Mechanical Properties of Dilated Human Ascending Aorta
12
Mechanical Properties of Dilated Human Ascending Aorta RUTH J. OKAMOTO, 1,2 JESSICA E. WAGENSEIL, 2 WILLIAM R. DELONG, 1 SARA J. PETERSON, 2 NICHOLAS T. KOUCHOUKOS, 3 and THORALF M. SUNDT III 4 1 Department of Mechanical Engineering, and 2 Department of Biomedical Engineering, 3 Missouri Baptist Medical Center, St. Louis, MO, and 4 Division of Cardiothoracic Surgery, Washington University, St. Louis, MO 63130 (Received 16 July 2001; accepted 4 April 2002) Abstract—Dilation of the ascending aorta, associated with Marfan Syndrome, bicuspid aortic valve, or advanced age, may lead to aortic dissection and rupture. Mathematical models can be used to assess the relative importance of increased wall stresses and decreased strength in these mechanical failures. To obtain needed inputs for such models, mechanical properties of dilated human ascending aorta were measured in vitro. Speci- mens for opening angle, biaxial elastic, and uniaxial circumfer- ential strength tests were cut from excised tissue obtained from 54 patients ~age 18–81 years! undergoing elective aortic graft replacement surgery. Opening angle was significantly greater in patients older than 50 years ~262°676°, n 521! compared to younger patients ~202°670°, n 513!. All biaxial elastic speci- mens ~n 540! exhibited nonlinear stress-strain behavior. Rapid increases in circumferential and axial stresses occurred at lower strains in the older patient group than in the younger. Mean strength was significantly lower in older patients ~1.3560.37 MPa, n 514! than younger ~2.0460.46 MPa, n 511, age ,50 years!. These changes in mechanical properties suggest that age may influence the risk of aortic dissection or rupture of dilated ascending aorta. © 2002 Biomedical Engineering Society. @DOI: 10.1114/1.1484220# Keywords—Vascular mechanics, Elasticity, Strength, Aortic disease. INTRODUCTION Dilation of the ascending aorta, in particular of the aortic root, increases the likelihood of aortic dissection and rupture. The term aneurysm is commonly used when the aortic transverse diameter exceeds twice the normal diameter for age and height of the patient. 33 Ascending aortic aneurysms occur in patients with congenital or inherited conditions such as Marfan Syndrome 15 and bi- cuspid aortic valve ~BAV! 9 and in some elderly patients with tricuspid aortic valve ~TAV!, usually with chronic hypertension. Graft replacement of the ascending aorta or the aortic root is recommended when the maximum di- ameter of the aorta exceeds 5 cm. 33 Robiscek and Thubrikar 29 have proposed that the three primary biological mechanisms in aortic dissection are decreased strength of the inner layer of the aortic wall, increased blood pressure, and increased average wall stress due to increased aortic diameter and de- creased wall thickness. They suggest that the intima tears because circumferential stress is highest at the inner wall. However, their analysis assumes the aorta is cylin- drical and isotropic and does not contain circumferential residual stress, assumptions which are not consistent with experimental data from animal blood vessels. 13 Thus, while the three proposed mechanisms seem reasonable, more detailed mathematical models are needed to assess their relative importance in different classes of patients. Such modeling, in turn, requires information on the ge- ometry and mechanical properties of the human ascend- ing aorta, including its strength, elastic properties, and residual stresses. Data on the mechanical properties of the human as- cending aorta are limited. The incremental elastic moduli and distensibility of normal and dilated ~Marfan! ascend- ing aorta have been measured in vivo 11,15 but these data can only be used to predict the mechanical behavior within the measured physiologic range. Furthermore, they do not provide any information on the strength of the tissue or on the state of residual stress. The opening angle of nondilated human ascending aorta obtained postmortem have been measured by Saini et al., 31 and the geometry and elastic properties of thoracic aorta by Learoyd and Taylor. 18 The strength of the descending, but not ascending, thoracic aorta has been measured by investigators in both the normal 21 and dilated ~Marfan! 24 aorta. The objective of the present study was to measure elastic properties, strength, and residual stress of dilated ascending aorta in Marfan, BAV, and TAV patients in order to provide inputs to mathematical models of aortic dilation, dissection, and rupture. Address correspondence to Ruth J. Okamoto, DSc, Washington University, Campus Box 1185, One Brookings Drive, St. Louis, MO 63130-4899. Electronic mail: [email protected] Annals of Biomedical Engineering, Vol. 30, pp. 624–635, 2002 0090-6964/2002/30~5!/624/12/$15.00 Printed in the USA. All rights reserved. Copyright © 2002 Biomedical Engineering Society 624
Transcript of Mechanical Properties of Dilated Human Ascending Aorta

Annals of Biomedical Engineering,Vol. 30, pp. 624–635, 2002 0090-6964/2002/30~5!/624/12/$15.00Printed in the USA. All rights reserved. Copyright © 2002 Biomedical Engineering Society
Mechanical Properties of Dilated Human Ascending Aorta
RUTH J. OKAMOTO,1,2 JESSICA E. WAGENSEIL,2 WILLIAM R. DELONG,1 SARA J. PETERSON,2
NICHOLAS T. KOUCHOUKOS,3 and THORALF M. SUNDT III 4
1Department of Mechanical Engineering, and2Department of Biomedical Engineering,3Missouri Baptist Medical Center, St. Louis,MO, and4Division of Cardiothoracic Surgery, Washington University, St. Louis, MO 63130
(Received 16 July 2001; accepted 4 April 2002)
ithay
canwas.s o
er-romtr in
idwean
t agedy.
ic
eonhenma
or
s
a odi-
eionrticragede-arsnerlin-tialwith
able,sessts.e-nd-nd
as-uli
iorre,ofningned
by,
d by
ureted
intic
gtonO
Abstract—Dilation of the ascending aorta, associated wMarfan Syndrome, bicuspid aortic valve, or advanced age, mlead to aortic dissection and rupture. Mathematical modelsbe used to assess the relative importance of increasedstresses and decreased strength in these mechanical failureobtain needed inputs for such models, mechanical propertiedilated human ascending aorta were measuredin vitro. Speci-mens for opening angle, biaxial elastic, and uniaxial circumfential strength tests were cut from excised tissue obtained f54 patients~age 18–81 years! undergoing elective aortic grafreplacement surgery. Opening angle was significantly greatepatients older than 50 years~262°676°, n521! compared toyounger patients~202°670°, n513!. All biaxial elastic speci-mens~n540! exhibited nonlinear stress-strain behavior. Rapincreases in circumferential and axial stresses occurred at lostrains in the older patient group than in the younger. Mestrength was significantly lower in older patients~1.3560.37MPa, n514! than younger~2.0460.46 MPa,n511, age,50years!. These changes in mechanical properties suggest thamay influence the risk of aortic dissection or rupture of dilatascending aorta. ©2002 Biomedical Engineering Societ@DOI: 10.1114/1.1484220#
Keywords—Vascular mechanics, Elasticity, Strength, Aortdisease.
