
Inducible amp C β-lactamase producing gram-negative bacilli from blood stream infections:...
9
ELSEVIER SURVEILLANCE OF ANTIMICROBIAL RESISTANCE Inducible Amp C P-Lactamase Producing Gram-Negative Bacilli from Blood Stream Infections: Frequency, Antimicrobial Susceptibility, and Molecular Epidemiology in a National Surveillance Program (SCOPE) Michael A. Pfaller, Ronald N. Jones, Steven A. Marshall, Stacy L. Coffman, Richard J. Hollis, Michael B. Edmond, and Richard P. Wenzel A surveillance study of nosocomial blood stream infections [Sur- veillance and Control of Pathogens of Epidemiologic Importance (SCOPE)] was conducted during a 14month period in 199.5 to 1996 in approximately 50 American medical centers. Among the 4725 blood stream infections, the etiologic agent was Enter- obacter spp. in 230, Citrobacter freundii in 24, and Serratia marcescens in 65. The vast majority of these isolates (89%) had been sent to the University of Iowa including 198 Enterobacter spp. (46 Enterobacter aerogenes, 141 Enterobacter cloacae, 17 other Enterobacter spp), 23 C. freundii, and 62 S. marc- escens. Because these species are capable of producing Amp C p-lactamase, we examined their susceptibility to 12 broad- spectrum antimicrobial agents. The frequency of resistance to cefiazidime and the molecular epidemiology of cefazidime- resistarzt strains was also examined. Among the Enterobacter spp. and C. freundii isolates, resistance to third generation ceph- alosporins (ceflazidime, cqtriaxone) and broad-spectrum semisyn- thetic penicillins (piperacillin), zuith or without an enzyme inhibi- From the Department of Pathology (MAP, RNJ, SAM, SLC, RJH), University of Iowa College of Medicine, Iowa City, Iowa; and the Department of Internal Medicine (MBE, RPW), Medical College of Virginia, Virginia Commonwealth University, Rich- mond, Virginia, USA. Address reprint requests to Dr. Michael A. Pfaller, Medical Mi- crobiology Division, Department of Pathology, 273 MRC, Univer- sity of Iowa College of Medicine, Iowa City, Iowa 52242, USA. Received 10 March 1997; revised and accepted 7 April 1997. tor (piperacillin/tazobactam), was high, e.g., 35 to 50%. The S. marcescens isolates were quite susceptible to all agents tested. Both imipenem and ct$pime were active against virtually all iso- lates tested including 84 stably derepressed Amp C-producing ceflazidime-resistant strains of Enterobacter spy. and C. freun- dii. The overall rank order of activity for the six best agents against these Am ,C-producing strains was: imipenem (100% susceptible) > a I kacin = cefepime (98.6%) > ciprojloxacin = gentamicin = ojloxacin (93.6 to 94.0%). Molecular typing stud- ies of c$tazidime-resistant E. cloacae using an automated ri- botyping system, as well as pulsed-field gel electrophoresis, indi- cated that although clonal spread of a single strain occurred in some of the medical centers, most of the episodes of bacteremia were caused by patient-unique strains. Control of these resistant organisms will require attention to microbiologic recognition of phenotypes, to infection control practices, and to limiting the overuse of certain extended spectrum p-lactams. 0 1997 Elsmier Science Inc. INTRODUCTION Antimicrobial-resistant bacteria are the cause of nu- merous clinical problems world wide. Although the development of some resistance is the inevitable re- sult of the clinical use of antimicrobials, the extent of resistance, and the variety of resistance mechanisms that are now relatively common among many bacte- ria are truly astounding (Ballow and Schentag 1992; Brown et al. 1990; DeGheldre et al. 1997; Jones et al. 1994, 1997). Among the more serious antimicrobial DIAGN MICROBIOL INFECT DIS 1997;28:211-219 0 1997 Eisevier Science Inc. All rights reserved. 655 Avenue of the Americas, New York, NY 10010 0732-8893/97/$17.00 PI1 SO732-8893(97)00064-3
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Inducible amp C β-lactamase producing gram-negative bacilli from blood stream infections:...
ELSEVIER
SURVEILLANCE OF ANTIMICROBIAL RESISTANCE
Inducible Amp C P-Lactamase Producing Gram-Negative Bacilli from Blood Stream Infections: Frequency, Antimicrobial Susceptibility, and Molecular Epidemiology in a National Surveillance Program (SCOPE)
Michael A. Pfaller, Ronald N. Jones, Steven A. Marshall, Stacy L. Coffman, Richard J. Hollis, Michael B. Edmond, and Richard P. Wenzel
A surveillance study of nosocomial blood stream infections [Sur- veillance and Control of Pathogens of Epidemiologic Importance (SCOPE)] was conducted during a 14month period in 199.5 to 1996 in approximately 50 American medical centers. Among the 4725 blood stream infections, the etiologic agent was Enter- obacter spp. in 230, Citrobacter freundii in 24, and Serratia marcescens in 65. The vast majority of these isolates (89%) had been sent to the University of Iowa including 198 Enterobacter spp. (46 Enterobacter aerogenes, 141 Enterobacter cloacae, 17 other Enterobacter spp), 23 C. freundii, and 62 S. marc- escens. Because these species are capable of producing Amp C p-lactamase, we examined their susceptibility to 12 broad- spectrum antimicrobial agents. The frequency of resistance to cefiazidime and the molecular epidemiology of cefazidime- resistarzt strains was also examined. Among the Enterobacter spp. and C. freundii isolates, resistance to third generation ceph- alosporins (ceflazidime, cqtriaxone) and broad-spectrum semisyn- thetic penicillins (piperacillin), zuith or without an enzyme inhibi-
From the Department of Pathology (MAP, RNJ, SAM, SLC, RJH), University of Iowa College of Medicine, Iowa City, Iowa; and the Department of Internal Medicine (MBE, RPW), Medical College of Virginia, Virginia Commonwealth University, Rich- mond, Virginia, USA.
Address reprint requests to Dr. Michael A. Pfaller, Medical Mi- crobiology Division, Department of Pathology, 273 MRC, Univer- sity of Iowa College of Medicine, Iowa City, Iowa 52242, USA.
Received 10 March 1997; revised and accepted 7 April 1997.
tor (piperacillin/tazobactam), was high, e.g., 35 to 50%. The S. marcescens isolates were quite susceptible to all agents tested. Both imipenem and ct$pime were active against virtually all iso- lates tested including 84 stably derepressed Amp C-producing ceflazidime-resistant strains of Enterobacter spy. and C. freun- dii. The overall rank order of activity for the six best agents against these Am ,C-producing strains was: imipenem (100% susceptible) > a I kacin = cefepime (98.6%) > ciprojloxacin = gentamicin = ojloxacin (93.6 to 94.0%). Molecular typing stud- ies of c$tazidime-resistant E. cloacae using an automated ri- botyping system, as well as pulsed-field gel electrophoresis, indi- cated that although clonal spread of a single strain occurred in some of the medical centers, most of the episodes of bacteremia were caused by patient-unique strains. Control of these resistant organisms will require attention to microbiologic recognition of phenotypes, to infection control practices, and to limiting the overuse of certain extended spectrum p-lactams. 0 1997 Elsmier Science Inc.
