
Dofetilide-Induced Long QT and Torsades de Pointes
6
Dofetilide-Induced Long QT and Torsades de Pointes Mehmet K. Aktas, M.D., ∗ Abrar H. Shah, M.D., ∗ and Toshio Akiyama, M.D.† From the ∗ University of Rochester, Strong Memorial Hospital, Department of Cardiovascular Diseases, Rochester, NY; and †Formerly Professor of Medicine (Cardiology), Director of Heart Station, University of Rochester. Currently Co-director, Cardiovascular Sciences, Covance, Reno, Nevada Dofetilide, a new class III antiarrhythmic agent, has been approved as an antiarrhythmic agent for the treatment of atrial fibrillation and atrial flutter. Dofetilide selectively inhibits the rapid component of the delayed rectifier potassium current resulting in a prolongation of the effective refractory period. Like other drugs that affect potassium currents, the prolonged QT interval occurring in the patients treated with dofetilide can be complicated by torsades de pointes. We report four cases of dofetilide- induced QT prolongation and torsades de pointes. We discuss the risk factors for the development of dofetilide-induced long QT and torsades de pointes and review the current literature. A.N.E. 2007;12(3):197–202 dofetilide; Tikosyn; torsades de pointes; atrial fibrillation Dofetilide is a novel class III antiarrhythmic drug that selectively inhibits the rapid component of the delayed rectifier potassium current and prolongs the refractory period without any significant effect on the atrioventricular nodal conduction system. 1,2 As a pure class III agent, it has no negative in- otropic effect even in patients with markedly re- duced left ventricular function. 3 In patients with atrial fibrillation (AF), dofetilide has been shown to frequently restore and maintain sinus rhythm. 4,5 In patients with left-ventricular dysfunction with recent myocardial infarction and congestive heart failure with left ventricular dysfunction, treatment with dofetilide does not affect all cause mortality, cardiac mortality, or total arrhythmic deaths. 6–8 Dofetilide is effective in treating AF and atrial flutter (AFL) in this population. Like other drugs that affect potassium currents, dofetilide is known to prolong the QT interval and induce malignant ventricular tachyarrhythmias including torsade de pointes. 2, 5,7,8 We present a series of patients, admit- ted to Strong Memorial Hospital, with dofetilide- induced QT prolongation and torsades de pointes. CASE PRESENTATION Patients started on dofetilide at our institution are closely monitored by the Heart Station for Address for reprints: Mehmet K. Aktas, University of Rochester, Strong Memorial Hospital, Department of Cardiovascular Diseases, 601 Elmwood Avenue, Box 679-C, Rochester, NY 14642. Fax: +(585)-242-9549; E-mail: Mehmet [email protected] QT prolongation and/or torsades de pointes. Since October 2001, 268 patients with AF or AFL have been treated with dofetilide. Four patients devel- oped prolonged QT and torsades de pointes corre- sponding to an incidence of 1.5%. The first patient is a 51-year-old man with non- ischemic cardiomyopathy (NICM), a left ventric- ular ejection fraction (LVEF) of 20%, chronic left bundle branch block (LBBB), who developed symp- tomatic AF and was admitted to the hospital for dofetilide initiation. His baseline QTc was 0.46 sec- onds and he was started on dofetilide, 500 micro- grams (mcg) twice daily. He converted to normal si- nus rhythm (NSR) after two doses. After the fourth dose of dofetilide, he developed multiple runs of nonsustained ventricular tachycardia (VT) during which time his QTc was calculated to be 0.8 sec- onds (Fig. 1). His potassium level was 3.7 meq/L and his magnesium level was 1.8 meq/L, which were both corrected intravenously. Dofetilide was discontinued and his QTc normalized and the pa- tient did not have any further episodes of VT. The second patient is a 46-year-old man with an NICM, LVEF of 8%, who was admitted with de- compensated, New York Heart Association Class IV heart failure. He had a chronic LBBB, persis- tent AF and underwent a successful transesopha- geal echocardiography guided cardioversion. He C 2007, Copyright the Authors Journal compilation C 2007, Blackwell Publishing, Inc. 197
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Dofetilide-Induced Long QT and Torsades de Pointes
Dofetilide-Induced Long QT and Torsades de Pointes
Mehmet K. Aktas, M.D.,∗ Abrar H. Shah, M.D.,∗ and Toshio Akiyama, M.D.†From the ∗University of Rochester, Strong Memorial Hospital, Department of Cardiovascular Diseases, Rochester,NY; and †Formerly Professor of Medicine (Cardiology), Director of Heart Station, University of Rochester.Currently Co-director, Cardiovascular Sciences, Covance, Reno, Nevada
Dofetilide, a new class III antiarrhythmic agent, has been approved as an antiarrhythmic agent for thetreatment of atrial fibrillation and atrial flutter. Dofetilide selectively inhibits the rapid component ofthe delayed rectifier potassium current resulting in a prolongation of the effective refractory period.Like other drugs that affect potassium currents, the prolonged QT interval occurring in the patientstreated with dofetilide can be complicated by torsades de pointes. We report four cases of dofetilide-induced QT prolongation and torsades de pointes. We discuss the risk factors for the developmentof dofetilide-induced long QT and torsades de pointes and review the current literature.
