Interventions for the prevention and management of neck/upper extremity musculoskeletal conditions:...
14
REVIEW Interventions for the prevention and management of neck/ upper extremity musculoskeletal conditions: a systematic review M G Boocock, P J McNair, P J Larmer, B Armstrong, J Collier, M Simmonds, N Garrett ................................................................................................................................... Occup Environ Med 2007;64:291–303. doi: 10.1136/oem.2005.025593 Considered from medical, social or economic perspectives, the cost of musculoskeletal injuries experienced in the workplace is substantial, and there is a need to identify the most efficacious interventions for their effective prevention, management and rehabilitation. Previous reviews have highlighted the limited number of studies that focus on upper extremity intervention programmes. The aim of this study was to evaluate the findings of primary, secondary and/or tertiary intervention studies for neck/upper extremity conditions undertaken between 1999 and 2004 and to compare these results with those of previous reviews. Relevant studies were retrieved through the use of a systematic approach to literature searching and evaluated using a standardised tool. Evidence was then classified according to a ‘‘pattern of evidence’’ approach. Studies were categorised into subgroups depending on the type of intervention: mechanical exposure interventions; production systems/organisational culture interventions and modifier interventions. 31 intervention studies met the inclusion criteria. The findings provided evidence to support the use of some mechanical and modifier interventions as approaches for preventing and managing neck/upper extremity musculoskeletal conditions and fibromyalgia. Evidence to support the benefits of production systems/organisational culture interventions was found to be lacking. This review identified no single-dimensional or multi- dimensional strategy for intervention that was considered effective across occupational settings. There is limited information to support the establishment of evidence-based guidelines applicable to a number of industrial sectors. ............................................................................. See end of article for authors’ affiliations ........................ Correspondence to: Dr M G Boocock, Physical Rehabilitation Research Centre, Auckland University of Technology, Private Bag 92006, Auckland 1020, New Zealand; [email protected] Accepted 17 August 2006 Published Online First 14 September 2006 ........................ O ne of the major problems facing industrial countries is work-related musculoskeletal disorders. 1 Recent literature suggests that the incidence of such injuries may continue to rise owing to increased exposure to workplace risk factors, 2 more segmented and repetitive work, increased mechanisation and shifts in working practices towards the service and information sector. 3 There are direct health costs associated with the rehabilitation of workers with musculoskeletal injuries, and also significant economic costs are imposed on the industry as a result of compensa- tion, lost productivity and retraining. 4 The magni- tude of the problem in financial terms has been estimated in the US to be as much as US$54 billion per year. 1 Workers affected by work-related musculo- skeletal disorders are often afflicted by long-term pain, loss of function and disability. For the effective prevention and management of such disorders, national organisations (eg, National Institute for Occupational Safety and Health, USA; Health and Safety Executive, UK; Occupational Safety and Health, New Zealand) have often implemented a variety of single- dimensional and multi-dimensional programmes involving medical, physical and psychosocial inter- ventions. As intervention approaches within an industrial setting are often complex and evolving, they require evidenced-based models to be effective. 1 Any evaluation of the potential benefits of interventions is difficult. However, the work of Westgaard and Winkel 5 provides a model for the classification of interventions, thereby allowing a review of the literature to be undertaken in a structured manner. Westgaard and Winkel 5 cate- gorised intervention strategies into three main groups: mechanical exposure, production systems/ organisational culture and modifier interventions. Mechanical exposure interventions typically focus on changing the design of tools, such as the computer mouse or keyboard. Production systems interventions, however, generally implement changes to the material production and/or the organisational culture of a company. The latter may involve team building and increased worker participation in the problem-solving of workplace production (ie, participatory ergonomics). Finally, interventions that incorporate specific training of workers to manage exposure levels to physical and psychosocial stressors are termed modifier interventions. These may involve an exercise programme and/or ergonomic education. Previous reviews have highlighted a dearth of literature examining the effectiveness of interven- tion approaches for the prevention and manage- ment of neck/upper extremity musculoskeletal conditions. 6–9 Furthermore, many of the experi- mental studies included in these reviews have been of low quality and few have included randomised controlled trials (RCT). Thus, the opportunity to establish effective evidence-based management programmes for work-related Abbreviations: GATE, generic appraisal tool for epidemiology; RCT, randomised controlled trials; VDU, visual display unit 291 www.occenvmed.com group.bmj.com on May 14, 2011 - Published by oem.bmj.com Downloaded from
Transcript of Interventions for the prevention and management of neck/upper extremity musculoskeletal conditions:...

REVIEW
Interventions for the prevention and management of neck/upper extremity musculoskeletal conditions: a systematicreviewM G Boocock, P J McNair, P J Larmer, B Armstrong, J Collier, M Simmonds, N Garrett. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Occup Environ Med 2007;64:291–303. doi: 10.1136/oem.2005.025593
Considered from medical, social or economic perspectives, thecost of musculoskeletal injuries experienced in the workplace issubstantial, and there is a need to identify the most efficaciousinterventions for their effective prevention, management andrehabilitation. Previous reviews have highlighted the limitednumber of studies that focus on upper extremity interventionprogrammes. The aim of this study was to evaluate the findingsof primary, secondary and/or tertiary intervention studies forneck/upper extremity conditions undertaken between 1999and 2004 and to compare these results with those of previousreviews. Relevant studies were retrieved through the use of asystematic approach to literature searching and evaluated usinga standardised tool. Evidence was then classified according to a‘‘pattern of evidence’’ approach. Studies were categorised intosubgroups depending on the type of intervention: mechanicalexposure interventions; production systems/organisationalculture interventions and modifier interventions. 31 interventionstudies met the inclusion criteria. The findings providedevidence to support the use of some mechanical and modifierinterventions as approaches for preventing and managingneck/upper extremity musculoskeletal conditions andfibromyalgia. Evidence to support the benefits of productionsystems/organisational culture interventions was found to belacking. This review identified no single-dimensional or multi-dimensional strategy for intervention that was consideredeffective across occupational settings. There is limitedinformation to support the establishment of evidence-basedguidelines applicable to a number of industrial sectors.. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
See end of article forauthors’ affiliations. . . . . . . . . . . . . . . . . . . . . . . .
Correspondence to:Dr M G Boocock, PhysicalRehabilitation ResearchCentre, Auckland Universityof Technology, Private Bag92006, Auckland 1020,New Zealand;[email protected]
Accepted 17 August 2006Published Online First14 September 2006. . . . . . . . . . . . . . . . . . . . . . . .
One of the major problems facing industrialcountries is work-related musculoskeletaldisorders.1 Recent literature suggests that
the incidence of such injuries may continue to riseowing to increased exposure to workplace riskfactors,2 more segmented and repetitive work,increased mechanisation and shifts in workingpractices towards the service and informationsector.3
There are direct health costs associated with therehabilitation of workers with musculoskeletalinjuries, and also significant economic costs areimposed on the industry as a result of compensa-tion, lost productivity and retraining.4 The magni-tude of the problem in financial terms has been
estimated in the US to be as much as US$54 billionper year.1
Workers affected by work-related musculo-skeletal disorders are often afflicted by long-termpain, loss of function and disability. For theeffective prevention and management of suchdisorders, national organisations (eg, NationalInstitute for Occupational Safety and Health,USA; Health and Safety Executive, UK;Occupational Safety and Health, New Zealand)have often implemented a variety of single-dimensional and multi-dimensional programmesinvolving medical, physical and psychosocial inter-ventions. As intervention approaches within anindustrial setting are often complex and evolving,they require evidenced-based models to be effective.1
Any evaluation of the potential benefits ofinterventions is difficult. However, the work ofWestgaard and Winkel5 provides a model for theclassification of interventions, thereby allowing areview of the literature to be undertaken in astructured manner. Westgaard and Winkel5 cate-gorised intervention strategies into three maingroups: mechanical exposure, production systems/organisational culture and modifier interventions.Mechanical exposure interventions typically focuson changing the design of tools, such as thecomputer mouse or keyboard. Production systemsinterventions, however, generally implementchanges to the material production and/or theorganisational culture of a company. The lattermay involve team building and increased workerparticipation in the problem-solving of workplaceproduction (ie, participatory ergonomics). Finally,interventions that incorporate specific training ofworkers to manage exposure levels to physical andpsychosocial stressors are termed modifierinterventions. These may involve an exerciseprogramme and/or ergonomic education.
Previous reviews have highlighted a dearth ofliterature examining the effectiveness of interven-tion approaches for the prevention and manage-ment of neck/upper extremity musculoskeletalconditions.6–9 Furthermore, many of the experi-mental studies included in these reviews havebeen of low quality and few have includedrandomised controlled trials (RCT). Thus, theopportunity to establish effective evidence-basedmanagement programmes for work-related
Abbreviations: GATE, generic appraisal tool forepidemiology; RCT, randomised controlled trials; VDU,visual display unit
291
www.occenvmed.com
group.bmj.com on May 14, 2011 - Published by oem.bmj.comDownloaded from

musculoskeletal disorders has been restricted. Therefore, thereis a need to update our current knowledge using a systematicapproach. The aim of this study was to fulfil this need byconducting a systematic review and evaluation of the findingsof primary/secondary and/or tertiary intervention studies forneck/upper extremity musculoskeletal conditions undertakenbetween 1999 and 2004.
METHODSSearch strategyAn initial search of the literature integrated a variety of sourcesincluding textbooks and conference proceedings, national andinternational health and safety organisation websites, and ageneral internet search. From this initial search, an extensivekeyword list was developed to incorporate nationally andinternationally recognised work-related musculoskeletal termsand definitions (eg, musculoskeletal disorder, repetitive straininjuries and occupational overuse syndrome), inclusive ofdiagnostic conditions (eg, thoracic outlet syndrome and cubitaltunnel syndrome). Keywords specific to intervention studieswere generated, which used a combination of generic labels (eg,musculoskeletal control and ergonomic intervention) andspecific intervention approaches (eg, workstation design, jobrotation and physical training).
Four researchers (BA, MGB, JC and MS), guided by a libraryand information manager, carried out the literature search. Thekeyword list and all combinations of keywords were useduniformly by all four researchers to ensure a standardisedapproach to the search procedure. An initial check of thekeyword list was made against each of the subject headingsfrom 15 electronic databases (CINAHL (including CochraneReviews); EBSCO Megafile Premier (including Medline, HealthSource: Consumer Edition and Nursing/Academic Edition);Embase; Ergonomics Abstracts; Index NZ; AMED (Allied andComplementary Medicine); Annual reviews; Psych INFO(including PsycARTICLES); ProQuest 5000 (includingProQuest Health and Medical Complete); Expanded AcademicASAP; Sports Discus; Science Direct; Blackwell Synergy;Lippincott 100; OSH Reference Collection (includingOSHLINE with NIOSHTIC and NIOSHTIC2)). An examinationof review articles (unrestricted by date of publication), as wellas the personal libraries of the contributing authors, wasundertaken to identify further studies. Personal communica-tions with national and international representatives or expertswithin the field of musculoskeletal conditions were also made.Where appropriate, additional keywords were added andmodifications made to the keyword list.
