Longitudinal Associations Between Changes in Physical Activity and Depressive Symptoms in Adulthood:...
10
Longitudinal Associations Between Changes in Physical Activity and Depressive Symptoms in Adulthood: The Young Finns Study Xiaolin Yang & Mirja Hirvensalo & Mirka Hintsanen & Taina Hintsa & Laura Pulkki-Råback & Markus Jokela & Risto Telama & Tuija Tammelin & Nina Hutri-Kähönen & Jorma S. A. Viikari & Olli T. Raitakari # International Society of Behavioral Medicine 2013 Abstract Background Although previous studies have associated phys- ical activity (PA) with lower depressive symptoms, the combined effects of the (1) frequency, (2) intensity, and (3) duration of long-term PA have not been examined in detail. Purpose We examined the dose–response association be- tween changes in frequency, intensity, and duration of PA and depressive symptoms in men and women over 6 years. Methods Participants comprised 1,959 healthy adults (833 men and 1,126 women), aged 24–39 years in 2001, drawn from the ongoing Young Finns Study. PA was assessed using a self-report questionnaire completed in connection with a medical examination in 2001 and 2007. Depres- sive symptoms were simultaneously assessed using a modified version of Beck’ s Depression Inventory in both phases. Results High doses of PA at baseline were prospectively associated with fewer depressive symptoms in men, while moderate doses of PA at baseline were inversely associated with the prevalence of depressive symptoms in women. As- sociations between baseline PA and depressive symptom changes were mediated by social and health-related factors which differed between men and women. Long-term partici- pation in regular PA in all dimensions remained remarkably stable (all p <0.001). Compared to those who remained inac- tive, the persistently active participants in all dimensions, with the exception of women’ s intensity group, were more likely to show decreases in depressive symptoms independent of the included confounders. An increase in PA in certain groups was also independently associated with fewer depressive symptoms, particularly in women. Conclusions Regular and persistent participation in different doses of PA may provide short-term and long-term beneficial effects on depressive symptom changes. The results imply that the moderate to high doses of PA may serve as a buffer against depression in early midlife. X. Yang (*) : T. Tammelin LIKES—Research Center for Sport and Health Sciences, Viitaniementie 15a, 40720 Jyväskylä, Finland e-mail: [email protected] M. Hirvensalo : R. Telama Department of Sport Sciences, University of Jyväskylä, Jyväskylä, Finland M. Hintsanen Helsinki Collegium for Advanced Studies and Unit of Personality, Work and Health Psychology, University of Helsinki, Helsinki, Finland T. Hintsa : L. Pulkki-Råback : M. Jokela Unit of Personality, Work and Health Psychology, University of Helsinki, Helsinki, Finland N. Hutri-Kähönen Department of Pediatrics, Tampere University Hospital, Tampere, Finland J. S. A. Viikari Department of Medicine, University of Turku and Turku University Hospital, Turku, Finland O. T. Raitakari Department of Clinical Physiology, Turku University Hospital and Research Centre of Applied and Preventive Cardiovascular Medicine, University of Turku, Turku, Finland Int.J. Behav. Med. DOI 10.1007/s12529-013-9376-0
Transcript of Longitudinal Associations Between Changes in Physical Activity and Depressive Symptoms in Adulthood:...

Longitudinal Associations Between Changes in PhysicalActivity and Depressive Symptoms in Adulthood: The YoungFinns Study
Xiaolin Yang & Mirja Hirvensalo & Mirka Hintsanen & Taina Hintsa &
Laura Pulkki-Råback & Markus Jokela & Risto Telama & Tuija Tammelin &
Nina Hutri-Kähönen & Jorma S. A. Viikari & Olli T. Raitakari
# International Society of Behavioral Medicine 2013
AbstractBackground Although previous studies have associated phys-ical activity (PA) with lower depressive symptoms, thecombined effects of the (1) frequency, (2) intensity, and(3) duration of long-term PA have not been examined indetail.
Purpose We examined the dose–response association be-tween changes in frequency, intensity, and duration ofPA and depressive symptoms in men and women over6 years.Methods Participants comprised 1,959 healthy adults (833men and 1,126 women), aged 24–39 years in 2001, drawnfrom the ongoing Young Finns Study. PA was assessedusing a self-report questionnaire completed in connectionwith a medical examination in 2001 and 2007. Depres-sive symptoms were simultaneously assessed using amodified version of Beck’s Depression Inventory in bothphases.Results High doses of PA at baseline were prospectivelyassociated with fewer depressive symptoms in men, whilemoderate doses of PA at baseline were inversely associatedwith the prevalence of depressive symptoms in women. As-sociations between baseline PA and depressive symptomchanges were mediated by social and health-related factorswhich differed between men and women. Long-term partici-pation in regular PA in all dimensions remained remarkablystable (all p <0.001). Compared to those who remained inac-tive, the persistently active participants in all dimensions, withthe exception of women’s intensity group, were more likely toshow decreases in depressive symptoms independent of theincluded confounders. An increase in PA in certain groupswas also independently associated with fewer depressivesymptoms, particularly in women.Conclusions Regular and persistent participation in differentdoses of PA may provide short-term and long-term beneficialeffects on depressive symptom changes. The results imply thatthe moderate to high doses of PAmay serve as a buffer againstdepression in early midlife.
X. Yang (*) : T. TammelinLIKES—Research Center for Sport and Health Sciences,Viitaniementie 15a, 40720 Jyväskylä, Finlande-mail: [email protected]
M. Hirvensalo :R. TelamaDepartment of Sport Sciences, University of Jyväskylä, Jyväskylä,Finland
M. HintsanenHelsinki Collegium for Advanced Studies and Unit of Personality,Work and Health Psychology, University of Helsinki, Helsinki,Finland
T. Hintsa : L. Pulkki-Råback :M. JokelaUnit of Personality, Work and Health Psychology, University ofHelsinki, Helsinki, Finland
N. Hutri-KähönenDepartment of Pediatrics, Tampere University Hospital, Tampere,Finland
J. S. A. ViikariDepartment of Medicine, University of Turku and Turku UniversityHospital, Turku, Finland
O. T. RaitakariDepartment of Clinical Physiology, Turku University Hospital andResearch Centre of Applied and Preventive CardiovascularMedicine, University of Turku, Turku, Finland
Int.J. Behav. Med.DOI 10.1007/s12529-013-9376-0

Keywords Physicalactivity .Depressivesymptoms .Adults .
Follow-up
Introduction
Depressive symptoms increase the risk for developing psy-chological and physical disabilities, including the risk fordeveloping chronic diseases [1]. The lifetime prevalence ofmajor depressive disorders is estimated to be between 15 and20 % in developed countries [2]; an additional 20 % experi-ence elevated depressive symptoms [3]. Thus, the harmfuleffects of depression affect society considerably on at a largescale. Several systematic reviews, including meta-analyses,have shown that low physical activity (PA) during leisure timeis consistently supported as an important predictor of higherdepressive symptoms among youth [4, 5] and adults [6–8],particularly among young and middle-aged women [9–12].PA refers to sport and recreational PA during leisure time thatenhances health, including activities that vary in frequency,intensity, duration, type, and total amount [13].
