
Impact of Medical Errors and Malpractice on Health ...
347
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Impact of Medical Errors and Malpractice on Health ...


Marina RigaHealth Economist-Researcher, Greece
Impact of Medical Errors and Malpractice on Health Economics, Quality, and Patient Safety
A volume in the Advances in Medical Education, Research, and Ethics (AMERE) Book Series

Published in the United States of America byIGI Global Medical Information Science Reference (an imprint of IGI Global)701 E. Chocolate AvenueHershey PA 17033Tel: 717-533-8845Fax: 717-533-8661 E-mail: [email protected] site: http://www.igi-global.com
Copyright © 2017 by IGI Global. All rights reserved. No part of this publication may be reproduced, stored or distributed in any form or by any means, electronic or mechanical, including photocopying, without written permission from the publisher.Product or company names used in this set are for identification purposes only. Inclusion of the names of the products or companies does not indicate a claim of ownership by IGI Global of the trademark or registered trademark. Library of Congress Cataloging-in-Publication Data
British Cataloguing in Publication DataA Cataloguing in Publication record for this book is available from the British Library.
All work contributed to this book is new, previously-unpublished material. The views expressed in this book are those of the authors, but not necessarily of the publisher.
Names: Riga, Marina, 1982- editor. Title: Impact of medical errors and malpractice on health economics, quality, and patient safety / Marina Riga, editor. Description: Hershey, PA : Medical Information Science Reference, [2017] | Includes bibliographical references. Identifiers: LCCN 2016059043| ISBN 9781522523376 (h/c) | ISBN 9781522523383 (eISBN) Subjects: | MESH: Medical Errors--adverse effects | Malpractice--economics | Medical Errors--economics | Quality Assurance, Health Care--methods | Patient Safety | Patient Harm--prevention & control Classification: LCC R729.8 | NLM WB 100 | DDC 610.28/9--dc23 LC record available at https://lccn.loc.gov/2016059043
This book is published in the IGI Global book series Advances in Medical Education, Research, and Ethics (AMERE) (ISSN: Pending; eISSN: Pending)

Advances in Medical Education,
Research, and Ethics (AMERE)
Book SeriesMission
The Advances in Medical Education, Research, and Ethics (AMERE) Book Series (ISSN Pending) is pub-lished by IGI Global, 701 E. Chocolate Avenue, Hershey, PA 17033-1240, USA, www.igi-global.com. This series is composed of titles available for purchase individually; each title is edited to be contextually exclusive from any other title within the series. For pricing and ordering information please visit http://www.igi-global.com/book-series/advances-medical-education-research-ethics/132365. Postmaster: Send all address changes to above address. Copyright © 2017 IGI Global. All rights, including translation in other languages reserved by the publisher. No part of this series may be reproduced or used in any form or by any means – graphics, electronic, or mechanical, including photocopying, recording, taping, or information and retrieval systems – without written permission from the publisher, except for non commercial, educational use, including classroom teaching purposes. The views expressed in this series are those of the authors, but not necessarily of IGI Global.
IGI Global is currently accepting manuscripts for publication within this series. To submit a proposal for a volume in this series, please contact our Acquisition Editors at [email protected] or visit: http://www.igi-global.com/publish/.
Coverage
ISSN:Pending EISSN:Pending
Humans are living longer now than ever as a result of advances in the medical field. Having the tools available to train knowledgeable and ethical future genera-tions of doctors and medical researchers is essential to continuing to advance our understanding of the human body and develop new ways of treating and curing sickness and disease.
The Advances in Medical Education, Research, and Ethics (AMERE) book series highlights publications pertaining to advancements in pedagogical practice for developing future healthcare professionals, research methods, and advancements in 10 the medical field, as well as moral behavior and practice of healthcare profes-sionals, students, and researchers. Featuring research-based book publications that are highly relevant to the healthcare community, this series is ideally designed for library inclusion at medical universities and research institutions as well as personal use by medical professionals, researchers, and upper-level students entering the field.
• Clinical Research• Conflicts of Interest• Ethics in Medicine• Healthcare Pedagogy• Medical Curricula• Medical Simulation• Patient Data• Professional Development• Research Methods• Scientific Misconduct

Titles in this SeriesFor a list of additional titles in this series, please visit: www.igi-global.com
Advancing Medical Education Through Strategic Instructional DesignJill Stefaniak (Old Dominion University, USA) Medical Information Science Reference • copyright 2017 • 349pp • H/C (ISBN: 9781522520986) • US $205.00 (our price)Organizational Culture and Ethics in Modern MedicineAnna Rosiek (Nicolaus Copernicus University in Toruń, Collegium Medicum in Bydgoszcz, Poland) and Krzysztof Leksowski (Nicolaus Copernicus University in Toruń, Collegium Medicum in Bydgoszcz, Poland) Medical Information Science Reference • copyright 2016 • 448pp • H/C (ISBN: 9781466696587) • US $225.00 (our price)Handbook of Research on Advancing Health Education through TechnologyVictor C.X. Wang (Florida Atlantic University, USA) Medical Information Science Reference • copyright 2016 • 588pp • H/C (ISBN: 9781466694941) • US $335.00 (our price)Optimizing Medicine Residency Training ProgramsJayita Poduval (Pondicherry Institute of Medical Sciences, India) Medical Information Science Reference • copyright 2016 • 300pp • H/C (ISBN: 9781466695276) • US $220.00 (our price)
701 E. Chocolate Ave., Hershey, PA 17033Order online at www.igi-global.com or call 717-533-8845 x100
To place a standing order for titles released in this series, contact: [email protected]
Mon-Fri 8:00 am - 5:00 pm (est) or fax 24 hours a day 717-533-8661

Preface;...................................................................................................................xi;
Chapter 1;
Clinical.Pathways.and.the.Human.Factor:.Approaches.to.Control.and.Reduction.of.Human.Error.Risk;............................................................................. 1;
Vaughan Michell;, Reading University, UK;
Jasmine Tehrani;, Reading University, UK;
Chapter 2;
Medical.Errors:.Impact.on.Health.Care.Quality;................................................... 33;
Jayita Poduval;, Pondicherry Institute of Medical Sciences, India;
Chapter 3;
Patient.Safety.and.Medical.Errors:.Building.Safer.Healthcare.Systems.for.Better.Care;............................................................................................................ 61;
Vasiliki Kapaki;, University of Peloponnese, Greece;
Kyriakos Souliotis;, University of Peloponnese, Greece;
Chapter 4;
Application.of.Quality.Management.in.Promoting.Patient.Safety.and.Preventing.Medical.Errors;.................................................................................... 91;
Ali Mohammad Mosadeghrad;, Tehran University of Medical Sciences, Iran;
Abraha Woldemichael;, Mekelle University, Ethiopia;
Chapter 5;
The.Perspectives.of.Medical.Errors.in.the.Health.Care.Industry;....................... 113;
Kijpokin Kasemsap;, Suan Sunandha Rajabhat University, Thailand;
Table of Contents

Chapter 6;
The.Role.of.Forensic.Medicine.in.Medical.Errors;............................................. 144;
Grigorios Leon;, Hellenic Society of Forensic Medicine, Greece;
Chapter 7;
The.Psychological.Impact.of.Medical.Error.on.Patients,.Family.Members,.and.Health.Professionals;..................................................................................... 171;
Mary I. Gouva;, TEI of Epirus, Greece;
Chapter 8;
The.Second.Victim.Phenomenon:.The.Way.Out;................................................ 197;
Paraskevi K. Skourti;, National and Kapodistrian University of Athens, Greece;
Andreas Pavlakis;, Neapolis University Pafos, Cyprus;
Related References;............................................................................................ 223;
Compilation of References;............................................................................... 259;
About the Contributors;.................................................................................... 328;
Index;................................................................................................................... 332;

Preface;...................................................................................................................xi;
Chapter 1;
Clinical.Pathways.and.the.Human.Factor:.Approaches.to.Control.and.Reduction.of.Human.Error.Risk;............................................................................. 1;
Vaughan Michell;, Reading University, UK;
Jasmine Tehrani;, Reading University, UK;
A.key.approach.to.improving.patient.safety.is.to.seek.to.modify.both.formal.and.informal.behaviours.in.response.to.the.extensive.reporting.of.error.causes.in.the.literature..This.response.is.primarily.in.two.parts;.a).actions.to.minimise.the.risk.of.error.or.b).actions.to.control.against.error..For.a).very.valuable.work.has.also.been.undertaken.in.running.human.factors.courses.to.demonstrate.and.try.to.change.poor.behaviour.via.best.practice.models..In.the.case.of.b).much.work.has.been.done.on.increasing.control.regimes.such.as.checklists.and.also.formal.rules.in.formal.procedures..However,.these.actions.tend.to.be.specific.to.specific.health.units,.are.often.piecemeal.and.are.not.integrated.to.complement.each.other..Little.work.has.been. done. to. integrate. these. formal. and. informal/social. behaviour. into. clinical.pathways.or.health.activities..This.chapter.reviews.current.thinking.and.develops.a.methodology.and.proposal.for.identification.and.control.of.human.error.in.clinical.pathways.based.on.the.research.of.the.two.authors.;
Chapter 2;
Medical.Errors:.Impact.on.Health.Care.Quality;................................................... 33;
Jayita Poduval;, Pondicherry Institute of Medical Sciences, India;
The. impact. of. medical. errors. on. the. delivery. of. health. care. is. massive,. and. it.significantly.reduces.health.care.quality..They.could.be.largely.attributed.to.system.failures. and. not. human. weakness.. Therefore. improving. health. care. quality. and.ensuring.quality.control.in.health.care.would.mean.making.systems.function.in.a.better.manner..In.order.to.achieve.this.all.sections.of.society.as.well.as.industry.must. be. involved.. Reporting. of. medical. error. needs. to. be. encouraged. and. this.
Detailed Table of Contents

may.be.ensured.if.health.care.professionals.as.well.as.administrators.and.health.consumers.come.forward.without.fear.of.being.blamed..To.get.to.the.root.of.the.problem-.literally.and.metaphorically-.a.root.cause.analysis.and.audit.must.be.carried.out.whenever.feasible..Persons.outside.the.medical.care.establishment.also.need.to.work.with.medical.service.providers.to.set.standards.of.performance,.competence.and.excellence.;
Chapter 3;
Patient.Safety.and.Medical.Errors:.Building.Safer.Healthcare.Systems.for.Better.Care;............................................................................................................ 61;
Vasiliki Kapaki;, University of Peloponnese, Greece;
Kyriakos Souliotis;, University of Peloponnese, Greece;
Patient.Safety.is.considered.to.be.the.most.important.parameter.of.quality.that.every.contemporary.healthcare.system.should.be.aiming.at..The.terms.“Patient.Safety”.and.“Medical.Errors”.are.directly.linked.to.the.“Safety.Culture.and.Climate”.in.every.organization..It.is.widely.accepted.that.medical.errors.constitute.an.index.of.insufficient.safety.and.are.defined.as.any.unintentional.event.that.diminishes.or.could.diminish.the.level.of.patient.safety..This.chapter.indicates.that.a.beneficial.safety.culture.is.essential.to.enhance.and.assure.patient.safety..Furthermore,.health.care.staff.with.a.positive.safety.culture.is.more.probable.to.learn.openly.and.successfully.from.errors.and.injuries.;
Chapter 4;
Application.of.Quality.Management.in.Promoting.Patient.Safety.and.Preventing.Medical.Errors;.................................................................................... 91;
Ali Mohammad Mosadeghrad;, Tehran University of Medical Sciences, Iran;
Abraha Woldemichael;, Mekelle University, Ethiopia;
The. combination. of. healthcare. professionals,. processes. and. technologies. bring.significant. benefits. for. patients.. However,. it. also. involves. an. inevitable. risk. of.adverse.events..Patients.receiving.health.care.in.health.institutions.have.the.potential.to.experience.some.forms.of.medical.errors..The.word.medical.error.commonly.encompasses. terms.such.as.mistakes,.near.misses,.active.and. latent.errors..This.signifies.the.complexity.and.multidimensional.nature.of.the.error..The.consequences.can.be.costly.to.the.patients,.the.health.professionals,.the.health.care.institutions,.and.the.entire.health.care.system..The.costs.may.involve.human,.economic,.and.social.aspects..Thus,.ensuring.quality.health.care.can.contribute.to.patients’.safety.by. reducing.potential.medical.errors. in.practice..This.chapter.aims. to. introduce.a.quality.management.framework.for. improving.the.quality.and.effectiveness.of.services,.reducing.medical.errors.and.making.the.healthcare.system.safer.for.patients. ;

Chapter 5;
The.Perspectives.of.Medical.Errors.in.the.Health.Care.Industry;....................... 113;
Kijpokin Kasemsap;, Suan Sunandha Rajabhat University, Thailand;
This.chapter.presents.the.overview.of.medical.errors;.drug.prescription.errors.and.prescribing;.the.overview.of.medical.error.disclosure;.medical.errors.and.telemedicine;.medical.errors.and.medical.education;.the.overview.of.nursing.medication.errors;.and. the.aspects.of.medical.errors. in. the.health.care. industry..Reducing.medical.errors,.increasing.patient.safety,.and.improving.the.quality.of.health.care.are.the.major.goals.in.the.health.care.industry..Medical.errors.are.caused.by.mistakes.in.drug.prescription,.dosing,.and.medical.administration.in.inpatient.and.outpatient.settings..Heath.care-related.guidelines,.institutional.safety.practices,.and.modern.health.care.technologies.must.be.applied.in.hospitals,.clinics,.and.medical.offices.to.reduce.the.occurrence.of.medical.errors..The.chapter.argues.that.understanding.the.perspectives.of.medical.errors.has.the.potential.to.enhance.health.care.performance.and.reach.strategic.goals.in.the.health.care.industry.;
Chapter 6;
The.Role.of.Forensic.Medicine.in.Medical.Errors;............................................. 144;
Grigorios Leon;, Hellenic Society of Forensic Medicine, Greece;
This.chapter.presents.the.importance.of.Legal.and.Forensic.Medicine.in.medical.malpractice.and.explains.how.autopsies.have.a.crucial.role.for.the.evaluation.and.the.prevention.of.medical.errors..Health.systems.vary.from.country.to.country;.however,.experts.are.indispensable.in.each.system..In.fact,.experts’.opinions.are.asked.for.resolution.of.specific.court.cases..Standard.of.care.is.often.assessed.by.expert.medical.witnesses.who.testify.for.one.of.the.litigants..The.physician.who.acts.as.an.expert.witness.is.one.of.the.most.important.figures.in.malpractice.litigation..Therefore,.a.doctor.who.is.an.expert.witness.has.to.have.certain.training.and.qualifications.and.to.act.under.common.recommendations..The.ideal.medical.expert.seems.to.be.the.forensic.doctor..In.the.future,.a.harmonization.of.practices.could.be.applied.in.medical.liability.cases.and.the.guidelines.provided.by.the.medico-legal.community.could.constitute.a.stable.base.for.their.evaluation.;
Chapter 7;
The.Psychological.Impact.of.Medical.Error.on.Patients,.Family.Members,.and.Health.Professionals;..................................................................................... 171;
Mary I. Gouva;, TEI of Epirus, Greece;
The.current.chapter.examines.the.psychological.implications.emerging.from.medical.errors..Whilst.the.psychological.effects.have.studied,.nonetheless.the.consequent.impacts.and.the.underlying.psychological.causes.have.not.been.sufficiently.analysed.and/.or.interpreted..The.chapter.will.add.to.the.literate.by.using.a.psychodynamic.

approach. in. analysing. the. psychological. impact. of. medical. errors. and. provide.interpretations.of.the.underlying.causes..The.chapter.concludes.that.medical.errors.lead.to.a.series.of.implications..For.the.patient.the.quality.of.interactions.with.health.professionals.are.directly.affected.and.usually.have.immediate.consequences..The.impact.of.these.consequences.in.the.patient.is.mediated.by.the.patient’s.personality,.history.of.the.individual.and.the.psychoanalytic.destiny.of.the.patient..For.the.patient’s.relatives.medical.errors.create.emotional.cracks.leading.to.regression.and.eventual.transference.of.the.medical.errors.as.a.“bad”.object..For.health.professionals.medical.errors.impact.upon.the.psychological.defence.mechanisms.of.the.psychic.Ego. ;
Chapter 8;
The.Second.Victim.Phenomenon:.The.Way.Out;................................................ 197;
Paraskevi K. Skourti;, National and Kapodistrian University of Athens, Greece;
Andreas Pavlakis;, Neapolis University Pafos, Cyprus;
Medical.error.happens.when.an.action.within.the.medical.field.is.not.fulfilled.as.planned,.or.the.plan.is.performed.incorrectly..Patient.and.family.are.the.first.victim.of.an.adverse.event..The.damage.in.a.patient’s.health,.leads.in.a.distressing.situation.not.only.for.the.patient,.but.also.for.the.clinician.who.is.responsible.for.this.outcome..The.term.“second.victim”.refers.to.the.trauma.that.a.health.professional.sustains.due.to.a.serious.adverse.event.in.the.healthcare.system..After.a.medical.error.the.caregivers.are.experiencing.the.aftermath.in.their.personal.and.professional.life..They.feel.isolated.and.abandoned,.and.some.of.them.are.coming.up.against.the.law.with.penal.and.disciplinary.ramifications.as.a.consequence.of.the.blame.culture.in.the.health.care.system..Some.health.professionals.experienced.the.consequences.of.an.unfortunate.incident.even.if.it.did.not.lead.in.harm.to.the.patient’s.health.;
Related References;............................................................................................ 223;
Compilation of References;............................................................................... 259;
About the Contributors;.................................................................................... 328;
Index;................................................................................................................... 332;

xi
Preface
Medical errors exist and can provoke discussion and debate about quality and patient safety issues of health care provision, with multiple and complex social and eco-nomic implications. The starting point for bringing them to the forefront of public attention was the reports of Institute of Medicine titled “To Err is Human: Building a Safer Health System” and “Crossing the Quality Chasm: A New Health System for the 21st Century”. On the report of Quality Interagency Coordination Task Force (n.d.), a medical error was determined as “the failure of a planned action to be completed as intended or the use of a wrong plan to achieve an aim. Errors can include problems in practice, products, procedures, and systems”. Researches worldwide revealed that the number of patients who have experienced a medical error in healthcare is worryingly high, while a significant proportion of harm refers to medical errors reasonably preventable. Under the burden of serious economic and social implications of physical harms and the finding that the root causes are mainly systemic in the overall health system, it is essential to take strategically designed actions to reduce medical errors, involving the health care professionals and patients, using Information Technology for detecting, reporting and analyzing the medical errors.
This book explores the impact of medical errors on patient safety, healthcare quality and on fiscal consolidation and cost containment on healthcare systems and looks to initiate a debate among health decision makers, health professionals and patients about accurate reporting of medical errors for empowering the culture of patient safety and healthcare quality. Additionally, chapters address the hidden weaknesses, failures and malpractices existing in healthcare systems globally, the variety of medical errors’ measurement methods, and the different aspects of inci-dent reporting systems implementation. This book aims to be an essential reference source, building on the available literature in the field of the detection and analysis of the various implications of medical errors while providing for further research opportunities in this dynamic field.

xii
Health decision makers, health managers, health professionals, patients, medical malpractice lawyers, academicians, researchers, advanced-level students, healthcare information technology developers, and government officials will find this book useful in furthering their research exposure to pertinent topics in the various impli-cations of medical errors.
It is hoped that this book will provide the resources necessary for health deci-sion makers and health professionals to adopt a culture of openness and implement a systematic review of medical errors in order to improve the quality of care and patients’ safety in the healthcare system, worldwide as well as to achieve the health care cost containment.
Marina RigaHealth Economist-Research, Greece
REFERENCES
Quality Interagency Coordination Task Force. (n.d.). Retrieved from https://archive.ahrq.gov/quic/

Copyright ©2017, IGI Global. Copying or distributing in print or electronic forms without written permission of IGI Global is prohibited.
DOI: 10.4018/978-1-5225-2337-6.ch001
Chapter 1
1
Clinical Pathways and the Human Factor:
Approaches to Control and Reduction of Human Error Risk
ABSTRACT
A key approach to improving patient safety is to seek to modify both formal and informal behaviours in response to the extensive reporting of error causes in the literature. This response is primarily in two parts; a) actions to minimise the risk of error or b) actions to control against error. For a) very valuable work has also been undertaken in running human factors courses to demonstrate and try to change poor behaviour via best practice models. In the case of b) much work has been done on increasing control regimes such as checklists and also formal rules in formal procedures. However, these actions tend to be specific to specific health units, are often piecemeal and are not integrated to complement each other. Little work has been done to integrate these formal and informal/social behaviour into clinical pathways or health activities. This chapter reviews current thinking and develops a methodology and proposal for identification and control of human error in clinical pathways based on the research of the two authors.
Vaughan MichellReading University, UK
Jasmine TehraniReading University, UK

Clinical Pathways and the Human Factor
2
1. INTRODUCTION AND BACKGROUND
1.1 Patient Safety
Although large numbers of people continue to be successfully cared for and treated in the National Health Service, a significant number of errors and other forms of harm occur. It has been calculated that up to 10% of patients admitted to NHS hospitals are subject to a patient safety incident and that up to half of these incidents could have been prevented ((Osborn and Williams, 2004; Vincent et al., 2001). Surprisingly, up to half of the 10% of Iatrogenic or accidental errors could have been prevented (Michell et al, 2012). It was estimated by a Bristol Royal Infirmary Inquiry (Bristol HMSO, 2001) that around 25,000 preventable deaths occur in the NHS each year due to patient safety incidents. These incidents also generate a significant financial burden that includes avoidably prolonged care, additional treatment and litigation costs.
Avoidable unintended or accidental outcomes of medical care, medical errors are also a serious and challenging issue in many other countries including North America. The influential Institute of Medicine‘s (IOM‘s) report, To Err Is Human highlighted the extent of the problem and the need for remediation was documented in Building a Safer Health System (1999), where between 44,000 and 98,000 people die in hospitals each year as the result of medical errors. There is broad international agreement on the importance of achieving improvements to quality in this area (Milligan, 2007). The recorded event where an error is noticed ie a safety incident is defined by the National Patient Safety Agency (NPSA, 2004) as: any unintended or unexpected incident which could have or did lead to harm for one or more patients receiving NHS funded care‘‘. These types of incidents are also referred to in the literature as adverse events/incidents, medical error, clinical error, and include the concept of near miss. The latter is a situation in which an error or some other form of patient safety incident is averted, such as noticing and therefore avoiding giving the wrong drug to a patient.
In the UK, the terminology for self-inflicted errors by clinicians and health work-ers has evolved from serious untoward incident to ‘significant event’ or in extreme cases ‘never events’ with examples of over 1600 serious incidents occurring in one NHS region in one single year (Rosenorn-Lanng, 2014)
However, whatever the terminology these events are all dependent on the human in the room and in the loop, clearly driving the need to understand the human as a source of error. The study of the effect of the human condition on safety events and human errors is often termed ‘human factors’ and is clearly important in the understanding of safety problems since the care and intervention activities are primarily human driven.

Clinical Pathways and the Human Factor
3
1.2 Human Factors
Chapanis defines human factors as ‘a body of information about human abilities, limitations and characteristics that are relevant to the design process’ (Chapanis, 1996). In a work context, human factors include environmental, organisational and job factors, and individual characteristics which influence behaviour in a work environment. Clinicians have suggested ‘Human factors relate to the aspects of human behaviour that reduce certainty of actions and can set conditions for, and create, human errors. This alludes to the fact that human factors not only relate to the way the error is driven by human actions, or inaction, but also a human failing may be a precursor and contributing factor to an error by other individuals and indeed machines that are predicated on human decisions.
Human factors can perhaps be more simply understood as all the factors or condi-tions that affect human behaviour and particularly human fallibility or the propensity for error and unintended outcomes. Sadly, whilst human fallibility leading to errors can be moderated, they cannot be eliminated. It is inevitable that errors will occur in healthcare, as they do in other safety critical industries, because they are an intrinsic human trait – to err is human (Kohn et al., 2000).
There have been a number of attempts to propose a categorisation of human fac-tors that lead to errors and patient safety issues. Reason (1995) analysed conditions under which human factors can contribute to safety failures and proposed a generic model of accident causation (Reason, 1995). (Chang et al, 2005) conducted a series of similar studies and presented an evaluation of existing patient safety terminologies and classifications and grouped the findings into five complementary root nodes: impact, type, domain, cause and prevention. In this paper, cause and type root nodes are further analysed for the purpose of better understanding of human factors and towards a generic taxonomy and classification schema of human factors influencing near misses and adverse events. As a basis for understanding the range of human factors Rosenorn-Lanng & Michell developed the ‘SHEEP’ structured factor model as an acronym for classifying the human factor variables that influence error into five groups; (S) systems, (H) human interaction, (E) environment, equipment, (P) personal (Rosenorn-Lanng & Michell, 2014). This approach can provide a useful l checklist of human factors, both causal and influential that safety events and errors can be categorised against to understand the influence of human factors on activ-ity and task failures. Ongoing capture and categorisation of these events can then yield a database of human factor patterns in a specific clinical environment that can be statistically analysed to focus sparse improvement resources to resolve them. Example factors from the SHEEP model are used to illustrate this chapter and can also be integrated with the other models mentioned. Our concern is to understand the human factors affecting human clinical actions and seek ways to moderate the

Clinical Pathways and the Human Factor
4
impact of these factors. The following sections investigate the cause of error and the range of human factor drivers. To develop the approach we adopt a modified form of Jackson & Flin’s model of factors affecting patient safety (Figure 1) (Flin et al, 2009).
2. ERRORS
2.1 Individual Human Error Factors
Reason defined an error as ‘a failure of a planned action’ (Reason, 1995) and identi-fied 3 key types of individual human error. He distinguished between slips – failure to do something and mistakes or failures to do the thing right. Leape suggested slips were due to attention issues or intention failures (Leape, 1994). Mistakes relate mainly to errors in the conscious human mind’s judgement and decision making and cover rule based and knowledge based types. Rule based errors involve either applying the correct rule, to the wrong context due to incorrect situation perception or applying a rule that has been recorded incorrectly, to the right situation (Leape, 1994). Knowledge based errors resulted from cognitive processing failures of us-ing an incorrect, familiar or incomplete mental model that does not represent the actual situation.
Figure 1. Factors affecting patent safety outcomes (adapted from (Flin et al, 2009)

Clinical Pathways and the Human Factor
5
Perception Errors
Some errors due to forgetfulness (slips- P1) or incorrect decision making (mistakes) are due to perception errors where a specific pattern may not be noticed or the clinician forgot to search for it or the pattern was not recognised correctly (Michell et al, 2012). A good example of forgetting is given by the clinical case of missing an obvious elbow injury when a patient was brought in for treatment (Smits et al, 2009; Panella et al, 2003). Another type of perception error is where the focus of the action is on the wrong object- i.e. description errors (P2). Individuals usually have a plan or model of what they expect to perceive and another source of error relates to the wrong plan or expected perception (P3). A final source of perception error is seeing a specific cue eg bruised skin and taking the wrong action by making assumptions about the implications from the perceived visual cue (P4).
Rule Based Errors
Work activities that are often repeated as routine clinical actions or experienced activities are often encoded by human cognitive rules (Rasmussen, 1983) (Shap-pel and Wiegmann, 2000). Leape (Leape, 1994) defined three types of rule based errors. Firstly the correct rule may be used in wrong context (C1), for example due to a perception error eg mis-assigning a clinician with an inappropriate skill to a specific patient problem (Smits et al, 2009). Alternatively it may involve applying a rule that has been understood by the individual incorrectly (c2), to the right situ-ation, for example the mis calculation of medical doses (Smits et al, 2009). Further details can be found in Michell 201444 IGI Book
Knowledge Based Errors
Knowledge based errors are errors in cognitive action plans due to incorrect or incomplete mental models (C4)/ (c5) of the clinical situation and context (Michell IOT 2014). This is often due to lack of experience or the problem of applying and extrapolating existing experience and knowledge in novel or new situations (Smits et al, 2009). For example human factor compulsion to revert to a (see i)) familiar mental model and decision, rather than a realistic one produced by cognitively as-sessing all the facts to select a superior decision (Reason, 2000). Other drivers of knowledge based errors are the human impulse to re-use and fit the situation facts to a pre-existing and well known habitual cognitive response (C3) (Reason, 2000). A summary of the personal error types is given in Figure 2. Hence identifying the points and situations in which these types of errors may be more prevalent can help in reducing patient safety risk.

Clinical Pathways and the Human Factor
6
2.2 Cognitive and Physiological Abilities
The importance of the condition of the human in the action loop suggests that actors in clinical processes must become self-aware of their own condition that may affect the state or outcome of a situation that could lead to error. Research has identified a large number of factors that can act as error contributors. These include physiologi-cal conditions including stress, fatigue, cognitive workload, time pressure, lack of knowledge and the need for help (Rosenorn-Lanng, 2014). Within clinician self-awareness a number of clinically specific conditions have been identified that are important to our discussion.
Situational Awareness and Coning of Attention
Some key errors have been caused by clinicians being too focused on their task and missing a deteriorating situation around them that results in error and patient harm. For example the process for intubating patients can so focus the clinician that they can ignore the fact that a patient cannot breath (Rosenorn-Lanng & Michell, 2014). This is the human factor of situational awareness (Reason 1990), first identified by German First World War flying ace Oswald Boelke (Stanton et al, 2001). It relates to awareness of what is going on about the person – or the perception, comprehension of meaning and projection of the status of elements of a person’s environment (Flin et al, 2009). It can include lack of recognition of critical cues for decisions, failure to interpret meanings, lack of understanding of individual task responsibilities and failure to communicate (Stanton et al, 2001). These human factor tendencies seem to
Figure 2. Individual Errors (Adapted from Michell, 2014)

Clinical Pathways and the Human Factor
7
occur where a cognitive task requiring focused attention by an individual is required. Such tasks are typical of most medical interventions. However, the issue here is ensuring salient events, states or information relevant to the activity focus are noticed by the concentrating clinicians. One solution is to encourage clinicians to vocalise their thoughts and actions to make it clear what their focus is on and enable others to raise awareness of missing critical factors and concerns (Rosenorn-Lanng, 2014).
A factor related to situational awareness is the coning of attention of a typical surgeon, used to focusing on the detail of a surgical intervention. Three types of attention cones have been proposed
1. The eye focus cone of vision2. A side cone of peripheral vision for example in checking machine readings
and locations of devices and individuals and3. The auditory cone or focus of hearing that can sometimes block out important
information as well as noise (Rosenorn-Lanng, 2014).
An additional factor in coning may be related to habit. Leape identified that slips resulted from failures in automatic skills for example a tendency for humans to follow the most habitual rather than the correct routine (Leape, 1994).
2.3 Personal and Physiological factors: Stress and Fatigue
Humans live and work in complex environments that can affect our physiology and hence alter our cognitive and perception responses and decision making. Stress, or an individual’s negative response to the pressure of work is the key driver of these changes (Flin et al, 2009). Stress varies with an individual’s balance of their capabil-ity vs. what is demanded of them, which in turn depends on their skills, education and training. Examples of personal factors that increase stress and impact safety are low job satisfaction and morale, high workload (Rosenorn-Lanng & Michell, 2014). A good example of the very wide range of factors that were found to affect performance are given in Figure 3.
2.4 Organisational Factors
A combination of process, human and system controls constitute a defence against errors in depth. Organisational errors result from errors in systems or people and resources and represent a failure of multiple checks and controls due to ‘active and passive failures’ and gaps in safety defences in depth’ as defined by reason in his ‘Swiss Cheese model’ (Reason, 1998). Work on the sheep model identified a wide range of factors that influence physiology and stress.

Clinical Pathways and the Human Factor
8
The Impact of Culture
Swidler identified the impact of culture on actions : ‘Culture provides the material from which individuals and groups construct strategies of action’ and ‘groups and individuals call upon these resources selectively bringing to bear different styles and habits of action selectively (Swidler, 1986). This is particularly visible in the impact of important influence of the hospital and the professional clinical group and even the cross cultural team to which clinicians belong. Safety culture ideally involves everyone focusing on the ‘value and priority of the patient’ (Weigmann et al, 2010).
The culture of an organisation therefore provides a set of standards of behaviour to which its members follow and aspire. Hence a culture in which procedures and standards are flouted and there is little concern and management and control of slack practices can provide a fertile environment for a multitude of quality problems and errors.
A key weapon in error reduction and quality improvement in healthcare is the adjustment of culture (Davies et al, 2000). The World Health Organisation defined safety culture in terms of individual and group attitudes, competencies and patterns of behaviour (Flin et al, 2009). Critically this culture must be open to views and findings and ideally a culture that encourages learning and improvement (Reason, 1998). However, culture, as Davis et al suggest has imprecise definitions but can be described as ‘the emergent property of that organisation’s constituent parts; the
Figure 3. Example personal factors (adapted from (Rosenorn-Lanng, 2014))

Clinical Pathways and the Human Factor
9
behaviour of the organisation at different levels does impact actions and their out-comes as seen in well-known phrases such as ‘it is the way things are done around here as well as the way things are understood, judged and valued’ (Davies et al, 2000). Culture drives behaviour and hence is a precursor to the human factor fail-ings we seek to avoid.
Managing Clinical Activities: Workload
Managing and controlling clinical behaviour and activity is however itself open to human factor failings. The focus on managing human in their activities relies on a) allocating work efficiently and effectively, i.e. ‘planning, scheduling and forecasting’ and b) observing and controlling violations of process and appropriate behaviour to avoid error and patient risk situations. With increased medical demands it is no surprise that increase in task workload and the cognitive complexity of the task are both error-inducing factors (Weigmann et al, 2010). Also mis-scheduling of the right staff can also be an issue (Helmreich, 2000). Good management and control requires accurate, timely and appropriate situational information in the right context. Cognitive and workload overload and the inability to be aware of everything can also lead to additional or ‘knock on’ errors (Smits et al, 2009).
2.5 Team/Unit Culture
Leadership and Role Errors in Teams
Leadership - the process of influencing individuals to achieve goals (Flin et al, 2009) for clinical tasks can be vital in directing the clinical intervention towards the desired solution. Leadership in a medical situation is de-factor a case of safety leadership – ie responsibility for encouraging everyone to make the right decisions to ensure safety. But all too often in a complex and hectic clinical emergency situation it is unclear who is in charge. This can lead to the assumption that others are or have already made critical decisions or to delays in action. A lack of clear leadership can result in decisions being deferred, tasks not delegated and completed and a lack of information flow and coordination that can lead to serious errors (Rosenorn-Lanng, 2014) (Mohr et al, 2002).

Clinical Pathways and the Human Factor
10
Role Conflict
Role conflict, where an individual is uncertain of their role, has unreasonable job demands or incompatible requests on them, is a well known driver of stress (Piko, 2006). Even ignoring stress, role conflict in team situations where it is uncertain whose task it is to lead or act can result in the task being left undone and hence turn into a potential safety error by default. Ideally any clinical process must ensure there is a clear definition and understanding of roles in terms of who is responsible for and who must undertake each action or activity. The technique of process mapping using swim lanes to identify responsibilities vs. activities within a process helps to identify who performs what actions and where there is ambiguity or duplication that may lead to delay in action, inaction or error (Wohed et al, 2006).
Communication
Communication – ‘the transfer of information, ideas, feelings’ (Flin et al, 2009) is often critical to efficient and effective task execution in a medical environment. Communication failures are a major contributor to medical errors, particularly in operating theatres. However communication covers many forms both in human and machine transfer of information and the lack of it or the type and comprehension of the message to whether the message is timely and appropriate [Debbie sheep igi]. Problem identification, for example in a surgical situation requires the free input of open views that may be inhibited by human factors such as [Debbie book]. Similarly critical decision making as in medical diagnosis requires the generation, understanding and communication of alternative solutions that can be affected by human error factors. Normal workload and task allocation and reporting relies on clear and unambiguous communication that may be affected by personal and envi-ronmental factors (Davies, 2005). Macintosh et al identified five key characteristics of communication in healthcare: communication is necessary to reduce morbidity, must be used by all team members, must be able to occur in the situation, and must be effective ie focused on the salient points and must be the right type of commu-nication (Davies, 2005).

Clinical Pathways and the Human Factor
11
Handover Error
Particular error examples often concern the problem of miscommunication or mis-interpretation of meanings when transferring information between teams (Noble and Donaldson, 2011). This leads to the need for clear communication and handover points of information in medical processes and also clear responsibility for com-municating and ideally guidelines on what to communicate if these errors are to be reduced. The World Health Organisation actively promotes pre task briefings via a checklist (Flin et al, 2009) and the format for ensure efficient and effective communication is given in the SBAR (Situation, Background, Assessment, recom-mendation) format that is widely promoted among clinicians, but in many cases not always used (Haig et al, 2006).
Systems and Human Factors
The human within a clinical situation almost always operates within a framework of information and organisational structures that we refer to as ‘systems’ in this context. A health organisation operates within an arrangement of informal behaviour rules, driven by values and beliefs, formal behaviour rules as dictated by standard procedures and technical behaviours driven by the technology used within the health enterprise. Formal information artefacts within a hospital may range from detailed protocols and procedures to care bundles and pathways. Typical sources of information error are multiple and confusing copies of information and ambiguous information leading to different perceptions and action (Rosenorn-Lanng & Michell, 2014).
2.6 The Work Environment
Reason coined the term ‘local traps’ to identify working environment conditions that in conjunction with violations of procedures and human error can create unsafe and risky patient situations (Reason, 1998). Rosenorn-Lanng, an experienced clinical practitioner in her research stratified the environmental conditions into static ele-ments of the physical structure and location and arrangement of resources and the dynamic elements relating to interruptions to process and location issues as being contributors to error conditions (Rosenorn-Lanng, 2014). Environmental factors such as lack of resources due to lack of knowledge of their location or being unable to access them can be instrumental in denying vital and sometime lifesaving care. Hospitals also have a frequent need to move clinicians and patients and dynamic issues such as journey time or blockages and delays in the movement of resources can also reduce decision time and lead to pressure to make mistakes and slips. A simplified set of environmental factors is illustrated in Figure 4.

Clinical Pathways and the Human Factor
12
The main goal of introducing human factor controls in to clinical pathways is not so much to minimise that particular error but to enhance human performance at different levels of system.
2.7 Clinical Pathways
The key means of management of planned clinical intervention in many hospitals is the grouping of procedures, information and guidelines around a route or path of treatment for a specific medical condition – what are often known as clinical pathways. There are a range of definitions of clinical pathways. Clinical pathways are also known as care maps, anticipated recovery pathways were introduced in 1985 and are an attempt at developing practical standard operating procedures for clinical processes (Li et al, 2014). Clinical pathways (CP) represent an approach by healthcare organisations to develop an ideal planned sequence of steps to minimise risks and variations in clinical intervention (Cabitza et al, 2008). Despite the lack of formal industrial type process design of pathways in many health organisations, other than formalisation by committee, their specifications involve the proven clini-cal best practices from medical guidelines (Cabitza et al, 2008) and are an attempt to standardise care processes (Ye et al 2008). In reality CPs are often realised as collections of often disparate and abbreviated blocks of information for use by many disciplines, nurses, surgeons, anaesthetists that represent the distillation of best clinical practice for the treatment of a specific medical condition., but are specific
Figure 4. Static environment factors (adapted from (Rosenorn-Lanng, 2014)

Clinical Pathways and the Human Factor
13
to each institution and are generally used as an organisational management tool for coordinating clinicians actions for a specific patient condition (Audimoolam et al, 2005). Most clinical pathways are still paper-based and designed for the ideal patient scenarios and include both planning information as well as mechanisms to record variations in actual clinical interventions (Michell et al, 2012). A CP serves as a useful guide for more detailed analysis of activities and human factor relationships to clinical work. Formal clinical pathways, using and enforcing well documented tasks and protocols and specified goals, are known to reduce slips because of the structured support information for activities in the pathway documentation (Panella et al, 2003). A correctly identified and disseminated clinical pathway can act as a scaffold onto which human factor knowledge and controls can be welded to better manage their outcomes.
3 MODELLING HUMAN BEHAVIOUR AND ERROR
This section addresses how we can model human behaviour by utilising how hu-mans use cultural rules. These cultural rules take the form of behavioural norms that drive many human actions and mistakes as a precursor to better identification of human factor and their influence on the safety outcome of clinical pathways. We follow this by a review what are human factors and risk measurements that can be applied to enable the discovery of where human factor errors are most likely to occur within pathways.
3.1 Rules and Human Norms
An organization can be visualised as a social system in which people behave in an organized manner conforming to a certain system of norms. These norms relate to rules, regulations and patterns (Wright 1963). Norms are often referred to as rules that are shared by and defined by a culture, such as norms in religion, law and social convention. In an organisation, norms reflect the regular behaviour of members that enable g co-ordination of their actions. Norms are developed through practical experiences of agents in a society and in turn have functions of directing, coordinating and controlling actions within society (Liu, 2000).
An organisation can be modelled as a system of social agents where people conduct themselves in an organised way by conforming to regularities of percep-tion, behaviour, belief and value. The function of a norm is to determine whether patterns of behaviour are lawful or acceptable in the context of the society. Norms thus can be seen as a form of standards for executing behaviour for the members of a cultural group that wishes to conform to these norms to coordinate their actions.

Clinical Pathways and the Human Factor
14
Identifying, capturing and modelling norms or human rules governing behaviour enables us to partly predict and anticipate human actions and human co-ordination with other agents. Norms can be categorised in a variety of ways. Five types of norms that govern substantive human actions or behaviour can be identified in this way, each of which controls an aspect of human behaviour. They are perceptual norms, evaluative norms, cognitive norms and behavioural norms. Perceptual norms are human rules to guide pattern recognition, for example how a clinician might perceive a cancerous lump. Perceptual norms need to be used in conjunction with evaluative norms which are essentially rules that identify relative value and ranking necessary for decision making between for example the importance of one pattern or view over another. Cognitive norms relate to cause and effect and logic such as in norms that relate to evidence based medical treatments and the knowledge and implications of specific perceptions and beliefs. Finally behavioural norms are essentially human rules for performing specific activities. Norms can also be categorised according to whether they reflect the human rule for a specific action (substantive), or a rule to communicate only (communication norms) or a human rule that dictates the control of actions (control norm) (Stamper, 1994). For a complete description of different types of norms, see (Stamper, 1994)
Norms relate to human behaviour which can be categorised according to the interaction. Firstly informal human behaviour enables norms related to living such as religion, laws and cultural rules. Secondly the evolution of industry has led to formal norms seen as standard operating procedures and rules regarding business interaction. These formal norms are governed by roles and organisational sanctions. Thirdly in operating technical equipment technical norms have been developed such as the need to swipe the screen of an iphone in order to operate it.
Identifying these repeated rules can help provide a type of formal logic around what can sometimes be seen as complex human behaviour. But formalisation has limits even when the norms can be defined explicitly. This is because members of an organisation need to interpret them. As we have seen with human error, hu-man interpretation, even of important and life critical rules can be prone to error. Also many norms defy formalisation because of their complexity and sensitivity to human values, views and beliefs which are subject to many dynamic factors in a situation. Hence, any formalisation devised must include agents (authorities of action who can take explicit responsibility for their actions) whom are part of the system and cannot be expressed in mathematical and logical symbols. Identifying implicit norms in human factor behaviour examples help us to understand and de-velop appropriate controls. ie control norms to counteract the influence of human factor driven errors and slips.

Clinical Pathways and the Human Factor
15
Modelling Norms
Norms can be modelled as: If <condition> then <consequent. The typical model of a norm is seen below (Liu and Dix, 1997). Whenever <condition> If <state> Then <agent> Is <deontic operator> To <action>. The condition clause, describes the matching mechanism to apply that refer to the context in which norm can be ap-plied and defines the data the norm subject requires. The state clause refers to the conditions that must be present for the deontic operator to apply.
The deontic operator” is derived from Deontic Logic and can be one of the fol-lowing: “obliged”, “permitted” and “prohibited” which prescribes what people must, may, and must not do and refers to the human ability to choose and adjust decisions. It is essential to recognize that norms are not as rigid as logical conditions therefore they allow to model situations were decisions are made solely based on human judg-ment and there is a degree of flexibility in patterns of actual behaviour The agent clause describes authority (s) of action that is responsible for the action. The action clause specifies the consequence of norm, which can be an action, or generation of information. The system of norms for a community determines essential informa-tion required by its subjects, who are the agents in the organisation, to conform to its norms and enables the modelling and handling of alternative behaviour of agents within a business domain (Stamper 1980, Stamper and Liu 1994). Norms with their deontic option therefore reflect the dynamics of people’s behaviour in a business context hence are more suitable for modelling human focused behaviours in clinical processes that lead to risk and human error.
Methods for Capturing Norms
Organisational semiotics methods have been developed for capturing norms in human and technology systems using a formal methodology called MEASUR - Methods for Eliciting, Analyzing and Specifying Users‘ Requirements (Stamper et al., 1988). This involves three procedures that firstly identifies stakeholders and their influence on the system being investigated and then the ontology of information and activi-ties and then a final stage that analyses the patterns of human behaviour and leads to the development of the formal models of norms defined earlier. Identification of norms enables the capture of the form of rules that influence human behaviour.

Clinical Pathways and the Human Factor
16
3.2 Risk Modelling and Human Factors
Various methods are available for assessing risks of process failure. The scope of the chapter prevents a discussion of risk modelling methods and so we have selected the FMEA model as a vehicle as it is one of the most commonly used approaches in health practice and easy to understand.
Failure Mode and Effects Analysis
The Failure Mode and Effects Analysis method of identifying failures in products and processes has been widely used both in industry as part of Six Sigma process analysis methodology and more recently has been applied to medicine (Chiozza and Ponzetti 2009). In summary it involves the identification of the ways in which a process can fail and the apportioning of the risk via three elements. Information regarding failure points for a process can be mapped via a process mapping method (Wohed et al, 2006). Typically block diagrams/narrative functional statements can be used to determine the success/failure ways or modes and its effect or impact in the process together with root cause analysis to identify the driver of the failure (Dhillon, 2003). The FMEA method provides a simple three factor multiplier to establish the seriousness of the risk of failure on a relative scale. Firstly the prob-ability of a specific failure (P), the impact of the specific failure (I) and the pos-sibility of detection of the failure in order to correct it (D). Each of these metrics is typically measured on a scale of 1-10 and then multiplied to provide an overall risk number as high as 1000 as a ranking measure of the risk (Zur Muehlen, 2004). Typically any factor > 7 is considered a high risk factor contributor. FMEA assumes a process model or documentation is available and that events leading to failure can be identified and that remedial risk reduction actions are also identifiable (Reason, Manstead et al., 1990).
Muehlen et al advocate a technique for risk aware process modelling by taking into account the a risk structural model for risk composition, a goal model relating risks of missing goals and a risk state model to evaluate dynamic risk combina-tions (Rosemann and Zur Muehlen, 2005). Reason reminds us that successful high reliability organisations use tools and reminders to help them remember the safe approach to actions (Reason, 2000). Human behaviour factors are factor that other authors suggest should be borne in mind when both patient safety problems are mapped and tools chosen (Chiozza and Ponzetti 2009). It is well known that clinical risk can be contained by risk management initiatives provided they cover all areas in which can emerge (Verbano and Turra, 2010), thus necessitating the inclusion of a process that considers and wide range of risk factors in an accessible form. However, little work has been undertaken to integrate these methods. Our approach

Clinical Pathways and the Human Factor
17
builds on Muehlen’s three model and FMEA risk analysis to a) identify the safety risks in clinical pathways l. and b) identify the specific human factor risks based on a knowledge of human factors in an accessible form such as the SHEEP model human factors that c) can complement traditional hard predictive controls and softer human behaviour controls..
4. INTEGRATING HUMAN FACTORS INTO CLINICAL PATHWAY MANAGEMENT
4.1 Controls
Controls involve the management of a goal situation by understanding and perceiv-ing a difference between the desired and actual goal state (the control error) and then identifying an action – ‘the control action or ‘control’ to move the undesired state back towards the desired state. Muehlen identified four business risk reduction approaches of which 3 apply in the case of clinical processes. A risk relates to the probability that some undesired state that may occur, such as the opportunity for an error. Firstly risks can be reduced by the introduction of controls to better ensure goal outcomes and reduce risk events (Roseman and Muehlin, 2005). Secondly risks can be avoided by altering/redesigning the process for specific actions and resources. Finally risks could be accepted and their impact reduced by pre-prepared contingency plans.
Sadiq et al (Sadiq et al, 2007) suggest the need to ensure a systematic approach to business objectives and control objectives in process design. Although Sadiq’s focus was compliance controls, it applies equally well to error controls. What is needed is explicit analysis and modelling of the process and defined and reasoned control objectives against a defined clinical risk and set of internal controls to reduce the risk. What often happens is that for clinical processes controls in the form of checklists (Grieshaber et al, 2009) etc are often added after errors occur and a root cause analysis occurs as a system of reminders to prevent reoccurrence.
Muehlen advocating the use of business process management (Roseman and Muehlin, 2005) identified four business risk reduction approaches of which 3 apply in the case of clinical processes. Firstly risks could be reduced by the introduction of controls to reduce and mitigate risk events. Secondly risks could be avoided by altering/redesigning the process for specific actions and resources. Finally risks could be accepted and their impact reduced by pre-prepared contingency plans. We will focus on controls – that mainly relate to quality controls after the event and process changes which relate to integrating quality assurance into the process by removing or significantly reducing the possibility of error.

Clinical Pathways and the Human Factor
18
4.2 Predictive, Personal and Cultural Controls
Predictive Controls
The use of FMEA or other methods can produce a set of ‘predictive error control points’ ie Muehlens’ ‘controls to reduce and mitigate risk events’ where predictive controls are defined as controls able to be set up for a known process ‘a priori’ or ahead of time to catch predicted failures. Many medical procedures are designed as sets of formal rules or norms as predictive controls identified when reviewing evidence based practice or experience. There are two main types. Firstly those con-trols that focus on control of quality by checking it after the activity or state change has occurred ie quality controls. One of the most frequent examples is the use of checklists or check points to affirm that the control goal has been reached (Semel et al, 2010). Another type of predictive control is a quality assurance based control where the process and activities are designed to actively prevent the error occurring, ie ensuring the quality by not allowing error outcomes to occur, ie through process design or change (Roseman and Muehlin, 2005). Predictive controls require a good knowledge of the actual activities and behaviours and their variations, actions and states of the stakeholders and known failure modes. This enables the identification of control objectives and needed controls at appropriate risk points. Predictive controls can be modelled as formal control norms or standard operating procedures.
Control of Perception Errors
Perception activities can be identified in clinical process models by use of verb-noun combinations such as ‘check’, ‘monitor’, ‘review’, ‘evaluate’. Typically clinical activities relating to perception may involve diagnosis and assessment using the clinician’s knowledge and experience of similar patterns and their meaning. Errors of perception such as a slip can often be controlled by the inclusion of checklists to reduce or remove forgetfulness and to ensure the clinician focuses on specific features that fit the pattern. Checklists are widely used in medicine [ref] and often included as part of clinical pathway paperwork. However, repeated use can numb the cogni-tive need for the checklist and result in simple box ticking or reverse engineering of the checklist after the event. Incorrect action plans can be reduced by cues and guides such as protocols and phone apps that can provide assurance of the right ac-tion given specific cues as can visual pattern charts to reduce perception cue error.

Clinical Pathways and the Human Factor
19
Control of Rule Based Errors
Context and rule error points are more difficult to identify, often because they are part of the tacit knowledge of the physician or clinician and their internal decision process. However, they are highly likely to occur at clinical decision points of di-agnosis and substantive intervention. Peleg and Tu advocate formal specification of clinical guidelines and detailed checking and update to detect rule based and related errors in clinical guideline and pathway documents (Peleg and Tu, 2009). The introduction of electronic records and related automation and personal phone apps is likely to render this more automatic, especially with the increasing use of artificial intelligence and the development of internet of things applications in medi-cal systems (For more details see Michell IOT 2014). However, one partial control is to make the rule and decision making process by ensuring clinicians verbalise their decision rule thoughts and make them explicit and open to feedback.
Control of Knowledge Based Errors
Knowledge based error is also difficult to plan for and manage due to its tacit nature. However, it can often be identified in clinical simulations where there is possibility of discussion and analysis of the thought process and knowledge required for the activity. In future the use of the Internet of Things (IoT) and sensor information may enable the detection of such errors from the record of follow on activities (Michell, 2014).
A potential solution to knowledge based errors is increased planning and de-sign of the process or clinical pathway and work activities to facilitate a predictive common shared understanding that by default (provided there is a minimum risk of group think or dominance by one party) should enable reasoned mental models to be developed that can survive error situations (Jalote-Parmar et al, 2008). This often involves extensive training and simulation to ensure the shared knowledge is identified, integrated and indeed used effectively as the varying situations occur.

Clinical Pathways and the Human Factor
20
Identifying Predictive Control Points
A key issue is to identify where specific failures may occur and where specific pre-dictive controls can occur. The use of the SHEEP model at one hospital has helped by providing a checklist of factors and categories of failure (Rosenorn-Lanng & Michell, 2014). When a medical department develops an error report the SHEEP human factor groups and types can be used to categorise the contributing factors and the weight of their contribution. Analysing the contributing factors enables a measure of the highest or most frequently occurring human factor and their impact. This information can then be used to identify where in a clinical pathway such human factor failures are likely to occur and to develop the predictive controls mentioned above.
4.3 Formal and Informal Norms
As we have seen modification and control of human behaviours ultimately depends on the individual and their adherence to rules. Hence to increase the control over human factors we can develop and apply more formal norms by the training and enforcement of new procedures and role specifications as part of a process improve-ment or redesign exercise.
Control Norms for Situational Awareness and Coning of Attention.
Both situational awareness and coming of attention suggest a need to be aware of where there is a high risk of these situations in clinical activities. Solutions to reduce situational awareness include organising information to ease understanding and match personal goals and the addition of cues, and training in pattern recogni-tion and multi-tasking (Stanton et al, 2001). This suggests a general rule or norm of whenever < high risk action> and < focused cognitive work by a single individual or specialist> then < ensure an independent second observer with knowledge and authority to enable the effective transmission of salient events, states or information to the cognitive work individual or team>. Other solutions involve more elaborate rule sets.

Clinical Pathways and the Human Factor
21
Personal Controls
Whilst formal controls can be enforced by the organisation the human focus of medical processes can also be moderated by the use of the humans themselves. Benabou & Tirole’s research on personal commitment and self-control identified personal rules that individuals used to manage their behaviour [(Bénabou and Ti-role, 2004). Ainslee 1992 (in (Bénabou and Tirole, 2004)) defined personal rules as willpower impulse controls that prevent temptation to act in a damaging way to the individual. We adapt Benabou and Tirole and Ainslee’s view to identify a generic set of personal norms. However, norms are subject to the willpower and lack of perfect recall that can alter their use and effectivity. Nevertheless in our research we identified good examples of personal rules that clinicians had used, that were driven by strong willpower (an important self-regulating mechanism advocated by Baumeister et al. (1994)) due to the bad event or ‘near miss’ that emphasised the need for their personal control over future events of this type.
We therefore define a second set of controls as personal controls. We define personal controls as informal control rules or heuristics - ie behavioural norms used by the individual to ensure the correct outcome of an action. Personal controls are informal as they are tacit and not formally codified by the organisation. Personal controls depend on the individual’s character and self-discipline for their introduc-tion and are typically the result of experience and concern about the outcome of an activity. They are part of the individual’s set of behavioural norms. For example one interviewee from a patient safety survey (Rosenorn-Lanng & Michell, 2014) always verbally repeated drug volume and strength information and asked for a second check whenever they knew themselves to be tired and hence the possibility of a perception or epistemic error was reduced. Hence an applicable norm might be:
Whenever< administering a drug> If <tired> must <repeat calculations and ensure a second clinician confirms my thinking>
Another clinical medical practitioner suggested their personal control norms for the parts of the clinical pathway (CP) they were responsible for involved care-ful checking; ‘It is easy to become blasé and so I check each stage carefully and I ensure that I involve others and their views’
Whenever< reviewing a clinical pathway > If < responsible physician > must <check each stage to minimise risk and involve others in reviewing my opinion

Clinical Pathways and the Human Factor
22
However, as above, the enactment of a ‘personal patient safety control norm’ depends on the discipline and awareness, or ‘strength of character’ of the individual. Such norms unless sanctioned and enforced by fear or personal lessons of past failure, are also subject to human factor failings such as stress. Hence we suggest the need for personal controls at stress points or points of high risk needs to be highlighted within clinical pathways. A good example is when additional factors such as noise or tiredness can reduce the willpower and motivation to apply the personal norm.
Cultural Controls
We have discussed the effect of culture on errors in the earlier section. We therefore identify a third set of controls as culturally driven controls resulting from national, organisation, professional, or team driven learnt and repeated behaviours. These relate to cultural norms and behaviours, but are not a formal part of the organisation rules or are not specific enough to be used directly, but enable the development of habitual norms related to them or traditional ways or working in groups or parts of an organisation. As Reason asserts organisational methods, actions and traditional working practices can create a communal safety culture (Reason, 1998). The existence of cultural norm beliefs and accepted behaviours creates discomfort and dissonance if the cultural behaviour or belief is violated. However, it can be difficult to measure or define a safety culture and the ’norms’ of safety behaviour (Pronovost and Sexton, 2005). Repeated training, examples and practice and consistent control behaviour can develop cultural controls. Examples of cultural controls are:
Cultural controls can be developed and disseminated through human factors training and repeated application of good practices and reflection and discussion within the groups affected by the actions (Rosenorn-Lanng & Michell, 2014).
For example, a discussion with a renal physician identified the levels of profes-sional and renal team culture norms that actively enforce the use of existing protocols:
‘The department norms can be summed up as: a) strongly that all Renal protocols must be followed b) any deviations must be discussed c) use of anecdotal alterna-tives are discouraged’
These rules actively reduced any thought of alternative workarounds and focused the clinicians only on evidence based best practice and official protocols as a se-ries of formal work and behaviour norms. This is an example of a culture type as defined by Davis et al (Davies et al, 2000) of uniformity rather than diversity and of central direction and avoidance of risk. However such a culture is less flexible to change and the discovery of improved ways of managing risk unless authorised by central authority.

Clinical Pathways and the Human Factor
23
Summary
A combination of process, human and system controls can constitute a defence against errors in depth. Organisational errors result from errors in systems or people and resources and represent a failure of multiple checks and formal controls due to ‘active and passive failures’ and gaps in safety defences in depth’ (Reason, 1998). Identifying potential human factor failure points and the corresponding predictive controls, cultural and personal controls in an integrated manner can help reduce safety risk. To aid this task suggested groups of controls are summarised in Figure 5.
5. HUMAN FACTORS AND THE CONTROL PROBLEM
5.1 Human Factors Requirements and Human Failure Modes and Effects Analysis (HFFMEA)
To develop a measure to rank identified potential failure points we use the FMEA approach mentioned earlier. Most FMEA analysis covers human and technology error, but rarely classifies human factors. We extend FMEA for clinical risks by identifying a set of human factor potential failure modes based on table 1 and 2, a range of predictive, personal and cultural controls. The innumerable ways in which human factors can impact a process make it extremely difficult to identify all the
Figure 5. Suggested control groups
Clinical Pathways and the Human Factor
24
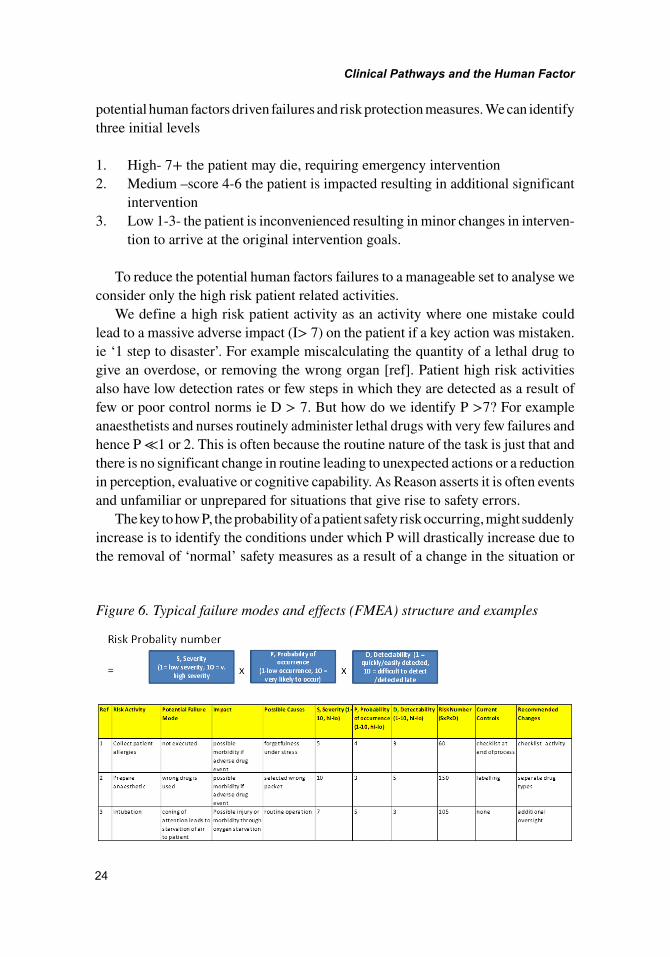
potential human factors driven failures and risk protection measures. We can identify three initial levels
1. High- 7+ the patient may die, requiring emergency intervention2. Medium –score 4-6 the patient is impacted resulting in additional significant
intervention3. Low 1-3- the patient is inconvenienced resulting in minor changes in interven-
tion to arrive at the original intervention goals.
To reduce the potential human factors failures to a manageable set to analyse we consider only the high risk patient related activities.
We define a high risk patient activity as an activity where one mistake could lead to a massive adverse impact (I> 7) on the patient if a key action was mistaken. ie ‘1 step to disaster’. For example miscalculating the quantity of a lethal drug to give an overdose, or removing the wrong organ [ref]. Patient high risk activities also have low detection rates or few steps in which they are detected as a result of few or poor control norms ie D > 7. But how do we identify P >7? For example anaesthetists and nurses routinely administer lethal drugs with very few failures and hence P ≪1 or 2. This is often because the routine nature of the task is just that and there is no significant change in routine leading to unexpected actions or a reduction in perception, evaluative or cognitive capability. As Reason asserts it is often events and unfamiliar or unprepared for situations that give rise to safety errors.
The key to how P, the probability of a patient safety risk occurring, might suddenly increase is to identify the conditions under which P will drastically increase due to the removal of ‘normal’ safety measures as a result of a change in the situation or
Figure 6. Typical failure modes and effects (FMEA) structure and examples

Clinical Pathways and the Human Factor
25
human behaviour. This requires identifying the human factor failure points and the controls employed in the formal process – typically a codified clinical pathway. If we can define these high risk points for each elective clinical process we can then define the human factors behaviours that could lead to the catastrophic result and design countermeasures to them. An excellent example is the risk of cabin pressure failure due to external cabin doors not being correctly locked resulting in the now universal safety control countermeasure of ensuring each cabin crew member that checks a door check their opposite number’s doors are safely locked or unlocked.
To identify the human factor risks and their respective controls a multistep pro-cess is proposed. Firstly a clinical pathway process model needs to be made available or developed. This should typically be in BPMN swim lane format to show the activities and roles responsible together with any necessary metrics such as timings and decision conditions. The traditional traditional Failure Modes and Effects Analysis (FMEA) method is used to identify failure points and modes within pro-cesses and activities and their relative probability of occurrence and level of impact to produce the risk assessment number. Existing formal controls (quality control and assurance measures) should also be identified to determine the detectability and impact of the error, given many errors may be contained by existing pre- event quality assurance controls. This is the first pass. A second review or pass of the process is then made to identify human factor drivers of failure modes, ie what
Figure 7. The proposed HF-FMEA process

Clinical Pathways and the Human Factor
26
possible factors are likely to occur that could stimulate error. This covers the percep-tion and cognitive error types and the different levels of Jackson and flin’s model ie cognitive skills and personal resources through to team and unit culture and or-ganisational factors. Use should be made of models and lists of situational factors affecting safety such as the SHEEP model to identify which factors may occur at specific activities in the process. For example the environmental and systems factor list will always have some relevance in any process. A third pass is then made to assess any dangerous combinations of failure modes that could cause knock on ef-fects and increase high impacts. For example where a minor error may drive or lead to a bigger impact and probability of occurrence – eg an incorrect patient name may lead to an incorrect and incorrectable operation if a single further control point is missed or such an event occurs in conjunction with human factors such as tired surgeons in an emergency situation.
The FMEA risk priority number based list should then be re-prioritised to con-firm the major risks and the major human factor drivers. The high risk human factor driven parts of the process/activities are then studied to identify predictive controls in the form of active checks on quality and or process redesign to provide quality assurance. Where possible personal and cultural control points should be identi-fied and the related behaviour norms should be extracted to support training and discussion. These behaviour norms and details of the potential human factor driven failure mechanisms should then be used to develop relevant training and simulation exercises and workshops organised to develop these behaviours. For example the non-technical skills training often provided to healthcare professionals to ensure human factors awareness (Rosenorn-lanng, 2014b).
6 CONCLUSION
This chapter has reviewed current thinking and develops a methodology for identifi-cation and control of human error in clinical pathways based on the research of the two authors. Using examples from the literature we have proposed and described a method of identifying and integrating the study and control of human factors into a traditional FMEA method of process and clinical risk analysis. We have suggested a semiotic norm based approach for the identification of human factor behaviours and norm based controls. We have explained how traditional predictive controls and risk avoidance by process redesign can be combined with the identification of human factor controls. We have shown how the use of the HF-FMEA approach and

Clinical Pathways and the Human Factor
27
the identification of organisational, team and individual risks and errors can be used to define risk points and how new cultural and personal controls can augment tradi-tional formal control regimes to reduce human factor error. This is achieved through application of an adapted risk model to identify the human factor risks, modelling and integration of human factor and controls in clinical pathways as demonstrated by an actual simulation example. We hope this will result in more rigorous control the care process ensuring completeness, consistency and patient safety by enabling the mapping of formal and informal/safety controls into clinical pathways.

Clinical Pathways and the Human Factor
28
REFERENCES
Audimoolam, S., Nair, M., Gaikwad, R., & Qing, C. (2005). The Role of Clinical Pathways in Improving Patient Outcomes. Retrieved from cs.dal.ca
Bénabou, R., & Tirole, J. (2004). Willpower and personal rules. Journal of Political Economy, 112(4), 848–886. doi:10.1086/421167
Cabitza, F., Simone, C., & Sarini, M. (2008). Knowledge artifacts as bridges between theory and practice: the clinical pathway case. In Knowledge Management in Action (pp. 37-50). Springer US.
Chapanis, A. (1996). Human factors in systems engineering. John Wiley & Sons, Inc.
Chang, A., Schyve, P. M., Croteau, R. J., OLeary, D. S., & Loeb, J. M. (2005). The JCAHO patient safety event taxonomy: A standardized terminology and classifica-tion schema for near misses and adverse events. International Journal for Quality in Health Care, 17(2), 95–105. doi:10.1093/intqhc/mzi021 PMID:15723817
Davies, H. T., Nutley, S. M., & Mannion, R. (2000). Organisational culture and qual-ity of health care. Quality in Health Care, 9(2), 111–119. doi:10.1136/qhc.9.2.111 PMID:11067249
Dhillon, B. S. (2003). Methods for performing human reliability and error analysis in health care. International Journal of Health Care Quality Assurance, 16(6), 306–317. doi:10.1108/09526860310495697
Flin, R., Winter, J., & Cakil Sarac, M. R. (2009). Human factors in patient safety: Review of topics and tools. World Health, 2.
Grieshaber, D. C., Armstrong, T. J., Chaffin, D. B., Keyserling, W. M., & Ashton-Miller, J. (2009). The effects of insertion method and force on hand clearance en-velopes for rubber hose insertion tasks. Human Factors: The Journal of the Human Factors and Ergonomics Society, 51(2), 152–163. doi:10.1177/0018720809336414 PMID:19653480
Haig, K.M., Sutton, S., & Whittington, J. (2006). SBAR: A shared mental model for improving communication between clinicians. Joint Commission Journal on Quality and Patient Safety, 32(3), 167-75.
Kohn, L. T., Corrigan, J. M., & Donaldson, M. S. (Eds.). (2000). To err is human: building a Safer Health System (Vol. 6). National Academies Press.
Leape, L. L. (1994). Error in medicine. Journal of the American Medical Associa-tion, 272(23), 1851–1857. doi:10.1001/jama.1994.03520230061039 PMID:7503827

Clinical Pathways and the Human Factor
29
Li, W., Liu, K., Yang, H., & Yu, C. (2014). Integrated clinical pathway management for medical quality improvement–based on a semiotically inspired systems architecture. European Journal of Information Systems, 23(4), 400–417. doi:10.1057/ejis.2013.9
Liu, K., & Dix, A. (1997, May). Norm governed agents in CSCW. In The First International Workshop on Computational Semiotics. IGI.
Michell, V., Tehrani, J., & Liu, K. (2012). Are clinical documents optimised for patient safety? A critical analysis of patient safety outcomes using the EDA error model. Health Policy and Technology, 1(4), 214–227. doi:10.1016/j.hlpt.2012.10.003
Michell, V. (2014). The Internet of Things and Opportunities for Pervasive Safety Monitored Health Environments. In Patient Safety and Quality Care through Health Informatics. IGI. doi:10.4018/978-1-4666-4546-2.ch020
Milligan, F. J. (2007). Establishing a culture for patient safety–The role of edu-cation. Nurse Education Today, 27(2), 95–102. doi:10.1016/j.nedt.2006.03.003 PMID:16713030
Mohr, J. J., Abelson, H. T., & Barach, P. (2002). Creating effective leadership for improving patient safety. Quality Management in Health Care, 11(1), 69–78. doi:10.1097/00019514-200211010-00010 PMID:12455344
Noble, D. J., & Donaldson, L. J. (2011). Republished paper: The quest to eliminate intrathecal vincristine errors: a 40-year journey. Postgraduate Medical Journal, 87(1023), 71–74. doi:10.1136/qshc.2008.030874rep PMID:21173052
Osborn, S., & Williams, S. (2004). Seven steps to patient safety. An overview guide for NHS staff. Retrieved from http://www. npsa. nhs. uk/nrls/improvingpatientsafety/patient-safety-tools-and-guidance/7steps/
Panella, M., Marchisio, S., & Di Stanislao, F. (2003). Reducing clinical variations with clinical pathways: Do pathways work? International Journal for Quality in Health Care, 15(6), 509–521. doi:10.1093/intqhc/mzg057 PMID:14660534
Peleg, M., & Tu, S. W. (2009). Design patterns for clinical guidelines. Artificial Intel-ligence in Medicine, 47(1), 1–24. doi:10.1016/j.artmed.2009.05.004 PMID:19500956
Piko, B. F. (2006). Burnout, role conflict, job satisfaction and psychosocial health among Hungarian health care staff: A questionnaire survey. International Journal of Nursing Studies, 43(3), 311–318. doi:10.1016/j.ijnurstu.2005.05.003 PMID:15964005
Pronovost, P., & Sexton, B. (2005). Assessing safety culture: Guidelines and rec-ommendations. Quality & Safety in Health Care, 14(4), 231–233. doi:10.1136/qshc.2005.015180 PMID:16076784

Clinical Pathways and the Human Factor
30
Rasmussen, J. (1983). Skills, rules, and knowledge; signals, signs, and symbols, and other distinctions in human performance models. Systems, Man and Cybernetics, IEEE Transactions on, (3), 257-266.
Reason, J., Manstead, A., Stradling, S., Baxter, J., & Campbell, K. (1990). Errors and violations on the roads: A real distinction? Ergonomics, 33(10-11), 1315–1332. doi:10.1080/00140139008925335 PMID:20073122
Reason, J. (2000). Human error: Models and management. BMJ (Clinical Research Ed.), 320(7237), 768–770. doi:10.1136/bmj.320.7237.768 PMID:10720363
Rosemann, M., & Zur Muehlen, M. (2005). Integrating risks in business process models. ACIS 2005 Proceedings, 50.
Rosenorn-Lanng, D., & Michell, V. (2014). The SHEEP Model; Applying Near Miss Analysis. In Patient Safety and Quality Care through Health Informatics. IGI.
Reason, J. (1995a). Understanding adverse events: Human factors. Quality in Health Care, 4(2), 80–89.
Rosenorn-Lanng, D. (2014). Human Factors in Healthcare: Level One. Oxford University Press.
Reason, J. (1995b). Safety in the operating theatre—Part 2: Human error and organi-sational failure. Current Anaesthesia and Critical Care, 6(2), 121–126. doi:10.1016/S0953-7112(05)80010-9
Reason, J. (1998). Achieving a safe culture: Theory and practice. Work and Stress, 12(3), 293–306. doi:10.1080/02678379808256868
Sadiq, S., Governatori, G., & Namiri, K. (2007). Modeling control objectives for business process compliance. In Business process management (pp. 149–164). Springer Berlin Heidelberg. doi:10.1007/978-3-540-75183-0_12
Semel, M. E., Resch, S., Haynes, A. B., Funk, L. M., Bader, A., Berry, W. R., & Gawande, A. A. et al. (2010). Adopting a surgical safety checklist could save money and improve the quality of care in US hospitals. Health Affairs, 29(9), 1593–1599. doi:10.1377/hlthaff.2009.0709 PMID:20820013
Shappel, S. A., & Wiegmann, D. A. (2000). The human factors analysis and clas-sification system--HFACS (No. DOT/FAA/AM-00/7). US Federal Aviation Admin-istration, Office of Aviation Medicine.

Clinical Pathways and the Human Factor
31
Smits, M., Groenewegen, P., Timmermans, D., van der Wal, G., & Wagner, C. (2009). The nature and causes of unintended events reported at ten emergency departments. BMC Emergency Medicine, 9(1), 16. doi:10.1186/1471-227X-9-16 PMID:19765275
Spath, P. L. (2003). Using failure mode and effects analysis to improve patient safety. AORN Journal, 78(1), 15–37. doi:10.1016/S0001-2092(06)61343-4 PMID:12885066
Stanton, N. A., Chambers, P. R., & Piggott, J. (2001). Situational awareness and safety. Safety Science, 39(3), 189–204. doi:10.1016/S0925-7535(01)00010-8
Stamper, R. (1994). Social norms in requirements analysis: an outline of MEASUR. Academic Press Professional, Inc.
Swidler, A. (1986). Culture in action: Symbols and strategies. American Sociologi-cal Review, 51(2), 273–286. doi:10.2307/2095521
Verbano, C., & Turra, F. (2010). A human factors and reliability approach to clini-cal risk management: Evidence from Italian cases. Safety Science, 48(5), 625–639. doi:10.1016/j.ssci.2010.01.014
Vincent, C., Neale, G., & Woloshynowych, M. (2001). Adverse events in British hospitals: Preliminary retrospective record review. BMJ (Clinical Research Ed.), 322(7285), 517–519. doi:10.1136/bmj.322.7285.517 PMID:11230064
Wiegmann, D. A., Eggman, A. A., ElBardissi, A. W., Parker, S. H., & Sundt, T. M. III. (2010). Improving cardiac surgical care: A work systems approach. Applied Ergonomics, 41(5), 701–712. doi:10.1016/j.apergo.2009.12.008 PMID:20202623
Wohed, P., van der Aalst, W. M., Dumas, M., ter Hofstede, A. H., & Russell, N. (2006, September). On the suitability of BPMN for business process modelling. In International conference on business process management (pp. 161-176). Springer Berlin Heidelberg. doi:10.1007/11841760_12
Ye, Y., Jiang, Z., & Yang, D.-A. (2008). Semantics-Based Clinical Pathway Work-flow and Variance Management Framework. IEEE/SOLI 2008.IEEE International Conference on Service Operations and Logistics, and Informatics.
Zur Muehlen, M. (2002). Workflow-Based Process Controlling: Foundation. Design, and application of Workflow-driven Process information system.

Clinical Pathways and the Human Factor
32
APPENDIX
Figure 8. Index to Key Acronyms

Copyright ©2017, IGI Global. Copying or distributing in print or electronic forms without written permission of IGI Global is prohibited.
DOI: 10.4018/978-1-5225-2337-6.ch002
Chapter 2
33
Medical Errors:Impact on Health Care Quality
ABSTRACT
The impact of medical errors on the delivery of health care is massive, and it sig-nificantly reduces health care quality. They could be largely attributed to system failures and not human weakness. Therefore improving health care quality and ensuring quality control in health care would mean making systems function in a better manner. In order to achieve this all sections of society as well as industry must be involved. Reporting of medical error needs to be encouraged and this may be ensured if health care professionals as well as administrators and health con-sumers come forward without fear of being blamed. To get to the root of the prob-lem- literally and metaphorically- a root cause analysis and audit must be carried out whenever feasible. Persons outside the medical care establishment also need to work with medical service providers to set standards of performance, competence and excellence.
Jayita PoduvalPondicherry Institute of Medical Sciences, India

Medical Errors
34
INTRODUCTION
The objectives of this chapter are to recognize health as a basic human right, and to define the issues of quality and costs of health care in this context. It is not a luxury but a basic privilege of the poorest individual. Poor, sick and suffering citizens, besides being denied this basic human dignity, add considerably to the economic burden of a nation in terms of lack of productivity and the considerable drain on economic resources as well. On the other hand, poor health for the rich and afflu-ent means a plethora of illnesses known as lifestyle disorders- again affecting both productivity and resources. Thus, quality in health care is not just about access to health care or limited by social and economic factors and problems of affordability. Publicly funded health care, insurance schemes and a robust primary health care infrastructure are the basic necessities for access and affordability. Safety and ef-ficacy then determine whether the utilization of health services is optimum, and thereby cost- effective.
BACKGROUND
While almost all manner of drugs or procedural intervention comes with the dis-claimer of a ‘side effect’, the quantum and severity of this sees wide disparities across communities and societies. There are medical facilities where such side effects are virtually unheard of and others where the same are a perfectly acceptable part of medical treatment. So it is absolutely possible that side effects of medical therapy could be minimized and the quality of such therapy maximized.
These undesirable effects may be broadly classified into the known therapeutic extensions of drugs and interventions, adverse drug reactions or harmful effects of a drug given in therapeutic doses, medication errors, and the most serious of them all- medical malpractice and negligence (Grober & Bohnen, 2005; Keriel-Gascou, Figon, Letrilliart, Chaneliére, & Colin, 2011). A new dimension has been added to this, such as when a potential or incipient undesirable effect of medical treatment has been identified and prevented- the near miss (Kessels-Habraken, Van der Schaaf, De Jonge, & Rutte, 2010).
What might be the reasons for medical error to occur and thereby negatively impact the quality of health care?

Medical Errors
35
The two most common reasons, and also the easiest to explain, are the twin effects of the speed of scientific technology and the rising perceptions and expectations of health care consumers. Technology brings with it more gadgetry and less human interaction. While computerized systems might seem to offer errorless functioning, one must appreciate that at some point human presence might be required, and this is where room for error might exist. The same argument could be extended to patient expectations- more advanced technology does raise the hopes of the consumers of health, even though serious limitations of this technology might exist, and these would be by and large unknown to the end user. Thus health and medical care are very often compromised even when all infrastructure and technology exist to deliver high quality medical care.
MAIN FOCUS OF THE CHAPTER
Issues, Controversies, Problems
The process of making the diagnosis itself is a highly variable one- with a dispro-portional higher component being the human factor. In fact, all of it could be con-sidered entirely dependent on the human factor- what is better known as the doctor’s clinical acumen. Much could go wrong right at this very first step. The doctor’s ability to assess the patient’s illness in a precise manner by skilful history taking and examination, and then making a probable diagnosis and following it up with the relevant tests and investigations, rests entirely on the professional competence of the doctor. And this in itself could be fraught with almost every kind of error possible. The worst form of medical error is therefore one in which the incompetence of the medical professional becomes highly obvious, and forms the crux of a claim of medical negligence or malpractice. The glut of technology has further complicated the situation, with the common belief or assumption that what the doctor cannot diagnose, the machine will.
It is not difficult to understand why making a diagnosis could be such an onerous task. History taking as a science and art is paid scant attention to in modern times, but something every doctor is expected to possess in the finest degree. It is, or should be, ingrained in the training of every medical professional until it becomes second nature and gives the medical profession the tag of ‘noble’ (Aronson, Henderson, Webb, & Rawlins, 2006; FitzGerald, 2009). But the rapid march of technology has somewhat confused the picture and compounded the problem areas in patient care- those that require time, humility, discipline, patience and a “listening ear”- literally and figuratively. Issues with the allocation of time to each patient, the seniority and experience of the doctor, the stratification of medical care services into primary,

Medical Errors
36
secondary and tertiary, billing protocols involving insurance and other service pro-viders and consumer awareness are important factors which could impact the depth to which a reliable medical history is obtained. As more and more globalization takes place, methods and patterns of training of medical professionals must also follow standardized systems. The influx of technology however, and the business model of medical education, has introduced a disproportionate increase in scientific methodology as compared to artistic skill in the process of history taking. This could make things look a little too simple, and also the assumption that every doctor is a good one. For example, in many facilities the medical history of the patient might be obtained by a very junior doctor, a doctor in training, a nurse or paramedic, or simply a computerized checklist or patient questionnaire. An arbitrary conglomera-tion of symptoms is then teamed up with an equally cursory or illogical clinical examination, and then an entire battery of tests is ordered. It is hoped that one of these tests would yield the correct answer.
So the words of George Bernard Shaw might not be out of place in this kind of a situation:
The single biggest problem in communication is the illusion that it has taken place.
In other words, the most essential form of communication between the patient and doctor- the fact that the patient has been able to convey his or her problem to the doctor, and that the doctor has understood this fully and acted on it- is often incomplete, illogical and even fallacious. Apart from the patient being subjected to an array of tests without having undergone a proper evaluation, there could be serious lapses in communication across the hierarchy of a medical establishment. Doctors- in training and those training the former- nurses, paramedics, administrators- could all be speaking a different language, in a manner of speaking. This practice and culture is perhaps the root cause of the problem of medical errors (Digitale, 2014; Khairat & Gong, 2010). Without the common bridge of an efficient primary care facility, a definitive diagnosis often eludes the patient even when top notch technology is available at higher levels of care. Doctors avoid ‘crucial conversation’ and general communication, ranging from poor clinical decision making to serious lapses in teamwork in patient care services.
Of late, electronic medical record systems (EMRs) have further complicated this aspect of medical care. While it is an undisputed fact that digital technology is the way of the future, the way this technology is used leaves much to be desired, at least in the health care industry. EMRs for the documentation of clinical history and examination commonly follow a template or checklist pattern, with subtle nuances vital to the patient completely left out. Such templates, furthermore, are largely dependent on the vendors of such services and the sophistication of the software

Medical Errors
37
they use. Large variations in standardization might exist and some specialty subjects under represented. Diagrammatic representation might be inadequate, thus reducing the speed and accuracy of cross checking such information.
Even where electronic information has been recorded accurately, serious over-sight might occur when it comes to the actual dispensing of medication. Drop down boxes in the EMRs typically list medications in alphabetical order, with entire lists of similar sounding names of widely different classes of drugs. Carelessly ticking off a particular drug results in what is known as a substitution error. While this could happen in the hands of a trainee or even qualified doctor, it is most often seen when non- medical persons such as nurses, paramedics or pharmacists make such entries. The administration of the wrong drug, if not detected in time, could result in a seri-ous adverse effect or even a fatality, and the price to be paid could be enormous.
Also, clinical practice guidelines (CPGs) may not be followed in many places. CPGs may not be uniformly or universally adhered to, for example, treatment of chronic rhinosinusitis sees wide variations, some of which may harbour scope for medical error (Dubin, Liu, Lin, & Senior, 2007) Clinical practice patterns may vary from place to place and case to case but nevertheless have serious medicolegal out-comes (Carter, 1999; Nash, Nash, Leach, & Poetker, 2011; Poetker and Smith, 2015; Ward and Allen, 2008). Prescription and use of seemingly harmless medications such as analgesics, and also more judicious use of drugs such as corticosteroids, should be considered more seriously in order to avoid medico legal hassles (Christensen, Nielsen, & Nielsen, 1990; Crane, 1993; Fink, 1983; Goldenbaum et al, 2008; Kuehn and Doyle, 1990; McAbee, 1998). Medical errors arising from such common lapses in clinical decision making occur across the board in almost all specialties and can prove extremely costly (Bettman, 1990; Rothschild et al, 2002). They in turn push up the cost of such specialist services, and lead to poor utilization of such services.
Therefore, the practice and use of evidence based medicine (EBM) may leave a lot to be desired. This culture or philosophy is known as suboptimal practice (Bates et al, 2001). This study describes in detail the limitations of traditional practice without the modernizing and standardizing effect of information technology (IT). It cites instances by which safe delivery of medical care could be ensured by the adoption of computerized systems and suggests ways and means by which this could be carried out.
The flip side of IT- substitution error, MARs (medication administration records), and unsafe order alerts- must also be taken into consideration (Bates et al, 2001). The authors strongly recommend improvement of vendor developed systems. They also explain the challenges of digitization of health care from the technical, administra-tive, and economic standpoints. For example, integration of information technology

Medical Errors
38
is often hampered by what is known as ‘silo accounting’, that is, the expenditure on different components of this integration is difficult from the financial point of view. It requires both competence and cleverness on the part of the cost accountant to convince the administrators of the cost utility of these systems. This fact is also not helped by the current financial crisis in the health industry and indeed overall in virtually all industries. There is thus a lack of interest and investment in IT wizards, and the extremely talented personnel who can maintain such IT systems. Technical hitches such as format and interface issues of clinical decision support (CDS) systems continue to plague the health care industry, especially the failure to integrate into a web viewing system that could facilitate real time supervision of medical interven-tions. There is also a lack of consensus among health professionals regarding the extent to which information technology might prove useful in health care delivery.
Medical Errors and Health Care Quality
The twin issues of quality and safety are intimately related and were first examined in extremely high risk establishments such as nuclear power stations and the avia-tion industry (Norman, 1988; Rasmussen, 1982; Reason, 1990; Senders and Moray, 1991). It is these industries where actual safety protocols were first designed and tested, and eventually put into practice and organizational culture. Gradually and inevitably, it became the norm rather than exception that safety protocols be applied to all industries (Fischman, 2000). It was not long before the health care industry also took cognizance of such measures, and the now famous “To Err is Human” report was put forth by the Institutes of Medicine in North America (Kohn, Corri-gan, & Donaldson, 1999). Several authors have pointed out that medical errors exist because it is human to err. There is also the belief that such errors do not occur at the individual level, but are the consequences of what are termed’ system failures’. Perhaps this notion is itself paradoxical and seems to contradict itself. If ‘to err is human’ then how can there be a ‘systems failure’?
Therefore, what is probably more important in this message is that ‘doctors are human’ but the ‘system fails’ owing to the environment or culture in which doctors must work. And this is where the hard part begins- the system must change from inside if systems failures are to be avoided and medical errors reduced. One of the elements of designing safety, especially with regard to the health care industry, is to find ways and means to enhance what is known as “situational awareness”. This means, literally, that “transparency” is created in all settings where medical care is being delivered. This, in particular, pertains to areas in the health care establish-ment considered extremely high risk, such as critical or intensive care and operation
Medical Errors
39
theaters. It is proposed that the combination of man and machine produces the best results, and not when they work individually. Systems changes are therefore the need to the hour (Macklis, Meier, & Weinhous, 1998; Senders and Moray, 1991). Figure 1 illustrates how medical errors and health care quality are inter-related and influenced by systems changes.
SOLUTIONS AND RECOMMENDATIONS
Systems Changes to Combat Medical Errors: The Role of ‘Communication’
Everything becomes a little different as soon as it is spoken out loud, said Hermann Hesse. Nowhere other the health care industry are these words more pertinent. If health care providers do not sufficiently speak out loud to each other and ensure clear channels of communication, it is more or less guaranteed that someone will- the health consumer and the media. It is virtually impossible, especially in the current highly charged climate in health care, to hide a medical error. And when out in the
Figure 1. To Err is Human

Medical Errors
40
open, the repercussions are enormous- lives and reputations are always at stake- and the quality of life poor.
Similarly, professional medical education has seen recent changes such as working time directives and shift duties for doctors in training. While debates still continue over the supposed advantages of these developments, one thing that is undisputed is the scope for serious oversight that comes in with the changes of shift from one staff or resident doctor to another. Handoffs are treatment orders that must be com-municated to the next doctor on call rotation. Most of the time, one simply needs to check the patient’s treatment chart to follow what is happening and what might need to be done further. But many a time, important changes or developments in the patient’s status occur and this means that some radical changes would have to be made to the treatment or essential investigations or tests must be carried out. Lack of proper communication at this juncture naturally leads to suboptimal treatment and sometimes serious lapses in treatment. It is strongly recommended that hand-offs be in both written and digital format- sometimes cross checking with the next on call in real time- so that medical errors can be minimized (Perna, 2014). While this protocol seems to suggest that it is a time consuming, laborious and disruptive procedure, it has been found not to interfere with the overall flow of work, and still reduce the rate of error significantly (Digitale, 2014).
Communication is also paramount when the diagnosis or any other aspect of the patient’s illness is in doubt or is disputed by other members of the team. In the case of independent practice, this means that the treating doctor must liaise with and seek help from colleagues and peers outside the immediate medical establishment to carry out the optimal treatment of the patient, or to refer to another establishment if required. In an academic or multidisciplinary setting, it involves transparency, humility, respect, vigilance and concern for the patient to ensure that all the members of the team work in a cohesive and seamless manner to execute the correct treatment (Shahrokhi, Ebrahimpour, & Ghodousi, 2013). In particular, a respectful attitude towards all members of a health care establishment is paramount and ensures good quality medical care at most times, if not all. It ensures teamwork, which is a virtue and necessity in today’s chaotic world of hi tech medical establishments. Not only medical professionals but other members of the team such as nursing and paramedi-cal personnel need to bear this in mind and always act in a spirit of cooperation (Garrett, 2008; Kyung and Barbara, 2011).

Medical Errors
41
In fact, the nursing staffs occupy a pivotal role in the detection and prevention of medical mishaps. An intelligent and vigilant nursing staff is in a position to pick up areas of obvious oversight in a patient’s treatment chart, and convey this information to the doctor concerned, or even any other available member of the team (Garrett, 2008) (Kyung, Barbara, 2011; Shahrokhi, Ebrahimpour, & Ghodousi, 2013). Nurses are also the cornerstone for ensuring continuum in care. This means that the patient is not only given good quality care while undergoing treatment in the hospital, but has also been given a proper list of medications to take and any other advice at the time of discharge. Apart from the doctor, it is the nurse who must reinforce the need for timely follow up and also give specific instructions about what to do should the patient encounter any expected or even untoward adverse event. Similarly, a quali-fied, concerned pharmacist could also pick up obvious substitution errors where there is a mismatch between the diagnosis and the treatment advised. It is not to be taken lightly that a competent pharmacist can even decipher a doctor’s notorious scrawl on a handwritten prescription and proceed to take due action such as quickly checking back with the prescribing doctor.
Communication across all levels must be ensured and constantly improved. This translates into immense patient satisfaction, apart from facilitating all members of the medical care workforce to be consciously aware of their individual duties and responsibilities. Communication as a gift and as an obligation must be inculcated into the training of all medical, paramedical, nursing and administrative personnel. There are several examples whereby errors of omission or commission are pre-empted by proper communication. When these are actually highlighted it seems both silly and sad that such lapses in communication could lead to serious medical error (Swaminath and Raguram, 2010).
Some other researchers have specifically studied medication errors, wound in-fections and technical lapses in hospital settings (Leape et al, 1991). Even outside the hospital, that is, in domiciliary or non hospital settings, medication errors are mainly related to deficiencies in prescription advice at the time of discharge, and also a lackadaisical attitude among health care staff in giving instructions to the patient or family regarding future follow up and post treatment surveillance (Gurwitz et al, 2000). It is also sobering to note the impact of medication errors due to missing a dose- something that is perhaps not taken as seriously as it should be (Bates et al, 1995). Insufficient advice to patients regarding the importance of following the prescription judiciously is rather common.

Medical Errors
42
Communication and Patient Consent
The process of procuring consent sees huge variations across the globe. In develop-ing countries where consumer awareness is often subliminal and sketchy, ‘consent’ is just another word in the dictionary. Neither patient nor doctor understands fully the implications of giving or taking consent respectively, and a formal consent sheet may be even unheard of. This scenario is rapidly changing, like the radical changes taking place in the health care industry today. Consent now includes an informed, verbal and written consent. The extent to which all the three components are adhered to may vary slightly from region to region. Likewise, patients that are educated may sign their consent in full, while the unlettered could be allowed to sign with their thumbprint.
Informed and written consent also has slight variations from country to country. For instance, in North America, this includes almost every sort of information per-taining to the patient’s illness, and for which the patient might seek a thorough and detailed explanation. In Australia, however, the extent to which informed consent is expected is only as far as specific ‘information’ regarding that particular patient is valid. For example, a surgical procedure involving a particular organ, or one of a set of paired organs, could have specific implications that need to be clearly understood by the patient.
Medical Error: The Role of Information Technology (IT)
Estimates of medical error and major morbidity and mortality may be difficult to calculate with precision (Sox and Woloshin, 2000). Nevertheless, the speed and regularity with which medical errors occur does not escape notice easily by providers and consumers alike. In many health care setups, doctors still practice in the tradi-tional ‘paternal’ philosophy. They ‘cannot be seen’ to commit an error; therefore, the tendency is to hush matters up. No matter how deep the reach of technology, this mindset is not easily changed. Reporting of error is almost nonexistent and therefore its eradication a no brainer. If the end user or patient is equally unquestioning, there would not even be the concept of a ‘medical error’. Globalization, of course, is en-suring that this does not happen, and all over the world, a medical error is coming to be more and more easily recognizable by a lay person.

