
Knowledge and Perceptions of Newly Graduated Medical Practitioners in Malaysia of Their Role in...
11
Knowledge and Perceptions of Newly Graduated Medical Practitioners in Malaysia of Their Role in Medical Care of People With Developmental DisabilitiesJudith L. Moyle*, Teresa Iacono*, and Merilyn Liddell* † *Centre for Developmental Disability Health, Monash University; and † RMIT University, Melbourne, Vic., Australia Abstract Improving content and consistency on developmental disabilities in undergraduate medical curricula has been recom- mended as a means of improving health outcomes for people with developmental disabilities. Although often the subject of studies in Western countries, little is known about content on developmental disabilities in undergraduate curricula in developing countries. A study was undertaken to: (1) explore content and experience with developmental disabilities received in undergraduate training by medical practitioners in Malaysia; and (2) explore perceptions of their role in the identification and management of developmental disabilities in practice. Comparisons were made according to location of training. Data were collected using a 107-item questionnaire that was administered to 230 newly graduated house officers on their first rotations in seven public hospitals in Peninsula Malaysia. Deficits and inconsistencies were indicated in both content and experience of developmental disabilities during training. Uncertainty about their role in the identification and management of developmental disabilities was evident. Greater inconsistencies and deficits were evident for respondents trained in Eastern and Middle Eastern countries compared with those trained in Malaysia and Western countries. Results suggest a need for increased content, consistency, and intentional exposure in relation to developmental disabilities during undergraduate training across all training settings. Keywords: clinical experience, developmental disabilities, intellectual disabilities, Malaysia, undergraduate medical training INTRODUCTION A major barrier to quality primary medical care for people with intellectual and developmental disabilities (DD) has been lack of knowledge of and experience with this group by primary medical practitioners (e.g., Burge, Ouellette-Kuntz, Isaacs, & Lunsky, 2008; Lian, Ho, & Yeo, 2003; Millar, Chorlton, & Lennox, 2004). Links between poor health status of people with such disabilities and problems with access to quality primary medical care have been well documented (e.g., Durvasula & Beange, 2001; Lin, Wu, & Lee, 2003; Millar et al., 2004). Researchers have argued that caring for people with DD is complex, with numerous factors impacting on the outcomes of their health care (e.g., Beange & Bauman, 1990; Sutherland, Couch, & Iacono, 2002). Knowledge of and experience with DD, however, appears to be a pivotal factor in the provision of effective primary health care to this group. A common recommendation by researchers for improving health outcomes for people with DD has been to improve medical training (e.g., Burge et al., 2008; Lennox, Diggens, & Ugoni, 1997). This issue, however, has attracted only limited direct research attention (e.g., Kerr, 1997; Kerr, Fraser, & Felce, 1996; Lennox & Diggens, 1999a; 1999b). Research focused on under- graduate medical curricula has indicated many inconsistencies in material on DD and associated health conditions (e.g., Burge etal., 2008; Piachaud, 2002; Veltman, Stewart, Tardiff, & Brani- gan, 2001). Furthermore, such studies do exist and have been conducted in Western countries. In examining understanding of the range of developmental delay or disabilities in developing countries, traditional beliefs may need to be considered. In Malaysia, for example, DD have been viewed, historically, according to traditional beliefs where strange appearance or behaviors may be attributed to the influence of evil spirits, spells from jealous neighbors, or punish- ment from deceased ancestors or angry gods (Chen, 2000; Colson, 1971a; 1971b; Groce, 1999). Many people will seek treat- ment from traditional healers (or “bomohs”) when a disability is suspected (Ariff & Lieng, 2002; Edman & Koon, 2000; Heggenhoughen, 1980). Currently, many students from developing countries study away from their country of birth Received March 31, 2009; accepted September 27, 2009 Correspondence: Judith L. Moyle, Centre for Developmental Disability Health, Monash University, Building 1, 270 Ferntree Gully Road, Notting Hill, Vic. 3168, Australia. Tel: +61 3 9501 2400; Fax: +61 3 8575 2270; E-mail: [email protected] Journal of Policy and Practice in Intellectual Disabilities Volume 7 Number 2 pp 85–95 June 2010 © 2010 International Association for the Scientific Study of Intellectual Disabilities and Wiley Periodicals, Inc.
Transcript of Knowledge and Perceptions of Newly Graduated Medical Practitioners in Malaysia of Their Role in...

Knowledge and Perceptions of Newly GraduatedMedical Practitioners in Malaysia of TheirRole in Medical Care of People WithDevelopmental Disabilitiesjppi_252 85..95
Judith L. Moyle*, Teresa Iacono*, and Merilyn Liddell*†
*Centre for Developmental Disability Health, Monash University; and †RMIT University, Melbourne, Vic., Australia
Abstract Improving content and consistency on developmental disabilities in undergraduate medical curricula has been recom-mended as a means of improving health outcomes for people with developmental disabilities. Although often the subject of studiesin Western countries, little is known about content on developmental disabilities in undergraduate curricula in developing countries.A study was undertaken to: (1) explore content and experience with developmental disabilities received in undergraduate training bymedical practitioners in Malaysia; and (2) explore perceptions of their role in the identification and management of developmentaldisabilities in practice. Comparisons were made according to location of training. Data were collected using a 107-item questionnairethat was administered to 230 newly graduated house officers on their first rotations in seven public hospitals in Peninsula Malaysia.Deficits and inconsistencies were indicated in both content and experience of developmental disabilities during training. Uncertaintyabout their role in the identification and management of developmental disabilities was evident. Greater inconsistencies and deficitswere evident for respondents trained in Eastern and Middle Eastern countries compared with those trained in Malaysia and Westerncountries. Results suggest a need for increased content, consistency, and intentional exposure in relation to developmental disabilitiesduring undergraduate training across all training settings.
Keywords: clinical experience, developmental disabilities, intellectual disabilities, Malaysia, undergraduate medical training
INTRODUCTION
A major barrier to quality primary medical care for peoplewith intellectual and developmental disabilities (DD) has beenlack of knowledge of and experience with this group by primarymedical practitioners (e.g., Burge, Ouellette-Kuntz, Isaacs, &Lunsky, 2008; Lian, Ho, & Yeo, 2003; Millar, Chorlton, & Lennox,2004). Links between poor health status of people with suchdisabilities and problems with access to quality primary medicalcare have been well documented (e.g., Durvasula & Beange, 2001;Lin, Wu, & Lee, 2003; Millar et al., 2004). Researchers have arguedthat caring for people with DD is complex, with numerous factorsimpacting on the outcomes of their health care (e.g., Beange &Bauman, 1990; Sutherland, Couch, & Iacono, 2002). Knowledgeof and experience with DD, however, appears to be a pivotalfactor in the provision of effective primary health care to thisgroup.
A common recommendation by researchers for improvinghealth outcomes for people with DD has been to improve medicaltraining (e.g., Burge et al., 2008; Lennox, Diggens, & Ugoni,1997). This issue, however, has attracted only limited directresearch attention (e.g., Kerr, 1997; Kerr, Fraser, & Felce, 1996;Lennox & Diggens, 1999a; 1999b). Research focused on under-graduate medical curricula has indicated many inconsistencies inmaterial on DD and associated health conditions (e.g., Burgeet al., 2008; Piachaud, 2002; Veltman, Stewart, Tardiff, & Brani-gan, 2001). Furthermore, such studies do exist and have beenconducted in Western countries.
