
aspects of dose, dose rate and radioisotopes in brachytherapy ...

Improved targeting device and computer navigation for accurate placementof brachytherapy needles
Ion P. I. Pappas and Paul RyanM.E. Müller Research Center, University of Bern, Stauffacherstr. 78, CH-3014 Bern, Switzerland
Peter CossmannHirslanden Klinik Aarau, Department of Radiation Oncology, Rain 34, CH-5000 Aarau, Switzerland
Jens Kowal and Blake BorgesonM.E. Müller Research Center, University of Bern, Stauffacherstr. 78, CH-3014 Bern, Switzerland
Marco Caversaccioa!
Inselspital, Department of ORL, Head and Neck Surgery, University of Bern, CH-3010 Bern, Switzerland
sReceived 26 November 2004; revised 15 March 2005; accepted for publication 16 March 2005;published 26 May 2005d
Successful treatment of skull base tumors with interstitial brachytherapy requires high targetingaccuracy for the brachytherapy needles to avoid harming vital anatomical structures. To enable safeplacement of the needles in this area, we developed an image-based planning and navigation systemfor brachytherapy, which includes a custom-made mechanical positioning arm that allows roughand fine adjustment of the needle position. The fine-adjustment mechanism consists of an XYZmicrostage at the base of the arm and a needle holder with two fine-adjustable inclinations. Therotation axes of the inclinations cross at the tip of the needle so that the inclinational adjustments donot interfere with the translational adjustments. A vacuum cushion and a noninvasive fixation frameare used for the head immobilization. To avoid mechanical bending of the needles due to the weightof attached tracking markers, which would be detrimental for targeting accuracy, only a single LEDmarker on the tail of the needle is used. An experimental phantom-based targeting study with thissetup demonstrated that a positioning accuracy of 1.4 mmsrmsd can be achieved. The study showedthat the proposed setup allows brachytherapy needles to be easily aligned and inserted with hightargeting accuracy according to a preliminary plan. The achievable accuracy is higher than if theneedles are inserted manually. The proposed system can be linked to a standard afterloader andstandard dosimetry planning module. The associated additional effort is reasonable for the clinicalpractice and therefore the proposed procedure provides a promising tool for the safe treatment oftumors in the skull base area. ©2005 American Association of Physicists in Medicine.fDOI: 10.1118/1.1901363g
Key words: brachytherapy, navigation, needle, positioning, targeting, tumor, skull base
y raes dpy,ffectftdar
elladiour-audood
l an-
f theciswhil
are-llentlasticn anddio--
y
hree-im-
ionalCT
n isand
oseof
nicalit is
I. INTRODUCTION
Brachytherapy is a method of radiation therapy wherebdioactive sources are inserted with percutaneous needlrectly within or very close to the tumor. In brachytherahigh radiation dosages can be delivered with minimal eto the surrounding healthy tissue, thanks to the 1/r2 decay ogamma rays, to the surrounding healthy tissue.1,2 The moscommon uses of brachytherapy are for primary or secontreatment of prostate cancer, cervical cancer3,4 and certainhead and neck cancers.5 Tumors at the skull base are wsuited for brachytherapy treatment, since conventional rtherapy steletherapyd leads to too high dose rates for srounding critical organs such as the cranial nerves, thetory nerve, the salivary glands, the orbita and the brain. Gresults have been reported for the treatment of residuarecurrent tumors of the nasopharynx area.6–8 Besides the adequate radio-dosage administration, the success obrachytherapy treatment largely depends on the prplacement of the needles at the desired target points,
9–11
avoiding harm to nearby critical structures. Brachy-1796 Med. Phys. 32 „6…, June 2005 0094-2405/2005/32 „6…
-i-
y
-
i-
d
eee
therapy requires excellent knowledge of the anatomy, awness of the radiosensitivity of critical structures and excemanual dexterity. Steel needles are preferred over pneedles because they bend less. To improve the precisioreproducible placement of the radioactive sources, raoncologists use templates,12,13fluoroscopic or ultrasound image guidance,14,15 direct CT control,16,17 and more recentlthree-dimensional stereotactic navigation.11,18–21 Previousstudies in the head and neck region have shown that tdimensional navigation of brachytherapy needles canprove the targeting accuracy compared to conventbrachytherapy or needle insertion performed undercontrol.18 The essential benefit of stereotactic navigatiothat the needle insertion paths, implant target locationsradiodoses can be planned on preoperative imagessCT orMRd prior to the needle application. Thereby optimal ddistribution fields and insertion paths minimizing the riskharming surrounding structures can be planned. In cliuse, to be able to apply a homogenous dosage field,
usually desired to place the needles in parallel orientation, in1796/1796/6/$22.50 © 2005 Am. Assoc. Phys. Med.