Medical Errors
43
‘Patient- centered’ medicine is therefore the only way to go, and more and more medical professionals and systems must accept and adopt this paradigm and actively practice evidence- based medicine. In institutional and training centers, the work culture must encourage transparency, change, ethics and professionalism amongst all health care workers. For example, even when doctors are enthusiastic and proactive about reporting error, there may be reluctance and reservation among nursing and other staff about what proportion of blame they are to burden. Often, this becomes a contentious issue because the doctor is considered the final author-ity in the dispensation of treatment to his or her patient, and therefore also the one person to fix responsibility on. At times, this could also mean that an inflated rate of error is reported. This could not however be half as detrimental as not recognizing error at all. Strategies to improve communication by adopting active surveillance of hospital medical errors and adverse events using information technology have been discussed (Szekendi et al, 2006). Communication and the use of information technology can also be extended to the issue of actual reporting of medical errors.
Digitization of medicine and computerized systems in health care has a positive impact on the industry and this has been extensively researched in the last several decades. How medical information helps to improve both the safety and quality of health care has been discussed specifically with regard to the prevention of medi-cal errors and the adverse effects of medical interventions (Leape et al, 1995). The many applications of IT in the health care industry have been described in the light of their positive impact on health care quality (Glaser, Teich, & Kuperman, 1996). Cost effectiveness of physician entry in computer workstations has also been studied consistently for the last few decades (Tierney, Miller, Overhage, & McDonald, 1993).
Clinical decision support forms an essential component in the reduction of medical error and enhancement of health care quality. This could be executed by several mechanisms-
1. Computerized records and entry of patient data including medication prescription can be done, and is already being practiced in many medical establishments, both stand alone nursing homes and large multispecialty hospitals and corporate chains. This might initially be a time consuming affair as staff make the shift from manual to computerized documentation but eventually prove to be user friendly and time saving. Besides being impressive and greatly contributing to consumer satisfaction, such practice has been shown to significantly reduce error while ensuring continuum of care (Glaser, Teich, & Kuperman, 1996; Tierney, Miller, Overhage, & McDonald, 1993).

Medical Errors
44
2. Alerting system(s) combining physician, lab and pharmacy data can be in-corporated in specific settings such as critical care and emergency situations (Karve, Ou, Lytle, & Peterson, 2008; Lindenauer et al, 2007). Such measures are not only essential in such settings but also greatly beneficial in the long run in terms of cost savings accrued from the conscious avoidance of medical error.
3. Algorithms, order sets, clinical practice guidelines, trend monitors, co- sign forcers are other ways and means to streamline and make systems more effec-tive and efficient in the delivery of good care and in minimizing error.
Computerized physician order entry has been found to be by and large helpful, especially when it comes to the avoidance of medical errors (Koppel et al, 2005). Also, the role of good teamwork cannot be overemphasized and it involves close communication and cooperation of all members of the medical establishment so that serious lapses in delivery and continuum of care are prevented (Bates et al, 1998). Alerts in real top on personal computer devices such as palm tops- and in the current era, mobile smart phones- could go a long way in keeping physicians and nursing staff up to date and keyed in to the progress of their patients, especially in high risk areas (Shabot and LoBue, 1995) Wireless alerts for patients on life saving medical and requiring lab investigations in critical care can be delivered in real time, thus foreseeing and avoiding a medical error (Shabot, LoBue, & Chen, 2000).
While the above measures appear to be rather simple and straightforward to implement from the technical point of view, this does not happen principally because the management of many medical establishments does not prioritize the issue of medication errors, and adopt appropriate information technology methods to ad-dress this issue (Kavanagh, 2011; O’Brien, Kumar, Metersky, 2013). However, it is interesting to learn that the return of investment (ROI) of IT based systems and the value proposition is generally positive with regard to the computerized entry of prescription and physician orders, though there may be a negative balance with regard to the actual cost savings in the management of medical error (Gregory, 2013; Morey, Fine, Loree, Retzlaff-Roberts, & Tsubakitani, 1992).
Incentivizing Health Care
In many countries, doctors are compelled to practice what is known as defensive medicine. This means that instead of a straightforward but judicious treatment approach, an exhaustive battery of tests and procedures is employed so as not to leave anything to chance. The culture of defensive medicine is pervasive all across the globe, from the highly developed United States of America, to the emerging superpowers of Asia.

Medical Errors
45
Part of this stems from the demands and expectations of health consumers, but most of it arises out of suboptimal competence of practicing doctors, combined with a lax regulatory system where aggrieved patients find it difficult to seek legal remediation. A climate of fear of litigation, retaliation, violence and vandalism means that medical professionals take cover- literally and figuratively- under the umbrella of medical indemnity insurance. While this seems to protect consumer interests, what it actually does is push up the costs of health care and thereby reduce its quality in the long run.
Transparency and a systems approach therefore help to ensure that the practice of defensive medicine is discouraged. Awareness of consumer rights must be tem-pered with regulatory measures, professional and safe practice methods, and holistic training of health care professionals. One method to design a better health system has been to provide incentives for safe practice and a low rate of medical error. This again seems to give the impression those medical professionals and health care systems would function better when induced to do so with incentives in cash and kind. But this fails to take into account the very essence of a medical error- that it is human to err- and that it is most often an involuntary and unintentional act. An incentive is unlikely to reduce this very human frailty, and on closer introspection, one might be led to believe that it would actually put doctors and other medical personnel on edge, and encourage the practice of defensive medicine (Kapp, 1997; Studdert, Mello, & Gawande, 2006).
On the other hand, what might be an effective deterrent is the idea of value based purchasing (VBP) (O’Brien, Kumar, & Metersky, 2013). Health care facilities with a higher rate of error might be penalized and thus forced to explore, establish and ensure better and safer practice methods (Kavanagh, 2011). This process must however be implemented in a methodical and systematic manner over a long period of time, while ensuring continuum in care. So far, the issue of incentives and value based purchasing has been investigated in a variety of settings from primary and community care to critical care and emergency medicine. The research conducted has showed initial promise but lacks a cost benefit analysis. It may even be that quality health care actually comes at a price (Morey et al, 1992). This means that medical establishments would have to invest more in order to improve quality, safety and care, unless efficient systems are put into place. This would then make health care affordable to a select few, and thus would be contrary to the global health care goals of quality and equity in health care. Simple solutions must be sought and put into practice and involve all the stakeholders.
In many countries such as the USA, the insurance enabled medical care system has introduced pay for performance incentives. Patient outcomes are analyzed for customer satisfaction and cost effectiveness and doctors and/or hospitals incentiv-ized accordingly. This naturally translates into better quality medical care and has

Medical Errors
46
an in built system of reducing medical error, though much research is still pending in this sector.
Incentives to hospitals for safe practice have been extensively discussed and debated in both the public and professional arenas (Stratton, 2011; Whitten, Dutta, Carpenter, & Bodie, n. d.). Incentives such as pay for performance may be poten-tially beneficial but have not been seriously researched, or robust conclusions drawn. Many different settings for performance incentives have been explored- primary care, emergency medicine, critical care, centers catering to a large number of minority patients, as well as with respect to developing and underdeveloped countries (Andel, Davidow, Hollander, & Moreno, 2012; Glickman, Schulman, Peterson, Hocker, & Cairns, 2008; Karve, Ou, Lytle, & Peterson, 2008; Khanduja, Scales, & Adhikari, 2009; Kmucha, 2010; Petersen, Woodard, Urech, Daw, & Sookanan, 2006; Scott et al, 2011; Sura and Shah, 2010; Witter, Fretheim, Kessy, & Lindahl, 2012).
Performance incentives when combined with the risk of public reporting and negative publicity were also studied. Both together show promising results but there is yet no cost benefit analysis to be able draw conclusive arguments from the same (Lindenauer et al, 2007).
Medical Error Reporting
No doctor wishes to commit an error, but what is often overlooked is that most doctors do not even understand what a medical error is. There may be confusion about when to actually recognize and report an error. Many a time, a side effect or adverse event takes place irrespective of a right clinical decision or medical judgment. Such incidents are not deemed suitable for reporting by many medical professionals who might be unaware of the concept of clinical pharmacovigilance. Indeed, this topic itself has only recently made its presence felt in most hospital settings- both corporate and academic- in the developing world at least. Continuing efforts in this direction are needed to increase awareness about the importance of reporting of any untoward or unexpected medical misfortune.
In this regard, the media reporting of a medical error- and the public reaction to it- must be given a special mention. Medical professionals, health establishments, the public and the media are invariably at loggerheads with each other (Gallagher, Waterman, Ebers, Fraser, & Levinson, 2003; Whitten, Dutta, Carpenter, & Bodie, n. d.). Also, the medical community, the general public and the mass media may seriously misinterpret and misrepresent each other (Blendon, DesRoches, & Bro-die, 2002). But this situation need not be so, and every effort must be made to see that misreporting does not occur. In many countries, especially in the developing world, there is an increasing culture of vigilantism. Lack of good governance and governmental regulations in all aspects of daily living, including health care services,

Medical Errors
47
means that there is heightened anger and frustration in the community and this can spill over into the health care establishment. Any untoward medical event- a drug overdose, death due to a drug past its expiry date, administration of the wrong drug, a surgical complication or a botched surgery- is quickly seized by the general public to vent their ire and indulge in vandalism. This is simply because they know that there might not be an adequate legal recourse. Add sensationalization of the event by the media, and the situation could even become riot like and result in destruction of innocent lives and property owing to a violent attack on the hospital or nursing home where such an event has taken place.
Thus the mass media such as television and newspapers have a specific respon-sibility in portraying the facts in as impartial a manner as possible (Jackson and Harper, 2001; Miller, Nelson, & Spurlock, 2001; Stump, 2000). Because what the media says could have a powerful- almost hypnotic- impact on the public, self regu-lation, governmental authority, law and order, and of course, the moral fiber of the community, are always matters that the media should take into consideration. Media trial of a doctor or medical establishment makes matters worse and rarely brings the truth to light. The doctor’s career and reputation are often ruined beyond redemption and the suffering patient or family, apart from getting their fifteen minutes of fame, very rarely get anything more.
It must be understood that even the culture of media reporting is influenced by not only governmental regulations but also the level of professionalism and trans-parency in the system. The timing of information to be released to the public, the amount and nature of such information, a generalized caution or alert regarding a medical error or disease outbreak, et cetera, must at all times ensure confidential-ity of both the erring doctor and the aggrieved patient. (Gregory, 2013; Stratton, 2011). Balance, reserve, and a non judgmental attitude are not only necessary in terms of containing public anger but also when exploring ways to make positive changes to the system. Also, a sincere attempt must be made to see whether a true human error occurred or an act of obvious negligence on the part of the doctor. The report can then conclude with a firm statement as to how such a lapse is going to be addressed as far as the patient is concerned, and also how to foresee and prevent similar events in the future. In short, the right message must be communicated to the public (Mazor, Simon, & Gurwitz, 2004). Blame games and finger pointing are best avoided as far as media reporting is concerned, but assurance needs to be given that sufficient steps would be taken to rectify the problem.
In India, most of the health care industry currently operates in the private sec-tor. As far as medical errors go, this scenario may be considered both good and bad. Hospitals in the academic setting- the teaching hospitals- have been keenly studied and suggestions put forward to minimize and avoid medical errors (Sharma, Awasthi, Dixit, & Sharma, 2011). The bad news is that governmental regulation

Medical Errors
48
may be deficient or even absent in many of these hospitals and health care centers. Medical errors or negligence may be rampant and unchecked, especially in regions where public awareness is not at par with technological progress, and cultural norms enable morbidity and mortality to be accepted with a fair degree of karmic philosophy. Even though such mishaps are coming to light more and more, the only common outcome is an outpouring of anger and the threat of litigation. Sometimes, public anger results in vandalism and violent attacks against doctors and hospitals. Legal recourse is generally slow and tedious, enough for the family to give up too soon, and for things to go back to status quo. In the more developed towns and cit-ies, consumer courts do prove to be very active, and are a major deterrent against individual doctors committing medical error. The practice of defensive medicine is on the rise, and doctors not only take large insurance covers but patients are also subjected to numerous unnecessary tests and procedures. The ‘system’ per se does not see any major change, as voluntary reporting is unheard of and mandatory re-porting is virtually absent, or at best erratic (Kumar and Chaudhary, 2009).
The good news is that private health care capitalizes on brand equity and quality assurance. To do this, a culture of professionalism must exist in the entire health care setup, as is true for the large hospital chains across the country. Vigilance, de-fensive medicine and sheer hard work at every level ensure that errors of omission and commission are minimized. Not only is the doctor rewarded but the hospital also profits and the market value of both increases. Most of the big hospital brands thus flourish on the dynamism and caliber of individual doctors, who in turn benefit from being part of a famous brand. It is a mutually convenient arrangement, and everyone is aware of the stakes, which means that in any actual event of serious medical error, the onus is usually on the doctor. Many a time, the legal hassles are handled by the parent hospital, but in the event of a malpractice case that is lost in courts it is the doctor that must pay the price by quitting or being terminated from service. Again, the system does not really go through an overhaul.
Fortunately, change is setting in. In both the service, and also educational and training centers, in the public sector as well as private, the clamor for accreditation has paved the way for safety protocols and guidelines to be instituted. A major chunk of these is the adoption of checklists and regular CMEs (continuing medical educa-tion) to build confidence and raise awareness about safety concerns and reducing medical errors (Sewal, Singh, Prakash, Kumar, & Medhi, 2014).
At certain centers in India, there is an active pharmacological surveillance sys-tem that is engaged in medical error reporting (Thakur, Thawani, Raina, Kothiyal, & Chakarabarty, 2013). Awareness of the same is however sporadic and it would yet be several years before such vigilance systems find their way into widespread acceptance and enthusiastic practice. Many others, such as the author’s, conduct regular M&M (morbidity and mortality) meetings and departmental audits or chart

Medical Errors
49
reviews to document medical errors (Gommans, McIntosh, Bee, & Allan, 2008; Hearnshaw, Harker, Cheater, Baker, & Grimshaw, 2002; Montesi and Lechi, 2009). While transparency is encouraged, blame mongering is not, unless there has been a serious lapse in care amounting to gross negligence.
The Role of the Public
The media is also largely responsible for education of the general public, even without the actual reporting of a medical error (Walsh-Childers, 1994). Newspapers, maga-zines, books and journals on matters of health and medicine are always of interest to the community. It is important to ensure that such material is of sound quality and not spurious literature that has the potential to contribute to the practice of quackery. The media must be especially careful about the accuracy and interpretation of the reports of professional bodies (Dentzer, 2000). This is actually an ongoing process- the consumer equivalent of a ‘continuing medical education’. The language adopted, is of course, simple and shorn of the medical jargon that the general public would have little use of. Medical professionals are constantly encouraged to be active participants and advocates of the cause of medical education of the lay population. In this manner, they could not only reach out to the community and display the real and human side of the medical doctor, but also help health consumers take better charge of their own well being.
Patients and health consumers are thus empowered to identify and address many a medical side effect or adverse effect to the best extent possible at their level (Brit-ten, 2009). Such a prospect is especially enabled in today’s digitized world, but here again there is a word of caution. Wrong information or hype could do more harm than good and cause panic among health consumers. It is like walking a tightrope- how much is good information, and when would it be called too much information? Nevertheless, with better levels of education and awareness in modern society, one hopes that a fine balance would be reached between patient responsibility and vulnerability. This could help reduce the rate of hospital visits required manage the problem, thereby reducing further expenditure and improving quality. Patient reporting of medical errors is therefore highly encouraged in the current era, and many mobile apps and other avenues have been developed and exist in most urban areas and even some rural areas.
Reporting by patients is especially pertinent in the case of those availing of OTC (over the counter) medications, and those that need to be on long term medication for a particular medical condition such as diabetes or high blood pressure. Even medication advised for a recent illness often requires a minimum period of time for review, during which the patient could monitor the progress and report any adverse drug event that might occur.

Medical Errors
50
Education of the public and governmental regulation is paramount when looking to ensure both the quality and safety of medical care. In North America, the Food and Drug Administration (FDA) has a pivotal role in not only ensuring the develop-ment and marketing of drugs and medications, but also ensures checks and balances in the actual delivery of medical care at both the level of caregivers and consumers (Meadows, 2003). Risk factors that patients might have for medical error to occur are of particular interest and should be a point of concern for medical professionals looking after patients in the hospital setting (Bates et al, 1999).
Patient education and awareness must be encouraged both by the medical fra-ternity as well as the broader media. Sensationalism is detrimental to medical error reporting, and this is where the governmental machinery and the judicial process ensure that professionalism is maintained by all sections of society (Riga, Vozikis, & Pollalis, 2014).
Thus it becomes more and more evident that medical errors and their impact could be minimized with the help of a systems approach to the practice of health care. This would involve co-operation and co-ordination of almost all the stakeholders- doctors, patients, suppliers, administrators and the media (Meadows, 2003). Better ways of designing and streamlining the health care industry need to be explored, instead of a knee jerk approach wherein the doctor is put in the dock and subjected to a media trial, and the bigger picture overlooked (Gandhi, Kachalia, Yoon, Puopolo, & Brennan, 2009; Ioannidis and Lau, 2001).
The Role of Holistic Health Care
One of the things hardly ever discussed is the role of holistic care in modern medicine. Health education, better lifestyle choices, easy and effective home remedies, and even appropriate use of alternative medicine, would ensure that every component of the health care industry is optimized, and the occurrence of error minimized.
Many societies actively practise an integrative or holistic approach to health care. In the United States of America, the Henry Ford Foundation and the Henry Ford (Holistic) Health (care) System in the state of Michigan offers integrative health and medical care under a single roof. In India, organizations such as “Soukya”, based in Bangalore, offer homeopathic, Ayurvedic and other traditional treatments for com-mon as well as serious illnesses and are hugely popular with the public. Figure 2 sums up the essential components of the “system” for improving health care quality

Medical Errors
51
FUTURE RESEARCH DIRECTIONS
By inviting and incorporating other health care systems such as alternative and in-tegrative medicine, more patient involvement and autonomy could be ensured. This might also facilitate more comprehensive medicine and a greater focus on preven-tive and primary health care. Promotion of better health would naturally reduce the scope for medical error and enhance health care quality.
CONCLUSION
A renewed emphasis on ethics and professionalism is paramount. Communication, standardization, accreditation and clinical governance form the cornerstone of such remediation. It includes better practice methods such as evidence based medicine and adherence to clinical practice guidelines, checklists, pharmacological surveil-lance and vigilance, audits and patient advocacy. All these would then contribute to a climate where a highly litigious practice environment and popularity of ‘defensive medicine’ gives way to a systems approach and correction of systems errors, thereby improving the quality of health care.
Figure 2. Quality in a nutshell

Medical Errors
52
REFERENCES
Andel, C., Davidow, S. L., Hollander, M., & Moreno, D. A. (2012). The economics of health care quality and medical errors. Journal of Health Care Finance, 39(1), 39–50. PMID:23155743
Aronson, J. K., Henderson, G., Webb, D. J., & Rawlins, M. D. (2006). A prescription for better prescribing. British Medical Journal, 333(7566), 459–460. doi:10.1136/bmj.38946.491829.BE PMID:16946321
Bates, D. W., Boyle, D. L., Vander Vliet, M. B., Schneider, J., & Leape, L. L. (1995). Relationship between medication errors and adverse drug events. Journal of Gen-eral Internal Medicine, 10(4), 199–205. doi:10.1007/BF02600255 PMID:7790981
Bates, D. W., Cohen, M., Leape, L. L., Overhage, J. M., Shabot, M. M., & Sheridan, T. (2001). Reducing the Frequency of Errors in Medicine Using Information Tech-nology. Journal of the American Medical Informatics Association, 8(4), 299–308. doi:10.1136/jamia.2001.0080299 PMID:11418536
Bates, D. W., Leape, L. L., Cullen, D. J., Laird, N., Petersen, L. A., Teich, J. M., & Seger, D. L. et al. (1998). Effect of computerized physician order entry and a team intervention on prevention of serious medication errors. Journal of the American Medi-cal Association, 280(15), 1311–1316. doi:10.1001/jama.280.15.1311 PMID:9794308
Bates, D. W., Miller, E. B., Cullen, D. J., Burdick, L., Williams, L., Laird, N., & Leape, L. L. et al. (1999). Patient risk factors for adverse drug events in hospital-ized patients. Archives of Internal Medicine, 159(21), 2553–2660. doi:10.1001/archinte.159.21.2553 PMID:10573045
Bettman, J. W. (1990). Seven hundred medicolegal cases in ophthalmology. Ophthal-mology, 97(10), 1379–1384. doi:10.1016/S0161-6420(90)32406-5 PMID:2243691
Blendon, R., DesRoches, C. M., Brodie, M., Benson, J. M., Rosen, A. B., Sch-neider, E., & Steffenson, A. E. et al. (2002). Views of practicing physicians and the public on medical adverse events. The New England Journal of Medicine, 347(24), 1933–1940. doi:10.1056/NEJMsa022151 PMID:12477944
Britten, N. (2009). Medication errors: The role of the patient. British Journal of Clinical Pharmacology, 67(6), 646–650. doi:10.1111/j.1365-2125.2009.03421.x PMID:19594532

Medical Errors
53
Carter, R. M. (1999). Malpractice and avascular necrosis: Legal outcomes. Ca-nadian Journal of Gastroenterology, 13(1), 79–84. doi:10.1155/1999/517893 PMID:10099819
Christensen, L. Q., Nielsen, L. M., & Nielsen, S. L. (1990). Traffic accidents and drivers suspected for drug influence. Forensic Science International, 45(3), 273–280. doi:10.1016/0379-0738(90)90184-Z PMID:2361649
Crane, M. (1993). The medication errors that get doctors sued. Medical Economics, 22, 36–41. PMID:10171740
Dentzer, S. (2000). Media mistakes in coverage of the Institute of Medicine’s error report. Effective Clinical Practice, 3, 305–308. PMID:11151532
Digitale, E. (2014). Better communication between caregivers reduces medical er-rors, study finds. Retrieved from https://med.stanford.edu/news/all-news/2014/12/better-communication-between-caregivers-reduces-medical-errors.html
Dubin, M. G., Liu, C., Lin, S. Y., & Senior, B. A. (2007). American Rhinology Society member survey on maximal medical therapy for chronic rhinosinusitis. American Journal of Rhinology, 21(4), 483–488. doi:10.2500/ajr.2007.21.3047 PMID:17882920
Fink, J. L. (1983). Liability claims based on drug use. Drug Intelligence & Clinical Pharmacy, 17, 667–670. PMID:6617491
Fischman, J. (2000, July17). Industry Preaches Safety in Pittsburgh. U.S. News & World Report.
FitzGerald, R. J. (2009). Medication errors: The importance of an accurate drug his-tory. British Journal of Clinical Pharmacology, 67(6), 671–675. doi:10.1111/j.1365-2125.2009.03424.x PMID:19594536
Gallagher, T. H., Waterman, A. D., Ebers, A. G., Fraser, V. J., & Levinson, W. (2003). Patients and physicians attitudes regarding the disclosure of medical adverse events. Journal of the American Medical Association, 289(8), 1001–1007. doi:10.1001/jama.289.8.1001 PMID:12597752
Gandhi, T. K., Kachalia, A., Yoon, C., Puopolo, A. L., & Brennan, T. A. (2009). Identifying steps that are more prone to error and then designing studies that would reduce error rates, instead of just pursuing litigation. British Journal of Clinical Pharmacology, 67(6), 651–655. PMID:19594533
Garrett, C. (2008) The effect of nurse staffing patterns on medical errors and nurse burnout. Association of periOerative Registered Nurses Journal, 87, 1191–1204.

Medical Errors
54
Glaser, J., Teich, J. M., & Kuperman, G. (1996) Impact of information events on medical care.Proceedings of the 1996 HIMSS Annual Conference. Chicago, IL: Healthcare Information and Management Systems Society.
Glickman, S. W., Schulman, K. A., Peterson, E. D., Hocker, M. B., & Cairns, C. B. (2008). Evidence-based perspectives on pay for performance and quality of patient care and outcomes in emergency medicine. Annals of Emergency Medicine, 51(5), 622–631. doi:10.1016/j.annemergmed.2008.01.010 PMID:18358566
Goldenbaum, D. M., Christopher, M., Gallagher, R. M., Fishman, S., Payne, R., Joranson, D., & Thexton, A. et al. (2008). Physician charged with opioid anal-gesic- prescribing offences. Pain Medicine, 9(6), 737–747. doi:10.1111/j.1526-4637.2008.00482.x PMID:18657218
Gommans, J., McIntosh, P., Bee, S., & Allan, W. (2008). Improving the quality of written prescriptions in a general hospital: The influence of 10 years of se-rial audits and targeted interventions. Internal Medicine Journal, 38(4), 243–248. doi:10.1111/j.1445-5994.2007.01518.x PMID:18298560
Gregory, A. (2013). Jeremy Hunt unveils new NHS guidelines but doctors who cover up their mistakes won’t be liable. Retrieved from http://www.mirror.co.uk/news/uk-news/new-nhs-guidelines-doctors-who-1786689
Grober, E. D., & Bohnen, J. M. A. (2005). Defining medical error. Canadian Journal of Surgery, 48(1), 39–44. PMID:15757035
Gurwitz, J. H., Field, T. S., Avorn, J., McCormick, D., Jain, S., Eckler, M., & Bates, D. W. et al. (2000). Incidence and preventability of adverse drug events in nursing homes. The American Journal of Medicine, 109(2), 87–94. doi:10.1016/S0002-9343(00)00451-4 PMID:10967148
Hearnshaw, H., Harker, R., Cheater, F., Baker, R., & Grimshaw, G. (2002). A study of the methods used to select review criteria for clinical audit. Health Technology Assessment, 6, 1–78. PMID:11809128
Ioannidis, J. P. A., & Lau, J. (2001). Evidence on Interventions to Reduce Medi-cal Errors: An Overview and Recommendations for Future Research. Journal of General Internal Medicine, 16(5), 325–334. doi:10.1046/j.1525-1497.2001.00714.x PMID:11359552
Jackson, T., & Harper, A. (2001). Blunders will never cease: How the media re-port medical errors – A risky business. British Medical Journal, 322(7285), 562. doi:10.1136/bmj.322.7285.562

Medical Errors
55
Kapp, M. B. (1997). Legal Anxieties and Medical Mistakes: Barriers and Pretexts. Journal of General Internal Medicine, 12(12), 787–788. doi:10.1046/j.1525-1497.1997.07167.x PMID:9436901
Karve, A. M., Ou, F. S., Lytle, B. L., & Peterson, E. D. (2008). Potential unintended financial consequences of pay-for-performance on the quality of care for minority patients. American Heart Journal, 155(3), 571–576. doi:10.1016/j.ahj.2007.10.043 PMID:18294498
Kavanagh, K. T. (2011). Financial incentives to promote health care quality: The hospital acquired conditions nonpayment policy. Social Work in Public Health, 26(5), 524–541. doi:10.1080/19371918.2011.533554 PMID:21902485
Keriel-Gascou, M., Figon, S., Letrilliart, L., Chaneliére, M., & Colin, C. (2011). Classifications and definitions of adverse events in primary care: A systematic review. La Presse Medicale, 40(11), e499–e505. doi:10.1016/j.lpm.2011.05.014 PMID:21802248
Kessels-Habraken, M., Van der Schaaf, T., De Jonge, J., & Rutte, C. (2010). Defin-ing near misses: Towards a sharpened definition based on empirical data about error handling processes. Social Science & Medicine, 70(9), 1301–1308. doi:10.1016/j.socscimed.2010.01.006 PMID:20153573
Khairat, S., & Gong, Y. (2010). Understanding effective clinical communication in medical errors. Studies in Health Technology and Informatics, 160, 704–708. PMID:20841777
Khanduja, K., Scales, D. C., & Adhikari, N. K. (2009). Pay for performance in the intensive care unitopportunity or threat? Critical Care Medicine, 37(3), 852–858. doi:10.1097/CCM.0b013e3181962b0b PMID:19237887
Kmucha, S. T. (2010). The Many Challenges of Pay-for-Performance Programs. American Health and Drug Benefits, 3(2), 135–142. PMID:25126315
Kohn, L. T., Corrigan, J. M., & Donaldson, M. S. (Eds.). (1999). To err is human: building a safer health system. Washington, DC: National Academy Press, Institute of Medicine.
Koppel, R., Metlay, J. P., Cohen, A., Abaluck, B., Localio, A. R., Kimmel, S. E., & Strom, B. L. (2005). Role of computerised physician order entry systems in facili-tating medication errors. Journal of the American Medical Association, 293(10), 1197–1203. doi:10.1001/jama.293.10.1197 PMID:15755942

Medical Errors
56
Kuehn, S. L., & Doyle, M. J. (1990). Medication errors: 1977 to 1988. Experience in medical malpractice claims. New Jersey Medicine, 87, 27–34. PMID:2300277
Kumar, S., & Chaudhary, S. (2009). Medical errors and consequent adverse events in critically ill surgical patients in a tertiary care teaching hospital in Delhi. Journal of Emergencies. Trauma and Shock, 2(2), 80–84. doi:10.4103/0974-2700.50740
Kyung, C. Y., & Barbara, M. (2011). Moderating effects of learning climate on the impact of RN staffing on medication errors. Nursing Research, 60, 32–39. doi:10.1097/NNR.0b013e3181ff73cc PMID:21127452
Leape, L. L., Bates, D. W., Cullen, D. J., Cooper, J., Demonaco, H. J., & Gallivan, T. et al.. (1995). Systems analysis of adverse drug events. ADE Prevention Study Group. Journal of the American Medical Association, 274(1), 35–43. doi:10.1001/jama.1995.03530010049034 PMID:7791256
Leape, L. L., Brennan, T. A., Laird, N. M., Lawthers, A. G., Localio, A. R., Barnes, B. A., & Hiatt, H. et al. (1991). The nature of adverse events in hospitalized patients: Results from the Harvard Medical Practice Study II. The New England Journal of Medicine, 324(6), 377–384. doi:10.1056/NEJM199102073240605 PMID:1824793
Lindenauer, P. K., Remus, D., Roman, S., Rothberg, M. B., Benjamin, E. M., Ma, A., & Bratzler, D. W. (2007). Public reporting and pay for performance in hospital quality improvement. The New England Journal of Medicine, 356(5), 486–496. doi:10.1056/NEJMsa064964 PMID:17259444
Macklis, R. M., Meier, T., & Weinhous, M. S. (1998). Error rates in clinical radio-therapy. Journal of Clinical Oncology, 16, 551–556. PMID:9469340
Mazor, K. K., Simon, S. R., & Gurwitz, J. H. (2004). Communicating with patients about medical adverse events. Archives of Internal Medicine, 164(15), 1690–1697. doi:10.1001/archinte.164.15.1690 PMID:15302641
McAbee, G. N. (1998). Malpractice risks associated with prescribing medi-cation for chronic headaches. Headache, 38(1), 53–55. doi:10.1046/j.1526-4610.1998.3801053.x PMID:9505005
Meadows, M. (2003). Strategies to reduce medication errors. How the FDA is work-ing to improve medication safety and what you can do to help. FDA Consumer, 37(3), 20–27. PMID:12793389
Miller, L. K., Nelson, M. S., & Spurlock, B. W. (2001). A compendium of suggested practices for preventing and reducing medication errors. Roseville, CA: California Institute for Health System Performance.

Medical Errors
57
Montesi, G., & Lechi, A. (2009). Prevention of medication errors: Detection and audit. British Journal of Clinical Pharmacology, 67(6), 651–655. doi:10.1111/j.1365-2125.2009.03422.x PMID:19594533
Morey, R. C., Fine, D. J., Loree, S. W., Retzlaff-Roberts, D. L., & Tsubakitani, S. (1992). The trade-off between hospital cost and quality of care. An exploratory em-pirical analysis. Medical Care, 30(8), 677–698. doi:10.1097/00005650-199208000-00002 PMID:1640765
Nash, J. J., Nash, A. G., Leach, M. E., & Poetker, D. M. (2011). Medical malpractice and corticosteroid use. Otolaryngology - Head and Neck Surgery, 144(1), 10–15. doi:10.1177/0194599810390470 PMID:21493380
Norman, D. A. (1988). The Design of Everyday Things. New York: Basic Books.
OBrien, J. M. Jr, Kumar, A., & Metersky, M. L. (2013). Does value-based purchas-ing enhance quality of care and patient outcomes in the ICU? Critical Care Clinics, 29(1), 91–112. doi:10.1016/j.ccc.2012.10.002 PMID:23182530
Perna, G. (2014). Study: Better Verbal, Written Communication During Provider Handoffs Reduces Medical Errors. Retrieved from http://www.healthcare-informatics.com/news-item/study-better-verbal-written-communication-during-provider-hand-offs-reduces-medical-errors
Petersen, L. A., Woodard, L. D., Urech, T., Daw, C., & Sookanan, S. (2006). Does pay-for-performance improve the quality of health care? Annals of Internal Medicine, 145(4), 265–272. doi:10.7326/0003-4819-145-4-200608150-00006 PMID:16908917
Poetker, D. M., & Smith, T. L. (2015). Medicolegal Implications of Common Rhi-nologic Medications. Otolaryngologic Clinics of North America, 48(5), 817–826. doi:10.1016/j.otc.2015.05.009 PMID:26117297
Rasmussen, J. (1982). Human errors: A taxonomy for describing human malfunc-tion in industrial installations. Journal of Occupational Accidents, 4(2-4), 311–335. doi:10.1016/0376-6349(82)90041-4
Reason, J. (1990). Human Error. Cambridge, UK: Cambridge University Press. doi:10.1017/CBO9781139062367
Riga, M., Vozikis, A., & Pollalis, Y. (2014). Medical Errors in Greece: An Economic Analysis of Compensations Awarded by Civil Courts (20002009). Open Journal of Applied Sciences, 4(04), 168–175. doi:10.4236/ojapps.2014.44017

Medical Errors
58
Rothschild, J. M., Federico, F. A., Gandhi, T. K., Kaushal, R., Williams, D. H., & Bates, D. W. (2002). Analysis of medication- related malpractice claims: Causes, preventability, and costs. Archives of Internal Medicine, 162(21), 2414–2420. doi:10.1001/archinte.162.21.2414 PMID:12437399
Scott, A., Sivey, P., Ait Ouakrim, D., Willenberg, L., Naccarella, L., Furler, J., & Young, D. (2011). The effect of financial incentives on the quality of health care provided by primary care physicians. Cochrane Database of Systematic Reviews, (9): CD008451. PMID:21901722
Senders, J., & Moray, N. (1991). Human Error: Cause, Prediction and Reduction. Mahwah, NJ: Lawrence Erlbaum.
Sewal, R. K., Singh, P. K., Prakash, A., Kumar, B., & Medhi, B. (2014). A pro-spective study to evaluate awareness about medication errors amongst health-care personnel representing North, East, West Regions of India. International Journal of Applied and Basic Medical Research, 4(1), 43–46. doi:10.4103/2229-516X.125694 PMID:24600578
Shabot, M., & LoBue, M. (1995). Real-time wireless decision support alerts on a palmtop PDA. Proceedings of the Annual Symposium on Computer Applications in Medical Care, 19, 174–177. PMID:8563261
Shabot, M., LoBue, M., & Chen, J. (2000) Wireless clinical alerts for critical medica-tion, laboratory and physiologic data.Proceedings of the 33rd Hawaii International Conference on System Sciences (HICSS, Washington, DC: IEEE Computer Society. doi:10.1109/HICSS.2000.926784
Shahrokhi, A., Ebrahimpour, F., & Ghodousi, A. (2013). Factors effective on medi-cation errors: A nursing view. Journal of Research in Pharmacy Practice, 2(1), 18–23. doi:10.4103/2279-042X.114084 PMID:24991599
Sharma, G., Awasthi, S., Dixit, A., & Sharma, G. (2011). Patient safety risk as-sessment and risk management: A review on Indian hospitals. Chronicles of Young Scientists, 2(4), 186–191. doi:10.4103/2229-5186.93022
Sox, H. C., & Woloshin, S. (2000). How many deaths are due to medical error? Get-ting the number right. Effective Clinical Practice, 3(6), 277–283. PMID:11151524
Stratton, A. (2011). Hospitals will be forced to admit medical errors, says govern-ment. Retrieved from http://www.theguardian.com/politics/2011/jun/20/hospitals-forced-to-admit-errors

Medical Errors
59
Studdert, D. M., Mello, M. M., Gawande, A. A., Gandhi, T. K., Kachalia, A., Yoon, C., & Brennan, T. A. et al. (2006). Claims, errors, and compensation payments in medical malpractice litigation. The New England Journal of Medicine, 354(19), 2024–2033. doi:10.1056/NEJMsa054479 PMID:16687715
Stump, S. (2000). Re-engineering the medication error-reporting process: Removing the blame and improving the system. American Journal of Health-System Pharmacy, 57(4), S10–S17. PMID:11148939
Sura, A., & Shah, N. R. (2010). Pay-for-Performance Initiatives: Modest Benefits for Improving Healthcare Quality. American Health and Drug Benefits, 3(2), 135–142. PMID:25126315
Swaminath, G., & Raguram, R. (2010). Medical errors – I: The problem. Indian Jour-nal of Psychiatry, 52(2), 110–112. doi:10.4103/0019-5545.64580 PMID:20838497
Szekendi, M. K., Sullivan, C., Bobb, A., Feinglass, J., Rooney, D., Barnard, C., & Noskin, G. A. (2006). Active surveillance using electronic triggers to detect adverse events in hospitalized patients. Quality & Safety in Health Care, 15(3), 184–190. doi:10.1136/qshc.2005.014589 PMID:16751468
Thakur, H., Thawani, V., Raina, R. S., Kothiyal, G., & Chakarabarty, M. (2013). Non-compliance pattern due to medication errors at a Teaching Hospital in Srikot, India. Indian Journal of Pharmacology, 45(3), 289–292. doi:10.4103/0253-7613.111899 PMID:23833376
Tierney, W. M., Miller, M. E., Overhage, J. M., & McDonald, C. J. (1993). Physician inpatient order writing on microcomputer workstations: Effects on resource utiliza-tion. Journal of the American Medical Association, 269(3), 379–383. doi:10.1001/jama.1993.03500030077036 PMID:8418345
Walsh-Childers, K. (1994). Newspaper influence on health policy development. Newspaper Research Journal, 15, 89–101.
Ward, T. N., & Allen, W. R. (2008). Case 3. The steroid complication. Headache, 48(6), 866–870. doi:10.1111/j.1526-4610.2008.01164_3.x PMID:18549368
Whitten, P., Dutta, M. J., Carpenter, S., & Bodie, G. D. (n.d.). News Media and Health Care Providers at the Crossroads of Medical Adverse Events. Retrieved from http://www.ncbi.nlm.nih.gov/books/NBK43609/
Witter, S., Fretheim, A., Kessy, F. L., & Lindahl, A. K. (2012). Paying for perfor-mance to improve the delivery of health interventions in low- and middle-income countries. Cochrane Database of Systematic Reviews, 2, CD007899. PMID:22336833

Medical Errors
60
KEY TERMS AND DEFINITIONS
Cost-Effectiveness: The economic efficiency of health care services.Evidence-Based Medicine: The use of scientific literature to guide medical
and health care decisions.Health Care Quality: The minimum acceptable standard of health services.Medical Error: An act of omission or commission in health care service delivery.Medication Error: An act of omission or commission in administering a drug.

Copyright ©2017, IGI Global. Copying or distributing in print or electronic forms without written permission of IGI Global is prohibited.
DOI: 10.4018/978-1-5225-2337-6.ch003
Chapter 3
61
Patient Safety and Medical Errors:
Building Safer Healthcare Systems for Better Care
ABSTRACT
Patient Safety is considered to be the most important parameter of quality that every contemporary healthcare system should be aiming at. The terms “Patient Safety” and “Medical Errors” are directly linked to the “Safety Culture and Climate” in every organization. It is widely accepted that medical errors constitute an index of insufficient safety and are defined as any unintentional event that diminishes or could diminish the level of patient safety. This chapter indicates that a beneficial safety culture is essential to enhance and assure patient safety. Furthermore, health care staff with a positive safety culture is more probable to learn openly and suc-cessfully from errors and injuries.
Vasiliki KapakiUniversity of Peloponnese, Greece
Kyriakos SouliotisUniversity of Peloponnese, Greece

Patient Safety and Medical Errors
62
INTRODUCTION
The adverse events in healthcare constitute a major issue of global interest since they could be traced in the healthcare systems of every country regardless of their level of development. Worldwide, millions of patients suffer or get injured and die annually due to the provision of unsafe care and treatment. Hospital infections, inadequate diagnosis, delays in treatment, adverse drug events and omissions of surgical procedures make up the most common root causes of medical errors or adverse events that may be avoided.
Donabedian (1980) suggested the evaluation of healthcare quality and linked it directly to the patient safety. Moreover, he suggested that the assessment of quality should be applied according to the structure (resources and administration), the pro-cess (culture and professional co-operation) and outcome (competence development and goal achievement). Twenty years after the Donabedian’s model, the managers of healthcare services adopted the principles of Total Quality Management (TQM) from Deming’s work. TQM promotes not only the team spirit and the coordination but also the clarification of the procedures, the commitment to the goals of the or-ganization and the change, ultimately aiming at the constant pursuit and assurance of quality services. In healthcare, the Continuous Quality Improvement (CQI) has been considered as interdependent with the integrated implementation of a program which is based on a trustworthy risk management policy aimed at minimizing the chances of further instance of a preventable medical error (Donabedian, 1980). According to McFadden, Stock and Gowen (2014) although CQI initiatives are extremely associated with improved process quality, they are also connected with higher hospital-acquired condition rates, a measure of patient safety (McFadden, Stock, & Gowen, 2014).
Within the discussion framework about medical error prevention, European and non-European Organizations keep talking about methods and tools, which will effec-tively contribute to the assurance of a safe and high quality healthcare environment. According to Nix, Coopey and Clancy (2006) the quality tools include websites, protocols, data bases, newsletters, guidelines and other mechanisms in order to help healthcare professionals, legislators in the healthcare sector and patients to create, promote and cultivate quality conditions in healthcare organizations or in their daily lives. The significance of the above methods in CQI and patient safety is obvious (Nix, Coopey, & Clancy, 2006).
The main objectives of this chapter are first of all, the discription of “safety” as a parameter of healthcare quality as well as the categorization of concepts regard-ing the “patient safety”. Secondly, the clarification of the terms “patient safety

Patient Safety and Medical Errors
63
culture” and “patient safety climate”, revealing the relation between them as well as the role of “patient safety culture” in the analysis of medical errors and adverse events and the presentation of the parameters linked to it. Finally, the authors give prominence to the importance of “safety culture” evaluation within the healthcare units and clearly present the methods of research for the evaluation of “Patient Safety Culture”, which are internationally used.
BACKGROUND
Research by Cameron and Quain (2011) and Talbot (2008) argued that the term of “safety” is mentioned to the degree to which organizations provide the required responsibility to meet the demands of
1. The citizens’ satisfaction,2. The justice in employment, and3. The implementation of standards and controls, through bureaucratic procedures
(Cameron & Quain, 2011; Talbot, 2008).
Patient safety, as a term, appears for the first time in literature in 1960 (Lauter-stein & Mustoe, 1960). However, the systematic study of this acceptation has started the last two decades. Legido – Quigley et al. (2008) argued that patient safety is traditionally considered one of the aspects of high quality healthcare environment just as the efficiency, the effectiveness, the accessibility, the equality, the patients satisfaction, the improvement of the health and wellbeing, the continuation of the provided care, the adequacy and the acceptance of healthcare on an individual and social level (Legido – Quigley et al., 2008).
According to Rice (2003) “safe care”, from one hand, is the care that is provided without errors and omissions, which have negative impact on the patients’ wellbe-ing and has objective parameters. On the other hand, quality healthcare expresses perfection and is subjective naturally (Rice, 2003).
National Patient Safety Foundation (NPSF) in the United States determines the patient safety as the avoidance, the prevention, and the improvement of unfortunate events or and personal injuries during healthcare provision. Brewer and Colditz (1999) claimed that the acceptation of safety is relevant and suggest that the acceptance of an unfortunate event depends on the severity of the disease and the availability of alternative therapies (Brewer & Colditz, 1999). In the report which was entitled “To err is human: Building a Safer Health System” and was published in 2000 by

Patient Safety and Medical Errors
64
The Institute of Medicine (IOM) the patient safety is defined as the exemption from the risk of accidental injury during healthcare provision (Homsted, 2000). The assurance of patient safety entails the development of functional systems and procedures which minimize the possibility of error and increase the possibility of its prevention when this occurs. The above interpretation of “patient safety” has been adopted by Agency for Healthcare Research and Quality (AHRQ) and World Health Organization (WHO).
Furthermore, relevant definition has been attributed to patient safety, by Card (2014) according to which, patient safety is the freedom from accidental injuries, throughout healthcare provision, and the activities that are carried out for the avoid-ance, prevention or correction of the adverse outcomes, which may result from the healthcare provision (Card, 2014). Spath (2000) argued that patient safety refers to actions undertaken by individuals and organizations to protect health care recipients from being harmed by the effects of health care services (Spath, 2000).
The acceptation of patient safety is also included in the dictionary of the European Society for Quality in Healthcare, ESQH as the constant recognition, analysis and management of risks and events related to the patients, in order to make healthcare provision safer and minimize the harm which is caused to patients. Safety is the result of the interaction between the additional parts and the procedures of the system (Kristensen, Bartels, Sabroe & Mainz, 2014; Kristensen, Mainz & Bartels, 2007).
In any case, the signification of patient safety is much wider than the simple absence of errors and adverse events, throughout the healthcare provision. As an acceptation, it is multidimensional, and taking into consideration that, the health sector is defined by the increased complexity and risk. In addition, the solutions of patient safety problems could be found in the broader environment of the healthcare system. It should be underlined that patient safety constitutes a set of procedures which express, evaluate, minimize the dangers and are constantly improved. The result could be presented by less medical errors and limited risks (Homsted, 2000).
The term of safety culture was used for the first time in 1987 by the Nuclear Agency, concerning the accident that happened in Chernobyl in 1986. In the re-port of International Nuclear Safety Advisory Group (2001) the safety culture is described as following:
Safety culture is defined as the set of characteristics and attitudes which determines that safety issues of nuclear plants are of paramount significance and that safety should be getting the appropriate attention, due to its significance, so much for individuals as well as for organizations.
Patient Safety and Medical Errors
65
This meaning was entered in order to explain the way by which the luck of knowl-edge and understanding of risk and safety so much on the side of the employees as much as on the side of the organizations as a whole, contributed to the result of the destruction (International Nuclear Safety Advisory Group, 2001, p.4). In addition, according to the Advisory Committee on the Safety of Nuclear Facilities, “safety culture” is defined as
the result of individual and collective values, attitudes, views, abilities and patterns of behavior, which determines the level of commitment, the style and the effective-ness of the organizations and risk management (ACSNI, 1993, p.15).
In health sector, a widely known definition which refers to “safety culture” is the one which was developed by the Health and Safety Executive (HSE) in UK and describes it as “the product of collective and individual values, mindsets, abilities and attitudes which determine the devotion, the style and the experience of organiza-tions’ Health and Safety Management system” (Human Engineering for the Health and Safety Executive, 2005, pp.3-4).
The above mentioned definitions are among the dominant and the most used ones that could be found in literature. Although, many studies, regarding the perception of safety culture, have been carried out, no unanimity in a common definition has been achieved.
As a consequence, the term “safety culture” having achieved international use in the previous decade, is generally used to describe a corporate culture, which the safety has become perceptible and accessible as the main priority. In the light of this evidence, it is clear that “safety culture” constitutes a subset of the overall organiza-tional culture. This means that safety performance in organizations is significantly influenced by the parameters of management, which are traditionally not approached as “part of the safety” (Institution of Engineering and Technology, 2009).
From 1980 and on, there is a variety of researches on the issues regarding culture of safety, but as it has already been mentioned previously, the “concept” remains “indistinctly defined” to a great extent. There are, however, some common character-istics, which can be recognized in most of the terms. These common characteristics, which are linked to safety culture, incorporate the concepts of beliefs, values, and attitudes shared by a group of people. Glendon, Clarke and Mckenna (2006) pointed out that a number of terms regarding safety culture depend on the views, shared by the members of a team within organizations or the social environment. Therefore it becomes obvious that there is a trend to express safety culture in terms of mindsets and attitudes. Moreover they highlight the fact that in the attempt to define culture of safety, the intention of some researchers focuses on mindsets whereas others

Patient Safety and Medical Errors
66
emphasize on the culture of safety through attitudes and working activities. In their point of view, the culture of safety in organizations serves as a guide regarding the way that employees shall behave within the work environment. The attitudes of the employees are influenced or/and defined by which number of them is accepted and rewarded at the same time. Therefore it is important to define the organizations’ perception of culture safety, since it constitutes the most decisive factor of human performance and organizational safety (Glendon, Clarke & Mckenna 2006).
On the other side, the acceptation of “safety climate” has been widely researched over the last decades in the industries in order to prevent unsafe attitudes and to ascertain the incidence of injuries and accidents (Sexton et al., 2011). The term “safety climate” was used for the first time by Zohar (1980) in his attempt to have described the perceptions of the employees on the value and the role of safety in their organizations. To be more precise, Huang, Chen and Grosch (2010) and Zohar (1980) argued that “the safety climate” states the perceptions of the employees on the policies, the procedures and the practices applied in the organizations, as they are linked to the value, the significance and the real priority of safety within the organizations (Huang, Chen & Grosch 2010; Zohar, 1980). Furthermore, according to Pronovost et al. (2003) “safety climate” refers to the characteristics of “safety cul-ture” which are distinguished for the attitudes and the perceptions of the employees at a given time. It is considered that it is an indicator of the dominant safety culture by a working group or generally organizations. It includes factors which are related to the powerful and preventive commitment to “patient safety”. The term “power-ful” includes the way in which issues of “patient safety” and “adverse events” are being mentioned, managed and treated whereas the term “commitment” relates to the attitudes of the executives in organizations towards “patient safety” (Pronovost et al., 2003). In other words, Blegen, Pepper and Rosse (2005) claimed that the “safety climate” refers to the perceptions of the personnel regarding the protection of patients from medical errors and injuries, occurring during the healthcare provi-sion and at the work environment (Blegen, Pepper & Rosse 2005).
Strong commitments of the executives within the organizations suggest an inte-gral part of the agency’s safety. Edmondson (2004) argued that in “positive safety climate”, the agencies are mainly guided by the commitment to “patient safety” and the improvement of quality more than by other issues of the organizations such as budgets (Edmondson, 2004).
Niskanen defined “safety climate” as the “set of attitudes that may be perceived for a specific task within organizations, which may arise from policies and practices that same organizations impose on the employees and their superiors” (as cited in Guldenmund, 2000, pp. 227 - 229). Research by Olsson, Forsberg and Bjerså (2016) shows recent knowledge regarding the safety climate and willingness to put into effect evidence-based practice and person centered care in general surgical wards in
Patient Safety and Medical Errors
67
university hospitals and points out significant connections between the above two areas. The inferred safety climate is extremely related to evidence-based practice and person centered care. While registered nurses for the most part reported af-firmative job satisfaction and a worthy team work culture in their units, there were signs that betterments in organizational management are needed (Olsson, Forsberg, & Bjerså, 2016).
According to Ginsburg and Gilin Oore (2016) organizations or units wishing to acquire a view of their safety climate(s) will have a much more complete picture if they investigate both the level and the strength of climate scores, and consider also the shape of units’ climate profiles. Examining a unit’s mean score (ie, level), the standard deviation of the climate score and a simple histogram of the scores can provide this comprehensive picture. Focusing on patient safety culture level and strength can also further knowledge of the extent to which patient safety culture is a key variable in the domain of PS (Ginsburg & Gilin Oore, 2016).
Yule (2003) highlighted the fact that, the definitions of “safety climate” were directly related to the definitions of “safety culture” (Yule, 2003). Guldenmund (2000) recognized common points in both of these definitions (Guldenmund, 2000). However, there are some important differences to be distinguished since “safety culture” refers more to subjectively common beliefs, values and attitudes towards employment and the organizations in general, whereas the “safety climate” is closer to the operations of the organizations. Specifically it is characterized by the casual beliefs in relation to the work environment, the working practices, the policies of the organizations and the administrative activities.
Safety as Priority for Organizations
As the more ardent proponents of safety and CQI are the managers and the leaders, as higher is the level of the employees’ commitment, which has a positive influ-ence on the performance of the employees and the prevention of errors and adverse events. The tangible commitment includes the provision of sufficient human and financial resources in a constant effort towards the direction of safety and quality. Researches by Cooper (2000) and Leape (2000) illustrated that the desired behaviors are often developed through the assimilation of the observed behaviors of others and the body of suggestions which provide almost imperceptible messages for the acceptance of the particular behaviors (Cooper, 2000; Leape, 2000).
Additionally, it is necessary to redefine the acceptation of the one “accountable” and the one “responsible” therefore significantly limiting the punitive aspect of errors. What is a contradiction in terms of the adoption of such an approach is that every member of organizations undertakes even bigger responsibility as to safety. Accord-ing to Leape (2000) it was a fact that there must be no delay in demonstrating who

Patient Safety and Medical Errors
68
was responsible for the errors and this burden should be equally allocated among the employees, who must be alert in order to trace and report any imperfections of the system, which create unsafe conditions and work together for the improvement of the procedures and the prevention of errors and adverse events (Leape, 2000).
Taking everything into account, both safety and quality could not be treated as a supplementary process to the strategic decisions but they should constitute a priority and have a central role in every level of the organizations.
Classification of the Concepts in Relation to Patient Safety
There are many definitions in literature, regarding patient safety, which bear many similarities but also important differences, as it has already been mentioned. Their differentiation is not always obvious and distinct. Simultaneously, there is also a practical difficulty regarding the classification of adverse events and the determi-nation of the indexes for the measuring of the safety. Taking under consideration the above mentioned difficulties, it was deemed necessary to create the third axis in relation to the activities of a “World Alliance for Patient Safety”, which is titled “Taxonomy for patient safety” (WHO, 2005a). Efforts of equal importance have been scheduled and realized apart from WHO and AHRQ, also by ESQH which has a guiding role in the program “Safety improvement for Patients in Europe, SimPatIE” which is funded by the European Union.
In autumn of 2003, WHO Working Group on Patient Safety Taxonomy was held in Geneva, firstly in order to discuss the need to adopt a common terminology for everything related to patient safety, secondly to present the various definitions regarding patient safety and thirdly to help the classification methods of adverse events and near misses among various countries become known. Last but not least, the development of a common classification framework for patient safety is among the main objectives of the specific working group. In this meeting it was also sug-gested to create three working groups, in order to initiate the implementation of the above mentioned goals (WHO, 2003).
One of the six goals of World Alliance for Patient Safety of WHO, was the real-ization of a program for International Patient Safety Event Taxonomy, based on the work which has already been realized by the above mentioned working group. The first meeting took place in Vancouver in 2005, in order to set the goals and the im-portance of classification and strategic planning for its development (WHO, 2005b).
Within the same year, a literature review by WHO (2005) for the years 2003 - 2005 was published regarding the taxonomies which were related to patient safety. Seventeen classifications were found in the review, eleven of which were carried out for specific issues related to patient safety, such as diagnosis, laboratory test results

Patient Safety and Medical Errors
69
etc. and the other six were specifically carried out to be used along with adverse effects reporting systems (WHO, 2005a).
Two years later in 2007, WHO published the Conceptual Framework for the International Classification for Patient Safety (ICPS) (WHO, 2007). This report, apart from the framework analysis, included a set of definitions for 46 terms, which were related to the framework and the patient safety. The terms were the following: classification, concept, class, semantic relationship, patient, healthcare, health, safety, hazard, circumstance, event, agent, patient safety, health-care associated harm, patient safety incident, error, violation, risk, adverse event, harm, disease, injury, suffer-ing, disability, near-miss, contributing factor, incident type, patient characteristics, attributes, incident characteristics, adverse reaction, side effect, preventable, detec-tion, mitigating factor, patient outcome, degree of harm, organizational outcome, ameliorating action, actions taken to reduce risk, resilience, accountable, quality, system failure, system improvement, root cause analysis (WHO, 2007).
Kristensen, Mainz and Bartels (2007) claimed that the SimPatIE program of the European Union entails the completion of a vocabulary which includes twenty four terms related to the acceptation of patient safety. The purpose of its development is multiple: (a) to determine the basic terms and acceptation related to patient safety, (b) to facilitate communication and understanding in the whole Europe, (c) to make sure that these are easily understandable even by people who are not native English speakers (d) to take under consideration the various European views regarding the different cultures. The grouping of the above mentioned terms becomes as follows (Kristensen, Mainz &Bartels, 2007):
1. Detection Risk:a. Patient Safety,b. Adverse Event,c. Actual Event,d. Near Miss,e. Complication,f. Sentinel Event,g. Critical Incident,h. Complaint,i. Reporting System, andj. Professional Standard.
2. Analysis of Risk:a. Harm,b. Adverse Outcome,c. Risk,d. Calculated Risk,

Patient Safety and Medical Errors
70
e. Barrier, andf. Situational Awareness.
3. Resulting Actions:a. Risk Management,b. Error Management,c. Action Plan,d. Culture of Safety, ande. Human Factor.
4. Failure Mode:a. Negligence,b. Situational Factor, andc. Error.
Another classification which is just as useful and effective for the estimation of patient safety, is the one that related to quantitative indicators, part of which are also the various kinds of errors. In 2006, OECD published a relevant technical text which included twenty one measurable indicators for patient safety which are presented below (McLoughlin et al., 2006):
1. Hospital – Acquired Infections:a. Ventilator pneumonia,b. Wound infection,c. Infection due to medical care, andd. Decubitus ulcer.
2. Operative and Post-Operative Complications:a. Complications of anesthesia,b. Postoperative hip fracture,c. Postoperative pulmonary embolism (PE) or deep vein thrombosis (DVT),d. Postoperative sepsis, ande. Technical difficulty with procedure.
3. Sentinel Events:a. Transfusion reaction,b. Wrong blood type,c. Wrong-site surgery,d. Foreign body left in during procedure,e. Medical equipment-related adverse events, andf. Medication errors.
4. Obstetrics:a. Birth trauma - injury to neonate,b. Obstetric trauma – vaginal delivery,

Patient Safety and Medical Errors
71
c. Obstetric trauma - caesarean section, andd. Problems with childbirth.
5. Other Care-Related Adverse Events:a. Patient falls, andb. In-hospital hip fracture or fall.
The first results of part of SimPatIE program were published in 2007. The primary goal of SimPatIE, was the development of a set of patient safety indicators. Kris-tensen, Mainz and Bartels (2007) claimed that forty two indicators were registered, twenty nine of which were classified in the following thematic subsections: infection control, surgical implications, pharmaceutical errors, topics of obstetrics, patient falls. The other nine were general indicators regarding the operation of organizations such as, mortality rates and the other four concerned specialized diseases such as the risk of suicide for schizophrenic patients etc (Kristensen, Mainz & Bartels, 2007).
Simultaneously AHRQ (2007) has published a list with ten exhortations for patient safety in hospitals, which is being constantly updated. These exhortations with direct practical implementation aim at minimizing the adverse events, so as to insure the maximum level of patient safety. These exhortations are the following (AHQR, 2007):
1. Evaluate and improve the patient safety culture in your hospital.2. Cultivate the team spirit and create constructive partnerships.3. Limit the shifts of the personnel as much as possible.4. Place tubes in the chest safely.5. Prevent the occurrence of hospital infections6. Utilize appropriately the department directors and particularly of ICU.7. Use credible tools which support the clinical decision making.8. Create an adverse events reporting system.9. Minimize the use of urinary catheters to three days.10. Minimize the unnecessary interruptions of health care professionals during
the performance of their tasks.
The Role of Safety Culture in the Expansion of the Accidents
Over time special value has been given to the causes of professional accidents and the research in high risk industries has contributed a lot to the understanding of the impact of the systems and the human factors to the organizational safety. At this point, the reference to new theoretical approaches for human errors, which arose from the research studies of the accidents, is important.

Patient Safety and Medical Errors
72
According to the Systems Theory, the majority of errors are not caused by neg-ligence or inability but by the vulnerabilities of the systems, rendering the work environment prone to errors. Latent conditions arise from insufficiencies or defects in organizational functions, such as the development of policies and protocols, budgets, employment, equipment maintenance and process management. Such insufficiencies are possible to create working conditions which cause the human tendency to errors and additionally they challenge the limits of human efficiency (as cited in Reason, 1990).
According to Reason (1990) “The Human Factors Theory” is based on the fol-lowing principle: “the change of human nature is not possible, but what is possible is the change of the conditions within which humans work.” The relation of “Human Factors Theory” with the development of “safety culture” is based on 3 principles guiding the systems design as follows:
1. Prevention of errors by designing such systems, which eliminate the predict-able human weaknesses, making it harder to make an error.
2. Not concealing errors aiming at their management.3. The development of methods which moderate the consequences of the errors
upon their occurrence (Reason, 1990).
The Characteristics of Positive Safety Culture
Many publications aim at the examination of specific management policies, which serve as a prediction for safety efficiency. Reason (1998) argued that
the ideal culture of safety constitutes an “engine” that guides the system through the achievement of the goal of maintaining the highest possible resistance against the corporate risks.
The researcher himself also believes that in periods of adequate safety efficiency, the best way to remain cautious is to “collect the appropriate information.” That means that it is necessary to create a culture of information and communication in general within the work environment. A culture of communication requires the administration on matters of safety to be alert for various factors (for example hu-man, technical, organizational and environmental), which influence the systems of safety (Reason, 1998, p.294).
Ultimately one could say that the organizational culture of safety reflects the way in which safety is addressed in the work environment. It is however important to note that a safety management system does not simply consist of a set of policies and processes on a library shelf, but it is safety management and the way in which

Patient Safety and Medical Errors
73
the policies and the processes are applied in everyday practice in the work environ-ment. In addition, the nature of safety management in the work environment (for example resources, policies, practices and processes, control etc.) influences the culture and the safety climate in organizations.
The findings of a recent study forcefully point out that investing in activities and procedures that strengthen organizational learning and enhancing safety climate can importantly contribute to increased cognizance about the theme and, as a con-sequence, make safer processes not only for patients, but for the organization as a whole (Silva, Barbosa, Padilha, & Malik, 2016).
Shanon, Mayr and Haines (1997) conducted a review of 10 studies, which exam-ined the relation between organizational factors and the incidence rate of accidents. In their review they included only the studies which made comparisons among at least 20 work environments. In order for a variable to considered, firmly associated with the accidents rate or relation it should:
1. Be statistically important in the direction of at least the two thirds of the stud-ies under examination, and
2. Not be significant in the opposite direction in another study. The variables which were classified by various organizations were 17.
What was found was that every variable met the criteria of being firmly associated with a low incidence rate of accidents. Some of those variables include (Shanon, Mayr & Haines 1997):
• The training received by the Committee for Health and Safety.• The good relation between the administration and the employees.• The monitoring and the control of unsafe working attitudes.• The low departure rate of the personnel from the companies / organizations.• The safety control of the equipment.
There is also a level of agreement as to which practices of safety management are considered ideal. Mearns, Whitaker and Flin (2003) reassured that some issues of general interest which emerge from literature are for example (Mearns, Whitaker & Flin 2003):
• The commitment of management to safety, which includes: ◦ The priority of safety in the phase of production.
• The maintenance of safety’s high profile in the conferences: ◦ Personal participation of the owners in the conferences regarding safety. ◦ Particular descriptions of job positions which also include safety terms.

Patient Safety and Medical Errors
74
• The communication on safety issues also including among others: ◦ Channels of official and unofficial communication. ◦ Regular communication between the administration, the auditors and
the human resources.• The involvement of employees includes:
◦ Strengthening/Authorization. ◦ A Delegation responsible for safety. ◦ Encouragement for commitment to the organizations.
At this point, it is also important to mention that the nature and the number of accidents, which have occurred as a result of insufficient safety management, led to the development of inspection tools which make sure that these management practices are ultimately successful. Mearns et al. (2003) argued that the evaluation of these practices contributes to the estimation of a safety climate (Mearns et al., 2003).
Finally, Reason (1998) claimed that organizational culture cannot be instantly created, but it is developed over time. The safety culture of organizations is a result of the between the working environment, the human resources, the health practices, the safety and the leadership (Reason, 1998).
The Parameters Linked to the “Patient Safety Culture”
The safety culture in the healthcare sector is influenced by various factors, which are mentioned as factors or parameters with specific characteristics. These factors are linked to the leadership, the work environment, the personnel and the safety factors and constitute additional parameters of “safety culture”.
Kristensen et al. (2015) supported that more clinical leaders than frontline clini-cians have a positive sensory awareness of teamwork and safety climate (Kristensen et al., 2015). Moreover, Moutier et al. (2016) claim that in order to improve a culture of respect in the learning environment, institutions can successfully involve academic leaders and ability at all levels to give attention to disruptive behavior and improve affirmative climate factors (Moutier et al., 2016).
According to the research of Sammer, Lykens, Singh, Mains and Lackan (2010) the above parameters were leadership, team work, the integration of knowledge based on evidence, communication, the organizations that learn from its mistakes, the ac-countability of the system and not individuals for the errors as well as the heath care focused on the patient (Sammer, Lykens, Singh, Mains, & Lackan, 2010). Similar results were also shown in the research of El-Jardali, Dimassi, Jamal, Jaafar and Hemadeh (2011) according to which the factors which contribute to the achievement of a “positive culture of safety” are the report of adverse events and the non-punitive reaction to errors, the appropriate communication, the commitment of leadership

Patient Safety and Medical Errors
75
and management to the development of a safety culture, the sufficient employment and the accreditation of the hospital (El-Jardali, Dimassi, Jamal, Jaafar, & Hemadeh, 2011). In addition, according to the evaluation tool created by Sorra and Nieva in the United States in 2004, “safety culture” is examined through twelve parameters which are presented below (Sorra & Nieva, 2004):
• Teamwork Within Units.• Supervisor/Manager Expectations & Actions Promoting Patient Safety.• Organizational Learning—Continuous Improvement.• Management Support for Patient Safety.• Overall Perceptions of Patient Safety.• Feedback & Communication About Error.• Communication Openness.• Frequency of Events Reported.• Teamwork Across Units.• Staffing.• Handoffs & Transitions.• No punitive Response to Errors.
The Significance of Safety Culture Evaluation by the Patient
Research by Hellings, Schrooten, Klazinga and Vleugels (2010) illustrated that the evaluation of “safety climate” constitutes the first stage in the development of a culture of safety, since it constitutes an indication of the level of safety of the orga-nizations and contributes to the prevention of errors (Hellings, Schrooten, Klazinga & Vleugels, 2010). Zohar, Livne, Tenne –Gazit, Admi and Donchin (2007) argued that the evaluation of “safety climate” requires its measurement, which is mainly carried out by the use of structured questionnaires or interviews. The questionnaires are completed anonymously by health professors and their scores are summed up for the overall evaluation of safety climate in the organizations and the identifica-tion of the basic parameters that influence it (Zohar, Livne, Tenne-Gazit, Admi, & Donchin, 2007). The evaluation results include the views of the employees regard-ing the parameters of safety culture, their wish to report the adverse events and the overall score given by them to the departments they work at (Sorra &Nieva, 2004). This process shows the level to which patient safety constitutes a priority in the organizations and reveals information for the attitude of health care professionals towards the errors.

Patient Safety and Medical Errors
76
The benefits from the evaluation of the “safety climate” are many so much on an individual as well as an organizational level. Researches by Smits, Wagner, Spreeuwenberg, van der Wal and Groenewegen, (2009) and Nieva and Sorra, (2003) illustrated that on an individual level, the information of the personnel is enhanced from the parameters and the attitudes, which influence the “patient safety”. Simulta-neously they give feedback regarding the errors and the omissions that occur. On an organizational level, the evaluation of a safety climate is required by the international accreditation organizations, and it is used as a diagnostic tool for the identification of the parameters of “safety culture” which need to be improved. Also, it is used for the evaluation of the safety improvement programs, as well as for the comparative evaluation of safety climate at the hospital in comparison to other hospitals (Smits, Wagner, Spreeuwenberg, van der Wal, & Groenewegen, 2009; Nieva & Sorra, 2003). Additionally, Neal and Griffin (2004) claimed that it is one of the means of improvement of the hospitals credibility, since it contributes to the redesign of the existed processes and the correction of the organizational factors, which make health professionals more prone to errors (Neal & Griffin, 2004).
Sources of “Patient Safety Culture” Evaluation Tools
In December of 2003, AHRQ developed a webpage, which hosts the quality tools for health. This webpage was established as a data base, and a web portal about practices and ready for use tools for the evaluation, measurement, promotion and improvement of health care quality in America. This service aims at providing the health care providers, the political leadership of every Ministry of Health, the patients – consumers of health services and the researchers an accessible mechanism, which can provide suggestions, initiations and principles for the improvement of quality, improve medical treatment provision and receipt, help the decisions, regarding medical treatment, and train each of the customers separately regarding the needs of healthcare (Nix et al., 2006).
Quality Tools include summaries of tools, which constitute an easy to use mechanism for obtaining standardized information on tools, while at the same time they include external links for other websites dedicated to each tool separately (Nix et al., 2006).

Patient Safety and Medical Errors
77
National Guideline Clearinghouse
National Guideline Clearinghouse (NGC,www.guideline.gov) of AHRQ, the online repository of practical guides, based on evidences which were created on 1998, con-stitutes an additional source of tools. Although Quality Tools and NGC are similar websites, one of the criteria of Quality Tools is that the tool must be accessible from the internet, which does not apply for NGC. Therefore, the nursing stuff can find tools in NGC which are not available in Quality Tools. The tools, which are available in NGC have been developed in combination with the instructions in order to help health care providers (nurses, doctors, hospitals) implement them. NGC includes more than 1.500 tools accompanied by instructions. Clinical algorithms, pocket guides and short helping guides constitute more than the 2/3 of the total number of tools. Most of those in charge for the creation and the development of guidelines and the relevant tools, usually develop more than 1 tools. Just like Quality Tools, NGC is updated every week with new improved tools and guidelines (Nix et al., 2006).
Patient Safety Network
The tools, which were developed for use in program related to patient safety, may be downloaded from the webpage Patient Safety Network» of AHRQ PSNet (http://psnet.ahrq.gov/). This webpage constitutes a portal of paramount value for the improvement of patient safety and the prevention of medical errors, whereas it also constitutes the first overall effort, in order to enlight health care providers, managers, and consumers – patients on every aspect of patient safety. The webpage includes summaries of tools and research findings on patient safety, information regarding oncoming meetings and conferences as well as links with articles, books and references. The following type of tools along with their available number are among the categories in this page: 23 audiovisual means, 108 books/references, 8 clinical guiding instructions and 154 web pages, which include links to courses of study / curriculums, data bases, forums and government WebPages (Nix et al., 2006).
Modification of Federal Tools
In addition, federally funded guidelines and tools are provided by the public sector, which means that they can be used without the acquisition of relevant permission, that subjects to copyright law. Some of them, however, are likely to include particu-lar tables or content, which subject to copyright restrictions. In the event that the authors maintain the copyright of their product, they must grand their permission for the use of their material or ask for a monetary exchange. Every page refers to its

Patient Safety and Medical Errors
78
requirements for downloading and using its tools, and to what extend a copyright license is required (Nix et al., 2006).
Research Tools for the Evaluation of Patient Safety Culture
Research by Sexton et al. (2006) illustrated that the initial efforts for the evaluation and the improvement of “safety culture” and later the more clearly defined role of “patient safety” are facilitated by the measurements regarding safety culture. By determining the characteristics of organizations, which are negative for the clients and perhaps they are linked to safety, the supervisors have the ability to intervene so as to improve the quality of healthcare (Sexton et al., 2006).
Moreover Sexton et al. (2006) argued that the existed tools for the evaluation of patient safety culture are many, whereas there are few references in literature, which provide guidance to the users or the researchers regarding the selection of research tools or initiations in relation to measurements for the improvement of safety (Sexton et al., 2006).
The variety of tools are confirmed by the results of the extended literature review, which was carried out by EUNetPas (2009), 24 patient safety culture evaluation tools were identified and used immediately within and outside the European Union and they are the following (EUNeTPaS, 2009):
• Checklist for Assessing Institutional Resilience.• Culture of Safety Survey.• Danish Patient Safety Culture Questionnaire.• Error Orientation Questionnaire.• Hospital Culture Questionnaire.• Hospital Survey on Patient Safety.• Hospital Survey on Patient Safety Culture.• Manchester Patient Safety Assessment Framework.• Nursing Unit Cultural Assessment Instrument.• Patient Safety Climate in Aesthesia.• Patient Safety Culture Questionnaire.• Patient Safety Culture in Healthcare Organizations Survey.• Safety Attitudes Questionnaire.• Safety Climate Assessment Tool.• Safety Climate Scale.• Safety Climate Survey.• Stanford Safety Culture Instrument.• Teamwork and Patient Safety Attitudes Questionnaire.• Trainee Supplemental Survey.

Patient Safety and Medical Errors
79
• TUKU – Safety Culture in Health Care Survey.• Veteran Affairs Palo Alto / Stanford Patient Safety Center for Inquiry.• Veterans Health Administration Patient Safety Culture Questionnaire.• Vienna Safety Culture Questionnaire.• World Alliance for Patient Safety Hand Hygiene Campaigns Healthcare -
Units Survey on Patient Safety Culture.
The majority of these tools have been designed and applied for the evaluation of patient safety culture in hospitals, but few of them have been applied to Primary Health Care structures, nursing homes and Emergency Departments. According to a report which was elaborated and published by EUNetPaS (2009), the tools for the assessing of patient safety culture, which are widely used in the European Union are the following (EUNeTPaS, 2009):
• Clinical Risk Management: ◦ Austria.
• Drug risk perception with respect to NSAIDs: ◦ Slovakia.
• Error Orientation Questionnaire: ◦ Denmark.
• Healthcare workers’ perception of adverse events and incident reporting: ◦ Italy.
• Hospital Survey on Patient Safety Culture: ◦ Belgium, ◦ United Kingdom (Scotland), ◦ Switzerland, ◦ Netherlands, ◦ Italy, ◦ Spain, ◦ Croatia, ◦ Sweden, ◦ Iceland, ◦ France, ◦ Norway, and ◦ Finland.
• Information System for Surveillance and Control of Adverse Events: ◦ Spain.
• Manchester Patient Safety Assessment Framework: ◦ United Kingdom, ◦ Germany, and

Patient Safety and Medical Errors
80
◦ Netherlands.• Patient perception of safety in health services. CASSES Questionnaire:
◦ Spain.• Patient safety care in healthcare organizations - Quality Standards:
◦ Spain.• Safety Attitudes Questionnaire (different versions):
◦ Hungary, ◦ Norway, ◦ Germany, and ◦ United Kingdom.
• Safety Climate Assessment Instrument: ◦ United Kingdom by European Federation of Nurses.
• The Danish Patient Safety Culture Questionnaire: ◦ Denmark.
• TUKU – Safety culture in health care survey: ◦ Finland.
• Vienna Safety Culture Questionnaire: ◦ Austria.
• World Alliance for Patient Safety Hand Hygiene Campaigns Healthcare - Units Survey on Patient Safety Culture: ◦ Portugal.
According to the results of a recent study, important variation and opportunities for enhancement in patient safety culture exist across neonatal Intensive Care Unit. Significant systematic differences exist between Safety Attitudes Questionnaire and Hospital Survey on Patient Safety Culture such that these tools should not be used interchangeably (Profit et al., 2015). The above findings are ensured by another study which was concluded that there were differences in perception regarding patient safety among ICUs, which confirms the existence of local micro cultures. The study did not illustrate equality between the Safety Attitudes Questionnaire and the Hospital Survey on Patient Safety Culture (Santiago & Turrini, 2015).
The Internal Market Information System (IMI) was developed by the European Union, and aims at contributing to patient safety through the prompt and modern information exchange among the regulatory nursing bodies, regarding its well-functioning and the activity of their members. Through the IMI system, the Euro-pean Federation of Nursing Regulators will improve its electronic database, which refers to nurses, so as to allow the national regulatory nursing bodies to exchange the information required for the recognition of the educational and professional qualifications and skills of the nurses. According to Stievano, Jurado, Rocco and Sasso (2009) this process enables the mobility of professionals, and ensures the high

Patient Safety and Medical Errors
81
quality of nursing care in a smooth and consistent way throughout the European Union (Stievano, Jurado, Rocco, & Sasso, 2009).
In 2004, the head of patient safety at the Health Service of the University of Pennsylvania set up a specific task force which consisted of people responsible for the quality and the patient safety at the hospitals-members. This taskforce undertook the development of a learning program for those who support this purpose regard-ing patient safety, so as to take action and develop a program to ensure safety in healthcare sector. That is how Delta were brought together with the vision that over time patient safety would be integrated in the safety culture of the organizations and the attitude of the nursing stuff, eliminating the need for a specific program. The role of each member in Delta was to participate in the meetings in order to be trained in the theoretical approach and the practice of safety principles, protect the patient safety in the work environment and cooperate with their colleagues to find ways for the improvement of patient safety (Schwoebel & Creely, 2010).
According to the Institute for Save Medication Practices, insulin, the hormone, which controls the blood sugar levels, is often involved in errors which put patients at risk. The patients who have gone through severe hypoglycemia are likely to have been granted wrong doses, wrong type of insulin or right doses in the wrong time. Bass, Will, Todd and Weatherford (2007) supported that In order to be able to comprehend how is it possible for all those errors to occur, one has to examine the various types of insulin, as well as the available medicine, which enhance insulin and additionally the fact that most patients have been subscribed more than one type of medicine. In addition, many of those products have similar names and package. Therefore, it is only a miracle the fact that even more errors don’t occur (Bass, Will, Todd, & Weatherford, 2007).
Bass et al. (2007) suggested the nurses’ familiarization with the new insulin therapies, the new methods and the precautions that must be taken, for patient safety. Initially it is suggested to develop Table, enumerating the insulin products, which are used in the hospital and the time of administration for each. In order to limit the confusion, the evolution of the insulin therapy from its older typical form to the most recent medication for the enhancement of insulin is recorded. The nurse must also confirm the existence of a practical table, so as to control the commencement, the peak and the duration of the action of every product before administration, whereas it is also suggested that the prescription and the doses are checked by a colleague before administering the medication (Bass et al., 2007).
According to the findings of the above French research in some cases, and in particular in cases of vulnerable patients with serious problems, the adherence to health care protocols is not always sufficient for the prevention of adverse events. Taking also under consideration the fact that, they may be found in emergency, their situation is not sufficiently covered by clinical guidance. The particular research,

Patient Safety and Medical Errors
82
with a sample of 8.754 patients in 292 rooms, in 71 hospitals over 35.234 days of hospitalization aimed at the estimation of adverse events in medical and surgical activity so much in public as well as in private hospitals, whereas it also aimed at the evaluation of the clinical condition of the patients and the active errors. The results showed that the prevention of adverse events is influenced by the compliance with the recommendations on correct practices (Bass, et al., 2007).
Michel, Quenon, Djihoud, Tricaud-Vialle and de Sarasqueta (2007) claimed that the complex nature of care as well as the increased use of technology consti-tutes factors which contribute to the increased risk of patients. Paediatric patients represent one of the most vulnerable populations of patients due to age, height, as well as their anatomical and natural development and the severity of the injury or disease. In addition children offen fail to protect themselves from possible risks and therefore they are based on their parents who many not feel sufficiently prepared to act on their behalf. These factors underline the need for a coordinated effort for the protection of this population from risks (Michel, Quenon, Djihoud, Tricaud-Vialle, & de Sarasqueta, 2007).
Moreover the plan of C&W hospital on safety in hospitals, expresss the need to develop a culture, which does not use punishment as a means to remove the stain of error and encourage the reporting of errors, allowing the organizations to learn from its mistakes and unpredictable events. Verschoor et al. (2007) argued that this safety culture is based on trust, which is built on the abolishment of individual accountability for the errors, awareness and the cautiousness, open communica-tion, learning and constant improvement (Verschoor et al., 2007). Notable is the contribution of the IHI which has developed methods to facilitate the development of safety culture in the hospital.
FUTURE RESEARCH DIRECTIONS
Recognizing the significance of “safety culture” as well as the importance of the opinion of healthcare professionals on the issues of safety constitutes dire need since they constitute the immediate and main healthcare providers. The assessment of safety culture is a process, which may contribute positively to the change of culture and signify the beginning of patient safety constant improvement. The combina-tion of safety culture assessment and safety management is a field that needs to be further developed.

Patient Safety and Medical Errors
83
Within the framework of a holistic intervention for the development of “safety culture” in hospitals, the three basic determining parameters (scope of work, work environment and particular individual characteristics) must be addressed in parallel and globally. The important thing is the final result to aim at the most appropriate activities for each category of employees and situation. The development of a positive safety culture is considered a prerequisite for the prevention of errors and patient safety. In the future, the development and use of psychometric tools, especially designed for the evaluation of the attitude of healthcare professionals on issues of safety for particular group of patients such as psychiatric patients or patients with cancer, would be useful since it would contribute generally to the improvement of quality of healthcare services.
CONCLUSION
An important body of evidence, points to medical errors as a leading cause of death and harm during the healthcare provision. The terms “patient safety” and “medical errors” were directly linked to “safety climate” in organizations. “Safety climate” in work environment is a complex variable which is influenced by inherent charac-teristics of health professions (tension – rate, work - stress, experience acquisition, type of events) as much as by parameters involving particular work conditions (the role of management, team work), and each of the health professionals (satisfaction from work, love for the profession).
Finally, patient safety appears to be a sector, which requires immediate action to be taken by all parties involved in the provision of health care. Health scientists owe to act according to Hippocratic admonition “Do no harm” attempting to adhere to all those rules and principles in the exercise of their task, which aim at not just the restoration of the patients’ physical and mental health but also to the prevention of additional emotional and personal injury.

Patient Safety and Medical Errors
84
REFERENCES
ACSNI. (1993). Advisory Committee on the Safety of Nuclear Installation: Human Factors Study Group Third Report: Organizing for safety. Sheffield, UK: HSE Books.
Agency for Healthcare Research and Quality. (2009). 10 Patient Safety Tips for Hospitals. Retrieved from http://www.ahrq.gov/patients-consumers/diagnosis-treatment/hospitals-clinics/10-tips/index.html
Bass, A., Will, T., Todd, M., & Weatherford, D. (2007). The latest tools for patients with diabetes. RN, 70(6), 39–43. PMID:17624061
Blegen, M. A., Pepper, G. A., & Rosse, J. (2005). Safety Climate on Hospital Units: A New Measure Advances in Patient Safety: From Research to Implementation (Vol. 4). Rockville, MD: Programs, Tools, and Products.
Brewer, T., & Colditz, G. A. (1999). Postmarketing surveillance and adverse drug reactions: Current perspectives and future needs. Journal of the American Medical Association, 281(9), 824–829. doi:10.1001/jama.281.9.824 PMID:10071004
Cameron, K., & Quinn, R. E. (2011). Diagnosing and changing organizational culture: based on the competing values framework. Reading, MA: Addison Wesley Longman.
Card, A. J. (2014). Patient safety: This is public health. Journal of Healthcare Risk Management, 34(1), 6–12. doi:10.1002/jhrm.21145 PMID:25070252
Cooper, M. D. (2000). Towards a model of safety culture. Safety Science, 36(2), 111–136. doi:10.1016/S0925-7535(00)00035-7
Donabedian, A. (1980). Explorations in Quality Assessment and Monitoring: The Definition of Quality and Approaches to Its Assessment.: Vol. III. The Methods and Findings of Quality Assessment Measurement and Monitoring. Ann Arbor, MI: Health Administration Press.
Edmondson, A. C. (2004). Learning from failure in health care: Frequent oppor-tunities, pervasive barriers. Quality & Safety in Health Care, 13(Suppl 2), ii3–ii9. doi:10.1136/qshc.2003.009597 PMID:15576689
El-Jardali, F., Dimassi, H., Jamal, D., Jaafar, M., & Hemadeh, N. (2011). Predictors and outcomes of patient safety culture in hospitals. BMC Health Services Research, 11(1), 45. doi:10.1186/1472-6963-11-45 PMID:21349179
EUNETPAS. (2009). Catalogue: currently used patient safety culture instruments in Europe. Aarthus.

Patient Safety and Medical Errors
85
Ginsburg, L., & Gilin Oore, D. (2016). Patient safety climate strength: A concept that requires more attention. BMJ Quality & Safety, 25(9), 680–687. doi:10.1136/bmjqs-2015-004150 PMID:26453636
Glendon, A. I., Clarke, S., & Mckenna, E. F. (2006). Human Safety and Risk Man-agement (2nd ed.). Boca Raton, FL: CRC Press.
Guldenmund, F. W. (2000). The nature of safety culture: A review of theory and research. Safety Science, 34(1–3), 215–257. doi:10.1016/S0925-7535(00)00014-X
Hellings, J., Schrooten, W., Klazinga, N. S., & Vleugels, A. (2010). Improving pa-tient safety culture. International Journal of Health Care Quality Assurance, 23(5), 489–506. doi:10.1108/09526861011050529 PMID:20845679
Homsted, L. (2000). Institute of Medicine report: to err is human: building a safer health care system. The Florida Nurse, 48(1), 6. PMID:11995167
Huang, Y. H., Chen, P. Y., & Grosch, J. W. (2010). Safety climate: New develop-ments in conceptualization, theory, and research. Accident; Analysis and Prevention, 42(5), 1421–1422. doi:10.1016/j.aap.2009.12.007 PMID:20538096
Human Engineering for the Health and Safety Executive. (2005). A review on safety culture and safety climate literature for the development of the safety culture inspec-tion toolkit. Bristol: Author.
Institution of Engineering and Technology. (2009). Health & Safety Briefing No. 07. Retrieved from: http:// www.theiet.org/factfiles
International Nuclear Safety Advisory Group –INSAG. (2001). Safety Culture. Report 75-INSAG 4. International Atomic Energy Agency.
Kristensen, S., Bartels, P., Sabroe, S., & Mainz, J. (2014). Patient safety culture can be a driver for high clinical quality. Ugeskrift for Laeger, 176(32), 1483–1486. PMID:25292469
Kristensen, S., Hammer, A., Bartels, P., Sunol, R., Groene, O., Thompson, C. A., & Wagner, C. et al. (2015). Quality management and perceptions of teamwork and safety climate in European hospitals. International Journal for Quality in Health Care, 27(6), 499–506. doi:10.1093/intqhc/mzv079 PMID:26443813
Kristensen, S., Mainz, J., & Bartels, P. A. (2007). A patient safety vocabulary: Safety improvement for patients in Europe. SimPatlE. Denmark: ESQH.
Lauterstein, R. H., & Mustoe, L. F. (1960). Accidents involve people. Nursing Outlook, 8, 96–98. PMID:14414610

Patient Safety and Medical Errors
86
Leape, L. (2000). Preventing mishaps team effort, error expert says. OR Manager, 16(2), 1, 12–13. PMID:10787891
Legido-Quigley, H., McKee, M., Walshe, K., Sunol, R., Nolte, E., & Klazinga, N. (2008). How can quality of health care be safeguarded across the European Union? BMJ (Clinical Research Ed.), 336(7650), 920–923. doi:10.1136/bmj.39538.584190.47 PMID:18436947
McFadden, K. L., Stock, G. N., & Gowen, C. R. III. (2014). Leadership, safety cli-mate, and continuous quality improvement: Impact on process quality and patient safety. The Journal of Nursing Administration, 44(10Suppl), S27–S37. doi:10.1097/nna.0000000000000119 PMID:25279509
McLoughlin, V., Millar, J., Mattke, S., Franca, M., Jonsson, P. M., Somekh, D., & Bates, D. (2006). Selecting indicators for patient safety at the health system level in OECD countries. International Journal for Quality in Health Care, 18(Suppl 1), 14–20. doi:10.1093/intqhc/mzl030 PMID:16954511
Mearns, K., Whitaker, S. M., & Flin, R. (2003). Safety climate, safety management practice and safety performance in offshore environments. Safety Science, 41(8), 641–680. doi:10.1016/S0925-7535(02)00011-5
Michel, P., Quenon, J. L., Djihoud, A., Tricaud-Vialle, S., & de Sarasqueta, A. M. (2007). French national survey of inpatient adverse events prospectively assessed with ward staff. Quality & Safety in Health Care, 16(5), 369–377. doi:10.1136/qshc.2005.016964 PMID:17913779
Moutier, C., Wingard, D., Gudea, M., Jeste, D., Goodman, S., & Reznik, V. (2016). The Culture of Academic Medicine: Faculty Behaviors Impacting the Learning En-vironment. Academic Psychiatry, 40(6), 912–918. doi:10.1007/s40596-016-0582-3 PMID:27368643
Neal, A., & Griffin, A. (2004). Safety climate and safety at work. In J. Barling & M. Frone (Eds.), The psychology of workplace safety. Washington, DC: American Psychological Association. doi:10.1037/10662-002
Nieva, V., & Sorra, J. (2003). Safety culture assessment: A tool for improving patient safety in healthcare organizations. Quality & Safety in Health Care, 12(Suppl 2), ii17–ii23. doi:10.1136/qhc.12.suppl_2.ii17 PMID:14645891
Nix, M. P., Coopey, M., & Clancy, C. M. (2006). Quality tools to improve care and prevent errors. Journal of Nursing Care Quality, 21(1), 1–4. doi:10.1097/00001786-200601000-00001 PMID:16340679

Patient Safety and Medical Errors
87
Olsson, C., Forsberg, A., & Bjerså, K. (2016). Safety climate and readiness for implementation of evidence and person centered practice – A national study of registered nurses in general surgical care at Swedish university hospitals. BMC Nursing, 15(1), 54. doi:10.1186/s12912-016-0174-2 PMID:27625589
Profit, J., Lee, H. C., Sharek, P. J., Kan, P., Nisbet, C. C., Thomas, E. J., & Sexton, B. et al. (2015). Comparing NICU teamwork and safety climate across two commonly used survey instruments. BMJ Quality & Safety. doi:10.1136/bmjqs-2014-003924 PMID:26700545
Pronovost, P. J., Weast, B., Holzmueller, C. G., Rosenstein, B. J., Kidwell, R. P., Haller, K. B., & Rubin, H. R. et al. (2003). Evaluation of the culture of safety: Sur-vey of clinicians and managers in an academic medical center. Quality & Safety in Health Care, 12(6), 405–410. doi:10.1136/qhc.12.6.405 PMID:14645754
Reason, J. (1990). Human Error. Cambridge University Press. doi:10.1017/CBO9781139062367
Reason, J. (1998). Achieving a safe culture: Theory and practice. Work and Stress, 12(3), 293–306. doi:10.1080/02678379808256868
Rice, R. B. (2003). Patient safety: Who guards the patient. Online Journal of Issues in Nursing, 8(3), 1. PMID:14656190
Sammer, C. E., Lykens, K., Singh, K. P., Mains, D. A., & Lackan, N. A. (2010). What is patient safety culture? A review of the literature. Journal of Nursing Schol-arship, 42(2), 156–165. doi:10.1111/j.1547-5069.2009.01330.x PMID:20618600
Santiago, T. H., & Turrini, R. N. (2015). Organizational culture and climate for patient safety in Intensive Care Units. Revista da Escola de Enfermagem da U S P., 49, 123–130. doi:10.1590/S0080-623420150000700018 PMID:26761702
Schwoebel, A., & Creely, J. (2010). Improving the safety of neonatal care through the development and implementation of a staff-focused delta team. The Journal of Perinatal & Neonatal Nursing, 24(1), 81–87. doi:10.1097/JPN.0b013e3181ce33ab PMID:20147835
Sexton, J. B., Berenholtz, S. M., Goeschel, C. A., Watson, S. R., Holzmueller, C. G., Thompson, D. A., & Pronovost, P. J. et al. (2011). Assessing and improving safety climate in a large cohort of intensive care units. Critical Care Medicine, 39(5), 934–939. doi:10.1097/CCM.0b013e318206d26c PMID:21297460

Patient Safety and Medical Errors
88
Sexton, J. B., Makary, M. A., Tersigni, A. R., Pryor, D., Hendrich, A., Thomas, E. J., & Pronovost, P. J. et al. (2006). Teamwork in the operating room: Frontline per-spectives among hospitals and operating room personnel. Anesthesiology, 105(5), 877–884. doi:10.1097/00000542-200611000-00006 PMID:17065879
Shannon, H. S., Mayr, J., & Haines, T. (1997). Overview of the relationship be-tween organizational and workplace factors and injury rates. Safety Science, 26(3), 201–217. doi:10.1016/S0925-7535(97)00043-X
Silva, N. D., Barbosa, A. P., Padilha, K. G., & Malik, A. M. (2016). Patient safety in organizational culture as perceived by leaderships of hospital institutions with different types of administration. Revista da Escola de Enfermagem da U S P., 50(3), 490–497. doi:10.1590/S0080-623420160000400016 PMID:27556721
Smits, M., Wagner, C., Spreeuwenberg, P., van der Wal, G., & Groenewegen, P. P. (2009). Measuring patient safety culture: An assessment of the clustering of responses at unit level and hospital level. Quality & Safety in Health Care, 18(4), 292–296. doi:10.1136/qshc.2007.025965 PMID:19651934
Sorra, J. S., & Nieva, V. F. (2004). Hospital survey on patient safety culture. Rock-ville, MD: Agency for Healthcare Research and Quality.
Spath, P. L. (2000). Patient safety improvement guidebook. Forest Grove, OR: Brown-Spath & Associates.
Stievano, A., Jurado, M. G., Rocco, G., & Sasso, L. (2009). A new information ex-change system for nursing professionals to enhance patient safety across Europe. Jour-nal of Nursing Scholarship, 41(4), 391–398. doi:10.1111/j.1547-5069.2009.01307.x PMID:19941585
Talbot, C. (2008). Measuring public value: A competitive value approach. Aca-demic Press.
Verschoor, K. N., Taylor, A., Northway, T. L., Hudson, D. G., Van Stolk, D. E., Shearer, K. J., & Miller, G. et al. (2007). Creating a safety culture at the Childrens and Womens Health Centre of British Columbia. Journal of Pediatric Nursing, 22(1), 81–86. doi:10.1016/j.pedn.2006.08.012 PMID:17234501
WHO. (2003). Executive board. Quality of care: patient safety. Retrieved from: http://apps.who.int/gb/archive/pdf_files/EB113/eeb11337.pdf
WHO. (2005). Project to develop the international patient safety Event taxonomy: updated review of the literature 2003 - 2005. Final report. Retrieved from: http://www.who.int/patientsafety/taxonomy/IPSET_Sept05_FINAL.pdf

Patient Safety and Medical Errors
89
WHO. (2005a). News release. Launch of the WHO Collaborating Center on patient safety solutions. WHO.
WHO. (2005b). World Alliance for patient safety. In WHO draft guidelines for adverse event reporting and learning systems. From information to action. Geneva, Switzer-land: WHO. Retrieved from: http://www.who.int/patientsafety/en/brochure_final.pdf
WHO. (2007). World Alliance for patient safety. The conceptual framework for the International Classification for patient safety. Version 1.0 for use in the field testing (ICPS). Retrieved from: http://www.who.int/patientsafety/ICPS%20-%20July%202007.pdf
Yule, S. (2003). Safety culture and safety climate: A review of the literature. Indus-trial Psychology Research Centre.
Zohar, D. (1980). Safety climate in industrial organizations: Theoretical and applied implications. The Journal of Applied Psychology, 65(1), 96–102. doi:10.1037/0021-9010.65.1.96 PMID:7364709
Zohar, D., Livne, Y., Tenne-Gazit, O., Admi, H., & Donchin, Y. (2007). Health-care climate: A framework for measuring and improving patient safety. Critical Care Medicine, 35(5), 1312–1317. doi:10.1097/01.CCM.0000262404.10203.C9 PMID:17414090

Patient Safety and Medical Errors
90
KEY TERMS AND DEFINITIONS
Adverse Events: Any kind of error, mistake, accident, failure or deviation from the safe treatment of the patients, whether or not causing harm on them.
Harm: Α negative consequence, whether or not it is obvious to the patient.Learning: The hospitals learn from their errors and look for new opportunities for
performance betterment. Learning is valued among a considerable number of staff.Patient-Centered Care: Patient care is centered around the patients and their
families. The patients are not only active participants in their own care, but also act as an intermediary between the hospital units and the community.
Patient Safety: The avoidance and prevention of patient injuries or adverse events that are the result of health care procedures.
Safety Culture: A complicated and enduring characteristic reflecting essential values, rules and suppositions.
Teamwork: A spirit of respect and cooperation among colleagues exists among executives and personnel. Relationships are unrestricted, secure, respectful and flexible.