In examining understanding of the range of developmentaldelay or disabilities in developing countries, traditional beliefsmay need to be considered. In Malaysia, for example, DD havebeen viewed, historically, according to traditional beliefs wherestrange appearance or behaviors may be attributed to theinfluence of evil spirits, spells from jealous neighbors, or punish-ment from deceased ancestors or angry gods (Chen, 2000;Colson, 1971a; 1971b; Groce, 1999). Many people will seek treat-ment from traditional healers (or “bomohs”) when a disabilityis suspected (Ariff & Lieng, 2002; Edman & Koon, 2000;Heggenhoughen, 1980). Currently, many students fromdeveloping countries study away from their country of birth
Received March 31, 2009; accepted September 27, 2009Correspondence: Judith L. Moyle, Centre for Developmental DisabilityHealth, Monash University, Building 1, 270 Ferntree Gully Road, NottingHill, Vic. 3168, Australia. Tel: +61 3 9501 2400; Fax: +61 3 8575 2270;E-mail: [email protected]
Journal of Policy and Practice in Intellectual DisabilitiesVolume 7 Number 2 pp 85–95 June 2010
© 2010 International Association for the Scientific Study of Intellectual Disabilities and Wiley Periodicals, Inc.

(Athimulum, 2002; Hawthorne, Minas, & Singh, 2004), orafter graduation, find employment in countries other than wherethey were trained (Birrell, 2004; Brechat, Hodges, & Segouin,2005; Hawthorne et al., 2004). In many communities, most prac-titioners will at some time provide treatment for people fromcultural backgrounds other than their own (Lynch, 1998; Yox,2003).
Malaysia has a strong public policy commitment to improv-ing support for people with DD (Jayasooria, Krishnan, & Ooi,1997; Jayasooria & Ooi, 1994). At the time of this study, Malay-sia supported some 10 medical training schools (Suleiman,2000). Now, because of a rapidly expanding education sector,there are some 21 medical schools in Malaysia (MalaysianMedical Resources, 2010). Like most other countries in Asia,Malaysia has a different healthcare history and cultural structurefrom that of Western countries (Suleiman, 1991; 1999; 2000).Little is known, however, about the knowledge of medical prac-titioners in Malaysia in relation to intellectual and DD or oftheir perceptions of their role in the medical care of this groupof people in their local communities. In order to improve theconsistency of knowledge of such disabilities in an increasinglyglobal environment, there is a need to understand how medicalstudents are taught about the range of DD, how medical prac-titioners perceive their role, and whether traditional culturalbeliefs impact treatment choices.
Deficits of knowledge of medical practitioners indicated inresearch conducted in Western settings have included lack ofknowledge or familiarity of particular DD (Lennox, Diggens, &Ugoni, 2000; Lian et al., 2003; Straetmans, 2007), health risksassociated with each (Hagerman & Hagerman, 2004; Jaquemontet al., 2003; Sutherland et al., 2002), the impact of communica-tion impairment(Iacono, Davis, Humphreys, & Chandler, 2003;Lennox et al., 2000; Millar et al., 2004), impact of such disabilitieson family and carers (Baxter, Cummins, & Yiolitis, 2000; Iaconoet al., 2003; Seltzer, Krauss, Orsmond, & Vestal, 2001), and theservices available to support them (Cook & Lennox, 2000; Dur-vasula & Beange, 2001). Furthermore, research has indicated thatmost medical students lack opportunities for face-to-face experi-ence with people with DD during their medical training (Lennoxet al., 2000). According to Paton and Cockburn (1995), the morerecent introduction of alternative modes of learning, such as“Problem-Based Learning” (PBL), may hinder such opportuni-ties. They argued that clinical teaching or a form of clinicalapprenticeship, whereby students observe and practice clinicalactivities under supervision of an experienced practitioner, is stillnecessary for activities such as performing a developmentalassessment. According to Paton and Cockburn (1995), the skillsnecessary for this important activity are not readily obtainedthrough PBL formats.
Face-to-face exposure and practical experience with childrenand adults with developmental delay or disabilities has also beenreported to positively influence attitudes of medical practitionerstoward this group (e.g., Handler et al., 1994; Wolraich & Siper-stein, 1986; Yuker and Hurley, 1987). Of particular interest arefindings indicating a connection between the level and length ofexposure to DD and attitudinal outcomes (Handler et al., 1994;Wolraich & Siperstein, 1986). Handler and his colleagues (1994),for example, argued that exposure combined with clinical expe-rience with people with DD during training was the factor most
likely to effect changes from lower to higher expectations ofoutlook. Lack of such exposure and experience therefore repre-sents an additional barrier to the ability of medical practitionersto provide adequate care for this group (Burge et al., 2008; Cook& Lennox, 2000; Millar et al., 2004).
Aims
The primary aims of this study were to obtain information onnewly graduated Malaysian medical practitioners’ knowledge ofDD, of their role in the care of people with DD, and the impactof traditional beliefs about disability on their treatment of thisgroup. An additional aim, given that many undergraduatestudents study overseas before returning to practice in Malaysia,was to explore differences in knowledge, perceptions of role, andtraditional beliefs according to location of training.
METHOD
Participants Recruitment and Description
Recruitment was from seven large regional and central gov-ernment hospitals throughout Peninsula Malaysia. Participantswere newly graduated medical practitioners (i.e., those indivi-duals having completed undergraduate medical training thatcommenced immediately after secondary school education) froma cohort of approximately 900 housemen on their first or secondpublic hospital rotations in Malaysia. Administrators identifiedcontact persons for each hospital, who distributed invitations tohouse officers and arranged dates and times within departmentsfor completion of questionnaires. In all, 230 (about 26%) newlygraduated house officers completed the survey. Of the responsegroup, 71% had received their training in Malaysia and 29% inother countries.
Instrument
A 107-item questionnaire composed of two main sections wasdeveloped for the purpose of the study. Section one explored (1)recollections of time spent studying DD during training; (2)medical disciplines in which DD were taught; (3) informationreceived about common and less common DD; (4) assessment ofnormal development; (5) face-to-face experience with peoplewith DD during training; and (6) opportunities to observe andpractice clinical activities. Formats of response for the sets ofquestions in this section varied: some used a three-, four-, orfive-point Likert scale; some used yes/no answers.
Section two addressed respondents’ perceptions of their rolein diagnosis and management of DD. Respondents were invitedto respond to an array of statements about identification andmanagement according to four-point Likert scales anchored by“Strongly Disagree” and “Strongly Agree.”
A separate section requested demographic information onage, ethnicity, location of birth, location of growing up, and
Journal of Policy and Practice in Intellectual Disabilities Volume 7 Number 2 June 2010
J. L. Moyle et al. • Disability Training of Malaysian Medical Practitioners
86

location of training. The questionnaire was tested by two medicalpractitioners in Australia prior to the survey being conducted inMalaysia. Minor alterations to wording were made at their sug-gestion. Questionnaire completion took from 20–30 min.
Administration
The survey was administered in Malaysia over a period of sixmonths during 2002 (July to December). At each site, approxi-mately 2 weeks lead-in time at each hospital was provided tosecure the cooperation of the administrator and to obtain poten-tial respondents. To collect the information, respondents at eachsite attended group sessions lasting approximately half an hour.The first researcher distributed the surveys at these sessions andcollected them at the end.
Data Analysis
Data in the form of survey responses were entered into SPSSv12.0 (SPSS Inc., Chicago, IL) and summarized using descriptivestatistics. Comparisons were made for most data according tolocation of training. In order to make comparisons, some loca-tions were combined into regions to increase cell sizes.