A.N.E. 2007;12(3):197–202
dofetilide; Tikosyn; torsades de pointes; atrial fibrillation
Dofetilide is a novel class III antiarrhythmic drugthat selectively inhibits the rapid component of thedelayed rectifier potassium current and prolongsthe refractory period without any significant effecton the atrioventricular nodal conduction system.1,2
As a pure class III agent, it has no negative in-otropic effect even in patients with markedly re-duced left ventricular function.3 In patients withatrial fibrillation (AF), dofetilide has been shown tofrequently restore and maintain sinus rhythm.4,5
In patients with left-ventricular dysfunction withrecent myocardial infarction and congestive heartfailure with left ventricular dysfunction, treatmentwith dofetilide does not affect all cause mortality,cardiac mortality, or total arrhythmic deaths.6–8
Dofetilide is effective in treating AF and atrialflutter (AFL) in this population. Like other drugsthat affect potassium currents, dofetilide is knownto prolong the QT interval and induce malignantventricular tachyarrhythmias including torsade depointes.2,5,7,8 We present a series of patients, admit-ted to Strong Memorial Hospital, with dofetilide-induced QT prolongation and torsades de pointes.
CASE PRESENTATION
Patients started on dofetilide at our institutionare closely monitored by the Heart Station for
Address for reprints: Mehmet K. Aktas, University of Rochester, Strong Memorial Hospital, Department of Cardiovascular Diseases, 601Elmwood Avenue, Box 679-C, Rochester, NY 14642. Fax: +(585)-242-9549; E-mail: Mehmet [email protected]
QT prolongation and/or torsades de pointes. SinceOctober 2001, 268 patients with AF or AFL havebeen treated with dofetilide. Four patients devel-oped prolonged QT and torsades de pointes corre-sponding to an incidence of 1.5%.
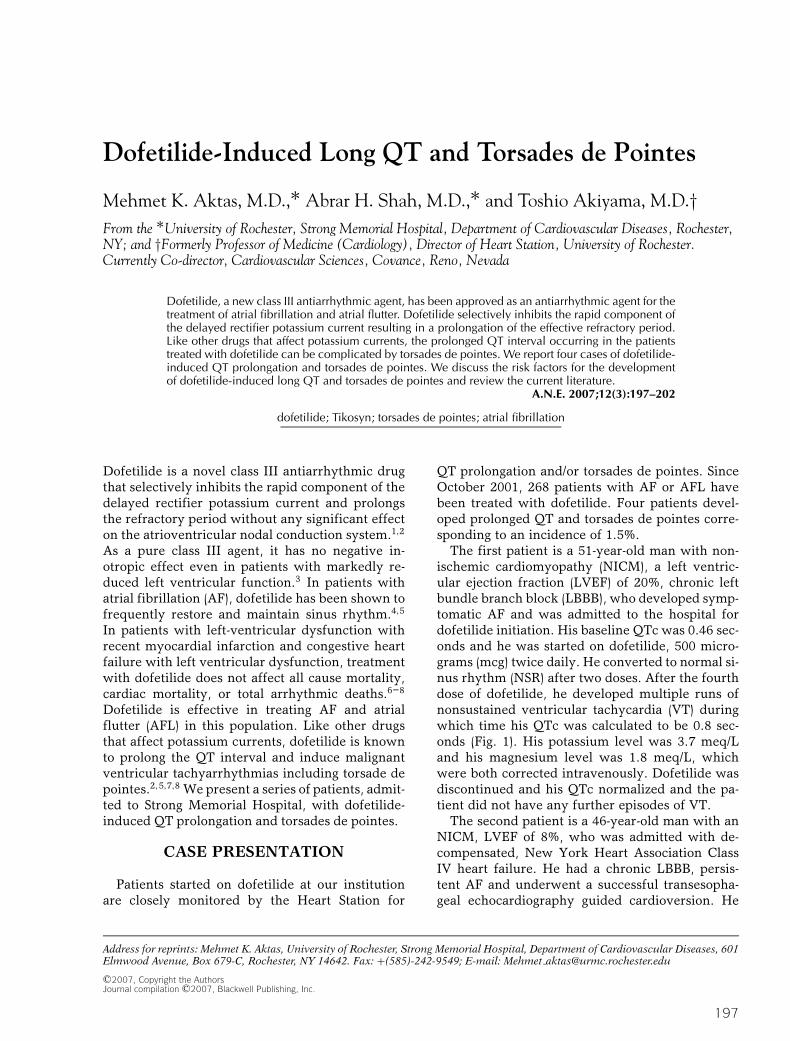
