Immunization of high-risk paediatric populations: Central European Vaccination Awareness Group...
15
Immunization of high-risk paediatric populations: Central European Vaccination Awareness Group (CEVAG) recommendations Expert Rev. Vaccines Early online, 1–15 (2014) Darko Richter*, Ioana Anca, Francis E Andre ´, Mustafa Bakir, Roman Chlibek, Milan C ˇ iz ˇ man, Atanas Mangarov, Zso ´ fia Me ´ szner, Marko Pokorn, Roman Prymula, Nuran Salman, Pavol S ˇ imurka, Eda Tamm, Goran Tes ˇovic ´, Ingrid Urbanc ˇı ´kova ´, Vytautas Usonis, Jacek Wysocki and Dace Zavadska *Author for correspondence: Tel.: +385 1237 6521 Fax: +385 1237 6573 [email protected] For a full list of author affiliations, please see page 15. Over the last decade, childhood immunization has substantially reduced morbidity and mortality from vaccine-preventable diseases. However, particular paediatric risk groups, such as those with comorbidities, may not be adequately vaccinated despite being more susceptible to complications and death from certain infectious diseases. This may be due to lack of immunization recommendations, lack of awareness, or incomplete adherence to existing guidelines. Furthermore, recommendations for immunization can be inconsistent across Europe. An expanded initiative from the Central European Vaccination Awareness Group aims to raise awareness of the different high-risk paediatric groups, differentiate them according to their specific risk, and formalise a guidance statement for the immunization of each population. KEYWORDS: Central Europe • high-risk • immunization • paediatric • recommendations Immunization programs represent one of the most impactful advances in medicine [1]. Uni- versal immunization schedules are primarily aimed at infants and young children because they suffer the highest incidence of disease and risk of complications and death. From 1900 to 1998, US childhood immunization pro- grams dramatically reduced pediatric mortality from infectious diseases from 62 to 2% [1]. In 2011, the CDC listed the worldwide preven- tion of an estimated 2.5 million deaths in chil- dren aged <5 years annually as one of the top 10 public health achievements in the last decade [2]. Pediatric subgroups at raised risk of severe disease and mortality from vaccine-preventable infections, such as influenza [3], may not be covered by universal national immunization programs (NIPs) or country-specific high-risk recommendations. Although herd immunity may effectively prevent the microbial circula- tion in the population, individual risks and circumstances should also be considered [1]. An expanded initiative to target specific high-risk pediatric populations could provide further protection from particular infections. Immuni- zation recommendations for high-risk groups vary between European countries, and the adoption of standardized recommendations could encourage the dissemination of appro- priate information about pediatric subgroups that are most at risk. This paper has therefore collated for the first time all recommendations for high-risk pediat- ric populations in Central European Vaccina- tion Awareness Group (CEVAG) countries to create an immunization guidance statement for adaptation to individual country needs. About CEVAG CEVAG comprises regional experts from 12 Central European countries: Bulgaria, Cro- atia, the Czech Republic, Estonia, Hungary, Latvia, Lithuania, Poland, Romania, Slovakia, Slovenia and Turkey [4]. The aim of CEVAG is to encourage the efficient and safe use of vaccines to prevent, control and, if possible, eliminate infectious diseases by raising informahealthcare.com 10.1586/14760584.2014.897615 Ó 2014 Informa UK Ltd ISSN 1476-0584 1 Review Expert Review of Vaccines Downloaded from informahealthcare.com by 87.110.161.216 on 03/22/14 For personal use only.
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of Immunization of high-risk paediatric populations: Central European Vaccination Awareness Group...

