The Paradigm of Complexity in Clinical Neurocognitive Science
Upload
manchesterCategory
view
1download
0
Research report
Impact of lingual gyrus volume on antidepressant responseand neurocognitive functions in Major Depressive Disorder:A voxel-based morphometry study
JeYoung Jung a, June Kang b, Eunsoo Won c, Kichun Namd, Min-Soo Lee b, Woo Suk Tae e,n,Byung-Joo Ham c,nn
a Neuroscience and Aphasia Research Unit, University of Manchester, Manchester, UKb Department of Biomedical Sciences, Korea University College of Medicine, Seoul, South Koreac Department of Psychiatry, Anam Hospital, Korea University College of Medicine, 126-1, Anam-Dong 5-ga, Sungbuk-Ku, Seoul 136-705, South Koread Department of Psychology, Korea University, Seoul, South Koreae Neuroscience Research Institute, Kangwon National University Hospital, Chuncheon, South Korea
a r t i c l e i n f o
Article history:Received 18 March 2014Received in revised form1 August 2014Accepted 11 August 2014Available online 20 August 2014
Keywords:Major Depressive Disorder (MDD)Antidepressant responsivenessLingual gyrusVoxel-based morphometry (VBM)Cognitive function
a b s t r a c t
Background: Voxel-based morphometry (VBM) has demonstrated structural brain changes betweenpatients with Major Depressive Disorder (MDD) and healthy individuals. The initial response toantidepressants is crucial to predict prognosis in the treatment of MDD. The aim of the present studywas to investigate gray matter abnormalities predicting antidepressant responsiveness and the relation-ships between volumetric differences and clinical/cognitive traits in MDD patients.Methods: Fifty MDD patients who received 8 week period antidepressant treatment and 29 healthycontrols participated in this study. VBM was applied to assess structural changes between MDD groupsand control group. Neuropsychological tests were conducted on all participants.Results: Both treatment responsive and non-responsive patients showed a significant volume reduction ofthe left insular, but only non-responsive patients had decreased volume in the right superior frontal gyruscompared to healthy controls. The comparison between treatment responsive and non-responsive patientgroups demonstrated a significant difference in gray matter volume in the lingual gyrus. The larger volumeof lingual gryus predicted early antidepressant response, which was attributable to better performance inneuropsychological tests.Limitation: This study included a small sample size and the patients received various antidepressants andbenzodiazepines.Conclusion: Our findings suggest that the patients who responded poorly to antidepressants weremorphologically and cognitively impaired, whereas the treatment responsive patients showed lessstructural changes and relatively preserved cognitive functions. The lingual gyrus may be a possiblecandidate region to predict antidepressant responsiveness and maintained cognition in MDD.
& 2014 Published by Elsevier B.V.
1. Introduction
Major Depressive Disorder (MDD) is a mental disorder prevalentworldwide, and leads to significant disability and suffering in dailyliving (Kessler et al., 2003). Antidepressants are an important andeffective treatment of depressive disorders. The treatment withantidepressants is encouraged to patients continually who respondto initial treatment (Anderson et al., 2000). About 50% of all MDD
patients initially receiving antidepressant treatment respond to it,whereas non-responsive patients to the treatment remain to beafflicted with symptoms and are functionally impaired (Fava andDavidson, 1996). This huge portion of initial non-responders toantidepressants is a momentous challenge in the treatment byclinicians who ought to find other additional therapies to obtainresponse (Fagiolini and Kupfer, 2003). Therefore, it is required toidentify markers for the early treatment response, which helpspatients who are less likely to respond to antidepressant treatmentat the early treatment stage.
Various factors contribute to the etiology of MDD such as stress,trauma, psychological and social influence (Fava and Kendler,2000). Moreover, recent neuroimaging studies have suggested
Contents lists available at ScienceDirect
journal homepage: www.elsevier.com/locate/jad
Journal of Affective Disorders
http://dx.doi.org/10.1016/j.jad.2014.08.0180165-0327/& 2014 Published by Elsevier B.V.
n Corresponding author.nn Corresponding author. Tel.: þ82 2 9206843; fax: þ82 2 9272836.E-mail addresses: [email protected] (W.S. Tae),
[email protected] (B.-J. Ham).
Journal of Affective Disorders 169 (2014) 179–187

that neurobiological factors including structural and functionalabnormalities also play a role in MDD (Fizgerald et al., 2008; Priceand Drevets, 2010; Bora et al., 2012). The pathology of MDD is stillunclear but it has been agreed that a distributed brain networkinvolved in mood regulation is structurally and functionallyimpaired by MDD (Mayberg, 1997; Drevets et al., 2007, 2008;Arnone et al., 2012a; Lai and Wu, 2014). The key brain areas of thisnetwork (limbic-cortical network) are amygdala, hippocampus,basal ganglia, cingulate cortex, insular, dorsolateral prefrontalcortex (DLPFC), and dorsolmedial frontal cortex. Above all, struc-tural findings have demonstrated various, and somewhat incon-sistent, results of decreased gray matter volumes in the mentionedregions.
Voxel-based morphometry (VBM) is an unbiased whole brainapproach for detecting structural differences in gray matterbetween different clinical populations (Ashburner and Friston,2000). VBM provides a systematic estimate of regional gray matterbased on voxel-by-voxel comparison through the whole brain.Previous VBM studies have reported somewhat inconsistent find-ings related to MDD. They have showed the loss of gray mattervolume in prefrontal cortex (Taki et al., 2005; Vasic et al., 2008),hippocampus and temporal lobe (Shah et al., 1998; Bergouignanet al., 2009; Vasic et al., 2008), and anterior cingulate cortex (ACC)and insular (Tang et al., 2007; Yuan et al., 2008; Lai, 2013; Lai andWu, 2014; Stratmann et al., 2014). These discordances may arisefrom differences in sample size, heterogeneous depression groupsor the condition of patients with or without antidepressants at thetime of study.
More recently, there have been increasing literatures investi-gating the neurobiological factors involved in achieving earlyresponse or remission of MDD. VBM studies have reportedstructural changes in MDD patients in relation to clinical responsefollowing pharmacological treatment. The hippocampal volume, inparticular, can be a potential biomarker for depressive episodes(Frodl et al., 2008; MacQueen and Frodl., 2011; Arnone et al., 2013).Arnone et al. (2013) have demonstrated that following 8 weeks ofantidepressant treatment, there was an increase in hippocampalvolume, which was reduced in MDD patients initially. Further-more, Smith et al. (2013) demonstrated an increase in volume ofthe DLPFC in depressed patients, after 12 weeks of antidepressanttreatment. Emerging findings from Positron Emission Tomography(PET) and functional magnetic resonance imaging (fMRI) studiessuggest activity changes in ACC (Mayberg et al., 1999; Gotlib et al.,2005), ventral striatum (Fu et al., 2004), visual cortices (Davidsonet al., 2003; Fu et al., 2004; Desseilles et al., 2009; Veer et al., 2010;Zeng et al., 2012), and amygdala (Sheline et al., 2001; Davidsonet al., 2003; Fu et al., 2007; Victor et al., 2010; Arnone et al., 2012b)during and after antidepressant treatment. These findings suggestthat antidepressant treatment can bring about structural andfunctional brain changes in brain areas of the limbic-corticalnetwork in relation to clinical improvement.