The first patient is a 51-year-old man with non-ischemic cardiomyopathy (NICM), a left ventric-ular ejection fraction (LVEF) of 20%, chronic leftbundle branch block (LBBB), who developed symp-tomatic AF and was admitted to the hospital fordofetilide initiation. His baseline QTc was 0.46 sec-onds and he was started on dofetilide, 500 micro-grams (mcg) twice daily. He converted to normal si-nus rhythm (NSR) after two doses. After the fourthdose of dofetilide, he developed multiple runs ofnonsustained ventricular tachycardia (VT) duringwhich time his QTc was calculated to be 0.8 sec-onds (Fig. 1). His potassium level was 3.7 meq/Land his magnesium level was 1.8 meq/L, whichwere both corrected intravenously. Dofetilide wasdiscontinued and his QTc normalized and the pa-tient did not have any further episodes of VT.
The second patient is a 46-year-old man with anNICM, LVEF of 8%, who was admitted with de-compensated, New York Heart Association ClassIV heart failure. He had a chronic LBBB, persis-tent AF and underwent a successful transesopha-geal echocardiography guided cardioversion. He
C©2007, Copyright the AuthorsJournal compilation C©2007, Blackwell Publishing, Inc.
197
198 � A.N.E. � July 2007 � Vol. 12, No. 3 � Aktas, et al. � Dofetilide-Induced Torsades de Pointes
Figure 1. ECG 1. Patient 1. Twelve-lead ECG showing sinus bradycardia, left atrial enlargement, leftbundle branch block, and severe QT prolongation with a QTc of 0.8 seconds. Telemetry 1. Patient1. Telemetry showing prolonged QTc and polymorphic ventricular tachycardia.
eventually received a biventricular-implantablecardioverter defibrillator (BiV-ICD) for cardiacresynchronization therapy but continued to haveintermittent AF. He was started on dofetilide 500mcg twice daily with a baseline QTc of 0.46 sec-onds (Fig. 2). Following the third dose of dofetilide,his QTc increased to 0.56 seconds and he devel-oped several episodes of torsades de pointes requir-ing multiple defibrillations (Fig. 3). His electrolyteswere within the normal range. Dofetilide was dis-continued and his BiV-ICD was reprogrammed topace at 100 beats/minute to decrease the risk of tor-sades de pointes. Two days later, his BiV-ICD wasreprogrammed to its nominal setting and the pa-tient was discharged home. He has since had nofurther ventricular arrhythmias at over 18 monthsof follow-up.
