
Lack of standardization in the procedures for mycological examination of sputum samples from CF...
10
Introduction Cystic fibrosis (CF) is the predominant genetic disease in the Caucasian population in European countries. While several organs may be affected, the severity of lesions involving the respiratory tract usually dictates both patient morbidity and eventually mortality [1]. Mutations in the Cystic Fibrosis Transmembrane Conductance Regulator All authors are members of the ISHAM Working group on Fungal Respiratory Infections in Cystic Fibrosis. Received 1 June 2010; Received in final revised form 21 July 2010; Accepted 24 July 2010 Correspondence: Andrew M. Borman, UK Mycology Reference Laboratory, Health Protection Agency South-West Regional Laborato- ries, Myrtle Road, Bristol BS2 8EL, UK. Tel: 44 117 9268683; Fax: 44 117 9226611; E-mail: [email protected] Lack of standardization in the procedures for mycological examination of sputum samples from CF patients: a possible cause for variations in the prevalence of filamentous fungi ANDREW M. BORMAN*, MICHAEL D. PALMER*, LAURENCE DELHAES †, JACQUELINE CARRÈRE ‡, LOÏC FAVENNEC §, STÉPHANE RANQUE#, JEAN-PIERRE GANGNEUX^, REGINE HORRÉ $ & JEAN-PHILIPPE BOUCHARA ¶ *UK Mycology Reference Laboratory, Health Protection Agency, Bristol, UK, †Parasitology-Mycology Service (EA3609 - BDEEP) Faculty of Medicine, Univ. Lille Nord de France (UDSL), University Hospital Centre & IFR-142, Institut Pasteur de Lille, France, ‡Laboratoire de Biologie, CRCM, Hôpital Renée Sabran, Giens, Hyères, France, §Laboratoire de Parasitologie-Mycologie, Centre Hospitalier Universitaire, Rouen, France, #Laboratoire de Parasitologie-Mycologie, AP-HM Timone, Marseille, France, ^Laboratoire de Parasitologie-Mycologie, Centre Hospitalier Universitaire de Rennes and UPRES-EA 4427, Université de Rennes 1, France, $Federal Institute for Drugs and Medical Devices, Bonn, Germany, and ¶Groupe d’Etude des Interactions Hôte-Pathogène, UPRES-EA 3142, Université d’Angers & Laboratoire de Parasitologie-Mycologie, Centre Hospitalier Universitaire, Angers, France Filamentous fungi and yeasts are increasingly isolated from respiratory secretions of patients with cystic fibrosis (CF), and persistent fungal colonization of the airways of such patients is thought to exacerbate lung damage. While many independent studies have identified Aspergillus fumigatus complex as the principal colonizing fungus in CF, increased awareness of the role of fungi in CF pathology coupled with improved mycological culture and identification methods have resulted in a number of other fungi being isolated and reported from CF sputum samples, including A. terreus, mem- bers of the Pseudallescheria boydii/ Scedosporium apiospermum complex, Exophiala dermatitidis, Paecilomyces and Penicillium species. However, the range of fungal path- ogens isolated and the relative prevalence of individual species vary widely between reports from different geographical CF centres, and as yet no standardized method for the mycological examination of CF sputum samples has been adopted. Here, we examine the potential contribution of the mycological methods employed to exam- ine CF respiratory secretions relative to the variability in the fungal biota reported. The role of direct microscopic examination of respiratory samples and the impact of the culture conditions used on the detection of specific fungal pathogens are addressed, and the potential significance of isolation of yeast species from CF patient airways is discussed. Keywords cystic fibrosis, filamentous fungi, yeasts, respiratory samples, culture methods © 2010 ISHAM DOI: 10.3109/13693786.2010.511287 Medical Mycology 2010, 48(Suppl. 1), S88–S97 Med Mycol Downloaded from informahealthcare.com by Hopital Salvator on 11/22/10 For personal use only.
Transcript of Lack of standardization in the procedures for mycological examination of sputum samples from CF...

Medical Mycology 2010, 48(Suppl. 1), S88–S97
Med
Myc
ol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y H
opita
l Sal
vato
r on
11/
22/1
0Fo
r pe
rson
al u
se o
nly.
Lack of standardization in the procedures for mycological
examination of sputum samples from CF patients:
a possible cause for variations in the prevalence of
fi lamentous fungi
All authors are members of the
Respiratory Infections in Cystic F
Received 1 June 2010; Received
Accepted 24 July 2010
Correspondence: Andrew M. B
Laboratory, Health Protection Age
ries, Myrtle Road, Bristol BS2 8E
� 44 117 9226611; E-mail: Andy.B
ANDREW M. BORMAN * , MICHAEL D. PALMER * , LAURENCE DELHAES † , JACQUELINE CARR È RE ‡ ,
LO Ï C FAVENNEC § , ST É PHANE RANQUE # , JEAN-PIERRE GANGNEUX ̂ , REGINE HORR É $
& JEAN-PHILIPPE BOUCHARA ¶
* UK Mycology Reference Laboratory, Health Protection Agency, Bristol, UK, † Parasitology-Mycology Service (EA3609 - BDEEP)
Faculty of Medicine, Univ. Lille Nord de France (UDSL), University Hospital Centre & IFR-142, Institut Pasteur de Lille, France,
‡ Laboratoire de Biologie, CRCM, H ô pital Ren é e Sabran, Giens, Hy è res, France, § Laboratoire de Parasitologie-Mycologie, Centre
Hospitalier Universitaire, Rouen, France, # Laboratoire de Parasitologie-Mycologie, AP-HM Timone, Marseille, France, ^Laboratoire de
Parasitologie-Mycologie, Centre Hospitalier Universitaire de Rennes and UPRES-EA 4427, Universit é de Rennes 1, France, $ Federal
Institute for Drugs and Medical Devices, Bonn, Germany, and ¶ Groupe d ’ Etude des Interactions H ô te-Pathog è ne, UPRES-EA 3142,
Universit é d ’ Angers & Laboratoire de Parasitologie-Mycologie, Centre Hospitalier Universitaire, Angers, France
© 2010 ISHAM
Filamentous fungi and yeasts are increasingly isolated from respiratory secretions of patients with cystic fi brosis (CF), and persistent fungal colonization of the airways of such patients is thought to exacerbate lung damage. While many independent studies have identifi ed Aspergillus fumigatus complex as the principal colonizing fungus in CF, increased awareness of the role of fungi in CF pathology coupled with improved mycological culture and identifi cation methods have resulted in a number of other fungi being isolated and reported from CF sputum samples, including A. terreus , mem-bers of the Pseudallescheria boydii / Scedosporium apiospermum complex, Exophiala dermatitidis , Paecilomyces and Penicillium species. However, the range of fungal path-ogens isolated and the relative prevalence of individual species vary widely between reports from different geographical CF centres, and as yet no standardized method for the mycological examination of CF sputum samples has been adopted. Here, we examine the potential contribution of the mycological methods employed to exam-ine CF respiratory secretions relative to the variability in the fungal biota reported. The role of direct microscopic examination of respiratory samples and the impact of the culture conditions used on the detection of specifi c fungal pathogens are addressed, and the potential signifi cance of isolation of yeast species from CF patient airways is discussed.
