Lipoprotein(a) as a cardiovascular risk factor: current status
Pharmacological Research Communications, Vol. 18, No. 5, 1986 471
LONG TERM-EFFECT OF FENOFIBRATE ON LIPOPROTEIN LEVEL AND
COMPOSITION IN DIFFERENT TYPES OF GENETIC HYPERLIPIDEMIAS
G. Baggio, A. Gasparotto, G. C i u f f e t t i * , G. Valer io,
R. Fe l l i n , U. Senin*, C. Gabel l i , G. Crepaldi
Department of Internal Medicine-Universi ty of Padua-Pol icl inico Univers i tar io
Via G ius t in ian i , 2 - 35128 PADOVA - I t a l y
* Cl in ica Medica-Universit~ di Perugia-Pol ic l in ico Monteluce-Perugia- l ta ly
Received in final form 21 March 1986
SUMMARY
Fenofibrate e f fec t on plasma l ip ids and l ipoprote ins was studied in 23
pat ients with primary hyperlipoproteinemias (HLP): 12 with fami l ia l
hypercholesterolemia (FH), 5 wi th combined HLP and 6 with Type I I I HLP. Tr ia l
lasted from 8 to 10 months.
Cholesterol and t r i g l yce r ides were s i gn i f i can t l y reduced in a l l pat ients
as fo l lows: cholesterol dropped 26% in FH (p<O. O01), 32% in combined HLP and
48% in type I I I HLP; t r i g l yce r ides dropped 29%, 64% and 72% respect ively.
This drop involved LDL in FH, VLDL and LDL in combined HLP and ~-VLDL in
type I I I HLP pat ients. In FH and combined HLP patients we observed a +10%
(p<O.01) and a +9% (n.s . ) increase of HDL, respect ive ly .
Two patients had a mild SGOT and SGPT increase and three had a vescicular
cutaneous erythema.
INTRODUCTION
Fenofibrate is very valuable among l i p i d lowering drugs since i t was
shown to be e f f i c i e n t in reducing atherogenic l ipoprote ins (VLDL, LDL and
~-VLDL) and increasing HDL in d i f f e ren t types of hyperl ipoproteinemia (HLP)
(1-8).
However, i t s long range e f fec t have not yet been studied and only one
0031-6989/86/050471-10/$03.00/0 © 1986 The Italian Pharmacological Society
472 Pharmaco~g~alResearch Commun~ation~VoL 1~ No. ~ 1986
publication reports on i ts ef fect on type I I I HLP (4)° This is why we'studied
for a period of 8-10 months fenofibrate ef fect and i ts tolerance with a dosage
of I00x3 mg/die in various types of primary hyperlipoproteinemia (HLP):
fami l ia l hypercholesterolemia (FH), combined HLP and fami l ia l type I I I HLP.
MATERIALS AND METHODS
I) Case Report
23 patients affected by fami l ia l hypercholesterolemia (HLP) were studied:
12 (7 females and 5 males) with fami l ia l hypercholesterolemia (FH), 5 (2
females and 3 males) with combined HLP and 6 (I female and 5 males) with type
I I I HLP. The patients have been informed about the treatment plan and gave
the i r consent to i t . Anthropometric parameters and cholesterol and
t r ig lycer ide basal levels are reported in Tab. I .
Familial HLP phenotypes were established on the basis of WHO c r i t e r i a (9):
cholesterol and t r ig lycer ides levels of plasma, and of LDL, VLDL and HDL
fractions obtained by preparative u l t racentr i fugat ion plus polyanions
precip i tat ion (11-12), agarose l ipoprotein electrophoresis, c l in ica l features
and fami l ia l h is tory. For type I I I HLP diagnosis, the VLDL cholesterol/Serum
Triglycerides ra t io was evaluated (always >O.30).Apo E2/E2 phenotype was
confirmed with isoelectr icfocusing (10) af ter the t r i a l in four of these
patients (patient No. 3-4-5-6). As regard the other two patients: patient No.