INTRODUCTION
Antimicrobial-resistant bacteria are the cause of nu- merous clinical problems world wide. Although the development of some resistance is the inevitable re- sult of the clinical use of antimicrobials, the extent of resistance, and the variety of resistance mechanisms that are now relatively common among many bacte- ria are truly astounding (Ballow and Schentag 1992; Brown et al. 1990; DeGheldre et al. 1997; Jones et al. 1994, 1997). Among the more serious antimicrobial
DIAGN MICROBIOL INFECT DIS 1997;28:211-219 0 1997 Eisevier Science Inc. All rights reserved. 655 Avenue of the Americas, New York, NY 10010
0732-8893/97/$17.00 PI1 SO732-8893(97)00064-3
212 M.A. Pfaller et al.
resistance issues facing hospitals is that of resistance to “third-generation” cephalosporins among the En- terobacferiucae (Brown et al. 1990; Burwen et al. 1994; Ehrhardt and Sanders 1993; Jones et al. 1997; Pitout et al. 1997; Quinn 1994; Sanders and Sanders 1988; Syn- dman 1991). This resistance is principally associated with the hyperproduction of Bush group 1, chromo- somally mediated (Amp C) cephalosporinases found among isolates of Enferobacter aerogenes, Enterobacfer cloacae, Citrobacter freundii, and Serrafia marcescens (Ehrhardt and Sanders 1993; Jones et al. 1997; Liver- more 1995; Pitout et al. 1997; Sanders 1984). These cephalosporinases confer resistance to almost all /3-lactams (including the “third-generation” cephalo- sporins and the /3-lactamase inhibitor combinations) except the carbapenems (imipenem and meropenem) and the “fourth-generation” cephalosporins (cefepime and cefpirome) (Ehrhardt and Sanders 1993; Gaston 1988; Jones et al. 1994, 1997; Livermore 1995; Quinn 1994; Sanders and Sanders 1988; Snydman 1991). The increased production of Amp C plactamase among species of Enterobacter, Citrobucter, and Serratiu may be induced by certain /3-lactam substrates, and spontane- ous mutation to a stably derepressed constitutive state may occur (Jones et al. 1997; Livermore 1995; Pitout et al. 1997; Sanders 1984; Sanders and Sanders 1986; Stapleton et al. 1995). The prevalence of these inducible or stably derepressed Amp C-producing strains is closely related to the use of extended spectrum p-lactam agents. They are most commonly observed among hospitalized patients, especially those in inten- sive care units (Ballow and Schentag 1992; Brown et al. 1990; Burwen et al. 1994; Ehrhardt and Sanders 1993; Gallagher 1990; Gaston 1988; Jarvis and Martone 1992; Sanders and Sanders 1988; Snydman 1991; Stapleton et
Epidemiologic Importance) Program (Voelker 1996), we describe the frequency of occurrence and antimi- crobial susceptibility profile of those species of En- terobacteriaceae (E. cloacae, E. aerogenes, C. freundii, and S. rnurcescens) capable of producing Amp C /3-lactamase. The frequency of ceftazidime resistance and the molecular epidemiology of these strains are also described.
MATERIALS AND METHODS
Study Design
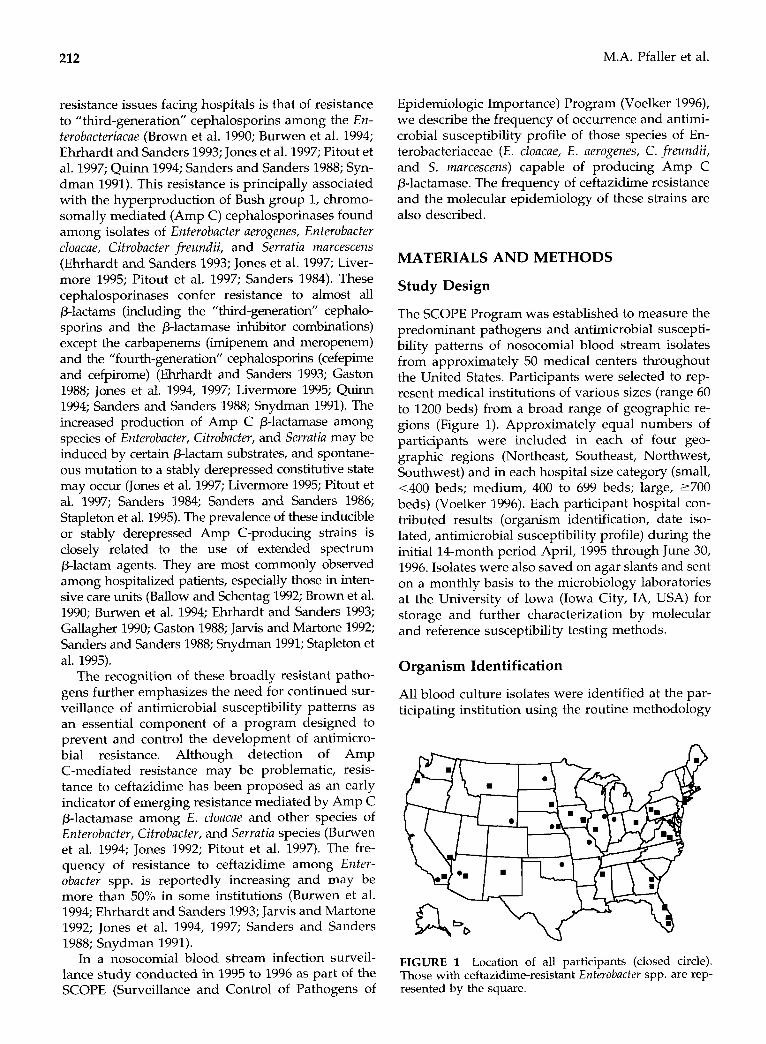
The SCOPE Program was established to measure the predominant pathogens and antimicrobial suscepti- bility patterns of nosocomial blood stream isolates from approximately 50 medical centers throughout the United States. Participants were selected to rep- resent medical institutions of various sizes (range 60 to 1200 beds) from a broad range of geographic re- gions (Figure 1). Approximately equal numbers of participants were included in each of four geo- graphic regions (Northeast, Southeast, Northwest, Southwest) and in each hospital size category (small, ~400 beds; medium, 400 to 699 beds; large, 2700 beds) (Voelker 1996). Each participant hospital con- tributed results (organism identification, date iso- lated, antimicrobial susceptibility profile) during the initial 14-month period April, 1995 through June 30, 1996. Isolates were also saved on agar slants and sent on a monthly basis to the microbiology laboratories at the University of Iowa (Iowa City, IA, USA) for storage and further characterization by molecular and reference susceptibility testing methods.
al. 1995). The recognition of these broadly resistant patho-
Organism Identification
gens furtheruemphasizes the need for continued sur- All blood culture isolates were identified at the par- veillance of antimicrobial susceptibility patterns as an essential component of a program designed to
ticipating institution using the routine methodology
prevent and control the development of antimicro- bial resistance. Although detection of Amp C-mediated resistance may be problematic, resis- tance to ceftazidime has been proposed as an early indicator of emerging resistance mediated by Amp C /3-lactamase among E. cloacae and other species of Enterobacfer, Cifrobacter, and Serrutia species (Burwen et al. 1994; Jones 1992; Pitout et al. 1997). The fre- quency of resistance to ceftazidime among Enter- obacter spp. is reportedly increasing and may be more than 50% in some institutions (Burwen et al. 1994; Ehrhardt and Sanders 1993; Jarvis and Martone 1992; Jones et al. 1994, 1997; Sanders and Sanders 1988; Snydman 1991).