The final search involved the previously mentioned 15electronic databases and an examination of the bibliographiesof recent review papers. To ensure that only high-quality paperswere included within the current literature review, strictinclusion/exclusion criteria were adopted. These criteria werebased on previous major reviews in this subject area(Bernard10).
Inclusion criteria
N Published within the past 5 years (Jan 1999–Oct 2004).
N Participation rate >70%.
N Health outcomes defined by symptoms and/or well-docu-mented questionnaires and/or physical examination.
N The body part in question was subjected to an independentexposure assessment—that is, direct observation or actualmeasurement of exposure.
N Musculoskeletal conditions of the neck, shoulder, elbow andhand/wrist (neck/upper extremities).
N Duration of subject follow-up >2 months.
N Sufficient documentation of intervention and interventionprocess.
N English language publications.
Exclusion criteria
N Back pain and lower extremity injuries.
N Laboratory-based studies.
N Clinical treatment of musculoskeletal disorders.
N Clinically based modifier interventions such as pharma-cological treatment, splinting, acupuncture and physiother-apy or chiropractic treatment.
Quality assessment and grading of studiesThe critical appraisal and grading of studies involved the use ofthe generic appraisal tool for epidemiology (GATE): appraisalmodules (effective practice, informatics and quality improve-ment).11 This tool focused specifically on issues of studyvalidity, quality of the study, the measure of occurrence, effectand precision of the study results and external validity.
After completion of the GATE checklists for interventionstudies, papers were graded according to the quality of thestudy using a modified version of the CochraneMusculoskeletal Injuries Group scoring system, in conjunctionwith the GATE tool, to provide an overall score for each study.12
The modified Cochrane Musculoskeletal Injuries Group scoringsystem comprised 13 separate questions graded between 0 and2, covering aspects of study design and outcome measures. Afinal overall score (quality rating), out of a possible 26, wasawarded to each intervention paper. Once each study had beenassigned a rating score, it was graded according to a three-pointrating scale: low, medium or high. The cut-off points for eachlevel of grading were based on the overall distribution of scoresacross the intervention studies: ,10 = ‘‘low’’-quality study;>10,19 = ‘‘medium’’-quality study; >19 = ‘‘high’’-qualitystudy.
Six reviewers (BA, MGB, JC, PJL, PJM and MS) were trainedin the review and scoring protocols. Two reviewers scored eachpaper independently, and if any discrepancy was foundbetween their scores a third person reviewed the paper toreach a consensus.
Evidence classificationA ‘‘pattern of evidence’’ approach for classifying the level ofevidence attached to intervention studies was adopted.1 Theterminology and criteria used to define these levels of evidencewere adapted from previous review papers6 7 10 13–15 and mod-ified according to the quality assessment procedure adopted bythis review (table 1). The overall level of evidence (ie, strong,moderate, some or insufficient) was then based on the numberof studies, study design and the quality rating ascribed to thatstudy.
Classification of intervention studiesUsing a format similar to Westgaard and Winkel,5 studies inthis review were categorised into subgroups depending on thetype of intervention: mechanical exposure interventions,production systems/organisational culture interventions andmodifier interventions. Interventions were also classified asprimary, secondary and/or tertiary according to the definitionsof the National Research Council1—that is, primary interven-tions before members of the population at risk having acquireda condition of concern; secondary interventions afteroccurrence of the condition within the population of concernand tertiary intervention strategies designed for individualswith chronically disabling conditions.
292 Boocock, McNair, Larmer, et al
www.occenvmed.com
group.bmj.com on May 14, 2011 - Published by oem.bmj.comDownloaded from

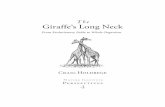
RESULTSIn excess of 5000 articles were identified from the initial search,of which 451 were suitable for abstract review; after a review ofthe abstracts, 102 intervention studies were considered. Intotal, 31 intervention studies were considered to have met theinclusion criteria and were suitable for full review (fig 1). Tenwere classified as mechanical exposure interventions, two asproduction systems/organisational culture interventions and 19as modifier interventions. On the basis of the type ofmechanical intervention involved and the group of workersreported upon, it was possible to further classify mechanicalinterventions into three subgroups: (1) work environment/workstation adjustments and visual display unit (VDU)
workers, (2) workstation equipment and VDU workers and(3) ergonomic equipment and manufacturing workers.Although no subgroups of production systems/organisationalculture interventions could be identified, it was possible togroup studies in the area of modifier interventions under sixbroad categories: (1) exercise and neck/upper extremityconditions; (2) exercise and fibromyalgia; (3) multiple modifier(including exercise) and neck/upper extremity conditions; (4)multiple modifier (including exercise) and fibromyalgia; (5)multiple modifier (excluding exercise) and neck/upper extre-mity conditions and (6) multiple modifier (excluding exercise)and fibromyalgia. Table 2 gives the tabulated informationpertaining to each paper.
Table 1 Level of evidence for evaluating the importance of intervention studies in the management of neck/upper extremitymusculoskeletal conditions
Level of evidence Definition
Strong When provided by generally consistent findings in multiple RCTs of high quality (QR>19)Moderate When provided by generally consistent findings in one RCT of high quality (QR>19) and in one or more RCTs of moderate or low quality, or by
generally consistent findings in multiple RCTs of moderate quality (QR,19>10).Some When limited evidence, with only one RCT (any quality rating). Some findings of a positive relationship between exposure to the intervention and
WRMD in one cohort or case–referent study, or consistent findings in multiple cross-sectional studies, of which at least one study was of mediumquality (QR>10,14)
Insufficient All other cases (ie, consistent findings in multiple low-quality (QR,10) cross-sectional studies, or inconsistent findings in multiple studies) orfindings of only one cross-sectional study, irrespective of the quality of the study
QR, quality rating; RCTs, randomised controlled trials; WRMD, work-related musculoskeletal disorders.
Figure 1 Overview of the literature search and review strategy.
Prevention and management of musculoskeletal conditions 293
www.occenvmed.com
group.bmj.com on May 14, 2011 - Published by oem.bmj.comDownloaded from

Mechanical exposure interventionsTen studies were classified as mechanical exposure interven-tions, and thereafter subdivided into three main groups asdescribed previously. Within the subgroup of work environ-ment/workstation adjustments (eg, modified lighting, newwork place, office layout and software application) in VDUworkers with neck/upper extremity conditions, four studies16–19
presented positive outcomes. Three were of medium qual-ity,16 17 19 and included an RCT,19 whereas one study18 was of lowquality. On the basis of the levels of evidence identified in table1, it was concluded that there was some evidence for positivehealth effects after work environment/workstation adjustmentsin VDU workers with neck/upper extremity conditions.
Three studies20–22 that involved changes to workstationequipment (ie, keyboards and mouse design) in VDU workerswith neck/upper extremity conditions reported positive out-comes resulting from these types of interventions. Rempel etal’s21 and Tittiranonda et al’s22 studies were RCTs of high andmedium quality, respectively, while Arras et al’s20 study was oflow quality. Hence, there was moderate evidence to support thistype of intervention.
Three studies23–25 that involved the introduction of ergonomicequipment (eg, adjustable chairs and vibration-proof tools) forworkers with neck/upper extremity conditions used in themanufacturing industry found positive health outcomes.However, all were rated as low quality. Thus, it was concludedthat there was insufficient evidence for positive health effectsresulting from this type of intervention.
Production systems/organisational cultureTwo studies26 27 did not find improvements in health outcomesassociated with organisational and work-task design changes inoffice workers and manufacturing assembly workers; bothstudies were of low quality. Thus, there was insufficientevidence to support production systems/organisational inter-vention strategies.
Modifier interventionsNineteen studies were classified under modifier interventions,and subsequently subclassified as described previously. Positivehealth outcomes were observed in three medium-qualitystudies28–30 that examined the effects of exercise (eg, strengthtraining, coordination and flexibility) in workers with neck/upper extremity conditions (excluding fibromyalgia). Thesestudies included an RCT.28 Thus, it was concluded that therewas some evidence that exercise has positive effects in workerswith neck/upper extremity conditions.
Of the four studies31–34 that investigated the effects of exercise(ie, aerobic, flexibility and biofeedback for relaxation) inpatients diagnosed with fibromyalgia, one study32 was ratedas high quality and three31 33 34 as medium quality. Schachter etal32 and van Santen34 found no significant differences acrosscontrol and experimental groups. Meiworm et al31 and Valim etal33 noted positive findings after the intervention, although acontrol group was lacking in the latter study. Overall, it wasconcluded that there was some evidence in support of the use ofexercise as an intervention for managing patients diagnosedwith fibromyalgia.
One RCT of medium quality38 and three of low quality35–37
provided some evidence that multiple modifier interventionsincluding exercise (ie, rest-breaks, Getsom programme, educa-tion and strengthening) can have positive effects in workerswith neck/upper extremity conditions (excluding fibromyalgia).Furthermore, four medium-quality studies40–43 that included anRCT,41 and one low-quality study39, provided some evidence thatmultiple modifier interventions including exercise (ie, land andpool exercises, relaxation, education and cognitive behaviouraltherapy) can have positive effects in workers with fibromyalgia.
An RCT of medium quality,44 which examined multiplemodifier interventions excluding exercise (ie, cognitive beha-vioural training and education), showed positive effects forworkers with neck/upper extremity conditions (excludingfibromyalgia). By contrast, one low-quality study45 examiningeducation found no significant effects. Therefore, there wassome evidence to support the use of this strategy. With respectto multiple modifier interventions excluding exercise (ie, socialsupport and education) for workers with fibromyalgia, therewas insufficient evidence from an RCT in a medium-qualitystudy46 to support this strategy.
DISCUSSIONThis review embodied the principles of a systematic review.Although some authors have suggested that an important facetof a systematic review might be to include a meta-analysis,47
this was not considered appropriate for this review due to theheterogeneity of study designs, the general poor quality ofstudies and the diversity of exposure and outcome measuresreported.
