Late potentials in a bradycardia-dependent long QT syndrome associated with sudden death during...
9
JACC Vol. 19, No.3 March I, 1992:541-9 541 Late Potentials in a Bradycardia-Dependent Long QT Syndrome Associated With Sudden Death During Sleep TOM J. M. TORE, MD, eEES D. J. DE LANGEN, PHD, MARGREET TH.E. BINK-BOELKENS, MD, PIET H. MOOK, PHD, JAN-WILLEM VIERSMA, MD, KONG 1. LIE, MD, HARRY WESSELING, MD Groningen, The Netherlands The purpose of this study was to determine the incidence of late potentials and their relation to QT prolongation in a family with a high incidence of sudden death during sleep at a young age and bradycardia-dependent QT prolongation (n = 9) and to compare the findings with those in consanguineous family members without QT prolongation (n =13). Six (67%) of the 9 family members with QT prolongation had late potentials on the signal-averaged elec- trocardiogram (ECG) compared with 1 of the 13 normal subjects (p < 0.007). Positive predictive accuracy of the signal-averaged ECG for the detection of subjects with QT prolongation was 86 %; negative predictive accuracy was 80%. During exercise testing, the QT interval normalized, whereas late potentials did not change significantly. Exercise testing did not reveal the presence of coronary artery disease as a possible cause of late potentials. Life-threatening ventricular arrhythmias are frequently found in the congenital long QT syndromes (1). Among our outpatients, there is a family with a high rate of sudden death during sleep at a young age. In contrast to the QT prolon- gation during exercise in the Romano-Ward and Jervell- Lange-Nielsen syndromes (2), in this family the QT interval is prolonged at rest and normalizes during exercise. The history taken from witnesses suggests that sudden death was due to cardiac arrhythmia. Because our previous efforts to detect ventricular arrhythmias that could clarify the cause of sudden death in this family were fruitless, we decided to look for factors like late potentials that indicate the presence of a possible substrate for ventricular arrhythmias. Late potentials are low amplitude signals at the end of the QRS complex that can be detected by signal-averaged elec- trocardiography (3). They are the body surface representa- tion of fractionated local electrical activity detected by endocardial mapping in coronary artery disease (4,5). After From the Departments of Pharmacology/Clinical Pharmacology, Paediat- rics, Thoraxcentre and Cardiology, University of Groningen, Groningen, The Netherlands. This study was presented in part at the 63rd Scientific Sessions of the American Heart Association, Dallas, Texas, November 1990. This study was supported by Grant 86.061 of The Netherlands Heart Foundation, The Hague, The Netherlands. Manuscript received February 12, 1991; revised manuscript received July 29, 1991, accepted August 9, 1991. Address for reprints: Tom J. M. Tobe, MD, the Department of Medicine, Sophia Hospital, P.O. Box 10.400, 8000 GK Zwolle, The Netherlands. © 1992 by the American College of Cardiology It is concluded that 1) compared with family members with a normal QT interval, patients with this type of bradycardia- dependent QT prolongation have a high incidence of late poten- tials; 2) late potentials persist despite normalization of the QT interval at high heart rates, indicating that there is no direct relation between late potentials and QT prolongation; and 3) late potentials are not caused by coronary artery disease in these subjects. Therefore, the detection of late potentials might be a new aid in the detection and risk stratification of patients with the long QT syndrome. Late potentials possibly indicate a substrate for ven- tricular tachyarrhythmias in this type of bradycardia-dependent QT prolongation. (J Am Coll CardioI1992;19:541-9) myocardial infarction, fractionated electrograms correlate, albeit not directly, with inducible ventricular tachycardia (6). In prospective studies (7,8) after myocardial infarction, late potentials were shown to be useful markers for sustained ventricular tachycardia and sudden death. The purpose of this study was to assess the presence of late potentials as markers for slow conduction and their relation to QT prolongation in this family with congenital bradycardia-dependent QT prolongation. Methods Study patients. Among our outpatients is a family in which 15 of 112 members died suddenly at a young age during sleep. A 12-lead electrocardiogram (ECG) from one of the patients who died suddenly showed marked QT interval prolongation and an abnormal T wave configuration. All patients who died suddenly were previously healthy, without a history of palpitation or syncope and with good exercise tolerance. In the surviving family members who have been studied in a standardized fashion since 1958 (9), no systolic murmur could be heard. Ventricular arrhythmias were not detected despite repeated 24-h ambulatory electro- cardiographic (ECG) monitoring. Atrioventricular (AV) block was not observed. Previous echocardiography did not reveal abnormalities. None of the subjects was deaf and audiograms were normal. Twenty-eight consanguineous family members gave in- 0735-1097/92/$5.00
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Late potentials in a bradycardia-dependent long QT syndrome associated with sudden death during...

JACC Vol. 19, No.3March I, 1992:541-9
541
Late Potentials in a Bradycardia-Dependent Long QT SyndromeAssociated With Sudden Death During Sleep
TOM J. M. TORE, MD, eEES D. J. DE LANGEN, PHD, MARGREET TH.E. BINK-BOELKENS, MD,PIET H. MOOK, PHD, JAN-WILLEM VIERSMA, MD, KONG 1. LIE, MD, HARRY WESSELING, MD
Groningen, The Netherlands
The purpose of this study was to determine the incidence of latepotentials and their relation to QT prolongation in a family with ahigh incidence of sudden death during sleep at a young age andbradycardia-dependent QT prolongation (n =9) and to comparethe findings with those in consanguineous family members withoutQT prolongation (n =13). Six (67%) of the 9family members withQT prolongation had late potentials on the signal-averaged electrocardiogram (ECG) compared with 1of the 13 normal subjects(p < 0.007). Positive predictive accuracy of the signal-averagedECG for the detection of subjects with QT prolongation was 86%;negative predictive accuracy was 80%. During exercise testing,the QT interval normalized, whereas late potentials did notchange significantly. Exercise testing did not reveal the presence ofcoronary artery disease as a possible cause of late potentials.
Life-threatening ventricular arrhythmias are frequentlyfound in the congenital long QT syndromes (1). Among ouroutpatients, there is a family with a high rate of sudden deathduring sleep at a young age. In contrast to the QT prolongation during exercise in the Romano-Ward and JervellLange-Nielsen syndromes (2), in this family the QT intervalis prolonged at rest and normalizes during exercise. Thehistory taken from witnesses suggests that sudden death wasdue to cardiac arrhythmia. Because our previous efforts todetect ventricular arrhythmias that could clarify the cause ofsudden death in this family were fruitless, we decided to lookfor factors like late potentials that indicate the presence of apossible substrate for ventricular arrhythmias.
