
Initial Diagnosis of Leprosy in Patients Treated by an Ophthalmologist and Confirmation by...
9
Initial Diagnosis of Leprosy in Patients Treated by an Ophthalmologist and Confirmation by Conventional Analysis and Polymerase Chain Reaction Imtiaz A. Chaudhry, MD, PhD, 1 Farrukh A. Shamsi, MPhil, PhD, 2 Elsanusi Elzaridi, MD, 3 Abdulaziz Awad, MD, 4 Hamad Al-Fraikh, MD, 5 Mohammed Al-Amry, MD, 5 Hassan Al-Dhibi, MD, 6 Fenwick C. Riley, MD 7 Purpose: To report the initial diagnosis of leprosy in patients seeking treatment from an ophthalmologist in a tertiary eye care center, its confirmation by histopathologic and polymerase chain reaction analysis, and review of literature. Design: Noncomparative retrospective case series. Participants: Patients with no known history of leprosy who were selected based on either a clinical suspicion or a histopathologic diagnosis and were found to have ocular or periocular lesions suggestive of leprosy. Methods: Review of clinical records of patients with no known history of leprosy seen by an ophthalmologist at a tertiary eye care referral center. Main Outcome Measures: Patient demographics, presenting symptoms and signs, diagnostic studies, complications, and treatment. Results: Among the 6 patients (5 women and 1 man; average age, 55 years), only 2 were found to have leprosy from clinical examination alone. Histopathologic characteristics or demonstration of acid-fast bacilli, suggestive of leprosy, were found in 5 patients. Definite confirmation of leprosy was made by polymerase chain reaction performed on formalin-fixed, paraffin-embedded tissues of 4 patients having suspected leprosy based on clinicohistopathologic examination results. Conclusions: The diagnosis of leprosy relies on the clinical symptom complex, epidemiologic factors, and demonstration of acid-fast bacilli in the tissue sample. Considering that the global leprosy population is 12 million, a patient with leprosy may be found anywhere. The ophthalmologist may be the first one to encounter such patient, in which case suspicion and detection of ocular findings may lead to early treatment of the infection. Polymerase chain reaction may be a new tool in the definite diagnosis of leprosy when suspicion of the diseases is raised by clinicohistopathologic studies. Ophthalmology 2007;114:1904 –1911 © 2007 by the American Academy of Ophthalmology. Leprosy, or Hansen’s disease, is a chronic contagious dis- ease caused by Mycobacterium leprae, a strongly acid-fast, rod-shaped bacterium. It is one of the oldest recorded in- fectious diseases affecting humans with potentially incapac- itating neurologic and social sequelae. 1,2 Leprosy has been reported to have the highest incidence of ocular involve- ment of any human bacterial infections and represents a leading cause of blindness in countries such as India, Nepal, and Brazil. 3–5 It is estimated that leprosy affects 10 to 12 Originally received: October 10, 2006. Final revision: February 11, 2007. Accepted: February 12, 2007. Available online: May 25, 2007. Manuscript no. 2006-1147. 1 Oculoplastic and Orbit Division, King Khaled Eye Specialist Hospital, Riyadh, Saudi Arabia. 2 Research Department, King Khaled Eye Specialist Hospital, Riyadh, Saudi Arabia. 3 Royal Victoria Eye Infirmary, Newcastle-upon-Tyne, United Kingdom. 4 Pediatric Division, King Khaled Eye Specialist Hospital, Riyadh, Saudi Arabia. 5 Anterior Segment Division, King Khaled Eye Specialist Hospital, Riy- adh, Saudi Arabia. 6 Vitreoretinal Division, King Khaled Eye Specialist Hospital, Riyadh, Saudi Arabia. 7 Department of Pathology, King Khaled Eye Specialist Hospital, Riyadh, Saudi Arabia. Drs Chaudhry and Shamsi were equal contributors. Presented at: American Academy of Ophthalmology Annual Meeting, November 2006, Las Vegas, Nevada. The authors have no propriety interests in the study. Correspondence to Imtiaz A. Chaudhry, MD, PhD, Oculoplastic and Orbit Division, King Khaled Eye Specialist Hospital, P.O. Box 7191, Riyadh 11462, Saudi Arabia. E-mail: [email protected]. 1904 © 2007 by the American Academy of Ophthalmology ISSN 0161-6420/07/$–see front matter Published by Elsevier Inc. doi:10.1016/j.ophtha.2007.02.011
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Initial Diagnosis of Leprosy in Patients Treated by an Ophthalmologist and Confirmation by...
Initial Diagnosis of Leprosy in PatientsTreated by an Ophthalmologist andConfirmation by Conventional Analysisand Polymerase Chain Reaction
Imtiaz A. Chaudhry, MD, PhD,1 Farrukh A. Shamsi, MPhil, PhD,2 Elsanusi Elzaridi, MD,3
Abdulaziz Awad, MD,4 Hamad Al-Fraikh, MD,5 Mohammed Al-Amry, MD,5 Hassan Al-Dhibi, MD,6
Fenwick C. Riley, MD7
Purpose: To report the initial diagnosis of leprosy in patients seeking treatment from an ophthalmologist ina tertiary eye care center, its confirmation by histopathologic and polymerase chain reaction analysis, and reviewof literature.
Design: Noncomparative retrospective case series.Participants: Patients with no known history of leprosy who were selected based on either a clinical suspicion
or a histopathologic diagnosis and were found to have ocular or periocular lesions suggestive of leprosy.Methods: Review of clinical records of patients with no known history of leprosy seen by an ophthalmologist
at a tertiary eye care referral center.Main Outcome Measures: Patient demographics, presenting symptoms and signs, diagnostic studies,
complications, and treatment.Results: Among the 6 patients (5 women and 1 man; average age, 55 years), only 2 were found to have
leprosy from clinical examination alone. Histopathologic characteristics or demonstration of acid-fast bacilli,suggestive of leprosy, were found in 5 patients. Definite confirmation of leprosy was made by polymerase chainreaction performed on formalin-fixed, paraffin-embedded tissues of 4 patients having suspected leprosy basedon clinicohistopathologic examination results.
Conclusions: The diagnosis of leprosy relies on the clinical symptom complex, epidemiologic factors, anddemonstration of acid-fast bacilli in the tissue sample. Considering that the global leprosy population is 12million, a patient with leprosy may be found anywhere. The ophthalmologist may be the first one to encountersuch patient, in which case suspicion and detection of ocular findings may lead to early treatment of the infection.Polymerase chain reaction may be a new tool in the definite diagnosis of leprosy when suspicion of the diseasesis raised by clinicohistopathologic studies. Ophthalmology 2007;114:1904–1911 © 2007 by the AmericanAcademy of Ophthalmology.
