
Performance of CFRP Wrapped Square Reinforced Concrete Columns Subjected to Eccentric Loading
Measurement Tools Used in the Study of EccentricContraction–Induced InjuryGordon L. Warren,1 Dawn A. Lowe2 and Robert B. Armstrong1
1 Muscle Biology Laboratory, Texas A&M University, College Station, Texas, USA2 Department of Anatomy, University of South Florida, Tampa, Florida, USA
ContentsAbstract . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 431. Evaluation of Measurement Tools in Human Studies . . . . . . . . . . . . . . . . . . . . . . . . . . . 45
1.1 Torque . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 451.2 Range of Motion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 471.3 Histology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 471.4 Blood Levels of Myofibre Proteins . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 481.5 Soreness . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 481.6 Other Measurement Tools . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 49
2. Evaluation of Measurement Tools in Animal Studies . . . . . . . . . . . . . . . . . . . . . . . . . . . 492.1 Force . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 512.2 Histology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 522.3 Release of Myofibre Proteins . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 542.4 Muscle Enzyme Activity . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 54
3. Recommendations for Future Studies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 543.1 Human Studies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 543.2 Animal Studies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 553.3 Induction of Injury . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 55
4. Conclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 56
Abstract The objective of this review is to evaluate the measurement tools currentlyused in the study of eccentric contraction–induced muscle injury, with emphasison their usefulness for quantifying the magnitude and duration of the injury andas indicators of muscle functional deficits. In studies in humans, it was concludedthat measurements of maximal voluntary contraction torque and range of motionprovide the best methods for quantifying muscle injury. Similarly, in animal stud-ies, the in vitro measurement of electrically elicited force under isometric condi-tions was considered to be the best of the measurement tools currently in use.
For future studies, more effort should be put into measuring other contractileparameters (e.g. force/torque-velocity and force/torque-length relationships,maximal shortening velocity and fatigue susceptibility) that may reflect injury-induced functional impairments. The use of histology, ratings of soreness and the
REVIEW ARTICLE Sports Med 1999 Jan; 27 (1): 43-590112-1642/99/0001-0043/$08.50/0
© Adis International Limited. All rights reserved.

measurement of blood or bath levels of myofibre proteins should be discouragedfor purposes of quantifying muscle injury and/or functional impairment.
There has been considerable interest in the med-ical literature regarding the phenomenon of eccen-tric contraction–induced skeletal muscle injury,particularly over the past 15 years. Numerous stud-ies have been published describing the injury, in-vestigating mechanisms underlying the pathologyand seeking preventative and therapeutic interven-tions. As with any clinical or scientific problem, itis important to develop ‘markers’ or measures thatpermit precise quantification of the phenomenon.However, even a cursory perusal of the literaturedemonstrates that a wide variety of criteria for mus-cle injury has been employed, and that there hasbeen no general agreement on the best methods forquantifying the pathology. This article aims to eval-uate the various markers for eccentric contraction–induced muscle injury and presents our recommen-dations on the most useful methods for quantifyingthis form of muscle injury.
From both basic and clinical science perspec-tives, injury criteria should relate to muscle func-tion. The clinical importance of considering thefunctional manifestations of the injury has beenemphasised by recent legislation in the US in-cluded in the Omnibus Budget Reconciliation Actsof 1989 and 1990 (PL 101-239 and 101-508). Theearlier act created the Agency for Health Care Pol-icy and Research (AHCPR), which has responsibil-ity for the study of outcomes and effectiveness ofdiagnostic, therapeutic and preventative healthcare services and procedures. A year later, a com-prehensive study of rehabilitation financing wasmandated and the National Center for Medical Re-habilitation Research (NCMRR) was created underthe National Institutes of Health (NIH). Both actshave resulted in a move in rehabilitation healthcaretowards ‘functional outcomes management’, withan emphasis on the development of functionalmeasurement tools.[1-3] Because of this emphasis,and the fact that work- and exercise-induced mus-cle injury have medical significance,[4,5] the func-
tional criteria used in evaluation of muscle injurywarrant critical review as a healthcare issue.
Basic science has been affected by this legisla-tion as well. In 1994, NIH/NCMRR and AHCPRco-sponsored a conference, ‘An Agenda for Medi-cal Rehabilitation Outcomes Research’, at whichthe improvement of functional measurement toolsand encouragement of uniformity in the use ofthese tools across all specialties was called for.[6]
The guidelines formalised at this conference, in ad-dition to others, will most likely dictate the direc-tion of future basic biomedical science research inthe US.
Thus, in this article, we take the view that meas-ures of muscle function provide the best means forevaluating the magnitude and time-course of mus-cle injuries resulting from eccentric contractions.Muscle function is operationally defined as theability to exert force under a given set of condi-tions, that is, over a given range of motion (ROM)or at a fixed muscle length, at a given velocity orat a given external load, at a given level of activa-tion and over a given number of contractions. Atool that assesses 1 or more of these components ofmuscle function is defined as a functional measure-ment tool. From a functional standpoint, muscleinjury may be defined as a prolonged (i.e. lastingdays or weeks) impairment of the ability of a mus-cle to produce force.
After describing methods for evaluating musclefunction in injured muscles, this article comparesother measurement tools that have been used. (Wereviewed only those studies in which the injury wasinduced by the performance of eccentric contrac-tions or exercise biased towards eccentric contrac-tions.) The article has been divided into an evalua-tion of those measurement tools used in humanstudies and those used in animal studies: 52 humanstudies conducted over the last 15 years and 46animal studies over the last 13 years were re-viewed. This selection of the literature, repre-sentative of this research field, was not intended to
44 Warren et al.
Adis International Limited. All rights reserved. Sports Med 1999 Jan; 27 (1)

be all-encompassing. After an evaluation of themeasurement tools currently in use, recommenda-tions for their use in future studies have been listed.Finally, recommendations have been provided onhow to induce the injury to maximise the validityand reliability of the measurement tools.
1. Evaluation of Measurement Tools inHuman Studies
Table I provides a list of the reviewed humanstudies along with a breakdown, by study, of thetools employed.
1.1 Torque
Maximal voluntary contraction (MVC) torquewas measured in 50% of the studies reviewed; itwas the third most frequently used measurementtool (see table I). MVC torque is directly propor-tional to force [muscle (or muscle group) force-producing capability equals torque divided by themoment arm of the muscle(s) attachment to thebone]; however, this moment arm is rarely deter-mined because it is joint angle–dependent. Never-theless, as long as torque measurements are madeat the same joint angle, valid comparisons can bemade within and among individuals. This is an im-portant point because peak torques are often re-ported and compared without consideration of thejoint angle at which they occurred. The sametorque produced at 2 different joint angles does notnecessarily require the same muscle force output.Also, by making the torque measurements at thesame joint angle, it is ensured that the ratio of mus-cle length/optimal muscle length is the same for thecomparisons.
Torque output is also velocity-dependent be-cause of the muscle force-velocity relationship.Ideally, all torque measurements should be madeat the same muscle shortening or lengthening ve-locity. In reality, this can only be achieved duringisometric contractions since isokinetic tests ensureconstant angular velocity only, and velocity is un-controlled during isotonic contractions.
Two shortcomings in the use of MVC torque asa functional measurement tool for assessing mus-
cle impairment are that torque output is affected byfatigue and by an individual’s motivation and pain.First, it is difficult to distinguish fatigue-relatedreductions in torque from injury-related reduc-tions.[59] This is particularly true during or imme-diately after the injury protocol (an exercise proto-col designed to elicit muscle injury). Second, evenwith highly motivated individuals, it is debatablewhether maximal effort elicits maximal recruit-ment of all motor units.[25,60,61] An attempt to cir-cumvent this problem has been made in 13% of thereviewed studies by employing percutaneous elec-trical stimulation (see table I). Because electricalstimulation does not recruit the entire muscle (ormuscle group), possible regional heterogeneity inthe injury compromises the validity of the ap-proach. However, electrical stimulation is usefulfor determination of the torque-frequency relation-ship and in evaluation of the muscular componentof fatigue.
Validity of a functional measurement tool is de-pendent on the reliability of that tool. Reliabilityof the MVC torque measurement is generally high(i.e. intraclass correlation coefficients ≥ 0.85).[62,63]
This has been discussed recently elsewhere.[62,63]
However, we wish to emphasise the importance ofestablishing reliability within each basic scienceand clinical research setting using similar individ-uals and conditions to the experimental settings. Itis also important that care be taken in the terminol-ogy employed when discussing MVC torque meas-urement. All too often it is inferred that the externalload equals the force produced by the muscle(s).This is inappropriate because the moment arms ofboth the muscle attachment and the external loadare usually unequal and are constantly changingas a function of joint angle. This may have led toerroneous conclusions about the relative effects offorce and muscle length on the extent of injury in1 study.[37]
We believe that MVC torque provides the bestmeasure of muscle injury resulting from eccentriccontractions. As described, it is relatively accurateand reliable and it provides the primary means fordetermining muscle function in human studies.
