
M ore than prim ary stability. - Implant Practice US
68
More than primary stability. The new tapered standard. Learn more about the Bone Level Tapered Implant at www.straumann.us/blt 800/448 8168 PAYING SUBSCRIBERS EARN 24 CONTINUING EDUCATION CREDITS PER YEAR! clinical articles • management advice • practice profiles • technology reviews October/November 2015 – Vol 8 No 5 PROMOTING EXCELLENCE IN IMPLANTOLOGY Practice profile Dr. John Crisler Ridge preservation in a case of severe periodontitis Drs. Roberto Rossi, Ulf Nannmark, Andrea Pilloni, and Nino Squadrito, CDT Surgery in prevention of inferior alveolar nerve damage Drs. Lira Rahman, Jacobus Hercules van den Heever, and Andre W. van Zyl Reconstruction of resected jaw assisted by 3D technologies Dr. Ronald Delmanto Step-by-Step Clinical Versatility of Osseodensification
-
Upload
khangminh22 -
Category
Documents
-
view
4 -
download
0
Transcript of M ore than prim ary stability. - Implant Practice US
More than prim
ary stability. The new
tapered standard.
Learn more about the
Bone Level Tapered Implant at
www.straumann.us/blt
800/448 8168
PAYING SUBSCRIBERS EARN 24 CONTINUING EDUCATION CREDITS PER YEAR!
clinical articles • management advice • practice profiles • technology reviews
October/November 2015 – Vol 8 No 5
P R O M O T I N G E X C E L L E N C E I N I M P L A N T O L O G Y
Practice profileDr. John Crisler
Ridge preservation in a case of severe periodontitisDrs. Roberto Rossi, Ulf Nannmark, Andrea Pilloni, and Nino Squadrito, CDT
Surgery in prevention of inferior alveolar nerve damageDrs. Lira Rahman, Jacobus Hercules van den Heever, and Andre W. van Zyl
Reconstruction of resected jaw assisted by 3D technologiesDr. Ronald Delmanto
Step-by-StepClinical Versatility of Osseodensification
PARTNERING WITH YOU IN THEADVANCEMENT OF OVERDENTURE TREATMENTBEST-IN-CLASS PRODUCTS. END-TO-END PATIENT SOLUTIONS.
Clinician preferredaround the globe.
STAY TUNEDfor the next generation
of the world’s leading
overdenture attachment
system coming in
JANUARY 2016!
Nearly 2 million satisfied patients.
ZEST Anchors, the global leader in products, education, and support for overdenture applications.
For more than 40 years, ZEST Anchors has been an innovator in the design and manufacturing of dental solutions for the treatment of fully or partially edentulous patients. We pioneered pivoting, self-aligning attachments that substantially reduced the damage caused by the improper seating of overdentures. Our flagship product, LOCATOR®, is a reliable restorative solution that the industry, clinician community, and patients have come to trust.
Today, ZEST Anchors continues to make innovating our priority by introducing products and services that provide clinicians with more support for the treatment
of their edentulous patients. From exceptionally designed overdenture implant systems, to dental tools and materials for overdenture modification and processing. Along with our 10-year implant warranty and unmatched technical support, you can trust ZEST Anchors to offer you the ultimate end-to-end solutions for overdenture applications.
And we are just getting started!Take a closer look at all the ways ZEST Anchors can help you enhance your patients’ lives — and expand your client base. As you will see, it’s a beneficial partnership now, and for future cutting-edge innovations.
Contact us today at www.zestanchors.com/6 or call 800-262-2310©2015 ZEST Anchors LLC. All rights reserved. CHAIRSIDE, LOCATOR, and ZEST are registered trademarks and SATURNO is a trademark of ZEST IP Holdings, LLC. InPlace is a trademark of ZEST Anchors LLC.

We have all had the experience of purchasing something only to realize we have been duped. Whether we were intentionally
taken advantage of or just didn’t do our homework, the result is the same — we feel unfulfilled. The results don’t live up to the promises.
When dealing with purchases in the dental field, it is the support that most often makes the biggest difference. When you buy a dental implant surgical kit and some implants, you may find yourself in a situ-ation in which the person giving you surgical advice has never actually placed an implant. A weekend course on implant placement doesn’t always give you the answers you need during your surgery. The number and combinations of factors can be daunting.
Mentor is defined as “someone who guides another to success.” If there is someone who is doing something you would like to do, then who better to learn from? If you would like to learn to play the guitar, find a teacher who can guide you through the process. However, not every skilled person is a good mentor. It is important to find someone who “speaks to your listening.” In other words, it is important that the relationship is based on trust.
In the field of dentistry, there can be disagreement about either treatment recommended or treatment rendered. Some dentists feel they are in competition with their colleagues. The truth is, there is room for everyone to succeed, and cooperation among peers raises the profession as a whole. Patients hate to go to a new dentist and have him/her say that the treatment they received at the previous dentist was not done properly. It is good practice to refrain from criticizing a procedure to which you were not present. Rather, simply provide patients with the information they request from you. There are, of course, circumstances in which the standard of care has been grossly ignored. As a colleague once told me, “No matter how good we think we are, sometimes you just have a bad outcome.” It is our responsibility to minimize those “bad outcomes.”
In implant dentistry, the technical skill required is not as demanding as most of the proce-dures dentists perform every day. It is usually the case selection that causes problems for the inexperienced clinician. The sales pitch of the implant representative can hypnotize us into thinking that placement is as easy as a buccal pit. I find that nothing replaces preparation.
While looking for good continuing education relating to implant placement, it’s nice to have someone close to you to consult. It is a little unrealistic to expect your local oral surgeon to train you to do something he/she would rather do for you, but we all have an interest in personal growth. The surgeons expand their procedures to experience this personal growth. Why should we be any different? The important thing is that it needs to be done with the patient’s best interests in mind. If this is always kept in mind, the path to growth is much easier.
The idea of mentoring is that you have someone with whom you can consult to help with case evaluation and surgical techniques. Unfortunately, we don’t get to choose the implant cases that present at our office. It is of great value to have an experienced person at your disposal to help with individual cases. The value is in the ability of the experienced person to foresee possible problems and avoid unwanted outcomes. There may be cases in which the recommendation is to refer to the surgeon for placement, and the clinician can restore the case. Your patients come to you because they trust you; they would rather not go to another office if you can provide them with what they need.
Mentoring programs are a great way to provide the service your patients deserve.
Terry L. Work, DMD
Build your implant practice through mentoring
Dr. Terry Work earned a Bachelor of Science degree at the University of Oregon before continuing on to dental school at Oregon Health Sciences University. After joining the U.S. Navy, he served as a Navy Dental Officer for 4 years before setting up his private practice in Scottsdale, Arizona. He has more than 20 years of experience as a practicing dentist and is an Ambassador for Neodent USA, a global provider of dental implantology and tooth restoration solutions. He also lectures on implant placement and bone grafting techniques. Dr. Work is a member of the American Academy of Implant Dentistry, American Dental Association, and Arizona State Dental Association, and is a Diplomate of the International Congress of Oral Implantologists.
Terry L. Work, DMD
INT
RO
DU
CT
ION
October/November 2015 - Volume 8 Number 5
EDITORIAL ADVISORSSteve Barter BDS, MSurgDent RCS Anthony Bendkowski BDS, LDS RCS, MFGDP, DipDSed, DPDS, MsurgDent Philip Bennett BDS, LDS RCS, FICOI Stephen Byfield BDS, MFGDP, FICD Sanjay Chopra BDS Andrew Dawood BDS, MSc, MRD RCS Professor Nikolaos Donos DDS, MS, PhD Abid Faqir BDS, MFDS RCS, MSc (MedSci) Koray Feran BDS, MSC, LDS RCS, FDS RCS Philip Freiburger BDS, MFGDP (UK) Jeffrey Ganeles, DMD, FACD Mark Hamburger BDS, BChD Mark Haswell BDS, MSc Gareth Jenkins BDS, FDS RCS, MScD Stephen Jones BDS, MSc, MGDS RCS, MRD RCS Gregori M. Kurtzman, DDS Jonathan Lack DDS, CertPerio, FCDS Samuel Lee, DDS David Little DDS Andrew Moore BDS, Dip Imp Dent RCS Ara Nazarian DDS Ken Nicholson BDS, MSc Michael R. Norton BDS, FDS RCS(ed) Rob Oretti BDS, MGDS RCS Christopher Orr BDS, BSc Fazeela Khan-Osborne BDS, LDS RCS, BSc, MSc Jay B. Reznick DMD, MD Nigel Saynor BDS Malcolm Schaller BDS Ashok Sethi BDS, DGDP, MGDS RCS, DUI Harry Shiers BDS, MSc, MGDS, MFDS Harris Sidelsky BDS, LDS RCS, MSc Paul Tipton BDS, MSc, DGDP(UK) Clive Waterman BDS, MDc, DGDP (UK) Peter Young BDS, PhD Brian T. Young DDS, MS
CE QUALITY ASSURANCE ADVISORY BOARDDr. Alexandra Day BDS, VTJulian English BA (Hons), editorial director FMCDr. Paul Langmaid CBE, BDS, ex chief dental officer to the Government
for WalesDr. Ellis Paul BDS, LDS, FFGDP (UK), FICD, editor-in-chief Private
DentistryDr. Chris Potts BDS, DGDP (UK), business advisor and ex-head of
Boots Dental, BUPA Dentalcover, VirginDr. Harry Shiers BDS, MSc (implant surgery), MGDS, MFDS, Harley St
referral implant surgeon
PUBLISHER | Lisa MolerEmail: [email protected]
GENERAL MANAGER | Adrienne Good Email: [email protected]
MANAGING EDITOR | Mali Schantz-Feld Email: [email protected] | Tel: (727) 515-5118
ASSISTANT EDITOR | Elizabeth RomanekEmail: [email protected]
EDITORIAL ASSISTANT | Mandi GrossEmail: [email protected]
NATIONAL ACCOUNT MANAGER | Michelle Manning Email: [email protected]
CREATIVE DIRECTOR/PRODUCTION MANAGER | Amanda Culver Email: [email protected]
FRONT OFFICE MANAGER | Theresa JonesEmail: [email protected]
MedMark, LLC15720 N. Greenway-Hayden Loop #9Scottsdale, AZ 85260Tel: (480) 621-8955 Fax: (480) 629-4002Toll-free: (866) 579-9496 Web: www.implantpracticeus.com
www.medmarkaz.com
SUBSCRIPTION RATES1 year (6 issues) $99* 3 years (18 issues) $239* * plus shipping
© FMC 2013. All rights reserved. FMC is part of the specialist
publishing group Springer Science+ Business Media. The publisher’s written consent must be obtained before any part of this publication may be reproducedvw in any form whatsoever, including photocopies and information retrieval systems. While every care has been taken in the preparation of this magazine, the publisher cannot be held responsible for the accuracy of the information printed herein, or in any consequence arising from it. The views expressed herein are those of the author(s) and not necessarily the opinion of either Implant Practice or the publisher.
Volume 8 Number 5 Implant practice 1

Practice profile John Crisler, DDS, MAGDFulfillment through serving people
Case reportReconstruction of resected jaw assisted by 3D technologiesDr. Ronald Delmanto required creative
treatment planning for a patient after
jaw resection ..................................16
Case studyImmediate implant placement: cutting treatment time in halfDr. Charles D. Schlesinger illustrates
a case involving immediate implant
placement ......................................20
Seeing the lightThe 10.6 µm SuperPulse CO2 laser may alleviate the late implant failure linked to tissue tensionDrs. Jack Krauser and Peter Vitruk
explore soft tissue recession
prevention with the CO2 laser ......... 26Case study 12Post extraction, immediate placement and restoration in the mandible using Neodent Drive® implantsDr. M. John Matos discusses an immediate placement technique to
produce a desirable outcome
6
ON THE COVER
Cover photo courtesy of Versah. Article begins on page 54.
2 Implant practice Volume 8 Number 5
TABLE OF CONTENTS

Follow nature‘s contour
www.dentsplyimplants.com
DEN
TSPL
Y Im
plan
ts d
oes
not w
aive
any
rig
ht to
its
trade
mar
ks b
y no
t usi
ng th
e sy
mbo
ls ®
or ™
. 326
7083
7-U
S150
5 ©
201
5 D
ENTS
PLY
Impl
ants
. All
right
s re
serv
ed
OsseoSpeed™ Profile EV—A unique implant specifically designed for sloped ridges
OsseoSpeed Profile EV is specially designed for efficient use of existing bone in sloped ridge situations.
• Provides 360 degrees of bone preservationmaintaining soft tissue esthetics
• Can help to reduce the need for bone augmentation
• Components designed to allow for accurateidentification of the implant position throughoutthe treatment process
OsseoSpeed Profile EV is an integral part of the new ASTRA TECH Implant System™ EV and is supported by the unique ASTRA TECH Implant System BioManagement Complex.
For more information visit www.jointheev.com
Continuing education
Surgery in prevention of inferior alveolar nerve damageDrs. Lira Rahman, Jacobus Hercules
van den Heever, and Andre W. van
Zyl present the application of guided
dental implant surgery in prevention
of inferior alveolar nerve damage in a
patient with compromised bone
................................................41
Practice developmentFive foolproof ways to get a “yes” to more treatment plansDee Dee Reid discusses ways to help
patients get the dental care they need
.................................................44
Materials & equipment ....................... 47
Practice developmentTarget practiceIn the second part of his series on
marketing, Toks Oyegunle explains
how creating the perfect patient avatar
can help move your practice forward
.................................................48
Implant insightsImplant retention: making the right choiceDr. Peter Sanders explores the pros
and cons of screw-, cement-, and
friction-retained restorations and
explains the appropriate methods
of all three .................................. 50
Step-by-step
Clinical Versatility of Osseodensification................54
ATLANTIS™ patient-specific solutions ................................. 56
A micro-thin forceps and simplified method for the placement of tunnel connective tissue grafts.................................................58
Industry news
...................................................... 59
Product profileSalvin® Renovix® Guided Healing Collagen Membrane.................................................60
On the horizon
Mentorship, more important than ever!Dr. Justin Moody reflects on the
importance of inspiring others .......62
AAID update
AAID Annual Conference blends classic with cutting edge ................................................64
Continuing educationRidge preservation in a case of severe periodontitisDrs. Roberto Rossi, Ulf Nannmark, Andrea Pilloni, and Nino Squadrito, CDT,
demonstrate how to preserve and condition the soft tissue with a combined
approach
34
4 Implant practice Volume 8 Number 5
TABLE OF CONTENTS

To learn more about how to work with our Patented Immediate Load Technology & Dual Stabilization® Implant Line, call 800-228-0477 or email us at [email protected].
Our products are designed by dentists for dentists, just like you!
Order Today! [email protected] Improves Your Dentistry
800-228-0477Complete Implant Solutions
PROVEN Immediate Load TechnologyWhether you want your patient to go home with a temporary crown, or have them wait during a conventional healing period, the TSI is designed and patented to give you that choice.
The TSI’s patented implant body with its 2mm Embedded Tapered Platform™, Bull Nose Auger™ tip, Mini Cortic-O™ threads and SLA surface provides the perfect support for all your restorative needs, whether they be a single restoration or a full mouth reconstruction.
See the TSI in action on page 20!
40min
Dental Implant with Provisional Restoration in 40 Minutes!
What can you tell us about your background?
I grew up in Anderson, Indiana, and was born and raised as a Hoosier. It was a great place to grow up. I learned to love outdoor activities with lots of camping and became an Eagle Scout. I attended Indiana University in Bloomington and graduated in Biological Sciences and Psychology in 1973. I attended Indiana University School of Dentistry in Indianapolis and graduated in 1977. I had several uncles who were physicians, and I knew I wanted to go into some field of medi-cine. Dentistry seemed to be just the right fit.
My high school girlfriend and wife of 38 years and I reacquainted while I was in dental school. We married 1 month after graduation, packed up a U-Haul®, and moved west to the Navajo Indian Reserva-tion in Window Rock, Arizona. I served with the Indian Health Service, U.S. Public Health Service for the next 3 years as a Facility
Dental Officer in a unique and fascinating cultural environment.
By then the West had grown on us, and we wouldn’t turn back. I established a private general dentistry practice in Rio Rancho, New Mexico, contiguous with Albuquerque, fueled with a 1980 bank loan with an interest rate of 24.25%. (Ouch!)
Is your practice limited solely to implants, or do you practice other types of dentistry?
I practice comprehensive dentistry and utilize implants as an integral part of my treat-ment planning. A significant part of my prac-tice is reconstruction using the principles of Orognathic Bioesthetics International (OBI).
Why did you decide to focus on implant dentistry?
I began restoring dental implants in 1984 after attending training at a Brånemark
course. A periodontist began using my office as a satellite in the 1980s, and he was placing the IMZ® implants with its intra-mobile element developed by Axel Kirsch in Germany. I saw the great opportunity to help patients with both fixed and removable dental prosthetics using implants, and I have developed my continuing education and training in that direction since then.
John Crisler, DDS, MAGD
Fulfillment through serving people
New Mexico Mission of Mercy
Dr. John Crisler
6 Implant practice Volume 8 Number 5
PRACTICE PROFILE

Long working time for you.Short setting time for them.
3M, ESPE, Imprint and Penta are trademarks of 3M or 3M Deutschland GmbH. Used under license in Canada. © 3M 2015. All rights reserved. 1. 3M ESPE internal data
Imprint™ 4 VPS Impression Material
The material that gives you more control for accurate results … and improves the patient experience.
• All the working time you need—no stressful race againstthe clock. Adequate working time is a factor for avoidingproblems and for making good impressions.
• The fastest intra-oral setting time on the market.1
Noticeably reduces chair time and stress for patients—without reducing the precision of your impressionresults. Available in Super Quick set (75 seconds) orRegular set (2 minutes).
www.3MESPE.com/Imprint4

Do your patients come through referrals?
We frequently receive referrals from existing patients, other dental professionals, and the State of New Mexico Workers’ Compensation Program, where I have helped people from all over our large state, primarily with TMJ-related injury issues. Many of these patients have benefited from implant-retained restorations.
How long have you been practicing implant dentistry, and what systems do you use?
I have been restoring dental implants for 31 years, and I began placing dental implants 13 years ago. I have accumulated no less than 15 different surgical and restorative systems during that time. I have had the most success with the internal connection systems. I currently use the Ossotanium implant system, which uses nanoparticle titanium implants. These implants are twice as strong as implants using conventional titanium, and the osseo-integration time and loading times are signifi-cantly reduced. This facilitates immediate loading and temporization, a much appreci-ated advantage to patients over removable appliances for temporization, especially in the esthetic zone. The Ossotanium system also offers bone level, tissue level, one-piece, and mini implants. We have been able to offer immediate temporization through immediate loading, utilizing the system’s temporary abut-ments and sleeves to fabricate provisional restorations.
What training have you undertaken?I have been an avid believer in continuing
education ever since graduation from dental school. I have sought and achieved Fellow-ship and Mastership in the Academy of General Dentistry and have completed over 3,000 hours of continuing dental education. Membership and training in courses offered by the AAID have also been very valuable to me. I was fortunate to have Dr. Walter Schuman, a principal with the BASIC Dental Implant System, mentor me and coach me in the actual placement of my first implants in my office. For the last 10 years, the greatest and most valuable source of my hands-on training has been through the New Mexico Dental Implant Study Club, which I helped initiate. Our study club has up to eight members at a time, and we meet 8 times per year, for treatment planning and surgical sessions. We have been privileged to have the mentorship and support of Dr. Steven Holbrook since our inception.
Who has inspired you?My personal inspiration has come from
my faith and clergy over the years who have guided me along the path of serving my fellow man with my God-given ability to help other people. Professionally, Dr. Steven Holbrook has been a great inspiration and mentor with his seemingly boundless energy and enthusiasm toward excellence in dental implantology.
What is the most satisfying aspect of your practice?
The heartfelt thanks and show of appre-ciation from patients whom we have served are the most satisfying aspects of my prac-tice. Dr. Albert Schweitzer said, “I don’t know what your destiny will be, but one thing I know; the only ones among you who will be really happy are those who will have sought and found how to serve.”
Professionally, what are you most proud of?
I have many patients who have placed their trust in me since the early 1980s when I opened my private practice. As I have acquired new technologies, and as the science of implantology has grown, I have been able to offer the benefits of implants
to an increasing number of patients. My patients now have children and grand- children who still consider me their dentist. I am also proud of the relationships I have devel-oped and nurtured with dental colleagues and specialists, as well as with my wonderful staff. I served as a Co-Chairman for the 2014 New Mexico Mission of Mercy, a large-scale, 2-day free dental clinic that provided just over $1 million of dental treatment. In 2 days of joyful giving, 1,344 volunteers, including dentists, hygienists, assistants, and commu-nity volunteers, served 1,055 patients with 8,633 procedures.
What do you think is unique about your practice?
We have a beautiful location with our operatories and balcony looking out over the Rio Grande Valley and onto the Sandia Mountains. We offer comprehensive care utilizing the diagnostic and reconstructive principles of Orognathic Bioesthetics Inter-national (OBI). We take the time to educate patients about ideal or optimum treatment after listening to their concerns, goals, and factors that influence their decisions about treatment. When patients have missing teeth, we offer them the same treatment we would want for ourselves and our families.
Front desk
Dr. Crisler and staff — Elisa, Marta, Leigh, Megan, Shaelee
Sandia Mountains
8 Implant practice Volume 8 Number 5
PRACTICE PROFILE

More than primary stability.
The new tapered standard.
In combination with:
1 Benic GI, Gallucci GO, Mokti M, Hämmerle CH, Weber HP, Jung RE. Titanium-zirconium narrow-diameter versus titanium regular diameter implants for anterior and premolar single crowns: 1-year results of a randomized controlled clinical study. Journal of Clinical Periodontology 2013 Nov;40(11):1052–61. Epub 2013 Sep 8.
Flexibility in challenging clinical and anatomical situations – the Straumann® Bone Level Tapered Implant:
• Roxolid® material – Permits the use of smaller-diameter implants with the same clinical performance as regular-diameter titanium implants1
• SLActive® surface – Designed to maximize treatment success and predictability in stability critical treatment protocols
• Apically tapered – Overcomes anatomical restrictions and is designed to enable placement in under-prepared sites
• Crossfit® Connection – Delivers simplified handling and assurance that the abutment is seated properly
straumann.us/blt

What has been your biggest challenge?
Balance and harmony in life are very important. It is easy for me to enjoy our profession so much that the other compo-nents of love, recreation, family, friends, and faith do not get an adequate share of time.
What would you have been if you had not become a dentist?
I think I would have enjoyed being an electronics engineer because of my love for gadgets. With the amazing improvements and technology in digital photography, I may still become a professional travel photog-rapher. But for now, I’m still getting a lot of enjoyment from the practice of dentistry.
What is the future of implants and dentistry?
I think we will see much more utilization of the nanoparticle-structured titanium implants because of their greater strength and faster integration time, which will permit us to provide excellent service in a shorter period of time. As patients become more educated about the benefits of dental implants in general, more demand will occur for the services of qualified and trained general-ists and specialists who can provide these services.
What are your top tips for maintaining a successful practice?
I imagine myself sitting in the dental chair every time I treat a patient. Whether I’m giving a super-gentle injection or discussing a potential treatment plan with a patient, I
want to treat patients with the same respect and dignity I would want for myself. I am currently blessed with having the best staff of my career in dentistry. They frequently speak of their appreciation for me, and I try to reciprocate with praise for a job well done to them. So much of the success of a dental practice depends on having a great supportive staff. I love going to work and treating people with the help of my dental family.
What advice would you give to a budding implant dentist?
Challenge yourself to move forward with your education and experience in implant dentistry. Ralph Waldo Emerson said, “Unless you try to do something beyond what you have already mastered, you will never grow.” Go to implant courses and participation training with different systems. Even though each system has its own unique qualities and selling points, you will discover and be reinforced by the commonalities among them. Find a mentor for support and learning, which is always a two-way street. Find a dental lab that gives you great support for implant cases. I have been blessed with having the support of two great labs in New Mexico — Esthetic Dental Arts laboratory and New West Dental Lab.
What are your hobbies, and what do you do in your spare time?
My wife and I have enjoyed traveling to many parts of the world, and we have many more to see. Planning our trips is an ongoing
pleasure in our spare time. I enjoy photog-raphy, and this has been an important part of our travels, internationally as well as within the United States, and our beautiful Land of Enchantment, New Mexico. We enjoy cruising both on river ships throughout the world and on oceangoing cruise ships. I had the pleasure of working with Holland America Line in the SeaDentist program for two or three cruises per year for 5 years, cruising in many parts of the world and doing dentistry onboard the ships. SCUBA diving has been an enjoyable hobby of mine since I was a teenager. Our yearly trips to Mexico include diving excursions.
Red Square, Moscow, Russia Dr. Crisler and family
Diving in Mexico
Top 10 favorites1. Time with my growing family2. Ossotanium implants3. World travel4. Digital photography5. Indiana Hoosiers6. Telescopes with illumination7. PreXion imaging for treatment planning8. Our Land of Enchantment, New Mexico9. DEXIS™ digital radiography 10. My wonderful staff
10 Implant practice Volume 8 Number 5
PRACTICE PROFILE
IP
Soft from the syringe.Hard in the defect.Prep. Dispense. Shape.
Placing bone graft has never been this easy. Once the coated granules of GUIDOR® easy-graft® are syringed into the bone defect and come in contact with blood, they change in approximately one minute from a moldable material to a rigid, porous scaffold.
• Designed for ease of useand predictability
• 100% synthetic andfully resorbable
• Ideal for ridge preservation andfilling voids around immediate implantplacements
This product should not be used in pregnant or nursing women.
easy-graft® CLASSICalloplastic bone grafting system
Want a demo? Sign up for a Sunstar representative visit at www.guidor.com/appointment or
To purchase or learn more, visit GUIDOR.com/easy-graft/ or call 1-877-484-3671. Instructions for Use (IFU), including indications, contraindications, precautions and potential adverse effects, are available at GUIDOR.com/IFU/.© 2015 Sunstar Americas, Inc. All rights reserved. GDR15041 07012015v1GUIDOR is a registered trademark of Sunstar Suisse, SA. easy-graft is a registered trademark of Degradable Solutions AG.
Visit the Sunstar booth at upcoming trade shows: AAOMS in Washington, DC (#846); ADA in Washington, DC (#1800); AAP in Orlando, FL (#1000); GNYDM in NY, NY (#3828)
IntroductionImmediate placement can produce
esthetic and functional comfort,1 while also preserving the width and height of the alveolar bone and providing a patient with a reduction in treatment time and expense. The following case demonstrates the preferred outcome to multiple tooth extractions using the imme-diate placement and loading technique.
Patient presentationA 49-year-old male presented to the
office with obvious advanced periodontal issues that were limited to the mandibular anterior teeth. The teeth were no longer func-tional due to increased mobility, significant flare, and patient discomfort. The patient had a medical history of atrial fibrillation, a knee arthroscopy without complications, hyper-tension, and hyperlipidemia. The patient had no known drug allergies and was taking sotalol, diltiazem, pravastatin, and lisinopril.
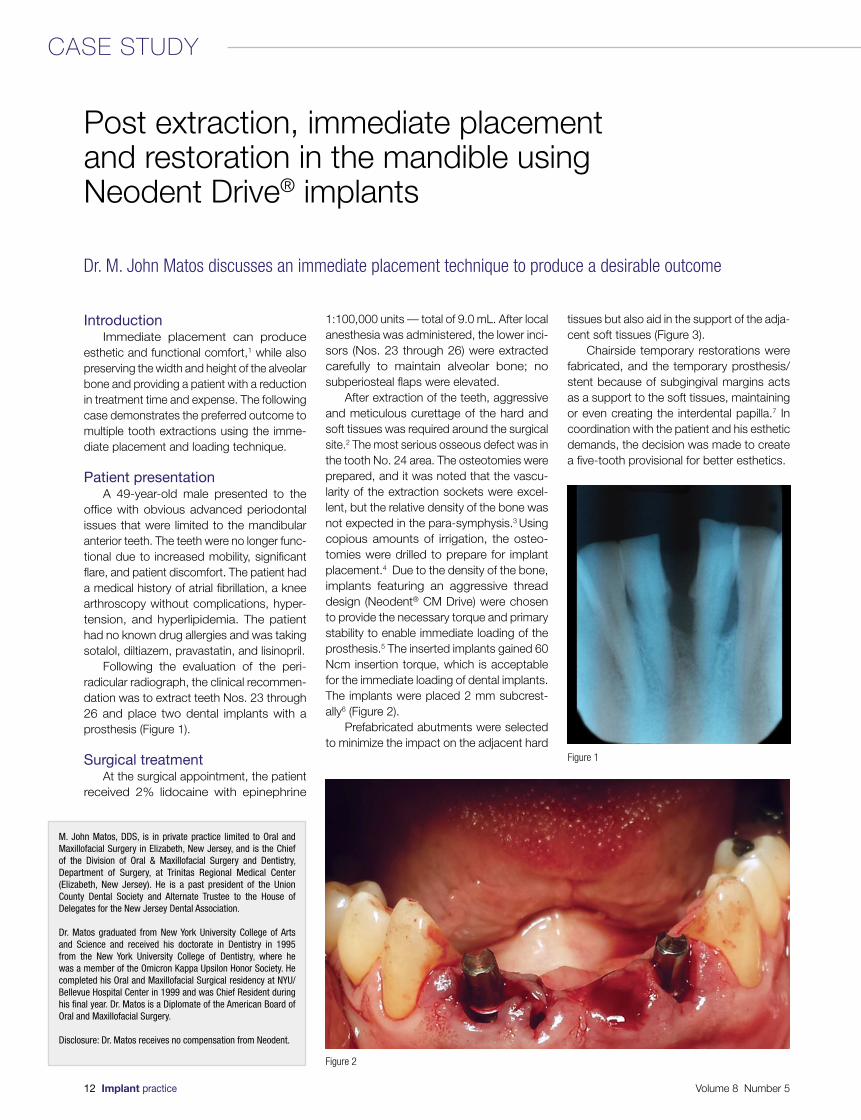
Following the evaluation of the peri- radicular radiograph, the clinical recommen-dation was to extract teeth Nos. 23 through 26 and place two dental implants with a prosthesis (Figure 1).
Surgical treatmentAt the surgical appointment, the patient
received 2% lidocaine with epinephrine
1:100,000 units — total of 9.0 mL. After local anesthesia was administered, the lower inci-sors (Nos. 23 through 26) were extracted carefully to maintain alveolar bone; no subperiosteal flaps were elevated.
After extraction of the teeth, aggressive and meticulous curettage of the hard and soft tissues was required around the surgical site.2 The most serious osseous defect was in the tooth No. 24 area. The osteotomies were prepared, and it was noted that the vascu-larity of the extraction sockets were excel-lent, but the relative density of the bone was not expected in the para-symphysis.3 Using copious amounts of irrigation, the osteo- tomies were drilled to prepare for implant placement.4 Due to the density of the bone, implants featuring an aggressive thread design (Neodent® CM Drive) were chosen to provide the necessary torque and primary stability to enable immediate loading of the prosthesis.5 The inserted implants gained 60 Ncm insertion torque, which is acceptable for the immediate loading of dental implants. The implants were placed 2 mm subcrest-ally6 (Figure 2).
Prefabricated abutments were selected to minimize the impact on the adjacent hard
tissues but also aid in the support of the adja-cent soft tissues (Figure 3).
Chairside temporary restorations were fabricated, and the temporary prosthesis/stent because of subgingival margins acts as a support to the soft tissues, maintaining or even creating the interdental papilla.7 In coordination with the patient and his esthetic demands, the decision was made to create a five-tooth provisional for better esthetics.
Post extraction, immediate placement and restoration in the mandible using Neodent Drive® implants
Dr. M. John Matos discusses an immediate placement technique to produce a desirable outcome
M. John Matos, DDS, is in private practice limited to Oral and Maxillofacial Surgery in Elizabeth, New Jersey, and is the Chief of the Division of Oral & Maxillofacial Surgery and Dentistry, Department of Surgery, at Trinitas Regional Medical Center (Elizabeth, New Jersey). He is a past president of the Union County Dental Society and Alternate Trustee to the House of Delegates for the New Jersey Dental Association.
Dr. Matos graduated from New York University College of Arts and Science and received his doctorate in Dentistry in 1995 from the New York University College of Dentistry, where he was a member of the Omicron Kappa Upsilon Honor Society. He completed his Oral and Maxillofacial Surgical residency at NYU/Bellevue Hospital Center in 1999 and was Chief Resident during his final year. Dr. Matos is a Diplomate of the American Board of Oral and Maxillofacial Surgery.
Disclosure: Dr. Matos receives no compensation from Neodent.
Figure 1
Figure 2
12 Implant practice Volume 8 Number 5
CASE STUDY
Select from a wide range of prosthetic
options for an aesthetic result
All CM Implants feature a reliable Platform
Switching designA variety of implantdiameters with oneconnection size
Ask about our Acqua Product Line featuring an innovative hydrophilic surface
A Morse Taper connection for a secure
and confident fit
For more than 20 years Neodent has invested in continuous research and product development to help you offer the best standard of care. Contact us today and ask about our new lines of hydrophilic and zygomatic implants along with our new Ti Base prosthetic components.
© Copyright 2015 All rights reserved.
www.instradent.us
We put innovation and confidence in your hands
Continuous Innovations and a 96.5 % Success Rateare only Some of the Reasons Why More Than
30,000 Dentists Choose Neodent.
Visit booth #801 at the AAI D Annual Conference in October for live in-booth demonstrations. You can also call 855/412-8883 or visit www.instradent.us.
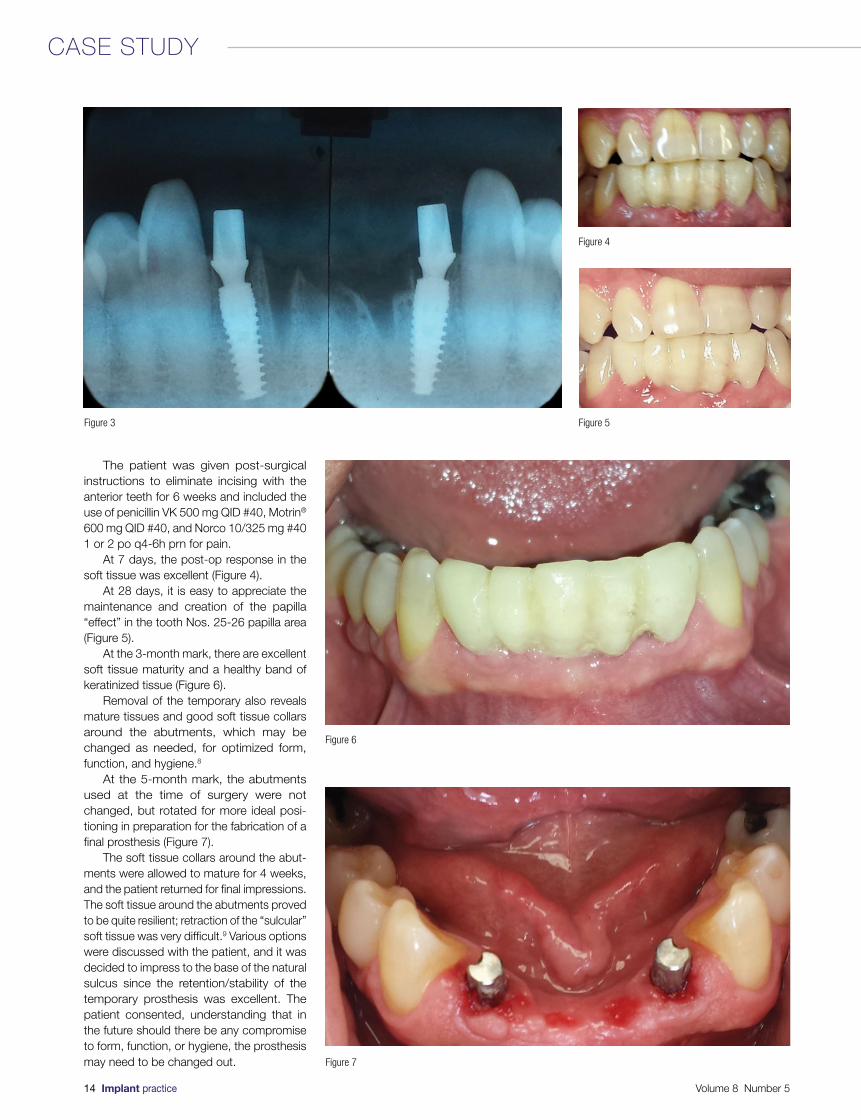
The patient was given post-surgical instructions to eliminate incising with the anterior teeth for 6 weeks and included the use of penicillin VK 500 mg QID #40, Motrin® 600 mg QID #40, and Norco 10/325 mg #40 1 or 2 po q4-6h prn for pain.
At 7 days, the post-op response in the soft tissue was excellent (Figure 4).
At 28 days, it is easy to appreciate the maintenance and creation of the papilla “effect” in the tooth Nos. 25-26 papilla area (Figure 5).
At the 3-month mark, there are excellent soft tissue maturity and a healthy band of keratinized tissue (Figure 6).
Removal of the temporary also reveals mature tissues and good soft tissue collars around the abutments, which may be changed as needed, for optimized form, function, and hygiene.8
At the 5-month mark, the abutments used at the time of surgery were not changed, but rotated for more ideal posi-tioning in preparation for the fabrication of a final prosthesis (Figure 7).
The soft tissue collars around the abut-ments were allowed to mature for 4 weeks, and the patient returned for final impressions. The soft tissue around the abutments proved to be quite resilient; retraction of the “sulcular” soft tissue was very difficult.9 Various options were discussed with the patient, and it was decided to impress to the base of the natural sulcus since the retention/stability of the temporary prosthesis was excellent. The patient consented, understanding that in the future should there be any compromise to form, function, or hygiene, the prosthesis may need to be changed out.
Figure 3
Figure 4
Figure 5
Figure 6
Figure 7
14 Implant practice Volume 8 Number 5
CASE STUDY