Ethical Approval
The study was approved by the Monash University StandingCommittee on Research involving Human Subjects. Consent wasimplied by completion and return of surveys. Permission wasobtained from the Director General of the Ministry of Health,Malaysia, Directors of Health of each state in which the study wasundertaken and the chief executive officers and department headswithin each of the hospitals approached.
FINDINGS
Demographic Characteristics of Respondents
Most respondents were of Malay ethnicity (60%) and mosttrained in Malaysia (71%). Smaller numbers were of Chinese
(21%), Indian (17%), and other (2%) ethnicity. Other respon-dents trained in Eastern and Middle Eastern countries (15%) orWestern countries, including Australia and New Zealand (14%).Most respondents were aged between 25 and 26 years (58%), 17%were aged 22–24 years, and 18% were aged 27–29 years; only a fewwere 30 years or older (4%).
Section One: Exposure and Experience
The underlying intent of questions in section one was toexplore knowledge that resulted through lecture content, expo-sure, and clinical experience during training. Where possible,chi-square was calculated to determine if differences according tolocation of training were significant. From exploration of theoverall length of lecture time exposure devoted to the topic ofDD, less than one-third of the respondents (28%) recalled receiv-ing more than 5 h of lecture time on DD; 65% recalled less than5 h and 7% recalled no lectures on DD during training. Respon-dents who trained in Eastern and Middle Eastern countries weresignificantly less likely to recall having received more than 5 h oflectures on DD compared with respondents trained in Malaysiaand Western countries (c2 = 10.38, df = 2, p = 0.006, standardresidual (SR) = -2.1).
Results from exploration of the level of detail on DD contentin lecture information received in different disciplines duringtraining are summarized in Table 1. Most detailed information ondevelopmental delay or disabilities was received during pediatricand psychiatric lectures. Some information was received duringmedical disciplines of family medicine and public health. Nocomparisons according to location of training reached a signifi-cance of p = 0.012 (adjusted for family-wise error). Resultsdescribing the amount of information received on commonlyoccurring DD are summarized in Table 2. Significant differences(set at p = 0.003 to adjust for family-wise error) in the amount ofinformation received on some disabilities were found when com-parisons were made for locations of training (see Table 3).
Training related to the assessment of children using normaldevelopmental milestones (NDMs) in written, lecture, observa-tion, and practice formats was explored. Most respondentsreceived written information (89%) and lectures (93%) onNDMs during training, and most both observed and practicedusing NDMs with a child, but there was variation in terms of thedisciplines in which they received face-to-face exposure. The per-
TABLE 1Level of detail of information on developmental disabilities received in lectures in different medical disciplines
Medical discipline Association with location of training N
Amount reported (%)
None Some Detailed
Pediatrics c2 = 6.48; df = 2; p = 0.039 223 0.9 39.3 58.9Psychiatry c2 = 7.11; df = 2; p = 0.029 219 14.2 49.8 36.1Family medicine c2 = 2.50; df = 4; p = 0.65 213 16.8 67.3 14.6Public health c2 = 7.11; df = 2; p = 0.029 217 36.9 53.5 9.7
Note: n = valid responses, % = percentage of respondents; df = degrees of freedom.
Journal of Policy and Practice in Intellectual Disabilities Volume 7 Number 2 June 2010
J. L. Moyle et al. • Disability Training of Malaysian Medical Practitioners
87

centages of respondents reporting face-to-face exposure withineach department were as follows: 98% in pediatric, 64% in psy-chiatric, 47% in medical, 17% in surgical, 30% in orthopedic,34% in public health, and 48% in family medicine departments.No significant association with location of training was foundfor written information received on NDMs (c2 = 8.13, df = 2,p = 0.017), or lectures received (c2 = 0.753, df = 1, p = 0.385),using p = 0.016 to account for family-wise error. A significantassociation was found, however, with observation of a develop-mental assessment using NDMs (c2 = 16.87; df = 2; p = 0.000).This association was accounted for by those medical personnelwho trained in Eastern and Middle Eastern countries who wereless likely to have observed a developmental assessment usingNDMs (SR = 3.2) compared with respondents who trained inMalaysia and Western countries. Chi-square is not reported forlocation of training and opportunity to practice developmentalassessment against NDMs because expected counts of some crosstabulations were less than five.
Opportunities to observe and practice clinical activities with achild or adult with a developmental delay or disability arereported in Table 4. Although most respondents had opportuni-ties to observe clinical activities with people with such disabilitiesduring training, other than when the activity was to assess a childagainst NDMs, far fewer had opportunities for practice.
Section Two: Perception of Role in Identification and Management
As the questionnaire was developed for the purpose of thecurrent study, the section on perceptions was analyzed for its
underlying constructs. Factor analyses were conducted on the 21items in the questionnaire for identification and the 25 itemsfor management of a developmental disability. As a first step,assumptions were tested to ensure the data were suitable forfactor analysis (Hutcheson & Sofroniou, 1999). Correlationmatrices were inspected to ensure correlation among items. Itemsthat correlated poorly with other items were deleted. To ensuresampling adequacy, items with poor Kaiser-Meyer-Olkin scores(less than 0.7) were deleted until an overall score of 0.7 wasobtained, thereby exceeding the minimum value of 0.6 recom-mended by Hutcheson and Sofroniou (1999). As a result, 15 itemsfor identification and 18 items for management were included inthe factor analysis. These items were subjected to principal com-ponents analysis using SPSS v 12.0. For items for identification, afive-factor solution explained 58% of the variance and capturedmost of the original intent of questions included. For items formanagement, a five-factor solution explained 52% of the varianceand captured most of the original intent of the questions.
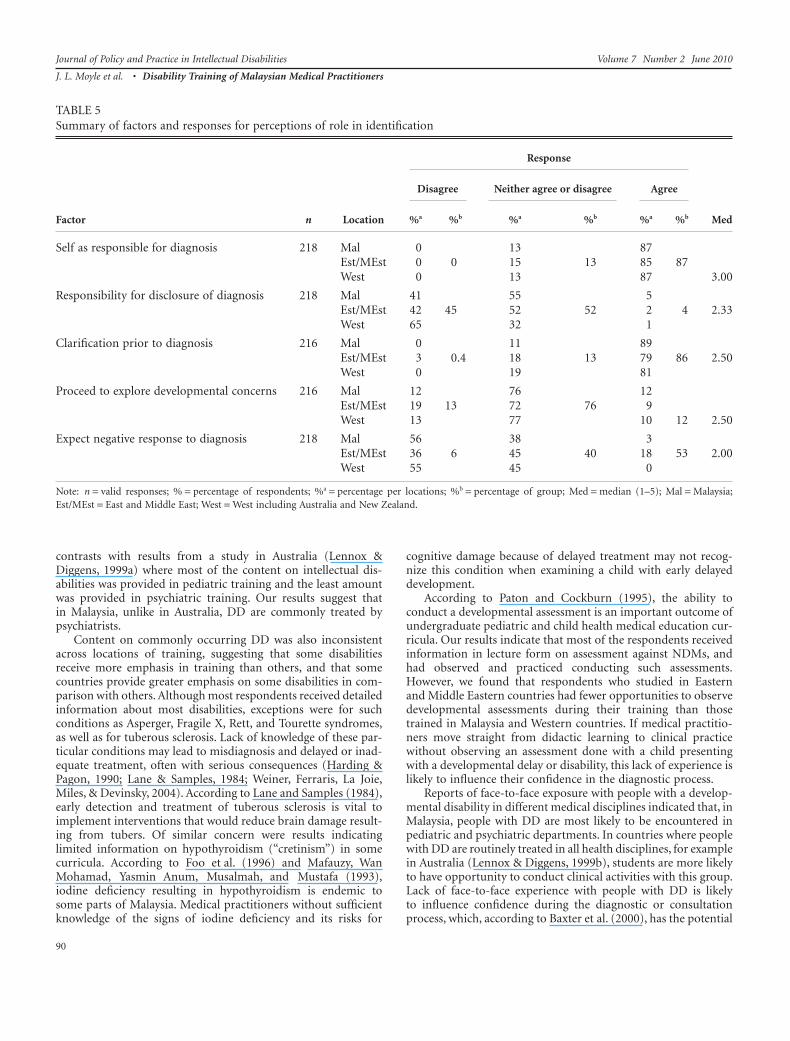
Results for factors describing perceptions of roles in identifi-cation of DD are summarized in Table 5. Patterns evident fromthis table include that although respondents irrespective of train-ing location agreed they should be responsible for making a diag-nosis, most were uncertain about, or would not disclose thisinformation to parents. Furthermore, although most agreed theywould explore further prior to making a diagnosis, they wereuncertain about when they should proceed to do so. Although alittle over half of the respondents felt parents would wish to knowabout their child’s disability, others were uncertain of howparents would respond.
