
The Immunomodulatory Role of Syncytiotrophoblast Microvesicles
Upload
vanderbiltCategory
view
0download
0
Tissue Antigens ISSN 0001-2815
REVIEW ARTICLE
Invariant natural killer T cells: innate-like T cells with potentimmunomodulatory activitiesL. Wu, C. L. Gabriel, V. V. Parekh & L. Van Kaer
Department of Microbiology and Immunology, Vanderbilt University School of Medicine, Nashville, TN, USA
Key words
a-galactosylceramide; adjuvant; CD1d;
glycolipids; immunomodulation;
immunotherapy; innate immunity; invariant
natural killer T cells
Correspondence
L. Van Kaer, PhD
Department of Microbiology and Immunology
Vanderbilt University School of Medicine
Medical Center North
Room A-5301
1161 21st Avenue South
Nashville
TN 37232-2363
USA
Tel: 11 615 343 2707
Fax: 11 615 343 2972
e-mail: [email protected]
Received 11 March 2009; accepted
11 March 2009
doi: 10.1111/j.1399-0039.2009.01256.x
Abstract
Invariant natural killer T (iNKT) cells are a subset of T lymphocytes that react with
glycolipid antigens presented by the major histocompatibility complex class
I-related glycoprotein CD1d. Although iNKT cells express an antigen-specific
receptor of the adaptive immune system, they behave more like cells of the innate
immune system. A hallmark of iNKT cells is their capacity to produce copious
amounts of immunoregulatory cytokines quickly after activation. The cytokines
produced by iNKT cells can influence the level of activation ofmany cell types of the
innate and adaptive immune systems as well as the quality of an adaptive immune
response. As such, iNKT cells have emerged as important regulators of immune
responses, playing a role in microbial immunity, autoimmunity, tumor immunity,
and a variety of inflammatory conditions. Although several endogenous and
exogenous glycolipid antigens of iNKT cells have been identified, how these
glycolipids orchestrate iNKT-cell functions remains poorly understood. Neverthe-
less, iNKT cells hold substantial promise as targets for development of vaccine
adjuvants and immunotherapies. These properties of iNKT cells have been
investigated most extensively in mouse models of human disease using the marine
sponge-derived agent a-galactosylceramide (a-GalCer) and related iNKT-cell
antigens. While these preclinical studies have raised enthusiasm for developing
iNKT-cell-based immunotherapies, they also showed potential health risks
associated with iNKT cell activation. Although a-GalCer treatment in humans
was shown to be safe in the short term, further studies are needed to develop safe and
effective iNKT-cell-based therapies.
Introduction
Cells of the innate immune system can sense microbial
pathogens through germ line-encoded receptors, called
pattern recognition receptors, which interact with con-
served pathogen-associated molecular patterns. In turn, the
cytokines and costimulatory molecules elaborated by cells
of the innate immune system are critically important for
initiating an effective adaptive immune response. B and T
cells of the adaptive immune system recognize microbial
pathogens through diverse, antigen-specific receptors that
are generated by somatic DNA rearrangement. Invariant
natural killer T (iNKT) cells are a distinct subset of T
lymphocytes that express a receptor of the adaptive immune
system, yet their specificity and behavior are more
reminiscent of cells of the innate immune system. Here, we
will review the salient characteristics and functions of
these fascinating cells and discuss their potential appli-
cations in the development of vaccine adjuvants and
immunotherapies.
iNKT cells and their cousins
Nearly two decades ago, it was reported that a small subset
of murine T lymphocytes expressed NK1.1 (also called
CD161), a marker that was previously considered to be
uniquely expressed by natural killer (NK) cells [reviewed in
(1)]. This finding, together with parallel studies from other
investigators characterizing a T-cell subset expressing
ª 2009 John Wiley & Sons A/S � Tissue Antigens 73, 535–545 535

intermediate T-cell receptor (TCR) surface levels with
a repertoire skewed toward Vb8 and a subset of
CD42CD82 (double-negative) T cells producing immuno-
regulatory cytokines, indicated the existence of a unique
subpopulation of T cells defined by NK1.1 expression.
Subsequent studies showed that the majority of these cells
were reactive with the major histocompatibility complex
(MHC) class I-related protein CD1d, and these cells were
called natural killer T (NKT) cells to reflect their hybrid
surface expression phenotype of conventional T cells and
NK cells. However, it soon became clear that not all NK1.1-
expressing cells recognized CD1d and that some CD1d-
restricted T cells failed to express the NK1.1 marker. The
need for a redefinition of these cells was further com-
pounded by the realization that the NK1.1 marker
(recognized by the PK136 antibody) is only expressed in
mouse strains such as C57BL/6 but not in many other
commonly used mouse strains (although these strains
express allelic variants of NK1.1 that are not recognized
by the PK136 antibody). These lymphocytes have now been
further categorized into three distinct subsets (1):
(a) Type I NKT cells, also called iNKT cells or
conventional NKT cells, are CD1d-restricted T cells
that express a semi-invariant TCR formed by the
combination of Va14–Ja18 and Vb8.2/Vb7/Vb2chains in mice and homologous Va24–Ja18 and
Vb11 chains in humans. The majority of these cells
express NK1.1 (CD161 in humans) (Figure 1A).
(b) Type II NKT cells, also called nonclassical NKT
cells, are also CD1d restricted but have a more
diverse TCR repertoire, and many of these cells
express NK1.1.
(c) NKT-like cells consist of a diverse range of cell
types, including CD1d-independent, NK1.1-expressing
T cells and multiple other T-cell subsets that express
semi-invariant TCRs. To avoid confusion with type I
and type II NKT cells, and because these cells are
CD1d independent, it has been recommended that
these cell types should not be called NKT cells (1).
This review paper focuses on type I NKT cells, which we
will call iNKT cells. A key issue in studying iNKT cells is to
reliably identify these cells, which can be accomplished in
mice and humans by usingmultimeric forms of CD1d (most
commonly CD1d tetramers) loaded with the prototypic
iNKT-cell antigen a-galactosylceramide (a-GalCer, see
below). Functional studies of iNKT cells in vivo can be
performed most reliably with TCR gene Ja18-deficientmice. Analysis of CD1d-deficient mice, together with Ja18-deficient mice, can be used to distinguish between type I and
type II NKT-cell functions.
iNKT cells are found with the highest frequency in the
liver and the bone marrow of mice and at significant
numbers in the thymus, spleen, and peripheral blood [for
reviews regarding iNKT cells, see (2–5)]. In humans, the
frequency of NKT cells is usually much lower and with
a high degree of variability between individuals. Most
murine iNKT cells express the coreceptor CD4, and the
remaining cells express neither CD4 nor CD8, whereas
a significant proportion of iNKT cells in humans express
CD8a. In addition to NK1.1 (or CD161), iNKT cells
express a variety of other receptors that are characteristic of
the NK-cell lineage, including NKG2D, CD94 and mem-
bers of the Ly49 family of NK-cell receptors. iNKT cells
also constitutively express a variety of markers such as
CD44, CD69 and CD122 that are typical of activated or
memory T cells.
