
Malaria and related environmental issues in India: a case study of Aligarh city
11
GeoJournal 89: 89–99, 2001. © 2002 Kluwer Academic Publishers. Printed in the Netherlands. 89 Malaria and related environmental issues in India: a case study of Aligarh city Abha Lakshmi Singh 1,∗ and Atiqur Rahman 2 1 Department of Geography, Aligarh Muslim University, Aligarh-202 002, U.P., India; 2 Department of Geography, Jamia Millia Islamia, New Delhi, India; ∗ Author for correspondence (Tel. 571-700683; Fax: 571-700683; E-mail: [email protected]) Received 11 June 2001; accepted 31 January 2002 Key words: malaria, environmental issues; small towns; income groups; water logging, open blocked drains Abstract Malaria is one of the most widespread diseases in the world. Endemic malaria no longer occurs in many temperate zones as a result of social and economic improvement. At present malaria is the Third World’s most dreaded killer. It kills over 1 million people and causes 300–500 million episodes of illness. In India, malaria-reported deaths have shown an upward trend. In 1955, a drive to eradicate malaria was launched in India. But after initial success it failed and malaria made a comeback. Malarial mosquitoes generally prefer unpolluted natural breeding sites but now they have adapted to the changed urban environment. In this paper, an attempt has been made to examine the occurrence of malaria and related environmental issues in a small town of India. Aligarh city, lying in the shadow of the country’s capital New Delhi, was selected as a case study. Data were collected mainly from household surveys with the help of questionnaire interviews. About 2,185 households belonging to different income groups were sampled. The differences in the occurrence of malaria in the different income households (in 87% low, 69% lower-middle, 65% middle, 14% upper-middle, and 5% upper) suggest that most of these differences are related to the environmental conditions existing inside and outside their homes, such as poor drainage system, poor sullage disposal, open blocked drains, waterlogging and indoor water storage in open containers. Commitment both by the Government and local residents is needed to improve the environmental conditions and eradicate malaria. Introduction Many cities in the Third World face insurmountable prob- lems. Environment-related diseases like diarrhoea, typhoid, cholera and food poisoning (caused by use of contaminated water and/or food), pneumonia and tuberculosis (airborne respiratory infections), malaria, dengue fever, filariasis (vec- tor borne diseases), scabies, trachoma, typhus etc. (due to lack of water for washing) are the leading causes of death and illness in most cities in the Third World (Hardoy and Satterthwaite, 1992). Malaria is one of the oldest chronic and most widespread diseases that have plagued mankind for centuries. More than 2,000 million people in about 100 countries now live in ar- eas where there is a definite risk (Elhadi and Others, 1991). India is one of these risk zones. Endemic malaria no longer occurs in temperate zones as a result of social and economic improvement. Malaria is mainly associated with tropical countries. At present, malaria is the Third World’s most dreaded killer. It kills over 1 million people and causes 300– 500 million episodes of illness each year (Agarwal, 2000). Efforts to control malaria in the last 50 years have met with little success. In many regions where malaria transmission had been almost eliminated, the disease has made a come- back and cases of malaria are on rise. It forces man to seek shelter behind bed nets, and wear long sleeved shirts and clothes that conceal. Malaria is a mosquito-borne disease. The female Anopheline mosquito plays a key role as a vector in the inci- dence of malaria. There are about 400 species of Anopheles mosquitoes, but only about 10 species are responsible for transmitting malaria (Park, 1997). Anopheline culicifacies is the main vector of the Indian heartland. It has the ability to adapt to breeding in water bodies of all shapes and sizes and all degrees of permanence over a couple of weeks or so. It is now reported to be resistant to DDT and HCH (Bruce and Global, 1970). Anophel stephenesi, long known as a species which had adapted to life in urban domestic cisterns etc. is probably more widespread and more significant. It has also developed resistance to DDT (Akhtar and Learmonth, 1985). In India, malaria-related deaths have shown an upward trend from 99 in 1975, to 207 in 1980, to 422 in 1992 and to 911 in 1998 (Ministry of Health and Family Welfare, 1998). Researchers claim that the actual numbers must be much higher (National Malaria Eradication Programme, 1999). In 1955, a drive to eradicate malaria was launched. After an initial success it failed. Plasmodium (malaria parasite) devel- oped a resistance to insecticides and chloroquine. In the late 1960s and early 1970s, malaria made a comeback. Attempts to control the second wave of the disease had limited suc- cess. In the late 1970s and early 1980s Plasmodium spread further. In the 1990s, industrial and agricultural projects caused ecological changes which favored transmission of
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of Malaria and related environmental issues in India: a case study of Aligarh city

GeoJournal 89: 89–99, 2001.© 2002 Kluwer Academic Publishers. Printed in the Netherlands.