Late potentials are low amplitude signals at the end of theQRS complex that can be detected by signal-averaged electrocardiography (3). They are the body surface representation of fractionated local electrical activity detected byendocardial mapping in coronary artery disease (4,5). After
From the Departments of Pharmacology/Clinical Pharmacology, Paediatrics, Thoraxcentre and Cardiology, University of Groningen, Groningen, TheNetherlands. This study was presented in part at the 63rd Scientific Sessionsof the American Heart Association, Dallas, Texas, November 1990. Thisstudy was supported by Grant 86.061 of The Netherlands Heart Foundation,The Hague, The Netherlands.
Manuscript received February 12, 1991; revised manuscript received July29, 1991, accepted August 9, 1991.
Address for reprints: Tom J. M. Tobe, MD, the Department of Medicine,Sophia Hospital, P.O. Box 10.400, 8000 GK Zwolle, The Netherlands.
© 1992 by the American College of Cardiology
It is concluded that 1) compared with family members with anormal QT interval, patients with this type of bradycardiadependent QT prolongation have a high incidence of late potentials; 2) late potentials persist despite normalization of the QTinterval at high heart rates, indicating that there is no directrelation between late potentials and QT prolongation; and 3) latepotentials are not caused by coronary artery disease in thesesubjects.
Therefore, the detection of late potentials might be a new aid inthe detection and risk stratification of patients with the long QTsyndrome. Late potentials possibly indicate a substrate for ventricular tachyarrhythmias in this type of bradycardia-dependentQT prolongation.
(J Am Coll CardioI1992;19:541-9)
myocardial infarction, fractionated electrograms correlate,albeit not directly, with inducible ventricular tachycardia (6).In prospective studies (7,8) after myocardial infarction, latepotentials were shown to be useful markers for sustainedventricular tachycardia and sudden death.
The purpose of this study was to assess the presence oflate potentials as markers for slow conduction and theirrelation to QT prolongation in this family with congenitalbradycardia-dependent QT prolongation.
MethodsStudy patients. Among our outpatients is a family in
which 15 of 112 members died suddenly at a young ageduring sleep. A 12-lead electrocardiogram (ECG) from oneof the patients who died suddenly showed marked QTinterval prolongation and an abnormal T wave configuration.All patients who died suddenly were previously healthy,without a history of palpitation or syncope and with goodexercise tolerance. In the surviving family members whohave been studied in a standardized fashion since 1958 (9),no systolic murmur could be heard. Ventricular arrhythmiaswere not detected despite repeated 24-h ambulatory electrocardiographic (ECG) monitoring. Atrioventricular (AV)block was not observed. Previous echocardiography did notreveal abnormalities. None of the subjects was deaf andaudiograms were normal.
Twenty-eight consanguineous family members gave in-
0735-1097/92/$5.00
542 TORE ET AL.LATE POTENTIALS AND QT PROLONGATION
JACC Vol. 19, No.3March I, 1992:541-9
formed consent for the study. Six of the 28 were excluded:I with QT prolongation because the QRS duration on the12-lead ECG was >120 ms, 2 without QT prolongation,because of a ventricular pacemaker (implanted for treatmentof sinus arrhythmia with pauses up to 7 s), 1 because ofpre-excitation, 1because the heart rate was not low enoughfor detection of bradycardia-dependent QT prolongation and1 without QT prolongation because a low noise signalaveraged ECG could not be obtained at rest. None of thesubjects received digitalis, antiarrhythmic drugs or otherdrugs with QT prolongation as a potential side effect. Nonehad electrolyte disturbances.
QT interval measurements. Measurement of the QT interval is difficult to standardize (10). We chose the methoddescribed by Cowan et al. (11), who showed that themaximal QT duration is predominantly measured in the rightprecordial leads. QT intervals were measured in lead V2
from the onset of the QRS complex to the end of the T wave.The end of the T wave was defined as a return to the TPbaseline. When a U wave interrupted the T wave beforereturn to baseline, the QT interval was measured to the nadirof the curve between T and U waves. Biphasic T waves weremeasured to the time of final return to baseline (11). The QTinterval corrected for heart rate (QTc) was calculated withuse of Bazett's equation (12) (QTc = QT/square root of RR).This interval was used only to compare the QT interval atdifferent heart rates.
RR.QT scattergrams. An RR-QT scattergram wasplotted for each patient on the basis of the QT intervalmeasurements (not corrected for heart rate) obtained fromexercise testing and ambulatory ECG monitoring. The normal values described by Lepeschkin (13) were used todiscriminate between subjects with normal or prolonged QTintervals. A patient was considered to have bradycardiadependent QT prolongation when the QT interval was consistently prolonged over a wide range of heart rates <60beats/min.
Ambulatory ECG monitoring. The Marquette Laser XPSystem was used. Electrodes were placed as follows: C1(modified VI): VI and at the left suprasternal notch; C2(modified V5): V5 and at the right suprasternal notch; C3(modified aVF): V3 and at the left clavicle. Positive electrodes were VI' V5 and V3'
Exercise testing. A modified bicycle exercise test wasperformed to shorten the RR and QT intervals physiologically. Exercise was started at 50 Wand was increased tomaximal capacity with increments of 10 W/30 s. Aftermaximal exercise was achieved, the subjects continued for5 min at a submaximal exercise level. During exercise, leadsV2, V4, V5, II, III and aVF were recorded continuously at a25-mm/s paper speed (Marquette CASE-12, frequency response 0.07 to 100 Hz).
