
intussusception of transverse colon - NCBI
24
INTUSSUSCEPTION OF TRANSVERSE COLON thrombin increased, so that on her return for follow-up, according to the blood examination she had bleeding rather than clotting tendencies. STATED MEETING HELD MARCH 27, 199.9 The President, DR. FRANK S. MATHEWS, in the Chair NON-MALIGNANT INTUSSUSCEPTION OF TRANSVERSE COLON IN ADULT DR. CONDICT \V. CUTLER. JR., presented a man, forty-seven years of age, who was a(lmitte(l to the Lincoln Hospital on February 25, 1928, complain1- ing of general abdominal pain, vomiting and diarrhea. Previously in good health, he began about a month before admission to complain of cramp-like pain in the abdomen. This pain was very persis- tent, was not localized, did not radiate and was not associated with meals. After the onset he was able to continue at work for a week, but then discon- tinued working because of the progressive character of his complaints. Two weeks before admission he began vomiting about ten to fifteen minutes after meals. The vomitus consisted of food just taken. Up to this time the bowels had been regular, but the stools now became diarrhoeal following catharsis anid continued so. Three days before admission the pain became more severe and spasmodic. The vomiting and diarrhcea also became more intense. The stools and vomitus were brown and fluid. The patient had never observed b)lood in either. Upon admission the patient was quite prostrated. His tem)erature was 100, pulse 130. With the exception of a distended abdomen which was every- where ten(ler, though not rigid, the physical findings were not significant. There was a suggestion of resistance to palpation in the upper right quad- rant, and slight rebound tenderness was referred there. The urine was nor- mal. Blood count: white blood cells I4,000, polymorphonuclears 78 per cent. As the diagnosis was not clear, further investigation was begun after the patient had been relieved of his vomiting by lavage and put on fluid (liet. During the succeeding few days, however, the distention, cramps and diarrhcea persisted. Tests of the stools with benzidine gave consistently positive reactions for blood. There was also considerable mucus in the passages. Gastric analysis was essentially normal in result. The \Vassermann was negative. X-rays showed a stomach normal in size and without filling defect or retention. There was practically a stoppage of the barium meal in the ascending colon, the caecum and terminal ileum showing marked distention. Barium enema showed obstruction distal to the hepatic flexure, though incomplete. The patient was operated upon Mlarch 2I. Exploration of the abdomen through a right rectus incision revealed a mass in the right upper quadrant. When adherent omentum had been separated from it this mass proved to be an intussusception of the first part of the transverse colon, just beyond the hepatic flexure. The mass was about the size of one's fist. The gut wall and surrounding intestinal coils showed evidence of active inflammation. The induration both of the affected intestine and adjacent mesentery was marked. There were several small firm glands in the mesentery suggesting malignant metastasis. 293
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of intussusception of transverse colon - NCBI
INTUSSUSCEPTION OF TRANSVERSE COLON
thrombin increased, so that on her return for follow-up, according to theblood examination she had bleeding rather than clotting tendencies.
STATED MEETING HELD MARCH 27, 199.9
The President, DR. FRANK S. MATHEWS, in the Chair
NON-MALIGNANT INTUSSUSCEPTION OF TRANSVERSE COLON INADULT
DR. CONDICT \V. CUTLER. JR., presented a man, forty-seven years of age,who was a(lmitte(l to the Lincoln Hospital on February 25, 1928, complain1-ing of general abdominal pain, vomiting and diarrhea.
Previously in good health, he began about a month before admission tocomplain of cramp-like pain in the abdomen. This pain was very persis-tent, was not localized, did not radiate and was not associated with meals.After the onset he was able to continue at work for a week, but then discon-tinued working because of the progressive character of his complaints. Twoweeks before admission he began vomiting about ten to fifteen minutes aftermeals. The vomitus consisted of food just taken. Up to this time the bowelshad been regular, but the stools now became diarrhoeal following catharsisanid continued so. Three days before admission the pain became more severeand spasmodic. The vomiting and diarrhcea also became more intense. Thestools and vomitus were brown and fluid. The patient had never observedb)lood in either.
Upon admission the patient was quite prostrated. His tem)erature was100, pulse 130. With the exception of a distended abdomen which was every-where ten(ler, though not rigid, the physical findings were not significant.There was a suggestion of resistance to palpation in the upper right quad-rant, and slight rebound tenderness was referred there. The urine was nor-mal. Blood count: white blood cells I4,000, polymorphonuclears 78 per cent.
As the diagnosis was not clear, further investigation was begun afterthe patient had been relieved of his vomiting by lavage and put on fluid(liet. During the succeeding few days, however, the distention, cramps anddiarrhcea persisted.
Tests of the stools with benzidine gave consistently positive reactions forblood. There was also considerable mucus in the passages. Gastric analysiswas essentially normal in result. The \Vassermann was negative. X-raysshowed a stomach normal in size and without filling defect or retention.There was practically a stoppage of the barium meal in the ascending colon,the caecum and terminal ileum showing marked distention. Barium enemashowed obstruction distal to the hepatic flexure, though incomplete.
The patient was operated upon Mlarch 2I. Exploration of the abdomenthrough a right rectus incision revealed a mass in the right upper quadrant.When adherent omentum had been separated from it this mass proved to bean intussusception of the first part of the transverse colon, just beyond thehepatic flexure. The mass was about the size of one's fist. The gut walland surrounding intestinal coils showed evidence of active inflammation.The induration both of the affected intestine and adjacent mesentery wasmarked. There were several small firm glands in the mesentery suggestingmalignant metastasis.
293
NEW YORK SURGICAL SOCIETY
An attempt was made to reduce the intussusception with partial suc-cess, about three inches of intussuscipiens being withdrawn. When this wasaccomplished the suggestion of any extensive malignancy was much lessmarked the gut appearing merely thickened and inflamed. On this accountit was decided not to subject the patient to a radical colectomy but to performa local resection of the Mikulicz type. The affected loop of intestine togetherwith adjacent normal gut and its mesentery was eventrated and fixed in theusual manner, terminating the first stage.
Three days later the second stage, removal of the eventrated mass,-wasperformed. A Kocher clamp was introduced to cut down the spur betweenthe parallel lumina of the ascending and transverse colon.
Pathological examination of the removed portion of gut and of its mesen-tery showed no evidence of malignancy. The firm nodular mass of the gutwall which had formed the apex of the intussuscipiens showed hypertrophyof the mucosa and marked chronic and acute inflammatory changes withsuperficial ulceration but no carcinomatous change. The other coats of theintestine showed corresponding pathology.
The patient, relieved of his svmptoms, progressed satisfactorily. Thespur was cut down joining the lumina and bowel movements began aboutone week after the second stage. June 6 closure of the peristent faecal fis-tula was done. To avoid peritoneal contamination the gut at the site of thestoma was not separated from the abdominal wall, but was tightly closed insitu and the muscles and fascia united over it in their normal relations. Heal-ing occurred without leakage, and the patient was discharged two weeks iaterin good condition. He has been well and gaining in weight since that time.
H2EMORRHAGE FROM MIDDLE MENINGEAL ARTERY
DOCTOR CUTLER presented also a woman, thirty-nine years of age,who was admitted to the First Surgical Division of the Roosevelt HospitalDecember 14, I928.
Forty-eight hours prior to admission the patient, while standing at thehead of the stairs fell without determined cause and was found lying uncon-scious at the foot of the stairs. This condition of unconsciousness persistedfor a few moments. Upon recovering it was noticed that her left arm washeld in a peculiar position and seemed weak. She was put to bed and seemedrather dazed, but could be readily aroused. She subsequently improved, buton walking there was noted to be a definite weakness in the left leg whilethe left arm also continued weak. Twelve hours before admission she lostconsciousness completely and her condition had become progressively worsesince that time.
When admitted she wats in a stuporous condition and tossing restlesslyin bed.
Examination of the head showed a moderate hematoma in the right sideof the scalp above the mastoid region. The eyes showed contraction of theright pupil as compared with the left and distinct divergent strabismus. Thepupils reacted to light, but sluggishly. Ophthalmoscopic examination was dif-ficult because of the constant rolling of the eyes, but there seemed to be someslight haziness in outline of the discs. There was no apparent paralysis ofthe face muscles and no marked twitching. In her unco6rdinated movementsthe patient used both the left arm and left leg, but muscular resistance inthe arm in particular was distinctly weaker than on the right side. The
294
H:EMORRHAGE FROM MIDDLE MENINGEAL ARTERY
reflexes at the knee were exaggerated, but apparently equal on both sides.There was no rigidity of the neck or Kernig sign.
Her temperature on admission was ioo.8°, respirations 32, pulse 78, bloodpressure I25/70.
An X-ray picture of the skull did not show a definite fracture at the firstexamination, but this was not conclusive because of the difficulty in keepingthe patient's head quiet during exposure.A lumbar puncture was done and six cubic centimetres of uniformly
bloody fluid was obtained under normal pressure.Subsequently, upon the day of admission, I50 cubic centimetres of 50
per cent. glucose were administered intravenously and there seemed to besome slight improvement on the following morning. During the day, how-ever, the patient became more stuporous and the breathing somewhat ster-torous in type, and movements in the left arm and leg were gradually lost,as also was the activity of the face muscles on the left side. Definite chokingof the optic discs was now observed and a diagnosis of extradural hxemor-rhage with fractured skull and laceration of the middle meningeal artery wasmade. December i6 the patient was operated upon. She was completelycomatose and no anaesthesia was necessary. A button trephine was done overthe bifurcation of the anterior branch of the right middle meningeal artery.A considerable amount of clot was discovered beneath the skull extendingin all directions in the parietal region. A temporal decompression was thenproceeded with and a flap of bone turned down. Its removal revealed a largeblood clot perhaps amounting to about six ounces and covering most of theanterior right hemisphere. Active bleeding was coming from the middlemeningeal artery and this was temporarily controlled with packing. The clotwas removed and the dura beneath found not to have been torn. It was, how-ever, very markedly depressed and the brain tissue beneath it felt very softand almost fluctuating. Attempt was now made to control the bleeding whichapparently came up from the area below the base of the flap. In order tosecure the bleeding point the opening was enlarged downward with a rongeurso that the inner table could be inspected all the way to the base of the skull.No definite point of bleeding could be observed, but blood continued to wellup from the base in the neighborhood of the foramen spinosum. As no speci-fic bleeding spot could be isolated, a small strip of packing was introducedinto this region, which, with moderate pressure, eventually controlled thebleeding. This packing was brought out at the lower angle of the woundanteriorly and flap of elevated bone, muscle and scalp replaced.