Although the associations of PAwith depressive symptomshave been widely demonstrated in both cross-sectional andprospective studies [4–8], details of the dose–responserelationship involving different dimensions of PA (fre-quency, intensity, duration) remain unclear because pre-vious studies have explored the dose–response effects ofPA using only one dimension of PA: either frequency orduration or intensity [11, 14–17].
In recent years, only a few longitudinal studies have exam-ined the effects of PA on depressive symptoms in youth [18]and adults [19–21], and all but one suggested that early PA isassociated with lower levels of depressive symptoms in adult-hood. Stavrakakis et al. [20] did not find a significant associ-ation between adolescent PA in various domains (nature,frequency, duration, and intensity) and onset of depressionin early adulthood. The dose–response relation was observedfor women but not for men [21]. However, these studies didnot measure the dose–response association of changes in eachdimension of PAwith depressive symptom changes over time.Thus, the dose–response effects of PA on mental health wouldneed to be more thoroughly taken into account in a longitudi-nal design [6].
It is important to note that changes in the dose of PA areassociated with the likelihood of depression, taking into ac-count potential preexisting depressive symptoms. It is plausi-ble that previous depressive symptoms are modifiable riskfactors for changes in PA, which could make a contributionto divergent trends in the relationship between changes in PAand risk for developing elevated depressive symptoms. Mostlongitudinal studies have excluded participants with a historyof depressive symptoms on the grounds that such symptomsmay confound accurate evaluation of changes in PA [21, 22].
There is scarcity of studies including participants withpreexisting depressive symptoms [12, 23], and none of thesehas investigated the role of long-term PA on depressive symp-tom changes over time. The best solution to this problem is toinclude previous depressive symptoms in full multivariateanalyses [24].
To our knowledge, no longitudinal studies have assessedthe associations of changes in dimensions of PA and overall ofPA with depressive symptom changes in adulthood. Under-standing the change in PA is vital to assessing significance ofPA for psychological health, especially from a preventivepoint of view, as adherence to a healthy lifestyle is a centralproblem in preventive medicine. Thus, in the present study,we examined the association of dimensions of PA (i.e., fre-quency, intensity, and duration) and overall of PAwith depres-sive symptom changes in early mid-life over a 6-year follow-up period, taking into account potential confounders such asage, education, occupation, marital status, smoking, and bodymass index (BMI).
Methods
Participants and Procedure
The Young Finns Study is an ongoing longitudinalpopulation-based study targeting children and adolescentswho were born in 1962, 1965, 1968, 1971, 1974, or 1977. Atotal of 4,320 children and adolescents aged 3, 6, 9, 12, 15,and 18 years were invited to participate in the initial survey in1980. Of these, 3,596 (83.2 %) participants participated. Thestudy was carried out in all five Finnish university cities withmedical schools (Helsinki, Kuopio, Oulu, Tampere, and Tur-ku) and their surrounding communities. The study participantswere randomly chosen from the national population registerfor these areas. They were followed up in 1983, 1986, 1989,1992, 2001, and 2007. The study protocol was reviewed andapproved by the ethics committee of each of the five partici-pating universities, and the subjects’ informed consent wasobtained [25].
The data for this study covered all six cohorts, aged from24 to 39 years in 2001 and hence, 30–45 years in 2007.Participants with missing information on PA and depressivesymptoms variables in either 2001 or 2007 (n =1,506) wereexcluded. Some of the reasons for the loss of participantsincluded lack of time, unwillingness to participate, absencefrom the place of residence at time of examination, and death[25]. Pregnant women, either currently (n =37) or previouslyin 2001(n =62), and participants who had a diagnosis ofdiabetes mellitus (n =15 for type I and n =17 for type II) orischemic heart disease (n =4) were also excluded from theseanalyses. Complete data on all variables were available for1,955 healthy adults (831 men and 1,124 women).
Int.J. Behav. Med.

Measures
Physical Activity
Physical activity was assessed using a self-report question-naire administered in connection with a medical examinationin 2001 and 2007 [26, 27]. Options in frequency of PA werecategorized as follows: (1) not at all or once a month, (2) oncea week, (3) 2–3 times a week, and (4) 4–6 times a week ordaily. Intensity of PAwas classified as follows: (1) not gettingout of breath and sweating, (2) getting out of breath andsweating moderately, and (3) getting out of breath and sweat-ing a lot. The intensity category has been shown to display amodest correlation with certain high-intensity sports such asjogging, ball games, racket games, and ice hockey [28]. Du-ration of PA was defined as follows: (1)<20 min, (2) 20–40 min, (3) 40–60 min, and (4)>60 min. Overall PAwas firstcomputed as the average product of frequency, intensity, andduration, and then categorized into quartiles (inactive, low,moderate, and high) in line with a widely used procedure [29].
In order to examine changes in dimensions of PA andoverall of PA over 6 years, participants were first classifiedas high (those who participated in moderate-intensity to high-intensity PA for≥20 min at least twice a week) and low (thosewhose participation in PAwas less intense and less frequent) attwo separate phases. The participants were then divided intofour groups: persistently high (in both phases), increasing(active in 2007 but not in 2001), decreasing (active in 2001but not in 2007), and persistently low (in both phases). Test-retest reliability for overall PA values over time, as indicatedby intraclass correlation coefficients (ICC), was acceptable formen (ICC=0.56) and women (ICC=0.57). The validity of PAwas tested by showing statistically significant correlation witha 7-day pedometer study (n =1,853) [30].
Depressive Symptoms
Depressive symptoms were assessed by using a modifiedversion of Beck’s Depression Inventory (BDI) [31, 32]. Inthe present study, the participants were asked to rate thesecond mildest description of the original 21 items (e.g., “Ioften feel sad”) on a 5-point scale (1=strongly disagree, 5=strongly agree). We then asked the participants to rate theiragreement with it on a 5-point Likert scale. Depressive symp-toms are characterized by negative mood, sadness, pessimism,decreased functioning (e.g., indecisiveness), work inhibition,and somatic problems (e.g., insomnia and fatigue) [32]. Amean score for the 21 items was calculated, resulting in adepressive symptom score ranging from 1 to 5, with higherscores indicating greater level of depressive symptoms. Thechange in depressive symptom score was calculated bysubtracting baseline depressive symptoms from follow-updepressive symptoms. The continuous depressive symptom
score was used for two reasons: (1) because prevalence ofclinical depression in this health population was low (3.8 %)fulfilling criteria for moderate to severe depression, and (2)because subthreshold symptoms are known to be importantpredictors of future depressive disorder [33].