The prosthesis was delivered with a knife-edge collar design with the intent of not violating the soft tissue that matured around the abutment since the time of placement and then rotation10 (Figure 8).
The patient was very pleased with all aspects of treatment and the final outcome and content with the design in both form and occlusion (function). The soft tissues are beautiful in their color, contour, and surface/keratinization — there is maintenance of the bone and excellent “fill” in the defect that was seen in the area of tooth No. 24 during extraction (Figure 9).
Figure 8 Figure 9
REFERENCES
1. Wöhrle PS . Single-tooth replacement in the aesthetic zone with immediate provisionalization: fourteen consecutive case reports. Pract Periodontics Aesthet Dent. 1998; 10(9):1107-1114.
2. da Rosa Jc, Rosa AC, Fadanelli MA, Sotto-Maior BS. Immediate implant placement, reconstruction of compromised sockets, and repair of gingival recession with a triple graft from the maxillary tuberosity: a variation of the immediate dentoalveolar restoration technique. J Prosthet Dent. 2014;112(4):717-722.
3. Möhlhenrich SC, Modabber A, Steiner T, Mitchell DA, Hölzle F. Heat generation and drill wear during dental implant site prepara-tion: systematic review. Br J Oral Maxillofac Surg. 2015;Jun 4 epub ahead of print. doi: 10.1016/j.bjoms.2015.05.004.
4. Bullon B, Bueno EF, Herrero M, Fernandez-Palacin A, Rios JV, Bullon P, Gil FJ. Effect of irrigation and stainless steel drills on dental implant bed heat generation. J Mater Sci Mater Med. 2015;26(2):75.
5. Javed F, Ahmed HB, Crespi R, and Romanos GE. Role of primary stability for successful osseointegration of dental implants: Factors of influence and evaluation. Interv Med Appl Sci. 2013;5(4):162–167.
6. Castro DS, Araujo MA, Benfatti CA, Araujo Cdos R, Piattelli A, Perrotti V, Iezzi G. Comparative histological and histomorpho-metrical evaluation of marginal bone resorption around external hexagon and Morse cone implants: an experimental study in dogs. Implant Dent. 2014;23(3):270-276.
7. Moy PK, Parminter PE. Chairside preparation of provisional restorations. J Oral Maxillofac Surg. 2005;63(9 Suppl 2):80-88.
8. Palacci P, Nowzari H. Soft tissue enhancement around dental implants. Periodontol 2000. 2008; 47:113–132.
9. Phatale S, Marawar PP, Byakod G, Lagdive SB, Kalburge JV. Effect of retraction materials on gingival health: A histopathological study. J Indian Soc Periodontol. 2010;14(1): 35–39.
10. DeHoff PH, Anusavice KJ. Effect of metal design on marginal distortion of metal-ceramic crowns. J Dent Res.1984;63(11):1327-1331.
7 BITS FREEWITH PURCHASE OF RIGHT ANGLED
DRIVER AND TORQUE ADAPTER
Volume 8 Number 5 Implant practice 15
CA
SE
ST
UD
Y
IP
When a patient named Al visited his general dentist several years ago,
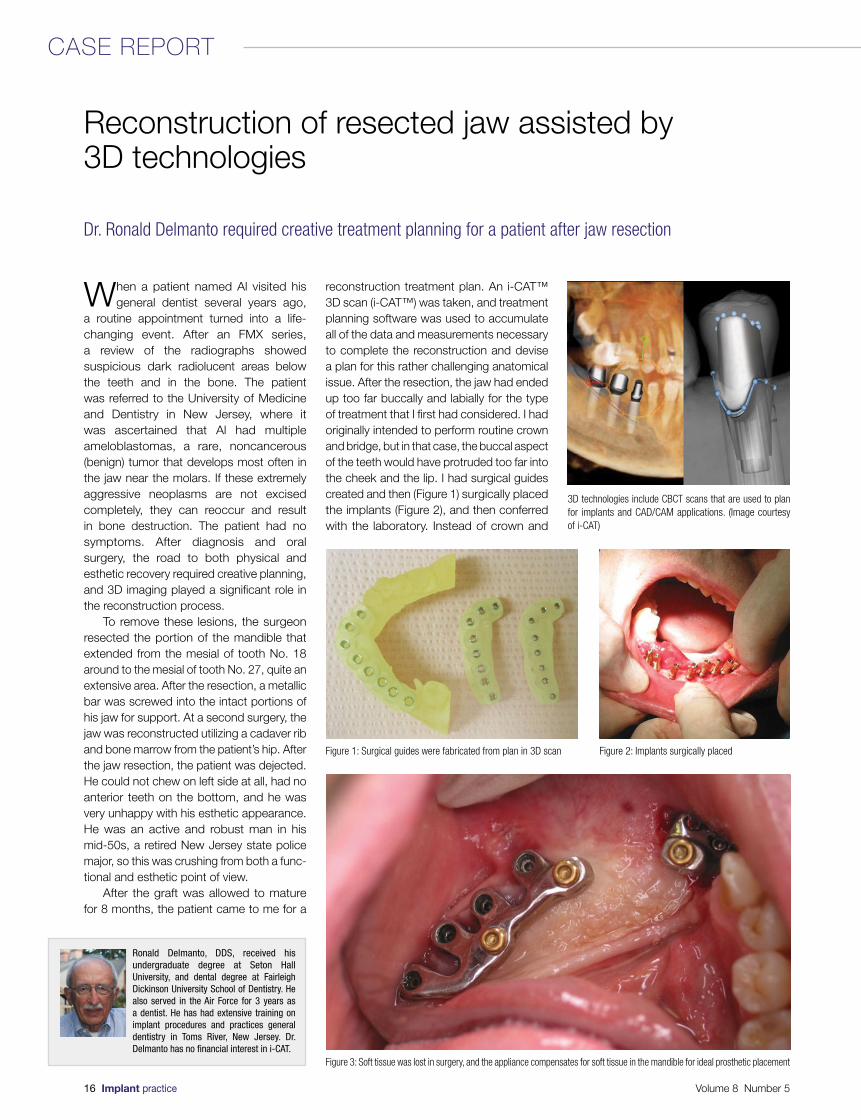
a routine appointment turned into a life-changing event. After an FMX series, a review of the radiographs showed suspicious dark radiolucent areas below the teeth and in the bone. The patient was referred to the University of Medicine and Dentistry in New Jersey, where it was ascertained that Al had multiple ameloblastomas, a rare, noncancerous (benign) tumor that develops most often in the jaw near the molars. If these extremely aggressive neoplasms are not excised completely, they can reoccur and result in bone destruction. The patient had no symptoms. After diagnosis and oral surgery, the road to both physical and esthetic recovery required creative planning, and 3D imaging played a significant role in the reconstruction process.
To remove these lesions, the surgeon resected the portion of the mandible that extended from the mesial of tooth No. 18 around to the mesial of tooth No. 27, quite an extensive area. After the resection, a metallic bar was screwed into the intact portions of his jaw for support. At a second surgery, the jaw was reconstructed utilizing a cadaver rib and bone marrow from the patient’s hip. After the jaw resection, the patient was dejected. He could not chew on left side at all, had no anterior teeth on the bottom, and he was very unhappy with his esthetic appearance. He was an active and robust man in his mid-50s, a retired New Jersey state police major, so this was crushing from both a func-tional and esthetic point of view.
After the graft was allowed to mature for 8 months, the patient came to me for a
reconstruction treatment plan. An i-CAT™ 3D scan (i-CAT™) was taken, and treatment planning software was used to accumulate all of the data and measurements necessary to complete the reconstruction and devise a plan for this rather challenging anatomical issue. After the resection, the jaw had ended up too far buccally and labially for the type of treatment that I first had considered. I had originally intended to perform routine crown and bridge, but in that case, the buccal aspect of the teeth would have protruded too far into the cheek and the lip. I had surgical guides created and then (Figure 1) surgically placed the implants (Figure 2), and then conferred with the laboratory. Instead of crown and
Reconstruction of resected jaw assisted by 3D technologies
Dr. Ronald Delmanto required creative treatment planning for a patient after jaw resection
Ronald Delmanto, DDS, received his undergraduate degree at Seton Hall University, and dental degree at Fairleigh Dickinson University School of Dentistry. He also served in the Air Force for 3 years as a dentist. He has had extensive training on implant procedures and practices general dentistry in Toms River, New Jersey. Dr. Delmanto has no financial interest in i-CAT.
3D technologies include CBCT scans that are used to plan for implants and CAD/CAM applications. (Image courtesy of i-CAT)
Figure 1: Surgical guides were fabricated from plan in 3D scan Figure 2: Implants surgically placed
Figure 3: Soft tissue was lost in surgery, and the appliance compensates for soft tissue in the mandible for ideal prosthetic placement
16 Implant practice Volume 8 Number 5
CASE REPORT

