Infliximab induction and maintenance therapy for moderate-to-severe psoriasis: a phase III,...
8
Articles Introduction Psoriasis is a chronic, immunologically based, inflammatory skin disease, of which plaque-type psoriasis is the most common form. 1,2 Cytokines released from cutaneous antigen-presenting cells, T cells, and keratinocytes are believed to play a key part in the formation of plaques in psoriasis. 3,4 Biological treatments that target cytokines represent a new option for the management of the disease. 5 Tumour necrosis factor (TNF), a key mediator in many inflammatory diseases, is thought to have an important role in the pathogenesis of psoriasis. In a novel mouse model, it has been shown that TNF is the primary cytokine mediating the activation and proliferation of resident T cells, which are essential in the development of psoriasis lesions. 6 Increased concentrations of TNF have been recorded in the serum samples 7 and skin lesions of patients with psoriasis, 8–10 and serum concentrations of TNF have been shown to correlate with disease activity. 11 Infliximab, a monoclonal antibody that binds with high affinity and specificity to TNF and neutralises its biological activity, is approved for the treatment of other chronic diseases characterised by TNF-mediated inflammation, such as rheumatoid arthritis, Crohn’s disease, ankylosing spondylitis, and psoriatic arthritis. Early studies have identified biological effects and clinical activity in psoriasis. 12,13 Here, we present the results of a phase III study, addressing the long-term safety and efficacy of infliximab for the treatment of skin and nail lesions in patients with psoriasis. Additional information was obtained on the potential effect of antibodies to infliximab and serum concentrations of infliximab on maintenance of the therapeutic response. Methods Patients Of 472 adult patients who were screened, 378 were enrolled at 32 centres in this phase III, multicentre, double-blind, placebo-controlled trial. Institutional review board or ethics committee approval and written informed consent were obtained before any protocol- specific procedures were undertaken. Patients had a diagnosis of moderate-to-severe plaque-type psoriasis for at least 6 months, were candidates for phototherapy or systemic therapy, had a psoriasis area and severity index (PASI) score of at least 12, and had at least 10% of their total body surface area affected by psoriasis. Those with a history or risk of serious infection, lymphoproliferative disease, or active tuberculosis were ineligible, and previous treatment with infliximab or any other TNF- antagonists was not allowed. All systemic treatments Lancet 2005; 366: 1367–74 See Comment page 1333 *Investigators are listed at the end of the report Department of Dermatology, Georg-August University, Göttingen, Germany (Prof K Reich MD); Department of Dermatology, University of Zurich Hospital, Zurich, Switzerland (F O Nestle MD); Probity Medical Research, Waterloo, and University of Western Ontario, London, Ontario, Canada (K Papp MD); Hôpital L’Archet, Nice, France (Prof J-P Ortonne MD); Scios Inc, Fremont, CA, USA (R Evans PharmD), Centocor, Malvern PA, USA (C Guzzo MD, S Li MS, L T Dooley DrPH); and Dermatology Centre, Hope Hospital, University of Manchester, Manchester, UK (Prof C E M Griffiths MD) Correspondence to: Prof C E M Griffiths, Dermatology Centre, Hope Hospital, Salford, Manchester M6 8HD, UK Christopher.griffiths@ manchester.ac.uk www.thelancet.com Vol 366 October 15, 2005 1367 Infliximab induction and maintenance therapy for moderate-to-severe psoriasis: a phase III, multicentre, double-blind trial Kristian Reich, Frank O Nestle, Kim Papp, Jean-Paul Ortonne, Robert Evans, Cynthia Guzzo, Shu Li, Lisa T Dooley, Christopher E M Griffiths, for the EXPRESS study investigators* Summary Background Tumour necrosis factor (TNF) is thought to play a part in the pathogenesis of psoriasis. We assessed the efficacy and safety of continuous treatment with infliximab, a monoclonal antibody that binds to and neutralises the activity of TNF, in patients with psoriasis. Methods In this phase III, multicentre, double-blind trial, 378 patients with moderate-to-severe plaque psoriasis were allocated in a 4:1 ratio to receive infusions of either infliximab 5 mg/kg or placebo at weeks 0, 2, and 6, then every 8 weeks to week 46. At week 24, placebo-treated patients crossed over to infliximab treatment. Skin and nail signs of psoriasis were assessed using the psoriasis area and severity index (PASI) and nail psoriasis severity index (NAPSI), respectively. The primary endpoint, analysed on an intention-to-treat-basis, was the proportion of patients achieving at least a 75% improvement in PASI from baseline to week 10. Findings At week 10, 80% (242/301) of patients treated with infliximab achieved at least a 75% improvement from their baseline PASI (PASI 75) and 57% (172/301) achieved at least a 90% improvement (PASI 90), compared with 3% and 1% in the placebo group, respectively (p0·0001). At week 24, PASI 75 (82% for infliximab vs 4% for placebo) and PASI 90 (58% vs 1%) were maintained (p0·0001). At week 50, 61% achieved PASI 75 and 45% achieved PASI 90 in the infliximab group. Infliximab was generally well tolerated in most patients. Interpretation Infliximab is effective in both an induction and maintenance regimen for the treatment of moderate- to-severe psoriasis, with a high percentage of patients achieving sustained PASI 75 and PASI 90 improvement through 1 year.
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of Infliximab induction and maintenance therapy for moderate-to-severe psoriasis: a phase III,...
Articles
IntroductionPsoriasis is a chronic, immunologically based,inflammatory skin disease, of which plaque-typepsoriasis is the most common form.1,2 Cytokinesreleased from cutaneous antigen-presenting cells,T cells, and keratinocytes are believed to play a key partin the formation of plaques in psoriasis.3,4 Biologicaltreatments that target cytokines represent a new optionfor the management of the disease.5 Tumour necrosisfactor � (TNF�), a key mediator in many inflammatorydiseases, is thought to have an important role in thepathogenesis of psoriasis. In a novel mouse model, ithas been shown that TNF� is the primary cytokinemediating the activation and proliferation of residentT cells, which are essential in the development ofpsoriasis lesions.6 Increased concentrations of TNF�have been recorded in the serum samples7 and skinlesions of patients with psoriasis,8–10 and serumconcentrations of TNF� have been shown to correlatewith disease activity.11
Infliximab, a monoclonal antibody that binds withhigh affinity and specificity to TNF� and neutralises itsbiological activity, is approved for the treatment of otherchronic diseases characterised by TNF�-mediatedinflammation, such as rheumatoid arthritis, Crohn’sdisease, ankylosing spondylitis, and psoriatic arthritis.