In the perspectives of brain structure–cognition relationship,Li et al. (2010) were the first to demonstrate that structuralabnormalities, such as postcentral gyrus and prefrontal cortex werecorrelated with cognitive function in remitting and non-remittingpatients with MDD. The remitters had milder impairments in visualattention correlating with gray matter volume of postcentral gyrusand superior/medial frontal gyrus, whereas the non-remittersshowed several regional abnormalities, such as the thalamus,amygdala/parahippocampal gyrus with more severe deficits incognition related to gray matter volume reduction in the left DLPFC.However, all subjects had recurrent MDD and a relatively longermean duration of illness (9.2 years). Several literatures reported thatchronicity or recurrence of MDD has influence on the observedbrain volumetric abnormalities in depressive patients. Therefore,further studies are required to elucidate these findings.
In this study, we investigated gray matter volume differencesassociated with antidepressant responsiveness over an 8 weekperiod in MDD patients with relatively a short period of illness anda small number of past episodes using the VBM method. Specifi-cally, we looked for regional gray matter differences predictingantidepressant response and correlated the structural differenceswith cognitive functions. We predicted that brain regions withinlimbic-cortical network showed volumetric abnormalities in MDDpatients compared to healthy controls. Specifically, we expectbrain structural changes in limbic areas such as amygdala, hippo-campus, and insular, and in cortices such as DLPFC, ACC, and visualcortices in relation to antidepressant responsiveness. Antidepres-sant responsive patients represented less volumetric changes aswell as better cognitive functions relative to non-responsivepatients. Similar to Li et al.'s (2010) findings that structuralalterations were correlated with cognitive functions in MDDpatients, we might expect that structural changes predictingtreatment outcome would be associated with cognitive functionsin MDD patients with a relatively short period of illness, even inthe early stage of treatment.
2. Methods
2.1. Participants
Fifty MDD patients (14 males and 36 females) were recruited fromKorea University Anam Hospital in Seoul, South Korea. Trainedpsychiatrists examined all subjects using the Structured ClinicalInterview for the fourth revision of the Diagnostic and StatisticalManual of Mental Disorders (DSM-IV) (Han and Hong, 2000). Patientswere required to have depressive symptoms for at least 2 monthsprior to enrollment and a higher score than 17 on the 17-itemHamilton Depression Rating Scale (HDRS-17) at enrollment (Yi et al.,2005). The exclusion criteria were: (1) MDD patients with anycomorbid major psychiatric illness (based on DSM-IV criteria) onAxis I or Axis II within the last 6 months; (2) MDD with psychoticfeatures; (3) concurrent serious medical illness or primary neurolo-gical illness, such as cerebrovascular disease, Parkinson's disease, orepilepsy; (4) and contraindication for MRI.
Clinical symptoms were evaluated using HDRS-17 scale at thefirst enrollment, and after 1, 2, 4, and 8 weeks of the antidepressanttreatment. All patients received open-label antidepressant treat-ment including serotonin reuptake inhibitors (SSRIs), serotoninnorepinephrine reuptake inhibitors (SNRIs), bupropion, and benzo-diazepines for 8 weeks. Of the patients taking medication, most ofpatients (n¼45) received escitalopram (10–20 mg), 1 received par-oxetine (25–50 mg), 2 received venlafaxine (75–225 mg), 1 receivedduloxetine (30–60 mg) and 2 received bupropion (150–300 mg).Among them 39 patients also received lorazepam (0.25–0.5 mg).After 8 weeks treatments, patients were divided into responder andnon-responder MDD groups according to the severity of theirdepression. Responders (R, 7 males and 19 females, mean age41713 years) were defined as those who showed a 50% decreaseof HDRS-17 score after treatment, compared to their initial score(Frank et al., 1991). The patients who did not reach the responsestatus after treatment were defined as non-responders (NR, 7 malesand 17 females, mean age 43710 years).
Twenty-nine healthy controls, age and gender matched, (HC,8 males and 21 females, mean age 44713 years) participated inthis study. HC was confirmed to have no Axis I or II disorders orfamily histories of psychiatric illness by a psychiatrist's interviewand was screened using HDRS-17 with a cut-off score below 7.
This study was approved by the Ethic Committee of KoreaUniversity, Seoul, South Korea. Written informed consent wasobtained from all participants.
J. Jung et al. / Journal of Affective Disorders 169 (2014) 179–187180

2.2. Neuropsychological assessments
History was taken to obtain demographic and clinical charac-teristic for all participants. Neuropsychological assessments wereconducted to evaluate cognitive functions (9 MDD patients refusedto be assessed).
Neuropsychological assessments included the modified versionof the Trail Making Test (TMT) for attention, the Rey–Kim MemoryBattery for memory, Stroop test, and a word fluency test for frontallobe function. TMT consists of two parts; numbers in part A andletters in part B. Rey–Kim Memory Battery is composed of verbalmemory tests and non-verbal memory tests. Memory Quotient(MQ) was calculated from all scores from subset tests. In Strooptest, the participants were asked to name the color of each item onthree tasks; the color dots (repetition), common words (neutralword) in color, and color words not corresponding to their namecolor. Error control in Stroop test was calculated from the numberof errors (if there was no error, the score was ‘6’, the perfect score).The word fluency test asked participants to speak words startingwith a consonant instructed by a psychiatrist as many as possiblein a given time.
2.3. Magnetic resonance imaging acquisition
MRI scan was performed on a 3T Siemens MRI system.T1-weighted images were acquired parallel to the anterior commis-sure–posterior commissure line using T1-weighted magnetization-prepared rapid gradient-echo (MP-RAGE (1900 ms repetition time,2.6 ms echo time, 220 mm field of view, 256�256 matrix size, 176coronal slices without gap, 1�1�1mm3 voxels, 161 flip angle,number of excitations¼1). For patients, the structural scan wasacquired at the beginning of the treatment (within 2 weeks of thetreatment, 11 patients were drug-naïve at the time of the scanning).
2.4. Voxel-based morphometry
Voxel-based morphometry was performed in order to investigatethe gray matter change using a VBM8 toolbox (http://dbm.neuro.uni-jena.de/vbm8/) in SPM8 (Wellcome Department of Neuroscience,London, UK; http://www.fil.ion.ucl.ac.uk/spm/software/spm8/). VBMprocessing is involved in the following steps. All MRI images werespatially normalized to SPM's T1 template and segmented into graymatter (GM), white matter (WM), and cerebrospinal fluid (CFS). TheVBM segmentation implements adaptive Maximum A Posterior (MAP)and partial volume estimation (PVE) to segment the native spaceimages into rigid-body aligned GM andWH images for all participantsthen warped them into the neighborhood of the Montreal Neurolo-gical Institute (MNI) coordinate space. To improve the segmentation,spatially adaptive nonlocal means (SANLM) denoising methods, andclassical Markov Random Field were employed. DiffeomorphicAnatomical Registration Through Exponentiated Lie Algebra (DARTEL)protocol was applied for normalization. DARTEL uses a large-deformation framework with a constant velocity generating deforma-tions. A DARTEL template was created during segmentation and eachindividual data was registered to this template. Using “Display oneslice for all images”module in VBM8, the registered data were visuallyinspected. Finally the images were smoothed with an 8mm full widthat half-maximum Gaussian kernel. Each voxel in the resulting imageshas an absolute amount of brain volume corresponding to the brainvolume per unit before the normalization.
