
INTERNATIONAL JOURNAL OF MEDICAL AND APPLIED SCIENCES CASE REPORT CARCINOSARCOMA OF BREAST: A RARE...
7
INTERNATIONAL JOURNAL OF MEDICAL AND APPLIED SCIENCES ISSN:2320‐3137 155 www.earthjournals.org Volume 2 Issue 3 2013 CASE REPORT CARCINOSARCOMA OF BREAST: A RARE CASE JAISWAL RIDDHI 1* , AGARWAL AKANKSHA 2 1 ASSISTANT PROFESSOR, KING GEORGE’S MEDICAL UNIVERSITY LUCKNOW 2 THIRD YEAR RESIDENT, KING GEORGE’S MEDICAL UNIVERSITY LUCKNOW ABSTRACT Carcinosarcoma of the breast, also called as metaplastic carcinoma, is a rare and aggressive tumour with two distinct cell lines comprising of epithelial and mesenchymal components, with few cases reported, incidence being 0.1% of all the breast tumours [1]. . The prognosis of carcinosarcoma breast is poor compared to more common types of breast cancers such as infiltrating ductal or lobular carcinomas. These tumours are a diagnostic and therapeutic challenge to both the clinician and pathologist. A case of carcinosarcoma breast in a 40 -years woman is presented here. KEY WORDS: Carcinoma,case report, breast , tumours INTRODUCTION Carcinosarcoma have been observed in various organs including the ovary and uterus. The true definition of metaplastic carcinoma of the breast is a tumour of malignant epithelial tissue (carcinoma) mixed with malignant cells of mesenchymal origin (sarcoma) without an apparent intermediate zone, with apparent histological and cytological features present on light microscopy and Immunohistochemical testing [2]. Recent studies indicate it to be a malignant mammary neoplasm probably with multipotential myoepithelial cell origin [3]. ‘Monophasic sarcomatoid carcinoma” term is used in presence of identifiable epithelial component. The term for biphasic tumours like’ biphasic sarcomatoid carcinoma’ or carcinosarcoma’ may be used. Rescent evidences suggest these tumours to originate
-
Upload
earthjournals -
Category
Documents
-
view
1 -
download
0
Transcript of INTERNATIONAL JOURNAL OF MEDICAL AND APPLIED SCIENCES CASE REPORT CARCINOSARCOMA OF BREAST: A RARE...

INTERNATIONAL JOURNAL OF MEDICAL AND APPLIED SCIENCES ISSN:2320‐3137
155 www.earthjournals.org Volume 2 Issue 3 2013
CASE REPORT
CARCINOSARCOMA OF BREAST: A RARE CASE
JAISWAL RIDDHI1*, AGARWAL AKANKSHA2
1 ASSISTANT PROFESSOR, KING GEORGE’S MEDICAL UNIVERSITY
LUCKNOW 2 THIRD YEAR RESIDENT, KING GEORGE’S MEDICAL UNIVERSITY
LUCKNOW
ABSTRACT Carcinosarcoma of the breast, also called as metaplastic carcinoma, is a rare and aggressive tumour with two distinct cell lines comprising of epithelial and mesenchymal components, with few cases reported, incidence being 0.1% of all the breast tumours [1].. The prognosis of carcinosarcoma breast is poor compared to more common types of breast cancers such as infiltrating ductal or lobular carcinomas. These tumours are a diagnostic and therapeutic challenge to both the clinician and pathologist. A case of carcinosarcoma breast in a 40 -years woman is presented here.
KEY WORDS: Carcinoma,case report, breast , tumours
INTRODUCTION Carcinosarcoma have been observed in various organs including the ovary and uterus. The true definition of metaplastic carcinoma of the breast is a tumour of malignant epithelial tissue (carcinoma) mixed with malignant cells of mesenchymal origin (sarcoma) without an apparent intermediate zone, with apparent histological and cytological features present on light microscopy and
Immunohistochemical testing [2]. Recent studies indicate it to be a malignant mammary neoplasm probably with multipotential myoepithelial cell origin [3]. ‘Monophasic sarcomatoid carcinoma” term is used in presence of identifiable epithelial component. The term for biphasic tumours like’ biphasic sarcomatoid carcinoma’ or carcinosarcoma’ may be used. Rescent evidences suggest these tumours to originate

INTERNATIONAL JOURNAL OF MEDICAL AND APPLIED SCIENCES ISSN:2320‐3137
156 www.earthjournals.org Volume 2 Issue 3 2013
from malignant myofibroblasts or from metaplastic differentiation of malignant epithelial cells into myofibroblasts [4]. The differential diagnoses include spindle cell sarcoma, malignant phyllodes tumour and stromal sarcomas [8]. Here we present a case of 40- years female who was diagnosed with carcinosarcoma breast on the basis of histological picture and supported by immunohistochemistry.