iNKT-cell antigens
Because of its limited diversity, the TCRof iNKT cells more
closely resembles the pattern recognition receptors ex-
pressed by cells of the innate immune system than the
diverse antigen-specific receptors expressed by cells of the
adaptive immune system. Because of their propensity to
react with autologous cells, it has been generally assumed
that iNKT cells recognize both endogenous and exogenous
glycolipid antigens. All iNKT cells from mice and humans
react with a-GalCer (6) (Figure 1B), a glycosphingolipid
that was isolated from the marine spongeAgelas mauritianus
during a screen of natural products with antimetastatic
activities in mice. a-GalCer is a very potent iNKT-cell
agonist and has been extensively studied with regard to its
interaction with CD1d and the invariant TCR of iNKT
cells, its immunomodulatory activities, and its therapeutic
properties. The trimolecular complex formed between
a-GalCer, CD1d and the invariant TCR has been investi-
gated at the atomic level and has shown an unusual and
unexpected recognition mode (7, 8). Numerous structural
variants of a-GalCer have been synthesized and analyzed
(see below and Figure 1B). Several of the known naturally
occurring exogenous iNKT-cell ligands are pathogen-
derived glycolipid antigens, such as glycosylceramides from
the cell wall of gram-negativeNovosphingobium (previously
called Sphingomonas) species (9–11) and diacylglycerols
from Lyme disease-causing Borrelia burgdorferi bacteria
(12) (Figure 1B). Interestingly, because the Novosphin-
gobium glycolipids are structurally similar to a-GalCer,
and because marine sponges are commonly colonized by
bacteria, includingNovosphingobium species, it is likely that
a-GalCer was isolated from Novosphingobium bacteria that
colonized the marine sponge. Several studies have also
shown reactivity of iNKT cells with select cellular, tumor-
derived, and other microbial glycolipids, but these reagents
were only recognized by small subsets of iNKT cells. An
endogenous, lysosomal glycosphingolipid, isoglobotrihex-
osylceramide (iGb3, Figure 1B) is capable of activating
murine and human iNKT cells (10), albeit at lower levels
iNKT cells L. Wu et al.
536 ª 2009 John Wiley & Sons A/S � Tissue Antigens 73, 535–545
than a-GalCer or the bacterial glycolipids, as would be
expected for an endogenous, physiological ligand. The role
of iGb3 in the development and function of iNKT cells is
still under investigation.
Presentation of glycolipid antigens to iNKTcells
CD1d molecules are expressed by professional antigen-
presenting cells (APCs), including dendritic cells (DCs),
macrophages, and B cells (CD1d is particularly abundant
on marginal zone B cells) as well as by double-positive
thymocytes and hepatocytes. Soon after synthesis in the
endoplasmic reticulum (ER), CD1d molecules bind with
endogenous phospholipids that facilitate the exit of CD1d
from the ER and its transport to the cell surface (13–15)
(Figure 2). Current evidence indicates that the loading of
phospholipids onto CD1d in the ER involves the action of
microsomal triglyceride transfer protein, which is a lipid
transfer protein (LTP) that plays an important role in the
assembly of apolipoprotein (apo) B with lipids in the ER.
Surface CD1d is then internalized by clathrin-mediated
endocytosis that depends on a tyrosine-based motif in the
cytoplasmic tail of CD1d. In addition to this pathway, it has
been reported that a subset of CD1d molecules reaches
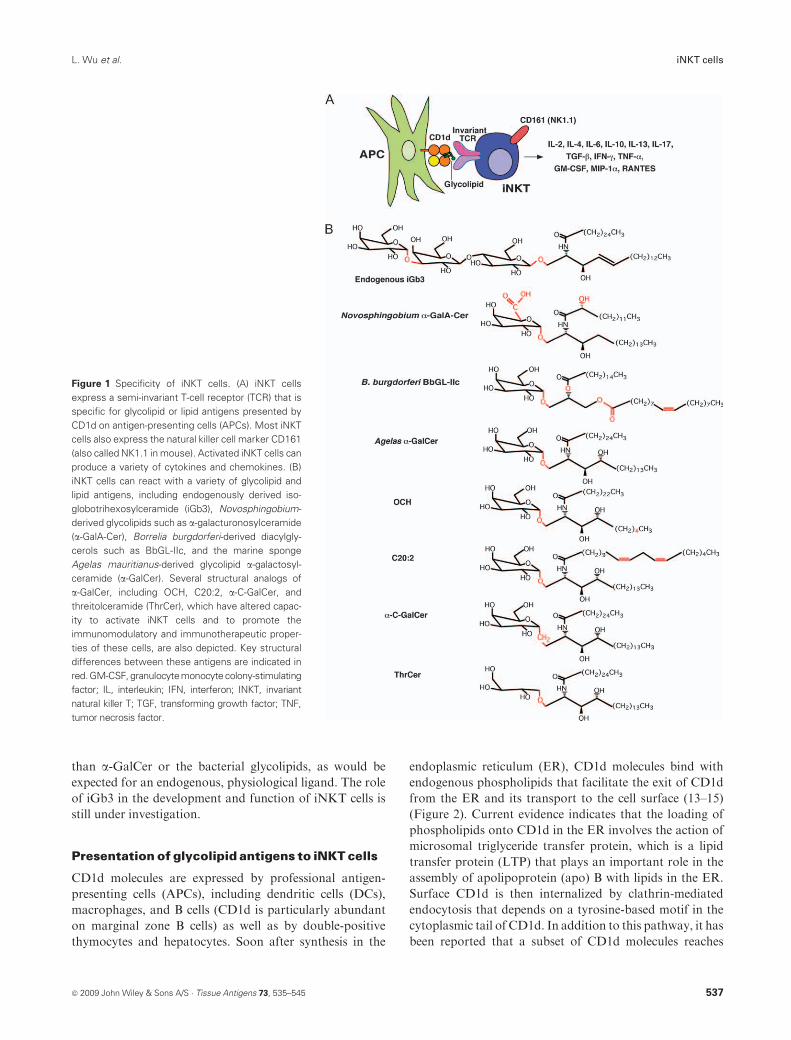
Figure 1 Specificity of iNKT cells. (A) iNKT cells
express a semi-invariant T-cell receptor (TCR) that is
specific for glycolipid or lipid antigens presented by
CD1d on antigen-presenting cells (APCs). Most iNKT
cells also express the natural killer cell marker CD161
(also called NK1.1 in mouse). Activated iNKT cells can
produce a variety of cytokines and chemokines. (B)
iNKT cells can react with a variety of glycolipid and
lipid antigens, including endogenously derived iso-
globotrihexosylceramide (iGb3), Novosphingobium-
derived glycolipids such as a-galacturonosylceramide
(a-GalA-Cer), Borrelia burgdorferi-derived diacylgly-
cerols such as BbGL-IIc, and the marine sponge
Agelas mauritianus-derived glycolipid a-galactosyl-ceramide (a-GalCer). Several structural analogs of
a-GalCer, including OCH, C20:2, a-C-GalCer, and
threitolceramide (ThrCer), which have altered capac-
ity to activate iNKT cells and to promote the
immunomodulatory and immunotherapeutic proper-
ties of these cells, are also depicted. Key structural
differences between these antigens are indicated in
red.GM-CSF, granulocytemonocytecolony-stimulating
factor; IL, interleukin; IFN, interferon; INKT, invariant
natural killer T; TGF, transforming growth factor; TNF,
tumor necrosis factor.