Early studies have identified biological effects andclinical activity in psoriasis.12,13 Here, we present theresults of a phase III study, addressing the long-termsafety and efficacy of infliximab for the treatment of skinand nail lesions in patients with psoriasis. Additionalinformation was obtained on the potential effect ofantibodies to infliximab and serum concentrations ofinfliximab on maintenance of the therapeutic response.
Methods PatientsOf 472 adult patients who were screened, 378 wereenrolled at 32 centres in this phase III, multicentre,double-blind, placebo-controlled trial. Institutionalreview board or ethics committee approval and writteninformed consent were obtained before any protocol-specific procedures were undertaken. Patients had adiagnosis of moderate-to-severe plaque-type psoriasis forat least 6 months, were candidates for phototherapy orsystemic therapy, had a psoriasis area and severity index(PASI) score of at least 12, and had at least 10% of theirtotal body surface area affected by psoriasis. Those with ahistory or risk of serious infection, lymphoproliferativedisease, or active tuberculosis were ineligible, andprevious treatment with infliximab or any other TNF�-antagonists was not allowed. All systemic treatments
Lancet 2005; 366: 1367–74
See Comment page 1333
*Investigators are listed at theend of the report
Department of Dermatology,Georg-August University,Göttingen, Germany(Prof K Reich MD); Departmentof Dermatology, University ofZurich Hospital, Zurich,Switzerland (F O Nestle MD);Probity Medical Research,Waterloo, and University ofWestern Ontario, London,Ontario, Canada (K Papp MD);Hôpital L’Archet, Nice, France(Prof J-P Ortonne MD); Scios Inc,Fremont, CA, USA (R Evans PharmD), Centocor,Malvern PA, USA (C Guzzo MD,S Li MS, L T Dooley DrPH); andDermatology Centre, HopeHospital, University ofManchester, Manchester, UK(Prof C E M Griffiths MD)
Correspondence to:Prof C E M Griffiths, DermatologyCentre, Hope Hospital, Salford,Manchester M6 8HD, [email protected]
www.thelancet.com Vol 366 October 15, 2005 1367
Infliximab induction and maintenance therapy formoderate-to-severe psoriasis: a phase III, multicentre,double-blind trialKristian Reich, Frank O Nestle, Kim Papp, Jean-Paul Ortonne, Robert Evans, Cynthia Guzzo, Shu Li, Lisa T Dooley, Christopher E M Griffiths, for theEXPRESS study investigators*
Summary Background Tumour necrosis factor � (TNF�) is thought to play a part in the pathogenesis of psoriasis. We assessed
the efficacy and safety of continuous treatment with infliximab, a monoclonal antibody that binds to and neutralises
the activity of TNF�, in patients with psoriasis.
Methods In this phase III, multicentre, double-blind trial, 378 patients with moderate-to-severe plaque psoriasis were
allocated in a 4:1 ratio to receive infusions of either infliximab 5 mg/kg or placebo at weeks 0, 2, and 6, then every
8 weeks to week 46. At week 24, placebo-treated patients crossed over to infliximab treatment. Skin and nail signs of
psoriasis were assessed using the psoriasis area and severity index (PASI) and nail psoriasis severity index (NAPSI),
respectively. The primary endpoint, analysed on an intention-to-treat-basis, was the proportion of patients achieving
at least a 75% improvement in PASI from baseline to week 10.
Findings At week 10, 80% (242/301) of patients treated with infliximab achieved at least a 75% improvement from
their baseline PASI (PASI 75) and 57% (172/301) achieved at least a 90% improvement (PASI 90), compared with
3% and 1% in the placebo group, respectively (p�0·0001). At week 24, PASI 75 (82% for infliximab vs 4% for
placebo) and PASI 90 (58% vs 1%) were maintained (p�0·0001). At week 50, 61% achieved PASI 75 and 45%
achieved PASI 90 in the infliximab group. Infliximab was generally well tolerated in most patients.
Interpretation Infliximab is effective in both an induction and maintenance regimen for the treatment of moderate-
to-severe psoriasis, with a high percentage of patients achieving sustained PASI 75 and PASI 90 improvement
through 1 year.
lhoff
I05277527

Articles
and phototherapies were stopped a month beforetreatment, and topical treatment was stopped 2 weeksbefore starting study treatment. Concomitant topicaltreatment, phototherapy, or any systemic treatment thatcould affect psoriasis was not allowed up to week 50, withthe exception of 2·5% hydrocortisone, or equivalent,applied topically to the face or groin, or both, after week10.
ProceduresAn adaptive treatment allocation (stratified by investigatorsite) was used to assign patients. Eligible patients wereallocated in a 4:1 ratio to receive infliximab 5 mg/kg(Remicade, Centocor, Malvern, PA, USA) or placebo.ClinPhone (Lawrenceville, NJ, USA) allocated patientsusing a minimisation algorithm with biased coinassignment by means of an interactive voice responsesystem. The treatment assignment was storedelectronically, and the stored data were used to allocatefuture patients in such a way that the imbalance betweentreatment groups was kept to a minimum. Thisinformation was distributed to the unblinded sitepharmacist, who then prepared the study drug. Theinvestigators, study site personnel, and patients remainedblinded until the database lock at week 50. Patients in theinfliximab group received intravenous infusions ofinfliximab 5 mg/kg at weeks 0, 2, and 6 and every 8 weeksthrough to week 46. Patients in the placebo groupreceived placebo at weeks 0, 2, 6, 14, and 22, crossing overin a double-blind fashion to infliximab 5 mg/kg at weeks24, 26, and 30 and every 8 weeks through to week 46.
