
Matrix Immobilization Enhances the Tissue Repair Activity of Growth Factor Gene Therapy Vectors
16
HUMAN GENE THERAPY 12:783–798 (May 1, 2001) Mary Ann Liebert, Inc. Matrix Immobilization Enhances the Tissue Repair Activity of Growth Factor Gene Therapy Vectors JOHN DOUKAS, 1 LOIS A. CHANDLER, 1 ANA MARIA GONZALEZ, 1 DANLING GU, 1 DIANA K. HOGANSON, 1 CHENGLIE MA, 1 THANH NGUYEN, 1 MARIE A. PRINTZ, 1 MARK NESBIT, 2 MEENHARD HERLYN, 2 TIMOTHY M. CROMBLEHOLME, 3 SHARON LEA AUKERMAN, 1 BARBARA A. SOSNOWSKI, 1 and GLENN F. PIERCE 1 ABSTRACT Although growth factor proteins display potent tissue repair activities, difficulty in sustaining localized ther- apeutic concentrations limits their therapeutic activity. We reasoned that enhanced histogenesis might be achieved by combining growth factor genes with biocompatible matrices capable of immobilizing vectors at delivery sites. When delivered to subcutaneously implanted sponges, a platelet-derived growth factor B-en- coding adenovirus (AdPDGF-B) formulated in a collagen matrix enhanced granulation tissue deposition 3- to 4-fold (p # 0.0002), whereas vectors encoding fibroblast growth factor 2 or vascular endothelial growth fac- tor promoted primarily angiogenic responses. By day 8 posttreatment of ischemic excisional wounds, colla- gen-formulated AdPDGF-B enhanced granulation tissue and epithelial areas up to 13- and 6-fold (p , 0.009), respectively, and wound closure up to 2-fold (p , 0.05). At longer times, complete healing without excessive scar formation was achieved. Collagen matrices were shown to retain both vector and transgene products within delivery sites, enabling the transduction and stimulation of infiltrating repair cells. Quantitative PCR and RT-PCR demonstrated both vector DNA and transgene mRNA within wound beds as late as 28 days posttreatment. By contrast, aqueous formulations allowed vector seepage from application sites, leading to PDGF-induced hyperplasia in surrounding tissues but not wound beds. Finally, repeated applications of PDGF- BB protein were required for neotissue induction approaching equivalence to a single application of collagen- immobilized AdPDGF-B, confirming the utility of this gene transfer approach. Overall, these studies demon- strate that immobilizing matrices enable the controlled delivery and activity of tissue promoting genes for the effective regeneration of injured tissues. 783 OVERVIEW SUMMARY This article describes the development of a new therapeu- tic approach to the repair of tissue defects. Adenovirus vectors encoding growth factor proteins were prepared in several biocompatible matrices, so as to allow for their con- trolled delivery to and retention at treatment sites. Using several animal models of tissue regeneration and repair, op- timum responses were seen with a platelet-derived growth factor B-encoding vector immobilized in type I collagen. This formulation induced the rapid generation of granula- tion tissue, and in ischemic excisional wounds also led to im- proved re-epithelialization and wound closure without ex- cess scar formation. The collagen matrix was shown both to provide a scaffold for infiltrating wound repair cells, which represent the target population for vector transduc- tion, and to localize vector and transgene product within the immediate delivery site. These preclinical studies sup- port the development of matrix-immobilized gene therapy approaches for regeneration of injured tissues. INTRODUCTION C URRENT MEDICAL SCIENCE inadequately addresses the repair and regeneration of injured tissues (Pierce and Mustoe, 1995; Steed, 1998; Singer and Clark, 1999). Extensive research has suggested that growth factor proteins are capable of induc- 1 Selective Genetics, San Diego, CA 92121. 2 Wistar Institute, Philadelphia, PA 19104. 3 Children’s Hospital of Philadelphia, Philadelphia, PA 19104.
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of Matrix Immobilization Enhances the Tissue Repair Activity of Growth Factor Gene Therapy Vectors

HUMAN GENE THERAPY 12783ndash798 (May 1 2001)Mary Ann Liebert Inc
Matrix Immobilization Enhances the Tissue Repair Activityof Growth Factor Gene Therapy Vectors
JOHN DOUKAS1 LOIS A CHANDLER1 ANA MARIA GONZALEZ1 DANLING GU1
DIANA K HOGANSON1 CHENGLIE MA1 THANH NGUYEN1 MARIE A PRINTZ1 MARK NESBIT2
MEENHARD HERLYN2 TIMOTHY M CROMBLEHOLME3 SHARON LEA AUKERMAN1
BARBARA A SOSNOWSKI1 and GLENN F PIERCE1
ABSTRACT
Although growth factor proteins display potent tissue repair activities difficulty in sustaining localized ther-apeutic concentrations limits their therapeutic activity We reasoned that enhanced histogenesis might beachieved by combining growth factor genes with biocompatible matrices capable of immobilizing vectors atdelivery sites When delivered to subcutaneously implanted sponges a platelet-derived growth factor B-en-coding adenovirus (AdPDGF-B) formulated in a collagen matrix enhanced granulation tissue deposition 3- to4-fold (p 00002) whereas vectors encoding fibroblast growth factor 2 or vascular endothelial growth fac-tor promoted primarily angiogenic responses By day 8 posttreatment of ischemic excisional wounds colla-gen-formulated AdPDGF-B enhanced granulation tissue and epithelial areas up to 13- and 6-fold (p 0009)respectively and wound closure up to 2-fold (p 005) At longer times complete healing without excessivescar formation was achieved Collagen matrices were shown to retain both vector and transgene productswithin delivery sites enabling the transduction and stimulation of infiltrating repair cells Quantitative PCRand RT-PCR demonstrated both vector DNA and transgene mRNA within wound beds as late as 28 daysposttreatment By contrast aqueous formulations allowed vector seepage from application sites leading toPDGF-induced hyperplasia in surrounding tissues but not wound beds Finally repeated applications of PDGF-BB protein were required for neotissue induction approaching equivalence to a single application of collagen-immobilized AdPDGF-B confirming the utility of this gene transfer approach Overall these studies demon-strate that immobilizing matrices enable the controlled delivery and activity of tissue promoting genes for theeffective regeneration of injured tissues
783
OVERVIEW SUMMARY
This article describes the development of a new therapeu-tic approach to the repair of tissue defects Adenovirus vectors encoding growth factor proteins were prepared inseveral biocompatible matrices so as to allow for their con-trolled delivery to and retention at treatment sites Usingseveral animal models of tissue regeneration and repair op-timum responses were seen with a platelet-derived growthfactor B-encoding vector immobilized in type I collagenThis formulation induced the rapid generation of granula-tion tissue and in ischemic excisional wounds also led to im-proved re-epithelialization and wound closure without ex-cess scar formation The collagen matrix was shown both
to provide a scaffold for infiltrating wound repair cellswhich represent the target population for vector transduc-tion and to localize vector and transgene product withinthe immediate delivery site These preclinical studies sup-port the development of matrix-immobilized gene therapyapproaches for regeneration of injured tissues
INTRODUCTION
CURRENT MEDICAL SCIENCE inadequately addresses the repairand regeneration of injured tissues (Pierce and Mustoe
1995 Steed 1998 Singer and Clark 1999) Extensive researchhas suggested that growth factor proteins are capable of induc-
1Selective Genetics San Diego CA 921212Wistar Institute Philadelphia PA 191043Childrenrsquos Hospital of Philadelphia Philadelphia PA 19104
ing the desired responses because of their ability to stimulatecellular proliferation migration and in some cases extracellu-lar matrix (ECM) deposition (Lynch et al 1989 Deuel et al1991) For the most part however growth factor proteins havenot achieved clinically significant improvements in tissue re-pair largely because of difficulties in establishing and main-taining therapeutic protein levels within treatment sites (Pierceand Mustoe 1995 Greenhalgh 1996)
Gene delivery represents a potential solution to these prob-lems as it can establish sustained protein production in situThis approach necessitates a careful therapeutic design partic-ularly as to the form in which genes are applied to injured tis-sues Although particle-mediated delivery of growth factorgenes is feasible (Andree et al 1994 Benn et al 1996 Em-ing et al 1999) the nonbiodegradable particles utilized mayeventually induce tissue damage Transplantation of growth fac-tor-transduced keratinocytes has been effective in animal mod-els (Vogt et al 1994 Eming et al 1998) However this ap-proach delivers transgenes only to the surface of treatment sitesminimizing their potential to influence deep wound beds andin addition the extensive ex vivo manipulations necessitatedlimit widespread clinical utility
A preferable strategy would be to directly apply gene vec-tors to treatment sites Direct injection however is suitable onlyfor accessing the outer margins of tissue defects and thereforeoffers minimal benefit to larger sized defects The formulationof growth factor genes in aqueous vehicles allows for their uni-form application to wound beds (Liechty et al 1999) how-ever such vehicles are unlikely to retain either gene vectors ortransgene products within delivery sites and therefore the ben-efit of gene therapy would be lost An alternative approachwhich we hypothesize is more appropriate for tissue repair in-volves the immobilization of growth factor genes within bio-compatible matrices (Bonadio et al 1999) This would permitvectorndashmatrix formulations to be directly applied to activewound beds where they could then serve as scaffolds for in-vading repair cells Subsequent transduction of these cellswould then allow for transgene expression and formation ofneotissues all within matrix scaffolds With appropriate designthese matrices would eventually be reabsorbed andor remod-eled during tissue repair and thus become fully integratedwithin final mature tissues
Taking these factors into consideration we formulated ade-novirus vectors encoding growth factor genes in several matri-ces and examined their ability to induce both neotissue for-mation and tissue defect repair Adenovirus was selected as thegene vector in order to achieve high but transient transgene ex-pression (Wilson 1996) characteristics that are well suited totissue repair needs We now report the use of select matrixndashvector combinations to induce robust tissue regeneration andrepair
MATERIALS AND METHODS
Vectors and growth factor protein
E1- E3-deleted human adenovirus type 5 vectors encodingindividual transgenes under the control of cytomegalovirus(CMV) promoters included AdLuc (firefly luciferase) Ad-
PDGF-B (160-amino acid open reading frame of humanplatelet-derived growth factor B) AdVEGF (121-amino acidform of vascular endothelial growth factor) and AdFGF2 (18-kDa form of fibroblast growth factor 2) Vectors were grownin 293 cells (American Type Culture Collection ManassasVA) purified by CsCl2 centrifugation dialyzed into virus buffer(20 mM Trisndash25 mM NaCl containing 25 glycerol pH 8)and stored at 280degC Virus particle concentration was deter-mined by comparing total DNA content (measured usingPicoGreen assay kits Molecular Probes Eugene OR) with aknown reference stock Plaque-forming units (PFU) were de-termined by plaque assay using 293 cells Human rPDGF-BBprotein (109 amino acid form) was produced in a eukaryoticexpression system and formulated in phosphate-buffered saline(PBS) containing 1 human albumin vehicle and doses wereselected to conform to those used in preclinical and clinicalstudies (Steed 1995 drsquoHemecourt et al 1998 Wieman 1998Wieman et al 1998)
Preparation of adenovirusndashmatrix treatments
Vectors were prepared as four different formulations For015 collagen formulations vectors were adjusted to the de-sired concentration in a vehicle of monomeric bovine type Icollagen (15 mgml Cohesion Technologies Palo Alto CA)053 minimal essential medium (Life Technologies Grand Is-land NY) and NaHCO3 (pH 74) at 18 mgml This materialis liquid at 4degC but quickly polymerizes to form a gel on warm-ing For 26 collagen formulations virus vectors were mixedwith 65 fibrillar bovine type I collagen (Matrix Contract Ser-vices San Diego CA) as follows Luer lock adapters were usedto connect two syringes (one loaded with vector in virus bufferand one with collagen) and the syringe contents were passedback and forth 30 times to achieve complete mixing This re-sults in a relatively thick but injectable single-phase materialFor carboxymethylcellulose (CMC) formulations vectors wereadjusted to the desired concentration in 25 aqueous sodiumCMC (Spectrum Quality Products Gardena CA) this mater-ial is a viscous liquid at body temperature Finally for aqueousformulations vectors were simply diluted to the desired con-centration in virus buffer Pilot studies were also performed toconfirm that all formulations prepared as described containeda uniform and homogeneous distribution of vector Briefly for-mulations were loaded into syringes samples were collectedfrom throughout the syringe contents and high-performanceliquid chromatography (HPLC) was used to confirm equivalentvirus particle concentrations among these samples
Vector stability and release assays
To determine matrix influences on vector activity AdLuc wasformulated at 5 3 1011 particlesml and held at 37degC for 60 minCMC matrices were then dissociated by vortexing in water015 collagen matrices by incubation with type I collagenase(01 mgml Worthington Biochemical Freehold NJ) at 37degCfor 45 min and 26 collagen matrices by digestion with col-lagenase (1 mgml) under these same conditions Control stud-ies established that exposure to collagenase as described hadminimal to no influence on vector structure as determined byreversed phase HPLC (data not shown) Sample aliquots wereapplied to 293 cells and cellular luciferase and protein contents
DOUKAS ET AL784
were determined as previously described (Doukas et al 1999)Samples were analyzed as serial dilutions to confirm linearityof assay responses Controls consisted of AdLuc freshly dilutedin virus buffer containing either CMC or collagenase at finaldoses equivalent to those of experimental samples In some ex-periments AdPDGF-B formulations were also incubated at 37degCfor 72 hr in an excess of either virus buffer or wound exudatefluid (taken from excisional wounds created in farm swine) af-ter which vectors were recovered as described and used to trans-duce 293 cells and cellular production of PDGF-BB determinedby enzyme-linked immunosorbent assay (ELISA)
To determine vector release from matrices 200-ml aliquotsof AdLucndashmatrix formulations were incubated in 800 ml of wa-ter at room temperature for 05 6 or 24 hr with gentle rock-ing After a brief centrifugation supernatants were sampled andassayed for DNA content using the PicoGreen assay Data werethen normalized to control values obtained when AdLuc for-mulated in virus buffer was directly added to water
PVA sponge model
All animal studies conformed to guidelines set forth in theGuide for the Care and Use of Laboratory Animals (NationalResearch Council Washington DC) and were approved byappropriate review committees Under anesthesia six full-thickness incisions 5 mm in length were placed on the ventralsurfaces of 400 to 450-g Sprague-Dawley rats after which asingle sterile polyvinyl alcohol (PVA) sponge (12 cm 3 3 mmgrade 3 M-PACT Eudora KS) was inserted per incision and
the incisions were closed with wound clips Four days post-sur-gery sponges were injected with 200-ml aliquots of either ad-enovirusndashmatrix formulations (2 3 109 or 2 3 1010 virus par-ticles per sponge) PDGF-BB protein or vehicle alone and thesponges were recovered on days 1ndash8 along with any surround-ing cellular capsules A single 3-mm section was taken fromthe center of each sponge fixed with 4 paraformaldehyde in02 M sodium phosphate buffer (pH 74) for 4 hr at 4degC andparaffin embedded The remaining sponge sections were thenprocessed for biochemical analyses as described below
Rabbit ear wound models
Male and female New Zealand White rabbits 4 kg in bodyweight (Western Oregon Rabbit Company Philomath OR)were anesthetized after which their ears were rendered bothischemic and insensitive to pain by ligation of the central androstral arteries and nerves respectively (Ahn and Mustoe1990) Using tissue biopsy punches 6- or 8-mm-diameterwounds were placed in the ventral surface extending throughthe perichondrium and additionally in some cases through theunderlying cartilage layer which was gently removed with for-ceps in order to expose the underlying dermis Larger sizedwounds were useful in creating greater tissue repair challengesas 6-mm wounds were found to exhibit considerable self-heal-ing under control conditions (see Results) Cartilage-intact mod-els were used for comparison with previous studies whereascartilage-removed models were used as more representative ofclinically encountered situations Adenovirusndashmatrix formula-
TISSUE REPAIR USING GROWTH FACTOR GENES 785
FIG 1 Adenovirus release from immobilizing matrices AdLuc was formulated in either saline 015 collagen 26 colla-gen or CMC Aliquots were then incubated in an excess of water for 05 6 or 24 hr and AdLuc released into the aqueous phasewas measured by a fluorescence-based DNA detection assay Data were normalized to the activity observed in saline-formulatedsamples (100 adenovirus release) and are shown as means 6 SD (n 5 3)
tions were then applied to wound beds as either 5-ml volumescontaining 2 3 109 virus particles (for 6-mm wounds) or 8-mlvolumes containing 4 3 109 virus particles (for 8-mm wounds)control treatments consisted of vehicles alone After treatmentapplications wounds were covered with occlusive dressings(OpSite Smith amp Nephew Largo FL) On days 7ndash10 post-surgery and treatment wounds were harvested and fixed as de-scribed above These time points were selected on the basis ofminimal self-healing in most untreated wounds as determinedin preliminary model development studies In general largerwounds allowed for longer study times as did cartilage intactmodels
Finally to assess the long-term effects of vector application6-mm wounds were placed in nonischemic rabbit ears to thelevel of underlying cartilage and treated as described aboveWounds were then harvested for analysis on days 28ndash180 post-treatment
Biolocalization studies
Two model systems were used to examine adenovirus vectorbiodistribution In the first model 6-mm-diameter wounds ex-
tending through the underlying cartilage were placed in rabbitears as described above nonischemic ears were used so as topresent the greatest opportunity for vascular dissemination ofvirus Wound beds were then treated with AdPDGF-B formu-lated in 015 collagen (2 3 109 virus particles per wound in a5-ml volume) after which animals were housed for 1 3 7 or14 days After blood collection via cardiac puncture animalswere perfused with 120 ml of PBS at a rate of 20 mlmin andwound beds and organs were harvested for polymerase chain re-action (PCR)-based detection of AdPDGF-B Forty cycles oftouchdown PCR were performed with oligonucleotide primersdesigned to amplify a 315-base pair fragment spanning the ma-jority of the human PDGF-B 109-amino acid coding region(sense 59-TTCCCTGACCATTGCTGAGCCGGCCA-39 anti-sense 59-ACAGGCCGTGCAGCTCCACTG-39) This ldquotouch-downrdquo strategy of thermocycling employs successively de-creasing annealing temperatures (four cycles performed at eachannealing temperature beginning at 72degC and decreasing in 1degCincrements down to 63degC with each cycle consisting of a 30-sec annealing step and a 1-min extension step) PCR ampliconswere then visualized on ethidium bromide-stained 08 agarosegels
DOUKAS ET AL786
FIG 2 Influence of adenovirusndashmatrix formulations on neotissue formation PVA sponges were implanted subcutaneously intorats and 4 days later were injected with either AdPDGF-B AdFGF2 AdVEGF or AdLuc (2 3 1010 virus particles per sponge)formulated in 015 collagen controls consisted of collagen alone Six days posttreatment sponges were processed as paraffinsections and stained as follows (A) AdPDGF-B trichrome stain (B) AdPDGF-B Ki-67 immunostain Note the positively stainedendothelial cells (arrowheads) and fibroblasts (arrows) (C) AdFGF2 trichrome stain (D) AdFGF2 BSL-I lectin stain (E) Ad-VEGF trichrome stain (F) AdVEGF BSL-I lectin stain (G) AdLuc trichrome stain (H) Collagen vehicle trichrome stainOriginal magnification (A C E and G) 3200 (B D F and H) 3400
TABLE 1 NEOTISSUE FORMATION AFTER DELIVERY OF ADENOVIRUSndashMATRIX FORMULATIONSa
Granulation Protein DNATreatment fill () (mgsponge) (mgsponge)
015 Collagen vehicle 26 6 18 13 6 2 79 6 21AdPDGF-B (2 3 109 particles) 62 6 22b 15 6 2 107 6 27AdPDGF-B (2 3 1010 particles) 93 6 6b 26 6 9b 215 6 109b
AdLuc (2 3 109 particles) 24 6 15 12 6 2 67 6 12AdLuc (2 3 1010 particles) 36 6 22 16 6 2 102 6 27
015 Collagen vehicle 29 6 8 15 6 2 69 6 10AdPDGF-B (2 3 1010 particles) 86 6 15c 25 6 3c 136 6 20c
AdVEGF (2 3 1010 particles) 44 6 16d 25 6 4c 144 6 24c
015 Collagen vehicle 18 6 8 10 6 1 65 6 12AdPDGF-B (2 3 1010 particles) 68 6 13c 23 6 5e 151 6 51c
AdFGF2 (2 3 1010 particles) 55 6 15c 18 6 3c 126 6 33f
aPVA sponges were implanted subcutaneously in rats and 4 days later injected with either 015 collagen alone or collagencontaining adenovirus vectors Vector doses are listed as the number of virus particles delivered per sponge Six days posttreat-ment sponges were recovered and processed to determine the percent sponge area filled with granulation tissue (0ndash100) aswell as total protein and DNA contents as described in Materials and Methods Data are presented as means 6 SD (n 5 8)
bp 00002 versus collagen control and p 0005 versus AdLuc groupscp 00001 versus collagen controldp 003 versus collagen controlep 00001 versus collagen control and p 0002 versus AdFGF2fp 0001 versus collagen control
TISSUE REPAIR USING GROWTH FACTOR GENES 787
A second model utilized 7-cm2 full-thickness excisionalwounds placed on the backs of anesthetized rabbits Woundswere treated with AdPDGF-B formulated in 26 collagen (2 3
109 or 2 3 1011 virus particles per wound in 700-ml volumes)and then covered with OpSite dressing On day 3 7 28 or 90posttreatment blood was collected animals were perfused asdescribed above and the following organs were recoveredwound bed brain heart lung liver spleen kidney gonad andlymph nodes (axillary cranial mesenteric and posterior medi-astinal) Real-time quantitative TaqMan PCR was performedusing 45 two-step cycles with primers designed to amplify se-quences bridging the vector backbone and the PDGF-B pre-proregion (sense 59-GGATCTTCGAGTCGACAAGCTT-3 9 an-tisense 59-TAAGGGCTCCTCGAAATACTCTA-3 9) The re-sulting amplicons were detected with an internal fluorogenicprobe (59-TAGTGGTACTTAGCGACGACCCGC-3 9) and anABI Prism 7700 sequence detector (PE Applied BiosystemsFoster City CA) The initial target copy numbers present ineach reaction were quantified by extrapolation from standardcurves of AdPDGF-B DNA in the background of 1 mg of rab-bit liver DNA per reaction Each PCR contained 1 mg of testDNA with the exception of wound bed which contained 500ng per reaction and blood which contained the equivalent of10 ml of original sample Each test sample was assayed in du-plicate to control for PCR inhibitory substances a third reac-tion was spiked with 100 copies of AdPDGF-B DNA PCR dataare presented as AdPDGF-B genome copies per wound thelimit of quantitation (LOQ) was 10 copiesmg DNA or an av-erage of 105 copieswound
For those tissues scoring positive for PCR-amplifiable vec-tor we further performed real-time quantitative reverse tran-scriptase (RT)-PCR Reverse transcriptase reactions were per-formed with 100 ng of each test RNA per reaction and randomhexamer primers The resulting cDNAs were then used to am-plify both rabbit 18S rRNA cDNA and PDGF-B cDNA in sep-arate PCRs The vector-specific primers were designed to am-plify full-length 160-amino acid human PDGF-B mRNA(sense 59-CAAGCACACGCATGACAAGA-3 9 antisense 59-TTTCGTTATCGTAGTGTTTAAAGTGT-3 9) The resulting131-nucleotide amplicons were detected with an internal fluo-rogenic probe (59-AAACAAGTTGCTCGATGGATCCTTAT-CAGGCT-39) RT-PCRs were then normalized for total RNAby 18S rRNA content with a second pair of PCR primers RT-PCR data are presented as the relative amount of PDGF-BmRNA per unit 18S rRNA (in arbitrary units)
Histochemical analyses
For routine morphological assessment paraffin sections werestained according to the Masson trichrome procedure In addi-tion a blinded observer using a microscope equipped with oc-ular micrometers measured the area within sponges filled bygranulation tissue these values are expressed as the percentageof sponge interior occupied by tissue ( granulation fill) Forexcisional wounds trichrome-stained sections and an imageanalysis software package (Image-Pro Plus software Media Cy-bernetics Silver Spring MD) were used to determine the cross-sectional areas of granulation tissue and epithelium per wound(in mm2) In addition the percentage of wound closure was cal-culated according to the following formula [(original wound
diameter 2 epithelial gap length) original wound diameter] 3100
For immunohistochemistry paraffin sections were stainedwith biotinylated Griffonia (Bandeiraea) simplicifolia lectin I(BSL-I) horseradish peroxidase (HRP)-labeled streptavidin anddiaminobenzidine (DAB Vector Laboratories BurlingameCA) in order to detect vascular endothelium Mouse anti-Ki-67and HRP-labeled rabbit anti-mouse IgG antibodies followed byDAB were used to detect proliferating cells Mouse anti-humanPDGF-BB (Z2703 American Type Culture Collection) andHRPndashanti-mouse IgG antibodies followed by DAB were usedto detect human PDGF-BB protein Fluorescein isothiocyanate(FITC)-conjugated anti-adenovirus antibody (Accurate Chemi-cals Westbury NY) and the nuclear stain 496-diamidino-2-phenylindole (DAPI Molecular Probes) were used to detectinternalized adenovirus vectors Finally fibroblasts were iden-tified with Cy3-labeled anti-vimentin (Sigma St Louis MO)
For in situ hybridization procedures an [a-35S] UTP-labeledriboprobe prepared from the full-length human PDGF-B cDNAwas used as previously described (Gonzalez et al 1995) Asense riboprobe was used to control for nonspecific hybridiza-tions
Biochemical analyses
Tissue samples not processed for paraffin embedding wereplaced in 100 mM phosphate buffer containing 02 Triton X-100 (pH 78) and agitated at 55 msec for 20 sec in a Fast-Prep system (BIO 101 Vista CA) After centrifugation su-pernatants were analyzed for protein using a bicinchoninic acidassay (Pierce Rockville IL) and for DNA using the PicoGreenassay PDGF-BB protein content was determined with a humanPDGF-BB-specific ELISA (RampD Systems Minneapolis MN)
Statistical Analyses
Data are presented as arithmetic means 6 1 SD Groups ofthree or more means within individual studies were comparedby one-way analysis of variance (ANOVA) and the Fisher pro-cedure for least significant differences (StatView softwareAbacus Concepts Berkeley CA)
RESULTS
Adenovirus vectors can be immobilized in an activeform within matrices
As an initial step to the in vivo assessment of adenovirusndashmatrix formulations we first determined the activity profilesand release kinetics for vectors formulated in type I collagenand carboxymethylcellulose (CMC) Collagen was selected onthe basis of its successful use as a delivery matrix for proteinsand DNA (Grotendorst et al 1985 Mustoe et al 1987 1991Sprugel et al 1987 Khouri et al 1994 Bonadio et al 1999)as well as its ability to enhance tissue repair responses in fi-broblasts (Xu and Clark 1996 1997) Relatively low (015)and high (26) concentrations were examined reasoning thatthis would allow for either relatively short or long retentiontimes at application sites respectively CMC was selected on
DOUKAS ET AL788
TISSUE REPAIR USING GROWTH FACTOR GENES 789
FIG 3 Localization of gene vector and transgene product within neotissues PVA sponges implanted in rats were injected withAdPDGF-B formulated in 015 collagen (2 3 1010 virus particles per sponge) and paraffin sections were stained as follows(A) Day 1 posttreatment anti-adenovirus immunostain to detect AdPDGF-B (green) DAPI stain to detect cell nuclei (blue) (B)Day 4 posttreatment in situ hybridization using human PDGF-B gene probe (C) Day 1 posttreatment anti-human PDGF-BBprotein immunostain positively stained leukocytes (arrowheads) and fibroblasts (arrows) are indicated (D) Day 6 posttreatmentanti-PDGF-BB immunostain (E) Day 8 posttreatment anti-PDGF-BB immunostain (F) Day 8 post- treatment immunostains todetect PDGF-BB protein (green) and vimentin (red) yellow fluorescence indicates PDGF-BB and vimentin colocalization bluefluorescence indicates cell nuclei (DAPI stain) Original magnifications (AndashC E and F)3 400 (D) 31000
the basis of its clinical use for the delivery of PDGF-BB pro-tein (Steed 1995)
Matrix influences on vector activity were examined by in-cubating AdLuc formulations at 37degC for 60 min followed bymatrix dissolution and vector bioassay (luciferase productionby 293 cells) This is an important test as adenoviruses arequickly inactivated under unfavorable physical and chemicalconditions (Nyberg-Hoffman and Aguilar-Cordova 1999)None of the matrices examined had a deleterious effect on vec-tor activity (90 6 12 106 6 5 and 139 6 37 of control ac-tivity for 015 collagen 26 collagen and CMC respec-tively) To further model in vivo vector stability we alsoincubated AdPDGF-B formulated in 26 collagen with woundfluid for 72 hr at 37degC prior to vector recovery and analysisWe observed no reduction in the level of PDGF-BB productionfrom cells transduced with AdPDGF-B exposed to wound fluidas compared with vector exposed to virus buffer (30 6 5 vs20 6 3 ng of PDGF-BB produced per milliliter of culturemedium respectively n 5 3)
As these data support the suitability of the selected matricesfor in vivo use we next determined their influence on vectorrelease kinetics (Fig 1) When placed in water collagen ma-trices retained the majority of their immobilized vectors with015 and 26 collagen releasing only 17 6 3 and 3 6 1 ofvector by 24 hr respectively By contrast 48 6 3 of AdLucwas released from CMC within 30 min and 61 6 2 by 6 hrThis was not unexpected as CMC is fairly water soluble andas both CMC and adenoviral particles are negatively chargedTherefore collagen matrices in a concentration-dependentfashion display more favorable kinetics for localizing and re-taining adenovirus vectors at delivery sites than does CMC
Collagen-immobilized adenoviruses induce distinctneotissues in vivo
Initial in vivo tests of matrix-immobilized vectors were per-formed with an established model of de novo tissue generation(Buckley et al 1985 Sprugel et al 1987 LeGrand et al1993) PVA sponges implanted subcutaneously in rats were in-jected with a single dose of adenovirus formulated in either col-lagen or CMC and then analyzed for tissue formation Forgrowth factor transgenes we selected platelet-derived growth
factor B (PDGF-B) vascular endothelial growth factor (VEGF)and fibroblast growth factor 2 (FGF2) because of their well-known mitogenic activities
AdPDGF-B formulated in 015 collagen induced granula-tion tissue formation in a dose-responsive manner (Table 1)Compared with vehicle controls delivering 2 3 1010 virus par-ticles induced a 17- to 23-fold increase in sponge protein con-tent (p 00002) a 2- to 27-fold increase in DNA content (p
00002) and a 29- to 43-fold increase in granulation tissue fill(p 00002) Trichrome-stained sections revealed the nearcomplete fill of sponge interiors with well-formed granulationtissue by day 6 posttreatment (Fig 2A) Expression of Ki-67a nuclear protein upregulated in proliferating cells (Gerdes etal 1983) established that both vascular endothelium (arrow-heads Fig 2B) and fibroblasts (arrows Fig 2B) had prolifer-ated in response to PDGF-B gene delivery AdFGF2 and Ad-VEGF also enhanced protein and DNA content within sponges(Table 1) However these vectors induced less granulation tis-sue deposition as compared with AdPDGF-B and the tissuesformed were histologically distinct
Tissues present in AdFGF2-treated sponges were highly vas-cular as revealed by the endothelial-reactive lectin BSL-I (Fig2D) Many of the infiltrating mononuclear cells also reactedpositively with BSL-I lectin suggesting that these cells wereendothelial cells or endothelial precursors AdFGF2 did nothowever induce the formation of classic granulation tissue aslittle collagen deposition was observed demonstrated by thepaucity of blue-staining material in trichrome-stained sections(Fig 2C) AdVEGF also induced heavily vascularized tissues(Fig 2E and F) but with greater extracellular collagen deposi-tion than AdFGF2 Relative to AdPDGF-B-induced tissueshowever AdVEGF-induced tissues were disorganized con-tained few fibroblasts and were markedly edematous Finallywhen AdLuc was delivered as a control treatment no signifi-cant increases in protein DNA or granulation tissue were ob-served compared with collagen vehicle alone (Table 1)Trichrome-stained sections revealed sparse inflammatory cellinfiltrates within AdLuc-treated sponges (Fig 2G) which com-pared with the near absence of infiltration after delivery of col-lagen vehicle alone (Fig 2H) suggested a limited antiviral response
Unlike the 015 collagen formulations described above
DOUKAS ET AL790
TABLE 2 NEOTISSUE FORMATION AFTER PDGF-B GENE OR PDGF-BB PROTEIN DELIVERYa
Granulation Protein DNATreatment fill () (mgsponge) (mgsponge)
015 Collagen vehicle 28 6 13b 16 6 2b 103 6 22b
AdPDGF-B 81 6 15b 30 6 6b 218 6 28b
PDGF-BB 100 mg 64 6 12c 22 6 4c 155 6 26c
PDGF-BB 10 mg qod 3 3d 77 6 9b0 31 6 8b 230 6 75b
aPVA sponges implanted in rats were injected with either 015 collagen vehicle or collagen containing AdPDGF-B as described in Table 1 Alternatively PDGF-BB protein was delivered as a single 100-mg dose on day 4 postimplantation or as10-mg doses on days 4 6 and 8 Sponges were removed on day 12 postimplantation and processed to determine the percent granulation fill as well as total protein and DNA contents Data are presented as means 6 SD (n 5 4ndash8)
bp 00001 versus collagen control and p 005 versus 100-mg PDGF-BBcp 003 versus collagen controldqod 3 3 Every other day three times
TISSUE REPAIR USING GROWTH FACTOR GENES 791
TABLE 3 INFLUENCE OF ADENOVIRUSndashMATRIX FORMULATIONS ON ISCHEMIC WOUND HEALINGa
Granulation Epithelial Wound closureTreatment Model system area (mm2) area (mm2) ( complete)
Aqueous buffer Cartilage intact 10 6 08 05 6 03 61 6 226 mm day 10
AdPDGF-B in Cartilage intact 24 6 22 05 6 01 73 6 28aqueous buffer 6 mm day 10
015 Collagen Cartilage intact 05 6 03 05 6 02 89 6 14vehicle 6 mm day 10
AdPDGF-B in Cartilage intact 16 6 09b 09 6 03c 97 6 7015 collagen 6 mm day 10
Aqueous buffer Cartilage removed 45 6 08 08 6 02 95 6 96 mm day 7
AdPDGF-B in Cartilage removed 40 6 15 11 6 05 82 6 22aqueous buffer 6 mm day 7
015 Collagen Cartilage removed 36 6 13 06 6 02 88 6 22vehicle 6 mm day 7
AdPDGF-B in Cartilage removed 70 6 14b 07 6 03 79 6 22015 collagen 6 mm day 7
26 Collagen Cartilage removed 04 6 05 01 6 01 24 6 15vehicle 8 mm day 8
AdPDGF-B in Cartilage removed 51 6 25b 06 6 03b 52 6 25c
26 collagen 8 mm day 8
aExcisional wounds (6 or 8 mm in diameter) were placed in ischemic rabbit ears with underlying cartilage left intact or re-moved Wounds were then treated with AdPDGF-B formulated in aqueous virus buffer or collagen control treatments consistedof vehicle alone For 6-mm wounds virus was applied as 2 3 109 particles per wound for 8-mm wounds as 4 3 109 particlesper wound On days 7ndash10 posttreatment wounds were harvested and processed as trichrome-stained paraffin sections whichwere then used to quantify newly formed granulation tissue and epithelium (cross-sectional area in mm2) and the degree of woundsurface closure (where 100 equals complete closure) Data are presented as means 6 SD (n 5 4ndash8)
bp 0009 versus vehicle controlcp 005 versus vehicle control
26 collagen formulations could not be reliably examined inthe PVA sponge model as their relatively high viscosity pre-vented uniform filling of sponges by syringe CMC-formulatedvectors were also unsuitable for this model system as theyproved highly inflammatory (data not shown) These formula-tions therefore were evaluated in more appropriate excisionalwound models (see below)
Tissue repair cells are transduced by collagen-immobilized adenoviruses
On the basis of the robust activity of collagen-formulatedAdPDGF-B we elected to further examine this vectorndashmatrixcombination first by seeking to correlate PDGF-B gene deliv-ery with subsequent transgene and protein expression WhenPVA sponges treated with 015 collagenndashAdPDGF-B werestained with both an anti-adenovirus antibody and the nuclearstain DAPI the majority of cells present 1 day after gene de-livery had bound andor internalized adenovirus (Fig 3A) Insitu hybridization revealed that these cells were successfullytransduced by virus as they contained human PDGF-B mRNA(Fig 3B) By contrast hybridization product was not detectedwith a sense riboprobe or when AdLuc-treated sponges wereexamined (data not shown)
We next used a human PDGF-BB-specific antibody to iden-tify the cell types responsible for transgene expression By day
1 postdelivery of 015 collagenndashAdPDGF-B PDGF-BB pro-tein was localized to leukocytes (arrowheads) and fibroblasts (ar-row Fig 3C) With time PDGF-BB protein was detected boundto the extracellular matrix (ECM) surrounding positively stainedcells (Fig 3D) This last observation indicates that a reservoir ofPDGF-BB protein develops within treated tissues and thus mayprolong the histogenic effects of this growth factor Finally byday 8 the majority of immunoreactivity had abated with pri-marily microvascular endothelium remaining positive (Fig 3E)However scattered fibroblasts could still be shown to producePDGF-BB protein by dual immunohistochemistry with anti-PDGF-BB and anti-vimentin antibodies (Fig 3F)
Multiple administrations of PDGF-BB protein are required to approximate the histogenic effects of collagenndashAdPDGF-B
To directly compare gene therapy with the more conven-tional approach of growth factor protein delivery we next quan-tified tissue formation in response to either PDGF gene or pro-tein delivery A single injection of 015 collagenndashAdPDGF-Benhanced granulation tissue filling of sponges by 3-fold versusvehicle alone (p 00001) and sponge protein and DNA lev-els by 2-fold (p 00001 Table 2) Using a human PDGF-BB-specific ELISA this growth factor was detected at 54 6 13ngsponge (n 5 8) By contrast when PDGF-BB protein was
delivered as a single dose nearly 2000-fold in excess of thisconcentration the tissue formation responses observed (proteinand DNA accumulation and granulation tissue formation) weresignificantly lower (p 005 Table 2) In fact repeated dos-ing with PDGF-BB protein was required in order to achieve re-sponses comparable to a single administration of the PDGF-Bgene These data therefore support our hypothesis that the abil-ity of gene delivery to establish prolonged in situ growth fac-tor production translates into greater histogenesis than that seenwith growth factor proteins
CollagenndashAdPDGF-B induces complete healing of ischemic wounds
Nonhealing wounds are a major risk in chronically ischemictissues as low oxygen tension greatly impairs tissue repair pro-cesses We therefore compared the ability of matrix versusaqueous formulated AdPDGF-B to repair ischemic excisionalwounds Several models were employed to compare variationsin wound size and condition so as to allow for a more com-plete picture of tissue repair
In the first model system 6-mm-diameter wounds were cre-ated in ischemic rabbit ears by removal of epidermal and der-mal layers but not underlying cartilage This model has beenused in previous studies of growth factor proteins and genes(Ahn and Mustoe 1990 Mustoe et al 1994 Liechty et al1999) and was therefore employed to allow comparison withthese reports However it represents an artificial system as thepresence of a cartilage layer restricts both treatment activity andhealing to wound margins and in addition the initially acellu-lar wound bed forms a cup that artifactually retains aqueoustreatments As would be predicted we found a trend towardgranulation tissue formation in this model after the applicationof AdPDGF-B formulated in aqueous buffer (Table 3) How-ever this response did not reach the level of statistical signifi-cance as tissue development was highly variable (note the highstandard deviation value) In addition epithelial regenerationand wound closure were minimal to unaffected By contrastAdPDGF-B formulated in 015 collagen enhanced granula-tion tissue area by 32-fold and epithelial area by 18-fold overthat achieved with vehicle alone (p 0009 and 005 respec-tively) Although near complete closure of epithelial gaps wasalso achieved the high level of self-healing in control-treatedgroups (89 wound closure) precluded statistical significance
In an alternative model design subdermal cartilage was com-pletely removed from excisional wounds creating beds whosefloors now consisted of dermal tissue (Pierce et al 1994b)This design allows for cellular responses from the entire woundbed as well as the opportunity for vector migration beyond
treatment areas We now observed that aqueous formulated Ad-PDGF-B failed to induce even a trend toward tissue regenera-tion (Table 3) Rather the vector appears to have seeped throughthe wound bed floor as inflammatory cell infiltrates and fociof fibroblast proliferation were observed in the underlying der-mis and at wound margins (Fig 4A) Immunohistochemistryconfirmed the production of human PDGF-BB at these sites(Fig 4B) CMC-formulated AdPDGF-B also failed to induceany meaningful tissue repair Wounds treated with this formu-lation showed a diffuse inflammatory response within thewound bed and wound surfaces were overlain with fibrin clotsrather than regenerating epithelium (Fig 4C and D) By con-trast AdPDGF-B formulated in 015 collagen enhanced gran-ulation tissue deposition 19-fold within wound beds versus ve-hicle controls (p 0002) and wounds were extensivelyepithelialized (Table 3) Neither epithelial regeneration norwound closure achieved significance however as the high de-gree of self-healing achieved in this particular model (see ve-hicle alone group) most likely masked transgene-stimulated re-sponses
To address these model limitations as our next system wecreated 8-mm wounds in ischemic rabbit ears by removingepidermal dermal and cartilage layers reasoning that largerexcisional wounds would display limited self-healing In ad-dition this model could readily accommodate 26 collagenformulations which proved difficult to reproducibly apply insmaller wounds Compared with control wounds treated withcollagen vehicle alone wounds treated with AdPDGF-B for-mulated in 26 collagen achieved a 12-fold enhancementin granulation tissue fill and a 6-fold enhancement in re-ep-ithelialization by day 8 posttreatment (p 0009 Table 3)In addition wound closure was only 24 complete in colla-gen vehicle-treated wounds by day 8 but 52 complete inwounds treated with collagen-formulated AdPDGF-B (p
005) Histologically AdPDGF-B-treated wounds showed nosigns of tissue hyperplasia or chronic inflammation but ratheran orderly repair process marked by a regenerated epitheliallayer overlying a wound bed filled with granulation tissue(Fig 4E and F)
CollagenndashAdPDGF-B induces normal long-term tissue repair
Our choice of adenoviruses for transgene delivery was partlybased on the reasoning that as these vectors establish transientgene expression they would not lead to hyperproliferative re-sponses or scar formation To test this hypothesis we treatedrabbit ear excisional wounds with AdPDGF-B formulated in015 collagen and examined tissue repair responses out to
DOUKAS ET AL792
FIG 4 Influence of adenovirusndashmatrix formulations on excisional wound repair Excisional wounds (6 or 8 mm in diameter andextending through underlying cartilage layers) were placed in ischemic rabbit ears bars indicate original wound depth (determinedfrom cartilage visible at wound margins) Wounds were then treated with AdPDGF-B formulated in either virus buffer CMC orcollagen and on day 7 or 8 posttreatment processed for histology or immunohistochemistry An identical design was used to ex-amine long-term healing on day 90 except that wounds were created in nonischemic ears (A) Day 7 buffer-formulated AdPDGF-B-treated 6-mm wound trichrome stain (B) Day 7 buffer-formulated AdPDGF-B-treated 6-mm wound anti-PDGF-BB proteinimmunostain (C and D) Day 7 CMC-formulated AdPDGF-B-treated 6-mm wound trichrome stains (E and F) Day 8 26 col-lagen-formulated AdPDGF-B-treated 8-mm wound trichrome stains (G and H) Day 90 015 collagen-formulated AdPDGF-B-treated 6-mm wound trichrome stains Original magnification (A C E and G) 340 (B D F and H) 3200
TISSUE REPAIR USING GROWTH FACTOR GENES 793
DOUKAS ET AL794
TABLE 4 BIODISTRIBUTION OF AdPDGF-B IN EXCISIONAL WOUNDSa
Positive samplestotal assayed
Tissue AdPDGF-B dose Day 3 Day 7 Day 28 Day 90
Wound bed 2 3 109 particles 66 66 66b 06Axillary lymph nodes 2 3 109 particles 02 ND 06 06
Wound bed 2 3 1011 particles 66 66 66 46c
Axillary lymph nodes 2 3 1011 particles 66 ND 66d 26e
aFull-thickness excisional wounds (7 cm2) were placed on the backs of rabbits and AdPDGF-B formulated in 26 collagenwas applied as either 2 3 109 or 2 3 1011 virus particles per wound On days 3ndash90 posttreatment wound beds and a panel oforgans were harvested for real-time PCR quantification of viral genome Data are shown for wound bed and axillary lymph nodesamples as the number of samples that yielded amplifiable signals per total number assayed ND not determined
bThree of six samples scored below the level of quantitation (LOQ 10ndash100 copiesmg DNA)cAll four positive samples scored below the LOQdThree of six samples scored below the LOQeBoth positive samples scored below the LOQ
180 days posttreatment (Fig 5) PDGF-B gene delivery en-hanced total ear thickness relative to controls on day 28 (229 6
020 vs 179 6 019 mm p 00001) and day 60 (192 6 001vs 182 6 011 mm p 0005) as anticipated on the basis ofthe ability of this formulation to induce granulation tissue for-mation By day 90 posttreatment however there was no mea-surable difference in ear thickness between AdPDGF-B andcontrol-treated groups and this relationship continued out today 180 indicating that growth factor gene delivery did not in-duce excessive scar formation This was also confirmed histo-logically AdPDGF-B-treated wounds on day 90 and beyondwere composed of a thin outer keratin layer an underlying ep-ithelial layer of equivalent thickness to nonwounded areas anda collagen-rich dermis devoid of any signs of tissue hyperpla-sia (Fig 4G and H)
Collagen immobilization limits adenovirus vectorbiodistribution beyond treatment sites
As a final measure of the value of matrix immobilization forgene delivery we determined the biodistribution patterns ofvectors after their in vivo delivery In the first model systemused AdPDGF-B formulated in 015 collagen was applied torabbit ear wounds at equivalent doses as previously describedwounds were extended through underlying cartilage but vas-cular supplies were not disturbed so as to permit maximal vec-tor dissemination By PCR no adenoviral DNA was detectablein lung spleen brain cervical lymph nodes or gonads on day1 3 7 or 14 (n 5 6 per group) In the liver one of six sam-ples was positive on days 3 and 7 but none on day 14 in serumonly one of six samples tested positive on day 14 (equivalentof 500-ml serum volume) By contrast adenovirus was detectedin eight of eight wound bed samples at all time points exam-ined
In a second model system excisional wounds placed on thebacks of rabbits were treated with AdPDGF-B formulated in26 collagen Because of their anatomical placement thismodel allowed for the creation of larger excisional wounds (7-cm2 total area) than those placed in rabbit ears (03 cm2) and
consequently larger treatment volumes and vector doses (2 3109 or 2 3 1011 virus particles per wound) At the lower doseof 2 3 109 particles PCR-amplifiable adenoviral DNA was notdetectable beyond wound beds on day 3 7 28 or 90 Tissuessampled and found not to contain vector included blood heartlung liver kidney brain spleen lymph nodes and gonads (n 5
6group) In wound beds adenoviral DNA was detected at alltime points except for day 90 (Table 4 and Fig 6) Vector lev-els did decrease however by 38-fold between days 7 and 28with three of six samples falling below the level of quantita-tion (LOQ) by real-time PCR at the latter time point (Fig 6)
At a 100-fold higher vector dose of 2 3 1011 particles perwound PCR-amplifiable adenoviral DNA was once again un-detectable in the majority of tissues sampled Except for a sin-gle day 7 liver sample and a single day 7 brain sample (bothbelow the LOQ) adenoviral DNA was only detectable directlyin wound beds or in the axillary lymph nodes that drain woundsites (Table 4) Moreover three of six positive axillary nodesamples scored below the LOQ on day 28 as did both positivesamples on day 90 indicating that they contained relatively lit-tle vector Within wound beds adenoviral DNA was detectedat quantifiable levels out to day 28 and at detectable but non-quantifiable levels on day 90 DNA copy numbers remainedsteady between days 3 and 7 dropped 107-fold between days7 and 28 and a further 1662-fold by day 90 Finally at eachtime point DNA copy numbers in wounds treated with 2 3
1011 particles were approximately 100-fold higher than thosefound in wounds treated with 2 3 109 particles thus confirm-ing the linearity of our assay system
To better define the time course of human PDGF-BB pro-duction we also quantified transgene mRNA levels in woundbed samples treated at 2 3 109 particles per wound This treat-ment dose was selected as representative of the virus particleconcentration capable of inducing complete healing in ischemicear wounds Quantifiable levels of human PDGF-B mRNAwere detectable in treated dorsal wounds at days 3 7 and 28(Fig 6) with levels decreasing 14-fold between days 3 and 7and 5-fold between days 7 and 28 The more sensitive tech-nique of real-time RT-PCR therefore demonstrates that trans-
TISSUE REPAIR USING GROWTH FACTOR GENES 795
gene expression extends well beyond the 8-day time period sug-gested using anti-PDGF-BB immunohistochemistry as a de-tection system (Fig 3)
DISCUSSION
These studies demonstrate that immobilization of gene ther-apy vectors in collagen-based matrices enables their efficientdelivery and activity in vivo Matrix immobilization achievedprolonged transgene-encoded growth factor production and asa consequence robust tissue repair By contrast aqueous vehi-cles failed to retain adenoviruses at application sites resultingin diffuse inflammation rather than productive tissue regenera-tion These observations confirm our basic hypothesis that ma-trix immobilization of growth factor-encoding gene therapyvectors represents a promising approach to tissue repair
Although de novo tissue deposition was achievable with sev-eral growth factor genes PDGF-B proved the most suitable forrepair of cutaneous defects A single administration of colla-gen-immobilized AdPDGF-B rapidly induced the formation ofhighly cellular and vascularized tissues with dense ECMs richin collagen By contrast AdFGF2 induced a primarily vascu-lar response with little collagen deposition FGF2 induces therelease of matrix metalloproteinase 1 or interstitial collagenase(Buckley-Sturrock et al 1989) and this may underlie the rel-ative paucity of ECM accumulation VEGF gene delivery alsoinduced highly vascular responses however the enhanced per-meability characteristic of VEGF-induced vasculature (Dvoraket al 1995) led to edema within nascent tissues In fact much
of the enhanced protein and DNA deposition observed in Ad-VEGF-treated PVA sponges may well derive from fluid exu-dates rather than actual tissue formation Finally the inabilityof AdLuc delivery to induce anything beyond a limited in-flammatory response confirms that tissue formation was de-pendent on growth factor gene delivery
The robust activity of PDGF-B gene delivery was expectedas PDGF-BB protein initiates multiple aspects of tissue forma-tion including cellular influx and proliferation ECM deposi-tion and tissue remodeling (Pierce et al 1988 1991 1994a)Indeed PDGF-BB is the only growth factor protein to have suc-cessfully completed human clinical trials and be approved forthe treatment of dermal wounds (Steed 1995 drsquoHemecourt etal 1998 Wieman 1998 Wieman et al 1998) We observedthat collagen-formulated AdPDGF-B induced the complete re-pair of excisional skin defects without unwanted long-term ef-fects such as the development of hypertrophic scars Endoge-nous growth factors other than PDGF-BB however most likelymediated the enhanced re-epithelialization observed in thesewounds as epithelial regeneration is driven by members of theepidermal growth factor and FGF families (Pierce et al 1994bDanilenko et al 1995) Our data indicate nonetheless that tis-sue regeneration and repair were initiated and to a great degreedriven by transgene-encoded PDGF-BB
Despite the known activity of PDGF-BB protein we wereable to demonstrate greater tissue deposition after gene deliv-ery as compared with the use of recombinant growth factor pro-tein A single application of PDGF-BB protein could not equalthe ability of PDGF-B gene therapy to induce neotissue for-mation even at doses well in excess of that induced in situ byAdPDGF-B and in excess of that used in human clinical trials
FIG 5 Influence of collagen-formulated AdPDGF-B on long-term tissue repair Excisional wounds (6 mm in diameter withcartilage remaining intact) were placed in nonischemic rabbit ears and treated with either 015 collagen alone (open columns)or AdPDGF-B formulated in this vehicle (solid columns) On days 28ndash180 posttreatment total ear thickness at the site of eachwound was measured (in mm) with calipers Data are presented as means 6 SD (n 5 3) Treatment groups differ by p 00001groups differ by p 0005
(Steed 1995 drsquoHemecourt et al 1998 Wieman 1998 Wie-man et al 1998) In fact repeated administrations of PDGF-BB protein were required to approach the level of tissue for-mation observed after a single administration of AdPDGF-BThese data support our hypothesis that sustained localizedgrowth factor production is required for robust tissue repair
In further support of this hypothesis we demonstrated thatmRNA encoding human PDGF-B was present in excisionalwounds as late as day 28 after collagen-formulated AdPDGF-B administration By contrast previous studies of PDGF-BBprotein found that the great majority of this growth factor wasgone from treated wounds 1 day postapplication and that anytissue maturation subsequently observed was most likely dueto the upregulation of endogenous growth factors (Pierce et al1992 1995) We also demonstrated that repair cells such asmononuclear leukocytes endothelial cells and fibroblasts pres-ent with developing neotissues represent the source of both
transgene transcription and PDGF-BB production In additiona depot of human PDGF-BB was detected bound to the colla-gen delivery matrix and ECM of these tissues This was antici-pated as PDGF-BB contains collagen-binding motifs (Soma-sundaram and Schuppan 1996) We hypothesize that subsequentmatrix metalloproteinase activity by repair cells will serve togenerate localized release of this sequestered growth factor pooland as a consequence further drive tissue regeneration Theseevents which are central to tissue remodeling should be directlyenhanced by collagen matrices as type I collagen stimulates me-talloproteinase production integrin expression and cellular ac-tivation in PDGF-stimulated fibroblasts (Xu and Clark 19961997)
An additional rationale for employing collagen matrices wasto physically immobilize vectors This was confirmed in vivowhere collagen matrices maintained AdPDGF-B at deliverysites for at least 28 days and limited vector migration to other
DOUKAS ET AL796
FIG 6 Persistence of collagen-formulated vector and transgene transcripts in excisional wounds Full-thickness excisionalwounds (7 cm2) were placed on the dorsal surface of rabbits and treated with AdPDGF-B formulated in 26 collagen at either2 3 109 or 2 3 1011 virus particles per wound (open and closed columns respectively) Wounds were then covered with OpSitedressing and on days 3 7 or 28 posttreatment wound beds were harvested for real-time quantitative PCR and RT-PCR analy-ses PCR data are presented in the upper graph as AdPDGF-B copies per wound RT-PCR data are presented in the lower graphas the relative amount of PDGF-B mRNA per unit 18S rRNA (in arbitrary units) All data points are means 6 SD (n 5 6)
tissues or organs In vitro tests also established that collagenmatrices not only prevent vector loss due to diffusion but pre-serve vector activity despite prolonged incubation in acutewound fluid Successful vector immobilization and tissue re-pair could be achieved with both 015 collagen and 26 col-lagen suggesting flexibility in the final vehicle formulation re-quired for effective vector delivery This flexibility was neededin the present studies as 26 collagen formulations proveddifficult to deliver to PVA sponges and 6-mm excisionalwounds This would not be of concern in clinical settings how-ever where wound beds are easily accessible and generally sev-eral square centimeters in area By contrast CMC was inef-fective at retaining vector in aqueous environments Moreimportantly this matrix was itself inflammatory and whencombined with adenovirus the net result was inflammationrather than tissue repair We are currently examining the util-ity of other matrices such as fibrin and hyaluronic acid whichbecause of their more provisional nature may offer yet greatercellular migration into wounds as compared with type I colla-gen
Although an aqueous-based AdPDGF-B formulation hasbeen previously shown to enhance tissue formation (Liechty etal 1999) this was achieved with a model system that artifi-cially retains vectors within treatment sites In fact the presentstudies demonstrate that any tissue repair observed after Ad-PDGF-B delivery in a nongelling liquid is dependent on the useof this model system In wounds not designed to retain appliedtreatments aqueous-formulated AdPDGF-B seeped into sur-rounding tissues and led to hyperplasia within these areas ratherthan to tissue regeneration within the active wound bed Colla-gen-immobilized AdPDGF-B on the other hand did persist inthese wound beds and led to significant enhancements in gran-ulation tissue formation as well as enhanced wound re-epithe-lialization and wound closure The significance of these activ-ities is further substantiated considering that they wereachievable in 8-mm-diameter ischemic wounds which withinthe time frame examined could not self-heal to any meaning-ful degree in the absence of gene therapy However as all theanimal models employed in these studies will eventually self-heal given sufficient time the full value of matrix-immobilizedgene therapy vectors remains to be confirmed in human clini-cal trials
In conclusion we present evidence that matrix-immobilizedgene therapy vectors encoding appropriate growth-promotinggenes represent a promising approach to tissue regeneration andrepair This basic concept can be expanded to include alterna-tive matrices such as controlled-release formulations as wellas tissue-specific growth factors Furthermore the addition oftargeting ligands to adenovirus vectors (eg FGF2) can en-hance their ability to transduce cells such that tissue repair re-sponses comparable to nontargeted vectors can be achieved butat significantly lower vector doses (Chandler et al 2000a)With appropriate design and application schedules one couldconceivably time the release of multiple growth factors to spe-cific stages of a tissue repair cascade In addition we have foundin preliminary studies that collagen-immobilized nonviral vec-tors such as PDGF-B plasmids which have potentially morefavorable safety profiles than adenovirus vectors can also en-hance tissue formation in vivo (Chandler et al 2000b Tyroneet al 2000) Such flexibility should allow for the widespreadapplication of gene therapy to the treatment of injured tissues
ACKNOWLEDGMENTS
We thank Jeff Davidson (Vanderbilt University School ofMedicine) for assistance in establishing the PVA sponge modelCarl-Henrik Heldin (Ludwig Institute for Cancer Research) forthe PDGF-B gene construct and Emelie Amburn Lara AsatoSharon Chang Gail Fieser Lydia Greenlees Rebecca Smokerand Linda Manza for excellent technical assistance This pub-lication was made possible in part by NIH grants 1R43AR46154(JD) and 5P01CA25874 (MH)
REFERENCES
AHN ST and MUSTOE TA (1990) Effects of ischemia on ulcerwound healing A new model in the rabbit ear Ann Plast Surg 2417ndash23
ANDREE C SWAIN WF PAGE CP MACKLIN MDSLAMA J HATZIS D and ERIKSSON E (1994) In vivo trans-fer and expression of a human epidermal growth factor gene accel-erates wound repair Proc Natl Acad Sci USA 91 12188ndash12192
BENN SI WHITSITT JS BROADLEY KN NANNEY LBPERKINS D HE L PATEL M MORGAN JR SWAIN WFand DAVIDSON JM (1996) Particle-mediated gene transfer withtransforming growth factor-b1 cDNAs enhances wound repair in ratskin J Clin Invest 98 2894ndash2902
BONADIO J SMILEY E PATIL P and GOLDSTEIN S (1999)Localized direct plasmid gene delivery in vivo Prolonged therapyresults in reproducible tissue regeneration Nat Med 5 753ndash759
BUCKLEY A DAVIDSON JM KAMERATH CD WOLT TBand WOODWARD SC (1985) Sustained release of epidermalgrowth factor accelerates wound repair Proc Natl Acad Sci USA82 7340ndash7344
BUCKLEY-STURROCK A WOODWARD SC SENIOR RMGRIFFIN GL KLAGSBRUN M and DAVIDSON JM (1989)Differential stimulation of collagenase and chemotactic activity in fi-broblasts derived from rat wound repair tissue and human skin bygrowth factors J Cell Physiol 138 70ndash78
CHANDLER LA DOUKAS J GONZALEZ AM HOGANSONDK GU DL MA C NESBIT M CROMBLEHOLME TMHERLYN M SOSNOWSKI BA and PIERCE GF (2000a)FGF2ndashTargeted adenovirus encoding platelet-derived growth factor-B enhances de novo tissue formation Mol Ther 2 153ndash160
CHANDLER LA MA C GONZALEZ AM DOUKAS JNGUYEN T PIERCE GF and PHILLIPS ML (2000b) Ma-trix-enabled gene transfer for cutaneous wound repair Wound Re-pair Regen 8 473ndash479
DANILENKO DM RING BD TARPLEY JE MORRIS BVAN GY MORAWIECKI A CALLAHAN W GOLDEN-BERG M HERSHENSON S and PIERCE GF (1995) Growthfactors in porcine full and partial thickness burn repair Differing tar-gets and effects of keratinocyte growth factor platelet-derivedgrowth factor-BB epidermal growth factor and neu differentiationfactor Am J Pathol 147 1261ndash1277
DEUEL TF KAWAHARA RS MUSTOE TA and PIERCE GF(1991) Growth factors and wound healing Platelet-derived growthfactor as a model cytokine Annu Rev Med 42 567ndash584
DrsquoHEMECOURT PA SMIELL JM and KARIM MR (1998) So-dium carboxymethylcellulose aqueous-based gel vs becaplermin gelin patients with nonhealing lower extremity diabetic ulcers Wounds10 69ndash75
DOUKAS J HOGANSON DK ONG M YING W LACEYDL BAIRD A PIERCE GF and SOSNOWSKI BA (1999)Retargeted delivery of adenoviral vectors through fibroblast growthfactor receptors involves unique cellular pathways FASEB J 131459ndash1466
TISSUE REPAIR USING GROWTH FACTOR GENES 797
DVORAK HF BROWN LF DETMAR M and DVORAK AM(1995) Vascular permeability factorvascular endothelial growth fac-tor microvascular hyperpermeability and angiogenesis Am JPathol 146 1029ndash1039
EMING SA MEDALIE DA TOMPKINS RG YARMUSHML and MORGAN JR (1998) Genetically modified human ker-atinocytes overexpressing PDGF-A enhance the performance of acomposite skin graft Hum Gene Ther 9 529ndash539
EMING SA WHITSITT JS HE L KRIEG T MORGAN JRand DAVIDSON JM (1999) Particle-mediated gene transfer ofPDGF isoforms promotes wound repair J Invest Dermatol 112297ndash302
GERDES J SCHWAB U LEMKE H and STEIN H (1983) Pro-duction of a mouse monoclonal antibody reactive with a human nu-clear antigen associated with cell proliferation Int J Cancer 3113ndash20
GONZALEZ AM BERRY M MAHER PA LOGAN A andBAIRD A (1995) A comprehensive analysis of the distribution ofFGF-2 and FGFR1 in the rat brain Brain Res 701 201ndash226
GREENHALGH DG (1996) The role of growth factors in woundhealing J Trauma 41 159ndash167
GROTENDORST GR MARTIN GR PENCEV D SODEK Jand HARVEY AK (1985) Stimulation of granulation tissue for-mation by platelet-derived growth factor in normal and diabetic ratsJ Clin Invest 76 2323ndash2329
KHOURI RK HONG SP DEUNE EG TARPLEY JE SONGSZ SERDAR CM and PIERCE GF (1994) De novo genera-tion of permanent neovascularized soft tissue appendages by platelet-derived growth factor J Clin Invest 94 1757ndash1763
LEGRAND EK SENTER LH GAMELLI RL and KIORPESTC (1993) Evaluation of PDGF-BB PDGF-AA bFGF IL-1 andEGF dose responses in polyvinyl alcohol sponge implants assessedby a rapid histologic method Growth Factors 8 315ndash329
LIECHTY KW NESBIT M HERLYN M RADU A ADZICKNS and CROMBLEHOLME TM (1999) Adenoviral-mediatedoverexpression of platelet-derived growth factor-B corrects ischemicimpaired wound healing J Invest Dermatol 113 375ndash383
LYNCH SE COLVIN RB and ANTONIADES HN (1989)Growth factors in wound healing J Clin Invest 84 640ndash646
MUSTOE TA PIERCE GF THOMASON A GRAMATES PSPORN MB and DEUEL TF (1987) Accelerated healing of in-cisional wounds in rats induced by transforming growth factor-betaScience 237 1333ndash1336
MUSTOE TA PIERCE GF MORISHIMA C and DEUEL TF(1991) Growth factor-induced acceleration of tissue repair throughdirect and inductive activities in a rabbit dermal ulcer model J ClinInvest 87 694ndash703
MUSTOE TA AHN ST TARPLEY JE and PIERCE GF(1994) Role of hypoxia in growth factor responses Differential ef-fects of basic fibroblast growth factor and platelet-derived growthfactor in an ischemic wound model Wound Rep Reg 2 277ndash283
NYBERG-HOFFMAN C and AGUILAR-CORDOVA E (1999) In-stability of adenoviral vectors during transport and its implication forclinical studies Nat Med 5 955ndash957
PIERCE GF and MUSTOE TA (1995) Pharmacologic enhance-ment of wound healing Annu Rev Med 46 467ndash481
PIERCE GF MUSTOE TA SENIOR RM REED J GRIFFINGL THOMASON A and DEUEL TF (1988) In vivo incisionalwound healing augmented by platelet-derived growth factor and re-combinant c-sis gene homodimeric proteins J Exp Med 167 974ndash987
PIERCE GF VANDE BERG J RUDOLPH R TARPLEY J andMUSTOE TA (1991) Platelet-derived growth factor-BB and trans-forming growth factor beta 1 selectively modulate glycosaminogly -cans collagen and myofibroblasts in excisional wounds Am JPathol 138 629ndash646
PIERCE GF TARPLEY JE YANAGIHARA D MUSTOE TA
FOX GM and THOMASON A (1992) Platelet-derived growthfactor (BB homodimer) transforming growth factor-b1 and basic fi-broblast growth factor in dermal wound healing Neovessel and ma-trix formation and cessation of repair Am J Pathol 140 1375ndash1388
PIERCE GF TARPLEY JE ALLMAN RM GOODE PS SER-DAR CM MORRIS B MUSTOE TA and VANDE BERG J(1994a) Tissue repair processes in healing chronic pressure ulcerstreated with recombinant platelet-derived growth factor BB Am JPathol 145 1399ndash1410
PIERCE GF YANAGIHARA D KLOPCHIN K DANILENKODM HSU E KENNEY WC and MORRIS CF (1994b) Stim-ulation of all epithelial elements during skin regeneration by kerati-nocyte growth factor J Exp Med 179 831ndash840
PIERCE GF TARPLEY JE TSENG J BREADY J CHANGD KENNEY WC RUDOLPH R ROBSON MC VANDEBERG J and REID P (1995) Detection of platelet-derived growthfactor (PDGF)-AA in actively healing human wounds treated withrecombinant PDGF-BB and absence of PDGF in chronic nonhealingwounds J Clin Invest 96 1336ndash1350
SINGER AJ and CLARK RA (1999) Cutaneous wound healingN Engl J Med 341 738ndash746
SOMASUNDARAM R and SCHUPPAN D (1996) Type I II IIIIV V and VI collagens serve as extracellular ligands for the iso-forms of platelet-derived growth factor (AA BB and AB) J BiolChem 271 26884ndash26891
SPRUGEL KH MCPHERSON JM CLOWES AW and ROSSR (1987) Effects of growth factors in vivo I Cell ingrowth intoporous subcutaneous chambers Am J Pathol 129 601ndash613
STEED DL (1995) Clinical evaluation of recombinant humanplatelet-derived growth factor for the treatment of lower extremitydiabetic ulcers Diabetic Ulcer Study Group J Vasc Surg 21 71ndash78
STEED DL (1998) Foundations of good ulcer care Am J Surg 17620S-25S
TYRONE JW MOGFORD JE CHANDLER LA MA C XIAY PIERCE GF and MUSTOE TA (2000) Collagen-embeddedplatelet-derived growth factor DNA plasmid promotes wound heal-ing in a dermal ulcer model J Surg Res 93 230ndash236
VOGT PM THOMPSON S ANDREE C LIU P BREUING KHATZIS D BROWN H MULLIGAN RC and ERIKSSON E(1994) Genetically modified keratinocytes transplanted to woundsreconstitute the epidermis Proc Natl Acad Sci USA 91 9307ndash9311
WIEMAN TJ (1998) Clinical efficacy of becaplermin (rhPDGF-BB)gel Becaplermin Gel Studies Group Am J Surg 176 74S-79S
WIEMAN TJ SMIELL JM and SU Y (1998) Efficacy and safetyof a topical gel formulation of recombinant human platelet-derivedgrowth factor-BB (becaplermin) in patients with chronic neuropathicdiabetic ulcers A phase III randomized placebo-controlled double-blind study Diabetes Care 21 822ndash827
WILSON JM (1996) Adenoviruses as gene-delivery vehicles NEngl J Med 334 1185ndash1187
XU J and CLARK RA (1996) Extracellular matrix alters PDGFregulation of fibroblast integrins J Cell Biol 132 239ndash249
XU J and CLARK RA (1997) A three-dimensional collagen latticeinduces protein kinase C-z activity Role in a2 integrin and collage-nase mRNA expression J Cell Biol 136 473ndash483
Address reprint requests toDr John Doukas
Selective Genetics Inc11035 Roselle Street
San Diego CA 92121
E-mail jdoukasselectivegeneticscom
Received for publication December 28 2000 accepted after re-vision February 23 2001
DOUKAS ET AL798

