relative
Present Review as appropriate by project

Ellis, Keith Head of Business Intelligence
No interest declared
Game, Lucy Head of NHS CHC - Operational Lead
Husband is Deputy Director of Finance Accounting & control for IES, WS & NEE CCGs
X Husband, indirect
Present
Garner, Sandra* Designated Nurse Safeguarding Children
No interest declared
Hawkes, Vicki Finance Manager No interest declared
Isaacs, Sarah Head of Primary Care Careers
No interest declared
Jayatilleka, Tehara Senior Finance Manager
Husband/Spouse is a consultant Psychiatrist employed by EPUT
X Husband, indirect
2010 Present Not involved in MH contracts/services and discussions
Jongepier, Lianne* Head of Transformation
Husband is a partner at Creffield Medical Group
X Spouse - Indirect Interest
2000 Present Remove self from relevant procurements & meetings. Where appropriate raise to chair
Joyce, Lianne Associate Director of Nursing SNEE CCG and SCC
(1) Married to Garry Joyce- Deputy director of CYP transformation (2) Joint role between CCG’s and Suffolk County council- my SCC role manages some services that are commissioned by CCG. LD behaviour support team, enuresis service and CHRIS service. .
(2) (1) (1) Indirect Interest (2) Financial Interest
(1) Ongoing (2) 2021
Present
Kent, Steven Finance Manager – Primary Care NHS England
No interest declared
Mackenzie, Charlotte Senior Management Accountant
No interest declared
Sawtell, Vicky Deputy Director of Performance & Contracts
Indirect- Close friend Joining GP Primary Choice as Chief Operating Officer from May 2022
X Friend – Indirect interest
May 2022 Present Review on project-by project basis. Exclude self from relevant procurements & meetings where possible or raise with Chair for agreed approach
Shiers, Debbie Business Support Officer (IPT)
No interest declared
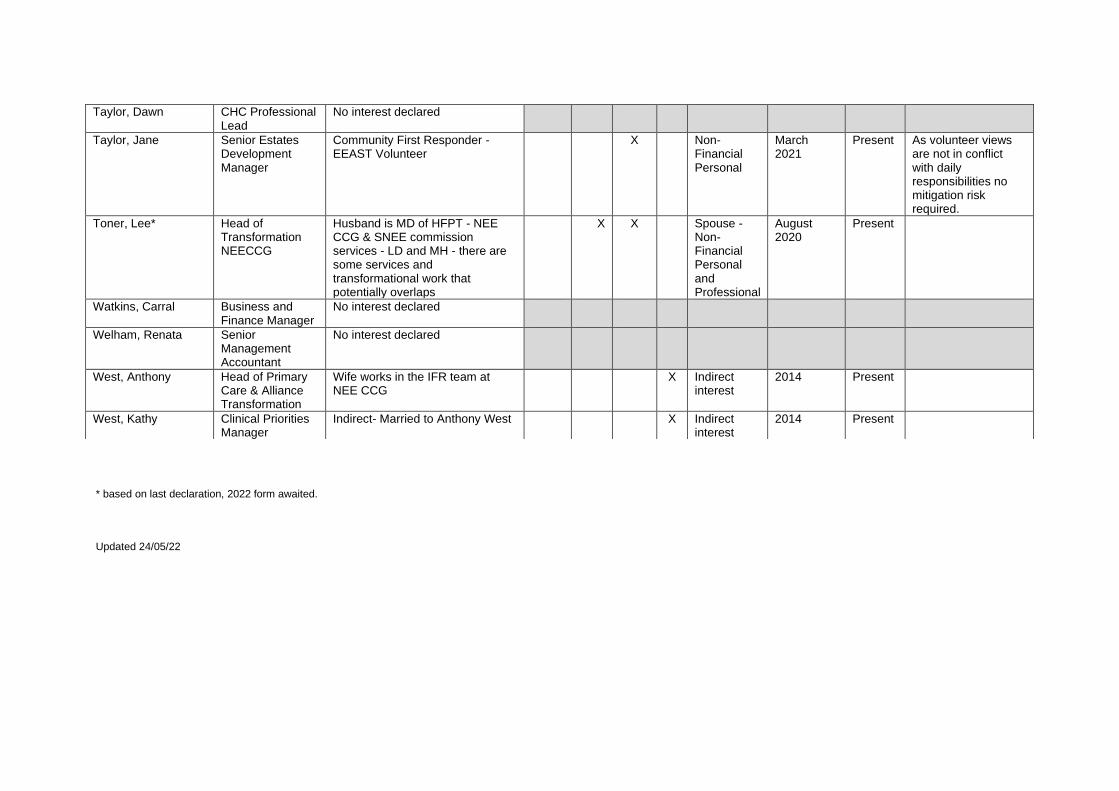
* based on last declaration, 2022 form awaited.
Updated 24/05/22
Taylor, Dawn CHC Professional Lead
No interest declared
Taylor, Jane Senior Estates Development Manager
Community First Responder - EEAST Volunteer
X Non-Financial Personal
March 2021
Present As volunteer views are not in conflict with daily responsibilities no mitigation risk required.
Toner, Lee* Head of Transformation NEECCG
Husband is MD of HFPT - NEE CCG & SNEE commission services - LD and MH - there are some services and transformational work that potentially overlaps
X X Spouse - Non-Financial Personal and Professional
August 2020
Present
Watkins, Carral Business and Finance Manager
No interest declared
Welham, Renata Senior Management Accountant
No interest declared
West, Anthony Head of Primary Care & Alliance Transformation
Wife works in the IFR team at NEE CCG
X Indirect interest
2014 Present
West, Kathy Clinical Priorities Manager
Indirect- Married to Anthony West X Indirect interest
2014 Present
Page 1 of 5
GOVERNING BODY
Agenda Item No. 23
Reference No. NEECCG 22-47
Date. 7 June 2022
Title
Governing Body Assurance Framework
Lead Director
Amanda Lyes, Director of Corporate Services and System Infrastructure
Author(s)
Risk Manager, Corporate Governance Officer
Purpose
To provide the Governing Body with the current strategic risks and a summary of the top risks from the Directorate Risk Register.
Applicable CCG Strategic Objectives:
1. To achieve our vision through an inclusive, holistic approach to patient and service user centred commissioning, embedding personalisation of care through integrated health and social care services.
x
2. To transform care and drive continuous improvement in quality and safety. Achieve the best possible outcomes for our service users through high quality care.
x
3. To use commissioning resources effectively and responsibly. To develop our organisation, teams and individual staff to be trusted, competent, well trained, talented, enthusiastic and dedicated.
x
4 To tackle the biggest health challenges in north east Essex including reducing health inequalities.
x
Recommendation: The Governing Body is asked to note the current strategic risks and a summary of the top risks from the Directorate Risk Register.

Page 2 of 5
1. Summary 1.1 This report provides the Governing Body with the current strategic risks (11) identified by the
CCG and what controls are in place to manage each risk. A summary of the top risks from the Directorate Risk Register is included in Appendix 1.
The Governing Body is asked to note the current strategic risks:
Risk Ref and
Owner Risk description and actions update
CCG001 Amanda Lyes
Delay in progressing the Clacton Hospital site redevelopment in accordance with the original bid criteria and stated spend profile could result in withdrawal of STP capital for the project. June 2022 Revised OBC is now all but complete and the formal review and approvals process is now commencing. This is likely to take a number of months due to the various groups and committees both at a local, regional and national level that it needs to be reviewed at.
CCG002 Amanda Lyes
Lack of workforce resource across heath and care, could create a risk to delivery of CCG statutory targets due to failure in providers to meet waiting time plans and destabilisation in primary care. May 2022 update: Staffing across Health and Care system remains a challenge. Despite falling covid-19 sickness levels, absences still high with worrying trends of staff leaving or expressing to leave. Plans being established and/or in situ to address issues i.e. H&WB interventions, activities to support career aspiration, education transformation, attracting people into health and care through school and college-based activities. The Reservist model is due to be launched in early Summer to support staffing.