2.5. Group comparisons of VBM
We used ANCOVA to compare gray matter volumes among thegroups. The total intracranial volume (TIV), ages, and genders wereentered in the analysis as covariates. Significance was set at an
uncorrected threshold of po0.005 with more than 100 contiguousvoxels for exploratory whole brain analysis. From the results of theexploratory whole brain analysis, we found the areas in the limbic-cortical network including bilateral amygdala, caudate, putamen,insular, ACC, visual cortex and DLPFC (Mayberg et al., 1999;Keedwell et al., 2009; Li et al., 2010). For the multiple comparisonscorrection, the significant clusters were performed by Small-Volume Correction (SVC) with an anatomically defined regionalmask from WFU PickAtlas Tool (http://www.fmri.wfubmc.edu) andBonferroni correction for regions in the limbic-cortical network(po0.007). We reported the clusters only meeting a SVC-FWE(Family-Wise Error) corrected po0.05 with more than 100 con-tiguous voxels.
2.6. Statistical analysis
Statistical analysis was performed by using SPSS 12 software.One-way ANOVA and Chi-square test were applied to compare thevalues among groups. For neuropsychological tests, we used t-testand ANOVA followed by post-hoc with Bonferroni correction(po0.05). Pearson's correlation test (two-tailed), with FDR (FalseDiscovery Rate) corrected pr0.05, was applied to explore and toobtain more power in the relationship between GM volume andneuropsychological test results (Benjamini and Hochberg, 1995).
3. Results
3.1. Clinical characteristics and neuropsychological profilesamong groups
We tested 26MDD NR, 24MDD R, and 29 HC. There were nosignificant differences in clinical variables including gender (χ2 (2)¼0.03, p¼0.984), age, and IQ among groups (Fo1.75, p40.182).Thirty-one patients were first episode MDD patients (20 patients inNR and 11 patients in R). Averaged illness duration was about 3 yearsfor NR (36.4733.2 months) and R (33.4743.1 months) patients.Both patients groups showed less than 1 past depressive episode onaverage. Between patient groups, there were no differences in age ofonset, illness duration, and past depressive episodes (to1.212,p40.231). However, the R group showed a significant decrease inpost-HDRS compared to the NR group (t(48)¼�7.09, po0.001).
ANOVA revealed that there were significant differences in pre-HDRS (F(2, 76)¼200.59, po0.001), Stroop test (repetition, F(2, 66)¼4.84, po0.05; neutral word, F(2, 66)¼6.75, po0.005; color word,F(2, 66)¼6.12, po0.005; error control, F(2, 66)¼5.41, po0.01) andMQ (F(2, 67)¼3.70, po0.05) among groups. The patient groups andthe control group did not show any differences in the TMT and theword fluency test (Fo1.09, p40.34). Post-hoc analysis substantiatedthat NR performed poorer than HC in Stroop test and Rey–KimMemory test (po0.05). However, R group completed the tests withno significant difference from the HC group (p40.48). Both R and NRgroups exhibited significantly higher scores in HDRS-17 compared toHC group before antidepressant treatment (po0.05) (Table 1).
3.2. Gray matter (GM) volume changes among groups
The exploratory whole brain analysis revealed that there weresignificant volumetric differences in MDD patients compared to HCssuch as insular, ACC, SFG, IFG, orbital frontal cortex, and amygdala.Between patient groups, lingual gyrus and precuneus showedsignificant gray matter volume difference (see the Supplementaryinformation).
To confirm the findings, we applied a more stringent threshold,pFWE-SVC-correctedo0.05, for the areas found in the exploratorywhole brain analysis. GM volumes of the NR group were
J. Jung et al. / Journal of Affective Disorders 169 (2014) 179–187 181
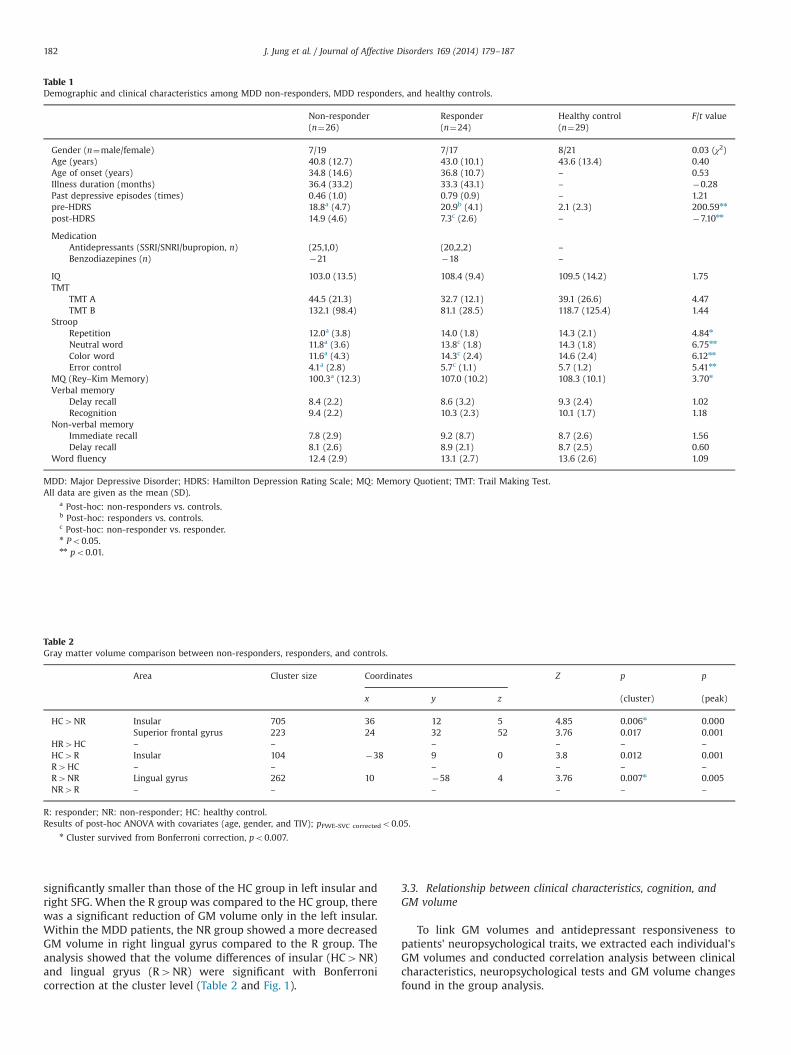
significantly smaller than those of the HC group in left insular andright SFG. When the R group was compared to the HC group, therewas a significant reduction of GM volume only in the left insular.Within the MDD patients, the NR group showed a more decreasedGM volume in right lingual gyrus compared to the R group. Theanalysis showed that the volume differences of insular (HC4NR)and lingual gryus (R4NR) were significant with Bonferronicorrection at the cluster level (Table 2 and Fig. 1).
