Increased risk of pre-eclampsia and fetal death in HIV-infected pregnant women receiving highly...
14
11th Conference on Retroviruses and Opportunistic Infections February 8-11, San Francisco, CA 11th Conference on Retroviruses and Opportunistic Infections February 8-11, San Francisco, CA Increased risk of pre-eclampsia and fetal death in HIV-infected pregnant women receiving highly active antiretroviral therapy Increased risk of pre Increased risk of pre - - eclampsia eclampsia and and fetal fetal death death in HIV in HIV - - infected pregnant women infected pregnant women receiving highly receiving highly active active antiretroviral therapy antiretroviral therapy O Coll, A Suy, E Martinez , M Lonca, E de Lazzari, S Pisa, M Larrousse, A Milinkovic, S Hernandez, J Mallolas, JL Blanco, F Garcia, JM Miró, V Cararach, JA Vanrell, JM Gatell. O Coll, A Suy, E Martinez , M Lonca, E de Lazzari, S Pisa, M Larrousse, A Milinkovic, S Hernandez, J Mallolas, JL Blanco, F Garcia, JM Miró, V Cararach, JA Vanrell, JM Gatell. Hospital Clinic, Barcelona, Spain. Hospital Clinic, Barcelona, Spain. e-mail: [email protected] e-mail: [email protected]
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Increased risk of pre-eclampsia and fetal death in HIV-infected pregnant women receiving highly...
11th Conference on Retroviruses and Opportunistic InfectionsFebruary 8-11, San Francisco, CA
11th Conference on Retroviruses and Opportunistic InfectionsFebruary 8-11, San Francisco, CA
Increased risk of pre-eclampsia and fetal
death in HIV-infected pregnant women
receiving highly active antiretroviral therapy
Increased risk of preIncreased risk of pre--eclampsiaeclampsia and and fetal fetal
death death in HIVin HIV--infected pregnant women infected pregnant women
receiving highly receiving highly activeactive antiretroviral therapyantiretroviral therapy
O Coll, A Suy, E Martinez, M Lonca, E de Lazzari, S Pisa,M Larrousse, A Milinkovic, S Hernandez, J Mallolas, JL Blanco,
F Garcia, JM Miró, V Cararach, JA Vanrell, JM Gatell.
O Coll, A Suy, E Martinez, M Lonca, E de Lazzari, S Pisa,M Larrousse, A Milinkovic, S Hernandez, J Mallolas, JL Blanco,
F Garcia, JM Miró, V Cararach, JA Vanrell, JM Gatell.
Hospital Clinic,Barcelona, Spain.Hospital Clinic,
Barcelona, Spain.
e-mail: [email protected]: [email protected]

Increased risk of pre-eclampsia and fetal death in HIV-infected women on HAART
BACKGROUNDIncreased risk of preIncreased risk of pre--eclampsiaeclampsia and and fetalfetal death death in HIVin HIV--infected women on infected women on HAARTHAART
BACKGROUND• A longer and better living and a reasonably low risk of mother-
to-child transmission have led to an increase in the number of pregnancies among HIV-infected women.
• Outcomes and adverse effects of antiretreoviral therapy in pregnant HIV-infected women have been mainly focused on the fetus and the infant, and rarely on the mother.
• Pre-eclampsia was a rare complication of pregnancy in HIV-infected women, even much less frequent than in the general population. However, we have detected an increase in the cases of pre-eclampsia and fetal death in HIV-infected women receiving HAART, and both conditions coexisted more commonly than expected.
• A longer and better living and a reasonably low risk of mother-to-child transmission have led to an increase in the number of pregnancies among HIV-infected women.
• Outcomes and adverse effects of antiretreoviral therapy in pregnant HIV-infected women have been mainly focused on the fetus and the infant, and rarely on the mother.
• Pre-eclampsia was a rare complication of pregnancy in HIV-infected women, even much less frequent than in the general population. However, we have detected an increase in the cases of pre-eclampsia and fetal death in HIV-infected women receiving HAART, and both conditions coexisted more commonly than expected.