Signal·averaged electrocardiography. Signal-averagingwas performed with the subjects supine. After the skin wasprepared with a mildly abrasive pad and washed with ether,seven self-adhesive silver-silver chloride electrodes (Red
600...,......-----------.,
520
440
~ 360-]~ 280sd 200 +--r-r-....---.-r-r----.--.--r-r-r-i
300 500 700 900 1100 1300 1500
RR - Interval Ims)i I I I I I I I
150 100 75 60 50 45 40 38heart rate I beats/mon)
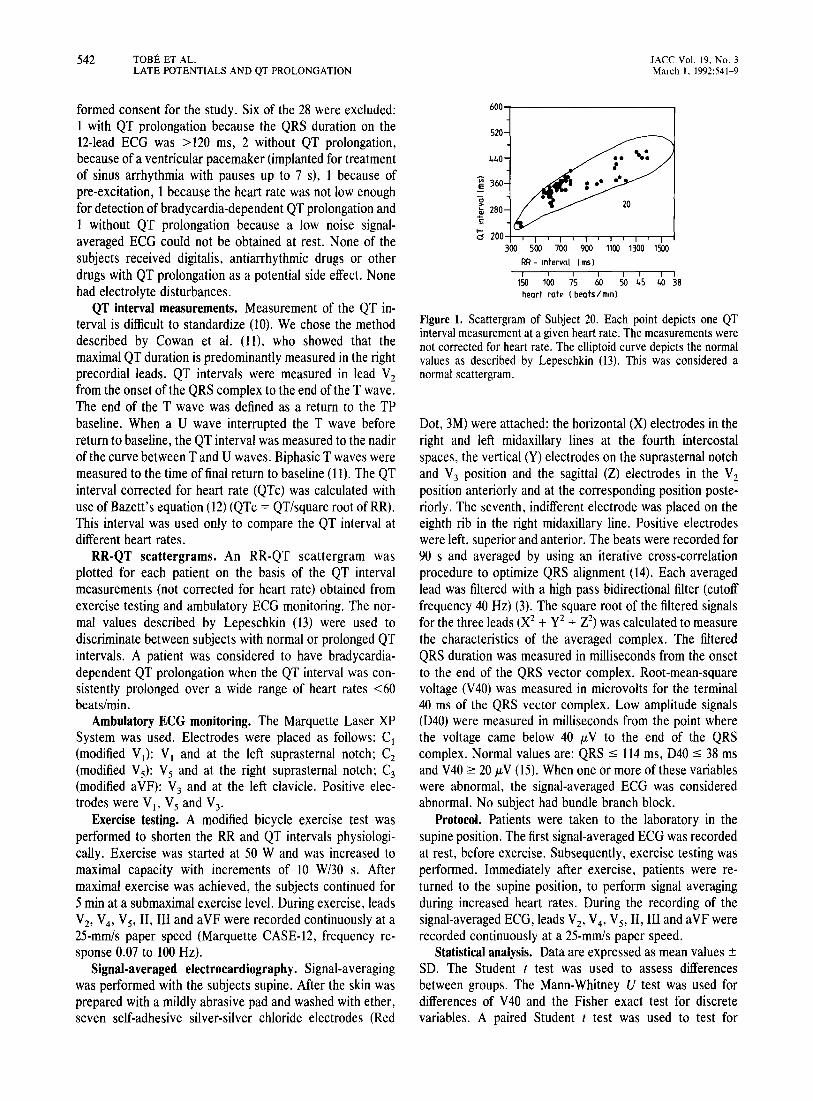
Figure 1. Scattergram of Subject 20. Each point depicts one QTinterval measurement at a given heart rate. The measurements werenot corrected for heart rate. The elliptoid curve depicts the normalvalues as described by Lepeschkin (13). This was considered anormal scattergram.
Dot, 3M) were attached: the horizontal (X) electrodes in theright and left midaxillary lines at the fourth intercostalspaces, the vertical (Y) electrodes on the suprasternal notchand V3 position and the sagittal (Z) electrodes in the V2
position anteriorly and at the corresponding position posteriorly. The seventh, indifferent electrode was placed on theeighth rib in the right midaxillary line. Positive electrodeswere left, superior and anterior. The beats were recorded for90 s and averaged by using an iterative cross-correlationprocedure to optimize QRS alignment (14). Each averagedlead was filtered with a high pass bidirectional filter (cutofffrequency 40 Hz) (3). The square root of the filtered signalsfor the three leads (X2 + y 2 + Z2) was calculated to measurethe characteristics of the averaged complex. The filteredQRS duration was measured in milliseconds from the onsetto the end of the QRS vector complex. Root-mean-squarevoltage (V40) was measured in microvolts for the terminal40 ms of the QRS vector complex. Low amplitude signals(D40) were measured in milliseconds from the point wherethe voltage came below 40 JLV to the end of the QRScomplex. Normal values are: QRS :s 114 ms, D40 :s 38 msand V40::=: 20 JLV (15). When one or more of these variableswere abnormal, the signal-averaged ECG was consideredabnormal. No subject had bundle branch block.
Protocol. Patients were taken to the laboratory in thesupine position. The first signal-averaged ECG was recordedat rest, before exercise. Subsequently, exercise testing wasperformed. Immediately after exercise, patients were returned to the supine position, to perform signal averagingduring increased heart rates. During the recording of thesignal-averaged ECG, leads V2, V4, V5, II, III and aVF wererecorded continuously at a 25-mm/s paper speed.
Statistical analysis. Data are expressed as mean values ±SD. The Student t test was used to assess differencesbetween groups. The Mann-Whitney U test was used fordifferences of V40 and the Fisher exact test for discretevariables. A paired Student t test was used to test for
lACC Vol. 19, No.3March I, 1992:541-9
TOBE ET AL.LATE POTENTIALS AND QT PROLONGATION
543
506
QTe(me)
aVF
V1
07:30:00 103 V5
06:00:50 51 V5
time helrt rate(beats/min)
S20
§ 360
~ 2805
1t40
iii I I I i I150 100 7S 60 50 4S 40 38heQrt rQte IbeQts/mlO I
600 .........---------~
5 200-+-....-..........--r--..,....~~~__r_~_.__I300 500 700 900 1100 1300 1500
RR -lOtervQI I ms)
Figure 2. Scattergram of Subject 4. This was considered to be anabnormal scattergram with QT prolongation over a wide range ofheart rates <60 beats/min.
differences before and after exercise. Differences were considered statistically significant when p was <0.05. Sensitivity was defined as True positive/[True positive + Falsenegative], specificity as True negative/[True negative +False positive], positive predictive accuracy as True positive/[True positive + False positive], and negative predictiveaccuracy as True negative/[True negative + False negative].
Figure 4. Subject 4. Ambulatory electrocardiogram. Paper speed is25 mm/s, 0.1 mV/mm. The upper panel was recorded during sleep.QT interval prolongation (QTc interval = 506 ms) and an abnormalT wave configuration are visible. The lower panel was recordedduring the awake state. The QT interval (QTc interval = 433 ms) andT wave configuration have normalized.
ResultsRR-QT scattergrams. With use of the normal values
described by Lepeschkin (13), the difference between normal subjects and those with QT prolongation could be seenunambiguously in each scattergram. In Figure 1(Subject 20)QT intervals are within the normal range at all heart rates,whereas in Figure 2 (Subject 4) considerable QT prolongation is present at heart rates <60 beats/min. The QT intervalis prolonged at low heart rates, whereas it normalizes at highheart rates (Fig. 3and 4). The scattergrams ofall subjects areshown in Figure 5. The heart rate below which the QT
interval is prolonged varies from 60 to 80 beats/min and thedegree of QT prolongation differs among subjects. Thus, 9subjects were characterized as having bradycardia-dependentQT prolongation and 13 as normal. The EeG characteristicsof all patients at rest are summarized in Table 1.