ª 2009 John Wiley & Sons A/S � Tissue Antigens 73, 535–545 537
L. Wu et al. iNKT cells

endosomal compartments after association with the MHC
class II-associated invariant chain in the ER. Within late
endosomes, theER-loaded phospholipids are exchanged for
antigenic lipids that can activate iNKT cells. These
glycolipids can be derived from endogenous sources, such
as lysosomal iGb3, or from exogenous sources. Multiple
pathwaysmight be engaged to deliver exogenous glycolipids
to the CD1d-loading compartment: (a) phagocytosis of
microbes or their products, (b) engagement of mannose
within glycolipids by mannose receptors, (c) engagement
of modified low-density lipoprotein (LDL) by scavenger
receptors, and (d) internalization of apoE-containing lipid
complexes through the LDL receptor or related lipoprotein
receptors. After their arrival in late endosomal compart-
ments, endogenous or exogenous glycolipidsmight undergo
processing (e.g. by carbohydrate hydrolases), followed by
loading onto CD1d with the assistance of a variety of LTPs,
including saposins, GM2 activator and Niemann–Pick C2
protein. These antigenic CD1d–glycolipid complexes are
then displayed at the cell surface for recognition by
iNKT cells.
In recent years, it has become clear that multiple viral
pathogens, including Kaposi sarcoma-associated herpes
virus, HIV-1, herpes simplex virus-1, vesicular stomatitis
virus, and vaccinia virus, can interfere with CD1d traffick-
ing and, thus, impede glycolipid antigen presentation to
iNKT cells (16). Furthermore, Chlamydia trachomatis
downregulates CD1d expression on human epithelial cells
by targeting its degradation by both cellular and chlamydial
proteasomes (17).
iNKT-cell development
Like conventional T cells, iNKT cells develop in the thymus
(18). iNKT cells develop relatively late during T-cell
ontogeny, owing to structural constraints in the recombi-
nation of TCRVa14 and Ja18 gene segments.Generation of
the canonical Va14–Ja18 rearrangement is a random event.
After expression of surface TCRs at the double-positive
thymocyte stage, iNKT cells diverge from conventional
T cells. iNKT cells require positive selection by CD1d–
glycolipid complexes in the thymus. However, in sharp
contrast with the positive selection of conventional T cells,
which is dependent on cortical thymic epithelial cells, iNKT
cells are selected by CD1d-expressing, double-positive
thymocytes. This selection likely involves endogenous
iNKT-cell antigens, and iGb3 has been suggested to play
such a role (10). This selection process also involves
homotypic interactions between members of the signaling
lymphocyte activation molecule (SLAM) family of recep-
tors (19). These receptors signal through the adaptor protein
SLAM-associated protein, the Src kinase Fyn, and the
downstreamtranscription factor nuclear factor (NF)-kB (20).
The selected iNKT cells subsequently expand and undergo
multiple maturation steps that ultimately result in the
characteristic surface phenotype and innate-like effector
functions of iNKT cells. These maturation steps involve
a variety of signal transducers, transcription factors, and
costimulatory molecules. Importantly, recent studies have
showna critical role of the transcription factor promyelocytic
leukemia zinc finger (PLZF) in directing the innate-like
effector differentiation of iNKT cells during thymic develop-
ment (21, 22). Furthermore, the licensing of mature iNKT
cells for cytokine production requires granulocyte monocyte
colony-stimulating factor (GM-CSF) signaling (23). After
Figure 2 The CD1d antigen processing and presentation pathway. After
its synthesis in the endoplasmic reticulum (ER), the CD1d heavy chain
associates with b2-microglobulin (b2m). This complex is loaded with ER-
resident phospholipids with the assistance of lipid transfer proteins
(LTPs) such asmicrosomal triglyceride transfer protein (MTP). These lipid
chaperones facilitate transport of CD1d to the cell surface. Surface CD1d
molecules are then endocytosed and enter endosomal and lysosomal
compartments, where the ER-derived lipids are replaced with endoge-
nous or exogenous glycolipids, with the assistance of LTPs such as the
saposin proteins (SAPs). Exogenous glycolipids can reach the CD1d-
loading compartment by multiple pathways, including carbohydrate
receptors, scavenger receptors, or lipoprotein receptors, or following
phagocytosis of microorganisms. Some glycolipid antigens might
undergo carbohydrate processing by carbohydrate hydrolases (Hy).
CD1d complexes loaded with lysosomal or exogenously derived
glycolipids are subsequently displayed at the cell surface.
538 ª 2009 John Wiley & Sons A/S � Tissue Antigens 73, 535–545
iNKT cells L. Wu et al.

acquisition of their innate-like phenotype, iNKT cells egress
from the thymus in amechanism that involves lymphotoxin-breceptor signaling. Nevertheless, in mouse, a significant
proportion of iNKT cells remain in the thymus, where they
become long-lived residents. Recruitment of iNKT cells to
peripheral tissues requires expression of the sphingosine
1-phosphate 1 receptor, and entry into the liver requires
expression of the chemokine receptor CXCR6.
Pathways of iNKT-cell activation
In most immune responses where iNKT cells have been
implicated, the mechanism of iNKT-cell activation remains
poorly understood. Nevertheless, studies with microbial
pathogens have shown two general pathways of iNKT-cell
activation (14, 24) (Figure 3). In the direct pathway of
iNKT-cell activation (Figure 1A), which is engaged by
Novosphingobium species and B. burgdorferi, cognate gly-
colipids bind CD1d and activate iNKT cells directly.
However, iNKT cells also become activated to many
microbes that lack cognate iNKT-cell antigens (25).
iNKT-cell activation during infection with such micro-
organisms is driven by cytokines. In this indirect pathway of
iNKT-cell activation (Figure 3B), engagement of signaling
pattern recognition receptors, most notably toll-like recep-
tors, with microbial products leads to the production of
cytokines such as interleukin (IL)-12, IL-18, and/or type I
interferons (IFNs) that can activate iNKT cells. The latter
mechanism has been implicated in the activation of iNKT
cells by several bacterial and viral microorganisms and their
products. For some microorganisms, iNKT-cell activation
also requires CD1d expression on the APCs, in which case
cytokines might function to amplify low-affinity interac-
tions of the iNKT-cell receptor with complexes between
CD1d and endogenous glycolipids such as iGb3. Similar
mechanisms might be involved in the activation of iNKT
cells during acute and chronic inflammatory conditions.
iNKT-cell functions
A hallmark of iNKT cells is to rapidly produce copious
amounts of cytokines quickly after TCR engagement (2–5).