Increased risk of pre-eclampsia and fetal death in HIV-infected women on HAART
OBJECTIVESIncreased risk of preIncreased risk of pre--eclampsiaeclampsia and and fetalfetal death death in HIVin HIV--infected women on infected women on HAARTHAART
OBJECTIVES
• To study the incidence and the risk factors
for pre-eclampsia and fetal death in the
general population of pregnant women and
in the population of pregnant HIV-infected
women followed in our institution.
• To study the incidence and the risk factors
for pre-eclampsia and fetal death in the
general population of pregnant women and
in the population of pregnant HIV-infected
women followed in our institution.

Increased risk of pre-eclampsia and fetal death in HIV-infected women on HAART
PATIENTS AND DESIGNIncreasedIncreased riskrisk ofof prepre--eclampsia eclampsia andand fetal fetal deathdeath in HIVin HIV--infectedinfected womenwomen onon HAARTHAART
PATIENTS AND DESIGNPATIENTS• Prospective database with all pregnant women cared in our institution starting January 1, 2001• Prospective database with all pregnant HIV-infected women cared in our institution starting November 1, 1985• Demographic and obstetrical variables for each woman, and variables on HIV infection, AIDS-related illnesses, and antiretroviral therapy for those HIV-infected were collected• Decisions regarding initiation of antiretroviral therapy and type of antiretrovirals included were done according recommendations existing and independent from the participation in this study• Informed consent
DESIGN• Prospective cohort study• 1 institution caring for pregnant women in an area of 2.5 million inhabitants in Barcelona, Spain• For the purpose of the study, censorship was established on July 31, 2003.
PATIENTSPATIENTS•• Prospective database with all pregnant women cared in our instiProspective database with all pregnant women cared in our institution tution starting January 1, 2001starting January 1, 2001•• Prospective database with all pregnant HIVProspective database with all pregnant HIV--infected women cared in our infected women cared in our institution starting November 1, 1985institution starting November 1, 1985•• Demographic and obstetrical variables for each woman, and variaDemographic and obstetrical variables for each woman, and variables on HIV bles on HIV infection, AIDSinfection, AIDS--related illnesses, and antiretroviral therapy for those HIVrelated illnesses, and antiretroviral therapy for those HIV--infected were collectedinfected were collected•• Decisions regarding initiation of antiretroviral therapy and tyDecisions regarding initiation of antiretroviral therapy and type of pe of antiretroviralsantiretrovirals included were done according recommendations existing and included were done according recommendations existing and independent from the participation in this studyindependent from the participation in this study•• Informed consentInformed consent
DESIGNDESIGN•• Prospective cohort studyProspective cohort study•• 1 institution caring for pregnant women in an area of 2.5 milli1 institution caring for pregnant women in an area of 2.5 million inhabitants in on inhabitants in Barcelona, SpainBarcelona, Spain•• For the purpose of the study, censorship was established on JulFor the purpose of the study, censorship was established on July 31, 2003.y 31, 2003.
GENERAL POPULATION•Periodical visits following current recommendations and routine blood chemistry and cells, and blood pressure and qualitative urine test for proteinuria in each visit.• At first visit, screening for hepatitis B and C viruses, CMV, rubella, syphilis, toxoplasmosis, asymptomatic bacteriuria, chlamydia and gonococci. Routine screening for HIV for women not previously known to be infected from January 1990; prior to this date, restricted to women at known risk for HIV.• Routine screening for gestational diabetes mellitus at 24-48 weeks, sonography for the assessment of age and fetal abnormalities at 12, 22, and 32 weeks, and for group B streptococcus before labor.•Additional standardised care was given to women with specific condictions.
HIV-INFECTED WOMEN• Information concerning decision to continue pregnancy according to Spanish law.• Antiretroviral therapy offered or maintaned according to the availability and recommendations at the time of pregnancy. Triple therapy (HAART) routinely offered from August 1998.
