iPlastics 2019 Volume 4 Issue 1.pdf - apsoprs
36
Vol. 4 Issue 1, July 2019 Lacrimal Issue Asia Pacific Society of Ophthalmic Plastic & Reconstructive Surgery Official Newsletter of Asia Pacific Society of Ophthalmic Plastic & Reconstructive Surgery
-
Upload
khangminh22 -
Category
Documents
-
view
4 -
download
0
Transcript of iPlastics 2019 Volume 4 Issue 1.pdf - apsoprs

1Asia Pacific Society of Ophthalmic Plastic & Reconstructive Surgery
Vol. 4 Issue 1, July 2019Lacrimal Issue
Asia Pacific Society of Ophthalmic Plastic & Reconstructive Surgery
Official Newsletter ofAsia Pacific Society of
Ophthalmic Plastic & Reconstructive Surgery
2 iPlastics : Vol. 4 Issue 1, Julu 2019 - Lacrimal Issue
Editor - In - ChiefBen Limbu (Nepal)
Editorial BoardRaoul Paolo D. Henson (Philippines)Sunny Shen (Singapore)David Liu (China)Dong Mei Li (China)Apjit Kaur (India)Mohammod Javed Ali (India)Yang Suk-Wu (South Korea)Jang Jae-Woo (South Korea)Yunia Irawati (Indonesia)Preamjit Saonanon (Thailand)Vanessa (Malaysia)
President Raoul Paolo D. Henson
Immediate Past President Yuen Kwok Lai Hunter
President ElectDong Mei Li
Vice PresidentsAudrey Looi Lee GeokSeah Lay LengRohit Saiju
SecretaryMary Rose Pe Yan
TreasurerStephanie Ming Young
CouncilorsCheng Pak ManNattawut WanumkarngWei LuHelen LewPreamjit SaonanonMasashi MimuraNaseem Vanessa MansuraliJuan YeSyeed Mehbub Ul KadirMark Anthony ImperialHuifang Zhou
Secretariat OfficeContact PersonBen [email protected] 066 MacArthur Hi-way, Angeles City, Philippines
Dear Colleagues,
Lacrimal disorders comprise a huge proportion of Ophthalmic Plastic & Reconstructive Surgery field in our day-to-day practice. Moreover, the amount of satisfaction is enormous if we can provide optimal management strategy for various lacrimal disorders.
This newsletter has been serving you with diverse information from the Oculoplastics world leaders and hopes to prove good guidelines regarding lacrimal disease and its management. Considering overwhelming responses to our previous issues, we are delighted to present our new issue of iPlastics with the focus on lacrimal system disorders.
Lacrimal system iPlastics newsletter is mainly focused first on tear production by main and accessory lacrimal glands and secondly the drainage system that contains puncta, the Canaliculi, the lacrimal sac and the nasolacrimal duct.
There can be number of conditions interfering with the normal function of this system such as inadequate production of tears, disturbance in drainage of tears due to pathologies such as punctual stenosis/atresia, Canalicular obstructions, nasolacrimal duct obstruction, various infections or inflammations associated with the lacrimal apparatus like dacryoadenitis, dacrocystitis or malignancies involving Lacrimal apparatus.
I would like to acknowledge Dr Nisha Shrestha, Dr Hom Gurung & Dr Triptesh Pandey for significant contribution to accomplish this newsletter and also Yalamber Limbu & Binesh Maharjan for design and layout of the newsletter.
Hope this issue provides a good insight on lacrimal disorders to the readers.
Happy Reading!
Editorial
Best Regards,Ben Limbu M.D.Editor – In – Chief APSOPRS 2019 -2020
3Asia Pacific Society of Ophthalmic Plastic & Reconstructive Surgery
Dear APSOPRS members,
It is indeed a privilege to serve as the 10th president of the Asia-Pacific Society of Ophthalmic Plastic and Reconstructive Surgery (APSOPRS) for the years 2019-2020. I remember in the year 2000 I was just fresh from fellowship when Professor Reynaldo Javate was organizing the inception of APSOPRS. We were tasked to help out in organizing the first ever meeting of the society in Manila. This was almost two decades ago. As a novice consultant the roster of speakers we had during that time amazed me. A couple of notable speakers were the late Dr. Albert Hornblass and Dr. Stephen Bosniak. Only a few member countries were present during that meeting and most of the founding members were mostly from the Philippines. Now almost all countries of the Asia-Pacific region are well represented in our society with more than 200 members and still increasing!
I was also fortunate to attend and witness all the APSOPRS biennial meetings in Sydney, Singapore, Seoul, Beijing, New Delhi, Osaka and last year in Hongkong. Having been there with the society from day one was a blessing for me. I was able to imbibe the camaraderie of our members and see first-hand how the society was being run. We are now going full circle and the APSOPRS meeting will be back in Manila next year. I want to thank our past presidents for paving the way in bringing our society to greater heights. We are now sister societies with ASOPRS, thanks to Dr. Ashok Grover and with ESOPRS, thanks to Dr. Hunter Yuen. We are now also acknowledged as experts in the field of oculoplastics and have been invited to organize sessions for the APAO, SOE and WOC.
Since January, my presidency has started tackling similar issues in the past. Among these are the secretariat, finances, memberships, website, fellowship trainings and scientific programs in international meetings. We had our first successful council meeting during the APAO in Bangkok last March. Much has been discussed and with the help of the current executive council we will be able to bring the society to the next level of excellence and professionalism.
I also bring bearer of some good news. This year’s ESOPRS meeting will be in Hamburg, Germany and I’m glad to inform our members that I will be one of the keynote speakers. On another note, I was also invited to speak at the 50th founding anniversary of the ASOPRS in San Francisco during their fall meeting in September. I will talk about the history of ASPSOPRS in one of their sessions entitled the “History of Oculoplastics – OPRS around the world.”
This year has been exciting and fruitful so far. We hope to continue to spread the influence of our society around the globe. Upcoming important big meetings next year will be the APAO in Xiamen, China, the WOC meeting in Capetown, South Africa and then our 11th APSOPRS meeting in Manila. See you!
Message from President
Raoul Paolo D. Henson, M.D.President
APSOPRS 2019-2020

4 iPlastics : Vol. 4 Issue 1, Julu 2019 - Lacrimal Issue
In this Issue Original Article1. Lacrimal Sac and Nasolacrimal Duct Anatomy in the Japanese Population
Tushar Sarbajna, MD; Hirohiko Kakizaki, MD, PhD; and Yasuhiro Takahashi, MD, PhD5
2. Prolactin and Prolactin-Inducible Protein (PIP) in the Pathogenesis of Primary Acquired Nasolacri-mal Duct Obstruction (PANDO)Mohammad Javed Ali, FRCS, Ph.D.
9
3. Endonasal Flap ManagementNattawut Wanumkarng, MD
12
Review Article4. External Dacrocystorhinostomy, endonasal endoscopic dacrocystorhinostomy and endocanalicular
LASER endoscopic dacryocystorhinostomy: A reviewBen Limbu,MD, Triptesh Raj Pandey MD, Hom Bahadur Gurung, MD
19
Case Report5. Lacrimal Gland Carcinosarcoma : A Case Report
Tan Chew-Ean, Vanessa N Mansurali23
6. Case Reports on Lacrimal Sac Tumors: Rare and MysteriousSyeed Mehbub Ul Kadir, Murtuza Nuruddin, Golam Haider
26
7. Malignant Hemangiopericytoma of The Lacrimal Sac (A Case Report)Purjanto Tepo Utomo, Banuaji Dibyasakti, Agus Supartoto
28
Tribute8. Jose Rizal, Martyr and Ophthalmologist, is the National Hero of the Philippines
Raoul Paolo D. Henson and Minguita Padilla
31
Event News9. 10th conference of Asia Pacific Society of Ophthalmic Plastic & Reconstructive Surgery and the
Hong Kong Ophthalmological Symposium 2018 Hunter Yuen
32
Photos
10. APSOPRS members speak at the meeting of the European Society of Ophthalmology 35
11. APSOPRS new secretariat office in Manila Philippines 36
Guidelines 36

5Asia Pacific Society of Ophthalmic Plastic & Reconstructive Surgery
INTRODUCTION
Nasolacrimal duct obstruction (NLDO) is the most common disorder of the lacrimal system. An in-depth knowledge of the anatomy of the lacrimal sac and NLD is of paramount importance to understand its pathophysiology and to perform a successful dacryocystorhinostomy (DCR) for NLDO. This study aims to provide a comprehensive review of the anatomy of the lacrimal sac and NLD in the Japanese population.
A REVIEW OF JAPANESE LACRIMAL SAC AND NLD ANATOMY
Lacrimal Sac and Its Fossa
Lacrimal sac fossa
The lacrimal sac fossa is a conical-shaped depression in the anteromedial orbital wall (Figure 1A).1,2 It comprises the frontal process of the maxillary bone and the lacrimal bone and is bordered by the anterior and posterior lacrimal crests, respectively. The lacrimo-maxillary suture lies between the crests (Figures 1A and B). Posterior to the suture, the lacrimal bone is thinner and can be easily punched out during DCR (Figure 1B).2 In a Japanese population, the proportion of the lacrimal bone appears to be larger than other races.2 The sutura notha is a vessel groove that runs nasally and parallel to the anterior lacrimal crest (Figure 1C). This is formed by a branch of the inferior orbital artery. The bone, nasal to the groove is thin and easy to break, and it can be helpful for
Tushar Sarbajna, MD; Hirohiko Kakizaki, MD, PhD; and Yasuhiro Takahashi, MD, PhD
Department of Oculoplastic, Orbital, and Lacrimal Surgery, Aichi Medical University Hospital, 1-1 Yazako-Karimata, Nagakute, Aichi, Japan
Corresponding Email: [email protected]
Lacrimal Sac and Nasolacrimal Duct Anatomy in the Japanese Population
surgeons to start the creation of a bony window here, during external DCR.3
The inclination of the lacrimal sac fossa is in the infero-postero-lateral direction (Table 1), and the dimension of the nose was correlated with the lateral angle (Figures 1D and E).5-7
Lacrimal sac
The lacrimal sac and NLD are, in reality, a continuous structure without a distinct histological boundary (Figure 2A), but the nasolacrimal canal entrance is the anatomical boundary. The part above (lying on the lacrimal sac fossa) and below the entrance are the lacrimal sac and NLD, respectively. The shape of the lacrimal sac is conical.1 Laterally, the sac is covered by the lacrimal fascia while its posterior aspect is covered by common fascia along with the Horner’s muscle and sac.8,9 These comprise the components of the “lacrimal diaphragm”. The medial canthal tendon (MCT) covers a part of the anterior surface of the sac. The superior aspect of the sac above the MCT is termed as the fundus of the lacrimal sac (Figure 2B). The mean height of the fundus from the MCT is 4.21 mm.10
The lacrimal sac is 7.5 mm in the anteroposterior diameter, 3.0 – 4.9 mm in the horizontal diameter, and 9.8 – 11.0 mm in height.11,12 The horizontal diameter of the lacrimal sac lumen is 1.0 – 2.0 mm, although intra-sac pressure can affect this.13 The lacrimal sac is lined with stratified columnar epithelium with goblet cells, cilia, and serous glands.12
Figure 1. The lacrimal fossa and bony nasolacrimal canal.A. The lacrimal sac fossa is a conically-shaped depression located between the anterior and posterior lacrimal crests. The lacrimo-maxillary suture runs between the crests (a right orbit, the photo taken laterally). B. An axial section of a computed tomographic image of the orbit showing the anterior and posterior lacrimal crests along with the lacrimo-maxillary suture. The maxillary and lacrimal bones can also be visualized. C. The sutura notha (a left orbit, the photo taken from the front). D and E. The inclination of the lacrimal fossa and bony nasolacrimal canal. D. The posterior type. The lacrimal sac is directed posteriorly (dotted line) and the bony nasolacrimal canal runs more posteriorly (solid line). E. The outward type. The lacrimal sac is inclined laterally (dotted line). The bony nasolacrimal canal is curved medially (solid line) against the long axis of the lacrimal sac and is inclined outward against the sagittal plane (D. a right orbit, the photo taken laterally; E. a left orbit, the photo taken from the front).
Original Article

6 iPlastics : Vol. 4 Issue 1, Julu 2019 - Lacrimal Issue
The wall of the lacrimal sac is cavernous in nature.14 It is regulated by the blood flow to the wall, causing the lacrimal mucosa to thicken or thin out, either through congestion in response to parasympathetic stimulation, or through decongestion in response to sympathetic stimulation to the cavernous body.15 However, in comparison to the NLD, the cavernous structure in the lacrimal sac is considerably thin and less developed.14
The elastic fibers play an important part in maintaining the
innate elasticity of the lacrimal sac for the pump function of tear drainage. Elastic fibers are distributed in the lamina propria of the lacrimal sac, with higher density observed in the upper and middle lacrimal sac levels.16
The lacrimal drainage-associated lymphoid tissue (LDALT) constitutes the main immune mechanism of the lacrimal system.17 The LDALT forms a functional unit along with the lacrimal gland, conjunctiva, and nasal mucosa and helps in maintaining ocular surface integrity through lymphocyte
Figure 2. The lacrimal sac and nasolacrimal duct. A. The lacrimal sac and nasolacrimal duct (NLD) are a continuous structure. A portion of NLD continues several millimeters beneath the nasal mucosa and is called the valve of Hasner (a right lacrimal drainage system, the photo taken medially).B. A part of the anterior surface of the lacrimal sac is covered by the medial canthal tendon (MCT). The part superior to the MCT is called the fundus of the lacrimal sac (a left orbit, the photo taken from the front).
A B
Table 1. Inclination of lacrimal sac (fossa) and nasolacrimal duct (canal).
Authors Study Method Angle Direction Type Mean Angle (degrees)
Narioka, et al (2007) Cadaveric study
Lacrimal Sac to Coronal Plane Posterior - 27.2°
Lacrimal Sac to Sagittal Plane Lateral 24.7°
NLD to Coronal Plane Posterior 22.5°
Lacrimal Sac to NLD Anterior (80.4%) 8.9°
Posterior (19.6%) -12.3°
NLD to Sagittal Plane Lateral Inward (63%) 10.2°
Outward (37%) 7.6°
Lacrimal Sac to NLD - 28.3°
Narioka, et al (2008) Cadaveric study
Lacrimal Sac to Supero-Medial Orbital Rim Posterior Anterior (46%) 6.5°
Posterior (54%) -7.6°
NLD to Supero-Medial Orbital Rim Posterior Anterior (72%) 7.9°
Posterior (28%) -7.5°
Park, et al (2012) Cadaveric study
Lacrimal Sac Fossa to Coronal Plane Posterior - 9.5°
Nasolacrimal Canal to Coronal Plane - 19.8°
Lacrimal Sac Fossa to Nasolacrimal Canal - 10.3°
Takahashi, et al (2013) Cadaveric study
Lacrimal Sac Fossa to Sagittal Plane Lateral - 11.9°
Nasolacrimal Canal to Sagittal Plane - 0.1°
Lacrimal Sac Fossa to Nasolacrimal Canal - 11.8°
Shigeta, et al (2007) CT Study Nasolacrimal Canal to Nasal Floor Posterior - 78.3°
CT, computed tomographic
Tushar et al : Lacrimal Sac and Nasolacrimal Duct Anatomy in the Japanese Population

7Asia Pacific Society of Ophthalmic Plastic & Reconstructive Surgery
B C
Figure 3. The bony nasolacrimal canal entrance and the narrowest part of the bony nasolacrimal canal. A. Elliptical bony nasolacrimal canal entrances (the photo taken superiorly).B. The funnel type. The narrowest point of the canal is at the entrance (arrow) (a left orbit, the photo taken laterally).C. The hourglass type. The narrowest point (arrowhead) is below the entrance (arrow) (a right orbit, the photo taken laterally).
recirculation.17 As the LDALT is located in the sub-epithelial layer of the sac, inflammatory changes due to autoimmune diseases can be observed in the sub-epithelial layer of the lacrimal sac.18,19
Nasolacrimal Canal and NLD
Nasolacrimal canal
The nasolacrimal canal is composed of the lacrimal bone superonasally, the inferior turbinate bone inferonasally, and the maxillary bone temporally. The bony canal length is around 12 mm. The inclination of the longitudinal axis of the nasolacrimal canal is shown in Table 1 (Figures 1D and E).4-7,20
The bony nasolacrimal canal entrance to the canal lies medial to the junction between the lacrimal tubercle of the maxillary bone and the lacrimal hamulus of the lacrimal bone. The entrance is elliptical (Figure 3A), and the anteroposterior and transverse diameters of the bony nasolacrimal canal entrance are 5.6 – 6.9 mm and 5.0 – 5.7 mm, respectively.20-22 These are generally longer in males and elderly patients.20,21
The shape of the nasolacrimal canal was divided into 2 types: funnel (the narrowest point at the entrance) (Figure 3B) and hourglass (the narrowest point below the entrance) (Figure 3C).22,23 The funnel type was more frequently observed in patients with primary acquired NLDO.22
NLD
The NLD is divided into 2 parts: the part running in the nasolacrimal canal (the intraosseous part) and that running in the mucosal tissue in the inferior meatus (the intrameatal part). The length of the duct is 15 – 18 mm, and it is 5 – 7 mm longer than the bony canal.11,12 Mucosal folds of eminences called the valve of Krause is occasionally present in the NLD lumen.11 The part where the NLD continues several millimeters beneath the nasal mucosa, after it leaves its
osseous channel is called the valve of Hasner (Figure 2A). It is essential in preventing the air or fluid within the nose from going up into the NLD. The shape of NLD opening into the inferior meatus can be variable and is classified into 4 main types: wide-open (12%), valve-like (8%), sleeve-like (14%), and adhesive (66%).24
The NLD is lined with stratified columnar epithelium with goblet cells, cilia, and serous glands, similar to the lacrimal sac.12 The distribution of goblet cells is more towards the inferior portion in the NLD.14 The NLD has more developed venous plexus and narrower cavity compared to the lacrimal sac, enabling reabsorption of lacrimal fluid.14
The intrameatal part contains dense amount of elastic fibers, similar to the lacrimal sac.16 This is helpful in the prevention of counterflow of the tears and air.16 The intraosseous part has lesser elastic fibers since it is free from mechanical stress.16
CONCLUSION
To the best of our knowledge, this is one of the very few comprehensive reviews on the lacrimal sac and the NLD anatomy in Japanese population. We believe that understanding the anatomy in the Japanese population is essential to provide insight as to how it is important to consider patients as individuals, with unique and varied anatomies, and uphold a patient-specific approach thus providing the best possible patient care.
ACKNOWLEDGEMENTS
The authors wish to acknowledge Professor Munekazu Naito and Professor Takashi Nakano at Department of Anatomy, for assisting the authors in cadaver dissection.
Tushar et al : Lacrimal Sac and Nasolacrimal Duct Anatomy in the Japanese Population