Following the patient's return to the ward there was a distinct hyper-pyrexia, her temperature reaching I070. This was associated with markedshock and the blood pressure fell to 70/45. She responded, however, to thetreatment employed for shock and by the following day showed distinctimprovement. Within twenty-four hours after operation the patient wasentirely conscious although a little confused. She was able to use the musclesof the left side, face, arm and leg at this time. During the succeeding daysthe improvement continued. The slight discharge from the wound subsidedfollowing the removal of the packing on the third day. She was allowedout of bed on the twenty-seventh post-operative day feeling entirely well.Since that time the patient has continued in excellent health and has had nosymptoms of weakness of the arm or leg and no alteration from her nor-mal mentality.
295
NEW YORK SURGICAL SOCIETY
OSTEOMYELITIS OF JAWDOCTOR CUTLER presetnted also a man, thirty-three years of age, who-
was admitted to the Lincoln Hospital May 26, I928. Ten days previously hehad, begun to have pain and swelling at the left side of the jaw. Two daysafter onset a left lower molar was extracted, and as the swelling did not sub-side his dentist had made several incisions within the mouth near the site ofextraction. The pain and swelling increased, however, and when the patientwas admitted there was a tense and brawny induration of the left lowercheek and side of the neck. There was also marked swelling within the mouth,suggestive of alveolar abscess, and from the site of extraction there was athin purulent discharge. The mouth could be opened but one-half inch.
At this time the patient's temperature was I02, pulse Io6. He'seemedvery sick and was markedly prostrated. Urine was normal. Blood count:white blood cells i8,0oo, polynuclears 8o per cent.
On the day following admission an incision was made in an area of soften-ing beneath the ramus of the left jaw and pus obtained. The alveolar abscesswas also opened. Subsequent incisions were made as localizations of theprocess or pocketing occurred. For a period of nearly six weeks the patient'stemperature continued of the septic type, ranging from 990 to I030 or1040 daily. During this period several transfusions were given. Blood cul-tures showed no growth. The patient was so depleted and septic that itwas feared he would not survive. The temperature began to subside, how-ever,' and'by the middle of July had reached normal and the patient was upand about with numerous d-raining sinuses about the jaw and neck.
At about-this time' the removal of'sequestra from the jaw began. As frag-ments of the bone. became demonstrably loose or were' shown by X-ray,they wer'e .removed, the sinuses being frequently enlarged for the purpose.This process continued u'ntil in October, the total fragments removed approxi-mating a considerable portion 'of the'lowet jaw. The sinuses closed until atthe present time but one remains discharging. There is at the bottom of thisa small sequestrum which requires -removal.
On November I 7 the patient was discharged to the dental clinic forremoval of the dead teeth and splinting of the jaw. From just below thearticulations no solid bone was palpable at this time, and in fact for a con-siderable period of time, while disintegration of the jaw was progressing,there was no stability to the structure. It was assumed that following a dentalclearing of the mouth and after an appropriate period for the subsidence of.exudate some grafting procedure would need to be attempted.
X-ray pictures which were taken about one month later showed someevidence of. bone regeneration.' This regeneration has been progressive tothe present time, and now has developed a fairly stable bony structure. It isnow possible for the patient to use his jaw a little, and he opens his mouthabout onie inch. The removal of dead teeth and the application of an appro-priate dental plate will improve his function considerably.
LARGE RETROPERITONEAL LIPOMADR. DEWITT STETTEN presented a man, forty-three years of age, who
was first seen by him December 5, 1923. He had been examined the weekpreviously for life insurance and a growth was discovered in the lower abdo-men. There were no symptoms. The patient had not lost any weight. Onexamination a large, ovoid, fluctuating mass was felt,- filling the right lowerquadrant of the abdomen, extending as high as the umbilicus, and somewhatto the left of the median line. It was insensitive and there was no rigidity.It was dull to percussion. The mass felt very much like a large cyst, possibly
296
STRANGULATED FEMORAL HERNIA WITH GANGRENE
of mesenteric or omental origin. Rectal examination was negative. On cathe-terizing the patient and emptying the bladder, no effect was noted on thesize or shape of the mass. X-ray examination showed no defect in the largeintestine, but the cwecum was displaced upward and to the left by the tumor.December I I, 1923, an operation was do^ne.- A median incision was made,and a large retroperitoneal, yellowish tumor was found, which had pushedthe cacum upward and inward, and the posterior parietal peritoneum forwardso that this had become attached and adherent to the lower leaf of the mesen-tery of the terminal ileum. There was a small, kinked and twisted appendixwith a club-shaped tip, bound down by adhesions between the tumor and thecaecum. The tumor was distinctly encapsulated and obviously lipomatous incharacter, springing apparently from the retroperitoneal fat in the, region ofthe brim of the pelvis near the right sacro-iliac joint. There was a lobulatedprolongation posteriorlynear the upper pole. The KA.tumor was enucleatedwithout much difficulty bysplitting the posterior pa-rietal peritoneum over it,and then dividing the cap-isule of the tumor. It wasmoderately adherent atthe lower pole and at thelo b u la t e d prolongationposteriorly near the upperpole. There was very lit-tle bleeding. The appen-dix was removed in theusual fashion. The tumor(Fig. I) measured twen-ty-two centimetres inlength, twelve centimetres FIG. i.-Large retroperitoneal lipoma.in width, and nine centi-metres in thickness, and weighed 7IO grams. It was encapsulated and therewas a small lobulation of the upper pole posteriorly. It was rather firmer andmore fibrous than the usual lipoma. On microscopic examination the tumorwas found to be an ordinary lipoma, composed.of mature fat cells, with nosuggestion of malignancy. The convalescence was uneventful and the patienthas remained perfectly well since.
STRANGULATED FEMORAL HERNIA WITH GANGRENE OF ILEUM INSEVENTY-NINE YEAR OLD PATIENT
DR. DEWITT STETTEN presented a woman, eighty years of age, whom hefirst saw on October I5, 1927. For twenty-five years the patient had had ahernia in the right groin, which had always been reducible, and which neverhad been previously incarcerated; A truss had been worn until five yearsago. About twenty hours previously patient developed abdominal crampsand vomiting which continued- in -spite of an effective enema. About threehours before Doctor Stetten's examination, she noticed that the swelling ofher right groin had become irreducible. The examination disclosed a hard,sensitive, globular swelling in the right groin, the size of a small orange. Itwas irreducible and tympanitic on percussion. The patient's condition wasgood. The temperature was normaf. The pulse was 8o, regular and of good
297
NEW YORK SURGICAL SOCIETY
quality. The presence of a right strangulated femoral hernia was evident.The patient was immediately transferred to the hospital and operated uponunder local anesthesia. In the hernial sac was found a four inch loop ofileum, dark bluish-black in color. In spite of about twenty minutes' nursingwith hot saline wipes, there was only slight improvement in the appearanceof the strangulated loop, although the peritoneum was glossy and thereappeared to be some peristalsis. It seemed rather certain that the loop wouldnot recover, but owing to the patient's age a primary resection was deemedinadvisable. The loop was therefore drawn out on the abdominal wall untilundoubtedly healthy intestine protruded beyond the peritoneal cavity; gauzetampons were packed around the loop. The patient ceased vomiting imme-diately upon the relief of the constriction. After the lapse of nineteen hoursexamination showed advanced gangrene of the strangulated loop. The patientwas again operated upon under nitrous oxide-oxygen-ethylene anaesthesia.The tampons were removed and the healthy ileum brought further out intothe wound. Deliberate resection with a lateral isoperistaltic ileo-ileostomy wasperformed in the usual manner, The anastomosed portion of the intestinewas then replaced into the abdominal cavity, a modified Lotheissen femoral-inguinal hernioplasty was done according to the method described by theauthor. The patient's convalescence was entirely uneventful and the woundhealed by primary union.
Doctor Stetten presented this case to demonstrate a plan of procedurein strangulated hernia with intestinal gangrene in the aged, which he believedto be worthy of commendation. By dividing the constriction, the intestinalobstruction and shock are relieved. The danger of primary resection, withintestinal anastomosis and hernioplasty is certainly reduced by performingthis operation after an elapsed period of time, during which the patient hashad some chance to recover. This method is certainly preferable and withoutmuch greater risk than the usual procedure of removing the gangrenous gutthat has been brought into the wound, leaving the resultant ileostomy for sub-sequent closure and then performing a secondary hernioplasty.
DR. HOWARD LILIENTHAL said that in hernia when gangrene is pres-ent, even though the constriction has been removed, the process may afterall be progressive and there may be spots of gangrene quite a distance fromthe primary necrotic area. Consequently, to avoid danger, he preferred to cutoff that loop of the gut as soon as possible. He has used a method exempli-fied in the following case: A little, thin, old woman had strangulated herniawith gangrene of the ileum. Doctor Lilienthal enlarged the opening, with-drew the gut until practically certain that nothing was left within of the gan-grene, placed half a Murphy button into each side of the loop through anopening in the gangrenous part, made a minute incision over the stem ofeach button and forced the two together. No suture was necessary, overlap-ping or otherwise. The walls of this gut were thin. The strangulation wasso acute that there was no hypertrophy of the gut walls. He crushed the gutwalls the same as he is in the habit of crushing the root of the appendix;ligated over the place where the clamp had crushed the two legs of the loopabout an inch and a half away from the Murphy button, which was nowclosed, and insured immediate passage of gas and liquid stool; cut the ileum
298
STRANGULATED) FEMORAL HERNIA WITH- GANGRENE
off and'carbolized the stumps 'thoroughly. -The silk ligature -was left withits ends in the wound and the remainder of the herniia was pushed back farenough to make sure it was in the abdomen, strapped there and left. It wasseven or eight days before the ligature came away with the stump and therewas at no time leakage or other trouble. The button came away in due timeand the patient was entirely cured. In feeble, vomiting, old individuals, whenone wishes to finish the operation as quickly as possible, this is a good methodand there is as little danger connected with it as there is in. any other pro-cedure with the same object. Contact has been established, not only thegangrenous loop has been gotten rid of but the unhealthy tissues intimatelyconnected with it. The danger point is near enough to the opening in theabdominal wall so there need be no fear if there should be some accident atthe point where the ligature was applied.