3.3. Relationship between clinical characteristics, cognition, andGM volume
To link GM volumes and antidepressant responsiveness topatients' neuropsychological traits, we extracted each individual'sGM volumes and conducted correlation analysis between clinicalcharacteristics, neuropsychological tests and GM volume changesfound in the group analysis.
Table 1Demographic and clinical characteristics among MDD non-responders, MDD responders, and healthy controls.
Non-responder Responder Healthy control F/t value(n¼26) (n¼24) (n¼29)
Gender (n¼male/female) 7/19 7/17 8/21 0.03 (χ2)Age (years) 40.8 (12.7) 43.0 (10.1) 43.6 (13.4) 0.40Age of onset (years) 34.8 (14.6) 36.8 (10.7) – 0.53Illness duration (months) 36.4 (33.2) 33.3 (43.1) – �0.28Past depressive episodes (times) 0.46 (1.0) 0.79 (0.9) – 1.21pre-HDRS 18.8a (4.7) 20.9b (4.1) 2.1 (2.3) 200.59nn
post-HDRS 14.9 (4.6) 7.3c (2.6) – �7.10nn
MedicationAntidepressants (SSRI/SNRI/bupropion, n) (25,1,0) (20,2,2) –
Benzodiazepines (n) �21 �18 –
IQ 103.0 (13.5) 108.4 (9.4) 109.5 (14.2) 1.75TMT
TMT A 44.5 (21.3) 32.7 (12.1) 39.1 (26.6) 4.47TMT B 132.1 (98.4) 81.1 (28.5) 118.7 (125.4) 1.44
StroopRepetition 12.0a (3.8) 14.0 (1.8) 14.3 (2.1) 4.84n
Neutral word 11.8a (3.6) 13.8c (1.8) 14.3 (1.8) 6.75nn
Color word 11.6a (4.3) 14.3c (2.4) 14.6 (2.4) 6.12nn
Error control 4.1a (2.8) 5.7c (1.1) 5.7 (1.2) 5.41nn
MQ (Rey–Kim Memory) 100.3a (12.3) 107.0 (10.2) 108.3 (10.1) 3.70n
Verbal memoryDelay recall 8.4 (2.2) 8.6 (3.2) 9.3 (2.4) 1.02Recognition 9.4 (2.2) 10.3 (2.3) 10.1 (1.7) 1.18
Non-verbal memoryImmediate recall 7.8 (2.9) 9.2 (8.7) 8.7 (2.6) 1.56Delay recall 8.1 (2.6) 8.9 (2.1) 8.7 (2.5) 0.60
Word fluency 12.4 (2.9) 13.1 (2.7) 13.6 (2.6) 1.09
MDD: Major Depressive Disorder; HDRS: Hamilton Depression Rating Scale; MQ: Memory Quotient; TMT: Trail Making Test.All data are given as the mean (SD).
a Post-hoc: non-responders vs. controls.b Post-hoc: responders vs. controls.c Post-hoc: non-responder vs. responder.n Po0.05.nn po0.01.
Table 2Gray matter volume comparison between non-responders, responders, and controls.
Area Cluster size Coordinates Z p p
x y z (cluster) (peak)
HC4NR Insular 705 36 12 5 4.85 0.006n 0.000Superior frontal gyrus 223 24 32 52 3.76 0.017 0.001
HR4HC – – – – – –
HC4R Insular 104 �38 9 0 3.8 0.012 0.001R4HC – – – – – –
R4NR Lingual gyrus 262 10 �58 4 3.76 0.007n 0.005NR4R – – – – – –
R: responder; NR: non-responder; HC: healthy control.Results of post-hoc ANOVA with covariates (age, gender, and TIV); pFWE-SVC correctedo0.05.
n Cluster survived from Bonferroni correction, po0.007.
J. Jung et al. / Journal of Affective Disorders 169 (2014) 179–187182

In the comparison of the R group against the NR group, we found asignificant volumetric difference in the right lingual gyrus. ANCOVAwith TIV, ages, and genders as covariates revealed that the averagevolume of lingual gyrus showed significant differences betweengroups (F(2, 73)¼11.09, po0.001). Post-hoc analysis demonstratedthat R group exhibited larger GM volume compared to NR (po0.001)and HC (pr0.001) group significantly. There was no differencebetween NR group and HC group (p40.28). The volume of lingualgyrus in MDD patients was correlated with the age of MDD onset(r¼�0.26, pFDR-corrected¼0.05) and post-HDRS (r¼�0.41, pFDR-correctedo0.001). Strikingly, the volume of lingual gyrus highly predicted theantidepressant treatment effect (post-HDRS score). Patients showinga lager reduction of HDRS after treatment had a greater volume oflingual gyrus. Moreover, patients having a greater volume of lingualgyrus performed better at the Stroop test (color word: r¼0.30,pFDR-corrected¼0.05, error control: r¼0.59, pFDR-correctedo0.001). Therewas a marginally significant correlation between the volume of lingualgyrus and MQ (r¼0.26, pFDR-corrected¼0.07). Specifically, the subsets ofthe Rey–Kim test (visual memory tests) including non-verbal immedi-ate memory test (r¼0.52, pFDR-correctedo0.001) and non-verbal delaymemory test (r¼0.50, pFDR-correctedo0.001) were significantly corre-lated with the volume of lingual gyrus. Also, the other verbal memorytests (delay recall: r¼0.30, pFDR-corrected¼0.07, recognition: r¼0.30,pFDR-corrected¼0.06) showed marginal correlations with the volume oflingual gyrus. These results suggest that the lingual gyrus volume isassociated with neuropsychological tests performance in MDDpatients. Thus, a relatively preserved cognitive function in antidepres-sant responders may be attributed to the larger GM volume of thelingual gyrus. There were no other significant correlations betweenclinical characteristics, cognitive functions, and other GM volumesfound in group comparison. These results are illustrated in Fig. 2.
4. Discussion
By recruiting MDD patients with a relatively short period ofillness and a small number of past episodes, we investigated how
antidepressant responsiveness is predicted by brain structure–cognition relationship. In the comparison of each MDD group withhealthy controls, antidepressant non-responsive patients showedsevere structural alterations and cognitive deficits in memory andattention control. However, treatment responsive patients had aminor structural change only in the left insular and exhibited acognitive level that was equal to healthy controls. The antidepres-sant responsive patients had a greater volume of lingual gyruscompared to non-responsive patients and healthy controls. Thevolume of the lingual gryus in MDD patients was correlated withantidepressant responsiveness and cognitive function, which sug-gests that a larger volume of the lingual gryus may contribute to apreserved cognitive function for antidepressant responders.