I died for myocardial in farct ion (he had severe CVD, PAD and CHD as well as
al l typical cutaneous features of type I I I hyperlipoproteinemia), patient No.
2 did not attend our l i p id c l i n i c af ter the end of the t r i a l . Renal, thyroid,
l i ve r function were normal; other causes of secondary hyperlipidemia were
excluded.
2) Treatment Plan
300 mg fenofibrate were administered in three dai ly doses (100mgx3) for 8
months to combined and type ] I I HLP, and for 10 months to FH patients. Two
months before and during the whole t r i a l the patients followed a standard
isocaloric diet (20% protein, 45% carbohydrates, 35% f a t ) , containing 300 mg
cholesterol per day, a P/S ra t io of 1.8, and 12-15 gr f ibre per day. FH
patients af ter 10 months treatment were studied for another 4 weeks only under
Pharmacological Research Communications, Vol. 18, No. 5, 1986 4?3
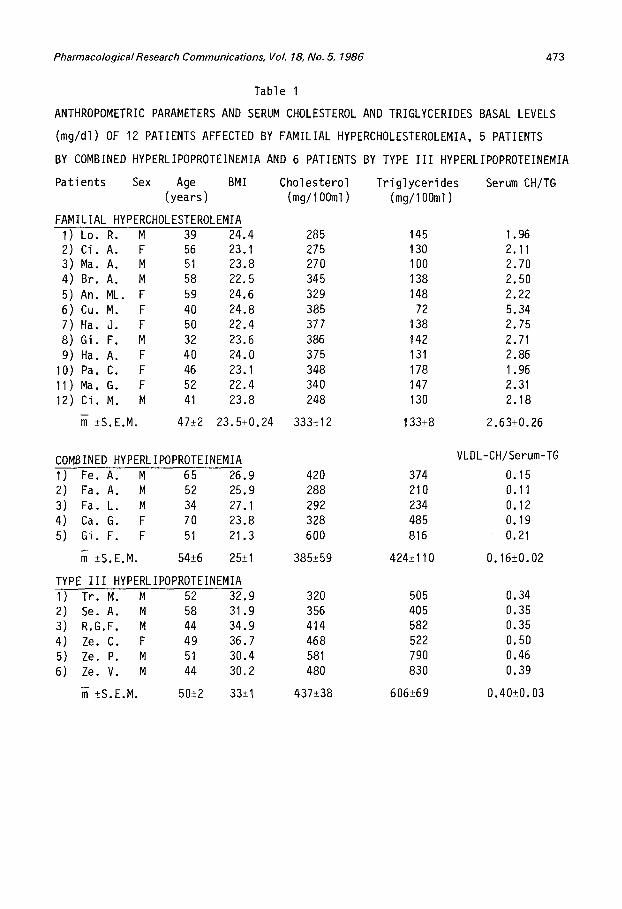
Table I
ANTHROPOMETRIC PARAMETERS AND SERUM CHOLESTEROL AND TRIGLYCERIDES BASAL LEVELS
(mg/dl) OF 12 PATIENTS AFFECTED BY FAMILIAL HYPERCHOLESTEROLEMIA, 5 PATIENTS
BY COMBINED HYPERLIPOPROTEINEMIA AND 6 PATIENTS BY TYPE I I I HYPERLIPOPROTEINEMIA
Patients Sex Age BMI Cholesterol Tr ig lycer ides (years) (mg/1OOml) (mg/1OOml)
FAMILIAL HYPERCHOLESTEROLEMIA I) Lo. R. M 39 24.4 285 145 2) Ci. A. F 56 23.1 275 130 3) Ma. A. M 51 23.8 270 100 4) Br. A. M 58 22.5 345 138 5) An. ML. F 59 24.6 329 148 6) Cu. M. F 40 24.8 385 72 7) Ha. J. F 50 22.4 377 138 8) Gi. F. M 32 23.6 386 142 9) Ha. A. F 40 24.0 375 131
10) Pa. C. F 46 23.1 348 178 11) Ma. G. F 52 22.4 340 147 12) Ci. M. M 41 23.8 248 130
• +S.E.M. 47_+2 23.5_+0.24 333±12 133_+8
Serum CH/TG
I . 96 2.11 2.70 2.50 2.22 5.34 2.75 2.71 2.86 I. 96 2.31 2.18
2.63_+0.26
COMBINED HYPERLIPOPROTEINEMIA I) Fe. A. M 65 26.9 420 374 2) Fa. A. M 52 25.9 288 210 3) Fao L. M 34 27.1 292 234 4) Ca. G. F 70 23.8 328 485 5) Gi. F. F 51 21.3 600 816