Data on respondents’ perceptions of role in medical caremanagement are presented in Table 6, inspection of which indi-cates a consistent lack of appreciation of the importance of earlyintervention for DD across the whole group. In contrast, percep-tions about where to access resources varied according to locationof training. Most respondents would be sensitive to the impact ofa developmental disability on the family; whereas, taking respon-sibility to follow-up after a diagnosis of a developmental delay ordisability varied according to location of training. Few of therespondents accepted traditionally held beliefs about the cause ofa disability or negative attitudes toward people with disabilities.
DISCUSSION
Our study indicated content received on the topic of develop-mental delay or disabilities during undergraduate medical train-ing was limited and inconsistent across training schools, therebyproviding support for similar findings of previous studies con-ducted in Western countries (e.g., Burge et al., 2008; Lennox &Diggens, 1999a; 1999b; Lennox et al., 1997). Perceptions thatnewly graduated medical practitioners in Malaysia had of theirrole in the medical care of children or adults with these types ofdisabilities were mixed, with most lacking awareness of theimportance of early intervention. Furthermore, although mostfelt they should be able to make a diagnosis, most would beunsure about when or how to explore developmental concerns,that is, the implications of that diagnosis, and reported that theywould be reluctant to disclose a diagnosis to family members. Infact, most would refer patients with a developmental disability to
TABLE 2Information received on commonly occurring developmentaldisabilities
Disability type n
Amount reported
None or some Detailed% %
Down syndrome 225 6 94Cerebral palsy 226 8 92Turner syndrome 226 19 81Spina bifida 225 20 80Hydrocephaly 225 20 80ADHD 225 35 65Autism 225 40 60Anencephaly 226 42 58Hypothyroidism (“Cretinism”) 225 47 53Tuberous sclerosis 225 53 47Fetal alcohol syndrome 225 64 36Fragile X 225 71 29Tourette syndrome 225 79 21Asperger syndrome 225 89 11Rett syndrome 225 93 7
Note: n = number of respondents who completed each item; ADHD =attention deficit hyperactivity disorder.
Journal of Policy and Practice in Intellectual Disabilities Volume 7 Number 2 June 2010
J. L. Moyle et al. • Disability Training of Malaysian Medical Practitioners
88

specialists for management, lacking the confidence to identifyand manage these conditions themselves. They tended to believeit is not their role to care for people with DD in primarypractice. Most respondents, however, denied that they were influ-enced by traditional beliefs about disability on the way theywould practice.
By exploring these issues in Malaysia, this study provided (1)an insight not available in previous studies into how training hasprepared medical practitioners in a developing country formedical care of people with developmental delay or disabilities;and (2) a basis for comparison of results for these issues betweenlocations of training in Malaysia, Eastern, Middle Eastern, andWestern countries.
Content on Developmental Disabilities in Curricula
Variation in the amount of content addressing DD in under-graduate medical education curricula across training schools, asfound in this study, has been reported previously (e.g., Claxton,1994; Lennox & Diggens, 1999a). Such variability has implica-tions for medical practitioners in a global environment wherestudents may have studied at locations other than where they willpractice after graduation and where expectations for knowledgeand responsibility in the care of DD may vary across settings. Insettings where a basic level of knowledge of DD is anticipated,newly graduated medical practitioners without such knowledgewill be unable to fulfill the expectations of people with DD andtheir families for an adequate level and quality of service.
We observed that content in lecture form was equally concen-trated in both pediatric and psychiatric curricula. This finding
TABLE 3Summary of differences of information received on disabilities according to locations of training
Condition and c2
Results
Significant comparisons for information received
West/Aust/NZ East/M-East Malaysia
Little or No Detailed Little or No Detailed Little or No Detailed
Asperger syndc2 = 14.25; df = 2;p = 0.001
Less likely thanothers
More likely thanothers
SR = -2.1 SR = 2.6
Autism c2 = 35.26;df = 2; p = 0.000
Less likely thanothers
More likely thanothers
More likely thanothers
Less likely thanothers
SR = -2.6 SR = 2.1 SR = 3.3 SR = -2.7
Fragile X c2 = 16.47;df = 2; p = 0.000
Less likely thanothers
More likely thanothers
SR = -2.1 SR = 3.1
Spina bifidac2 = 17.49; df = 2;p = 0.000
Less likely thanothers
More likely thanothers
SR = -2.1 SR = 3.5
ADHD c2 = 24.61;df = 2; p = 0.000
More likely thanothers
SR = 3.0
Tourette syndc2 = 16.41; df = 2;p = 0.000
Less likely thanothers
More likely thanothers
Less likely thanothers
SR = -4.0 SR = 2.1 SR = -2.1
Note: Synd = syndrome; SR = standard residual; East/M-East = Eastern and Middle Eastern; West/Aust/NZ = Western, including Australia and New Zealand;ADHD = attention deficit hyperactivity disorder; df = degrees of freedom.
TABLE 4Opportunity to observe and practice clinical activities with achild or adult with a developmental disability during training
Clinical activity (n)
Responses (%)
Observe Practice
Assessment of child against NDMs (226) 89 88Assessment for diagnosis (217) 59 41Giving management advice (219) 71 29Medical treatment (219) 80 20Consultation for illness (212) 80 20Surgical intervention (187) 94 6
Note: n = valid responses; % = percentage of respondents; NDM = normaldevelopmental milestones.
Journal of Policy and Practice in Intellectual Disabilities Volume 7 Number 2 June 2010
J. L. Moyle et al. • Disability Training of Malaysian Medical Practitioners
89
contrasts with results from a study in Australia (Lennox &Diggens, 1999a) where most of the content on intellectual dis-abilities was provided in pediatric training and the least amountwas provided in psychiatric training. Our results suggest thatin Malaysia, unlike in Australia, DD are commonly treated bypsychiatrists.