INTRODUCTION
Dilation of the ascending aorta, in particular of thaortic root, increases the likelihood of aortic dissectiand rupture. The term aneurysm is commonly used wthe aortic transverse diameter exceeds twice the nordiameter for age and height of the patient.33 Ascendingaortic aneurysms occur in patients with congenitalinherited conditions such as Marfan Syndrome15 and bi-cuspid aortic valve~BAV !9 and in some elderly patientwith tricuspid aortic valve~TAV !, usually with chronichypertension. Graft replacement of the ascending aortthe aortic root is recommended when the maximumameter of the aorta exceeds 5 cm.33
Address correspondence to Ruth J. Okamoto, DSc, WashinUniversity, Campus Box 1185, One Brookings Drive, St. Louis, M63130-4899. Electronic mail: [email protected]
624
llTof
r
e
l
r
Robiscek and Thubrikar29 have proposed that ththree primary biological mechanisms in aortic dissectare decreased strength of the inner layer of the aowall, increased blood pressure, and increased avewall stress due to increased aortic diameter andcreased wall thickness. They suggest that the intima tebecause circumferential stress is highest at the inwall. However, their analysis assumes the aorta is cydrical and isotropic and does not contain circumferenresidual stress, assumptions which are not consistentexperimental data from animal blood vessels.13 Thus,while the three proposed mechanisms seem reasonmore detailed mathematical models are needed to astheir relative importance in different classes of patienSuch modeling, in turn, requires information on the gometry and mechanical properties of the human asceing aorta, including its strength, elastic properties, aresidual stresses.
Data on the mechanical properties of the humancending aorta are limited. The incremental elastic modand distensibility of normal and dilated~Marfan! ascend-ing aorta have been measuredin vivo11,15 but these datacan only be used to predict the mechanical behavwithin the measured physiologic range. Furthermothey do not provide any information on the strengththe tissue or on the state of residual stress. The opeangle of nondilated human ascending aorta obtaipostmortem have been measured by Sainiet al.,31 andthe geometry and elastic properties of thoracic aortaLearoyd and Taylor.18 The strength of the descendingbut not ascending, thoracic aorta has been measureinvestigators in both the normal21 and dilated~Marfan!24
aorta.The objective of the present study was to meas
elastic properties, strength, and residual stress of dilaascending aorta in Marfan, BAV, and TAV patientsorder to provide inputs to mathematical models of aordilation, dissection, and rupture.

64raflveor
onordve,e-
–81Vto
ely
annts
ereer-enialerns
eeftertheandro-s
l-a
heeessu
fored
ap-ortaowtheumtom-ereue.
ting
sel
thecut
deed
ended,–2,
heen 5ere
625Mechanical Properties of Dilated Human Ascending Aorta
METHODS
Patients
Dilated ascending aortic tissue was removed frompatients undergoing composite root replacement or greplacement of the ascending aorta with or without vareplacement at Washington University Medical CenterMissouri Baptist Medical Center. Based on informatifrom preoperative exams, patients were classified accing the presence of a tricuspid or bicuspid aortic valor a prior diagnosis of Marfan Syndrome. Usable mchanical test data was obtained from 54 patients, 19years old~Table 1!. Because the age range of the BAgroup was so large, we subdivided the BAV patients inyounger~,50 years! and older~>50 years! subgroups.The mean ages of the BAV subgroups more closmatched the ages of the Marfan and TAV groups~Table1!. The study protocol was approved by the HumStudies Committees of both institutions and the patiegave informed consent.
Mechanical Testing
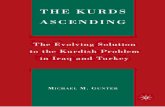
After harvesting, the aortic tissue specimens wstored in refrigerated saline at 4 °C. We intended to pform three types of measurements on each specimopening angle, planar biaxial stretching, and uniaxstrength. Because the tissue was excised during surgthe size, condition, and configuration of the specimevaried. It was often not possible to perform all thrmechanical tests on tissue from a single patient. Areceiving the tissue, we obtained digital images ofintact specimen, measured its overall dimensions,recorded its condition, including the presence of athesclerotic lesions. Generally, the tissue was received ashort tube~Fig. 1! cut from above the sinuses of Vasalva. In a few cases the tube was not complete andopening angle ring could not be cut. More frequently, taxial dimension of the tube was too short to cut all thrspecimens. In the latter case, a separate piece of ti
TABLE 1. Patient characteristics. Patients were dividedaccording to preoperative diagnosis of Marfan Syndrome,
BAV, or TAV.
Marfan(n56)
BAV
TAV(n515)
,50 years(n515)
>50 years(n518)
Age (years) 39 6 13 39 6 10 63 6 8 67 6 11Male Gender 5 11 15 7Aortic diam(cm)a
5.4 6 0.8 5.4 6 0.7 5.0 6 0.4 5.6 6 0.6
aMaximum preoperative diam reported by surgeon, computed to-mography, magnetic resonance imaging, or echocardiographicexam. Data were not available for four patients (1 BAV ,50years, 2 BAV >50 years, 1 TAV).
t
-
:
y,
a
n
e
from the noncoronary sinus that was large enoughbiaxial testing was sometimes provided. We decidwhich tests to perform and then cut the tissue intopropriate sections. The proximal human ascending ais enclosed in the pericardial sac up to a level just belthe innominate artery. The intrapericardial aorta andpulmonary trunk are sheathed with visceral pericardi~epicardium!.30 This epicardial layer adhered looselythe adventitia over most of the intact specimen’s circuference and was not removed before testing. Tests wnormally conducted 1–2 days after harvesting the tissResults from tests more than 5 days after harveswere excluded.
Circumferential Residual Stress
Circumferential residual stress in the blood veswall, noted by Fung and others in the middle 1980’s,2,35
has been characterized by an ‘‘opening angle,’’ i.e.,angle that a ring shaped specimen springs open whenradially.7 To measure opening angle, a 3–5 mm wiring was sliced from one end of the aortic tissue, placin room-temperature saline19 and allowed to equilibratefor at least 15 min. After obtaining a digital image of thclosed ring, a single radial cut was made. Han aFung10 found the opening angle of pig aorta reach95% of its final value within 10 min. In five early testswe measured opening angles from images obtained 15–7, and 10–15 min after making the radial cut. Tmeasured opening angle changed less than 1% betweand 7 min and 10–15 min. Thus, all opening angles w
FIGURE 1. The intact aortic specimen for a 47 year old bi-cuspid aortic valve patient. „A… whole specimen with adven-titial side out „B… intimal side up after removing openingangle ring and cutting specimen open to lay flat. Scale barÄ 1 cm.