89
Malaria and related environmental issues in India: a case study of Aligarh city
Abha Lakshmi Singh1,∗ and Atiqur Rahman2
1Department of Geography, Aligarh Muslim University, Aligarh-202 002, U.P., India; 2Department of Geography,Jamia Millia Islamia, New Delhi, India; ∗Author for correspondence (Tel. 571-700683; Fax: 571-700683; E-mail:[email protected])
Received 11 June 2001; accepted 31 January 2002
Key words: malaria, environmental issues; small towns; income groups; water logging, open blocked drains
Abstract
Malaria is one of the most widespread diseases in the world. Endemic malaria no longer occurs in many temperate zonesas a result of social and economic improvement. At present malaria is the Third World’s most dreaded killer. It kills over1 million people and causes 300–500 million episodes of illness. In India, malaria-reported deaths have shown an upwardtrend. In 1955, a drive to eradicate malaria was launched in India. But after initial success it failed and malaria made acomeback. Malarial mosquitoes generally prefer unpolluted natural breeding sites but now they have adapted to the changedurban environment. In this paper, an attempt has been made to examine the occurrence of malaria and related environmentalissues in a small town of India. Aligarh city, lying in the shadow of the country’s capital New Delhi, was selected asa case study. Data were collected mainly from household surveys with the help of questionnaire interviews. About 2,185households belonging to different income groups were sampled. The differences in the occurrence of malaria in the differentincome households (in 87% low, 69% lower-middle, 65% middle, 14% upper-middle, and 5% upper) suggest that most ofthese differences are related to the environmental conditions existing inside and outside their homes, such as poor drainagesystem, poor sullage disposal, open blocked drains, waterlogging and indoor water storage in open containers. Commitmentboth by the Government and local residents is needed to improve the environmental conditions and eradicate malaria.
Introduction
Many cities in the Third World face insurmountable prob-lems. Environment-related diseases like diarrhoea, typhoid,cholera and food poisoning (caused by use of contaminatedwater and/or food), pneumonia and tuberculosis (airbornerespiratory infections), malaria, dengue fever, filariasis (vec-tor borne diseases), scabies, trachoma, typhus etc. (due tolack of water for washing) are the leading causes of deathand illness in most cities in the Third World (Hardoy andSatterthwaite, 1992).
Malaria is one of the oldest chronic and most widespreaddiseases that have plagued mankind for centuries. More than2,000 million people in about 100 countries now live in ar-eas where there is a definite risk (Elhadi and Others, 1991).India is one of these risk zones. Endemic malaria no longeroccurs in temperate zones as a result of social and economicimprovement. Malaria is mainly associated with tropicalcountries. At present, malaria is the Third World’s mostdreaded killer. It kills over 1 million people and causes 300–500 million episodes of illness each year (Agarwal, 2000).Efforts to control malaria in the last 50 years have met withlittle success. In many regions where malaria transmissionhad been almost eliminated, the disease has made a come-back and cases of malaria are on rise. It forces man to seekshelter behind bed nets, and wear long sleeved shirts andclothes that conceal.
Malaria is a mosquito-borne disease. The femaleAnopheline mosquito plays a key role as a vector in the inci-dence of malaria. There are about 400 species of Anophelesmosquitoes, but only about 10 species are responsible fortransmitting malaria (Park, 1997). Anopheline culicifacies isthe main vector of the Indian heartland. It has the ability toadapt to breeding in water bodies of all shapes and sizes andall degrees of permanence over a couple of weeks or so. Itis now reported to be resistant to DDT and HCH (Bruce andGlobal, 1970). Anophel stephenesi, long known as a specieswhich had adapted to life in urban domestic cisterns etc. isprobably more widespread and more significant. It has alsodeveloped resistance to DDT (Akhtar and Learmonth, 1985).
In India, malaria-related deaths have shown an upwardtrend from 99 in 1975, to 207 in 1980, to 422 in 1992 and to911 in 1998 (Ministry of Health and Family Welfare, 1998).Researchers claim that the actual numbers must be muchhigher (National Malaria Eradication Programme, 1999). In1955, a drive to eradicate malaria was launched. After aninitial success it failed. Plasmodium (malaria parasite) devel-oped a resistance to insecticides and chloroquine. In the late1960s and early 1970s, malaria made a comeback. Attemptsto control the second wave of the disease had limited suc-cess. In the late 1970s and early 1980s Plasmodium spreadfurther. In the 1990s, industrial and agricultural projectscaused ecological changes which favored transmission of

90
Figure 1. Location of Aligarh city.
malaria (Agarwal, 2000). The Anopheles mosquito requiresa breeding ground, which has now developed because of anumber of environmental factors.
