Low-resolution data analysis for low-density lipoprotein particle
Upload
independentCategory
view
1download
0
Low recovery rates stabilize malaria endemicity in areas of lowtransmission in coastal Kenya
Weidong Gu a,*, Charles M. Mbogo b, John I. Githure c, James L. Regens d,Gerry F. Killeen g, Chris M. Swalm e, Guiyun Yan f, John C. Beier a
a Department of Tropical Medicine, School of Public Health and Tropical Medicine, Tulane University Health Sciences Center, New
Orleans, LA 70112, USAb Kenya Medical Research Institute (KEMRI), Kilifi, Kenya
c International Centre of Insect Physiology and Ecology (ICIPE), Nairobi, Kenyad Institute for Science and Public Policy, University of Oklahoma, Norman, OK 73019, USA
e Energy Spatial Analysis Research Laboratory, Tulane University Health Sciences Center, New Orleans, LA 70112, USAf Department of Biological Science, State University of New York, Buffalo, NY 14260, USA
g Department of Public Health and Epidemiology, Swiss Tropical Institute, Basel, Switzerland
Received 3 September 2002; received in revised form 10 September 2002; accepted 12 December 2002
Abstract
The prevalence of Plasmodium falciparum malaria in African communities can be high and stable even in areas of
relatively low transmission where people expose to only a few infectious bites per year. We show in this field study
conducted in 30 sites along the coastal Kenya that prevalence in school children was consistently high, although there
were many sites where transmission intensity measured by exposure to infectious bites was less than 10 per year.
Statistical analyses revealed that prevalence was significantly correlated with the infectious exposure occurring 10�/11
months previously, suggesting that long-lived infections were commonplace and one of the major contributors for the
stability of malaria in these sites. Using mechanistic models of malaria transmission, we found that the association of
high prevalence and low transmission could be due to low recovery rates. Therefore, significant reductions of malaria
prevalence and burden require substantial reductions of the duration of acquired infections, even in areas that have
quite low transmission intensities by the standards of sub-Saharan Africa. Infection control featured by active detection
and drug treatment as well as vector control is critical to combat malaria in areas of relatively low transmission
intensity.
# 2003 Elsevier Science B.V. All rights reserved.
Keywords: Epidemiology; Model; Logistic regression; Infection control; Case detection and drug treatment
1. Introduction
Over 90% of the global morbidity and mortality
caused by Plasmodium falciparum parasites occurs
in sub-Saharan Africa (Breman et al., 2001; Sachs
* Corresponding author. Present address: Medical
Entomology, Illinois Natural History Survey, 607 E Peabody
Drive, Champaign, IL 61820, USA. Tel.: �/1-217-333-1186; fax:
�/1-217-333-2359.
E-mail address: [email protected] (W. Gu).
Acta Tropica 86 (2003) 71�/81
www.elsevier.com/locate/actatropica
0001-706X/03/$ - see front matter # 2003 Elsevier Science B.V. All rights reserved.
doi:10.1016/S0001-706X(03)00020-2

and Malaney, 2002). Over the past two decades,malaria has deteriorated and mortality doubled or
more in most part of the continent (Trape et al.,
2002). It is increasingly realized that control
programs should be tailored to local epidemiolo-
gical and socioeconomic characteristics (Toure
and Coluzzi, 2000; Hamoudi and Sachs, 1999).
One of the important factors characterizing ma-
laria epidemiological patterns is transmission in-tensity (Beier et al., 1999). The intensity of
transmission is commonly defined as the average
number of infectious bites received during a given
period of time by an individual living in the area,
known as the entomological inoculation rate
(EIR). In practice, EIR is estimated as the product
of the proportion of mosquitoes with sporozoites
in their salivary glands and human-biting rateexperienced by exposed individuals. In Asia and
South America, people are exposed to low levels of
transmission. In contrast, Africa or Papua New
Guinea is the only part of the world where
transmission intensity is high enough to be mea-
sured directly with standard entomological meth-
ods. Although EIR levels often reach hundreds
and sometimes exceed a thousand infectious bitesper year in Africa, it is noteworthy that a
significant proportion of African communities
seems to have relatively low levels of transmission
represented by EIRs of 10 infectious bites per year
or less (Hay et al., 2000). Hereafter in the paper,
we refer low transmission to the situations where
EIR is less than 10 infectious bites per year,
although such levels would be regarded as extre-mely high almost anywhere outside of tropical
Africa.
P. falciparum prevalence in human usually
exceeds 20% in African settings where transmis-
sion is undetectable or below one infectious bite
per year and rapidly increases to exceed 50% at
annual EIRs of 15 or more (for review, see Beier et
al., 1999). In many arid parts of Africa, malariaparasites maintain high prevalence by surviving
and remaining infectious in their human hosts for
the duration of the long dry season, during which
there is little or no transmission (Babiker, 1998;
Theander, 1998; Zwetyenaga et al., 1999; Thomas
and Lindsay, 2000). The association of high
prevalence with low transmission indicates that
malaria control is extremely difficult because aconsiderable reduction in transmission is required
to have a significant impact on prevalence (Beier et
al., 1999).