Immunization of high-riskpaediatric populations:Central European VaccinationAwareness Group (CEVAG)recommendationsExpert Rev. Vaccines Early online, 1–15 (2014)
Darko Richter*,Ioana Anca,Francis E Andre,Mustafa Bakir,Roman Chlibek,Milan Cizman,Atanas Mangarov,Zsofia Meszner,Marko Pokorn,Roman Prymula,Nuran Salman,Pavol Simurka,Eda Tamm,Goran Tesovic,Ingrid Urbancıkova,Vytautas Usonis,Jacek Wysocki andDace Zavadska
*Author for correspondence:
Tel.: +385 1237 6521
Fax: +385 1237 6573
For a full list of author affiliations,
please see page 15.
Over the last decade, childhood immunization has substantially reduced morbidity andmortality from vaccine-preventable diseases. However, particular paediatric risk groups, suchas those with comorbidities, may not be adequately vaccinated despite being moresusceptible to complications and death from certain infectious diseases. This may be due tolack of immunization recommendations, lack of awareness, or incomplete adherence toexisting guidelines. Furthermore, recommendations for immunization can be inconsistentacross Europe. An expanded initiative from the Central European Vaccination AwarenessGroup aims to raise awareness of the different high-risk paediatric groups, differentiate themaccording to their specific risk, and formalise a guidance statement for the immunization ofeach population.
KEYWORDS: Central Europe • high-risk • immunization • paediatric • recommendations
Immunization programs represent one of themost impactful advances in medicine [1]. Uni-versal immunization schedules are primarilyaimed at infants and young children becausethey suffer the highest incidence of disease andrisk of complications and death. From 1900to 1998, US childhood immunization pro-grams dramatically reduced pediatric mortalityfrom infectious diseases from 62 to 2% [1]. In2011, the CDC listed the worldwide preven-tion of an estimated 2.5 million deaths in chil-dren aged <5 years annually as one of the top10 public health achievements in the lastdecade [2].
Pediatric subgroups at raised risk of severedisease and mortality from vaccine-preventableinfections, such as influenza [3], may not becovered by universal national immunizationprograms (NIPs) or country-specific high-riskrecommendations. Although herd immunitymay effectively prevent the microbial circula-tion in the population, individual risks andcircumstances should also be considered [1]. Anexpanded initiative to target specific high-risk
pediatric populations could provide furtherprotection from particular infections. Immuni-zation recommendations for high-risk groupsvary between European countries, and theadoption of standardized recommendationscould encourage the dissemination of appro-priate information about pediatric subgroupsthat are most at risk.
This paper has therefore collated for the firsttime all recommendations for high-risk pediat-ric populations in Central European Vaccina-tion Awareness Group (CEVAG) countries tocreate an immunization guidance statement foradaptation to individual country needs.
About CEVAGCEVAG comprises regional experts from12 Central European countries: Bulgaria, Cro-atia, the Czech Republic, Estonia, Hungary,Latvia, Lithuania, Poland, Romania, Slovakia,Slovenia and Turkey [4]. The aim of CEVAGis to encourage the efficient and safe use ofvaccines to prevent, control and, if possible,eliminate infectious diseases by raising
informahealthcare.com 10.1586/14760584.2014.897615 � 2014 Informa UK Ltd ISSN 1476-0584 1
Review
Exp
ert R
evie
w o
f V
acci
nes
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
87.1
10.1
61.2
16 o
n 03
/22/
14Fo
r pe
rson
al u
se o
nly.

awareness of immunization and compiling and distributingappropriate information. CEVAG is an established voluntaryassociation of national representatives and legal entities inter-ested in promoting immunization in Central Europe. CEVAGis organizationally independent of state administration and self-administration bodies, political parties and other civil associa-tions and initiatives. The association does, however, cooperatewith these groups to realize and promote common plansand interests.
What is a high-risk group?