ing the desired responses because of their ability to stimulatecellular proliferation migration and in some cases extracellu-lar matrix (ECM) deposition (Lynch et al 1989 Deuel et al1991) For the most part however growth factor proteins havenot achieved clinically significant improvements in tissue re-pair largely because of difficulties in establishing and main-taining therapeutic protein levels within treatment sites (Pierceand Mustoe 1995 Greenhalgh 1996)
Gene delivery represents a potential solution to these prob-lems as it can establish sustained protein production in situThis approach necessitates a careful therapeutic design partic-ularly as to the form in which genes are applied to injured tis-sues Although particle-mediated delivery of growth factorgenes is feasible (Andree et al 1994 Benn et al 1996 Em-ing et al 1999) the nonbiodegradable particles utilized mayeventually induce tissue damage Transplantation of growth fac-tor-transduced keratinocytes has been effective in animal mod-els (Vogt et al 1994 Eming et al 1998) However this ap-proach delivers transgenes only to the surface of treatment sitesminimizing their potential to influence deep wound beds andin addition the extensive ex vivo manipulations necessitatedlimit widespread clinical utility
A preferable strategy would be to directly apply gene vec-tors to treatment sites Direct injection however is suitable onlyfor accessing the outer margins of tissue defects and thereforeoffers minimal benefit to larger sized defects The formulationof growth factor genes in aqueous vehicles allows for their uni-form application to wound beds (Liechty et al 1999) how-ever such vehicles are unlikely to retain either gene vectors ortransgene products within delivery sites and therefore the ben-efit of gene therapy would be lost An alternative approachwhich we hypothesize is more appropriate for tissue repair in-volves the immobilization of growth factor genes within bio-compatible matrices (Bonadio et al 1999) This would permitvectorndashmatrix formulations to be directly applied to activewound beds where they could then serve as scaffolds for in-vading repair cells Subsequent transduction of these cellswould then allow for transgene expression and formation ofneotissues all within matrix scaffolds With appropriate designthese matrices would eventually be reabsorbed andor remod-eled during tissue repair and thus become fully integratedwithin final mature tissues
Taking these factors into consideration we formulated ade-novirus vectors encoding growth factor genes in several matri-ces and examined their ability to induce both neotissue for-mation and tissue defect repair Adenovirus was selected as thegene vector in order to achieve high but transient transgene ex-pression (Wilson 1996) characteristics that are well suited totissue repair needs We now report the use of select matrixndashvector combinations to induce robust tissue regeneration andrepair
MATERIALS AND METHODS
Vectors and growth factor protein
E1- E3-deleted human adenovirus type 5 vectors encodingindividual transgenes under the control of cytomegalovirus(CMV) promoters included AdLuc (firefly luciferase) Ad-
PDGF-B (160-amino acid open reading frame of humanplatelet-derived growth factor B) AdVEGF (121-amino acidform of vascular endothelial growth factor) and AdFGF2 (18-kDa form of fibroblast growth factor 2) Vectors were grownin 293 cells (American Type Culture Collection ManassasVA) purified by CsCl2 centrifugation dialyzed into virus buffer(20 mM Trisndash25 mM NaCl containing 25 glycerol pH 8)and stored at 280degC Virus particle concentration was deter-mined by comparing total DNA content (measured usingPicoGreen assay kits Molecular Probes Eugene OR) with aknown reference stock Plaque-forming units (PFU) were de-termined by plaque assay using 293 cells Human rPDGF-BBprotein (109 amino acid form) was produced in a eukaryoticexpression system and formulated in phosphate-buffered saline(PBS) containing 1 human albumin vehicle and doses wereselected to conform to those used in preclinical and clinicalstudies (Steed 1995 drsquoHemecourt et al 1998 Wieman 1998Wieman et al 1998)
Preparation of adenovirusndashmatrix treatments
Vectors were prepared as four different formulations For015 collagen formulations vectors were adjusted to the de-sired concentration in a vehicle of monomeric bovine type Icollagen (15 mgml Cohesion Technologies Palo Alto CA)053 minimal essential medium (Life Technologies Grand Is-land NY) and NaHCO3 (pH 74) at 18 mgml This materialis liquid at 4degC but quickly polymerizes to form a gel on warm-ing For 26 collagen formulations virus vectors were mixedwith 65 fibrillar bovine type I collagen (Matrix Contract Ser-vices San Diego CA) as follows Luer lock adapters were usedto connect two syringes (one loaded with vector in virus bufferand one with collagen) and the syringe contents were passedback and forth 30 times to achieve complete mixing This re-sults in a relatively thick but injectable single-phase materialFor carboxymethylcellulose (CMC) formulations vectors wereadjusted to the desired concentration in 25 aqueous sodiumCMC (Spectrum Quality Products Gardena CA) this mater-ial is a viscous liquid at body temperature Finally for aqueousformulations vectors were simply diluted to the desired con-centration in virus buffer Pilot studies were also performed toconfirm that all formulations prepared as described containeda uniform and homogeneous distribution of vector Briefly for-mulations were loaded into syringes samples were collectedfrom throughout the syringe contents and high-performanceliquid chromatography (HPLC) was used to confirm equivalentvirus particle concentrations among these samples
Vector stability and release assays
To determine matrix influences on vector activity AdLuc wasformulated at 5 3 1011 particlesml and held at 37degC for 60 minCMC matrices were then dissociated by vortexing in water015 collagen matrices by incubation with type I collagenase(01 mgml Worthington Biochemical Freehold NJ) at 37degCfor 45 min and 26 collagen matrices by digestion with col-lagenase (1 mgml) under these same conditions Control stud-ies established that exposure to collagenase as described hadminimal to no influence on vector structure as determined byreversed phase HPLC (data not shown) Sample aliquots wereapplied to 293 cells and cellular luciferase and protein contents
DOUKAS ET AL784
were determined as previously described (Doukas et al 1999)Samples were analyzed as serial dilutions to confirm linearityof assay responses Controls consisted of AdLuc freshly dilutedin virus buffer containing either CMC or collagenase at finaldoses equivalent to those of experimental samples In some ex-periments AdPDGF-B formulations were also incubated at 37degCfor 72 hr in an excess of either virus buffer or wound exudatefluid (taken from excisional wounds created in farm swine) af-ter which vectors were recovered as described and used to trans-duce 293 cells and cellular production of PDGF-BB determinedby enzyme-linked immunosorbent assay (ELISA)
To determine vector release from matrices 200-ml aliquotsof AdLucndashmatrix formulations were incubated in 800 ml of wa-ter at room temperature for 05 6 or 24 hr with gentle rock-ing After a brief centrifugation supernatants were sampled andassayed for DNA content using the PicoGreen assay Data werethen normalized to control values obtained when AdLuc for-mulated in virus buffer was directly added to water
PVA sponge model
All animal studies conformed to guidelines set forth in theGuide for the Care and Use of Laboratory Animals (NationalResearch Council Washington DC) and were approved byappropriate review committees Under anesthesia six full-thickness incisions 5 mm in length were placed on the ventralsurfaces of 400 to 450-g Sprague-Dawley rats after which asingle sterile polyvinyl alcohol (PVA) sponge (12 cm 3 3 mmgrade 3 M-PACT Eudora KS) was inserted per incision and
the incisions were closed with wound clips Four days post-sur-gery sponges were injected with 200-ml aliquots of either ad-enovirusndashmatrix formulations (2 3 109 or 2 3 1010 virus par-ticles per sponge) PDGF-BB protein or vehicle alone and thesponges were recovered on days 1ndash8 along with any surround-ing cellular capsules A single 3-mm section was taken fromthe center of each sponge fixed with 4 paraformaldehyde in02 M sodium phosphate buffer (pH 74) for 4 hr at 4degC andparaffin embedded The remaining sponge sections were thenprocessed for biochemical analyses as described below
Rabbit ear wound models
Male and female New Zealand White rabbits 4 kg in bodyweight (Western Oregon Rabbit Company Philomath OR)were anesthetized after which their ears were rendered bothischemic and insensitive to pain by ligation of the central androstral arteries and nerves respectively (Ahn and Mustoe1990) Using tissue biopsy punches 6- or 8-mm-diameterwounds were placed in the ventral surface extending throughthe perichondrium and additionally in some cases through theunderlying cartilage layer which was gently removed with for-ceps in order to expose the underlying dermis Larger sizedwounds were useful in creating greater tissue repair challengesas 6-mm wounds were found to exhibit considerable self-heal-ing under control conditions (see Results) Cartilage-intact mod-els were used for comparison with previous studies whereascartilage-removed models were used as more representative ofclinically encountered situations Adenovirusndashmatrix formula-
TISSUE REPAIR USING GROWTH FACTOR GENES 785
FIG 1 Adenovirus release from immobilizing matrices AdLuc was formulated in either saline 015 collagen 26 colla-gen or CMC Aliquots were then incubated in an excess of water for 05 6 or 24 hr and AdLuc released into the aqueous phasewas measured by a fluorescence-based DNA detection assay Data were normalized to the activity observed in saline-formulatedsamples (100 adenovirus release) and are shown as means 6 SD (n 5 3)
tions were then applied to wound beds as either 5-ml volumescontaining 2 3 109 virus particles (for 6-mm wounds) or 8-mlvolumes containing 4 3 109 virus particles (for 8-mm wounds)control treatments consisted of vehicles alone After treatmentapplications wounds were covered with occlusive dressings(OpSite Smith amp Nephew Largo FL) On days 7ndash10 post-surgery and treatment wounds were harvested and fixed as de-scribed above These time points were selected on the basis ofminimal self-healing in most untreated wounds as determinedin preliminary model development studies In general largerwounds allowed for longer study times as did cartilage intactmodels
Finally to assess the long-term effects of vector application6-mm wounds were placed in nonischemic rabbit ears to thelevel of underlying cartilage and treated as described aboveWounds were then harvested for analysis on days 28ndash180 post-treatment
Biolocalization studies
Two model systems were used to examine adenovirus vectorbiodistribution In the first model 6-mm-diameter wounds ex-
tending through the underlying cartilage were placed in rabbitears as described above nonischemic ears were used so as topresent the greatest opportunity for vascular dissemination ofvirus Wound beds were then treated with AdPDGF-B formu-lated in 015 collagen (2 3 109 virus particles per wound in a5-ml volume) after which animals were housed for 1 3 7 or14 days After blood collection via cardiac puncture animalswere perfused with 120 ml of PBS at a rate of 20 mlmin andwound beds and organs were harvested for polymerase chain re-action (PCR)-based detection of AdPDGF-B Forty cycles oftouchdown PCR were performed with oligonucleotide primersdesigned to amplify a 315-base pair fragment spanning the ma-jority of the human PDGF-B 109-amino acid coding region(sense 59-TTCCCTGACCATTGCTGAGCCGGCCA-39 anti-sense 59-ACAGGCCGTGCAGCTCCACTG-39) This ldquotouch-downrdquo strategy of thermocycling employs successively de-creasing annealing temperatures (four cycles performed at eachannealing temperature beginning at 72degC and decreasing in 1degCincrements down to 63degC with each cycle consisting of a 30-sec annealing step and a 1-min extension step) PCR ampliconswere then visualized on ethidium bromide-stained 08 agarosegels
DOUKAS ET AL786
FIG 2 Influence of adenovirusndashmatrix formulations on neotissue formation PVA sponges were implanted subcutaneously intorats and 4 days later were injected with either AdPDGF-B AdFGF2 AdVEGF or AdLuc (2 3 1010 virus particles per sponge)formulated in 015 collagen controls consisted of collagen alone Six days posttreatment sponges were processed as paraffinsections and stained as follows (A) AdPDGF-B trichrome stain (B) AdPDGF-B Ki-67 immunostain Note the positively stainedendothelial cells (arrowheads) and fibroblasts (arrows) (C) AdFGF2 trichrome stain (D) AdFGF2 BSL-I lectin stain (E) Ad-VEGF trichrome stain (F) AdVEGF BSL-I lectin stain (G) AdLuc trichrome stain (H) Collagen vehicle trichrome stainOriginal magnification (A C E and G) 3200 (B D F and H) 3400
TABLE 1 NEOTISSUE FORMATION AFTER DELIVERY OF ADENOVIRUSndashMATRIX FORMULATIONSa
Granulation Protein DNATreatment fill () (mgsponge) (mgsponge)
015 Collagen vehicle 26 6 18 13 6 2 79 6 21AdPDGF-B (2 3 109 particles) 62 6 22b 15 6 2 107 6 27AdPDGF-B (2 3 1010 particles) 93 6 6b 26 6 9b 215 6 109b
AdLuc (2 3 109 particles) 24 6 15 12 6 2 67 6 12AdLuc (2 3 1010 particles) 36 6 22 16 6 2 102 6 27
015 Collagen vehicle 29 6 8 15 6 2 69 6 10AdPDGF-B (2 3 1010 particles) 86 6 15c 25 6 3c 136 6 20c
AdVEGF (2 3 1010 particles) 44 6 16d 25 6 4c 144 6 24c
015 Collagen vehicle 18 6 8 10 6 1 65 6 12AdPDGF-B (2 3 1010 particles) 68 6 13c 23 6 5e 151 6 51c
AdFGF2 (2 3 1010 particles) 55 6 15c 18 6 3c 126 6 33f
aPVA sponges were implanted subcutaneously in rats and 4 days later injected with either 015 collagen alone or collagencontaining adenovirus vectors Vector doses are listed as the number of virus particles delivered per sponge Six days posttreat-ment sponges were recovered and processed to determine the percent sponge area filled with granulation tissue (0ndash100) aswell as total protein and DNA contents as described in Materials and Methods Data are presented as means 6 SD (n 5 8)
bp 00002 versus collagen control and p 0005 versus AdLuc groupscp 00001 versus collagen controldp 003 versus collagen controlep 00001 versus collagen control and p 0002 versus AdFGF2fp 0001 versus collagen control
TISSUE REPAIR USING GROWTH FACTOR GENES 787
A second model utilized 7-cm2 full-thickness excisionalwounds placed on the backs of anesthetized rabbits Woundswere treated with AdPDGF-B formulated in 26 collagen (2 3
109 or 2 3 1011 virus particles per wound in 700-ml volumes)and then covered with OpSite dressing On day 3 7 28 or 90posttreatment blood was collected animals were perfused asdescribed above and the following organs were recoveredwound bed brain heart lung liver spleen kidney gonad andlymph nodes (axillary cranial mesenteric and posterior medi-astinal) Real-time quantitative TaqMan PCR was performedusing 45 two-step cycles with primers designed to amplify se-quences bridging the vector backbone and the PDGF-B pre-proregion (sense 59-GGATCTTCGAGTCGACAAGCTT-3 9 an-tisense 59-TAAGGGCTCCTCGAAATACTCTA-3 9) The re-sulting amplicons were detected with an internal fluorogenicprobe (59-TAGTGGTACTTAGCGACGACCCGC-3 9) and anABI Prism 7700 sequence detector (PE Applied BiosystemsFoster City CA) The initial target copy numbers present ineach reaction were quantified by extrapolation from standardcurves of AdPDGF-B DNA in the background of 1 mg of rab-bit liver DNA per reaction Each PCR contained 1 mg of testDNA with the exception of wound bed which contained 500ng per reaction and blood which contained the equivalent of10 ml of original sample Each test sample was assayed in du-plicate to control for PCR inhibitory substances a third reac-tion was spiked with 100 copies of AdPDGF-B DNA PCR dataare presented as AdPDGF-B genome copies per wound thelimit of quantitation (LOQ) was 10 copiesmg DNA or an av-erage of 105 copieswound
For those tissues scoring positive for PCR-amplifiable vec-tor we further performed real-time quantitative reverse tran-scriptase (RT)-PCR Reverse transcriptase reactions were per-formed with 100 ng of each test RNA per reaction and randomhexamer primers The resulting cDNAs were then used to am-plify both rabbit 18S rRNA cDNA and PDGF-B cDNA in sep-arate PCRs The vector-specific primers were designed to am-plify full-length 160-amino acid human PDGF-B mRNA(sense 59-CAAGCACACGCATGACAAGA-3 9 antisense 59-TTTCGTTATCGTAGTGTTTAAAGTGT-3 9) The resulting131-nucleotide amplicons were detected with an internal fluo-rogenic probe (59-AAACAAGTTGCTCGATGGATCCTTAT-CAGGCT-39) RT-PCRs were then normalized for total RNAby 18S rRNA content with a second pair of PCR primers RT-PCR data are presented as the relative amount of PDGF-BmRNA per unit 18S rRNA (in arbitrary units)
Histochemical analyses
For routine morphological assessment paraffin sections werestained according to the Masson trichrome procedure In addi-tion a blinded observer using a microscope equipped with oc-ular micrometers measured the area within sponges filled bygranulation tissue these values are expressed as the percentageof sponge interior occupied by tissue ( granulation fill) Forexcisional wounds trichrome-stained sections and an imageanalysis software package (Image-Pro Plus software Media Cy-bernetics Silver Spring MD) were used to determine the cross-sectional areas of granulation tissue and epithelium per wound(in mm2) In addition the percentage of wound closure was cal-culated according to the following formula [(original wound
diameter 2 epithelial gap length) original wound diameter] 3100
For immunohistochemistry paraffin sections were stainedwith biotinylated Griffonia (Bandeiraea) simplicifolia lectin I(BSL-I) horseradish peroxidase (HRP)-labeled streptavidin anddiaminobenzidine (DAB Vector Laboratories BurlingameCA) in order to detect vascular endothelium Mouse anti-Ki-67and HRP-labeled rabbit anti-mouse IgG antibodies followed byDAB were used to detect proliferating cells Mouse anti-humanPDGF-BB (Z2703 American Type Culture Collection) andHRPndashanti-mouse IgG antibodies followed by DAB were usedto detect human PDGF-BB protein Fluorescein isothiocyanate(FITC)-conjugated anti-adenovirus antibody (Accurate Chemi-cals Westbury NY) and the nuclear stain 496-diamidino-2-phenylindole (DAPI Molecular Probes) were used to detectinternalized adenovirus vectors Finally fibroblasts were iden-tified with Cy3-labeled anti-vimentin (Sigma St Louis MO)
For in situ hybridization procedures an [a-35S] UTP-labeledriboprobe prepared from the full-length human PDGF-B cDNAwas used as previously described (Gonzalez et al 1995) Asense riboprobe was used to control for nonspecific hybridiza-tions
Biochemical analyses
Tissue samples not processed for paraffin embedding wereplaced in 100 mM phosphate buffer containing 02 Triton X-100 (pH 78) and agitated at 55 msec for 20 sec in a Fast-Prep system (BIO 101 Vista CA) After centrifugation su-pernatants were analyzed for protein using a bicinchoninic acidassay (Pierce Rockville IL) and for DNA using the PicoGreenassay PDGF-BB protein content was determined with a humanPDGF-BB-specific ELISA (RampD Systems Minneapolis MN)
Statistical Analyses
Data are presented as arithmetic means 6 1 SD Groups ofthree or more means within individual studies were comparedby one-way analysis of variance (ANOVA) and the Fisher pro-cedure for least significant differences (StatView softwareAbacus Concepts Berkeley CA)
RESULTS
Adenovirus vectors can be immobilized in an activeform within matrices
As an initial step to the in vivo assessment of adenovirusndashmatrix formulations we first determined the activity profilesand release kinetics for vectors formulated in type I collagenand carboxymethylcellulose (CMC) Collagen was selected onthe basis of its successful use as a delivery matrix for proteinsand DNA (Grotendorst et al 1985 Mustoe et al 1987 1991Sprugel et al 1987 Khouri et al 1994 Bonadio et al 1999)as well as its ability to enhance tissue repair responses in fi-broblasts (Xu and Clark 1996 1997) Relatively low (015)and high (26) concentrations were examined reasoning thatthis would allow for either relatively short or long retentiontimes at application sites respectively CMC was selected on
DOUKAS ET AL788
TISSUE REPAIR USING GROWTH FACTOR GENES 789
FIG 3 Localization of gene vector and transgene product within neotissues PVA sponges implanted in rats were injected withAdPDGF-B formulated in 015 collagen (2 3 1010 virus particles per sponge) and paraffin sections were stained as follows(A) Day 1 posttreatment anti-adenovirus immunostain to detect AdPDGF-B (green) DAPI stain to detect cell nuclei (blue) (B)Day 4 posttreatment in situ hybridization using human PDGF-B gene probe (C) Day 1 posttreatment anti-human PDGF-BBprotein immunostain positively stained leukocytes (arrowheads) and fibroblasts (arrows) are indicated (D) Day 6 posttreatmentanti-PDGF-BB immunostain (E) Day 8 posttreatment anti-PDGF-BB immunostain (F) Day 8 post- treatment immunostains todetect PDGF-BB protein (green) and vimentin (red) yellow fluorescence indicates PDGF-BB and vimentin colocalization bluefluorescence indicates cell nuclei (DAPI stain) Original magnifications (AndashC E and F)3 400 (D) 31000
the basis of its clinical use for the delivery of PDGF-BB pro-tein (Steed 1995)
Matrix influences on vector activity were examined by in-cubating AdLuc formulations at 37degC for 60 min followed bymatrix dissolution and vector bioassay (luciferase productionby 293 cells) This is an important test as adenoviruses arequickly inactivated under unfavorable physical and chemicalconditions (Nyberg-Hoffman and Aguilar-Cordova 1999)None of the matrices examined had a deleterious effect on vec-tor activity (90 6 12 106 6 5 and 139 6 37 of control ac-tivity for 015 collagen 26 collagen and CMC respec-tively) To further model in vivo vector stability we alsoincubated AdPDGF-B formulated in 26 collagen with woundfluid for 72 hr at 37degC prior to vector recovery and analysisWe observed no reduction in the level of PDGF-BB productionfrom cells transduced with AdPDGF-B exposed to wound fluidas compared with vector exposed to virus buffer (30 6 5 vs20 6 3 ng of PDGF-BB produced per milliliter of culturemedium respectively n 5 3)
As these data support the suitability of the selected matricesfor in vivo use we next determined their influence on vectorrelease kinetics (Fig 1) When placed in water collagen ma-trices retained the majority of their immobilized vectors with015 and 26 collagen releasing only 17 6 3 and 3 6 1 ofvector by 24 hr respectively By contrast 48 6 3 of AdLucwas released from CMC within 30 min and 61 6 2 by 6 hrThis was not unexpected as CMC is fairly water soluble andas both CMC and adenoviral particles are negatively chargedTherefore collagen matrices in a concentration-dependentfashion display more favorable kinetics for localizing and re-taining adenovirus vectors at delivery sites than does CMC
Collagen-immobilized adenoviruses induce distinctneotissues in vivo
Initial in vivo tests of matrix-immobilized vectors were per-formed with an established model of de novo tissue generation(Buckley et al 1985 Sprugel et al 1987 LeGrand et al1993) PVA sponges implanted subcutaneously in rats were in-jected with a single dose of adenovirus formulated in either col-lagen or CMC and then analyzed for tissue formation Forgrowth factor transgenes we selected platelet-derived growth
factor B (PDGF-B) vascular endothelial growth factor (VEGF)and fibroblast growth factor 2 (FGF2) because of their well-known mitogenic activities
AdPDGF-B formulated in 015 collagen induced granula-tion tissue formation in a dose-responsive manner (Table 1)Compared with vehicle controls delivering 2 3 1010 virus par-ticles induced a 17- to 23-fold increase in sponge protein con-tent (p 00002) a 2- to 27-fold increase in DNA content (p
00002) and a 29- to 43-fold increase in granulation tissue fill(p 00002) Trichrome-stained sections revealed the nearcomplete fill of sponge interiors with well-formed granulationtissue by day 6 posttreatment (Fig 2A) Expression of Ki-67a nuclear protein upregulated in proliferating cells (Gerdes etal 1983) established that both vascular endothelium (arrow-heads Fig 2B) and fibroblasts (arrows Fig 2B) had prolifer-ated in response to PDGF-B gene delivery AdFGF2 and Ad-VEGF also enhanced protein and DNA content within sponges(Table 1) However these vectors induced less granulation tis-sue deposition as compared with AdPDGF-B and the tissuesformed were histologically distinct
Tissues present in AdFGF2-treated sponges were highly vas-cular as revealed by the endothelial-reactive lectin BSL-I (Fig2D) Many of the infiltrating mononuclear cells also reactedpositively with BSL-I lectin suggesting that these cells wereendothelial cells or endothelial precursors AdFGF2 did nothowever induce the formation of classic granulation tissue aslittle collagen deposition was observed demonstrated by thepaucity of blue-staining material in trichrome-stained sections(Fig 2C) AdVEGF also induced heavily vascularized tissues(Fig 2E and F) but with greater extracellular collagen deposi-tion than AdFGF2 Relative to AdPDGF-B-induced tissueshowever AdVEGF-induced tissues were disorganized con-tained few fibroblasts and were markedly edematous Finallywhen AdLuc was delivered as a control treatment no signifi-cant increases in protein DNA or granulation tissue were ob-served compared with collagen vehicle alone (Table 1)Trichrome-stained sections revealed sparse inflammatory cellinfiltrates within AdLuc-treated sponges (Fig 2G) which com-pared with the near absence of infiltration after delivery of col-lagen vehicle alone (Fig 2H) suggested a limited antiviral response
Unlike the 015 collagen formulations described above
DOUKAS ET AL790
TABLE 2 NEOTISSUE FORMATION AFTER PDGF-B GENE OR PDGF-BB PROTEIN DELIVERYa
Granulation Protein DNATreatment fill () (mgsponge) (mgsponge)
015 Collagen vehicle 28 6 13b 16 6 2b 103 6 22b
AdPDGF-B 81 6 15b 30 6 6b 218 6 28b
PDGF-BB 100 mg 64 6 12c 22 6 4c 155 6 26c
PDGF-BB 10 mg qod 3 3d 77 6 9b0 31 6 8b 230 6 75b
aPVA sponges implanted in rats were injected with either 015 collagen vehicle or collagen containing AdPDGF-B as described in Table 1 Alternatively PDGF-BB protein was delivered as a single 100-mg dose on day 4 postimplantation or as10-mg doses on days 4 6 and 8 Sponges were removed on day 12 postimplantation and processed to determine the percent granulation fill as well as total protein and DNA contents Data are presented as means 6 SD (n 5 4ndash8)
bp 00001 versus collagen control and p 005 versus 100-mg PDGF-BBcp 003 versus collagen controldqod 3 3 Every other day three times
TISSUE REPAIR USING GROWTH FACTOR GENES 791
TABLE 3 INFLUENCE OF ADENOVIRUSndashMATRIX FORMULATIONS ON ISCHEMIC WOUND HEALINGa
Granulation Epithelial Wound closureTreatment Model system area (mm2) area (mm2) ( complete)
Aqueous buffer Cartilage intact 10 6 08 05 6 03 61 6 226 mm day 10
AdPDGF-B in Cartilage intact 24 6 22 05 6 01 73 6 28aqueous buffer 6 mm day 10
015 Collagen Cartilage intact 05 6 03 05 6 02 89 6 14vehicle 6 mm day 10
AdPDGF-B in Cartilage intact 16 6 09b 09 6 03c 97 6 7015 collagen 6 mm day 10
Aqueous buffer Cartilage removed 45 6 08 08 6 02 95 6 96 mm day 7
AdPDGF-B in Cartilage removed 40 6 15 11 6 05 82 6 22aqueous buffer 6 mm day 7
015 Collagen Cartilage removed 36 6 13 06 6 02 88 6 22vehicle 6 mm day 7
AdPDGF-B in Cartilage removed 70 6 14b 07 6 03 79 6 22015 collagen 6 mm day 7
26 Collagen Cartilage removed 04 6 05 01 6 01 24 6 15vehicle 8 mm day 8
AdPDGF-B in Cartilage removed 51 6 25b 06 6 03b 52 6 25c
26 collagen 8 mm day 8
aExcisional wounds (6 or 8 mm in diameter) were placed in ischemic rabbit ears with underlying cartilage left intact or re-moved Wounds were then treated with AdPDGF-B formulated in aqueous virus buffer or collagen control treatments consistedof vehicle alone For 6-mm wounds virus was applied as 2 3 109 particles per wound for 8-mm wounds as 4 3 109 particlesper wound On days 7ndash10 posttreatment wounds were harvested and processed as trichrome-stained paraffin sections whichwere then used to quantify newly formed granulation tissue and epithelium (cross-sectional area in mm2) and the degree of woundsurface closure (where 100 equals complete closure) Data are presented as means 6 SD (n 5 4ndash8)
bp 0009 versus vehicle controlcp 005 versus vehicle control
26 collagen formulations could not be reliably examined inthe PVA sponge model as their relatively high viscosity pre-vented uniform filling of sponges by syringe CMC-formulatedvectors were also unsuitable for this model system as theyproved highly inflammatory (data not shown) These formula-tions therefore were evaluated in more appropriate excisionalwound models (see below)
Tissue repair cells are transduced by collagen-immobilized adenoviruses
On the basis of the robust activity of collagen-formulatedAdPDGF-B we elected to further examine this vectorndashmatrixcombination first by seeking to correlate PDGF-B gene deliv-ery with subsequent transgene and protein expression WhenPVA sponges treated with 015 collagenndashAdPDGF-B werestained with both an anti-adenovirus antibody and the nuclearstain DAPI the majority of cells present 1 day after gene de-livery had bound andor internalized adenovirus (Fig 3A) Insitu hybridization revealed that these cells were successfullytransduced by virus as they contained human PDGF-B mRNA(Fig 3B) By contrast hybridization product was not detectedwith a sense riboprobe or when AdLuc-treated sponges wereexamined (data not shown)
We next used a human PDGF-BB-specific antibody to iden-tify the cell types responsible for transgene expression By day
1 postdelivery of 015 collagenndashAdPDGF-B PDGF-BB pro-tein was localized to leukocytes (arrowheads) and fibroblasts (ar-row Fig 3C) With time PDGF-BB protein was detected boundto the extracellular matrix (ECM) surrounding positively stainedcells (Fig 3D) This last observation indicates that a reservoir ofPDGF-BB protein develops within treated tissues and thus mayprolong the histogenic effects of this growth factor Finally byday 8 the majority of immunoreactivity had abated with pri-marily microvascular endothelium remaining positive (Fig 3E)However scattered fibroblasts could still be shown to producePDGF-BB protein by dual immunohistochemistry with anti-PDGF-BB and anti-vimentin antibodies (Fig 3F)
Multiple administrations of PDGF-BB protein are required to approximate the histogenic effects of collagenndashAdPDGF-B
To directly compare gene therapy with the more conven-tional approach of growth factor protein delivery we next quan-tified tissue formation in response to either PDGF gene or pro-tein delivery A single injection of 015 collagenndashAdPDGF-Benhanced granulation tissue filling of sponges by 3-fold versusvehicle alone (p 00001) and sponge protein and DNA lev-els by 2-fold (p 00001 Table 2) Using a human PDGF-BB-specific ELISA this growth factor was detected at 54 6 13ngsponge (n 5 8) By contrast when PDGF-BB protein was
delivered as a single dose nearly 2000-fold in excess of thisconcentration the tissue formation responses observed (proteinand DNA accumulation and granulation tissue formation) weresignificantly lower (p 005 Table 2) In fact repeated dos-ing with PDGF-BB protein was required in order to achieve re-sponses comparable to a single administration of the PDGF-Bgene These data therefore support our hypothesis that the abil-ity of gene delivery to establish prolonged in situ growth fac-tor production translates into greater histogenesis than that seenwith growth factor proteins
CollagenndashAdPDGF-B induces complete healing of ischemic wounds
Nonhealing wounds are a major risk in chronically ischemictissues as low oxygen tension greatly impairs tissue repair pro-cesses We therefore compared the ability of matrix versusaqueous formulated AdPDGF-B to repair ischemic excisionalwounds Several models were employed to compare variationsin wound size and condition so as to allow for a more com-plete picture of tissue repair
In the first model system 6-mm-diameter wounds were cre-ated in ischemic rabbit ears by removal of epidermal and der-mal layers but not underlying cartilage This model has beenused in previous studies of growth factor proteins and genes(Ahn and Mustoe 1990 Mustoe et al 1994 Liechty et al1999) and was therefore employed to allow comparison withthese reports However it represents an artificial system as thepresence of a cartilage layer restricts both treatment activity andhealing to wound margins and in addition the initially acellu-lar wound bed forms a cup that artifactually retains aqueoustreatments As would be predicted we found a trend towardgranulation tissue formation in this model after the applicationof AdPDGF-B formulated in aqueous buffer (Table 3) How-ever this response did not reach the level of statistical signifi-cance as tissue development was highly variable (note the highstandard deviation value) In addition epithelial regenerationand wound closure were minimal to unaffected By contrastAdPDGF-B formulated in 015 collagen enhanced granula-tion tissue area by 32-fold and epithelial area by 18-fold overthat achieved with vehicle alone (p 0009 and 005 respec-tively) Although near complete closure of epithelial gaps wasalso achieved the high level of self-healing in control-treatedgroups (89 wound closure) precluded statistical significance
In an alternative model design subdermal cartilage was com-pletely removed from excisional wounds creating beds whosefloors now consisted of dermal tissue (Pierce et al 1994b)This design allows for cellular responses from the entire woundbed as well as the opportunity for vector migration beyond
treatment areas We now observed that aqueous formulated Ad-PDGF-B failed to induce even a trend toward tissue regenera-tion (Table 3) Rather the vector appears to have seeped throughthe wound bed floor as inflammatory cell infiltrates and fociof fibroblast proliferation were observed in the underlying der-mis and at wound margins (Fig 4A) Immunohistochemistryconfirmed the production of human PDGF-BB at these sites(Fig 4B) CMC-formulated AdPDGF-B also failed to induceany meaningful tissue repair Wounds treated with this formu-lation showed a diffuse inflammatory response within thewound bed and wound surfaces were overlain with fibrin clotsrather than regenerating epithelium (Fig 4C and D) By con-trast AdPDGF-B formulated in 015 collagen enhanced gran-ulation tissue deposition 19-fold within wound beds versus ve-hicle controls (p 0002) and wounds were extensivelyepithelialized (Table 3) Neither epithelial regeneration norwound closure achieved significance however as the high de-gree of self-healing achieved in this particular model (see ve-hicle alone group) most likely masked transgene-stimulated re-sponses
To address these model limitations as our next system wecreated 8-mm wounds in ischemic rabbit ears by removingepidermal dermal and cartilage layers reasoning that largerexcisional wounds would display limited self-healing In ad-dition this model could readily accommodate 26 collagenformulations which proved difficult to reproducibly apply insmaller wounds Compared with control wounds treated withcollagen vehicle alone wounds treated with AdPDGF-B for-mulated in 26 collagen achieved a 12-fold enhancementin granulation tissue fill and a 6-fold enhancement in re-ep-ithelialization by day 8 posttreatment (p 0009 Table 3)In addition wound closure was only 24 complete in colla-gen vehicle-treated wounds by day 8 but 52 complete inwounds treated with collagen-formulated AdPDGF-B (p
005) Histologically AdPDGF-B-treated wounds showed nosigns of tissue hyperplasia or chronic inflammation but ratheran orderly repair process marked by a regenerated epitheliallayer overlying a wound bed filled with granulation tissue(Fig 4E and F)
CollagenndashAdPDGF-B induces normal long-term tissue repair
Our choice of adenoviruses for transgene delivery was partlybased on the reasoning that as these vectors establish transientgene expression they would not lead to hyperproliferative re-sponses or scar formation To test this hypothesis we treatedrabbit ear excisional wounds with AdPDGF-B formulated in015 collagen and examined tissue repair responses out to
DOUKAS ET AL792
FIG 4 Influence of adenovirusndashmatrix formulations on excisional wound repair Excisional wounds (6 or 8 mm in diameter andextending through underlying cartilage layers) were placed in ischemic rabbit ears bars indicate original wound depth (determinedfrom cartilage visible at wound margins) Wounds were then treated with AdPDGF-B formulated in either virus buffer CMC orcollagen and on day 7 or 8 posttreatment processed for histology or immunohistochemistry An identical design was used to ex-amine long-term healing on day 90 except that wounds were created in nonischemic ears (A) Day 7 buffer-formulated AdPDGF-B-treated 6-mm wound trichrome stain (B) Day 7 buffer-formulated AdPDGF-B-treated 6-mm wound anti-PDGF-BB proteinimmunostain (C and D) Day 7 CMC-formulated AdPDGF-B-treated 6-mm wound trichrome stains (E and F) Day 8 26 col-lagen-formulated AdPDGF-B-treated 8-mm wound trichrome stains (G and H) Day 90 015 collagen-formulated AdPDGF-B-treated 6-mm wound trichrome stains Original magnification (A C E and G) 340 (B D F and H) 3200
TISSUE REPAIR USING GROWTH FACTOR GENES 793
DOUKAS ET AL794
TABLE 4 BIODISTRIBUTION OF AdPDGF-B IN EXCISIONAL WOUNDSa
Positive samplestotal assayed
Tissue AdPDGF-B dose Day 3 Day 7 Day 28 Day 90
Wound bed 2 3 109 particles 66 66 66b 06Axillary lymph nodes 2 3 109 particles 02 ND 06 06
Wound bed 2 3 1011 particles 66 66 66 46c
Axillary lymph nodes 2 3 1011 particles 66 ND 66d 26e
aFull-thickness excisional wounds (7 cm2) were placed on the backs of rabbits and AdPDGF-B formulated in 26 collagenwas applied as either 2 3 109 or 2 3 1011 virus particles per wound On days 3ndash90 posttreatment wound beds and a panel oforgans were harvested for real-time PCR quantification of viral genome Data are shown for wound bed and axillary lymph nodesamples as the number of samples that yielded amplifiable signals per total number assayed ND not determined
bThree of six samples scored below the level of quantitation (LOQ 10ndash100 copiesmg DNA)cAll four positive samples scored below the LOQdThree of six samples scored below the LOQeBoth positive samples scored below the LOQ
180 days posttreatment (Fig 5) PDGF-B gene delivery en-hanced total ear thickness relative to controls on day 28 (229 6
020 vs 179 6 019 mm p 00001) and day 60 (192 6 001vs 182 6 011 mm p 0005) as anticipated on the basis ofthe ability of this formulation to induce granulation tissue for-mation By day 90 posttreatment however there was no mea-surable difference in ear thickness between AdPDGF-B andcontrol-treated groups and this relationship continued out today 180 indicating that growth factor gene delivery did not in-duce excessive scar formation This was also confirmed histo-logically AdPDGF-B-treated wounds on day 90 and beyondwere composed of a thin outer keratin layer an underlying ep-ithelial layer of equivalent thickness to nonwounded areas anda collagen-rich dermis devoid of any signs of tissue hyperpla-sia (Fig 4G and H)
Collagen immobilization limits adenovirus vectorbiodistribution beyond treatment sites
As a final measure of the value of matrix immobilization forgene delivery we determined the biodistribution patterns ofvectors after their in vivo delivery In the first model systemused AdPDGF-B formulated in 015 collagen was applied torabbit ear wounds at equivalent doses as previously describedwounds were extended through underlying cartilage but vas-cular supplies were not disturbed so as to permit maximal vec-tor dissemination By PCR no adenoviral DNA was detectablein lung spleen brain cervical lymph nodes or gonads on day1 3 7 or 14 (n 5 6 per group) In the liver one of six sam-ples was positive on days 3 and 7 but none on day 14 in serumonly one of six samples tested positive on day 14 (equivalentof 500-ml serum volume) By contrast adenovirus was detectedin eight of eight wound bed samples at all time points exam-ined
In a second model system excisional wounds placed on thebacks of rabbits were treated with AdPDGF-B formulated in26 collagen Because of their anatomical placement thismodel allowed for the creation of larger excisional wounds (7-cm2 total area) than those placed in rabbit ears (03 cm2) and
consequently larger treatment volumes and vector doses (2 3109 or 2 3 1011 virus particles per wound) At the lower doseof 2 3 109 particles PCR-amplifiable adenoviral DNA was notdetectable beyond wound beds on day 3 7 28 or 90 Tissuessampled and found not to contain vector included blood heartlung liver kidney brain spleen lymph nodes and gonads (n 5
6group) In wound beds adenoviral DNA was detected at alltime points except for day 90 (Table 4 and Fig 6) Vector lev-els did decrease however by 38-fold between days 7 and 28with three of six samples falling below the level of quantita-tion (LOQ) by real-time PCR at the latter time point (Fig 6)
At a 100-fold higher vector dose of 2 3 1011 particles perwound PCR-amplifiable adenoviral DNA was once again un-detectable in the majority of tissues sampled Except for a sin-gle day 7 liver sample and a single day 7 brain sample (bothbelow the LOQ) adenoviral DNA was only detectable directlyin wound beds or in the axillary lymph nodes that drain woundsites (Table 4) Moreover three of six positive axillary nodesamples scored below the LOQ on day 28 as did both positivesamples on day 90 indicating that they contained relatively lit-tle vector Within wound beds adenoviral DNA was detectedat quantifiable levels out to day 28 and at detectable but non-quantifiable levels on day 90 DNA copy numbers remainedsteady between days 3 and 7 dropped 107-fold between days7 and 28 and a further 1662-fold by day 90 Finally at eachtime point DNA copy numbers in wounds treated with 2 3
1011 particles were approximately 100-fold higher than thosefound in wounds treated with 2 3 109 particles thus confirm-ing the linearity of our assay system
To better define the time course of human PDGF-BB pro-duction we also quantified transgene mRNA levels in woundbed samples treated at 2 3 109 particles per wound This treat-ment dose was selected as representative of the virus particleconcentration capable of inducing complete healing in ischemicear wounds Quantifiable levels of human PDGF-B mRNAwere detectable in treated dorsal wounds at days 3 7 and 28(Fig 6) with levels decreasing 14-fold between days 3 and 7and 5-fold between days 7 and 28 The more sensitive tech-nique of real-time RT-PCR therefore demonstrates that trans-
TISSUE REPAIR USING GROWTH FACTOR GENES 795
gene expression extends well beyond the 8-day time period sug-gested using anti-PDGF-BB immunohistochemistry as a de-tection system (Fig 3)
DISCUSSION
These studies demonstrate that immobilization of gene ther-apy vectors in collagen-based matrices enables their efficientdelivery and activity in vivo Matrix immobilization achievedprolonged transgene-encoded growth factor production and asa consequence robust tissue repair By contrast aqueous vehi-cles failed to retain adenoviruses at application sites resultingin diffuse inflammation rather than productive tissue regenera-tion These observations confirm our basic hypothesis that ma-trix immobilization of growth factor-encoding gene therapyvectors represents a promising approach to tissue repair
Although de novo tissue deposition was achievable with sev-eral growth factor genes PDGF-B proved the most suitable forrepair of cutaneous defects A single administration of colla-gen-immobilized AdPDGF-B rapidly induced the formation ofhighly cellular and vascularized tissues with dense ECMs richin collagen By contrast AdFGF2 induced a primarily vascu-lar response with little collagen deposition FGF2 induces therelease of matrix metalloproteinase 1 or interstitial collagenase(Buckley-Sturrock et al 1989) and this may underlie the rel-ative paucity of ECM accumulation VEGF gene delivery alsoinduced highly vascular responses however the enhanced per-meability characteristic of VEGF-induced vasculature (Dvoraket al 1995) led to edema within nascent tissues In fact much
of the enhanced protein and DNA deposition observed in Ad-VEGF-treated PVA sponges may well derive from fluid exu-dates rather than actual tissue formation Finally the inabilityof AdLuc delivery to induce anything beyond a limited in-flammatory response confirms that tissue formation was de-pendent on growth factor gene delivery
The robust activity of PDGF-B gene delivery was expectedas PDGF-BB protein initiates multiple aspects of tissue forma-tion including cellular influx and proliferation ECM deposi-tion and tissue remodeling (Pierce et al 1988 1991 1994a)Indeed PDGF-BB is the only growth factor protein to have suc-cessfully completed human clinical trials and be approved forthe treatment of dermal wounds (Steed 1995 drsquoHemecourt etal 1998 Wieman 1998 Wieman et al 1998) We observedthat collagen-formulated AdPDGF-B induced the complete re-pair of excisional skin defects without unwanted long-term ef-fects such as the development of hypertrophic scars Endoge-nous growth factors other than PDGF-BB however most likelymediated the enhanced re-epithelialization observed in thesewounds as epithelial regeneration is driven by members of theepidermal growth factor and FGF families (Pierce et al 1994bDanilenko et al 1995) Our data indicate nonetheless that tis-sue regeneration and repair were initiated and to a great degreedriven by transgene-encoded PDGF-BB
Despite the known activity of PDGF-BB protein we wereable to demonstrate greater tissue deposition after gene deliv-ery as compared with the use of recombinant growth factor pro-tein A single application of PDGF-BB protein could not equalthe ability of PDGF-B gene therapy to induce neotissue for-mation even at doses well in excess of that induced in situ byAdPDGF-B and in excess of that used in human clinical trials
FIG 5 Influence of collagen-formulated AdPDGF-B on long-term tissue repair Excisional wounds (6 mm in diameter withcartilage remaining intact) were placed in nonischemic rabbit ears and treated with either 015 collagen alone (open columns)or AdPDGF-B formulated in this vehicle (solid columns) On days 28ndash180 posttreatment total ear thickness at the site of eachwound was measured (in mm) with calipers Data are presented as means 6 SD (n 5 3) Treatment groups differ by p 00001groups differ by p 0005
(Steed 1995 drsquoHemecourt et al 1998 Wieman 1998 Wie-man et al 1998) In fact repeated administrations of PDGF-BB protein were required to approach the level of tissue for-mation observed after a single administration of AdPDGF-BThese data support our hypothesis that sustained localizedgrowth factor production is required for robust tissue repair
In further support of this hypothesis we demonstrated thatmRNA encoding human PDGF-B was present in excisionalwounds as late as day 28 after collagen-formulated AdPDGF-B administration By contrast previous studies of PDGF-BBprotein found that the great majority of this growth factor wasgone from treated wounds 1 day postapplication and that anytissue maturation subsequently observed was most likely dueto the upregulation of endogenous growth factors (Pierce et al1992 1995) We also demonstrated that repair cells such asmononuclear leukocytes endothelial cells and fibroblasts pres-ent with developing neotissues represent the source of both
transgene transcription and PDGF-BB production In additiona depot of human PDGF-BB was detected bound to the colla-gen delivery matrix and ECM of these tissues This was antici-pated as PDGF-BB contains collagen-binding motifs (Soma-sundaram and Schuppan 1996) We hypothesize that subsequentmatrix metalloproteinase activity by repair cells will serve togenerate localized release of this sequestered growth factor pooland as a consequence further drive tissue regeneration Theseevents which are central to tissue remodeling should be directlyenhanced by collagen matrices as type I collagen stimulates me-talloproteinase production integrin expression and cellular ac-tivation in PDGF-stimulated fibroblasts (Xu and Clark 19961997)
An additional rationale for employing collagen matrices wasto physically immobilize vectors This was confirmed in vivowhere collagen matrices maintained AdPDGF-B at deliverysites for at least 28 days and limited vector migration to other
DOUKAS ET AL796
FIG 6 Persistence of collagen-formulated vector and transgene transcripts in excisional wounds Full-thickness excisionalwounds (7 cm2) were placed on the dorsal surface of rabbits and treated with AdPDGF-B formulated in 26 collagen at either2 3 109 or 2 3 1011 virus particles per wound (open and closed columns respectively) Wounds were then covered with OpSitedressing and on days 3 7 or 28 posttreatment wound beds were harvested for real-time quantitative PCR and RT-PCR analy-ses PCR data are presented in the upper graph as AdPDGF-B copies per wound RT-PCR data are presented in the lower graphas the relative amount of PDGF-B mRNA per unit 18S rRNA (in arbitrary units) All data points are means 6 SD (n 5 6)
tissues or organs In vitro tests also established that collagenmatrices not only prevent vector loss due to diffusion but pre-serve vector activity despite prolonged incubation in acutewound fluid Successful vector immobilization and tissue re-pair could be achieved with both 015 collagen and 26 col-lagen suggesting flexibility in the final vehicle formulation re-quired for effective vector delivery This flexibility was neededin the present studies as 26 collagen formulations proveddifficult to deliver to PVA sponges and 6-mm excisionalwounds This would not be of concern in clinical settings how-ever where wound beds are easily accessible and generally sev-eral square centimeters in area By contrast CMC was inef-fective at retaining vector in aqueous environments Moreimportantly this matrix was itself inflammatory and whencombined with adenovirus the net result was inflammationrather than tissue repair We are currently examining the util-ity of other matrices such as fibrin and hyaluronic acid whichbecause of their more provisional nature may offer yet greatercellular migration into wounds as compared with type I colla-gen
Although an aqueous-based AdPDGF-B formulation hasbeen previously shown to enhance tissue formation (Liechty etal 1999) this was achieved with a model system that artifi-cially retains vectors within treatment sites In fact the presentstudies demonstrate that any tissue repair observed after Ad-PDGF-B delivery in a nongelling liquid is dependent on the useof this model system In wounds not designed to retain appliedtreatments aqueous-formulated AdPDGF-B seeped into sur-rounding tissues and led to hyperplasia within these areas ratherthan to tissue regeneration within the active wound bed Colla-gen-immobilized AdPDGF-B on the other hand did persist inthese wound beds and led to significant enhancements in gran-ulation tissue formation as well as enhanced wound re-epithe-lialization and wound closure The significance of these activ-ities is further substantiated considering that they wereachievable in 8-mm-diameter ischemic wounds which withinthe time frame examined could not self-heal to any meaning-ful degree in the absence of gene therapy However as all theanimal models employed in these studies will eventually self-heal given sufficient time the full value of matrix-immobilizedgene therapy vectors remains to be confirmed in human clini-cal trials
In conclusion we present evidence that matrix-immobilizedgene therapy vectors encoding appropriate growth-promotinggenes represent a promising approach to tissue regeneration andrepair This basic concept can be expanded to include alterna-tive matrices such as controlled-release formulations as wellas tissue-specific growth factors Furthermore the addition oftargeting ligands to adenovirus vectors (eg FGF2) can en-hance their ability to transduce cells such that tissue repair re-sponses comparable to nontargeted vectors can be achieved butat significantly lower vector doses (Chandler et al 2000a)With appropriate design and application schedules one couldconceivably time the release of multiple growth factors to spe-cific stages of a tissue repair cascade In addition we have foundin preliminary studies that collagen-immobilized nonviral vec-tors such as PDGF-B plasmids which have potentially morefavorable safety profiles than adenovirus vectors can also en-hance tissue formation in vivo (Chandler et al 2000b Tyroneet al 2000) Such flexibility should allow for the widespreadapplication of gene therapy to the treatment of injured tissues
ACKNOWLEDGMENTS
We thank Jeff Davidson (Vanderbilt University School ofMedicine) for assistance in establishing the PVA sponge modelCarl-Henrik Heldin (Ludwig Institute for Cancer Research) forthe PDGF-B gene construct and Emelie Amburn Lara AsatoSharon Chang Gail Fieser Lydia Greenlees Rebecca Smokerand Linda Manza for excellent technical assistance This pub-lication was made possible in part by NIH grants 1R43AR46154(JD) and 5P01CA25874 (MH)
REFERENCES
AHN ST and MUSTOE TA (1990) Effects of ischemia on ulcerwound healing A new model in the rabbit ear Ann Plast Surg 2417ndash23
ANDREE C SWAIN WF PAGE CP MACKLIN MDSLAMA J HATZIS D and ERIKSSON E (1994) In vivo trans-fer and expression of a human epidermal growth factor gene accel-erates wound repair Proc Natl Acad Sci USA 91 12188ndash12192
BENN SI WHITSITT JS BROADLEY KN NANNEY LBPERKINS D HE L PATEL M MORGAN JR SWAIN WFand DAVIDSON JM (1996) Particle-mediated gene transfer withtransforming growth factor-b1 cDNAs enhances wound repair in ratskin J Clin Invest 98 2894ndash2902
BONADIO J SMILEY E PATIL P and GOLDSTEIN S (1999)Localized direct plasmid gene delivery in vivo Prolonged therapyresults in reproducible tissue regeneration Nat Med 5 753ndash759
BUCKLEY A DAVIDSON JM KAMERATH CD WOLT TBand WOODWARD SC (1985) Sustained release of epidermalgrowth factor accelerates wound repair Proc Natl Acad Sci USA82 7340ndash7344
BUCKLEY-STURROCK A WOODWARD SC SENIOR RMGRIFFIN GL KLAGSBRUN M and DAVIDSON JM (1989)Differential stimulation of collagenase and chemotactic activity in fi-broblasts derived from rat wound repair tissue and human skin bygrowth factors J Cell Physiol 138 70ndash78
CHANDLER LA DOUKAS J GONZALEZ AM HOGANSONDK GU DL MA C NESBIT M CROMBLEHOLME TMHERLYN M SOSNOWSKI BA and PIERCE GF (2000a)FGF2ndashTargeted adenovirus encoding platelet-derived growth factor-B enhances de novo tissue formation Mol Ther 2 153ndash160
CHANDLER LA MA C GONZALEZ AM DOUKAS JNGUYEN T PIERCE GF and PHILLIPS ML (2000b) Ma-trix-enabled gene transfer for cutaneous wound repair Wound Re-pair Regen 8 473ndash479
DANILENKO DM RING BD TARPLEY JE MORRIS BVAN GY MORAWIECKI A CALLAHAN W GOLDEN-BERG M HERSHENSON S and PIERCE GF (1995) Growthfactors in porcine full and partial thickness burn repair Differing tar-gets and effects of keratinocyte growth factor platelet-derivedgrowth factor-BB epidermal growth factor and neu differentiationfactor Am J Pathol 147 1261ndash1277
DEUEL TF KAWAHARA RS MUSTOE TA and PIERCE GF(1991) Growth factors and wound healing Platelet-derived growthfactor as a model cytokine Annu Rev Med 42 567ndash584
DrsquoHEMECOURT PA SMIELL JM and KARIM MR (1998) So-dium carboxymethylcellulose aqueous-based gel vs becaplermin gelin patients with nonhealing lower extremity diabetic ulcers Wounds10 69ndash75
DOUKAS J HOGANSON DK ONG M YING W LACEYDL BAIRD A PIERCE GF and SOSNOWSKI BA (1999)Retargeted delivery of adenoviral vectors through fibroblast growthfactor receptors involves unique cellular pathways FASEB J 131459ndash1466
TISSUE REPAIR USING GROWTH FACTOR GENES 797
DVORAK HF BROWN LF DETMAR M and DVORAK AM(1995) Vascular permeability factorvascular endothelial growth fac-tor microvascular hyperpermeability and angiogenesis Am JPathol 146 1029ndash1039
EMING SA MEDALIE DA TOMPKINS RG YARMUSHML and MORGAN JR (1998) Genetically modified human ker-atinocytes overexpressing PDGF-A enhance the performance of acomposite skin graft Hum Gene Ther 9 529ndash539
EMING SA WHITSITT JS HE L KRIEG T MORGAN JRand DAVIDSON JM (1999) Particle-mediated gene transfer ofPDGF isoforms promotes wound repair J Invest Dermatol 112297ndash302
GERDES J SCHWAB U LEMKE H and STEIN H (1983) Pro-duction of a mouse monoclonal antibody reactive with a human nu-clear antigen associated with cell proliferation Int J Cancer 3113ndash20
GONZALEZ AM BERRY M MAHER PA LOGAN A andBAIRD A (1995) A comprehensive analysis of the distribution ofFGF-2 and FGFR1 in the rat brain Brain Res 701 201ndash226
GREENHALGH DG (1996) The role of growth factors in woundhealing J Trauma 41 159ndash167
GROTENDORST GR MARTIN GR PENCEV D SODEK Jand HARVEY AK (1985) Stimulation of granulation tissue for-mation by platelet-derived growth factor in normal and diabetic ratsJ Clin Invest 76 2323ndash2329
KHOURI RK HONG SP DEUNE EG TARPLEY JE SONGSZ SERDAR CM and PIERCE GF (1994) De novo genera-tion of permanent neovascularized soft tissue appendages by platelet-derived growth factor J Clin Invest 94 1757ndash1763
LEGRAND EK SENTER LH GAMELLI RL and KIORPESTC (1993) Evaluation of PDGF-BB PDGF-AA bFGF IL-1 andEGF dose responses in polyvinyl alcohol sponge implants assessedby a rapid histologic method Growth Factors 8 315ndash329
LIECHTY KW NESBIT M HERLYN M RADU A ADZICKNS and CROMBLEHOLME TM (1999) Adenoviral-mediatedoverexpression of platelet-derived growth factor-B corrects ischemicimpaired wound healing J Invest Dermatol 113 375ndash383
LYNCH SE COLVIN RB and ANTONIADES HN (1989)Growth factors in wound healing J Clin Invest 84 640ndash646
MUSTOE TA PIERCE GF THOMASON A GRAMATES PSPORN MB and DEUEL TF (1987) Accelerated healing of in-cisional wounds in rats induced by transforming growth factor-betaScience 237 1333ndash1336
MUSTOE TA PIERCE GF MORISHIMA C and DEUEL TF(1991) Growth factor-induced acceleration of tissue repair throughdirect and inductive activities in a rabbit dermal ulcer model J ClinInvest 87 694ndash703
MUSTOE TA AHN ST TARPLEY JE and PIERCE GF(1994) Role of hypoxia in growth factor responses Differential ef-fects of basic fibroblast growth factor and platelet-derived growthfactor in an ischemic wound model Wound Rep Reg 2 277ndash283
NYBERG-HOFFMAN C and AGUILAR-CORDOVA E (1999) In-stability of adenoviral vectors during transport and its implication forclinical studies Nat Med 5 955ndash957
PIERCE GF and MUSTOE TA (1995) Pharmacologic enhance-ment of wound healing Annu Rev Med 46 467ndash481
PIERCE GF MUSTOE TA SENIOR RM REED J GRIFFINGL THOMASON A and DEUEL TF (1988) In vivo incisionalwound healing augmented by platelet-derived growth factor and re-combinant c-sis gene homodimeric proteins J Exp Med 167 974ndash987
PIERCE GF VANDE BERG J RUDOLPH R TARPLEY J andMUSTOE TA (1991) Platelet-derived growth factor-BB and trans-forming growth factor beta 1 selectively modulate glycosaminogly -cans collagen and myofibroblasts in excisional wounds Am JPathol 138 629ndash646
PIERCE GF TARPLEY JE YANAGIHARA D MUSTOE TA
FOX GM and THOMASON A (1992) Platelet-derived growthfactor (BB homodimer) transforming growth factor-b1 and basic fi-broblast growth factor in dermal wound healing Neovessel and ma-trix formation and cessation of repair Am J Pathol 140 1375ndash1388
PIERCE GF TARPLEY JE ALLMAN RM GOODE PS SER-DAR CM MORRIS B MUSTOE TA and VANDE BERG J(1994a) Tissue repair processes in healing chronic pressure ulcerstreated with recombinant platelet-derived growth factor BB Am JPathol 145 1399ndash1410
PIERCE GF YANAGIHARA D KLOPCHIN K DANILENKODM HSU E KENNEY WC and MORRIS CF (1994b) Stim-ulation of all epithelial elements during skin regeneration by kerati-nocyte growth factor J Exp Med 179 831ndash840
PIERCE GF TARPLEY JE TSENG J BREADY J CHANGD KENNEY WC RUDOLPH R ROBSON MC VANDEBERG J and REID P (1995) Detection of platelet-derived growthfactor (PDGF)-AA in actively healing human wounds treated withrecombinant PDGF-BB and absence of PDGF in chronic nonhealingwounds J Clin Invest 96 1336ndash1350
SINGER AJ and CLARK RA (1999) Cutaneous wound healingN Engl J Med 341 738ndash746
SOMASUNDARAM R and SCHUPPAN D (1996) Type I II IIIIV V and VI collagens serve as extracellular ligands for the iso-forms of platelet-derived growth factor (AA BB and AB) J BiolChem 271 26884ndash26891
SPRUGEL KH MCPHERSON JM CLOWES AW and ROSSR (1987) Effects of growth factors in vivo I Cell ingrowth intoporous subcutaneous chambers Am J Pathol 129 601ndash613
STEED DL (1995) Clinical evaluation of recombinant humanplatelet-derived growth factor for the treatment of lower extremitydiabetic ulcers Diabetic Ulcer Study Group J Vasc Surg 21 71ndash78
STEED DL (1998) Foundations of good ulcer care Am J Surg 17620S-25S
TYRONE JW MOGFORD JE CHANDLER LA MA C XIAY PIERCE GF and MUSTOE TA (2000) Collagen-embeddedplatelet-derived growth factor DNA plasmid promotes wound heal-ing in a dermal ulcer model J Surg Res 93 230ndash236
VOGT PM THOMPSON S ANDREE C LIU P BREUING KHATZIS D BROWN H MULLIGAN RC and ERIKSSON E(1994) Genetically modified keratinocytes transplanted to woundsreconstitute the epidermis Proc Natl Acad Sci USA 91 9307ndash9311
WIEMAN TJ (1998) Clinical efficacy of becaplermin (rhPDGF-BB)gel Becaplermin Gel Studies Group Am J Surg 176 74S-79S
WIEMAN TJ SMIELL JM and SU Y (1998) Efficacy and safetyof a topical gel formulation of recombinant human platelet-derivedgrowth factor-BB (becaplermin) in patients with chronic neuropathicdiabetic ulcers A phase III randomized placebo-controlled double-blind study Diabetes Care 21 822ndash827
WILSON JM (1996) Adenoviruses as gene-delivery vehicles NEngl J Med 334 1185ndash1187
XU J and CLARK RA (1996) Extracellular matrix alters PDGFregulation of fibroblast integrins J Cell Biol 132 239ndash249
XU J and CLARK RA (1997) A three-dimensional collagen latticeinduces protein kinase C-z activity Role in a2 integrin and collage-nase mRNA expression J Cell Biol 136 473ndash483
Address reprint requests toDr John Doukas
Selective Genetics Inc11035 Roselle Street
San Diego CA 92121
E-mail jdoukasselectivegeneticscom
Received for publication December 28 2000 accepted after re-vision February 23 2001
DOUKAS ET AL798