We therefore sought to further examine the
relationship between malaria prevalence and ex-
posure history in the coastal Kenya which has
been traditionally categorized as hyper-endemic
(Marsh, 1992) while experiencing relatively lowtransmission (Mbogo et al., 1995). Our primary
aims were to better understand the factors respon-
sible for the association of high prevalence and low
transmission, and to identify strategies that might
overcome some of these obstacles and allow such
communities to roll back malaria more success-
fully.
2. Material and methods
2.1. Entomological and parasitological field surveys
in Kenya
Thirty sites along the coast of Kenya (Fig. 1)
were selected for entomological and epidemiologi-
cal surveys during June 1997�/May 1998. This areahas been considered a typical hyper- to holo-
endemic area where the main vectors are mosquito
species in the Anopheles gambiae complex (A.
gambiae , A. arabiensis , and A. merus) and A.
funestus (Marsh, 1992; Mbogo et al., 1995). The
detailed description of the field study is presented
in another paper (Mbogo et al., accepted manu-
script). Briefly, indoor-resting mosquitoes weresampled using the pyrethrum spray collection
(PSC) method at each site once in every 2 months
inside 10 randomly selected houses situated within
a 2-km radius surrounding a primary school. At
the time of mosquito collection, the number of
individuals who slept in the house the previous
night was recorded. The heads and thoraces of all
anopheline mosquitoes were tested using P. falci-
parum sporozoite ELISA. Annual EIR for each
site was estimated as the product of the human-
biting rate and the proportion of sporozoite-
positive mosquitoes averaged over the whole study
period. The human-biting rate was calculated by
dividing the total number of blood-fed and half-
W. Gu et al. / Acta Tropica 86 (2003) 71�/8172

gravid mosquitoes caught in PSC catches by the
number of persons sleeping in the house the night
preceding the collection.
A cross-sectional parasitological survey was
carried out at 30 primary schools in the study
area in May 1998 after obtaining informed consent
from parents and teachers. Thick and thin blood
smears were collected from approximately 100
school children 6�/12 years of age. The thick smear
blood slides were stained with Giemsa and the
number of parasites were counted per 200 leuco-
cytes, and the parasite density was calculated
based on a mean leukocyte count of 8000 per
microliter of blood. A blood film was declared
negative if no parasites were found in 200 micro-
scopic fields of the thick smear examined.
2.2. Temporal correlation between prevalence and
previous exposure
The bimonthly entomological sampling preced-
ing the cross-sectional survey of prevalence al-
lowed us to examine temporal correlations
between prevalence and previous exposure to
infectious bites. We modeled the proportion of
infections in school children as logistic function oflagged exposures measured by EIR. For each site,
the data were aggregated for the periods of June�/
July, August�/October, and November�/December
in 1997, and January�/May in 1998 according to
transmission seasonality on the coastal Kenya
(Fig. 2). The exposure was estimated as the EIRs
averaged during these periods in each site, i.e.
E10�11, E7�9, E5�6, and E1�4 corresponding to thelagged exposures of 10�/11, 7�/9, 5�/6, and 1�/4
months for children in May 1998 (Table 1).
Prevalence (pi) of school children in site i is
logit(pi)�b0�b1Ei;10�11�b2Ei;7�9�b3Ei;5�6
�b4Ei;1�4;
where logit(pi )�/log(pi /(1�/pi)). The parameters
of b0,1,. . .,4 were estimated using the maximum
likelihood method. Note that the estimates of the
proportion of sporozoite infection for a particular
period were made separately based on the mos-
Fig. 1. The annual EIRs from 30 study sites sampled on the
coast of Kenya in East Africa from June 1997 to May 1998.
Fig. 2. Seasonal variation in average EIR over the 30 sites
located on the coast of Kenya.
W. Gu et al. / Acta Tropica 86 (2003) 71�/81 73

quito samples collected during the corresponding
period. The estimates of annual EIR were, how-
ever, obtained from the estimates based on all
mosquito samples aggregated for the whole study
period.