Measurements of Functional Muscle Injury 45
Adis International Limited. All rights reserved. Sports Med 1999 Jan; 27 (1)
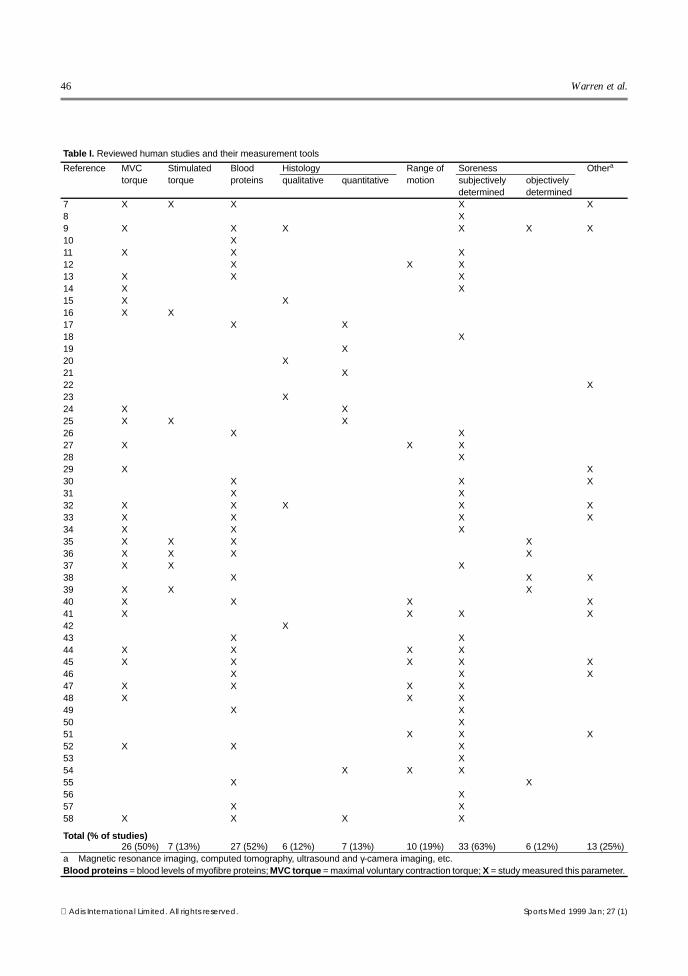
Table I. Reviewed human studies and their measurement tools
Reference MVCtorque
Stimulatedtorque
Bloodproteins
Histology Range ofmotion
Soreness Othera
qualitative quantitative subjectivelydetermined
objectivelydetermined
7 X X X X X8 X9 X X X X X X10 X11 X X X12 X X X13 X X X14 X X15 X X16 X X17 X X18 X19 X20 X21 X22 X23 X24 X X25 X X X26 X X27 X X X28 X29 X X30 X X X31 X X32 X X X X X33 X X X X34 X X X35 X X X X36 X X X X37 X X X38 X X X39 X X X40 X X X X41 X X X X42 X43 X X44 X X X X45 X X X X X46 X X X47 X X X X48 X X X49 X X50 X51 X X X52 X X X53 X54 X X X55 X X56 X57 X X58 X X X X
Total (% of studies)26 (50%) 7 (13%) 27 (52%) 6 (12%) 7 (13%) 10 (19%) 33 (63%) 6 (12%) 13 (25%)
a Magnetic resonance imaging, computed tomography, ultrasound and γ-camera imaging, etc.Blood proteins = blood levels of myofibre proteins; MVC torque = maximal voluntary contraction torque; X = study measured this parameter.
46 Warren et al.
Adis International Limited. All rights reserved. Sports Med 1999 Jan; 27 (1)

Also, the reductions in MVC torque resulting frominjury persist over the entire span of the progres-sion of the degenerative and regenerative pro-cesses, that is, until the muscle returns to its pre-injury condition. The prolonged reduction inmuscle function following injury induced by ec-centric contractions in humans is presented in fig-ure 1. As will be discussed in sections 1.3 to 1.6,other commonly used markers, including releaseof myofibre proteins, soreness and histopathology,are not in evidence over the entire time-course, andeven when in evidence, they may or may not becorrelated with the magnitude of the functionaldecrements.
1.2 Range of Motion
ROM is defined as the arc over which a jointmay operate, and this constrains the muscle lengthrange (for single joint muscles). ROM is deter-mined by skin, subcutaneous tissue, tendon, artic-ular capsule and bone properties, in addition tothose of muscle. ROM measurement was used in19% of the reviewed human studies (see table I)but in only 1 of the studies was the full ROMdetermined.[27] In several studies of the arm, ROMhas been underestimated by measuring the anglebetween maximal flexion and relaxed armhang.[12,40,41,44,45,47,48,51,54] For the purpose of in-terpreting ROM data, guidelines exist that describethe functional level of impairment associated witha given reduction in ROM.[65] We recommend thatthese guidelines be applied in the basic science lab-oratory as well as in rehabilitative medicine.
Reliability of the ROM measurement in muscleinjury research has not been well documented, butthere are reliability data in the rehabilitative med-icine field.[66-68] Passive ROM measurement typi-cally demonstrates poor-to-moderate inter-rater re-liability (i.e. intraclass correlation coefficients of0.3 to 0.9) but good intra-rater reliability (i.e. intra-class correlation coefficients ≥ 0.9).[66-68] Robersonand Giurintano[67] have proposed a more reliablealternative to the passive measurement. They rec-ommend rotating the joint to either extreme until apredetermined level of passive torque is attained,
measuring the angle, and then repeating the proce-dure at the other joint extreme.
1.3 Histology
Histological analysis using light or electronmicroscopy was used in 13 (25%) of the reviewedhuman studies (see table I). Only 7 out of these 13studies attempted to quantify histological abnor-malities. The use of histology as a measurementtool is discussed in detail in section 2.2, but in bothhuman and animal studies, the histopathology ofmuscle fibres following eccentric contractions hascorrelated poorly with functional measurements(e.g. MVC torque production), both in terms of themagnitude and time-course of the impairment. Inthis section, only the potential problems specific tohuman studies have been addressed.• Specimens are usually obtained from a small
(i.e. 10 to 50mg) percutaneous needle biopsy of1 muscle. This biopsy represents only a smallfraction of the involved muscle(s), so whetherthe specimen is representative of the muscleshould always be questioned.
• Since it has been reported that injury to the vas-tus lateralis muscle by a previous biopsy has notbeen repaired even after 2 weeks of recovery,[69]
1 2 3 4 5 6 7 8 9 10
6
8
10
12
14
16
18
20
Pre Post
Days after exercise
Isom
etric
str
engt
h (k
g)
Fig. 1. Isometric strength (mean ± standard error of the mean)of the forearm flexor muscles before (Pre), immediately after(Post) and 5 days post exercise for 109 individuals and meansfor 6 to 10 days post exercise for 15 individuals (reproducedfrom Clarkson et al.,[64] with permission).
Measurements of Functional Muscle Injury 47
Adis International Limited. All rights reserved. Sports Med 1999 Jan; 27 (1)

the validity and reliability of longitudinal stud-ies can be compromised.
• Needle biopsies have elevated blood creatinekinase levels,[70] thus potentially confoundingthe results of that commonly used injury marker.
• Decrements in MVC torque have not been tem-porally related to the number of affected fibres.[24]
Whereas MVC torque has been depressed im-mediately after the injury protocol, histologicalabnormalities in muscle cross-sections have notbeen evident until several days later.[24] It shouldbe pointed out that, at the electron microscopiclevel, these same investigators[24] observed le-sions in the muscle fibres in longitudinal sec-tions immediately after eccentric contractions.
1.4 Blood Levels of Myofibre Proteins
Blood levels of creatine kinase, lactate dehydro-genase, glutamic-oxaloacetic transaminase, slowmyosin heavy-chain fragments and/or myoglobinhave been used as markers of eccentric contraction–induced injury in 52% of the reviewed human stud-ies (see table I).
Changes in blood levels of myofibre proteinscorrelate poorly with decreases in muscle func-tion.[11,13,35,36] The greatest decrement in MVCtorque production usually occurs immediately afterthe initiation of the injury while peak blood levelsof creatine kinase, etc. normally occur no earlierthan 1 day later (fig. 2).
In contrast, Rodenburg et al.[44] reported thatblood levels of creatine kinase and myoglobin aresignificantly correlated with the decrements inMVC torque and ROM. However, at time pointsless than 1 day following the initiation of the injury,the variance of creatine kinase and myoglobin lev-els could not account for a significant portion ofthe variance in MVC torque. At time points ≥1 day,the percentage variance in either MVC torque orROM accounted for by variance in serum creatinekinase was only moderate (median 53%, range 12to 73%). Serum myoglobin level explained evenless of the variance of MVC torque or ROM (me-dian 38%, range 16 to 62%).