This review attempted to classify interventions according towhether they were primary, secondary or tertiary. Most studieswere considered to involve secondary and/or tertiary interven-tions, although the type of intervention was often difficult todetermine or not clearly stated, particularly for tertiaryinterventions (ie, studies often failed to define chronicallydisabling conditions). In most cases, tertiary interventions fellwithin the group of modifier interventions and, typically,involved subjects with fibromyalgia. Although some studiesincluded both subjects with pain (ie, secondary intervention)and those without pain (ie, primary intervention), thosewithout pain were rarely discussed independently within theresults sections of the respective studies. These difficulties,combined with the heterogeneity of outcome measures,prevented direct comparisons between interventions or theevaluation of the efficacy of certain intervention types.Furthermore, where studies failed to make a clear distinctionbetween subjects with and without pain, or to stratify theiranalysis according to the different participant groups, it isdifficult to fully appreciate whether an intervention wasbenefiting one group of subjects more than another—forexample, findings may well have been driven more by theprevention of new disorders than existing cases. The design offuture studies should clearly define the purpose and populationgroups targeted, clearly documenting those participants whobenefited most from the intervention.
To group intervention types and facilitate comparisons withprevious reviews, the classification system proposed byWestgaard and Winkel5 was adopted. This classified interven-tions according to whether they were mechanical, productionsystems/organisation culture or modifier interventions. In someinstances, further sub-grouping of interventions was possible,thereby enabling interventions to be more closely aligned tospecific industries, population groups and/or musculoskeletalconditions.
Mechanical interventionsTable 3 provides an overall summary of the effectiveness ofmechanical interventions based on the findings of the currentreview and makes comparisons with those of previous reviews.The finding that there was some evidence for work environ-ment/workstation adjustment for improved health outcomes inVDU workers with neck/upper extremity conditions wasconsistent with two previous reviews5 48 and similar to that ofVerhagen et al.9 With respect to the latter review, it should benoted that different levels for indicating evidence were adoptedand, on examination, their level denoted as ‘‘limited’’ can beconsidered similar to our level ‘‘some’’.
294 Boocock, McNair, Larmer, et al
www.occenvmed.com
group.bmj.com on May 14, 2011 - Published by oem.bmj.comDownloaded from

Table
2Su
mm
ary
ofin
terv
entio
nst
udie
s
Inte
rven
tion
class
ifica
tion
Aut
hor
Des
ign
Inte
rven
tion
Mea
sure
sFi
ndin
gs
Qua
lity
ofev
iden
ceD
esig
nty
peTy
peQ
ualit
ysc
ore
Con
trol
grou
pPr
imar
y/se
cond
ary/
tert
iary
Qua
lity
ratin
gSu
bjec
tsD
iagn
osis
/con
ditio
n
Mec
hani
cal
expos
ure
inte
rven
tions
Wor
ken
viro
nmen
t/w
orks
tatio
nadju
stm
ents
&V
DU
wor
kers
Aar
aset
al(2
001)1
6
Pros
pect
ive
para
llelg
roup
stud
yYes
(with
outin
terv
entio
n)150
VD
Uw
orke
rsV
isua
ldis
com
fort
,he
adac
he,
neck
,sh
ould
er&
fore
arm
pain
New
light
ing,
new
wor
kpla
ces
and
opto
met
ric
corr
ectio
ns(w
hen
requ
ired
)Pr
imar
y
Pain
inte
nsity
and
dura
tion
VA
S,St
anda
rdis
edN
ordi
cm
uscu
losk
elet
alqu
estio
nnai
re
Redu
ced
shou
lder
pain
No
redu
ctio
nin
neck
pain
Unc
hang
edfo
rear
man
dha
ndpa
in
11
Med
ium
Nev
ala-
Pura
nen
etal
(2003)1
7
Pre-
/pos
t-co
hort
with
para
llelg
roup
rand
omis
edw
ithre
spec
tto
inst
ruct
ion
No
20
VD
Uw
orke
rsN
eck,
shou
lder
and
uppe
rlim
bpa
in
Mod
ifica
tions
ofof
fice
layo
utan
dw
orks
tatio
n+/
2er
gono
mic
advi
cean
dup
per
limb
exer
cise
sSe
cond
ary
VA
Spa
insc
ore
Que
stio
nnai
re:
men
tals
trai
nan
dph
ysic
alex
erci
seou
tsid
eof
wor
k
Redu
ced
uppe
rlim
bV
AS
scor
esIm
prov
edw
ork
post
ure
(sho
ulde
rfle
xion
)A
ltere
dEM
Gac
tivity
duri
ngty
ping
and
the
use
ofth
em
ouse
No
diffe
renc
esbe
twee
ngr
oups
inw
ork
pace
,ch
ange
inm
enta
lstr
ain
atw
ork
orfr
eque
ncy
ofph
ysic
alex
erci
se
10
Med
ium
Mek
hora
etal
(2000)1
8
Rand
omis
edpr
ospe
ctiv
epa
ralle
lgr
oup
stud
yYes
(del
ayed
inte
rven
tion;
subj
ects
asow
nco
ntro
ls)
85
VD
Uw
orke
rsTe
nsio
nne
cksy
ndro
me
Wor
ksta
tion
adju
stm
entus
ing
com
pute
rso
ftwar
eap
plic
atio
n(In
telA
dve
rsio
n1.2
)Se
cond
ary
Ada
pted
Vis
ualA
nalo
gue
Dis
com
fort
Scal
e(V
AD
S)St
anda
rdis
edN
ordi
cm
uscu
losk
elet
alqu
estio
nnai
re
Redu
ced
VA
DS
No
diffe
renc
ebe
twee
nw
orkl
oad
and
wor
kdu
ratio
nth
roug
hout
stud
yan
d/or
betw
een
com
pani
es
9 Low
Ket
ola
etal
(2002)1
9
Rand
omis
edco
ntro
lled
tria
lYes
(with
outin
terv
entio
n)109
VD
Uw
orke
rsN
eck,
shou
lder
and
uppe
rlim
bpa
in
Wor
ksta
tion
adju
stm
ent&
/or
rede
sign
follo
win
gin
tens
ive
ergo
nom
iced
ucat
ion
Seco
ndar
y
Finn
ish
educ
atio
nsy
stem
ergo
nom
icra
ting
scal
eD
isco
mfo
rtdi
ary
Mod
ified
Nor
dic
mus
culo
skel
etal
ques
tionn
aire
Redu
ctio
nsin
disc
omfo
rtra
tings
at2
mon
ths
Impr
oved
ergo
nom
icra
ting,
inte
nsiv
egr
oup
grea
ter
than
educ
atio
nor
refe
renc
egr
oup
12
Med
ium
Wor
ksta
tion
equi
pm
ent
&V
DU
wor
kers
Aar
aset
al(2
001)2
0Pr
ospe
ctiv
epa
ralle
lgro
upst
udy
Yes
(with
outin
terv
entio
n)67
VD
Uw
orke
rsN
eck,
shou
lder
&fo
rear
mpa
in
VD
Uw
ork
utili
sing
the
Ani
rco
mpu
ter
mou
se(in
terv
entio
n)ve
rsus
atr
aditi
onal
mou
seSe
cond
ary
VA
Spa
insc
ore
Clin
ical
exam
inat
ion
Redu
ced
num
ber
ofte
nder
poin
tsin
the
neck
and
shou
lder
Redu
ced
neck
,sh
ould
er,
fore
arm
,w
rist
and
hand
pain
scor
es,
6,
12
mon
ths
Redu
ced
sick
leav
eRe
duce
dpa
inw
ithfle
xion
and
side
-fle
xion
pass
ive
ROM
ince
rvic
alsp
ine
9 Low
Rem
pele
tal
(1999)2
1
Rand
omis
edco
ntro
lled
tria
lYes
(with
outin
terv
entio
n;su
bjec
tsm
atch
ed)
24
keyb
oard
oper
ator
s(a
dmin
istr
ativ
eas
sist
ants
orte
chni
calw
rite
r/ed
itors
)C
arpa
lTun
nelS
yndr
ome
(CTS
)
Use
ofke
yboa
rdw
here
the
keys
diffe
red
inth
eir
forc
e-di
spla
cem
ent
char
acte
rist
ics.
Key
boar
d‘A
’–Pr
otou
ch(K
eyTr
onic
Cor
pora
tion)
.K
eybo
ard
‘B’–
Mac
Pro
Plus
with
2-o
unce
rubb
erdo
mes
(Key
Tron
icC
orpo
ratio
n)Se
cond
ary/
tert
iary
(?)
Self-
adm
inis
tere
dm
edic
alhi
stor
yqu
estio
nnai
reSy
mpt
omsu
rvey
(VA
Spa
insc
ore)
Que
stio
nnai
reof
hand
-fun
ctio
nst
atus
Stan
dard
ised
phys
ical
exam
inat
ion
Ner
veco
nduc
tion
test
Diff
eren
cein
pain
leve
lsbe
twee
nth
eke
yboa
rdgr
oups
,12
wee
ks;
notat
6w
eeks
.Re
duce
dpa
inat
12
wee
ksus
ing
keyb
oard
‘A’
No
diffe
renc
esin
mea
npa
lm-w
rist
med
ian
sens
ory
late
ncie
sbe
twee
n0
and
12
wee
ksN
odi
ffere
nces
betw
een
grou
psin
hand
-fun
ctio
nra
tings
,6
and
12
wee
ks
20
Hig
h
Prevention and management of musculoskeletal conditions 295
www.occenvmed.com
group.bmj.com on May 14, 2011 - Published by oem.bmj.comDownloaded from

Inte
rven
tion
class
ifica
tion
Aut
hor
Des
ign
Inte
rven
tion
Mea
sure
sFi
ndin
gs
Qua
lity
ofev
iden
ceD
esig
nty
peTy
peQ
ualit
ysc
ore
Con
trol
grou
pPr
imar
y/se
cond
ary/
tert
iary
Qua
lity
ratin
gSu
bjec
tsD
iagn
osis
/con
ditio
n
Titti
rano
nda
etal
(1999)2
2
Rand
omis
edco
ntro
lled
tria
lYes
(pla
cebo
inte
rven
tion;
subj
ects
mat
ched
)4
grou
ps,
20
keyb
oard
oper
ator
sin
each
Car
palT
unne
lSyn
drom
e(C
TS)
and/
orte
ndon
itis
4co
mpu
ter
keyb
oard
s:st
anda
rd(p
lace
bo),
App
leA
djus
tabl
eK
eybo
ard
(kb1
),C
omfo
rtK
eybo
ard
Syst
em(k
b2)
and
Mic
roso
ftN
atur
alK
eybo
ard
(kb3
)Se
cond
ary/
tert
iary
(?)
Phys
ical
exam
inat
ion
Han
d/ar
mdi
scom
fort
and
pain
ques
tionn
aire
VA
Sof
stiff
ness
,nu
mbn
ess
orpa
inJo
bC
onte
ntIn
stru
men
t(J
CI)
Wor
kIn
terp
erso
nal
Rela
tions
hips
Inve
ntor
y(W
IRI)
Sign
ifica
ntre
duct
ion
inov
eral
lpai
nse
veri
tyin
kb3
at6
mon
ths
Sign
ifica
ntin
crea
sein
func
tiona
lsta
tus
afte
r6
mon
ths
inkb
3gr
oup
com
pare
dto
plac
ebo.