Until recently malaria was considered to be a predomi-nant disease of rural areas in India but now it has becomea serious threat to urban life. High incidence of malariapatients, some of them victims of lethal celebral malaria,have been reported from various cities of India. Celebralmalaria accounts for almost 39% of the 2 million malariacases being reported in India every year (Times of India,1998). Congestion in cities has led to unhygienic living con-ditions, strain on urban resources – housing, water, lack of adisposal system of sewage, water from washing and bathing,
solid wastes, water stagnation, increased construction ac-tivities serve as excellent breeding grounds for mosquitoes.During the rainy season more breeding grounds are created.Almost every household, especially from the low-incomeand slum areas are found to be suffering from frequent boutsof malaria. Urban malaria has become more widespreadand more significant as an important public health prob-lem. Hence, the fight against malaria has become one of thebiggest tasks in the health care sector of the country. Thereis need for detailed local studies.
There are thousands of small towns in India lying outsidethe metropolitan veil. Such towns are destined to remain inthe shadow of mammoth cities like Delhi, Calcutta, Mum-
91
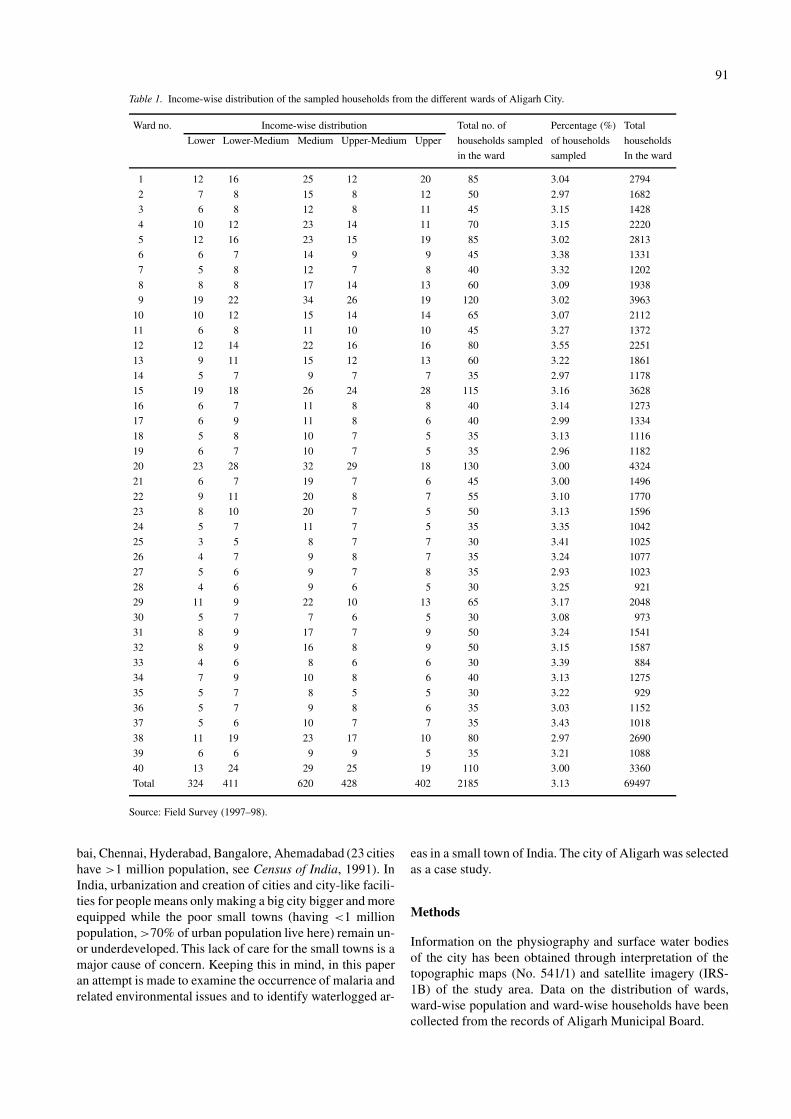
Table 1. Income-wise distribution of the sampled households from the different wards of Aligarh City.