GENERAL POPULATIONGENERAL POPULATION••Periodical visits following current recommendations and routine Periodical visits following current recommendations and routine blood chemistry and blood chemistry and cells, and blood pressure and qualitative urine test for cells, and blood pressure and qualitative urine test for proteinuriaproteinuria in each visit.in each visit.•• At first visit, screening for hepatitis B and C viruses, CMV, rAt first visit, screening for hepatitis B and C viruses, CMV, rubella, syphilis, ubella, syphilis, toxoplasmosis, asymptomatic toxoplasmosis, asymptomatic bacteriuriabacteriuria, chlamydia and gonococci. Routine screening , chlamydia and gonococci. Routine screening for HIV for women not previously known to be infected from Januafor HIV for women not previously known to be infected from January 1990; prior to this ry 1990; prior to this date, restricted to women at known risk for HIV.date, restricted to women at known risk for HIV.•• Routine screening for gestational diabetes mellitus at 24Routine screening for gestational diabetes mellitus at 24--48 weeks, 48 weeks, sonographysonography for the for the assessment of age and fetal abnormalities at 12, 22, and 32 weekassessment of age and fetal abnormalities at 12, 22, and 32 weeks, and for group B s, and for group B streptococcus before labor.streptococcus before labor.••Additional Additional standardisedstandardised care was given to women with specific care was given to women with specific condictionscondictions..
HIVHIV--INFECTED WOMENINFECTED WOMEN•• Information concerning decision to continue pregnancy accordingInformation concerning decision to continue pregnancy according to Spanish law.to Spanish law.•• Antiretroviral therapy offered or Antiretroviral therapy offered or maintanedmaintaned according to the availability and according to the availability and recommendations at the time of pregnancy. Triple therapy (HAART)recommendations at the time of pregnancy. Triple therapy (HAART) routinely offered routinely offered from August 1998.from August 1998.
Increased risk of pre-eclampsia and fetal death in HIV-infected women on HAART
CLINICAL ASSESSMENTIncreasedIncreased riskrisk ofof prepre--eclampsia eclampsia andand fetal fetal deathdeath in HIVin HIV--infectedinfected womenwomen onon HAARTHAART
CLINICAL ASSESSMENT

DEFINITIONS• The estimated date of pregnancy was calculated with the last menstruation and adjusted by sonography if discordance.• HAART was considered if antiretroviral therapy included at least 3 drugs.• Pre-eclampsia was routinely screened in all women through blood pressure and proteinuria assessment in all prenatal visits, during labor, and the immediate postpartum. Pre-eclampsia was defined as blood pressure ≥140/90 mmHg plus proteinuria ≥ 300mg/24h. In all cases coded as pregnancy hypertension or pre-eclampsia, clinical records and laboratory tests were reassessed. Only cases that fully met pre-eclampsia criteria were considered.• Fetal death (stillbirth) was considered as an intrauterine fetal death after 22 weeks of pregnancy. All cases of fetal demise are individually reviewed by the perinatally mortality hospital committee, and fetal necropsy and cariotype are done.
DEFINITIONSDEFINITIONS
•• The estimated date of pregnancy was calculated with the last meThe estimated date of pregnancy was calculated with the last menstruation nstruation and adjusted by and adjusted by sonographysonography if discordance.if discordance.
•• HAART was considered if antiretroviral therapy included at leasHAART was considered if antiretroviral therapy included at least 3 drugs.t 3 drugs.
•• PrePre--eclampsiaeclampsia was routinely screened in all women through blood pressure was routinely screened in all women through blood pressure and and proteinuriaproteinuria assessment in all prenatal visits, during labor, and the assessment in all prenatal visits, during labor, and the immediate postpartum. Preimmediate postpartum. Pre--eclampsiaeclampsia was defined as blood pressure was defined as blood pressure ≥≥140/90 140/90 mmHg plus mmHg plus proteinuriaproteinuria ≥≥ 300mg/24h. In all cases coded as pregnancy 300mg/24h. In all cases coded as pregnancy hypertension or prehypertension or pre--eclampsiaeclampsia, clinical records and laboratory tests were , clinical records and laboratory tests were reassessed. Only cases that fully met prereassessed. Only cases that fully met pre--eclampsiaeclampsia criteria were considered.criteria were considered.