Signal-averaged electrocardiography at rest. Six (67%) ofthe 9 subjects with bradycardia-dependent QT prolongationhad a late potential (Fig. 6A, Table 2) compared with only 1
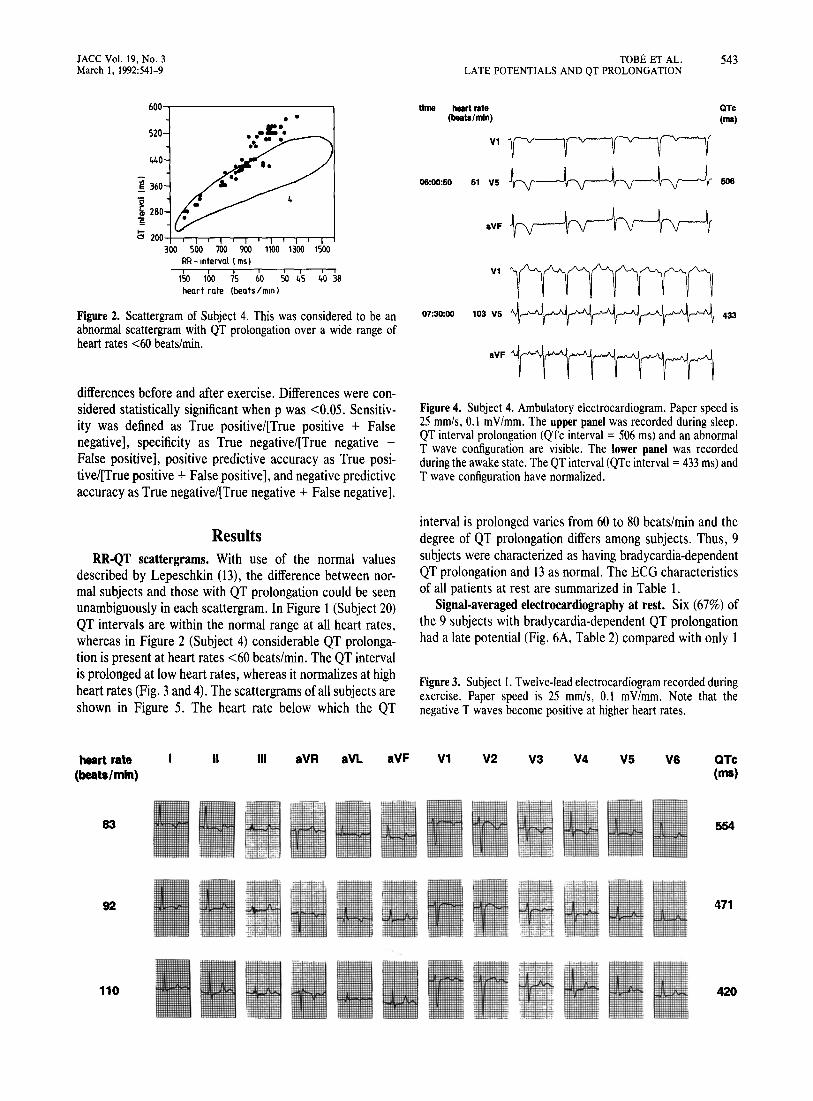
Figure 3. Subject I. Twelve-lead electrocardiogram recorded duringexercise. Paper speed is 25 mm/s, 0.1 mV/mm. Note that thenegative T waves become positive at higher heart rates.
heart rate(beats/min)
II III aVR aVL aVF V1 V2 V3 V4 V5 V6 QTe(rna)
83 554
92 471
110 II~-"'~ - I~. = ..": .- :=
420

'Axis: not indicated when between 0° and 90°; negative T waves in aVRand VI were not considered to be abnormal.
Exercise testing. Exercise testing was performed in 19subjects. The QT interval normalized in all subjects at aheart rate of >100 beats/min. Moreover, the abnormalconfiguration of the T waves normalized at high heart rates(Fig. 4). Such changes were similar in all subjects observed.The maximal heart rate achieved was similar in both groups:153 ± 27 beats/min in normal subjects versus 156 ± 19beats/min in subjects with QT prolongation; after correctionfor age the values were 76.9 ± 12.3% in normal subjectsversus 86.5 ± 7.5% in subjects with QT prolongation. Valuesfor maximal exercise capacity were also similar: 158 ± 58 Win normal subjects versus 126 ± 39 W in subjects with QTprolongation; after correction for age and gender thesevalues were 75 ± 22.7% in normal subjects versus 58.5 ±24.7% in subjects with QT prolongation. No subject reportedangina or manifested horizontal or downsloping ST segmentdepression. Neither rate-dependent bundle branch block norventricular arrhythmias were observed.
Signal-averaged electrocardiography after exercise. A signal-averaged ECG at a higher heart rate was obtained fromeight subjects with and from six subjects without QT prolongation (Table 3). It was based on the scattergrams
21
.• I. ,...-.. -
22
544 TOBE ET AL. lACC Vol. 19, No.3LATE POTENTIALS AND QT PROLONGATION March I, 1992:541-9
fTable 1. Twelve-Lead Electrocardiogram at Rest in 22 Subjects
.' p Biphasic Negative Flat..Subject No. Axis' T Wave T Wave TWave
2 • 3 QT prolongationI I,II,III,aVL, VI to V3.. : aVF,V4
??to V6... .. Vz, V3
;a, •• 3 Vz,V3,aVL• 4* 6* 4 150° II,III,aVF,V3
to V6
5 100° V3.. 6
P.J'__.I. .,. ,,,.. .-.- 7 120° II ,III,aVF,Vz
'..- to V6.8 120° II,III,aVF,V4 VI to V3:" 7* 8* 9*
to V6
9 aVL,V 1 toV4
Normal subjects.. ;._-:-f 10..II
10 12 II,III,aVF,V5, V6
13 120°14 100°
!"""... , '-" ..:... 15".. 16. ...
13* 14 17 120°18 Vz1920 100° II
.··i·· .. :., . 21. ..:..22
16 18
(8%) of the 13 normal subjects (p < 0.007). Late potentialswere absent in the three oldest subjects with QT prolongation (Subjects 1 to 3. mean age 61 years), whereas all youngpatients had late potentials. The sensitivity of the signalaveraged ECG for the detection of subjects with QT prolongation was 67% (6 of 9) and the specificity was 92% (12 of13). The positive predictive accuracy was 86% (6 of 7) andthe negative predictive accuracy was 80% (12 of 15).
Figure 5. Scattergrams of all 22 subjects. Scales are proportionateto Figures 1 and 2. Numbers indicate the subjects as shown inTables 1 and 2. Asterisks indicate subjects with late potentials.