8 iPlastics : Vol. 4 Issue 1, Julu 2019 - Lacrimal Issue
REFERENCES1. Kakizaki H, Ichinose A, Takahashi Y, Kang H, Ikeda H, Nakano T, et al. Horner’s muscle contribution to lacrimal sac drainage. Ophthalmic Plast
Reconstr Surg. 2012;28:145–48.
2. Sarbajna T, Takahashi Y, Valencia MRP, Ito M, Nishimura K, Kakizaki H. Computed tomographic assessment of the lacrimal sac fossa in the Japanese population. Ann Anat. 2019;224:23-27.
3. Kakizaki H, Iwaki M, Asamoto K, Nakano T. Anatomical basis for an appropriate initial osseous hole in external dacryocystorhinostomy. Nippon Ganka Gakkai Zasshi. 2008a;112:39–44 (Japanese).
4. Narioka J, Matsuda S, Ohashi Y. Inclination of the superomedial orbital rim in relation to that of the nasolacrimal drainage system. Ophthalmic Surg Lasers Imaging. 2008;39:167–70.
5. Narioka J, Matsuda S, Ohashi Y. Correlation between anthropometric facial features and characteristics of nasolacrimal drainage system in connection to false passage. Clin Experiment Ophthalmol. 2007;35:651–6.
6. Park J, Takahashi Y, Nakano T, Asamoto K, Masayoshi I, Selva D, et al. The orientation of the lacrimal fossa to the bony nasolacrimal canal: an anatomic study. Ophthalmic Plast Reconstr Surg. 2012;28:463–6.
7. Takahashi Y, Nakamura Y, Nakano T, Iwaki M, Kakizaki H. Horizontal orientation of the bony lacrimal passage: an anatomic study. Ophthalmic Plast Reconstr Surg. 2013;29:128–30.
8. Shinohara H, Taniguchi Y, Kominami R, Yasutaka S, Kawamata S. The lacrimal fascia redefined. Clin Anat. 2001b;6:401–5.
9. Kakizaki H, Asamoto K, Nakano T, Selva D, Leibovitch I. Lacrimal canaliculus. Ophthalmology. 2010;117:644.
10. Takahashi Y, Kinoshita H, Nakano T, Asamoto K, Ichinose A, Kakizaki H. Anatomy of the anterior ethmoidal foramen, medial canthal tendon, and lacrimal fossa for trasncutaneous anterior ethmoidal nerve block in Japanese individuals. Ophthalmic Plast Reconstr Surg. 2014;30:431–33.
11. Kurihashi K, Imada M, Yamashita A. Anatomical analysis of the human lacrimal drainage pathway under an operating microscope. Int Ophthalmol. 1991;15:411–6.
12. Yoshihashi R, Ishio K. Clinical anatomy for endoscopic endonasal dacryocystorhinostomy. Johns. 2008;24:421–4 (Japanese).
13. Takahashi Y, Suzuki T, Kakizaki H. Lacrimal sac movement under intrasac pressure changes observed with dacryoendoscopy. Ophthalmic Plast Reconstr Surg. 2014c;30:313–4.
14. Mito H, Takahashi Y, Nakano T, Asamoto K, Ikeda H, Kakizaki H. Consecutive microscopic anatomical characteristics of the lacrimal sac and nasolacrimal duct: cases with or without inflammation. Invest Ophthalmol Vis Sci. 2014;55:5233–7.
15. Narioka J, Ohashi Y. Changes in lumen width of nasolacrimal drainage system after adrenergic and cholinergic stimulation. Am J Ophthalmol. 2006;141:689–98.
16. Kitaguchi Y, Takahashi Y, Nakano T, Naito M, Ikeda H, Miyazaki H, et al. Distribution of elastic fibers in the lacrimal sac and nasolacrimal duct of Japanese cadavers. Ophthalmic Plast Reconstr Surg. 2018;34:86–9.
17. Ali MJ, Mulay K, Pujari A, Naik MN. Derangements of lacrimal drainage-associated lymphoid tissue (LDALT) in human chronic dacryocystitis. Ocul Immunol Inflamm. 2013;21:417–23.
18. Takahashi Y, Ikeda H, Takahashi E, Kakizaki H. Immunostain of immunoglobulin G4 in the lacrimal sac. Ocul Immunol Inflamm. 2018;26:1053–8.
19. Ishikawa E, Takahashi Y, Nishimura K, Ito M, Kakizaki H. Dacryocystitis and rhinosinusitis secondary to sarcoidosis. J Craniofac Surg. 2019;30:e52–4.
20. Shigeta K, Takegoshi H, Kikuchi S. Sex and age differences in the bony nasolacrimal canal. Arch Ophthalmol. 2007;125:1677–81.
21. Takahashi Y, Kakizaki H, Nakano T. Bony nasolacrimal duct entrance diameter: gender difference in cadaveric study. Ophthalmic Plast Reconstr Surg. 2011a;227:204–5.
22. Takahashi Y, Nakata K, Miyazaki H, Ichinose A, Kakizaki H. Comparison of bony nasolacrimal canal narrowing with or without primary acquired nasolacrimal duct obstruction in a Japanese population. Ophthalmic Plast Reconstr Surg. 2014b;30:434–8.
23. Takahashi Y, Nakamura Y, Nakano T, Asamoto K, Iwaki M, Selva D, et al. The narrowest part of the bony nasolacrimal canal: an anatomical study. Ophthalmic Plast Reconstr Surg. 2013b;29:318–22.
24. Onogi J. Nasal endoscopic findings of functional obstruction of nasolacrimal duct. Rinsho Ganka. 2012;55:650–4 (Japanese).
Tushar et al : Lacrimal Sac and Nasolacrimal Duct Anatomy in the Japanese Population

9Asia Pacific Society of Ophthalmic Plastic & Reconstructive Surgery
ABSTRACT
Primary acquired nasolacrimal duct obstruction (PANDO) is a syndrome of unknown etiology, predominantly affecting post-menopausal females, characterized by progressive inflammation, fibrosis and subsequent obstruction of the nasolacrimal duct. Numerous factors have been proposed as possible etiologic factors and include anatomical configuration, ocular and nasal infections, peri-lacrimal vascular disorders, hormonal influence, lacrimal drainage lymphoid tissue, gastroesophageal reflux disease, topical medications, swimming pool exposure, smoking, genetic factors, autonomic and lysosomal dysregulation. The authors hypothesize Prolactin (PRL) and Prolactin-inducible protein (PIP) play a role in the etiopathogenesis of primary acquired nasolacrimal duct obstruction.
INTRODUCTION
Primary acquired nasolacrimal duct obstruction (PANDO) is a syndrome of unknown etiology, predominantly affecting post-menopausal females, characterized by progressive inflammation, fibrosis and subsequent obstruction of the nasolacrimal duct.1-3 The resultant clinical manifestations include epiphora and discharge, occasional development of lacrimal sac mucocele or acute dacryocystitis.2 Numerous factors have been proposed as possible etiologic factors and include anatomical configuration, ocular and nasal infections, peri-lacrimal vascular disorders, hormonal influence, lacrimal drainage lymphoid tissue, gastroesophageal reflux disease, topical medications, swimming pool exposure, smoking, genetic factors, autonomic and lysosomal dysregulation.1-7 Prolactin receptors have been identified in the epithelia and submucosal glands of the lacrimal sac and nasolacrimal ducts.6 They have been proposed as possible extra-pituitary
Mohammad Javed Ali, FRCS, Ph.D.1,2
Govindram Seksaria Institute of Dacryology, L.V. Prasad Eye Institute, Hyderabad, India.
Corresponding Email: [email protected]
Prolactin and Prolactin-Inducible Protein (PIP) in the Pathogenesis of Primary
Acquired Nasolacrimal Duct Obstruction (PANDO)
Financial Disclosure: Mohammad Javed Ali received support from the Alexander von Humboldt Foundation for his research and he also receives royalties from Springer for the 2nd edition of the textbook 'Principles and Practice of Lacrimal Surgery' and treatise 'Atlas of Lacrimal Drainage Disorders'.
Declaration of Interests: The authors report no conflict of interests.
sites of prolactin synthesis. Significant proportions of Prolactin-inducible protein (PIP) has been detected in lacrimal sac extracts.7
Hypothesis
Prolactin and Prolactin-inducible protein play a role in the etiopathogenesis of primary acquired nasolacrimal duct obstruction.
Evaluation of Hypothesis
Prolactin
Prolactin (PRL) is a pituitary hormone secreted by the lactotrophs and its main function is during pregnancy and lactation and contributes to the development of mammary glands, synthesis of milk and its maintenance.8 However, PRL is known to be synthesized in extra-pituitary sites and has a significant immunomodulatory role. Cells of the immune system produce PRL, express PRL receptors (PRLR) and also respond to it, suggesting an autocrine or paracrine mechanism.6,9,10 PRL acts as a cytokine and inhibits the negative selection of autoreactive B-lymphocytes. Conversely PRL stimulates the proliferation of lymphocytes and modulates thymic actions.9 Apart from lymphocytes, PRLR have also been noted in macrophages and fibroblasts.10,11 PRL can enhance or inhibit pro-inflammatory mechanisms in a specific manner and hence maintains a crucial pro and anti-inflammatory balance. Hence, it would not be surprising that PRL has been linked to numerous auto-immune disorders like rheumatoid and psoriatic arthritis.10,11 In addition, PRL has demonstrated tropic action on lacrimal glands and regulates its secretion and protein content.12 In animal experiments, PRL has been shown to restore the lacrimal gland cholinergic neurotransmitter receptors.13 and
Original Article

10 iPlastics : Vol. 4 Issue 1, Julu 2019 - Lacrimal Issue
also augment the effects of testosterone.14
Hormonal influence as a factor in PANDO was mainly proposed because of the female predilection and more so in the post-menopausal age. Ali et al6 performed a qualitative hormonal profiling of the entire lacrimal drainage system in female and male subjects with PANDO and cadaveric controls. They studied expression of estrogen alpha (ERα), estrogen beta (ERβ), aromatase (CYP19), testosterone (TSTR), progesterone (PGR), oxytocin (OXTR), prolactin (PRL), and somatostatins 1 to 5. They found that PRL receptors in expression to be prominent in the lacrimal sac and NLD epithelia and also the submucosal glands but the canalicular epithelium showed minimal expression. Interestingly, this expression was less prominent in normal post-menopausal females as compared to normal males of comparable age. The diseased samples of PANDO showed reduced expression in the epithelia and absence in the submucosal glands. This possibly gives an indirect evidence reduced expression of PRL predisposes the nasolacrimal duct obstruction. The hypothesis can thus be that reduced PRL may hamper the physiological functions of the lacrimal epithelia and its submucosal glands, disturbs the cholinergic interactions, and facilitates an imbalance of the pro and anti-inflammatory modulatory effects. The possibility of local hormonal microenvironments in the lacrimal drainage, independent of the systemic levels have been hypothesized earlier.6 Since all these may be local effects, it can lead to regional inflammation and such recurrent attacks may predispose the nasolacrimal ducts to an obstruction and subsequent clinical syndrome of PANDO
Prolactin-inducible protein (PIP)
Prolactin-inducible protein is a single polypeptide chain expressed in salivary, sweat and lacrimal glands.15 PIP is upregulated by Prolactin and androgens. It has versatile functions in reproductive and immune systems.16 PIP is also overexpressed in malignancies and is being investigated as a potential biomarker for tumor detection and progression.15,16 Interestingly, it is also being considered as a good biomarker for the corneal disease, keratoconus17 and has also been hypothesized in the pathogenesis of dacryoliths.18 It can bind to many bacterial species and
inhibit their proliferation. It can also bind to CD4 cells, Fc portion of immunoglobulin G and zinc alpha-2 glycoprotein.7 Its abundance in mucosal tissues suggests a role in mucosal immunity.15 Immune dysfunctions have been demonstrated in PIP knock-out mice. Lacrimal drainage system (LDS) has a large mucosal surface and hence the presence of PIP is hence not surprising. It is possible that PIP in part protects the LDS from continuous onslaught of bacteria from ocular surface and also medial local immune responses. Disorders in PIP synthesis and regulation can be intricately associated with PRL and can potentially predispose the LDS to infections and inflammations. These may in turn make the narrow and vulnerable NLD to repeated attacks, healing by fibrosis and subsequent obstructions and clinical syndrome of PANDO.
Current Challenges and Consequences of the Hypothesis
Linking prolactin and PIP to PANDO would need extensive targeted investigations. It is yet to conclusively demonstrate local synthesis of PRL and PIP and whether it is the LDS cells themselves or immune cells as has been demonstrated in autoimmune diseases. Site-specific molecular interactions of PRL and PIP in NLD is to be ascertained. Animal experiments of the LDS involving PIP knock out mice would give insights into clinical pathophysiology. It is important to remember that hormonal influences are at most grossly involving the NLD and not lacrimal sac. Is this because of narrower dimensions of NLD or are the lacrimal sac effects being missed is yet to be deciphered. The lead of PRL and PIP in etiopathogenesis of PANDO is promising but may only partly explain the causative mechanisms involved unless all the interacting molecular pathways are deciphered. The discovery of molecular mechanisms in PANDO will have a massive impact on the way we treat them. It would not be audacious for us to believe that PANDO would one day have a medical treatment and there may even be preventive strategies in the future.
CONCLUSION
The presence of Prolactin receptors in the LDS and isolation of PIP from lacrimal extracts opens up exciting avenues to explore the pathogenesis of PANDO.
Mohammad et al : Prolactin and Prolactin-Inducible Protein (PIP) in the Pathogenesis of Primary Acquired Nasolacrimal Duct Obstruction (PANDO)

11Asia Pacific Society of Ophthalmic Plastic & Reconstructive Surgery
REFERENCES1. Ali MJ, Paulsen F. Etiopathogenesis of primary acquired nasolacrimal duct obstruction (PANDO): what we know and what we need to know.
Ophthal Plast Reconstr Surg 2019 (Epub).
2. Kamal S, Ali MJ. Primary acquired nasolacrimal duct obstruction (PANDO) and secondary acquired lacrimal duct obstruction (SALDO). In, ‘Principles and Practice of Lacrimal Surgery’, 2nd edition, Ali MJ (editor). Springer, Singapore. 2018, pp 163-171.
3. Das A, Rath S, Naik MN, Ali MJ. The incidence of lacrimal drainage disorders across a tertiary eye care network: Customization of an indigenously developed electronic medical record system – eyeSmart. Ophthal Plast Reconstr Surg 2018 (Epub).
4. Paulsen FP, Thale AB, Maune S, Tillmann BN. New insights into the pathophysiology of primary acquired dacryostenosis. Ophthalmology 2001;108:2329-2336.
5. Paulsen F, Schaudig U, Maune S, Thale AB. Loss of tear duct-associated lymphoid tissue in association with scarring of symptomatic dacryostenosis. Ophthalmology 2003;110:85-92.
6. Ali MJ, Schicht M, Paulsen F. Qualitative hormonal profiling of the lacrimal drainage system: potential insights into the etiopathogenesis of primary acquired nasolacrimal duct obstruction. Ophthal Plast Reconstr Surg 2017;33:381-388.
7. Ali MJ, Venugopal A, Ranganath KS, Jagannadham MV, Nadimpalli SK. Soluble glycoproteins of the lacrimal sac: role in defense with special reference to prolactin-inducible protein. Orbit 2018 (Epub).
8. Saleem M, Martin H, Coates P. Prolactin biology and laboratory measurement: An update on physiology and current analytical issues. Clin Biochem Rev 2018;39:3-16.
9. Savino W. Prolactin: An immunomodulator in health and disease. Front Horm Res 2017;48:69-75.
10. Tang MW, Garcia S, Gerlag DM, Tak PP, Reedquist KA. Insight into the endocrine system and the immune system: A review of the inflammatory role of prolactin in rheumatoid arthritis and psoriatic arthritis. Front Immunol 2017;8:720.
11. Borba VV, Zandman-Goddard G, Schoenfeld Y. Prolactin and auto-immunity. Front Immunol 2018;9:73.
12. Wang Y, Chiu CT, Nakamura T, Traffic of endogenous, transduced, and endocytosed prolactin in rabbit lacrimal acinar cells. Exp Eye Res 2007;85:749-761.
13. Azzarolo AM, Bjerrum K, Maves CA. Hypophsectomy-induced regression of female rat lacrimal glands: partial restoration and maintenance by dihydrotestosterone and prolactin. Invest Ophthalmol Vis Sci 1995;36:216-226.
14. Keenan EJ, Klase PA, Thomas JA. Interaction between prolactin and androgens in the accessory sex organs of male mice. J Endocrinol 1981;90:323-330.
15. Hassan MI, Waheed A, Yadav S, Singh TP, Ahmad F. Prolactin inducible protein in cancer, fertility and immunoregulation: structure, function and its clinical implications. Cell Mol Life Sci 2009;66:447-459.
16. Ihedioha OC, Shiu RPC, Uzonna JE, Myal Y. Prolactin-inducible protein: from breast cancer biomarker to immune modulator – novel insights from knockout mice. DNA Cell Biol 2016;35:537-541.
17. Sharif R, B.ak-Nielsen S, Sejersen H, Ding K, Hjortdal J, Karamichos D. Prolactin-inducible protein is a novel biomarker for keratoconus. Exp Eye Res 2018;179:55-63.
18. Mano F, Takimoto H, Masako Oe. Proteomic analysis of dacryoliths from patients with or without topical Rebamipide treatment. Biomed Hub 2018;3:487585.
Mohammad et al : Prolactin and Prolactin-Inducible Protein (PIP) in the Pathogenesis of Primary Acquired Nasolacrimal Duct Obstruction (PANDO)