Ward no. Income-wise distribution Total no. of Percentage (%) Total
Lower Lower-Medium Medium Upper-Medium Upper households sampled of households households
in the ward sampled In the ward
1 12 16 25 12 20 85 3.04 2794
2 7 8 15 8 12 50 2.97 1682
3 6 8 12 8 11 45 3.15 1428
4 10 12 23 14 11 70 3.15 2220
5 12 16 23 15 19 85 3.02 2813
6 6 7 14 9 9 45 3.38 1331
7 5 8 12 7 8 40 3.32 1202
8 8 8 17 14 13 60 3.09 1938
9 19 22 34 26 19 120 3.02 3963
10 10 12 15 14 14 65 3.07 2112
11 6 8 11 10 10 45 3.27 1372
12 12 14 22 16 16 80 3.55 2251
13 9 11 15 12 13 60 3.22 1861
14 5 7 9 7 7 35 2.97 1178
15 19 18 26 24 28 115 3.16 3628
16 6 7 11 8 8 40 3.14 1273
17 6 9 11 8 6 40 2.99 1334
18 5 8 10 7 5 35 3.13 1116
19 6 7 10 7 5 35 2.96 1182
20 23 28 32 29 18 130 3.00 4324
21 6 7 19 7 6 45 3.00 1496
22 9 11 20 8 7 55 3.10 1770
23 8 10 20 7 5 50 3.13 1596
24 5 7 11 7 5 35 3.35 1042
25 3 5 8 7 7 30 3.41 1025
26 4 7 9 8 7 35 3.24 1077
27 5 6 9 7 8 35 2.93 1023
28 4 6 9 6 5 30 3.25 921
29 11 9 22 10 13 65 3.17 2048
30 5 7 7 6 5 30 3.08 973
31 8 9 17 7 9 50 3.24 1541
32 8 9 16 8 9 50 3.15 1587
33 4 6 8 6 6 30 3.39 884
34 7 9 10 8 6 40 3.13 1275
35 5 7 8 5 5 30 3.22 929
36 5 7 9 8 6 35 3.03 1152
37 5 6 10 7 7 35 3.43 1018
38 11 19 23 17 10 80 2.97 2690
39 6 6 9 9 5 35 3.21 1088
40 13 24 29 25 19 110 3.00 3360
Total 324 411 620 428 402 2185 3.13 69497
Source: Field Survey (1997–98).
bai, Chennai, Hyderabad, Bangalore, Ahemadabad (23 citieshave >1 million population, see Census of India, 1991). InIndia, urbanization and creation of cities and city-like facili-ties for people means only making a big city bigger and moreequipped while the poor small towns (having <1 millionpopulation, >70% of urban population live here) remain un-or underdeveloped. This lack of care for the small towns is amajor cause of concern. Keeping this in mind, in this paperan attempt is made to examine the occurrence of malaria andrelated environmental issues and to identify waterlogged ar-
eas in a small town of India. The city of Aligarh was selectedas a case study.
Methods
Information on the physiography and surface water bodiesof the city has been obtained through interpretation of thetopographic maps (No. 541/1) and satellite imagery (IRS-1B) of the study area. Data on the distribution of wards,ward-wise population and ward-wise households have beencollected from the records of Aligarh Municipal Board.

92
Figure 2. Ward-wise division and location of sampled households in Aligarh city.
The data were collected mainly from primary sources.The methods used include:• site observation• survey of sampled households on the basis of question-
naire interviewsThe questionnaire used in the interviews was devel-
oped with the help of questionnaires used in similar studies
(Bradley et al., 1991; McGranahan, 1991; McGranahanet al. 1991; Stephens and Harpham, 1991; Ellegard andEgneus 1992; Benneh et al., 1993; Leitman, 1993; Mc-Granahan, 1993; Songsore and McGranahan, 1993, Jacobiet al., 1994, McGranahan and Songsore, 1994; Singhet al., 1995, 1996; Rahman, 1998). It covered the follow-ing topics: occurrence of malaria during the last one year,

93
Figure 3. Occurrence of malaria in the sampled households of Aligarh city.
drainage around the house, type of drainage, mode of dis-posal of household waste, waterlogging around the house,type of waterlogged, indoor storage of water in open con-tainers, presence of mosquitoes inside the house and use ofpreventive measures.
The data were drawn with the help of the questionnairefrom a comprehensive survey of the households. Aligarh cityhas 69,797 households (Census of India, 1991). About 30 to130 households were sampled from every ward of the city.Stratified random sampling has been done keeping in mindthat the households selected were a good representation ofpersons belonging to different income groups. In this way(3.15%) about 2,185 households (a household consists ofall those persons who occupy a housing unit collectively,
put their feet under one table or otherwise join togetherin an arrangement to provide food, clothing, shelter andother basic residential necessities) were sampled (Table 1,Figure 2).
About 402 households belonged to the upper incomegroup (earning more than Rs. 9,000 per month, 1 US $ =Rs. 43.00; 1 £ = Rs. 65.00), 428 households belonged tothe upper-middle income group (income ranging betweenRs. 5,000–9,000), 620 households belonged to the middle-income group (Rs. 3,000–4,999), 411 households belongedto the lower-middle income group (Rs. 1,500–2,999) and324 households belonged to the low-income group (incomeless than Rs. 1,500). The interviews were carried on during

94
Figure 4. Collection and disposal of wastewater by the Municipality in Aligarh city.
1997–98. The principal women were chosen as respondentsbecause they know more about their household conditions.