Q U A L I T Y, C O M PAT I B L E I M P L A N T S. U N B E ATA B L E VA L U E.
infinity TRI-CAM $149.99
NobelReplace® Tapered
MSRP $399*
infinity OCTAGON TL
$169.99
Straumann® Standard Plus
MSRP $355*
infinity INTERNAL HEX
$149.99
Zimmer Screw-Vent® MSRP $412*
infinity EXTERNAL HEX
$149.99
Brånemark System®
MSRP $399*
infinity OCTAGON BL
$169.99
Straumann® Bone LevelMSRP $355*
www.acesurgical.com • 800.441.3100
BUILT TO EXCITE YOUR REFERRALS. PRICED TO EXCITE YOUR PATIENTS.
infinity Dental Implant Systems are built to respect the relationship between your practice and your referring dentists. We understand the importance of delivering a truly compatible solution for your entire clinical network without having to over-pay for it. From surgical placement to final restoration, you can be assured that every infinity Dental Implant System will deliver quality, compatibility, and value to your implant practice.
To learn more, visit our website www.acesurgical.com or call to speak with one of our implant specialists at 800.441.3100.
PURCHASE ANY INFINITY IMPLANT
Be sure to visit ACE at theAAID • LAS VEGAS, NVBOOTH #708-710 • OCT. 21-24
Be sure to visit ACE at theAAP • ORLANDO, FLBOOTH #319 • NOV. 14-17
GET A HEALING ABUTMENT FREE*
* FREE Infinity Abutment of your choice and the Infinity Implant must be on the same order. Valid through November 2015. Price comparison based on 2014/2015 US list pricesfor comparable items by leading manufacturers. All trademarks are property of their respective owners. Copyright © 2015 ACE Surgical Supply Co., Inc., Brockton, MA U.S.A.
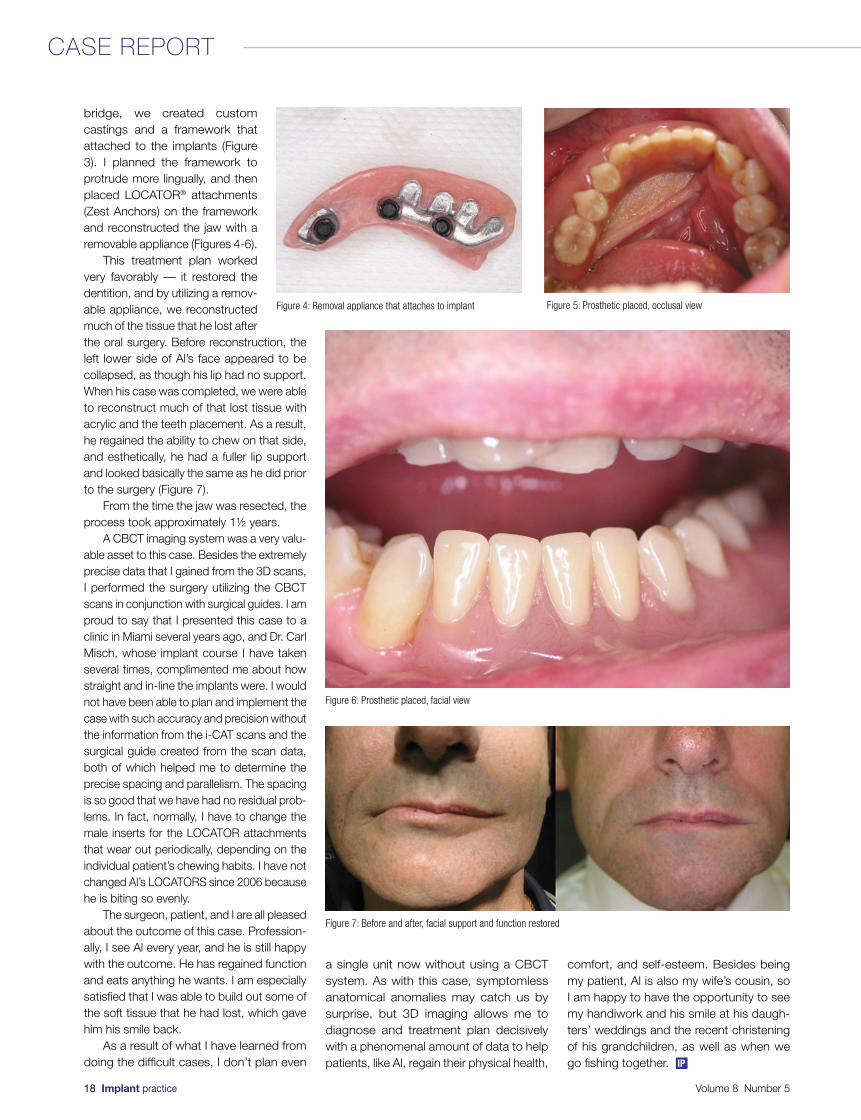
bridge, we created custom castings and a framework that attached to the implants (Figure 3). I planned the framework to protrude more lingually, and then placed LOCATOR® attachments (Zest Anchors) on the framework and reconstructed the jaw with a removable appliance (Figures 4-6).
This treatment plan worked very favorably — it restored the dentition, and by utilizing a remov-able appliance, we reconstructed much of the tissue that he lost after the oral surgery. Before reconstruction, the left lower side of Al’s face appeared to be collapsed, as though his lip had no support. When his case was completed, we were able to reconstruct much of that lost tissue with acrylic and the teeth placement. As a result, he regained the ability to chew on that side, and esthetically, he had a fuller lip support and looked basically the same as he did prior to the surgery (Figure 7).
From the time the jaw was resected, the process took approximately 1½ years.
A CBCT imaging system was a very valu-able asset to this case. Besides the extremely precise data that I gained from the 3D scans, I performed the surgery utilizing the CBCT scans in conjunction with surgical guides. I am proud to say that I presented this case to a clinic in Miami several years ago, and Dr. Carl Misch, whose implant course I have taken several times, complimented me about how straight and in-line the implants were. I would not have been able to plan and implement the case with such accuracy and precision without the information from the i-CAT scans and the surgical guide created from the scan data, both of which helped me to determine the precise spacing and parallelism. The spacing is so good that we have had no residual prob-lems. In fact, normally, I have to change the male inserts for the LOCATOR attachments that wear out periodically, depending on the individual patient’s chewing habits. I have not changed Al’s LOCATORS since 2006 because he is biting so evenly.
The surgeon, patient, and I are all pleased about the outcome of this case. Profession-ally, I see Al every year, and he is still happy with the outcome. He has regained function and eats anything he wants. I am especially satisfied that I was able to build out some of the soft tissue that he had lost, which gave him his smile back.
As a result of what I have learned from doing the difficult cases, I don’t plan even
a single unit now without using a CBCT system. As with this case, symptomless anatomical anomalies may catch us by surprise, but 3D imaging allows me to diagnose and treatment plan decisively with a phenomenal amount of data to help patients, like Al, regain their physical health,
comfort, and self-esteem. Besides being my patient, Al is also my wife’s cousin, so I am happy to have the opportunity to see my handiwork and his smile at his daugh-ters’ weddings and the recent christening of his grandchildren, as well as when we go fishing together.
Figure 4: Removal appliance that attaches to implant Figure 5: Prosthetic placed, occlusal view
Figure 6: Prosthetic placed, facial view
Figure 7: Before and after, facial support and function restored
18 Implant practice Volume 8 Number 5
CASE REPORT
IP
Immediate placement of dental implants has become a successful and dependable
treatment modality in today’s modern implant practice. One of the biggest advantages is the drastic decrease in overall treatment time for the patient. In today’s world of instant gratification, an average decrease in treatment time from 7-8 months in traditional extract/graft/wait/place/wait protocol to a much more palatable 3-4 months is a true practice builder. Though immediate temporization or restoration is the ultimate goal in mind when extracting a tooth, many times this does not constitute a prudent treatment plan. Factors to consider include primary stability sufficient enough to load, prosthetic considerations, and the size of the resulting extraction socket.
The success rate of immediate implant placement approaches the success rates of delayed placement1; therefore, with the right technique and the correct implant, this should be done as routine rather than the occasional treatment option.
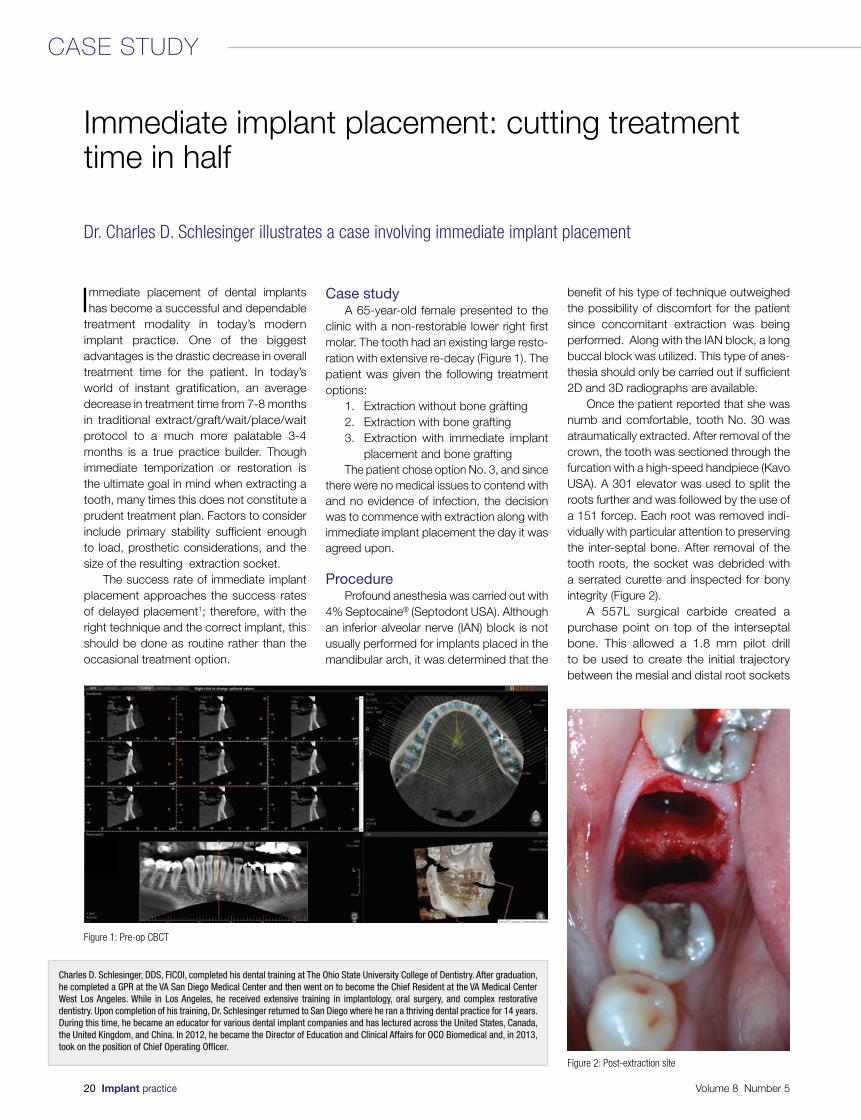
Case studyA 65-year-old female presented to the
clinic with a non-restorable lower right first molar. The tooth had an existing large resto-ration with extensive re-decay (Figure 1). The patient was given the following treatment options:
1. Extraction without bone grafting2. Extraction with bone grafting3. Extraction with immediate implant
placement and bone graftingThe patient chose option No. 3, and since
there were no medical issues to contend with and no evidence of infection, the decision was to commence with extraction along with immediate implant placement the day it was agreed upon.
ProcedureProfound anesthesia was carried out with
4% Septocaine® (Septodont USA). Although an inferior alveolar nerve (IAN) block is not usually performed for implants placed in the mandibular arch, it was determined that the
benefit of his type of technique outweighed the possibility of discomfort for the patient since concomitant extraction was being performed. Along with the IAN block, a long buccal block was utilized. This type of anes-thesia should only be carried out if sufficient 2D and 3D radiographs are available.
Once the patient reported that she was numb and comfortable, tooth No. 30 was atraumatically extracted. After removal of the crown, the tooth was sectioned through the furcation with a high-speed handpiece (Kavo USA). A 301 elevator was used to split the roots further and was followed by the use of a 151 forcep. Each root was removed indi-vidually with particular attention to preserving the inter-septal bone. After removal of the tooth roots, the socket was debrided with a serrated curette and inspected for bony integrity (Figure 2).
A 557L surgical carbide created a purchase point on top of the interseptal bone. This allowed a 1.8 mm pilot drill to be used to create the initial trajectory between the mesial and distal root sockets
Immediate implant placement: cutting treatment time in half
Dr. Charles D. Schlesinger illustrates a case involving immediate implant placement
Charles D. Schlesinger, DDS, FICOI, completed his dental training at The Ohio State University College of Dentistry. After graduation, he completed a GPR at the VA San Diego Medical Center and then went on to become the Chief Resident at the VA Medical Center West Los Angeles. While in Los Angeles, he received extensive training in implantology, oral surgery, and complex restorative dentistry. Upon completion of his training, Dr. Schlesinger returned to San Diego where he ran a thriving dental practice for 14 years. During this time, he became an educator for various dental implant companies and has lectured across the United States, Canada, the United Kingdom, and China. In 2012, he became the Director of Education and Clinical Affairs for OCO Biomedical and, in 2013, took on the position of Chief Operating Officer.
Figure 1: Pre-op CBCT
Figure 2: Post-extraction site
20 Implant practice Volume 8 Number 5
CASE STUDY
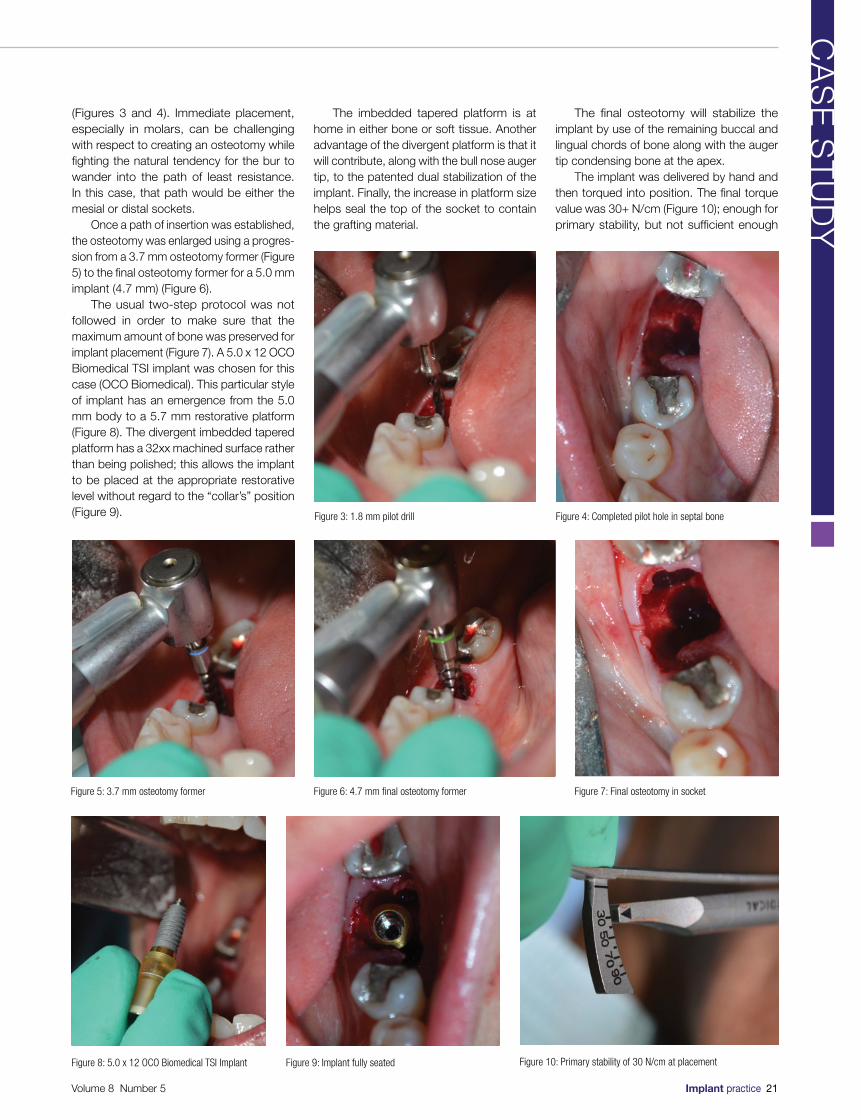
(Figures 3 and 4). Immediate placement, especially in molars, can be challenging with respect to creating an osteotomy while fighting the natural tendency for the bur to wander into the path of least resistance. In this case, that path would be either the mesial or distal sockets.
Once a path of insertion was established, the osteotomy was enlarged using a progres-sion from a 3.7 mm osteotomy former (Figure 5) to the final osteotomy former for a 5.0 mm implant (4.7 mm) (Figure 6).
The usual two-step protocol was not followed in order to make sure that the maximum amount of bone was preserved for implant placement (Figure 7). A 5.0 x 12 OCO Biomedical TSI implant was chosen for this case (OCO Biomedical). This particular style of implant has an emergence from the 5.0 mm body to a 5.7 mm restorative platform (Figure 8). The divergent imbedded tapered platform has a 32xx machined surface rather than being polished; this allows the implant to be placed at the appropriate restorative level without regard to the “collar’s” position (Figure 9).
The imbedded tapered platform is at home in either bone or soft tissue. Another advantage of the divergent platform is that it will contribute, along with the bull nose auger tip, to the patented dual stabilization of the implant. Finally, the increase in platform size helps seal the top of the socket to contain the grafting material.
The final osteotomy will stabilize the implant by use of the remaining buccal and lingual chords of bone along with the auger tip condensing bone at the apex.
The implant was delivered by hand and then torqued into position. The final torque value was 30+ N/cm (Figure 10); enough for primary stability, but not sufficient enough
Figure 3: 1.8 mm pilot drill Figure 4: Completed pilot hole in septal bone
Figure 5: 3.7 mm osteotomy former Figure 6: 4.7 mm final osteotomy former Figure 7: Final osteotomy in socket
Figure 8: 5.0 x 12 OCO Biomedical TSI Implant Figure 9: Implant fully seated Figure 10: Primary stability of 30 N/cm at placement
Volume 8 Number 5 Implant practice 21
CA
SE
ST
UD
Y
for immediate loading. In order to immediate load this implant, it would require at least 45 N/cm and/or at least an ISQ value of 64 with an Osstell meter.2
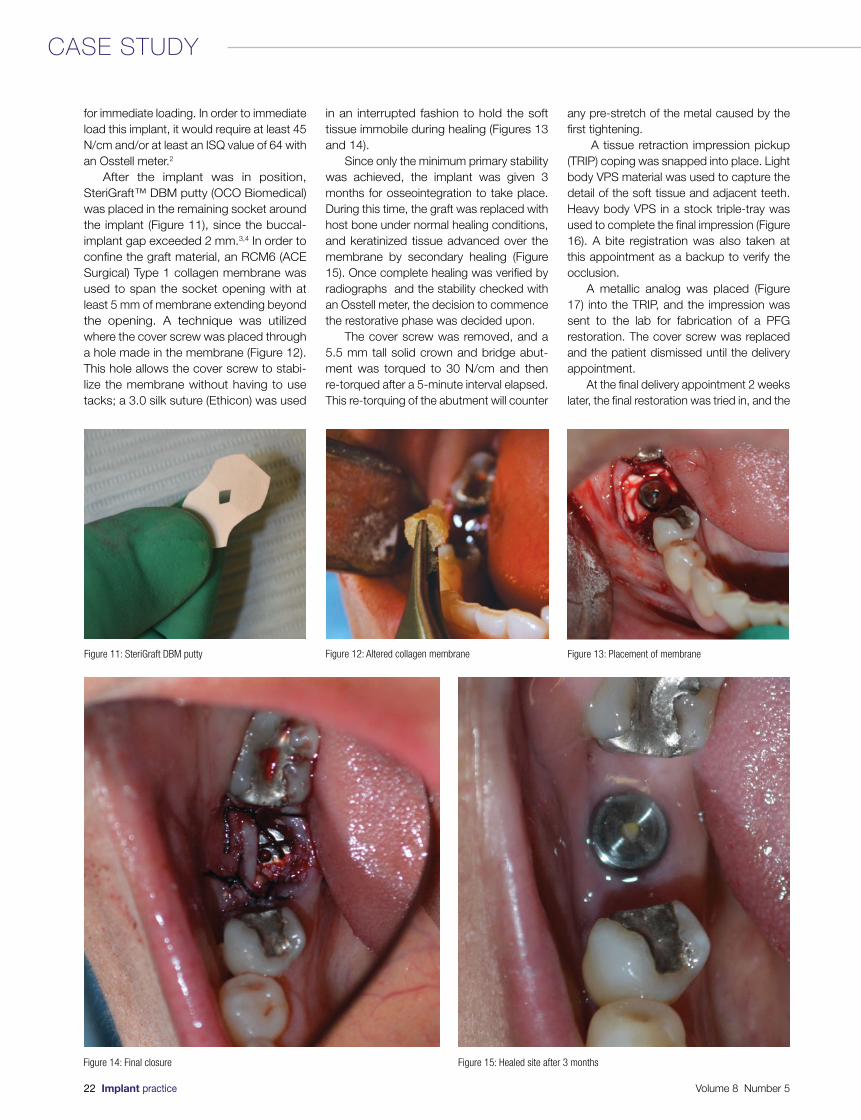
After the implant was in position, SteriGraft™ DBM putty (OCO Biomedical) was placed in the remaining socket around the implant (Figure 11), since the buccal-implant gap exceeded 2 mm.3,4 In order to confine the graft material, an RCM6 (ACE Surgical) Type 1 collagen membrane was used to span the socket opening with at least 5 mm of membrane extending beyond the opening. A technique was utilized where the cover screw was placed through a hole made in the membrane (Figure 12). This hole allows the cover screw to stabi-lize the membrane without having to use tacks; a 3.0 silk suture (Ethicon) was used
in an interrupted fashion to hold the soft tissue immobile during healing (Figures 13 and 14).
Since only the minimum primary stability was achieved, the implant was given 3 months for osseointegration to take place. During this time, the graft was replaced with host bone under normal healing conditions, and keratinized tissue advanced over the membrane by secondary healing (Figure 15). Once complete healing was verified by radiographs and the stability checked with an Osstell meter, the decision to commence the restorative phase was decided upon.
The cover screw was removed, and a 5.5 mm tall solid crown and bridge abut-ment was torqued to 30 N/cm and then re-torqued after a 5-minute interval elapsed. This re-torquing of the abutment will counter
any pre-stretch of the metal caused by the first tightening.
A tissue retraction impression pickup (TRIP) coping was snapped into place. Light body VPS material was used to capture the detail of the soft tissue and adjacent teeth. Heavy body VPS in a stock triple-tray was used to complete the final impression (Figure 16). A bite registration was also taken at this appointment as a backup to verify the occlusion.
A metallic analog was placed (Figure 17) into the TRIP, and the impression was sent to the lab for fabrication of a PFG restoration. The cover screw was replaced and the patient dismissed until the delivery appointment.
At the final delivery appointment 2 weeks later, the final restoration was tried in, and the
Figure 11: SteriGraft DBM putty
Figure 14: Final closure
Figure 13: Placement of membrane
Figure 15: Healed site after 3 months
Figure 12: Altered collagen membrane
22 Implant practice Volume 8 Number 5
CASE STUDY
TRUSTED PURITY FOR BONE REGENERATION.
YOUR PATIENTS DON’T KNOW ABOUT AlloOss,
BUT THEY’RE GLAD YOU DO.
ACE Surgical Supply Co., Inc.
allograft part iculates & blocks
ACE alloOss particulates and blocks combines natural collagen and minerals with the bony structure of allograft to promote new bone formation. alloOss grafts provide a scaffold for cell ingrowth and acts as a guide for rapid bone regeneration. The particulate remodels completely and is able to stabilize implants within 4-6 months. Block grafts maintain strength and volume with rapid remodeling within 5-6 months. To learn more and to take advantage of this amazing offer, visit our website www.acesurgical.com or call 800-441-3100.
* The least expensive of the 6 alloOss products on the same order is no charge. Not to be combined with other alloOss discounts or promotions. To get the no-chargeproduct online, please add at least 6 qualifying products to your cart before checkout. Use promo code “IMUSA”. Offer valid during October and November 2015.
Copyright © 2015 ACE Surgical Supply Co., Inc. alloOss is manufactured by ACE Surgical Supply Co, Inc. Brockton, MA, U.S.A.
BUY 6PAYFOR 5
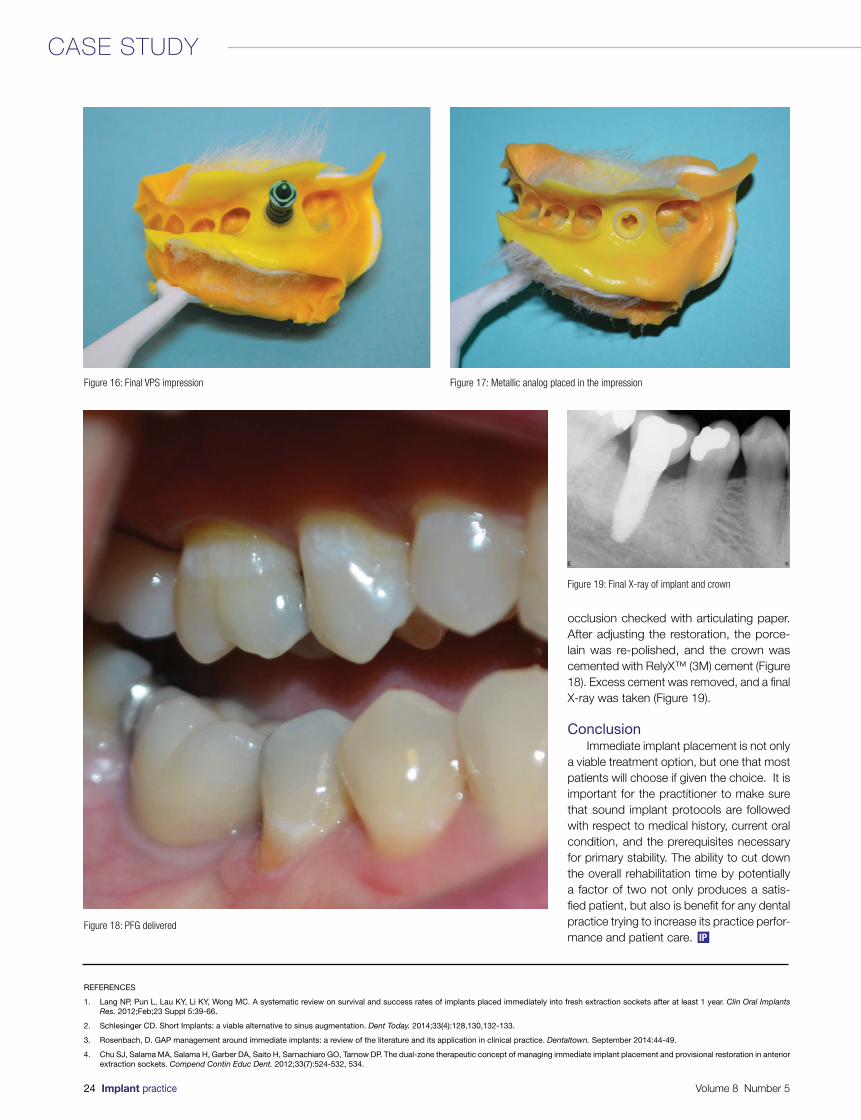
Figure 17: Metallic analog placed in the impression
occlusion checked with articulating paper. After adjusting the restoration, the porce-lain was re-polished, and the crown was cemented with RelyX™ (3M) cement (Figure 18). Excess cement was removed, and a final X-ray was taken (Figure 19).
ConclusionImmediate implant placement is not only
a viable treatment option, but one that most patients will choose if given the choice. It is important for the practitioner to make sure that sound implant protocols are followed with respect to medical history, current oral condition, and the prerequisites necessary for primary stability. The ability to cut down the overall rehabilitation time by potentially a factor of two not only produces a satis-fied patient, but also is benefit for any dental practice trying to increase its practice perfor-mance and patient care.
Figure 19: Final X-ray of implant and crown
Figure 18: PFG delivered
Figure 16: Final VPS impression
REFERENCES
1. Lang NP, Pun L, Lau KY, Li KY, Wong MC. A systematic review on survival and success rates of implants placed immediately into fresh extraction sockets after at least 1 year. Clin Oral Implants Res. 2012;Feb;23 Suppl 5:39-66.
2. Schlesinger CD. Short Implants: a viable alternative to sinus augmentation. Dent Today. 2014;33(4):128,130,132-133.
3. Rosenbach, D. GAP management around immediate implants: a review of the literature and its application in clinical practice. Dentaltown. September 2014:44-49.
4. Chu SJ, Salama MA, Salama H, Garber DA, Saito H, Sarnachiaro GO, Tarnow DP. The dual-zone therapeutic concept of managing immediate implant placement and provisional restoration in anterior extraction sockets. Compend Contin Educ Dent. 2012;33(7):524-532, 534.
24 Implant practice Volume 8 Number 5
CASE STUDY
IP
IntroductionIn 1986, Albrektsson, et al.,1 proposed
criteria for evaluating implant success based on clinical and radiographic evidence of osseointegration: the healing of bone around implants to produce direct anchorage of the implant that is then maintained during func-tional loading without the growth of fibrous tissue at the bone-implant interface.2 The extensive body of peer-reviewed literature published in the field of implantology since then offers a number of additional criteria to define implant success. These criteria include the absence of peri-implantitis, lack of pain and implant mobility, radiographic evidence of minimal crestal bone loss, clin-ical function, esthetic outcome, and patient satisfaction.1,3-5
Despite having predictable outcome and long-term success rate, implants sometimes fail — i.e., require removal or have already been lost.5 Implant failures may be classi-fied as early, when the implant body fails to get osseointegrated, or late, when the implant body is unable to sustain the osseo- integration.6 A number of clinical studies have identified various risk factors that may cause or contribute to implant failure.3,5,7 Among the factors associated with implant failures are bone quality and quantity, history of perio-dontal disease, edentulism, location of the implant, bacterial contamination, delayed wound healing, surgical trauma, implant-related factors (type of implant system, implant surface), and others.
Smoking, occlusal overload, and other biological and biomechanical factors have also been noted to compromise implant success.8,9 More recent studies have concluded that another significant factor of implant success is soft tissue thickness (or biotype).10-13 Some studies name lack of adequate keratinized tissue or attached mucosa among contrib-uting factors of implant failure.14-16 This topic is controversial, and more studies are needed to prove or disprove its validity.
Tension problem — alarming trend This article focuses on an alarming
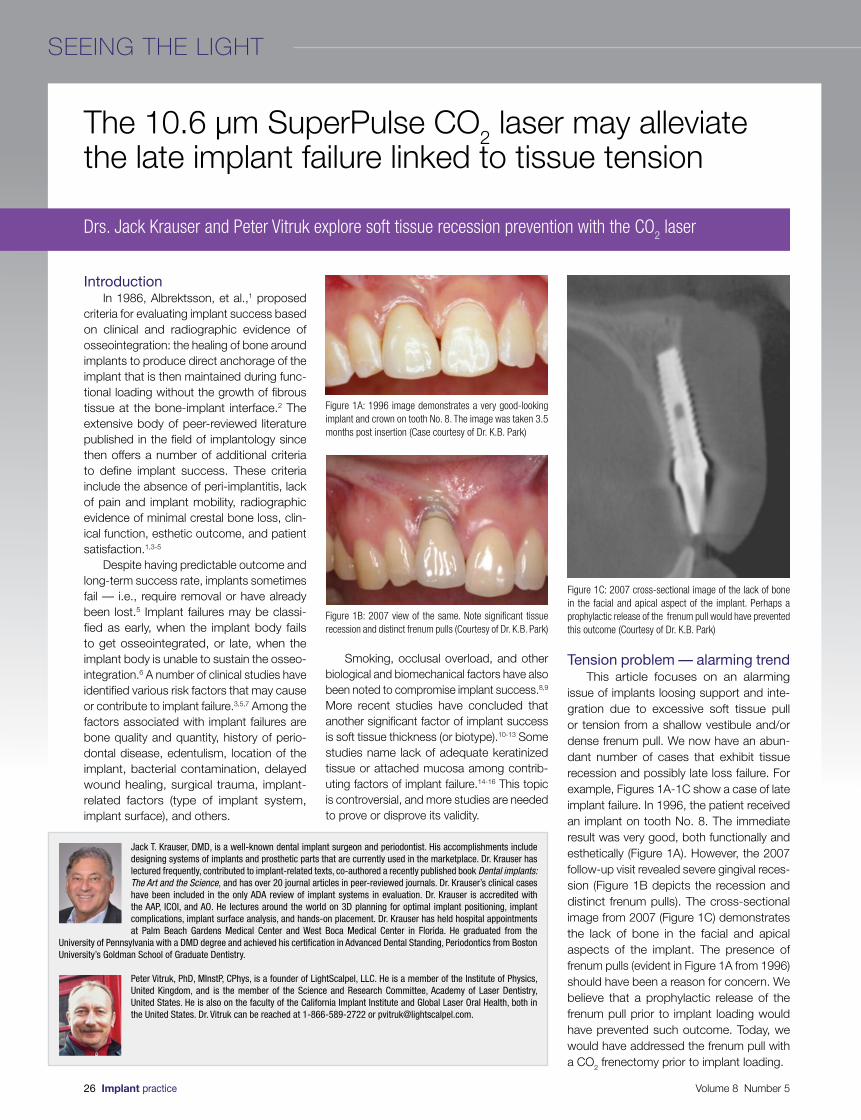
issue of implants loosing support and inte-gration due to excessive soft tissue pull or tension from a shallow vestibule and/or dense frenum pull. We now have an abun-dant number of cases that exhibit tissue recession and possibly late loss failure. For example, Figures 1A-1C show a case of late implant failure. In 1996, the patient received an implant on tooth No. 8. The immediate result was very good, both functionally and esthetically (Figure 1A). However, the 2007 follow-up visit revealed severe gingival reces-sion (Figure 1B depicts the recession and distinct frenum pulls). The cross-sectional image from 2007 (Figure 1C) demonstrates the lack of bone in the facial and apical aspects of the implant. The presence of frenum pulls (evident in Figure 1A from 1996) should have been a reason for concern. We believe that a prophylactic release of the frenum pull prior to implant loading would have prevented such outcome. Today, we would have addressed the frenum pull with a CO2 frenectomy prior to implant loading.
The 10.6 µm SuperPulse CO2 laser may alleviate the late implant failure linked to tissue tension
Jack T. Krauser, DMD, is a well-known dental implant surgeon and periodontist. His accomplishments include designing systems of implants and prosthetic parts that are currently used in the marketplace. Dr. Krauser has lectured frequently, contributed to implant-related texts, co-authored a recently published book Dental implants: The Art and the Science, and has over 20 journal articles in peer-reviewed journals. Dr. Krauser’s clinical cases have been included in the only ADA review of implant systems in evaluation. Dr. Krauser is accredited with the AAP, ICOI, and AO. He lectures around the world on 3D planning for optimal implant positioning, implant complications, implant surface analysis, and hands-on placement. Dr. Krauser has held hospital appointments at Palm Beach Gardens Medical Center and West Boca Medical Center in Florida. He graduated from the
University of Pennsylvania with a DMD degree and achieved his certification in Advanced Dental Standing, Periodontics from Boston University’s Goldman School of Graduate Dentistry.
Peter Vitruk, PhD, MInstP, CPhys, is a founder of LightScalpel, LLC. He is a member of the Institute of Physics, United Kingdom, and is the member of the Science and Research Committee, Academy of Laser Dentistry, United States. He is also on the faculty of the California Implant Institute and Global Laser Oral Health, both in the United States. Dr. Vitruk can be reached at 1-866-589-2722 or [email protected].
Drs. Jack Krauser and Peter Vitruk explore soft tissue recession prevention with the CO2 laser
Figure 1A: 1996 image demonstrates a very good-looking implant and crown on tooth No. 8. The image was taken 3.5 months post insertion (Case courtesy of Dr. K.B. Park)
Figure 1B: 2007 view of the same. Note significant tissue recession and distinct frenum pulls (Courtesy of Dr. K.B. Park)
Figure 1C: 2007 cross-sectional image of the lack of bone in the facial and apical aspect of the implant. Perhaps a prophylactic release of the frenum pull would have prevented this outcome (Courtesy of Dr. K.B. Park)
26 Implant practice Volume 8 Number 5
SEEING THE LIGHT