CASE:
a 40 -years female underwent modified radical mastectomy for malignant breast lump and the specimen was submitted in our department for Histopathological examination. Patient had a history of left breast lump since 7 months, gradually increasing in size and associated with pain. There was no significant obstetric or family history. Patient had breastfed all her children. Mammography revealed a high density cystic mass with irregular margins and foci of calcification. Fine needle aspiration cytology of the lesion, done at a private institute diagnosed the lesion as infiltrating ductal carcinoma and biopsy was advised for further confirmation.
Gross examination showed a 18X15X6 cm sized MRM specimen was received with attached skin flap measuring 17X14
cm.NAC was retracted and a nodule 5X5 cm was identified underlying the skin, which on cutting showed solid white areas. On serial sectioning a solid growth measuring 11X9X6 cm was identified. The growth cut soft to firm and on cutting a cystic cavity was identified. 5 lymph nodes were also identified in the axillary tail.
Microscopic examination of the tumour consisted of both the malignant epithelial and mesenchymal components disposed as sheets and lobules along with focal areas of necrosis and chondroid differentiation. Epithelial component was pleomorphic, round to oval cells, with high nucleo Cytoplasmic ratio, hyperchromatic to vesicular nuclei, inconspicuous to prominent nucleoli, surrounded by scant to abundant eosinophilic cytoplasm. Spindled mesenchymal cells had hyperchromatic, fusiform nuclei and moderate bipolar cytoplasm. Fair number of mitotic figures was also seen. All the lymph nodes were free from tumour cell invasion.
Immunohistochemistry showed Positivity for CK 7, Pan CK, Vimentin, Ki67, S100 but was Negative for desmin and SMA.
Further evaluation of hormonal receptor assay was ‘triple negative’ i.e. ER, PR, HER2Neu were negative.

INTERNATIONAL JOURNAL OF MEDICAL AND APPLIED SCIENCES ISSN:2320‐3137
157 www.earthjournals.org Volume 2 Issue 3 2013
FIGURE 1: GROSS PICTURE OF BREAST SPECIMEN SHOWING RETRACTED NIPPLES ALONG WITH A NODULAR GROWTH ON THE SURFACE.
FIGURE 2: GROSS PICTURE SHOWING CUT SURFACE OF THE TUMOUR. A FLESHY TUMOUR MASS WITH VARIEGATED APPEARANCE.
INTERNATIONAL JOURNAL OF MEDICAL AND APPLIED SCIENCES ISSN:2320‐3137
158 www.earthjournals.org Volume 2 Issue 3 2013
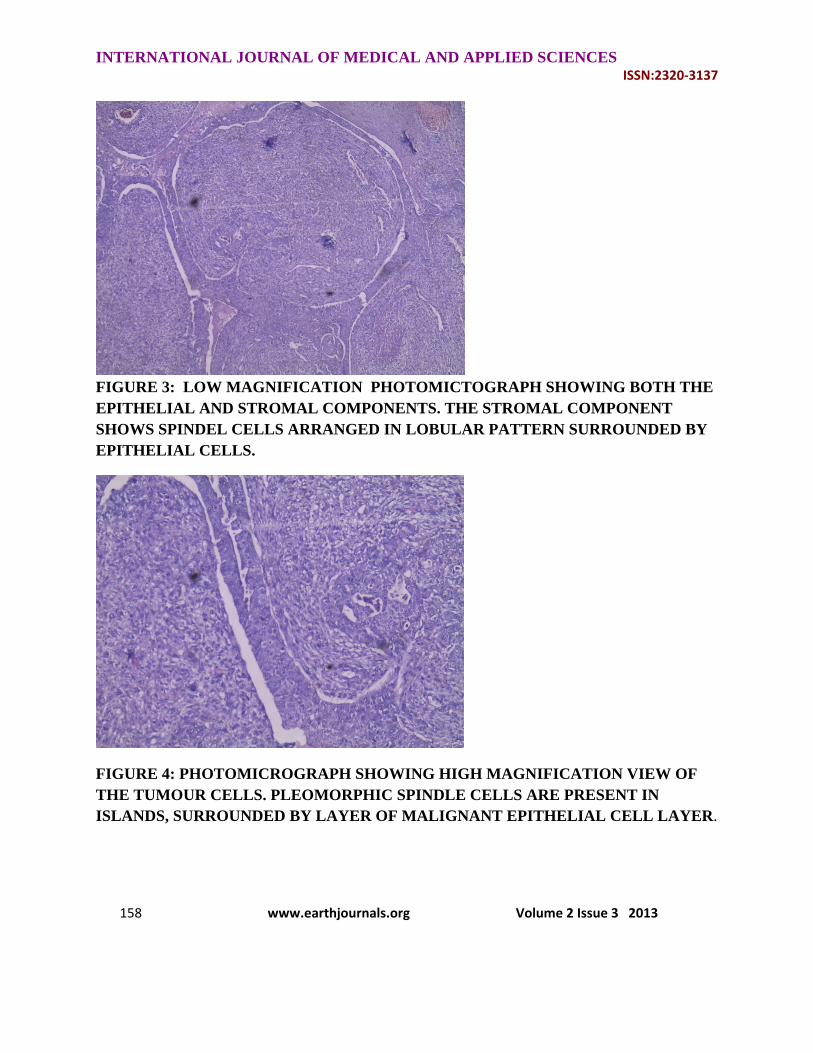
FIGURE 3: LOW MAGNIFICATION PHOTOMICTOGRAPH SHOWING BOTH THE EPITHELIAL AND STROMAL COMPONENTS. THE STROMAL COMPONENT SHOWS SPINDEL CELLS ARRANGED IN LOBULAR PATTERN SURROUNDED BY EPITHELIAL CELLS.
FIGURE 4: PHOTOMICROGRAPH SHOWING HIGH MAGNIFICATION VIEW OF THE TUMOUR CELLS. PLEOMORPHIC SPINDLE CELLS ARE PRESENT IN ISLANDS, SURROUNDED BY LAYER OF MALIGNANT EPITHELIAL CELL LAYER.