Keywords cystic fi brosis , fi lamentous fungi , yeasts , respiratory samples , culture methods
ISHAM Working group on Fungal
ibrosis.
in fi nal revised form 21 July 2010;
orman, UK Mycology Reference
ncy South-West Regional Laborato-
L, UK. Tel: � 44 117 9268683; Fax:
Introduction
Cystic fi brosis (CF) is the predominant genetic disease in
the Caucasian population in European countries. While
several organs may be affected, the severity of lesions
involving the respiratory tract usually dictates both patient
morbidity and eventually mortality [1]. Mutations in the
Cystic Fibrosis Transmembrane Conductance Regulator
DOI: 10.3109/13693786.2010.511287

Respiratory samples from CF patients: comparison of culture methods S89
Med
Myc
ol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y H
opita
l Sal
vato
r on
11/
22/1
0Fo
r pe
rson
al u
se o
nly.
( CFTR ) gene result in altered mucociliary clearance, and
characteristic excessively viscous bronchial mucus
[reviewed in 2]. This viscous mucus is frequently contam-
inated with a variety of bacterial and fungal facultative
pathogens, leading to extensive colonization of the respira-
tory tract, and to recurrent exacerbations of pulmonary
disease [3 – 6].
While a variety of moulds are frequently recovered
from CF respiratory secretions, Aspergillus fumigatus
is the principal fi lamentous fungus reported to colonize
the airways of CF patients, independent of the geo-
graphic region studied or the mycological methodolo-
gies employed [6 – 8]. Prolonged colonization with
Aspergillus spp. results in sensitization and eventually
allergic bronchopulmonary aspergillosis (ABPA) in a
signifi cant proportion of CF patients, which has been
associated with accelerated deterioration of lung function
[9 – 11]. Other common fungi repeatedly cultured from
CF patient samples include Aspergillus terreus , members
of the Scedosporium apiospermum complex, Geosmithia
spp., Paecilomyces spp. and Exophiala dermatitidis
[7,8,12 – 16; for review see 6]. At least certain of these
opportunistic fungal colonizers of CF respiratory tracts
have already been shown to be capable of causing inva-
sive and disseminated infections in CF patients after lung
transplantation [see for example 17,18].
Numerous studies have also reported extremely elevated
isolation rates for Candida species from CF respiratory
samples, with C. albicans being by far the predominant
yeast species identifi ed [8,16,19,20]. Controversy remains
as to the potential role of Candida species colonization in
the pathology of CF, and as to whether isolation of yeasts
from sputum samples truly refl ects colonization in CF
patients, or rather results from contamination of samples
from yeasts present commensally (or introduced from
food) in the oral cavity. However, the detection of
Candida -specifi c IgE responses in ABPA patients [21]
and data indicating that serologic IgE responses against
C. albicans correlated both with ABPA and culture positiv-
ity for this yeast [22] suggest that sensitization to coloniz-
ing Candida species may be a relevant immunological
marker for ABPA development.
Although a comparison of the fungi reported from CF
patients from various studies worldwide reveals a fairly
conserved epidemiological picture of the key fungal spe-
cies involved, the relative prevalence of individual spe-
cies varies considerably. This variation may stem from
actual geographical differences in the prevalence of cer-
tain individual species, temporal changes in the relative
prevalence of certain species driven by climatic or social
factors, or from population differences in the genetic
susceptibility to certain organisms. For example it has
been suggested that the elevated isolation frequencies of
© 2010 ISHAM, Medical Mycology, 48(Suppl. 1), S88–S97
Exophiala dermatitidis in German CF patients might
result from frequenting sauna facilities, in which this
thermophilic organism is known to thrive [6,16,23,24].
However, it is also likely that the insensitivity of the
culture methods employed in some studies coupled with
the absence of a consensus approach to examining CF
respiratory secretions at least partly underpins the
apparently variable fungal biota reported from different
CF patient cohorts. Several studies describing fungal
selective media for the culture of CF secretions support
this contention. Mycological media supplemented with
a cocktail of antibiotics active principally against
Gram-negative bacteria significantly increased the sen-
sitivity of culture for both yeasts and filamentous fungi
[25]. For example, erythritol-chloramphenicol agar
and extended incubation time improved the isolation of
E. dermatitidis [16] and two different semi-selective
media (yeast extract-peptone-dextrose-agar with cyclo-
heximide [12], or SceSel � [14,26]) greatly facilitated
the detection of species belonging to the P. boydii / S. apiospermum complex.
The current paper uses data drawn from several CF
centres and mycology laboratories in the UK and France
to lend further support to the idea that the major factors
determining the prevalence of individual fungal species
reported from CF patients are indeed the mycological
approaches employed for examination and culture of
respiratory samples from such patients. We also discuss
the relative merits of direct microscopic examination
of sputum samples for the detection and enumeration of
fi lamentous fungi and yeasts, and the urgent need for
a multi-centric collaborative approach to defi ne a stan-
dardized method for examining respiratory specimens
from CF patients.
Methods
The following mycological methods were employed in the
various centres for the examination and culture of sputum
samples from CF patients:
Mycology Reference Laboratory (MRL), Bristol, UK
Sputum samples were mixed with an equal volume of
sputasol (Oxoid, Basingstoke, UK) and incubated at 37 ° C
for 15 min. Volumes of 10 ml of treated sputum were then
centrifuged at 3000 rpm (1500 g ) for 10 min in a MSE
Centaur 2 bench-top centrifuge. Supernatants were dis-
carded, leaving approximately 0.5 ml of sputum and pel-
leted sediment. Sedimented material was resuspended in
the 0.5 ml of remaining sputum, and aliquots of 0.2 ml
each were inoculated onto duplicate Sabouraud ’ s glucose
peptone agar fl asks containing chloramphenicol (Cmp;

© 2010 ISHAM, Medical Mycology, 48(Suppl. 1), S88–S97
S90 Borman et al.
Med
Myc
ol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y H
opita
l Sal
vato
r on
11/
22/1
0Fo
r pe
rson
al u
se o
nly.
0.05 g/l) which were incubated at 30 ° C and 37 ° C for 3 – 4
weeks. Cultures were examined and reported after 48 h
and then re-incubated for a further 3 weeks and re-
examined periodically (usually weekly). Moulds were
identifi ed by examination of macroscopic and microscopic
features, according to standard descriptions. For yeasts,
Candida albicans was identifi ed by germ tube forma-
tion, with all germ tube negative isolates were reported as
Candida species.
The remaining 0.1 ml of resuspended sediment was
mixed with an equal volume of 20% KOH and a single
drop of Calcofl uor (Bactidrop, Remel), and examined
using a fl uorescence microscope with a V-2A fi lter (excita-
tion 380 – 420 nm; dichromatic mirror 430 nm; barrier fi lter
450 nm).
Bristol Royal Infi rmary, Microbiology Department, Bristol, UK
Data were collected for organisms referred to the MRL for
identifi cation. Sputum samples were mixed with an equal
volume of 0.1% dithiothreitol and incubated at 37 ° C for
15 min. After incubation, 1 μ l volumes of treated sputum
and sputum diluted 1/500 in sterile water were inoculate
in parallel onto; (a) Sabouraud ’ s glucose peptone agar
(incubation at 37 ° C for up to 6 weeks). (b) CLED agar
(incubation at 37 ° C for 48 h) (c) mannitol salt agar (incu-
bation at 37 ° C for 48 h), and (d) two Burkholderia cepacia
selective agar plates (incubation at 30 ° C for 5 days for one
plate and at 37 ° C for 48 h). All fi lamentous fungi, includ-
ing those from CF patients, were referred to the MRL for
identifi cation.