We used this modified BDI as it was thought to revealinterindividual variance in depressive symptoms in a healthy,young population in which rates of clinical depression areknown to be low [34]. The theoretical model of the revisedquestionnaire has been tested by confirmatory factor analyseson the Young Finns study data, with the results indicating thatthis model is empirically identifiable [35]. The modified BDIhas previously been associated with psychological character-istics that are known to be associated with depression, such asa difficult childhood temperament (negative emotionality andlow sociability), adulthood sentimentality and fatigability, andlow social support [35–37]. Moreover, our measure has beenassociated with metabolic and cardiovascular risk factors suchas obesity [38] and preclinical atherosclerosis [32] in theYoung Finns study. Cronbach α reliability for the modifiedBDI was 0.92 in both 2001 and 2007.
Confounders
Baseline age was considered as a potential confounder.Level of education was measured as the total number ofcompleted school years in 2001. Occupation was classi-fied into three categories on the basis of the criteria usedby the Central Statistical Office of Finland: 1=manual(builders, metal workers, nannies, etc.); 2=lower non-manual (civil servants, specialized and skilled workers,etc.); and 3=upper non-manual (administrators, managersand academics, etc.). Marital status was formed as twocategories: married (married, engaged, or cohabiting) andnon-married (single, divorced, or widowed). Smokingstatus was divided into three groups: (1) current smokers:participants smoking at least once a week or more fre-quently; (2) ever smokers: those smoking less than onceper week or quitting; and (3) never smokers. Weight wasmeasured with a Seca scale (Vogel & Halke, Hamburg,Germany), and height was measured with a Secaanthropometer. BMI was calculated as weight (kg)/height(m2).
Statistical Analyses
Descriptive characteristics are expressed as means (SD) forcontinuous variables and as proportions (%) for categoricalvariables. Gender comparisons of all variables were analyzedusing t tests or χ2 tests. A generalized linear model was usedto examine the association of dimensions of PA and overall ofPA at baseline, and its changes with depressive symptomchanges over a 6-year follow-up period, controlling for age,
Int.J. Behav. Med.
education, occupation, marital status, smoking, and BMI, withlow-active participants as the reference group. All analyseswere done separately for men and women. The level ofsignificance was p <0.05. All the statistical analyseswere performed using SPSS 20.0 for Window (SPSSInc., Chicago, IL).
Results
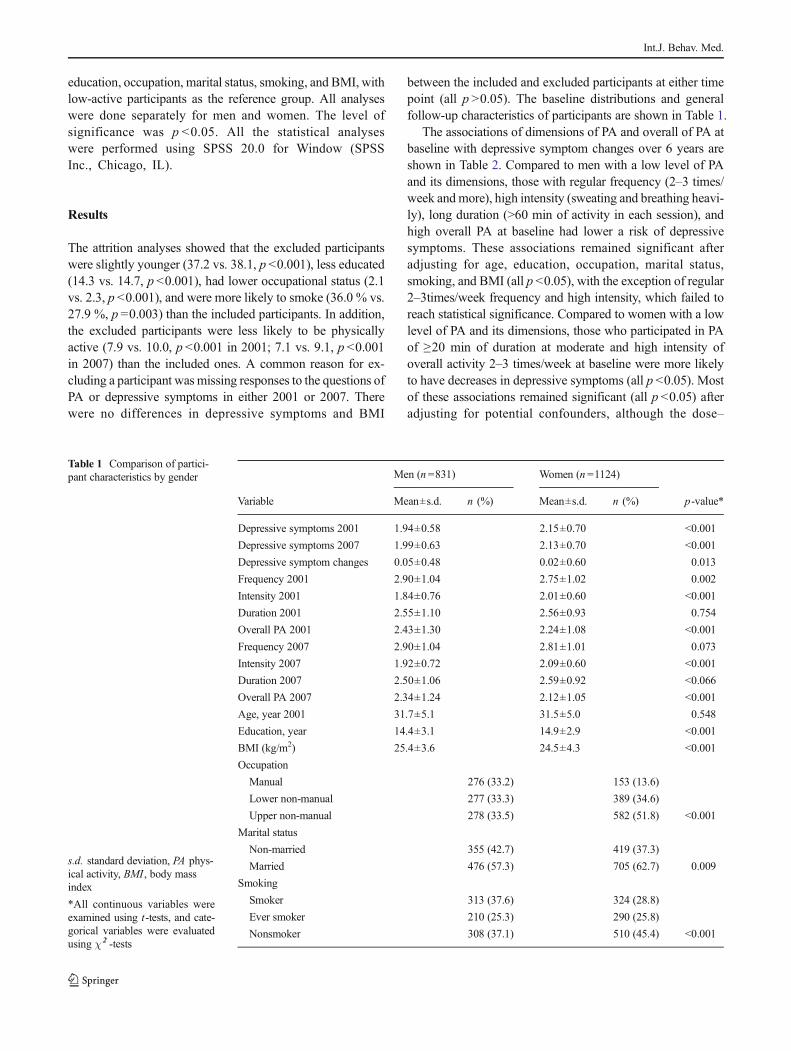
The attrition analyses showed that the excluded participantswere slightly younger (37.2 vs. 38.1, p <0.001), less educated(14.3 vs. 14.7, p <0.001), had lower occupational status (2.1vs. 2.3, p <0.001), and were more likely to smoke (36.0 % vs.27.9 %, p =0.003) than the included participants. In addition,the excluded participants were less likely to be physicallyactive (7.9 vs. 10.0, p <0.001 in 2001; 7.1 vs. 9.1, p <0.001in 2007) than the included ones. A common reason for ex-cluding a participant wasmissing responses to the questions ofPA or depressive symptoms in either 2001 or 2007. Therewere no differences in depressive symptoms and BMI
between the included and excluded participants at either timepoint (all p >0.05). The baseline distributions and generalfollow-up characteristics of participants are shown in Table 1.