Interestingly, however, iNKT cells are capable of producing
a wide array of cytokines (Figure 1A), including IL-2, IL-4,
IL-6, IL-10, IL-13, transforming growth factor (TGF)-b,IFN-g, and tumor necrosis factor (TNF)-a, and some iNKT
cells can also produce IL-17. iNKT cells also produce
growth factors for hematopoietic cells such asGM-CSF and
multiple chemokines such as macrophage inflammatory
protein (MIP)-1a and RANTES. In addition, these cells
have cytolytic activity, owing to high levels of granzyme B,
perforin, FasL, and TNF-related apoptosis-inducing
ligand. The effector functions exhibited by iNKT cells are
strongly influenced by the nature, strength, and context of
the stimulus as well as by the APC type and activation
status. For example, activation by cognate iNKT antigens
typically results in IFN-g and IL-4 production by iNKT
cells, whereas the cytokine-driven pathway of iNKT-cell
activation typically fails to induce substantial amounts of
IL-4, suggesting that IL-4 production by these cells largely
depends on TCR engagement. DCs appear to be the most
effective APCs in presenting glycolipids and activating
iNKT cells in vivo. Furthermore, although CD1d was
thought to lack significant polymorphism, a recent study
has identified severalmurineCD1d alleles that can affect the
presentation of endogenous and exogenous antigens to
iNKT cells (26).
iNKT cells can be divided into subsets based on CD4 and
NK1.1 (in mice) expression (27, 28). These distinct subsets of
iNKT cells show substantial diversity in their ability to
produce cytokines (29), which might explain their functional
differences. In humans, CD41 iNKT cells produce both Th1
and Th2 cytokines, whereas CD42 iNKT cells primarily
produce Th1 cytokines. Although differences in cytokine
production are less dramatic in mouse iNKT-cell subsets,
differences in the capacity of CD41 and CD42 iNKT cells to
regulate immune responses have been observed (28). IL-17
production by murine iNKT cells appears to be specific to
a subpopulation of CD42NK1.12 cells (29).
iNKT cells are capable of extensive cross talk with
a variety of other cell types, including DCs, macrophages,
neutrophils, NK cells, and conventional B and T cells, but
also B-1 B cells, marginal zone B cells, gd T cells, different
subsets of regulatory T (Treg) cells, type II NKT cells, and
myeloid-derived suppressor cells. In addition, because of
their capacity to promote cytokines that can bias adaptive
immune responses toward T helper type 1 (Th1), Th2, Th17,
or Treg-cell differentiation, iNKT cells can have a profound
impact on the quality of an immune response.
iNKT cells play important roles in a variety of immune
responses, as shown in studies with iNKT-cell-deficient
mice (because of CD1d or Ja18 gene disruption), Va14–Ja18 transgenic animals, and/orCD1d-blocking antibodies.
iNKT cells play a protective role in infections with a variety
of pathogens (25), including Pseudomonas aeruginosa,
B. burgdorferi, Ehrlichia muris, Chlamydia pneumoniae,
Novosphingobium capsulatum, Streptococcus pneumoniae,
Leishmania major, Schistosoma mansoni, Cryptococcus neo-
formans, influenza virus, Theiler’s murine encephalomyeli-
tis virus, and herpes simplex viruses 1 and 2. However,
iNKT cells can also play a pathogenic role during microbial
infection, such as during the immune response toChlamydia
muridarum. These studies also showed that the genetic
background of the animals used can have a significant
impact on the contribution of iNKT cells to antimicrobial
immunity. For example, iNKT cells protected against
cerebral malaria in BALB/c mice but exacerbated disease
in C57BL/6 mice. Likewise, iNKT cells played a protective
ª 2009 John Wiley & Sons A/S � Tissue Antigens 73, 535–545 539
L. Wu et al. iNKT cells

role in the immune response to respiratory syncytial virus
(RSV) in BALB/cmice, but exacerbated disease in C57BL/6
mice. In the case of infection with lymphocytic choriome-
ningitis virus, iNKT cells inhibited viral replication in the
pancreas and liver but not in the spleen (30), suggesting that
these cells can induce tissue-specific antiviral effects.
Because a significant proportion of human iNKT cells
express CD4 and the chemokine receptors CCR5 and
CXCR6, these cells are effective targets for HIV-1 infection
andmight serve as an early reservoir of HIV-1 replication in
infected individuals (31). iNKT cells play a protective role in
host immunity to tumors (32), which has been shown in
transplantable, chemically induced, and genetic tumor
models. iNKT cells generally also play a protective role in
autoimmunity (33), such as during the progression of
diabetes in nonobese diabetic (NOD) mice and in some
mouse models of multiple sclerosis (MS) and systemic lupus
erythematosus. However, iNKT cells can also contribute to
pathology in autoimmunity, as shown in models of
collagen-induced arthritis and antibody-mediated arthritis,
and during the development of primary biliary cirrhosis in
transgenic mice expressing a dominant-negative TGF-breceptor or in mice infected with Novosphingobium aroma-
ticivorans (34). iNKT cells also make an important
contribution to the development of tolerance in a variety
of experimental models, including anterior chamber-
associated immune deviation in the eye, anti-CD4-mediated
and costimulatory blockade in transplant tolerance, ultra-
violet- and burn-wound-induced immune suppression, fetal
tolerance, and graft-vs-host disease. iNKT cells play an
important pathogenic role in the development of a variety of
inflammatory diseases and hypersensitivities in mice, includ-
ing atherosclerosis, contact hypersensitivity, transplant
rejection, oxazolone-induced colitis, concanavalin-A-
induced hepatitis, lipopolysaccharide-induced inflamma-
tion and shock, hepatic ischemia–reperfusion injury, and
allergen-, ozone-, and virus-induced airway hyperreactivity.
Finally, iNKT cells, through their capacity to produce
colony-stimulating factors such as GM-CSF, also contrib-
ute to hematopoiesis during steady-state conditions and
situations of immune activation.
While these studies have shown critical roles of iNKT
cells in both health and disease, iNKT-cell-deficient mice do
not develop any obvious spontaneous pathologies, except
for lupus-like nephritis in aged Ja18 knockout mice (35). In
addition, iNKT cells appear to be absent in ruminants (36),
suggesting functional redundancy with other innate-like or
CD1-restricted T-cell subsets.
Response of iNKT cells to glycolipid antigens
The in vivo response of iNKT cells to glycolipid antigen
stimulation has been explored most extensively with
a-GalCer (37). Within hours after a-GalCer treatment,
iNKT cells produce copious amounts of cytokines, includ-
ing IL-2, IL-4, and IFN-g. Activated iNKT cells produce
IL-4 more rapidly than most other cytokines, and cytokine
production is short lived, lasting only a few days. iNKT cells
Figure 3 Two ways to activate an iNKT cell. (A) In the direct pathway of iNKT-cell activation, microbial antigens that reach CD1d-containing endosomal
compartments through any of the pathways depicted in Figure 2 are loaded onto CD1dwith the assistance of lipid transfer proteins such as the saposins
(SAPs). These complexes are then displayed at the cell surface for recognition by the invariant T-cell receptor (TCR) on iNKT cells. (B) In the indirect
pathway of iNKT-cell activation,microbial products engageextracellular or intracellular toll-like receptors (TLRs),which induce the production of cytokines
such as interleukin (IL)-12, IL-18, and/or type I interferons (IFN-a and IFN-b). These cytokines subsequently engage cytokine receptors on iNKT cells,
resulting in iNKT-cell activation. Different cytokines have been implicated in the activation of iNKT cells in response to distinct microbial products. For
somemicrobial products, iNKT-cell activation through this cytokine-drivenmechanism also requires engagement of the invariant TCR on iNKT cells with
CD1d molecules bound with endogenous antigens. INKT, invariant natural killer T.
