
Effect of seizures on the cognitive and behavioral phenotypes ...
Upload
independentCategory
view
2download
0
ORIGINAL ARTICLES
Independent Component Analysis in the Study ofFocal Seizures
Jorge Iriarte,* Elena Urrestarazu,* Julio Artieda,* Miguel Valencia,* Pierre LeVan,†Cesar Viteri,* and Manuel Alegre*
Summary: Independent component analysis (ICA) is a novel tech-nique that can separate statistically independent elements fromcomplex signals. It has demonstrated its utility in separating artifactsand analyzing interictal discharges in EEG. ICA has been usedrecently in ictal recordings, showing the possibility of isolating theictal activity. The goal of our study was to analyze focal seizureswith ICA, decomposing the elements of the seizures to understandtheir genesis and propagation, and to differentiate between varioustypes of focal seizures. We studied 26 focal seizures of temporal,frontal, or parietal origin. Only seizures with suspected focal onsetwere included in the study. The EEG recordings were acquired byusing standard video-EEG equipment, with scalp electrodes. All theoff-line analysis was carried out on a PC by means of specificsoftware developed in the Matlab environment. ICA componentswere calculated with the use of the JADE (Joint ApproximateDiagonalization of Eigen-matrices) algorithm. The decomposition ofthe seizures varied according to the EEG seizure pattern. In theseizures with focal rhythmic theta slow or sharp waves, the rhythmicactivity was separated into one to five components, having an initialcomponent with a clear concordance with the focus, whereas theothers had an onset a few milliseconds later and corresponded toneighboring areas. In the 6 frontal seizures with regional rhythmiclow voltage fast activity, 4 to 10 components were found, practicallywith a simultaneous timing, having a frontal distribution. In the threefrontal seizures with a diffuse attenuation of the EEG signal, it wasnot possible to differentiate components of cerebral origin from thecomponents of muscle artifact. ICA is an interesting tool to study thenature of focal seizures. The results depend on the EEG pattern. Inthe seizures with a clear EEG focal pattern, ICA may be useful toseparate components of the ictal onset from the propagated activity.
Key Words: Independent component analysis, Independent compo-nent analysis, Focal seizures.
(J Clin Neurophysiol 2006;23: 551–558)
BACKGROUNDIndependent component analysis (ICA) is a technique
that can separate statistically independent elements of a signal(Hyvarinen and Oja, 2000; Jung et al., 2001; Vigario et al.,2000). The Joint Approximate Diagonalization of Eigen-matrices (JADE) algorithm (Bartlett et al., 1995; Cardoso,1998) is based on the diagonalization of cumulant matrices.Fourth-order cross-cumulants between the extracted sourcesare jointly minimized, thus making them as independent aspossible. A strong point of JADE for ICA applications is thatit does not have any parameter-tuning requirement. ICA wasoriginally proposed as a method of separating different voicesspeaking at the same time, but can also be applied to otherkinds of biological and physical signals (Brown et al., 2001).In pregnant women, it has been used to separate EKG signalsof the mother and the child (De�Lathauwer et al., 2000; Hoyerand Hyvarinen, 2000). It has been used to analyze signals ofmagnetoencephalography, fMRI, audiograms, or others(Arfanakis et al., 2000; Ikeda and Toyama, 2000; McKeownet al., 1998; Wang et al., 1999). As EEG signals are acomplex sum of several sources of electrical brain activity,they might also benefit from an analysis with the use of ICA(Lagerlund et al., 1997). So far, in electroencephalography,ICA has been proposed as a tool to identify and eliminateartifacts and recently as a way to study spikes and seizures(Jung et al., 2000; Kobayashi et al., 1999; Kobayashi et al.,2001; Makeig et al., 1996; Makeig et al., 1997).
Focal seizures begin in an area called ictal focus andnormally spread to other areas, resulting in various ictalsymptoms (symptomatogenic areas) (Rosenow and Luders,2001). The patterns of propagation can have a prognosticvalue for the success of the epilepsy surgery (Schulz et al.,2000). The main prerequisite for epilepsy surgery is to de-termine the location of the ictal focus; assuming there is onlyone focus, then its removal will ensure the success of theresection. Nowadays, video-EEG monitoring with surfaceelectrodes, if concordant with neuroimaging data, is sufficientfor the purposes of presurgical evaluation. However, in animportant proportion of patients, when the EEG and neuro-imaging data are discordant, studies with intracranial elec-trodes should be performed (Diehl and Luders, 2000).
Since ICA can decompose statistically independentelements of a signal, its use in ictal recordings theoreticallymay be useful to separate components of the seizures. So far,only one study shows some results in focal ictal recordings,
*Clinical Neurophysiology Section, Department of Neurology, ClinicaUniversitaria/Foundation for Applied Medical Research, School of Med-icine, University of Navarra; †Montreal Neurological Institute, McGillUniversity, Montreal, Canada.
Address correspondence and reprint requests to Dr. Jorge Iriarte, ClinicalNeurophysiology Section, Department of Neurology, Clınica Universi-taria, University of Navarra, Avda Pıo XII 36, Pamplona 31008, Navarra,Spain; e-mail: [email protected].