Case study: Aligarh city
Aligarh is a small town in North India, which lies in theshadow of the country’s capital New Delhi (Figure 1). It isabout 130 km from New Delhi. This town has not benefitedfrom its proximity to the capital city. It is cracking under the
pressure of its growing population. The city’s population hasincreased from 0.4 millions in 1991 (Census of India, 1991)to 0.8 million in 2001 (Aligarh Municipal Board, 2001).Here clean water is a dream, flies breed in human excretain open, solid waste clogs drains, mosquitoes breed in poolsof dirty water and in drains which are open, paths are narrowand roads are full of pot-holes (Singh and Rahman, 1999).The city has a distinct demarcation between the old and thenew part. The Delhi–Calcutta railway line separates the oldand new part of the city (Figure 2). The old part of the
95
city spreads over 27 wards. The Upper Kot and the adjacentAchal Tal area is the core and the nucleus of the old part.It is very congested and has the highest population densi-ties. The old part of the city which lies on the west of therailway line presents a picture of decadence in the absenceof proper drainage. The place emits a vile stench and putriddrains provide a fertile ground for flies and mosquitoes. Thehouses are closely spaced and lanes are narrow. There is lackof civic amenities. The new parts of the city spread over13 wards. It spreads over the middle and outer fringe areas.It comprises the Civil Lines and the University area, whichappears remarkably clean but now with the springing up ofnew residential colonies and commercial complexes this partis also becoming congested and dirty (Singh et al., 1996).
Topographically the district of Aligarh represents a shal-low trough, sauce-pan shape-like appearance with the RiverGanga in the north-east and the River Yamuna in the north-west forming the highland peripheries. Through the centreof the district, a broad low lying belt runs from north-west tosouth-east. This belt is part of the extensive low lying tractwhich runs through the centre of the doab (inter-riverineplain). This depression is narrow in the north and gets widerin the south and it eventually passes into the adjoining dis-trict. This tract is characterized by imperfect drainage andnumerous lakes. Aligarh city lies in the centre of the low-lying tract (Figure 1). Because of lack of natural drainage,rain water and wastewater collect in the low-lying areas ofthe city. There is no outlet of water. The city not only getssubmerged during the rain season (from mid-June to mid-September, average annual rainfall is 77 mm) but remainssubmerged all the year round because of imperfect naturaldrainage.
Discussion
Malaria is not only one of the important diseases reportedby the respondents but it remains to be by far the mostfrequently reported health problem at the Out Patient De-partment of the University Medical College Hospital, Gov-ernment Civil Hospital and at various private clinics ofAligarh city. An analysis of malaria and its association withenvironmental conditions is difficult on the basis of house-hold questionnaires because self diagnosis of malaria isinaccurate, households cannot identify malarial mosquitoesand neither blood tests were undertaken during the sur-vey. Nevertheless, according to information collected fromthe University Medical College Hospital, Government CivilHospital and from various private clinics, malaria accountedfor between 41–53% of the cases reported between 1997–99.While such statistics may exaggerate the relative importanceof malaria there is little doubt that it still remains to be animportant cause of ill health in the city. Figure 3 is show-ing the percentage of sampled households belonging to thedifferent income groups reporting about the occurrence ofmalaria. About 87% of the low, 69% of the lower-middle,65% of the middle, 14% of the upper-middle and 5% of theupper-income households reported the occurrence of malariaduring the last one year.
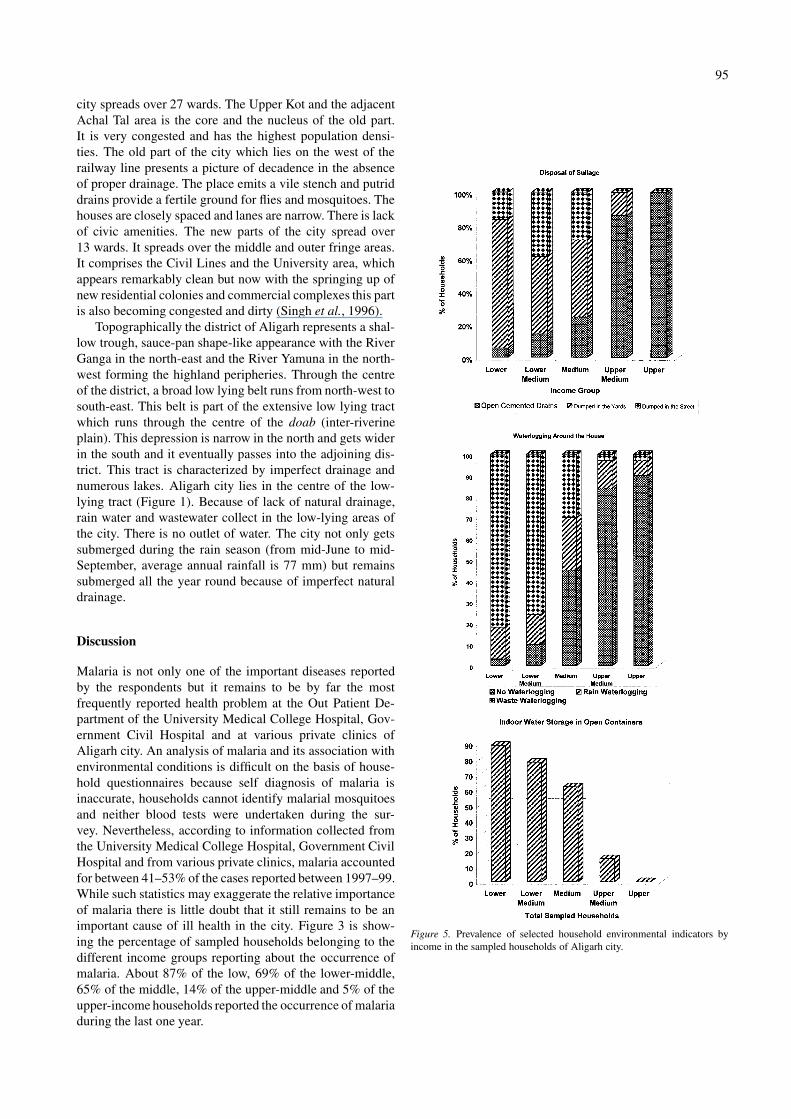
Figure 5. Prevalence of selected household environmental indicators byincome in the sampled households of Aligarh city.