Patients were assessed at all study visits through week50 with the PASI system, an index of the physical severityof psoriasis ranging from 0 to 72.14 Clinical response wasalso assessed by a static physician’s global assessment(PGA), which documented the physician’s assessment ofpsoriasis at each visit (scores from 0 to 5). Nail psoriasiswas assessed at weeks 0, 10, 24, 38, and 50 with the nailpsoriasis severity index (NAPSI).15 Briefly, a target nailthat represented the most severe nail psoriasis at baselinewas divided into quadrants that were graded for fourcharacteristics of both nail matrix psoriasis and nail bedpsoriasis, with a highest possible total score of 8. Safetyassessments comprised measurement of routinelaboratory parameters and reporting of adverse events atall study visits through week 50. Blood samples wereobtained from 169 patients to measure infliximab serumconcentrations before and after each infusion and atweeks 10 and 50. Additional blood samples were obtainedat weeks 0, 46, and 66 to identify antibodies toinfliximab.16 Antinuclear antibodies and anti-double-stranded DNA antibodies were assessed for samplesgathered at weeks 0, 24, and 50.
The primary efficacy endpoint was the proportion ofpatients achieving at least a 75% improvement in PASIfrom baseline (PASI 75) to week 10. Major secondaryendpoints included the proportion of patients achieving
PASI 75 at week 24 and the proportion of patientsachieving a PGA score of cleared (0) or minimal (1) atweek 10. Other endpoints included the proportion ofpatients achieving 50% improvement from baseline(PASI 50) and 90% improvement from baseline(PASI 90), the percentage improvement from baseline inPASI, the percentage improvement in NAPSI at weeks 10,24, and 50, and the proportion of patients achieving aPGA score of cleared or minimal at weeks 24 and 50.
Statistical analysisAll efficacy endpoints at weeks 10 and 24 were comparedbetween the two treatment groups. Pearson �2 tests wereused to compare the proportions of patients responding totreatment. Continuous response parameters wereanalysed with a two-sample t test on van der Waerdennormal scores (normal scores derived from ranks). Allstatistical tests were two-sided and done at an alpha levelof 0·05. For all secondary endpoints, nominal p valueswith no adjustment for multiplicity were reported.
Efficacy data from all patients were analysed accordingto assigned treatment groups. For patients in the placebogroup, only patients who crossed over to receiveinfliximab were included in efficacy summaries for visitsafter week 24. Safety data were summarised by the actualtreatment received in patients who had had at least onedose of study agent.
The primary efficacy endpoint (PASI 75 at week 10) aswell as PASI 50 and PASI 90 at week 10 were analysed onan intention-to-treat basis. Patients were regarded as notachieving the endpoints if they discontinued studytreatment because of lack of efficacy or loss of response,or were treated with prohibited treatments before week10. Additionally, patients who did not return forassessment or had insufficient data to calculate the PASIat week 10 were regarded as not achieving PASI 50, PASI75, or PASI 90. An intention-to-treat analysis was notdone for other efficacy analyses. Instead, the followingdata handling rules were applied (prespecified analysis):in patients who discontinued the study agent because oflack of efficacy or loss of response or who starteddisallowed medication, baseline values were used forcontinuous variables, or the patients were regarded as notachieving the endpoints for binary responses, irrespectiveof the observed data; in other patients, observed data wereused.
In the pre-specified analysis of PASI response overtime, all observed data were used irrespective of whetherthe drug was given. In the per protocol analysis, whichwas done post hoc, patients must have completed theinduction phase to be included in the analysis.Additionally, data after two missed infusions or afterstudy infusion discontinuation were excluded. In the perprotocol analysis, patients who discontinued because oflack of efficacy or loss of response, or who starteddisallowed non-topical medication were deemed non-responders.
1368 www.thelancet.com Vol 366 October 15, 2005
Articles
Serum infliximab concentrations were summarisedover time separately for patients in whom PASI 75 wasachieved at week 10 and maintained through week 50and those in whom the PASI 75 response was notmaintained. The distribution of patients acrosssubgroups categorised by antibody-to-infliximab statuswas summarised at weeks 46 and 66.
Role of the funding sourceA committee composed of employees of Centocor,Malvern, PA, USA, and members of the study steeringcommittee designed this study. Centocor staff gathereddata from all clinical sites to create the clinical databaseand did the statistical analyses. All authors participatedin the interpretation of data, the preparation of thepaper, and the decision to submit for publication.
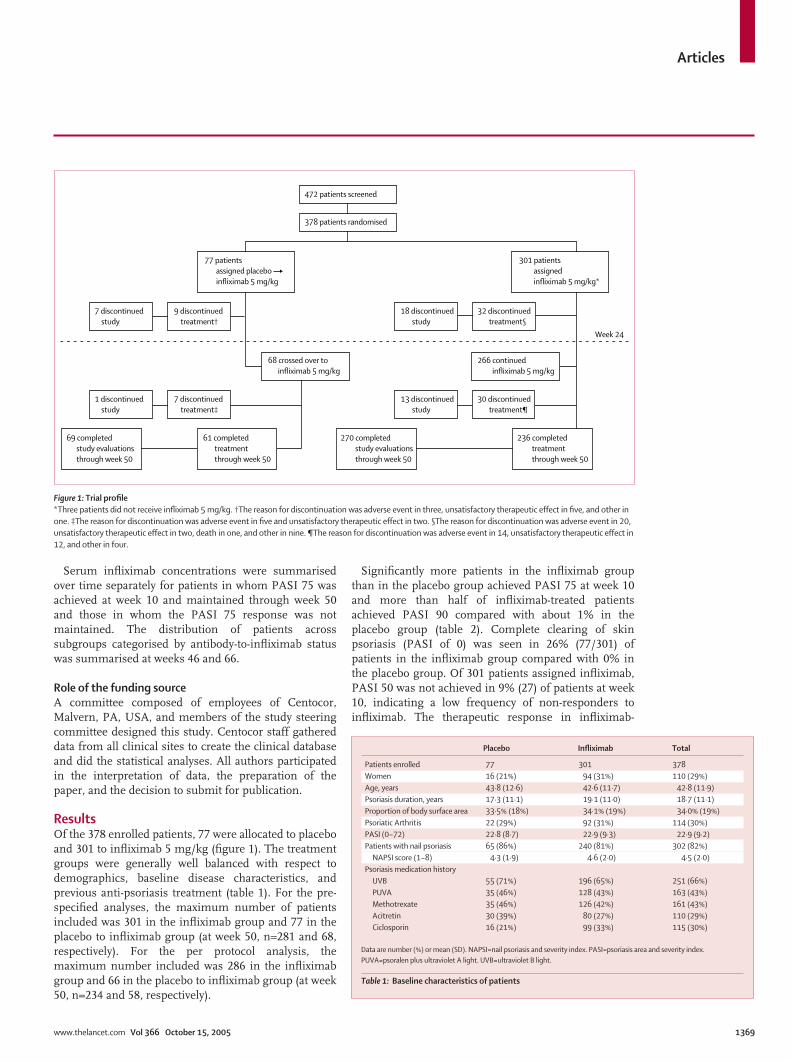
ResultsOf the 378 enrolled patients, 77 were allocated to placeboand 301 to infliximab 5 mg/kg (figure 1). The treatmentgroups were generally well balanced with respect todemographics, baseline disease characteristics, andprevious anti-psoriasis treatment (table 1). For the pre-specified analyses, the maximum number of patientsincluded was 301 in the infliximab group and 77 in theplacebo to infliximab group (at week 50, n=281 and 68,respectively). For the per protocol analysis, themaximum number included was 286 in the infliximabgroup and 66 in the placebo to infliximab group (at week50, n=234 and 58, respectively).