Copyright ©2017, IGI Global. Copying or distributing in print or electronic forms without written permission of IGI Global is prohibited.
DOI: 10.4018/978-1-5225-2337-6.ch004
Chapter 4
91
Application of Quality Management in
Promoting Patient Safety and Preventing
Medical Errors
ABSTRACT
The combination of healthcare professionals, processes and technologies bring significant benefits for patients. However, it also involves an inevitable risk of ad-verse events. Patients receiving health care in health institutions have the potential to experience some forms of medical errors. The word medical error commonly encompasses terms such as mistakes, near misses, active and latent errors. This signifies the complexity and multidimensional nature of the error. The consequences can be costly to the patients, the health professionals, the health care institutions, and the entire health care system. The costs may involve human, economic, and social aspects. Thus, ensuring quality health care can contribute to patients’ safety by reducing potential medical errors in practice. This chapter aims to introduce a quality management framework for improving the quality and effectiveness of ser-vices, reducing medical errors and making the healthcare system safer for patients.
Ali Mohammad MosadeghradTehran University of Medical Sciences, Iran
Abraha WoldemichaelMekelle University, Ethiopia

Application of Quality Management in Promoting Patient Safety
92
INTRODUCTION
Health care is not as safe and reliable as it might be. Healthcare delivery is a complex process involving multiple independent agents and clinical pathways. One component of the system is interdependent and interacts with other multiple components. The occurrence of errors during the healthcare services delivery is inevitable. Medical errors are frequently occurring, complex and pervasive public health concerns that pose serious challenges to patient safety and could cause death and injury. The prevalence of the issue is gaining immense attention in recent years.
Unfortunately, the deaths due to preventable medical errors exceed the number of death from road accidents, cancer, or AIDS. Evidence from hospitalized patients consistently revealed high rates of adverse events (McLean, 2015). Preventable medical errors and adverse events are commonly observed in patients receiving care in hospitals and healthcare facilities. For example, evidence from US shows the occurrence of an estimated 161,655 medical errors in 2008 and 170,201 medical errors in 2009. The extrapolated estimate showed that there were more than four million unique injury visits containing more than one million unique medical errors each year in the entire US population (David et al., 2013). Although reports from developing countries are limited, medical errors are worldwide concerns.
Insufficient technical skills and motivation of healthcare professionals, poor qual-ity of infrastructure, equipment, and drugs, and shortcomings in infection control and healthcare waste management particularly in developing countries make the probability of adverse events much higher than in industrialized nations.
Improving healthcare processes and enhancing health care quality are critical and enduring steps in promoting patient safety and reducing medical errors. This can be achieved through improving professional knowledge, meticulous health care delivery, adherence to policy and procedures and safe service delivery, improving institutional transparency and patient involvement in decisions, building good in-stitutional culture and functional monitoring and evaluation.
This chapter presents the details of aspects of medical errors in connection with health care quality, and possible approaches to reduce medical errors and improve patient safety. The overall purpose of this chapter is to introduce a quality management framework to assist healthcare practitioners to improve the quality and effectiveness of services and reduce medical errors and their consequences.

Application of Quality Management in Promoting Patient Safety
93
MEDICAL ERRORS AND ADVERSE EVENTS
Medical Errors
The concept of “medical error” encompasses many intertwined individual and healthcare system related factors that make describing it more challenging. Medical error is related to the supply side of the healthcare organization (i.e., the healthcare system and professionals). Reason (1990) defined medical error as “a failure of a planned action to be completed as intended (error of execution) or the use of a wrong plan to achieve an aim (error of planning)”. Van Den Bos and colleagues (2011) described medical error as a “preventable adverse outcome that results from improper medical management (a mistake of commission) rather than from the progression of an illness resulting from lack of care (a mistake of omission)”. Grober and Bohnen (2005) have also defined medical error as ‘an act of omission or commission in planning or execution that contributes or could contribute to an unintended result’. The concept of medical error, therefore, refers to a mistake in actions or thoughts (judgment) in healthcare settings whether or not harm the pa-tient. This definition includes the main domains of error causation (planning and execution; omission and commission), and captures faulty processes that can lead to errors, whether adverse outcomes occur or not.
Medical errors can be classified in many ways. One way of classifying medical errors is preventable or unpreventable errors. Preventable errors are those errors that can be predicted and remediated. For instance, errors related to malfunctioning of a technology can be prevented through routine monitoring and inspection of the technology. However, not all errors are predictable. Hence, certain errors remain out of the professional’s control. For example, a debilitated patient may develop a pressure sore after prolonged hours of surgical procedure despite meticulous care provided by the professionals to the patient’s best interest. Thus, in unpreventable errors, the professionals should take the opportunity to share such lessons with other caregivers to prevent similar consequences from occurring again (Hemingway et al., 2015).

Application of Quality Management in Promoting Patient Safety
94
Leape and colleagues (1991) classified medical errors as management errors and technical errors or negligent errors (errors of omission or errors of commission). Management errors involve the actions of individual professionals in a given health facility as well as the broader systems where the professionals operate. Technical errors relate to injury to a patient during operation, bleeding, etc. An error of com-mission occurs when an incorrect action is taken, such as prescribing ceftriaxone for a neonate who has hyperbilirubinemia. An error of omission results when a correct action is not taken such as failure or delay in making a diagnosis or starting treatment, and failure to use indicated tests or take precautions to prevent harm. The errors of omission can be more common than the occurrence of errors of commission.
The healthcare delivery process is characterized by the interdependence of one component of the system with multiple other components and the interactions are time dependent. Hence, error occurrence is inevitable. In this perspective, medi-cal errors are classified as either active or latent errors. Active errors occur at the level of the frontline professional operating in the complex healthcare system and produce immediate events. One such error can be the administration of wrong dose of a medication to a patient where the probability of occurrence of immediate harm is high. Hence, active errors are easier to measure because they are limited in time and space. However, a single active error can be the result of many latent errors. Latent errors refer to system defects such as poor purchasing decisions, incorrect equipment installation, inadequate maintenance of equipment, inadequate staffing, high workload, and insufficient training (Thomas & Petersen, 2003). These system factors can influence the frontline professional to commit active errors (Kalra et al., 2013). Latent errors occur over broad ranges of time and space and they may exist for days, months, or even years before they lead to a more apparent medical error or adverse event. Therefore, measuring latent errors is not straightforward (Thomas & Petersen, 2003).
The most frequent but avoidable medical errors include incorrect indications, incorrect dosages and incorrect administration of drugs, and inadequate selection of medical devices (Baker, et al. 2004). Medication errors are perhaps common forms of medical errors. Medication errors such as prescribing errors, dispensing errors, administering errors, monitoring patient for effects errors, medication administration record errors, etc. are commonly faced types of errors (Miller et al., 2007). Evidence from case-control study in two hospitals in New Jersey (US) reported medication errors rate of 0.8 per 100 admissions, or 1.6 per 1000 patient days. Most errors were occurred at the administration stage of the medication use process and the frequent types of errors included wrong time, wrong medication, wrong dose, and omission errors (Choi, et al., 2016).

Application of Quality Management in Promoting Patient Safety
95
Adverse Events
Medical injuries (adverse events) are different from medical errors not only because of their focus but also all errors do not necessarily cause harm. Medical injury is the medical care with an adverse outcome. The adverse outcome can be due to a medical error or due to unavoidable complications. The injury covers a wide range of outcomes, from a mild allergic reaction to a drug to death (Van Den et al., 2011). Thus, an adverse event is an injury, harm, or complication caused by medical man-agement rather than by the underlying disease process or patient conditions.
In health care, harm refers to an undesirable, or detrimental injury to a patient or to a healthcare process. The injury must involve or have some negative impact or potential impact on a patient or patients, and there must be some indication that the event is a result of some part of the healthcare process (either through commission or omission), rather than a result of events outside the healthcare process, such as the patient’s own actions or the natural progression of the disease (Walshe, 2000). Generally, adverse events refer to the harms that happen to patients (demand side) as a result of errors in the healthcare delivery (supply side). However, it is important to remember that most medical errors do not lead to adverse events.
Like medical errors, adverse events can be preventable or non-preventable and they cover a broad-spectrum of consequences involving surgical and non-surgical interventions. The consequences may again range from those that are unpredictable such as allergic reactions to drugs to which the patient had no known previous expo-sure, to those that might have been unavoidable such as bone marrow depression from cancer chemotherapy, to those that result from errors in medication administration or patient monitoring such as bleeding associated with the use of anticoagulants (Leape et al., 1991). Some adverse events may spontaneously resolve or neutralize before the consequences have time to develop to cause harm. Such adverse event is called a near miss (Garrouste-Orgeas et al, 2012).
Generally, non-preventable adverse events may refer to those consequences that are unavoidable and occur following certain appropriate medical care to patients. Preventable adverse events are those consequences due to serious medical errors that may involve negligence (Rothschild et al., 2005).

Application of Quality Management in Promoting Patient Safety
96
Causes of Medical Errors
Most medical injuries are rooted either in the inherent risk in the healthcare prac-tice, or in the healthcare system related errors or the result of a combination of human and organizational factors. Errors of omission are often cases of negligent errors. Consider a patient has presented with a classic history of acute appendicitis, typical findings on physical examination, and suggestive laboratory-test results. If the responsible physician misses the diagnosis, the case would be both an error in diagnosis (mistaken diagnosis) and a case of negligence. Furthermore, if the diagnosis was made but no appendicitis was found after a surgical intervention on the patient for appendectomy, there would have been an error in diagnosis but not negligent error. In this case the surgeon would have been blamed for not following the generally accepted standard of practice.
The mere occurrence of error could be a necessary but not sufficient condition for concluding negligence. Hence, medical negligence can be defined as failure to meet the standard of practice of an average qualified professional practicing in his or her specialty. Technical errors occur most frequently but relatively few of them are judged to result from negligence (Leape et al., 1991).
A variety of medical errors and adverse events related to improper transfusions, surgical injuries and wrong-site surgery, falls, burns, pressure ulcers, and mistaken patient identities happen to receiving health care services. The error rates with seri-ous consequences are usually high in patients admitted to the intensive care units, operating rooms, and emergency departments (Kohn et al., 1999). The errors may often result from improper management of patients, clinical workflow processes, and information systems (Bonney, 2013). Furthermore, the cause of medical errors or adverse events can be related to case complexity, discontinuity of care, failure to follow protocol or accepted practice, fatigue, gap in knowledge, high workload, insufficient information on pharmacologic properties of medication, medication side effects, relationship dynamics, and structural problems (Jacobs et al., 2007).
Effects of Medical Errors and Adverse Events
The burdens of medical errors and adverse events to patients, health profession-als, and to the healthcare organizations and other agencies is complex and may be described in terms of financial and non-financial effects.

Application of Quality Management in Promoting Patient Safety
97
Effects on Patients
A medical error may result in a serious harm to a patient, such as death, disability, or additional prolonged treatment (Northcott et al., 2008). Recent evidence shows that the number of premature deaths from preventable harm to patients in the US is estimated to be more than 400,000 per year. Besides, serious harm were found to be 10- to 20-fold more common than lethal harm (James, 2013).
Effects on Health Professionals
Health professionals are also prone to the consequences of medical errors they com-mitted during service delivery. Job-related emotional and psychosocial problems such as sleep disturbance, anxiety or fear of committing future errors, increased caution, loss of confidence, unnecessary security measures while performing du-ties, worsening of professional-patient relations, and loss of social trust and harm to reputation have been commonly identified adverse events on health professionals (Stangierski, 2012; Waterman, et al., 2007). These intense emotional distresses can lead to increased risk of burnout and depression (Schwappach and Boluarte, 2009). This condition leads to dissatisfaction and fatigue and keeps the vicious cycle of further error that causes AEs on patients.
The consequences of medical errors are usually prosecuted under the tort sys-tem. The tort system seeks to deter negligence by monetarily punishing negligent providers and compensating the injured parties with those monies. Evidence from US showed that about 7.4% of physicians had a malpractice claim, of which 1.6% of the claim led to a payment. However, the proportion of malpractice claim varied by specialty ranging from 2.6% claim in psychiatry to 19.1% in neurosurgery. By the age of 65 years, about 75% of physicians in low-risk specialties had faced a malpractice claim compared to 99% of physicians in high-risk specialties. The mean indemnity payment was about $274,887. The mean payments ranged from $117,832 for dermatology to $520,923 for pediatrics (Jena et al., 2011).
Effects on Healthcare Organizations
Despite the increasing commitment of healthcare managers and professionals to improve quality and reduce the likelihood of the human errors, the consequences of medical errors to healthcare facilities are yet very high. A pilot study on medical error reporting information system (MERIS) that engaged physicians, hospitals, citizens and various users in Greece found 35 adverse events in a public hospital, with about 12 additional hospital days and an extra healthcare cost of €12,000 per

Application of Quality Management in Promoting Patient Safety
98
adverse event or of about €312,000 per annum for intensive care unit (ICU) costs only (Riga, et al., 2015).
In US the total annual cost of measurable medical errors was about $985 mil-lion in 2008 and just over $1billion in 2009. The median cost of $892 per error to hospitals in 2008 increased to $939 in 2009. Medical errors directly affect patient outcomes and hospitals’ profit as the costs related to preventable medical errors may not be reimbursed. However, Mello, et al. (2007) reported that hospitals bear only about 22 per cent of the costs analyzing 465 hospital adverse events.
Approaches to Improve Health Care Quality and Safety
The negative consequence of medical errors on patients, healthcare personnel and healthcare organizations forces managers and practitioners to analyze the causes of medical errors and implement comprehensive preventative programs to reduce their occurrence. Both reactive and proactive methods have been applied to prevent or handle errors. However, reactive methods are blamed for focusing on events rather than processes. The proactive methods have been viewed positively and more readily accepted by clinicians as they focus on the entire process rather than mainly on errors.
In the past two decades, the acknowledgement of medical errors, leading to patient injury and even death, has generated potential healthcare legislation and consumer awareness about integrating quality into healthcare services. Concepts like clinical audit, continuous professional development, peer reviews, clinical governance and accreditation are examples of attempts to monitor and improve quality of healthcare services. However, interventions to reduce medical errors in the past decade have not been largely effective (McLean, 2015).
Quality management is a potential way to improve systems and procedures by using scientific methods to achieve an optimum outcome, i.e. quality services, customer satisfaction and better performance (Mosadeghrad, 2005). Quality has become an increasingly predominant part of our lives. People are constantly look-ing for quality products and services. Improving systems, structures and processes results in quality products.
Quality Healthcare
Quality, because of its subjective nature and intangible characteristics, is difficult to define. Definitions vary depending on whose perspective is taken and within which context it is considered. Quality, therefore, has been defined as ‘value’ (Feigenbaum, 1951); ‘excellence’ (Peters and Waterman, 1982); ‘conformance to specifications’ (Gilmore, 1974); ‘conformance to requirements’(Crosby, 1992); ‘fitness for use’

Application of Quality Management in Promoting Patient Safety
99
(Juran, 1988); loss avoidance (Taguchi, 1979) and ‘meeting and/or exceeding cus-tomers’ expectations’ (Parasuraman et al., 1985).
Healthcare service quality is even more difficult to define and measure than in other sectors. Distinct healthcare industry characteristics such as intangibility, heterogeneity and simultaneity make it difficult to define and measure quality (Mo-sadeghrad, 2014). Healthcare service is an intangible product and cannot physically be touched, felt, viewed, counted or measured like manufactured goods. Healthcare service quality depends on service process and customer and service provider in-teractions. Some healthcare quality attributes such as timeliness, consistency, and accuracy are hard to measure beyond a subjective assessment by the customer. It is often difficult to reproduce consistent healthcare services. Healthcare services can differ between producers. This ‘heterogeneity’ can occur because different profession-als (e.g., physicians, nurses, etc.) deliver the service to patients with varying needs. Quality standards are more difficult to establish in service operations. Healthcare professionals provide services differently because factors such as experience, indi-vidual abilities and personalities vary (McLaughlin and Kaluzny, 2006). Healthcare services are simultaneously produced and consumed and cannot be stored for later consumption. This makes quality control difficult because the customer cannot judge ‘quality’ prior to purchase and consumption. Unlike manufactured goods, it is less likely to have a final quality check in health sector. Therefore, healthcare outcomes cannot be guaranteed.
Donabedian(1980:5) defined healthcare quality as ‘the application of medical science and technology in a manner that maximizes its benefit to health without correspondingly increasing the risk’. He distinguishes three components of quality:
1. Technical quality,2. Interpersonal quality, and3. Amenities.
Technical quality relates to the effectiveness of care in producing achievable health gain. Interpersonal quality refers to the extent of accommodation of patient needs and preferences. Finally, amenities include features such as comfort of physical surroundings and attributes of the organization of service provision. Subsequently, Donabedian (1988) proposed the triad of structures, processes and outcomes as a framework for assessing quality of care. Structure refers to the attributes of the set-tings in which care is provided. It includes resources, staff and equipment. Process covers all aspects of delivering care and is related to interaction within and between practitioners and patients. Outcome focuses on the end result or the effect of the care provided.

Application of Quality Management in Promoting Patient Safety
100
Øvretveit (2009) defines quality care as the ‘Provision of care that exceeds patient expectations and achieves the highest possible clinical outcomes with the resources available’ (p.4). He developed a system for improving the quality of healthcare based on three dimensions of quality: professional, client and management qual-ity. Professional quality is based on professionals’ views of whether professionally assessed consumer needs have been met using correct techniques and procedures. Client quality is whether or not direct beneficiaries feel they get what they want from the services. Management quality is ensuring that services are delivered in a resource-efficient way.
Mosadeghrad (2012) in an attempt to measure healthcare service quality identi-fied 182 attributes of quality of healthcare services interviewing 700 healthcare stakeholders. The identified attributes of quality healthcare were grouped into five dimensions: efficacy, effectiveness, efficiency, environment and empathy (5Es). Efficiency refers to the extent to which resources are used well in achieving a given result. It shows the ratio of the benefits of services to the associated costs of producing those services. ‘Effectiveness’ and ‘efficacy’ of care refer to the degree to which desired results and outcomes of care are achieved. The former refers to meeting customer expectations and the latter deals with the extent to which the provider’s objective of providing the service has been achieved. Tangible attributes of healthcare services (Environment) refer to the physical facilities (e.g. structure, building, equipment) and personnel (quantity and quality) that create the capacity to provide healthcare services. Empathy refers to the ability of understanding and caring the healthcare setting provides its customers.
Mosadeghrad (2013a) defined quality healthcare as “Consistently delighting the patient by providing efficacious, effective and efficient healthcare services according to the latest clinical guidelines and standards, which meet patient needs and satisfies providers”. He argues that Eight Quality “Rights” should be integrated in the healthcare services to be considered high quality. Thus, quality healthcare means “Providing the right healthcare services in a right way in the right place at the right time by the right provider to the right individual for the right price to get the right results”.
Quality Management
Quality management migrated into the healthcare sector from the manufacturing sector of the economy during the 1980s. Consequently, in the last 30 years, many healthcare organizations utilized various industrial quality management strategies and techniques such as Continuous Quality Improvement, Total Quality Manage-ment, Business Process Reengineering, Quality function deployment, Benchmark-ing, Six Sigma, Five S, Balanced Score Card and lean production to improve the

Application of Quality Management in Promoting Patient Safety
101
quality of outcomes and efficiency of healthcare service delivery (Mosadeghrad and Ferlie, 2016).
Quality management enables healthcare organizations to identify customer re-quirements to deliver appropriate care, benchmark for best practices and improve processes to reduce the frequency and severity of medical errors. Implementation of Quality management will lead to improved employee collaboration, better employee morale, improved interdisciplinary working relationships, improved consistency of standards, higher quality patient care, reduced patient complaints, improved patient satisfaction, improved cost effectiveness,and increased productivity and profitability (Alexander et al., 2006; and Macinati, 2008).
A Practical Method for Improving Quality and Safety of Healthcare Services
Healthcare organizations can learn a great deal from industrial experiences of quality improvement and error prevention. Industrial management strategies and techniques can be adopted, adapted and implemented in health sector for enhancing the productivity and serve better the customers (Mosadeghrad and Ferlie, 2016).
Healthcare professionals are working with complex and complicated processes and technologies and high levels of uncertainty which can lead to medical errors. Therefore, managers should manage healthcare organizations through a compre-hensive framework and assess and evaluate the structures, processes and outcomes of healthcare services and continuously improve the quality and safety of services. A framework for improving healthcare quality and safety was proposed in Figure 1. Excellent results with respect to patients, employees and organization are achieved
Figure 1. A conceptual framework for improving healthcare quality and safetySource: Mosadeghrad 2013b

Application of Quality Management in Promoting Patient Safety
102
through leadership and management, planning, quality culture, education and training, employee management, patient management, resource management, and process management”.
Quality management enablers are categorized into primary (initial) enablers (i.e., employee management, patient management, resource management and process management) and secondary (supportive) enablers (i.e., leadership and manage-ment, planning, education and training and creating a quality culture). Healthcare professionals are not always directly responsible for medical errors and adverse events. Rather, dysfunctional and faulty systems are the reasons for delivery of unsafe, poor quality healthcare services. System or latent errors (i.e., organizational and managerial policies, working environment, equipment, and workload) influence the healthcare professionals to commit some forms of active errors (e.g., mistakes, negligent, incompetence).
Managers drive the organizations towards quality. Leadership is a key facilitator in establishing, fostering, nurturing and promoting a culture of quality and safety (Yates et al., 2005; Blake et al., 2006). Top-down authoritative leadership style must be replaced with a more supportive, democratic, charismatic and participative style that allows employees’ involvement in quality management programmes to improve their performance. Top management must create clear quality mission and vision for employees, from the boardroom to the frontline, and inspire them to continu-ously improve the quality and safety of their outcomes.
Quality improvement can only result from planned management actions. A well-defined plan for improving the quality and safety of healthcare services (time-frame, resources, training and supportive organizational structure) is important. Education and training are critical and help develop employees’ capabilities on a continuous basis. All those involved in patient care require educating and training about er-rors, their causes and prevention. Training and education secure commitment and behavioral change toward continuous quality improvement.
Preventing poor care depends on the culture and the values of healthcare provid-ers. Successful quality management requires building a supportive organizational culture. Improving healthcare quality and safety can be achieved by establishing a culture of trust, empowerment, teamwork, collaboration, cooperation and continu-ous improvement in healthcare organizations (Mosadeghrad, 2006). This culture is characterized by honesty, open, flexible, and respectful relationships, transparent error communication, and a systems approach to medical error prevention and sus-tained improvements in patient safety. Such a culture recognizes errors as system failures rather than individual failures.

Application of Quality Management in Promoting Patient Safety
103
Humans always err. Every health professional, as a human being, has the poten-tial to commit some forms of medical errors (Guillod, 2013). The responsibility for safety should be shared by all healthcare personnel. Well-treated staff treat patients well. Employee empowerment, commitment and engagement in quality manage-ment programs are essential in creating a culture of safe, effective, responsive and compassionate care, improving patient safety and preventing medical errors. The collaboration and teamwork among healthcare providers are crucial due to the complex nature of disease processes, treatments and technologies. The shortage of qualified healthcare providers is a key structural issue that impacts patient safety. Workload forces professionals to rely more on their memories to perform important actions and hinders effective communication among healthcare personnel. These conditions are likely to create an environment for unsafe processes. For example, doctors who work 24-hour shifts were found to be accountable for making 36% more serious medical errors in the care of their patients compared to doctors not doing extended shift work (Jha, et al., 2010).
Customer focus is the foundation of the quality management philosophy. The patient is the only reason for the existence of a healthcare institution. Healthcare practitioners should be more patient-centered, identify patients’ needs and meet them and show more caring and compassion. They should value patients, create a healing environment and promote their health and well being. Patients should be empowered and allowed to participate in their care decisions.
Healthcare managers should allocate necessary resources to quality improve-ment projects to be continued successfully. Collecting timely, reliable and relevant data and information from both inside and outside the organization for assessing, improving and evaluating purposes are fundamental. Such information is necessary for the effective resources usage, identification of patients’ requirements, evaluat-ing the effectiveness and efficiency of the operations and determining the cause of quality problems.
Quality management focuses on studying, understanding and improving the work processes to reduce variations and errors and enhance productivity. Process management involves defining, planning, optimizing and controlling the processes. Patient safety initiatives should focus more on process improvements affecting or-ganizational, technical, and human factors. Figure 2 shows an eight-step approach to sustain quality and safety of healthcare services through process management. These steps include:

Application of Quality Management in Promoting Patient Safety
104
1. Simplify, optimize and standardize the processes2. Develop objectives for processes3. Analyze the processes to identify opportunities for improvement4. Drive solution for substantial improvement5. Plan the change6. Deploy the plan7. Study the effects of implementation8. Act on the results and standardize the result
Simplify, Optimize and Standardize the Processes
Standardized processes, guidelines and protocols and evidence-based best practices lead to a culture of safety (Odwazny et al., 2005). Hence, it is necessary to define and document all core and critical processes that describe what needs to be done to achieve organizational goals. Employees should be trained in process mapping and documenting each step of the process using flowchart diagram. Healthcare processes should be analyzed and optimized to meet patients’ legitimate requirements. Con-sequently, processes should be simplified, standardized, stabilized and optimized to reduce variation and wasted steps and achieve high reliability. Processes should be ‘‘mistake-proof’’ and minimize the chances of errors. Evidence-based healthcare practices should be emphasized.
Figure 2. A ten-step approach for quality improvementSource: Mosadeghrad 2013b

Application of Quality Management in Promoting Patient Safety
105
Develop Objectives for Processes
Quality improvement teams should identify the main stakeholders of each core pro-cess, discover their needs and accordingly develop specific objectives for meeting them. Minimizing performance variability and defects should also be considered as an important objective for processes. Key performance indicators (KPIs) should be identified for operational objectives. It is important to identify benchmark standards for KPIs to be able to measure the compliance of processes with those standards.
Analyze the Processes to Identify Opportunities for Improvement
The next step is to analyze the performance of the processes and procedures us-ing KPIs and comparing the results with the predetermined objectives. Measuring KPIs helps quality improvement teams identify opportunities for improvement (e.g., safety problems). Employees should report safety related events. Medical errors and adverse events should be acknowledged and studied so that flawed systems and vulnerable processes can be identified and fixed. An effective reporting sys-tem should be developed as a medium of learning from the errors and modifying behaviors appropriately.
Employees including medical and nursing staff must value learning. They should learn from their mistakes and seek opportunities for performance improvement. In addition, using computerized reviews are more effective and efficient. According to Bates and colleagues (1994), more than 50%, and up to 89%, of adverse events can be identified electronically. A blame-free error-reporting and non punitive atmosphere should be created. The presence of a strong leadership supported by organizational commitment and individual accountability is essential in driving these changes. Organizational culture should be changed to increase employees’ comfort in report-ing errors. The incident reporting rates can be improved by providing feedback to employees through applying the necessary changes.
Drive Solution for Substantial Improvement
Quality improvement teams must understand the causes of the problem (e.g. medi-cal errors and adverse events) to develop solutions. Once the specific problem has been identified, its possible causes should be determined by using a cause and effect (Fishbone or Ishikawa) diagram and brainstorming. Root Cause Analysis (RCA) and Healthcare Failure Mode Effect Analysis (HFMEA) can also be used for process analysis. Quality improvement teams can use RCA to examine the underlying con-tributors to an adverse event and investigate further medical errors and near misses and take corrective actions.

Application of Quality Management in Promoting Patient Safety
106
As the quality improvement team matures, more preventive and proactive risk management techniques can be used for identifying and improving potentially unsafe processes to prevent errors. HFMEA is a proactive technique for error detection and reduction. This technique was initially introduced within the aerospace industry in the1960s. The application of this approach in the healthcare industry dates back to the 1990s for prospective risk analysis of high-risk processes and the prevention of medication errors. Finally, the quality improvement teams can use focus groups with personnel, customers and suppliers to find the most cost-effective solutions to remove the cause of the problem.
Plan the Change
A detailed action plan should be developed that identifies achievable targets within acceptable timelines. The action plan describes in great detail exactly how solu-tions will be implemented to accomplish the objectives developed earlier in this process. The plan should also describe the project’s process and how the tasks will be completed.
Deploy the Plan
Quality improvement teams should then implement the intervention plan to resolve the problem.
Study the Effects of Implementation
The implementation of intervention plan should be reviewed to measure the results and compare measured results against the pre-defined performance indicators to assess the actual quality situation.
Act on the Results and Standardize the Result
Appropriate actions required to improve the process must be taken to close the gaps between the required and actual performance. A revised flowchart should be drawn as it should work from now on. The changes should be communicated to the employees, customers and suppliers involved.

Application of Quality Management in Promoting Patient Safety
107
CONCLUSION, FUTURE DIRECTIONS AND RECOMMENDATIONS
Although medical interventions benefit patients, they can also cause harm. Generally, medical errors pose negative consequences on patients, healthcare providers, and organizations. The consequences of medical errors and adverse events to health-care organizations is substantial and, to a large extent, avoidable. The emphasis should be on preventing preventable medical errors and adverse events and improving patient safety rather than relying on the perfectionist view of professionalism that assumes qualified health professionals commit no medical errors.
Risk management and quality management help avoid and prevent injuries and adverse outcomes stemming from the process of health care delivery, minimize deviations and variations from accepted standards of medical practices and reduce consequently healthcare expenditure. Healthcare providers particularly clinicians should be equipped with necessary resources, standardized procedures, education and training, and timely and robust information to achieve quality and patient safety. A system-wide approach and a blame-free environment, aimed at better organizational performance, lead to much better results than focusing on individuals. Furthermore, use of technology, information accessibility, evidence-based practices, communication skills, multi-professional team-work, patient collaboration, managing uncertainties and functional monitoring and evaluation are necessary for patient safety within healthcare organizations.

Application of Quality Management in Promoting Patient Safety
108
REFERENCES
Alexander, J. A., Weiner, B. J., & Griffith, J. (2006). Quality improvement and hos-pital financial performance. Journal of Organizational Behavior, 27(7), 1003–1029. doi:10.1002/job.401
Baker, G. R. (2004). The Canadian Adverse Events Study: The incidence of adverse events among hospital patients in Canada. Canadian Medical Association Journal, 170(11), 1678–1686. doi:10.1503/cmaj.1040498 PMID:15159366
Bates, D. W., ONeil, A. C., Boyle, D., Teich, J., Chertow, G. M., Komaroff, A. L., & Brennan, T. A. (1994). Potential identifiability and preventability of adverse events using information systems. Journal of the American Medical Informatics Associa-tion, 1(5), 404–411. doi:10.1136/jamia.1994.95153428 PMID:7850564
Blake, S. C., Kohler, S., Rask, K., Davis, A., & Naylor, D. V. (2006). Facilitators and barriers to 10 national quality forum safe practices. American Journal of Medical Quality, 21(5), 323–334. doi:10.1177/1062860606291781 PMID:16973949
Bonney, W. (2013). Medical errors: Moral and ethical considerations. Journal of Hospital Administration, 3(2), 80–88. doi:10.5430/jha.v3n2p80
Choi, I., Lee, S., Flynn, L., Kim, C. M., & Suh, D. C. (2016). Incidence and treatment costs attributable to medication errors in hospitalized patients. Research in Social & Administrative Pharmacy, 12(3), 428–437. doi:10.1016/j.sapharm.2015.08.006 PMID:26361821
Crosby, P. (1992). Quality is free. New York: McGraw-Hill.
David, G., Gunnarsson, C. L., Waters, H. C., Horblyuk, R., & Kaplan, H. S. (2013). Economic Measurement of Medical Errors Using a Hospital Claims Database. Value in Health, 16(2), 305–310. doi:10.1016/j.jval.2012.11.010 PMID:23538182
Donabedian, A. (1980). The definition of quality and approaches to its assessment. Ann Arbor: Michigan Health Administration Press.
Donabedian, A. (1988). The quality of care: How can it be assessed? Jour-nal of the American Medical Association, 260(12), 1743–1748. doi:10.1001/jama.1988.03410120089033 PMID:3045356
Feigenbaum, A. V. (1951). Quality control: Principles, practice, and administra-tion. New York: McGraw-Hill.
Application of Quality Management in Promoting Patient Safety
109
Garrouste-Orgeas, M., Philippart, F., Bruel, C., Max, A., Lau, N., & Misset, B. (2012). Overview of medical errors and adverse events. Annals of Intensive Care, 2(1), 2. doi:10.1186/2110-5820-2-2 PMID:22339769
Gilmore, H. L. (1974). Product conformance. Quality Progress, 7(5), 16–19.
Grober, E. D., & Bohnen, J. M. A. (2005). Defining medical error. Canadian Journal of Surgery, 48(1), 39–44. PMID:15757035
Guillod, O. (2013). Medical error disclosure and patient safety: Legal aspects. Journal of Public Health Research, 2(3), 182–185. doi:10.4081/jphr.2013.e31 PMID:25170502
Hemingway, M. W., OMalley, C., & Silvestri, S. (2015). Safety culture and care: A program to prevent surgical errors. AORN Journal, 101(4), 404–415. doi:10.1016/j.aorn.2015.01.002 PMID:25835006
Jacobs, S., O’Beirne, M., Derflingher, L. P., Vlach, L., Rosser, W., & Drummond, N. (2007). Errors and adverse events in family medicine: Developing and validating a Canadian taxonomy of errors. Canadian Family Physician Medecin de Famille Canadien, 53(2), 270–276. PMID:17872644
James, J. T. (2013). A new, evidence-based estimate of patient harms associ-ated with hospital care. Journal of Patient Safety, 9(3), 122–128. doi:10.1097/PTS.0b013e3182948a69 PMID:23860193
Jena, A. B., Seabury, S., Lakdawalla, D., & Chandra, A. (2011). Malpractice Risk According to Physician Specialty. The New England Journal of Medicine, 365(7), 629–636. doi:10.1056/NEJMsa1012370 PMID:21848463
Jha, A. K., Prasopa-Plaizier, N., Larizgoitia, I., & Bates, D. W. (2010). Patient safety research: An overview of the global evidence. Quality & Safety in Health Care, 19(1), 42–47. doi:10.1136/qshc.2008.029165 PMID:20172882
Juran, J. (1988). Quality control handbook (4th ed.). New York: McGraw-Hill.
Kalra, J., Kalra, N., & Baniak, N. (2013). Medical error, disclosure and patient safety : A global view of quality care. Clinical Biochemistry, 46(13-14), 1161–1169. doi:10.1016/j.clinbiochem.2013.03.025 PMID:23578740
Kohn, L. T., Corrigan, J. M., & Molla, S. (1999). To Err Is Human. Medicine, 126(November), 312.

Application of Quality Management in Promoting Patient Safety
110
Leape, L. L., Brennan, T. A., Laird, N., Lawthers, A. G., Localio, A. R., Barnes, B. A., & Hiatt, H. et al. (1991). The nature of adverse events in hospitalized pa-tients. The New England Journal of Medicine, 324(6), 377–384. doi:10.1056/NEJM199102073240605 PMID:1824793
Macinati, M. S. (2008). The relationship between quality management systems and organisational performance in the Italian National Health Service. Health Policy (Amsterdam), 85(2), 228–241. doi:10.1016/j.healthpol.2007.07.013 PMID:17825941
McLaughlin, C. P., & Kaluzny, A. D. (2006). Continuous quality improvement in health care (3rd ed.). Jones & Bartlett Publishers.
McLean, T. R. (2015). Why the distribution of medical errors matters. American Journal of Surgery, 210(1), 188–192.
Mello, M. M., Studdert, D. M., Thomas, E. J., Yoon, C. S., & Brennan, T. A. (2007). Who pays for medical errors? An analysis of adverse event costs, the medical liability system, and incentives for patient safety improvement. Journal of Empirical Legal Studies, 4(4), 835–860. doi:10.1111/j.1740-1461.2007.00108.x
Miller, M. R., Robinson, K. A., Lubomski, L. H., Rinke, M. L., & Pronovost, P. J. (2007). Medication errors in paediatric care: A systematic review of epidemiology and an evaluation of evidence supporting reduction strategy recommendations. Quality & Safety in Health Care, 16(2), 116–126. doi:10.1136/qshc.2006.019950 PMID:17403758
Mosadeghrad, A. M. (2005). A survey of total quality management in Iran: Barriers to successful implementation in health care organizations. International Journal of Health Care Quality Assurance Incorporating Leadership in Health Services, 18(3), 12–34. doi:10.1108/13660750510611189
Mosadeghrad, A. M. (2006). The impact of organizational culture on the success-ful implementation of Total Quality Management. TQM Journal, 18(6), 606–625. doi:10.1108/09544780610707101
Mosadeghrad, A. M. (2012). A conceptual framework for quality of care. Mat Soc Med, 24(4), 251–261. doi:10.5455/msm.2012.24.251-261 PMID:23922534
Mosadeghrad, A. M. (2013a). Healthcare service quality: Towards a broad defini-tion. International Journal of Health Care Quality Assurance, 26(3), 203–219. doi:10.1108/09526861311311409 PMID:23729125
Application of Quality Management in Promoting Patient Safety
111
Mosadeghrad, A. M. (2013b). Verification of a quality management theory: Us-ing a Delphi study. International Journal of Health Policy and Management, 1(4), 261–271. doi:10.15171/ijhpm.2013.55 PMID:24596883
Mosadeghrad, A. M. (2014). Factors influencing health care service quality. Inter-national Journal of Health Policy and Management, 3(2), 77–89. doi:10.15171/ijhpm.2014.65 PMID:25114946
Mosadeghrad, A. M., & Ferlie, E. (2016). Total Quality Management in Healthcare. In A. Ortenblad, C. Abrahamson Lofstrom, & R. Sheaff (Eds.), Management in-novations for healthcare organizations: adopt, abandon or adapt? (pp. 378–396). Routledge.
Northcott, H., Vanderheyden, L., Northcott, J., Adair, C., McBrien-Morrison, C., Norton, P., & Cowell, J. (2008). Perceptions of preventable medical errors in Al-berta, Canada. International Journal for Quality in Health Care, 20(2), 115–122. doi:10.1093/intqhc/mzm067 PMID:18158295
Odwazny, R., Hasler, S., Abrams, R., & McNutt, R. (2005). Organizational and cultural changes for providing safe patient care. Quality Management in Health Care, 14(3), 132–143. doi:10.1097/00019514-200507000-00002 PMID:16027591
Øvretveit, J. (2009). Does improving quality save money? A review of evidence of which improvements to quality reduce costs to health service providers. London: The Health Foundation.
Parasuraman, A., Zeithaml, V. A., & Berry, L. L. (1985). A conceptual model of service quality and its implications for future research. Journal of Marketing, 49(4), 41–50. doi:10.2307/1251430
Peters, T., & Waterman, R. (1982). In search of excellence: lessons from America’s best run companies. New York: Harper and Rowe.
Reason, J. (1990). Human error. Cambridge, UK: Cambridge University Press. doi:10.1017/CBO9781139062367
Riga, M., Vozikis, A., Pollalis, Y., & Souliotis, K. (2015). Medical Error Reporting Information System as an innovative patient safety intervention : A health policy perspective. Health Policy (Amsterdam), 119(4), 539–548. doi:10.1016/j.health-pol.2014.12.006 PMID:25554702

Application of Quality Management in Promoting Patient Safety
112
Rothschild, J. M., Landrigan, C. P., Cronin, J. W., Kaushal, R., Lockley, S. W., Burdick, E., & Bates, D. W et al.. (2005). The Critical Care Safety Study: The in-cidence and nature of adverse events and serious medical errors in intensive care. Critical Care Medicine, 33(8), 1694–1700. doi:10.1097/01.CCM.0000171609.91035.BD PMID:16096443
Schwappach, D. L., & Boluarte, T. A. (2009). The emotional impact of medical error involvement on physicians: A call for leadership and organizational accountability. Swiss Medical Weekly, 139(1), 9. PMID:18951201
Stangierski, A., Warmuz-Stangierska, I., Ruchala, M., Zdanowska, J., Glowacka, M. D., Sowinski, J., & Ruchala, P. (2012). Short communication: Medical errors-not only patients problem. Archives of Medical Science, 8(3), 569–574. doi:10.5114/aoms.2012.29539 PMID:22852017
Taguchi, G. (1979). Introduction to Off-line Quality Control. Magaya, Japan: Central Japan Quality Control Association.
Thomas, E. J., & Petersen, L. A. (2003). Measuring errors and adverse events in health care. Journal of General Internal Medicine, 18(1), 61–67. doi:10.1046/j.1525-1497.2003.20147.x PMID:12534766
Van Den Bos, J., Rustagi, K., Gray, T., Halford, M., Ziemkiewicz, E., & Shreve, J. (2011). The $17.1 billion problem: The annual cost of measurable medical errors. Health Affairs, 30(4), 596–603. doi:10.1377/hlthaff.2011.0084 PMID:21471478
Walshe, K. (2000). Adverse events in health care: Issues in measurement. Quality in Health Care : QHC, 9(1), 47–52. doi:10.1136/qhc.9.1.47 PMID:10848370
Waterman, A. D., Garbutt, J., Hazel, E., Dunagan, W. C., Levinson, W., Fraser, V. J., & Gallagher, T. H. (2007). The emotional impact of medical errors on practic-ing physicians in the United States and Canada. Joint Commission Journal on Quality and Patient Safety, 33(8), 467–476. doi:10.1016/S1553-7250(07)33050-X PMID:17724943
Yates, G. R., Bernd, D. L., Sayles, S. M., Stockmeier, C. A., Burke, G., & Merti, G. E. (2005). Building and sustaining a systemwide culture of safety. Journal of Quality and Patient Safety, 31(12), 684–689. doi:10.1016/S1553-7250(05)31089-0 PMID:16430021

Copyright ©2017, IGI Global. Copying or distributing in print or electronic forms without written permission of IGI Global is prohibited.
DOI: 10.4018/978-1-5225-2337-6.ch005
Chapter 5
113
The Perspectives of Medical Errors in the Health Care Industry
ABSTRACT
This chapter presents the overview of medical errors; drug prescription errors and prescribing; the overview of medical error disclosure; medical errors and telemedi-cine; medical errors and medical education; the overview of nursing medication er-rors; and the aspects of medical errors in the health care industry. Reducing medical errors, increasing patient safety, and improving the quality of health care are the major goals in the health care industry. Medical errors are caused by mistakes in drug prescription, dosing, and medical administration in inpatient and outpatient settings. Heath care-related guidelines, institutional safety practices, and modern health care technologies must be applied in hospitals, clinics, and medical offices to reduce the occurrence of medical errors. The chapter argues that understanding the perspectives of medical errors has the potential to enhance health care performance and reach strategic goals in the health care industry.
Kijpokin KasemsapSuan Sunandha Rajabhat University, Thailand

The Perspectives of Medical Errors in the Health Care Industry
114
INTRODUCTION
Health care organizations face a wide range of internal and external factors that enable their ability to provide safe, quality, and reliable health care services (Pate & Swofford, 2016). Medical errors are one of the major threats for patient safety in all countries (Pazokian, Tafreshi, & Rassouli, 2014). Medical errors remain the most commonly occurring error in the health care area (Absulem & Hardin, 2011). The avoidable sources of medical errors include the failure to take a biopsy despite suspicious clinical findings, or incorrect clinicopathological correlations resulting in deleterious effects for the patient (Lehmann, Wesselmann, Weber, & Sment-kowski, 2015). Clinicians involved in medical errors can experience significant distress (McLennan et al., 2015). The review and analysis of medical errors have emphasized their preventable potential for reoccurrence (Olaniyan, Ghaleb, Dhil-lon, & Robinson, 2015).
There is evidence that providers are reluctant to make the compensation for medical errors until a lawsuit is filed (Gawande, 2007). The rising health care costs, partially due to preventable medical errors, lead many hospitals to redouble their process improvement efforts (Gowen, McFadden, & Settaluri, 2012). The impact of digitization has important effect on teleexpertise, where a medical professional can remotely ask health care advices through the utilization of information and communication technology (ICT) toward providing medical treatment to a patient in remote environment (Doumbouya, Kamsu-Foguem, Kenfack, & Foguem, 2015). However, the outcome of such advice remotely obtained can lead to medical errors. It is important to determine whether the causes of the errors can be avoidable or not for the purposes of establishing the truth and assuring justice for the victims of medical errors (Doumbouya et al., 2015).
Providing effective health care service gains an increasing attention over the past few years (Chetouane & Ibraheem, 2016). There is an increasing need for the process improvement in health care systems regarding quality, safety, effectiveness, suitability, speed, efficiency, and uniformity (Institute of Medicine, 2001). Health care managers can make a major impact on safety culture development by promot-ing the patient safety-related strategies and fostering their employees’ motivation to implement the health care improvement programs at the individual and departmental levels (Kagan & Barnoy, 2013). To improve patient safety, hospital managers should establish the reporting mechanisms at the national and international levels (Brady, Malone, & Fleming, 2009).

The Perspectives of Medical Errors in the Health Care Industry
115
The chapter is based on a literature review of medical errors. The extensive lit-erature of medical errors provides a contribution to practitioners and researchers by presenting the advanced issues of medical errors in order to minimize the medical errors in global health care.
BACKGROUND
For years, health care experts have recognized that medical errors exist and com-promise health care quality (Vozikis, 2012). Errors are defined as any deviation from established standard operating procedures (Maskens et al., 2014). Studies of medical errors demonstrate that errors and adverse events are common in hospitals (Shah et al., 2009). Preventable error, malpractice, and complications can be con-sidered as adverse events (Zientek, 2010). The adverse events rates and medical lawsuits are on the rise, whereas many medical errors are mostly due to negligence or malpractices which are preventable (Wong & Balasingam, 2013). Being able to understand health information and make decisions from that information is vital to patients’ well-being (Kasemsap, 2017a).
Medical errors are the medical mistakes that can lead to serious consequences and even death of patients (Pazokian et al., 2014). Ammouri et al. (2015) indicated that patient safety is considered to be crucial to health care quality and is one of the major parameters monitored by all health care organizations around the world. Patient safety is a central issue of health care provision (Lehmann et al., 2015). Many quality improvement education programs have been introduced over the last decade with the purpose of enhancing patient safety (Gordon, Darbyshire, & Baker, 2012).
Patient safety remains a global challenge affecting many patients throughout the world (Schwappach, 2014). There are various approaches toward improving health care provision and patient safety in the health care industry (Lehmann et al., 2015). Critically ill patients need life saving treatments and are often exposed to medications requiring careful titration (Manias, Williams, & Liew, 2012). Improving patient safety hinges on the ability of health care providers to accurately identify, disclose, and report medical errors (Hobgood, Weiner, & Tamayo-Sarver, 2006). Learning and continuous improvement, hospital management support, supervisor expectations, communications about error, teamwork, and hospital handoffs are the major predictors of patient safety culture (Ammouri et al., 2015).

The Perspectives of Medical Errors in the Health Care Industry
116
Medical interventions must account for differences in medical error identifica-tion, disclosure, and reporting by medicine provider type (Hobgood et al., 2006). Palmero et al. (2016) indicated that inexpensive and simple medication interven-tions can improve the intelligibility of prescriptions and reduce medication errors. Targeting the susceptible population groups and the dangerous aspects of the health care systems can be the effective approach to both medical error management and prevention (Olaniyan et al., 2015). In the digital society, there is a shift in the issue of designing and implementing health information system (Doumbouya et al., 2015).
Clinical practitioners play an essential role in the medical error reduction through providing accurate clinical information, procuring high-quality specimens, providing timely follow-up task on test results, effectively communicating on the potentially discrepant diagnoses, and advocating second opinions on the pathological diagnosis in specific situations (Raab & Grzybicki, 2010). Health professionals and patients must prepare themselves to take advantage of the established health care processes that improve the quality of health care service (Doumbouya et al., 2015). High self-efficacy and perceived effectiveness of the specific preventive actions considerably increase the likelihood of participation in medical error prevention (Schwappach & Wernli, 2010).
ADVANCED ISSUES OF MEDICAL ERRORS IN GLOBAL HEALTH CARE
This section provides the overview of medical errors; drug prescription errors and prescribing; the overview of medical error disclosure; medical errors and telemedi-cine; medical errors and medical education; the overview of nursing medication errors; and the aspects of medical errors in the health care industry.
Overview of Medical Errors
Medical errors are the consequence of multiple actions of the whole chain of or-ganizational and individual interactions in which the individual does not have the intention of doing wrong (Garrouste-Orgeas, Flaatten, & Moreno, 2016). Medication errors can occur by patients and their health care providers in any stage of health care pathway (Gavgani, Oskouei, & Salehi, 2015). The ability to decrease medical errors depends on an understanding of the types and patterns of medical errors that occur in various settings (Henneman, Blank, Gattasso, Williamson, & Henneman, 2006). Clinical decisions based on the inaccurate sources of information can lead to medical errors, high treatment costs, and poor patient outcomes (Zaheer, 2015).
The Perspectives of Medical Errors in the Health Care Industry
117
Since the 1970s, scientists have studied clinical decision making in order to im-prove its processes. Clinical decision making is called clinical reasoning, diagnostic reasoning, clinical judgment, and clinical inference (Ge et al., 2012). In scientific context, clinical decision making can be categorized into two modes (i.e., deductive mode and empirical mode). Clinical decision making is a critical aspect of clini-cal performance, having a high impact on quality and safety of care (Lucchiari & Pravettoni, 2012). Regarding deductive mode, when decisions are based on theoreti-cal knowledge of diseases and the mechanisms of different treatments. Regarding empirical mode, when decisions are based on past experiences (Ge et al., 2012).
Different techniques are utilized in clinical decision-making process. The practical techniques include decision trees, Markov models, and simulation. Decision support systems play an important role in medical decision making (Azar & El-Metwally, 2013). Clinical reasoning is an important contributor to the quality of health care, but to achieve this quality of health care, the provided decisions in the clinical rea-soning have to be safe. Goal Structuring Notation (GSN) is proposed to encourage communication among medical professionals and is more suitable for the analysis of medical errors (Doumbouya et al., 2015). Lawson and Daniel (2011) proposed a work in which they attempted to reduce and even eliminate diagnosis errors. The diagnosis errors encountered in health care systems are caused by cognitive errors.
Doumbouya et al. (2015) indicated that two categories of medical errors include process errors and knowledge errors. Process errors cover care system errors coordina-tion, errors due to complementary examinations, such as drug prescription, results’ management, errors related to medications, errors related to non-medications, and communication problems. Knowledge errors involve three concepts (i.e., errors in the execution of clinical tasks, errors in diagnosis, and wrong treatment decision with right diagnosis). Another area where medical errors have been explored is e-health cardiology (Gortzis & Nikiforidis, 2008). In e-health cardiology, two types of knowledge processes include knowledge tracing and knowledge cataloguing. Knowledge tracing demonstrates how a system executes and produces knowledge. Knowledge cataloguing classifies the knowledge that exists within the information system (Gortzis & Nikiforidis, 2008).
Based on knowledge processes, Gortzis and Nikiforidis (2008) proposed an important system (e.g., e-health cardiology environment) to minimize the medical errors in health care systems. Their approach is quite similar to teleexpertise since it allows collaboration among medical professionals. Gortzis and Nikiforidis (2008) achieved their goal by considering both knowledge tracing process and knowledge cataloguing process. Concerning knowledge tracing process that shows how the health care system executes and produces the knowledge, Gortzis and Nikiforidis (2008) demonstrated how the collected data is accepted or rejected. The collected data consists of a set of variables provided by the patients through portable de-

The Perspectives of Medical Errors in the Health Care Industry
118
vices. Each variable is related to the upper threshold and the lower threshold. The developed software performs the first filter by discarding data that is unrelated to the patients and then the data supposed to be valid can be systematically stored in the knowledge base.
Drug Prescription Errors and Prescribing
Prescribing is a complex task and a high-risk area of clinical practice (Brennan & Mattick, 2013). Celebi et al. (2010) indicated that prescribing correctly represents one of the most essential skills of a physician when it comes to patient safety. The prescribing errors that occur in hospitals are a source of health care concern (Tully, 2012). In 2007, the National Patient Safety Agency performed a study demonstrat-ing that errors in prescribing led to nearly 12,000 adverse clinical incidents a year (Davies et al., 2011). Medical errors are common in health care settings, and the prescribing errors are the most common type (Harding, Britten, & Bristow, 2010). The tasks of prescribing, preparation, and administration of drugs are executed within a complex health care system (McDowell, Ferner, & Ferner, 2009). Ross et al. (2009) indicated that the prescribing errors account for a substantial proportion of medication errors and cause the significant medication problems.
Patients observe medical errors in the administration of drugs and they can be a valuable resource in the prevention of medical errors (Schwappach & Wernli, 2010). Drug prescription errors are a common and persistent problem in health care (Armitage, Newell, & Wright, 2010) and can be detrimental to patient care (Lewis et al., 2014). Electronic prescribing has a significant effect on the reduction of the prescribing errors (Shawahna et al., 2011). With the increasing number of adverse effects of drugs and the prescribing errors, the clinical pharmacologist plays an important role in introducing new drugs and in improving the effective use of cur-rent drugs (Williams, 2012).
Health professionals should establish the specific health care goals toward improving health literacy in strategic plans, programs, and educational initiatives (Kasemsap, 2017b). There is a need for more applied learning to develop the skill-based and applied aspects of drug prescribing toward improving the preparedness for drug prescription (Rothwell et al., 2012). National data regarding drug prescrip-tion is required in order to benchmark the independent nurses’ prescribing practices in critical care (Carberry, Connelly, & Murphy, 2013). Insufficient knowledge is a significant factor in the nurses’ drug administration errors (Hsaio et al., 2010).
Active failures are the unsafe acts committed by people who are in contact with the patient or system (Reason, 1990). Active failures take a wide variety of forms, such as slips, lapses, fumbles, mistakes, and procedural violations (Reason, 1990). Medical errors in drug prescription are frequently studied, but analyzing the data

The Perspectives of Medical Errors in the Health Care Industry
119
regarding drug administration is scarce (Niemann et al., 2015). Among all medica-tion errors and adverse drug events, medication administration errors are common (Schwappach & Wernli, 2010). Medication administration errors are reported to occur in critical care settings, and can be associated with severe consequences (Mansour, James, & Edgley, 2012).
Overview of Medical Error Disclosure
Perception and satisfaction of patients with health care services are considered as the important parameters to evaluate the quality and competence of health care provid-ers and the outcomes of their health care services in patients’ health (Dias-Souza, 2016). The disclosure of medical error is useful in raising patient awareness, reducing their suffering, improving the quality of care, and limiting the consequences of the health care failure. Disclosing the medical errors to patients is an important part of patient care (Kaldjian et al., 2007). Kaldjian et al. (2006) indicated that four major domains of facilitating medical error disclosure include responsibility to patient, responsibility to self, responsibility to profession, and responsibility to community.
Effective risk management depends on establishing a reporting culture (Reason, 1997). The underreporting of medical administration errors is a threat to the qual-ity of nursing care (Lin & Ma, 2009). The training and support of medical error disclosure can inform health care staff that the organization appreciates the honesty and integrity (Rathert & Phillips, 2010). Accreditation agencies (e.g., the Joint Commission on Accreditation of Healthcare Organization) encourage hospitals to voluntarily disclose information about medical errors (Rouse & Kaplan, 2008). The Joint Commission on Accreditation of Healthcare Organization has placed a great deal of emphasis on the patient safety-related strategies to reduce patient’s identification errors (Koshy, 2005).
The disclosure of harmful errors to patients is recommended, but appears to be uncommon (White et al., 2011). Regarding medical error disclosure, the implemen-tation of the anonymous reporting system with training is related to a statistically significant increase in the rate of reported medical errors (Taylor, Brownstein, Klein, & Strandjord, 2007). Nordén-Hägg et al. (2012) stated that introducing a web-based system for reporting the dispensing errors has a positive impact on the quantity of medical reports and completeness. Electronic reporting systems are the important components of the patient-safety movement, but are problematic, particularly in capturing information from physicians (Foster, Sidhu, Gadhia, & DeMusis, 2008).
Health care-related risk managers play a crucial role in promoting transparency in health care and enhancing patient safety (Gallagher et al., 2006). The organizational safety culture can encourage the medical error reporting by health care staff and can improve patient safety (Kagan & Barnoy, 2013). Shame and guilt are the subjective

The Perspectives of Medical Errors in the Health Care Industry
120
emotional responses that occur in response to the negative events (e.g., the making of medical mistakes and an experience of mistreatment), and are extensively studied in the field of psychology (Bynum & Goodie, 2014).
Sevdalis et al. (2010) stated that diagnostic errors present a particular challenge for medical error-related reporting systems because they involve clinical reasoning. Medical error reporting can be strengthened by human error theory, capturing a wide range of contributory medication factors to facilitate learning and encourage supportive medication actions (Armitage et al., 2010). Anoosheh et al. (2008) stated that medical outcomes that are identified from the process of practice error manage-ment should promote interventions designed to prevent future practice errors based on the contributory medication factors.
The reporting of near-miss medication events is significantly increased, suggesting that this is a beneficial format for gathering data on this type of medical error (Taylor et al., 2007). Guidance for nurses indicates that all medical errors and near misses should be immediately reported in order to facilitate the development of a learning culture (Haw, Stubbs, & Dickens, 2014). The supervisory discussion, the informal discussion, and near-miss reporting contain important information for improving clinical care (Rosenthal, Cornett, Sutcliffe, & Lewton, 2005). The registration of near misses prevents medical errors with serious consequences and thus improves the quality of care (Bosma, Veen, & Roukema, 2011).
Medical Errors and Telemedicine
Telemedicine is the use of telecommunication systems to deliver health care at a distance. Telemedicine can facilitate the efficient provision of health care services. Telemedicine bridges the challenges often encountered across different service levels including primary care, regional, and national care services, coordination between health care institutions, mobile medicine, medical and medical-social ac-tors, promotion of virtual clustering, and new modalities for collaboration among medical partner organizations (Kamsu-Foguem & Foguem, 2014).
Elkin et al. (2013) described the usability-error ontology to handle medical errors in clinical contexts. The ontology can be employed to help improve the patients’ treatment outcomes while ensuring the interoperability of the medical systems. In their ontology, the top level is categorized into two levels (i.e., cognitive errors and non-cognitive errors) since several medical errors are caused by human being. This work is interesting since it reveals the usability errors in the health information technology (health IT) or its interaction with users. However, the study of Elkin et al. (2013) does not explicitly discuss how medical professionals can collaborate with the important aspect in telemedicine.

The Perspectives of Medical Errors in the Health Care Industry
121
Medical Errors and Medical Education
During the last decade, there has been a drive to improve the medical quality of patient care and prevent the occurrence of avoidable errors (Wong, Levinson, & Shojania, 2012). Accreditation standards and assessment methods, both during training and at end-of-training certification examinations, should explicitly target these medical competencies (Wong et al., 2012). Härkänen et al. (2015) indicated that observing real situations in clinical practice can provide undetected information regarding problems in the medication process. Although it is clear that the cur-riculum in medical schools should encompass quality and safety training to reduce patient safety in health care settings, many medical schools are slow to implement the reforms of medical education that are necessary to accomplish such a goal (DesHarnais & Nash, 2011).
Medical educators should increase exposure to exemplary responses to medical errors and help medical students learn from medical errors toward reducing medical errors in the future (Martinez & Lo, 2008). Training programs and managerial sup-port, focusing on improving patient safety, need to be emphasized to prevent medical errors in the health care industry (Hwang & Hwang, 2011). Use of current health care equipment for medical procedures (e.g., central-line insertion and central-line care) is primarily dependent on the cognition of the health care staff (Bakdash & Drews, 2012). Deficiencies in the prescribing education and training are closely linked to the high frequency of medication errors (Sandilands et al., 2011). Meth-ods for estimating the prevalence of physician dyscompetence include evaluating available data on medical errors, malpractice claims, disciplinary actions, quality control studies, medical record-related review studies, and physician’s performance evaluation (Williams, 2006).
In medical education, medical trainees’ perceptions and attitudes toward medical errors vary depending on whether the severity of outcome and whether the medi-cal error is attributable to an individual or a team (Muller & Ornstein, 2007). Safe prescribing is a core competency in undergraduate medical education (Harding et al., 2010). The lack of preparedness of graduates for medical practice is related to a lack of exposure and preparation for clinical practice (Rothwell et al., 2012). Ac-cepting responsibility for medical errors is recognized as prerequisite to medical education (Mazor, Fischer, Haley, Hatem, & Quirk, 2005).
The integration of simulation into the training of health care professionals pro-vides the health care-related context for decision making and procedural skills in a high-fidelity environment, without having risk to patients (Gardner & Rich, 2014). Medical simulation can be applied in the training efforts to reduce medical errors concerning medical knowledge and patient care (Issenberg, Chung, & Devine, 2011). Medical simulation exhibits the causes of teamwork errors, latent errors, and error-

The Perspectives of Medical Errors in the Health Care Industry
122
producing conditions in emergency medical services (EMS) pediatric care (Lammers, Byrwa, & Fales, 2012). Woodfield et al. (2014) indicated that simulating cases and utilizing real drug charts are the effective methods for improving medical students’ prescribing ability and confidence in medical emergencies.
Overview of Nursing Medication Errors
The nursing error relating to clinical management (NECM taxonomy) provides direc-tion to clinicians and health care managers on various areas in clinical management that are most vulnerable to medical error (Tran & Johnson, 2010). Contributory medication factors to the nurse’s medical errors include the reconciliation of medi-cal errors, the types of drug distribution system, the quality of prescriptions, and the distractions during administration, excessive workloads, and nurse’s medical knowledge (Brady et al., 2009).
Abdi et al. (2015) indicated that nurse managers can contribute to promoting a safety culture by encouraging staff to report medical errors, promoting learning from medical errors, and addressing inter-professional communication problems. When supported by their practice environments, nurses employ practices that can assist in interrupting medical errors before they reach the patients (Flynn, Liang, Dickson, Xie, & Suh, 2012). Nurses should carefully check medical administration in the high-alert situations toward reducing medical errors (Sheu, Wei, Chen, Yu, & Tang, 2009). Effective nursing handover is an opportunity for nurses to prevent medical errors by implementing more risk-aware handover strategies (Drach-Zahavy & Hadid, 2015).
Knowledge about nurses’ error perception is crucial for establishing a sustainable risk management (Habermann, Foraita, & Cramer, 2013). There is a need to decrease the number and severity of medical administration errors, by increasing both nurse awareness and medical error reporting (Kelly & Wright, 2012). Identification of the conditions contributing to medication errors allows clinical nurses and administra-tion systems to eliminate medical errors and to incorporate the changes that create a safer patient environment (Tang, Sheu, Yu, Wei, & Chen, 2007).
Aspects of Medical Errors in the Health Care Industry
Medication errors are a significant cause of morbidity and mortality in hospital-ized patients (Brady et al., 2009). There is an increasing recognition that medical errors cause a global health problem, as many medical errors result in patient harm and increase costs to health care providers (Wheeler & Wheeler, 2005). Medical errors are affected by individual and work environment characteristics (Hwang & Hwang, 2011). Efforts to mitigate risk in the emergency department should include

The Perspectives of Medical Errors in the Health Care Industry
123
the diverse clinical specialties who work in this complex environment, with atten-tion to those health conditions and potential errors with the highest risk (Brown, McCarthy, Kelen, & Levy, 2010).
The analysis of medical error patterns, contributory medication factors, and sug-gestions for error prevention can help reduce the frequency of medication events and improve patient care (Haw & Cahill, 2011). Medical errors have a serious effect on clinicians (McLennan et al., 2015). The implementation of the existing interven-tions at points within the system significantly offers the cost-effective approaches to improving medication safety in primary care (Olaniyan et al., 2015). Promoting the consistency between health care professionals as to what constitutes medica-tion error contributes to the increased accuracy and compliance in the reporting of medical errors, thus creating effective health care policies toward reducing the occurrence of medical errors (Brady et al., 2009).
Measuring medical error typically results in the biased estimates of exposure-disease associations, the severity of the bias, and the nature of the bias concerning medical error patterns (Keogh & White, 2014). The quality function deployment matrix is used to translate the desired improvement in the malpractice costs into both medical decisions and diagnostic tests (Dror & Margol, 2015). The methods of Incident reporting (IR) and failure mode and effective analysis (FMEA) are widely used to detect and analyze the medical errors in health care settings (Daverio et al., 2015).
Computerized medication management systems are found to improve the medica-tion safety (Redley & Botti, 2013). Standardized IT in the health care industry can reduce the preventable errors and increase patient safety (Koshy, 2005). Barcode labels, radio frequency identification tags (RFID), and palm vein-scanning technol-ogy are increasingly utilized in patient identification (Fastman & Kaplan, 2011). RFID solutions can be utilized to reduce the operating costs through decreasing labor costs, enhancing automation, improving the tracing procedure, and prevent-ing the material loss (Kasemsap, 2015a). Concerning health care operations, RFID monitors the operating instruments and medical equipment during procedures to ensure all materials are accounted for (Kasemsap, 2017c).
Medical liability reform is viewed by many physician groups as a method of reducing medical malpractice litigation and lowering health care costs (Pegalis & Bal, 2012). Physicians cannot avoid the responsibilities and liabilities as a profession, when they provide the inappropriate advice to patients (Nakayasu & Sato, 2012). The lack of cooperation among health care providers and the poor continuity of health care significantly contribute to medical errors (Kroll, Singleton, Collier, & Jones, 2008). Medication-ordering error rates are higher for the overnight and post-call physicians, particularly on the medical wards (Hendey, Barth, & Soliz, 2005).

The Perspectives of Medical Errors in the Health Care Industry
124
Many medical errors are reported with the utilization of the paper-based tool than with the existing computerized error-reporting system (Kolovos, Bratton, & Levy, 2008). It can be more effective when the computerization of physicians’ orders links to other computerized systems toward detecting and preventing the medical prescription errors (Shamliyan, Duval, Du, & Kane, 2008). Clinical decision sup-port systems utilize IT to improve the quality of care by supporting the physician’s decision-making process (Laing et al., 2015).
The medication errors found in many hospitals in Australia are the prescription-related ordering errors, dispensing, administration, and medication recording errors (Hodgkinson, Koch, Nay, & Nichols, 2006). Hodgkinson et al. (2006) stated that medical strategies to reduce medical errors include the establishment of comput-erized physician ordering entry systems combined with clinical decision support systems; individual medication supply systems when compared with other dispens-ing systems (e.g., ward stock approaches); the utilization of clinical pharmacists in the inpatient setting; and the checking of medication orders by nurses before dispensing medication.
Workload and lack of medical experience at the current ward are two impor-tant conditions that can lead to medical errors (Seki & Yamasaki, 2006). Health care organizations need to support clinicians in coping with the stress concerning medical errors (McLennan et al., 2015). In order to constitute a practical action to counteract the medical errors, it is necessary to consider major elements (e.g., human, technological, and organizational perspectives) that contribute to the oc-currence of a critical medication event (Smorti, Cappelli, Zarantonello, Tani, & Gensini, 2014). Incorporating the apology into conversations between physicians and patients can address the needs of both parties and can play an important role in the effective resolution of disputes concerning the occurrence of medical errors (Robbennolt, 2009).
FUTURE RESEARCH DIRECTIONS
The classification of the extensive literature in the domains of medical errors will provide the potential opportunities for future research. Telemedicine is the utili-zation of medical information exchanged from one site to another via electronic communications to improve a patient’s clinical health status. Telemedicine offers important benefits (e.g., improved access, cost efficiencies, improved quality, and patient demand). Telemedicine brings the health care value through its ability for the remote visits with patients, immediate access to health care professionals, real-time access to health data, and health monitoring capabilities (Kasemsap, 2017d).

The Perspectives of Medical Errors in the Health Care Industry
125
Electronic health record (EHR) provides the ability to exchange complete health information about a patient in real time. EHR systems are very important in health care settings and have the potential to transform the health care system from a mostly paper-based industry to the one that utilizes the clinical data and other pieces of information to assist the health care providers in delivering the higher quality of care to their patients (Kasemsap, 2017e). Accurate, updated, and thorough information through EHR leads to a higher quality of care, from better diagnoses to reduced medication errors. The integration of health IT into primary care includes a wide variety of electronic methods that are used to manage information about people’s health and health care, for both individual patients and groups of patients. Effec-tive health IT can lower costs, improve efficiency, and reduce medical error, while providing better patient care and service (Kasemsap, 2017f). An examination of linkages among telemedicine, EHR, health IT, TQM, and medical error reduction would seem to be viable for future research efforts.
Quality of performance is the numerical measurement of the performance of an organization or process assessed through measurement of physical products and statistical sampling of the output of processes (Kasemsap, 2014). In order to facilitate quality performance and achieve the effectiveness of the whole quality management system, researchers and managers should develop and maintain their organization’s total quality management (TQM) practices related to quality performance in organi-zation (Kasemsap, 2015b). Implementing Six Sigma within global operations offers a number of benefits, such as the improved customer loyalty, reduced cycle time, better time management, better employee motivation, improved strategic planning, and the reduced risk of defects (Kasemsap, 2016). Successful Lean health care ef-forts result in the measurable improvements in patient outcomes, such as improved quality, less harm due to preventable errors, better access, shorter waiting times, and better service (Kasemsap, 2017g). Recent developments in the robotic age have made robots and robotics more intelligent, affordable, and user-friendly in modern operations, ranging from manufacturing to health care (Kasemsap, 2017h). Reduc-ing medical errors through the applications of TQM, Six Sigma, Lean health care, and robotics would be beneficial for future research directions.

The Perspectives of Medical Errors in the Health Care Industry
126
CONCLUSION
This chapter explained the overview of medical errors; drug prescription errors and prescribing; the overview of medical error disclosure; medical errors and telemedi-cine; medical errors and medical education; the overview of nursing medication errors; and the aspects of medical errors in the health care industry. Reducing medi-cal errors, increasing patient safety, and improving the quality of health care are the major goals in the health care industry. Medical errors are caused by mistakes in drug prescription, dosing, and medical administration in inpatient and outpatient settings. Heath care-related guidelines, institutional safety practices, and modern health care technologies must be applied in hospitals, clinics, and medical offices to reduce the occurrence of medical errors.
Health care organizations must clearly communicate with all health care provid-ers that patient safety is their responsibility, and health care managers must define how the health care organizations deal with the unsafe practitioners toward reducing the medical errors. The perspective to effectively implement a safe medication-use process is the need for the well-defined, consistently applied, and highly standardized system process. The successful approach to the implementation of a safe medication-use process is the effective collaboration among health care leadership, health care providers, and patients. Health care organizations must provide the leadership, expec-tations, training, and structure to promote the coordinated functioning of caregivers and patients to enhance the quality of health care and reduce the medical errors.
Health care providers and health care organizations must adopt a proactive approach to the reduction of medical errors. The technologies and processes of health care systems must be continuously evaluated regarding the potential risks to patient safety. Understanding the perspectives of medical errors is necessary for health care organizations that seek to serve patients, increase health care perfor-mance, strengthen competitiveness, and achieve continuous success in the health care industry. Therefore, it is essential for health care organizations to understand their perspectives of medical errors and develop a strategic plan to regularly check their practical advancements toward minimizing the medical errors in the health care industry. Understanding the perspectives of medical errors has the potential to enhance health care performance and reach strategic goals in the health care industry.

The Perspectives of Medical Errors in the Health Care Industry
127
REFERENCES
Abdi, Z., Delgoshaei, B., Ravaghi, H., Abbasi, M., & Heyrani, A. (2015). The culture of patient safety in an Iranian intensive care unit. Journal of Nursing Management, 23(3), 333–345. doi:10.1111/jonm.12135 PMID:23902287
Absulem, S., & Hardin, H. (2011). Home health nurses’ perceived care errors. Rehabilitation Nursing, 36(3), 98–105. doi:10.1002/j.2048-7940.2011.tb00073.x PMID:21675394
Ammouri, A. A., Tailakh, A. K., Muliira, J. K., Geethakrishnan, R., & Al Kindi, S. N. (2015). Patient safety culture among nurses. International Nursing Review, 62(1), 102–110. doi:10.1111/inr.12159 PMID:25495946
Anoosheh, M., Ahmadi, F., Faghihzadeh, S., & Vaismoradi, M. (2008). Causes and management of nursing practice errors: A questionnaire survey of hospital nurses in Iran. International Nursing Review, 55(3), 288–295. doi:10.1111/j.1466-7657.2008.00623.x PMID:19522944
Armitage, G., Newell, R., & Wright, J. (2010). Improving the quality of drug error reporting. Journal of Evaluation in Clinical Practice, 16(6), 1189–1197. doi:10.1111/j.1365-2753.2009.01293.x PMID:20807298
Azar, A. T., & El-Metwally, S. M. (2013). Decision tree classifiers for automated medical diagnosis. Neural Computing & Applications, 23(7), 2387–2403. doi:10.1007/s00521-012-1196-7
Bakdash, J. Z., & Drews, F. A. (2012). Using knowledge in the world to improve patient safety: Designing affordances in health care equipment to specify a sequential “checklist”. Human Factors and Ergonomics in Manufacturing & Service Industries, 22(1), 7–20. doi:10.1002/hfm.20289
Bosma, E., Veen, E. J., & Roukema, J. A. (2011, November). Incidence, nature and impact of error in surgery. British Journal of Surgery, 98(11), 1654–1659. PMID: 21706475 doi:10.1002/bjs.7594
Brady, A. M., Malone, A. M., & Fleming, S. (2009). A literature review of the individual and systems factors that contribute to medication errors in nursing practice. Journal of Nursing Management, 17(6), 679–697. doi:10.1111/j.1365-2834.2009.00995.x PMID:19694912
The Perspectives of Medical Errors in the Health Care Industry
128
Brennan, N., & Mattick, K. (2013). A systematic review of educational interventions to change behaviour of prescribers in hospital settings, with a particular emphasis on new prescribers. British Journal of Clinical Pharmacology, 75(2), 359–372. doi:10.1111/j.1365-2125.2012.04397.x PMID:22831632
Brown, T. W., McCarthy, M. L., Kelen, G. D., & Levy, F. (2010). An epidemiologic study of closed emergency department malpractice claims in a national database of physician malpractice insurers. Academic Emergency Medicine, 17(5), 553–560. doi:10.1111/j.1553-2712.2010.00729.x PMID:20536812
Bynum, W. E. IV, & Goodie, J. L. (2014). Shame, guilt, and the medical learner: Ignored connections and why we should care. Medical Education, 48(11), 1045–1054. doi:10.1111/medu.12521 PMID:25307632
Carberry, M., Connelly, S., & Murphy, J. (2013). A prospective audit of a nurse in-dependent prescribing within critical care. Nursing in Critical Care, 18(3), 135–141. doi:10.1111/j.1478-5153.2012.00534.x PMID:23577948
Celebi, N., Kirchhoff, K., Lammerding-Köppel, M., Riessen, R., & Weyrich, P. (2010). Medical clerkships do not reduce common prescription errors among medi-cal students. Naunyn-Schmiedeberg’s Archives of Pharmacology, 382(2), 171–176. doi:10.1007/s00210-010-0530-9 PMID:20535451
Chetouane, F., & Ibraheem, E. (2016). Surgery operations modeling and schedul-ing in healthcare systems. In P. Manolitzas, E. Grigoroudis, N. Matsatsinis, & D. Yannacopoulos (Eds.), Effective methods for modern healthcare service quality and evaluation (pp. 90–108). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-9961-8.ch005
Daverio, M., Fino, G., Luca, B., Zaggia, C., Pettenazzo, A., Parpaiola, A., & Ami-goni, A. et al. (2015). Failure mode and effective analysis ameliorate awareness of medical errors: A 4-year prospective observational study in critically ill children. Paediatric Anaesthesia, 25(12), 1227–1234. doi:10.1111/pan.12772 PMID:26432066
Davies, E. D., Schneider, F., Childs, S., Hucker, T., Krikos, D., Peh, J., & Cash-man, J. et al. (2011). A prevalence study of errors in opioid prescribing in a large teaching hospital. International Journal of Clinical Practice, 65(9), 923–929. doi:10.1111/j.1742-1241.2011.02705.x PMID:21752165
DesHarnais, S. I., & Nash, D. B. (2011). Reforming way medical students and physicians are taught about quality and safety. Mount Sinai Journal of Medicine: A Journal of Translational and Personalized Medicine, 78(6), 834–841. doi:10.1002/msj.20302

The Perspectives of Medical Errors in the Health Care Industry
129
Dias-Souza, M. V. (2016). Strategies for expanding access and improving the qual-ity of pharmaceutical services. In P. Manolitzas, E. Grigoroudis, N. Matsatsinis, & D. Yannacopoulos (Eds.), Effective methods for modern healthcare service quality and evaluation (pp. 168–201). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-9961-8.ch008
Doumbouya, M. B., Kamsu-Foguem, B., Kenfack, H., & Foguem, C. (2015). Argu-mentative reasoning and taxonomic analysis for the identification of medical errors. Engineering Applications of Artificial Intelligence, 46, 166–179. doi:10.1016/j.engappai.2015.08.009
Drach-Zahavy, A., & Hadid, N. (2015). Nursing handovers as resilient points of care: Linking handover strategies to treatment errors in the patient care in the follow-ing shift. Journal of Advanced Nursing, 71(5), 1135–1145. doi:10.1111/jan.12615 PMID:25641374
Dror, S., & Margol, D. (2015). Framework for analyzing malpractice cases to im-prove healthcare systems. Quality and Reliability Engineering International, 31(7), 1103–1113. doi:10.1002/qre.1851
Elkin, P. L., Beuscart-zephir, M. C., Pelayo, S., Patel, V., & Nøhr, C. (2013). The usability-error ontology. In M. Beuscart-Zéphir, M. Jaspers, C. Kuziemsky, C. Nøhr, & J. Aarts (Eds.), Context sensitive health informatics: Human and sociotechnical approaches (pp. 91–96). Amsterdam, The Netherlands: IOS Press.
Fastman, B. R., & Kaplan, H. S. (2011). Errors in transfusion medicine: Have we learned our lesson? Mount Sinai Journal of Medicine: A Journal of Translational and Personalized Medicine, 78(6), 854–864. doi:10.1002/msj.20296
Flynn, L., Liang, Y., Dickson, G. L., Xie, M., & Suh, D. C. (2012). Nurses’ practice environments, error interception practices, and inpatient medication errors. Journal of Nursing Scholarship, 44(2), 180–186. doi:10.1111/j.1547-5069.2012.01443.x PMID:22510244
Foster, P. N., Sidhu, R., Gadhia, D. A., & DeMusis, M. (2008). Leveraging com-puterized sign-out to increase error reporting and addressing patient safety in graduate medical education. Journal of General Internal Medicine, 23(4), 481–484. doi:10.1007/s11606-007-0503-y PMID:18373149
Gallagher, T. H., Brundage, G., Summy, E. A., Bommarito, K. M., Ebers, A. G., Waterman, A. D., & Dunagan, C. et al. (2006). National survey: Risk managers’ attitudes and experiences regarding patient safety and error disclosure. Journal of Healthcare Risk Management, 26(3), 11–16. doi:10.1002/jhrm.5600260305

The Perspectives of Medical Errors in the Health Care Industry
130
Gardner, A., & Rich, M. (2014). Error management training and simulation educa-tion. The Clinical Teacher, 11(7), 537–540. doi:10.1111/tct.12217 PMID:25417983
Garrouste-Orgeas, M., Flaatten, H., & Moreno, R. (2016). Understanding medical errors and adverse events in ICU patients. Intensive Care Medicine, 42(1), 107–109. doi:10.1007/s00134-015-3968-x PMID:26248952
Gavgani, V. Z., Oskouei, M. M., & Salehi, R. (2015). Patients’ medication errors: How patients’ inadequate information about their prosthetic heart valve diseases affects their healthcare. In Healthcare administration: Concepts, methodologies, tools, and applications (pp. 1081–1087). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-6339-8.ch057
Gawande, A. (2007). Better: A surgeon’s notes on performance. New York, NY: Metropolitan Books.
Ge, X., Rijo, R., Paige, R. F., Kelly, T. P., & McDermid, J. A. (2012). Introducing goal structuring notation to explain decisions in clinical practice. Procedia Technol-ogy, 5, 686–695. doi:10.1016/j.protcy.2012.09.076
Gordon, M., Darbyshire, D., & Baker, P. (2012). Non-technical skills training to enhance patient safety: A systematic review. Medical Education, 46(11), 1042–1054. doi:10.1111/j.1365-2923.2012.04343.x PMID:23078681
Gortzis, L. G., & Nikiforidis, G. (2008). Tracing and cataloguing knowledge in an e-health cardiology environment. Journal of Biomedical Informatics, 41(2), 217–223. doi:10.1016/j.jbi.2007.09.001 PMID:17945541
Gowen, C. R. III, McFadden, K. L., & Settaluri, S. (2012). Contrasting con-tinuous quality improvement, Six Sigma, and Lean management for enhanced outcomes in US hospitals. American Journal of Business, 27(2), 133–153. doi:10.1108/19355181211274442
Habermann, M., Foraita, R., & Cramer, H. (2013). Categories of errors and error frequencies as identified by nurses: Results of a cross-sectional study in German nursing homes and hospitals. Journal of Public Health, 21(1), 3–13. doi:10.1007/s10389-012-0531-x
Harding, S., Britten, N., & Bristow, D. (2010). The performance of junior doctors in applying clinical pharmacology knowledge and prescribing skills to standard-ized clinical cases. British Journal of Clinical Pharmacology, 69(6), 598–606. doi:10.1111/j.1365-2125.2010.03645.x PMID:20565451
The Perspectives of Medical Errors in the Health Care Industry
131
Härkänen, M., Ahonen, J., Kervinen, M., Turunen, H., & Vehviläinen-Julkunen, K. (2015). The factors associated with medication errors in adult medical and surgical inpatients: A direct observation approach with medication record reviews. Scandinavian Journal of Caring Sciences, 29(2), 297–306. doi:10.1111/scs.12163 PMID:25213297
Haw, C., & Cahill, C. (2011). A computerized system for reporting medication events in psychiatry: The first two years of operation. Journal of Psychiatric and Mental Health Nursing, 18(4), 308–315. doi:10.1111/j.1365-2850.2010.01664.x PMID:21418430
Haw, C., Stubbs, J., & Dickens, G. L. (2014). Barriers to the reporting of medication administration errors and near misses: An interview study of nurses at a psychiat-ric hospital. Journal of Psychiatric and Mental Health Nursing, 21(9), 797–805. PMID:24646372
Hendey, G. W., Barth, B. E., & Soliz, T. (2005). Overnight and postcall er-rors in medication orders. Academic Emergency Medicine, 12(7), 629–634. doi:10.1111/j.1553-2712.2005.tb00919.x PMID:15995095
Henneman, E. A., Blank, F. S. J., Gattasso, S., Williamson, K., & Henneman, P. L. (2006). Testing a classification model for emergency department errors. Jour-nal of Advanced Nursing, 55(1), 90–99. doi:10.1111/j.1365-2648.2006.03878.x PMID:16768743
Hobgood, C., Weiner, B., & Tamayo-Sarver, J. H. (2006). Medical error identifi-cation, disclosure, and reporting: Do emergency medicine provider groups differ? Academic Emergency Medicine, 13(4), 443–451. doi:10.1111/j.1553-2712.2006.tb00324.x PMID:16531598
Hodgkinson, B., Koch, S., Nay, R., & Nichols, K. (2006). Strategies to reduce medi-cation errors with reference to older adults. International Journal of Evidence-Based Healthcare, 4(1), 2–41. PMID:21631752
Hsaio, G. Y., Chen, I. J., Yu, S., Wei, I. L., Fang, Y. Y., & Tang, F. I. (2010). Nurses’ knowledge of high-alert medications: Instrument development and validation. Jour-nal of Advanced Nursing, 66(1), 177–190. doi:10.1111/j.1365-2648.2009.05164.x PMID:20423443
Hwang, J. I., & Hwang, E. J. (2011). Individual and work environment charac-teristics associated with error occurrences in Korean public hospitals. Journal of Clinical Nursing, 20(21/22), 3256–3266. doi:10.1111/j.1365-2702.2011.03773.x PMID:21733027

The Perspectives of Medical Errors in the Health Care Industry
132
Institute of Medicine. (2001). Crossing in the quality chasm: A new health system for the 21st century. Washington, DC: National Academies Press.
Issenberg, S. B., Chung, H. S., & Devine, L. A. (2011). Patient safety training simulations based on competency criteria of the Accreditation Council for Graduate Medical Education. Mount Sinai Journal of Medicine: A Journal of Translational and Personalized Medicine, 78(6), 842–853. doi:10.1002/msj.20301
Kagan, I., & Barnoy, S. (2013). Organizational safety culture and medical er-ror reporting by Israeli nurses. Journal of Nursing Scholarship, 45(3), 273–280. PMID:23574516
Kaldjian, L. C., Jones, E. W., Rosenthal, G. E., Tripp-Reimer, T., & Hillis, S. L. (2006). An empirically derived taxonomy of factors affecting physicians’ willingness to disclose medical errors. Journal of General Internal Medicine, 21(9), 942–948. doi:10.1007/BF02743142 PMID:16918739
Kaldjian, L. C., Jones, E. W., Wu, B. J., Forman-Hoffman, V. L., Levi, B. H., & Rosenthal, G. E. (2007). Disclosing medical errors to patients: Attitudes and practices of physicians and trainees. Journal of General Internal Medicine, 22(7), 988–996. doi:10.1007/s11606-007-0227-z PMID:17473944
Kamsu-Foguem, B., & Foguem, C. (2014). Telemedicine and mobile health with integrative medicine in developing countries. Health Policy and Technology, 3(4), 264–271. doi:10.1016/j.hlpt.2014.08.008
Kasemsap, K. (2014). Unifying a framework of organizational culture, organiza-tional climate, knowledge management, and job performance. In R. Perez-Castillo & M. Piattini (Eds.), Uncovering essential software artifacts through business process archeology (pp. 336–362). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4667-4.ch013
Kasemsap, K. (2015a). The role of radio frequency identification in modern libraries. In S. Thanuskodi (Ed.), Handbook of research on inventive digital tools for collec-tion management and development in modern libraries (pp. 361–385). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-8178-1.ch021
Kasemsap, K. (2015b). The role of total quality management practices on quality performance. In A. Moumtzoglou, A. Kastania, & S. Archondakis (Eds.), Labora-tory management information systems: Current requirements and future perspec-tives (pp. 1–31). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-6320-6.ch001

The Perspectives of Medical Errors in the Health Care Industry
133
Kasemsap, K. (2016). Applying Lean Production and Six Sigma in global opera-tions. In U. Akkucuk (Ed.), Handbook of research on waste management techniques for sustainability (pp. 44–74). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-9723-2.ch003
Kasemsap, K. (2017a). The fundamentals of health literacy. In N. Wickramasinghe (Ed.), Handbook of research on healthcare administration and management (pp. 507–527). Hershey, PA: IGI Global. doi:10.4018/978-1-5225-0920-2.ch030
Kasemsap, K. (2017b). Promoting health literacy in global health care. In N. Wickra-masinghe (Ed.), Handbook of research on healthcare administration and management (pp. 485–506). Hershey, PA: IGI Global. doi:10.4018/978-1-5225-0920-2.ch029
Kasemsap, K. (2017c). Radio frequency identification and mobile ad-hoc network: Theories and applications. In S. Bhattacharyya, N. Das, D. Bhattacharjee, & A. Mukherjee (Eds.), Handbook of research on recent developments in intelligent communication application (pp. 63–95). Hershey, PA: IGI Global. doi:10.4018/978-1-5225-1785-6.ch003
Kasemsap, K. (2017d). The importance of telemedicine in global health care. In N. Wickramasinghe (Ed.), Handbook of research on healthcare administration and management (pp. 157–177). Hershey, PA: IGI Global. doi:10.4018/978-1-5225-0920-2.ch010
Kasemsap, K. (2017e). Mastering electronic health record in global health care. In N. Wickramasinghe (Ed.), Handbook of research on healthcare administration and management (pp. 222–242). Hershey, PA: IGI Global. doi:10.4018/978-1-5225-0920-2.ch014
Kasemsap, K. (2017f). Analyzing the role of health information technology in global health care. In N. Wickramasinghe (Ed.), Handbook of research on health-care administration and management (pp. 287–307). Hershey, PA: IGI Global. doi:10.4018/978-1-5225-0920-2.ch017
Kasemsap, K. (2017g). Lean thinking in global health care: Theory and applications. In N. Wickramasinghe (Ed.), Handbook of research on healthcare administration and management (pp. 120–141). Hershey, PA: IGI Global. doi:10.4018/978-1-5225-0920-2.ch008
Kasemsap, K. (2017h). Robotics: Theory and applications. In M. Moore (Ed.), Cy-bersecurity breaches and issues surrounding online threat protection (pp. 311–345). Hershey, PA: IGI Global. doi:10.4018/978-1-5225-1941-6.ch013

The Perspectives of Medical Errors in the Health Care Industry
134
Kelly, J., & Wright, D. (2012). Medicine administration errors and their severity in secondary care older persons’ ward: A multi-centre observational study. Journal of Clinical Nursing, 21(13/14), 1806–1815. doi:10.1111/j.1365-2702.2011.03760.x PMID:21733025
Keogh, R. H., & White, I. R. (2014). A toolkit for measurement error correction, with a focus on nutritional epidemiology. Statistics in Medicine, 33(12), 2137–2155. doi:10.1002/sim.6095 PMID:24497385
Kolovos, N. S., Bratton, S. L., & Levy, F. H. (2008). A novel error-reporting tool in pediatric intensive care. Journal for Healthcare Quality, 30(3), 43–50. doi:10.1111/j.1945-1474.2008.tb01142.x PMID:18507240
Koshy, R. (2005). Navigating the information technology highway: Computer solutions to reduce errors and enhance patient safety. Transfusion, 45(Suppl. 4), 189S–205S. doi:10.1111/j.1537-2995.2005.00619.x PMID:16181403
Kroll, L., Singleton, A., Collier, J., & Jones, I. R. (2008). Learning not to take it seriously: Junior doctors’ accounts of error. Medical Education, 42(10), 982–990. doi:10.1111/j.1365-2923.2008.03151.x PMID:18823517
Laing, G., Bruce, J., Skinner, D., Allorto, N., Aldous, C., Thomson, S., & Clarke, D. (2015). Using a hybrid electronic medical record system for the surveillance of adverse surgical events and human error in a developing world surgical service. World Journal of Surgery, 39(1), 70–79. doi:10.1007/s00268-014-2766-x PMID:25167900
Lammers, R., Byrwa, M., & Fales, W. (2012). Root causes of errors in a simulated prehospital pediatric emergency. Academic Emergency Medicine, 19(1), 37–47. doi:10.1111/j.1553-2712.2011.01252.x PMID:22251191
Lawson, A. E., & Daniel, E. S. (2011). Inferences of clinical diagnostic reasoning and diagnostic error. Journal of Biomedical Informatics, 44(3), 402–412. doi:10.1016/j.jbi.2010.01.003 PMID:20093196
Lehmann, L., Wesselmann, U., Weber, B., & Smentkowski, U. (2015). Medical error analysis in dermatology according to the reports of the North Rhine Medical Association from 2004–2013. JDDG: Journal der Deutschen Dermatologischen Gesellschaft, 13(9), 903–908. PMID:26882381
Lewis, P. J., Ashcroft, D. M., Dornan, T., Taylor, D., Wass, V., & Tully, M. P. (2014). Exploring the causes of junior doctors’ prescribing mistakes: A qualitative study. British Journal of Clinical Pharmacology, 78(2), 310–319. doi:10.1111/bcp.12332 PMID:24517271