12 iPlastics : Vol. 4 Issue 1, Julu 2019 - Lacrimal Issue
SUMMARY
In the current day, the popularity of endoscopic dacryocystorhinostomy (DCR) has been increased among the oculoplastic surgeons, ophthalmologists and ENT specialists. The various techniques of sutured flap have been discussed that they are quite difficult because of the narrow nasal cavity and trans-nasal flap suturing consumes high learning curve. The author has discovered that appropriate choosing endonasal flap type and the intranasal flap suturing techniques promote the primary intentional healing and provide the better success rate comparing to the conventional endoscopic DCR without flap suturing. There were several literatures described various techniques for intranasal flap management without suturing during endoscopic DCR.1-15 The purpose of the surgery is to create the bypass tract (nasal ostium) from the eye to the nose without external scar tissue. The chapter would describe the classification of flap management for trans-nasal endoscopic DCR with flap suturing in depth.
Factors for the success of endoscopic DCR with flap suturing
1. Adequate size of an osteotomy Creating a large bony ostium with a diameter of about 1.5 cm is the primary key to success.9 After creating C-shaped flap (posterior base) on nasal mucosa 2-3 mm in front of the axillar of middle turbinate and extending 8 mm above and below axilla of
Nattawut Wanumkarng, MD
Department of Ophthalmology, Bumrungrad International Hospital, Bangkok
Corresponding Email: [email protected]
Endonasal Flap Management
middle turbinate. Then the nasal mucosa was removed conservatively. The incision is quite parallel and along the frontal process of maxillary bone. Then all bone covering lacrimal sac and upper part of the nasolacrimal duct were removed to get an osteotomy of around 15 mm x 15 mm.1 At this point, the bone and surrounding nasal mucosa should be removed conservatively. Too much bony removal and mucosal removal could lead to bony gap that could provoke the granulation tissue and scar at a new ostium.
2. Approximation of lacrimal flap mucosa and surrounding nasal mucosa with flap suturing.16
Classification of lacrimal flap for endoscopic DCR with flap suturing (Fig.1)
1. Anterior and Posterior Flap 2. Superior and Inferior Flap 3. Superior and Anterior Flap (Combined Flap)
Flap Suturing for Endoscopic Dacryocystorhinostomy
Kirtane17 reported the endoscopic DCR with flap suturing for the first time in 2013 in 20 patients (23 Endoscopic DCRs). Suturing with 5-0 vicryl was done 18 18 Endoscopic DCRs and a vascular clip was used in 2 DCRs to put the mucosal flap and medial wall sac together. His technique provided a primary success rate of 95% and ultimate rate of 100% and there is not only minimally invasive but has minimal complications.
Lacrimal Flap Classification
Superior - Inferior FlapAnterior - Posterior Flap (Combined Flap)Anterior - Superior Flap
Figure 1: Lacrimal Flap Classification. Anterior - Posterior Flap (Left), Superior – Inferior Flap (center), Anterior – Superior Flap (right)
Original Article

13Asia Pacific Society of Ophthalmic Plastic & Reconstructive Surgery
Surgical Techniques
Each patient has various dimension of nasal cavity depends on the ethnic groups and degree of septal deviation. There is quite steep learning curve for flap suturing during endoscopic DCR.18 The beginners may consume 15-20 minutes initially. After the practicing, the lacrimal surgeon could finish flap suturing with in 3-5 minutes.
Concepts s of Flap Suturing during the Endoscopic DCR
1. Adequate Osteotomy
The lacrimal surgeon needs to have well understandings of the lacrimal system, frontal process of maxillary bone, lacrimal bone and ethmoidal bone properly. The appropriate size of Osteotomy (bony ostium) which include removed bone of frontal process of maxillary bone, lacrimal bone and anterior part of ethmoidal bone (uncinate process) is recommended at the point to get the complete exposure of the lacrimal sac including the fundus.19 If the size of bony ostium is too small, the ability to approach to completely open the medial aspect of lacrimal sac wall would be difficult or inadequate. If the size of the bony ostium is too large, the nasal mucosa would be removed too much inevitably which would lead to too large bony gap between lacrimal mucosal flap and surrounding nasal mucosa. Secondary intention healing would occur instead of primary intention healing. The more cicatricial tissue develops, the more chance of contracted nasal ostium or granulation tissue which may lead to failure of Endoscopic DCR.20-22
2. Classification of Lacrimal Flap Suturing for Endoscopic DCR
After completion of bony ostium creation, the next step is choosing the type of lacrimal flap. The conventional endoscopic DCR without flap preservation or flap preservation without flap suturing may have more granulation or cicatricial tissue at the gap between the lacrimal flap and nasal mucosa.23 The author practically classifies lacrimal flap classification for endoscopic flap suturing according to the benefits of maximal approximation allowed by the anatomical tissues of lacrimal and nasal mucosal approximation during the surgery. The types of the created lacrimal flap depend on the shape of lacrimal sac and incision which is made on the medial aspect of lacrimal sac wall. Below are the concepts for considering which types of lacrimal flap for endoscopic flap suturing.
2.1 Anterior - Posterior Flap (A-P Flap)
This type of lacrimal flap is appropriate for most of conventional endoscopic DCR. In normal lacrimal sac without acute or chronic dacryocystitis, the lacrimal mucosa
would be thin, no inflammation and no distention which the creation of A-P flap is practicable. After the creation of appropriate bony ostium with preservation of nasal mucosa, the I-shaped incision was created on the medial wall of exposed lacrimal sac with 15-degree blade <Figure 2a-h>. The author would recommend creating the I-shaped incision slightly more posteriorly which this would create a larger anterior flap and a smaller posterior flap. Then the larger anterior lacrimal flap was flipped anteriorly to approximate the nasal mucosa anteriorly. At this point, the author always opens 2-3 mm of proximal part of nasolacrimal bone and overlying nasal mucosa. This would allow the whole anterior lacrimal sac flap and very proximal part of nasolacrimal duct mucosa could be rotated anteriorly to approximate to nasal mucosa. With this technique, the author believes that it would prevent the Sump syndrome.20 2 stitches of 6-0 vicryl flap suturing with 11 mm S-14 bended spatula needle are always performed. Posterior flap suturing is occasionally performed in some conditions such as wide nasal cavity without marked septal deviation or demonstrated surgery.
2.2 Superior - Inferior Flap (S-I Flap)
This type of flap is suitable in some condition and not done frequently such as chronic dacryocystitis with dacryocystocele. In this condition, the size of lacrimal sac
Figure 2: Anterior and Posterior Flap Suturing.Fig. 2a Show medial wall of lacrimal sac after creation of appropriate
bony ostium with preservation of nasal mucosa. Fig. 2b-c I-shaped incision was done with 15-degree blade. Fig 2d Anterior and posterior
lacrimal flap were created. Fig. 2e Anterior lacrimal flap was sutured with 8 mm, 6-0 vicryl bended spatula needle. Fig. 2f Nasal mucosa (anterior to anterior lacrimal sac flap) was sutured with the same needle. Fig. 2g
with good cooperation by assistant holding the endoscope, the surgeon could perform trans-nasal flap suturing with 2 hand technique. Fig. 2h
Simple square knot tying was tightened. Fig. 2i 2 stitches of anterior flap suturing and 1 stitch of posterior flap suturing were performed.
Nattawat Wanumkang : Endonasal Flap Management

14 iPlastics : Vol. 4 Issue 1, Julu 2019 - Lacrimal Issue
is usually distended with accumulated lacrimal sac content and lacrimal mucosa may be thicker than usual. H-shaped incision is done on the medial wall of lacrimal sac (Figure. 3b). In the author’s series (unpublished data), the S-I flap was used in small percent of patients such as chronic dacryocystocele (Figure 3a-d) or revision surgery.
The superior lacrimal flap is rotated superiorly, and the inferior flap is flipped inferiorly according to the gravitational effect. Mostly, the author performs the superior lacrimal flap suturing to the nasal mucosa superiorly. The author believes that the fixation by flap suturing on superior flap would provide prevention of cicatricial tissue or granulation tissue on the area of common canaliculi which this concept could be applied to use in the critical condition such as revision in severe cicatricial tissue over common canaliculus (severe contracted nasal ostium) from previous failed DCR.23 (Figure 3a-d). 1 or 2 stitches of 6-0 vicryl flap suturing with 11 mm S-14 bended spatula needle could be performed according to the width of nasal cavity. There is no need for inferior lacrimal flap suturing because of the inferior lacrimal flap usually lies down by the gravity.
2.3 Combined flap anterior and superior flap (A-S Flap)
With the concepts of superior flap suturing, the author has discovered that the combination of anterior flap and superior flap suturing provide the marked benefits in the difficult
revision surgery. The author has observed and applied in the cases with very thick cicatricial tissue surrounding the lacrimal sac wall or at area of common canaliculus. If there is adequate lacrimal tissue or cicatricial tissue (pseudo-superior lacrimal flap) over the area of common canaliculi of lacrimal sac, this would allow the surgeon to perform superior lacrimal flap suturing to surrounding nasal mucosa additional to conventional anterior lacrimal flap suturing. This would provide the great benefits for preventing the late contraction of nasal ostium or Sump syndrome after the endoscopic DCR or revision surgery23 (Figure 4a-i).
3. Concepts of intranasal suturing
To perform intranasal flap suturing and flap management is not easy and routinely done as the external DCR24,25 because of many factors such as narrow nasal cavity especially caused by septal deviation, swelling of nasal mucosa or nasal mass. To achieve intranasal flap suturing needs time for practicing initially after the lacrimal surgeon feels comfortable with the techniques, the experienced surgeon could achieve intranasal flap suturing within 3-5 minutes. The author does believe that this concepts and techniques could be applied to increase the success rate of endoscopic DCR and for failed DCR revision practically.
Figure 3: Superior and Inferior Flap Suturing and H-shaped Incision.
Fig. 3a Medial wall of distended lacrimal sac was exposed after the well bony ostium was done. Fig. 3b H-shaped incision was done. Fig. 3c Supe-rior and inferior intranasal flap suturing was done with 8 mm bended 6-0 vicryl spatula needle. Fig. 3d Silicone tube intubation was done which
showed area of common canaliculi.
Figure 4: Anterior and Superior Flap Suturing (Combinded Flap Suturing).
Fig. 4a Show medial wall of lacrimal sac on left side after creation of ap-propriate bony ostium with nasal mucosal tissue preservation. Bowman’s probe was introduced and tented the medial wall of lacrimal sac. Fig.
4b-d Vertical incision was done by 15-degree blade for creating anterior and posterior lacrimal flap. Fig. 4e-f Anterior lacrimal flap was sutured to nasal mucosa anteriorly with 6-0 bended vicryl suture and tied with
simple surgical knot. Fig. 4 g-i Superior lacrimal flap was flipped superiorly and sutured to nasal mucosa superiorly with the same technique.
.
Nattawat Wanumkang : Endonasal Flap Management

15Asia Pacific Society of Ophthalmic Plastic & Reconstructive Surgery
3.1 Position of lacrimal surgeon and assistant during intranasal flap suturing
Otorhinolaryngologists usually perform endoscopic surgery with holding rigid endoscope with the left hand and surgical instruments with right hand and stand on the right-hand side of the operating table. The author recommends the lacrimal surgeon stands on the right-hand side of operating table and the well-trained assistant stands on the left-hand side of operating table and holds the operating endoscope with two-hand technique (Figure 5f). This would allow the lacrimal surgeon could use both hands for performing intranasal flap suturing easily and fast. The important issues to stress with the assistant are moving rigid endoscope unit gradually as 1-2 mm for each movement according to the surgeon movement and the rigid endoscope unit should be placed on infero-medial aspect of nasal cavity all the time which would allow enough space above then the surgeon could perform intranasal surgery comfortably and provide the stability of surgical image for the surgeon.
Concept for stability of holding the 30-degree, 16 mm length, 4 mm diameter, rigid endoscope unit are
- One side of endoscope camera unit is hold by the assistant’s left hand and the rigid endoscope lens is hold by the assistant’s right hand (Figure 5f)
- The distal part of rigid endoscope lens is placed on the
infero-medial aspect of nasal cavity all the time during the operation.
3.2 Type of surgical needle for intranasal flap suturing
The author uses 6-0 coated vicryl S-14, 8 mm, 1/4c and 45 cm spatula needle (Ethicon W9552, polyglactin 910, Johnson & Johnson international) for the intranasal flap suturing. The reasons are 6-0 vicryl is slow absorbable material, strong enough to keep strength during suturing, easy handling and there is no infection found after using this for the past 13 years. Because of the narrowing of nasal cavity including the concept of suturing inside narrow cavity, the appropriate curvature of needle should be 180 degrees instead of 90 degree. The author always bends the original 8mm and 90 degrees (1/4c) spatula (S-14) needle to 180 degrees needle (Figure 5a-d) which is suitable for intranasal flap suturing. The benefit of spatula needle is its sharpness is on both sides of needle which would penetrate through the lacrimal or nasal mucosa without cutting through tissue too much as cutting or reverse cutting needle. The 8 mm length of needle is suitable and easy for manipulating needle in small and narrow nasal cavity either forehand suturing or backhand suturing.
3.3 Benefits of Flap Suturing during Endoscopic DCR
Flap suturing for external DCR has been the basic principle and standard more than hundred years. Various techniques for approximation flap in external DCR have been discussed.23-33 There were a few literatures that described the details and techniques for intranasal lacrimal and nasal mucosal flap approximation by flap suturing techniques. The author has discovered that the intranasal flap suturing is the challenging task and could increase the success rate and be applied for primary and revision endoscopic DCR practically.
3.3.1 For proper approximation of lacrimal and nasal mucosa as primary intention healing. If the surgeon understands the concept of flap classification and flap suturing techniques for intranasal endoscopic DCR, the surgeon could choose one of the above flap classifications for designing types of lacrimal mucosal flap and perform intranasal flap suturing.
3.3.2 Flap Suturing for Failed DCR
From the author’s experience, the cicatricial tissue that covers the created nasal osmium could be found as 2 types.
3.3.2.1. Thin cicatricial tissue on medial wall of lacrimal sac with well healed internal lacrimal sac wall mucosa (SUMP Syndrome).20-22
Figure 5: Needle & Surgeon.Fig. 5a Package of original S-14 6-0 vicryl Fig. 5b Original 8 mm
90-degree (1/4c) spatula needle with 6-0 coated vicryl. Fig. 5c Bended 8 mm 180-degree (1/2c) spatula needle with forehand grasp Fig. 5d
The same needle with backhand grasp Fig. 5e Handling the Castroviejo needle holder with palm down position Fig. 5f The position of surgeon
and assistant during endoscopic DCR.
Nattawat Wanumkang : Endonasal Flap Management