JACC Vol. 19, No.3March I, 1992:541-9
TOBE ET AL.LATE POTENTIALS AND QT PROLONGATION
545
100-r---------:-----nr-------------,
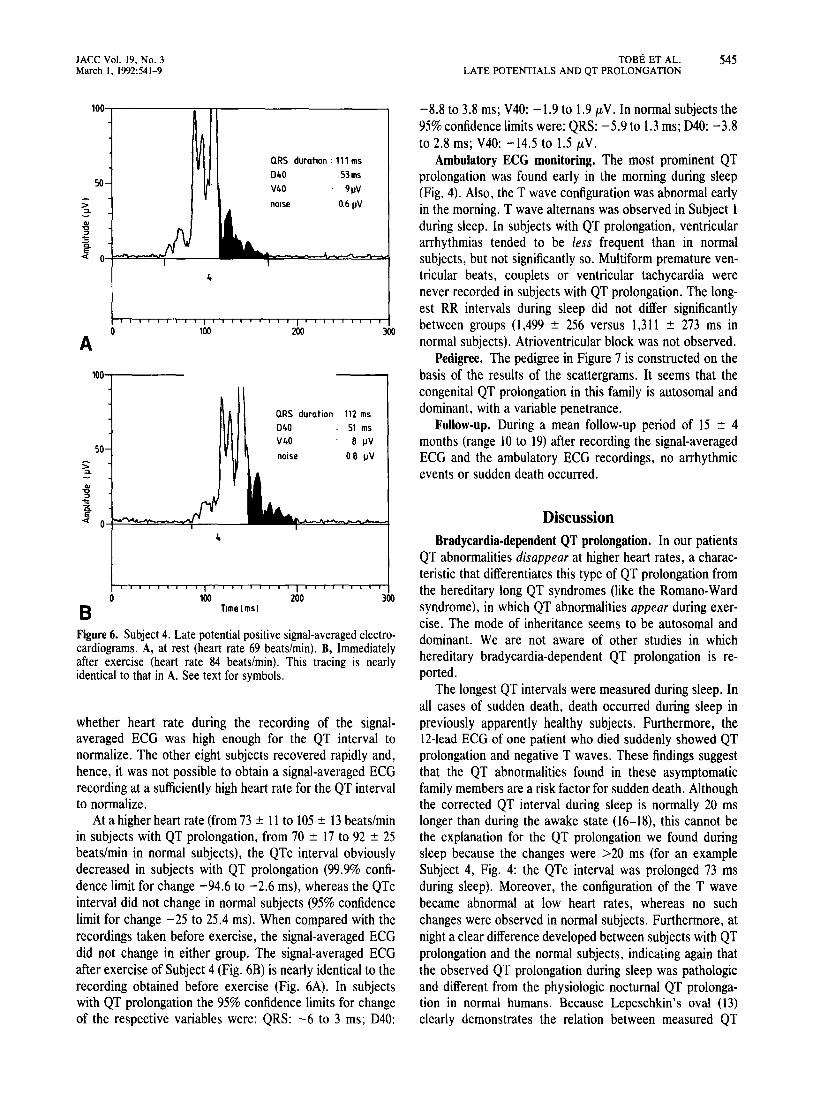
Figure 6. Subject 4. Late potential positive signal-averaged electrocardiograms. A, at rest (heart rate 69 beats/min). B, ImmediatelYafter exercise (heart rate 84 beats/min). This tracing is nearlyidentical to that in A. See text for symbols.
DiscussionBradycardia-dependent QT prolongation. In our patients
QT abnormalities disappear at higher heart rates, a characteristic that differentiates this type of QT prolongation fromthe hereditary long QT syndromes (like the Romano-Wardsyndrome), in which QT abnormalities appear during exercise. The mode of inheritance seems to be autosomal anddominant. We are not aware of other studies in whichhereditary bradycardia-dependent QT prolongation is reported.
The longest QT intervals were measured during sleep. Inall cases of sudden death, death occurred during sleep inpreviously apparently healthy subjects. Furthermore, theIHead ECG of one patient who died suddenly showed QTprolongation and negative T waves. These findings suggestthat the QT abnormalities found in these asymptomaticfamily members are a risk factor for sudden death. Althoughthe corrected QT interval during sleep is normally 20 mslonger than during the awake state (16-18), this cannot bethe explanation for the QT prolongation we found duringsleep because the changes were >20 ms (for an exampleSubject 4, Fig. 4: the QTc interval was prolonged 73 msduring sleep). Moreover, the configuration of the T wavebecame abnormal at low heart rates, whereas no suchchanges were observed in normal subjects. Furthermore, atnight a clear difference developed between subjects with QTprolongation and the normal subjects, indicating again thatthe observed QT prolongation during sleep was pathologicand different from the physiologic nocturnal QT prolongation in normal humans. Because Lepeschkin's oval (13)clearly demonstrates the relation between measured QT
-8.8 to 3.8 ms; V40: -1.9 to 1.9 /LV. In normal subjects the95% confidence limits were: QRS: - 5.9 to 1.3 ms; D40: -3.8to 2.8 ms; V40: -14.5 to 1.5 /LV.
Ambulatory ECG monitoring. The most prominent QTprolongation was found early in the morning during sleep(Fig. 4). Also, the T wave configuration was abnormal earlyin the morning. T wave altemans was observed in Subject 1during sleep. In subjects with QT prolongation, ventriculararrhythmias tended to be less frequent than in normalsubjects, but not significantly so. Multiform premature ventricular beats, couplets or ventricular tachycardia werenever recorded in subjects with QT prolongation. The longest RR intervals during sleep did not differ significantlybetween groups (1,499 ± 256 versus 1,311 ± 273 ms innormal subjects). Atrioventricular block was not observed.
Pedigree. The pedigree in Figure 7 is constructed on thebasis of the results of the scattergrams. It seems that thecongenital QT prolongation in this family is autosomal anddominant, with a variable penetrance.
Follow-up. During a mean follow-up period of 15 ± 4months (range 10 to 19) after recording the signal-averagedECG and the ambulatory ECG recordings, no arrhythmicevents or sudden death occurred.
300200
200 300
QRS duration 112 ms040 51 msV40 8 IJV
noise 0.8 IJV
Q.RS duration: 111 ms040 53msV40 . 91N
nOise 0.61JV
Time (ms)
4
4
100
100
50
>::L..~~« O-f:>=~~~--
A1001...-----
o
o
50
B
whether heart rate during the recording of the signalaveraged ECG was high enough for the QT interval tonormalize. The other eight subjects recovered rapidly and,hence, it was not possible to obtain a signal-averaged ECGrecording at a sufficiently high heart rate for the QT intervalto normalize.