minof
u-intsdid
inx-utthele oed
ofedir-ereo teci
nd
eshewith
heus
tod inM
rs
ing
v-ci-onsnu-
ed-rednedch
i-a
ofgere
ff-s,
ali-are
yof
i-
as
tch
e-
ex-
d-re
i-as00
herialrgy
,rial
626 OKAMOTO et al.
measured on images of the open ring obtained 5–7after making the radial cut. The inner circumferencethe wall was digitized using Scion Image 4.0~ScionCorp., Frederick MD! and the opening angle was calclated from the angle created between the two endpoand the midpoint of the circumference. Some ringsnot remain on edge after the radial cut, and any ringswhich more than half of the length fell over were ecluded from the analysis. When a portion of the ring, bless than half, had fallen over, the opening angle ofupright segment was measured and the opening angthe full ring was calculated using the method describin the Appendix.
Elastic Properties
We chose planar biaxial testing20 to characterize theelastic properties of the tissue. Unlike uniaxial testingcircumferential rings or strips, biaxial tests can be usto determine if tissue properties differ between the ccumferential and axial directions. Planar specimens wused because pressure-diameter tests are unsuited tdilated ascending aorta where the diameter of the spmen exceeds its axial length.
The excised aortic tissue was cut along its length aapproximately square specimens~2.0–2.5 cm per side!were cut from the excised aortic tissue with edgaligned to the circumferential and axial directions of taorta. The thickness of the specimen was measuredcalipers ~0.01 mm/div, Mitutoyu! while holding it be-tween glass slides. The specimen was attached to txand y carriages of a biaxial tester using continuolengths of 3–0~0.2 mm diam! silk suture placed throughat least four and usually five attachment points closeeach edge of the specimen. The specimens floateroom-temperature Krebs–Ringer solution with 0.1 mpapaverine and bubbled with 95% O2, 5% CO2 to main-tain a pH of 7.2–7.4 during testing. Four small markeforming a quadrilateral~3–4 mm per side! were glued tothe intima in the central region of the specimen uscynoacrylate glue~Superglue, Duro!.
Initial, unloaded dimensions were obtained by remoing all tension on the sutures while allowing the spemen to float in the bath. The marker square dimensiwere obtained from a video tracking system that contiously monitored thex andy position of each marker. Thetester’s motorized carriages were controlled using feback from the tracking system to produce the desistretching protocols. The specimen was preconditiofor ten cycles at 10% equibiaxial stretch. Then easpecimen was subject to strip biaxial~one directionstretched while the other was held constant! in the cir-cumferential and axial direction followed by an equibaxial stretching protocol. All protocols consisted oftriangular displacement waveform~20 s period! with
f
he-
stretch varying between a base line~1.02! and the pre-scribed stretch ratio resulting in applied strain rates2%–4% per second. Following ten preconditionincycles of the prescribed stretches for each protocol, thxand y marker positions and corresponding forces weacquired at 30 Hz for three loading cycles. Two obiaxial protocols~simultaneous stretch in both directionwith one magnitude larger than the other! were also run;the resulting data were used for material parameter vdation. The unloaded dimensions of the marker squwere periodically rechecked between protocols.
Green’s~finite! strain in the central region defined bthe markers was calculated following the methodHumphreyet al.14 First, the in-plane deformation gradent tensorF was obtained from thex and y coordinatesof the markers at each sample point. The tissue wassumed to be incompressible, so that the radial~out-of-plane! stretch ratio was obtained from det~F!51. Thismethod accounts for in-plane shearing. Green’s strainEis then obtained fromF using
E5 12 ~FTF21!. ~1!
The Cauchy stresses were calculated from the streratioslx andly and the applied forcesFx andFy usingthe undeformed specimen thicknessT and the lengthsover which the forces were applied:
sX5lX
FX
TLY; sY5lY
FY
TLX. ~2!
The lengthsLx and Ly are the measured distances btween the sutures~i.e. the ‘‘suture square’’! in the un-loaded specimen as described by Nielsenet al.22
Stress-strain data for each patient were fit to anponential constitutive relation. First, following May–Newman and Yin,20 stress-strain data from a single loaing cycle of the equibiaxial stretching protocol wesmoothed using a running median of span 15 to elimnate outliers. Then every third smoothed datapoint wselected, resulting in a dataset of approximately 1stress-strain data points. Data from thex and y stripbiaxial protocols was reduced in a similar manner. Tthree datasets were combined and used to fit mateparameters in an exponential, anisotropic, strain enedensity function proposed for blood vessels3,36 assumingincompressibility
r0W5c
2exp~b1ECC
2 1b2EZZ2 12b3ECCEZZ!, ~3!
where W is the strain energy per unit volume$c,b1 ,b2 ,b3% are the parameters describing the mate

leial,
c-
byedrewn
be-theredce
luerifyialcal
ri-cmhexi-
hat
sinoxi-as
wasthearethethehegerst-
c-en
ataneth,
,
th,
tsageto
ses
ts.ngs
dred
re-d
inegleasmher-
r-ents
aterofm-
t sohein-
s.
627Mechanical Properties of Dilated Human Ascending Aorta
behavior andECC and EZZ are circumferential and axiastrains. For this form of strain energy function, thCauchy stress components in the circumferential, axand radial directions are calculated from
sCC2sRR5lC2 ]W
]ECC, sZZ2sRR5lZ
2 ]W
]EZZ. ~4!
For planar biaxial tests, the radial~i.e., out-of-plane!stress,sRR, is zero. The circumferential and axial diretions are the same as the experimentalx andy directions,respectively. When the strain energy function givenEq. ~3! is used to model an artery as a thick-wallcylinder, the equation of radial equilibrium and pressuboundary conditions are used to solve for the unknoradial stress distribution in Eq.~4!.12
A Levenberg–Marquardt algorithm26 was used tominimize the sum of the squares of the differencestween the predicted and experimental stresses ofcombined dataset using the experimentally measustrains as independent variables. The optimization produre was repeated using a wide range of starting vafor the parameters. This procedure enabled us to vethat the fitted material parameters for each biaxspecimen tested resulted in a global, rather than lominimum.
Strength Testing
We measured the strength of a circumferentially oented specimen approximately 3.5 cm in length and 1wide cut from the aortic tissue. The middle region of tspecimen was narrowed and had a width of appromately 4 mm. The necked shape was similar to tdescribed by Mohan and Melvin21 but our overall speci-men size was smaller. The thickness was measured uthe same method as the biaxial test specimen. Apprmately 4–7 mm of each end of the specimen wclamped into sandpaper-lined grips. A marker squareglued to the center of the specimen, and as withbiaxial specimen, the dimensions of this marker squwere used to determine the amount of stretch incircumferential direction. The grips were attached tox axis of the testing machine used for biaxial testing. Tspecimen floated in a bath of oxygenated Krebs–Rinsolution with the same composition used for biaxial teing. After ten preconditioning cycles~10 s period, trian-gular force waveform of 0.10–0.49 N!, a force ramp of0.59 N/s was applied for up to 30 s until failure ocurred. A test was considered successful if the specimfailed in the narrower region of the specimen. Test dwere converted to stress-strain data in a similar manto the biaxial test protocols, and the ultimate strengdefined as the Cauchy stress at failure,s f , was calcu-lated from
-s
,
g
r
s f5Fl f
TW, ~5!
whereF is the maximum force attained prior to failurel f is the circumferential stretch ratio at failure, andTand W are the undeformed thickness and necked widrespectively.