Additional evidence for the dissociation be-tween blood levels of myofibre proteins and con-tractile function includes the observation that re-peated bouts of eccentric contractions eliminate theelevation in blood creatine kinase level while thecontractile decrements are only minimally attenu-ated.[35] Also, extreme variations in blood levels ofcreatine kinase occur among individuals despitesimilar decrements in contractile function in re-sponse to a bout of eccentric contractions.[13] Fur-thermore, blood levels of creatine kinase are disso-ciated from histological signs of injury.[17]
A relationship between losses of muscle func-tion and changes in blood levels of myofibre pro-teins in the early phases of eccentric contraction–induced injury can be hypothesised. If one assumesthat the reduction in the force-producing capabilityof a muscle is due to disruption of force-bearingstructural elements, then cell membrane integritymight be lost because force-bearing elements con-stitute and/or cross the cell membrane. Loss of cellmembrane integrity might then permit diffusion ofmyofibre proteins into the extracellular space and,eventually, the general circulation. One majorproblem with this hypothesis is that blood levels ofmyofibre proteins reflect not only their release intothe blood but also their removal. Alterations infunction of, and/or blood flow to, the tissues thatclear these proteins affect the blood levels ofmyofibre proteins, as does exercise-induced haemo-concentration or haemodilution. Thus, there is nocompelling reason to expect that blood levels ofmyofibre proteins accurately reflect functionallosses resulting from injury.
1.5 Soreness
Soreness was the most commonly used markerof injury, used in 73% of the reviewed human stud-ies (see table I). 12% of the studies used an objec-tive means of measuring soreness (i.e. measuringforce applied to a muscle group at the pain thresh-old) while 63% used a visual analogue or numericalscale for subjective evaluation of soreness. Never-theless, soreness has correlated poorly withchanges in muscle function,[29,33,45,48] both in terms
48 Warren et al.
Adis International Limited. All rights reserved. Sports Med 1999 Jan; 27 (1)

of magnitude and time-course. As with the bloodlevels of myofibre proteins, soreness onset occursafter the onset of contractile decrements and thechange in ROM (fig. 2).
1.6 Other Measurement Tools
Other types of measurement tool were used in25% of the reviewed human studies. Most of theseemployed some sort of noninvasive imaging device[e.g. magnetic resonance imaging (MRI), com-puted tomography (CT), ultrasound and γ-cameraimaging]. Changes in the measurements obtainedusing these tools have not correlated temporallywith those of muscle function,[29,33,45] which is notparticularly surprising. For example, MRI detectsspatial variations in the local magnetic fields ofprotons in the body while CT measures spatial vari-ations in x-ray attenuation coefficients. Ultrasoundmeasures distances between structures reflectingradio waves in the MHz range. Nuclear medicine
techniques provide a measure of the spatial distri-bution of a γ-emitting radionuclide in the body.Thus, there is no reason to expect that data fromthese imaging modalities would necessarily be in-dicative of loss of contractile function; that is, it isnot possible to determine whether an ‘abnormal-appearing’ region in an image coincides with a re-gion of altered muscle function. From the few stud-ies conducted, abnormalities detected by MRI or99mTc γ-camera imaging seem to peak at 3 to 6 daysfollowing initiation of the injury,[30,33,38,45,51] againtemporally lagging behind the functional impair-ment.
2. Evaluation of Measurement Tools inAnimal Studies
Functional measurement tools that have beenused in animal studies of muscle injury induced byeccentric contractions are listed in table II.
0
10
20
30
40
50
60
70
80
90
100
0-0.99 1-1.99 2-2.99 3-3.99 4-4.99 5-5.99 ≥ 6
Time of peak impairment (days)
Per
cent
age
of s
tudi
es
MVC torqueRange of motionBlood levels of myofibre proteinsSoreness
Fig. 2. Percentage of reviewed human studies showing peak impairment at each of 7 time intervals following initiation of eccentriccontraction–induced injury. Data for 4 measures are presented: maximal voluntary contraction (MVC) torque (n = 23 studies), rangeof motion (n = 6 studies), blood levels of myofibre proteins (n = 25 studies) and soreness (n = 33 studies). Data are from studieslisted in table I that made ≥3 measurements over ≥3 days. [Where possible, any decrements/changes in a given measure werecorrected for those observed in the control condition (e.g. subtraction of an isometric contraction protocol torque decrement fromthat measured for the eccentric contraction protocol)].
Measurements of Functional Muscle Injury 49
Adis International Limited. All rights reserved. Sports Med 1999 Jan; 27 (1)

Table II. Reviewed animal studies and their measurement tools
Reference Po invitro
Po/torquein situ
Torque invivo
Force-frequencyrelationship
Othercontractileparameters
Histology Proteinrelease
Muscleenzymecontenta
Otherqualitative quantitative
71 X X X72 X73 X X X74 X X X75 X X76 X X X77 X X X X7879 X X X80 X X X X81 X8283 X84 X X X X85 X86 X X X87 X X X88 X X89 X90 X X X X91 X X92 X X X X X X X93 X X X X94 X X X95 X X X X96 X X X97 X X X98 X X X X X X99 X X X X100 X X X101 X X102 X103 X X X104 X X X X105 X X106107 X108 X109 X X X X110 X X111 X X X112 X X X X113 X X X114 X X X X115 X X116 X X X
Total (% of studies)19 (41%) 14 (30%) 3 (7%) 13 (28%) 16 (35%) 11 (24%) 18 (39%) 17 (37%) 5 (11%) 8 (17%)
a β-Glucuronidase or glucose-6-phosphate dehydrogenase.Po = maximal isometric tetanic force; X = study measured this parameter.
50 Warren et al.
Adis International Limited. All rights reserved. Sports Med 1999 Jan; 27 (1)

2.1 Force
Maximal isometric tetanic force (Po) is a com-monly used muscle function parameter. It wasmeasured in 67% of the reviewed studies; isotonicor isokinetic forces were not measured in any ofthese studies.
Po or maximal isometric torque was measuredin situ (i.e. the muscle retains normal vascular sup-ply but the nerve and/or distal tendon are exposed)in 30% of the studies, and in vitro (i.e. the muscleis completely isolated from the animal) in 41% ofthe studies reviewed (see table II). An advantageof these 2 muscle preparations, as opposed to invivo muscle preparations, is that the force outputof a specific muscle can be determined. In in vivopreparations, torque is measured across a joint and,normally, multiple synergistic muscles are acti-vated.
Po measurements in animal studies are depend-ent on the elicitation of true maximal force outputby the muscle(s). For example, the effects of an-aesthesia on muscle contractile function need to beconsidered with in situ and in vivo preparations.The type of anaesthetic regimen, the depth of an-aesthesia and the time-course of induction relativeto the functional measurements all influence mus-cle force or torque production.[117] In addition,some of the more commonly used anaesthetics(e.g. pentobarbital and ketamine) have been shownto have adverse effects on contractility in themouse.[117]
Muscle contractions in the in situ and in vitromuscle preparations (and some in vivo protocols)are ‘involuntary’; that is, the muscle(s) is stimu-lated directly (in vitro) or indirectly through thenerve (in situ or in vivo). For maximal forces to beobtained in these muscle preparations, stimulationparameters (i.e. voltage/current, frequency andpulse duration) must be optimised. For example,the optimal frequency of stimulation needs to bedetermined both before and after injury inductionbecause of a rightward shift of the force-frequencycurve following muscle injury,[97,98] especially atlow frequencies.[104] Therefore, higher stimulationfrequencies may be necessary to obtain Po follow-
ing injury. Force-frequency curves were determinedin 28% of the studies reviewed (see table II) butthey were determined both before and after injuryin only 9 of those 13 studies.[73,74,76,86,90,92,93,98,104]
If the muscle is stimulated through the nerve, caremust also be taken to avoid injury to the nerve. Thiscan be minimised by using balanced (or slightlyimbalanced) biphasic pulses and noble metal elec-trodes.[118,119]
Another consideration in determining Po afterinitiation of the injury is that muscles must havemetabolically recovered from the injury-inducingcontractions. This is necessary to ensure that anydecrement in Po reflects injury to the muscle andnot fatigue. For in vitro muscle preparations, thetime needed for recovery can be estimated.[109] Theinterval between contractions and the duration ofcontractions can be adjusted to minimise the meta-bolic demands placed upon the muscle as well.Whenever possible, it is helpful to include iso-metric or concentric controls; if the isometric orconcentric protocol is the same (stimulation pa-rameters and contraction time) as the eccentric pro-tocol, and there is minimal reduction in force, onecan be reasonably certain that metabolic fatigue isnot responsible for the force loss in the eccentriccontraction group. Both concentric and isometriccontractions require higher energy expenditurethan eccentric contractions.[120-122]
Adverse anaesthetic effects are normally not amajor consideration when using in vitro musclepreparations; however, there are other factors thatmust be considered to ensure validity of the meas-urements. First and foremost is the viability of themuscle preparation. Only muscles that weigh<30mg should be studied in vitro at physiologicaltemperatures,[123] although it is possible to main-tain larger muscles (70 to 90mg) in vitro at lowertemperatures.[124] The primary concern regardingmuscle size is to ensure that sufficient quantities ofnutrients, including oxygen, are able to diffuse tothe muscle core. Muscles studied in vitro must alsobe maintained at optimal muscle length (Lo); mus-cles incubated at shorter lengths have elevatedrates of protein degradation.[125] Lo has been found
Measurements of Functional Muscle Injury 51
Adis International Limited. All rights reserved. Sports Med 1999 Jan; 27 (1)
to shift towards longer lengths following inductionof injury.[116] Additionally, Lo may differ if the fre-quency of stimulation is changed (e.g. if stimula-tion frequency is increased following injury, thenLo may be decreased).[126] In all muscle prepara-tions, muscle length should be maintained withinthe anatomical range of the muscle (preferablywithin the physiological range) before, during andafter the induction of muscle injury.