Leprosy, or Hansen’s disease, is a chronic contagious dis-ease caused by Mycobacterium leprae, a strongly acid-fast,rod-shaped bacterium. It is one of the oldest recorded in-fectious diseases affecting humans with potentially incapac-
Originally received: October 10, 2006.Final revision: February 11, 2007.Accepted: February 12, 2007.Available online: May 25, 2007. Manuscript no. 2006-1147.1 Oculoplastic and Orbit Division, King Khaled Eye Specialist Hospital,Riyadh, Saudi Arabia.2 Research Department, King Khaled Eye Specialist Hospital, Riyadh,Saudi Arabia.3 Royal Victoria Eye Infirmary, Newcastle-upon-Tyne, United Kingdom.4 Pediatric Division, King Khaled Eye Specialist Hospital, Riyadh, SaudiArabia.5 Anterior Segment Division, King Khaled Eye Specialist Hospital, Riy-
adh, Saudi Arabia.1904 © 2007 by the American Academy of OphthalmologyPublished by Elsevier Inc.
itating neurologic and social sequelae.1,2 Leprosy has beenreported to have the highest incidence of ocular involve-ment of any human bacterial infections and represents aleading cause of blindness in countries such as India, Nepal,and Brazil.3–5 It is estimated that leprosy affects 10 to 12
6 Vitreoretinal Division, King Khaled Eye Specialist Hospital, Riyadh,Saudi Arabia.7 Department of Pathology, King Khaled Eye Specialist Hospital, Riyadh,Saudi Arabia.
Drs Chaudhry and Shamsi were equal contributors.
Presented at: American Academy of Ophthalmology Annual Meeting,November 2006, Las Vegas, Nevada.
The authors have no propriety interests in the study.
Correspondence to Imtiaz A. Chaudhry, MD, PhD, Oculoplastic and OrbitDivision, King Khaled Eye Specialist Hospital, P.O. Box 7191, Riyadh
11462, Saudi Arabia. E-mail: [email protected].ISSN 0161-6420/07/$–see front matterdoi:10.1016/j.ophtha.2007.02.011

Chaudhry et al � Initial Diagnosis of Ocular Leprosy
million people worldwide, of whom 3% to 7% becomevisually disabled as a result of the disease.2,4–7 The diseaseis widespread in tropical and subtropical countries of Asia,Africa, and Latin America. Because of the rarity of leprosyin developed countries, there is a lack of awareness of themanifestations of ocular and periocular leprosy, and signssuch as corneal scarring, uveitis, and eyelid anomalies sel-dom are considered in the differential diagnosis. Consider-ing current levels of travel between countries and global-ization, patients with leprosy may be seen anywhere in theworld.
The diagnosis of leprosy frequently is delayed becauseclinicians fail to recognize the early symptoms and signsof the disease.8 An important feature of M. leprae is that itis the only mycobacterium that cannot be grown in vitro andtherefore cannot be diagnosed by culture studies. Further,the diagnosis often relies on microscopic detection of acid-fast bacilli in tissue samples. Unfortunately, the sensitivityof acid-fast bacilli staining is low and requires at least 104
organisms per gram of tissue for reliable detection.9 Inaddition, acid-fast staining detects the organism only at thedegeneration phase of its development, therefore limitingthe identification of all the organisms that may be present inthe tissue. Serologic tests based on specific M. leprae anti-gens may be helpful in the detection of M. leprae infec-tions.10 However, these assays do not reflect all clinicalinfections because most of the patients at the paucibacillarystage of infection do not develop significant levels of anti-body response.11 However, molecular probes have shown agreat potential for detection and identification of M. lepraein tissues with more sensitivity than any other method.12–14
In particular, DNA amplification of various genomic se-quences of M. leprae through polymerase chain reaction hasbeen found to be useful in detecting very low numbers ofbacteria.15–18 More recently, the detection of M. leprae, itscomponents, or both by polymerase chain reaction in fixedtissues has been found to be useful in examining nonocularspecimens for the presence of M. leprae, which along withhistologic analysis has helped in arriving at a definitive andrapid diagnosis in clinically suspected cases.19,20 Herein, theauthors present their experience in the diagnosis of ocularand periocular leprosy in patients seeking treatment at atertiary eye care center with no known prior history ofleprosy. These patients were suspected of having leprosybased on clinical or histopathologic examination results,and 4 of them were confirmed to have leprosy by the useof conventional polymerase chain reaction performed onformalin-fixed paraffin-embedded tissues.
Patients and Methods
Medical records of patients seen at King Khaled Eye Spe-cialist Hospital in Riyadh, Saudi Arabia, a tertiary eye carecenter, over a 5-year period with a final diagnosis of leprosywere reviewed for the presenting clinical symptoms, signs,diagnostic studies, and surgical procedures performed. Pa-tients were included in the study if there was clinical,histopathologic, or positive polymerase chain reaction find-
ings consistent with leprosy. The clinical charts were re-viewed for the patients’ demographics such as age, gender,and presence of clinical, histopathologic, or genetic evi-dence of leprosy. Only patients fulfilling the clinical, his-topathologic, or genetic criteria for leprosy were included inthe study. Information regarding their past medical or sur-gical history was recorded. Best-corrected Snellen visualacuity, as well as ocular examination results, of these pa-tients were reviewed from their first presentation until thelast follow-up examination. Operative notes were reviewedfor procedures performed in patients in whom any surgeryhad been performed. In patients in whom leprosy was sus-pected based on the presence of acid-fast bacilli or charac-teristic granulomatous tissue reaction from the paraffin-embedded slides, further genetic testing was carried out.Specifically, DNA from the formalin-fixed, paraffin-embeddedtissue was extracted by standard proteinase K digestionfollowed by phenolchloroform extraction and precipitationby isopropanol and ammonium acetate. Each specimen wasamplified by the polymerase chain reaction method using apair of commercially synthesized (Sigma-Genosys Ltd.,Poole, United Kingdom) primers to produce a 250-bp frag-ment of the M. leprae 85 A–C intergenic region (sense5=-ATA CTG TTC ACG CAG CAT CG-3= and antisense5=-GTT GAA GGC ATC AAG CAG GT-3=). The 85 A–Cproduct comprises the region between the fbpA and fbpCgenes. Polymerase chain reaction was performed in a DyadDNA engine (MJ Research) thermal cycler. The positivecontrols used were 85 A–C cloned fragments of M. lepraeand purified DNA from M. leprae.