Statistical Methods
All statistics are presented as mean values61 stan-dard deviation. Unpaired, two-tailed Student’s t-teswere used to compare means between the twogroups. Single-factor analysis of variance was usedcompare mean values between patient groups.P values,0.05 were considered significant. Statistical analywere carried out using Statview 5.0~SAS Institute Inc.,Cary, NC!.
RESULTS
Circumferential Residual Stress
We cut rings from tissue obtained from 55 patienWe were able to measure an opening angle from 34 ri~4 Marfan, 8 younger BAV, 10 older BAV, 12 TAV!.Figures 2~A!–2~D! illustrates the range of measureopening angles. Opening angles could not be measuin 21 rings. For 15 patients~2 Marfan, 8 younger BAV,3 older BAV, 2 TAV! more than half of the ring fell over@Fig. 2~E!#. In rings from three patients~2 TAV, 1 BAV!the local curvature of the ring changed abruptly orversed@Fig. 2~F!#, and in three other rings we observeapparent damage during cutting or insufficient salcovering the ring. The mean measured opening anwas 239°679° and the mean age of the 34 patients w55617 years. We determined the opening angle fromeasured partial segments for 9 of the 34 rings. Tratio of the upright circumference to the total circumfeence was 0.7360.06. There was not a significant diffeence in the opening angles measured from segm~219°662°, n59! and complete rings~246°684°, n525!.
For 25 rings, the measured opening angle was grethan 180° so that the adventitia was on the inner sidethe curved open ring. The ends of the open ring froone TAV patient~age 74 years! crossed so that the opening angle was 367°. Closed rings from eight patients~2Marfan, 1 older BAV, 5 TAV, mean age 63618 years!,spontaneously inverted before we made the radial cuthat the adventitia was on the inner side of the ring. Tmean opening angle of the rings that spontaneouslyverted ~316°642°! was significantly~p,0.001! greaterthan those that did not invert~215°672°!, suggesting thisphenomenon is associated with larger opening angle

e
0
Figof
gerups
l
heastanallovelly
e ofthe
ss-ger-the
forn int.ial
eon-
628 OKAMOTO et al.
Opening angle,a, was positively correlated with ag@Fig. 3~A!#. Linear regression yieldeda591.9812.68* Age~years!, R250.33. The meana forpatients younger than 50 years~202°670°, n513!, wassignificantly ~p,0.05! less than the mean for patients 5years and older~262°676°, n521!. Mean openingangles for the different disease groups are shown in3~B!. Somewhat surprisingly, the mean opening anglethe Marfan group was 52° larger than that of the younBAV group, but the differences between disease gro
FIGURE 2. Open rings of ascending aorta. The dark lineindicates the digitized intimal edge of the upright portion ofthe ring. Scale bars Ä1 cm. „A…–„D… Typical measured open-ing angles „a…. „A… aË180°, 34 year old TAV patient, „B… aÌ180°, 45 year old BAV patient, „C… aÌ360°, 74 year old TAVpatient, „D… a f measured from sector of ring „aÄ157°…, 25year old Marfan patient. „E…–„F… Rings where opening anglecould not be measured. „E… Most of ring fell over, 47 year oldBAV patient. „F… Nonuniform curvature, 35 year old BAV pa-tient.
.
were not significant~p50.23!, possibly due to the smalsize of the Marfan group~n54!.
Elastic Properties
The biaxial specimens were cut from regions of taortic specimen that had an axial dimension of at le2.0 cm. Biaxial test specimens for three of six Marfpatients came from the noncoronary sinus, whileother specimens came from the ascending aorta abthe sinuses of Valsalva. The biaxial specimen typicaencompassed about 1/4–1/6 of the total circumferencthe intact aortic specimen, and the mean thickness ofunloaded biaxial specimens was 2.660.5 mm.
Tissue from all patients exhibited a nonlinear strestrain response as shown for a representative younand older patient in Fig. 4. After an initially linear region, the stress increased rapidly. The strain at whichstress became nonlinear decreased with age.
Material parameters were optimized separatelyeach patient. The data used for optimization are showFigs. 5~A! and 5~B! for the representative older patienThe data and the predicted stresses for two off-biaxprotocols~not included in the optimization! are shown inFigs. 5~C! and 5~D!. The predicted stresses from thexponential fit are able to accurately reproduce the n
FIGURE 3. „A… Opening angle, a, as a function of age.Dashed line shows linear fit to data. Markers show patientgroups listed in Table 1. Diamonds: Marfan. Filled triangles:younger BAV. Open triangles: older BAV. Circles: TAV. „B…
Mean opening angle for each patient group „values listed incolumn …; error bars show ¿1 SD.

forin
isr ausm-
tedomhes
ior.on-
otimu-ss
heeci-thataas
m
aseisthehential
629Mechanical Properties of Dilated Human Ascending Aorta
linear behavior of the data. Fitted parameter valuesthe representative patients shown in Fig. 4 are givenTable 2.
For an exponential form of constitutive relation, itnot possible to use mean values of the coefficients fogroup of patients to simulate the mean behavior becaof interactions between coefficients. Therefore, to exa
FIGURE 4. Circumferential and axial Cauchy stress vs. strainfrom equibiaxial stretching protocols for an older and ayounger patient. Filled circles: 65 year old tricuspid aorticvalve patient. Filled triangles: 49 year old bicuspid aorticvalve patient.
e
ine the effect of age and type of aortic disease, prediccircumferential and axial stresses were calculated frthe material parameters at simulated equibiaxial stretc~leq! of 1.25 and 1.35~Fig. 6!, the range at which wegenerally observed the onset of the nonlinear behavIn specimens from some older patients however, theset of nonlinear behavior occurred belowleq51.25 andthe simulated values of stress were as high as 106 kPa atleq51.25 orleq51.35. In those cases, the tissue had nbeen tested at equibiaxial stretches as high as the slated leq. We further reasoned that the simulated strevalues could not actually be reached physically in ttissue because failure was observed in our older spmens at stresses of 103 kPa, as explained in the strengtesting results later. We thus excluded specimen dwhere either predicted circumferential or axial stress wgreater than 103 kPa. This occurred in specimens frothree patients atleq51.25 ~1 older BAV, 2 TAV! andfrom six patients~2 older BAV, 4 TAV! at leq51.35.