No
sign
ifica
ntde
crea
sein
prev
alen
ceof
clin
ical
mea
sure
saf
ter
6m
onth
s
18
Med
ium
Ergon
omic
equi
pm
ent
&m
anu
fact
urin
gw
orke
rs
Her
bert
etal
(2001)2
3
Coh
ortst
udy
No
N=
56
fem
ale
His
pani
can
dIn
dian
spoo
ling
wor
kers
atse
quin
man
ufac
turi
ngco
mpa
nyU
pper
extr
emity
Mus
culo
skel
etal
Dis
orde
rs(M
SDs)
Ergo
nom
iced
ucat
ion
and
intr
oduc
tion
ofad
just
able
chai
r(in
clud
ing
trai
ning
inco
rrec
tch
air
use)
Prim
ary/
seco
ndar
y
Sym
ptom
spo
rtio
nof
the
1993
NIO
SHqu
estio
nnai
rePr
e-/P
ostvi
deo-
anal
ysis
ofup
per
extr
emity
post
ures
usin
gth
eM
odifi
edEx
posu
reA
sses
smen
tM
etho
d
Redu
ced
pain
scor
esaf
ter
intr
oduc
tion
ofad
just
able
chai
rsat
mos
tan
atom
icsi
tes
Redu
ced
prev
alen
ceof
pain
inth
eri
ght
shou
lder
,le
ftel
bow
,an
dle
ftfo
rear
maf
ter
intr
oduc
tion
ofad
just
able
chai
r.Im
prov
edup
per
limb
post
ure
follo
win
gch
air
inte
rven
tion
8 Low
Aib
aet
al(1
999)2
4
Pros
pect
ive
long
itudi
nalc
ohor
tN
o383
man
ufac
turi
ngw
orke
rsus
ing
impa
ctw
renc
hes
Vib
ratio
nW
hite
Fing
er(V
WF)
Intr
oduc
tion
ofvi
brat
ion-
dam
ped
wre
nch
Prim
ary
Stoc
khol
mW
orks
hop
Scal
efo
rV
WF
Que
stio
nnai
res
onw
ork
hist
orie
s,m
edic
alhi
stor
ies
and
subj
ectiv
esy
mpt
oms,
incl
udin
gV
WF
Med
ical
doct
orco
nfir
med
VW
Fby
show
ing
the
subj
ecta
phot
ogra
phof
typi
calV
WF
cond
ition
s
Prev
alen
ceof
VW
Fel
imin
ated
3 Low
Jetz
eret
al(2
003)2
5
Coh
ortst
udy
No
165
man
ufac
ture
rs&
inst
alle
rsof
conc
rete
roof
ing
tiles
Han
d-A
rmV
ibra
tion
Synd
rom
e(H
AV
S)or
CTS
Intr
oduc
tion
ofne
wto
ols
with
decr
ease
dle
vels
ofH
and-
Arm
vibr
atio
nex
posu
rean
d/or
ISO
10
819
glov
esPr
imar
y
Que
stio
nnai
reon
med
ical
and
wor
khi
stor
yC
linic
alha
ndex
amin
atio
nby
occu
patio
nalh
ealth
nurs
esV
ascu
lar
test
sde
pend
ing
onre
spon
ses
tom
edic
alqu
estio
nnai
rean
dSt
ockh
olm
Wor
ksho
pSc
ale
Tren
dto
war
dde
crea
sing
prev
alen
ceof
HA
VS
Wor
kers
who
used
new
low
-vib
ratio
nto
ols
and
wor
eIS
O10
819
glov
essh
owed
mos
tim
prov
emen
tan
dle
ast
decr
emen
tin
sym
ptom
s
6 Low
Prod
uctio
nsy
stem
s/or
gani
satio
ncu
lture
inte
rven
tions
Prod
uctio
nsy
stem
s/or
gani
satio
ncu
lture
inte
rven
tion
Chr
istm
anss
onet
al(1
999)2
6
Pre-
/pos
t-ca
se-s
tudi
esN
o17
win
dow
and
door
asse
mbl
yw
orke
rsU
pper
extr
emity
pain
diso
rder
s
Org
anis
atio
nal
tera
tions
,co
ntro
lsy
stem
san
dw
ork
desi
gn(d
istr
ibut
ion
ofw
ork
task
s)Pr
imar
y
Stru
ctur
edin
terv
iew
sV
ideo
anal
yses
usin
gH
and-
Arm
-Mov
emen
t-A
naly
sis
(HA
MA
)Ps
ycho
-soc
ialq
uest
ionn
aire
sM
edic
alex
amin
atio
n
No
impr
ovem
ent
inpr
eval
ence
ofup
per
extr
emity
MSD
sdu
ring
stud
ype
riod
Som
eps
ycho
soci
alfa
ctor
sim
prov
ed(e
g‘‘i
nflu
ence
onan
dco
ntro
lof
wor
k’’),
som
ew
orse
ned
(eg
‘‘rel
atio
nshi
pw
ithfe
llow
wor
kers
’’)
4 Low
Fern
stro
m&
Abo
rg(1
999)2
7
Coh
ort
No
22
fem
ale
offic
ew
orke
rspe
rfor
min
gda
taen
try
task
sN
eck,
shou
lder
,ar
man
dha
ndpa
in
Org
anis
atio
nal
tera
tions
and
diffe
rent
wor
kta
sks
Prim
ary/
seco
ndar
y
Clin
ical
exam
inat
ion
byph
ysio
ther
apis
tD
iagn
oses
acco
rdin
gto
ado
cum
ente
dsc
reen
ing
met
hod
Subj
ects
vide
otap
edth
roug
hout
test
days
No
impr
ovem
ent
inne
ck,
shou
lder
and/
orar
mpa
inN
odi
ffere
nce
innu
mbe
ror
dura
tion
ofre
stpe
riod
sbe
twee
nye
ars
Incr
ease
dno
n-co
mpu
ter
wor
kfr
om50
min
in1991
to93
min
in1992
8 Low
Table
2C
ontin
ued
296 Boocock, McNair, Larmer, et al
www.occenvmed.com
group.bmj.com on May 14, 2011 - Published by oem.bmj.comDownloaded from

Inte
rven
tion
class
ifica
tion
Aut
hor
Des
ign
Inte
rven
tion
Mea
sure
sFi
ndin
gs
Qua
lity
ofev
iden
ceD
esig
nty
peTy
peQ
ualit
ysc
ore
Con
trol
grou
pPr
imar
y/se
cond
ary
/ter
tiary
Qua
lity
ratin
gSu
bjec
tsD
iagn
osis
/con
ditio
n
Mod
ifier
inte
rven
tions
Exer
cise
and
upper
extr
emity
cond
ition
sLu
dew
igan
dBo
rsta
d(2
003)
28
Rand
omis
edco
ntro
lled
tria
lYes
(with
outin
terv
entio
nan
dw
ithou
tco
nditi
ons)
92
mal
eco
nstr
uctio
nw
orke
rspe
rfor
min
gov
erhe
adw
ork
Shou
lder
Impi
ngem
ent
Synd
rom
e
Stre
tchi
ngan
dpr
ogre
ssiv
est
reng
thtr
aini
ngpr
ogra
mm
eSe
cond
ary/
tert
iary
(?)
Self-
repo
rted
Shou
lder
Ratin
gQ
uest
ionn
aire
(SRQ
)M
odifi
edSh
ould
erPa
inan
dD
isab
ility
Inde
x(S
PAD
I)Q
uest
ionn
aire
Impr
ovem
ent
inse
lf-re
port
edSh
ould
erRa
ting
Que
stio
nnai
re(S
RQ)
and
Shou
lder
Satis
fact
ion
Scor
es
16
Med
ium
Hag
berg
etal
(2000)2
9
Rand
omis
edtr
ial
No
69
wom
enin
dust
rial
wor
kers
Cer
vico
-bra
chia
lsy
ndro
me
ICD
-10
code
M53.1
Isom
etri
csh
ould
eren
dura
nce
vers
usst
reng
th16
wee
ktr
aini
ngpr
ogra
mm
eTe
rtia
ry
VA
Spa
insc
ores
Sick
leav
e&
NSA
IDus
eSt
anda
rise
dph
ysic
alex
amin
atio
nSt
reng
th,
rang
eof
mot
ion
and
endu
ranc
ete
sts
Redu
ced
pain
,no
diffe
renc
eby
trai
ning
type
No
redu
ctio
nin
sick
leav
eIm
prov
edar
mm
otio
npe
rfor
man
cete
stIn
crea
sed
shou
lder
stre
ngth
14
Med
ium
Wal
ing
etal
(2002)3
0
Pros
pect
ive
quas
i-ra
ndom
ised
tria
lN
o126
fem
ale
adm
inis
trat
ive
wor
kers
Trap
eziu
sM
yalg
ia
Gro
uptr
aini
ngpr
ogra
mm
es:
a)St
reng
thgr
oup
b)En
dura
nce
grou
pc)
Coo
rdin
atio
ngr
oup
d)St
ress
man
agem
ent
(non
-tra
inin
g)re
fere
nce
grou
pTe
rtia
ry
VA
Spa
insc
ores
Freq
uenc
yof
pain
Pres
sure
pain
thre
shol
dsD
egre
eof
wor
ryU
seof
anal
gesi
csSi
ckle
ave
Redu
ced
freq
uenc
yof
pain
and
VA
Sin
allg
roup
sov
ertim
eN
och
ange
inpr
essu
repa
inth
resh
olds
No
diffe
renc
esbe
twee
ntr
aini
nggr
oups
and
refe
renc
egr
oup
onan
yva
riab
le
12
Med
ium
Exer
cise
&Fi
bro
mya
lgia
Mei
wor
met
al(2
000)3
1
Expe
rim
enta
ltri
alYes
(with
outin