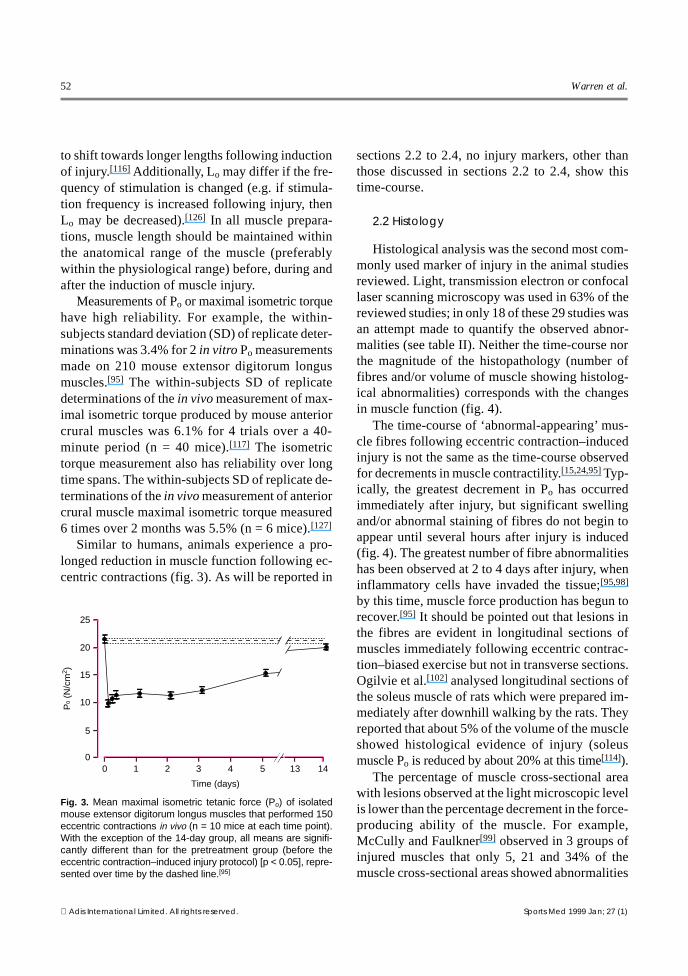
Measurements of Po or maximal isometric torquehave high reliability. For example, the within-subjects standard deviation (SD) of replicate deter-minations was 3.4% for 2 in vitro Po measurementsmade on 210 mouse extensor digitorum longusmuscles.[95] The within-subjects SD of replicatedeterminations of the in vivo measurement of max-imal isometric torque produced by mouse anteriorcrural muscles was 6.1% for 4 trials over a 40-minute period (n = 40 mice).[117] The isometrictorque measurement also has reliability over longtime spans. The within-subjects SD of replicate de-terminations of the in vivo measurement of anteriorcrural muscle maximal isometric torque measured6 times over 2 months was 5.5% (n = 6 mice).[127]
Similar to humans, animals experience a pro-longed reduction in muscle function following ec-centric contractions (fig. 3). As will be reported in
sections 2.2 to 2.4, no injury markers, other thanthose discussed in sections 2.2 to 2.4, show thistime-course.
2.2 Histology
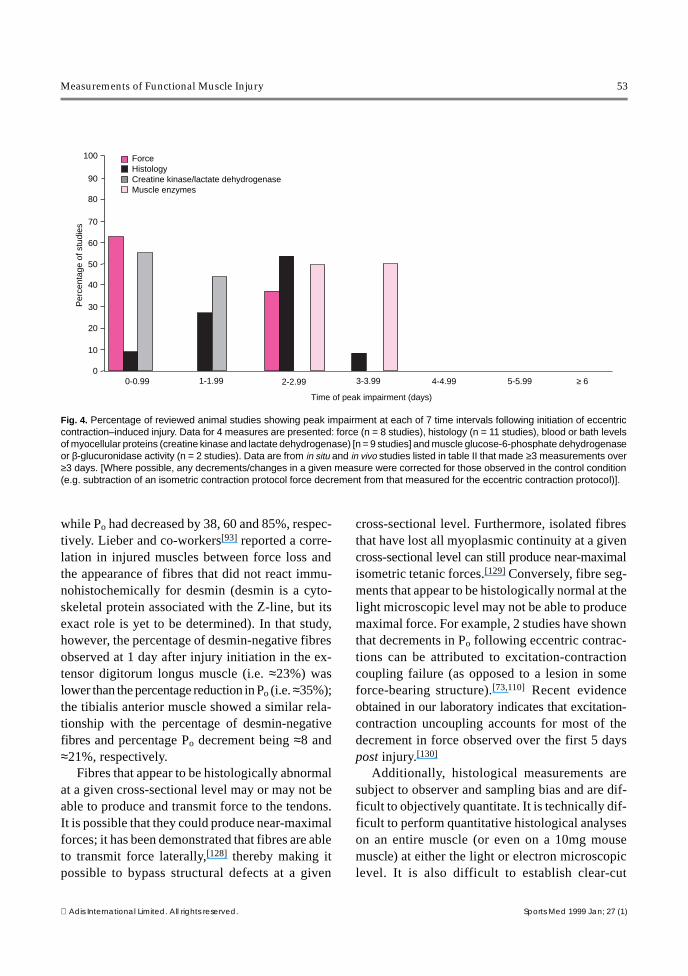
Histological analysis was the second most com-monly used marker of injury in the animal studiesreviewed. Light, transmission electron or confocallaser scanning microscopy was used in 63% of thereviewed studies; in only 18 of these 29 studies wasan attempt made to quantify the observed abnor-malities (see table II). Neither the time-course northe magnitude of the histopathology (number offibres and/or volume of muscle showing histolog-ical abnormalities) corresponds with the changesin muscle function (fig. 4).
The time-course of ‘abnormal-appearing’ mus-cle fibres following eccentric contraction–inducedinjury is not the same as the time-course observedfor decrements in muscle contractility.[15,24,95] Typ-ically, the greatest decrement in Po has occurredimmediately after injury, but significant swellingand/or abnormal staining of fibres do not begin toappear until several hours after injury is induced(fig. 4). The greatest number of fibre abnormalitieshas been observed at 2 to 4 days after injury, wheninflammatory cells have invaded the tissue;[95,98]
by this time, muscle force production has begun torecover.[95] It should be pointed out that lesions inthe fibres are evident in longitudinal sections ofmuscles immediately following eccentric contrac-tion–biased exercise but not in transverse sections.Ogilvie et al.[102] analysed longitudinal sections ofthe soleus muscle of rats which were prepared im-mediately after downhill walking by the rats. Theyreported that about 5% of the volume of the muscleshowed histological evidence of injury (soleusmuscle Po is reduced by about 20% at this time[114]).
The percentage of muscle cross-sectional areawith lesions observed at the light microscopic levelis lower than the percentage decrement in the force-producing ability of the muscle. For example,McCully and Faulkner[99] observed in 3 groups ofinjured muscles that only 5, 21 and 34% of themuscle cross-sectional areas showed abnormalities
0 1 2 3 4 5 13 140
5
10
15
20
25
Po
(N/c
m2 )
Time (days)
Fig. 3. Mean maximal isometric tetanic force (Po) of isolatedmouse extensor digitorum longus muscles that performed 150eccentric contractions in vivo (n = 10 mice at each time point).With the exception of the 14-day group, all means are signifi-cantly different than for the pretreatment group (before theeccentric contraction–induced injury protocol) [p < 0.05], repre-sented over time by the dashed line.[95]
52 Warren et al.
Adis International Limited. All rights reserved. Sports Med 1999 Jan; 27 (1)
while Po had decreased by 38, 60 and 85%, respec-tively. Lieber and co-workers[93] reported a corre-lation in injured muscles between force loss andthe appearance of fibres that did not react immu-nohistochemically for desmin (desmin is a cyto-skeletal protein associated with the Z-line, but itsexact role is yet to be determined). In that study,however, the percentage of desmin-negative fibresobserved at 1 day after injury initiation in the ex-tensor digitorum longus muscle (i.e. ≈23%) waslower than the percentage reduction in Po (i.e. ≈35%);the tibialis anterior muscle showed a similar rela-tionship with the percentage of desmin-negativefibres and percentage Po decrement being ≈8 and≈21%, respectively.