540 ª 2009 John Wiley & Sons A/S � Tissue Antigens 73, 535–545
iNKT cells L. Wu et al.

activated in thismanner also profoundly downregulate their
surface TCRs, which become nearly undetectable by 8–12 h
but are mostly restored by 24 h after a-GalCer injection.
This phenomenon is largely responsible for the transient
‘disappearance’ of iNKT cells following a-GalCer injection
when these cells are identified with reagents that bind with
surface TCRs (anti-TCR-b antibodies or CD1d tetramers).
Activated iNKT cells also downregulate the surface
expression of the NK1.1 marker, and this downregulation
is long lasting (up to 6 months). a-GalCer-activated iNKT
cells also rapidly proliferate in vivo, resulting in profound
expansion of the iNKT-cell population in multiple organs,
which peaks around day 3 after a-GalCer treatment. In
some studies, the iNKT-cell population was shown to
expand up to 10- to 15-fold in the spleen and 2- to 3-fold in
liver. After this expansion phase, the iNKT-cell population
contracts through homeostatic mechanisms that involve the
proapoptotic Bcl-2 family member Bim, reaching pre-
treatment levels around 10–15 days.
A cardinal feature of adaptive immunity is the develop-
ment of immunological memory. However, this is not the
case for iNKT cells, which develop an anergic phenotype
after a-GalCer treatment (37). This anergic phenotype
persists for up to 6 weeks after the initial a-GalCer
treatment. A similar anergic phenotype is seen following
challenge of mice with multiple bacterial pathogens or their
products (38–40) and following injection of sulfatide (41),
a ligand of type II NKT cells. Thus, the development of
anergy might be a common outcome of iNKT-cell
activation. Acquisition of an anergic phenotype by acti-
vated iNKT cells likely provides a means to avoid chronic
cytokine production by these cells that could cause
uncontrolled inflammation. The anergic phenotype induced
by a-GalCerwas intrinsic to these cells, and the proliferative
defect could be overcome by culture in the presence of IL-2.
iNKT-cell anergy was associated with sustained expression
of the inhibitory, costimulatory receptor programmed
death-1 (PD-1) (42, 43). Blockade of PD-1 interactions with
its ligands, PD-L1 and PD-L2, was able to prevent the
generation of iNKT-cell anergy by a-GalCer but not by
bacteria or sulfatide. The critical role of the PD-1/PD-L
pathway in the induction of iNKT-cell anergy was further
shown in PD-1 knockout animals, which are resistant to
a-GalCer-induced iNKT-cell anergy (43). Furthermore,
certain glycolipid treatment modalities can effectively
activate iNKT cells while avoiding the induction of anergy.
This includes the delivery ofa-GalCer in the context ofDCs,
loaded onto a recombinant CD1d molecule, formulated as
a nanoparticle, or injected subcutaneously at low doses.
Numerous structural analogs of a-GalCer have been
synthesized and analyzed (37). Some reagents, such as the
sphingosine-truncated a-GalCer analog called ‘OCH’
(Figure 1B) and the C20:2 variant containing a diunsatu-
rated N-acyl chain (Figure 1B), induce a Th2-biased
cytokine production profile by iNKT cells. Conversely,
the C-glycoside analog a-C-GalCer (Figure 1B) promotes
a Th1 bias in the cytokine production profile of iNKT cells.
Furthermore, iNKT cells stimulated with threitolceramide
(Figure 1B), a nonglycosidic a-GalCer analog, produce
a cytokine profile similar to that of a-GalCer but recover
more quickly from activation-induced anergy (44).
Immunomodulatory activities ofiNKT-cell ligands
The cytokines secreted by a-GalCer-activated iNKT cells
can rapidly activate a variety of other cell types, including
DCs, macrophages, NK cells, B cells, and conventional
T cells (37, 45). This is evidenced by expression of activation
markers such as CD69 on NK cells, B cells, and T cells and
induction of costimulatory molecules on DCs, macro-
phages, and B cells. Activation of DCs involves interactions
between CD40 and OX40 ligand on these cells with CD40
ligand and OX40, respectively, on iNKT cells. Activated
DCs subsequently produce proinflammatory cytokines
such as IL-12 and TNF-a, which further contribute to the
cytokine storm. IL-12 derived fromDCs and IFN-g derivedfrom iNKT cells also induce NK cells to produce IFN-g.Furthermore, a-GalCer-activated iNKT cells enhance the
immune responses mediated by cytotoxic T cells (CTL),
CD41 T cells, and B cells. a-GalCer promotes not only
T-cell-dependent but also T-cell-independent antibody
responses, probably owing to the capacity of iNKT cells
to interact withCD1donB cells, includingB-1 andmarginal
zone B cells. These characteristics of activated iNKT cells
form the basis for the adjuvant activities of iNKT-cell
ligands (46).
a-GalCer also influences the quality of an adaptive
immune response (37, 45). A single a-GalCer injection
induces a substantial rise in serum immunoglobulin E levels,
suggesting Th2 deviation of the adaptive immune response.
Th2 deviation is characteristically observed in chronic
a-GalCer injection protocols, which might be associated
with the capacity of anergic iNKT cells to produce residual
amounts of Th2 but not of Th1 cytokines.
The cytokine storm that ensues following a-GalCer
treatment can also lead to significant pathology (47).
Because many iNKT cells reside in the liver, a single
a-GalCer treatment induces transient hepatitis in mice.
a-GalCer treatment in some mouse strains can also induce
abortion, probably because a substantial number of iNKT
cells reside in the uterus. Furthermore, a single intranasal
administration of a-GalCer sensitizes mice to the develop-
ment of airway hypersensitivity. Nevertheless, a-GalCer
treatment in humans, who have fewer iNKT cells thanmice,
has proven to be safe, at least in the short term (48).
However, at present, it is unclear whether a-GalCer
treatment in humans can elicit sufficiently strong biological
ª 2009 John Wiley & Sons A/S � Tissue Antigens 73, 535–545 541
L. Wu et al. iNKT cells

responses to bring forth its adjuvant and therapeutic
activities.
iNKT-cell antigens as vaccine adjuvants
The capacity of iNKT-cell ligands to enhance the efficacy of
vaccines against multiple microbial pathogens has been
tested (46, 49). Inclusion of a-GalCer in a malaria vaccine
resulted in enhanced antimalarial immunity, in a manner
that was dependent on IFN-g production by iNKT cells.
a-C-GalCer, which induces a Th1-biased cytokine pro-
duction profile in iNKT cells, showed profoundly enhanced
adjuvant activity in the malaria vaccine compared with
a-GalCer. a-GalCer was also effective as a mucosal
adjuvant in different vaccine formulations directed against
influenza virus. Likewise, a-GalCer enhanced the immuno-
genicity of an HIV-1 DNA vaccine, enhancing CD4 and
CD8 T-cell responses as well as humoral immunity.