terv
entio
n)39,
mos
tlyfe
mal
esFi
brom
yalg
ia(F
M)
12
wee
kpr
ogre
ssiv
eae
robi
cen
dura
nce
exer
cise
prog
ram
me
incl
udin
gw
alki
ng,
jogg
ing,
cycl
ing
and/
orsw
imm
ing
Seco
ndar
y/te
rtia
ry
Body
diag
ram
ofpa
inV
AS
pain
scor
ePr
essu
repa
inth
resh
olds
Dec
reas
edpa
infu
lbod
yar
eaRe
duce
dm
ean
num
ber
ofte
nder
poin
tsM
ean
pain
thre
shol
dun
chan
ged
VA
Ssc
ore
unch
ange
dN
och
ange
sin
cont
rolg
roup
10
Med
ium
Scha
chte
ret
al(2
003)3
2
Rand
omis
edco
ntro
lled
tria
lYes
(with
outin
terv
entio
n)143
fem
ales
FM
Diff
erin
gex
erci
sedu
ratio
n:a)
Long
Bout
ofEx
erci
se(L
BE)
b)Sh
ortBo
utof
Exer
cise
(SBE
)c)
No
exer
cise
(NE)
(con
trol
)Te
rtia
ry
Body
pain
diag
ram
sA
IMS2
Que
stio
nnai
reA
ffect
Scal
eSc
ore
Fibr
omya
lgia
Impa
ctQ
uest
ionn
aire
(FIQ
)V
AS
pain
scor
eC
PSS
Redu
ced
dise
ase
seve
rity
and
impr
oved
self-
effic
acy
with
inSB
Egr
oup
and
com
pare
dto
NE
grou
pIm
prov
emen
tsin
phys
ical
func
tion,
dise
ase
seve
rity
,sy
mpt
oms,
self-
effic
acy
and
psyc
holo
gica
lwel
l-bei
ngin
LBE
grou
p
19
Hig
h
Val
imet
al(2
003)3
3
Rand
omis
edtr
ial
No
76
fem
ales
FM
Two
exer
cise
mod
aliti
es:
a)A
erob
icex
erci
se(A
E)w
alki
ngpr
ogra
mm
e,b)
Stre
tchi
ngex
erci
se(S
E)Te
rtia
ry
Sitan
dre
ach
(flex
ibili
ty)
test
Fibr
omya
lgia
Impa
ctQ
uest
ionn
aire
(FIQ
)Sh
ortFo
rm–3
6(S
F-36)
Que
stio
n-na
ire
Beck
Dep
ress
ion
Inve
ntor
y(B
DI)
Trac
e-St
ate
Anx
iety
Inve
ntor
yPa
insc
ore
from
tend
erpo
ints
VA
Spa
insc
ore
Impr
ovem
ents
inA
Egr
oup
com
pare
dto
SEgr
oup
ofto
talF
IQsc
ore
and
role
emot
iona
land
men
talh
ealth
dom
ains
ofFI
Q,
the
men
talc
ompo
nent
sum
mar
yof
SF-3
6,
BDI,
VA
Ssc
ore
and
num
ber
ofte
nder
poin
tsN
oim
prov
emen
tin
SEgr
oup
inm
enta
lhe
alth
orro
leem
otio
nald
omai
nsan
dth
eM
enta
lCom
pone
ntSu
mm
ary
ofth
eSF
-36
orBD
I
17
Med
ium
Table
2C
ontin
ued
Prevention and management of musculoskeletal conditions 297
www.occenvmed.com
group.bmj.com on May 14, 2011 - Published by oem.bmj.comDownloaded from

Inte
rven
tion
class
ifica
tion
Aut
hor
Des
ign
Inte
rven
tion
Mea
sure
sFi
ndin
gs
Qua
lity
ofev
iden
ceD
esig
nty
peTy
peQ
ualit
ysc
ore
Con
trol
grou
pPr
imar
y/se
cond
ary
/ter
tiary
Qua
lity
ratin
gSu
bjec
tsD
iagn
osis
/con
ditio
n
van
Sant
enet
al(2
002)3
4
Pre-
/pos
t-te
sttr
ial
Yes
(with
outin
terv
entio
n)143
Fem
ales
FM
Two
inte
rven
tion
mod
aliti
es:
a)G
roup
supe
rvis
edfit
ness
prog
ram
me,
(aer
obic
exer
cise
and
isom
etri
cst
reng
then
ing)
b)Bi
ofee
dbac
ktr
aini
ngfo
rm
uscl
ere
laxa
tion
Tert
iary
VA
Spa
insc
ore
VA
Sfa
tigue
scal
eH
ealth
stat
us:
Art
hriti
sIm
pact
Mea
sure
men
tSc
ale,
Sick
ness
Impa
ctPr
ofile
(SIP
)Ps
ycho
logi
caldi
stre
ss:
Sym
ptom
Che
cklis
t-90-
Revi
sed
(SC
L-90)
Phys
ical
fitne
ss-
bicy
cle
ergo
met
er
No
sign
ifica
ntfin
ding
sex
cept
phys
ical
fitne
ssw
orse
ned
for
allg
roup
sov
erth
est
udy
peri
od.
Dec
reas
ew
asle
ssin
fitne
ssgr
oup
com
pare
dto
cont
rolg
roup
14
Med
ium
Mul
tiple
mod
ifier
inte
rven
tions
(incl
udin
gex
erci
se)
&up
per
extr
emity
cond
ition
s
deG
reef
etal
(2003)3
5
Rand
omis
edco
ntro
lled
tria
lYes
(with
outin
terv
entio
n)53
Sym
phon
yO
rche
stra
Mus
icia
nsPR
MD
s
Spec
ific
mob
ilisi
ng,
stre
ngth
enin
g,an
dco
nditi
onin
gpr
ogra
mm
e(th
eG
roni
ngen
Exer
cise
Ther
apy
for
Sym
phon
yO
rche
stra
Mus
icia
ns(G
ETSO
M)
prog
ram
me)
Seco
ndar
y/te
rtia
ry(?
)
Phys
ical
Com
pete
nce
Scal
e(P
CS)
Wor
ldH
ealth
Que
stio
nnai
refo
rM
usic
ians
(WH
QM
)
Mus
culo
skel
etal
diso
rder
sde
crea
sed
Perc
eive
dph
ysic
alco
mpe
tenc
ein
crea
sed
9 Low
Cha
net
al(2
000)3
6
Pre-
/pos
t-te
sttr
ial
No
12
Wor
k-re
late
dla
tera
lepi
cond
yliti
sof
elbo
w
Educ
atio
non
path
olog
yan
der
gono
mic
sre
late
dto
WRM
DS,
stre
tchi
ng&
stre
ngth
enin
gex
erci
ses
tobe
perf
orm
edat
hom
ean
dw
ork
hard
enin
gpr
otoc
ols
Seco
ndar
y/te
rtia
ry(?
)
VA
Spa
insc
ores
LLU
MC
(Lom
aLi
nda
Uni
vers
ityM
edic
alC
entr
e)A
ctiv
itySo
rtBa
ltim
ore
Ther
apeu
ticEq
uipm
ent
(BTE
)Pr
imus
mea
sure
sD
exte
rEv
alua
tion
Com
pute
rSy
stem
Satis
fact
ion
with
Perf
orm
ance
Scal
edQ
uest
ionn
aire
Redu
ctio
nsin
pre/
post
VA
Spa
insc
ores
mai
ntai
ned
at4
and
12
wee
kfo
llow
-up
Incr
ease
dBT
EPr
imus
mea
sure
sIn
crea
ses
inLL
UM
CA
ctiv
itySo
rtSc
ores
and
Satis
fact
ion
with
Perf
orm
ance
Scal
edQ
uest
ionn
aire
Scor
esm
aint
aine
dat
4th
and
12th
wee
ksof
follo
w-u
p
7 Low
Om
eret
al(2
003/2
004)3
7
Rand
omis
edco
ntro
lled
tria
lN
otr
ueco
ntro
lgro
up50
VD
Uw
orke
rsC
umul
ativ
eTr
aum
aD
isor
ders
(CTD
s)in
clud
ing
Myo
fasc
ialP
ain
Synd
rom
e(M
PS)
and
Car
palT
unne
lSyn
drom
e(C
TS)
Ergo
nom
ican
dhe
alth
educ
atio
n(‘co
ntro
l’gr
oup)
vers
usan
exer
cise
prog
ram
me
(flex
ibili
ty,
RoM
,re
laxa
tion,
stre
ngth
enin
gan
dpo
stur
alex
erci
ses
invo
lvin
gth
ene
cksh
ould
ers
and
wri
sts
perf
orm
ed3
days
per
wee
kat
lunc
htim
e)(tr
eatm
ent
grou
p)Se
cond
ary/
tert
iary
(?)
Pain
asse
ssm
ent
usin
gN
umer
icRa
ting
Scal
e(N
RS)
Pain
Dis
abili
tyIn
dex
(PD
I)Ti
redn
ess
Scal
e(T
S)Be
ckD
epre
ssio
nIn
vent
ory
BDI)
Scal
e
Impr
oved
NRS
,PD
Iand
BDIs
core
sfo
rtr
eatm
ent
grou
p9 Lo
w
van
den
Heu
vel
etal
(2003)3
8Ra
ndom
ised
cont
rolle
dtr
ial
Yes
(with
outin
terv
entio
n)268
VD
Uw
orke
rsW
ork-
rela
ted
uppe
rlim
bre
petit
ive
stra
inin
juri
esac
cord
ing
toth
eH
ealth
Cou
ncil
ofth
eN
ethe
rlan
ds
Mic
robr
eaks
prom
pted
byco
mpu
ter
softw
are
and
‘‘nat
ural
’’re
stbr
eaks
vers
usm
icro
brea
ksan
dna
tura
lres
tbr
eaks
com
bine
dw
ithth
epe
rfor
man
ceof
regu
lar
exer
cise
spe
rfor
med
atth
ew
orks
tatio
nal
sopr
ompt
edby
the
softw
are
Seco
ndar
y/te
rtia
ry(?