Results
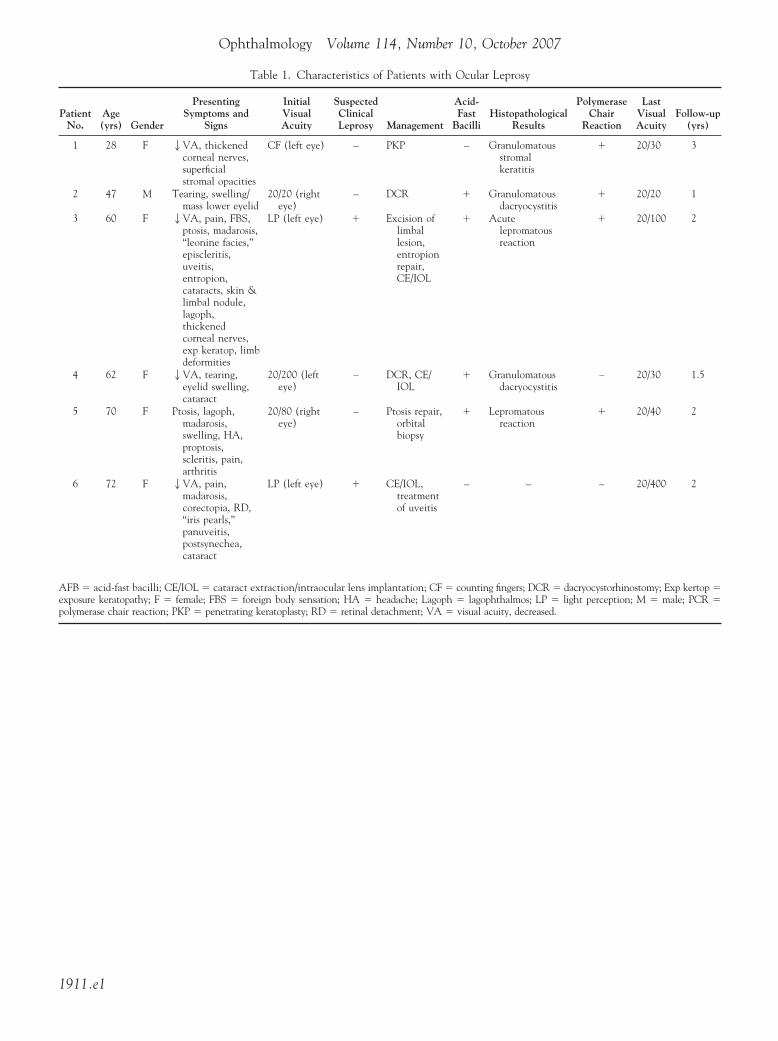
The characteristics of the 6 patients (5 women and 1 man)in whom the final diagnosis of leprosy was made are pre-sented in Table 1 (available at http://aaojournal.org). Theaverage age of these patients was 55 years (range, 28–72years). Presenting symptoms and signs included decreasedvisual acuity in 4 patients, swelling and mass lesions in 4patients, pain in 3 patients, cataracts in 3 patients, andthickened corneal nerves, lagophthalmos, tearing, ptosis,madarosis, and uveitis in 2 patients each. Other symptomsand signs included proptosis, corneal stromal opacities,limbal and skin nodules, iris pearls (Fig 1), panuveitis andretinal detachment, limbs deformities, and leonine facies(Fig 2) in 1 patient each. Presenting visual acuity rangedfrom 20/20 in 1 patient to light perception vision in 2patients. Only 2 patients (patients 3 and 6; Table 1) weresuspected of having leprosy based on clinical evidence ofiris pearls, or leonine facies. One patient underwent pene-trating keratoplasty to improve her vision, and 3 patientsunderwent cataract surgery and implantation of intraocularlenses. Two patients required dacryocystorhinostomies and1 patient required ptosis repair and underwent an orbitalbiopsy, performed at the same time. Two patients requiredlimbal or eyelid margin lesion excision. One patient re-quired entropion repair and 1 patient was treated for panu-veitis. A clinical diagnosis of leprosy was made in only 2patients based on history and clinicalexamination results,
including slit-lamp biomicroscopy (patients 3 and 6; Table 1).1905
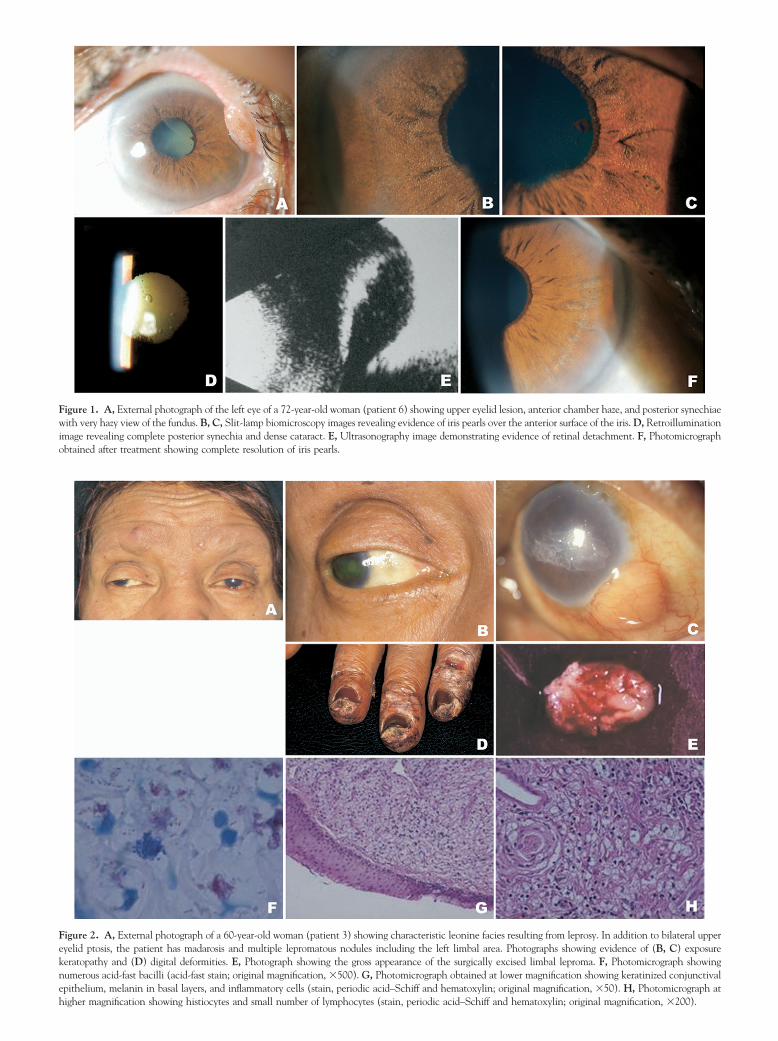
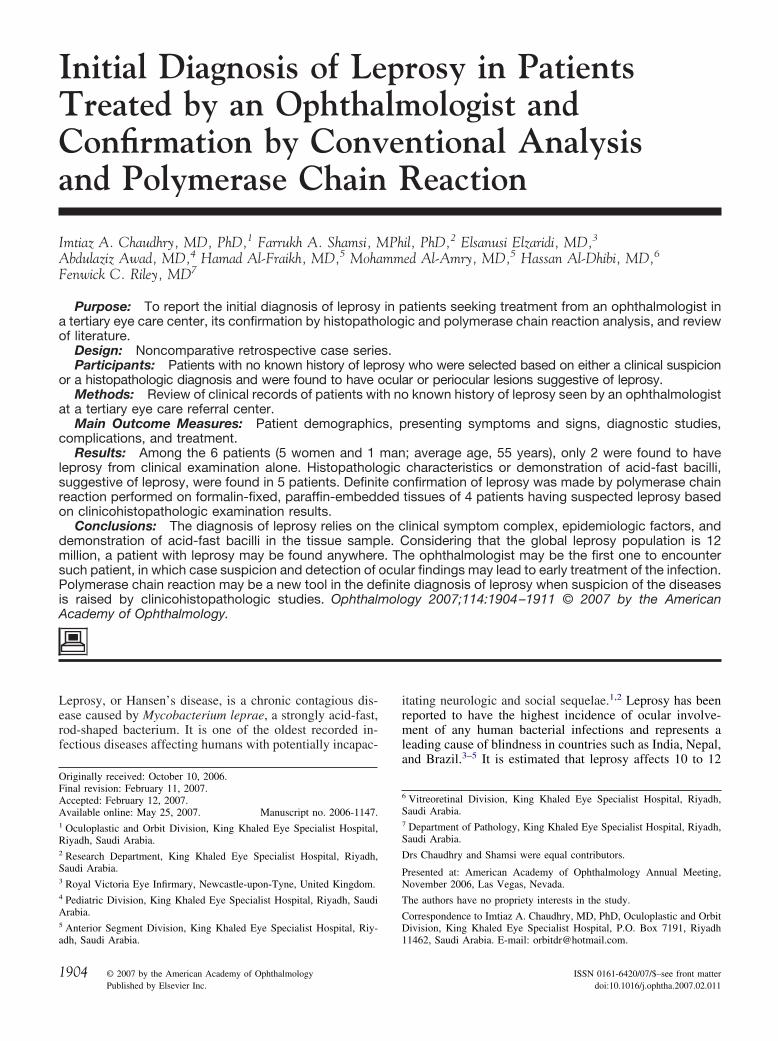
Figure 1. A, External photograph of the left eye of a 72-year-old woman (patient 6) showing upper eyelid lesion, anterior chamber haze, and posterior synechiaewith very hazy view of the fundus. B, C, Slit-lamp biomicroscopy images revealing evidence of iris pearls over the anterior surface of the iris. D, Retroilluminationimage revealing complete posterior synechia and dense cataract. E, Ultrasonography image demonstrating evidence of retinal detachment. F, Photomicrograph