In a nosocomial blood stream infection surveil- lance study conducted in 1995 to 1996 as part of the SCOPE (Surveillance and Control of Pathogens of
FIGURE 1 Location of all participants (closed circle). Those with ceftazidime-resistant Enterobacter spp. are rep- resented by the square.
Blood Stream Infections 213
in use at each laboratory. Upon receipt at the Uni- versity of Iowa, isolates were subcultured onto blood agar to ensure viability and to examine for purity. Confirmation of species identification was per- formed using Vitek (bioMerieux Vitek, St. Louis, MO, USA), and API (bioMerieux) products, or con- ventional methods as required. Isolates were frozen at -70°C until needed.
Susceptibility Testing
Antimicrobial susceptibility testing of isolates of Enterobacter spp., Citrobacter freundii, and Serratia marcescens was performed using the reference broth microdilution method as described by the NCCLS (1997). Antimicrobial agents were ob- tained from the respective manufacturers and included: piperacillin, piperacillin/tazobactam, amikacin, gentamicin, tobramycin, ciprofloxacin, ofloxacin, trimethoprim/sulfamethoxazole, ceftri- axone, ceftazidime, cefepime, and imipenem. Quality control was performed by testing Esche- richia coli ATCC 25922, Staphylococcus uureus ATCC 29213, Pseudomonas aeruginosa ATCC 27853, and Enterococcus faecalis ATCC 29212. Interpretive cri- teria for each antimicrobial tested was that pub- lished by NCCLS (1997).
Molecular Typing
RESULTS
Frequency of Occurrence of Blood Stream Pathogens
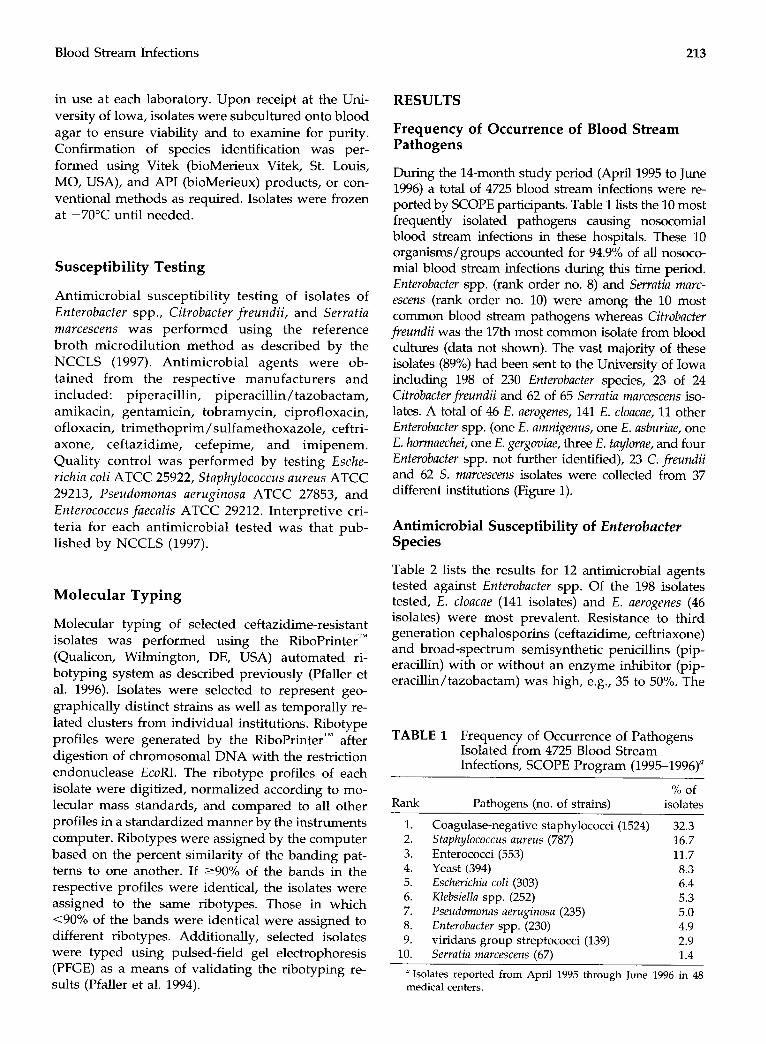
During the 14-month study period (April 1995 to June 1996) a total of 4725 blood stream infections were re- ported by SCOPE participants. Table 1 lists the 10 most frequently isolated pathogens causing nosocomial blood stream infections in these hospitals. These 10 organisms/groups accounted for 94.9% of all nosoco- mial blood stream infections during this time period. Enterobacter spp. (rank order no. 8) and Serrutia marc- escens (rank order no. 10) were among the 10 most common blood stream pathogens whereas Citrobacter freundii was the 17th most common isolate from blood cultures (data not shown). The vast majority of these isolates (89%) had been sent to the University of Iowa including 198 of 230 Enterobucfer species, 23 of 24 Cifrobacter fieundii and 62 of 65 Serratia marcescens iso- lates. A total of 46 E. aerogenes, 141 E. cloacue, 11 other Enferobacter spp. (one E. arnnigenus, one E. asburiae, one E. hormaechei, one E. gergoviae, three E. taylorue, and four Enterobucter spp. not further identified), 23 C. fieundii and 62 S. marcescens isolates were collected from 37 different institutions (Figure 1).