Centre Hospitalier R é gional Universitaire, Lille, France
Sputum samples were treated with an equal volume of a
1 � solution of 2,3-dihydroxy-1,4-dithiolbutane in sterile
water (Digest-EUR ® , Eurobio, France), followed by incu-
bation for 30 min at 37 ° C. After direct microscopic exam-
ination of either Giemsa or Ortho-Toluidin blue stained
samples, 50 ml volumes of treated sputum were inocu-
lated in parallel onto CandiSelectTM 4 (Bio-Rad; incu-
bation at 37 ° C for 3 weeks), Sabouraud ’ s glucose peptone
agar with 0.5 g/l amikacin (incubation at 25 ° C for 3
weeks) and ½ diluted Sabouraud ’ s glucose agar with 0.5
g/l amikacin (incubation at 25 ° C for 3 weeks). Moulds
were identifi ed by examination of macroscopic and
microscopic features. For isolates with atypical morphol-
ogy, identifi cation was confi rmed by amplifi cation and
sequencing of the ITS1-ITS2 region of the nuclear ribo-
somal repeat region. For yeasts, Candida albicans was
identifi ed by latex agglutination testing, tentative IDs for
non- C. albicans Candida species were obtained using
CHROMagar chromagenic media.
Laboratoire de Parasitologie-Mycologie, Centre Hospitalier
Universitaire, Angers, France
Prior to 1996, after direct examination, aliquots (10 μ l)
were plated on two yeast extract-peptone-dextrose-agar
(YPDA) plates containing 0.5 g/l chloramphenicol (Cmp),
and for one of them 0.5 g/l cycloheximide. Each sample
was also digested with an equal volume of mucolytic agent
(Digest-EUR ® , Eurobio) for 30 min at room temperature.
The digested mix was then diluted 1:5 (fi nal dilution of the
sample 1:10), and 10 μ l aliquots were inoculated onto two
YPDA plates containing Cmp and for one of them cyclo-
heximide was also included in the agar medium. All plates
were incubated at 37 ° C for 3 weeks even if some rapidly
growing fungi like A. fumigatus were detected.
From 1996, the procedure was slightly modifi ed. Before
digestion, aliquots of the sample were inoculated in paral-
lel onto CHROMAgar Candida (Becton-Dickinson, UK)
incubation at 37 ° C for 3 weeks), and YPDA with Cmp and
cycloheximide (incubation at 37 ° C for 3 weeks). After
digestion and dilution, the procedure was unchanged.
From 2006, cultures were performed exclusively after
digestion and dilution. All samples were inoculated (10 μ l
aliquots) in parallel onto (a) CHROMAgar Candida (incuba-
tion at 37 ° C for 3 weeks), (b) in-house prepared YPDA-Cmp-
cycloheximide (incubation at 37 ° C for 3 weeks), (c) in-house
prepared DRBC-benomyl (dichloran-rose bengal chloram-
phenicol agar containing 0.1 g/l Cmp and supplemented with
0,008 g/l benomyl; incubation at 37 ° C for 3 weeks), (d) in-
house prepared Erythritol agar supplemented with Cmp (incu-
bation at 37 ° C for 3 weeks), (e) Sabouraud ’ s glucose agar
containing Cmp and gentamicin (Becton-Dickinson; incuba-
tion at 20 – 25 ° C for 3 weeks), (f) in-house prepared YPDA-
Cmp-cycloheximide (incubation at 20 – 25 ° C for 3 weeks) and
(g) in-house prepared Erythritol agar � Cmp (incubation at
20 – 25 ° C for 3 weeks). Yeasts were identifi ed according to
colony colour on CHROMagar Candida (Becton-Dickinson)
and, for non-green colonies, by their carbohydrate assimila-
tion pattern using ID 32C test strips (bioM é rieux). Moulds
were identifi ed morphologically according to standard mac-
roscopic and microscopic descriptions.
Laboratoire de Parasitologie-Mycologie, Centre Hospitalier
Universitaire, Rouen, France
Digestion of the samples by mixing with an equal volume
of Digest-EUR (Eurobio), following which, 20- μ l aliquots
of the digested sample were inoculated in parallel onto a
commercial Sabouraud ’ s glucose peptone agar slant con-
taining 0.04g/l gentamicin (Bio-Rad, France) and a second
Sabouraud ’ s glucose peptone agar slant containing gen-
tamicin and cycloheximide (Bio-Rad France), both of
which were incubated at 30 ° C for 2 weeks. Identifi cation

Respiratory samples from CF patients: comparison of culture methods S91
Med
Myc
ol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y H
opita
l Sal
vato
r on
11/
22/1
0Fo
r pe
rson
al u
se o
nly.
of yeasts was achieved by establishing their auxanographic
profi les using ID 32C test strips and mould isolates were
identifi ed morphologically, according to standard macro-
scopic and microscopic descriptions.
Laboratoire de Biologie, H ô pital Ren é e Sabran, Giens, France
Samples were digested by mixing with an equal volume of
Sputasol (Oxoid) and after 20-min incubation at room tem-
perature, 30- μ l aliquots of the digested sample were inoc-
ulated in parallel onto an in-house prepared DRBC-benomyl
agar plate and a gentamicin-containing Sabouraud ’ s glu-
cose peptone agar plate (bioM é rieux, France). All plates
were incubated at 37 ° C for one week. Yeasts were identi-
fi ed according to their carbohydrate assimilation pattern
using Api 20C Aux test strips (bioM é rieux) and moulds
were identifi ed morphologically according to standard
macroscopic and microscopic descriptions. For suspected
isolates of G. argillacea , the morphological identifi cation
was confi rmed by gene sequencing.
Laboratoire de Parasitologie-Mycologie, Centre Hospitalier
Universitaire, Rennes, France
All samples were fi rst digested by mixing with Digest-
EUR (Eurobio). After 30 min of incubation under constant
shaking, the digested samples were centrifuged, and por-
tions of the resulting pellets were inoculated in parallel on
two Sabouraud glucose agar slants with 50 mg/l Cmp (AES
Chemunex, Combourg, France), one of which was incu-
bated at 37 ° C and the other 30 ° C for 7 days. Moulds were
identifi ed by examination of macroscopic and microscopic
features, according to standard macroscopic and micro-
scopic descriptions. For yeasts, non- C. albicans Candida
species were identifi ed by a combination of chromogenic
agars (CHROMagar, Bekton Dickinson, France) and the
mini Api system (BioM é rieux, France).
Laboratoire de Parasitologie-Mycologie, Centre Hospitalier
Universitaire, Marseille, France
Thick mucous samples were digested with an equal volume
of Sputagest Selectavial (Mast Diagnostic, France) for 10
min at room temperature and were then processed as fl uid
samples. Direct examination of the sample was performed
using chloral-lactophenol cotton blue (VWR, France)
staining. A volume of 500 μ l of fl uid sample (or digested
mucous sample) was inoculated onto one Sabouraud dex-
trose agar slant with chloramphenicol and gentamicin
(AES Chemunex or BioM é rieux, France) and incubated
at 27 – 30 ° C for 10 days. The purity of yeast isolates was
checked by subculture on CHROMAgarTM Candida
© 2010 ISHAM, Medical Mycology, 48(Suppl. 1), S88–S97
medium. Candida albicans and Candida krusei were
identifi ed using the rapid agglutination test, i.e., Bichro-
latex albicans and Bichrolatex krusei (Fumouze Diagnos-
tics, France), respectively. Other yeast species were
identifi ed on the basis of the color of the colonies on chro-
mogenic medium, microscopic morphology on PCB
medium and carbohydrate assimilation profi les on Auxa-
color 2 (Sanofi Diagnostic, Pasteur, France). Moulds were
identifi ed on the basis of macroscopic and microscopic
morphological characteristics, according to standard
descriptions.