The Perspectives of Medical Errors in the Health Care Industry
135
Lin, Y. H., & Ma, S. M. (2009). Willingness of nurses to report medication ad-ministration errors in Southern Taiwan: A cross-sectional survey. Worldviews on Evidence-Based Nursing, 6(4), 237–245. doi:10.1111/j.1741-6787.2009.00169.x PMID:19747183
Lucchiari, C., & Pravettoni, G. (2012). Cognitive balanced model: A conceptual scheme of diagnostic decision making. Journal of Evaluation in Clinical Practice, 18(1), 82–88. doi:10.1111/j.1365-2753.2011.01771.x PMID:21999310
Manias, E., Williams, A., & Liew, D. (2012). Interventions to reduce medication errors in adult intensive care: A systematic review. British Journal of Clinical Phar-macology, 74(3), 411–423. doi:10.1111/j.1365-2125.2012.04220.x PMID:22348303
Mansour, M., James, V., & Edgley, A. (2012). Investigating the safety of medica-tion administration in adult critical care settings. Nursing in Critical Care, 17(4), 189–197. doi:10.1111/j.1478-5153.2012.00500.x PMID:22698161
Martinez, W., & Lo, B. (2008). Medical students’ experiences with medical er-rors: An analysis of medical student essays. Medical Education, 42(7), 733–741. doi:10.1111/j.1365-2923.2008.03109.x PMID:18507766
Maskens, C., Downie, H., Wendt, A., Lima, A., Merkley, L., Lin, Y., & Callum, J. (2014). Hospital-based transfusion error tracking from 2005 to 2010: Identifying the key errors threatening patient transfusion safety. Transfusion, 54(1), 66–73. doi:10.1111/trf.12240 PMID:23672511
Mazor, K. M., Fischer, M. A., Haley, H. L., Hatem, D., & Quirk, M. E. (2005). Teaching and medical errors: Primary care preceptors’ views. Medical Education, 39(10), 982–990. doi:10.1111/j.1365-2929.2005.02262.x PMID:16178824
McDowell, S. E., Ferner, H. S., & Ferner, R. E. (2009). The pathophysiology of medication errors: How and where they arise. British Journal of Clinical Pharma-cology, 67(6), 605–613. doi:10.1111/j.1365-2125.2009.03416.x PMID:19594527
McLennan, S. R., Engel-Glatter, S., Meyer, A. H., Schwappach, D. L. B., Schei-degger, D. H., & Elger, B. S. (2015). The impact of medical errors on Swiss an-aesthesiologists: A cross-sectional survey. Acta Anaesthesiologica Scandinavica, 59(8), 990–998. doi:10.1111/aas.12517 PMID:25952281
Muller, D., & Ornstein, K. (2007). Perceptions of and attitudes towards medical errors among medical trainees. Medical Education, 41(7), 645–652. doi:10.1111/j.1365-2923.2007.02784.x PMID:17614884

The Perspectives of Medical Errors in the Health Care Industry
136
Nakayasu, K., & Sato, C. (2012). Liability for telemedicine. International Journal of E-Health and Medical Communications, 3(1), 1–21. doi:10.4018/jehmc.2012010101
Niemann, D., Bertsche, A., Meyrath, D., Koepf, E. D., Traiser, C., Seebald, K., & Bertsche, T. et al. (2015). A prospective three-step intervention study to prevent medication errors in drug handling in paediatric care. Journal of Clinical Nursing, 24(1/2), 101–114. doi:10.1111/jocn.12592 PMID:24890332
Nordén-Hägg, A., Kettis-Lindblad, Å., Ring, L., & Kälvemark-Sporrong, S. (2012). Experiences of a nationwide web-based system: Reporting dispensing errors in Swedish pharmacies. International Journal of Pharmacy Practice, 20(1), 25–32. doi:10.1111/j.2042-7174.2011.00159.x PMID:22236177
Olaniyan, J. O., Ghaleb, M., Dhillon, S., & Robinson, P. (2015). Safety of medica-tion use in primary care. International Journal of Pharmacy Practice, 23(1), 3–20. doi:10.1111/ijpp.12120 PMID:24954018
Palmero, D., Di Paolo, E. R., Beauport, L., Pannatier, A., & Tolsa, J. F. (2016). A bundle with a preformatted medical order sheet and an introductory course to reduce prescription errors in neonates. European Journal of Pediatrics, 175(1), 113–119. doi:10.1007/s00431-015-2607-4 PMID:26272253
Pate, C. L., & Swofford, M. D. (2016). Organizational integration of decision analytic methods in healthcare settings. In P. Manolitzas, E. Grigoroudis, N. Matsatsinis, & D. Yannacopoulos (Eds.), Effective methods for modern healthcare service quality and evaluation (pp. 45–73). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-9961-8.ch003
Pazokian, M., Tafreshi, M. Z., & Rassouli, M. (2014). Iranian nurses’ perspectives on factors influencing medication errors. International Nursing Review, 61(2), 246–254. doi:10.1111/inr.12086 PMID:24571495
Pegalis, S. E., & Bal, B. S. (2012). Closed medical negligence claims can drive patient safety and reduce litigation. Clinical Orthopaedics and Related Research, 470(5), 1398–1404. doi:10.1007/s11999-012-2308-5 PMID:22419349
Raab, S. S., & Grzybicki, D. M. (2010). Quality in cancer diagnosis. CA: a Cancer Journal for Clinicians, 60(3), 139–165. doi:10.3322/caac.20068 PMID:20444999
Rathert, C., & Phillips, W. (2010). Medical error disclosure training: Evidence for values-based ethical environments. Journal of Business Ethics, 97(3), 491–503. doi:10.1007/s10551-010-0520-3

The Perspectives of Medical Errors in the Health Care Industry
137
Reason, J. (1990). Human error. Cambridge, UK: Cambridge University Press. doi:10.1017/CBO9781139062367
Reason, J. (1997). Managing the risks of organizational accidents. Aldershot, UK: Ashgate.
Redley, B., & Botti, M. (2013). Reported medication errors after introducing an electronic medication management system. Journal of Clinical Nursing, 22(3/4), 579–589. doi:10.1111/j.1365-2702.2012.04326.x PMID:22998067
Robbennolt, J. K. (2009). Apologies and medical error. Clinical Orthopaedics and Re-lated Research, 467(2), 376–382. doi:10.1007/s11999-008-0580-1 PMID:18972177
Rosenthal, M. M., Cornett, P. L., Sutcliffe, K. M., & Lewton, E. (2005). Beyond the medical record. Journal of General Internal Medicine, 20(5), 404–409. doi:10.1111/j.1525-1497.2005.0098.x PMID:15963161
Ross, S., Bond, C., Rothnie, H., Thomas, S., & Macleod, M. J. (2009). What is the scale of prescribing errors committed by junior doctors? A systematic review. British Journal of Clinical Pharmacology, 67(6), 629–640. doi:10.1111/j.1365-2125.2008.03330.x PMID:19094162
Rothwell, C., Burford, B., Morrison, J., Morrow, G., Allen, M., Davies, C., & Illing, J. et al. (2012). Junior doctors prescribing: Enhancing their learning in practice. British Journal of Clinical Pharmacology, 73(2), 194–202. doi:10.1111/j.1365-2125.2011.04061.x PMID:21752067
Rouse, R. A., & Kaplan, J. B. (2008). Why do some hospital leaders “speak no evil” about their organizations’ medical errors? The Journal of Leadership Studies, 2(3), 6–16. doi:10.1002/jls.20070
Sandilands, E. A., Reid, K., Shaw, L., Bateman, D. N., Webb, D. J., Dhaun, N., & Kluth, D. C. (2011). Impact of a focussed teaching programme on practical prescribing skills among final year medical students. British Journal of Clinical Pharmacology, 71(1), 29–33. doi:10.1111/j.1365-2125.2010.03808.x PMID:21143498
Schwappach, D. L. B. (2014). Risk factors for patient-reported medical errors in eleven countries. Health Expectations, 17(3), 321–331. doi:10.1111/j.1369-7625.2011.00755.x PMID:22296575
Schwappach, D. L. B., & Wernli, M. (2010). Medication errors in chemotherapy: Incidence, types and involvement of patients in prevention. A review of the lit-erature. European Journal of Cancer Care, 19(3), 285–292. doi:10.1111/j.1365-2354.2009.01127.x PMID:19708929

The Perspectives of Medical Errors in the Health Care Industry
138
Seki, Y., & Yamasaki, Y. (2006). Effects of working conditions on intravenous medication errors in a Japanese hospital. Journal of Nursing Management, 14(2), 128–139. doi:10.1111/j.1365-2934.2006.00597.x PMID:16487424
Sevdalis, N., Jacklin, R., Arora, S., Vincent, C. A., & Thomson, R. G. (2010). Diag-nostic error in a national incident reporting system in the UK. Journal of Evaluation in Clinical Practice, 16(6), 1276–1281. doi:10.1111/j.1365-2753.2009.01328.x PMID:20727061
Shah, R. K., Lander, L., Forbes, P., Jenkins, K., Healy, G. B., & Roberson, D. W. (2009). Safety on an inpatient pediatric otolaryngology service: Many small errors, few adverse events. The Laryngoscope, 119(5), 871–879. doi:10.1002/lary.20208 PMID:19358191
Shamliyan, T. A., Duval, S., Du, J., & Kane, R. L. (2008). Just what the doctor or-dered. Review of the evidence of the impact of computerized physician order entry system on medication errors. Health Services Research, 43(1p1), 32–53.
Shawahna, R., Rahman, N. U., Ahmad, M., Debray, M., Yliperttula, M., & Declèves, X. (2011). Electronic prescribing reduces prescribing error in public hospitals. Journal of Clinical Nursing, 20(21/22), 3233–3245. doi:10.1111/j.1365-2702.2011.03714.x PMID:21627699
Sheu, S. J., Wei, I. L., Chen, C. H., Yu, S., & Tang, F. I. (2009). Using snowball sampling method with nurses to understand medication administration errors. Jour-nal of Clinical Nursing, 18(4), 559–569. doi:10.1111/j.1365-2702.2007.02048.x PMID:18298506
Smorti, A., Cappelli, F., Zarantonello, R., Tani, F., & Gensini, G. F. (2014). Medical error and systems of signaling: Conceptual and linguistic definition. In-ternal and Emergency Medicine, 9(6), 681–688. doi:10.1007/s11739-014-1108-1 PMID:25034521
Tang, F. I., Sheu, S. J., Yu, S., Wei, I. L., & Chen, C. H. (2007). Nurses relate the contributing factors involved in medication errors. Journal of Clinical Nursing, 16(3), 447–457. doi:10.1111/j.1365-2702.2005.01540.x PMID:17335520
Taylor, J. A., Brownstein, D., Klein, E. J., & Strandjord, T. P. (2007). Evaluation of an anonymous system to report medical errors in pediatric inpatients. Journal of Hospital Medicine, 2(4), 226–233. doi:10.1002/jhm.208 PMID:17683099
Tran, D. T., & Johnson, M. (2010). Classifying nursing errors in clinical manage-ment within an Australian hospital. International Nursing Review, 57(4), 454–462. doi:10.1111/j.1466-7657.2010.00846.x PMID:21050197

The Perspectives of Medical Errors in the Health Care Industry
139
Tully, M. P. (2012). Prescribing errors in hospital practice. British Journal of Clinical Pharmacology, 74(4), 668–675. doi:10.1111/j.1365-2125.2012.04313.x PMID:22554316
Vozikis, A. (2012). Adverse events and medical errors in Greece: Knowledge cre-ation and capture methods. In P. Ordóñez de Pablos & M. Lytras (Eds.), Knowledge management and drivers of innovation in services industries (pp. 95–101). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-0948-8.ch009
Wheeler, S. J., & Wheeler, D. W. (2005). Medication errors in anaesthesia and critical care. Anaesthesia, 60(3), 257–273. doi:10.1111/j.1365-2044.2004.04062.x PMID:15710011
White, A. A., Bell, S. K., Krauss, M. J., Garbutt, J., Dunagan, W. C., Fraser, V. J., & Gallagher, T. H. et al. (2011). How trainees would disclose medical errors: Edu-cational implications for training programmes. Medical Education, 45(4), 372–380. doi:10.1111/j.1365-2923.2010.03875.x PMID:21401685
Williams, B. W. (2006). The prevalence and special educational requirements of dyscompetent physicians. The Journal of Continuing Education in the Health Pro-fessions, 26(3), 173–191. doi:10.1002/chp.68 PMID:16986149
Williams, D. (2012). Monitoring medicines use: The role of the clinical pharmacolo-gist. British Journal of Clinical Pharmacology, 74(4), 685–690. doi:10.1111/j.1365-2125.2012.04316.x PMID:22554404
Wong, B. M., Levinson, W., & Shojania, K. G. (2012). Quality improvement in medical education: Current state and future directions. Medical Education, 46(1), 107–119. doi:10.1111/j.1365-2923.2011.04154.x PMID:22150202
Wong, R. S. Y., & Balasingam, U. (2013). Teaching medical law in medical educa-tion. Journal of Academic Ethics, 11(2), 121–138. doi:10.1007/s10805-013-9184-9
Woodfield, G., O’Sullivan, M., Haddington, N., & Stanton, A. (2014). Using simula-tion for prescribing: An evaluation. The Clinical Teacher, 11(1), 24–28. doi:10.1111/tct.12056 PMID:24405915
Zaheer, S. (2015). Implementation of evidence-based practice and the PARIHS framework. In Healthcare administration: Concepts, methodologies, tools, and applications (pp. 323–340). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-6339-8.ch017
Zientek, D. M. (2010). Medical error, malpractice and complications: A moral geogra-phy. HEC Forum, 22(2), 145–157. doi:10.1007/s10730-010-9130-9 PMID:20480208

The Perspectives of Medical Errors in the Health Care Industry
140
ADDITIONAL READING
Al-Zahrani, W., & Sheikh, M. (2015). Detection of pre-analytical laboratory test-ing errors: Leads and lessons for patient safety. In M. Sheikh, A. Mahamoud, & M. Househ (Eds.), Transforming public health in developing nations (pp. 241–263). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-8702-8.ch011
Buetow, S., Kiata, L., Liew, T., Kenealy, T., Dovey, S., & Elwyn, G. (2010). Ap-proaches to reducing the most important patient errors in primary health-care: Patient and professional perspectives. Health & Social Care in the Community, 18(3), 296–303. PMID:20141539
Caruba, T., Boussadi, A., Lenain, E., Korb-Savoldelli, V., Gillaizeau, F., Durieux, P., & Sabatier, B. (2015). A simulation study of the interception of prescribing er-rors by clinical pharmacists in an acute hospital setting. Journal of Evaluation in Clinical Practice, 21(4), 673–680. doi:10.1111/jep.12363 PMID:25907983
Choo, J., Johnston, L., & Manias, E. (2014). Effectiveness of an electronic inpatient medication record in reducing medication errors in Singapore. Nursing & Health Sciences, 16(2), 245–254. doi:10.1111/nhs.12078 PMID:23855683
Conte, D. (2013). Recognizing errors in medical literature. Internal and Emergency Medicine, 8(2), 97–98. doi:10.1007/s11739-012-0887-5 PMID:23269531
Cottney, A., & Innes, J. (2015). Medication-administration errors in an urban mental health hospital: A direct observation study. International Journal of Mental Health Nursing, 24(1), 65–74. doi:10.1111/inm.12096 PMID:25394525
Davis, R. E., Joshi, D., Patel, K., Briggs, M., & Vincent, C. A. (2013). The medical student as a patient: Attitudes towards involvement in the quality and safety of health care. Journal of Evaluation in Clinical Practice, 19(5), 812–818. PMID:22620283
de Feijter, J. M., de Grave, W. S., Koopmans, R. P., & Scherpbier, A. J. J. A. (2013). Informal learning from error in hospitals: What do we learn, how do we learn and how can informal learning be enhanced? A narrative review. Advances in Health Sciences Education: Theory and Practice, 18(4), 787–805. doi:10.1007/s10459-012-9400-1 PMID:22948951
Dumitrescu, A., & Ryan, C. A. (2014). Addressing the taboo of medical error through IGBOs: I got burnt once! European Journal of Pediatrics, 173(4), 503–508. doi:10.1007/s00431-013-2168-3 PMID:24240665

The Perspectives of Medical Errors in the Health Care Industry
141
Fyhr, A., & Akselsson, R. (2012). Characteristics of medication errors with parenteral cytotoxic drugs. European Journal of Cancer Care, 21(5), 606–613. doi:10.1111/j.1365-2354.2012.01331.x PMID:22335508
Groszkruger, D. (2014). Diagnostic error: Untapped potential for improving pa-tient safety? Journal of Healthcare Risk Management, 34(1), 38–43. doi:10.1002/jhrm.21149 PMID:25070255
Huckels-Baumgart, S., & Manser, T. (2014). Identifying medication error chains from critical incident reports: A new analytic approach. Journal of Clinical Phar-macology, 54(10), 1188–1197. doi:10.1002/jcph.319 PMID:24782100
Ison, M. G., Holl, J. L., & Ladner, D. (2012). Preventable errors in organ transplanta-tion: An emerging patient safety issue? American Journal of Transplantation, 12(9), 2307–2312. doi:10.1111/j.1600-6143.2012.04139.x PMID:22703471
Kalbfleisch, J. D., & Wolfe, R. A. (2013). On monitoring outcomes of medical providers. Statistics in Biosciences, 5(2), 286–302. doi:10.1007/s12561-013-9093-x
Khalili, H., Farsaei, S., Rezaee, H., & Dashti-Khavidaki, S. (2011). Role of clini-cal pharmacists’ interventions in detection and prevention of medication errors in a medical ward. International Journal of Clinical Pharmacology, Therapy and Toxicology, 33(2), 281–284. PMID:21394569
Kooienga, S., & Stewart, V. T. (2011). Putting a face on medical errors: A patient perspective. Journal for Healthcare Quality, 33(4), 37–41. doi:10.1111/j.1945-1474.2010.00121.x PMID:21733023
Lawton, R., Carruthers, S., Gardner, P., Wright, J., & McEachan, R. R. C. (2012). Identifying the latent failures underpinning medication administration errors: An exploratory study. Health Services Research, 47(4), 1437–1459. doi:10.1111/j.1475-6773.2012.01390.x PMID:22375850
Leroy, P. (2011). Medical errors: The importance of the bullet’s blunt end. Eu-ropean Journal of Pediatrics, 170(2), 251–252. doi:10.1007/s00431-010-1283-7 PMID:20809247
Manias, E., Kinney, S., Cranswick, N., & Williams, A. (2014). Medication errors in hospitalised children. Journal of Paediatrics and Child Health, 50(1), 71–77. doi:10.1111/jpc.12412 PMID:24397451
Menon, S., Singh, H., Meyer, A. N. D., Belmont, E., & Sittig, D. F. (2014). Electronic health record–related safety concerns: A cross-sectional survey. Journal of Health-care Risk Management, 34(1), 14–26. doi:10.1002/jhrm.21146 PMID:25070253

The Perspectives of Medical Errors in the Health Care Industry
142
Palmieri, P. A., Peterson, L. T., & Noeding, M. N. (2015). Health information tech-nology: Anticipating, recognizing, and preventing disruptions in complex adaptive healthcare systems. In Healthcare administration: Concepts, methodologies, tools, and applications (pp. 1–22). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-6339-8.ch001
Seidling, H. M., Lampert, A., Lohmann, K., Schiele, J. T., Send, A. J. F., Witticke, D., & Haefeli, W. E. (2013). Safeguarding the process of drug administration with an emphasis on electronic support tools. British Journal of Clinical Pharmacology, 76(Suppl. 1), 25–36. doi:10.1111/bcp.12191 PMID:24007450
Siklósi, B., Novák, A., & Prószéky, G. (2016). Context-aware correction of spell-ing errors in Hungarian medical documents. Computer Speech & Language, 35, 219–233. doi:10.1016/j.csl.2014.09.001
Tallentire, V. R., & Smith, S. E. (2012). Medical error: Time to get real? Medical Education, 46(7), 632–634. doi:10.1111/j.1365-2923.2012.04292.x PMID:22691143
Thomas, L., Cordonnier-Jourdin, C., Benhamou-Jantelet, G., Diviné, C., & Le Louët, H. (2011). Medication errors management process in hospital: A 6-month pilot study. Fundamental & Clinical Pharmacology, 25(6), 768–775. doi:10.1111/j.1472-8206.2010.00907.x PMID:21210845
Varjavand, N., Nair, S., & Gracely, E. (2012). A call to address the curricular provi-sion of emotional support in the event of medical errors and adverse events. Medical Education, 46(12), 1149–1151. doi:10.1111/medu.12074 PMID:23171256
Zhang, Q., Li, Y., Li, J., Mao, X., Zhang, L., Ying, Q., & Zhang, M. et al. (2012). Patients for patient safety in China: A cross sectional study. Journal of Evidence-Based Medicine, 5(1), 6–11. doi:10.1111/j.1756-5391.2012.01164.x PMID:23528115

The Perspectives of Medical Errors in the Health Care Industry
143
KEY TERMS AND DEFINITIONS
Health Care: The act of taking preventative or necessary medical procedures to improve a person’s well-being.
Information: The data that is specific and organized for a purpose.Information Technology: The set of tools, processes, and equipment employed
to collect, process, and present the information.Medication: The set of drugs, used to improve a particular condition or illness.Medicine: A substance, especially in the form of a liquid or a pill, that is a treat-
ment for illness or injury.Patient: A person who is receiving medical care.Physician: A medical doctor, especially one who has the health care skill.Prescription: A piece of paper on which a physician writes the details of drugs
that patient requires.

Copyright ©2017, IGI Global. Copying or distributing in print or electronic forms without written permission of IGI Global is prohibited.
DOI: 10.4018/978-1-5225-2337-6.ch006
Chapter 6
144
The Role of Forensic Medicine in Medical Errors
ABSTRACT
This chapter presents the importance of Legal and Forensic Medicine in medical malpractice and explains how autopsies have a crucial role for the evaluation and the prevention of medical errors. Health systems vary from country to country; however, experts are indispensable in each system. In fact, experts’ opinions are asked for resolution of specific court cases. Standard of care is often assessed by expert medical witnesses who testify for one of the litigants. The physician who acts as an expert witness is one of the most important figures in malpractice litiga-tion. Therefore, a doctor who is an expert witness has to have certain training and qualifications and to act under common recommendations. The ideal medical expert seems to be the forensic doctor. In the future, a harmonization of practices could be applied in medical liability cases and the guidelines provided by the medico-legal community could constitute a stable base for their evaluation.
Grigorios LeonHellenic Society of Forensic Medicine, Greece

The Role of Forensic Medicine in Medical Errors
145
INTRODUCTION
Medical malpractice is defined as any act or omission by a physician during treat-ment of a patient that deviates from accepted norms of practice in the medical com-munity and causes an injury to the patient. Medical malpractice is a specific subset of tort law that deals with professional negligence. “Tort” is the Norman word for “wrong,” and tort law is a body of law that creates and provides remedies for civil wrongs that are distinct from contractual duties or criminal wrongs. “Negligence” is generally defined as conduct that falls short of a standard; the most commonly used standard in tort law is that of a so-called “reasonable person”. The reasonable person standard is a legal fiction, created so that the law can have a reference stan-dard of reasoned conduct that a person in similar circumstances would adopt, or not in order to protect another person from a foreseeable risk of harm (Bal, 2009a). The objectives of this chapter are to present the autopsy as a tool for the evaluation of lethal cases of medical malpractice, to explain the role of the expert witness and the medical testimony and finally to make a proposal for the role of the Legal and Forensic Medicine in medical liability cases.
BACKGROUND
According to Black’s Law Dictionary, medical negligence requires that the plaintiff establishes the following elements:
1. The existence of the physician’s duty to the plaintiff, usually based on the pre-existence of the physician-patient relationship;
2. The applicable standard of care and its violation;3. Damages (a compensable injury); and4. A causal connection between the violation of the standard of care and the harm
complained of, generally defined as “that degree of care which a reasonably prudent person should exercise in same or similar circumstances.”
If the defendant’s conduct falls outside the standards, then he or she may be found liable for any damages that resulted from his or her conduct (Black’s Law Dictionary, 1991).
The plaintiff in a tort claim generally pursues monetary damages, compensatory or punitive (or both), from the defendant. The traditional goals of medical malpractice are to ensure that the injured patient is made whole again, usually through monetary award, or that the relatives of a dead patient receive a moral satisfaction through a compensation and, in all cases, to deter other physicians from similar breaches of duty.

The Role of Forensic Medicine in Medical Errors
146
However, the current system across the world of malpractice does a poor job of serving the interests of physicians or patients. The malpractice process is slow, frustrating patients and negating any impact on deterring poor physician behaviors or on improving patient outcomes. The administrative costs of the current system are significant, as large amounts of compensation are taken by attorney fees. Most importantly, an atmosphere of “deny and defend” remains in which patients’ ques-tions and concerns often go unanswered, medical errors go unrecognized, and patient safety is not addressed (Stamm, Korzick, Beech & Wood, 2016).
Thus, most physicians will face a malpractice claim during their career, a reality that likely leads to the practice of defensive medicine (Stamm, Korzick, Beech & Wood, 2016). Defensive medicine may be defined as “the use of diagnostic procedures/testing or treatments undertaken explicitly for the purpose of averting malpractice suits” (Tancredi & Barondess, 1978). In addition, lawsuits against resident doctors are not rare. Resident doctors are frequently brought into a lawsuit as a co-defendant with the attending physician and hospital. Often at the beginning of a malpractice claim, the lawyer will include all potentially responsible parties and then eventu-ally remove those who are not necessary when more information is obtained during the investigative process. If a resident doctor is sued for malpractice, the attending physician is often sued as well because he or she has the ultimate responsibility in supervising the resident (Ott & Houry, 2000; Wegman & Stannard, 2012).
Overall, just because residents are trainees does not mean they cannot be held liable for medical malpractice. Residents can and do get sued. If a resident is sued, it is likely that his or her malpractice insurance coverage will cover most of the claim. Lawsuits are time consuming and stressful and, regardless of outcome, will affect the remainder of a medical career. To avoid being sued, residents should keep up to date with the recent guidelines, communicate well with patients, document well, and ask for help when they need it (Bailey, 2013).
“High-liability risk specialty” or “High-risk specialty” are terms commonly utilized within the medical professional liability system’s (i.e. medical malpractice system) research literature (Carroll & Buddenbaum, 2013). In Kessler and col-leagues’ study on the impact of malpractice reform and physician supply, high-risk specialties were identified based on malpractice insurance premiums (Kessler, Sage & Becker, 2005). In this case five specialties were identified – obstetrics/gynecology, surgery, anesthesiology, emergency medicine, and radiology. The same specialties are also identified in further studies (Hudson & Moore, 2011; Studdert, Mello, Sage, DesRoches, Peugh, Zapert & Brennan, 2005; Jena, Seabury, Lakdawalla & Chandra, 2011).

The Role of Forensic Medicine in Medical Errors
147
On the basis of a research study from Greece, we note that the main compensation for the specialty Obstetrics-Gynecology scaled up to €612,561. This is consistent with the findings of a study which mentions that both the Emergency Department and the specialty of Obstetrics-Gynecology cover 28% of all financial demands or €1,9 million. Other recent research from Utah shows that 58% of adverse events are surgical, of which 25% refer to foreign objects retained after surgery, especially in surgeries of Obstetrics-Gynecology. The remaining cases deal with nonsurgical events like healthcare management and hospital environment (Riga, Vozikis & Pollalis, 2014).
Malpractice fears are believed to influence various aspects of obstetrical practice. They seem to have contributed in small part to the rising primary caesarean section rate, but have also played a considerable role in the downtrend in vaginal birth after caesarean (VBAC) statistics (Schifrin & Cohen, 2013).
Unnecessary caesarean sections, increase the costs of care, expose patients to significant risks of harm in current and future pregnancies, and are a major public health concern (Main, Morton, Melsop, Hopkins, Giuliani & Gould, 2012; MacKay, Berg, Duran, Chang & Rosenberg, 2005). A study of the relation between malpractice insurance premiums and obstetrical care in a cohort of 890,266 women across the US in 2006 found that an average state malpractice premium of over $100,000 was associated with a higher caesarean delivery rate and a lower incidence of VBAC, and instrumental delivery when compared with states in which the premium was less than $50,000. It is obvious that fear of litigation had a marked effect on obstetric practice when premiums were high (Zwecker, Azoulay & Abenhaim, 2011).
Other investigators have similarly found that the perceived risk of malpractice litigation was a clear determinant of obstetricians’ choice of caesarean delivery in various clinical scenarios, and that a correlation exists between the caesarean rate and malpractice insurance costs (Ryan, Schnatz, Greene & Curry, 2005). The size of this effect on practice patterns is difficult to quantify. Studies in Florida, USA, suggest that clinicians who have had a significant indemnity payment on their behalf responded by a modest change in their caesarean rates (Grant & McInnes, 2004). Evidence shows that the rising caesarean section rate in the USA has been associ-ated with increased maternal mortality and higher rates of hemorrhage, infection and infertility (Blanchette, 2011).
Many believe that by revealing doctors their errors to the patients, we’ll be better equipped to learn from their mistakes (Tevlin, Doherty & Traynor, 2013). However, disclosure following a medical error does not always happen (Kaldjian, Jones, Wu, Forman-Hoffman, Levi & Rosenthal, 2007; Gallagher, Mello, Levinson, Wynia, Sachdeva, Snyder Sulmasy, Truog, Conway, Mazor, Lembitz, Bell, Sokol-Hessner, Shapiro, Puopolo & Arnold, 2013). The primary reasons that appear to prevent dis-closure from reliably occurring are simple: reputational and legal fears both posing

The Role of Forensic Medicine in Medical Errors
148
a formidable barrier (Gallagher, Studdert & Levinson, 2007). Admitting mistakes is a difficult thing for individuals to do in any setting whether personal or profes-sional. In the United States, the challenge to be open with patients is substantially amplified by concerns over potentially increased medical liability risk. These repu-tational and legal barriers may not only be impeding the safety benefits associated with disclosure of medical error, but also interfering with the fulfillment of ethical obligations physicians have to their patients (Kachalia & Bates, 2014).
Interest has been bolstered by the first “disclosure and offer” programs that have demonstrated improved liability outcomes for doing the right thing (Kraman & Hamm, 1999; Kachalia, Kaufman, Boothman, Anderson, Welch, Saint & Rogers, 2010). The first program to publish its results was a Veterans Affairs hospital that implemented a disclosure, apology, and offer program and found that it dropped from being in the top quartile of liability payments down to the bottom quartile as compared to its peers (Kraman & Hamm, 1999). The University of Michigan pro-gram, which has received tremendous attention, also found very favorable results after implementation (Kachalia, Kaufman, Boothman, Anderson, Welch, Saint & Rogers, 2010; Clinton & Obama, 2006). Liability payouts and legal costs associ-ated with defense attorneys both dropped by 60 percent. In addition, the University experienced fewer liability claims overall with a 36 percent decrease in the claims it was paying or defending (Kachalia, Kaufman, Boothman, Anderson, Welch, Saint & Rogers, 2010; Clinton & Obama, 2006). The reasons for the decrease are unclear, but what is certain is that as the University started disclosing errors and making offers of compensation, its malpractice experience improved, including beating actuarial predictions as well as outperforming national trends on compensation and defense costs (Kachalia & Bates, 2014).
MAIN FOCUS OF THE CHAPTER
Forensic medicine today is a large medical field that includes many subareas, in-cluding the investigation of medical malpractice. Legal and Forensic Medicine is the application of medical knowledge and methodology for the resolution of legal questions and problems for individuals and society. It involves the observation, documentation, collection, assessment, and scientific interpretation of medical evidence deriving from clinical and post mortem investigations required for the different fields of law, including criminal, civil, work, family, and administrative.
Medicolegal systems are different around the world. In the United States, the situation can vary within states from one county to another. However, there are two well-defined main systems, the coroner system and the medical examiner system. Worth noting that in the States, during this past half century, there has been remarkable

The Role of Forensic Medicine in Medical Errors
149
increase in the role of forensic pathologists and medical examiners in the determi-nation of cause and manner of deaths in health care facilities and investigations of quality of patient care. Autopsy data are an essential part of this quality assurance (QA) program in patient care, especially in trauma centers’ QA programs. Forensic pathologists participate in evaluating appropriateness of patient care where death occurs during or following therapeutic and diagnostic procedures. Continuous quality improvement programs now extend into data sharing in child and elder abuse cases, monitoring of defective medical devices and consumer products which contributed to deaths. In recent years, forensic pathologists are increasingly requested directly by family members to conduct private autopsies to provide independent opinions as to quality of patient care. Thus forensic pathologists are contributing expertise to an ever widening circle of influence in prevention of unnecessary deaths with quality assurance programs and peer review processes.
In England and Wales the coroner system developed from the twelfth century, at which time the coroner was largely responsible for supervising the material interests of the Crown in criminal cases. It is impossible to generalize about the comparable systems in Continental Europe; the procedures for investigating sudden and unexpected death vary not only from country to country but also within national boundaries although the legal code based on Roman law operates in many states. Currently the Legal and Forensic Medicine is a thematic federation in the European Union of Medical Specialists (UEMS).
The European Council of Legal Medicine has published a document called “De-scription of Legal and Forensic Medicine as a medical specialty in the EU” which is submitted to the UEMS (European Council of Legal Medicine, 2011). Among the core activities of Forensic Medicine, according to this document, is also the medical liability, especially relative to the civil and criminal systems, guidance on evidence, medical negligence and medical malpractice. In fact, autopsies made by forensic doctors in malpractice cases are very important for a number of reasons.
1. THE IMPORTANCE OF THE AUTOPSY IN LETHAL CASES
Autopsy, a surgical procedure performed on a recently deceased patient, is the last and most complete diagnostic procedure. Carefully performed by a thoughtful, interested, and experienced psysician, it should reveal much of the truth about the health of the deceased patient and the mechanism of death. During the latter half of the 19th and the first half of the 20th centuries, the autopsy was widely acknowledged to be the cornerstone of medical practice and education in Europe and America. It was considered essential for monitoring the accuracy of clinical diagnoses, establishing accurate causes of death, and educating both clinicians and students. The hospital

The Role of Forensic Medicine in Medical Errors
150
autopsy rate—the number of autopsies per number of deaths in a given hospital—was an important measure of quality medical care in both academic and nonacademic hospitals. The autopsy rate in US hospitals was approximately 50% before World War II, reached a high of about 60% in the 1960s, then rapidly declined to its current level of about 5% to 10%. It is likely 0% in many hospitals. It is important to note that clinically unsuspected medical errors in deceased patients will not be detected if autopsies are not performed.
The medical malpractice is today a central item for the forensic pathology and the lethal medical malpractice is a specific subgroup of a wider phenomenon and a rising and central topic for the forensic pathologist. Forensic autopsies are a manda-tory step in the judicial evaluation of the suspected medical malpractice. Reliable national and international registers about the medical malpractice are still missing. Therefore, nowadays the necroscopic archives are one of the best sources of data about such a complex phenomenon. The judicial autopsy is a fundamental step in the forensic investigation on lethal malpractice cases and therefore the best data on this topic usually come from the necroscopic archives.
The forensic investigation on lethal medical malpractice cases must determine the cause of the patient’s death, must analyze all the actions of the involved clinicians and must eventually state a causal relationship between the patient’s death and the identified malpractice. The forensic investigation about a medical malpractice case should be performed – according to the Recommendation R(99)3 of the Council of Europe – by a team of two physicians of whom at least one should be qualified in forensic pathology and no definite forensic diagnosis of medical malpractice should be done without a thorough technical investigation (Council of Europe,1999). In Italy the second physician has to be a specialized doctor of the branch which is involved in the malpractice case (Casali, Mobilia, Sordo, Blandino & Genovese, 2014).
Autopsy studies identify major diagnostic discrepancies in 10–20% of cases. Most cases in autopsy series derive from inpatient settings, but they also include deaths from the emergency department which, for many reasons, is considered to be the natural laboratory for studying diagnostic error. Although autopsies have a significant decline in the USA, they are still common in many other countries, and despite the availability of modern imaging, continue to show diagnoses being missed that might have been lifesaving, particularly infections and cardiovascular conditions (Graber, 2013).
Although autopsy data is considered the “gold standard” in terms of provid-ing the most definitive data on the accuracy of diagnosis, only a subset of cases ever reach autopsy, and in many cases, the relationship between clinical diagnoses and autopsy findings remains unclear. Autopsies also discover a large number of incidental findings that were not suspected during life, but that were clinically ir-relevant (Graber, 2013).

The Role of Forensic Medicine in Medical Errors
151
In general, the percentage of autopsies due to malpractice claims on all autop-sies is varying widely between 1.9 and 20%. According to a China study, 36.7% of forensic evaluations performed in the Wuhan University School of Medicine, Department of Forensic Medicine, were medical malpractice claims over the past 10 years (He, Li, Bynum, Meng, Yan, Li & Liu, 2015). This is higher than other countries, such as Germany, where maximally 20% of the total autopsies involved malpractice claims. Among the malpractice claims, the rate of approved cases was strikingly high (51.1%) in China (He, Li, Bynum, Meng, Yan, Li & Liu, 2015). Ac-cording to the annual report of the arbitration committees of the medical councils in Germany, only maximally 28.6% of malpractice claims were confirmed, whereas in the United States, there were even fewer confirmed cases (Jena, 2011; Madea & Preuss, 2009; Studdert, Mello & Brennan, 2004).
Autopsy is even nowadays a very efficient method of clarifying medical mal-practice claims (Bove & Iery, 2002; Juvin, Teissiere, Brion, Desmonts & Durigon 2000; Perkins, McAuley, Davies & Gao, 2003; Shojania & Burton, 2008; Shojania, Burton, McDonald & Goldmann, 2003). 64.3% of all cases were clarified after autopsy. This is not only of special interest to the prosecutor but for the accused doctors as well, since immediate clarification means that in two third of cases the preliminary investigation can be terminated already after autopsy (Madea, 2009). The great value of autopsies for verifying medical malpractice becomes also evident by a recent study from the UK (Start & Cross, 1999). The National Confidential Enquiry into Peri-Operative Deaths (NCEPOD) has been auditing data on deaths within 30 days of any surgical operation or invasive diagnostic procedure under local or general anesthesia in England and Wales since 1987. Autopsy often yields findings not suspected when a person was alive. For instance major discrepancies between clinical diagnosis and postmortem findings are encountered in 20.3% (81 of 346) of autopsies. Similar results are known from other studies (Nichols, Aronica & Babe, 1998; Shojania & Burton, 2008; Shojania, Burton, McDonald & Goldmann, 2003). 21% of surgeons received a copy of the autopsy report indicating that clini-cally unexpected findings had emerged. More unexpected findings have continued to be provided by autopsy examination over the years. This has also been confirmed by other studies (Shojania, Burton, McDonald & Goldmann, 2003).
According to a US American evaluation of autopsy reports in litigation cases doctors sued for medical malpractice do not have to fear the autopsy (Bove & Iery, 2002). A retrospective evaluation revealed that even in cases where the autopsy report was in favour of the plaintiff the cases were often settled. In the same study it is concluded that the findings support the proposition that autopsy information is generally not harmful for defendants in law suits alleging medical malpractice. Fear of autopsy findings is unbecoming to the medical profession and an obstacle

The Role of Forensic Medicine in Medical Errors
152
to the pursuit of excellence through uninhibited outcome analysis (Bove & Iery, 2002). Without autopsies many cases cannot be properly clarified.
To use medical malpractice claims in lethal cases and their objective clarifica-tion by autopsies as additional sources for the evaluation and prevention of errors requires sampling of cases, but sampling not only on a local but on a national or, better, international level. The special value of objective data that exist in forensic pathology and toxicology becomes also evident from a study on adverse drug events: ‘‘Thus, without having access to autopsy data and drug analysis data clinicians are ‘‘walking in the fog’’ as far as detecting fatal adverse drug events is concerned.’’ (Ebbesen, Buajordet, Erikssen, Brors, Hilberg, Svaar & Sandvik, 2001).
A multicentre retrospective analysis of 4450 autopsies carried out due to suspicion of medical malpractice in 17 German institutes of forensic medicine from 1990 to 2000 was performed for the German Federal Ministry of Health (Madea & Preuss, 2009). During the time period analyzed, an increase of cases was noted. The main results of the study are: in the cooperating institutes the total number of autopsies due to suspected medical malpractice ranged from 1.4 to 20%. In more than 40% of the cases preliminary proceedings were started because the manner of death was certified as non-natural or not clarified (Madea & Preuss, 2009).
Hospital doctors were more affected by medical malpractice claims than doctors in private practice. However, the number of confirmed cases of medical malpractice was higher for doctors in private practice than for hospital doctors. Although surgery is still at the top of the disciplines involved in medical malpractice claims, the number of confirmed surgical cases was below the average. Mistakes in care were confirmed to be above the average. Medico-legal autopsies are still a very sufficient method to evaluate cases of medical malpractice: in this study 2863 cases could already be clarified by autopsy. Up to now there is no systematic registration of medical malpractice charges in Germany. A systematic registration should be initiated to build up and/or improve error reporting systems and, thus, to improve patient safety. Compared to other sources of medical malpractice claims (arbitration committees of the medical chambers, reference material of health and insurance companies, files of civil courts) the data of this multicentre study are in so far unique as only lethal cases were evaluated and a complete autopsy report was available as basis of an expert opinion in alleged medical malpractice cases (Madea & Preuss, 2009).
A similar study was performed in Italy, where the archive of the Institute of Fo-rensic Medicine of the Milan University was analyzed focusing on all the suspicious cases for medical malpractice that had undergone a judicial autopsy from January 1996 to December 2009 (Casali, Mobilia, Sordo, Blandino & Genovese, 2014). For all the selected 317 cases, general epidemiological (sex, age, death settings), clinical (comorbidities, anamnestic notes) and necroscopic (cause of death) data were available, while for just 71 cases occurring from 2007 to 2009 a full forensic
The Role of Forensic Medicine in Medical Errors
153
report was also available that extended to the ultimate technical articulation about the suspected malpractice. Analyzing the chronological trend of the malpractice claims in Milan, there is clearly a historical bipartition between a low prevalence period (before 2001) and a great prevalence period (after 2001) (Casali, Mobilia, Sordo, Blandino & Genovese, 2014).
As mentioned above, the best available data source on lethal cases is in the files of the institutes of forensic medicine. This subgroup is of special importance since death is the most severe outcome of medical malpractice and the reproach to have caused the death of a patient by medical malpractice is the most severe malpractice claim. An advantage of these investigations compared to epidemiological investiga-tions on adverse events, etc. is that the cause of death was qualified on an objective basis (by autopsy). Furthermore forensic pathologists are familiar with giving expert evidence in penal law, especially concerning a causal connection, as most of the malpractice cases arrive in court.
The main task of the forensic pathologist is to give an opinion on the cause, manner and causation of death. Forensic pathologists are not prejudiced against any field of medicine. In most participating institutes, forensic pathologists already had access to the relevant clinical records before autopsy. When a comprehensive written report was necessary, all clinical data were available since they were nec-essary for subsequent clinico-pathological correlations. Based just on the autopsy findings the forensic pathologist is often able to rule out medical negligence, e.g. since a natural cause of death is evident. In all other cases it is standard that reports of clinical experts in the appropriate specialty are recommended. In some areas the forensic pathologist raises already the questions which should be addressed by the clinicians, based on the autopsy findings. In rare cases pathologist and clinician prepare a common final report.
2. EXPERT MEDICAL WITNESSES
Expert witnesses are “Men of science educated in the art, or persons possessing special or peculiar knowledge, acquired from practical experience.”
An expert is anyone with special knowledge, skill, experience, training or educa-tion in a particular field or discipline that permits them to testify to an opinion that will aid a judge or jury in resolving a question that is beyond the understanding or competence of laypersons. An expert witness is an expert who makes his or her knowledge available to a court (a tribunal or any other forum where formal rules of evidence apply) to help it understand the issues of a case and reach a sound and just decision. (Grobler, 2007)

The Role of Forensic Medicine in Medical Errors
154
Perioperative deaths necessitate medicolegal investigations in many countries. Medicolegal evaluations of the medical malpractice claims are initiated by the pa-tient/ relatives or by the legal authorities. Unfortunately, medical malpractice claims cannot be investigated within the framework of specific legal practices. Malpractice claims, which are considered criminal law suits, are assessed within the scope of causing death as a result of recklessness, carelessness, unskillfulness, failure to follow orders and directions; illegal conduct; and negligence. Suing for damages and opening a criminal suit is possible on grounds of medical malpractice claims. Legal authorities have to take medical expert opinion. Due to the fact that there are no expert institutions specifically dealing with medical malpractice in most of the countries, the choice of the medical expert (a specialist and/or a council) who has a great role in the assessment of malpractice claims, lies with the judge and/or the prosecutor.
Some countries use official organizations whose expert opinion needs to be taken in claims related to criminal law suits as in Turkey with the Supreme Health Council (SHC), which is under the frame of the Ministry of Health (Ozdemir, Cekin, Can & Hilal, 2005). The council examines medical files sent by legal authorities only. The council makes their assessments through careful examination of the medical records in those files. They later send the statements (reports) containing their opin-ions to the court. In practice, the opinions stated by this council directly affect the verdicts to be given by these courts (Ozdemir, Cekin, Can & Hilal, 2005; Tümer & Dener, 2006). Health systems vary from country to country; however, experts are indispensable in each system. In fact, experts’ opinions are asked for resolution of specific court cases.
The resolution of a medical malpractice case depends in large part on whether the defending physician met the standard of care. This standard is as follows:
The law exacts of physicians and surgeons in the practice of their profession only that they possess and exercise that reasonable degree of skill, knowledge, and care ordinarily possessed and exercised by members of their profession under similar circumstances, and does not exact from them the utmost degree of care and skill attainable or known to the profession. (Drechsler, 1999)
Standard-of-care arguments in the courtrooms of industrialized nations have recently begun to focus on evidence-based guidelines, also referred to as practice parameters. Evidence-based guidelines provide the legal standard in Dutch and French courts (Johnston & Sartwelle, 2013). In the United Kingdom, the Bolam test (enshrining the standard of care based on conformity to accepted practice), modified through the Bolitho holding that courts are not bound by expert opinion, allows greater reliance on clinical guidelines in malpractice proceedings (Johnston

The Role of Forensic Medicine in Medical Errors
155
& Sartwelle, 2013). Arguments were recently emerged that deviation from guide-lines should be proof of negligence. (Wassem, Mehil & Upile, 2011) Australia initially rejected the Bolam physician-based standard of care testimony in favor of court-determined concepts of negligence. Subsequent legislation, however, restored physician opinions as the source of determination of negligence, thereby allowing discretion in acceptance of various evidence-based guidelines (Johnston & Sartwelle, 2013). In New Zealand, the codified duty of reasonable care and skill incorporates but is not limited to the Bolam test; reasonable care can require a higher standard than currently accepted practice. Moreover, physicians must comply with ‘‘legal, professional, ethical and other relevant standards,’’ which includes practice guide-lines. Canada shares similar common law standards allowing consideration of prac-tice guidelines (Johnston & Sartwelle, 2013). In the United States, evidence-based guidelines have received increasing attention in the medical profession since first introduced to clinical medicine in the 1980s. Presently evidence-based guidelines are widely used in medical education, hospitals, clinics, and almost every aspect of clinical medicine. Evidence-based guidelines were a national concomitant of medicine’s transition from experience-based anecdotal practices to scientifically guided treatments. Thousands of guidelines have now been published (Johnston & Sartwelle, 2013).
Standard of care is often assessed by expert medical witnesses who testify for one of the litigants (Graber, Hartz, James, Nugent & Green, 2005). The lack of respect with which experts are treated, causes some good physicians to refuse to be wit-nesses, which further damages the prestige and quality of experts who participate in legal proceedings (Gross, 1991). Concern about the credibility of medical expert testimony in malpractice litigation is not new. Despite efforts by medical and legal authorities for the past two centuries, cooperation between the two professions fre-quently degenerates and acrimony between physicians and attorneys is commonplace. An editorial in JAMA as far back as 1892 addressed this sad state of affairs and its impact on the quality of expert medical testimony by lashing out at the “disgraceful exhibition of medical experts who are hired...[to give] paid theories and opinions”. Harvard Law Review 1897 also made reference to the low esteem in which expert medical testimony was held by creating a hypothetic opening statement from an at-torney to a jury: “Gentlemen of the jury, there are three kinds of liars: the common liar, the damned liar, and the scientific expert!” (Grobler, 2007)
Because testimony from adversarial experts may be biased, unreliable, or invalid, alternatives have been suggested. These include court-appointed experts, malpractice screening panels, and practice guidelines. Although these approaches reduce error, they have other limitations: court appointed experts have been difficult to fund, malpractice screening panels cannot legally substitute for jury trials, and practice

The Role of Forensic Medicine in Medical Errors
156
guidelines often conflict with each other or give only very general information that is difficult to apply in a specific case.
In essence, under the modern evidence rules there are very few formalities of expert testimony. An expert can give opinions in any manner the trial court allows and the expert chooses, as long as the opinion is relevant, reliable, and confined to the expert’s field of expertise. All US states have differences in their evidence rules and court procedures, but virtually all have updated their rules and procedures so that in litigation today expert witnesses dominate the courtroom as never before, in both civil and criminal trials. Studies have documented experts of some kind being called in more than 80% of civil cases, with an average of four experts per case (Johnston & Sartwelle, 2013). Expert domination should not be surprising given our complex society, the dominance of the civil and criminal court system for solving cultural problems, and the dominance of science and medicine in daily life. Entire new fields of expertise have been developed as a result of litigation—life care planners, accident reconstruction experts, forensic psychiatrists, and many others.
Even more important to our inquiry is physician courtroom testimony. Physicians of all specialties are a staple of trials of all kinds, but especially personal injuries, product liability, vehicle accidents, workers’ compensation, medical malpractice suits, and even legal malpractice suits, because of the case within –a case require-ment- and even certain criminal cases (child abuse, sexual assault). All these have a common element— medical evidence is essential.
3. EXPERT MEDICAL TESTIMONY AND CRITERIA OF QUALIFICATION
Definition of expert testimony goes beyond the usual thought of what constitutes expert involvement:
1. Medical evaluation of a party to a legal proceeding, including personal inter-view and examination and/or review of medical records or other pertinent data (including laboratory tests and imaging studies);
2. Formulating an expert opinion based on such evaluation; and3. Communicating such an opinion to attorneys, courts, licensing boards, peer
review bodies, or other agencies, whether in the form of testimony in court, deposition, answers to interrogatories, or affidavit (American Academy of Neurology, 2005).

The Role of Forensic Medicine in Medical Errors
157
The interests of the public and the medical profession are best served when scientifically sound and unbiased expert witness testimony is readily available to plaintiffs and defendants in medical negligence suits. Generally, the purpose of expert witness testimony in medical malpractice is to describe standards of care relevant to a given case, identify any breaches in those standards, and if so noted, render an opinion as to whether those breaches are the most likely cause of injury (Localio, Lawthers, Brennan, Laird, Hebert, Peterson, Newhouse, Weiler & Hiatt, 1991). In addition, an expert may be needed to testify about the current clinical state of a patient to assist the process of determining damages.
In civil litigation, expert witness testimony is much different from that of other witnesses. In legal proceedings involving allegations of medical negligence, “witnesses of fact” (those testifying because they have personal knowledge of the incident or people involved in the lawsuit) must restrict their testimony to the facts of the case at issue. The expert witness is given more latitude. The expert witness is allowed to compare the applicable standards of care with the facts of the case and interpret whether the evidence indicates a deviation from the standards of care. The medical expert also provides an opinion (within a reasonable degree of medical certainty) as to whether that breach in care is the most likely cause of the patient’s injury. Without the expert’s explanation of the range of acceptable treatment modalities within the standard of care and interpretation of medical facts, juries would not have the technical expertise needed to distinguish malpractice (an adverse event caused by negligent care or “bad care”) from maloccurrence (an adverse event or “bad outcome”) (Localio, Lawthers, Brennan, Laird, Hebert, Peterson, Newhouse, Weiler & Hiatt, 1991).
While Anesthesiologists, as well as Hematologist–Oncologists, were the most commonly utilized expert witnesses, it should also be noted that other specialities appeared to play a significant role in plaintiff strategies. Otolaryngologists appeared as expert witnesses on behalf of both plaintiffs and defendants equally. Although the identities of these experts varied, it should be noted that some practitioners repeatedly testify for one side or another. For example, there was one Otolaryngologist involved as an expert witness for the plaintiff in six cases, likely representing a substantial time contribution (Svider, Husain, Kovalerchik, Mauro, Setzen, Baredes & Eloy, 2013).
Physicians may find serving as an expert witness to be interesting, intellectually stimulating, and financially beneficial. However, potential expert witnesses should be aware of the increased legal scrutiny being applied to expert witness testimony in medical malpractice litigation. In the past, expert witnesses received absolute immunity from civil litigation regarding their testimony. This is no longer the case. Expert witnesses may be subject to disciplinary sanctions from professional orga-nizations and state medical boards (Bal, 2009 b).

The Role of Forensic Medicine in Medical Errors
158
Codes of conduct to which medical experts should adhere and the goals to which they should aspire are clearly spelled out by representative medical organizations in the USA, UK and Australia. The following is a combination of similar statements on medical expert witness by professional representative bodies in the USA (the American Medical Association, American College of Surgeons, the Society for Vascular Surgery and American Academy of Pediatrics). (American Academy of Pediatrics, 2002; Grobler, 2007).
Doctors have an obligation to testify in court as expert witnesses on behalf of the plaintiff or defendant as appropriate. The physician who acts as an expert wit-ness is one of the most important figures in malpractice litigation. Recommended qualifications for doctors acting as an expert witness are:
• Have a current, valid and unrestricted license to practice medicine and ac-knowledged specialty qualifications.
• Be knowledgeable by recent and substantive experience or demonstrated competence appropriate to the subject matter of the case. Should limit testi-mony to their sphere of medical expertise. Be able to demonstrate evidence of continuing medical education relevant to the specialty or the subject matter.
• Be adequately prepared and should testify honestly and truthfully to the best of their medical knowledge. The medical witness must not become an advo-cate or partisan in the legal proceeding.
• Be familiar with the standard of care provided at the time of the alleged oc-currence and should be actively involved in the clinical practice of the spe-cialty or the subject matter of the case during the time the testimony or opin-ion is provided.
• Be prepared to document the percentage of time that is involved in serving as an expert witness, as well as willing to disclose the fees or compensation obtained for such activities and the total number of times he or she has testi-fied for the plaintiff or defendant.
The American Trial Lawyers’ Association has reported a recent difficulty in retaining plaintiff expert witnesses (Gorney, 2003). This may be attributed to the potential for disciplinary action by medical societies against their members. The American College of Surgeons (ACS) has previously issued statements regarding recommended guidelines for physicians acting as expert witnesses, with failure to comply being a possible violation of bylaws. Several of these qualifications deal with having an active and unrestricted license, and demonstrating competence in the procedures about which the surgeon is testifying. Other obligations include a willingness to disclose the amount of compensation they are being provided with, as well as an emphasis on the consequences for misleading and false testimony,

The Role of Forensic Medicine in Medical Errors
159
including prosecution for perjury, and suspension of his or her professional license. Within these statements, the guidelines explicitly state that physicians are obligated to testify truthfully, and do not outline disciplinary action for witnesses that do not adhere to these recommendations (Svider, Husain, Kovalerchik, Mauro, Setzen, Baredes & Eloy, 2013).
Participation in the legal system should be both selective and obligatory, so that testifying becomes an honor and a duty and is performed by people with the greatest knowledge and integrity. Scientific and legal organizations should confer together and develop qualifications for witnesses that should include expertise in how to evaluate all aspects of scientific investigations. Expert witnesses should also be trained in legal principles and processes so that they can give adequate testimony, particularly on cross-examination. As part of pre-trial discovery, experts should be required to explain precisely why their testimony was different from that of oppos-ing experts. In addition, fees should be limited, so that there is no financial motive that might bias the expert. More innovative reforms would have a court appointed expert review regularly for the court or even have judges trained in science do this (Kaufman, 2001).
Despite ethical codes, expert witness guidelines, and statements about trials being the pursuit of truth and justice, a great many judges, jurors, and lawyers perceive expert witnesses on both sides as bias partisans (Johnston, 2010). This perception is not new. As early as the 19th century, after parties were allowed to call experts to support their arguments, observers criticized the use of experts pointing to the common perception that an ‘‘expert could be found who would testify to anything absurd” (Johnston & Sartwelle, 2013). In the 20th century in the United States, sub-stantial discussion occurred about parties’ uses of experts, with one Yale professor likening lawyers’ manipulation of experts to playing the saxophone, the lawyer not only picking the tune but then manipulating the expert as if the expert were a musical instrument on which the lawyer sounded the desired notes (Johnston & Sartwelle, 2013). Following English law, physicians were called as expert witnesses by the parties. The rules related to expert testimony became increasingly refined as more and more malpractice cases reached the courts, so that by the turn of the 20th century medical malpractice suits were being tried much like they are today (Annas, 2012).
Nowadays, as an “independent” expert witness the doctor will not be the treating doctor who gives evidence primarily on fact (such as what the patient stated, what symptoms were reported, what examination was undertaken, and what advice or treatment was offered). The expert witness provides an opinion on the facts of the case, either as provided in written form, or based on the expert doctor’s own exami-nation of the patient. This is at the request, almost always, of one or other party to a claim, or a case once in court. The report, however, is for the benefit of the court, and is entirely independent of that party. Whilst a party can make a request for an

The Role of Forensic Medicine in Medical Errors
160
opinion on certain specified questions, and it is legitimate to comment upon the answers given and to ask for matters to be considered further, or reconsidered, the opinion must both be and be seen to be independent, objective and unbiased. It is liable to be tested in cross examination. The independence of thought of an expert witness must be jealously guarded.
An opinion will be based on the doctor’s expertise (i.e. his or her technical knowledge and experience) and will assist the court in deciding the matter before it. The expert doctor’s role is to assist the court by providing independent opinion, and his or her opinion may be used to diminish the other side’s case. The qualifica-tion and knowledge of the expert doctor must be established in court. Often, but not always, there is a competing opinion prepared on behalf of the opponents of those who instructed that doctor.
Expert evidence should be – and should be seen to be – independent, objective and unbiased. In particular, an expert witness must not be biased towards the party responsible for paying his or her fee. The evidence should be consistent regardless of who is paying for it. In the event of any connection with any party to a claim or case that might be considered to be prejudicial to any degree to impartiality, it ought to be disclosed.
An expert must remember that expert fees are always a subject of inquiry by the opposition. An expert will have to produce bills and payments as part of the deposi-tion and trial process. Questions are always asked concerning hourly fees, with the veiled implication that the witness’s real motivation is not an honest opinion, but rather an opinion for sale to the highest bidder. Rather, an expert witness should deal with such questions sincerely, remembering what the lawyer is forgetting— the lawyer’s witnesses are also being paid.
The expert can greatly assist a direct examination by preparing a direct exami-nation outline and working with the lawyer to make the testimony clear, effective, and persuasive. The lawyer, on the other hand, needs to prepare the expert for cross examination and, in particular, for cross-examination by learned treatises. Attorneys’ work in an adversarial system is to sway the trier of fact with the most articulate, understandable, presentable, and persuasive expert, rather than the best scientist. In contrast, science requires that the expert focus solely on the evidence without the influence of the parties’ goals. Recent rulings in the USA and UK have redefined the courts’ role in ensuring the quality of expert testimony (Cecil, 2005; Kassirer, 2002; Editorial, 2005). In Australia expert witnesses have to undergo training and accreditation (Vinen, 2005).
Ideally, expert witnesses should be unbiased conveyers of information. The pivotal factor in the medical tort process is the integrity of the expert witness testimony. It should be reliable, objective and accurate and provide a truthful analysis of the standard of care. Regrettably, not all medical experts testify within these boundar-

The Role of Forensic Medicine in Medical Errors
161
ies. The medical community has long been aware that not all experts testify within scientific standards and ethical guidelines.
Physicians agreeing to testify as experts in medical negligence cases should conduct themselves as follows:
1. Regardless of the source of the request for testimony (plaintiff or defendant physician), expert witnesses should lend their knowledge, experience, and best judgment to all relevant facts of the case.
2. Expert witnesses should take necessary steps to ensure that they have access to all documents used to establish the facts of the case and the circumstances surrounding the occurrence.
3. Relevant information should not be excluded for any reason and certainly not to create a perspective favoring the plaintiff or the defendant.
4. The expert witness’s opinion should be fair and objective. The expert witness should be comfortable with his or her testimony regardless of whether it is to be used by the plaintiff or defendant.
A witness does not need to possess total knowledge of a subject—neurology, for example—but knowledge of the discrete area of the testimony involved. Having qualified as an expert in another case does not automatically qualify him or her as an expert in every case. On the other hand, a person is not disqualified as an expert merely because he or she is not a specialist. Forensic pathologists are familiar with giving expert evidence in penal and civil law and are not prejudiced against any field of medicine. Furthermore, the requirements of Legal and Forensic Medicine specialization make forensic doctors the ideal expert witnesses in malpractice cases.
SOLUTIONS AND RECOMMENDATIONS
The role of Legal and Forensic Medicine has become increasingly specific, essential and ineluctable in the judicial setting in order to prevent and avoid erroneous inter-pretations and hasty scientific verdicts. The multiplicity of regulatory frameworks and operative systems and the literature on medical malpractice, as well as a recent exploratory supranational survey, prove the absence of international medico-legal guidelines and/or recommendations governing the ascertainment and evaluation process in cases of suspected medical liability.
There are also no EU regulations, guidelines, and recommendations to prevent, or at least reduce, the multiplicity of regulatory frameworks and national operative systems. Today, one sees the co-existence of systems anchored in the common law juridical models or, more directly, traceable to Roman law, such as, respectively,

The Role of Forensic Medicine in Medical Errors
162
the Nordic countries and Great Britain, the Mediterranean countries, and Central and Eastern Europe, where dissimilar legislative-juridical models exist, from which diverse operating systems of dispute resolution arise, on a judicial, criminal, civil and/or administrative, or, mostly, extra-judicial basis (Ferrara, 2013).
As has often happened in other scientific and disciplinary contexts, the medico-legal community has provided the first example by:
1. Respecting the Hippocratic oath of the third millennium, of knowledge, know-how and again the “search for the truth,” through the identification and self-report to the medical community of errors committed during the performance of one’s work and assistance;
2. Posing an initial remedy to the externally caused detriment of the patient’s rights, through the triggering of a positive process aimed at “European con-sensus on ascertainment methodology and criteria for evaluating damage from medical malpractice,” on living and deceased persons (Ferrara, 2013).
The “Consensus Guidelines Document”, elaborated by the European Academy of Legal Medicine Working Group on Medical Malpractice, is the just first step towards the complex and multifaceted harmonization process of the legislative–juridi-cal, operational and institutional practices of medical liability cases in the different European countries (Ferrara, Baccino, Bajanowski, Boscolo-Berto, Castellano, De Angel, Pauliukevičius, Ricci, Vanezis, Vieira, Viel & Villanueva, 2013)
It is recommended that the appointed expert is a specialist in Legal Medicine and/or Forensic Pathology or that the expert has fully completed postgraduate training in legal medicine, preferably at university level and is recognized as a medico-legal expert by the supervising authority in his or her country and habitually practices that specialty.
The expert should demonstrate adequate training (preferably at university level) in the following areas:
1. Basic competence in criminal, civil and administrative law, with particular reference to those regulations in the field of medical health.
2. Theoretical and practical experience of medicolegal semeiotics and of the medico-legal evaluation of psychophysical validity in the areas of civil law and private/public insurance.
3. In the case of ascertainment on corpses, theoretical and practical notions of forensic pathology with a thorough first-hand and in-depth experience of many years as well as considerable expertise in forensic autopsies.

The Role of Forensic Medicine in Medical Errors
163
4. Theoretical notions and practical experience on the subject of the causal value/link, with particular reference to the demonstration of the causal link between a medical error and the damage, subsuming the phenomena under scientific laws.
Cases of medical liability lawsuits are quite varied and occur in all specialties, although with different frequencies and degrees of seriousness. In order to present a lawsuit, it is necessary to have suffered some kind of injury or loss. In the case of a living person, that person is the one who sustains the injury. In normal condi-tions, that person files the claim, but when the person in question is a minor or one whose mental capacities are affected, family members will represent that person in the lawsuit.
FUTURE RESEARCH DIRECTIONS
Although the regulations in various European countries are extremely heteroge-neous—as, indeed, are the operational procedures in the same countries—medico-legal experts are involved in the majority of cases of presumed Medical Responsibility and/or Liability on living persons. Apart from the juridical framework (penal, civil) or extra juridical in which the medico-legal professional works and apart from the fact that that person acts as a consultant for the judge, insurance company, injured party or other institution or figure, the method of ascertainment to be followed is the same, including analysis of clinical and documentary data and execution of clinical and medico-legal examination, described in the abovementioned document.
This exemplary process of harmonization, triggered by the European Academy and Community of Legal Medicine, is certainly strengthened and enhanced by the contribution of other International Experts and Communities of various disciplines, as well as facilitated by a legislative reform, likely to be promoted by the European Council, which, in addition to the ascertainment methodology and criteria of evalua-tion, aims to standardize the structure of the juridical–legislative medical malpractice lawsuits in the various European states.
The role of medicolegal experts and the need for medico-legal experts worldwide will increase, because liability claims against doctors were increasing in the last 20 years. This is a reality described also in the Eurobarometer entitled “Medical errors” which express the above tendency by the results presented. In fact, medi-cal errors are perceived as a prominent problem in Europe. In all countries polled, except Finland, majority of citizens ranks medical errors as an important issue in their country. Citizens of Europe appear to be well aware of the existence of medi-cal errors since 78% indicate that they have at least sometimes read or heard about

The Role of Forensic Medicine in Medical Errors
164
them. In all countries polled, at least half of the respondents belong to this group (European Commission, 2006).
The implementation of the European Guidelines on Methods of Ascertainment and Criteria of Evaluation in Medical Liability cases brings improvements in claims handling practice and ensures reliable data for research in this field. Current research based on the analysis of claims is insufficient and data arising from negligence claims are not being used effectively to learn from failures in care.
CONCLUSION
Although change in attitudes is gradual, professionals should get used to this dif-ferent way of learning from errors, the main liability insurers worldwide should rigorously address this point and medico-legal experts should be involved and lead this change. In the future, a harmonization of the practices of medical liability cases could be applied in a wider level worldwide.
Whatever man does, wherever he is living, deaths and body damages will continue to occur, often by medical malpractice. Legal and Forensic Medicine is expected to explain them and to propose measures that might have prevented unnecessary outcomes. Countries have to invest in Legal and Forensic Medicine, as the stronger and more powerful it is, the more useful will be for the justice, the patients, the physicians, the health system and the society as a whole.

The Role of Forensic Medicine in Medical Errors
165
REFERENCES
American Academy of Neurology. (2005). Qualifications and guidelines for the expert witness. Retrieved from https://www.aan.com/uploadedFiles/Website_Li-brary_Assets/Documents/8.Membership/5.Ethics/1.Code_of_Conduct/Membership-Ethics-American%20Academy%20of%20Neurology%20Qualifications%20and%20Guidelines%20for%20the%20Physician%20Expert%20Witness%20(2).pdf
American Academy of Pediatrics. (2002). Guidelines for Expert Witness Testimony in Medical Malpractice Litigation. Pediatrics, 109(5).
Annas, G. J. (2012). Doctors, patients, and lawyers--two centuries of health law. The New England Journal of Medicine, 367(5), 445–450.
Bailey, R. A. (2013). Resident liability in medical malpractice. Annals of Emer-gency Medicine, 61(1), 114–117. doi:10.1016/j.annemergmed.2012.04.024 PMID:22632773
Bal, B.S. (2009a). An Introduction to Medical Malpractice in the United States. Clinical Orthopaedics and Related Research, 467(2), 339-47.
Bal, B. S. (2009b). The Expert Witness in Medical Malpractice Litigation. Clinical Orthopaedics and Related Research, 467(2), 383–391. doi:10.1007/s11999-008-0634-4 PMID:19052827
Black’s Law Dictionary. (1991). 6th ed.). St Paul, MN: West Publishing Co.
Blanchette, H. (2011). The rising cesarean delivery rate in America: What are the consequences? Obstetrics and Gynecology, 118(3), 687–690. doi:10.1097/AOG.0b013e318227b8d9 PMID:21860302
Bove, K. E., & Iery, C. (2002). The role of the autopsy in medical malpractice cases. I. A review of 99 appeals court decisions. Archives of Pathology & Laboratory Medicine, 126(9), 1023–1031. PMID:12204050
Carroll, A.E., & Buddenbaum, J.L. (2013). High and low-risk specialties experience with the U.S. medical malpractice system. BMC Health Services Research, 13, 465.
Casali, M. B., Mobilia, F., Del Sordo, S., Blandino, A., & Genovese, U. (2014). The medical malpractice in Milan-Italy. A retrospective survey on 14 years of judicial autopsies. Forensic Science International, 242, 38–43. doi:10.1016/j.forsciint.2014.06.002 PMID:25023215
Cecil, J. S. (2005). Ten years of judicial gatekeeping under Daubert. American Journal of Public Health, 95(S1), S74–S80. doi:10.2105/AJPH.2004.044776 PMID:16030342

The Role of Forensic Medicine in Medical Errors
166
Clinton, H. R., & Obama, B. (2006). Making patient safety the centerpiece of medi-cal liability reform. The New England Journal of Medicine, 354(21), 2205–2208. doi:10.1056/NEJMp068100 PMID:16723612
Council of Europe, Committee of Ministers. (1999). Recommendation no. R (99) 3 of the Committee of Ministers to Member States on the Harmonisation of Med-ico-Legal Autopsy Rules. Retrieved from http://www.coe.int/t/dg3/healthbioethic/texts_and_documents/RecR(99)3.pdf
Drechsler, C. T. (1999). Duty of care: liability for malpractice. In American Juris-prudence: Physicians, Surgeons, and Other Healers (2nd ed.; Vol. 61). St. Paul, MN: West Press.
Ebbesen, J., Buajordet, I., Erikssen, J., Brors, O., Hilberg, T., Svaar, H., & Sandvik, L. (2001). Drug related deaths in a department of internal medicine. Archives of Internal Medicine, 161(19), 2317–2323. doi:10.1001/archinte.161.19.2317 PMID:11606147
Editorial. (2005). Roles and responsibilities of medical expert witnesses. British Medical Journal, 331(7512), 305.
European Commission. (2006). Special Eurobarometer. Medical Errors. Retrieved from http://ec.europa.eu/health/ph_information/documents/eb_64_en.pdf
European Council of Legal Medicine. (2011). Description of Legal and Forensic Medicine as a Medical Specialty in the EU. Retrieved from http://eclm.info/docs/Documents/ECLM_UEMS_document._Approved_ECLM_GA_140911.pdf
Ferrara, S. D. (2013). Medical malpractice and legal medicine. International Journal of Legal Medicine, 127(3), 541–543. doi:10.1007/s00414-013-0839-2 PMID:23455848
Ferrara, S. D., Baccino, E., Bajanowski, T., Boscolo-Berto, R., Castellano, M., De Angel, R., & Villanueva, E. et al. (2013). EALM Working Group on Medical Malpractice. Malpractice and medical liability. European Guidelines on Methods of Ascertainment and Criteria of Evaluation. International Journal of Legal Medicine, 127(3), 545–557. doi:10.1007/s00414-013-0836-5 PMID:23564275
Gallagher, T. H., Studdert, D., & Levinson, W. (2007). Disclosing harmful medi-cal errors to patients. The New England Journal of Medicine, 356(26), 2713–2719. doi:10.1056/NEJMra070568 PMID:17596606
Gallagher, T. H., Mello, M. M., Levinson, W., Wynia, M. K., Sachdeva, A. K., Snyder Sulmasy, L., & Arnold, R. et al. (2013). Talking with patients about other clinicians errors. The New England Journal of Medicine, 369(18), 1752–1757. doi:10.1056/NEJMsb1303119 PMID:24171522

The Role of Forensic Medicine in Medical Errors
167
Gorney, M. (2003). Expert witnesses: Caught in a moral and ethical dilemma. Bul-letin of the American College of Surgeons, 88, 12–14. PMID:23593721
Graber, M.A., Hartz, A., James, P., Nugent, A., & Green, M.D. (2005). An alterna-tive method of determining standard of care in alleged cases of malpractice. Journal of the American Board of Family Medicine, 18(6), 453-8.
Graber, M.L. (2013). The incidence of diagnostic error in medicine. BMJ Quality & Safety, 22(2), ii21-ii27.
Grant, D., & McInnes, M. M. (2004). Malpractice experience and the incidence of cesarean delivery: A physician-level longitudinal analysis. Inquiry, 41(2), 170–188. doi:10.5034/inquiryjrnl_41.2.170 PMID:15449432
Grobler, S. (2007, March). The role of the expert witness. The South African Gas-troenterology Review, 11-14.
Gross, S. (1991). Expert evidence. Wisconsin Law Review, 1113–1232.
Hudson, M. J., & Moore, G. P. (2011). Defenses to malpractice: What every emer-gency physician should know. The Journal of Emergency Medicine, 41(6), 598–606. doi:10.1016/j.jemermed.2010.07.001 PMID:21094012
Jena, A. B., Seabury, S., Lakdawalla, D., & Chandra, A. (2011). Malpractice risk according to physician specialty. The New England Journal of Medicine, 365(7), 629–636. doi:10.1056/NEJMsa1012370 PMID:21848463
Jerjes, W., Mahil, J., & Upile, T. (2011). English law for the surgeon II: clinical negligence. Head & Neck Oncology, 3, 52.
Johnston, J.C., & Sartwelle, T.P. (2013). The expert witness in medical malpractice litigation: through the looking glass. Journal of Child Neurology, 28(4), 484-501.
Johnston, J. C. (2010). Neurological malpractice and nonmalpractice liability. Neu-rologic Clinics, 28(2), 441–458. doi:10.1016/j.ncl.2009.11.008 PMID:20202503
Juvin, P., Teissiere, F., Brion, F., Desmonts, J. M., & Durigon, M. (2000). Postop-erative death and malpractice suits: Is autopsy useful? Anesthesia and Analgesia, 91, 344–346. PMID:10910845
Kachalia, A., & Bates, D. W. (2014). Disclosing medical errors: The view from the USA. The Surgeon, 12(2), 64–67. doi:10.1016/j.surge.2013.12.002 PMID:24461211

The Role of Forensic Medicine in Medical Errors
168
Kachalia, A., Kaufman, S. R., Boothman, R., Anderson, S., Welch, K., Saint, S., & Rogers, M. A. (2010). Liability claims and costs before and after implementation of a medical error disclosure program. Annals of Internal Medicine, 153(4), 213–221. doi:10.7326/0003-4819-153-4-201008170-00002 PMID:20713789
Kaldjian, L. C., Jones, E. W., Wu, B. J., Forman-Hoffman, V. L., Levi, B. H., & Kassirer, J. P. (2002). Inconsistency in evidentiary standards for medical testimony. Disorder in the Courts. Journal of the American Medical Association, 288(11), 1382. doi:10.1001/jama.288.11.1382 PMID:12234232
Kaufman, H. H. (2001). The expert witness. Neither Frye nor Daubert solved the problem: What can be done? Science & Justice, 41(1), 7–20. doi:10.1016/S1355-0306(01)71844-8 PMID:11215302
Kessler, D. P., Sage, W. M., & Becker, D. J. (2005). Impact of malpractice reforms on the supply of physician services. Journal of the American Medical Association, 293(21), 2618–2625. doi:10.1001/jama.293.21.2618 PMID:15928283
Kraman, S. S., & Hamm, G. (1999). Risk management: Extreme honesty may be the best policy. Annals of Internal Medicine, 131(12), 963–967. doi:10.7326/0003-4819-131-12-199912210-00010 PMID:10610649
Localio, A.R., Lawthers, A.G., Brennan, T.A., Laird, N.M., Hebert, L.E., Peterson, L.M., … Hiatt, H.H. (1991). Relation between malpractice claims and adverse events due to negligence. Results of the Harvard Medical Practice Study III. New England Journal of Medicine, 325(4), 245-51.
MacKay, A. P., Berg, C. J., Duran, C., Chang, J., & Rosenberg, H. (2005). An assessment of pregnancy-related mortality in the United States. Paediatric and Perinatal Epidemiology, 19(3), 206–214. doi:10.1111/j.1365-3016.2005.00653.x PMID:15860079
Madea, B. (2009). Medico-legal autopsies as a source of information to improve patient safety. Legal Medicine, 11, 76–79. doi:10.1016/j.legalmed.2009.01.108 PMID:19289305
Madea, B., & Preuss, J. (2009). Medical malpractice as reflected by the forensic evaluation of 4450 autopsies. Forensic Science International, 190(1-3), 58–66. doi:10.1016/j.forsciint.2009.05.013 PMID:19524380
Main, E.K., Morton, C.H., Melsop, K., Hopkins, D., Giuliani, G., & Gould, J.B. (2012). Creating a public agenda for maternity safety and quality in cesarean delivery. Obstetrics & Gynecology, 120(5), 1194-8.

The Role of Forensic Medicine in Medical Errors
169
Nichols, L., Aronica, P., & Babe, C. (1998). Are autopsies obsolete? American Journal of Clinical Pathology, 110(2), 210–218. doi:10.1093/ajcp/110.2.210 PMID:9704620
Noguchi T., & Sathyavagiswaran, L. (2005). The role of the forensic pathologist in quality assurance and safety of patient care. Medicine and Law, 24(3), 535-47.
Ott, C. J., & Houry, D. E. (2000). Medical malpractice and the emergency medicine resident. Annals of Emergency Medicine, 36(6), 631–633. doi:10.1067/mem.2000.111063 PMID:11097709
Ozdemir, M. H., Cekin, N., Can, I. O., & Hilal, A. (2005). Malpractice and system of expertise in anaesthetic procedures in Turkey. Forensic Science International, 153(2-3), 161–167. doi:10.1016/j.forsciint.2004.08.016 PMID:16139105
Perkins, G. D., McAuley, D. F., Davies, S., & Gao, F. (2003). Discrepancies between clinical and postmortem diagnoses in critically ill patients: An observational study. Journal of Critical Care, 7(6), 129–132. doi:10.1186/cc2359 PMID:14624686
Riga, M., Vozikis, A., & Pollalis, Y. (2014). Medical Errors in Greece: An Economic Analysis of Compensations Awarded by Civil Courts (20002009). Open Journal of Applied Sciences., 4(04), 168–175. doi:10.4236/ojapps.2014.44017
Rosenthal, G. E. (2007). Disclosing medical errors to patients: Attitudes and practices of physicians and trainees. Journal of General Internal Medicine, 22(7), 988–996. doi:10.1007/s11606-007-0227-z PMID:17473944
Ryan, K., Schnatz, P., Greene, J., & Curry, S. (2005). Change in cesarean section rate as a reflection of the present malpractice crisis. Connecticut Medicine, 69, 139–141. PMID:15861999
Schifrin, B. S., & Cohen, W. R. (2013). The effect of malpractice claims on the use of caesarean section. Best Practice & Research. Clinical Obstetrics & Gynaecology, 27(2), 269–283. doi:10.1016/j.bpobgyn.2012.10.004 PMID:23206669
Shojania, K. G., & Burton, E. C. (2008). The vanishing non forensic autopsy. The New England Journal of Medicine, 358(9), 873–875. doi:10.1056/NEJMp0707996 PMID:18305264
Shojania, K. G., Burton, E. C., McDonald, K. M., & Goldmann, L. (2003). Changes in rates of autopsy-detected diagnostic errors over time: A systematic review. Journal of the American Medical Association, 289(21), 2849–2856. doi:10.1001/jama.289.21.2849 PMID:12783916

The Role of Forensic Medicine in Medical Errors
170
Stamm, J.A., Korzick, K.A., Beech, K., & Wood, K.E. (2016). Medical Malpractice: Reform for Today’s Patients and Clinicians. The American Journal of Medicine, 129(1), 20-5.
Start, R. D., & Cross, S. S. (1999). Pathological investigation of deaths following surgery, anesthesia, and medical procedures. Journal of Clinical Pathology, 52, 640–652. doi:10.1136/jcp.52.9.640 PMID:10655984
Studdert, D. M., Mello, M. M., Sage, W. M., DesRoches, C. M., Peugh, J., Zapert, K., & Brennan, T. A. (2005). Defensive medicine among high-risk specialist phy-sicians in a volatile malpractice environment. Journal of the American Medical Association, 293(21), 2609–2617. doi:10.1001/jama.293.21.2609 PMID:15928282
Studdert, D. M., Mello, M. M., & Brennan, T. A. (2004). Medical malpractice. The New England Journal of Medicine, 350(3), 283–292. doi:10.1056/NEJMhpr035470 PMID:14724310
Tancredi, L. R., & Barondess, J. A. (1978). The problem of defensive medicine. Science, 200(4344), 879–882. doi:10.1126/science.644329 PMID:644329
Tevlin, R., Doherty, E., & Traynor, O. (2013). Improving disclosure and manage-ment of medical error e an opportunity to transform the surgeons of tomorrow. The Surgeon: Journal of the Royal Colleges of Surgeons of Edinburgh and Ireland, 11(6), 338-43.
Tümer, A. R., & Dener, C. (2006). Evaluation of surgical malpractice in Turkey. Legal Medicine, 8(1), 11–15. doi:10.1016/j.legalmed.2005.06.006 PMID:16157500
Vinen, J. (2005). Negligence of medical experts. British Medical Journal, 330(7498), 1027. doi:10.1136/bmj.330.7498.1027-a
Wegman, B., Stannard, J., & Bal, B. S. (2012). Medical liability of the physician in training. Clinical Orthopaedics and Related Research, 470(5), 1379–1385. doi:10.1007/s11999-012-2244-4 PMID:22278849
Copyright ©2017, IGI Global. Copying or distributing in print or electronic forms without written permission of IGI Global is prohibited.
DOI: 10.4018/978-1-5225-2337-6.ch007
Chapter 7
171
The Psychological Impact of Medical Error on Patients,
Family Members, and Health Professionals
ABSTRACT
The current chapter examines the psychological implications emerging from medical errors. Whilst the psychological effects have studied, nonetheless the consequent impacts and the underlying psychological causes have not been sufficiently analysed and/ or interpreted. The chapter will add to the literate by using a psychodynamic approach in analysing the psychological impact of medical errors and provide in-terpretations of the underlying causes. The chapter concludes that medical errors lead to a series of implications. For the patient the quality of interactions with health professionals are directly affected and usually have immediate consequences. The impact of these consequences in the patient is mediated by the patient’s personal-ity, history of the individual and the psychoanalytic destiny of the patient. For the patient’s relatives medical errors create emotional cracks leading to regression and eventual transference of the medical errors as a “bad” object. For health profes-sionals medical errors impact upon the psychological defence mechanisms of the psychic Ego.
Mary I. GouvaTEI of Epirus, Greece

The Psychological Impact of Medical Error
172
INTRODUCTION
Medical errors have been identified as the most common type of error affecting the safety of patients (Brady, Malone, & Fleming, 2009). The majority of people that are in contact with the health services, either as services users or service pro-viders, have experiences of a medical error. However, dealing with the aftermath of a medical error and the manner in which this impacts on each individual is not identical or repeatable. The medical error from a psychological perspective to a great degree depends on its ‘history, on the story of its protagonists and on the spatial-temporal features whereby the medical error occurred. Furthermore, whilst there is an immediate and possibly long term effect of the medical error to patients, family members and health professionals, nonetheless this effect is very different. Patient and family members experience the medical errors as victims, whereas health professionals experience the medical errors not just as perpetrators but according to several studies (Pratt & Jachna, 2015; Panella, et al., 2014; Seys, et al., 2013) and as second victims.
The social representations of medical errors from patients, family members and health professionals, and the somatic and psychological effects of medical errors have been widely discussed in the literature. However, the analysis of the underlying psychological causality of medical errors and the interpretation of its consequences based on a psychodynamic approach is currently lacking in the wider literature. The current chapter aims at highlighting the psychological causes of the medical error and interpreting via a psychodynamic approach the impact these have on patients, family members and health professionals.
BACKGROUND
While there are some studies investigating the psychological effects of medical errors on family members (Worsham, 2009; Delbanco & Bell, 2007; Gallagher et al., 2003), and some other studies exploring health professionals experiences and roles in medical errors (Waterman, et al., 2007; Vincent, 2003; Duclos, et al., 2005), nonetheless the literature concedes that there are insufficient available evidence to explicitly determine the impact of medical errors on patients (Elder, et al., 2005; Mazor, et al., 2004).

The Psychological Impact of Medical Error
173
The few available studies on the topic have concluded that after the occurrence of a medical error patients express lack of confidence towards health professionals and consequently avoid using the health system, and if they end up using the health system they become much more persistent for a second medical opinion (Elder, Ja-cobson, Zink, & Hasse, 2005). On the other hand, the family members following a medical error express thoughts, feelings and behaviors that are comparable to those of individuals that have been exposed to other sorts of psychosocial traumas. However, family members in addition to exhibiting behaviors similar to psychosocial trauma they as well report a sense of increased fear, horror, helplessness, guilt, humiliation, shame, dissociation, and/or detachment from emotions (Worsham, 2012). Finally, health professionals involved in medical errors often express emotional distress, depression, guilt, shame and decreased job satisfaction, and display signs of physical fatigue, sleeplessness, difficulties of concentration, tachycardia and hypertension (Waterman, et al. 2007; Pratt & Jachna, 2015). Furthermore, many health profes-sionals do not feel free to report the error, and this inhibition of reporting errors is often a result of what the literature defines as medical narcissism, whereby health professionals find the disclosure of an error to be too challenging for their self-image of competence, control, and “treatment-oriented focus, hence rationalizing the error as unavoidable, unimportant, or unnecessary to reveal because it will not change the outcome and instead try to forget about the error and go about issues as the error never occurred (Banja 2005; Anderson, et al., 2009; Panella, et al., 2014).
Both, the emotional impact and the psychological effects of a medical error is depended on the way that the incident was addressed and the strategies used for the disclosing the medical error if this is disclosed (Vincent, 2003). Some typical reactions portraying the emotional impact of medical errors on health professionals are expressions of apology, demonstration of an apparent and conscious effort to avoid the repetition of similar medical error in future cases and the compensation, material or otherwise, to the patient (Lamb, et al., 2003). Literature suggests that thorough disclosure of a medical errors improves the understanding of the patterns of errors, and in this way otherwise characterised “unavoidable” errors become preventable, thus increasing patient satisfaction, re-establishing trust amongst the patient and the health professional, and forging a positive emotional reaction (Mazor et al., 2004; Banja 2005). Furthermore, the disclosure of a medical error reduces the expressed need for change of doctors and reduces litigation disputes. Also, research data demonstrates that family members wish as much as possible information regarding the medical errors to be given during the care of their beloved one, and they want information about the avoidance of similar errors in the future, as well as an apology and the restoration of the damage suffered due the medical error (Allan & McKillop, 2010; Blendon et al., 2002; Gallagher et al., 2005; Mazor et al., 2004; Lamb et al, 2003).

The Psychological Impact of Medical Error
174
From the above is highlighted that the psychological consequences of medical errors are directly related to patient safety and the quality of healthcare.
INTERPRETING THE PSYCHOLOGICAL ASPECTS OF MEDICAL ERRORS
The psychological effect of a medical error relates to the historicity of the error and the uniqueness of both the error and the individual experiencing the error, as well as the specific role the individual has in the error. It appears that it is not so much the medical error in itself as a fact that has the most forceful impact, but its conse-quences that result in a crisis of meaning and interpretation attached to a medical error. Based on clinical experience it can be obeserved that both the patient’s and their family’s responses towards a medical error is subjective and notrelated to the error itself nor to its seriousness.
1. Psychological Implications of Patients Following a Medical Error
In the literature it appears that there are significantly less studies relating to the emo-tional and psychological impacts of medical errors on patients, than there are relating to the emotional and psychological impact of medical errors on health professionals. Furthermore, the available studies on patient experiences of medical errors focus primarily on the practical ways in which the patients react when confronted with a medical error and the ways they would like to be dealt by health professionals. There are limited numbers of studies that focus on the emotional and psychological effects of medical errors on patients. These limited studies converge to the fact that the aftermath of a medical error leaves patients’ with a sense of angry sentiments, with reduced confidence towards health professionals and with avoidance of the health system and increased persistence for a second medical opinion (Elder, Jacobson, Zink, & Hasse, 2005). Furthermore, patients also expressed their wish to be made directly and immediately aware of the medical errors, even if there is nothing that can be done about it (Mazor, et al., 2004). Also, Vincent, Pincus, and Scurr (1993) assert that surgical accidents have a major adverse psychological impact on patients, and the poor communication after the accident increases patients’ distress.
Janssen et al. (2007) study indicates that psychosocial aspects of physician-patient interaction is of great significance in the health care of seriously injured Accord-ing to Gallagher et al. (2003), patients believe that the way in which the medical error will be presented to them has a significant impact on their levels of distress. However, the notion of discomfort increases when the presentation and explanation

The Psychological Impact of Medical Error
175
of medical errors are incomplete or when there are efforts from health personal to become evasive in relation to the medical error. On the other hand, patient anxi-ety is reduced when the medical error is revealed candidly and compassionately with a genuine effort from health professionals to seek forgiveness. Mazor, et al.’s (2006) study examining the factors influencing patients’ responses to medical er-rors concluded that full disclosure is likely to have a positive effect or no effect on how patients respond to medical errors, and that there is an uncertain association between an existing positive physician-patient relationship and the waiving of costs associated with the medical error.
Therefore the point of interest from a psychological aspect of medical errors is why are there limited studies concerning the emotional and psychological effects of medical errors on patients and why they main emphasis of studies remain the practi-cal ways patients react when confronted with a medical error and the consequent negative effect between patient and health professional relationships. Firstly, the simplistic assumption is that some patients as a result of a medical error have major health effects or even die as consequence of the medical error rendering them un-able to communicate their experiences and feelings of the medical error. Secondly, patients that survived the medical error and are capable of sharing experiences and feelings may express unwillingness to participate in relevant studies as the narration and revival of the experience is similar to scratching an old wound and potential lead to memory reconstructions thus re-living a traumatic experience.
Reflecting on our own clinical experience with patients that have experienced a medical error we concur with Elder et al. (2005) that anger is a psychological effect that is usually present, but feelings such as guilt, shame, fear of symptoms, anxiety and distress are not usually present in patients or family members and in minor cases that they may appear they are circumstantial and very quickly fade away.
In the subsequent sub-headings the psychological issues that arise in patients after the medical error will be presented and analysed, beginning chronologically from that which would be occurred immediately after the disclosure of medical error.
A. The Presentation of the Medical Error and the Acquisition of Knowledge
The patient, when faced with a medical error, his first and greatest need is to establish a level of certainty with regard to the degree and extent of the medical error, and the consequences that this medical error will have on health. The result of this process and lack of knowledge leads to sentiments of insecurity, anguish, fear and anxiety. The manner in which the medical error is disclosed to the patient has significant psychological consequences on the levels of patient anxiety (Gallagher, et al., 2003). Truog et al. (2010) in their book entitled “Talking with patients and families about

The Psychological Impact of Medical Error
176
medical error: A guide for education and practice” emphasized that five features of the physician-patient relationship deserve special attention, namely; 1) transparency, 2) respect, 3) accountability, 4) continuity, and 5) kindness.
Furthermore, when a medical error occurs, patients wish to have this information conveyed to them by the person responsible for the medical error and not delegate to someone else the responsibility to communicate this information (Delbanco & Bell, 2007). However, even when the health professional responsible for the medical error provides directly information of the occurrence of the medical error to the patient there still may be cases of distress, fear and anxiety exhibited by patients until the patient acquires relevant knowledge of the consequences and develops a degree of certainty with regard to the positive outcomes of the medical error. Once, however, the symptoms of the body permits, then the psyche will need to take over and do the next step. This next step that relies on the psychic is depended on one hand on the manner by which the medical error will be dealt with, and on the other hand on the psychic maturity of the specific patient. Most patients feel humbled by the admittance of the error from the person responsible and therefore are ready even to forgive the person responsible for the medical error. They feel by forgiving that they are doing something “good” and to a point expect a symbolic reward from the doctor-parent, from the therapeutic group-family, from the institution-society, but above all expecting a symbolic reward from life itself.
B. The Hidden Injustice
After the immediacy of the situation concerning a medical error and initial forgive-ness from the patient, follows the aftermath of the medical error that is usually accompanied by feelings of frustration. This frustration for some patients is often expressed with anger and allocation of blame. Similarly, Elder et al. (2005) concur that the sentiment of anger follows the immediacy of a medical error. But if distanced from the situations it becomes obvious that this anger has various characteristics and is expressed in multi-various ways. It is both a frightened anger and a polite anger. The wrathful anger is usually and typically expressed by the family members. The patient as bearer of the disease and its exhibiting symptoms has firmly moved into a new self with a transformed behaviour and a different psychology. Some patients may as well express bitterness about what happened to them and this is usually communicated primarily with non-verbal cues, such as sighs, head bowing, think-ing look etc. The answer-begging questions are; what is hidden in this anger and bitterness? Towards what direction are they both heading? Forward or backward?
Mr. Peter was a 65 years old that undergone a surgical removal of a malignancy from the stomach, after a medical error that occurred during the surgery led him to undergo an obligatory second surgery. When asked “how do you feel about what

The Psychological Impact of Medical Error
177
happened to you?” he replied “you are asking what I feel? It is obvious that the doctor would make a medical error during my surgery. Who else could this hap-pen? This is the story of my life. It goes from error to error. I was the eldest son in my family and my parents learned how to become parents on me. My younger siblings for my mother were always those that needed more help and needs. By an accident I was almost left homeless, but fortunately I managed to recover. Due to my parents’ omission to write up a will, my siblings shared the family fortune in an unjust manner, leaving me out of the sharing. And in spite this injustice done on me by them, nonetheless I am the one that have ill health. Even God treated me unfair. I cannot understand why do as a result of my ill-health my children have to suffer? This is what is of concern to me”. Usually, behind sentiments of anger and bitterness lurks a sense of injustice. This sense of injustice and bitterness is rationalised by the patient and is expanded as to apply to his entire life. It is easier for the patient to discuss the injustice of life with family members than discuss his illness. The medical error in this case covered up the uneasiness of talking about the illness and temporarily even repressed the illness.
C. The Medical Error as a Decorative Medal
As noted above it has been found that some patients following a medical error develop a more dynamic communication with healthcare providers, decrease their trust towards health professionals, avoid the health system and become much more persistent for a second medical opinion (Elder et al., 2005). Indeed, there are pa-tients that usually take it upon themselves in acquiring the capacity at their com-munication and behaviour change. It appears as if the medical error became their reason d’etre of their existence and their license to rebel against the health system, health professionals and parental symbols. It is as if the medical error signifies the termination of a predestined punishment and leads to secondary narcissistic satisfactions enabling the individual that until recently was able to speak only with his body to start speaking with his mouth, and especially with his actions. It is as if the patient from feeling as being persecuted from life is transformed to becom-ing the persecutor of the entire health system. It is as if the patient is redeeming himself/ herself for all errors and oversights in his/her life. In this way the medical error becomes in its own right the decorative medal that can be worn and become distinguish from others. Essentially the medical error when worn as a decorative medal the individual feels valued. The victory over the medical error, since it was unable to destroy the individual, is transformed to a tool that highlights the self as a warrior that has seized the opportunity to change.