The associations of dimensions of PA and overall of PA atbaseline with depressive symptom changes over 6 years areshown in Table 2. Compared to men with a low level of PAand its dimensions, those with regular frequency (2–3 times/week andmore), high intensity (sweating and breathing heavi-ly), long duration (>60 min of activity in each session), andhigh overall PA at baseline had lower a risk of depressivesymptoms. These associations remained significant afteradjusting for age, education, occupation, marital status,smoking, and BMI (all p <0.05), with the exception of regular2–3times/week frequency and high intensity, which failed toreach statistical significance. Compared to women with a lowlevel of PA and its dimensions, those who participated in PAof ≥20 min of duration at moderate and high intensity ofoverall activity 2–3 times/week at baseline were more likelyto have decreases in depressive symptoms (all p <0.05). Mostof these associations remained significant (all p <0.05) afteradjusting for potential confounders, although the dose–
Table 1 Comparison of partici-pant characteristics by gender
s.d. standard deviation, PA phys-ical activity, BMI , body massindex
*All continuous variables wereexamined using t-tests, and cate-gorical variables were evaluatedusing χ2 -tests
Men (n =831) Women (n =1124)
Variable Mean±s.d. n (%) Mean±s.d. n (%) p-value*
Depressive symptoms 2001 1.94±0.58 2.15±0.70 <0.001
Depressive symptoms 2007 1.99±0.63 2.13±0.70 <0.001
Depressive symptom changes 0.05±0.48 0.02±0.60 0.013
Frequency 2001 2.90±1.04 2.75±1.02 0.002
Intensity 2001 1.84±0.76 2.01±0.60 <0.001
Duration 2001 2.55±1.10 2.56±0.93 0.754
Overall PA 2001 2.43±1.30 2.24±1.08 <0.001
Frequency 2007 2.90±1.04 2.81±1.01 0.073
Intensity 2007 1.92±0.72 2.09±0.60 <0.001
Duration 2007 2.50±1.06 2.59±0.92 <0.066
Overall PA 2007 2.34±1.24 2.12±1.05 <0.001
Age, year 2001 31.7±5.1 31.5±5.0 0.548
Education, year 14.4±3.1 14.9±2.9 <0.001
BMI (kg/m2) 25.4±3.6 24.5±4.3 <0.001
Occupation
Manual 276 (33.2) 153 (13.6)
Lower non-manual 277 (33.3) 389 (34.6)
Upper non-manual 278 (33.5) 582 (51.8) <0.001
Marital status
Non-married 355 (42.7) 419 (37.3)
Married 476 (57.3) 705 (62.7) 0.009
Smoking
Smoker 313 (37.6) 324 (28.8)
Ever smoker 210 (25.3) 290 (25.8)
Nonsmoker 308 (37.1) 510 (45.4) <0.001
Int.J. Behav. Med.

response associations of duration and intensity with depres-sive symptom changes were attenuated or even disappeared.
The associations between long-term participation in regularPA and depressive symptom changes are shown in Table 3.Both men and women who participated regularly in morefrequent, higher intensity, longer duration, and higher overallof PA during the 6 years had a lower risk for depressivesymptoms compared to those who were inactive. As shownin Fig. 1, the significant difference between the doses ofoverall PA in depressive symptom changes persisted acrosstime among men and women. Similar results were observed ineach dimension (data not shown).
With regard to changes in levels of dimensions of PA andoverall of PA, persistently active men were less likely todevelop depressive symptoms than their persistently inactivecounterparts over 6 years, independent of potential con-founders (Table 4). Increasing PA frequency was independent-ly associated with low risk of depressive symptoms. Menclassified as increasingly active or decreasingly active didnot differ significantly from those in the persistently inactivegroup in depressive symptoms. In comparison to persistently
inactive women, the persistently active women who partici-pated more frequently and with longer duration had a lowerrisk for depressive symptoms. Increasing and persistently highfrequency and duration of PA remained inversely associatedwith depressive symptoms after adjustments were made forpotential confounders, but the associations of decreasing fre-quency and duration of PA disappeared when control variableswere added. With respect to overall PA, persistent activity andincreasing activity remained inversely associatedwith depressivesymptom changes after adjustments were made for all con-founders. There were no significant differences between changesin PA intensity and changes in depressive symptoms in women.
Discussion
We found that men and women with greater frequency, longerduration, and higher overall level of PA, but not intensity, atbaseline indicated lower risk for depressive symptom changesafter adjustment were made for potential confounders. Genderdifferences in the association between PA level at baseline and
Table 2 Generalized linear models to examine the association between frequency, intensity, duration, and overall of physical activity at baseline anddepressive symptom changes by gender
Baseline Men Women
Physical activity Model 1 Model 2 Model 1a Model 2b
β (95 % CI) β (95 % CI) β (95 % CI) β (95 % CI)
Frequency
Inactive Reference Reference Reference Reference
1 time/week −0.08 (−0.12, −0.04) −0.06 (−0.10, −0.03) −0.09 (−0.13, −0.04) −0.05 (−0.09, −0.01)2–3 times/week −0.10 (−0.14, −0.06)* −0.10 (−0.14, −0.06) −0.17 (−0.21, −0.13)** −0.15 (−0.18, −0.11)*≥4 times/week −0.22 (−0.25, −0.15)** −0.21 (−0.24, −0.14)** −0.12 (−0.17, −0.07) −0.08 (−0.13, −0.03)
Intensity
Low Reference Reference Reference Reference
Moderate −0.03 (−0.02, 0.08) 0.03 (−0.02, 0.09) −0.01 (−0.06, 0.04) 0.01 (−0.04, 0.06)High −0.15 (−0.20, −0.10)* −0.13 (−0.16, −0.09) −0.17 (−0.22, −0.11)* −0.12 (−0.18, −0.06)
Duration
<20 min Reference Reference Reference Reference
20–40 min −0.05 (−0.09, 0.01) −0.03 (−0.08, 0.02) −0.15 (−0.19, −0.11)* −0.08 (−0.12, −0.03)40–60 min −0.11 (−0.15, −0.06) −0.10 (−0.14, −0.05) −0.20 (−0.24, −0.17)*** −0.12 (−0.16, −0.08)*>60 min −0.20 (−0.25, −0.15)** −0.18 (−0.23, −0.13)* −0.17 (−0.22, −0.12)* −0.08 (−0.14, −0.03)
Overall
Inactive Reference Reference Reference Reference
Low −0.10 (−0.15, −0.04) −0.10 (−0.15, −0.04) 0.04 (−0.02, 0.09) 0.06 (0.01, 0.13)
Moderate −0.08 (−0.12, −0.04) −0.07 (−0.11, −0.03) −0.15 (−0.19, −0.12)** −0.12 (−0.16, −0.09)*High −0.18 (−0.22, −0.15)*** −0.18 (−0.22, −0.14)** −0.17 (−0.22, −0.13)** −0.14 (−0.18, −0.10)*
CI confidence interval
*p <0.05, **p<0.01, and ***p <0.001aAdjusted for agebAdditional adjusted for education, occupation, marital status, smoking, and body mass index
Int.J. Behav. Med.