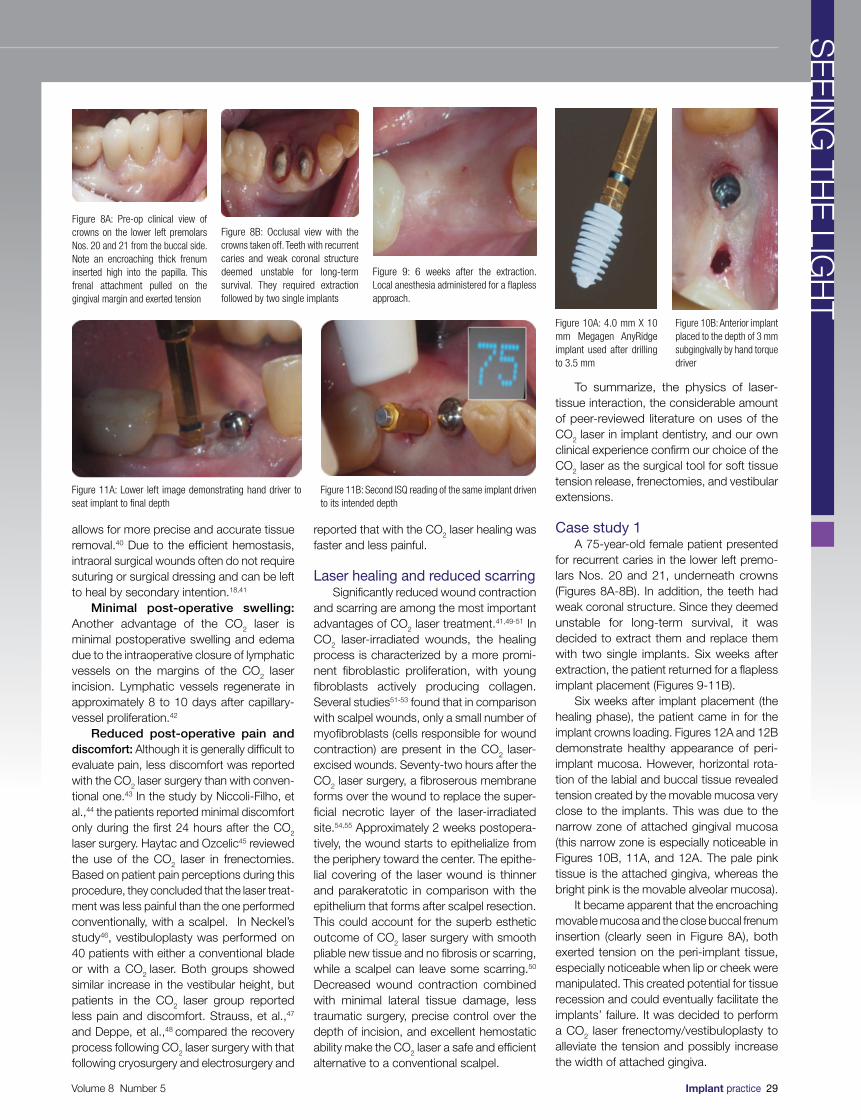
Figure 2 demonstrates two single Brånemark implants placed nearly 15 years prior. Natural buccal and lingual narrowing of the alveolar ridge and high mucogingival junction combined with frenum pull could possibly contribute to the buccal gingival recession and, consequently, the implant failure. In this case, the patient could have benefited from the tissue tension release.
Figure 3 presents the occlusal view of a modern design Megagen AnyRidge® implant with its early maintenance of the buccolingual ridge form. In other words, the buccal frenum pull was prophylactically released to alleviate tissue tension and lower the risk of marginal tissue recession in the future. Figure 3 clearly demonstrates healthy gingival mucosa in the absence of any frenum pulls or tension.
This article identifies the tissue tension problem and demonstrates a quick, effec-tive, and relatively painless concept to prophy-lactically address this issue with the adjunctive use of a 10.6 micron SuperPulse CO2 laser.
Sources of pull and tensionHigh muscle attachment: Sometimes,
muscle attachment extends onto the crest of the ridge, which results in a shallow vestibule. Such muscle attachment can create space inadequate for a substantial implant-supported denture (or any denture, for that matter). In addition, muscle fibers exert considerable tension on peri-implant mucosa, which may eventually result in gingival recession. In such cases, a simple vestibular extension procedure can solve the problem. Small penetration depth of the CO2
laser is important for the vestibular extension procedure because it affords the clinician precise control over the depth of incision.
Frenum pull: Frena are folds of mucous membrane containing fibrous connective tissue that attach lips and cheeks to the alve-olar mucosa, the gingiva, and the underlying
periosteum.17 Some frenal attachments can be dense, pulling on the attached gingiva. Tissue tension caused by the presence of frenum pull can be an important etiological factor in progressive gingival recession around posts and in eventual strut expo-sure.18,19 In the case of implant-retained denture prosthesis, frenum can limit denture extensions and even affect the seal and reten-tion of the denture.18,20 The CO2 laser frenec-tomy procedure that releases tension exerted by the frenum pull creates a better chance of long-term success for a dental implant without sutures pulling, less postoperative swelling, and only minor pain or discomfort.
Lack of keratinized mucosa or attached gingival mucosa: Another risk factor is lack of attached gingiva. The width of attached gingival mucosa varies for different patients and even for different teeth in the same patient. In the oral cavity, attached gingiva (keratinized masticatory mucosa) meets movable alveolar mucosa (lining mucosa) at the mucogingival junc-tion (MGJ). Clinically, the MGJ is identified by a mucogingival groove and the change from the pale pink of the attached gingiva to the bright pink of the movable alveolar mucosa.20 Width of keratinized mucosa is the distance between the mucogingival junction (MGJ) and the coronal aspect of the kera-tinized mucosa.14 There is no unequivocal consensus on the role the presence of kera-tinized mucosa plays in maintaining implant health.21-23 Literature suggests that a greater width of keratinized mucosa is advantageous due to the following:
• It provides a resistant barrier to plaque-induced inflammation
• It replaces non-keratinized margins to prevent recession
• It deepens vestibules to provide better access for tooth brushing
• It dissipates functional and mastica-tory stress placed on the gingival margin of a restoration
• It facilitates oral hygiene, and improves esthetics and patient comfort14,16,22
Clinicians generally agree about the link between the insufficient amount of kera-tinized mucosa or attached gingiva and marginal tissue recession. A study by Chung, et al.,14 has found that dental implants with insufficient attached gingiva show more plaque accumulation and mucosal inflam-mation than implants with adequate attached gingiva. If attached gingiva is insufficient (less than 4 mm), and the MGJ is positioned high, mucosa surrounding the implant is mobile and easily retractable during mastication and speech.24 Such tissue retraction can
facilitate the introduction of plaque into the peri-implant pocket14,24 and lead to gingival recession. The presence of adequate (approximately 4 mm) attached gingiva correlates with mucosal health and can help prevent inflammation in peri-implant tissues. Al-Sabbagh and Bhavsar24 pointed out that wide zone of attached peri-implant gingiva provides better gingival seal around the implant. Another study has shown the correlation between lack of attached gingiva and crestal bone loss of 2 mm or more.25 These findings lead many clinicians, the authors included, to believe that the creation of sufficient amount of attached gingiva around implants is important and can potentially prevent implant failure. Width of the attached gingiva may be increased by a local vestibuloplasty.
To summarize, tissue tension or pull due to a shallow vestibule (caused by high muscle attachment), dense frenum, or lack of keratinized/attached mucosa can contribute to gingival recession. In addition to causing an esthetic problem, mucosal recession that denudes threads or a rough implant surface might impede the ability of the patient to maintain the implant clean from plaque. The resulting inflammation and infection create the risk of potential peri-implant bone loss and eventual implant failure.26,27
Proposed solution In order to effectively release tension
created either by a high muscle attachment and/or dense frenum, or high mucogingival junction with only a small amount of gingival mucosa, we recommend performing a CO2
laser frenectomy and/or vestibuloplasty with secondary epithelialization.
Why CO2 laser? Not all lasers are equally efficient at
both tissue vaporization (i.e., ablation or cutting) and coagulation. The difference is illustrated in the absorption spectra for main soft tissue chromophores28,29 in Figure 4. Some dental laser wavelengths (around 3,000 nm, such as Erbium lasers) are well absorbed by the water-rich soft tissue and are great at cutting but are not as efficient at coagulating.29 Other dental laser wave-lengths (around 1,000 nm, such as diodes and Nd:YAG) are efficient coagulators, but inefficient scalpels30 since they are poorly absorbed by the soft tissue.
The 10,600 nm CO2 laser wavelength is efficient at both vaporizing and coagulating the soft tissue simultaneously (Figure 4), although it is not as good as Erbium laser at cutting and not as good as diode/Nd:YAG at coagulating. Most importantly, the CO2 laser’s
Figure 3: Occlusal view of a modern design implant Megagen AnyRidge® with its early maintenance of the buccal-lingual ridge form
Figure 2: Occlusal view of a Brånemark implant site at close to 15 years’ placement. Note the buccal-lingual ridge narrowing. This, coupled with frenum pull, may contribute to a buccal recession
Volume 8 Number 5 Implant practice 27
SE
EIN
G TH
E LIG
HT
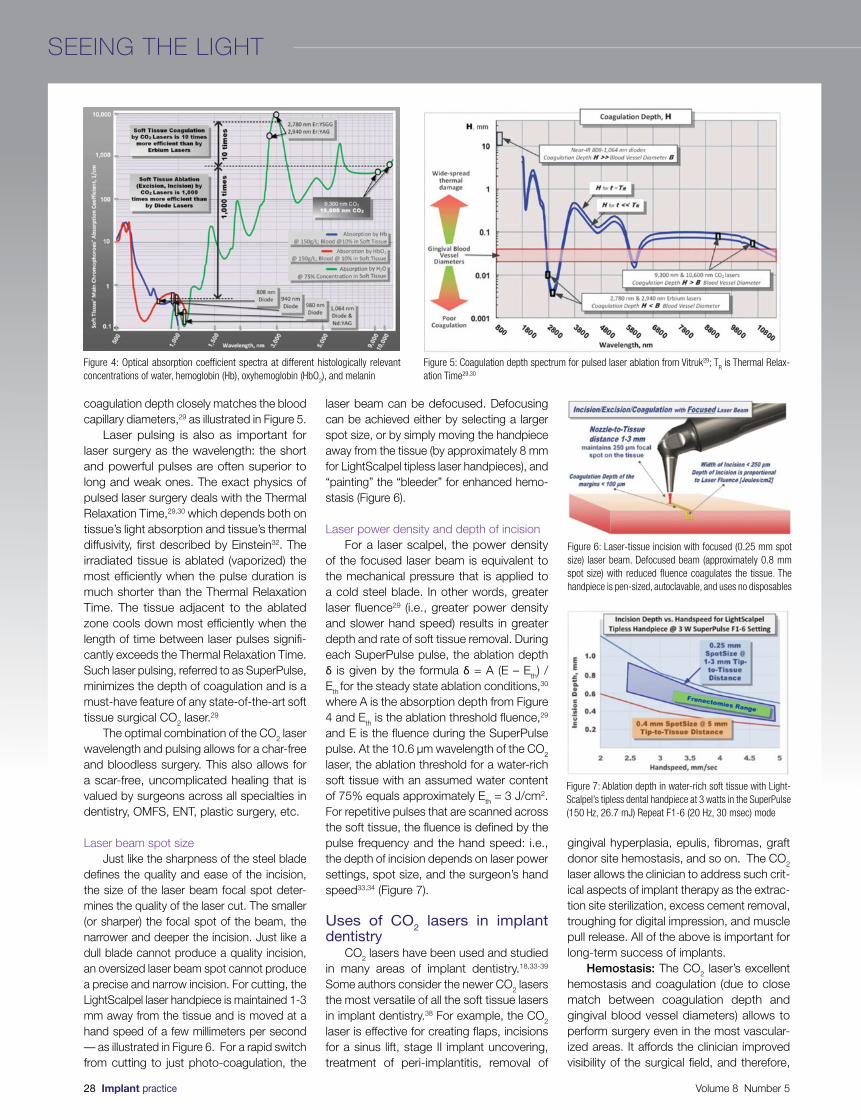
coagulation depth closely matches the blood capillary diameters,29 as illustrated in Figure 5.
Laser pulsing is also as important for laser surgery as the wavelength: the short and powerful pulses are often superior to long and weak ones. The exact physics of pulsed laser surgery deals with the Thermal Relaxation Time,29,30 which depends both on tissue’s light absorption and tissue’s thermal diffusivity, first described by Einstein32. The irradiated tissue is ablated (vaporized) the most efficiently when the pulse duration is much shorter than the Thermal Relaxation Time. The tissue adjacent to the ablated zone cools down most efficiently when the length of time between laser pulses signifi-cantly exceeds the Thermal Relaxation Time. Such laser pulsing, referred to as SuperPulse, minimizes the depth of coagulation and is a must-have feature of any state-of-the-art soft tissue surgical CO2 laser.29
The optimal combination of the CO2 laser wavelength and pulsing allows for a char-free and bloodless surgery. This also allows for a scar-free, uncomplicated healing that is valued by surgeons across all specialties in dentistry, OMFS, ENT, plastic surgery, etc.
Laser beam spot sizeJust like the sharpness of the steel blade
defines the quality and ease of the incision, the size of the laser beam focal spot deter-mines the quality of the laser cut. The smaller (or sharper) the focal spot of the beam, the narrower and deeper the incision. Just like a dull blade cannot produce a quality incision, an oversized laser beam spot cannot produce a precise and narrow incision. For cutting, the LightScalpel laser handpiece is maintained 1-3 mm away from the tissue and is moved at a hand speed of a few millimeters per second — as illustrated in Figure 6. For a rapid switch from cutting to just photo-coagulation, the
laser beam can be defocused. Defocusing can be achieved either by selecting a larger spot size, or by simply moving the handpiece away from the tissue (by approximately 8 mm for LightScalpel tipless laser handpieces), and “painting” the “bleeder” for enhanced hemo-stasis (Figure 6).
Laser power density and depth of incisionFor a laser scalpel, the power density
of the focused laser beam is equivalent to the mechanical pressure that is applied to a cold steel blade. In other words, greater laser fluence29 (i.e., greater power density and slower hand speed) results in greater depth and rate of soft tissue removal. During each SuperPulse pulse, the ablation depth δ is given by the formula δ = A (E – Eth) / Eth for the steady state ablation conditions,30
where A is the absorption depth from Figure 4 and Eth is the ablation threshold fluence,29 and E is the fluence during the SuperPulse pulse. At the 10.6 µm wavelength of the CO2
laser, the ablation threshold for a water-rich soft tissue with an assumed water content of 75% equals approximately Eth = 3 J/cm2. For repetitive pulses that are scanned across the soft tissue, the fluence is defined by the pulse frequency and the hand speed: i.e., the depth of incision depends on laser power settings, spot size, and the surgeon’s hand speed33,34 (Figure 7).
Uses of CO2 lasers in implant dentistry
CO2 lasers have been used and studied in many areas of implant dentistry.18,33-39
Some authors consider the newer CO2 lasers the most versatile of all the soft tissue lasers in implant dentistry.38 For example, the CO2
laser is effective for creating flaps, incisions for a sinus lift, stage II implant uncovering, treatment of peri-implantitis, removal of
gingival hyperplasia, epulis, fibromas, graft donor site hemostasis, and so on. The CO2
laser allows the clinician to address such crit-ical aspects of implant therapy as the extrac-tion site sterilization, excess cement removal, troughing for digital impression, and muscle pull release. All of the above is important for long-term success of implants.
Hemostasis: The CO2 laser’s excellent hemostasis and coagulation (due to close match between coagulation depth and gingival blood vessel diameters) allows to perform surgery even in the most vascular-ized areas. It affords the clinician improved visibility of the surgical field, and therefore,
Figure 4: Optical absorption coefficient spectra at different histologically relevant concentrations of water, hemoglobin (Hb), oxyhemoglobin (HbO
2), and melanin
Figure 5: Coagulation depth spectrum for pulsed laser ablation from Vitruk29; TR is Thermal Relax-
ation Time29,30
Figure 6: Laser-tissue incision with focused (0.25 mm spot size) laser beam. Defocused beam (approximately 0.8 mm spot size) with reduced fluence coagulates the tissue. The handpiece is pen-sized, autoclavable, and uses no disposables
Figure 7: Ablation depth in water-rich soft tissue with Light-Scalpel’s tipless dental handpiece at 3 watts in the SuperPulse (150 Hz, 26.7 mJ) Repeat F1-6 (20 Hz, 30 msec) mode
28 Implant practice Volume 8 Number 5
SEEING THE LIGHT
allows for more precise and accurate tissue removal.40 Due to the efficient hemostasis, intraoral surgical wounds often do not require suturing or surgical dressing and can be left to heal by secondary intention.18,41
Minimal post-operative swelling: Another advantage of the CO2 laser is minimal postoperative swelling and edema due to the intraoperative closure of lymphatic vessels on the margins of the CO2 laser incision. Lymphatic vessels regenerate in approximately 8 to 10 days after capillary-vessel proliferation.42
Reduced post-operative pain and discomfort: Although it is generally difficult to evaluate pain, less discomfort was reported with the CO2 laser surgery than with conven-tional one.43 In the study by Niccoli-Filho, et al.,44 the patients reported minimal discomfort only during the first 24 hours after the CO2 laser surgery. Haytac and Ozcelic45 reviewed the use of the CO2 laser in frenectomies. Based on patient pain perceptions during this procedure, they concluded that the laser treat-ment was less painful than the one performed conventionally, with a scalpel. In Neckel’s study46, vestibuloplasty was performed on 40 patients with either a conventional blade or with a CO2 laser. Both groups showed similar increase in the vestibular height, but patients in the CO2 laser group reported less pain and discomfort. Strauss, et al.,47 and Deppe, et al.,48 compared the recovery process following CO2 laser surgery with that following cryosurgery and electrosurgery and
reported that with the CO2 laser healing was faster and less painful.
Laser healing and reduced scarringSignificantly reduced wound contraction
and scarring are among the most important advantages of CO2 laser treatment.41,49-51 In CO2 laser-irradiated wounds, the healing process is characterized by a more promi-nent fibroblastic proliferation, with young fibroblasts actively producing collagen. Several studies51-53 found that in comparison with scalpel wounds, only a small number of myofibroblasts (cells responsible for wound contraction) are present in the CO2 laser-excised wounds. Seventy-two hours after the CO2 laser surgery, a fibroserous membrane forms over the wound to replace the super-ficial necrotic layer of the laser-irradiated site.54,55 Approximately 2 weeks postopera-tively, the wound starts to epithelialize from the periphery toward the center. The epithe-lial covering of the laser wound is thinner and parakeratotic in comparison with the epithelium that forms after scalpel resection. This could account for the superb esthetic outcome of CO2 laser surgery with smooth pliable new tissue and no fibrosis or scarring, while a scalpel can leave some scarring.50 Decreased wound contraction combined with minimal lateral tissue damage, less traumatic surgery, precise control over the depth of incision, and excellent hemostatic ability make the CO2 laser a safe and efficient alternative to a conventional scalpel.
To summarize, the physics of laser-tissue interaction, the considerable amount of peer-reviewed literature on uses of the CO2 laser in implant dentistry, and our own clinical experience confirm our choice of the CO2 laser as the surgical tool for soft tissue tension release, frenectomies, and vestibular extensions.
Case study 1A 75-year-old female patient presented
for recurrent caries in the lower left premo-lars Nos. 20 and 21, underneath crowns (Figures 8A-8B). In addition, the teeth had weak coronal structure. Since they deemed unstable for long-term survival, it was decided to extract them and replace them with two single implants. Six weeks after extraction, the patient returned for a flapless implant placement (Figures 9-11B).
Six weeks after implant placement (the healing phase), the patient came in for the implant crowns loading. Figures 12A and 12B demonstrate healthy appearance of peri-implant mucosa. However, horizontal rota-tion of the labial and buccal tissue revealed tension created by the movable mucosa very close to the implants. This was due to the narrow zone of attached gingival mucosa (this narrow zone is especially noticeable in Figures 10B, 11A, and 12A. The pale pink tissue is the attached gingiva, whereas the bright pink is the movable alveolar mucosa).
It became apparent that the encroaching movable mucosa and the close buccal frenum insertion (clearly seen in Figure 8A), both exerted tension on the peri-implant tissue, especially noticeable when lip or cheek were manipulated. This created potential for tissue recession and could eventually facilitate the implants’ failure. It was decided to perform a CO2 laser frenectomy/vestibuloplasty to alleviate the tension and possibly increase the width of attached gingiva.
Figure 8A: Pre-op clinical view of crowns on the lower left premolars Nos. 20 and 21 from the buccal side. Note an encroaching thick frenum inserted high into the papilla. This frenal attachment pulled on the gingival margin and exerted tension
Figure 8B: Occlusal view with the crowns taken off. Teeth with recurrent caries and weak coronal structure deemed unstable for long-term survival. They required extraction followed by two single implants
Figure 9: 6 weeks after the extraction. Local anesthesia administered for a flapless approach.
Figure 10A: 4.0 mm X 10 mm Megagen AnyRidge implant used after drilling to 3.5 mm
Figure 10B: Anterior implant placed to the depth of 3 mm subgingivally by hand torque driver
Figure 11A: Lower left image demonstrating hand driver to seat implant to final depth
Figure 11B: Second ISQ reading of the same implant driven to its intended depth
Volume 8 Number 5 Implant practice 29
SE
EIN
G TH
E LIG
HT
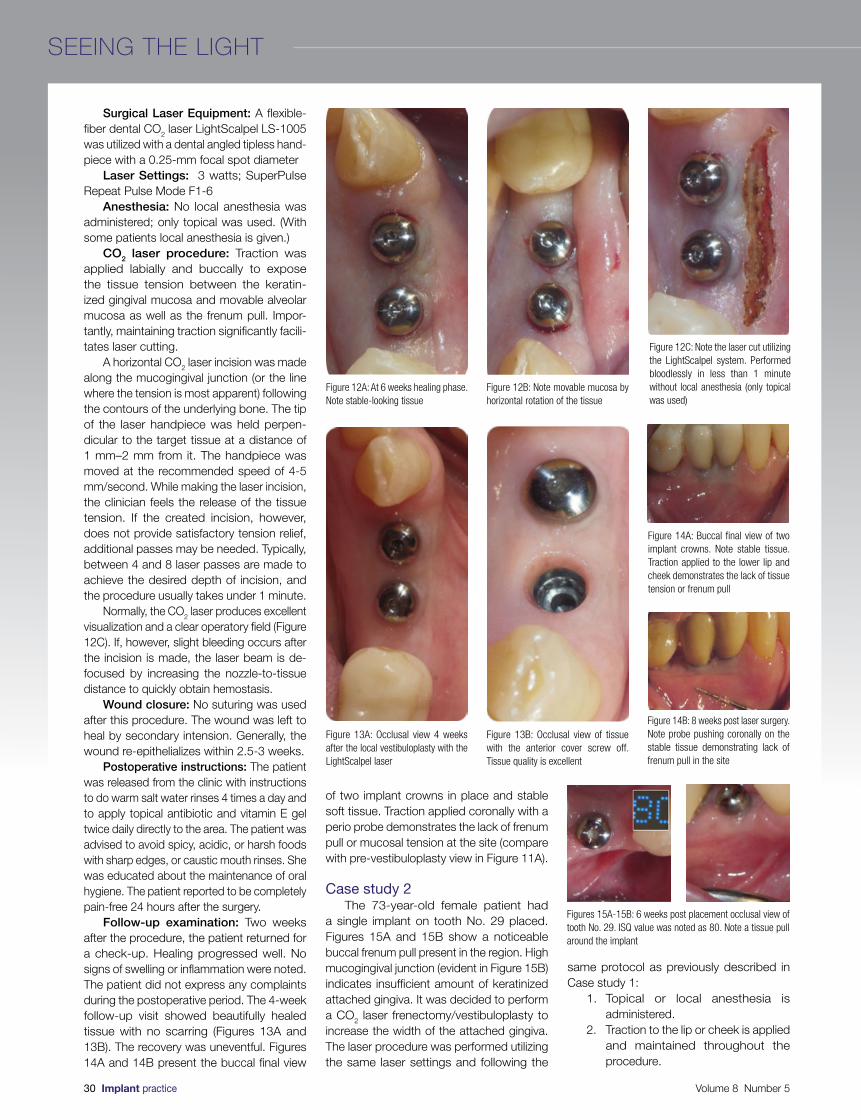
Surgical Laser Equipment: A flexible-fiber dental CO2 laser LightScalpel LS-1005 was utilized with a dental angled tipless hand-piece with a 0.25-mm focal spot diameter
Laser Settings: 3 watts; SuperPulse Repeat Pulse Mode F1-6
Anesthesia: No local anesthesia was administered; only topical was used. (With some patients local anesthesia is given.)
CO2 laser procedure: Traction was applied labially and buccally to expose the tissue tension between the keratin-ized gingival mucosa and movable alveolar mucosa as well as the frenum pull. Impor-tantly, maintaining traction significantly facili-tates laser cutting.
A horizontal CO2 laser incision was made along the mucogingival junction (or the line where the tension is most apparent) following the contours of the underlying bone. The tip of the laser handpiece was held perpen-dicular to the target tissue at a distance of 1 mm–2 mm from it. The handpiece was moved at the recommended speed of 4-5 mm/second. While making the laser incision, the clinician feels the release of the tissue tension. If the created incision, however, does not provide satisfactory tension relief, additional passes may be needed. Typically, between 4 and 8 laser passes are made to achieve the desired depth of incision, and the procedure usually takes under 1 minute.
Normally, the CO2 laser produces excellent visualization and a clear operatory field (Figure 12C). If, however, slight bleeding occurs after the incision is made, the laser beam is de- focused by increasing the nozzle-to-tissue distance to quickly obtain hemostasis.
Wound closure: No suturing was used after this procedure. The wound was left to heal by secondary intension. Generally, the wound re-epithelializes within 2.5-3 weeks.
Postoperative instructions: The patient was released from the clinic with instructions to do warm salt water rinses 4 times a day and to apply topical antibiotic and vitamin E gel twice daily directly to the area. The patient was advised to avoid spicy, acidic, or harsh foods with sharp edges, or caustic mouth rinses. She was educated about the maintenance of oral hygiene. The patient reported to be completely pain-free 24 hours after the surgery.
Follow-up examination: Two weeks after the procedure, the patient returned for a check-up. Healing progressed well. No signs of swelling or inflammation were noted. The patient did not express any complaints during the postoperative period. The 4-week follow-up visit showed beautifully healed tissue with no scarring (Figures 13A and 13B). The recovery was uneventful. Figures 14A and 14B present the buccal final view
of two implant crowns in place and stable soft tissue. Traction applied coronally with a perio probe demonstrates the lack of frenum pull or mucosal tension at the site (compare with pre-vestibuloplasty view in Figure 11A).
Case study 2The 73-year-old female patient had
a single implant on tooth No. 29 placed. Figures 15A and 15B show a noticeable buccal frenum pull present in the region. High mucogingival junction (evident in Figure 15B) indicates insufficient amount of keratinized attached gingiva. It was decided to perform a CO2 laser frenectomy/vestibuloplasty to increase the width of the attached gingiva. The laser procedure was performed utilizing the same laser settings and following the
same protocol as previously described in Case study 1:
1. Topical or local anesthesia is administered.
2. Traction to the lip or cheek is applied and maintained throughout the procedure.
Figure 12A: At 6 weeks healing phase. Note stable-looking tissue
Figure 12B: Note movable mucosa by horizontal rotation of the tissue
Figure 12C: Note the laser cut utilizing the LightScalpel system. Performed bloodlessly in less than 1 minute without local anesthesia (only topical was used)
Figure 13A: Occlusal view 4 weeks after the local vestibuloplasty with the LightScalpel laser
Figure 13B: Occlusal view of tissue with the anterior cover screw off. Tissue quality is excellent
Figure 14A: Buccal final view of two implant crowns. Note stable tissue. Traction applied to the lower lip and cheek demonstrates the lack of tissue tension or frenum pull
Figure 14B: 8 weeks post laser surgery. Note probe pushing coronally on the stable tissue demonstrating lack of frenum pull in the site
Figures 15A-15B: 6 weeks post placement occlusal view of tooth No. 29. ISQ value was noted as 80. Note a tissue pull around the implant
30 Implant practice Volume 8 Number 5
SEEING THE LIGHT

© Carestream Health, Inc. 2015. WinOMS is a registered trademark of Carestream Health. iPad is a trademark of Apple, Inc., registered in the U.S. and other countries. 12993 OM AD 0915
CS WinOMS Cloud
CLOUDCOVERAGE
ANYTIME, ANYWHERE ACCESSAFFORDABILITY AND CONTROL
Now CS WinOMS Cloud brings cutting-edge speed, security and redundancy to your practice – providing you peace of mind so you can focus on what you do best. Avoid IT hassles, cut costs and run your software on more devices – including PCs, Macs, iPads and other tablets.
• Store and share 2D/3D images between of� ces
• HIPAA-compliant, secure data backup
• One predictable monthly fee – pay as you go with no long-term contracts
• 24/7 access from almost any Web-enabled device
LET’S REDEFINE OMS
Call 800.944.6365 today, or visit www.carestreamdental.com
Carestream Dental is a proud supporter of AAOMS.

IP
3. Laser handpiece is directed at 90º to the target tissue.
4. Laser-tissue distance is kept at 1 mm-2 mm for an incision and 3 mm-4 mm for coagulation.
5. Hand speed is maintained at 4-5 mm/second.
6. An incision is made at the point where tissue tension is most apparent.
7. The incision should follow the contours of the underlying bone.
8. The incision is extended to the desired depth.
9. No sutures are required.10. Patient is released from the clinic
immediately after the procedure with instructions on how to maintain oral hygiene, to avoid acidic, caustic or harsh foods, drinks or mouth rinses. We recommend warm salt rinses 4 times a day; NSAIDs, if needed, topical antibiotic and vitamin E gel twice daily.
Figure 16 demonstrates immediate postoperative view of the CO2 laser frenec-tomy/vestibuloplasty completed in less than 1 minute, bloodlessly, and without local anesthesia.
Follow-up evaluation: At 4 weeks, the surgical site appeared completely healed (Figure 17). The patient gained 3 mm-4 mm of the vestibule depth, and although the frenum was still present, its attachment moved apically and further away from the implant (Figure 17).
Conclusion The CO2 laser was chosen for this proce-
dure for several reasons, such as the laser’s ability to provide instant hemostasis with a minuscule zone of thermal injury (sub 50 microns),31 lack of need for sutures, reduced wound contraction, smooth healing, and only minor pain and discomfort reported by patients.
The CO2 laser frenectomy/vestibuloplasty is a simple, neat, and quick procedure with minimal postoperative pain or discomfort for the patient. While by no means a panacea against implant failure, this procedure allows the clinician to remove one of the many risk factors — i.e., tissue tension, that can poten-tially compromise the long-term success of dental implants. Due to the above and based on years of clinical experience, the authors recommend the CO2 laser frenectomy/vestibu-loplasty as an effective surgical solution.
AcknowledgmentAuthors greatly appreciate the support and contribution from Anna (Anya) Glazkova, PhD, in preparing this material for publication.
REFERENCES:
1. Albrektsson T, Zarb G, Worthington P, Eriksson AR. The long-term efficacy of currently used dental implants: a review and proposed criteria of success. Int J Oral Maxillofac Implants. 1986;1(1):11-25.
2. Brånemark PI, Hansson BO, Adell R, Breine U, Lindström J, Hallén O, Ohman A. Osseointegrated implants in the treatment of the edentulous jaw. Experience from a 10-year period. Scand J Plast Reconstr Surg Suppl. 1977;16:1-132.
3. Smith DE, Zarb GA. Criteria for success of osseointegrated endos-seous implants. J Prosthet Dent. 1989;62(5):567–572.
4. Proskin HM, Jeffcoat RL, Catlin A, Campbell J, Jeffcoat MK. A meta-analytic approach to determine the state of the science on implant dentistry. Int J Oral Maxillofac Implants. 2007;22 suppl:11-18.
5. Misch CE, Perel ML, Wang HL, Sammartino G, Galindo-Moreno P, Trisi P, Steigmann M, Rebaudi A, Palti A, Pikos MA, Schwartz-Arad D, Choukroun J, Gutierrez-Perez JL, Marenzi G, Valavanis DK. Implant success, survival, and failure: the International Congress of Oral Implantologists (ICOI) Pisa Consensus Conference. Implant Dent. 2008;17(1):5-15.
6. Heydenrijk K, Meijer HJ, van der Reijden WA, Raghoebar GM, Vissink A, Stegenga B. Microbiota around root-form endosseous implants: a review of the literature. Int J Oral Maxillofac Implants. 2002;17(6):829–838.
7. Moy PK, Medina D, Shetty V, Aghaloo TL. Dental implant failure rates and associated risk factors. Int J Oral Maxillofac Implants. 2005;20(4):569–577.
8. Steigenga J, Al-Shammari K, Misch C, Nociti FH Jr, Wang HL. Effects of implant thread geometry on percentage of osseointe-gration and resistance to reverse torque in the tibia of rabbits. J Periodontol. 2004;75(9):1233-1241.
9. Kim Y, Oh TJ, Misch CE, Wang HL. Occlusal considerations in implant therapy: clinical guidelines with biomechanical rationale. Clin Oral Implants Res. 2005;16(1):26-35.
10. Evans CD, Chen ST. Esthetic outcomes of immediate implant place-ments. Clin Oral Implants Res. 2008;19(1):73-80.
11. Jung RE, Sailer I, Hammerle CH, Attin T, Schmidlin P. In vitro color changes of soft tissues caused by restorative materials. Int J Peri-odontics Restorative Dent. 2007;27(3):251-257.
12. Levine RA, Huynh-Ba G, Cochran DL. Soft tissue augmentation procedures for mucogingival defects in esthetic sites. Int J Oral Maxillofac Implants. 2014;29 Suppl:155-185.
13. Lee A, Fu JH, Wang HL. Soft tissue biotype affects implant success. Implant Dent. 2011;20(3):e38-47. doi: 10.1097/ID.0b013e3182181d3d.
14. Chung DM, Oh TJ, Shotwell JL, Misch CE, Wang HL. Significance of keratinized mucosa in maintenance of dental implants with different surfaces. J Periodontol. 2006;77(8):1410–1420.
15. Bengazi F, Wennström JL, Lekholm U. Recession of the soft tissue margin at oral implants. A 2-year longitudinal prospective study. Clin Oral Implants Res. 1996;7(4):303-310.
16. Greenstein G, Cavallaro J. The clinical significance of keratinized gingiva around dental implants. Compend Contin Educ Dent. 201;32(8):24-31;quiz 32, 34.
17. Devishree SKG, Shubhashini PV. Frenectomy: A Review with the Reports of Surgical Techniques. J Clin Diagn Res. 2012 Nov; 6(9): 1587–1592. Published online 2012 Nov 15. doi: 10.7860/JCDR/2012/4089.2572
18. Namour S. Atlas of Current Oral Laser Surgery. Boca Raton, FL:Universal Publishers;2011.
19. Weber SP. A mucobuccal fold extension for implant and other surgical procedures. J Prosthet Dent. 1972;27(4):423-433.
20. Nanci A. Oral mucosa. In: Nanci A, ed. Ten cate’s oral histology: development, structure, and function. 7th ed. St.Louis, MO:Mosby;2008:319-357.
21. Cairo F, Pagliaro U, Nieri M. Soft tissue management at implant sites. J Clin Periodontol. 2008;35(8 suppl):163-167.
22. Bouri A Jr, Bissada N, Al-Zahrani MS, Faddoul F, Nouneh I. Width of keratinized gingiva and the health status of the supporting tissues around dental implants. Int J Oral Maxillofac Implants. 2008;23(2):323-326.
23. Yeung SC. Biological basis for soft tissue management in implant dentistry. Aust Dent J. 2008;53(suppl 1):S39-S42.
24. Al-Sabbagh M, Bhavsar I. Key local and surgical factors related to implant failure. Dent Clin North Am. 2015;59(1):1-23. doi: 10.1016/j.cden.2014.09.001.
25. Block MS, Kent JN. Factors associated with soft- and hard-tissue compromise of endosseous implants. J Oral Maxillofac Surg. 1990;48(11):1153–1160.
26. Albrektsson T, Dahlin C, Jemt T, Sennerby L, Turri A, Wennerberg A. Is marginal bone loss around oral implants the result of a provoked foreign body reaction? Clin Implant Dent Relat Res. 2014;16(2):155-165. doi: 10.1111/cid.12142. Epub 2013 Sep 4.
27. Dibart S, Warbington M, Su MF, Skobe Z. In vitro evaluation of the implant-abutment bacterial seal: the locking taper system. Int J Oral Maxillofac Implants. 2005;20(5):732-737.
28. Jacques SL. Optical properties of biological tissues: a review. Phys Med Biol. 2013;58(11):R37-61.
29. Vitruk P. Oral soft tissue laser ablative and coagulative efficiencies spectra. Implant Practice US. 2014;7(6):22-27.
30. Vogel A, Venugopalan V. Mechanisms of pulsed laser ablation of biological tissues. Chem Rev. 2003;103(2):577-644.
31. Wilder-Smith P, Arrastia AM, Liaw LH, Berns M. Incision properties and thermal effects of three CO2 lasers in soft tissue. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1995; 79(6):685-691.
32. Einstein A. Über die von der molekularkinetischen theorie der wärme geforderte bewegung von in ruhenden flüssigkeiten suspendierten teilchen (translation: On the movement of small particles suspended in a stationary liquid demanded by the molecular-kinetic theory of heat). Ann Phys. 1905;2(Doc. 16):549-560.
33. Linden E, Vitruk P. SuperPulse 10.6 um CO2 laser-assisted, closed flap treatment of peri-implantitis. Implant Practice US. 2015: 8(4):30-34.
34. Cobb C, Vitruk P. Effectiveness of a super pulsed CO2 laser for removal of biofilm from three different types of implant surfaces: an in vitro study. Implant Practice US. 2015;8(3):20-28.
35. Romanos G. Laser surgical tools in implant dentistry for long-time prognosis of oral implants. Int Congress Series. 2003;1248:111.
36. Deppe H, Horch H, Helmut G, Brill T, Wagenpfeil S, Donath, K. Peri-implant care with the CO2 laser: in vitro and in vivo results. Med Laser Appl. 2005;20:61-70.
37. Deppe H, Horch H. Laser applications in oral surgery and implant dentistry. Lasers Med Sci. 2007;22:217-221.
38. Julian J. Lasers in implant dentistry. In: Convissar RA. Principles and Practices of Laser Dentistry. St. Louis, MO: Mosby; 2011:114-38.
39. Romanos G, Ko HH, Froum S, Tarnow D. The Use of CO2 Laser in the Treatment of Peri-implantitis. Photomed Laser Surg. 2009;27(3):381-386.
40. Kotlow LA. Lasers in pediatric dentistry. Dent Clin North Am. 2004;48(4):889-922.
41. Zaffe D, Vitale MC, Martignone A, Scarpelli F, Botticelli AR. Morpho-logical histochemical and immunocytochemical study of CO2 and Er:YAG laser effect on oral soft tissues. Photomed Laser Surg. 2004;22(3):185-189.
42. Lambrecht JT, Stübinger S, Hodel Y. Treatment of intraoral heman-giomas with the CO2 laser. J Oral Laser Appl. 2004;4:89-96.
43. Pogrel MA. The carbon dioxide laser in soft tissue preprosthetic surgery. J Prosthet Dent. 1989;61(2):203-208.
44. Niccoli-Filho W, Neves ACC, Penna LAP, Seraidarian PI, Riva R. Removal of epulis fissuratum associated to vestibuloplasty with carbon dioxide laser. Lasers in Med Sci. 1999;14(3):203–206.
45. Haytac MC, Ozcelik O. Evaluation of patient perceptions after frenectomy operations: a comparison of carbon dioxide laser and scalpel techniques. J Periodontol. 2006;77(11):1815-1819.
46. Neckel CP. Vestibuloplasty: a retrospective study on conven-tional and laser operation techniques. Lasers in Dentistry. 1999;76(5)18–23.
47. Strauss RA, Fallon SD. Lasers in contemporary oral and maxillofa-cial surgery. Dent Clin North Am. 2004;48(4):861-888.
48. Deppe H, Horch HH. Current status of laser applications in oral and cranio-maxillofacial surgery. Med Laser Appl. 2007;22(1):39-42.
49. Zeinoun T, Nammour S, Dourov N, Aftimos G, Luomanen M. Myofibroblasts in healing laser excision wounds. Lasers Surg Med. 2001;28(1):74-79.
50. Wang X, Ishizaki NT, Matsumoto K. Healing process of skin after CO2 laser ablation at low radiance: a comparison of continuous-wave and pulsed mode. Photomed Laser Surg. 2005;23(1):20-26.
51. Grbavac RA, Veeck EB, Bernard JP, Ramalho LM, Pinheiro AL. Effects of laser therapy in CO2 laser wounds in rats. Photomed Laser Surg. 2006;24(3):389-396.
52. de Freitas AC, Pinheiro AL, de Oliveira MG, Ramalho LM. Assess-ment of the behavior of myofibroblasts on scalpel and CO2 laser wounds: an immunohistochemical study in rats. J Clin Laser Med Surg. 2002;20(4):221-225.
53. Fisher SE, Frame JW, Browne RM, Tranter RM. A comparative histological study of wound healing following CO2 laser and conventional surgical excision of canine buccal mucosa. Arch Oral Biol. 1983;28(4):287-291.
54. Basu MK, Frame JW, Rhys Evans PH. Wound healing following partial glossectomy using the CO2 laser, diathermy and scalpel: a histological study in rats. J Laryngol Otol. 1988;102(4):322-327.
55. Tambuwala A, Sangle A, Khan A, Sayed A. Excision of oral leuko-plakia by CO2 lasers versus traditional scalpel: A comparative study. J Maxillofac Oral Surg. 2014;13(3):320-327.
Figure 16: Immediate postoperative view of LightScalpel frenectomy/vestibuloplasty performed in less than 1 minute, bloodlessly, and without local anesthesia
Figure 17: Healed laser frenectomy/vestibuloplasty site 4 weeks after the surgery. Note the 3 mm-4 mm gain in the attached gingiva width and no pull at the margin
32 Implant practice Volume 8 Number 5
SEEING THE LIGHT
convenience is keyAvailable in a variety of options, MinerOss® X is an anorganic bovine bone mineral matrix that is physically and chemically comparable to the mineral structure of human bone. The MinerOss® X family of xenografts* can be used in a wide variety of grafting applications, including:
• extraction socket grafting
• ridge and sinus augmentation
• grafting for implant placement
• infrabony periodontal defects
MinerOss® X CollagenMinerOss® X Collagen is a combination of 95% anorganic cancellous bovine bone and approximately 5% bovine collagen. This block form allows for convenience during placement and an ideal solution for many applications.
MinerOss® X Syringe MinerOss® X Syringe is cancellous particulate pre-loaded into a delivery syringe to assist with optimal placement at the defect site.
MinerOss® X Particulate MinerOss® X Particulate is available in either cancellous or cortical form. The complex trabecular architecture and natural consistency allow for ideal bone formation at the defect site.
*Family of xenograft-derived bone graft matrices..MinerOss® is a registered trademark of BioHorizons. MinerOss® X is manufactured by Collagen Matrix, Inc. Not all products are available in all countries. ©BioHorizons. All Rights Reserved. SPMP14168 REV C MAY 2015
MinerOss® Xfamily of xenografts
For more information, contact BioHorizonsCustomer Care: 888.246.8338 or shop online at www.biohorizons.com