Results and discussion
The impact of variable culture methods on the prevalence
of fungal species reported from CF respiratory secretions
The published literature contains extensive data concerning
the range of mould species associated with respiratory
samples from CF patients. Principal among the more com-
monly encountered organisms are A. fumigatus , other
Aspergillus species (especially A. terreus and A. fl avus ),
members of the Scedosporium apiospermum complex, and
in certain CF centres Exophiala dermatitidis , Paecilomyces
spp. and Penicillium spp. (see for example [6,14]). An
examination of data collected recently from different Euro-
pean CF centres supports this general pattern (Tables 1 and
2), and confi rms the predominance of A. fumigatus in such
samples. All centres reported high prevalence rates for this
organism, both in terms of total respiratory secretions pro-
cessed and in terms of the number of CF patients sampled,
although signifi cant variation was observed in absolute
positivity rates for this organism (10.1 – 80.4% of samples;
8.6 – 88.9% of patients). Similarly, most centres also
reported the isolation of A. terreus , A. fl avus , S. apiosper-mum complex from a smaller, but signifi cant number of
patients and samples (Tables 1 and 2), in agreement with
most existing reports. Many centres also reported the isola-
tion of Penicillium spp. from patients in the various cohorts.
To date, it is unclear whether the isolation of this organism
has relevance to clinical exacerbation in CF, or rather
serves as a marker for exposure to air generally contami-
nated with fi lamentous fungi.
Repeated isolation of Aspergillus and Scedosporium
spp. from patient samples is accepted to be an indicator
of colonization with those organisms. However, an appre-
ciation of the exact burden of colonization within the CF
population as a whole is diffi cult, principally because
absolute prevalence rates vary signifi cantly between even
geographically close CF centres (compare for example
data for A. fumigatus and S. apiospermum ; Table 1; and
for A. fl avus, A. terreus and S. apiospermum reported
from the CF centres in Angers, Rouen and Lille for 2006;
S92 Borman et al.
Study Centre
Bristold Bristole Giens Hospital Rennes Hospital Marseille Hospital
Cultures S (156) P (69) S (102) P (36) S (1033) P (238) S (471) P (135) S (932) P (442)
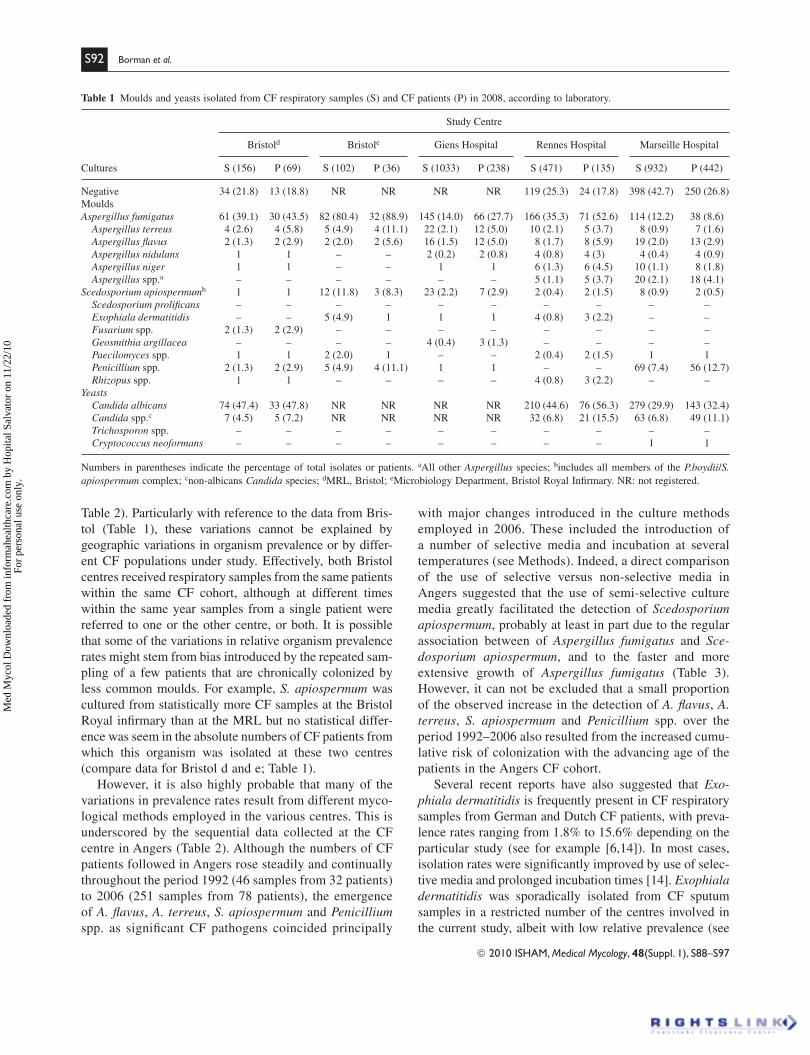
Negative 34 (21.8) 13 (18.8) NR NR NR NR 119 (25.3) 24 (17.8) 398 (42.7) 250 (26.8) Moulds Aspergillus fumigatus 61 (39.1) 30 (43.5) 82 (80.4) 32 (88.9) 145 (14.0) 66 (27.7) 166 (35.3) 71 (52.6) 114 (12.2) 38 (8.6)
Aspergillus terreus 4 (2.6) 4 (5.8) 5 (4.9) 4 (11.1) 22 (2.1) 12 (5.0) 10 (2.1) 5 (3.7) 8 (0.9) 7 (1.6) Aspergillus fl avus 2 (1.3) 2 (2.9) 2 (2.0) 2 (5.6) 16 (1.5) 12 (5.0) 8 (1.7) 8 (5.9) 19 (2.0) 13 (2.9) Aspergillus nidulans 1 1 – – 2 (0.2) 2 (0.8) 4 (0.8) 4 (3) 4 (0.4) 4 (0.9) Aspergillus niger 1 1 – – 1 1 6 (1.3) 6 (4.5) 10 (1.1) 8 (1.8) Aspergillus spp.a – – – – – – 5 (1.1) 5 (3.7) 20 (2.1) 18 (4.1)
Scedosporium apiospermum b 1 1 12 (11.8) 3 (8.3) 23 (2.2) 7 (2.9) 2 (0.4) 2 (1.5) 8 (0.9) 2 (0.5) Scedosporium prolifi cans – – – – – – – – – – Exophiala dermatitidis – – 5 (4.9) 1 1 1 4 (0.8) 3 (2.2) – – Fusarium spp. 2 (1.3) 2 (2.9) – – – – – – – – Geosmithia argillacea – – – – 4 (0.4) 3 (1.3) – – – – Paecilomyces spp. 1 1 2 (2.0) 1 – – 2 (0.4) 2 (1.5) 1 1 Penicillium spp. 2 (1.3) 2 (2.9) 5 (4.9) 4 (11.1) 1 1 – – 69 (7.4) 56 (12.7) Rhizopus spp. 1 1 – – – – 4 (0.8) 3 (2.2) – –
Yeasts Candida albicans 74 (47.4) 33 (47.8) NR NR NR NR 210 (44.6) 76 (56.3) 279 (29.9) 143 (32.4) Candida spp.c 7 (4.5) 5 (7.2) NR NR NR NR 32 (6.8) 21 (15.5) 63 (6.8) 49 (11.1) Trichosporon spp. – – – – – – – – – – Cryptococcus neoformans – – – – – – – – 1 1
Med
Myc
ol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y H
opita
l Sal
vato
r on
11/
22/1
0Fo
r pe
rson
al u
se o
nly.