2.3. Mechanistic models of malaria transmission
We further examined the relationship between
malaria prevalence and transmission intensity
using Macdonald’s (1957) models. Human hosts
Table 1
Exposure to EIR from A. gambiae and A. funestus , and logistic regression of prevalence of school children on lagged exposure in some
study sites in coastal Kenya
Site code Prevalence (%) Previous exposure (infectious bites)
Ei ,10 � 11 Ei ,7 � 9 Ei ,5 � 6 Ei ,0 � 4 Annual (Ei ,0 � 11)
AMA 73 72.24 0.75 0.00 10.93 121.06
BAR 65 4.50 2.96 1.76 3.33 16.29
CHA 40 0.00 0.00 0.00 0.00 0.00
DAB 38 0.00 0.00 0.56 0.00 0.58
DIN 60 14.15 5.02 27.30 2.00 52.98
DUM 82 21.95 0.00 0.00 0.46 28.00
GAR 79 7.92 0.89 12.04 1.27 21.78
GAZ 60 0.00 0.83 5.78 0.00 6.18
JAR 55 13.38 2.37 3.26 5.84 30.12
KAG 73 0.00 12.23 11.73 0.00 24.98
KIS 69 9.77 1.54 7.20 0.00 33.13
KIT 71 0.00 0.00 0.00 0.00 0.00
MAG 82 29.64 7.78 5.51 27.18 74.65
MAJ 59 0.00 7.35 15.92 4.70 40.01
MAS 65 3.54 6.69 18.40 3.71 39.67
MAZ 48 0.00 6.70 7.23 0.00 13.09
MBC 60 0.00 0.00 1.57 0.00 1.67
MJA 49 0.00 9.52 3.63 3.18 17.44
MJB 64 0.00 0.00 7.33 3.08 10.64
MJJ 74 10.08 5.42 15.46 3.89 36.81
MOY 78 7.17 0.00 0.00 5.13 14.42
MTE 84 22.77 2.63 0.00 2.71 36.38
MWA 51 1.94 0.00 0.00 0.00 2.12
PAZ 71 0.00 3.54 1.55 1.03 7.69
SHA 54 0.71 0.00 0.26 0.00 1.11
TAK 52 0.00 0.00 0.00 0.00 0.00
TSU 68 14.87 10.46 0.00 7.12 42.36
VIN 66 5.12 0.00 11.84 7.16 26.66
VUG 44 0.00 0.00 7.65 0.00 7.81
ZIW 59 1.97 0.00 0.00 0.00 4.00
Proportion of exposure (%) 0.41 0.15 0.28 0.16
Logistic regression
b 0.017 0.009 0.006 0.018
bS.D. 0.004 0.012 0.006 0.011
Wald statistic 4.370 0.749 0.919 1.725
P -value B/0.001 0.45 0.36 0.08
Annual EIRs were estimated by averaging proportion of sporozoite infection in mosquito samples over the entire period of the
study.
W. Gu et al. / Acta Tropica 86 (2003) 71�/8174

are categorized as either susceptible or infected.Assuming that human�/mosquito contact occurs
randomly, susceptible human become infected at a
rate of b EIR, where b is a constant representing
transmission efficiency between infectious mosqui-
toes and susceptible individuals. Infected indivi-
duals clear their infections and become susceptible
again at a constant daily recovery rate (r),
equivalent to the reciprocal of mean infectionperiod. Thus, the change in malaria prevalence
over time is modeled as (Macdonald, 1957)
dy
dt�b EIR(1�y)�ry: (1)
The relationship between prevalence (y*) and EIR
at equilibrium (i.e. dy /dt�/0) is
y��b EIR
b EIR � r: (2)
This simplistic model suggests that the relationship
between prevalence and EIR is dictated by the
recovery rate. The smaller the r , the higher is
prevalence, no matter what values of b and EIR
are. In reality, both b and r vary as a function of
exposure history, reflecting the effects of immunity(Dietz et al., 1974; Bekessy et al., 1976; Molineaux
and Gramiccia, 1980). We assume constant b and
r for school children living in the study areas and
thus ignore the influence of acquired immunity.
These simplifications are necessary to derive the
general relationship between prevalence and trans-
mission intensity in low transmission areas, while
we nevertheless recognize that the consistentlyhigh prevalence observed at these sites is asso-
ciated with considerable levels of acquired immu-
nity against clinic incidence of malaria (Mbogo et
al., 1995; Gupta et al., 1999). It is difficult to
estimate b or r from experimental studies. For
coefficient b , it was reported that only less than
20% bites from gland-positive mosquitoes pro-
duced infections in residents of endemic areas (Pulland Grab, 1974). Experimental infection by A.
stephensi on volunteers demonstrated that 5 of 10
volunteers developed parasitamae after challenged
by one or two infective mosquitoes (Rickman et
al., 1990). Empirical studies suggested similar
patterns of transmission of sporozoites between
A. stephensi and A. gambiae (Beier et al., 1991).Therefore, we approximated b as 0.5. With the
value of b fixed, we could explore what possible
values of r fitted to our field observations using
Eq. (2). We did not statistically estimate the
recovery rate because our focus was to explore
the factors responsible for the observed pattern of
association of high prevalence with low transmis-
sion rather than to accurately estimate r using thissimplistic model.
Since estimating EIR needs data on human-
biting rates and proportions of sporozoite infec-
tions in mosquitoes, it is not commonly available
and difficult to estimate because the proportion of
sporozoite infection in mosquito populations is
often low even for the most efficient African
vectors, especially in areas of low transmissionwhere it is often difficult to obtain sufficient
mosquito samples for analysis (Gu, 1995). For
example, in Sudan where malaria is endemic and
highly prevalent, it was reported that only one
infected mosquito was identified during a survey
lasted for several years (Theander, 1998). We
further investigated the relationship between pre-
valence and the human-biting rate that was oftensurveyed in many epidemiological studies. We
used Macdonald’s (1952) model of sporozoite
infection in mosquitoes that involved explicitly
modeling transmission dynamics in mosquito
populations. The proportion (s ) of sporozoites’
infection in mosquitoes is modeled as
s�pnacy
acy � loge p; (3)
where a is human-biting habit, c the transmissioncoefficient between an infected person and a
susceptible mosquito, p the daily survival rate of
mosquitoes, and n the number of days taken for
completion of extrinsic parasite development in
mosquitoes.