CCG003 Amanda Lyes
A target Cyber-attack on the NHS corporate and primary care estate. This could have an impact on Resource, Service, Reputation and Finances. 22 March 2022 update: 1. Regular communications to users re phishing threats. Target date: Ongoing Completion: Proposed further actions as implementation plans progress: Procure and rollout new network switching system with NAC (stage 1). Procure and rollout identity management system. In light of events in the Ukraine and the potential for increased cyber-attacks, the safeguards the CCGs currently have in place are compliant with NHSE directives
CCG004 Richard Watson
Failure to meet the outcomes within the NHS constitution - Cancer standards May 2022 update: All diagnostic waits improving. CT Diagnostic walk around services now in place for LGI/UGI. The trust have implemented super Saturdays and a Vanguard has been in place in Ipswich. In the trust only Cancer/Urgent and inpatient activity is being undertaken, all routine endoscopy is being done at other independent sector providers. 104 day position – The overall trust position is impacted by the backlog in surgery (colorectal, UGI and urology) All other tumour sites have recovered their backlog position. Colchester are at pre-Covid levels, Ipswich are better than pre-Covid levels Issues remain with patients being referred with FIT tests either completed or taken. This is creating patients being referred onto incorrect pathway and delaying treatment, additional triage now in place at front end of pathway to vague symptoms clinic. Breast pain pathway now up and running and currently is
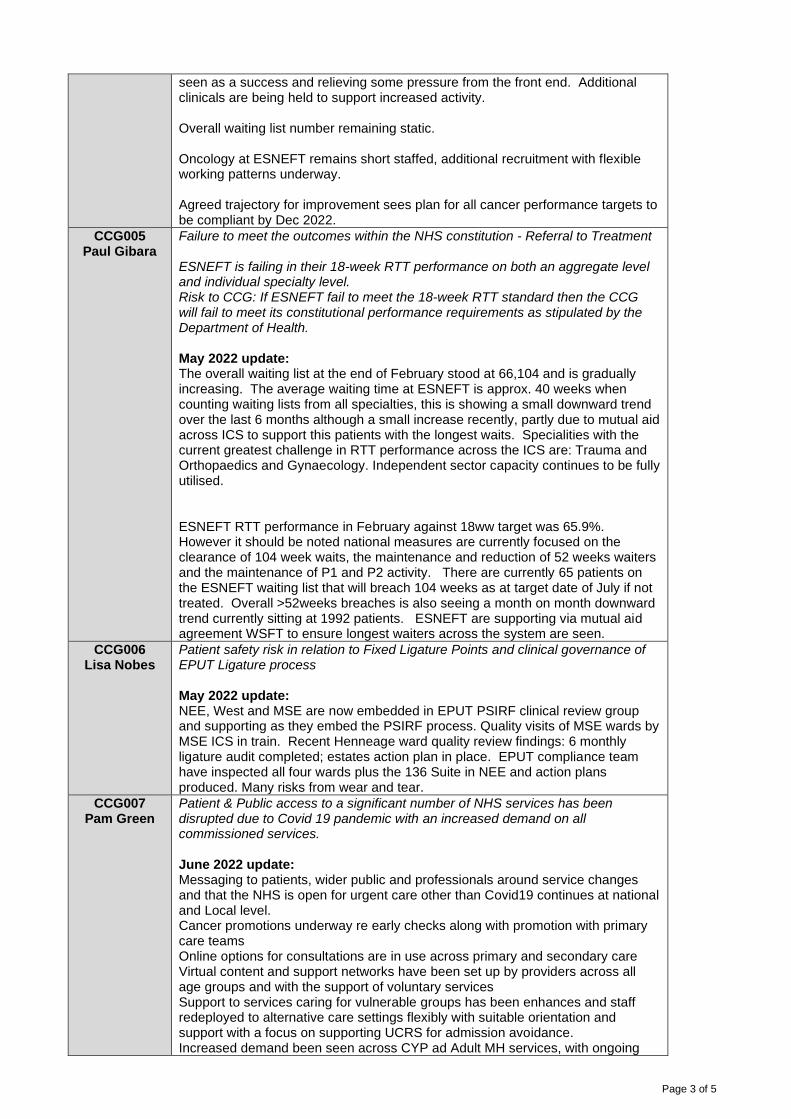
Page 3 of 5
seen as a success and relieving some pressure from the front end. Additional clinicals are being held to support increased activity. Overall waiting list number remaining static. Oncology at ESNEFT remains short staffed, additional recruitment with flexible working patterns underway. Agreed trajectory for improvement sees plan for all cancer performance targets to be compliant by Dec 2022.
CCG005 Paul Gibara
Failure to meet the outcomes within the NHS constitution - Referral to Treatment ESNEFT is failing in their 18-week RTT performance on both an aggregate level and individual specialty level. Risk to CCG: If ESNEFT fail to meet the 18-week RTT standard then the CCG will fail to meet its constitutional performance requirements as stipulated by the Department of Health. May 2022 update: The overall waiting list at the end of February stood at 66,104 and is gradually increasing. The average waiting time at ESNEFT is approx. 40 weeks when counting waiting lists from all specialties, this is showing a small downward trend over the last 6 months although a small increase recently, partly due to mutual aid across ICS to support this patients with the longest waits. Specialities with the current greatest challenge in RTT performance across the ICS are: Trauma and Orthopaedics and Gynaecology. Independent sector capacity continues to be fully utilised. ESNEFT RTT performance in February against 18ww target was 65.9%. However it should be noted national measures are currently focused on the clearance of 104 week waits, the maintenance and reduction of 52 weeks waiters and the maintenance of P1 and P2 activity. There are currently 65 patients on the ESNEFT waiting list that will breach 104 weeks as at target date of July if not treated. Overall >52weeks breaches is also seeing a month on month downward trend currently sitting at 1992 patients. ESNEFT are supporting via mutual aid agreement WSFT to ensure longest waiters across the system are seen.
CCG006 Lisa Nobes
Patient safety risk in relation to Fixed Ligature Points and clinical governance of EPUT Ligature process May 2022 update: NEE, West and MSE are now embedded in EPUT PSIRF clinical review group and supporting as they embed the PSIRF process. Quality visits of MSE wards by MSE ICS in train. Recent Henneage ward quality review findings: 6 monthly ligature audit completed; estates action plan in place. EPUT compliance team have inspected all four wards plus the 136 Suite in NEE and action plans produced. Many risks from wear and tear.
CCG007 Pam Green
Patient & Public access to a significant number of NHS services has been disrupted due to Covid 19 pandemic with an increased demand on all commissioned services. June 2022 update: Messaging to patients, wider public and professionals around service changes and that the NHS is open for urgent care other than Covid19 continues at national and Local level. Cancer promotions underway re early checks along with promotion with primary care teams Online options for consultations are in use across primary and secondary care Virtual content and support networks have been set up by providers across all age groups and with the support of voluntary services Support to services caring for vulnerable groups has been enhances and staff redeployed to alternative care settings flexibly with suitable orientation and support with a focus on supporting UCRS for admission avoidance. Increased demand been seen across CYP ad Adult MH services, with ongoing
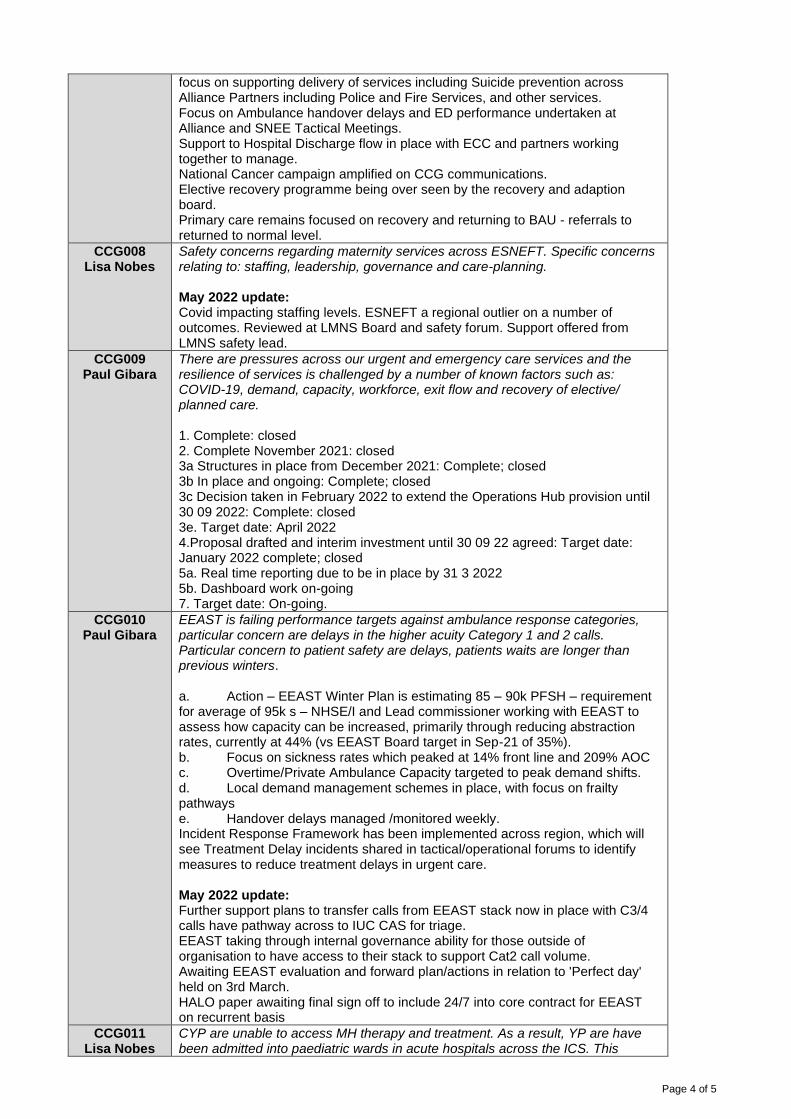
Page 4 of 5
focus on supporting delivery of services including Suicide prevention across Alliance Partners including Police and Fire Services, and other services. Focus on Ambulance handover delays and ED performance undertaken at Alliance and SNEE Tactical Meetings. Support to Hospital Discharge flow in place with ECC and partners working together to manage. National Cancer campaign amplified on CCG communications. Elective recovery programme being over seen by the recovery and adaption board. Primary care remains focused on recovery and returning to BAU - referrals to returned to normal level.