The adjuvant activities of iNKT cells have also been
tested in multiple cancer vaccines (46, 49). a-GalCer
substantially enhanced the priming and boosting of CD8
T cells directed against ovalbumin antigens or the human
cancer/testis antigen NY-ESO-1, resulting in the eradica-
tion of established tumors bearing these antigens. Coad-
ministration of a-GalCer with irradiated plasmacytoma
cells also enhanced tumor immunity, in a manner that
involved DC maturation. Similarly, injection of a-GalCer-
loaded and CD1d-transfected B16melanoma cells provided
protection against rechallenge of the melanoma cells.
iNKT cells as targets for immunotherapy
a-GalCer was originally discovered by Kirin Brewery
Company, Ltd. (Gunma, Japan) as a natural product with
antimetastatic activities in mice (50). The antitumor
activities of a-GalCer have been shown in a variety of
transplantable, chemically induced, and genetic tumor
models (48). Although iNKT cells themselves have cytolytic
activity, the tumor target cells do not need to express CD1d
for therapeutic efficacy, suggesting that iNKT cells are not
the relevant effector cells. Instead, NK cells and antigen-
specific CTLs appear to be the critical effector cells through
their cytolytic activities and their capacity to produce
IFN-g, which has antiangiogenic activities. Delivery of
a-GalCer in the context of DCs provided superior anti-
metastatic activities, in part because this treatment avoids
the induction of iNKT-cell anergy. Likewise, combined
treatment with a-GalCer and antibodies that block the
PD-1/PD-L pathway, thus avoiding anergy induction, was
superior to a-GalCer treatment alone (42, 43). Further-
more, a-C-GalCer wasmore effective than a-GalCer, which
is probably because of its superior capacity to induce IFN-gproduction by iNKT cells, to prime DCs, and to trans-
activate NK cells and CD8 T cells. These preclinical studies
have paved the way for phase I and phase II trials in cancer
patients (48). These studies used free a-GalCer, a-GalCer
presented byDCs, or transfer of cells expanded in vitro from
peripheral bloodmononuclear cells culturedwith a-GalCer.
Although these treatments were safe, it has generally been
challenging to obtain strong biological responses, which is
likely because of the low frequency of iNKT cells in humans,
as well as the iNKT-cell dysfunction that has been observed
in cancer patients. The most encouraging trial to date
involved a study where patients with non-small cell lung
cancer were administered four times with peripheral blood
mononuclear cells cultured in the presence of a-GalCer, IL-2,
and GM-CSF (51). This treatment was well tolerated and
was accompanied by the induction of iNKT-cell-dependent
responses. The patients with increased IFN-g-producingcells, compared with poor responders, had an increased
median survival time (responders: 31.9 months, n ¼ 10;
poor responders: 9.7 months, n ¼ 7; P ¼ 0.0015).
The capacity of a-GalCer tomodulatemicrobial infection
has also been investigated (52). a-GalCer treatment was
generally associated with enhanced pathogen clearance and
an improved disease course, as shown for Mycobacterium
tuberculosis, S. pneumoniae, P. aeruginosa, Trypanosoma
cruzi, C. neoformans, hepatitis B virus, and influenza virus.
However, for C. muridarum infection, delayed rather than
enhanced clearance was observed. Mechanisms of action
appeared to be diverse. In some cases, divergent results were
obtainedwith regard to pathogen clearance and disease. For
example, a-GalCer treatment of RSV-infected mice delayed
viral clearance but improved weight loss. For Plasmodium
species, a-GalCer treatment promoted the clearance of
organisms from mice infected with the sporozoite stages of
the parasite but delayed clearance of mice infected with
erythrocyte stages. This is likely because of the critical role
of IFN-g and CD81 T cells in clearing the liver but not
blood stages of the organism, which is consistent with the
enhanced capacity of a-C-GalCer to clear malaria parasites
from sporozoite-infected mice. Importantly, the time
window in which a-GalCer treatment was effective is rather
narrow, typically within a few days of infection. As such,
iNKT-cell activation will likely provide little benefit to
established infections. No benefit of a-GalCer treatment
was observed in patients chronically infected with hepatitis
C virus (53).
Because of its capacity to promote Th2 immune responses,
particularly when injected repeatedly, a-GalCer has been
tested in multiple mouse models of autoimmunity (33, 50).
Chronic a-GalCer treatment protected NOD mice against
diabetes, in a manner that involved Th2 deviation of auto-
antigen-specific immune responses, but the role of Th2 cyto-
kines in this process remains unproven. Foxp3-expressing
Treg cells, tolerogenic DCs, and anergy induction in
pathogenic T cells all have been implicated as factors
542 ª 2009 John Wiley & Sons A/S � Tissue Antigens 73, 535–545
iNKT cells L. Wu et al.

contributing to disease protection. OCH also protected
against disease, and C20:2 appeared to be more effective
than botha-GalCer andOCH.a-GalCer andOCHwere also
effective in protecting mice against the development of
experimental autoimmune encephalomyelitis (EAE) in mice,
a model forMS.However, these studies also showed that the
timing of iNKT-cell activation can significantly impact
treatment efficacy, with early treatment ameliorating disease
and late treatment exacerbating disease in some studies. In
these EAE models, disease amelioration was typically
associated with Th2 deviation and disease exacerbation was
associated with Th1 deviation. Nevertheless, both Th1 and
Th2 cytokines have been implicated in disease protection,
which is consistent with a pathogenic role of Th17 cells in
EAE. a-GalCer also protected mice against experimental
autoimmune myasthenia gravis, an antibody-dependent
disease, in a mechanism that appeared to rely on Foxp3-
expressing Treg cells. a-GalCer and OCH were able to
protectC57BL/6mice against collagen-induced arthritis, and
this was associated with Th2 deviation. a-GalCer also
attenuated collagen-induced arthritis in DBA/1 mice, with
a critical role for IL-10. Surprisingly, however, a single
injection of a-C-GalCer was also protective in the DBA/1
model of collagen-induced arthritis, and thiswas suggested to
be because of general suppression of T-cell responses. In
contrast with its effects on collagen-induced arthritis,
a-GalCer moderately enhanced joint inflammation in an
antibody-mediated arthritis model. a-GalCer, OCH, and
a-C-GalCer were all protective in an experimental model of
ocular autoimmunity, and surprisingly, a-C-GalCer was
most effective (54). This protective effect of a-C-GalCer was
associated with dampening of Th1 and Th17 effector
functions. a-GalCer was generally protective in chemically
induced and geneticmodels of lupus-like disease, but in some
mouse strains, or when administered late in the disease
process, it exacerbated disease (55). Disease protection was
typically associated with Th2 deviation. a-GalCer was also
protective inamodel for autoimmune thyroiditis, in amanner
that correlated with reduced IFN-g and reduced autoanti-
body production. Collectively, these studies have shown that
iNKT-cell activation typically protects against autoimmu-
nity but that treatment efficacy is influenced by a variety of
parameters, including the nature and dose of the iNKT-cell
antigens, the frequency and route of injections, the timing of
treatment relative to disease initiation and progression, the
particular animalmodel used, and the genetic background of
the animals (33, 50). Many of these issues pose problems for
translation to treatment of human autoimmunity.