_+S.E.M. 54_+6 25_+I 385_+59 424_+110
TYPE I I I HYPERLIPOPROTEINEMIA I) Tr. M. M 52 32.9 320 505 2) Se. A. M 58 31.9 356 405 3) R.G.F. M 44 34.9 414 582 4) Ze. C. F 49 36.7 468 522 5) Ze. P. M 51 30.4 581 790 6) Ze. V. M 44 30.2 480 830
_+S.E.M. 50_+2 33_+I 437_+38 606_+69
VLDL-CH/Serum-TG
0.15 0. I I 0.12 0.19 0.21
0.16_+0.02
0.34 0.35 0.35 0.50 0.46 0.39
0.40_+0.03
474 Pharmacological Research Communications, VoI. 18, No. 5, 1986
diet . Plasma cholesterol and t r ig lycer ides and l ipoprotein fract ions were
evaluated monthly. Al l safety parameters (hepatic and renal function, blood
sugar, uricemia, alkal ine phosphatase, hematology, CPK, LDH, iron, urine
analysis) were control led before and af ter 4 and 8 months t r i a l s .
Every month al l patients underwent c l in ica l examination. Compliance to
d iet and to drug therapy was control led by dietary enquires and p i l l s count.
Patients were not taking other drugs during the study. Any other
pharmacological hypolipidemic treatment was suspended 3 months before the
fenofibrate t r i a l .
3) L_iipoprotein isolat ion and chemical analysis
Lipoprotein fract ions were isolated by a combination of preparative
u l t racentr i fugat ion and polyanions precip i tat ion (11,12). Cholesterol and
t r ig lycer ides were measured by enzymatic methods (13,14).
Lipoprotein electrophoresis in agarose was done according to Seidel et al.
(15).
4) S ta t is t i ca l analysis
Sta t is t i ca l analysis for the evaluation of results was made with the
Student two ta i l s t test only for data of FH patients (16).
Due to a low number of patients studied, 5 with combined HLP and 6 with
type I I I HLP, the i r s ta t i s t i ca l evaluation was not possible. Only variat ions of
percentages are reported.