were determined as previously described (Doukas et al 1999)Samples were analyzed as serial dilutions to confirm linearityof assay responses Controls consisted of AdLuc freshly dilutedin virus buffer containing either CMC or collagenase at finaldoses equivalent to those of experimental samples In some ex-periments AdPDGF-B formulations were also incubated at 37degCfor 72 hr in an excess of either virus buffer or wound exudatefluid (taken from excisional wounds created in farm swine) af-ter which vectors were recovered as described and used to trans-duce 293 cells and cellular production of PDGF-BB determinedby enzyme-linked immunosorbent assay (ELISA)
To determine vector release from matrices 200-ml aliquotsof AdLucndashmatrix formulations were incubated in 800 ml of wa-ter at room temperature for 05 6 or 24 hr with gentle rock-ing After a brief centrifugation supernatants were sampled andassayed for DNA content using the PicoGreen assay Data werethen normalized to control values obtained when AdLuc for-mulated in virus buffer was directly added to water
PVA sponge model
All animal studies conformed to guidelines set forth in theGuide for the Care and Use of Laboratory Animals (NationalResearch Council Washington DC) and were approved byappropriate review committees Under anesthesia six full-thickness incisions 5 mm in length were placed on the ventralsurfaces of 400 to 450-g Sprague-Dawley rats after which asingle sterile polyvinyl alcohol (PVA) sponge (12 cm 3 3 mmgrade 3 M-PACT Eudora KS) was inserted per incision and
the incisions were closed with wound clips Four days post-sur-gery sponges were injected with 200-ml aliquots of either ad-enovirusndashmatrix formulations (2 3 109 or 2 3 1010 virus par-ticles per sponge) PDGF-BB protein or vehicle alone and thesponges were recovered on days 1ndash8 along with any surround-ing cellular capsules A single 3-mm section was taken fromthe center of each sponge fixed with 4 paraformaldehyde in02 M sodium phosphate buffer (pH 74) for 4 hr at 4degC andparaffin embedded The remaining sponge sections were thenprocessed for biochemical analyses as described below
Rabbit ear wound models
Male and female New Zealand White rabbits 4 kg in bodyweight (Western Oregon Rabbit Company Philomath OR)were anesthetized after which their ears were rendered bothischemic and insensitive to pain by ligation of the central androstral arteries and nerves respectively (Ahn and Mustoe1990) Using tissue biopsy punches 6- or 8-mm-diameterwounds were placed in the ventral surface extending throughthe perichondrium and additionally in some cases through theunderlying cartilage layer which was gently removed with for-ceps in order to expose the underlying dermis Larger sizedwounds were useful in creating greater tissue repair challengesas 6-mm wounds were found to exhibit considerable self-heal-ing under control conditions (see Results) Cartilage-intact mod-els were used for comparison with previous studies whereascartilage-removed models were used as more representative ofclinically encountered situations Adenovirusndashmatrix formula-
TISSUE REPAIR USING GROWTH FACTOR GENES 785
FIG 1 Adenovirus release from immobilizing matrices AdLuc was formulated in either saline 015 collagen 26 colla-gen or CMC Aliquots were then incubated in an excess of water for 05 6 or 24 hr and AdLuc released into the aqueous phasewas measured by a fluorescence-based DNA detection assay Data were normalized to the activity observed in saline-formulatedsamples (100 adenovirus release) and are shown as means 6 SD (n 5 3)
tions were then applied to wound beds as either 5-ml volumescontaining 2 3 109 virus particles (for 6-mm wounds) or 8-mlvolumes containing 4 3 109 virus particles (for 8-mm wounds)control treatments consisted of vehicles alone After treatmentapplications wounds were covered with occlusive dressings(OpSite Smith amp Nephew Largo FL) On days 7ndash10 post-surgery and treatment wounds were harvested and fixed as de-scribed above These time points were selected on the basis ofminimal self-healing in most untreated wounds as determinedin preliminary model development studies In general largerwounds allowed for longer study times as did cartilage intactmodels
Finally to assess the long-term effects of vector application6-mm wounds were placed in nonischemic rabbit ears to thelevel of underlying cartilage and treated as described aboveWounds were then harvested for analysis on days 28ndash180 post-treatment
Biolocalization studies
Two model systems were used to examine adenovirus vectorbiodistribution In the first model 6-mm-diameter wounds ex-
tending through the underlying cartilage were placed in rabbitears as described above nonischemic ears were used so as topresent the greatest opportunity for vascular dissemination ofvirus Wound beds were then treated with AdPDGF-B formu-lated in 015 collagen (2 3 109 virus particles per wound in a5-ml volume) after which animals were housed for 1 3 7 or14 days After blood collection via cardiac puncture animalswere perfused with 120 ml of PBS at a rate of 20 mlmin andwound beds and organs were harvested for polymerase chain re-action (PCR)-based detection of AdPDGF-B Forty cycles oftouchdown PCR were performed with oligonucleotide primersdesigned to amplify a 315-base pair fragment spanning the ma-jority of the human PDGF-B 109-amino acid coding region(sense 59-TTCCCTGACCATTGCTGAGCCGGCCA-39 anti-sense 59-ACAGGCCGTGCAGCTCCACTG-39) This ldquotouch-downrdquo strategy of thermocycling employs successively de-creasing annealing temperatures (four cycles performed at eachannealing temperature beginning at 72degC and decreasing in 1degCincrements down to 63degC with each cycle consisting of a 30-sec annealing step and a 1-min extension step) PCR ampliconswere then visualized on ethidium bromide-stained 08 agarosegels
DOUKAS ET AL786
FIG 2 Influence of adenovirusndashmatrix formulations on neotissue formation PVA sponges were implanted subcutaneously intorats and 4 days later were injected with either AdPDGF-B AdFGF2 AdVEGF or AdLuc (2 3 1010 virus particles per sponge)formulated in 015 collagen controls consisted of collagen alone Six days posttreatment sponges were processed as paraffinsections and stained as follows (A) AdPDGF-B trichrome stain (B) AdPDGF-B Ki-67 immunostain Note the positively stainedendothelial cells (arrowheads) and fibroblasts (arrows) (C) AdFGF2 trichrome stain (D) AdFGF2 BSL-I lectin stain (E) Ad-VEGF trichrome stain (F) AdVEGF BSL-I lectin stain (G) AdLuc trichrome stain (H) Collagen vehicle trichrome stainOriginal magnification (A C E and G) 3200 (B D F and H) 3400
TABLE 1 NEOTISSUE FORMATION AFTER DELIVERY OF ADENOVIRUSndashMATRIX FORMULATIONSa
Granulation Protein DNATreatment fill () (mgsponge) (mgsponge)
015 Collagen vehicle 26 6 18 13 6 2 79 6 21AdPDGF-B (2 3 109 particles) 62 6 22b 15 6 2 107 6 27AdPDGF-B (2 3 1010 particles) 93 6 6b 26 6 9b 215 6 109b
AdLuc (2 3 109 particles) 24 6 15 12 6 2 67 6 12AdLuc (2 3 1010 particles) 36 6 22 16 6 2 102 6 27
015 Collagen vehicle 29 6 8 15 6 2 69 6 10AdPDGF-B (2 3 1010 particles) 86 6 15c 25 6 3c 136 6 20c
AdVEGF (2 3 1010 particles) 44 6 16d 25 6 4c 144 6 24c
015 Collagen vehicle 18 6 8 10 6 1 65 6 12AdPDGF-B (2 3 1010 particles) 68 6 13c 23 6 5e 151 6 51c
AdFGF2 (2 3 1010 particles) 55 6 15c 18 6 3c 126 6 33f
aPVA sponges were implanted subcutaneously in rats and 4 days later injected with either 015 collagen alone or collagencontaining adenovirus vectors Vector doses are listed as the number of virus particles delivered per sponge Six days posttreat-ment sponges were recovered and processed to determine the percent sponge area filled with granulation tissue (0ndash100) aswell as total protein and DNA contents as described in Materials and Methods Data are presented as means 6 SD (n 5 8)
bp 00002 versus collagen control and p 0005 versus AdLuc groupscp 00001 versus collagen controldp 003 versus collagen controlep 00001 versus collagen control and p 0002 versus AdFGF2fp 0001 versus collagen control
TISSUE REPAIR USING GROWTH FACTOR GENES 787
A second model utilized 7-cm2 full-thickness excisionalwounds placed on the backs of anesthetized rabbits Woundswere treated with AdPDGF-B formulated in 26 collagen (2 3
109 or 2 3 1011 virus particles per wound in 700-ml volumes)and then covered with OpSite dressing On day 3 7 28 or 90posttreatment blood was collected animals were perfused asdescribed above and the following organs were recoveredwound bed brain heart lung liver spleen kidney gonad andlymph nodes (axillary cranial mesenteric and posterior medi-astinal) Real-time quantitative TaqMan PCR was performedusing 45 two-step cycles with primers designed to amplify se-quences bridging the vector backbone and the PDGF-B pre-proregion (sense 59-GGATCTTCGAGTCGACAAGCTT-3 9 an-tisense 59-TAAGGGCTCCTCGAAATACTCTA-3 9) The re-sulting amplicons were detected with an internal fluorogenicprobe (59-TAGTGGTACTTAGCGACGACCCGC-3 9) and anABI Prism 7700 sequence detector (PE Applied BiosystemsFoster City CA) The initial target copy numbers present ineach reaction were quantified by extrapolation from standardcurves of AdPDGF-B DNA in the background of 1 mg of rab-bit liver DNA per reaction Each PCR contained 1 mg of testDNA with the exception of wound bed which contained 500ng per reaction and blood which contained the equivalent of10 ml of original sample Each test sample was assayed in du-plicate to control for PCR inhibitory substances a third reac-tion was spiked with 100 copies of AdPDGF-B DNA PCR dataare presented as AdPDGF-B genome copies per wound thelimit of quantitation (LOQ) was 10 copiesmg DNA or an av-erage of 105 copieswound
For those tissues scoring positive for PCR-amplifiable vec-tor we further performed real-time quantitative reverse tran-scriptase (RT)-PCR Reverse transcriptase reactions were per-formed with 100 ng of each test RNA per reaction and randomhexamer primers The resulting cDNAs were then used to am-plify both rabbit 18S rRNA cDNA and PDGF-B cDNA in sep-arate PCRs The vector-specific primers were designed to am-plify full-length 160-amino acid human PDGF-B mRNA(sense 59-CAAGCACACGCATGACAAGA-3 9 antisense 59-TTTCGTTATCGTAGTGTTTAAAGTGT-3 9) The resulting131-nucleotide amplicons were detected with an internal fluo-rogenic probe (59-AAACAAGTTGCTCGATGGATCCTTAT-CAGGCT-39) RT-PCRs were then normalized for total RNAby 18S rRNA content with a second pair of PCR primers RT-PCR data are presented as the relative amount of PDGF-BmRNA per unit 18S rRNA (in arbitrary units)
Histochemical analyses
For routine morphological assessment paraffin sections werestained according to the Masson trichrome procedure In addi-tion a blinded observer using a microscope equipped with oc-ular micrometers measured the area within sponges filled bygranulation tissue these values are expressed as the percentageof sponge interior occupied by tissue ( granulation fill) Forexcisional wounds trichrome-stained sections and an imageanalysis software package (Image-Pro Plus software Media Cy-bernetics Silver Spring MD) were used to determine the cross-sectional areas of granulation tissue and epithelium per wound(in mm2) In addition the percentage of wound closure was cal-culated according to the following formula [(original wound
diameter 2 epithelial gap length) original wound diameter] 3100
For immunohistochemistry paraffin sections were stainedwith biotinylated Griffonia (Bandeiraea) simplicifolia lectin I(BSL-I) horseradish peroxidase (HRP)-labeled streptavidin anddiaminobenzidine (DAB Vector Laboratories BurlingameCA) in order to detect vascular endothelium Mouse anti-Ki-67and HRP-labeled rabbit anti-mouse IgG antibodies followed byDAB were used to detect proliferating cells Mouse anti-humanPDGF-BB (Z2703 American Type Culture Collection) andHRPndashanti-mouse IgG antibodies followed by DAB were usedto detect human PDGF-BB protein Fluorescein isothiocyanate(FITC)-conjugated anti-adenovirus antibody (Accurate Chemi-cals Westbury NY) and the nuclear stain 496-diamidino-2-phenylindole (DAPI Molecular Probes) were used to detectinternalized adenovirus vectors Finally fibroblasts were iden-tified with Cy3-labeled anti-vimentin (Sigma St Louis MO)
For in situ hybridization procedures an [a-35S] UTP-labeledriboprobe prepared from the full-length human PDGF-B cDNAwas used as previously described (Gonzalez et al 1995) Asense riboprobe was used to control for nonspecific hybridiza-tions
Biochemical analyses
Tissue samples not processed for paraffin embedding wereplaced in 100 mM phosphate buffer containing 02 Triton X-100 (pH 78) and agitated at 55 msec for 20 sec in a Fast-Prep system (BIO 101 Vista CA) After centrifugation su-pernatants were analyzed for protein using a bicinchoninic acidassay (Pierce Rockville IL) and for DNA using the PicoGreenassay PDGF-BB protein content was determined with a humanPDGF-BB-specific ELISA (RampD Systems Minneapolis MN)
Statistical Analyses
Data are presented as arithmetic means 6 1 SD Groups ofthree or more means within individual studies were comparedby one-way analysis of variance (ANOVA) and the Fisher pro-cedure for least significant differences (StatView softwareAbacus Concepts Berkeley CA)
RESULTS
Adenovirus vectors can be immobilized in an activeform within matrices
As an initial step to the in vivo assessment of adenovirusndashmatrix formulations we first determined the activity profilesand release kinetics for vectors formulated in type I collagenand carboxymethylcellulose (CMC) Collagen was selected onthe basis of its successful use as a delivery matrix for proteinsand DNA (Grotendorst et al 1985 Mustoe et al 1987 1991Sprugel et al 1987 Khouri et al 1994 Bonadio et al 1999)as well as its ability to enhance tissue repair responses in fi-broblasts (Xu and Clark 1996 1997) Relatively low (015)and high (26) concentrations were examined reasoning thatthis would allow for either relatively short or long retentiontimes at application sites respectively CMC was selected on
DOUKAS ET AL788
TISSUE REPAIR USING GROWTH FACTOR GENES 789
FIG 3 Localization of gene vector and transgene product within neotissues PVA sponges implanted in rats were injected withAdPDGF-B formulated in 015 collagen (2 3 1010 virus particles per sponge) and paraffin sections were stained as follows(A) Day 1 posttreatment anti-adenovirus immunostain to detect AdPDGF-B (green) DAPI stain to detect cell nuclei (blue) (B)Day 4 posttreatment in situ hybridization using human PDGF-B gene probe (C) Day 1 posttreatment anti-human PDGF-BBprotein immunostain positively stained leukocytes (arrowheads) and fibroblasts (arrows) are indicated (D) Day 6 posttreatmentanti-PDGF-BB immunostain (E) Day 8 posttreatment anti-PDGF-BB immunostain (F) Day 8 post- treatment immunostains todetect PDGF-BB protein (green) and vimentin (red) yellow fluorescence indicates PDGF-BB and vimentin colocalization bluefluorescence indicates cell nuclei (DAPI stain) Original magnifications (AndashC E and F)3 400 (D) 31000
the basis of its clinical use for the delivery of PDGF-BB pro-tein (Steed 1995)
Matrix influences on vector activity were examined by in-cubating AdLuc formulations at 37degC for 60 min followed bymatrix dissolution and vector bioassay (luciferase productionby 293 cells) This is an important test as adenoviruses arequickly inactivated under unfavorable physical and chemicalconditions (Nyberg-Hoffman and Aguilar-Cordova 1999)None of the matrices examined had a deleterious effect on vec-tor activity (90 6 12 106 6 5 and 139 6 37 of control ac-tivity for 015 collagen 26 collagen and CMC respec-tively) To further model in vivo vector stability we alsoincubated AdPDGF-B formulated in 26 collagen with woundfluid for 72 hr at 37degC prior to vector recovery and analysisWe observed no reduction in the level of PDGF-BB productionfrom cells transduced with AdPDGF-B exposed to wound fluidas compared with vector exposed to virus buffer (30 6 5 vs20 6 3 ng of PDGF-BB produced per milliliter of culturemedium respectively n 5 3)
As these data support the suitability of the selected matricesfor in vivo use we next determined their influence on vectorrelease kinetics (Fig 1) When placed in water collagen ma-trices retained the majority of their immobilized vectors with015 and 26 collagen releasing only 17 6 3 and 3 6 1 ofvector by 24 hr respectively By contrast 48 6 3 of AdLucwas released from CMC within 30 min and 61 6 2 by 6 hrThis was not unexpected as CMC is fairly water soluble andas both CMC and adenoviral particles are negatively chargedTherefore collagen matrices in a concentration-dependentfashion display more favorable kinetics for localizing and re-taining adenovirus vectors at delivery sites than does CMC
Collagen-immobilized adenoviruses induce distinctneotissues in vivo
Initial in vivo tests of matrix-immobilized vectors were per-formed with an established model of de novo tissue generation(Buckley et al 1985 Sprugel et al 1987 LeGrand et al1993) PVA sponges implanted subcutaneously in rats were in-jected with a single dose of adenovirus formulated in either col-lagen or CMC and then analyzed for tissue formation Forgrowth factor transgenes we selected platelet-derived growth
factor B (PDGF-B) vascular endothelial growth factor (VEGF)and fibroblast growth factor 2 (FGF2) because of their well-known mitogenic activities
AdPDGF-B formulated in 015 collagen induced granula-tion tissue formation in a dose-responsive manner (Table 1)Compared with vehicle controls delivering 2 3 1010 virus par-ticles induced a 17- to 23-fold increase in sponge protein con-tent (p 00002) a 2- to 27-fold increase in DNA content (p
00002) and a 29- to 43-fold increase in granulation tissue fill(p 00002) Trichrome-stained sections revealed the nearcomplete fill of sponge interiors with well-formed granulationtissue by day 6 posttreatment (Fig 2A) Expression of Ki-67a nuclear protein upregulated in proliferating cells (Gerdes etal 1983) established that both vascular endothelium (arrow-heads Fig 2B) and fibroblasts (arrows Fig 2B) had prolifer-ated in response to PDGF-B gene delivery AdFGF2 and Ad-VEGF also enhanced protein and DNA content within sponges(Table 1) However these vectors induced less granulation tis-sue deposition as compared with AdPDGF-B and the tissuesformed were histologically distinct
Tissues present in AdFGF2-treated sponges were highly vas-cular as revealed by the endothelial-reactive lectin BSL-I (Fig2D) Many of the infiltrating mononuclear cells also reactedpositively with BSL-I lectin suggesting that these cells wereendothelial cells or endothelial precursors AdFGF2 did nothowever induce the formation of classic granulation tissue aslittle collagen deposition was observed demonstrated by thepaucity of blue-staining material in trichrome-stained sections(Fig 2C) AdVEGF also induced heavily vascularized tissues(Fig 2E and F) but with greater extracellular collagen deposi-tion than AdFGF2 Relative to AdPDGF-B-induced tissueshowever AdVEGF-induced tissues were disorganized con-tained few fibroblasts and were markedly edematous Finallywhen AdLuc was delivered as a control treatment no signifi-cant increases in protein DNA or granulation tissue were ob-served compared with collagen vehicle alone (Table 1)Trichrome-stained sections revealed sparse inflammatory cellinfiltrates within AdLuc-treated sponges (Fig 2G) which com-pared with the near absence of infiltration after delivery of col-lagen vehicle alone (Fig 2H) suggested a limited antiviral response
Unlike the 015 collagen formulations described above
DOUKAS ET AL790
TABLE 2 NEOTISSUE FORMATION AFTER PDGF-B GENE OR PDGF-BB PROTEIN DELIVERYa
Granulation Protein DNATreatment fill () (mgsponge) (mgsponge)
015 Collagen vehicle 28 6 13b 16 6 2b 103 6 22b
AdPDGF-B 81 6 15b 30 6 6b 218 6 28b
PDGF-BB 100 mg 64 6 12c 22 6 4c 155 6 26c
PDGF-BB 10 mg qod 3 3d 77 6 9b0 31 6 8b 230 6 75b
aPVA sponges implanted in rats were injected with either 015 collagen vehicle or collagen containing AdPDGF-B as described in Table 1 Alternatively PDGF-BB protein was delivered as a single 100-mg dose on day 4 postimplantation or as10-mg doses on days 4 6 and 8 Sponges were removed on day 12 postimplantation and processed to determine the percent granulation fill as well as total protein and DNA contents Data are presented as means 6 SD (n 5 4ndash8)
bp 00001 versus collagen control and p 005 versus 100-mg PDGF-BBcp 003 versus collagen controldqod 3 3 Every other day three times
TISSUE REPAIR USING GROWTH FACTOR GENES 791
TABLE 3 INFLUENCE OF ADENOVIRUSndashMATRIX FORMULATIONS ON ISCHEMIC WOUND HEALINGa
Granulation Epithelial Wound closureTreatment Model system area (mm2) area (mm2) ( complete)
Aqueous buffer Cartilage intact 10 6 08 05 6 03 61 6 226 mm day 10
AdPDGF-B in Cartilage intact 24 6 22 05 6 01 73 6 28aqueous buffer 6 mm day 10
015 Collagen Cartilage intact 05 6 03 05 6 02 89 6 14vehicle 6 mm day 10
AdPDGF-B in Cartilage intact 16 6 09b 09 6 03c 97 6 7015 collagen 6 mm day 10
Aqueous buffer Cartilage removed 45 6 08 08 6 02 95 6 96 mm day 7
AdPDGF-B in Cartilage removed 40 6 15 11 6 05 82 6 22aqueous buffer 6 mm day 7
015 Collagen Cartilage removed 36 6 13 06 6 02 88 6 22vehicle 6 mm day 7
AdPDGF-B in Cartilage removed 70 6 14b 07 6 03 79 6 22015 collagen 6 mm day 7
26 Collagen Cartilage removed 04 6 05 01 6 01 24 6 15vehicle 8 mm day 8
AdPDGF-B in Cartilage removed 51 6 25b 06 6 03b 52 6 25c
26 collagen 8 mm day 8
aExcisional wounds (6 or 8 mm in diameter) were placed in ischemic rabbit ears with underlying cartilage left intact or re-moved Wounds were then treated with AdPDGF-B formulated in aqueous virus buffer or collagen control treatments consistedof vehicle alone For 6-mm wounds virus was applied as 2 3 109 particles per wound for 8-mm wounds as 4 3 109 particlesper wound On days 7ndash10 posttreatment wounds were harvested and processed as trichrome-stained paraffin sections whichwere then used to quantify newly formed granulation tissue and epithelium (cross-sectional area in mm2) and the degree of woundsurface closure (where 100 equals complete closure) Data are presented as means 6 SD (n 5 4ndash8)
bp 0009 versus vehicle controlcp 005 versus vehicle control
26 collagen formulations could not be reliably examined inthe PVA sponge model as their relatively high viscosity pre-vented uniform filling of sponges by syringe CMC-formulatedvectors were also unsuitable for this model system as theyproved highly inflammatory (data not shown) These formula-tions therefore were evaluated in more appropriate excisionalwound models (see below)
Tissue repair cells are transduced by collagen-immobilized adenoviruses
On the basis of the robust activity of collagen-formulatedAdPDGF-B we elected to further examine this vectorndashmatrixcombination first by seeking to correlate PDGF-B gene deliv-ery with subsequent transgene and protein expression WhenPVA sponges treated with 015 collagenndashAdPDGF-B werestained with both an anti-adenovirus antibody and the nuclearstain DAPI the majority of cells present 1 day after gene de-livery had bound andor internalized adenovirus (Fig 3A) Insitu hybridization revealed that these cells were successfullytransduced by virus as they contained human PDGF-B mRNA(Fig 3B) By contrast hybridization product was not detectedwith a sense riboprobe or when AdLuc-treated sponges wereexamined (data not shown)
We next used a human PDGF-BB-specific antibody to iden-tify the cell types responsible for transgene expression By day
1 postdelivery of 015 collagenndashAdPDGF-B PDGF-BB pro-tein was localized to leukocytes (arrowheads) and fibroblasts (ar-row Fig 3C) With time PDGF-BB protein was detected boundto the extracellular matrix (ECM) surrounding positively stainedcells (Fig 3D) This last observation indicates that a reservoir ofPDGF-BB protein develops within treated tissues and thus mayprolong the histogenic effects of this growth factor Finally byday 8 the majority of immunoreactivity had abated with pri-marily microvascular endothelium remaining positive (Fig 3E)However scattered fibroblasts could still be shown to producePDGF-BB protein by dual immunohistochemistry with anti-PDGF-BB and anti-vimentin antibodies (Fig 3F)
Multiple administrations of PDGF-BB protein are required to approximate the histogenic effects of collagenndashAdPDGF-B
To directly compare gene therapy with the more conven-tional approach of growth factor protein delivery we next quan-tified tissue formation in response to either PDGF gene or pro-tein delivery A single injection of 015 collagenndashAdPDGF-Benhanced granulation tissue filling of sponges by 3-fold versusvehicle alone (p 00001) and sponge protein and DNA lev-els by 2-fold (p 00001 Table 2) Using a human PDGF-BB-specific ELISA this growth factor was detected at 54 6 13ngsponge (n 5 8) By contrast when PDGF-BB protein was
delivered as a single dose nearly 2000-fold in excess of thisconcentration the tissue formation responses observed (proteinand DNA accumulation and granulation tissue formation) weresignificantly lower (p 005 Table 2) In fact repeated dos-ing with PDGF-BB protein was required in order to achieve re-sponses comparable to a single administration of the PDGF-Bgene These data therefore support our hypothesis that the abil-ity of gene delivery to establish prolonged in situ growth fac-tor production translates into greater histogenesis than that seenwith growth factor proteins
CollagenndashAdPDGF-B induces complete healing of ischemic wounds
Nonhealing wounds are a major risk in chronically ischemictissues as low oxygen tension greatly impairs tissue repair pro-cesses We therefore compared the ability of matrix versusaqueous formulated AdPDGF-B to repair ischemic excisionalwounds Several models were employed to compare variationsin wound size and condition so as to allow for a more com-plete picture of tissue repair
In the first model system 6-mm-diameter wounds were cre-ated in ischemic rabbit ears by removal of epidermal and der-mal layers but not underlying cartilage This model has beenused in previous studies of growth factor proteins and genes(Ahn and Mustoe 1990 Mustoe et al 1994 Liechty et al1999) and was therefore employed to allow comparison withthese reports However it represents an artificial system as thepresence of a cartilage layer restricts both treatment activity andhealing to wound margins and in addition the initially acellu-lar wound bed forms a cup that artifactually retains aqueoustreatments As would be predicted we found a trend towardgranulation tissue formation in this model after the applicationof AdPDGF-B formulated in aqueous buffer (Table 3) How-ever this response did not reach the level of statistical signifi-cance as tissue development was highly variable (note the highstandard deviation value) In addition epithelial regenerationand wound closure were minimal to unaffected By contrastAdPDGF-B formulated in 015 collagen enhanced granula-tion tissue area by 32-fold and epithelial area by 18-fold overthat achieved with vehicle alone (p 0009 and 005 respec-tively) Although near complete closure of epithelial gaps wasalso achieved the high level of self-healing in control-treatedgroups (89 wound closure) precluded statistical significance
In an alternative model design subdermal cartilage was com-pletely removed from excisional wounds creating beds whosefloors now consisted of dermal tissue (Pierce et al 1994b)This design allows for cellular responses from the entire woundbed as well as the opportunity for vector migration beyond
treatment areas We now observed that aqueous formulated Ad-PDGF-B failed to induce even a trend toward tissue regenera-tion (Table 3) Rather the vector appears to have seeped throughthe wound bed floor as inflammatory cell infiltrates and fociof fibroblast proliferation were observed in the underlying der-mis and at wound margins (Fig 4A) Immunohistochemistryconfirmed the production of human PDGF-BB at these sites(Fig 4B) CMC-formulated AdPDGF-B also failed to induceany meaningful tissue repair Wounds treated with this formu-lation showed a diffuse inflammatory response within thewound bed and wound surfaces were overlain with fibrin clotsrather than regenerating epithelium (Fig 4C and D) By con-trast AdPDGF-B formulated in 015 collagen enhanced gran-ulation tissue deposition 19-fold within wound beds versus ve-hicle controls (p 0002) and wounds were extensivelyepithelialized (Table 3) Neither epithelial regeneration norwound closure achieved significance however as the high de-gree of self-healing achieved in this particular model (see ve-hicle alone group) most likely masked transgene-stimulated re-sponses
To address these model limitations as our next system wecreated 8-mm wounds in ischemic rabbit ears by removingepidermal dermal and cartilage layers reasoning that largerexcisional wounds would display limited self-healing In ad-dition this model could readily accommodate 26 collagenformulations which proved difficult to reproducibly apply insmaller wounds Compared with control wounds treated withcollagen vehicle alone wounds treated with AdPDGF-B for-mulated in 26 collagen achieved a 12-fold enhancementin granulation tissue fill and a 6-fold enhancement in re-ep-ithelialization by day 8 posttreatment (p 0009 Table 3)In addition wound closure was only 24 complete in colla-gen vehicle-treated wounds by day 8 but 52 complete inwounds treated with collagen-formulated AdPDGF-B (p
005) Histologically AdPDGF-B-treated wounds showed nosigns of tissue hyperplasia or chronic inflammation but ratheran orderly repair process marked by a regenerated epitheliallayer overlying a wound bed filled with granulation tissue(Fig 4E and F)
CollagenndashAdPDGF-B induces normal long-term tissue repair
Our choice of adenoviruses for transgene delivery was partlybased on the reasoning that as these vectors establish transientgene expression they would not lead to hyperproliferative re-sponses or scar formation To test this hypothesis we treatedrabbit ear excisional wounds with AdPDGF-B formulated in015 collagen and examined tissue repair responses out to
DOUKAS ET AL792
FIG 4 Influence of adenovirusndashmatrix formulations on excisional wound repair Excisional wounds (6 or 8 mm in diameter andextending through underlying cartilage layers) were placed in ischemic rabbit ears bars indicate original wound depth (determinedfrom cartilage visible at wound margins) Wounds were then treated with AdPDGF-B formulated in either virus buffer CMC orcollagen and on day 7 or 8 posttreatment processed for histology or immunohistochemistry An identical design was used to ex-amine long-term healing on day 90 except that wounds were created in nonischemic ears (A) Day 7 buffer-formulated AdPDGF-B-treated 6-mm wound trichrome stain (B) Day 7 buffer-formulated AdPDGF-B-treated 6-mm wound anti-PDGF-BB proteinimmunostain (C and D) Day 7 CMC-formulated AdPDGF-B-treated 6-mm wound trichrome stains (E and F) Day 8 26 col-lagen-formulated AdPDGF-B-treated 8-mm wound trichrome stains (G and H) Day 90 015 collagen-formulated AdPDGF-B-treated 6-mm wound trichrome stains Original magnification (A C E and G) 340 (B D F and H) 3200
TISSUE REPAIR USING GROWTH FACTOR GENES 793
DOUKAS ET AL794
TABLE 4 BIODISTRIBUTION OF AdPDGF-B IN EXCISIONAL WOUNDSa
Positive samplestotal assayed
Tissue AdPDGF-B dose Day 3 Day 7 Day 28 Day 90
Wound bed 2 3 109 particles 66 66 66b 06Axillary lymph nodes 2 3 109 particles 02 ND 06 06
Wound bed 2 3 1011 particles 66 66 66 46c
Axillary lymph nodes 2 3 1011 particles 66 ND 66d 26e
aFull-thickness excisional wounds (7 cm2) were placed on the backs of rabbits and AdPDGF-B formulated in 26 collagenwas applied as either 2 3 109 or 2 3 1011 virus particles per wound On days 3ndash90 posttreatment wound beds and a panel oforgans were harvested for real-time PCR quantification of viral genome Data are shown for wound bed and axillary lymph nodesamples as the number of samples that yielded amplifiable signals per total number assayed ND not determined
bThree of six samples scored below the level of quantitation (LOQ 10ndash100 copiesmg DNA)cAll four positive samples scored below the LOQdThree of six samples scored below the LOQeBoth positive samples scored below the LOQ
180 days posttreatment (Fig 5) PDGF-B gene delivery en-hanced total ear thickness relative to controls on day 28 (229 6
020 vs 179 6 019 mm p 00001) and day 60 (192 6 001vs 182 6 011 mm p 0005) as anticipated on the basis ofthe ability of this formulation to induce granulation tissue for-mation By day 90 posttreatment however there was no mea-surable difference in ear thickness between AdPDGF-B andcontrol-treated groups and this relationship continued out today 180 indicating that growth factor gene delivery did not in-duce excessive scar formation This was also confirmed histo-logically AdPDGF-B-treated wounds on day 90 and beyondwere composed of a thin outer keratin layer an underlying ep-ithelial layer of equivalent thickness to nonwounded areas anda collagen-rich dermis devoid of any signs of tissue hyperpla-sia (Fig 4G and H)
Collagen immobilization limits adenovirus vectorbiodistribution beyond treatment sites
As a final measure of the value of matrix immobilization forgene delivery we determined the biodistribution patterns ofvectors after their in vivo delivery In the first model systemused AdPDGF-B formulated in 015 collagen was applied torabbit ear wounds at equivalent doses as previously describedwounds were extended through underlying cartilage but vas-cular supplies were not disturbed so as to permit maximal vec-tor dissemination By PCR no adenoviral DNA was detectablein lung spleen brain cervical lymph nodes or gonads on day1 3 7 or 14 (n 5 6 per group) In the liver one of six sam-ples was positive on days 3 and 7 but none on day 14 in serumonly one of six samples tested positive on day 14 (equivalentof 500-ml serum volume) By contrast adenovirus was detectedin eight of eight wound bed samples at all time points exam-ined
In a second model system excisional wounds placed on thebacks of rabbits were treated with AdPDGF-B formulated in26 collagen Because of their anatomical placement thismodel allowed for the creation of larger excisional wounds (7-cm2 total area) than those placed in rabbit ears (03 cm2) and
consequently larger treatment volumes and vector doses (2 3109 or 2 3 1011 virus particles per wound) At the lower doseof 2 3 109 particles PCR-amplifiable adenoviral DNA was notdetectable beyond wound beds on day 3 7 28 or 90 Tissuessampled and found not to contain vector included blood heartlung liver kidney brain spleen lymph nodes and gonads (n 5
6group) In wound beds adenoviral DNA was detected at alltime points except for day 90 (Table 4 and Fig 6) Vector lev-els did decrease however by 38-fold between days 7 and 28with three of six samples falling below the level of quantita-tion (LOQ) by real-time PCR at the latter time point (Fig 6)
At a 100-fold higher vector dose of 2 3 1011 particles perwound PCR-amplifiable adenoviral DNA was once again un-detectable in the majority of tissues sampled Except for a sin-gle day 7 liver sample and a single day 7 brain sample (bothbelow the LOQ) adenoviral DNA was only detectable directlyin wound beds or in the axillary lymph nodes that drain woundsites (Table 4) Moreover three of six positive axillary nodesamples scored below the LOQ on day 28 as did both positivesamples on day 90 indicating that they contained relatively lit-tle vector Within wound beds adenoviral DNA was detectedat quantifiable levels out to day 28 and at detectable but non-quantifiable levels on day 90 DNA copy numbers remainedsteady between days 3 and 7 dropped 107-fold between days7 and 28 and a further 1662-fold by day 90 Finally at eachtime point DNA copy numbers in wounds treated with 2 3
1011 particles were approximately 100-fold higher than thosefound in wounds treated with 2 3 109 particles thus confirm-ing the linearity of our assay system
To better define the time course of human PDGF-BB pro-duction we also quantified transgene mRNA levels in woundbed samples treated at 2 3 109 particles per wound This treat-ment dose was selected as representative of the virus particleconcentration capable of inducing complete healing in ischemicear wounds Quantifiable levels of human PDGF-B mRNAwere detectable in treated dorsal wounds at days 3 7 and 28(Fig 6) with levels decreasing 14-fold between days 3 and 7and 5-fold between days 7 and 28 The more sensitive tech-nique of real-time RT-PCR therefore demonstrates that trans-
TISSUE REPAIR USING GROWTH FACTOR GENES 795
gene expression extends well beyond the 8-day time period sug-gested using anti-PDGF-BB immunohistochemistry as a de-tection system (Fig 3)
DISCUSSION
These studies demonstrate that immobilization of gene ther-apy vectors in collagen-based matrices enables their efficientdelivery and activity in vivo Matrix immobilization achievedprolonged transgene-encoded growth factor production and asa consequence robust tissue repair By contrast aqueous vehi-cles failed to retain adenoviruses at application sites resultingin diffuse inflammation rather than productive tissue regenera-tion These observations confirm our basic hypothesis that ma-trix immobilization of growth factor-encoding gene therapyvectors represents a promising approach to tissue repair
Although de novo tissue deposition was achievable with sev-eral growth factor genes PDGF-B proved the most suitable forrepair of cutaneous defects A single administration of colla-gen-immobilized AdPDGF-B rapidly induced the formation ofhighly cellular and vascularized tissues with dense ECMs richin collagen By contrast AdFGF2 induced a primarily vascu-lar response with little collagen deposition FGF2 induces therelease of matrix metalloproteinase 1 or interstitial collagenase(Buckley-Sturrock et al 1989) and this may underlie the rel-ative paucity of ECM accumulation VEGF gene delivery alsoinduced highly vascular responses however the enhanced per-meability characteristic of VEGF-induced vasculature (Dvoraket al 1995) led to edema within nascent tissues In fact much
of the enhanced protein and DNA deposition observed in Ad-VEGF-treated PVA sponges may well derive from fluid exu-dates rather than actual tissue formation Finally the inabilityof AdLuc delivery to induce anything beyond a limited in-flammatory response confirms that tissue formation was de-pendent on growth factor gene delivery
The robust activity of PDGF-B gene delivery was expectedas PDGF-BB protein initiates multiple aspects of tissue forma-tion including cellular influx and proliferation ECM deposi-tion and tissue remodeling (Pierce et al 1988 1991 1994a)Indeed PDGF-BB is the only growth factor protein to have suc-cessfully completed human clinical trials and be approved forthe treatment of dermal wounds (Steed 1995 drsquoHemecourt etal 1998 Wieman 1998 Wieman et al 1998) We observedthat collagen-formulated AdPDGF-B induced the complete re-pair of excisional skin defects without unwanted long-term ef-fects such as the development of hypertrophic scars Endoge-nous growth factors other than PDGF-BB however most likelymediated the enhanced re-epithelialization observed in thesewounds as epithelial regeneration is driven by members of theepidermal growth factor and FGF families (Pierce et al 1994bDanilenko et al 1995) Our data indicate nonetheless that tis-sue regeneration and repair were initiated and to a great degreedriven by transgene-encoded PDGF-BB
Despite the known activity of PDGF-BB protein we wereable to demonstrate greater tissue deposition after gene deliv-ery as compared with the use of recombinant growth factor pro-tein A single application of PDGF-BB protein could not equalthe ability of PDGF-B gene therapy to induce neotissue for-mation even at doses well in excess of that induced in situ byAdPDGF-B and in excess of that used in human clinical trials
FIG 5 Influence of collagen-formulated AdPDGF-B on long-term tissue repair Excisional wounds (6 mm in diameter withcartilage remaining intact) were placed in nonischemic rabbit ears and treated with either 015 collagen alone (open columns)or AdPDGF-B formulated in this vehicle (solid columns) On days 28ndash180 posttreatment total ear thickness at the site of eachwound was measured (in mm) with calipers Data are presented as means 6 SD (n 5 3) Treatment groups differ by p 00001groups differ by p 0005
(Steed 1995 drsquoHemecourt et al 1998 Wieman 1998 Wie-man et al 1998) In fact repeated administrations of PDGF-BB protein were required to approach the level of tissue for-mation observed after a single administration of AdPDGF-BThese data support our hypothesis that sustained localizedgrowth factor production is required for robust tissue repair
In further support of this hypothesis we demonstrated thatmRNA encoding human PDGF-B was present in excisionalwounds as late as day 28 after collagen-formulated AdPDGF-B administration By contrast previous studies of PDGF-BBprotein found that the great majority of this growth factor wasgone from treated wounds 1 day postapplication and that anytissue maturation subsequently observed was most likely dueto the upregulation of endogenous growth factors (Pierce et al1992 1995) We also demonstrated that repair cells such asmononuclear leukocytes endothelial cells and fibroblasts pres-ent with developing neotissues represent the source of both
transgene transcription and PDGF-BB production In additiona depot of human PDGF-BB was detected bound to the colla-gen delivery matrix and ECM of these tissues This was antici-pated as PDGF-BB contains collagen-binding motifs (Soma-sundaram and Schuppan 1996) We hypothesize that subsequentmatrix metalloproteinase activity by repair cells will serve togenerate localized release of this sequestered growth factor pooland as a consequence further drive tissue regeneration Theseevents which are central to tissue remodeling should be directlyenhanced by collagen matrices as type I collagen stimulates me-talloproteinase production integrin expression and cellular ac-tivation in PDGF-stimulated fibroblasts (Xu and Clark 19961997)
An additional rationale for employing collagen matrices wasto physically immobilize vectors This was confirmed in vivowhere collagen matrices maintained AdPDGF-B at deliverysites for at least 28 days and limited vector migration to other
DOUKAS ET AL796
FIG 6 Persistence of collagen-formulated vector and transgene transcripts in excisional wounds Full-thickness excisionalwounds (7 cm2) were placed on the dorsal surface of rabbits and treated with AdPDGF-B formulated in 26 collagen at either2 3 109 or 2 3 1011 virus particles per wound (open and closed columns respectively) Wounds were then covered with OpSitedressing and on days 3 7 or 28 posttreatment wound beds were harvested for real-time quantitative PCR and RT-PCR analy-ses PCR data are presented in the upper graph as AdPDGF-B copies per wound RT-PCR data are presented in the lower graphas the relative amount of PDGF-B mRNA per unit 18S rRNA (in arbitrary units) All data points are means 6 SD (n 5 6)
tissues or organs In vitro tests also established that collagenmatrices not only prevent vector loss due to diffusion but pre-serve vector activity despite prolonged incubation in acutewound fluid Successful vector immobilization and tissue re-pair could be achieved with both 015 collagen and 26 col-lagen suggesting flexibility in the final vehicle formulation re-quired for effective vector delivery This flexibility was neededin the present studies as 26 collagen formulations proveddifficult to deliver to PVA sponges and 6-mm excisionalwounds This would not be of concern in clinical settings how-ever where wound beds are easily accessible and generally sev-eral square centimeters in area By contrast CMC was inef-fective at retaining vector in aqueous environments Moreimportantly this matrix was itself inflammatory and whencombined with adenovirus the net result was inflammationrather than tissue repair We are currently examining the util-ity of other matrices such as fibrin and hyaluronic acid whichbecause of their more provisional nature may offer yet greatercellular migration into wounds as compared with type I colla-gen
Although an aqueous-based AdPDGF-B formulation hasbeen previously shown to enhance tissue formation (Liechty etal 1999) this was achieved with a model system that artifi-cially retains vectors within treatment sites In fact the presentstudies demonstrate that any tissue repair observed after Ad-PDGF-B delivery in a nongelling liquid is dependent on the useof this model system In wounds not designed to retain appliedtreatments aqueous-formulated AdPDGF-B seeped into sur-rounding tissues and led to hyperplasia within these areas ratherthan to tissue regeneration within the active wound bed Colla-gen-immobilized AdPDGF-B on the other hand did persist inthese wound beds and led to significant enhancements in gran-ulation tissue formation as well as enhanced wound re-epithe-lialization and wound closure The significance of these activ-ities is further substantiated considering that they wereachievable in 8-mm-diameter ischemic wounds which withinthe time frame examined could not self-heal to any meaning-ful degree in the absence of gene therapy However as all theanimal models employed in these studies will eventually self-heal given sufficient time the full value of matrix-immobilizedgene therapy vectors remains to be confirmed in human clini-cal trials
In conclusion we present evidence that matrix-immobilizedgene therapy vectors encoding appropriate growth-promotinggenes represent a promising approach to tissue regeneration andrepair This basic concept can be expanded to include alterna-tive matrices such as controlled-release formulations as wellas tissue-specific growth factors Furthermore the addition oftargeting ligands to adenovirus vectors (eg FGF2) can en-hance their ability to transduce cells such that tissue repair re-sponses comparable to nontargeted vectors can be achieved butat significantly lower vector doses (Chandler et al 2000a)With appropriate design and application schedules one couldconceivably time the release of multiple growth factors to spe-cific stages of a tissue repair cascade In addition we have foundin preliminary studies that collagen-immobilized nonviral vec-tors such as PDGF-B plasmids which have potentially morefavorable safety profiles than adenovirus vectors can also en-hance tissue formation in vivo (Chandler et al 2000b Tyroneet al 2000) Such flexibility should allow for the widespreadapplication of gene therapy to the treatment of injured tissues
ACKNOWLEDGMENTS
We thank Jeff Davidson (Vanderbilt University School ofMedicine) for assistance in establishing the PVA sponge modelCarl-Henrik Heldin (Ludwig Institute for Cancer Research) forthe PDGF-B gene construct and Emelie Amburn Lara AsatoSharon Chang Gail Fieser Lydia Greenlees Rebecca Smokerand Linda Manza for excellent technical assistance This pub-lication was made possible in part by NIH grants 1R43AR46154(JD) and 5P01CA25874 (MH)
REFERENCES
AHN ST and MUSTOE TA (1990) Effects of ischemia on ulcerwound healing A new model in the rabbit ear Ann Plast Surg 2417ndash23
ANDREE C SWAIN WF PAGE CP MACKLIN MDSLAMA J HATZIS D and ERIKSSON E (1994) In vivo trans-fer and expression of a human epidermal growth factor gene accel-erates wound repair Proc Natl Acad Sci USA 91 12188ndash12192
BENN SI WHITSITT JS BROADLEY KN NANNEY LBPERKINS D HE L PATEL M MORGAN JR SWAIN WFand DAVIDSON JM (1996) Particle-mediated gene transfer withtransforming growth factor-b1 cDNAs enhances wound repair in ratskin J Clin Invest 98 2894ndash2902
BONADIO J SMILEY E PATIL P and GOLDSTEIN S (1999)Localized direct plasmid gene delivery in vivo Prolonged therapyresults in reproducible tissue regeneration Nat Med 5 753ndash759
BUCKLEY A DAVIDSON JM KAMERATH CD WOLT TBand WOODWARD SC (1985) Sustained release of epidermalgrowth factor accelerates wound repair Proc Natl Acad Sci USA82 7340ndash7344
BUCKLEY-STURROCK A WOODWARD SC SENIOR RMGRIFFIN GL KLAGSBRUN M and DAVIDSON JM (1989)Differential stimulation of collagenase and chemotactic activity in fi-broblasts derived from rat wound repair tissue and human skin bygrowth factors J Cell Physiol 138 70ndash78
CHANDLER LA DOUKAS J GONZALEZ AM HOGANSONDK GU DL MA C NESBIT M CROMBLEHOLME TMHERLYN M SOSNOWSKI BA and PIERCE GF (2000a)FGF2ndashTargeted adenovirus encoding platelet-derived growth factor-B enhances de novo tissue formation Mol Ther 2 153ndash160
CHANDLER LA MA C GONZALEZ AM DOUKAS JNGUYEN T PIERCE GF and PHILLIPS ML (2000b) Ma-trix-enabled gene transfer for cutaneous wound repair Wound Re-pair Regen 8 473ndash479
DANILENKO DM RING BD TARPLEY JE MORRIS BVAN GY MORAWIECKI A CALLAHAN W GOLDEN-BERG M HERSHENSON S and PIERCE GF (1995) Growthfactors in porcine full and partial thickness burn repair Differing tar-gets and effects of keratinocyte growth factor platelet-derivedgrowth factor-BB epidermal growth factor and neu differentiationfactor Am J Pathol 147 1261ndash1277
DEUEL TF KAWAHARA RS MUSTOE TA and PIERCE GF(1991) Growth factors and wound healing Platelet-derived growthfactor as a model cytokine Annu Rev Med 42 567ndash584
DrsquoHEMECOURT PA SMIELL JM and KARIM MR (1998) So-dium carboxymethylcellulose aqueous-based gel vs becaplermin gelin patients with nonhealing lower extremity diabetic ulcers Wounds10 69ndash75
DOUKAS J HOGANSON DK ONG M YING W LACEYDL BAIRD A PIERCE GF and SOSNOWSKI BA (1999)Retargeted delivery of adenoviral vectors through fibroblast growthfactor receptors involves unique cellular pathways FASEB J 131459ndash1466
TISSUE REPAIR USING GROWTH FACTOR GENES 797
DVORAK HF BROWN LF DETMAR M and DVORAK AM(1995) Vascular permeability factorvascular endothelial growth fac-tor microvascular hyperpermeability and angiogenesis Am JPathol 146 1029ndash1039
EMING SA MEDALIE DA TOMPKINS RG YARMUSHML and MORGAN JR (1998) Genetically modified human ker-atinocytes overexpressing PDGF-A enhance the performance of acomposite skin graft Hum Gene Ther 9 529ndash539
EMING SA WHITSITT JS HE L KRIEG T MORGAN JRand DAVIDSON JM (1999) Particle-mediated gene transfer ofPDGF isoforms promotes wound repair J Invest Dermatol 112297ndash302
GERDES J SCHWAB U LEMKE H and STEIN H (1983) Pro-duction of a mouse monoclonal antibody reactive with a human nu-clear antigen associated with cell proliferation Int J Cancer 3113ndash20
GONZALEZ AM BERRY M MAHER PA LOGAN A andBAIRD A (1995) A comprehensive analysis of the distribution ofFGF-2 and FGFR1 in the rat brain Brain Res 701 201ndash226
GREENHALGH DG (1996) The role of growth factors in woundhealing J Trauma 41 159ndash167
GROTENDORST GR MARTIN GR PENCEV D SODEK Jand HARVEY AK (1985) Stimulation of granulation tissue for-mation by platelet-derived growth factor in normal and diabetic ratsJ Clin Invest 76 2323ndash2329
KHOURI RK HONG SP DEUNE EG TARPLEY JE SONGSZ SERDAR CM and PIERCE GF (1994) De novo genera-tion of permanent neovascularized soft tissue appendages by platelet-derived growth factor J Clin Invest 94 1757ndash1763
LEGRAND EK SENTER LH GAMELLI RL and KIORPESTC (1993) Evaluation of PDGF-BB PDGF-AA bFGF IL-1 andEGF dose responses in polyvinyl alcohol sponge implants assessedby a rapid histologic method Growth Factors 8 315ndash329
LIECHTY KW NESBIT M HERLYN M RADU A ADZICKNS and CROMBLEHOLME TM (1999) Adenoviral-mediatedoverexpression of platelet-derived growth factor-B corrects ischemicimpaired wound healing J Invest Dermatol 113 375ndash383
LYNCH SE COLVIN RB and ANTONIADES HN (1989)Growth factors in wound healing J Clin Invest 84 640ndash646
MUSTOE TA PIERCE GF THOMASON A GRAMATES PSPORN MB and DEUEL TF (1987) Accelerated healing of in-cisional wounds in rats induced by transforming growth factor-betaScience 237 1333ndash1336
MUSTOE TA PIERCE GF MORISHIMA C and DEUEL TF(1991) Growth factor-induced acceleration of tissue repair throughdirect and inductive activities in a rabbit dermal ulcer model J ClinInvest 87 694ndash703
MUSTOE TA AHN ST TARPLEY JE and PIERCE GF(1994) Role of hypoxia in growth factor responses Differential ef-fects of basic fibroblast growth factor and platelet-derived growthfactor in an ischemic wound model Wound Rep Reg 2 277ndash283
NYBERG-HOFFMAN C and AGUILAR-CORDOVA E (1999) In-stability of adenoviral vectors during transport and its implication forclinical studies Nat Med 5 955ndash957
PIERCE GF and MUSTOE TA (1995) Pharmacologic enhance-ment of wound healing Annu Rev Med 46 467ndash481
PIERCE GF MUSTOE TA SENIOR RM REED J GRIFFINGL THOMASON A and DEUEL TF (1988) In vivo incisionalwound healing augmented by platelet-derived growth factor and re-combinant c-sis gene homodimeric proteins J Exp Med 167 974ndash987
PIERCE GF VANDE BERG J RUDOLPH R TARPLEY J andMUSTOE TA (1991) Platelet-derived growth factor-BB and trans-forming growth factor beta 1 selectively modulate glycosaminogly -cans collagen and myofibroblasts in excisional wounds Am JPathol 138 629ndash646
PIERCE GF TARPLEY JE YANAGIHARA D MUSTOE TA
FOX GM and THOMASON A (1992) Platelet-derived growthfactor (BB homodimer) transforming growth factor-b1 and basic fi-broblast growth factor in dermal wound healing Neovessel and ma-trix formation and cessation of repair Am J Pathol 140 1375ndash1388
PIERCE GF TARPLEY JE ALLMAN RM GOODE PS SER-DAR CM MORRIS B MUSTOE TA and VANDE BERG J(1994a) Tissue repair processes in healing chronic pressure ulcerstreated with recombinant platelet-derived growth factor BB Am JPathol 145 1399ndash1410
PIERCE GF YANAGIHARA D KLOPCHIN K DANILENKODM HSU E KENNEY WC and MORRIS CF (1994b) Stim-ulation of all epithelial elements during skin regeneration by kerati-nocyte growth factor J Exp Med 179 831ndash840
PIERCE GF TARPLEY JE TSENG J BREADY J CHANGD KENNEY WC RUDOLPH R ROBSON MC VANDEBERG J and REID P (1995) Detection of platelet-derived growthfactor (PDGF)-AA in actively healing human wounds treated withrecombinant PDGF-BB and absence of PDGF in chronic nonhealingwounds J Clin Invest 96 1336ndash1350
SINGER AJ and CLARK RA (1999) Cutaneous wound healingN Engl J Med 341 738ndash746
SOMASUNDARAM R and SCHUPPAN D (1996) Type I II IIIIV V and VI collagens serve as extracellular ligands for the iso-forms of platelet-derived growth factor (AA BB and AB) J BiolChem 271 26884ndash26891
SPRUGEL KH MCPHERSON JM CLOWES AW and ROSSR (1987) Effects of growth factors in vivo I Cell ingrowth intoporous subcutaneous chambers Am J Pathol 129 601ndash613
STEED DL (1995) Clinical evaluation of recombinant humanplatelet-derived growth factor for the treatment of lower extremitydiabetic ulcers Diabetic Ulcer Study Group J Vasc Surg 21 71ndash78
STEED DL (1998) Foundations of good ulcer care Am J Surg 17620S-25S
TYRONE JW MOGFORD JE CHANDLER LA MA C XIAY PIERCE GF and MUSTOE TA (2000) Collagen-embeddedplatelet-derived growth factor DNA plasmid promotes wound heal-ing in a dermal ulcer model J Surg Res 93 230ndash236
VOGT PM THOMPSON S ANDREE C LIU P BREUING KHATZIS D BROWN H MULLIGAN RC and ERIKSSON E(1994) Genetically modified keratinocytes transplanted to woundsreconstitute the epidermis Proc Natl Acad Sci USA 91 9307ndash9311
WIEMAN TJ (1998) Clinical efficacy of becaplermin (rhPDGF-BB)gel Becaplermin Gel Studies Group Am J Surg 176 74S-79S
WIEMAN TJ SMIELL JM and SU Y (1998) Efficacy and safetyof a topical gel formulation of recombinant human platelet-derivedgrowth factor-BB (becaplermin) in patients with chronic neuropathicdiabetic ulcers A phase III randomized placebo-controlled double-blind study Diabetes Care 21 822ndash827
WILSON JM (1996) Adenoviruses as gene-delivery vehicles NEngl J Med 334 1185ndash1187
XU J and CLARK RA (1996) Extracellular matrix alters PDGFregulation of fibroblast integrins J Cell Biol 132 239ndash249
XU J and CLARK RA (1997) A three-dimensional collagen latticeinduces protein kinase C-z activity Role in a2 integrin and collage-nase mRNA expression J Cell Biol 136 473ndash483
Address reprint requests toDr John Doukas
Selective Genetics Inc11035 Roselle Street
San Diego CA 92121
E-mail jdoukasselectivegeneticscom
Received for publication December 28 2000 accepted after re-vision February 23 2001
DOUKAS ET AL798

tions were then applied to wound beds as either 5-ml volumescontaining 2 3 109 virus particles (for 6-mm wounds) or 8-mlvolumes containing 4 3 109 virus particles (for 8-mm wounds)control treatments consisted of vehicles alone After treatmentapplications wounds were covered with occlusive dressings(OpSite Smith amp Nephew Largo FL) On days 7ndash10 post-surgery and treatment wounds were harvested and fixed as de-scribed above These time points were selected on the basis ofminimal self-healing in most untreated wounds as determinedin preliminary model development studies In general largerwounds allowed for longer study times as did cartilage intactmodels
Finally to assess the long-term effects of vector application6-mm wounds were placed in nonischemic rabbit ears to thelevel of underlying cartilage and treated as described aboveWounds were then harvested for analysis on days 28ndash180 post-treatment
Biolocalization studies
Two model systems were used to examine adenovirus vectorbiodistribution In the first model 6-mm-diameter wounds ex-
tending through the underlying cartilage were placed in rabbitears as described above nonischemic ears were used so as topresent the greatest opportunity for vascular dissemination ofvirus Wound beds were then treated with AdPDGF-B formu-lated in 015 collagen (2 3 109 virus particles per wound in a5-ml volume) after which animals were housed for 1 3 7 or14 days After blood collection via cardiac puncture animalswere perfused with 120 ml of PBS at a rate of 20 mlmin andwound beds and organs were harvested for polymerase chain re-action (PCR)-based detection of AdPDGF-B Forty cycles oftouchdown PCR were performed with oligonucleotide primersdesigned to amplify a 315-base pair fragment spanning the ma-jority of the human PDGF-B 109-amino acid coding region(sense 59-TTCCCTGACCATTGCTGAGCCGGCCA-39 anti-sense 59-ACAGGCCGTGCAGCTCCACTG-39) This ldquotouch-downrdquo strategy of thermocycling employs successively de-creasing annealing temperatures (four cycles performed at eachannealing temperature beginning at 72degC and decreasing in 1degCincrements down to 63degC with each cycle consisting of a 30-sec annealing step and a 1-min extension step) PCR ampliconswere then visualized on ethidium bromide-stained 08 agarosegels
DOUKAS ET AL786
FIG 2 Influence of adenovirusndashmatrix formulations on neotissue formation PVA sponges were implanted subcutaneously intorats and 4 days later were injected with either AdPDGF-B AdFGF2 AdVEGF or AdLuc (2 3 1010 virus particles per sponge)formulated in 015 collagen controls consisted of collagen alone Six days posttreatment sponges were processed as paraffinsections and stained as follows (A) AdPDGF-B trichrome stain (B) AdPDGF-B Ki-67 immunostain Note the positively stainedendothelial cells (arrowheads) and fibroblasts (arrows) (C) AdFGF2 trichrome stain (D) AdFGF2 BSL-I lectin stain (E) Ad-VEGF trichrome stain (F) AdVEGF BSL-I lectin stain (G) AdLuc trichrome stain (H) Collagen vehicle trichrome stainOriginal magnification (A C E and G) 3200 (B D F and H) 3400
TABLE 1 NEOTISSUE FORMATION AFTER DELIVERY OF ADENOVIRUSndashMATRIX FORMULATIONSa
Granulation Protein DNATreatment fill () (mgsponge) (mgsponge)
015 Collagen vehicle 26 6 18 13 6 2 79 6 21AdPDGF-B (2 3 109 particles) 62 6 22b 15 6 2 107 6 27AdPDGF-B (2 3 1010 particles) 93 6 6b 26 6 9b 215 6 109b
AdLuc (2 3 109 particles) 24 6 15 12 6 2 67 6 12AdLuc (2 3 1010 particles) 36 6 22 16 6 2 102 6 27
015 Collagen vehicle 29 6 8 15 6 2 69 6 10AdPDGF-B (2 3 1010 particles) 86 6 15c 25 6 3c 136 6 20c
AdVEGF (2 3 1010 particles) 44 6 16d 25 6 4c 144 6 24c
015 Collagen vehicle 18 6 8 10 6 1 65 6 12AdPDGF-B (2 3 1010 particles) 68 6 13c 23 6 5e 151 6 51c
AdFGF2 (2 3 1010 particles) 55 6 15c 18 6 3c 126 6 33f
aPVA sponges were implanted subcutaneously in rats and 4 days later injected with either 015 collagen alone or collagencontaining adenovirus vectors Vector doses are listed as the number of virus particles delivered per sponge Six days posttreat-ment sponges were recovered and processed to determine the percent sponge area filled with granulation tissue (0ndash100) aswell as total protein and DNA contents as described in Materials and Methods Data are presented as means 6 SD (n 5 8)
bp 00002 versus collagen control and p 0005 versus AdLuc groupscp 00001 versus collagen controldp 003 versus collagen controlep 00001 versus collagen control and p 0002 versus AdFGF2fp 0001 versus collagen control
TISSUE REPAIR USING GROWTH FACTOR GENES 787
A second model utilized 7-cm2 full-thickness excisionalwounds placed on the backs of anesthetized rabbits Woundswere treated with AdPDGF-B formulated in 26 collagen (2 3
109 or 2 3 1011 virus particles per wound in 700-ml volumes)and then covered with OpSite dressing On day 3 7 28 or 90posttreatment blood was collected animals were perfused asdescribed above and the following organs were recoveredwound bed brain heart lung liver spleen kidney gonad andlymph nodes (axillary cranial mesenteric and posterior medi-astinal) Real-time quantitative TaqMan PCR was performedusing 45 two-step cycles with primers designed to amplify se-quences bridging the vector backbone and the PDGF-B pre-proregion (sense 59-GGATCTTCGAGTCGACAAGCTT-3 9 an-tisense 59-TAAGGGCTCCTCGAAATACTCTA-3 9) The re-sulting amplicons were detected with an internal fluorogenicprobe (59-TAGTGGTACTTAGCGACGACCCGC-3 9) and anABI Prism 7700 sequence detector (PE Applied BiosystemsFoster City CA) The initial target copy numbers present ineach reaction were quantified by extrapolation from standardcurves of AdPDGF-B DNA in the background of 1 mg of rab-bit liver DNA per reaction Each PCR contained 1 mg of testDNA with the exception of wound bed which contained 500ng per reaction and blood which contained the equivalent of10 ml of original sample Each test sample was assayed in du-plicate to control for PCR inhibitory substances a third reac-tion was spiked with 100 copies of AdPDGF-B DNA PCR dataare presented as AdPDGF-B genome copies per wound thelimit of quantitation (LOQ) was 10 copiesmg DNA or an av-erage of 105 copieswound
For those tissues scoring positive for PCR-amplifiable vec-tor we further performed real-time quantitative reverse tran-scriptase (RT)-PCR Reverse transcriptase reactions were per-formed with 100 ng of each test RNA per reaction and randomhexamer primers The resulting cDNAs were then used to am-plify both rabbit 18S rRNA cDNA and PDGF-B cDNA in sep-arate PCRs The vector-specific primers were designed to am-plify full-length 160-amino acid human PDGF-B mRNA(sense 59-CAAGCACACGCATGACAAGA-3 9 antisense 59-TTTCGTTATCGTAGTGTTTAAAGTGT-3 9) The resulting131-nucleotide amplicons were detected with an internal fluo-rogenic probe (59-AAACAAGTTGCTCGATGGATCCTTAT-CAGGCT-39) RT-PCRs were then normalized for total RNAby 18S rRNA content with a second pair of PCR primers RT-PCR data are presented as the relative amount of PDGF-BmRNA per unit 18S rRNA (in arbitrary units)
Histochemical analyses
For routine morphological assessment paraffin sections werestained according to the Masson trichrome procedure In addi-tion a blinded observer using a microscope equipped with oc-ular micrometers measured the area within sponges filled bygranulation tissue these values are expressed as the percentageof sponge interior occupied by tissue ( granulation fill) Forexcisional wounds trichrome-stained sections and an imageanalysis software package (Image-Pro Plus software Media Cy-bernetics Silver Spring MD) were used to determine the cross-sectional areas of granulation tissue and epithelium per wound(in mm2) In addition the percentage of wound closure was cal-culated according to the following formula [(original wound
diameter 2 epithelial gap length) original wound diameter] 3100
For immunohistochemistry paraffin sections were stainedwith biotinylated Griffonia (Bandeiraea) simplicifolia lectin I(BSL-I) horseradish peroxidase (HRP)-labeled streptavidin anddiaminobenzidine (DAB Vector Laboratories BurlingameCA) in order to detect vascular endothelium Mouse anti-Ki-67and HRP-labeled rabbit anti-mouse IgG antibodies followed byDAB were used to detect proliferating cells Mouse anti-humanPDGF-BB (Z2703 American Type Culture Collection) andHRPndashanti-mouse IgG antibodies followed by DAB were usedto detect human PDGF-BB protein Fluorescein isothiocyanate(FITC)-conjugated anti-adenovirus antibody (Accurate Chemi-cals Westbury NY) and the nuclear stain 496-diamidino-2-phenylindole (DAPI Molecular Probes) were used to detectinternalized adenovirus vectors Finally fibroblasts were iden-tified with Cy3-labeled anti-vimentin (Sigma St Louis MO)
For in situ hybridization procedures an [a-35S] UTP-labeledriboprobe prepared from the full-length human PDGF-B cDNAwas used as previously described (Gonzalez et al 1995) Asense riboprobe was used to control for nonspecific hybridiza-tions
Biochemical analyses
Tissue samples not processed for paraffin embedding wereplaced in 100 mM phosphate buffer containing 02 Triton X-100 (pH 78) and agitated at 55 msec for 20 sec in a Fast-Prep system (BIO 101 Vista CA) After centrifugation su-pernatants were analyzed for protein using a bicinchoninic acidassay (Pierce Rockville IL) and for DNA using the PicoGreenassay PDGF-BB protein content was determined with a humanPDGF-BB-specific ELISA (RampD Systems Minneapolis MN)
Statistical Analyses
Data are presented as arithmetic means 6 1 SD Groups ofthree or more means within individual studies were comparedby one-way analysis of variance (ANOVA) and the Fisher pro-cedure for least significant differences (StatView softwareAbacus Concepts Berkeley CA)
RESULTS
Adenovirus vectors can be immobilized in an activeform within matrices
As an initial step to the in vivo assessment of adenovirusndashmatrix formulations we first determined the activity profilesand release kinetics for vectors formulated in type I collagenand carboxymethylcellulose (CMC) Collagen was selected onthe basis of its successful use as a delivery matrix for proteinsand DNA (Grotendorst et al 1985 Mustoe et al 1987 1991Sprugel et al 1987 Khouri et al 1994 Bonadio et al 1999)as well as its ability to enhance tissue repair responses in fi-broblasts (Xu and Clark 1996 1997) Relatively low (015)and high (26) concentrations were examined reasoning thatthis would allow for either relatively short or long retentiontimes at application sites respectively CMC was selected on
DOUKAS ET AL788
TISSUE REPAIR USING GROWTH FACTOR GENES 789
FIG 3 Localization of gene vector and transgene product within neotissues PVA sponges implanted in rats were injected withAdPDGF-B formulated in 015 collagen (2 3 1010 virus particles per sponge) and paraffin sections were stained as follows(A) Day 1 posttreatment anti-adenovirus immunostain to detect AdPDGF-B (green) DAPI stain to detect cell nuclei (blue) (B)Day 4 posttreatment in situ hybridization using human PDGF-B gene probe (C) Day 1 posttreatment anti-human PDGF-BBprotein immunostain positively stained leukocytes (arrowheads) and fibroblasts (arrows) are indicated (D) Day 6 posttreatmentanti-PDGF-BB immunostain (E) Day 8 posttreatment anti-PDGF-BB immunostain (F) Day 8 post- treatment immunostains todetect PDGF-BB protein (green) and vimentin (red) yellow fluorescence indicates PDGF-BB and vimentin colocalization bluefluorescence indicates cell nuclei (DAPI stain) Original magnifications (AndashC E and F)3 400 (D) 31000
the basis of its clinical use for the delivery of PDGF-BB pro-tein (Steed 1995)
Matrix influences on vector activity were examined by in-cubating AdLuc formulations at 37degC for 60 min followed bymatrix dissolution and vector bioassay (luciferase productionby 293 cells) This is an important test as adenoviruses arequickly inactivated under unfavorable physical and chemicalconditions (Nyberg-Hoffman and Aguilar-Cordova 1999)None of the matrices examined had a deleterious effect on vec-tor activity (90 6 12 106 6 5 and 139 6 37 of control ac-tivity for 015 collagen 26 collagen and CMC respec-tively) To further model in vivo vector stability we alsoincubated AdPDGF-B formulated in 26 collagen with woundfluid for 72 hr at 37degC prior to vector recovery and analysisWe observed no reduction in the level of PDGF-BB productionfrom cells transduced with AdPDGF-B exposed to wound fluidas compared with vector exposed to virus buffer (30 6 5 vs20 6 3 ng of PDGF-BB produced per milliliter of culturemedium respectively n 5 3)
As these data support the suitability of the selected matricesfor in vivo use we next determined their influence on vectorrelease kinetics (Fig 1) When placed in water collagen ma-trices retained the majority of their immobilized vectors with015 and 26 collagen releasing only 17 6 3 and 3 6 1 ofvector by 24 hr respectively By contrast 48 6 3 of AdLucwas released from CMC within 30 min and 61 6 2 by 6 hrThis was not unexpected as CMC is fairly water soluble andas both CMC and adenoviral particles are negatively chargedTherefore collagen matrices in a concentration-dependentfashion display more favorable kinetics for localizing and re-taining adenovirus vectors at delivery sites than does CMC
Collagen-immobilized adenoviruses induce distinctneotissues in vivo
Initial in vivo tests of matrix-immobilized vectors were per-formed with an established model of de novo tissue generation(Buckley et al 1985 Sprugel et al 1987 LeGrand et al1993) PVA sponges implanted subcutaneously in rats were in-jected with a single dose of adenovirus formulated in either col-lagen or CMC and then analyzed for tissue formation Forgrowth factor transgenes we selected platelet-derived growth
factor B (PDGF-B) vascular endothelial growth factor (VEGF)and fibroblast growth factor 2 (FGF2) because of their well-known mitogenic activities
AdPDGF-B formulated in 015 collagen induced granula-tion tissue formation in a dose-responsive manner (Table 1)Compared with vehicle controls delivering 2 3 1010 virus par-ticles induced a 17- to 23-fold increase in sponge protein con-tent (p 00002) a 2- to 27-fold increase in DNA content (p
00002) and a 29- to 43-fold increase in granulation tissue fill(p 00002) Trichrome-stained sections revealed the nearcomplete fill of sponge interiors with well-formed granulationtissue by day 6 posttreatment (Fig 2A) Expression of Ki-67a nuclear protein upregulated in proliferating cells (Gerdes etal 1983) established that both vascular endothelium (arrow-heads Fig 2B) and fibroblasts (arrows Fig 2B) had prolifer-ated in response to PDGF-B gene delivery AdFGF2 and Ad-VEGF also enhanced protein and DNA content within sponges(Table 1) However these vectors induced less granulation tis-sue deposition as compared with AdPDGF-B and the tissuesformed were histologically distinct
Tissues present in AdFGF2-treated sponges were highly vas-cular as revealed by the endothelial-reactive lectin BSL-I (Fig2D) Many of the infiltrating mononuclear cells also reactedpositively with BSL-I lectin suggesting that these cells wereendothelial cells or endothelial precursors AdFGF2 did nothowever induce the formation of classic granulation tissue aslittle collagen deposition was observed demonstrated by thepaucity of blue-staining material in trichrome-stained sections(Fig 2C) AdVEGF also induced heavily vascularized tissues(Fig 2E and F) but with greater extracellular collagen deposi-tion than AdFGF2 Relative to AdPDGF-B-induced tissueshowever AdVEGF-induced tissues were disorganized con-tained few fibroblasts and were markedly edematous Finallywhen AdLuc was delivered as a control treatment no signifi-cant increases in protein DNA or granulation tissue were ob-served compared with collagen vehicle alone (Table 1)Trichrome-stained sections revealed sparse inflammatory cellinfiltrates within AdLuc-treated sponges (Fig 2G) which com-pared with the near absence of infiltration after delivery of col-lagen vehicle alone (Fig 2H) suggested a limited antiviral response
Unlike the 015 collagen formulations described above
DOUKAS ET AL790
TABLE 2 NEOTISSUE FORMATION AFTER PDGF-B GENE OR PDGF-BB PROTEIN DELIVERYa
Granulation Protein DNATreatment fill () (mgsponge) (mgsponge)
015 Collagen vehicle 28 6 13b 16 6 2b 103 6 22b
AdPDGF-B 81 6 15b 30 6 6b 218 6 28b
PDGF-BB 100 mg 64 6 12c 22 6 4c 155 6 26c
PDGF-BB 10 mg qod 3 3d 77 6 9b0 31 6 8b 230 6 75b
aPVA sponges implanted in rats were injected with either 015 collagen vehicle or collagen containing AdPDGF-B as described in Table 1 Alternatively PDGF-BB protein was delivered as a single 100-mg dose on day 4 postimplantation or as10-mg doses on days 4 6 and 8 Sponges were removed on day 12 postimplantation and processed to determine the percent granulation fill as well as total protein and DNA contents Data are presented as means 6 SD (n 5 4ndash8)
bp 00001 versus collagen control and p 005 versus 100-mg PDGF-BBcp 003 versus collagen controldqod 3 3 Every other day three times
TISSUE REPAIR USING GROWTH FACTOR GENES 791
TABLE 3 INFLUENCE OF ADENOVIRUSndashMATRIX FORMULATIONS ON ISCHEMIC WOUND HEALINGa
Granulation Epithelial Wound closureTreatment Model system area (mm2) area (mm2) ( complete)
Aqueous buffer Cartilage intact 10 6 08 05 6 03 61 6 226 mm day 10
AdPDGF-B in Cartilage intact 24 6 22 05 6 01 73 6 28aqueous buffer 6 mm day 10
015 Collagen Cartilage intact 05 6 03 05 6 02 89 6 14vehicle 6 mm day 10
AdPDGF-B in Cartilage intact 16 6 09b 09 6 03c 97 6 7015 collagen 6 mm day 10
Aqueous buffer Cartilage removed 45 6 08 08 6 02 95 6 96 mm day 7
AdPDGF-B in Cartilage removed 40 6 15 11 6 05 82 6 22aqueous buffer 6 mm day 7
015 Collagen Cartilage removed 36 6 13 06 6 02 88 6 22vehicle 6 mm day 7
AdPDGF-B in Cartilage removed 70 6 14b 07 6 03 79 6 22015 collagen 6 mm day 7
26 Collagen Cartilage removed 04 6 05 01 6 01 24 6 15vehicle 8 mm day 8
AdPDGF-B in Cartilage removed 51 6 25b 06 6 03b 52 6 25c
26 collagen 8 mm day 8
aExcisional wounds (6 or 8 mm in diameter) were placed in ischemic rabbit ears with underlying cartilage left intact or re-moved Wounds were then treated with AdPDGF-B formulated in aqueous virus buffer or collagen control treatments consistedof vehicle alone For 6-mm wounds virus was applied as 2 3 109 particles per wound for 8-mm wounds as 4 3 109 particlesper wound On days 7ndash10 posttreatment wounds were harvested and processed as trichrome-stained paraffin sections whichwere then used to quantify newly formed granulation tissue and epithelium (cross-sectional area in mm2) and the degree of woundsurface closure (where 100 equals complete closure) Data are presented as means 6 SD (n 5 4ndash8)
bp 0009 versus vehicle controlcp 005 versus vehicle control
26 collagen formulations could not be reliably examined inthe PVA sponge model as their relatively high viscosity pre-vented uniform filling of sponges by syringe CMC-formulatedvectors were also unsuitable for this model system as theyproved highly inflammatory (data not shown) These formula-tions therefore were evaluated in more appropriate excisionalwound models (see below)
Tissue repair cells are transduced by collagen-immobilized adenoviruses
On the basis of the robust activity of collagen-formulatedAdPDGF-B we elected to further examine this vectorndashmatrixcombination first by seeking to correlate PDGF-B gene deliv-ery with subsequent transgene and protein expression WhenPVA sponges treated with 015 collagenndashAdPDGF-B werestained with both an anti-adenovirus antibody and the nuclearstain DAPI the majority of cells present 1 day after gene de-livery had bound andor internalized adenovirus (Fig 3A) Insitu hybridization revealed that these cells were successfullytransduced by virus as they contained human PDGF-B mRNA(Fig 3B) By contrast hybridization product was not detectedwith a sense riboprobe or when AdLuc-treated sponges wereexamined (data not shown)
We next used a human PDGF-BB-specific antibody to iden-tify the cell types responsible for transgene expression By day
1 postdelivery of 015 collagenndashAdPDGF-B PDGF-BB pro-tein was localized to leukocytes (arrowheads) and fibroblasts (ar-row Fig 3C) With time PDGF-BB protein was detected boundto the extracellular matrix (ECM) surrounding positively stainedcells (Fig 3D) This last observation indicates that a reservoir ofPDGF-BB protein develops within treated tissues and thus mayprolong the histogenic effects of this growth factor Finally byday 8 the majority of immunoreactivity had abated with pri-marily microvascular endothelium remaining positive (Fig 3E)However scattered fibroblasts could still be shown to producePDGF-BB protein by dual immunohistochemistry with anti-PDGF-BB and anti-vimentin antibodies (Fig 3F)
Multiple administrations of PDGF-BB protein are required to approximate the histogenic effects of collagenndashAdPDGF-B
To directly compare gene therapy with the more conven-tional approach of growth factor protein delivery we next quan-tified tissue formation in response to either PDGF gene or pro-tein delivery A single injection of 015 collagenndashAdPDGF-Benhanced granulation tissue filling of sponges by 3-fold versusvehicle alone (p 00001) and sponge protein and DNA lev-els by 2-fold (p 00001 Table 2) Using a human PDGF-BB-specific ELISA this growth factor was detected at 54 6 13ngsponge (n 5 8) By contrast when PDGF-BB protein was
delivered as a single dose nearly 2000-fold in excess of thisconcentration the tissue formation responses observed (proteinand DNA accumulation and granulation tissue formation) weresignificantly lower (p 005 Table 2) In fact repeated dos-ing with PDGF-BB protein was required in order to achieve re-sponses comparable to a single administration of the PDGF-Bgene These data therefore support our hypothesis that the abil-ity of gene delivery to establish prolonged in situ growth fac-tor production translates into greater histogenesis than that seenwith growth factor proteins
CollagenndashAdPDGF-B induces complete healing of ischemic wounds
Nonhealing wounds are a major risk in chronically ischemictissues as low oxygen tension greatly impairs tissue repair pro-cesses We therefore compared the ability of matrix versusaqueous formulated AdPDGF-B to repair ischemic excisionalwounds Several models were employed to compare variationsin wound size and condition so as to allow for a more com-plete picture of tissue repair
In the first model system 6-mm-diameter wounds were cre-ated in ischemic rabbit ears by removal of epidermal and der-mal layers but not underlying cartilage This model has beenused in previous studies of growth factor proteins and genes(Ahn and Mustoe 1990 Mustoe et al 1994 Liechty et al1999) and was therefore employed to allow comparison withthese reports However it represents an artificial system as thepresence of a cartilage layer restricts both treatment activity andhealing to wound margins and in addition the initially acellu-lar wound bed forms a cup that artifactually retains aqueoustreatments As would be predicted we found a trend towardgranulation tissue formation in this model after the applicationof AdPDGF-B formulated in aqueous buffer (Table 3) How-ever this response did not reach the level of statistical signifi-cance as tissue development was highly variable (note the highstandard deviation value) In addition epithelial regenerationand wound closure were minimal to unaffected By contrastAdPDGF-B formulated in 015 collagen enhanced granula-tion tissue area by 32-fold and epithelial area by 18-fold overthat achieved with vehicle alone (p 0009 and 005 respec-tively) Although near complete closure of epithelial gaps wasalso achieved the high level of self-healing in control-treatedgroups (89 wound closure) precluded statistical significance
In an alternative model design subdermal cartilage was com-pletely removed from excisional wounds creating beds whosefloors now consisted of dermal tissue (Pierce et al 1994b)This design allows for cellular responses from the entire woundbed as well as the opportunity for vector migration beyond
treatment areas We now observed that aqueous formulated Ad-PDGF-B failed to induce even a trend toward tissue regenera-tion (Table 3) Rather the vector appears to have seeped throughthe wound bed floor as inflammatory cell infiltrates and fociof fibroblast proliferation were observed in the underlying der-mis and at wound margins (Fig 4A) Immunohistochemistryconfirmed the production of human PDGF-BB at these sites(Fig 4B) CMC-formulated AdPDGF-B also failed to induceany meaningful tissue repair Wounds treated with this formu-lation showed a diffuse inflammatory response within thewound bed and wound surfaces were overlain with fibrin clotsrather than regenerating epithelium (Fig 4C and D) By con-trast AdPDGF-B formulated in 015 collagen enhanced gran-ulation tissue deposition 19-fold within wound beds versus ve-hicle controls (p 0002) and wounds were extensivelyepithelialized (Table 3) Neither epithelial regeneration norwound closure achieved significance however as the high de-gree of self-healing achieved in this particular model (see ve-hicle alone group) most likely masked transgene-stimulated re-sponses
To address these model limitations as our next system wecreated 8-mm wounds in ischemic rabbit ears by removingepidermal dermal and cartilage layers reasoning that largerexcisional wounds would display limited self-healing In ad-dition this model could readily accommodate 26 collagenformulations which proved difficult to reproducibly apply insmaller wounds Compared with control wounds treated withcollagen vehicle alone wounds treated with AdPDGF-B for-mulated in 26 collagen achieved a 12-fold enhancementin granulation tissue fill and a 6-fold enhancement in re-ep-ithelialization by day 8 posttreatment (p 0009 Table 3)In addition wound closure was only 24 complete in colla-gen vehicle-treated wounds by day 8 but 52 complete inwounds treated with collagen-formulated AdPDGF-B (p
005) Histologically AdPDGF-B-treated wounds showed nosigns of tissue hyperplasia or chronic inflammation but ratheran orderly repair process marked by a regenerated epitheliallayer overlying a wound bed filled with granulation tissue(Fig 4E and F)
CollagenndashAdPDGF-B induces normal long-term tissue repair
Our choice of adenoviruses for transgene delivery was partlybased on the reasoning that as these vectors establish transientgene expression they would not lead to hyperproliferative re-sponses or scar formation To test this hypothesis we treatedrabbit ear excisional wounds with AdPDGF-B formulated in015 collagen and examined tissue repair responses out to
DOUKAS ET AL792
FIG 4 Influence of adenovirusndashmatrix formulations on excisional wound repair Excisional wounds (6 or 8 mm in diameter andextending through underlying cartilage layers) were placed in ischemic rabbit ears bars indicate original wound depth (determinedfrom cartilage visible at wound margins) Wounds were then treated with AdPDGF-B formulated in either virus buffer CMC orcollagen and on day 7 or 8 posttreatment processed for histology or immunohistochemistry An identical design was used to ex-amine long-term healing on day 90 except that wounds were created in nonischemic ears (A) Day 7 buffer-formulated AdPDGF-B-treated 6-mm wound trichrome stain (B) Day 7 buffer-formulated AdPDGF-B-treated 6-mm wound anti-PDGF-BB proteinimmunostain (C and D) Day 7 CMC-formulated AdPDGF-B-treated 6-mm wound trichrome stains (E and F) Day 8 26 col-lagen-formulated AdPDGF-B-treated 8-mm wound trichrome stains (G and H) Day 90 015 collagen-formulated AdPDGF-B-treated 6-mm wound trichrome stains Original magnification (A C E and G) 340 (B D F and H) 3200
TISSUE REPAIR USING GROWTH FACTOR GENES 793
DOUKAS ET AL794
TABLE 4 BIODISTRIBUTION OF AdPDGF-B IN EXCISIONAL WOUNDSa
Positive samplestotal assayed
Tissue AdPDGF-B dose Day 3 Day 7 Day 28 Day 90
Wound bed 2 3 109 particles 66 66 66b 06Axillary lymph nodes 2 3 109 particles 02 ND 06 06
Wound bed 2 3 1011 particles 66 66 66 46c
Axillary lymph nodes 2 3 1011 particles 66 ND 66d 26e
aFull-thickness excisional wounds (7 cm2) were placed on the backs of rabbits and AdPDGF-B formulated in 26 collagenwas applied as either 2 3 109 or 2 3 1011 virus particles per wound On days 3ndash90 posttreatment wound beds and a panel oforgans were harvested for real-time PCR quantification of viral genome Data are shown for wound bed and axillary lymph nodesamples as the number of samples that yielded amplifiable signals per total number assayed ND not determined
bThree of six samples scored below the level of quantitation (LOQ 10ndash100 copiesmg DNA)cAll four positive samples scored below the LOQdThree of six samples scored below the LOQeBoth positive samples scored below the LOQ
180 days posttreatment (Fig 5) PDGF-B gene delivery en-hanced total ear thickness relative to controls on day 28 (229 6
020 vs 179 6 019 mm p 00001) and day 60 (192 6 001vs 182 6 011 mm p 0005) as anticipated on the basis ofthe ability of this formulation to induce granulation tissue for-mation By day 90 posttreatment however there was no mea-surable difference in ear thickness between AdPDGF-B andcontrol-treated groups and this relationship continued out today 180 indicating that growth factor gene delivery did not in-duce excessive scar formation This was also confirmed histo-logically AdPDGF-B-treated wounds on day 90 and beyondwere composed of a thin outer keratin layer an underlying ep-ithelial layer of equivalent thickness to nonwounded areas anda collagen-rich dermis devoid of any signs of tissue hyperpla-sia (Fig 4G and H)
Collagen immobilization limits adenovirus vectorbiodistribution beyond treatment sites
As a final measure of the value of matrix immobilization forgene delivery we determined the biodistribution patterns ofvectors after their in vivo delivery In the first model systemused AdPDGF-B formulated in 015 collagen was applied torabbit ear wounds at equivalent doses as previously describedwounds were extended through underlying cartilage but vas-cular supplies were not disturbed so as to permit maximal vec-tor dissemination By PCR no adenoviral DNA was detectablein lung spleen brain cervical lymph nodes or gonads on day1 3 7 or 14 (n 5 6 per group) In the liver one of six sam-ples was positive on days 3 and 7 but none on day 14 in serumonly one of six samples tested positive on day 14 (equivalentof 500-ml serum volume) By contrast adenovirus was detectedin eight of eight wound bed samples at all time points exam-ined
In a second model system excisional wounds placed on thebacks of rabbits were treated with AdPDGF-B formulated in26 collagen Because of their anatomical placement thismodel allowed for the creation of larger excisional wounds (7-cm2 total area) than those placed in rabbit ears (03 cm2) and
consequently larger treatment volumes and vector doses (2 3109 or 2 3 1011 virus particles per wound) At the lower doseof 2 3 109 particles PCR-amplifiable adenoviral DNA was notdetectable beyond wound beds on day 3 7 28 or 90 Tissuessampled and found not to contain vector included blood heartlung liver kidney brain spleen lymph nodes and gonads (n 5
6group) In wound beds adenoviral DNA was detected at alltime points except for day 90 (Table 4 and Fig 6) Vector lev-els did decrease however by 38-fold between days 7 and 28with three of six samples falling below the level of quantita-tion (LOQ) by real-time PCR at the latter time point (Fig 6)
At a 100-fold higher vector dose of 2 3 1011 particles perwound PCR-amplifiable adenoviral DNA was once again un-detectable in the majority of tissues sampled Except for a sin-gle day 7 liver sample and a single day 7 brain sample (bothbelow the LOQ) adenoviral DNA was only detectable directlyin wound beds or in the axillary lymph nodes that drain woundsites (Table 4) Moreover three of six positive axillary nodesamples scored below the LOQ on day 28 as did both positivesamples on day 90 indicating that they contained relatively lit-tle vector Within wound beds adenoviral DNA was detectedat quantifiable levels out to day 28 and at detectable but non-quantifiable levels on day 90 DNA copy numbers remainedsteady between days 3 and 7 dropped 107-fold between days7 and 28 and a further 1662-fold by day 90 Finally at eachtime point DNA copy numbers in wounds treated with 2 3
1011 particles were approximately 100-fold higher than thosefound in wounds treated with 2 3 109 particles thus confirm-ing the linearity of our assay system
To better define the time course of human PDGF-BB pro-duction we also quantified transgene mRNA levels in woundbed samples treated at 2 3 109 particles per wound This treat-ment dose was selected as representative of the virus particleconcentration capable of inducing complete healing in ischemicear wounds Quantifiable levels of human PDGF-B mRNAwere detectable in treated dorsal wounds at days 3 7 and 28(Fig 6) with levels decreasing 14-fold between days 3 and 7and 5-fold between days 7 and 28 The more sensitive tech-nique of real-time RT-PCR therefore demonstrates that trans-
TISSUE REPAIR USING GROWTH FACTOR GENES 795
gene expression extends well beyond the 8-day time period sug-gested using anti-PDGF-BB immunohistochemistry as a de-tection system (Fig 3)
DISCUSSION
These studies demonstrate that immobilization of gene ther-apy vectors in collagen-based matrices enables their efficientdelivery and activity in vivo Matrix immobilization achievedprolonged transgene-encoded growth factor production and asa consequence robust tissue repair By contrast aqueous vehi-cles failed to retain adenoviruses at application sites resultingin diffuse inflammation rather than productive tissue regenera-tion These observations confirm our basic hypothesis that ma-trix immobilization of growth factor-encoding gene therapyvectors represents a promising approach to tissue repair
Although de novo tissue deposition was achievable with sev-eral growth factor genes PDGF-B proved the most suitable forrepair of cutaneous defects A single administration of colla-gen-immobilized AdPDGF-B rapidly induced the formation ofhighly cellular and vascularized tissues with dense ECMs richin collagen By contrast AdFGF2 induced a primarily vascu-lar response with little collagen deposition FGF2 induces therelease of matrix metalloproteinase 1 or interstitial collagenase(Buckley-Sturrock et al 1989) and this may underlie the rel-ative paucity of ECM accumulation VEGF gene delivery alsoinduced highly vascular responses however the enhanced per-meability characteristic of VEGF-induced vasculature (Dvoraket al 1995) led to edema within nascent tissues In fact much
of the enhanced protein and DNA deposition observed in Ad-VEGF-treated PVA sponges may well derive from fluid exu-dates rather than actual tissue formation Finally the inabilityof AdLuc delivery to induce anything beyond a limited in-flammatory response confirms that tissue formation was de-pendent on growth factor gene delivery
The robust activity of PDGF-B gene delivery was expectedas PDGF-BB protein initiates multiple aspects of tissue forma-tion including cellular influx and proliferation ECM deposi-tion and tissue remodeling (Pierce et al 1988 1991 1994a)Indeed PDGF-BB is the only growth factor protein to have suc-cessfully completed human clinical trials and be approved forthe treatment of dermal wounds (Steed 1995 drsquoHemecourt etal 1998 Wieman 1998 Wieman et al 1998) We observedthat collagen-formulated AdPDGF-B induced the complete re-pair of excisional skin defects without unwanted long-term ef-fects such as the development of hypertrophic scars Endoge-nous growth factors other than PDGF-BB however most likelymediated the enhanced re-epithelialization observed in thesewounds as epithelial regeneration is driven by members of theepidermal growth factor and FGF families (Pierce et al 1994bDanilenko et al 1995) Our data indicate nonetheless that tis-sue regeneration and repair were initiated and to a great degreedriven by transgene-encoded PDGF-BB
Despite the known activity of PDGF-BB protein we wereable to demonstrate greater tissue deposition after gene deliv-ery as compared with the use of recombinant growth factor pro-tein A single application of PDGF-BB protein could not equalthe ability of PDGF-B gene therapy to induce neotissue for-mation even at doses well in excess of that induced in situ byAdPDGF-B and in excess of that used in human clinical trials
FIG 5 Influence of collagen-formulated AdPDGF-B on long-term tissue repair Excisional wounds (6 mm in diameter withcartilage remaining intact) were placed in nonischemic rabbit ears and treated with either 015 collagen alone (open columns)or AdPDGF-B formulated in this vehicle (solid columns) On days 28ndash180 posttreatment total ear thickness at the site of eachwound was measured (in mm) with calipers Data are presented as means 6 SD (n 5 3) Treatment groups differ by p 00001groups differ by p 0005
(Steed 1995 drsquoHemecourt et al 1998 Wieman 1998 Wie-man et al 1998) In fact repeated administrations of PDGF-BB protein were required to approach the level of tissue for-mation observed after a single administration of AdPDGF-BThese data support our hypothesis that sustained localizedgrowth factor production is required for robust tissue repair
In further support of this hypothesis we demonstrated thatmRNA encoding human PDGF-B was present in excisionalwounds as late as day 28 after collagen-formulated AdPDGF-B administration By contrast previous studies of PDGF-BBprotein found that the great majority of this growth factor wasgone from treated wounds 1 day postapplication and that anytissue maturation subsequently observed was most likely dueto the upregulation of endogenous growth factors (Pierce et al1992 1995) We also demonstrated that repair cells such asmononuclear leukocytes endothelial cells and fibroblasts pres-ent with developing neotissues represent the source of both
transgene transcription and PDGF-BB production In additiona depot of human PDGF-BB was detected bound to the colla-gen delivery matrix and ECM of these tissues This was antici-pated as PDGF-BB contains collagen-binding motifs (Soma-sundaram and Schuppan 1996) We hypothesize that subsequentmatrix metalloproteinase activity by repair cells will serve togenerate localized release of this sequestered growth factor pooland as a consequence further drive tissue regeneration Theseevents which are central to tissue remodeling should be directlyenhanced by collagen matrices as type I collagen stimulates me-talloproteinase production integrin expression and cellular ac-tivation in PDGF-stimulated fibroblasts (Xu and Clark 19961997)
An additional rationale for employing collagen matrices wasto physically immobilize vectors This was confirmed in vivowhere collagen matrices maintained AdPDGF-B at deliverysites for at least 28 days and limited vector migration to other
DOUKAS ET AL796
FIG 6 Persistence of collagen-formulated vector and transgene transcripts in excisional wounds Full-thickness excisionalwounds (7 cm2) were placed on the dorsal surface of rabbits and treated with AdPDGF-B formulated in 26 collagen at either2 3 109 or 2 3 1011 virus particles per wound (open and closed columns respectively) Wounds were then covered with OpSitedressing and on days 3 7 or 28 posttreatment wound beds were harvested for real-time quantitative PCR and RT-PCR analy-ses PCR data are presented in the upper graph as AdPDGF-B copies per wound RT-PCR data are presented in the lower graphas the relative amount of PDGF-B mRNA per unit 18S rRNA (in arbitrary units) All data points are means 6 SD (n 5 6)
tissues or organs In vitro tests also established that collagenmatrices not only prevent vector loss due to diffusion but pre-serve vector activity despite prolonged incubation in acutewound fluid Successful vector immobilization and tissue re-pair could be achieved with both 015 collagen and 26 col-lagen suggesting flexibility in the final vehicle formulation re-quired for effective vector delivery This flexibility was neededin the present studies as 26 collagen formulations proveddifficult to deliver to PVA sponges and 6-mm excisionalwounds This would not be of concern in clinical settings how-ever where wound beds are easily accessible and generally sev-eral square centimeters in area By contrast CMC was inef-fective at retaining vector in aqueous environments Moreimportantly this matrix was itself inflammatory and whencombined with adenovirus the net result was inflammationrather than tissue repair We are currently examining the util-ity of other matrices such as fibrin and hyaluronic acid whichbecause of their more provisional nature may offer yet greatercellular migration into wounds as compared with type I colla-gen
Although an aqueous-based AdPDGF-B formulation hasbeen previously shown to enhance tissue formation (Liechty etal 1999) this was achieved with a model system that artifi-cially retains vectors within treatment sites In fact the presentstudies demonstrate that any tissue repair observed after Ad-PDGF-B delivery in a nongelling liquid is dependent on the useof this model system In wounds not designed to retain appliedtreatments aqueous-formulated AdPDGF-B seeped into sur-rounding tissues and led to hyperplasia within these areas ratherthan to tissue regeneration within the active wound bed Colla-gen-immobilized AdPDGF-B on the other hand did persist inthese wound beds and led to significant enhancements in gran-ulation tissue formation as well as enhanced wound re-epithe-lialization and wound closure The significance of these activ-ities is further substantiated considering that they wereachievable in 8-mm-diameter ischemic wounds which withinthe time frame examined could not self-heal to any meaning-ful degree in the absence of gene therapy However as all theanimal models employed in these studies will eventually self-heal given sufficient time the full value of matrix-immobilizedgene therapy vectors remains to be confirmed in human clini-cal trials
In conclusion we present evidence that matrix-immobilizedgene therapy vectors encoding appropriate growth-promotinggenes represent a promising approach to tissue regeneration andrepair This basic concept can be expanded to include alterna-tive matrices such as controlled-release formulations as wellas tissue-specific growth factors Furthermore the addition oftargeting ligands to adenovirus vectors (eg FGF2) can en-hance their ability to transduce cells such that tissue repair re-sponses comparable to nontargeted vectors can be achieved butat significantly lower vector doses (Chandler et al 2000a)With appropriate design and application schedules one couldconceivably time the release of multiple growth factors to spe-cific stages of a tissue repair cascade In addition we have foundin preliminary studies that collagen-immobilized nonviral vec-tors such as PDGF-B plasmids which have potentially morefavorable safety profiles than adenovirus vectors can also en-hance tissue formation in vivo (Chandler et al 2000b Tyroneet al 2000) Such flexibility should allow for the widespreadapplication of gene therapy to the treatment of injured tissues
ACKNOWLEDGMENTS
We thank Jeff Davidson (Vanderbilt University School ofMedicine) for assistance in establishing the PVA sponge modelCarl-Henrik Heldin (Ludwig Institute for Cancer Research) forthe PDGF-B gene construct and Emelie Amburn Lara AsatoSharon Chang Gail Fieser Lydia Greenlees Rebecca Smokerand Linda Manza for excellent technical assistance This pub-lication was made possible in part by NIH grants 1R43AR46154(JD) and 5P01CA25874 (MH)
REFERENCES
AHN ST and MUSTOE TA (1990) Effects of ischemia on ulcerwound healing A new model in the rabbit ear Ann Plast Surg 2417ndash23
ANDREE C SWAIN WF PAGE CP MACKLIN MDSLAMA J HATZIS D and ERIKSSON E (1994) In vivo trans-fer and expression of a human epidermal growth factor gene accel-erates wound repair Proc Natl Acad Sci USA 91 12188ndash12192
BENN SI WHITSITT JS BROADLEY KN NANNEY LBPERKINS D HE L PATEL M MORGAN JR SWAIN WFand DAVIDSON JM (1996) Particle-mediated gene transfer withtransforming growth factor-b1 cDNAs enhances wound repair in ratskin J Clin Invest 98 2894ndash2902
BONADIO J SMILEY E PATIL P and GOLDSTEIN S (1999)Localized direct plasmid gene delivery in vivo Prolonged therapyresults in reproducible tissue regeneration Nat Med 5 753ndash759
BUCKLEY A DAVIDSON JM KAMERATH CD WOLT TBand WOODWARD SC (1985) Sustained release of epidermalgrowth factor accelerates wound repair Proc Natl Acad Sci USA82 7340ndash7344
BUCKLEY-STURROCK A WOODWARD SC SENIOR RMGRIFFIN GL KLAGSBRUN M and DAVIDSON JM (1989)Differential stimulation of collagenase and chemotactic activity in fi-broblasts derived from rat wound repair tissue and human skin bygrowth factors J Cell Physiol 138 70ndash78
CHANDLER LA DOUKAS J GONZALEZ AM HOGANSONDK GU DL MA C NESBIT M CROMBLEHOLME TMHERLYN M SOSNOWSKI BA and PIERCE GF (2000a)FGF2ndashTargeted adenovirus encoding platelet-derived growth factor-B enhances de novo tissue formation Mol Ther 2 153ndash160
CHANDLER LA MA C GONZALEZ AM DOUKAS JNGUYEN T PIERCE GF and PHILLIPS ML (2000b) Ma-trix-enabled gene transfer for cutaneous wound repair Wound Re-pair Regen 8 473ndash479
DANILENKO DM RING BD TARPLEY JE MORRIS BVAN GY MORAWIECKI A CALLAHAN W GOLDEN-BERG M HERSHENSON S and PIERCE GF (1995) Growthfactors in porcine full and partial thickness burn repair Differing tar-gets and effects of keratinocyte growth factor platelet-derivedgrowth factor-BB epidermal growth factor and neu differentiationfactor Am J Pathol 147 1261ndash1277
DEUEL TF KAWAHARA RS MUSTOE TA and PIERCE GF(1991) Growth factors and wound healing Platelet-derived growthfactor as a model cytokine Annu Rev Med 42 567ndash584
DrsquoHEMECOURT PA SMIELL JM and KARIM MR (1998) So-dium carboxymethylcellulose aqueous-based gel vs becaplermin gelin patients with nonhealing lower extremity diabetic ulcers Wounds10 69ndash75
DOUKAS J HOGANSON DK ONG M YING W LACEYDL BAIRD A PIERCE GF and SOSNOWSKI BA (1999)Retargeted delivery of adenoviral vectors through fibroblast growthfactor receptors involves unique cellular pathways FASEB J 131459ndash1466
TISSUE REPAIR USING GROWTH FACTOR GENES 797
DVORAK HF BROWN LF DETMAR M and DVORAK AM(1995) Vascular permeability factorvascular endothelial growth fac-tor microvascular hyperpermeability and angiogenesis Am JPathol 146 1029ndash1039
EMING SA MEDALIE DA TOMPKINS RG YARMUSHML and MORGAN JR (1998) Genetically modified human ker-atinocytes overexpressing PDGF-A enhance the performance of acomposite skin graft Hum Gene Ther 9 529ndash539
EMING SA WHITSITT JS HE L KRIEG T MORGAN JRand DAVIDSON JM (1999) Particle-mediated gene transfer ofPDGF isoforms promotes wound repair J Invest Dermatol 112297ndash302
GERDES J SCHWAB U LEMKE H and STEIN H (1983) Pro-duction of a mouse monoclonal antibody reactive with a human nu-clear antigen associated with cell proliferation Int J Cancer 3113ndash20
GONZALEZ AM BERRY M MAHER PA LOGAN A andBAIRD A (1995) A comprehensive analysis of the distribution ofFGF-2 and FGFR1 in the rat brain Brain Res 701 201ndash226
GREENHALGH DG (1996) The role of growth factors in woundhealing J Trauma 41 159ndash167
GROTENDORST GR MARTIN GR PENCEV D SODEK Jand HARVEY AK (1985) Stimulation of granulation tissue for-mation by platelet-derived growth factor in normal and diabetic ratsJ Clin Invest 76 2323ndash2329
KHOURI RK HONG SP DEUNE EG TARPLEY JE SONGSZ SERDAR CM and PIERCE GF (1994) De novo genera-tion of permanent neovascularized soft tissue appendages by platelet-derived growth factor J Clin Invest 94 1757ndash1763
LEGRAND EK SENTER LH GAMELLI RL and KIORPESTC (1993) Evaluation of PDGF-BB PDGF-AA bFGF IL-1 andEGF dose responses in polyvinyl alcohol sponge implants assessedby a rapid histologic method Growth Factors 8 315ndash329
LIECHTY KW NESBIT M HERLYN M RADU A ADZICKNS and CROMBLEHOLME TM (1999) Adenoviral-mediatedoverexpression of platelet-derived growth factor-B corrects ischemicimpaired wound healing J Invest Dermatol 113 375ndash383
LYNCH SE COLVIN RB and ANTONIADES HN (1989)Growth factors in wound healing J Clin Invest 84 640ndash646
MUSTOE TA PIERCE GF THOMASON A GRAMATES PSPORN MB and DEUEL TF (1987) Accelerated healing of in-cisional wounds in rats induced by transforming growth factor-betaScience 237 1333ndash1336
MUSTOE TA PIERCE GF MORISHIMA C and DEUEL TF(1991) Growth factor-induced acceleration of tissue repair throughdirect and inductive activities in a rabbit dermal ulcer model J ClinInvest 87 694ndash703
MUSTOE TA AHN ST TARPLEY JE and PIERCE GF(1994) Role of hypoxia in growth factor responses Differential ef-fects of basic fibroblast growth factor and platelet-derived growthfactor in an ischemic wound model Wound Rep Reg 2 277ndash283
NYBERG-HOFFMAN C and AGUILAR-CORDOVA E (1999) In-stability of adenoviral vectors during transport and its implication forclinical studies Nat Med 5 955ndash957
PIERCE GF and MUSTOE TA (1995) Pharmacologic enhance-ment of wound healing Annu Rev Med 46 467ndash481
PIERCE GF MUSTOE TA SENIOR RM REED J GRIFFINGL THOMASON A and DEUEL TF (1988) In vivo incisionalwound healing augmented by platelet-derived growth factor and re-combinant c-sis gene homodimeric proteins J Exp Med 167 974ndash987
PIERCE GF VANDE BERG J RUDOLPH R TARPLEY J andMUSTOE TA (1991) Platelet-derived growth factor-BB and trans-forming growth factor beta 1 selectively modulate glycosaminogly -cans collagen and myofibroblasts in excisional wounds Am JPathol 138 629ndash646
PIERCE GF TARPLEY JE YANAGIHARA D MUSTOE TA
FOX GM and THOMASON A (1992) Platelet-derived growthfactor (BB homodimer) transforming growth factor-b1 and basic fi-broblast growth factor in dermal wound healing Neovessel and ma-trix formation and cessation of repair Am J Pathol 140 1375ndash1388
PIERCE GF TARPLEY JE ALLMAN RM GOODE PS SER-DAR CM MORRIS B MUSTOE TA and VANDE BERG J(1994a) Tissue repair processes in healing chronic pressure ulcerstreated with recombinant platelet-derived growth factor BB Am JPathol 145 1399ndash1410
PIERCE GF YANAGIHARA D KLOPCHIN K DANILENKODM HSU E KENNEY WC and MORRIS CF (1994b) Stim-ulation of all epithelial elements during skin regeneration by kerati-nocyte growth factor J Exp Med 179 831ndash840
PIERCE GF TARPLEY JE TSENG J BREADY J CHANGD KENNEY WC RUDOLPH R ROBSON MC VANDEBERG J and REID P (1995) Detection of platelet-derived growthfactor (PDGF)-AA in actively healing human wounds treated withrecombinant PDGF-BB and absence of PDGF in chronic nonhealingwounds J Clin Invest 96 1336ndash1350
SINGER AJ and CLARK RA (1999) Cutaneous wound healingN Engl J Med 341 738ndash746
SOMASUNDARAM R and SCHUPPAN D (1996) Type I II IIIIV V and VI collagens serve as extracellular ligands for the iso-forms of platelet-derived growth factor (AA BB and AB) J BiolChem 271 26884ndash26891
SPRUGEL KH MCPHERSON JM CLOWES AW and ROSSR (1987) Effects of growth factors in vivo I Cell ingrowth intoporous subcutaneous chambers Am J Pathol 129 601ndash613
STEED DL (1995) Clinical evaluation of recombinant humanplatelet-derived growth factor for the treatment of lower extremitydiabetic ulcers Diabetic Ulcer Study Group J Vasc Surg 21 71ndash78
STEED DL (1998) Foundations of good ulcer care Am J Surg 17620S-25S
TYRONE JW MOGFORD JE CHANDLER LA MA C XIAY PIERCE GF and MUSTOE TA (2000) Collagen-embeddedplatelet-derived growth factor DNA plasmid promotes wound heal-ing in a dermal ulcer model J Surg Res 93 230ndash236
VOGT PM THOMPSON S ANDREE C LIU P BREUING KHATZIS D BROWN H MULLIGAN RC and ERIKSSON E(1994) Genetically modified keratinocytes transplanted to woundsreconstitute the epidermis Proc Natl Acad Sci USA 91 9307ndash9311
WIEMAN TJ (1998) Clinical efficacy of becaplermin (rhPDGF-BB)gel Becaplermin Gel Studies Group Am J Surg 176 74S-79S
WIEMAN TJ SMIELL JM and SU Y (1998) Efficacy and safetyof a topical gel formulation of recombinant human platelet-derivedgrowth factor-BB (becaplermin) in patients with chronic neuropathicdiabetic ulcers A phase III randomized placebo-controlled double-blind study Diabetes Care 21 822ndash827
WILSON JM (1996) Adenoviruses as gene-delivery vehicles NEngl J Med 334 1185ndash1187
XU J and CLARK RA (1996) Extracellular matrix alters PDGFregulation of fibroblast integrins J Cell Biol 132 239ndash249
XU J and CLARK RA (1997) A three-dimensional collagen latticeinduces protein kinase C-z activity Role in a2 integrin and collage-nase mRNA expression J Cell Biol 136 473ndash483
Address reprint requests toDr John Doukas
Selective Genetics Inc11035 Roselle Street
San Diego CA 92121
E-mail jdoukasselectivegeneticscom
Received for publication December 28 2000 accepted after re-vision February 23 2001
DOUKAS ET AL798