A single injection of a-GalCer into recipient mice
significantly reduced morbidity and mortality of graft-vs-
host disease (56). This was dependent on stimulation of host
iNKT cells and Th2 deviation of donor T cells.
Although iNKT cells exhibit potent therapeutic proper-
ties in a number of diseases, iNKT-cell activation can also
exacerbate disease such as allergic reactions and atheroscle-
rosis in mice (33, 55).
Conclusions and outlook
iNKT cells are unique lymphocytes that bridge the innate
and adaptive immune systems. These cells acquire their
innate-like phenotype during thymic development by
interaction with CD1d–glycolipid complexes on double-
positive cells and under direction of the transcription factor
PLZF. iNKT cells can respond to endogenous and exo-
genous glycolipid antigens but can also become activated
indirectly by cytokine-driven mechanisms. Quickly after
activation, these cells produce a variety of cytokines with
potent immunomodulatory activities, but they then enter
a period of quiescence. iNKT cells regulate a variety of
immune responses. iNKT-cell ligands exhibit potent
immune-enhancing properties that are being exploited for
the development of vaccine adjuvants. iNKT-cell activation
also has therapeutic effects in mice, and clinical trials with
a-GalCer for cancer are underway. The preclinical studies
with a-GalCer and related iNKT-cell antigens have also
shown potential risks associated with iNKT-cell activation
that will need to be overcome in order to develop safe and
effective iNKT-cell-based vaccine adjuvants and therapies.
Future studies should focus on developing means to better
control the outcome of iNKT-cell activation on immune
responses and disease using diverse treatment modalities
and within genetically diverse hosts.
Acknowledgments
We apologize to colleagues whose work we did not cite
because of space constraints or omission. We thank many
colleagues, especially Dr Sebastian Joyce (Vanderbilt
University School of Medicine), for helpful discussions.
The authors’ work was supported by grants from the
National Institutes of Health (to LVK), a discovery grant
from the Diabetes Research and Training Center at
Vanderbilt University School of Medicine (to LW), a pre-
doctoral fellowship from the National Institutes of Health
(to CLG), and a postdoctoral fellowship from the National
Multiple Sclerosis Society (to VVP).
References
1. Godfrey DI, MacDonald HR, Kronenberg M, Smyth MJ,
Van Kaer L. NKT cells: what’s in a name? Nat Rev Immunol
2004: 4: 231–7.
2. Taniguchi M, Harada M, Kojo S, Nakayama T, Wakao H.
The regulatory role of Va14 NKT cells in innate and
acquired immune response. Annu Rev Immunol 2003: 21:
483–513.
3. Brigl M, Brenner MB. CD1: antigen presentation and T cell
function. Annu Rev Immunol 2004: 22: 817–90.
ª 2009 John Wiley & Sons A/S � Tissue Antigens 73, 535–545 543
L. Wu et al. iNKT cells

4. Kronenberg M. Toward an understanding of NKT cell
biology: progress and paradoxes. Annu Rev Immunol 2005: 26:
877–900.
5. Bendelac A, Savage PB, Teyton L. The biology of NKT cells.
Annu Rev Immunol 2007: 25: 297–336.
6. Kawano T, Cui J, Koezuka Y et al. CD1d-restricted and
TCR-mediated activation of Va14 NKT cells by
glycosylceramides. Science 1997: 278: 1626–9.
7. Borg NA, Wun KS, Kjer-Nielsen L et al. CD1d-lipid-antigen
recognition by the semi-invariant NKTT-cell receptor.Nature
2007: 448: 44–9.
8. Matsuda JL, Mallevaey T, Scott-Browne J, Gapin L.
CD1d-restricted iNKT cells, the ‘Swiss-Army knife’ of the
immune system. Curr Opin Immunol 2008: 20: 358–68.
9. Kinjo Y, Wu DY, Kim G et al. Recognition of bacterial
glycosphingolipids by natural killer T cells. Nature 2005: 434:
520–5.
10. Mattner J, DeBord KL, Ismail N et al. Exogenous and
endogenous glycolipid antigens activate NKT cells during
microbial infections. Nature 2005: 434: 525–9.
11. Sriram V, Du W, Gervay-Hague J, Brutkiewicz RR. Cell wall
glycosphingolipids of Sphingomonas paucimobilis are
CD1d-specific ligand for NKT cells. Eur J Immunol 2005: 35:
1692–701.
12. Kinjo Y, Tupin E, Wu D et al. Natural killer T cells recognize
diacylglycerol antigens from pathogenic bacteria. Nat
Immunol 2006: 7: 978–86.
13. Joyce S, Van Kaer L. CD1-restricted antigen presentation: an
oily matter. Curr Opin Immunol 2003: 15: 95–104.
14. Barral DC, Brenner MB. CD1 antigen presentation: how it
works. Nat Rev Immunol 2007: 7: 929–41.
15. Major AS, Joyce S, Van Kaer L. Lipid metabolism,
atherogenesis andCD1-restricted antigen presentation.Trends
Mol Med 2006: 12: 270–8.
16. VanKaer L, Joyce S. Viral evasion of antigen presentation: not
just for peptides anymore. Nat Immunol 2006: 7: 795–7.
17. Kawana K, Quayle AJ, Ficarra M et al. CD1d degradation in
Chlamydia trachomatis-infected epithelial cells is the result of
both cellular and chlamydial proteasomal activity. JBiol Chem
2007: 282: 7368–75.
18. Godfrey DI, Berzins SP. Control points in NKT-cell
development. Nat Rev Immunol 2007: 7: 505–18.
19. Griewank K, Borowski C, Rietdijk S et al. Homotypic
interactions mediated by Slamf1 and Slamf6 receptors control
NKT cell lineage development. Immunity 2007: 27: 751–62.
20. Borowski C, Bendelac A. Signaling forNKT cell development:
the SAP-FynT connection. J Exp Med 2005: 201: 833–6.
21. Kovalovsky D, Uche OU, Eladad S et al. The BTB-zinc finger
transcriptional regulator PLZF controls the development of
invariant natural killer T cell effector functions. Nat Immunol
2008: 9: 1055–64.
22. SavageAK,ConstantinidesMG,Han J et al. The transcription
factor PLZF directs the effector program of the NKT cell
lineage. Immunity 2008: 29: 391–403.