•• Fetal death (stillbirth) was considered as an intrauterine fetaFetal death (stillbirth) was considered as an intrauterine fetal death after 22 l death after 22 weeks of pregnancy. All cases of fetal demise are individually rweeks of pregnancy. All cases of fetal demise are individually reviewed by the eviewed by the perinatallyperinatally mortality hospital committee, and fetal necropsy and mortality hospital committee, and fetal necropsy and cariotypecariotype are are done.done.
Increased risk of pre-eclampsia and fetal death in HIV-infected women on HAART
DEFINITIONSIncreasedIncreased riskrisk ofof prepre--eclampsia eclampsia andand fetal fetal deathdeath in HIVin HIV--infectedinfected womenwomen onon HAARTHAART
DEFINITIONS
• The incidences of pre-eclampsia, stillbirth and both were calculated in
the general and in the HIV-infected populations of pregnant women at
different time points.
• The risk for pre-eclampsia, stillbirth, or any of them were calculated in
the general population including HIV-infected women, in HIV-infected
women, and in HIV-infected women receiving HAART.
• Risk factors were estimated through logistic regression models.
Multivariate models were constructed through stepwise selection of
those variables showing an univariate P value <0.1. A significance level
of 95% was considered in all statistical procedures.
•• The incidences of preThe incidences of pre--eclampsiaeclampsia, stillbirth and both were calculated in , stillbirth and both were calculated in
the general and in the HIVthe general and in the HIV--infected populations of pregnant women at infected populations of pregnant women at
different time points.different time points.
•• The risk for preThe risk for pre--eclampsiaeclampsia, stillbirth, or any of them were calculated in , stillbirth, or any of them were calculated in
the general population including HIVthe general population including HIV--infected women, in HIVinfected women, in HIV--infected infected
women, and in HIVwomen, and in HIV--infected women receiving HAART. infected women receiving HAART.