Antimicrobial Susceptibility of Enterobacter Species
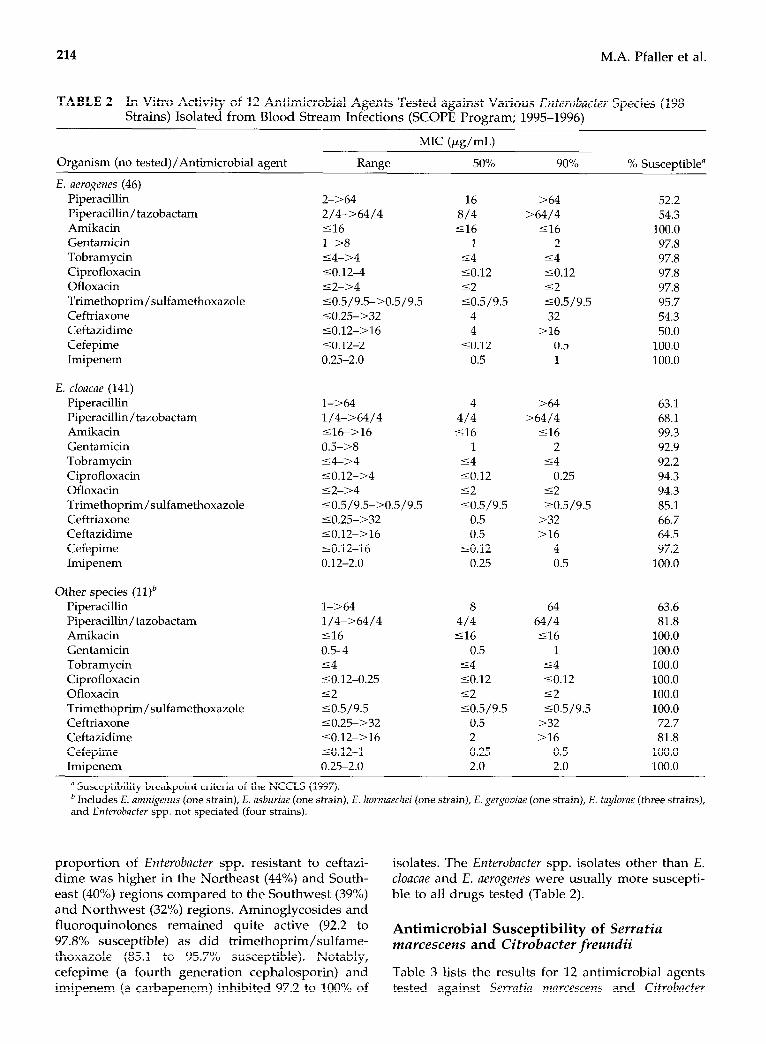
Table 2 lists the results for 12 antimicrobial agents tested against Enterobacter spp. Of the 198 isolates tested, E. cloacae (141 isolates) and E. aerogenes (46 isolates) were most prevalent. Resistance to third generation cephalosporins (ceftazidime, ceftriaxone) and broad-spectrum semisynthetic penicillins (pip- eracillin) with or without an enzyme inhibitor (pip- eracillin/tazobactam) was high, e.g., 35 to 50%. The
TABLE 1 Frequency of Occurrence of Pathogens Isolated from 4725 Blood Stream Infections, SCOPE Program (1995-1996)
Molecular typing of selected ceftazidime-resistant isolates was performed using the RiboPrinterrM (Qualicon, Wilmington, DE, USA) automated ri- botyping system as described previously (Pfaller et al. 1996). Isolates were selected to represent geo- graphically distinct strains as well as temporally re- lated clusters from individual institutions. Ribotype profiles were generated by the RiboPrinterTM after digestion of chromosomal DNA with the restriction endonuclease EcoRI. The ribotype profiles of each isolate were digitized, normalized according to mo- lecular mass standards, and compared to all other profiles in a standardized manner by the instruments computer. Ribotypes were assigned by the computer based on the percent similarity of the banding pat- terns to one another. If 290% of the bands in the respective profiles were identical, the isolates were assigned to the same ribotypes. Those in which ~90% of the bands were identical were assigned to different ribotypes. Additionally, selected isolates were typed using pulsed-field gel electrophoresis (PFGE) as a means of validating the ribotyping re- sults (Pfaller et al. 1994).
% of Rank Pathogens (no. of strains) isolates
1. Coagulase-negative staphylococci (1524) 32.3 2. Staphylococcus aureus (787) 16.7 3. Enterococci (553) 11.7 4. Yeast (394) 8.3 5. Esckerickia coli (303) 6.4 6. Klebsiella spp. (252) 5.3 7. Pseudomonas aeruginosa (235) 5.0 8. Enterobactev spp. (230) 4.9 9. viridans group streptococci (139) 2.9
10. Serratia marcescens (67) 1.4
“Isolates reported from April 1995 through June 1996 in 48
medical centers.
214 M.A. Pfaller et al.
TABLE 2 In Vitro Activity of 12 Antimicrobial Agents Tested against Various Enterobacter Species (198 Strains) Isolated from Blood Stream Infections (SCOPE Program; 1995-1996)
MIC (pg/mL)
Organism (no tested)/Antimicrobial agent Range 50% 90%
E. aerogenes (46)
Piperacillin Piperacillin/tazobactam Amikacin Gentamicin Tobramycin Ciprofloxacin Ofloxacin Trimethoprim/sulfamethoxazole Ceftriaxone Ceftazidime Cefepime Imipenem
E. cloacae (141) Piperacillin Piperacillin/tazobactam Amikacin Gentamicin Tobramycin Ciprofloxacin Ofloxacin Trimethoprim/sulfamethoxazole Ceftriaxone Ceftazidime Cefepime Imipenem
Other species (1 l)b Piperacillin Piperacillin/tazobactam Amikacin Gentamicin Tobramycin Ciprofloxacin Ofloxacin Trimethoprim/sulfamethoxazole Ceftriaxone Ceftazidime Cefepime Imipenem
2-X4 2/4->64/4 516 l->8 54-->4 ~0.124 ~2->4 %0.5/9.5->0.5/9.5 <0.25->32 <0.12->16 50.12-2 0.25-2.0
l-X&l 1/4-x4/4 ~16>16 0.55>8 %4->4 ~0.12->4 <2->4 SO.5/9.5->0.5/9.5 ~0.25->32 ~0.12->16 ~0.12-16 0.12-2.0
l->64 l/4->64/4 516 0.54 54 ~0.12-0.25 52 50.5/9.5 ~0.255>32 ~0.12->16 SO.12-1 0.25-2.0
16 >64 52.2 8/4 >64/4 54.3 ~16 ~16 100.0
1 2 97.8 54 54 97.8 SO.12 SO.12 97.8 52 52 97.8 SO.5/9.5 50.5/9.5 95.7
4 32 54.3 4 >16 50.0
SO.12 0.5 100.0 0.5 1 100.0
4 >64 63.1 4/4 >64/4 68.1 ~16 ~16 99.3
1 2 92.9 54 54 92.2 SO.12 0.25 94.3 52 52 94.3 50.5/9.5 ?0.5/9.5 85.1
0.5 >32 66.7 0.5 >16 64.5
SO.12 4 97.2 0.25 0.5 100.0
8 64 63.6 4/4 64/4 81.8 516 ~16 100.0
0.5 1 100.0 54 54 100.0 SO.12 SO.12 100.0 52 52 100.0 50.5/9.5 50.5/9.5 100.0
0.5 >32 72.7 2 >16 81.8 0.25 0.5 100.0 2.0 2.0 100.0
a Susceptibility breakpoint criteria of the NCCLS (1997). b Includes E. amni,penus (one strain), E. asburiae (one strain), E. hormaechei (one strain), E. gergoviae (one strain), E. faylorae (three strains), and Enferobacfer Lpp. not speciated (four strains).