As expected from the test data, there was an increin both circumferential and axial stress with age. Thincrease did not appear to be linear, but insteadstresses remained fairly constant until 50 years and tbegan to increase rapidly. We found that an exponen
TABLE 2. Fitted material parameters in the exponentialconstitutive relation †Eq. „3…‡ for the representative younger
and older patients shown in Fig. 4.
Patientgroup
Age(years)
c(KPa) b1 b2 b3 R2
BAV 49 29.2 2.31 1.85 0.55 0.983TAV 65 19.6 6.13 5.84 2.01 0.992
FIGURE 5. Stress-strain data used for material parameter optimization †„A… and „B…‡ and resulting fits to off-biaxial protocols †„C…
and „D…‡ for the 65 year old patient shown in Fig. 4.

630 OKAMOTO et al.
FIGURE 6. Circumferential and axial Cauchy stress at simulated equibiaxial stretching protocols plotted vs. age on a log scale.Dashed lines show exponential fit to data. Markers show different patient groups listed in Table 1. Diamonds: Marfan. Filledtriangles: younger BAV. Open triangles: older BAV. Circles: TAV.
etchbe-noteennd
rom
hel-ex
pslurethe
upred
tesla-
tion
asialfrom
this
ticend-
regression of stress vs. age fit the data at both strratios reasonably well. When data were comparedtween the patient groups shown in Table 1, we didfind significant differences in the stress values betwpatient groups of similar age, e.g., younger BAV aMarfan or older BAV and TAV.
Strength Testing
We performed successful strength tests on tissue f25 patients~3 Marfan, 7 younger BAV, 8 older BAV, 7TAV !. The response to the ramp force input in tstrength test protocol was initially rapid stretching folowed by a period where the tissue became almost intensible. Tissue strength decreased with age@Fig. 7~A!#.The extensibility~stretch ratio at failure! also decreasedwith age, consistent with biaxial test results@Fig. 7~B!#.A linear fit of failure stress,s f , as a function of ageyielded s f ~MPa!52.87520.023* Age ~years!, R2
50.42. When the patients were divided into two groubased on age, circumferential Cauchy stress at faiwas significantly greater in the younger group thanolder group~single-tailed, unpaired t-test,p,0.005! andextensibility was significantly reduced in the older groas shown in the bar graphs of Fig. 7. We had measuopening angle in 19 of the 25 successful strengthpatients. Although our data indicated a negative corretion between strength and opening angle, this correlawas not significant~p50.20!. Biaxial test results wereavailable for 11 of the 25 patients. Failure stress wnegatively correlated with predicted circumferentstress at stretch ratios of 1.25 and 1.35 as expected
-
t
the dependence of both these quantities on age, butcorrelation did not reach significance~p50.06!.
DISCUSSION
Our results show that residual stress, biaxial elasproperties, and strength measured in the dilated asc
FIGURE 7. „A… Cauchy stress at failure, s f , as a function ofage with means shown for younger „Ë50 years … and older„Ð50 years … age groups. „B… Stretch ratio at failure, l f , as afunction of age with means shown for the same age groups.Symbols same as Fig. 6. Significant „pË0.05… differences aredenoted by * .

ltsantheted
thee iheerou
agend
onsere
intheage
to
tureed
al
thing
lesterainiglein-u-
.ildthal
er-ngtheallygthticwa
in-ble
in-nt
we
sis.age,e
edsly.alhatilarhatthe
ingtheon.anditsertius
ghis
en
re. Inro-gsioninge.
eenta.rstic
gere
-
for
ll as
631Mechanical Properties of Dilated Human Ascending Aorta
ing aorta all change significantly with age. These resuare consistent with previous studies on normal humthoracic aorta. To our knowledge, however, these arefirst in vitro mechanical property measurements reporfor dilated human ascending aorta.
Fifty years was used as the cutoff age to dividepatients into younger and older age groups becauswas also the age used to subdivide the BAV group. Tmean and median ages of the patients in the study w54.4 and 56 years, respectively. When we repeatedstatistical analyses using 55 or 60 years as the cutoffall significant statistical differences between younger aolder age groups retained their significance. Conclusifrom statistical analyses between patient groups walso unaffected.
Circumferential Residual Stress
Liu and Fung19 and Badreck-Amoudiet al.1 measuredopening angles at various positions along the aortarats. Both studies found the ascending aorta hadhighest opening angle. Liu and Fung reported an avervalue of 160°, while Badreck-Amoudiet al. found thatthe opening angle increased from 120° at 6 weeks140° at 52 weeks of age. Badreck-Amoudiet al. alsofound the opening angle was independent of temperain the range of 10°–40 °C and, like our study, performtests in isotonic saline at room temperature.
Saini et al.31 reported mean opening angle in normhuman ascending aorta of 220° for 18 males~23–74years, mean age 48 years! and 140° for 12 females~3months–87 years, mean age 49 years!. They observed asignificant increase in opening angle with age for bosexes, consistent with our results. The mean openangle of 221°670° for the males in our study~n525,51615 years! was similar to Sainiet al. In contrast, themean opening angle of 289°683° ~n59, 66618 years!for the females in our study was greater than the femain Saini et al. although their mean age was also greathan either the males in our study or the females in Set al. The underlying cause of increased opening anwith age in humans is not known. Presumably thecrease reflects alterations in aortic wall structure inflenced by factors including hypertension and disease
During our examination of the intact specimens, mto moderate atherosclerosis was observed in many ofspecimens, generally appearing as clusters of sm~, than 3 mm diam!, yellowish patches or streaks on thintima that were not raised significantly from the surounding tissue. Larger patches or intimal thickeniwere noted in some specimens. While we recordedpresence of atherosclerosis, we did not systematiccharacterize its severity. We chose biaxial and strenspecimens from regions with few or no atheroscleropatches. However, because the opening angle ring
t
er,
el
s
cut from one end of the specimen, and because itcluded the entire circumference, we were not always ato avoid these regions. Sainiet al.31 observed a relationbetween the presence of atherosclerotic lesions andcreased opening angle, but did not find a significaincrease with the severity of the lesions. In our study,measured opening angles.300° in ten rings~5 TAV, 4BAV, 1 Marfan, mean age 70 years!. Of these ten rings,five came from patients where we noted atheroscleroSince atherosclerosis was associated with advancedit is difficult to isolate the individual effects of thesinterrelated factors in our study.
To our knowledge, spontaneous inversion of closrings of arterial tissue has not been described previouStergiopuloset al.32 measured opening angles in normand inverted pig carotid artery segments and found tthe inverted segment returned to a configuration simto the normal segment after cutting. This suggests tthe measured opening angles are not affected byspontaneous inversion of the closed ring. If the openangle is greater than 180°, the inverted state ofclosed ring would be closer to the stress-free conditiWe hypothesize that when the opening angle is large,when the height of the ring is small compared tomidwall radius, the specimen may spontaneously invand reach a lower energy state. The large midwall radof the closed rings in our study~1.5460.33 mm, n534! compared to the ring height of 3–5 mm, alonwith the large opening angles, could have allowed tprocess to occur.