•• Risk factors were estimated through logistic regression models.Risk factors were estimated through logistic regression models.
Multivariate models were constructed through stepwise selection Multivariate models were constructed through stepwise selection of of
those variables showing an those variables showing an univariateunivariate P value <0.1. A significance level P value <0.1. A significance level
of 95% was considered in all statistical procedures. of 95% was considered in all statistical procedures.
Increased risk of pre-eclampsia and fetal death in HIV-infected women on HAART
STATISTICAL ANALYSISIncreasedIncreased riskrisk ofof prepre--eclampsia eclampsia andand fetal fetal deathdeath in HIVin HIV--infectedinfected womenwomen onon HAARTHAART
STATISTICAL ANALYSIS
Increased risk of pre-eclampsia and fetal death in HIV-infected women on HAART
POPULATION AND CASESIncreasedIncreased riskrisk ofof prepre--eclampsia eclampsia andand fetal fetal deathdeath in HIVin HIV--infectedinfected womenwomen onon HAARTHAART
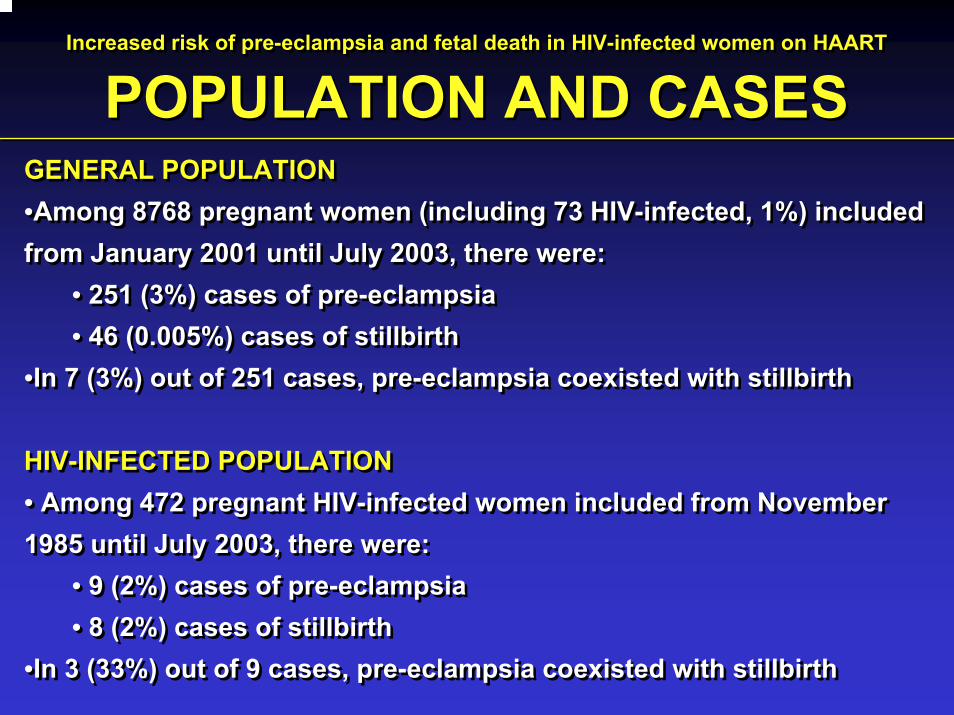
POPULATION AND CASESGENERAL POPULATION•Among 8768 pregnant women (including 73 HIV-infected, 1%) includedfrom January 2001 until July 2003, there were:
• 251 (3%) cases of pre-eclampsia• 46 (0.005%) cases of stillbirth
•In 7 (3%) out of 251 cases, pre-eclampsia coexisted with stillbirth
HIV-INFECTED POPULATION• Among 472 pregnant HIV-infected women included from November 1985 until July 2003, there were:
• 9 (2%) cases of pre-eclampsia• 8 (2%) cases of stillbirth
•In 3 (33%) out of 9 cases, pre-eclampsia coexisted with stillbirth
GENERAL POPULATION•Among 8768 pregnant women (including 73 HIV-infected, 1%) includedfrom January 2001 until July 2003, there were:
• 251 (3%) cases of pre-eclampsia• 46 (0.005%) cases of stillbirth
•In 7 (3%) out of 251 cases, pre-eclampsia coexisted with stillbirth
HIV-INFECTED POPULATION• Among 472 pregnant HIV-infected women included from November 1985 until July 2003, there were:
• 9 (2%) cases of pre-eclampsia• 8 (2%) cases of stillbirth
•In 3 (33%) out of 9 cases, pre-eclampsia coexisted with stillbirth