obtained after treatment showing complete resolution of iris pearls.Figure 2. A, External photograph of a 60-year-old woman (patient 3) showing characteristic leonine facies resulting from leprosy. In addition to bilateral uppereyelid ptosis, the patient has madarosis and multiple lepromatous nodules including the left limbal area. Photographs showing evidence of (B, C) exposurekeratopathy and (D) digital deformities. E, Photograph showing the gross appearance of the surgically excised limbal leproma. F, Photomicrograph showingnumerous acid-fast bacilli (acid-fast stain; original magnification, �500). G, Photomicrograph obtained at lower magnification showing keratinized conjunctivalepithelium, melanin in basal layers, and inflammatory cells (stain, periodic acid–Schiff and hematoxylin; original magnification, �50). H, Photomicrograph at
higher magnification showing histiocytes and small number of lymphocytes (stain, periodic acid–Schiff and hematoxylin; original magnification, �200).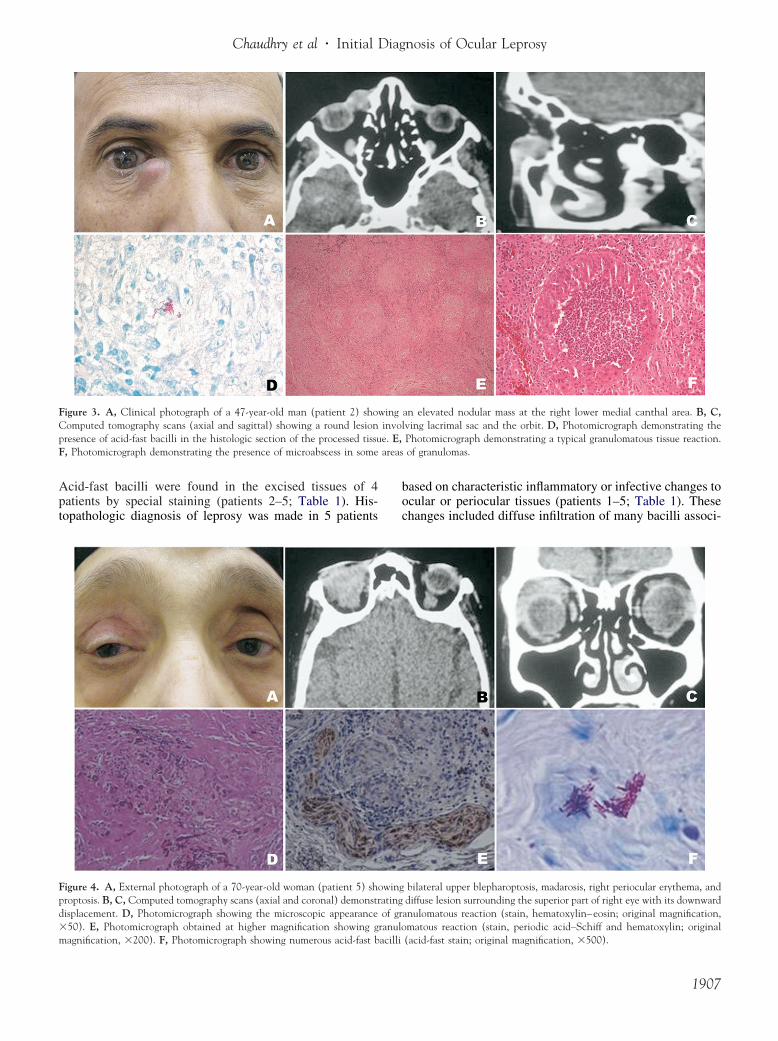
areas
Chaudhry et al � Initial Diagnosis of Ocular Leprosy
Acid-fast bacilli were found in the excised tissues of 4patients by special staining (patients 2–5; Table 1). His-topathologic diagnosis of leprosy was made in 5 patients
Figure 3. A, Clinical photograph of a 47-year-old man (patient 2) shoComputed tomography scans (axial and sagittal) showing a round lesionpresence of acid-fast bacilli in the histologic section of the processed tissuF, Photomicrograph demonstrating the presence of microabscess in some
Figure 4. A, External photograph of a 70-year-old woman (patient 5) shproptosis. B, C, Computed tomography scans (axial and coronal) demonstrdisplacement. D, Photomicrograph showing the microscopic appearance�50). E, Photomicrograph obtained at higher magnification showing g
magnification, �200). F, Photomicrograph showing numerous acid-fast bacillibased on characteristic inflammatory or infective changes toocular or periocular tissues (patients 1–5; Table 1). Thesechanges included diffuse infiltration of many bacilli associ-
an elevated nodular mass at the right lower medial canthal area. B, C,lving lacrimal sac and the orbit. D, Photomicrograph demonstrating thePhotomicrograph demonstrating a typical granulomatous tissue reaction.of granulomas.