The Psychological Impact of Medical Error
178
In conclusion, the manner by which patients responds to the medical error itself seems to depend upon both the type of the error and of the ways this is managed and treated by health care provider, the treatment group and the health organisation. The managing and treatment of the medical error always develop and is based upon the personality, personal history and psychoanalytic destiny of the patient.
2. Family Members and Medical Errors
Family members’ experiences of medical errors when occur in their beloved ones has recently drawn the interest of many scholars. Whilst, family members senti-ments to medical errors has drawn attention of research, nonetheless there is no explicit or sufficient explanations of these experience, but there is a convergence of most studies about the multifactorial nature of this situation. Several studies have highlighted the burden of relatives focusing on the psychological symptoms such as guilt, fear and feelings of isolation (Delbanco & Bell, 2007; Worsham, 2009). Other studies have highlighted that family member’s experiencing a medical error on their beloved one report symptoms that are similar to those of people exposed to other psychosocial traumas (Worsham, 2009). Furthermore, these studies also indicated that family members experience display an intense emotional reaction, exhibiting even feelings of horror, helplessness, humiliation, shame, dissociation or detachment from emotions, emotional numbing, increased anxiety, heightened arousal, avoidance of situations reminiscent of the experience and that they suffered from intrusive memories (Worsham, 2009).
Based on the above study conclusions family members experiences will be ana-lyzed and their symptoms interpreted. The time at which the event of medical error is occurred is already a difficult time as the fact of the disease has already disturbed the family health structure and has caused an imbalance that has been diffused within the whole family system, affecting both the system’s operation and family system’s people. In other words, the medical error triggers a family crisis without available solution from its internal system and it is forced to seek solutions outside the fam-ily and primarily from professionals. This is the place where the medical error will meet a family creating yet another crisis on the current one and some of the already existing symptoms are intensified and some new ones are added. Nevertheless, all the old and new symptoms are magnified emanate from the same event, which is not the original illness, but the medical error.

The Psychological Impact of Medical Error
179
The medical error becomes for the family members the main focus and problem, rather than the original illness. The medical error becomes for family members the main obstacle in satisfying the family needs and re-balancing the family system and for each family member at personal level to establish libidinal satisfaction. The family members lack the unique satisfaction that they require at the specific spatial-temporal context and feel frustrated. Family frustration puts at stake not only appropriate individual treatment and care, but also the answer to a question requir-ing a given mode of satisfaction. Furthermore, there is an expectation that health professionals do their duty, as dealing with the original illness appears to be easier than dealing with the side-effects of this medical.
A. The Presence of Guilt and Shame
According Delbanco & Bell (2007) patient’s family members following a medical error often accuse themselves as responsible for the medical error and feel guilty about that they have not managed to adequately and closely monitor their beloved one. These feelings are present despite the fact that most recognize that they could not have prevented the medical error.
The feeling of guilt may trigger emotional states varying from remorse to the apparently ridiculous self-reproach, which follows acts that the subject deems rep-rehensible, though the reasons he gives for doing so may or may not be adequate ones. Or again, it may refer to a vague sense of personal unworthiness unconnected with any particular act for which the subject blames himself (Laplanche & Pontalis, 1973). The feeling of guilt of family members identifies the emotional state which follows a medical error. This bestows the family members a responsibility they do not have or could control and avoid self-punishing in this way themselves with self-accusations and self-devaluations. Sometimes we have been witness of this self–punishment listening words like “I ought to have understand that something bad will happen” and “I should have disagreed to the hospitalization” and “I should have insisted in choosing another doctor” and “I should have get and a second opinion” and “I should not agree for the operation and to change his opinion”. The omnipotent superego, the known accuser and punisher of the psychic organ, in dif-ferentiation with the ego in the process of defensive psychic conflict, which follows the event of the medical error. The self attacks itself and it is worth to be noted that this feeling of guilt is partly unconscious, to the extent that the real nature of this self-punishment is not known to person. The feeling of guilt can as well occur in the form of shame which is associated with protective measures that the family members were unable to take for avoiding the medical error.

The Psychological Impact of Medical Error
180
The experienced of shame on family members is as well quite intense and is included with the psychological symptoms that family members feel (Worsham, 2009). The feeling of shame in medical error manifests both as internal shame and as external shame. Shame because the family members was unable to help the beloved one and shame in relation to the social environment which may consider that the family members were uncaring towards their beloved one. According Benn et al. (2005) internal shame concerns the negative evaluations of the self for the self and feelings which are addressed to self (such as disgust for the self). While the external shame is associated with assessments which focus on the aspects of ourselves which we believe that others will reject (Gilbert, 2000).
The social factor that triggers the feeling of shame is the gaze of the Other and the gaze of the community. The emotions alone are not related to ethics, but they are associated with actions which are stem from them (Heller, 2003). The gaze of the Other according to Heller (2003) acts as a moral authority and the gaze of the Self we could add that it acts as a prosecuting authority, since as we have seen it runs the superego commands. In the case of medical error the family is faced with both the gaze of the Other and the constitute gazes of the Self of each family member. Gilbert (1998) says that it is likely the emotions which are associated with shame to affect the sympathetic and the parasympathetic system in different ways that is difficult to untangle and fully understand.
Individuals experience feelings of shame when they perceive themselves as victims of injustice because they are very passive and powerless to prevent the self from becoming a victim (Gilligan, 2003). This sense of injustice is something that inevitably happens when medical error occur creating feelings such as victims of injustice combined with feelings of hopelessness, helplessness and weakness. According to Tangney & Dearing (2002) shame can cause anger, which is usually directed towards others.
B. Family Members in the Nest of Fear
According to Worsham’s (2009) study family members tend to report symptoms of fear and anxiety. The fear is always present in situations of uncertainty, desperation and deadlock, such as it is a psychic process which is mobilized in order to rejoin the stress which is released and which has a specific object, the consequences of the medical error. Family members feel fear due to psychological distress that the medical error caused their beloved one. This physiological desperation and the fear is rooted psychological and biological past existence of the individual and for this reason memories are activated from the pre-speaking period of his life that they had managed to push back.

The Psychological Impact of Medical Error
181
Delbanco & Bell (2007) highlight additional causes of real or imaginary fears of family members regarding further damages and risks, including the punishment of the healthcare workers insomuch they express their emotions or even and the future mistreatment. It is expected throughout the period of the experience of medical error relatives feel anxiety that creates fear and fear in return creates more anxiety. Their anxiety is their psychological reaction to the traumatic condition of the medi-cal error. This is a traumatic condition that is impossible to manage to control it. The released stress that results from the psychological trauma may in some cases to act and as a releasing agent for revealing the existence of a pre-existing neurotic structure. While in other cases this psychological trauma acts as a way of defusing and plays a decisive role even with regard the manifestation of family members’ symptoms (such symptoms are dissociation or detachment from emotions, intrusive memories, emotional numbing, heightened arousal and avoidance of situations reminiscent of the experience).
C. The Psychological Trauma that becomes Angry and Aggressive
Although, in none of the studies reviewed mentioned anger and aggression, none-theless we consider appropriate to highlight their presence, since many times they are the main protagonist or co-protagonist in cases of medical error. Aggression, according to Laplanche & Pontalis (1973) is the tendency or cluster of tendencies that find expression in real or fantasy behavior intended to harm other people, or to destroy, humiliate or constrain them. For example aggression may find expression as violent, destructive motor action, but can also find expression as the refusal to lend assistance or as a symbolic action (e.g. irony). Psycho-analysis has gradually come to give great importance to aggressiveness, showing it to be at work in the early stages of the individual’s development and the culmination of this increasing stress on aggressiveness is the attempt to find a single and basic instinctual under-pinning for it in the idea of the death instinct. Aggression and anger may occur from the frustration that the family members feel and from the sense of injustice felt for the whole family. Furthermore, according to Gilbert (1998), anger can along with anxiety and disgust be the key elements of the experience of shame, and be part of the non-verbal behavioral reactions of the family members. It is important to separate the anger from aggression. As Tangney & Dearing (2002) report, anger is concerned with a negative emotional state and it is an emotion which involves the attribution of blame, whereas aggressiveness is a behavioral reaction which intends to cause harm or distress to someone else.

The Psychological Impact of Medical Error
182
In our book “psychological issues in care stories” (Gouva & Kotrotsiou, 2011) we presented a story entitled “the bearer of their pain” where family members reacted with aggressiveness and even violence towards health professionals that cared for their beloved one because they considered them as sole responsible for the medical error. This was interpreted that via process of transference an awaken of instinctual impulses occurred, which were expressed impulsively, with acting out and becoming violent shortly after the announcement of the death of their beloved one.
Since the psychic does not undergo the effort of manifesting a behavior and a symptom for just a single reason, family members may express violent behavior because of their unconscious desire to exert violence to death and in the process become violent towards the doctor. They transfer to doctor death itself, in contrast to their initial meeting (prior the medical error) that they transferred the miracle of medical science or even God. Furthermore, family members may express violent behavior due to their unconscious desire to replace feelings of shame and lived humiliation with the feelings of pride. Gilligan (2003) argues that people resort to violence when they feel that they can wash away the shame by shaming those who feel that shamed them. The most powerful way to make one to feel ashamed is through violence as the most powerful way to push someone to commit violence is to make him to feel ashamed. Finally, family members that have experienced a medical error and display symptoms of anger and aggression, these symptoms can also take on the characteristics of domestic violence shifting the anger, aggression and narcissistic injury towards more safe persons.
Concluding, family members after a medical error are at the beginning of a crisis. They are fixated in a situation that creates emotional cracks, regressions, transfers, introjection of bad objects and a situation that is fundamental in their lives, and usually becomes the defining moment by which their lives are organized as the pre-event and post-event of medical error. Worsham (2009), in his study found that for some family members it felt as if time stopped at the moment of the medical error and the sense of distress commenced for the family members that in some cases was prolonged as long as ten years following the medical error.
3. The Psychological Consequences of a Medical Error on Physicians and Healthcare Professionals
The emotional world of doctors and the health professionals is overwhelmed by mixed feelings which arise from the duality of victory and defeat. Victory consists of the times they manage to help a patient and alleviate symptoms, and defeat consists of the times in which they fail to help and alleviate symptoms. Health professionals are daily obliged to live their professionals lives burdened with this duality and strive to come to terms with issues beyond human logic and endurance. Within this difficult

The Psychological Impact of Medical Error
183
and stressful daily routine of practice when faced with the possibility of a medical error on their part or from their participation in it, then unexpectedly they go into a blizzard of frozen emotions that can create to them unknown until those moment, behaviours and reactions without having any known mechanism of psychological and emotional survival in such situations.
A lot of studies have highlighted the psychological burden for second victims - doctors and health care professionals - (Pratt & Jachna, 2015; Panella, et al., 2014; Seys, et al., 2013) which is expressed by symptoms of fear. This fear takes the form of fear for their career, fear for the loss of their relationship with their colleagues (Delbanco & Bell, 2007), guilt (Pratt & Jachna, 2015; Sirriyeh, Lawton, Gardner, & Armitage, 2010; Delbanco & Bell, 2007; Gallagher, Waterman, Ebers, Fraser, & Levinson, 2003), anxiety (Waterman et al., 2007; Sirriyeh, Lawton, Gardner, & Armitage, 2010), emotional distress (Schwappach & Boluarteb, 2008; Waterman et al., 2007), risk for burnout and depression (Pratt & Jachna, 2015; Panella, et al., 2014; Schwappach & Boluarteb, 2008), distancing from patients who have suffered damage, anxiety and reduced confidence, avoiding of personal responsibility for the medical error (Delbanco & Bell, 2007), increased anxiety about future errors, loss of confidence, difficulties at sleeping, decreased satisfaction from their work and insult to their reputation (Waterman et al., 2007). Finally, Sirriyeh et al. (2010) study find evidences for the wide impact of medical error on health professionals with psychological effects which can include negatives conditions, such as shame, self-doubt, anxiety and guilt.
Based on the above research findings analysis of what ways and why both doctors and health care professionals react as they do with these psychological symptoms towards medical error?
Having worked with many doctors and health professionals for many years, we have concluded that the medical error is considered by many health professionals as failure and defeat. However, this failure and defeat is not confronted by all in the same way. There are some doctors and health professionals who perceive the medical error as the “great evil” and the emotional charging which they feel can lead them to emotional drain, stress, fear, guilt, shame, frustration and feelings of frustration. For others, again, the refusal to realize the medical error as therapeutic error regresses them to a child state of the self. Finally, there are those who express ambivalence with part of themselves blaming themselves and the other part defending themselves that eventually leads them at the end to psychic maturity of assuming responsibility. These three types of reaction to a medical error from health profes-sionals are not firm and unchangeable, but it is possible to move amongst reactions and this mobility depends on both the management and treatment of medical error by the patient and his family members, and the working environment that allows for a friendly and professional support or not.

The Psychological Impact of Medical Error
184
4. Introjection and Projection of Medical Error as a Bad Object
Health professionals and particularly doctors experience great stress as a result of a medical error, especially if they are implicated personally. They feel crushed by the negativity of the event and fail to appropriately distance themselves from the event and view it within its pragmatic dimensions. Consequently, they introject the medi-cal error as a “bad” object. This introjected “bad” object, than becomes a magnet for all their negativity relating to both their professional and the personal lives and eventually the medical error ends up defining the health professional.
This leads the health professional to exist in a reality that is lived in an inter-mediate space where at the one spectrum is the space of “I was someone” and the other spectrum the space “I will be nothing”. This intermediate space is defined by guilt and shame. Even if health professionals manage to overcome in the short term the guilt and shame and come out of this interim transitional space, the result is to be led to something even worse, which is the a vacant space. There is the contrast of the almost ideal self they considered until the time of the medical error and the now vacant space. And because the vacuum creates chaos and sense of absence, they rapidly return to the negative and painful sentiments that at least allow the psychic existence and the feeling of suffering, which consequently leads to a sense of existence.
Once the medical error is introjected as a “bad” object by the health professional it becomes situated in the psyche of the health professional and becomes a terrify-ing stalker that exposes the health professional to internal disaster risks. The “bad” object was described by Melanie Klein (1952) as a privative maternal breast, which can be a terrifying stalker and with the introjection the child is exposed to internal hazards. Similarly, the doctor and the health professional in an imaginary world of loss and of prosecution fears are led to not only to introject as partial bad breast the medical error, but also fantasize in a negative manner the entire health system and the medical science.
The result of a medical error for health professionals leads the Ego of the psy-chic body to become “heavily wounded” and therefore have limited abilities of deal with the stress emerging from the whole situation. According to Freud’s theory of anxiety, a situation of distress is the model of a traumatic experience. According to Freud, (1936), the internal risks have as a common denominator the loss or the separation. This leads to a gradual increase of intensity being unable to control this tension and is flooded by stimuli that lead individual to distress.
In our book entitled “psychological issues in care stories” (Gouva & Kotrotsiou, 2011) a series of similar stories are presented with doctors and health professionals experiencing guilt that increased the excitation in their psychic life. These experi-ences that they are processed by the usual methods failed and created feelings of

The Psychological Impact of Medical Error
185
guilt and disorder in their subjective stability. A doctor from these stories, after experiencing a patient’s death decided that it was his sole fault and he states the “narcissistic wound which I received with the incident that I share with you, it is not the first in my life. I have experienced others, equally if not more painful. Nor it is the first time that I react with flight from the problem. I do not know why I feel so guilty every time that something goes wrong with my patients. Maybe it is the fault of my mother with particular weakness at her son, with very developed sense of “duty” and “perfectionism” in her work and a father loving, sensitive, but absent when difficulties were presented in the family. Maybe it is my fault that from the time I was a child my mother made me to feel as a kind of saviour. The little saviour who would grow and would save everyone else, such he saved her with his birth. Maybe the psychologically helpless men of my family are at fault that never put someone over of their salvation and passed to me all the debt. That they did not only have to start me, and to finish it. My day is worth when I’m useful”. Similarly, Gallagher et al. (2003) note that many doctors are experiencing strong emotions after a medical error and they feel guilty for the fact of this error and the most difficult challenge for themselves is to forgive themselves.
5. Backtracking to Child State of the Self
According to Delbanco & Bell (2007) some of the doctors who were associated with medical errors felt the need to be removed from patients who had suffered an injury as a result of their medical error. In other cases, other doctors avoided their personal responsibility for the medical error. These doctors emotionally were led to the denial of the medical error and tried to decline any responsibility for the medical error because at that point of time and context it was the only psychological response they could exert. That was the only psychic way that could choose to support not only their external self but also their internal self. They felt the need to leave their patients, who had suffered the loss as not to come in contact with the principle of reality and not to enable the emergence of painful memories and second thoughts that will lead to new knowledge and new meaning of the medical error event. For their psychic economy backtracked to earlier times of the evolution of their Ego of the psychic, passed in modes of expression and behavior belonging to immature stages of self, less complex, less structured and less diversified. To avoid confront-ing themselves, they refused themselves. Backtracking to their child state of Self and using the defence mechanism of denial they managed to free themselves, even temporarily, and get rid of the unwanted event of the medical error. Anna Freud (1966) is curious with the easiness that adults are ready to use the same mechanism in their interaction with children or those that their narcissistic self sees as children as to fool them in denying a reality. The narcissistic self of the particular doctor

The Psychological Impact of Medical Error
186
i the above story, whom we try to describe in this category, somehow he behaves defensively and denies any involvement with the event of the medical error. Banja (2005) in his book “Medical Errors and Medical Narcissism” describes this medi-cal narcissism and the need of health professionals to undermine the disclosure of a medical error to the relatives and their families with the aim of maintaining their self-esteem.
6. Looking at the Past and Future
It would be a material omission for this sub-chapter not to discuss those doctors and healthcare professionals when faced with a medical error, whilst initially feel terrified by the incident, consequently becomes an opportunity for psychosocial maturation and to go on a journey to a place where the psychic impulses are transformed into altruistic processes. These health professionals in the short term may refuse to participate in medical error and attempt to protect themselves. Their personality, however, does not allow them to deny their past and all that has been psychologically achieved and therefore quickly depart from this immature renunciation of the event.
Subsequently, it is possible they go through sentiments of anger and displacement. They displace and transfer all the blame of the medical error, not on the patient and their relatives, but on the system, on the institutional failure of safeguarding patient safety and preventing medical errors, on the long hours and on the lack of care due to financial cuts. However, they will not anchor in this anger, but will accept their involvement in the medical error, they will try to negotiate either a good care of the patient suffered a medical error, or if that is not possible, they will advocate for an honest vindication of relatives and of the self. Because their future expects from these types of health professionals many other patients to be cared for and have a chance for a healthy and quality of life.
An example of a doctor in his attempt to defend himself in a mock jury organised by his lawyer stated that “is it possible that I am accused for the loose of life, me who saved thousands of lives, me that night and day am in the hospital and answer to so urgent requests? I have given my whole life for patients and their families?”. He remained speechless to his lawyers - “You are wrong, and this is the wrong way to defend yourself. You should not tell these things to the court. If it was so, as you say, should someone who kills with his car a man to defend himself, saying I drive so many years and never I killed someone, this is the first time it happens to me.” The doctor left the lawyer’s office feeling angry and overworked, but very troubled and with a sense of guilt. Ιt was a very tough week, without a clear mind and pow-ers to perform his duties at the hospital. At the end of this week he felt the need to find the patient’s family members to ask for their forgiveness, even though his lawyer had advised him to avoid such a meeting. He was free, now, to return to the

The Psychological Impact of Medical Error
187
work and new patients, but taking decisions for new ways both medical and human directions. This difficult week and the guilt led him to repentance. Tangney & Dear-ing (2002) state that guilt concerns to repentance and is associated with a specific behavior rather than the entire self, so it looks more adaptive and less pathogenic than shame. This separation of self leads to behaviour which are witnessed in guilt protects the self from diminishing its value, while leaves the door open for change of the negative behaviour.
In the current sub-heading the psychological effects of a medical error for doc-tors and health professionals were analysed and it is found that any involvement of health professionals with a medical error involve numerous psychic mechanisms that are important to understand the components that relate to the personality of each professional and psychic and their intellectual maturity. Their unique tool in addressing at the psychological challenges of a medical error is their scientific past, their personality and the psychic and spiritual maturity that they have developed by the process. A personality and a maturity that leads them to relate to this predica-ment engagement based on a subjective existential meaning.
SOLUTIONS AND RECOMMENDATIONS
In the wake of the psychological impacts of a medical error the question that is raised and asks urgently not only answers but also the best possible solutions is “in the here and now of a medical error what should be done?”. Responding directly to this question it would be as if we accept with ease the medical error, whereas it is suggested that all efforts be made as to reduce medical errors as much as pos-sible. To avoid medical errors it is necessary to develop a better undergraduate and postgraduate education in relation to medical errors. According to Bonney (2014) continuous and high quality education is necessary for the prevention of future medical errors. According to Paxton & Rubinfeld (2010) education must develop students’ awareness on the impacts of medical errors and facilitate the critical analysis which must be directed to the disclosure of medical errors to patients and their relatives.
The psychological effects on patients, relatives and doctors and health profes-sionals can be met in a common place. The place of the Other. This common place is only achieved via empathy. Empathy implies feel as the other feels, to be in his/her place, but not try to wear his/her shoes but retracting memories that lead the individual to feel or even understand how much pain the shoes can cause to the feet. For empathy to occur communication is essential and not only in verbal com-munication, but mainly non-verbal, body language. According to Delbanco & Bell (2007) all involved in a medical error need an organized structure that will restore the communication and support the emotional needs. Worsham (2009) indicates

The Psychological Impact of Medical Error
188
that good communication is fundamental to medicine and better communication ratings are associated with reduced symptoms of trauma reported by family mem-bers, however, data related to communication indicate that healthcare professionals consistently failed at communicating important information to family.
Communication, however, means first of all disclosure of medical error. It is particularly important the time when this revelation will take place and what will follow this disclosure. According to Worsham (2009) the quality of the disclosure is associated with reduced trauma symptoms in family members. The effective disclo-sure of the medical error mitigates the family’s response, while according Delbanco & Bell (2007) withholding information during the process of disclosure of medical error can lead to lawsuits on the part of relatives. Two distinct but interactive phases occur during the communication with family before and after an unexpected death of their beloved one. According to the findings of Taylor et al. (2008) study there is the dynamic phase of “CARE” and reactionary phase of “SHARE”. The phase of “CARE” relates to: a) creating credibility and establishing fiduciary responsibility b) articulating the purpose and plan of an operation c) relating to the whole person in body, mind, and spirit, and d) empathizing and aiming to developing a positive therapeutic relationship. The phase of “SHARE” relates to: a) scrutinizing the care provided perioperatively, b) honestly and humbly acknowledging errors c) articu-lating the circumstances of the death d) reassuring and consoling and e) Ensuring self-care, and aims at tackling the crisis in a compassionate and respectful manner and to ensure self-care for the doctor.
While disclosure implies the assumption of medical error, this does not mean acceptance of responsibility and in no way it represents repentance of this and the need for forgiveness. The repent and the need for forgiveness involve both verbal and practical obligations to the concept of fair compensation. However, Allan & McKillop (2010) recommends that an apology that incorporates an admission of responsibility, an expression of regret and some action by professionals to deal with the needs of patients may promote forgiveness. Robbennolt (2009) suggests that the sincere apology can lead to reduction of suffering so for both the patients and the doctors, and also helps in improving the relations between doctors and patients, so that these relationships have continuity and to be achieved facilitation of valid claims, thereby reducing the cost of lawsuits. Similar proposals for forgiveness and fair compensation is proposed by Berlinger (2011) who goes on to say that the doc-tor can work toward self-forgiveness, taking the responsibility for the past, working towards the understanding of role of the medical error and responding to the needs that have been created as a result of this error.
Berlinger (2011) proposal is of importance, since as we saw in the analysis of the psychological effects of medical errors on doctors and health professionals in the main part of this chapter, there are a series of effects that can afflict them both at the

The Psychological Impact of Medical Error
189
short and long term. Furthermore a medical error can lead to additional errors and a vicious cycle of error and health care systems have a moral responsibility to care for second victims (Pratt & Jachna, 2015). However, the coping strategies used by health professionals may have an impact on their patients, colleagues, and themselves, and it is crucial that a set of supportive mechanisms are in place to protect both the patient and involved health care providers (Seys et al., 2013). According to Harri-son, Lawton, and Stewart (2014) such formal supportive mechanisms as feedback, systems change and local improvements are lacking. Gallagher et al. (2003) argue that a better institutional support for caregivers involved in medical errors will help them to focus their attention on the affected patient, something that in our view is considered particularly necessary. We firmly believe that the problems and the psy-chological effects of medical errors could be addressed by ensuring the development of interdisciplinary groups of care and support as for patients and their relatives as well as for doctors and health professionals in each treatment and care provider.
FUTURE RESEARCH DIRECTIONS
From our study is indicated the need for a continuously research effort on the psy-chological effects of medical errors which will illuminate various aspects and will help all to better deal with medical errors. The psychological impacts of medical errors relate to the time that the medical error happened, the time of disclosure of the medical error, the time of admission of the medical error, the time of response to the medical error and finally the time in which this medical error makes meaning. These different times lead to different ways in dealing with the medical error, with different ways of expressing the medical error and with different rationalizations and meaning-making of the medical error. Many of these expressions of psychologi-cal effects, such as repression, of medical error, the identifications which can take place, the pressures, the posteriori experience cannot be studied with the method of quantitative research, but require primarily qualitative methodologies. Although many of the findings of existing studies are resulted from qualitative studies, these failed to develop in-depth understandings, as this would be feasible only with case studies and narratives both from patients and their relatives, and from doctors and health professionals.

The Psychological Impact of Medical Error
190
CONCLUSION
At the completion of this chapter medical errors cause complicated and always painful psychological effects on those who in one way or another are involved in them. The arguments of our analysis and interpretation are not physically integrated but can illuminate hidden expression and causes and demonstrate new approaches in relation to medical errors.
Patients who have experienced medical error feel angry, and often complain about the treatment they had from their doctor or health care team. The psychological effects which are observed on patients differ from those of their family members and are related to both the quality and the ways of dealing with the medical error from the treatment group, based always on their personality, personal history and their psychoanalytic destiny.
A medical error occurring on a beloved one appears to disrupt the health of the entire family and can cause an imbalance of the whole family system creating an internal disorder and a deregulation of the stability in each of the members, affecting both the operation of the family system and its’ members. Most of the time beyond the psychological symptoms the medical error threatens the very balance within the family and the family members go into a crisis situation and it is not the mere existence of the medical error that leads to this crisis, but primarily the interpreta-tions which the family members attribute to this error, which eventually affects their attitudes towards the situation. Therefore, family members’ perceptions with regards the disease and its implications is greatly determined by the ways in which the family will strife to overcome the crisis.
Remembering and following the multimode paths of psychological manifestations of doctors and health professionals it is determined that the psychological defence and mechanisms involved in the Ego, lead sometimes reprimand psychological effects for patients and relatives and sometimes reprimanding effects against the Self and these defences mechanisms are depended upon the health professionals’ personality, patient’s behaviours and his family and the organisational structure where practice takes place.

The Psychological Impact of Medical Error
191
REFERENCES
Allan, A., & McKillop, D. (2010). The health implications of apologizing after an adverse event. International Journal for Quality in Health Care, 22(2), 126–131. doi:10.1093/intqhc/mzq001 PMID:20139148
Anderson, B., Stumpf, P. G., & Schulkin, J. (2009). Medical error reporting, patient safety, and the physician. Journal of Patient Safety, 5(3), 176–179. doi:10.1097/PTS.0b013e3181b320b0 PMID:19927051
Banja, J. (2005). Medical Errors and Medical Narcissism. Sudbury, MA: Jones and Bartlett Publishers Inc.
Berlinger, N. (2011). Resolving Harmful Medical Mistakes - Is There a Role for Forgiveness? AMA Virtual Mentor, 13(9), 647–654. doi:10.1001/virtualmentor.2011.13.9.msoc1-1109 PMID:23137480
Blendon, R. J., DesRoches, C. M., Brodie, M., Benson, J. M., Rosen, A. B., Schneider, E., & Steffenson, A. E. et al. (2002). Patient safety: Views of practicing physicians and the public on medical errors. The New England Journal of Medicine, 347(24), 1933–1940. doi:10.1056/NEJMsa022151 PMID:12477944
Bonney, W. (2014). Medical errors: Moral and ethical considerations. Journal of Hospital Administration, 3(2), 80–88.
Brady, A. M., Malone, A. M., & Fleming, S. (2009). A literature review of the individual and systems factors that contribute to medication errors in nursing practice. Journal of Nursing Management, 17(6), 679–697. doi:10.1111/j.1365-2834.2009.00995.x PMID:19694912
Delbanco, T., & Bell, S. K. (2007). Guilty, Afraid, and Alone — Struggling with Medical Error. The New England Journal of Medicine, 357(17), 1682–1683. doi:10.1056/NEJMp078104 PMID:17960011
Duclos, C., Eichler, M., Taylor, L., Quintela, J., Main, D., Pace, W., & Staton, E. (2005). Patient perspectives of patient-provider communication after adverse events. International Journal for Quality in Health Care, 17(6), 479–486. doi:10.1093/intqhc/mzi065 PMID:16037100
The Psychological Impact of Medical Error
192
Elder, N. C., Jacobson, C. J., Zink, T., & Hasse, L. (2005). How experiencing pre-ventable medical problems changed patients interactions with primary health care. Annals of Family Medicine, 3(6), 537–544. doi:10.1370/afm.346 PMID:16338918
Freud, A. (1966). The Ego and the Mechanisms of Defense (Rev. Ed.). New York: International Universities Press.
Freud, S. (1936). Inhibitions, symptoms and anxiety. The Psychoanalytic Quarterly, 5, 415–443.
Gallagher, T., & Lucas, M. (2005). Should we disclose harmful medical errors to patients? If so, how? Journal of Clinical Outcomes Management, 12(5), 253–259.
Gallagher, T., Studdert, D., & Levinson, W. (2007). Disclosing harmful medical errors to patients. The New England Journal of Medicine, 356(26), 2713–2719. doi:10.1056/NEJMra070568 PMID:17596606
Gallagher, T. H., Waterman, A. D., Ebers, A. G., Fraser, V. J., & Levinson, W. (2003). Patients and physicians attitudes regarding the disclosure of medical errors. Journal of the American Medical Association, 289(8), 1001–1007. doi:10.1001/jama.289.8.1001 PMID:12597752
Gallagher, T. H., Waterman, A. D., Ebers, A. G., Fraser, V. J., & Levinson, W. (2003). Patients and physicians attitudes regarding the disclosure of medical errors. Journal of the American Medical Association, 289(8), 1001–1007. doi:10.1001/jama.289.8.1001 PMID:12597752
Gilbert, P. (1998). Some Core Issues and Controversies. In Shame; Interpersonal Behavior: Psychopathology and Culture (pp. 3-38). New York: Oxford University Press.
Gilbert, P. (2000). The Relationship of Shame, Social Anxiety and Depression: The Role of the Evaluation of Social Rank. Clinical Psychology & Psychotherapy, 7(3), 174–189. doi:10.1002/1099-0879(200007)7:3<174::AID-CPP236>3.0.CO;2-U
Gilbert, P. (2003). Evolution, Social Roles, and the Differences in Shame and Guilt. Social Research, 70, 1205–1230.
Gilligan, J. (2003). Shame, Guilt, and Violence. Social Research, 70, 1149–1180.

The Psychological Impact of Medical Error
193
Gouva, M., & Kotrotsiou, E. (2011). Psychological Issues in Care Stories. Athens: Medical Publications Lagos.
Harrison, R., Lawton, R., & Stewart, K. (2014). Doctors experiences of adverse events in secondary care: The professional and personal impact. Clinical Medicine, 14(6), 585–590. doi:10.7861/clinmedicine.14-6-585 PMID:25468840
Heller, A. (2003). Five approaches to the phenomenon of shame. Social Research, 70, 1016–1030.
Janssen, C., Ommen, O., Neugebauer, E., Lefering, R., & Pfaff, H. (2007). How to improve satisfaction with hospital stay of severely injured patients. Langen-becks Archives of Surgery, 392(6), 747–760. doi:10.1007/s00423-007-0186-1 PMID:17384957
Klein, M. (1952). Some theoretical conclusions regarding the emotional life of the infant. The Writings of Melanie Klein, 3, 61–93.
Lamb, R. M., Studdert, D. M., Bohmer, R. M., Berwick, D. M., & Brennan, T. A. (2003). Hospital disclosure practices: Results of a national survey. Health Affairs, 22(2), 73–83. doi:10.1377/hlthaff.22.2.73 PMID:12674409
Laplanche, J., & Pontalis, J. B. (1973). The language of psycho-analysis (D. Nich-olson-Smith, Trans.). Oxford, UK: W. W. Norton.
Mazor, K., Simon, S., Yood, R., Gurwitz, J., Martinson, B., Gunter, M., & Reed, G. (2004). Health plan members views about disclosure of medical errors. Annals of Internal Medicine, 140(6), 409–418. doi:10.7326/0003-4819-140-6-200403160-00006 PMID:15023706
Mazor, K. M., Reed, G. W., Yood, R. A., Fischer, M. A., Baril, J., & Gurwitz, J. H. (2006). Disclosure of Medical Errors: What Factors Influence How Patients Re-spond? Journal of General Internal Medicine, 21(7), 704–710. doi:10.1111/j.1525-1497.2006.00465.x PMID:16808770
Panella, M., Rinaldi, C., Vanhaecht, K., Donnarumma, C., Tozzi, Q., & Di Stanislao, F. (2014). Second victims of medical errors: A systematic review of the literature. Igiene e Sanita Pubblica, 70(1), 9–28. PMID:24770362

The Psychological Impact of Medical Error
194
Paxton, J. H., & Rubinfeld, I. S. (2010). Medical errors education: A prospective study of a new educational tool. American Journal of Medical Quality, 25(2), 135–142. doi:10.1177/1062860609353345 PMID:20110456
Pratt, S. D., & Jachna, B. R. (2015). Care of the clinician after an adverse event. International Journal of Obstetric Anesthesia, 24(1), 54–63. doi:10.1016/j.ijoa.2014.10.001 PMID:25499810
Robbennolt, J. K. (2009). Apologies and Medical Error. Clinical Orthopaedics and Re-lated Research, 467(2), 376–382. doi:10.1007/s11999-008-0580-1 PMID:18972177
Schwappach, D. L. B., & Boluarteb, T. A. (2008). The emotional impact of medical error involvement on physicians: A call for leadership and organisational account-ability. Swiss Medical Weekly, 138(1–2), 9–15. PMID:18951201
Seys, D., Wu, A. W., Van Gerven, E., Vleugels, A., Euwema, M., Panella, M., & Vanhaecht, K. (2013). Health care professionals as second victims after adverse events: A systematic review. Evaluation & the Health Professions, 36(2), 135–162. doi:10.1177/0163278712458918 PMID:22976126
Sirriyeh, R., Lawton, R., Gardner, P., & Armitage, G. (2010). Coping with medical error: A systematic review of papers to assess the effects of involvement in medi-cal errors on healthcare professionals’ psychological well-being. BMJ Quality and Safety in Health Care, 19(6), 1–8. PMID:20513788
Tangney, J. P., & Dearing, R. L. (2002). Shame and Guilt. New York: The Guilford Press. doi:10.4135/9781412950664.n388
Taylor, D., Hassan, M. A., Luterman, A., & Rodning, C. B. (2008). Unexpected intraoperative patient death: The imperatives of family- and surgeon-centered care. Archives of Surgery, 143(1), 87–92. doi:10.1001/archsurg.2007.27 PMID:18209158
Truog, R. D., Browning, D. M., Johnson, J. A., & Gallagher, T. H. (2010). Talking with patients and families about medical error: A guide for education and practice. Baltimore, MD: JHU Press.
Vincent, C. (2003). Understanding and Responding to Adverse Events. The New England Journal of Medicine, 348(11), 1051–1056. doi:10.1056/NEJMhpr020760 PMID:12637617

The Psychological Impact of Medical Error
195
Vincent, C. A., & Coulter, A. (2002). Patient safety: What about the patient? Quality & Safety in Health Care, 11(1), 76–80. doi:10.1136/qhc.11.1.76 PMID:12078376
Vincent, C. A., Pincus, T., & Scurr, J. H. (1993). Patients experience of surgical acci-dents. Quality in Health Care, 2(2), 77–82. doi:10.1136/qshc.2.2.77 PMID:10171783
Waterman, A., Garbutt, J., Hazel, E., Dunagan, W., Levinson, W., Fraser, V., & Gal-lagher, T. (2007). The emotional impact of medical errors on practicing physicians in the United States and Canada. Joint Commission Journal on Quality and Patient Safety, 33(8), 467–476. doi:10.1016/S1553-7250(07)33050-X PMID:17724943
Waterman, A. D., Garbutt, J., Hazel, E., Dunagan, W. C., Levinson, W., Fraser, V. J., & Gallagher, T. H. (2007). The Emotional Impact of Medical Errors on Prac-ticing Physicians in the United States and Canada. Joint Commission Journal on Quality and Patient Safety, 33(8), 467–476. doi:10.1016/S1553-7250(07)33050-X PMID:17724943
Worsham, S. L. (2009). The Psychological Impact of Medical Error: Symptoms of Trauma in Family Members of the Injured (Doctoral dissertation). Harvard University. Available from ProQuest Dissertations and Theses database. (UMI No. 1518406)

The Psychological Impact of Medical Error
196
KEY TERMS AND DEFINITIONS
Ambivalence: The simultaneous existence of love and hate.Denial: When individuals find it difficult to recognize a situation that is unpleas-
ant for them and capable of causing them anxiety and therefore unconsciously deny it by activating the negation (denial) mechanism.
Displacement: When individuals to project their feelings and their psychic content to another or to other people and even more to objects or situations, in order to reduce the intensity of certain representations, activating the mechanism of displacement.
Identification: Psychological process where by the subject assimilates an aspect, property or attribute of the other and is transformed, wholly or partially, after the model the other provides.
Projection: When individuals attribute to attribute to another or to other people properties, desires and emotions which while they are theirs they do not recognize them, thus activating the mechanism of projection.
Psychological Trauma: An event in the person’s life defined by the person’s incapacity to respond adequately to it, and by the effects that it brings about in the psychical organization of person.
Repression: Is a process where by the subject attempts to repel, or to confine to the unconscious, representations (thoughts, images, memories) which are bound to a pressure.
Transference: Is a process of actualization of unconscious wishes and use spe-cific objects and operates in the framework of a specific relationship established with these objects.

Copyright ©2017, IGI Global. Copying or distributing in print or electronic forms without written permission of IGI Global is prohibited.
DOI: 10.4018/978-1-5225-2337-6.ch008
Chapter 8
197
The Second Victim Phenomenon:
The Way Out
ABSTRACT
Medical error happens when an action within the medical field is not fulfilled as planned, or the plan is performed incorrectly. Patient and family are the first victim of an adverse event. The damage in a patient’s health, leads in a distressing situation not only for the patient, but also for the clinician who is responsible for this outcome. The term “second victim” refers to the trauma that a health professional sustains due to a serious adverse event in the healthcare system. After a medical error the caregivers are experiencing the aftermath in their personal and professional life. They feel isolated and abandoned, and some of them are coming up against the law with penal and disciplinary ramifications as a consequence of the blame culture in the health care system. Some health professionals experienced the consequences of an unfortunate incident even if it did not lead in harm to the patient’s health.
Paraskevi K. SkourtiNational and Kapodistrian University of Athens, Greece
Andreas PavlakisNeapolis University Pafos, Cyprus

The Second Victim Phenomenon
198
INTRODUCTION
Cost containment and the quality of a healthcare system are substantial elements contributing to patient safety. The “second victim phenomenon” negatively impacts healthcare quality and cost. A culture of blame exists in a majority of healthcare organizations and impacts the doctor-patient relationship. In addition, patient safety is under intense scrutiny. It is essential that a solution is found to restore the trust between a doctor and a patient. An adverse event is a potential “threat” for this relationship and can be the cause of victimization for both patient and clinician. Literature quests after solutions that can result in restoration of the relationship between patient and clinician and lead to reduction of the unfavorable implications this mistrust provoke in the health system.
BACKGROUND
According to several publications, roots of the second victim phenomenon extend beyond the healthcare profession. The phenomenon has its causes in the latent sys-temic factors in health care system that literally push health professional to err. Health professional victimization factors include: exhaustion of a health professional due to the understaffing of an organization; a professional’s burnout or depression; and blame culture in organizations. This situation is intensified by the current systems of patient compensation including possible litigation on behalf of the patient. This puts both the professional and patient in an ongoing venture. In turn, the situation can lead to low quality of the healthcare services and high healthcare expenses. Literature suggests several ways to confront the phenomenon. These include: es-tablishing teams to help the wounded professionals; changing the blame culture; and redefining the compensation systems.
MAIN FOCUS OF THE CHAPTER
The main issue resulting from the second victim phenomenon is the need for a structured peer or institutional support for the clinician. A poorly-structured or non-existent support system may result in a professional becoming a second victim following an adverse event (Ullstrom, Sachs, Hansson, Ovretveit, & Brommels, 2014). The support system should include guidelines and educational programming to practice disclosing skills (Wu, Boyle, Wallace, & Mazor, 2013).

The Second Victim Phenomenon
199
Tort reform could change the blame culture in healthcare organizations, which intensifies the second victim phenomenon. Tort reform is key to rendering functional programs (Catino, 2009). A clinician will not seek support if there is uncertainty surrounding legal protection (de Wit, Marks, Nattermann, & Wu, 2013). Education for clinicians and information for patients could strengthen this aim. Tort reform could decrease defensive medicine because it is the major cause of it (Hermer & Brody, 2010). These reforms could achieve cost containment in healthcare by reduc-ing litigation and compensation expenses, reducing costs from defensive behavior, and avoiding expenditures for the clinician’s treatment and rehabilitation.
SECOND VICTIM PHENOMENON
Human Error
A variety of things can cause harm to a patient. These include medical errors, an underlying disease, complications, or inherent treatment risks (Wu et al., 2013). Complications are adverse outcomes in a patient’s health and are possible even if the care is provided in the best way (Wu et al., 2013).
Scientific publications define medical errors in a variety of ways. Kalra, Kalra, and Baniak (2013) describe a medical error as a failure to properly carry out a planned action in the medical field or the fulfillment of an incorrect plan. Two types of errors can be distinguished: errors of planning and errors of execution (Zientek, 2010). A medical error does not always engender a harmful outcome to a patient (Sharpe, 2015). An error that may harm a patient but is avoided, either coincidentally, either it was not harmful, or it simply was precluded, is termed as a “near miss.” A “harmful event” is commonly defined in literature as an “adverse event.” This leads to a patient’s impairment within the care process and is free of intention. Harm to a patient that is caused by a professional’s unsafe or inadequate handling is called a “preventable adverse event” (Smorti, Cappelli, Zarantonello, Tani, & Gensini, 2014). According to Wu et al. (2013), it confirms the definition of a “harmful error.” An error in the medical field is not considered an action or omission originated exclusively by an individual. The system’s susceptibility to the error is contributed to by the complexity and high-risk nature of the health system (Taib, McIntosch, Caponecchia, & Baysari, 2011). The errors can be classified in two categories in healthcare systems: The active errors that are apparently carried out by an individual with immediate consequences, and the latent errors, that are not apparent, with roots inherent to systemic inadequacies, such as workload, fatigue, lack of equipment (Kalra et al., 2013).

The Second Victim Phenomenon
200
Latent or systemic factors are critical for the error commitment because in their “field” are lying the vulnerabilities of the health system (Kalra et al., 2013). Systemic errors are considered more significant than errors committed by individuals (Zientek, 2010). Due to the complexity of systemic factors, the World Health Organization (WHO) proposed the term “harmful patient safety incident” rather than “error” to divert the attachment to the individual errors (Sharpe, 2015).
The human factor is critical for the subsistence of the error. The error is part of the systemic inadequacies impacting clinicians. It is not the consequence of a negligent or unfortunate situation where a health professional may be held liable (Kohn, Corrigan, & Donaldson, 2000).
Who is the Second Victim?
A significant consequence of an adverse event is the harm caused to the patient’s health. Patients suffer physical and psychological ramifications. Apart from the prolonged hospitalization, which has both societal and economic consequences, the health system is burdened with societal costs from reduced productivity of the harmed individuals and the low quality level of the public health (Rafter et al., 2014).
According to research, one in seven patients experiences the effects of an adverse event (Seys et al., 2013). According to 2008 data from the United States Department of Health and Human Services, these events are due to: medication (31%); an event during the patient’s care (28%); surgery or another procedure (26%); and infection (15%) (Clancy, 2012). Patients and families are the first victims of the event. They experience a decline in their health, a prolonged hospitalization, or additional in-terventions inducing a considerable economic impact on their care. The injury—or even fatality—can cause permanent changes to a patient’s and/or patient’s family’s quality of life (Elwahab & Doherty, 2014).
The harmed patient and/or family are undoubtedly the main victim(s) of a harm-ful error in healthcare. However, they are not the sole victim. The involved health professional in an adverse incident can also be traumatized by the event. The event may impact his/her professional and personal life; it can potentially cause an emer-gency situation similar to post-traumatic disorders (Grissinger, 2014).
One of the first uses of the term “second victim” was by Wu (2000). In Scott (2011) a second victim of an adverse event is defined as “a healthcare provider involved in an unanticipated adverse patient event, medical error, and/or patient-related injury who becomes victimized in the sense that the provider is traumatized by the event” (para. 7). Some health professionals also experience the consequences of a medical error after an unfortunate incident, even if it did not cause harm to the patient (Elwahab & Doherty, 2014).

The Second Victim Phenomenon
201
Features of the Phenomenon
The second victim phenomenon presents in a variety of ways in suffering clinicians because it chronically stigmatizes their life (Grissinger, 2014). It is highly possible that a clinician will experience the phenomenon (Scott, 2015a). Estimates show that 50% of providers will experience impacts of the phenomenon at least once in their professional lives (Seys et al., 2012). Medical errors cause 400,000 deaths annually in the U.S. (Marmon & Heiss, 2015). With approximately 600,000 medical doctors in the U.S., at least one death hypothetically corresponds to every doctor annually (Marmon & Heiss, 2015).
In 2007, a qualitative study was conducted among different types of health professionals (Scott, 2011). The study intended to understand the impact of these events on clinicians. A participant described a particular adverse event as “… the darkest hour of his professional career” (Scott, 2011, para. 6). In the same research, many of the second victims recalled devastating details of the day of the event, such as the “color of the scrubs worn” (Scott, 2011, para. 8). Undeniably, an adverse event is important to the healthcare professional and is a “possible career-ending circumstance” (Scott, 2015a, para. 1).
Emotional Impact: Health professionals who are involved in an adverse event experience a strong emotional impact. According to Scott (2015b), they feel angry, ashamed, guilty, isolated, and humiliated; they develop low self-confidence and depression. The suffering clinicians feel responsible for the incident, discredit their skills and education (McCay & Wu, 2012), and doubt their career choice (Marmon & Heiss, 2015). Initially, they feel paralyzed as they withdraw and constantly relive the incident (Wu, 2000). They may struggle to concentrate and fulfill common obligations (Wu, 2000).
Depression from an adverse event may cause the provider to feel anxiety sur-rounding their professional performance. In 2011, members of the American Col-lege of Surgeons were asked about experiencing suicidal ideations in the past year. More than 6% answered positively which is double the rate of the general population and is interrelated to an adverse event (Pratt, Kenney, Scott, & Wu, 2012). Doctors from different specialties referred to several symptoms, including: persistent fear of errors (82%); loss of social trust (67%); and low-quality professional and personal lives (Elwahab & Doherty, 2014).

The Second Victim Phenomenon
202
Correlation has been observed between the second victim phenomenon and depression. In 2007, research in a pediatric U.S. hospital revealed that 20% of resi-dents (according to the Harvard National Depression Screening Day scale) were at high risk for depression (Fahrenkopf et al., 2008). Twenty-six percent had suffered depression in the past. Eleven (out of the 123 participants) were using antidepres-sant medication; three were suffering from depression. These rates are double the general population rate. Conclusively, a medical error was committed six times more frequently by a depressed resident (Fahrenkopf et al., 2008).
This research also measured the impact of burnout syndrome in the sample. Almost all of the depressed residents experienced burnout despite the lack of rela-tionship between this syndrome and the prevalence of errors. Burnout rates were 74% (Fahrenkopf et al., 2008). According to research, it is possible that an error makes the provider a second victim, therefore creating a vicious cycle between depression and medical errors (Fahrenkopf et al., 2008). The relationship between residents who suffer from both depression and burnout causes one to ask: Which came first? (Fahrenkopf et al., 2008).
Adverse events cause panic of job loss and reputation loss, as well as fear of litigation. The practitioner fears losing the respect of colleagues, faces enormous financial impacts, and worries about losing their professional license (Grissinger, 2014).
Physical impact: Second victims encounter problems perceived as physical dys-functions. These include nightmares (Wu & Steckelberg, 2012), insomnia (Grissinger, 2014), eating dysfunctions, diarrhea, nausea, vomiting, headaches, muscle tension, fatigue, a rapid heart rate, rapid breathing, and difficulties in concentration (Miller, Scott, & Hirschinger, 2015). Elwahab and Doherty (2014) state that surgeons re-ported “sweating, heart pounding, headache, and physical tension symptoms” (p. 298). This stressful reaction while performing an operation may impact the surgeon’s dexterity and surgical technique.
Causes Leading to the Phenomenon
Why would a clinician involved in an adverse event become a second victim? Suf-fering in silence, a blame culture, or insufficient, delayed, or absent institutional help leads to isolation and punishment. Researchers at the University of Missouri Health Care (MUHC) revealed that 68% of participants who experienced a patient safety event did not utilize institutional help (Scott, 2011). In a survey of the Agency for Healthcare Research and Quality (AHRQ) Hospital Survey on Patient Safety Culture, only 44% of participants believed that their institution “responds to clinician error in a non-punitive and supporting way” (Pratt et al., 2012, p. 235).

The Second Victim Phenomenon
203
Research from the United Kingdom demonstrated that 291 (out of 700) obstetric anesthetists were involved in a maternal death event. Sixty percent did not have support, 65% were not informed about the availability of support, and 5% were informed about the supporting structures within their institution (Pratt et al., 2012). Organizational and peer support, combined with research of the event, decrease the level of negative emotions experienced by a clinician after an adverse event.
Lack of support introduces a long-lasting emotional load to a professional. A non-judgmental form of confrontation is needed (Ullstrom et al., 2014). Risk man-agers should be informed about the available help and provide quality support to professionals. It is possible that risk managers are not receiving accurate statistics about the usefulness of the programs. Therefore, they wrongly conclude that the support is unnecessary or inefficient. Mistrust of existing support programs is re-lated to confidentiality issues, program effectiveness, and judgment of colleagues.
Both a culture change and improvement of organizational referral systems are needed (White et al., 2015). Even with the high incidence of adverse events, an organization may fail to routinely offer programs because they do not know how to construct a supportive mechanism (Van Gerven et al., 2014).
Dissatisfied by the error-free expectations, clinicians feel an increased burden of responsibilities. Due to the insufficiency of the system, they may seek dysfunc-tional manners to heal themselves. They may blame themselves, the patient, or the healthcare team for the incident. Some of the clinicians will experience burnout and turn to alcohol or drug abuse (Macleod, 2014). Subsequently, the fear of litigation exacerbates the clinician’s emotional situation (Zientek, 2010). The complexity of care in combination with personal responsibility generates a relationship between litigation risk and the physician’s behavior (Renkema, Broekhuis, & Ahaus, 2014).
The blame culture—the avoidance of risks in an organizational environment due to fear of punitive consequences—provokes medical errors and results in poor patient quality (Kalra et al., 2013). An adverse event for a clinician may be traumatic, with second victims feeling isolated in their personal and professional lives. The result of this isolation is unpropitious for healthcare professionals, a patient, a patient’s family, and healthcare organizations (Seys et al., 2012).
Ramifications
There are multiple consequences to a physician becoming a second victim. They can be summarized in two categories: economic consequences and legal consequences.
Systemic or latent errors are more important in relation to individual errors. This category of errors includes insufficient economic resources that, according to experts, presents significant obstacles to a healthcare system. The economic aspect of medical errors is an unenviable by-product of healthcare.

The Second Victim Phenomenon
204
An expensive premium allows an adverse event to be covered by an insurance policy for medical liability. Insurance coverage for medical liability is compulsory for every doctor due to increased expenses for compensation. The social cost in-cludes the rising expenses in the justice field as distributed to the patient and the state. This includes loss of social and individual profit due to a possible disability. One of the targets of the economic analysis of the tort law is the decrease of this social cost (Vliamos & Hatziplaton, 2008).
The physical and psychological problems of second victims also have eco-nomic consequences. These include lost working days, expenses related to loss of the professional’s confidence in their medical judgment, and the defensive way in which they practice medicine in fear of adverse events and litigation risk (Mira et al., 2015). Another economic problem is the decision of many second victims to relinquish their job. The economic impact is not minimized should the second victim decide to stay in their job. The psychological symptoms can generate low productivity and low quality levels reflecting in patient safety (Marmon & Heiss, 2015; White et al., 2015).
It is difficult and costly for an organization to replace a healthcare professional. In 2004, an estimated median cost for the loss of a physician was US$123,000 in recruiting fees and US$2 million in lost revenue. The loss of a nurse (medical/surgical or specialty) cost approximately US$47,403 and US$85,197, respectively. The problem is intensified because of the shortage of doctors and nurses (White et al., 2015).
DEFENSIVE MEDICINE
Defensive medicine occurs when the doctor deviates from what is considered “good practice” so that complaints from patients and/or family members is reduced, pre-vented, or avoided (Ortashi, Virdee, Hassan, Mutrynowski, & Abu-Zidan, 2013). Defensive behavior is characterized as positive when the physician uses unnecessary tests and treatments; it is characterized as negative when the physician abstains from high-risk health procedures (Ortashi et al., 2013).
The practice of defensive medicine is done in order to avoid litigation/complaints rather than to benefit the patient (Burdon, 2013; Catino, 2009). This critical element connects defensive medicine to the second victim phenomenon. According to Wu et al. (2013), a survey on barriers in the disclosure of adverse events mentions that, “Not surprisingly, the biggest barrier was the fear of litigation” (p. 188). In an educational session among professionals with second victim symptoms, the following was noted: “Error is uncomfortable for doctors. Participants noted some overreactions (I will send every single patient for a scan in future) …” (Lea & Danczak, 2014, p. 115).

The Second Victim Phenomenon
205
Second victim symptoms can also be observed in professionals who practice defensive medicine. This unsafe behavior emerges from the physician’s fear of dis-rupting the trust balance between him/herself and the patient, the financial burden of possible litigation, and the high cost of insurance premiums (Renkema et al., 2014). Healthcare professionals practice defensive medicine due to an increasingly complex system and the litigation risk increase related to higher mortality rates (Renkema et al., 2014).
Organizations are implementing a “punitive approach” to the instance of error. In turn, healthcare professionals are encouraged to practice defensive medicine. A research study in Pennsylvania was conducted among 824 specialists of high litiga-tion risk specialties. It revealed that 93% of the specialists declared the practice of defensive medicine; 43% admitted that they practiced medicine in a narrow field in order to avoid complications (Burdon, 2013; Catino, 2009). An Italian study concluded that 77.9% of participants practiced some form of defensive medicine within the last working month, 80% acted this way out of fear of involvement in possible legal action, and 60% feared a damages claim (Catino, 2009).
Another important element of this research is the negative publicity and accusatory media approach related to these events. Forty-three percent of the physicians that practiced defensive medicine were deeply concerned about this issue (Catino, 2009).
In a UK research study among 202 participants, 86% of physicians responded that they believe they do not work in a blame-free environment despite the efforts made in the UK to create a blame-free environment (Ortashi et al., 2013). Seventy-eight percent of physicians reported that they have practiced some form of defensive medicine; senior-grade doctors appeared to be distinguishably less associated to defensive medicine (Ortashi et al., 2013). A 2012 study out of the U.S. revealed that, in order to avoid litigation, practitioners use defensive medicine as a standard practice, especially in imaging studies (Nahed, Babu, Smith, & Heary, 2012). For defensive purposes, 76% of the respondents ordered imaging studies, 67% ordered laboratory tests, and 66% requested consultation from other physicians (Nahed et al., 2012).
If defensive medicine was a shield against litigation, statistics would show a reduced number of malpractice cases. On the contrary, an increasing rate of litiga-tions is observed, creating an economic burden for the health system (Pellino & Pellino, 2015).
Aside from the commonly supported aspect that practicing defensive medicine results from the fear of litigation, there is another opinion in the literature. A sur-vey by Cunningham and Wilson (2011) presented the response of a doctor to the complaints. After a complaint on behalf of a patient, a doctor reacts with symptoms identical to those of the second victim: anger, depression, reduced enjoyment level in practicing medicine, guilt, and shame (Cunningham & Wilson, 2011). The basic

The Second Victim Phenomenon
206
principle of defensive medicine is, until now, that it is a reaction of a clinician to the fear of litigation. Blame is then ascribed to the tort system.
According to the authors, defensive medicine also exists in New Zealand where the legal system is not tort-based. Therefore, defensive medicine is an unintended outcome of the process of complaints. The underlying reason is an internal response to shame rather than the litigious environment. The person who is ashamed has an intense desire to hide and withdraw. It is a reaction of “perceived assault or threat to one’s sense of self … [and] has been described as global attribution of failure” (Cunningham & Wilson, 2011, p. 451).
Consequently, the use of complaints as an opportunity to improve the health system has become dysfunctional (Cunningham & Wilson, 2011).
It is difficult to perform case-by-case research to find out if tests are necessary. It is taken for granted that it is an existing problem with a high cost to the health-care system and potentially dangerous impacts on the patients. Increased costs and limited values are characteristics of defensive medicine. The Pacific Research Institute revealed that defensive medicine has little benefits and costs more than US$120 billion per year (Healey, Kopen, & Smith, 2011). In the 2008, healthcare system expenditures due to defensive medicine are estimated to be US$55.6 billion (Nahed et al., 2012). The national cost for defensive practice in orthopedic surgery is estimated to be US$2 billion per year (Ortashi et al., 2013). Another study in the U.S. (Thomas, Ziller, & Thayer, 2010) showed that defensive medicine is an existing widespread problem with only a small impact on medical care costs.
Concerning the tort reform, as a way to change the perception of the doctors about practicing defensive medicine because of fear of litigation, Thomas, Ziller and Thayer (2010) conclude that the expected savings are overstated (Thomas et al., 2010, pp. 1578-1584). Hermer and Brody (2010) stated that tort reform is a necessary but not sufficient element in cost containment. However, tort reform is used to persuade physicians to accept substantial cost control measures impacting the practice of defensive medicine (Hermer & Brody, 2010). Studdert, Mello, and Brennan (2010) concurred with this assessment and suggested that non-conventional reforms are needed to feature system breakdowns rather than individual culpabil-ity. The limitation of economic consequences of litigation cannot decrease the risk of litigation or its adversarial aspects. The main problem is that the trust between patients and doctors ruptures. The social pressure of litigation and their increasing rates have caused a disturbance in this relationship (Pellino & Pellino, 2015).

The Second Victim Phenomenon
207
Compensation
Estimation of human life so as to appoint compensation to an individual as a result of a medical error injury depends on: (1) why the evaluation is made and (2) what frame should it be made into (Vliamos & Hatzis, 2009). There are suggestions in literature on ways to evaluate human life. These could be useful for the court of law to make decisions on the compensation for damages experienced by an injured patient. The philosophy is the maintenance of the patient’s situation at the same “util-ity level” as before the injury. This is called “perfect” compensation. The “value of statistical life” approach is an evaluation system relying on the “statistical life year.” It estimates the amount of reimbursement and traditional damages fundamental for compensation and deterrence relies on the economic damages based on the income, and on the non-economic damages based on elements of pain, suffering, grief, and loss of welfare (Vliamos & Hatzis, 2009).
No Fault Compensation: Compensation cannot always fulfill its mission if it is appointed years later or is smaller than requested. Literature proposes several ways to confront compensation without litigation. A program run by the University of Michigan encourages open disclosure policies and resolution programs (Wu et al., 2013). The outcome is a reduction of compensation claims from $3 million to $1million. COPIC®, a medical liability company in the U.S., has provided an aver-age payment of $5,400 to more than 3,000 patients by encouraging conversations about the incident between doctor and patient (Wu et al., 2013). A 2011 publication suggested that the US$150 billion cost of the malpractice system could afford to pay US$200,000 for every case of fatality and US$20,000 for injuries depending on the severity of each case (Goodman, Villarreal, & Jones, 2011). It is also proposed that prior to every treatment or surgery, a patient can be offered a voluntary no-fault insurance in case of suffering an adverse event, as an alternative to a possible lawsuit. Nobody is forced to quit the legal rights in the traditional way, but it is possible that most of the components are willing to do so (Goodman et al., 2011). An independent commission could determine the basic compensation; the patient could raise this amount by paying an additional premium from their own money. The basic premium has been overwhelmed by physicians and hospitals. It reflects the record of the provider or the institution in adverse events and it operates as an economic incentive for the deterrence of the injuries in the medical field.

The Second Victim Phenomenon
208
Economic Aspect of the Tort Law
The aim of the tort law is economic efficiency, namely the minimization of the cost of accidents. The types of costs include (Vliamos & Hatzis, 2009):
• Primary Costs: These reveal the costs of an error in the medical field, in-cluding costs for care after the injury, the loss of income capacity, and non-economic damages.
• Secondary Costs: These are the societal costs of an accident.• Tertiary Costs: These are costs related to the tort system, including admin-
istrative costs, lawyers/expert fees, and legal error fees.
Another type of cost, “cost of precaution,” targets the minimization of the cost of medical errors and the cost of prevention. In economic terms:
We should invest in preventing medical errors as long as the marginal benefit of precaution in minimizing the other types of costs is greater or equal to the marginal cost of preventive measures (such as insurance, self-insurance, avoidance of difficult or high-risk procedures, etc.) (Vliamos & Hatzis, 2009, p.244).
LEGAL CONSEQUENCES
Institutions often consider the second victims as individually responsible for an adverse event. An important coping strategy for the clinician is the disclosure of the event to the patient and family in order to provide explanation and apologize. Nevertheless, there is confusion regarding enacted mandatory laws on disclosure. Healthcare professionals are afraid of being liable upon disclosure. Legal protection for disclosure exists. In more than 30 U.S. states, the apology conversations are not accepted as evidence in the court of law.
Information exchanged by the medical review committee is also protected. The request for psychological support of the second victim by their institution is em-phatic; organizations are starting to respond by enacting support programs. There is uncertainty regarding the legal protection of these support programs. The clinician is uncertain about whether they can be used as evidence. The issue remains unsettled and clinicians are reluctant to seek support. Communication under the aegis of a support program should be covered by legal privilege.
The Second Victim Phenomenon
209
In a 2008 study, 60% of healthcare professionals declared that this fear is rep-resentative of their emotions (de Wit et al., 2013). This chapter suggests that all conversations between the clinician and the patient and/or supportive team should be covered by legal privilege. In particular, the privilege that the law provides to these conversations should not be used as evidence. The legal disunion among the states, as well as the differences in protection from state to state, is criticized. “Clear legislation” is needed to protect communication in the second victim programs Federal law statutes should be applied without any doubt (de Wit et al., 2013).
Therapeutic Jurisprudence
Therapeutic jurisprudence is a legal theory to support on characteristics of the legal process, accentuating the improvement of quality in the healthcare field (Dauer, 2003). According to research, a malpractice claim can bring an increased risk to future patients because of the negative effects of the claim on the physician.
Alternatives to this system are suggested to eliminate the defects and abolish their future negative impacts (Dauer, 2003). These include no-fault liability, enter-prise liability, and alterations to the reporting rules (disclosure and confidentiality) (Dauer, 2003).
MEDIATION
Mediation is conducted confidentially between the parties in a setting away from the hostility of the legal process. It is based in honest communication, aimed at understanding and hearing the other’s preoccupations. The outcome may refer to suggested procedural changes or the expectations of re-education of the physician. It is an opportunity to alert the other party to the conditions contributing to the adverse outcome. Finally, there is no certainty that compensation would be paid (Dauer, 2003).
Means of Confrontation
Confronting the impact of an adverse event is a complicated situation. However, a healthcare professional can be helped by structures at the individual and institutional level. Literature suggests coping mechanisms to be implemented by the organization. A healthcare professional is impacted by both the adverse event and the organiza-tion’s inadequate, often unstructured, and unsystematic manner of providing support (Ullstrom et al., 2014).

The Second Victim Phenomenon
210
Individual Needs Post-Event: A qualitative research study at a Swedish university hospital was conducted among 21 healthcare professionals (Ullstrom et al., 2014). It revealed that most of the participants characterized negative emotions as “long lasting” after an adverse event. They continued to remember the event and believed that they would never be free from it (Ullstrom et al., 2014).
Post-event support distinguished two response categories. The first concerned the need to discuss the event and receive emotional support. The majority of individuals needed a “free form” conversation surrounding the event. Few expressed their need for a structured dialog. The most important element was their need for empathy. Despite their support from colleagues and family, they emphasized the need for a follow-up by management. They expected long- and short-term leadership support.
The second category concerned the need to understand because this was needed in order to learn from the error. This procedure should be fulfilled both on an indi-vidual and an organizational level. The participants wanted to report the direct or indirect conditions contributing to the adverse outcome, including understaffing and poor routines. They were disappointed by the inquiry procedure since it did not reveal the root cause (Ullstrom et al., 2014). The second victims sought individual support from other members of the organization, including managers, supervisors, counselors, therapists, and colleagues. Emotional support was the main reason why a clinician discussed the adverse event with colleagues. Disclosure and open discussion surrounding the event decreases psychological stress, improved the patient-provider relationship, and aimed to improve long-term healthcare delivery. Positive effects can be seen if the second victim has quality colleague support and maintains a good relationship with the patient post-event (Seys et al., 2013).
Rights of the Second Victims: Clinicians who had an involvement in an adverse event often confront this traumatic situation in isolation and with fear of punishment. This reflects the blame culture that dominates healthcare organizations. However, these healthcare professionals should be handled with respect and the system should provide them the chance to learn from the error (Grissinger, 2014). According to Denham (2007), the acronym TRUST can be applied to the rights of second victims. Denham (2007) focused on the institution’s response to a suffering clinician.
• Treatment that is just.• Respect.• Understanding and compassion.• Supportive care.• Transparency and the opportunity to contribute.

The Second Victim Phenomenon
211
The “Recovery Trajectory”: The Office of Clinical Effectiveness of the MUHC conducted a study that included patient safety event investigations from 2003 to 2007 (Scott et al., 2009). The research studied the reactions of clinicians who have been involved in an adverse event and who experienced second victim phenomenon symptoms. Researchers found that clinicians confront the event in an individual way. Nevertheless, participants followed a “predictable recovery trajectory” during the coping process (Scott, 2015b). According to Scott (2015b), the stages of recovery are:
• Chaos and accident response.• Intrusive reflections.• Restoring personal integrity.• Enduring the inquisition.• Obtaining emotional first aid.• Moving on (in this stage, the clinician has three choices):
◦ Drop out of the profession. ◦ Survive and continue a professional life (due to the strong impact of the
adverse event, the clinician can never perform as s/he did before). ◦ Thrive (the clinician has learned from the adverse event and makes sure
that the same inexpediencies will never happen again).
Institutional Support and Patient Safety
The emotional situation experienced by the second victim is extremely strong. If help from the institution is inadequate or non-existent, the victim cannot recover. The physical and psychological symptoms will not be confronted and the possibility of abandonment of the profession will loom (Scott, 2015b). Promoting a systematic approach to support second victims within an organization is crucial to the recovery and rehabilitation in their formal professional situation (Wu & Steckelberg, 2012). In a survey conducted in the U.S. and Canada with 3,000 participants (Macleod, 2014), 80% reported that they would care about receiving support after an adverse event. Ninety percent declared that their health institution provides inadequate sup-port to help victims cope with stress from an error (Macleod, 2014).
Cost containment efforts lead to a reduction in healthcare professionals; the provision of accomplishing more services with fewer staff increases the possibil-ity of an adverse event. Yet, only a few programs support second victims in the U.S. There is also lack of best practice guidelines. This results in mistrust by the staff who, in turn, are reluctant to use existing support programs. Reasons for this

The Second Victim Phenomenon
212
reluctance include: reduced confidence in the effectiveness of the program; doubts about confidentiality; negative credential records; a raise in liability premiums; and litigation risk (Macleod, 2014). An important step toward support and protection for traumatized clinicians due to an adverse event is to have acquaintance with the second victim phenomenon and enact proactive coping strategies in health care organizations (Scott, 2011). If institutions do not offer support to their healthcare professionals after an adverse event, they will not be trustworthy or respectful and moreover, they will probably witness negative consequences in the organizational culture (Seys et al., 2013).
Despite the increase in the prevalence of adverse events, organizations are not in a position to offer support to healthcare professionals (Van Gerven et al., 2014). In this survey research is published about the existence or lack of support in Dutch-speaking protocols in Belgium. The research questions focused on: (1) the prevalence of the second victim support protocols; (2) the main organizational contact person for the second victims; and (3) whether these protocols are due to published international recommendations. The results showed that a small number of participant organiza-tions had a protocol in place to support the second victims. More than half of the organizations pointed to the chief nursing officer or a combination of individuals as appropriate for contact after an adverse event. None of the protocols conformed to international recommendations (Van Gerven et al., 2014).
Organizational Structures
Some programs have been established to provide emotional support to health professionals who are suffering after an involvement with an unanticipated event. Examples include:
The MUHC for YOU Team: The MUHC implemented the tool, “Theory of Transpersonal Caring and the Critical Incident Stress Management Model,” to reduce suffering. It is a complete infrastructure providing support at an organiza-tional level (Seys et al., 2013). The mission, accomplished by a “YOU” team, is performed in three tiers:
• Tier 1: This tier provides immediate emotional aid by educated leaders and peers in the second victim phenomenon.
• Tier 2: This tier is a provision of immediate support by the utilization of two structural interventions: one-on-one second victim caring moments and col-lective sessions.
• Tier 3: This tier provides professional counseling to the suffering person when his/her condition requires specialized support beyond the help of a trained peer. (Seys et al., 2013)

The Second Victim Phenomenon
213
The “YOU” team provides services to the second victims for five years to minimize negative impacts on a healthcare professional after an adverse event (Hirschinger, Scott, & Hahn-Cover, 2015).
Some other support structures found in the healthcare field are:
• Medically Induced Trauma Support Services (MITSS).• Critical Incident Stress Management (CISM).• Institute for Healthcare Improvement (IHI).
High Reliability Organizations (HROs) and the Safety Culture
The concept of HROs was first used in high-risk industries where the safety of the public and the workers depended on undeviating compliance to the safety rules (for example, nuclear industries). Healthcare is a field of multifaceted regulations, complex diagnoses, and management or treatment. It is a field in which humans experience high rates of stress. Three characteristics must be implemented to achieve a high level of reliability in a culture of safety: trust, reporting, and improvement. A sub-stantial characteristic for quality and improvement of performance is safety culture:
… the product of individual and group values, attitudes, perceptions, competencies, and patterns of behavior that determine the commitment to, and the style and pro-ficiency of, an organization’s health and safety management.” (Health and Safety Commission of Great Britain 1993) as cited in Miller et al. (2015) (Miller et al., 2015, p. 2)
A just culture occurs when a health professional is handled fairly and the orga-nization confronts a reduction of safety risks. Professionals seek potential dangers that could threaten the organization. They also strive to complete their job in the most reliable way (Denham, 2007). Managers look for the best system features in order to create the valuable circumstances for a professional’s highest perfor-mance. Theoretically, risks loom in every action. However, professionals are only responsible for things that they can control. System design is the management’s responsibility; every professional in the organization is responsible for behavioral choices (Denham, 2007).

The Second Victim Phenomenon
214
DISCLOSURE OF ADVERSE EVENTS AND PATIENT SAFETY
Healthcare professionals should be transparent about their errors to their patients, their colleagues, and themselves. This is one way to achieve patient safety. A social and ethical convention exists between healthcare professionals and patients. A basic element in disclosure is the realization that errors in the medical field are unavoid-able. It should be an aim of the professional to understand the institutional factors supporting the disclosure procedure (Denham, 2007). Basic patient safety procedures include the identification, report, and open disclosure of errors. Learning from er-rors is a principle of healthcare management with the prerequisite that errors are reported. A professional with previous adverse event experience has an increased possibility to participate in the prevention and non-recurrence of errors if s/he has been offered support rather than blame. Healthcare organizations should learn from every dimension of the event rather than take statements, hide information, and with-hold conversations in fear of a lawsuit. When a patient is unintentionally harmed, a healthcare organization should redress the situation, allowing everybody the oppor-tunity to learn from the mistake in order to prevent future events (Denham, 2007).
Open Disclosure
Open disclosure is communication about an adverse event in order to acknowledge suffering and inform patients and family. Open disclosure includes information about the event, its consequences, and possible corrective actions. It also includes apologies and information on preventing the same incident from happening again.
According to Manser (2011), a survey with 958 participants showed that non-disclosure was connected to low rates of patient satisfaction. Ninety-eight percent of the participants expected acknowledgment after an adverse event irrespective of the severity of harm (Manser, 2011). The information should be timely and ac-curate because silence by the professional may be interpreted as an effort to hide information and/or show disrespect. Full disclosure also offers relief to the clinician (Manser, 2011).

The Second Victim Phenomenon
215
Key Elements
Key elements are tools to help the researchers understand the way that patients are affected by the disclosing procedure (Wu et al., 2013):
• Explanations to patient and family about the event.• Acknowledgement of responsibility (this is positively accepted by patients).• Expressions of sincere regret (apologizing maintains a strong patient-provider
relationship).• Commitment to preventing recurrences.
Barriers to Disclosure
Even with supportive policies for disclosure, clinicians face barriers when disclosing information. According to Wu et al. (2013), barriers to full disclosure are:
• Fear of legal and financial consequences accompanied by emotional distress resulting in the clinician becoming the second victim
• Attitudes surrounding disclosure• Lack of skills with inadequate training on effective disclosure• No role models• Lack of institutional and peer support
Policy Solution to Support Disclosure: Healthcare providers need a policy with detailed instructions on disclosure and adverse events. Wu et al. (2013) propose policies on educational efforts, as well as disclosure training in medical school, a residency, and all grades of education. Professionals with prior disclosure experi-ence also need a refreshment course on disclosure skills. Patients should obtain information about an organization’s policies and the expectation of openness after an unanticipated event. Consequently, the barriers are emotional, cultural, and attitudinal. For this reason, the gap between the recommendations of policy and implementation still exist.

The Second Victim Phenomenon
216
SOLUTIONS AND RECOMMENDATIONS
Adverse events cannot be avoided in healthcare. The second victim phenomenon is an outcome of the loss of trust between the doctor and the patient. The blame culture, the clinicians’ unreal expectations to be infallible, and the fear of litigation intimidates healthcare professionals and impacts the quality of healthcare services (Pellino & Pellino, 2015).
Confronting this problem is difficult. On a national level, interventions should be made in healthcare systems. Leadership should take preventative measures toward imminent adverse events. Manser (2011) suggests ways to help an organization meet the needs of a healthcare professional:
• Construct effective support systems for clinicians.• Establish guidelines to manage critical incidents.• Follow immediate measures in case of an adverse event.• Construct standards for disclosure.• Prepare educational interventions.
FUTURE RESEARCH DIRECTIONS
Additional research on adverse events will be a major contribution to patient safety and quality healthcare services. It will also be valuable to thoroughly understand the impact that these events have on the clinician’s mental and physical health. Research on institutional support is useful to manage the second victim phenomenon since the provisions for supportive management is fairly recent.
CONCLUSION
The second victim phenomenon does not only include the suffering healthcare pro-fessional. It impacts patients, the patient’s family, and the healthcare system. The patient experiences an injury, the clinician experiences serious psychological and physical consequences, and the healthcare system deals with the impact of defen-sive medicine costs and an obligation to punish a “wounded” clinician suffering the consequences of an unanticipated event. Organizational reform is needed to prevent systemic and latent adverse events. Structures should be established to support the second victim and provide education to cope with the negative impacts of an ad-verse event. Providing support to the clinicians, as well as teaching disclosure and apology techniques avoids “silence.”

The Second Victim Phenomenon
217
REFERENCES
Burdon, J. (2013). Defensive medicine and clinical risk management. In R. G. Beran (Ed.), Legal and forensic medicine (pp. 621–628). Berlin: Springer. doi:10.1007/978-3-642-32338-6_109
Catino, M. (2009, July). Blame culture and defensive medicine. Cognition Technol-ogy and Work, 11(4), 245–253. doi:10.1007/s10111-009-0130-y
Clancy, C. M. (2012, January/March). Alleviating second victim syndrome. How we should handle patient harm. Journal of Nursing Care Quality, 27(1), 1–5. doi:10.1097/NCQ.0b013e3182366b53 PMID:22124276
Cunningham, W., & Wilson, H. (2011, March). Complaints, shame and defensive medicine. BMJ Quality & Safety, 20(5), 449–452. doi:10.1136/bmjqs.2011.051722 PMID:21441601
Dauer, E. A. (2003). A therapeutic jurisprudence perspective on legal responses to medical error. Journal of Legal Medicine, 24(1), 37–50. doi:10.1080/713832126 PMID:12623695
de Wit, M. E., Marks, C. M., Nattermann, J. P., & Wu, A. W. (2013, December). Supporting second victims of patient safety events: Shouldnt these communica-tions be covered by legal privilege? The Journal of Law, Medicine & Ethics, 41(4), 852–858. doi:10.1111/jlme.12095 PMID:24446943
Denham, C. (2007). TRUST: The 5 rights of the second victim. Journal of Patient Safety, 3(2), 107–119. doi:10.1097/01.jps.0000236917.02321.fd
Elwahab, A. S., & Doherty, E. (2014). What about doctors? The impact of medical er-rors. The Surgeon, 12(6), 297–300. doi:10.1016/j.surge.2014.06.004 PMID:25056239
Fahrenkopf, A., Barger, L., Sharek, P., Lewin, D., Chiang, V., Edwards, S., … Landrigan, C. (2008, February). Rates of medication errors among depressed and burnt out residents: Prospective cohort study. British Medical Journal. Retrieved from http://www.bmj.com/content/336/7642/488
Goodman, J. C., Villarreal, P., & Jones, B. (2011, April). The social cost of ad-verse medical events, and what we can do about it. Health Affairs, 30(4), 590–595. doi:10.1377/hlthaff.2010.1256 PMID:21471477
Grissinger, M. (2014). Too many abandon the “second victims” of medical errors. Pharmacy & Therapeutics, 39(9), 591–592. PMID:25210409

The Second Victim Phenomenon
218
Healey, B., Kopen, D., & Smith, J. (2011). Physicians, defensive medicine and eth-ics. Academy of Health Care Management Journal, 7(1), 59–78.
Hermer, L. D., & Brody, H. (2010). Defensive medicine, cost containment, and reform. Journal of General Internal Medicine, 25(5), 470–473. doi:10.1007/s11606-010-1259-3 PMID:20143176
Hirschinger, L. E., Scott, S. D., & Hahn-Cover, K. (2015, April 3). Clinician support: Five years of lessons learned. Patient Safety and Quality Healthcare. Retrieved from http://psqh.com/march-april-2015/clinician-support-five-years-of-lessons-learned
Kalra, J., Kalra, N., & Baniak, N. (2013, September). Medical error, disclosure and patient safety: A global view of quality care. Clinical Biochemistry, 46(13-14), 1161–1169. doi:10.1016/j.clinbiochem.2013.03.025 PMID:23578740
Kohn, L. T., Corrigan, J. M., & Donaldson, M. S. (2000). To err is human: Building a safer health system. Washington, DC: National Academy Press.
Lea, A., & Danczak, A. (2014). Medical error: A dirty little secret or a great learn-ing opportunity? Education for Primary Care, 25(2), 114–118. PMID:24593978
Macleod, L. (2014, January/February). “Second victim” casualties and how physi-cian leaders can help. Physician Executive Journal, 40, 8–12. PMID:24575696
Manser, T. (2011). Managing the aftermath of critical incidents: Meeting the needs of health-care providers and patients. Best Practice & Research. Clinical Anaesthe-siology, 25(2), 169–179. doi:10.1016/j.bpa.2011.02.004 PMID:21550542
Marmon, L. M., & Heiss, K. (2015). Improving surgeon wellness: The second vic-tim syndrome and quality of care. Seminars in Pediatric Surgery, 24(6), 315–318. doi:10.1053/j.sempedsurg.2015.08.011 PMID:26653167
McCay, L., & Wu, A. (2012). Medical error: The second victim. British Journal of Hospital Medicine, 73(Sup10), C146–C148. doi:10.12968/hmed.2012.73.Sup10.C146 PMID:23124197
Miller, R., Scott, S., & Hirschinger, L. (2015, September). Improving patient safety: The intersection of safety culture, clinician and staff support, and patient safety organizations. Retrieved from http://www.centerforpatientsafety.org/wp-content/themes/patient-safety/pdf/Second-Victims-White-Paper.pdf
Mira, J. J., Lorenzo, S., Carrillo, I., Ferrus, L., Perez-Perez, P., Iglesias, F., & Astier, P. et al. (2015, August). Interventions in health organisations to reduce the impact of adverse events in second and third victims. BMC Health Services Research, 15(341), 1–9. doi:10.1186/s12913-015-0994-x PMID:26297015

The Second Victim Phenomenon
219
Nahed, B. V., Babu, M. A., Smith, T. R., & Heary, R. F. (2012, June 22). Malprac-tice liability and defensive medicine: A national survey of neurosurgeons. PLOS ONE. Retrieved from http://journals.plos.org/plosone/article?id=10.1371/journal.pone.0039237
Ortashi, O., Virdee, V., Hassan, R., Mutrynowski, T., & Abu-Zidan, F. (2013, October). The practice of defensive medicine among hospital doctors in the United Kingdom. BMC Medical Ethics, 14(42). Retrieved from http://bmcmedethics.biomedcentral.com/articles/10.1186/1472-6939-14-42 PMID:24168064
Pellino, I. M., & Pellino, G. (2015, December). Consequences of defensive medicine, second victims, and clinical-judicial syndrome on surgeons medical practice and on health service. Updates in Surgery, 67(4), 331–337. doi:10.1007/s13304-015-0338-8 PMID:26650202
Pratt, S., Kenney, L., Scott, S. D., & Wu, A. W. (2012, April). How to develop a second victim support program: A toolkit for health care organizations. Joint Commission Journal on Quality and Patient Safety, 38(5), 235–240. doi:10.1016/S1553-7250(12)38030-6 PMID:22649864
Rafter, N., Hickey, A., Condell, S., Conroy, R., O’Connor, P., Vaughan, D., & Williams, D. (2014, July). Adverse events in healthcare: Learning from mistakes. Quarterly Journal of Medicine: An International Journal of Medicine. doi:10.1093/qjmed/hcu145
Renkema, E., Broekhuis, M., & Ahaus, K. (2014, January). Conditions that influ-ence the impact of malpractice litigation risk on physicians’ behavior regarding patient safety. BMC Health Services Research, 14(38). Retrieved from http://www.biomedcentral.com/1472-6963/14/38 PMID:24460754
Scott, S. D. (2011, May). The second victim phenomenon: A harsh reality of health care professions. Patient Safety Network. Retrieved from https://psnet.ahrq.gov/perspectives/perspective/102
Scott, S. D. (2015a, October). Second victim support: Implications for patient safety attitudes and perceptions. PSQH. Retrieved from http://www.psqh.com/analysis/second-victim-support-implications-for-patient-safety-attitudes-and-perceptions/
Scott, S. D. (2015b, September). The second victim experience: Mitigating the harm. American Nurse Today, 10(9), 8-11. Retrieved from http://www.americannursetoday.com/wp-content/uploads/2015/09/ant9-Second-victim-820.pdf

The Second Victim Phenomenon
220
Scott, S. D., Hirschinger, L. E., Cox, K. R., McCoig, M., Brandt, J., & Hall, L. W. (2009). The natural history of recovery for the healthcare provider second victim after adverse patient events. Quality & Safety in Health Care, 18(5), 325–330. doi:10.1136/qshc.2009.032870 PMID:19812092
Seys, D., Scott, S., Wu, A., Van Garven, E., Vleugels, A., Euwema, M., & Vanhaecht, K. et al. (2013). Supporting involved health care professionals (second victims) fol-lowing an adverse health event: A literature review. International Journal of Nurs-ing Studies, 50(5), 678–687. doi:10.1016/j.ijnurstu.2012.07.006 PMID:22841561
Seys, D., Wu, A., Van Gerven, E., Vlaugels, A., Euwema, M., Panella, M., & Vanhaecht, K. et al. (2012, June). Health care professionals as second victims after adverse events: A systematic review. Evaluation & the Health Professions, 36(2), 135–162. doi:10.1177/0163278712458918 PMID:22976126
Sharpe, V. A. (2015, January). Mistakes, medical. In H. ten Have (Ed.), Encyclopedia of global bioethics (pp. 1–8). Springer International Publishing. doi:10.1007/978-3-319-05544-2_296-1
Smorti, A., Cappelli, F., Zarantonello, R., Tani, F., & Gensini, G. F. (2014). Medical error and systems of signaling: Conceptual and linguistic definition. In-ternal and Emergency Medicine, 9(6), 681–688. doi:10.1007/s11739-014-1108-1 PMID:25034521
Studdert, D., Mello, M., & Brennan, T. (2010). Defensive medicine and tort reform: A wide view. Journal of General Internal Medicine, 25(5), 380–381. doi:10.1007/s11606-010-1319-8 PMID:20349156
Taib, I. A., McIntosch, A. S., Caponecchia, C., & Baysari, M. (2011). A review of medical error taxonomies: A human factors perspective. Safety Science, 49(5), 607–615. doi:10.1016/j.ssci.2010.12.014
Thomas, J. W., Ziller, E., & Thayer, D. (2010). Low costs of defensive medicine, small savings from tort reform. Health Affairs, 29(9), 1578–1584. doi:10.1377/hlthaff.2010.0146 PMID:20820011
Ullstrom, S., Sachs, M. A., Hansson, J., Ovretveit, J., & Brommels, M. (2014). Suffering in silence: A qualitative study of second victims of adverse events. BMJ Quality & Safety, 23(4). doi:10:1136, 325-331
Van Gerven, E., Seys, D., Panella, M., Sermeus, W., Euwema, M., Federico, F., & Vanhaet, K. et al. (2014). Involvement of health-care professionals in an adverse event: The role of management in supporting their workforce. Polskie Archiwum Medycyny Wewnetrznej, 124(6), 313–319. PMID:24781784

The Second Victim Phenomenon
221
Vliamos, S., & Hatziplaton, M. (2008). Economic analysis of medical errors. Chronicles of Private Law (offprint), 584-590.
Vliamos, S., & Hatzis, A. (2009). The assesment of compensatory damages for medical error by the Greek courts: An economic analysis. In N. B. James Brox (Ed.), The global economics of a changing environment (pp. 239–251). Waterloo, Ontario, Canada: North Waterloo Academic Press.
White, A. A., Brock, D., McCotter, P. I., Hofeldt, R., Edrees, H. H., Wu, A. W., & Gallagher, T. H. et al. (2015). Risk managers descriptions of programs to support second victims after adverse events. Journal of Healthcare Risk Management, 34(4), 30–40. doi:10.1002/jhrm.21169 PMID:25891288
Wu, A. W. (2000, March). Medical error: The second victim. The doctor who makes the mistake needs help too. British Medical Journal, 320(7237), 726–727. doi:10.1136/bmj.320.7237.726 PMID:10720336
Wu, A. W., Boyle, D. J., Wallace, G., & Mazor, K. M. (2013). Disclosure of adverse events in the United States and Canada: An update, and a proposed framework for improvement. Journal of Public Health Research, 2(3), 186–193. doi:10.4081/jphr.2013.e32 PMID:25170503
Wu, A. W., & Steckelberg, R. C. (2012). Medical error, incident investigation and the second victim: Doing better but feeling worse? BMJ Quality & Safety, 21(4), 267–269. doi:10.1136/bmjqs-2011-000605 PMID:22213379
Zientek, D. M. (2010). Medical error, malpractice and complications: A moral geogra-phy. HEC Forum, 22(2), 145–157. doi:10.1007/s10730-010-9130-9 PMID:20480208

The Second Victim Phenomenon
222
KEY TERMS AND DEFINITIONS
Adverse Event: An unintentional and unenviable action of a healthcare profes-sional leading to a harmful outcome in a patient’s health.
Defensive Medicine: The clinician’s deviation from “good practice” to avoid a patient’s or family’s complaints.
Disclosure: A structured procedure following an adverse event in which the clinician offers explanations, apologies, and reassurance of non-recurrence.
First Victim: The patient and family who experience a harmful outcome of an adverse medical event.
Medical Error: Failed performance of a properly planned action or the proper fulfillment of an incorrect plan in the medical field.
Second Victim: The healthcare professional who is involved in a harmful out-come and is regarded as another victim of the adverse outcome.
Third Victim: The healthcare organization that experiences a reputation or financial harm after an adverse event.