RESULTS
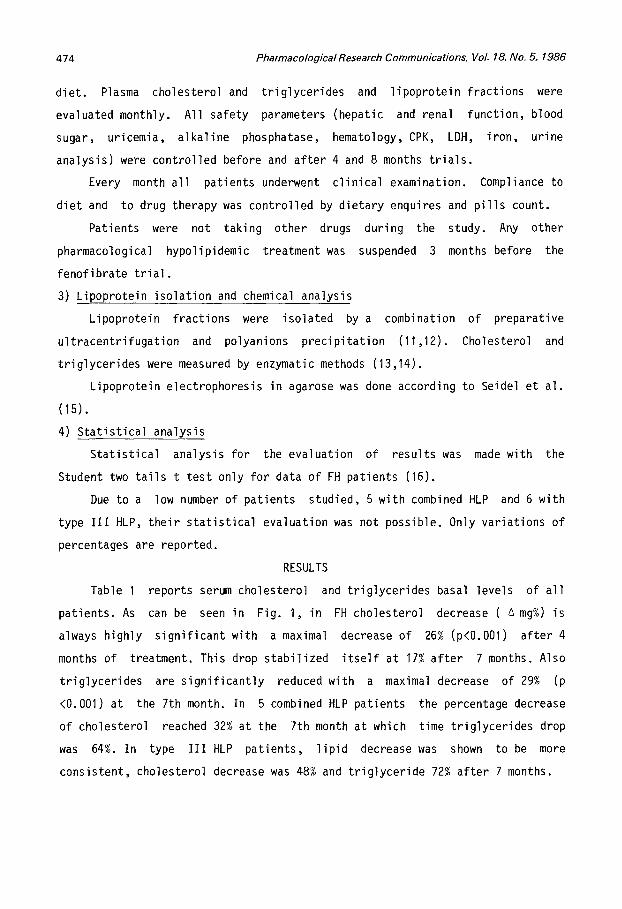
Table I reports serum cholesterol and t r ig lycer ides basal levels of a l l
patients. As can be seen in Fig. I , in FH cholesterol decrease ( ~ mg%) is
always highly s ign i f icant with a maximal decrease of 26% (p<O.O01) af ter 4
months of treatment. This drop stabi l ized i t s e l f at 17% af ter 7 months. Also
t r ig lycer ides are s ign i f i can t l y reduced with a maximal decrease of 29% (p
<0.001) at the 7th month. In 5 combined HLP patients the percentage decrease
of cholesterol reached 32% at the 7th month at which time t r ig lycer ides drop
was 64%. In type I I I HLP pat ients, l i p id decrease was shown to be more
consistent, cholesterol decrease was 48% and t r ig lycer ide 72% af ter 7 months.
PharmacologicalResearch Communications, VoL 18, No. 5, 1986
.~" ----
hl
o
iii
iii -I
o z o
0.
J
~/////////////////////////~
~//////////////////~
~//////////////////~
W
~/////////////////~ .J 0
l~'lllllh, "/////I////////////~
"////~ "//////////////////A
~//////////////////~,
~/I/////////III///////II/~
"I/////////////////////////~
~//////////////////////////~ I " o , . •
~ 0 0 0 0 0 0 0 0 0 ~ 0 m 0 0 0 0
~ m
. m
° ~
0
i : oi~ o ! ~ , ~ i . ~ , o,o ! ) ¢ , >
°i,~f ° ~ " I ~ i , ~,
I~ 0 0 0 0 0 0 0 0 0 0 0 0 < ° ° I o o o o o o . o o o o
0
• (,1 i~
m W IN
"io
, , , , , " , a "J
m----
m l ~ " Q rO
r - . 0 ~ .~ 0
I',. t~ 0 1.~ V
¢D LJ c" • ~ <~
0
° ~ ~ •
O.J ..c: V U ~ D. .
- 'E dg 0
_ . J o ~ ~ g
~ 5 • , ~ o ~
~ E ~ 4 . - ~
0 o
~ I - < 3
0 m " v '
0 4 - V <:1 4 - e-~
(1.) ~ ~T~
475

476 Pharmacological Research Communications, VoL 18, No. 5, 1986
Fig. 2 shows that in FH pat ients , LDL cholesterol has a decrease s imi lar
to that of serum (-31% at the 4th month, p<O.O01; -20% at the 10th month,
p<O.01). However, HDL cholesterol increased s i g n i f i c a n t l y a f te r 6 months
treatment, reaching a 10% increment at the 7th month (p<0.01).
