
INTERNATIONAL JOURNAL OF MEDICAL AND APPLIED SCIENCES CLOSED DIAPHYSEAL FRACTURES OF TIBIA MANAGED...
12
INTERNATIONAL JOURNAL OF MEDICAL AND APPLIED SCIENCES ISSN:2320‐3137 179 www.earthjournals.org Volume 2 Issue 3 2013 ORIGINAL ARTICLE CLOSED DIAPHYSEAL FRACTURES OF TIBIA MANAGED BY CLOSED INTRAMEDULLARY INTERLOCKING NAILING USING DISTAL LOCKING JIG: A PROSPECTIVE STUDY Maruthi CV* 1 , Roshan Pais 2 , Sujai S 3 , Ravi Kumar K 4 ,Shiva Prakash SU 5 , Nanjundappa HC 6 1. Assistant professor , Dept of Orthopaedics, MVJ MC and RH, Hoskote, Bangalore, India 2. Assistant professor , Dept of Orthopaedics, MVJ MC and RH, Hoskote, Bangalore, India 3. Assistant professor , Dept of Orthopaedics, MVJ MC and RH, Hoskote, Bangalore, India 4. Associate professor , Dept of Orthopaedics, MVJ MC and RH, Hoskote, Bangalore, India 5. Assistant professor , Dept of Orthopaedics, MVJ MC and RH, Hoskote, Bangalore, India 6. Professor , Dept of Orthopaedics, MVJ MC and RH, Hoskote, Bangalore, India ABSTRACT Diaphyseal fractures of tibia are most common due to increase in road traffic accidents and fall from height from building constructions. Interlocking is the surgical treatment of choice for the closed fractures. In most of the institutions image intensifier is used to perform the procedure. Using distal locking jig avoids the usage of image intensifier and its hazards. Thirty cases of closed diaphyseal fracture of tibia were managed with interlocking nail without using image intensifier and using distal locking jig between March 2010 and October 2012. And post operatively followed at 6, 12, 24 weeks and results were evaluated using Johner and Wruh’s criteria.We achieved results as 80% excellent, 13.33% good and 6.66% fair.Interlocking nailing using distal locking jig is an excellent method for the diaphyseal fractures of tibia. This has excellent functional outcome and further, reduces the hazards of image intensifier to the patient and surgical team. Key words: Diaphyseal fracture, Distal locking jig, Image intensifier, Interlocking nail. INTRODUCTION Diaphyseal fractures of tibia are most common injuries encountered in casualty department, probably due to the increased incidence of road traffic accidents and fall from height from the building constructions. The treatment for closed fractures ranging from closed manipulation and cast application to the intramedullary nailing. Intramedullary nailing is the surgical technique of choice. In most of the institutions image intensifier is used to perform the procedure. But its use is superimposed with hazards of radiation to the patient and surgical team. Using distal locking jig is an alternative approach for the fixation which is free from such hazard. Here we have made an attempt to study the functional outcome in patients with closed diaphyseal fractures of tibia managed by closed intramedullary interlocking nailing using distal locking jig.
-
Upload
earthjournals -
Category
Documents
-
view
1 -
download
0
Transcript of INTERNATIONAL JOURNAL OF MEDICAL AND APPLIED SCIENCES CLOSED DIAPHYSEAL FRACTURES OF TIBIA MANAGED...
INTERNATIONAL JOURNAL OF MEDICAL AND APPLIED SCIENCES ISSN:2320‐3137
179 www.earthjournals.org Volume 2 Issue 3 2013
ORIGINAL ARTICLE
CLOSED DIAPHYSEAL FRACTURES OF TIBIA MANAGED BY CLOSED INTRAMEDULLARY INTERLOCKING NAILING USING DISTAL LOCKING JIG: A PROSPECTIVE STUDY
Maruthi CV*1, Roshan Pais2, Sujai S3, Ravi Kumar K4,Shiva Prakash SU5, Nanjundappa HC6
1. Assistant professor , Dept of Orthopaedics, MVJ MC and RH, Hoskote, Bangalore, India 2. Assistant professor , Dept of Orthopaedics, MVJ MC and RH, Hoskote, Bangalore, India 3. Assistant professor , Dept of Orthopaedics, MVJ MC and RH, Hoskote, Bangalore, India 4. Associate professor , Dept of Orthopaedics, MVJ MC and RH, Hoskote, Bangalore, India 5. Assistant professor , Dept of Orthopaedics, MVJ MC and RH, Hoskote, Bangalore, India 6. Professor , Dept of Orthopaedics, MVJ MC and RH, Hoskote, Bangalore, India
ABSTRACT Diaphyseal fractures of tibia are most common due to increase in road traffic accidents and fall from height from building constructions. Interlocking is the surgical treatment of choice for the closed fractures. In most of the institutions image intensifier is used to perform the procedure. Using distal locking jig avoids the usage of image intensifier and its hazards. Thirty cases of closed diaphyseal fracture of tibia were managed with interlocking nail without using image intensifier and using distal locking jig between March 2010 and October 2012. And post operatively followed at 6, 12, 24 weeks and results were evaluated using Johner and Wruh’s criteria.We achieved results as 80% excellent, 13.33% good and 6.66% fair.Interlocking nailing using distal locking jig is an excellent method for the diaphyseal fractures of tibia. This has excellent functional outcome and further, reduces the hazards of image intensifier to the patient and surgical team. Key words: Diaphyseal fracture, Distal locking jig, Image intensifier, Interlocking nail.