23. Bezbradica JS, Gordy LE, Stanic AK et al.
Granulocyte-macrophage colony-stimulating factor regulates
effector differentiation of invariant natural killer T cells during
thymic ontogeny. Immunity 2006: 25: 487–97.
24. Van Kaer L, Joyce S. Innate immunity: NKT cells in the
spotlight. Curr Biol 2005: 15: R429–31.
25. Tupin E, Kinjo T, Kronenberg M. The unique role of natural
killer T cells in the response to microorganisms. Nat Rev
Microbiol 2007: 5: 405–17.
26. Zimmer MI, Nguyen HP, Wang B et al. Polymorphisms in
CD1d affect antigen presentation and the activation of
CD1d-restricted T cells. Proc Natl Acad Sci U S A 2009: 106:
1909–14.
27. Godfrey DI, Kronenberg M. Going both ways: immune
regulation via CD1d-dependent NKT cells. J Clin Invest 2004:
114: 1379–88.
28. Seino K, Taniguchi M. Functionally distinct NKT cell subsets
and subtypes. J Exp Med 2005: 202: 1623–6.
29. Coquet JM, Chakravarti S, Kyparissoudis K et al. Diverse
cytokine production by NKT cell subsets and identification of
an IL-17-producing CD4-NK1.1- NKT cell population. Proc
Natl Acad Sci U S A 2008: 105: 11287–92.
30. Diana J, Griseri T, Lagaye S et al. NKT cell-plasmacytoid
dendritic cell cooperation via OX40 controls viral infection in
a tissue-specific manner. Immunity 2009: 30: 289–99.
31. Unutmaz D. NKT cells and HIV infection. Microbes Infect
2003: 5: 1041–7.
32. Terabe M, Berzofsky JA. The role of NKT cells in tumor
immunity. Adv Cancer Res 2008: 101: 277–348.
33. Wu L, Van Kaer L. Natural killer T cells and autoimmune
disease. Curr Mol Med 2009: 9: 4–14.
34. Joyce S, Van Kaer L. Invariant natural killer T cells trigger
adaptive lymphocytes to churn up bile. Cell Host Microbe
2008: 3: 275–7.
35. Sireci G, Russo D, Dieli F et al. Immunoregulatory role of
Ja281 T cells in aged mice developing lupus-like nephritis.
Eur J Immunol 2007: 37: 425–33.
36. Looringh van Beeck FA, Reinink P, Hermsen R et al.
Functional CD1d and/or NKT cell invariant chain transcript
in horse, pig, African elephant and guinea pig, but not in
ruminants. Mol Immunol 2009: 46: 1424–31.
37. Parekh VV, Lalani S, Van Kaer L. The in vivo response of
invariant natural killer T cells to glycolipid antigens. Int Rev
Immunol 2006: 26: 31–48.
38. Kim S, Lalani S, Parekh VV, Vincent TL, Wu L, Van Kaer L.
Impact of bacteria on the phenotype, functions and
therapeutic activities of iNKT cells in mice. J Clin Invest 2008:
118: 2301–15.
39. Chiba A, Dascher CC, Besra GS, Brenner MB. Rapid NKT
cell responses are self-terminating during the course of
microbial infection. J Immunol 2008: 181: 2292–302.
40. Choi HJ, Xu H, Geng Y, Colmone A, Cho H, Wang CR.
Bacterial infection alters the kinetics and function of iNKT cell
responses. J Leukoc Biol 2008: 84: 1462–71.
41. Halder RC, Aguilera C, Maricic I, Kumar V. Type II NKT
cell-mediated anergy induction in type I NKT cells prevents
inflammatory liver disease. J Clin Invest 2007: 117:
2302–12.
42. ChangWS, Kim JY, Kim YJ et al. Cutting edge: programmed
death-1/programmed death ligand 1 interaction regulates the
induction and maintenance of invariant NKT cell anergy.
J Immunol 2008: 181: 6707–10.
544 ª 2009 John Wiley & Sons A/S � Tissue Antigens 73, 535–545
iNKT cells L. Wu et al.

43. Parekh VV, Lalani S, Kim S et al. PD-1/PD-L blockade
prevents anergy induction and enhances the anti-tumor
activities of glycolipid-activated invariant NKT cells.
J Immunol 2009: 182: 2816–26.
44. Silk JD, Salio M, Reddy BG et al. Cutting edge: nonglycosidic
CD1d lipid ligands activate human andmurine invariantNKT
cells. J Immunol 2008: 180: 6452–6.
45. Van Kaer L. Regulation of immune responses by
CD1d-restricted natural killer T cells. Immunol Res 2004: 30:
139–53.
46. Kim S, Lalani S, Parekh VV, Wu L, Van Kaer L. Glycolipid
ligands of invariant natural killer T cells as vaccine adjuvants.
Expert Rev Vaccines 2008: 7: 1519–32.
47. Parekh VV, Wilson MT, Van Kaer L. iNKT-cell responses to
glycolipids. Crit Rev Immunol 2005: 25: 183–213.
48. Motohashi S, Nakayama T. Clinical applications of natural
killer T cell-based immunotherapy for cancer.Cancer Sci 2008:
99: 638–45.
49. Cerundolo V, Silk JD, Masri SH, Salio M. Harnessing
invariant NKT cells in vaccination strategies. Nat Rev
Immunol 2009: 9: 28–38.
50. Van Kaer L. a-Galactosylceramide therapy for autoimmune
diseases: prospects and obstacles. Nat Rev Immunol 2005: 5:
31–42.
51. Motohashi S, Nagato K, Kunii N et al. A phase I-II study of
a-galactosylceramide-pulsed IL-2/GM-CSF-cultured
peripheral blood mononuclear cells in patients with advanced
and recurrent non-small cell lung cancer. J Immunol 2009: 182:
2492–501.
52. Behar SM, Porcelli SA. CD1-restricted T cells in host defense
to infectious diseases. Curr Top Microbiol Immunol 2007: 314:
215–50.
53. Veldt BJ, van der Vliet HJ, von Blomberg BM et al.
Randomized placebo controlled phase I/II trial of
a-galactosylceramide for the treatment of chronic hepatitis C.
J Hepatol 2007: 47: 356–65.
54. Grajewski RS, Hansen AM, Agarwal RK et al. Activation of
invariant NKT cells ameliorates experimental ocular
autoimmunity by a mechanism involving innate IFN-gamma
production and dampening of the adaptive Th1 and Th17
responses. J Immunol 2008: 181: 4791–7.
55. Major AS, Singh RR, Joyce S, Van Kaer L. The role of
invariant natural killer T cells in lupus and atherogenesis.
Immunol Res 2006: 34: 49–66.
56. Hashimoto D, Asakura S, Miyake S et al. Stimulation of host
NKT cells by synthetic glycolipid regulates acute
graft-versus-host disease by inducing Th2 polarization of
donor T cells. J Immunol 2005: 174: 551–6.
ª 2009 John Wiley & Sons A/S � Tissue Antigens 73, 535–545 545
L. Wu et al. iNKT cells
Copyright © 2022 FDOKUMEN




