Significantly more patients in the infliximab groupthan in the placebo group achieved PASI 75 at week 10and more than half of infliximab-treated patientsachieved PASI 90 compared with about 1% in theplacebo group (table 2). Complete clearing of skinpsoriasis (PASI of 0) was seen in 26% (77/301) ofpatients in the infliximab group compared with 0% inthe placebo group. Of 301 patients assigned infliximab,PASI 50 was not achieved in 9% (27) of patients at week10, indicating a low frequency of non-responders toinfliximab. The therapeutic response in infliximab-
www.thelancet.com Vol 366 October 15, 2005 1369
472 patients screened
378 patients randomised
77 patients assigned placebo infliximab 5 mg/kg
7 discontinued study
1 discontinued study
18 discontinued study
9 discontinued treatment†
7 discontinued treatment‡
32 discontinued treatment§
30 discontinued treatment¶
13 discontinued study
68 crossed over to infliximab 5 mg/kg
Week 24
301 patients assigned infliximab 5 mg/kg*
266 continued infliximab 5 mg/kg
236 completed treatment through week 50
270 completed study evaluations through week 50
61 completed treatment through week 50
69 completed study evaluations through week 50
Figure 1: Trial profile*Three patients did not receive infliximab 5 mg/kg. †The reason for discontinuation was adverse event in three, unsatisfactory therapeutic effect in five, and other inone. ‡The reason for discontinuation was adverse event in five and unsatisfactory therapeutic effect in two. §The reason for discontinuation was adverse event in 20,unsatisfactory therapeutic effect in two, death in one, and other in nine. ¶The reason for discontinuation was adverse event in 14, unsatisfactory therapeutic effect in12, and other in four.
Placebo Infliximab Total
Patients enrolled 77 301 378Women 16 (21%) 94 (31%) 110 (29%)Age, years 43·8 (12·6) 42·6 (11·7) 42·8 (11·9)Psoriasis duration, years 17·3 (11·1) 19·1 (11·0) 18·7 (11·1)Proportion of body surface area 33·5% (18%) 34·1% (19%) 34·0% (19%)Psoriatic Arthritis 22 (29%) 92 (31%) 114 (30%)PASI (0–72) 22·8 (8·7) 22·9 (9·3) 22·9 (9·2)Patients with nail psoriasis 65 (86%) 240 (81%) 302 (82%)
NAPSI score (1–8) 4·3 (1·9) 4·6 (2·0) 4·5 (2·0)Psoriasis medication history
UVB 55 (71%) 196 (65%) 251 (66%)PUVA 35 (46%) 128 (43%) 163 (43%)Methotrexate 35 (46%) 126 (42%) 161 (43%)Acitretin 30 (39%) 80 (27%) 110 (29%)Ciclosporin 16 (21%) 99 (33%) 115 (30%)
Data are number (%) or mean (SD). NAPSI=nail psoriasis and severity index. PASI=psoriasis area and severity index.PUVA=psoralen plus ultraviolet A light. UVB=ultraviolet B light.
Table 1: Baseline characteristics of patients

Articles
treated patients was rapid, with significant differences(p�0·0001) recorded between the treatment groups asearly as week 2 for the proportion of patients achievingPASI 50 (figure 2). By week 6, significantly moreinfliximab-treated patients than placebo-treated patientsachieved PASI 75 and PASI 90 (p�0·0001). The PASI 75and PASI 90 responses were sustained through week 24and most patients achieved PASI 75 and 90 responsesthrough week 50 (table 2). Results of the per protocolanalysis showed a better maintenance of PASI responsethan with the pre-specified analysis. Based on a pre-specified analysis on PASI 75 responders at week 10, theresponse to infliximab was sustained, with most PASI 75responders at week 10 maintaining this responsethrough week 24 (203/229 patients; 89%) and week 50(153/225; 68%). The efficacy of infliximab, as shown byPASI reductions, was paralleled by PGA results. Clinicalimprovement of psoriasis was evident in the infliximabgroup (figure 3).
The percentage reduction from baseline of the NAPSIwas significantly greater in infliximab-treated patientsthan in placebo-treated patients at weeks 10 and 24(table 2). Improvement of nail psoriasis continuedbetween weeks 10 and 24 in the infliximab group,indicating a delayed response of nail signs comparedwith skin response (figure 3). Improvements of nailpsoriasis achieved at week 24 in infliximab-treatedpatients were generally maintained at week 50 (table 2).