Periodontal disease is often responsible for the loss of attachment around teeth and
therefore a major cause of ridge deficiency after the teeth are extracted. The world has become more and more aware of esthetics in dentistry, and any procedure aimed to preserve the hard and soft tissue becomes useful to satisfy the needs of increasingly demanding patients.
This article will present a case of advanced periodontitis treated with a ridge preservation technique and later planned and finalized with the use of guided implant surgery, immediate loading, and thus, soft tissue conditioning in order to minimize the effects of the disease.
The literatureTooth loss in many cases is one of the
primary causes of alveolar bone remodeling and loss. Schropp and colleagues showed the changes in the soft and hard tissues after teeth extraction in clinical and radiographic prospective study (2003).
The tissue changes after removal of a premolar or a molar in 46 patients were evaluated over a period of 12 months by measuring study casts, linear radiographic analysis, and subtraction radiography. Their results showed that the major changes occurred during 1 year after extraction.
Jahangiri and colleagues reviewed the understanding of the biology of tooth extraction, wound healing, and residual ridge remodeling (1988). Defects in socket matrix formation or cellular activity will lead to stalled healing. The review of residual ridge remodeling describes the long-term result of tooth extraction and formation of
residual ridges in which the quantity of bone tissue continuously decreases. The authors suggested that any potential regulatory factor of residual ridge resorption should have an adverse effect either on the increased catabolic activity by osteoclasts or on the decreased anabolic activity by osteoblasts.
A recent study by Barone and colleagues described the tissue changes of extraction sockets with a comparison of spontaneous healing versus a ridge preservation technique with secondary soft tissue healing (2013). The study group was treated with careful extraction and insertion of corticocancellous porcine bone and a collagen membrane, while the control sites received only sutures to stabilize the blood clot. Test sites showed a vertical bone remodeling of 0.3 ± 0.76 mm, 1.1 ± 0.96 mm, and 0.9 ± 0.98 mm at the mesial, buccal, and distal sites, while the control group showed a remodeling of 1 ± 0.7 mm, 2.1 ± 0.6 mm, and 1 ± 0.8 mm at the same sites. Horizontal changes were 3.6 ± 0.72 mm in the control sites and 1.6 ± 0.55 mm in the study group.
This study concluded that alveolar ridge preservation technique performed with collagenated porcine bone graft and a resorbable membrane was able to limit the contour changes after tooth extraction. Another important issue was that test sites
showed a better preservation of facial kera-tinized gingiva when compared to control sites. Also, grafted sites allowed the place-ment of longer implants and wider implants when compared to non-grafted sites.
In 2008, Allegrini and colleagues reviewed the literature on socket preserva-tion and concluded that the maintenance of the alveolar bone after extraction depends on a careful surgical procedure and the use of a biomaterial capable of maintaining the prior space, which is helpful in bone tissue healing.
In 2012, Lindhe and colleagues evaluated an important factor: changes in the pattern of bone resorption in periodontitis and non- periodontitis subjects. The paper was to discuss the tissue of the fully healed extrac-tion sites in patients who had lost teeth as a result of periodontal disease or from other causes. This study indicated that the edentu-lous posterior maxilla was comprised of 58% lamellar bone, 15% woven bone, 7% osteoid, and 10% bone marrow. More than 50% was mineralized bone. Also, Vignoletti and colleagues presented a systematic review of the surgical protocols for ridge preservation after tooth extraction (2012).
Fourteen publications on PubMed, Embase, and the Cochrane Central Register of Controlled Trials (CENTRAL) were evalu-ated, each looking at randomized controlled
Ridge preservation in a case of severe periodontitis
Drs. Roberto Rossi, Ulf Nannmark, Andrea Pilloni, and Nino Squadrito, CDT, demonstrate how to preserve and condition the soft tissue with a combined approach
Roberto Rossi, DDS, MScD, is in private practice in Genova, Italy.
Ulf Nannmark, DDS, PhD, is an associate professor in the Department of Oral and Maxillofacial Surgery at the Sahlgrenska Academy, University of Gothenburg, in Sweden.
Andrea Pilloni, DDS, MScD, is the chairman of the Department of Periodontology at the Sapienza University of Rome in Rome, Italy.
Nino Squadrito, CDT, is head of the Golden Smile Laboratory in Genova, Italy.
Educational aims and objectivesThis article aims to present a case of advanced periodontitis treated with implants and a ridge preservation technique to help preserve and improve the soft tissue.
Expected outcomesImplant Practice US subscribers can answer the CE questions on page 40 to earn 2 hours of CE from reading this article. Correctly answering the questions will demonstrate the reader can:• Identify a technique for approaching implant treatment in severe periodontitis
in order to minimize the collapse of the soft and hard tissue and thus try to preserve the natural esthetics.
• Review the biology of tooth extractions, wound healing, and residual ridge modeling.• See how this technique with the materials used limited contour changes after tooth extraction and
preserved facial keratinized gingiva.• Realize the differences in the pattern of bone resorption in periodontitis and non-periodontitis subjects.• Recognize that the combination of presurgical computed planning and immediate loading might lead to
excellent soft tissue conditioning and minimal surgical traumatism for the hard and soft tissue. • Realize the importance of the relationship between the height of the interproximal bone peak and the
teeth’s contact point to emphasize the importance of maintenance or reconstruction of the bone to support the soft tissue.
34 Implant practice Volume 8 Number 5
CONTINUING EDUCATION
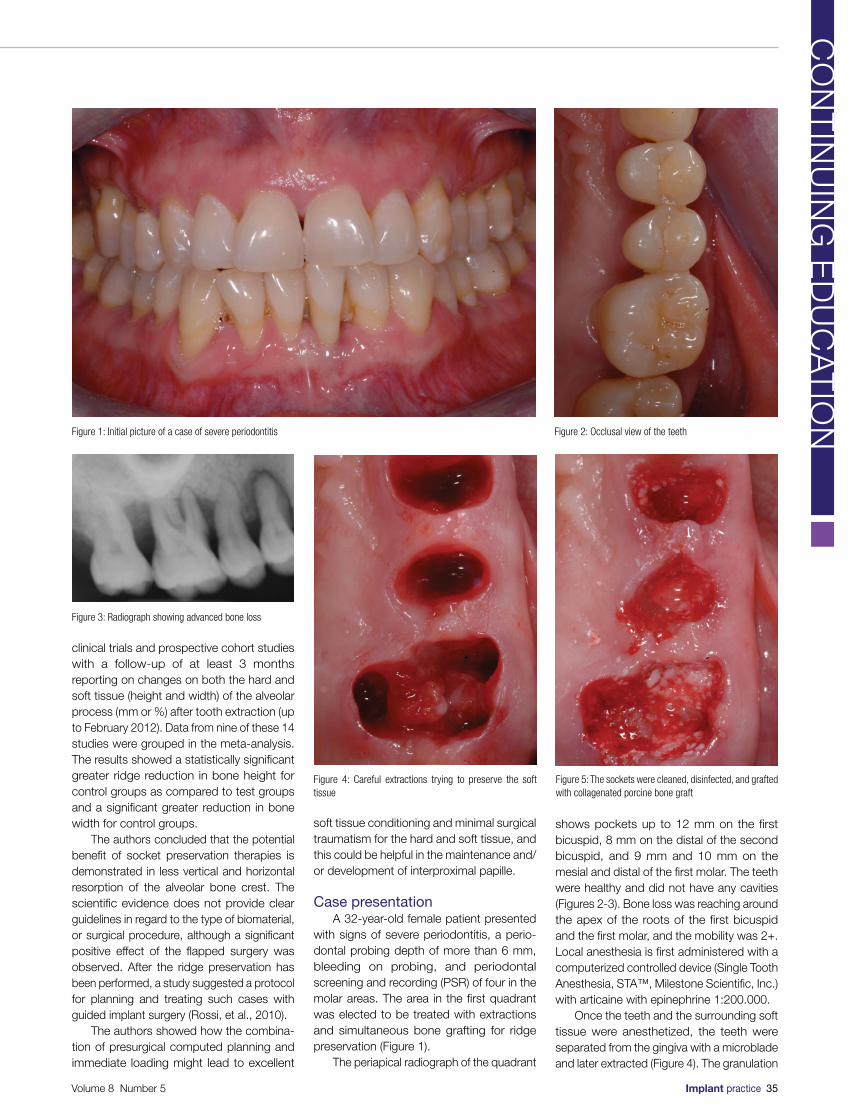
clinical trials and prospective cohort studies with a follow-up of at least 3 months reporting on changes on both the hard and soft tissue (height and width) of the alveolar process (mm or %) after tooth extraction (up to February 2012). Data from nine of these 14 studies were grouped in the meta-analysis. The results showed a statistically significant greater ridge reduction in bone height for control groups as compared to test groups and a significant greater reduction in bone width for control groups.
The authors concluded that the potential benefit of socket preservation therapies is demonstrated in less vertical and horizontal resorption of the alveolar bone crest. The scientific evidence does not provide clear guidelines in regard to the type of biomaterial, or surgical procedure, although a significant positive effect of the flapped surgery was observed. After the ridge preservation has been performed, a study suggested a protocol for planning and treating such cases with guided implant surgery (Rossi, et al., 2010).
The authors showed how the combina-tion of presurgical computed planning and immediate loading might lead to excellent
soft tissue conditioning and minimal surgical traumatism for the hard and soft tissue, and this could be helpful in the maintenance and/or development of interproximal papille.
Case presentationA 32-year-old female patient presented
with signs of severe periodontitis, a perio-dontal probing depth of more than 6 mm, bleeding on probing, and periodontal screening and recording (PSR) of four in the molar areas. The area in the first quadrant was elected to be treated with extractions and simultaneous bone grafting for ridge preservation (Figure 1).
The periapical radiograph of the quadrant
shows pockets up to 12 mm on the first bicuspid, 8 mm on the distal of the second bicuspid, and 9 mm and 10 mm on the mesial and distal of the first molar. The teeth were healthy and did not have any cavities (Figures 2-3). Bone loss was reaching around the apex of the roots of the first bicuspid and the first molar, and the mobility was 2+. Local anesthesia is first administered with a computerized controlled device (Single Tooth Anesthesia, STA™, Milestone Scientific, Inc.) with articaine with epinephrine 1:200.000.
Once the teeth and the surrounding soft tissue were anesthetized, the teeth were separated from the gingiva with a microblade and later extracted (Figure 4). The granulation
Figure 1: Initial picture of a case of severe periodontitis Figure 2: Occlusal view of the teeth
Figure 3: Radiograph showing advanced bone loss
Figure 4: Careful extractions trying to preserve the soft tissue
Figure 5: The sockets were cleaned, disinfected, and grafted with collagenated porcine bone graft
Volume 8 Number 5 Implant practice 35
CO
NT
INU
ING
ED
UC
AT
ION
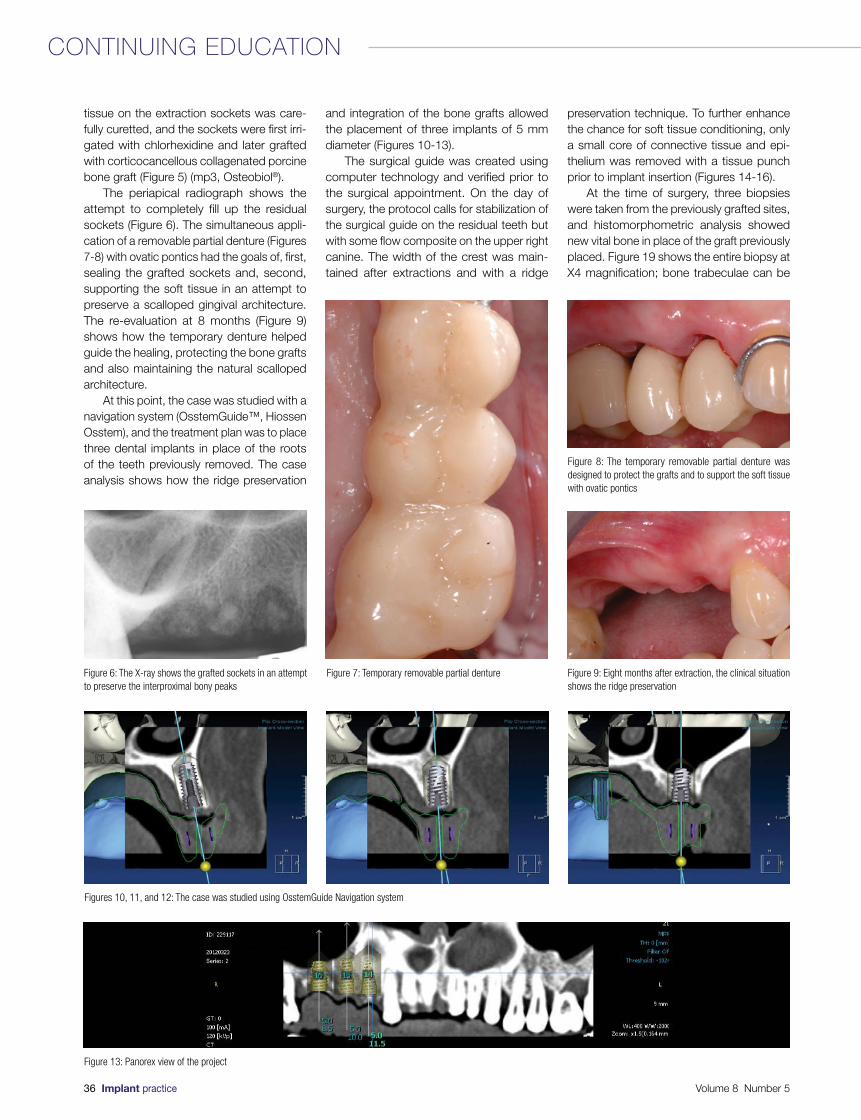
tissue on the extraction sockets was care-fully curetted, and the sockets were first irri-gated with chlorhexidine and later grafted with corticocancellous collagenated porcine bone graft (Figure 5) (mp3, Osteobiol®).
The periapical radiograph shows the attempt to completely fill up the residual sockets (Figure 6). The simultaneous appli-cation of a removable partial denture (Figures 7-8) with ovatic pontics had the goals of, first, sealing the grafted sockets and, second, supporting the soft tissue in an attempt to preserve a scalloped gingival architecture. The re-evaluation at 8 months (Figure 9) shows how the temporary denture helped guide the healing, protecting the bone grafts and also maintaining the natural scalloped architecture.
At this point, the case was studied with a navigation system (OsstemGuide™, Hiossen Osstem), and the treatment plan was to place three dental implants in place of the roots of the teeth previously removed. The case analysis shows how the ridge preservation
and integration of the bone grafts allowed the placement of three implants of 5 mm diameter (Figures 10-13).
The surgical guide was created using computer technology and verified prior to the surgical appointment. On the day of surgery, the protocol calls for stabilization of the surgical guide on the residual teeth but with some flow composite on the upper right canine. The width of the crest was main-tained after extractions and with a ridge
preservation technique. To further enhance the chance for soft tissue conditioning, only a small core of connective tissue and epi-thelium was removed with a tissue punch prior to implant insertion (Figures 14-16).
At the time of surgery, three biopsies were taken from the previously grafted sites, and histomorphometric analysis showed new vital bone in place of the graft previously placed. Figure 19 shows the entire biopsy at X4 magnification; bone trabeculae can be
Figure 6: The X-ray shows the grafted sockets in an attempt to preserve the interproximal bony peaks
Figure 7: Temporary removable partial denture
Figure 8: The temporary removable partial denture was designed to protect the grafts and to support the soft tissue with ovatic pontics
Figure 9: Eight months after extraction, the clinical situation shows the ridge preservation
Figures 10, 11, and 12: The case was studied using OsstemGuide Navigation system
Figure 13: Panorex view of the project
36 Implant practice Volume 8 Number 5
CONTINUING EDUCATION
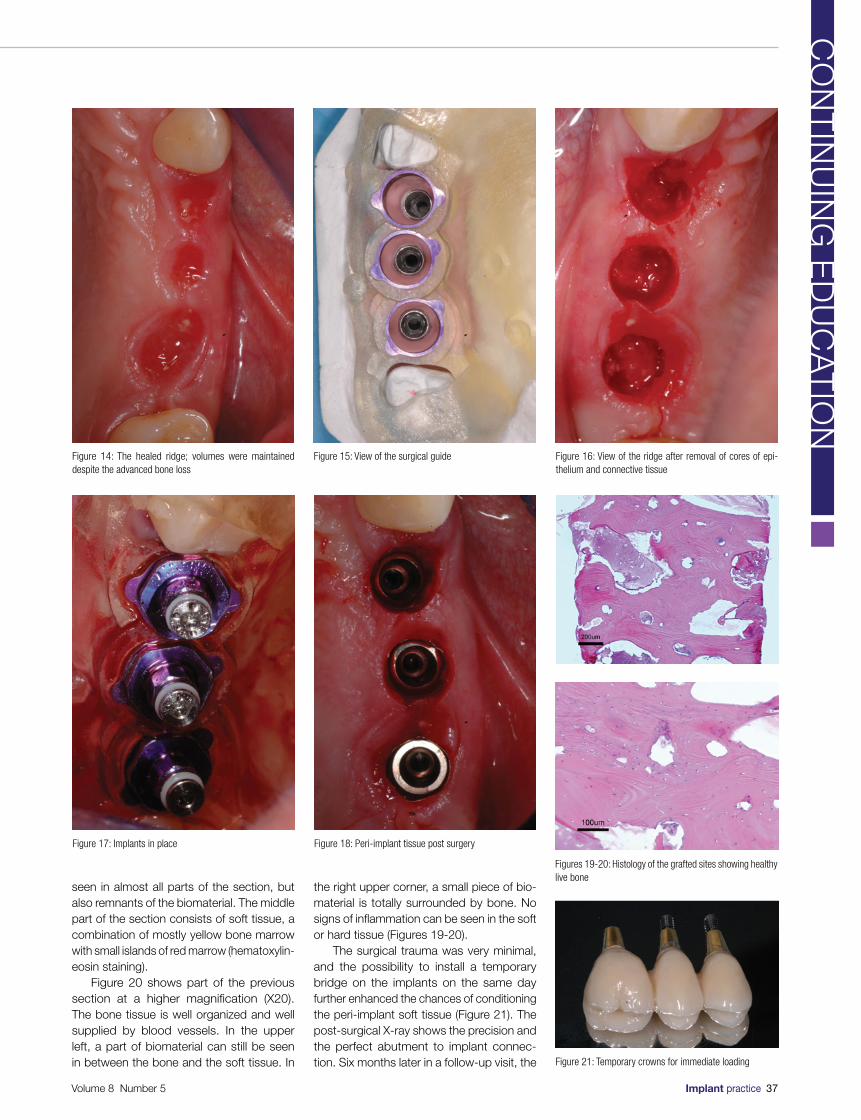
seen in almost all parts of the section, but also remnants of the biomaterial. The middle part of the section consists of soft tissue, a combination of mostly yellow bone marrow with small islands of red marrow (hematoxylin- eosin staining).
Figure 20 shows part of the previous section at a higher magnification (X20). The bone tissue is well organized and well supplied by blood vessels. In the upper left, a part of biomaterial can still be seen in between the bone and the soft tissue. In
the right upper corner, a small piece of bio-material is totally surrounded by bone. No signs of inflammation can be seen in the soft or hard tissue (Figures 19-20).
The surgical trauma was very minimal, and the possibility to install a temporary bridge on the implants on the same day further enhanced the chances of conditioning the peri-implant soft tissue (Figure 21). The post-surgical X-ray shows the precision and the perfect abutment to implant connec-tion. Six months later in a follow-up visit, the
Figure 14: The healed ridge; volumes were maintained despite the advanced bone loss
Figure 15: View of the surgical guide Figure 16: View of the ridge after removal of cores of epi-thelium and connective tissue
Figure 17: Implants in place Figure 18: Peri-implant tissue post surgery
Figures 19-20: Histology of the grafted sites showing healthy live bone
Figure 21: Temporary crowns for immediate loading
Volume 8 Number 5 Implant practice 37
CO
NT
INU
ING
ED
UC
AT
ION
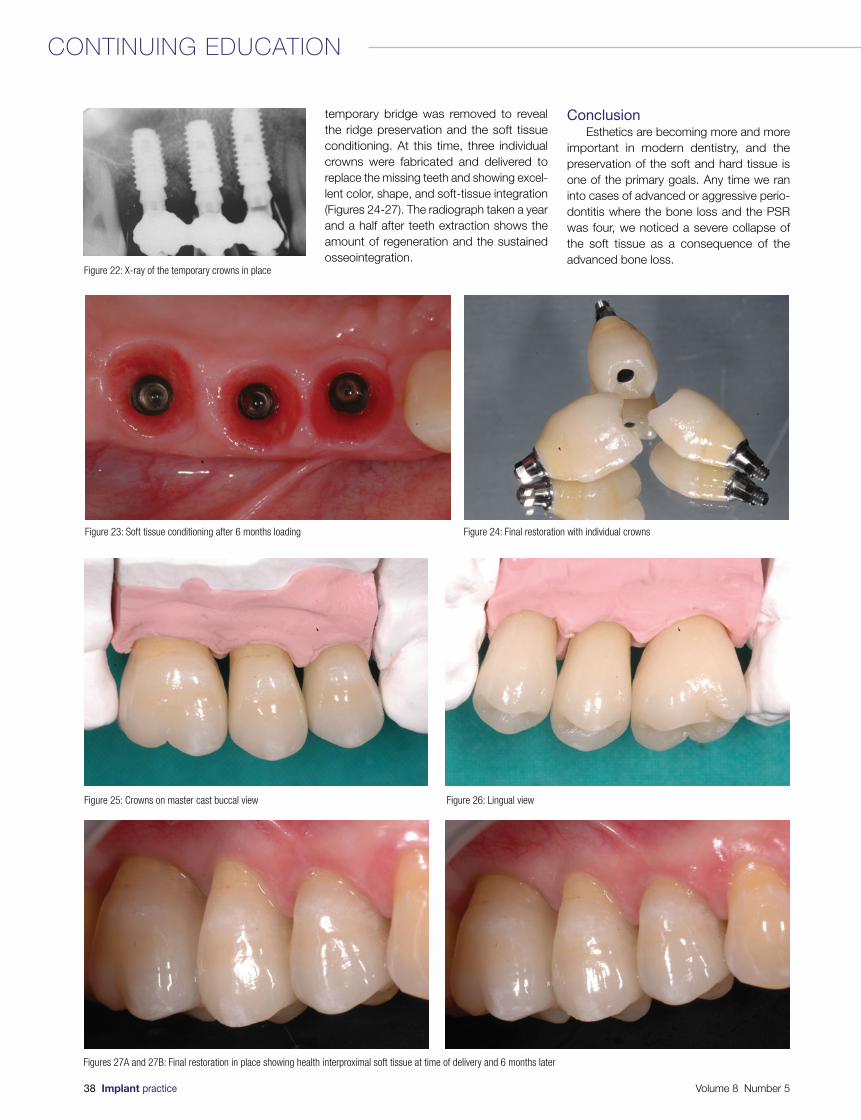
temporary bridge was removed to reveal the ridge preservation and the soft tissue conditioning. At this time, three individual crowns were fabricated and delivered to replace the missing teeth and showing excel-lent color, shape, and soft-tissue integration (Figures 24-27). The radiograph taken a year and a half after teeth extraction shows the amount of regeneration and the sustained osseointegration.
ConclusionEsthetics are becoming more and more
important in modern dentistry, and the preservation of the soft and hard tissue is one of the primary goals. Any time we ran into cases of advanced or aggressive perio- dontitis where the bone loss and the PSR was four, we noticed a severe collapse of the soft tissue as a consequence of the advanced bone loss.
Figure 22: X-ray of the temporary crowns in place
Figure 23: Soft tissue conditioning after 6 months loading Figure 24: Final restoration with individual crowns
Figure 25: Crowns on master cast buccal view Figure 26: Lingual view
Figures 27A and 27B: Final restoration in place showing health interproximal soft tissue at time of delivery and 6 months later
38 Implant practice Volume 8 Number 5
CONTINUING EDUCATION
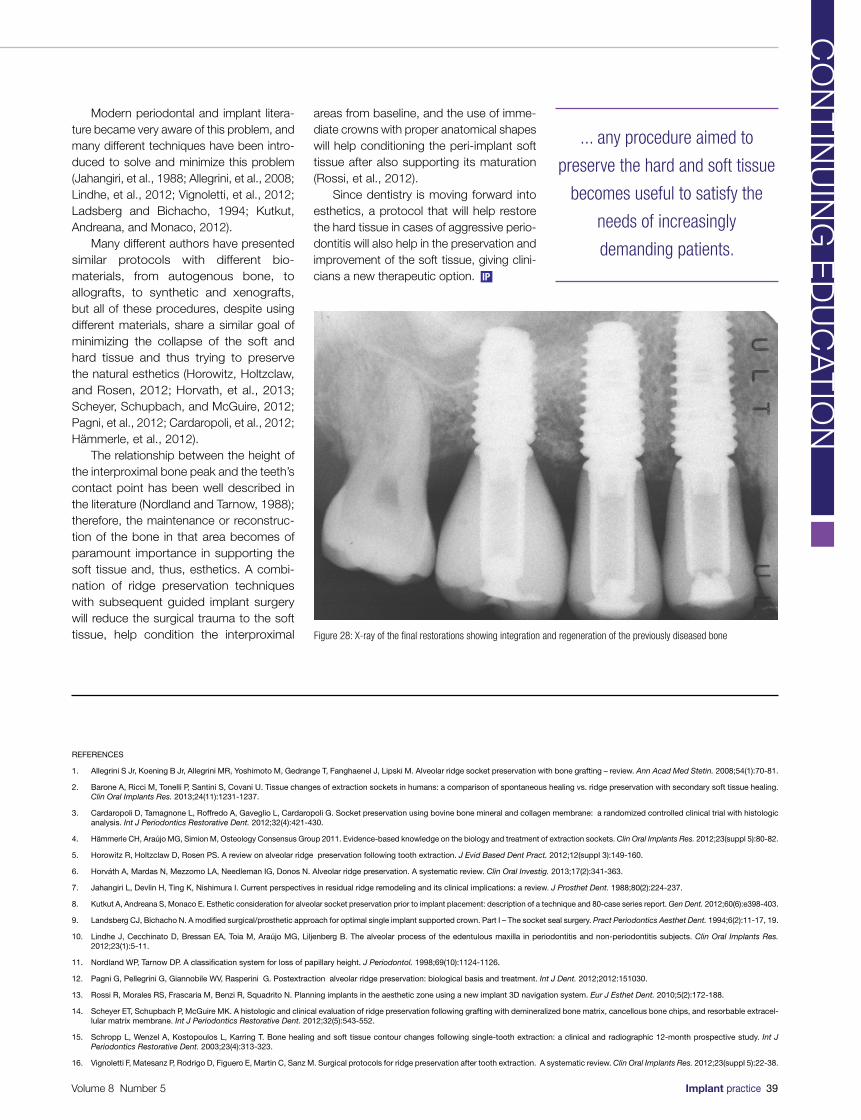
REFERENCES
1. Allegrini S Jr, Koening B Jr, Allegrini MR, Yoshimoto M, Gedrange T, Fanghaenel J, Lipski M. Alveolar ridge socket preservation with bone grafting – review. Ann Acad Med Stetin. 2008;54(1):70-81.
2. Barone A, Ricci M, Tonelli P, Santini S, Covani U. Tissue changes of extraction sockets in humans: a comparison of spontaneous healing vs. ridge preservation with secondary soft tissue healing. Clin Oral Implants Res. 2013;24(11):1231-1237.
3. Cardaropoli D, Tamagnone L, Roffredo A, Gaveglio L, Cardaropoli G. Socket preservation using bovine bone mineral and collagen membrane: a randomized controlled clinical trial with histologic analysis. Int J Periodontics Restorative Dent. 2012;32(4):421-430.
4. Hämmerle CH, Araújo MG, Simion M, Osteology Consensus Group 2011. Evidence-based knowledge on the biology and treatment of extraction sockets. Clin Oral Implants Res. 2012;23(suppl 5):80-82.
5. Horowitz R, Holtzclaw D, Rosen PS. A review on alveolar ridge preservation following tooth extraction. J Evid Based Dent Pract. 2012;12(suppl 3):149-160.
6. Horváth A, Mardas N, Mezzomo LA, Needleman IG, Donos N. Alveolar ridge preservation. A systematic review. Clin Oral Investig. 2013;17(2):341-363.
7. Jahangiri L, Devlin H, Ting K, Nishimura I. Current perspectives in residual ridge remodeling and its clinical implications: a review. J Prosthet Dent. 1988;80(2):224-237.
8. Kutkut A, Andreana S, Monaco E. Esthetic consideration for alveolar socket preservation prior to implant placement: description of a technique and 80-case series report. Gen Dent. 2012;60(6):e398-403.
9. Landsberg CJ, Bichacho N. A modified surgical/prosthetic approach for optimal single implant supported crown. Part I – The socket seal surgery. Pract Periodontics Aesthet Dent. 1994;6(2):11-17, 19.
10. Lindhe J, Cecchinato D, Bressan EA, Toia M, Araújo MG, Liljenberg B. The alveolar process of the edentulous maxilla in periodontitis and non-periodontitis subjects. Clin Oral Implants Res. 2012;23(1):5-11.
11. Nordland WP, Tarnow DP. A classification system for loss of papillary height. J Periodontol. 1998;69(10):1124-1126.
12. Pagni G, Pellegrini G, Giannobile WV, Rasperini G. Postextraction alveolar ridge preservation: biological basis and treatment. Int J Dent. 2012;2012:151030.
13. Rossi R, Morales RS, Frascaria M, Benzi R, Squadrito N. Planning implants in the aesthetic zone using a new implant 3D navigation system. Eur J Esthet Dent. 2010;5(2):172-188.
14. Scheyer ET, Schupbach P, McGuire MK. A histologic and clinical evaluation of ridge preservation following grafting with demineralized bone matrix, cancellous bone chips, and resorbable extracel-lular matrix membrane. Int J Periodontics Restorative Dent. 2012;32(5):543-552.
15. Schropp L, Wenzel A, Kostopoulos L, Karring T. Bone healing and soft tissue contour changes following single-tooth extraction: a clinical and radiographic 12-month prospective study. Int J Periodontics Restorative Dent. 2003;23(4):313-323.
16. Vignoletti F, Matesanz P, Rodrigo D, Figuero E, Martin C, Sanz M. Surgical protocols for ridge preservation after tooth extraction. A systematic review. Clin Oral Implants Res. 2012;23(suppl 5):22-38.
Figure 28: X-ray of the final restorations showing integration and regeneration of the previously diseased bone
Modern periodontal and implant litera-ture became very aware of this problem, and many different techniques have been intro-duced to solve and minimize this problem (Jahangiri, et al., 1988; Allegrini, et al., 2008; Lindhe, et al., 2012; Vignoletti, et al., 2012; Ladsberg and Bichacho, 1994; Kutkut, Andreana, and Monaco, 2012).
Many different authors have presented similar protocols with different bio- materials, from autogenous bone, to allografts, to synthetic and xenografts, but all of these procedures, despite using different materials, share a similar goal of minimizing the collapse of the soft and hard tissue and thus trying to preserve the natural esthetics (Horowitz, Holtzclaw, and Rosen, 2012; Horvath, et al., 2013; Scheyer, Schupbach, and McGuire, 2012; Pagni, et al., 2012; Cardaropoli, et al., 2012; Hämmerle, et al., 2012).
The relationship between the height of the interproximal bone peak and the teeth’s contact point has been well described in the literature (Nordland and Tarnow, 1988); therefore, the maintenance or reconstruc-tion of the bone in that area becomes of paramount importance in supporting the soft tissue and, thus, esthetics. A combi-nation of ridge preservation techniques with subsequent guided implant surgery will reduce the surgical trauma to the soft tissue, help condition the interproximal
areas from baseline, and the use of imme-diate crowns with proper anatomical shapes will help conditioning the peri-implant soft tissue after also supporting its maturation (Rossi, et al., 2012).
Since dentistry is moving forward into esthetics, a protocol that will help restore the hard tissue in cases of aggressive perio-dontitis will also help in the preservation and improvement of the soft tissue, giving clini-cians a new therapeutic option.
... any procedure aimed to
preserve the hard and soft tissue
becomes useful to satisfy the
needs of increasingly
demanding patients.
Volume 8 Number 5 Implant practice 39
CO
NT
INU
ING
ED
UC
AT
ION
IP