INTERNATIONAL JOURNAL OF MEDICAL AND APPLIED SCIENCES ISSN:2320‐3137
159 www.earthjournals.org Volume 2 Issue 3 2013
FIGURE 5: IHC STAINING FOR CYTOKERATIN MARKER SHOW POSITIVITY IN THE EPITHELIAL COMPONENT
DISCUSSION
Carcinosarcoma of the breast (metaplastic, biphasic metaplastic, metaplastic sarcomatoid carcinoma, sarcomatoid carcinoma) is an aggressive, rare neoplasm. The true definition of metaplastic carcinoma of the breast is a tumour of malignant epithelial tissue (carcinoma) mixed with malignant cells of mesenchymal origin (sarcoma) with apparent histologic and cytologic features present on light microscopy and Immunohistochemical testing [3]. Indeed, this tumour type is often referred to as metaplastic breast cancer, characterized as an unusual and uncommon neoplasm that is comprised by an admixture of two or more components [7] The tumour components may be homogeneously adenosquamous, or heterogeneously epithelial (adenocarcinoma) and mesenchymal (matrix, spindle cell and sarcomatous) in origin [7]. However, it seems more appropriate to term all breast
carcinomas with obvious carcinomatous and sarcomatous features as biphasic metaplastic sarcomatoid carcinoma (MSC)
Regardless of the name given to this entity, most metaplastic tumours of the breast are poorly differentiated, high grade, highly cellular, with mitotically active pleomorphic spindle cells. The majority are estrogen and progesterone receptor negative, and HER2-neu negative by immunohistochemistry [9]. The clinical and pathologic features of metaplastic breast carcinomas are important to distinguish from other types of uncommon breast malignancies such as spindle cell carcinoma, matrix producing carcinoma, fibrosarcoma, osteosarcoma, malignant fibrous histiocytoma, phylloides tumor and stromal sarcoma as their behavior, response to treatment and survival rates differ greatly. Clinical features of metaplastic breast cancer are similar to those patients with invasive ductal carcinoma. Recurrence can be rapid as the primary tumour is aggressive, thus mandating close interval follow-up after resection. Pulmonary metastasis is more common than

INTERNATIONAL JOURNAL OF MEDICAL AND APPLIED SCIENCES ISSN:2320‐3137
160 www.earthjournals.org Volume 2 Issue 3 2013
brain, skeletal or hepatic metastasis, and the prognosis for these patients is poor [3]. Outcomes for local recurrences are somewhat improved when surgical resection is achievable. In general, the recommended treatment options have followed the established NCCN guidelines for patients with invasive breast cancer. In the majority of the reported cases, mastectomy with or without axillary node dissection was performed, followed by post-operative chemotherapy and radiation therapy in various combinations.