Increased risk of pre-eclampsia and fetal death in HIV-infected women on HAART
INCIDENCE IN GENERAL POPULATIONIncreasedIncreased riskrisk ofof prepre--eclampsia eclampsia andand fetal fetal deathdeath in HIVin HIV--infectedinfected womenwomen onon HAARTHAART
INCIDENCE IN GENERAL POPULATION
Calendar year
0
10
20
30
40
50
2001 2002 2003
%
3113 3634 2021At risk
Pre-eclampsia Stillbirth Bad Outcome (either)
Test for trend p-value: 0.434 0.862 0.575

Increased risk of pre-eclampsia and fetal death in HIV-infected women on HAART
INCIDENCE IN HIV-INFECTED POPULATIONIncreasedIncreased riskrisk ofof prepre--eclampsia eclampsia andand fetal fetal deathdeath in HIVin HIV--infectedinfected womenwomen onon HAARTHAART
INCIDENCE IN HIV-INFECTED POPULATION
Calendaryear
0
10
20
30
40
50
85-86-87 88-89 90-91 92-93 94-95 96-97 98-99 00-01 02-03
%
54 64 72 56 45 36 33 60 52At risk
Pre-eclampsia Stillbirth Bad Outcome (either)
Test for trend p-value: <0.001 0.006 <0.001
Increased risk of pre-eclampsia and fetal death in HIV-infected women on HAART
RISK FACTORS ALL WOMEN (n=8768)IncreasedIncreased riskrisk ofof prepre--eclampsia eclampsia andand fetal fetal deathdeath in HIVin HIV--infectedinfected womenwomen onon HAARTHAART
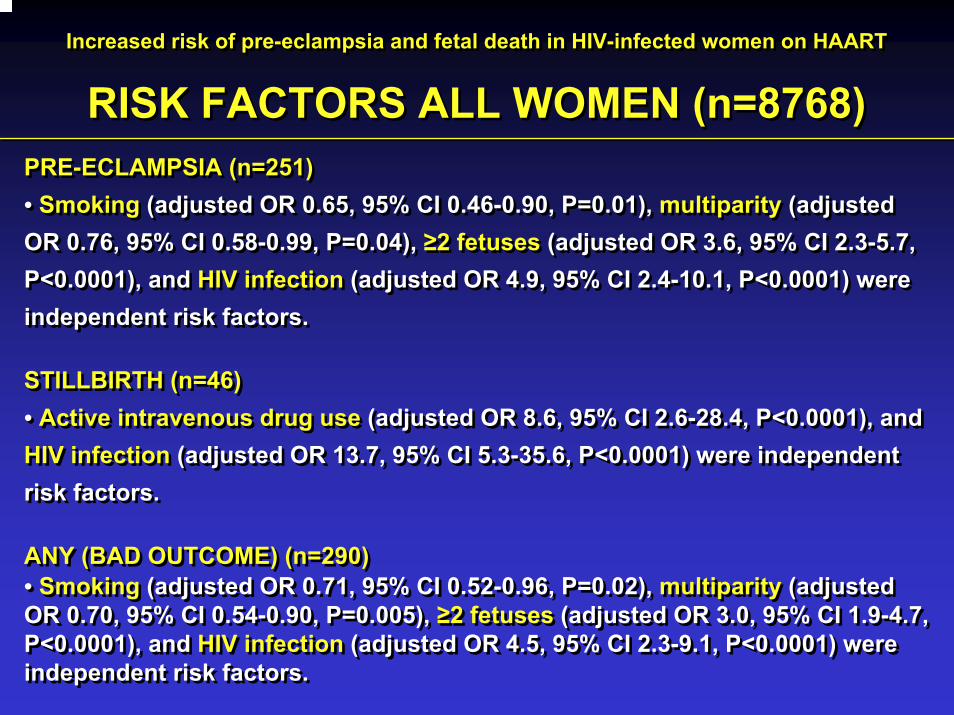
RISK FACTORS ALL WOMEN (n=8768)PRE-ECLAMPSIA (n=251)• Smoking (adjusted OR 0.65, 95% CI 0.46-0.90, P=0.01), multiparity (adjusted OR 0.76, 95% CI 0.58-0.99, P=0.04), ≥2 fetuses (adjusted OR 3.6, 95% CI 2.3-5.7, P<0.0001), and HIV infection (adjusted OR 4.9, 95% CI 2.4-10.1, P<0.0001) were independent risk factors.
STILLBIRTH (n=46)• Active intravenous drug use (adjusted OR 8.6, 95% CI 2.6-28.4, P<0.0001), and HIV infection (adjusted OR 13.7, 95% CI 5.3-35.6, P<0.0001) were independent risk factors.
ANY (BAD OUTCOME) (n=290)• Smoking (adjusted OR 0.71, 95% CI 0.52-0.96, P=0.02), multiparity (adjusted OR 0.70, 95% CI 0.54-0.90, P=0.005), ≥2 fetuses (adjusted OR 3.0, 95% CI 1.9-4.7, P<0.0001), and HIV infection (adjusted OR 4.5, 95% CI 2.3-9.1, P<0.0001) were independent risk factors.