INTRODUCTION Diaphyseal fractures of tibia are most common injuries encountered in casualty department, probably due to the increased incidence of road traffic accidents and fall from height from the building constructions. The treatment for closed fractures ranging from closed manipulation and cast application to the intramedullary nailing. Intramedullary nailing is the surgical technique of choice. In most of the
institutions image intensifier is used to perform the procedure. But its use is superimposed with hazards of radiation to the patient and surgical team. Using distal locking jig is an alternative approach for the fixation which is free from such hazard. Here we have made an attempt to study the functional outcome in patients with closed diaphyseal fractures of tibia managed by closed intramedullary interlocking nailing using distal locking jig.

INTERNATIONAL JOURNAL OF MEDICAL AND APPLIED SCIENCES ISSN:2320‐3137
180 www.earthjournals.org Volume 2 Issue 3 2013
Materials and methods We studied thirty cases of closed diaphyseal fractures of tibia (Pic. 1) admitted in Department of Orthopaedics between March 2010 and October 2012. This included both males and females within the age group of
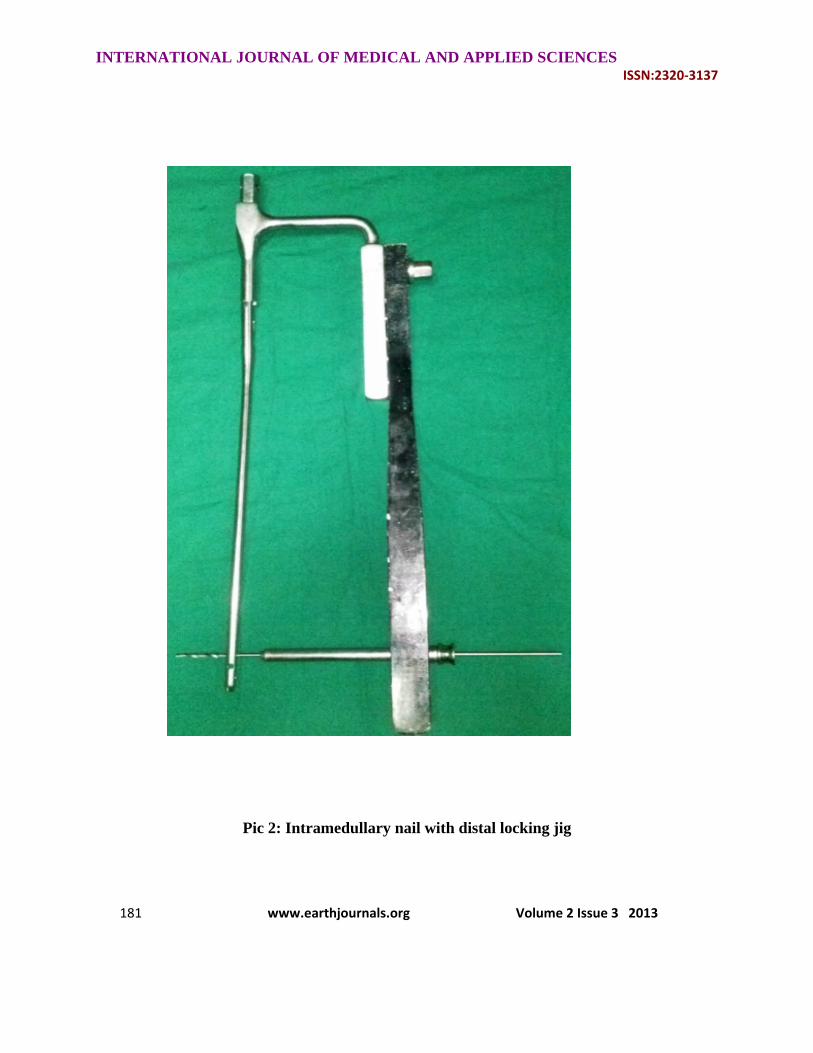
20 – 50 years. Fractures were classified using OTA (Table 1) and Tscherne (Table 2) classification. All cases were operated by closed intramedullary interlocking using distal locking jig (Pic. 2).