TISSUE REPAIR USING GROWTH FACTOR GENES 787
A second model utilized 7-cm2 full-thickness excisionalwounds placed on the backs of anesthetized rabbits Woundswere treated with AdPDGF-B formulated in 26 collagen (2 3
109 or 2 3 1011 virus particles per wound in 700-ml volumes)and then covered with OpSite dressing On day 3 7 28 or 90posttreatment blood was collected animals were perfused asdescribed above and the following organs were recoveredwound bed brain heart lung liver spleen kidney gonad andlymph nodes (axillary cranial mesenteric and posterior medi-astinal) Real-time quantitative TaqMan PCR was performedusing 45 two-step cycles with primers designed to amplify se-quences bridging the vector backbone and the PDGF-B pre-proregion (sense 59-GGATCTTCGAGTCGACAAGCTT-3 9 an-tisense 59-TAAGGGCTCCTCGAAATACTCTA-3 9) The re-sulting amplicons were detected with an internal fluorogenicprobe (59-TAGTGGTACTTAGCGACGACCCGC-3 9) and anABI Prism 7700 sequence detector (PE Applied BiosystemsFoster City CA) The initial target copy numbers present ineach reaction were quantified by extrapolation from standardcurves of AdPDGF-B DNA in the background of 1 mg of rab-bit liver DNA per reaction Each PCR contained 1 mg of testDNA with the exception of wound bed which contained 500ng per reaction and blood which contained the equivalent of10 ml of original sample Each test sample was assayed in du-plicate to control for PCR inhibitory substances a third reac-tion was spiked with 100 copies of AdPDGF-B DNA PCR dataare presented as AdPDGF-B genome copies per wound thelimit of quantitation (LOQ) was 10 copiesmg DNA or an av-erage of 105 copieswound
For those tissues scoring positive for PCR-amplifiable vec-tor we further performed real-time quantitative reverse tran-scriptase (RT)-PCR Reverse transcriptase reactions were per-formed with 100 ng of each test RNA per reaction and randomhexamer primers The resulting cDNAs were then used to am-plify both rabbit 18S rRNA cDNA and PDGF-B cDNA in sep-arate PCRs The vector-specific primers were designed to am-plify full-length 160-amino acid human PDGF-B mRNA(sense 59-CAAGCACACGCATGACAAGA-3 9 antisense 59-TTTCGTTATCGTAGTGTTTAAAGTGT-3 9) The resulting131-nucleotide amplicons were detected with an internal fluo-rogenic probe (59-AAACAAGTTGCTCGATGGATCCTTAT-CAGGCT-39) RT-PCRs were then normalized for total RNAby 18S rRNA content with a second pair of PCR primers RT-PCR data are presented as the relative amount of PDGF-BmRNA per unit 18S rRNA (in arbitrary units)
Histochemical analyses
For routine morphological assessment paraffin sections werestained according to the Masson trichrome procedure In addi-tion a blinded observer using a microscope equipped with oc-ular micrometers measured the area within sponges filled bygranulation tissue these values are expressed as the percentageof sponge interior occupied by tissue ( granulation fill) Forexcisional wounds trichrome-stained sections and an imageanalysis software package (Image-Pro Plus software Media Cy-bernetics Silver Spring MD) were used to determine the cross-sectional areas of granulation tissue and epithelium per wound(in mm2) In addition the percentage of wound closure was cal-culated according to the following formula [(original wound
diameter 2 epithelial gap length) original wound diameter] 3100
For immunohistochemistry paraffin sections were stainedwith biotinylated Griffonia (Bandeiraea) simplicifolia lectin I(BSL-I) horseradish peroxidase (HRP)-labeled streptavidin anddiaminobenzidine (DAB Vector Laboratories BurlingameCA) in order to detect vascular endothelium Mouse anti-Ki-67and HRP-labeled rabbit anti-mouse IgG antibodies followed byDAB were used to detect proliferating cells Mouse anti-humanPDGF-BB (Z2703 American Type Culture Collection) andHRPndashanti-mouse IgG antibodies followed by DAB were usedto detect human PDGF-BB protein Fluorescein isothiocyanate(FITC)-conjugated anti-adenovirus antibody (Accurate Chemi-cals Westbury NY) and the nuclear stain 496-diamidino-2-phenylindole (DAPI Molecular Probes) were used to detectinternalized adenovirus vectors Finally fibroblasts were iden-tified with Cy3-labeled anti-vimentin (Sigma St Louis MO)
For in situ hybridization procedures an [a-35S] UTP-labeledriboprobe prepared from the full-length human PDGF-B cDNAwas used as previously described (Gonzalez et al 1995) Asense riboprobe was used to control for nonspecific hybridiza-tions
Biochemical analyses
Tissue samples not processed for paraffin embedding wereplaced in 100 mM phosphate buffer containing 02 Triton X-100 (pH 78) and agitated at 55 msec for 20 sec in a Fast-Prep system (BIO 101 Vista CA) After centrifugation su-pernatants were analyzed for protein using a bicinchoninic acidassay (Pierce Rockville IL) and for DNA using the PicoGreenassay PDGF-BB protein content was determined with a humanPDGF-BB-specific ELISA (RampD Systems Minneapolis MN)
Statistical Analyses
Data are presented as arithmetic means 6 1 SD Groups ofthree or more means within individual studies were comparedby one-way analysis of variance (ANOVA) and the Fisher pro-cedure for least significant differences (StatView softwareAbacus Concepts Berkeley CA)
RESULTS
Adenovirus vectors can be immobilized in an activeform within matrices
As an initial step to the in vivo assessment of adenovirusndashmatrix formulations we first determined the activity profilesand release kinetics for vectors formulated in type I collagenand carboxymethylcellulose (CMC) Collagen was selected onthe basis of its successful use as a delivery matrix for proteinsand DNA (Grotendorst et al 1985 Mustoe et al 1987 1991Sprugel et al 1987 Khouri et al 1994 Bonadio et al 1999)as well as its ability to enhance tissue repair responses in fi-broblasts (Xu and Clark 1996 1997) Relatively low (015)and high (26) concentrations were examined reasoning thatthis would allow for either relatively short or long retentiontimes at application sites respectively CMC was selected on
DOUKAS ET AL788
TISSUE REPAIR USING GROWTH FACTOR GENES 789
FIG 3 Localization of gene vector and transgene product within neotissues PVA sponges implanted in rats were injected withAdPDGF-B formulated in 015 collagen (2 3 1010 virus particles per sponge) and paraffin sections were stained as follows(A) Day 1 posttreatment anti-adenovirus immunostain to detect AdPDGF-B (green) DAPI stain to detect cell nuclei (blue) (B)Day 4 posttreatment in situ hybridization using human PDGF-B gene probe (C) Day 1 posttreatment anti-human PDGF-BBprotein immunostain positively stained leukocytes (arrowheads) and fibroblasts (arrows) are indicated (D) Day 6 posttreatmentanti-PDGF-BB immunostain (E) Day 8 posttreatment anti-PDGF-BB immunostain (F) Day 8 post- treatment immunostains todetect PDGF-BB protein (green) and vimentin (red) yellow fluorescence indicates PDGF-BB and vimentin colocalization bluefluorescence indicates cell nuclei (DAPI stain) Original magnifications (AndashC E and F)3 400 (D) 31000
the basis of its clinical use for the delivery of PDGF-BB pro-tein (Steed 1995)
Matrix influences on vector activity were examined by in-cubating AdLuc formulations at 37degC for 60 min followed bymatrix dissolution and vector bioassay (luciferase productionby 293 cells) This is an important test as adenoviruses arequickly inactivated under unfavorable physical and chemicalconditions (Nyberg-Hoffman and Aguilar-Cordova 1999)None of the matrices examined had a deleterious effect on vec-tor activity (90 6 12 106 6 5 and 139 6 37 of control ac-tivity for 015 collagen 26 collagen and CMC respec-tively) To further model in vivo vector stability we alsoincubated AdPDGF-B formulated in 26 collagen with woundfluid for 72 hr at 37degC prior to vector recovery and analysisWe observed no reduction in the level of PDGF-BB productionfrom cells transduced with AdPDGF-B exposed to wound fluidas compared with vector exposed to virus buffer (30 6 5 vs20 6 3 ng of PDGF-BB produced per milliliter of culturemedium respectively n 5 3)
As these data support the suitability of the selected matricesfor in vivo use we next determined their influence on vectorrelease kinetics (Fig 1) When placed in water collagen ma-trices retained the majority of their immobilized vectors with015 and 26 collagen releasing only 17 6 3 and 3 6 1 ofvector by 24 hr respectively By contrast 48 6 3 of AdLucwas released from CMC within 30 min and 61 6 2 by 6 hrThis was not unexpected as CMC is fairly water soluble andas both CMC and adenoviral particles are negatively chargedTherefore collagen matrices in a concentration-dependentfashion display more favorable kinetics for localizing and re-taining adenovirus vectors at delivery sites than does CMC
Collagen-immobilized adenoviruses induce distinctneotissues in vivo
Initial in vivo tests of matrix-immobilized vectors were per-formed with an established model of de novo tissue generation(Buckley et al 1985 Sprugel et al 1987 LeGrand et al1993) PVA sponges implanted subcutaneously in rats were in-jected with a single dose of adenovirus formulated in either col-lagen or CMC and then analyzed for tissue formation Forgrowth factor transgenes we selected platelet-derived growth
factor B (PDGF-B) vascular endothelial growth factor (VEGF)and fibroblast growth factor 2 (FGF2) because of their well-known mitogenic activities
AdPDGF-B formulated in 015 collagen induced granula-tion tissue formation in a dose-responsive manner (Table 1)Compared with vehicle controls delivering 2 3 1010 virus par-ticles induced a 17- to 23-fold increase in sponge protein con-tent (p 00002) a 2- to 27-fold increase in DNA content (p
00002) and a 29- to 43-fold increase in granulation tissue fill(p 00002) Trichrome-stained sections revealed the nearcomplete fill of sponge interiors with well-formed granulationtissue by day 6 posttreatment (Fig 2A) Expression of Ki-67a nuclear protein upregulated in proliferating cells (Gerdes etal 1983) established that both vascular endothelium (arrow-heads Fig 2B) and fibroblasts (arrows Fig 2B) had prolifer-ated in response to PDGF-B gene delivery AdFGF2 and Ad-VEGF also enhanced protein and DNA content within sponges(Table 1) However these vectors induced less granulation tis-sue deposition as compared with AdPDGF-B and the tissuesformed were histologically distinct
Tissues present in AdFGF2-treated sponges were highly vas-cular as revealed by the endothelial-reactive lectin BSL-I (Fig2D) Many of the infiltrating mononuclear cells also reactedpositively with BSL-I lectin suggesting that these cells wereendothelial cells or endothelial precursors AdFGF2 did nothowever induce the formation of classic granulation tissue aslittle collagen deposition was observed demonstrated by thepaucity of blue-staining material in trichrome-stained sections(Fig 2C) AdVEGF also induced heavily vascularized tissues(Fig 2E and F) but with greater extracellular collagen deposi-tion than AdFGF2 Relative to AdPDGF-B-induced tissueshowever AdVEGF-induced tissues were disorganized con-tained few fibroblasts and were markedly edematous Finallywhen AdLuc was delivered as a control treatment no signifi-cant increases in protein DNA or granulation tissue were ob-served compared with collagen vehicle alone (Table 1)Trichrome-stained sections revealed sparse inflammatory cellinfiltrates within AdLuc-treated sponges (Fig 2G) which com-pared with the near absence of infiltration after delivery of col-lagen vehicle alone (Fig 2H) suggested a limited antiviral response
Unlike the 015 collagen formulations described above
DOUKAS ET AL790
TABLE 2 NEOTISSUE FORMATION AFTER PDGF-B GENE OR PDGF-BB PROTEIN DELIVERYa
Granulation Protein DNATreatment fill () (mgsponge) (mgsponge)
015 Collagen vehicle 28 6 13b 16 6 2b 103 6 22b
AdPDGF-B 81 6 15b 30 6 6b 218 6 28b
PDGF-BB 100 mg 64 6 12c 22 6 4c 155 6 26c
PDGF-BB 10 mg qod 3 3d 77 6 9b0 31 6 8b 230 6 75b
aPVA sponges implanted in rats were injected with either 015 collagen vehicle or collagen containing AdPDGF-B as described in Table 1 Alternatively PDGF-BB protein was delivered as a single 100-mg dose on day 4 postimplantation or as10-mg doses on days 4 6 and 8 Sponges were removed on day 12 postimplantation and processed to determine the percent granulation fill as well as total protein and DNA contents Data are presented as means 6 SD (n 5 4ndash8)
bp 00001 versus collagen control and p 005 versus 100-mg PDGF-BBcp 003 versus collagen controldqod 3 3 Every other day three times
TISSUE REPAIR USING GROWTH FACTOR GENES 791
TABLE 3 INFLUENCE OF ADENOVIRUSndashMATRIX FORMULATIONS ON ISCHEMIC WOUND HEALINGa
Granulation Epithelial Wound closureTreatment Model system area (mm2) area (mm2) ( complete)
Aqueous buffer Cartilage intact 10 6 08 05 6 03 61 6 226 mm day 10
AdPDGF-B in Cartilage intact 24 6 22 05 6 01 73 6 28aqueous buffer 6 mm day 10
015 Collagen Cartilage intact 05 6 03 05 6 02 89 6 14vehicle 6 mm day 10
AdPDGF-B in Cartilage intact 16 6 09b 09 6 03c 97 6 7015 collagen 6 mm day 10
Aqueous buffer Cartilage removed 45 6 08 08 6 02 95 6 96 mm day 7
AdPDGF-B in Cartilage removed 40 6 15 11 6 05 82 6 22aqueous buffer 6 mm day 7
015 Collagen Cartilage removed 36 6 13 06 6 02 88 6 22vehicle 6 mm day 7
AdPDGF-B in Cartilage removed 70 6 14b 07 6 03 79 6 22015 collagen 6 mm day 7
26 Collagen Cartilage removed 04 6 05 01 6 01 24 6 15vehicle 8 mm day 8
AdPDGF-B in Cartilage removed 51 6 25b 06 6 03b 52 6 25c
26 collagen 8 mm day 8
aExcisional wounds (6 or 8 mm in diameter) were placed in ischemic rabbit ears with underlying cartilage left intact or re-moved Wounds were then treated with AdPDGF-B formulated in aqueous virus buffer or collagen control treatments consistedof vehicle alone For 6-mm wounds virus was applied as 2 3 109 particles per wound for 8-mm wounds as 4 3 109 particlesper wound On days 7ndash10 posttreatment wounds were harvested and processed as trichrome-stained paraffin sections whichwere then used to quantify newly formed granulation tissue and epithelium (cross-sectional area in mm2) and the degree of woundsurface closure (where 100 equals complete closure) Data are presented as means 6 SD (n 5 4ndash8)
bp 0009 versus vehicle controlcp 005 versus vehicle control
26 collagen formulations could not be reliably examined inthe PVA sponge model as their relatively high viscosity pre-vented uniform filling of sponges by syringe CMC-formulatedvectors were also unsuitable for this model system as theyproved highly inflammatory (data not shown) These formula-tions therefore were evaluated in more appropriate excisionalwound models (see below)
Tissue repair cells are transduced by collagen-immobilized adenoviruses
On the basis of the robust activity of collagen-formulatedAdPDGF-B we elected to further examine this vectorndashmatrixcombination first by seeking to correlate PDGF-B gene deliv-ery with subsequent transgene and protein expression WhenPVA sponges treated with 015 collagenndashAdPDGF-B werestained with both an anti-adenovirus antibody and the nuclearstain DAPI the majority of cells present 1 day after gene de-livery had bound andor internalized adenovirus (Fig 3A) Insitu hybridization revealed that these cells were successfullytransduced by virus as they contained human PDGF-B mRNA(Fig 3B) By contrast hybridization product was not detectedwith a sense riboprobe or when AdLuc-treated sponges wereexamined (data not shown)
We next used a human PDGF-BB-specific antibody to iden-tify the cell types responsible for transgene expression By day
1 postdelivery of 015 collagenndashAdPDGF-B PDGF-BB pro-tein was localized to leukocytes (arrowheads) and fibroblasts (ar-row Fig 3C) With time PDGF-BB protein was detected boundto the extracellular matrix (ECM) surrounding positively stainedcells (Fig 3D) This last observation indicates that a reservoir ofPDGF-BB protein develops within treated tissues and thus mayprolong the histogenic effects of this growth factor Finally byday 8 the majority of immunoreactivity had abated with pri-marily microvascular endothelium remaining positive (Fig 3E)However scattered fibroblasts could still be shown to producePDGF-BB protein by dual immunohistochemistry with anti-PDGF-BB and anti-vimentin antibodies (Fig 3F)
Multiple administrations of PDGF-BB protein are required to approximate the histogenic effects of collagenndashAdPDGF-B
To directly compare gene therapy with the more conven-tional approach of growth factor protein delivery we next quan-tified tissue formation in response to either PDGF gene or pro-tein delivery A single injection of 015 collagenndashAdPDGF-Benhanced granulation tissue filling of sponges by 3-fold versusvehicle alone (p 00001) and sponge protein and DNA lev-els by 2-fold (p 00001 Table 2) Using a human PDGF-BB-specific ELISA this growth factor was detected at 54 6 13ngsponge (n 5 8) By contrast when PDGF-BB protein was
delivered as a single dose nearly 2000-fold in excess of thisconcentration the tissue formation responses observed (proteinand DNA accumulation and granulation tissue formation) weresignificantly lower (p 005 Table 2) In fact repeated dos-ing with PDGF-BB protein was required in order to achieve re-sponses comparable to a single administration of the PDGF-Bgene These data therefore support our hypothesis that the abil-ity of gene delivery to establish prolonged in situ growth fac-tor production translates into greater histogenesis than that seenwith growth factor proteins
CollagenndashAdPDGF-B induces complete healing of ischemic wounds
Nonhealing wounds are a major risk in chronically ischemictissues as low oxygen tension greatly impairs tissue repair pro-cesses We therefore compared the ability of matrix versusaqueous formulated AdPDGF-B to repair ischemic excisionalwounds Several models were employed to compare variationsin wound size and condition so as to allow for a more com-plete picture of tissue repair
In the first model system 6-mm-diameter wounds were cre-ated in ischemic rabbit ears by removal of epidermal and der-mal layers but not underlying cartilage This model has beenused in previous studies of growth factor proteins and genes(Ahn and Mustoe 1990 Mustoe et al 1994 Liechty et al1999) and was therefore employed to allow comparison withthese reports However it represents an artificial system as thepresence of a cartilage layer restricts both treatment activity andhealing to wound margins and in addition the initially acellu-lar wound bed forms a cup that artifactually retains aqueoustreatments As would be predicted we found a trend towardgranulation tissue formation in this model after the applicationof AdPDGF-B formulated in aqueous buffer (Table 3) How-ever this response did not reach the level of statistical signifi-cance as tissue development was highly variable (note the highstandard deviation value) In addition epithelial regenerationand wound closure were minimal to unaffected By contrastAdPDGF-B formulated in 015 collagen enhanced granula-tion tissue area by 32-fold and epithelial area by 18-fold overthat achieved with vehicle alone (p 0009 and 005 respec-tively) Although near complete closure of epithelial gaps wasalso achieved the high level of self-healing in control-treatedgroups (89 wound closure) precluded statistical significance
In an alternative model design subdermal cartilage was com-pletely removed from excisional wounds creating beds whosefloors now consisted of dermal tissue (Pierce et al 1994b)This design allows for cellular responses from the entire woundbed as well as the opportunity for vector migration beyond
treatment areas We now observed that aqueous formulated Ad-PDGF-B failed to induce even a trend toward tissue regenera-tion (Table 3) Rather the vector appears to have seeped throughthe wound bed floor as inflammatory cell infiltrates and fociof fibroblast proliferation were observed in the underlying der-mis and at wound margins (Fig 4A) Immunohistochemistryconfirmed the production of human PDGF-BB at these sites(Fig 4B) CMC-formulated AdPDGF-B also failed to induceany meaningful tissue repair Wounds treated with this formu-lation showed a diffuse inflammatory response within thewound bed and wound surfaces were overlain with fibrin clotsrather than regenerating epithelium (Fig 4C and D) By con-trast AdPDGF-B formulated in 015 collagen enhanced gran-ulation tissue deposition 19-fold within wound beds versus ve-hicle controls (p 0002) and wounds were extensivelyepithelialized (Table 3) Neither epithelial regeneration norwound closure achieved significance however as the high de-gree of self-healing achieved in this particular model (see ve-hicle alone group) most likely masked transgene-stimulated re-sponses
To address these model limitations as our next system wecreated 8-mm wounds in ischemic rabbit ears by removingepidermal dermal and cartilage layers reasoning that largerexcisional wounds would display limited self-healing In ad-dition this model could readily accommodate 26 collagenformulations which proved difficult to reproducibly apply insmaller wounds Compared with control wounds treated withcollagen vehicle alone wounds treated with AdPDGF-B for-mulated in 26 collagen achieved a 12-fold enhancementin granulation tissue fill and a 6-fold enhancement in re-ep-ithelialization by day 8 posttreatment (p 0009 Table 3)In addition wound closure was only 24 complete in colla-gen vehicle-treated wounds by day 8 but 52 complete inwounds treated with collagen-formulated AdPDGF-B (p
005) Histologically AdPDGF-B-treated wounds showed nosigns of tissue hyperplasia or chronic inflammation but ratheran orderly repair process marked by a regenerated epitheliallayer overlying a wound bed filled with granulation tissue(Fig 4E and F)
CollagenndashAdPDGF-B induces normal long-term tissue repair
Our choice of adenoviruses for transgene delivery was partlybased on the reasoning that as these vectors establish transientgene expression they would not lead to hyperproliferative re-sponses or scar formation To test this hypothesis we treatedrabbit ear excisional wounds with AdPDGF-B formulated in015 collagen and examined tissue repair responses out to
DOUKAS ET AL792
FIG 4 Influence of adenovirusndashmatrix formulations on excisional wound repair Excisional wounds (6 or 8 mm in diameter andextending through underlying cartilage layers) were placed in ischemic rabbit ears bars indicate original wound depth (determinedfrom cartilage visible at wound margins) Wounds were then treated with AdPDGF-B formulated in either virus buffer CMC orcollagen and on day 7 or 8 posttreatment processed for histology or immunohistochemistry An identical design was used to ex-amine long-term healing on day 90 except that wounds were created in nonischemic ears (A) Day 7 buffer-formulated AdPDGF-B-treated 6-mm wound trichrome stain (B) Day 7 buffer-formulated AdPDGF-B-treated 6-mm wound anti-PDGF-BB proteinimmunostain (C and D) Day 7 CMC-formulated AdPDGF-B-treated 6-mm wound trichrome stains (E and F) Day 8 26 col-lagen-formulated AdPDGF-B-treated 8-mm wound trichrome stains (G and H) Day 90 015 collagen-formulated AdPDGF-B-treated 6-mm wound trichrome stains Original magnification (A C E and G) 340 (B D F and H) 3200
TISSUE REPAIR USING GROWTH FACTOR GENES 793
DOUKAS ET AL794
TABLE 4 BIODISTRIBUTION OF AdPDGF-B IN EXCISIONAL WOUNDSa
Positive samplestotal assayed
Tissue AdPDGF-B dose Day 3 Day 7 Day 28 Day 90
Wound bed 2 3 109 particles 66 66 66b 06Axillary lymph nodes 2 3 109 particles 02 ND 06 06
Wound bed 2 3 1011 particles 66 66 66 46c
Axillary lymph nodes 2 3 1011 particles 66 ND 66d 26e
aFull-thickness excisional wounds (7 cm2) were placed on the backs of rabbits and AdPDGF-B formulated in 26 collagenwas applied as either 2 3 109 or 2 3 1011 virus particles per wound On days 3ndash90 posttreatment wound beds and a panel oforgans were harvested for real-time PCR quantification of viral genome Data are shown for wound bed and axillary lymph nodesamples as the number of samples that yielded amplifiable signals per total number assayed ND not determined
bThree of six samples scored below the level of quantitation (LOQ 10ndash100 copiesmg DNA)cAll four positive samples scored below the LOQdThree of six samples scored below the LOQeBoth positive samples scored below the LOQ
180 days posttreatment (Fig 5) PDGF-B gene delivery en-hanced total ear thickness relative to controls on day 28 (229 6
020 vs 179 6 019 mm p 00001) and day 60 (192 6 001vs 182 6 011 mm p 0005) as anticipated on the basis ofthe ability of this formulation to induce granulation tissue for-mation By day 90 posttreatment however there was no mea-surable difference in ear thickness between AdPDGF-B andcontrol-treated groups and this relationship continued out today 180 indicating that growth factor gene delivery did not in-duce excessive scar formation This was also confirmed histo-logically AdPDGF-B-treated wounds on day 90 and beyondwere composed of a thin outer keratin layer an underlying ep-ithelial layer of equivalent thickness to nonwounded areas anda collagen-rich dermis devoid of any signs of tissue hyperpla-sia (Fig 4G and H)
Collagen immobilization limits adenovirus vectorbiodistribution beyond treatment sites
As a final measure of the value of matrix immobilization forgene delivery we determined the biodistribution patterns ofvectors after their in vivo delivery In the first model systemused AdPDGF-B formulated in 015 collagen was applied torabbit ear wounds at equivalent doses as previously describedwounds were extended through underlying cartilage but vas-cular supplies were not disturbed so as to permit maximal vec-tor dissemination By PCR no adenoviral DNA was detectablein lung spleen brain cervical lymph nodes or gonads on day1 3 7 or 14 (n 5 6 per group) In the liver one of six sam-ples was positive on days 3 and 7 but none on day 14 in serumonly one of six samples tested positive on day 14 (equivalentof 500-ml serum volume) By contrast adenovirus was detectedin eight of eight wound bed samples at all time points exam-ined
In a second model system excisional wounds placed on thebacks of rabbits were treated with AdPDGF-B formulated in26 collagen Because of their anatomical placement thismodel allowed for the creation of larger excisional wounds (7-cm2 total area) than those placed in rabbit ears (03 cm2) and
consequently larger treatment volumes and vector doses (2 3109 or 2 3 1011 virus particles per wound) At the lower doseof 2 3 109 particles PCR-amplifiable adenoviral DNA was notdetectable beyond wound beds on day 3 7 28 or 90 Tissuessampled and found not to contain vector included blood heartlung liver kidney brain spleen lymph nodes and gonads (n 5
6group) In wound beds adenoviral DNA was detected at alltime points except for day 90 (Table 4 and Fig 6) Vector lev-els did decrease however by 38-fold between days 7 and 28with three of six samples falling below the level of quantita-tion (LOQ) by real-time PCR at the latter time point (Fig 6)
At a 100-fold higher vector dose of 2 3 1011 particles perwound PCR-amplifiable adenoviral DNA was once again un-detectable in the majority of tissues sampled Except for a sin-gle day 7 liver sample and a single day 7 brain sample (bothbelow the LOQ) adenoviral DNA was only detectable directlyin wound beds or in the axillary lymph nodes that drain woundsites (Table 4) Moreover three of six positive axillary nodesamples scored below the LOQ on day 28 as did both positivesamples on day 90 indicating that they contained relatively lit-tle vector Within wound beds adenoviral DNA was detectedat quantifiable levels out to day 28 and at detectable but non-quantifiable levels on day 90 DNA copy numbers remainedsteady between days 3 and 7 dropped 107-fold between days7 and 28 and a further 1662-fold by day 90 Finally at eachtime point DNA copy numbers in wounds treated with 2 3
1011 particles were approximately 100-fold higher than thosefound in wounds treated with 2 3 109 particles thus confirm-ing the linearity of our assay system
To better define the time course of human PDGF-BB pro-duction we also quantified transgene mRNA levels in woundbed samples treated at 2 3 109 particles per wound This treat-ment dose was selected as representative of the virus particleconcentration capable of inducing complete healing in ischemicear wounds Quantifiable levels of human PDGF-B mRNAwere detectable in treated dorsal wounds at days 3 7 and 28(Fig 6) with levels decreasing 14-fold between days 3 and 7and 5-fold between days 7 and 28 The more sensitive tech-nique of real-time RT-PCR therefore demonstrates that trans-
TISSUE REPAIR USING GROWTH FACTOR GENES 795
gene expression extends well beyond the 8-day time period sug-gested using anti-PDGF-BB immunohistochemistry as a de-tection system (Fig 3)
DISCUSSION
These studies demonstrate that immobilization of gene ther-apy vectors in collagen-based matrices enables their efficientdelivery and activity in vivo Matrix immobilization achievedprolonged transgene-encoded growth factor production and asa consequence robust tissue repair By contrast aqueous vehi-cles failed to retain adenoviruses at application sites resultingin diffuse inflammation rather than productive tissue regenera-tion These observations confirm our basic hypothesis that ma-trix immobilization of growth factor-encoding gene therapyvectors represents a promising approach to tissue repair
Although de novo tissue deposition was achievable with sev-eral growth factor genes PDGF-B proved the most suitable forrepair of cutaneous defects A single administration of colla-gen-immobilized AdPDGF-B rapidly induced the formation ofhighly cellular and vascularized tissues with dense ECMs richin collagen By contrast AdFGF2 induced a primarily vascu-lar response with little collagen deposition FGF2 induces therelease of matrix metalloproteinase 1 or interstitial collagenase(Buckley-Sturrock et al 1989) and this may underlie the rel-ative paucity of ECM accumulation VEGF gene delivery alsoinduced highly vascular responses however the enhanced per-meability characteristic of VEGF-induced vasculature (Dvoraket al 1995) led to edema within nascent tissues In fact much
of the enhanced protein and DNA deposition observed in Ad-VEGF-treated PVA sponges may well derive from fluid exu-dates rather than actual tissue formation Finally the inabilityof AdLuc delivery to induce anything beyond a limited in-flammatory response confirms that tissue formation was de-pendent on growth factor gene delivery
The robust activity of PDGF-B gene delivery was expectedas PDGF-BB protein initiates multiple aspects of tissue forma-tion including cellular influx and proliferation ECM deposi-tion and tissue remodeling (Pierce et al 1988 1991 1994a)Indeed PDGF-BB is the only growth factor protein to have suc-cessfully completed human clinical trials and be approved forthe treatment of dermal wounds (Steed 1995 drsquoHemecourt etal 1998 Wieman 1998 Wieman et al 1998) We observedthat collagen-formulated AdPDGF-B induced the complete re-pair of excisional skin defects without unwanted long-term ef-fects such as the development of hypertrophic scars Endoge-nous growth factors other than PDGF-BB however most likelymediated the enhanced re-epithelialization observed in thesewounds as epithelial regeneration is driven by members of theepidermal growth factor and FGF families (Pierce et al 1994bDanilenko et al 1995) Our data indicate nonetheless that tis-sue regeneration and repair were initiated and to a great degreedriven by transgene-encoded PDGF-BB
Despite the known activity of PDGF-BB protein we wereable to demonstrate greater tissue deposition after gene deliv-ery as compared with the use of recombinant growth factor pro-tein A single application of PDGF-BB protein could not equalthe ability of PDGF-B gene therapy to induce neotissue for-mation even at doses well in excess of that induced in situ byAdPDGF-B and in excess of that used in human clinical trials
FIG 5 Influence of collagen-formulated AdPDGF-B on long-term tissue repair Excisional wounds (6 mm in diameter withcartilage remaining intact) were placed in nonischemic rabbit ears and treated with either 015 collagen alone (open columns)or AdPDGF-B formulated in this vehicle (solid columns) On days 28ndash180 posttreatment total ear thickness at the site of eachwound was measured (in mm) with calipers Data are presented as means 6 SD (n 5 3) Treatment groups differ by p 00001groups differ by p 0005
(Steed 1995 drsquoHemecourt et al 1998 Wieman 1998 Wie-man et al 1998) In fact repeated administrations of PDGF-BB protein were required to approach the level of tissue for-mation observed after a single administration of AdPDGF-BThese data support our hypothesis that sustained localizedgrowth factor production is required for robust tissue repair
In further support of this hypothesis we demonstrated thatmRNA encoding human PDGF-B was present in excisionalwounds as late as day 28 after collagen-formulated AdPDGF-B administration By contrast previous studies of PDGF-BBprotein found that the great majority of this growth factor wasgone from treated wounds 1 day postapplication and that anytissue maturation subsequently observed was most likely dueto the upregulation of endogenous growth factors (Pierce et al1992 1995) We also demonstrated that repair cells such asmononuclear leukocytes endothelial cells and fibroblasts pres-ent with developing neotissues represent the source of both
transgene transcription and PDGF-BB production In additiona depot of human PDGF-BB was detected bound to the colla-gen delivery matrix and ECM of these tissues This was antici-pated as PDGF-BB contains collagen-binding motifs (Soma-sundaram and Schuppan 1996) We hypothesize that subsequentmatrix metalloproteinase activity by repair cells will serve togenerate localized release of this sequestered growth factor pooland as a consequence further drive tissue regeneration Theseevents which are central to tissue remodeling should be directlyenhanced by collagen matrices as type I collagen stimulates me-talloproteinase production integrin expression and cellular ac-tivation in PDGF-stimulated fibroblasts (Xu and Clark 19961997)
An additional rationale for employing collagen matrices wasto physically immobilize vectors This was confirmed in vivowhere collagen matrices maintained AdPDGF-B at deliverysites for at least 28 days and limited vector migration to other
DOUKAS ET AL796
FIG 6 Persistence of collagen-formulated vector and transgene transcripts in excisional wounds Full-thickness excisionalwounds (7 cm2) were placed on the dorsal surface of rabbits and treated with AdPDGF-B formulated in 26 collagen at either2 3 109 or 2 3 1011 virus particles per wound (open and closed columns respectively) Wounds were then covered with OpSitedressing and on days 3 7 or 28 posttreatment wound beds were harvested for real-time quantitative PCR and RT-PCR analy-ses PCR data are presented in the upper graph as AdPDGF-B copies per wound RT-PCR data are presented in the lower graphas the relative amount of PDGF-B mRNA per unit 18S rRNA (in arbitrary units) All data points are means 6 SD (n 5 6)
tissues or organs In vitro tests also established that collagenmatrices not only prevent vector loss due to diffusion but pre-serve vector activity despite prolonged incubation in acutewound fluid Successful vector immobilization and tissue re-pair could be achieved with both 015 collagen and 26 col-lagen suggesting flexibility in the final vehicle formulation re-quired for effective vector delivery This flexibility was neededin the present studies as 26 collagen formulations proveddifficult to deliver to PVA sponges and 6-mm excisionalwounds This would not be of concern in clinical settings how-ever where wound beds are easily accessible and generally sev-eral square centimeters in area By contrast CMC was inef-fective at retaining vector in aqueous environments Moreimportantly this matrix was itself inflammatory and whencombined with adenovirus the net result was inflammationrather than tissue repair We are currently examining the util-ity of other matrices such as fibrin and hyaluronic acid whichbecause of their more provisional nature may offer yet greatercellular migration into wounds as compared with type I colla-gen
Although an aqueous-based AdPDGF-B formulation hasbeen previously shown to enhance tissue formation (Liechty etal 1999) this was achieved with a model system that artifi-cially retains vectors within treatment sites In fact the presentstudies demonstrate that any tissue repair observed after Ad-PDGF-B delivery in a nongelling liquid is dependent on the useof this model system In wounds not designed to retain appliedtreatments aqueous-formulated AdPDGF-B seeped into sur-rounding tissues and led to hyperplasia within these areas ratherthan to tissue regeneration within the active wound bed Colla-gen-immobilized AdPDGF-B on the other hand did persist inthese wound beds and led to significant enhancements in gran-ulation tissue formation as well as enhanced wound re-epithe-lialization and wound closure The significance of these activ-ities is further substantiated considering that they wereachievable in 8-mm-diameter ischemic wounds which withinthe time frame examined could not self-heal to any meaning-ful degree in the absence of gene therapy However as all theanimal models employed in these studies will eventually self-heal given sufficient time the full value of matrix-immobilizedgene therapy vectors remains to be confirmed in human clini-cal trials
In conclusion we present evidence that matrix-immobilizedgene therapy vectors encoding appropriate growth-promotinggenes represent a promising approach to tissue regeneration andrepair This basic concept can be expanded to include alterna-tive matrices such as controlled-release formulations as wellas tissue-specific growth factors Furthermore the addition oftargeting ligands to adenovirus vectors (eg FGF2) can en-hance their ability to transduce cells such that tissue repair re-sponses comparable to nontargeted vectors can be achieved butat significantly lower vector doses (Chandler et al 2000a)With appropriate design and application schedules one couldconceivably time the release of multiple growth factors to spe-cific stages of a tissue repair cascade In addition we have foundin preliminary studies that collagen-immobilized nonviral vec-tors such as PDGF-B plasmids which have potentially morefavorable safety profiles than adenovirus vectors can also en-hance tissue formation in vivo (Chandler et al 2000b Tyroneet al 2000) Such flexibility should allow for the widespreadapplication of gene therapy to the treatment of injured tissues
ACKNOWLEDGMENTS
We thank Jeff Davidson (Vanderbilt University School ofMedicine) for assistance in establishing the PVA sponge modelCarl-Henrik Heldin (Ludwig Institute for Cancer Research) forthe PDGF-B gene construct and Emelie Amburn Lara AsatoSharon Chang Gail Fieser Lydia Greenlees Rebecca Smokerand Linda Manza for excellent technical assistance This pub-lication was made possible in part by NIH grants 1R43AR46154(JD) and 5P01CA25874 (MH)
REFERENCES
AHN ST and MUSTOE TA (1990) Effects of ischemia on ulcerwound healing A new model in the rabbit ear Ann Plast Surg 2417ndash23
ANDREE C SWAIN WF PAGE CP MACKLIN MDSLAMA J HATZIS D and ERIKSSON E (1994) In vivo trans-fer and expression of a human epidermal growth factor gene accel-erates wound repair Proc Natl Acad Sci USA 91 12188ndash12192
BENN SI WHITSITT JS BROADLEY KN NANNEY LBPERKINS D HE L PATEL M MORGAN JR SWAIN WFand DAVIDSON JM (1996) Particle-mediated gene transfer withtransforming growth factor-b1 cDNAs enhances wound repair in ratskin J Clin Invest 98 2894ndash2902
BONADIO J SMILEY E PATIL P and GOLDSTEIN S (1999)Localized direct plasmid gene delivery in vivo Prolonged therapyresults in reproducible tissue regeneration Nat Med 5 753ndash759
BUCKLEY A DAVIDSON JM KAMERATH CD WOLT TBand WOODWARD SC (1985) Sustained release of epidermalgrowth factor accelerates wound repair Proc Natl Acad Sci USA82 7340ndash7344
BUCKLEY-STURROCK A WOODWARD SC SENIOR RMGRIFFIN GL KLAGSBRUN M and DAVIDSON JM (1989)Differential stimulation of collagenase and chemotactic activity in fi-broblasts derived from rat wound repair tissue and human skin bygrowth factors J Cell Physiol 138 70ndash78
CHANDLER LA DOUKAS J GONZALEZ AM HOGANSONDK GU DL MA C NESBIT M CROMBLEHOLME TMHERLYN M SOSNOWSKI BA and PIERCE GF (2000a)FGF2ndashTargeted adenovirus encoding platelet-derived growth factor-B enhances de novo tissue formation Mol Ther 2 153ndash160
CHANDLER LA MA C GONZALEZ AM DOUKAS JNGUYEN T PIERCE GF and PHILLIPS ML (2000b) Ma-trix-enabled gene transfer for cutaneous wound repair Wound Re-pair Regen 8 473ndash479
DANILENKO DM RING BD TARPLEY JE MORRIS BVAN GY MORAWIECKI A CALLAHAN W GOLDEN-BERG M HERSHENSON S and PIERCE GF (1995) Growthfactors in porcine full and partial thickness burn repair Differing tar-gets and effects of keratinocyte growth factor platelet-derivedgrowth factor-BB epidermal growth factor and neu differentiationfactor Am J Pathol 147 1261ndash1277
DEUEL TF KAWAHARA RS MUSTOE TA and PIERCE GF(1991) Growth factors and wound healing Platelet-derived growthfactor as a model cytokine Annu Rev Med 42 567ndash584
DrsquoHEMECOURT PA SMIELL JM and KARIM MR (1998) So-dium carboxymethylcellulose aqueous-based gel vs becaplermin gelin patients with nonhealing lower extremity diabetic ulcers Wounds10 69ndash75
DOUKAS J HOGANSON DK ONG M YING W LACEYDL BAIRD A PIERCE GF and SOSNOWSKI BA (1999)Retargeted delivery of adenoviral vectors through fibroblast growthfactor receptors involves unique cellular pathways FASEB J 131459ndash1466
TISSUE REPAIR USING GROWTH FACTOR GENES 797
DVORAK HF BROWN LF DETMAR M and DVORAK AM(1995) Vascular permeability factorvascular endothelial growth fac-tor microvascular hyperpermeability and angiogenesis Am JPathol 146 1029ndash1039
EMING SA MEDALIE DA TOMPKINS RG YARMUSHML and MORGAN JR (1998) Genetically modified human ker-atinocytes overexpressing PDGF-A enhance the performance of acomposite skin graft Hum Gene Ther 9 529ndash539
EMING SA WHITSITT JS HE L KRIEG T MORGAN JRand DAVIDSON JM (1999) Particle-mediated gene transfer ofPDGF isoforms promotes wound repair J Invest Dermatol 112297ndash302
GERDES J SCHWAB U LEMKE H and STEIN H (1983) Pro-duction of a mouse monoclonal antibody reactive with a human nu-clear antigen associated with cell proliferation Int J Cancer 3113ndash20
GONZALEZ AM BERRY M MAHER PA LOGAN A andBAIRD A (1995) A comprehensive analysis of the distribution ofFGF-2 and FGFR1 in the rat brain Brain Res 701 201ndash226
GREENHALGH DG (1996) The role of growth factors in woundhealing J Trauma 41 159ndash167
GROTENDORST GR MARTIN GR PENCEV D SODEK Jand HARVEY AK (1985) Stimulation of granulation tissue for-mation by platelet-derived growth factor in normal and diabetic ratsJ Clin Invest 76 2323ndash2329
KHOURI RK HONG SP DEUNE EG TARPLEY JE SONGSZ SERDAR CM and PIERCE GF (1994) De novo genera-tion of permanent neovascularized soft tissue appendages by platelet-derived growth factor J Clin Invest 94 1757ndash1763
LEGRAND EK SENTER LH GAMELLI RL and KIORPESTC (1993) Evaluation of PDGF-BB PDGF-AA bFGF IL-1 andEGF dose responses in polyvinyl alcohol sponge implants assessedby a rapid histologic method Growth Factors 8 315ndash329
LIECHTY KW NESBIT M HERLYN M RADU A ADZICKNS and CROMBLEHOLME TM (1999) Adenoviral-mediatedoverexpression of platelet-derived growth factor-B corrects ischemicimpaired wound healing J Invest Dermatol 113 375ndash383
LYNCH SE COLVIN RB and ANTONIADES HN (1989)Growth factors in wound healing J Clin Invest 84 640ndash646
MUSTOE TA PIERCE GF THOMASON A GRAMATES PSPORN MB and DEUEL TF (1987) Accelerated healing of in-cisional wounds in rats induced by transforming growth factor-betaScience 237 1333ndash1336
MUSTOE TA PIERCE GF MORISHIMA C and DEUEL TF(1991) Growth factor-induced acceleration of tissue repair throughdirect and inductive activities in a rabbit dermal ulcer model J ClinInvest 87 694ndash703
MUSTOE TA AHN ST TARPLEY JE and PIERCE GF(1994) Role of hypoxia in growth factor responses Differential ef-fects of basic fibroblast growth factor and platelet-derived growthfactor in an ischemic wound model Wound Rep Reg 2 277ndash283
NYBERG-HOFFMAN C and AGUILAR-CORDOVA E (1999) In-stability of adenoviral vectors during transport and its implication forclinical studies Nat Med 5 955ndash957
PIERCE GF and MUSTOE TA (1995) Pharmacologic enhance-ment of wound healing Annu Rev Med 46 467ndash481
PIERCE GF MUSTOE TA SENIOR RM REED J GRIFFINGL THOMASON A and DEUEL TF (1988) In vivo incisionalwound healing augmented by platelet-derived growth factor and re-combinant c-sis gene homodimeric proteins J Exp Med 167 974ndash987
PIERCE GF VANDE BERG J RUDOLPH R TARPLEY J andMUSTOE TA (1991) Platelet-derived growth factor-BB and trans-forming growth factor beta 1 selectively modulate glycosaminogly -cans collagen and myofibroblasts in excisional wounds Am JPathol 138 629ndash646
PIERCE GF TARPLEY JE YANAGIHARA D MUSTOE TA
FOX GM and THOMASON A (1992) Platelet-derived growthfactor (BB homodimer) transforming growth factor-b1 and basic fi-broblast growth factor in dermal wound healing Neovessel and ma-trix formation and cessation of repair Am J Pathol 140 1375ndash1388
PIERCE GF TARPLEY JE ALLMAN RM GOODE PS SER-DAR CM MORRIS B MUSTOE TA and VANDE BERG J(1994a) Tissue repair processes in healing chronic pressure ulcerstreated with recombinant platelet-derived growth factor BB Am JPathol 145 1399ndash1410
PIERCE GF YANAGIHARA D KLOPCHIN K DANILENKODM HSU E KENNEY WC and MORRIS CF (1994b) Stim-ulation of all epithelial elements during skin regeneration by kerati-nocyte growth factor J Exp Med 179 831ndash840
PIERCE GF TARPLEY JE TSENG J BREADY J CHANGD KENNEY WC RUDOLPH R ROBSON MC VANDEBERG J and REID P (1995) Detection of platelet-derived growthfactor (PDGF)-AA in actively healing human wounds treated withrecombinant PDGF-BB and absence of PDGF in chronic nonhealingwounds J Clin Invest 96 1336ndash1350
SINGER AJ and CLARK RA (1999) Cutaneous wound healingN Engl J Med 341 738ndash746
SOMASUNDARAM R and SCHUPPAN D (1996) Type I II IIIIV V and VI collagens serve as extracellular ligands for the iso-forms of platelet-derived growth factor (AA BB and AB) J BiolChem 271 26884ndash26891
SPRUGEL KH MCPHERSON JM CLOWES AW and ROSSR (1987) Effects of growth factors in vivo I Cell ingrowth intoporous subcutaneous chambers Am J Pathol 129 601ndash613
STEED DL (1995) Clinical evaluation of recombinant humanplatelet-derived growth factor for the treatment of lower extremitydiabetic ulcers Diabetic Ulcer Study Group J Vasc Surg 21 71ndash78
STEED DL (1998) Foundations of good ulcer care Am J Surg 17620S-25S
TYRONE JW MOGFORD JE CHANDLER LA MA C XIAY PIERCE GF and MUSTOE TA (2000) Collagen-embeddedplatelet-derived growth factor DNA plasmid promotes wound heal-ing in a dermal ulcer model J Surg Res 93 230ndash236
VOGT PM THOMPSON S ANDREE C LIU P BREUING KHATZIS D BROWN H MULLIGAN RC and ERIKSSON E(1994) Genetically modified keratinocytes transplanted to woundsreconstitute the epidermis Proc Natl Acad Sci USA 91 9307ndash9311
WIEMAN TJ (1998) Clinical efficacy of becaplermin (rhPDGF-BB)gel Becaplermin Gel Studies Group Am J Surg 176 74S-79S
WIEMAN TJ SMIELL JM and SU Y (1998) Efficacy and safetyof a topical gel formulation of recombinant human platelet-derivedgrowth factor-BB (becaplermin) in patients with chronic neuropathicdiabetic ulcers A phase III randomized placebo-controlled double-blind study Diabetes Care 21 822ndash827
WILSON JM (1996) Adenoviruses as gene-delivery vehicles NEngl J Med 334 1185ndash1187
XU J and CLARK RA (1996) Extracellular matrix alters PDGFregulation of fibroblast integrins J Cell Biol 132 239ndash249
XU J and CLARK RA (1997) A three-dimensional collagen latticeinduces protein kinase C-z activity Role in a2 integrin and collage-nase mRNA expression J Cell Biol 136 473ndash483
Address reprint requests toDr John Doukas
Selective Genetics Inc11035 Roselle Street
San Diego CA 92121
E-mail jdoukasselectivegeneticscom
Received for publication December 28 2000 accepted after re-vision February 23 2001
DOUKAS ET AL798