CCG008 Lisa Nobes
Safety concerns regarding maternity services across ESNEFT. Specific concerns relating to: staffing, leadership, governance and care-planning. May 2022 update: Covid impacting staffing levels. ESNEFT a regional outlier on a number of outcomes. Reviewed at LMNS Board and safety forum. Support offered from LMNS safety lead.
CCG009 Paul Gibara
There are pressures across our urgent and emergency care services and the resilience of services is challenged by a number of known factors such as: COVID-19, demand, capacity, workforce, exit flow and recovery of elective/ planned care. 1. Complete: closed 2. Complete November 2021: closed 3a Structures in place from December 2021: Complete; closed 3b In place and ongoing: Complete; closed 3c Decision taken in February 2022 to extend the Operations Hub provision until 30 09 2022: Complete: closed 3e. Target date: April 2022 4.Proposal drafted and interim investment until 30 09 22 agreed: Target date: January 2022 complete; closed 5a. Real time reporting due to be in place by 31 3 2022 5b. Dashboard work on-going 7. Target date: On-going.
CCG010 Paul Gibara
EEAST is failing performance targets against ambulance response categories, particular concern are delays in the higher acuity Category 1 and 2 calls. Particular concern to patient safety are delays, patients waits are longer than previous winters. a. Action – EEAST Winter Plan is estimating 85 – 90k PFSH – requirement for average of 95k s – NHSE/I and Lead commissioner working with EEAST to assess how capacity can be increased, primarily through reducing abstraction rates, currently at 44% (vs EEAST Board target in Sep-21 of 35%). b. Focus on sickness rates which peaked at 14% front line and 209% AOC c. Overtime/Private Ambulance Capacity targeted to peak demand shifts. d. Local demand management schemes in place, with focus on frailty pathways e. Handover delays managed /monitored weekly. Incident Response Framework has been implemented across region, which will see Treatment Delay incidents shared in tactical/operational forums to identify measures to reduce treatment delays in urgent care. May 2022 update: Further support plans to transfer calls from EEAST stack now in place with C3/4 calls have pathway across to IUC CAS for triage. EEAST taking through internal governance ability for those outside of organisation to have access to their stack to support Cat2 call volume. Awaiting EEAST evaluation and forward plan/actions in relation to 'Perfect day' held on 3rd March. HALO paper awaiting final sign off to include 24/7 into core contract for EEAST on recurrent basis
CCG011 Lisa Nobes
CYP are unable to access MH therapy and treatment. As a result, YP are have been admitted into paediatric wards in acute hospitals across the ICS. This

Page 5 of 5
creates a risk to staff, patients and families on these wards. May 2022 update: Escalation pathway drafted and undergoing system scrutiny/sign off. CYP MH Ipswich and WSH posts - recruitment underway with NHSE monies and additional CCG investment.
2. Resource Implications
This report does not seek any resources. 3. Engagement and Communication
Each individual risk has been evaluated, including the requirement to communicate with relevant stakeholders.
4. Equality and Diversity
The proposed approach will ensure that risk is assessed from a quality perspective including equality and diversity.

Like
lihoo
d
Con
sequ
enc
e
Ris
k sc
ore
Like
lihoo
d
Con
sequ
enc
e
Ris
k sc
ore
Like
lihoo
d
Con
sequ
enc
e
Ris
k sc
ore
CCG001 01-Apr-22 Delay in progressing the Clacton Hospital site redevelopment in accordance with the original bid criteria and stated spend profile could result in withdrawal of STP capital for the project. This in turn could cause reputational damage to the hospital and wider NHS system
If significant monies are not obtained through the bidding process for the STP Capital the primary care estate in Clacton will not be fit for purpose for the future model of primary care. The initial financial risk gives rise to a variety of other risks, so grip on the project and its finances acts to control the other risks.
SO3 AL 4 4 16 Controls over quality, performance, reputational and financial risk: Programme governance established with project board, which includes representation from NHSE via SEA.NHSE Regional team engaged in early page turns of business case to ensure correct content and context provided. Wider master planning taking place to look at options beyond phase one project and ensure maximum efficiencies are implemented. NHSE to explore potential of site ownership from NHS PS to a NHS Provider organisation which may reduce costs of the scheme. Full business case being developed at risk to reduce overall programme.
June 2022 Revised OBC is now all but complete and the formal review and approvals process is now commencing. This is likely to take a number of months due to the various groups and committees both at a local, regional and national level that it needs to be reviewed at.
4 5 20 4 3 12 End 2023
CCG002 01-Apr-22 Lack of workforce resource across heath and care, could create a risk to delivery of CCG statutory targets due to failure in providers to meet waiting time plans and destabilisation in primary care.
The system has ageing clinical workforce with insufficient younger workforce to replace, leading to clinical risk of patients not being seen in appropriate timescales and inability to meet clinical and performance quality targets. Covid-19 impact on staffing levels due to sickness and/or isolation.Staff redeployed to resource Covid-19 vaccination centres. Retention risk due to burnout and other factors such as work life balance Inability to maintain safer staffing levels in accordance with NICE and National Quality Board guidance.Potential sickness absence of staff due to workload further impact on patient safety, care and services impact on staff retention, losing staff due to increased workload.The loss of staff due to the need to be vaccinated by April 2022.Risk of breaching constitutional obligations. Primary care risk of some practices not being able to function and list closures. EEAST unable to recruit against ISR plan impacting on the level of PFSH available to d l
SO3 AL 4 5 20 Controls over quality and performance: SNEE Can Do People Plan in place. SNEE People Board established to implement the system People Plan and associated initiatives. Local workforce transformation groups established in each Alliance, as well as PC WIG and GPCC that report into People Board for Primary Care. Recovery planning is in place, retention planning in place both regionally and across SNEE. Fully linked in. Health and Care Academy in place to inspire people to work in health and care. Apprenticeship strategy in place to grow our own
IESCCG, NEE and WSCCG Local Workforce Transformation groups, PC WIG and GPCC reporting to SNEE People Board, also various steering groups that are topic specific e.g. retention group.
May 2022 Staffing across Health and Care system remains a challenge. Despite falling covid-19 sickness levels, absences still high with worrying trends of staff leaving or expressing to leave. Plans being established and/or in situ to address issues i.e. H&WB interventions, activities to support career aspiration, education transformation, attracting people into health and care through school and college-based activities. The Reservist model is due to be launched in early Summer to support staffing.
4 4 16 4 2 8 31-Mar-22
CCG003 01-Apr-22 Potential impact of cyber security incident could lead to wide scale IT system outages, meaning no access to patient records, e-dispensing services etc
Risk to the CCGThe CCGs would suffer significant service disruption and potential patient harm and financial loss
National requirements have increased, in respect of the need to achieve cyber essentials + accreditation.No national funding has been identified specifically for cyber security work to mitigate against the increased risk, and the increased requirements. No access to systems – would require frontline services to fully enact Business Continuity and Disaster Recovery procedures.Potential for lack of access to relevant IT skills and insight to develop a recovery plan (dependent on type of attack).Restoration of services complex, would involve multiple vendors and take a significant period of time
SO2 SO3 AL 4 5 20 Controls in place over Quality, performance, finance and reputation:NB - eliminating risk of cyber-attack completely is not possible.Following external cyber assessment (post-Wannacry cyber-attack local review); a number of areas to be addressed to reduce risk of an attack and any potential impacts (see actions). In progress:Service provider (NEL) undergoing wide scale review of cyber assurance, have achieved cyber essentials accreditation and cyber essentials + accreditation. CCG has own domain (green) under NEL and has achieved cyber essentials accreditation for the CCG.RSM reviewed cyber controls. Assurance received. Additional ETTF (GP Capital) funds have been successful to implement a NAC solution, details being worked up with NEL.Board level training to IESCCG and WSCCG Board and Lay Members.W10 rollout 99.95% complete. Handful of remaining W10 PCs will be decommissioned in service transition, they remain supported. Improved access controls and enabling multi-factor authentication with OKTA.Implementation of effective incident response plan via ICC.Regular patch of systems as part of BAU and planned forced machine restarts.Ensure that backups, restore mechanisms and online defences are working - monitored as BAU, monthly reporting and live dashboards.NEL have team to keep up to date with latest threat and mitigation information.
External Audit.
Internal audit complete
Monthly SLA provider meetings.