Pic 1: Diaphyseal fracture of both bones left leg
INTERNATIONAL JOURNAL OF MEDICAL AND APPLIED SCIENCES ISSN:2320‐3137
181 www.earthjournals.org Volume 2 Issue 3 2013
Pic 2: Intramedullary nail with distal locking jig
INTERNATIONAL JOURNAL OF MEDICAL AND APPLIED SCIENCES ISSN:2320‐3137
182 www.earthjournals.org Volume 2 Issue 3 2013
Table 1: Orthopaedic Trauma Association (OTA)[1] AO classification of tibial diaphyseal fractures.
Type A : Unifocal fractures Group A1 Spiral fractures
Subgroups A1.1 Intact fibula A1.2 Tibia and fibula fractures at different level A1.3 Tibia and fibula fractures at same level
Group A2 Oblique fractures (fracture line >30degrees)
Subgroups A2.1 Intact fibula A2.2 Tibia and fibula fractures at different level A2.3 Tibia and fibula fractures at same level
Group A3 Transverse fractures (fracture line <30degrees)
Subgroups A3.1 Intact fibula A3.2 Tibia and fibula fractures at different level A3.3 Tibia and fibula fractures at same level
Type B : Wedge fractures Group B1 Intact Spiral wedge fractures
Subgroups B1.1 Intact fibula B1.2 Tibia and fibula fractures at different level B1.3 Tibia and fibula fractures at same level
Group B2 Intact bending wedge fractures
Subgroups B2.1 Intact fibula B2.2 Tibia and fibula fractures at different level B2.3 Tibia and fibula fractures at same level
Group B3 Communited wedge fractures
Subgroups B3.1 Intact fibula B3.2 Tibia and fibula fractures at different level B3.3 Tibia and fibula fractures at same level
Type C : Complex fractures (multifragmentary, segmental or comminuted fractures) Group C1 Spiral Wedge fractures
Subgroups C 1.1 Two intermediate fragments C 1.2 Three intermediate fragments C 1.3 More than three intermediate fragments
Group C2 Segmental fractures
Subgroups C2.1 One segmental fragment C2.2 Segmental fragment and additional wedge fragment C2.3 Two segmental fragments
Group C3 Communited fractures
Subgroups C3.1 Two or three intermediate fragments C3.2 Limited communition (<4cm) C3.3 Extensive communition

INTERNATIONAL JOURNAL OF MEDICAL AND APPLIED SCIENCES ISSN:2320‐3137
183 www.earthjournals.org Volume 2 Issue 3 2013
Table 2: Tscherne[2] classification of closed fractures.
C0 Fracture has little or no soft tissue injury
C1 The fracture has mild-to-moderate severe fracture configuration with superficial abrasions