DR. RICHARD LEWI$OHN referred to a patient whom he had presentedbefore this Society in I926. He had operated on the man in I920 for stran-gulated inguinal hernia of six hours' duration. The patient was- eighty-twoyears of age at the time of operation. Parts of the transverse colon werecompletely gangrenous and he performed a primary resection. The man, asidefrom pneumonia, made an uneventful recovery. These old people, when theyare in good general condition such as absence of marked pathology in heart,lungs or kidneys, are not very grave operative risks. In view of the fact thatDoctor Stetten was doubtful as to the viability of the strangulated intestine,"vorlagerung" was the correct procedure. In the presence of definite gan-grene, primary resection would be preferable to a two-stage operation.
Doctor Stetten in closing said that he had presented this case just becausehe thought it illustrated the value of not doing a primary resection in thesecases. It is true that at the time of the first operation he was slightly doubt-ful of the condition of the gut and that he thought that there was a pos-sibility that it might recover. Nevertheless, he believes that even if the cer-tainty of gangrene is present it would be advisable to follow this procedureand not do the resection until a later date when the patient has recoveredsomewhat from the shock and obstruction after the constriction has beenrelieved. He thinks that by this means the risk of operation and the mor-tality might be reduced. Although his patient was in good condition at thetime of the first operation and might have stood a primary resection, sheceased vomiting immediately after the release of constriction and was instill better condition at the end of the nineteen hours when the resectionwas performed.
As to the possibility of gangrene extending further along the intestine, inthis case this was out of the question, as the ileum was brought out on theabdominal wall well beyond the gangrenous area. He felt that this dangercould easily be overcome and that there was no particular need for worryabout absorption from the loop of extra-abdominal intestinal gangrene whenwell walled off by tampons and only left for a relatively short period of -time.A similar situation is frequently met with in the Mikulicz "vorlagerung"
299,
NEW YORK SURGICAL SOCIETY
operation where the mesenteric vessels must be ligated. Here there is neverany trouble provided the gangrene which follows the arrest of the circulationis entirely extra-abdominal.
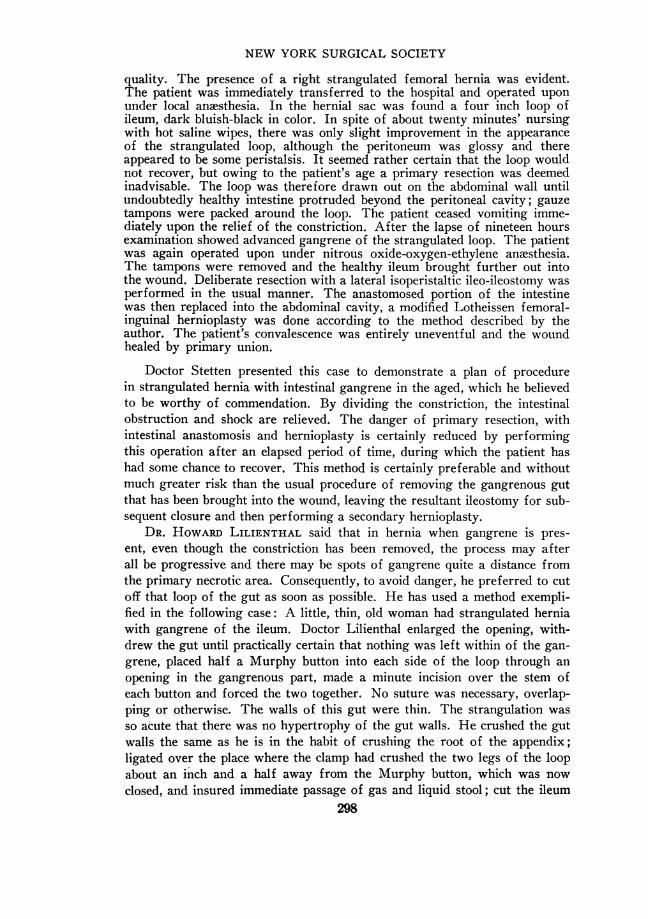
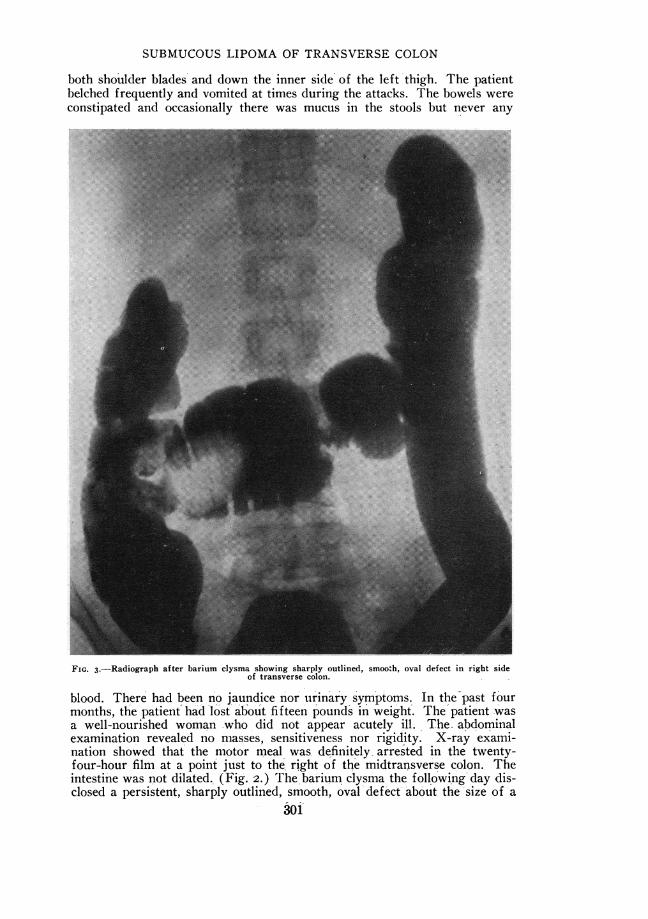
FIG. 2.-Radiograph twenty-four hours after motor meal showing arrest of meal in right side oftransverse colon.
SUBMUCOUS LIPOMA OF TRANSVERSE COLON WITH RECURRENTINTUSSUSCEPTION
DR. DEWITT STETTEN presented a woman, forty years of age, who firstcame under his observation February 5, I929. She gave a history of havinghad during the previous seven weeks repeated attacks of severe cramp-likeabdominal pain with rather vague localization. The pain apparently startedsomewhere in the left lower abdomen and radiated all over the abdomen, to
300-
SUBMUCOUS LIPOMA OF TRANSVERSE COLON
both shoulder blades and down the inner side' of the left thigh. The patientbelched frequently and vomited at times during the attacks. The bowels wereconstipated and occasionally there was mucus in the stools but never any
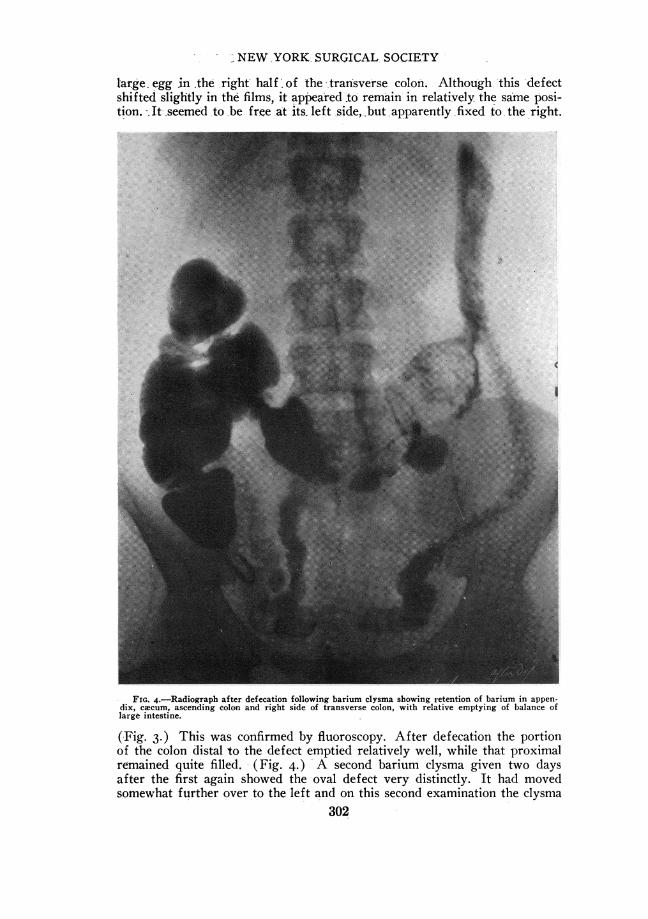
FIG. 3.-Radiograph after barium clysma showing sharply outlined, smooth, oval defect in right sideof transverse colon.
blood. There had been no jaundice nor urinary symptoms. In the past fourmonths, the patient had lost about fifteen pounds in weight. The patient wasa well-nourished woman .who did not appear acutely ill. The. abdominalexamination revealed no masses, sensitiveness nor rigidity. X-ray exami-nation showed that the motor meal was definitely- arrested in the twenty-four-hour film at a point just to the. right of the midtransverse colon. Theintestine was not dilated., (Fig. 2.) The barium clysma the following day dis-closed a persistent, sharply outlined, smooth, oval'defect about the size of a
301
-NEW YORK- SURGICAL SOCIETY
large egg in .the right half of the -transverse colon. -Although -this defectshifted slightly in the films, it appeared to remain in relatively the same posi-tion. It- seemed to be free at its- left side, but apparently fixed to, the right.