Copyright © 2006 by the American Clinical Neurophysiology SocietyISSN: 0736-0258/06/2306-0551
Journal of Clinical Neurophysiology • Volume 23, Number 6, December 2006 551
and it only indicated that ICA might separate one or severalcomponents of the ictal changes from other activities intemporal seizures (Nam et al., 2002). The goal of our studywas to apply ICA with several types of seizures, at differentlocations and with a variety of EEG patterns, to studywhether ICA can be useful in investigating how the seizuresoriginate and develop and if it can indicate the location of theprimary focus. These data could be valuable in understandingthe evolution of seizures and might simplify the presurgicalevaluation of epilepsy.
METHODSWe studied 26 focal seizures of 12 different patients (1
to 3 per patient). Twelve seizures were temporal seizuresfrom seven presurgical patients (five with mesiotemporalsclerosis (MTS), one with an arteriovenous malformation,and one with a residual lesion to an abscess). Four of thepatients with MTS underwent epilepsy surgery, and after 2years, three of them were seizure-free and one had infrequentsimple partial seizures. Another 12 seizures corresponded to4 patients with frontal epilepsy caused by cortical dysplasia(n � 3) or by cryptogenic epilepsy (normal MRI, n � 1).Finally, the last patient had two seizures related to a parietaloligodendroglioma.
The EEGs were acquired by using the standard video-EEG equipment in our epilepsy unit (64-channel digital EEGwith LaMont amplifiers [LaMont, WI, USA] and Harmoniesoftware [Stellate, Montreal, Canada]). The sampling fre-quency was 200 Hz. Electrodes were placed according to the10 to 20 system, with additional anterotemporal electrodes inT1/T2 and both mastoids as reference. The duration of thesamples was 10 to 40 seconds, to ensure the inclusion of thefirst seconds of the ictal changes. The samples were analyzedin the referential montage referred to the average of bothmastoids.
We included in the study exclusively focal seizures inpatients with interictal spikes concordant with an obvious
MRI abnormality, except for one patient with simple motorpartial seizures involving the right leg. In this patient, thediagnosis was of cryptogenic epilepsy, but the focus wassuspected clinically to be very well defined, and the EEGs,interictal and ictal, were very focal.
The ictal EEGs were categorized into one of threedifferent patterns. The most frequent pattern consisted offocal rhythmic theta slow or sharp waves (12 temporal, 2parietal, 3 frontal). Six frontal seizures appeared as regionalrhythmic low voltage fast activity. The other three frontalseizures showed a diffuse attenuation of the EEG signal.
All the off-line analysis was carried out on a PC bymeans of specific software developed in the Matlab environ-ment. ICA was applied by using the JADE algorithm imple-mented in this Matlab platform. We calculated the maximumpossible number of components (as many as electrodes used,n � 23). The components with likely ictal activity (ictalcomponents) were visually identified by the appearance ofrhythmic activity or low voltage fast activity. The samemorphologic criteria used to identify seizures in the clinicalpractice were applied. EEGs were reconstructed from each ofthe ictal components to facilitate their identification and studytheir localization. To ensure that normal brain activity, suchas occipital alpha rhythm, and muscle artifact would not beerroneously classified as ictal activity, the reconstructedEEGs were visually compared with the original EEG. Onlythe components that were clearly identified as containing ictalactivity, as described above, were included in the study. Thetime of ictal onset was determined in each component byvisually labeling the time in which the ictal activity firstappeared, using an expanded time scale if necessary. Thiswas done independent of the time of ictal onset observed inthe original EEG. To study the spatiotemporal evolution ofthe ictal components, they were ordered, if possible, accord-ing to the time of onset of the ictal activity, and isopotentialmaps of the components were generated from the recon-structed EEGs. A more detailed explanation of the procedure