Since EIR is a product of human-biting rate
(ma) and s , substituting Eq. (3) into Eq. (1) and
solving for the equilibrium prevalence in human,we obtain
y��ma2 bcpn � r loge p
ma2 bcpn � rac: (4)
W. Gu et al. / Acta Tropica 86 (2003) 71�/81 75

The relationship between prevalence and the hu-man-biting rate is shaped by many parameters
governing the transmission. Empirical data were
available for some of these parameters on the coast
of Kenya (Mbogo et al., 1996), and the values of
the other parameters were extracted from other
studies in which A. gambiae and A. funestus were
involved and ideally conducted on the Kenyan
coast. Specifically, a was set as 0.4 because theoviposition cycle was estimated to be 2 days
(Ijumba et al., 1990; Mutero and Birley, 1987)
and human blood indices for A. gambiae on the
coastal Kenya is consistently greater than 80%
(Mbogo et al., 1996); p was estimated to be 0.85
based on a parous rate of ca. 0.65 for A. gambiae
and A. funestus in the study areas (Mbogo et al.,
1996) and an oviposition cycle of 2 days; and theextrinsic incubation period n was set to be 10 days
(Lines et al., 1991). The infectious reservoir is
usually estimated to be around 5% of the whole
population in areas with stable endemic malaria
(Drakeley et al., 2000; Graves et al., 1988; Haji et
al., 1996; Killeen et al., 2000). We therefore set c as
0.15, reflecting the approximate mean infectious-
ness of infected individuals that would be requiredto maintain typical levels of infectiousness in the
population as a whole at the levels of prevalence
observed here. By fixing the values of a , b , c , p ,
and n as 0.4, 0.5, 0.15, 0.85, and 10, respectively,
we could examine how the relationship between
prevalence and human-biting rates (ma) is affected
by the recovery rate using Eq. (4). Although the
specific curves of the predictions do change inresponse to adjustments to the values of these
parameters, exploring the parameter space shows
that our conclusions are valid to reasonable ranges
in these values of the parameters most likely
encountered in the field.
3. Results
Transmission intensity on the coast of Kenya
varied widely from place to place with annual
EIRs ranging from B/1 to 121 infectious bites,
with several adjacent sites experiencing consider-
ably different transmission levels (Fig. 1). There
were 16 sites with annual EIRs of less than 20, and
12 sites of less than 10. Malaria parasite transmis-
sion was detected all year-round with two peaks
appearing during June�/July and November�/De-
cember (Fig. 2). P. falciparum malaria infection
prevalence was consistently high in school children
at all 30 sites, regardless of local EIR estimates
(Fig. 3a). The average prevalence from the sites
with annual EIR values of less than 5 was 53%.
Compared to the three orders of magnitude
variation in annual EIR among the 30 sites, the
variation in prevalence was relatively small.
The summaries of sporozoite infection in A.
gambiae and A. funestus for each period are
tabulated (Table 2). Logistic regression of preva-
lence to previous exposure shows that prevalence
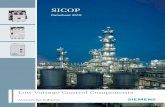
Fig. 3. The relationships between malaria prevalence and
transmission intensity, measured by annual EIR (a) and the
man-biting rate (b) under various recovery rates: (*/ - - */)
0.005; (*/ - */) 0.01; (. . .) 0.02; (*/) 0.05, and (m) the
observations in the coast of Kenya.
W. Gu et al. / Acta Tropica 86 (2003) 71�/8176

was only significantly related to the exposure that
lagged 10�/11 months (Table 1). The significant
relationship between prevalence and exposure
taking place more than 10 months previously
suggests long periods of infection for many
children residing in low transmission areas on the
coast of Kenya.
Fig. 3a displays the relationship between pre-
valence and EIR with the estimated parameters
under various recovery rates. This model predicts
that given the estimated recovery rate of 0.005,
substantial reductions of prevalence can only
occur when EIR is reduced below one infectious
bite per year. However, substantial increase in the
recovery rate from 0.005 to 0.05 could significantly
reduce prevalence from 75 to 23% when annual
EIR is 10 (Fig. 3a).
The predicted prevalence as a function of the
human-biting rate is displayed under various
recovery rates (Fig. 3b). The predictions based
on the recovery rate of 0.005 capture the empiri-
cally observed steep rise to high prevalence once
transmission potential exceeds the threshold re-
quired for stable transmission (Beier et al., 1999).