Content on commonly occurring DD was also inconsistentacross locations of training, suggesting that some disabilitiesreceive more emphasis in training than others, and that somecountries provide greater emphasis on some disabilities in com-parison with others. Although most respondents received detailedinformation about most disabilities, exceptions were for suchconditions as Asperger, Fragile X, Rett, and Tourette syndromes,as well as for tuberous sclerosis. Lack of knowledge of these par-ticular conditions may lead to misdiagnosis and delayed or inad-equate treatment, often with serious consequences (Harding &Pagon, 1990; Lane & Samples, 1984; Weiner, Ferraris, La Joie,Miles, & Devinsky, 2004). According to Lane and Samples (1984),early detection and treatment of tuberous sclerosis is vital toimplement interventions that would reduce brain damage result-ing from tubers. Of similar concern were results indicatinglimited information on hypothyroidism (“cretinism”) in somecurricula. According to Foo et al. (1996) and Mafauzy, WanMohamad, Yasmin Anum, Musalmah, and Mustafa (1993),iodine deficiency resulting in hypothyroidism is endemic tosome parts of Malaysia. Medical practitioners without sufficientknowledge of the signs of iodine deficiency and its risks for
cognitive damage because of delayed treatment may not recog-nize this condition when examining a child with early delayeddevelopment.
According to Paton and Cockburn (1995), the ability toconduct a developmental assessment is an important outcome ofundergraduate pediatric and child health medical education cur-ricula. Our results indicate that most of the respondents receivedinformation in lecture form on assessment against NDMs, andhad observed and practiced conducting such assessments.However, we found that respondents who studied in Easternand Middle Eastern countries had fewer opportunities to observedevelopmental assessments during their training than thosetrained in Malaysia and Western countries. If medical practitio-ners move straight from didactic learning to clinical practicewithout observing an assessment done with a child presentingwith a developmental delay or disability, this lack of experience islikely to influence their confidence in the diagnostic process.
Reports of face-to-face exposure with people with a develop-mental disability in different medical disciplines indicated that, inMalaysia, people with DD are most likely to be encountered inpediatric and psychiatric departments. In countries where peoplewith DD are routinely treated in all health disciplines, for examplein Australia (Lennox & Diggens, 1999b), students are more likelyto have opportunity to conduct clinical activities with this group.Lack of face-to-face experience with people with DD is likelyto influence confidence during the diagnostic or consultationprocess, which, according to Baxter et al. (2000), has the potential
TABLE 5Summary of factors and responses for perceptions of role in identification
Factor n Location
Response
Med
Disagree Neither agree or disagree Agree
%a %b %a %b %a %b
Self as responsible for diagnosis 218 Mal 0 13 87Est/MEst 0 0 15 13 85 87West 0 13 87 3.00
Responsibility for disclosure of diagnosis 218 Mal 41 55 5Est/MEst 42 45 52 52 2 4 2.33West 65 32 1
Clarification prior to diagnosis 216 Mal 0 11 89Est/MEst 3 0.4 18 13 79 86 2.50West 0 19 81
Proceed to explore developmental concerns 216 Mal 12 76 12Est/MEst 19 13 72 76 9West 13 77 10 12 2.50
Expect negative response to diagnosis 218 Mal 56 38 3Est/MEst 36 6 45 40 18 53 2.00West 55 45 0
Note: n = valid responses; % = percentage of respondents; %a = percentage per locations; %b = percentage of group; Med = median (1–5); Mal = Malaysia;Est/MEst = East and Middle East; West = West including Australia and New Zealand.
Journal of Policy and Practice in Intellectual Disabilities Volume 7 Number 2 June 2010
J. L. Moyle et al. • Disability Training of Malaysian Medical Practitioners
90

to impact negatively on patients and their families, and lead todistrust of practitioners.
Many respondents noted that they had lacked opportunities toconduct clinical activities with people with DD during their train-ing. It might be concluded that clinical experience with any popu-lation could be transferred to people with disabilities, but sucha conclusion has been challenged by previous researchers (Lennox& Diggens, 1999a; 1999b; Taplin, 1994). Clinical activities withpeople with DD differ in many ways to those of the generalpopulation. For example, people with DD with speech or cognitivedeficits are frequently unable to either identify or describe theirhealth problems to practitioners (Iacono et al., 2003; Lennox et al.,1997). Furthermore, according to Lennox et al. (1997), other bar-riers such as difficulties of access, dependence on carers, financialhardships, and challenging behaviors will impact on the success ofconsultations with this group. Newly graduated medical practitio-ners with no previous clinical experience with DD may be over-whelmed by the challenges they face in identifying problemsand making care management recommendations (Taplin, 1994).When lack of experience and confidence is combined with lack ofknowledge about commonly occurring disabilities, people withDD and their families are likely to be left with unmet health andemotional needs and children at risk of further developmentaldamage (Baxter et al., 2000; Lane & Samples, 1984).
Another concern which may arise because of the lack ofclinical practice is that, in many instances, families are isolatedfrom medical practitioners because of vast distance to the nearestmedical center or a lack access to suitable transport. Conse-
quently, some patients may present only once for consultationwith a medical practitioner (Colson, 1971a; 1971b; Iacono et al.,2003). According to Baxter et al. (2000) and Cahill and Masters-Glidden (1996), the quality of the first consultation will oftenaffect how families or carers view the role of medicine in theirfuture management of their family member. Additionally, withinsettings such as in Malaysia, where there are few allied therapysupports, families may expect medical practitioners to provide allof the information they require for the management of theirfamily member (e.g., Ariff, 2000, Ariff & Lieng, 2002; Colson,1971a). Should the medical practitioner lack the knowledge,experience, and resources to provide adequate support, familiesare likely to experience great hardship in the care of their child oradult with a disability. Compulsory inclusion of clinical encoun-ters with people presenting with DD as a routine part of under-graduate curricula may ensure that many of the necessaryskills for the healthcare of people with DD are addressed duringtraining,
Perception of Role in Identification
The overall picture of uncertainty on the role the respondentswould play in identification of DD, as indicated by the results,suggested that the respondents felt ill-prepared to attempt a diag-nosis of a developmental disability. Despite their confusionaround how and when a diagnosis should be made, most indi-cated that they ought to be able to do so. Reports of positive
TABLE 6Summary of factors and responses for perceptions of role in management
Factor n Location
Response
Med
Disagree Neither agree or disagree Agree
%a %b %a %b %a %b
Access to resources and advice Mal 0.64 68 32217 Est/MEst 6 1 47 65 47 34
West 0 68 32 2.75
Early intervention and support important in management 214 Mal 24 74 2Est/Mest 32 26 61 65 6 42 2.33West 29 71 0
Take responsibility after diagnosis 217 Mal 1 18 81Est/MEst 3 1 22 18 75 72 3.00West 0 10 90
Sensitive to the impact of disability on families 215 Mal 0 54 46Est/MEst 0 0 45 52 55 48 2.83West 0 45 55
Traditional beliefs about cause and attitudes aboutdisabilities
215 Mal 56Est/MEst 36 90 9 0.5 1.6West 55
Note. n = valid responses; % = percentage of respondents; %a = percentage per locations; %b = percentage of group; Med = median; Mal = Malaysia;Est/MEst = East and Middle East; West = West including Australia and New Zealand.
Journal of Policy and Practice in Intellectual Disabilities Volume 7 Number 2 June 2010
J. L. Moyle et al. • Disability Training of Malaysian Medical Practitioners
91

intentions toward the provision of primary care to people withdisabilities have been reported in previous research (e.g., Cham-bers, Milsom, Evans, Lucking, & Campbell, 1998; Dovey & Webb,2000; Kerr et al., 1996). According to Chambers et al. (1998),however, few practitioners were able to follow through on theirgood intentions. Barriers, such as lack of knowledge, lack of time,financial impost, dependence on others to bring patients toappointments, and other practice pressures, were cited by Cham-bers and colleagues as reasons for not following up after initialconsultation. Such reports suggest that, despite their good inten-tions, our respondents were likely to encounter similar barriers tothe provision of quality primary care for people with DD as theyprogress in primary practice.