Adjuvant hormonal therapy and chemotherapy is based upon the receptor status of the primary tumor and is an important tool in treatment recommendations. The HER1/EGFR receptor is reported to be over-expressed in the majority of metaplastic sarcomatoid carcinomas of the breast and should be included in the initial evaluation of the various tumors which are described under this classification. The results may then be utilized to tailor the adjuvant therapy based upon these findings. New treatment opportunities may exist with the development of agents targeting the EGFR receptor such as gefitinib (ZD1839, Iressa) and cetuximab (Erbitux)[11,12]
CONCLUSION
Appropriate diagnosis of carcinosarcoma requires a calculated approach on the part of clinician and pathologist. Histopathology, supplemented by immunohistochemistry and hormonal status are mandatory for proper treatment planning.
REFERENCES:
1. Hennessy BT, Giordano S, Broglio K, Duan Z, Trent J, Buchholz TA et al (2006) Biphasic metaplastic sarcomatoid carcinoma of the breast. Annals of Oncology 17:605
2. Wick MR, Swanson PE (1993) Carcinosarcomas: current perspectives and an historical review of nosological concepts. Semin Diagn Pathol 10:118
3. Tokudome N, Sakamoto G, Sakai T, Sarumaru S, Okuyama N, Hori F et al (2005) A case of carcinosarcoma of the breast. Breast Cancer 12:149
4. Gogas J, Kouskos E, Markopoulos C, Mantas D, Antonopoulou Z, Kontzoglou K et al (2003) Carcinosarcoma of the breast: report of two cases. Eur J Gynaecol Oncol 24:93
5. Wada H, Enomoto T, Tsujimoto M, Nomura T, Murata Y, Shroyer KR (1998) Carcinosarcoma of the breast: molecular-biological study for analysis of histogenesis. Human Pathol 29:1324
6. Perret L, Chaubert P, Hessler D, Guillou L (1998) Primary heterologous carcinosarcoma (metaplastic carcinoma) of the urinary bladder: a clinicopathologic, immunohistochemical, and ultrastructural analysis of eight cases and a review of the literature. Cancer 82:1535
7. Tsekeris P, Dimou S (2000) Synchronous endometrial carcinosarcoma and breast carcinoma: a case report. Eur J Gynaecol Oncol 21:309
8. Cornette J, Tjalma WA, Buytaert P (2005) Biphasic sarcomatoid carcinoma or carcinosarcoma of the breast: prognosis and therapy. Eur J Gynaecol Oncol 26:514
9. Beatty JD, Atwood M, Tickman R, Reiner M. Metaplastic breast cancer: clinical significance. The American Journal of Surgery. 2006;191:657–664. doi: 10.1016/j.amjsurg.2006.01.038.
10. Tse GM, Tan PH, Putti TC, Lui PCW, Chaiwun B, Law BKB. Metaplastic carcinoma of the breast: a clinicopathologic review. J Clin Pathol. 2006;59:1079–1083. doi: 10.1136/jcp.2005.030536.

INTERNATIONAL JOURNAL OF MEDICAL AND APPLIED SCIENCES ISSN:2320‐3137
161 www.earthjournals.org Volume 2 Issue 3 2013
11. Leibl S, Moinfar F. Metaplastic breast carcinomas are negative for Her-2 but frequently express EGFR (Her-1): potential relevance to adjuvant treatment with EGFR tyrosine kinase inhibitors? J Clin Pathol. 2005;58:700–704. doi: 10.1136/jcp.2004.025
12. Okumo S, Kurebayashi J, Otsuki T, Yamamoto Y, Tanaka K, Sonoo H. Additive antitumor effect of the epidermal growth factor receptor tyrosine kinase inhibitor gefitinib (Iressa, ZD1839) and the antioestrogen fulvestrant (Faslodex, ICI 182,780) in breast cancer cells. Br J Cancer. 2004;12;90(1):236–244.




