)
Perc
eive
dov
eral
lrec
over
yfr
omco
mpl
aint
sFr
eque
ncy
ofco
mpl
aint
sSe
veri
tyof
pain
VA
Ssc
ale
Self-
repo
rted
sick
leav
ePr
oduc
tivity
Self-
repo
rted
reco
very
high
erin
inte
rven
tion
grou
pN
odi
ffere
nces
betw
een
the
grou
psfo
rsi
ckle
ave
Impr
oved
prod
uctiv
ityin
Gro
up1
(bre
aks
and
noex
erci
ses)
com
pare
dto
cont
rolg
roup
Impr
oved
accu
racy
rate
inin
terv
entio
ngr
oups
com
pare
dto
cont
rolg
roup
13
Med
ium
Table
2C
ontin
ued
298 Boocock, McNair, Larmer, et al
www.occenvmed.com
group.bmj.com on May 14, 2011 - Published by oem.bmj.comDownloaded from

Inte
rven
tion
class
ifica
tion
Aut
hor
Des
ign
Inte
rven
tion
Mea
sure
sFi
ndin
gs
Qua
lity
ofev
iden
ceD
esig
nty
peTy
peQ
ualit
ysc
ore
Con
trol
grou
pPr
imar
y/se
cond
ary/
tert
iary
Qua
lity
ratin
gSu
bjec
tsD
iagn
osis
/con
ditio
n
Mul
tiple
mod
ifier
inte
rven
tions
(incl
udin
gex
erci
se)
&Fi
bro
mya
lgia
Baile
yet
al(1
999)3
9
Pros
pect
ive
pre-
/pos
t-co
hort
stud
yN
o106
FM
Fibr
o-Fi
tPr
ogra
mm
e:12-w
eek
out-pa
tient
exer
cise
and
mul
tidis
cipl
inar
ypr
ogra
mm
eTe
rtia
ry
Fibr
o-Fi
tse
lf-ef
ficac
yqu
estio
nnai
reC
anad
ian
Stan
dard
ised
Test
ofFi
tnes
s(C
STF)
Fibr
omya
lgia
Impa
ctQ
uest
ionn
aire
(FIQ
)C
anad
ian
Occ
upat
iona
lPe
rfor
man
ceM
easu
re(C
OPM
)Fa
mily
Cri
sis
Ori
ente
dPe
rson
alEv
alua
tion
Scal
es(F
-CO
PES)
Impr
ovem
ents
inal
lout
com
em
easu
res
Rela
tions
hip
betw
een
smok
ing
and
pain
.i.e
.sm
oker
sha
dle
ssim
prov
emen
tin
pain
Atte
ndan
cera
teof
FMsu
ppor
tgr
oup
rela
ted
togr
eate
rim
prov
emen
tin
pain
Patie
nts
who
refu
sed
pain
oran
ti-de
pres
sant
med
icat
ions
had
poor
erou
tcom
es
8 Low
Ced
rasc
hiet
al(2
004)4
0
Pre-
/pos
t-te
sttr
ial
Yes
(with
outin
terv
entio
n)61
FM
Gro
uptr
aini
ngpr
ogra
mm
e.C
onsi
sted
ofpo
olex
erci
se,
rela
xatio
n,lo
wim
pact
land
exer
cise
,ac
tiviti
esof
daily
livin
gan
ded
ucat
ion.
Tert
iary
Num
ber
ofte
nder
poin
tsan
dm
yalg
icsc
ore
Glo
balr
atin
gby
phys
icia
nQ
uest
ionn
aire
s
Impr
ovem
ent
inFi
brom
yalg
iaIm
pact
Que
stio
nnai
re(F
IQ)
and
Psyc
holo
gica
lG
ener
alW
ell-B
eing
(PG
WB)
Inde
xN
och
ange
inob
ject
ive
phys
icia
nm
easu
res
14
Med
ium
Gow
ans
etal
(1999)4
1
Rand
omis
edco
ntro
lled
tria
lYes
(del
ayed
inte
rven
tion;
subj
ects
asow
nco
ntro
ls)
41
FM
6-w
eek
exer
cise
and
educ
atio
npr
ogra
mm
e(tw
oex
erci
sean
dtw
om
ultid
isci
plin
ary
educ
atio
nals
essi
ons
per
wee
k)Te
rtia
ry
Fibr
omya
lgia
Impa
ctQ
uest
ionn
aire
(FIQ
)A
rthr
itis
Self-
Effic
acy
Scal
e(A
SES)
Kno
wle
dge
ofFM
man
agem
ent
Que
stio
nnai
re6
min
wal
kte
st
Impr
ovem
ent
in6
min
wal
kdi
stan
ce,
wel
l-bei
ng,
self-
effic
acy,
and
FMkn
owle
dge
Redu
ced
mor
ning
fatig
ueA
llga
ins
mai
ntai
ned
atfo
llow
-up
exce
ptm
orni
ngfa
tigue
and
subj
ects
’kn
owle
dge
ofFM
man
agem
ent
whi
chre
sum
edto
base
line
leve
ls
11
Med
ium
Man
nerk
orpi
etal
(2000)4
2
Pre-
/pos
t-te
sttr
ial
No
true
cont
rolg
roup
used
69
fem
ales
FM
Two
inte
rven
tion
mod
aliti
es:
a)G
roup
pool
exer
cise
prog
ram
me
b)Ed
ucat
ion
prog
ram
me
Tert
iary
Fibr
omya
lgia
Impa
ctQ
uest
ionn
aire
(FIQ
)Sh
ortFo
rm-3
6Q
uest
ionn
aire
(SF-
36)
Swed
ish
Mul
ti-di
men
sion
alPa
inIn
vent
ory
(MPI
-S)
Art
hriti
sSe
lf-Ef
ficac
ySc
ale
(ASE
S-S)
Art
hriti
sIm
pact
Mea
sure
men
tSc
ales
(AIM
S)Q
ualit
yof
Life
Que
stio
nnai
re(Q
OLS
)
Impr
oved
FIQ
scor
ean
dw
alk
dist
ance
com
pare
dw
ithed
ucat
ion
grou
pIm
prov
edFI
Qph
ysic
alfu
nctio
ning
and
anxi
ety
scor
esin
exer
cise
com
pare
dw
ithed
ucat
ion
grou
pIm
prov
edSf
-36
gene
ralh
ealth
scor
e,so
cial
func
tioni
ng,
pain
seve
rity
and
affe
ctiv
edi
stre
ssco
mpo
nent
sof
MPI
-Sin
exer
cise
grou
pIm
prov
edA
IMS
depr
essi
onan
dQ
OLS
inex
erci
seco
mpa
red
toed
ucat
ion
grou
p
14
Med
ium
Table
2C
ontin
ued
Prevention and management of musculoskeletal conditions 299
www.occenvmed.com
group.bmj.com on May 14, 2011 - Published by oem.bmj.comDownloaded from

Inte
rven
tion
class
ifica
tion
Aut
hor
Des
ign
Inte
rven
tion
Mea
sure
sFi
ndin
gs
Qua
lity
ofev
iden
ceD
esig
nty
peTy
peQ
ualit
ysc
ore
Con
trol
grou
pPr
imar
y/se
cond
ary
/ter
tiary
Qua
lity
ratin
gSu
bjec
tsD
iagn
osis
/con
ditio
n
Redo
ndo
etal
(2004)4
3
Pros
pect
ive,
long
itudi
nal,
quas
i-ra
ndom
ised
,pa
ralle
ltri
alN
o40
fem
ales
FM
Two
inte
rven
tion
mod
aliti
es:
a)Ph
ysic
alEx
erci
se(P
E)an
dca
rdio
vasc
ular
fitne
sspr
ogra
mm
eb)
Cog
nitiv
e-be
havi
oura
lth
erap
y(C
BT)
Tert
iary
Fibr
omya
lgia
Que
stio
nnai
re(F
IQ)
Shor
tFo
rm-3
6(S
F-36)
Beck
Anx
iety
Inve
ntor
yC
hron
icPa
inSe
lf-Ef
ficac
ySc
ale
(CPS
S)C
hron
icPa
inC
opin
gIn
vent
ory
Rang
eof
Mot
ion
and
Pain
scal
e
PEG
roup
:Im
prov
emen
tsin
mos
tite
ms
and
tota
lsco
reof
FIQ
Impr
ovem
ent
inth
ebo
dily
pain
dom
ain
ofSF
-36
Aton
eye
arfo
llow
-up
none
ofcl
inic
alva
riab
les
wer
esi
gnifi
cant
lybe
tter
than
the
initi
alas
sess
men
tC
BTG
roup
:Im
prov
edite
ms
ofFI
Q(s
tiffn
ess,
tota
lsco
re)
at8
wee
ksA
t6
mon
than
don
eye
arch
ange
sno
tm
aint
aine
d,ex
cept
impr
oved
gene
ral
heal
thdo
mai
nsof
SF-3
6ED
UC
grou
p:sy
mpt
oms
and
pain
impr
oved
0–6
wee
ks;
retu
rned
toba
selin
e6–3
2w
eeks
16
Med
ium
Mul
tiple
mod
ifier
inte
rven
tions
(exc
ludin
gex
erci
se)
&up
per
extr
emity
cond
ition
s
Fauc
ettet
al(2
002)4
4
Rand
omis
edco
ntro
lled
tria
lYes
(with
outin
terv
entio
n)139
engi
neer
san
dm
icro
scop
icas
sem
bly
wor
kers
ofel
ectr
onic
man
ufac
turi
ngco
rpor
atio
nU
pper
limb
Wor
k-Re
late
dM
uscu
losk
elet
alD
isor
ders
(WRM
SDs)
Mus
cle
Lear
ning
Ther
apy
(MLT
)or
educ
atio
nalg
roup
(ED
UC
)co
nsis
ting
ofO
HN
-del
iver
eded
ucat
ion
and
Cog
nitiv
eBe
havi
oura
lTra
inin
g(C
BT)
that
addr
esse
dsy
mpt
oman
dst
ress
man
agem
ent
and
prob
lem
solv
ing
Prim
ary
Sym
ptom
Dia
ryD
ata
VA
Spa
inm
easu
res
Surf
ace
Elec
trom
yogr
aphy
(EM
G)
MLT
grou
p:0–6
wee
ksno
chan
gein
sym
ptom
san
dpa
in;
6–3
2w
eeks
wor
sene
dC
ontr
olgr
oup:
0–6
–32
wee
kssy
mpt
oms
and
pain
stea
dily
wor
sene
dD
iffer
ence
sat
6w
eeks
sign
ifica
nt,
butno
tov
eral
ltim
epe
riod
s
10
Med
ium
Bohr
(2000)4
5Ra
ndom
ised
cont
rolle
dtr
ial
No,
com
pari
son
oftw
oin
terv
entio
ngr
oups
102
VD
Uw
orke
rsN
eck,
shou
lder
and
uppe
rlim
bpa
in
Trad
ition
aler
gono
mic
educ
atio
nve
rsus
part
icip
ator
yer
gono
mic
educ
atio
nPr
imar
y
Pape
ran
dpe
ncil
surv
eys
Obs
erva
tiona
lche
cklis
tsSt
anda
rdis
edN
ordi
cm
uscu
losk
elet
alqu
estio
nnai
reW
ork
AG
PAR
scor
e
No
diffe
renc
ebe
twee
ntw
ogr
oups
for
obse
rvat
ion
data
scor
esfo
rth
ew
ork
area
conf
igur
atio
n,w
orke
rpo
stur
es,
orov
eral
lsco
res
No
diffe
renc
ebe
twee
ntw
ogr
oups
for
uppe
rbo
dypa
in/d
isco
mfo
rtor
APG
AR
scor
es
9 Low
Mul
tiple
mod
ifier
inte
rven
tions
(exc
ludin
gex
erci
se)
&Fi
bro
mya
lgia
Oliv
eret
al(2
001)4
6
Rand
omis
edco
ntro
lled
tria
lYes
(with
outin
terv
entio
n)600
patie
nts
FM
Soci
alsu
ppor
tve
rsus
soci
alsu
ppor
tco
mbi
ned
with
heal
than
dse
lf-he
lped
ucat
ion
Tert
iary
Hea
lthC
are
Cos
tsK
now
ledg
eof
FM‘G
uttm
an-li
ke’
Gro
upC
ohes
iven
ess
Scal
eA
dapt
edA
rthr
itis
Self-
Effic
acy
Scal
e
Redu
ced
help
less
ness
for
part
icip
ants
inal
lgro
ups
butm
ore
mar
kedl
yin
soci
alsu
ppor
tan
ded
ucat
ion
grou
p
12
Med
ium
Table
2C
ontin
ued
300 Boocock, McNair, Larmer, et al
www.occenvmed.com
group.bmj.com on May 14, 2011 - Published by oem.bmj.comDownloaded from

In this study, there was moderate evidence that workstationequipment (mouse and keyboard design) can lead to positivehealth benefits in VDU workers with neck/upper extremitymusculoskeletal conditions. However, there was insufficientevidence for equipment interventions among manufacturingworkers with neck/upper extremity musculoskeletal conditions.Previous reviews have not delineated according to types ofoccupation. With respect to the findings for VDU workers,Williams et al8 reported a trend towards positive benefits forseveral workplace interventions associated with modificationsto keyboard designs, while our findings showed strongersupport for this intervention strategy. This difference mayreflect the more objective approach to grading evidence used inthis review. In contrast to our conclusions related to VDUworkers were those of Verhagen et al,9 who found limitedevidence for the efficacy of some keyboards in people withcarpal tunnel syndrome. However, it should be noted thatVerhagen et al9 reported that the RCT study by Tittiranonda etal22 provided no evidence to support modifications to keyboarddesign, a finding in contrast with our appraisal of the paper andalso that of Williams et al.8
Production systems interventionsThe finding of insufficient evidence for the benefits ofproduction systems/organisation culture interventions wasconsistent with one previous review.5 Westgaard and Winkel5
identified seven Swedish production systems interventionstudies and concluded that ‘‘this group of papers providedlittle evidence to suggest that improved health can be achievedthrough redesign of the production systems’’.