Uncertainty about when to explore clinical concerns wasconsistent across all locations of training. Implied by items inthe questionnaire that formed this factor (in the factoranalysis—Hutcheson & Sofroniou, 1999) was a “wait-and-see”approach on the part of practitioners to concerns expressed byparents. Such hesitancy suggested (1) a lack of teaching duringundergraduate medical training on the commonly agreed prac-tice to intervene as soon as possible after a developmental delay issuspected; and (2) lack of knowledge of the possible conse-quences of delayed exploration (e.g., Weiner et al., 2004).
Uncertainty about the process for the diagnosis of a develop-mental delay or disability may therefore arise from a combinedlack of knowledge about such conditions, limited exposure andclinical experience with people with DD during training, andpoor understanding of the importance for urgency. In addition,unwillingness to disclose a diagnosis might reflect a commonlyheld belief that the responsibility for diagnosis resides with spe-cialist physicians. Support for this explanation is found in previ-ous studies (e.g., Bernard & Bates, 1994; Cumella, Corbett,Clarke, & Smith, 1992), where, under medical models of care inWestern countries, DD were considered to fall into the domain ofspecialist practitioners, usually pediatricians and/or psychiatrists.Given our results which suggest that DD in Malaysia are morelikely to be treated in pediatric and psychiatric departments, itcould be concluded that respondents may expect that it will be theresponsibility of a specialist in these disciplines to confirm adiagnosis.
Perception of Role in Management
We also found that most respondents were unsure aboutwhere to access resources about DD and that most tended not tosee early intervention as an important care management strategy.This provides further support to the overall picture of uncertaintyabout managing DD. Nevertheless, encouraging was that mostrespondents indicated they would provide follow-up medicalmanagement after a diagnosis, and, although most were unsureabout the impact of a developmental disability on the family,many tended toward being sensitive to the impact it might have.This result indicated that, despite their lack of knowledge aboutsuch disabilities, most respondents had positive attitudes aboutcaring for this group. Further support for this is provided in thatmost respondents did not accept traditional beliefs about thecause of DD and other negative attitudes about disability knownto be held by some people in communities in Malaysia.
The importance to families of the provision of informationand resources by their primary medical practitioners has beenreported in previous research (Baxter et al., 2000; Hasnat &Graves, 2000). Inconsistency of access to information andresources on DD suggested that, on the whole, undergraduatemedical students received insufficient training on where to accessinformation and resources in order to manage DD in primarypractice. Similar deficits have been reported by medical practitio-ners in studies conducted in Western countries (e.g., Cook &Lennox, 2000; Iacono et al., 2003; Marshall et al., 1996).
With respect to a sense of responsibility after diagnosis along-side that of an intention to disclose a diagnosis suggest that newlygraduated medical practitioners in Malaysia feel they would beresponsible for the general healthcare of a person with a disability,but may not feel responsible for the management of the disabil-ity itself. Such an interpretation or explanation could be drawnfrom results if they reflected the belief that responsibility formanaging DD resides with specialists rather than with primarypractitioners.
Lack of teaching on the importance of early intervention mayrepresent an example of a failure, because of lack of resources insome countries, to upgrade undergraduate medical training cur-ricula in line with advances of knowledge gained by research. Ofconcern is that the value of intervening early has been describedin research in Western countries for a number of decades (Cen-terwall, 1971; Haber, 1991; Marfo, 1991). Furthermore, earlyintervention centers for children with a developmental delay havebeen established in Malaysia since the early 1990s (Lim, 2007;Wong, 1993; Young, 1991). Lack of emphasis on this issue inundergraduate medical curricula in Malaysia and elsewhere istherefore puzzling.
Decisions by medical practitioners to delay exploration ofparental concerns, when considered with results indicating lack ofknowledge of some DD that pose a risk to the ongoing health ordevelopment of a child (e.g., tuberous sclerosis, hypothyroidism),suggest that such delays may lead to some children in Malaysiasuffering further, albeit preventable, damage (Mafauzy et al.,1993; Weiner et al., 2004), and parents therefore suffering greaterdistress than might otherwise have been expected (Baxter et al.,2000; Nursey, Rohde, & Farmer, 1992).
Lack of practice in the assessment of children with suspectedDD was evident for some of the respondents. The results indicat-ing a lack of confidence to disclose a diagnosis suggest support forthe recommendations made by Paton and Cockburn (1995) oneof which was the retention in training of observation and practiceof some clinical activities under the supervision of experiencedmedical practitioners. With this in mind, we observed that, whileslightly less than half of the respondents indicated sensitivity tothe impact of diagnosis of a developmental disability on a family,slightly more than half were unsure of the impact a diagnosis ofDD would have. Using Paton and Cockburn’s argument, skills insensitivity and empathy are more likely to be obtained if modeledby experienced practitioners in a clinical situation with peoplewith DD and their families.
Although there is a strong history of traditional beliefs aboutthe cause of DD in Malaysian communities (Azhar, Varma, &Hakim, 1995; Edman & Koon, 2000), few respondents in thecurrent study held those beliefs themselves. Furthermore, fewwould approach people with a developmental disability with
Journal of Policy and Practice in Intellectual Disabilities Volume 7 Number 2 June 2010
J. L. Moyle et al. • Disability Training of Malaysian Medical Practitioners
92

negative attitudes or negative perceptions of their value as a resultof the beliefs and attitudes held in the community. Although therespondents strongly rejected traditional interpretations aboutthe causes of disabilities, evidence that such interpretations arestill common in Malaysia is nevertheless strong in the literature(Ariff, 2000; Chen, 2000). It is important therefore that under-graduate curricula for medical practitioners in Malaysia containinformation on how traditional beliefs about DD may impact onfamilies attending for consultation, and who may also consulttraditional healers alongside modern medical practitioners (e.g.,Razali, Khan, & Hasanah, 1996).
Clinical Implications
Without a core level of disability knowledge, it is unlikelythat newly graduated medical practitioners will be able to meetthe basic healthcare needs of children with developmental delayor intellectual disabilities. Strategies are therefore needed toavoid delaying assessment and intervention of infants and youngchildren with delayed development, thereby reducing the risk offurther damage. In countries with limited allied health serviceswhere medical practitioners are likely to be the sole providers ofinformation for people with disabilities, it is important for prac-titioners to have sufficient knowledge and information to passon. Furthermore, in settings where DD are routinely treated inpsychiatric and pediatric departments, strategies should beintroduced to ensure health conditions common to young andolder adults with DD (e.g., metabolic disorders, heart disease)are able to be recognized often by practitioners as the source ofchallenging behaviors and deteriorating mental health. Withoutsufficient knowledge and information about appropriate care,people with DD will continue to experience poorer health statusand quality of life compared with people who do not havedisabilities.
Research Implications
The current study was limited by a lack of pretesting of thequestionnaire prior to the study. As a consequence, when factoranalyses were conducted to explore construct validity, a numberof questions were omitted. Pretesting would have removed prob-lematic questions prior to data collection, thus reducing ques-tionnaire completion time. A second limitation was that thequestionnaire was developed in a Western context and was pre-sented in English. Although all respondents were English speak-ing, for most it was their second language. Finally, because thestudy was conducted in the hospitals where the respondents werepracticing, response rates were limited by pressures of work andthe willingness of department heads to release respondents fromtheir duties.