Increasing the recovery rate not only reduces
predicted prevalence but also increases the thresh-
old of transmission. There is an evident bias in the
model fit that predictions with the recovery rate of
Table 2
Summary of sporozoite examination from sampled mosquitoes aggregated for four periods during June 1997�/May 1998 from the 30
sites on the coast of Kenya
Mosquito species Sampling period
June�/July August�/October November�/December 1997 January�/May 1998
A. gambiae
Sites with annual EIRB/10
Positive 5 8 10 2
Total examined 64 197 933 66
Proportion of sporozoites 0.08 0.04 0.11 0.03
Sites with annual EIR�/10
Positive 121 66 93 28
Total examined 1027 531 2215 347
Proportion of sporozoites 0.12 0.12 0.04 0.08
All sites
Positive 126 74 103 30
Total examined 1091 728 3148 413
Proportion of sporozoites 0.12 0.10 0.03 0.07
A. funestus
Sites with annual EIRB/10
Positive 1 1 7 1
Total examined 22 46 386 153
Proportion of sporozoites 0.05 0.02 0.02 0.01
Sites with annual EIR�/10
Positive 48 30 13 28
Total examined 721 595 695 679
Proportion of sporozoites 0.07 0.05 0.02 0.04
All sites
Positive 49 31 20 29
Total examined 743 641 1081 832
Proportion of sporozoites 0.07 0.05 0.02 0.03
W. Gu et al. / Acta Tropica 86 (2003) 71�/81 77

0.005 underestimate prevalence at the low end oftransmission intensity while overestimate preva-
lence at high transmission intensity.
4. Discussion
Previous studies reported discrepancies between
predicted and observed prevalence due to failure
to account for exposure-induced immunity(Koella, 1991). The models we have applied
underestimate prevalence at low EIR values and
overestimate prevalence at high EIR values.
Therefore, infections likely last longer than 200
days at EIRs of 1 or less and shorter periods where
annual EIR�/10. Although sampling errors asso-
ciated with limitations of the indoor PSC catch for
estimating transmission intensity may contributeto these biases, increasing immunity in response to
previous blood-stage infection (Charlwook et al.,
1998) is the most likely explanation for this bias
and indicates that the estimated threshold for
transmission stability is probably overestimated
by our analysis. This is because the estimated rate
of recovery approximates the mean of values
encountered over the range of transmission in-tensity and prevalence observed here. Thus,
although mean recovery rate may be substantially
higher at EIRs of 10 or more, at transmission
intensities of 1 or less, the recovery rate might be
considerably less than 0.005 as indicated by visual
inspection of model fitting (Fig. 3a). Modeling of
the EIR�/prevalence relationship at increasing
rates of recovery demonstrates that substantialreductions in the mean duration of infections
could reduce prevalence in many sites and could
increase the threshold vector density required to
maintain transmission (Fig. 3b).
It should be noted that EIRs are only measur-
able by conventional entomological methods when
they are moderate to high (Theander, 1998). For
areas where people are exposed to only a fewinfectious bites per year, intensive sampling sur-
veys, especially covering most of the transmission
seasons, are required to accurately estimate EIRs.
If transmission is temporally concentrated during
short seasons like that observed on the coast (Fig.
2), the estimates of EIRs with limited sampling
effort are biased, especially in areas of lowtransmission. Therefore, it is not surprising to
find high prevalences in three sites where no
transmission was detected. It is difficult to assess
the effect of the bias on our estimation of the
recovery rate. In this study, we believe that the
results are qualitatively valid in the presence of the
bias. First of all, both logistic regression of
prevalence on previous exposures and fitting thefield data to dynamical models (Eqs. (2) and (4))
generated consistently low recovery rates. Addi-
tionally, the model (Eq. (4)) without estimates of
EIR displayed a consistent pattern.
Substantial transmission had occurred on the
coastal Kenya during the short rains of
November�/December in 1997. The significant
association between prevalence and exposure dur-ing the previous long rains, almost a whole year
previously, indicates that long-lived infections are
important features on the coast of Kenya as they
are in more arid parts of Africa (Babiker, 1998;
Theander, 1998; Zwetyenaga et al., 1999). Long-
term persistence of infections may be one of the
major mechanisms for P. falciparum that enables
it to maintain high stable prevalence across muchof its range where transmission is seasonal or
intermittent.
The pattern of high prevalence in areas of
relatively low transmission and low recovery rates
of untreated malaria infections in Africa is not
uncommon to malaria epidemiologists. By exam-
ining the link between these two characteristics of
malaria epidemiology, here we have further ex-plored its implications for public health policy to
identify strategies that could enable drastic reduc-
tions of malaria burden in many parts of Africa
where transmission intensity is relatively low by
the standards of this most malaria-afflicted con-
tinent. The implication of this result for malaria
control is that we should reconsider our long-term
goals and control strategies for African commu-nities where, for example, EIR is below 10
infectious bites per year. Besides conventional
vector control to reduce transmission intensity,
aggressive and sustained efforts to increase recov-
ery rates through active case detection and drug
treatment should also be considered in these areas.
By developing an individual-based model, we were
W. Gu et al. / Acta Tropica 86 (2003) 71�/8178

able to incorporate effects of immunity on bothsusceptibility and recovery rate as a function of
individuals’ exposure history (Gu et al., 2003). The
results of the individual-based model are indicative
that infection control characterized by active
detection and drug treatment as well as vector
control is feasible to eliminate malaria from many
sites on the coast of Kenya (Gu et al., 2003).