This is the first volumetric MRI study which demonstrated thatthe volume of lingual gyrus is associated with antidepressantresponsiveness in MDD patients. The lingual gyrus was not com-monly identified in previous volumetric studies on MDD. However,functional imaging studies have revealed abnormal activation in thelingual gyrus and altered visual network including the lingual gyrusin depressed patients compared to healthy controls (Desseilles et al.,2009; Veer et al., 2010; Laurent and Ablow., 2012; Zeng et al., 2012).Especially, Keedwell et al. (2009) demonstrated the activity changeof the lingual gyrus and primary visual cortex after an open labelantidepressant treatments. Before treatment, depressed patientsshowed increased responses in visual areas to sad faces, whereasthe response of visual cortices was increased to happy faces aftertreatment with clinical improvement. This finding suggested thatantidepressants shifted emotional processing bias for negativeinformation toward a positive direction by modulating the func-tional activity in visual areas. Besides, Yatham et al. (2010) reportedthat electroconvulsive therapy in MDD patients diminished 5-HT2receptors in the right lingual gyrus, which correlated with depres-sive symptoms. These studies suggested that MDD would lead tothe functional abnormality of visual areas and antidepressanttreatment can shift the abnormal activity into a normal level. Also,visual cortices could be susceptible to antidepressant treatment.Taken together, our data first demonstrated that the volume of
Fig. 1. Gray matter (GM) volume changes from group analysis. (A) Statistical parametric map showing GM volume reduction in NR group compared to HC group. (B) Statisticalparametric map showing GM volume reduction in R group compared to HC group. (C) Statistical parametric map showing GM volume reduction in NR group compared to Rgroup. Red indicates significant areas thresholded at the voxel level puncorrectedo0.005 and yellow indicates significant regions thresholded at the cluster level pFWE-SVC
correctedo0.05. (D) Bar graph showing the averaged GM volume of the lingual gyrus. Green bar represents R group. Red bar represents NR group. White bar represents HC group.Error bars indicates standard error. nnpr0.001. (For interpretation of the references to color in this figure legend, the reader is referred to the web version of this article.)
J. Jung et al. / Journal of Affective Disorders 169 (2014) 179–187 183

lingual gyrus highly predicted the antidepressant treatment effect.Therefore, in accordance with the functional alteration of lingualgyrus responsive to antidepressant treatment, our finding suggeststhe lingual gyrus might be a potential marker of early antidepres-sant response in MDD patients with a short illness period, even atthe early stage of treatment.
The volume of lingual gyrus was also associated with neurop-sychological features of depression in our analysis. The lingual
gyrus plays an important role in visual processing and liesbetween the calcarine sulcus next to the fusiform gyrus, and thecollateral sulcus reaches the temporal lobe which joins the para-hippocampal gyrus (Mendoza and Anne, 2008). Also, the lingualgyrus is directly connected to the limbic system (Conrad andStumpf., 1975). Damage to this area particularly is involved invisual memory dysfunction and visuo-limbic disconnection syn-drome (Bogousslavsky et al., 1987). In visual attention control, the
Fig. 2. Relationship between the GM volume of lingual gyrus in MDD patients and clinical/neuropsychological measurements. (a) Correlation between the age of onset andthe GM volume of lingual gyrus. (b) Correlation between post-HDRS and the GM volume of lingual gyrus. (c) Correlation between color word score in Stroop test and the GMvolume of lingual gyrus. (d) Correlation between error control in Stroop test and the GM volume of lingual gyrus. (e) Correlation between non-verbal immediate recall in theRey–Kim test and the GM volume of lingual gyrus. (f) Correlation between non-verbal delay recall in the Rey–Kim test and the GM volume of lingual gyrus. Redmultiplication represents the individual of non-responders. Blue circle represents the responders. (For interpretation of the references to color in this figure legend, thereader is referred to the web version of this article.)
J. Jung et al. / Journal of Affective Disorders 169 (2014) 179–187184

activity of lingual gyrus is mediated by a top-down attentioncontrol system which includes the frontoparietal network(Hopfinger et al., 2000). Desseilles et al. (2009) demonstratedthe interaction between mood regulation and cognition in MDDpatients focusing on visual information processing. They found anabnormal filtering of irrelevant information in visual cortices aswell as altered functional connectivity between frontoparietalnetwork and visual cortices. Based on these fMRI findings, theyargued that the abnormal visual processing interfered with therecruitment of executive/attention neural network in MDDpatients. Consequently, the abnormal state of visual corticesinfluences cognitive functions for depressive patients. Recently,Peterson et al. (2009) investigated the cortical thickness of 131people who were at high familial risk for developing MDD. Theyfound that individuals with a higher risk had significant corticalthinning in frontal, parietal, temporal, and occipital areas in theright hemisphere. Especially, cortical thinning in the posterior partof the right hemisphere including inferior parietal and occipitalcortex predicted worse attention and visual memory performance.These findings support the suggestion of Drevets (2007) thatalterations in the functional balance between top-down controland emotion-limbic circuits may underlie the pathophysiology ofMDD. In other words, top-down influences from frontoparietalnetworks were altered in MDD patients, leading to an abnormalneural processing in visual cortices and the modulation of thelimbic system. In our data, the decreased volume of lingual gyrusas well as SFG in non-responsive patients resulted in impairedvisual memory and attention functions. On the other hand,the larger volume of lingual gyrus and relatively intact frontalregions enabled responsive patients to achieve a normal level ofcognitive functions. Therefore, the structural change of lingualgyrus in responsive patients might contribute to their cognitivefunctions by interacting with frontoparietal network and limbicnetwork.
The decreased gray matter volume in the right SFG in non-responsive MDD patients in our study has been reported in previousstudies (Yuan et al., 2008; Koolschijn et al., 2009; Li et al., 2010;Bora et al., 2012; Serra-Blasco et al., 2013). As a major region in thecortico-limbic network, the abnormal morphology of SFG isinvolved in dysfunctional mood and emotional regulation in MDD(Mayberg, 2003). A recent meta-analysis with VBM studies demon-strated that MDD patients compared to healthy controls haddecreased gray matter in the right dosromedial frontal cortex(Bora et al., 2012). Specifically, only chronic patients showed SFGreduction, compared to healthy controls, and first-episode patientsdid not show such reduction. Mwangi et al. (2012) attempted toclassify which brain region is associated with MDD using machinelearning techniques. They showed that volume reduction in thefrontal lobe including SFG highly predicted MDD and the severityof depression at an individual level. With all these findings, ourresult suggests that SFG can be a biomarker of MDD, which maydevelop into a chronic form or treatment-resistant form of MDD.In addition, it was observed that the gray matter volume in SFGwas correlated with cognitive functions in MDD patients (Li et al.,2010). This may explain the finding of our study, that only non-responsive patients with cognitive impairments had structuralchanges in SFG.