223
Related References
To continue our tradition of advancing information science and technology research, we have compiled a list of recommended IGI Global readings. These references will provide additional information and guidance to further enrich your knowledge and assist you with your own research and future publications.
Aas, I. H. (2013). Improving patient safety with telemedicine: Exploring organiza-tional factors. In A. Moumtzoglou & A. Kastania (Eds.), E-health technologies and improving patient safety: Exploring organizational factors (pp. 56–70). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2657-7.ch004
Aboelfotoh, M. H., Martin, P., & Hassanein, H. (2013). Ubiquitous multimedia data access in electronic health care systems. In D. Tjondronegoro (Ed.), Tools for mobile multimedia programming and development (pp. 191–227). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4054-2.ch011
Abreu, J. F., Almeida, P., & Silva, T. (2013). iNeighbour TV: A social TV application to promote wellness of senior citizens. In R. Martinho, R. Rijo, M. Cruz-Cunha, & J. Varajão (Eds.), Information systems and technologies for enhancing health and social care (pp. 1-19). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3667-5.ch001
Aceti, V., & Luppicini, R. (2013). Exploring the effect of mhealth technologies on communication and information sharing in a pediatric critical care unit: A case study. In J. Tan (Ed.), Healthcare information technology innovation and sustainability: Frontiers and adoption (pp. 88–108). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2797-0.ch006
Adami, I., Antona, M., & Stephanidis, C. (2014). Ambient assisted living for people with motor impairments. In G. Kouroupetroglou (Ed.), Disability informatics and web accessibility for motor limitations (pp. 76–104). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4442-7.ch003

Related References
224
Åkerberg, A., Lindén, M., & Folke, M. (2013). Pedometer cell phone applications and future trends in measuring physical activity. In R. Martinho, R. Rijo, M. Cruz-Cunha, & J. Varajão (Eds.), Information systems and technologies for enhancing health and social care (pp. 324–339). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3667-5.ch021
Al Hamouche, V. (2014). Making quality control decisions in radiology department: A decision support system for radiographers’ performance appraisal using PACS. In C. El Morr (Ed.), Research perspectives on the role of informatics in health policy and management (pp. 48–61). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4321-5.ch004
Al-Khudairy, S. (2014). Caring for our aging population: Using CPOE and tele-homecare systems as a response to health policy concerns. In C. El Morr (Ed.), Research perspectives on the role of informatics in health policy and management (pp. 153–166). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4321-5.ch010
Albuquerque, C. (2013). The study of social needs as a strategic tool for the in-novation of the social care sector: The contribution of new technologies. In M. Cruz-Cunha, I. Miranda, & P. Gonçalves (Eds.), Handbook of research on ICTs for human-centered healthcare and social care services (pp. 347–365). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3986-7.ch018
Alexandrou, D. A., & Pardalis, K. V. (2013). SEMantic PATHways: Modeling, executing, and monitoring intra-organizational healthcare business processes to-wards personalized treatment. In A. Moumtzoglou & A. Kastania (Eds.), E-health technologies and improving patient safety: Exploring organizational factors (pp. 98–123). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2657-7.ch007
Algarín, A. D., Demurjian, S. A., Ziminski, T. B., Sánchez, Y. K., & Kuykendall, R. (2014). Securing XML with role-based access control: Case study in health care. In A. Ruiz-Martinez, R. Marin-Lopez, & F. Pereniguez-Garcia (Eds.), Architectures and protocols for secure information technology infrastructures (pp. 334–365). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4514-1.ch013
Almeida, L., Menezes, P., & Dias, J. (2013). Augmented reality framework for the socialization between elderly people. In M. Cruz-Cunha, I. Miranda, & P. Gonçalves (Eds.), Handbook of research on ICTs for human-centered healthcare and social care services (pp. 430–448). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3986-7.ch023

Related References
225
Amer, M. B., Amawi, M., & El-Khatib, H. (2013). A novel neural fuzzy approach for diagnosis of potassium disturbances. In J. Tan (Ed.), Healthcare information technology innovation and sustainability: Frontiers and adoption (pp. 208–218). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2797-0.ch013
Andersen, S. T., & Jansen, A. (2013). Innovation in ICT-based health care provision. In J. Tan (Ed.), Healthcare information technology innovation and sustainability: Frontiers and adoption (pp. 58–72). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2797-0.ch004
Angjellari-Dajci, F., Lawless, W. F., Stachura, M. E., Wood, E. A., & DiBattisto, C. (2013). Economic evaluations for service delivery in autism spectrum disorders: benefit-cost analysis for emerging telehealth systems. In M. Cruz-Cunha, I. Miranda, & P. Gonçalves (Eds.), Handbook of research on ICTs and management systems for improving efficiency in healthcare and social care (pp. 16–42). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3990-4.ch002
Archibald, D., MacDonald, C. J., Hogue, R., & Mercer, J. (2013). Accessing knowledge from the bedside: Introducing the tablet computer to clinical teaching. In C. Rückemann (Ed.), Integrated information and computing systems for natural, spatial, and social sciences (pp. 96–109). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2190-9.ch005
Archondakis, S. (2013). Static telecytological applications for proficiency testing. In V. Gulla, A. Mori, F. Gabbrielli, & P. Lanzafame (Eds.), Telehealth networks for hospital services: New methodologies (pp. 228–239). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2979-0.ch015
Arling, P. A., Doebbeling, B. N., & Fox, R. L. (2013). Improving the implementa-tion of evidence-based practice and information systems in healthcare: A social network approach. In J. Tan (Ed.), Healthcare information technology innovation and sustainability: Frontiers and adoption (pp. 247–270). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2797-0.ch016
Arriaga, P., Esteves, F., & Fernandes, S. (2013). Playing for better or for worse?: Health and social outcomes with electronic gaming. In M. Cruz-Cunha, I. Miranda, & P. Gonçalves (Eds.), Handbook of research on ICTs for human-centered healthcare and social care services (pp. 48–69). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3986-7.ch003

Related References
226
Arslan, P. (2014). Collaborative participation in personalized health through mobile diaries. In K. Rızvanoğlu & G. Çetin (Eds.), Research and design innovations for mobile user experience (pp. 150–181). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4446-5.ch009
Assis-Hassid, S., Reychav, I., Pliskin, J. S., & Heart, T. H. (2013). The effects of electronic medical record (EMR) use in primary care on the physician-patient relation-ship. In M. Cruz-Cunha, I. Miranda, & P. Gonçalves (Eds.), Handbook of research on ICTs for human-centered healthcare and social care services (pp. 130–150). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3986-7.ch007
Baladrón, C., Aguiar, J. M., Calavia, L., Carro, B., & Sánchez-Esguevillas, A. (2014). Learning on the move in the web 2.0: New initiatives in m-learning. In K-12 educa-tion: Concepts, methodologies, tools, and applications (pp. 1693–1714). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4502-8.ch097
Belsis, P., Skourlas, C., & Gritzalis, S. (2013). Secure electronic healthcare records management in wireless environments. In M. Khosrow-Pour (Ed.), Interdisciplin-ary advances in information technology research (pp. 202–219). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3625-5.ch015
Benito, R. V., Vega-Colado, C., Coco, M. B., Cuadrado, R., Torres-Zafra, J. C., Sánchez-Pena, J. M., & López-Miguel, A. et al. (2013). New electro-optic and display technology for visually disabled people. In M. Cruz-Cunha, I. Miranda, & P. Gonçalves (Eds.), Handbook of research on ICTs for human-centered healthcare and social care services (pp. 687–718). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3986-7.ch036
Bergenti, F., Poggi, A., & Tomaiuolo, M. (2013). Using multi-agent systems to support e-health services. In M. Cruz-Cunha, I. Miranda, & P. Gonçalves (Eds.), Handbook of research on ICTs for human-centered healthcare and social care services (pp. 549–567). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3986-7.ch029
Berler, A., & Apostolakis, I. (2014). Normalizing cross-border healthcare in Europe via new e-prescription paradigms. In C. El Morr (Ed.), Research perspectives on the role of informatics in health policy and management (pp. 168–208). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4321-5.ch011
Bernhard, S., Al Zoukra, K., & Schtte, C. (2013). From non-invasive hemodynamic measurements towards patient-specific cardiovascular diagnosis. In Data mining: Concepts, methodologies, tools, and applications (pp. 2069–2093). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2455-9.ch106

Related References
227
Best, C., O’Neill, B., & Gillespie, A. (2013). Assistive technology for cognition: Enabling activities of daily living. In M. Cruz-Cunha, I. Miranda, & P. Gonçalves (Eds.), Handbook of research on ICTs for human-centered healthcare and social care services (pp. 112–129). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3986-7.ch006
Boboc, C., & Ţiţan, E. (2014). Migration of medical doctors, health, medical education, and employment in eastern and central Europe. In A. Driouchi (Ed.), Labor and health economics in the Mediterranean region: Migration and mobility of medical doctors (pp. 158–191). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4723-7.ch007
Bradai, N., Chaari, L., & Kamoun, L. (2013). A comprehensive overview of wireless body area networks (WBAN). In J. Rodrigues (Ed.), Digital advances in medicine, e-health, and communication technologies (pp. 1–32). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2794-9.ch001
Brown, K. E., Bayley, J., & Newby, K. (2013). Serious game for relationships and sex education: Application of an intervention mapping approach to development. In S. Arnab, I. Dunwell, & K. Debattista (Eds.), Serious games for healthcare: Applica-tions and implications (pp. 135–166). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-1903-6.ch007
Burns, J., Blanchard, M., & Metcalf, A. (2013). Bridging the digital divide in Aus-tralia: The potential implications for the mental health of young people experiencing marginalisation. In Digital literacy: Concepts, methodologies, tools, and applications (pp. 772–793). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-1852-7.ch040
Buyurgan, N., Rardin, R. L., Jayaraman, R., Varghese, V. M., & Burbano, A. (2013). A novel GS1 data standard adoption roadmap for healthcare providers. In J. Tan (Ed.), Healthcare information technology innovation and sustainability: Frontiers and adoption (pp. 41–57). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2797-0.ch003
Cabrita, M. D., & Cabrita, M. (2014). Applying social marketing to healthcare: Challenges and opportunities. In A. Kapoor & C. Kulshrestha (Eds.), Dynamics of competitive advantage and consumer perception in social marketing (pp. 78–97). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4430-4.ch004

Related References
228
Carroll, J. M., & Rosson, M. B. (2013). Community networks: Infrastructure and models for therapeutic support. In M. Cruz-Cunha, I. Miranda, & P. Gonçalves (Eds.), Handbook of research on ICTs for human-centered healthcare and social care services (pp. 187–207). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3986-7.ch010
Castiglioni, I., Gilardi, M. C., & Gallivanone, F. (2013). E-health decision support systems for the diagnosis of dementia diseases. In A. Moumtzoglou & A. Kastania (Eds.), E-health technologies and improving patient safety: Exploring organizational factors (pp. 84–97). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2657-7.ch006
Catley, C., Smith, K., McGregor, C., James, A., & Eklund, J. M. (2013). A frame-work for multidimensional real-time data analysis: A case study for the detection of apnoea of prematurity. In A. Gangopadhyay (Ed.), Methods, models, and computation for medical informatics (pp. 16–35). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2653-9.ch002
Chaari, L., & Kamoun, L. (2013). QoS concepts and architecture over wireless body area networks for healthcare applications. In J. Rodrigues (Ed.), Digital advances in medicine, e-health, and communication technologies (pp. 114–130). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2794-9.ch007
Chamberlin, B., Maloney, A., Gallagher, R. R., & Garza, M. L. (2013). Active video games: Potential for increased activity, suggestions for use, and guidelines for implementation. In S. Arnab, I. Dunwell, & K. Debattista (Eds.), Serious games for healthcare: Applications and implications (pp. 191–212). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-1903-6.ch009
Charisi, A., Korvesis, P., & Megalooikonomou, V. (2013). Similarity searching of medical image data in distributed systems: Facilitating telemedicine applications. In A. Gangopadhyay (Ed.), Methods, models, and computation for medical informat-ics (pp. 58–77). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2653-9.ch004
Chen, Y. (2013). Construction of digital statistical atlases of the liver and their ap-plications to computer-aided diagnosis. In J. Wu (Ed.), Technological advancements in biomedicine for healthcare applications (pp. 68–79). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2196-1.ch008
Cheng, B., Stanley, R. J., De, S., Antani, S., & Thoma, G. R. (2013). Automatic detection of arrow annotation overlays in biomedical images. In J. Tan (Ed.), Health-care information technology innovation and sustainability: Frontiers and adoption (pp. 219–236). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2797-0.ch014

Related References
229
Cherian, E. J., & Ryan, T. W. (2014). Incongruent needs: Why differences in the iron-triangle of priorities make health information technology adoption and use dif-ficult. In C. El Morr (Ed.), Research perspectives on the role of informatics in health policy and management (pp. 209–221). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4321-5.ch012
Chun, S. A., Kwon, J. H., & Lee, H. (2013). Social credential-based role recom-mendation and patient privacy control in medical emergency. In A. Gangopadhyay (Ed.), Methods, models, and computation for medical informatics (pp. 215–237). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2653-9.ch013
Cohen, J. F., Bancilhon, J., & Sergay, S. (2013). An empirical study of patient will-ingness to use self-service technologies in the healthcare context. In M. Cruz-Cunha, I. Miranda, & P. Gonçalves (Eds.), Handbook of research on ICTs and management systems for improving efficiency in healthcare and social care (pp. 378–395). Her-shey, PA: IGI Global. doi:10.4018/978-1-4666-3990-4.ch019
Corrigan, D., Hederman, L., Khan, H., Taweel, A., Kostopoulou, O., & Delaney, B. (2013). An ontology-driven approach to clinical evidence modelling implement-ing clinical prediction rules. In A. Moumtzoglou & A. Kastania (Eds.), E-health technologies and improving patient safety: Exploring organizational factors (pp. 257–284). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2657-7.ch016
Costa, Â., Andrade, F., & Novais, P. (2013). Privacy and data protection towards elderly healthcare. In M. Cruz-Cunha, I. Miranda, & P. Gonçalves (Eds.), Handbook of research on ICTs for human-centered healthcare and social care services (pp. 330–346). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3986-7.ch017
Coughlan, J., & Brinkman, W. (2013). Design considerations for delivering e-learning to surgical trainees. In J. Rodrigues (Ed.), Digital advances in medicine, e-health, and communication technologies (pp. 341–350). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2794-9.ch020
D’Abundo, M. L. (2013). Electronic health record implementation in the United States healthcare industry: Making the process of change manageable. In V. Wang (Ed.), Handbook of research on technologies for improving the 21st century workforce: Tools for lifelong learning (pp. 272–286). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2181-7.ch018
D’Andrea, A., Ferri, F., & Grifoni, P. (2013). RFID technologies in the health sector. In A. Moumtzoglou & A. Kastania (Eds.), E-health technologies and improving patient safety: Exploring organizational factors (pp. 140–147). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2657-7.ch009

Related References
230
D’Astolfo, C. (2014). Investing in a “rehabilitation model” to improve the decision-making process in long-term care. In C. El Morr (Ed.), Research perspectives on the role of informatics in health policy and management (pp. 37–47). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4321-5.ch003
Dasgupta, S. S. (2013). Cyber capability framework: A tool to evaluate ICT for development projects. In M. Cruz-Cunha, I. Miranda, & P. Gonçalves (Eds.), Hand-book of research on ICTs for human-centered healthcare and social care services (pp. 399–406). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3986-7.ch021
Davis, S. A. (2013). Global telemedicine and ehealth: Advances for future healthcare – Using a systems approach to integrate healthcare functions. In V. Gulla, A. Mori, F. Gabbrielli, & P. Lanzafame (Eds.), Telehealth networks for hospital services: New methodologies (pp. 15–32). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2979-0.ch002
Deng, M., Petkovic, M., Nalin, M., & Baroni, I. (2013). Home healthcare in cloud computing. In M. Cruz-Cunha, I. Miranda, & P. Gonçalves (Eds.), Handbook of research on ICTs and management systems for improving efficiency in healthcare and social care (pp. 614–634). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3990-4.ch032
DeVany, M., Knobloch-Ludwig, K., Penticoff, M., Assimacopoulos, A., & Speedie, S. (2013). Telehealth implementation: The voice of experience. In S. Sarnikar, D. Bennett, & M. Gaynor (Eds.), Cases on healthcare information technology for pa-tient care management (pp. 126–139). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2671-3.ch008
Dingli, A., Abela, C., & D’Ambrogio, I. (2013). PINATA: Taking e-health a step forward. In A. Moumtzoglou & A. Kastania (Eds.), E-health technologies and im-proving patient safety: Exploring organizational factors (pp. 173–195). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2657-7.ch012
Dogra, D. P., Nandam, K., Majumdar, A. K., Sural, S., Mukhopadhyay, J., Majum-dar, B., & Mukherjee, S. et al. (2013). A tool for automatic hammersmith infant neurological examination. In J. Rodrigues (Ed.), Digital advances in medicine, e-health, and communication technologies (pp. 301–311). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2794-9.ch017
Doyle, J., Bertolotto, M., & Wilson, D. (2013). Towards multimodal mobile GIS for the elderly. In Digital literacy: Concepts, methodologies, tools, and applications (pp. 590–609). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-1852-7.ch031

Related References
231
Dragoni, A. F. (2013). Health services through digital terrestrial television. In V. Gulla, A. Mori, F. Gabbrielli, & P. Lanzafame (Eds.), Telehealth networks for hospital services: New methodologies (pp. 207–227). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2979-0.ch014
Dragoni, A. F. (2013). Virtual carer: A first prototype. In V. Gulla, A. Mori, F. Gabbrielli, & P. Lanzafame (Eds.), Telehealth networks for hospital services: New methodologies (pp. 290–299). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2979-0.ch019
Driouchi, A. (2014). Introduction to labor and health economics: Mobility of medi-cal doctors in the Mediterranean region. In A. Driouchi (Ed.), Labor and health economics in the Mediterranean region: Migration and mobility of medical doctors (pp. 1–22). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4723-7.ch001
Driouchi, A. (2014). Medical knowledge, north-south cooperation, and mobility of medical doctors. In A. Driouchi (Ed.), Labor and health economics in the Mediter-ranean region: Migration and mobility of medical doctors (pp. 376–395). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4723-7.ch015
Driouchi, A. (2014). Skilled human resources in the health sectors and impacts of new health technologies on health workforce in developing economies. In A. Driou-chi (Ed.), Labor and health economics in the Mediterranean region: Migration and mobility of medical doctors (pp. 23–50). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4723-7.ch002
Duan, X., Wang, X., & Huang, Q. (2013). Medical manipulators for surgical appli-cations. In J. Wu (Ed.), Technological advancements in biomedicine for healthcare applications (pp. 111–122). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2196-1.ch012
Dunwell, I., & Jarvis, S. (2013). A serious game for on-the-ward infection control awareness training: Ward off infection. In S. Arnab, I. Dunwell, & K. Debattista (Eds.), Serious games for healthcare: Applications and implications (pp. 233–246). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-1903-6.ch011
Durant, K. T., McCray, A. T., & Safran, C. (2013). Identifying temporal changes and topics that promote growth within online communities: A prospective study of six online cancer forums. In A. Gangopadhyay (Ed.), Methods, models, and computation for medical informatics (pp. 78–97). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2653-9.ch005

Related References
232
El-Farargy, N. (2013). Refresher training in clinical psychology supervision: A blended learning approach. In A. Benson, J. Moore, & S. Williams van Rooij (Eds.), Cases on educational technology planning, design, and implementation: A project management perspective (pp. 295–317). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4237-9.ch016
Ervin, K. (2014). Legal and ethical considerations in the implementation of elec-tronic health records. In J. Krueger (Ed.), Cases on electronic records and resource management implementation in diverse environments (pp. 193–210). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4466-3.ch012
Fakhar, A. (2014). Beyond brain drain: A case study of the benefits of cooperation on medical immigration. In A. Driouchi (Ed.), Labor and health economics in the Mediterranean region: Migration and mobility of medical doctors (pp. 294–313). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4723-7.ch012
Falan, S. L., Han, B., Zoeller, L. H., Tarn, J. M., & Roach, D. M. (2013). Sustaining healthcare through waste elimination: A taxonomic analysis with case illustrations. In J. Tan (Ed.), Healthcare information technology innovation and sustainability: Frontiers and adoption (pp. 18–39). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2797-0.ch002
Farinha, C., & Mira da Silva, M. (2013). Identifying requirements for healthcare information systems with focus groups. In M. Cruz-Cunha, I. Miranda, & P. Gon-çalves (Eds.), Handbook of research on ICTs for human-centered healthcare and social care services (pp. 491–510). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3986-7.ch026
Ferreira, L., Teixeira, A., & Cunha, J. P. (2013). Medical information extraction in European Portuguese. In M. Cruz-Cunha, I. Miranda, & P. Gonçalves (Eds.), Hand-book of research on ICTs for human-centered healthcare and social care services (pp. 607–626). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3986-7.ch032
Forrestal, E. J., Cellucci, L. W., Zeng, X., Kennedy, M. H., & Smith, D. (2013). Health information technology collaboration in community health centers: The community partners HealthNet, Inc. In S. Sarnikar, D. Bennett, & M. Gaynor (Eds.), Cases on healthcare information technology for patient care management (pp. 171–196). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2671-3.ch011
Frederico, C. (2013). Nutrition games. In S. Arnab, I. Dunwell, & K. Debattista (Eds.), Serious games for healthcare: Applications and implications (pp. 167–190). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-1903-6.ch008

Related References
233
Freitas, L., Pereira, R. T., Pereira, H. G., Martini, R., Mozzaquatro, B. A., Kasper, J., & Librelotto, G. (2013). Ontological representation and an architecture for homecare pervasive systems. In R. Martinho, R. Rijo, M. Cruz-Cunha, & J. Varajão (Eds.), Information systems and technologies for enhancing health and social care (pp. 215–234). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3667-5.ch015
Frigo, C. A., & Pavan, E. E. (2014). Prosthetic and orthotic devices. In Assistive technologies: Concepts, methodologies, tools, and applications (pp. 549–613). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4422-9.ch028
Fukami, T., & Wu, J. (2013). Image fusion method and the efficacy of multimodal cardiac images. In J. Wu (Ed.), Technological advancements in biomedicine for healthcare applications (pp. 47–54). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2196-1.ch006
Furdu, I., & Patrut, B. (2013). ICT applications and solutions in healthcare: Present and perspectives. In M. Cruz-Cunha, I. Miranda, & P. Gonçalves (Eds.), Handbook of research on ICTs and management systems for improving efficiency in healthcare and social care (pp. 559–576). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3990-4.ch029
Gabbrielli, F. (2013). Telemedicine R&D influencing incoming strategies and organization models. In V. Gulla, A. Mori, F. Gabbrielli, & P. Lanzafame (Eds.), Telehealth networks for hospital services: New methodologies (pp. 250–264). Her-shey, PA: IGI Global. doi:10.4018/978-1-4666-2979-0.ch017
Gaivéo, J. M. (2013). Security of ICTs supporting healthcare activities. In M. Cruz-Cunha, I. Miranda, & P. Gonçalves (Eds.), Handbook of research on ICTs for human-centered healthcare and social care services (pp. 208–228). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3986-7.ch011
Gallo, C. (2013). A multichannel framework for multimedia content deployment in e-health environments. In M. Cruz-Cunha, I. Miranda, & P. Gonçalves (Eds.), Handbook of research on ICTs and management systems for improving efficiency in healthcare and social care (pp. 872–891). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3990-4.ch045
Gao, Y., Yang, W., Yang, J., Satoshi, T., & Wu, J. (2013). Neural mechanisms of audiovisual integration in integrated processing for verbal perception and spatial factors. In J. Wu (Ed.), Biomedical engineering and cognitive neuroscience for healthcare: Interdisciplinary applications (pp. 327–336). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2113-8.ch034

Related References
234
Gatzidis, C. (2013). First-person shooter game engines and healthcare: An examina-tion of the current state of the art and future potential. In S. Arnab, I. Dunwell, & K. Debattista (Eds.), Serious Games for Healthcare: Applications and Implications (pp. 76–89). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-1903-6.ch004
Gaughan, M. (2013). The hybridized nature of America’s health care system: Medi-care as a case of both market and public failure. In M. Merviö (Ed.), Healthcare management and economics: Perspectives on public and private administration (pp. 154–164). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3982-9.ch012
Gavgani, V. Z. (2013). Information therapy (ix) service and patients’ preference. In A. Gangopadhyay (Ed.), Methods, models, and computation for medical informatics (pp. 117–125). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2653-9.ch007
Gholson, J., & Tennyson, H. (2013). One system of care, one electronic chart. In S. Sarnikar, D. Bennett, & M. Gaynor (Eds.), Cases on healthcare information technology for patient care management (pp. 55–69). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2671-3.ch003
Ghosh, B. (2013). Healthcare systems using clinical data: Addressing data in-teroperability challenges. In S. Sarnikar, D. Bennett, & M. Gaynor (Eds.), Cases on healthcare information technology for patient care management (pp. 208–223). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2671-3.ch013
Gillies, A. C., & Howard, J. (2013). Information as change agent or barrier in health care reform? In J. Tan (Ed.), Healthcare information technology innovation and sustainability: Frontiers and adoption (pp. 1–17). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2797-0.ch001
Glusker, A., & Hoelscher, E. (2014). Transitioning from print to online-only resources: The experience of a medium-sized healthcare organization library. In J. Krueger (Ed.), Cases on electronic records and resource management implementation in diverse environments (pp. 226–242). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4466-3.ch014
Gofuku, A., Fukumori, S., & Sato, K. (2013). A mirror visual feedback therapy system applying virtual reality technology. In J. Wu (Ed.), Biomedical engineer-ing and cognitive neuroscience for healthcare: Interdisciplinary applications (pp. 73–80). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2113-8.ch008

Related References
235
Gomes, C., Sperandio, F., Peles, A., Borges, J., Brito, A. C., & Almada-Lobo, B. (2013). An operating theater planning decision support system. In R. Martinho, R. Rijo, M. Cruz-Cunha, & J. Varajão (Eds.), Information systems and technolo-gies for enhancing health and social care (pp. 69–86). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3667-5.ch005
Grissom, T. E., DuKatz, A., Kordylewski, H. A., & Dutton, R. P. (2013). Bring out your data: The evolution of the national anesthesia clinical outcomes registry (NACOR). In A. Gangopadhyay (Ed.), Methods, models, and computation for medical informatics (pp. 126–145). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2653-9.ch008
Guimarães, C., Antunes, D. R., García, L. S., & Fernandes, S. (2013). Information challenges of the deaf in their health and social care needs. In M. Cruz-Cunha, I. Miranda, & P. Gonçalves (Eds.), Handbook of research on ICTs for human-cen-tered healthcare and social care services (pp. 93–111). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3986-7.ch005
Guinalíu, M., Marta, J., & Subero, J. M. (2013). Social networks as a tool to improve the life quality of chronic patients and their relatives. In M. Cruz-Cunha, I. Miranda, & P. Gonçalves (Eds.), Handbook of research on ICTs for human-centered healthcare and social care services (pp. 172–186). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3986-7.ch009
Gullà, V. (2013). Leading the technological innovation in healthcare systems: The telematic medicine approach. In V. Gulla, A. Mori, F. Gabbrielli, & P. Lanzafame (Eds.), Telehealth networks for hospital services: New methodologies (pp. 134–153). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2979-0.ch009
Gullà, V., & Cancellotti, C. (2013). Telemedicine in emergency: A first aid hospital network experience. In V. Gulla, A. Mori, F. Gabbrielli, & P. Lanzafame (Eds.), Telehealth networks for hospital services: New methodologies (pp. 240–248). Her-shey, PA: IGI Global. doi:10.4018/978-1-4666-2979-0.ch016
Guo, M., Yu, Y., Yang, J., & Wu, J. (2013). The crossmodal between the visual and tactile for motion perception. In J. Wu (Ed.), Biomedical engineering and cognitive neuroscience for healthcare: Interdisciplinary applications (pp. 99–108). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2113-8.ch011
Hafeez-Baig, A., & Gururajan, R. (2013). Phenomena of adoption of wireless hand-held devices: A case of healthcare setting. In H. Muga & K. Thomas (Eds.), Cases on the diffusion and adoption of sustainable development practices (pp. 20–43). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2842-7.ch002

Related References
236
Haida, M. (2013). Implications of NIRS brain signals. In J. Wu (Ed.), Biomedical engineering and cognitive neuroscience for healthcare: Interdisciplinary applications (pp. 120–128). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2113-8.ch013
Han, D., & Braun, K. L. (2013). Promoting active ageing through technology train-ing in Korea. In Digital literacy: Concepts, methodologies, tools, and applications (pp. 572–589). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-1852-7.ch030
Hareva, D. H., Okada, H., & Oka, H. (2013). Ecological momentary assessment us-ing a mobile phone. In J. Wu (Ed.), Technological advancements in biomedicine for healthcare applications (pp. 398–407). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2196-1.ch039
Hatton, J. D., Schmidt, T. M., & Jelen, J. (2013). Adoption of electronic health care records: Physician heuristics and hesitancy. In R. Martinho, R. Rijo, M. Cruz-Cunha, & J. Varajão (Eds.), Information systems and technologies for enhancing health and social care (pp. 148–165). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3667-5.ch010
Heinrichs, L., Fellander-Tsai, L., & Davies, D. (2013). Clinical virtual worlds: The wider implications for professional development in healthcare. In K. Bredl & W. Bösche (Eds.), Serious games and virtual worlds in education, professional devel-opment, and healthcare (pp. 221–240). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3673-6.ch014
Heinrichs, W. L., Davies, D., & Davies, J. (2013). Virtual worlds in healthcare: Applications and implications. In S. Arnab, I. Dunwell, & K. Debattista (Eds.), Serious games for healthcare: Applications and implications (pp. 1–22). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-1903-6.ch001
Hirata, M., Yanagisawa, T., Matsushita, K., Sugata, H., Kamitani, Y., & Suzuki, T. … Yoshimine, T. (2013). Brain–machine interface using brain surface electrodes: Real-time robotic control and a fully implantable wireless system. In J. Wu (Ed.), Technological advancements in biomedicine for healthcare applications (pp. 362-374). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2196-1.ch036
Hocine, N., & Gouaïch, A. (2013). Difficulty and scenario adaptation: An approach to customize therapeutic games. In S. Arnab, I. Dunwell, & K. Debattista (Eds.), Serious games for healthcare: Applications and implications (pp. 107–134). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-1903-6.ch006

Related References
237
Hoonakker, P., Cartmill, R. S., Carayon, P., & Walker, J. M. (2013). Development and psychometric qualities of the SEIPS survey to evaluate CPOE/EHR implemen-tation in ICUs. In J. Tan (Ed.), Healthcare information technology innovation and sustainability: Frontiers and adoption (pp. 161–179). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2797-0.ch010
Igrejas, G., Amaral, J. S., & Rodrigues, P. J. (2013). Fall detection systems to be used by elderly people. In M. Cruz-Cunha, I. Miranda, & P. Gonçalves (Eds.), Handbook of research on ICTs for human-centered healthcare and social care services (pp. 449–473). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3986-7.ch024
Inomata, C., & Nitta, S. (2013). Nursing in integrative medicine and nurses’ en-gagement in caring-healing: A discussion based on the practice and study of music therapy and nursing care for patients with neurodegenerative disorders. In J. Wu (Ed.), Technological advancements in biomedicine for healthcare applications (pp. 235–239). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2196-1.ch025
Iwaki, S. (2013). Multimodal neuroimaging to visualize human visual processing. In J. Wu (Ed.), Biomedical engineering and cognitive neuroscience for health-care: Interdisciplinary applications (pp. 274–282). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2113-8.ch028
Ji, Z., Sugi, T., Goto, S., Wang, X., & Nakamura, M. (2013). Multi-channel template extraction for automatic EEG spike detection. In J. Wu (Ed.), Biomedical engineer-ing and cognitive neuroscience for healthcare: Interdisciplinary applications (pp. 255–265). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2113-8.ch026
Jiang, Y., Wang, S., Tan, R., Ishida, K., Ando, T., & Fujie, M. G. (2013). Motor cortex activation during mental imagery of walking: An fNIRS study. In J. Wu (Ed.), Biomedical engineering and cognitive neuroscience for healthcare: Interdisciplin-ary applications (pp. 29–37). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2113-8.ch004
Kalina, J., & Zvárová, J. (2013). Decision support systems in the process of improving patient safety. In A. Moumtzoglou & A. Kastania (Eds.), E-health technologies and improving patient safety: Exploring organizational factors (pp. 71–83). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2657-7.ch005
Kato, P. M. (2013). The role of the researcher in making serious games for health. In S. Arnab, I. Dunwell, & K. Debattista (Eds.), Serious games for healthcare: Applica-tions and implications (pp. 213–231). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-1903-6.ch010

Related References
238
Katsura, S. (2013). Preservation and reproduction of human motion based on a motion-copying system. In J. Wu (Ed.), Technological advancements in biomedicine for healthcare applications (pp. 375–384). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2196-1.ch037
Kikuchi, T. (2013). Human-friendly mechatronics systems with functional fluids and elastomers. In J. Wu (Ed.), Technological advancements in biomedicine for healthcare applications (pp. 94–101). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2196-1.ch010
Kimura, T., Miura, T., Shinohara, K., & Doi, S. (2013). Visual attention in 3-D space while moving forward. In J. Wu (Ed.), Biomedical engineering and cognitive neuroscience for healthcare: Interdisciplinary applications (pp. 81–88). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2113-8.ch009
Kldiashvili, E. (2013). Implementation of telecytology in Georgia. In V. Gulla, A. Mori, F. Gabbrielli, & P. Lanzafame (Eds.), Telehealth networks for hospital services: New methodologies (pp. 341–361). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2979-0.ch022
Koppar, A. R., & Sridhar, V. (2013). Malaria parasite detection: Automated method using microscope color image. In J. Rodrigues (Ed.), Digital advances in medicine, e-health, and communication technologies (pp. 289–300). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2794-9.ch016
Krishnaswamy, K., & Oates, T. (2014). Pathway to independence: Past, present, and beyond via robotics. In G. Kouroupetroglou (Ed.), Disability informatics and web accessibility for motor limitations (pp. 153–201). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4442-7.ch005
Kurita, Y., Ikeda, A., Nagata, K., Okajima, M., & Ogasawara, T. (2013). Biomedical robotics for healthcare. In J. Wu (Ed.), Technological advancements in biomedicine for healthcare applications (pp. 160–169). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2196-1.ch017
Lakkaraju, S., & Lakkaraju, S. (2013). Mobile device application in healthcare. In S. Sarnikar, D. Bennett, & M. Gaynor (Eds.), Cases on healthcare information technology for patient care management (pp. 276–307). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2671-3.ch016
Laskowski, M. (2013). A prototype agent based model and machine learning hybrid system for healthcare decision support. In J. Rodrigues (Ed.), Digital advances in medicine, e-health, and communication technologies (pp. 230–253). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2794-9.ch013

Related References
239
Lee, T. (2014). Mobile healthcare computing in the cloud. In J. Rodrigues, K. Lin, & J. Lloret (Eds.), Mobile networks and cloud computing convergence for progressive services and applications (pp. 275–294). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4781-7.ch015
Lelardeux, C., Alvarez, J., Montaut, T., Galaup, M., & Lagarrigue, P. (2013). Health-care games and the metaphoric approach. In S. Arnab, I. Dunwell, & K. Debattista (Eds.), Serious games for healthcare: Applications and implications (pp. 23–49). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-1903-6.ch002
Lhotska, L., Bursa, M., Huptych, M., Chudacek, V., & Havlik, J. (2013). Interoper-ability of medical devices and information systems. In M. Cruz-Cunha, I. Miranda, & P. Gonçalves (Eds.), Handbook of research on ICTs for human-centered healthcare and social care services (pp. 749–762). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3986-7.ch039
Li, X., Lin, Z., & Wu, J. (2013). Language processing in the human brain of literate and illiterate subjects. In J. Wu (Ed.), Biomedical engineering and cognitive neuro-science for healthcare: Interdisciplinary applications (pp. 201–209). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2113-8.ch021
Liao, H. (2013). Biomedical information processing and visualization for minimally invasive neurosurgery. In J. Wu (Ed.), Technological advancements in biomedicine for healthcare applications (pp. 36–46). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2196-1.ch005
Libreri, C., & Graffigna, G. (2014). How web 2.0 shapes patient knowledge shar-ing: The case of diabetes in Italy. In C. El Morr (Ed.), Research perspectives on the role of informatics in health policy and management (pp. 238–260). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4321-5.ch014
Lin, L., Chen, Y., Wu, J., & Tennyson, R. D. (2013). What skill/knowledge is im-portant to a nursing professional? In P. Ordóñez de Pablos (Ed.), Business, technol-ogy, and knowledge management in Asia: Trends and innovations (pp. 234–249). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2652-2.ch018
Liu, G. (2014). Using case costing data and case mix for funding and benchmarking in rehabilitation hospitals. In C. El Morr (Ed.), Research perspectives on the role of informatics in health policy and management (pp. 62–78). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4321-5.ch005

Related References
240
Lixun, Z., Dapeng, B., & Lei, Y. (2013). Design of and experimentation with a walk-ing assistance robot. In J. Wu (Ed.), Technological advancements in biomedicine for healthcare applications (pp. 123–127). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2196-1.ch013
Ma, X., Chen, G., & Xiao, J. (2013). Understanding weight change behaviors through online social networks. In A. Gangopadhyay (Ed.), Methods, models, and computation for medical informatics (pp. 189–214). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2653-9.ch012
Makikawa, M., Okada, S., Fujiwara, Y., & Esaki, M. (2013). Sleep monitoring system equipped with a flexible non-contact ECG, respiration, and body motion sensor. In J. Wu (Ed.), Technological advancements in biomedicine for healthcare applications (pp. 287–297). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2196-1.ch030
Malindretos, G. (2013). Distribution and logistics outsourcing in the pharmaceutical sector. In D. Folinas (Ed.), Outsourcing management for supply chain operations and logistics service (pp. 202–222). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2008-7.ch012
Manvi, S. S., & B., M. R. (2013). A survey on health care services using wireless sensor networks. In M. Cruz-Cunha, I. Miranda, & P. Gonçalves (Eds.), Handbook of research on ICTs for human-centered healthcare and social care services (pp. 587-606). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3986-7.ch031
Marshall, S., & Hogan, J. (2013). The use of medical simulation to improve patient safety. In A. Moumtzoglou & A. Kastania (Eds.), E-health technologies and improv-ing patient safety: Exploring organizational factors (pp. 155–172). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2657-7.ch011
Martin, J., & McKay, E. (2013). Mental health, post-secondary education, and information communications technology. In J. Lannon & E. Halpin (Eds.), Human rights and information communication technologies: Trends and consequences of use (pp. 196–213). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-1918-0.ch012
Martin, J., & McKay, E. (2014). Mental health, post-secondary education, and information communications technology. In Assistive technologies: Concepts, methodologies, tools, and applications (pp. 1209–1226). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4422-9.ch063

Related References
241
Masayuki, K., Eiji, K., Tetsuo, T., & Nozomu, M. (2013). Evaluation of olfactory impairment in Parkinson’s disease using near-infrared spectroscopy. In J. Wu (Ed.), Biomedical engineering and cognitive neuroscience for healthcare: Interdisciplinary applications (pp. 293–302). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2113-8.ch030
Mazzanti, I., Maolo, A., & Antonicelli, R. (2013). E-health and telemedicine in the elderly: State of the art. In V. Gulla, A. Mori, F. Gabbrielli, & P. Lanzafame (Eds.), Telehealth Networks for Hospital Services: New Methodologies (pp. 33–43). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2979-0.ch003
Mazzanti, I., Maolo, A., & Antonicelli, R. (2014). E-health and telemedicine in the elderly: State of the art. In Assistive technologies: Concepts, methodologies, tools, and applications (pp. 693–704). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4422-9.ch034
McCrossan, B. A., & Casey, F. A. (2013). The role of telemedicine in paediatric cardiology. In V. Gulla, A. Mori, F. Gabbrielli, & P. Lanzafame (Eds.), Telehealth networks for hospital services: New methodologies (pp. 44–88). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2979-0.ch004
McGinnes, S., & Burke, M. (2013). Hoping for the best: A qualitative study of infor-mation technology in primary care. In M. Cruz-Cunha, I. Miranda, & P. Gonçalves (Eds.), Handbook of research on ICTs and management systems for improving ef-ficiency in healthcare and social care (pp. 1088–1108). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3990-4.ch057
Medhekar, A., Wong, H. Y., & Hall, J. (2014). Innovation in medical tourism service marketing: A case of India. In A. Goyal (Ed.), Innovations in services marketing and management: Strategies for emerging economies (pp. 49–66). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4671-1.ch003
Medhekar, A., Wong, H. Y., & Hall, J. (2014). Medical tourism: A conceptual framework for an innovation in global healthcare provision. In A. Goyal (Ed.), In-novations in services marketing and management: Strategies for emerging economies (pp. 148–169). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4671-1.ch009
Mendes, D., & Rodrigues, I. P. (2013). A semantic web pragmatic approach to de-velop clinical ontologies, and thus semantic interoperability, based in HL7 v2.xml messaging. In R. Martinho, R. Rijo, M. Cruz-Cunha, & J. Varajão (Eds.), Informa-tion systems and technologies for enhancing health and social care (pp. 205–214). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3667-5.ch014

Related References
242
Mettler, T. (2013). Transformation of the hospital supply chain: How to measure the maturity of supplier relationship management systems in hospitals? In J. Tan (Ed.), Healthcare information technology innovation and sustainability: Frontiers and adoption (pp. 180–192). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2797-0.ch011
Miesenberger, K., Nussbaum, G., & Ossmann, R. (2014). AsTeRICS: A framework for including sensor technology into AT solutions for people with motor disabilities. In G. Kouroupetroglou (Ed.), Assistive technologies and computer access for mo-tor disabilities (pp. 154–179). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4438-0.ch006
Miller, K., & Sankaranarayanan, S. (2013). Applications of policy based agents in wireless body sensor mesh networks for patient health monitoring. In J. Rodrigues (Ed.), Digital advances in medicine, e-health, and communication technologies (pp. 85–101). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2794-9.ch005
Mohammadian, M., & Jentzsch, R. (2013). User and data classification for a se-cure and practical approach for patient-doctor profiling using an RFID framework in hospital. In S. Sarnikar, D. Bennett, & M. Gaynor (Eds.), Cases on healthcare information technology for patient care management (pp. 224–253). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2671-3.ch014
Montazemi, A. R., Pittaway, J. J., & Keshavjee, K. (2013). State of IS integration in the context of patient-centered care: A network analysis and research directions. In J. Tan (Ed.), Healthcare information technology innovation and sustainability: Frontiers and adoption (pp. 127–144). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2797-0.ch008
Mori, A. R., Contenti, M., & Verbicaro, R. (2013). Policies on telemedicine-enhanced hospital services: Prioritization criteria for the interventions at regional level. In V. Gulla, A. Mori, F. Gabbrielli, & P. Lanzafame (Eds.), Telehealth networks for hospital services: New methodologies (pp. 1–14). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2979-0.ch001
Morita, A. (2013). The quantitative EEG change in Parkinson’s disease. In J. Wu (Ed.), Biomedical engineering and cognitive neuroscience for healthcare: Interdis-ciplinary applications (pp. 225–234). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2113-8.ch023

Related References
243
Moromugi, S., & Ishimatsu, T. (2013). A strength training machine with a dynamic resistance control function based on muscle activity level. In J. Wu (Ed.), Techno-logical advancements in biomedicine for healthcare applications (pp. 102–110). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2196-1.ch011
Morrow, D., & Chin, J. (2013). Technology as a bridge between health care systems and older adults. In R. Zheng, R. Hill, & M. Gardner (Eds.), Engaging older adults with modern technology: Internet use and information access needs (pp. 59–79). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-1966-1.ch004
Mostafa, R., Hasan, G. M., Kabir, A. A., & Rahman, M. A. (2013). Proposed frame-work for the deployment of telemedicine centers in rural Bangladesh. In J. Rodrigues (Ed.), Digital advances in medicine, e-health, and communication technologies (pp. 254–270). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2794-9.ch014
Motoi, K., Ogawa, M., Yamakoshi, T., & Yamakoshi, K. (2013). Fusion physiologi-cal sensing system for healthcare. In J. Wu (Ed.), Technological advancements in biomedicine for healthcare applications (pp. 298–313). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2196-1.ch031
Motorny, S. P. (2013). Big information technology bet of a small community hospital. In S. Sarnikar, D. Bennett, & M. Gaynor (Eds.), Cases on healthcare information technology for patient care management (pp. 70–94). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2671-3.ch004
Moumtzoglou, A. (2013). Risk perception as a patient safety dimension. In A. Moumtzoglou & A. Kastania (Eds.), E-health technologies and improving patient safety: Exploring organizational factors (pp. 285–299). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2657-7.ch017
Msanjila, S. S. (2013). Emerging ICT challenges on provision of online HIV/AIDS advisory services. In M. Cruz-Cunha, I. Miranda, & P. Gonçalves (Eds.), Handbook of research on ICTs for human-centered healthcare and social care services (pp. 248–269). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3986-7.ch013
Müller, A. (2013). Improving the identification of medication names by increasing phonological awareness via a language-teaching computer game (medicina). In S. Arnab, I. Dunwell, & K. Debattista (Eds.), Serious games for healthcare: Applica-tions and implications (pp. 283–295). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-1903-6.ch014

Related References
244
Murakami, S., Kim, H., Tan, J. K., Ishikawa, S., & Aoki, T. (2013). The develop-ment of a quantitative method for the detection of periarticular osteoporosis using density features within ROIs from computed radiography images of the hand. In J. Wu (Ed.), Technological advancements in biomedicine for healthcare applications (pp. 55–67). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2196-1.ch007
Nadathur, S. G., & Warren, J. R. (2013). Formal-transfer in and out of stroke care units: An analysis using Bayesian networks. In J. Tan (Ed.), Healthcare information technology innovation and sustainability: Frontiers and adoption (pp. 193–207). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2797-0.ch012
Naidoo, V., & Naidoo, Y. (2014). Home telecare, medical implant, and mobile tech-nology: Evolutions in geriatric care. In C. El Morr (Ed.), Research perspectives on the role of informatics in health policy and management (pp. 222–237). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4321-5.ch013
Nakagawa, S. (2013). Bone-conducted ultrasonic perception: An elucidation of per-ception mechanisms and the development of a novel hearing aid for the profoundly deaf. In J. Wu (Ed.), Technological advancements in biomedicine for healthcare applications (pp. 148–159). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2196-1.ch016
Nakai, M., & Niinomi, M. (2013). Recent progress in mechanically biocompat-ible titanium-based materials. In J. Wu (Ed.), Technological advancements in biomedicine for healthcare applications (pp. 206–212). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2196-1.ch022
Nakakuki, T., & Okada-Hatakeyama, M. (2013). Methods for the analysis of intra-cellular signal transduction systems. In J. Wu (Ed.), Technological advancements in biomedicine for healthcare applications (pp. 347–353). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2196-1.ch034
Nalin, M., Verga, M., Sanna, A., & Saranummi, N. (2013). Directions for ICT research in disease prevention. In M. Cruz-Cunha, I. Miranda, & P. Gonçalves (Eds.), Hand-book of research on ICTs for human-centered healthcare and social care services (pp. 229–247). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3986-7.ch012
Nap, H. H., & Diaz-Orueta, U. (2013). Rehabilitation gaming. In S. Arnab, I. Dunwell, & K. Debattista (Eds.), Serious games for healthcare: Applications and implica-tions (pp. 50–75). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-1903-6.ch003

Related References
245
Narushima, T., & Ueda, K. (2013). Calcium phosphate coating on titanium by RF magnetron sputtering. In J. Wu (Ed.), Technological advancements in biomedicine for healthcare applications (pp. 223–233). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2196-1.ch024
Nava-Muñoz, S., & Morán, A. L. (2013). A review of notifications systems in elder care environments: Challenges and opportunities. In M. Cruz-Cunha, I. Miranda, & P. Gonçalves (Eds.), Handbook of research on ICTs for human-centered healthcare and social care services (pp. 407–429). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3986-7.ch022
Nganji, J. T., & Nggada, S. H. (2014). Adoption of blended learning technologies in selected secondary schools in Cameroon and Nigeria: Challenges in disability inclusion. In N. Ololube (Ed.), Advancing technology and educational development through blended learning in emerging economies (pp. 159–173). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4574-5.ch009
Nishiguchi, H. (2013). Description of and applications for a motion analysis method for upper limbs. In J. Wu (Ed.), Technological advancements in biomedicine for healthcare applications (pp. 1–10). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2196-1.ch001
Nokata, M. (2013). Small medical robot. In J. Wu (Ed.), Technological advance-ments in biomedicine for healthcare applications (pp. 170–179). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2196-1.ch018
Noritsugu, T. (2013). Wearable power assist robot driven with pneumatic rubber artificial muscles. In J. Wu (Ed.), Technological advancements in biomedicine for healthcare applications (pp. 139–147). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2196-1.ch015
Noteboom, C. (2013). Physician interaction with EHR: The importance of stakeholder identification and change management. In S. Sarnikar, D. Bennett, & M. Gaynor (Eds.), Cases on healthcare information technology for patient care management (pp. 95–112). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2671-3.ch005
O’Hanlon, S. (2013). Avoiding adverse consequences of e-health. In A. Moumtzoglou & A. Kastania (Eds.), E-health technologies and improving patient safety: Exploring organizational factors (pp. 13–26). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2657-7.ch002

Related References
246
Ogawa, K., Nishio, S., Minato, T., & Ishiguro, H. (2013). Android robots as telepres-ence media. In J. Wu (Ed.), Biomedical engineering and cognitive neuroscience for healthcare: Interdisciplinary applications (pp. 54–63). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2113-8.ch006
Ohashi, M., Sakimura, N., Fujimoto, M., Hori, M., & Kurata, N. (2013). Technical perspective of authentication policy extension for the adaptive social services and e-health care management. In M. Cruz-Cunha, I. Miranda, & P. Gonçalves (Eds.), Handbook of research on ICTs for human-centered healthcare and social care services (pp. 719–726). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3986-7.ch037
Ohta, Y., & Uchida, M. (2013). Non-contact pulse monitoring using live imaging. In J. Wu (Ed.), Technological advancements in biomedicine for healthcare applications (pp. 240–246). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2196-1.ch026
Ohuchida, K., & Hashizume, M. (2013). Biomedical robotics for healthcare. In J. Wu (Ed.), Technological advancements in biomedicine for healthcare applications (pp. 200–205). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2196-1.ch021
Oikonomou, D., Moulianitis, V., Lekkas, D., & Koutsabasis, P. (2013). DSS for health emergency response: A contextual, user-centred approach. In R. Biswas (Ed.), Clinical solutions and medical progress through user-driven healthcare (pp. 51–69). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-1876-3.ch006
Okamoto, S., Hirotomi, T., Aoki, K., & Hosomi, Y. (2013). Evaluation of walking motions with the aid of walkers using acceleration sensors. In J. Wu (Ed.), Biomedical engineering and cognitive neuroscience for healthcare: Interdisciplinary applications (pp. 346–354). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2113-8.ch036
Okamura, H. (2013). Rehabilitation of elderly people with dementia. In J. Wu (Ed.), Biomedical engineering and cognitive neuroscience for healthcare: Interdisciplinary applications (pp. 235–242). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2113-8.ch024
Olvera-Lobo, M., & Gutiérrez-Artacho, J. (2013). Searching health information in question-answering systems. In M. Cruz-Cunha, I. Miranda, & P. Gonçalves (Eds.), Handbook of research on ICTs for human-centered healthcare and social care services (pp. 474–490). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3986-7.ch025
Padovani, E., Orelli, R. L., Agnoletti, V., & Buccioli, M. (2013). Low cost and human-centered innovations in healthcare services: A case of excellence in Italy. In S. Saeed & C. Reddick (Eds.), Human-centered system design for electronic governance (pp. 239–252). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3640-8.ch014

Related References
247
Paninchukunnath, A. (2014). Healthcare services delivery in India: special reference to mother and child health. In A. Goyal (Ed.), Innovations in services marketing and management: Strategies for emerging economies (pp. 170–189). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4671-1.ch010
Parentela, G., Mancini, P., Naccarella, F., Feng, Z., & Rinaldi, G. (2013). Tele-medicine, the European space agency, and the support to the african population for infectious disease problems: Potentiality and perspectives for Asia countries and China. In V. Gulla, A. Mori, F. Gabbrielli, & P. Lanzafame (Eds.), Telehealth networks for hospital services: New methodologies (pp. 89–96). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2979-0.ch005
Paterson, G. I., MacDonald, J. M., & Mensink, N. N. (2014). The administrative policy quandary in Canada’s health service organizations. In C. El Morr (Ed.), Research perspectives on the role of informatics in health policy and management (pp. 116–134). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4321-5.ch008
Pereira, O. R., Caldeira, J. M., & Rodrigues, J. J. (2013). An advanced and secure symbian-based mobile approach for body sensor networks interaction. In J. Rodrigues (Ed.), Digital advances in medicine, e-health, and communication technologies (pp. 33–48). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2794-9.ch002
Phua, C., Roy, P. C., Aloulou, H., Biswas, J., Tolstikov, A., & Foo, V. S. … Xu, D. (2014). State-of-the-art assistive technology for people with dementia. In Assistive technologies: Concepts, methodologies, tools, and applications (pp. 1606-1625). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4422-9.ch085
Pino, A. (2014). Augmentative and alternative communication systems for the motor disabled. In G. Kouroupetroglou (Ed.), Disability informatics and web accessibility for motor limitations (pp. 105–152). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4442-7.ch004
Portela, F., Cabral, A., Abelha, A., Salazar, M., Quintas, C., Machado, J., & Santos, M. F. et al. (2013). Knowledge acquisition process for intelligent decision support in critical health care. In R. Martinho, R. Rijo, M. Cruz-Cunha, & J. Varajão (Eds.), Information systems and technologies for enhancing health and social care (pp. 55–68). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3667-5.ch004
Previtali, P. (2013). Grid technology for archive solutions in health care organizations. In A. Moumtzoglou & A. Kastania (Eds.), E-health technologies and improving patient safety: Exploring organizational factors (pp. 148–154). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2657-7.ch010

Related References
248
Qi, G., & Wu, J. (2013). Functional role of the left ventral occipito-temporal cortex in reading. In J. Wu (Ed.), Biomedical engineering and cognitive neuroscience for healthcare: Interdisciplinary applications (pp. 192–200). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2113-8.ch020
Queirós, A., Alvarelhão, J., Silva, A. G., Teixeira, A., & Pacheco da Rocha, N. (2013). A conceptual framework for the design and development of AAL services. In M. Cruz-Cunha, I. Miranda, & P. Gonçalves (Eds.), Handbook of research on ICTs for human-centered healthcare and social care services (pp. 568–586). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3986-7.ch030
Ravka, N. (2014). Informatics and health services: The potential benefits and chal-lenges of electronic health records and personal electronic health records in patient care, cost control, and health research – An overview. In C. El Morr (Ed.), Research perspectives on the role of informatics in health policy and management (pp. 89–114). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4321-5.ch007
Reibling, N., & Wendt, C. (2013). Regulating patients’ access to healthcare services. In M. Merviö (Ed.), Healthcare management and economics: Perspectives on public and private administration (pp. 53–68). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3982-9.ch005
Reis, C. I., Freire, C. S., Fernández, J., & Monguet, J. M. (2013). Patient centered design: Challenges and lessons learned from working with health professionals and schizophrenic patients in e-therapy contexts. In R. Martinho, R. Rijo, M. Cruz-Cunha, & J. Varajão (Eds.), Information systems and technologies for enhancing health and social care (pp. 120–135). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3667-5.ch008
Ricketts, M. (2014). Making health information personal: How anecdotes bring concepts to life. In S. Hai-Jew (Ed.), Packaging digital information for enhanced learning and analysis: Data visualization, spatialization, and multidimensionality (pp. 1–36). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4462-5.ch001
Rocha, Á. (2013). Evolution of information systems and technologies maturity in healthcare. In J. Tan (Ed.), Healthcare information technology innovation and sustainability: Frontiers and adoption (pp. 238–246). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2797-0.ch015
Rodríguez-Gómez, D., & Gairín, J. (2014). Communities of practice in the Catalan public administration: Promoting their improvement. In Y. Al-Bastaki & A. Shajera (Eds.), Building a competitive public sector with knowledge management strategy (pp. 383–402). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4434-2.ch018

Related References
249
Rodríguez-Solano, C., Lezcano, L., & Sicilia, M. (2013). Automated generation of SNOMED CT subsets from clinical guidelines. In R. Martinho, R. Rijo, M. Cruz-Cunha, & J. Varajão (Eds.), Information systems and technologies for enhancing health and social care (pp. 190–204). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3667-5.ch013
Rosu, S. M., & Dragoi, G. (2014). E-health sites development using open source software and OMT methodology as support for family doctors’ activities: A Roma-nian case study. In M. Cruz-Cunha, F. Moreira, & J. Varajão (Eds.), Handbook of research on enterprise 2.0: Technological, social, and organizational dimensions (pp. 72–88). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4373-4.ch004
Saha, P. (2014). Systemic enterprise architecture as future: Tackling complexity in governments in the cusp of change. In P. Saha (Ed.), A systemic perspective to managing complexity with enterprise architecture (pp. 1–70). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4518-9.ch001
Saijo, Y. (2013). Biomedical application of multimodal ultrasound microscope. In J. Wu (Ed.), Technological advancements in biomedicine for healthcare applica-tions (pp. 27–35). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2196-1.ch004
Santos, M., Bastião, L., Costa, C., Silva, A., & Rocha, N. (2013). Clinical data min-ing in small hospital PACS: Contributions for radiology department improvement. In R. Martinho, R. Rijo, M. Cruz-Cunha, & J. Varajão (Eds.), Information systems and technologies for enhancing health and social care (pp. 236–251). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3667-5.ch016
Santos, M. F., Portela, F., Miranda, M., Machado, J., Abelha, A., Silva, Á., & Rua, F. (2013). Grid data mining strategies for outcome prediction in distributed intensive care units. In R. Martinho, R. Rijo, M. Cruz-Cunha, & J. Varajão (Eds.), Informa-tion systems and technologies for enhancing health and social care (pp. 87–101). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3667-5.ch006
Santos, R. J., Bernardino, J., & Vieira, M. (2013). A hypotension surveillance and prediction system for critical care. In M. Cruz-Cunha, I. Miranda, & P. Gonçalves (Eds.), Handbook of research on ICTs and management systems for improving efficiency in healthcare and social care (pp. 341–355). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3990-4.ch017

Related References
250
Sanz, P. R., Mezcua, B. R., & Pena, J. M. (2013). ICTs for orientation and mobility for blind people: A state of the art. In M. Cruz-Cunha, I. Miranda, & P. Gonçalves (Eds.), Handbook of research on ICTs for human-centered healthcare and social care services (pp. 646–669). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3986-7.ch034
Sasayama, T., Hamada, S., & Kobayashi, T. (2013). Application of prewhitening beamformer with linear constraints for correlated EEG signal source estimation. In J. Wu (Ed.), Biomedical engineering and cognitive neuroscience for health-care: Interdisciplinary applications (pp. 243–254). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2113-8.ch025
Sato, T., & Minato, K. (2013). Differences in analysis methods of the human uncinate fasciculus using diffusion tensor MRI. In J. Wu (Ed.), Biomedical engineering and cognitive neuroscience for healthcare: Interdisciplinary applications (pp. 162–170). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2113-8.ch017
Satoh, J. (2013). Molecular network analysis of target RNAs and interacting proteins of TDP-43, a causative gene for the neurodegenerative diseases ALS/FTLD. In J. Wu (Ed.), Technological advancements in biomedicine for healthcare applications (pp. 314–335). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2196-1.ch032
Schafer, S. B. (2013). Fostering psychological coherence: With ICTs. In M. Cruz-Cunha, I. Miranda, & P. Gonçalves (Eds.), Handbook of research on ICTs for human-centered healthcare and social care services (pp. 29–47). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3986-7.ch002
Schmeida, M., & McNeal, R. (2013). Bridging the inequality gap to accessing medicare and medicaid information online: An empirical analysis of e-government success 2002 through 2010. In J. Gil-Garcia (Ed.), E-government success around the world: Cases, empirical studies, and practical recommendations (pp. 60–78). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4173-0.ch004
Scholl, J. C., & Olaniran, B. A. (2013). ICT use and multidisciplinary healthcare teams. In M. Cruz-Cunha, I. Miranda, & P. Gonçalves (Eds.), Handbook of research on ICTs for human-centered healthcare and social care services (pp. 627–645). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3986-7.ch033
Serrano, M., Elmisery, A., Foghlú, M. Ó., Donnelly, W., Storni, C., & Fernström, M. (2013). Pervasive computing support in the transition towards personalised health systems. In J. Rodrigues (Ed.), Digital advances in medicine, e-health, and com-munication technologies (pp. 49–64). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2794-9.ch003

Related References
251
Shibata, T. (2013). A human-like cognitive computer based on a psychologically inspired VLSI brain model. In J. Wu (Ed.), Technological advancements in bio-medicine for healthcare applications (pp. 247–266). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2196-1.ch027
Shimada, S. (2013). Self-body recognition and its impairment. In J. Wu (Ed.), Bio-medical engineering and cognitive neuroscience for healthcare: Interdisciplinary applications (pp. 156–161). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2113-8.ch016
Shimogonya, Y., Ishikawa, T., Yamaguchi, T., Kumamaru, H., & Itoh, K. (2013). Computational study of the hemodynamics of cerebral aneurysm initiation. In J. Wu (Ed.), Technological advancements in biomedicine for healthcare applications (pp. 267–277). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2196-1.ch028
Shimonomura, K. (2013). A neuromorphic robot vision system to predict the response of visual neurons. In J. Wu (Ed.), Technological advancements in biomedicine for healthcare applications (pp. 193–199). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2196-1.ch020
Shrestha, S. (2013). Clinical decision support system for diabetes prevention: An illustrative case. In S. Sarnikar, D. Bennett, & M. Gaynor (Eds.), Cases on health-care information technology for patient care management (pp. 308–329). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2671-3.ch017
Siddiqui, Z. S., & Jonas-Dwyer, D. R. (2013). Mobile learning in health professions education: A systematic review. In J. Keengwe (Ed.), Pedagogical applications and social effects of mobile technology integration (pp. 193–205). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2985-1.ch011
Silvana de Rosa, A., Fino, E., & Bocci, E. (2014). Addressing healthcare on-line demand and supply relating to mental illness: Knowledge sharing about psychiatry and psychoanalysis through social networks in Italy and France. In A. Kapoor & C. Kulshrestha (Eds.), Dynamics of competitive advantage and consumer perception in social marketing (pp. 16–55). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4430-4.ch002
Sobol, M., & Prater, E. (2013). Adoption, usage and efficiency: Benchmarking healthcare IT in private practices. In J. Tan (Ed.), Healthcare information technol-ogy innovation and sustainability: Frontiers and adoption (pp. 145–159). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2797-0.ch009

Related References
252
Sobrinho, Á. A., Dias da Silva, L., Melo de Medeiros, L., & Pinheiro, M. E. (2013). A mobile assistant to aid early detection of chronic kidney disease. In R. Martinho, R. Rijo, M. Cruz-Cunha, & J. Varajão (Eds.), Information systems and technolo-gies for enhancing health and social care (pp. 309–323). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3667-5.ch020
Soomlek, C., & Benedicenti, L. (2013). Agent-based wellness indicator. In V. Gulla, A. Mori, F. Gabbrielli, & P. Lanzafame (Eds.), Telehealth networks for hospital services: New methodologies (pp. 300–330). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2979-0.ch020
Spadaro, L., Timpano, F., Marino, S., & Bramanti, P. (2013). Telemedicine and Alzheimer disease: ICT-based services for people with Alzheimer disease and their caregivers. In V. Gulla, A. Mori, F. Gabbrielli, & P. Lanzafame (Eds.), Telehealth networks for hospital services: New methodologies (pp. 191–206). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2979-0.ch013
Stefaniak, J. E. (2013). Resuscitating team roles within wayburn health system. In A. Ritzhaupt & S. Kumar (Eds.), Cases on educational technology implementation for facilitating learning (pp. 130–145). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3676-7.ch008
Sugiura, M. (2013). A cognitive neuroscience approach to self and mental health. In J. Wu (Ed.), Biomedical engineering and cognitive neuroscience for healthcare: Interdisciplinary applications (pp. 1–10). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2113-8.ch001
Supnithi, T., Buranarach, M., Thatphithakkul, N., Junsirimongkol, B., Wongrocha-nanan, S., Kulnawan, N., & Jiamjarasrangsi, W. (2014). A self-management service framework to support chronic disease patients’ self-management. In M. Kosaka & K. Shirahada (Eds.), Progressive trends in knowledge and system-based science for service innovation (pp. 425–450). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4663-6.ch023
Takahashi, K., & Watanabe, K. (2013). Crossmodal interactions in visual com-petition. In J. Wu (Ed.), Biomedical engineering and cognitive neuroscience for healthcare: Interdisciplinary applications (pp. 64–72). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2113-8.ch007
Tamiya, T., Kawanishi, M., Miyake, K., Kawai, N., & Guo, S. (2013). Neurosurgical operations using navigation microscope integration system. In J. Wu (Ed.), Tech-nological advancements in biomedicine for healthcare applications (pp. 128–138). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2196-1.ch014

Related References
253
Tan, R., Wang, S., Jiang, Y., Ishida, K., & Fujie, M. G. (2013). Motion control of an omni-directional walker for walking support. In J. Wu (Ed.), Biomedical engineer-ing and cognitive neuroscience for healthcare: Interdisciplinary applications (pp. 20–28). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2113-8.ch003
Tanaka, H., & Furutani, M. (2013). Sleep management promotes healthy lifestyle, mental health, QOL, and a healthy brain. In J. Wu (Ed.), Biomedical engineering and cognitive neuroscience for healthcare: Interdisciplinary applications (pp. 211–224). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2113-8.ch022
Tang, X., Gao, Y., Yang, W., Zhang, M., & Wu, J. (2013). Audiovisual integration of natural auditory and visual stimuli in the real-world situation. In J. Wu (Ed.), Biomedical engineering and cognitive neuroscience for healthcare: Interdisciplinary applications (pp. 337–344). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2113-8.ch035
Targowski, A. (2013). Well-being, wisdom, health, and IT: From the big-picture to the small-picture. In M. Cruz-Cunha, I. Miranda, & P. Gonçalves (Eds.), Handbook of research on ICTs for human-centered healthcare and social care services (pp. 1–28). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3986-7.ch001
Tayabali, S., & Martin, C. M. (2013). The need to transform the core values of medical care and health organizations. In R. Biswas (Ed.), Clinical solutions and medical progress through user-driven healthcare (pp. 85–92). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-1876-3.ch009
Taylor, B. W. (2014). Decision-making and decision support in acute care. In C. El Morr (Ed.), Research perspectives on the role of informatics in health policy and management (pp. 1–18). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4321-5.ch001
Teixeira, C., Pinto, J. S., Ferreira, F., Oliveira, A., Teixeira, A., & Pereira, C. (2013). Cloud computing enhanced service development architecture for the living usability lab. In R. Martinho, R. Rijo, M. Cruz-Cunha, & J. Varajão (Eds.), Information sys-tems and technologies for enhancing health and social care (pp. 33–53). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3667-5.ch003
Teixeira, L., Saavedra, V., Ferreira, C., & Santos, B. S. (2013). The role of ICTs in the management of rare chronic diseases: The case of hemophilia. In M. Cruz-Cunha, I. Miranda, & P. Gonçalves (Eds.), Handbook of research on ICTs and manage-ment systems for improving efficiency in healthcare and social care (pp. 635–649). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3990-4.ch033

Related References
254
Tiwari, S., & Srivastava, R. (2014). Research and developments in medical image reconstruction methods and its applications. In R. Srivastava, S. Singh, & K. Shukla (Eds.), Research developments in computer vision and image processing: Method-ologies and applications (pp. 274–312). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4558-5.ch014
Tobolcea, I. (2013). The psychosocial impact of ICT efficiency on speech disorders-treatment. In M. Cruz-Cunha, I. Miranda, & P. Gonçalves (Eds.), Handbook of re-search on ICTs for human-centered healthcare and social care services (pp. 70–92). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3986-7.ch004
Toda, T., Chen, P., Ozaki, S., Fujita, K., & Ideguchi, N. (2013). A simple web-based image database system for facilitating medical care in dermatological clinics. In J. Wu (Ed.), Technological advancements in biomedicine for healthcare applications (pp. 385–397). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2196-1.ch038
Trudeau, S. (2013). CoRDS registry: An HIT case study concerning setup and main-tenance of a disease registry. In S. Sarnikar, D. Bennett, & M. Gaynor (Eds.), Cases on healthcare information technology for patient care management (pp. 197–207). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2671-3.ch012
Tseng, R., & Yi-Luen Do, E. (2013). The role of information and computer technol-ogy for children with autism spectrum disorder and the facial expression wonderland (FEW). In A. Gangopadhyay (Ed.), Methods, models, and computation for medical informatics (pp. 98–116). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2653-9.ch006
Uchitomi, H., Suzuki, K., Nishi, T., Hove, M. J., Miyake, Y., Orimo, S., & Wada, Y. (2013). Gait rhythm of Parkinson’s disease patients and an interpersonal synchrony emulation system based on cooperative gait. In J. Wu (Ed.), Biomedical engineer-ing and cognitive neuroscience for healthcare: Interdisciplinary applications (pp. 38–53). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2113-8.ch005
Van Genderen, E. (2014). Intensive care. In V. Jham & S. Puri (Eds.), Cases on consumer-centric marketing management (pp. 53–67). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4357-4.ch006
Vidal, B., Pereira, J. M., & Santos, G. (2013). SimBody: An interactive simula-tor for health education. In S. Arnab, I. Dunwell, & K. Debattista (Eds.), Serious games for healthcare: Applications and implications (pp. 265–282). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-1903-6.ch013

Related References
255
Vivekananda-Schmidt, P. (2013). Ethics in the design of serious games for healthcare and medicine. In S. Arnab, I. Dunwell, & K. Debattista (Eds.), Serious games for healthcare: Applications and implications (pp. 91–106). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-1903-6.ch005
Wahbeh, A. (2013). Application of handheld computing and mobile phones in dia-betes self-care. In S. Sarnikar, D. Bennett, & M. Gaynor (Eds.), Cases on healthcare information technology for patient care management (pp. 254–275). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2671-3.ch015
Waidyanatha, N., & Dekker, S. (2013). The RTBP – Collective intelligence driving health for the user. In R. Biswas (Ed.), Clinical solutions and medical progress through user-driven healthcare (pp. 70–78). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-1876-3.ch007
Waidyanatha, N., Dubrawski, A. M. G., & Gow, G. (2013). Affordable system for rapid detection and mitigation of emerging diseases. In J. Rodrigues (Ed.), Digital advances in medicine, e-health, and communication technologies (pp. 271–288). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2794-9.ch015
Walker, D. (2013). How would a ban on prescriber-identifying information impact pharmaceutical marketing? In M. Merviö (Ed.), Healthcare management and eco-nomics: Perspectives on public and private administration (pp. 141–153). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3982-9.ch011
Wang, B., Yan, T., & Wu, J. (2013). Neuronal function in the cortical face perception network. In J. Wu (Ed.), Biomedical engineering and cognitive neuroscience for healthcare: Interdisciplinary applications (pp. 171–182). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2113-8.ch018
Wang, Y., & Wang, Q. (2013). Evaluating the IEEE 802.15.6 2.4GHz WBAN pro-posal on medical multi-parameter monitoring under WiFi/bluetooth interference. In J. Rodrigues (Ed.), Digital advances in medicine, e-health, and communication technologies (pp. 312–325). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2794-9.ch018
Watanabe, T., & Miura, N. (2013). Functional electrical stimulation (FES) control for restoration and rehabilitation of motor function. In J. Wu (Ed.), Technological advancements in biomedicine for healthcare applications (pp. 80–93). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2196-1.ch009

Related References
256
Watanabe, Y., Tanaka, H., & Hirata, K. (2013). Evaluation of cognitive function in migraine patients: A study using event-related potentials. In J. Wu (Ed.), Biomedical engineering and cognitive neuroscience for healthcare: Interdisciplinary applications (pp. 303–310). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2113-8.ch031
Wesorick, B. (2013). Essential steps for successful implementation of the EHR to achieve sustainable, safe, quality care. In A. Moumtzoglou & A. Kastania (Eds.), E-health technologies and improving patient safety: Exploring organizational fac-tors (pp. 27–55). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2657-7.ch003
Whitaker, R. (2013). Securing health-effective medicine in practice: A critical perspective on user-driven healthcare. In R. Biswas (Ed.), Clinical solutions and medical progress through user-driven healthcare (pp. 35–50). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-1876-3.ch005
Wickramasinghe, N., Troshani, I., Hill, S. R., Hague, W., & Goldberg, S. (2013). A transaction cost assessment of a pervasive technology solution for gestational diabetes. In J. Tan (Ed.), Healthcare information technology innovation and sustainability: Frontiers and adoption (pp. 109–126). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2797-0.ch007
Wu, Q., Li, C., Takahashi, S., & Wu, J. (2013). Visual-tactile bottom-up and top-down attention. In J. Wu (Ed.), Biomedical engineering and cognitive neuroscience for healthcare: Interdisciplinary applications (pp. 183–191). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2113-8.ch019
Yamaguchi, S., Onoda, K., & Abe, S. (2013). Feedback-related negativity and its clinical implications. In J. Wu (Ed.), Biomedical engineering and cognitive neuro-science for healthcare: Interdisciplinary applications (pp. 283–292). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2113-8.ch029
Yan, B., Lei, Y., Tong, L., & Chen, K. (2013). Functional neuroimaging of acupunc-ture: A systematic review. In J. Wu (Ed.), Biomedical engineering and cognitive neuroscience for healthcare: Interdisciplinary applications (pp. 142–155). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2113-8.ch015
Yang, J. (2014). Towards healthy public policy: GIS and food systems analysis. In C. El Morr (Ed.), Research perspectives on the role of informatics in health policy and management (pp. 135–152). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4321-5.ch009

Related References
257
Yang, J., Li, Q., Gao, Y., & Wu, J. (2013). Temporal dependency of multisensory audiovisual integration. In J. Wu (Ed.), Biomedical engineering and cognitive neu-roscience for healthcare: Interdisciplinary applications (pp. 320–326). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2113-8.ch033
Yang, J. J., Liu, J. F., Kurokawa, T., Kitamura, N., Yasuda, K., & Gong, J. P. (2013). Tough double-network hydrogels as scaffolds for tissue engineering: Cell behavior in vitro and in vivo test. In J. Wu (Ed.), Technological advancements in biomedicine for healthcare applications (pp. 213–222). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2196-1.ch023
Yang, W., Gao, Y., & Wu, J. (2013). Effects of selective and divided attention on audiovisual interaction. In J. Wu (Ed.), Biomedical engineering and cognitive neu-roscience for healthcare: Interdisciplinary applications (pp. 311–319). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2113-8.ch032
Yano, Y. (2013). An EMG control system for an ultrasonic motor using a PSoC microcomputer. In J. Wu (Ed.), Technological advancements in biomedicine for healthcare applications (pp. 11–17). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2196-1.ch002
Yokoi, H., Kato, R., Mori, T., Yamamura, O., & Kubota, M. (2013). Functional electri-cal stimulation based on interference-driven PWM signals for neuro-rehabilitation. In J. Wu (Ed.), Technological advancements in biomedicine for healthcare applications (pp. 180–192). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2196-1.ch019
York, A. M., & Nordengren, F. R. (2013). E-learning and web 2.0 case study: The role of gender in contemporary models of health care leadership. In H. Yang & S. Wang (Eds.), Cases on formal and informal e-learning environments: Opportunities and practices (pp. 292–313). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-1930-2.ch016
Yu, W. D., & Bhagwat, R. (2013). Modeling emergency and telemedicine health support system: A service oriented architecture approach using cloud computing. In J. Rodrigues (Ed.), Digital advances in medicine, e-health, and communication technologies (pp. 187–213). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2794-9.ch011
Yu, Y., Yang, J., & Wu, J. (2013). Cognitive functions and neuronal mechanisms of tactile working memory. In J. Wu (Ed.), Biomedical engineering and cognitive neuroscience for healthcare: Interdisciplinary applications (pp. 89–98). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2113-8.ch010

Related References
258
Zaheer, S. (2014). Implementation of evidence-based practice and the PARIHS framework. In C. El Morr (Ed.), Research perspectives on the role of informatics in health policy and management (pp. 19–36). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4321-5.ch002
Zapirain, B. G., & Zorrilla, A. M. (2013). Independent living support for disabled and elderly people using cell phones. In M. Cruz-Cunha, I. Miranda, & P. Gonçalves (Eds.), Handbook of research on ICTs for human-centered healthcare and social care services (pp. 379–397). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3986-7.ch020
Zhou, X., & Ren, X. (2013). Speed-accuracy tradeoff models of target-based and trajectory-based movements. In J. Wu (Ed.), Biomedical engineering and cognitive neuroscience for healthcare: Interdisciplinary applications (pp. 355–368). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2113-8.ch037
Zouag, N., & Driouchi, A. (2014). Trends and prospects of the Moroccan health system: 2010-2030. In A. Driouchi (Ed.), Labor and health economics in the mediter-ranean region: Migration and mobility of medical doctors (pp. 314–336). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4723-7.ch013

259
Compilation of References
Aas, I. H. (2013). Improving patient safety with telemedicine: Exploring organizational factors. In A. Moumtzoglou & A. Kastania (Eds.), E-health technologies and improving patient safety: Exploring organizational factors (pp. 56–70). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2657-7.ch004
Abdi, Z., Delgoshaei, B., Ravaghi, H., Abbasi, M., & Heyrani, A. (2015). The culture of pa-tient safety in an Iranian intensive care unit. Journal of Nursing Management, 23(3), 333–345. doi:10.1111/jonm.12135 PMID:23902287
Aboelfotoh, M. H., Martin, P., & Hassanein, H. (2013). Ubiquitous multimedia data access in elec-tronic health care systems. In D. Tjondronegoro (Ed.), Tools for mobile multimedia programming and development (pp. 191–227). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4054-2.ch011
Abreu, J. F., Almeida, P., & Silva, T. (2013). iNeighbour TV: A social TV application to pro-mote wellness of senior citizens. In R. Martinho, R. Rijo, M. Cruz-Cunha, & J. Varajão (Eds.), Information systems and technologies for enhancing health and social care (pp. 1-19). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3667-5.ch001
Absulem, S., & Hardin, H. (2011). Home health nurses’ perceived care errors. Rehabilitation Nursing, 36(3), 98–105. doi:10.1002/j.2048-7940.2011.tb00073.x PMID:21675394
Aceti, V., & Luppicini, R. (2013). Exploring the effect of mhealth technologies on communication and information sharing in a pediatric critical care unit: A case study. In J. Tan (Ed.), Healthcare information technology innovation and sustainability: Frontiers and adoption (pp. 88–108). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2797-0.ch006
ACSNI. (1993). Advisory Committee on the Safety of Nuclear Installation: Human Factors Study Group Third Report: Organizing for safety. Sheffield, UK: HSE Books.
Adami, I., Antona, M., & Stephanidis, C. (2014). Ambient assisted living for people with motor impairments. In G. Kouroupetroglou (Ed.), Disability informatics and web accessibility for mo-tor limitations (pp. 76–104). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4442-7.ch003

Compilation of References
260
Agency for Healthcare Research and Quality. (n.d.). Patient Safety Tips for Hospitals. Retrieved from http://www.ahrq.gov/patients-consumers/diagnosis-treatment/hospitals-clinics/10-tips/index.html
Åkerberg, A., Lindén, M., & Folke, M. (2013). Pedometer cell phone applications and future trends in measuring physical activity. In R. Martinho, R. Rijo, M. Cruz-Cunha, & J. Varajão (Eds.), Information systems and technologies for enhancing health and social care (pp. 324–339). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3667-5.ch021
Al Hamouche, V. (2014). Making quality control decisions in radiology department: A deci-sion support system for radiographers’ performance appraisal using PACS. In C. El Morr (Ed.), Research perspectives on the role of informatics in health policy and management (pp. 48–61). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4321-5.ch004
Albuquerque, C. (2013). The study of social needs as a strategic tool for the innovation of the social care sector: The contribution of new technologies. In M. Cruz-Cunha, I. Miranda, & P. Gonçalves (Eds.), Handbook of research on ICTs for human-centered healthcare and social care services (pp. 347–365). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3986-7.ch018
Alexander, J. A., Weiner, B. J., & Griffith, J. (2006). Quality improvement and hospital finan-cial performance. Journal of Organizational Behavior, 27(7), 1003–1029. doi:10.1002/job.401
Alexandrou, D. A., & Pardalis, K. V. (2013). SEMantic PATHways: Modeling, executing, and monitoring intra-organizational healthcare business processes towards personalized treatment. In A. Moumtzoglou & A. Kastania (Eds.), E-health technologies and improving patient safety: Exploring organizational factors (pp. 98–123). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2657-7.ch007
Algarín, A. D., Demurjian, S. A., Ziminski, T. B., Sánchez, Y. K., & Kuykendall, R. (2014). Securing XML with role-based access control: Case study in health care. In A. Ruiz-Martinez, R. Marin-Lopez, & F. Pereniguez-Garcia (Eds.), Architectures and protocols for secure information technology infrastructures (pp. 334–365). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4514-1.ch013
Al-Khudairy, S. (2014). Caring for our aging population: Using CPOE and telehomecare sys-tems as a response to health policy concerns. In C. El Morr (Ed.), Research perspectives on the role of informatics in health policy and management (pp. 153–166). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4321-5.ch010
Allan, A., & McKillop, D. (2010). The health implications of apologizing after an adverse event. International Journal for Quality in Health Care, 22(2), 126–131. doi:10.1093/intqhc/mzq001 PMID:20139148
Almeida, L., Menezes, P., & Dias, J. (2013). Augmented reality framework for the socialization between elderly people. In M. Cruz-Cunha, I. Miranda, & P. Gonçalves (Eds.), Handbook of research on ICTs for human-centered healthcare and social care services (pp. 430–448). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3986-7.ch023

Compilation of References
261
American Academy of Neurology. (2005). Qualifications and guidelines for the expert witness. Retrieved from https://www.aan.com/uploadedFiles/Website_Library_Assets/Documents/8.Membership/5.Ethics/1.Code_of_Conduct/Membership-Ethics-American%20Academy%20of%20Neurology%20Qualifications%20and%20Guidelines%20for%20the%20Physician%20Expert%20Witness%20(2).pdf
American Academy of Pediatrics. (2002). Guidelines for Expert Witness Testimony in Medical Malpractice Litigation. Pediatrics, 109(5).
Amer, M. B., Amawi, M., & El-Khatib, H. (2013). A novel neural fuzzy approach for diagnosis of potassium disturbances. In J. Tan (Ed.), Healthcare information technology innovation and sustainability: Frontiers and adoption (pp. 208–218). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2797-0.ch013
Ammouri, A. A., Tailakh, A. K., Muliira, J. K., Geethakrishnan, R., & Al Kindi, S. N. (2015). Patient safety culture among nurses. International Nursing Review, 62(1), 102–110. doi:10.1111/inr.12159 PMID:25495946
Andel, C., Davidow, S. L., Hollander, M., & Moreno, D. A. (2012). The economics of health care quality and medical errors. Journal of Health Care Finance, 39(1), 39–50. PMID:23155743
Andersen, S. T., & Jansen, A. (2013). Innovation in ICT-based health care provision. In J. Tan (Ed.), Healthcare information technology innovation and sustainability: Frontiers and adoption (pp. 58–72). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2797-0.ch004
Anderson, B., Stumpf, P. G., & Schulkin, J. (2009). Medical error reporting, patient safety, and the physician. Journal of Patient Safety, 5(3), 176–179. doi:10.1097/PTS.0b013e3181b320b0 PMID:19927051
Angjellari-Dajci, F., Lawless, W. F., Stachura, M. E., Wood, E. A., & DiBattisto, C. (2013). Economic evaluations for service delivery in autism spectrum disorders: benefit-cost analysis for emerging telehealth systems. In M. Cruz-Cunha, I. Miranda, & P. Gonçalves (Eds.), Handbook of research on ICTs and management systems for improving efficiency in healthcare and social care (pp. 16–42). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3990-4.ch002
Annas, G. J. (2012). Doctors, patients, and lawyers--two centuries of health law. The New England Journal of Medicine, 367(5), 445–450.
Anoosheh, M., Ahmadi, F., Faghihzadeh, S., & Vaismoradi, M. (2008). Causes and management of nursing practice errors: A questionnaire survey of hospital nurses in Iran. International Nursing Review, 55(3), 288–295. doi:10.1111/j.1466-7657.2008.00623.x PMID:19522944
Archibald, D., MacDonald, C. J., Hogue, R., & Mercer, J. (2013). Accessing knowledge from the bedside: Introducing the tablet computer to clinical teaching. In C. Rückemann (Ed.), Inte-grated information and computing systems for natural, spatial, and social sciences (pp. 96–109). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2190-9.ch005

Compilation of References
262
Archondakis, S. (2013). Static telecytological applications for proficiency testing. In V. Gulla, A. Mori, F. Gabbrielli, & P. Lanzafame (Eds.), Telehealth networks for hospital services: New methodologies (pp. 228–239). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2979-0.ch015
Arling, P. A., Doebbeling, B. N., & Fox, R. L. (2013). Improving the implementation of evidence-based practice and information systems in healthcare: A social network approach. In J. Tan (Ed.), Healthcare information technology innovation and sustainability: Frontiers and adoption (pp. 247–270). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2797-0.ch016
Armitage, G., Newell, R., & Wright, J. (2010). Improving the quality of drug error reporting. Jour-nal of Evaluation in Clinical Practice, 16(6), 1189–1197. doi:10.1111/j.1365-2753.2009.01293.x PMID:20807298
Aronson, J. K., Henderson, G., Webb, D. J., & Rawlins, M. D. (2006). A prescription for better prescribing. British Medical Journal, 333(7566), 459–460. doi:10.1136/bmj.38946.491829.BE PMID:16946321
Arriaga, P., Esteves, F., & Fernandes, S. (2013). Playing for better or for worse?: Health and social outcomes with electronic gaming. In M. Cruz-Cunha, I. Miranda, & P. Gonçalves (Eds.), Handbook of research on ICTs for human-centered healthcare and social care services (pp. 48–69). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3986-7.ch003
Arslan, P. (2014). Collaborative participation in personalized health through mobile diaries. In K. Rızvanoğlu & G. Çetin (Eds.), Research and design innovations for mobile user experience (pp. 150–181). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4446-5.ch009
Assis-Hassid, S., Reychav, I., Pliskin, J. S., & Heart, T. H. (2013). The effects of electronic medical record (EMR) use in primary care on the physician-patient relationship. In M. Cruz-Cunha, I. Miranda, & P. Gonçalves (Eds.), Handbook of research on ICTs for human-centered healthcare and social care services (pp. 130–150). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3986-7.ch007
Audimoolam, S., Nair, M., Gaikwad, R., & Qing, C. (2005). The Role of Clinical Pathways in Improving Patient Outcomes. Retrieved from cs.dal.ca
Azar, A. T., & El-Metwally, S. M. (2013). Decision tree classifiers for automated medical diag-nosis. Neural Computing & Applications, 23(7), 2387–2403. doi:10.1007/s00521-012-1196-7
Bailey, R. A. (2013). Resident liability in medical malpractice. Annals of Emergency Medicine, 61(1), 114–117. doi:10.1016/j.annemergmed.2012.04.024 PMID:22632773
Bakdash, J. Z., & Drews, F. A. (2012). Using knowledge in the world to improve patient safety: Designing affordances in health care equipment to specify a sequential “checklist”. Human Factors and Ergonomics in Manufacturing & Service Industries, 22(1), 7–20. doi:10.1002/hfm.20289
Baker, G. R. (2004). The Canadian Adverse Events Study: The incidence of adverse events among hospital patients in Canada. Canadian Medical Association Journal, 170(11), 1678–1686. doi:10.1503/cmaj.1040498 PMID:15159366

Compilation of References
263
Bal, B.S. (2009a). An Introduction to Medical Malpractice in the United States. Clinical Ortho-paedics and Related Research, 467(2), 339-47.
Baladrón, C., Aguiar, J. M., Calavia, L., Carro, B., & Sánchez-Esguevillas, A. (2014). Learning on the move in the web 2.0: New initiatives in m-learning. In K-12 education: Concepts, meth-odologies, tools, and applications (pp. 1693–1714). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4502-8.ch097
Bal, B. S. (2009b). The Expert Witness in Medical Malpractice Litigation. Clinical Orthopae-dics and Related Research, 467(2), 383–391. doi:10.1007/s11999-008-0634-4 PMID:19052827
Banja, J. (2005). Medical Errors and Medical Narcissism. Sudbury, MA: Jones and Bartlett Publishers Inc.
Bass, A., Will, T., Todd, M., & Weatherford, D. (2007). The latest tools for patients with diabetes. RN, 70(6), 39–43. PMID:17624061
Bates, D. W., Boyle, D. L., Vander Vliet, M. B., Schneider, J., & Leape, L. L. (1995). Relation-ship between medication errors and adverse drug events. Journal of General Internal Medicine, 10(4), 199–205. doi:10.1007/BF02600255 PMID:7790981
Bates, D. W., Cohen, M., Leape, L. L., Overhage, J. M., Shabot, M. M., & Sheridan, T. (2001). Reducing the Frequency of Errors in Medicine Using Information Technology. Journal of the American Medical Informatics Association, 8(4), 299–308. doi:10.1136/jamia.2001.0080299 PMID:11418536
Bates, D. W., Leape, L. L., Cullen, D. J., Laird, N., Petersen, L. A., Teich, J. M., & Seger, D. L. et al. (1998). Effect of computerized physician order entry and a team intervention on prevention of serious medication errors. Journal of the American Medical Association, 280(15), 1311–1316. doi:10.1001/jama.280.15.1311 PMID:9794308
Bates, D. W., Miller, E. B., Cullen, D. J., Burdick, L., Williams, L., Laird, N., & Leape, L. L. et al. (1999). Patient risk factors for adverse drug events in hospitalized patients. Archives of Internal Medicine, 159(21), 2553–2660. doi:10.1001/archinte.159.21.2553 PMID:10573045
Bates, D. W., ONeil, A. C., Boyle, D., Teich, J., Chertow, G. M., Komaroff, A. L., & Brennan, T. A. (1994). Potential identifiability and preventability of adverse events using information systems. Journal of the American Medical Informatics Association, 1(5), 404–411. doi:10.1136/jamia.1994.95153428 PMID:7850564
Belsis, P., Skourlas, C., & Gritzalis, S. (2013). Secure electronic healthcare records management in wireless environments. In M. Khosrow-Pour (Ed.), Interdisciplinary advances in information technology research (pp. 202–219). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3625-5.ch015
Bénabou, R., & Tirole, J. (2004). Willpower and personal rules. Journal of Political Economy, 112(4), 848–886. doi:10.1086/421167

Compilation of References
264
Benito, R. V., Vega-Colado, C., Coco, M. B., Cuadrado, R., Torres-Zafra, J. C., Sánchez-Pena, J. M., & López-Miguel, A. et al. (2013). New electro-optic and display technology for visually disabled people. In M. Cruz-Cunha, I. Miranda, & P. Gonçalves (Eds.), Handbook of research on ICTs for human-centered healthcare and social care services (pp. 687–718). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3986-7.ch036
Bergenti, F., Poggi, A., & Tomaiuolo, M. (2013). Using multi-agent systems to support e-health services. In M. Cruz-Cunha, I. Miranda, & P. Gonçalves (Eds.), Handbook of research on ICTs for human-centered healthcare and social care services (pp. 549–567). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3986-7.ch029
Berler, A., & Apostolakis, I. (2014). Normalizing cross-border healthcare in Europe via new e-prescription paradigms. In C. El Morr (Ed.), Research perspectives on the role of informatics in health policy and management (pp. 168–208). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4321-5.ch011
Berlinger, N. (2011). Resolving Harmful Medical Mistakes - Is There a Role for Forgiveness? AMA Virtual Mentor, 13(9), 647–654. doi:10.1001/virtualmentor.2011.13.9.msoc1-1109 PMID:23137480
Bernhard, S., Al Zoukra, K., & Schtte, C. (2013). From non-invasive hemodynamic measurements towards patient-specific cardiovascular diagnosis. In Data mining: Concepts, methodologies, tools, and applications (pp. 2069–2093). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2455-9.ch106
Best, C., O’Neill, B., & Gillespie, A. (2013). Assistive technology for cognition: Enabling activi-ties of daily living. In M. Cruz-Cunha, I. Miranda, & P. Gonçalves (Eds.), Handbook of research on ICTs for human-centered healthcare and social care services (pp. 112–129). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3986-7.ch006
Bettman, J. W. (1990). Seven hundred medicolegal cases in ophthalmology. Ophthalmology, 97(10), 1379–1384. doi:10.1016/S0161-6420(90)32406-5 PMID:2243691
Black’s Law Dictionary. (1991). 6th ed.). St Paul, MN: West Publishing Co.
Blake, S. C., Kohler, S., Rask, K., Davis, A., & Naylor, D. V. (2006). Facilitators and barriers to 10 national quality forum safe practices. American Journal of Medical Quality, 21(5), 323–334. doi:10.1177/1062860606291781 PMID:16973949
Blanchette, H. (2011). The rising cesarean delivery rate in America: What are the conse-quences? Obstetrics and Gynecology, 118(3), 687–690. doi:10.1097/AOG.0b013e318227b8d9 PMID:21860302
Blegen, M. A., Pepper, G. A., & Rosse, J. (2005). Safety Climate on Hospital Units: A New Measure Advances in Patient Safety: From Research to Implementation (Vol. 4). Rockville, MD: Programs, Tools, and Products.

Compilation of References
265
Blendon, R., DesRoches, C. M., Brodie, M., Benson, J. M., Rosen, A. B., Schneider, E., & Stef-fenson, A. E. et al. (2002). Views of practicing physicians and the public on medical adverse events. The New England Journal of Medicine, 347(24), 1933–1940. doi:10.1056/NEJMsa022151 PMID:12477944
Boboc, C., & Ţiţan, E. (2014). Migration of medical doctors, health, medical education, and employment in eastern and central Europe. In A. Driouchi (Ed.), Labor and health economics in the Mediterranean region: Migration and mobility of medical doctors (pp. 158–191). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4723-7.ch007
Bonney, W. (2013). Medical errors: Moral and ethical considerations. Journal of Hospital Ad-ministration, 3(2), 80–88. doi:10.5430/jha.v3n2p80
Bosma, E., Veen, E. J., & Roukema, J. A. (2011, November). Incidence, nature and impact of error in surgery. British Journal of Surgery, 98(11), 1654–1659. PMID: 21706475 doi:10.1002/bjs.7594
Bove, K. E., & Iery, C. (2002). The role of the autopsy in medical malpractice cases. I. A review of 99 appeals court decisions. Archives of Pathology & Laboratory Medicine, 126(9), 1023–1031. PMID:12204050
Bradai, N., Chaari, L., & Kamoun, L. (2013). A comprehensive overview of wireless body area networks (WBAN). In J. Rodrigues (Ed.), Digital advances in medicine, e-health, and communi-cation technologies (pp. 1–32). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2794-9.ch001
Brady, A. M., Malone, A. M., & Fleming, S. (2009). A literature review of the individual and systems factors that contribute to medication errors in nursing practice. Journal of Nursing Management, 17(6), 679–697. doi:10.1111/j.1365-2834.2009.00995.x PMID:19694912
Brennan, N., & Mattick, K. (2013). A systematic review of educational interventions to change behaviour of prescribers in hospital settings, with a particular emphasis on new prescribers. Brit-ish Journal of Clinical Pharmacology, 75(2), 359–372. doi:10.1111/j.1365-2125.2012.04397.x PMID:22831632
Brewer, T., & Colditz, G. A. (1999). Postmarketing surveillance and adverse drug reactions: Current perspectives and future needs. Journal of the American Medical Association, 281(9), 824–829. doi:10.1001/jama.281.9.824 PMID:10071004
Britten, N. (2009). Medication errors: The role of the patient. British Journal of Clinical Phar-macology, 67(6), 646–650. doi:10.1111/j.1365-2125.2009.03421.x PMID:19594532
Brown, K. E., Bayley, J., & Newby, K. (2013). Serious game for relationships and sex education: Application of an intervention mapping approach to development. In S. Arnab, I. Dunwell, & K. Debattista (Eds.), Serious games for healthcare: Applications and implications (pp. 135–166). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-1903-6.ch007

Compilation of References
266
Brown, T. W., McCarthy, M. L., Kelen, G. D., & Levy, F. (2010). An epidemiologic study of closed emergency department malpractice claims in a national database of physician malpractice insurers. Academic Emergency Medicine, 17(5), 553–560. doi:10.1111/j.1553-2712.2010.00729.x PMID:20536812
Burdon, J. (2013). Defensive medicine and clinical risk management. In R. G. Beran (Ed.), Legal and forensic medicine (pp. 621–628). Berlin: Springer. doi:10.1007/978-3-642-32338-6_109
Burns, J., Blanchard, M., & Metcalf, A. (2013). Bridging the digital divide in Australia: The potential implications for the mental health of young people experiencing marginalisation. In Digital literacy: Concepts, methodologies, tools, and applications (pp. 772–793). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-1852-7.ch040
Buyurgan, N., Rardin, R. L., Jayaraman, R., Varghese, V. M., & Burbano, A. (2013). A novel GS1 data standard adoption roadmap for healthcare providers. In J. Tan (Ed.), Healthcare information technology innovation and sustainability: Frontiers and adoption (pp. 41–57). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2797-0.ch003
Bynum, W. E. IV, & Goodie, J. L. (2014). Shame, guilt, and the medical learner: Ignored connec-tions and why we should care. Medical Education, 48(11), 1045–1054. doi:10.1111/medu.12521 PMID:25307632
Cabitza, F., Simone, C., & Sarini, M. (2008). Knowledge artifacts as bridges between theory and practice: the clinical pathway case. In Knowledge Management in Action (pp. 37-50). Springer US.
Cabrita, M. D., & Cabrita, M. (2014). Applying social marketing to healthcare: Challenges and opportunities. In A. Kapoor & C. Kulshrestha (Eds.), Dynamics of competitive advantage and consumer perception in social marketing (pp. 78–97). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4430-4.ch004
Cameron, K., & Quinn, R. E. (2011). Diagnosing and changing organizational culture: based on the competing values framework. Reading, MA: Addison Wesley Longman.
Carberry, M., Connelly, S., & Murphy, J. (2013). A prospective audit of a nurse independent prescribing within critical care. Nursing in Critical Care, 18(3), 135–141. doi:10.1111/j.1478-5153.2012.00534.x PMID:23577948
Card, A. J. (2014). Patient safety: This is public health. Journal of Healthcare Risk Management, 34(1), 6–12. doi:10.1002/jhrm.21145 PMID:25070252
Carroll, A.E., & Buddenbaum, J.L. (2013). High and low-risk specialties experience with the U.S. medical malpractice system. BMC Health Services Research, 13, 465.
Carroll, J. M., & Rosson, M. B. (2013). Community networks: Infrastructure and models for therapeutic support. In M. Cruz-Cunha, I. Miranda, & P. Gonçalves (Eds.), Handbook of research on ICTs for human-centered healthcare and social care services (pp. 187–207). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3986-7.ch010

Compilation of References
267
Carter, R. M. (1999). Malpractice and avascular necrosis: Legal outcomes. Canadian Journal of Gastroenterology, 13(1), 79–84. doi:10.1155/1999/517893 PMID:10099819
Casali, M. B., Mobilia, F., Del Sordo, S., Blandino, A., & Genovese, U. (2014). The medical malpractice in Milan-Italy. A retrospective survey on 14 years of judicial autopsies. Forensic Science International, 242, 38–43. doi:10.1016/j.forsciint.2014.06.002 PMID:25023215
Castiglioni, I., Gilardi, M. C., & Gallivanone, F. (2013). E-health decision support systems for the diagnosis of dementia diseases. In A. Moumtzoglou & A. Kastania (Eds.), E-health technologies and improving patient safety: Exploring organizational factors (pp. 84–97). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2657-7.ch006
Catino, M. (2009, July). Blame culture and defensive medicine. Cognition Technology and Work, 11(4), 245–253. doi:10.1007/s10111-009-0130-y
Catley, C., Smith, K., McGregor, C., James, A., & Eklund, J. M. (2013). A framework for multi-dimensional real-time data analysis: A case study for the detection of apnoea of prematurity. In A. Gangopadhyay (Ed.), Methods, models, and computation for medical informatics (pp. 16–35). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2653-9.ch002
Cecil, J. S. (2005). Ten years of judicial gatekeeping under Daubert. American Journal of Public Health, 95(S1), S74–S80. doi:10.2105/AJPH.2004.044776 PMID:16030342
Celebi, N., Kirchhoff, K., Lammerding-Köppel, M., Riessen, R., & Weyrich, P. (2010). Medi-cal clerkships do not reduce common prescription errors among medical students. Naunyn-Schmiedeberg’s Archives of Pharmacology, 382(2), 171–176. doi:10.1007/s00210-010-0530-9 PMID:20535451
Chaari, L., & Kamoun, L. (2013). QoS concepts and architecture over wireless body area net-works for healthcare applications. In J. Rodrigues (Ed.), Digital advances in medicine, e-health, and communication technologies (pp. 114–130). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2794-9.ch007
Chamberlin, B., Maloney, A., Gallagher, R. R., & Garza, M. L. (2013). Active video games: Po-tential for increased activity, suggestions for use, and guidelines for implementation. In S. Arnab, I. Dunwell, & K. Debattista (Eds.), Serious games for healthcare: Applications and implications (pp. 191–212). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-1903-6.ch009
Chang, A., Schyve, P. M., Croteau, R. J., OLeary, D. S., & Loeb, J. M. (2005). The JCAHO patient safety event taxonomy: A standardized terminology and classification schema for near misses and adverse events. International Journal for Quality in Health Care, 17(2), 95–105. doi:10.1093/intqhc/mzi021 PMID:15723817
Chapanis, A. (1996). Human factors in systems engineering. John Wiley & Sons, Inc.