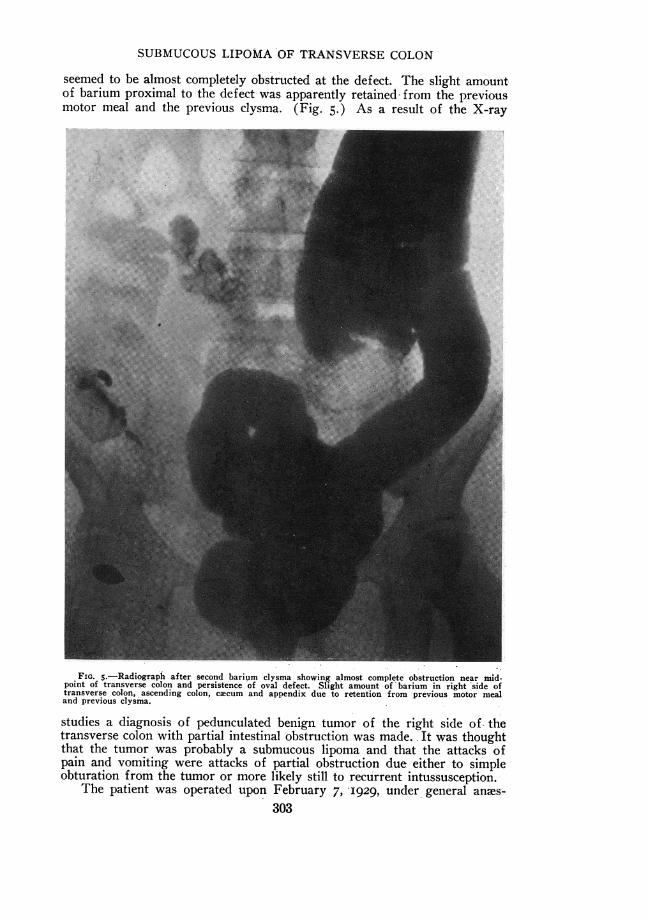
FIG. 4.-Radiograph after defecation following barium clysma showing retention of barium in appen-dix, caecum, ascending colon and right side of transverse colon, with relative emptying of balance oflarge intestine.
(Fig. 3.) This was confirmed by fluoroscopy. After defecation the portionof the colon distal to the defect emptied relatively well, while that proximalremained quite filled. (Fig. 4.) A second barium clysma given two daysafter the first again showed the oval defect very distinctly. It had movedsomewhat further over to the left and on this second examination the clysma
302
SUBMUCOUS LIPOMA OF TRANSVERSE COLON
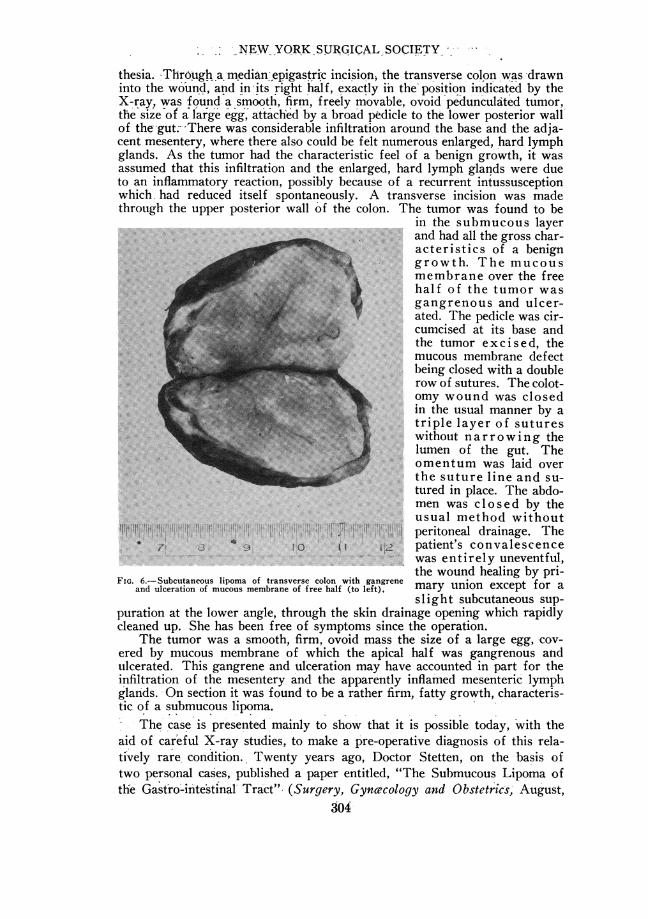
seemed to be almost completely obstructed at the defect. The slight amountof barium proximal to the defect-was apparently retained from the previousmotor meal and the previous clysma. (Fig. 5.) As a result of the X-ray
FIG. S.-Radiograph after second barium clysma showing almost complete obstruction near mid-point of transverse colon and persistence of oval defect. Slight amount of barium in right 'side oftransverse colon, ascending colon, cacum and appendix due to retention from previous motor mealand previous clysma.
studies a diagnosis of pedunculated benign tumor of the right side of, thetransverse colon with partial intestinal obstruction was made. It was thoughtthat the tumor was probably a submucous lipoma and that the attacks ofpain and vomiting were attacks of partial obstruction due either to simpleobturation from the tumor or more likely still to recurrent intussusception.-
The patient was operated upon February 7, '1929, under general anes-303
; NEW YORK SURGICAL SOCIETY
thesia. Through a median epigastric incision, the transverse colon was -drawninto the wound, and in its right half, exactly iin the position indicated by theX-ray, was found a smooth, firm, freely movable, ovoid pedunculated tumor,the size of a large egg, attach'ed by a broad pedicle to the lower posterior wallof the gut -There was considerable infiltration around the base and the adja-cent mesentery, where there also could be felt numerous enlarged, hard lymphglands. As the tumor had the characteristic feel of a benign growth, it wasassumed that this infiltration and the enlarged, hard lymph glands were dueto an inflammatory reaction, possibly because of a recurrent intussusceptionwhich. had reduced itself spontaneously. A transverse incision was madethrough the upper posterior wall of the colon. The tumor was found to be
in the submucous layerand had all the gross char-acteristics of a benign~~~~~~~~.............'i ' ' ' o
grwth. The mucousmembrane over the freehalf of the tumor was
MJ~~~Jfll-~~ ~ ~ ~ gangenos and ulcer-ated The pedicle was circumcised at its base and
.. ",','',,'' '? i "J lu, >' ' 'the tumor exc ised,themucous membrane de ect
* being closed with a doublerow of sutures, The colot-omy wound was closedin the usual manner by a
:'lI `iN' triple layer of sutureswithout narrowing thelumen of the gut. The
..::
omentum was laid overthe suture line and su-tured in place. The abdo-* : :. ....men was closed by theusual method without
~~ ~ ~ ~ peritoneal ~~~~~~~~~~~~drainage. Thet?:~~~~~~~~~~~~~1 T.18 l1.:.. peritonealt!t !111:i| !III 71 3 9 1` 1 qi. patient's convalescence
wase ntirely uneventful,the wound healing by pri-
FIG. 6.- Subcutaneous lipoma of transverse colon with gangrene f rand ulceration of mucous membrane of free half (to left). maryslight subcutaneous sup-
puration at the lower angle, through the skin drainage opening which rapidlycleaned up. She has been free of symptoms since the operation.
The tumor was a smooth, firm, ovoid mass the size of a large egg, cov-ered by mucous membrane of which the apical half was gangrenous andulcerated. This gangrene and ul'ceration may have accounted in part for theinfiltration of the mesentery and the apparently inflamed mesenteric lymphglands. On section it was found to be a rather firm, fatty growth, characteris-tic of a submucous lipoma.
The case is presented mainly to show that it is possible today, 'with theaid of careful X-ray studies, to make a pre-operative diagnosis of this rela-tively rare condition. Twenty years ago, Doctor Stetten, on the basis oftwo personal cases, published a paper entitled, "The Submucous Lipoma ofthe Gast-ro-inte'stinal' Tract" (Surgery, Gynwccology and Obstetrics, August,
304
RADICAL AMPUTATION OF BREAST FOR CARCINOMA
Vol. ix, PP. I56-I75, I909). In this paper he made a complete analysis ofthe literature up to that time and found that seventy-seven cases had beenreported from all portions of the gastro-intestinal tract, of which thirty-fourwere in the colon, excluding the rectal cases. In fifteen of these an intussus-ception occurred-nine chronic and six acute. It is curious to note that in thispaper there is no reference whatsoever to X-ray studies as a diagnostic mea-sure. Of course twenty years ago the radiographic study of gastro-intestinallesions was in its infancy, and although studies of the stomach were begin-ning to be made, the intestine was still considerably neglected for a numberof years. When the paper was published, a definite, correct, pre-operativediagnosis was regarded as an almost impossible achievement. As a result ofthe strides that have been made in intestinal radiography in the past yearsit must be admitted that the exact'diagnosis in this case was neither fantas-tic nor difficult, but rather obvious. Its mobility definitely suggested thepedunculation and even the probable pre-operative diagnosis of the pathologyof the tumor was not so far-fetched, as it is well known that the submucouslipoma is by far the most common form of benign growth in this region.
DR. JOHN DOUGLAS said there were two reasons perhaps why correctdiagnosis in this case had been possible. One, that Doctor Stetten had hada similar case before and that helps in making a diagnosis of rare conditions.The other, that it was a submucous tumor. These lipomata of the large intes-tine are not always submucous. Some two or three years ago Doctor Doug-las said he had shown before the Society a case of lipoma of the large intes-tines. The tumor was not pedunculated in this case. An X-ray of the colonwas taken. In the radiograph the shadow was exactly that which would beshown by a carcinoma and it was not until a section of the sigmoid had beenremoved and an anastomosis done and the gut cut open afterward that thefact that it was a lipoma rather than a carcinoma could be recognized.
DR. FRANK S. MATHEWS recalled a case with pelvic tumor well circum-scribed and suggesting an ovarian cyst. It was, however, attached to the wallof the pelvis. At operation it proved to be a lipoma, for the most part easilyenucleated, but it extended downward and evidently had its origin in thefemoral canal.