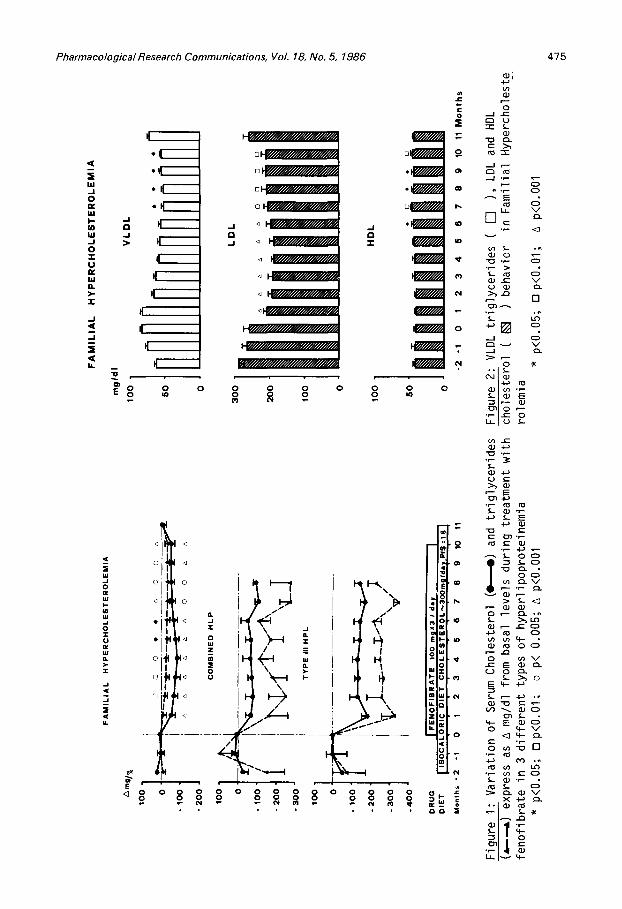
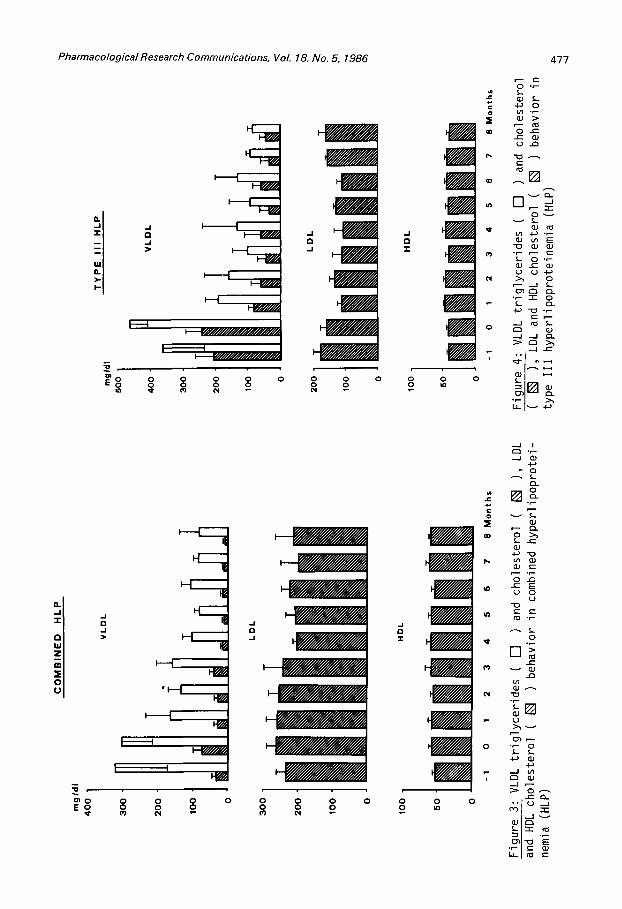
In combined HLP (Fig. 3) the most important var ia t ions occurred wi th in
VLDL f rac t ions : at the 8th month -73% t r i g l yce r i de and -87% cholestero l . LDL
cholesterol also showed a decrease during the whole t r i a l reaching -22% at the
7th month. HDL cholesterol had a tendency to increase reaching a +9% at the
end of the t r i a l . In type I I I HLP disappearance of ~-VLDL occurred as noted
from the reduction of t r i g l yce r i des : cholesterol ra t io in the f rac t ion with
d<I.006 g/ml from 0.48 to 0.10 (Table 2).