96
Figure 6. Occurrence of mosquitoes inside the house and use of preventivemeasures in the sampled household of Aligarh city.
Malaria is closely related to a number of environmentalfactors and efforts should be made to identify them so thatsolutions to the problem may be found.
Water is the most influential factor because mosquitoesbreed in water. In India, Anopheles mosquitoe has developedinto an urban species and is found in much higher numbers inmany cities than in the countryside (WHO, 1988). AlthoughAnopheles mosquitoes generally prefer unpolluted naturalbreeding sites, it has now adapted to the urban environmentof Aligarh city. Congestion, increased constructional activ-ities, poor drainage system (both natural and man made),disposal of sullage in open drains, open drains which are per-manently blocked by garbage, polythene, etc. Since the cityis located in a depression there is no or a very sluggish flowof water in the drains. The water seems to be either standingin the drains or overflowing, waterlogging, and indoor water
storage in open containers are some of the important causeswhich facilitate mosquito breeding in the city.
While one might expect mosquitoes to be largely preva-lent in the rainy season, it remains high all the year roundbecause Aligarh city provides an ideal breeding ground formosquitoes. Overcrowding, coupled with sauce-pan shapedtopography, poor drainage system (both natural and munici-pal), increase in industrial, commercial establishments (likerestaurants, hotels, hospitals), multistoried buildings (likeresidential apartments, shopping complexes) and construc-tion sites (which use large amounts of water) has led to thecollection of water in the low-lying areas. The constructionsites are a heaven for mosquitoes as they maintain large wa-ter storage tanks for construction work. The left out ditches,overhead tanks, ornamental tanks, and cisterns of the mul-tistoried buildings help in the breeding of malaria vectorAnopheles stephensi. The city is dotted with pools of wastewater and drains which are choked and overflowing all theyear round.
An examination of the Aligarh’s civic system revealedthat the municipality collects and disposes the waste waterthrough a system of open drains and covered sewers (Fig-ure 4). Zone 1, 2 and 3 are partly severed while zone 4is totally unsevered. The main sewer from zone 2 and 3 iscompletely choked resulting in spread of sewage and over-flowing of surface drains. The open drains which carry thesullage are partly tapped into the sewage system which alsocauses choking of the sewer lines. The drains are connectedto a main drain along the periphery of the city which joinsa small tributary of the River Yamuna. Since there is hardlyany ground slope available (Figure 1), the flow in the drainsis sluggish and there is large-scale spreading of sewage. Theopen putrid drains and waste waterlogging also provide aheaven for mosquitoes.
The environment in and around homes is more criticalto people’s health. A detailed examination of the malaria-related household environmental factors was conducted.Perusal of Figure 5 shows that sullage (household wastewater) was normally discharged in open cemented drains ordumped in the yard or dumped in the street. Better methodsincluding discharge in closed separate drains and in sewer-ages or septic tanks were hardly used. Sullage was disposedin open cemented drains by 98% of the upper, 86% of theupper-middle, 22% of the middle, 14% of the lower-middleand 5% of the low-income sampled households. Sullage dis-posal in the streets or in the yard is more common in thelow, lower-middle and middle-income households. In poorneighborhoods, inadequate sullage disposal gives rise to wa-terlogging in and around homes. About 97% of the low, 91%of the lower-middle, 55% of the middle, 14% of the upper-middle and 10% of the upper-income sampled householdsreported waterlogging in and around their homes. This wa-terlogging occurs due to collection of waste and rain water.This shows the poor drainage conditions and no provision ofa proper drainage system by the Aligarh municipality in thepoor localities or in the newly developed parts of the city.