% Susceptible”
proportion of Entevobactev spp. resistant to ceftazi- dime was higher in the Northeast (44%) and South- east (40%) regions compared to the Southwest (39%) and Northwest (32%) regions. Aminoglycosides and fluoroquinolones remained quite active (92.2 to 97.8% susceptible) as did trimethoprim/sulfame- thoxazole (85.1 to 95.7% susceptible). Notably, cefepime (a fourth generation cephalosporin) and imipenem (a carbapenem) inhibited 97.2 to 100% of
isolates. The Enterobacter spp. isolates other than E. cloacae and E. aerogmes were usually more suscepti- ble to all drugs tested (Table 2).
Antimicrobial Susceptibility of Servatia marcescens and Citrobacter freundii
Table 3 lists the results for 12 antimicrobial agents tested against Serratia marcescens and Citrobacter

Blood Stream Infections 215
TABLE 3 Antimicrobial Activity of 12 Broad-Spectrum Antimicrobial Agents Tested against Blood Stream Isolates of Serratia ma~ce~cen~ and Citrobacter freundii (SCOPE Study 1995-1996)
Organism (no tested)/Antimicrobial agent Range
MIC (&mL)
50% 90% % Susceptible”
S. marcescens (62) Piperacillin Piperacillin/tazobactam Amikacin Gentamicin Tobramycin Ciprofloxacin Ofloxacin Trimethoprim/sulfamethoxazole Ceftriaxone Ceftazidime Cefepime Imipenem
C. fwundii (23) Piperacillin Piperacillin/tazobactam Amikacin Gentamicin Tobramycin Ciprofloxacin Ofloxacin Trimethoprim/sulfamethoxazole Ceftriaxone Ceftazidime Cefepime Imipenem
l-%4 2 l/4->64/4 214 S16->16 516 l->8 2 sl->4 54 %0.12->4 so.12 s2->4 52 <0.5/9.5->0.5/9.5 50.5/9.5 <0.25>32 ~0.25 50.12-8 0.25 50.12-8 so.12 0.12-l 0.25
2-164 16 2/P>64/4 16/4 S16->16 516 sO.5->8 1 s4->4 54 sO.12->4 so.12 s2->4 52 <0.5/9.5->0.5/9.5 50.5/9.5 sO.25->32 1 %0.12->16 1 ~0.124 so.12 0.12-0.5 0.25
a Interpretation of the NCCLS (1997).
freundii blood stream isolates from 29 different hos- pitals. A total of 62 S. mdrcescens and 23 C. freundii were tested. The S. marcescens isolates were remark- ably susceptible with only piperacillin (85.5%), tobra- mycin (69.4), and trimethoprim/sulfamethoxazole (88.7%) falling below the 90% susceptible level. Ceftazidime, cefepime, and imipenem were the most active agents inhibiting 100% of all isolates at con- centrations of 58 pg/mL (51 pg/mL of imipenem). Among the C. fieundii isolates, resistance to “third- generation” cephalosporins (ceftazidime, ceftriax- one), piperacillin, and piperacillin/tazobactam was high, 39.1 to 47.8%. The proportion of C. jkeundii resistant to ceftazidime was greatest in the Northeast and Southwest (50% each) and lowest in the South- east (33%). The aminoglycosides and ciprofloxacin were quite active (91.3 to 95.7% susceptible). Ofloxa- tin was slightly less active than ciprofloxacin against two isolates, but more active than ciprofloxacin against one strain of S. marcescens. As with the En- terobacter spp., cefepime (100% susceptible) and imi- penem (100% susceptible) were very active against all isolates of C. freundii (MI&,, 10.12 pg/mL and 0.25 pg/mL, respectively).
64
8/4 516
4 >4
0.5 52 >0.5/9.5
2
0.5 0.5
>64 >64/4
516 1
54
4 >0.5/9.5
>32 >16
so.12 0.25
85.5 93.5 98.4 90.3 69.4 90.3 91.9 88.7 98.4
100.0 100.0 100.0
52.2 60.9 95.7 91.3 91.3 91.3 82.6 87.0 56.5 60.9
100.0 100.0
Susceptibility of Ceftazidime-Resistant Isolates to Selected Antimicrobial Agents
A total of 84 ceftazidime-resistant isolates from 25 geographically separate medical centers (Figure 1) were further evaluated (Table 4). These isolates were also resistant to ceftriaxone, piperacillin, and pip- eracillin/tazobactam and likely represented stably derepressed Amp C-producing strains of E. aerogenes (23 isolates, 50% of total for the species), E. cloacae (50 isolates, 35% of total for the species), and C. freztndii (nine isolates, 39% of total for the species). The rate in descending order of documented ceftazidime- resistant isolates was Northeast (36% of all docu- mented resistant isolates) = Southeast (36%) > Southwest (15%) > Northwest (13%).
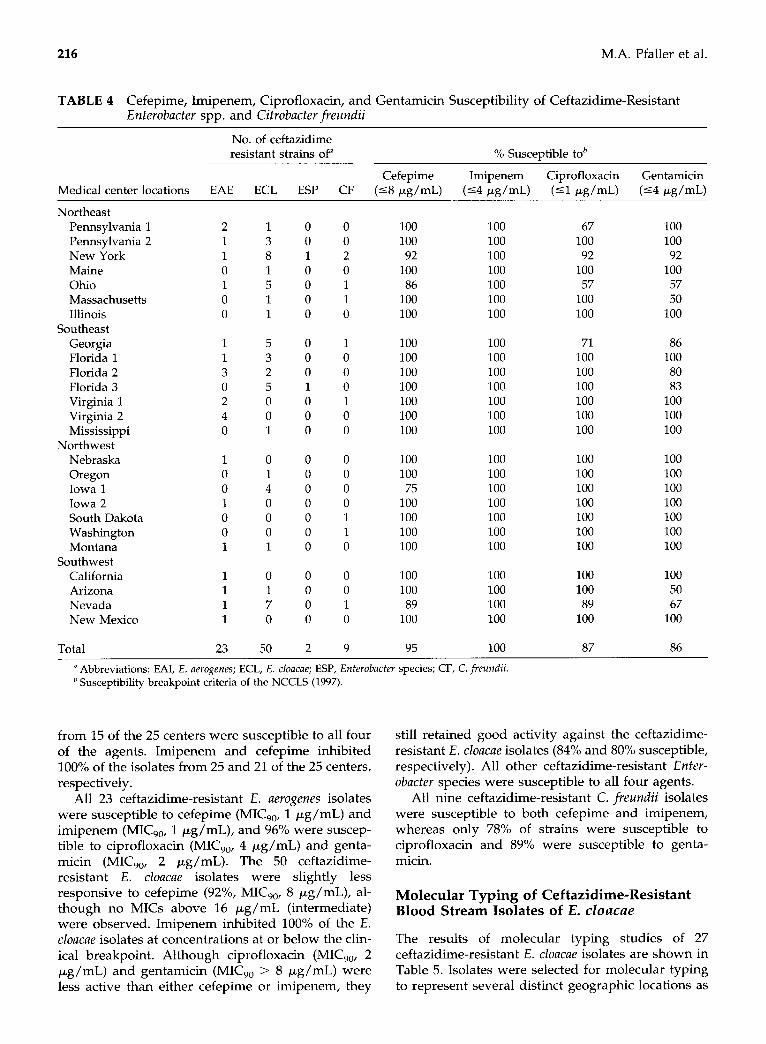
The susceptibility of the 84 ceftazidime-resistant isolates to cefepime, imipenem, ciprofloxacin, and gentamicin is shown in Table 4. Imipenem was the most active agent inhibiting 100% of all ceftazidime- resistant isolates (MIC,,, 1 pg/mL) followed by cefepime (95%; MI&,, 8 pg/mL), ciprofloxacin (87%; MIC,,, 2 pg/mL), and gentamicin (86%; MIC,,, > 8 pg/mL). All of the ceftazidime-resistant isolates