C2 The fracture has a moderately severe fracture configuration and deep contamination with local skin or muscle contusion
C3 The fracture has severe fracture configuration and extensive contusion or crushing of skin or destruction of muscle
Surgical technique Under spinal anaesthesia with appropriate aseptic precautions and tourniquet control, anterior midline patellar tendon splitting approach was used. An awl was introduced proximal to the medial half of the tibial tuberosity or LAP (lateral anterior and proximal) entry for the proximal one third fractures [3], perpendicular to the long axis of tibia 1cm to 1.5cm depth. Awl was made vertical along the axis of the tibia and introduced into the medullary canal with swivel movements. A beaded guide wire was introduced after closed reduction. The position confirmed by reduced mobility at the fracture site, bony end feel of guide wire and by passing rigid cannulated reamers over the guide wire. Reaming done using cannulated rigid reamers up till one to two mm more than the predetermined nail size which was calculated by preoperative radiographs. Guide wire was exchanged and the predetermined nail is introduced with proximal and distal jig assembly. Length was assessed by preoperative contralateral tibial measurements and intraoperative guide
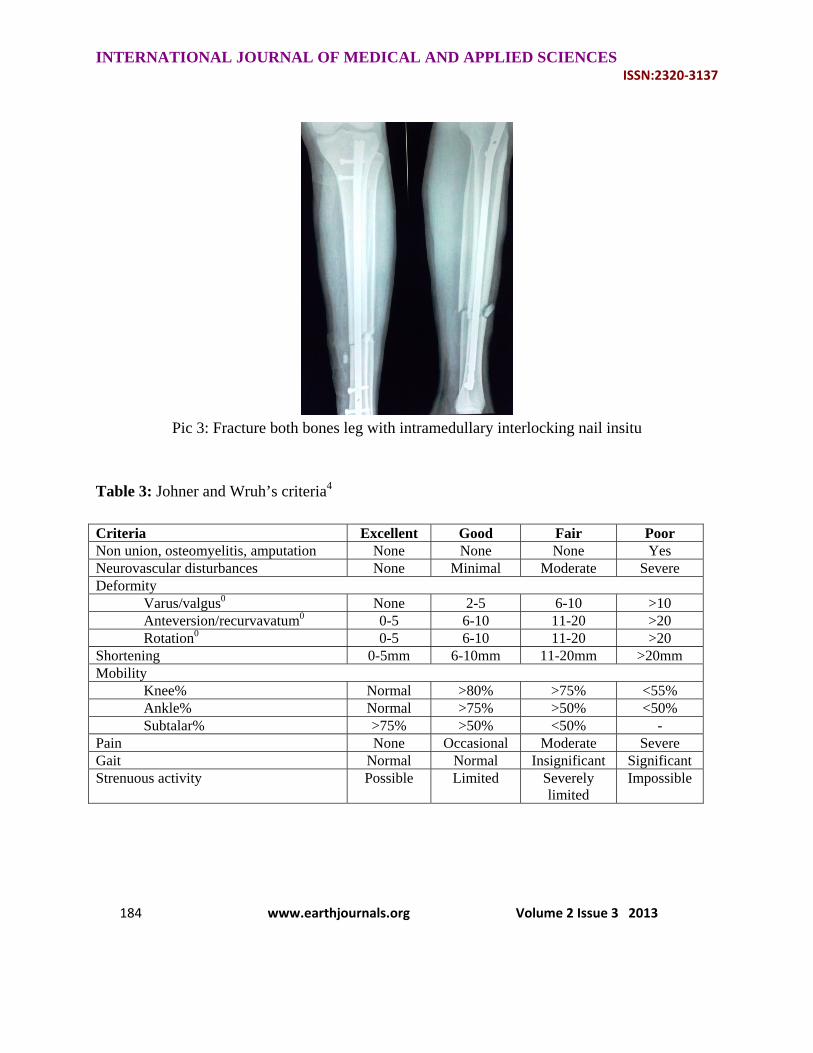
wire length difference. Locking started from distal to proximal, all the while using the guide wire to confirm placement of bolts. Wounds were closed in layers after a saline wash. Post operative protocol Patient was given parentral antibiotics for two days and oral antibiotics for another three days. Check x ray was taken immediately after the surgery (Pic 3). Wound inspected two days after the surgery. Sutures were removed on 12th day. Meantime physiotherapy started with active quadriceps strengthening, range of motion and non weight bearing ambulation with the support of crutches. And patient’s were followed up at 6, 12 and 24 weeks and assessed for subjective, clinical, radiological sign of union and ability to do strenuous activity. Fracture Union was considered when patient was full weight bearing without pain; fracture site was not tender on palpation and radiograph showed osseous union. Finally, functional assessment was done at 6 months using the Johner and Wruh’s criteria[4] (Table 3).