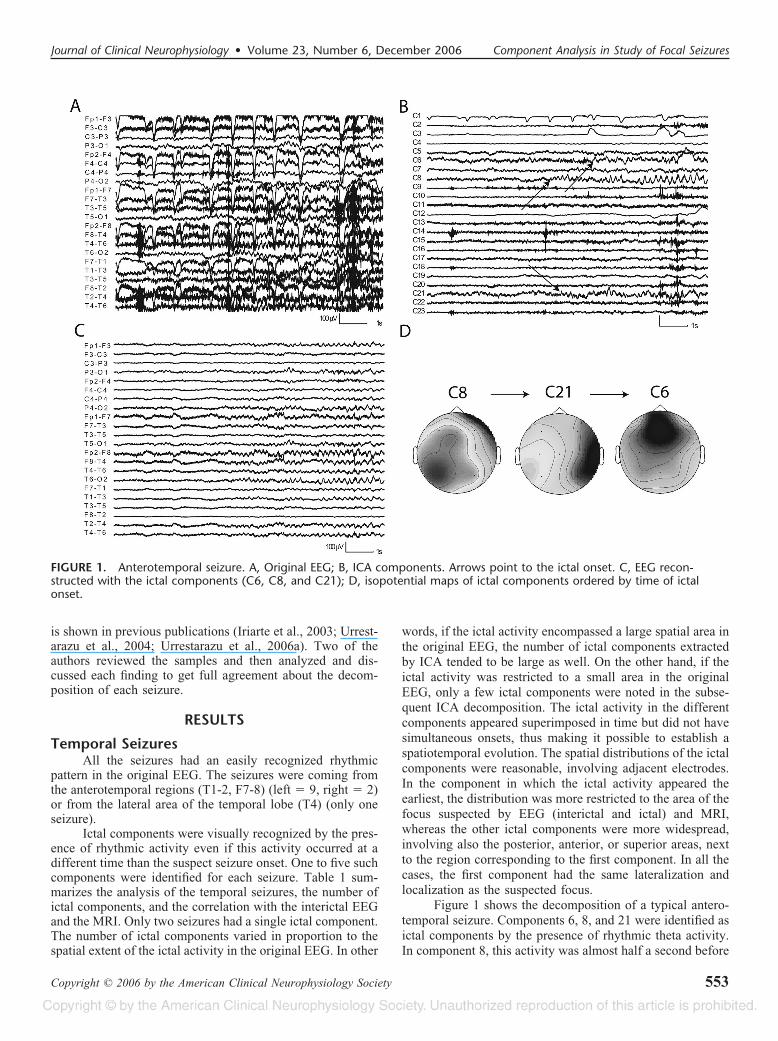
TABLE 1. Summary of the Data of Temporal Seizures: EEG and MRI Findings
Seizure C Topography 1st Comp. Topography During Seizure Evolution Interictal EEG MRI Qx
A1 3 AT right ¡ posterior ipsilateral ¡ central AT right MTS right Yes
A2 2 AT right ¡ posterior ipsilateral
B3 5 AT right ¡ posterior ipsilateral ¡ central ¡ temporal contralateral AT right MTS right Yes
B4 3 AT right ¡ posterior ipsilateral ¡ central
B5 3 AT right ¡ central ¡ temporal contralateral
C5 3 AT right ¡ posterior ipsilateral ¡ temporal contralateral AT right MTS right Yes CPS
C6 3 AT right ¡ central ¡ central, mainly left
D7 3 AT right ¡ posterior ipsilateral AT right MTS right —
D8 3 AT right ¡ central ¡ temporal contralateral
E9 1 AT left AT left MTS left Yes
E10 1 AT left
F11 3 AT right ¡ central ¡ central, mainly left AT right AVM right temporal No
G12 4 LT right ¡ anterior ¡ temporal contralateral LT right (T4) Abscess —
The letter (A ¡ G) indicates the patient. C � number of components. Topography 1st comp., Isopotential map of the ictal component with earliest onset. Topography duringthe seizure evolution � topography of the other components. AT, Anterotemporal; LT, laterotemporal; MTS, mesiotemporal sclerosis; AVM, arteriovenous malformation; Qx, surgeryperformed; Yes � seizure free; Yes, CPS � complex partial seizures persist after surgery; —, sent to another center.
Iriarte et al. Journal of Clinical Neurophysiology • Volume 23, Number 6, December 2006
Copyright © 2006 by the American Clinical Neurophysiology Society552
is shown in previous publications (Iriarte et al., 2003; Urrest-arazu et al., 2004; Urrestarazu et al., 2006a). Two of theauthors reviewed the samples and then analyzed and dis-cussed each finding to get full agreement about the decom-position of each seizure.
RESULTS
Temporal SeizuresAll the seizures had an easily recognized rhythmic
pattern in the original EEG. The seizures were coming fromthe anterotemporal regions (T1-2, F7-8) (left � 9, right � 2)or from the lateral area of the temporal lobe (T4) (only oneseizure).
Ictal components were visually recognized by the pres-ence of rhythmic activity even if this activity occurred at adifferent time than the suspect seizure onset. One to five suchcomponents were identified for each seizure. Table 1 sum-marizes the analysis of the temporal seizures, the number ofictal components, and the correlation with the interictal EEGand the MRI. Only two seizures had a single ictal component.The number of ictal components varied in proportion to thespatial extent of the ictal activity in the original EEG. In other
words, if the ictal activity encompassed a large spatial area inthe original EEG, the number of ictal components extractedby ICA tended to be large as well. On the other hand, if theictal activity was restricted to a small area in the originalEEG, only a few ictal components were noted in the subse-quent ICA decomposition. The ictal activity in the differentcomponents appeared superimposed in time but did not havesimultaneous onsets, thus making it possible to establish aspatiotemporal evolution. The spatial distributions of the ictalcomponents were reasonable, involving adjacent electrodes.In the component in which the ictal activity appeared theearliest, the distribution was more restricted to the area of thefocus suspected by EEG (interictal and ictal) and MRI,whereas the other ictal components were more widespread,involving also the posterior, anterior, or superior areas, nextto the region corresponding to the first component. In all thecases, the first component had the same lateralization andlocalization as the suspected focus.