Monthly service review provider meetings.
Monthly Joint Digital and IT Services Board.
Audit Committee review.
Scrutiny Committee review
Governing Body Board level training to IESCCG and WSCCG Governing Body’s and Lay Members.
22 March 2022 1. Regular communications to users re phishing threats.Target date: OngoingCompletion:
Proposed further actions as implementation plans progress:Procure and rollout new network switching system with NAC (stage 1).Procure and rollout identity management system.
In light of events in the Ukraine and the potential for increased cyber-attacks, the safeguards the CCGs currently have in place are compliant with NHSE directives
4 5 20 3 4 12 31-Mar-22
CCG004 01-Apr-22 Failure to meet the outcomes within the NHS constitution - Cancer standards
Risk to CCG: If ESNEFT fail to meet62 day target then the CCG would have failed to meet its constitutional performance requirements as stipulated by the Department of Health.
Specific risks also include:
• Clinical risk of patients not being seen in appropriate timescales• Risk of deteriorating patient outcomes and experience due to long waits.• Risk of breaching constitutional obligations.• Risk of increasing patient harm bothphysically and mentally due to being on Cancer pathway for extended period oftime. In addition to the above there is a new risk emerging relating to patients notattending cancer appointments.
Failure to diagnose and treat within the cancer waiting times standard leading to potentially reduced clinical outcomes for patients
Failure to achieve the 62 day standard of 85% consistently during 2021/22Failure to achieve the 62 day Screening standard of 90% consistently during 2021/22Failure to achieve the 31 day 1st standard of 96% consistently during 2021/22Failure to achieve the 31 day sub Surgery standard of 94% consistently during 2021/22Failure to achieve the 31 day Radiotherapy standard of 94% consistently during 2021/22Failure to achieve the 31 day Drug standard of 98% consistently during 2021/22Failure to achieve the 2WW standard of 93% consistently during2021/22Failure to achieve the 2WW Breast standard of 93% consistently during 2021/22
SO2 & SO4 RW 4 4 16 High level controls to mitigate risks in relation to quality, performance and reputation include: Contractual arrangementsMDT tracking MDT oversight of clinical diagnostics and treatment datesSOP for diagnostic reporting and next step actioning SI reporting procedures and LEAPSMortality Review CommitteeESNEFT Cancer board ESNEFT Breach reporting Process to board levelEast of England Cancer Quality Task and Finish Group SNEE Cancer System Oversight MeetingsCancer Programme Delivery Board ESNEFT elective care programme BoardTime Matters board Programme, STP cancer Transformation programmeWeekly specialty reporting and cancer focused ESNEFT PTL in placeDetailed controls include:• Super-green wards are in place with all patients level 1 or level 2 but not suitable for ISP to be listed once isolation period and swabs completed.• Dermatology team (high volumes with delays area) working through list of patients offering new dates whilst continuing to book new referrals.• Additional cancer reporting and information being received by CCG.• Activity and monitoring of cancer continues (colorectal referrals now back to pre-covid levels), capacity to support these patients being utilised with IP.• Some transformation activities will be delayed• Cancer priority treatment lists will continue to be reviewed and managed.
All these controls work to improve quality and performance at ESNEFT and therefore
ESNEFT elective care programme Board.Time Matters Board Programme oversight of the elective care programme Board ESNEFT cancer Board.ESNEFT breach reporting process to board levelEast of England Cancer Quality Task and Finish Group
Monthly Performance and Quality Review Meetings and monthly NHSE/I/CCG/ESNEFT cancer meetings in place.
May 2022 All diagnostic waits improving. CT Diagnostic walk around services now in place for LGI/UGI. The trust have implemented super Saturdays and a Vanguard has been in place in Ipswich. In the trust only Cancer/Urgent and inpatient activity is being undertaken, all routine endoscopy is being done at other independent sector providers.
104 day position – The overall trust position is impacted by the backlog in surgery (colorectal, UGI and urology) All other tumour sites have recovered their backlog position. Colchester are at pre-Covid levels, Ipswich are better than pre-Covid levels
Issues remain with patients being referred with FIT tests either completed or taken. This is creating patients being referred onto incorrect pathway and delaying treatment, additional triage now in place at front end of pathway to vague symptoms clinic. Breast pain pathway now up and running and currently is seen as a success and relieving some pressure from the front end. Additional clinicals are being held to support increased activity.
Overall waiting list number remaining static.
Oncology at ESNEFT remains short staffed, additional recruitment with flexible working patterns underway.
Agreed trajectory for improvement sees plan for all cancer performance targets to be compliant by Dec 2022.
4 4 16 2 2 4 To be agreed / revisited post Covid
NEE Governing Body Assurance Framework
Target date
Initial Risk Rating
Current Risk Rating
Target Risk Rating
Ref Date added Risk HazardLink to
Assurance Framework
Risk Owner Controls Assurance of Controls Progress
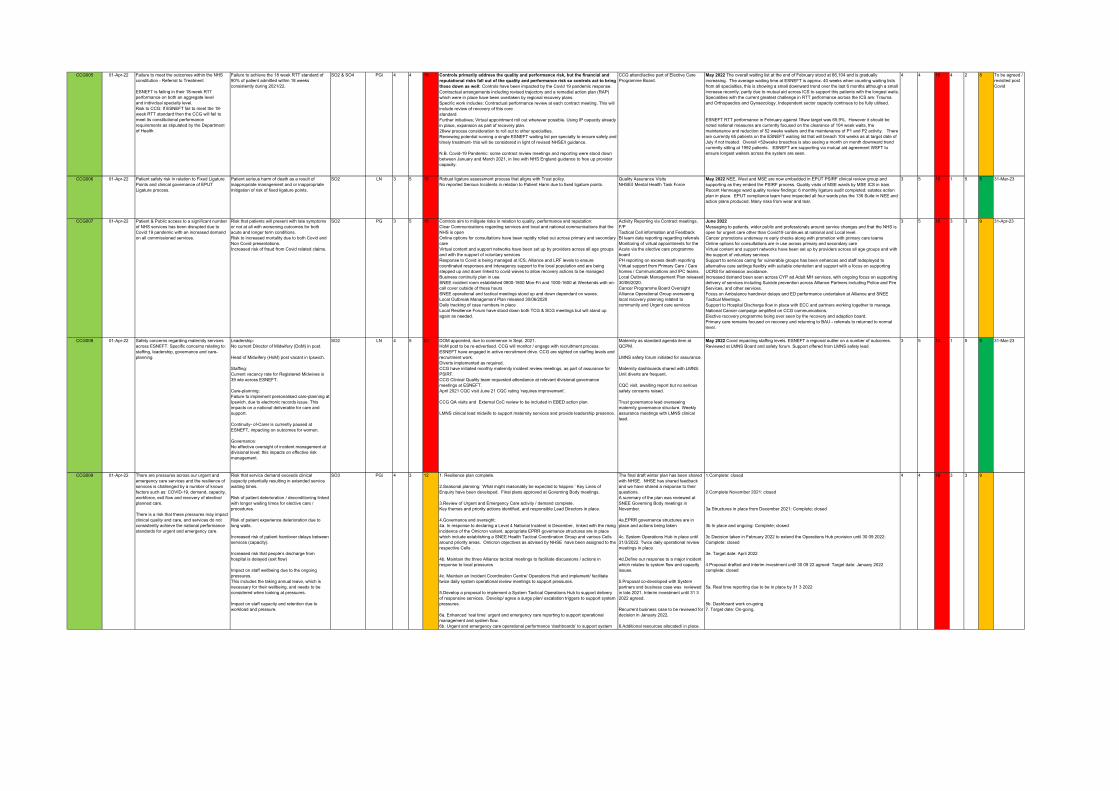
CCG005 01-Apr-22 Failure to meet the outcomes within the NHS constitution - Referral to Treatment
ESNEFT is failing in their 18-week RTTperformance on both an aggregate leveland individual specialty level.Risk to CCG: If ESNEFT fail to meet the 18-week RTT standard then the CCG will fail to meet its constitutional performance requirements as stipulated by the Department of Health.
Failure to achieve the 18 week RTT standard of 90% of patient admitted within 18 weeks consistently during 2021/22.
SO2 & SO4 PGi 4 4 16 Controls primarily address the quality and performance risk, but the financial and reputational risks fall out of the quality and performance risk so controls act to bring these down as well: Controls have been impacted by the Covid 19 pandemic response. Contractual arrangements including revised trajectory and a remedial action plan (RAP) which were in place have been overtaken by regional recovery plans. Specific work includes: Contractual performance review at each contract meeting. This will include review of recovery of this corestandard. Further initiatives; Virtual appointment roll out wherever possible. Using IP capacity already in place, expansion as part of recovery plan.26ww process consideration to roll out to other specialties.Reviewing potential running a single ESNEFT waiting list per specialty to ensure safety and timely treatment- this will be considered in light of revised NHSE/I guidance.