In patients in whom serum concentrations ofinfliximab were measured, the median pre-infusionconcentration of infliximab stabilised from week 22 toweek 46 between 2·8 �g/mL and 3·7 �g/mL, and asteady-state concentration was maintained through week46. However, in 26–29% of patients, pre-infusionconcentrations of infliximab were undetectable between
1370 www.thelancet.com Vol 366 October 15, 2005
Week 10 Week 24 Week 50
Placebo Infliximab p Placebo Infliximab p Placebo/infliximab Infliximab
PASI responseNumber (pre-specified) 77 301 77 276 68 281
�90% improvement 1 (1%) 172 (57%) �0·0001 1 (1%) 161 (58%) �0·0001 34 (50%) 127 (45%) �75% improvement 2 (3%) 242 (80%) �0·0001 3 (4%) 227 (82%) �0·0001 52 (77%) 170 (61%)�50% improvement 6 (8%) 274 (91%) �0·0001 6 (6%) 248 (90%) �0·0001 61 (90%) 193 (69%)
Number (per protocol) 66 277 65 260 58 234�90% improvement 0 167 (60%) NC 1 (2%) 160 (62%) NC 30 (52%) 129 (55%)�75% improvement 1 (2%) 236 (85%) NC 3 (5%) 224 (86%) NC 48 (83%) 165 (71%)�50% improvement 5 (8%) 266 (96%) NC 4 (6%) 243 (94%) NC 54 (93%) 186 (80%)
PASI Number 77 292 77 276 68 281
Percent improvement 6·1 (29·9) 85·5 (21·4) �0·0001 4·4 (40·1) 83·9 (25·2) �0·0001 80·7 (26·3) 64·3 (41·2)NAPSI*Number 65 235 65 223 58 226
Percent improvement –5·9 (54·3) 26·0 (42·3) �0·0001 –3·2 (62·3) 56·3 (43·4) �0·0001 72·5 (38·9) 56·3 (52·0)PGA responseNumber 77 292 77 276 68 281
Minimal or cleared 3 (4%) 242 (83%) �0·0001 2 (3%) 203 (74%) �0·0001 46 (68%) 149 (53%)
Data are number (%) or mean (SD). NAPSI=nail psoriasis and severity index. NC=not calculated. PASI=psoriasis area and severity index. PGA=physician’s global assessment. *NAPSI was assessed only in patients with nailpsoriasis at baseline.
Table 2: Clinical responses at week 10, week 24, and week 50
Infliximab 5 mg/kg (per protocol)Infliximab 5 mg/kg (per pre-specified)
Placebo to infliximab 5 mg/kg (per protocol)Placebo to infliximab 5 mg/kg (pre-specified)
50% improvement in PASI 50% improvement in PASI
75% improvement in PASI 75% improvement in PASI
90% improvement in PASI 90% improvement in PASI
A D
B E
C F
Pati
ents
(%)
100
75
50
25
0
Pati
ents
(%)
Pati
ents
(%)
100
75
50
25
0
100
75
50
25
00 2 6 10 14 22 2426
Weeks Weeks
30 38 46 50 0 2 6 10 14 22 2426 30 38 46 50
Figure 2: Skin response as measured by PASI improvement in 378 patients with moderate-to-severe plaquepsoriasis allocated to infliximab or placebo with crossover to infliximab at week 24Data were analysed on both a pre-specified and per protocol basis in the infliximab (A–C) and placebo (D–F) groups.

Articles
week 30 and week 46. There was evidence that themaintenance of clinical response was related to theachievement of stable infliximab serum concentrations.Of 75 patients for whom week 0 post-infusion serumconcentration data were available and who achievedPASI 75 at week 10, 56 maintained their PASI improve-ment through week 50, and these patients had medianpre-infusion serum infliximab concentrations above1·0 �g/mL at week 30 and thereafter. By contrast, the19 patients who lost response by week 50 had medianpre-infusion serum infliximab concentrations less than1·0 �g/mL (figure 4).
Cumulative analysis of the 264 infliximab-treatedpatients who had appropriate samples for analysis ofantibodies to infliximab through week 66 showed thatmost samples (168; 64%) were antibody negative,whereas 27% (70) were positive and 10% (26) wereinconclusive for antibodies to infliximab. In addition tothe analysis of antibodies to infliximab at week 66 (ie, 20weeks after the last infusion), an earlier sample wasobtained before the week 46 infusion to assess the effectof continued dosing on the incidence of antibodies toinfliximab. The incidences of antibodies to infliximab atweeks 46 and 66 were 22% and 19%, respectively,thereby indicating that the number of antibody-positivepatients did not increase with continued dosing
(figure 5). Antibody-to-infliximab status, as assessedthrough week 66, did have an effect on the maintenanceof response through week 50. Among patients whoachieved PASI 75 at week 10, 39% (20) who were positivefor antibodies to infliximab maintained this responsethrough week 50 compared with 81% (106) and 96% (22)of antibody-negative and inconclusive patients,respectively. Although fewer antibody-positive patientsachieved PASI 75 or maintained clinical responsethrough week 50, an antibody-positive status did notpreclude a clinical response to infliximab.
Through week 24, the proportion of patients whoexperienced at least one adverse event was slightlyhigher in the infliximab group (82%) than in the placebogroup (71%). Similar proportions of patients in each
www.thelancet.com Vol 366 October 15, 2005 1371
Figure 3: Significant improvement in skin (A, B) and nail (C, D) psoriasisactivity after treatment with infliximab 5 mg/kg from baseline (A and C) toweek 24 (B and D)
Responders at week 10 and week 50Responders at week 10 but not week 50
100
10
1
0 2 6
Med
ium
ser
um in
flixi
mab
con
cent
rati
on (�
g/m
L)
10 14 22 30 38 46 50
�0·1
Weeks
Infusion
Figure 4: Pre-infusion serum infliximab concentration in patients who achieved PASI 75 at week 10(responders) and who maintained the response to week 50 (n=56) or who did not maintain the response atweek 50 (n=19) Vertical lines indicate IQR.
0
Positive
Negative
Week 46 Week 66
Inconclu
sive
Positive
Negative
Inconclu
sive
20
40Pati
ents
(%)
60
80
100
Figure 5: Proportion of patients treated with infliximab, categorised aspositive, negative, and inconclusive for antibody status at week 46 and 66Patients were classified as negative (no antibodies detected and undetectableserum infliximab), positive (antibodies detected irrespective of infliximab serumconcentrations), or inconclusive (no antibodies detected but detectable seruminfliximab).