A second model utilized 7-cm2 full-thickness excisionalwounds placed on the backs of anesthetized rabbits Woundswere treated with AdPDGF-B formulated in 26 collagen (2 3
109 or 2 3 1011 virus particles per wound in 700-ml volumes)and then covered with OpSite dressing On day 3 7 28 or 90posttreatment blood was collected animals were perfused asdescribed above and the following organs were recoveredwound bed brain heart lung liver spleen kidney gonad andlymph nodes (axillary cranial mesenteric and posterior medi-astinal) Real-time quantitative TaqMan PCR was performedusing 45 two-step cycles with primers designed to amplify se-quences bridging the vector backbone and the PDGF-B pre-proregion (sense 59-GGATCTTCGAGTCGACAAGCTT-3 9 an-tisense 59-TAAGGGCTCCTCGAAATACTCTA-3 9) The re-sulting amplicons were detected with an internal fluorogenicprobe (59-TAGTGGTACTTAGCGACGACCCGC-3 9) and anABI Prism 7700 sequence detector (PE Applied BiosystemsFoster City CA) The initial target copy numbers present ineach reaction were quantified by extrapolation from standardcurves of AdPDGF-B DNA in the background of 1 mg of rab-bit liver DNA per reaction Each PCR contained 1 mg of testDNA with the exception of wound bed which contained 500ng per reaction and blood which contained the equivalent of10 ml of original sample Each test sample was assayed in du-plicate to control for PCR inhibitory substances a third reac-tion was spiked with 100 copies of AdPDGF-B DNA PCR dataare presented as AdPDGF-B genome copies per wound thelimit of quantitation (LOQ) was 10 copiesmg DNA or an av-erage of 105 copieswound
For those tissues scoring positive for PCR-amplifiable vec-tor we further performed real-time quantitative reverse tran-scriptase (RT)-PCR Reverse transcriptase reactions were per-formed with 100 ng of each test RNA per reaction and randomhexamer primers The resulting cDNAs were then used to am-plify both rabbit 18S rRNA cDNA and PDGF-B cDNA in sep-arate PCRs The vector-specific primers were designed to am-plify full-length 160-amino acid human PDGF-B mRNA(sense 59-CAAGCACACGCATGACAAGA-3 9 antisense 59-TTTCGTTATCGTAGTGTTTAAAGTGT-3 9) The resulting131-nucleotide amplicons were detected with an internal fluo-rogenic probe (59-AAACAAGTTGCTCGATGGATCCTTAT-CAGGCT-39) RT-PCRs were then normalized for total RNAby 18S rRNA content with a second pair of PCR primers RT-PCR data are presented as the relative amount of PDGF-BmRNA per unit 18S rRNA (in arbitrary units)
Histochemical analyses
For routine morphological assessment paraffin sections werestained according to the Masson trichrome procedure In addi-tion a blinded observer using a microscope equipped with oc-ular micrometers measured the area within sponges filled bygranulation tissue these values are expressed as the percentageof sponge interior occupied by tissue ( granulation fill) Forexcisional wounds trichrome-stained sections and an imageanalysis software package (Image-Pro Plus software Media Cy-bernetics Silver Spring MD) were used to determine the cross-sectional areas of granulation tissue and epithelium per wound(in mm2) In addition the percentage of wound closure was cal-culated according to the following formula [(original wound
diameter 2 epithelial gap length) original wound diameter] 3100
For immunohistochemistry paraffin sections were stainedwith biotinylated Griffonia (Bandeiraea) simplicifolia lectin I(BSL-I) horseradish peroxidase (HRP)-labeled streptavidin anddiaminobenzidine (DAB Vector Laboratories BurlingameCA) in order to detect vascular endothelium Mouse anti-Ki-67and HRP-labeled rabbit anti-mouse IgG antibodies followed byDAB were used to detect proliferating cells Mouse anti-humanPDGF-BB (Z2703 American Type Culture Collection) andHRPndashanti-mouse IgG antibodies followed by DAB were usedto detect human PDGF-BB protein Fluorescein isothiocyanate(FITC)-conjugated anti-adenovirus antibody (Accurate Chemi-cals Westbury NY) and the nuclear stain 496-diamidino-2-phenylindole (DAPI Molecular Probes) were used to detectinternalized adenovirus vectors Finally fibroblasts were iden-tified with Cy3-labeled anti-vimentin (Sigma St Louis MO)
For in situ hybridization procedures an [a-35S] UTP-labeledriboprobe prepared from the full-length human PDGF-B cDNAwas used as previously described (Gonzalez et al 1995) Asense riboprobe was used to control for nonspecific hybridiza-tions
Biochemical analyses
Tissue samples not processed for paraffin embedding wereplaced in 100 mM phosphate buffer containing 02 Triton X-100 (pH 78) and agitated at 55 msec for 20 sec in a Fast-Prep system (BIO 101 Vista CA) After centrifugation su-pernatants were analyzed for protein using a bicinchoninic acidassay (Pierce Rockville IL) and for DNA using the PicoGreenassay PDGF-BB protein content was determined with a humanPDGF-BB-specific ELISA (RampD Systems Minneapolis MN)
Statistical Analyses
Data are presented as arithmetic means 6 1 SD Groups ofthree or more means within individual studies were comparedby one-way analysis of variance (ANOVA) and the Fisher pro-cedure for least significant differences (StatView softwareAbacus Concepts Berkeley CA)
RESULTS
Adenovirus vectors can be immobilized in an activeform within matrices
As an initial step to the in vivo assessment of adenovirusndashmatrix formulations we first determined the activity profilesand release kinetics for vectors formulated in type I collagenand carboxymethylcellulose (CMC) Collagen was selected onthe basis of its successful use as a delivery matrix for proteinsand DNA (Grotendorst et al 1985 Mustoe et al 1987 1991Sprugel et al 1987 Khouri et al 1994 Bonadio et al 1999)as well as its ability to enhance tissue repair responses in fi-broblasts (Xu and Clark 1996 1997) Relatively low (015)and high (26) concentrations were examined reasoning thatthis would allow for either relatively short or long retentiontimes at application sites respectively CMC was selected on
DOUKAS ET AL788
TISSUE REPAIR USING GROWTH FACTOR GENES 789
FIG 3 Localization of gene vector and transgene product within neotissues PVA sponges implanted in rats were injected withAdPDGF-B formulated in 015 collagen (2 3 1010 virus particles per sponge) and paraffin sections were stained as follows(A) Day 1 posttreatment anti-adenovirus immunostain to detect AdPDGF-B (green) DAPI stain to detect cell nuclei (blue) (B)Day 4 posttreatment in situ hybridization using human PDGF-B gene probe (C) Day 1 posttreatment anti-human PDGF-BBprotein immunostain positively stained leukocytes (arrowheads) and fibroblasts (arrows) are indicated (D) Day 6 posttreatmentanti-PDGF-BB immunostain (E) Day 8 posttreatment anti-PDGF-BB immunostain (F) Day 8 post- treatment immunostains todetect PDGF-BB protein (green) and vimentin (red) yellow fluorescence indicates PDGF-BB and vimentin colocalization bluefluorescence indicates cell nuclei (DAPI stain) Original magnifications (AndashC E and F)3 400 (D) 31000
the basis of its clinical use for the delivery of PDGF-BB pro-tein (Steed 1995)
Matrix influences on vector activity were examined by in-cubating AdLuc formulations at 37degC for 60 min followed bymatrix dissolution and vector bioassay (luciferase productionby 293 cells) This is an important test as adenoviruses arequickly inactivated under unfavorable physical and chemicalconditions (Nyberg-Hoffman and Aguilar-Cordova 1999)None of the matrices examined had a deleterious effect on vec-tor activity (90 6 12 106 6 5 and 139 6 37 of control ac-tivity for 015 collagen 26 collagen and CMC respec-tively) To further model in vivo vector stability we alsoincubated AdPDGF-B formulated in 26 collagen with woundfluid for 72 hr at 37degC prior to vector recovery and analysisWe observed no reduction in the level of PDGF-BB productionfrom cells transduced with AdPDGF-B exposed to wound fluidas compared with vector exposed to virus buffer (30 6 5 vs20 6 3 ng of PDGF-BB produced per milliliter of culturemedium respectively n 5 3)
As these data support the suitability of the selected matricesfor in vivo use we next determined their influence on vectorrelease kinetics (Fig 1) When placed in water collagen ma-trices retained the majority of their immobilized vectors with015 and 26 collagen releasing only 17 6 3 and 3 6 1 ofvector by 24 hr respectively By contrast 48 6 3 of AdLucwas released from CMC within 30 min and 61 6 2 by 6 hrThis was not unexpected as CMC is fairly water soluble andas both CMC and adenoviral particles are negatively chargedTherefore collagen matrices in a concentration-dependentfashion display more favorable kinetics for localizing and re-taining adenovirus vectors at delivery sites than does CMC
Collagen-immobilized adenoviruses induce distinctneotissues in vivo
Initial in vivo tests of matrix-immobilized vectors were per-formed with an established model of de novo tissue generation(Buckley et al 1985 Sprugel et al 1987 LeGrand et al1993) PVA sponges implanted subcutaneously in rats were in-jected with a single dose of adenovirus formulated in either col-lagen or CMC and then analyzed for tissue formation Forgrowth factor transgenes we selected platelet-derived growth
factor B (PDGF-B) vascular endothelial growth factor (VEGF)and fibroblast growth factor 2 (FGF2) because of their well-known mitogenic activities
AdPDGF-B formulated in 015 collagen induced granula-tion tissue formation in a dose-responsive manner (Table 1)Compared with vehicle controls delivering 2 3 1010 virus par-ticles induced a 17- to 23-fold increase in sponge protein con-tent (p 00002) a 2- to 27-fold increase in DNA content (p
00002) and a 29- to 43-fold increase in granulation tissue fill(p 00002) Trichrome-stained sections revealed the nearcomplete fill of sponge interiors with well-formed granulationtissue by day 6 posttreatment (Fig 2A) Expression of Ki-67a nuclear protein upregulated in proliferating cells (Gerdes etal 1983) established that both vascular endothelium (arrow-heads Fig 2B) and fibroblasts (arrows Fig 2B) had prolifer-ated in response to PDGF-B gene delivery AdFGF2 and Ad-VEGF also enhanced protein and DNA content within sponges(Table 1) However these vectors induced less granulation tis-sue deposition as compared with AdPDGF-B and the tissuesformed were histologically distinct
Tissues present in AdFGF2-treated sponges were highly vas-cular as revealed by the endothelial-reactive lectin BSL-I (Fig2D) Many of the infiltrating mononuclear cells also reactedpositively with BSL-I lectin suggesting that these cells wereendothelial cells or endothelial precursors AdFGF2 did nothowever induce the formation of classic granulation tissue aslittle collagen deposition was observed demonstrated by thepaucity of blue-staining material in trichrome-stained sections(Fig 2C) AdVEGF also induced heavily vascularized tissues(Fig 2E and F) but with greater extracellular collagen deposi-tion than AdFGF2 Relative to AdPDGF-B-induced tissueshowever AdVEGF-induced tissues were disorganized con-tained few fibroblasts and were markedly edematous Finallywhen AdLuc was delivered as a control treatment no signifi-cant increases in protein DNA or granulation tissue were ob-served compared with collagen vehicle alone (Table 1)Trichrome-stained sections revealed sparse inflammatory cellinfiltrates within AdLuc-treated sponges (Fig 2G) which com-pared with the near absence of infiltration after delivery of col-lagen vehicle alone (Fig 2H) suggested a limited antiviral response
Unlike the 015 collagen formulations described above
DOUKAS ET AL790
TABLE 2 NEOTISSUE FORMATION AFTER PDGF-B GENE OR PDGF-BB PROTEIN DELIVERYa
Granulation Protein DNATreatment fill () (mgsponge) (mgsponge)
015 Collagen vehicle 28 6 13b 16 6 2b 103 6 22b
AdPDGF-B 81 6 15b 30 6 6b 218 6 28b
PDGF-BB 100 mg 64 6 12c 22 6 4c 155 6 26c
PDGF-BB 10 mg qod 3 3d 77 6 9b0 31 6 8b 230 6 75b
aPVA sponges implanted in rats were injected with either 015 collagen vehicle or collagen containing AdPDGF-B as described in Table 1 Alternatively PDGF-BB protein was delivered as a single 100-mg dose on day 4 postimplantation or as10-mg doses on days 4 6 and 8 Sponges were removed on day 12 postimplantation and processed to determine the percent granulation fill as well as total protein and DNA contents Data are presented as means 6 SD (n 5 4ndash8)
bp 00001 versus collagen control and p 005 versus 100-mg PDGF-BBcp 003 versus collagen controldqod 3 3 Every other day three times
TISSUE REPAIR USING GROWTH FACTOR GENES 791
TABLE 3 INFLUENCE OF ADENOVIRUSndashMATRIX FORMULATIONS ON ISCHEMIC WOUND HEALINGa
Granulation Epithelial Wound closureTreatment Model system area (mm2) area (mm2) ( complete)
Aqueous buffer Cartilage intact 10 6 08 05 6 03 61 6 226 mm day 10
AdPDGF-B in Cartilage intact 24 6 22 05 6 01 73 6 28aqueous buffer 6 mm day 10
015 Collagen Cartilage intact 05 6 03 05 6 02 89 6 14vehicle 6 mm day 10
AdPDGF-B in Cartilage intact 16 6 09b 09 6 03c 97 6 7015 collagen 6 mm day 10
Aqueous buffer Cartilage removed 45 6 08 08 6 02 95 6 96 mm day 7
AdPDGF-B in Cartilage removed 40 6 15 11 6 05 82 6 22aqueous buffer 6 mm day 7
015 Collagen Cartilage removed 36 6 13 06 6 02 88 6 22vehicle 6 mm day 7
AdPDGF-B in Cartilage removed 70 6 14b 07 6 03 79 6 22015 collagen 6 mm day 7
26 Collagen Cartilage removed 04 6 05 01 6 01 24 6 15vehicle 8 mm day 8
AdPDGF-B in Cartilage removed 51 6 25b 06 6 03b 52 6 25c
26 collagen 8 mm day 8
aExcisional wounds (6 or 8 mm in diameter) were placed in ischemic rabbit ears with underlying cartilage left intact or re-moved Wounds were then treated with AdPDGF-B formulated in aqueous virus buffer or collagen control treatments consistedof vehicle alone For 6-mm wounds virus was applied as 2 3 109 particles per wound for 8-mm wounds as 4 3 109 particlesper wound On days 7ndash10 posttreatment wounds were harvested and processed as trichrome-stained paraffin sections whichwere then used to quantify newly formed granulation tissue and epithelium (cross-sectional area in mm2) and the degree of woundsurface closure (where 100 equals complete closure) Data are presented as means 6 SD (n 5 4ndash8)
bp 0009 versus vehicle controlcp 005 versus vehicle control
26 collagen formulations could not be reliably examined inthe PVA sponge model as their relatively high viscosity pre-vented uniform filling of sponges by syringe CMC-formulatedvectors were also unsuitable for this model system as theyproved highly inflammatory (data not shown) These formula-tions therefore were evaluated in more appropriate excisionalwound models (see below)
Tissue repair cells are transduced by collagen-immobilized adenoviruses
On the basis of the robust activity of collagen-formulatedAdPDGF-B we elected to further examine this vectorndashmatrixcombination first by seeking to correlate PDGF-B gene deliv-ery with subsequent transgene and protein expression WhenPVA sponges treated with 015 collagenndashAdPDGF-B werestained with both an anti-adenovirus antibody and the nuclearstain DAPI the majority of cells present 1 day after gene de-livery had bound andor internalized adenovirus (Fig 3A) Insitu hybridization revealed that these cells were successfullytransduced by virus as they contained human PDGF-B mRNA(Fig 3B) By contrast hybridization product was not detectedwith a sense riboprobe or when AdLuc-treated sponges wereexamined (data not shown)
We next used a human PDGF-BB-specific antibody to iden-tify the cell types responsible for transgene expression By day
1 postdelivery of 015 collagenndashAdPDGF-B PDGF-BB pro-tein was localized to leukocytes (arrowheads) and fibroblasts (ar-row Fig 3C) With time PDGF-BB protein was detected boundto the extracellular matrix (ECM) surrounding positively stainedcells (Fig 3D) This last observation indicates that a reservoir ofPDGF-BB protein develops within treated tissues and thus mayprolong the histogenic effects of this growth factor Finally byday 8 the majority of immunoreactivity had abated with pri-marily microvascular endothelium remaining positive (Fig 3E)However scattered fibroblasts could still be shown to producePDGF-BB protein by dual immunohistochemistry with anti-PDGF-BB and anti-vimentin antibodies (Fig 3F)
Multiple administrations of PDGF-BB protein are required to approximate the histogenic effects of collagenndashAdPDGF-B
To directly compare gene therapy with the more conven-tional approach of growth factor protein delivery we next quan-tified tissue formation in response to either PDGF gene or pro-tein delivery A single injection of 015 collagenndashAdPDGF-Benhanced granulation tissue filling of sponges by 3-fold versusvehicle alone (p 00001) and sponge protein and DNA lev-els by 2-fold (p 00001 Table 2) Using a human PDGF-BB-specific ELISA this growth factor was detected at 54 6 13ngsponge (n 5 8) By contrast when PDGF-BB protein was
delivered as a single dose nearly 2000-fold in excess of thisconcentration the tissue formation responses observed (proteinand DNA accumulation and granulation tissue formation) weresignificantly lower (p 005 Table 2) In fact repeated dos-ing with PDGF-BB protein was required in order to achieve re-sponses comparable to a single administration of the PDGF-Bgene These data therefore support our hypothesis that the abil-ity of gene delivery to establish prolonged in situ growth fac-tor production translates into greater histogenesis than that seenwith growth factor proteins
CollagenndashAdPDGF-B induces complete healing of ischemic wounds
Nonhealing wounds are a major risk in chronically ischemictissues as low oxygen tension greatly impairs tissue repair pro-cesses We therefore compared the ability of matrix versusaqueous formulated AdPDGF-B to repair ischemic excisionalwounds Several models were employed to compare variationsin wound size and condition so as to allow for a more com-plete picture of tissue repair
In the first model system 6-mm-diameter wounds were cre-ated in ischemic rabbit ears by removal of epidermal and der-mal layers but not underlying cartilage This model has beenused in previous studies of growth factor proteins and genes(Ahn and Mustoe 1990 Mustoe et al 1994 Liechty et al1999) and was therefore employed to allow comparison withthese reports However it represents an artificial system as thepresence of a cartilage layer restricts both treatment activity andhealing to wound margins and in addition the initially acellu-lar wound bed forms a cup that artifactually retains aqueoustreatments As would be predicted we found a trend towardgranulation tissue formation in this model after the applicationof AdPDGF-B formulated in aqueous buffer (Table 3) How-ever this response did not reach the level of statistical signifi-cance as tissue development was highly variable (note the highstandard deviation value) In addition epithelial regenerationand wound closure were minimal to unaffected By contrastAdPDGF-B formulated in 015 collagen enhanced granula-tion tissue area by 32-fold and epithelial area by 18-fold overthat achieved with vehicle alone (p 0009 and 005 respec-tively) Although near complete closure of epithelial gaps wasalso achieved the high level of self-healing in control-treatedgroups (89 wound closure) precluded statistical significance
In an alternative model design subdermal cartilage was com-pletely removed from excisional wounds creating beds whosefloors now consisted of dermal tissue (Pierce et al 1994b)This design allows for cellular responses from the entire woundbed as well as the opportunity for vector migration beyond
treatment areas We now observed that aqueous formulated Ad-PDGF-B failed to induce even a trend toward tissue regenera-tion (Table 3) Rather the vector appears to have seeped throughthe wound bed floor as inflammatory cell infiltrates and fociof fibroblast proliferation were observed in the underlying der-mis and at wound margins (Fig 4A) Immunohistochemistryconfirmed the production of human PDGF-BB at these sites(Fig 4B) CMC-formulated AdPDGF-B also failed to induceany meaningful tissue repair Wounds treated with this formu-lation showed a diffuse inflammatory response within thewound bed and wound surfaces were overlain with fibrin clotsrather than regenerating epithelium (Fig 4C and D) By con-trast AdPDGF-B formulated in 015 collagen enhanced gran-ulation tissue deposition 19-fold within wound beds versus ve-hicle controls (p 0002) and wounds were extensivelyepithelialized (Table 3) Neither epithelial regeneration norwound closure achieved significance however as the high de-gree of self-healing achieved in this particular model (see ve-hicle alone group) most likely masked transgene-stimulated re-sponses
To address these model limitations as our next system wecreated 8-mm wounds in ischemic rabbit ears by removingepidermal dermal and cartilage layers reasoning that largerexcisional wounds would display limited self-healing In ad-dition this model could readily accommodate 26 collagenformulations which proved difficult to reproducibly apply insmaller wounds Compared with control wounds treated withcollagen vehicle alone wounds treated with AdPDGF-B for-mulated in 26 collagen achieved a 12-fold enhancementin granulation tissue fill and a 6-fold enhancement in re-ep-ithelialization by day 8 posttreatment (p 0009 Table 3)In addition wound closure was only 24 complete in colla-gen vehicle-treated wounds by day 8 but 52 complete inwounds treated with collagen-formulated AdPDGF-B (p
005) Histologically AdPDGF-B-treated wounds showed nosigns of tissue hyperplasia or chronic inflammation but ratheran orderly repair process marked by a regenerated epitheliallayer overlying a wound bed filled with granulation tissue(Fig 4E and F)
CollagenndashAdPDGF-B induces normal long-term tissue repair
Our choice of adenoviruses for transgene delivery was partlybased on the reasoning that as these vectors establish transientgene expression they would not lead to hyperproliferative re-sponses or scar formation To test this hypothesis we treatedrabbit ear excisional wounds with AdPDGF-B formulated in015 collagen and examined tissue repair responses out to
DOUKAS ET AL792
FIG 4 Influence of adenovirusndashmatrix formulations on excisional wound repair Excisional wounds (6 or 8 mm in diameter andextending through underlying cartilage layers) were placed in ischemic rabbit ears bars indicate original wound depth (determinedfrom cartilage visible at wound margins) Wounds were then treated with AdPDGF-B formulated in either virus buffer CMC orcollagen and on day 7 or 8 posttreatment processed for histology or immunohistochemistry An identical design was used to ex-amine long-term healing on day 90 except that wounds were created in nonischemic ears (A) Day 7 buffer-formulated AdPDGF-B-treated 6-mm wound trichrome stain (B) Day 7 buffer-formulated AdPDGF-B-treated 6-mm wound anti-PDGF-BB proteinimmunostain (C and D) Day 7 CMC-formulated AdPDGF-B-treated 6-mm wound trichrome stains (E and F) Day 8 26 col-lagen-formulated AdPDGF-B-treated 8-mm wound trichrome stains (G and H) Day 90 015 collagen-formulated AdPDGF-B-treated 6-mm wound trichrome stains Original magnification (A C E and G) 340 (B D F and H) 3200
TISSUE REPAIR USING GROWTH FACTOR GENES 793
DOUKAS ET AL794
TABLE 4 BIODISTRIBUTION OF AdPDGF-B IN EXCISIONAL WOUNDSa
Positive samplestotal assayed
Tissue AdPDGF-B dose Day 3 Day 7 Day 28 Day 90
Wound bed 2 3 109 particles 66 66 66b 06Axillary lymph nodes 2 3 109 particles 02 ND 06 06
Wound bed 2 3 1011 particles 66 66 66 46c
Axillary lymph nodes 2 3 1011 particles 66 ND 66d 26e
aFull-thickness excisional wounds (7 cm2) were placed on the backs of rabbits and AdPDGF-B formulated in 26 collagenwas applied as either 2 3 109 or 2 3 1011 virus particles per wound On days 3ndash90 posttreatment wound beds and a panel oforgans were harvested for real-time PCR quantification of viral genome Data are shown for wound bed and axillary lymph nodesamples as the number of samples that yielded amplifiable signals per total number assayed ND not determined
bThree of six samples scored below the level of quantitation (LOQ 10ndash100 copiesmg DNA)cAll four positive samples scored below the LOQdThree of six samples scored below the LOQeBoth positive samples scored below the LOQ
180 days posttreatment (Fig 5) PDGF-B gene delivery en-hanced total ear thickness relative to controls on day 28 (229 6
020 vs 179 6 019 mm p 00001) and day 60 (192 6 001vs 182 6 011 mm p 0005) as anticipated on the basis ofthe ability of this formulation to induce granulation tissue for-mation By day 90 posttreatment however there was no mea-surable difference in ear thickness between AdPDGF-B andcontrol-treated groups and this relationship continued out today 180 indicating that growth factor gene delivery did not in-duce excessive scar formation This was also confirmed histo-logically AdPDGF-B-treated wounds on day 90 and beyondwere composed of a thin outer keratin layer an underlying ep-ithelial layer of equivalent thickness to nonwounded areas anda collagen-rich dermis devoid of any signs of tissue hyperpla-sia (Fig 4G and H)
Collagen immobilization limits adenovirus vectorbiodistribution beyond treatment sites
As a final measure of the value of matrix immobilization forgene delivery we determined the biodistribution patterns ofvectors after their in vivo delivery In the first model systemused AdPDGF-B formulated in 015 collagen was applied torabbit ear wounds at equivalent doses as previously describedwounds were extended through underlying cartilage but vas-cular supplies were not disturbed so as to permit maximal vec-tor dissemination By PCR no adenoviral DNA was detectablein lung spleen brain cervical lymph nodes or gonads on day1 3 7 or 14 (n 5 6 per group) In the liver one of six sam-ples was positive on days 3 and 7 but none on day 14 in serumonly one of six samples tested positive on day 14 (equivalentof 500-ml serum volume) By contrast adenovirus was detectedin eight of eight wound bed samples at all time points exam-ined
In a second model system excisional wounds placed on thebacks of rabbits were treated with AdPDGF-B formulated in26 collagen Because of their anatomical placement thismodel allowed for the creation of larger excisional wounds (7-cm2 total area) than those placed in rabbit ears (03 cm2) and
consequently larger treatment volumes and vector doses (2 3109 or 2 3 1011 virus particles per wound) At the lower doseof 2 3 109 particles PCR-amplifiable adenoviral DNA was notdetectable beyond wound beds on day 3 7 28 or 90 Tissuessampled and found not to contain vector included blood heartlung liver kidney brain spleen lymph nodes and gonads (n 5
6group) In wound beds adenoviral DNA was detected at alltime points except for day 90 (Table 4 and Fig 6) Vector lev-els did decrease however by 38-fold between days 7 and 28with three of six samples falling below the level of quantita-tion (LOQ) by real-time PCR at the latter time point (Fig 6)
At a 100-fold higher vector dose of 2 3 1011 particles perwound PCR-amplifiable adenoviral DNA was once again un-detectable in the majority of tissues sampled Except for a sin-gle day 7 liver sample and a single day 7 brain sample (bothbelow the LOQ) adenoviral DNA was only detectable directlyin wound beds or in the axillary lymph nodes that drain woundsites (Table 4) Moreover three of six positive axillary nodesamples scored below the LOQ on day 28 as did both positivesamples on day 90 indicating that they contained relatively lit-tle vector Within wound beds adenoviral DNA was detectedat quantifiable levels out to day 28 and at detectable but non-quantifiable levels on day 90 DNA copy numbers remainedsteady between days 3 and 7 dropped 107-fold between days7 and 28 and a further 1662-fold by day 90 Finally at eachtime point DNA copy numbers in wounds treated with 2 3
1011 particles were approximately 100-fold higher than thosefound in wounds treated with 2 3 109 particles thus confirm-ing the linearity of our assay system
To better define the time course of human PDGF-BB pro-duction we also quantified transgene mRNA levels in woundbed samples treated at 2 3 109 particles per wound This treat-ment dose was selected as representative of the virus particleconcentration capable of inducing complete healing in ischemicear wounds Quantifiable levels of human PDGF-B mRNAwere detectable in treated dorsal wounds at days 3 7 and 28(Fig 6) with levels decreasing 14-fold between days 3 and 7and 5-fold between days 7 and 28 The more sensitive tech-nique of real-time RT-PCR therefore demonstrates that trans-
TISSUE REPAIR USING GROWTH FACTOR GENES 795
gene expression extends well beyond the 8-day time period sug-gested using anti-PDGF-BB immunohistochemistry as a de-tection system (Fig 3)
DISCUSSION
These studies demonstrate that immobilization of gene ther-apy vectors in collagen-based matrices enables their efficientdelivery and activity in vivo Matrix immobilization achievedprolonged transgene-encoded growth factor production and asa consequence robust tissue repair By contrast aqueous vehi-cles failed to retain adenoviruses at application sites resultingin diffuse inflammation rather than productive tissue regenera-tion These observations confirm our basic hypothesis that ma-trix immobilization of growth factor-encoding gene therapyvectors represents a promising approach to tissue repair
Although de novo tissue deposition was achievable with sev-eral growth factor genes PDGF-B proved the most suitable forrepair of cutaneous defects A single administration of colla-gen-immobilized AdPDGF-B rapidly induced the formation ofhighly cellular and vascularized tissues with dense ECMs richin collagen By contrast AdFGF2 induced a primarily vascu-lar response with little collagen deposition FGF2 induces therelease of matrix metalloproteinase 1 or interstitial collagenase(Buckley-Sturrock et al 1989) and this may underlie the rel-ative paucity of ECM accumulation VEGF gene delivery alsoinduced highly vascular responses however the enhanced per-meability characteristic of VEGF-induced vasculature (Dvoraket al 1995) led to edema within nascent tissues In fact much
of the enhanced protein and DNA deposition observed in Ad-VEGF-treated PVA sponges may well derive from fluid exu-dates rather than actual tissue formation Finally the inabilityof AdLuc delivery to induce anything beyond a limited in-flammatory response confirms that tissue formation was de-pendent on growth factor gene delivery
The robust activity of PDGF-B gene delivery was expectedas PDGF-BB protein initiates multiple aspects of tissue forma-tion including cellular influx and proliferation ECM deposi-tion and tissue remodeling (Pierce et al 1988 1991 1994a)Indeed PDGF-BB is the only growth factor protein to have suc-cessfully completed human clinical trials and be approved forthe treatment of dermal wounds (Steed 1995 drsquoHemecourt etal 1998 Wieman 1998 Wieman et al 1998) We observedthat collagen-formulated AdPDGF-B induced the complete re-pair of excisional skin defects without unwanted long-term ef-fects such as the development of hypertrophic scars Endoge-nous growth factors other than PDGF-BB however most likelymediated the enhanced re-epithelialization observed in thesewounds as epithelial regeneration is driven by members of theepidermal growth factor and FGF families (Pierce et al 1994bDanilenko et al 1995) Our data indicate nonetheless that tis-sue regeneration and repair were initiated and to a great degreedriven by transgene-encoded PDGF-BB
Despite the known activity of PDGF-BB protein we wereable to demonstrate greater tissue deposition after gene deliv-ery as compared with the use of recombinant growth factor pro-tein A single application of PDGF-BB protein could not equalthe ability of PDGF-B gene therapy to induce neotissue for-mation even at doses well in excess of that induced in situ byAdPDGF-B and in excess of that used in human clinical trials
FIG 5 Influence of collagen-formulated AdPDGF-B on long-term tissue repair Excisional wounds (6 mm in diameter withcartilage remaining intact) were placed in nonischemic rabbit ears and treated with either 015 collagen alone (open columns)or AdPDGF-B formulated in this vehicle (solid columns) On days 28ndash180 posttreatment total ear thickness at the site of eachwound was measured (in mm) with calipers Data are presented as means 6 SD (n 5 3) Treatment groups differ by p 00001groups differ by p 0005
(Steed 1995 drsquoHemecourt et al 1998 Wieman 1998 Wie-man et al 1998) In fact repeated administrations of PDGF-BB protein were required to approach the level of tissue for-mation observed after a single administration of AdPDGF-BThese data support our hypothesis that sustained localizedgrowth factor production is required for robust tissue repair
In further support of this hypothesis we demonstrated thatmRNA encoding human PDGF-B was present in excisionalwounds as late as day 28 after collagen-formulated AdPDGF-B administration By contrast previous studies of PDGF-BBprotein found that the great majority of this growth factor wasgone from treated wounds 1 day postapplication and that anytissue maturation subsequently observed was most likely dueto the upregulation of endogenous growth factors (Pierce et al1992 1995) We also demonstrated that repair cells such asmononuclear leukocytes endothelial cells and fibroblasts pres-ent with developing neotissues represent the source of both
transgene transcription and PDGF-BB production In additiona depot of human PDGF-BB was detected bound to the colla-gen delivery matrix and ECM of these tissues This was antici-pated as PDGF-BB contains collagen-binding motifs (Soma-sundaram and Schuppan 1996) We hypothesize that subsequentmatrix metalloproteinase activity by repair cells will serve togenerate localized release of this sequestered growth factor pooland as a consequence further drive tissue regeneration Theseevents which are central to tissue remodeling should be directlyenhanced by collagen matrices as type I collagen stimulates me-talloproteinase production integrin expression and cellular ac-tivation in PDGF-stimulated fibroblasts (Xu and Clark 19961997)
An additional rationale for employing collagen matrices wasto physically immobilize vectors This was confirmed in vivowhere collagen matrices maintained AdPDGF-B at deliverysites for at least 28 days and limited vector migration to other
DOUKAS ET AL796
FIG 6 Persistence of collagen-formulated vector and transgene transcripts in excisional wounds Full-thickness excisionalwounds (7 cm2) were placed on the dorsal surface of rabbits and treated with AdPDGF-B formulated in 26 collagen at either2 3 109 or 2 3 1011 virus particles per wound (open and closed columns respectively) Wounds were then covered with OpSitedressing and on days 3 7 or 28 posttreatment wound beds were harvested for real-time quantitative PCR and RT-PCR analy-ses PCR data are presented in the upper graph as AdPDGF-B copies per wound RT-PCR data are presented in the lower graphas the relative amount of PDGF-B mRNA per unit 18S rRNA (in arbitrary units) All data points are means 6 SD (n 5 6)
tissues or organs In vitro tests also established that collagenmatrices not only prevent vector loss due to diffusion but pre-serve vector activity despite prolonged incubation in acutewound fluid Successful vector immobilization and tissue re-pair could be achieved with both 015 collagen and 26 col-lagen suggesting flexibility in the final vehicle formulation re-quired for effective vector delivery This flexibility was neededin the present studies as 26 collagen formulations proveddifficult to deliver to PVA sponges and 6-mm excisionalwounds This would not be of concern in clinical settings how-ever where wound beds are easily accessible and generally sev-eral square centimeters in area By contrast CMC was inef-fective at retaining vector in aqueous environments Moreimportantly this matrix was itself inflammatory and whencombined with adenovirus the net result was inflammationrather than tissue repair We are currently examining the util-ity of other matrices such as fibrin and hyaluronic acid whichbecause of their more provisional nature may offer yet greatercellular migration into wounds as compared with type I colla-gen
Although an aqueous-based AdPDGF-B formulation hasbeen previously shown to enhance tissue formation (Liechty etal 1999) this was achieved with a model system that artifi-cially retains vectors within treatment sites In fact the presentstudies demonstrate that any tissue repair observed after Ad-PDGF-B delivery in a nongelling liquid is dependent on the useof this model system In wounds not designed to retain appliedtreatments aqueous-formulated AdPDGF-B seeped into sur-rounding tissues and led to hyperplasia within these areas ratherthan to tissue regeneration within the active wound bed Colla-gen-immobilized AdPDGF-B on the other hand did persist inthese wound beds and led to significant enhancements in gran-ulation tissue formation as well as enhanced wound re-epithe-lialization and wound closure The significance of these activ-ities is further substantiated considering that they wereachievable in 8-mm-diameter ischemic wounds which withinthe time frame examined could not self-heal to any meaning-ful degree in the absence of gene therapy However as all theanimal models employed in these studies will eventually self-heal given sufficient time the full value of matrix-immobilizedgene therapy vectors remains to be confirmed in human clini-cal trials
In conclusion we present evidence that matrix-immobilizedgene therapy vectors encoding appropriate growth-promotinggenes represent a promising approach to tissue regeneration andrepair This basic concept can be expanded to include alterna-tive matrices such as controlled-release formulations as wellas tissue-specific growth factors Furthermore the addition oftargeting ligands to adenovirus vectors (eg FGF2) can en-hance their ability to transduce cells such that tissue repair re-sponses comparable to nontargeted vectors can be achieved butat significantly lower vector doses (Chandler et al 2000a)With appropriate design and application schedules one couldconceivably time the release of multiple growth factors to spe-cific stages of a tissue repair cascade In addition we have foundin preliminary studies that collagen-immobilized nonviral vec-tors such as PDGF-B plasmids which have potentially morefavorable safety profiles than adenovirus vectors can also en-hance tissue formation in vivo (Chandler et al 2000b Tyroneet al 2000) Such flexibility should allow for the widespreadapplication of gene therapy to the treatment of injured tissues
ACKNOWLEDGMENTS
We thank Jeff Davidson (Vanderbilt University School ofMedicine) for assistance in establishing the PVA sponge modelCarl-Henrik Heldin (Ludwig Institute for Cancer Research) forthe PDGF-B gene construct and Emelie Amburn Lara AsatoSharon Chang Gail Fieser Lydia Greenlees Rebecca Smokerand Linda Manza for excellent technical assistance This pub-lication was made possible in part by NIH grants 1R43AR46154(JD) and 5P01CA25874 (MH)
REFERENCES
AHN ST and MUSTOE TA (1990) Effects of ischemia on ulcerwound healing A new model in the rabbit ear Ann Plast Surg 2417ndash23
ANDREE C SWAIN WF PAGE CP MACKLIN MDSLAMA J HATZIS D and ERIKSSON E (1994) In vivo trans-fer and expression of a human epidermal growth factor gene accel-erates wound repair Proc Natl Acad Sci USA 91 12188ndash12192
BENN SI WHITSITT JS BROADLEY KN NANNEY LBPERKINS D HE L PATEL M MORGAN JR SWAIN WFand DAVIDSON JM (1996) Particle-mediated gene transfer withtransforming growth factor-b1 cDNAs enhances wound repair in ratskin J Clin Invest 98 2894ndash2902
BONADIO J SMILEY E PATIL P and GOLDSTEIN S (1999)Localized direct plasmid gene delivery in vivo Prolonged therapyresults in reproducible tissue regeneration Nat Med 5 753ndash759
BUCKLEY A DAVIDSON JM KAMERATH CD WOLT TBand WOODWARD SC (1985) Sustained release of epidermalgrowth factor accelerates wound repair Proc Natl Acad Sci USA82 7340ndash7344
BUCKLEY-STURROCK A WOODWARD SC SENIOR RMGRIFFIN GL KLAGSBRUN M and DAVIDSON JM (1989)Differential stimulation of collagenase and chemotactic activity in fi-broblasts derived from rat wound repair tissue and human skin bygrowth factors J Cell Physiol 138 70ndash78
CHANDLER LA DOUKAS J GONZALEZ AM HOGANSONDK GU DL MA C NESBIT M CROMBLEHOLME TMHERLYN M SOSNOWSKI BA and PIERCE GF (2000a)FGF2ndashTargeted adenovirus encoding platelet-derived growth factor-B enhances de novo tissue formation Mol Ther 2 153ndash160
CHANDLER LA MA C GONZALEZ AM DOUKAS JNGUYEN T PIERCE GF and PHILLIPS ML (2000b) Ma-trix-enabled gene transfer for cutaneous wound repair Wound Re-pair Regen 8 473ndash479
DANILENKO DM RING BD TARPLEY JE MORRIS BVAN GY MORAWIECKI A CALLAHAN W GOLDEN-BERG M HERSHENSON S and PIERCE GF (1995) Growthfactors in porcine full and partial thickness burn repair Differing tar-gets and effects of keratinocyte growth factor platelet-derivedgrowth factor-BB epidermal growth factor and neu differentiationfactor Am J Pathol 147 1261ndash1277
DEUEL TF KAWAHARA RS MUSTOE TA and PIERCE GF(1991) Growth factors and wound healing Platelet-derived growthfactor as a model cytokine Annu Rev Med 42 567ndash584
DrsquoHEMECOURT PA SMIELL JM and KARIM MR (1998) So-dium carboxymethylcellulose aqueous-based gel vs becaplermin gelin patients with nonhealing lower extremity diabetic ulcers Wounds10 69ndash75
DOUKAS J HOGANSON DK ONG M YING W LACEYDL BAIRD A PIERCE GF and SOSNOWSKI BA (1999)Retargeted delivery of adenoviral vectors through fibroblast growthfactor receptors involves unique cellular pathways FASEB J 131459ndash1466
TISSUE REPAIR USING GROWTH FACTOR GENES 797
DVORAK HF BROWN LF DETMAR M and DVORAK AM(1995) Vascular permeability factorvascular endothelial growth fac-tor microvascular hyperpermeability and angiogenesis Am JPathol 146 1029ndash1039
EMING SA MEDALIE DA TOMPKINS RG YARMUSHML and MORGAN JR (1998) Genetically modified human ker-atinocytes overexpressing PDGF-A enhance the performance of acomposite skin graft Hum Gene Ther 9 529ndash539
EMING SA WHITSITT JS HE L KRIEG T MORGAN JRand DAVIDSON JM (1999) Particle-mediated gene transfer ofPDGF isoforms promotes wound repair J Invest Dermatol 112297ndash302
GERDES J SCHWAB U LEMKE H and STEIN H (1983) Pro-duction of a mouse monoclonal antibody reactive with a human nu-clear antigen associated with cell proliferation Int J Cancer 3113ndash20
GONZALEZ AM BERRY M MAHER PA LOGAN A andBAIRD A (1995) A comprehensive analysis of the distribution ofFGF-2 and FGFR1 in the rat brain Brain Res 701 201ndash226
GREENHALGH DG (1996) The role of growth factors in woundhealing J Trauma 41 159ndash167
GROTENDORST GR MARTIN GR PENCEV D SODEK Jand HARVEY AK (1985) Stimulation of granulation tissue for-mation by platelet-derived growth factor in normal and diabetic ratsJ Clin Invest 76 2323ndash2329
KHOURI RK HONG SP DEUNE EG TARPLEY JE SONGSZ SERDAR CM and PIERCE GF (1994) De novo genera-tion of permanent neovascularized soft tissue appendages by platelet-derived growth factor J Clin Invest 94 1757ndash1763
LEGRAND EK SENTER LH GAMELLI RL and KIORPESTC (1993) Evaluation of PDGF-BB PDGF-AA bFGF IL-1 andEGF dose responses in polyvinyl alcohol sponge implants assessedby a rapid histologic method Growth Factors 8 315ndash329
LIECHTY KW NESBIT M HERLYN M RADU A ADZICKNS and CROMBLEHOLME TM (1999) Adenoviral-mediatedoverexpression of platelet-derived growth factor-B corrects ischemicimpaired wound healing J Invest Dermatol 113 375ndash383
LYNCH SE COLVIN RB and ANTONIADES HN (1989)Growth factors in wound healing J Clin Invest 84 640ndash646
MUSTOE TA PIERCE GF THOMASON A GRAMATES PSPORN MB and DEUEL TF (1987) Accelerated healing of in-cisional wounds in rats induced by transforming growth factor-betaScience 237 1333ndash1336
MUSTOE TA PIERCE GF MORISHIMA C and DEUEL TF(1991) Growth factor-induced acceleration of tissue repair throughdirect and inductive activities in a rabbit dermal ulcer model J ClinInvest 87 694ndash703
MUSTOE TA AHN ST TARPLEY JE and PIERCE GF(1994) Role of hypoxia in growth factor responses Differential ef-fects of basic fibroblast growth factor and platelet-derived growthfactor in an ischemic wound model Wound Rep Reg 2 277ndash283
NYBERG-HOFFMAN C and AGUILAR-CORDOVA E (1999) In-stability of adenoviral vectors during transport and its implication forclinical studies Nat Med 5 955ndash957
PIERCE GF and MUSTOE TA (1995) Pharmacologic enhance-ment of wound healing Annu Rev Med 46 467ndash481
PIERCE GF MUSTOE TA SENIOR RM REED J GRIFFINGL THOMASON A and DEUEL TF (1988) In vivo incisionalwound healing augmented by platelet-derived growth factor and re-combinant c-sis gene homodimeric proteins J Exp Med 167 974ndash987
PIERCE GF VANDE BERG J RUDOLPH R TARPLEY J andMUSTOE TA (1991) Platelet-derived growth factor-BB and trans-forming growth factor beta 1 selectively modulate glycosaminogly -cans collagen and myofibroblasts in excisional wounds Am JPathol 138 629ndash646
PIERCE GF TARPLEY JE YANAGIHARA D MUSTOE TA
FOX GM and THOMASON A (1992) Platelet-derived growthfactor (BB homodimer) transforming growth factor-b1 and basic fi-broblast growth factor in dermal wound healing Neovessel and ma-trix formation and cessation of repair Am J Pathol 140 1375ndash1388
PIERCE GF TARPLEY JE ALLMAN RM GOODE PS SER-DAR CM MORRIS B MUSTOE TA and VANDE BERG J(1994a) Tissue repair processes in healing chronic pressure ulcerstreated with recombinant platelet-derived growth factor BB Am JPathol 145 1399ndash1410
PIERCE GF YANAGIHARA D KLOPCHIN K DANILENKODM HSU E KENNEY WC and MORRIS CF (1994b) Stim-ulation of all epithelial elements during skin regeneration by kerati-nocyte growth factor J Exp Med 179 831ndash840
PIERCE GF TARPLEY JE TSENG J BREADY J CHANGD KENNEY WC RUDOLPH R ROBSON MC VANDEBERG J and REID P (1995) Detection of platelet-derived growthfactor (PDGF)-AA in actively healing human wounds treated withrecombinant PDGF-BB and absence of PDGF in chronic nonhealingwounds J Clin Invest 96 1336ndash1350
SINGER AJ and CLARK RA (1999) Cutaneous wound healingN Engl J Med 341 738ndash746
SOMASUNDARAM R and SCHUPPAN D (1996) Type I II IIIIV V and VI collagens serve as extracellular ligands for the iso-forms of platelet-derived growth factor (AA BB and AB) J BiolChem 271 26884ndash26891
SPRUGEL KH MCPHERSON JM CLOWES AW and ROSSR (1987) Effects of growth factors in vivo I Cell ingrowth intoporous subcutaneous chambers Am J Pathol 129 601ndash613
STEED DL (1995) Clinical evaluation of recombinant humanplatelet-derived growth factor for the treatment of lower extremitydiabetic ulcers Diabetic Ulcer Study Group J Vasc Surg 21 71ndash78
STEED DL (1998) Foundations of good ulcer care Am J Surg 17620S-25S
TYRONE JW MOGFORD JE CHANDLER LA MA C XIAY PIERCE GF and MUSTOE TA (2000) Collagen-embeddedplatelet-derived growth factor DNA plasmid promotes wound heal-ing in a dermal ulcer model J Surg Res 93 230ndash236
VOGT PM THOMPSON S ANDREE C LIU P BREUING KHATZIS D BROWN H MULLIGAN RC and ERIKSSON E(1994) Genetically modified keratinocytes transplanted to woundsreconstitute the epidermis Proc Natl Acad Sci USA 91 9307ndash9311
WIEMAN TJ (1998) Clinical efficacy of becaplermin (rhPDGF-BB)gel Becaplermin Gel Studies Group Am J Surg 176 74S-79S
WIEMAN TJ SMIELL JM and SU Y (1998) Efficacy and safetyof a topical gel formulation of recombinant human platelet-derivedgrowth factor-BB (becaplermin) in patients with chronic neuropathicdiabetic ulcers A phase III randomized placebo-controlled double-blind study Diabetes Care 21 822ndash827
WILSON JM (1996) Adenoviruses as gene-delivery vehicles NEngl J Med 334 1185ndash1187
XU J and CLARK RA (1996) Extracellular matrix alters PDGFregulation of fibroblast integrins J Cell Biol 132 239ndash249
XU J and CLARK RA (1997) A three-dimensional collagen latticeinduces protein kinase C-z activity Role in a2 integrin and collage-nase mRNA expression J Cell Biol 136 473ndash483
Address reprint requests toDr John Doukas
Selective Genetics Inc11035 Roselle Street
San Diego CA 92121
E-mail jdoukasselectivegeneticscom
Received for publication December 28 2000 accepted after re-vision February 23 2001
DOUKAS ET AL798

TISSUE REPAIR USING GROWTH FACTOR GENES 789
FIG 3 Localization of gene vector and transgene product within neotissues PVA sponges implanted in rats were injected withAdPDGF-B formulated in 015 collagen (2 3 1010 virus particles per sponge) and paraffin sections were stained as follows(A) Day 1 posttreatment anti-adenovirus immunostain to detect AdPDGF-B (green) DAPI stain to detect cell nuclei (blue) (B)Day 4 posttreatment in situ hybridization using human PDGF-B gene probe (C) Day 1 posttreatment anti-human PDGF-BBprotein immunostain positively stained leukocytes (arrowheads) and fibroblasts (arrows) are indicated (D) Day 6 posttreatmentanti-PDGF-BB immunostain (E) Day 8 posttreatment anti-PDGF-BB immunostain (F) Day 8 post- treatment immunostains todetect PDGF-BB protein (green) and vimentin (red) yellow fluorescence indicates PDGF-BB and vimentin colocalization bluefluorescence indicates cell nuclei (DAPI stain) Original magnifications (AndashC E and F)3 400 (D) 31000
the basis of its clinical use for the delivery of PDGF-BB pro-tein (Steed 1995)
Matrix influences on vector activity were examined by in-cubating AdLuc formulations at 37degC for 60 min followed bymatrix dissolution and vector bioassay (luciferase productionby 293 cells) This is an important test as adenoviruses arequickly inactivated under unfavorable physical and chemicalconditions (Nyberg-Hoffman and Aguilar-Cordova 1999)None of the matrices examined had a deleterious effect on vec-tor activity (90 6 12 106 6 5 and 139 6 37 of control ac-tivity for 015 collagen 26 collagen and CMC respec-tively) To further model in vivo vector stability we alsoincubated AdPDGF-B formulated in 26 collagen with woundfluid for 72 hr at 37degC prior to vector recovery and analysisWe observed no reduction in the level of PDGF-BB productionfrom cells transduced with AdPDGF-B exposed to wound fluidas compared with vector exposed to virus buffer (30 6 5 vs20 6 3 ng of PDGF-BB produced per milliliter of culturemedium respectively n 5 3)
As these data support the suitability of the selected matricesfor in vivo use we next determined their influence on vectorrelease kinetics (Fig 1) When placed in water collagen ma-trices retained the majority of their immobilized vectors with015 and 26 collagen releasing only 17 6 3 and 3 6 1 ofvector by 24 hr respectively By contrast 48 6 3 of AdLucwas released from CMC within 30 min and 61 6 2 by 6 hrThis was not unexpected as CMC is fairly water soluble andas both CMC and adenoviral particles are negatively chargedTherefore collagen matrices in a concentration-dependentfashion display more favorable kinetics for localizing and re-taining adenovirus vectors at delivery sites than does CMC
Collagen-immobilized adenoviruses induce distinctneotissues in vivo
Initial in vivo tests of matrix-immobilized vectors were per-formed with an established model of de novo tissue generation(Buckley et al 1985 Sprugel et al 1987 LeGrand et al1993) PVA sponges implanted subcutaneously in rats were in-jected with a single dose of adenovirus formulated in either col-lagen or CMC and then analyzed for tissue formation Forgrowth factor transgenes we selected platelet-derived growth
factor B (PDGF-B) vascular endothelial growth factor (VEGF)and fibroblast growth factor 2 (FGF2) because of their well-known mitogenic activities
AdPDGF-B formulated in 015 collagen induced granula-tion tissue formation in a dose-responsive manner (Table 1)Compared with vehicle controls delivering 2 3 1010 virus par-ticles induced a 17- to 23-fold increase in sponge protein con-tent (p 00002) a 2- to 27-fold increase in DNA content (p
00002) and a 29- to 43-fold increase in granulation tissue fill(p 00002) Trichrome-stained sections revealed the nearcomplete fill of sponge interiors with well-formed granulationtissue by day 6 posttreatment (Fig 2A) Expression of Ki-67a nuclear protein upregulated in proliferating cells (Gerdes etal 1983) established that both vascular endothelium (arrow-heads Fig 2B) and fibroblasts (arrows Fig 2B) had prolifer-ated in response to PDGF-B gene delivery AdFGF2 and Ad-VEGF also enhanced protein and DNA content within sponges(Table 1) However these vectors induced less granulation tis-sue deposition as compared with AdPDGF-B and the tissuesformed were histologically distinct
Tissues present in AdFGF2-treated sponges were highly vas-cular as revealed by the endothelial-reactive lectin BSL-I (Fig2D) Many of the infiltrating mononuclear cells also reactedpositively with BSL-I lectin suggesting that these cells wereendothelial cells or endothelial precursors AdFGF2 did nothowever induce the formation of classic granulation tissue aslittle collagen deposition was observed demonstrated by thepaucity of blue-staining material in trichrome-stained sections(Fig 2C) AdVEGF also induced heavily vascularized tissues(Fig 2E and F) but with greater extracellular collagen deposi-tion than AdFGF2 Relative to AdPDGF-B-induced tissueshowever AdVEGF-induced tissues were disorganized con-tained few fibroblasts and were markedly edematous Finallywhen AdLuc was delivered as a control treatment no signifi-cant increases in protein DNA or granulation tissue were ob-served compared with collagen vehicle alone (Table 1)Trichrome-stained sections revealed sparse inflammatory cellinfiltrates within AdLuc-treated sponges (Fig 2G) which com-pared with the near absence of infiltration after delivery of col-lagen vehicle alone (Fig 2H) suggested a limited antiviral response
Unlike the 015 collagen formulations described above
DOUKAS ET AL790
TABLE 2 NEOTISSUE FORMATION AFTER PDGF-B GENE OR PDGF-BB PROTEIN DELIVERYa
Granulation Protein DNATreatment fill () (mgsponge) (mgsponge)
015 Collagen vehicle 28 6 13b 16 6 2b 103 6 22b
AdPDGF-B 81 6 15b 30 6 6b 218 6 28b
PDGF-BB 100 mg 64 6 12c 22 6 4c 155 6 26c
PDGF-BB 10 mg qod 3 3d 77 6 9b0 31 6 8b 230 6 75b
aPVA sponges implanted in rats were injected with either 015 collagen vehicle or collagen containing AdPDGF-B as described in Table 1 Alternatively PDGF-BB protein was delivered as a single 100-mg dose on day 4 postimplantation or as10-mg doses on days 4 6 and 8 Sponges were removed on day 12 postimplantation and processed to determine the percent granulation fill as well as total protein and DNA contents Data are presented as means 6 SD (n 5 4ndash8)
bp 00001 versus collagen control and p 005 versus 100-mg PDGF-BBcp 003 versus collagen controldqod 3 3 Every other day three times
TISSUE REPAIR USING GROWTH FACTOR GENES 791
TABLE 3 INFLUENCE OF ADENOVIRUSndashMATRIX FORMULATIONS ON ISCHEMIC WOUND HEALINGa
Granulation Epithelial Wound closureTreatment Model system area (mm2) area (mm2) ( complete)
Aqueous buffer Cartilage intact 10 6 08 05 6 03 61 6 226 mm day 10
AdPDGF-B in Cartilage intact 24 6 22 05 6 01 73 6 28aqueous buffer 6 mm day 10
015 Collagen Cartilage intact 05 6 03 05 6 02 89 6 14vehicle 6 mm day 10
AdPDGF-B in Cartilage intact 16 6 09b 09 6 03c 97 6 7015 collagen 6 mm day 10
Aqueous buffer Cartilage removed 45 6 08 08 6 02 95 6 96 mm day 7
AdPDGF-B in Cartilage removed 40 6 15 11 6 05 82 6 22aqueous buffer 6 mm day 7
015 Collagen Cartilage removed 36 6 13 06 6 02 88 6 22vehicle 6 mm day 7
AdPDGF-B in Cartilage removed 70 6 14b 07 6 03 79 6 22015 collagen 6 mm day 7
26 Collagen Cartilage removed 04 6 05 01 6 01 24 6 15vehicle 8 mm day 8
AdPDGF-B in Cartilage removed 51 6 25b 06 6 03b 52 6 25c
26 collagen 8 mm day 8
aExcisional wounds (6 or 8 mm in diameter) were placed in ischemic rabbit ears with underlying cartilage left intact or re-moved Wounds were then treated with AdPDGF-B formulated in aqueous virus buffer or collagen control treatments consistedof vehicle alone For 6-mm wounds virus was applied as 2 3 109 particles per wound for 8-mm wounds as 4 3 109 particlesper wound On days 7ndash10 posttreatment wounds were harvested and processed as trichrome-stained paraffin sections whichwere then used to quantify newly formed granulation tissue and epithelium (cross-sectional area in mm2) and the degree of woundsurface closure (where 100 equals complete closure) Data are presented as means 6 SD (n 5 4ndash8)
bp 0009 versus vehicle controlcp 005 versus vehicle control
26 collagen formulations could not be reliably examined inthe PVA sponge model as their relatively high viscosity pre-vented uniform filling of sponges by syringe CMC-formulatedvectors were also unsuitable for this model system as theyproved highly inflammatory (data not shown) These formula-tions therefore were evaluated in more appropriate excisionalwound models (see below)
Tissue repair cells are transduced by collagen-immobilized adenoviruses
On the basis of the robust activity of collagen-formulatedAdPDGF-B we elected to further examine this vectorndashmatrixcombination first by seeking to correlate PDGF-B gene deliv-ery with subsequent transgene and protein expression WhenPVA sponges treated with 015 collagenndashAdPDGF-B werestained with both an anti-adenovirus antibody and the nuclearstain DAPI the majority of cells present 1 day after gene de-livery had bound andor internalized adenovirus (Fig 3A) Insitu hybridization revealed that these cells were successfullytransduced by virus as they contained human PDGF-B mRNA(Fig 3B) By contrast hybridization product was not detectedwith a sense riboprobe or when AdLuc-treated sponges wereexamined (data not shown)
We next used a human PDGF-BB-specific antibody to iden-tify the cell types responsible for transgene expression By day
1 postdelivery of 015 collagenndashAdPDGF-B PDGF-BB pro-tein was localized to leukocytes (arrowheads) and fibroblasts (ar-row Fig 3C) With time PDGF-BB protein was detected boundto the extracellular matrix (ECM) surrounding positively stainedcells (Fig 3D) This last observation indicates that a reservoir ofPDGF-BB protein develops within treated tissues and thus mayprolong the histogenic effects of this growth factor Finally byday 8 the majority of immunoreactivity had abated with pri-marily microvascular endothelium remaining positive (Fig 3E)However scattered fibroblasts could still be shown to producePDGF-BB protein by dual immunohistochemistry with anti-PDGF-BB and anti-vimentin antibodies (Fig 3F)
Multiple administrations of PDGF-BB protein are required to approximate the histogenic effects of collagenndashAdPDGF-B
To directly compare gene therapy with the more conven-tional approach of growth factor protein delivery we next quan-tified tissue formation in response to either PDGF gene or pro-tein delivery A single injection of 015 collagenndashAdPDGF-Benhanced granulation tissue filling of sponges by 3-fold versusvehicle alone (p 00001) and sponge protein and DNA lev-els by 2-fold (p 00001 Table 2) Using a human PDGF-BB-specific ELISA this growth factor was detected at 54 6 13ngsponge (n 5 8) By contrast when PDGF-BB protein was
delivered as a single dose nearly 2000-fold in excess of thisconcentration the tissue formation responses observed (proteinand DNA accumulation and granulation tissue formation) weresignificantly lower (p 005 Table 2) In fact repeated dos-ing with PDGF-BB protein was required in order to achieve re-sponses comparable to a single administration of the PDGF-Bgene These data therefore support our hypothesis that the abil-ity of gene delivery to establish prolonged in situ growth fac-tor production translates into greater histogenesis than that seenwith growth factor proteins
CollagenndashAdPDGF-B induces complete healing of ischemic wounds
Nonhealing wounds are a major risk in chronically ischemictissues as low oxygen tension greatly impairs tissue repair pro-cesses We therefore compared the ability of matrix versusaqueous formulated AdPDGF-B to repair ischemic excisionalwounds Several models were employed to compare variationsin wound size and condition so as to allow for a more com-plete picture of tissue repair
In the first model system 6-mm-diameter wounds were cre-ated in ischemic rabbit ears by removal of epidermal and der-mal layers but not underlying cartilage This model has beenused in previous studies of growth factor proteins and genes(Ahn and Mustoe 1990 Mustoe et al 1994 Liechty et al1999) and was therefore employed to allow comparison withthese reports However it represents an artificial system as thepresence of a cartilage layer restricts both treatment activity andhealing to wound margins and in addition the initially acellu-lar wound bed forms a cup that artifactually retains aqueoustreatments As would be predicted we found a trend towardgranulation tissue formation in this model after the applicationof AdPDGF-B formulated in aqueous buffer (Table 3) How-ever this response did not reach the level of statistical signifi-cance as tissue development was highly variable (note the highstandard deviation value) In addition epithelial regenerationand wound closure were minimal to unaffected By contrastAdPDGF-B formulated in 015 collagen enhanced granula-tion tissue area by 32-fold and epithelial area by 18-fold overthat achieved with vehicle alone (p 0009 and 005 respec-tively) Although near complete closure of epithelial gaps wasalso achieved the high level of self-healing in control-treatedgroups (89 wound closure) precluded statistical significance
In an alternative model design subdermal cartilage was com-pletely removed from excisional wounds creating beds whosefloors now consisted of dermal tissue (Pierce et al 1994b)This design allows for cellular responses from the entire woundbed as well as the opportunity for vector migration beyond
treatment areas We now observed that aqueous formulated Ad-PDGF-B failed to induce even a trend toward tissue regenera-tion (Table 3) Rather the vector appears to have seeped throughthe wound bed floor as inflammatory cell infiltrates and fociof fibroblast proliferation were observed in the underlying der-mis and at wound margins (Fig 4A) Immunohistochemistryconfirmed the production of human PDGF-BB at these sites(Fig 4B) CMC-formulated AdPDGF-B also failed to induceany meaningful tissue repair Wounds treated with this formu-lation showed a diffuse inflammatory response within thewound bed and wound surfaces were overlain with fibrin clotsrather than regenerating epithelium (Fig 4C and D) By con-trast AdPDGF-B formulated in 015 collagen enhanced gran-ulation tissue deposition 19-fold within wound beds versus ve-hicle controls (p 0002) and wounds were extensivelyepithelialized (Table 3) Neither epithelial regeneration norwound closure achieved significance however as the high de-gree of self-healing achieved in this particular model (see ve-hicle alone group) most likely masked transgene-stimulated re-sponses
To address these model limitations as our next system wecreated 8-mm wounds in ischemic rabbit ears by removingepidermal dermal and cartilage layers reasoning that largerexcisional wounds would display limited self-healing In ad-dition this model could readily accommodate 26 collagenformulations which proved difficult to reproducibly apply insmaller wounds Compared with control wounds treated withcollagen vehicle alone wounds treated with AdPDGF-B for-mulated in 26 collagen achieved a 12-fold enhancementin granulation tissue fill and a 6-fold enhancement in re-ep-ithelialization by day 8 posttreatment (p 0009 Table 3)In addition wound closure was only 24 complete in colla-gen vehicle-treated wounds by day 8 but 52 complete inwounds treated with collagen-formulated AdPDGF-B (p
005) Histologically AdPDGF-B-treated wounds showed nosigns of tissue hyperplasia or chronic inflammation but ratheran orderly repair process marked by a regenerated epitheliallayer overlying a wound bed filled with granulation tissue(Fig 4E and F)
CollagenndashAdPDGF-B induces normal long-term tissue repair
Our choice of adenoviruses for transgene delivery was partlybased on the reasoning that as these vectors establish transientgene expression they would not lead to hyperproliferative re-sponses or scar formation To test this hypothesis we treatedrabbit ear excisional wounds with AdPDGF-B formulated in015 collagen and examined tissue repair responses out to
DOUKAS ET AL792
FIG 4 Influence of adenovirusndashmatrix formulations on excisional wound repair Excisional wounds (6 or 8 mm in diameter andextending through underlying cartilage layers) were placed in ischemic rabbit ears bars indicate original wound depth (determinedfrom cartilage visible at wound margins) Wounds were then treated with AdPDGF-B formulated in either virus buffer CMC orcollagen and on day 7 or 8 posttreatment processed for histology or immunohistochemistry An identical design was used to ex-amine long-term healing on day 90 except that wounds were created in nonischemic ears (A) Day 7 buffer-formulated AdPDGF-B-treated 6-mm wound trichrome stain (B) Day 7 buffer-formulated AdPDGF-B-treated 6-mm wound anti-PDGF-BB proteinimmunostain (C and D) Day 7 CMC-formulated AdPDGF-B-treated 6-mm wound trichrome stains (E and F) Day 8 26 col-lagen-formulated AdPDGF-B-treated 8-mm wound trichrome stains (G and H) Day 90 015 collagen-formulated AdPDGF-B-treated 6-mm wound trichrome stains Original magnification (A C E and G) 340 (B D F and H) 3200
TISSUE REPAIR USING GROWTH FACTOR GENES 793
DOUKAS ET AL794
TABLE 4 BIODISTRIBUTION OF AdPDGF-B IN EXCISIONAL WOUNDSa
Positive samplestotal assayed
Tissue AdPDGF-B dose Day 3 Day 7 Day 28 Day 90
Wound bed 2 3 109 particles 66 66 66b 06Axillary lymph nodes 2 3 109 particles 02 ND 06 06
Wound bed 2 3 1011 particles 66 66 66 46c
Axillary lymph nodes 2 3 1011 particles 66 ND 66d 26e
aFull-thickness excisional wounds (7 cm2) were placed on the backs of rabbits and AdPDGF-B formulated in 26 collagenwas applied as either 2 3 109 or 2 3 1011 virus particles per wound On days 3ndash90 posttreatment wound beds and a panel oforgans were harvested for real-time PCR quantification of viral genome Data are shown for wound bed and axillary lymph nodesamples as the number of samples that yielded amplifiable signals per total number assayed ND not determined
bThree of six samples scored below the level of quantitation (LOQ 10ndash100 copiesmg DNA)cAll four positive samples scored below the LOQdThree of six samples scored below the LOQeBoth positive samples scored below the LOQ
180 days posttreatment (Fig 5) PDGF-B gene delivery en-hanced total ear thickness relative to controls on day 28 (229 6
020 vs 179 6 019 mm p 00001) and day 60 (192 6 001vs 182 6 011 mm p 0005) as anticipated on the basis ofthe ability of this formulation to induce granulation tissue for-mation By day 90 posttreatment however there was no mea-surable difference in ear thickness between AdPDGF-B andcontrol-treated groups and this relationship continued out today 180 indicating that growth factor gene delivery did not in-duce excessive scar formation This was also confirmed histo-logically AdPDGF-B-treated wounds on day 90 and beyondwere composed of a thin outer keratin layer an underlying ep-ithelial layer of equivalent thickness to nonwounded areas anda collagen-rich dermis devoid of any signs of tissue hyperpla-sia (Fig 4G and H)
Collagen immobilization limits adenovirus vectorbiodistribution beyond treatment sites
As a final measure of the value of matrix immobilization forgene delivery we determined the biodistribution patterns ofvectors after their in vivo delivery In the first model systemused AdPDGF-B formulated in 015 collagen was applied torabbit ear wounds at equivalent doses as previously describedwounds were extended through underlying cartilage but vas-cular supplies were not disturbed so as to permit maximal vec-tor dissemination By PCR no adenoviral DNA was detectablein lung spleen brain cervical lymph nodes or gonads on day1 3 7 or 14 (n 5 6 per group) In the liver one of six sam-ples was positive on days 3 and 7 but none on day 14 in serumonly one of six samples tested positive on day 14 (equivalentof 500-ml serum volume) By contrast adenovirus was detectedin eight of eight wound bed samples at all time points exam-ined
In a second model system excisional wounds placed on thebacks of rabbits were treated with AdPDGF-B formulated in26 collagen Because of their anatomical placement thismodel allowed for the creation of larger excisional wounds (7-cm2 total area) than those placed in rabbit ears (03 cm2) and
consequently larger treatment volumes and vector doses (2 3109 or 2 3 1011 virus particles per wound) At the lower doseof 2 3 109 particles PCR-amplifiable adenoviral DNA was notdetectable beyond wound beds on day 3 7 28 or 90 Tissuessampled and found not to contain vector included blood heartlung liver kidney brain spleen lymph nodes and gonads (n 5
6group) In wound beds adenoviral DNA was detected at alltime points except for day 90 (Table 4 and Fig 6) Vector lev-els did decrease however by 38-fold between days 7 and 28with three of six samples falling below the level of quantita-tion (LOQ) by real-time PCR at the latter time point (Fig 6)
At a 100-fold higher vector dose of 2 3 1011 particles perwound PCR-amplifiable adenoviral DNA was once again un-detectable in the majority of tissues sampled Except for a sin-gle day 7 liver sample and a single day 7 brain sample (bothbelow the LOQ) adenoviral DNA was only detectable directlyin wound beds or in the axillary lymph nodes that drain woundsites (Table 4) Moreover three of six positive axillary nodesamples scored below the LOQ on day 28 as did both positivesamples on day 90 indicating that they contained relatively lit-tle vector Within wound beds adenoviral DNA was detectedat quantifiable levels out to day 28 and at detectable but non-quantifiable levels on day 90 DNA copy numbers remainedsteady between days 3 and 7 dropped 107-fold between days7 and 28 and a further 1662-fold by day 90 Finally at eachtime point DNA copy numbers in wounds treated with 2 3
1011 particles were approximately 100-fold higher than thosefound in wounds treated with 2 3 109 particles thus confirm-ing the linearity of our assay system
To better define the time course of human PDGF-BB pro-duction we also quantified transgene mRNA levels in woundbed samples treated at 2 3 109 particles per wound This treat-ment dose was selected as representative of the virus particleconcentration capable of inducing complete healing in ischemicear wounds Quantifiable levels of human PDGF-B mRNAwere detectable in treated dorsal wounds at days 3 7 and 28(Fig 6) with levels decreasing 14-fold between days 3 and 7and 5-fold between days 7 and 28 The more sensitive tech-nique of real-time RT-PCR therefore demonstrates that trans-
TISSUE REPAIR USING GROWTH FACTOR GENES 795
gene expression extends well beyond the 8-day time period sug-gested using anti-PDGF-BB immunohistochemistry as a de-tection system (Fig 3)
DISCUSSION
These studies demonstrate that immobilization of gene ther-apy vectors in collagen-based matrices enables their efficientdelivery and activity in vivo Matrix immobilization achievedprolonged transgene-encoded growth factor production and asa consequence robust tissue repair By contrast aqueous vehi-cles failed to retain adenoviruses at application sites resultingin diffuse inflammation rather than productive tissue regenera-tion These observations confirm our basic hypothesis that ma-trix immobilization of growth factor-encoding gene therapyvectors represents a promising approach to tissue repair
Although de novo tissue deposition was achievable with sev-eral growth factor genes PDGF-B proved the most suitable forrepair of cutaneous defects A single administration of colla-gen-immobilized AdPDGF-B rapidly induced the formation ofhighly cellular and vascularized tissues with dense ECMs richin collagen By contrast AdFGF2 induced a primarily vascu-lar response with little collagen deposition FGF2 induces therelease of matrix metalloproteinase 1 or interstitial collagenase(Buckley-Sturrock et al 1989) and this may underlie the rel-ative paucity of ECM accumulation VEGF gene delivery alsoinduced highly vascular responses however the enhanced per-meability characteristic of VEGF-induced vasculature (Dvoraket al 1995) led to edema within nascent tissues In fact much
of the enhanced protein and DNA deposition observed in Ad-VEGF-treated PVA sponges may well derive from fluid exu-dates rather than actual tissue formation Finally the inabilityof AdLuc delivery to induce anything beyond a limited in-flammatory response confirms that tissue formation was de-pendent on growth factor gene delivery
The robust activity of PDGF-B gene delivery was expectedas PDGF-BB protein initiates multiple aspects of tissue forma-tion including cellular influx and proliferation ECM deposi-tion and tissue remodeling (Pierce et al 1988 1991 1994a)Indeed PDGF-BB is the only growth factor protein to have suc-cessfully completed human clinical trials and be approved forthe treatment of dermal wounds (Steed 1995 drsquoHemecourt etal 1998 Wieman 1998 Wieman et al 1998) We observedthat collagen-formulated AdPDGF-B induced the complete re-pair of excisional skin defects without unwanted long-term ef-fects such as the development of hypertrophic scars Endoge-nous growth factors other than PDGF-BB however most likelymediated the enhanced re-epithelialization observed in thesewounds as epithelial regeneration is driven by members of theepidermal growth factor and FGF families (Pierce et al 1994bDanilenko et al 1995) Our data indicate nonetheless that tis-sue regeneration and repair were initiated and to a great degreedriven by transgene-encoded PDGF-BB
Despite the known activity of PDGF-BB protein we wereable to demonstrate greater tissue deposition after gene deliv-ery as compared with the use of recombinant growth factor pro-tein A single application of PDGF-BB protein could not equalthe ability of PDGF-B gene therapy to induce neotissue for-mation even at doses well in excess of that induced in situ byAdPDGF-B and in excess of that used in human clinical trials
FIG 5 Influence of collagen-formulated AdPDGF-B on long-term tissue repair Excisional wounds (6 mm in diameter withcartilage remaining intact) were placed in nonischemic rabbit ears and treated with either 015 collagen alone (open columns)or AdPDGF-B formulated in this vehicle (solid columns) On days 28ndash180 posttreatment total ear thickness at the site of eachwound was measured (in mm) with calipers Data are presented as means 6 SD (n 5 3) Treatment groups differ by p 00001groups differ by p 0005
(Steed 1995 drsquoHemecourt et al 1998 Wieman 1998 Wie-man et al 1998) In fact repeated administrations of PDGF-BB protein were required to approach the level of tissue for-mation observed after a single administration of AdPDGF-BThese data support our hypothesis that sustained localizedgrowth factor production is required for robust tissue repair
In further support of this hypothesis we demonstrated thatmRNA encoding human PDGF-B was present in excisionalwounds as late as day 28 after collagen-formulated AdPDGF-B administration By contrast previous studies of PDGF-BBprotein found that the great majority of this growth factor wasgone from treated wounds 1 day postapplication and that anytissue maturation subsequently observed was most likely dueto the upregulation of endogenous growth factors (Pierce et al1992 1995) We also demonstrated that repair cells such asmononuclear leukocytes endothelial cells and fibroblasts pres-ent with developing neotissues represent the source of both
transgene transcription and PDGF-BB production In additiona depot of human PDGF-BB was detected bound to the colla-gen delivery matrix and ECM of these tissues This was antici-pated as PDGF-BB contains collagen-binding motifs (Soma-sundaram and Schuppan 1996) We hypothesize that subsequentmatrix metalloproteinase activity by repair cells will serve togenerate localized release of this sequestered growth factor pooland as a consequence further drive tissue regeneration Theseevents which are central to tissue remodeling should be directlyenhanced by collagen matrices as type I collagen stimulates me-talloproteinase production integrin expression and cellular ac-tivation in PDGF-stimulated fibroblasts (Xu and Clark 19961997)
An additional rationale for employing collagen matrices wasto physically immobilize vectors This was confirmed in vivowhere collagen matrices maintained AdPDGF-B at deliverysites for at least 28 days and limited vector migration to other
DOUKAS ET AL796
FIG 6 Persistence of collagen-formulated vector and transgene transcripts in excisional wounds Full-thickness excisionalwounds (7 cm2) were placed on the dorsal surface of rabbits and treated with AdPDGF-B formulated in 26 collagen at either2 3 109 or 2 3 1011 virus particles per wound (open and closed columns respectively) Wounds were then covered with OpSitedressing and on days 3 7 or 28 posttreatment wound beds were harvested for real-time quantitative PCR and RT-PCR analy-ses PCR data are presented in the upper graph as AdPDGF-B copies per wound RT-PCR data are presented in the lower graphas the relative amount of PDGF-B mRNA per unit 18S rRNA (in arbitrary units) All data points are means 6 SD (n 5 6)
tissues or organs In vitro tests also established that collagenmatrices not only prevent vector loss due to diffusion but pre-serve vector activity despite prolonged incubation in acutewound fluid Successful vector immobilization and tissue re-pair could be achieved with both 015 collagen and 26 col-lagen suggesting flexibility in the final vehicle formulation re-quired for effective vector delivery This flexibility was neededin the present studies as 26 collagen formulations proveddifficult to deliver to PVA sponges and 6-mm excisionalwounds This would not be of concern in clinical settings how-ever where wound beds are easily accessible and generally sev-eral square centimeters in area By contrast CMC was inef-fective at retaining vector in aqueous environments Moreimportantly this matrix was itself inflammatory and whencombined with adenovirus the net result was inflammationrather than tissue repair We are currently examining the util-ity of other matrices such as fibrin and hyaluronic acid whichbecause of their more provisional nature may offer yet greatercellular migration into wounds as compared with type I colla-gen
Although an aqueous-based AdPDGF-B formulation hasbeen previously shown to enhance tissue formation (Liechty etal 1999) this was achieved with a model system that artifi-cially retains vectors within treatment sites In fact the presentstudies demonstrate that any tissue repair observed after Ad-PDGF-B delivery in a nongelling liquid is dependent on the useof this model system In wounds not designed to retain appliedtreatments aqueous-formulated AdPDGF-B seeped into sur-rounding tissues and led to hyperplasia within these areas ratherthan to tissue regeneration within the active wound bed Colla-gen-immobilized AdPDGF-B on the other hand did persist inthese wound beds and led to significant enhancements in gran-ulation tissue formation as well as enhanced wound re-epithe-lialization and wound closure The significance of these activ-ities is further substantiated considering that they wereachievable in 8-mm-diameter ischemic wounds which withinthe time frame examined could not self-heal to any meaning-ful degree in the absence of gene therapy However as all theanimal models employed in these studies will eventually self-heal given sufficient time the full value of matrix-immobilizedgene therapy vectors remains to be confirmed in human clini-cal trials
In conclusion we present evidence that matrix-immobilizedgene therapy vectors encoding appropriate growth-promotinggenes represent a promising approach to tissue regeneration andrepair This basic concept can be expanded to include alterna-tive matrices such as controlled-release formulations as wellas tissue-specific growth factors Furthermore the addition oftargeting ligands to adenovirus vectors (eg FGF2) can en-hance their ability to transduce cells such that tissue repair re-sponses comparable to nontargeted vectors can be achieved butat significantly lower vector doses (Chandler et al 2000a)With appropriate design and application schedules one couldconceivably time the release of multiple growth factors to spe-cific stages of a tissue repair cascade In addition we have foundin preliminary studies that collagen-immobilized nonviral vec-tors such as PDGF-B plasmids which have potentially morefavorable safety profiles than adenovirus vectors can also en-hance tissue formation in vivo (Chandler et al 2000b Tyroneet al 2000) Such flexibility should allow for the widespreadapplication of gene therapy to the treatment of injured tissues
ACKNOWLEDGMENTS
We thank Jeff Davidson (Vanderbilt University School ofMedicine) for assistance in establishing the PVA sponge modelCarl-Henrik Heldin (Ludwig Institute for Cancer Research) forthe PDGF-B gene construct and Emelie Amburn Lara AsatoSharon Chang Gail Fieser Lydia Greenlees Rebecca Smokerand Linda Manza for excellent technical assistance This pub-lication was made possible in part by NIH grants 1R43AR46154(JD) and 5P01CA25874 (MH)
REFERENCES
AHN ST and MUSTOE TA (1990) Effects of ischemia on ulcerwound healing A new model in the rabbit ear Ann Plast Surg 2417ndash23
ANDREE C SWAIN WF PAGE CP MACKLIN MDSLAMA J HATZIS D and ERIKSSON E (1994) In vivo trans-fer and expression of a human epidermal growth factor gene accel-erates wound repair Proc Natl Acad Sci USA 91 12188ndash12192
BENN SI WHITSITT JS BROADLEY KN NANNEY LBPERKINS D HE L PATEL M MORGAN JR SWAIN WFand DAVIDSON JM (1996) Particle-mediated gene transfer withtransforming growth factor-b1 cDNAs enhances wound repair in ratskin J Clin Invest 98 2894ndash2902
BONADIO J SMILEY E PATIL P and GOLDSTEIN S (1999)Localized direct plasmid gene delivery in vivo Prolonged therapyresults in reproducible tissue regeneration Nat Med 5 753ndash759
BUCKLEY A DAVIDSON JM KAMERATH CD WOLT TBand WOODWARD SC (1985) Sustained release of epidermalgrowth factor accelerates wound repair Proc Natl Acad Sci USA82 7340ndash7344
BUCKLEY-STURROCK A WOODWARD SC SENIOR RMGRIFFIN GL KLAGSBRUN M and DAVIDSON JM (1989)Differential stimulation of collagenase and chemotactic activity in fi-broblasts derived from rat wound repair tissue and human skin bygrowth factors J Cell Physiol 138 70ndash78
CHANDLER LA DOUKAS J GONZALEZ AM HOGANSONDK GU DL MA C NESBIT M CROMBLEHOLME TMHERLYN M SOSNOWSKI BA and PIERCE GF (2000a)FGF2ndashTargeted adenovirus encoding platelet-derived growth factor-B enhances de novo tissue formation Mol Ther 2 153ndash160
CHANDLER LA MA C GONZALEZ AM DOUKAS JNGUYEN T PIERCE GF and PHILLIPS ML (2000b) Ma-trix-enabled gene transfer for cutaneous wound repair Wound Re-pair Regen 8 473ndash479
DANILENKO DM RING BD TARPLEY JE MORRIS BVAN GY MORAWIECKI A CALLAHAN W GOLDEN-BERG M HERSHENSON S and PIERCE GF (1995) Growthfactors in porcine full and partial thickness burn repair Differing tar-gets and effects of keratinocyte growth factor platelet-derivedgrowth factor-BB epidermal growth factor and neu differentiationfactor Am J Pathol 147 1261ndash1277
DEUEL TF KAWAHARA RS MUSTOE TA and PIERCE GF(1991) Growth factors and wound healing Platelet-derived growthfactor as a model cytokine Annu Rev Med 42 567ndash584
DrsquoHEMECOURT PA SMIELL JM and KARIM MR (1998) So-dium carboxymethylcellulose aqueous-based gel vs becaplermin gelin patients with nonhealing lower extremity diabetic ulcers Wounds10 69ndash75
DOUKAS J HOGANSON DK ONG M YING W LACEYDL BAIRD A PIERCE GF and SOSNOWSKI BA (1999)Retargeted delivery of adenoviral vectors through fibroblast growthfactor receptors involves unique cellular pathways FASEB J 131459ndash1466
TISSUE REPAIR USING GROWTH FACTOR GENES 797
DVORAK HF BROWN LF DETMAR M and DVORAK AM(1995) Vascular permeability factorvascular endothelial growth fac-tor microvascular hyperpermeability and angiogenesis Am JPathol 146 1029ndash1039
EMING SA MEDALIE DA TOMPKINS RG YARMUSHML and MORGAN JR (1998) Genetically modified human ker-atinocytes overexpressing PDGF-A enhance the performance of acomposite skin graft Hum Gene Ther 9 529ndash539
EMING SA WHITSITT JS HE L KRIEG T MORGAN JRand DAVIDSON JM (1999) Particle-mediated gene transfer ofPDGF isoforms promotes wound repair J Invest Dermatol 112297ndash302
GERDES J SCHWAB U LEMKE H and STEIN H (1983) Pro-duction of a mouse monoclonal antibody reactive with a human nu-clear antigen associated with cell proliferation Int J Cancer 3113ndash20
GONZALEZ AM BERRY M MAHER PA LOGAN A andBAIRD A (1995) A comprehensive analysis of the distribution ofFGF-2 and FGFR1 in the rat brain Brain Res 701 201ndash226
GREENHALGH DG (1996) The role of growth factors in woundhealing J Trauma 41 159ndash167
GROTENDORST GR MARTIN GR PENCEV D SODEK Jand HARVEY AK (1985) Stimulation of granulation tissue for-mation by platelet-derived growth factor in normal and diabetic ratsJ Clin Invest 76 2323ndash2329
KHOURI RK HONG SP DEUNE EG TARPLEY JE SONGSZ SERDAR CM and PIERCE GF (1994) De novo genera-tion of permanent neovascularized soft tissue appendages by platelet-derived growth factor J Clin Invest 94 1757ndash1763
LEGRAND EK SENTER LH GAMELLI RL and KIORPESTC (1993) Evaluation of PDGF-BB PDGF-AA bFGF IL-1 andEGF dose responses in polyvinyl alcohol sponge implants assessedby a rapid histologic method Growth Factors 8 315ndash329
LIECHTY KW NESBIT M HERLYN M RADU A ADZICKNS and CROMBLEHOLME TM (1999) Adenoviral-mediatedoverexpression of platelet-derived growth factor-B corrects ischemicimpaired wound healing J Invest Dermatol 113 375ndash383
LYNCH SE COLVIN RB and ANTONIADES HN (1989)Growth factors in wound healing J Clin Invest 84 640ndash646
MUSTOE TA PIERCE GF THOMASON A GRAMATES PSPORN MB and DEUEL TF (1987) Accelerated healing of in-cisional wounds in rats induced by transforming growth factor-betaScience 237 1333ndash1336
MUSTOE TA PIERCE GF MORISHIMA C and DEUEL TF(1991) Growth factor-induced acceleration of tissue repair throughdirect and inductive activities in a rabbit dermal ulcer model J ClinInvest 87 694ndash703
MUSTOE TA AHN ST TARPLEY JE and PIERCE GF(1994) Role of hypoxia in growth factor responses Differential ef-fects of basic fibroblast growth factor and platelet-derived growthfactor in an ischemic wound model Wound Rep Reg 2 277ndash283
NYBERG-HOFFMAN C and AGUILAR-CORDOVA E (1999) In-stability of adenoviral vectors during transport and its implication forclinical studies Nat Med 5 955ndash957
PIERCE GF and MUSTOE TA (1995) Pharmacologic enhance-ment of wound healing Annu Rev Med 46 467ndash481
PIERCE GF MUSTOE TA SENIOR RM REED J GRIFFINGL THOMASON A and DEUEL TF (1988) In vivo incisionalwound healing augmented by platelet-derived growth factor and re-combinant c-sis gene homodimeric proteins J Exp Med 167 974ndash987
PIERCE GF VANDE BERG J RUDOLPH R TARPLEY J andMUSTOE TA (1991) Platelet-derived growth factor-BB and trans-forming growth factor beta 1 selectively modulate glycosaminogly -cans collagen and myofibroblasts in excisional wounds Am JPathol 138 629ndash646
PIERCE GF TARPLEY JE YANAGIHARA D MUSTOE TA
FOX GM and THOMASON A (1992) Platelet-derived growthfactor (BB homodimer) transforming growth factor-b1 and basic fi-broblast growth factor in dermal wound healing Neovessel and ma-trix formation and cessation of repair Am J Pathol 140 1375ndash1388
PIERCE GF TARPLEY JE ALLMAN RM GOODE PS SER-DAR CM MORRIS B MUSTOE TA and VANDE BERG J(1994a) Tissue repair processes in healing chronic pressure ulcerstreated with recombinant platelet-derived growth factor BB Am JPathol 145 1399ndash1410
PIERCE GF YANAGIHARA D KLOPCHIN K DANILENKODM HSU E KENNEY WC and MORRIS CF (1994b) Stim-ulation of all epithelial elements during skin regeneration by kerati-nocyte growth factor J Exp Med 179 831ndash840
PIERCE GF TARPLEY JE TSENG J BREADY J CHANGD KENNEY WC RUDOLPH R ROBSON MC VANDEBERG J and REID P (1995) Detection of platelet-derived growthfactor (PDGF)-AA in actively healing human wounds treated withrecombinant PDGF-BB and absence of PDGF in chronic nonhealingwounds J Clin Invest 96 1336ndash1350
SINGER AJ and CLARK RA (1999) Cutaneous wound healingN Engl J Med 341 738ndash746
SOMASUNDARAM R and SCHUPPAN D (1996) Type I II IIIIV V and VI collagens serve as extracellular ligands for the iso-forms of platelet-derived growth factor (AA BB and AB) J BiolChem 271 26884ndash26891
SPRUGEL KH MCPHERSON JM CLOWES AW and ROSSR (1987) Effects of growth factors in vivo I Cell ingrowth intoporous subcutaneous chambers Am J Pathol 129 601ndash613
STEED DL (1995) Clinical evaluation of recombinant humanplatelet-derived growth factor for the treatment of lower extremitydiabetic ulcers Diabetic Ulcer Study Group J Vasc Surg 21 71ndash78
STEED DL (1998) Foundations of good ulcer care Am J Surg 17620S-25S
TYRONE JW MOGFORD JE CHANDLER LA MA C XIAY PIERCE GF and MUSTOE TA (2000) Collagen-embeddedplatelet-derived growth factor DNA plasmid promotes wound heal-ing in a dermal ulcer model J Surg Res 93 230ndash236
VOGT PM THOMPSON S ANDREE C LIU P BREUING KHATZIS D BROWN H MULLIGAN RC and ERIKSSON E(1994) Genetically modified keratinocytes transplanted to woundsreconstitute the epidermis Proc Natl Acad Sci USA 91 9307ndash9311
WIEMAN TJ (1998) Clinical efficacy of becaplermin (rhPDGF-BB)gel Becaplermin Gel Studies Group Am J Surg 176 74S-79S
WIEMAN TJ SMIELL JM and SU Y (1998) Efficacy and safetyof a topical gel formulation of recombinant human platelet-derivedgrowth factor-BB (becaplermin) in patients with chronic neuropathicdiabetic ulcers A phase III randomized placebo-controlled double-blind study Diabetes Care 21 822ndash827
WILSON JM (1996) Adenoviruses as gene-delivery vehicles NEngl J Med 334 1185ndash1187
XU J and CLARK RA (1996) Extracellular matrix alters PDGFregulation of fibroblast integrins J Cell Biol 132 239ndash249
XU J and CLARK RA (1997) A three-dimensional collagen latticeinduces protein kinase C-z activity Role in a2 integrin and collage-nase mRNA expression J Cell Biol 136 473ndash483
Address reprint requests toDr John Doukas
Selective Genetics Inc11035 Roselle Street
San Diego CA 92121
E-mail jdoukasselectivegeneticscom
Received for publication December 28 2000 accepted after re-vision February 23 2001
DOUKAS ET AL798