The third patient is a 64-year-old woman withrheumatic valvular heart disease, with an LVEF of10% who was admitted with decompensated heartfailure. ECG on admission showed atrial tachy-cardia with 2:1 atrioventricular block, a QRS du-ration of 0.11 seconds and a QTc of 0.43 sec-onds (Fig. 4). She was started on dofetilide at
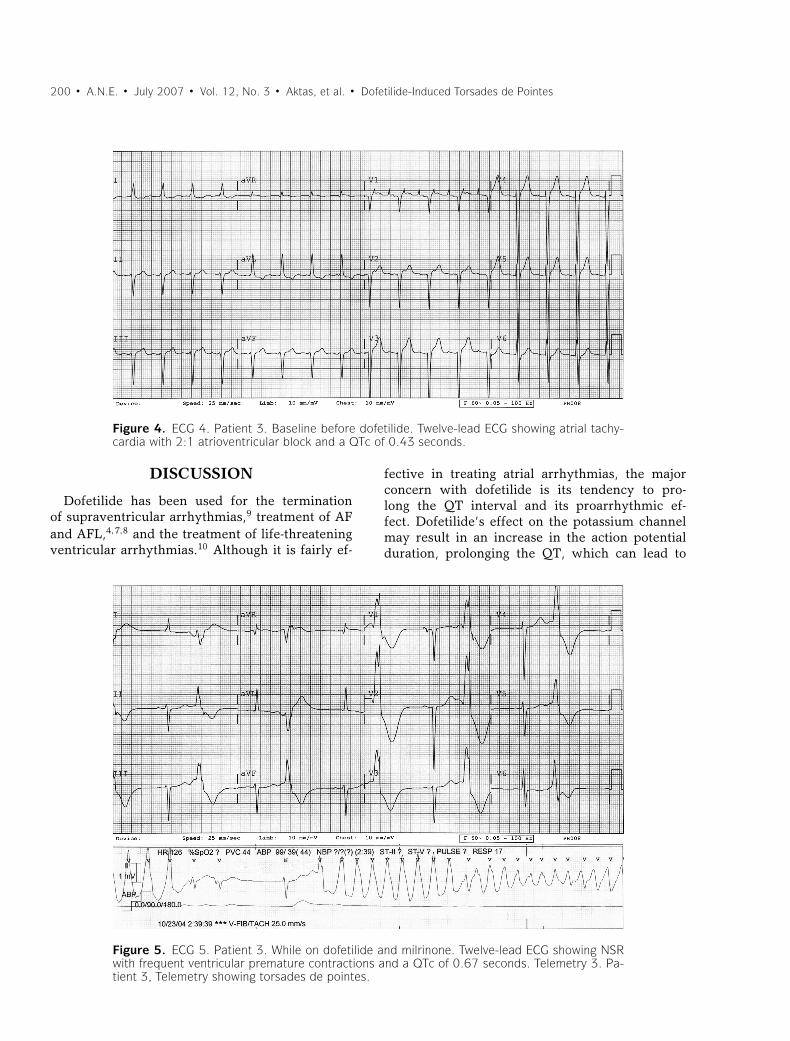
125 mcg twice daily due to renal insufficiencyand she converted to NSR. On hospital day 7,while on dofetilide, she was started on milrinonedue to worsening pulmonary edema. On hospi-tal day 8 she developed torsades de pointes re-quiring multiple external defibrillations (Teleme-try 3). She was successfully resuscitated and bothdofetilide and milrinone were discontinued. TheQTc measured immediately after the cardiac ar-rest was 0.67 seconds (Fig. 5). Laboratory evalu-ation revealed normal potassium and magnesiumlevels. An ICD was implanted for the primary pre-vention of sudden cardiac death and she was even-tually discharged to home. She has not had anyfurther ventricular arrhythmias during 10 monthsof follow-up.
The fourth patient, an 80-year-old woman withcoronary artery disease and valvular heart diseasebut with preserved left ventricular systolic func-tion was admitted with AF and a rapid ventricularresponse. She was started on dofetilide at whichtime her QTc was calculated as 0.45 seconds. Threehours after the first dose of dofetilide she had QTprolongation with a QTc calculated as 0.68 seconds

A.N.E. � July 2007 � Vol. 12, No. 3 � Aktas, et al. � Dofetilide-Induced Torsades de Pointes � 199
Figure 2. ECG 2. Patient 2. Before initiation of dofetilide. Twelve-lead ECG showing atrial fibril-lation, left bundle branch block, and QTc of 0.46 seconds.
and she subsequently developed recurrent but self-terminating torsades de pointes (Fig. 6). Dofetilidewas discontinued however she continued to haverecurrent torsades de pointes. A temporary transve-
Figure 3. ECG 3. Patient 2. After third dose of dofetilide. Twelve-lead ECG showing NSR withventricular capture spikes and a QTc of 0.57 seconds. Telemetry 2. Patient 2. Telemetry showingtorsades de pointes.
nous pacemaker was placed and she was paced at85 beats/minute to decrease the risk of torsades depointes. Eventually the pacer was removed and shehad no further recurrence of torsades de pointes.