Compilation of References
268
Charisi, A., Korvesis, P., & Megalooikonomou, V. (2013). Similarity searching of medical image data in distributed systems: Facilitating telemedicine applications. In A. Gangopadhyay (Ed.), Methods, models, and computation for medical informatics (pp. 58–77). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2653-9.ch004
Cheng, B., Stanley, R. J., De, S., Antani, S., & Thoma, G. R. (2013). Automatic detection of arrow annotation overlays in biomedical images. In J. Tan (Ed.), Healthcare information technology innovation and sustainability: Frontiers and adoption (pp. 219–236). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2797-0.ch014
Chen, Y. (2013). Construction of digital statistical atlases of the liver and their applications to computer-aided diagnosis. In J. Wu (Ed.), Technological advancements in biomedicine for health-care applications (pp. 68–79). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2196-1.ch008
Cherian, E. J., & Ryan, T. W. (2014). Incongruent needs: Why differences in the iron-triangle of priorities make health information technology adoption and use difficult. In C. El Morr (Ed.), Research perspectives on the role of informatics in health policy and management (pp. 209–221). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4321-5.ch012
Chetouane, F., & Ibraheem, E. (2016). Surgery operations modeling and scheduling in healthcare systems. In P. Manolitzas, E. Grigoroudis, N. Matsatsinis, & D. Yannacopoulos (Eds.), Effective methods for modern healthcare service quality and evaluation (pp. 90–108). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-9961-8.ch005
Choi, I., Lee, S., Flynn, L., Kim, C. M., & Suh, D. C. (2016). Incidence and treatment costs attributable to medication errors in hospitalized patients. Research in Social & Administrative Pharmacy, 12(3), 428–437. doi:10.1016/j.sapharm.2015.08.006 PMID:26361821
Christensen, L. Q., Nielsen, L. M., & Nielsen, S. L. (1990). Traffic accidents and drivers sus-pected for drug influence. Forensic Science International, 45(3), 273–280. doi:10.1016/0379-0738(90)90184-Z PMID:2361649
Chun, S. A., Kwon, J. H., & Lee, H. (2013). Social credential-based role recommendation and patient privacy control in medical emergency. In A. Gangopadhyay (Ed.), Methods, models, and computation for medical informatics (pp. 215–237). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2653-9.ch013
Clancy, C. M. (2012, January/March). Alleviating second victim syndrome. How we should handle patient harm. Journal of Nursing Care Quality, 27(1), 1–5. doi:10.1097/NCQ.0b013e3182366b53 PMID:22124276
Clinton, H. R., & Obama, B. (2006). Making patient safety the centerpiece of medical liability reform. The New England Journal of Medicine, 354(21), 2205–2208. doi:10.1056/NEJMp068100 PMID:16723612
Compilation of References
269
Cohen, J. F., Bancilhon, J., & Sergay, S. (2013). An empirical study of patient willingness to use self-service technologies in the healthcare context. In M. Cruz-Cunha, I. Miranda, & P. Gonçalves (Eds.), Handbook of research on ICTs and management systems for improving efficiency in healthcare and social care (pp. 378–395). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3990-4.ch019
Cooper, M. D. (2000). Towards a model of safety culture. Safety Science, 36(2), 111–136. doi:10.1016/S0925-7535(00)00035-7
Corrigan, D., Hederman, L., Khan, H., Taweel, A., Kostopoulou, O., & Delaney, B. (2013). An ontology-driven approach to clinical evidence modelling implementing clinical prediction rules. In A. Moumtzoglou & A. Kastania (Eds.), E-health technologies and improving patient safety: Exploring organizational factors (pp. 257–284). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2657-7.ch016
Costa, Â., Andrade, F., & Novais, P. (2013). Privacy and data protection towards elderly health-care. In M. Cruz-Cunha, I. Miranda, & P. Gonçalves (Eds.), Handbook of research on ICTs for human-centered healthcare and social care services (pp. 330–346). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3986-7.ch017
Coughlan, J., & Brinkman, W. (2013). Design considerations for delivering e-learning to surgi-cal trainees. In J. Rodrigues (Ed.), Digital advances in medicine, e-health, and communication technologies (pp. 341–350). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2794-9.ch020
Council of Europe, Committee of Ministers. (1999). Recommendation no. R (99) 3 of the Com-mittee of Ministers to Member States on the Harmonisation of Medico-Legal Autopsy Rules. Retrieved from http://www.coe.int/t/dg3/healthbioethic/texts_and_documents/RecR(99)3.pdf
Crane, M. (1993). The medication errors that get doctors sued. Medical Economics, 22, 36–41. PMID:10171740
Crosby, P. (1992). Quality is free. New York: McGraw-Hill.
Cunningham, W., & Wilson, H. (2011, March). Complaints, shame and defensive medicine. BMJ Quality & Safety, 20(5), 449–452. doi:10.1136/bmjqs.2011.051722 PMID:21441601
D’Abundo, M. L. (2013). Electronic health record implementation in the United States healthcare industry: Making the process of change manageable. In V. Wang (Ed.), Handbook of research on technologies for improving the 21st century workforce: Tools for lifelong learning (pp. 272–286). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2181-7.ch018
D’Andrea, A., Ferri, F., & Grifoni, P. (2013). RFID technologies in the health sector. In A. Moumtzoglou & A. Kastania (Eds.), E-health technologies and improving patient safety: Exploring organizational factors (pp. 140–147). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2657-7.ch009

Compilation of References
270
D’Astolfo, C. (2014). Investing in a “rehabilitation model” to improve the decision-making process in long-term care. In C. El Morr (Ed.), Research perspectives on the role of informatics in health policy and management (pp. 37–47). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4321-5.ch003
Dasgupta, S. S. (2013). Cyber capability framework: A tool to evaluate ICT for development projects. In M. Cruz-Cunha, I. Miranda, & P. Gonçalves (Eds.), Handbook of research on ICTs for human-centered healthcare and social care services (pp. 399–406). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3986-7.ch021
Dauer, E. A. (2003). A therapeutic jurisprudence perspective on legal responses to medical error. Journal of Legal Medicine, 24(1), 37–50. doi:10.1080/713832126 PMID:12623695
Daverio, M., Fino, G., Luca, B., Zaggia, C., Pettenazzo, A., Parpaiola, A., & Amigoni, A. et al. (2015). Failure mode and effective analysis ameliorate awareness of medical errors: A 4-year pro-spective observational study in critically ill children. Paediatric Anaesthesia, 25(12), 1227–1234. doi:10.1111/pan.12772 PMID:26432066
David, G., Gunnarsson, C. L., Waters, H. C., Horblyuk, R., & Kaplan, H. S. (2013). Economic Measurement of Medical Errors Using a Hospital Claims Database. Value in Health, 16(2), 305–310. doi:10.1016/j.jval.2012.11.010 PMID:23538182
Davies, E. D., Schneider, F., Childs, S., Hucker, T., Krikos, D., Peh, J., & Cashman, J. et al. (2011). A prevalence study of errors in opioid prescribing in a large teaching hospital. International Journal of Clinical Practice, 65(9), 923–929. doi:10.1111/j.1742-1241.2011.02705.x PMID:21752165
Davies, H. T., Nutley, S. M., & Mannion, R. (2000). Organisational culture and quality of health care. Quality in Health Care, 9(2), 111–119. doi:10.1136/qhc.9.2.111 PMID:11067249
Davis, S. A. (2013). Global telemedicine and ehealth: Advances for future healthcare – Using a systems approach to integrate healthcare functions. In V. Gulla, A. Mori, F. Gabbrielli, & P. Lanzafame (Eds.), Telehealth networks for hospital services: New methodologies (pp. 15–32). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2979-0.ch002
de Wit, M. E., Marks, C. M., Nattermann, J. P., & Wu, A. W. (2013, December). Supporting second victims of patient safety events: Shouldnt these communications be covered by legal privilege? The Journal of Law, Medicine & Ethics, 41(4), 852–858. doi:10.1111/jlme.12095 PMID:24446943
Delbanco, T., & Bell, S. K. (2007). Guilty, Afraid, and Alone — Struggling with Medical Er-ror. The New England Journal of Medicine, 357(17), 1682–1683. doi:10.1056/NEJMp078104 PMID:17960011
Deng, M., Petkovic, M., Nalin, M., & Baroni, I. (2013). Home healthcare in cloud computing. In M. Cruz-Cunha, I. Miranda, & P. Gonçalves (Eds.), Handbook of research on ICTs and manage-ment systems for improving efficiency in healthcare and social care (pp. 614–634). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3990-4.ch032

Compilation of References
271
Denham, C. (2007). TRUST: The 5 rights of the second victim. Journal of Patient Safety, 3(2), 107–119. doi:10.1097/01.jps.0000236917.02321.fd
Dentzer, S. (2000). Media mistakes in coverage of the Institute of Medicine’s error report. Ef-fective Clinical Practice, 3, 305–308. PMID:11151532
DesHarnais, S. I., & Nash, D. B. (2011). Reforming way medical students and physicians are taught about quality and safety. Mount Sinai Journal of Medicine: A Journal of Translational and Personalized Medicine, 78(6), 834–841. doi:10.1002/msj.20302
DeVany, M., Knobloch-Ludwig, K., Penticoff, M., Assimacopoulos, A., & Speedie, S. (2013). Telehealth implementation: The voice of experience. In S. Sarnikar, D. Bennett, & M. Gaynor (Eds.), Cases on healthcare information technology for patient care management (pp. 126–139). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2671-3.ch008
Dhillon, B. S. (2003). Methods for performing human reliability and error analysis in health care. International Journal of Health Care Quality Assurance, 16(6), 306–317. doi:10.1108/09526860310495697
Dias-Souza, M. V. (2016). Strategies for expanding access and improving the quality of pharma-ceutical services. In P. Manolitzas, E. Grigoroudis, N. Matsatsinis, & D. Yannacopoulos (Eds.), Effective methods for modern healthcare service quality and evaluation (pp. 168–201). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-9961-8.ch008
Digitale, E. (2014). Better communication between caregivers reduces medical errors, study finds. Retrieved from https://med.stanford.edu/news/all-news/2014/12/better-communication-between-caregivers-reduces-medical-errors.html
Dingli, A., Abela, C., & D’Ambrogio, I. (2013). PINATA: Taking e-health a step forward. In A. Moumtzoglou & A. Kastania (Eds.), E-health technologies and improving patient safety: Exploring organizational factors (pp. 173–195). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2657-7.ch012
Dogra, D. P., Nandam, K., Majumdar, A. K., Sural, S., Mukhopadhyay, J., Majumdar, B., & Mukherjee, S. et al. (2013). A tool for automatic hammersmith infant neurological examination. In J. Rodrigues (Ed.), Digital advances in medicine, e-health, and communication technologies (pp. 301–311). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2794-9.ch017
Donabedian, A. (1980). Explorations in Quality Assessment and Monitoring: The Definition of Quality and Approaches to Its Assessment.: Vol. III. The Methods and Findings of Quality As-sessment Measurement and Monitoring. Ann Arbor, MI: Health Administration Press.
Donabedian, A. (1980). The definition of quality and approaches to its assessment. Ann Arbor: Michigan Health Administration Press.
Donabedian, A. (1988). The quality of care: How can it be assessed? Journal of the American Medi-cal Association, 260(12), 1743–1748. doi:10.1001/jama.1988.03410120089033 PMID:3045356

Compilation of References
272
Doumbouya, M. B., Kamsu-Foguem, B., Kenfack, H., & Foguem, C. (2015). Argumentative reasoning and taxonomic analysis for the identification of medical errors. Engineering Applica-tions of Artificial Intelligence, 46, 166–179. doi:10.1016/j.engappai.2015.08.009
Doyle, J., Bertolotto, M., & Wilson, D. (2013). Towards multimodal mobile GIS for the elderly. In Digital literacy: Concepts, methodologies, tools, and applications (pp. 590–609). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-1852-7.ch031
Drach-Zahavy, A., & Hadid, N. (2015). Nursing handovers as resilient points of care: Linking handover strategies to treatment errors in the patient care in the following shift. Journal of Ad-vanced Nursing, 71(5), 1135–1145. doi:10.1111/jan.12615 PMID:25641374
Dragoni, A. F. (2013). Health services through digital terrestrial television. In V. Gulla, A. Mori, F. Gabbrielli, & P. Lanzafame (Eds.), Telehealth networks for hospital services: New methodolo-gies (pp. 207–227). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2979-0.ch014
Dragoni, A. F. (2013). Virtual carer: A first prototype. In V. Gulla, A. Mori, F. Gabbrielli, & P. Lanzafame (Eds.), Telehealth networks for hospital services: New methodologies (pp. 290–299). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2979-0.ch019
Drechsler, C. T. (1999). Duty of care: liability for malpractice. In American Jurisprudence: Physicians, Surgeons, and Other Healers (2nd ed.; Vol. 61). St. Paul, MN: West Press.
Driouchi, A. (2014). Introduction to labor and health economics: Mobility of medical doctors in the Mediterranean region. In A. Driouchi (Ed.), Labor and health economics in the Mediter-ranean region: Migration and mobility of medical doctors (pp. 1–22). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4723-7.ch001
Driouchi, A. (2014). Medical knowledge, north-south cooperation, and mobility of medical doc-tors. In A. Driouchi (Ed.), Labor and health economics in the Mediterranean region: Migration and mobility of medical doctors (pp. 376–395). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4723-7.ch015
Driouchi, A. (2014). Skilled human resources in the health sectors and impacts of new health technologies on health workforce in developing economies. In A. Driouchi (Ed.), Labor and health economics in the Mediterranean region: Migration and mobility of medical doctors (pp. 23–50). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4723-7.ch002
Dror, S., & Margol, D. (2015). Framework for analyzing malpractice cases to improve healthcare systems. Quality and Reliability Engineering International, 31(7), 1103–1113. doi:10.1002/qre.1851
Duan, X., Wang, X., & Huang, Q. (2013). Medical manipulators for surgical applications. In J. Wu (Ed.), Technological advancements in biomedicine for healthcare applications (pp. 111–122). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2196-1.ch012

Compilation of References
273
Dubin, M. G., Liu, C., Lin, S. Y., & Senior, B. A. (2007). American Rhinology Society member survey on maximal medical therapy for chronic rhinosinusitis. American Journal of Rhinology, 21(4), 483–488. doi:10.2500/ajr.2007.21.3047 PMID:17882920
Duclos, C., Eichler, M., Taylor, L., Quintela, J., Main, D., Pace, W., & Staton, E. (2005). Patient perspectives of patient-provider communication after adverse events. International Journal for Quality in Health Care, 17(6), 479–486. doi:10.1093/intqhc/mzi065 PMID:16037100
Dunwell, I., & Jarvis, S. (2013). A serious game for on-the-ward infection control aware-ness training: Ward off infection. In S. Arnab, I. Dunwell, & K. Debattista (Eds.), Serious games for healthcare: Applications and implications (pp. 233–246). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-1903-6.ch011
Durant, K. T., McCray, A. T., & Safran, C. (2013). Identifying temporal changes and topics that promote growth within online communities: A prospective study of six online cancer forums. In A. Gangopadhyay (Ed.), Methods, models, and computation for medical informatics (pp. 78–97). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2653-9.ch005
Ebbesen, J., Buajordet, I., Erikssen, J., Brors, O., Hilberg, T., Svaar, H., & Sandvik, L. (2001). Drug related deaths in a department of internal medicine. Archives of Internal Medicine, 161(19), 2317–2323. doi:10.1001/archinte.161.19.2317 PMID:11606147
Editorial. (2005). Roles and responsibilities of medical expert witnesses. British Medical Journal, 331(7512), 305.
Edmondson, A. C. (2004). Learning from failure in health care: Frequent opportunities, pervasive barriers. Quality & Safety in Health Care, 13(Suppl 2), ii3–ii9. doi:10.1136/qshc.2003.009597 PMID:15576689
Elder, N. C., Jacobson, C. J., Zink, T., & Hasse, L. (2005). How experiencing preventable medical problems changed patients interactions with primary health care. Annals of Family Medicine, 3(6), 537–544. doi:10.1370/afm.346 PMID:16338918
El-Farargy, N. (2013). Refresher training in clinical psychology supervision: A blended learning approach. In A. Benson, J. Moore, & S. Williams van Rooij (Eds.), Cases on educational technol-ogy planning, design, and implementation: A project management perspective (pp. 295–317). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4237-9.ch016
El-Jardali, F., Dimassi, H., Jamal, D., Jaafar, M., & Hemadeh, N. (2011). Predictors and outcomes of patient safety culture in hospitals. BMC Health Services Research, 11(1), 45. doi:10.1186/1472-6963-11-45 PMID:21349179
Elkin, P. L., Beuscart-zephir, M. C., Pelayo, S., Patel, V., & Nøhr, C. (2013). The usability-error ontology. In M. Beuscart-Zéphir, M. Jaspers, C. Kuziemsky, C. Nøhr, & J. Aarts (Eds.), Context sensitive health informatics: Human and sociotechnical approaches (pp. 91–96). Amsterdam, The Netherlands: IOS Press.

Compilation of References
274
Elwahab, A. S., & Doherty, E. (2014). What about doctors? The impact of medical errors. The Surgeon, 12(6), 297–300. doi:10.1016/j.surge.2014.06.004 PMID:25056239
Ervin, K. (2014). Legal and ethical considerations in the implementation of electronic health records. In J. Krueger (Ed.), Cases on electronic records and resource management implementa-tion in diverse environments (pp. 193–210). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4466-3.ch012
EUNETPAS. (2009). Catalogue: currently used patient safety culture instruments in Europe. Aarthus.
European Commission. (2006). Special Eurobarometer. Medical Errors. Retrieved from http://ec.europa.eu/health/ph_information/documents/eb_64_en.pdf
European Council of Legal Medicine. (2011). Description of Legal and Forensic Medicine as a Medical Specialty in the EU. Retrieved from http://eclm.info/docs/Documents/ECLM_UEMS_document._Approved_ECLM_GA_140911.pdf
Fahrenkopf, A., Barger, L., Sharek, P., Lewin, D., Chiang, V., Edwards, S., … Landrigan, C. (2008, February). Rates of medication errors among depressed and burnt out residents: Prospective cohort study. British Medical Journal. Retrieved from http://www.bmj.com/content/336/7642/488
Fakhar, A. (2014). Beyond brain drain: A case study of the benefits of cooperation on medi-cal immigration. In A. Driouchi (Ed.), Labor and health economics in the Mediterranean region: Migration and mobility of medical doctors (pp. 294–313). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4723-7.ch012
Falan, S. L., Han, B., Zoeller, L. H., Tarn, J. M., & Roach, D. M. (2013). Sustaining healthcare through waste elimination: A taxonomic analysis with case illustrations. In J. Tan (Ed.), Health-care information technology innovation and sustainability: Frontiers and adoption (pp. 18–39). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2797-0.ch002
Farinha, C., & Mira da Silva, M. (2013). Identifying requirements for healthcare information systems with focus groups. In M. Cruz-Cunha, I. Miranda, & P. Gonçalves (Eds.), Handbook of research on ICTs for human-centered healthcare and social care services (pp. 491–510). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3986-7.ch026
Fastman, B. R., & Kaplan, H. S. (2011). Errors in transfusion medicine: Have we learned our lesson? Mount Sinai Journal of Medicine: A Journal of Translational and Personalized Medicine, 78(6), 854–864. doi:10.1002/msj.20296
Feigenbaum, A. V. (1951). Quality control: Principles, practice, and administration. New York: McGraw-Hill.
Ferrara, S. D. (2013). Medical malpractice and legal medicine. International Journal of Legal Medicine, 127(3), 541–543. doi:10.1007/s00414-013-0839-2 PMID:23455848

Compilation of References
275
Ferrara, S. D., Baccino, E., Bajanowski, T., Boscolo-Berto, R., Castellano, M., De Angel, R., & Villanueva, E. et al. (2013). EALM Working Group on Medical Malpractice. Malpractice and medical liability. European Guidelines on Methods of Ascertainment and Criteria of Evaluation. International Journal of Legal Medicine, 127(3), 545–557. doi:10.1007/s00414-013-0836-5 PMID:23564275
Ferreira, L., Teixeira, A., & Cunha, J. P. (2013). Medical information extraction in European Portuguese. In M. Cruz-Cunha, I. Miranda, & P. Gonçalves (Eds.), Handbook of research on ICTs for human-centered healthcare and social care services (pp. 607–626). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3986-7.ch032
Fink, J. L. (1983). Liability claims based on drug use. Drug Intelligence & Clinical Pharmacy, 17, 667–670. PMID:6617491
Fischman, J. (2000, July17). Industry Preaches Safety in Pittsburgh. U.S. News & World Report.
FitzGerald, R. J. (2009). Medication errors: The importance of an accurate drug history. British Journal of Clinical Pharmacology, 67(6), 671–675. doi:10.1111/j.1365-2125.2009.03424.x PMID:19594536
Flin, R., Winter, J., & Cakil Sarac, M. R. (2009). Human factors in patient safety: Review of topics and tools. World Health, 2.
Flynn, L., Liang, Y., Dickson, G. L., Xie, M., & Suh, D. C. (2012). Nurses’ practice environments, error interception practices, and inpatient medication errors. Journal of Nursing Scholarship, 44(2), 180–186. doi:10.1111/j.1547-5069.2012.01443.x PMID:22510244
Forrestal, E. J., Cellucci, L. W., Zeng, X., Kennedy, M. H., & Smith, D. (2013). Health informa-tion technology collaboration in community health centers: The community partners HealthNet, Inc. In S. Sarnikar, D. Bennett, & M. Gaynor (Eds.), Cases on healthcare information technology for patient care management (pp. 171–196). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2671-3.ch011
Foster, P. N., Sidhu, R., Gadhia, D. A., & DeMusis, M. (2008). Leveraging computerized sign-out to increase error reporting and addressing patient safety in graduate medical education. Journal of General Internal Medicine, 23(4), 481–484. doi:10.1007/s11606-007-0503-y PMID:18373149
Frederico, C. (2013). Nutrition games. In S. Arnab, I. Dunwell, & K. Debattista (Eds.), Serious games for healthcare: Applications and implications (pp. 167–190). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-1903-6.ch008
Freitas, L., Pereira, R. T., Pereira, H. G., Martini, R., Mozzaquatro, B. A., Kasper, J., & Librelotto, G. (2013). Ontological representation and an architecture for homecare pervasive systems. In R. Martinho, R. Rijo, M. Cruz-Cunha, & J. Varajão (Eds.), Information systems and technologies for enhancing health and social care (pp. 215–234). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3667-5.ch015

Compilation of References
276
Freud, A. (1966). The Ego and the Mechanisms of Defense (Rev. Ed.). New York: International Universities Press.
Freud, S. (1936). Inhibitions, symptoms and anxiety. The Psychoanalytic Quarterly, 5, 415–443.
Frigo, C. A., & Pavan, E. E. (2014). Prosthetic and orthotic devices. In Assistive technologies: Concepts, methodologies, tools, and applications (pp. 549–613). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4422-9.ch028
Fukami, T., & Wu, J. (2013). Image fusion method and the efficacy of multimodal cardiac im-ages. In J. Wu (Ed.), Technological advancements in biomedicine for healthcare applications (pp. 47–54). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2196-1.ch006
Furdu, I., & Patrut, B. (2013). ICT applications and solutions in healthcare: Present and per-spectives. In M. Cruz-Cunha, I. Miranda, & P. Gonçalves (Eds.), Handbook of research on ICTs and management systems for improving efficiency in healthcare and social care (pp. 559–576). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3990-4.ch029
Gabbrielli, F. (2013). Telemedicine R&D influencing incoming strategies and organization models. In V. Gulla, A. Mori, F. Gabbrielli, & P. Lanzafame (Eds.), Telehealth networks for hospital services: New methodologies (pp. 250–264). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2979-0.ch017
Gaivéo, J. M. (2013). Security of ICTs supporting healthcare activities. In M. Cruz-Cunha, I. Miranda, & P. Gonçalves (Eds.), Handbook of research on ICTs for human-centered healthcare and social care services (pp. 208–228). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3986-7.ch011
Gallagher, T. H., Brundage, G., Summy, E. A., Bommarito, K. M., Ebers, A. G., Waterman, A. D., & Dunagan, C. et al. (2006). National survey: Risk managers’ attitudes and experiences regarding patient safety and error disclosure. Journal of Healthcare Risk Management, 26(3), 11–16. doi:10.1002/jhrm.5600260305
Gallagher, T. H., Mello, M. M., Levinson, W., Wynia, M. K., Sachdeva, A. K., Snyder Sulmasy, L., & Arnold, R. et al. (2013). Talking with patients about other clinicians errors. The New Eng-land Journal of Medicine, 369(18), 1752–1757. doi:10.1056/NEJMsb1303119 PMID:24171522
Gallagher, T. H., Studdert, D., & Levinson, W. (2007). Disclosing harmful medical errors to pa-tients. The New England Journal of Medicine, 356(26), 2713–2719. doi:10.1056/NEJMra070568 PMID:17596606
Gallagher, T. H., Waterman, A. D., Ebers, A. G., Fraser, V. J., & Levinson, W. (2003). Patients and physicians attitudes regarding the disclosure of medical adverse events. Journal of the Ameri-can Medical Association, 289(8), 1001–1007. doi:10.1001/jama.289.8.1001 PMID:12597752
Gallagher, T., & Lucas, M. (2005). Should we disclose harmful medical errors to patients? If so, how? Journal of Clinical Outcomes Management, 12(5), 253–259.

Compilation of References
277
Gallo, C. (2013). A multichannel framework for multimedia content deployment in e-health environments. In M. Cruz-Cunha, I. Miranda, & P. Gonçalves (Eds.), Handbook of research on ICTs and management systems for improving efficiency in healthcare and social care (pp. 872–891). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3990-4.ch045
Gandhi, T. K., Kachalia, A., Yoon, C., Puopolo, A. L., & Brennan, T. A. (2009). Identifying steps that are more prone to error and then designing studies that would reduce error rates, instead of just pursuing litigation. British Journal of Clinical Pharmacology, 67(6), 651–655. PMID:19594533
Gao, Y., Yang, W., Yang, J., Satoshi, T., & Wu, J. (2013). Neural mechanisms of audiovisual integration in integrated processing for verbal perception and spatial factors. In J. Wu (Ed.), Bio-medical engineering and cognitive neuroscience for healthcare: Interdisciplinary applications (pp. 327–336). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2113-8.ch034
Gardner, A., & Rich, M. (2014). Error management training and simulation education. The Clini-cal Teacher, 11(7), 537–540. doi:10.1111/tct.12217 PMID:25417983
Garrett, C. (2008) The effect of nurse staffing patterns on medical errors and nurse burnout. Association of periOerative Registered Nurses Journal, 87, 1191–1204.
Garrouste-Orgeas, M., Flaatten, H., & Moreno, R. (2016). Understanding medical errors and adverse events in ICU patients. Intensive Care Medicine, 42(1), 107–109. doi:10.1007/s00134-015-3968-x PMID:26248952
Garrouste-Orgeas, M., Philippart, F., Bruel, C., Max, A., Lau, N., & Misset, B. (2012). Overview of medical errors and adverse events. Annals of Intensive Care, 2(1), 2. doi:10.1186/2110-5820-2-2 PMID:22339769
Gatzidis, C. (2013). First-person shooter game engines and healthcare: An examination of the current state of the art and future potential. In S. Arnab, I. Dunwell, & K. Debattista (Eds.), Serious Games for Healthcare: Applications and Implications (pp. 76–89). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-1903-6.ch004
Gaughan, M. (2013). The hybridized nature of America’s health care system: Medicare as a case of both market and public failure. In M. Merviö (Ed.), Healthcare management and econom-ics: Perspectives on public and private administration (pp. 154–164). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3982-9.ch012
Gavgani, V. Z. (2013). Information therapy (ix) service and patients’ preference. In A. Gangopad-hyay (Ed.), Methods, models, and computation for medical informatics (pp. 117–125). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2653-9.ch007
Gavgani, V. Z., Oskouei, M. M., & Salehi, R. (2015). Patients’ medication errors: How patients’ inadequate information about their prosthetic heart valve diseases affects their healthcare. In Healthcare administration: Concepts, methodologies, tools, and applications (pp. 1081–1087). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-6339-8.ch057

Compilation of References
278
Gawande, A. (2007). Better: A surgeon’s notes on performance. New York, NY: Metropolitan Books.
Ge, X., Rijo, R., Paige, R. F., Kelly, T. P., & McDermid, J. A. (2012). Introducing goal structuring notation to explain decisions in clinical practice. Procedia Technology, 5, 686–695. doi:10.1016/j.protcy.2012.09.076
Gholson, J., & Tennyson, H. (2013). One system of care, one electronic chart. In S. Sarnikar, D. Bennett, & M. Gaynor (Eds.), Cases on healthcare information technology for patient care management (pp. 55–69). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2671-3.ch003
Ghosh, B. (2013). Healthcare systems using clinical data: Addressing data interoperability challenges. In S. Sarnikar, D. Bennett, & M. Gaynor (Eds.), Cases on healthcare information technology for patient care management (pp. 208–223). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2671-3.ch013
Gilbert, P. (1998). Some Core Issues and Controversies. In Shame; Interpersonal Behavior: Psychopathology and Culture (pp. 3-38). New York: Oxford University Press.
Gilbert, P. (2000). The Relationship of Shame, Social Anxiety and Depression: The Role of the Evaluation of Social Rank. Clinical Psychology & Psychotherapy, 7(3), 174–189. doi:10.1002/1099-0879(200007)7:3<174::AID-CPP236>3.0.CO;2-U
Gilbert, P. (2003). Evolution, Social Roles, and the Differences in Shame and Guilt. Social Research, 70, 1205–1230.
Gillies, A. C., & Howard, J. (2013). Information as change agent or barrier in health care reform? In J. Tan (Ed.), Healthcare information technology innovation and sustainability: Frontiers and adoption (pp. 1–17). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2797-0.ch001
Gilligan, J. (2003). Shame, Guilt, and Violence. Social Research, 70, 1149–1180.
Gilmore, H. L. (1974). Product conformance. Quality Progress, 7(5), 16–19.
Ginsburg, L., & Gilin Oore, D. (2016). Patient safety climate strength: A concept that requires more attention. BMJ Quality & Safety, 25(9), 680–687. doi:10.1136/bmjqs-2015-004150 PMID:26453636
Glaser, J., Teich, J. M., & Kuperman, G. (1996) Impact of information events on medical care.Proceedings of the 1996 HIMSS Annual Conference. Chicago, IL: Healthcare Information and Management Systems Society.
Glendon, A. I., Clarke, S., & Mckenna, E. F. (2006). Human Safety and Risk Management (2nd ed.). Boca Raton, FL: CRC Press.
Glickman, S. W., Schulman, K. A., Peterson, E. D., Hocker, M. B., & Cairns, C. B. (2008). Evidence-based perspectives on pay for performance and quality of patient care and outcomes in emergency medicine. Annals of Emergency Medicine, 51(5), 622–631. doi:10.1016/j.annemerg-med.2008.01.010 PMID:18358566

Compilation of References
279
Glusker, A., & Hoelscher, E. (2014). Transitioning from print to online-only resources: The experience of a medium-sized healthcare organization library. In J. Krueger (Ed.), Cases on elec-tronic records and resource management implementation in diverse environments (pp. 226–242). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4466-3.ch014
Gofuku, A., Fukumori, S., & Sato, K. (2013). A mirror visual feedback therapy system applying virtual reality technology. In J. Wu (Ed.), Biomedical engineering and cognitive neuroscience for healthcare: Interdisciplinary applications (pp. 73–80). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2113-8.ch008
Goldenbaum, D. M., Christopher, M., Gallagher, R. M., Fishman, S., Payne, R., Joranson, D., & Thexton, A. et al. (2008). Physician charged with opioid analgesic- prescribing offences. Pain Medicine, 9(6), 737–747. doi:10.1111/j.1526-4637.2008.00482.x PMID:18657218
Gomes, C., Sperandio, F., Peles, A., Borges, J., Brito, A. C., & Almada-Lobo, B. (2013). An operating theater planning decision support system. In R. Martinho, R. Rijo, M. Cruz-Cunha, & J. Varajão (Eds.), Information systems and technologies for enhancing health and social care (pp. 69–86). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3667-5.ch005
Gommans, J., McIntosh, P., Bee, S., & Allan, W. (2008). Improving the quality of written prescriptions in a general hospital: The influence of 10 years of serial audits and targeted inter-ventions. Internal Medicine Journal, 38(4), 243–248. doi:10.1111/j.1445-5994.2007.01518.x PMID:18298560
Goodman, J. C., Villarreal, P., & Jones, B. (2011, April). The social cost of adverse medical events, and what we can do about it. Health Affairs, 30(4), 590–595. doi:10.1377/hlthaff.2010.1256 PMID:21471477
Gordon, M., Darbyshire, D., & Baker, P. (2012). Non-technical skills training to enhance pa-tient safety: A systematic review. Medical Education, 46(11), 1042–1054. doi:10.1111/j.1365-2923.2012.04343.x PMID:23078681
Gorney, M. (2003). Expert witnesses: Caught in a moral and ethical dilemma. Bulletin of the American College of Surgeons, 88, 12–14. PMID:23593721
Gortzis, L. G., & Nikiforidis, G. (2008). Tracing and cataloguing knowledge in an e-health cardiology environment. Journal of Biomedical Informatics, 41(2), 217–223. doi:10.1016/j.jbi.2007.09.001 PMID:17945541
Gouva, M., & Kotrotsiou, E. (2011). Psychological Issues in Care Stories. Athens: Medical Publications Lagos.
Gowen, C. R. III, McFadden, K. L., & Settaluri, S. (2012). Contrasting continuous quality im-provement, Six Sigma, and Lean management for enhanced outcomes in US hospitals. American Journal of Business, 27(2), 133–153. doi:10.1108/19355181211274442
Compilation of References
280
Graber, M.A., Hartz, A., James, P., Nugent, A., & Green, M.D. (2005). An alternative method of determining standard of care in alleged cases of malpractice. Journal of the American Board of Family Medicine, 18(6), 453-8.
Graber, M.L. (2013). The incidence of diagnostic error in medicine. BMJ Quality & Safety, 22(2), ii21-ii27.
Grant, D., & McInnes, M. M. (2004). Malpractice experience and the incidence of cesarean delivery: A physician-level longitudinal analysis. Inquiry, 41(2), 170–188. doi:10.5034/inqui-ryjrnl_41.2.170 PMID:15449432
Gregory, A. (2013). Jeremy Hunt unveils new NHS guidelines but doctors who cover up their mistakes won’t be liable. Retrieved from http://www.mirror.co.uk/news/uk-news/new-nhs-guidelines-doctors-who-1786689
Grieshaber, D. C., Armstrong, T. J., Chaffin, D. B., Keyserling, W. M., & Ashton-Miller, J. (2009). The effects of insertion method and force on hand clearance envelopes for rubber hose insertion tasks. Human Factors: The Journal of the Human Factors and Ergonomics Society, 51(2), 152–163. doi:10.1177/0018720809336414 PMID:19653480
Grissinger, M. (2014). Too many abandon the “second victims” of medical errors. Pharmacy & Therapeutics, 39(9), 591–592. PMID:25210409
Grissom, T. E., DuKatz, A., Kordylewski, H. A., & Dutton, R. P. (2013). Bring out your data: The evolution of the national anesthesia clinical outcomes registry (NACOR). In A. Gangopadhyay (Ed.), Methods, models, and computation for medical informatics (pp. 126–145). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2653-9.ch008
Grober, E. D., & Bohnen, J. M. A. (2005). Defining medical error. Canadian Journal of Surgery, 48(1), 39–44. PMID:15757035
Grobler, S. (2007, March). The role of the expert witness. The South African Gastroenterology Review, 11-14.
Gross, S. (1991). Expert evidence. Wisconsin Law Review, 1113–1232.
Guillod, O. (2013). Medical error disclosure and patient safety: Legal aspects. Journal of Public Health Research, 2(3), 182–185. doi:10.4081/jphr.2013.e31 PMID:25170502
Guimarães, C., Antunes, D. R., García, L. S., & Fernandes, S. (2013). Information challenges of the deaf in their health and social care needs. In M. Cruz-Cunha, I. Miranda, & P. Gonçalves (Eds.), Handbook of research on ICTs for human-centered healthcare and social care services (pp. 93–111). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3986-7.ch005
Guinalíu, M., Marta, J., & Subero, J. M. (2013). Social networks as a tool to improve the life quality of chronic patients and their relatives. In M. Cruz-Cunha, I. Miranda, & P. Gonçalves (Eds.), Handbook of research on ICTs for human-centered healthcare and social care services (pp. 172–186). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3986-7.ch009

Compilation of References
281
Guldenmund, F. W. (2000). The nature of safety culture: A review of theory and research. Safety Science, 34(1–3), 215–257. doi:10.1016/S0925-7535(00)00014-X
Gullà, V. (2013). Leading the technological innovation in healthcare systems: The telematic medicine approach. In V. Gulla, A. Mori, F. Gabbrielli, & P. Lanzafame (Eds.), Telehealth networks for hospital services: New methodologies (pp. 134–153). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2979-0.ch009
Gullà, V., & Cancellotti, C. (2013). Telemedicine in emergency: A first aid hospital network experience. In V. Gulla, A. Mori, F. Gabbrielli, & P. Lanzafame (Eds.), Telehealth networks for hospital services: New methodologies (pp. 240–248). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2979-0.ch016
Guo, M., Yu, Y., Yang, J., & Wu, J. (2013). The crossmodal between the visual and tactile for motion perception. In J. Wu (Ed.), Biomedical engineering and cognitive neuroscience for health-care: Interdisciplinary applications (pp. 99–108). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2113-8.ch011
Gurwitz, J. H., Field, T. S., Avorn, J., McCormick, D., Jain, S., Eckler, M., & Bates, D. W. et al. (2000). Incidence and preventability of adverse drug events in nursing homes. The American Journal of Medicine, 109(2), 87–94. doi:10.1016/S0002-9343(00)00451-4 PMID:10967148
Habermann, M., Foraita, R., & Cramer, H. (2013). Categories of errors and error frequencies as identified by nurses: Results of a cross-sectional study in German nursing homes and hospitals. Journal of Public Health, 21(1), 3–13. doi:10.1007/s10389-012-0531-x
Hafeez-Baig, A., & Gururajan, R. (2013). Phenomena of adoption of wireless handheld devices: A case of healthcare setting. In H. Muga & K. Thomas (Eds.), Cases on the diffusion and adoption of sustainable development practices (pp. 20–43). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2842-7.ch002
Haida, M. (2013). Implications of NIRS brain signals. In J. Wu (Ed.), Biomedical engineering and cognitive neuroscience for healthcare: Interdisciplinary applications (pp. 120–128). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2113-8.ch013
Haig, K.M., Sutton, S., & Whittington, J. (2006). SBAR: A shared mental model for improving communication between clinicians. Joint Commission Journal on Quality and Patient Safety, 32(3), 167-75.
Han, D., & Braun, K. L. (2013). Promoting active ageing through technology training in Korea. In Digital literacy: Concepts, methodologies, tools, and applications (pp. 572–589). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-1852-7.ch030
Harding, S., Britten, N., & Bristow, D. (2010). The performance of junior doctors in applying clinical pharmacology knowledge and prescribing skills to standardized clinical cases. British Journal of Clinical Pharmacology, 69(6), 598–606. doi:10.1111/j.1365-2125.2010.03645.x PMID:20565451

Compilation of References
282
Hareva, D. H., Okada, H., & Oka, H. (2013). Ecological momentary assessment using a mobile phone. In J. Wu (Ed.), Technological advancements in biomedicine for healthcare applications (pp. 398–407). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2196-1.ch039
Härkänen, M., Ahonen, J., Kervinen, M., Turunen, H., & Vehviläinen-Julkunen, K. (2015). The factors associated with medication errors in adult medical and surgical inpatients: A direct ob-servation approach with medication record reviews. Scandinavian Journal of Caring Sciences, 29(2), 297–306. doi:10.1111/scs.12163 PMID:25213297
Harrison, R., Lawton, R., & Stewart, K. (2014). Doctors experiences of adverse events in second-ary care: The professional and personal impact. Clinical Medicine, 14(6), 585–590. doi:10.7861/clinmedicine.14-6-585 PMID:25468840
Hatton, J. D., Schmidt, T. M., & Jelen, J. (2013). Adoption of electronic health care records: Physician heuristics and hesitancy. In R. Martinho, R. Rijo, M. Cruz-Cunha, & J. Varajão (Eds.), Information systems and technologies for enhancing health and social care (pp. 148–165). Her-shey, PA: IGI Global. doi:10.4018/978-1-4666-3667-5.ch010
Haw, C., & Cahill, C. (2011). A computerized system for reporting medication events in psychia-try: The first two years of operation. Journal of Psychiatric and Mental Health Nursing, 18(4), 308–315. doi:10.1111/j.1365-2850.2010.01664.x PMID:21418430
Haw, C., Stubbs, J., & Dickens, G. L. (2014). Barriers to the reporting of medication administra-tion errors and near misses: An interview study of nurses at a psychiatric hospital. Journal of Psychiatric and Mental Health Nursing, 21(9), 797–805. PMID:24646372
Healey, B., Kopen, D., & Smith, J. (2011). Physicians, defensive medicine and ethics. Academy of Health Care Management Journal, 7(1), 59–78.
Hearnshaw, H., Harker, R., Cheater, F., Baker, R., & Grimshaw, G. (2002). A study of the methods used to select review criteria for clinical audit. Health Technology Assessment, 6, 1–78. PMID:11809128
Heinrichs, L., Fellander-Tsai, L., & Davies, D. (2013). Clinical virtual worlds: The wider im-plications for professional development in healthcare. In K. Bredl & W. Bösche (Eds.), Serious games and virtual worlds in education, professional development, and healthcare (pp. 221–240). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3673-6.ch014
Heinrichs, W. L., Davies, D., & Davies, J. (2013). Virtual worlds in healthcare: Applications and implications. In S. Arnab, I. Dunwell, & K. Debattista (Eds.), Serious games for healthcare: Applications and implications (pp. 1–22). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-1903-6.ch001
Heller, A. (2003). Five approaches to the phenomenon of shame. Social Research, 70, 1016–1030.
Hellings, J., Schrooten, W., Klazinga, N. S., & Vleugels, A. (2010). Improving patient safety culture. International Journal of Health Care Quality Assurance, 23(5), 489–506. doi:10.1108/09526861011050529 PMID:20845679

Compilation of References
283
Hemingway, M. W., OMalley, C., & Silvestri, S. (2015). Safety culture and care: A program to prevent surgical errors. AORN Journal, 101(4), 404–415. doi:10.1016/j.aorn.2015.01.002 PMID:25835006
Hendey, G. W., Barth, B. E., & Soliz, T. (2005). Overnight and postcall errors in medication orders. Academic Emergency Medicine, 12(7), 629–634. doi:10.1111/j.1553-2712.2005.tb00919.x PMID:15995095
Henneman, E. A., Blank, F. S. J., Gattasso, S., Williamson, K., & Henneman, P. L. (2006). Testing a classification model for emergency department errors. Journal of Advanced Nursing, 55(1), 90–99. doi:10.1111/j.1365-2648.2006.03878.x PMID:16768743
Hermer, L. D., & Brody, H. (2010). Defensive medicine, cost containment, and reform. Journal of General Internal Medicine, 25(5), 470–473. doi:10.1007/s11606-010-1259-3 PMID:20143176
Hirata, M., Yanagisawa, T., Matsushita, K., Sugata, H., Kamitani, Y., & Suzuki, T. … Yoshimine, T. (2013). Brain–machine interface using brain surface electrodes: Real-time robotic control and a fully implantable wireless system. In J. Wu (Ed.), Technological advancements in biomedicine for healthcare applications (pp. 362-374). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2196-1.ch036
Hirschinger, L. E., Scott, S. D., & Hahn-Cover, K. (2015, April 3). Clinician support: Five years of lessons learned. Patient Safety and Quality Healthcare. Retrieved from http://psqh.com/march-april-2015/clinician-support-five-years-of-lessons-learned
Hobgood, C., Weiner, B., & Tamayo-Sarver, J. H. (2006). Medical error identification, disclosure, and reporting: Do emergency medicine provider groups differ? Academic Emergency Medicine, 13(4), 443–451. doi:10.1111/j.1553-2712.2006.tb00324.x PMID:16531598
Hocine, N., & Gouaïch, A. (2013). Difficulty and scenario adaptation: An approach to customize therapeutic games. In S. Arnab, I. Dunwell, & K. Debattista (Eds.), Serious games for healthcare: Applications and implications (pp. 107–134). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-1903-6.ch006
Hodgkinson, B., Koch, S., Nay, R., & Nichols, K. (2006). Strategies to reduce medication errors with reference to older adults. International Journal of Evidence-Based Healthcare, 4(1), 2–41. PMID:21631752
Homsted, L. (2000). Institute of Medicine report: to err is human: building a safer health care system. The Florida Nurse, 48(1), 6. PMID:11995167
Hoonakker, P., Cartmill, R. S., Carayon, P., & Walker, J. M. (2013). Development and psycho-metric qualities of the SEIPS survey to evaluate CPOE/EHR implementation in ICUs. In J. Tan (Ed.), Healthcare information technology innovation and sustainability: Frontiers and adoption (pp. 161–179). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2797-0.ch010

Compilation of References
284
Hsaio, G. Y., Chen, I. J., Yu, S., Wei, I. L., Fang, Y. Y., & Tang, F. I. (2010). Nurses’ knowledge of high-alert medications: Instrument development and validation. Journal of Advanced Nursing, 66(1), 177–190. doi:10.1111/j.1365-2648.2009.05164.x PMID:20423443
Huang, Y. H., Chen, P. Y., & Grosch, J. W. (2010). Safety climate: New developments in con-ceptualization, theory, and research. Accident; Analysis and Prevention, 42(5), 1421–1422. doi:10.1016/j.aap.2009.12.007 PMID:20538096
Hudson, M. J., & Moore, G. P. (2011). Defenses to malpractice: What every emergency physician should know. The Journal of Emergency Medicine, 41(6), 598–606. doi:10.1016/j.jemermed.2010.07.001 PMID:21094012
Human Engineering for the Health and Safety Executive. (2005). A review on safety culture and safety climate literature for the development of the safety culture inspection toolkit. Bristol: Author.
Hwang, J. I., & Hwang, E. J. (2011). Individual and work environment characteristics associ-ated with error occurrences in Korean public hospitals. Journal of Clinical Nursing, 20(21/22), 3256–3266. doi:10.1111/j.1365-2702.2011.03773.x PMID:21733027
Igrejas, G., Amaral, J. S., & Rodrigues, P. J. (2013). Fall detection systems to be used by elderly people. In M. Cruz-Cunha, I. Miranda, & P. Gonçalves (Eds.), Handbook of research on ICTs for human-centered healthcare and social care services (pp. 449–473). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3986-7.ch024
Inomata, C., & Nitta, S. (2013). Nursing in integrative medicine and nurses’ engagement in caring-healing: A discussion based on the practice and study of music therapy and nursing care for patients with neurodegenerative disorders. In J. Wu (Ed.), Technological advancements in biomedicine for healthcare applications (pp. 235–239). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2196-1.ch025
Institute of Medicine. (2001). Crossing in the quality chasm: A new health system for the 21st century. Washington, DC: National Academies Press.
Institution of Engineering and Technology. (2009). Health & Safety Briefing No. 07. Retrieved from: http:// www.theiet.org/factfiles
International Nuclear Safety Advisory Group –INSAG. (2001). Safety Culture. Report 75-INSAG 4. International Atomic Energy Agency.
Ioannidis, J. P. A., & Lau, J. (2001). Evidence on Interventions to Reduce Medical Errors: An Overview and Recommendations for Future Research. Journal of General Internal Medicine, 16(5), 325–334. doi:10.1046/j.1525-1497.2001.00714.x PMID:11359552
Issenberg, S. B., Chung, H. S., & Devine, L. A. (2011). Patient safety training simulations based on competency criteria of the Accreditation Council for Graduate Medical Education. Mount Sinai Journal of Medicine: A Journal of Translational and Personalized Medicine, 78(6), 842–853. doi:10.1002/msj.20301

Compilation of References
285
Iwaki, S. (2013). Multimodal neuroimaging to visualize human visual processing. In J. Wu (Ed.), Biomedical engineering and cognitive neuroscience for healthcare: Interdisciplinary applications (pp. 274–282). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2113-8.ch028
Jackson, T., & Harper, A. (2001). Blunders will never cease: How the media report medical er-rors – A risky business. British Medical Journal, 322(7285), 562. doi:10.1136/bmj.322.7285.562
Jacobs, S., O’Beirne, M., Derflingher, L. P., Vlach, L., Rosser, W., & Drummond, N. (2007). Errors and adverse events in family medicine: Developing and validating a Canadian taxonomy of errors. Canadian Family Physician Medecin de Famille Canadien, 53(2), 270–276. PMID:17872644
James, J. T. (2013). A new, evidence-based estimate of patient harms associated with hospital care. Journal of Patient Safety, 9(3), 122–128. doi:10.1097/PTS.0b013e3182948a69 PMID:23860193
Janssen, C., Ommen, O., Neugebauer, E., Lefering, R., & Pfaff, H. (2007). How to improve satisfaction with hospital stay of severely injured patients. Langenbecks Archives of Surgery, 392(6), 747–760. doi:10.1007/s00423-007-0186-1 PMID:17384957
Jena, A. B., Seabury, S., Lakdawalla, D., & Chandra, A. (2011). Malpractice Risk According to Physician Specialty. The New England Journal of Medicine, 365(7), 629–636. doi:10.1056/NEJMsa1012370 PMID:21848463
Jerjes, W., Mahil, J., & Upile, T. (2011). English law for the surgeon II: clinical negligence. Head & Neck Oncology, 3, 52.
Jha, A. K., Prasopa-Plaizier, N., Larizgoitia, I., & Bates, D. W. (2010). Patient safety research: An overview of the global evidence. Quality & Safety in Health Care, 19(1), 42–47. doi:10.1136/qshc.2008.029165 PMID:20172882
Jiang, Y., Wang, S., Tan, R., Ishida, K., Ando, T., & Fujie, M. G. (2013). Motor cortex activation during mental imagery of walking: An fNIRS study. In J. Wu (Ed.), Biomedical engineering and cognitive neuroscience for healthcare: Interdisciplinary applications (pp. 29–37). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2113-8.ch004
Ji, Z., Sugi, T., Goto, S., Wang, X., & Nakamura, M. (2013). Multi-channel template extraction for automatic EEG spike detection. In J. Wu (Ed.), Biomedical engineering and cognitive neuro-science for healthcare: Interdisciplinary applications (pp. 255–265). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2113-8.ch026
Johnston, J.C., & Sartwelle, T.P. (2013). The expert witness in medical malpractice litigation: through the looking glass. Journal of Child Neurology, 28(4), 484-501.
Johnston, J. C. (2010). Neurological malpractice and nonmalpractice liability. Neurologic Clinics, 28(2), 441–458. doi:10.1016/j.ncl.2009.11.008 PMID:20202503
Juran, J. (1988). Quality control handbook (4th ed.). New York: McGraw-Hill.
Juvin, P., Teissiere, F., Brion, F., Desmonts, J. M., & Durigon, M. (2000). Postoperative death and malpractice suits: Is autopsy useful? Anesthesia and Analgesia, 91, 344–346. PMID:10910845

Compilation of References
286
Kachalia, A., & Bates, D. W. (2014). Disclosing medical errors: The view from the USA. The Surgeon, 12(2), 64–67. doi:10.1016/j.surge.2013.12.002 PMID:24461211
Kachalia, A., Kaufman, S. R., Boothman, R., Anderson, S., Welch, K., Saint, S., & Rogers, M. A. (2010). Liability claims and costs before and after implementation of a medical error disclo-sure program. Annals of Internal Medicine, 153(4), 213–221. doi:10.7326/0003-4819-153-4-201008170-00002 PMID:20713789
Kagan, I., & Barnoy, S. (2013). Organizational safety culture and medical error reporting by Israeli nurses. Journal of Nursing Scholarship, 45(3), 273–280. PMID:23574516
Kaldjian, L. C., Jones, E. W., Rosenthal, G. E., Tripp-Reimer, T., & Hillis, S. L. (2006). An em-pirically derived taxonomy of factors affecting physicians’ willingness to disclose medical errors. Journal of General Internal Medicine, 21(9), 942–948. doi:10.1007/BF02743142 PMID:16918739
Kaldjian, L. C., Jones, E. W., Wu, B. J., Forman-Hoffman, V. L., Levi, B. H., & Kassirer, J. P. (2002). Inconsistency in evidentiary standards for medical testimony. Disorder in the Courts. Journal of the American Medical Association, 288(11), 1382. doi:10.1001/jama.288.11.1382 PMID:12234232
Kaldjian, L. C., Jones, E. W., Wu, B. J., Forman-Hoffman, V. L., Levi, B. H., & Rosenthal, G. E. (2007). Disclosing medical errors to patients: Attitudes and practices of physicians and train-ees. Journal of General Internal Medicine, 22(7), 988–996. doi:10.1007/s11606-007-0227-z PMID:17473944
Kalina, J., & Zvárová, J. (2013). Decision support systems in the process of improving patient safety. In A. Moumtzoglou & A. Kastania (Eds.), E-health technologies and improving patient safety: Exploring organizational factors (pp. 71–83). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2657-7.ch005
Kalra, J., Kalra, N., & Baniak, N. (2013). Medical error, disclosure and patient safety : A global view of quality care. Clinical Biochemistry, 46(13-14), 1161–1169. doi:10.1016/j.clin-biochem.2013.03.025 PMID:23578740
Kamsu-Foguem, B., & Foguem, C. (2014). Telemedicine and mobile health with integrative medicine in developing countries. Health Policy and Technology, 3(4), 264–271. doi:10.1016/j.hlpt.2014.08.008
Kapp, M. B. (1997). Legal Anxieties and Medical Mistakes: Barriers and Pretexts. Journal of Gen-eral Internal Medicine, 12(12), 787–788. doi:10.1046/j.1525-1497.1997.07167.x PMID:9436901
Karve, A. M., Ou, F. S., Lytle, B. L., & Peterson, E. D. (2008). Potential unintended financial consequences of pay-for-performance on the quality of care for minority patients. American Heart Journal, 155(3), 571–576. doi:10.1016/j.ahj.2007.10.043 PMID:18294498

Compilation of References
287
Kasemsap, K. (2014). Unifying a framework of organizational culture, organizational climate, knowledge management, and job performance. In R. Perez-Castillo & M. Piattini (Eds.), Uncov-ering essential software artifacts through business process archeology (pp. 336–362). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4667-4.ch013
Kasemsap, K. (2015a). The role of radio frequency identification in modern libraries. In S. Thanuskodi (Ed.), Handbook of research on inventive digital tools for collection management and development in modern libraries (pp. 361–385). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-8178-1.ch021
Kasemsap, K. (2015b). The role of total quality management practices on quality performance. In A. Moumtzoglou, A. Kastania, & S. Archondakis (Eds.), Laboratory management informa-tion systems: Current requirements and future perspectives (pp. 1–31). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-6320-6.ch001
Kasemsap, K. (2016). Applying Lean Production and Six Sigma in global operations. In U. Akkucuk (Ed.), Handbook of research on waste management techniques for sustainability (pp. 44–74). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-9723-2.ch003
Kasemsap, K. (2017a). The fundamentals of health literacy. In N. Wickramasinghe (Ed.), Hand-book of research on healthcare administration and management (pp. 507–527). Hershey, PA: IGI Global. doi:10.4018/978-1-5225-0920-2.ch030
Kasemsap, K. (2017b). Promoting health literacy in global health care. In N. Wickramasinghe (Ed.), Handbook of research on healthcare administration and management (pp. 485–506). Hershey, PA: IGI Global. doi:10.4018/978-1-5225-0920-2.ch029
Kasemsap, K. (2017c). Radio frequency identification and mobile ad-hoc network: Theories and applications. In S. Bhattacharyya, N. Das, D. Bhattacharjee, & A. Mukherjee (Eds.), Handbook of research on recent developments in intelligent communication application (pp. 63–95). Hershey, PA: IGI Global. doi:10.4018/978-1-5225-1785-6.ch003
Kasemsap, K. (2017d). The importance of telemedicine in global health care. In N. Wickramas-inghe (Ed.), Handbook of research on healthcare administration and management (pp. 157–177). Hershey, PA: IGI Global. doi:10.4018/978-1-5225-0920-2.ch010
Kasemsap, K. (2017e). Mastering electronic health record in global health care. In N. Wick-ramasinghe (Ed.), Handbook of research on healthcare administration and management (pp. 222–242). Hershey, PA: IGI Global. doi:10.4018/978-1-5225-0920-2.ch014
Kasemsap, K. (2017f). Analyzing the role of health information technology in global health care. In N. Wickramasinghe (Ed.), Handbook of research on healthcare administration and management (pp. 287–307). Hershey, PA: IGI Global. doi:10.4018/978-1-5225-0920-2.ch017
Kasemsap, K. (2017g). Lean thinking in global health care: Theory and applications. In N. Wickramasinghe (Ed.), Handbook of research on healthcare administration and management (pp. 120–141). Hershey, PA: IGI Global. doi:10.4018/978-1-5225-0920-2.ch008

Compilation of References
288
Kasemsap, K. (2017h). Robotics: Theory and applications. In M. Moore (Ed.), Cybersecurity breaches and issues surrounding online threat protection (pp. 311–345). Hershey, PA: IGI Global. doi:10.4018/978-1-5225-1941-6.ch013
Kato, P. M. (2013). The role of the researcher in making serious games for health. In S. Arnab, I. Dunwell, & K. Debattista (Eds.), Serious games for healthcare: Applications and implications (pp. 213–231). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-1903-6.ch010
Katsura, S. (2013). Preservation and reproduction of human motion based on a motion-copying system. In J. Wu (Ed.), Technological advancements in biomedicine for healthcare applications (pp. 375–384). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2196-1.ch037
Kaufman, H. H. (2001). The expert witness. Neither Frye nor Daubert solved the problem: What can be done? Science & Justice, 41(1), 7–20. doi:10.1016/S1355-0306(01)71844-8 PMID:11215302
Kavanagh, K. T. (2011). Financial incentives to promote health care quality: The hospital acquired conditions nonpayment policy. Social Work in Public Health, 26(5), 524–541. doi:10.1080/19371918.2011.533554 PMID:21902485
Kelly, J., & Wright, D. (2012). Medicine administration errors and their severity in secondary care older persons’ ward: A multi-centre observational study. Journal of Clinical Nursing, 21(13/14), 1806–1815. doi:10.1111/j.1365-2702.2011.03760.x PMID:21733025
Keogh, R. H., & White, I. R. (2014). A toolkit for measurement error correction, with a focus on nutritional epidemiology. Statistics in Medicine, 33(12), 2137–2155. doi:10.1002/sim.6095 PMID:24497385
Keriel-Gascou, M., Figon, S., Letrilliart, L., Chaneliére, M., & Colin, C. (2011). Classifications and definitions of adverse events in primary care: A systematic review. La Presse Medicale, 40(11), e499–e505. doi:10.1016/j.lpm.2011.05.014 PMID:21802248
Kessels-Habraken, M., Van der Schaaf, T., De Jonge, J., & Rutte, C. (2010). Defining near misses: Towards a sharpened definition based on empirical data about error handling processes. Social Science & Medicine, 70(9), 1301–1308. doi:10.1016/j.socscimed.2010.01.006 PMID:20153573
Kessler, D. P., Sage, W. M., & Becker, D. J. (2005). Impact of malpractice reforms on the sup-ply of physician services. Journal of the American Medical Association, 293(21), 2618–2625. doi:10.1001/jama.293.21.2618 PMID:15928283
Khairat, S., & Gong, Y. (2010). Understanding effective clinical communication in medical errors. Studies in Health Technology and Informatics, 160, 704–708. PMID:20841777
Khanduja, K., Scales, D. C., & Adhikari, N. K. (2009). Pay for performance in the inten-sive care unitopportunity or threat? Critical Care Medicine, 37(3), 852–858. doi:10.1097/CCM.0b013e3181962b0b PMID:19237887
Kikuchi, T. (2013). Human-friendly mechatronics systems with functional fluids and elastomers. In J. Wu (Ed.), Technological advancements in biomedicine for healthcare applications (pp. 94–101). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2196-1.ch010

Compilation of References
289
Kimura, T., Miura, T., Shinohara, K., & Doi, S. (2013). Visual attention in 3-D space while mov-ing forward. In J. Wu (Ed.), Biomedical engineering and cognitive neuroscience for healthcare: Interdisciplinary applications (pp. 81–88). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2113-8.ch009
Kldiashvili, E. (2013). Implementation of telecytology in Georgia. In V. Gulla, A. Mori, F. Gab-brielli, & P. Lanzafame (Eds.), Telehealth networks for hospital services: New methodologies (pp. 341–361). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2979-0.ch022
Klein, M. (1952). Some theoretical conclusions regarding the emotional life of the infant. The Writings of Melanie Klein, 3, 61–93.
Kmucha, S. T. (2010). The Many Challenges of Pay-for-Performance Programs. American Health and Drug Benefits, 3(2), 135–142. PMID:25126315
Kohn, L. T., Corrigan, J. M., & Donaldson, M. S. (2000). To err is human: Building a safer health system. Washington, DC: National Academy Press.
Kohn, L. T., Corrigan, J. M., & Donaldson, M. S. (Eds.). (1999). To err is human: building a safer health system. Washington, DC: National Academy Press, Institute of Medicine.
Kohn, L. T., Corrigan, J. M., & Donaldson, M. S. (Eds.). (2000). To err is human: building a Safer Health System (Vol. 6). National Academies Press.
Kohn, L. T., Corrigan, J. M., & Molla, S. (1999). To Err Is Human. Medicine, 126(November), 312.
Kolovos, N. S., Bratton, S. L., & Levy, F. H. (2008). A novel error-reporting tool in pediatric intensive care. Journal for Healthcare Quality, 30(3), 43–50. doi:10.1111/j.1945-1474.2008.tb01142.x PMID:18507240
Koppar, A. R., & Sridhar, V. (2013). Malaria parasite detection: Automated method using microscope color image. In J. Rodrigues (Ed.), Digital advances in medicine, e-health, and communication technologies (pp. 289–300). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2794-9.ch016
Koppel, R., Metlay, J. P., Cohen, A., Abaluck, B., Localio, A. R., Kimmel, S. E., & Strom, B. L. (2005). Role of computerised physician order entry systems in facilitating medication errors. Journal of the American Medical Association, 293(10), 1197–1203. doi:10.1001/jama.293.10.1197 PMID:15755942
Koshy, R. (2005). Navigating the information technology highway: Computer solutions to reduce errors and enhance patient safety. Transfusion, 45(Suppl. 4), 189S–205S. doi:10.1111/j.1537-2995.2005.00619.x PMID:16181403
Kraman, S. S., & Hamm, G. (1999). Risk management: Extreme honesty may be the best policy. Annals of Internal Medicine, 131(12), 963–967. doi:10.7326/0003-4819-131-12-199912210-00010 PMID:10610649

Compilation of References
290
Krishnaswamy, K., & Oates, T. (2014). Pathway to independence: Past, present, and beyond via robotics. In G. Kouroupetroglou (Ed.), Disability informatics and web accessibility for motor limitations (pp. 153–201). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4442-7.ch005
Kristensen, S., Bartels, P., Sabroe, S., & Mainz, J. (2014). Patient safety culture can be a driver for high clinical quality. Ugeskrift for Laeger, 176(32), 1483–1486. PMID:25292469
Kristensen, S., Hammer, A., Bartels, P., Sunol, R., Groene, O., Thompson, C. A., & Wagner, C. et al. (2015). Quality management and perceptions of teamwork and safety climate in European hospitals. International Journal for Quality in Health Care, 27(6), 499–506. doi:10.1093/intqhc/mzv079 PMID:26443813
Kristensen, S., Mainz, J., & Bartels, P. A. (2007). A patient safety vocabulary: Safety improve-ment for patients in Europe. SimPatlE. Denmark: ESQH.
Kroll, L., Singleton, A., Collier, J., & Jones, I. R. (2008). Learning not to take it seriously: Junior doctors’ accounts of error. Medical Education, 42(10), 982–990. doi:10.1111/j.1365-2923.2008.03151.x PMID:18823517
Kuehn, S. L., & Doyle, M. J. (1990). Medication errors: 1977 to 1988. Experience in medical malpractice claims. New Jersey Medicine, 87, 27–34. PMID:2300277
Kumar, S., & Chaudhary, S. (2009). Medical errors and consequent adverse events in critically ill surgical patients in a tertiary care teaching hospital in Delhi. Journal of Emergencies. Trauma and Shock, 2(2), 80–84. doi:10.4103/0974-2700.50740
Kurita, Y., Ikeda, A., Nagata, K., Okajima, M., & Ogasawara, T. (2013). Biomedical robotics for healthcare. In J. Wu (Ed.), Technological advancements in biomedicine for healthcare applica-tions (pp. 160–169). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2196-1.ch017
Kyung, C. Y., & Barbara, M. (2011). Moderating effects of learning climate on the impact of RN staffing on medication errors. Nursing Research, 60, 32–39. doi:10.1097/NNR.0b013e3181ff73cc PMID:21127452
Laing, G., Bruce, J., Skinner, D., Allorto, N., Aldous, C., Thomson, S., & Clarke, D. (2015). Using a hybrid electronic medical record system for the surveillance of adverse surgical events and human error in a developing world surgical service. World Journal of Surgery, 39(1), 70–79. doi:10.1007/s00268-014-2766-x PMID:25167900
Lakkaraju, S., & Lakkaraju, S. (2013). Mobile device application in healthcare. In S. Sarnikar, D. Bennett, & M. Gaynor (Eds.), Cases on healthcare information technology for patient care management (pp. 276–307). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2671-3.ch016
Lamb, R. M., Studdert, D. M., Bohmer, R. M., Berwick, D. M., & Brennan, T. A. (2003). Hospi-tal disclosure practices: Results of a national survey. Health Affairs, 22(2), 73–83. doi:10.1377/hlthaff.22.2.73 PMID:12674409

Compilation of References
291
Lammers, R., Byrwa, M., & Fales, W. (2012). Root causes of errors in a simulated prehospi-tal pediatric emergency. Academic Emergency Medicine, 19(1), 37–47. doi:10.1111/j.1553-2712.2011.01252.x PMID:22251191
Laplanche, J., & Pontalis, J. B. (1973). The language of psycho-analysis (D. Nicholson-Smith, Trans.). Oxford, UK: W. W. Norton.
Laskowski, M. (2013). A prototype agent based model and machine learning hybrid system for healthcare decision support. In J. Rodrigues (Ed.), Digital advances in medicine, e-health, and communication technologies (pp. 230–253). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2794-9.ch013
Lauterstein, R. H., & Mustoe, L. F. (1960). Accidents involve people. Nursing Outlook, 8, 96–98. PMID:14414610
Lawson, A. E., & Daniel, E. S. (2011). Inferences of clinical diagnostic reasoning and diag-nostic error. Journal of Biomedical Informatics, 44(3), 402–412. doi:10.1016/j.jbi.2010.01.003 PMID:20093196
Lea, A., & Danczak, A. (2014). Medical error: A dirty little secret or a great learning opportunity? Education for Primary Care, 25(2), 114–118. PMID:24593978
Leape, L. (2000). Preventing mishaps team effort, error expert says. OR Manager, 16(2), 1, 12–13. PMID:10787891
Leape, L. L. (1994). Error in medicine. Journal of the American Medical Association, 272(23), 1851–1857. doi:10.1001/jama.1994.03520230061039 PMID:7503827
Leape, L. L., Bates, D. W., Cullen, D. J., Cooper, J., Demonaco, H. J., & Gallivan, T. et al.. (1995). Systems analysis of adverse drug events. ADE Prevention Study Group. Journal of the American Medical Association, 274(1), 35–43. doi:10.1001/jama.1995.03530010049034 PMID:7791256
Leape, L. L., Brennan, T. A., Laird, N. M., Lawthers, A. G., Localio, A. R., Barnes, B. A., & Hiatt, H. et al. (1991). The nature of adverse events in hospitalized patients: Results from the Harvard Medical Practice Study II. The New England Journal of Medicine, 324(6), 377–384. doi:10.1056/NEJM199102073240605 PMID:1824793
Lee, T. (2014). Mobile healthcare computing in the cloud. In J. Rodrigues, K. Lin, & J. Lloret (Eds.), Mobile networks and cloud computing convergence for progressive services and applica-tions (pp. 275–294). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4781-7.ch015
Legido-Quigley, H., McKee, M., Walshe, K., Sunol, R., Nolte, E., & Klazinga, N. (2008). How can quality of health care be safeguarded across the European Union? BMJ (Clinical Research Ed.), 336(7650), 920–923. doi:10.1136/bmj.39538.584190.47 PMID:18436947
Lehmann, L., Wesselmann, U., Weber, B., & Smentkowski, U. (2015). Medical error analysis in dermatology according to the reports of the North Rhine Medical Association from 2004–2013. JDDG: Journal der Deutschen Dermatologischen Gesellschaft, 13(9), 903–908. PMID:26882381

Compilation of References
292
Lelardeux, C., Alvarez, J., Montaut, T., Galaup, M., & Lagarrigue, P. (2013). Healthcare games and the metaphoric approach. In S. Arnab, I. Dunwell, & K. Debattista (Eds.), Serious games for healthcare: Applications and implications (pp. 23–49). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-1903-6.ch002
Lewis, P. J., Ashcroft, D. M., Dornan, T., Taylor, D., Wass, V., & Tully, M. P. (2014). Exploring the causes of junior doctors’ prescribing mistakes: A qualitative study. British Journal of Clinical Pharmacology, 78(2), 310–319. doi:10.1111/bcp.12332 PMID:24517271
Lhotska, L., Bursa, M., Huptych, M., Chudacek, V., & Havlik, J. (2013). Interoperability of medical devices and information systems. In M. Cruz-Cunha, I. Miranda, & P. Gonçalves (Eds.), Handbook of research on ICTs for human-centered healthcare and social care services (pp. 749–762). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3986-7.ch039
Liao, H. (2013). Biomedical information processing and visualization for minimally invasive neurosurgery. In J. Wu (Ed.), Technological advancements in biomedicine for healthcare applica-tions (pp. 36–46). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2196-1.ch005
Libreri, C., & Graffigna, G. (2014). How web 2.0 shapes patient knowledge sharing: The case of diabetes in Italy. In C. El Morr (Ed.), Research perspectives on the role of informatics in health policy and management (pp. 238–260). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4321-5.ch014
Lindenauer, P. K., Remus, D., Roman, S., Rothberg, M. B., Benjamin, E. M., Ma, A., & Bratzler, D. W. (2007). Public reporting and pay for performance in hospital quality improvement. The New England Journal of Medicine, 356(5), 486–496. doi:10.1056/NEJMsa064964 PMID:17259444
Lin, L., Chen, Y., Wu, J., & Tennyson, R. D. (2013). What skill/knowledge is important to a nursing professional? In P. Ordóñez de Pablos (Ed.), Business, technology, and knowledge management in Asia: Trends and innovations (pp. 234–249). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2652-2.ch018
Lin, Y. H., & Ma, S. M. (2009). Willingness of nurses to report medication administration errors in Southern Taiwan: A cross-sectional survey. Worldviews on Evidence-Based Nursing, 6(4), 237–245. doi:10.1111/j.1741-6787.2009.00169.x PMID:19747183
Liu, G. (2014). Using case costing data and case mix for funding and benchmarking in rehabilitation hospitals. In C. El Morr (Ed.), Research perspectives on the role of informatics in health policy and management (pp. 62–78). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4321-5.ch005
Liu, K., & Dix, A. (1997, May). Norm governed agents in CSCW. In The First International Workshop on Computational Semiotics. IGI.
Li, W., Liu, K., Yang, H., & Yu, C. (2014). Integrated clinical pathway management for medical quality improvement–based on a semiotically inspired systems architecture. European Journal of Information Systems, 23(4), 400–417. doi:10.1057/ejis.2013.9

Compilation of References
293
Li, X., Lin, Z., & Wu, J. (2013). Language processing in the human brain of literate and illiter-ate subjects. In J. Wu (Ed.), Biomedical engineering and cognitive neuroscience for healthcare: Interdisciplinary applications (pp. 201–209). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2113-8.ch021
Lixun, Z., Dapeng, B., & Lei, Y. (2013). Design of and experimentation with a walking assistance robot. In J. Wu (Ed.), Technological advancements in biomedicine for healthcare applications (pp. 123–127). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2196-1.ch013
Localio, A.R., Lawthers, A.G., Brennan, T.A., Laird, N.M., Hebert, L.E., Peterson, L.M., … Hiatt, H.H. (1991). Relation between malpractice claims and adverse events due to negligence. Results of the Harvard Medical Practice Study III. New England Journal of Medicine, 325(4), 245-51.
Lucchiari, C., & Pravettoni, G. (2012). Cognitive balanced model: A conceptual scheme of diagnostic decision making. Journal of Evaluation in Clinical Practice, 18(1), 82–88. doi:10.1111/j.1365-2753.2011.01771.x PMID:21999310
Macinati, M. S. (2008). The relationship between quality management systems and organisational performance in the Italian National Health Service. Health Policy (Amsterdam), 85(2), 228–241. doi:10.1016/j.healthpol.2007.07.013 PMID:17825941
MacKay, A. P., Berg, C. J., Duran, C., Chang, J., & Rosenberg, H. (2005). An assessment of pregnancy-related mortality in the United States. Paediatric and Perinatal Epidemiology, 19(3), 206–214. doi:10.1111/j.1365-3016.2005.00653.x PMID:15860079
Macklis, R. M., Meier, T., & Weinhous, M. S. (1998). Error rates in clinical radiotherapy. Journal of Clinical Oncology, 16, 551–556. PMID:9469340
Macleod, L. (2014, January/February). “Second victim” casualties and how physician leaders can help. Physician Executive Journal, 40, 8–12. PMID:24575696
Madea, B. (2009). Medico-legal autopsies as a source of information to improve patient safety. Legal Medicine, 11, 76–79. doi:10.1016/j.legalmed.2009.01.108 PMID:19289305
Madea, B., & Preuss, J. (2009). Medical malpractice as reflected by the forensic evaluation of 4450 autopsies. Forensic Science International, 190(1-3), 58–66. doi:10.1016/j.forsciint.2009.05.013 PMID:19524380
Main, E.K., Morton, C.H., Melsop, K., Hopkins, D., Giuliani, G., & Gould, J.B. (2012). Creating a public agenda for maternity safety and quality in cesarean delivery. Obstetrics & Gynecology, 120(5), 1194-8.
Makikawa, M., Okada, S., Fujiwara, Y., & Esaki, M. (2013). Sleep monitoring system equipped with a flexible non-contact ECG, respiration, and body motion sensor. In J. Wu (Ed.), Techno-logical advancements in biomedicine for healthcare applications (pp. 287–297). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2196-1.ch030

Compilation of References
294
Malindretos, G. (2013). Distribution and logistics outsourcing in the pharmaceutical sector. In D. Folinas (Ed.), Outsourcing management for supply chain operations and logistics service (pp. 202–222). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2008-7.ch012
Manias, E., Williams, A., & Liew, D. (2012). Interventions to reduce medication errors in adult intensive care: A systematic review. British Journal of Clinical Pharmacology, 74(3), 411–423. doi:10.1111/j.1365-2125.2012.04220.x PMID:22348303
Manser, T. (2011). Managing the aftermath of critical incidents: Meeting the needs of health-care providers and patients. Best Practice & Research. Clinical Anaesthesiology, 25(2), 169–179. doi:10.1016/j.bpa.2011.02.004 PMID:21550542
Mansour, M., James, V., & Edgley, A. (2012). Investigating the safety of medication administra-tion in adult critical care settings. Nursing in Critical Care, 17(4), 189–197. doi:10.1111/j.1478-5153.2012.00500.x PMID:22698161
Manvi, S. S., & B., M. R. (2013). A survey on health care services using wireless sensor net-works. In M. Cruz-Cunha, I. Miranda, & P. Gonçalves (Eds.), Handbook of research on ICTs for human-centered healthcare and social care services (pp. 587-606). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3986-7.ch031
Marmon, L. M., & Heiss, K. (2015). Improving surgeon wellness: The second victim syndrome and quality of care. Seminars in Pediatric Surgery, 24(6), 315–318. doi:10.1053/j.semped-surg.2015.08.011 PMID:26653167
Marshall, S., & Hogan, J. (2013). The use of medical simulation to improve patient safety. In A. Moumtzoglou & A. Kastania (Eds.), E-health technologies and improving patient safety: Exploring organizational factors (pp. 155–172). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2657-7.ch011
Martinez, W., & Lo, B. (2008). Medical students’ experiences with medical errors: An analysis of medical student essays. Medical Education, 42(7), 733–741. doi:10.1111/j.1365-2923.2008.03109.x PMID:18507766
Martin, J., & McKay, E. (2013). Mental health, post-secondary education, and information communications technology. In J. Lannon & E. Halpin (Eds.), Human rights and information communication technologies: Trends and consequences of use (pp. 196–213). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-1918-0.ch012
Martin, J., & McKay, E. (2014). Mental health, post-secondary education, and information communications technology. In Assistive technologies: Concepts, methodologies, tools, and applications (pp. 1209–1226). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4422-9.ch063
Masayuki, K., Eiji, K., Tetsuo, T., & Nozomu, M. (2013). Evaluation of olfactory impairment in Parkinson’s disease using near-infrared spectroscopy. In J. Wu (Ed.), Biomedical engineering and cognitive neuroscience for healthcare: Interdisciplinary applications (pp. 293–302). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2113-8.ch030

Compilation of References
295
Maskens, C., Downie, H., Wendt, A., Lima, A., Merkley, L., Lin, Y., & Callum, J. (2014). Hos-pital-based transfusion error tracking from 2005 to 2010: Identifying the key errors threatening patient transfusion safety. Transfusion, 54(1), 66–73. doi:10.1111/trf.12240 PMID:23672511
Ma, X., Chen, G., & Xiao, J. (2013). Understanding weight change behaviors through online social networks. In A. Gangopadhyay (Ed.), Methods, models, and computation for medical informatics (pp. 189–214). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2653-9.ch012
Mazor, K. K., Simon, S. R., & Gurwitz, J. H. (2004). Communicating with patients about medical adverse events. Archives of Internal Medicine, 164(15), 1690–1697. doi:10.1001/archinte.164.15.1690 PMID:15302641
Mazor, K. M., Fischer, M. A., Haley, H. L., Hatem, D., & Quirk, M. E. (2005). Teaching and medical errors: Primary care preceptors’ views. Medical Education, 39(10), 982–990. doi:10.1111/j.1365-2929.2005.02262.x PMID:16178824
Mazor, K. M., Reed, G. W., Yood, R. A., Fischer, M. A., Baril, J., & Gurwitz, J. H. (2006). Dis-closure of Medical Errors: What Factors Influence How Patients Respond? Journal of General Internal Medicine, 21(7), 704–710. doi:10.1111/j.1525-1497.2006.00465.x PMID:16808770
Mazor, K., Simon, S., Yood, R., Gurwitz, J., Martinson, B., Gunter, M., & Reed, G. (2004). Health plan members views about disclosure of medical errors. Annals of Internal Medicine, 140(6), 409–418. doi:10.7326/0003-4819-140-6-200403160-00006 PMID:15023706
Mazzanti, I., Maolo, A., & Antonicelli, R. (2013). E-health and telemedicine in the elderly: State of the art. In V. Gulla, A. Mori, F. Gabbrielli, & P. Lanzafame (Eds.), Telehealth Networks for Hospital Services: New Methodologies (pp. 33–43). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2979-0.ch003
Mazzanti, I., Maolo, A., & Antonicelli, R. (2014). E-health and telemedicine in the elderly: State of the art. In Assistive technologies: Concepts, methodologies, tools, and applications (pp. 693–704). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4422-9.ch034
McAbee, G. N. (1998). Malpractice risks associated with prescribing medication for chronic headaches. Headache, 38(1), 53–55. doi:10.1046/j.1526-4610.1998.3801053.x PMID:9505005
McCay, L., & Wu, A. (2012). Medical error: The second victim. British Journal of Hospital Medicine, 73(Sup10), C146–C148. doi:10.12968/hmed.2012.73.Sup10.C146 PMID:23124197
McCrossan, B. A., & Casey, F. A. (2013). The role of telemedicine in paediatric cardiology. In V. Gulla, A. Mori, F. Gabbrielli, & P. Lanzafame (Eds.), Telehealth networks for hospital services: New methodologies (pp. 44–88). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2979-0.ch004
McDowell, S. E., Ferner, H. S., & Ferner, R. E. (2009). The pathophysiology of medication errors: How and where they arise. British Journal of Clinical Pharmacology, 67(6), 605–613. doi:10.1111/j.1365-2125.2009.03416.x PMID:19594527

Compilation of References
296
McFadden, K. L., Stock, G. N., & Gowen, C. R. III. (2014). Leadership, safety climate, and con-tinuous quality improvement: Impact on process quality and patient safety. The Journal of Nursing Administration, 44(10Suppl), S27–S37. doi:10.1097/nna.0000000000000119 PMID:25279509
McGinnes, S., & Burke, M. (2013). Hoping for the best: A qualitative study of information technology in primary care. In M. Cruz-Cunha, I. Miranda, & P. Gonçalves (Eds.), Handbook of research on ICTs and management systems for improving efficiency in healthcare and social care (pp. 1088–1108). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3990-4.ch057
McLaughlin, C. P., & Kaluzny, A. D. (2006). Continuous quality improvement in health care (3rd ed.). Jones & Bartlett Publishers.
McLean, T. R. (2015). Why the distribution of medical errors matters. American Journal of Surgery, 210(1), 188–192.
McLennan, S. R., Engel-Glatter, S., Meyer, A. H., Schwappach, D. L. B., Scheidegger, D. H., & Elger, B. S. (2015). The impact of medical errors on Swiss anaesthesiologists: A cross-sectional survey. Acta Anaesthesiologica Scandinavica, 59(8), 990–998. doi:10.1111/aas.12517 PMID:25952281
McLoughlin, V., Millar, J., Mattke, S., Franca, M., Jonsson, P. M., Somekh, D., & Bates, D. (2006). Selecting indicators for patient safety at the health system level in OECD countries. In-ternational Journal for Quality in Health Care, 18(Suppl 1), 14–20. doi:10.1093/intqhc/mzl030 PMID:16954511
Meadows, M. (2003). Strategies to reduce medication errors. How the FDA is working to improve medication safety and what you can do to help. FDA Consumer, 37(3), 20–27. PMID:12793389
Mearns, K., Whitaker, S. M., & Flin, R. (2003). Safety climate, safety management practice and safety performance in offshore environments. Safety Science, 41(8), 641–680. doi:10.1016/S0925-7535(02)00011-5
Medhekar, A., Wong, H. Y., & Hall, J. (2014). Innovation in medical tourism service market-ing: A case of India. In A. Goyal (Ed.), Innovations in services marketing and management: Strategies for emerging economies (pp. 49–66). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4671-1.ch003
Medhekar, A., Wong, H. Y., & Hall, J. (2014). Medical tourism: A conceptual framework for an innovation in global healthcare provision. In A. Goyal (Ed.), Innovations in services marketing and management: Strategies for emerging economies (pp. 148–169). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4671-1.ch009
Mello, M. M., Studdert, D. M., Thomas, E. J., Yoon, C. S., & Brennan, T. A. (2007). Who pays for medical errors? An analysis of adverse event costs, the medical liability system, and incentives for patient safety improvement. Journal of Empirical Legal Studies, 4(4), 835–860. doi:10.1111/j.1740-1461.2007.00108.x

Compilation of References
297
Mendes, D., & Rodrigues, I. P. (2013). A semantic web pragmatic approach to develop clinical ontologies, and thus semantic interoperability, based in HL7 v2.xml messaging. In R. Martinho, R. Rijo, M. Cruz-Cunha, & J. Varajão (Eds.), Information systems and technologies for enhanc-ing health and social care (pp. 205–214). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3667-5.ch014
Mettler, T. (2013). Transformation of the hospital supply chain: How to measure the maturity of supplier relationship management systems in hospitals? In J. Tan (Ed.), Healthcare information technology innovation and sustainability: Frontiers and adoption (pp. 180–192). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2797-0.ch011
Michell, V. (2014). The Internet of Things and Opportunities for Pervasive Safety Monitored Health Environments. In Patient Safety and Quality Care through Health Informatics. IGI. doi:10.4018/978-1-4666-4546-2.ch020
Michell, V., Tehrani, J., & Liu, K. (2012). Are clinical documents optimised for patient safety? A critical analysis of patient safety outcomes using the EDA error model. Health Policy and Technology, 1(4), 214–227. doi:10.1016/j.hlpt.2012.10.003
Michel, P., Quenon, J. L., Djihoud, A., Tricaud-Vialle, S., & de Sarasqueta, A. M. (2007). French national survey of inpatient adverse events prospectively assessed with ward staff. Quality & Safety in Health Care, 16(5), 369–377. doi:10.1136/qshc.2005.016964 PMID:17913779
Miesenberger, K., Nussbaum, G., & Ossmann, R. (2014). AsTeRICS: A framework for including sensor technology into AT solutions for people with motor disabilities. In G. Kouroupetroglou (Ed.), Assistive technologies and computer access for motor disabilities (pp. 154–179). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4438-0.ch006
Miller, R., Scott, S., & Hirschinger, L. (2015, September). Improving patient safety: The intersec-tion of safety culture, clinician and staff support, and patient safety organizations. Retrieved from http://www.centerforpatientsafety.org/wp-content/themes/patient-safety/pdf/Second-Victims-White-Paper.pdf
Miller, K., & Sankaranarayanan, S. (2013). Applications of policy based agents in wireless body sensor mesh networks for patient health monitoring. In J. Rodrigues (Ed.), Digital advances in medicine, e-health, and communication technologies (pp. 85–101). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2794-9.ch005
Miller, L. K., Nelson, M. S., & Spurlock, B. W. (2001). A compendium of suggested practices for preventing and reducing medication errors. Roseville, CA: California Institute for Health System Performance.
Miller, M. R., Robinson, K. A., Lubomski, L. H., Rinke, M. L., & Pronovost, P. J. (2007). Medication errors in paediatric care: A systematic review of epidemiology and an evaluation of evidence supporting reduction strategy recommendations. Quality & Safety in Health Care, 16(2), 116–126. doi:10.1136/qshc.2006.019950 PMID:17403758

Compilation of References
298
Milligan, F. J. (2007). Establishing a culture for patient safety–The role of education. Nurse Education Today, 27(2), 95–102. doi:10.1016/j.nedt.2006.03.003 PMID:16713030
Mira, J. J., Lorenzo, S., Carrillo, I., Ferrus, L., Perez-Perez, P., Iglesias, F., & Astier, P. et al. (2015, August). Interventions in health organisations to reduce the impact of adverse events in second and third victims. BMC Health Services Research, 15(341), 1–9. doi:10.1186/s12913-015-0994-x PMID:26297015
Mohammadian, M., & Jentzsch, R. (2013). User and data classification for a secure and practi-cal approach for patient-doctor profiling using an RFID framework in hospital. In S. Sarnikar, D. Bennett, & M. Gaynor (Eds.), Cases on healthcare information technology for patient care management (pp. 224–253). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2671-3.ch014
Mohr, J. J., Abelson, H. T., & Barach, P. (2002). Creating effective leadership for improving patient safety. Quality Management in Health Care, 11(1), 69–78. doi:10.1097/00019514-200211010-00010 PMID:12455344
Montazemi, A. R., Pittaway, J. J., & Keshavjee, K. (2013). State of IS integration in the context of patient-centered care: A network analysis and research directions. In J. Tan (Ed.), Healthcare information technology innovation and sustainability: Frontiers and adoption (pp. 127–144). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2797-0.ch008
Montesi, G., & Lechi, A. (2009). Prevention of medication errors: Detection and audit. British Journal of Clinical Pharmacology, 67(6), 651–655. doi:10.1111/j.1365-2125.2009.03422.x PMID:19594533
Morey, R. C., Fine, D. J., Loree, S. W., Retzlaff-Roberts, D. L., & Tsubakitani, S. (1992). The trade-off between hospital cost and quality of care. An exploratory empirical analysis. Medical Care, 30(8), 677–698. doi:10.1097/00005650-199208000-00002 PMID:1640765
Mori, A. R., Contenti, M., & Verbicaro, R. (2013). Policies on telemedicine-enhanced hospital services: Prioritization criteria for the interventions at regional level. In V. Gulla, A. Mori, F. Gabbrielli, & P. Lanzafame (Eds.), Telehealth networks for hospital services: New methodologies (pp. 1–14). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2979-0.ch001
Morita, A. (2013). The quantitative EEG change in Parkinson’s disease. In J. Wu (Ed.), Biomedi-cal engineering and cognitive neuroscience for healthcare: Interdisciplinary applications (pp. 225–234). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2113-8.ch023
Moromugi, S., & Ishimatsu, T. (2013). A strength training machine with a dynamic resistance control function based on muscle activity level. In J. Wu (Ed.), Technological advancements in biomedicine for healthcare applications (pp. 102–110). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2196-1.ch011
Morrow, D., & Chin, J. (2013). Technology as a bridge between health care systems and older adults. In R. Zheng, R. Hill, & M. Gardner (Eds.), Engaging older adults with modern technology: Internet use and information access needs (pp. 59–79). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-1966-1.ch004

Compilation of References
299
Mosadeghrad, A. M. (2005). A survey of total quality management in Iran: Barriers to successful implementation in health care organizations. International Journal of Health Care Quality Assur-ance Incorporating Leadership in Health Services, 18(3), 12–34. doi:10.1108/13660750510611189
Mosadeghrad, A. M. (2006). The impact of organizational culture on the successful implementation of Total Quality Management. TQM Journal, 18(6), 606–625. doi:10.1108/09544780610707101
Mosadeghrad, A. M. (2012). A conceptual framework for quality of care. Mat Soc Med, 24(4), 251–261. doi:10.5455/msm.2012.24.251-261 PMID:23922534
Mosadeghrad, A. M. (2013a). Healthcare service quality: Towards a broad definition. International Journal of Health Care Quality Assurance, 26(3), 203–219. doi:10.1108/09526861311311409 PMID:23729125
Mosadeghrad, A. M. (2013b). Verification of a quality management theory: Using a Delphi study. International Journal of Health Policy and Management, 1(4), 261–271. doi:10.15171/ijhpm.2013.55 PMID:24596883
Mosadeghrad, A. M. (2014). Factors influencing health care service quality. International Journal of Health Policy and Management, 3(2), 77–89. doi:10.15171/ijhpm.2014.65 PMID:25114946
Mosadeghrad, A. M., & Ferlie, E. (2016). Total Quality Management in Healthcare. In A. Orten-blad, C. Abrahamson Lofstrom, & R. Sheaff (Eds.), Management innovations for healthcare organizations: adopt, abandon or adapt? (pp. 378–396). Routledge.
Mostafa, R., Hasan, G. M., Kabir, A. A., & Rahman, M. A. (2013). Proposed framework for the deployment of telemedicine centers in rural Bangladesh. In J. Rodrigues (Ed.), Digital advances in medicine, e-health, and communication technologies (pp. 254–270). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2794-9.ch014
Motoi, K., Ogawa, M., Yamakoshi, T., & Yamakoshi, K. (2013). Fusion physiological sensing system for healthcare. In J. Wu (Ed.), Technological advancements in biomedicine for healthcare applications (pp. 298–313). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2196-1.ch031
Motorny, S. P. (2013). Big information technology bet of a small community hospital. In S. Sarnikar, D. Bennett, & M. Gaynor (Eds.), Cases on healthcare information technology for patient care management (pp. 70–94). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2671-3.ch004
Moumtzoglou, A. (2013). Risk perception as a patient safety dimension. In A. Moumtzoglou & A. Kastania (Eds.), E-health technologies and improving patient safety: Exploring organizational factors (pp. 285–299). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2657-7.ch017
Moutier, C., Wingard, D., Gudea, M., Jeste, D., Goodman, S., & Reznik, V. (2016). The Culture of Academic Medicine: Faculty Behaviors Impacting the Learning Environment. Academic Psychiatry, 40(6), 912–918. doi:10.1007/s40596-016-0582-3 PMID:27368643