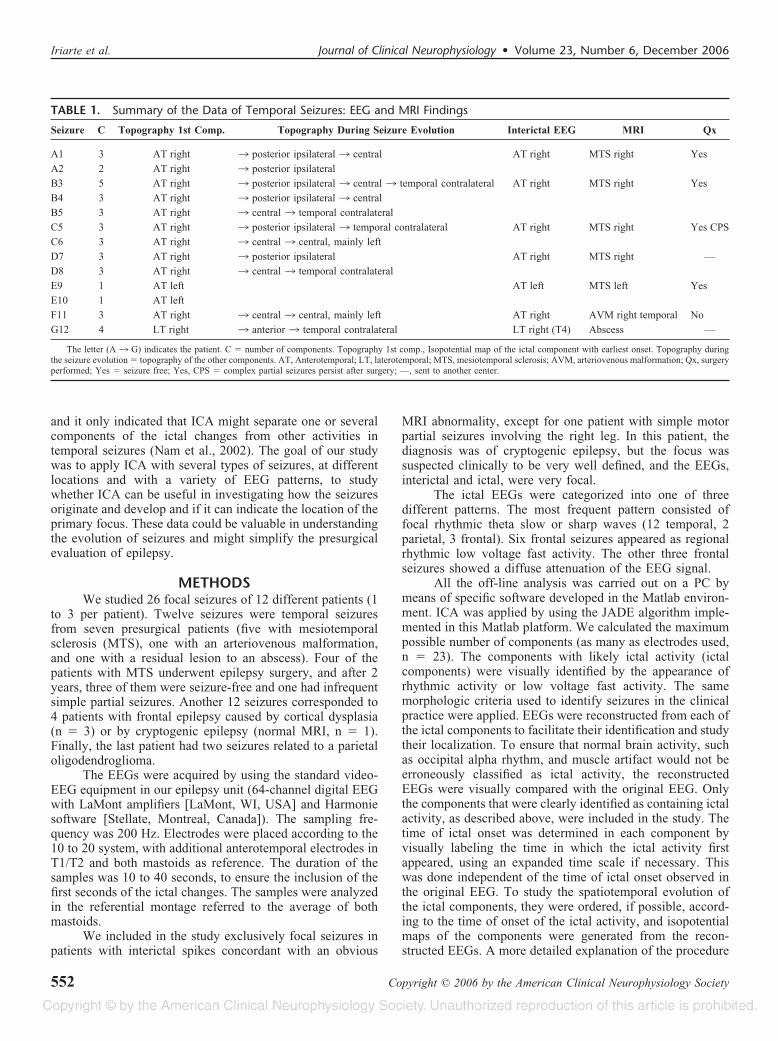
Figure 1 shows the decomposition of a typical antero-temporal seizure. Components 6, 8, and 21 were identified asictal components by the presence of rhythmic theta activity.In component 8, this activity was almost half a second before
FIGURE 1. Anterotemporal seizure. A, Original EEG; B, ICA components. Arrows point to the ictal onset. C, EEG recon-structed with the ictal components (C6, C8, and C21); D, isopotential maps of ictal components ordered by time of ictalonset.
Journal of Clinical Neurophysiology • Volume 23, Number 6, December 2006 Component Analysis in Study of Focal Seizures
Copyright © 2006 by the American Clinical Neurophysiology Society 553

the onset in component 21 and more than 1 second before theonset in component 6. Component 8 was located in the rightanterotemporal region, component 21 had a wider extent andwas located over more posterior aspects of the right temporalareas, and component 4 was bilateral frontal. Figure 2 showsthe analysis of the laterotemporal seizure from the patientwith a sequel to an abscess. Components 1, 7, and 23 wereidentified as ictal components by the presence of rhythmictheta activity. A spatiotemporal evolution of the componentswas also established. Ictal onset in component 1 was a fewmilliseconds before the onsets in components 23 and 7; theonset in these latter components was almost simultaneous.The ictal onset was identified in the EEGs reconstructed fromeach of these components (not shown in the figure), usingdifferent time scales to obtain accurate measurements. Com-ponent 1 was located in the right midtemporal area, andcomponents 23 and 7 were progressively more anterior. Afinal component (component 17) involved contralateral re-gions.
Frontal SeizuresThe ictal recordings of frontal seizures were classified
into three different patterns: rhythmic 1-Hz sharp waves inthe central regions (Cz, C4) (pattern A: three seizures fromone patient), low-voltage focal rhythmic fast activity (patternB: six seizures from two patients), or no obvious changeswith low voltage diffuse activity and muscle artifact (patternC: three seizures from one patient). Table 2 summarizes thefindings in the frontal seizures, with the correlation with theEEG and MRI.