cy fontly
to bre-nsence
dia-ntethe92for
h ats tg ostem
an-
rtionthe
se i-l-
brar
ntor
oca-iticalcan
hy-en of
ed inles0.1
otrakah islableeec-nive
edle
rana-ameplete
rapywith
g
T
1797 Pappas et al. : Targeting device for navigation in brachytherapy 1797
an equidistant arrangement. The aimed targeting accurathe needles is around ±1 mm. For deviations significagreater than 1 mm, the needle geometry would needreassessedse.g., via CTd and applied dosages should becalculated. However, the purpose of navigated needle ition is precisely to plan trajectories and dosages in advaA further advantage of navigation is that the applied ration dosages and dose distribution can be easily docume
The clinical focus of this paper is tumor treatment atfrontal skull base with HDR brachytherapy using Ir 1sgamma radiationd sources. We present an accuracy studythe placement of navigated brachytherapy needles witoptimized targeting system and procedure, which attempminimize the errors due to needle misalignment, bendinthe needle, tracking, and patient registration. The syconsists of sad a noninvasive head-fixation frame withvacuum head cushion,sbd a fine-adjustable needle positioing mechanism,scd a tracking camera for navigation, andsdddedicated software allowing planning of the needle insetrajectories and providing interventional guidance forneedle insertion. The targeting system is intended for ucombination with a commercial afterloaderse.g., Microselectron, Nucletron, or Varisource, Variand and a commerciabrachytherapy planner/dosimetry modulese.g., Plato, Nucletron, or Brachyvision, Variand.
II. MATERIALS AND METHODS
A. System description
1. Planning and navigation system
A new customplanningandnavigationsoftware programwas developed in C++ using the open source software liies VTK sVisualization Toolkitd, ITK sInsight Toolkitd,Coin3D sopen-source implementation of the Open Inve
APId and Qt. This software evolved from an earlier imple-Medical Physics, Vol. 32, No. 6, June 2005
r
e
r-.
d.
nof
n
-
mentation used for ENT surgery.22 The planning moduleal-lows the user to specify on a CT or MR dataset target ltions and needle insertion paths such that harm to cranatomical structures is avoided. The planning modulebe linked to a commercial dosimetry module for bractherapy. Thenavigation moduleprovides real-time imagguidance during the needle insertion. The current positiothe needle and the planned insertion path are visualizreal timesFig. 1d. Deviations in the alignment of the needare indicated numerically with a resolution of 0.1° andmm. To track the needles in three dimensions, the Opttracking camerasNorthern Digital Inc., Ontario, Canadd,which tracks active infrared LED markers was used, whicone of the most accurate tracking devices currently avaisrms of 0.1 mm inx,y and 0.15 mm inz, according to thmanufacturer’s specificationsd. Other authors have used eltromagnetic tracking devices,18–20 mechanical positiodigitizers11 and infrared optical cameras with passmarkers.11
2. Head immobilization
To avoid motion of the patient’s head during the neinsertion, the head is placed on a special cushionsMedicalIntelligence, Schwabmünchen, Germanyd from which the aiis evacuated by a vacuum pump, resulting in a rigid,tomically shaped head support. Additionally, a head frwith three noninvasive rubber stamps provides a comimmobilization of the headsFig. 2d.