1. Tooth loss in many cases is ________ of alveolar bone remodeling and loss.a. not a factorb. one of the primary causes c. not related to the outcomes d. the only cause
2. The tissue changes after removal of a premolar or a molar in 46 patients were evaluated over a period of 12 months by measuring study casts, linear radio-graphic analysis, and subtraction radiography. Their results showed that the major changes occurred during ________ after extraction.a. 1 year b. 2 yearsc. 3 years d. 4 years
3. (In study by Jahangiri and colleagues) Defects in socket matrix formation or cellular activity will lead to __________.a. stabilization of the blood clotb. stalled healingc. decreased catabolic activityd. increase of osteoblasts
4. The authors (Jahangiri and colleagues) suggested that any potential regulatory factor of residual ridge resorption should have ________ either on the increased catabolic activity by osteoclasts or on the decreased anabolic activity by osteoblasts.a. an adverse effect
b. a positive effectc. no effectd. the desired effect
5. This study (by Barone and colleagues) concluded that alveolar ridge preservation technique performed with collagenated porcine bone graft and a resorb-able membrane _________ the contour changes after tooth extraction.a. completely eliminatedb. was unable to limitc. was able to limit d. enhanced
6. In 2008, Allegrini and colleagues reviewed the litera-ture on socket preservation and concluded that the maintenance of the alveolar bone after extraction depends on _________, which is helpful in bone tissue healing.a. a careful surgical procedureb. the use of a biomaterial capable of maintaining
the prior spacec. decreasing catabolic activityd. both a and b
7. Esthetics are becoming more and more important in modern dentistry, and _________ is one of the primary goals.a. the preservation of the soft tissueb. the preservation of the hard tissuec. fabrication of a temporary bridged. both a and b
8. Any time we ran into cases of advanced or aggres-sive periodontitis where the bone loss and the PSR was _______, we noticed a severe collapse of the soft tissue as a consequence of the advanced bone loss.a. twob. four c. six d. eight
9. Many different authors have presented similar proto-cols with different biomaterials, from autogenous bone, to allografts, to synthetic and xenografts, but all of these procedures, despite using different mate-rials, share a similar goal of ___________.a. only using the most cost-effective materialsb. minimizing the collapse of the soft and hard
tissuec. trying to preserve the natural estheticsd. both b and c
10. The relationship between the height of the inter-proximal bone peak and the teeth’s contact point has been well described in the literature; therefore, the maintenance or reconstruction of the bone in that area becomes of paramount importance in __________ and, thus, esthetics.a. supporting the soft tissueb. excising the soft tissuec. hardening the graftd. preventing infection
IMPLANT PRACTICE CEC
E C
RE
DIT
S
Each article is equivalent to two CE credits. Available only to paid subscribers. Free subscriptions do not qualify for the CE credits. Subscribe and receive up to 16 CE credits for only $99. To receive credit, complete the 10-question test by circling the correct answer, then either:
n Post the completed questionnaire to: Implant Practice US CE15720 N. Greenway-Hayden Loop. #9Scottsdale, AZ 85260n Fax to (480) 629-4002.To provide feedback on this article and CE, please email us at [email protected]
Legal disclaimer: The CE provider uses reasonable care in selecting and providing accurate content. The CE provider, however, does not independently verify the content or materials. Any opinions expressed in the materials are those of the author and not the CE provider. The instructional materials are intended to supplement, but are not a substitute for, the knowledge, skills, expertise and judgement of a trained healthcare professional.
FULL NAME
AGD REGISTRATION NUMBER
LICENSE NUMBER
ADDRESS
CITY, STATE, AND ZIP CODE
TELEPHONE/FAX
REF: IP V8.5 ROSSI
Please allow 28 days for the issue of the certificates to be posted.
CONTINUING EDUCATION BROUGHT TO YOU BY
Approved PACE Program ProviderFAGD/MAGD Credit Approval does not imply acceptance by a state or provincial board of dentistry or AGD endorsement12/1/2012 to 11/30/2016Provider ID# 325231
Ridge preservation in a case of severe periodontitisROSSI, ET AL.
40 Implant practice Volume 8 Number 5

IntroductionIatrogenic injuries to the inferior alve-
olar nerve (IAN) can impact significantly on patients’ lives. Altered sensation and pain in the orofacial region may interfere with speaking, eating, kissing, shaving, applying makeup, tooth brushing, drinking, and just about every social interaction (Renton, 2010).
IAN injury is the most problematic consequence of dental surgical procedures and has major medico-legal implications (Renton, 2011).
Causes of inferior alveolar nerve injury include placement of dental implants, local anesthetic injections, third molar surgery, endodontics, trauma, and orthognathic surgery.
Case history
A healthy 53-year-old female patient presented with a collapsed occlusion. Her main complaints were difficulty in chewing, esthetic dissatisfaction, and a desire not to lose more teeth. Function was limited to the seven anterior teeth with no posterior support (Figures 1-3). Loss of posterior occlusion may result in the loss of neuromuscular stability of the mandible, temporomandibular joint (TMJ) dysfunction, reduced mastica-tory efficiency, loss of vertical dimension, and poor esthetics. Rehabilitation should aim to address all of these concerns.
Further complications were lack of attached keratinized tissues and reduced mandibular alveolar ridge volume. Keratin-ized attached tissue, although a conten-tious topic, may have long-term benefits
with regard to plaque control at the implant site (Bouri and Nouneh, 2008; Lang and Loe, 1972).
This case highlights multidisciplinary comprehensive treatment planning of a complex case using cone beam computed tomography (CBCT) and computer-designed surgical guides.
The International Team of Implantology (ITI) SAC Assessment tool determined this case as complex.
Methods and materialsA diagnostic wax-up determined the
final 3D result that could be achieved in both arches. A CBCT revealed a very thick lingual cortex with poor cancellous bone, and close proximity of the mental foramina in planned positions LL5 and LR5. Simplant® Pro (Materialise Dental) was used to create the 3D representation of the anatomical struc-tures (Figures 4A-4B).
A stereolithographic stent (Classic SurgiGuide®, Materialise Dental) was printed
from the final treatment plan. This guides the surgeon with the position and angulation of implant placement, but not placement depth.
A tooth-supported, Classic SurgiGuide was decided upon for the following reasons.
Due to the close proximity of the mental foramina to the planned implant sites in posi-tions LL5 and LR5 and a very thick lingual cortex with almost no cancellous bone, it
Surgery in prevention of inferior alveolar nerve damage
Drs. Lira Rahman, Jacobus Hercules van den Heever, and Andre W. van Zyl present the application of guided dental implant surgery in prevention of inferior alveolar nerve damage in a patient with compromised bone
Lira Rahman, BChD (Stell), is Periodontics registrar at the Department of Periodontics and Oral Medicine, University of Pretoria, Pretoria, South Africa.
Jacobus Hercules van den Heever, BChD, MChD (Prost) (Pret), is a Prosthodontist in the Department of Prosthodontics, University of Pretoria, Pretoria, South Africa.
Professor Andre W. van Zyl, BChD, MChD(OMP)(Stell), is a Periodontist in the Department of Periodontics and Oral Medicine, University of Pretoria, Pretoria, South Africa.
Educational aims and objectivesThis article aims to present the application of guided dental implant surgery in prevention of inferior alveolar nerve damage in a patient with compromised bone.
Expected outcomesImplant Practice US subscribers can answer the CE questions on page 43 to earn 2 hours of CE from reading this article. Correctly answering the questions will demonstrate the reader can:• Identify some symptoms of inferior alveolar nerve (IAN) damage.• Recognize some causes of IAN.• See a case where IAN was prevented.• Realize the benefit of the surgical guide in planning the case.
Figure 1: Preoperative panoramic radiograph
Figure 2: Preoperative view maxilla
Figure 3: Preoperative view mandible
Volume 8 Number 5 Implant practice 41
CO
NT
INU
ING
ED
UC
AT
ION

was planned that the implants would need to be angled toward the lingual cortex to avoid the mental foramina and the inferior alveolar nerve (IAN). It was anticipated that angling the implant lingually in a controlled manner would result in a slight deviation of the implant toward the buccal direction.
The implication of this is that the surgeon requires a guide with a degree of “play,” which will allow him/her to make corrections during surgical placement of the implants.
The lack of attached keratinized tissue was addressed by performing bilateral mandibular vestibuloplasty procedures and free gingival grafts.
Straumann® Roxolid® Tissue Level Implants were placed with a 2-mm safety zone between implant and nerve (Greestein and Tarnow, 2006). Two 3.3 mm x 10 mm implants were inserted in the LL5 and LR5 sites and two 3.3 mm x 8 mm implants in the LL6 and LR6 sites using the Classic SurgiGuide. Roxolid is 50% stronger than pure titanium and shows improved integra-tion with bone and is thus ideally suited for reduced bone situations (www.straumann.us, 2008).
Provisional implant supported crowns are shown in Figure 5. Maxillary implants were subsequently inserted as planned (Figure 6). No postoperative nerve fallout or complica-tions were experienced.
Data set mappingA postoperative CBCT was taken and
mapped with the preoperative scan to deter-mine the correlation between planned and final implant positions (Table 1). Angular
deviations of this case are within the expected deviations for Classic SurgiGuide systems (Cassetta, et al. 2013; Park, et al., 2009). The postoperative CBCT mapping of the planned and eventual positions of the implants are shown in Figure 7.
ConclusionsThe preoperative planning
and use of a surgical guide were beneficial in this case as it provided knowledge of the exact location of the mental foramina, IAN, alveolar ridge dimensions, and the quality and quantity of bone available. This case demonstrates the importance of correctly diagnosing complex cases using the ITI SAC Assessment tool.
The only alternative to this treatment would have been bone block augmentation in the area of the mental foramen, a proce-dure too risky to undertake.
Complications with such complex cases can significantly impact the lives of patients and should be approached with extreme caution by experienced clinicians only.
AcknowledgmentsThe authors recognize Nicolette Schroeder, Simplant S.A., and Materialise Dental (Leuven, Belgium) for assistance and contribution toward the planning of this complex case. This article was adapted from the poster, ”The application of guided dental implant surgery in prevention of inferior alveolar nerve damage in a patient with compromized bone,” which won First Prize at the ITI Congress Southern Africa 2013, July.
REFERENCES
1. Bouri A Jr, Bissada N, Al-Zahrani MS, Faddoul F, Nouneh I. Width of keratinized gingiva and the health status of the supporting tissues around dental Implants. Int J Oral Maxillofac Implants. 2008;23(2):323-326
2. Cassetta M, Giansanti M, Di Mambro A, Calasso S, Barbato E. Accuracy of two stereolithographic surgical templates: a retrospective study. Clin Implant Dent Relat Res. 2013;15(3):448-459.
3. Greestein G, Tarnow D. The mental foramen and nerve: Clinical and anatomical factors related to dental implant placement: A literature review. J Periodontol. 2006;77(12):1933-1943.
4. Lang NP, Löe H. The relationship between the width of keratinized gingiva and gingival health. J Periodontal. 1972;43(10): 623-627.
5. Park C, Raigrodski AJ, Rosen J, Spiekerman C, London RM. Accuracy of implant placement using precision surgical guides with varying occlusogingival heights: An in vitro study. J Prosthet Dent. 2009;101(6):372-381.
6. Renton T. Prevention of Iatrogenic Inferior Alveolar Nerve Injuries in Relation to Dental Procedures. Dent Update. 2010; 37(6):350–366.
7. Renton T. Minimizing and managing nerve injuries in dental surgical procedures. Faculty Dent J. 2011;2(4):164-171.
8. Gottlow J, Dard M, Kjellson F, Obrecht M, Sennerby L. Eval-uation of a new titanium-zirconium implant.A biomechanical and histological comparative study in minipigs. Strau-mann. Study presented at Academy of Osseointegration 23rd Annual Meeting. Boston, MA. February 28-March 1 2008. http://www.straumann.us/content/dam/internet/straumann_us/resources/whitepaper/en/USLIT_285.pdf. Accessed September 17, 2015.
Figure 4A: Virtual implant planning Figure 4B: Implants planned lingual to the IAN Figure 5: Mandibular provisional crowns
Figure 6: Postoperative panoramic radiograph
Figure 7: Angular deviations demonstrated with mapping. Yellow — planned implant position. Red — final implant position
Table 1: Results of data set mapping
Angular deviation (degrees) Lateral deviation (mm)
Implant LR6 4,9956 1,4608
Implant LR5 2,5615 0,3925
Implant LL5 7,6647 0,2229
Implant LL6 3,5797 1,0744
42 Implant practice Volume 8 Number 5
CONTINUING EDUCATION
IP
1. _______ in the orofacial region may inter-fere with speaking, eating, kissing, shaving, applying makeup, tooth brushing, drinking, and just about every social interaction.a. Altered sensationb. Painc. Dermatological issuesd. both a and b
2. ____ is the most problematic consequence of dental surgical procedures and has major medico-legal implications.a. IAN injuryb. Pain at the injection sitec. MRSAd. TMJ
3. Causes of inferior alveolar nerve injury include placement of dental implants, __________, trauma, and orthognathic surgery.a. local anesthetic injectionsb. third molar surgeryc. endodonticsd. all of the above
4. This (stereolithic stent) guides the surgeon with ______ placement, but not placement depth.a. the position of the implant
b. the angulation of implantc. both a and bd. none of the above
5. (In this case history) It was anticipated that _______ in a controlled manner would result in a slight deviation of the implant toward the buccal direction.a. angling the implant buccallyb. angling the implant linguallyc. rotating the implantd. torquing down the implant
6. The lack of attached keratinized tissue was addressed by performing __________.a. root planing and curettageb. bilateral mandibular vestibuloplasty
proceduresc. free gingival graftsd. both b and c
7. Straumann® Roxolid® Tissue Level Implants were placed with a _________ between implant and nerve.a. .5-mm safety zoneb. 2-mm safety zone c. 3-mm safety zoned. 4-mm safety zone
8. Roxolid is _____ stronger than pure titanium and shows improved integration with bone and is thus ideally suited for reduced bone situations. a. 25%b. 35%c. 50%d. 64%
9. The preoperative planning and use of a surgical guide were beneficial in this case as it provided knowledge of _________, and the quality and quantity of bone available.a. the exact location of the mental foraminab. the location of the IANc. alveolar ridge dimensionsd. all of the above
10. The only alternative to this treatment would have been bone block augmentation in the area of the _______, a procedure too risky to undertake.a. TMJb. mental foramenc. lingual cortexd. hypoglossal nerve
IMPLANT PRACTICE CEC
E C
RE
DIT
S
Each article is equivalent to two CE credits. Available only to paid subscribers. Free subscriptions do not qualify for the CE credits. Subscribe and receive up to 16 CE credits for only $99. To receive credit, complete the 10-question test by circling the correct answer, then either:
n Post the completed questionnaire to: Implant Practice US CE15720 N. Greenway-Hayden Loop. #9Scottsdale, AZ 85260n Fax to (480) 629-4002.To provide feedback on this article and CE, please email us at [email protected]
Legal disclaimer: The CE provider uses reasonable care in selecting and providing accurate content. The CE provider, however, does not independently verify the content or materials. Any opinions expressed in the materials are those of the author and not the CE provider. The instructional materials are intended to supplement, but are not a substitute for, the knowledge, skills, expertise and judgement of a trained healthcare professional.
FULL NAME
AGD REGISTRATION NUMBER
LICENSE NUMBER
ADDRESS
CITY, STATE, AND ZIP CODE
TELEPHONE/FAX
REF: IP V8.5 RAHMAN
Please allow 28 days for the issue of the certificates to be posted.
CONTINUING EDUCATION BROUGHT TO YOU BY
Approved PACE Program ProviderFAGD/MAGD Credit Approval does not imply acceptance by a state or provincial board of dentistry or AGD endorsement12/1/2012 to 11/30/2016Provider ID# 325231
Surgery in prevention of inferior alveolar nerve damageRAHMAN, ET AL.
Volume 8 Number 5 Implant practice 43

Dee Dee Reid has focused her 20-plus year career in dentistry, and her experience spans the spectrum of care. Ms. Reid began her career in the back office where she gained a deep understanding of clinical details and practice dynamics. She connects with patients as a top-producing patient care coordinator. Ms. Reid helps doctors explain and schedule large cases and works alongside general dentists, dental specialists, and their teams to advance practice goals and get results. Most recently, she was a guest lecturer and workshop coordinator for the Functional Aesthetics series with Dr. Mark Montgomery and Dr. David Hornbrook. She frequently leads team programs for Contemporary Products Solutions related to team development for Invisalign® office systems. She has iTunes® podcasts available from the Thriving Dentist Show with Gary Takacs (The Relationship-Driven Practice) and from Dental Up with Dr. David Hornbrook (Increasing Your
Practice Exponentially). Ms. Reid currently works with Dr. Lincoln Parker in Orange County, California, as a Patient Concierge. She is also Principal at D2 Coaching and Consulting. You can email her at [email protected].
Let’s face it, no one likes to hear the word “no.” But the reality is, despite the
economic upturn, patients are still reluctant to say “yes” to larger treatment plans. A 2014 American Dental Association (ADA) study found that 40% of adults indicated that they will forgo dental care due to cost.1 Clearly, a healthy mouth shouldn’t be an “either/or” proposition for patients, but no one wants to be a pushy salesperson either.
So what can you do?
For over 20 years, I’ve helped dental practices from Texas to California realize profitable growth. The key to getting higher acceptance rates lies in how your office approaches the treatment plan presenta-tion. Try using these five proven techniques, and you’ll have more patients saying “yes.”
1. Listen and learnDid your last case presentation seem a
little one-sided? Was the patient nodding as you talked, but then at the end of the
exam, he/she just left without commit-ting to the procedure? The problem starts with the communication technique. Often, patients don’t fully comprehend what you’re proposing and how they can afford to pay for it. Remember, it’s hard to focus on anything when your mouth is full of equipment.
I recommend to my clients that they modify their consultation process. Start by conducting the usual exam, but pause before delivering the prognosis. Ask patients what’s important to them. Ask about their goals and their overall health, not just their oral health. Ask if they are happy with their appearance and their confidence level when they smile. Then, just listen. Let patients tell you what they are feeling.
Performing this simple step will provide valuable tips on how to position your treat-ment plan in a way that directly aligns with the patient’s personal goals. Discuss “why” and “how” your treatment plan addresses their concerns. Avoid simply listing “what”
Five foolproof ways to get a “yes” to more
treatment plans
Dee Dee Reid discusses ways to help patients get the dental care they need
44 Implant practice Volume 8 Number 5
PRACTICE DEVELOPMENT
©2015 Lending Club Patient Solutions products and services provided through Springstone Financial, LLC, a subsidiary of LendingClub Corporation. Payment plans made by issuing bank partners.
Isn’t it time your patient fi nancingmeasured up to your patient care?
“ Same-day treatment acceptance has gone up since incorporating Lending Club Patient Solutions into our treatment presentation.”—Christina C., Senior Treatment Coordinator, Georgia
“ Their high-quality customer service is unbeatable, plus they cost less than any other patient-fi nancing providers—a win for our patients and our practice.”
—Dee Dee R., Patient Concierge, Texas
Discover a new approach to patient fi nancing and see why we continue to get rave reviews. To learn how easy patient fi nancing can be:
Call 844.936.6673 or visit lendingclub.com/providers.
Formerly Springstone Patient Financing