In the seizures with pattern A, ICA isolated the ictalrhythmic sharp waves in a single component (Fig. 3). Thetopography of this component was maximal over the centralareas. In the seizures with pattern B, the ictal activity wasrecognized in 4 to 10 components. The visual identification ofictal components was straightforward, as there was a cleardifferentiation between these and the components with arti-facts or with normal brain activity. The ictal activity in the
FIGURE 2. Laterotemporal seizure. A, Original EEG; B, ICA components. Arrows point to the ictal onset. Vertical lines indicatethe times of ictal onset in the different components. C, Magnified view of the seizure onset section shown in B. Only compo-nents C1, C7, and C23 are shown. D, EEG reconstructed with the ictal components (C1, C7, C17, and C23); E, isopotentialmaps of ictal components ordered by time of ictal onset.
Iriarte et al. Journal of Clinical Neurophysiology • Volume 23, Number 6, December 2006
Copyright © 2006 by the American Clinical Neurophysiology Society554
different components appeared superimposed in time withsimultaneous or almost simultaneous onset, and their topog-raphy was not focal but regional, over a large area on thefrontal lobe. In the three seizures with low-voltage fastactivity (pattern C), it was not possible to differentiate thecomponents with the ictal activity from the components withmuscle activity, because the morphologies of both types ofactivities were very similar.
Parietal SeizuresThe original EEG showed a distinctive focal rhythmic
beta pattern despite high-voltage artifacts caused by eyemovements and muscle. ICA was able to separate the activityin an initial parietal component, followed by other compo-nents with a more diffuse location (as seen in Fig. 4).
DISCUSSIONA focal seizure is an electroclinical event caused by an
activation of an area of cerebral cortex. This activation arisesfrom a specific area and then spreads to other regions,producing the signs and symptoms of the seizure. The ictalEEG recording, especially with intracranial electrodes, is anappropriate method to detect the presence of a seizure andcan help in understanding the nature of this phenomenon(Alarcon et al., 1994; Park et al., 1996; Spencer et al., 1992).However, the EEG is the sum of the electrical activityrecorded simultaneously from several cortical areas. Currentfields of development in EEG include the use of mathematicalanalysis and the combination with other neuroimaging tech-niques (Gotman, 2003; Merlet et al., 1996;; Picton et al.,2000; Scherg and Berg, 1996; Scherg et al., 1999; van derMeij et al., 2001). Thanks to these methods, applied to ictaland interictal discharges, not only in focal but also in gener-alized epilepsies, an evolution of the discharges to different
brain areas with hypersynchrony phenomena has been found(Duckrow and Spencer, 1992; Millan et al., 2001; Santiago-Rodriguez et al., 2002; Stefan et al., 1991). ICA is onemethod of high interest because of its ability to separate theEEG activity into independent components mixed in spaceand time. Each component would represent an independentsource or brain generator.
Nam et al. (2002) could separate components of focalictal activity from artifact activity in temporal seizures. Inthat study, the reconstruction of the EEG with the appropriatecomponents fitted very well with the original seizure, andother rhythmic components were also found. They suggestedthat these other components corresponded to propagatedactivity. This group proposed that ICA could be of interest inthe study of focal seizures. In our study, our goals wereextended to study seizures of other localizations and EEGpatterns to facilitate their identification and interpretation andto study their localization and propagation.