bilateral upper blepharoptosis, madarosis, right periocular erythema, anddiffuse lesion surrounding the superior part of right eye with its downward
anulomatous reaction (stain, hematoxylin–eosin; original magnification,matous reaction (stain, periodic acid–Schiff and hematoxylin; original
winginvoe. E,
owingatingof gr
ranulo
(acid-fast stain; original magnification, �500).1907
Ophthalmology Volume 114, Number 10, October 2007
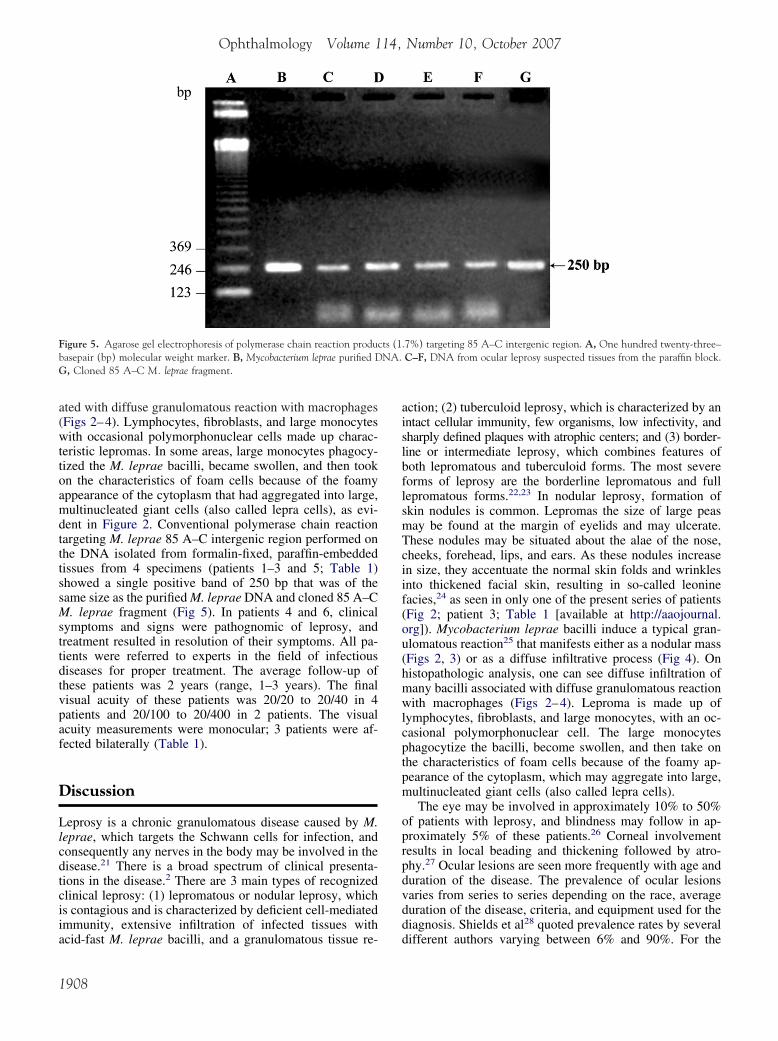
ated with diffuse granulomatous reaction with macrophages(Figs 2–4). Lymphocytes, fibroblasts, and large monocyteswith occasional polymorphonuclear cells made up charac-teristic lepromas. In some areas, large monocytes phagocy-tized the M. leprae bacilli, became swollen, and then tookon the characteristics of foam cells because of the foamyappearance of the cytoplasm that had aggregated into large,multinucleated giant cells (also called lepra cells), as evi-dent in Figure 2. Conventional polymerase chain reactiontargeting M. leprae 85 A–C intergenic region performed onthe DNA isolated from formalin-fixed, paraffin-embeddedtissues from 4 specimens (patients 1–3 and 5; Table 1)showed a single positive band of 250 bp that was of thesame size as the purified M. leprae DNA and cloned 85 A–CM. leprae fragment (Fig 5). In patients 4 and 6, clinicalsymptoms and signs were pathognomic of leprosy, andtreatment resulted in resolution of their symptoms. All pa-tients were referred to experts in the field of infectiousdiseases for proper treatment. The average follow-up ofthese patients was 2 years (range, 1–3 years). The finalvisual acuity of these patients was 20/20 to 20/40 in 4patients and 20/100 to 20/400 in 2 patients. The visualacuity measurements were monocular; 3 patients were af-fected bilaterally (Table 1).
Discussion
Leprosy is a chronic granulomatous disease caused by M.leprae, which targets the Schwann cells for infection, andconsequently any nerves in the body may be involved in thedisease.21 There is a broad spectrum of clinical presenta-tions in the disease.2 There are 3 main types of recognizedclinical leprosy: (1) lepromatous or nodular leprosy, whichis contagious and is characterized by deficient cell-mediatedimmunity, extensive infiltration of infected tissues with
Figure 5. Agarose gel electrophoresis of polymerase chain reaction produbasepair (bp) molecular weight marker. B, Mycobacterium leprae purified DG, Cloned 85 A–C M. leprae fragment.
acid-fast M. leprae bacilli, and a granulomatous tissue re-
1908
action; (2) tuberculoid leprosy, which is characterized by anintact cellular immunity, few organisms, low infectivity, andsharply defined plaques with atrophic centers; and (3) border-line or intermediate leprosy, which combines features ofboth lepromatous and tuberculoid forms. The most severeforms of leprosy are the borderline lepromatous and fulllepromatous forms.22,23 In nodular leprosy, formation ofskin nodules is common. Lepromas the size of large peasmay be found at the margin of eyelids and may ulcerate.These nodules may be situated about the alae of the nose,cheeks, forehead, lips, and ears. As these nodules increasein size, they accentuate the normal skin folds and wrinklesinto thickened facial skin, resulting in so-called leoninefacies,24 as seen in only one of the present series of patients(Fig 2; patient 3; Table 1 [available at http://aaojournal.org]). Mycobacterium leprae bacilli induce a typical gran-ulomatous reaction25 that manifests either as a nodular mass(Figs 2, 3) or as a diffuse infiltrative process (Fig 4). Onhistopathologic analysis, one can see diffuse infiltration ofmany bacilli associated with diffuse granulomatous reactionwith macrophages (Figs 2–4). Leproma is made up oflymphocytes, fibroblasts, and large monocytes, with an oc-casional polymorphonuclear cell. The large monocytesphagocytize the bacilli, become swollen, and then take onthe characteristics of foam cells because of the foamy ap-pearance of the cytoplasm, which may aggregate into large,multinucleated giant cells (also called lepra cells).