DR. HERMANN FISCHER said that these retroperitoneal lipomata are some-times of tremendous size. Although they are benign tumors they have thetendency to recur. There are on record several of these tumors that haverecurred two and even three times. They are potentially malignant as theycan endanger the life of the patient by their huge size and the difficulty oftheir removal. Every case of retroperitoneal tumor ought to be' carefullywatched for possible recurrence.
RADICAL AMPUTATION OF BREAST FOR CARCINOMA AFTER CLOSUREOF LARGE DEFECT
DR. DEWITT STETTEN presented a woman, forty years of age, whom hefirst saw March I5, I928. She had noticed a growth in her right breast fornearly a year. This had been growing rather rapidly for about four months.
20 305
NEW YORK SURGICAL SOCIETY
Examination disclosed a large, irregular, hard tumor in the outer upper quad-rant of the right breast extending toward the axilla. The tumor was firmlyand broadly adherent to the skin, and in the axilla several large, hard lymphglands could be palpated. The patient was operated on March 2I, I928, theusual radical amputation of the breast being performed. Owing to the exten-sive skin involvement, a very wide skin excision was necessary, especiallylaterally, so that there was an extremely small axillary flap left and a verylarge resulting defect, which, even with extensive undermining and mobiliza-tion of the skin of both sides, could not be closed. Instead of doing a Thierschgraft on this defect which has the disadvantage of leaving a very thin, deli-cate scar directly over the ribs, lateral crescentic incisions were made on eachside some distance away from the wound edge to relieve tension. After thiswas done the main wound could be easily closed without tension and the gapsproduced by the lateral crescentic incisions- were tamponed with gauze. Thepatient made an uneventful convalescence and the sutured portion of thewound healed by primary union, both- medial and lateral flaps maintainingexcellent nutrition. The gaps produced by the lateral incisions granulatednicely and on April 9, I928, these granulating areas were successfully Thierschgrafted. Doctor Stetten presents this case to demonstrate what he considersa practical method of closing large defects after radical amputation of thebreast. The scar from the main wound is a linear one, and there is a normalskin covering over the ribs. Function of- the arm was rapidly restored almostto normal except for a slight restriction to backward motion when the armis elevated. -Doctor Stetten believes that this method is superior to the graft-ing of the original defect as it leaves a normal skin covering with its padof subcutaneous fat over the anterior and more exposed portion of the chestand in no way increases the disturbance of function of the arm. Of coursethe Thiersch grafting of the lateral gaps could be done as a primary measure.This perhaps may even be more advisable than doing it as a secondary pro-cedure, as was done in this case.
DR. RICHARD LEWISOHN said that the Kocher incision, as used by Doc-tor Stetten, required plastic surgery in a large 'number of cases. With theStewart incision, which is now the incision of choice of a number of sur-geons at Mount Sinai Hospital, the skin can always be sutured without unduetension and without resorting to plastic correction. For this reason, the Stew-art incision, aside from its better cosmetic effect, is preferable to theKocher incision.
DR. ALEXIS MOSCHCOWITZ said that personally he objected to the Stew-art incision for a radical amputation of the breast. When he heard DoctorStewart read his paper describing the new incision, he was the first one touse it, but after trying it out on a few cases, he abandoned it. While cos-metically, very beautiful, he has never had as perfect an exposure as with theordinary incision extending a short distance down the arm; on that account,he is afraid of being less radical than with the ordinary incision.
HERNIA THROUGH THE FORAMEN OF WINSLOW
DR. JOHN DOUGLAS presented a man, fifty-three years of age, who hadan attack of severe pain during the night of October 26, I927. The painbegan in the region of the navel and then located in the epigastrium. Hevomited for four hours that night and the most severe pain was then relieved.
306
HERNIA THROUGH FORAMEN OF WINSLOW
He was admitted to ..
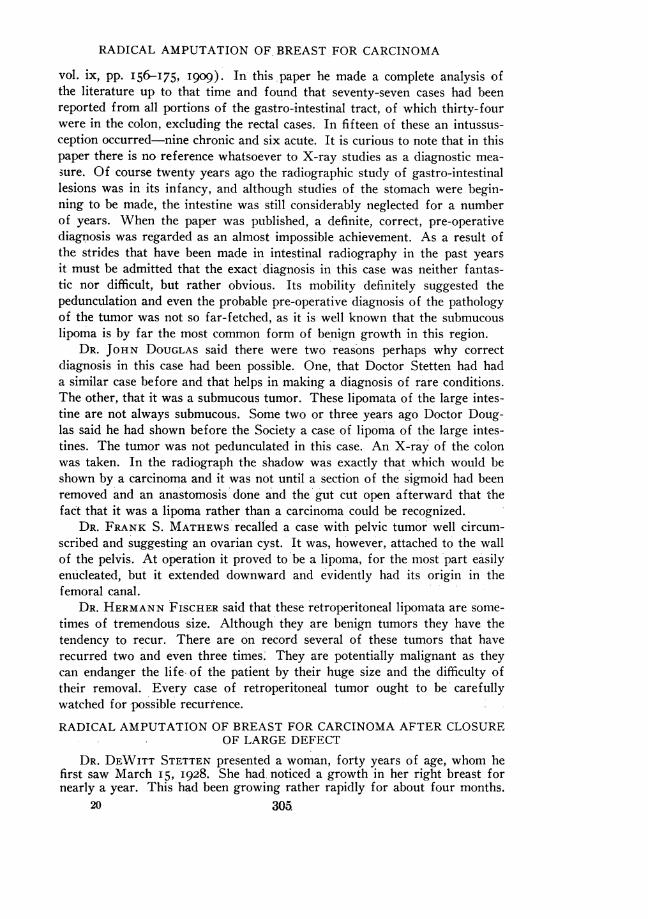
St. Luke's Hospital on ethe morning of October27. There was no eleva-tion of temperature orblood count, no rigidity orloss of liver dulness and *only moderate tendernessin the epigastrium.
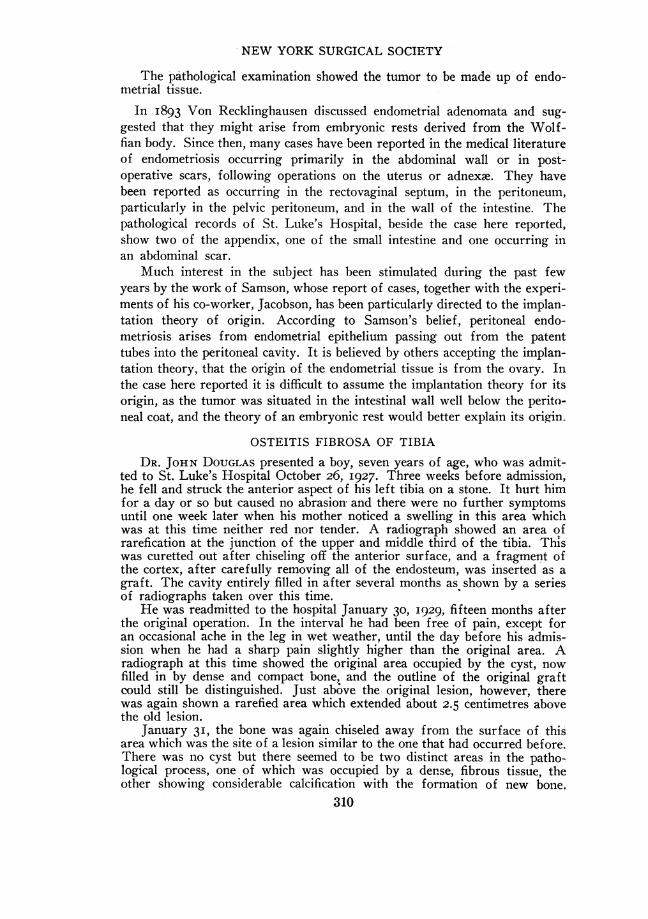
The following day theradiographs showed quite .obviously a displacementof the pylorus and duo-denal cap to the left witha defect along their rightmargins (see Figs. 7, 8,9), and a loop of smalli-testine which apparentlyhad passed through theforamen of Winslow intothe lesser sac. At the end .,f..of six hours the stomachwas emptied, but theshadow of this loop ofsmall intestine could stillbe seen, distended with FIG. 7.-Hernia through the foramen of Winslow five minutes
gas, occupyingthesa after barium meal. Note deformity of pylorus and duodenum andgas, occupying the same loop of small intestine in lesser sac.
location and well above.5 _the transverse colon,
which was outlined bythe bismuth filling it. This
'A ~~~~~was also shown, but less'"K_ _plainly, in a twenty-four-
hour film. Therefore, a. _ \ /M_ diagnosis was made of
hernia through the fora-mien of Winslow.