3. Targeting device
To improve the positioning accuracy, the brachytheneedles were mounted on an improved targeting devicefive fine-adjustable degrees of freedomsX,Y,Z,w ,ud. The
FIG. 1. Navigation interface showinin real-time the needleswhited over-laid on the three cutviews of the Cimage.
targeting device consists primarily of an articulated mechani-
,si-ue tongarm-ofa-t thethe
denceas
icaltione of
ead-
fine-t thethanriliz-
s forldo notthe, the
edle
rkeringlee
thethe
nser-er to
-n
eedleation
rence
1798 Pappas et al. : Targeting device for navigation in brachytherapy 1798
cal arm used for medical applicationssBaitella AG, ZürichSwitzerlandd. However, it is difficult to achieve a high potioning accuracy with these types of mechanical arms dslipping in the joints during the tightening of the lockiscrew. To enable fine-tuning of the needle position thewas mounted on anXYZ microstagesFig. 2d and a custommade needle holdersFig. 3d was mounted at the extremitythe armsFig. 3d, allowing the fine adjustment of the inclintions sw ,ud. The needle holder was designed such tharotation axes of the two inclinations cross at the tip of
FIG. 2. s1d Head fixation frame,s2d articulated mechanical arm,s3d brachy-therapy needle,s4d XYZpositioning stage,s5d needle holder with two fineadjustable angular degrees of freedom,s6d LED reference marker shield oneedle holder,s7d LED reference marker-shield on patient,s8d vacuumcushion.
needle. Thus, the adjustment of the needle’s inclination doe
Medical Physics, Vol. 32, No. 6, June 2005
not influence theXYZposition of its tip, i.e. inclination antranslation can be adjusted separately without interferscross talkd. The total travel of the fine positioning w±5 mm in XYZdirections and ±10° forsw ,ud. With the mi-crostage being roughly aligned to the principal anatomaxes of the patient and by aligning one of the inclinaplanes of the needle holder parallel to the sagittal planthe patient, it was straightforward to convert numerical rings provided by the navigation system intoXYZ,w ,u dis-placements. A trained user needed less than 1–2 min totune a needle on its planed insertion path, such thamisalignment given by the navigation system was less0.1 mm and 0.1°. The complete targeting device is steable since it consists of sterilizable metallic parts.
4. Tracking of the needle
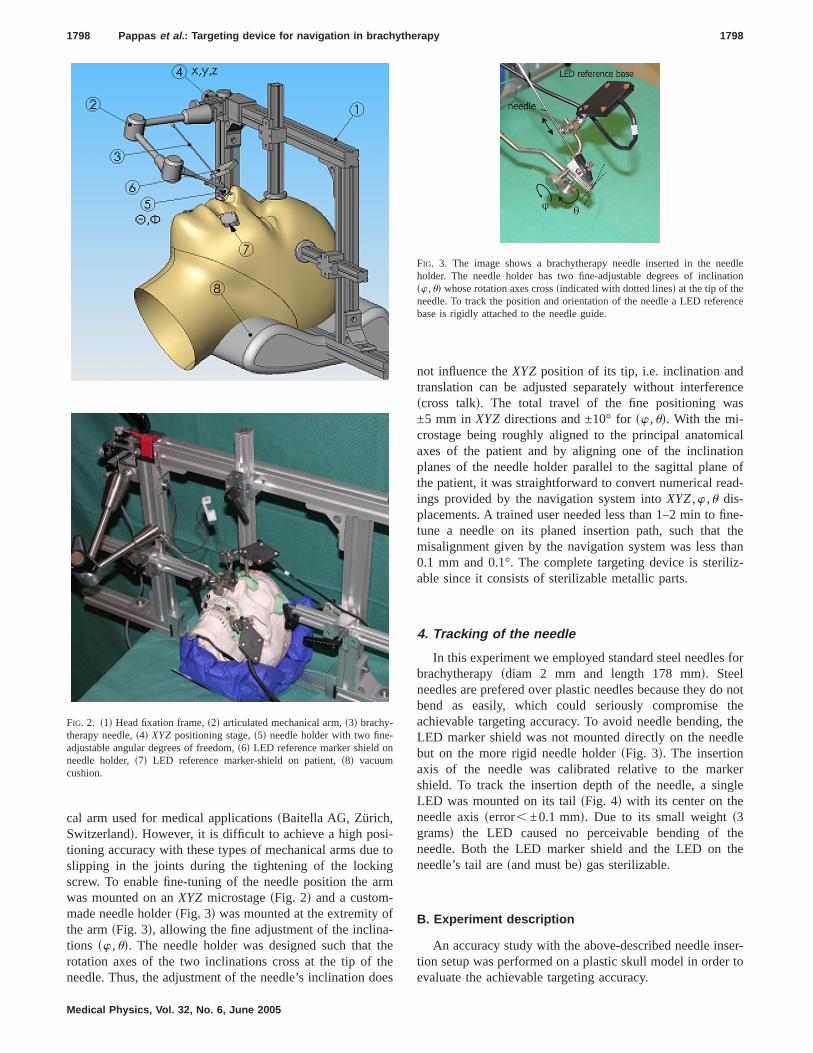
In this experiment we employed standard steel needlebrachytherapysdiam 2 mm and length 178 mmd. Steeneedles are prefered over plastic needles because theybend as easily, which could seriously compromiseachievable targeting accuracy. To avoid needle bendingLED marker shield was not mounted directly on the nebut on the more rigid needle holdersFig. 3d. The insertionaxis of the needle was calibrated relative to the mashield. To track the insertion depth of the needle, a sLED was mounted on its tailsFig. 4d with its center on thneedle axisserror, ±0.1 mmd. Due to its small weights3gramsd the LED caused no perceivable bending ofneedle. Both the LED marker shield and the LED onneedle’s tail aresand must bed gas sterilizable.