At a higher heart rate (from 73 ± 11 to 105 ± 13 beats/minin subjects with QT prolongation, from 70 ± 17 to 92 ± 25beats/min in normal subjects), the QTc interval obviouslydecreased in subjects with QT prolongation (99.9% confidence limit for change -94.6 to -2.6 ms), whereas the QTcinterval did not change in normal subjects (95% confidencelimit for change -25 to 25.4 ms). When compared with therecordings taken before exercise, the signal-averaged ECGdid not change in either group. The signal-averaged ECGafter exercise of Subject 4 (Fig. 6B) is nearly identical to therecording obtained before exercise (Fig. 6A). In subjectswith QT prolongation the 95% confidence limits for changeof the respective variables were: QRS: -6 to 3 ms; D40:
546 TOBE ET AL.LATE POTENTIALS AND QT PROLONGATION
JACC Vol. 19, No.3March I, 1992:541-9
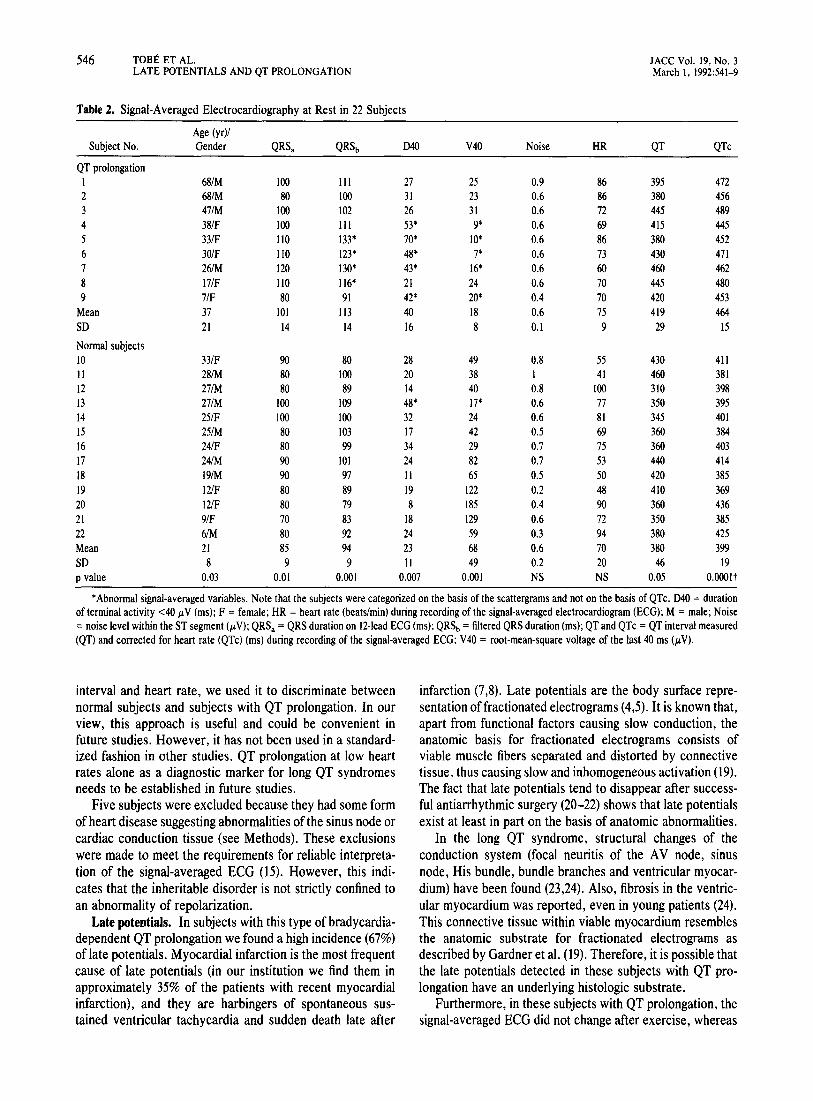
Table 2. Signal-Averaged Electrocardiography at Rest in 22 Subjects
Age (yr)1Subject No. Gender QRSa QRSb 040 V40 Noise HR QT QTc
QT prolongation1 68/M 100 III 27 25 0.9 86 395 4722 68/M 80 100 31 23 0.6 86 380 4563 47/M 100 102 26 31 0.6 72 445 4894 38/F 100 III 53* 9* 0.6 69 415 4455 33/F 110 133* 70* 10* 0.6 86 380 4526 30/F 110 123* 48* 7* 0.6 73 430 4717 261M 120 130* 43* 16* 0.6 60 460 4628 17/F 110 116* 21 24 0.6 70 445 4809 7/F 80 91 42* 20* 0.4 70 420 453
Mean 37 101 113 40 18 0.6 75 419 464SO 21 14 14 16 8 0.1 9 29 15
Normal subjects10 33/F 90 80 28 49 0.8 55 430 411II 281M 80 100 20 38 1 41 460 38112 271M 80 89 14 40 0.8 100 310 39813 271M 100 109 48* 17* 0.6 77 350 39514 251F 100 100 32 24 0.6 81 345 40115 251M 80 103 17 42 0.5 69 360 38416 24/F 80 99 34 29 0.7 75 360 40317 241M 90 101 24 82 0.7 53 440 41418 191M 90 97 II 65 0.5 50 420 38519 12/F 80 89 19 122 0.2 48 410 36920 12/F 80 79 8 185 0.4 90 360 43621 9/F 70 83 18 129 0.6 72 350 38522 6/M 80 92 24 59 OJ 94 380 425Mean 21 85 94 23 68 0.6 70 380 399SO 8 9 9 II 49 0.2 20 46 19P value 0.03 0.01 0.001 0.007 0.001 NS NS 0.05 O.OOOlt
*Abnormal signal-averaged variables. Note that the subjects were categorized on the basis of the scattergrams and not on the basis of QTc. 040 = durationof terminal activity <40 j.LV (ms); F = female; HR = heart rate (beats/min) during recording of the signal-averaged electrocardiogram (ECG); M= male; Noise=noise level within the ST segment (j.LV); QRSa =QRS duration on l2-Iead ECG (ms); QRSb =filtered QRS duration (ms); QT and QTc = QT interval measured(QT) and corrected for heart rate (QTc) (ms) during recording of the signal-averaged ECG; V40 = root-mean-square voltage of the last 40 ms (j.LV).
interval and heart rate, we used it to discriminate betweennormal subjects and subjects with QT prolongation. In ourview, this approach is useful and could be convenient infuture studies. However, it has not been used in a standardized fashion in other studies. QT prolongation at low heartrates alone as a diagnostic marker for long QT syndromesneeds to be established in future studies.
Five subjects were excluded because they had some formof heart disease suggesting abnormalities of the sinus node orcardiac conduction tissue (see Methods). These exclusionswere made to meet the requirements for reliable interpretation of the signal-averaged ECG (15). However, this indiocates that the inheritable disorder is not strictly confined toan abnormality of repolarization.
Late potentials. In subjects with this type of bradycardiadependent QT prolongation we found a high incidence (67%)of late potentials. Myocardial infarction is the most frequentcause of late potentials (in our institution we find them inapproximately 35% of the patients with recent myocardialinfarction), and they are harbingers of spontaneous sustained ventricular tachycardia and sudden death late after
infarction (7,8). Late potentials are the body surface representation offractionated electrograms (4,5). It is known that,apart from functional factors causing slow conduction, theanatomic basis for fractionated electrograms consists ofviable muscle fibers separated and distorted by connectivetissue, thus causing slow and inhomogeneous activation (19).The fact that late potentials tend to disappear after success·ful antiarrhythmic surgery (20-22) shows that late potentialsexist at least in part on the basis of anatomic abnormalities.