the basis of its clinical use for the delivery of PDGF-BB pro-tein (Steed 1995)
Matrix influences on vector activity were examined by in-cubating AdLuc formulations at 37degC for 60 min followed bymatrix dissolution and vector bioassay (luciferase productionby 293 cells) This is an important test as adenoviruses arequickly inactivated under unfavorable physical and chemicalconditions (Nyberg-Hoffman and Aguilar-Cordova 1999)None of the matrices examined had a deleterious effect on vec-tor activity (90 6 12 106 6 5 and 139 6 37 of control ac-tivity for 015 collagen 26 collagen and CMC respec-tively) To further model in vivo vector stability we alsoincubated AdPDGF-B formulated in 26 collagen with woundfluid for 72 hr at 37degC prior to vector recovery and analysisWe observed no reduction in the level of PDGF-BB productionfrom cells transduced with AdPDGF-B exposed to wound fluidas compared with vector exposed to virus buffer (30 6 5 vs20 6 3 ng of PDGF-BB produced per milliliter of culturemedium respectively n 5 3)
As these data support the suitability of the selected matricesfor in vivo use we next determined their influence on vectorrelease kinetics (Fig 1) When placed in water collagen ma-trices retained the majority of their immobilized vectors with015 and 26 collagen releasing only 17 6 3 and 3 6 1 ofvector by 24 hr respectively By contrast 48 6 3 of AdLucwas released from CMC within 30 min and 61 6 2 by 6 hrThis was not unexpected as CMC is fairly water soluble andas both CMC and adenoviral particles are negatively chargedTherefore collagen matrices in a concentration-dependentfashion display more favorable kinetics for localizing and re-taining adenovirus vectors at delivery sites than does CMC
Collagen-immobilized adenoviruses induce distinctneotissues in vivo
Initial in vivo tests of matrix-immobilized vectors were per-formed with an established model of de novo tissue generation(Buckley et al 1985 Sprugel et al 1987 LeGrand et al1993) PVA sponges implanted subcutaneously in rats were in-jected with a single dose of adenovirus formulated in either col-lagen or CMC and then analyzed for tissue formation Forgrowth factor transgenes we selected platelet-derived growth
factor B (PDGF-B) vascular endothelial growth factor (VEGF)and fibroblast growth factor 2 (FGF2) because of their well-known mitogenic activities
AdPDGF-B formulated in 015 collagen induced granula-tion tissue formation in a dose-responsive manner (Table 1)Compared with vehicle controls delivering 2 3 1010 virus par-ticles induced a 17- to 23-fold increase in sponge protein con-tent (p 00002) a 2- to 27-fold increase in DNA content (p
00002) and a 29- to 43-fold increase in granulation tissue fill(p 00002) Trichrome-stained sections revealed the nearcomplete fill of sponge interiors with well-formed granulationtissue by day 6 posttreatment (Fig 2A) Expression of Ki-67a nuclear protein upregulated in proliferating cells (Gerdes etal 1983) established that both vascular endothelium (arrow-heads Fig 2B) and fibroblasts (arrows Fig 2B) had prolifer-ated in response to PDGF-B gene delivery AdFGF2 and Ad-VEGF also enhanced protein and DNA content within sponges(Table 1) However these vectors induced less granulation tis-sue deposition as compared with AdPDGF-B and the tissuesformed were histologically distinct
Tissues present in AdFGF2-treated sponges were highly vas-cular as revealed by the endothelial-reactive lectin BSL-I (Fig2D) Many of the infiltrating mononuclear cells also reactedpositively with BSL-I lectin suggesting that these cells wereendothelial cells or endothelial precursors AdFGF2 did nothowever induce the formation of classic granulation tissue aslittle collagen deposition was observed demonstrated by thepaucity of blue-staining material in trichrome-stained sections(Fig 2C) AdVEGF also induced heavily vascularized tissues(Fig 2E and F) but with greater extracellular collagen deposi-tion than AdFGF2 Relative to AdPDGF-B-induced tissueshowever AdVEGF-induced tissues were disorganized con-tained few fibroblasts and were markedly edematous Finallywhen AdLuc was delivered as a control treatment no signifi-cant increases in protein DNA or granulation tissue were ob-served compared with collagen vehicle alone (Table 1)Trichrome-stained sections revealed sparse inflammatory cellinfiltrates within AdLuc-treated sponges (Fig 2G) which com-pared with the near absence of infiltration after delivery of col-lagen vehicle alone (Fig 2H) suggested a limited antiviral response
Unlike the 015 collagen formulations described above
DOUKAS ET AL790
TABLE 2 NEOTISSUE FORMATION AFTER PDGF-B GENE OR PDGF-BB PROTEIN DELIVERYa
Granulation Protein DNATreatment fill () (mgsponge) (mgsponge)
015 Collagen vehicle 28 6 13b 16 6 2b 103 6 22b
AdPDGF-B 81 6 15b 30 6 6b 218 6 28b
PDGF-BB 100 mg 64 6 12c 22 6 4c 155 6 26c
PDGF-BB 10 mg qod 3 3d 77 6 9b0 31 6 8b 230 6 75b
aPVA sponges implanted in rats were injected with either 015 collagen vehicle or collagen containing AdPDGF-B as described in Table 1 Alternatively PDGF-BB protein was delivered as a single 100-mg dose on day 4 postimplantation or as10-mg doses on days 4 6 and 8 Sponges were removed on day 12 postimplantation and processed to determine the percent granulation fill as well as total protein and DNA contents Data are presented as means 6 SD (n 5 4ndash8)
bp 00001 versus collagen control and p 005 versus 100-mg PDGF-BBcp 003 versus collagen controldqod 3 3 Every other day three times
TISSUE REPAIR USING GROWTH FACTOR GENES 791
TABLE 3 INFLUENCE OF ADENOVIRUSndashMATRIX FORMULATIONS ON ISCHEMIC WOUND HEALINGa
Granulation Epithelial Wound closureTreatment Model system area (mm2) area (mm2) ( complete)
Aqueous buffer Cartilage intact 10 6 08 05 6 03 61 6 226 mm day 10
AdPDGF-B in Cartilage intact 24 6 22 05 6 01 73 6 28aqueous buffer 6 mm day 10
015 Collagen Cartilage intact 05 6 03 05 6 02 89 6 14vehicle 6 mm day 10
AdPDGF-B in Cartilage intact 16 6 09b 09 6 03c 97 6 7015 collagen 6 mm day 10
Aqueous buffer Cartilage removed 45 6 08 08 6 02 95 6 96 mm day 7
AdPDGF-B in Cartilage removed 40 6 15 11 6 05 82 6 22aqueous buffer 6 mm day 7
015 Collagen Cartilage removed 36 6 13 06 6 02 88 6 22vehicle 6 mm day 7
AdPDGF-B in Cartilage removed 70 6 14b 07 6 03 79 6 22015 collagen 6 mm day 7
26 Collagen Cartilage removed 04 6 05 01 6 01 24 6 15vehicle 8 mm day 8
AdPDGF-B in Cartilage removed 51 6 25b 06 6 03b 52 6 25c
26 collagen 8 mm day 8
aExcisional wounds (6 or 8 mm in diameter) were placed in ischemic rabbit ears with underlying cartilage left intact or re-moved Wounds were then treated with AdPDGF-B formulated in aqueous virus buffer or collagen control treatments consistedof vehicle alone For 6-mm wounds virus was applied as 2 3 109 particles per wound for 8-mm wounds as 4 3 109 particlesper wound On days 7ndash10 posttreatment wounds were harvested and processed as trichrome-stained paraffin sections whichwere then used to quantify newly formed granulation tissue and epithelium (cross-sectional area in mm2) and the degree of woundsurface closure (where 100 equals complete closure) Data are presented as means 6 SD (n 5 4ndash8)
bp 0009 versus vehicle controlcp 005 versus vehicle control
26 collagen formulations could not be reliably examined inthe PVA sponge model as their relatively high viscosity pre-vented uniform filling of sponges by syringe CMC-formulatedvectors were also unsuitable for this model system as theyproved highly inflammatory (data not shown) These formula-tions therefore were evaluated in more appropriate excisionalwound models (see below)
Tissue repair cells are transduced by collagen-immobilized adenoviruses
On the basis of the robust activity of collagen-formulatedAdPDGF-B we elected to further examine this vectorndashmatrixcombination first by seeking to correlate PDGF-B gene deliv-ery with subsequent transgene and protein expression WhenPVA sponges treated with 015 collagenndashAdPDGF-B werestained with both an anti-adenovirus antibody and the nuclearstain DAPI the majority of cells present 1 day after gene de-livery had bound andor internalized adenovirus (Fig 3A) Insitu hybridization revealed that these cells were successfullytransduced by virus as they contained human PDGF-B mRNA(Fig 3B) By contrast hybridization product was not detectedwith a sense riboprobe or when AdLuc-treated sponges wereexamined (data not shown)
We next used a human PDGF-BB-specific antibody to iden-tify the cell types responsible for transgene expression By day
1 postdelivery of 015 collagenndashAdPDGF-B PDGF-BB pro-tein was localized to leukocytes (arrowheads) and fibroblasts (ar-row Fig 3C) With time PDGF-BB protein was detected boundto the extracellular matrix (ECM) surrounding positively stainedcells (Fig 3D) This last observation indicates that a reservoir ofPDGF-BB protein develops within treated tissues and thus mayprolong the histogenic effects of this growth factor Finally byday 8 the majority of immunoreactivity had abated with pri-marily microvascular endothelium remaining positive (Fig 3E)However scattered fibroblasts could still be shown to producePDGF-BB protein by dual immunohistochemistry with anti-PDGF-BB and anti-vimentin antibodies (Fig 3F)
Multiple administrations of PDGF-BB protein are required to approximate the histogenic effects of collagenndashAdPDGF-B
To directly compare gene therapy with the more conven-tional approach of growth factor protein delivery we next quan-tified tissue formation in response to either PDGF gene or pro-tein delivery A single injection of 015 collagenndashAdPDGF-Benhanced granulation tissue filling of sponges by 3-fold versusvehicle alone (p 00001) and sponge protein and DNA lev-els by 2-fold (p 00001 Table 2) Using a human PDGF-BB-specific ELISA this growth factor was detected at 54 6 13ngsponge (n 5 8) By contrast when PDGF-BB protein was
delivered as a single dose nearly 2000-fold in excess of thisconcentration the tissue formation responses observed (proteinand DNA accumulation and granulation tissue formation) weresignificantly lower (p 005 Table 2) In fact repeated dos-ing with PDGF-BB protein was required in order to achieve re-sponses comparable to a single administration of the PDGF-Bgene These data therefore support our hypothesis that the abil-ity of gene delivery to establish prolonged in situ growth fac-tor production translates into greater histogenesis than that seenwith growth factor proteins
CollagenndashAdPDGF-B induces complete healing of ischemic wounds
Nonhealing wounds are a major risk in chronically ischemictissues as low oxygen tension greatly impairs tissue repair pro-cesses We therefore compared the ability of matrix versusaqueous formulated AdPDGF-B to repair ischemic excisionalwounds Several models were employed to compare variationsin wound size and condition so as to allow for a more com-plete picture of tissue repair
In the first model system 6-mm-diameter wounds were cre-ated in ischemic rabbit ears by removal of epidermal and der-mal layers but not underlying cartilage This model has beenused in previous studies of growth factor proteins and genes(Ahn and Mustoe 1990 Mustoe et al 1994 Liechty et al1999) and was therefore employed to allow comparison withthese reports However it represents an artificial system as thepresence of a cartilage layer restricts both treatment activity andhealing to wound margins and in addition the initially acellu-lar wound bed forms a cup that artifactually retains aqueoustreatments As would be predicted we found a trend towardgranulation tissue formation in this model after the applicationof AdPDGF-B formulated in aqueous buffer (Table 3) How-ever this response did not reach the level of statistical signifi-cance as tissue development was highly variable (note the highstandard deviation value) In addition epithelial regenerationand wound closure were minimal to unaffected By contrastAdPDGF-B formulated in 015 collagen enhanced granula-tion tissue area by 32-fold and epithelial area by 18-fold overthat achieved with vehicle alone (p 0009 and 005 respec-tively) Although near complete closure of epithelial gaps wasalso achieved the high level of self-healing in control-treatedgroups (89 wound closure) precluded statistical significance
In an alternative model design subdermal cartilage was com-pletely removed from excisional wounds creating beds whosefloors now consisted of dermal tissue (Pierce et al 1994b)This design allows for cellular responses from the entire woundbed as well as the opportunity for vector migration beyond
treatment areas We now observed that aqueous formulated Ad-PDGF-B failed to induce even a trend toward tissue regenera-tion (Table 3) Rather the vector appears to have seeped throughthe wound bed floor as inflammatory cell infiltrates and fociof fibroblast proliferation were observed in the underlying der-mis and at wound margins (Fig 4A) Immunohistochemistryconfirmed the production of human PDGF-BB at these sites(Fig 4B) CMC-formulated AdPDGF-B also failed to induceany meaningful tissue repair Wounds treated with this formu-lation showed a diffuse inflammatory response within thewound bed and wound surfaces were overlain with fibrin clotsrather than regenerating epithelium (Fig 4C and D) By con-trast AdPDGF-B formulated in 015 collagen enhanced gran-ulation tissue deposition 19-fold within wound beds versus ve-hicle controls (p 0002) and wounds were extensivelyepithelialized (Table 3) Neither epithelial regeneration norwound closure achieved significance however as the high de-gree of self-healing achieved in this particular model (see ve-hicle alone group) most likely masked transgene-stimulated re-sponses
To address these model limitations as our next system wecreated 8-mm wounds in ischemic rabbit ears by removingepidermal dermal and cartilage layers reasoning that largerexcisional wounds would display limited self-healing In ad-dition this model could readily accommodate 26 collagenformulations which proved difficult to reproducibly apply insmaller wounds Compared with control wounds treated withcollagen vehicle alone wounds treated with AdPDGF-B for-mulated in 26 collagen achieved a 12-fold enhancementin granulation tissue fill and a 6-fold enhancement in re-ep-ithelialization by day 8 posttreatment (p 0009 Table 3)In addition wound closure was only 24 complete in colla-gen vehicle-treated wounds by day 8 but 52 complete inwounds treated with collagen-formulated AdPDGF-B (p
005) Histologically AdPDGF-B-treated wounds showed nosigns of tissue hyperplasia or chronic inflammation but ratheran orderly repair process marked by a regenerated epitheliallayer overlying a wound bed filled with granulation tissue(Fig 4E and F)
CollagenndashAdPDGF-B induces normal long-term tissue repair
Our choice of adenoviruses for transgene delivery was partlybased on the reasoning that as these vectors establish transientgene expression they would not lead to hyperproliferative re-sponses or scar formation To test this hypothesis we treatedrabbit ear excisional wounds with AdPDGF-B formulated in015 collagen and examined tissue repair responses out to
DOUKAS ET AL792
FIG 4 Influence of adenovirusndashmatrix formulations on excisional wound repair Excisional wounds (6 or 8 mm in diameter andextending through underlying cartilage layers) were placed in ischemic rabbit ears bars indicate original wound depth (determinedfrom cartilage visible at wound margins) Wounds were then treated with AdPDGF-B formulated in either virus buffer CMC orcollagen and on day 7 or 8 posttreatment processed for histology or immunohistochemistry An identical design was used to ex-amine long-term healing on day 90 except that wounds were created in nonischemic ears (A) Day 7 buffer-formulated AdPDGF-B-treated 6-mm wound trichrome stain (B) Day 7 buffer-formulated AdPDGF-B-treated 6-mm wound anti-PDGF-BB proteinimmunostain (C and D) Day 7 CMC-formulated AdPDGF-B-treated 6-mm wound trichrome stains (E and F) Day 8 26 col-lagen-formulated AdPDGF-B-treated 8-mm wound trichrome stains (G and H) Day 90 015 collagen-formulated AdPDGF-B-treated 6-mm wound trichrome stains Original magnification (A C E and G) 340 (B D F and H) 3200
TISSUE REPAIR USING GROWTH FACTOR GENES 793
DOUKAS ET AL794
TABLE 4 BIODISTRIBUTION OF AdPDGF-B IN EXCISIONAL WOUNDSa
Positive samplestotal assayed
Tissue AdPDGF-B dose Day 3 Day 7 Day 28 Day 90
Wound bed 2 3 109 particles 66 66 66b 06Axillary lymph nodes 2 3 109 particles 02 ND 06 06
Wound bed 2 3 1011 particles 66 66 66 46c
Axillary lymph nodes 2 3 1011 particles 66 ND 66d 26e
aFull-thickness excisional wounds (7 cm2) were placed on the backs of rabbits and AdPDGF-B formulated in 26 collagenwas applied as either 2 3 109 or 2 3 1011 virus particles per wound On days 3ndash90 posttreatment wound beds and a panel oforgans were harvested for real-time PCR quantification of viral genome Data are shown for wound bed and axillary lymph nodesamples as the number of samples that yielded amplifiable signals per total number assayed ND not determined
bThree of six samples scored below the level of quantitation (LOQ 10ndash100 copiesmg DNA)cAll four positive samples scored below the LOQdThree of six samples scored below the LOQeBoth positive samples scored below the LOQ
180 days posttreatment (Fig 5) PDGF-B gene delivery en-hanced total ear thickness relative to controls on day 28 (229 6
020 vs 179 6 019 mm p 00001) and day 60 (192 6 001vs 182 6 011 mm p 0005) as anticipated on the basis ofthe ability of this formulation to induce granulation tissue for-mation By day 90 posttreatment however there was no mea-surable difference in ear thickness between AdPDGF-B andcontrol-treated groups and this relationship continued out today 180 indicating that growth factor gene delivery did not in-duce excessive scar formation This was also confirmed histo-logically AdPDGF-B-treated wounds on day 90 and beyondwere composed of a thin outer keratin layer an underlying ep-ithelial layer of equivalent thickness to nonwounded areas anda collagen-rich dermis devoid of any signs of tissue hyperpla-sia (Fig 4G and H)
Collagen immobilization limits adenovirus vectorbiodistribution beyond treatment sites
As a final measure of the value of matrix immobilization forgene delivery we determined the biodistribution patterns ofvectors after their in vivo delivery In the first model systemused AdPDGF-B formulated in 015 collagen was applied torabbit ear wounds at equivalent doses as previously describedwounds were extended through underlying cartilage but vas-cular supplies were not disturbed so as to permit maximal vec-tor dissemination By PCR no adenoviral DNA was detectablein lung spleen brain cervical lymph nodes or gonads on day1 3 7 or 14 (n 5 6 per group) In the liver one of six sam-ples was positive on days 3 and 7 but none on day 14 in serumonly one of six samples tested positive on day 14 (equivalentof 500-ml serum volume) By contrast adenovirus was detectedin eight of eight wound bed samples at all time points exam-ined
In a second model system excisional wounds placed on thebacks of rabbits were treated with AdPDGF-B formulated in26 collagen Because of their anatomical placement thismodel allowed for the creation of larger excisional wounds (7-cm2 total area) than those placed in rabbit ears (03 cm2) and
consequently larger treatment volumes and vector doses (2 3109 or 2 3 1011 virus particles per wound) At the lower doseof 2 3 109 particles PCR-amplifiable adenoviral DNA was notdetectable beyond wound beds on day 3 7 28 or 90 Tissuessampled and found not to contain vector included blood heartlung liver kidney brain spleen lymph nodes and gonads (n 5
6group) In wound beds adenoviral DNA was detected at alltime points except for day 90 (Table 4 and Fig 6) Vector lev-els did decrease however by 38-fold between days 7 and 28with three of six samples falling below the level of quantita-tion (LOQ) by real-time PCR at the latter time point (Fig 6)
At a 100-fold higher vector dose of 2 3 1011 particles perwound PCR-amplifiable adenoviral DNA was once again un-detectable in the majority of tissues sampled Except for a sin-gle day 7 liver sample and a single day 7 brain sample (bothbelow the LOQ) adenoviral DNA was only detectable directlyin wound beds or in the axillary lymph nodes that drain woundsites (Table 4) Moreover three of six positive axillary nodesamples scored below the LOQ on day 28 as did both positivesamples on day 90 indicating that they contained relatively lit-tle vector Within wound beds adenoviral DNA was detectedat quantifiable levels out to day 28 and at detectable but non-quantifiable levels on day 90 DNA copy numbers remainedsteady between days 3 and 7 dropped 107-fold between days7 and 28 and a further 1662-fold by day 90 Finally at eachtime point DNA copy numbers in wounds treated with 2 3
1011 particles were approximately 100-fold higher than thosefound in wounds treated with 2 3 109 particles thus confirm-ing the linearity of our assay system
To better define the time course of human PDGF-BB pro-duction we also quantified transgene mRNA levels in woundbed samples treated at 2 3 109 particles per wound This treat-ment dose was selected as representative of the virus particleconcentration capable of inducing complete healing in ischemicear wounds Quantifiable levels of human PDGF-B mRNAwere detectable in treated dorsal wounds at days 3 7 and 28(Fig 6) with levels decreasing 14-fold between days 3 and 7and 5-fold between days 7 and 28 The more sensitive tech-nique of real-time RT-PCR therefore demonstrates that trans-
TISSUE REPAIR USING GROWTH FACTOR GENES 795
gene expression extends well beyond the 8-day time period sug-gested using anti-PDGF-BB immunohistochemistry as a de-tection system (Fig 3)
DISCUSSION
These studies demonstrate that immobilization of gene ther-apy vectors in collagen-based matrices enables their efficientdelivery and activity in vivo Matrix immobilization achievedprolonged transgene-encoded growth factor production and asa consequence robust tissue repair By contrast aqueous vehi-cles failed to retain adenoviruses at application sites resultingin diffuse inflammation rather than productive tissue regenera-tion These observations confirm our basic hypothesis that ma-trix immobilization of growth factor-encoding gene therapyvectors represents a promising approach to tissue repair
Although de novo tissue deposition was achievable with sev-eral growth factor genes PDGF-B proved the most suitable forrepair of cutaneous defects A single administration of colla-gen-immobilized AdPDGF-B rapidly induced the formation ofhighly cellular and vascularized tissues with dense ECMs richin collagen By contrast AdFGF2 induced a primarily vascu-lar response with little collagen deposition FGF2 induces therelease of matrix metalloproteinase 1 or interstitial collagenase(Buckley-Sturrock et al 1989) and this may underlie the rel-ative paucity of ECM accumulation VEGF gene delivery alsoinduced highly vascular responses however the enhanced per-meability characteristic of VEGF-induced vasculature (Dvoraket al 1995) led to edema within nascent tissues In fact much
of the enhanced protein and DNA deposition observed in Ad-VEGF-treated PVA sponges may well derive from fluid exu-dates rather than actual tissue formation Finally the inabilityof AdLuc delivery to induce anything beyond a limited in-flammatory response confirms that tissue formation was de-pendent on growth factor gene delivery
The robust activity of PDGF-B gene delivery was expectedas PDGF-BB protein initiates multiple aspects of tissue forma-tion including cellular influx and proliferation ECM deposi-tion and tissue remodeling (Pierce et al 1988 1991 1994a)Indeed PDGF-BB is the only growth factor protein to have suc-cessfully completed human clinical trials and be approved forthe treatment of dermal wounds (Steed 1995 drsquoHemecourt etal 1998 Wieman 1998 Wieman et al 1998) We observedthat collagen-formulated AdPDGF-B induced the complete re-pair of excisional skin defects without unwanted long-term ef-fects such as the development of hypertrophic scars Endoge-nous growth factors other than PDGF-BB however most likelymediated the enhanced re-epithelialization observed in thesewounds as epithelial regeneration is driven by members of theepidermal growth factor and FGF families (Pierce et al 1994bDanilenko et al 1995) Our data indicate nonetheless that tis-sue regeneration and repair were initiated and to a great degreedriven by transgene-encoded PDGF-BB
Despite the known activity of PDGF-BB protein we wereable to demonstrate greater tissue deposition after gene deliv-ery as compared with the use of recombinant growth factor pro-tein A single application of PDGF-BB protein could not equalthe ability of PDGF-B gene therapy to induce neotissue for-mation even at doses well in excess of that induced in situ byAdPDGF-B and in excess of that used in human clinical trials
FIG 5 Influence of collagen-formulated AdPDGF-B on long-term tissue repair Excisional wounds (6 mm in diameter withcartilage remaining intact) were placed in nonischemic rabbit ears and treated with either 015 collagen alone (open columns)or AdPDGF-B formulated in this vehicle (solid columns) On days 28ndash180 posttreatment total ear thickness at the site of eachwound was measured (in mm) with calipers Data are presented as means 6 SD (n 5 3) Treatment groups differ by p 00001groups differ by p 0005
(Steed 1995 drsquoHemecourt et al 1998 Wieman 1998 Wie-man et al 1998) In fact repeated administrations of PDGF-BB protein were required to approach the level of tissue for-mation observed after a single administration of AdPDGF-BThese data support our hypothesis that sustained localizedgrowth factor production is required for robust tissue repair
In further support of this hypothesis we demonstrated thatmRNA encoding human PDGF-B was present in excisionalwounds as late as day 28 after collagen-formulated AdPDGF-B administration By contrast previous studies of PDGF-BBprotein found that the great majority of this growth factor wasgone from treated wounds 1 day postapplication and that anytissue maturation subsequently observed was most likely dueto the upregulation of endogenous growth factors (Pierce et al1992 1995) We also demonstrated that repair cells such asmononuclear leukocytes endothelial cells and fibroblasts pres-ent with developing neotissues represent the source of both
transgene transcription and PDGF-BB production In additiona depot of human PDGF-BB was detected bound to the colla-gen delivery matrix and ECM of these tissues This was antici-pated as PDGF-BB contains collagen-binding motifs (Soma-sundaram and Schuppan 1996) We hypothesize that subsequentmatrix metalloproteinase activity by repair cells will serve togenerate localized release of this sequestered growth factor pooland as a consequence further drive tissue regeneration Theseevents which are central to tissue remodeling should be directlyenhanced by collagen matrices as type I collagen stimulates me-talloproteinase production integrin expression and cellular ac-tivation in PDGF-stimulated fibroblasts (Xu and Clark 19961997)
An additional rationale for employing collagen matrices wasto physically immobilize vectors This was confirmed in vivowhere collagen matrices maintained AdPDGF-B at deliverysites for at least 28 days and limited vector migration to other
DOUKAS ET AL796
FIG 6 Persistence of collagen-formulated vector and transgene transcripts in excisional wounds Full-thickness excisionalwounds (7 cm2) were placed on the dorsal surface of rabbits and treated with AdPDGF-B formulated in 26 collagen at either2 3 109 or 2 3 1011 virus particles per wound (open and closed columns respectively) Wounds were then covered with OpSitedressing and on days 3 7 or 28 posttreatment wound beds were harvested for real-time quantitative PCR and RT-PCR analy-ses PCR data are presented in the upper graph as AdPDGF-B copies per wound RT-PCR data are presented in the lower graphas the relative amount of PDGF-B mRNA per unit 18S rRNA (in arbitrary units) All data points are means 6 SD (n 5 6)
tissues or organs In vitro tests also established that collagenmatrices not only prevent vector loss due to diffusion but pre-serve vector activity despite prolonged incubation in acutewound fluid Successful vector immobilization and tissue re-pair could be achieved with both 015 collagen and 26 col-lagen suggesting flexibility in the final vehicle formulation re-quired for effective vector delivery This flexibility was neededin the present studies as 26 collagen formulations proveddifficult to deliver to PVA sponges and 6-mm excisionalwounds This would not be of concern in clinical settings how-ever where wound beds are easily accessible and generally sev-eral square centimeters in area By contrast CMC was inef-fective at retaining vector in aqueous environments Moreimportantly this matrix was itself inflammatory and whencombined with adenovirus the net result was inflammationrather than tissue repair We are currently examining the util-ity of other matrices such as fibrin and hyaluronic acid whichbecause of their more provisional nature may offer yet greatercellular migration into wounds as compared with type I colla-gen
Although an aqueous-based AdPDGF-B formulation hasbeen previously shown to enhance tissue formation (Liechty etal 1999) this was achieved with a model system that artifi-cially retains vectors within treatment sites In fact the presentstudies demonstrate that any tissue repair observed after Ad-PDGF-B delivery in a nongelling liquid is dependent on the useof this model system In wounds not designed to retain appliedtreatments aqueous-formulated AdPDGF-B seeped into sur-rounding tissues and led to hyperplasia within these areas ratherthan to tissue regeneration within the active wound bed Colla-gen-immobilized AdPDGF-B on the other hand did persist inthese wound beds and led to significant enhancements in gran-ulation tissue formation as well as enhanced wound re-epithe-lialization and wound closure The significance of these activ-ities is further substantiated considering that they wereachievable in 8-mm-diameter ischemic wounds which withinthe time frame examined could not self-heal to any meaning-ful degree in the absence of gene therapy However as all theanimal models employed in these studies will eventually self-heal given sufficient time the full value of matrix-immobilizedgene therapy vectors remains to be confirmed in human clini-cal trials
In conclusion we present evidence that matrix-immobilizedgene therapy vectors encoding appropriate growth-promotinggenes represent a promising approach to tissue regeneration andrepair This basic concept can be expanded to include alterna-tive matrices such as controlled-release formulations as wellas tissue-specific growth factors Furthermore the addition oftargeting ligands to adenovirus vectors (eg FGF2) can en-hance their ability to transduce cells such that tissue repair re-sponses comparable to nontargeted vectors can be achieved butat significantly lower vector doses (Chandler et al 2000a)With appropriate design and application schedules one couldconceivably time the release of multiple growth factors to spe-cific stages of a tissue repair cascade In addition we have foundin preliminary studies that collagen-immobilized nonviral vec-tors such as PDGF-B plasmids which have potentially morefavorable safety profiles than adenovirus vectors can also en-hance tissue formation in vivo (Chandler et al 2000b Tyroneet al 2000) Such flexibility should allow for the widespreadapplication of gene therapy to the treatment of injured tissues
ACKNOWLEDGMENTS
We thank Jeff Davidson (Vanderbilt University School ofMedicine) for assistance in establishing the PVA sponge modelCarl-Henrik Heldin (Ludwig Institute for Cancer Research) forthe PDGF-B gene construct and Emelie Amburn Lara AsatoSharon Chang Gail Fieser Lydia Greenlees Rebecca Smokerand Linda Manza for excellent technical assistance This pub-lication was made possible in part by NIH grants 1R43AR46154(JD) and 5P01CA25874 (MH)
REFERENCES
AHN ST and MUSTOE TA (1990) Effects of ischemia on ulcerwound healing A new model in the rabbit ear Ann Plast Surg 2417ndash23
ANDREE C SWAIN WF PAGE CP MACKLIN MDSLAMA J HATZIS D and ERIKSSON E (1994) In vivo trans-fer and expression of a human epidermal growth factor gene accel-erates wound repair Proc Natl Acad Sci USA 91 12188ndash12192
BENN SI WHITSITT JS BROADLEY KN NANNEY LBPERKINS D HE L PATEL M MORGAN JR SWAIN WFand DAVIDSON JM (1996) Particle-mediated gene transfer withtransforming growth factor-b1 cDNAs enhances wound repair in ratskin J Clin Invest 98 2894ndash2902
BONADIO J SMILEY E PATIL P and GOLDSTEIN S (1999)Localized direct plasmid gene delivery in vivo Prolonged therapyresults in reproducible tissue regeneration Nat Med 5 753ndash759
BUCKLEY A DAVIDSON JM KAMERATH CD WOLT TBand WOODWARD SC (1985) Sustained release of epidermalgrowth factor accelerates wound repair Proc Natl Acad Sci USA82 7340ndash7344
BUCKLEY-STURROCK A WOODWARD SC SENIOR RMGRIFFIN GL KLAGSBRUN M and DAVIDSON JM (1989)Differential stimulation of collagenase and chemotactic activity in fi-broblasts derived from rat wound repair tissue and human skin bygrowth factors J Cell Physiol 138 70ndash78
CHANDLER LA DOUKAS J GONZALEZ AM HOGANSONDK GU DL MA C NESBIT M CROMBLEHOLME TMHERLYN M SOSNOWSKI BA and PIERCE GF (2000a)FGF2ndashTargeted adenovirus encoding platelet-derived growth factor-B enhances de novo tissue formation Mol Ther 2 153ndash160
CHANDLER LA MA C GONZALEZ AM DOUKAS JNGUYEN T PIERCE GF and PHILLIPS ML (2000b) Ma-trix-enabled gene transfer for cutaneous wound repair Wound Re-pair Regen 8 473ndash479
DANILENKO DM RING BD TARPLEY JE MORRIS BVAN GY MORAWIECKI A CALLAHAN W GOLDEN-BERG M HERSHENSON S and PIERCE GF (1995) Growthfactors in porcine full and partial thickness burn repair Differing tar-gets and effects of keratinocyte growth factor platelet-derivedgrowth factor-BB epidermal growth factor and neu differentiationfactor Am J Pathol 147 1261ndash1277
DEUEL TF KAWAHARA RS MUSTOE TA and PIERCE GF(1991) Growth factors and wound healing Platelet-derived growthfactor as a model cytokine Annu Rev Med 42 567ndash584
DrsquoHEMECOURT PA SMIELL JM and KARIM MR (1998) So-dium carboxymethylcellulose aqueous-based gel vs becaplermin gelin patients with nonhealing lower extremity diabetic ulcers Wounds10 69ndash75
DOUKAS J HOGANSON DK ONG M YING W LACEYDL BAIRD A PIERCE GF and SOSNOWSKI BA (1999)Retargeted delivery of adenoviral vectors through fibroblast growthfactor receptors involves unique cellular pathways FASEB J 131459ndash1466
TISSUE REPAIR USING GROWTH FACTOR GENES 797
DVORAK HF BROWN LF DETMAR M and DVORAK AM(1995) Vascular permeability factorvascular endothelial growth fac-tor microvascular hyperpermeability and angiogenesis Am JPathol 146 1029ndash1039
EMING SA MEDALIE DA TOMPKINS RG YARMUSHML and MORGAN JR (1998) Genetically modified human ker-atinocytes overexpressing PDGF-A enhance the performance of acomposite skin graft Hum Gene Ther 9 529ndash539
EMING SA WHITSITT JS HE L KRIEG T MORGAN JRand DAVIDSON JM (1999) Particle-mediated gene transfer ofPDGF isoforms promotes wound repair J Invest Dermatol 112297ndash302
GERDES J SCHWAB U LEMKE H and STEIN H (1983) Pro-duction of a mouse monoclonal antibody reactive with a human nu-clear antigen associated with cell proliferation Int J Cancer 3113ndash20
GONZALEZ AM BERRY M MAHER PA LOGAN A andBAIRD A (1995) A comprehensive analysis of the distribution ofFGF-2 and FGFR1 in the rat brain Brain Res 701 201ndash226
GREENHALGH DG (1996) The role of growth factors in woundhealing J Trauma 41 159ndash167
GROTENDORST GR MARTIN GR PENCEV D SODEK Jand HARVEY AK (1985) Stimulation of granulation tissue for-mation by platelet-derived growth factor in normal and diabetic ratsJ Clin Invest 76 2323ndash2329
KHOURI RK HONG SP DEUNE EG TARPLEY JE SONGSZ SERDAR CM and PIERCE GF (1994) De novo genera-tion of permanent neovascularized soft tissue appendages by platelet-derived growth factor J Clin Invest 94 1757ndash1763
LEGRAND EK SENTER LH GAMELLI RL and KIORPESTC (1993) Evaluation of PDGF-BB PDGF-AA bFGF IL-1 andEGF dose responses in polyvinyl alcohol sponge implants assessedby a rapid histologic method Growth Factors 8 315ndash329
LIECHTY KW NESBIT M HERLYN M RADU A ADZICKNS and CROMBLEHOLME TM (1999) Adenoviral-mediatedoverexpression of platelet-derived growth factor-B corrects ischemicimpaired wound healing J Invest Dermatol 113 375ndash383
LYNCH SE COLVIN RB and ANTONIADES HN (1989)Growth factors in wound healing J Clin Invest 84 640ndash646
MUSTOE TA PIERCE GF THOMASON A GRAMATES PSPORN MB and DEUEL TF (1987) Accelerated healing of in-cisional wounds in rats induced by transforming growth factor-betaScience 237 1333ndash1336
MUSTOE TA PIERCE GF MORISHIMA C and DEUEL TF(1991) Growth factor-induced acceleration of tissue repair throughdirect and inductive activities in a rabbit dermal ulcer model J ClinInvest 87 694ndash703
MUSTOE TA AHN ST TARPLEY JE and PIERCE GF(1994) Role of hypoxia in growth factor responses Differential ef-fects of basic fibroblast growth factor and platelet-derived growthfactor in an ischemic wound model Wound Rep Reg 2 277ndash283
NYBERG-HOFFMAN C and AGUILAR-CORDOVA E (1999) In-stability of adenoviral vectors during transport and its implication forclinical studies Nat Med 5 955ndash957
PIERCE GF and MUSTOE TA (1995) Pharmacologic enhance-ment of wound healing Annu Rev Med 46 467ndash481
PIERCE GF MUSTOE TA SENIOR RM REED J GRIFFINGL THOMASON A and DEUEL TF (1988) In vivo incisionalwound healing augmented by platelet-derived growth factor and re-combinant c-sis gene homodimeric proteins J Exp Med 167 974ndash987
PIERCE GF VANDE BERG J RUDOLPH R TARPLEY J andMUSTOE TA (1991) Platelet-derived growth factor-BB and trans-forming growth factor beta 1 selectively modulate glycosaminogly -cans collagen and myofibroblasts in excisional wounds Am JPathol 138 629ndash646
PIERCE GF TARPLEY JE YANAGIHARA D MUSTOE TA
FOX GM and THOMASON A (1992) Platelet-derived growthfactor (BB homodimer) transforming growth factor-b1 and basic fi-broblast growth factor in dermal wound healing Neovessel and ma-trix formation and cessation of repair Am J Pathol 140 1375ndash1388
PIERCE GF TARPLEY JE ALLMAN RM GOODE PS SER-DAR CM MORRIS B MUSTOE TA and VANDE BERG J(1994a) Tissue repair processes in healing chronic pressure ulcerstreated with recombinant platelet-derived growth factor BB Am JPathol 145 1399ndash1410
PIERCE GF YANAGIHARA D KLOPCHIN K DANILENKODM HSU E KENNEY WC and MORRIS CF (1994b) Stim-ulation of all epithelial elements during skin regeneration by kerati-nocyte growth factor J Exp Med 179 831ndash840
PIERCE GF TARPLEY JE TSENG J BREADY J CHANGD KENNEY WC RUDOLPH R ROBSON MC VANDEBERG J and REID P (1995) Detection of platelet-derived growthfactor (PDGF)-AA in actively healing human wounds treated withrecombinant PDGF-BB and absence of PDGF in chronic nonhealingwounds J Clin Invest 96 1336ndash1350
SINGER AJ and CLARK RA (1999) Cutaneous wound healingN Engl J Med 341 738ndash746
SOMASUNDARAM R and SCHUPPAN D (1996) Type I II IIIIV V and VI collagens serve as extracellular ligands for the iso-forms of platelet-derived growth factor (AA BB and AB) J BiolChem 271 26884ndash26891
SPRUGEL KH MCPHERSON JM CLOWES AW and ROSSR (1987) Effects of growth factors in vivo I Cell ingrowth intoporous subcutaneous chambers Am J Pathol 129 601ndash613
STEED DL (1995) Clinical evaluation of recombinant humanplatelet-derived growth factor for the treatment of lower extremitydiabetic ulcers Diabetic Ulcer Study Group J Vasc Surg 21 71ndash78
STEED DL (1998) Foundations of good ulcer care Am J Surg 17620S-25S
TYRONE JW MOGFORD JE CHANDLER LA MA C XIAY PIERCE GF and MUSTOE TA (2000) Collagen-embeddedplatelet-derived growth factor DNA plasmid promotes wound heal-ing in a dermal ulcer model J Surg Res 93 230ndash236
VOGT PM THOMPSON S ANDREE C LIU P BREUING KHATZIS D BROWN H MULLIGAN RC and ERIKSSON E(1994) Genetically modified keratinocytes transplanted to woundsreconstitute the epidermis Proc Natl Acad Sci USA 91 9307ndash9311
WIEMAN TJ (1998) Clinical efficacy of becaplermin (rhPDGF-BB)gel Becaplermin Gel Studies Group Am J Surg 176 74S-79S
WIEMAN TJ SMIELL JM and SU Y (1998) Efficacy and safetyof a topical gel formulation of recombinant human platelet-derivedgrowth factor-BB (becaplermin) in patients with chronic neuropathicdiabetic ulcers A phase III randomized placebo-controlled double-blind study Diabetes Care 21 822ndash827
WILSON JM (1996) Adenoviruses as gene-delivery vehicles NEngl J Med 334 1185ndash1187
XU J and CLARK RA (1996) Extracellular matrix alters PDGFregulation of fibroblast integrins J Cell Biol 132 239ndash249
XU J and CLARK RA (1997) A three-dimensional collagen latticeinduces protein kinase C-z activity Role in a2 integrin and collage-nase mRNA expression J Cell Biol 136 473ndash483
Address reprint requests toDr John Doukas
Selective Genetics Inc11035 Roselle Street
San Diego CA 92121
E-mail jdoukasselectivegeneticscom
Received for publication December 28 2000 accepted after re-vision February 23 2001
DOUKAS ET AL798

TISSUE REPAIR USING GROWTH FACTOR GENES 791
TABLE 3 INFLUENCE OF ADENOVIRUSndashMATRIX FORMULATIONS ON ISCHEMIC WOUND HEALINGa
Granulation Epithelial Wound closureTreatment Model system area (mm2) area (mm2) ( complete)
Aqueous buffer Cartilage intact 10 6 08 05 6 03 61 6 226 mm day 10
AdPDGF-B in Cartilage intact 24 6 22 05 6 01 73 6 28aqueous buffer 6 mm day 10
015 Collagen Cartilage intact 05 6 03 05 6 02 89 6 14vehicle 6 mm day 10
AdPDGF-B in Cartilage intact 16 6 09b 09 6 03c 97 6 7015 collagen 6 mm day 10
Aqueous buffer Cartilage removed 45 6 08 08 6 02 95 6 96 mm day 7
AdPDGF-B in Cartilage removed 40 6 15 11 6 05 82 6 22aqueous buffer 6 mm day 7
015 Collagen Cartilage removed 36 6 13 06 6 02 88 6 22vehicle 6 mm day 7
AdPDGF-B in Cartilage removed 70 6 14b 07 6 03 79 6 22015 collagen 6 mm day 7
26 Collagen Cartilage removed 04 6 05 01 6 01 24 6 15vehicle 8 mm day 8
AdPDGF-B in Cartilage removed 51 6 25b 06 6 03b 52 6 25c
26 collagen 8 mm day 8
aExcisional wounds (6 or 8 mm in diameter) were placed in ischemic rabbit ears with underlying cartilage left intact or re-moved Wounds were then treated with AdPDGF-B formulated in aqueous virus buffer or collagen control treatments consistedof vehicle alone For 6-mm wounds virus was applied as 2 3 109 particles per wound for 8-mm wounds as 4 3 109 particlesper wound On days 7ndash10 posttreatment wounds were harvested and processed as trichrome-stained paraffin sections whichwere then used to quantify newly formed granulation tissue and epithelium (cross-sectional area in mm2) and the degree of woundsurface closure (where 100 equals complete closure) Data are presented as means 6 SD (n 5 4ndash8)
bp 0009 versus vehicle controlcp 005 versus vehicle control
26 collagen formulations could not be reliably examined inthe PVA sponge model as their relatively high viscosity pre-vented uniform filling of sponges by syringe CMC-formulatedvectors were also unsuitable for this model system as theyproved highly inflammatory (data not shown) These formula-tions therefore were evaluated in more appropriate excisionalwound models (see below)
Tissue repair cells are transduced by collagen-immobilized adenoviruses
On the basis of the robust activity of collagen-formulatedAdPDGF-B we elected to further examine this vectorndashmatrixcombination first by seeking to correlate PDGF-B gene deliv-ery with subsequent transgene and protein expression WhenPVA sponges treated with 015 collagenndashAdPDGF-B werestained with both an anti-adenovirus antibody and the nuclearstain DAPI the majority of cells present 1 day after gene de-livery had bound andor internalized adenovirus (Fig 3A) Insitu hybridization revealed that these cells were successfullytransduced by virus as they contained human PDGF-B mRNA(Fig 3B) By contrast hybridization product was not detectedwith a sense riboprobe or when AdLuc-treated sponges wereexamined (data not shown)
We next used a human PDGF-BB-specific antibody to iden-tify the cell types responsible for transgene expression By day
1 postdelivery of 015 collagenndashAdPDGF-B PDGF-BB pro-tein was localized to leukocytes (arrowheads) and fibroblasts (ar-row Fig 3C) With time PDGF-BB protein was detected boundto the extracellular matrix (ECM) surrounding positively stainedcells (Fig 3D) This last observation indicates that a reservoir ofPDGF-BB protein develops within treated tissues and thus mayprolong the histogenic effects of this growth factor Finally byday 8 the majority of immunoreactivity had abated with pri-marily microvascular endothelium remaining positive (Fig 3E)However scattered fibroblasts could still be shown to producePDGF-BB protein by dual immunohistochemistry with anti-PDGF-BB and anti-vimentin antibodies (Fig 3F)
Multiple administrations of PDGF-BB protein are required to approximate the histogenic effects of collagenndashAdPDGF-B
To directly compare gene therapy with the more conven-tional approach of growth factor protein delivery we next quan-tified tissue formation in response to either PDGF gene or pro-tein delivery A single injection of 015 collagenndashAdPDGF-Benhanced granulation tissue filling of sponges by 3-fold versusvehicle alone (p 00001) and sponge protein and DNA lev-els by 2-fold (p 00001 Table 2) Using a human PDGF-BB-specific ELISA this growth factor was detected at 54 6 13ngsponge (n 5 8) By contrast when PDGF-BB protein was
delivered as a single dose nearly 2000-fold in excess of thisconcentration the tissue formation responses observed (proteinand DNA accumulation and granulation tissue formation) weresignificantly lower (p 005 Table 2) In fact repeated dos-ing with PDGF-BB protein was required in order to achieve re-sponses comparable to a single administration of the PDGF-Bgene These data therefore support our hypothesis that the abil-ity of gene delivery to establish prolonged in situ growth fac-tor production translates into greater histogenesis than that seenwith growth factor proteins
CollagenndashAdPDGF-B induces complete healing of ischemic wounds
Nonhealing wounds are a major risk in chronically ischemictissues as low oxygen tension greatly impairs tissue repair pro-cesses We therefore compared the ability of matrix versusaqueous formulated AdPDGF-B to repair ischemic excisionalwounds Several models were employed to compare variationsin wound size and condition so as to allow for a more com-plete picture of tissue repair
In the first model system 6-mm-diameter wounds were cre-ated in ischemic rabbit ears by removal of epidermal and der-mal layers but not underlying cartilage This model has beenused in previous studies of growth factor proteins and genes(Ahn and Mustoe 1990 Mustoe et al 1994 Liechty et al1999) and was therefore employed to allow comparison withthese reports However it represents an artificial system as thepresence of a cartilage layer restricts both treatment activity andhealing to wound margins and in addition the initially acellu-lar wound bed forms a cup that artifactually retains aqueoustreatments As would be predicted we found a trend towardgranulation tissue formation in this model after the applicationof AdPDGF-B formulated in aqueous buffer (Table 3) How-ever this response did not reach the level of statistical signifi-cance as tissue development was highly variable (note the highstandard deviation value) In addition epithelial regenerationand wound closure were minimal to unaffected By contrastAdPDGF-B formulated in 015 collagen enhanced granula-tion tissue area by 32-fold and epithelial area by 18-fold overthat achieved with vehicle alone (p 0009 and 005 respec-tively) Although near complete closure of epithelial gaps wasalso achieved the high level of self-healing in control-treatedgroups (89 wound closure) precluded statistical significance
In an alternative model design subdermal cartilage was com-pletely removed from excisional wounds creating beds whosefloors now consisted of dermal tissue (Pierce et al 1994b)This design allows for cellular responses from the entire woundbed as well as the opportunity for vector migration beyond
treatment areas We now observed that aqueous formulated Ad-PDGF-B failed to induce even a trend toward tissue regenera-tion (Table 3) Rather the vector appears to have seeped throughthe wound bed floor as inflammatory cell infiltrates and fociof fibroblast proliferation were observed in the underlying der-mis and at wound margins (Fig 4A) Immunohistochemistryconfirmed the production of human PDGF-BB at these sites(Fig 4B) CMC-formulated AdPDGF-B also failed to induceany meaningful tissue repair Wounds treated with this formu-lation showed a diffuse inflammatory response within thewound bed and wound surfaces were overlain with fibrin clotsrather than regenerating epithelium (Fig 4C and D) By con-trast AdPDGF-B formulated in 015 collagen enhanced gran-ulation tissue deposition 19-fold within wound beds versus ve-hicle controls (p 0002) and wounds were extensivelyepithelialized (Table 3) Neither epithelial regeneration norwound closure achieved significance however as the high de-gree of self-healing achieved in this particular model (see ve-hicle alone group) most likely masked transgene-stimulated re-sponses
To address these model limitations as our next system wecreated 8-mm wounds in ischemic rabbit ears by removingepidermal dermal and cartilage layers reasoning that largerexcisional wounds would display limited self-healing In ad-dition this model could readily accommodate 26 collagenformulations which proved difficult to reproducibly apply insmaller wounds Compared with control wounds treated withcollagen vehicle alone wounds treated with AdPDGF-B for-mulated in 26 collagen achieved a 12-fold enhancementin granulation tissue fill and a 6-fold enhancement in re-ep-ithelialization by day 8 posttreatment (p 0009 Table 3)In addition wound closure was only 24 complete in colla-gen vehicle-treated wounds by day 8 but 52 complete inwounds treated with collagen-formulated AdPDGF-B (p
005) Histologically AdPDGF-B-treated wounds showed nosigns of tissue hyperplasia or chronic inflammation but ratheran orderly repair process marked by a regenerated epitheliallayer overlying a wound bed filled with granulation tissue(Fig 4E and F)
CollagenndashAdPDGF-B induces normal long-term tissue repair
Our choice of adenoviruses for transgene delivery was partlybased on the reasoning that as these vectors establish transientgene expression they would not lead to hyperproliferative re-sponses or scar formation To test this hypothesis we treatedrabbit ear excisional wounds with AdPDGF-B formulated in015 collagen and examined tissue repair responses out to
DOUKAS ET AL792
FIG 4 Influence of adenovirusndashmatrix formulations on excisional wound repair Excisional wounds (6 or 8 mm in diameter andextending through underlying cartilage layers) were placed in ischemic rabbit ears bars indicate original wound depth (determinedfrom cartilage visible at wound margins) Wounds were then treated with AdPDGF-B formulated in either virus buffer CMC orcollagen and on day 7 or 8 posttreatment processed for histology or immunohistochemistry An identical design was used to ex-amine long-term healing on day 90 except that wounds were created in nonischemic ears (A) Day 7 buffer-formulated AdPDGF-B-treated 6-mm wound trichrome stain (B) Day 7 buffer-formulated AdPDGF-B-treated 6-mm wound anti-PDGF-BB proteinimmunostain (C and D) Day 7 CMC-formulated AdPDGF-B-treated 6-mm wound trichrome stains (E and F) Day 8 26 col-lagen-formulated AdPDGF-B-treated 8-mm wound trichrome stains (G and H) Day 90 015 collagen-formulated AdPDGF-B-treated 6-mm wound trichrome stains Original magnification (A C E and G) 340 (B D F and H) 3200
TISSUE REPAIR USING GROWTH FACTOR GENES 793
DOUKAS ET AL794
TABLE 4 BIODISTRIBUTION OF AdPDGF-B IN EXCISIONAL WOUNDSa
Positive samplestotal assayed
Tissue AdPDGF-B dose Day 3 Day 7 Day 28 Day 90
Wound bed 2 3 109 particles 66 66 66b 06Axillary lymph nodes 2 3 109 particles 02 ND 06 06
Wound bed 2 3 1011 particles 66 66 66 46c
Axillary lymph nodes 2 3 1011 particles 66 ND 66d 26e
aFull-thickness excisional wounds (7 cm2) were placed on the backs of rabbits and AdPDGF-B formulated in 26 collagenwas applied as either 2 3 109 or 2 3 1011 virus particles per wound On days 3ndash90 posttreatment wound beds and a panel oforgans were harvested for real-time PCR quantification of viral genome Data are shown for wound bed and axillary lymph nodesamples as the number of samples that yielded amplifiable signals per total number assayed ND not determined
bThree of six samples scored below the level of quantitation (LOQ 10ndash100 copiesmg DNA)cAll four positive samples scored below the LOQdThree of six samples scored below the LOQeBoth positive samples scored below the LOQ
180 days posttreatment (Fig 5) PDGF-B gene delivery en-hanced total ear thickness relative to controls on day 28 (229 6
020 vs 179 6 019 mm p 00001) and day 60 (192 6 001vs 182 6 011 mm p 0005) as anticipated on the basis ofthe ability of this formulation to induce granulation tissue for-mation By day 90 posttreatment however there was no mea-surable difference in ear thickness between AdPDGF-B andcontrol-treated groups and this relationship continued out today 180 indicating that growth factor gene delivery did not in-duce excessive scar formation This was also confirmed histo-logically AdPDGF-B-treated wounds on day 90 and beyondwere composed of a thin outer keratin layer an underlying ep-ithelial layer of equivalent thickness to nonwounded areas anda collagen-rich dermis devoid of any signs of tissue hyperpla-sia (Fig 4G and H)
Collagen immobilization limits adenovirus vectorbiodistribution beyond treatment sites
As a final measure of the value of matrix immobilization forgene delivery we determined the biodistribution patterns ofvectors after their in vivo delivery In the first model systemused AdPDGF-B formulated in 015 collagen was applied torabbit ear wounds at equivalent doses as previously describedwounds were extended through underlying cartilage but vas-cular supplies were not disturbed so as to permit maximal vec-tor dissemination By PCR no adenoviral DNA was detectablein lung spleen brain cervical lymph nodes or gonads on day1 3 7 or 14 (n 5 6 per group) In the liver one of six sam-ples was positive on days 3 and 7 but none on day 14 in serumonly one of six samples tested positive on day 14 (equivalentof 500-ml serum volume) By contrast adenovirus was detectedin eight of eight wound bed samples at all time points exam-ined
In a second model system excisional wounds placed on thebacks of rabbits were treated with AdPDGF-B formulated in26 collagen Because of their anatomical placement thismodel allowed for the creation of larger excisional wounds (7-cm2 total area) than those placed in rabbit ears (03 cm2) and
consequently larger treatment volumes and vector doses (2 3109 or 2 3 1011 virus particles per wound) At the lower doseof 2 3 109 particles PCR-amplifiable adenoviral DNA was notdetectable beyond wound beds on day 3 7 28 or 90 Tissuessampled and found not to contain vector included blood heartlung liver kidney brain spleen lymph nodes and gonads (n 5
6group) In wound beds adenoviral DNA was detected at alltime points except for day 90 (Table 4 and Fig 6) Vector lev-els did decrease however by 38-fold between days 7 and 28with three of six samples falling below the level of quantita-tion (LOQ) by real-time PCR at the latter time point (Fig 6)
At a 100-fold higher vector dose of 2 3 1011 particles perwound PCR-amplifiable adenoviral DNA was once again un-detectable in the majority of tissues sampled Except for a sin-gle day 7 liver sample and a single day 7 brain sample (bothbelow the LOQ) adenoviral DNA was only detectable directlyin wound beds or in the axillary lymph nodes that drain woundsites (Table 4) Moreover three of six positive axillary nodesamples scored below the LOQ on day 28 as did both positivesamples on day 90 indicating that they contained relatively lit-tle vector Within wound beds adenoviral DNA was detectedat quantifiable levels out to day 28 and at detectable but non-quantifiable levels on day 90 DNA copy numbers remainedsteady between days 3 and 7 dropped 107-fold between days7 and 28 and a further 1662-fold by day 90 Finally at eachtime point DNA copy numbers in wounds treated with 2 3
1011 particles were approximately 100-fold higher than thosefound in wounds treated with 2 3 109 particles thus confirm-ing the linearity of our assay system
To better define the time course of human PDGF-BB pro-duction we also quantified transgene mRNA levels in woundbed samples treated at 2 3 109 particles per wound This treat-ment dose was selected as representative of the virus particleconcentration capable of inducing complete healing in ischemicear wounds Quantifiable levels of human PDGF-B mRNAwere detectable in treated dorsal wounds at days 3 7 and 28(Fig 6) with levels decreasing 14-fold between days 3 and 7and 5-fold between days 7 and 28 The more sensitive tech-nique of real-time RT-PCR therefore demonstrates that trans-
TISSUE REPAIR USING GROWTH FACTOR GENES 795
gene expression extends well beyond the 8-day time period sug-gested using anti-PDGF-BB immunohistochemistry as a de-tection system (Fig 3)
DISCUSSION
These studies demonstrate that immobilization of gene ther-apy vectors in collagen-based matrices enables their efficientdelivery and activity in vivo Matrix immobilization achievedprolonged transgene-encoded growth factor production and asa consequence robust tissue repair By contrast aqueous vehi-cles failed to retain adenoviruses at application sites resultingin diffuse inflammation rather than productive tissue regenera-tion These observations confirm our basic hypothesis that ma-trix immobilization of growth factor-encoding gene therapyvectors represents a promising approach to tissue repair
Although de novo tissue deposition was achievable with sev-eral growth factor genes PDGF-B proved the most suitable forrepair of cutaneous defects A single administration of colla-gen-immobilized AdPDGF-B rapidly induced the formation ofhighly cellular and vascularized tissues with dense ECMs richin collagen By contrast AdFGF2 induced a primarily vascu-lar response with little collagen deposition FGF2 induces therelease of matrix metalloproteinase 1 or interstitial collagenase(Buckley-Sturrock et al 1989) and this may underlie the rel-ative paucity of ECM accumulation VEGF gene delivery alsoinduced highly vascular responses however the enhanced per-meability characteristic of VEGF-induced vasculature (Dvoraket al 1995) led to edema within nascent tissues In fact much
of the enhanced protein and DNA deposition observed in Ad-VEGF-treated PVA sponges may well derive from fluid exu-dates rather than actual tissue formation Finally the inabilityof AdLuc delivery to induce anything beyond a limited in-flammatory response confirms that tissue formation was de-pendent on growth factor gene delivery
The robust activity of PDGF-B gene delivery was expectedas PDGF-BB protein initiates multiple aspects of tissue forma-tion including cellular influx and proliferation ECM deposi-tion and tissue remodeling (Pierce et al 1988 1991 1994a)Indeed PDGF-BB is the only growth factor protein to have suc-cessfully completed human clinical trials and be approved forthe treatment of dermal wounds (Steed 1995 drsquoHemecourt etal 1998 Wieman 1998 Wieman et al 1998) We observedthat collagen-formulated AdPDGF-B induced the complete re-pair of excisional skin defects without unwanted long-term ef-fects such as the development of hypertrophic scars Endoge-nous growth factors other than PDGF-BB however most likelymediated the enhanced re-epithelialization observed in thesewounds as epithelial regeneration is driven by members of theepidermal growth factor and FGF families (Pierce et al 1994bDanilenko et al 1995) Our data indicate nonetheless that tis-sue regeneration and repair were initiated and to a great degreedriven by transgene-encoded PDGF-BB
Despite the known activity of PDGF-BB protein we wereable to demonstrate greater tissue deposition after gene deliv-ery as compared with the use of recombinant growth factor pro-tein A single application of PDGF-BB protein could not equalthe ability of PDGF-B gene therapy to induce neotissue for-mation even at doses well in excess of that induced in situ byAdPDGF-B and in excess of that used in human clinical trials
FIG 5 Influence of collagen-formulated AdPDGF-B on long-term tissue repair Excisional wounds (6 mm in diameter withcartilage remaining intact) were placed in nonischemic rabbit ears and treated with either 015 collagen alone (open columns)or AdPDGF-B formulated in this vehicle (solid columns) On days 28ndash180 posttreatment total ear thickness at the site of eachwound was measured (in mm) with calipers Data are presented as means 6 SD (n 5 3) Treatment groups differ by p 00001groups differ by p 0005
(Steed 1995 drsquoHemecourt et al 1998 Wieman 1998 Wie-man et al 1998) In fact repeated administrations of PDGF-BB protein were required to approach the level of tissue for-mation observed after a single administration of AdPDGF-BThese data support our hypothesis that sustained localizedgrowth factor production is required for robust tissue repair
In further support of this hypothesis we demonstrated thatmRNA encoding human PDGF-B was present in excisionalwounds as late as day 28 after collagen-formulated AdPDGF-B administration By contrast previous studies of PDGF-BBprotein found that the great majority of this growth factor wasgone from treated wounds 1 day postapplication and that anytissue maturation subsequently observed was most likely dueto the upregulation of endogenous growth factors (Pierce et al1992 1995) We also demonstrated that repair cells such asmononuclear leukocytes endothelial cells and fibroblasts pres-ent with developing neotissues represent the source of both
transgene transcription and PDGF-BB production In additiona depot of human PDGF-BB was detected bound to the colla-gen delivery matrix and ECM of these tissues This was antici-pated as PDGF-BB contains collagen-binding motifs (Soma-sundaram and Schuppan 1996) We hypothesize that subsequentmatrix metalloproteinase activity by repair cells will serve togenerate localized release of this sequestered growth factor pooland as a consequence further drive tissue regeneration Theseevents which are central to tissue remodeling should be directlyenhanced by collagen matrices as type I collagen stimulates me-talloproteinase production integrin expression and cellular ac-tivation in PDGF-stimulated fibroblasts (Xu and Clark 19961997)
An additional rationale for employing collagen matrices wasto physically immobilize vectors This was confirmed in vivowhere collagen matrices maintained AdPDGF-B at deliverysites for at least 28 days and limited vector migration to other
DOUKAS ET AL796
FIG 6 Persistence of collagen-formulated vector and transgene transcripts in excisional wounds Full-thickness excisionalwounds (7 cm2) were placed on the dorsal surface of rabbits and treated with AdPDGF-B formulated in 26 collagen at either2 3 109 or 2 3 1011 virus particles per wound (open and closed columns respectively) Wounds were then covered with OpSitedressing and on days 3 7 or 28 posttreatment wound beds were harvested for real-time quantitative PCR and RT-PCR analy-ses PCR data are presented in the upper graph as AdPDGF-B copies per wound RT-PCR data are presented in the lower graphas the relative amount of PDGF-B mRNA per unit 18S rRNA (in arbitrary units) All data points are means 6 SD (n 5 6)
tissues or organs In vitro tests also established that collagenmatrices not only prevent vector loss due to diffusion but pre-serve vector activity despite prolonged incubation in acutewound fluid Successful vector immobilization and tissue re-pair could be achieved with both 015 collagen and 26 col-lagen suggesting flexibility in the final vehicle formulation re-quired for effective vector delivery This flexibility was neededin the present studies as 26 collagen formulations proveddifficult to deliver to PVA sponges and 6-mm excisionalwounds This would not be of concern in clinical settings how-ever where wound beds are easily accessible and generally sev-eral square centimeters in area By contrast CMC was inef-fective at retaining vector in aqueous environments Moreimportantly this matrix was itself inflammatory and whencombined with adenovirus the net result was inflammationrather than tissue repair We are currently examining the util-ity of other matrices such as fibrin and hyaluronic acid whichbecause of their more provisional nature may offer yet greatercellular migration into wounds as compared with type I colla-gen
Although an aqueous-based AdPDGF-B formulation hasbeen previously shown to enhance tissue formation (Liechty etal 1999) this was achieved with a model system that artifi-cially retains vectors within treatment sites In fact the presentstudies demonstrate that any tissue repair observed after Ad-PDGF-B delivery in a nongelling liquid is dependent on the useof this model system In wounds not designed to retain appliedtreatments aqueous-formulated AdPDGF-B seeped into sur-rounding tissues and led to hyperplasia within these areas ratherthan to tissue regeneration within the active wound bed Colla-gen-immobilized AdPDGF-B on the other hand did persist inthese wound beds and led to significant enhancements in gran-ulation tissue formation as well as enhanced wound re-epithe-lialization and wound closure The significance of these activ-ities is further substantiated considering that they wereachievable in 8-mm-diameter ischemic wounds which withinthe time frame examined could not self-heal to any meaning-ful degree in the absence of gene therapy However as all theanimal models employed in these studies will eventually self-heal given sufficient time the full value of matrix-immobilizedgene therapy vectors remains to be confirmed in human clini-cal trials
In conclusion we present evidence that matrix-immobilizedgene therapy vectors encoding appropriate growth-promotinggenes represent a promising approach to tissue regeneration andrepair This basic concept can be expanded to include alterna-tive matrices such as controlled-release formulations as wellas tissue-specific growth factors Furthermore the addition oftargeting ligands to adenovirus vectors (eg FGF2) can en-hance their ability to transduce cells such that tissue repair re-sponses comparable to nontargeted vectors can be achieved butat significantly lower vector doses (Chandler et al 2000a)With appropriate design and application schedules one couldconceivably time the release of multiple growth factors to spe-cific stages of a tissue repair cascade In addition we have foundin preliminary studies that collagen-immobilized nonviral vec-tors such as PDGF-B plasmids which have potentially morefavorable safety profiles than adenovirus vectors can also en-hance tissue formation in vivo (Chandler et al 2000b Tyroneet al 2000) Such flexibility should allow for the widespreadapplication of gene therapy to the treatment of injured tissues
ACKNOWLEDGMENTS
We thank Jeff Davidson (Vanderbilt University School ofMedicine) for assistance in establishing the PVA sponge modelCarl-Henrik Heldin (Ludwig Institute for Cancer Research) forthe PDGF-B gene construct and Emelie Amburn Lara AsatoSharon Chang Gail Fieser Lydia Greenlees Rebecca Smokerand Linda Manza for excellent technical assistance This pub-lication was made possible in part by NIH grants 1R43AR46154(JD) and 5P01CA25874 (MH)
REFERENCES
AHN ST and MUSTOE TA (1990) Effects of ischemia on ulcerwound healing A new model in the rabbit ear Ann Plast Surg 2417ndash23
ANDREE C SWAIN WF PAGE CP MACKLIN MDSLAMA J HATZIS D and ERIKSSON E (1994) In vivo trans-fer and expression of a human epidermal growth factor gene accel-erates wound repair Proc Natl Acad Sci USA 91 12188ndash12192
BENN SI WHITSITT JS BROADLEY KN NANNEY LBPERKINS D HE L PATEL M MORGAN JR SWAIN WFand DAVIDSON JM (1996) Particle-mediated gene transfer withtransforming growth factor-b1 cDNAs enhances wound repair in ratskin J Clin Invest 98 2894ndash2902
BONADIO J SMILEY E PATIL P and GOLDSTEIN S (1999)Localized direct plasmid gene delivery in vivo Prolonged therapyresults in reproducible tissue regeneration Nat Med 5 753ndash759
BUCKLEY A DAVIDSON JM KAMERATH CD WOLT TBand WOODWARD SC (1985) Sustained release of epidermalgrowth factor accelerates wound repair Proc Natl Acad Sci USA82 7340ndash7344
BUCKLEY-STURROCK A WOODWARD SC SENIOR RMGRIFFIN GL KLAGSBRUN M and DAVIDSON JM (1989)Differential stimulation of collagenase and chemotactic activity in fi-broblasts derived from rat wound repair tissue and human skin bygrowth factors J Cell Physiol 138 70ndash78
CHANDLER LA DOUKAS J GONZALEZ AM HOGANSONDK GU DL MA C NESBIT M CROMBLEHOLME TMHERLYN M SOSNOWSKI BA and PIERCE GF (2000a)FGF2ndashTargeted adenovirus encoding platelet-derived growth factor-B enhances de novo tissue formation Mol Ther 2 153ndash160
CHANDLER LA MA C GONZALEZ AM DOUKAS JNGUYEN T PIERCE GF and PHILLIPS ML (2000b) Ma-trix-enabled gene transfer for cutaneous wound repair Wound Re-pair Regen 8 473ndash479
DANILENKO DM RING BD TARPLEY JE MORRIS BVAN GY MORAWIECKI A CALLAHAN W GOLDEN-BERG M HERSHENSON S and PIERCE GF (1995) Growthfactors in porcine full and partial thickness burn repair Differing tar-gets and effects of keratinocyte growth factor platelet-derivedgrowth factor-BB epidermal growth factor and neu differentiationfactor Am J Pathol 147 1261ndash1277
DEUEL TF KAWAHARA RS MUSTOE TA and PIERCE GF(1991) Growth factors and wound healing Platelet-derived growthfactor as a model cytokine Annu Rev Med 42 567ndash584
DrsquoHEMECOURT PA SMIELL JM and KARIM MR (1998) So-dium carboxymethylcellulose aqueous-based gel vs becaplermin gelin patients with nonhealing lower extremity diabetic ulcers Wounds10 69ndash75
DOUKAS J HOGANSON DK ONG M YING W LACEYDL BAIRD A PIERCE GF and SOSNOWSKI BA (1999)Retargeted delivery of adenoviral vectors through fibroblast growthfactor receptors involves unique cellular pathways FASEB J 131459ndash1466
TISSUE REPAIR USING GROWTH FACTOR GENES 797
DVORAK HF BROWN LF DETMAR M and DVORAK AM(1995) Vascular permeability factorvascular endothelial growth fac-tor microvascular hyperpermeability and angiogenesis Am JPathol 146 1029ndash1039
EMING SA MEDALIE DA TOMPKINS RG YARMUSHML and MORGAN JR (1998) Genetically modified human ker-atinocytes overexpressing PDGF-A enhance the performance of acomposite skin graft Hum Gene Ther 9 529ndash539
EMING SA WHITSITT JS HE L KRIEG T MORGAN JRand DAVIDSON JM (1999) Particle-mediated gene transfer ofPDGF isoforms promotes wound repair J Invest Dermatol 112297ndash302
GERDES J SCHWAB U LEMKE H and STEIN H (1983) Pro-duction of a mouse monoclonal antibody reactive with a human nu-clear antigen associated with cell proliferation Int J Cancer 3113ndash20
GONZALEZ AM BERRY M MAHER PA LOGAN A andBAIRD A (1995) A comprehensive analysis of the distribution ofFGF-2 and FGFR1 in the rat brain Brain Res 701 201ndash226
GREENHALGH DG (1996) The role of growth factors in woundhealing J Trauma 41 159ndash167
GROTENDORST GR MARTIN GR PENCEV D SODEK Jand HARVEY AK (1985) Stimulation of granulation tissue for-mation by platelet-derived growth factor in normal and diabetic ratsJ Clin Invest 76 2323ndash2329
KHOURI RK HONG SP DEUNE EG TARPLEY JE SONGSZ SERDAR CM and PIERCE GF (1994) De novo genera-tion of permanent neovascularized soft tissue appendages by platelet-derived growth factor J Clin Invest 94 1757ndash1763
LEGRAND EK SENTER LH GAMELLI RL and KIORPESTC (1993) Evaluation of PDGF-BB PDGF-AA bFGF IL-1 andEGF dose responses in polyvinyl alcohol sponge implants assessedby a rapid histologic method Growth Factors 8 315ndash329
LIECHTY KW NESBIT M HERLYN M RADU A ADZICKNS and CROMBLEHOLME TM (1999) Adenoviral-mediatedoverexpression of platelet-derived growth factor-B corrects ischemicimpaired wound healing J Invest Dermatol 113 375ndash383
LYNCH SE COLVIN RB and ANTONIADES HN (1989)Growth factors in wound healing J Clin Invest 84 640ndash646
MUSTOE TA PIERCE GF THOMASON A GRAMATES PSPORN MB and DEUEL TF (1987) Accelerated healing of in-cisional wounds in rats induced by transforming growth factor-betaScience 237 1333ndash1336
MUSTOE TA PIERCE GF MORISHIMA C and DEUEL TF(1991) Growth factor-induced acceleration of tissue repair throughdirect and inductive activities in a rabbit dermal ulcer model J ClinInvest 87 694ndash703
MUSTOE TA AHN ST TARPLEY JE and PIERCE GF(1994) Role of hypoxia in growth factor responses Differential ef-fects of basic fibroblast growth factor and platelet-derived growthfactor in an ischemic wound model Wound Rep Reg 2 277ndash283
NYBERG-HOFFMAN C and AGUILAR-CORDOVA E (1999) In-stability of adenoviral vectors during transport and its implication forclinical studies Nat Med 5 955ndash957
PIERCE GF and MUSTOE TA (1995) Pharmacologic enhance-ment of wound healing Annu Rev Med 46 467ndash481
PIERCE GF MUSTOE TA SENIOR RM REED J GRIFFINGL THOMASON A and DEUEL TF (1988) In vivo incisionalwound healing augmented by platelet-derived growth factor and re-combinant c-sis gene homodimeric proteins J Exp Med 167 974ndash987
PIERCE GF VANDE BERG J RUDOLPH R TARPLEY J andMUSTOE TA (1991) Platelet-derived growth factor-BB and trans-forming growth factor beta 1 selectively modulate glycosaminogly -cans collagen and myofibroblasts in excisional wounds Am JPathol 138 629ndash646
PIERCE GF TARPLEY JE YANAGIHARA D MUSTOE TA
FOX GM and THOMASON A (1992) Platelet-derived growthfactor (BB homodimer) transforming growth factor-b1 and basic fi-broblast growth factor in dermal wound healing Neovessel and ma-trix formation and cessation of repair Am J Pathol 140 1375ndash1388
PIERCE GF TARPLEY JE ALLMAN RM GOODE PS SER-DAR CM MORRIS B MUSTOE TA and VANDE BERG J(1994a) Tissue repair processes in healing chronic pressure ulcerstreated with recombinant platelet-derived growth factor BB Am JPathol 145 1399ndash1410
PIERCE GF YANAGIHARA D KLOPCHIN K DANILENKODM HSU E KENNEY WC and MORRIS CF (1994b) Stim-ulation of all epithelial elements during skin regeneration by kerati-nocyte growth factor J Exp Med 179 831ndash840
PIERCE GF TARPLEY JE TSENG J BREADY J CHANGD KENNEY WC RUDOLPH R ROBSON MC VANDEBERG J and REID P (1995) Detection of platelet-derived growthfactor (PDGF)-AA in actively healing human wounds treated withrecombinant PDGF-BB and absence of PDGF in chronic nonhealingwounds J Clin Invest 96 1336ndash1350
SINGER AJ and CLARK RA (1999) Cutaneous wound healingN Engl J Med 341 738ndash746
SOMASUNDARAM R and SCHUPPAN D (1996) Type I II IIIIV V and VI collagens serve as extracellular ligands for the iso-forms of platelet-derived growth factor (AA BB and AB) J BiolChem 271 26884ndash26891
SPRUGEL KH MCPHERSON JM CLOWES AW and ROSSR (1987) Effects of growth factors in vivo I Cell ingrowth intoporous subcutaneous chambers Am J Pathol 129 601ndash613
STEED DL (1995) Clinical evaluation of recombinant humanplatelet-derived growth factor for the treatment of lower extremitydiabetic ulcers Diabetic Ulcer Study Group J Vasc Surg 21 71ndash78
STEED DL (1998) Foundations of good ulcer care Am J Surg 17620S-25S
TYRONE JW MOGFORD JE CHANDLER LA MA C XIAY PIERCE GF and MUSTOE TA (2000) Collagen-embeddedplatelet-derived growth factor DNA plasmid promotes wound heal-ing in a dermal ulcer model J Surg Res 93 230ndash236
VOGT PM THOMPSON S ANDREE C LIU P BREUING KHATZIS D BROWN H MULLIGAN RC and ERIKSSON E(1994) Genetically modified keratinocytes transplanted to woundsreconstitute the epidermis Proc Natl Acad Sci USA 91 9307ndash9311
WIEMAN TJ (1998) Clinical efficacy of becaplermin (rhPDGF-BB)gel Becaplermin Gel Studies Group Am J Surg 176 74S-79S
WIEMAN TJ SMIELL JM and SU Y (1998) Efficacy and safetyof a topical gel formulation of recombinant human platelet-derivedgrowth factor-BB (becaplermin) in patients with chronic neuropathicdiabetic ulcers A phase III randomized placebo-controlled double-blind study Diabetes Care 21 822ndash827
WILSON JM (1996) Adenoviruses as gene-delivery vehicles NEngl J Med 334 1185ndash1187
XU J and CLARK RA (1996) Extracellular matrix alters PDGFregulation of fibroblast integrins J Cell Biol 132 239ndash249
XU J and CLARK RA (1997) A three-dimensional collagen latticeinduces protein kinase C-z activity Role in a2 integrin and collage-nase mRNA expression J Cell Biol 136 473ndash483
Address reprint requests toDr John Doukas
Selective Genetics Inc11035 Roselle Street
San Diego CA 92121
E-mail jdoukasselectivegeneticscom
Received for publication December 28 2000 accepted after re-vision February 23 2001
DOUKAS ET AL798