Wide accessibility to health cares and effectivetreatment of malaria infections have played a
significant role in reducing malaria morbidity
and mortality in Asian countries (Alles et al.,
1998). In Sri Lanka, point prevalence was less than
1% in areas with EIR of one per annum, whereas
similar inoculation rates in Africa are associated
with much high prevalence (Carter et al., 2000).
Similarly, low prevalences have also been reportedin peri-urban communities in Senegal exposed to
an annual EIR of approximately 14 but who have
good access to screening and treatment (Ver-
cruysse et al., 1983). Furthermore, the successful
interruption of malaria transmission by African
vectors with a combination of rigorous vector
control, and intensive case detection and drug
treatment has been clearly demonstrated on theisland of Mauritius (Julvez, 1995; Kaneko et al.,
2000). The arrival of A. gambiae in Mauritius in
the mid-19th century brought with it catastrophic
epidemics, followed by stable endemic malaria
similar to that experienced by much of mainland
Africa today (Julvez, 1995). During the Global
Malaria Eradication campaign, malaria was suc-
cessfully eradicated from this island with a combi-nation of aggressive vector control and rigorous
case surveillance. Mauritius remains free of ma-
laria today despite the continued presence of
highly efficient vectors, predominantly A. arabien-
sis , because of a relentless system for screening,
treating, and following immigrants from malarious
regions (Julvez, 1995).
Closer examination of Fig. 3b reveals that undercurrent conditions on the coast of Kenya, where
poor access to good clinical facilities and effective
drugs allows most chronic infections to persist for
10 months, vector densities would probably have
to be reduced to less than one bite per week or
possibly less, for transmission to be destabilized
and eliminated. This is clearly beyond the reach of
vector control methods currently applied in Kenyaand available more broadly in Africa (Mbogo et
al., 1995; Molineaux and Gramiccia, 1980; Killeen
et al., 2000). Conversely, even increasing the mean
recovery rate so that most infections are cleared in
50 days more or less is similarly unlikely to
destabilize transmission at vector densities of
more than one bite per person per day. In reality,
malaria is likely to be even more intransigent thanindicated by these steady-state models because
they assume homogenous, random mixing of the
vector and human populations. In the real-world
of malaria transmission, exposure and transmis-
sion are highly aggregated in space and time,
resulting in greatly stabilized transmission and
the concentration of most transmission within
foci which are much more intense than the localaverage and considerably more robust to control
(Carter et al., 2000; Woolhouse et al., 1997; Dye
and Hasibeder, 1986). Furthermore, strategies
aiming at elimination of malaria are sensitive to
introduction of new infections into infection-free
communities and even a single introduced infec-
tion can cause an epidemic in an infection-free
community (Arez et al., 1999; Gu et al., 2003).Thus, it seems that if our ambitions for malaria
control in Africa are to go beyond clinical manage-
ment of cases and partial reductions of incidence,
both intensive vector control and active suppres-
sion of human infection prevalence will be re-
quired, even in areas where transmission intensity
is considered relatively low by African standards.
Macdonald developed the theory of malariastability that emphasized the role of mosquito-
related parameters in characterizing malaria sta-
bility such as survival rate and human-biting habit
(Macdonald, 1952, 1957). The emphasis on ma-
laria-related parameters is derived from the gen-
eral understanding that these parameters are
subject to greater variation in nature than the
recovery rate (Macdonald, 1952). This is notsurprising since most of the studies upon which
that observation was based do have high levels of
transmission (Molineaux and Gramiccia, 1980).
This mosquito-oriented characterization of ma-
laria stability has led to the generalization that
malaria is unstable in areas of low and seasonal
transmission. However, malaria transmission in
W. Gu et al. / Acta Tropica 86 (2003) 71�/81 79

Africa is clearly very stable even where transmis-sion is relatively low due to slow recovery from
infection. Unless substantial reductions of trans-
mission intensity and increases in the recovery rate
of human are both achieved and immigrants
monitored, stable malaria will continue unabated
in Africa, even in areas where transmission poten-
tial is relatively moderate. We suggest that our
long-term goals for effective control of malaria inAfrica must therefore go beyond bednets and
clinical case management to include active case
detection, treatment, and rigorous follow-up of
asymptomatic infections so that the reservoir of
parasites to initiate new infections can be substan-
tially reduced without forcing the emergence of
drug resistance.
Acknowledgements
We thank A. Spielman, P. Carnevale, and C.Rogier for inspiring discussions about malaria
epidemiology that led to the present work. Special
thanks are due to A. Saul, V. Robert, and J. Lines
for their critical and constructive suggestions.
Financial support came from NIH (U19
AI45511, D43 TW01142, D43 TW00920) and
NSF (DEB-0083602).
References
Alles, H.K., Mendis, K.N., Carter, R., 1998. Maleria mortality
rates in South Asia and in Africa: implications for malaria
control. Parasitol Today 14, 369�/375.
Arez, A.P., Snounou, G., Pinto, J., Sousa, C.A., Modiano, D.,
Ribeiro, H., Franco, A.S., Alves, J., Rosario, V.E., 1999. A
clonal Plasmodium falciparum population in an isolated
outbreak of malaria in the Republic of Cabo Verde.