Articles
treatment group reported infections and infusionreactions (table 3). Three serious infections (ie, definedas any infection meeting the regulatory definition for aserious adverse event) were reported in infliximab-treated patients. Additionally, three patients in theinfliximab group had delayed hypersensitivity reactions,generally characterised by myalgia, arthralgia, fever, orrash, which improved within 2 weeks in all but onepatient for whom follow-up information was notavailable. There were no demyelinating events,tuberculosis, or serious opportunistic infections and nonew onset congestive heart failure or haematologicalevents of interest (pancytopenia, aplastic anaemia,agranulocytosis). Through week 24, two patients in theinfliximab group reported a lupus-like syndrome witharthralgias and anti-double-stranded DNA antibodies.Through week 50, four serious infusion reactions werereported in infliximab-treated patients.
No clinically significant changes were noted inhaematological or chemical values, with the exception ofaspartate aminotransferase and alanine aminotrans-ferase. Through week 24, 6% and 2% of patients in theinfliximab group had generally asymptomatic markedlyabnormal increases in alanine aminotransferase and
aspartate aminotransferase, respectively (ie, defined as�150 U/L and �100% increase from baseline) comparedwith none in the placebo group. No patients had amarkedly abnormal total bilirubin (�3·0 mg/dL and�100% increase) or alkaline phosphatase (�250 IU/Land �100% increase) value, and no adverse events ofjaundice or hyperbilirubinaemia were reported. Theseincreases resolved with continuation or interruption oftreatment and, in certain cases, discontinuation oftreatment; however, most patients were able to completeinfusions.
DiscussionIn this phase III study of infliximab in patients withmoderate-to-severe psoriasis, we show the high efficacy,rapid onset, and long-term maintenance of therapeuticresponse for skin as well as nail lesions. Maintenance oftherapeutic response seemed to be related to theachievement of stable serum infliximab concentrationsand was more common in patients negative forantibodies to infliximab than in antibody-positivepatients. These data establish intravenous infliximabmonotherapy as an effective anti-psoriatic treatment andprovide insights into potential parameters that affect thelong-term clinical response.
About two-thirds of patients achieved a PASI 75response and around a third achieved a PASI 90response by week 6; the proportions of patientscontinued to increase, with more than three-quartersachieving PASI 75 and a half achieving PASI 90responses at the end of the induction period (week 10).Complete clearing of psoriasis at week 10 was reportedin about a quarter of patients. Importantly, the study alsoshowed that extended treatment with infliximab5 mg/kg every 8 weeks is effective in maintaining thisresponse and is generally well tolerated in most patients.The substantial efficacy of infliximab, as documented byPASI reductions, was paralleled by PGA responses.These results indicate that infliximab is an effectivetreatment for psoriasis when compared with data fromstudies of other biological treatments, includingalefacept,17 etanercept,18 and efalizumab,19–22 as well assystemic treatments, such as ciclosporin andmethotrexate.23
Nail psoriasis, often recognised as a treatment-resistantdisease manifestation, improved to a much greater extentin patients treated with infliximab than in placebo-treatedpatients. Significant improvements of nail psoriasis wereseen as early as week 10. At week 24, there was a 56%mean decrease of the NAPSI in the infliximab group andthis response was maintained through week 50. Theseresults warrant further investigation.
At 6 months, based on pre-specified analyses, theproportions of patients achieving PASI 50, 75, and 90were consistent with the improvements achieved at week10 after the induction regimen, and most infliximab-treated patients achieved PASI 75 at week 50. With a per
1372 www.thelancet.com Vol 366 October 15, 2005
Placebo Infliximab
Patients treated 76 298Common adverse events*
Upper respiratory tract infection 12 (16%) 46 (15%)Headache 9 (12%) 43 (14%)Fatigue 3 (4%) 25 (8%)Hepatic enzymes increased 0 26 (9%)Pruritus 5 (7%) 22 (7%)Arthralgia 3 (4%) 21 (7%)Rhinitis 1 (1%) 18 (6%)Pain 4 (5%) 17 (6%)Pharyngitis 6 (8%) 17 (6%)Herpes simplex 4 (5%) 10 (3%)Psoriasis 10 (13%) 9 (3%)Sinusitis 4 (5%) 4 (1%)
Serious adverse events† 2 (3%) 17 (6%)Adverse events leading to withdrawal 5 (7%) 27 (9%)Infections 30 (40%) 125 (42%)
Treated infections 11 (15%) 44 (15%)Infusion reactions‡ 7 (2%) 38 (3%)Neoplasms § 0 3 (1%)
Squamous cell carcinoma 0 2 (1%)Basal cell carcinoma 0 1 (0%)
Data are number (%). *Absolute numbers and percentages of patients with one ormore adverse event reported in 5% or more patients in the placebo or infliximab group.The WHOART preferred terms are sorted by decreasing frequency in the infliximabgroup. †One patient in the infliximab treatment group died 25 days after the week 2infusion as a result of sepsis secondary to necrotising fasciitis. This patient suffered asevere burn on his hand about 1 week before hospital admission but did not seekmedical attention. On admission, this patient was diagnosed with cellulitis and treatedwith intravenous cephalosporin but died 12 h later. ‡Infusion reactions were defined asadverse events occurring during or within one hour after the infusion was completed.Numbers and percentages refer to the total number of infusions (347 in the placebogroup and 1416 in the infliximab group). §A total of three patients had adverse eventscoded to malignancies, all of which were associated with the skin. The verbatimdiagnosis of one case of squamous cell carcinoma was bowenoid actinic keratosis.
Table 3: Adverse events during the placebo-controlled phase(weeks 0–24)

Articles
protocol approach to assess maintenance of response,86% and 71% of infliximab patients achieved PASI 75after 6 months and one year, respectively. To providesome perspective on maintenance of response amongthe biological treatments, the data from this study can becompared with other approved biological treatments. Ananalysis of responders based on prespecified datahandling rules in the present study indicates that 89% ofpatients achieving a PASI 75 response at week 10maintained this response at 6 months and 65%maintained this response at 1 year. These resultscompare favourably to efalizumab and etanercept, withwhich about 77% of PASI 75 responders at the primaryendpoint (week 12) maintained this response atweek 24.19,24 Of note, no dose escalation or concomitanttreatment was allowed in our study, apart from very lowpotency topical corticosteroids on the face or groin afterweek 10. To our knowledge, no data spanning a year oftreatment without the use of concomitant therapy ordose escalation have been published for other biologicaltreatments.