TABLE 2
VLDL-CHOLESTEROL (CH)/TRIGLYCERIDES (TG) AND VLDL-CH/SERUM-TG RATIOS
DURING TREATMENT WITH FENOFIBRATE IN TYPE I I I HYPERLIPOPROTEINEMIA
Months -I 0 +4 +8
VLDL CH m ± 0.57± 0.48± 0.35± 0.01± TG S.E.M. 0.08 0.03 0.10 0.06
VLDL-CH m ± 0.39± 0.40± 0.21± 0.14± Serum-TG S.E.M. 0.06 0.03 0.12 0.04
LDL cholesterol (Fig. 4) demonstrates var iat ions during the whole t r i a l
even i f i t remained wi th in normal range.
Also HDL cholesterol presented mild var iat ions ranging from 40 to 46
mg/dl.
Lipid and l ipoprote in levels in FH pat ients reached normal basal values
a f te r 4 weeks of wash-out.
Body weight was kept stable in FH and type I I I HLP pat ients , whereas i t
increased on the 4th and 6th month in combined HLP pat ients.
SIDE EFFECTS
Two FH patients suspended t r i a l due to SGOT and SGPT increase to about
100 U/L (normal value <40 U/L). The SGOT and SGPT levels decreased wi th in
Pharmacological Research Communications, Vol. 18, No. 5, 1986
m
i
m I
"o
~o
- I 0 - I
I
c ~ i [ - - - - - - -
I - - F # ' / / ~
c=~ r - -
I
HP'//////~
I t ~--..~// / f / f / / / / / / f / / / / f f / /~' /~/~
I I r~////////////////////~
0 0 0 0 0 0 0 0
0
m m
0 0 0 0 0 P
c o
0 0 t~
4 7 7
O " ~
4--) 0
0 e- ..C= U r'~
e--
D~ ~, - r -
~ m E
~ 0
• ~ - r - 0
- - J . - I n
~ J
m
m m m
"0 ,
E o
I
I - - IV / / / / / /~
0 0 0 0 0 0 0 ¢~3 tW
!
0 0 0 0 0 0 0 0 0
ul J=
c o
E W
m
i
0 0 In
.r.,
oJ r~
c-- E 0
" 0
0
rn~ e -
u
• .12 ~--~- I ~ ~-

478 PharmacologicalResearch Communications, Vol. 18, No. 5, 1986
normal range in few days a f te r the drug suspension.
Three pat ients (I with combined HLP and 2 with t y p e l l l HLP) during f ina l
stage of t r i a l had a cutaneous vescicular erythema which disappeared a f te r drug
treatment.
DISCUSSION
Results of our study are in agreement with those of other authors ( I -8 ) .
Fenofibrate was very e f f i c i e n t in reducing both cholesterol and t r i g l yce r i de
levels in hyperlipidemias with d i f f e ren t pathogenesis.
In FH i t reduces LDL, in combined HLP both LDL and VLDL, in type I I I HLP
i t causes the disappearance of B-VLDL. These data seems to indicate that th is
drug acts on various steps of the l ipoprote in catabol ic cascade.
Treatment of combined HLP with other drugs resul ts in a decrease of VLDL
but in an increase of LDL (17,18). As well the disappearance of ~-VLDL should
resu l t in an increase of LDL. This phenomenon was not seen under fenof ibrate
treatment. We think that fenof ibrate acts on catabolism of VLDL and B-VLDL as
well as of LDL with the same strength and ve loc i ty .
Concerning HDL behavior under fenof ibrate treatment data are
contradictory. In our study we observed an HDL cholesterol increase both in FH
and combined HLP. No var ia t ion of HDL cholesterol was observed in type I I I HLP
patients as was instead reported by R6ssner et al . (4).