Fibres that appear to be histologically abnormalat a given cross-sectional level may or may not beable to produce and transmit force to the tendons.It is possible that they could produce near-maximalforces; it has been demonstrated that fibres are ableto transmit force laterally,[128] thereby making itpossible to bypass structural defects at a given
cross-sectional level. Furthermore, isolated fibresthat have lost all myoplasmic continuity at a givencross-sectional level can still produce near-maximalisometric tetanic forces.[129] Conversely, fibre seg-ments that appear to be histologically normal at thelight microscopic level may not be able to producemaximal force. For example, 2 studies have shownthat decrements in Po following eccentric contrac-tions can be attributed to excitation-contractioncoupling failure (as opposed to a lesion in someforce-bearing structure).[73,110] Recent evidenceobtained in our laboratory indicates that excitation-contraction uncoupling accounts for most of thedecrement in force observed over the first 5 dayspost injury.[130]
Additionally, histological measurements aresubject to observer and sampling bias and are dif-ficult to objectively quantitate. It is technically dif-ficult to perform quantitative histological analyseson an entire muscle (or even on a 10mg mousemuscle) at either the light or electron microscopiclevel. It is also difficult to establish clear-cut
0
10
20
30
40
50
60
70
80
90
100
Per
cent
age
of s
tudi
es
0-0.99 1-1.99 2-2.99 3-3.99 4-4.99 5-5.99 ≥ 6
Time of peak impairment (days)
ForceHistologyCreatine kinase/lactate dehydrogenaseMuscle enzymes
Fig. 4. Percentage of reviewed animal studies showing peak impairment at each of 7 time intervals following initiation of eccentriccontraction–induced injury. Data for 4 measures are presented: force (n = 8 studies), histology (n = 11 studies), blood or bath levelsof myocellular proteins (creatine kinase and lactate dehydrogenase) [n = 9 studies] and muscle glucose-6-phosphate dehydrogenaseor β-glucuronidase activity (n = 2 studies). Data are from in situ and in vivo studies listed in table II that made ≥3 measurements over≥3 days. [Where possible, any decrements/changes in a given measure were corrected for those observed in the control condition(e.g. subtraction of an isometric contraction protocol force decrement from that measured for the eccentric contraction protocol)].
Measurements of Functional Muscle Injury 53
Adis International Limited. All rights reserved. Sports Med 1999 Jan; 27 (1)

criteria for the presence or extent of a histologicalabnormality.
2.3 Release of Myofibre Proteins
The release of creatine kinase and/or lactate de-hydrogenase was utilised as a criterion for muscleinjury in 37% of the animal studies reviewed (seetable II). Measuring blood levels of myofibreproteins in animals (in studies that induced muscleinjury in vivo or in situ) is problematic, as describedin section 1.4. That is, blood levels reflect the re-lease and clearance of proteins in circulation, andrelease and clearance can vary independently.
For in vitro muscle preparations, release of pro-teins into the bathing medium may be measured.However, one must be cautious because of enzymeinactivation over time.[109] It is also possible to getelevated protein release if the muscle is not dis-sected carefully, as any damage to the peripheralfibres results in the release of intracellular proteins.
The time-course of protein release from injuredmuscles is not the same as that for muscle func-tional impairments (fig. 4). First, the appearance ofmyofibre proteins in the blood from injured mus-cles in vivo is biphasic. There is an immediate in-crease in these proteins in the blood, which hasbeen associated with initial injury to the muscle,and then a second peak, 2 to 4 days later.[71] Thesecond elevation has been attributed to the infiltra-tion of phagocytic cells. This biphasic response hasalso been observed in muscles injured in vivo butstudied in vitro.[95] Second, muscles that are injuredand studied in vitro lose proteins progressivelyover time;[112] that is, there is no sudden release ofenzymes corresponding with the immediate forcedecrement.[111] Third, the extent of lactate dehydro-genase release does not match the extent of redis-tribution of lipophilic and hydrophilic cell mem-brane probes.[113]
The mechanical factor that best explains the lossof Po (i.e. peak force produced during eccentriccontractions) is not the most important factor af-fecting release of creatine kinase.[109] Investigatorsfound that release of creatine kinase was affected
only by the lengthening velocity of the eccentriccontractions.[109]
2.4 Muscle Enzyme Activity
The activity of β-glucuronidase or glucose-6-phosphate dehydrogenase in injured muscle wasdetermined in 11% of the animal studies reviewed.The activities of these enzymes is thought to reflectdegenerative/inflammatory processes in the tis-sue.[62] Changes in the activities of these enzymeshave not reflected the changes in muscle functionbecause the increases in enzyme activities occurafter the decrement in force production by a num-ber of days. Glucose-6-phosphate dehydrogenaseis not elevated until 2 to 3 days post injury.[71] Sim-ilarly, β-glucuronidase activity is not increaseduntil 2 to 4 days following induction of injury.[88]
3. Recommendations for Future Studies
3.1 Human Studies
We recommend that investigators studying ec-centric contraction–induced injury include meas-urements of MVC torque and ROM because thesevariables provide a reliable means of quantifyingthe functional decrements resulting from the in-jury. Ideally, torque should be measured under iso-metric and isokinetic conditions to define the torque–angular velocity relationship. So-called ‘isotonic’contractions are not so useful because they are nottruly isotonic; the external resistance is not con-stant throughout the ROM because the effectivemoment arm of the external load changes as a func-tion of joint angle. It is highly desirable that themeasurement conditions (e.g. joint angle and vel-ocity) be carefully controlled.
We believe that measures of soreness and bloodlevels of myofibre proteins have limitations in theirusefulness as criteria for injury. They are more labileand less consistent variables compared with MVCtorque and ROM and their time-course does notcorrespond with the decrements in muscle function.
If treatment for soreness was to be based solelyon reducing pain, it is possible that functional re-covery could be impaired. For example, administra-
54 Warren et al.
Adis International Limited. All rights reserved. Sports Med 1999 Jan; 27 (1)

tion of flurbiprofen has been found to impair func-tional recovery in the rabbit following eccentriccontraction–induced injury.[131] In addition, Krot-kiewski and co-workers[32] found that antioxidantsmarkedly reduce soreness and serum creatine kin-ase levels but have no effect on the recovery of mus-cle strength. The efficacy of any treatment for in-jured muscles should include consideration of therecovery of muscle function. Whereas pain affectsthe quality of life as well as the rehabilitative pro-cess, it is clear that the trend is for medical rehab-ilitative funding to be directed primarily towardsimproving function, as discussed in the introduc-tory portion of this article.
Histology has long been considered the ‘goldstandard’ as an injury criterion. This may havebeen justified in the past when accurate and precisemeasurements of isometric and isokinetic muscletorque could not be easily obtained. However, thedifficulty in quantifying the histopathology and thefact that its progression in injured muscles does notclearly track the force deficits limit its usefulnessfor reliably quantifying muscle injury. Histologyand other imaging modalities continue to be usefulfor probing the mechanisms of the reductions intorque and ROM. For example, one can use MRIand spectroscopy to detect regional variations inmuscle activity. Also, immunofluorescence andimmunohistochemistry at the light and electronmicroscopic levels might be exploited to determinethe force-bearing and membrane structures subjectto disruption.
3.2 Animal Studies
We recommend that measures of the contractilefunction of muscle, such as Po, force-frequency andforce-velocity relationships, and maximal shorten-ing velocity be used as the primary measurementtools for quantifying the extent of muscle injury.An in vitro muscle preparation is the preferredmeans with which to determine muscle functionafter initiation of eccentric contraction–inducedinjury. Advantages of this type of muscle prepara-tion are that the observations are generally un-
affected by anaesthetic effects and not affected byinjury to the nerve or neuromuscular junction.
With all types of muscle preparations, stimula-tion parameters need to be optimised in order toobtain true maximal functional measures. Themeasured forces (or torques) may be reported in avariety of ways such as, for example, in absoluteunits, per cross-sectional area or normalised to thecontralateral control muscle. For long term studies,the latter is preferable since it corrects for anygrowth that occurs. Forces produced by musclesthat are studied in vitro or in situ may need to becorrected for oedema if the force is expressed percross-sectional area.[132]
As with the human studies, we also recommendthat release of myocellular proteins not be used toestimate the extent of muscle injury. Histology atthe light and electron microscopic levels, includingthe study of living tissue with the confocal laserscanning microscope, is valuable in terms oflocalising abnormal structures and possibly the al-tered force-bearing proteins themselves. However,we do not recommend its use for assessing the ex-tent of muscle injury.