depressive symptom changes were also observed. Regularparticipation in any amount of PA was inversely and signifi-cantly associated with reduced likelihood of depressive symp-toms in both genders. Men and women who remained
physically active in all dimensions over 6 years, with oneexception, had significantly lower levels of depressive symp-toms compared to those who remained inactive, independentof potential confounders. Increased frequency, duration and
Mea
ns o
f de
pres
sive
sym
ptom
cha
nges
Year of measurement
Fig. 1 Adjusted mean differencein depressive symptom scores bythe doses of overall physicalactivity over a 6-year period inmen and women
Table 3 Generalized linear models to examine the association between regular frequency, intensity, duration, and overall of physical activity anddepressive symptom changes by gender
6-year physical activity Men Women
Model 1 Model 2 Model 1a Model 2b
β (95 % CI) β (95 % CI) β (95 % CI) β (95 % CI)
Frequency
Low Reference Reference Reference Reference
High −0.16 (−0.17, −0.15)*** −0.13 (−0.14, −0.12)*** −0.19 (−0.20, −0.18)*** −0.14 (−0.15, −0.12)***Intensity
Low Reference Reference Reference Reference
High −0.13 (−0.14, −0.11)*** −0.11 (−0.12, −0.10)*** −0.17 (−0.18, −0.15)*** −0.14 (−0.16, −0.13)***Duration
Low Reference Reference Reference Reference
High −0.15 (−0.16, −0.14)*** −0.11 (−0.12, −0.10)*** −0.21 (−0.23, −0.20)*** −0.15 (−0.16, −0.13)***Overall
Low Reference Reference Reference Reference
High −0.17 (−0.20, −0.15)*** −0.15 (−0.18, −0.14)*** −0.22 (−0.24, −0.20)*** −0.17 (−0.20, −0.15)***
CI confidence interval
***p <0.001aAdjusted for agebAdditional adjusted for education, occupation, marital status, smoking, and body mass index
Int.J. Behav. Med.
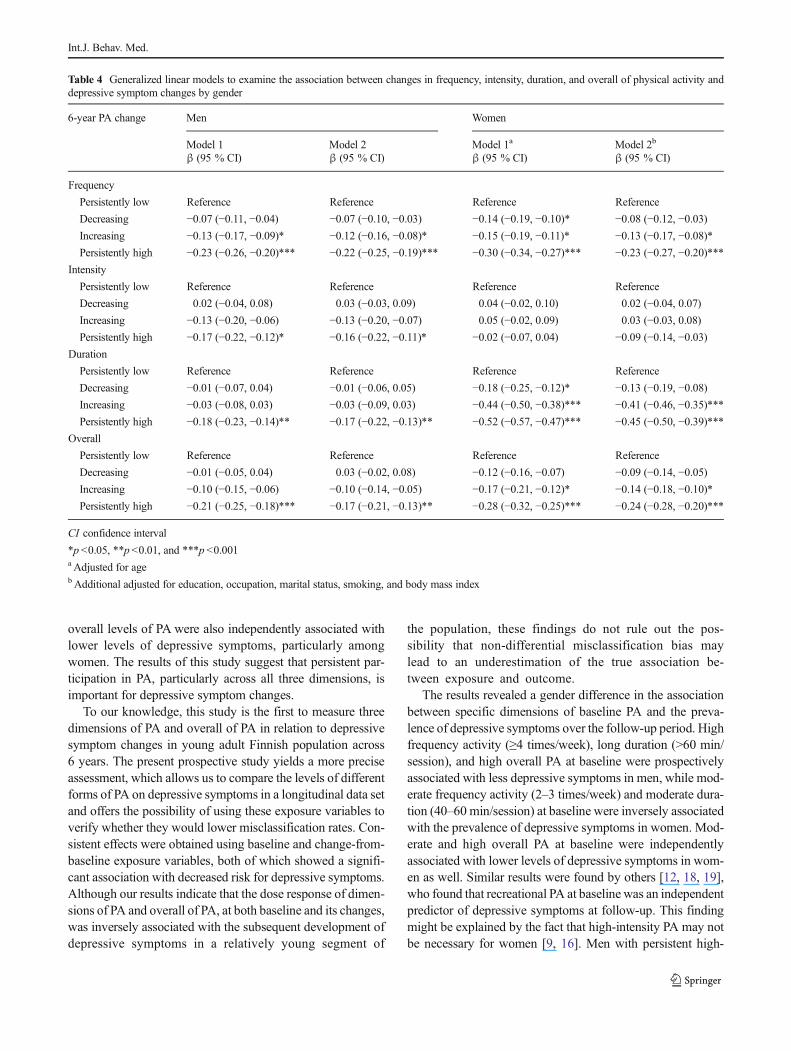
overall levels of PA were also independently associated withlower levels of depressive symptoms, particularly amongwomen. The results of this study suggest that persistent par-ticipation in PA, particularly across all three dimensions, isimportant for depressive symptom changes.
To our knowledge, this study is the first to measure threedimensions of PA and overall of PA in relation to depressivesymptom changes in young adult Finnish population across6 years. The present prospective study yields a more preciseassessment, which allows us to compare the levels of differentforms of PA on depressive symptoms in a longitudinal data setand offers the possibility of using these exposure variables toverify whether they would lower misclassification rates. Con-sistent effects were obtained using baseline and change-from-baseline exposure variables, both of which showed a signifi-cant association with decreased risk for depressive symptoms.Although our results indicate that the dose response of dimen-sions of PA and overall of PA, at both baseline and its changes,was inversely associated with the subsequent development ofdepressive symptoms in a relatively young segment of
the population, these findings do not rule out the pos-sibility that non-differential misclassification bias maylead to an underestimation of the true association be-tween exposure and outcome.