A high-risk group includes individuals who are at a higher thanaverage risk of acquiring infection or those at higher risk ofhaving adverse outcomes [3]. In epidemiology, it is ‘a group ofpeople in the community with a higher-than-expected risk fordeveloping a particular disease, which may be defined on ameasurable parameter, for example, an inherited genetic defect,physical attribute, lifestyle, habit, socioeconomic and/or educa-tional feature, as well as environment’ [5]. This paper definesindividuals as ‘high risk’ when their physiological, medical,social, ethnic, occupational, environmental or economic condi-tions result in a higher than average risk of acquiring certaininfectious diseases. These groups are also at increased risk ofhospitalization, complications, severe disease progressionor death.
Why vaccinate high-risk groups?
Mortality from vaccine-preventable disease is sometimes higherin children with pre-existing disorders than in healthy children.
In 2009–2010, children with moderate and severe pre-existing conditions accounted for 11 and 64% of the 70 pediat-ric pandemic influenza (H1N1)-related deaths in England andWales, respectively, with most deaths (87%) among those<2 years [6]. A German observational study reported comorbid-ities (e.g., chronic respiratory or cardiac disease; neurodevelop-mental disorder) in 75% of intensive care unit pediatricadmissions due to pandemic influenza (H1N1) [7]. In a Belgianmulticenter survey, 47% of children hospitalized with pan-demic influenza had similar comorbidities [8].
In 2009, due to the ongoing burden of influenza, theEuropean Council of ministers recommended that EU MemberStates implement national action plans to achieve an influenzaimmunization coverage rate of 75% in high-risk groups by thewinter season of 2014/2015 [9]. This includes all individualswith the following comorbidities: chronic respiratory and car-diovascular diseases, chronic metabolic disorders, chronic renaland hepatic diseases and congenital or acquired immune systemdisorders [9].
Who vaccinates high-risk groups?
Overall, the CEVAG countries practice the system of manda-tory NIPs with full financial coverage by the state. In mostCEVAG countries, immunizations are implemented by primarycare pediatricians/general practitioners. In some countries(e.g., Hungary, Slovakia), a ‘Special Immunization Services’
network provides individual immunization plans for high-riskpatients. Current mandatory NIPs of CEVAG countries aresummarized in TABLE 1. USA recommendations issued annuallyby the Advisory Committee on Immunization Practices (ACIP)are included for comparison. Exceptions to the mandatory orfully reimbursed immunizations are given in the footnotes (6,22, 23, 26, 31, 33) to TABLE 1.
High-risk group categoriesNeonates, infants & very young children
The initial protection provided by maternal antibodies ininfants eventually wanes, and their immature or naıve immunesystems leave them vulnerable to infection [1]. Consequently,neonates, infants and very young children are the principalrecipients of most universally recommended or mandatory vac-cinations (TABLE 1).
WHO recommends annual influenza vaccination or revacci-nation, particularly for high-risk groups (i.e., children aged6–59 months and individuals with defined comorbidities) [10].Children aged 6–23 months have a high burden of severe dis-ease from influenza, and the WHO recommends targeting thisgroup when sufficient resources are available. Children aged2–5 years have a lower burden of disease than those aged<2 years and respond better to vaccination, resulting in broaderand higher levels of protection [10].
Premature & low birth-weight infants
Preterm babies (<37 weeks’ gestation) are at increased risk ofcomplications and morbidity from vaccine-preventable diseases,but are less likely to receive timely immunizations [11,12]. Thisis partially due to high rates of medical complications andphysicians’ concerns regarding fragility and impaired vaccineimmune responses in preterm babies [12]. All vaccines routinelyrecommended for full-term infants are safe to use in preterm,low birthweight (<2500 g) and even very low birthweightinfants (<1500 g) [12,13]. Medically stable preterm and lowbirthweight infants are recommended to receive full doses ofpneumococcal conjugate vaccine (PCV), Haemophilus influenzaetype b (Hib), diphtheria, tetanus and pertussis (DTaP), hepatitisB (HepB), rotavirus and poliovirus vaccines at a chronologicalage consistent with the standard schedules for full-terminfants [12]. Larger premature infants have similar immuneresponses to full-term infants although responses may bereduced in very premature infants (<28–32 weeks’ gestation atbirth) [14]. Surprisingly, antibody titers with the inactivated tri-valent influenza vaccine in extremely low birthweight infants(birthweight <1000 g) vaccinated at 6–17 months of age weretiters or more in matched full-term infants [15]. The traditionalexception to this practice of early immunization regardless ofgestational age is the Bacillus Calmette–Guerin (BCG) vaccineagainst tuberculosis (TB). If recommended at birth, then BCGis usually given to infants weighing ‡2000 g or 34–35 weekspostmenstrual age, despite recent data that preterm (31–34weeks) and full-term infants have a similar response to thetuberculin test post-BCG vaccination [16]. BCG is universally
Review Richter, Anca, Andre et al.