Parasitology 118, 347�/355.
Babiker, H.A., 1998. Unstable malaria in Sudan: the influence
of the dry season. Plasmodium falciparum population in the
unstable malaria area of eastern Sudan is stable and
genetically complex. Trans. R. Soc. Trop. Med. Hyg. 92,
585�/589.
Beier, J.C., Davis, J.R., Vaughan, J.A., Noden, B.H., Beier,
M.S., 1991. Quantitation of Plasmodium falciparum spor-
ozoites transmitted in vitro by experimentally infected
Anopheles gambiae and Anopheles stephensi . Am. J. Trop.
Med. Hyg. 44, 564�/570.
Beier, J.C., Killeen, G.F., Githure, J.I., 1999. Entomologic
inoculation rates and Plasmodium falciparum malaria pre-
valence in Africa. Am. J. Trop. Med. Hyg. 61, 109�/113.
Bekessy, A., Molineaux, L., Storey, J., 1976. Estimation of
incidence and recovery rates of Plasmodium falciparum
parasitaemia from longitudinal data. Bull. World Health
Organ. 54, 685�/693.
Breman, J.G., Egan, A., Keusch, G.T., 2001. The intolerable
burden of malaria: a new look at the numbers. Am. J. Trop.
Med. Hyg. Suppl. 64, 4�/7.
Carter, R., Mendis, K.N., Roberts, D., 2000. Spatial targeting
of interventions against malaria. Bull. World Health Organ.
78, 1401�/1411.
Charlwook, J.D., Smith, T., Lyimo, E., Kitua, A.Y., Masanja,
H., Booth, M., Alonso, P.L., Tanner, M., 1998. Incidence of
Plasmodium falciparum infection in infants in relation to
exposure to sporozoite-infected anophelines. Am. J. Trop.
Med. Hyg. 59, 243�/251.
Dietz, K., Molineaux, L., Thomas, A., 1974. A malaria model
tested in the African Savannah. Bull. World Health Organ.
50, 347�/357.
Drakeley, C.J., Akim, N.I.J., Sauerwein, R.W., Greenwood,
B.M., Targett, G.A.T., 2000. Estimates of the infectious
reservoir of Plasmodium falciparum malaria in the Gambia
and in Tanzania. Trans. R. Soc. Trop. Med. Hyg. 94, 472�/
476.
Dye, C., Hasibeder, G., 1986. Population dynamics of mos-
quito-borne disease: effects of flies which bite some people
more frequently than others. Trans. R. Soc. Trop. Med.
Hyg. 80, 69�/77.
Graves, P.M., Burkot, T.R., Carter, R., Cattani, J.A., Lagog,
M., Parker, J., Brabin, B.J., Gibson, F.D., Bradley, D.J.,
Alpers, M.P., 1988. Measurement of malarial infectivity of
human populations to mosquitoes in the Madang area,
Papua New Guinea. Parasitology 96, 251�/263.
Gu, W., 1995. Estimating sporozoite rates by examining pooled
samples of mosquitoes. Trans. R. Soc. Trop. Med. Hyg. 89,
359�/360.
Gu, W., Killeen, G.F., Mbogo, C.M., Regens, J.L., Githure,
J.I., Beier, J.C., 2003. An individual-based model of
Plasmodium falciparum malaria transmission on the coast
of Kenya. Trans. R. Soc. Trop. Med. Hyg. 97, 1�/8.
Gupta, S., Snow, R.W., Donnelly, C.A., Marsh, K., Newbold,
C., 1999. Immunity to non-cerebral severe malaria is
acquired after one or two infections. Nat. Med. 5, 340�/343.
Haji, H., Smith, T., Meuwissen, J.T., Sauerwein, R., Charl-
wood, J.D., 1996. Estimation of the infectious reservoir of
Plasmodium falciparum in natural vector populations based
on oocyst size. Trans. R. Soc. Trop. Med. Hyg. 90, 494�/
497.
Hamoudi, A., Sachs, J.D., 1999. The changing global distribu-
tion of malaria: a review. Working Papers. Center for
International Development at Harvard University.
Hay, S.I., Rogers, D.J., Toomer, J.F., Snow, R.W., 2000.
Annual Plasmodium falciparum entomological inoculation
rates (EIR) across Africa: literature survey, internet access
and review. Trans. R. Soc. Trop. Med. Hyg. 94, 113�/127.
W. Gu et al. / Acta Tropica 86 (2003) 71�/8180

Ijumba, J.N., Mwangi, R.W., Beier, J.C., 1990. Malaria
transmission potential of Anopheles mosquitoes in the
Mwea-Tebere irrigation scheme, Kenya. Med. Vet. Ento-
mol. 4, 425�/432.
Julvez, J., 1995. History of insular malaria in the southwestern
Indian Ocean: an eco-epidemiological approach. Sante 5,
353�/358.
Kaneko, A., Taleo, G., Kalkoa, M., Yamar, S., Kobayakawa,
T., Bjorkman, A., 2000. Malaria eradication on islands.