Biaxial testing was performed on tissue from sevpatients with inverted closed rings~4 TAV, 1 BAV, 2Marfan!. The elastic properties of the specimens wesimilar to noninverted specimens of comparable agerings from ten patients for whom we had noted athesclerosis of the intact specimens, we found five rininverted and five did not. Thus, spontaneous inversappeared to be primarily associated with larger openangles that were in turn associated with advanced ag
Elastic Properties
Alterations in the elastic response with age have bpreviously reported for descending thoracic aorLearoyd and Taylor18 used in vitro pressure-diametetesting to estimate the circumferential incremental elamodulus~Einc! of 5 ‘‘young’’ ~mean age 17 years! and 6‘‘old’’ ~mean age 45 years! human upper descendinthoracic aortas obtained at autopsy. The segments wstretched to the measuredin situ length and then pressurized. At 120 mm Hg, the meanEinc for the old group,was approximately 3.5 MPa, compared to 1.2 MPathe younger group. These age-related changes inEinc
depend upon vessel radius and wall thickness as wethe intrinsic properties of the tissue tested, however.

op-
arain
-essalat
andperss-
mmin
atrmanlinbe
de-rta
be-ss-tessti
hedatalwapoon
ftionterngthhengvener
n-ni-
iale o
herar-
r-nd
ap-t andre-urtheas-omndtede-
isxial
-e
gearef they
d aisbe
tasl
ts,ioner-
irein-hisontheth-e
iallyas
632 OKAMOTO et al.
There are few previous studies of arterial elastic prerties using planar biaxial testing. Debes and Fung4 mea-sured elastic properties of excised canine pulmonaryteries and found an approximately linear stress-strrelationship in the physiologic range of stress~,25 kPa!and strain. Zhou and Fung38 characterized canine descending thoracic aorta and observed nonlinear strstrain behavior in both circumferential and longitudindirections. While the nonlinear behavior occurredhigher strains~EC.0.8 andEZ.0.5! than those in ourstudy, Zhou and Fung used fitted material propertiesmeasured geometry to conclude that canine aorta oates in the nonlinear range of the circumferential strestrain relationship.
For human descending thoracic aorta,Einc has beenshown to increase with pressure between 50 and 150Hg,17,18 suggesting that nonlinear behavior is reachednormal human aorta. In the dilated aorta, it is likely ththe mean wall stresses are even higher than in the noaorta because of the increased lumen radius. The noear behavior could cause smaller changes in radiustween diastolic and systolic pressures, leading tocreased compliance and reducing the ability of the aoto dampen pulsatile flow.
We observed only a small amount of hysteresistween loading and unloading curves. Equibiaxial strestrain curves were similar when stretching at strain rabetween 0.5%/s and 6%/s. Thus, we felt a pseudoelaconstitutive formulation was suitable for this tissue. Tnonlinear stress-strain behavior suggested fitting theto either a polynomial or exponential form. Equibiaxistress-stretch results also indicated that the tissuesomewhat anisotropic. We selected an orthotropic, exnential form proposed by previous investigators basedpressure-diameter testing of arteries.
We found that a combined data set~equibiaxial plustwo strip biaxial protocols! resulted in a unique set oparameters for each patient using the constitutive relain Eq. ~3!. Humphrey12 showed that the seven parameexponential constitutive relation proposed by Chuoand Fung3 allows the degree of anisotropy to vary wistrain. However, we did not obtain unique values for toptimized material parameters from multiple startiguesses when fitting our experimental data to that separameter form using the Lagrange multipliapproach.12
The constitutive relation of Eq.~3! has the propertythat, for equibiaxial stretching, the ratio of circumferetial to axial stress is independent of the stretch magtude and is given byscc /szz5(b11b3)/(b21b3).12
This ratio defines the degree of in-plane anisotropy.When we calculated this ratio from the fitted mater
parameters for each patient, we obtained a mean valu1.0960.29, but did not find a consistent direction to tanisotropy, as the ratio ranged from 0.64 to 2.00. Fe
-
-
-
l--
c
a
s-
f
resi et al.6 performed uniaxial tensile tests on circumfeential and axial strips of porcine ascending aorta aaortic sinus. The circumferential elastic modulus wasproximately 1.2–1.5 times the longitudinal modulus anominal strain of 30% for ascending aortic tissue, a0.6–2.0 times the longitudinal modulus in the sinusgion, depending upon circumferential location. In ostudy, three Marfan biaxial test specimens came fromnoncoronary sinus, while all others came from thecending aorta. The in-plane anisotropy ratio ranged fr0.7 to 1.2 for the three sinus specimens. We did not fithat the degree of anisotropy was significantly correlawith age, or a particular type of aortic disease, but dcreased with the unloaded wall thickness~scc /szz
51.1760.31, T<2.6 mm, n521; scc /szz50.9660.22, T.2.6 mm,n519, p,0.05!.
Strength Testing
Our observation that strength decreases with ageconsistent with other studies that have measured uniastrength of normal,21,23 aneurysmal,27 and Marfanaorta.24 Perejdaet al. studied rings of descending thoracic aorta in 21 controls~age 19–48 years, mean ag34.6 years! and five Marfan patients~3169 years! andreported nominal~force/unit undeformed area! stress atfailure. A significant decrease in failure stress with awas observed in the control group. When their valuesconverted to Cauchy stresses, the average strength ocontrol group~3.4 MPa! is greater than that predicted bour linear fit of strength to age~2.1 MPa!. Since theirmeasurements were from a different location and usedifferent method, one must be careful in interpreting thdifference, but it does suggest that dilated aorta mayweaker than nondilated aorta. Mohan and Melvin21 re-ported a mean strength of 1.7 MPa for 18 normal aor~age559618 years!. This mean is closer to, but stilgreater than, our linear fit~1.5 MPa! for that mean age.It is also important to note that, due to size constrainwe measured strength in the circumferential directonly. Mohan and Melvin found lower strength in thlongitudinal than circumferential direction when peforming dynamic~i.e., high strain rate! strength testing.