Indoor water storage in open containers also facilitatesbreeding of mosquitoes. Most of the houses built in richer

97
Figure 7. Identification of areas under water logging in Aligarh city.
residential areas have overhead tanks or other relatively effi-cient water storage facilities, while in poorer residential ar-eas, with inadequate service facilities, individual householdshave devised coping strategies by providing their own smallstorage containers such as buckets, barrels cans, pots etc. Aircoolers and cisterns, mostly used by the upper-middle, mid-dle and lower-middle income households, facilitate breedingof mosquitoes because water is stored in the open tanks ofthe coolers. The high incidence of indoor water storage inopen containers among the lower and middle-income house-holds is seen in Figure 5. About 89% of the low, 78% ofthe lower-middle, 62% of the middle, and 15% of the upper-
middle income sampled households were storing water inopen containers inside their homes.
The survey undertaken for this study does not provideinformation on mosquito species but the results indicate thatin 69% of the low, 57% of the lower-middle, 51% of the mid-dle, 10% of the upper-middle and 1% of the upper-incomesampled households reported the presence of mosquitoes in-side their homes (Figure 6). The respondents reported beingbitten by mosquitoes throughout the year, especially duringthe night. During the rainy season the mosquito populationincreases enormously as these conditions provide breedinggrounds in the form of pits, garbage bins, left-out containers,open tanks, open drains etc. where water gets stagnated. Ex-

98
cluding households with full screening, the responses werequite similar in different areas of the city and among thedifferent income groups. Indoor water storage in open con-tainers has emerged as an influential factor which should beassociated with the presence of mosquitoes inside the houseor with more mosquito biting. If the presence of malarialmosquito breeding in household water containers is increas-ing, these findings also indicate that indoor water storagemay be increasing malaria prevalence.
Regarding the use of preventive measures, the most pop-ular methods include the use of fly doors and windows(screening), mosquito mats and coils, pump cans etc. by theupper, upper-middle and middle-income households. Use ofmosquito coils, bed nets, and dependency on the Govern-ment agencies to spray are the most common means amongthe poor households.
Conclusions
The study has revealed that malarial mosquitoes are un-doubtedly a major health risk for the residents of small citieslike Aligarh. It is the principal health problem reported bythe Out Patient Department of University Medical CollegeHospital, Government Civil Hospital and by various privateclinics. Mosquitoes are a known health risk, especially whenthe city is congested, constructional activities are going on,drainage conditions are poor, disposal of sullage is poor,drains are open and choked, when there is no flow of water,when there is waterlogging and when residents store waterindoors in open containers.
The results clearly indicate that the lower-income house-holds are at greater risk than the wealthier households.Most differences in the occurrence of malaria in the dif-ferent income households are related to the environmentalconditions. The poor surroundings of the lower and lower-middle income households offer a fertile breeding groundfor Anopheles mosquitoes. Lack of health knowledge anda lowered resistance due to malnutrition have been some ofthe predisposing causes of a number of cases of malaria inthese poor households. The poor suffer the most and becauseof their poor physical environment they tend to remain sick.
The results also indicate that malaria is closely relatedto a number of environmental factors. Water is the mostinfluential factor because mosquitoes breed in any type ofwater–fresh or brackish water. Anopheles mosquitoes gen-erally prefer unpolluted natural breeding sites but they havenow adapted to the changed urban environment. They arenow found breeding in open stagnant drains, in pools of wa-ter collected in the yard or in the streets or in pits and in waterstored indoors in open containers, coolers or cisterns. Thus,collection of water or waterlogging aggravates this problem.Alleviating the waterlogging problem should be given toppriority. Such areas should be identified because it will be ofgreat help in the malaria eradication programme. An attemptis made to identify the malaria-prone areas. Figure 7 hasbeen prepared with the help of topographical sheets, satelliteimageries and a survey of the 40 wards of Aligarh city. This
figure is showing the areas suffering from waterlogging (per-manent, seasonal and occasional) and areas where there isno waterlogging. Permanent waterlogging is a very commonfeature of the city. Lal Diggi, Kali Deh, Nai Abadi, Gamb-hirpura, ADA colony, Bihari colony, Shakti Nagar, Industrialcolony, Loco colony, Hamdard Nagar, Friends colony etc.are areas under permanent waterlogging. Seasonal and occa-sional waterlogging is caused by rain, overflowing of opendrains, collection of household waste water in low-lyingareas like on roads and yards, excessive constructional ac-tivities etc. Since the city is situated in a low-lying area, itgets submerged during the rains.