N.B. Covid-19 Pandemic: some contract review meetings and reporting were stood down between January and March 2021, in line with NHS England guidance to free up provider capacity.
CCG attend/active part of Elective Care Programme Board.
May 2022 The overall waiting list at the end of February stood at 66,104 and is gradually increasing. The average waiting time at ESNEFT is approx. 40 weeks when counting waiting lists from all specialties, this is showing a small downward trend over the last 6 months although a small increase recently, partly due to mutual aid across ICS to support this patients with the longest waits. Specialities with the current greatest challenge in RTT performance across the ICS are: Trauma and Orthopaedics and Gynaecology. Independent sector capacity continues to be fully utilised.
ESNEFT RTT performance in February against 18ww target was 65.9%. However it should be noted national measures are currently focused on the clearance of 104 week waits, the maintenance and reduction of 52 weeks waiters and the maintenance of P1 and P2 activity. There are currently 65 patients on the ESNEFT waiting list that will breach 104 weeks as at target date of July if not treated. Overall >52weeks breaches is also seeing a month on month downward trend currently sitting at 1992 patients. ESNEFT are supporting via mutual aid agreement WSFT to ensure longest waiters across the system are seen.
4 4 16 4 2 8 To be agreed / revisited post Covid
CCG006 01-Apr-22 Patient safety risk in relation to Fixed Ligature Points and clinical governance of EPUT Ligature process.
Patient serious harm of death as a result of inappropriate management and or inappropriate mitigation of risk of fixed ligature points.
SO2 LN 3 5 15 Robust ligature assessment process that aligns with Trust policy.No reported Serious Incidents in relation to Patient Harm due to fixed ligature points.
Quality Assurance VisitsNHSE/I Mental Health Task Force
May 2022 NEE, West and MSE are now embedded in EPUT PSIRF clinical review group and supporting as they embed the PSIRF process. Quality visits of MSE wards by MSE ICS in train. Recent Henneage ward quality review findings: 6 monthly ligature audit completed; estates action plan in place. EPUT compliance team have inspected all four wards plus the 136 Suite in NEE and action plans produced. Many risks from wear and tear.
3 5 15 1 5 5 31-Mar-23
CCG007 01-Apr-22 Patient & Public access to a significant number of NHS services has been disrupted due to Covid 19 pandemic with an increased demand on all commissioned services.
Risk that patients will present with late symptoms or not at all with worsening outcomes for both acute and longer term conditions.Risk to increased mortality due to both Covid and Non Covid presentations.Increased risk of fraud from Covid related claims.
SO2 PG 3 5 15 Controls aim to mitigate risks in relation to quality, performance and reputation:Clear Communications regarding services and local and national communications that the NHS is openOnline options for consultations have been rapidly rolled out across primary and secondary care Virtual content and support networks have been set up by providers across all age groups and with the support of voluntary servicesResponse to Covid is being managed at ICS, Alliance and LRF levels to ensure coordinated responses and interagency support to the local population and are being stepped up and down linked to covid waves to allow recovery actions to be managedBusiness continuity plan in use.SNEE incident room established 0800-1800 Mon-Fri and 1000-1600 at Weekends with on-call cover outside of these hoursSNEE operational and tactical meetings stood up and down dependant on waves.Local Outbreak Management Plan released 30/06/2020Daily tracking of case numbers in placeLocal Resilience Forum have stood down both TCG & SCG meetings but will stand up again as needed.
Activity Reporting via Contract meetings, F/P Tactical Cell information and FeedbackBI team data reporting regarding referrals Monitoring of virtual appointments for the Acute via the elective care programme board PH reporting on excess death reportingVirtual support from Primary Care / Care homes / Communications and IPC teams.Local Outbreak Management Plan released 30/06/2020.Cancer Programme Board Oversight Alliance Operational Group overseeing local recovery planning related to community and Urgent care services
June 2022 Messaging to patients, wider public and professionals around service changes and that the NHS is open for urgent care other than Covid19 continues at national and Local level.Cancer promotions underway re early checks along with promotion with primary care teamsOnline options for consultations are in use across primary and secondary careVirtual content and support networks have been set up by providers across all age groups and with the support of voluntary servicesSupport to services caring for vulnerable groups has been enhances and staff redeployed to alternative care settings flexibly with suitable orientation and support with a focus on supporting UCRS for admission avoidance.Increased demand been seen across CYP ad Adult MH services, with ongoing focus on supporting delivery of services including Suicide prevention across Alliance Partners including Police and Fire Services, and other services.Focus on Ambulance handover delays and ED performance undertaken at Alliance and SNEE Tactical Meetings.Support to Hospital Discharge flow in place with ECC and partners working together to manage.National Cancer campaign amplified on CCG communications.Elective recovery programme being over seen by the recovery and adaption board.Primary care remains focused on recovery and returning to BAU - referrals to returned to normal level.
3 5 15 3 3 9 31-Apr-23
CCG008 01-Apr-22 Safety concerns regarding maternity services across ESNEFT. Specific concerns relating to: staffing, leadership, governance and care-planning.
Leadership: No current Director of Midwifery (DoM) in post.
Head of Midwifery (HoM) post vacant in Ipswich.
Staffing: Current vacancy rate for Registered Midwives is 39 wte across ESNEFT.
Care-planning: Failure to implement personalised care-planning at Ipswich, due to electronic records issue. This impacts on a national deliverable for care and support.
Continuity- of-Carer is currently paused at ESNEFT, impacting on outcomes for women.
Governance: No effective oversight of incident management at divisional level; this impacts on effective risk management.
SO2 LN 4 5 20 DOM appointed, due to commence in Sept. 2021. HoM post to be re-advertised. CCG will monitor / engage with recruitment process. ESNEFT have engaged in active recruitment drive. CCG are sighted on staffing levels and recruitment work. Diverts implemented as required. CCG have initiated monthly maternity incident review meetings, as part of assurance for PSIRF. CCG Clinical Quality team requested attendance at relevant divisional governance meetings at ESNEFT.April 2021 CQC visit June 21 CQC rating ‘requires improvement’.
CCG QA visits and External CoC review to be included in EBED action plan.
LMNS clinical lead midwife to support maternity services and provide leadership presence.
Maternity as standard agenda item at QCPM.
LMNS safety forum initiated for assurance.
Maternity dashboards shared with LMNS.Unit diverts are frequent.
CQC visit, awaiting report but no serious safety concerns raised.
Trust governance lead overseeing maternity governance structure. Weekly assurance meetings with LMNS clinical lead.
May 2022 Covid impacting staffing levels. ESNEFT a regional outlier on a number of outcomes. Reviewed at LMNS Board and safety forum. Support offered from LMNS safety lead.
3 5 15 1 5 5 31-Mar-23
CCG009 01-Apr-22 There are pressures across our urgent and emergency care services and the resilience of services is challenged by a number of known factors such as: COVID-19, demand, capacity, workforce, exit flow and recovery of elective/ planned care.
There is a risk that these pressures may impact clinical quality and care, and services do not consistently achieve the national performance standards for urgent and emergency care.
Risk that service demand exceeds clinical capacity potentially resulting in extended service waiting times.
Risk of patient deterioration / deconditioning linked with longer waiting times for elective care / procedures.
Risk of patient experience deterioration due to long waits.
Increased risk of patient handover delays between services (capacity).
Increased risk that people’s discharge from hospital is delayed (exit flow)
Impact on staff wellbeing due to the ongoing pressures. This includes the taking annual leave, which is necessary for their wellbeing, and needs to be considered when looking at pressures.
Impact on staff capacity and retention due to workload and pressure.
SO3 PGi 4 3 12 1. Resilience plan complete.
2.Seasonal planning: ‘What might reasonably be expected to happen.’ Key Lines of Enquiry have been developed. Final plans approved at Governing Body meetings.
3.Review of Urgent and Emergency Care activity / demand complete. Key themes and priority actions identified, and responsible Lead Directors in place.
4.Governance and oversight:4a. In response to declaring a Level 4 National Incident in December, linked with the rising incidence of the Omicron variant, appropriate EPRR governance structures are in place which include establishing a SNEE Health Tactical Coordination Group and various Cells around priority areas. Omicron objectives as advised by NHSE have been assigned to the respective Cells .
4b. Maintain the three Alliance tactical meetings to facilitate discussions / actions in response to local pressures
4c. Maintain an Incident Coordination Centre/ Operations Hub and implement/ facilitate twice daily system operational review meetings to support pressures.
5.Develop a proposal to implement a System Tactical Operations Hub to support delivery of responsive services. Develop/ agree a surge plan/ escalation triggers to support system pressures.
6a. Enhanced ‘real time’ urgent and emergency care reporting to support operational management and system flow.6b. Urgent and emergency care operational performance ‘dashboards’ to support system
The final draft winter plan has been shared with NHSE. NHSE has shared feedback and we have shared a response to their questions. A summary of the plan was reviewed at SNEE Governing Body meetings in November.