Results from this study suggest a need for a more direct studyof the curricula for DD currently provided by medical schools,both in Malaysia and in other countries from which studentsfrom Malaysia obtain their training, rather than relying onrespondent recall and report. A second issue for future researcharising from this study is a need to explore the most effective waysto teach knowledge and management of DD to undergraduate
medical students. In particular, consideration needs to be given tohow best to prepare students to practice in locations with limitedresources and/or diverse cultural beliefs and health practices.Finally, in recognition of the increasingly global nature of medicaleducation, research is needed to identify ways to develop interna-tional standards for the inclusion of DD in undergraduatemedical education curricular.
Conclusions
The overall impression gleaned from this study is that under-graduate medical training of Malaysian medical practitionersvaried, was inconsistent across training settings, and did notequip newly graduated medical practitioners with sufficientknowledge and experience to effectively care for people with DDin primary practice. Lacking were knowledge of particular dis-abilities, experience in conducting clinical activities with thisgroup, skills on how to access information and resources relatedto DD, awareness of the importance of early intervention, andknowledge about when to intervene. Uncertainty about thesemany aspects of the care of people with DD suggests that theindecisiveness of newly graduated medical practitioners in theircare is likely to adversely influence health outcomes of this groupin Malaysia, and in other countries where respondents to thisstudy practice.
REFERENCES
Ariff, K. M. (2000). Preferential utilisation of healthcare systems by aMalaysian rural community for the treatment of musculoskeletalinjuries. The Medical Journal of Malaysia, 55, 451–458.
Ariff, K. M., & Lieng, T. C. (2002). Rural health care in Malaysia. TheAustralian Journal of Rural Health, 10, 99–103.
Athimulum, N. (2002, July 3). Malaysian students in foreign medicalinstitutions. Malaysian Medical Association News, 21.
Azhar, M. Z., Varma, S. L., & Hakim, H. R. (1995). Phenomenologicaldifferences of delusions between schizophrenic patients of two cul-tures in Malaysia. Singapore Medical Journal, 36, 273–275.
Baxter, C., Cummins, R. A., & Yiolitis, L. (2000). Parental stress attributedto family members with and without disability: A longitudinal study.Journal of Intellectual and Developmental Disability, 25, 105–118.
Beange, H., & Bauman, A. (1990). Caring for the developmentallydisabled in the community. Australian Family Physician, 19, 1555,1558–1563.
Bernard, S., & Bates, R. (1994). The role of the psychiatrist in learningdisability: How it is perceived by the general practitioner. PsychiatricBulletin, 18, 205–206.
Birrell, R. J. (2004). Australian policy on overseas trained doctors. MedicalJournal of Australia, 181, 635–639.
Brechat, P. H., Hodges, B., & Segouin, C. (2005). Globalization in healthcare: Is international standardization of quality a step toward out-sourcing? International Journal for Quality in Health Care, 17, 277–279.
Burge, P., Ouellette-Kuntz, H., Isaacs, B., & Lunsky, Y. (2008). Medicalstudent’s views on training in intellectual disabilities. CanadianFamily Physician, 54, 568–571.
Cahill, B. M., & Masters-Glidden, L. (1996). Influence of child diagnosison family and parental functioning: Down syndrome versus otherdisabilities. American Journal on Mental Retardation, 101(2), 149–160.
Journal of Policy and Practice in Intellectual Disabilities Volume 7 Number 2 June 2010
J. L. Moyle et al. • Disability Training of Malaysian Medical Practitioners
93

Centerwall, S. A. (1971). The mentally retarded and the family physician:Results of a survey of Michigan doctors. Michigan Medicine, 69, 597–602.
Chambers, R., Milsom, G., Evans, N., Lucking, A., & Campbell, I. (1998).The primary care workload and prescribing costs associated withpatients with learning disability discharged from long-stay care to thecommunity. British Journal of Learning Disabilities, 26, 9–12.
Chen, P. C. Y. (2000). Traditional and modern medicine in Malaysia.Medical Journal of Malaysia, 55 (Suppl B), 5–8.
Claxton, A. (1994). Teaching medical students about disability. BritishMedical Journal, 308, 805–806.
Colson, A. C. (1971a). The differential use of medical resources in devel-oping countries. Journal of Health and Social Behaviour, 12, 226–237.
Colson, A. C. (1971b). The prevention of illness in a Malay village: Ananalysis of concepts and behaviour. Monograph Series 2. WinstonSalem: Wake Forest University.
Cook, A., & Lennox, N. (2000). General practice registars’ care of peoplewith intellectual disabilities. Journal of Intellectual and DevelopmentalDisability, 25, 69–77.
Cumella, S., Corbett, J., Clarke, D., & Smith, B. (1992). Primary healthcarefor people with a learning disability. Mental Handicap, 20, 123–125.
Dovey, S., & Webb, O. J. (2000). General practitioners’ perception of theirrole in care for people with intellectual disability. Journal of Intellec-tual Disability Research, 44, 553–561.
Durvasula, S., & Beange, H. (2001). Health inequalities in people withintellectual disability: Strategies for improvement. Health PromotionJournal of Australia, 11, 27–31.
Edman, J. L., & Koon, T. Y. (2000). Mental illness beliefs in Malaysia:Ethnic and intergenerational comparisons. The International Journalof Social Psychiatry, 46, 101–109.
Foo, L. C., Zainah, T., Goh, S. Y., Letchuman, G. R., Nafikudin, M.,Doraisingam, P., et al. (1996). Iodisation of village water supply in thecontrol of endemic iodine deficiency in rural Sarawak, Malaysia.Biomedical and Environmental Science, 9, 236–241.
Groce, N. E. (1999). Disability in cross-cultural perspective: Rethinkingdisability. Lancet, 354, 756–757.
Haber, J. (1991). Early diagnosis and referral of children with develop-mental disabilities. American Family Physician, 43, 132–140.
Hagerman, P. J., & Hagerman, R. J. (2004). The fragileX premutation: Amaturing perspective. American Journal of Human Genetics, 74, 805–816.
Handler, E. G., Bhardwaj A., & Jackson, D. S. (1994). Medical students’and allied health care professionals’ perceptions toward the mentallyretarded population. Journal of Developmental & Physical Disabilities,6(3), 291–297.
Harding, C. O., & Pagon, R. A. (1990). Incidence of tuberous sclerosis inpatients with cardiac rhabdomyoma. American Journal of MedicalGenetics, 37, 443–446.
Hasnat, M. J., & Graves, P. (2000). Disclosure of developmental disability:A study of parent satisfaction and the determinants of satisfaction.Journal of Paediatrics and Child Health, 36, 32–35.
Hawthorne, L., Minas, H., & Singh, B. (2004). A case study in the global-ization of medical education: Assisting overseas-born students at theUniversity of Melbourne. Medical Teacher, 26, 150–159.
Heggenhoughen, H. K. (1980). Bomohs, doctors and sinsehs: Medicalpluralism in Malaysia. Social Science and Medicine (Medical Anthro-pology), 14B, 235–244.
Hutcheson, G., & Sofroniou, N. (1999). Factor analysis. In K. A. Bollen &J. S. Long (Eds.), The multivariate social scientist (pp. 217–251).London: Sage.
Iacono, T., Davis, R., Humphreys, J., & Chandler, N. (2003). GP andsupport people’s concerns and priorities for meeting the health careneeds of individuals with developmental disabilities: A metropolitanand non-metropolitan comparison. Journal of Intellectual and Devel-opmental Disability, 28, 353–368.