Drug e f f icacy remained stable during t r i a l as was already reported by
others (4). I ts tolerance was good during the whole t r i a l .
These resul ts underl ine the important e f f icacy of fenof ibrate on d i f f e ren t
types of genetic hyperlipidemias and makes fenof ibrate nowadays one of the
f i r s t choice l i p i d lowering drugs.
AKNOWLEDGEMENTS
This study was supported in part by grants from Progetto Final izzato CNR:
Ingegneria Genetica e Basi Molecolari del le Malat t ie Ered i tar ie ; Sottoprogetto
Basi Molecolari del le Malat t ie Ered i tar ie .

Pharmacological Research Communications, Vol. 18, No. 5, 1986 479
REFERENCES
I~ Drouin, P., Mejan, L., Lambert, D., W~Ifert, E., and Debry, G. (1980) Curr. Ther. Res. 28: 728.
Rouffy, J. , Sauvanet, J.P., Chanu, B., Bakir, R., Goy-Loeper, J. , Saya, C., and Pinarol i , F. (1980).
Nouv. Presse Med. 9: 3747.
Ducobu, J. (1980) Acta Clin. Belg. 35: 148.
R~ssner, S., and Oro, L. (1981) Atherosclerosis 38: 273.
5. Lehtonen, A., and V i ikar i , J. (1982) Artery 10: 353.
Micheli, H., Pometta, D., and Gustafson, A. (1980) Nouv. Presse Med. 9:3759.
Avogaro, P., Bi t to lo Bon, G., Belussi, F., Pontoglio, E., and Cazzolato, G. (I 983)
Atherosclerosis 47." 95.
Mordasini, R., Grandjean, E.M., Nobile, P.C., Paumgartner, G., and Riva, G. (1979)
Schweiz. Med. Wschr. 109: 1140.
9. Beaumont, J.L. , Carlson, L.A., Cooper, G.R., Fejfar , Z., Fredrickson, D.S. and Strasser, T. (1970)
WHO Bull. 43." 891.
10. Marcel, Y.L., Bergseth, M., and Nestruck, A.C. (1979) Biochim. Biophys. Acta 573: 175.
11. Havel, R.J., Eder, H.A., and Bragdon, J.H. (1955) J. Clin. Invest. 34: 1345.
12. National Inst i tutes of Health (1974): Manual of Laboratory Operations, Vol. I . , DHEW publication No. 75-628.
13. Roschlau, P. von, Bernt, E., and Gruber, W. (1974) Z. Klin. Chem. Klin. Biochem. 12: 403.
14. Wahlefeld, A.W. (1976) in Methods of Enzymatic Analysis (Bergmeyer, H.U., ed.), Vol. 4, pp. 1831-1835, Verlag Chemie Weiheim, Academic Press Inc., New York and London.
15. Seidel, D., Wieland, H., and Ruppert, C. (1973) Clin. Chem. 19: 737.
16. Snedecor, G.W., and Cochran, W.G. (1967) Stat is t ica l Methods, 6th ed. lowa State University Press, Ames, IA.
17. Crepaldi, G., Fel l in , R., Baggio, G., Manzato, E. (1980) in Atherosclerosis Reviews, Raven Press, New York, Vol. 7, pp. 203-211.
2.
3.
4.
6.
7.
8.

480 Pharmacological Research Communications, VoL 18, No. 5, 1986
18. Fell in, R., Martini, S., Valerio, G., Baggio, G., Gasparotto, A., Baiocchi, M.R., Baldo, G., and Crepaldi, G. (1983)
in Atherosclerotic Brain Disease (Crepaldi, G., Fel l in, R., Olsson, A.G., Toffano, G. eds.), Raven Press, New York, pp. 207-216.
Copyright © 2022 FDOKUMEN