In the long QT syndrome, structural changes of theconduction system (focal neuritis of the AV node, sinusnode, His bundle, bundle branches and ventricular myocardium) have been found (23,24), Also, fibrosis in the ventricular myocardium was reported, even in young patients (24).This connective tissue within viable myocardium resemblesthe anatomic substrate for fractionated electrograms asdescribed by Gardner et al. (19). Therefore, it is possible thatthe late potentials detected in these subjects with QT prolongation have an underlying histologic substrate.
Furthermore, in these subjects with QT prolongation, thesignal-averaged ECG did not change after exercise, whereas

JACC Vol. 19, No.3March I, 1992:541-9
Table 3. Signal-Averaged Electrocardiography Immediately AfterExercise in 14 Subjects
Subject No. QRSb 040 V40 Noise HR QT QTc
QT prolongationI 110 27 25 0.6 114 295 4072 99 31 21 0.6 96 315 4003 106 28 29 0.6 104 315 4124 112 51 8 0.8 84 360 4295 123 50 II 0.5 118 310 4336 114 42 8 0.8 94 345 4387 133 44 13 0.7 117 295 4158 119 22 28 0.6 112 295 404
Mean 115 37 18 0.7 105 316 417SO II 11 9 0.1 13 24 14
Normal subjects10 84 30 38 0.9 70 360 391II 95 19 37 1.2 62 385 39113 106 45 8 0.7 124 300 42915 99 21 25 0.8 105 300 39816 98 34 23 0.6 111 290 39517 96 19 87 1.6 80 330 383Mean 96 28 36 1 92 328 398SO 7 10 27 0.4 25 38 16p value 0.004 NS NS 0.02 NS NS 0.04
Abbreviations and measurement units as in Table 2.
the QT interval normalized. This observation suggests thatthere is no direct relation between late potentials (that is,delayed depolarization) and repolarization. This finding is inaccordance with data on patients with coronary arterydisease (25,26). It is unlikely that coronary artery disease isthe cause of late potentials detected in this family because1) the a priori likelihood is low in these young subjects;2) no subject had an episode of acute chest pain suggestive ofacute myocardial infarction; 3) no subject reported angina;4) there were no abnormal Q waves on the 12-lead ECG;5) the T wave abnormalities at rest always normalized duringexercise; and 6) there was no horizontal ST segment depression during exercise. Moreover, the good exercise tolerancemakes other heart diseases unlikely. Therefore, late potentials seem to be part of the disease itself and it is unlikely thatthey are caused by concomitant coronary artery disease or
TORE ET AL. 547LATE POTENTIALS AND QT PROLONGATION
myocardial infarction. The relative absence of late potentialsin the family members with normal QT intervals supportsthis view.
Possible significance of late potentials in long QT syndromes. Although late potentials are established risk factorsfor arrhythmic events late after myocardial infarction, weare not aware of such evidence in the congenital long QTsyndromes. The subjects who died suddenly were young andit is interesting that late potentials were not found in ourthree oldest subjects. Although it is tempting to say thatthese three subjects are still alive because they do not havea late potential, we appreciate that in this study prospectivedata that confirm that hypothesis are lacking. Because thisstudy does not contribute to the understanding of suddendeath in these patients, a larger prospective study is necessary to assess the prognostic value of late potentials forarrhythmic events in these syndromes.
From a theoretical point of view, the two prerequisites forreentry could be met by the combination of late potentials(as markers for slow conduction) and QT prolongation (as amarker for prolonged refractoriness) (27,28). Because thesetwo prerequisites for reentry seem to be present, it is evenmore striking that ventricular tachycardia was never recorded. Moreover, ventricular tachycardia could not beinduced at programmed electrical stimulation in Subjects 4and 8 in a previous study (unpublished results). This findingmay indicate that reentry does not playa major role in thesesubjects, and that other arrhythmogenic factors like autonomic influences (1) or afterdepolarizations (29), or both, aremore important.
Implications. The 12-lead ECG of two subjects with QTprolongation (Subjects 5 and 6) showed a normal T wave
Figure 7. Pedigree. Circles = female subjects; squares = malesubjects. The Roman numerals at left refer to the generation, theArabic numerals indicate the age at which sudden death during sleepoccurred. The subjects of this study were (from left to right) asfollows (bold Arabic numerals refer to the subject number shown inTables 1 to 3; the light Arabic numerals refer to the position at thepedigree at a line): 1: III-2; 2: III-I; 3: III-IO; 4: IV-I; 5: IV-4; 6:IV-5; 7: IV-6; 8: IV-17; 9: V-2; 10: IV·8; 11: IV-9; 12: IV-12; 13:IV-18; 14: IV-16; 15: IV-l3; 16: IV-19; 17: IV-IO; 18: IV-20; 19:IV-21; 20: V-4; 21: V-I; 22: V-6.
II
III
IV
v
E:j SUDDEN DEATH DURING SLEEP o NO QT PROLONGATION • QT PROLONGATION

548 TOBE ET AL.LATE POTENTIALS AND QT PROLONGATION
JACC Vol. 19, No.3March I, 1992:541-9
configuration that was not prolonged at first glance. Bothsubjects had a late potential, which was the only abnormalfinding at rest. Therefore, in some cases this kind of QTprolongation will be found only after an active search forabnormalities on 24-h ECG recordings because at low heartrates during sleep QT prolongation is obvious. In this familywith a high incidence of QT prolongation, the signalaveraged ECG had rather good positive (86%) and negative(80%) predictive values with respect to the presence orabsence of QT prolongation. However, the predictive valuein the general population will be lower because the incidenceof QT prolongation is lower. Therefore, the value of signalaveraged electrocardiography as a new aid in both thedetection and subsequent risk stratification of long QTsyndromes needs to be established in future studies.
Previously, some family members were treated with aventricular pacemaker, because of sinus arrhythmia or QTprolongation at low heart rates, or both. Our patients are nottreated with beta-adrenergic blocking agents, because thesewill cause even lower heart rates at night with concomitantlyeven more pronounced QT prolongation. Although betablocking agents are known to slow the heart rate, it is theireffect on autonomic balance that renders benefit. Perhapsbeta-blocking or other autonomic agents would be beneficialin this particular group of patients. However, this treatmentcannot be based on reported data, because we are not awareof other reports of this or a similar type of bradycardiadependent QT prolongation.
Conclusions. From our data, we conclude that 1) whencompared with family members with a normal QT interval,subjects with bradycardia-dependent QT prolongation havea high incidence of late potentials; 2) late potentials persistdespite normalization of the QT interval at high heart rates,indicating that there is no direct relation between latepotentials and QT prolongation; 3) as there is no sign ofcoronary artery disease and the probability of coronaryartery disease is very low in this age group, the presence oflate potentials seems to be part of the disease itself;4) spontaneous ventricular arrhythmias are rare in thesesubjects; 5) inheritance of this type of bradycardiadependent QT prolongation seems to be of the autosomal,dominant type; and 6) in this family late potentials wereuseful predictors of the presence of QT prolongation.