Jaquemont, S., Hagerman, R. J., Leehey, M., Grigsby, J., Zhang, L., Brun-berg, J. A., et al. (2003). Fragile X premutation tremor/ataxia syn-drome: Molecular, clinical and imaging correlates. American Journalof Human Genetics, 72, 869–878.
Jayasooria, D., Krishnan, B., & Ooi, G. (1997). Disabled people in a newlyindustrialised economy: Opportunities and challenges in Malaysia.Disability and Society, 12, 445–463.
Jayasooria, D., & Ooi, G. (1994). Disabled people’s movement inMalaysia. Disability and Society, 9, 97–100.
Kerr, M., Fraser, W., & Felce, D. (1996). Primary health care for peoplewith a learning disability. Mental Handicap, 24, 2–8.
Kerr, M. P. (1997). Primary health care for people with anintellectual disability. Journal of Intellectual Disability Research, 41,363–364.
Lane, W., & Samples, J. (1984). Tuberous sclerosis: Case study of earlyseizure control and subsequent normal development. Journal ofAutism and Developmental Disorders, 14, 423–427.
Lennox, N., & Diggens, J. (1999a). Medical education and intellectualdisability: A survey of Australian medical schools. Journal of Intellec-tual and Developmental Disability, 24, 333–340.
Lennox, N., & Diggens, J. (1999b). Knowledge, skills and attitudes:Medical schools’ coverage of an ideal curriculum on intellectual dis-ability. Journal of Intellectual and Developmental Disability, 24, 341–347.
Lennox, N., Diggens, J., & Ugoni, A. (1997). Barriers and solutions to thegeneral practice care of people with an intellectual disability. Journalof Intellectual Disability Research, 41, 380–390.
Lennox, N., Diggens, J., & Ugoni, A. (2000). Health care for people withan intellectual disability: General Practitioners’ attitudes, and provi-sion of care. Journal of Intellectual and Developmental Disability, 25,127–133.
Lian, W. B., Ho, S. K. Y., & Yeo, L. Y. (2003). General practitioner’sknowledge on childhood developmental and behavioural disorders.Singapore Medical Journal, 44, 397–403.
Lim, B. H. (2007). From the ground up: Constructing an early interventionprogram in Malaysia. Unpublished doctoral disseration, Departmentof Education, Deakin University, Geelong, Australia.
Lin, J. D., Wu, J. L., & Lee, P. N. (2003). Healthcare needs of people withintellectual disability in institutions in Taiwan. Journal of IntellectualDisability Research, 47, 169–180.
Lynch, E. W. (1998). Developing cross-cultural competence. In E. W.Lynch & M. J. Hanson (Eds.), Developing cross-cultural competence: Aguide to working with young children and their families (pp. 47–90).Baltimore: Paul H. Brookes.
Mafauzy, M., Wan Mohamad, W. B., Yasmin Anum, M. Y., Musalmah,M., & Mustafa, B. E. (1993). The prevalence of endemic goitre inKelantan, Malaysia. Medical Journal of Malaysia, 48, 64–70.
Malaysian Medical Resources. (2010). Medical schools. Retrieved March19, 2010, from http://medicine.com.my/wp/?page_id=19
Marfo, K. (1991). Early intervention in transition: current perspectives onprograms for handicapped children. New York: Praeger Publishers.
Marshall, S., Martin, D., & Myles, F. (1996). Survey of GPs’ views oflearning disability services. British Journal of Nursing, 5(13), 798–800.
Millar, L., Chorlton, M. C., & Lennox, N. (2004). People with intellec-tual disability: Barriers to the provision of good primary care.Journal of the Royal Australian College of General Practitioners, 33,657–658.
Nursey, A. D., Rohde, J. R., & Farmer, R. D. (1992). Ways of telling parentsabout their child and his or her mental handicap: A comparison ofdoctors’ and parents’ views. Journal of Mental Deficiency Research, 35,48–57.
Paton, J. Y., & Cockburn, F. (1995). Core knowledge, skills and attitudes inchild health for undergraduates. Archives of Disease in Childhood, 73,263–265.
Journal of Policy and Practice in Intellectual Disabilities Volume 7 Number 2 June 2010
J. L. Moyle et al. • Disability Training of Malaysian Medical Practitioners
94

Piachaud, J. (2002). Teaching learning disability to undergraduatemedical students. Advances in Psychiatric Treatment, 8, 334–341.
Razali, M. S., Khan, U. A., & Hasanah, C. I. (1996). Belief in supernaturalcauses of mental illness among Malay patients: Impact on treatment.Acta Psychiatrica Scandinavica, 94, 229–233.
Seltzer, M. M., Krauss, M. W., Orsmond, G. I., & Vestal, C. (2001).Families of adolescents and adults with autism: Uncharted territory.International Review of Research in Mental Retardation, 23, 267–294.
SPSS Inc., an IBM Company, Chicago, IL, USA.Straetmans, J. (2007). Health problems of people with intellectual dis-
abilities: The impact for general practice. British Journal of GeneralPractice, 57, 64–66.
Suleiman, A. B. (1991). The organisation of family practice services andcareer in family medicine: Rationale for family medicine programme inMalaysia. Kuala Lumpur: Ministry of Health Malaysia, GovernmentPress.
Suleiman, A. B. (1999). Missions of a medical school: An Asian perspec-tive. Academy of Medicine, 78 (8 Suppl), S45–S52.
Suleiman, A. B. (2000). Health sector reform: Ethical issues and chal-lenges. Medical Journal of Malaysia, 55 (Suppl B), 5–8.
Sutherland, G., Couch, M. A., & Iacono, T. (2002). Health issues for adultswith developmental disability. Research in Developmental Disabilities,23, 422–445.
Taplin, J. E. (1994). Proposal for multidisciplinary academic centres forteaching and research in developmental disabilities. Journal of Intel-lectual and Developmental Disability, 19, 281–286.
Veltman, A., Stewart, D. E., Tardiff, G. S., & Branigan, M. (2001). Percep-tion of primary healthcare services among people with physicaldisabilities—Part 1: Access issues. Medscape General Medicine, 3(2),18.
Weiner, H. L., Ferraris, N., La Joie, J., Miles, D., & Devinsky, O. (2004).Epilepsy surgery in young children with tuberous sclerosis: Results ofa novel approach. Journal of Child Neurology, 19, 687–689.
Wolraich, M. L., & Siperstein, G. N. (1986). Physicians and otherprofessional’s expectations and prognoses for mentally retardedindividuals. American Journal of Mental Deficiency, 9, 244–249.
Wong, P. W. (1993). Parental attitudes towards early intervention programsfor preschool children with developmental delays in Malaysia.Manchester: University of Manchester.
Young, B. (1991). Who cares: The story of Malaysian Care. Kuala Lumpur:Malaysian Care.
Yox, S. (2003). Cultural responsiveness improves healing. MedscapeMedical News. Retrieved November 26, 2003, from http://www.medscape.com/viewarticle/452137
Yuker, H. E., & Hurley, M. K. (1987). Contact with and attitudes towardpersons with disabilities: The measurement of inter-group contact.Rehabilitation Psychology, 32, 145–154.
Journal of Policy and Practice in Intellectual Disabilities Volume 7 Number 2 June 2010
J. L. Moyle et al. • Disability Training of Malaysian Medical Practitioners
95




