B. Experiment description
An accuracy study with the above-described needle ition setup was performed on a plastic skull model in ord
FIG. 3. The image shows a brachytherapy needle inserted in the nholder. The needle holder has two fine-adjustable degrees of inclinsw ,ud whose rotation axes crosssindicated with dotted linesd at the tip of theneedle. To track the position and orientation of the needle a LED refebase is rigidly attached to the needle guide.
sevaluate the achievable targeting accuracy.

rizedsticrap
rtion
tra-nondelCTre
digi-ted
tionded t
aseFi-
l the
dica-eated
ve to
gles
rgettwotionree-
arget
n inance
uredtheica-
lennedesulting itt that
f the
ringe armage
its
a rms
1799 Pappas et al. : Targeting device for navigation in brachytherapy 1799
1. Definition of the target pointsand insertion paths
Eight 1 mm-diameter spheres, embedded in polymesilicone were placed at the frontal skull base of the plaskull and were used as target points for the brachytheneedles. A CT scan of the plastic skuIl was obtainedsGELighting, spiral CT, 0.65 mm slice thicknessd and with thehelp of the planning software, intranasal needle insepaths to these target points were defined.
2. Patient to image registration
The first step in any navigated intervention is the registion of the preoperative data to the patient. In our case,invasive registration of the CT to the phantom skull mowas achieved using a maxillary occlusal splint with fourmarkerssFig. 5d. During the intervention, the markers areplaced by registration markers, which can be easilytized with a pointer. This registration method is well-adapfor clinical use and leads to high registration accuracy.23
3. Targeting trials
First, the preoperative plan was loaded into the navigamodule and registration of the CT was performed asscribed above. Then, the needle position was fine-tunematch the starting point of the planned insertion path, bon the information provided by the navigation system.nally, the needle was pushed forward along its axis unti
FIG. 4. Brachytherapy needle with a LED mounted axially on the tail oneedle, used to monitor the insertion depth of the needle.sad Side view;sbdback view.
FIG. 5. Picture shows the occlusion splint mounted on the maxilla. Duthe CT scanning, four CT markers are mounted on the splint, thesreplaced by registration markers to perform the registration of the CT i
to the patient.Medical Physics, Vol. 32, No. 6, June 2005
y
-
-od
desired insertion depth was reached, according to the intions of the navigation system. The procedure was rep20 times, for different targets.
4. Measurement of targeting accuracy
To measure the accuracy of the needle position relatithe target point, a navigated X-ray fluoroscopesC armd wasused. Two fluoroscopic images from two different anwere captured, showing the needle tip and targetsFig. 6d.The position of the needle tip and the position of the tacould be reconstructed in three dimensions from thefluoroscopic images using our in-house C-arm navigasoftware.24 The targeting error was measured as the thdimensional distance of the needle tip to the desired tpoint.
III. RESULTS
The results of the targeting experiments are showFig. 7. The targeting error, defined by the average distfrom the needle tip to the target, was 1.4 mmsrmsd with astandard deviation of 0.5 mm and with a maximal measerror of 2.4 mm. The available microscrews facilitatedfine-tuning of the needle alignment according to the indtions of the navigation system with resolution,0.1 mm inXYZ and ,0.1° in w and u at the entry point of the needpath. However, some of the insertion paths were plawith the axis too close to bone structures and as a rduring the insertion, the needle touched the bone, causto deviate from the straight path. It thus became eviden
e
FIG. 6. FluoroscopesC-armd image showing the brachytherapy needle infinal position and the 1 mm diameter target sphere.