216 M.A. Pfaller et al.
TABLE 4 Cefepime, Imipenem, Ciprofloxacin, and Gentamicin Susceptibility of Ceftazidime-Resistant Enterobacter spp. and Citrobacter fieundii
No. of ceftazidime resistant strains Of” % Susceptible tab
Cefepime Imipenem Ciprofloxacin Gentamicin Medical center locations EAE ECL ESP CF (58 &mL) (54 pg/mL) (51 &mL) (<4 PglmL)
Northeast Pennsylvania 1 Pennsylvania 2 New York Maine Ohio Massachusetts Illinois
Southeast Georgia Florida 1 Florida 2 Florida 3 Virginia 1 Virginia 2 Mississippi
Northwest Nebraska Oregon Iowa 1 Iowa 2 South Dakota Washington Montana
Southwest California Arizona Nevada New Mexico
Total 23
5 3 2 5 0 0 1
0 1 4 0 0 0 1
0 1 7 0
50
0
0
1 0 0 0 0
0 0 0 1 0 0 0
0 0 0 0 0 0 0
0 0 0 0
2
0 100 100 67 100 0 100 100 100 100 2 92 100 92 92 0 100 100 100 100 1 86 100 57 57 1 100 100 100 50 0 100 100 100 100
1 100 100 71 86 0 100 100 100 100 0 100 100 100 80 0 100 100 100 83 1 100 100 100 100 0 100 100 100 100 0 100 100 100 100
0 100 100 100 100 0 100 100 100 100 0 75 100 100 100 0 100 100 100 100 1 100 100 100 100 1 100 100 100 100 0 100 100 100 100
0 100 100 100 100 0 100 100 100 50 1 89 100 89 67 0 100 100 100 100
9 95 100 87 86 -
a Abbreviations: EAI, E. aerogenes; ECL, E. cloacae; ESP, Enterobacter species; CF, C. freundii. b Susceptibility breakpoint criteria of the NCCLS (1997).
from 15 of the 25 centers were susceptible to all four still retained good activity against the ceftazidime- of the agents. Imipenem and cefepime inhibited resistant E. cloacae isolates (84% and 80% susceptible, 100% of the isolates from 25 and 21 of the 25 centers, respectively). All other ceftazidime-resistant Enter- respectively. obacter species were susceptible to all four agents.
All 23 ceftazidime-resistant E. aerogenes isolates were susceptible to cefepime (MI&, 1 &mL) and imipenem (MI&,, 1 &mL), and 96% were suscep- tible to ciprofloxacin (MI&, 4 pg/mL) and genta- micin (MI&,, 2 pg/mL). The 50 ceftazidime- resistant E. cloacae isolates were slightly less responsive to cefepime (92%, MI&,, 8 pg/mL), al- though no MICs above 16 pg/mL (intermediate) were observed. Imipenem inhibited 100% of the E. cloacae isolates at concentrations at or below the clin- ical breakpoint. Although ciprofloxacin (MI&,, 2 pg/mL) and gentamicin (MIC,, > 8 pg/mL) were less active than either cefepime or imipenem, they
All nine ceftazidime-resistant C. freundii isolates were susceptible to both cefepime and imipenem, whereas only 78% of strains were susceptible to ciprofloxacin and 89% were susceptible to genta- micin.
Molecular Typing of Ceftazidime-Resistant Blood Stream Isolates of E. cZoacne
The results of molecular typing studies of 27 ceftazidime-resistant E. cloacae isolates are shown in Table 5. Isolates were selected for molecular typing to represent several distinct geographic locations as

Location Site Ribotype No. of isolates
Pennsylvania 1 225-4 1 2 224-l 2
Ohio 1 224-7 3 396-4 1
New York 1 229-5 1 229-2 1 226-8 1 265-l 1 250-B 1
2 459-l 1
1 229-l 1 228-8 1
2 357-5 1 3 376-8 1
225-5 1 323-8 1 204-4 1
Iowa 1 264-7 1
Nevada 1 226-4 1 225-6 3 224-l 1 225-4 1
Florida
Blood Stream Infections
TABLE 5 Strain Variation among Ceftazidime- Resistant Blood Stream Isolates of Enterobacter cloacae
well as temporally related clusters of isolates from individual institutions.
Genetic discrimination among the 27 ceftazidime- resistant isolates of E. cloacae was achieved by ri- botyping using the restriction enzyme EcoRI and an automated system (RiboPrinterTM, Qualicon, Wilm- ington, DE, USA) (Figure 2). A total of 20 distinct ribotyping profiles were identified among the 27 iso- lates. Generally, each ribotype represented an indi- vidual patient, and epidemiologically unrelated iso- lates of E. cloacae had distinctly different ribotype profiles (Table 5 and Figure 2). Even within the same institution, phenotypically similar (ceftazidime- resistant) isolates were usually distinctly different based on the results of ribotyping and PFGE (data not shown) analysis. Although two ribotypes, 224-l and 225-4, were each observed in two different insti- tutions, there was no evidence for any geographic clustering of resistant strains.
In three instances, the same ribotype of ceftazidime-resistant E. cloacae was isolated from pa- tients hospitalized in the same institution. Ribotype 225-6 included three isolates from a cluster of six bacteremias caused by ceftazidime-resistant E. doa- cue over a period of 146 days at a hospital in the
217
A 1 2 3 4 5 6 MW
B 1 2 3 4 5
FIGURE 2 Ribotype profiles of ceftazidime-resistant iso- lates of E. cloacue. A, isolates from Nevada site 1 (see Table 5); lanes 1 to 3, ribotype 225-6; lane 4, ribotype 224-l; lane 5, ribotype 225-4; lane 6, ribotype 226-4. B, isolates from New York site 1 (see Table 5); lane 1, ribotype 250-8; lane 2, ribotype 229-5; lane 3, ribotype 229-2; lane 4, ribotype 265-l; lane 5, ribotype 226-8.