INTERNATIONAL JOURNAL OF MEDICAL AND APPLIED SCIENCES ISSN:2320‐3137
184 www.earthjournals.org Volume 2 Issue 3 2013
Pic 3: Fracture both bones leg with intramedullary interlocking nail insitu
Table 3: Johner and Wruh’s criteria4
Criteria Excellent Good Fair Poor Non union, osteomyelitis, amputation None None None Yes Neurovascular disturbances None Minimal Moderate Severe Deformity
Varus/valgus0 None 2-5 6-10 >10 Anteversion/recurvavatum0 0-5 6-10 11-20 >20 Rotation0 0-5 6-10 11-20 >20
Shortening 0-5mm 6-10mm 11-20mm >20mm Mobility
Knee% Normal >80% >75% <55% Ankle% Normal >75% >50% <50% Subtalar% >75% >50% <50% -
Pain None Occasional Moderate Severe Gait Normal Normal Insignificant Significant Strenuous activity Possible Limited Severely
limited Impossible

INTERNATIONAL JOURNAL OF MEDICAL AND APPLIED SCIENCES ISSN:2320‐3137
185 www.earthjournals.org Volume 2 Issue 3 2013
Observations and Results: In our study 17(56.67%) patients were between 20 and 30 years, 8(26.66%) between 31 and 40 years and 5(16.67%) between 41 and 50 years. Most of them were males 24(80%), females 6 (20%). Majority of the injuries were due to road traffic accident, i.e., in 19 (63.33%) followed by fall from height in 8 (26.66%), fall of a heavy object in 2(6.66%) and history of assault in 1 (3.33%) case. The right leg was affected in 21 cases (70%) and the left leg in remaining 9 (30%). Fracture at mid 1/3rd constituted the majority at 17(56.66%), lower third 11(36.66%), upper third and junction of upper and mid third constituted 3.33% each. Radiologically oblique type was common with 12(40%), spiral and transverse constituted 7 (23.33%) each, wedge fragment in 3(10%) and communited in 1(3.33%). Using the AO classification type A constituted 26(86.66%), B 3(10%) and C 1(3.33%). Tscherne type C1 19(53.33%), C0 16(36.66%) and C2 5(10%). Based on the clinical and radiological parameters, patients were started on partial weight bearing and full weight bearing. We started partial weight bearing for 24 patients at 4 weeks, 3 patients at 6weeks and for remaining 3 at 8 week. Dynamization was done in four transverse and one oblique fracture at eight weeks as there was no signs of healing. Full weight bearing was started by 10weeks in 24 patients, 12 weeks in 4, 14 and 16 in the remaining 2. Complete
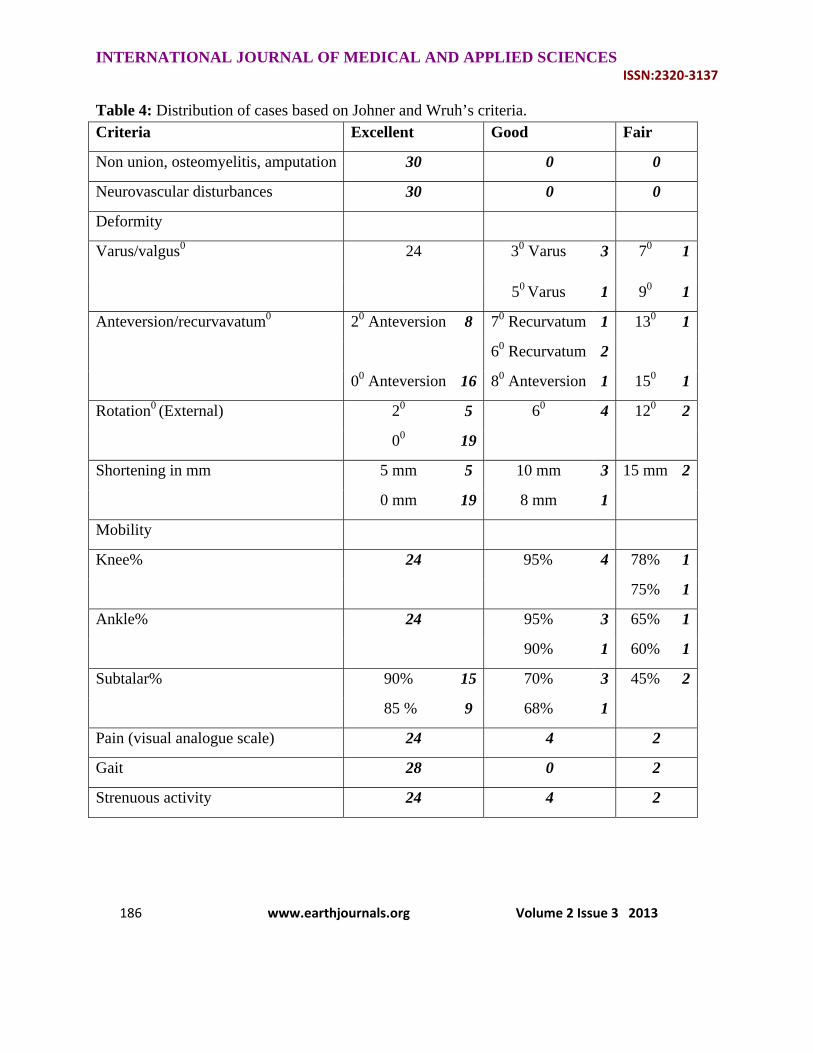
radiological healing of fracture was noted by 20 weeks in 20 patients, 16 weeks in 8 and 22 weeks in remaining 2. In our series, majority of fractures united within 20weeks (24 patients). The average time of union was 17 weeks. Complications like non union, osteomyelitis and patients undergoing for amputation was not seen in any of our patients, but we found delayed union in 2 patients. Neurovascular disturbances were not seen in any of our patients. Complications: Two patients had superficial wound infection which subsided by regular dressings and antibiotics according to the culture report. Anterior knee pain in two patients with proximal and junction of proximal and mid third fractures, probably due to high entry point (Picture 4) caused prominent proximal nail with impingement on the patellar tendon. In one patient impending compartment syndrome noted, postoperatively probably due to communited fracture and treated by limb elevation, active toe and ankle movements and anti oedema measures. One patient went to fat embolism intraoperatively, managed in ICU by appropriate measures, patient recovered by 13 days and shifted to the ward. Results were evaluated using Johner and Wruh’s criteria. We achieved 80% excellent, 13.33% good and 6.66% fair results (Table-4).