Table 2). Particularly with reference to the data from Bris-
tol (Table 1), these variations cannot be explained by
geographic variations in organism prevalence or by differ-
ent CF populations under study. Effectively, both Bristol
centres received respiratory samples from the same patients
within the same CF cohort, although at different times
within the same year samples from a single patient were
referred to one or the other centre, or both. It is possible
that some of the variations in relative organism prevalence
rates might stem from bias introduced by the repeated sam-
pling of a few patients that are chronically colonized by
less common moulds. For example, S. apiospermum was
cultured from statistically more CF samples at the Bristol
Royal infi rmary than at the MRL but no statistical differ-
ence was seem in the absolute numbers of CF patients from
which this organism was isolated at these two centres
(compare data for Bristol d and e; Table 1).
However, it is also highly probable that many of the
variations in prevalence rates result from different myco-
logical methods employed in the various centres. This is
underscored by the sequential data collected at the CF
centre in Angers (Table 2). Although the numbers of CF
patients followed in Angers rose steadily and continually
throughout the period 1992 (46 samples from 32 patients)
to 2006 (251 samples from 78 patients), the emergence
of A. fl avus , A. terreus , S. apiospermum and Penicillium
spp. as signifi cant CF pathogens coincided principally
with major changes introduced in the culture methods
employed in 2006. These included the introduction of
a number of selective media and incubation at several
temperatures (see Methods). Indeed, a direct comparison
of the use of selective versus non-selective media in
Angers suggested that the use of semi-selective culture
media greatly facilitated the detection of Scedosporium
apiospermum , probably at least in part due to the regular
association between of Aspergillus fumigatus and Sce-dosporium apiospermum , and to the faster and more
extensive growth of Aspergillus fumigatus (Table 3).
However, it can not be excluded that a small proportion
of the observed increase in the detection of A. fl avus , A. terreus , S. apiospermum and Penicillium spp. over the
period 1992 – 2006 also resulted from the increased cumu-
lative risk of colonization with the advancing age of the
patients in the Angers CF cohort.
Several recent reports have also suggested that Exo-phiala dermatitidis is frequently present in CF respiratory
samples from German and Dutch CF patients, with preva-
lence rates ranging from 1.8% to 15.6% depending on the
particular study (see for example [6,14]). In most cases,
isolation rates were signifi cantly improved by use of selec-
tive media and prolonged incubation times [14]. Exophiala
dermatitidis was sporadically isolated from CF sputum
samples in a restricted number of the centres involved in
the current study, albeit with low relative prevalence (see
Table 1 Moulds and yeasts isolated from CF respiratory samples (S) and CF patients (P) in 2008, according to laboratory.
Numbers in parentheses indicate the percentage of total isolates or patients. aAll other Aspergillus species; bincludes all members of the P.boydii / S. apiospermum complex; cnon-albicans Candida species; dMRL, Bristol; eMicrobiology Department, Bristol Royal Infi rmary. NR: not registered.
© 2010 ISHAM, Medical Mycology, 48(Suppl. 1), S88–S97

© 2010 ISHAM, Medical Mycology, 48(Suppl. 1), S88–S97
Respiratory samples from CF patients: comparison of culture methods S93
Tabl
e 2
Mo
uld
s an
d y
east
s is
ola
ted f
rom
CF
res
pir
atory
sam
ple
s (S
) an
d C
F p
atie
nts
(P
) in
lab
ora
tori
es i
n t
hre
e U
niv
ersi
ty h
osp
ital
s fr
om
Fra
nce
, ac
cord
ing t
o l
abora
tory
. N
um
ber
s in
par
enth
eses
indic
ate
the
per
centa
ge
of
tota
l is
ola
tes
or
pat
ients
.
Anger
s 1992
Anger
s 1996
Anger
s 2000
Anger
s 2
006
Lil
le 2
006
Rouen
2006
S (
46)
P (
32)
S (
143)
P (
44)
S (
148)
P (
52)
S (
251)
P (
78)
S (
333)
P (
76)
S (
646)
P (
137)
Yea
sts
Can
dida
alb
ican
s 26 (
56.5
)17 (
53.1
)94 (
65.7
)29 (
65.9
)87 (
58.8
)27 (
51.9
)132 (
52.3
)41 (
52.6
)80 (
24.0
)55 (
72.4
)233 (
36.1
)78 (
56.9
) C
andi
da d
ubli
nien
sis
––
––
––
––
2 (
0.6
)2 (
2.6
)–
– C
andi
da fa
mat
a –
––
––
––
––
–1
1 C
andi
da g
labr
ata
––
12 (
8.4
)3 (
6.8
)11 (
7.4
)2 (
3.9
)15 (
6.0
)4 (
5.1
)8 (
2.4
)5 (
6.6
) 2 (
0.3
)1
Can
dida
inte
rmed
ia
–
–
–
–
–
–
–
–
–
–
11
Can
dida
kef
yr
––
––
––
2 (
0.8
)2 (
2.6
)1
1–
– C
andi
da p
arap
silo
sis
––
4 (
2.8
)4 (
9.1
)6 (
4.1
)4 (
7.7
) 32 (
12.8
) 9 (
11.5
)2 (
0.6
)2 (
2.6
) 5 (
0.8
)2 (
1.5
) C
andi
da li
poly
tica
–
––
––
–1
1–
– 3 (
0.4
)3 (
2.2
) C
andi
da in
cons
picu
a –
––
–1
1–
––
––
– C
andi
da s
phae
rica
–
––
––
–1
1–
––
– C
andi
da tr
opic
alis
–
––
–1
11
1–
–1
1 C
andi
da s
pp.
––
––
––
––
11
11
Geo
tric
hum
spp.
––
––
––
6 (
2.4
)5 (
6.4
)1
1 6 (
0.9
)6 (
4.4
) P
ichi
a et
sche
llsi
i –
––
––
–1
1–
––
– Sa
ccha
rom
yces
cer
evis
iae
––
––
––
2 (
0.8
)2 (
2.6
)–
–1
1 M
ould
s A
sper
gill
us fu
mig
atus
14 (
30.4
) 9
(28.1
)49 (
34.3
)17 (
38.6
)66 (
44.6
)22 (
42.3
) 93 (
37.1
)27 (
34.6
)55 (
16.5
)28 (
36.8
) 65 (
10.1
)39 (
28.5
) A
sper
gill
us fl
avus
–
––
–1
1 26 (
10.4
)10 (
12.8
)2 (
0.6
)2 (
2.6
) 4 (
0.6
)4 (
2.9
) A
sper
gill
us n
idul
ans
11
––
11
2 (
0.8
)1
––
––
Asp
ergi
llus
nig
er
––
11
––
––
––
2 (
0.3
)2 (
1.5
) A
sper
gill
us o
chra
ceus
–
––
––
–1
1–
––
– A
sper
gill
us te
rreu
s 1
12 (
1.4
)2 (
4.5
)7 (
4.7
)4 (
7.7
)22 (
8.8
) 8 (
10.3
)–
– 5 (
0.8
)3 (
2.2
) A
sper
gill
us v
ersi
colo
r –
––
––
– 4 (
1.6
)4 (
5.1
)–
– 3 (
0.5
)3 (
2.2
) Sc
edos
pori
um a
pios
perm
um
11
––
11
48 (
19.1
)10 (
12.9
)17 (
5.1
)4 (
5.2
) 5 (
0.8
)2 (
1.5
) Sc
edos
pori
um p
roli
fi can
s –
––
––
– 4 (
1.6
)1
––
––
Alt
erna
ria
spp.
––
––
––
2 (
0.8
)2 (
2.6
)–
– 2 (
0.3
)2 (
1.5
) C
lado
spor
ium
spp.
11
––
––
3 (
1.2
)3 (
3.9
)–
– 3 (
0.5
)2 (
1.5
) B
eauv
eria
spp.
––
––
––
11
––
––
Cer
atoc
ysti
s sp
p.