In our analysis, there was a decreased GM volume in the leftinsular in both antidepressant responsive and non-responsivepatients. Only recently has the structural abnormality of the leftinsular been found in relation to depressed patients (Takahashi et al.,2010; Lee et al., 2011; Soriano-Mas et al., 2011; Serra-Blasco et al.,2013; Lai, 2013; Lai andWu, 2014; Stratmann et al., 2014). The insularhas been described to be a key component of the limbic integrationcortex and plays a role in emotion and cognitive functions(Augustine, 1996). Evidence from functional neuroimaging studies
in both healthy controls (Reiman et al., 1997; Shin et al., 2000) anddepressed patients (Mayberg et al., 1999; Liotti et al., 2002) hasrevealed that the insular is involved in regulation of emotional state,especially in sadness and guilt. Moreover, Soriano-Mas et al. (2011)demonstrated a decreased volume of the left posterior insular in asizable MDD population (70 patients) in comparison with a healthypopulation. In particular, Takahashi et al. (2010) reported a significantreduction in the left insular cortex in both current and remitted MDDpatients as compared to healthy controls. They argued that thevolumetric reduction in the left insular may represent a biomarkerof vulnerability to depression. Our findings are consistent with theseresults and support Mayberg's proposal (2003) that dysfunctionallimbic-cortical circuit including the insular is related to pathogenicmechanisms underlying MDD.
The limitations of our study are as follows. First, our samplesize is relatively small. Also, we could not replicate an overall graymatter volume reduction in the limbic-cortical network. However,this can be explained by the fact that over half of our patients (31/50) were first-episode MDD patients and many patients had arelatively small number of past episodes. Therefore, it is possiblethat the volume loss in patients may not have progressed yet (seethe Supplementary information. The exploratory analysis showedvolume reduction in limbic-cortical network including amygdalaand ACC). Second, we did not control the type of antidepressant,and use of benzodiazepines. Although most patients receivedescitalpram, 6 patients received other antidepressants, includingparoxetine, venlafaxine, duloxetine, and bupropion. A majority ofpatients also received lorazepam. However, such diversity inmedication did not influence our finding. We examined the effectof medication diversities such as the number of medications, thecombination of medications that the patients were taking, andintake of sedative medication, using non-parametric tests. Theresults showed that there was no difference between the patientsgroups (p40.844). Moreover, the goal of the current study was toexplore a potential structural biomarker predicting the antide-pressant effect in naturalistic treatment conditions, and not topursue the effect of a certain type of antidepressant. This limita-tion applies to a majority of MRI studies on treatment response inMDD patients (Chen et al., 2007; Keedwell et al., 2009; Li et al.,2010). Third, the imaging data of patients were acquired at thebeginning of treatment (within 2 weeks). However, 11 patientswere drug-naïve at the time of the scanning and most of thepatients (38/50) took the scanning within 7 days after the treat-ment. Inter-rate reliability was not controlled in the current study.Finally, we also could not control psychosocial factors (e.g. stress,trauma or family problems), which could affect antidepressantresponse. Therefore, further studies that have controlled theseissues are needed to confirm our results.
In conclusion, we demonstrated that there were significantstructural differences between patients who responded to anti-depressants and those who responded poorly to them. Thetreatment responsive MDD patients showed preserved cognitivefunctions and a significant gray matter reduction only in the leftinsular when compared to the healthy group. In contrast, thepatients who responded poorly to antidepressants had severalfunctional deficits in neuropsychological tests and greater graymatter volume loss in the left insular and the right SFGcompared to healthy controls. Antidepressant responsivenesswas involved in gray matter volume difference in the lingualgyrus. Moreover, the lingual gyrus volume of MDD patients wascorrelated with treatment responsiveness and cognitive func-tions. The larger volume of the lingual gyrus in treatmentresponsive patients may attribute to their intact cognitivefunction. Therefore, we suggest that the lingual gyrus may bean important area in early antidepressant responsiveness andcognitive ability in depressed patients.
J. Jung et al. / Journal of Affective Disorders 169 (2014) 179–187 185

Conflict of interestNo conflicts of interest.
Role of funding sourceThis study was supported by a grant of the Korean Health Technology R&D
Project, Ministry of Health & Welfare, Republic of Korea (A120004).
AcknowledgmentWe thank all patients for participation in this study.
Appendix A. Supporting information
Supplementary data associated with this article can be found inthe online version at http://dx.doi.org/10.1016/j.jad.2014.08.018.
References
Anderson, I.M., Nutt, D.J., Deakin, J.F., 2000. Evidence-based guidelines for treatingdepressive disorders with antidepressants: a revision of the 1993 BritishAssociation for Psychopharmacology guidelines. British Association for Psycho-pharmacology. J. Psychopharmacol. 14, 3–20.
Arnone, D., McIntosh, A.M., Ebmeier, K.P., Munafo, M.R., Anderson, I.M., 2012a.Magnetic resonance imaging studies in unipolar depression: systematic reviewand meta-regression analyses. Eur. Neuropsychopharmacol. 22, 1–16.
Arnone, D., McKie, S., Elliott, R., Thomas, E.J., Downey, D., Juhasz, G., Williams, S.R.,Deakin, J.F., Anderson, I.M., 2012b. Increased amygdala responses to sad but notfearful faces in major depression: relation to mood state and pharmacologicaltreatment. Am. J. Psychiatry 169, 841–850.
Arnone, D., McKie, S., Elliott, R., Juhasz, G., Thomas, E.J., Downey, D., Williams, S.,Deakin, J.F., Anderson, I.M., 2013. State-dependent changes in hippocampal greymatter in depression. Mol. Psychiatry 18, 1265–1272.
Ashburner, J., Friston, K.J., 2000. Voxel-based morphometry—the methods. Neuro-image 11, 805–821.
Augustine, J.R., 1996. Circuitry and functional aspects of the insular lobe in primatesincluding humans. Brain Res. Brain Res. Rev. 22, 229–244.
Benjamini, Y., Hochberg, Y., 1995. Controlling the false discovery rate: a practicaland powerful approach to multiple testing. J. R. Stat. Soc. B 1, 289–300.
Bergouignan, L., Chupin, M., Czechowska, Y., Kinkingnehun, S., Lemogne, C.,Le Bastard, G., Lepage, M., Garnero, L., Colliot, O., Fossati, P., 2009. Can voxelbased morphometry, manual segmentation and automated segmentationequally detect hippocampal volume differences in acute depression? Neuro-image 45, 29–37.
Bogousslavsky, J., Miklossy, J., Deruaz, J.P., Assal, G., Regli, F., 1987. Lingual andfusiform gyri in visual processing: a clinico-pathologic study of superioraltitudinal hemianopia. J. Neurol. Neurosurg. Psychiatry 50, 607–614.
Bora, E., Fornito, A., Pantelis, C., Yucel, M., 2012. Gray matter abnormalities in MajorDepressive Disorder: a meta-analysis of voxel based morphometry studies.J. Affect. Disord. 138, 9–18.
Chen, C.H., Ridler, K., Suckling, J., Williams, S., Fu, C.H., Merlo-Pich, E., Bullmore, E.,2007. Brain imaging correlates of depressive symptom severity and predictorsof symptom improvement after antidepressant treatment. Biol. Psychiatry 62,407–414.
Conrad, C.D., Stumpf, W.E., 1975. Direct visual input to the limbic system: crossedretinal projections to the nucleus anterodorsalis thalami in the tree shrew. Exp.Brain Res. 23, 141–149.