3.3 Induction of Injury
For a functional measurement to be valid ineither animals or humans, it should possess speci-ficity. For example, the measurement tool lacksspecificity when a person runs downhill to induceinjury and then is tested on an isokinetic device.Muscles (or portions of muscles) recruited (andpotentially injured) during downhill running maynot be the same as those tested during isokinetictesting. Injuring and testing on the same deviceincreases the specificity of the testing. Eight out of25 studies in humans that conducted both pre- andpostinjury testing did not use the same device forinducing injury and testing.[7,9,16,24,32,34,36,39] Weare not advocating that the mode of testing be lim-ited to that used to induce the injury (i.e. eccentric),although the test specificity would be predictablylower during testing in isometric and concentricmodes.
Measurements of Functional Muscle Injury 55
Adis International Limited. All rights reserved. Sports Med 1999 Jan; 27 (1)
It is also important to quantify the injury induc-tion procedure in terms of mechanical factors. Itis known that factors such as peak torque/force,muscle length change and/or initial muscle lengthaffect the extent of muscle injury.[90,99,109] Thesefactors should be carefully controlled so that func-tional measurement comparisons among and/orwithin individuals will be valid. It is much moredifficult to quantify these factors for some modal-ities (e.g. downhill running).
4. Conclusions
When attempting to quantify muscle injury inboth human and animal studies, an effort should bemade to obtain measurements of force/torque-producing capability. In addition to the ‘standard’isometric force/torque measurement, characteris-ation of the force-producing capability as a func-tion of velocity, activation, muscle length and boutduration should be pursued. Ideally, measurementsof ROM should be included in human studies. Fur-thermore, we recommend a de-emphasis on the useof other commonly used markers (e.g. blood levelsof myofibre proteins, soreness and histology) toquantify the magnitude and time-course of themuscle injury.
References1. Harada N, Kominiski G, Sofaer S. Development of resource-
based patient classification scheme for rehabilitation. Inquiry1993; 30: 54-63
2. Harada N, Sofaer S, Kominski G. Functional status outcomesin rehabilitation: implications for prospective payment. MedCare 1993; 31: 345-57
3. Johnston MV, Keith RA, Hinderer SR. Measurement standardsfor interdisciplinary medical rehabilitation. Arch Phys MedRehabil 1992; 73: S3-23
4. Anonymous. Occupational injuries and illnesses in the UnitedStates, 1992. Washington, DC: US Department of Labor, Bu-reau of Labor Statistics, 1994. Government Document No.L2.2:OC1/153
5. Slätis P, Ruusinen A. Orthopedic diseases and trauma in Fin-land: trends in consumption of health services 1970-1985.Acta Orthopaed Scand 1991; 62 Suppl. 241: 13-6
6. Fuhrer MJ. Conference report: an agenda for medical rehabili-tation outcomes research. J Allied Health 1995; 24: 79-87
7. Balnave CD, Thompson MW. Effect of training on eccentricexercise-induced muscle damage. J Appl Physiol 1993; 75:1545-51
8. Berry, CB, Moritani T, Tolson H. Electrical activity and sore-ness in muscles after exercise. Am J Phys Med Rehabil 1990;69: 60-6
9. Buroker KC, Schwane JA. Does postexercise static stretchingalleviate delayed muscle soreness? Physician Sportsmed1989; 17: 65-83
10. Cannon JG, Fiatarone MA, Fielding RA, et al. Aging and stress-induced changes in complement activation and neutrophilmobilization. J Appl Physiol 1994; 76: 2616-20
11. Clarkson PM, Byrnes WC, McCormick KM, et al. Muscle sore-ness and serum creatine kinase activity following isometric,eccentric, and concentric exercise. Int J Sports Med 1986; 7:152-5
12. Clarkson PM, Dedrick, ME. Exercise-induced muscle damage,repair, and adaptation in old and young subjects. J Gerontol1988; 43: M91-6
13. Clarkson PM, Ebbeling C. Investigation of serum creatine ki-nase variability after muscle-damaging exercise. Clin Sci1988; 75: 257-61
14. Crenshaw AG, Karlsson S, Styf J, et al. Knee extension torqueand intramuscular pressure of the vastus lateralis muscle dur-ing eccentric and concentric activities. Eur J Appl Physiol1995; 70: 13-9
15. Crenshaw AG, Thornell LE, Fridén J. Intramuscular pressure,torque, and swelling for the exercise-induced sore vastuslateralis muscle. Acta Physiol Scand 1994; 152: 265-77
16. Davies CTM, White MJ. Muscle weakness following eccentricwork in man. Pflugers Arch 1981; 392: 168-71
17. Fielding RA, Manfredi TJ, Ding WJ, et al. Acute phase responsein exercise: 3. neutrophil and IL-1-beta accumulation in skel-etal muscle. Am J Physiol 1993; 265: R166-72
18. Fitzgerald GK, Rothstein JM, Mayhew TP, et al. Exercise-induced muscle soreness after concentric and eccentricisokinetic contractions. Phys Ther 1991; 71: 505-13
19. Fridén J. Changes in human skeletal muscle induced by long-term eccentric exercise. Cell Tissue Res 1984; 236: 365-72
20. Fridén J, Kjörell U, Thornell LE. Delayed muscle soreness andcytoskeletal alterations: an immunocytological study in man.Int J Sports Med 1984; 5: 15-8
21. Fridén J, Seger J, Ekblom B. Sublethal muscle fibre injuriesafter high-tension anaerobic exercise. Eur J Appl Physiol1988; 57: 360-8
22. Fridén J, Sfakianos PN, Hargens AR. Muscle soreness and in-tramuscular fluid pressure: comparison between eccentric andconcentric load. J Appl Physiol 1986; 61: 2175-9
23. Fridén J, Sfakianos PN, Hargens AR, et al. Residual muscularswelling after repetitive eccentric contractions. J OrthopaedRes 1988; 6: 493-8
24. Fridén J, Sjöström M, Ekblom B. Myofibrillar damage follow-ing intense eccentric exercise in man. Int J Sports Med 1983;4: 170-6
25. Gibala MJ, MacDougall JD, Tarnopolsky MA, et al. Changesin human skeletal muscle ultrastructure and force productionafter acute resistance exercise. J Appl Physiol 1995; 78: 702-8
26. Gleeson M, Almey J, Brooks S, et al. Hematological and acute-phase responses associated with delayed-onset muscle sore-ness in humans. Eur J Appl Physiol 1995; 71: 137-42
27. Grossman JM, Arnold BL, Perrin DH, et al. Effect of ibuprofenuse on delayed-onset muscle soreness of the elbow flexors. JSports Rehabil 1995; 4: 253-63