Compilation of References
300
Msanjila, S. S. (2013). Emerging ICT challenges on provision of online HIV/AIDS advisory services. In M. Cruz-Cunha, I. Miranda, & P. Gonçalves (Eds.), Handbook of research on ICTs for human-centered healthcare and social care services (pp. 248–269). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3986-7.ch013
Müller, A. (2013). Improving the identification of medication names by increasing phonological awareness via a language-teaching computer game (medicina). In S. Arnab, I. Dunwell, & K. Debattista (Eds.), Serious games for healthcare: Applications and implications (pp. 283–295). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-1903-6.ch014
Muller, D., & Ornstein, K. (2007). Perceptions of and attitudes towards medical errors among medical trainees. Medical Education, 41(7), 645–652. doi:10.1111/j.1365-2923.2007.02784.x PMID:17614884
Murakami, S., Kim, H., Tan, J. K., Ishikawa, S., & Aoki, T. (2013). The development of a quan-titative method for the detection of periarticular osteoporosis using density features within ROIs from computed radiography images of the hand. In J. Wu (Ed.), Technological advancements in biomedicine for healthcare applications (pp. 55–67). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2196-1.ch007
Nadathur, S. G., & Warren, J. R. (2013). Formal-transfer in and out of stroke care units: An analysis using Bayesian networks. In J. Tan (Ed.), Healthcare information technology inno-vation and sustainability: Frontiers and adoption (pp. 193–207). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2797-0.ch012
Nahed, B. V., Babu, M. A., Smith, T. R., & Heary, R. F. (2012, June 22). Malpractice liability and defensive medicine: A national survey of neurosurgeons. PLOS ONE. Retrieved from http://journals.plos.org/plosone/article?id=10.1371/journal.pone.0039237
Naidoo, V., & Naidoo, Y. (2014). Home telecare, medical implant, and mobile technology: Evo-lutions in geriatric care. In C. El Morr (Ed.), Research perspectives on the role of informatics in health policy and management (pp. 222–237). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4321-5.ch013
Nakagawa, S. (2013). Bone-conducted ultrasonic perception: An elucidation of perception mechanisms and the development of a novel hearing aid for the profoundly deaf. In J. Wu (Ed.), Technological advancements in biomedicine for healthcare applications (pp. 148–159). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2196-1.ch016
Nakai, M., & Niinomi, M. (2013). Recent progress in mechanically biocompatible titanium-based materials. In J. Wu (Ed.), Technological advancements in biomedicine for healthcare applications (pp. 206–212). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2196-1.ch022
Nakakuki, T., & Okada-Hatakeyama, M. (2013). Methods for the analysis of intracellular signal transduction systems. In J. Wu (Ed.), Technological advancements in biomedicine for healthcare applications (pp. 347–353). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2196-1.ch034

Compilation of References
301
Nakayasu, K., & Sato, C. (2012). Liability for telemedicine. International Journal of E-Health and Medical Communications, 3(1), 1–21. doi:10.4018/jehmc.2012010101
Nalin, M., Verga, M., Sanna, A., & Saranummi, N. (2013). Directions for ICT research in disease prevention. In M. Cruz-Cunha, I. Miranda, & P. Gonçalves (Eds.), Handbook of research on ICTs for human-centered healthcare and social care services (pp. 229–247). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3986-7.ch012
Nap, H. H., & Diaz-Orueta, U. (2013). Rehabilitation gaming. In S. Arnab, I. Dunwell, & K. Debattista (Eds.), Serious games for healthcare: Applications and implications (pp. 50–75). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-1903-6.ch003
Narushima, T., & Ueda, K. (2013). Calcium phosphate coating on titanium by RF magnetron sputtering. In J. Wu (Ed.), Technological advancements in biomedicine for healthcare applica-tions (pp. 223–233). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2196-1.ch024
Nash, J. J., Nash, A. G., Leach, M. E., & Poetker, D. M. (2011). Medical malpractice and corticoste-roid use. Otolaryngology - Head and Neck Surgery, 144(1), 10–15. doi:10.1177/0194599810390470 PMID:21493380
Nava-Muñoz, S., & Morán, A. L. (2013). A review of notifications systems in elder care envi-ronments: Challenges and opportunities. In M. Cruz-Cunha, I. Miranda, & P. Gonçalves (Eds.), Handbook of research on ICTs for human-centered healthcare and social care services (pp. 407–429). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3986-7.ch022
Neal, A., & Griffin, A. (2004). Safety climate and safety at work. In J. Barling & M. Frone (Eds.), The psychology of workplace safety. Washington, DC: American Psychological Association. doi:10.1037/10662-002
Nganji, J. T., & Nggada, S. H. (2014). Adoption of blended learning technologies in selected secondary schools in Cameroon and Nigeria: Challenges in disability inclusion. In N. Ololube (Ed.), Advancing technology and educational development through blended learning in emerg-ing economies (pp. 159–173). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4574-5.ch009
Nichols, L., Aronica, P., & Babe, C. (1998). Are autopsies obsolete? American Journal of Clini-cal Pathology, 110(2), 210–218. doi:10.1093/ajcp/110.2.210 PMID:9704620
Niemann, D., Bertsche, A., Meyrath, D., Koepf, E. D., Traiser, C., Seebald, K., & Bertsche, T. et al. (2015). A prospective three-step intervention study to prevent medication errors in drug handling in paediatric care. Journal of Clinical Nursing, 24(1/2), 101–114. doi:10.1111/jocn.12592 PMID:24890332
Nieva, V., & Sorra, J. (2003). Safety culture assessment: A tool for improving patient safety in healthcare organizations. Quality & Safety in Health Care, 12(Suppl 2), ii17–ii23. doi:10.1136/qhc.12.suppl_2.ii17 PMID:14645891

Compilation of References
302
Nishiguchi, H. (2013). Description of and applications for a motion analysis method for upper limbs. In J. Wu (Ed.), Technological advancements in biomedicine for healthcare applications (pp. 1–10). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2196-1.ch001
Nix, M. P., Coopey, M., & Clancy, C. M. (2006). Quality tools to improve care and prevent er-rors. Journal of Nursing Care Quality, 21(1), 1–4. doi:10.1097/00001786-200601000-00001 PMID:16340679
Noble, D. J., & Donaldson, L. J. (2011). Republished paper: The quest to eliminate intrathecal vincristine errors: a 40-year journey. Postgraduate Medical Journal, 87(1023), 71–74. doi:10.1136/qshc.2008.030874rep PMID:21173052
Noguchi T., & Sathyavagiswaran, L. (2005). The role of the forensic pathologist in quality as-surance and safety of patient care. Medicine and Law, 24(3), 535-47.
Nokata, M. (2013). Small medical robot. In J. Wu (Ed.), Technological advancements in bio-medicine for healthcare applications (pp. 170–179). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2196-1.ch018
Nordén-Hägg, A., Kettis-Lindblad, Å., Ring, L., & Kälvemark-Sporrong, S. (2012). Experiences of a nationwide web-based system: Reporting dispensing errors in Swedish pharmacies. Inter-national Journal of Pharmacy Practice, 20(1), 25–32. doi:10.1111/j.2042-7174.2011.00159.x PMID:22236177
Noritsugu, T. (2013). Wearable power assist robot driven with pneumatic rubber artificial muscles. In J. Wu (Ed.), Technological advancements in biomedicine for healthcare applications (pp. 139–147). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2196-1.ch015
Norman, D. A. (1988). The Design of Everyday Things. New York: Basic Books.
Northcott, H., Vanderheyden, L., Northcott, J., Adair, C., McBrien-Morrison, C., Norton, P., & Cowell, J. (2008). Perceptions of preventable medical errors in Alberta, Canada. International Journal for Quality in Health Care, 20(2), 115–122. doi:10.1093/intqhc/mzm067 PMID:18158295
Noteboom, C. (2013). Physician interaction with EHR: The importance of stakeholder iden-tification and change management. In S. Sarnikar, D. Bennett, & M. Gaynor (Eds.), Cases on healthcare information technology for patient care management (pp. 95–112). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2671-3.ch005
O’Hanlon, S. (2013). Avoiding adverse consequences of e-health. In A. Moumtzoglou & A. Kastania (Eds.), E-health technologies and improving patient safety: Exploring organizational factors (pp. 13–26). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2657-7.ch002
OBrien, J. M. Jr, Kumar, A., & Metersky, M. L. (2013). Does value-based purchasing enhance quality of care and patient outcomes in the ICU? Critical Care Clinics, 29(1), 91–112. doi:10.1016/j.ccc.2012.10.002 PMID:23182530

Compilation of References
303
Odwazny, R., Hasler, S., Abrams, R., & McNutt, R. (2005). Organizational and cultural changes for providing safe patient care. Quality Management in Health Care, 14(3), 132–143. doi:10.1097/00019514-200507000-00002 PMID:16027591
Ogawa, K., Nishio, S., Minato, T., & Ishiguro, H. (2013). Android robots as telepresence media. In J. Wu (Ed.), Biomedical engineering and cognitive neuroscience for healthcare: Interdisciplin-ary applications (pp. 54–63). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2113-8.ch006
Ohashi, M., Sakimura, N., Fujimoto, M., Hori, M., & Kurata, N. (2013). Technical perspective of authentication policy extension for the adaptive social services and e-health care manage-ment. In M. Cruz-Cunha, I. Miranda, & P. Gonçalves (Eds.), Handbook of research on ICTs for human-centered healthcare and social care services (pp. 719–726). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3986-7.ch037
Ohta, Y., & Uchida, M. (2013). Non-contact pulse monitoring using live imaging. In J. Wu (Ed.), Technological advancements in biomedicine for healthcare applications (pp. 240–246). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2196-1.ch026
Oikonomou, D., Moulianitis, V., Lekkas, D., & Koutsabasis, P. (2013). DSS for health emergency response: A contextual, user-centred approach. In R. Biswas (Ed.), Clinical solutions and medical progress through user-driven healthcare (pp. 51–69). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-1876-3.ch006
Okamoto, S., Hirotomi, T., Aoki, K., & Hosomi, Y. (2013). Evaluation of walking motions with the aid of walkers using acceleration sensors. In J. Wu (Ed.), Biomedical engineering and cogni-tive neuroscience for healthcare: Interdisciplinary applications (pp. 346–354). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2113-8.ch036
Okamura, H. (2013). Rehabilitation of elderly people with dementia. In J. Wu (Ed.), Biomedi-cal engineering and cognitive neuroscience for healthcare: Interdisciplinary applications (pp. 235–242). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2113-8.ch024
Olaniyan, J. O., Ghaleb, M., Dhillon, S., & Robinson, P. (2015). Safety of medication use in primary care. International Journal of Pharmacy Practice, 23(1), 3–20. doi:10.1111/ijpp.12120 PMID:24954018
Olsson, C., Forsberg, A., & Bjerså, K. (2016). Safety climate and readiness for implementation of evidence and person centered practice – A national study of registered nurses in general surgical care at Swedish university hospitals. BMC Nursing, 15(1), 54. doi:10.1186/s12912-016-0174-2 PMID:27625589
Olvera-Lobo, M., & Gutiérrez-Artacho, J. (2013). Searching health information in question-answering systems. In M. Cruz-Cunha, I. Miranda, & P. Gonçalves (Eds.), Handbook of research on ICTs for human-centered healthcare and social care services (pp. 474–490). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3986-7.ch025

Compilation of References
304
Ortashi, O., Virdee, V., Hassan, R., Mutrynowski, T., & Abu-Zidan, F. (2013, October). The practice of defensive medicine among hospital doctors in the United Kingdom. BMC Medical Ethics, 14(42). Retrieved from http://bmcmedethics.biomedcentral.com/articles/10.1186/1472-6939-14-42 PMID:24168064
Osborn, S., & Williams, S. (2004). Seven steps to patient safety. An overview guide for NHS staff. Retrieved from http://www. npsa. nhs. uk/nrls/improvingpatientsafety/patient-safety-tools-and-guidance/7steps/
Ott, C. J., & Houry, D. E. (2000). Medical malpractice and the emergency medicine resident. Annals of Emergency Medicine, 36(6), 631–633. doi:10.1067/mem.2000.111063 PMID:11097709
Øvretveit, J. (2009). Does improving quality save money? A review of evidence of which im-provements to quality reduce costs to health service providers. London: The Health Foundation.
Ozdemir, M. H., Cekin, N., Can, I. O., & Hilal, A. (2005). Malpractice and system of exper-tise in anaesthetic procedures in Turkey. Forensic Science International, 153(2-3), 161–167. doi:10.1016/j.forsciint.2004.08.016 PMID:16139105
Padovani, E., Orelli, R. L., Agnoletti, V., & Buccioli, M. (2013). Low cost and human-centered innovations in healthcare services: A case of excellence in Italy. In S. Saeed & C. Reddick (Eds.), Human-centered system design for electronic governance (pp. 239–252). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3640-8.ch014
Palmero, D., Di Paolo, E. R., Beauport, L., Pannatier, A., & Tolsa, J. F. (2016). A bundle with a preformatted medical order sheet and an introductory course to reduce prescription errors in neonates. European Journal of Pediatrics, 175(1), 113–119. doi:10.1007/s00431-015-2607-4 PMID:26272253
Panella, M., Marchisio, S., & Di Stanislao, F. (2003). Reducing clinical variations with clinical pathways: Do pathways work? International Journal for Quality in Health Care, 15(6), 509–521. doi:10.1093/intqhc/mzg057 PMID:14660534
Panella, M., Rinaldi, C., Vanhaecht, K., Donnarumma, C., Tozzi, Q., & Di Stanislao, F. (2014). Second victims of medical errors: A systematic review of the literature. Igiene e Sanita Pubblica, 70(1), 9–28. PMID:24770362
Paninchukunnath, A. (2014). Healthcare services delivery in India: special reference to mother and child health. In A. Goyal (Ed.), Innovations in services marketing and management: Strate-gies for emerging economies (pp. 170–189). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4671-1.ch010
Parasuraman, A., Zeithaml, V. A., & Berry, L. L. (1985). A conceptual model of service quality and its implications for future research. Journal of Marketing, 49(4), 41–50. doi:10.2307/1251430

Compilation of References
305
Parentela, G., Mancini, P., Naccarella, F., Feng, Z., & Rinaldi, G. (2013). Telemedicine, the Eu-ropean space agency, and the support to the african population for infectious disease problems: Potentiality and perspectives for Asia countries and China. In V. Gulla, A. Mori, F. Gabbrielli, & P. Lanzafame (Eds.), Telehealth networks for hospital services: New methodologies (pp. 89–96). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2979-0.ch005
Pate, C. L., & Swofford, M. D. (2016). Organizational integration of decision analytic methods in healthcare settings. In P. Manolitzas, E. Grigoroudis, N. Matsatsinis, & D. Yannacopoulos (Eds.), Effective methods for modern healthcare service quality and evaluation (pp. 45–73). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-9961-8.ch003
Paterson, G. I., MacDonald, J. M., & Mensink, N. N. (2014). The administrative policy quan-dary in Canada’s health service organizations. In C. El Morr (Ed.), Research perspectives on the role of informatics in health policy and management (pp. 116–134). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4321-5.ch008
Paxton, J. H., & Rubinfeld, I. S. (2010). Medical errors education: A prospective study of a new educa-tional tool. American Journal of Medical Quality, 25(2), 135–142. doi:10.1177/1062860609353345 PMID:20110456
Pazokian, M., Tafreshi, M. Z., & Rassouli, M. (2014). Iranian nurses’ perspectives on factors influencing medication errors. International Nursing Review, 61(2), 246–254. doi:10.1111/inr.12086 PMID:24571495
Pegalis, S. E., & Bal, B. S. (2012). Closed medical negligence claims can drive patient safety and reduce litigation. Clinical Orthopaedics and Related Research, 470(5), 1398–1404. doi:10.1007/s11999-012-2308-5 PMID:22419349
Peleg, M., & Tu, S. W. (2009). Design patterns for clinical guidelines. Artificial Intelligence in Medicine, 47(1), 1–24. doi:10.1016/j.artmed.2009.05.004 PMID:19500956
Pellino, I. M., & Pellino, G. (2015, December). Consequences of defensive medicine, second victims, and clinical-judicial syndrome on surgeons medical practice and on health service. Updates in Surgery, 67(4), 331–337. doi:10.1007/s13304-015-0338-8 PMID:26650202
Pereira, O. R., Caldeira, J. M., & Rodrigues, J. J. (2013). An advanced and secure symbian-based mobile approach for body sensor networks interaction. In J. Rodrigues (Ed.), Digital advances in medicine, e-health, and communication technologies (pp. 33–48). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2794-9.ch002
Perkins, G. D., McAuley, D. F., Davies, S., & Gao, F. (2003). Discrepancies between clinical and postmortem diagnoses in critically ill patients: An observational study. Journal of Critical Care, 7(6), 129–132. doi:10.1186/cc2359 PMID:14624686
Perna, G. (2014). Study: Better Verbal, Written Communication During Provider Handoffs Reduces Medical Errors. Retrieved from http://www.healthcare-informatics.com/news-item/study-better-verbal-written-communication-during-provider-handoffs-reduces-medical-errors
Compilation of References
306
Petersen, L. A., Woodard, L. D., Urech, T., Daw, C., & Sookanan, S. (2006). Does pay-for-performance improve the quality of health care? Annals of Internal Medicine, 145(4), 265–272. doi:10.7326/0003-4819-145-4-200608150-00006 PMID:16908917
Peters, T., & Waterman, R. (1982). In search of excellence: lessons from America’s best run companies. New York: Harper and Rowe.
Phua, C., Roy, P. C., Aloulou, H., Biswas, J., Tolstikov, A., & Foo, V. S. … Xu, D. (2014). State-of-the-art assistive technology for people with dementia. In Assistive technologies: Concepts, methodologies, tools, and applications (pp. 1606-1625). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4422-9.ch085
Piko, B. F. (2006). Burnout, role conflict, job satisfaction and psychosocial health among Hun-garian health care staff: A questionnaire survey. International Journal of Nursing Studies, 43(3), 311–318. doi:10.1016/j.ijnurstu.2005.05.003 PMID:15964005
Pino, A. (2014). Augmentative and alternative communication systems for the motor disabled. In G. Kouroupetroglou (Ed.), Disability informatics and web accessibility for motor limitations (pp. 105–152). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4442-7.ch004
Poetker, D. M., & Smith, T. L. (2015). Medicolegal Implications of Common Rhinologic Medica-tions. Otolaryngologic Clinics of North America, 48(5), 817–826. doi:10.1016/j.otc.2015.05.009 PMID:26117297
Portela, F., Cabral, A., Abelha, A., Salazar, M., Quintas, C., Machado, J., & Santos, M. F. et al. (2013). Knowledge acquisition process for intelligent decision support in critical health care. In R. Martinho, R. Rijo, M. Cruz-Cunha, & J. Varajão (Eds.), Information systems and technologies for enhancing health and social care (pp. 55–68). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3667-5.ch004
Pratt, S. D., & Jachna, B. R. (2015). Care of the clinician after an adverse event. International Journal of Obstetric Anesthesia, 24(1), 54–63. doi:10.1016/j.ijoa.2014.10.001 PMID:25499810
Pratt, S., Kenney, L., Scott, S. D., & Wu, A. W. (2012, April). How to develop a second victim support program: A toolkit for health care organizations. Joint Commission Journal on Qual-ity and Patient Safety, 38(5), 235–240. doi:10.1016/S1553-7250(12)38030-6 PMID:22649864
Previtali, P. (2013). Grid technology for archive solutions in health care organizations. In A. Moumtzoglou & A. Kastania (Eds.), E-health technologies and improving patient safety: Exploring organizational factors (pp. 148–154). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2657-7.ch010
Profit, J., Lee, H. C., Sharek, P. J., Kan, P., Nisbet, C. C., Thomas, E. J., & Sexton, B. et al. (2015). Comparing NICU teamwork and safety climate across two commonly used survey instruments. BMJ Quality & Safety. doi:10.1136/bmjqs-2014-003924 PMID:26700545

Compilation of References
307
Pronovost, P. J., Weast, B., Holzmueller, C. G., Rosenstein, B. J., Kidwell, R. P., Haller, K. B., & Rubin, H. R. et al. (2003). Evaluation of the culture of safety: Survey of clinicians and managers in an academic medical center. Quality & Safety in Health Care, 12(6), 405–410. doi:10.1136/qhc.12.6.405 PMID:14645754
Pronovost, P., & Sexton, B. (2005). Assessing safety culture: Guidelines and recommendations. Quality & Safety in Health Care, 14(4), 231–233. doi:10.1136/qshc.2005.015180 PMID:16076784
Qi, G., & Wu, J. (2013). Functional role of the left ventral occipito-temporal cortex in reading. In J. Wu (Ed.), Biomedical engineering and cognitive neuroscience for healthcare: Interdisciplinary applications (pp. 192–200). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2113-8.ch020
Quality Interagency Coordination Task Force. (n.d.). Retrieved from https://archive.ahrq.gov/quic/
Queirós, A., Alvarelhão, J., Silva, A. G., Teixeira, A., & Pacheco da Rocha, N. (2013). A concep-tual framework for the design and development of AAL services. In M. Cruz-Cunha, I. Miranda, & P. Gonçalves (Eds.), Handbook of research on ICTs for human-centered healthcare and social care services (pp. 568–586). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3986-7.ch030
Raab, S. S., & Grzybicki, D. M. (2010). Quality in cancer diagnosis. CA: a Cancer Journal for Clinicians, 60(3), 139–165. doi:10.3322/caac.20068 PMID:20444999
Rafter, N., Hickey, A., Condell, S., Conroy, R., O’Connor, P., Vaughan, D., & Williams, D. (2014, July). Adverse events in healthcare: Learning from mistakes. Quarterly Journal of Medicine: An International Journal of Medicine. doi:10.1093/qjmed/hcu145
Rasmussen, J. (1983). Skills, rules, and knowledge; signals, signs, and symbols, and other dis-tinctions in human performance models. Systems, Man and Cybernetics, IEEE Transactions on, (3), 257-266.
Rasmussen, J. (1982). Human errors: A taxonomy for describing human malfunction in in-dustrial installations. Journal of Occupational Accidents, 4(2-4), 311–335. doi:10.1016/0376-6349(82)90041-4
Rathert, C., & Phillips, W. (2010). Medical error disclosure training: Evidence for values-based ethical environments. Journal of Business Ethics, 97(3), 491–503. doi:10.1007/s10551-010-0520-3
Ravka, N. (2014). Informatics and health services: The potential benefits and challenges of elec-tronic health records and personal electronic health records in patient care, cost control, and health research – An overview. In C. El Morr (Ed.), Research perspectives on the role of informatics in health policy and management (pp. 89–114). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4321-5.ch007
Reason, J. (1990). Human Error. Cambridge, UK: Cambridge University Press. doi:10.1017/CBO9781139062367
Reason, J. (1995a). Understanding adverse events: Human factors. Quality in Health Care, 4(2), 80–89.

Compilation of References
308
Reason, J. (1995b). Safety in the operating theatre—Part 2: Human error and organisational failure. Current Anaesthesia and Critical Care, 6(2), 121–126. doi:10.1016/S0953-7112(05)80010-9
Reason, J. (1997). Managing the risks of organizational accidents. Aldershot, UK: Ashgate.
Reason, J. (1998). Achieving a safe culture: Theory and practice. Work and Stress, 12(3), 293–306. doi:10.1080/02678379808256868
Reason, J. (2000). Human error: Models and management. BMJ (Clinical Research Ed.), 320(7237), 768–770. doi:10.1136/bmj.320.7237.768 PMID:10720363
Reason, J., Manstead, A., Stradling, S., Baxter, J., & Campbell, K. (1990). Errors and violations on the roads: A real distinction? Ergonomics, 33(10-11), 1315–1332. doi:10.1080/00140139008925335 PMID:20073122
Redley, B., & Botti, M. (2013). Reported medication errors after introducing an electronic medi-cation management system. Journal of Clinical Nursing, 22(3/4), 579–589. doi:10.1111/j.1365-2702.2012.04326.x PMID:22998067
Reibling, N., & Wendt, C. (2013). Regulating patients’ access to healthcare services. In M. Merviö (Ed.), Healthcare management and economics: Perspectives on public and private administration (pp. 53–68). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3982-9.ch005
Reis, C. I., Freire, C. S., Fernández, J., & Monguet, J. M. (2013). Patient centered design: Chal-lenges and lessons learned from working with health professionals and schizophrenic patients in e-therapy contexts. In R. Martinho, R. Rijo, M. Cruz-Cunha, & J. Varajão (Eds.), Information systems and technologies for enhancing health and social care (pp. 120–135). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3667-5.ch008
Renkema, E., Broekhuis, M., & Ahaus, K. (2014, January). Conditions that influence the im-pact of malpractice litigation risk on physicians’ behavior regarding patient safety. BMC Health Services Research, 14(38). Retrieved from http://www.biomedcentral.com/1472-6963/14/38 PMID:24460754
Rice, R. B. (2003). Patient safety: Who guards the patient. Online Journal of Issues in Nursing, 8(3), 1. PMID:14656190
Ricketts, M. (2014). Making health information personal: How anecdotes bring concepts to life. In S. Hai-Jew (Ed.), Packaging digital information for enhanced learning and analysis: Data visualization, spatialization, and multidimensionality (pp. 1–36). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4462-5.ch001
Riga, M., Vozikis, A., & Pollalis, Y. (2014). Medical Errors in Greece: An Economic Analysis of Compensations Awarded by Civil Courts (20002009). Open Journal of Applied Sciences, 4(04), 168–175. doi:10.4236/ojapps.2014.44017
Riga, M., Vozikis, A., Pollalis, Y., & Souliotis, K. (2015). Medical Error Reporting Information System as an innovative patient safety intervention : A health policy perspective. Health Policy (Amsterdam), 119(4), 539–548. doi:10.1016/j.healthpol.2014.12.006 PMID:25554702

Compilation of References
309
Robbennolt, J. K. (2009). Apologies and medical error. Clinical Orthopaedics and Related Re-search, 467(2), 376–382. doi:10.1007/s11999-008-0580-1 PMID:18972177
Rocha, Á. (2013). Evolution of information systems and technologies maturity in healthcare. In J. Tan (Ed.), Healthcare information technology innovation and sustainability: Frontiers and adoption (pp. 238–246). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2797-0.ch015
Rodríguez-Gómez, D., & Gairín, J. (2014). Communities of practice in the Catalan public ad-ministration: Promoting their improvement. In Y. Al-Bastaki & A. Shajera (Eds.), Building a competitive public sector with knowledge management strategy (pp. 383–402). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4434-2.ch018
Rodríguez-Solano, C., Lezcano, L., & Sicilia, M. (2013). Automated generation of SNOMED CT subsets from clinical guidelines. In R. Martinho, R. Rijo, M. Cruz-Cunha, & J. Varajão (Eds.), Information systems and technologies for enhancing health and social care (pp. 190–204). Her-shey, PA: IGI Global. doi:10.4018/978-1-4666-3667-5.ch013
Rosemann, M., & Zur Muehlen, M. (2005). Integrating risks in business process models. ACIS 2005 Proceedings, 50.
Rosenorn-Lanng, D., & Michell, V. (2014). The SHEEP Model; Applying Near Miss Analysis. In Patient Safety and Quality Care through Health Informatics. IGI.
Rosenorn-Lanng, D. (2014). Human Factors in Healthcare: Level One. Oxford University Press.
Rosenthal, M. M., Cornett, P. L., Sutcliffe, K. M., & Lewton, E. (2005). Beyond the medical record. Journal of General Internal Medicine, 20(5), 404–409. doi:10.1111/j.1525-1497.2005.0098.x PMID:15963161
Ross, S., Bond, C., Rothnie, H., Thomas, S., & Macleod, M. J. (2009). What is the scale of prescribing errors committed by junior doctors? A systematic review. British Journal of Clini-cal Pharmacology, 67(6), 629–640. doi:10.1111/j.1365-2125.2008.03330.x PMID:19094162
Rosu, S. M., & Dragoi, G. (2014). E-health sites development using open source software and OMT methodology as support for family doctors’ activities: A Romanian case study. In M. Cruz-Cunha, F. Moreira, & J. Varajão (Eds.), Handbook of research on enterprise 2.0: Technological, social, and organizational dimensions (pp. 72–88). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4373-4.ch004
Rothschild, J. M., Federico, F. A., Gandhi, T. K., Kaushal, R., Williams, D. H., & Bates, D. W. (2002). Analysis of medication- related malpractice claims: Causes, preventability, and costs. Archives of Internal Medicine, 162(21), 2414–2420. doi:10.1001/archinte.162.21.2414 PMID:12437399
Rothschild, J. M., Landrigan, C. P., Cronin, J. W., Kaushal, R., Lockley, S. W., Burdick, E., & Bates, D. W et al.. (2005). The Critical Care Safety Study: The incidence and nature of adverse events and serious medical errors in intensive care. Critical Care Medicine, 33(8), 1694–1700. doi:10.1097/01.CCM.0000171609.91035.BD PMID:16096443

Compilation of References
310
Rothwell, C., Burford, B., Morrison, J., Morrow, G., Allen, M., Davies, C., & Illing, J. et al. (2012). Junior doctors prescribing: Enhancing their learning in practice. British Journal of Clini-cal Pharmacology, 73(2), 194–202. doi:10.1111/j.1365-2125.2011.04061.x PMID:21752067
Rouse, R. A., & Kaplan, J. B. (2008). Why do some hospital leaders “speak no evil” about their organizations’ medical errors? The Journal of Leadership Studies, 2(3), 6–16. doi:10.1002/jls.20070
Ryan, K., Schnatz, P., Greene, J., & Curry, S. (2005). Change in cesarean section rate as a re-flection of the present malpractice crisis. Connecticut Medicine, 69, 139–141. PMID:15861999
Sadiq, S., Governatori, G., & Namiri, K. (2007). Modeling control objectives for business pro-cess compliance. In Business process management (pp. 149–164). Springer Berlin Heidelberg. doi:10.1007/978-3-540-75183-0_12
Saha, P. (2014). Systemic enterprise architecture as future: Tackling complexity in governments in the cusp of change. In P. Saha (Ed.), A systemic perspective to managing complexity with en-terprise architecture (pp. 1–70). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4518-9.ch001
Saijo, Y. (2013). Biomedical application of multimodal ultrasound microscope. In J. Wu (Ed.), Technological advancements in biomedicine for healthcare applications (pp. 27–35). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2196-1.ch004
Sammer, C. E., Lykens, K., Singh, K. P., Mains, D. A., & Lackan, N. A. (2010). What is patient safety culture? A review of the literature. Journal of Nursing Scholarship, 42(2), 156–165. doi:10.1111/j.1547-5069.2009.01330.x PMID:20618600
Sandilands, E. A., Reid, K., Shaw, L., Bateman, D. N., Webb, D. J., Dhaun, N., & Kluth, D. C. (2011). Impact of a focussed teaching programme on practical prescribing skills among final year medical students. British Journal of Clinical Pharmacology, 71(1), 29–33. doi:10.1111/j.1365-2125.2010.03808.x PMID:21143498
Santiago, T. H., & Turrini, R. N. (2015). Organizational culture and climate for patient safety in Intensive Care Units. Revista da Escola de Enfermagem da U S P., 49, 123–130. doi:10.1590/S0080-623420150000700018 PMID:26761702
Santos, M. F., Portela, F., Miranda, M., Machado, J., Abelha, A., Silva, Á., & Rua, F. (2013). Grid data mining strategies for outcome prediction in distributed intensive care units. In R. Martinho, R. Rijo, M. Cruz-Cunha, & J. Varajão (Eds.), Information systems and technologies for enhancing health and social care (pp. 87–101). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3667-5.ch006
Santos, M., Bastião, L., Costa, C., Silva, A., & Rocha, N. (2013). Clinical data mining in small hospital PACS: Contributions for radiology department improvement. In R. Martinho, R. Rijo, M. Cruz-Cunha, & J. Varajão (Eds.), Information systems and technologies for enhancing health and social care (pp. 236–251). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3667-5.ch016

Compilation of References
311
Santos, R. J., Bernardino, J., & Vieira, M. (2013). A hypotension surveillance and prediction system for critical care. In M. Cruz-Cunha, I. Miranda, & P. Gonçalves (Eds.), Handbook of re-search on ICTs and management systems for improving efficiency in healthcare and social care (pp. 341–355). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3990-4.ch017
Sanz, P. R., Mezcua, B. R., & Pena, J. M. (2013). ICTs for orientation and mobility for blind people: A state of the art. In M. Cruz-Cunha, I. Miranda, & P. Gonçalves (Eds.), Handbook of research on ICTs for human-centered healthcare and social care services (pp. 646–669). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3986-7.ch034
Sasayama, T., Hamada, S., & Kobayashi, T. (2013). Application of prewhitening beamformer with linear constraints for correlated EEG signal source estimation. In J. Wu (Ed.), Biomedi-cal engineering and cognitive neuroscience for healthcare: Interdisciplinary applications (pp. 243–254). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2113-8.ch025
Satoh, J. (2013). Molecular network analysis of target RNAs and interacting proteins of TDP-43, a causative gene for the neurodegenerative diseases ALS/FTLD. In J. Wu (Ed.), Technological advancements in biomedicine for healthcare applications (pp. 314–335). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2196-1.ch032
Sato, T., & Minato, K. (2013). Differences in analysis methods of the human uncinate fasciculus using diffusion tensor MRI. In J. Wu (Ed.), Biomedical engineering and cognitive neurosci-ence for healthcare: Interdisciplinary applications (pp. 162–170). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2113-8.ch017
Schafer, S. B. (2013). Fostering psychological coherence: With ICTs. In M. Cruz-Cunha, I. Mi-randa, & P. Gonçalves (Eds.), Handbook of research on ICTs for human-centered healthcare and social care services (pp. 29–47). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3986-7.ch002
Schifrin, B. S., & Cohen, W. R. (2013). The effect of malpractice claims on the use of caesar-ean section. Best Practice & Research. Clinical Obstetrics & Gynaecology, 27(2), 269–283. doi:10.1016/j.bpobgyn.2012.10.004 PMID:23206669
Schmeida, M., & McNeal, R. (2013). Bridging the inequality gap to accessing medicare and med-icaid information online: An empirical analysis of e-government success 2002 through 2010. In J. Gil-Garcia (Ed.), E-government success around the world: Cases, empirical studies, and practical recommendations (pp. 60–78). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4173-0.ch004
Scholl, J. C., & Olaniran, B. A. (2013). ICT use and multidisciplinary healthcare teams. In M. Cruz-Cunha, I. Miranda, & P. Gonçalves (Eds.), Handbook of research on ICTs for human-centered healthcare and social care services (pp. 627–645). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3986-7.ch033
Schwappach, D. L. B. (2014). Risk factors for patient-reported medical errors in eleven countries. Health Expectations, 17(3), 321–331. doi:10.1111/j.1369-7625.2011.00755.x PMID:22296575

Compilation of References
312
Schwappach, D. L. B., & Boluarteb, T. A. (2008). The emotional impact of medical error in-volvement on physicians: A call for leadership and organisational accountability. Swiss Medical Weekly, 138(1–2), 9–15. PMID:18951201
Schwappach, D. L. B., & Wernli, M. (2010). Medication errors in chemotherapy: Incidence, types and involvement of patients in prevention. A review of the literature. European Journal of Cancer Care, 19(3), 285–292. doi:10.1111/j.1365-2354.2009.01127.x PMID:19708929
Schwappach, D. L., & Boluarte, T. A. (2009). The emotional impact of medical error involvement on physicians: A call for leadership and organizational accountability. Swiss Medical Weekly, 139(1), 9. PMID:18951201
Schwoebel, A., & Creely, J. (2010). Improving the safety of neonatal care through the develop-ment and implementation of a staff-focused delta team. The Journal of Perinatal & Neonatal Nursing, 24(1), 81–87. doi:10.1097/JPN.0b013e3181ce33ab PMID:20147835
Scott, S. D. (2011, May). The second victim phenomenon: A harsh reality of health care profes-sions. Patient Safety Network. Retrieved from https://psnet.ahrq.gov/perspectives/perspective/102
Scott, S. D. (2015a, October). Second victim support: Implications for patient safety attitudes and perceptions. PSQH. Retrieved from http://www.psqh.com/analysis/second-victim-support-implications-for-patient-safety-attitudes-and-perceptions/
Scott, S. D. (2015b, September). The second victim experience: Mitigating the harm. American Nurse Today, 10(9), 8-11. Retrieved from http://www.americannursetoday.com/wp-content/uploads/2015/09/ant9-Second-victim-820.pdf
Scott, A., Sivey, P., Ait Ouakrim, D., Willenberg, L., Naccarella, L., Furler, J., & Young, D. (2011). The effect of financial incentives on the quality of health care provided by primary care physicians. Cochrane Database of Systematic Reviews, (9): CD008451. PMID:21901722
Scott, S. D., Hirschinger, L. E., Cox, K. R., McCoig, M., Brandt, J., & Hall, L. W. (2009). The natural history of recovery for the healthcare provider second victim after adverse patient events. Quality & Safety in Health Care, 18(5), 325–330. doi:10.1136/qshc.2009.032870 PMID:19812092
Seki, Y., & Yamasaki, Y. (2006). Effects of working conditions on intravenous medication errors in a Japanese hospital. Journal of Nursing Management, 14(2), 128–139. doi:10.1111/j.1365-2934.2006.00597.x PMID:16487424
Semel, M. E., Resch, S., Haynes, A. B., Funk, L. M., Bader, A., Berry, W. R., & Gawande, A. A. et al. (2010). Adopting a surgical safety checklist could save money and improve the qual-ity of care in US hospitals. Health Affairs, 29(9), 1593–1599. doi:10.1377/hlthaff.2009.0709 PMID:20820013
Senders, J., & Moray, N. (1991). Human Error: Cause, Prediction and Reduction. Mahwah, NJ: Lawrence Erlbaum.

Compilation of References
313
Serrano, M., Elmisery, A., Foghlú, M. Ó., Donnelly, W., Storni, C., & Fernström, M. (2013). Pervasive computing support in the transition towards personalised health systems. In J. Rodrigues (Ed.), Digital advances in medicine, e-health, and communication technologies (pp. 49–64). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2794-9.ch003
Sevdalis, N., Jacklin, R., Arora, S., Vincent, C. A., & Thomson, R. G. (2010). Diagnostic error in a national incident reporting system in the UK. Journal of Evaluation in Clinical Practice, 16(6), 1276–1281. doi:10.1111/j.1365-2753.2009.01328.x PMID:20727061
Sewal, R. K., Singh, P. K., Prakash, A., Kumar, B., & Medhi, B. (2014). A prospective study to evaluate awareness about medication errors amongst health-care personnel representing North, East, West Regions of India. International Journal of Applied and Basic Medical Research, 4(1), 43–46. doi:10.4103/2229-516X.125694 PMID:24600578
Sexton, J. B., Berenholtz, S. M., Goeschel, C. A., Watson, S. R., Holzmueller, C. G., Thompson, D. A., & Pronovost, P. J. et al. (2011). Assessing and improving safety climate in a large cohort of in-tensive care units. Critical Care Medicine, 39(5), 934–939. doi:10.1097/CCM.0b013e318206d26c PMID:21297460
Sexton, J. B., Makary, M. A., Tersigni, A. R., Pryor, D., Hendrich, A., Thomas, E. J., & Pronovost, P. J. et al. (2006). Teamwork in the operating room: Frontline perspectives among hospitals and operating room personnel. Anesthesiology, 105(5), 877–884. doi:10.1097/00000542-200611000-00006 PMID:17065879
Seys, D., Scott, S., Wu, A., Van Garven, E., Vleugels, A., Euwema, M., & Vanhaecht, K. et al. (2013). Supporting involved health care professionals (second victims) following an adverse health event: A literature review. International Journal of Nursing Studies, 50(5), 678–687. doi:10.1016/j.ijnurstu.2012.07.006 PMID:22841561
Seys, D., Wu, A. W., Van Gerven, E., Vleugels, A., Euwema, M., Panella, M., & Vanhaecht, K. (2013). Health care professionals as second victims after adverse events: A systematic re-view. Evaluation & the Health Professions, 36(2), 135–162. doi:10.1177/0163278712458918 PMID:22976126
Shabot, M., & LoBue, M. (1995). Real-time wireless decision support alerts on a palmtop PDA. Proceedings of the Annual Symposium on Computer Applications in Medical Care, 19, 174–177. PMID:8563261
Shabot, M., LoBue, M., & Chen, J. (2000) Wireless clinical alerts for critical medication, labora-tory and physiologic data.Proceedings of the 33rd Hawaii International Conference on System Sciences (HICSS, Washington, DC: IEEE Computer Society. doi:10.1109/HICSS.2000.926784
Shah, R. K., Lander, L., Forbes, P., Jenkins, K., Healy, G. B., & Roberson, D. W. (2009). Safety on an inpatient pediatric otolaryngology service: Many small errors, few adverse events. The Laryngoscope, 119(5), 871–879. doi:10.1002/lary.20208 PMID:19358191
Compilation of References
314
Shahrokhi, A., Ebrahimpour, F., & Ghodousi, A. (2013). Factors effective on medication errors: A nursing view. Journal of Research in Pharmacy Practice, 2(1), 18–23. doi:10.4103/2279-042X.114084 PMID:24991599
Shamliyan, T. A., Duval, S., Du, J., & Kane, R. L. (2008). Just what the doctor ordered. Review of the evidence of the impact of computerized physician order entry system on medication errors. Health Services Research, 43(1p1), 32–53.
Shannon, H. S., Mayr, J., & Haines, T. (1997). Overview of the relationship between organi-zational and workplace factors and injury rates. Safety Science, 26(3), 201–217. doi:10.1016/S0925-7535(97)00043-X
Shappel, S. A., & Wiegmann, D. A. (2000). The human factors analysis and classification system--HFACS (No. DOT/FAA/AM-00/7). US Federal Aviation Administration, Office of Avia-tion Medicine.
Sharma, G., Awasthi, S., Dixit, A., & Sharma, G. (2011). Patient safety risk assessment and risk management: A review on Indian hospitals. Chronicles of Young Scientists, 2(4), 186–191. doi:10.4103/2229-5186.93022
Sharpe, V. A. (2015, January). Mistakes, medical. In H. ten Have (Ed.), Encyclopedia of global bioethics (pp. 1–8). Springer International Publishing. doi:10.1007/978-3-319-05544-2_296-1
Shawahna, R., Rahman, N. U., Ahmad, M., Debray, M., Yliperttula, M., & Declèves, X. (2011). Electronic prescribing reduces prescribing error in public hospitals. Journal of Clinical Nursing, 20(21/22), 3233–3245. doi:10.1111/j.1365-2702.2011.03714.x PMID:21627699
Sheu, S. J., Wei, I. L., Chen, C. H., Yu, S., & Tang, F. I. (2009). Using snowball sampling method with nurses to understand medication administration errors. Journal of Clinical Nursing, 18(4), 559–569. doi:10.1111/j.1365-2702.2007.02048.x PMID:18298506
Shibata, T. (2013). A human-like cognitive computer based on a psychologically inspired VLSI brain model. In J. Wu (Ed.), Technological advancements in biomedicine for healthcare applica-tions (pp. 247–266). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2196-1.ch027
Shimada, S. (2013). Self-body recognition and its impairment. In J. Wu (Ed.), Biomedical engi-neering and cognitive neuroscience for healthcare: Interdisciplinary applications (pp. 156–161). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2113-8.ch016
Shimogonya, Y., Ishikawa, T., Yamaguchi, T., Kumamaru, H., & Itoh, K. (2013). Computational study of the hemodynamics of cerebral aneurysm initiation. In J. Wu (Ed.), Technological ad-vancements in biomedicine for healthcare applications (pp. 267–277). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2196-1.ch028
Shimonomura, K. (2013). A neuromorphic robot vision system to predict the response of visual neurons. In J. Wu (Ed.), Technological advancements in biomedicine for healthcare applications (pp. 193–199). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2196-1.ch020

Compilation of References
315
Shojania, K. G., & Burton, E. C. (2008). The vanishing non forensic autopsy. The New England Journal of Medicine, 358(9), 873–875. doi:10.1056/NEJMp0707996 PMID:18305264
Shojania, K. G., Burton, E. C., McDonald, K. M., & Goldmann, L. (2003). Changes in rates of autopsy-detected diagnostic errors over time: A systematic review. Journal of the American Medical Association, 289(21), 2849–2856. doi:10.1001/jama.289.21.2849 PMID:12783916
Shrestha, S. (2013). Clinical decision support system for diabetes prevention: An illustrative case. In S. Sarnikar, D. Bennett, & M. Gaynor (Eds.), Cases on healthcare information technology for patient care management (pp. 308–329). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2671-3.ch017
Siddiqui, Z. S., & Jonas-Dwyer, D. R. (2013). Mobile learning in health professions education: A systematic review. In J. Keengwe (Ed.), Pedagogical applications and social effects of mobile technology integration (pp. 193–205). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2985-1.ch011
Silva, N. D., Barbosa, A. P., Padilha, K. G., & Malik, A. M. (2016). Patient safety in orga-nizational culture as perceived by leaderships of hospital institutions with different types of administration. Revista da Escola de Enfermagem da U S P., 50(3), 490–497. doi:10.1590/S0080-623420160000400016 PMID:27556721
Silvana de Rosa, A., Fino, E., & Bocci, E. (2014). Addressing healthcare on-line demand and supply relating to mental illness: Knowledge sharing about psychiatry and psychoanalysis through social networks in Italy and France. In A. Kapoor & C. Kulshrestha (Eds.), Dynamics of competitive advantage and consumer perception in social marketing (pp. 16–55). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4430-4.ch002
Sirriyeh, R., Lawton, R., Gardner, P., & Armitage, G. (2010). Coping with medical error: A systematic review of papers to assess the effects of involvement in medical errors on healthcare professionals’ psychological well-being. BMJ Quality and Safety in Health Care, 19(6), 1–8. PMID:20513788
Smits, M., Groenewegen, P., Timmermans, D., van der Wal, G., & Wagner, C. (2009). The na-ture and causes of unintended events reported at ten emergency departments. BMC Emergency Medicine, 9(1), 16. doi:10.1186/1471-227X-9-16 PMID:19765275
Smits, M., Wagner, C., Spreeuwenberg, P., van der Wal, G., & Groenewegen, P. P. (2009). Measuring patient safety culture: An assessment of the clustering of responses at unit level and hospital level. Quality & Safety in Health Care, 18(4), 292–296. doi:10.1136/qshc.2007.025965 PMID:19651934
Smorti, A., Cappelli, F., Zarantonello, R., Tani, F., & Gensini, G. F. (2014). Medical error and systems of signaling: Conceptual and linguistic definition. Internal and Emergency Medicine, 9(6), 681–688. doi:10.1007/s11739-014-1108-1 PMID:25034521

Compilation of References
316
Sobol, M., & Prater, E. (2013). Adoption, usage and efficiency: Benchmarking healthcare IT in private practices. In J. Tan (Ed.), Healthcare information technology innovation and sustain-ability: Frontiers and adoption (pp. 145–159). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2797-0.ch009
Sobrinho, Á. A., Dias da Silva, L., Melo de Medeiros, L., & Pinheiro, M. E. (2013). A mobile assistant to aid early detection of chronic kidney disease. In R. Martinho, R. Rijo, M. Cruz-Cunha, & J. Varajão (Eds.), Information systems and technologies for enhancing health and social care (pp. 309–323). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3667-5.ch020
Soomlek, C., & Benedicenti, L. (2013). Agent-based wellness indicator. In V. Gulla, A. Mori, F. Gabbrielli, & P. Lanzafame (Eds.), Telehealth networks for hospital services: New methodologies (pp. 300–330). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2979-0.ch020
Sorra, J. S., & Nieva, V. F. (2004). Hospital survey on patient safety culture. Rockville, MD: Agency for Healthcare Research and Quality.
Sox, H. C., & Woloshin, S. (2000). How many deaths are due to medical error? Getting the number right. Effective Clinical Practice, 3(6), 277–283. PMID:11151524
Spadaro, L., Timpano, F., Marino, S., & Bramanti, P. (2013). Telemedicine and Alzheimer disease: ICT-based services for people with Alzheimer disease and their caregivers. In V. Gulla, A. Mori, F. Gabbrielli, & P. Lanzafame (Eds.), Telehealth networks for hospital services: New methodologies (pp. 191–206). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2979-0.ch013
Spath, P. L. (2000). Patient safety improvement guidebook. Forest Grove, OR: Brown-Spath & Associates.
Spath, P. L. (2003). Using failure mode and effects analysis to improve patient safety. AORN Journal, 78(1), 15–37. doi:10.1016/S0001-2092(06)61343-4 PMID:12885066
Stamm, J.A., Korzick, K.A., Beech, K., & Wood, K.E. (2016). Medical Malpractice: Reform for Today’s Patients and Clinicians. The American Journal of Medicine, 129(1), 20-5.
Stamper, R. (1994). Social norms in requirements analysis: an outline of MEASUR. Academic Press Professional, Inc.
Stangierski, A., Warmuz-Stangierska, I., Ruchala, M., Zdanowska, J., Glowacka, M. D., Sowin-ski, J., & Ruchala, P. (2012). Short communication: Medical errors-not only patients problem. Archives of Medical Science, 8(3), 569–574. doi:10.5114/aoms.2012.29539 PMID:22852017
Stanton, N. A., Chambers, P. R., & Piggott, J. (2001). Situational awareness and safety. Safety Science, 39(3), 189–204. doi:10.1016/S0925-7535(01)00010-8
Start, R. D., & Cross, S. S. (1999). Pathological investigation of deaths following surgery, anesthesia, and medical procedures. Journal of Clinical Pathology, 52, 640–652. doi:10.1136/jcp.52.9.640 PMID:10655984

Compilation of References
317
Stefaniak, J. E. (2013). Resuscitating team roles within wayburn health system. In A. Ritzhaupt & S. Kumar (Eds.), Cases on educational technology implementation for facilitating learning (pp. 130–145). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3676-7.ch008
Stievano, A., Jurado, M. G., Rocco, G., & Sasso, L. (2009). A new information exchange system for nursing professionals to enhance patient safety across Europe. Journal of Nursing Scholarship, 41(4), 391–398. doi:10.1111/j.1547-5069.2009.01307.x PMID:19941585
Stratton, A. (2011). Hospitals will be forced to admit medical errors, says government. Retrieved from http://www.theguardian.com/politics/2011/jun/20/hospitals-forced-to-admit-errors
Studdert, D. M., Mello, M. M., & Brennan, T. A. (2004). Medical malpractice. The New England Journal of Medicine, 350(3), 283–292. doi:10.1056/NEJMhpr035470 PMID:14724310
Studdert, D. M., Mello, M. M., Gawande, A. A., Gandhi, T. K., Kachalia, A., Yoon, C., & Brennan, T. A. et al. (2006). Claims, errors, and compensation payments in medical malpractice litiga-tion. The New England Journal of Medicine, 354(19), 2024–2033. doi:10.1056/NEJMsa054479 PMID:16687715
Studdert, D. M., Mello, M. M., Sage, W. M., DesRoches, C. M., Peugh, J., Zapert, K., & Brennan, T. A. (2005). Defensive medicine among high-risk specialist physicians in a volatile malpractice environment. Journal of the American Medical Association, 293(21), 2609–2617. doi:10.1001/jama.293.21.2609 PMID:15928282
Studdert, D., Mello, M., & Brennan, T. (2010). Defensive medicine and tort reform: A wide view. Journal of General Internal Medicine, 25(5), 380–381. doi:10.1007/s11606-010-1319-8 PMID:20349156
Stump, S. (2000). Re-engineering the medication error-reporting process: Removing the blame and improving the system. American Journal of Health-System Pharmacy, 57(4), S10–S17. PMID:11148939
Sugiura, M. (2013). A cognitive neuroscience approach to self and mental health. In J. Wu (Ed.), Biomedical engineering and cognitive neuroscience for healthcare: Interdisciplinary applications (pp. 1–10). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2113-8.ch001
Supnithi, T., Buranarach, M., Thatphithakkul, N., Junsirimongkol, B., Wongrochananan, S., Kulnawan, N., & Jiamjarasrangsi, W. (2014). A self-management service framework to support chronic disease patients’ self-management. In M. Kosaka & K. Shirahada (Eds.), Progressive trends in knowledge and system-based science for service innovation (pp. 425–450). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4663-6.ch023
Sura, A., & Shah, N. R. (2010). Pay-for-Performance Initiatives: Modest Benefits for Improv-ing Healthcare Quality. American Health and Drug Benefits, 3(2), 135–142. PMID:25126315
Swaminath, G., & Raguram, R. (2010). Medical errors – I: The problem. Indian Journal of Psychiatry, 52(2), 110–112. doi:10.4103/0019-5545.64580 PMID:20838497

Compilation of References
318
Swidler, A. (1986). Culture in action: Symbols and strategies. American Sociological Review, 51(2), 273–286. doi:10.2307/2095521
Szekendi, M. K., Sullivan, C., Bobb, A., Feinglass, J., Rooney, D., Barnard, C., & Noskin, G. A. (2006). Active surveillance using electronic triggers to detect adverse events in hospitalized patients. Quality & Safety in Health Care, 15(3), 184–190. doi:10.1136/qshc.2005.014589 PMID:16751468
Taguchi, G. (1979). Introduction to Off-line Quality Control. Magaya, Japan: Central Japan Quality Control Association.
Taib, I. A., McIntosch, A. S., Caponecchia, C., & Baysari, M. (2011). A review of medical er-ror taxonomies: A human factors perspective. Safety Science, 49(5), 607–615. doi:10.1016/j.ssci.2010.12.014
Takahashi, K., & Watanabe, K. (2013). Crossmodal interactions in visual competition. In J. Wu (Ed.), Biomedical engineering and cognitive neuroscience for healthcare: Interdisciplinary ap-plications (pp. 64–72). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2113-8.ch007
Talbot, C. (2008). Measuring public value: A competitive value approach. Academic Press.
Tamiya, T., Kawanishi, M., Miyake, K., Kawai, N., & Guo, S. (2013). Neurosurgical operations using navigation microscope integration system. In J. Wu (Ed.), Technological advancements in biomedicine for healthcare applications (pp. 128–138). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2196-1.ch014
Tanaka, H., & Furutani, M. (2013). Sleep management promotes healthy lifestyle, mental health, QOL, and a healthy brain. In J. Wu (Ed.), Biomedical engineering and cognitive neurosci-ence for healthcare: Interdisciplinary applications (pp. 211–224). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2113-8.ch022
Tancredi, L. R., & Barondess, J. A. (1978). The problem of defensive medicine. Science, 200(4344), 879–882. doi:10.1126/science.644329 PMID:644329
Tang, F. I., Sheu, S. J., Yu, S., Wei, I. L., & Chen, C. H. (2007). Nurses relate the contributing factors involved in medication errors. Journal of Clinical Nursing, 16(3), 447–457. doi:10.1111/j.1365-2702.2005.01540.x PMID:17335520
Tangney, J. P., & Dearing, R. L. (2002). Shame and Guilt. New York: The Guilford Press. doi:10.4135/9781412950664.n388
Tang, X., Gao, Y., Yang, W., Zhang, M., & Wu, J. (2013). Audiovisual integration of natural auditory and visual stimuli in the real-world situation. In J. Wu (Ed.), Biomedical engineering and cognitive neuroscience for healthcare: Interdisciplinary applications (pp. 337–344). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2113-8.ch035

Compilation of References
319
Tan, R., Wang, S., Jiang, Y., Ishida, K., & Fujie, M. G. (2013). Motion control of an omni-directional walker for walking support. In J. Wu (Ed.), Biomedical engineering and cognitive neuroscience for healthcare: Interdisciplinary applications (pp. 20–28). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2113-8.ch003
Targowski, A. (2013). Well-being, wisdom, health, and IT: From the big-picture to the small-picture. In M. Cruz-Cunha, I. Miranda, & P. Gonçalves (Eds.), Handbook of research on ICTs for human-centered healthcare and social care services (pp. 1–28). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3986-7.ch001
Tayabali, S., & Martin, C. M. (2013). The need to transform the core values of medical care and health organizations. In R. Biswas (Ed.), Clinical solutions and medical progress through user-driven healthcare (pp. 85–92). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-1876-3.ch009
Taylor, B. W. (2014). Decision-making and decision support in acute care. In C. El Morr (Ed.), Research perspectives on the role of informatics in health policy and management (pp. 1–18). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4321-5.ch001
Taylor, D., Hassan, M. A., Luterman, A., & Rodning, C. B. (2008). Unexpected intraoperative patient death: The imperatives of family- and surgeon-centered care. Archives of Surgery, 143(1), 87–92. doi:10.1001/archsurg.2007.27 PMID:18209158
Taylor, J. A., Brownstein, D., Klein, E. J., & Strandjord, T. P. (2007). Evaluation of an anony-mous system to report medical errors in pediatric inpatients. Journal of Hospital Medicine, 2(4), 226–233. doi:10.1002/jhm.208 PMID:17683099
Teixeira, C., Pinto, J. S., Ferreira, F., Oliveira, A., Teixeira, A., & Pereira, C. (2013). Cloud comput-ing enhanced service development architecture for the living usability lab. In R. Martinho, R. Rijo, M. Cruz-Cunha, & J. Varajão (Eds.), Information systems and technologies for enhancing health and social care (pp. 33–53). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3667-5.ch003
Teixeira, L., Saavedra, V., Ferreira, C., & Santos, B. S. (2013). The role of ICTs in the management of rare chronic diseases: The case of hemophilia. In M. Cruz-Cunha, I. Miranda, & P. Gonçalves (Eds.), Handbook of research on ICTs and management systems for improving efficiency in healthcare and social care (pp. 635–649). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3990-4.ch033
Tevlin, R., Doherty, E., & Traynor, O. (2013). Improving disclosure and management of medical error e an opportunity to transform the surgeons of tomorrow. The Surgeon: Journal of the Royal Colleges of Surgeons of Edinburgh and Ireland, 11(6), 338-43.
Thakur, H., Thawani, V., Raina, R. S., Kothiyal, G., & Chakarabarty, M. (2013). Noncompli-ance pattern due to medication errors at a Teaching Hospital in Srikot, India. Indian Journal of Pharmacology, 45(3), 289–292. doi:10.4103/0253-7613.111899 PMID:23833376
Thomas, E. J., & Petersen, L. A. (2003). Measuring errors and adverse events in health care. Journal of General Internal Medicine, 18(1), 61–67. doi:10.1046/j.1525-1497.2003.20147.x PMID:12534766

Compilation of References
320
Thomas, J. W., Ziller, E., & Thayer, D. (2010). Low costs of defensive medicine, small savings from tort reform. Health Affairs, 29(9), 1578–1584. doi:10.1377/hlthaff.2010.0146 PMID:20820011
Tierney, W. M., Miller, M. E., Overhage, J. M., & McDonald, C. J. (1993). Physician inpatient order writing on microcomputer workstations: Effects on resource utilization. Journal of the American Medical Association, 269(3), 379–383. doi:10.1001/jama.1993.03500030077036 PMID:8418345
Tiwari, S., & Srivastava, R. (2014). Research and developments in medical image reconstruction methods and its applications. In R. Srivastava, S. Singh, & K. Shukla (Eds.), Research develop-ments in computer vision and image processing: Methodologies and applications (pp. 274–312). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4558-5.ch014
Tobolcea, I. (2013). The psychosocial impact of ICT efficiency on speech disorders-treatment. In M. Cruz-Cunha, I. Miranda, & P. Gonçalves (Eds.), Handbook of research on ICTs for human-centered healthcare and social care services (pp. 70–92). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3986-7.ch004
Toda, T., Chen, P., Ozaki, S., Fujita, K., & Ideguchi, N. (2013). A simple web-based image database system for facilitating medical care in dermatological clinics. In J. Wu (Ed.), Techno-logical advancements in biomedicine for healthcare applications (pp. 385–397). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2196-1.ch038
Tran, D. T., & Johnson, M. (2010). Classifying nursing errors in clinical management within an Australian hospital. International Nursing Review, 57(4), 454–462. doi:10.1111/j.1466-7657.2010.00846.x PMID:21050197
Trudeau, S. (2013). CoRDS registry: An HIT case study concerning setup and maintenance of a disease registry. In S. Sarnikar, D. Bennett, & M. Gaynor (Eds.), Cases on healthcare information technology for patient care management (pp. 197–207). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2671-3.ch012
Truog, R. D., Browning, D. M., Johnson, J. A., & Gallagher, T. H. (2010). Talking with patients and families about medical error: A guide for education and practice. Baltimore, MD: JHU Press.
Tseng, R., & Yi-Luen Do, E. (2013). The role of information and computer technology for children with autism spectrum disorder and the facial expression wonderland (FEW). In A. Gangopadhyay (Ed.), Methods, models, and computation for medical informatics (pp. 98–116). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2653-9.ch006
Tully, M. P. (2012). Prescribing errors in hospital practice. British Journal of Clinical Pharma-cology, 74(4), 668–675. doi:10.1111/j.1365-2125.2012.04313.x PMID:22554316
Tümer, A. R., & Dener, C. (2006). Evaluation of surgical malpractice in Turkey. Legal Medicine, 8(1), 11–15. doi:10.1016/j.legalmed.2005.06.006 PMID:16157500

Compilation of References
321
Uchitomi, H., Suzuki, K., Nishi, T., Hove, M. J., Miyake, Y., Orimo, S., & Wada, Y. (2013). Gait rhythm of Parkinson’s disease patients and an interpersonal synchrony emulation system based on cooperative gait. In J. Wu (Ed.), Biomedical engineering and cognitive neuroscience for healthcare: Interdisciplinary applications (pp. 38–53). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2113-8.ch005
Ullstrom, S., Sachs, M. A., Hansson, J., Ovretveit, J., & Brommels, M. (2014). Suffering in silence: A qualitative study of second victims of adverse events. BMJ Quality & Safety, 23(4). doi:10:1136, 325-331
Van Den Bos, J., Rustagi, K., Gray, T., Halford, M., Ziemkiewicz, E., & Shreve, J. (2011). The $17.1 billion problem: The annual cost of measurable medical errors. Health Affairs, 30(4), 596–603. doi:10.1377/hlthaff.2011.0084 PMID:21471478
Van Genderen, E. (2014). Intensive care. In V. Jham & S. Puri (Eds.), Cases on consumer-centric marketing management (pp. 53–67). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4357-4.ch006
Van Gerven, E., Seys, D., Panella, M., Sermeus, W., Euwema, M., Federico, F., & Vanhaet, K. et al. (2014). Involvement of health-care professionals in an adverse event: The role of manage-ment in supporting their workforce. Polskie Archiwum Medycyny Wewnetrznej, 124(6), 313–319. PMID:24781784
Verbano, C., & Turra, F. (2010). A human factors and reliability approach to clinical risk manage-ment: Evidence from Italian cases. Safety Science, 48(5), 625–639. doi:10.1016/j.ssci.2010.01.014
Verschoor, K. N., Taylor, A., Northway, T. L., Hudson, D. G., Van Stolk, D. E., Shearer, K. J., & Miller, G. et al. (2007). Creating a safety culture at the Childrens and Womens Health Centre of British Columbia. Journal of Pediatric Nursing, 22(1), 81–86. doi:10.1016/j.pedn.2006.08.012 PMID:17234501
Vidal, B., Pereira, J. M., & Santos, G. (2013). SimBody: An interactive simulator for health educa-tion. In S. Arnab, I. Dunwell, & K. Debattista (Eds.), Serious games for healthcare: Applications and implications (pp. 265–282). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-1903-6.ch013
Vincent, C. (2003). Understanding and Responding to Adverse Events. The New England Journal of Medicine, 348(11), 1051–1056. doi:10.1056/NEJMhpr020760 PMID:12637617
Vincent, C. A., & Coulter, A. (2002). Patient safety: What about the patient? Quality & Safety in Health Care, 11(1), 76–80. doi:10.1136/qhc.11.1.76 PMID:12078376
Vincent, C. A., Pincus, T., & Scurr, J. H. (1993). Patients experience of surgical accidents. Qual-ity in Health Care, 2(2), 77–82. doi:10.1136/qshc.2.2.77 PMID:10171783
Vincent, C., Neale, G., & Woloshynowych, M. (2001). Adverse events in British hospitals: Preliminary retrospective record review. BMJ (Clinical Research Ed.), 322(7285), 517–519. doi:10.1136/bmj.322.7285.517 PMID:11230064

Compilation of References
322
Vinen, J. (2005). Negligence of medical experts. British Medical Journal, 330(7498), 1027. doi:10.1136/bmj.330.7498.1027-a
Vivekananda-Schmidt, P. (2013). Ethics in the design of serious games for healthcare and medi-cine. In S. Arnab, I. Dunwell, & K. Debattista (Eds.), Serious games for healthcare: Applications and implications (pp. 91–106). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-1903-6.ch005
Vliamos, S., & Hatziplaton, M. (2008). Economic analysis of medical errors. Chronicles of Private Law (offprint), 584-590.
Vliamos, S., & Hatzis, A. (2009). The assesment of compensatory damages for medical error by the Greek courts: An economic analysis. In N. B. James Brox (Ed.), The global economics of a changing environment (pp. 239–251). Waterloo, Ontario, Canada: North Waterloo Academic Press.
Vozikis, A. (2012). Adverse events and medical errors in Greece: Knowledge creation and capture methods. In P. Ordóñez de Pablos & M. Lytras (Eds.), Knowledge management and drivers of innovation in services industries (pp. 95–101). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-0948-8.ch009
Wahbeh, A. (2013). Application of handheld computing and mobile phones in diabetes self-care. In S. Sarnikar, D. Bennett, & M. Gaynor (Eds.), Cases on healthcare information technology for patient care management (pp. 254–275). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2671-3.ch015
Waidyanatha, N., & Dekker, S. (2013). The RTBP – Collective intelligence driving health for the user. In R. Biswas (Ed.), Clinical solutions and medical progress through user-driven healthcare (pp. 70–78). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-1876-3.ch007
Waidyanatha, N., Dubrawski, A. M. G., & Gow, G. (2013). Affordable system for rapid detection and mitigation of emerging diseases. In J. Rodrigues (Ed.), Digital advances in medicine, e-health, and communication technologies (pp. 271–288). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2794-9.ch015
Walker, D. (2013). How would a ban on prescriber-identifying information impact pharmaceuti-cal marketing? In M. Merviö (Ed.), Healthcare management and economics: Perspectives on public and private administration (pp. 141–153). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3982-9.ch011
Walsh-Childers, K. (1994). Newspaper influence on health policy development. Newspaper Research Journal, 15, 89–101.
Walshe, K. (2000). Adverse events in health care: Issues in measurement. Quality in Health Care : QHC, 9(1), 47–52. doi:10.1136/qhc.9.1.47 PMID:10848370
Wang, B., Yan, T., & Wu, J. (2013). Neuronal function in the cortical face perception network. In J. Wu (Ed.), Biomedical engineering and cognitive neuroscience for healthcare: Interdisciplinary applications (pp. 171–182). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2113-8.ch018

Compilation of References
323
Wang, Y., & Wang, Q. (2013). Evaluating the IEEE 802.15.6 2.4GHz WBAN proposal on medi-cal multi-parameter monitoring under WiFi/bluetooth interference. In J. Rodrigues (Ed.), Digital advances in medicine, e-health, and communication technologies (pp. 312–325). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2794-9.ch018
Ward, T. N., & Allen, W. R. (2008). Case 3. The steroid complication. Headache, 48(6), 866–870. doi:10.1111/j.1526-4610.2008.01164_3.x PMID:18549368
Watanabe, T., & Miura, N. (2013). Functional electrical stimulation (FES) control for restoration and rehabilitation of motor function. In J. Wu (Ed.), Technological advancements in biomedicine for healthcare applications (pp. 80–93). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2196-1.ch009
Watanabe, Y., Tanaka, H., & Hirata, K. (2013). Evaluation of cognitive function in migraine patients: A study using event-related potentials. In J. Wu (Ed.), Biomedical engineering and cognitive neuroscience for healthcare: Interdisciplinary applications (pp. 303–310). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2113-8.ch031
Waterman, A. D., Garbutt, J., Hazel, E., Dunagan, W. C., Levinson, W., Fraser, V. J., & Gallagher, T. H. (2007). The emotional impact of medical errors on practicing physicians in the United States and Canada. Joint Commission Journal on Quality and Patient Safety, 33(8), 467–476. doi:10.1016/S1553-7250(07)33050-X PMID:17724943
Wegman, B., Stannard, J., & Bal, B. S. (2012). Medical liability of the physician in training. Clinical Orthopaedics and Related Research, 470(5), 1379–1385. doi:10.1007/s11999-012-2244-4 PMID:22278849
Wesorick, B. (2013). Essential steps for successful implementation of the EHR to achieve sus-tainable, safe, quality care. In A. Moumtzoglou & A. Kastania (Eds.), E-health technologies and improving patient safety: Exploring organizational factors (pp. 27–55). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2657-7.ch003
Wheeler, S. J., & Wheeler, D. W. (2005). Medication errors in anaesthesia and critical care. Anaesthesia, 60(3), 257–273. doi:10.1111/j.1365-2044.2004.04062.x PMID:15710011
Whitaker, R. (2013). Securing health-effective medicine in practice: A critical perspective on user-driven healthcare. In R. Biswas (Ed.), Clinical solutions and medical progress through user-driven healthcare (pp. 35–50). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-1876-3.ch005
White, A. A., Bell, S. K., Krauss, M. J., Garbutt, J., Dunagan, W. C., Fraser, V. J., & Gallagher, T. H. et al. (2011). How trainees would disclose medical errors: Educational implications for training programmes. Medical Education, 45(4), 372–380. doi:10.1111/j.1365-2923.2010.03875.x PMID:21401685
White, A. A., Brock, D., McCotter, P. I., Hofeldt, R., Edrees, H. H., Wu, A. W., & Gallagher, T. H. et al. (2015). Risk managers descriptions of programs to support second victims after ad-verse events. Journal of Healthcare Risk Management, 34(4), 30–40. doi:10.1002/jhrm.21169 PMID:25891288

Compilation of References
324
Whitten, P., Dutta, M. J., Carpenter, S., & Bodie, G. D. (n.d.). News Media and Health Care Providers at the Crossroads of Medical Adverse Events. Retrieved from http://www.ncbi.nlm.nih.gov/books/NBK43609/
WHO. (2003). Executive board. Quality of care: patient safety. Retrieved from: http://apps.who.int/gb/archive/pdf_files/EB113/eeb11337.pdf
WHO. (2005). Project to develop the international patient safety Event taxonomy: updated review of the literature 2003 - 2005. Final report. Retrieved from: http://www.who.int/patientsafety/taxonomy/IPSET_Sept05_FINAL.pdf
WHO. (2005a). News release. Launch of the WHO Collaborating Center on patient safety solu-tions. WHO.
WHO. (2005b). World Alliance for patient safety. In WHO draft guidelines for adverse event reporting and learning systems. From information to action. Geneva, Switzerland: WHO. Re-trieved from: http://www.who.int/patientsafety/en/brochure_final.pdf
WHO. (2007). World Alliance for patient safety. The conceptual framework for the International Classification for patient safety. Version 1.0 for use in the field testing (ICPS). Retrieved from: http://www.who.int/patientsafety/ICPS%20-%20July%202007.pdf
Wickramasinghe, N., Troshani, I., Hill, S. R., Hague, W., & Goldberg, S. (2013). A transaction cost assessment of a pervasive technology solution for gestational diabetes. In J. Tan (Ed.), Healthcare information technology innovation and sustainability: Frontiers and adoption (pp. 109–126). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2797-0.ch007
Wiegmann, D. A., Eggman, A. A., ElBardissi, A. W., Parker, S. H., & Sundt, T. M. III. (2010). Improving cardiac surgical care: A work systems approach. Applied Ergonomics, 41(5), 701–712. doi:10.1016/j.apergo.2009.12.008 PMID:20202623
Williams, B. W. (2006). The prevalence and special educational requirements of dyscompetent physicians. The Journal of Continuing Education in the Health Professions, 26(3), 173–191. doi:10.1002/chp.68 PMID:16986149
Williams, D. (2012). Monitoring medicines use: The role of the clinical pharmacologist. Brit-ish Journal of Clinical Pharmacology, 74(4), 685–690. doi:10.1111/j.1365-2125.2012.04316.x PMID:22554404
Witter, S., Fretheim, A., Kessy, F. L., & Lindahl, A. K. (2012). Paying for performance to improve the delivery of health interventions in low- and middle-income countries. Cochrane Database of Systematic Reviews, 2, CD007899. PMID:22336833
Wohed, P., van der Aalst, W. M., Dumas, M., ter Hofstede, A. H., & Russell, N. (2006, September). On the suitability of BPMN for business process modelling. In International conference on busi-ness process management (pp. 161-176). Springer Berlin Heidelberg. doi:10.1007/11841760_12

Compilation of References
325
Wong, B. M., Levinson, W., & Shojania, K. G. (2012). Quality improvement in medical education: Current state and future directions. Medical Education, 46(1), 107–119. doi:10.1111/j.1365-2923.2011.04154.x PMID:22150202
Wong, R. S. Y., & Balasingam, U. (2013). Teaching medical law in medical education. Journal of Academic Ethics, 11(2), 121–138. doi:10.1007/s10805-013-9184-9
Woodfield, G., O’Sullivan, M., Haddington, N., & Stanton, A. (2014). Using simulation for prescrib-ing: An evaluation. The Clinical Teacher, 11(1), 24–28. doi:10.1111/tct.12056 PMID:24405915
Worsham, S. L. (2009). The Psychological Impact of Medical Error: Symptoms of Trauma in Family Members of the Injured (Doctoral dissertation). Harvard University. Available from ProQuest Dissertations and Theses database. (UMI No. 1518406)
Wu, A. W. (2000, March). Medical error: The second victim. The doctor who makes the mistake needs help too. British Medical Journal, 320(7237), 726–727. doi:10.1136/bmj.320.7237.726 PMID:10720336
Wu, A. W., Boyle, D. J., Wallace, G., & Mazor, K. M. (2013). Disclosure of adverse events in the United States and Canada: An update, and a proposed framework for improvement. Journal of Public Health Research, 2(3), 186–193. doi:10.4081/jphr.2013.e32 PMID:25170503
Wu, A. W., & Steckelberg, R. C. (2012). Medical error, incident investigation and the second victim: Doing better but feeling worse? BMJ Quality & Safety, 21(4), 267–269. doi:10.1136/bmjqs-2011-000605 PMID:22213379
Wu, Q., Li, C., Takahashi, S., & Wu, J. (2013). Visual-tactile bottom-up and top-down attention. In J. Wu (Ed.), Biomedical engineering and cognitive neuroscience for healthcare: Interdisciplin-ary applications (pp. 183–191). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2113-8.ch019
Yamaguchi, S., Onoda, K., & Abe, S. (2013). Feedback-related negativity and its clinical im-plications. In J. Wu (Ed.), Biomedical engineering and cognitive neuroscience for healthcare: Interdisciplinary applications (pp. 283–292). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2113-8.ch029
Yan, B., Lei, Y., Tong, L., & Chen, K. (2013). Functional neuroimaging of acupuncture: A sys-tematic review. In J. Wu (Ed.), Biomedical engineering and cognitive neuroscience for healthcare: Interdisciplinary applications (pp. 142–155). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2113-8.ch015
Yang, J. (2014). Towards healthy public policy: GIS and food systems analysis. In C. El Morr (Ed.), Research perspectives on the role of informatics in health policy and management (pp. 135–152). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4321-5.ch009
Yang, J. J., Liu, J. F., Kurokawa, T., Kitamura, N., Yasuda, K., & Gong, J. P. (2013). Tough double-network hydrogels as scaffolds for tissue engineering: Cell behavior in vitro and in vivo test. In J. Wu (Ed.), Technological advancements in biomedicine for healthcare applications (pp. 213–222). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2196-1.ch023
Compilation of References
326
Yang, J., Li, Q., Gao, Y., & Wu, J. (2013). Temporal dependency of multisensory audiovisual integration. In J. Wu (Ed.), Biomedical engineering and cognitive neuroscience for healthcare: Interdisciplinary applications (pp. 320–326). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2113-8.ch033
Yang, W., Gao, Y., & Wu, J. (2013). Effects of selective and divided attention on audiovisual interaction. In J. Wu (Ed.), Biomedical engineering and cognitive neuroscience for healthcare: Interdisciplinary applications (pp. 311–319). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2113-8.ch032
Yano, Y. (2013). An EMG control system for an ultrasonic motor using a PSoC microcomputer. In J. Wu (Ed.), Technological advancements in biomedicine for healthcare applications (pp. 11–17). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2196-1.ch002
Yates, G. R., Bernd, D. L., Sayles, S. M., Stockmeier, C. A., Burke, G., & Merti, G. E. (2005). Building and sustaining a systemwide culture of safety. Journal of Quality and Patient Safety, 31(12), 684–689. doi:10.1016/S1553-7250(05)31089-0 PMID:16430021
Ye, Y., Jiang, Z., & Yang, D.-A. (2008). Semantics-Based Clinical Pathway Workflow and Variance Management Framework. IEEE/SOLI 2008.IEEE International Conference on Service Operations and Logistics, and Informatics.
Yokoi, H., Kato, R., Mori, T., Yamamura, O., & Kubota, M. (2013). Functional electrical stimulation based on interference-driven PWM signals for neuro-rehabilitation. In J. Wu (Ed.), Technological advancements in biomedicine for healthcare applications (pp. 180–192). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2196-1.ch019
York, A. M., & Nordengren, F. R. (2013). E-learning and web 2.0 case study: The role of gender in contemporary models of health care leadership. In H. Yang & S. Wang (Eds.), Cases on formal and informal e-learning environments: Opportunities and practices (pp. 292–313). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-1930-2.ch016
Yule, S. (2003). Safety culture and safety climate: A review of the literature. Industrial Psychol-ogy Research Centre.
Yu, W. D., & Bhagwat, R. (2013). Modeling emergency and telemedicine health support system: A service oriented architecture approach using cloud computing. In J. Rodrigues (Ed.), Digital advances in medicine, e-health, and communication technologies (pp. 187–213). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2794-9.ch011
Yu, Y., Yang, J., & Wu, J. (2013). Cognitive functions and neuronal mechanisms of tactile work-ing memory. In J. Wu (Ed.), Biomedical engineering and cognitive neuroscience for healthcare: Interdisciplinary applications (pp. 89–98). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2113-8.ch010

Compilation of References
327
Zaheer, S. (2014). Implementation of evidence-based practice and the PARIHS framework. In C. El Morr (Ed.), Research perspectives on the role of informatics in health policy and management (pp. 19–36). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4321-5.ch002
Zaheer, S. (2015). Implementation of evidence-based practice and the PARIHS framework. In Healthcare administration: Concepts, methodologies, tools, and applications (pp. 323–340). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-6339-8.ch017
Zapirain, B. G., & Zorrilla, A. M. (2013). Independent living support for disabled and elderly people using cell phones. In M. Cruz-Cunha, I. Miranda, & P. Gonçalves (Eds.), Handbook of research on ICTs for human-centered healthcare and social care services (pp. 379–397). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-3986-7.ch020
Zhou, X., & Ren, X. (2013). Speed-accuracy tradeoff models of target-based and trajectory-based movements. In J. Wu (Ed.), Biomedical engineering and cognitive neuroscience for healthcare: Interdisciplinary applications (pp. 355–368). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-2113-8.ch037
Zientek, D. M. (2010). Medical error, malpractice and complications: A moral geography. HEC Forum, 22(2), 145–157. doi:10.1007/s10730-010-9130-9 PMID:20480208
Zohar, D. (1980). Safety climate in industrial organizations: Theoretical and applied implications. The Journal of Applied Psychology, 65(1), 96–102. doi:10.1037/0021-9010.65.1.96 PMID:7364709
Zohar, D., Livne, Y., Tenne-Gazit, O., Admi, H., & Donchin, Y. (2007). Healthcare climate: A framework for measuring and improving patient safety. Critical Care Medicine, 35(5), 1312–1317. doi:10.1097/01.CCM.0000262404.10203.C9 PMID:17414090
Zouag, N., & Driouchi, A. (2014). Trends and prospects of the Moroccan health system: 2010-2030. In A. Driouchi (Ed.), Labor and health economics in the mediterranean region: Migration and mobility of medical doctors (pp. 314–336). Hershey, PA: IGI Global. doi:10.4018/978-1-4666-4723-7.ch013
Zur Muehlen, M. (2002). Workflow-Based Process Controlling: Foundation. Design, and ap-plication of Workflow-driven Process information system.

328
About the Contributors
Marina T. Riga is a Health Economist. The main theme of her PhD thesis fo-cuses on the impact of medical errors on healthcare quality, patient safety, fiscal consolidation and cost containment on Healthcare Systems. Under this burden of serious economic and social implications of medical errors, the Information Tech-nology implementation for detecting, reporting and analyzing the preventablee errors can lead to continuous learning for the multi-professionals involved, improve-ment in quality of care, patients’ safety and reduction of medical errors on Health-care Systems, worldwide. Her relevant international publications include: MERIS (Medical Error Reporting Information System) as an innovative patient safety in-tervention: a health policy perspective (Health Policy, 2015), Medical Errors in Greece: An Economic Analysis of Compensations Awarded by Civil Courts (2000-2009) (Open Journal of Applied Sciences, 2014). Dr. Riga has mainly taught and published in the area of health economics, policy, quality assurance and health care management. She has been collaborating with researchers in EU health projects. Dr. Riga and her work received a notable award, titled: The Best Published Research Paper on issue of medical errors and adverse events.
* * *
Mary Gouva is Associate Professor of Psychology of the School of Health & Social Welfare, at the Technological Educational Institute of Epirus and is Head of the Research Laboratory Psychology of Patients, Families and Health Professionals. She has specialized in Social Psychiatry and her research interests of her scientific work in the context of her Ph.D. studies relate to the Psychological Characteristics of patients with Acute Leukemia and of their families. Her studies and her research interest concern the investigation of the psychological factors in somatic diseases, the patients’ and their families’ psychological profile and the psychological charac-

About the Contributors
teristics of the health professionals. Her clinical work has psychodynamic direction and include psychological support and counseling intervention on patients and their family members and participation in therapeutic groups of hospital clinics at the University Hospital of Ioannina. Her published scientific work concerns articles, announcements and books.
Kijpokin Kasemsap received his BEng degree in Mechanical Engineering from King Mongkut’s University of Technology, Thonburi, his MBA degree from Ramkhamhaeng University, and his DBA degree in Human Resource Management from Suan Sunandha Rajabhat University. He is a Special Lecturer in the Faculty of Management Sciences, Suan Sunandha Rajabhat University, based in Bangkok, Thailand. He is a Member of the International Association of Engineers (IAENG), the International Association of Engineers and Scientists (IAEST), the International Economics Development and Research Center (IEDRC), the International Associa-tion of Computer Science and Information Technology (IACSIT), the International Foundation for Research and Development (IFRD), and the International Innovative Scientific and Research Organization (IISRO). He also serves on the International Advisory Committee (IAC) for International Association of Academicians and Researchers (INAAR). He has had numerous original research articles in top in-ternational journals, conference proceedings, and books on the topics of business management, human resource management, and knowledge management, published internationally.
Grigorios Leon is the President of the Hellenic Society of Forensic Medicine. As a certified Forensic Pathologist and a sole trader, he maintains one of the few private medico-legal consulting practices in Greece. He is a graduate (MD) of the Medical School of the University of Rome “La Sapienza”, where he also obtained two Master Degrees (MSc). In 2009 he received his PhD from the Medical School of the National and Kapodistrian University of Athens. He has trained and worked in the Department of Legal Medicine and Toxicology at the University of Athens, in the Children’s hospital “Agia Sophia” as well as in the Office of Medical Examiner and trauma services of Broward County in the State of Florida, USA. He is a Profes-sor of Forensic Pathology at the Police Academy of Greece. His research interests are in the areas of Forensic Pathology, Medical Deontology and Bioethics. For his scientific work, he has been awarded scholarships from, amongst others, UNESCO and the European Committee.
329

About the Contributors
Vaughan Michell is an Informatics Lecturer and Business Technology Consult-ing Programme Director within the Informatics Research Centre at Henley Business School. He is also an honorary Senior Lecturer in Health Informatics in the Simulation Unit at the Royal Berkshire Hospital. Vaughan’s research focuses on the informat-ics of the business and technology interface at the design and operational level. He supervises PhD students in health informatics and related areas and has published papers in the areas of health informatics & semiotics, patient safety, clinical path-ways, medical device capability and cognition. Research interests include: semiotics, affordance and human and machine capability, knowledge intensive processes and cognition, device design and invention and man-machine interaction. Vaughan has a BSc in mechanical engineering from UCL, an MBA from Warwick University and a D.Phil in Robotics Image Processing from Oxford University.
Ali Mohammad Mosadeghrad is an Assistant Professor of Health Policy, Management and Economics at Tehran University of Medical Sciences. He received his PhD from University of London in Health Policy and Management. He has a wealth of experience in health policy, management and economics. He is an author, speaker, and a professional management consultant and trainer. Mosadeghrad has written extensively on many aspects of organization and management covering a full spectrum of subjects in strategy formulation, implementation and evaluation. His research work appears in international journals such as International Journal of Health Care Quality Assurance, International Journal of Strategic Change Manage-ment, International Journal of Health Policy and Management, and Health Services Management Research Journal. He has also contributed to many international conferences. His research interests include public sector management, strategic management, quality management, knowledge mobilization, Organisational health, and organisational change. His latest research is focused on international strategies.
Andreas Pavlakis studied Nursing at the School of Nursing in Nicosia, Cyprus; in 1982 he was awarded a Degree in Law (Major in Public Law and Social Sciences) by the Aristotelion University of Thessaloniki, Greece. He then proceeded with his post-degree studies in “Open and Distance Learning” at the Hellenic Open University (1999) and in Legislative Drafting (Commonwealth Distance Training Programme) which was awarded to him by the Commonwealth of Learning. In 1991 he completed his Doctorial Studies at the National and Kapodistrian University of Athens, Greece in the field of nursing. In 2003 he was appointed by the Council of Ministers as
330

About the Contributors
331
a Member of the Secretariat of the Open University of Cyprus until 2005. From August 2006 - 2015 he was an Assistant Professor of Health Care Management at the OUC. He has participated in a number of research projects dealing with health in public and private sector. Since October 2015 he is an Associate Professor at the University Neapolis of Pafos.
Jayita Poduval is a practicing otolaryngologist based in India. She completed her training from Mumbai in 1997 and has since been working in academic practice, medical research and postgraduate education in various places in India, with brief stints in Nepal and Malaysia. She also writes on medical and social issues and has several publications on these topics. She is also a trekker, amateur photographer and travel blogger.
Paraskevi K. Skourti is a R.N. She studied nursing in the Technological Edu-cational Foundation in Athens. She received her Magister Artium degree in “Health Units Management” from Open University of Cyprus in July of 2015. Today, she studies in Law Faculty in National and Kapodistrian University of Athens.
Jasmine Tehrani recently completed her PhD in the area of clinical pathways and health informatics.
Abraha Woldemichael is currently a Ph.D. student in Health Policy at Tehran University of Medical Sciences. He is also a lecturer at Mekelle University, School of Public Health, Ethiopia where he is teaching Healthcare management, Funda-mentals of public health, Public health law and ethics, Health economics and Health monitoring and evaluation both to undergraduate and postgraduate students. He has a B.Sc. in Nursing, BA in Management, Bachelor in Legal Law and M.Sc in Health Monitoring and Evaluation.

332
Index
A Adverse Events 2, 3, 28-31, 43, 52-75, 79-
82, 86, 90-98, 102-115, 130, 138-142, 147, 153, 168, 191-194, 202-207, 212-221
AHRQ 61, 64, 68, 71, 76, 77, 84, 202, 219Ambivalence 183, 196American Health Association (AHA) 61autopsy 145, 150-153, 165-169
B Bad Object 171, 184Blame Culture 197-203, 210, 216, 217
C Compensation 59, 114, 145-148, 156, 158,
173, 188, 198, 199, 204-209Control norms 1, 14, 18-24Cost-Effectiveness 60Cultural controls 1, 18, 22, 23Culture 8, 9, 13, 22, 26-31, 36-38, 43-48,
61-92, 102-105, 109-115, 119-122, 127, 132, 192, 197-203, 210-218
D Decisions 3-9, 15, 60, 68, 76, 92, 94, 103,
113-117, 123, 130, 165, 187, 207Defensive Medicine 44-51, 146, 170, 199,
204-206, 216-222Denial 185, 196
Disclosure 53, 109, 113-119, 126-131, 136, 147, 148, 168-175, 186-193, 197, 204-210, 214-222
Displacement 171, 186, 196
E EUNetPaS 78, 79, 84Evidence-Based Medicine 60, 142expert witness 144, 145, 153, 157-161,
165-168
F First Victim 197, 222Forensic Medicine 144-153, 161-166, 217
G guidelines 11, 12, 19, 29, 37, 44, 48-54,
62, 77, 89, 100, 104, 113, 126, 144, 146, 154-166, 198, 211, 216
H Harm 2, 6, 49, 64, 69, 83, 90-97, 107, 122,
125, 145, 147, 181, 197-200, 214-222Health Care 28-64, 71, 75-98, 107-127,
133, 140, 143, 149, 174, 178, 183, 189-198, 202, 212, 218-220
Health Care Quality 28, 33, 38, 39, 43, 50-55, 60, 76, 85, 92, 98, 110, 115
Helplessness 171, 173, 178, 180Human factors 1-3, 10-31, 71, 72, 84, 103,
127, 220

333
Index
I Identification 1, 10-18, 26, 27, 75, 76, 103,
116-123, 129-133, 162, 196, 214Incentive 45, 207Information 3, 7-21, 29-33, 37-54, 72-80,
88, 89, 96, 97, 103, 107-125, 130-134, 142-146, 151, 156, 160, 161, 166, 168, 173, 176, 188, 199, 208, 214, 215
Information Technology 33, 37, 38, 42-44, 52, 120, 133, 134, 142, 143
Interventions 7, 13, 34, 38, 43, 54, 59, 95, 98, 107, 113, 116, 120, 123, 128, 135, 141, 200, 212, 216, 218
IOM 2, 64
K Knowledge 4-6, 11-20, 28, 30, 65-67, 74,
92, 96, 113, 117-122, 127-132, 139, 148, 153-162, 175, 176, 185
L Learning 8, 56, 73-75, 81-90, 105, 115-
122, 134-140, 164, 214, 218, 219Legal Medicine 144, 149, 162-170, 217Litigation Risk 203-205, 212, 219
M Malpractice 34, 35, 48, 53-59, 97, 109,
113, 115, 121, 123, 128, 129, 139, 144-170, 205-209, 219, 221
Mechanisms of Defence 171Medical Errors 2, 10, 33-66, 77, 83, 91-
146, 150, 163-178, 185-195, 199-203, 208, 217, 221
medical expert 144, 154-158, 166Medication 34, 37, 41-44, 49-60, 70, 81,
94-96, 106-131, 135-143, 191, 200, 202, 217
Medication Error 60, 123, 141Medicine 2, 16, 18, 28-31, 37, 38, 43-60,
64, 81, 85-89, 109-116, 120, 128-170, 188-194, 199, 204-206, 216-222
N Narcissism 171, 173, 186, 191National Patient Safety Foundation (NPSF)
63
P Patient 1-16, 21-31, 35, 36, 40-103, 107-
136, 140-162, 166-222Patient-Centered Care 90Patient Safety 1-5, 16, 21-31, 58-92, 102,
103, 107-136, 140-142, 146, 152, 166, 168, 174, 186, 191, 195-204, 211-219
Personal controls 1, 21-23, 27Personality 178, 186-190Physician 19-22, 43, 44, 52-55, 59, 96,
109, 118-124, 128, 138, 143-146, 150, 154-161, 165-170, 191, 203-205, 209, 218
Prescription 37, 41-44, 52, 81, 113-118, 124-128, 136, 143
Pressure 6, 7, 11, 25, 49, 93, 96, 196, 206Principle of Reality 185Processes 6, 11-17, 21, 25, 55, 72-76,
91-106, 116, 117, 125, 126, 143, 149, 159, 186
Projection 6, 184, 196Psychic Maturity 176, 183Psychological Trauma 181, 196
Q Quality 2, 8, 17, 18, 25-69, 76-92, 97-141,
149, 150, 155, 160, 167-174, 186-204, 209-221
Quality management 29, 62, 85, 91, 92, 98-103, 107-111, 125, 132
Quality of Care 30, 55, 57, 88, 99, 108, 110, 119, 120, 124, 125, 197, 218
R Regression 171Reporting 1, 10, 33, 42-50, 56, 69, 71, 79,
82, 89, 97, 105, 111-123, 127-132, 136, 138, 152, 173, 191, 209, 213
Repression 189, 196

334
Index
S Safety Culture 8, 22, 29, 61-67, 71-90,
109, 114, 115, 119, 122, 127, 132, 202, 213, 218
Second Victim 197-222Suffering Clinician 197, 210
T Teamwork 36, 40, 44, 74-78, 85-90, 102,
103, 115, 121
testimony 145, 155-161, 165, 168Third Victim 222Tort Reform 199, 206, 220Transference 171, 182, 196
W WHO 9, 10, 14, 15, 38, 41, 46, 48, 54, 64-
69, 81, 82, 87-89, 94, 103, 110, 118, 123, 143-147, 153-163, 177, 182-190, 197-206, 210-212, 221, 222




