Limitations
Some limitations of our experimental methods requdiscussion. Perhaps foremost was the difficulty in obtaing all three types of test data from a single patient. Tdifficulty was due to the quantity, shape, and conditiof the excised tissue and to technical problems withopening angle and strength testing. In patients with aerosclerosis, most commonly elderly TAV patients, wcould not always find a homogeneous region for biaxor strength testing. Occasionally, we found a relativehomogeneous region for biaxial testing but the tissue w

r-atre-V
notheunataledg
edp.
ingrvaion
xi--
s.a-ess
inut,ullc-ss.thead-tothe
redally
enage9°,
tic
of
re-engund-
hussingthe
alltheol-
di--e-
hn
en-eseheallof
ersn an
the
ate-s ade-
ag-a
ande at
thisad-
aorad-o ag-belay-tress.
tiessedea-
ofe-
d into
t isand-
hi-
633Mechanical Properties of Dilated Human Ascending Aorta
so stiff that even our preconditioning protocols~10%equibiaxial stretch! could not be performed without teaing the sutures from the specimen. Thus, it is likely thour reported biaxial mechanical properties do not repsent the behavior of tissue from some older TApatients.
Because the shape of the specimen varied, it wasalways possible to cut a smooth ring from the end ofspecimen for opening angle measurements. Rings ofeven thickness tended to fall over. Strength test dwere excluded when the specimen slipped from or faiat a clamp. We found by trial and error that placinapproximately 4 mm of tissue in each clamp providsufficient clamping force and reduced failures at a clam
The method we employed to determine the openangle of a ring from a segment assumed that the cuture of the ring was uniform. We tested this assumptby determininga using segments~f 50.7! of six ringswhere the entire ring had remained upright. The mamum difference between thea determined from the segments and the measureda from the full ring was 30°,with the values being within 20° for five of the six ring
The ‘‘unloaded’’ reference for our stress-strain mesurements assumed that the tissue lay flat in its strfree state. In practice, some specimens curled slightlyboth the circumferential and axial directions when crequiring a small, but unknown, amount of stress to pthe specimen flat. The curl in the circumferential diretion can be explained by circumferential residual streWhen the opening angle was greater than 180°,specimen curved toward the adventitial surface. Theventitial surface was thus slightly stretched in orderflatten the specimen. However, because the ratio ofmidwall radius of the opened rings to the measuthickness was large, the flattening strain was genersmall. In the most extreme case wherea.360°, weestimated the circumferential Green’s strain at the advtitia due to flattening was less than 8%, and the averstrain less than 4%. At the mean opening angle of 23the average strain would be approximately 1%–2%.
Mechanical testing of arteries to determine elasproperties has been carried out at either room4,38 or bodytemperature.17,36 At room temperatures, the responsesmooth muscle is diminished.34 Kang et al.16 found ves-sel behavior of passive bovine coronary arteriesmained the same at temperatures from 21 to 55 °C. Det al.5 measured the shear modulus of rat aorta and foa small decrease~,10%! in shear modulus when measurements were made at 37 °C rather than 24 °C. Twe believe our room temperature measurements, u0.1 mM papaverine in the bath solution, representpassive response of the aorta to biaxial stretching.
In our analysis we have assumed that the aortic wis homogeneous. Due to the different composition ofmedia ~smooth muscle cells, elastic laminae and c
t
-
-
-
-
,
lagen!, adventitia ~primarily interwoven collagenfibrils!28 and attached visceral pericardium~mesothelialcells with underlying vasa vasorum, connective and apose tissue!,30 it is likely that they have different mechanical properties. Differences in the properties of mdia and adventitia were observed by von Maltzaet al.36 and Xie et al.37 In this study, it was observed inthe failed strength specimens that the media and advtitia often separated, suggesting that the strength of thlayers may be different. Different elastic properties of tlayers could also explain the correlation between wthickness and in-plane anisotropy. If the anisotropythe layers differs and the relative thickness of the laychanges as the unloaded wall thickness increases, theincrease in thickness might alter the anisotropy ofintact wall.
The large opening angles also suggest varying mrial properties. When a blood vessel is modeled ahomogeneous cylinder, the transmural stress gradientpends on the opening angle. It is thought that the mnitude of the opening angle is appropriate to provideuniform stress distribution through the wall.8 For a givenvessel geometry, applied pressure and axial stretch,material parameters, there is a unique opening anglwhich the stress becomes uniform.25 Using a homoge-neous model with the opening angles measured instudy, the stresses would generally be higher at theventitia. The predicted nonuniform stresses may bepathological condition associated with aortic dilationage. However, different properties of the media andventitia could reduce stress in the adventitia, leading tmore uniform transmural stress distribution. This sugests that a more detailed model of the wall mayneeded. Thus, mechanical test data on the individualers may be necessary to obtain more accurate local sdistributions needed for predicting rupture of the wall
CONCLUSIONS
In summary, we have reported mechanical properfor dilated human ascending aorta obtained from excisurgical tissue. Our results show age influences all msured mechanical properties, regardless of the typedisease that led to the dilatation. With appropriately dfined geometry, the mechanical properties can be usemathematical models of the dilated ascending aortapredict regional and transmural stress distributions. Ihoped that these models may lead to a better understing of the causes of aortic dissection and rupture.
ACKNOWLEDGMENTS
This research was supported by grants from the Wtaker Foundation~R. J. O.! and the National MarfanFoundation and a Whitaker Graduate Fellowship~J. E.

erancr-.-Pst
. 8.
e
E.rat
rter
ess
sed
ew
.ter-
g
our
e-t,
the
F.al
ors
nd
n
F.eriale.
edar-
rd.20l.
e
ies.
e-
ve
alnd
L.pe
on,nd
ressrial
P.
634 OKAMOTO et al.
W.!. The authors would like to thank Sadaf Toor for hassistance in mechanical testing and data analysis, NNickerson and Marci Bailey for gathering patient infomation and obtaining patient consent, and Dr. Frank CYin who graciously loaned the authors his biaxial teapparatus.
APPENDIX
Opening Angle Determined from a Segment of aCircular Ring
The opening angle of an open ring,a, can be deter-mined by measuring the opening angle of a segment,a f ,shown as the shaded portion of the open ring in FigThe included angle of the segment,u f , is related toa f
~in radians! by u f52up2a f u. Similarly, the includedangle of the ring,u, is given byu52up2au. Let f bethe ratio of the segment circumference,L f , to the cir-cumference of the open ring,L. Then f u5u f , so that2 f up2au52up2a f u. Noting that the absolute valubars can be dropped becausea anda f will both be eithergreater or less thanp and solving fora yields
a5a f2p~12 f !
f. ~A1!
This relation is valid for 0,a,2p.
REFERENCES
1Badreck-Amoudi, A., C. K. Patel, T. P. Kane, and S.Greenwald. The effect of age on residual strain in theaorta.ASME J. Biomech. Eng.118:440–444, 1996.
2Chuong, C. J., and Y. C. Fung. On residual stresses in aies. ASME J. Biomech. Eng.108:189–192, 1986.
3Chuong, C. J., and Y. C. Fung. Three-dimensional strdistribution in arteries.ASME J. Biomech. Eng.105:268–274, 1983.
4Debes, J. C., and Y. C. Fung. Biaxial mechanics of excicanine pulmonary arteries.Am. J. Physiol.269:H433–H442,1995.