Therefore, the detection of late potentials on the signalaveraged ECG might be a new aid in the risk stratification ofpatients with congenital QT prolongation. Late potentialspossibly indicate a substrate for ventricular tachyarrhythmias in this type of bradycardia-dependent QT prolongation.
We thank Jaap Haaksma and Roelie Boerema for careful analysis of theambulatory ECG recordings.
ReferencesI. Schwartz PJ, Locati E. The idiopathic long QT syndrome: pathogenetic
mechanisms and therapy. Eur Heart J 1985;6(suppl D): 103-14.
2. Jackman WM, Friday KJ, Anderson JL, Aliot EM, Clark M, Lazzara R.The long QT syndromes: a critical review, new clinical observations anda unifying hypothesis. Prog Cardiovasc Dis 1988;31:115-72.
3. Simson MB. Use of signals in the terminal QRS complex to Identifypatients with ventricular tachycardia after myocardial infarction. Circulation 1981;64:235-42.
4. Simson MB, Untereker WJ, Spielman SR, et al. Relation between latepotentials on the body surface and directly recorded fragmented electrograms in patients with ventricular tachycardia. Am J Cardiol1983 ;51: 10512.
5. Schwarzmaier HJ, Karbenn U, Borggrefe M, Ostermeyer J, Breithardt G.Relation between ventricular late endocardial activity during intraoperative endocardial mapping and low-amplitude signals within the terminalQRS complex on the signal-averaged surface electrocardiogram. Am JCardiol 1990;66:308-14.
6. Janse MJ. Reentry rhythms. In: Fozzard HA, Haber E, Jennings RB,Katz AM, Morgan HE, eds. The Heart and Cardiovascular System. NewYork: Raven Press, 1986:1203-38.
7. Gomes JA, Winters SL, Stewart D, Horowitz S, Milner M, Barreca P. Anew noninvasive index to predict sustained ventricular tachycardia andsudden death in the first year after myocardial infarction: based on thesignal-averaged electrocardiogram, radionuclide ejection fraction andHolter monitoring. J Am Coll CardioI1987;10:349-57.
8. Denniss AR, Richards DA, Cody DV, et al. Prognostic significance ofventricular tachycardia and fibrillation induced at programmed electricalstimulation and delayed potentials detected on the Signal-averaged electrocardiograms of survivors of acute myocardial infarction. Circulation1986;74:731-45.
9. Viersma JW, May JF, de Jongste MJL, Woude AA, Sijbring P, Lie KI.Long-QT syndrome and sudden death during sleep in one family (abstr).Eur Heart J 1988;9:45.
10. Butrous GS, Dabbas N, Patel PR, Cochrane T, Camm AJ. Measurementof the QT interval. In: Butrous GS, Schwartz PJ, eds. Clinical Aspects ofVentricular Repolarization. London: Farrand Press, 1989:41-8.
II. Cowan JC, Yusoff K, Moore M, et al. Importance oflead selection in QTinterval measurement. Am J CardioI1988;61:83-7.
12. Ahnve S. Correction of the QT interval for heart rate: review of differentformulas and the use of Bazell's formula in myocardial infarction. AmHeart J 1985;109:568-74.
13. Lepeschkin E. Modern Electrocardiography, Vol I. Baltimore: Williams& Wilkins, 1951: 184.
14. Denniss AR, Richards DA, Farrow RH, Davison A, Ross DL, Uther JB.Technique for maximizing the frequency response of the signal averagedFrank vectorcardiogram. J Biomed Eng 1986;8:207-12.
15. Breithardt G, Cain ME, EI-Sherif N, et al. Standards for analysis ofventricular late potentials using high resolution or signal-averaged electrocardiography. J Am Coll Cardioll99I;17:999-1OO6.
16. Gillis AM, Maclean KE, Guilleminault C. The QT interval during wakeand sleep in patients with ventricular arrhythmias. Sleep 1988;11:333-9.
17. Browne KF, Prystowsky E, Heger n, Chilson DA, Zipes DP. Prolongation of the Q-T interval in man during sleep. Am J CardioI1983;52:55-9.
18. Rasmussen V, Jensen G, Hansen JF. QT interval in 24-hour ambulatoryECG recordings from 60 healthy adult subjects. J Electrocardioll991 ;24:91-5.
19. Gardner PI, Ursell PC, Fenoglio n, Wit AL. Electrophysiologic andanatomic basis for fractionated electrograms recorded from healed myocardial infarcts. Circulation 1985;72:596-611.
20. Breithardt G, Seipel L, Ostermeyer J, et al. Effects of antiarrhythmicsurgery on late ventricular potentials recorded by precordial signalaveraging in patients with ventricular tachycardia. Am Heart J 1982;104:996-1003.
21. Marcus NH, Falcone RA, Harken AH, Josephson ME, Simson MB.Body surface late potentials: effects of endocardial resection in patientswith ventricular tachycardia. Circulation 1984;70:632-7.
22. Denniss AR, Johnson DC, Richards DA, Ross DL, Uther JB. Effect ofexcision of ventricular myocardium on delayed potentials detected by thesignal-averaged electrocardiogram in patients with ventricular tachycardia. Am J Cardiol 1987;59:591-5.
23. James TN, Froggatt P, Atkinson WJ, et al. De subitaneis mortibus. XXX.Observations on the pathophysiology of the long QT syndromes withspecial reference to the neuropathology of the heart. Circulation 1978;57:1221-31.

JACC Vol. 19, No.3March 1, 1992:541-9
TOBE ET AL.LATE POTENTIALS AND QT PROLONGATION
549
24. Bharati S, Dreifus L, Bucheleres G, et al. The conduction system inpatients with a prolonged QT interval. J Am Coli Cardiol 1985;6: 1110-9.
25. Caref EB, Goldberg N, Mendelson L, et al. Effects of exercise on thesignal-averaged electrocardiogram in coronary artery disease. Am JCardiol 1990;66:54-8.
26. Greenspon AJ, Volosin K. The effects of atrial pacing on the signalaveraged electrocardiogram in patients with coronary artery disease. AmHeart J 1990;119:29-34.
27. Kuo CS, Munakata K, Reddy CP, Surawicz B. Characteristics and
possible mechanism of ventricular arrhythmia dependent on the dispersion of action potential durations. Circulation 1983;67: 1356-67.
28. Vassallo JA, Cassidy DM, Kindwall KE, Marchlinski FE, Josephson ME.Nonuniform recovery of excitability in the left ventricle. Circulation1988;78: 1365-72.
29. Surawicz B. Electrophysiologic substrate of torsade de pointes: dispersion of repolarization or early afterdepolarizations? J Am Coli Cardiol1989;14:172-84.