––
––
––
11
––
––
Fus
ariu
m s
pp.
––
––
––
––
––
11
Geo
smit
hia
argi
llac
ea
––
––
––
11
––
––
Paec
ilom
yces
var
iott
ii
11
––
––
11
––
––
Peni
cill
ium
spp.
11
4 (
2.8
)3 (
6.8
)–
– 26 (
10.4
)20 (
25.7
)1
112 (
1.9
)9 (
6.5
) Pa
ecil
omyc
es s
pp.
––
––
––
––
––
11
Tric
hode
rma
spp.
––
––
––
11
––
––
Muc
or s
pp.
––
11
––
2 (
0.8
)2 (
2.6
)–
––
– E
xoph
iala
der
mat
itid
is
––
––
––
––
––
––
Ste
rile
mould
s–
–1
1–
–14 (
5.6
)10 (
12.8
)–
– 2 (
0.3
)2 (
1.5
)
Med
Myc
ol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y H
opita
l Sal
vato
r on
11/
22/1
0Fo
r pe
rson
al u
se o
nly.

S94 Borman et al.
2006 2007
Total number of samples (patients) 51 (78) 253 (84) S. apiospermum positive cultures:
Non-selective culture media 23 (7) 15 (7)
YPDA � cycloheximide 35 (8) 24 (7)
DRBC-benomyl 41 (8) 35 (10)
Med
Myc
ol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y H
opita
l Sal
vato
r on
11/
22/1
0Fo
r pe
rson
al u
se o
nly.
Tables 1 and 2). However, this organism was not detected
in samples by the majority of centres involved in this inves-
tigation. While this may again refl ect variations in the cul-
ture techniques and media employed, it is worth noting that
a least one of the centres that failed to detect signifi cant
numbers of E. dermatitidis isolates has employed appropri-
ate (ECA) selective media since 2006 (see data for Angers,
2006 ; Table 2). Conversely, no specifi c media likely to
improve isolation rates of Exophiala spp. were used for
samples analyzed in Bristol (Table 1), yet fi ve sequential
respiratory samples from a single patient were positive for
this organism in 2008.
An analysis of the methods employed by the various CF
centres participating in the current study also reveals a lack
of standardization in the absolute volumes of respiratory
samples that are subjected to examination, and especially
culture. Whilst all laboratories currently treat sputum sam-
ples with an equal volume of an appropriate mucolytic
agent, the volumes of treated sample that are then cultured
range from as little as 0.001 and 0.5 μ l (Bristol Royal Infi r-
mary), through 10 μ l (Angers), 20 μ l (Rouen) , 30 μ l
(Giens), 50 μ l (Lille) to 500 μ l (Marseille). At the MRL,
Bristol, and in Rennes, sputum is concentrated by cen-
trifugation and the pellet of the centrifuged, treated sputum
is cultured. It is clear that such variations in methodologies
are likely to signifi cantly infl uence the numbers and variety
of organisms isolated from a sample, and the subsequent
relative prevalence of the various fungal species. Con-
trolled studies are required to determine whether increas-
ing the sample volumes that are cultured will signifi cantly
increase isolation rates, or whether culture of excessive
volumes of respiratory secretions might actually inhibit the
growth of some or all fungal species (for example via com-
petition for nutrients or due to the presence of elevated
concentrations of inhibitory substances/bacteria). Impor-
tant variations also exist in both the nature and concentra-
tions of antibiotics employed in the mycological media
used by the various centres that have contributed to the
current study (see Materials and Methods). Studies per-
formed in Angers demonstrated a marked decrease in the
recovery of moulds from respiratory samples (presumably
due to overgrowth of bacteria) when the cycloheximide
concentration in media was reduced from 0.5 g/l to 0.05
g/l (data not shown). These fi ndings are in keeping with
suggestions that the selectivity of SceSel � culture media
is related in part to the mix of antibiotics used to inhibit
bacterial growth [25,26], and serve to highlight a further
aspect of culture media which requires standardization.
Finally, consideration should be given to whether the iden-
tifi cation methods used by the various centres might also
result in some variability in the organisms reported from
CF respiratory secretions. While this is certainly a possibil-
ity for yeast isolates, where the different participating cen-
tres employ a wide range of chromogenic and biochemical
approaches (see Materials and Methods), it is much less
likely for fi lamentous fungi (moulds), since most centres
that participated in the current study identifi ed isolates of
mould by macro-and microscopic examination using com-
mon and well established methodologies (see Materials
and Methods).
Yeast species isolated from CF sputum samples
Although Candida species, and principally C. albicans ,
are regularly recovered from samples of CF patients
[19,27,28], uncertainty remains as to whether this refl ects
transient contamination of the respiratory tract by com-
mensal fl ora or persistent colonization. Based primarily
on the poor predictive value of the isolation of Candida
species from respiratory secretions for invasive diseases
in non-neutropenic (non-CF) patients and on the rarity of
Candida pneumonia despite the extremely common
recovery of Candida from respiratory samples [29,30],
recent updates to IDSA guidelines concluded that anti-
fungal therapy should not be considered on the basis of
the isolation of Candida from the respiratory tract alone
for neutropenic or non-neutropenic patients, but did not
specifi cally address the CF population [31]. However,
both signifi cant long-term persistence and strain mainte-
nance of Candida species has been shown in CF respira-
tory tracts [19], and specifi c anti- Candida IgE responses
in CF patients appear to correlate with repeated isolation
of the yeast [22].
In agreement with all previous reports, C. albicans was
the predominant yeast isolated in the CF centres participat-
ing in the current study. Candida albicans accounted for
greater than 60% of all Candida species recovered (range
68.4 – 100%; Tables 1 and 2), and had been isolated at least
once in approximately 50% of the patients, irrespective of
the particular study centre (range 47.8 – 72.4%). The other
most frequent Candida species found in respiratory sam-
ples from CF patients were C. glabrata and C. parapsilosis
complex, with prevalence rates in the order of 2 – 10%
depending on the species and the CF centre (Table 2).
Indeed, the variations in prevalence rates amongst the var-
ious Candida species were less than those observed with
Table 3 Comparison of the use of non-selective versus semi-selective media
for the isolation of S. apiospermum complex in Angers, 2006 – 2007.
© 2010 ISHAM, Medical Mycology, 48(Suppl. 1), S88–S97

Respiratory samples from CF patients: comparison of culture methods S95
Microscopy result
Organism isolated N
Negative
(%)
Yeast
(%)
Filamentous
fungus (%)
A. fumigatus alone 30 10 (33.3) 1 (3.3) 19 (63.3)
A. fumigatus � C. albicans 27 2 (7.4) 8 (29.6) 17 (63.0)
A. fumigatus � Other mould 4 0 0 4 (100)
C. albicans alone 47 26 (55.3) 17 (36.2) 4 (8.5)Other Aspergillus spp. 8 2 (25) 3 (37.5) 3 (37.5)Other Candida spp. 7 4 (57.1) 3 (42.9) 0
Med
Myc
ol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y H
opita
l Sal
vato
r on
11/
22/1
0Fo
r pe
rson
al u
se o
nly.
fi lamentous fungi reported from the same CF centres for
the same time periods, and agreed fairly closely with previ-
ous reports [14,27]. It is possible that this lack of variation
refl ects the effi cacy of the standard mycological media
commonly employed in most CF centres for the isolation
of yeasts from clinical samples. Candida dubliniensis was
also reported from several CF centres participating in the
present study, but never approached the 11% colonization
rate reported by Peltroche-Llacsahuanga et al . [28].