Southwest. Although three of the bacteremias were caused by distinctly different (patient-unique) strains, the clustering of three infections due to iso- lates of the same DNA type and resistance profile suggests possible nosocomial transmission in that institution. The ribotyping results in this instance were also confirmed by PFGE. Similar clustering was observed in hospitals in Pennsylvania (ribotype 224-l) and Ohio (ribotype 224-7). In contrast, each of the remaining three hospitals with two or more bac- teremias caused by ceftazidime-resistant E. cloacae had strains that were patient-unique without any evidence for nosocomial transmission.
DISCUSSION
The results of this study confirm those of other inves- tigators suggesting that resistance rates to extended spectrum (“third-generation”) cephalosporins, other Plactams and klactamase inhibitor combinations among Enterobacteriaceae such as Enterobacter spp. and Citrobacterfreundii are quite high and may be increasing (Burwen et al. 1994; Quinn 1994; Sanders and Sanders 1988). In a nation wide survey of nosocomial blood

218 M.A. Pfaller et al.
stream infections we observed that the genera most likely to produce Bush group 1 (Amp C) plactamase, Enterobacter, Citrobacter, and Serratia, accounted for ap- proximately 7% of all nosocomial bacteremias and that 30% of these isolates were resistant to ceftazidime and other extended spectrum P-lactams and P-lactamase inhibitor combinations. Resistance was even higher among the Enterobacter species where 50% of E. aero- genes isolates and 36% of E. cloacae isolates were resis- tant to ceftazidime. These findings are similar to those of the National Nosocomial Infection Surveillance Pro- gram conducted by the Centers for Disease Control that indicated that ceftazidime resistance among all Enterobacter spp. isolates was 38% in the United States by 1991, but can markedly vary by geographic region (Burwen et al. 1994).
It is encouraging to note that several antimicrobial agents retain potent activity against these highly re- sistant organisms. Importantly, the carbapenem and the new “fourth-generation” cephalosporin tested were active against virtually all isolates including those stably derepressed Amp C-producing ceftazidime-resistant strains of Enterobacter spp. and C. freundii (Table 4). It is also notable that the fluo- roquinolones, aminoglycosides, and trimethoprim/ sulfamethoxazole retained good activity against these isolates. Although ceftazidime-resistant Enter- obacter and Citrobacter species are frequently cross- resistant to other antimicrobial classes such as fluo- roquinolones and aminoglycosides, ciprofloxacin and gentamicin (as representatives of these classes) inhibited 86% to 87% of the ceftazidime-resistant strains at their respective breakpoint concentrations (Table 4). The overall rank order of activity for the six best agents was: imipenem (100% susceptible) > amikacin = cefepime (98.6%) > ciprofloxacin = gen- tamicin = ofloxacin (93.6 to 94.0%).
The molecular epidemiology of inducible or stably derepressed Amp C-producing Gram-negative ba- cilli has not been well studied. In our investigation, we selected a group of ceftazidime-resistant E. cloacae isolates that represented both geographically distinct locations, as well as isolates from several different patient-episodes of bacteremia within specific insti- tutions. The isolates were typed using a highly stan- dardized and automated ribotyping system that fa- cilitated data analysis and comparison of ribotype profiles (Pfaller et al. 1996). Ribotyping results were also supported by typing with PFGE (Pfaller et al. 1994, 1996; Papasian et al. 1996). The molecular typ- ing results indicated that although clonal spread of a single strain was observed within a given institution, most of the episodes of bacteremia were caused by patient-unique strains of E. cloacae. This suggests that selection of mutant subpopulations within each pa- tient (endogenous infection) by exposure to P-lactam
agents was an important factor in the development of these resistant strains (Jones et al. 1997).
Nosocomial transmission of Amp C-producing E. cloacae may also occur to a limited extent and may be documented by molecular typing coupled with care- ful epidemiologic investigation. These findings have important implications for the control of Amp C P-lactamase-producing E. cloacae and suggest that both formulary restriction of broad spectrum agents (such as ceftazidime) and rigorous attention to infec- tion control procedures will be necessary.
In summary, we have documented the contempo- rary frequency of Amp C p-lactamase producing species of Enterobacter, Citrobacter, and Serratia among nosocomial blood stream isolates in the United States and have demonstrated the potent ac- tivity of drugs in several therapeutic classes against these highly resistant pathogens. We have also used molecular typing methods to demonstrate that al- though spread of a single resistant clone may occur within an institution, the majority of infections caused by ceftazidime-resistant E. cloacae are patient- unique and most likely have been selected by expo- sure to therapeutic p-lactam agents. For control of these resistant organisms we suggest attention to microbiologic recognition of phenotypes, to infection control practices, and to limiting the overuse of cer- tain extended spectrum /3-lactams.
The authors thank Kay Meyer for secretarial assistance in the preparation of this manuscript. This study was partially sup- ported by a grant from Wyeth-Ayerst. We acknowledge the excellent cooperation and participation of all member institu tions of the SCOPE Program. Participants contributing data/ isolates to our study include: Chandler Hospital, Savannah, GA (A. Davis, L. Formby), St. Joseph Hospital, Omaha, NE (S. Cavalieri, A. Lorenzen), St. Jude Medical Center, Fuller- ton, CA (D. Koga, P. Wardell), St. Alexus Medical Center, Bismark, ND (R. Baltzer, S. Ziemann), Sf. Mary’s Hospital, Enid, OK (C. Williams, J Word), Western Pennsylvania Hos- pital, Pittsburgh, PA (K. Gartner, T. Montgomery), Geisinger Medical Center, Danville, PA (P. Bourbeau, M. Dahlman), Mt. Sinai Medical Center, Miami, FL (J. Moore, S. Sharp), Broward General Hospital, Ft. Lauderdale, FL (P. Johnson, J. Stone), Memorial Medical Center, Savannah, GA (M. Mc- Nally, M. Shapiro), VA Medical Center, Portland, OR (R. Tjoelker, D. Sewell), Mercy Hospital Medical Center, Des Moines, IA (M. L. Davenport, C. Grout), Sioux Valley Hospi- tal, Sioux Falls, SD CL. Docken, D. Ohrt), Sacred Heart Medi- cal Center, Spokane, WA (D. Anderson, D. Leo@, Immanuel Medical Center, Omaha, NE (V. Oczki, G. Pullen), Maricopa Medical Center, Phoenix, AZ (J. Chapman, S. Gamble), Co- lumbia Presbyterian Hospital, New York, NY (P. Della-Latta, M. Fracaro), Florida Hospital and Medical Center, Orlando, FL (H. Ferwerda, T. Otal, S. Hernandez), University of lowa Hospitals and Clinics, Iowa City, IA (L. Herwaldt, R. N. Jones, M. A. Pfaller), St. John’s Mercy Medical Center, St.