The eye may be involved in approximately 10% to 50%of patients with leprosy, and blindness may follow in ap-proximately 5% of these patients.26 Corneal involvementresults in local beading and thickening followed by atro-phy.27 Ocular lesions are seen more frequently with age andduration of the disease. The prevalence of ocular lesionsvaries from series to series depending on the race, averageduration of the disease, criteria, and equipment used for thediagnosis. Shields et al28 quoted prevalence rates by several
.7%) targeting 85 A–C intergenic region. A, One hundred twenty-three–C–F, DNA from ocular leprosy suspected tissues from the paraffin block.
cts (1NA.
different authors varying between 6% and 90%. For the

Chaudhry et al � Initial Diagnosis of Ocular Leprosy
most part, they found that the patients with more severephysical deformities had more severe ocular involvement.Hornblass,29 however, did not find any correlation betweenthe severity of the systemic disease and ocular signs. Healso did not find any difference between lepromatous, tu-berculoid, or mixed types of leprosy in his study of SouthVietnamese patients. The reasons for this difference may bebias in the populations studied, the efficiency of the controlprogram, racial variation, the average duration of the dis-ease, or the average age of the group studied.30 A survey of100 patients with leprosy from Brazil revealed that 72% ofthem had ocular involvement, among whom 38% had sight-threatening complications that included, keratitis, iritis, lag-ophthalmos, and secondary glaucoma.28 Lagophthalmoswas found in 13% of these patients and was attributed topalsy of the orbicularis oculi muscle, and most of them hadectropion of lower eyelid.28 Hornblass29 examined the eyesof 51 randomly selected patients with biopsy-proven lep-rosy and found that 76% of them had ocular involvement.All the patients in the studies by Shields et al and Hornblasshad known leprosy, and the ocular complications usuallywere quite apparent. The current study is different fromprevious studies because none of the patients had a knownhistory of leprosy and sought treatment from an ophthal-mologist for ocular symptoms. Leprosy is not prevalent inthe Kingdom of Saudi Arabia; however, migrant workersfrom India, Nepal, and other African countries may infectthe local population.31–33 At present, leprosy is one of thereportable diseases in the kingdom, and when new cases arediscovered, they are treated according to World HealthOrganization guidelines.
In leprosy, ophthalmic manifestations may include ex-ternal ocular signs such as lagophthalmos as well as intraoc-ular findings such as uveitis. From the largest survey ofNorth American outpatients in the multidrug therapy era,48% of subjects had one or more sight-threatening compli-cations as a result of their disease.2 Lagophthalmos wasfound in 11% of these patients. Uveitis was found in 7% ofthe patients, either as a result of viable organisms infiltratingthe anterior chamber or due to type II reaction that producesa local inflammatory reaction.2 Although a degree of cor-neal sensory loss can be detected in some patients withlagophthalmos of several years’ duration, sensory loss onthe cornea is more a feature of long-standing lepromatousdisease where bacillary infiltration is more likely to befound in the ciliary nerve endings running toward the lim-bus, where there may have been repeated episodes of iri-tis.34 Leprosy produces a variety of corneal changes thatinclude corneal hypoesthesia, thickened corneal nerves, su-perficial stromal keratitis, pannus, interstitial keratitis, nod-ular keratitis, exposure keratitis, and other secondarychanges. Corneal involvement by leprosy begins peripher-ally. Characteristically, the inflammation initially involvesthe superotemporal quadrant and progresses to more gener-alized corneal involvement.35
Ocular complications resulting from leprosy are the re-sult of primary infection of the eye, and secondary damageis the result of neural involvement. Primary infection of theeye may result in prominent corneal nerves, conjunctivitis,
punctate keratitis, scleral nodules, and chronic uveitis. Thecornea seems to be the most vulnerable of the ocular tissues;5 of the 6 patients in the present study had corneal involve-ment either directly or because of exposure keratopathy(Table 1 [available at http://aaojournal.org]). Inflammationof the corneal nerves produces opacification and beadingcharacteristic of leprosy. Central corneal stromal infiltrationby macrophages that phagocytose M. leprae bacilli eventu-ally form small lepromas in the superficial stroma that arepathognomonic of leprosy. These characteristic histopatho-logic changes were observed in the corneal button of apatient in the present study after keratoplasty for stromalopacities (patient 1; Table 1). Because no acid-fast bacilliwere seen on histopathologic sections of the excised tissue,polymerase chain reaction on the fixed tissue was carriedout to confirm the definite diagnosis of leprosy. However,patient 6 had pathognomic leprosy (Fig 1) and iris pearlsthat disappeared, and the patient’s visual acuity improvedafter treatment. In one of the studies, the most commonlyobserved corneal lesions were superficial keratitis, whichoccurred in more than 34% of the cases.36 The superficialkeratitis of leprosy may be overlooked easily. Loss of cor-neal sensitivity, exposure, and diminished tear productionmake the cornea susceptible to secondary bacterial, viral,and fungal infections. Involvement of the ophthalmic divisionof the trigeminal nerve further results in corneal anesthesia.
After the cornea, the iris is the structure that is mostcommonly involved clinically in ocular leprosy. Iris atrophyis a common finding and is represented by flattening of theiris pattern as a whole and loss of the anterior iris architec-ture or stroma. As seen in 2 of the patients (patients 3 and6; Table 1 [available at http://aaojournal.org]), acute uveitismay be a common ophthalmic manifestation of leprosy.Direct bacterial invasion of the iris ciliary body producesthe chronic iritis that is considered to be the most commoncause of visual impairment in leprosy. A distinguishingcharacteristic of chronic leprous iritis is the presence of irislepromas, clinically called iris pearls. They typically appearas numerous discrete small white bodies in the pupillaryportion of the iris stroma, which are pathognomonic ofleprous iritis.37 These iris pearls were noted in only 1 of thepatients at initial presentation, which helped in pinpointingthe correct diagnosis (Fig 1). Histologically, the iris pearlsconsist of tightly packed bacilli within mononuclear cellswith little accompanying foreign body reaction or inflam-matory changes. Electron microscopy shows M. leprae cellsinfiltrating the iris stroma and destroying nonmyelinatednerve fibers.38 Frequently, chronic uveitis can lead to visualimpairment through the development of cataracts, glau-coma, or macular edema.39 According to a 10-year follow-up study, cataracts were found to be the main progressivelesions in patients with leprosy who had undergone multi-drug therapy.40 Cataract remains a major problem in lep-rosy; 3 of the patients required cataract surgery to improvetheir vision. Chronic granulomatous iridocyclitis probablyrepresents an antigen–antibody reaction and can be severe,resulting in exudative retinal detachment, as seen in 1 of thepatients (patient 6; Table 1).
Ocular adnexa including eyebrows and eyelids are in-volved frequently with loss of hair (madarosis), as seen in 3
of the patients. The eyelids and adnexa may be damaged in1909

Ophthalmology Volume 114, Number 10, October 2007
a variety of ways that include impairment of lacrimal sys-tem drainage and impairment of eyelid closure,41 as ob-served in 5 of the 6 patients. Some authors have reported theoccurrence of chronic dacryocystitis and dacryoadenitis inleprosy.35 Harley36 found 4 patients with purulent dacryo-cystitis in his review of 150 patients with ocular leprosyfrom Panama, but he suspected that the involvement of thelacrimal system was much more common. Paralytic ectro-pion may result from atonicity and relaxation of the lowereyelid.42 Ptosis, as seen in 2 of the patients, is an unusualmanifestation of the disease. Ptosis may result from eitherIIIrd cranial nerve involvement or infiltration of the eye-lid.25,43,44 Neural involvement of the IIIrd cranial nerve isexceedingly rare.