INTERNATIONAL JOURNAL OF MEDICAL AND APPLIED SCIENCES ISSN:2320‐3137
186 www.earthjournals.org Volume 2 Issue 3 2013
Table 4: Distribution of cases based on Johner and Wruh’s criteria. Criteria Excellent Good Fair
Non union, osteomyelitis, amputation 30 0 0
Neurovascular disturbances 30 0 0
Deformity
Varus/valgus0 24 30 Varus 3 70 1
50 Varus 1 90 1
Anteversion/recurvavatum0 20 Anteversion 8 70 Recurvatum 1 130 1
60 Recurvatum 2
00 Anteversion 16 80 Anteversion 1 150 1
Rotation0 (External) 20 5 60 4 120 2
00 19
Shortening in mm 5 mm 5 10 mm 3 15 mm 2
0 mm 19 8 mm 1
Mobility
Knee% 24 95% 4 78% 1
75% 1
Ankle% 24 95% 3 65% 1
90% 1 60% 1
Subtalar% 90% 15 70% 3 45% 2
85 % 9 68% 1
Pain (visual analogue scale) 24 4 2
Gait 28 0 2
Strenuous activity 24 4 2

INTERNATIONAL JOURNAL OF MEDICAL AND APPLIED SCIENCES ISSN:2320‐3137
187 www.earthjournals.org Volume 2 Issue 3 2013
DISCUSSION Fracture shaft of tibia is one of the most common fractures encountered by the orthopaedic surgeon. Over the years, various modalities of treatment have been used. The principle of biological osteosynthesis is rightly applied in long bone fracture healing and hence the selection of closed intra-medullary interlocking nailing with distal locking jig in this study. Arne Ekeland et al[5] (1988), in their study series of 45 patients noted the mean age of patients to be 35 years. Similar studies by Court Brown et al[6] (1990) noted the mean age to be 32.4 years & Court Brown et al[7] (1995) was 37 years. In our study, 56.63% of the patients were in the age group of 21-30 years with the mean age being 30.8 years. Tibial shaft diaphyseal fractures were seen in the younger age group probably because they are the people who are physically active, were engaged in increased various outdoor activities and as a result most of the injuries sustained were high-velocity injuries. Hooper et al[8] (1991) showed that the incidence of fracture had male preponderance (82%). Similarly, Court Brown et al[6](1990) showed the incidence among males was 81.3%. In our study, incidence in male was 80% in concordance to the other studies, pointing to the face that incidence in male is higher probably because of their more outdoor activities, while women majorly confined themselves to the domestic activities. Court Brown et al[7] (1995), showed that the commonest mode of injury was Road Traffic Accident accounting for an incidence of 37.5%. Lawtence B. Bone et al[9] (1986), reported in an earlier series a 90% incidence
of road traffic accidents tibial shaft fractures while Hooper et al8 (1991), reported a 59% incidence in his series. In our study, we have found that 19 patients of the tibial diaphyseal fractures occurred due to road traffic accidents which accounted for an incidence of 63.33%. In majority of cases, they involved the patients who were the motorists, while the remaining patients tended to be pedestrians. This could be attributed to the poor road traffic sense and poor quality of roads, leading to a higher incidence of road traffic accidents in our country. Anatomical Location of Fractures: In our series, the anatomical location of the fracture was in the middle-third of the shaft of tibia in 17 (56.66%) patients, followed by the lower third in 11 (36.66%) of the cases. This is comparable to Lawrence B Bone et al[9] (1986) series, where 53.5% were middle - third fractures. Similarly Court Brown et al[7] (1995), showed 44% were middle - third fractures. The middle third fractures are common because of anatomical features of more rigidity of the bone and its subcutaneous nature makes it more vulnerable to the injuring force. Type of Fracture: In our series Type A fractures were the commonest, they constituted 26 (86.66%). Type A fractures are unifocal fractures and in our series the incidence was higher than the series of Court Brown et al[7] (1995), who found that Type A accounted for 54% of all tibial fractures. Our series had a higher incidence of oblique fractures 40%, transverse fractures made up 23.33% , which was comparable to a study by Sankarsan Patro et al[10] (1998), in whose series, there were 59% of these fractures. Court Brown et al[7] reported 37.2% and Arne Ekeland[5] (1988)

INTERNATIONAL JOURNAL OF MEDICAL AND APPLIED SCIENCES ISSN:2320‐3137
188 www.earthjournals.org Volume 2 Issue 3 2013