For any plan which aims at tackling malaria,• the first step should be to identify mosquito breeding
grounds;• the second step should be to set up the staffing pattern for
care detection and subsequent treatment also for vectorcontrol pattern;
• and the third step should be to chalk out a suitable planof action.Large-scale planning by the government is needed. The
responsibility of keeping the household and neighborhoodclean lies on the shoulder of the residents. The governmentcannot tackle every problem, so the choices have to be madewith the help of local residents, NGO’s, local institutions andvoluntary organizations. An integrated strategy for improv-ing the waterlogging conditions, drainage conditions anderadication of mosquitoes is needed so that the residents ofThird World cities get relief from frequent bouts of malaria.
References
Agarwal A., 2000: Fighting malaria. Down to Earth, 15: 14–15.Agarwal A., 2000: Heading off fever. Down to Earth, 30: 29–39.Aligarh Municipal Board, 2001: Aligarh.Akhtar R. and Learmonth A.T.A., 1985: The resurgence of malaria in India
1965–76. In: Rais Akhtar (ed.), Geographical Aspects of Health andDisease in India. Concept Publication, New Delhi.
Benneh, G., Songsore J., Nabila J.S., Amuzu A.T., Tutu K.A., YangyuoruY. and McGranahan G, 1993: Environmental problems and the urbanhousehold in the Greater Accra metropolitan area – Ghana. StockholmEnvironment Institute, Stockholm, Sweden.
Bradley D., Cairncron S., Harpham T. and Stephens C., 1991: A review ofenvironmental health impacts in developing country cities. Urban Man-agement Programme. Discussion Paper, World Bank/UNDP/UNCHS(6).
Bruce-Chwatt L.J., 1970: Review of malaria control and eradication byattack on the vector. Misc. Publ. Entomol. Soc. Am., 7 (1): 7–27.
Census of India, 1991: District Census Handbook: Primary Census Ab-stract. XIII B.
Elhadi H., Benzerroung and Elom B., 1991: The world’s malaria situation.World Health, September–October: 6–7.
Ellegard A. and Egneus H., 1992: Health effects of charcoal and wood fuelin low income households in Lusaka. SEI, Sweden.
Hardoy J.E. and Satterthwaite D., 1992: Environmental problems in ThirdWorld cities, an agenda for the poor and the planet. InternationalInstitute for Environment and Development, London.
Jacobi P. and Camara L.M., 1994: Environmental problems facing urbanhouseholds in the city of São Paulo. Stockholm Environment Institute,Stockholm.
Leitmann J., 1993: Rapid urban environmental assessment: lessons fromcities in the developing world. Urb. Manag. Environ., 15, World Bank,Washington.

99
McGranahan G., 1991: Environmental problems and the urban householdsin Third World cities. Stockholm Environment Institute, Sweden.
McGranahan G. and Kaiser A., 1991: Household energy: problems, policiesand prospects. Stockholm Environment Institute, Sweden.
Ministry of Health and Family Welfare, 1998: Report on health informationof India, Directorate General of Health Services. Government of India,New Delhi.
McGranahan G., 1993: Household environmental problems in low-incomecities, an overview of problems and perspects for improvement. HabitatInternl., 7(2): 105–121.
McGranahan G. and Songsore, J. 1994: Wealth, health and urban house-holds: weighting environmental burdens in Accra, Jakarta and SãoPaulo. Stockholm Environment Institute, Sweden, 36(6): 4–11, 40–50.
National Malaria Eradication Programme Report, 1999, New Delhi.Park K., 1997: Park’s text book of preventive and social medicine. Fifth
edition. Banarsidas Bhanot Publishers, Jabalpur.Rahman A., 1998: Household environment and health. B.R. Publishers,
New Delhi.Report on the Adhoc Committee on Remote Sensing, 1977: Resource sens-
ing from space prospects for developing countries, National Academy ofSciences, Washington D.C.
Singh A.L., Siddiqui R.H. and Aziz A., 1995: Aligarh environment studyproject. IIED, London.
Singh A.L., Fazal S., Azam S.F. and Rahman A., 1996: Income, environ-ment and health: a household level study of Aligarh city, India. HabitatIntern., 29(1): 77–91.
Singh A.L. and Rahman, A. 1999: Household water supply, sanitation con-ditions and the occurrence of diarrhoea/dysentery in Aligarh city. In:Singh A.L. (ed.), Resources Management. B.R. Publishers, New Delhi.
Stephens C. and Harpham T., 1991: Environment and health in poor urbanareas of developing countries towards measurement at household level.Stockholm Environment Institute, Sweden.
Songsore J. and McGranahan G., 1993: Environment, wealth and health,towards an analysis of intra-urban differentials within Greater Accrametropolitan area. Environ. Urb., 5: 10–34.
Times of India, 1998, New Delhi.WHO 1988: Urban vector pest control. Technical report series no. 167.
Geneva.




