delivered as a single dose nearly 2000-fold in excess of thisconcentration the tissue formation responses observed (proteinand DNA accumulation and granulation tissue formation) weresignificantly lower (p 005 Table 2) In fact repeated dos-ing with PDGF-BB protein was required in order to achieve re-sponses comparable to a single administration of the PDGF-Bgene These data therefore support our hypothesis that the abil-ity of gene delivery to establish prolonged in situ growth fac-tor production translates into greater histogenesis than that seenwith growth factor proteins
CollagenndashAdPDGF-B induces complete healing of ischemic wounds
Nonhealing wounds are a major risk in chronically ischemictissues as low oxygen tension greatly impairs tissue repair pro-cesses We therefore compared the ability of matrix versusaqueous formulated AdPDGF-B to repair ischemic excisionalwounds Several models were employed to compare variationsin wound size and condition so as to allow for a more com-plete picture of tissue repair
In the first model system 6-mm-diameter wounds were cre-ated in ischemic rabbit ears by removal of epidermal and der-mal layers but not underlying cartilage This model has beenused in previous studies of growth factor proteins and genes(Ahn and Mustoe 1990 Mustoe et al 1994 Liechty et al1999) and was therefore employed to allow comparison withthese reports However it represents an artificial system as thepresence of a cartilage layer restricts both treatment activity andhealing to wound margins and in addition the initially acellu-lar wound bed forms a cup that artifactually retains aqueoustreatments As would be predicted we found a trend towardgranulation tissue formation in this model after the applicationof AdPDGF-B formulated in aqueous buffer (Table 3) How-ever this response did not reach the level of statistical signifi-cance as tissue development was highly variable (note the highstandard deviation value) In addition epithelial regenerationand wound closure were minimal to unaffected By contrastAdPDGF-B formulated in 015 collagen enhanced granula-tion tissue area by 32-fold and epithelial area by 18-fold overthat achieved with vehicle alone (p 0009 and 005 respec-tively) Although near complete closure of epithelial gaps wasalso achieved the high level of self-healing in control-treatedgroups (89 wound closure) precluded statistical significance
In an alternative model design subdermal cartilage was com-pletely removed from excisional wounds creating beds whosefloors now consisted of dermal tissue (Pierce et al 1994b)This design allows for cellular responses from the entire woundbed as well as the opportunity for vector migration beyond
treatment areas We now observed that aqueous formulated Ad-PDGF-B failed to induce even a trend toward tissue regenera-tion (Table 3) Rather the vector appears to have seeped throughthe wound bed floor as inflammatory cell infiltrates and fociof fibroblast proliferation were observed in the underlying der-mis and at wound margins (Fig 4A) Immunohistochemistryconfirmed the production of human PDGF-BB at these sites(Fig 4B) CMC-formulated AdPDGF-B also failed to induceany meaningful tissue repair Wounds treated with this formu-lation showed a diffuse inflammatory response within thewound bed and wound surfaces were overlain with fibrin clotsrather than regenerating epithelium (Fig 4C and D) By con-trast AdPDGF-B formulated in 015 collagen enhanced gran-ulation tissue deposition 19-fold within wound beds versus ve-hicle controls (p 0002) and wounds were extensivelyepithelialized (Table 3) Neither epithelial regeneration norwound closure achieved significance however as the high de-gree of self-healing achieved in this particular model (see ve-hicle alone group) most likely masked transgene-stimulated re-sponses
To address these model limitations as our next system wecreated 8-mm wounds in ischemic rabbit ears by removingepidermal dermal and cartilage layers reasoning that largerexcisional wounds would display limited self-healing In ad-dition this model could readily accommodate 26 collagenformulations which proved difficult to reproducibly apply insmaller wounds Compared with control wounds treated withcollagen vehicle alone wounds treated with AdPDGF-B for-mulated in 26 collagen achieved a 12-fold enhancementin granulation tissue fill and a 6-fold enhancement in re-ep-ithelialization by day 8 posttreatment (p 0009 Table 3)In addition wound closure was only 24 complete in colla-gen vehicle-treated wounds by day 8 but 52 complete inwounds treated with collagen-formulated AdPDGF-B (p
005) Histologically AdPDGF-B-treated wounds showed nosigns of tissue hyperplasia or chronic inflammation but ratheran orderly repair process marked by a regenerated epitheliallayer overlying a wound bed filled with granulation tissue(Fig 4E and F)
CollagenndashAdPDGF-B induces normal long-term tissue repair
Our choice of adenoviruses for transgene delivery was partlybased on the reasoning that as these vectors establish transientgene expression they would not lead to hyperproliferative re-sponses or scar formation To test this hypothesis we treatedrabbit ear excisional wounds with AdPDGF-B formulated in015 collagen and examined tissue repair responses out to
DOUKAS ET AL792
FIG 4 Influence of adenovirusndashmatrix formulations on excisional wound repair Excisional wounds (6 or 8 mm in diameter andextending through underlying cartilage layers) were placed in ischemic rabbit ears bars indicate original wound depth (determinedfrom cartilage visible at wound margins) Wounds were then treated with AdPDGF-B formulated in either virus buffer CMC orcollagen and on day 7 or 8 posttreatment processed for histology or immunohistochemistry An identical design was used to ex-amine long-term healing on day 90 except that wounds were created in nonischemic ears (A) Day 7 buffer-formulated AdPDGF-B-treated 6-mm wound trichrome stain (B) Day 7 buffer-formulated AdPDGF-B-treated 6-mm wound anti-PDGF-BB proteinimmunostain (C and D) Day 7 CMC-formulated AdPDGF-B-treated 6-mm wound trichrome stains (E and F) Day 8 26 col-lagen-formulated AdPDGF-B-treated 8-mm wound trichrome stains (G and H) Day 90 015 collagen-formulated AdPDGF-B-treated 6-mm wound trichrome stains Original magnification (A C E and G) 340 (B D F and H) 3200
TISSUE REPAIR USING GROWTH FACTOR GENES 793
DOUKAS ET AL794
TABLE 4 BIODISTRIBUTION OF AdPDGF-B IN EXCISIONAL WOUNDSa
Positive samplestotal assayed
Tissue AdPDGF-B dose Day 3 Day 7 Day 28 Day 90
Wound bed 2 3 109 particles 66 66 66b 06Axillary lymph nodes 2 3 109 particles 02 ND 06 06
Wound bed 2 3 1011 particles 66 66 66 46c
Axillary lymph nodes 2 3 1011 particles 66 ND 66d 26e
aFull-thickness excisional wounds (7 cm2) were placed on the backs of rabbits and AdPDGF-B formulated in 26 collagenwas applied as either 2 3 109 or 2 3 1011 virus particles per wound On days 3ndash90 posttreatment wound beds and a panel oforgans were harvested for real-time PCR quantification of viral genome Data are shown for wound bed and axillary lymph nodesamples as the number of samples that yielded amplifiable signals per total number assayed ND not determined
bThree of six samples scored below the level of quantitation (LOQ 10ndash100 copiesmg DNA)cAll four positive samples scored below the LOQdThree of six samples scored below the LOQeBoth positive samples scored below the LOQ
180 days posttreatment (Fig 5) PDGF-B gene delivery en-hanced total ear thickness relative to controls on day 28 (229 6
020 vs 179 6 019 mm p 00001) and day 60 (192 6 001vs 182 6 011 mm p 0005) as anticipated on the basis ofthe ability of this formulation to induce granulation tissue for-mation By day 90 posttreatment however there was no mea-surable difference in ear thickness between AdPDGF-B andcontrol-treated groups and this relationship continued out today 180 indicating that growth factor gene delivery did not in-duce excessive scar formation This was also confirmed histo-logically AdPDGF-B-treated wounds on day 90 and beyondwere composed of a thin outer keratin layer an underlying ep-ithelial layer of equivalent thickness to nonwounded areas anda collagen-rich dermis devoid of any signs of tissue hyperpla-sia (Fig 4G and H)
Collagen immobilization limits adenovirus vectorbiodistribution beyond treatment sites
As a final measure of the value of matrix immobilization forgene delivery we determined the biodistribution patterns ofvectors after their in vivo delivery In the first model systemused AdPDGF-B formulated in 015 collagen was applied torabbit ear wounds at equivalent doses as previously describedwounds were extended through underlying cartilage but vas-cular supplies were not disturbed so as to permit maximal vec-tor dissemination By PCR no adenoviral DNA was detectablein lung spleen brain cervical lymph nodes or gonads on day1 3 7 or 14 (n 5 6 per group) In the liver one of six sam-ples was positive on days 3 and 7 but none on day 14 in serumonly one of six samples tested positive on day 14 (equivalentof 500-ml serum volume) By contrast adenovirus was detectedin eight of eight wound bed samples at all time points exam-ined
In a second model system excisional wounds placed on thebacks of rabbits were treated with AdPDGF-B formulated in26 collagen Because of their anatomical placement thismodel allowed for the creation of larger excisional wounds (7-cm2 total area) than those placed in rabbit ears (03 cm2) and
consequently larger treatment volumes and vector doses (2 3109 or 2 3 1011 virus particles per wound) At the lower doseof 2 3 109 particles PCR-amplifiable adenoviral DNA was notdetectable beyond wound beds on day 3 7 28 or 90 Tissuessampled and found not to contain vector included blood heartlung liver kidney brain spleen lymph nodes and gonads (n 5
6group) In wound beds adenoviral DNA was detected at alltime points except for day 90 (Table 4 and Fig 6) Vector lev-els did decrease however by 38-fold between days 7 and 28with three of six samples falling below the level of quantita-tion (LOQ) by real-time PCR at the latter time point (Fig 6)
At a 100-fold higher vector dose of 2 3 1011 particles perwound PCR-amplifiable adenoviral DNA was once again un-detectable in the majority of tissues sampled Except for a sin-gle day 7 liver sample and a single day 7 brain sample (bothbelow the LOQ) adenoviral DNA was only detectable directlyin wound beds or in the axillary lymph nodes that drain woundsites (Table 4) Moreover three of six positive axillary nodesamples scored below the LOQ on day 28 as did both positivesamples on day 90 indicating that they contained relatively lit-tle vector Within wound beds adenoviral DNA was detectedat quantifiable levels out to day 28 and at detectable but non-quantifiable levels on day 90 DNA copy numbers remainedsteady between days 3 and 7 dropped 107-fold between days7 and 28 and a further 1662-fold by day 90 Finally at eachtime point DNA copy numbers in wounds treated with 2 3
1011 particles were approximately 100-fold higher than thosefound in wounds treated with 2 3 109 particles thus confirm-ing the linearity of our assay system
To better define the time course of human PDGF-BB pro-duction we also quantified transgene mRNA levels in woundbed samples treated at 2 3 109 particles per wound This treat-ment dose was selected as representative of the virus particleconcentration capable of inducing complete healing in ischemicear wounds Quantifiable levels of human PDGF-B mRNAwere detectable in treated dorsal wounds at days 3 7 and 28(Fig 6) with levels decreasing 14-fold between days 3 and 7and 5-fold between days 7 and 28 The more sensitive tech-nique of real-time RT-PCR therefore demonstrates that trans-
TISSUE REPAIR USING GROWTH FACTOR GENES 795
gene expression extends well beyond the 8-day time period sug-gested using anti-PDGF-BB immunohistochemistry as a de-tection system (Fig 3)
DISCUSSION
These studies demonstrate that immobilization of gene ther-apy vectors in collagen-based matrices enables their efficientdelivery and activity in vivo Matrix immobilization achievedprolonged transgene-encoded growth factor production and asa consequence robust tissue repair By contrast aqueous vehi-cles failed to retain adenoviruses at application sites resultingin diffuse inflammation rather than productive tissue regenera-tion These observations confirm our basic hypothesis that ma-trix immobilization of growth factor-encoding gene therapyvectors represents a promising approach to tissue repair
Although de novo tissue deposition was achievable with sev-eral growth factor genes PDGF-B proved the most suitable forrepair of cutaneous defects A single administration of colla-gen-immobilized AdPDGF-B rapidly induced the formation ofhighly cellular and vascularized tissues with dense ECMs richin collagen By contrast AdFGF2 induced a primarily vascu-lar response with little collagen deposition FGF2 induces therelease of matrix metalloproteinase 1 or interstitial collagenase(Buckley-Sturrock et al 1989) and this may underlie the rel-ative paucity of ECM accumulation VEGF gene delivery alsoinduced highly vascular responses however the enhanced per-meability characteristic of VEGF-induced vasculature (Dvoraket al 1995) led to edema within nascent tissues In fact much
of the enhanced protein and DNA deposition observed in Ad-VEGF-treated PVA sponges may well derive from fluid exu-dates rather than actual tissue formation Finally the inabilityof AdLuc delivery to induce anything beyond a limited in-flammatory response confirms that tissue formation was de-pendent on growth factor gene delivery
The robust activity of PDGF-B gene delivery was expectedas PDGF-BB protein initiates multiple aspects of tissue forma-tion including cellular influx and proliferation ECM deposi-tion and tissue remodeling (Pierce et al 1988 1991 1994a)Indeed PDGF-BB is the only growth factor protein to have suc-cessfully completed human clinical trials and be approved forthe treatment of dermal wounds (Steed 1995 drsquoHemecourt etal 1998 Wieman 1998 Wieman et al 1998) We observedthat collagen-formulated AdPDGF-B induced the complete re-pair of excisional skin defects without unwanted long-term ef-fects such as the development of hypertrophic scars Endoge-nous growth factors other than PDGF-BB however most likelymediated the enhanced re-epithelialization observed in thesewounds as epithelial regeneration is driven by members of theepidermal growth factor and FGF families (Pierce et al 1994bDanilenko et al 1995) Our data indicate nonetheless that tis-sue regeneration and repair were initiated and to a great degreedriven by transgene-encoded PDGF-BB
Despite the known activity of PDGF-BB protein we wereable to demonstrate greater tissue deposition after gene deliv-ery as compared with the use of recombinant growth factor pro-tein A single application of PDGF-BB protein could not equalthe ability of PDGF-B gene therapy to induce neotissue for-mation even at doses well in excess of that induced in situ byAdPDGF-B and in excess of that used in human clinical trials
FIG 5 Influence of collagen-formulated AdPDGF-B on long-term tissue repair Excisional wounds (6 mm in diameter withcartilage remaining intact) were placed in nonischemic rabbit ears and treated with either 015 collagen alone (open columns)or AdPDGF-B formulated in this vehicle (solid columns) On days 28ndash180 posttreatment total ear thickness at the site of eachwound was measured (in mm) with calipers Data are presented as means 6 SD (n 5 3) Treatment groups differ by p 00001groups differ by p 0005
(Steed 1995 drsquoHemecourt et al 1998 Wieman 1998 Wie-man et al 1998) In fact repeated administrations of PDGF-BB protein were required to approach the level of tissue for-mation observed after a single administration of AdPDGF-BThese data support our hypothesis that sustained localizedgrowth factor production is required for robust tissue repair
In further support of this hypothesis we demonstrated thatmRNA encoding human PDGF-B was present in excisionalwounds as late as day 28 after collagen-formulated AdPDGF-B administration By contrast previous studies of PDGF-BBprotein found that the great majority of this growth factor wasgone from treated wounds 1 day postapplication and that anytissue maturation subsequently observed was most likely dueto the upregulation of endogenous growth factors (Pierce et al1992 1995) We also demonstrated that repair cells such asmononuclear leukocytes endothelial cells and fibroblasts pres-ent with developing neotissues represent the source of both
transgene transcription and PDGF-BB production In additiona depot of human PDGF-BB was detected bound to the colla-gen delivery matrix and ECM of these tissues This was antici-pated as PDGF-BB contains collagen-binding motifs (Soma-sundaram and Schuppan 1996) We hypothesize that subsequentmatrix metalloproteinase activity by repair cells will serve togenerate localized release of this sequestered growth factor pooland as a consequence further drive tissue regeneration Theseevents which are central to tissue remodeling should be directlyenhanced by collagen matrices as type I collagen stimulates me-talloproteinase production integrin expression and cellular ac-tivation in PDGF-stimulated fibroblasts (Xu and Clark 19961997)
An additional rationale for employing collagen matrices wasto physically immobilize vectors This was confirmed in vivowhere collagen matrices maintained AdPDGF-B at deliverysites for at least 28 days and limited vector migration to other
DOUKAS ET AL796
FIG 6 Persistence of collagen-formulated vector and transgene transcripts in excisional wounds Full-thickness excisionalwounds (7 cm2) were placed on the dorsal surface of rabbits and treated with AdPDGF-B formulated in 26 collagen at either2 3 109 or 2 3 1011 virus particles per wound (open and closed columns respectively) Wounds were then covered with OpSitedressing and on days 3 7 or 28 posttreatment wound beds were harvested for real-time quantitative PCR and RT-PCR analy-ses PCR data are presented in the upper graph as AdPDGF-B copies per wound RT-PCR data are presented in the lower graphas the relative amount of PDGF-B mRNA per unit 18S rRNA (in arbitrary units) All data points are means 6 SD (n 5 6)
tissues or organs In vitro tests also established that collagenmatrices not only prevent vector loss due to diffusion but pre-serve vector activity despite prolonged incubation in acutewound fluid Successful vector immobilization and tissue re-pair could be achieved with both 015 collagen and 26 col-lagen suggesting flexibility in the final vehicle formulation re-quired for effective vector delivery This flexibility was neededin the present studies as 26 collagen formulations proveddifficult to deliver to PVA sponges and 6-mm excisionalwounds This would not be of concern in clinical settings how-ever where wound beds are easily accessible and generally sev-eral square centimeters in area By contrast CMC was inef-fective at retaining vector in aqueous environments Moreimportantly this matrix was itself inflammatory and whencombined with adenovirus the net result was inflammationrather than tissue repair We are currently examining the util-ity of other matrices such as fibrin and hyaluronic acid whichbecause of their more provisional nature may offer yet greatercellular migration into wounds as compared with type I colla-gen
Although an aqueous-based AdPDGF-B formulation hasbeen previously shown to enhance tissue formation (Liechty etal 1999) this was achieved with a model system that artifi-cially retains vectors within treatment sites In fact the presentstudies demonstrate that any tissue repair observed after Ad-PDGF-B delivery in a nongelling liquid is dependent on the useof this model system In wounds not designed to retain appliedtreatments aqueous-formulated AdPDGF-B seeped into sur-rounding tissues and led to hyperplasia within these areas ratherthan to tissue regeneration within the active wound bed Colla-gen-immobilized AdPDGF-B on the other hand did persist inthese wound beds and led to significant enhancements in gran-ulation tissue formation as well as enhanced wound re-epithe-lialization and wound closure The significance of these activ-ities is further substantiated considering that they wereachievable in 8-mm-diameter ischemic wounds which withinthe time frame examined could not self-heal to any meaning-ful degree in the absence of gene therapy However as all theanimal models employed in these studies will eventually self-heal given sufficient time the full value of matrix-immobilizedgene therapy vectors remains to be confirmed in human clini-cal trials
In conclusion we present evidence that matrix-immobilizedgene therapy vectors encoding appropriate growth-promotinggenes represent a promising approach to tissue regeneration andrepair This basic concept can be expanded to include alterna-tive matrices such as controlled-release formulations as wellas tissue-specific growth factors Furthermore the addition oftargeting ligands to adenovirus vectors (eg FGF2) can en-hance their ability to transduce cells such that tissue repair re-sponses comparable to nontargeted vectors can be achieved butat significantly lower vector doses (Chandler et al 2000a)With appropriate design and application schedules one couldconceivably time the release of multiple growth factors to spe-cific stages of a tissue repair cascade In addition we have foundin preliminary studies that collagen-immobilized nonviral vec-tors such as PDGF-B plasmids which have potentially morefavorable safety profiles than adenovirus vectors can also en-hance tissue formation in vivo (Chandler et al 2000b Tyroneet al 2000) Such flexibility should allow for the widespreadapplication of gene therapy to the treatment of injured tissues
ACKNOWLEDGMENTS
We thank Jeff Davidson (Vanderbilt University School ofMedicine) for assistance in establishing the PVA sponge modelCarl-Henrik Heldin (Ludwig Institute for Cancer Research) forthe PDGF-B gene construct and Emelie Amburn Lara AsatoSharon Chang Gail Fieser Lydia Greenlees Rebecca Smokerand Linda Manza for excellent technical assistance This pub-lication was made possible in part by NIH grants 1R43AR46154(JD) and 5P01CA25874 (MH)
REFERENCES
AHN ST and MUSTOE TA (1990) Effects of ischemia on ulcerwound healing A new model in the rabbit ear Ann Plast Surg 2417ndash23
ANDREE C SWAIN WF PAGE CP MACKLIN MDSLAMA J HATZIS D and ERIKSSON E (1994) In vivo trans-fer and expression of a human epidermal growth factor gene accel-erates wound repair Proc Natl Acad Sci USA 91 12188ndash12192
BENN SI WHITSITT JS BROADLEY KN NANNEY LBPERKINS D HE L PATEL M MORGAN JR SWAIN WFand DAVIDSON JM (1996) Particle-mediated gene transfer withtransforming growth factor-b1 cDNAs enhances wound repair in ratskin J Clin Invest 98 2894ndash2902
BONADIO J SMILEY E PATIL P and GOLDSTEIN S (1999)Localized direct plasmid gene delivery in vivo Prolonged therapyresults in reproducible tissue regeneration Nat Med 5 753ndash759
BUCKLEY A DAVIDSON JM KAMERATH CD WOLT TBand WOODWARD SC (1985) Sustained release of epidermalgrowth factor accelerates wound repair Proc Natl Acad Sci USA82 7340ndash7344
BUCKLEY-STURROCK A WOODWARD SC SENIOR RMGRIFFIN GL KLAGSBRUN M and DAVIDSON JM (1989)Differential stimulation of collagenase and chemotactic activity in fi-broblasts derived from rat wound repair tissue and human skin bygrowth factors J Cell Physiol 138 70ndash78
CHANDLER LA DOUKAS J GONZALEZ AM HOGANSONDK GU DL MA C NESBIT M CROMBLEHOLME TMHERLYN M SOSNOWSKI BA and PIERCE GF (2000a)FGF2ndashTargeted adenovirus encoding platelet-derived growth factor-B enhances de novo tissue formation Mol Ther 2 153ndash160
CHANDLER LA MA C GONZALEZ AM DOUKAS JNGUYEN T PIERCE GF and PHILLIPS ML (2000b) Ma-trix-enabled gene transfer for cutaneous wound repair Wound Re-pair Regen 8 473ndash479
DANILENKO DM RING BD TARPLEY JE MORRIS BVAN GY MORAWIECKI A CALLAHAN W GOLDEN-BERG M HERSHENSON S and PIERCE GF (1995) Growthfactors in porcine full and partial thickness burn repair Differing tar-gets and effects of keratinocyte growth factor platelet-derivedgrowth factor-BB epidermal growth factor and neu differentiationfactor Am J Pathol 147 1261ndash1277
DEUEL TF KAWAHARA RS MUSTOE TA and PIERCE GF(1991) Growth factors and wound healing Platelet-derived growthfactor as a model cytokine Annu Rev Med 42 567ndash584
DrsquoHEMECOURT PA SMIELL JM and KARIM MR (1998) So-dium carboxymethylcellulose aqueous-based gel vs becaplermin gelin patients with nonhealing lower extremity diabetic ulcers Wounds10 69ndash75
DOUKAS J HOGANSON DK ONG M YING W LACEYDL BAIRD A PIERCE GF and SOSNOWSKI BA (1999)Retargeted delivery of adenoviral vectors through fibroblast growthfactor receptors involves unique cellular pathways FASEB J 131459ndash1466
TISSUE REPAIR USING GROWTH FACTOR GENES 797
DVORAK HF BROWN LF DETMAR M and DVORAK AM(1995) Vascular permeability factorvascular endothelial growth fac-tor microvascular hyperpermeability and angiogenesis Am JPathol 146 1029ndash1039
EMING SA MEDALIE DA TOMPKINS RG YARMUSHML and MORGAN JR (1998) Genetically modified human ker-atinocytes overexpressing PDGF-A enhance the performance of acomposite skin graft Hum Gene Ther 9 529ndash539
EMING SA WHITSITT JS HE L KRIEG T MORGAN JRand DAVIDSON JM (1999) Particle-mediated gene transfer ofPDGF isoforms promotes wound repair J Invest Dermatol 112297ndash302
GERDES J SCHWAB U LEMKE H and STEIN H (1983) Pro-duction of a mouse monoclonal antibody reactive with a human nu-clear antigen associated with cell proliferation Int J Cancer 3113ndash20
GONZALEZ AM BERRY M MAHER PA LOGAN A andBAIRD A (1995) A comprehensive analysis of the distribution ofFGF-2 and FGFR1 in the rat brain Brain Res 701 201ndash226
GREENHALGH DG (1996) The role of growth factors in woundhealing J Trauma 41 159ndash167
GROTENDORST GR MARTIN GR PENCEV D SODEK Jand HARVEY AK (1985) Stimulation of granulation tissue for-mation by platelet-derived growth factor in normal and diabetic ratsJ Clin Invest 76 2323ndash2329
KHOURI RK HONG SP DEUNE EG TARPLEY JE SONGSZ SERDAR CM and PIERCE GF (1994) De novo genera-tion of permanent neovascularized soft tissue appendages by platelet-derived growth factor J Clin Invest 94 1757ndash1763
LEGRAND EK SENTER LH GAMELLI RL and KIORPESTC (1993) Evaluation of PDGF-BB PDGF-AA bFGF IL-1 andEGF dose responses in polyvinyl alcohol sponge implants assessedby a rapid histologic method Growth Factors 8 315ndash329
LIECHTY KW NESBIT M HERLYN M RADU A ADZICKNS and CROMBLEHOLME TM (1999) Adenoviral-mediatedoverexpression of platelet-derived growth factor-B corrects ischemicimpaired wound healing J Invest Dermatol 113 375ndash383
LYNCH SE COLVIN RB and ANTONIADES HN (1989)Growth factors in wound healing J Clin Invest 84 640ndash646
MUSTOE TA PIERCE GF THOMASON A GRAMATES PSPORN MB and DEUEL TF (1987) Accelerated healing of in-cisional wounds in rats induced by transforming growth factor-betaScience 237 1333ndash1336
MUSTOE TA PIERCE GF MORISHIMA C and DEUEL TF(1991) Growth factor-induced acceleration of tissue repair throughdirect and inductive activities in a rabbit dermal ulcer model J ClinInvest 87 694ndash703
MUSTOE TA AHN ST TARPLEY JE and PIERCE GF(1994) Role of hypoxia in growth factor responses Differential ef-fects of basic fibroblast growth factor and platelet-derived growthfactor in an ischemic wound model Wound Rep Reg 2 277ndash283
NYBERG-HOFFMAN C and AGUILAR-CORDOVA E (1999) In-stability of adenoviral vectors during transport and its implication forclinical studies Nat Med 5 955ndash957
PIERCE GF and MUSTOE TA (1995) Pharmacologic enhance-ment of wound healing Annu Rev Med 46 467ndash481
PIERCE GF MUSTOE TA SENIOR RM REED J GRIFFINGL THOMASON A and DEUEL TF (1988) In vivo incisionalwound healing augmented by platelet-derived growth factor and re-combinant c-sis gene homodimeric proteins J Exp Med 167 974ndash987
PIERCE GF VANDE BERG J RUDOLPH R TARPLEY J andMUSTOE TA (1991) Platelet-derived growth factor-BB and trans-forming growth factor beta 1 selectively modulate glycosaminogly -cans collagen and myofibroblasts in excisional wounds Am JPathol 138 629ndash646
PIERCE GF TARPLEY JE YANAGIHARA D MUSTOE TA
FOX GM and THOMASON A (1992) Platelet-derived growthfactor (BB homodimer) transforming growth factor-b1 and basic fi-broblast growth factor in dermal wound healing Neovessel and ma-trix formation and cessation of repair Am J Pathol 140 1375ndash1388
PIERCE GF TARPLEY JE ALLMAN RM GOODE PS SER-DAR CM MORRIS B MUSTOE TA and VANDE BERG J(1994a) Tissue repair processes in healing chronic pressure ulcerstreated with recombinant platelet-derived growth factor BB Am JPathol 145 1399ndash1410
PIERCE GF YANAGIHARA D KLOPCHIN K DANILENKODM HSU E KENNEY WC and MORRIS CF (1994b) Stim-ulation of all epithelial elements during skin regeneration by kerati-nocyte growth factor J Exp Med 179 831ndash840
PIERCE GF TARPLEY JE TSENG J BREADY J CHANGD KENNEY WC RUDOLPH R ROBSON MC VANDEBERG J and REID P (1995) Detection of platelet-derived growthfactor (PDGF)-AA in actively healing human wounds treated withrecombinant PDGF-BB and absence of PDGF in chronic nonhealingwounds J Clin Invest 96 1336ndash1350
SINGER AJ and CLARK RA (1999) Cutaneous wound healingN Engl J Med 341 738ndash746
SOMASUNDARAM R and SCHUPPAN D (1996) Type I II IIIIV V and VI collagens serve as extracellular ligands for the iso-forms of platelet-derived growth factor (AA BB and AB) J BiolChem 271 26884ndash26891
SPRUGEL KH MCPHERSON JM CLOWES AW and ROSSR (1987) Effects of growth factors in vivo I Cell ingrowth intoporous subcutaneous chambers Am J Pathol 129 601ndash613
STEED DL (1995) Clinical evaluation of recombinant humanplatelet-derived growth factor for the treatment of lower extremitydiabetic ulcers Diabetic Ulcer Study Group J Vasc Surg 21 71ndash78
STEED DL (1998) Foundations of good ulcer care Am J Surg 17620S-25S
TYRONE JW MOGFORD JE CHANDLER LA MA C XIAY PIERCE GF and MUSTOE TA (2000) Collagen-embeddedplatelet-derived growth factor DNA plasmid promotes wound heal-ing in a dermal ulcer model J Surg Res 93 230ndash236
VOGT PM THOMPSON S ANDREE C LIU P BREUING KHATZIS D BROWN H MULLIGAN RC and ERIKSSON E(1994) Genetically modified keratinocytes transplanted to woundsreconstitute the epidermis Proc Natl Acad Sci USA 91 9307ndash9311
WIEMAN TJ (1998) Clinical efficacy of becaplermin (rhPDGF-BB)gel Becaplermin Gel Studies Group Am J Surg 176 74S-79S
WIEMAN TJ SMIELL JM and SU Y (1998) Efficacy and safetyof a topical gel formulation of recombinant human platelet-derivedgrowth factor-BB (becaplermin) in patients with chronic neuropathicdiabetic ulcers A phase III randomized placebo-controlled double-blind study Diabetes Care 21 822ndash827
WILSON JM (1996) Adenoviruses as gene-delivery vehicles NEngl J Med 334 1185ndash1187
XU J and CLARK RA (1996) Extracellular matrix alters PDGFregulation of fibroblast integrins J Cell Biol 132 239ndash249
XU J and CLARK RA (1997) A three-dimensional collagen latticeinduces protein kinase C-z activity Role in a2 integrin and collage-nase mRNA expression J Cell Biol 136 473ndash483
Address reprint requests toDr John Doukas
Selective Genetics Inc11035 Roselle Street
San Diego CA 92121
E-mail jdoukasselectivegeneticscom
Received for publication December 28 2000 accepted after re-vision February 23 2001
DOUKAS ET AL798
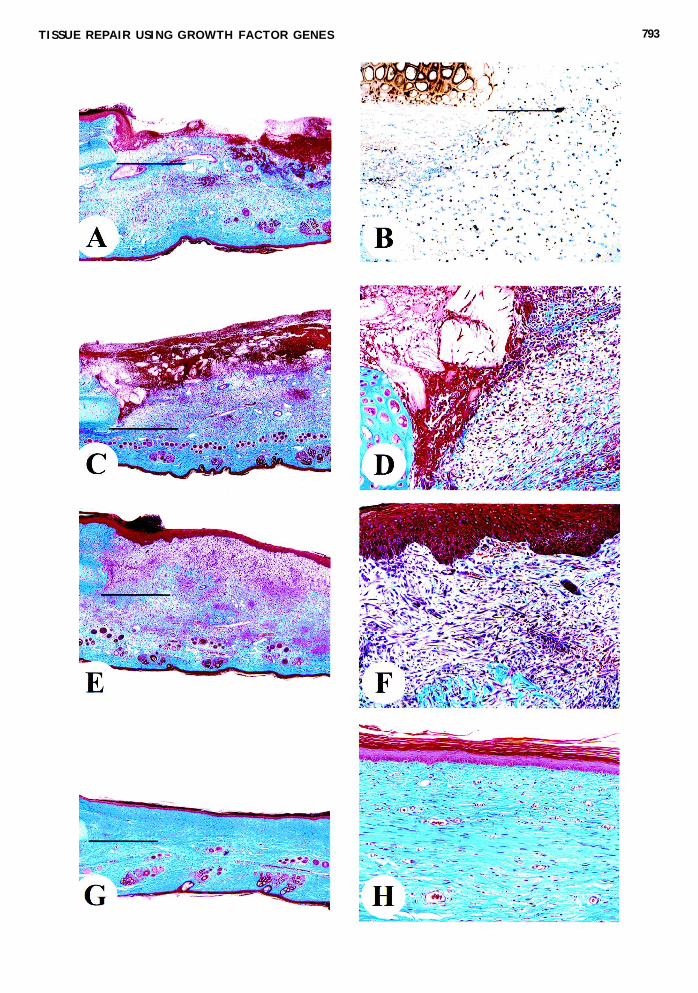
TISSUE REPAIR USING GROWTH FACTOR GENES 793
DOUKAS ET AL794
TABLE 4 BIODISTRIBUTION OF AdPDGF-B IN EXCISIONAL WOUNDSa
Positive samplestotal assayed
Tissue AdPDGF-B dose Day 3 Day 7 Day 28 Day 90
Wound bed 2 3 109 particles 66 66 66b 06Axillary lymph nodes 2 3 109 particles 02 ND 06 06
Wound bed 2 3 1011 particles 66 66 66 46c
Axillary lymph nodes 2 3 1011 particles 66 ND 66d 26e
aFull-thickness excisional wounds (7 cm2) were placed on the backs of rabbits and AdPDGF-B formulated in 26 collagenwas applied as either 2 3 109 or 2 3 1011 virus particles per wound On days 3ndash90 posttreatment wound beds and a panel oforgans were harvested for real-time PCR quantification of viral genome Data are shown for wound bed and axillary lymph nodesamples as the number of samples that yielded amplifiable signals per total number assayed ND not determined
bThree of six samples scored below the level of quantitation (LOQ 10ndash100 copiesmg DNA)cAll four positive samples scored below the LOQdThree of six samples scored below the LOQeBoth positive samples scored below the LOQ
180 days posttreatment (Fig 5) PDGF-B gene delivery en-hanced total ear thickness relative to controls on day 28 (229 6
020 vs 179 6 019 mm p 00001) and day 60 (192 6 001vs 182 6 011 mm p 0005) as anticipated on the basis ofthe ability of this formulation to induce granulation tissue for-mation By day 90 posttreatment however there was no mea-surable difference in ear thickness between AdPDGF-B andcontrol-treated groups and this relationship continued out today 180 indicating that growth factor gene delivery did not in-duce excessive scar formation This was also confirmed histo-logically AdPDGF-B-treated wounds on day 90 and beyondwere composed of a thin outer keratin layer an underlying ep-ithelial layer of equivalent thickness to nonwounded areas anda collagen-rich dermis devoid of any signs of tissue hyperpla-sia (Fig 4G and H)
Collagen immobilization limits adenovirus vectorbiodistribution beyond treatment sites
As a final measure of the value of matrix immobilization forgene delivery we determined the biodistribution patterns ofvectors after their in vivo delivery In the first model systemused AdPDGF-B formulated in 015 collagen was applied torabbit ear wounds at equivalent doses as previously describedwounds were extended through underlying cartilage but vas-cular supplies were not disturbed so as to permit maximal vec-tor dissemination By PCR no adenoviral DNA was detectablein lung spleen brain cervical lymph nodes or gonads on day1 3 7 or 14 (n 5 6 per group) In the liver one of six sam-ples was positive on days 3 and 7 but none on day 14 in serumonly one of six samples tested positive on day 14 (equivalentof 500-ml serum volume) By contrast adenovirus was detectedin eight of eight wound bed samples at all time points exam-ined
In a second model system excisional wounds placed on thebacks of rabbits were treated with AdPDGF-B formulated in26 collagen Because of their anatomical placement thismodel allowed for the creation of larger excisional wounds (7-cm2 total area) than those placed in rabbit ears (03 cm2) and
consequently larger treatment volumes and vector doses (2 3109 or 2 3 1011 virus particles per wound) At the lower doseof 2 3 109 particles PCR-amplifiable adenoviral DNA was notdetectable beyond wound beds on day 3 7 28 or 90 Tissuessampled and found not to contain vector included blood heartlung liver kidney brain spleen lymph nodes and gonads (n 5
6group) In wound beds adenoviral DNA was detected at alltime points except for day 90 (Table 4 and Fig 6) Vector lev-els did decrease however by 38-fold between days 7 and 28with three of six samples falling below the level of quantita-tion (LOQ) by real-time PCR at the latter time point (Fig 6)
At a 100-fold higher vector dose of 2 3 1011 particles perwound PCR-amplifiable adenoviral DNA was once again un-detectable in the majority of tissues sampled Except for a sin-gle day 7 liver sample and a single day 7 brain sample (bothbelow the LOQ) adenoviral DNA was only detectable directlyin wound beds or in the axillary lymph nodes that drain woundsites (Table 4) Moreover three of six positive axillary nodesamples scored below the LOQ on day 28 as did both positivesamples on day 90 indicating that they contained relatively lit-tle vector Within wound beds adenoviral DNA was detectedat quantifiable levels out to day 28 and at detectable but non-quantifiable levels on day 90 DNA copy numbers remainedsteady between days 3 and 7 dropped 107-fold between days7 and 28 and a further 1662-fold by day 90 Finally at eachtime point DNA copy numbers in wounds treated with 2 3
1011 particles were approximately 100-fold higher than thosefound in wounds treated with 2 3 109 particles thus confirm-ing the linearity of our assay system
To better define the time course of human PDGF-BB pro-duction we also quantified transgene mRNA levels in woundbed samples treated at 2 3 109 particles per wound This treat-ment dose was selected as representative of the virus particleconcentration capable of inducing complete healing in ischemicear wounds Quantifiable levels of human PDGF-B mRNAwere detectable in treated dorsal wounds at days 3 7 and 28(Fig 6) with levels decreasing 14-fold between days 3 and 7and 5-fold between days 7 and 28 The more sensitive tech-nique of real-time RT-PCR therefore demonstrates that trans-
TISSUE REPAIR USING GROWTH FACTOR GENES 795
gene expression extends well beyond the 8-day time period sug-gested using anti-PDGF-BB immunohistochemistry as a de-tection system (Fig 3)
DISCUSSION
These studies demonstrate that immobilization of gene ther-apy vectors in collagen-based matrices enables their efficientdelivery and activity in vivo Matrix immobilization achievedprolonged transgene-encoded growth factor production and asa consequence robust tissue repair By contrast aqueous vehi-cles failed to retain adenoviruses at application sites resultingin diffuse inflammation rather than productive tissue regenera-tion These observations confirm our basic hypothesis that ma-trix immobilization of growth factor-encoding gene therapyvectors represents a promising approach to tissue repair
Although de novo tissue deposition was achievable with sev-eral growth factor genes PDGF-B proved the most suitable forrepair of cutaneous defects A single administration of colla-gen-immobilized AdPDGF-B rapidly induced the formation ofhighly cellular and vascularized tissues with dense ECMs richin collagen By contrast AdFGF2 induced a primarily vascu-lar response with little collagen deposition FGF2 induces therelease of matrix metalloproteinase 1 or interstitial collagenase(Buckley-Sturrock et al 1989) and this may underlie the rel-ative paucity of ECM accumulation VEGF gene delivery alsoinduced highly vascular responses however the enhanced per-meability characteristic of VEGF-induced vasculature (Dvoraket al 1995) led to edema within nascent tissues In fact much
of the enhanced protein and DNA deposition observed in Ad-VEGF-treated PVA sponges may well derive from fluid exu-dates rather than actual tissue formation Finally the inabilityof AdLuc delivery to induce anything beyond a limited in-flammatory response confirms that tissue formation was de-pendent on growth factor gene delivery
The robust activity of PDGF-B gene delivery was expectedas PDGF-BB protein initiates multiple aspects of tissue forma-tion including cellular influx and proliferation ECM deposi-tion and tissue remodeling (Pierce et al 1988 1991 1994a)Indeed PDGF-BB is the only growth factor protein to have suc-cessfully completed human clinical trials and be approved forthe treatment of dermal wounds (Steed 1995 drsquoHemecourt etal 1998 Wieman 1998 Wieman et al 1998) We observedthat collagen-formulated AdPDGF-B induced the complete re-pair of excisional skin defects without unwanted long-term ef-fects such as the development of hypertrophic scars Endoge-nous growth factors other than PDGF-BB however most likelymediated the enhanced re-epithelialization observed in thesewounds as epithelial regeneration is driven by members of theepidermal growth factor and FGF families (Pierce et al 1994bDanilenko et al 1995) Our data indicate nonetheless that tis-sue regeneration and repair were initiated and to a great degreedriven by transgene-encoded PDGF-BB
Despite the known activity of PDGF-BB protein we wereable to demonstrate greater tissue deposition after gene deliv-ery as compared with the use of recombinant growth factor pro-tein A single application of PDGF-BB protein could not equalthe ability of PDGF-B gene therapy to induce neotissue for-mation even at doses well in excess of that induced in situ byAdPDGF-B and in excess of that used in human clinical trials
FIG 5 Influence of collagen-formulated AdPDGF-B on long-term tissue repair Excisional wounds (6 mm in diameter withcartilage remaining intact) were placed in nonischemic rabbit ears and treated with either 015 collagen alone (open columns)or AdPDGF-B formulated in this vehicle (solid columns) On days 28ndash180 posttreatment total ear thickness at the site of eachwound was measured (in mm) with calipers Data are presented as means 6 SD (n 5 3) Treatment groups differ by p 00001groups differ by p 0005
(Steed 1995 drsquoHemecourt et al 1998 Wieman 1998 Wie-man et al 1998) In fact repeated administrations of PDGF-BB protein were required to approach the level of tissue for-mation observed after a single administration of AdPDGF-BThese data support our hypothesis that sustained localizedgrowth factor production is required for robust tissue repair
In further support of this hypothesis we demonstrated thatmRNA encoding human PDGF-B was present in excisionalwounds as late as day 28 after collagen-formulated AdPDGF-B administration By contrast previous studies of PDGF-BBprotein found that the great majority of this growth factor wasgone from treated wounds 1 day postapplication and that anytissue maturation subsequently observed was most likely dueto the upregulation of endogenous growth factors (Pierce et al1992 1995) We also demonstrated that repair cells such asmononuclear leukocytes endothelial cells and fibroblasts pres-ent with developing neotissues represent the source of both
transgene transcription and PDGF-BB production In additiona depot of human PDGF-BB was detected bound to the colla-gen delivery matrix and ECM of these tissues This was antici-pated as PDGF-BB contains collagen-binding motifs (Soma-sundaram and Schuppan 1996) We hypothesize that subsequentmatrix metalloproteinase activity by repair cells will serve togenerate localized release of this sequestered growth factor pooland as a consequence further drive tissue regeneration Theseevents which are central to tissue remodeling should be directlyenhanced by collagen matrices as type I collagen stimulates me-talloproteinase production integrin expression and cellular ac-tivation in PDGF-stimulated fibroblasts (Xu and Clark 19961997)
An additional rationale for employing collagen matrices wasto physically immobilize vectors This was confirmed in vivowhere collagen matrices maintained AdPDGF-B at deliverysites for at least 28 days and limited vector migration to other
DOUKAS ET AL796
FIG 6 Persistence of collagen-formulated vector and transgene transcripts in excisional wounds Full-thickness excisionalwounds (7 cm2) were placed on the dorsal surface of rabbits and treated with AdPDGF-B formulated in 26 collagen at either2 3 109 or 2 3 1011 virus particles per wound (open and closed columns respectively) Wounds were then covered with OpSitedressing and on days 3 7 or 28 posttreatment wound beds were harvested for real-time quantitative PCR and RT-PCR analy-ses PCR data are presented in the upper graph as AdPDGF-B copies per wound RT-PCR data are presented in the lower graphas the relative amount of PDGF-B mRNA per unit 18S rRNA (in arbitrary units) All data points are means 6 SD (n 5 6)
tissues or organs In vitro tests also established that collagenmatrices not only prevent vector loss due to diffusion but pre-serve vector activity despite prolonged incubation in acutewound fluid Successful vector immobilization and tissue re-pair could be achieved with both 015 collagen and 26 col-lagen suggesting flexibility in the final vehicle formulation re-quired for effective vector delivery This flexibility was neededin the present studies as 26 collagen formulations proveddifficult to deliver to PVA sponges and 6-mm excisionalwounds This would not be of concern in clinical settings how-ever where wound beds are easily accessible and generally sev-eral square centimeters in area By contrast CMC was inef-fective at retaining vector in aqueous environments Moreimportantly this matrix was itself inflammatory and whencombined with adenovirus the net result was inflammationrather than tissue repair We are currently examining the util-ity of other matrices such as fibrin and hyaluronic acid whichbecause of their more provisional nature may offer yet greatercellular migration into wounds as compared with type I colla-gen
Although an aqueous-based AdPDGF-B formulation hasbeen previously shown to enhance tissue formation (Liechty etal 1999) this was achieved with a model system that artifi-cially retains vectors within treatment sites In fact the presentstudies demonstrate that any tissue repair observed after Ad-PDGF-B delivery in a nongelling liquid is dependent on the useof this model system In wounds not designed to retain appliedtreatments aqueous-formulated AdPDGF-B seeped into sur-rounding tissues and led to hyperplasia within these areas ratherthan to tissue regeneration within the active wound bed Colla-gen-immobilized AdPDGF-B on the other hand did persist inthese wound beds and led to significant enhancements in gran-ulation tissue formation as well as enhanced wound re-epithe-lialization and wound closure The significance of these activ-ities is further substantiated considering that they wereachievable in 8-mm-diameter ischemic wounds which withinthe time frame examined could not self-heal to any meaning-ful degree in the absence of gene therapy However as all theanimal models employed in these studies will eventually self-heal given sufficient time the full value of matrix-immobilizedgene therapy vectors remains to be confirmed in human clini-cal trials
In conclusion we present evidence that matrix-immobilizedgene therapy vectors encoding appropriate growth-promotinggenes represent a promising approach to tissue regeneration andrepair This basic concept can be expanded to include alterna-tive matrices such as controlled-release formulations as wellas tissue-specific growth factors Furthermore the addition oftargeting ligands to adenovirus vectors (eg FGF2) can en-hance their ability to transduce cells such that tissue repair re-sponses comparable to nontargeted vectors can be achieved butat significantly lower vector doses (Chandler et al 2000a)With appropriate design and application schedules one couldconceivably time the release of multiple growth factors to spe-cific stages of a tissue repair cascade In addition we have foundin preliminary studies that collagen-immobilized nonviral vec-tors such as PDGF-B plasmids which have potentially morefavorable safety profiles than adenovirus vectors can also en-hance tissue formation in vivo (Chandler et al 2000b Tyroneet al 2000) Such flexibility should allow for the widespreadapplication of gene therapy to the treatment of injured tissues
ACKNOWLEDGMENTS
We thank Jeff Davidson (Vanderbilt University School ofMedicine) for assistance in establishing the PVA sponge modelCarl-Henrik Heldin (Ludwig Institute for Cancer Research) forthe PDGF-B gene construct and Emelie Amburn Lara AsatoSharon Chang Gail Fieser Lydia Greenlees Rebecca Smokerand Linda Manza for excellent technical assistance This pub-lication was made possible in part by NIH grants 1R43AR46154(JD) and 5P01CA25874 (MH)
REFERENCES
AHN ST and MUSTOE TA (1990) Effects of ischemia on ulcerwound healing A new model in the rabbit ear Ann Plast Surg 2417ndash23
ANDREE C SWAIN WF PAGE CP MACKLIN MDSLAMA J HATZIS D and ERIKSSON E (1994) In vivo trans-fer and expression of a human epidermal growth factor gene accel-erates wound repair Proc Natl Acad Sci USA 91 12188ndash12192
BENN SI WHITSITT JS BROADLEY KN NANNEY LBPERKINS D HE L PATEL M MORGAN JR SWAIN WFand DAVIDSON JM (1996) Particle-mediated gene transfer withtransforming growth factor-b1 cDNAs enhances wound repair in ratskin J Clin Invest 98 2894ndash2902
BONADIO J SMILEY E PATIL P and GOLDSTEIN S (1999)Localized direct plasmid gene delivery in vivo Prolonged therapyresults in reproducible tissue regeneration Nat Med 5 753ndash759
BUCKLEY A DAVIDSON JM KAMERATH CD WOLT TBand WOODWARD SC (1985) Sustained release of epidermalgrowth factor accelerates wound repair Proc Natl Acad Sci USA82 7340ndash7344
BUCKLEY-STURROCK A WOODWARD SC SENIOR RMGRIFFIN GL KLAGSBRUN M and DAVIDSON JM (1989)Differential stimulation of collagenase and chemotactic activity in fi-broblasts derived from rat wound repair tissue and human skin bygrowth factors J Cell Physiol 138 70ndash78
CHANDLER LA DOUKAS J GONZALEZ AM HOGANSONDK GU DL MA C NESBIT M CROMBLEHOLME TMHERLYN M SOSNOWSKI BA and PIERCE GF (2000a)FGF2ndashTargeted adenovirus encoding platelet-derived growth factor-B enhances de novo tissue formation Mol Ther 2 153ndash160
CHANDLER LA MA C GONZALEZ AM DOUKAS JNGUYEN T PIERCE GF and PHILLIPS ML (2000b) Ma-trix-enabled gene transfer for cutaneous wound repair Wound Re-pair Regen 8 473ndash479
DANILENKO DM RING BD TARPLEY JE MORRIS BVAN GY MORAWIECKI A CALLAHAN W GOLDEN-BERG M HERSHENSON S and PIERCE GF (1995) Growthfactors in porcine full and partial thickness burn repair Differing tar-gets and effects of keratinocyte growth factor platelet-derivedgrowth factor-BB epidermal growth factor and neu differentiationfactor Am J Pathol 147 1261ndash1277
DEUEL TF KAWAHARA RS MUSTOE TA and PIERCE GF(1991) Growth factors and wound healing Platelet-derived growthfactor as a model cytokine Annu Rev Med 42 567ndash584
DrsquoHEMECOURT PA SMIELL JM and KARIM MR (1998) So-dium carboxymethylcellulose aqueous-based gel vs becaplermin gelin patients with nonhealing lower extremity diabetic ulcers Wounds10 69ndash75
DOUKAS J HOGANSON DK ONG M YING W LACEYDL BAIRD A PIERCE GF and SOSNOWSKI BA (1999)Retargeted delivery of adenoviral vectors through fibroblast growthfactor receptors involves unique cellular pathways FASEB J 131459ndash1466
TISSUE REPAIR USING GROWTH FACTOR GENES 797
DVORAK HF BROWN LF DETMAR M and DVORAK AM(1995) Vascular permeability factorvascular endothelial growth fac-tor microvascular hyperpermeability and angiogenesis Am JPathol 146 1029ndash1039
EMING SA MEDALIE DA TOMPKINS RG YARMUSHML and MORGAN JR (1998) Genetically modified human ker-atinocytes overexpressing PDGF-A enhance the performance of acomposite skin graft Hum Gene Ther 9 529ndash539
EMING SA WHITSITT JS HE L KRIEG T MORGAN JRand DAVIDSON JM (1999) Particle-mediated gene transfer ofPDGF isoforms promotes wound repair J Invest Dermatol 112297ndash302
GERDES J SCHWAB U LEMKE H and STEIN H (1983) Pro-duction of a mouse monoclonal antibody reactive with a human nu-clear antigen associated with cell proliferation Int J Cancer 3113ndash20
GONZALEZ AM BERRY M MAHER PA LOGAN A andBAIRD A (1995) A comprehensive analysis of the distribution ofFGF-2 and FGFR1 in the rat brain Brain Res 701 201ndash226
GREENHALGH DG (1996) The role of growth factors in woundhealing J Trauma 41 159ndash167
GROTENDORST GR MARTIN GR PENCEV D SODEK Jand HARVEY AK (1985) Stimulation of granulation tissue for-mation by platelet-derived growth factor in normal and diabetic ratsJ Clin Invest 76 2323ndash2329
KHOURI RK HONG SP DEUNE EG TARPLEY JE SONGSZ SERDAR CM and PIERCE GF (1994) De novo genera-tion of permanent neovascularized soft tissue appendages by platelet-derived growth factor J Clin Invest 94 1757ndash1763
LEGRAND EK SENTER LH GAMELLI RL and KIORPESTC (1993) Evaluation of PDGF-BB PDGF-AA bFGF IL-1 andEGF dose responses in polyvinyl alcohol sponge implants assessedby a rapid histologic method Growth Factors 8 315ndash329
LIECHTY KW NESBIT M HERLYN M RADU A ADZICKNS and CROMBLEHOLME TM (1999) Adenoviral-mediatedoverexpression of platelet-derived growth factor-B corrects ischemicimpaired wound healing J Invest Dermatol 113 375ndash383
LYNCH SE COLVIN RB and ANTONIADES HN (1989)Growth factors in wound healing J Clin Invest 84 640ndash646
MUSTOE TA PIERCE GF THOMASON A GRAMATES PSPORN MB and DEUEL TF (1987) Accelerated healing of in-cisional wounds in rats induced by transforming growth factor-betaScience 237 1333ndash1336
MUSTOE TA PIERCE GF MORISHIMA C and DEUEL TF(1991) Growth factor-induced acceleration of tissue repair throughdirect and inductive activities in a rabbit dermal ulcer model J ClinInvest 87 694ndash703
MUSTOE TA AHN ST TARPLEY JE and PIERCE GF(1994) Role of hypoxia in growth factor responses Differential ef-fects of basic fibroblast growth factor and platelet-derived growthfactor in an ischemic wound model Wound Rep Reg 2 277ndash283
NYBERG-HOFFMAN C and AGUILAR-CORDOVA E (1999) In-stability of adenoviral vectors during transport and its implication forclinical studies Nat Med 5 955ndash957
PIERCE GF and MUSTOE TA (1995) Pharmacologic enhance-ment of wound healing Annu Rev Med 46 467ndash481
PIERCE GF MUSTOE TA SENIOR RM REED J GRIFFINGL THOMASON A and DEUEL TF (1988) In vivo incisionalwound healing augmented by platelet-derived growth factor and re-combinant c-sis gene homodimeric proteins J Exp Med 167 974ndash987
PIERCE GF VANDE BERG J RUDOLPH R TARPLEY J andMUSTOE TA (1991) Platelet-derived growth factor-BB and trans-forming growth factor beta 1 selectively modulate glycosaminogly -cans collagen and myofibroblasts in excisional wounds Am JPathol 138 629ndash646
PIERCE GF TARPLEY JE YANAGIHARA D MUSTOE TA
FOX GM and THOMASON A (1992) Platelet-derived growthfactor (BB homodimer) transforming growth factor-b1 and basic fi-broblast growth factor in dermal wound healing Neovessel and ma-trix formation and cessation of repair Am J Pathol 140 1375ndash1388
PIERCE GF TARPLEY JE ALLMAN RM GOODE PS SER-DAR CM MORRIS B MUSTOE TA and VANDE BERG J(1994a) Tissue repair processes in healing chronic pressure ulcerstreated with recombinant platelet-derived growth factor BB Am JPathol 145 1399ndash1410
PIERCE GF YANAGIHARA D KLOPCHIN K DANILENKODM HSU E KENNEY WC and MORRIS CF (1994b) Stim-ulation of all epithelial elements during skin regeneration by kerati-nocyte growth factor J Exp Med 179 831ndash840
PIERCE GF TARPLEY JE TSENG J BREADY J CHANGD KENNEY WC RUDOLPH R ROBSON MC VANDEBERG J and REID P (1995) Detection of platelet-derived growthfactor (PDGF)-AA in actively healing human wounds treated withrecombinant PDGF-BB and absence of PDGF in chronic nonhealingwounds J Clin Invest 96 1336ndash1350
SINGER AJ and CLARK RA (1999) Cutaneous wound healingN Engl J Med 341 738ndash746
SOMASUNDARAM R and SCHUPPAN D (1996) Type I II IIIIV V and VI collagens serve as extracellular ligands for the iso-forms of platelet-derived growth factor (AA BB and AB) J BiolChem 271 26884ndash26891
SPRUGEL KH MCPHERSON JM CLOWES AW and ROSSR (1987) Effects of growth factors in vivo I Cell ingrowth intoporous subcutaneous chambers Am J Pathol 129 601ndash613
STEED DL (1995) Clinical evaluation of recombinant humanplatelet-derived growth factor for the treatment of lower extremitydiabetic ulcers Diabetic Ulcer Study Group J Vasc Surg 21 71ndash78
STEED DL (1998) Foundations of good ulcer care Am J Surg 17620S-25S
TYRONE JW MOGFORD JE CHANDLER LA MA C XIAY PIERCE GF and MUSTOE TA (2000) Collagen-embeddedplatelet-derived growth factor DNA plasmid promotes wound heal-ing in a dermal ulcer model J Surg Res 93 230ndash236
VOGT PM THOMPSON S ANDREE C LIU P BREUING KHATZIS D BROWN H MULLIGAN RC and ERIKSSON E(1994) Genetically modified keratinocytes transplanted to woundsreconstitute the epidermis Proc Natl Acad Sci USA 91 9307ndash9311
WIEMAN TJ (1998) Clinical efficacy of becaplermin (rhPDGF-BB)gel Becaplermin Gel Studies Group Am J Surg 176 74S-79S
WIEMAN TJ SMIELL JM and SU Y (1998) Efficacy and safetyof a topical gel formulation of recombinant human platelet-derivedgrowth factor-BB (becaplermin) in patients with chronic neuropathicdiabetic ulcers A phase III randomized placebo-controlled double-blind study Diabetes Care 21 822ndash827
WILSON JM (1996) Adenoviruses as gene-delivery vehicles NEngl J Med 334 1185ndash1187
XU J and CLARK RA (1996) Extracellular matrix alters PDGFregulation of fibroblast integrins J Cell Biol 132 239ndash249
XU J and CLARK RA (1997) A three-dimensional collagen latticeinduces protein kinase C-z activity Role in a2 integrin and collage-nase mRNA expression J Cell Biol 136 473ndash483
Address reprint requests toDr John Doukas
Selective Genetics Inc11035 Roselle Street
San Diego CA 92121
E-mail jdoukasselectivegeneticscom
Received for publication December 28 2000 accepted after re-vision February 23 2001
DOUKAS ET AL798