4a.EPRR governance structures are in place and actions being taken
4c. System Operations Hub in place until 31/3/2022. Twice daily operational review meetings in place
4d.Define our response to a major incident which relates to system flow and capacity issues.
5.Proposal co-developed with System partners and business case was reviewed in late 2021. Interim investment until 31 3 2022 agreed.
Recurrent business case to be reviewed for decision in January 2022.
6.Additional resources allocated/ in place.
1.Complete: closed
2.Complete November 2021: closed
3a Structures in place from December 2021: Complete; closed
3b In place and ongoing: Complete; closed
3c Decision taken in February 2022 to extend the Operations Hub provision until 30 09 2022: Complete: closed
3e. Target date: April 2022
4.Proposal drafted and interim investment until 30 09 22 agreed: Target date: January 2022 complete; closed
5a. Real time reporting due to be in place by 31 3 2022
5b. Dashboard work on-going7. Target date: On-going.
4 4 16 3 3 9
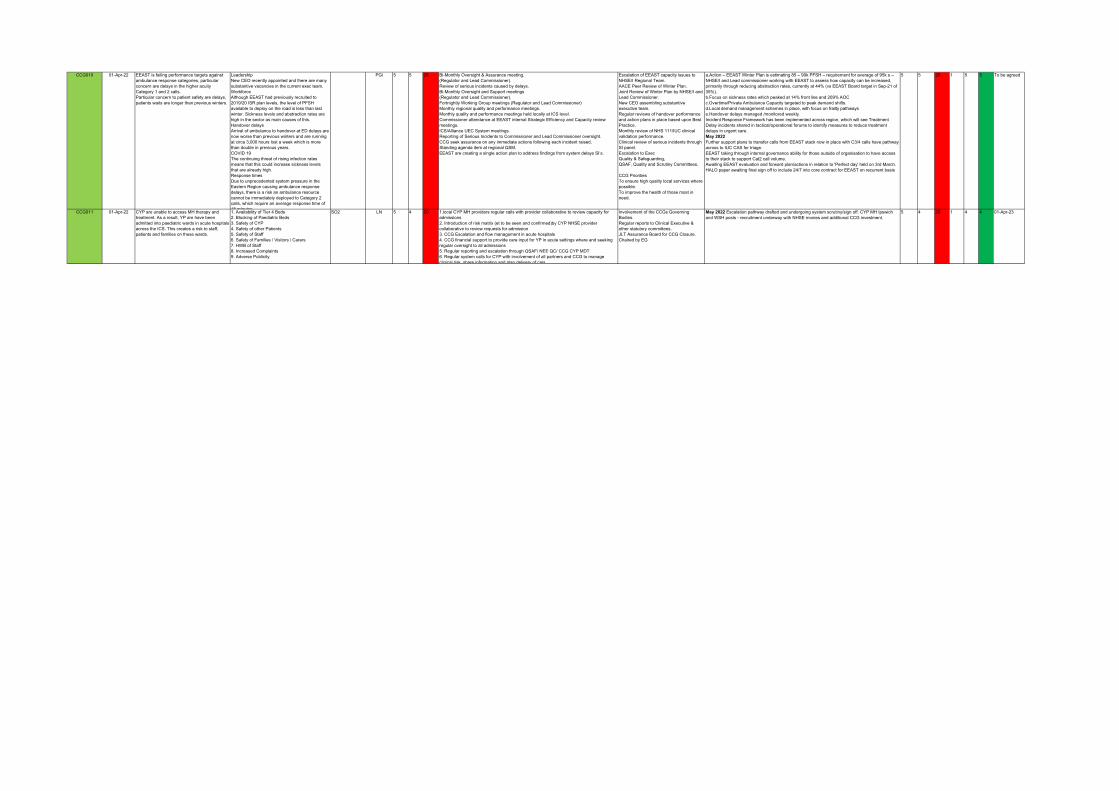
CCG010 01-Apr-22 EEAST is failing performance targets against ambulance response categories, particular concern are delays in the higher acuity Category 1 and 2 calls.Particular concern to patient safety are delays, patients waits are longer than previous winters.
LeadershipNew CEO recently appointed and there are many substantive vacancies in the current exec team.WorkforceAlthough EEAST had previously recruited to 2019/20 ISR plan levels, the level of PFSH available to deploy on the road is less than last winter. Sickness levels and abstraction rates are high in the sector as main causes of this. Handover delaysArrival of ambulance to handover at ED delays are now worse than previous winters and are running at circa 3,000 hours lost a week which is more than double in previous years.COVID 19The continuing threat of rising infection rates means that this could increase sickness levels that are already high.Response timesDue to unprecedented system pressure in the Eastern Region causing ambulance response delays, there is a risk an ambulance resource cannot be immediately deployed to Category 2 calls, which require an average response time of 18 minutes
PGi 5 5 25 Bi-Monthly Oversight & Assurance meeting.(Regulator and Lead Commissioner).Review of serious incidents caused by delays.Bi-Monthly Oversight and Support meetings(Regulator and Lead Commissioner).Fortnightly Working Group meetings (Regulator and Lead Commissioner)Monthly regional quality and performance meetings.Monthly quality and performance meetings held locally at ICS level. Commissioner attendance at EEAST internal Strategic Efficiency and Capacity review meetings.ICS/Alliance UEC System meetings.Reporting of Serious Incidents to Commissioner and Lead Commissioner oversight.CCG seek assurance on any immediate actions following each incident raised.Standing agenda item at regional QSM.EEAST are creating a single action plan to address findings from system delays SI’s.
Escalation of EEAST capacity issues to NHSE/I Regional Team.AACE Peer Review of Winter Plan.Joint Review of Winter Plan by NHSE/I and Lead Commissioner. New CEO assembling substantive executive team.Regular reviews of handover performance and action plans in place based upon Best Practice.Monthly review of NHS 111/IUC clinical validation performance.Clinical review of serious incidents through SI panel.Escalation to ExecQuality & Safeguarding,QSAF, Quality and Scrutiny Committees.
CCG PrioritiesTo ensure high quality local services where possible.To improve the health of those most in need.
a.Action – EEAST Winter Plan is estimating 85 – 90k PFSH – requirement for average of 95k s – NHSE/I and Lead commissioner working with EEAST to assess how capacity can be increased, primarily through reducing abstraction rates, currently at 44% (vs EEAST Board target in Sep-21 of 35%).
b.Focus on sickness rates which peaked at 14% front line and 209% AOC c.Overtime/Private Ambulance Capacity targeted to peak demand shifts. d.Local demand management schemes in place, with focus on frailty pathways e.Handover delays managed /monitored weekly.
Incident Response Framework has been implemented across region, which will see Treatment Delay incidents shared in tactical/operational forums to identify measures to reduce treatment delays in urgent care. May 2022Further support plans to transfer calls from EEAST stack now in place with C3/4 calls have pathway across to IUC CAS for triage.EEAST taking through internal governance ability for those outside of organisation to have access to their stack to support Cat2 call volume.Awaiting EEAST evaluation and forward plan/actions in relation to 'Perfect day' held on 3rd March.HALO paper awaiting final sign off to include 24/7 into core contract for EEAST on recurrent basis
5 5 25 1 5 5 To be agreed
CCG011 01-Apr-22 CYP are unable to access MH therapy and treatment. As a result, YP are have been admitted into paediatric wards in acute hospitals across the ICS. This creates a risk to staff, patients and families on these wards.
1. Availability of Tier 4 Beds2. Blocking of Paediatric Beds3. Safety of CYP4. Safety of other Patients5. Safety of Staff6. Safety of Families / Visitors / Carers7. HWB of Staff8. Increased Complaints9. Adverse Publicity
SO2 LN 5 4 20 1.local CYP MH providers regular calls with provider collaborative to review capacity for admissions2. Introduction of risk matrix (et to be seen and confirmed)by CYP NHSE provider collaborative to review requests for admission3. CCG Escalation and flow management in acute hospitals 4. CCG financial support to provide care input for YP in acute settings where and seeking regular oversight to all admissions 5. Regular reporting and escalation through QSAF/ NEE QC/ CCG CYP MDT6. Regular system calls for CYP with involvement of all partners and CCG to manage clinical risk, share information and plan delivery of care
Involvement of the CCGs Governing Bodies. Regular reports to Clinical Executive & other statutory committees.JLT Assurance Board for CCG Closure. Chaired by EG
May 2022 Escalation pathway drafted and undergoing system scrutiny/sign off. CYP MH Ipswich and WSH posts - recruitment underway with NHSE monies and additional CCG investment.
5 4 20 1 4 4 01-Apr-23

Directorate Risk Register summary of top risks
Date: June 2022
Department Risk Description / consequences
Current controls / assurance RAG Actions with status Completion date
Responsible person
1. Corporate Services
Lack of access to NEE / Suffolk tenancy
NEE staff are reliant of Suffolk colleagues to assist
16 Actions taken by NHSE will prevent any work being progressed on this until after the transition work is completed
June 2022 Amanda Lyes
2. Corporate Services
EU Exit - Consequences arising from ending of the Transition Period.