16 iPlastics : Vol. 4 Issue 1, Julu 2019 - Lacrimal Issue
For this condition, the surgeon could perform simple vertical incision along cicatricial tissue on medial wall of lacrimal sac and then rotate the anterior cicatricial flap anteriorly and posterior flap posteriorly. Performing anterior or posterior flap suturing could be applied according variation of surgical anatomy. Figure 6a-d shows performing flap suturing between anterior lacrimal flap to nasal mucosa anteriorly.
3.3.2.2. Thick cicatricial tissue on medial wall of lacrimal sac without well healed internal lacrimal sac wall.
The author usually found that this condition was always found with inadequate bony osmium and previous surgery initiated abnormal cicatricial tissue from secondary intentional healing (healing of lacrimal and nasal mucosal tissue between bony gap). In revision surgery, the surgeon needs to open the thick cicatricial tissue and create the new adequate bony osmium. The thick cicatricial tissue of residual lacrimal tissue could be found significantly. To try performing intranasal flap suturing by approximation between thick residual lacrimal sac cicatricial tissue (pseudo mucosal flap) including the
bottom part of lacrimal sac mucosa20 to the surrounding nasal tissue could provide the better approximation for the new nasal ostium as primary intention healing. This would provide the better success rate for revision DCR (Figure 7a-i).
My personal Techniques for Intranasal Flap Suturing
Tips for Intranasal Flap Suturing for Endoscopic DCR
- Adequate size of bony ostium is important factor (1.2-1.5 cm in diameter).
- Vertical incision on medial wall of lacrimal sac (I-shaped incision) should be created more posteriorly (anterior 2/3 and posterior 1/3). This would create more tissue for anterior lacrimal flap and less tissue on posterior lacrimal flap (Figure 2b-d). Because of the anterior lacrimal flap is practically be sutured easier than posterior lacrimal flap. The author recommended to perform 2 stitches for anterior flap suturing (Figure 2e-i). Upper half and lower half of anterior lacrimal flap would be secured to nasal mucosa anteriorly, this would help to approximate the lacrimal sac wall (including fundus, body and lower part) and very proximal part of nasolacrimal canal mucosa to nasal mucosa. The posterior lacrimal sac mucosa could be sutures occasionally. The author believes that if the
Figure 6: Correction for Sump syndrome on left side by simple posterior flap suturing.
Fig. 6a A tiny and high opening of contracted ostium after the failed endoscopic DCR Fig. 6b A vertical cut was done with 15-degree blade
Fig. 6c After the vertical incision, the anterior and posterior flap were created. A simple posterior lacrimal flap was sutured to nasal mucosa
of middle turbinate posteriorly. Fig. 6d After simple posterior lacrimal flap suturing, well healed internal lacrimal sac mucosa could be seen from
endoscopic view.
Figure 7: A Flap suturing for Failed DCR.Fig. 7a Correction for Failed DCR with thick cicatricial tissue on medial
wall of lacrimal sac by Anterior lacrimal flap suturing on right side Fig. 7b After enlarging the too small bony ostium from previous failed DCR, the medial wall of lacrimal sac wall could be seen. Fig.7c-d Vertical incision
was done on medial wall of thick lacrimal sac tissue then the anterior and posterior lacirmal flap was created. Fig. 7e Thick and cicatricial anterior lacrimal sac flap was rotated anteriorly with cupped forceps
Fig.7f-i Anterior lacrimal sac flap was sutured to nasal mucosa anteriorly with 2 stitches of bended 180 degree (1/2c) 8 mm spatula needle with
6- vicryl suture.
Nattawat Wanumkang : Endonasal Flap Management

17Asia Pacific Society of Ophthalmic Plastic & Reconstructive Surgery
anterior flap suturing could be done practically and routinely, the posterior flap suturing may not need to be done routinely.31
- The surrounding nasal mucosa should be preserved as much as possible during the removal. Because of excessive removal would lead to too much space between the lacrimal and nasal flap which would lead to more bleeding postoperatively and more cicatricial tissue or granulation tissue.
- The well-trained assistant who holds the endoscope during the surgery is required.
- The well-trained assistant should hold the endoscope stably and move synchronously with the surgeon’s hands. The rigid endoscope lens should be placed on the infero-medial aspect of nasal cavity all the time which this allows the enough space superiorly for the surgeon to perform intranasal flap suturing.
- During anterior flap suturing for Endoscopic DCR on right side, the author would recommend holding the needle holder as forehand grasp (palm down) (Figure. 5e). For anterior flap suturing for Endoscopic DCR on left side, the author would recommend holding the needle holder as backhand grasp (palm down). With the good
cooperation between the surgeon and the assistant for holding and moving the endoscope unit synchronously, the surgeon could perform the flap suturing (simple square knot) with both hands comfortably.
- In the condition of septal deviation on the operated side, the author does not perform the septal deviation routinely. the deviated septal bone was pushed to the opposite side and small cotton ball or tip of cotton bud were used to place on the upmost position of nasal cavity to allow temporary expansion of nasal cavity during the surgery. Only a few millimeters are expanded, the surgeon could perform intranasal endoscopic DCR and flap suturing comfortably. The small cotton ball or tip of cotton bud would be removed at the end of surgery.
- In the case of endoscopic DCR with flap suturing with marked septal deviation, the mucosal tissue of nasal mucosa, lacrimal mucosa and septal tissue could be injured, the author prefers to place silastic sheet (1mm thick) and sutures the silastic sheet with the septal mucosa anteriorly for preventing the intranasal adhesion band between the lacrimal flap, nasal mucosa and septal mucosa. The silastic sheet would be kept for 1-2 weeks then removed easily in office.
Nattawat Wanumkang : Endonasal Flap Management

18 iPlastics : Vol. 4 Issue 1, Julu 2019 - Lacrimal Issue
REFERENCES1. Tsirbas, A. and P.J. Wormald, Mechanical endonasal dacryocystorhinostomy with mucosal flaps. Br J Ophthalmol, 2003. 87(1): p. 43-7.
2. Massegur, H., E. Trias, and J.M. Adema, Endoscopic dacryocystorhinostomy: modified technique. Otolaryngol Head Neck Surg, 2004. 130(1): p. 39-46.
3. Yuen, K.S., et al., Modified endoscopic dacryocystorhinostomy with posterior lacrimal sac flap for nasolacrimal duct obstruction. Hong Kong Med J, 2004. 10(6): p. 394-400.
4. Jin, H.R., J.Y. Yeon, and M.Y. Choi, Endoscopic dacryocystorhinostomy: creation of a large marsupialized lacrimal sac. J Korean Med Sci, 2006. 21(4): p. 719-23.
5. Kansu, L., et al., Comparison of surgical outcomes of endonasal dacryocystorhinostomy with or without mucosal flaps. Auris Nasus Larynx, 2009. 36(5): p. 555-9.
6. Sonkhya, N. and P. Mishra, Endoscopic transnasal dacryocystorhinostomy with nasal mucosal and posterior lacrimal sac flap. J Laryngol Otol, 2009. 123(3): p. 320-6.
7. Ji, Q.S., et al., New mucosal flap modification for endonasal endoscopic dacryocystorhinostomy in Asians. Int J Ophthalmol, 2012. 5(6): p. 704-7.
8. Khalifa, M.A., et al., Endoscopic dacryocystorhinostomy with double posteriorly based nasal and lacrimal flaps: a prospective randomized controlled trial. Otolaryngol Head Neck Surg, 2012. 147(4): p. 782-7.
9. Cukurova, I., et al., Endoscopic dacryocystorhinostomy: outcomes using mucosal flap preserving technique. Eur Arch Otorhinolaryngol, 2013. 270(5): p. 1661-6.
10. Hodgson, N., et al., Outcomes of endonasal dacryocystorhinostomy without mucosal flap preservation. Ophthalmic Plast Reconstr Surg, 2014. 30(1): p. 24-7.
11. Prakash, M.D., B. Viswanatha, and R. Rasika, Powered Endoscopic Endonasal Dacryocystorhinostomy with Mucosal Flaps and Trimming of Anterior End of Middle Turbinate. Indian J Otolaryngol Head Neck Surg, 2015. 67(4): p. 333-7.
12. Green, R., R. Gohil, and P. Ross, Mucosal and lacrimal flaps for endonasal dacryocystorhinostomy: a systematic review. Clin Otolaryngol, 2017. 42(3): p. 514-520.
13. Peng, W., et al., A Modified Preserved Nasal and Lacrimal Flap Technique in Endoscopic Dacryocystorhinostomy. Sci Rep, 2017. 7(1): p. 6809.
14. Pradhan, P., et al., Double Posterior Based Flap Technique in Primary Endoscopic Dacryocystorhinostomy With and Without Using Powered Instrument. Indian J Otolaryngol Head Neck Surg, 2017. 69(4): p. 474-479.
15. Mueller, S.K., et al., Endoscopic DCR using bipedicled interlacing mucosal flaps. Laryngoscope, 2018. 128(4): p. 794-797.
16. Trimarchi, M., et al., Anastomosis of nasal mucosal and lacrimal sac flaps in endoscopic dacryocystorhinostomy. Eur Arch Otorhinolaryngol, 2009. 266(11): p. 1747-52.
17. Kirtane, M.V., et al., Endoscopic dacryocystorhinostomy with flap suturing. Indian J Otolaryngol Head Neck Surg, 2013. 65(Suppl 2): p. 236-41.
18. Lee, J.J., et al., Learning Curve for Endoscopic Endonasal Dacryocystorhinostomy. Korean J Ophthalmol, 2017. 31(4): p. 299-305.
19. Ali, M.J., et al., Endoscopic assessment of the dacryocystorhinostomy ostium after powered endoscopic surgery: behaviour beyond 4 weeks. Clin Exp Ophthalmol, 2015. 43(2): p. 152-5.
20. Jordan, D.R. and H. McDonald, Failed dacryocystorhinostomy: the sump syndrome. Ophthalmic Surg, 1993. 24(10): p. 692-3.
21. Qian, Z., et al., A Lacrimal Sump Syndrome With a Large Intranasal Ostium. J Craniofac Surg, 2015. 26(5): p. e386-8.
22. Sng, J., et al., Late dacryocystorhinostomy failure from lacrimal sump syndrome with pseudo-sac formation. Can J Ophthalmol, 2018. 53(4): p. e144-e148.
23. Kakizaki, H., et al., Prevention of re-obstruction in watery eye treatment: three-flap technique in external dacryocystorhinostomy. Graefes Arch Clin Exp Ophthalmol, 2016. 254(12): p. 2455-2460.
24. Serin, D., et al., External dacryocystorhinostomy: Double-flap anastomosis or excision of the posterior flaps? Ophthalmic Plast Reconstr Surg, 2007. 23(1): p. 28-31.
25. Takahashi, Y., H. Mito, and H. Kakizaki, External Dacryocystorhinostomy With or Without Double Mucosal Flap Anastomosis: Comparison of Surgical Outcomes. J Craniofac Surg, 2015. 26(4): p. 1290-3.
26. Evereklioglu, C., et al., Figure-of-eight vertical mattress suture technique for anterior flap suspension to overlying tissues in external dacryocystorhinostomy. Am J Ophthalmol, 2007. 143(2): p. 328-333.
27. Deka, A., S.P. Saikia, and S.K. Bhuyan, Combined posterior flap and anterior suspended flap dacryocystorhinostomy: A modification of external dacryocystorhinostomy. Oman J Ophthalmol, 2010. 3(1): p. 18-20.
28. Erdogan, G., et al., Inferior flap anastomosis in external dacryocystorhinostomy. Ophthalmic Plast Reconstr Surg, 2010. 26(4): p. 277-80.
29. Gupta, V.P., P. Gupta, and R. Gupta, Combined posterior flap and anterior suspended flap external dacryocystorhinostomy. Oman J Ophthalmol, 2011. 4(1): p. 40-1.
30. Bukhari, A.A., Meta-analysis of the effect of posterior mucosal flap anastomosis in primary external dacryocystorhinostomy. Clin Ophthalmol, 13. 7: p. 2281-5.
31. Katuwal, S., et al., External dacryocystorhinostomy: do we really need to repair the posterior flap? Orbit, 2013. 32(2): p. 102-6.
32. Dirim, B., et al., Comparison of Modifications in Flap Anastomosis Patterns and Skin Incision Types for External Dacryocystorhinostomy: Anterior-Only Flap Anastomosis with W Skin Incision versus Anterior and Posterior Flap Anastomosis with Linear Skin Incision. ScientificWorldJournal, 2015. 2015: p. 170841.
33. akahashi, Y., Y. Nakamura, and H. Kakizaki, Eight-flap anastomosis in external dacryocystorhinostomy. Br J Ophthalmol, 2015. 99(11): p. 1527-30.
Nattawat Wanumkang : Endonasal Flap Management