200 � A.N.E. � July 2007 � Vol. 12, No. 3 � Aktas, et al. � Dofetilide-Induced Torsades de Pointes
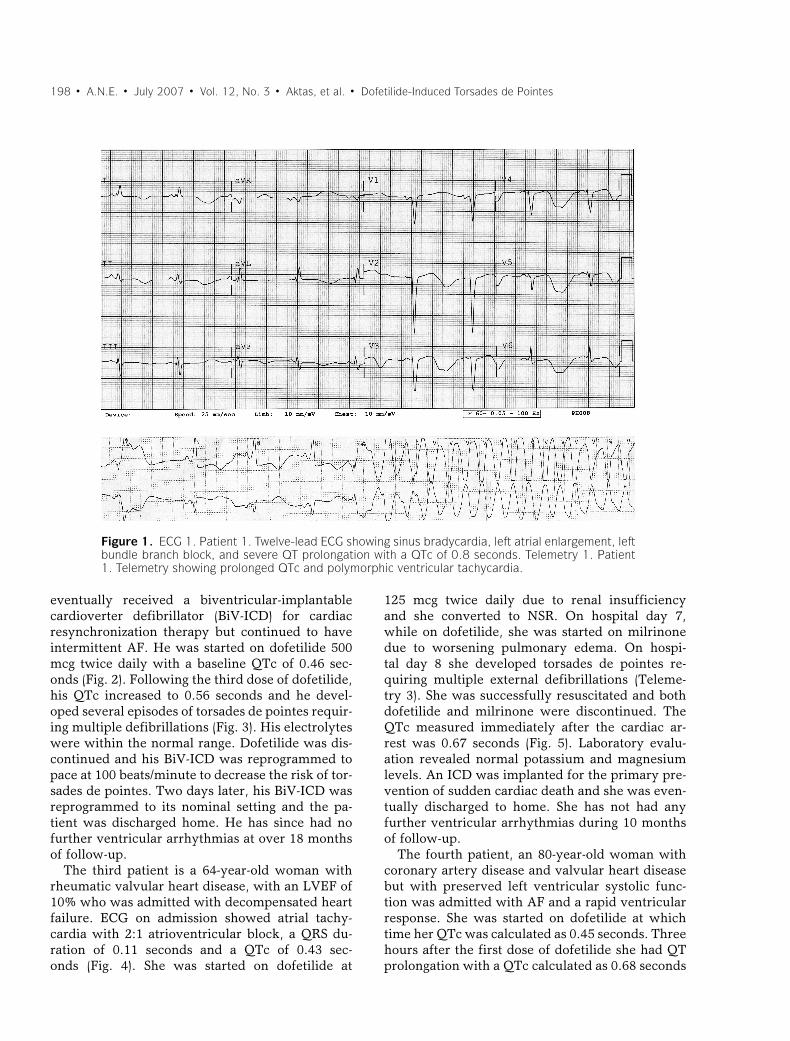
Figure 4. ECG 4. Patient 3. Baseline before dofetilide. Twelve-lead ECG showing atrial tachy-cardia with 2:1 atrioventricular block and a QTc of 0.43 seconds.
DISCUSSION
Dofetilide has been used for the terminationof supraventricular arrhythmias,9 treatment of AFand AFL,4,7,8 and the treatment of life-threateningventricular arrhythmias.10 Although it is fairly ef-
Figure 5. ECG 5. Patient 3. While on dofetilide and milrinone. Twelve-lead ECG showing NSRwith frequent ventricular premature contractions and a QTc of 0.67 seconds. Telemetry 3. Pa-tient 3, Telemetry showing torsades de pointes.
fective in treating atrial arrhythmias, the majorconcern with dofetilide is its tendency to pro-long the QT interval and its proarrhythmic ef-fect. Dofetilide’s effect on the potassium channelmay result in an increase in the action potentialduration, prolonging the QT, which can lead to

A.N.E. � July 2007 � Vol. 12, No. 3 � Aktas, et al. � Dofetilide-Induced Torsades de Pointes � 201
Figure 6. ECG 6. Patient 4. Twelve-lead ECG showing NSR followed by torsades de pointes. Telemetry4. Patient 4. Telemetry showing torsades de pointes.