Recommendations for systemic treatment for leprosydepend on the histopathologic form of the disease. Multi-drug treatment regimens are recommended by the WorldHealth Organization because of dapsone-resistant strains ofM. leprae.45–47 The World Health Organization initiativewith multidrug therapy for treating leprosy has resulted inreduction of the numbers of infected individuals world-wide.24,47 Multidrug regimens for treating leprosy combinedaily treatment with 100 mg dapsone and 50 mg clofazi-mine (plus 300 mg every month), with intermittent treat-ment with 600 mg rifampin every month for multibacillarydisease (full lepromatous, borderline lepromatous, and bor-derline disease) and daily treatment with dapsone withintermittent treatment with rifampin for paucibacillary dis-ease (full tuberculoid and borderline tuberculoid disease).Treatment of erythema nodosum leprosum depends on itsseverity. Treatment is successful with thalidomide (300 mgdaily tapered to 50–100 mg), prednisone (60–80 mg dailytapered as condition permits), or 300 mg clofazimine daily.24
High-dose corticosteroids and clofazimine is effective in thetreatment of reversal reaction. Surgical intervention often isnecessary to prevent exposure keratopathy in chronic cases.For repeated iridocyclitis, clofazimine and thalidomide canbe valuable. Even after completed multidrug therapy, pa-tients may continue to experience new ocular complicationsthat require periodic monitoring.48
The diagnosis of leprosy frequently is delayed becauseclinicians fail to recognize the early symptoms and signs ofthe disease. Suspicion of the disease, proper elicitation ofhistory, careful ocular examination, and appropriate diag-nostic tests may help with early diagnosis and treatment ofleprosy to prevent permanent damage to the ocular andperiocular adnexa. The ophthalmologist may be the first oneto encounter a leprosy patient because of corneal ulcerationresulting from exposure or uveitis. It is important to exam-ine such patients for characteristic features of leprosy, suchas skin-thickening facial features, limb deformities, andswollen peripheral nerves. The detection of these clinicalfindings can lead to early diagnosis of leprosy, which maylimit ocular damage and prevent potential infection inhousehold contacts. The role of the ophthalmologist there-fore should be extended beyond the traditional provision ofcare at a tertiary level. Ophthalmologists need to be awarethat ocular complications often arise from inattention orneglect of simple problems early in the disease. This study
is an effort to maintain a level of necessary awareness of the1910
problem of leprosy among the ophthalmologists. High levelof suspicion and early diagnosis and treatment may preventsystemic and ocular complications. Because the organismcannot be grown in vitro, the diagnosis of leprosy relies onthe clinical symptom complex, epidemiologic factors, anddemonstration of acid-fast bacilli in the tissue sample. Thepresent results suggest that polymerase chain reaction on theformalin-fixed, paraffin-embedded ocular tissue may bepractical in the diagnosis of suspected leprosy when othermeans of identification are not helpful. To the authors’knowledge, this is the first study that reports the confirma-tion of leprosy by genetic methods by the use of polymerasechain reaction on formalin-fixed, paraffin-embedded tissuein cases of suspected ocular leprosy based on clinicohis-topathologic evaluation results.
References
1. Sears ML. Ocular leprosy. Am J Ophthalmol 1958;46:359–61.2. Dana MR, Hochman MA, Viana MA, et al. Ocular manifes-
tations of leprosy in a noninstitutionalized community in theUnited States. Arch Ophthalmol 1994;112:626–9.
3. Barros JM DE. The ocular complications of leprosy. Am JOphthalmol 1946;29:162–5.
4. Ffytche TJ. The continuing challenge of ocular leprosy. Br JOphthalmol 1991;75:123–4.
5. World Health Organization. Leprosy: fact sheet no. 101.Available at: http://www.who.int/mediacentre/factsheets/fs101/en/index.html. Accessed February 6, 2007.
6. Ffytche TJ, Brandt F, Cerchez J, et al. Ocular complicationsobserved in leprosy patients in Romania. BMJ 1992;305:240–2.
7. Binford CH, Meyers WM, Walsh GP. Leprosy. JAMA 1982;247:2283–92.
8. Richards WW, Arrington JM. Unsuspected ocular leprosy.Am J Ophthalmol 1969;68:492–9.
9. Shepard CC, McRae DH. A method for counting acid-fastbacteria. Int J Lepr Other Mycobact Dis 1968;36:78–82.
10. Buhrer-Sekula S, Smits HL, Gussenhoven GC, et al. Simpleand fast lateral flow test for classification of leprosy patientsand identification of contacts with high risk of developingleprosy. J Clin Microbiol 2003;41:1991–5.
11. Douglas JT, Steven LM, Fajardo T, et al. The effects ofchemotherapy on antibody levels in lepromatous patients.Lepr Rev 1988;59:127–35.
12. Clark-Curtiss JE, Docherty MA. A species-specific repetitivesequence in Mycobacterium leprae DNA. J Infect Dis 1989;159:7–15.
13. Katoch VM. Newer diagnostic techniques for tuberculosis.Indian J Med Res 2004;120:418–28.
14. McFadden J, Kunze Z, Seechum P. DNA probes for detectionand identification. In: McFadden J, ed. Molecular Biology ofthe Mycobacteria. Guildford, United Kingdom: Surrey Uni-versity Press; 1990:139–72.
15. Torres P, Camarena JJ, Gomez JR, et al. Comparison of PCRmediated amplification of DNA and the classical methods fordetection of Mycobacterium leprae in different types of clin-ical samples in leprosy patients and contacts. Lepr Rev 2003;74:18–30.
16. Beige J, Lokies J, Schaberg T, et al. Clinical evaluation of aMycobacterium tuberculosis PCR assay. J Clin Microbiol1995;33:90–5.
17. Li JY, Lo ST, Ng CS. Molecular detection of Mycobacterium
Chaudhry et al � Initial Diagnosis of Ocular Leprosy
tuberculosis in tissues showing granulomatous inflammationwithout demonstrable acid-fast bacilli. Diagn Mol Pathol2000;9:67–74.
18. Kramme S, Bretzel G, Panning M, et al. Detection and quan-tification of Mycobacterium leprae in tissue samples by real-time PCR. Med Microbiol Immunol 2004;193:189–93.
19. Park DY, Kim JY, Choi KU, et al. Comparison of polymerasechain reaction with histopathologic features for diagnosis oftuberculosis in formalin-fixed, paraffin-embedded histologicspecimens. Arch Pathol Lab Med 2003;127:326–30.
20. Singh HB, Katoch VM, Natrajan M, et al. Improved protocolfor PCR detection of Mycobacterium leprae in bufferedformalin-fixed skin biopsies. Intl J Lepr Other Mycobact Dis2004;72:175–8.