The results revealed a gender difference in the associationbetween specific dimensions of baseline PA and the preva-lence of depressive symptoms over the follow-up period. Highfrequency activity (≥4 times/week), long duration (>60 min/session), and high overall PA at baseline were prospectivelyassociated with less depressive symptoms in men, while mod-erate frequency activity (2–3 times/week) and moderate dura-tion (40–60 min/session) at baseline were inversely associatedwith the prevalence of depressive symptoms in women. Mod-erate and high overall PA at baseline were independentlyassociated with lower levels of depressive symptoms in wom-en as well. Similar results were found by others [12, 18, 19],who found that recreational PA at baseline was an independentpredictor of depressive symptoms at follow-up. This findingmight be explained by the fact that high-intensity PA may notbe necessary for women [9, 16]. Men with persistent high-
Table 4 Generalized linear models to examine the association between changes in frequency, intensity, duration, and overall of physical activity anddepressive symptom changes by gender
6-year PA change Men Women
Model 1 Model 2 Model 1a Model 2b
β (95 % CI) β (95 % CI) β (95 % CI) β (95 % CI)
Frequency
Persistently low Reference Reference Reference Reference
Decreasing −0.07 (−0.11, −0.04) −0.07 (−0.10, −0.03) −0.14 (−0.19, −0.10)* −0.08 (−0.12, −0.03)Increasing −0.13 (−0.17, −0.09)* −0.12 (−0.16, −0.08)* −0.15 (−0.19, −0.11)* −0.13 (−0.17, −0.08)*Persistently high −0.23 (−0.26, −0.20)*** −0.22 (−0.25, −0.19)*** −0.30 (−0.34, −0.27)*** −0.23 (−0.27, −0.20)***
Intensity
Persistently low Reference Reference Reference Reference
Decreasing 0.02 (−0.04, 0.08) 0.03 (−0.03, 0.09) 0.04 (−0.02, 0.10) 0.02 (−0.04, 0.07)Increasing −0.13 (−0.20, −0.06) −0.13 (−0.20, −0.07) 0.05 (−0.02, 0.09) 0.03 (−0.03, 0.08)Persistently high −0.17 (−0.22, −0.12)* −0.16 (−0.22, −0.11)* −0.02 (−0.07, 0.04) −0.09 (−0.14, −0.03)
Duration
Persistently low Reference Reference Reference Reference
Decreasing −0.01 (−0.07, 0.04) −0.01 (−0.06, 0.05) −0.18 (−0.25, −0.12)* −0.13 (−0.19, −0.08)Increasing −0.03 (−0.08, 0.03) −0.03 (−0.09, 0.03) −0.44 (−0.50, −0.38)*** −0.41 (−0.46, −0.35)***Persistently high −0.18 (−0.23, −0.14)** −0.17 (−0.22, −0.13)** −0.52 (−0.57, −0.47)*** −0.45 (−0.50, −0.39)***
Overall
Persistently low Reference Reference Reference Reference
Decreasing −0.01 (−0.05, 0.04) 0.03 (−0.02, 0.08) −0.12 (−0.16, −0.07) −0.09 (−0.14, −0.05)Increasing −0.10 (−0.15, −0.06) −0.10 (−0.14, −0.05) −0.17 (−0.21, −0.12)* −0.14 (−0.18, −0.10)*Persistently high −0.21 (−0.25, −0.18)*** −0.17 (−0.21, −0.13)** −0.28 (−0.32, −0.25)*** −0.24 (−0.28, −0.20)***
CI confidence interval
*p <0.05, **p<0.01, and ***p <0.001aAdjusted for agebAdditional adjusted for education, occupation, marital status, smoking, and body mass index
Int.J. Behav. Med.

intensity activity were less likely to have depressive symp-toms compared to those with low-intensity activity. This wasnot found in women. Increased bout duration and overall ofPA were independently and inversely associated with theprevalence of depressive symptoms only in women. This isconsistent with findings from a longitudinal study [12] whichobserved those with increased PA to have lower depressivesymptoms than those who had remained inactive. On the otherhand, the present study showed that women were more likelythan men to report having elevated depressive symptoms atbaseline and follow-up. In order for women to get the mostbeneficial effects from PA, the short-term moderate amount ofPAwas also considered enough to be an effective for reducingdepressive symptoms.
Consistent with previous prospective research [12, 18, 19],we found that maintaining the recommended level of PA had aprotective role in reducing the incidence of depressive symp-toms. A dose–response relation was also observed not only inwomen [12, 21] but also in men. However, our findings werenot in agreement with those of recent studies reporting thateven light exercise (e.g., walking 1–3 times/week or PA≥1.25 h/week) resulted in a significant reduction of depression,compared to inactivity, in women [14, 39] and in men [40].These results were also not in agreement with a recent studythat has shown a major depressive episode to be unaffected byany of the PA dimensions across the adolescent period [20].These inconsistent findings may be caused by different as-sessments of PA, each tapping into different aspects of varia-tion in the dose–response relationship. Our data support theclear preventive role of persistent high PA in depressivesymptoms in both genders and provide some evidence thatthe type of dose–response association between the amount oflong-term PA and depressive symptoms prevention variesbetween men and women.
This study supports previous research [10, 18] which foundthat young adults are also at risk for depression and indicatesthat PA is inversely associated with depressive symptoms,particularly in young women. Regular PA appears to be aseffective for depression prevention as other treatments such asmedication and psychotherapy [8]. Our results are also inaccordance with previous research showing a longitudinalinverse association between PA and depressive symptoms inpopulation-based studies [19, 21].
Almost all the impacts of the dimensions of high PAwereunlikely to be affected by potential confounders, includingsocioeconomic factors (education and occupation), demo-graphic factors (age and marital status), and health-relatedfactors (smoking and BMI). Some but not all of these factorswere potentially associated with depressive symptoms. Wefound that men with less education, lower SES, and morefrequent smoking had a higher risk of depressive symptoms.High levels of depressive symptoms were common in marriedwomen. An association was observed between depressive
symptoms and BMI in both genders (data not shown). In thepresent analysis, however, the dose–response associations ofregular frequency (2–3 times/week), duration (varying bygender, with 20–40 min for men and >60 min for women),and high intensity in both genders at baseline were explainedby the potential confounders. In particular, the associations ofdecreasing frequency and duration in women disappearedafter adjusting for the confounders. The possible pathwayrelating PA and depressive symptoms may be mediatedthrough health status, particularly among women [12]. It ispossible that poor health status may affect both low PA anddepression. Individuals with poor health status may be lesslikely to participate in PA, which, in turn, increases the risk ofdepressive symptoms. On the other hand, poor health statusmay contribute to depressive symptoms and depressed indi-viduals are likely to be less willing to participate in PA.Finally, participants with a diagnosis of diabetes mellitus orischemic heart disease were not included in the present anal-yses. The attrition analyses showed that the participants ex-cluded for the health reason were more likely to be depressedcompared to those who were included.
It is noteworthy that the present observational data couldnot establish causality because there may be unmeasuredconfounders (e.g., unusual fatigue, lack of motivation, andpoor health status) that impacted the causal effect of PA ondepressive symptoms. In the present study, both the exposureand outcome variables were measured through self-ratings,which may introduce common-rater bias. Future research isneeded to establish the predominant causal association be-tween PA and depressive symptoms across different timepoints using cross-lagged panel models. It is important to testreverse causality so that the association between PA anddepressive symptoms can be properly evaluated.
Recently, some systematic reviews summarized the evi-dence supporting the possible mechanisms of PA for depres-sive symptoms [7, 41, 42]. Several possible mechanisms havebeen proposed, including improving self-efficacy in the psy-chological pathway, changes in the monoamine neurotrans-mitter systems, increasing the synthesis of serotonin, promot-ing social interaction, and strengthening social support. Theseproposed mechanisms have been suggested to explain howregular PAmay reduce depressive symptoms and examinationof precise mechanisms underlying the role of genetic andenvironmental factors in the association between PA anddepressive symptoms still need further clarification. On theother hand, the relationship between PA and depressive symp-toms may also be bidirectional: that is, symptoms of depres-sion may reduce levels of PA and thus increase sedentarylifestyle, along with unusual fatigue, low energy level, anddecreased motivation [43–46]. The present findings suggestthat regular participation in PAmay have a beneficial effect onpsychosocial well-being and may be recommended as ameans to improve mood, which may result in enhancing
Int.J. Behav. Med.