torsades de pointes.2 QT interval prolongation isdirectly related to the dose and plasma concentra-tion of the drug.1 Oral bioavailability of the drugis greater than 90% and peak concentrations arereached in 2–3 hours in an empty stomach and3–4 hours when taken with food.2 About 70–80%of the drug is excreted through the kidneys and theremainder is metabolized by the liver.1
Several clinical trials were directed to thestudy of the efficacy and the safety of dofetilide.Dofetilide was associated with torsades de pointesin 1.6% of patients with a recent myocardial in-farction and left ventricular dysfunction7 and in3.3% of patients with heart failure.8 In the DI-AMOND MI trial the frequency of torsades depointes dropped from 3% to 0.6% after the protocolwas changed to adjust the dose of dofetilide basedon creatinine clearance.6 A linear logistic regressionanalysis of the DIAMOND CHF study showed thatonly female sex (odds ratio, 3.2) and a NYHA classof III or IV (odds ratio, 3.9) were significantly asso-ciated with the occurrence of torsades de pointes.8
Dofetilide did not increase mortality in multiplerandomized clinical trials.6–8 However, there was adifference in mortality when analyzed by baselineQTc interval. In a substudy of the DIAMOND-CHFtrial there was a significant mortality benefit whendofetilide was used in patients with baseline QTcintervals less than 429 ms (risk ratio 0.3), while anincrease in mortality was seen with dofetilide ther-apy in patients with baseline QTc intervals greaterthan 429 ms (risk ratio 1.3).11 All four of the patientspresented in this series had baseline QTc intervalsthat were greater than 429 ms. Moreover, all fourpatients had a wide QRS duration at baseline; twopatients had LBBB and the other two had intraven-tricular conduction delays. To our knowledge thereare no studies showing an increased tendency to QTprolongation and/or torsades de pointes in patientswith a wider baseline QRS complex. Our obser-vation suggests that dofetilide induced torsades depointes is more common after conversion to NSR,and therefore, patients should be observed for atleast 24 hours after conversion to sinus rhythm.

202 � A.N.E. � July 2007 � Vol. 12, No. 3 � Aktas, et al. � Dofetilide-Induced Torsades de Pointes
One reason for this observation could be that therelatively slower heart rates seen in NSR comparedto AF may result in bradycardia-related QT prolon-gation and torsades de pointes.
Although dofetilide has been specifically studiedand approved for the pharmacologic treatment ofAF and AFL, it is associated with a real risk for QTprolongation and torsades de pointes. Appropriatepatient selection and close monitoring of the QT in-terval, electrolytes, and creatinine clearance shouldbe undertaken when administering dofetilide.
REFERENCES
1. Mounsey JP, DiMarco JP. Cardiovascular drugs. Dofetilide.Circulation 2000;102:2665–2670.
2. Falk RH, Decara JM. Dofetilide: A new pure class III an-tiarrhythmic agent. Am Heart J 2000;140:697–706.
3. Rousseau MF, Massart PE, van Eyll C, et al. Cardiacand hemodynamic effects of intravenous dofetilide in pa-tients with heart failure. Am J Cardiol 2001;87:1250–1254.
4. Singh S, Zoble RG, Yellen L, et al. Efficacy and safety of oraldofetilide in converting to and maintaining sinus rhythm inpatients with chronic atrial fibrillation or atrial flutter: Thesymptomatic atrial fibrillation investigative research ondofetilide (SAFIRE-D) study. Circulation 2000;102:2385–2390.
5. Guanzon AV, Crouch MA. Phase IV trial evaluating theeffectiveness and safety of dofetilide. Ann Pharmacother2004;38(7–8):1142–1147.
6. Kober L, Bloch Thomsen PE, Moller M, et al. Effect ofdofetilide in patients with recent myocardial infarction andleft-ventricular dysfunction: A randomised trial. Lancet.2000;356:2052–2058.
7. Pedersen OD, Bagger H, Keller N, Marchant B,et al. Efficacy of dofetilide in the treatment of atrialfibrillation-flutter in patients with reduced left ventricu-lar function: A Danish investigations of arrhythmia andmortality on dofetilide (diamond) substudy. Circulation2001;104:292–296.
8. Torp-Pedersen C, Moller M, Bloch-Thomsen PE, et al.Dofetilide in patients with congestive heart failure and leftventricular dysfunction. Danish investigations of arrhyth-mia and mortality on Dofetilide Study Group. N Engl J Med.1999;341:857–865.
9. Tendera M, Wnuk-Wojnar AM, Kulakowski P, et al. Ef-ficacy and safety of dofetilide in the prevention of symp-tomatic episodes of paroxysmal supraventricular tachycar-dia: A 6-month double-blind comparison with propafenoneand placebo. Am Heart J 2001;142:93–98.
10. Boriani G, Biffi M, Bacchi L, et al. A randomised cross-over study on the haemodynamic effects of oral dofetilidecompared with oral sotalol in patients with ischaemic heartdisease and sustained ventricular tachycardia. Eur J ClinPharmacol 2002;58:165–169.
11. Brendorp B, Elming H, Jun L, et al. QTc interval as a guideto select those patients with congestive heart failure andreduced left ventricular systolic function who will benefitfrom antiarrhythmic treatment with dofetilide. Circulation.2001;103:1422–1427.




