FIG. 7. The targeting experiment on a phantom skull model revealed
accuracy of 1.4 mm.
forision
oseng taineinceegate
mon
o,herhe
dthethe
ED
theeldalslipad-tingionsof-
osedre
canst btiontiononet arinse
oringand
neesed
US
bema-icaly bs ing th
jec-ring
viceg to
of an
fine-p al-edlespro-
reat-ead.
nical
Na-ce in
uldG.
indart-Gar-ur-y of
tmentern,.
ain
d B.y,”
cta
F Xl and
igh-l head
chy-rs,” J.
anditaryy
itialaled
and
1800 Pappas et al. : Targeting device for navigation in brachytherapy 1800
during the CT-based planning it is important to accountthe needle thickness and alert the user if a potential collbetween needle and bone becomes evident.
IV. DISCUSSION
The experimental results demonstrated that the propmethod allows convenient and accurate needle positionipredefined targets in the frontal skull base area. The obtresults are comparable11 or better18–20 than those reportedthe navigated brachytherapy literature and confirm or exaccuracies that could be obtained in other areas of navisurgery sneurosurgery, dental or ENT surgery22–25d. Giventhe high accuracy demands, we chose to use one of theaccuratesbut also expensived tracking devices available othe market sOptotrak, Northern Digital Inc, OntariCanadad, which was not the system of choice in otstudies.11,18–21 The problem of needle flexion due to tweight of the attached reference markerssor receiver coil incase of electromagnetic tracking systemsd, is not addresseby other authors. The proposed solution of attachingtracking markers on the needle holder rather than onneedle and monitoring the insertion depth with a single Lon the needle, proved to be efficient. Furthermore, theXYZand w ,u microscrews facilitated the fine alignment ofneedle. In other studies the needles were either hand-hmounted on an articulated arm.11,18–21 These mechanicarms, however, are difficult to fine-tune as they generallya few millimeters when the locking screw is tightened, leing to significant targeting errors. The proposed targeprocedure and accuracy are suitable for clinical applicatAn additional benefit of navigation is the opportunity itfers to document the radiation dosages and treatment.20 Toachieve high patient registration accuracy with the propocclusal splint at least three healthy maxillary teeth arequired. In case of edentulous patients, the dental splintnot be used, therefore other registration alternatives muused, e.g., by using anatomical landmarks in combinawith surface points digitization. The presented navigatechnique is suitable for tumors which are fixed to bstructure, such as tumors of the skull base. Tumors thaembedded in soft tissues can shift and therefore needletion should be performed and verified with fluoroscopicultrasoundsUSd imaging. In the skull base area, US imagis ergonomically difficult due to the narrow access pathsdue to the presence of anatomical cavities which wouldto be filled with gel. Generally, combined US- and CT-baneedle guidance can be achieved by 3D tracking of theprobe and registering its images to the CT.26 However, forreal-time applications only rigid transformations canhandled since the computational cost for nonrigid defortions is prohibitive. The next step to complete the preclinexperiments is a realistic study with cadaver heads. It madifficult to reach the same level of targeting accuracy athe phantom models, due to tissue displacements durin
advancement of the needle. This may cause deviations fromMedical Physics, Vol. 32, No. 6, June 2005
dod
dd
st
or
.
--e
er-
d
e
e
the planned needle trajectory. Potentially, the effect of tratory deviation may be reduced by rotating the needle duits advancement through the tissues.
V. CONCLUSION
In this paper we presented an improved targeting defor navigated insertion of brachytherapy needles leadinhigh targeting accuracy. The targeting device consistsarticulated mechanical arm for rough positioning, anXYZmicrostage and a custom-made needle holder with twoadjustable inclinational degrees of freedom. This setulows accurate, stable alignment and insertion of the neaccording to the computer-based preoperative plan. Thiscedure provides a promising tool for better and safer tment of tumors especially in critical areas such as the hThe associated additional effort is reasonable for the clipractice and routine.