DOUKAS ET AL794
TABLE 4 BIODISTRIBUTION OF AdPDGF-B IN EXCISIONAL WOUNDSa
Positive samplestotal assayed
Tissue AdPDGF-B dose Day 3 Day 7 Day 28 Day 90
Wound bed 2 3 109 particles 66 66 66b 06Axillary lymph nodes 2 3 109 particles 02 ND 06 06
Wound bed 2 3 1011 particles 66 66 66 46c
Axillary lymph nodes 2 3 1011 particles 66 ND 66d 26e
aFull-thickness excisional wounds (7 cm2) were placed on the backs of rabbits and AdPDGF-B formulated in 26 collagenwas applied as either 2 3 109 or 2 3 1011 virus particles per wound On days 3ndash90 posttreatment wound beds and a panel oforgans were harvested for real-time PCR quantification of viral genome Data are shown for wound bed and axillary lymph nodesamples as the number of samples that yielded amplifiable signals per total number assayed ND not determined
bThree of six samples scored below the level of quantitation (LOQ 10ndash100 copiesmg DNA)cAll four positive samples scored below the LOQdThree of six samples scored below the LOQeBoth positive samples scored below the LOQ
180 days posttreatment (Fig 5) PDGF-B gene delivery en-hanced total ear thickness relative to controls on day 28 (229 6
020 vs 179 6 019 mm p 00001) and day 60 (192 6 001vs 182 6 011 mm p 0005) as anticipated on the basis ofthe ability of this formulation to induce granulation tissue for-mation By day 90 posttreatment however there was no mea-surable difference in ear thickness between AdPDGF-B andcontrol-treated groups and this relationship continued out today 180 indicating that growth factor gene delivery did not in-duce excessive scar formation This was also confirmed histo-logically AdPDGF-B-treated wounds on day 90 and beyondwere composed of a thin outer keratin layer an underlying ep-ithelial layer of equivalent thickness to nonwounded areas anda collagen-rich dermis devoid of any signs of tissue hyperpla-sia (Fig 4G and H)
Collagen immobilization limits adenovirus vectorbiodistribution beyond treatment sites
As a final measure of the value of matrix immobilization forgene delivery we determined the biodistribution patterns ofvectors after their in vivo delivery In the first model systemused AdPDGF-B formulated in 015 collagen was applied torabbit ear wounds at equivalent doses as previously describedwounds were extended through underlying cartilage but vas-cular supplies were not disturbed so as to permit maximal vec-tor dissemination By PCR no adenoviral DNA was detectablein lung spleen brain cervical lymph nodes or gonads on day1 3 7 or 14 (n 5 6 per group) In the liver one of six sam-ples was positive on days 3 and 7 but none on day 14 in serumonly one of six samples tested positive on day 14 (equivalentof 500-ml serum volume) By contrast adenovirus was detectedin eight of eight wound bed samples at all time points exam-ined
In a second model system excisional wounds placed on thebacks of rabbits were treated with AdPDGF-B formulated in26 collagen Because of their anatomical placement thismodel allowed for the creation of larger excisional wounds (7-cm2 total area) than those placed in rabbit ears (03 cm2) and
consequently larger treatment volumes and vector doses (2 3109 or 2 3 1011 virus particles per wound) At the lower doseof 2 3 109 particles PCR-amplifiable adenoviral DNA was notdetectable beyond wound beds on day 3 7 28 or 90 Tissuessampled and found not to contain vector included blood heartlung liver kidney brain spleen lymph nodes and gonads (n 5
6group) In wound beds adenoviral DNA was detected at alltime points except for day 90 (Table 4 and Fig 6) Vector lev-els did decrease however by 38-fold between days 7 and 28with three of six samples falling below the level of quantita-tion (LOQ) by real-time PCR at the latter time point (Fig 6)
At a 100-fold higher vector dose of 2 3 1011 particles perwound PCR-amplifiable adenoviral DNA was once again un-detectable in the majority of tissues sampled Except for a sin-gle day 7 liver sample and a single day 7 brain sample (bothbelow the LOQ) adenoviral DNA was only detectable directlyin wound beds or in the axillary lymph nodes that drain woundsites (Table 4) Moreover three of six positive axillary nodesamples scored below the LOQ on day 28 as did both positivesamples on day 90 indicating that they contained relatively lit-tle vector Within wound beds adenoviral DNA was detectedat quantifiable levels out to day 28 and at detectable but non-quantifiable levels on day 90 DNA copy numbers remainedsteady between days 3 and 7 dropped 107-fold between days7 and 28 and a further 1662-fold by day 90 Finally at eachtime point DNA copy numbers in wounds treated with 2 3
1011 particles were approximately 100-fold higher than thosefound in wounds treated with 2 3 109 particles thus confirm-ing the linearity of our assay system
To better define the time course of human PDGF-BB pro-duction we also quantified transgene mRNA levels in woundbed samples treated at 2 3 109 particles per wound This treat-ment dose was selected as representative of the virus particleconcentration capable of inducing complete healing in ischemicear wounds Quantifiable levels of human PDGF-B mRNAwere detectable in treated dorsal wounds at days 3 7 and 28(Fig 6) with levels decreasing 14-fold between days 3 and 7and 5-fold between days 7 and 28 The more sensitive tech-nique of real-time RT-PCR therefore demonstrates that trans-
TISSUE REPAIR USING GROWTH FACTOR GENES 795
gene expression extends well beyond the 8-day time period sug-gested using anti-PDGF-BB immunohistochemistry as a de-tection system (Fig 3)
DISCUSSION
These studies demonstrate that immobilization of gene ther-apy vectors in collagen-based matrices enables their efficientdelivery and activity in vivo Matrix immobilization achievedprolonged transgene-encoded growth factor production and asa consequence robust tissue repair By contrast aqueous vehi-cles failed to retain adenoviruses at application sites resultingin diffuse inflammation rather than productive tissue regenera-tion These observations confirm our basic hypothesis that ma-trix immobilization of growth factor-encoding gene therapyvectors represents a promising approach to tissue repair
Although de novo tissue deposition was achievable with sev-eral growth factor genes PDGF-B proved the most suitable forrepair of cutaneous defects A single administration of colla-gen-immobilized AdPDGF-B rapidly induced the formation ofhighly cellular and vascularized tissues with dense ECMs richin collagen By contrast AdFGF2 induced a primarily vascu-lar response with little collagen deposition FGF2 induces therelease of matrix metalloproteinase 1 or interstitial collagenase(Buckley-Sturrock et al 1989) and this may underlie the rel-ative paucity of ECM accumulation VEGF gene delivery alsoinduced highly vascular responses however the enhanced per-meability characteristic of VEGF-induced vasculature (Dvoraket al 1995) led to edema within nascent tissues In fact much
of the enhanced protein and DNA deposition observed in Ad-VEGF-treated PVA sponges may well derive from fluid exu-dates rather than actual tissue formation Finally the inabilityof AdLuc delivery to induce anything beyond a limited in-flammatory response confirms that tissue formation was de-pendent on growth factor gene delivery
The robust activity of PDGF-B gene delivery was expectedas PDGF-BB protein initiates multiple aspects of tissue forma-tion including cellular influx and proliferation ECM deposi-tion and tissue remodeling (Pierce et al 1988 1991 1994a)Indeed PDGF-BB is the only growth factor protein to have suc-cessfully completed human clinical trials and be approved forthe treatment of dermal wounds (Steed 1995 drsquoHemecourt etal 1998 Wieman 1998 Wieman et al 1998) We observedthat collagen-formulated AdPDGF-B induced the complete re-pair of excisional skin defects without unwanted long-term ef-fects such as the development of hypertrophic scars Endoge-nous growth factors other than PDGF-BB however most likelymediated the enhanced re-epithelialization observed in thesewounds as epithelial regeneration is driven by members of theepidermal growth factor and FGF families (Pierce et al 1994bDanilenko et al 1995) Our data indicate nonetheless that tis-sue regeneration and repair were initiated and to a great degreedriven by transgene-encoded PDGF-BB
Despite the known activity of PDGF-BB protein we wereable to demonstrate greater tissue deposition after gene deliv-ery as compared with the use of recombinant growth factor pro-tein A single application of PDGF-BB protein could not equalthe ability of PDGF-B gene therapy to induce neotissue for-mation even at doses well in excess of that induced in situ byAdPDGF-B and in excess of that used in human clinical trials
FIG 5 Influence of collagen-formulated AdPDGF-B on long-term tissue repair Excisional wounds (6 mm in diameter withcartilage remaining intact) were placed in nonischemic rabbit ears and treated with either 015 collagen alone (open columns)or AdPDGF-B formulated in this vehicle (solid columns) On days 28ndash180 posttreatment total ear thickness at the site of eachwound was measured (in mm) with calipers Data are presented as means 6 SD (n 5 3) Treatment groups differ by p 00001groups differ by p 0005
(Steed 1995 drsquoHemecourt et al 1998 Wieman 1998 Wie-man et al 1998) In fact repeated administrations of PDGF-BB protein were required to approach the level of tissue for-mation observed after a single administration of AdPDGF-BThese data support our hypothesis that sustained localizedgrowth factor production is required for robust tissue repair
In further support of this hypothesis we demonstrated thatmRNA encoding human PDGF-B was present in excisionalwounds as late as day 28 after collagen-formulated AdPDGF-B administration By contrast previous studies of PDGF-BBprotein found that the great majority of this growth factor wasgone from treated wounds 1 day postapplication and that anytissue maturation subsequently observed was most likely dueto the upregulation of endogenous growth factors (Pierce et al1992 1995) We also demonstrated that repair cells such asmononuclear leukocytes endothelial cells and fibroblasts pres-ent with developing neotissues represent the source of both
transgene transcription and PDGF-BB production In additiona depot of human PDGF-BB was detected bound to the colla-gen delivery matrix and ECM of these tissues This was antici-pated as PDGF-BB contains collagen-binding motifs (Soma-sundaram and Schuppan 1996) We hypothesize that subsequentmatrix metalloproteinase activity by repair cells will serve togenerate localized release of this sequestered growth factor pooland as a consequence further drive tissue regeneration Theseevents which are central to tissue remodeling should be directlyenhanced by collagen matrices as type I collagen stimulates me-talloproteinase production integrin expression and cellular ac-tivation in PDGF-stimulated fibroblasts (Xu and Clark 19961997)
An additional rationale for employing collagen matrices wasto physically immobilize vectors This was confirmed in vivowhere collagen matrices maintained AdPDGF-B at deliverysites for at least 28 days and limited vector migration to other
DOUKAS ET AL796
FIG 6 Persistence of collagen-formulated vector and transgene transcripts in excisional wounds Full-thickness excisionalwounds (7 cm2) were placed on the dorsal surface of rabbits and treated with AdPDGF-B formulated in 26 collagen at either2 3 109 or 2 3 1011 virus particles per wound (open and closed columns respectively) Wounds were then covered with OpSitedressing and on days 3 7 or 28 posttreatment wound beds were harvested for real-time quantitative PCR and RT-PCR analy-ses PCR data are presented in the upper graph as AdPDGF-B copies per wound RT-PCR data are presented in the lower graphas the relative amount of PDGF-B mRNA per unit 18S rRNA (in arbitrary units) All data points are means 6 SD (n 5 6)
tissues or organs In vitro tests also established that collagenmatrices not only prevent vector loss due to diffusion but pre-serve vector activity despite prolonged incubation in acutewound fluid Successful vector immobilization and tissue re-pair could be achieved with both 015 collagen and 26 col-lagen suggesting flexibility in the final vehicle formulation re-quired for effective vector delivery This flexibility was neededin the present studies as 26 collagen formulations proveddifficult to deliver to PVA sponges and 6-mm excisionalwounds This would not be of concern in clinical settings how-ever where wound beds are easily accessible and generally sev-eral square centimeters in area By contrast CMC was inef-fective at retaining vector in aqueous environments Moreimportantly this matrix was itself inflammatory and whencombined with adenovirus the net result was inflammationrather than tissue repair We are currently examining the util-ity of other matrices such as fibrin and hyaluronic acid whichbecause of their more provisional nature may offer yet greatercellular migration into wounds as compared with type I colla-gen
Although an aqueous-based AdPDGF-B formulation hasbeen previously shown to enhance tissue formation (Liechty etal 1999) this was achieved with a model system that artifi-cially retains vectors within treatment sites In fact the presentstudies demonstrate that any tissue repair observed after Ad-PDGF-B delivery in a nongelling liquid is dependent on the useof this model system In wounds not designed to retain appliedtreatments aqueous-formulated AdPDGF-B seeped into sur-rounding tissues and led to hyperplasia within these areas ratherthan to tissue regeneration within the active wound bed Colla-gen-immobilized AdPDGF-B on the other hand did persist inthese wound beds and led to significant enhancements in gran-ulation tissue formation as well as enhanced wound re-epithe-lialization and wound closure The significance of these activ-ities is further substantiated considering that they wereachievable in 8-mm-diameter ischemic wounds which withinthe time frame examined could not self-heal to any meaning-ful degree in the absence of gene therapy However as all theanimal models employed in these studies will eventually self-heal given sufficient time the full value of matrix-immobilizedgene therapy vectors remains to be confirmed in human clini-cal trials
In conclusion we present evidence that matrix-immobilizedgene therapy vectors encoding appropriate growth-promotinggenes represent a promising approach to tissue regeneration andrepair This basic concept can be expanded to include alterna-tive matrices such as controlled-release formulations as wellas tissue-specific growth factors Furthermore the addition oftargeting ligands to adenovirus vectors (eg FGF2) can en-hance their ability to transduce cells such that tissue repair re-sponses comparable to nontargeted vectors can be achieved butat significantly lower vector doses (Chandler et al 2000a)With appropriate design and application schedules one couldconceivably time the release of multiple growth factors to spe-cific stages of a tissue repair cascade In addition we have foundin preliminary studies that collagen-immobilized nonviral vec-tors such as PDGF-B plasmids which have potentially morefavorable safety profiles than adenovirus vectors can also en-hance tissue formation in vivo (Chandler et al 2000b Tyroneet al 2000) Such flexibility should allow for the widespreadapplication of gene therapy to the treatment of injured tissues
ACKNOWLEDGMENTS
We thank Jeff Davidson (Vanderbilt University School ofMedicine) for assistance in establishing the PVA sponge modelCarl-Henrik Heldin (Ludwig Institute for Cancer Research) forthe PDGF-B gene construct and Emelie Amburn Lara AsatoSharon Chang Gail Fieser Lydia Greenlees Rebecca Smokerand Linda Manza for excellent technical assistance This pub-lication was made possible in part by NIH grants 1R43AR46154(JD) and 5P01CA25874 (MH)
REFERENCES
AHN ST and MUSTOE TA (1990) Effects of ischemia on ulcerwound healing A new model in the rabbit ear Ann Plast Surg 2417ndash23
ANDREE C SWAIN WF PAGE CP MACKLIN MDSLAMA J HATZIS D and ERIKSSON E (1994) In vivo trans-fer and expression of a human epidermal growth factor gene accel-erates wound repair Proc Natl Acad Sci USA 91 12188ndash12192
BENN SI WHITSITT JS BROADLEY KN NANNEY LBPERKINS D HE L PATEL M MORGAN JR SWAIN WFand DAVIDSON JM (1996) Particle-mediated gene transfer withtransforming growth factor-b1 cDNAs enhances wound repair in ratskin J Clin Invest 98 2894ndash2902
BONADIO J SMILEY E PATIL P and GOLDSTEIN S (1999)Localized direct plasmid gene delivery in vivo Prolonged therapyresults in reproducible tissue regeneration Nat Med 5 753ndash759
BUCKLEY A DAVIDSON JM KAMERATH CD WOLT TBand WOODWARD SC (1985) Sustained release of epidermalgrowth factor accelerates wound repair Proc Natl Acad Sci USA82 7340ndash7344
BUCKLEY-STURROCK A WOODWARD SC SENIOR RMGRIFFIN GL KLAGSBRUN M and DAVIDSON JM (1989)Differential stimulation of collagenase and chemotactic activity in fi-broblasts derived from rat wound repair tissue and human skin bygrowth factors J Cell Physiol 138 70ndash78
CHANDLER LA DOUKAS J GONZALEZ AM HOGANSONDK GU DL MA C NESBIT M CROMBLEHOLME TMHERLYN M SOSNOWSKI BA and PIERCE GF (2000a)FGF2ndashTargeted adenovirus encoding platelet-derived growth factor-B enhances de novo tissue formation Mol Ther 2 153ndash160
CHANDLER LA MA C GONZALEZ AM DOUKAS JNGUYEN T PIERCE GF and PHILLIPS ML (2000b) Ma-trix-enabled gene transfer for cutaneous wound repair Wound Re-pair Regen 8 473ndash479
DANILENKO DM RING BD TARPLEY JE MORRIS BVAN GY MORAWIECKI A CALLAHAN W GOLDEN-BERG M HERSHENSON S and PIERCE GF (1995) Growthfactors in porcine full and partial thickness burn repair Differing tar-gets and effects of keratinocyte growth factor platelet-derivedgrowth factor-BB epidermal growth factor and neu differentiationfactor Am J Pathol 147 1261ndash1277
DEUEL TF KAWAHARA RS MUSTOE TA and PIERCE GF(1991) Growth factors and wound healing Platelet-derived growthfactor as a model cytokine Annu Rev Med 42 567ndash584
DrsquoHEMECOURT PA SMIELL JM and KARIM MR (1998) So-dium carboxymethylcellulose aqueous-based gel vs becaplermin gelin patients with nonhealing lower extremity diabetic ulcers Wounds10 69ndash75
DOUKAS J HOGANSON DK ONG M YING W LACEYDL BAIRD A PIERCE GF and SOSNOWSKI BA (1999)Retargeted delivery of adenoviral vectors through fibroblast growthfactor receptors involves unique cellular pathways FASEB J 131459ndash1466
TISSUE REPAIR USING GROWTH FACTOR GENES 797
DVORAK HF BROWN LF DETMAR M and DVORAK AM(1995) Vascular permeability factorvascular endothelial growth fac-tor microvascular hyperpermeability and angiogenesis Am JPathol 146 1029ndash1039
EMING SA MEDALIE DA TOMPKINS RG YARMUSHML and MORGAN JR (1998) Genetically modified human ker-atinocytes overexpressing PDGF-A enhance the performance of acomposite skin graft Hum Gene Ther 9 529ndash539
EMING SA WHITSITT JS HE L KRIEG T MORGAN JRand DAVIDSON JM (1999) Particle-mediated gene transfer ofPDGF isoforms promotes wound repair J Invest Dermatol 112297ndash302
GERDES J SCHWAB U LEMKE H and STEIN H (1983) Pro-duction of a mouse monoclonal antibody reactive with a human nu-clear antigen associated with cell proliferation Int J Cancer 3113ndash20
GONZALEZ AM BERRY M MAHER PA LOGAN A andBAIRD A (1995) A comprehensive analysis of the distribution ofFGF-2 and FGFR1 in the rat brain Brain Res 701 201ndash226
GREENHALGH DG (1996) The role of growth factors in woundhealing J Trauma 41 159ndash167
GROTENDORST GR MARTIN GR PENCEV D SODEK Jand HARVEY AK (1985) Stimulation of granulation tissue for-mation by platelet-derived growth factor in normal and diabetic ratsJ Clin Invest 76 2323ndash2329
KHOURI RK HONG SP DEUNE EG TARPLEY JE SONGSZ SERDAR CM and PIERCE GF (1994) De novo genera-tion of permanent neovascularized soft tissue appendages by platelet-derived growth factor J Clin Invest 94 1757ndash1763
LEGRAND EK SENTER LH GAMELLI RL and KIORPESTC (1993) Evaluation of PDGF-BB PDGF-AA bFGF IL-1 andEGF dose responses in polyvinyl alcohol sponge implants assessedby a rapid histologic method Growth Factors 8 315ndash329
LIECHTY KW NESBIT M HERLYN M RADU A ADZICKNS and CROMBLEHOLME TM (1999) Adenoviral-mediatedoverexpression of platelet-derived growth factor-B corrects ischemicimpaired wound healing J Invest Dermatol 113 375ndash383
LYNCH SE COLVIN RB and ANTONIADES HN (1989)Growth factors in wound healing J Clin Invest 84 640ndash646
MUSTOE TA PIERCE GF THOMASON A GRAMATES PSPORN MB and DEUEL TF (1987) Accelerated healing of in-cisional wounds in rats induced by transforming growth factor-betaScience 237 1333ndash1336
MUSTOE TA PIERCE GF MORISHIMA C and DEUEL TF(1991) Growth factor-induced acceleration of tissue repair throughdirect and inductive activities in a rabbit dermal ulcer model J ClinInvest 87 694ndash703
MUSTOE TA AHN ST TARPLEY JE and PIERCE GF(1994) Role of hypoxia in growth factor responses Differential ef-fects of basic fibroblast growth factor and platelet-derived growthfactor in an ischemic wound model Wound Rep Reg 2 277ndash283
NYBERG-HOFFMAN C and AGUILAR-CORDOVA E (1999) In-stability of adenoviral vectors during transport and its implication forclinical studies Nat Med 5 955ndash957
PIERCE GF and MUSTOE TA (1995) Pharmacologic enhance-ment of wound healing Annu Rev Med 46 467ndash481
PIERCE GF MUSTOE TA SENIOR RM REED J GRIFFINGL THOMASON A and DEUEL TF (1988) In vivo incisionalwound healing augmented by platelet-derived growth factor and re-combinant c-sis gene homodimeric proteins J Exp Med 167 974ndash987
PIERCE GF VANDE BERG J RUDOLPH R TARPLEY J andMUSTOE TA (1991) Platelet-derived growth factor-BB and trans-forming growth factor beta 1 selectively modulate glycosaminogly -cans collagen and myofibroblasts in excisional wounds Am JPathol 138 629ndash646
PIERCE GF TARPLEY JE YANAGIHARA D MUSTOE TA
FOX GM and THOMASON A (1992) Platelet-derived growthfactor (BB homodimer) transforming growth factor-b1 and basic fi-broblast growth factor in dermal wound healing Neovessel and ma-trix formation and cessation of repair Am J Pathol 140 1375ndash1388
PIERCE GF TARPLEY JE ALLMAN RM GOODE PS SER-DAR CM MORRIS B MUSTOE TA and VANDE BERG J(1994a) Tissue repair processes in healing chronic pressure ulcerstreated with recombinant platelet-derived growth factor BB Am JPathol 145 1399ndash1410
PIERCE GF YANAGIHARA D KLOPCHIN K DANILENKODM HSU E KENNEY WC and MORRIS CF (1994b) Stim-ulation of all epithelial elements during skin regeneration by kerati-nocyte growth factor J Exp Med 179 831ndash840
PIERCE GF TARPLEY JE TSENG J BREADY J CHANGD KENNEY WC RUDOLPH R ROBSON MC VANDEBERG J and REID P (1995) Detection of platelet-derived growthfactor (PDGF)-AA in actively healing human wounds treated withrecombinant PDGF-BB and absence of PDGF in chronic nonhealingwounds J Clin Invest 96 1336ndash1350
SINGER AJ and CLARK RA (1999) Cutaneous wound healingN Engl J Med 341 738ndash746
SOMASUNDARAM R and SCHUPPAN D (1996) Type I II IIIIV V and VI collagens serve as extracellular ligands for the iso-forms of platelet-derived growth factor (AA BB and AB) J BiolChem 271 26884ndash26891
SPRUGEL KH MCPHERSON JM CLOWES AW and ROSSR (1987) Effects of growth factors in vivo I Cell ingrowth intoporous subcutaneous chambers Am J Pathol 129 601ndash613
STEED DL (1995) Clinical evaluation of recombinant humanplatelet-derived growth factor for the treatment of lower extremitydiabetic ulcers Diabetic Ulcer Study Group J Vasc Surg 21 71ndash78
STEED DL (1998) Foundations of good ulcer care Am J Surg 17620S-25S
TYRONE JW MOGFORD JE CHANDLER LA MA C XIAY PIERCE GF and MUSTOE TA (2000) Collagen-embeddedplatelet-derived growth factor DNA plasmid promotes wound heal-ing in a dermal ulcer model J Surg Res 93 230ndash236
VOGT PM THOMPSON S ANDREE C LIU P BREUING KHATZIS D BROWN H MULLIGAN RC and ERIKSSON E(1994) Genetically modified keratinocytes transplanted to woundsreconstitute the epidermis Proc Natl Acad Sci USA 91 9307ndash9311
WIEMAN TJ (1998) Clinical efficacy of becaplermin (rhPDGF-BB)gel Becaplermin Gel Studies Group Am J Surg 176 74S-79S
WIEMAN TJ SMIELL JM and SU Y (1998) Efficacy and safetyof a topical gel formulation of recombinant human platelet-derivedgrowth factor-BB (becaplermin) in patients with chronic neuropathicdiabetic ulcers A phase III randomized placebo-controlled double-blind study Diabetes Care 21 822ndash827
WILSON JM (1996) Adenoviruses as gene-delivery vehicles NEngl J Med 334 1185ndash1187
XU J and CLARK RA (1996) Extracellular matrix alters PDGFregulation of fibroblast integrins J Cell Biol 132 239ndash249
XU J and CLARK RA (1997) A three-dimensional collagen latticeinduces protein kinase C-z activity Role in a2 integrin and collage-nase mRNA expression J Cell Biol 136 473ndash483
Address reprint requests toDr John Doukas
Selective Genetics Inc11035 Roselle Street
San Diego CA 92121
E-mail jdoukasselectivegeneticscom
Received for publication December 28 2000 accepted after re-vision February 23 2001
DOUKAS ET AL798

TISSUE REPAIR USING GROWTH FACTOR GENES 795
gene expression extends well beyond the 8-day time period sug-gested using anti-PDGF-BB immunohistochemistry as a de-tection system (Fig 3)
DISCUSSION
These studies demonstrate that immobilization of gene ther-apy vectors in collagen-based matrices enables their efficientdelivery and activity in vivo Matrix immobilization achievedprolonged transgene-encoded growth factor production and asa consequence robust tissue repair By contrast aqueous vehi-cles failed to retain adenoviruses at application sites resultingin diffuse inflammation rather than productive tissue regenera-tion These observations confirm our basic hypothesis that ma-trix immobilization of growth factor-encoding gene therapyvectors represents a promising approach to tissue repair
Although de novo tissue deposition was achievable with sev-eral growth factor genes PDGF-B proved the most suitable forrepair of cutaneous defects A single administration of colla-gen-immobilized AdPDGF-B rapidly induced the formation ofhighly cellular and vascularized tissues with dense ECMs richin collagen By contrast AdFGF2 induced a primarily vascu-lar response with little collagen deposition FGF2 induces therelease of matrix metalloproteinase 1 or interstitial collagenase(Buckley-Sturrock et al 1989) and this may underlie the rel-ative paucity of ECM accumulation VEGF gene delivery alsoinduced highly vascular responses however the enhanced per-meability characteristic of VEGF-induced vasculature (Dvoraket al 1995) led to edema within nascent tissues In fact much
of the enhanced protein and DNA deposition observed in Ad-VEGF-treated PVA sponges may well derive from fluid exu-dates rather than actual tissue formation Finally the inabilityof AdLuc delivery to induce anything beyond a limited in-flammatory response confirms that tissue formation was de-pendent on growth factor gene delivery
The robust activity of PDGF-B gene delivery was expectedas PDGF-BB protein initiates multiple aspects of tissue forma-tion including cellular influx and proliferation ECM deposi-tion and tissue remodeling (Pierce et al 1988 1991 1994a)Indeed PDGF-BB is the only growth factor protein to have suc-cessfully completed human clinical trials and be approved forthe treatment of dermal wounds (Steed 1995 drsquoHemecourt etal 1998 Wieman 1998 Wieman et al 1998) We observedthat collagen-formulated AdPDGF-B induced the complete re-pair of excisional skin defects without unwanted long-term ef-fects such as the development of hypertrophic scars Endoge-nous growth factors other than PDGF-BB however most likelymediated the enhanced re-epithelialization observed in thesewounds as epithelial regeneration is driven by members of theepidermal growth factor and FGF families (Pierce et al 1994bDanilenko et al 1995) Our data indicate nonetheless that tis-sue regeneration and repair were initiated and to a great degreedriven by transgene-encoded PDGF-BB
Despite the known activity of PDGF-BB protein we wereable to demonstrate greater tissue deposition after gene deliv-ery as compared with the use of recombinant growth factor pro-tein A single application of PDGF-BB protein could not equalthe ability of PDGF-B gene therapy to induce neotissue for-mation even at doses well in excess of that induced in situ byAdPDGF-B and in excess of that used in human clinical trials
FIG 5 Influence of collagen-formulated AdPDGF-B on long-term tissue repair Excisional wounds (6 mm in diameter withcartilage remaining intact) were placed in nonischemic rabbit ears and treated with either 015 collagen alone (open columns)or AdPDGF-B formulated in this vehicle (solid columns) On days 28ndash180 posttreatment total ear thickness at the site of eachwound was measured (in mm) with calipers Data are presented as means 6 SD (n 5 3) Treatment groups differ by p 00001groups differ by p 0005
(Steed 1995 drsquoHemecourt et al 1998 Wieman 1998 Wie-man et al 1998) In fact repeated administrations of PDGF-BB protein were required to approach the level of tissue for-mation observed after a single administration of AdPDGF-BThese data support our hypothesis that sustained localizedgrowth factor production is required for robust tissue repair
In further support of this hypothesis we demonstrated thatmRNA encoding human PDGF-B was present in excisionalwounds as late as day 28 after collagen-formulated AdPDGF-B administration By contrast previous studies of PDGF-BBprotein found that the great majority of this growth factor wasgone from treated wounds 1 day postapplication and that anytissue maturation subsequently observed was most likely dueto the upregulation of endogenous growth factors (Pierce et al1992 1995) We also demonstrated that repair cells such asmononuclear leukocytes endothelial cells and fibroblasts pres-ent with developing neotissues represent the source of both
transgene transcription and PDGF-BB production In additiona depot of human PDGF-BB was detected bound to the colla-gen delivery matrix and ECM of these tissues This was antici-pated as PDGF-BB contains collagen-binding motifs (Soma-sundaram and Schuppan 1996) We hypothesize that subsequentmatrix metalloproteinase activity by repair cells will serve togenerate localized release of this sequestered growth factor pooland as a consequence further drive tissue regeneration Theseevents which are central to tissue remodeling should be directlyenhanced by collagen matrices as type I collagen stimulates me-talloproteinase production integrin expression and cellular ac-tivation in PDGF-stimulated fibroblasts (Xu and Clark 19961997)
An additional rationale for employing collagen matrices wasto physically immobilize vectors This was confirmed in vivowhere collagen matrices maintained AdPDGF-B at deliverysites for at least 28 days and limited vector migration to other
DOUKAS ET AL796
FIG 6 Persistence of collagen-formulated vector and transgene transcripts in excisional wounds Full-thickness excisionalwounds (7 cm2) were placed on the dorsal surface of rabbits and treated with AdPDGF-B formulated in 26 collagen at either2 3 109 or 2 3 1011 virus particles per wound (open and closed columns respectively) Wounds were then covered with OpSitedressing and on days 3 7 or 28 posttreatment wound beds were harvested for real-time quantitative PCR and RT-PCR analy-ses PCR data are presented in the upper graph as AdPDGF-B copies per wound RT-PCR data are presented in the lower graphas the relative amount of PDGF-B mRNA per unit 18S rRNA (in arbitrary units) All data points are means 6 SD (n 5 6)
tissues or organs In vitro tests also established that collagenmatrices not only prevent vector loss due to diffusion but pre-serve vector activity despite prolonged incubation in acutewound fluid Successful vector immobilization and tissue re-pair could be achieved with both 015 collagen and 26 col-lagen suggesting flexibility in the final vehicle formulation re-quired for effective vector delivery This flexibility was neededin the present studies as 26 collagen formulations proveddifficult to deliver to PVA sponges and 6-mm excisionalwounds This would not be of concern in clinical settings how-ever where wound beds are easily accessible and generally sev-eral square centimeters in area By contrast CMC was inef-fective at retaining vector in aqueous environments Moreimportantly this matrix was itself inflammatory and whencombined with adenovirus the net result was inflammationrather than tissue repair We are currently examining the util-ity of other matrices such as fibrin and hyaluronic acid whichbecause of their more provisional nature may offer yet greatercellular migration into wounds as compared with type I colla-gen
Although an aqueous-based AdPDGF-B formulation hasbeen previously shown to enhance tissue formation (Liechty etal 1999) this was achieved with a model system that artifi-cially retains vectors within treatment sites In fact the presentstudies demonstrate that any tissue repair observed after Ad-PDGF-B delivery in a nongelling liquid is dependent on the useof this model system In wounds not designed to retain appliedtreatments aqueous-formulated AdPDGF-B seeped into sur-rounding tissues and led to hyperplasia within these areas ratherthan to tissue regeneration within the active wound bed Colla-gen-immobilized AdPDGF-B on the other hand did persist inthese wound beds and led to significant enhancements in gran-ulation tissue formation as well as enhanced wound re-epithe-lialization and wound closure The significance of these activ-ities is further substantiated considering that they wereachievable in 8-mm-diameter ischemic wounds which withinthe time frame examined could not self-heal to any meaning-ful degree in the absence of gene therapy However as all theanimal models employed in these studies will eventually self-heal given sufficient time the full value of matrix-immobilizedgene therapy vectors remains to be confirmed in human clini-cal trials
In conclusion we present evidence that matrix-immobilizedgene therapy vectors encoding appropriate growth-promotinggenes represent a promising approach to tissue regeneration andrepair This basic concept can be expanded to include alterna-tive matrices such as controlled-release formulations as wellas tissue-specific growth factors Furthermore the addition oftargeting ligands to adenovirus vectors (eg FGF2) can en-hance their ability to transduce cells such that tissue repair re-sponses comparable to nontargeted vectors can be achieved butat significantly lower vector doses (Chandler et al 2000a)With appropriate design and application schedules one couldconceivably time the release of multiple growth factors to spe-cific stages of a tissue repair cascade In addition we have foundin preliminary studies that collagen-immobilized nonviral vec-tors such as PDGF-B plasmids which have potentially morefavorable safety profiles than adenovirus vectors can also en-hance tissue formation in vivo (Chandler et al 2000b Tyroneet al 2000) Such flexibility should allow for the widespreadapplication of gene therapy to the treatment of injured tissues
ACKNOWLEDGMENTS
We thank Jeff Davidson (Vanderbilt University School ofMedicine) for assistance in establishing the PVA sponge modelCarl-Henrik Heldin (Ludwig Institute for Cancer Research) forthe PDGF-B gene construct and Emelie Amburn Lara AsatoSharon Chang Gail Fieser Lydia Greenlees Rebecca Smokerand Linda Manza for excellent technical assistance This pub-lication was made possible in part by NIH grants 1R43AR46154(JD) and 5P01CA25874 (MH)
REFERENCES
AHN ST and MUSTOE TA (1990) Effects of ischemia on ulcerwound healing A new model in the rabbit ear Ann Plast Surg 2417ndash23
ANDREE C SWAIN WF PAGE CP MACKLIN MDSLAMA J HATZIS D and ERIKSSON E (1994) In vivo trans-fer and expression of a human epidermal growth factor gene accel-erates wound repair Proc Natl Acad Sci USA 91 12188ndash12192
BENN SI WHITSITT JS BROADLEY KN NANNEY LBPERKINS D HE L PATEL M MORGAN JR SWAIN WFand DAVIDSON JM (1996) Particle-mediated gene transfer withtransforming growth factor-b1 cDNAs enhances wound repair in ratskin J Clin Invest 98 2894ndash2902
BONADIO J SMILEY E PATIL P and GOLDSTEIN S (1999)Localized direct plasmid gene delivery in vivo Prolonged therapyresults in reproducible tissue regeneration Nat Med 5 753ndash759
BUCKLEY A DAVIDSON JM KAMERATH CD WOLT TBand WOODWARD SC (1985) Sustained release of epidermalgrowth factor accelerates wound repair Proc Natl Acad Sci USA82 7340ndash7344
BUCKLEY-STURROCK A WOODWARD SC SENIOR RMGRIFFIN GL KLAGSBRUN M and DAVIDSON JM (1989)Differential stimulation of collagenase and chemotactic activity in fi-broblasts derived from rat wound repair tissue and human skin bygrowth factors J Cell Physiol 138 70ndash78
CHANDLER LA DOUKAS J GONZALEZ AM HOGANSONDK GU DL MA C NESBIT M CROMBLEHOLME TMHERLYN M SOSNOWSKI BA and PIERCE GF (2000a)FGF2ndashTargeted adenovirus encoding platelet-derived growth factor-B enhances de novo tissue formation Mol Ther 2 153ndash160
CHANDLER LA MA C GONZALEZ AM DOUKAS JNGUYEN T PIERCE GF and PHILLIPS ML (2000b) Ma-trix-enabled gene transfer for cutaneous wound repair Wound Re-pair Regen 8 473ndash479
DANILENKO DM RING BD TARPLEY JE MORRIS BVAN GY MORAWIECKI A CALLAHAN W GOLDEN-BERG M HERSHENSON S and PIERCE GF (1995) Growthfactors in porcine full and partial thickness burn repair Differing tar-gets and effects of keratinocyte growth factor platelet-derivedgrowth factor-BB epidermal growth factor and neu differentiationfactor Am J Pathol 147 1261ndash1277
DEUEL TF KAWAHARA RS MUSTOE TA and PIERCE GF(1991) Growth factors and wound healing Platelet-derived growthfactor as a model cytokine Annu Rev Med 42 567ndash584
DrsquoHEMECOURT PA SMIELL JM and KARIM MR (1998) So-dium carboxymethylcellulose aqueous-based gel vs becaplermin gelin patients with nonhealing lower extremity diabetic ulcers Wounds10 69ndash75
DOUKAS J HOGANSON DK ONG M YING W LACEYDL BAIRD A PIERCE GF and SOSNOWSKI BA (1999)Retargeted delivery of adenoviral vectors through fibroblast growthfactor receptors involves unique cellular pathways FASEB J 131459ndash1466
TISSUE REPAIR USING GROWTH FACTOR GENES 797
DVORAK HF BROWN LF DETMAR M and DVORAK AM(1995) Vascular permeability factorvascular endothelial growth fac-tor microvascular hyperpermeability and angiogenesis Am JPathol 146 1029ndash1039
EMING SA MEDALIE DA TOMPKINS RG YARMUSHML and MORGAN JR (1998) Genetically modified human ker-atinocytes overexpressing PDGF-A enhance the performance of acomposite skin graft Hum Gene Ther 9 529ndash539
EMING SA WHITSITT JS HE L KRIEG T MORGAN JRand DAVIDSON JM (1999) Particle-mediated gene transfer ofPDGF isoforms promotes wound repair J Invest Dermatol 112297ndash302
GERDES J SCHWAB U LEMKE H and STEIN H (1983) Pro-duction of a mouse monoclonal antibody reactive with a human nu-clear antigen associated with cell proliferation Int J Cancer 3113ndash20
GONZALEZ AM BERRY M MAHER PA LOGAN A andBAIRD A (1995) A comprehensive analysis of the distribution ofFGF-2 and FGFR1 in the rat brain Brain Res 701 201ndash226
GREENHALGH DG (1996) The role of growth factors in woundhealing J Trauma 41 159ndash167
GROTENDORST GR MARTIN GR PENCEV D SODEK Jand HARVEY AK (1985) Stimulation of granulation tissue for-mation by platelet-derived growth factor in normal and diabetic ratsJ Clin Invest 76 2323ndash2329
KHOURI RK HONG SP DEUNE EG TARPLEY JE SONGSZ SERDAR CM and PIERCE GF (1994) De novo genera-tion of permanent neovascularized soft tissue appendages by platelet-derived growth factor J Clin Invest 94 1757ndash1763
LEGRAND EK SENTER LH GAMELLI RL and KIORPESTC (1993) Evaluation of PDGF-BB PDGF-AA bFGF IL-1 andEGF dose responses in polyvinyl alcohol sponge implants assessedby a rapid histologic method Growth Factors 8 315ndash329
LIECHTY KW NESBIT M HERLYN M RADU A ADZICKNS and CROMBLEHOLME TM (1999) Adenoviral-mediatedoverexpression of platelet-derived growth factor-B corrects ischemicimpaired wound healing J Invest Dermatol 113 375ndash383
LYNCH SE COLVIN RB and ANTONIADES HN (1989)Growth factors in wound healing J Clin Invest 84 640ndash646
MUSTOE TA PIERCE GF THOMASON A GRAMATES PSPORN MB and DEUEL TF (1987) Accelerated healing of in-cisional wounds in rats induced by transforming growth factor-betaScience 237 1333ndash1336
MUSTOE TA PIERCE GF MORISHIMA C and DEUEL TF(1991) Growth factor-induced acceleration of tissue repair throughdirect and inductive activities in a rabbit dermal ulcer model J ClinInvest 87 694ndash703
MUSTOE TA AHN ST TARPLEY JE and PIERCE GF(1994) Role of hypoxia in growth factor responses Differential ef-fects of basic fibroblast growth factor and platelet-derived growthfactor in an ischemic wound model Wound Rep Reg 2 277ndash283
NYBERG-HOFFMAN C and AGUILAR-CORDOVA E (1999) In-stability of adenoviral vectors during transport and its implication forclinical studies Nat Med 5 955ndash957
PIERCE GF and MUSTOE TA (1995) Pharmacologic enhance-ment of wound healing Annu Rev Med 46 467ndash481
PIERCE GF MUSTOE TA SENIOR RM REED J GRIFFINGL THOMASON A and DEUEL TF (1988) In vivo incisionalwound healing augmented by platelet-derived growth factor and re-combinant c-sis gene homodimeric proteins J Exp Med 167 974ndash987
PIERCE GF VANDE BERG J RUDOLPH R TARPLEY J andMUSTOE TA (1991) Platelet-derived growth factor-BB and trans-forming growth factor beta 1 selectively modulate glycosaminogly -cans collagen and myofibroblasts in excisional wounds Am JPathol 138 629ndash646
PIERCE GF TARPLEY JE YANAGIHARA D MUSTOE TA
FOX GM and THOMASON A (1992) Platelet-derived growthfactor (BB homodimer) transforming growth factor-b1 and basic fi-broblast growth factor in dermal wound healing Neovessel and ma-trix formation and cessation of repair Am J Pathol 140 1375ndash1388
PIERCE GF TARPLEY JE ALLMAN RM GOODE PS SER-DAR CM MORRIS B MUSTOE TA and VANDE BERG J(1994a) Tissue repair processes in healing chronic pressure ulcerstreated with recombinant platelet-derived growth factor BB Am JPathol 145 1399ndash1410
PIERCE GF YANAGIHARA D KLOPCHIN K DANILENKODM HSU E KENNEY WC and MORRIS CF (1994b) Stim-ulation of all epithelial elements during skin regeneration by kerati-nocyte growth factor J Exp Med 179 831ndash840
PIERCE GF TARPLEY JE TSENG J BREADY J CHANGD KENNEY WC RUDOLPH R ROBSON MC VANDEBERG J and REID P (1995) Detection of platelet-derived growthfactor (PDGF)-AA in actively healing human wounds treated withrecombinant PDGF-BB and absence of PDGF in chronic nonhealingwounds J Clin Invest 96 1336ndash1350
SINGER AJ and CLARK RA (1999) Cutaneous wound healingN Engl J Med 341 738ndash746
SOMASUNDARAM R and SCHUPPAN D (1996) Type I II IIIIV V and VI collagens serve as extracellular ligands for the iso-forms of platelet-derived growth factor (AA BB and AB) J BiolChem 271 26884ndash26891
SPRUGEL KH MCPHERSON JM CLOWES AW and ROSSR (1987) Effects of growth factors in vivo I Cell ingrowth intoporous subcutaneous chambers Am J Pathol 129 601ndash613
STEED DL (1995) Clinical evaluation of recombinant humanplatelet-derived growth factor for the treatment of lower extremitydiabetic ulcers Diabetic Ulcer Study Group J Vasc Surg 21 71ndash78
STEED DL (1998) Foundations of good ulcer care Am J Surg 17620S-25S
TYRONE JW MOGFORD JE CHANDLER LA MA C XIAY PIERCE GF and MUSTOE TA (2000) Collagen-embeddedplatelet-derived growth factor DNA plasmid promotes wound heal-ing in a dermal ulcer model J Surg Res 93 230ndash236
VOGT PM THOMPSON S ANDREE C LIU P BREUING KHATZIS D BROWN H MULLIGAN RC and ERIKSSON E(1994) Genetically modified keratinocytes transplanted to woundsreconstitute the epidermis Proc Natl Acad Sci USA 91 9307ndash9311
WIEMAN TJ (1998) Clinical efficacy of becaplermin (rhPDGF-BB)gel Becaplermin Gel Studies Group Am J Surg 176 74S-79S
WIEMAN TJ SMIELL JM and SU Y (1998) Efficacy and safetyof a topical gel formulation of recombinant human platelet-derivedgrowth factor-BB (becaplermin) in patients with chronic neuropathicdiabetic ulcers A phase III randomized placebo-controlled double-blind study Diabetes Care 21 822ndash827
WILSON JM (1996) Adenoviruses as gene-delivery vehicles NEngl J Med 334 1185ndash1187
XU J and CLARK RA (1996) Extracellular matrix alters PDGFregulation of fibroblast integrins J Cell Biol 132 239ndash249
XU J and CLARK RA (1997) A three-dimensional collagen latticeinduces protein kinase C-z activity Role in a2 integrin and collage-nase mRNA expression J Cell Biol 136 473ndash483
Address reprint requests toDr John Doukas
Selective Genetics Inc11035 Roselle Street
San Diego CA 92121
E-mail jdoukasselectivegeneticscom
Received for publication December 28 2000 accepted after re-vision February 23 2001
DOUKAS ET AL798

(Steed 1995 drsquoHemecourt et al 1998 Wieman 1998 Wie-man et al 1998) In fact repeated administrations of PDGF-BB protein were required to approach the level of tissue for-mation observed after a single administration of AdPDGF-BThese data support our hypothesis that sustained localizedgrowth factor production is required for robust tissue repair
In further support of this hypothesis we demonstrated thatmRNA encoding human PDGF-B was present in excisionalwounds as late as day 28 after collagen-formulated AdPDGF-B administration By contrast previous studies of PDGF-BBprotein found that the great majority of this growth factor wasgone from treated wounds 1 day postapplication and that anytissue maturation subsequently observed was most likely dueto the upregulation of endogenous growth factors (Pierce et al1992 1995) We also demonstrated that repair cells such asmononuclear leukocytes endothelial cells and fibroblasts pres-ent with developing neotissues represent the source of both
transgene transcription and PDGF-BB production In additiona depot of human PDGF-BB was detected bound to the colla-gen delivery matrix and ECM of these tissues This was antici-pated as PDGF-BB contains collagen-binding motifs (Soma-sundaram and Schuppan 1996) We hypothesize that subsequentmatrix metalloproteinase activity by repair cells will serve togenerate localized release of this sequestered growth factor pooland as a consequence further drive tissue regeneration Theseevents which are central to tissue remodeling should be directlyenhanced by collagen matrices as type I collagen stimulates me-talloproteinase production integrin expression and cellular ac-tivation in PDGF-stimulated fibroblasts (Xu and Clark 19961997)
An additional rationale for employing collagen matrices wasto physically immobilize vectors This was confirmed in vivowhere collagen matrices maintained AdPDGF-B at deliverysites for at least 28 days and limited vector migration to other
DOUKAS ET AL796
FIG 6 Persistence of collagen-formulated vector and transgene transcripts in excisional wounds Full-thickness excisionalwounds (7 cm2) were placed on the dorsal surface of rabbits and treated with AdPDGF-B formulated in 26 collagen at either2 3 109 or 2 3 1011 virus particles per wound (open and closed columns respectively) Wounds were then covered with OpSitedressing and on days 3 7 or 28 posttreatment wound beds were harvested for real-time quantitative PCR and RT-PCR analy-ses PCR data are presented in the upper graph as AdPDGF-B copies per wound RT-PCR data are presented in the lower graphas the relative amount of PDGF-B mRNA per unit 18S rRNA (in arbitrary units) All data points are means 6 SD (n 5 6)
tissues or organs In vitro tests also established that collagenmatrices not only prevent vector loss due to diffusion but pre-serve vector activity despite prolonged incubation in acutewound fluid Successful vector immobilization and tissue re-pair could be achieved with both 015 collagen and 26 col-lagen suggesting flexibility in the final vehicle formulation re-quired for effective vector delivery This flexibility was neededin the present studies as 26 collagen formulations proveddifficult to deliver to PVA sponges and 6-mm excisionalwounds This would not be of concern in clinical settings how-ever where wound beds are easily accessible and generally sev-eral square centimeters in area By contrast CMC was inef-fective at retaining vector in aqueous environments Moreimportantly this matrix was itself inflammatory and whencombined with adenovirus the net result was inflammationrather than tissue repair We are currently examining the util-ity of other matrices such as fibrin and hyaluronic acid whichbecause of their more provisional nature may offer yet greatercellular migration into wounds as compared with type I colla-gen
Although an aqueous-based AdPDGF-B formulation hasbeen previously shown to enhance tissue formation (Liechty etal 1999) this was achieved with a model system that artifi-cially retains vectors within treatment sites In fact the presentstudies demonstrate that any tissue repair observed after Ad-PDGF-B delivery in a nongelling liquid is dependent on the useof this model system In wounds not designed to retain appliedtreatments aqueous-formulated AdPDGF-B seeped into sur-rounding tissues and led to hyperplasia within these areas ratherthan to tissue regeneration within the active wound bed Colla-gen-immobilized AdPDGF-B on the other hand did persist inthese wound beds and led to significant enhancements in gran-ulation tissue formation as well as enhanced wound re-epithe-lialization and wound closure The significance of these activ-ities is further substantiated considering that they wereachievable in 8-mm-diameter ischemic wounds which withinthe time frame examined could not self-heal to any meaning-ful degree in the absence of gene therapy However as all theanimal models employed in these studies will eventually self-heal given sufficient time the full value of matrix-immobilizedgene therapy vectors remains to be confirmed in human clini-cal trials
In conclusion we present evidence that matrix-immobilizedgene therapy vectors encoding appropriate growth-promotinggenes represent a promising approach to tissue regeneration andrepair This basic concept can be expanded to include alterna-tive matrices such as controlled-release formulations as wellas tissue-specific growth factors Furthermore the addition oftargeting ligands to adenovirus vectors (eg FGF2) can en-hance their ability to transduce cells such that tissue repair re-sponses comparable to nontargeted vectors can be achieved butat significantly lower vector doses (Chandler et al 2000a)With appropriate design and application schedules one couldconceivably time the release of multiple growth factors to spe-cific stages of a tissue repair cascade In addition we have foundin preliminary studies that collagen-immobilized nonviral vec-tors such as PDGF-B plasmids which have potentially morefavorable safety profiles than adenovirus vectors can also en-hance tissue formation in vivo (Chandler et al 2000b Tyroneet al 2000) Such flexibility should allow for the widespreadapplication of gene therapy to the treatment of injured tissues
ACKNOWLEDGMENTS
We thank Jeff Davidson (Vanderbilt University School ofMedicine) for assistance in establishing the PVA sponge modelCarl-Henrik Heldin (Ludwig Institute for Cancer Research) forthe PDGF-B gene construct and Emelie Amburn Lara AsatoSharon Chang Gail Fieser Lydia Greenlees Rebecca Smokerand Linda Manza for excellent technical assistance This pub-lication was made possible in part by NIH grants 1R43AR46154(JD) and 5P01CA25874 (MH)
REFERENCES
AHN ST and MUSTOE TA (1990) Effects of ischemia on ulcerwound healing A new model in the rabbit ear Ann Plast Surg 2417ndash23
ANDREE C SWAIN WF PAGE CP MACKLIN MDSLAMA J HATZIS D and ERIKSSON E (1994) In vivo trans-fer and expression of a human epidermal growth factor gene accel-erates wound repair Proc Natl Acad Sci USA 91 12188ndash12192
BENN SI WHITSITT JS BROADLEY KN NANNEY LBPERKINS D HE L PATEL M MORGAN JR SWAIN WFand DAVIDSON JM (1996) Particle-mediated gene transfer withtransforming growth factor-b1 cDNAs enhances wound repair in ratskin J Clin Invest 98 2894ndash2902
BONADIO J SMILEY E PATIL P and GOLDSTEIN S (1999)Localized direct plasmid gene delivery in vivo Prolonged therapyresults in reproducible tissue regeneration Nat Med 5 753ndash759
BUCKLEY A DAVIDSON JM KAMERATH CD WOLT TBand WOODWARD SC (1985) Sustained release of epidermalgrowth factor accelerates wound repair Proc Natl Acad Sci USA82 7340ndash7344
BUCKLEY-STURROCK A WOODWARD SC SENIOR RMGRIFFIN GL KLAGSBRUN M and DAVIDSON JM (1989)Differential stimulation of collagenase and chemotactic activity in fi-broblasts derived from rat wound repair tissue and human skin bygrowth factors J Cell Physiol 138 70ndash78
CHANDLER LA DOUKAS J GONZALEZ AM HOGANSONDK GU DL MA C NESBIT M CROMBLEHOLME TMHERLYN M SOSNOWSKI BA and PIERCE GF (2000a)FGF2ndashTargeted adenovirus encoding platelet-derived growth factor-B enhances de novo tissue formation Mol Ther 2 153ndash160
CHANDLER LA MA C GONZALEZ AM DOUKAS JNGUYEN T PIERCE GF and PHILLIPS ML (2000b) Ma-trix-enabled gene transfer for cutaneous wound repair Wound Re-pair Regen 8 473ndash479
DANILENKO DM RING BD TARPLEY JE MORRIS BVAN GY MORAWIECKI A CALLAHAN W GOLDEN-BERG M HERSHENSON S and PIERCE GF (1995) Growthfactors in porcine full and partial thickness burn repair Differing tar-gets and effects of keratinocyte growth factor platelet-derivedgrowth factor-BB epidermal growth factor and neu differentiationfactor Am J Pathol 147 1261ndash1277
DEUEL TF KAWAHARA RS MUSTOE TA and PIERCE GF(1991) Growth factors and wound healing Platelet-derived growthfactor as a model cytokine Annu Rev Med 42 567ndash584
DrsquoHEMECOURT PA SMIELL JM and KARIM MR (1998) So-dium carboxymethylcellulose aqueous-based gel vs becaplermin gelin patients with nonhealing lower extremity diabetic ulcers Wounds10 69ndash75
DOUKAS J HOGANSON DK ONG M YING W LACEYDL BAIRD A PIERCE GF and SOSNOWSKI BA (1999)Retargeted delivery of adenoviral vectors through fibroblast growthfactor receptors involves unique cellular pathways FASEB J 131459ndash1466
TISSUE REPAIR USING GROWTH FACTOR GENES 797
DVORAK HF BROWN LF DETMAR M and DVORAK AM(1995) Vascular permeability factorvascular endothelial growth fac-tor microvascular hyperpermeability and angiogenesis Am JPathol 146 1029ndash1039
EMING SA MEDALIE DA TOMPKINS RG YARMUSHML and MORGAN JR (1998) Genetically modified human ker-atinocytes overexpressing PDGF-A enhance the performance of acomposite skin graft Hum Gene Ther 9 529ndash539
EMING SA WHITSITT JS HE L KRIEG T MORGAN JRand DAVIDSON JM (1999) Particle-mediated gene transfer ofPDGF isoforms promotes wound repair J Invest Dermatol 112297ndash302
GERDES J SCHWAB U LEMKE H and STEIN H (1983) Pro-duction of a mouse monoclonal antibody reactive with a human nu-clear antigen associated with cell proliferation Int J Cancer 3113ndash20
GONZALEZ AM BERRY M MAHER PA LOGAN A andBAIRD A (1995) A comprehensive analysis of the distribution ofFGF-2 and FGFR1 in the rat brain Brain Res 701 201ndash226
GREENHALGH DG (1996) The role of growth factors in woundhealing J Trauma 41 159ndash167
GROTENDORST GR MARTIN GR PENCEV D SODEK Jand HARVEY AK (1985) Stimulation of granulation tissue for-mation by platelet-derived growth factor in normal and diabetic ratsJ Clin Invest 76 2323ndash2329
KHOURI RK HONG SP DEUNE EG TARPLEY JE SONGSZ SERDAR CM and PIERCE GF (1994) De novo genera-tion of permanent neovascularized soft tissue appendages by platelet-derived growth factor J Clin Invest 94 1757ndash1763
LEGRAND EK SENTER LH GAMELLI RL and KIORPESTC (1993) Evaluation of PDGF-BB PDGF-AA bFGF IL-1 andEGF dose responses in polyvinyl alcohol sponge implants assessedby a rapid histologic method Growth Factors 8 315ndash329
LIECHTY KW NESBIT M HERLYN M RADU A ADZICKNS and CROMBLEHOLME TM (1999) Adenoviral-mediatedoverexpression of platelet-derived growth factor-B corrects ischemicimpaired wound healing J Invest Dermatol 113 375ndash383
LYNCH SE COLVIN RB and ANTONIADES HN (1989)Growth factors in wound healing J Clin Invest 84 640ndash646
MUSTOE TA PIERCE GF THOMASON A GRAMATES PSPORN MB and DEUEL TF (1987) Accelerated healing of in-cisional wounds in rats induced by transforming growth factor-betaScience 237 1333ndash1336
MUSTOE TA PIERCE GF MORISHIMA C and DEUEL TF(1991) Growth factor-induced acceleration of tissue repair throughdirect and inductive activities in a rabbit dermal ulcer model J ClinInvest 87 694ndash703
MUSTOE TA AHN ST TARPLEY JE and PIERCE GF(1994) Role of hypoxia in growth factor responses Differential ef-fects of basic fibroblast growth factor and platelet-derived growthfactor in an ischemic wound model Wound Rep Reg 2 277ndash283
NYBERG-HOFFMAN C and AGUILAR-CORDOVA E (1999) In-stability of adenoviral vectors during transport and its implication forclinical studies Nat Med 5 955ndash957
PIERCE GF and MUSTOE TA (1995) Pharmacologic enhance-ment of wound healing Annu Rev Med 46 467ndash481
PIERCE GF MUSTOE TA SENIOR RM REED J GRIFFINGL THOMASON A and DEUEL TF (1988) In vivo incisionalwound healing augmented by platelet-derived growth factor and re-combinant c-sis gene homodimeric proteins J Exp Med 167 974ndash987
PIERCE GF VANDE BERG J RUDOLPH R TARPLEY J andMUSTOE TA (1991) Platelet-derived growth factor-BB and trans-forming growth factor beta 1 selectively modulate glycosaminogly -cans collagen and myofibroblasts in excisional wounds Am JPathol 138 629ndash646
PIERCE GF TARPLEY JE YANAGIHARA D MUSTOE TA
FOX GM and THOMASON A (1992) Platelet-derived growthfactor (BB homodimer) transforming growth factor-b1 and basic fi-broblast growth factor in dermal wound healing Neovessel and ma-trix formation and cessation of repair Am J Pathol 140 1375ndash1388
PIERCE GF TARPLEY JE ALLMAN RM GOODE PS SER-DAR CM MORRIS B MUSTOE TA and VANDE BERG J(1994a) Tissue repair processes in healing chronic pressure ulcerstreated with recombinant platelet-derived growth factor BB Am JPathol 145 1399ndash1410
PIERCE GF YANAGIHARA D KLOPCHIN K DANILENKODM HSU E KENNEY WC and MORRIS CF (1994b) Stim-ulation of all epithelial elements during skin regeneration by kerati-nocyte growth factor J Exp Med 179 831ndash840
PIERCE GF TARPLEY JE TSENG J BREADY J CHANGD KENNEY WC RUDOLPH R ROBSON MC VANDEBERG J and REID P (1995) Detection of platelet-derived growthfactor (PDGF)-AA in actively healing human wounds treated withrecombinant PDGF-BB and absence of PDGF in chronic nonhealingwounds J Clin Invest 96 1336ndash1350
SINGER AJ and CLARK RA (1999) Cutaneous wound healingN Engl J Med 341 738ndash746
SOMASUNDARAM R and SCHUPPAN D (1996) Type I II IIIIV V and VI collagens serve as extracellular ligands for the iso-forms of platelet-derived growth factor (AA BB and AB) J BiolChem 271 26884ndash26891
SPRUGEL KH MCPHERSON JM CLOWES AW and ROSSR (1987) Effects of growth factors in vivo I Cell ingrowth intoporous subcutaneous chambers Am J Pathol 129 601ndash613
STEED DL (1995) Clinical evaluation of recombinant humanplatelet-derived growth factor for the treatment of lower extremitydiabetic ulcers Diabetic Ulcer Study Group J Vasc Surg 21 71ndash78
STEED DL (1998) Foundations of good ulcer care Am J Surg 17620S-25S
TYRONE JW MOGFORD JE CHANDLER LA MA C XIAY PIERCE GF and MUSTOE TA (2000) Collagen-embeddedplatelet-derived growth factor DNA plasmid promotes wound heal-ing in a dermal ulcer model J Surg Res 93 230ndash236
VOGT PM THOMPSON S ANDREE C LIU P BREUING KHATZIS D BROWN H MULLIGAN RC and ERIKSSON E(1994) Genetically modified keratinocytes transplanted to woundsreconstitute the epidermis Proc Natl Acad Sci USA 91 9307ndash9311
WIEMAN TJ (1998) Clinical efficacy of becaplermin (rhPDGF-BB)gel Becaplermin Gel Studies Group Am J Surg 176 74S-79S
WIEMAN TJ SMIELL JM and SU Y (1998) Efficacy and safetyof a topical gel formulation of recombinant human platelet-derivedgrowth factor-BB (becaplermin) in patients with chronic neuropathicdiabetic ulcers A phase III randomized placebo-controlled double-blind study Diabetes Care 21 822ndash827
WILSON JM (1996) Adenoviruses as gene-delivery vehicles NEngl J Med 334 1185ndash1187
XU J and CLARK RA (1996) Extracellular matrix alters PDGFregulation of fibroblast integrins J Cell Biol 132 239ndash249
XU J and CLARK RA (1997) A three-dimensional collagen latticeinduces protein kinase C-z activity Role in a2 integrin and collage-nase mRNA expression J Cell Biol 136 473ndash483
Address reprint requests toDr John Doukas
Selective Genetics Inc11035 Roselle Street
San Diego CA 92121
E-mail jdoukasselectivegeneticscom
Received for publication December 28 2000 accepted after re-vision February 23 2001
DOUKAS ET AL798

tissues or organs In vitro tests also established that collagenmatrices not only prevent vector loss due to diffusion but pre-serve vector activity despite prolonged incubation in acutewound fluid Successful vector immobilization and tissue re-pair could be achieved with both 015 collagen and 26 col-lagen suggesting flexibility in the final vehicle formulation re-quired for effective vector delivery This flexibility was neededin the present studies as 26 collagen formulations proveddifficult to deliver to PVA sponges and 6-mm excisionalwounds This would not be of concern in clinical settings how-ever where wound beds are easily accessible and generally sev-eral square centimeters in area By contrast CMC was inef-fective at retaining vector in aqueous environments Moreimportantly this matrix was itself inflammatory and whencombined with adenovirus the net result was inflammationrather than tissue repair We are currently examining the util-ity of other matrices such as fibrin and hyaluronic acid whichbecause of their more provisional nature may offer yet greatercellular migration into wounds as compared with type I colla-gen
Although an aqueous-based AdPDGF-B formulation hasbeen previously shown to enhance tissue formation (Liechty etal 1999) this was achieved with a model system that artifi-cially retains vectors within treatment sites In fact the presentstudies demonstrate that any tissue repair observed after Ad-PDGF-B delivery in a nongelling liquid is dependent on the useof this model system In wounds not designed to retain appliedtreatments aqueous-formulated AdPDGF-B seeped into sur-rounding tissues and led to hyperplasia within these areas ratherthan to tissue regeneration within the active wound bed Colla-gen-immobilized AdPDGF-B on the other hand did persist inthese wound beds and led to significant enhancements in gran-ulation tissue formation as well as enhanced wound re-epithe-lialization and wound closure The significance of these activ-ities is further substantiated considering that they wereachievable in 8-mm-diameter ischemic wounds which withinthe time frame examined could not self-heal to any meaning-ful degree in the absence of gene therapy However as all theanimal models employed in these studies will eventually self-heal given sufficient time the full value of matrix-immobilizedgene therapy vectors remains to be confirmed in human clini-cal trials
In conclusion we present evidence that matrix-immobilizedgene therapy vectors encoding appropriate growth-promotinggenes represent a promising approach to tissue regeneration andrepair This basic concept can be expanded to include alterna-tive matrices such as controlled-release formulations as wellas tissue-specific growth factors Furthermore the addition oftargeting ligands to adenovirus vectors (eg FGF2) can en-hance their ability to transduce cells such that tissue repair re-sponses comparable to nontargeted vectors can be achieved butat significantly lower vector doses (Chandler et al 2000a)With appropriate design and application schedules one couldconceivably time the release of multiple growth factors to spe-cific stages of a tissue repair cascade In addition we have foundin preliminary studies that collagen-immobilized nonviral vec-tors such as PDGF-B plasmids which have potentially morefavorable safety profiles than adenovirus vectors can also en-hance tissue formation in vivo (Chandler et al 2000b Tyroneet al 2000) Such flexibility should allow for the widespreadapplication of gene therapy to the treatment of injured tissues
ACKNOWLEDGMENTS
We thank Jeff Davidson (Vanderbilt University School ofMedicine) for assistance in establishing the PVA sponge modelCarl-Henrik Heldin (Ludwig Institute for Cancer Research) forthe PDGF-B gene construct and Emelie Amburn Lara AsatoSharon Chang Gail Fieser Lydia Greenlees Rebecca Smokerand Linda Manza for excellent technical assistance This pub-lication was made possible in part by NIH grants 1R43AR46154(JD) and 5P01CA25874 (MH)
REFERENCES
AHN ST and MUSTOE TA (1990) Effects of ischemia on ulcerwound healing A new model in the rabbit ear Ann Plast Surg 2417ndash23
ANDREE C SWAIN WF PAGE CP MACKLIN MDSLAMA J HATZIS D and ERIKSSON E (1994) In vivo trans-fer and expression of a human epidermal growth factor gene accel-erates wound repair Proc Natl Acad Sci USA 91 12188ndash12192
BENN SI WHITSITT JS BROADLEY KN NANNEY LBPERKINS D HE L PATEL M MORGAN JR SWAIN WFand DAVIDSON JM (1996) Particle-mediated gene transfer withtransforming growth factor-b1 cDNAs enhances wound repair in ratskin J Clin Invest 98 2894ndash2902
BONADIO J SMILEY E PATIL P and GOLDSTEIN S (1999)Localized direct plasmid gene delivery in vivo Prolonged therapyresults in reproducible tissue regeneration Nat Med 5 753ndash759
BUCKLEY A DAVIDSON JM KAMERATH CD WOLT TBand WOODWARD SC (1985) Sustained release of epidermalgrowth factor accelerates wound repair Proc Natl Acad Sci USA82 7340ndash7344
BUCKLEY-STURROCK A WOODWARD SC SENIOR RMGRIFFIN GL KLAGSBRUN M and DAVIDSON JM (1989)Differential stimulation of collagenase and chemotactic activity in fi-broblasts derived from rat wound repair tissue and human skin bygrowth factors J Cell Physiol 138 70ndash78
CHANDLER LA DOUKAS J GONZALEZ AM HOGANSONDK GU DL MA C NESBIT M CROMBLEHOLME TMHERLYN M SOSNOWSKI BA and PIERCE GF (2000a)FGF2ndashTargeted adenovirus encoding platelet-derived growth factor-B enhances de novo tissue formation Mol Ther 2 153ndash160
CHANDLER LA MA C GONZALEZ AM DOUKAS JNGUYEN T PIERCE GF and PHILLIPS ML (2000b) Ma-trix-enabled gene transfer for cutaneous wound repair Wound Re-pair Regen 8 473ndash479
DANILENKO DM RING BD TARPLEY JE MORRIS BVAN GY MORAWIECKI A CALLAHAN W GOLDEN-BERG M HERSHENSON S and PIERCE GF (1995) Growthfactors in porcine full and partial thickness burn repair Differing tar-gets and effects of keratinocyte growth factor platelet-derivedgrowth factor-BB epidermal growth factor and neu differentiationfactor Am J Pathol 147 1261ndash1277
DEUEL TF KAWAHARA RS MUSTOE TA and PIERCE GF(1991) Growth factors and wound healing Platelet-derived growthfactor as a model cytokine Annu Rev Med 42 567ndash584
DrsquoHEMECOURT PA SMIELL JM and KARIM MR (1998) So-dium carboxymethylcellulose aqueous-based gel vs becaplermin gelin patients with nonhealing lower extremity diabetic ulcers Wounds10 69ndash75
DOUKAS J HOGANSON DK ONG M YING W LACEYDL BAIRD A PIERCE GF and SOSNOWSKI BA (1999)Retargeted delivery of adenoviral vectors through fibroblast growthfactor receptors involves unique cellular pathways FASEB J 131459ndash1466
TISSUE REPAIR USING GROWTH FACTOR GENES 797
DVORAK HF BROWN LF DETMAR M and DVORAK AM(1995) Vascular permeability factorvascular endothelial growth fac-tor microvascular hyperpermeability and angiogenesis Am JPathol 146 1029ndash1039
EMING SA MEDALIE DA TOMPKINS RG YARMUSHML and MORGAN JR (1998) Genetically modified human ker-atinocytes overexpressing PDGF-A enhance the performance of acomposite skin graft Hum Gene Ther 9 529ndash539
EMING SA WHITSITT JS HE L KRIEG T MORGAN JRand DAVIDSON JM (1999) Particle-mediated gene transfer ofPDGF isoforms promotes wound repair J Invest Dermatol 112297ndash302
GERDES J SCHWAB U LEMKE H and STEIN H (1983) Pro-duction of a mouse monoclonal antibody reactive with a human nu-clear antigen associated with cell proliferation Int J Cancer 3113ndash20
GONZALEZ AM BERRY M MAHER PA LOGAN A andBAIRD A (1995) A comprehensive analysis of the distribution ofFGF-2 and FGFR1 in the rat brain Brain Res 701 201ndash226
GREENHALGH DG (1996) The role of growth factors in woundhealing J Trauma 41 159ndash167
GROTENDORST GR MARTIN GR PENCEV D SODEK Jand HARVEY AK (1985) Stimulation of granulation tissue for-mation by platelet-derived growth factor in normal and diabetic ratsJ Clin Invest 76 2323ndash2329
KHOURI RK HONG SP DEUNE EG TARPLEY JE SONGSZ SERDAR CM and PIERCE GF (1994) De novo genera-tion of permanent neovascularized soft tissue appendages by platelet-derived growth factor J Clin Invest 94 1757ndash1763
LEGRAND EK SENTER LH GAMELLI RL and KIORPESTC (1993) Evaluation of PDGF-BB PDGF-AA bFGF IL-1 andEGF dose responses in polyvinyl alcohol sponge implants assessedby a rapid histologic method Growth Factors 8 315ndash329
LIECHTY KW NESBIT M HERLYN M RADU A ADZICKNS and CROMBLEHOLME TM (1999) Adenoviral-mediatedoverexpression of platelet-derived growth factor-B corrects ischemicimpaired wound healing J Invest Dermatol 113 375ndash383
LYNCH SE COLVIN RB and ANTONIADES HN (1989)Growth factors in wound healing J Clin Invest 84 640ndash646
MUSTOE TA PIERCE GF THOMASON A GRAMATES PSPORN MB and DEUEL TF (1987) Accelerated healing of in-cisional wounds in rats induced by transforming growth factor-betaScience 237 1333ndash1336
MUSTOE TA PIERCE GF MORISHIMA C and DEUEL TF(1991) Growth factor-induced acceleration of tissue repair throughdirect and inductive activities in a rabbit dermal ulcer model J ClinInvest 87 694ndash703
MUSTOE TA AHN ST TARPLEY JE and PIERCE GF(1994) Role of hypoxia in growth factor responses Differential ef-fects of basic fibroblast growth factor and platelet-derived growthfactor in an ischemic wound model Wound Rep Reg 2 277ndash283
NYBERG-HOFFMAN C and AGUILAR-CORDOVA E (1999) In-stability of adenoviral vectors during transport and its implication forclinical studies Nat Med 5 955ndash957
PIERCE GF and MUSTOE TA (1995) Pharmacologic enhance-ment of wound healing Annu Rev Med 46 467ndash481
PIERCE GF MUSTOE TA SENIOR RM REED J GRIFFINGL THOMASON A and DEUEL TF (1988) In vivo incisionalwound healing augmented by platelet-derived growth factor and re-combinant c-sis gene homodimeric proteins J Exp Med 167 974ndash987
PIERCE GF VANDE BERG J RUDOLPH R TARPLEY J andMUSTOE TA (1991) Platelet-derived growth factor-BB and trans-forming growth factor beta 1 selectively modulate glycosaminogly -cans collagen and myofibroblasts in excisional wounds Am JPathol 138 629ndash646
PIERCE GF TARPLEY JE YANAGIHARA D MUSTOE TA
FOX GM and THOMASON A (1992) Platelet-derived growthfactor (BB homodimer) transforming growth factor-b1 and basic fi-broblast growth factor in dermal wound healing Neovessel and ma-trix formation and cessation of repair Am J Pathol 140 1375ndash1388
PIERCE GF TARPLEY JE ALLMAN RM GOODE PS SER-DAR CM MORRIS B MUSTOE TA and VANDE BERG J(1994a) Tissue repair processes in healing chronic pressure ulcerstreated with recombinant platelet-derived growth factor BB Am JPathol 145 1399ndash1410
PIERCE GF YANAGIHARA D KLOPCHIN K DANILENKODM HSU E KENNEY WC and MORRIS CF (1994b) Stim-ulation of all epithelial elements during skin regeneration by kerati-nocyte growth factor J Exp Med 179 831ndash840
PIERCE GF TARPLEY JE TSENG J BREADY J CHANGD KENNEY WC RUDOLPH R ROBSON MC VANDEBERG J and REID P (1995) Detection of platelet-derived growthfactor (PDGF)-AA in actively healing human wounds treated withrecombinant PDGF-BB and absence of PDGF in chronic nonhealingwounds J Clin Invest 96 1336ndash1350
SINGER AJ and CLARK RA (1999) Cutaneous wound healingN Engl J Med 341 738ndash746
SOMASUNDARAM R and SCHUPPAN D (1996) Type I II IIIIV V and VI collagens serve as extracellular ligands for the iso-forms of platelet-derived growth factor (AA BB and AB) J BiolChem 271 26884ndash26891
SPRUGEL KH MCPHERSON JM CLOWES AW and ROSSR (1987) Effects of growth factors in vivo I Cell ingrowth intoporous subcutaneous chambers Am J Pathol 129 601ndash613
STEED DL (1995) Clinical evaluation of recombinant humanplatelet-derived growth factor for the treatment of lower extremitydiabetic ulcers Diabetic Ulcer Study Group J Vasc Surg 21 71ndash78
STEED DL (1998) Foundations of good ulcer care Am J Surg 17620S-25S
TYRONE JW MOGFORD JE CHANDLER LA MA C XIAY PIERCE GF and MUSTOE TA (2000) Collagen-embeddedplatelet-derived growth factor DNA plasmid promotes wound heal-ing in a dermal ulcer model J Surg Res 93 230ndash236
VOGT PM THOMPSON S ANDREE C LIU P BREUING KHATZIS D BROWN H MULLIGAN RC and ERIKSSON E(1994) Genetically modified keratinocytes transplanted to woundsreconstitute the epidermis Proc Natl Acad Sci USA 91 9307ndash9311
WIEMAN TJ (1998) Clinical efficacy of becaplermin (rhPDGF-BB)gel Becaplermin Gel Studies Group Am J Surg 176 74S-79S
WIEMAN TJ SMIELL JM and SU Y (1998) Efficacy and safetyof a topical gel formulation of recombinant human platelet-derivedgrowth factor-BB (becaplermin) in patients with chronic neuropathicdiabetic ulcers A phase III randomized placebo-controlled double-blind study Diabetes Care 21 822ndash827
WILSON JM (1996) Adenoviruses as gene-delivery vehicles NEngl J Med 334 1185ndash1187
XU J and CLARK RA (1996) Extracellular matrix alters PDGFregulation of fibroblast integrins J Cell Biol 132 239ndash249
XU J and CLARK RA (1997) A three-dimensional collagen latticeinduces protein kinase C-z activity Role in a2 integrin and collage-nase mRNA expression J Cell Biol 136 473ndash483
Address reprint requests toDr John Doukas
Selective Genetics Inc11035 Roselle Street
San Diego CA 92121
E-mail jdoukasselectivegeneticscom
Received for publication December 28 2000 accepted after re-vision February 23 2001
DOUKAS ET AL798

DVORAK HF BROWN LF DETMAR M and DVORAK AM(1995) Vascular permeability factorvascular endothelial growth fac-tor microvascular hyperpermeability and angiogenesis Am JPathol 146 1029ndash1039
EMING SA MEDALIE DA TOMPKINS RG YARMUSHML and MORGAN JR (1998) Genetically modified human ker-atinocytes overexpressing PDGF-A enhance the performance of acomposite skin graft Hum Gene Ther 9 529ndash539
EMING SA WHITSITT JS HE L KRIEG T MORGAN JRand DAVIDSON JM (1999) Particle-mediated gene transfer ofPDGF isoforms promotes wound repair J Invest Dermatol 112297ndash302
GERDES J SCHWAB U LEMKE H and STEIN H (1983) Pro-duction of a mouse monoclonal antibody reactive with a human nu-clear antigen associated with cell proliferation Int J Cancer 3113ndash20
GONZALEZ AM BERRY M MAHER PA LOGAN A andBAIRD A (1995) A comprehensive analysis of the distribution ofFGF-2 and FGFR1 in the rat brain Brain Res 701 201ndash226
GREENHALGH DG (1996) The role of growth factors in woundhealing J Trauma 41 159ndash167
GROTENDORST GR MARTIN GR PENCEV D SODEK Jand HARVEY AK (1985) Stimulation of granulation tissue for-mation by platelet-derived growth factor in normal and diabetic ratsJ Clin Invest 76 2323ndash2329
KHOURI RK HONG SP DEUNE EG TARPLEY JE SONGSZ SERDAR CM and PIERCE GF (1994) De novo genera-tion of permanent neovascularized soft tissue appendages by platelet-derived growth factor J Clin Invest 94 1757ndash1763
LEGRAND EK SENTER LH GAMELLI RL and KIORPESTC (1993) Evaluation of PDGF-BB PDGF-AA bFGF IL-1 andEGF dose responses in polyvinyl alcohol sponge implants assessedby a rapid histologic method Growth Factors 8 315ndash329
LIECHTY KW NESBIT M HERLYN M RADU A ADZICKNS and CROMBLEHOLME TM (1999) Adenoviral-mediatedoverexpression of platelet-derived growth factor-B corrects ischemicimpaired wound healing J Invest Dermatol 113 375ndash383
LYNCH SE COLVIN RB and ANTONIADES HN (1989)Growth factors in wound healing J Clin Invest 84 640ndash646
MUSTOE TA PIERCE GF THOMASON A GRAMATES PSPORN MB and DEUEL TF (1987) Accelerated healing of in-cisional wounds in rats induced by transforming growth factor-betaScience 237 1333ndash1336
MUSTOE TA PIERCE GF MORISHIMA C and DEUEL TF(1991) Growth factor-induced acceleration of tissue repair throughdirect and inductive activities in a rabbit dermal ulcer model J ClinInvest 87 694ndash703
MUSTOE TA AHN ST TARPLEY JE and PIERCE GF(1994) Role of hypoxia in growth factor responses Differential ef-fects of basic fibroblast growth factor and platelet-derived growthfactor in an ischemic wound model Wound Rep Reg 2 277ndash283
NYBERG-HOFFMAN C and AGUILAR-CORDOVA E (1999) In-stability of adenoviral vectors during transport and its implication forclinical studies Nat Med 5 955ndash957
PIERCE GF and MUSTOE TA (1995) Pharmacologic enhance-ment of wound healing Annu Rev Med 46 467ndash481
PIERCE GF MUSTOE TA SENIOR RM REED J GRIFFINGL THOMASON A and DEUEL TF (1988) In vivo incisionalwound healing augmented by platelet-derived growth factor and re-combinant c-sis gene homodimeric proteins J Exp Med 167 974ndash987
PIERCE GF VANDE BERG J RUDOLPH R TARPLEY J andMUSTOE TA (1991) Platelet-derived growth factor-BB and trans-forming growth factor beta 1 selectively modulate glycosaminogly -cans collagen and myofibroblasts in excisional wounds Am JPathol 138 629ndash646
PIERCE GF TARPLEY JE YANAGIHARA D MUSTOE TA
FOX GM and THOMASON A (1992) Platelet-derived growthfactor (BB homodimer) transforming growth factor-b1 and basic fi-broblast growth factor in dermal wound healing Neovessel and ma-trix formation and cessation of repair Am J Pathol 140 1375ndash1388
PIERCE GF TARPLEY JE ALLMAN RM GOODE PS SER-DAR CM MORRIS B MUSTOE TA and VANDE BERG J(1994a) Tissue repair processes in healing chronic pressure ulcerstreated with recombinant platelet-derived growth factor BB Am JPathol 145 1399ndash1410
PIERCE GF YANAGIHARA D KLOPCHIN K DANILENKODM HSU E KENNEY WC and MORRIS CF (1994b) Stim-ulation of all epithelial elements during skin regeneration by kerati-nocyte growth factor J Exp Med 179 831ndash840
PIERCE GF TARPLEY JE TSENG J BREADY J CHANGD KENNEY WC RUDOLPH R ROBSON MC VANDEBERG J and REID P (1995) Detection of platelet-derived growthfactor (PDGF)-AA in actively healing human wounds treated withrecombinant PDGF-BB and absence of PDGF in chronic nonhealingwounds J Clin Invest 96 1336ndash1350
SINGER AJ and CLARK RA (1999) Cutaneous wound healingN Engl J Med 341 738ndash746
SOMASUNDARAM R and SCHUPPAN D (1996) Type I II IIIIV V and VI collagens serve as extracellular ligands for the iso-forms of platelet-derived growth factor (AA BB and AB) J BiolChem 271 26884ndash26891
SPRUGEL KH MCPHERSON JM CLOWES AW and ROSSR (1987) Effects of growth factors in vivo I Cell ingrowth intoporous subcutaneous chambers Am J Pathol 129 601ndash613
STEED DL (1995) Clinical evaluation of recombinant humanplatelet-derived growth factor for the treatment of lower extremitydiabetic ulcers Diabetic Ulcer Study Group J Vasc Surg 21 71ndash78
STEED DL (1998) Foundations of good ulcer care Am J Surg 17620S-25S
TYRONE JW MOGFORD JE CHANDLER LA MA C XIAY PIERCE GF and MUSTOE TA (2000) Collagen-embeddedplatelet-derived growth factor DNA plasmid promotes wound heal-ing in a dermal ulcer model J Surg Res 93 230ndash236
VOGT PM THOMPSON S ANDREE C LIU P BREUING KHATZIS D BROWN H MULLIGAN RC and ERIKSSON E(1994) Genetically modified keratinocytes transplanted to woundsreconstitute the epidermis Proc Natl Acad Sci USA 91 9307ndash9311
WIEMAN TJ (1998) Clinical efficacy of becaplermin (rhPDGF-BB)gel Becaplermin Gel Studies Group Am J Surg 176 74S-79S
WIEMAN TJ SMIELL JM and SU Y (1998) Efficacy and safetyof a topical gel formulation of recombinant human platelet-derivedgrowth factor-BB (becaplermin) in patients with chronic neuropathicdiabetic ulcers A phase III randomized placebo-controlled double-blind study Diabetes Care 21 822ndash827
WILSON JM (1996) Adenoviruses as gene-delivery vehicles NEngl J Med 334 1185ndash1187
XU J and CLARK RA (1996) Extracellular matrix alters PDGFregulation of fibroblast integrins J Cell Biol 132 239ndash249
XU J and CLARK RA (1997) A three-dimensional collagen latticeinduces protein kinase C-z activity Role in a2 integrin and collage-nase mRNA expression J Cell Biol 136 473ndash483
Address reprint requests toDr John Doukas
Selective Genetics Inc11035 Roselle Street
San Diego CA 92121
E-mail jdoukasselectivegeneticscom
Received for publication December 28 2000 accepted after re-vision February 23 2001
DOUKAS ET AL798




