19Asia Pacific Society of Ophthalmic Plastic & Reconstructive Surgery
Dacryocystorhinostomy (DCR) has been the standard of treatment for saccal or postsaccal nasolacrimal duct obstruction in adults. Since the advent of modern DCR by Totti 1904,1,2 external DCR has been the gold standard of management. There were few modifications by Dupuy-Dutemps and Bourget, 19203 and the surgical approach entertained nearly 100 years of high success rate. With the rise of minimally invasive techniques in various subspecialty, new approaches were seeked forth and researched. cutaneous scar, long operation time, intraoperative bleeding and injury to lacrimal pump were few drawbacks of external dcr. though Caldwell had advocated endonasal DCR long ago,1893;4 it wasn’t popular due to lack of proper instruments and illumination sources. Endoscopic endonasal DCR approach took pace along with development of rigid endoscopes, Functional endoscopic sinus surgery (FESS) and various bright and malleable light sources. While lacrimal bones, nasal mucosa and lacrimal sac were still debrided mechanically, LASER was seen to produce dry and controlled surgical field. The laser DCR was developed and first described by Massaro et al. 1990.5,6 The uses of LASER are vast and is scrutinized for use in dacryology day by day.
This review of literature for last ten years was done to see the changing pattern of DCR surgery and compare the effectiveness of different surgical approaches against saccal and post saccal nasolacrimal duct obstruction in adults.
METHODOLOGY
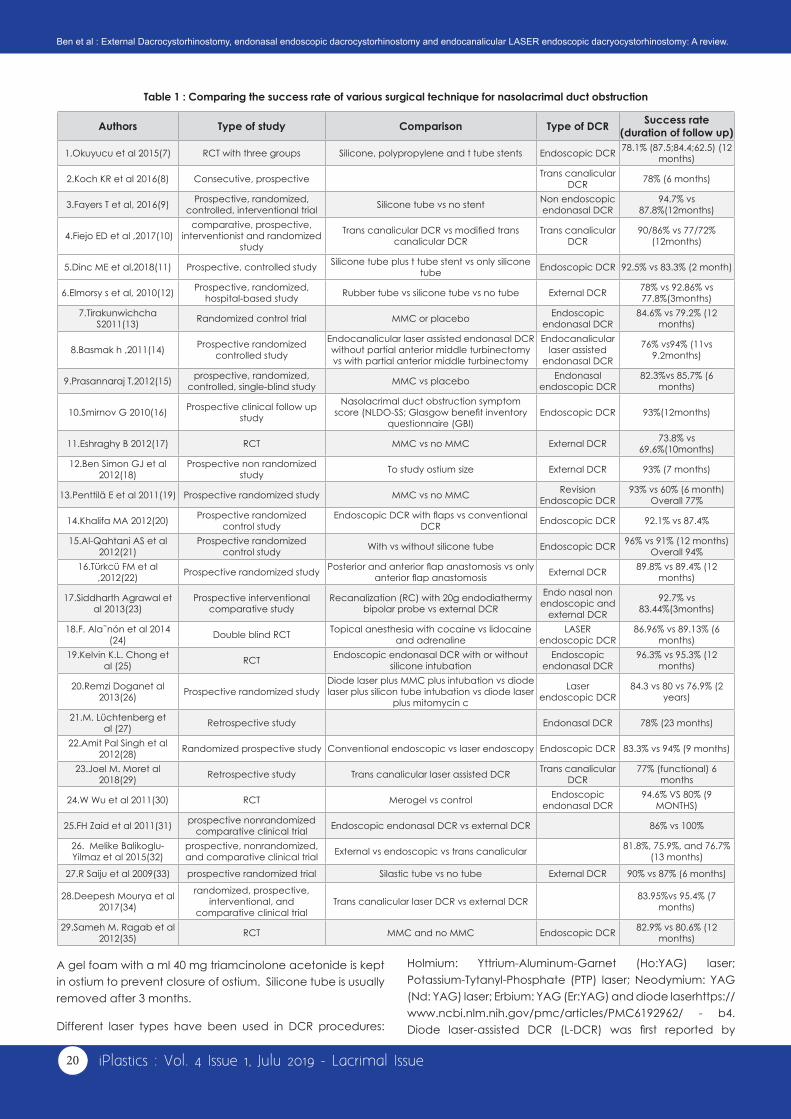
A PubMed online search with dacryocystorhinostomy was done with clinical trials and 10 years as filters. Of the 56 articles published in the duration, 29 articles were directly or indirectly involved with different approaches of adult DCR and had success rates (either anatomical or functional). Table 1. The published data were not homogenous and only one article had RCT comparing the three approaches. The duration of follow up were different. It is difficult to compare between a heterogenous group of studies with different follow up but we could study the individual success rates, common surgeries done, list advantages and disadvantages of different surgical approaches.
TECHNIQUES
External DCR are usually done under Local anesthesia with or without sedation. Infraorbital, anterior ethmoidal nerve block and local infiltration at incision site using 2% Lidocaine
Ben Limbu,MD,1 Triptesh Raj Pandey MD,2 Hom Bahadur Gurung, MD3
1Tilganga Institute Of Ophthalmology, 2Mechi Netralaya , 3Hetauda Community Eye Hospital
Corresponding Email: [email protected]
External Dacrocystorhinostomy, endonasal endoscopic dacrocystorhinostomy and
endocanalicular LASER endoscopic dacryocystorhinostomy: A review.
with Adrenaline 1: 100,000 and 0.5% Bupivacaine are given. Nasal packing is done with gauge ribbon soaked in 4% Lidocaine with Adrenaline 1:100,000 and Oxymetazoline 0.05% w. skin incision sites differ to different surgeons; the goal is to avoid visible scar as much as possible and avoid angular veins usually situated 8 mm medial to medial canthus. The orbicularis is usually dissected with blunt scissors up to periosteum. Medial canthus is cut or scrapped off to expose the lacrimal sac. It is pushed laterally and bone window is created through the naturally thin juncture of maxillary and lacrimal suture. Bones are nibbled by different sizes of Kerrison bone punch. Nasal mucosa is reached and cut into anterior and posterior flaps. Lacrimal sac is opened like a book from apex to neck and relaxing incisions given to form anterior and posterior flaps. Silicon tubes may or may not be placed. Some surgeons prefer suturing both flaps while most suture only the anterior flaps. Studies have shown no significant difference in results comparing posterior flap resection versus posterior flap anastomosis. Orbicularis and skin are sutured in layers. silicone tube is traditionally removed after 6 weeks.
Endoscopic DCR requires added machines and instrumentation. Light source, endoscopes of different sizes, motorized drill, tissue scraper, taka Yashi forceps and visual system. General anesthesia is the preferred anesthesia but surgeons have done even under local anesthesia with or without sedation. Nasal packing with ribbon gauge soaked in 4%Lidocaine with Adrenaline 1:100,000 and Oxymetazoline 0.05% was done for at least five minutes. A vitreoretinal light pipe or A bowman probe is inserted through the upper punctum and the common canaliculus into the lacrimal sac to identify the location of sac. The probe can be pricked through the lacrimal bone bringing it out from the sac through the mucosa of the lateral wall of the nasal cavity anterior to the middle turbinate. Local infiltration is given at and above the medial turbinate. The axilla of middle turbinate is the landmark corresponding the lacrommaxillary suture line. A C-shaped nasal flap is created for exposing frontal process of maxilla. Some surgeons use motorized tissue scrapper to remove the lateral mucosa flap. Boney ostium is created after removing the frontal process of maxillae and lacrimal bone with Kerrison rongeur of size 2 mm, 3 mm and oscillating diamond burr. Lateral wall of lacrimal sac is opened and widened with sickle blade with radial incisions superiorly and inferiorly. A Silicon tube is intubated from the upper and lower puncta and fixed onto the nasal mucosa near the nostril with a 5-0 polypropylene.
Review Article
20 iPlastics : Vol. 4 Issue 1, Julu 2019 - Lacrimal Issue
Table 1 : Comparing the success rate of various surgical technique for nasolacrimal duct obstruction
Authors Type of study Comparison Type of DCR Success rate (duration of follow up)
1.Okuyucu et al 2015(7) RCT with three groups Silicone, polypropylene and t tube stents Endoscopic DCR 78.1% (87.5;84.4;62.5) (12 months)
2.Koch KR et al 2016(8) Consecutive, prospective Trans canalicular DCR 78% (6 months)
3.Fayers T et al, 2016(9) Prospective, randomized, controlled, interventional trial Silicone tube vs no stent Non endoscopic
endonasal DCR94.7% vs
87.8%(12months)
4.Fiejo ED et al ,2017(10)comparative, prospective,
interventionist and randomized study
Trans canalicular DCR vs modified trans canalicular DCR
Trans canalicular DCR
90/86% vs 77/72% (12months)
5.Dinc ME et al,2018(11) Prospective, controlled study Silicone tube plus t tube stent vs only silicone tube Endoscopic DCR 92.5% vs 83.3% (2 month)
6.Elmorsy s et al, 2010(12) Prospective, randomized, hospital-based study Rubber tube vs silicone tube vs no tube External DCR 78% vs 92.86% vs
77.8%(3months)7.Tirakunwichcha
S2011(13) Randomized control trial MMC or placebo Endoscopic endonasal DCR
84.6% vs 79.2% (12 months)
8.Basmak h ,2011(14) Prospective randomized controlled study
Endocanalicular laser assisted endonasal DCR without partial anterior middle turbinectomy vs with partial anterior middle turbinectomy
Endocanalicular laser assisted
endonasal DCR
76% vs94% (11vs 9.2months)
9.Prasannaraj T,2012(15) prospective, randomized, controlled, single-blind study MMC vs placebo Endonasal
endoscopic DCR82.3%vs 85.7% (6
months)
10.Smirnov G 2010(16) Prospective clinical follow up study
Nasolacrimal duct obstruction symptom score (NLDO-SS; Glasgow benefit inventory
questionnaire (GBI) Endoscopic DCR 93%(12months)
11.Eshraghy B 2012(17) RCT MMC vs no MMC External DCR 73.8% vs 69.6%(10months)
12.Ben Simon GJ et al 2012(18)
Prospective non randomized study To study ostium size External DCR 93% (7 months)
13.Penttilä E et al 2011(19) Prospective randomized study MMC vs no MMC Revision Endoscopic DCR
93% vs 60% (6 month) Overall 77%
14.Khalifa MA 2012(20) Prospective randomized control study
Endoscopic DCR with flaps vs conventional DCR Endoscopic DCR 92.1% vs 87.4%
15.Al-Qahtani AS et al 2012(21)
Prospective randomized control study With vs without silicone tube Endoscopic DCR 96% vs 91% (12 months)
Overall 94%16.Türkcü FM et al
,2012(22) Prospective randomized study Posterior and anterior flap anastomosis vs only anterior flap anastomosis External DCR 89.8% vs 89.4% (12
months)
17.Siddharth Agrawal et al 2013(23)
Prospective interventional comparative study
Recanalization (RC) with 20g endodiathermy bipolar probe vs external DCR
Endo nasal non endoscopic and
external DCR
92.7% vs 83.44%(3months)
18.F. Ala˜nón et al 2014 (24) Double blind RCT Topical anesthesia with cocaine vs lidocaine
and adrenaline LASER
endoscopic DCR86.96% vs 89.13% (6
months)19.Kelvin K.L. Chong et
al (25) RCT Endoscopic endonasal DCR with or without silicone intubation
Endoscopic endonasal DCR
96.3% vs 95.3% (12 months)
20.Remzi Doganet al 2013(26) Prospective randomized study
Diode laser plus MMC plus intubation vs diode laser plus silicon tube intubation vs diode laser
plus mitomycin c
Laser endoscopic DCR
84.3 vs 80 vs 76.9% (2 years)
21.M. Lüchtenberg et al (27) Retrospective study Endonasal DCR 78% (23 months)
22.Amit Pal Singh et al 2012(28) Randomized prospective study Conventional endoscopic vs laser endoscopy Endoscopic DCR 83.3% vs 94% (9 months)
23.Joel M. Moret al 2018(29) Retrospective study Trans canalicular laser assisted DCR Trans canalicular
DCR77% (functional) 6
months
24.W Wu et al 2011(30) RCT Merogel vs control Endoscopic endonasal DCR
94.6% VS 80% (9 MONTHS)
25.FH Zaid et al 2011(31) prospective nonrandomized comparative clinical trial Endoscopic endonasal DCR vs external DCR 86% vs 100%
26. Melike Balikoglu-Yilmaz et al 2015(32)
prospective, nonrandomized, and comparative clinical trial External vs endoscopic vs trans canalicular 81.8%, 75.9%, and 76.7%
(13 months)
27.R Saiju et al 2009(33) prospective randomized trial Silastic tube vs no tube External DCR 90% vs 87% (6 months)
28.Deepesh Mourya et al 2017(34)
randomized, prospective, interventional, and
comparative clinical trialTrans canalicular laser DCR vs external DCR 83.95%vs 95.4% (7
months)
29.Sameh M. Ragab et al 2012(35) RCT MMC and no MMC Endoscopic DCR 82.9% vs 80.6% (12
months)
A gel foam with a ml 40 mg triamcinolone acetonide is kept in ostium to prevent closure of ostium. Silicone tube is usually removed after 3 months.
Different laser types have been used in DCR procedures:
Holmium: Yttrium-Aluminum-Garnet (Ho:YAG) laser; Potassium-Tytanyl-Phosphate (PTP) laser; Neodymium: YAG (Nd: YAG) laser; Erbium: YAG (Er:YAG) and diode laserhttps://www.ncbi.nlm.nih.gov/pmc/articles/PMC6192962/ - b4. Diode laser-assisted DCR (L-DCR) was first reported by
Ben et al : External Dacrocystorhinostomy, endonasal endoscopic dacrocystorhinostomy and endocanalicular LASER endoscopic dacryocystorhinostomy: A review.

21Asia Pacific Society of Ophthalmic Plastic & Reconstructive Surgery
Eloy et al in 2000. It used more and more because L-DCR had less tissue damage and sufficient osteotomy can be created using diode laser. The advantages of diode laser are; no external facial skin scar, local anesthesia possibility, less hemorrhage, fast procedure and minimal intra- and postoperative complications. After cleansing and draping the surgical site, the upper and lower canaliculi are dilated using Bowman probes. A rigid nasal endoscope with a 0-degree angle is inserted into the nose. Multidiode laser is used. The radius of the diode laser fiberoptic probe used is 600 µm. This probe is introduced into the lacrimal sac through the upper and lower canaliculi, until the transillumination of the aiming beam could be seen via the nasal endoscope just lateral and superior to the middle turbinate. Of 980 nm diode laser is applied until the largest possible osteotomy is achieved. The area of osteotomy is expanded to approximately 8-10 mm in diameter, and coagulated using diode-laser, carbonized tissue is removed under endoscopic guidance. Lacrimal passage is irrigated and silicon tube intubation is done at the end of the surgery.6,34,36,37
ADVANTAGES AND DISADVANTAGE
External DCR has been the time-tested gold standard procedure for years. It boasts a good success rate up to 100%, has short learning curve, cheaper instrumentation
Table 2 : Success rate of external DCR, endoscopic DCR and trans canalicular LASER DCR
Type of DCR Success rates (maximum and anatomical taken wherever available) Average (range)EXTERNAL DCR 92.86;93%;89.8%;83.44%;100%;81.8%;90%;95.4% 90.79% (81.8%-100%)
Endo nasal Endoscopic DCR 82.9%;75.9%;86%;94.6%;83.3%;96.3%;96%;92.1%;93%;93%;85.7%;84.6%;92.5%;87.5%;94.7% 89.21% (75.9%-96.3%)
Trans canalicular LASER endoscopic DCR 78%;86%;94%;89.13%;84.3%;77%;76.7%;83.95% 83.635(76.5%-94%)
and availability and affordability to all centers. Though cutaneous scars, long surgical time and injury to lacrimal pump mechanism is of high concern in minimally invasive surgery era. Endoscopic endonasal approach in DCR have no cutaneous scars and theoretically preserve the lacrimal pump. It is also said to be effective in acute dacryocystitis and handy for revision DCR. The downside of it is of course the costly instruments (one-time investment) and a steeper learning curve. The recovery time is quite less than external DCR. LASER trans canalicular DCR came with promising hopes of faster and precise ostium with less bleeding. It is costly and steep learning curve with fair success rates.31,32,37,38
CONCLUSION
The 10 years studies show that there are fairly consistent results with external and endoscopic DCR surgery with short surgical time. One reason may be people are getting used to with endoscopes and better instruments are developed like debrider and burr. The adjuncts like mitomycin C, silicone stent and merogel have shown inconsistent results. Different type of LASER has been used and diode LASER has shown better perspective in better hands. Endoscopic DCR is certainly getting more popular and effective day by day.
Table 3 : Comparision of different factors among External DCR, endoscopic DCR and trans canalicular LASER DCR
Sn Characteristics External
Dacryocystorhinostomy (Ex-DCR)
Endoscopic Endonasal Dacryocystorhinostomy
(EE-DCR)
Endocanalicular LASER Endoscopic Dacryocystorhinostomy
(EL-DCR)1. Surgicallly invasive High Less Very less
2. Operation time * More Less Less
3. External cutaneous scar Present Absent Absent
4. Lacrimal pump May be damaged Preserved Preserved
5. Post-operative rehabilitation Long Short Short
6. Cost of surgery Less High Very high
7. Learning curve Smooth Moderate Steep
8. Bony ostium Big Moderate Small
9. Success rate High High Moderate
10. Availability Common Fairly common Less common
REFERENCES1. Harish V, Benger RS. Origins of lacrimal surgery, and evolution of dacryocystorhinostomy to the present. Clinical & experimental ophthalmology.
2014;42(3):284-7.2. A. T. Nuovo metodo conservatore di cura radicale delle suppurazioni croniche del sacco lacrimale (dacriocistorinostomia). Clin Mod Firenze.
1904(10):385–7.3. Dupuy-Dutemps L, Bourguet M. Procede plastique de dacryocystorhinostomie et ses resultats1921. 241-61 p.4. GW C. Two new operations for obstruction of the nasal duct with preservation of the canaliculi, and an incidental description of a new lachrymal
probe. N Y Med J 1893(57):581.5. Massaro BM, Gonnering RS, Harris GJ. Endonasal laser dacryocystorhinostomy. A new approach to nasolacrimal duct obstruction. Archives of
ophthalmology (Chicago, Ill : 1960). 1990;108(8):1172-6.
Ben et al : External Dacrocystorhinostomy, endonasal endoscopic dacrocystorhinostomy and endocanalicular LASER endoscopic dacryocystorhinostomy: A review.