ACKNOWLEDGMENTS
The authors would like to acknowledge the Swisstional Foundation and the National Center of CompetenResearch, CO-MEshttp://www.co-me.chd, which providedthe financial support for this project. Moreover, we wolike to acknowledge the inspirational discussions withFichtinger from John’s Hopkins University, USA, the khelp of Mrs. Spielvogel from the Neuroradiology Depment, Inselspital and the valuable help of J. Chapuis, J.cia, and R. Walther from the M.E. Müller Institute for Sgical Technologies and Biomechanics at the UniversitBern, Switzerland.
adCorresponding author. Marco Caversaccio, Inselspital Bern, Deparof ENT, Head and Neck Surgery, University of Bern, CH-3010 BSwitzerland. Telephone:141-31-632-4174. Fax:141-31-632-4900Electronic mail: [email protected]
1F. Alesch, R. Hawliczek, and W. T. Koos, “Interstitial irradiation of brmetastases,” Acta Neurochir. Suppl.sWiend 63, 29–34s1995d.
2G. Kovacs, D. Hebbinghaus, P. Dennert, P. Kohr, R. Wilhelm, anKimmig, “Conformal treatment planning for interstitial brachytherapStrahlenther. Onkol.172, 469–474s1996d.
3C. B. Ostertag, “Brachytherapy—interstitial implant radiosurgery,” ANeurochir. Suppl.sWiend 58, 79–84s1993d.
4N. Zamboglou, “Interstitial brachytherapy possibilities,” inZamboglouBrachytherapy, 1st ed. Wien:sZuckschwerdt-Verlag, Wien, 1997d, pp.174–180.
5L. Pfreundner, K. Schwager, J. Willner, K. Baier, K. Bratengeier,Brunner, and M. Flentje, “Carcinoma of the external auditory canamiddle ear,” Int. J. Radiat. Oncol., Biol., Phys.,44, 777–88s1999d.
6M. Glatzel, J. Buntzel, D. Schroder, K. Kuttner, and D. Frohlich, “Hdose-rate brachytherapy in the treatment of recurrent and residuaand neck cancer, “Laryngoscope,”112, 1366–1371s2002d.
7J. D. Russell, N. R. Bleach, M. Glaser, and A. D. Cheesman, “Bratherapy for recurrent nasopharyngeal and naso-ethmoidal tumouLaryngol. Otol. 107, 115–120s1993d.
8N. Lee, R. Hoffman, T. L. Phillips, P. Xia, J. M. Quivey, V. Weinberg,I. C. Hsu, “Managing nasopharyngeal carcinoma with intracavbrachytherapy: One institution’s 45-year experience,” Brachytherap1,74–82s2002d.
9G. Ezzell, “Physical principles of treatment planning in interstbrachytherapy: Role of optimization,” inNew Developments in InterstitiRemote Controlled Brachytherapy, edited by N. Zamboglou, 1stsZuckschwerdt-Verlag, Wien, 1997d, pp. 35–37.
10H. Meertens, J. Borger, M. Steegerda, and A. Blom, “Evaluation
optimization of interstitial brachytherapy dose distributions,” inBrachy-
a-
r, P.fart,otact
d R.plate/ized
. E.im-ach,”
ai,g ofngue
. S.ctu-inte
,” Int
lou,alig-
al-icini,rapy
n, H.for
er, G.viga-ther.
er, N.ith a
chy-
nd R.stem,”
eze,tion of
.-P.ty,”
pera-
re-ized
r 03,
1801 Pappas et al. : Targeting device for navigation in brachytherapy 1801
therapy From Radium to Optimization, edited by R. F. Mould, J. J. Bterman, A. A. Matinezn, and B. L. Speiser, editors. 1st edsNucleotronInternational B.V., Veenedaal, The Netherlands, 1994d, pp. 300–306.
11R. Bale, W. Freysinger, A. Gunkel, M. Vogele, A. Sztankay, T. AueEichberger, A. Martin, T. Auberger, A. Scholtz, W. Jaschke, W. Thumand P. Lukas, “Head and neck tumors: Fractionated frameless stereinterstitial brachytherapy—initial experience” Radiology214, 591–595s2000d.