Operation was per-formed the following day,
Q1. : S .ffl >...........[there being no obstructionapparent in this loop of
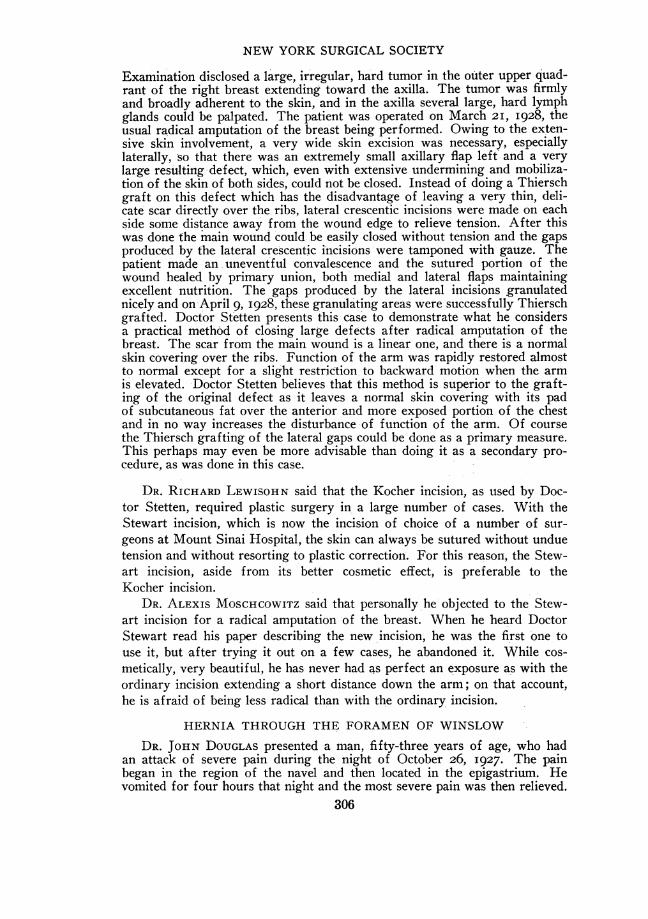
ONE _ .''-smallintestine. At thetime of operation no in-testine was found occupy-ing the lesser sac. How-ever, a loop of ileum, teninches long and about two
,,04 feet from the ileocaecalvalve, was found, at bothends of which could beeasily demonstrated a nar-
FIG. 8.-Hernia through the foramen of Winslow six hours row compressed area com-after meal. Note air-filled loop of small intestine in lesser saccontinuous with barium-filled loop below. pletely encircling the in-
307
NEW YORK SURGICAL SOCIETY
testine and extending well down into the mesentery, such as one sees in a loopof intestine which has been pulled out of a hernial sac after it has been pinchedby the margins of the ring. The foramen of Winslow admitted three fingers.As a later radiograph showed the absence of this shadow, it would appearfrom the evidence present that this loop of intestine had been herniatedthrough the foramen of Winslow into the lesser sac.
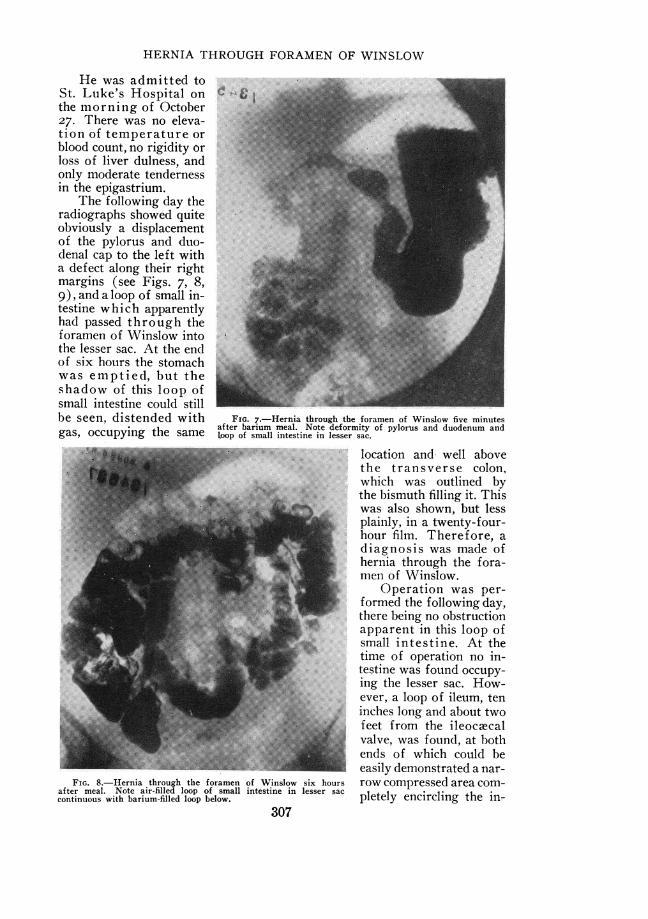
It being impossible to narrow the foramen of Winslow on account ofits surrounding structures and as the loop of intestine had apparently passedeither to the right of the hepatic flexure or in front of the transverse colon,
an attempt was madeto prevent a recurrence
7. of the lesion by causingadhesions between thegreater omentum and an-terior abdominal wall, sothat the small intestinecould not again pass infront of the transversecolon. Since the timeof operation, seventeenmonths ago, the patientas had no recurrence of
__ i t ... ^ ~~~~~~his symptoms.
= | - i ... In May, I924, thespeaker reported a case ofhernia through the fora-men of Winslow in theJournal of the AnmericanMedical Association. Atthat time there had been
FIG. 9.-Hernia through the foramen of Winslow. Twenty-four- collected by Ullman thirtyhour film: Note air-filled loop above colon. cases from the literature.
My case then recorded was the thirty-first case in the literature and the thirdcase in the American literature. Since then, a number of cases have beenreported, one series by Dewis and Miller, who added to Ullman's group onecase of their own and two additional cases not reported by Ullman, making atotal of thirty-three cases, not including the case previously reported by me.In a rather superficial search of the literature since then, I have found threeadditional cases reported-one by Shapiro, one by Carling and Smith andone by Green. These, together with the case here reported and the one pre-viously reported by me, make a total of thirty-eight cases.
The excellent articles and a review of the literature published by Dewisand Miller, and also by Ullman, make it unnecessary to again go throughthis part of the subject. However, while it is recognized that the occurrenceof a hernia through the foramen of Winslow usually causes symptoms ofacute strangulation and necessitates immediate operation, it was the disap-pearance of these acute symptoms which made possible the radiographic
308
ENDOMETRIOSIS OF THE SIGMOID
examination in this case which allowed a diagnosis to be made, which would,of course, be impossible in the presence of acute symptoms. As it is statedin one article on the subject that a diagnosis of this condition has never beenmade before operation and rarely even suspected, it seemed worth while toreport this case in which the diagnosis was made previous to operation, foralthough the intestine was not found in the lesser sac, there was ample evi-dence of its having been there at the time the radiograph was taken.
BIBLIOGRAPHY
1Shapiro, A.: Ztrbl. fur Chir., July 21, 1925.2Carling and Smith: British Journal of Surgery, January, I926.5Dewis, J. W., and Miller, R. H.: Surgery, Gynaecology and Obstetrics, vol. xlv., p.
95, I927.'Green, E. K.: Minn. Med., vol. x, p. 456, July, i927.Ullman, A.: Surgery, Gynaecology and Obstetrics, vol. xxxviii, p. 225, 1924.
ENDOMETRIOSIS OF THE SIGMOID-INTESTINAL OBSTRUCTION
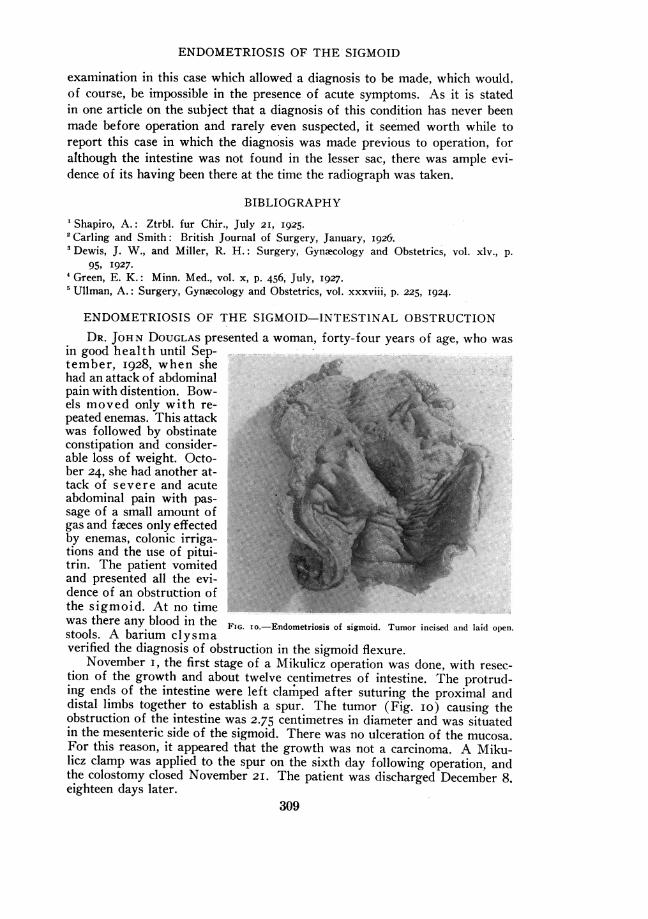
DR. JOHN DOUGLAS presented a woman, forty-four years of age, who wasin good health until Sep-tember, I928, when shehad an attack of abdominalpain with distention. Bow-els moved only with rekpeated enemas. This attackwas followed by obstinateconstipation and consider-able loss of weight. Octo- '.'ber 24, she had another at-tack of severe and acuteabdominal pain with pas-sage of a small amount ofgas and ftaces only effectedby enemas, colonic irriga-tions and the use of pitui-trin. The patient vomitedand presented all the evi-dence of an obstruttion ofthe sigmoid. At no timewas there any blood in the FIG. IO.-Endometriosis of sigmoid. Tumor incised and laid open.stools. A barium clysmaverified the diagnosis of obstruction in the sigmoid flexure.
November i, the first stage of a Mikulicz operation was done, with resec-tion of the growth and about twelve centimetres of intestine. The protrud-ing ends of the intestine were left clarmped after suturing the proximal anddistal limbs together to establish a spur. The tumor (Fig. io) causing theobstruction of the intestine was 2.75 centimetres in diameter and was situatedin the mesenteric side of the sigmoid. There was no ulceration of the mucosa.For this reason, it appeared that the growth was not a carcinoma. A Miku-licz clamp was applied to the spur on the sixth day following operation, andthe colostomy closed November 2I. The patient was discharged December 8.eighteen days later.
309
INEW YORK SURGICAL SOCIETY
The pathological examination showed the tumor to be made up' of endo-metrial tissue.
In I893 Von Recklinghausen discussed endometrial adenomata and sug-gested that they might arise from embryonic rests derived from the Wolf-fian body. Since then, many cases have been reported in the medical literatureof endometriosis occurring primarily in the abdominal wall or in post-operative scars, following operations on the uterus or adnexae. They havebeen reported as occurring in the rectovaginal septum, in the peritoneum,particularly in the pelvic peritoneum, and in the wall of the intestine. Thepathological records of St. Luke's Hospital, beside the case here reported,show two of the appendix, one of the small intestine and one occurring inan abdominal scar.