reported 42% of transverse and oblique fractures. In our series, Tscherne Cl type of fracture constituted 53.33% (16) of closed fractures. This is comparable to 53%in the series by Court Brown et al[7] (1995). C l type of closed fractures is commonly seen in road traffic accidents. The fibula was fractured along with the shaft of tibia in our series in 66.66% of cases. This is comparable to the series of Court Brown et al[7] (1995), where the associated fibula fracture was noted in 77.7% of the cases. The associated fracture of the fibula, in most of the cases reflects on the high - velocity injury pattern in our series, as in most the mode of injury was road traffic accident. Preoperative, Operative and Complications: All patients in our series were operated under spinal anaesthesia. In our series, we have used intramedullay nails ranging from 8 to 10 mm in diameter and from 280 to 360 mm in length. Static locking was done for all 30 cases in our series. Recently, Tsalafoutas et al[11] reported an average 137 ± 111 mGy and 5.7 ± 3.5 minutes of radiation exposure for tibial fracture nailing. We used distal locking jig, which has the advantage of avoiding radiation exposure due to image intensifier. In majority of our patients, active Hip, Knee, ankle movements and quadriceps exercises were started on the first postoperative day. These post-operative exercises were delayed in 4 patients who had head injury. Majority of patients were mobilized with the walker from the third postoperative day, without bearing weight on the operated leg. Suture removal was done in all patients on 12th day. Complete relief of pain was seen in majority of patients in two weeks.
Depending upon the type of fracture and stable fixation of fracture, partial weight bearing was started. In our series, partial weight bearing was started in 20 patients by the end of 4th week. Superficial infections occurred in 2 patients at the site of proximal surgical incision and healed by dressing and antibiotics, and 2 patients had anterior knee pain due to impingement of nail. Studies by Lawrence B. Bone et al[9] (1986), Arne Ekeland et al[5] (1988) and Blachut P.A. et al[12](1997) noted an infection rate of 6.25%, 4.4% and 1% respectively. Anterior knee pain was a common complication as depicted by Hernigou P. et al[13] (2000), who noted improper entry of nail into medullary canal caused anterior knee pain. Jarmo A.K. Toivnnen et al[14] (2002), noted anterior knee pain to be common in tibial intramedullary nailing. In 1996, Christie[15] noted embolic phenomenon during nailing. In our series one case had intraoperative fat embolism. In 1998 Utvag et al[16] quoted that there is no evidence to show that the degree of reaming significantly affect healing pattern. We had no neurological or vascular injury in our study. One patient had impending compartment syndrome managed by conservative measures. Full Weight bearing: Full weight bearing in our series was started at 10th week in 19 patients (63.33%) and at 12th week in 10 patients (33.33%). The appearance of bridging callus on radiographs and clinical assessment was done before the patient has borne full weight. The average time of full weight bearing was 10.81 weeks. Full weight bearing has been delayed in 1 patient as there was communited fracture. This is comparable to Lawrence B. Bone et al[9] (1986), where in his study weight bearing has been delayed in unstable fractures.

INTERNATIONAL JOURNAL OF MEDICAL AND APPLIED SCIENCES ISSN:2320‐3137
189 www.earthjournals.org Volume 2 Issue 3 2013
Grosse and Kempf[17] (1991), allowed full weight bearing at 8.5 weeks. Fracture Union: In our series, majority of fractures united within 20weeks (24 patients). The average time of union was 17.36 weeks. This is comparable to Anglen J.O. et al[18] (1995), Lawrence B. Bone et al[9], Court Brown et al[6] (1990) and Arne Ekeland et al[5] (1988) where they reported average union time of 22.5 weeks, 19 weeks, 16.7 weeks and 16 weeks, respectively. Second surgery: Dynamization was successful in four cases of transverse fracture and one case of oblique fracture. Wu and Shih[19] demonstrated only a 54% success rate in tibial and femoral fractures after dynamization. Functional Outcome Functional outcome was done at 6 months using the Johner and Wruh’s criteria which was graded into excellent, good, fair and poor. In our study, 80% (24 patients) had excellent, 13.33% (4 patients) good, 6.66% (2 patients) fair outcome. Klemet al[20] (1986), reported 62.50% excellent, 31.8% good, 4.5% fair and 1.2% poor results. ArneEkeland et al[5] (1988), reported 64.4% excellent, 28.8% good and 4.4% as fair. Conclusion: By our study we have come to the conclusion that Intramedullary interlocking for the diaphyseal fracture of tibia is excellent method of fracture fixation, helps in early mobilization of limb and patient, without disturbing the periosteal blood supply. Further, use of a distal locking jig would avoid radiation exposure and its hazard to patient and surgical team. But, for proximal third fractures plating may be a better alternative, as the high entry point causes prominence of the nail and anterior
knee pain. Communitted fractures may also treated with the same method to regain the near normal alignment and length of the bone. Finally, if there are no signs of healing by eight weeks, it is better to dynamize in transverse and short oblique fractures. REFERENCES
1. Müller ME, Koch P, Nazarian S, Schatzker J. The comprehensive classification of fractures of long bones. Berlin: Springer-Verlag; 1990.