5Deng, S. X., J. Tomioka, J. C. Debes, and Y. C. Fung. N
FIGURE 8. Measurement of opening angle from a segment„shaded region … of an arterial ring.
y
.
-
experiments on shear modulus of elasticity of arteries.Am. J.Physiol. 266:H1–H10, 1994.
6Ferraresi, C., A. M. Bertetto, L. Mazza, D. Maffiodo, and WFranco. One-dimensional experimental mechanical characization of porcine aortic root wall.Med. Biol. Eng. Comput.37:202–207, 1999.
7Fung, Y. C. Biomechanics: Mechanical Properties of LivinTissues, 2nd ed. New York: Springer, 1993, p. 568.
8Fung, Y. C. What are the residual stresses doing inarteries?Ann. Biomed. Eng.19:237–249, 1991.
9Hahn, R. T., M. J. Roman, A. H. Mogtader, and R. B. Dvereux. Association of aortic dilation with regurgitanstenotic and functionally normal bicuspid aortic valves.J.Am. Coll. Cardiol.19:283–288, 1992.
10Han, H. C., and Y. C. Fung. Species dependence ofzero-stress state of aorta: Pig versus rat.ASME J. Biomech.Eng. 113:446–451, 1991.
11Hirata, K., F. Triposkiadis, E. Sparks, J. Bowen, C.Wooley, and H. Boudoulas. The Marfan syndrome: Abnormaortic elastic properties.J. Am. Coll. Cardiol. 18:57–63,1991.
12Humphrey, J. D. An evaluation of pseudoelastic descriptused in arterial mechanics.ASME J. Biomech. Eng.121:259–262, 1999.
13Humphrey, J. D. Mechanics of the arterial wall: Review adirections.Crit. Rev. Biomed. Eng.23:1–162, 1995.
14Humphrey, J. D., D. L. Vawter, and R. P. Vito. Quantificatioof strains in biaxially tested soft tissues.J. Biomech.20:59–65, 1987.
15Jeremy, R. W., H. Huang, J. Hwa, H. McCarron, C.Hughes, and J. G. Richards. Relation between age, artdistensibility, and aortic dilatation in the Marfan syndromAm. J. Cardiol.74:369–373, 1994.
16Kang, T., J. Resar, and J. D. Humphrey. Heat-inducchanges in the mechanical behavior of passive coronaryteries.ASME J. Biomech. Eng.117:86–93, 1995.
17Langewouters, G. J., K. H. Wesseling, and W. J. GoedhaThe static elastic properties of 45 human thoracic andabdominal aortasin vitro and the parameters of a new modeJ. Biomech.17:425–435, 1984.
18Learoyd, B. M., and M. G. Taylor. Alterations with age in thviscoelastic properties of human arterial walls.Circ. Res.18:278–292, 1966.
19Liu, S. Q., and Y. C. Fung. Zero-stress states of arterASME J. Biomech. Eng.110:82–84, 1988.
20May-Newman, K., and F. C. P. Yin. Biaxial mechanical bhavior of excised porcine mitral valve leaflets.Am. J.Physiol. 269:H1319–H1327, 1995.
21Mohan, D., and J. W. Melvin. Failure properties of passihuman aortic tissue. I—uniaxial tension tests.J. Biomech.1:887–902, 1982.
22Nielsen, P. M. F., P. J. Hunter, and B. H. Smaill. Biaxitesting of membrane biomaterials: Testing equipment aprocedures.ASME J. Biomech. Eng.113:295–300, 1991.
23Oxlund, H., L. M. Rasmussen, T. T. Andreassen, andHeickendorff. Increased aortic stiffness in patients with ty1 ~insulin-dependent! diabetes mellitus. Diabetologia32:748–752, 1989.
24Perejda, A. J., P. A. Abraham, W. H. Carnes, W. F. Coulsand J. Uitto. Marfan’s syndrome: Structural, biochemical, amechanical studies of the aortic media.J. Lab. Clin. Med.106:376–383, 1985.
25Peterson, S. J., and R. J. Okamoto. Effect of residual stand heterogeneity on circumferential stress in the artewall. ASME J. Biomech. Eng.122:454–456, 2000.
26Press, W. H., S. A. Teukolsky, W. T. Vetterling, and B.

ficss,
s-
of2,
an
er-dis-
1th
ex
ter.nd
e
ndun-
a-nts
train
r.dia
seltial
nd
635Mechanical Properties of Dilated Human Ascending Aorta
Flannery. Numerical Recipes in Fortran: The Art of ScientiComputing, 2nd ed. New York: Cambridge University Pre1992.
27Raghavan, M. L., M. W. Webster, and D. A. Vorp.Ex vivobiomechanical behavior of abdominal aortic aneurysm: Asessment using a new mathematical model.Ann. Biomed.Eng. 24:573–582, 1996.
28Rhodin, J. Architecture of the vessel wall, in HandbookPhysiology, Section 2, The Cardiovascular System, Vol.Vascular Smooth Muscle, edited by R. M. Berne. AmericPhysiological Society, 1979, pp. 1–31.
29Robicsek, F., and M. J. Thubrikar. Hemodynamic considations regarding the mechanism and prevention of aorticsection.Ann. Thoracic Surgery58:1247–1253, 1994.
30Romanes, G. J. Cunningham’s Textbook of Anatomy, 1ed. London: Oxford University Press, 1972.
31Saini, A., C. Berry, and S. Greenwald. Effect of age and son residual stress in the aorta.J. Vasc. Res.32:398–405,1995.
32Stergiopulos, N., A. Pannatier, A. Rachev, and J. MeisElastic response of the arterial wall under physiologic a
nonphysiologic initial stress distribution: applicability of thstrain energy function.1994 ASME Adv. Bioeng.28:67–68,1994.
33Svensson, L. G., and E. S. Crawford. Cardiovascular aVascular Disease of the Aorta. Philadelphia, PA: W. B. Saders Company, 1997, p. 472.
34Toda, N., M. Hojo, and K. Sakae. Modification by temperture of the response of isolated aorta to stimulatory ageand transmural stimulation.Blood Vessels13:210–221, 1976.
35Vaishnav, R. N., and J. Vossoughi. Residual stress and sin aortic segments.J. Biomech.20:235–239, 1987.
36von Maltzahn, W. W., R. G. Warriyar, and W. F. KeitzeExperimental measurements of elastic properties of meand adventitia of bovine carotid arteries.J. Biomech.17:839–847, 1984.
37Xie, J. P., J. Zhou, and Y. C. Fung. Bending of blood veswall: Stress-strain laws of the intima-media and adventilayers.ASME J. Biomech. Eng.117:136–145, 1995.
38Zhou, J., and Y. C. Fung. The degree of nonlinearity aanisotropy of blood vessel elasticity.Proc. Natl. Acad. Sci.U.S.A.94:14255–14260, 1997.