PRE-ECLAMPSIA (n=251)• Smoking (adjusted OR 0.65, 95% CI 0.46-0.90, P=0.01), multiparity (adjusted OR 0.76, 95% CI 0.58-0.99, P=0.04), ≥2 fetuses (adjusted OR 3.6, 95% CI 2.3-5.7, P<0.0001), and HIV infection (adjusted OR 4.9, 95% CI 2.4-10.1, P<0.0001) were independent risk factors.
STILLBIRTH (n=46)• Active intravenous drug use (adjusted OR 8.6, 95% CI 2.6-28.4, P<0.0001), and HIV infection (adjusted OR 13.7, 95% CI 5.3-35.6, P<0.0001) were independent risk factors.
ANY (BAD OUTCOME) (n=290)• Smoking (adjusted OR 0.71, 95% CI 0.52-0.96, P=0.02), multiparity (adjusted OR 0.70, 95% CI 0.54-0.90, P=0.005), ≥2 fetuses (adjusted OR 3.0, 95% CI 1.9-4.7, P<0.0001), and HIV infection (adjusted OR 4.5, 95% CI 2.3-9.1, P<0.0001) were independent risk factors.

Increased risk of pre-eclampsia and fetal death in HIV-infected women on HAART
RISK FACTORS HIV-INFECTED (n=472)IncreasedIncreased riskrisk ofof prepre--eclampsia eclampsia andand fetal fetal deathdeath in HIVin HIV--infectedinfected womenwomen onon HAARTHAART
RISK FACTORS HIV-INFECTED (n=472)PRE-ECLAMPSIA (n=9)• Smoking (adjusted OR 0.05, 95% CI 0.006-0.40, P=0.005), and the months from the diagnosis of HIV infection (per 1-month increase) (adjusted OR 1.02, 95% CI 1.005-1.03, P=0.005) were independent risk factors.
STILLBIRTH (n=8)• Age (per 1-year increase) (adjusted OR 1.2, 95% CI 1.0-1.3, P=0.02), the months from the diagnosis of HIV infection (per 1-month increase) (adjusted OR 1.02, 95% CI 1.008-1.03, P=0.001), and HAART prior to pregnancy (adjusted OR 7.9, 95% CI 1.8-33.6, P=0.005) and during pregnancy (adjusted OR 6.1, 95% CI 1.2-31.9, P=0.05) were independent risk factors.
ANY (BAD OUTCOME) (n=14)• Smoking (adjusted OR 0.2, 95% CI 0.05-0.5, P=0.002), and the months from the diagnosis of HIV infection (per 1-month increase) (adjusted OR 1.02, 95% CI 1.007-1.03, P=0.001) were independent risk factors.
PRE-ECLAMPSIA (n=9)• Smoking (adjusted OR 0.05, 95% CI 0.006-0.40, P=0.005), and the months from the diagnosis of HIV infection (per 1-month increase) (adjusted OR 1.02, 95% CI 1.005-1.03, P=0.005) were independent risk factors.
STILLBIRTH (n=8)• Age (per 1-year increase) (adjusted OR 1.2, 95% CI 1.0-1.3, P=0.02), the months from the diagnosis of HIV infection (per 1-month increase) (adjusted OR 1.02, 95% CI 1.008-1.03, P=0.001), and HAART prior to pregnancy (adjusted OR 7.9, 95% CI 1.8-33.6, P=0.005) and during pregnancy (adjusted OR 6.1, 95% CI 1.2-31.9, P=0.05) were independent risk factors.
ANY (BAD OUTCOME) (n=14)• Smoking (adjusted OR 0.2, 95% CI 0.05-0.5, P=0.002), and the months from the diagnosis of HIV infection (per 1-month increase) (adjusted OR 1.02, 95% CI 1.007-1.03, P=0.001) were independent risk factors.