2. Oestern HJ, Tscherne H. Pathophysiology and classification of soft tissue injuries associated with fractures. In: Tscherne H, Gotzen L, eds. Fractures with soft tissues injuries. Berlin: Springer-Verlag; 1984.
3. Tanna DD. Text book of interlocking nailing. Third edition, Jaypee Brothers, New Delhi; 2010:3-16.
4. Johner R, Wruhs O .Classiffication of tibial shaft fractures and correlation with results after rigid internal fixation. Clin Orthop. 1983; 178:7-25.
5. Arne Ekeland, B Jorn, O Thoresen, Antti Alho, Kuntstromsoe, Gunnar et al. Interlocking intramedullary nailing in the treatment of tibial fractures. CORR. 1988; 231:208-15.
6. Court Brown CM, Christie JMC, Queen MM. Closed intramedullary tibial nailing. Journal of bone and joint surgery. 1990;72b:605-11.
7. Court Brown CM, Brine JMC. The epidemiology of tibial fractures. Journal of bone and joint surgery. 1995; 77b:417-21.
8. Hooper GJ, Kidellp G, Pennaji D. Conservative management or closed nailing for tibial shaft fractures: Randomized prospective trial. Journal of bone and joint surgery. 1991; 73b:83-5.
9. Lawrence B Bone, Kenneth D Johnson. Treatment of tibial fractures by reaming

INTERNATIONAL JOURNAL OF MEDICAL AND APPLIED SCIENCES ISSN:2320‐3137
190 www.earthjournals.org Volume 2 Issue 3 2013
and intramedullary nailing. Journal of bone and joint surgery.1986; 68a:877-86.
10. Sankarsanpatro, Sadangi BK, Mohapatro BM, Misra UN, Mohanty SM, Mohanpatro MR. Interlocking nailing in tibial fractures without C- arm. Indian journal of orthopaedics. 1998; 33: 175-8.
11. Tsalafoutas IA, Tsapaki V, Kaliakmanis A, Pneumaticos S, Tsoronis F, Koulentianos ED. Estimation of radiation doses to patients and surgeons from various fluoroscopically guided orthopaedic surgeries. Radiat Prot Dosimetry. 2007; June 11.
12. Blachut PA, Brien PJ, Meekmh RN, Broekhuyse M. Interlocking nailing with or without reaming further treatment of closed fractures of tibial shaft. Journal of bone and joint surgery. 1997; 79a:640-6.
13. Hernigou P, Cohen D. Proximal entry for intramedullary nailing of tibia. Journal of bone and joint surgery. 2000; 82b:33-41.
14. Toivanen JA, Vaisto O, Kannus P, Latvala K, Honkonen SE, Jarvinen MJ. Anterior knee pain after intramedullary nailing of fractures of tibial shaft. Journal of bone and joint surgery Am. 2002; 84a:580-5.
15. Christie J. The coagulativeaffects of fat embolization during intramedulary manipulative procedures. Tech Orthop. 1996; 11:14-7.
16. Utvag SE, Grundness O, Reikeras O. Effects of degrees of reaming on healing of segmental fractures in rats. J Orthop trauma. 1998; 12: 192-9.
17. Grosse A, Taglang G and Kempf GK. Locking system. Howmedica. 1991;28.
18. Anglenj O. A comparison of reamed and undreamed nailing of tibia. Journal of trauma. 1995;351.
19. Wu CC, Shih CH. Effective dynamisation of a static interlocking nailing on fracture healing. Can J Surg. 1993; 36:302.
20. Klemmk W, Borner M. Interlocking nailing of complex fractures of the femur and tibia. Clinical orthopaedics.1986; 212:89.




