Davidson, R.J., Irwin, W., Anderle, M.J., Kalin, N.H., 2003. The neural substrates of affectiveprocessing in depressed patients treated with venlafaxine. Am. J. Psychiatry160, 64–75.
Desseilles, M., Balteau, E., Sterpenich, V., Dang-Vu, T.T., Darsaud, A., Vandewalle, G.,Albouy, G., Salmon, E., Peters, F., Schmidt, C., Schabus, M., Gais, S., Degueldre, C.,Phillips, C., Luxen, A., Ansseau, M., Maquet, P., Schwartz, S., 2009. Abnormalneural filtering of irrelevant visual information in depression. J. Neurosci. 29,1395–1403.
Drevets, W.C., 2007. Orbitofrontal cortex function and structure in depression. Ann.N. Y. Acad. Sci. 1121, 499–527.
Drevets, W.C., Price, J.L., Furey, M.L., 2008. Brain structural and functional abnorm-alities in mood disorders: implications for neurocircuitry models of depression.Brain. Struct. Funct. 213, 93–118.
Fagiolini, A., Kupfer, D.J., 2003. Is treatment-resistant depression a unique subtypeof depression? Biol. Psychiatry 53, 640–648.
Fava, M., Davidson, K.G., 1996. Definition and epidemiology of treatment-resistantdepression. Psychiatr. Clin. N. Am. 19, 179–200.
Fava, M., Kendler, K.S., 2000. Major depressive disorder. Neuron 28, 335–341.Fizgerald, P.B., Laird, A.R., Maller, J., Daskalakis, Z.J., 2008. A meta-analytic study of
changes in brain activation in depression. Hum. Brain Mapp. 29, 683–695.Frank, E., Prien, R.F., Jarrett, R.B., Keller, M.B., Kupfer, D.J., Lavori, P.W., Rush, A.J.,
Weissman, M.M., 1991. Conceptualization and rationale for consensus defini-tions of terms in major depressive disorder. Remission, recovery, relapse, andrecurrence. Arch. Gen. Psychiatry 48, 851–855.
Frodl, T.S., Koutsouleris, N., Bottlender, R., Born, C., Jager, M., Scupin, I., Reiser, M.,Moller, H.J., Meisenzahl, E.M., 2008. Depression-related variation in brainmorphology over 3 years: effects of stress? Arch. Gen. Psychiatry 65, 1156–1165.
Fu, C.H., Williams, S.C., Brammer, M.J., Suckling, J., Kim, J., Cleare, A.J., Walsh, N.D.,Mitterschiffthaler, M.T., Andrew, C.M., Pich, E.M., Bullmore, E.T., 2007. Neuralresponses to happy facial expressions in major depression following antide-pressant treatment. Am. J. Psychiatry 164, 599–607.
Fu, C.H., Williams, S.C., Cleare, A.J., Brammer, M.J., Walsh, N.D., Kim, J., Andrew, C.M.,Pich, E.M., Williams, P.M., Reed, L.J., Mitterschiffthaler, M.T., Suckling, J.,Bullmore, E.T., 2004. Attenuation of the neural response to sad faces in majordepression by antidepressant treatment: a prospective, event-related func-tional magnetic resonance imaging study. Arch. Gen. Psychiatry 61, 877–889.
Gotlib, I.H., Sivers, H., Gabrieli, J.D., Whitfield-Gabrieli, S., Goldin, P., Minor, K.L.,Canli, T., 2005. Subgenual anterior cingulate activation to valenced emotionalstimuli in major depression. Neuroreport 16, 1731–1734.
Han, O., Hong, J., 2000. Structured Clinical Interview for DSM-IV Axis Disorder—Korean Version. Hana Medical Publishing, Seoul.
Hopfinger, J.B., Buonocore, M.H., Mangun, G.R., 2000. The neural mechanisms oftop-down attentional control. Nat. Neurosci. 3, 284–291.
Keedwell, P., Drapier, D., Surguladze, S., Giampietro, V., Brammer, M., Phillips, M.,2009. Neural markers of symptomatic improvement during antidepressanttherapy in severe depression: subgenual cingulate and visual cortical responsesto sad, but not happy, facial stimuli are correlated with changes in symptomscore. J. Psychopharmacol. 23, 775–788.
Kessler, R.C., Berglund, P., Demler, O., Jin, R., Koretz, D., Merikangas, K.R., Rush, A.J.,Walters, E.E., Wang, P.S., 2003. The epidemiology of major depressive disorder:results from the National Comorbidity Survey Replication (NCS-R). J. Am. Med.Assoc. 289, 3095–3105.
Koolschijn, P.C., van Haren, N.E., Lensvelt-Mulders, G.J., Hulshoff Pol, H.E., Kahn, R.S.,2009. Brain volume abnormalities in major depressive disorder: a meta-analysisof magnetic resonance imaging studies. Hum. Brain Mapp. 30, 3719–3735.
Laurent, H.K., Ablow, J.C., 2012. A cry in the dark: depressed mothers show reducedneural activation to their own infant's cry. Soc. Cogn. Affect. Neurosci. 7,125–134.
Lai, C.H., 2013. Gray matter volume in major depressive disorder: a meta-analysis ofvoxel-based morphometry studies. Psychiatry Res. 211, 37–46.
Lai, C.H., Wu, Y.T., 2014. Frontal-insula gray matter deficits in first-episodemedication-naive patients with major depressive disorder. J. Affect. Disord.160, 74–79.
Lee, H.Y., Tae, W.S., Yoon, H.K., Lee, B.T., Paik, J.W., Son, K.R., Oh, Y.W., Lee, M.S.,Ham, B.J., 2011. Demonstration of decreased gray matter concentration in themidbrain encompassing the dorsal raphe nucleus and the limbic subcorticalregions in major depressive disorder: an optimized voxel-based morphometrystudy. J. Affect. Disord. 133, 128–136.
Li, C.T., Lin, C.P., Chou, K.H., Chen, I.Y., Hsieh, J.C., Wu, C.L., Lin, W.C., Su, T.P., 2010.Structural and cognitive deficits in remitting and non-remitting recurrentdepression: a voxel-based morphometric study. Neuroimage 50, 347–356.
Liotti, M., Mayberg, H.S., McGinnis, S., Brannan, S.L., Jerabek, P., 2002. Unmaskingdisease-specific cerebral blood flow abnormalities: mood challenge in patientswith remitted unipolar depression. Am. J. Psychiatry 159, 1830–1840.
MacQueen, G., Frodl, T., 2011. The hippocampus in major depression: evidence forthe convergence of the bench and bedside in psychiatric research? Mol.Psychiatry 16, 252–264.
Mayberg, H.S., 1997. Limbic-cortical dysregulation: a proposed model of depres-sion. J. Neuropsychiatry Clin. Neurosci. 9, 471–481.
Mayberg, H.S., 2003. Modulating dysfunctional limbic-cortical circuits in depres-sion: towards development of brain-based algorithms for diagnosis andoptimised treatment. Br. Med. Bull. 65, 193–207.