Lancet 356, 1560�/1564.
Killeen, G.F., McKenzie, F.E., Foy, B.D., Schieffelin, C.,
Billingsley, P.F., Beier, J.C., 2000. The availability of
potential hosts as a determinant of feeding behaviours and
malaria transmission by African mosquito populations.
Am. J. Trop. Med. Hyg. 62, 545�/551.
Koella, J.C., 1991. On the use of mathematical models of
malaria transmission. Acta Trop. 49, 1�/25.
Lines, J.D., Wilkes, T.J., Lyimo, E.O., 1991. Human malaria
infectiousness measured by age-specific sporozoite rates in
Anopheles gambiae in Tanzania. Parasitology 102, 167�/177.
Macdonald, G., 1952. The analysis of equilibrium in malaria.
Trop. Dis. Bull. 49, 813�/828.
Macdonald, G., 1957. The Epidemiology and Control of
Malaria. Oxford University Press, London.
Marsh, K., 1992. Malaria*/a neglected disease. Parasitology
104, S53�/S69.
Mbogo, C.N., Snow, R.W., Khamala, C.P., Kabiru, E.W.,
Ouma, J.H., Githure, J.I., Marsh, K., Beier, J.C., 1995.
Relationships between Plasmodium falciparum transmission
by vector populations and the incidence of severe disease at
nine sites on the Kenyan coast. Am. J. Trop. Med. Hyg. 52,
201�/206.
Mbogo, C.N., Baya, N.M., Ofulla, A.V.O., Githure, J.I., Snow,
R.W., 1996. The impact of permethrin-impregnated bednets
on malaria vectors of the Kenyan coast. Med. Vet.
Entomol. 10, 251�/259.
Mbogo, C.N., Mwangangi, J.M., Nzovu, J., Gu, W., Yan, G.,
Gunter, J., Swalm, C., Keating, J., Regens, J.L., Shililu, J.I.,
Githure, J.I., Beier, J.C., accepted manuscript. Spatial and
temporal heterogeneity of Anopheles mosquitoes and Plas-
modium falciparum transmission along the Kenyan coast.
Am. J. Trop. Med. Hyg.
Molineaux, L., Gramiccia, G., 1980. The Garki Project. World
Health Organization, Geneva.
Mutero, C.M., Birley, M.H., 1987. Estimation of the survival
rate and oviposition cycle of field populations of malaria
vectors in Kenya. J. Appl. Ecol. 24, 853�/863.
Pull, J.H., Grab, B., 1974. A simple epidemiological model for
evaluating the malaria inoculation rate and the risk of
infection in infants. Bull. World Health Organ. 51, 507�/516.
Rickman, L.S., Jones, T.R., Long, G.W., Paparello, S.,
Schneider, I., Paul, C.F., Beaudoin, R.L., Hoffman, S.L.,
1990. Plasmodium falciparum -infected Anopheles stephensi
inconsistently transmit malaria to humans. Am. J. Trop.
Med. Hyg. 43, 441�/445.
Sachs, J., Malaney, P., 2002. The economic and social burden
of malaria. Nature 415, 680�/685.
Theander, T.G., 1998. Malaria in areas of unstable and
seasonal transmission: lessons from Daraweesh. Trans. R.
Soc. Trop. Med. Hyg. 92, 589�/592.
Thomas, C.J., Lindsay, S.W., 2000. Local-scale variation in
malaria infection amongst rural Gambian children esti-
mated by satellite remote sensing. Trans. R. Soc. Trop.
Med. Hyg. 94, 159�/163.
Toure, Y.T., Coluzzi, M., 2000. The challenges of doing more
against malaria. Bull. World Health Organ. 78, 1376.
Trape, J.-F., Pison, G., Spiegel, A., Enel, C., Rogier, C., 2002.
Combating malaria in Africa. Trends Parasitol. 18, 224�/
230.
Vercruysse, J., Jancloes, M., van de Velden, L., 1983. Epide-
miology of seasonal falciparum malaria in an urban area of
Senegal. Bull. World Health Organ. 61, 821�/831.
Woolhouse, M.E.J., Dye, C., Etard, J.-F., Charlwood, J.D.,
Garnett, G.P., Hagan, P., Hil, J.L.K., Ndhlovu, P.D.,
Quinnell, R.J., Watts, C.H., Chandiwana, S.K., Anderson,
R.M., 1997. Heterogeneities in the transmission of infec-
tious agents: implications for the design of control pro-
grams. Proc. Natl. Acad. Sci. USA 94, 338�/342.
Zwetyenaga, J., Rogier, C., Spiegel, A., Fontenille, D., Trape,
J.-F., Mercereau-Puijalon, O., 1999. A cohort study of
Plasmodium falciparum diversity during the dry season in
Ndiop, a Senegalese village with seasonal, mesoendemic
malaria. Trans. R. Soc. Trop. Med. Hyg. 93, 375�/380.
W. Gu et al. / Acta Tropica 86 (2003) 71�/81 81
Copyright © 2022 FDOKUMEN