you’re going to do (too much procedural or technical information can be off-putting). This active listening technique is far more collab-orative. When patients feel understood, it naturally follows that they are more likely to say “yes” to the treatment plan you’ve devel-oped together.
2. Show, don’t just tellShowing your patients what’s going on
inside their mouth is a lot more powerful than simply telling them. That’s why I strongly recommend using intraoral digital photog-raphy during the diagnostic phase. Pointing to a problem area with a digital image makes any issue become immediately clear.
Remember, for most patients, if it doesn’t hurt, it isn’t a problem. That’s because patients see only what’s in the bathroom mirror. Once patients see full-mouth photog-raphy, it’s so much easier to have a construc-tive dialogue. Showing patients a photo of their own dental issue lets them understand the need for even the most preemptive of treatment plans.
3. Success takes teamworkNo matter how hardworking or talented,
every dentist needs a good support team. That’s why (if you don’t already have one), I strongly recommend creating the posi-tion of Patient Coordinator. I’ve also seen this role called “Patient Care Counselor,” “Patient Procedure Manager,” or as in my case, “Patient Concierge”— but call it what you like, this position is key. You see, once the dentist has defined the treatment plan, it’s the Coordinator who works out the details with the patient.
I’ve found many patients are more comfortable talking to the Coordinators. That’s because they can use layperson’s terms to review procedures, insurance coverage, and the ease of third-party financing options. For many patients, how to pay is just as important as understanding what they’re paying for. Patients also like that Coordinators understand the need for affordability and financing options. Ultimately, a good Coordinator can make all the differ-ence in closing the case.
But what about the cost of this new position? The good news is that adding a skilled Treatment Coordinator can pay for itself. Here’s the math: A skilled Coordinator will cost between $3,500-$5,000 per month (depending on where your practice is located). But that same Coordinator can schedule and close an average of $2,000-$5,000 per day. Plus, the increase in practice collections is
often between $25,000-$75,000 per month. All this while freeing up the clinical team and the doctor to do what they do best — proce-dures. Now that’s a healthy ROI!
4. Educate everyone, not just the patient
Clearly, creating a Patient Coordinator position is important. But I reinforce with my clients the need to educate the entire support staff on frequently performed procedures, treatment schedules, common medical terms, financing option details, and practice protocols. That way, no matter who inter-acts with the patient, the conversation is seamless.
As a practice becomes more successful (and everyone becomes busier), an office-wide communication strategy is essential. This can be accomplished a number of ways: weekly staff meetings, office-wide emails or memos, even a company newsletter. It’s your choice, just as long as everyone is kept up-to-date on important practice developments.
5. Make it easy to say “yes” I started this story with news of an ADA
study. The fact is that over 40% of adults are still concerned about paying for dental care. Clearly, ease of obtaining affordable financing is an important factor for getting patients to say “yes.”
Many doctors don’t feel comfortable talking about money — but I always discuss third-party financing with patients. I also recommend my D2 Coaching and Consulting clients do the same. You see, as Concierge, it’s my job to make it as easy as possible for the patient to say “yes” to the doctor’s treatment plan. That’s why I love working with Lending Club Patient Solutions (formerly Springstone Patient Financing).
Honestly, they’re great partners. I’ve worked with Lending Club Patient Solutions for over 8 years now because they do an amazing job of empowering patients with more responsible and convenient financing options. Patients get what they want: fast approvals, True No-Interest Plans2 that avoid unwelcome surprises, and Extended Plans with great rates for low monthly payments. Your practice gets convenient selling tools,
helpful email updates with the patient’s funding status, five-star customer service, and some of the lowest practice fees in the industry.
Some dental practices do still use self-funded patient financing. But the half-now/half-later business can be a recipe for disaster. No one wants to have the tough “your payment is late” conversation — after all, you’re not in the debt collection business. With a good financing partner, you can avoid all of that. Their no-default risk means the office receives payment upfront, so collec-tions never cross your mind. Plus, working with an exceptional vendor like Lending Club Patient Solutions says a lot for your practice’s reputation and helps you build lasting patient relationships to grow your business.
You can find out more about Lending Club Patient Solutions at lendingclub.com/providers.
Time to put the steps into practiceNaturally, there are lots of ways to help
patients get the dental care they need and the services they want. But I hope you’ve found the tips I’ve covered here helpful, including honing your listening skills, using visuals, adding the role of Patient Coordi-nator, and recommending patient-friendly financing like plans offered through Lending Club Patient Solutions.
Imagine how successful your practice would be if just 50% more of your patients actually scheduled a procedure after their consultation? This type of conversion rate is possible when you follow these five easy steps.
REFERENCES
1. Yarbrough C, Nasseh K, Vujicic M. Why adults forgo dental care: evidence from a new national survey. [research brief]. American Dental Association, Health Policy Institute. http://www.ada.org/media/ADA/Science%20and%20Research/HPI/Files/HPIBrief_1114_1.ashx. Published November 2014. Accessed September 16, 2015.
2. No Interest for 6, 12, 18 or 24 months, after that 22.98% variable APR. Interest will be charged to your account at the standard variable APR of 22.98% (based on the Prime Rate) from the end of the promotional period on the remaining balance if the purchase balance is not paid in full within the promotional period. Minimum monthly payments for this plan during the promotional period will be the greater of: the amount of the purchase divided by the number of months in the promotional period (rounded up to the nearest $1.00); or $5. Required minimum purchase of $499 for the 6-month plan; $999 for the 12-month plan; $1,499 for the 18-month plan; $2,499 for the 24-month plan. Lending Club Patient Solutions credit accounts are offered by Comenity Capital Bank who determines qualifications for credit and promo-tion eligibility. Minimum Interest Charge is $1.00 per credit plan. Standard variable APR of 22.98%.
The key to getting higher acceptance rates lies in how your
office approaches the treatment plan presentation.
46 Implant practice Volume 8 Number 5
PRACTICE DEVELOPMENT
IP
Volume 8 Number 5 Implant practice 47
DENTSPLY and Sirona enter into definitive merger agreement
DENTSPLY International Inc. and Sirona Dental Systems, Inc., announced today that Boards of Directors of both companies have unanimously approved a definitive merger agreement, which will result in the world’s leading manufacturer of professional dental products and technologies. The combination will create a combined company with the largest sales and service infra-structure in dental with 15,000 employees globally. The combined company, supported by its leading platforms in consumables, equipment, and technology, will offer a powerful set of compli-mentary offerings and end-to-end solutions to enhance patient care. Dental professionals across the globe will be supported by the largest sales and service infrastructure in the industry, supported by leading distributors, to deliver an optimized product range that will meet the increasing global demand for digital dentistry and integrated solutions.
Read more about the companies at www.DENTSPLY.com or www.sirona.com.
Brasseler USA® creates iPhone® application for dental professionals
Brasseler USA®, a leading manufacturer of innovative, quality dental instrumentation, announces the wide release of the new Solutions Finder application, helping dental professionals iden-tify the right solution kit for their patients and procedures. The application is currently available in the iTunes® store at no cost to all iPhone® and iPad® users and is designed to be used by dental and laboratory professionals when they need to find the appropriate Brasseler bur systems for a specific procedure. Once they have found the best kit for the task at hand, the application allows them to request a price quote or to purchase the kit online.
The Brasseler USA Procedure Solutions application is efficient and easy to use:
• Dental professionals input information based on the specific procedure they are working on, including crowns, veneers, inlay/onlays, composites, amalgams, removable prosthetics, laboratory procedures, and more.
• The user can then choose between a wide variety of mate-rial choices within the procedure category.
• Once the material is selected, the application displays a selection of recommended procedure systems for the specified material.
• The user can then view detailed information about each recommended solution kit, including photos, system components, and various complimentary items.
To download the new Brasseler USA Procedure Solutions application, please visit http://brasselerusa.com/app.
KaVo Kerr Group Imaging introduces Invivo 5.4
KaVo Kerr Group Imaging has released Invivo 5.4, an enhance-ment to the award-winning CCT 3D imaging treatment-planning software. The new upgrade is fully integrated and exclusively used with Instrumentarium™ Dental, Gendex™, and SOREDEX™ 3D imaging systems. Upgraded, feature-rich software offers more control when designing crowns, abutments, and implants right from the cone beam 3D scan. Invivo 5.4 simplifies the entire implant selection process. With the ability to adjust and size the implant directly within the 3D rendering, you can now set implants individually or in parallel groups.
The upgraded Invivo 5.4 offers:• Quick and easy bone-grafting simulation• Advanced tools to design crowns fitting prepped teeth,
abutments, or pontics• Enhanced abutment design • Accurate jaw articulation simulation• Richer and more detailed airway analysisFor more information, visit http://www.gendex.com/invivo.
MD Guide 2 in 1 – Pilot drill and surgical guide
The MD Guide is a simple alternative to fabricating a conven-tional surgical guide — because 1 millimeter can make a real difference.
• Don’t change anything with your current procedure.• Minimize the stress and the frustration of a misplaced
implant.• Provides for accurate mesio-distal spacing and parallelism.• Use with any implant system or brand.For more information, visit www.endotechnic.com or call
877-477-8899.
M A T E R I A L S&
E Q U I P M E N Tlllllllllllll lllllllllllll
Toks Oyegunle is a leading business coach in the United Kingdom who enjoys helping dentists achieve success using proven techniques and strategies.
What target market do you currently attract — and why do you attract it?
This question should hopefully make you think of the current effect of your past marketing efforts. The simple fact is that the leads and patients you attract are a direct reflection of the target market you choose to focus on.
To answer this question — and many others related to your marketing activities, I am going to use a tool that I call the “triple M” profitable marketing framework. This frame-work is about getting the right message to the right market using the right media and methods effectively, efficiently, and profit-ably. It can help you to simplify, understand, and apply the essence of what profitable marketing really is.
The power of threeTo fully understand the market you
currently attract, there is a simple, but extremely valuable, exercise you can do.
Create a project to review your patient database going back as far as you can, and group all your patients into three distinct categories:
1. Best patients2. Average patients3. Worst patientsYou should have your own criteria for
deciding what constitutes the definition of patients in each category, but you may wish to consider the following.
Your “best patients” category should consist of people you really love to see for one reason or another; typically they will be the most profitable patients your practice has.
The “average patients” will be just that — they are not the most profitable, but they are probably loyal, relatively easy to treat
and satisfy with minimum stress to you and your team.
The “worst patients” are the ones that give you headaches — I am sure some may come to mind already. They are the ones that are regularly late for appointments, thereby messing up your work schedule. They regu-larly complain about your prices, staff, or services. You actually dread treating these patients as you have come to realize they are just very difficult to satisfy.
Nurturing patientsHaving done this exercise, I would urge
you to nurture all the best patients you can identify. Make them feel special in all inter-actions with your practice; explore the many ways you can provide more value to them while also extracting more revenue from the relationship. You will generate the most revenue from this group directly and sub-sequently from their referrals, assuming your practice has the appropriate referral- generating systems in place.
Study the average patients carefully; seek to understand them better as there is a good chance of converting between 10% and 40% of them to your best patient category, depending on their profiles and the marketing strategies you deploy to this effect.
Most of them will, however, remain average patients, so you need to make sure they are profitable, reliable, and to keep them loyal to your practice for as long as possible. There are a number of patient retention strategies you should seek to deploy in this regard.
With the group you identify as your “worst patients,” you should realistically consider “firing” as many of them as you can, as soon as possible. While this may sound somewhat harsh, you should realize it’s most likely the best thing you can do for your practice; you will save money, time, and improve team morale in the long term. In the short term, however, you should try to understand why
they are in the worst patient category and convert those that have similar profiles as your perfect patients. There are a number of ways to do this, but really, you should be sure they are worth this effort, hence the need to limit the exercise only to the ones that match your perfect patient profile.
Please understand that the process of categorizing your existing patients is very important and a necessary part of fully under-standing who you have been attracting with your existing marketing. You can actually do this yourself; you can delegate it to your practice manager or get a consultant to help you with the process. How you do it doesn’t really matter, but it is something you simply must do if you are serious about creating a thriving dental practice.
With a good understanding of your current patient base, we should explore creating a profile of who you really want to attract as a patient moving forward. The previous exercise will be quite helpful as you should have observed some trends among the best patients you have already identified.
This next exercise requires you to think in futuristic terms and develop a crystal-clear profile, or what I call the “perfect patient avatar,” a detailed description of the ideal patient you want to attract to your practice.
Having identified the best patients you currently have, the next step is to describe what a perfect patient would look like to you. How much do they earn? How old are they? Are they married or single? What do they do for a living? How important is their appear-ance to them? What car do they drive? Where do they go on holiday? What party do they vote for? These questions are to give you a general idea of how much you need to know about your perfect patients in order to attract them effortlessly to your practice.
The simple goal here is to develop an avatar — a profile that describes a very clear picture of who you really want as perfect patients for your practice. You will need to
Target practice
In the second part of his series on marketing, Toks Oyegunle explains how creating the perfect patient avatar can help move your practice forward
48 Implant practice Volume 8 Number 5
PRACTICE DEVELOPMENT
understand and apply the demographics and psychographics of the market.
The dictionary defines demographics as the statistical data of a population, especially those showing average age, income, education, and so on. It defines psychographics as the study and grouping of people according to their attitudes and tastes, especially for market research.
DemographicsWith demographics you are able
to describe people by groups that they belong to. This may range from gender, age, ethnicity, disabilities, mobility, home ownership, employment, status, location, and even sexuality. For example, will your perfect patient be in the age range of 25-35, 35-45, 45-55, or 55-plus? Will your perfect patient be male or female? Will he/she be a self-employed tycoon, a high-ranking execu-tive, or a celebrity?
PsychographicsOn the other hand, psychographics
helps you describe the interests, opinions,
attitudes, values, and behavior of your perfect patients. What are their likes and dislikes? What are their opinions on politics, religion, and money? What is their attitude about health and lifestyle?
The key to your success here is the ability to describe your perfect patient in as much detail as possible. Your whole team should be crystal clear on whom exactly you are looking for as a potential perfect patient.
The other side to this is that with such a detailed understanding of whom you are looking for, identifying them and locating them becomes relatively easier in terms of your lead generation advertising. For example, if your perfect patient is a BMW-driving corporate executive, it’s relatively easy to locate all the corporate executives with a BMW in the country for a laser-targeted marketing campaign. A perfect patient avatar will also help make your referrals more profitable, as people tend to know people who are similar to themselves professionally and financially.
Marketing foundationIf you haven’t created a perfect patient
avatar for your practice before, get one developed as soon as possible. If you have one already, now may be a good time to review it and establish if it is still ideal for your practice. Getting this right is critical, as it is the foundation on which you can build the marketing strategy of a thriving dental practice.
Volume 8 Number 5 Implant practice 49
PR
AC
TIC
E D
EV
ELO
PM
EN
T
IP
The perfect patient avatar
To help create profiles of your ideal patients, ask yourself:
• Are they male or female?• How old are they?• What is their marital status?• How do they earn a living?• Do they value their appearance?• What car do they drive?• What opinions do they have about
politics, religion, and money?• Where do they go on holiday?
Biodenta North America LLC | 11E Firstfield Rd. | Gaithersburg, MD 20878 | USA | Tel +1 240 482 8484 | [email protected]
www.biodenta.com/learnmore
Your Total Solution Provider
Scan Body
Biodenta has established its position within the dental field on the concept of the Total Solution Provider. This is a systems based approach to dentistry. Our two main product groups are Dental Implant System (DIS) and Digital Dentistry System (DDS). We believe that the future belongs to those who successfully can integrate these modules in a smart and efficient way. Our mission is to help clinicians to do this through advancements in products, workflows, and clinical procedures.
Biodenta stands for the highest Swiss quality and precision. Our staff collaborates with dental professionals and specialists from other industries on a daily basis in order to improve products and solutions for increased reliability, predictability, and simplicity. We invite you to learn more about Your Total Solution Provider and how we can work together to improve implant dentistry.
Fabrication
Prosthetic Materials & Solutions
Implant
Planning and Design
Digital Impression

When placing implants, choosing the right method of component retention
can be a complicated decision. Whether you choose screw-, friction-, or cement-retention, each method has great strengths and weaknesses; therefore, your selection should be made in accordance with each individual clinical situation.
Retrievability, stress, esthetics, and accessibility are just a few of the elements that enter the equation of suitability for optimal implant placement, as the clinical success of the restoration can be significantly influenced by your choice.
Strengths and weaknessesOver the years, the formula for the ideal
method of restoration has divided opinion among dental implantologists, many of whom have a strong preference for a single particular method. These preferences have been known to change depending on current trends, what we read and, of course, the failures we may have experienced in the past.
The truth is, screw-, cement-, and fric-tion-retained implants have many both pros and cons, and while some may be consid-ered to be more advantageous, certain methods may be more appropriate than others in specific circumstances.
For example, while cement retention is often considered to be the most successful method by reducing stress in the restora-tion and bone, there are still certain dis- advantages to this technique. Cement retention, for example, can cause issues
that occur with excess cement application leading to bone loss and peri-implant disease — particularly if standard components place the restorative margin deeper than would be ideal. Debonding — which can lead to the repeated loosening of the prosthesis and patient dissatisfaction — using a permanent cement may reduce debonding episodes but makes recovery more difficult or impossible.
Screw-retained implants also present disadvantages in certain cases; achieving a passive fit is significantly more difficult to attain with a screw-retained restoration due to stress being introduced into the resto-ration through the tightening of screws. If,
however, the prosthesis is cemented, a thin layer of the cement will offset a level of the stress offering compensation for any minor discrepancies in the fit, which would ordi-narily contribute to lack of passivity. So, cement-retained restorations are more likely to reduce stress and therefore the likelihood of stress related implant failure or peri-implantitis. Nonetheless, if retrievability is a factor that must be considered, then the likelihood of damaging the crown or bridge during removal is extremely high; a soft or temporary cement can be used if removal is necessary, but if frequent access is required, it is not the best method of retention.
Implant retention: making the right choice
Dr. Peter Sanders explores the pros and cons of screw-, cement-, and friction-retained restorations and explains the appropriate methods of all three
Peter Sanders, FFGDP RCS (Eng), MSc ImpDent (Lond), DipImpDent RCS (Eng) (Advanced certificate), MFGDP, BDS, LDSRCS, has been placing and replacing implants since 1987. For the past 8 years, his practice in Southampton has focused solely on implant dentistry. He completed the implant diploma at the Royal College of Surgeons in 2005 and obtained an MSc in implantology in 2009. He was awarded the fellowship by the FGDP RCS in 2011. He is currently a course director for the implant diploma at the Royal College of Surgeons in London and prior to this acted as an examiner for the diploma.
As an implant dentist,
I am frequently asked
which is the best method
of post retention. My
answer is always the
same: No single method
is superior to another.
50 Implant practice Volume 8 Number 5
IMPLANT INSIGHTS
All Smiles. Every Step of the Way.From a first dental visit to hygiene, orthodontics and
implants, the CareCredit credit card can make it
easier for families — mom, dad and the kids — to get
care when they want and need it. And CareCredit
gives them a financing resource they can use again
and again* as credit becomes available.
carecredit.com
IMPLT0815DA
Help more familiesachieve healthy, happy smiles. For more ways to optimize
CareCredit in your practice, contact your
Practice Development Team by calling
800-859-9975, option 1, then 6.
Not yet enrolled? Call 866-246-6401
*Subject to credit approval.

Friction-retained implant systems (where the abutment and/or prosthesis are retained by the force of friction between compo-nents) can provide a high level of stability and allow for a tension-free fit, without cement — this method has many advan-tages when it comes to ease of handling, use, and retrieval.
However, friction retention can also have disadvantages in certain circumstances. If the friction-retained prosthesis is designed to be removable by the patient, then the age or the dexterity of the patient should always be considered. If (for this or any other reason) the patient has ongoing issues with removing the retained prosthesis for hygiene reasons, it then becomes a de facto fixed restoration and will, therefore, need to be re- designed accordingly to facilitate oral hygiene procedures.
RetrievabilityMany clinicians consider screw-retained
implants to be the most effective solution if easy removal or access is a requirement. Retrievability is an important factor if the patient requires assistance with hygiene, or if the crown is fractured and needs to be repaired. However, while screw-retained implants can be easily accessed and removed, there is a risk that stress-related tension on the superstructure may be caused when re-tightening the screws in the process of replacement.
In terms of retrievability in cement-retained implants, one of the most commonly cited disadvantages is the diffi-culty in removal of the prosthesis. If the patient requires a great deal of hygienic maintenance, or has a personal prefer-ence to be able to easily remove the superstructure to clean the prosthesis, friction-retained implants allow for this kind of access. Using a milled bar with a milled superstructure and by using tight angles (of around 4 degrees), the superstructure will gain retention through the friction applied to the bar. This will allow for the patient to easily access and remove the structure to aid the cleaning process.
One of the biggest advantages of the friction-retained implant prosthesis is that, if the patient has maxillary atrophy and there-fore requires volume in the super-structure to deliver soft tissue or lip support, this tissue can be built, providing a more secure place-ment. If the superstructure is fixed, excess tissue support would normally be avoided due to the fact that the patient would not
be able to efficiently clean it. With friction-retained implants, the gums can be over-lapped and cleaned with ease.
Esthetics: screw versus cementWhile the screw system may have
advanced over many years, it is still at a disadvantage when it comes to esthetic results. With an implant angled to optimize bone availability and a system that allows only screw retention in line with the implant, the access hole in the prosthesis needs to be filled, and therefore, the esthetics of the crown are compromised from the outset. In addition, the hole filled in the prosthesis may also deteriorate over time.
Clearly, this is more of an issue in the esthetic zone at the front of the mouth where the flared maxilla inevitably results in the extension of the implant axis emerging through the facial surface of the crown. To overcome this, an angled abutment is screwed into the implant and the crown, and then cemented. The cementation of the implant restoration eliminates the unsightly screw holes, resulting in a much more esthet-ically pleasing result.
Often, in order to achieve optimum results, combining methods of retention can be most effective. For example, systems such as ANKYLOS® SynCone® (Dentsply Implants) combine the use of screws and friction to provide a tension-free retention with optimum hygiene capability. With such systems, 4-, 5- or 6-degree tapers are used, and here, gold caps are locked on to the abutments. These components are connected in the mouth to ensure passivity, but removal of the pros-thesis for daily cleaning can be a challenge for less dexterous elderly patients.
Intraoral welding is also a technique that uses a combination of friction- or screw-retention methods. Here, the abutments are connected to the implants and matching screw- or friction-retained components are tapped on to these. A titanium bar is then welded to these welding components while in the patient’s mouth. This means the fit is completely accurate from the outset,
and a more passive, stress-free structure is created.
With intraoral welding, friction compo-nents, which are inherently less bulky and easier to fit in the prosthetic envelope, are used around the front area of the mouth. The emergence of unsightly screw holes is also avoided. Farther back in the mouth, where more space is available, screw retention is used, giving the superstructure excellent stability.
Such combinations of retention are ideal if a patient has a fixed restoration but wants the benefits of having smaller volume components that provide friction retention toward the front of the mouth in the esthetic zone. Screws can then be used to lock the superstructure down in an area where there is space, and therefore, the esthetics of the prosthesis are not compromised.
Finding the right solutionAs an implant dentist, I am frequently
asked which is the best method of post retention. My answer is always the same: No single method is superior to another. A well-experienced and adept implant dentist will understand the features, benefits, and risks of each of the methods of retention, and will apply the most suitable method (or combination of methods) to meet each patient’s specific requirements.
For example, there may be functional and occlusal considerations; lip support and bone volume may need to be considered, as well as the space available for each patient. You may need to consider where the bone is best in relation to the prosthetic envelope, what angles you have to compensate for, and what the patient’s capacities are for hygiene and maintenance.
These all factor into whether screw-, cement-, or friction-retained implants should be selected for optimum placement. Having a broad knowledge and understanding of all three methods will enable you to provide a treatment plan that specifically suits your patient, ensuring successful long-term results are achieved.
A well-experienced and adept implant dentist ... will apply the
most suitable method (or combination of methods) to meet
each patient’s specific requirements.
52 Implant practice Volume 8 Number 5
IMPLANT INSIGHTS
IP