The application of ICA does not use any a priori spatialinformation. Therefore, the separation obtained by ICA dependson the EEG pattern and not on the location of the focus. In theseizures with a distinct rhythmic activity, ICA demonstrated ahigh capacity to separate the ictal activity from the normal brainactivity and artifacts. In most cases, more than one of thecalculated components contained ictal activity. Our interpreta-tion is that different components correspond to different braingenerators that become activated sequentially or simultaneously.Each generator would be, to some extent, independent from therest and would remain active, whereas others are recruited. ICAdoes not separate sources having the same spatial topography,even if they have widely evolving morphologies. Therefore, wedo not expect to see multiple components corresponding to asingle spatially stationary generator. In very focal seizures,
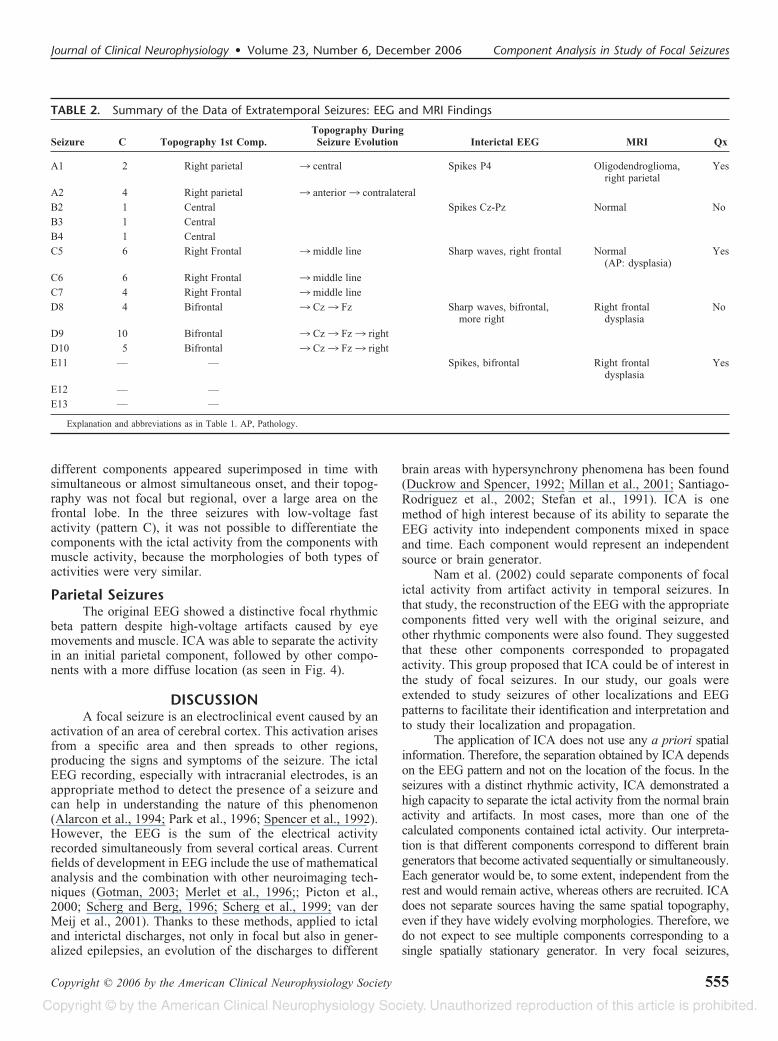
TABLE 2. Summary of the Data of Extratemporal Seizures: EEG and MRI Findings
Seizure C Topography 1st Comp.Topography During
Seizure Evolution Interictal EEG MRI Qx
A1 2 Right parietal ¡ central Spikes P4 Oligodendroglioma,right parietal
Yes
A2 4 Right parietal ¡ anterior ¡ contralateral
B2 1 Central Spikes Cz-Pz Normal No
B3 1 Central
B4 1 Central
C5 6 Right Frontal ¡ middle line Sharp waves, right frontal Normal(AP: dysplasia)
Yes
C6 6 Right Frontal ¡ middle line
C7 4 Right Frontal ¡ middle line
D8 4 Bifrontal ¡ Cz ¡ Fz Sharp waves, bifrontal,more right
Right frontaldysplasia
No
D9 10 Bifrontal ¡ Cz ¡ Fz ¡ right
D10 5 Bifrontal ¡ Cz ¡ Fz ¡ right
E11 — — Spikes, bifrontal Right frontaldysplasia
Yes
E12 — —
E13 — —
Explanation and abbreviations as in Table 1. AP, Pathology.
Journal of Clinical Neurophysiology • Volume 23, Number 6, December 2006 Component Analysis in Study of Focal Seizures
Copyright © 2006 by the American Clinical Neurophysiology Society 555

however, we identified only a single ictal component, supportingthe hypothesis of a single focus. It cannot be excluded that theappearance of multiple ictal components extracted by ICA is dueto a single generator that gradually spreads and is thus notspatially stationary. However, we think that this is unlikelybecause the spatial topographies of the multiple ictal compo-nents were nonoverlapping.
For seizures with an easily recognized rhythmic patternin the original EEG, it was possible to identify one ictalcomponent whose seizure onset occurred earlier than theother components and whose topography corresponded withthe main focus of the patient (as suspected by the interictalEEG and the MRI abnormalities). Other later componentsaccounted for ictal activity in other areas around this focus.Although the ictal activity was clearly visible in the originalEEG, the application of ICA facilitated the identification ofthe ictal focus and revealed the pattern of propagation of theseizure. Our results match adequately with findings obtainedby using simultaneous surface and intracranial recordings(Pacia and Ebersole, 1997). The onset of the ictal activity inthe later components had a clear time organization, support-ing the possibility of the sequential activation of different
generators as a basis for seizure propagation. The samespatiotemporal evolution of the ICA components had beenreported previously in one study realized with depth elec-trodes in patients with temporal lobe epilepsy; it was pro-posed that ICA could be used to understand better thespatiotemporal sequence of the activated connections (Urrest-arazu et al., 2006b). Our study also supports the differentia-tion between mesial and lateral temporal seizures studiedusing EEG (Ebersole and Pacia, 1996).
In some frontal seizures with regional changes withlow-voltage fast activity, ICA also found several components.However, the ictal activity of these components had a simul-taneous onset and their topography was regional over a bigarea of the frontal lobe. This kind of decomposition could beexplained by the simultaneous activation of different gener-ators that would give place to a regional ictal onset. Anotherexplanation for this finding could be that the ictal activityoccurs in a distant area, unrecorded by scalp electrodes(Sharbrough, 1993). The multiple sources extracted by ICAwould thus correspond to the activation of generators bypropagated activity from the original distant focus. In theother seizures with diffuse changes, ICA was unable to
FIGURE 3. Frontal seizure with pattern A. A, Original EEG; B, ICA components; C, EEG reconstructed with the ictal compo-nents (C9); D, isopotential map.