Much interest in the subject has been stimulated during the past fewyears by the work of Samson, whose report of cases, together with the experi-ments of his co-worker, Jacobson, has been particularly directed to the implan-tation theory of origin. According to Samson's belief, peritoneal endo-metriosis arises from endometrial epithelium passing out from the patenttubes into the peritoneal cavity. It'is believed by others accepting the implan-tation theory, that the origin of the endometrial tissue is from the ovary. Inthe case here reported it is difficult to assume the implantation theory for itsorigin, as the tumor was situated in the intestinal wall well below the perito-neal coat, and the theory of an embryonic rest would better explain its origin.
OSTEITIS FIBROSA OF TIBIA
DR. JOHN DOUGLAS presented a boy, seven years of age, who was admit-ted to St. Luke's Hospital October 26, I927. Three weeks before admission,he fell and struck the anterior aspect of his left tibia on a stone. It hurt himfor a day or so but caused no abrasion and there were no further symptomsuntil one week later when his mother noticed a swelling in this area whichwas at this time neither red nor tender. A radiograph showed an area ofrarefication at the junction of the upper and middle third of the tibia. Thiswas curetted out after chiseling off the anterior surface, and a fragment ofthe cortex, after carefully removing all of the endosteum, was inserted as agraft. The cavity entirely filled in after several months as shown by a seriesof radiographs taken over this time.
He was readmitted to the hospital January 30, I929, fifteen months afterthe original operation. In the interval he had been free of pain, except foran occasional ache in the leg in wet weather, until the day before his admis-sion when he had a sharp pain slightly higher than the original area. Aradiograph at this time showed the original area occupied by the cyst, nowfilled in by dense and compact bone, and the outline of the original graftcould still be distinguished. Just above the original lesion, however, therewas again shown a rarefied area which extended about 2.5 centimetres abovethe old lesion.
January 31, the bone was again chiseled away from the surface of thisarea which was the site of a lesion similar to the one that had occurred before.There was no cyst but there seemed to be two distinct areas in the patho-logical process, one of which was occupied by a dense, fibrous tissue, theother showing considerable calcification with the formation of new bone.
310
FRACTURES FROM OSTEITIS FIBROSA OF HUMERUS
This area was again chiseled out and filled with chips of bone removed fromthe cortex, which were carefully scraped so as to remove any endosteum orany bone which appeared diseased. He has again healed up and a radiographtaken a few days ago shows considerable calcification and regeneration inthis area.
The patient was shown to demonstrate a repair of the original area ofosteitis fibrosa by means of curetting together with insertion of a graft,and the development of a new area of the same process above and apparentlycontinuous with the old lesion.
FRACTURES FROM OSTEITIS FIBROSA OF HUMERUSDR. JOHN DOUGLAS presented a boy, thirteen and a half years of age.
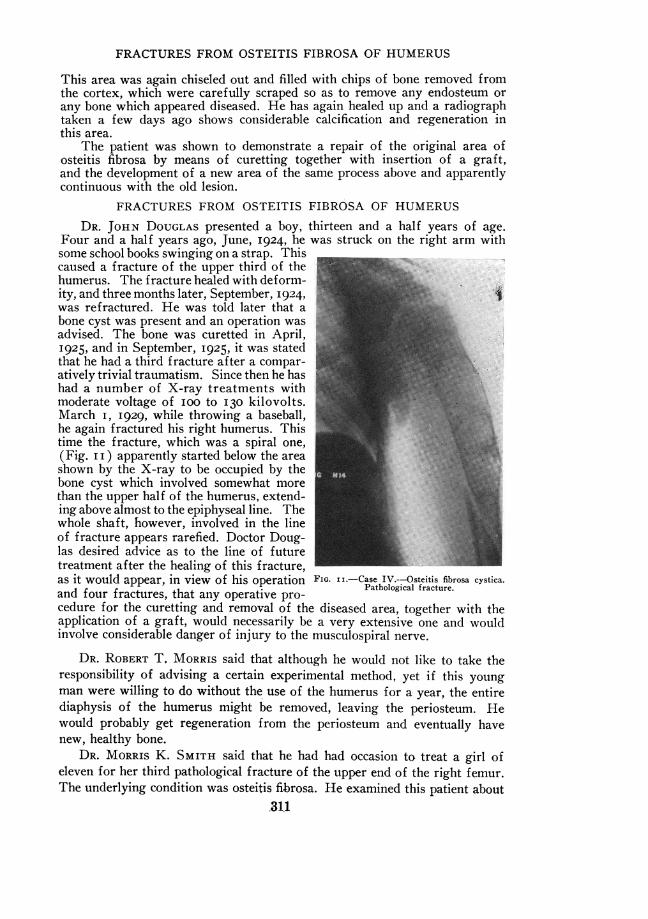
Four and a half years ago, June, I924, he was struck on the right arm withsome school books swinging on a strap. Thiscaused a fracture of the upper third of thehumerus. The fracture healed with deform-ity, and three months later, September, I924, _was refractured. He was told later that abone cyst was present and an operation wasadvised. The bone was curetted in April,1925, and in September, I925, it was statedthat he had a third fracture after a compar-atively trivial traumatism. Since then he hashad a number of X-ray treatments withmoderate voltage of IOO to I30 kilovolts.March I, I929, while throwing a baseball,he again fractured his right humerus. Thistime the fracture, which was a spiral one,(Fig. I I ) apparently started below the areashown by the X-ray to be occupied by thebone cyst which involved somewhat morethan the upper half of the humerus, extend-ing above almost to the epiphyseal line. Thewhole shaft, however, involved in the lineof fracture appears rarefied. Doctor Doug-las desired advice as to the line of futuretreatment after the healing of this fracture,as it would appear, in view of his operation FIG. ii.-Case WY-csteitisfibrosa cystica.and four fractures, that any operative pro-cedure for the curetting and removal of the diseased area, together with theapplication of a graft, would necessarily be a very extensive one and wouldinvolve considerable danger of injury to the musculospiral nerve.
DR. ROBERT T. MORRIS said that although he would not like to take theresponsibility of advising a certain experimental method, yet if this youngman were willing to do without the use of the humerus for a year, the entirediaphysis of the humerus might be removed, leaving the periosteum. Hewould probably get regeneration from the periosteum and eventually havenew, healthy bone.
DR. MORRIS K. SMITH said that he had had occasion to treat a girl ofeleven for her third pathological fracture of the upper end of the right femur.The underlying condition was osteitis fibrosa. He examined this patient about
311
NEW YORK SURGICAL SOCIETY
ten years later. She had had no subsequent fractures. There was markedshortening of the extremity. Doctor Douglas had called attention to theapparent new bone formation in the cyst in his case and Doctor Smith won-dered whether an eventual cure as far as strength of the arm was concernedmight not be anticipated if the patient were not operated upon.
DR. HERMANN FISCHER said that many years ago he observed a case,together with Dr. Frederick Kammerer, of an extensive osteofibrosis whichhad its seat in the diaphysis of the femur. The femur consisted of a mereshell of bone with a complete fibrosis of the cancellous tissue from the greatertrochanter down to the condyles. The man had suffered a pathological frac-ture in the middle of the femur which was the first symptom of the diseasein this case. All the diseased tissue in this case was removed. The man finallyleft the hospital with a consolidated fracture and a useful leg. He thoughtDoctor Douglas' case should be operated upon. One need not fear an injuryto the musculospiral, if it is carefully dissected and held out of the way.
DR. DEWITT STETTEN said that he had presented a similar case involvingthe femur before this Society November I2, I9I9.
The patient originally came to him about nine and a half years previouslywith a fracture of the neck of the femur. X-ray examination showed a con-dition that looked like a cyst, involving the neck, greater trochanter, and upperpart of the shaft. This was originally treated conservatively, but as therarefaction increased operation was eventually decided upon and performed,and a tumor-like mass was removed which consisted largely of undifferenti-ated osteoid or chondroid tissue with cartilaginous islands of various size.He made a good recovery and was well for about six and a half years whenhe developed a recurrence. The process subsequently extended down theshaft of the femur and required a second operation, from which he also madea satisfactory recovery. About nine months later he sustained a fracture ofthe neck of the femur and six months after that a transverse fracture ofthe shaft. Both of these fractures united satisfactorily and since that timehe has had no further trouble.
DOCTOR DOUGLAS in closing said that regarding the X-ray treatment ofthese cases he had seen two cases where radiotherapy had been used, oneinvolving the lower end of the radius, the other located in the femur. Theone in the radius has been quite successful and has markedly diminished insize. The one of the upper end of the femur is considerably improved. Thelast patient presented here has been treated for a year and a half and DoctorDouglas said he believed re-operation would be necessary as the X-rayappears to have done little good. He had asked for an' expression of opinionas to the advisability and danger of operating in this case as the processapparently involved most of the shaft of the'bone; there had already beenthree fractures and one operation; and because the danger of injury to themusculospiral nerve was particularly great in view of the changes resultingfrom the conditions which had gone before. It seems, however, that the prog-nosis without operation justifies this risk.
312
SUBPHRENIC ABSCESS
SUBPHRENIC ABSCESS
DR. THOMAS H. RUSSELL presented a man, thirty-eight years of age, whowas admitted to the Post-Graduate Hospital October 25, 192 1. He wasoperated upon for a perforated duodenal ulcer bv Doctor Russell during themonth of March, 192I. After the operation he made a satisfactory recoveryand felt exceptionally well, gained forty pounds in weight and was not trou-bled with symptoms of stomach trouble, which he had suffered from for along time before the operation. He remained well until six weeks before hisreception into the hospital when he suddenly began to have pain in the upperright abdomen. The pain was stabbing and very severe, and was not influ-enced by food. He began to lose weight rapidly. Three or four days ago thepain became very severe and was much worse after taking food. No nauseaor vomiting. He has had an irritating cough for several weeks. Pain is verysevere when he coughs.
The chest examination is negative. There is muscular rigidity and a senseof fulness in the right upper quadrant of abdomen. Tenderness is presentwhen the ribs are tapped over the right lower chest.