long-term maintenance of PA. Furthermore, increased andmaintained regular PA may lead to enhanced overall physicalcapacity and fitness and act as a buffer that delays the onset ofdepressive symptoms or helps prevent the symptoms ofdepression.
The strength of the study is the longitudinal population-based design, which has allowed examination of the effects ofthe frequency, intensity, and duration of PA, as well as overallPA at baseline and at follow-up, and its effects on depressivesymptoms over a 6-year period in several cohorts. There arealso several limitations that should be taken into account.First, the participants were relatively young and healthy menand women with a relatively small variance in depressivesymptoms. Prevalence of depression is known to peak inmiddle age or older populations [47, 48]. However, it isnotable that even at this age, the prevalence of depressivesymptomswas just enough to allow analysis of the associationbetween PA and depressive symptoms and that the associationwas significant [6–12]. Second, the excluded participantswere more often women than men and were slightly younger,less educated, and less physically active than the participants;however, they did not differ from participants in depressivesymptoms. Thus, a selection bias in the participants seemsunlikely. Third, we studied only PA during leisure time andthus, did not include work-related, transport-related, and do-mestic PA. It has been shown that leisure-time PA was in-versely associated with the risk of depressive symptomsamong women, but no associations were found for work-related, transport-related, or domestic PA [9, 15]. Furtherresearch, which takes these variables into account, will needto be undertaken in this important target group. In this study,however, the frequency, intensity, and duration of PA andoverall PA at both baseline and follow-up seemed to have apreventive influence on depressive symptoms. The physicalloads in occupation and housework are rather low and henceleisure-time PA forms a major proportion of total PA.
Finally, the study was conducted with a predominantlyhomogeneous Finnish sample, representative of the generalpopulation of similar age in Finland. Finland is a high-incomecountry with a higher level of education and occupationalstatus than many other countries. For these reasons, our find-ings cannot be generalized to populations with different so-cioeconomic strata or with substantial ethnic minoritypopulations.
In conclusion, the results show that the impact of PA ondeveloping depressive symptoms varies by gender, dose, andtime. Certain doses of baseline PA for developing depressivesymptoms were mediated by social and health-related factorsthat differed for men and women. The dose–response relationwas found for high-intensity PA in men and for moderateintensity PA in women. Overall PA and its maintenance ratherthan any single dimension of PA may help to reduce depres-sive symptoms over 6 years in adulthood. This study finds
evidence for the effectiveness of the moderate and high dosesof PA in reducing risk for depressive symptoms, raisingawareness of the benefits of PA, and in particular, increasingthe level of participation in PA.
Acknowledgments This study was financially supported by theAcademy of Finland [grant nos. 77841, 210283, 123621 (L.P.-R.),258578 (M.H.), 121584, 124282], Social Insurance Institution ofFinland, Ministry of Education and Culture (X.Y.), Turku UniversityFoundation, Special Federal Grants for Turku University Hospital, Re-search Funds of the University of Helsinki (M.H.), Juho Vainio Founda-tion (L.P.-R.; X.Y.), Finnish Foundation for Cardiovascular Research,Emil Aaltonen Foundation (M.H.), Alli Paasikivi Foundation (M.H.),Finnish Medical Foundation, Finnish Cultural Foundation, and YrjöJahnsson Foundation.
Conflicts of interest None declared.
References
1. Moussavi S, Chatterji S, Verdes E, Tandon A, Patel V, Ustun B.Depression, chronic diseases, and decrements in health: results fromthe World Health Surveys. Lancet. 2007;370:851–8.
2. Kessler RC, Berglund P, Demler O, Jin R, Merikangas KR, WaltersEE. Lifetime prevalence and age-of-onset distributions of DSM-IVdisorders in the national comorbidity survey replication. Arch GenPsychiatry. 2005;62:593–602.
3. Blumenthal JA, Sherwood A, Babyak MA, et al. Exercise andpharmacological treatment of depressive symptoms in patients withcoronary heart disease: results from the UPBEAT (Understanding thePrognostic Benefits of Exercise and Antidepressant Therapy) study. JAm Coll Cardiol. 2012;60:1053–63.
4. Biddle SJH, Asare M. Physical activity and mental health in childrenand adolescents: a review of reviews. Br J SportsMed. 2011;45:886–95.
5. Johnson KE, Taliaferro LA. Relationships between physical activityand depressive symptoms among middle and older adolescents: areview of the research literature. J Spec Pediatr Nurs. 2011;16:235–51.
6. Mead G, Morley W, Campbell P, Greig CA, Mcmurdo M, LawlorDA. Exercise for depression (Review). Cochrane Database Syst Rev.2009;3, CD004366.
7. Teychenne M, Ball K, Salmon J. Physical activity and likelihood ofdepression in adults: a review. Prev Med. 2008;46:397–411.
8. Phillips WT, Kiernan M, King AC. Physical activity as anonpharmacological treatment for depression: a review.Complement Health Pract Rev. 2003;8:139–52.
9. Teychenne M, Ball K, Salmon J. Associations between physicalactivity and depressive symptoms in women. Int J Behav Nutr PhysAct. 2008;5:27.
10. Azar D, Ball K, Salmon J, Cleland V. The association betweenphysical activity and depressive symptoms in young women: areview. Ment Health Phys Act. 2008;1:82–8.
11. Chu I-H, Buckworth J, Kirby TE, Emery CF. Effect of exerciseintensity on depressive symptoms in women. Ment Health PhysAct. 2009;2:37–43.
12. Brown WJ, Ford JH, Burton NW, Marshall AL, Dobson AJ.Prospective study of physical activity and depressive symptoms inmiddle-aged women. Am J Prev Med. 2005;29:265–72.
13. USDHHS. 2008 Physical Activity Guidelines for Americans. U.S.Department of Health and Human Services. 2008. www.health.gov/paguidelines. 2008.
Int.J. Behav. Med.
14. McKercher CM, Schmidt MD, Sanderson KA, Patton GC, Dwyer T,Venn AJ. Physical activity and depression in young adults. Am J PrevMed. 2009;36:161–4.
15. TeychenneM, Ball K, Salmon J. Physical activity, sedentary behaviorand depression among disadvantaged women. Health Educ Res.2010;25:632–44.
16. Dunn AL, Trivedi MH, Kampert JB, Clark CG, Chambliss HO.Exercise treatment for depression: efficacy and dose response. AmJ Prev Med. 2005;28:1–8.
17. Mutrie N, HannahM. The importance of both setting and intensity ofphysical activity in relation to non-clinical anxiety and depression. IntJ Health Promot Educ. 2007;45:24–32.
18. Jacka FN, Pasco JA,Williams LJ, Leslie ER, Dodd S, Nicholson GC,et al. Lower levels of physical activity in childhood associated withadult depression. J Sci Med Sport. 2011;14:222–6.