22 iPlastics : Vol. 4 Issue 1, Julu 2019 - Lacrimal Issue
6. Doğan M, Alizada A, Yavaş GF, Kahveci OK, Bakan O. Laser-assisted dacryocystorhinostomy in nasolacrimal duct obstruction: 5-year follow-up. Int J Ophthalmol. 2018;11(10):1616-20.
7. Okuyucu S, Gorur H, Oksuz H, Akoglu E. Endoscopic dacryocystorhinostomy with silicone, polypropylene, and T-tube stents; randomized controlled trial of efficacy and safety. American journal of rhinology & allergy. 2015;29(1):63-8.
8. KR, Cursiefen C, Heindl LM. [Transcanalicular Laser Dacryocystorhinostomy: One-Year-Experience in the Treatment of Acquired Nasolacrimal Duct Obstructions]. Klinische Monatsblatter fur Augenheilkunde. 2016;233(2):182-6.
9. Fayers T, Dolman PJ. Bicanalicular Silicone Stents in Endonasal Dacryocystorhinostomy: Results of a Randomized Clinical Trial. Ophthalmology. 2016;123(10):2255-9.
10. Feijo ED, Caixeta JA, de Souza Nery AC, Limongi RM, Matayoshi S. A comparative study of modified transcanalicular diode laser dacryocystorhinostomy versus conventional transcanalicular diode laser dacryocystorhinostomy. European archives of oto-rhino-laryngology : official journal of the European Federation of Oto-Rhino-Laryngological Societies (EUFOS) : affiliated with the German Society for Oto-Rhino-Laryngology - Head and Neck Surgery. 2017;274(8):3129-34.
11. Dinc ME, Ulusoy S, Sahin E, Bozan N, Avincsal MO, Tutar B, et al. The use of an ostial stent does not increase the success rate of endoscopic dacryocystorhinostomy. The Journal of laryngology and otology. 2018;132(8):718-23.
12. Elmorsy S, Fayek HM. Rubber tube versus silicone tube at the osteotomy site in external dacryocystorhinostomy. Orbit (Amsterdam, Netherlands). 2010;29(2):76-82.
13. Tirakunwichcha S, Aeumjaturapat S, Sinprajakphon S. Efficacy of mitomycin C in endonasal endoscopic dacryocystorhinostomy. The Laryngoscope. 2011;121(2):433-6.
14. Basmak H, Cakli H, Sahin A, Gursoy H, Ozer A, Colak E. What is the role of partial middle turbinectomy in endocanalicular laser-assisted endonasal dacryocystorhinostomy? American journal of rhinology & allergy. 2011;25(4):e160-5.
15. Prasannaraj T, Kumar BY, Narasimhan I, Shivaprakash KV. Significance of adjunctive mitomycin C in endoscopic dacryocystorhinostomy. American journal of otolaryngology. 2012;33(1):47-50.
16. Smirnov G, Tuomilehto H, Kokki H, Kemppainen T, Kiviniemi V, Nuutinen J, et al. Symptom score questionnaire for nasolacrimal duct obstruction in adults--a novel tool to assess the outcome after endoscopic dacryocystorhinostomy. Rhinology. 2010;48(4):446-51.
17. Eshraghy B, Raygan F, Tabatabaie SZ, Tari AS, Kasaee A, Rajabi MT. Effect of mitomycin C on success rate in dacryocystorhinostomy with silicone tube intubation and improper flaps. European journal of ophthalmology. 2012;22(3):326-9.
18. Ben Simon GJ, Brown C, McNab AA. Larger Osteotomies Result in Larger Ostia in External DacryocystorhinostomiesLarger Ostia in External Dacryocystorhinostomies. JAMA Facial Plastic Surgery. 2012;14(2):127-31.
19. Penttila E, Smirnov G, Seppa J, Kaarniranta K, Tuomilehto H. Mitomycin C in revision endoscopic dacryocystorhinostomy: a prospective randomized study. American journal of rhinology & allergy. 2011;25(6):425-8.
20. Khalifa MA, Ragab SM, Saafan ME, El-Guindy AS. Endoscopic dacryocystorhinostomy with double posteriorly based nasal and lacrimal flaps: a prospective randomized controlled trial. Otolaryngology--head and neck surgery : official journal of American Academy of Otolaryngology-Head and Neck Surgery. 2012;147(4):782-7.
21. Al-Qahtani AS. Primary endoscopic dacryocystorhinostomy with or without silicone tubing: a prospective randomized study. American journal of rhinology & allergy. 2012;26(4):332-4.
22. Turkcu FM, Oner V, Tas M, Alakus F, Iscan Y. Anastomosis of both posterior and anterior flaps or only anterior flaps in external dacryocystorhinostomy. Orbit (Amsterdam, Netherlands). 2012;31(6):383-5.
23. Siddharth Agrawal SKG, Vinita Singh, and Saurabh Agrawa. A novel technique to recanalize the nasolacrimal duct with endodiathermy bipolar probe. Indian J Ophthalmol. 2013;12(61):718–21.`
24. Alañón F AM, Jiménez JA, Calero B, Noriega A, Plaza G. Comparison between topical anaesthesia with cocaine versus lidocaine plus adrenaline for outpatient laser dacryocystorhinostomy. Arch Soc Esp Oftalmol. 2014 Feb;2(89):53-7.
25. Chong KK, Lai FH, Ho M, Luk A, Wong BW, Young A. Randomized trial on silicone intubation in endoscopic mechanical dacryocystorhinostomy (SEND) for primary nasolacrimal duct obstruction. Ophthalmology. 2013;120(10):2139-45.
26. Dogan R, Meric A, Ozsutcu M, Yenigun A. Diode laser-assisted endoscopic dacryocystorhinostomy: a comparison of three different combinations of adjunctive procedures. European archives of oto-rhino-laryngology : official journal of the European Federation of Oto-Rhino-Laryngological Societies (EUFOS) : affiliated with the German Society for Oto-Rhino-Laryngology - Head and Neck Surgery. 2013;270(8):2255-61.
27. Lüchtenberg M, Tratz F, Schalnus R, Helbig M, May A. Endonasale mikroskopische Dakryozystorhinostomie mit Endoillumination und Intubation bei Patienten mit kombinierten Tränenwegspathologien oder Revisionen. Klin Monatsbl Augenheilkd. 2013;230(01):46-50.
28. Singh AP, Narula V, Meher R. Uma nova abordagem para a dacriocistorrinostomia endoscópica. Brazilian Journal of Otorhinolaryngology. 2012;78:7-11.
29. Mor JM, Matthaei M, Schrumpf H, Koch KR, Bölke E, Heindl LM. Transcanalicular laser dacryocystorhinostomy for acquired nasolacrimal duct obstruction: an audit of 104 patients. Eur J Med Res. 2018;23(1):58-.
30. Wu W, Cannon PS, Yan W, Tu Y, Selva D, Qu J. Effects of Merogel coverage on wound healing and ostial patency in endonasal endoscopic dacryocystorhinostomy for primary chronic dacryocystitis. Eye (London, England). 2011;25(6):746-53.
31. Zaidi FH, Symanski S, Olver JM. A clinical trial of endoscopic vs external dacryocystorhinostomy for partial nasolacrimal duct obstruction. Eye (Lond). 2011;25(9):1219-24.
32. Balikoglu-Yilmaz M, Yilmaz T, Taskin U, Taskapili M, Akcay M, Oktay MF, et al. Prospective comparison of 3 dacryocystorhinostomy surgeries: external versus endoscopic versus transcanalicular multidiode laser. Ophthalmic plastic and reconstructive surgery. 2015;31(1):13-8.
33. Saiju R, Morse LJ, Weinberg D, Shrestha MK, Ruit S. Prospective randomised comparison of external dacryocystorhinostomy with and without silicone intubation. The British journal of ophthalmology. 2009;93(9):1220-2.
34. Mourya D, Rijal RK. Transcanalicular laser-assisted dacryocystorhinostomy with diode laser. Orbit (Amsterdam, Netherlands). 2017;36(6):370-4.35. Ragab SM, Elsherif HS, Shehata EM, Younes A, Gamea AM. Mitomycin C-enhanced revision endoscopic dacryocystorhinostomy: a prospective
randomized controlled trial. Otolaryngology--head and neck surgery : official journal of American Academy of Otolaryngology-Head and Neck Surgery. 2012;147(5):937-42.
36. Mor JM, Guo Y, Koch KR, Heindl LM. Transcanalicular Diode Laser-assisted Dacryocystorhinostomy for the Treatment of Primary Acquired Nasolacrimal Duct Obstruction. Journal of visualized experiments : JoVE. 2017(128).
37. Mirza S. JN. Laser-Assisted Dacryocystorhinostomy. Weber R.K. KR, Schaefer S.D., Della Rocca R.C., editor. Berlin, Heidelberg: Springer; 2007.38. Waly MA, Shalaby OE, Elbakary MA, Hashish AA. The cosmetic outcome of external dacryocystorhinostomy scar and factors affecting it. Indian
journal of ophthalmology. 2016;64(4):261-5.
Ben et al : External Dacrocystorhinostomy, endonasal endoscopic dacrocystorhinostomy and endocanalicular LASER endoscopic dacryocystorhinostomy: A review.
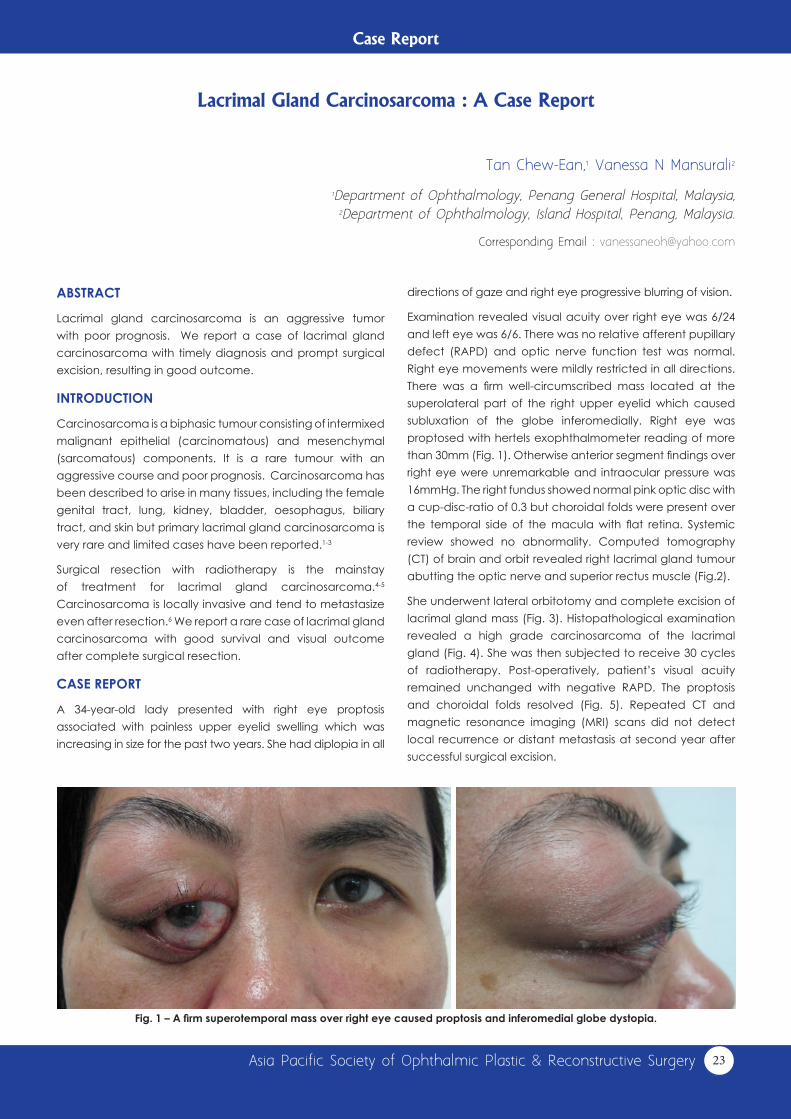
23Asia Pacific Society of Ophthalmic Plastic & Reconstructive Surgery
Case Report
ABSTRACT
Lacrimal gland carcinosarcoma is an aggressive tumor with poor prognosis. We report a case of lacrimal gland carcinosarcoma with timely diagnosis and prompt surgical excision, resulting in good outcome.
INTRODUCTION
Carcinosarcoma is a biphasic tumour consisting of intermixed malignant epithelial (carcinomatous) and mesenchymal (sarcomatous) components. It is a rare tumour with an aggressive course and poor prognosis. Carcinosarcoma has been described to arise in many tissues, including the female genital tract, lung, kidney, bladder, oesophagus, biliary tract, and skin but primary lacrimal gland carcinosarcoma is very rare and limited cases have been reported.1-3
Surgical resection with radiotherapy is the mainstay of treatment for lacrimal gland carcinosarcoma.4-5
Carcinosarcoma is locally invasive and tend to metastasize even after resection.6 We report a rare case of lacrimal gland carcinosarcoma with good survival and visual outcome after complete surgical resection.
CASE REPORT
A 34-year-old lady presented with right eye proptosis associated with painless upper eyelid swelling which was increasing in size for the past two years. She had diplopia in all
Tan Chew-Ean,1 Vanessa N Mansurali2
1Department of Ophthalmology, Penang General Hospital, Malaysia, 2Department of Ophthalmology, Island Hospital, Penang, Malaysia.
Corresponding Email : [email protected]
Lacrimal Gland Carcinosarcoma : A Case Report
directions of gaze and right eye progressive blurring of vision.
Examination revealed visual acuity over right eye was 6/24 and left eye was 6/6. There was no relative afferent pupillary defect (RAPD) and optic nerve function test was normal. Right eye movements were mildly restricted in all directions. There was a firm well-circumscribed mass located at the superolateral part of the right upper eyelid which caused subluxation of the globe inferomedially. Right eye was proptosed with hertels exophthalmometer reading of more than 30mm (Fig. 1). Otherwise anterior segment findings over right eye were unremarkable and intraocular pressure was 16mmHg. The right fundus showed normal pink optic disc with a cup-disc-ratio of 0.3 but choroidal folds were present over the temporal side of the macula with flat retina. Systemic review showed no abnormality. Computed tomography (CT) of brain and orbit revealed right lacrimal gland tumour abutting the optic nerve and superior rectus muscle (Fig.2).
She underwent lateral orbitotomy and complete excision of lacrimal gland mass (Fig. 3). Histopathological examination revealed a high grade carcinosarcoma of the lacrimal gland (Fig. 4). She was then subjected to receive 30 cycles of radiotherapy. Post-operatively, patient’s visual acuity remained unchanged with negative RAPD. The proptosis and choroidal folds resolved (Fig. 5). Repeated CT and magnetic resonance imaging (MRI) scans did not detect local recurrence or distant metastasis at second year after successful surgical excision.
Fig. 1 – A firm superotemporal mass over right eye caused proptosis and inferomedial globe dystopia.

24 iPlastics : Vol. 4 Issue 1, Julu 2019 - Lacrimal Issue
Fig. 2 – CT scan of axial view (A) and coronal view (B) revealed right lacrimal gland tumour abutting the optic nerve and superior rectus muscle.
Fig. 3 – Lacrimal gland tumour excised measuring 40mm x 30mm.
Fig. 4 – Histopathological examination demonstrated high grade carcinosarcoma of the lacrimal gland.
Fig. 5 – No recurrence noted after two years surgical excision of lacrimal gland tumour.
DISCUSSION
Carcinosarcoma is a highly aggressive and infiltrative tumor. It can occur in the epithelium of any part of the body. There is limited published data regarding carcinosarcoma, most of which involves the respiratory system (1% of all lung
malignancies) and urinary system (0.11% of all bladder malignancies).8-10 Orbital and lacrimal gland carcinosarcoma are rarely reported. Recent literature identified only 7 cases of primary orbital carcinosarcoma and 3 of them were lacrimal gland carcinosarcoma.1-3,6,7 Table 1 summarizes the
Tan et al : Lacrimal Gland Carcinosarcoma : A Case Report

25Asia Pacific Society of Ophthalmic Plastic & Reconstructive Surgery
published data of lacrimal gland carcinosarcoma and our patient outcomes.
Lacrimal gland carcinosarcoma is extremely rare and the overall prognosis is poor as patients usually present with late-stage disease, frequent nodal involvement and distant metastatic spread. Advanced patient age, female sex and the evidence of distant metastases adversely affect prognosis.11 Most of the lacrimal gland carcinosarcoma patients were female including our patient.2-3 Carcinosarcoma usually occurs in post-menopausal women with reported cases being aged 56 -91 years old.6 However, our patient is the youngest among them. Our patient presented with the similar presentation of Takahira’s patient which was eyelid mass, proptosis and reduced vision.3
Management of lacrimal gland carcinoma requires aggressive surgical excision along with adjuvant chemotherapy and radiation therapy. It appears that the carcinomatous component of the tumour is more sensitive than the sarcomatous component to radiation and chemotherapy.12 Our patient underwent surgical resection and histopathological examination showed high grade carcinosarcoma. She then completed 30 cycles of radiotherapy. Apart from radiotherapy, treatment using
chemotherapy such as vincristine, etoposide, ifosfamide, doxorubicin, 5-fluorouracil, and cisplatin have been applied in other extraorbital carcinosarcoma.6
Reported 5-year survival rates of carcinosarcoma range between 63 and 94%; overall mortality is 30 to 34%.11 Patients with extraorbital carcinosarcoma or metastasis to orbit region have been reported to have higher mortality and recurrence rate.13 In our patient, neither local recurrence nor distant metastasis has been observed after 2 years post excision, similar with Takahira’s patient.3
However, Font et al. reported that their patient with lacrimal gland carcinoma had defaulted follow-up and was found to have lung metastasis eventually.
CONCLUSIONCarcinosarcoma is an aggressive neoplasm that exhibits local tissue invasion and often metastasizes. Carcinosarcoma of the orbit may locally invade the intracranial cavity, and thus be related to a high rate of mortality. The length of time between presentation and treatment influences the prognosis; a delay in treatment could adversely affect the patient’s outcome. Hence, timely diagnosis and prompt institution of aggressive treatment are vital in improving the patient’s survival and visual outcome.
REFERENCES1. Ni C, Kuo PK, Dryja TP. Histopathological classification of 272 primary epithelial tumors of the lacrimal gland. Chin Med J (Engl) 1992;105:481–5. 2. Font RL, Smith SL, Bryan RG. Malignant epithelial tumors of the lacrimal gland: a clinicopathologic study of 21 cases. Arch Ophthalmol.
1998;116:613–6.3. Takahira M, Nakamura Y, Shimizu S, et al. Carcinosarcoma of the lacrimal gland arising from a pleomorphic adenoma. Am J Ophthalmol.
2005;140:337–40.4. Ushiro K. A case of carcinosarcoma of the maxillary sinus [in Japanese] Jibiinkoka. 1983;55:529–33. 5. Hafiz MA, Mira J, Toker C. Postirradiation carcinosarcoma of the nasal cavity. Otolaryngol Head Neck Surg. 1987;97:319–21.6. Prakalapakorn SG, Bernardino CR, Auclair PL, Grossniklaus HE. Carcinosarcoma of the Orbit: Report of Two Cases and Review of the Literature.
Ophthalmology. 2008; 115(11): 2065–70. 7. Mathew N, Mathew M, Farrah J. Sarcomatous Carcinoma of the Orbit: A Case Report and Review of the Literature. Case Rep Ophthalmol.
2015; 6:180-5. 8. Franks TJ, Galvin JR. Sarcomatoid carcinoma of the lung: histologic criteria and common lesions in the differential diagnosis. Arch Pathol Lab
Med 2010;134:49-54.9. Kumar M, Goyal S, Bahl A, Das P, Sharma DN, Ray R, Rath GK. Sarcomatoid carcinoma of the maxillary sinus: a rare head and neck tumor. J
Cancer Res Ther 2008;4:131-133.10. Wang J, Wang FW, Lagrange CA, Hemstreet Iii GPH, Kessinger A. Clinical features of sarcomatoid carcinoma (carcinosarcoma) of the urinary
bladder: analysis of 221 cases. Sarcoma 2010;2010:1-7.11. Van Marck VL, BM. Epithelial-mesenchymal transitions in human cancer: Rise and Fall of Epithelial Phenotype: Concepts of Epithelial-
Mesenchymal Transition. P. Savagner, Ed, Springer: Berlin 2005:111 - 34.12. Sonobe H, Hayashi K, Takahashi K, Ohtsuki Y, Kishimoto S, Saito H, Honjo I. True carcinosarcoma of the maxillary sinus. Pathol Res Pract.
1989;185:488–92.13. Gnepp DR, Henley JD, Simpson RHW, Eveson J. Salivary and Lacrimal Glands. Diagnostic Surgical Pathology of the Head and Neck. 2009;413–562.
Table 1 – Published data of lacrimal gland carcinosarcoma and our patient.
Authors, Year Age (years) Race Sex Laterality Symptoms Pathology Immunohisto-
chemical Stains Treatment Mortality Meta-stasis
Ni et al,1 1992 NA NA NA NA NA NA NA NA NA NA
Font et al,2 1998 NA NA F NA NA NA NA NA Defaulted
follow-up Lung
Takahira et al,3 2005 80 Japanese F Right Eyelid swelling Proptosis
Reduced vision
Arising from pleomorphic adenoma: carcinoma,
osteosarcoma
Cytokeratin AE1,3 +,
CAM5.2 +
Surgical resection
No recurrence 10 months
post-excsionNone
Our patient, 2019 34 Indonesian F Right
Superotemporal orbital mass ProptosisReduced vision
carcinosarcoma NA Surgical resection
No recurrence24 months
post-excisionNone
CAM, cell adhesion molecule; F, female; NA, not available; +, positive staining.
Tan et al : Lacrimal Gland Carcinosarcoma : A Case Report
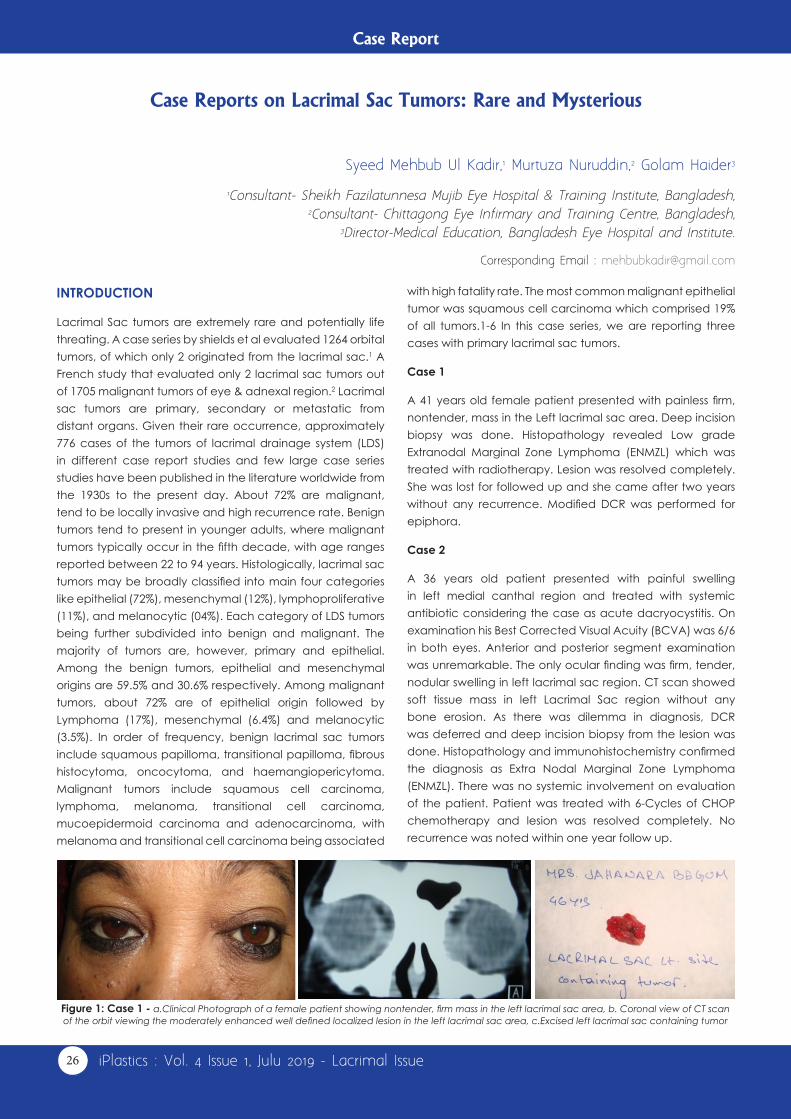
26 iPlastics : Vol. 4 Issue 1, Julu 2019 - Lacrimal Issue
Case Report
INTRODUCTION
Lacrimal Sac tumors are extremely rare and potentially life threating. A case series by shields et al evaluated 1264 orbital tumors, of which only 2 originated from the lacrimal sac.1 A French study that evaluated only 2 lacrimal sac tumors out of 1705 malignant tumors of eye & adnexal region.2 Lacrimal sac tumors are primary, secondary or metastatic from distant organs. Given their rare occurrence, approximately 776 cases of the tumors of lacrimal drainage system (LDS) in different case report studies and few large case series studies have been published in the literature worldwide from the 1930s to the present day. About 72% are malignant, tend to be locally invasive and high recurrence rate. Benign tumors tend to present in younger adults, where malignant tumors typically occur in the fifth decade, with age ranges reported between 22 to 94 years. Histologically, lacrimal sac tumors may be broadly classified into main four categories like epithelial (72%), mesenchymal (12%), lymphoproliferative (11%), and melanocytic (04%). Each category of LDS tumors being further subdivided into benign and malignant. The majority of tumors are, however, primary and epithelial. Among the benign tumors, epithelial and mesenchymal origins are 59.5% and 30.6% respectively. Among malignant tumors, about 72% are of epithelial origin followed by Lymphoma (17%), mesenchymal (6.4%) and melanocytic (3.5%). In order of frequency, benign lacrimal sac tumors include squamous papilloma, transitional papilloma, fibrous histocytoma, oncocytoma, and haemangiopericytoma. Malignant tumors include squamous cell carcinoma, lymphoma, melanoma, transitional cell carcinoma, mucoepidermoid carcinoma and adenocarcinoma, with melanoma and transitional cell carcinoma being associated
Syeed Mehbub Ul Kadir,1 Murtuza Nuruddin,2 Golam Haider3
1Consultant- Sheikh Fazilatunnesa Mujib Eye Hospital & Training Institute, Bangladesh, 2Consultant- Chittagong Eye Infirmary and Training Centre, Bangladesh,
3Director-Medical Education, Bangladesh Eye Hospital and Institute.
Corresponding Email : [email protected]
Case Reports on Lacrimal Sac Tumors: Rare and Mysterious
with high fatality rate. The most common malignant epithelial tumor was squamous cell carcinoma which comprised 19% of all tumors.1-6 In this case series, we are reporting three cases with primary lacrimal sac tumors.
Case 1
A 41 years old female patient presented with painless firm, nontender, mass in the Left lacrimal sac area. Deep incision biopsy was done. Histopathology revealed Low grade Extranodal Marginal Zone Lymphoma (ENMZL) which was treated with radiotherapy. Lesion was resolved completely. She was lost for followed up and she came after two years without any recurrence. Modified DCR was performed for epiphora.
Case 2
A 36 years old patient presented with painful swelling in left medial canthal region and treated with systemic antibiotic considering the case as acute dacryocystitis. On examination his Best Corrected Visual Acuity (BCVA) was 6/6 in both eyes. Anterior and posterior segment examination was unremarkable. The only ocular finding was firm, tender, nodular swelling in left lacrimal sac region. CT scan showed soft tissue mass in left Lacrimal Sac region without any bone erosion. As there was dilemma in diagnosis, DCR was deferred and deep incision biopsy from the lesion was done. Histopathology and immunohistochemistry confirmed the diagnosis as Extra Nodal Marginal Zone Lymphoma (ENMZL). There was no systemic involvement on evaluation of the patient. Patient was treated with 6-Cycles of CHOP chemotherapy and lesion was resolved completely. No recurrence was noted within one year follow up.
Figure 1: Case 1 - a.Clinical Photograph of a female patient showing nontender, firm mass in the left lacrimal sac area, b. Coronal view of CT scan of the orbit viewing the moderately enhanced well defined localized lesion in the left lacrimal sac area, c.Excised left lacrimal sac containing tumor