21. Lucas SB. Histopathology of leprosy and tuberculosis: anoverview. Br Med Bull 1988;44:584–99.
22. Ridley DS, Jopling WH. Classification of leprosy according toimmunity: a five-group system. Int J Lep Other Mycobact Dis1966;34:255–73.
23. Leiker DL. Classification of leprosy. Lepr Res 1966;37:7–15.24. Trucksis M. Mycobacterial diseases: tuberculosis and leprosy.
In: Albert DM, Jakobiec FA, eds. Principles and Practice ofOphthalmology. 2nd ed. Vol. 5. Philadelphia: Saunders; 2000:4842–52.
25. Collins T. Acute and chronic inflammation. In: Cotran RS,Kumar V, Collins T, eds. Robbins Pathologic Basis of Dis-ease. 6th ed. Philadelphia: Saunders; 1999:50–88.
26. Kagame GK. Ocular leprosy in Africa. Soc Sci Med 1983;17:1737–42.
27. Ffytche TJ. Role of iris changes as a cause of blindness inlepromatous leprosy. Br J Ophthalmol 1981;65:231–9.
28. Shields JA, Warring GO III, Monte LG. Ocular findings inleprosy. Am J Ophthalmol 1974;77:880–90.
29. Hornblass A. Ocular leprosy in South Vietnam. Am J Oph-thalmol 1973;75:478–80.
30. Dethlefs R. Prevalence of ocular manifestations of leprosy in PortMoresby, Papua New Guinea. Br J Ophthalmol 1981;65:223–5.
31. Daniel E, Koshy S, Rao GS, Rao PS. Ocular complications innewly diagnosed borderline lepromatous and lepromatous lep-rosy patients: baseline profile of the Indian cohort. Br J Oph-thalmol 2002;86:1336–40.
32. Courtright P, Daniel E, Rao S, et al. Eye disease in multiba-cillary leprosy patients at the time of their leprosy diagnosis:
findings from the Longitudinal Study of Ocular Leprosy(LOSOL) in India, the Philippines and Ethiopia. Lepr Rev2002;73:225–38.
33. Lubbers WJ, Schipper A, Hogeweg M, De Soldenhoff R. Eyedisease in newly diagnosed leprosy patients in eastern Nepal.Lepr Rev 1994;65:231–8.
34. Karacorlu MA, Cakiner T, Saylan T. Corneal sensitivity andcorrelation between decreased sensitivity and anterior segmentpathology in ocular leprosy. Br J Ophthalmol 1991;75:117–9.
35. Emiru VP. Ocular leprosy in Uganda. Br J Ophthalmol 1970;54:740–3.
36. Harley RD. Ocular leprosy in Panama. Am J Ophthalmol1946;29:295–316.
37. Daniel E, Ebenezer GJ, Job CK. Pathology of iris in leprosy.Br J Ophthalmol 1997;81:490–2.
38. Hashizume H, Shionuma E. Electron microscopic studies oflepromatous changes in the iris. Int J Lepr 1965;33:61–82.
39. Espiritu CG, Gelber R, Ostler HB. Chronic anterior uveitis inleprosy: an insidious cause of blindness. Br J Ophthalmol1991;75:273–5.
40. Hogeweg M, Faber WR. Progression of eye lesions in leprosy:ten-year follow-up study in the Netherlands. Int J Lepr OtherMycobact Dis 1991;59:392–7.
41. Orentreich DS, Orentreich N. Dermatology of the eyelids(Excluding neoplasms). In: Smith BC, Della Rocca RC, NesiFA, Lisman RD, eds. Ophthalmic Plastic and ReconstructiveSurgery. Vol. 2. St. Louis: Mosby; 1987:855–906.
42. Guimaraes FC, Cruz AA. Eyelid changes in long-standingleprosy. Ophthalmic Plast Reconstr Surg 1998;14:239–43.
43. Carus NH, Raizman MB, Williams DL, Baker AS. Relapse ofMycobacterium leprae infection with ocular manifestations.Clin Infect Dis 1995;20:776–80.
44. Schwab IR. Hansen’s disease (ocular leprosy). In: TabbaraKF, Hyndiuk RA, eds. Infections of the Eye. Boston: Little,Brown; 1986:615–24.
45. Jacobson RR. The treatment of leprosy (Hansen’s disease).Hosp Formul 1982;17:1076–91.
46. Chemotherapy of leprosy for control programmes. WorldHealth Organ Tech Rep Ser 1982;675:1–33.
47. World Health Organization. Leprosy elimination. Availableat: http://www.who.int/lep/en. Assessed February 10, 2007.
48. Daniel E, Ffytche TJ, Kempen JH, et al. Incidence of ocularcomplications in patients with multibacillary leprosy aftercompletion of a 2 year course of multidrug therapy. Br J
Ophthalmol 2006;90:949–54.1911
tachment; VA � visual acuity, decreased.
Ophthalmology Volume 114, Number 10, October 2007
Table 1. Characteristics o
PatientNo.
Age(yrs) Gender
PresentingSymptoms and
Signs
InitialVisualAcuity
SuspectedClinicalLeprosy
1 28 F 2VA, thickenedcorneal nerves,superficialstromal opacities
CF (left eye) –
2 47 M Tearing, swelling/mass lower eyelid
20/20 (righteye)
–
3 60 F 2VA, pain, FBS,ptosis, madarosis,“leonine facies,”episcleritis,uveitis,entropion,cataracts, skin &limbal nodule,lagoph,thickenedcorneal nerves,exp keratop, limbdeformities
LP (left eye) �
4 62 F 2VA, tearing,eyelid swelling,cataract
20/200 (lefteye)
–
5 70 F Ptosis, lagoph,madarosis,swelling, HA,proptosis,scleritis, pain,arthritis
20/80 (righteye)
–
6 72 F 2VA, pain,madarosis,corectopia, RD,“iris pearls,”panuveitis,postsynechea,cataract
LP (left eye) �
AFB � acid-fast bacilli; CE/IOL � cataract extraction/intraocular lens imexposure keratopathy; F � female; FBS � foreign body sensation; HA � hpolymerase chair reaction; PKP � penetrating keratoplasty; RD � retinal de
f Patients with Ocular Leprosy
Management
Acid-Fast
BacilliHistopathological
Results
PolymeraseChair
Reaction
LastVisualAcuity
Follow-up(yrs)
PKP – Granulomatousstromalkeratitis
� 20/30 3
DCR � Granulomatousdacryocystitis
� 20/20 1
Excision oflimballesion,entropionrepair,CE/IOL
� Acutelepromatousreaction
� 20/100 2
DCR, CE/IOL
� Granulomatousdacryocystitis
– 20/30 1.5
Ptosis repair,orbitalbiopsy
� Lepromatousreaction
� 20/40 2
CE/IOL,treatmentof uveitis
– – – 20/400 2
plantation; CF � counting fingers; DCR � dacryocystorhinostomy; Exp kertop �eadache; Lagoph � lagophthalmos; LP � light perception; M � male; PCR �
1911.e1




