However, since at least several of the centres in the current
study did not attempt the complete identifi cation of non-
C. albicans Candida species, or reported all germ tube
positive yeasts as C. albicans , it is possible that the true
prevalence rate of this organism might indeed be higher in
our CF patient cohorts.
Direct microscopic examination of CF respiratory samples
Respiratory samples that are submitted to certain CF cen-
tres are examined microscopically for the presence of
fungal elements (see Methods). At the MRL, Bristol, all
samples are subjected to direct microscopic examination
using Calcofl uor fl uorescent brightener (see Methods).
An analysis of the data correlating microscopic fi ndings
with culture results allows a crude evaluation of the util-
ity of this approach for the detection of potential coloni-
zation of patients with moulds and yeasts (Tables 4 and
5). Forty-one of 45 samples from 45 different CF patients
that were microscopy-positive for fi lamentous fungus
yielded at least one species of mould upon culture, and
all 12 samples in which moderate or large amounts of
fi lamentous fungi was reported proved to be culture pos-
itive for moulds (Table 4), demonstrating the potential
utility of direct microscopy examination as a marker for
mould isolation/colonization in CF respiratory samples.
Indeed, more than 65% of isolates (40/61) of A. fumigatus
were cultured from samples which had been found to
© 2010 ISHAM, Medical Mycology, 48(Suppl. 1), S88–S97
Culture result
Microscopy N
Culture
negative
(%)
Mould
isolated
(%)
Yeast
isolated
(%)
Mould �
Yeast
isolated (%)
Negative 76 28 (36.8) 15 (19.7) 30 (39.5) 3 (3.9)Yeast detected 33 3 (9.1) 2 (6.1) 17 (51.5) 11 (33.3)Small amounts of
fi lamentous fungus
33 3 (9.1) 13 (39.4) 1 (3.0) 16 (48.5)
Moderate amounts of
fi lamentous fungus
6 0 6 (100) 0 0
Large amounts of
fi lamentous fungus
6 0 3 (50) 0 3 (50)
be microscopy positive for fi lamentous fungal hyphae/
hyphal fragments (Table 5). Interestingly, A.fumigatus
grew but was not recorded microscopically from nearly
30% of samples that were culture and microscopy posi-
tive for yeasts, as compared to only 3% of samples that
were microscopy positive but culture negative for yeast
(Table 5). This suggests that high concentrations of
Candida albicans blastospores/hyphae in certain CF res-
piratory secretions might hinder the microscopic detec-
tion of mould hyphae. It will be interesting to determine
if samples that are microscopy-negative but culture posi-
tive for A. fumigatus contain recently ‘ acquired ’ , non-
germinated fungal conidia as opposed to growing fungal
hyphae, and if so, whether such conidia are an indicative
precursor of future colonization.
For yeasts, the value of direct microscopy examination
of sputum samples appears somewhat less clear. Yeasts
were recovered from almost 40% of microscopy negative
samples (Table 4) and only 33.8% (25/74) of the C. albi-cans isolates were from samples in which yeasts had been
seen by direct microscopy (Table 5), suggesting that micro-
scopic examination is less sensitive for the detection of
yeasts, and/or that a high proportion of samples contain
very low numbers of yeast cells. Data from the MRL con-
cerning the yeasts isolated from sputum samples from non-
CF patients, and those isolated from mucosal sites and sites
indicative of systemic Candida infections (blood, tissue
etc) reveals a similar range of organisms and relative prev-
alences to those seen in CF populations (data not shown).
Thus, the signifi cance of isolation of a particular yeast
from CF secretions cannot be assessed on the basis of the
identity of the organism alone. It remains to be determined
whether those samples that are microscopy-negative but
culture-positive for yeasts correspond to samples that have
been ‘ contaminated ’ by low numbers of food yeasts/com-
mensal organisms from the oropharynx. Finally, any dis-
cussion on the potential utility of direct examination of
respiratory secretions should include an assessment of the
likelihood that the results would impact favourably on
Table 4 Correlation between results of direct microscopic examination
and culture of CF respiratory secretions, data from CF secretions
examined at the MRL in 2008.
Table 5 Fungi isolated from CF respiratory secretions ( N � 123) at
the MRL in 2008, as a function of the results of direct microscopic
examination.

S96 Borman et al.
Med
Myc
ol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y H
opita
l Sal
vato
r on
11/
22/1
0Fo
r pe
rson
al u
se o
nly.
patient management, especially since any correlations
between the result of direct examination and culture and
clinical condition are likely to be considerably complicated
in patients receiving antifungal therapy.
Conclusions
A considerable volume of data now supports the conten-
tion that a number of key fungal species regularly and
persistently colonize the respiratory tract of patients with
CF. However, a true picture of the prevalence of different
fungal species in CF lungs, and of the signifi cance of their
isolation is hindered by the absence of a standardized
approach to examining such samples. While several stud-
ies have identifi ed semi-selective media that improve the
isolation of certain of the fungal pathogens associated
with CF, these media are not employed routinely in many
laboratories, and the number of different media that would
be required to effectively capture the complete fungal
biota remains unknown. It is becoming clear that once a
standardized approach has been implemented, it will be
possible to accurately analyze the role of some of the
‘ rarer ’ fi lamentous fungi in the exacerbation of the
clinical picture in CF, and the possibility that there are
regional or population-driven variations in the fungi that
colonize CF patients. In this respect, it is worth noting
that several recent taxonomic studies have identifi ed
cryptic species within key clinical morpho-species of
both moulds and yeasts [32 – 36], including Aspergillus fumigatus species complex, S. apiospermum complex and
C. parapsilosis complex. To date, correct identifi cation
of members of these species complexes necessitates
molecular approaches, including sequencing of various
conserved fungal target genes [36], and as such is not
routinely available to many laboratories. It remains to
be determined whether discrimination of such cryptic
species will provide signifi cant clinical benefi t or epide-
miological impact in the context of CF.
We would suggest that the development of a standardized
approach to the culture of respiratory samples from CF
patients will require a two stage process. The fi rst stage
would involve a limited number of key CF centres and be
aimed at developing a defi nitive and easily implementable
approach to the processing and culture of respiratory speci-
mens. This could be achieved in a step-wise fashion (perhaps
using selected CF respiratory samples that are distributed
across these pilot centres), in which fi rst the optimal sample
volume/processing method is determined, followed by a par-
allel comparison of appropriateness of the available semi-
selective media for the isolation of the key fungal pathogens
currently implicated in colonization of CF patients. The sec-
ond stage would then involve adoption of this standardized
methodology in CF centres across the globe, and rigorous
comparison of the epidemiological data on CF biota collected
in different geographic locations. Irrespective of the exact
approach that is chosen, it is undeniable that there is a press-
ing requirement for a concerted effort towards defi ning the
optimal methods for the mycological analysis of the fungal
component of CF microbiology.
Acknowledgments
We wish to thank all of the members of the laboratories
that have contributed data to this study.
Declaration of interest: The authors report no confl icts of
interest. The authors alone are responsible for the content
and writing of this paper.
References
Koch C, H ø iby N. Diagnosis and treatment of cystic fi brosis. 1 Respira-tion 2000; 67 : 239 – 247.
Lommatzsch ST, Aris R. Genetics of cystic fi brosis. 2 Semin Respir Crit Care Med 2009; 30 : 531 – 538.
Sibley CD, Rabin H, Surette MG. Cystic fi brosis: a polymicrobial 3
infectious disease. Future Microbiol 2006; 1 : 53 – 61.
Goss CH, Burns JL. Exacerbations in cystic fi brosis. 1: Epidemiology 4
and pathogenesis. Thorax 2007; 62 : 360 – 367.