Iriarte et al. Journal of Clinical Neurophysiology • Volume 23, Number 6, December 2006
Copyright © 2006 by the American Clinical Neurophysiology Society556

separate muscle artifact from low voltage brain activity; wecould not clearly identify the ictal activity among the ex-tracted components.
An important issue when using ICA is that there is nodefinitive proof that the separated components correspondto actual independent generators of brain activity. Never-theless, other studies, using ICA for artifact removal orapplying ICA to interictal discharges and comparing theresults with findings from intracranial recordings, supportthe use of ICA to isolate the various sources constitutingthe EEG signal (Iriarte et al., 2003; Kobayashi et al., 2001;Urrestarazu et al., 2006a). However, these results shouldnot necessarily be extrapolated to other kinds of experi-ments; a correct separation of sources is not guaranteedand thus cannot be taken for granted.
Taking into consideration these limitations, our studyshows that ICA could be a useful tool to better understandthe spatiotemporal evolution of the generators in focalseizures with different electroencephalographic patterns,
providing insights into their physiopathogenesis. More-over, ICA can contribute to a better localization of theseizure onset and could be considered as a noninvasivetechnique that may diminish the need for more aggressivesteps in the planning of epilepsy surgery. Further studiesare needed to corroborate the accuracy of ICA in recon-structing the spatiotemporal evolution of focal seizuresand in localizing the ictal focus.
ACKNOWLEDGMENTSThis project was partially funded through the “UTE
project CIMA” and by the Government of Navarra, grants forresearch in Health 12/2003 and 16/2003. Dr. Urrestarazu isa Research Fellow supported by a grant of the Department ofEducation of the Basque Government; her current address isMontreal Neurologic Institute, McGill University, Montreal,Canada.
FIGURE 4. Parietal seizure. A, Original EEG; B, ICA components. Arrows point to the ictal onset. C, Magnified view of theseizure onset section shown in B. Only components C15 and C16 are shown. D, EEG reconstructed with the ictal components(C15 and C16); E, isopotential maps of ictal components ordered by time of ictal onset.
Journal of Clinical Neurophysiology • Volume 23, Number 6, December 2006 Component Analysis in Study of Focal Seizures
Copyright © 2006 by the American Clinical Neurophysiology Society 557
REFERENCESAlarcon G, Guy CN, Binnie CD, et al. Intracerebral propagation of interictal
activity in partial epilepsy: implications for source localisation. J NeurolNeurosurg Psychiatry. 1994;57:435–449.
Arfanakis K, Cordes D, Haughton VM, et al. Combining independentcomponent analysis and correlation analysis to probe interregionalconnectivity in fMRI task activation datasets. Magn Reson Imaging.2000;18:921–930.
Bartlett MS, Makeig S, Bell AJ, et al. Independent component analysis ofEEG data. Abstr Soc Neurosci. 1995;21:437.
Brown GD, Yamada S, Sejnowski TJ. Independent component analysis at theneural cocktail party. Trends Neurosci. 2001;24:54–63.
Cardoso JF. Blind signal separation: statistical principles. Proceedings of theIEEE. 1998;9:2009–2025.
De-Lathauwer L, De-Moor B, Vandewalle J. Fetal electrocardiogram extrac-tion by blind source subspace separation. IEEE Trans Biomed Eng.2000;47:567–572.
Diehl B, Luders HO. Temporal lobe epilepsy: when are invasive recordingsneeded? Epilepsia. 2000;41(Suppl 3):S61–S74.
Duckrow RB, Spencer SS. Regional coherence and the transfer of ictalactivity during seizure onset in the medial temporal lobe. Electroen-cephalogr Clin Neurophysiol. 1992;82:415–422.
Ebersole JS, Pacia SV. Localization of temporal lobe foci by ictal EEGpatterns. Epilepsia. 1996;37:386–399.
Gotman J. Noninvasive methods for evaluating the localization and propa-gation of epileptic activity. Epilepsia. 2003;44(Suppl 12):21–29.
Hoyer PO, Hyvarinen A. Independent component analysis applied to featureextraction from colour and stereo images. Network. 2000;11:191–210.
Hyvarinen A, Oja E. Independent component analysis: algorithms andapplications. Neural Netw. 2000;13:411–430.
Ikeda S, Toyama K. Independent component analysis for noisy data: MEGdata analysis. Neural Netw. 2000;13:1063–1074.
Iriarte J, Urrestarazu E, Valencia M, et al. Independent component analysisas a tool to eliminate artifacts in EEG: a quantitative study. J ClinNeurophysiol. 2003;20:249–257.
Jung TP, Makeig S, Humphries C, et al. Removing electroencephalographicartifacts by blind source separation. Psychophysiology. 2000;37:163–178.
Jung TP, Makeig S, McKeown MJ, et al. Imaging brain dynamics usingindependent component analysis. Proc IEEE. 2001;89:1107–1120.
Kobayashi K, James CJ, Nakahori T, et al. Isolation of epileptiform dis-charges from unaveraged EEG by independent component analysis.Clin Neurophysiol. 1999;110:1755–1763.