12B. W. Corn, R. M. Lanciano, N. Rosenblum, M. Schnall, S. King, anEpperson, “Improved treatment planning for the Syed–Neblett temusing endorectal-coil magnetic resonance and intraoperativeslaparotomylaparoscopyd guidance: a new integrated technique for hysterectomwomen with vaginal tumors,” Gynecol. Oncol.56, 255–261s1995d
13P. J. Paley, W. J. Koh, K. J. Stelzer, B. A. Goff, H. K. Tamimi, and BGreer, “A new technique for performing Syed template interstitialplants for anterior vaginal tumors using an open retropubic approGynecol. Oncol.73, 121–125s1999d.
14K. Yoshida, K. Shimizutani, E. Tanaka, H. Shiomi, H. Yamazaki, A. ImY. Yoshioka, S. Nakamura, and T. Inoue, “Ultrasonographic monitorinhigh dose rate interstitial implant using template technique for oral tocancer,” Radiat. Med.17, 337–341s1999d.
15G. L. Grado, T. R. Larson, C. S. Balch, M. M. Grado, J. M. Collins, JKriegshauser, G. P. Swanson, R. J. Navickis, and M. M. Wilkes, “Aarial disease-free survival after prostate cancer brachytherapy usingactive techniques with biplane ultrasound and fluoroscopic guidanceJ. Radiat. Oncol., Biol., Phys.42, 289–298s1998d.
16C. Kolotas, G. Birn, D. Baltas, B. Rogge, P. Ulrich, and N. Zambog“CT guided interstitial high dose rate brachytherapy for recurrent mnant gliomas”, Br. J. Radiol.72, 805–808s1999d.
17A. A. Martinez, L. L. Kestin, J. S. Stromberg, J. A. Gonzalez, M. Wlace, G. S. Gustafson, G. K. Edmudson, W. Spencer, and F. A. V“Interim report of image-guided conformal high-dose-rate brachythe
for patients with unfavorable prostate cancer the William Beaumont phaseMedical Physics, Vol. 32, No. 6, June 2005
ic
r-.
II dose-escalating trial,” Int. J. Radiat. Oncol., Biol., Phys.,47, 343–352s2000d.
18G. Strassmann, C. Kolotas, R. Heyd, S. Walter, D. Baltas, T. MartiVogt, G. Ioannidis, G. Sakas, and N. Zamboglou, “Navigation systeminterstitial brachytherapy,” Radiother. Oncol.56, 49–57s2000d.
19G. Strassmann, R. Heyd, R. Cabillic-Engenhard, C. Kolotas, S. WaltSakas, D. Richter, and N. Zamboglou, “Accuracy of 3-D needle nation in interstitial brachytherapy in various body regions,” StrahlenOnkol. 178, 644–647s2002d.
20C. Tonus, G. Strassmann, D. Debertshauser, C. Kolotas, S. WaltZamboglou, and H. Nier, “Intraoperative radiotherapy—Progress wCT-assisted navigation system,” Chirurg72, 731–735s2001d.
21T. Aueret al., “3D navigation in der interstiellen stereotaktischen bratherapie,” Strahlenther. Onkol.174, 82–87s1998d.
22M. Caversaccio, R. Baechler, K. Ladrach, G. Schroth, L.-P. Nolte, aHausler, “The Bernese frameless optical computer aided surgery syComput. Aided Surg.4, 328–334s1999d.
23N. C. Gellrich, A. Schramm, B. Hammer, S. Rojas, D. Cufi, W. Lagrand R. Schmelzeisen, “Computer-assisted secondary reconstrucunilateral posttraumatic orbital deformity,” Plast. Reconstr. Surg.110,1417–1429s2002d.
24G. Zheng, A. Marx, U. Langlotz, K. H. Widmer, M. Buttaro, and LNolte. “A hybrid CT-free navigation system for total hip arthroplasComput. Aided Surg.7, 129–145s2002d.
25M. Caversaccio and W. Freysinger, “Computer assistance for intraotive navigation in ENT surgery,” Min. Invas. Ther. Allied. Technol.1–2,36–51s2003d.
26L. Solbiati, “Real-time ultrasound-CT fusion: How to quickly and pcisely perform radiofrequency ablation for small or poorly visualliver tumors,” The Radiol. Soc. of N. AmericasRSNAd, 90th ScientificAssembly & Annual Meeting, Chicago, IL, November 28–Decembe
2004.Copyright © 2022 FDOKUMEN




