The X-ray showed subphrenic abscess. (The films have been destroyed.)With gas-oxygen anesthesia an incision was made in the right upper quad-rant of abdomen parallel to right rectus muscle, just as incision ordinarilyused for gall-bladder operations.
Abdomen opened and explored. A large abscess was found in front of andabove the liver extending down over the margin of the liver. With finger dis-section the abscess was opened and pus removed by means of suction. Tworubber tube drains were inserted and wound closed with silkworm sutures.Patient made an uneventful recovery and was discharged from hospitalNovember 23, 192I. He has been in excellent health since.
DOCTOR RUSSELL presented a second patient, a man, thirty-five years ofage, who was admitted to hospital July 25, I919. He had suffered from painin his right upper abdomen since the preceding July 12, on which date hewas struck on the right side of lower chest and upper abdomen by a fallingspring iron. There was severe pain at the time which subsided somewhat ina short while. The next day pain became worse and has gradually increasedin severity. He has noticed fulness over right lower ribs. He coughs agreat deal but cannot get relief by coughing. Cough is very painful.
Examination of chest negative. There is a decided fulness with tender-ness and rigidity over the right costal margin and in epigastrium. Increasedliver dulness which extends up to the third rib. There is sense of increasedlieat over right upper abdomen and over swelling in right lower chest.
Operation under gas-oxygen anaesthesia. Incision parallel to right costalmargin down to peritoneum. Peritoneum stripped downward and fingersgradually inserted into abscess cavity extending above liver and below dia-phragm. A large amount of thick yellow pus evacuated. Not foul in odor.Two rubber tube drains inserted. Dry dressing applied.
Culture Report.-Specimen shows numerous pus cells with irregularpieces of tissue about eight millimetres thick and resemble echinococcuscyst formation.
Mlicroscopic.-Cyst wall shows hyaline lamellar structure of concentricrings similar to echinococcus cyst but no parasite found. Discharged Sep-tember 30, I919.
DOCTOR RUSSELL presented also a man, thirty-five years of age, who wasadmitted to hospital June 30, 1921, complaining of pain in his epigastrium.The man had had pneumonia seven years ago on left side. He was operated
313
NEW YORK SURGICAL SOCIETY
upon by Doctor Deaver, in Philadelphia, seven months ago for intestinalobstruction; a colostomy being performed in left side at that time. He wasthought to have cancer of the bowel which proved to be inflammatory; thencolostomy was closed. Six weeks ago was operated upon by Doctor Russellin,the Post-Graduate Hospital fQr intestinal obstruction and general peri-tonitis-obstruction due to a band-no perforation found after careful search.Peritoneal cavity washed out with saline and drained. Patient in very poorcondition. Prognosis bad. The man improved after this last operation buthad a stormy convalescence. Was discharged from hospital eighteen dayslater in good condition.
Readmitted to Post-Graduate Hospital June 30, I921, complaining of painin right upper quadrant of abdomen referred to back and right lower chest.Nausea but no vomiting. Is losing weight rapidly and cannot eat. Feelsvery weak.
Physical examination reveals numerous rales in right lower base. Ten-derness over liver region and right upper quadrant of abdomen. X-ray showsright diaphragm elevated and flattened with obstruction of the costophrenicangle. Absent illumination is seen at right base, this having a cup-shapedappearance bounded above by a straight line with a definite wave suggest-ing a hydropneumothorax, this probably encapsulated. The quantity of fluidis estimated at about a pint. Blood count I4,400, with 88 per cent. polynu-clear cells; temperature ioi0; pulse II8. Under nitrous oxide anaesthesia anincision was made in right upper quadrant of abdomen. A large subdiaphrag-matic abscess was found on the right side. Abscess extends from upper sur-face of right lobe of liver to the suspensory ligament, then follows down tounder surface'of liver. Opened with fingers. Pus removed by suction. Rub-ber tube and cigarette drain inserted. Wound closed with silkworm gut. Pusshows pneumococcus. Patient discharged August 8, I921.
SUBPHRENIC ABSCESS WITH SPECIAL REFERENCE TO TREATMENT
DR. THOMAS H. RUSSELL read a paper with the above title, for whichsee page 238.
DR. HoWARD LILIENTHAL said that he was more convinced than everthat the abdominal route is not to be preferred to the supraphrenic, but hetries to avoid entering the pleura. Doctor Russell had shown very clearlythat thoracic complications are not uncommon in subphrenic abscess. There-fore, Doctor Lilienthal believes that by making an exploration above thediaphragm certain of these complications could be discovered in their incipi-ency. For example, empyema may have resulted from the perforation ofa small subphrenic abscess. By the supraphrenic route such sacculated empy-emas can be drained without infecting the general pleural cavity. The speakeroperated, using local anaesthetic, by the following method:
The patient lies prone with a pillow underneath his abdomen and withhis head lower than the location of the proposed incision. This posture wasfirst recommended by Dr. Charles A. Elsberg. A portion of the ninth rib issubperiosteally resected, the'pleura pushed away from the diaphragm and thesubphrenic abscess then aspirated and drained. Supraphrenic collections ofpus in the neighborhood of the subphrenic abscess will be found and can alsobe drained. If during the approach the pleura should be accidently opened,very little air will enter because of the posture of the patient. It is then pos-
314
SUBPHRENIC ABSCESS WITH REFERENCE TO TREATMENT
sible to suture the upper edge of the pleura to the diaphragm at a distancefrom the wound of entrance so that a large area is exposed through whichaspiration and then drainage can be accomplished. It has even been possibleto use a rib spreader and thus thoroughly expose the phrenic dome. Explora-tory puncture through the unopened skin is not advisable in these cases butwith the exposure made as outlined above the needle may be used and onegets an idea from the density of the tissues traversed that the abscess is near.The mortality in cases treated by this method must be very low. If there ispain in reaching a low sacculated empyema it may be necessary to supple-ment the local anaesthetic with general anaesthesia. Once having entered asupraphrenic empyema it should be widely opened and the region toward themediastinal side should be explored for these cases often form mesial empy-emas connected with the supraphrenic.
To illustrate one advantage of the high approach Doctor Lilienthal brieflyoutlined the case of a young man who in the course of paratyphoid feverdeveloped a subphrenic abscess which perforated the diaphragm and, goingstill further, involved the lung itself in the suppurative process. By themethod here described it was possible to drain the lung abscess as well asthe subphrenic.
From long experience in abdominal, as well as in thoracic surgery, DoctorLilienthal expressed his conviction that, other things being equal, the shockfollowing an operation for thoracic suppuration is less than that which is seenin similar abdominal infections. Drainage from below secured by dissectingup over the dome of the liver is by no means always satisfactory and counterdrainage posteriorly must often be made.
DR. SEWARD ERDMAN said that as Doctor Russell had so definitely con-demned the commonly tised method of draining subphrenic abscesses byapproach laterally, between or through the ribs, and recommended an anterior,transperitoneal, drainage, it seenmed unfortunate that Doctor Russell did notgive the mortality in his series of cases.
In order to carry conviction that the abdominal approach was superior,a very convincing lowering of the mortality rate must be shown.
He thought Doctor Russell had included several cases of abscess follow-ing operations on the biliary tract where the local collection of pus or retainedbile would naturally call for approach through the operative incision, and itwould seem that there could be little difference of opinion about this.
But for true subphrenic collections well up on the superior surface of theliver, Doctor Erdman still believes that the lateral approach through the ribsafforded the most direct and satisfactory drainage and he felt that the explora-tory needle used at the time of operation was most helpful in locating the pus.
On the Second Surgical Division of the New York Hospital a consecu-tive series of twenty-one operations for subphrenic abscess showed sevendeaths (33 per cent.).
Sixteen of the cases were complications of other serious conditions:315
NEW; YORK SURGICAL SOCIETY
iI cases of appen(dicitis with peritonitis (5 deaths)2 perforated duodenal ulcers (2 deaths)I actite cholecystitisI suppurative pleurisyI spleinic anoemia
It is seen that all the (leatlhs occurre(l in cases whlere peritonitis was theunderlying cause of the subphrenic abscess, and( largely responsible forthe deaths.
The remiiaininig five cases were primarily (liagnose(l as sul)phrenic abscess;these were all (lrained througlh the ribs anid all of them recovered; the nee(dlewas used in each of these cases.
DR. ROBERT T. MORRIS said that in the group) of cases suitable forabdominal approach there is one instrumenit especially useful and that is abig urethral sound. It is curved just right to curve up over the (lome of theliver. When pus escapes a large, hard tube can be inserted, following thiswith the use of Dakin's solution. These cases will do very well under thatsort of treatment.
DR. JOHN DOUGLAS said as to the questioni of diagniosis in these casesDoctor Russell spoke of the gas which usually forms unlder the diaphragm.Gas usually does form in these cases when the infection is due to anaerobicbacteria. The bubble of gas which collects under the diaphragm with thepatient in the erect positioni, or at the highest point with the patient lying onthe side, is one of the greatest helps that he knows of in helping make thediagnosis. As far as the incision is concerned he doubted as to the particularadvantage of an anterior incision. He remembered having a case where asubphrenic abscess formed after an appendix operation and he made ananterior incision and had great difficulty in keeping the tube in place fotdrainage. By a posterior inicision andl approach he believes, as Doctor Lilien-thal has said, it can be done with very little or no more than a moderateamount of difficulty under local anxesthesia. He believed that if one (loesaccidentally open the pleural cavity it is alm-iost always possible to wall thatoff at the time and wait twenty-four hours before going into the abscess cavity
DOCTOR RUSSELL, in closing, said he thought, summed up, the point is, allagree these abscesses come from intra-abdominal diseases and it seems strangeto him to go through the chest to help a condition following an abdomi-nal infection. In answer to question about mortality rate Doctor -Russellreplied that he had not intended to convey the impression that these casesat the Post-Graduate Hospital were all opened through the front; someof them were opened through the side. A review of these cases had beenmade to arrive at the causes of the abscesses. He has been able to communi-cate with six cases he operated upon through the abdomen and they arewell today.
316




