Increased risk of pre-eclampsia and fetal death in HIV-infected women on HAART
RISK FACTORS HIV-INFECTED ON HAART (n=120)IncreasedIncreased riskrisk ofof prepre--eclampsia eclampsia andand fetal fetal deathdeath in HIVin HIV--infectedinfected womenwomen onon HAARTHAART
RISK FACTORS HIV-INFECTED ON HAART (n=120)
PRE-ECLAMPSIA (n=8)
• White race (adjusted OR 0.2, 95% CI 0.03-0.90, P=0.04), and the months on
HAART (per 1-month increase) (adjusted OR 1.01, 95% CI 1.001-1.02, P=0.04)
were independent risk factors.
STILLBIRTH (n=5)
• No significative model could be found.
ANY (BAD OUTCOME) (n=11)
• Smoking (adjusted OR 0.3, 95% CI 0.07-0.08, P=0.05), the months from the
diagnosis of HIV infection (per 1-month increase) (adjusted OR 1.01, 95% CI
1.001-1.03, P=0.04) and the months on HAART (per 1-month increase) (adjusted
OR 1.01, 95% CI 1.001-1.02, P=0.03) were independent risk factors.
PRE-ECLAMPSIA (n=8)
• White race (adjusted OR 0.2, 95% CI 0.03-0.90, P=0.04), and the months on
HAART (per 1-month increase) (adjusted OR 1.01, 95% CI 1.001-1.02, P=0.04)
were independent risk factors.
STILLBIRTH (n=5)
• No significative model could be found.
ANY (BAD OUTCOME) (n=11)
• Smoking (adjusted OR 0.3, 95% CI 0.07-0.08, P=0.05), the months from the
diagnosis of HIV infection (per 1-month increase) (adjusted OR 1.01, 95% CI
1.001-1.03, P=0.04) and the months on HAART (per 1-month increase) (adjusted
OR 1.01, 95% CI 1.001-1.02, P=0.03) were independent risk factors.

Risk of lipoatrophy in antiretroviral-naive HIV-infected adults
CONCLUSIONSRiskRisk ofof lipoatrophylipoatrophy in in antiretroviralantiretroviral--naivenaive HIVHIV--infectedinfected adultsadults
CONCLUSIONS• We have witnessed an unexpected increase in the incidence of pre-eclampsia and stillbirth in HIV-infected pregnant women on HAART, while the incidence of these conditions remained stable in the general population.
• Pre-eclampsia and stillbirth were associated in a frequency higher than in the general population.
• HIV infection was identified as a risk factor for pre-eclampsia , stillbirth, or any of them in the general population.
• The known duration of HIV infection was identified as a risk factor for pre-eclampsia , stillbirth, or any of them in HIV-infected pregnant women.
• The known duration of HIV infection and the duration of exposure to HAART were risk factors for pre-eclampsia , stillbirth, or any of them in HIV-infected pregnant women receiving HAART.
• Potential pathogenic factors, including exposure to specific antiretroviral classes, will be further studied. If our findings are confirmed by other investigators, it may lead to caution in the recommendations of care for HIV-infected women who wish to become pregnant.
• We have witnessed an unexpected increase in the incidence of pre-eclampsia and stillbirth in HIV-infected pregnant women on HAART, while the incidence of these conditions remained stable in the general population.
• Pre-eclampsia and stillbirth were associated in a frequency higher than in the general population.
• HIV infection was identified as a risk factor for pre-eclampsia , stillbirth, or any of them in the general population.
• The known duration of HIV infection was identified as a risk factor for pre-eclampsia , stillbirth, or any of them in HIV-infected pregnant women.
• The known duration of HIV infection and the duration of exposure to HAART were risk factors for pre-eclampsia , stillbirth, or any of them in HIV-infected pregnant women receiving HAART.
• Potential pathogenic factors, including exposure to specific antiretroviral classes, will be further studied. If our findings are confirmed by other investigators, it may lead to caution in the recommendations of care for HIV-infected women who wish to become pregnant.