27Asia Pacific Society of Ophthalmic Plastic & Reconstructive Surgery
Case 3
A 21-year-old young male patient presented with a nontender lesion in the right lacrimal sac area of 2 years’ duration. CT scan of the orbit revealed mildly enhanced homogeneous lesion in the right lacrimal sac. Clinical diagnosis was squamous papilloma in the lacrimal sac. Excision biopsy was performed and histopathology reported the diagnosis of the lacrimal sac lesion as haemangiopericytoma.
Discussion: Recurrence and mortality rates for lacrimal sac tumors are varied. Benign tumours of the lacrimal sac have a good prognosis if completely excised but benign papillomas with inverted pattern have a tendency to recur 10 to 40%. The recurrence rate of invasive squamous cell and transitional cell carcinoma appears to be about 50%. The malignant potential of hemangiopericytoma can be unpredictable. Lymphoid lesions respond to radiotherapy and chemotherapy and have a variable prognosis depending on the extent of the disease and the type of tumor. The most terrible prognosis is that of malignant melanoma despite aggressive treatment.1,5-7
The best management for the suspected tumors
confined to the lacrimal sac, is total excision of the tumor (Dacryocystectomy without osteotomy). A planned DCR or reconstruction may take place at a later date after histological confirmation. Adjuvant (Radiotherapy and or chemotherapy) can be an effective to reduce the rate of recurrence and for incomplete resection.
CONCLUSIONSuccessful management of lacrimal sac tumors requires the following- a high index of suspicion, as these are fatal tumor and often misdiagnosed as dacryocystitis. Early and appropriate aggressive intervention will help to complete resolution of the tumor as well as to reduce the recurrence. It is an important tool for the surgeon to carefully inspect the lacrimal sac during DCR to prevent missing a neoplasm. Careful long term follows up is required, as recurrence and/or metastases may occur even after years of primary treatment.
ACKNOWLEDGMENTThe authors thank Professor Subrahmanyam Mallajosyula, professor and head, department of Ophthalmology, Maharaja Institute of Medical Sciences, India for guide and inspires us to do research work and academic activities.
REFERENCES1. Sheilds JA et al., Survey of 1264 patients with orbital tumors and simulating lesions.Ophthalmology. 2004:; 111(5): 997-1008.2. Scat Y et al. Epidemiological study of 1705 malignant tumors of the eye and adnexa. J Fr Ophthalmol. 1996; 19(2): 83-88.3. Ni C, D’Amico DJ, Fan CQ, Kuo PK. Tumors of the lacrimal sac: A clinicopathological analysis of 82 cases. Int Ophthalmol Clin 1982: 22: 121–140.4. Stefanyszyn M.A et al. Lacrimal Sac Tumors. Journal of Ophthalmic Plastic and Reconstructive Surgery. 1994; 10 (3): 169-94.5. Parmar DN, Rose GE. Management of Lacrimal Sac tumors. Eye. 2003; 17: 599-606.6. Montalban A, Lietin B, Louvier C, et al. Malignant lacrimal sac tumors. Eur Ann Otorhinolaryngol Head and Neck Dis. 2010;127;165-727. Savino G, Battendieri R, Gari M et al. Long term outcomes of primary ocular adnexal lymphoma treatment with intraorbital rituximab injections.
J Cancer Res Clin Oncol. 2013;139: 1251-55.
Figure 2: Case2 - a. Patients with Nodular, firm, tender lesion in the left medial canthal area like as acute dacryocystitis. b. Axial CT scan of the orbit showing soft tissue mass in right Lacrimal Sac region without any bone erosion. c. Resolved left lacrimal sac tumor after completion of treatment.
Figure 3: Case 3 - a. Young patient with a nontender lesion in the right lacrimal sac area, b. Axial CT scan of the orbit showing mild enhanced soft tissue lesion involving the right lacrimal sac area, c. Excised tumor from the right lacrimal sac area
Tan et al : Lacrimal Gland Carcinosarcoma : A Case Report

28 iPlastics : Vol. 4 Issue 1, Julu 2019 - Lacrimal Issue
Case Report
ABSTRACTHemangiopericytoma is a malignant vascular tumor arises from pericapillary cells or pericytes of Zimmerman that may developes anywhere where capillaries are found. Orbital hemangiopericytoma is a rare, potentially malignant vascular tumor, which can affect any part of the orbit. Difficulties in correctly diagnosing this tumor preoperatively compound this problem. Incomplete excision is associated with increased risk of local recurrence and metastatic disease. Treatment options for orbital recurrence include orbital excenteration further attempts at complete excision, or local excision and adjuvant therapy with radiotherapy, brachytherapy, or chemotherapy. Case report. A 33-year old female since the pass 12 years had been complained of a slowly enlarging painless lump on the right medial canthus of her right eye with epiphora. Firstly she felt her right eye was tearing and then a slowly enlarging painless lump on the medial canthus was noted. Neither bloody reflux nor bloody tears had been observed. Patient underwent external DCR. One week after the surgery, the Pathological Anatomy examination showed Malignant Hemangiopericytoma. 35-fractions of Co 60 radiotherapy were applied as adjuvant therapy. One year follow-up was made and no signs of recurrence were noted.
Keywords : Hemangiopericytoma, lacrimal sac, external DCR, radiotherapy
Purjanto Tepo Utomo, Banuaji Dibyasakti, Agus Supartoto
1Ophthalmology Dept, Dr. Sardjito Hospital/ Faculty of Medicine, Public Health and Nursing Universitas Gadjah Mada, Yogyakarta, Indonesia
Corresponding Email : [email protected]
Malignant Hemangiopericytoma of The Lacrimal Sac (A Case Report)
Hemangiopericytoma is a malignant vascular tumor arising from pericapillary cells or pericytes of Zimmerman that may develops in any organs where capillaries are found.1,2 The concept was first introduced by Stout and Murray in 1942, its occurrence has been reported in many parts of the body, most often in the head and neck.3 The tumor mainly develops in the lower extremities, retroperitoneum or pelvis and rarely occurs in the larynx, spleen, bone, meninges or thorax. The peak of incidence of hemangiopericytoma is in the fourth and fifth decades of life. The natural history of this tumor can be very long. However, it is sometimes a locally aggressive, potentially malignant tumor that produces late local recurrences and distant metastase mainly to bone, lung and liver.1
Orbital hemangiopericytoma is a rare, potentially malignant vascular tumor, which can affect any part of the orbit. The frequency of hemangiopericytoma in five orbital series was 0.1 to 1.2%.4 Hemangiopericytoma rarely originates in the lacrimal sac. The onset of the lacrimal sac hemangioperycitoma is found in younger age group than that in other orbital location,5 7 cases had been reported previously. The treatment of choice is complete surgical excision but because of its vascular nature and tissue friability during surgery this is frequently can not be achieved. Difficulties in correctly diagnosing this tumor preoperatively compound this problem. Incomplete excision is associated with increased risk of local recurrence and metastatic disease. Treatment options for orbital recurrence include orbital excenteration further attempts at complete excision, or local excision and adjuvant therapy with radiotherapy, brachytherapy, or chemotherapy.6
Case Report
A 33-year old female came to the eye clinic of Sardjito General Hospital with a chief complain of a lump on the right medial canthus of her right eye. Since the past 12 years, she has been suffered from tearing on her right eye and a slowly enlarging painless lump was observed accordingly. There were no bloody reflux or bloody tears had been observed. Furthermore, since 1 year ago the lump had been getting inflame and pain frequently. In spite of taking antibiotic there was no improvement. Where as, tearing became worse.
On her first visit, the ophthalmic examinations showed : the visual acuity were 6/6 for both eyes, There was a tumor on the medial canthus of the right eye with the measure 3x2x0.5 cm,3 firm, fixed and no pain on palpation while the left eye was normal. The anterior segments were normal for both eyes, as well as the lenses and the fundus examinations. Like the IOP measurement, the ocular motilities were normal for both eyes.
Unlike the left eye, a reflux was observed on the right eye when the anel tests were performed on both eyes. Due to the clinical finding, probing examination was conducted on the right eye, and an obstruction in the part of lacrimal canal was suspected. Afterwards, dacryocistografy was undertaken and an obstruction was identified in the lacrimal canal portion. Noticed that an obstruction was present in the lacrimal canal, the External DCR procedure was indicated for this patient.
The External DCR Report• Having confirmed the obstruction by sondase, the skin
was incised to expose the lacrimal sac
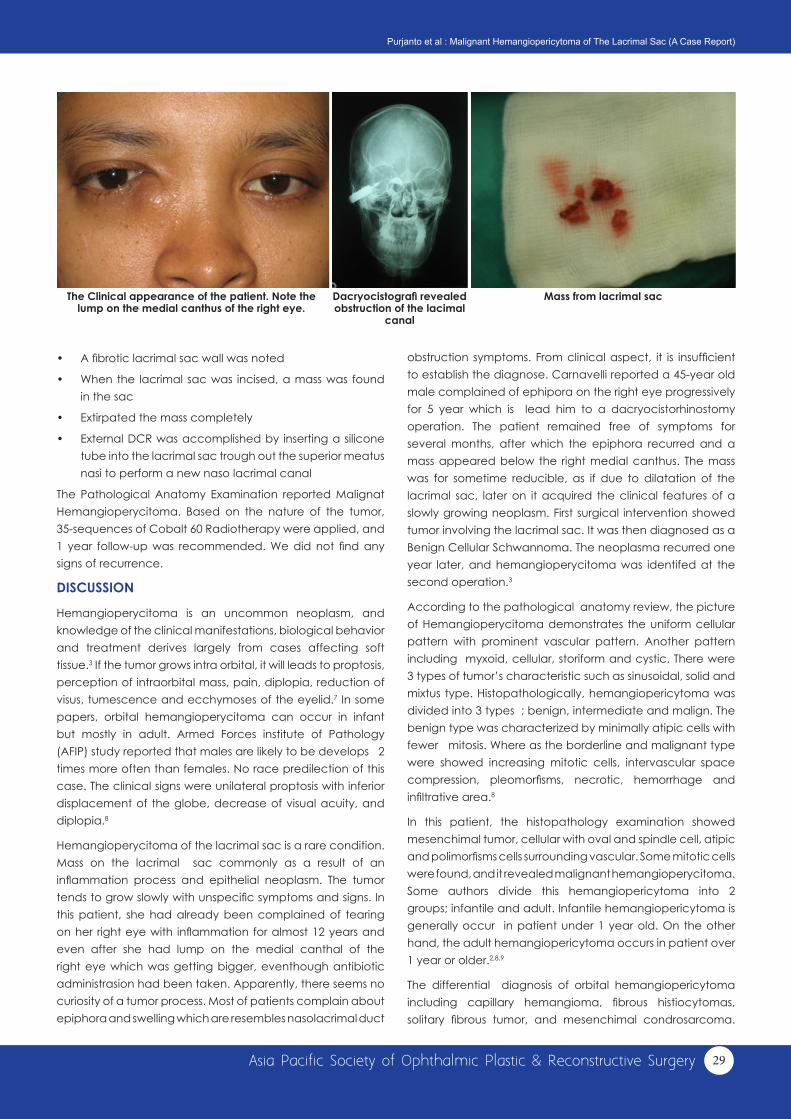
29Asia Pacific Society of Ophthalmic Plastic & Reconstructive Surgery
• A fibrotic lacrimal sac wall was noted
• When the lacrimal sac was incised, a mass was found in the sac
• Extirpated the mass completely
• External DCR was accomplished by inserting a silicone tube into the lacrimal sac trough out the superior meatus nasi to perform a new naso lacrimal canal
The Pathological Anatomy Examination reported Malignat Hemangioperycitoma. Based on the nature of the tumor, 35-sequences of Cobalt 60 Radiotherapy were applied, and 1 year follow-up was recommended. We did not find any signs of recurrence.
DISCUSSION
Hemangioperycitoma is an uncommon neoplasm, and knowledge of the clinical manifestations, biological behavior and treatment derives largely from cases affecting soft tissue.3 If the tumor grows intra orbital, it will leads to proptosis, perception of intraorbital mass, pain, diplopia, reduction of visus, tumescence and ecchymoses of the eyelid.7 In some papers, orbital hemangioperycitoma can occur in infant but mostly in adult. Armed Forces institute of Pathology (AFIP) study reported that males are likely to be develops 2 times more often than females. No race predilection of this case. The clinical signs were unilateral proptosis with inferior displacement of the globe, decrease of visual acuity, and diplopia.8
Hemangioperycitoma of the lacrimal sac is a rare condition. Mass on the lacrimal sac commonly as a result of an inflammation process and epithelial neoplasm. The tumor tends to grow slowly with unspecific symptoms and signs. In this patient, she had already been complained of tearing on her right eye with inflammation for almost 12 years and even after she had lump on the medial canthal of the right eye which was getting bigger, eventhough antibiotic administrasion had been taken. Apparently, there seems no curiosity of a tumor process. Most of patients complain about epiphora and swelling which are resembles nasolacrimal duct
The Clinical appearance of the patient. Note the lump on the medial canthus of the right eye.
Mass from lacrimal sacDacryocistografi revealed obstruction of the lacimal
canal
obstruction symptoms. From clinical aspect, it is insufficient to establish the diagnose. Carnavelli reported a 45-year old male complained of ephipora on the right eye progressively for 5 year which is lead him to a dacryocistorhinostomy operation. The patient remained free of symptoms for several months, after which the epiphora recurred and a mass appeared below the right medial canthus. The mass was for sometime reducible, as if due to dilatation of the lacrimal sac, later on it acquired the clinical features of a slowly growing neoplasm. First surgical intervention showed tumor involving the lacrimal sac. It was then diagnosed as a Benign Cellular Schwannoma. The neoplasma recurred one year later, and hemangioperycitoma was identifed at the second operation.3
According to the pathological anatomy review, the picture of Hemangioperycitoma demonstrates the uniform cellular pattern with prominent vascular pattern. Another pattern including myxoid, cellular, storiform and cystic. There were 3 types of tumor’s characteristic such as sinusoidal, solid and mixtus type. Histopathologically, hemangiopericytoma was divided into 3 types ; benign, intermediate and malign. The benign type was characterized by minimally atipic cells with fewer mitosis. Where as the borderline and malignant type were showed increasing mitotic cells, intervascular space compression, pleomorfisms, necrotic, hemorrhage and infiltrative area.8
In this patient, the histopathology examination showed mesenchimal tumor, cellular with oval and spindle cell, atipic and polimorfisms cells surrounding vascular. Some mitotic cells were found, and it revealed malignant hemangioperycitoma. Some authors divide this hemangiopericytoma into 2 groups; infantile and adult. Infantile hemangiopericytoma is generally occur in patient under 1 year old. On the other hand, the adult hemangiopericytoma occurs in patient over 1 year or older.2,8,9
The differential diagnosis of orbital hemangiopericytoma including capillary hemangioma, fibrous histiocytomas, solitary fibrous tumor, and mesenchimal condrosarcoma.
Purjanto et al : Malignant Hemangiopericytoma of The Lacrimal Sac (A Case Report)