Continued focus on strong financial & contract management. ICS engagement on coordinated management of issues arising. Engagement with NHSE full Incident Coordination Centre DHSC EU Exit Operational Readiness Guidance including Action Card for Commissioners Senior Responsible Officer identified and supported by Emergency Planning and Resilience Manager.
12 SNEE APC meetings discuss implications of EU Exit in relation to medicines.
June 2022 Amanda Lyes
3. Corporate Services
New grant agreement process presents a risk to the delivery of estates projects.
Scheme business case development / approvals accelerated to maximize available build times on site. Regular engagement and meetings established with practice, consultants and contractors to manage build program and for any options for acceleration once on site. Operational risks escalated to, CCG Directors and NHSE regional and national teams for assistance. Estates leads working closely with NHSE and practices to address questions / issues raised through the new grant agreement process
10 Work with practices and NHS England to have grant agreements signed and in place to allow projects to start on site as quickly as possible or seek agreement for alternative arrangement to allow works to commence.
June 2022 Closed
Amanda Lyes
Risk Description / consequences
Current controls / assurance RAG Actions with status Completion date
Responsible person
1. COO Ipswich & East and West
A practice in IES have encountered significant GP staffing issues which may impact on their ability to see patients in a timely manner
CCG is working with local practices and the current provider to develop a plan to deal with this issue.
12
Work on the way with the practice in respect of building project. Staffing issues have stabilised
Ongoing David Brown

Risk Description / consequences
Current controls / assurance RAG Actions with status Completion date
Responsible person
1. Performance Improvement
Suffolk CYP Community services There have been longstanding concerns around the waiting times for autism spectrum disorder assessment & diagnosis for CYP up to 11 yrs. The pandemic has exacerbated waiting times. >400 CYP are waiting over 12 months for an autism assessment vs NICE guidance which is assessment/diagnosis within 6 months
A progress summary paper was shared by the trust in April 2022 and several areas of concern have been identified. Concerns have been shared with the trust and a meeting has been scheduled for 27 April to discuss the concerns. Concerns were raised at the April Community contract meeting and on-going discussions with the trust will be supported by colleagues from clinical quality and transformation. Concerns will be summarised at the CYP MDT in April to understand any other mitigation options. There is currently limited assurance that WSFT has implemented the service restoration plan.
16
Waiting list restoration plan developed and CCG investment agreed in October 2021. Restoration plan implemented by WSFT. A progress summary paper was shared by the trust in April 2022 and several areas of concern have been identified. These concerns have been shared with the trust Families have been provided with information/signposted to support resources. Additional resources due to be available from summer 2021 following the completion of the NDD procurement. Service has contacted all families to support signposting.
No end date Nicola Brunning
2. Performance Improvement
Pandemic Disease Hazard: On both the Suffolk and Essex Community Risk Registers Pandemic Influenza is the highest noted. During an outbreak we could see significant staff shortages from the CCG and provider organisations, disruption to supply chains. Changes in both local and national priorities for NHS Care that will translate in to changes within teams to deliver them. Consequences include inability to provide services, temporary loss of staff (through sickness/ caring for relatives), permanent loss of staff. Inability to discharge from hospitals due to lack of care facilities (inclusive of domiciliary care, residential and nursing homes). Increase in deaths likely
UKHSA monitoring for potential outbreaks. Resilience Forum Pandemic Plans. Resilience Forum Mass Fatality and excess death plans. CCG Business Continuity Plan, CCG Emergency Response Plan, Provider business continuity plans. NHS EPRR Core Standards process.
15
Annual CCG Business Continuity exercise. Annual flu vaccination campaign.
01/04/2023 Chris Chapman
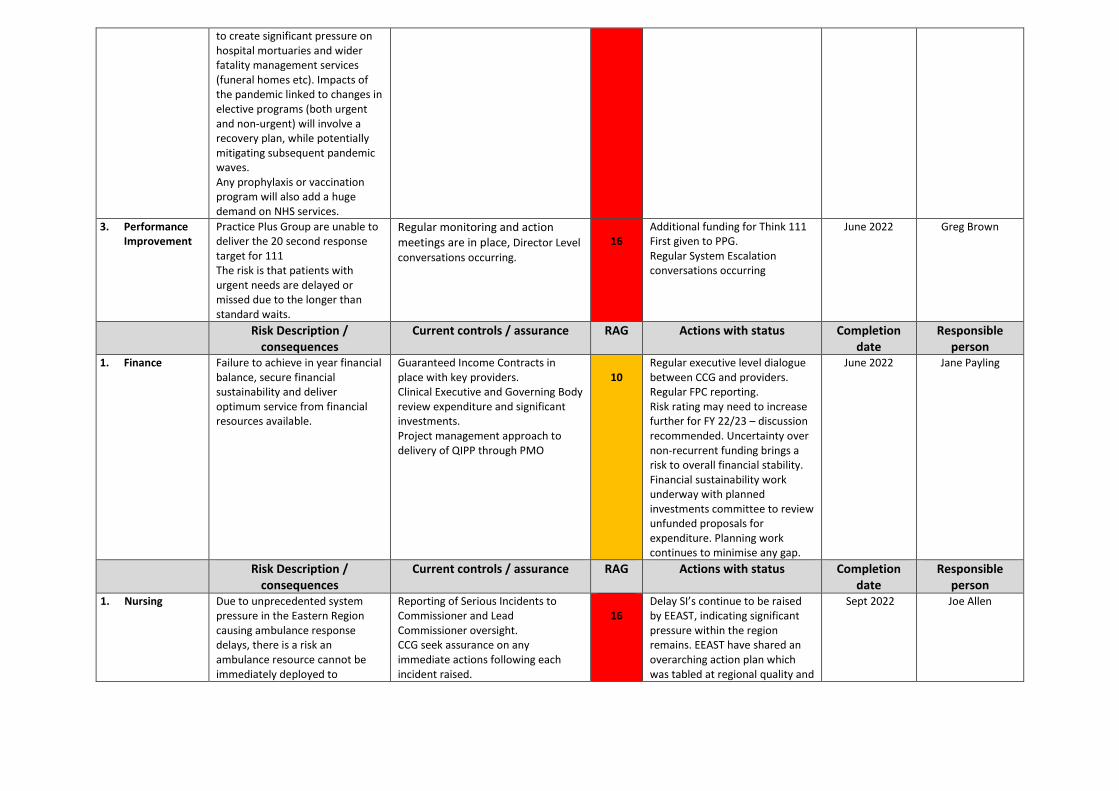
to create significant pressure on hospital mortuaries and wider fatality management services (funeral homes etc). Impacts of the pandemic linked to changes in elective programs (both urgent and non-urgent) will involve a recovery plan, while potentially mitigating subsequent pandemic waves. Any prophylaxis or vaccination program will also add a huge demand on NHS services.
3. Performance Improvement
Practice Plus Group are unable to deliver the 20 second response target for 111 The risk is that patients with urgent needs are delayed or missed due to the longer than standard waits.
Regular monitoring and action meetings are in place, Director Level conversations occurring.
16
Additional funding for Think 111 First given to PPG. Regular System Escalation conversations occurring
June 2022 Greg Brown
Risk Description / consequences
Current controls / assurance RAG Actions with status Completion date
Responsible person
1. Finance Failure to achieve in year financial balance, secure financial sustainability and deliver optimum service from financial resources available.
Guaranteed Income Contracts in place with key providers. Clinical Executive and Governing Body review expenditure and significant investments. Project management approach to delivery of QIPP through PMO
10
Regular executive level dialogue between CCG and providers. Regular FPC reporting. Risk rating may need to increase further for FY 22/23 – discussion recommended. Uncertainty over non-recurrent funding brings a risk to overall financial stability. Financial sustainability work underway with planned investments committee to review unfunded proposals for expenditure. Planning work continues to minimise any gap.
June 2022 Jane Payling
Risk Description / consequences
Current controls / assurance RAG Actions with status Completion date
Responsible person
1. Nursing Due to unprecedented system pressure in the Eastern Region causing ambulance response delays, there is a risk an ambulance resource cannot be immediately deployed to
Reporting of Serious Incidents to Commissioner and Lead Commissioner oversight. CCG seek assurance on any immediate actions following each incident raised.
16
Delay SI’s continue to be raised by EEAST, indicating significant pressure within the region remains. EEAST have shared an overarching action plan which was tabled at regional quality and
Sept 2022 Joe Allen

Category 2 calls, which require an average response time of 18 minutes.
Standing agenda item at regional QSM. EEAST are creating a single action plan to address findings from system delays SI’s. CCG co-ordinating system response to facilitate improved response times across the region.
safeguarding meeting in January 2022. A framework has been written to take system SI's for discussion and action at operational and tactical forums in each locality. This is in order to stimulate a collective system response in order to improve treatment times for patients accessing emergency care. The framework is currently being rolled out across the region.