19. Korniloff K, Vanhala M, Kautiainen H, Koponen H, Peltonen M,Mäntyselkä P, et al. Lifetime leisure-time physical activity and therisk of depressive symptoms at the ages of 65–74 years: the FIN-D2Dsurvey. Prev Med. 2012;54:313–5.
20. Stavrakakis N, Roest A, Verhulst F, Ormel J, de Jonge P, OldehinkelA. Physical activity and onset of depression in adolescents: A pro-spective study in the general population cohort TRAILS. J PsychiatrRev. 2013;47:1304–8.
21. Wang F, DesMeules M, Luo W, Dai S, Lagace C, Morrison H.Leisure-time physical activity and marital status in relation to depres-sion between men and women: a prospective study. Health Psychol.2011;30:204–11.
22. Heesch KC, Burton NW, Brown WJ. Concurrent and prospectiveassociations between physical activity, walking and mental health inolder women. J Epidemiol Community Health. 2011;65:807–13.
23. Kritz-Silverstein D, Barrett-Connor E, Corbeau C. Cross-sectionaland prospective study of exercise and depressed mood in the elderly:the Rancho Bernardo study. Am J Epidemiol. 2001;153:596–603.
24. Smith PM, Bielecky A. The impact of changes in job strain and itscomponents on the risk of depression. Am J Public Health. 2012;102:352–8.
25. Raitakari OT, Juonala M, Rönnemaa T, Keltikangas-Järvinen L,Räsänen L, Pietikäinen M, et al. Cohort profile: the cardiovascularrisk in Young Finns Study. Int J Epidemiol. 2008;37:1220–6.
26. Telama R, Yang X, Viikari J, Välimäki I, Wanne O, Raitakari O.Physical activity from childhood to adulthood: a 21-year trackingstudy. Am J Prev Med. 2005;28:267–73.
27. Yang X, Telama R, Hirvensalo M, Hintsa T, Pulkki-Råback L,Hintsanen M, et al. Leadership component of type A behaviorpredicts physical activity in early midlife. Int J Behav Med.2012;19:48–55.
28. Mansikkaniemi K, Juonala M, Taimela S, Hirvensalo M, Telama R,Huupponen R, et al. Cross-sectional associations between physicalactivity and selected coronary heart disease risk factors in youngadults. The Cardiovascular Risk in Young Finns Study. Ann Med.2012;44:733–44.
29. Haskell WL, I-Min L, Pate RR, Powell KE, Blair SN, Franklin BA,et al. Physical activity and public health: updated recommendation foradults from the American College of Sports Medicine and theAmericanHeart Association.Med Sci Sports Exerc. 2007;39:1423–34.
30. Hirvensalo M, Telama R, Schmidt MD, Tammelin TH, Yang X,Magnussen CG, et al. Daily steps among Finnish adults: variationby age, sex, and socioeconomic position. Scand J Public Health.2011;39:669–77.
31. Beck A, Steer R. Manual for the revised Beck Depression Inventory.TX: Psychological Corp.: San Antonio; 1987.
32. Elovainio M, Keltikangas-Järvinen L, Kivimäki M, Pulkki L,Puttonen S, Heponiemi T, et al. Depressive symptoms and carotidartery intima-media thickness in young adults: the CardiovascularRisk in Young Finns Study. Psychosom Med. 2005;67:561–7.
33. Karsten J, Hartman CA, Smit JH, Zitman FG, Beekman AT, CuijpersP, et al. Psychiatric history and subthreshold symptoms as predictorsof the occurrence of depressive or anxiety disorder within 2 years. BrJ Psychiatry. 2011;198:206–12.
34. Salmela-Aro K, Nurmi J-E. Depressive symptoms and personalproject appraisals: a cross-lagged longitudinal study. Pers IndividDif. 1996;21:373–81.
35. Katainen S, Räikkönen K, Keltikangas-jarvinen L. Adolescent tem-perament, perceived social support, and depressive tendencies aspredictors of depressive tendencies in young adulthood. Eur J Pers.1999;13:183–207.
36. Elovainio M, Kivimäki M, Puttonen S, Heponiemi T, Pulkki L,Keltikangas-Järvinen L. Temperament and depressive symptoms: apopulation-based longitudinal study on Cloninger’s psychobiologicaltemperament model. J Affect Disord. 2004;83:227–32.
37. Heponiemi T, Elovainio M, Kivimäki M, Pulkki L, Puttonen S,Keltikangas-Järvinen L. The longitudinal effects of social supportand hostility on depressive tendencies. Soc Sci Med. 2006;63:1374–82.
38. Pulkki-Råback L, Elovainio M, Kivimäki M, Mattsson N, RaitakariOT, Puttonen S, et al. Depressive symptoms and the metabolicsyndrome in childhood and adulthood. Health Psychol. 2009;28:108–16.
39. Lindwall M, Rennemark M, Halling A, Berglund J, Hassmén P.Depression and exercise in elderly men and women: findings fromthe Swedish national study on aging and care. J Aging Phys Act.2007;15:41–55.
40. Sieverdes JC, Ray BM, Sui X, Lee D-C, Hand GA, Baruth M, et al.Association between leisure time physical activity and depressivesymptoms in men. Med Sci Sports Exerc. 2012;44:260–5.
41. Bernard P, Ninot G, Moullec G, Guillaume S, Courtet P, Quantin X.Smoking cessation, depression, and exercise: empirical evidence,clinical needs, and mechanisms. Nicotine Tob Res. 2013;15:1635–50.
42. Uebelacker L, Epstein-Lubow G, Gaudiano B, Tremont G, Battle C,Miller I. Hatha yoga for depression: critical review of the evidence forefficacy, plausible mechanisms of action, and directions for futureresearch. J Psychiatr Pract. 2010;16:22–33.
43. Ruo B, Rumsfeld JS, Pipkin S, Whooley MA. Relation betweendepressive symptoms and treadmill exercise capacity in the Heartand Soul Study. Am J Cardiol. 2004;94:96–9.
44. Roshanaei-Moghaddam B, Katon WJ, Russo J. The longitudinaleffects of depression on physical activity. Gen Hosp Psychiatry.2009;31:306–15.
45. De Moor MHM, Beem AL, Stubbe JH, Boomsma DI, De Geus EJC.Regular exercise, anxiety, depression and personality: a population-based study. Prev Med. 2006;42:273–9.
46. Harvey SB, Hotopf M, Overland S, Mykletun A. Physical activityand common mental disorders. Br J Psychiatry. 2010;197:357–64.
47. National Association of Chronic Disease Directors. Centers forDisease Control and Prevention and National Association ofChronic Disease Directors. The state of mental health and aging inAmerica issue brief 1: What do the data tell us? Atlanta, GA: Nati.;2008.
48. Adults in later life with mental health problems, mental health foun-dation quoting psychiatry in the elderly (3rd edition), OxfordUniversity Press 2002. Available at: www.mentalhealth.org.uk.;2002.
Int.J. Behav. Med.