The two production systems/organisation culture interven-tions26 27 identified in this review were of low quality, showedno improvements in outcome measures and involved non-RCT.Although RCTs are considered the most powerful study design,ensuring randomisation and control within the workplace,particularly with respect to changes in production systems orthe organisational culture within a company, is not alwayspossible or ethical.1 49 This raises the question as to whetherthese types of interventions should be subjected to the samerigour as those used to evaluate the efficacy of mechanical ormodifier interventions, and whether different criteria on whichto base evidence classification should be adopted.
Modifier interventionsTable 4 provides an overall summary of the efficacy of modifierinterventions based on the findings of the current review andalso makes comparisons with the findings of previous reviews.Westgaard and Winkel5 concluded that modifier interventionsinvolving the worker (eg, physical training) often achievepositive benefits. The current study concurred with theseconclusions in that it found there was some evidence thatexercise alone had positive effects in workers with neck/upperextremity musculoskeletal conditions. This finding was similarto Verhagen et al,9 but in contrast to Williams et al8 who foundinsufficient evidence for the effectiveness of exercise pro-grammes when managing neck/upper extremity musculoske-letal conditions. With respect to Williams et al,8 only one paperwith a low sample size and without a control group formed thebasis of their conclusion. However, in this study, evidence wasbased on the findings from three medium-quality studies, one
Table 3 A comparison between the current and previous reviews for the level of evidence in support of mechanical interventions forneck/upper extremity musculoskeletal conditions
Intervention condition/industry group
Evidence
Strong Moderate Some Insufficient
Mechanical exposure interventionsWork environment/work station adjustments and VDU workers with neck/upperextremity musculoskeletal conditions
* � � �
Work station equipment and VDU workers with neck/upper extremitymusculoskeletal conditions
* � �
Work station equipment and manufacturing workers with neck/upper extremitymusculoskeletal conditions
*
VDU, visual display unit.*Current review.�Previous reviews (NB: includes multiple findings from different reviews. As descriptions for ratings of evidence may have varied between review papers, these havebeen aligned with the current rating system based on the wording used).
Table 4 A comparison between the current and previous reviews for the level of evidence in support of modifier interventions forneck/upper extremity conditions
Intervention condition/industry group
Evidence
Strong Moderate Some Insufficient
Modifier interventionsExercise and neck/upper extremity musculoskeletal conditions (excludingfibromyalgia)
* � � �
Exercise and fibromyalgia *Multiple modifier interventions (including exercise) and neck/upper extremitymusculoskeletal conditions (excluding fibromyalgia)
* � �
Multiple modifier interventions (including exercise) and fibromyalgia * �Multiple modifier interventions (excluding exercise) and neck/upper extremitymusculoskeletal conditions (excluding fibromyalgia)
* � �
Multiple modifier interventions (excluding exercise) and fibromyalgia * �
*Current review.�Previous reviews (NB: includes multiple findings from different reviews. As descriptions for ratings of evidence may have varied between review papers, these havebeen aligned with the current rating system based on the wording used).
Prevention and management of musculoskeletal conditions 301
www.occenvmed.com
group.bmj.com on May 14, 2011 - Published by oem.bmj.comDownloaded from

of which was an RCT. With regard to fibromyalgia, someevidence for exercise interventions was found, although itshould be noted that contrasting findings led to this conclusion.No other reviews have focused upon the effects of exercise andfibromyalgia.
The current review found some evidence for multiplemodifier interventions, inclusive and exclusive of exercise, inpatients with neck/upper limb conditions. Such programmesincluded a combination of various types of low-intensity groupexercise training, education, relaxation techniques and/orcognitive behavioural therapy. A review by Karjalainen et al7
focused upon multidisciplinary biopsychosocial rehabilitationstudies and found insufficient evidence to support theseprogrammes in the rehabilitation of adult patients with upperlimb repetitive strain injuries. However, only two studies werereported upon in this review and these were published in 1994–5. Similarly, Verhagen et al9 concluded that there was a clearlack of evidence for multidisciplinary treatment. However, thisconclusion was based on a single study, whereas the currentreview identified 12 studies examining multiple modifiers.Some evidence was found to support the use of multi-disciplinary rehabilitation inclusive of exercise for fibromyalgia.Multiple modifier interventions exclusive of exercise were noteffective in improving musculoskeletal health in patients withfibromyalgia, although there was an indication that somepsychological factors, such as feelings of helplessness, may beimproved. Similarly, Karjalainen et al14 considered the effects ofmultidisciplinary rehabilitation exclusive of exercise for fibro-myalgia, reviewing seven studies of which four were of lowquality, and concluded that there was insufficient evidence tosupport these programmes.
Limitations of the reviewAlthough this review included those studies that used well-documented questionnaires for pain symptom outcomes, thevalidity and reliability of these measures could not always bedetermined. Unpublished studies, conference proceedings,reports and PhD theses were not reviewed. Reviewers werenot blinded to authors or affiliations of published articles and,finally, the review was restricted to studies written in English.
CONCLUSIONThis review identified no one single strategy for interventionthat was considered effective for all types of industrial settings.The findings provided evidence to support the use of somemechanical and modifier interventions as approaches for theprevention and management of neck/upper extremity muscu-loskeletal conditions and fibromyalgia. With respect to thelatter, there was a distinct lack of well-designed modifierintervention studies where the intervention was specificallytailored for the work environment and the tasks performed bythe workers. Evidence to support the benefits of productionsystems/organisational culture interventions was lacking. Thesefindings may be a reflection of the difficulty of undertakingstudies within the workplace that include interventions focusedupon health benefits compared with increased productivity andperformance.
Overall, there seemed to be no clearly defined researchstrategy targeted at the identification of effective interventionsspecific to high-risk industrial workers or individual neck/upperextremity musculoskeletal conditions. At present, there are onlyisolated studies, often of low quality, that provide limitedinformation for the establishment of new evidence-basedguidelines applicable across a number of industrial sectors.Future consideration should be given to a national/internationalresearch strategy plan targeted at specific groups (industries) orneck/upper extremity musculoskeletal conditions. In this respect,a series of well-designed, related projects will improve our
understanding of the complexity of issues related to injury andoccupational health management. Until then, we will continue tobe faced with isolated research projects, the findings of which donot provide sufficient evidence for changing existing injuryprevention and management practices.
ACKNOWLEDGEMENTSThe financial support of the Accident Compensation Corporation ofNew Zealand in funding this research project is greatly appreciated. Weacknowledge the valuable assistance and guidance of AUT’sInformation and Education Services, in particular Andrew South.
Authors’ affiliations. . . . . . . . . . . . . . . . . . . . . . .
M G Boocock, P J McNair, P J Larmer, B Armstrong, J Collier,M Simmonds, N Garrett, Physical Rehabilitation Research Centre,Auckland University of Technology, Auckland, New Zealand
Competing interests: None declared.
REFERENCES1 Panel on Musculoskeletal Disorders and the Workplace, Commission on
Behavioral and Social Sciences and Education, National Research Council andInstitute of Medicine. Musculoskeletal disorders and the workplace: low back andupper extremities. Washington, DC: National Academy Press, 2001:17–37.
2 Buckle P, Devereux J. Work-related neck and upper limb musculoskeletaldisorders. Bilbao, Spain: European Agency for Safety and Health at Work,1999:7–10.
3 Yassi A. Repetitive strain injuries. Lancet 1997;349:943–7.4 Boden LI, Biddle EA, Spieler EA. Social and economic impacts of workplace
illness and injury: current and future directions for research. Am J Ind Med2001;40:398–402.
5 Westgaard RH, Winkel J. Ergonomic intervention research for improvedmusculoskeletal health: a critical review. Int J Ind Ergon 1997;20:463–500.
Main messages
N An international systematic review of contemporaryliterature (within the past 5 years) found 31 ergonomicinterventions for the prevention and management ofneck/upper extremity musculoskeletal conditions
N Findings support the use of some mechanical andmodifier interventions for managing upper extremityconditions and fibromyalgia
N Although evidence is lacking to support the benefits ofproduction systems/organisational culture interventions,new quality criteria to replace that of blinding andrandomisation may be necessary if the efficacy of theseinterventions is to be properly understood
N Future consideration should be given to a national/international research strategy plan targeted at specifichigh-risk industry groups and/or neck/upper extremityconditions.
Policy implications
N Until such evidence is available, interventions for theprevention and management of neck/upper extremitymusculoskeletal conditions should continue to use multi-factorial approaches
N The use of production systems/organisational culturechanges should not be viewed as a single specificintervention that will bring about improved outcomes inthose workers with neck/upper extremity musculoskeletalconditions.