2. Nursing Risk of reputational impact as the lead commissioner of NSFT services, which show organisational risks in relation to clinical safety of services, timeliness of access to commissioned clinical services and the quality of care planning and risk assessments. This also create a risk of lack of public confidence including stakeholders in the ability of NSFT to provide the service.
Quality assurance reviews of all 41 service lines within Suffolk NSFT. Actions from visits shared with NSFT, progress monitored through CQRM. CCG support with trust quality and safety review process. Monthly CQRM meetings focus on quality / contractual requirements / appropriate actions / trajectories to meet required quality and contractual requirements. Joint support process from alliance system, with the allocation of SRO and project lead roles to support NSFT with progress for operational delivery to enable MCP process in 2022.
15
Safe and Wellbeing reviews for LD inpatients completed. Minor learning points very positive feedback from patients and families. Currently waiting for the CQC inspection report to be published.
Sept 2022 Wendy Scott
Risk Description / consequences
Current controls / assurance RAG Actions with status Completion date
Responsible person
1. Transformation Failure to achieve national Dementia diagnosis target for WSCCG of 67% in line with the Prime Minister's Challenge on Dementia 2020.
Dementia action plans in place for each locality agreed at Clinical Executive. Full Programme of work underway as agreed with NHSE. Workstreams as follows: 1. Leadership and Governance, including clinical leadership 2. Improving Memory Assessment Services 3. Case finding in acute settings 4. Case finding in care homes 5. Engaging primary care in diagnosis.
9
Transformation programme active with additional NHSE/I funding received as part of Covid recovery which includes supporting primary care, memory services and support services in addressing capacity, pathway flow and navigation of the system.
30 June 2022
Rob Chandler
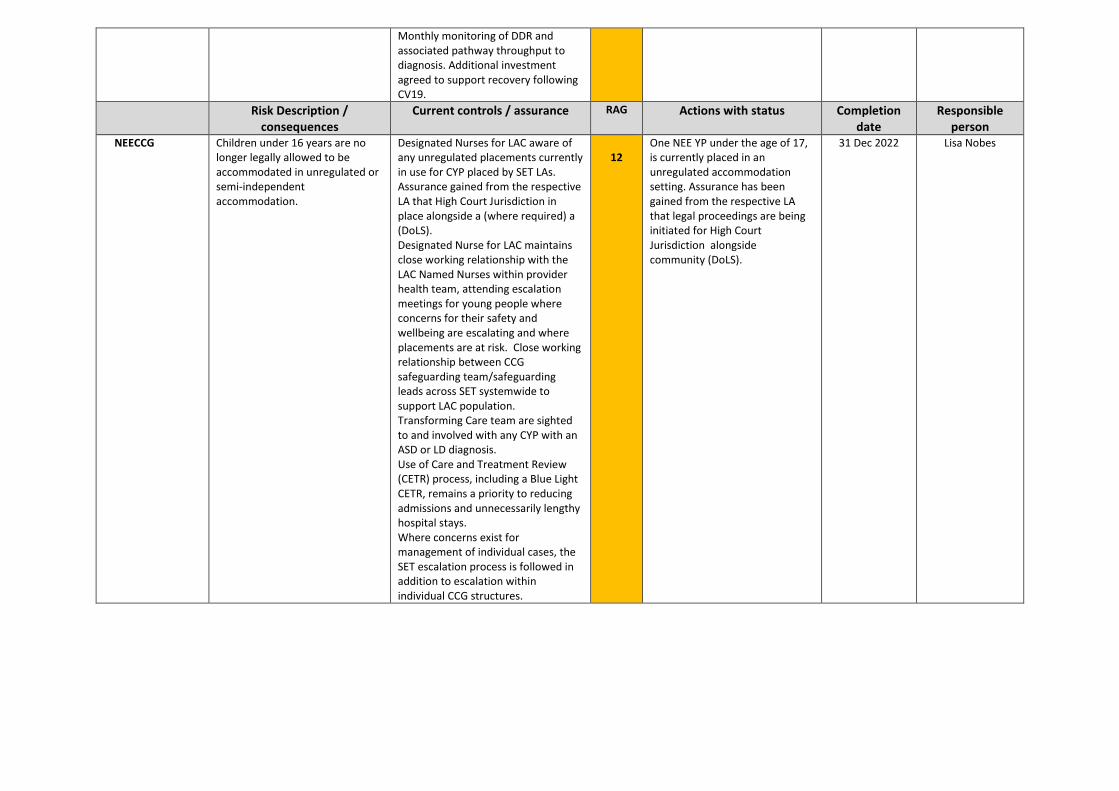
Monthly monitoring of DDR and associated pathway throughput to diagnosis. Additional investment agreed to support recovery following CV19.
Risk Description / consequences
Current controls / assurance RAG Actions with status Completion date
Responsible person
NEECCG Children under 16 years are no longer legally allowed to be accommodated in unregulated or semi-independent accommodation.
Designated Nurses for LAC aware of any unregulated placements currently in use for CYP placed by SET LAs. Assurance gained from the respective LA that High Court Jurisdiction in place alongside a (where required) a (DoLS). Designated Nurse for LAC maintains close working relationship with the LAC Named Nurses within provider health team, attending escalation meetings for young people where concerns for their safety and wellbeing are escalating and where placements are at risk. Close working relationship between CCG safeguarding team/safeguarding leads across SET systemwide to support LAC population. Transforming Care team are sighted to and involved with any CYP with an ASD or LD diagnosis. Use of Care and Treatment Review (CETR) process, including a Blue Light CETR, remains a priority to reducing admissions and unnecessarily lengthy hospital stays. Where concerns exist for management of individual cases, the SET escalation process is followed in addition to escalation within individual CCG structures.
12
One NEE YP under the age of 17, is currently placed in an unregulated accommodation setting. Assurance has been gained from the respective LA that legal proceedings are being initiated for High Court Jurisdiction alongside community (DoLS).
31 Dec 2022 Lisa Nobes
Page 1 of 2
GOVERNING BODY Agenda Item No. 24
Reference No. NEECCG 22-48
Date. 7 June 2022 Title
Health and Wellbeing Update
Lead Director
Amanda Lyes - Interim Director of Workforce, Suffolk and North East Essex Integrated Care System & Director of Corporate Services and System Infrastructure
Author(s)
Nick Oldfield – HR Business Partner
Purpose
To update Health and Wellbeing actions across SNEE CCGs’
Applicable CCG Strategic Objectives: 1. To achieve our vision through an inclusive, holistic approach to patient and service user centred commissioning, embedding personalisation of care through integrated health and social care services.
2. To transform care and drive continuous improvement in quality and safety. Achieve the best possible outcomes for our service users through high quality care.
3. To use commissioning resources effectively and responsibly. To develop our organisation, teams and individual staff to be trusted, competent, well trained, talented, enthusiastic and dedicated.
x
4 To tackle the biggest health challenges in north east Essex including reducing health inequalities.
Recommendation: The NEE Governing Body is asked to note and comment on current Health and Wellbeing interventions across SNEE CCGs’

Page 2 of 2
1. Summary 1.1 Please find a summary update of work currently underway to support staff Health and
Wellbeing across SNEE CCGs’ 2. Key Points to Note
Health and Wellbeing Ambassadors: • We now have 24 Health and Wellbeing Ambassadors across the 3 CCGs’ • The Ambassadors are currently being encouraged to undertake training in the role –
free e-learning course supplied by NHS England. • The Ambassadors have been encouraged to think of ways to promote H&W in their
teams. Some have introduced a monthly H&W section in team meetings and have been actively promoting national ‘walking week’ and ‘stress awareness week’.
Mental Health First Aiders: • The CCGs’ now have 13 trained MHFA’s Recent/planned initiatives: • Launched Disability and LGBTQ+ network groups – February/March 22. The
LGBTQ+ group, in particular, has grown and now has an active cohort of staff involved.
• Looking to start and are promoting a Menopause and Women’s network group. • Working alongside the sustainability lead and the RSPB to promote spending time in
nature sessions for staff – this has started to gain traction and the H&W ambassadors are soon to be updated on how we can progress and promote this in teams.
Domestic Abuse Awareness: • Working with local charity, Alpha Vesta, to deliver 2 Domestic Abuse Awareness
sessions in June and July 22. • Alpha Vesta are also supporting us in the writing a Domestic Abuse Awareness
Policy. ICS H&W Team: • Forging closer links with the ICS H&W Team. • Looking to introduce to staff the free H&W advice platform – My Health My Way -
which has been promoted by the ICS H&W Team. • Also supporting with the creation of the ICS H&W Strategy.
3. Recommendation 3.1 The NEE Governing Body is asked to note and comment on current Health and Wellbeing
interventions across SNEE CCGs’.
Copyright © 2022 FDOKUMEN