56 Warren et al.
Adis International Limited. All rights reserved. Sports Med 1999 Jan; 27 (1)
28. High DM, Howley ET, Franks BD. The effects of static stretch-ing and warm-up on prevention of delayed-onset muscle sore-ness. Res Q Exerc Sport 1989; 60: 357-61
29. Howell JN, Chleboun G, Conatser R. Muscle stiffness, strengthloss, swelling and soreness following exercise-induced injuryin humans. J Physiol (Lond) 1993; 464: 183-96
30. Jones DA, Newham DJ, Round JM, et al. Experimental humanmuscle damage: morphological changes in relation to otherindices of damage. J Physiol (Lond) 1986; 375: 435-48
31. Kirwan JP, Hichner RC, Yarasheski KE, et al. Eccentric exerciseinduces transient insulin resistance in healthy individuals. JAppl Physiol 1992; 72: 2197-202
32. Krotkiewski M, Brzezinska Z, Liu B, et al. Prevention of mus-cle soreness by pretreatment with antioxidants. Scand J MedSci Sport 1994; 4: 191-9
33. Mair J, Koller A, Artner-Dworzak E, et al. Effects of exerciseon plasma myosin heavy chain fragments and MRI of skeletalmuscle. J Appl Physiol 1992; 72: 656-63
34. Mair J, Mayr M, Müller E, et al. Rapid adaptation to eccentricexercise-induced muscle damage. Int J Sport Med 1995; 16:352-6
35. Newham DJ, Jones DA, Clarkson PM. Repeated high-forceeccentric exercise: effects on muscle pain and damage. J ApplPhysiol 1987; 63: 1381-6
36. Newham DJ, Jones DA, Edwards RHT. Large delayed plasmacreatine kinase changes after stepping exercise. MuscleNerve 1983; 6: 380-5
37. Newham DJ, Jones DA, Ghosh G, et al. Muscle fatigue and painafter eccentric contractions at long and short length. Clin Sci1988; 74: 553-7
38. Newham DJ, Jones DA, Tolfree SEJ, et al. Skeletal muscledamage: a study of isotope uptake, enzyme efflux and painafter stepping. Eur J Appl Physiol 1986; 55: 106-12
39. Newham DJ, Mills KR, Quigley BM, et al. Pain and fatigueafter concentric and eccentric muscle contractions. Clin Sci1983; 64: 55-62
40. Nosaka K, Clarkson PM. Effect of eccentric exercise on plasmaenzyme activities previously elevated by eccentric exercise.Eur J Appl Physiol 1994; 69: 492-7
41. Nosaka K, Clarkson PM. Muscle damage following repeatedbouts of high force eccentric exercise. Med Sci Sports Exerc1995; 27: 1263-9
42. O’Reilly K, Warhol MJ, Fielding RA, et al. Eccentric exercise-induced muscle damage impairs muscle glycogen repletion.J Appl Physiol 1987; 63: 252-6
43. Pizza FX, Mitchell JB, Davis BH, et al. Exercise-induced mus-cle damage: effect on circulating leukocyte and lymphocytesubsets. Med Sci Sports Exerc 1995; 27: 363-70
44. Rodenburg JB, Bär PR, Deboer RW. Relations between musclesoreness and biochemical and functional outcomes of eccen-tric exercise. J Appl Physiol 1993; 74: 2976-83
45. Rodenburg JB, Deboer RW, Schiereck P, et al. Changes in phos-phorus compounds and water content in skeletal muscle dueto eccentric exercise. Eur J Appl Physiol 1994; 68: 205-13
46. Rodenburg JB, Degroot MCH, Van Echteld CJA, et al. Phos-phate metabolism of prior eccentrically loaded vastusmedialis muscle during exercise in humans. Acta PhysiolScand 1995; 153: 97-108
47. Rodenburg JB, Steenbeek D, Schiereck P, et al. Warm-up,stretching and massage diminish harmful effects of eccentricexercise. Int J Sports Med 1994; 15: 414-9
48. Saxton JM, Clarkson PM, James R, et al. Neuromuscular dys-function following eccentric exercise. Med Sci Sports Exerc1995; 27: 1185-93
49. Schwane JA, Johnson SR, Vandenakker CB, et al. Delayed-onsetmuscular soreness and plasma CK and LDH activities afterdownhill running. Med Sci Sports Exerc 1983; 15: 51-6
50. Schwane JA, Watrous BG, Johnson SR, et al. Is lactic acidrelated to delayed-onset muscle soreness? Physician Sportsmed1983; 11: 124-31
51. Shellock FG, Fukunaga T, Mink JH, et al. Exertional muscleinjury: evaluation of concentric versus eccentric actions withserial MR imaging. Radiology 1991; 179: 659-64
52. Smith LL, Fulmer MG, Holbert D, et al. The impact of a re-peated bout of eccentric exercise on muscular strength, mus-cle soreness and creatine kinase. Br J Sports Med 1994; 28:267-71
53. Smith LL, McCammon M, Smith S, et al. White blood cellresponse to uphill walking and downhill jogging at similarmetabolic loads. Eur J Appl Physiol 1989; 58: 833-7
54. Stauber WT, Clarkson PM, Fritz VR, et al. Extracellular matrixdisruption and pain after eccentric muscle action. J ApplPhysiol 1990; 69: 868-74
55. Tiidus PM, Ianuzzo CD. Effects of intensity and duration ofmuscular exercise on delayed soreness and serum enzymeactivities. Med Sci Sports Exerc 1983; 15: 461-5
56. Wessel J, Wan A. Effect of stretching on the intensity of delayed-onset muscle soreness. Clin Sports Med 1994; 4: 83-7
57. Westerlind KC, Byrnes WC, Harris C, et al. Alterations in oxygenconsumption during and between bouts of level and downhillrunning. Med Sci Sports Exerc 1994; 26: 1144-52
58. Widrick JJ, Costill DL, McConell GR, et al. Time course ofglycogen accumulation after eccentric exercise. J Appl Phys-iol 1992; 72: 1999-2004
59. Fitts RH. Cellular mechanisms of fatigue. Physiol Rev 1994;74: 49-94
60. Sale DG. Influence of exercise and training on motor unit acti-vation. Exerc Sport Sci Rev 1987; 15: 95-151
61. Tesch PA, Dudley GA, Duvoisin MR, et al. Force and EMGsignal patterns during repeated bouts of concentric or eccen-tric muscle actions. Acta Physiol Scand 1990; 138: 263-71
62. Abernethy P, Wilson G, Logan P. Strength and power assess-ment: issues, controversies and challenges. Sports Med 1995;19: 401-17
63. Kellis E, Baltzopoulos V. Isokinetic eccentric exercise. SportsMed 1995; 19: 202-22
64. Clarkson PM, Nosaka K, Braun B. Muscle function after exercise-induced muscle damage and rapid adaptation. Med Sci SportsExerc 1992; 24: 512-20
65. Anonymous. Guides to the evaluation of permanent impair-ment. 4th ed. Chicago: American Medical Association, 1993
66. Gajdosik RL, Bohannon RW. Clinical measurement of range ofmotion: review of goniometry emphasizing reliability and va-lidity. Phys Ther 1987; 67: 1867-72
67. Roberson L, Giurintano DJ. Objective measures of joint stiff-ness. J Hand Ther 1995; 8: 163-6
Measurements of Functional Muscle Injury 57
Adis International Limited. All rights reserved. Sports Med 1999 Jan; 27 (1)

68. Rothstein JM, Miller PJ, Roettger RF. Goniometry reliability ina clinical setting: elbow and knee measurements. Phys Ther1983; 63: 1611-5
69. Staron RS, Hikida RS, Murray TF, et al. Assessment of skeletalmuscle damage in successive biopsies from strength-trainedand untrained men and women. Eur J Appl Phsiol 1992; 65:258-64
70. Hikida RS, Staron RS, Hagerman FC, et al. Serum creatinekinase activity and its changes after a muscle biopsy. ClinPhysiol 1991; 11: 51-9
71. Armstrong RB, Ogilvie RW, Schwane JA. Eccentric exercise-induced injury to rat skeletal muscle. J Appl Physiol 1983; 54:80-93
72. Asp S, Kristiansen S, Richter EA. Eccentric muscle damagetransiently decreases rat skeletal muscle GLUT-4 protein. JAppl Physiol 1995; 79: 1338-45
73. Balnave CD, Allen DG. Intracellular calcium and force in singlemouse muscle fibres following repeated contractions withstretch. J Physiol (Lond) 1995; 488: 25-36
74. Brooks SV, Faulkner JA. Contraction-induced injury: recoveryof skeletal muscles in young and old mice. Am J Physiol 1990;258: C436-42
75. Brooks SV, Faulkner JA. Isometric, shortening, and lengtheningcontractions of muscle fiber segments from adult and oldmice. Am J Physiol 1994; 267: C507-13
76. Brooks SV, Zerba E, Faulkner JA. Injury to muscle fibres aftersingle stretches of passive and maximally stimulated musclesin mice. J Physiol (Lond) 1995; 488: 459-69
77. Carter GT, Kikuchi N, Abresch RT, et al. Effects of exhaustiveconcentric and eccentric exercise on murine skeletal muscle.Arch Phys Med Rehabil 1994; 75: 555-9
78. Darr S. Exercise-induced satellite cell activation in growing andmature skeletal muscle. J Appl Physiol 1987; 63: 1816-21
79. Duan C, Delp MD, Hayes DA, et al. Rat skeletal muscle mito-chondrial [Ca2+] and injury from downhill walking. J ApplPhysiol 1990; 68: 1241-51
80. Faulkner JA, Jones DA, Round JM. Injury to skeletal musclesof mice by forced lengthening during contractions. Q J ExpPhysiol 1989; 74: 661-70
81. Fridén J, Lieber RL, Thornell LE. Subtle indications of muscledamage following eccentric contractions. Acta Physiol Scand1991; 142: 523-4
82. Fritz VK, Stauber WT. Characterization of muscles injured byforced lengthening. II. proteoglycans. Med Sci Sports Exerc1988; 20: 354-61