302 Boocock, McNair, Larmer, et al
www.occenvmed.com
group.bmj.com on May 14, 2011 - Published by oem.bmj.comDownloaded from

6 Karjalainen K, Malmivaara A, van TM, et al. Multidisciplinary biopsychosocialrehabilitation for neck and shoulder pain among working age adults: asystematic review within the framework of the Cochrane Collaboration BackReview Group. Spine 2001;26:174–81.
7 Karjalainen K, Malmivaara A, van Tulder M, et al. Biopsychosocial rehabilitationfor upper limb repetitive strain injuries in working age adults (Cochrane Review).The Cochrane Library. Chichester, UK: John Wiley & Sons, 2004:3.
8 Williams RM, Westmorland MG, Schmuck G, et al. Effectiveness of workplacerehabilitation interventions in the treatment of work-related upper extremitydisorders: a systematic review. J Hand Ther 2004;17:267–73.
9 Verhagen AP, Bierma-Zeinstra SM, Feleus A, et al. Ergonomic andphysiotherapeutic interventions for treating upper extremity work relateddisorders in adults (Cochrane Review). The Cochrane Library. Chichester, UK:John Wiley & Sons, 2004:3.
10 Bernard BP. Musculoskeletal disorders and workplace factors: a critical review ofepidemiologic evidence for work-related musculoskeletal disorders of the neck,upper extremity, and low back. Cincinnati: National Institute for OccupationalSafety and Health (NIOSH), 1997:1–14.
11 EPIQ. Generic Appraisal Tool for Epidemiology (GATE), AppraisalModules.UoA, 2004. http://www.epiq.co.nz (accessed 2 Feb 2007).
12 Thomson LC, Handoll HHG, Cunningham A, et al. Physiotherapist-ledprogrammes and interventions for rehabilitation of anterior cruciate ligament,medial collateral ligament and meniscal injuries of the knee in adults (CochraneReview). The Cochrane Library. Chichester, UK: John Wiley & Sons, 2004:4.
13 Ariens GA, van Mechelen W, Bongers PM, et al. Physical risk factors for neckpain. Scand J Work Environ Health 2000;26:7–19.
14 Karjalainen K, Malmivaara A, van Tulder M, et al. Multidisciplinaryrehabilitation for fibromyalgia and musculoskeletal pain in working age adults(Cochrane Review). Cochrane Library. Chichester, UK: John Wiley & Sons,2004:3.
15 O’Connor D, Marshall S, Massy-Westropp N. Non-surgical treatment (other thansteroid injection) for carpal tunnel syndrome (Cochrane Review). The CochraneLibrary. Chichester, UK: John Wiley & Sons, 2004:3.
16 Aaras A, Horgen G, Bjorset HH, et al. Musculoskeletal, visual and psychosocialstress in VDU operators before and after multidisciplinary ergonomicinterventions. A 6 years prospective study—part II. Appl Ergon2001;32:559–71.
17 Nevala-Puranen N, Pakarinen K, Louhevaara V. Ergonomic intervention onneck, shoulder and arm symptoms of newspaper employees in work with visualdisplay units. Int J Ind Ergon 2003;31:1–10.
18 Mekhora K, Liston CB, Nanthavanij S, et al. The effect of ergonomic interventionon discomfort in computer users with tension neck syndrome. Int J Ind Ergon2000;26:367–79.
19 Ketola R, Toivonen R, Hakkanen M, et al. Effects of ergonomic intervention inwork with video display units. Scand J Work Environ Health 2002;28:18–24.
20 Aaras A, Dainoff M, Ro O, et al. Can a more neutral position of the forearmwhen operating a computer mouse reduce the pain level for visual display unitoperators? A prospective epidemiological intervention study: part II. Int J HumComput Interact 2001;13:13–40.
21 Rempel D, Tittiranonda P, Burastero S, et al. Effect of keyboard keyswitch designon hand pain. J Occup Environ Med 1999;41:111–19.
22 Tittiranonda P, Rempel D, Armstrong T, et al. Effect of four computer keyboardsin computer users with upper extremity musculoskeletal disorders. Am J Ind Med1999;35:647–61.
23 Herbert R, Dropkin J, Warren N, et al. Impact of a joint labor-managementergonomics program on upper extremity musculoskeletal symptoms amonggarment workers. Appl Ergon 2001;32:453–60.
24 Aiba Y, Ohshiba S, Ishizuka H, et al. Study on the effects of countermeasures forvibrating tool workers using an impact wrench. Ind Health 1999;37:426–31.
25 Jetzer T, Haydon P, Reynolds D. Effective intervention with ergonomics,antivibration gloves, and medical surveillance to minimize hand-arm vibrationhazards in the workplace. J Occup Environ Med 2003;45:1312–17.
26 Christmansson M, Friden J, Sollerman C. Task design, psycho-social workclimate and upper extremity pain disorders—effects of an organisationalredesign on manual repetitive assembly jobs. Appl Ergon 1999;30:463–72.
27 Fernstrom EA, Aborg CM. Alterations in shoulder muscle activity due to changesin data entry organisation. Int J Ind Ergon 1999;23:231–40.
28 Ludewig PM, Borstad JD. Effects of a home exercise programme on shoulderpain and functional status in construction workers. Occup Environ Med2003;60:841–9.
29 Hagberg M, Harms-Ringdahl K, Nisell R, et al. Rehabilitation of neck-shoulderpain in women industrial workers: a randomized trial comparing isometricshoulder endurance training with isometric shoulder strength training. Arch PhysMed Rehabil 2000;81:1051–8.
30 Waling K, Javholm B, Sundelin G. Effects of training on female trapeziusmyalgia: an intervention study with a 3-year follow-up period. Spine2002;27:789–96, [With commentary by A Malmivaara]..
31 Meiworm L, Jakob E, Walker U, et al. Patients with fibromyalgia benefit fromaerobic endurance exercise. Clin Rheumatol 2000;19:253–7.
32 Schachter CL, Busch AJ, Peloso PM, et al. Effects of short versus long bouts ofaerobic exercise in sedentary women with fibromyalgia: a randomizedcontrolled trial. Phys Ther 2003;83:340–58.
33 Valim V, Oliveira L, Suda A, et al. Aerobic fitness effects in fibromyalgia.J Rheumatol 2003;30:1060–9.
34 van Santen M, Bolwijn P, Verstappen F, et al. A randomized clinical trialcomparing fitness and biofeedback training versus basic treatment in patientswith fibromyalgia. J Rheumatol 2002;29:575–81.
35 de Greef M, van Wijck R, Reynders K, et al. Impact of the Groningen exercisetherapy for symphony orchestra musicians program on perceived physicalcompetence and playing-related musculoskeletal disorders of professionalmusicians. Med Probl Perform Art 2003;18:156–60.
36 Chan CCH, Li CWP, Hung L, et al. A standardized clinical series for work-relatedlateral epicondylitis. J Occup Rehabil 2000;10:143–52.
37 Omer SR, Ozcan E, Karan A, et al. Musculoskeletal system disorders in computerusers: effectiveness of training and exercise programs. J Back MusculoskeletalRehabil 2003;17:9–13.
38 van den Heuvel SG, de Looze MP, Hildebrandt VH, et al. Effects of softwareprograms stimulating regular breaks and exercises on work-related neck andupper-limb disorders. Scand J Work Environ Health 2003;29:106–16.
39 Bailey A, Starr L, Alderson M, et al. A comparative evaluation of a fibromyalgiarehabilitation program. Arthritis Care Res 1999;12:336–40.
40 Cedraschi C, Desmeules J, Rapiti E, et al. Fibromyalgia: a randomised, controlledtrial of a treatment programme based on self management. Ann Rheum Dis2004;63:290–6.
41 Gowans SE, deHueck A, Voss S, et al. A randomized, controlled trial of exerciseand education for individuals with fibromyalgia. Arthritis Care Res1999;12:120–8.
42 Mannerkorpi K, Nyberg B, Ahlmen M, et al. Pool exercise combined with aneducation program for patients with fibromyalgia syndrome. A prospective,randomized study. J Rheumatol 2000;27:2473–81.
43 Redondo JR, Justo CM, Moraleda FV, et al. Long-term efficacy of therapy inpatients with fibromyalgia: a physical exercise-based program and a cognitive-behavioral approach. Arthritis Rheum 2004;51:184–92.
44 Faucett J, Garry M, Nadler D, et al. A test of two training interventions to preventwork-related musculoskeletal disorders of the upper extremity. Appl Ergon2002;33:337–48.
45 Bohr PC. Office ergonomics education: a comparison of traditional andparticipatory methods. Work 2002;19:185–91.
46 Oliver K, Cronan TA, Walen HR, et al. Effects of social support and education onhealth care costs for patients with fibromyalgia. J Rheumatol 2001;28:2711–19.
47 NHS Centre for Reviews and Dissemination. Undertaking systematic reviews ofresearch on effectiveness. CRD guidelines for those carrying out orcommissioning reviews. York: University of York, 1996.
48 Lincoln AE, Vernick JS, Ogaitis S, et al. Interventions for the primary preventionof work-related carpal tunnel syndrome. Am J Prev Med 2000;18(Suppl4):37–50.
49 Zwerling C, Daltroy LH, Fine LJ, et al. Design and conduct of occupational injuryintervention studies: a review of evaluation strategies. Am J Ind Med1997;32:164–79.
Answers (true (T), false (F)) to the questions on How to undertake a systematicreview in an occupational setting by Nicholson, on pages 361–6
1. a) T; b) T; c) F; d) F; e) T.2. a) F; b) F; c) T; d) T; e) F.3. a) F; b) T; c) T; d) T; e) T.4. a) T; b) F; c) T; d) T; e) F.5. a) T; b) F; c) T; d) T; e) T.
Prevention and management of musculoskeletal conditions 303
www.occenvmed.com
group.bmj.com on May 14, 2011 - Published by oem.bmj.comDownloaded from

doi: 10.1136/oem.2005.025593September 14, 2006
2007 64: 291-303 originally published onlineOccup Environ Med M G Boocock, P J McNair, P J Larmer, et al. reviewmusculoskeletal conditions: a systematicmanagement of neck/upper extremity Interventions for the prevention and
http://oem.bmj.com/content/64/5/291.full.htmlUpdated information and services can be found at:
These include:
References
http://oem.bmj.com/content/64/5/291.full.html#related-urlsArticle cited in:
http://oem.bmj.com/content/64/5/291.full.html#ref-list-1This article cites 39 articles, 6 of which can be accessed free at:
serviceEmail alerting
box at the top right corner of the online article.Receive free email alerts when new articles cite this article. Sign up in the
Notes
http://group.bmj.com/group/rights-licensing/permissionsTo request permissions go to:
http://journals.bmj.com/cgi/reprintformTo order reprints go to:
http://group.bmj.com/subscribe/To subscribe to BMJ go to:
group.bmj.com on May 14, 2011 - Published by oem.bmj.comDownloaded from