As psoriasis is a chronic disease that usually needslong-term treatment, understanding why some patientslost response from week 30 to one year is important.This finding can be attributed, in part, to patients whodiscontinued treatment but continued to be followed upfor safety reasons. Other possible explanations for thisloss in PASI 75 response include changes in seruminfliximab concentrations or the presence of neutral-ising antibodies. A pharmacokinetic analysis showedthat those with detectable pre-infusion serum infliximabconcentrations generally maintained their PASI 75response over time. Patients with undetectable seruminfliximab concentrations (�0·1 �g/mL), includingthose developing antibodies to infliximab, were lesslikely to maintain response. Therefore, maintaining anextended PASI response seemed to depend on achievingmeasurable concentrations of infliximab in serum andsuggests that a subgroup of patients could require morefrequent administration to maintain response. Variabledosage frequency is currently being assessed in anotherstudy.
Overall, infliximab 5 mg/kg was generally welltolerated, with around 80% of patients completing allinfusions. With equal follow up, similar proportions ofpatients in the placebo and infliximab groups hadinfections as well as treated infections. Serious adverseevents occurred more frequently in infliximab-treatedpatients than in placebo-treated patients during thecontrolled phase of the study; this observation includedserious infections, which are known to occur with allTNF� inhibitors. In fact, increased susceptibility tofungal and bacterial infections has been reported withTNF-inhibitors.25,26 However, there were no cases oftuberculosis, demyelinating events, heart failure, ormalignancies other than skin cancers. The proportion ofinfusions with reactions was similar in the placebo and
infliximab groups through week 24, and the rate in theinfliximab group was similar to previous findings ininfliximab studies of patients with rheumatoid arthritisor Crohn’s disease.27,28 The serious infusion reaction rateof 1% in this study is also consistent with the rate forstudies of infliximab in other diseases.29 Therefore,patients with psoriasis treated with infliximab, as forother indications, must be monitored closely forinfection, infusion reactions, and other serious un-common events.
The only important laboratory finding was an increasein aminotransferase concentrations, which occurredmore commonly in alanine aminotransferase thanaspartate aminotransferase and which were usually lessthan three times the upper limit of normal. Suchincreases have been reported in patients withrheumatoid arthritis or Crohn’s disease treated withinfliximab. By contrast with the psoriasis population,increases in alanine aminotransferase of at least twotimes the upper limit of normal in patients withrheumatoid arthritis have occurred with similarfrequency in the infliximab groups compared with thatof placebo.27 Of note, rises in aminotransferaseconcentrations have been reported with infliximab in thepsoriatic arthritis population.30 Psoriasis patients couldbe predisposed to such increases. However, this findingwill need long-term follow up in large groups of treatedpsoriasis patients.
In conclusion, infliximab monotherapy is highlyeffective in the treatment of skin and nail disease inpatients with moderate-to-severe psoriasis, with a rapidonset of action and a sustained effect in most patients.Treatment is generally well tolerated, with a safetyprofile similar to that established in approvedindications. This study documents the long-term efficacyand safety of infliximab and provides novel insights intothe relevance of serum concentrations of infliximab aswell as antibody-to-infliximab status for maintenance ofresponse in psoriasis.
ContributorsK Reich and F O Nestle contributed equally to this study. K Reich,F O Nestle, C E M Griffiths, C Guzzo, R Evans, S Li, and L T Dooleyparticipated in the development of the study, had full access to all datafor interpretation, and had final responsibility for the decision to submitfor publication. K Reich, C E M Griffiths, and F O Nestle comprised theSteering Committee and had main responsibility for writing the article,with clinical input from C Guzzo and R Evans and statistical supportfrom S Li and L T Dooley. K Papp and J-P Ortonne, who participated inthe conduct of the trial, provided review and approval of the manuscript.
Express study investigators P Altmeyer, Bochum, Germany; G Burg, Zurich, Switzerland;M Friedrich, Berlin, Germany; R Gniadecki, Copenhagen, Denmark;C Griffiths, Manchester, UK; F Groenhoej Larsen, Copenhagen,Denmark; G Guillet, Poitiers, France; W Gulliver, New Foundland,Canada; A Gupta, Ontario, Canada; M Heenen, Brussels, Belgium;R Kaufmann, Frankfurt, Germany; H Kerl, Gras, Austria; K Kragballe,Aarhus, Denmark; J Lambert, Edegem, Belgium; R Langley,Nova Scotia, Canada; T Luger, Munster, Germany; C Lynde, Ontario,Canada; L Marot, Brussels, Belgium; J-M Naeyaert, Gent, Belgium;J-F Nicolas, Pierre-Bénite, France; J-P Ortonne, Nice, France; K Papp,Ontario, Canada; Y Poulin, Quebec, Canada; N Provost, Quebec,
www.thelancet.com Vol 366 October 15, 2005 1373

Articles
Canada; K Reich, Gottingen, Germany; J Revuz, Créteil, France;L Robertson, Alberta, Canada; L Rosoph, Ontario, Canada; M Rustin,London, UK; J-H Saurat, Geneva, Switzerland; R Schopf, Mainz,Germany; M Sticherling, Leipzig, Germany.
Conflict of interest statement K Reich has served as a consultant and paid speaker for Centocor andSchering-Plough. C E M Griffiths has served as a consultant and paidspeaker and received grant funding from Centocor and Schering-Plough. F O Nestle has served as a consultant for Centocor and paidspeaker for Centocor and Schering-Plough. K Papp received grants andhas acted as a consultant for Centocor and Schering-Plough. C Guzzo, S Li, and L T Dooley are employees of Centocor. R Evans was anemployee of Centocor at the time this study was conducted and iscurrently an employee of Scios.
AcknowledgmentsThis study (C0168T38) was funded by Centocor, and Schering-Plough,Kenilworth, NJ, USA. We thank C Marano for drafting the antibodysection of this manuscript and C Arnold for her writing support; bothare employees of Centocor.