Gilligan PH. Microbiology of airway disease in patients with cystic 5
fi brosis. Clin Microbiol Rev 1991; 4 : 35 – 51.
Pihet M, Carr è re J, Cimon B, 6 et al . Occurrence and relevance of
fi lamentous fungi in respiratory secretions of patients with cystic
fi brosis. Med Mycol 2009; 47 : 387 – 397.
Cimon B, Carr è re J, Chazalette JP, 7 et al . Fungal colonisation and immune
response to fungi in cystic fi brosis. J Mycol M é d 1995; 5 : 211 – 216.
Bakare N, Rickerts V, Bargon J, Just-N ü bling, G. Prevalence of 8
Aspergillus fumigatus and other fungal species in the sputum of adult
patients with cystic fi brosis. Mycoses 2003; 46 : 19 – 23.
Elphick H, Southern K. Antifungal therapies for allergic broncho-9
pulmonary aspergillosis in people with cystic fi brosis. Cochrane Database Syst Rev 2000; 4 : CD002204.
De Almeida MB, Bussamra MH, Rodrigues JC. Allergic bronchopul-10
monary apsergillosis in paediatric cystic fi brosis patients. Paediatr Repir Rev 2006; 7 : 67 – 72.
Laufer P, Fink JN, Bruns WT, 11 et al . Allergic bronchopulmonary asper-
gillosis in cystic fi brosis. J Allergy Clin Immunol 1984; 73 : 44 – 48.
Cimon B, Carr è re J, Vinatier JF, 12 et al . Clinical signifi cance of
Scedosporium apiospermum in patients with cystic fi brosis. Eur J Clin Microbiol Infect 2000; 19 : 53 – 56.
Cimon B, Zouhair R, Symoens F 13 et al . Aspergillus terreus in a
cystic fi brosis clinic: environmental distribution and patient colonisa-
tion pattern. J Hosp Infect 2003; 53 : 81 – 82.
Horr é R, Marklein G, Siekmeier R, Nidermajer S, Reiffert SM. 14
Selective isolation of Pseudallescheria and Scedosporium species
from respiratory tract specimens of cystic fi brosis patients. Respira-tion 2009; 77 : 320 – 324.
Barton RC, Borman AM, Johnson EM, 15 et al . Isolation of the fungus
Geosmithia argillacea in the sputum of people with cystic fi brosis. J Clin Microbiol 2010; 48 : 2615–2617.
Horr é R, Schaal KP, Siekmeier R, 16 et al . Isolation of fungi, especially
Exophiala dermatitidis , in patients suffering from cystic fi brosis.
Respiration 2004; 71 : 360 – 366.
© 2010 ISHAM, Medical Mycology, 48(Suppl. 1), S88–S97

Respiratory samples from CF patients: comparison of culture methods S97
Med
Myc
ol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y H
opita
l Sal
vato
r on
11/
22/1
0Fo
r pe
rson
al u
se o
nly.
Symoens F, Knoop C, Schrooyen M, 17 et al . Disseminated
Scedosporium apiospermum infection in a cystic fi brosis patient
after double-lung transplantation. J Heart Lung Transplant 2006;
25 : 603 – 607.
Iversen M, Burton CM, Vand S, 18 et al . Aspergillus infection in lung
transplant patients: incidence and prognosis. Eur J Clin Microbiol Infect Dis 2007; 26 : 879 – 886.
Muthig M, Hebestreit A, Ziegler U, Seidler M, Muller F-MC. 19
Persistence of Candida species in the respiratory tract of cystic fi brosis
patients. Med Mycol 2010; 48 : 56 – 63.
Nagano Y, Elborn JS, Millar BC, 20 et al . Comparison of techniques to
examine the diversity of fungi in adult patients with cystic fi brosis.
Med Mycol 2010; 48 : 166 – 176.
Roig E, Malo JL, Montplaisir S, Anti- 21 Candida albicans IgE and
IgG subclasses in sera of patients with allergic bronchopulmonary
aspergillosis (ABPA). Allergy 1997; 52 : 394 – 403.
M á iz L, Cuevas M, Quirce S 22 et al . Serologic IgE immune responses
against Aspergillus fumigatus and Candida albicans in patients with
cystic fi brosis. Chest 2002; 121 : 782 – 788.
Haase G, Shopnik H, Kusenbach G. 23 Exophiala dermatitidis infec-
tion in cystic fi brosis. Lancet 1990; 336 : 188 – 189.
Matos T, de Hoog GS, de Boer AG, de Crom I, Haase G. High preva-24
lence of the neurotropic Exophiala dermatitidis and related olig-
otrophic black yeasts in sauna facilities. Mycoses 2002; 45 : 373 – 377.
Nagano Y, Milar BC, Goldsmith CE, 25 et al . Development of selective
media for the isolation of yeasts and fi lamentous fungi from the spu-
tum of adult patients with cystic fi brosis (CF). J Cyst Fibros 2008; 7 :
566 – 572.
Rainer J, Kaltseis J, de Hoog GS, Summerbell RC. Effi cacy of a selec-26
tive isolation procedure for members of the Pseudallescheria boydii complex. Antonie van Leeuwenhoek 2008; 93 : 315 – 322.
© 2010 ISHAM, Medical Mycology, 48(Suppl. 1), S88–S97
Doern GV, Brogden-Torres B. Optimum use of selective plated 27
media in primary processing of respiratory tract specimens from
patients with cystic fi brosis. J Clin Microbiol 1992; 30 : 2740 – 2742.
Peltroche-Llacsahuanga H, Dohmen H, Haase G. Recovery of 28
Candida dubliniensis from sputum of cystic fi brosis patients. Mycoses
2002; 45 : 15 – 18.
Kontoyiannis DP, Reddy BT, Torres HA, 29 et al . Pulmonary candidiasis
in patients with cancer: an autopsy study. Clin Infect Dis 2002; 34 :
400 – 403.
Wood GC, Mueller EW, Croce MA, Boucher BA, Fabian TC. 30 Candida
sp. isolated from bronchoalveolar lavage: clinical signifi cance in criti-
cally ill trauma patients. Intensive Care Med 2006; 32 : 599 – 603.
Pappas PG, Kauffman CA, Andes D, 31 et al . Clinical practice guidelines
for the management of candidiasis: 2009 update by the Infectious
Diseases Society of America. Clin Infect Dis 2009; 48 : 503 – 505.
Tavanti, A, Davidson AD, Gow NAR, Maiden MCJ, Odds FC. 32 Can-dida orthopsilosis and Candida metapsilosis spp. nov . to replace
Candida parapsilosis groups II and III. J Clin Microbiol 2005, 43 :
284 – 292.
Balajee SA, Gribskov JL, Hanley E, 33 et al . Aspergillus lentulus sp. nov.,
a new sibling species of A . fumigatus . Eukaryot Cell 2005; 4 : 625 – 632.
Balajee SA, Houbraken J, Verweij PE, 34 et al . Aspergillus species
identifi cation in the clinical setting. Stud Mycol 2007, 59 :39 – 46.
Gilgado F, Cano J, Gen é J, Sutton DA, Guarro J. Molecular and phe-35
notypic data supporting distinct species statuses for Scedosporium apiospermum and Pseudallescheria boydii and the proposed new
species Scedosporium dehoogii . J Clin Microbiol 2008, 46 : 766 – 771.
Balajee SA, Borman AM, Brandt ME, 36 et al . Sequence-based identi-
fi cation of Aspergillus , Fusarium and the Mucorales in the clinical
mycology laboratory: where are we and where should we go from
here? J Clin Microbiol 2009; 47 : 877 – 884.




