30 iPlastics : Vol. 4 Issue 1, Julu 2019 - Lacrimal Issue
Pathological anatomy figure 1 year after therapy
Fibrous histiocytoma was dominated with high cellular storyform pattern without vascular component. Where as in the condrosarcoma, the mesenchim consists of condroid area or catilage.2,8
The best management for hemangiopericytoma was complete removal of the tumor. Espat reported that 5 years survival was 100% if the tumor were completely removed. Some authors remind to be more careful in doing the surgery, because sometimes it is difficult to gain complete removal of the tumor. Chemotherapy and radiotherapy are still effective. Especially for the patients with incomplete removal of the tumor, big tumor mass or invasive case, chemotherapy and radiotherapy were a must. Someya reported that post operative adjuvant radiothetrapy 50 Gry in 20 – 30 fractions doses gave good significant result. In this patient, after underwent tumor removal and external dacryocistorhinostomy, an adjuvant radiotherapy using 35 fractions of Co 60 for 50 Gy are applied. One year post operative follow up revealed good condition, both the epiphora and the mass was absent.1,8
The prognosis of adult hemangiopericytoma is poorer compare with the infantile type. In a study of 106 cases, 93
with complete follow up data, 10 years survival rate was 70%. Mac Master reported that of 60 patients, 48% were died. Auguste found that of 19 patients 53% were developed lung metastases, the 5 years survival rate was 59% and 10 years survival rate was 47%.8 Metastatic was found mostly in the lung and bone, and it account for 10-60% of the cases depending of the tumor location. In orbital site, almost 30% developed metastases. Recurrence may occured in a long time, 20 years or more, so the long follow-up is highly recommended. In this patient, after 1 year follow-up, the condition was still good. However, a long term observation is still needed. Since the tumor is slowly progress, beside the clinical symptoms and signs, CT- Scan evaluations were recommended.
CONCLUSION
Hemangiopericytoma of the lacrimal sac is rare, but it tends to be malignant. The clinical signs can mimic a lacrimal duct obstruction, so thorough evaluation of the clinical signs and symptoms were important. The ancillary test such as CT-Scan or MRI can help to established the diagnose. Post operative chemotherapy or radiotherapy are recommended as the adjuvant therapy. Long term observation is needed.
REFERENCES1. Someya M, Sakata K, Oouchi A, Nagakura H, Satoh M, Hareyama M, Four cases of meningeal hemangiopericytoma treated with surgery and
radiotherapy, Jpn J Clin Oncol, 2001, vol 31, 548-5522. Marec-Berard PM, Malignant hemangiopericytoma, Orphanet encyclopedia, 2004. 1-33. Carnavelli L, Trimarchi F, Rosso R, stringa M, Hemangiopericytoma of the lacrimal sac: a case report, Br.J.Ophthalmol, 1988 vol 72, 782-7854. Karcioglu ZA (editor) ,Orbital tumors: diagnosis and treatment, Springer Scince, China 20055. Carles NC, Palu RN, Jagirdar JS, Hemangiopericytoma of the lacrimal sac, Clinicopathology report, Arcophthalmol, 1998, Vol 116, 1677-16806. Gear HC, Kemp EG, Kacperek A, Errington RD, Treatment of recurrent orbital hemangiopericytoma with surgery and proton beam therapy,
Br.J.Ophtahalmol, 2005, vol 89, 123-1247. Valentini V, Gianluca N, Francesco F, Andrea T, Mario P, Andrea B, Surgical treatment of recurrent orbital hemangiopericytoma, Journal of
craniosurgical surgery, 2004, vol 15, 106-1138. Jakobiec FA, Albert DM, Vascular lesion of the orbit, Principles and practice of Ophthalmology Volume 3, 1994 pp 1971-729. Rootman J, Vascular Disease of the orbit, 2003 pp 544-46
Purjanto et al : Malignant Hemangiopericytoma of The Lacrimal Sac (A Case Report)

31Asia Pacific Society of Ophthalmic Plastic & Reconstructive Surgery
Raoul Paolo D. Henson and Minguita Padilla
Corresponding Email : [email protected]
Jose Rizal, Martyr and Ophthalmologist, is the National Hero of the Philippines
Most of us from APSOPRS do not know Dr. Jose Rizal. Maybe some of you may know him through the APAO Jose Rizal International Medal. But Rizal was more than just a martyr and an ophthalmologist. He was an agriculturist, poet, novelist, educator, fencer, horticulturist, linguist, journalist, musician, polyglot, sculptor and sharp shooter. As a polyglot, he knew and was well versed with more than 20 languages. Rizal was also well travelled. He journeyed all around Europe most notably in Spain, France and Germany. But little did we know that he also travelled to America reaching the shores of San Francisco in 1888 going cross country visiting many states along the way including Nevada, Utah, Colorado, Nebraska, Chicago, and Niagara Falls until he reached the city of New York en route to Europe.
Jose Rizal became an ophthalmologist to treat the ailing eyesight of his beloved mother but he also showed the light of freedom
For detail article of Dr. Jose Rizal - https://paojournal.com/article/yes-dr-jose-rizal-was-a-real-ophthalmologist/
Tribute
to his fellow Filipinos through his writings. Below is an article about Rizal by Dr. Minguita Padilla, past president of the Philippine Academy of Ophthalmology. She not only discussed in detail Rizal’s early education and excursion in Europe for his ophthalmology training, but she also revealed his excruciating journey on how he wanted to achieve Philippine independence
from the o p p r e s s i v e g o v e r n m e n t during his time. Dr. Minguita Padilla wrote this article for the 150th birth anniversary of Dr. Jose Rizal.

32 iPlastics : Vol. 4 Issue 1, Julu 2019 - Lacrimal Issue
The 10th conference of the Asia Pacific Society of Ophthalmic Plastic & Reconstructive Surgery was a successful and memorable meeting creating many ‘firsts’ in Hong Kong – It was the first international Oculoplastic meeting in Hong Kong. It is also the first time for the Hong Kong Ophthalmological Society and the College of Ophthalmologists of Hong Kong to cohost an international Oculoplastic meeting. Being the first large scale international Oculoplastics meeting to be hosted in Hong Kong, the event brought together ophthalmologists from around the world and especially those from the Asia Pacific Region, receiving a record number of more than 800 participants with more than 200 actively practicing international ophthalmologists from 45 countries (including Romania, Brazil and Israel among others) attending.
Delegates enjoyed a busy schedule packed with more than 120 invited speakers and a high volume of submitted posters and paper presentations covering a wide variety of latest research and updates in the area of functional and aesthetic Oculoplastics. This year’s conference was also the first to showcase a 3D video symposium with high definition viewing of eyelid, orbit and endoscopic surgeries. It was definitely an eye opening experience and brought forth a new angle in ophthalmic surgery, education and training by incorporating innovative technology.
Following the APSOPRS AGM on 16th December, we have a formal handover ceremony to Dr. Raoul Henson. We
have made a first APSOPRS president medal and hope this president medal can be passed to future presidents. We are also delighted to share with you that our members of good standing have, for the first time, approached around 200. Another ‘first’ of this meeting included the hosting of a local press conference on 16th December focusing especially on the area of ptosis and thyroid eye disease. The heartfelt sharing from real patients shone light on the impact both physically and psychosocially of disfiguring conditions ranging from ptosis to Dysthyroid Ophthalmopathy. The event was well attended and publicized widely by the press, spreading the importance of seeking early medical attention from ophthalmologists when it comes to eye diseases and the treatments available that we can readily offer to our patients. Advocating the importance and value of Oculoplastics subspecialty will certainly enhance the overall care of our patients.
Besides the fruitful scientific programs, the social aspect of the conference was certainly a highlight too. The conference kicked off with a welcoming dinner where we received and welcomed all our invited speakers, distinguished guests and our keynote speakers Prof Don Kikkawa, Professor of Clinical Ophthalmology, University of California at San Diego and Prof Geoffrey Rose, Director of Adnexal Service at Moorfields Eye Hospital. To showcase the vibrant side of Hong Kong, it was the first time we organized a lunchtime cruise party and a tram party for participants to see another side of
10th conference of Asia Pacific Society of Ophthalmic Plastic &
Reconstructive Surgery and the Hong Kong Ophthalmological Symposium 2018 Hunter Yuen
Chairman, APSOPRS 2018 HK Organizing CommitteeAPSOPRS Past President
Event News

33Asia Pacific Society of Ophthalmic Plastic & Reconstructive Surgery
Hong Kong. Both were well attended by overseas and local ophthalmologists and the light hearted events received positive reviews, providing an opportunity for old friends to catch up and to meet new ones against the spectacular background of the Hong Kong skyline. The annual gala dinner was again a fun-filled event with a chance for our talented colleagues to showcase their musicality through memorable performances by our one and only Eye Band.
The success of this event could not have been possible without the hard work of the organizing committee, the support of the Hong Kong Ophthalmological Society, the College of Ophthalmologists of Hong Kong, Asia Pacific Society of Ophthalmic Plastic & Reconstructive Surgery and last but not least, the generous donations from corporate sponsors and individual donors. With the generosity from individual donors we were able to present 12 travel grants to
deserving young ophthalmologists from overseas to support and encourage international conference attendance.
I would like to thanks the support from all the past presidents for their support especially Prof Reynaldo Javate, Prof Yoon-Duck Kim, Prof XQ Fan, Prof Chee-Chew Yip who has helped us for the scientific program. Also, I would like to thanks all my OC team especially Dr George Cheng and Prof Kelvin Chong. Of course, support from all the APSOPRS 2016-2018 council members and all APSOPRS members of utmost importance as well.
The 30th Hong Kong Ophthalmological Symposium was a meeting of many firsts and we look forward to many more to come in the future. On behalf of the organizing committee, we would like to express our sincere thanks again to all colleagues for your participation and support to the event.

34 iPlastics : Vol. 4 Issue 1, Julu 2019 - Lacrimal Issue
SPONSORSHIP AND EXHIBITION
Diamond sponsor Novartis Pharmaceuticals (HK) Ltd / Alcon Hong Kong Limited
Platinum sponsor Bayer HealthCare Limited Carl Zeiss Far East Co LtdSanten Pharmaceuticals (HK) Ltd.
Gold SponsorJohnson and Johnson
Silver SponsorsBausch & Lomb (Hong Kong) Ltd Global Vision CorporationLoyal Tech Group Ltd.Rich Plan International Ltd.Topcon Beijing (HK) Ltd
Exhibitors Allergan Hong Kong Limited Focus Mercantile (HK) Co. Ltd.Skyview Optical Co. Ltd.Starz Tech International Ltd.The Vita Co. Ltd.
Sunday lunch (invited speakers) Dr. John Chang
Travel Grant Donors1. Dr. George Cheng 2. Dr. Alvin Kwok 3. Dr. Dexter Leung 4. Dr. Donald Woo 5. Dr. Victor Woo 6. Dr. Emily Yeung 7. Dr. Carol Yu 8. Dr. Can Yuen 9. The College of Ophthalmologists of Hong Kong 10. The Hong Kong Ophthalmological Society
Special thanks and acknowledgements
Travel grant recipients1. Dr. Ardining Rejeki Sastrosatomo Indonesia 2. Dr. Akshay Nair India 3. Dr. Sharmin Ahmed Bangladesh 4. Dr. Ankit singh Tomar India 5. Dr. Dikshya Bista Nepal 6. Dr. Datu Respatika Indonesia 7. Dr. Shahid Alam India 8. Dr. Tazbir Ahmed Bangladesh 9. Dr. Ha Ha Thi Thu Viet Nam 10. Dr. Mutmainah Mahyuddin Indonesia 11. Dr. Abhishek Onkar India 12. Dr. Hasan Jawad Bangladesh
EYE BANDDr. Patrick Tong Bass/ guitarDr. Nancy Yuen VocalsDr. Jeffrey Pong Vocals/ drumsDr. Kenneth Ng Vocals/ keyboardDr. Desmund Yip Guitar/ bassDr. Leslie Cheng Vocals/ keyboardMr. Alex Bucks Saxophone
AWARDS PRESENTED
Best Oral Presenter Dr. Jasmine Chuang (Hong Kong Eye Hospital) Title: Comparison of Peripapillary Vessel Density of Acute Non-arteritic Anterior Ischemic Optic Neuropathy and Other Optic Neuropathies with Disc Swelling
Best Poster Presenter Dr. Yim Cheuk Ling (Hong Kong Eye Hospital) Title: Sebaceous Carcinoma can mimic Ocular Cicatricial Pemphigoid
Resident’s ChallengeDr. Cherie Wong (Hong Kong Eye Hospital)

35Asia Pacific Society of Ophthalmic Plastic & Reconstructive Surgery
A few of our APSOPRS members attended the European Society of Ophthalmology (SOE) meeting held in Nice, France last June 14-16, 2019. Our immediate past president, Dr. Hunter Yuen, headed our delegation of speakers. He was responsible for linking up with the SOE and was able to organize a joint session with our sister society ESOPRS. The
APSOPRS members speak at
the meeting of the European Society of Ophthalmology
other notable APSOPRS speakers in this meeting were Dr. Reynaldo Javate, Dr. Gangadhara Sundar, Dr. Kelvin Chong, Dr. Dong Mei Li, Dr. Wei Lu, and Dr. Raoul Henson. It was a very fruitful meeting and we can’t wait to participate in the next SOE meeting in 2021 in the beautiful city of Prague.
Promoting APSOPRS Manila 2020
Congress dinner with SOE President Dr. Jan Tjeerd De Faber Wei Lu, Dongmei Li, Reynaldo Javate, Raoul Henson, Hunter Yuen, Gangadhara Sundar, Kelvin Chong

36 iPlastics : Vol. 4 Issue 1, Julu 2019 - Lacrimal Issue
With our new secretary Jenna Cruz APSOPRS secretariat Office
APSOPRS council meeting in The 34th Congress of Asia Pacific Academy of Ophthalmology, 6-9 March, 2019, Bangkok.
Below are the formats for the different categories of articles:
Invited/Original/Review Articles (no more than 1600 words; include images where appropriate) Case Highlights This refers to the written presentation of an interesting or challenging case in the following format: • History (no more than 100 words) • Examination (no more than 150 words; include
clinical photos) • Investigations (include imaging where appropriate) • Management (no more than 100 words; include
pathology images where appropriate) • Discussion (no more than 200 words; including
challenges encountered in diagnosis or management)
APSOPRS new secretariat office in Manila Philippines
Guidelines Operative Pearls This refers purely to advice that allows the reader to improve on his or her intraoperative technique and can include immediate post-op advice (no more than 600 words; include images where appropriate)
Meetings or Social Visits
All meetings organized by APSOPRS members as well as social visits to each other’s’ centers are eligible for inclusion in the newsletter (no more than 1000 words for the main APSOPRS biennial meeting and no more than 500 words for other meetings or visits).
Philosophical Notes
No more than 800 words; include images where appropriate