83. Garrett WE, Safran MR, Seaber AV, et al. Biomechanical com-parison of stimulated and nonstimulated skeletal musclepulled to failure. Am J Sports Med 1987; 15: 448-54
84. Hasselman CT, Best TM, Seaber AV, et al. A threshold and con-tinuum of injury during active stretch of rabbit skeletal mus-cle. Am J Sports Med 1995; 23: 65-73
85. Head SI, Williams DA, Stephenson DG. Abnormalities in struc-ture and function of limb skeletal muscle fibres of dystrophicmdx mice. Proc R Soc Lond B Biol Sci 1992; 248: 163-9
86. Hutchins MO, Skjonsby HS, Brazeau GA, et al. Weakness inmouse masticatory muscles by repetitive contractions withforced lengthening. J Dent Res 1995; 74: 642-8
87. Komulainen J, Kytola J, Vihko V. Running-induced muscle in-jury and myocellular enzyme release in rats. J Appl Physiol1994; 77: 2299-304
88. Komulainen J, Takala TES, Vihko V. Does increased serum cre-atine-kinase activity reflect exercise-induced muscle damagein rats. Int J Sports Med 1995; 16: 150-4
89. Lapier TK, Burton HW, Almon R, et al. Alterations in intramus-cular connective tissue after limb casting affect contraction-induced muscle injury. J Appl Physiol 1995; 78: 1065-9
90. Lieber RL, Fridén J. Muscle damage is not a function of muscleforce but active muscle strain. J Appl Physiol 1993; 74: 520-6
91. Lieber RL, Fridén J. Selective damage of fast glycolytic musclefibres with eccentric contraction of the rabbit tibialis anterior.Acta Physiol Scand 1988; 133: 587-8
92. Lieber RL, Schmitz MC, Mishra DK, et al. Contractile and cel-lular remodeling in rabbit skeletal muscle after cyclic eccen-tric contractions. J Appl Physiol 1994; 77: 1926-34
93. Lieber RL, Woodburn TM, Fridén J. Muscle damage inducedby eccentric contractions of 25% strain. J Appl Physiol 1991;70: 2498-507
94. Lowe DA, Warren GL, Hayes DA, et al. Eccentric contractioninduced injury of mouse soleus muscle: effect of varying[Ca2+]o. J Appl Physiol 1994; 76: 1445-53
95. Lowe DA, Warren GL, Ingalls CP, et al. Muscle function andprotein metabolism after initiation of eccentric contraction-induced injury. J Appl Physiol 1995; 79: 1260-70
96. McArdle A, Edwards RHT, Jackson MJ. Effects of contractileactivity on muscle damage in the dystrophin-deficient mdxmouse. Clin Sci 1991; 80: 367-71
97. McBride TA, Gorin FA, Carlsen RC. Prolonged recovery andreduced adaptation in aged rat muscle following eccentricexercise. Mech Ageing Dev 1995; 83: 185-200
98. McCully KK, Faulkner JA. Injury to skeletal muscle fibers ofmice following lengthening contractions. J Appl Physiol1985; 59: 119-26
99. McCully KK, Faulkner JA. Characteristics of lengthening con-tractions associated with injury to skeletal muscle fibers. JAppl Physiol 1986; 61: 293-9
100. McNeil PL, Khakee R. Disruptions of muscle fiber plasmamembranes – role in exercise-induced damage. Am J Pathol1992; 140: 1097-109
101. Moens P, Baatsen PHWW, Marechal G. Increased susceptibilityof EDL muscles from mdx mice to damage induced by con-traction with stretch. J Muscle Res Cell Motil 1993; 14: 446-51
102. Ogilvie RW, Armstrong RB, Baird KE, et al. Lesions in the ratsoleus muscle following eccentrically biased exercise. Am JAnat 1988; 182: 335-46
103. Sacco P, Jones DA. The protective effect of damaging eccentricexercise against repeated bouts of exercise in the mousetibialis anterior muscle. Exp Physiol 1992; 77: 757-60
104. Sacco P, Jones DA, Dick JRT, et al. Contractile properties andsusceptibility to exercise-induced damage of normal and mdxmouse tibialis anterior muscle. Clin Sci 1992; 82: 227-36
105. Schwane JA, Armstrong RB. Effect of training on skeletal mus-cle injury from downhill running in rats. J Appl Physiol 1983;55: 969-75
106. Snyder AC, Lamb DR, Salm CP, et al. Myofibrillar protein deg-radation after eccentric exercise. Experientia 1984; 40: 69-70
107. Stauber WT, Miller GR, Grimmet JG, et al. Adaptation of ratsoleus muscles to 4-wk of intermittent strain. J Appl Physiol1994; 77: 58-62
108. Van Der Meulen JH, Kuipers H, Stassen FRM, et al. High en-ergy phosphates and related compounds, glycogen levels and
58 Warren et al.
Adis International Limited. All rights reserved. Sports Med 1999 Jan; 27 (1)

histology in the rat tibialis anterior muscle after forced length-ening and isometric exercise. Pflugers Arch 1992; 420: 354-8
109. Warren GL, Hayes DA, Lowe DA, et al. Mechanical factors inthe initiation of eccentric contraction-induced injury in ratsoleus muscle. J Physiol (Lond) 1993; 464: 457-75
110. Warren GL, Hayes DA, Lowe DA, et al. Excitation failure inmouse soleus muscle injured by eccentric contractions. JPhysiol (Lond) 1993; 468: 487-99
111. Warren GL, Hayes DA, Lowe DA, et al. Materials fatigue ini-tiates eccentric contraction-induced injury in rat soleus mus-cle. J Physiol (Lond) 1993; 464: 477-89
112. Warren GL, Hayes DA, Lowe DA, et al. Eccentric contraction-induced injury in normal and hindlimb-suspended mouse so-leus and EDL muscles. J Appl Physiol 1994; 77: 1421-30
113. Warren GL, Lowe DA, Hayes DA, et al. Redistribution of cellmembrane probes following contraction-induced injury ofmouse soleus muscle. Cell Tissue Res 1995; 282: 311-20
114. Warren JA, Jenkins RR, Packer L, et al. Elevated muscle vita-min E does not attenuate eccentric exercise-induced muscleinjury. J Appl Physiol 1992; 72: 2168-75
115. Watchko JF, Johnson BD, Gosselin LE, et al. Age-related dif-ferences in diaphragm muscle injury after lengthening acti-vations. J Appl Physiol 1994; 77: 2125-33
116. Wood SA, Morgan DL, Proske U. Effects of repeated eccentriccontractions on structure and mechanical properties of toadsartorius muscle. Am J Physiol 1993; 265: C792-800
117. Ingalls CP, Warren GL, Lowe DA, et al. Differential effects ofanesthetics on in vivo skeletal muscle contractile function inthe mouse. J Appl Physiol 1996; 80: 332-40
118. Brummer SB, Robble LS. Criteria for selecting electrodes forelectrical stimulation: theoretical and practical considera-tions. Ann N Y Acad Sci 1983; 77: 159-71
119. Scheiner A, Mortimer JT. Imbalanced biphasic electrical stim-ulation: muscle tissue damage. Ann Biomed Eng 1990; 18:407-25
120. Bonde-Petersen F, Knuttgen HG, Henriksson J. Muscle meta-bolism during exercise with concentric and eccentric contrac-tions. J Appl Physiol 1972; 33: 792-5
121. Curtin NA, Davies RE. Chemical and mechanical changes dur-ing stretching of activated frog skeletal muscle. Cold SpringHarb Symp Quant Biol 1970; 37: 619-26
122. Infante AA, Klaupiks D, Davies RE. Adenosine triphosphate:changes in muscles doing negative work. Science 1964; 144:1577-8
123. Goldberg AL, Martel SB, Kushmerick MJ. In vitro preparationsof the diaphragm and other skeletal muscles. Meth Enzymol1975; 39: 82-94
124. Seagal SS, Faulkner JA. Temperature-dependent physiologicalstability of rat skeletal muscle in vitro. Am J Physiol 1985;248: C265-70
125. Baracos V, Goldberg AL. Maintenance of normal length im-proves protein balance and energy status in isolated rat skel-etal muscle. Am J Physiol 1986; 251: C588-96
126. Roszek B, Bann GC, Huijing PA. Decreasing stimulationfrequency-dependent length-force characteristics of rat mus-cle. J Appl Physiol 1994; 77: 2115-24
127. Warren GL, Ingalls CP, Armstrong RB. A stimulating nerve cufffor chronic in vivo measurements of torque produced aboutthe ankle in the mouse. J Appl Physiol 1998; 84: 2171-6
128. Street SF. Lateral transmission of tension in frog myofibers: amyofibrillar network and transverse cytoskeletal connectionsare possible transmitters. J Cell Physiol 1986; 114: 346-64
129. Street SF, Ramsey RW. Sarcolemma: transmitter of active ten-sion in frog skeletal muscle. Science 1965; 149: 1379-80
130. Ingalls CP, Warren GL, Williams JH, et al. E-C coupling failurein mouse EDL muscle after in vivo eccentric contractions. JAppl Physiol 1998; 85: 58-67
131. Mishra DK, Fridén J, Schmitz MC, et al. Anti-inflammatorymedication after muscle injury. J Bone Joint Surg 1995; 77-A:1510-9
132. Kandarian SC, Boushel RC, Schulte LM. Elevated interstitialfluid volume in rat soleus muscles by hindlimb unweighting.J Appl Physiol 1991; 71: 910-4
Correspondence and reprints: Dr Gordon L. Warren, Depart-ment of Physical Therapy, University Plaza, Georgia StateUniversity, Atlanta, GA 30303-3083, USA.E-mail: [email protected]
Measurements of Functional Muscle Injury 59
Adis International Limited. All rights reserved. Sports Med 1999 Jan; 27 (1)

Copyright © 2022 FDOKUMEN




