Blood Stream Infections
Louis, MO (J. Block, L. Meyer), St. Vincent Hospital and Health Center, Billings, MT (L. Temme, S. Skates), University Medical Center of S. Nevada, Las Vegas, NV (J. Bingkam, V. Leslie), Central Maine Medical Center, Lewiston, ME (M. A. Johnson, P. Noddin), United Medical Center, Cheyenne, WY (S. Garner, C. Halverson), Walter 0. Boswell Hospital, Sun City, AZ (J Tkeis, V. Verkoeren), Lutheran General Hospital, Park Ridge, IL (N. Bkarani, C. Galaviz), Akron General Medi- cal Center, Akron, OH (D. Sailsbury, P. Sfeckel), Sentara Norfolk General Hospital, Novfolk, VA (B. Greene, L. Howell), San Bernadino County Medical Center, San Bernadino, CA
REFERENCES
Ballow CH, Schentag JJ (1992) Trends in antimicrobial utilization and bacterial resistance: Report of the Na- tional Resistance Surveillance Group. Diagn Microbial Infect Dis 15(suppl):37S42S.
Brown EH, Spencer RC, Brown JMC (1990) The emergence of bacterial resistance in hospitals: A need for continu- ous surveillance. 1 Hosp Infect 125(suppl A):3539.
Burwen DR, Banejee SN, Gaynes RF, the National Noso- comial Infections Surveillance System (1994) Ceftazi- dime resistance among selected nosocomial Gram- negative bacilli in the United States. 1 Infect Dis 170: 1622-1625.
DeGheldre Y, Maes N, Rost F, DeRyck R, Clevenbergh P, Vincent JL, Struelens MJ (1997) Molecular epidemiology of an outbreak of multidrug-resistant Enterobacter aero- genes infections and in vi,vo emergence of imipenem resistance. ] Clin Microbial 35:152-160.
Ehrhardt AF, Sanders CC (1993) f3-lactam resistance amongst Enterobactev species. j Antimicrob Ckemotker 32(suppl B):l-11.
Gallagher PG (1990) Enterobacfer bacteremia in pediatric patients. Rev lnfecf Dis 12808-812.
Gaston MA (1988) Enterobacter: An emerging nosocomial pathogen. I Hosp Infect 11:197-208.
Jarvis WR, Martone WJ (1992) Predominant pathogens in hospital infections. I Antimicrob Ckemotker 29(suppl A): 19-24.
Jones RN (1992) The current and future impact of antimi- crobial resistance among nosocomial bacterial patho- gens. Diagn Microbial Infect Dis 15(suppl):3%1OS.
Jones RN, Kehrberg EN, Erwin ME, Anderson SC, and the Fluoroquinolone Resistance Surveillance Group (1994) Prevalence of important pathogens and antimicrobial activity of parenteral drugs at numerous medical cen- ters in the United States. Study on the threat of emerg- ing resistance: Real or perceived? Diagn Microbial Infect Dis 19:203-215.
Jones RN, Baquero F, Privitera G, Inoue M, Wiedemann B (1997) Inducible P-lactamase-mediated resistance to third- generation cephalosporins. Clin Microbial Infect. 3(suppl l):S7-520.
Livermore DM (1995) f3-lactamases in laboratory and clin- ical resistance. Clin Microbial Rev 8:557-584.
National Committee for Clinical Laboratory Standards
(M. Tomasulo), Baystate Medical Center, Springfield, MA (M. Gardner, M. Sckulte), Beth Israel Medical Center, New York, NY (W. McKinley, M. Mofyl), United Samaritans Medical Center, Danville, IL (M. Lampman, B. Morris, D. Page,, Parkview Regional Medical Center, Vicksburg, MS (L. Bane, G. Pierce, N. Taylor), Community Hospitals of Indianapolis, Indianapolis, IN (P. Gielerak), Medical College of Virginia, Richmond, VA (M. Edmond, S. Wallace, R. Wenzel), 89th Medical Group, Andrews Air Force Base, MD (A. Varlijen), Presbyterian Health Services, Albuquerque, NM (J. Ferranti).
(1997) Methods for Dilution Antimicrobial Susceptibility Tests for Bacteria that Grow Aerobically, M7-A4, 4th ed. Wayne, PA: National Committee for Clinical Labora- tory Standards.
Papasian CJ, Kinney J, Coffrnan S, Hollis RJ, Pfaller MA (1996) Transmission of Cifrobacter koseri from mother to infant documented by ribotyping and pulsed-field gel electrophoresis. Diagn Microbial Infect Dis 26:63-67.
Pfaller MA, Hollis RJ, Sader HS (1994) Chromosomal re- striction fragment analysis by pulsed-field gel electro- phoresis. In Clinical Microbiology Procedures Handbook, Supplement 1. Ed, HD Isenberg. Washington, DC: American Society for Microbiology, pp 10.5.c.l- 10.5.c.12.
Pfaller MA, Wendt C, Hollis RJ, Wenzel RI’, Fritschel SJ, Neubauer JJ, Herwaldt LA (1996) Comparative evalua- tion of an automated ribotyping system versus pulsed- field gel electrophoresis for epidemiological typing of clinical isolates of Esckerickia coli and Pseudomonas aeruginosa from patients with recurrent Gram-negative bacteremia. Diagn Microbial Infect Dis 25:1-S.
Pitout JDD, Moland ES, Sanders CC, Thomson KS, Fitzsim- mons SR (1997) f3-Lactamases and detection of p-lactam resistance in Enterobacter spp. Anfimicrob Agents Cke- mother 41:35-39.
Quinn JP (1994) Clinical significance of extended-spectrum beta-lactamases. Eur J Clin Microbial Infect Dis 1:3942.
Sanders CC (1984) p-lactamase and non-hydrolytic resis- tance mechanisms. I Antimicrob Ckemofker 13:1-3.
Sanders CC, Sanders WE (1986) Type 1 /3-lactamases of Gram-negative bacteria: Interactions with p-lactam an- tibiotics. I Infect Dis 159:792-800.
Sanders CC, Sanders WE Jr (1988) Clinical and epidemio- logical implications for use of newer cephalosporins. Rev Infect Dis 10:830-836.
Snydman DR (1991) Clinical implications of multi-drug resistance in the intensive care unit. Stand J Infect Dis 22(suppl 78):5463.
Stapleton I’, Shannon K, Phillips I (1995) The ability of /3-lactam antimicrobials to select mutants with dere- pressed /3-lactamase synthesis from Citrobacteufreundii. j Antimicrob Chemotker 361483496.
Voelker R (1996) New group tracks hospital’s drug- resistant bugs. JAMA 275:177-178.




