References1 Lebwohl M. Psoriasis. Lancet 2003; 361: 1197–204. 2 Schon MP, Boehncke WH. Psoriasis. N Engl J Med 2005; 352:
1899–912.3 Nickoloff BJ, Nestle FO. Recent insights into the
immunopathogenesis of psoriasis provide new therapeuticopportunities. J Clin Invest 2004; 113: 1664–75.
4 Gottlieb AB. Psoriasis: emerging therapeutic strategies. Nat Rev2005; 4: 19–34.
5 Sterry W, Barker J, Boehncke WH, et al. Biological therapies in thesystemic management of psoriasis: International ConsensusConference. Br J Dermatol 2004; 151 (suppl 69): 3–17.
6 Boyman O, Hefti HP, Conrad C, Nickoloff BJ, Suter M, Nestle FO.Spontaneous development of psoriasis in a new animal modelshows an essential role for resident T-cells and tumor necrosisfactor-�. J Exp Med 2004;199: 731–36.
7 Bonifati C, Carducci M, Cordiali Fei P, et al. Correlated increases oftumour necrosis factor-alpha, interleukin-6 and granulocytemonocyte-colony-stimulating factor levels in suction blister fluidsand sera of psoriatic patients—relationships with disease severity.Clin Exp Dermatol 1994; 19: 383–87.
8 Nickoloff BJ, Karabin GD, Barker JNWN, et al. Cellular localizationof interleukin-8 and its inducer, tumor necrosis factor-alpha inpsoriasis. Am J Pathol 1991; 138: 129–40.
9 Kristensen M, Chu CQ, Eedy DJ, Feldmann M, Brennan FM,Breathnach SM. Localization of tumour necrosis factor-alpha(TNF-alpha) and its receptors in normal and psoriatic skin:epidermal cells express the 55-kD but not the 75kD TNF receptor.Clin Exp Immunol 1993; 94: 354–62.
10 Reich K, Garbe C, Blaschke V, et al. Response of psoriasis tointerleukin-10 is associated with suppression of cutaneous type 1inflammation, downregulation of the epidermal interleukin-8/CXCR2 pathway and normalization of keratinocyte maturation.J Invest Dermatol 2001; 116: 319–29.
11 Mussi A, Bonifati C, Carducci M, et al. Serum TNF-alpha levelscorrelate with disease severity and are reduced by effective therapy inplaque-type psoriasis. J Biol Regul Homeost Agents 1997; 11: 115–18.
12 Chaudhari U, Romano P, Mulcahy LD, Dooley LT, Baker DG,Gottlieb AB. Efficacy and safety of infliximab monotherapy forplaque-type psoriasis: a randomised trial. Lancet 2001; 357:1842–47.
13 Gottlieb AB, Evans R, Li S, Dooley LT, Guzzo C, Baker D.Infliximab induction therapy for patients with severe plaque-typepsoriasis: a randomized, double-blind, placebo-controlled trial.J Am Acad Dermatol 2004; 51: 534–42.
14 Fredriksson T, Pettersson U. Severe psoriasis: oral therapy with anew retinoid. Dermatologica 1978; 157: 238–44.
15 Rich P and Scher RK. Nail psoriasis severity index: a useful tool forevaluation of nail psoriasis. J Am Acad Dermatol 2003; 49: 206–12.
16 Hanauer SB, Wagner CL, Bala M, et al. Incidence and importanceof antibody responses to infliximab after maintenance or episodictreatment in Crohn’s disease. Clin Gastroenterol Hepatol 2004; 2:542–53.
17 Lebwohl M, Christophers E, Langley R, Ortonne JP, Roberts J,Griffiths CE. Alefacept Clinical Study Group: an international,randomized, double-blind, placebo-controlled phase 3 trial ofintramuscular alefacept in patients with chronic plaque psoriasis.Arch Dermatol 2003; 139: 719–27.
18 Leonardi CL, Powers JL, Matheson RT, et al. Etanercept asmonotherapy in patients with psoriasis. N Engl J Med 2003; 349:2014–22.
19 Lebwohl M, Tyring SK, Hamilton TK, et al. A novel targeted T-cellmodulator, efalizumab, for plaque psoriasis. N Engl J Med 2003;349: 2004–13.
20 Gordon KB, Papp, KA, Hamilton TK, et al. Efalizumab for patientswith moderate to severe plaque psoriasis: a randomized controlledtrial. JAMA 2003; 290: 3073–80.
21 Menter A, Gordon K, Carey W, et al. Efficacy and safety observedduring 24 weeks of efalizumab therapy in patients with moderateto severe plaque psoriasis. Arch Dermatol 2005; 141: 31–38.
22 Leonardi CL, Papp KA, Gordon KB, et al. Extended efalizumabtherapy improves chronic plaque psoriasis: results from arandomized phase III trial. J Am Acad Dermatol 2005; 52: 425–33.
23 Heydendael VMR, Spuls PI, Opmeer BC, et al. Methotrexate versuscyclosporine in moderate-to-severe chronic plaque psoriasis.N Engl J Med 2003; 349: 658–65.
24 ENBREL [package insert]. Thousand Oaks, CA: ImmunexCorporation, 2003.
25 Bakleh M, Tleyjeh I, Matteson EL, Osmon DR, Berbari EF.Infectious complications of tumor necrosis factor-� antagonists.Int J Derm 2005; 44: 443–48.
26 Khanna D, McMahon M, Furst DE. Safety of tumour necrosisfactor-� antagonists. Drug Safety 2004; 27: 307–24.
27 Maini R, St Clair EW, Breedveld F, et al. Infliximab (chimeric anti-tumour necrosis factor � monoclonal antibody) versus placebo inrheumatoid arthritis patients receiving concomitant methotrexate:a randomized phase III trial. Lancet 1999; 354: 1932–39.
28 Hanauer SB, Feagan BG, Lichtenstein GR, et al. Maintenanceinfliximab for Crohn’s disease: the ACCENT I randomized trial.Lancet 2002; 359: 1541–49.
29 Remicode (Inliximab). Physicians Desk Reference. Montvale, USA:Medical Economics Company, 2005.
30 Antoni C, Krueger GG, de Vlam K, et al. Infliximab improves signsand symptoms of psoriatic arthritis: results of the IMPACT 2 trial.Ann Rheum Dis 2005; 64: 1150–57.
1374 www.thelancet.com Vol 366 October 15, 2005