The Densah® Bur is based on a new technology for osteotomy preparation that we have called “osseodensification”. Unlike traditional bone drilling technologies, osseodensification does not excavate bone tissue. Rather, it preserves bone bulk so bone tissue is simultaneously compacted and auto-grafted in an outwardly expanding direction to form the osteotomy.
When a Densah® Bur is rotated at 800-1500 RPM in a reversed, counterclockwise direction with steady external irrigation, called “Densifying Mode”, a dense compacted layer of bone tissue is formed along the walls and base of the osteotomy. Scientific literature has suggested that dense compacted bone tissue produces stronger purchase for dental implants, higher implant stability, and may facilitate faster healing.
Each Densah® Bur features patented multiple, precision-ground flutes within a tapered geometry designed to produce a fast feed rate in two modes of operation. The taper design allows the surgeon to constantly modulate pressure and regulate irrigation.
The flutes are tipped with a proprietary chisel edge that concentrates thrust force while reducing tool chatter to produce smooth haptic feedback that intuitively allows the surgeon to make “on the fly” adjustments.
In the “Densifying Mode”, downward surgical pressure coupled with steady external irrigation creates a gentle hydrodynamic pressure wave, which expands a pilot osteotomy without excavating bone tissue with minimal heat elevation. A densified zone of surrounding bone is generated while plastically expanding the bony ridge at the same time.
In the “Cutting Mode”, the Bur is rotated at 800-1500 RPM in a clockwise (CW) direction to precisely cut bone if needed.
A Densah® Bur kit contains Densah® Burs of progressively larger diameter, which are to be used sequentially to achieve the desired osteotomy size. Densah® Burs can be used with all standard engines and implants.
Densah® Bur Technology Preserves and Enhances Bone
Traditional Drill Bits Extract and Diminish BoneReplace Your Bits with Burs One by One
www.versah.com©2015 Huwais IP Holdings LLC. All rights reserved. Versah and Densah are registered trademarks of Huwais IP Holdings LLC. REV 01
Ø (2.0 mm) Ø (3.0 mm) Ø (4.0 mm) Ø (5.0 mm) Ø (2.3 mm) Ø (3.3 mm) Ø (4.3 mm) Ø (5.3 mm) Ø (2.5 mm) Ø (3.5 mm) Ø (4.5 mm) Ø (5.5 mm)
Scan this QR Code to view our Versahtility
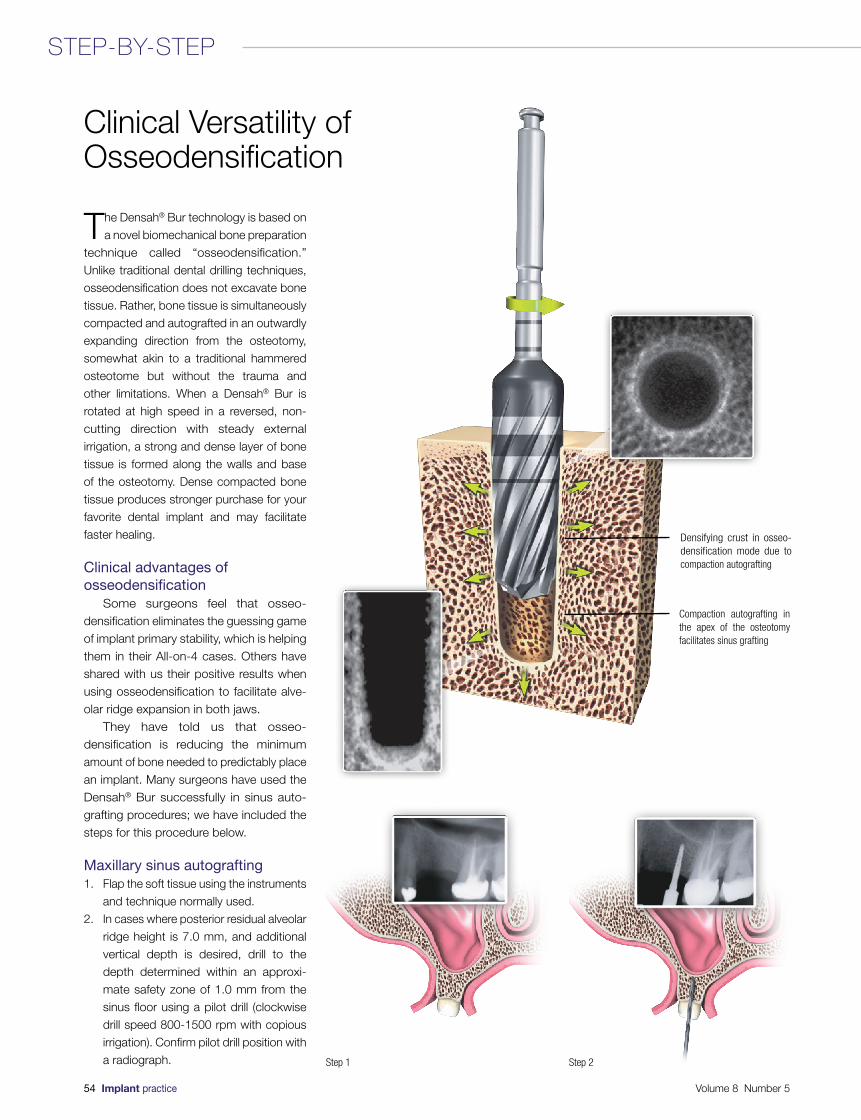
The Densah® Bur technology is based on a novel biomechanical bone preparation
technique called “osseodensification.” Unlike traditional dental drilling techniques, osseodensification does not excavate bone tissue. Rather, bone tissue is simultaneously compacted and autografted in an outwardly expanding direction from the osteotomy, somewhat akin to a traditional hammered osteotome but without the trauma and other limitations. When a Densah® Bur is rotated at high speed in a reversed, non-
cutting direction with steady external irrigation, a strong and dense layer of bone tissue is formed along the walls and base of the osteotomy. Dense compacted bone tissue produces stronger purchase for your favorite dental implant and may facilitate faster healing.
Clinical advantages of osseodensification
Some surgeons feel that osseo- densification eliminates the guessing game of implant primary stability, which is helping
them in their All-on-4 cases. Others have shared with us their positive results when using osseodensification to facilitate alve-olar ridge expansion in both jaws.
They have told us that osseo- densification is reducing the minimum amount of bone needed to predictably place an implant. Many surgeons have used the Densah® Bur successfully in sinus auto-grafting procedures; we have included the steps for this procedure below.
Maxillary sinus autografting1. Flap the soft tissue using the instruments
and technique normally used.2. In cases where posterior residual alveolar
ridge height is 7.0 mm, and additional vertical depth is desired, drill to the depth determined within an approxi-mate safety zone of 1.0 mm from the sinus floor using a pilot drill (clockwise drill speed 800-1500 rpm with copious irrigation). Confirm pilot drill position with a radiograph.
Clinical Versatility of Osseodensification
Densifying crust in osseo- densification mode due to compaction autografting
Compaction autografting in the apex of the osteotomy facilitates sinus grafting
Step 1 Step 2
54 Implant practice Volume 8 Number 5
STEP-BY-STEP
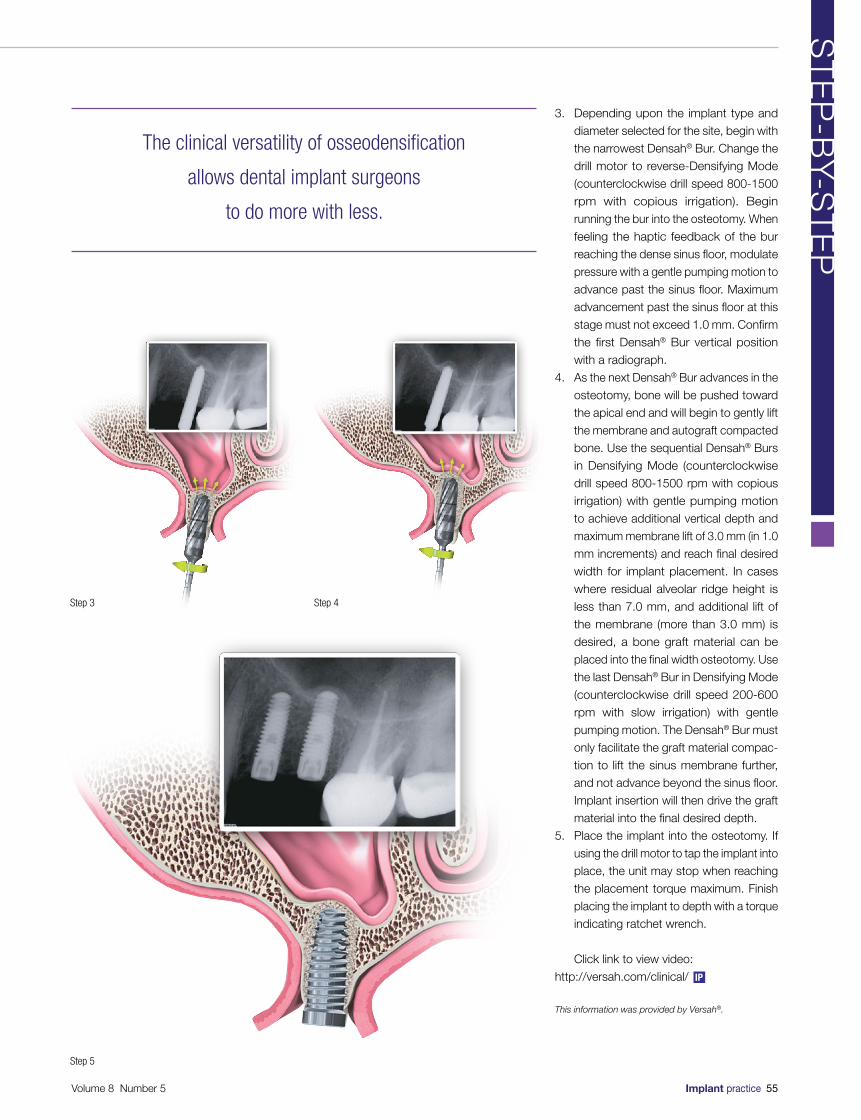
3. Depending upon the implant type and diameter selected for the site, begin with the narrowest Densah® Bur. Change the drill motor to reverse-Densifying Mode (counterclockwise drill speed 800-1500 rpm with copious irrigation). Begin running the bur into the osteotomy. When feeling the haptic feedback of the bur reaching the dense sinus floor, modulate pressure with a gentle pumping motion to advance past the sinus floor. Maximum advancement past the sinus floor at this
stage must not exceed 1.0 mm. Confirm the first Densah® Bur vertical position with a radiograph.
4. As the next Densah® Bur advances in the osteotomy, bone will be pushed toward the apical end and will begin to gently lift
the membrane and autograft compacted bone. Use the sequential Densah® Burs in Densifying Mode (counterclockwise drill speed 800-1500 rpm with copious irrigation) with gentle pumping motion to achieve additional vertical depth and maximum membrane lift of 3.0 mm (in 1.0 mm increments) and reach final desired width for implant placement. In cases where residual alveolar ridge height is
less than 7.0 mm, and additional lift of the membrane (more than 3.0 mm) is desired, a bone graft material can be
placed into the final width osteotomy. Use the last Densah® Bur in Densifying Mode (counterclockwise drill speed 200-600 rpm with slow irrigation) with gentle pumping motion. The Densah® Bur must only facilitate the graft material compac-tion to lift the sinus membrane further, and not advance beyond the sinus floor. Implant insertion will then drive the graft material into the final desired depth.
5. Place the implant into the osteotomy. If
using the drill motor to tap the implant into place, the unit may stop when reaching the placement torque maximum. Finish
placing the implant to depth with a torque indicating ratchet wrench.
Click link to view video: http://versah.com/clinical/
This information was provided by Versah®.
Step 3 Step 4
Step 5
The clinical versatility of osseodensification
allows dental implant surgeons
to do more with less.
Volume 8 Number 5 Implant practice 55
ST
EP
-BY-S
TE
P
IP
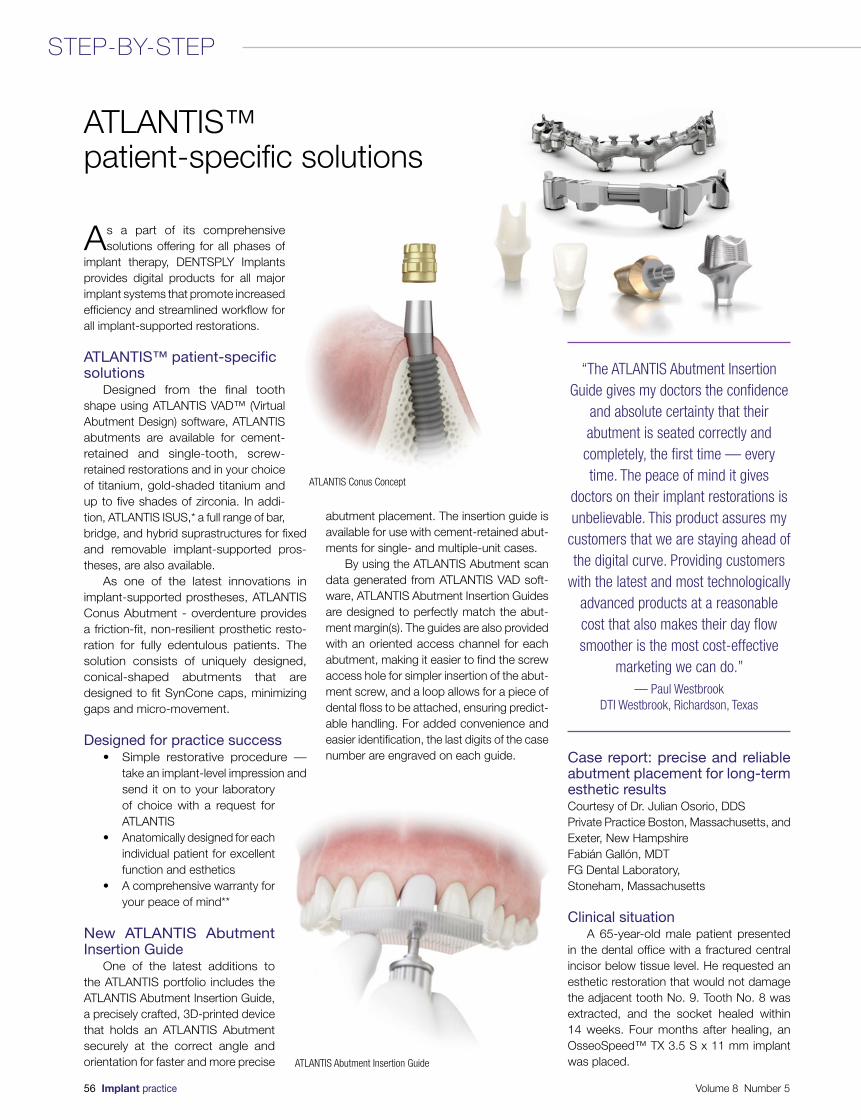
As a part of its comprehensive solutions offering for all phases of
implant therapy, DENTSPLY Implants provides digital products for all major implant systems that promote increased efficiency and streamlined workflow for all implant-supported restorations.
ATLANTIS™ patient-specific solutions
Designed from the final tooth shape using ATLANTIS VAD™ (Virtual Abutment Design) software, ATLANTIS abutments are available for cement-retained and single-tooth, screw-retained restorations and in your choice of titanium, gold-shaded titanium and up to five shades of zirconia. In addi-tion, ATLANTIS ISUS,* a full range of bar, bridge, and hybrid suprastructures for fixed and removable implant-supported pros-theses, are also available.
As one of the latest innovations in implant-supported prostheses, ATLANTIS Conus Abutment - overdenture provides a friction-fit, non-resilient prosthetic resto-ration for fully edentulous patients. The solution consists of uniquely designed, conical-shaped abutments that are designed to fit SynCone caps, minimizing gaps and micro-movement.
Designed for practice success• Simple restorative procedure —
take an implant-level impression and send it on to your laboratory of choice with a request for ATLANTIS
• Anatomically designed for each individual patient for excellent function and esthetics
• A comprehensive warranty for your peace of mind**
New ATLANTIS Abutment Insertion Guide
One of the latest additions to the ATLANTIS portfolio includes the ATLANTIS Abutment Insertion Guide, a precisely crafted, 3D-printed device that holds an ATLANTIS Abutment securely at the correct angle and orientation for faster and more precise
abutment placement. The insertion guide is available for use with cement-retained abut-ments for single- and multiple-unit cases.
By using the ATLANTIS Abutment scan data generated from ATLANTIS VAD soft-ware, ATLANTIS Abutment Insertion Guides are designed to perfectly match the abut-ment margin(s). The guides are also provided with an oriented access channel for each abutment, making it easier to find the screw access hole for simpler insertion of the abut-ment screw, and a loop allows for a piece of dental floss to be attached, ensuring predict-able handling. For added convenience and easier identification, the last digits of the case number are engraved on each guide. Case report: precise and reliable
abutment placement for long-term esthetic resultsCourtesy of Dr. Julian Osorio, DDSPrivate Practice Boston, Massachusetts, and Exeter, New HampshireFabián Gallón, MDTFG Dental Laboratory, Stoneham, Massachusetts
Clinical situationA 65-year-old male patient presented
in the dental office with a fractured central incisor below tissue level. He requested an esthetic restoration that would not damage the adjacent tooth No. 9. Tooth No. 8 was extracted, and the socket healed within 14 weeks. Four months after healing, an OsseoSpeed™ TX 3.5 S x 11 mm implant was placed.
ATLANTIS™ patient-specific solutions
ATLANTIS Conus Concept
ATLANTIS Abutment Insertion Guide
“The ATLANTIS Abutment Insertion Guide gives my doctors the confidence
and absolute certainty that their abutment is seated correctly and completely, the first time — every time. The peace of mind it gives
doctors on their implant restorations is unbelievable. This product assures my
customers that we are staying ahead of the digital curve. Providing customers
with the latest and most technologically advanced products at a reasonable cost that also makes their day flow smoother is the most cost-effective
marketing we can do.”— Paul Westbrook
DTI Westbrook, Richardson, Texas
56 Implant practice Volume 8 Number 5
STEP-BY-STEP
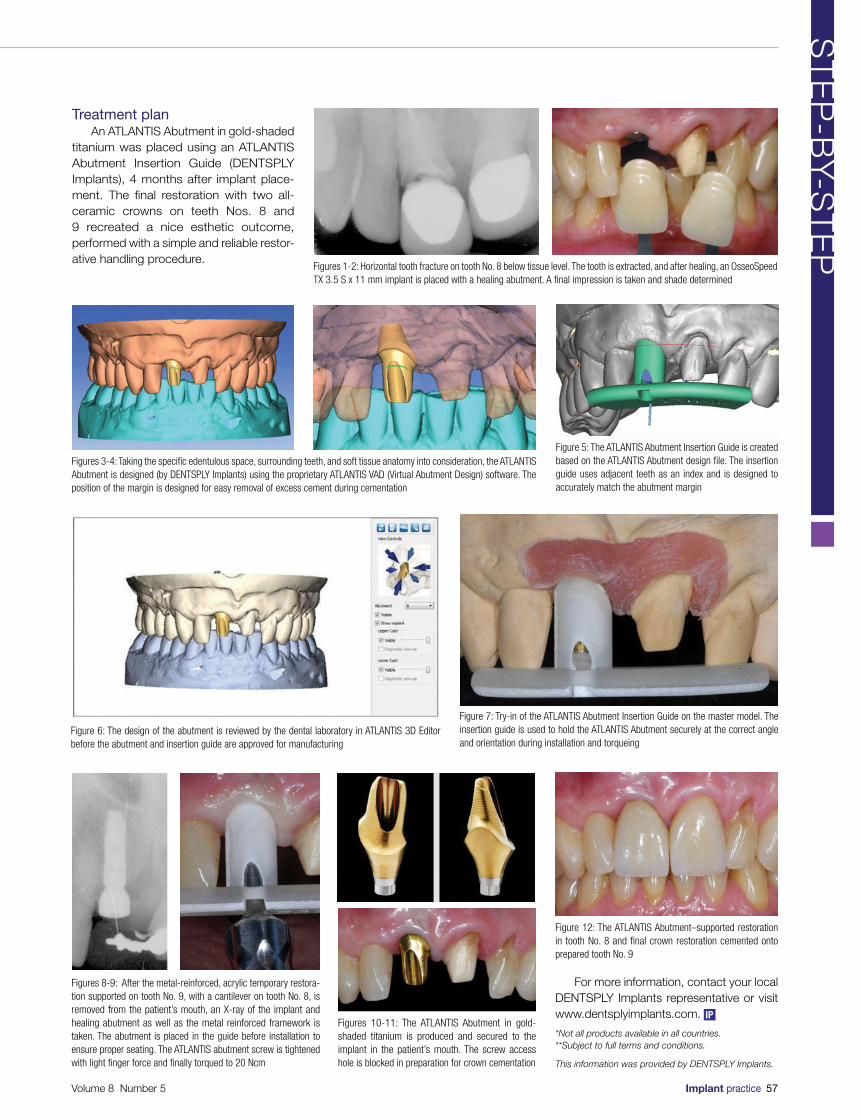
Treatment planAn ATLANTIS Abutment in gold-shaded
titanium was placed using an ATLANTIS Abutment Insertion Guide (DENTSPLY Implants), 4 months after implant place-ment. The final restoration with two all-ceramic crowns on teeth Nos. 8 and 9 recreated a nice esthetic outcome, performed with a simple and reliable restor-ative handling procedure.
Figures 1-2: Horizontal tooth fracture on tooth No. 8 below tissue level. The tooth is extracted, and after healing, an OsseoSpeed TX 3.5 S x 11 mm implant is placed with a healing abutment. A final impression is taken and shade determined
Figures 3-4: Taking the specific edentulous space, surrounding teeth, and soft tissue anatomy into consideration, the ATLANTIS Abutment is designed (by DENTSPLY Implants) using the proprietary ATLANTIS VAD (Virtual Abutment Design) software. The position of the margin is designed for easy removal of excess cement during cementation
Figure 5: The ATLANTIS Abutment Insertion Guide is created based on the ATLANTIS Abutment design file. The insertion guide uses adjacent teeth as an index and is designed to accurately match the abutment margin
Figure 6: The design of the abutment is reviewed by the dental laboratory in ATLANTIS 3D Editor before the abutment and insertion guide are approved for manufacturing
Figure 7: Try-in of the ATLANTIS Abutment Insertion Guide on the master model. The insertion guide is used to hold the ATLANTIS Abutment securely at the correct angle and orientation during installation and torqueing
Figures 8-9: After the metal-reinforced, acrylic temporary restora-tion supported on tooth No. 9, with a cantilever on tooth No. 8, is removed from the patient’s mouth, an X-ray of the implant and healing abutment as well as the metal reinforced framework is taken. The abutment is placed in the guide before installation to ensure proper seating. The ATLANTIS abutment screw is tightened with light finger force and finally torqued to 20 Ncm
Figures 10-11: The ATLANTIS Abutment in gold-shaded titanium is produced and secured to the implant in the patient’s mouth. The screw access hole is blocked in preparation for crown cementation
Figure 12: The ATLANTIS Abutment–supported restoration in tooth No. 8 and final crown restoration cemented onto prepared tooth No. 9
For more information, contact your local DENTSPLY Implants representative or visit www.dentsplyimplants.com.
*Not all products available in all countries.**Subject to full terms and conditions.
This information was provided by DENTSPLY Implants.
Volume 8 Number 5 Implant practice 57
ST
EP
-BY-S
TE
P
IP
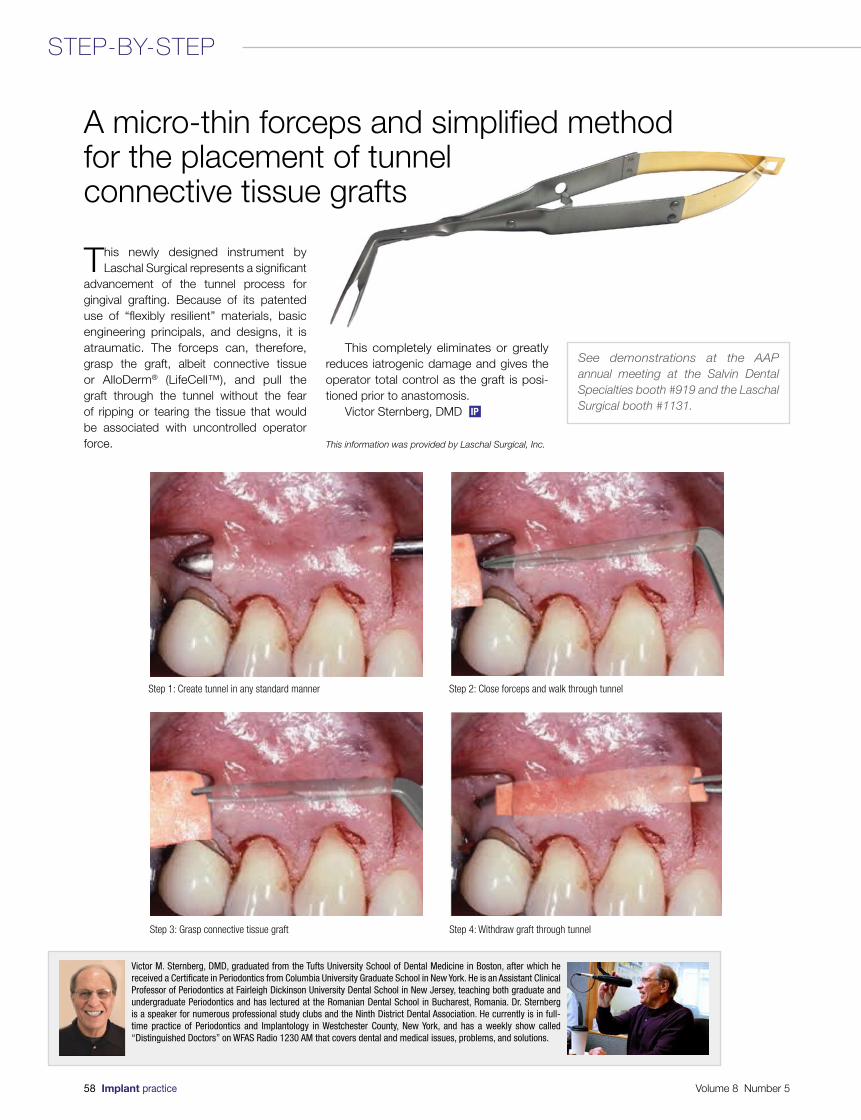
This newly designed instrument by Laschal Surgical represents a significant
advancement of the tunnel process for gingival grafting. Because of its patented use of “flexibly resilient” materials, basic engineering principals, and designs, it is atraumatic. The forceps can, therefore, grasp the graft, albeit connective tissue or AlloDerm® (LifeCell™), and pull the graft through the tunnel without the fear of ripping or tearing the tissue that would be associated with uncontrolled operator force.
This completely eliminates or greatly reduces iatrogenic damage and gives the operator total control as the graft is posi-tioned prior to anastomosis.
Victor Sternberg, DMD
This information was provided by Laschal Surgical, Inc.
A micro-thin forceps and simplified methodfor the placement of tunnel connective tissue grafts
Step 1: Create tunnel in any standard manner Step 2: Close forceps and walk through tunnel
Step 3: Grasp connective tissue graft Step 4: Withdraw graft through tunnel
Victor M. Sternberg, DMD, graduated from the Tufts University School of Dental Medicine in Boston, after which he received a Certificate in Periodontics from Columbia University Graduate School in New York. He is an Assistant Clinical Professor of Periodontics at Fairleigh Dickinson University Dental School in New Jersey, teaching both graduate and undergraduate Periodontics and has lectured at the Romanian Dental School in Bucharest, Romania. Dr. Sternberg is a speaker for numerous professional study clubs and the Ninth District Dental Association. He currently is in full-time practice of Periodontics and Implantology in Westchester County, New York, and has a weekly show called “Distinguished Doctors” on WFAS Radio 1230 AM that covers dental and medical issues, problems, and solutions.
See demonstrations at the AAP annual meeting at the Salvin Dental Specialties booth #919 and the Laschal Surgical booth #1131.
58 Implant practice Volume 8 Number 5
STEP-BY-STEP
IP
Volume 8 Number 5 Implant practice 59
IND
US
TR
Y N
EW
S
25 years of assessing osseointegration with ISQ diagnostics
At the European Association of Osseointegration (EAO) Congress in September 2015 in Stockholm, Sweden, Osstell, together with leading clinicians, reviewed ISQ diagnostic tech-nology — the objective and noninvasive way to measure implant stability. The proprietary method celebrates 25 years in practice and 700 successful studies and publications.
Osstell brought together Professor Daniel Buser (Switzerland), Professor Peter Moy (United States), and Dr. Marcus Dagnelid (Sweden) to discuss the clinical context of ISQ diagnostics as well as the advantages of using ISQ measurements in daily practice. The focus of ISQ diagnostics is to reduce treatment time, manage patients with risk factors, and reduce unnecessary costs related to premature loading.
For more information, visit www.osstell.com
Academy of Osseointegration 2016 Annual Meeting grows to include hands-on workshop sessions
To accommodate the growing demand for dental implant training and education, the Academy of Osseointegration (AO) has expanded its 31st Annual Meeting to include hands-on-workshop sessions. These sessions will be held the afternoon of February 17, 2016, the day before the Opening Symposium and Welcome Reception. For the next 3 days (February 18-20), specialists, and general dentists will continue to learn together about the latest in science and technology from the world’s leading clini-cians and researchers. The meeting, themed “Globalization of Implant Dentistry: A World Collaboration,” will be held at the San Diego Convention Center in San Diego. Registration will open this fall. Follow AO on Facebook and Twitter using #AO2016 to stay up-to-date.
Share your good (implant) news!
Submit your press release for consideration to managing editor Mali Schantz-Feld via email at [email protected].

The Renovix® Guided Healing Collagen Membrane from Salvin Dental is getting
excellent reviews from doctors using it for pre-implant grafting procedures, including socket preservation, ridge augmentation, and sinus lifts. It combines the ability to drape and conform to the specific anatomy of a grafted defect, while maintaining structural integrity and elasticity. This combination of ideal handling characteristics helps make grafting procedures easier and more predictable.
When it comes to selecting the perfect membrane for guided bone and tissue regeneration, there are many choices. Yet most clinicians are still looking for the ideal barrier that combines the best handling and performance characteristics. Some collagen membranes remain stiff even after being hydrated, making it difficult to place over a ridge and conform to the shape of the defect. Other membranes have no memory and resemble wet tissue paper, making it extremely difficult to manipulate during surgery.
Renovix® was originally created for use in repairing pediatric cardiac defects. Cardiac surgeons needed a resorbable membrane to protect the surgical site without migration, and to have it cross-linked in a way that significantly reduced the chance of an inflammatory response. Based on these specific requests, the material used for Renovix® was developed.
Renovix® is fabricated from Type 1 porcine collagen, known to be one of the purest forms of collagen available. It is cross-linked with polysaccharide, a naturally occurring sugar, with excellent biocompatibility. The combined performance and handling characteristics of this membrane, along with specific requests from many implant surgeons, encouraged Salvin Dental to introduce Renovix® for guided bone-regeneration procedures.
Case reports and clinical documenta-tion are an important part of the decision-making process when determining how regenerative products will perform. Steve Wallace, DDS, MHS, from Wilmington, North Carolina, has used Renovix® in over 25 cases as a guided regeneration barrier after extraction and grafting of maxillary first and second molars in preparation for implant placement. Dr. Wallace made the following statement detailing his clinical experience with Renovix®: “Primary flap closure over maxillary molar extraction sites is always difficult to achieve. I have been using Renovix® as my barrier over these
grafted sites to exclude soft tissue ingrowth. I have seen that Renovix® remains intact up to 13 weeks and consistently promotes soft tissue closure over it with minimal inflammation.”
When it is first removed from its sterile packaging, Renovix® is transparent and fairly rigid. Once hydrated, Renovix® becomes opaque, making it easy to identify when brought into the surgical field, and very easy to manipulate. Doctors have said that they get their best results when trimming it after it has been hydrated.
Renovix® is very thin, yet has remark-able tensile strength. This characteristic provides several clinical advantages. First and foremost, it can easily be tacked or sutured to the surgical site if needed. Next, it can be tucked into small tunnel incisions using a micro periosteal elevator without concern that the instrument will easily puncture through the membrane. Finally, the fact that Renovix® is thin and resilient enables the clinician to elevate smaller flaps, leaving more of the periosteum and blood supply undisturbed for faster healing and less patient discomfort.
James Woodyard, DMD, MS, from Newburgh, Indiana, made the following statement regarding his experience with Renovix®: “The thinness and excellent tensile strength of Renovix® allows me to create small tunnel incisions and tuck it under the tissue without tearing the membrane. With thicker membranes that I used in the past, I had to create large full-thickness flaps, and many of the other thin membranes had a tendency to tear when I tried to tuck them. When I decrease the size of the flap elevated and exposure of bone, I decrease postoperative swelling, pain, bone loss, and discomfort for the patient. The less invasive I can be, the less complications I have. I
am extremely pleased with the results that I have seen when using Renovix®.”
Renovix® is available in three different sizes and is individually packaged sterile for immediate use. Many doctors like 15 mm x 25 mm size because it will typically fully cover a grafted extraction socket from the buccal to the opposing lingual plate, main-taining full coverage over the ridge, without having to select a larger size. This unique size reduces waste and saves money by of-ten eliminating the need to select the next larger size.
For more information about Renovix®, check out the product video on the company’s website at www.salvin.com, or contact the team of experts at Salvin Dental at 800-535-6566. They’ll take great care of you!
This information was provided by Salvin Dental.
Salvin® Renovix® Guided Healing Collagen Membrane
Elastic handling
Conforms to the surgical site when hydratedPhoto: Dr. Steve Wallace, DDS, MHS – Wilmington, North Carolina
60 Implant practice Volume 8 Number 5
PRODUCT PROFILE
IP
Socket Graft Without Primary Closure
Grafted Extraction Socket
Renovix® Draped Over Surgical Site
Sutured Without Primary Closure
4 Week Post-Op Mature Tissue Closure
16 Week X-Ray Ideal Bone Formation
Surgery & Photos: Dr. Steve Wallace, Periodontist, Wilmington, NC
Mineralized Cancellous+
• ResorbablePorcineCollagenMembraneFor Guided Tissue & Bone Regeneration
• OptimalMechanical&ElasticHandlingCharacteristics
• BiocompatibilityWithNoInflammatoryResponse
• EasilySuturedOrTackedOverYourSurgicalSite
• EasilyCut&ShapeToYourDesiredSize
• CompareToOssix™OrBio-Gide® Ossix™ is a registered trademark of Johnson & Johnson Bio-Gide® is a registered trademark of Geistlich
Socket Graft Without Primary Closure
Grafted Extraction Socket
Renovix® Placed DoubleLayer
Sutured Without Primary Closure
16 Week Post-Op Mature Tissue Closure
16 Week X-Ray Ideal Bone Formation
Surgery & Photos: Dr. James Woodyard, Periodontist, Newburgh, IN
Mineralized Cortical / Cancellous+
Guided Healing Collagen Membrane
Salvin Dental Specialties, IncToll Free (US & Canada) 800-535-6566 • www.salvin.com
Phone 704-442-5400 • Fax 704-442-5424 • Email: [email protected] Latrobe Drive • Charlotte, NC 28211 • USA
© 2015 Salvin Dental Specialties, Inc. All Rights Reserved. REV. 08-26-2015

Yesterday one of my patients asked me how I became interested in dentistry,
and I told her that my childhood dentist encouraged me to look into the profession. She then asked me, what about implants? How did I become interested in dental implants, and did I ever think that I would one day be teaching others? I answered that a dentist named Dr. Roger Plooster inspired my passion for dental implants, and no, I never really had thought about teaching others.
As I sat in my office that night finishing up my notes, I kept thinking about my conversation earlier that day. How I got to this desk was truly through a lot of hard work and help from some key people along the way, my MENTORS. We have many mentors in life — parents, teachers, and friends who guide us, mold us, and push us to be the very best.
Over the years, I have had many associ-ates come through my practices; early on it was about getting some help in a time when I was too busy. Sadly, these doctors moved on to work elsewhere and to establish their
own practices. Today, I realize that I failed them for it wasn’t really about the nice office, fancy technology, or even the money … It was about mentorship. Dental school has always been hard, but now it’s even harder with the kinds of debt today’s young dentists have.
Mentorship is so much more than showing someone how to do a procedure. It’s about showing them that it’s truly an honor and a privilege to call someone a patient, that you should always treat patients how you yourself would want to be treated,
and that compassion and humility are good for the profession.
Years ago, I thought that success was measured in money and material things; today those items don’t register on my list. Opening an email to see an X-ray of the first dental implant one of my students placed or a phone call from someone who tells me that I made a difference in his/her life — that’s success! It is true that I love my job, and I love helping my patients improve their lives with dental implants, but I am the most humbled by those that call me their mentor.
Mentorship, more important than ever!
Justin Moody, DDS, DICOI, DABOI, is a Diplomate of the American Board of Oral Implantology and of the International Congress of Oral Implantologists, Fellow and Associate Fellow of the American Academy of Implant Dentistry, and Adjunct Professor at the University of Nebraska Medical College. He is an international speaker and
is in private practice at The Dental Implant Center in Rapid City, South Dakota. He can be reached at [email protected] or at www.justinmoodydds.com.
Dr. Justin Moody reflects on the importance of inspiring others
Dr. Justin Moody and Jim Perry, the COO of Affordable Care, Inc.
Implant 101 in Birmingham, Alabama
Live Implant Training Mentorship
Hands-on implant training in Rapid City, South Dakota
We have many mentors in life — parents, teachers, and friends
who guide us, mold us, and push us to be the very best.
62 Implant practice Volume 8 Number 5
ON THE HORIZON
IP

The science of implant dentistry sees improvements and innovation every day.
The American Academy of Implant Dentistry’s 64th Annual Educational Conference at Caesars Palace™ in Las Vegas, Nevada, on October 21-24, 2015, blends the classic with tomorrow’s innovations.
Attendees have the opportunity to earn as many as 20 hours of continuing educa-tion credit focused on implant dentistry. The theme of the conference, “Where Classic Principles Support Cutting-Edge Implant Dentistry,” serves as a reminder of the groundwork laid over 60 years ago by the dental implant pioneers. Caesars Palace serves as a classic Las Vegas backdrop to fit the classic educational theme of the conference.
Over 1,000 implant dentistry profes-sionals will hear from Dr. Carl Misch, one of the pioneers in implant dentistry, as he delivers one of our keynote addresses on Thursday afternoon, October 22. Back by popular demand is Dr. Daniel Alam, who was the leading microsurgeon on the first face transplant performed in the United States. Dr. Alam brought the audience to its feet at the 2010 AAID Annual Conference. This year, he will inspire attendees with his presenta-tion on Face Transplantation: Past, Present, Future, as the closing keynote speaker of the Conference.
Over 3½ days, world-renowned clini-cians will review time-honored dental implant techniques and explore cutting-edge dental implants. They will evaluate the latest concepts in dental implant treatment plan-ning and rethink the science and practice of implant dentistry.
“The AAID is known for providing prac-tical education for the practicing implant dentist. Not only is that found in the didactic and hands-on sessions, but through the interaction of peers in the halls and at the social events during our Conference,” pointed out Dr. John Da Silva, president of the AAID.
“What happens in Vegas at AAID’s Annual Educational Conference is not intended to stay in Vegas. Bring it home, and put it to use immediately in your practice,” he added.
In addition to Main Podium presentations, attendees can choose from 16 hands-on workshops as well as 16 didactic seminars. Two days of team-oriented training are also offered.
A post-conference, full-day course on advanced soft and hard tissue grafting will
be offered. This course includes hands-on experience on cadaver heads.
Next year’s Annual Conference will be held in New Orleans, October 26-29, 2016.
Established in 1951, the AAID is the only dental implant organization that offers credentials recognized by federal and state courts as bona fide. Its membership, which exceeds 5,000, includes general dentists, oral surgeons, periodontists, and prostho-dontists from across the United States and in 40 other countries.
The Academy is known worldwide for its bona fide credentialing program in implant dentistry. The rigorous requirements — coupled with AAID’s commitment to educate patients about implant dentistry and the importance of using a knowledgeable, experi-enced, and trained implant dentist such as an
AAID-credentialed member — sets the Academy apart.
More information about AAID’s consumer outreach can be found at www.aaid-implant.org. Informa-tion about the educational offerings, valuable member benefits, the credentialing program, and other offerings from the AAID can be found online at www.aaid.com.
This information was provided by the AAID.
AAID Annual Conference blends classic with cutting edge
AAID’s Annual Conference is known for clinically-relevant hands-on learning
AAID offers practical education for the practicing implant dentistAttendees have the chance to interact with leading clinicians
64 Implant practice Volume 8 Number 5
AAID UPDATE
IP

• Inclusive® Tapered Implant
• Inclusive® Titanium Healing Abutment and Impression Coping
• Choose from a BruxZir® Solid Zirconia Crown with Inclusive® Custom Implant Abutment or BruxZir Screw-Retained Implant Crown
BruxZir® Implant Bundle
$395* includes
Save Time and Money by the Bundle
BruxZir Solid Zirconia, the world’s most prescribed zirconia restoration, now comes as a complete tooth replacement solution. For about the same price as a crown and custom abutment, everything needed to replace a missing tooth is included. The bundle provides convenience and predictable treatment costs, and reduces the need to keep a supply of implants and prosthetic components on hand.
*Price does not include shipping or applicable taxes. Inclusive is a registered trademark of Prismatik Dentalcraft, Inc.
877-708-7972www.glidewelldental.com
For more information GLIDEWELLLABORATORIES
Premium Products - Outstanding Value

simply brilliantSWISH™
Straumann®-compatible1 design
NEW SwishTapered™Tissue- or Bone-Level Implant with Internal Octagon Connection
All-in-1 Packagingincludes implant, cover screw, healing collar & carrier/transfer – $150 SBM
NEW SwishActive™Bone-Level Implant with 12° Conical Hex Connection
SwishPlus™Tissue-Level Implant with Internal Octagon Connection
With 1 surgical tray, All-in-1 Packaging and 1 price at any level, the simplicity of the Swish™ Implant System is evident. The design enhancements combined with Straumann-compatibility1 are what make it truly brilliant.
Each implant body design promotes self-tapping, initial stability and reduced crestal bone stress
The NEW SwishActive also features a platform-shifting conical hex connection with six indexing positions for precise prosthetic placement. Matched transgingival profiles on prosthetics allow for consistent soft tissue management throughout treatment.
All this with TRUE SAVINGS of $435 compared to Straumann. Now that’s simply brilliant.
Call to schedule a FREE trial www.implantdirect.com | 888-649-6425
1SwishPlus and SwishTapered fully compatible with Straumann tissue level implants, with some restrictions for 3.3mm and 5.7mm diameter implants. SwishActive surgically compatible with Straumann drills with exception of profiling drills and Bone-Level Tapered drills. All trademarks are property of their respective companies.




