Mayberg, H.S., Liotti, M., Brannan, S.K., McGinnis, S., Mahurin, R.K., Jerabek, P.A.,Silva, J.A., Tekell, J.L., Martin, C.C., Lancaster, J.L., Fox, P.T., 1999. Reciprocallimbic-cortical function and negative mood: converging PET findings indepression and normal sadness. Am. J. Psychiatry 156, 675–682.
Mendoza, J.E., Foundas, Anne L., 2008. Clinical Neuroanatomy: A NeurobehavioralApproach. Springer, New York.
Mwangi, B., Ebmeier, K.P., Matthews, K., Steele, J.D., 2012. Multi-centre diagnosticclassification of individual structural neuroimaging scans from patients withmajor depressive disorder. Brain 135, 1508–1521.
Peterson, B.S., Warner, V., Bansal, R., Zhu, H., Hao, X., Liu, J., Durkin, K., Adams, P.B.,Wickramaratne, P., Weissman, M.M., 2009. Cortical thinning in persons atincreased familial risk for major depression. Proc. Natl. Acad. Sci. USA 106,6273–6278.
Price, J.L., Drevets, W.C., 2010. Neurocircuitry of mood disorders. Neuropsycho-pharmacology 35, 192–216.
Reiman, E.M., Lane, R.D., Ahern, G.L., Schwartz, G.E., Davidson, R.J., Friston, K.J.,Yun, L.S., Chen, K., 1997. Neuroanatomical correlates of externally and internallygenerated human emotion. Am. J. Psychiatry 154, 918–925.
Serra-Blasco, M., Portella, M.J., Gomez-Anson, B., de Diego-Adelino, J., Vives-Gilabert, Y.,Puigdemont, D., Granell, E., Santos, A., Alvarez, E., Perez, V., 2013. Effects of illnessduration and treatment resistance on grey matter abnormalities in major depres-sion. Br. J. Psychiatry 202, 434–440.
Shah, P.J., Ebmeier, K.P., Glabus, M.F., Goodwin, G.M., 1998. Cortical grey matterreductions associated with treatment-resistant chronic unipolar depression.Controlled magnetic resonance imaging study. Br. J. Psychiatry 172, 527–532.
Sheline, Y.I., Barch, D.M., Donnelly, J.M., Ollinger, J.M., Snyder, A.Z., Mintun, M.A.,2001. Increased amygdala response to masked emotional faces in depressed
J. Jung et al. / Journal of Affective Disorders 169 (2014) 179–187186

subjects resolves with antidepressant treatment: an fMRI study. Biol. Psychiatry50, 651–658.
Shin, L.M., Dougherty, D.D., Orr, S.P., Pitman, R.K., Lasko, M., Macklin, M.L., Alpert, N.M.,Fischman, A.J., Rauch, S.L., 2000. Activation of anterior paralimbic structures duringguilt-related script-driven imagery. Biol. Psychiatry 48, 43–50.
Smith, R., Chen, K., Baxter, L., Fort, C., Lane, R.D., 2013. Antidepressant effects ofsertraline associated with volume increases in dorsolateral prefrontal cortex.J. Affect. Disord. 146, 414–419.
Soriano-Mas, C., Hernandez-Ribas, R., Pujol, J., Urretavizcaya, M., Deus, J., Harrison, B.J.,Ortiz, H., Lopez-Sola, M., Menchon, J.M., Cardoner, N., 2011. Cross-sectional andlongitudinal assessment of structural brain alterations in melancholic depression.Biol. Psychiatry 69, 318–325.
Stratmann, M., Konrad, C., Kugel, H., Krug, A., Schoning, S., Ohrmann, P., Uhlmann, C.,Postert, C., Suslow, T., Heindel, W., et al., 2014. Insular and hippocampal graymatter volume reductions in patients with major depressive disorder. PLoS One 9,e102692.
Takahashi, T., Yucel, M., Lorenzetti, V., Tanino, R., Whittle, S., Suzuki, M., Walterfang,M., Pantelis, C., Allen, N.B., 2010. Volumetric MRI study of the insular cortex inindividuals with current and past major depression. J. Affect. Disord. 121,231–238.
Taki, Y., Kinomura, S., Awata, S., Inoue, K., Sato, K., Ito, H., Goto, R., Uchida, S., Tsuji, I., Arai,H., Kawashima, R., Fukuda, H., 2005. Male elderly subthreshold depression patientshave smaller volume of medial part of prefrontal cortex and precentralgyruscompared with age-matched normal subjects: a voxel-based morphometry.J. Affect. Disord. 88, 313–320.
Tang, Y., Wang, F., Xie, G., Liu, J., Li, L., Su, L., Liu, Y., Hu, X., He, Z., Blumberg, H.P.,2007. Reduced ventral anterior cingulate and amygdala volumes in medication-
naive females with major depressive disorder: a voxel-based morphometricmagnetic resonance imaging study. Psychiatry Res. 156, 83–86.
Vasic, N., Walter, H., Hose, A., Wolf, R.C., 2008. Gray matter reduction associatedwith psychopathology and cognitive dysfunction in unipolar depression: avoxel-based morphometry study. J. Affect. Disord. 109, 107–116.
Veer, I.M., Beckmann, C.F., van Tol, M.J., Ferrarini, L., Milles, J., Veltman, D.J., Aleman, A.,van Buchem, M.A., van der Wee, N.J., Rombouts, S.A., 2010. Whole brain resting-state analysis reveals decreased functional connectivity in major depression. Front.Syst. Neurosci. 4, 1–10.
Victor, T.A., Furey, M.L., Fromm, S.J., Ohman, A., Drevets, W.C., 2010. Relationshipbetween amygdala responses to masked faces and mood state and treatment inmajor depressive disorder. Arch. Gen. Psychiatry 67, 1128–1138.
Yatham, L.N., Liddle, P.F., Lam, R.W., Zis, A.P., Stoessl, A.J., Sossi, V., Adam, M.J., Ruth, T.J.,2010. Effect of electroconvulsive therapy on brain 5-HT(2) receptors in majordepression. Br. J. Psychiatry 196, 474–479.
Yi, J., Bae, S.O., Ahn, Y.M., Park, D.B., Noh, K.S., Shin, H.K., et al., 2005. Validity andreliability of the Korean version of the Hamilton Depression Rating Scale(K-HDRS). J. Korean Neuropsychiatr. Assoc. 44, 456–465.
Yuan, Y., Zhu, W., Zhang, Z., Bai, F., Yu, H., Shi, Y., Qian, Y., Liu, W., Jiang, T., You, J., Liu, Z.,2008. Regional gray matter changes are associated with cognitive deficits inremitted geriatric depression: an optimized voxel-based morphometry study. Biol.Psychiatry 64, 541–544.
Zeng, L.L., Shen, H., Liu, L., Wang, L., Li, B., Fang, P., Zhou, Z., Li, Y., Hu, D., 2012.Identifying major depression using whole-brain functional connectivity: amultivariate pattern analysis. Brain 135, 1498–1507.
J. Jung et al. / Journal of Affective Disorders 169 (2014) 179–187 187
Copyright © 2022 FDOKUMEN