Kobayashi K, Merlet I, Gotman J. Separation of spikes from background byindependent component analysis with dipole modeling and comparisonto intracranial recording. Clin Neurophysiol. 2001;112:405–413.
Lagerlund TD, Sharbrough FW, Busacker NE. Spatial filtering of multichan-nel electroencephalographic recordings through principal componentanalysis by singular value decomposition. J Clin Neurophysiol. 1997;14:73–82.
Makeig S, Bell AJ, Jung TP, Sejnowski TJ. Independent component analysisof electroencephalographic data. Adv Neurol Info Process Syst. 1996;8:145–151.
Makeig S, Jung TP, Bell AJ, et al. Blind separation of auditory event-related brain responses into independent components. Proc NatlAcad Sci U S A. 1997;94:10979–10984.
McKeown MJ, Makeig S, Brown GG, et al. Analysis of fMRI data by blind
separation into independent spatial components. Hum Brain Mapping.1998;6:160–188.
Merlet I, Garcia-Larrea L, Gregoire MC, et al. Source propagation ofinterictal spikes in temporal lobe epilepsy. Correlations between spikedipole modelling and [18F]fluorodeoxyglucose PET data. Brain. 1996;119(Pt 2):377–392.
Millan E, Abou-Khalil B, Delbeke D, Konrad P. Frontal localization ofabsence seizures demonstrated by ictal positron emission tomography.Epilepsy Behav. 2001;2:54–60.
Nam H, Yim TG, Han SK, et al. Independent component analysis of ictalEEG in medial temporal lobe epilepsy. Epilepsia. 2002;43:160–164.
Pacia SV, Ebersole JS. Intracranial EEG substrates of scalp ictal patternsfrom temporal lobe foci. Epilepsia. 1997;38:642–654.
Park YD, Murro AM, King DW, et al. The significance of ictal depth EEGpatterns in patients with temporal lobe epilepsy. ElectroencephalogrClin Neurophysiol. 1996;99:412–415.
Picton TW, van Roon P, Armilio ML, et al. The correction of ocular artifacts:a topographic perspective. Clin Neurophysiol. 2000;111:53–65.
Rosenow F, Luders H. Presurgical evaluation of epilepsy. Brain. 2001;124:1683–1700.
Santiago-Rodriguez E, Harmony T, Fernandez-Bouzas A, et al. Sourceanalysis of polyspike and wave complexes in juvenile myoclonicepilepsy. Seizure. 2002;11:320–324.
Scherg M, Bast T, Berg P. Multiple source analysis of interictal spikes: goals,requirements, and clinical value. J Clin Neurophysiol. 1999;16:214–224.
Scherg M, Berg P. New concepts of brain source imaging and localization.Electroencephalogr Clin Neurophysiol Suppl. 1996;46:127–37.
Schulz R, Luders HO, Hoppe M, et al. Interictal EEG and ictal scalp EEGpropagation are highly predictive of surgical outcome in mesial tempo-ral lobe epilepsy. Epilepsia. 2000;41:564–570.
Sharbrough FW. Scalp-recorded ictal patterns in focal epilepsy. J ClinNeurophysiol. 1993;10:262–267.
Spencer SS, Guimaraes P, Katz A, et al . Morphological patterns of seizuresrecorded intracranially. Epilepsia. 1992;33:537–545.
Stefan H, Schneider S, Abraham-Fuchs K, et al. The neocortico to mesio-basal limbic propagation of focal epileptic activity during the spike-wave complex. Electroencephalogr Clin Neurophysiol. 1991;79:1–10.
Urrestarazu E, Iriarte J, Alegre M, et al. Independent component analysisremoving artifacts in ictal recordings. Epilepsia. 2004;45:1071–1078.
Urrestarazu E, Iriarte J, Artieda J, et al. Independent component analysisseparates spikes of different origin in the EEG. J Clin Neurophysiol.2006a;23:72–78.
Urrestarazu E, LeVan P, Gotman G. Independent component analysis iden-tifies ictal bitemporal activity in intracranial recordings at the time ofunilateral discharges. Clin Neurophysiol. 2006b;117:549–561.
van der Meij W, Huiskamp GJ, Rutten GJ, et al. The existence of two sourcesin rolandic epilepsy: confirmation with high resolution EEG, MEG andfMRI. Brain Topogr. 2001;13:275–282.
Vigario R, Sarela J, Jousmaki V, et al. Independent component approach tothe analysis of EEG and MEG recordings. IEEE Trans Biomed Eng.2000;47:589–593.
Wang ZS, Cheung JY, Chen JD. Blind separation of multichannel electro-gastrograms using independent component analysis based on a neuralnetwork. Med Biol Eng Comput. 1999;37:80–86.
Iriarte et al. Journal of Clinical Neurophysiology • Volume 23, Number 6, December 2006
Copyright © 2006 by the American Clinical Neurophysiology Society558
Copyright © 2022 FDOKUMEN




