doi: 10.1586/14760584.2014.897615 Expert Rev. Vaccines
Exp
ert R
evie
w o
f V
acci
nes
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
87.1
10.1
61.2
16 o
n 03
/22/
14Fo
r pe
rson
al u
se o
nly.

Table
1.Pediatric
nationalim
munizationprogrammeschedulesin
CentralEuropeanVaccinationAwareness
Groupco
untriesandUSA
Advisory
CommitteeonIm
munizationPracticesreco
mmendations(upto
date
2014).
Vaccine
BG
HR
CZE
EE
HU
LVLT
PO
RO
SK
SI
TR
USA35
BCG
0d1
0d,13y2
1–5
d0d
2–5
d2–3
d0d
2–7
d0d3
2m
DTaP
2m,3m,
4m,
16m
4,6y
2m,4m,
6m,1y,
5y
9w,13w,
17w
11–18m,
5–6
y
3m,4.5
m,
6m,2y,
6–7
y
2m,3m,
4m,18m,
6y,
2m,4m,
6m,12–
15m,7y
2m,4m,
6m,18m,
6–7
y
2m,4m,
6m,16m
5
5y
2m,4m,
6m,12m,
4y,
6y
2m,4m,
10–11m,
5y
3m,
4–5
m,
6m,
12–24m
2m,
4m,
6m,
18m,6y
2m,4m,
6m,
15–18m,
4–6
y
dT/DTaP
12y,
17y6
dT:
14y,
18y
10–11y7
17y8
11y9
14y1
015–16y
14y,
19y1
1
14y1
212y1
38–9
y,
16–18y1
4
14y
11–12y
HepatitisB
0d,1m,
6m
0d,2m,
6m,12y1
5
9w,13w,
17w
11–18m
16
0d,1m,
6m,12y1
7
0d18,14y
0d19,2m,
4m,6m,
12–15m,
14y1
5
0d,1m,
6m
0d,2m,
7m
0d,2m,
6m
0d20,2m,
4m,10–
11m
0d21,
5–6
y
0d,1m,
6m
0d,
1–2
m,
6–1
8m
HepatitisA
2y2
218m,
24m
12–23m
Hib
2m,3m,
4m,16m
4
2m,4m,
6m,1y
9w,13w,
17w
11–18m
3m,4.5
m,
6m,2y
2m,3m,
4m,18m
2m,4m,
6m,12–
15m
2m,4m,
6m,18m
2m,4m,
6m,16m,
2m,4m,
6m,12m
2m,4m,
10–11m
3m,
4–5
m,
6m,
12–24m
2m,
4m,
6m,
18m
2m,4m,
6m,
12–15m
HPV
12y2
313y
12y2
412y2
512y2
611–12y
11–12y
MMR
13m,12y
1y,
6y
15m,21–
25m
1y,
13y
15m,11y
12–15m,
7y,
12y2
7
15–16m,
6–7
y,
12y2
8
13m,10y
12m,7y
14–17m,
10y
12–18m,
5–6
y
12m,6y
12–18m,
4–6
y
Pneu
mococcal
(PCV)
2m,3m,
4m,
12m
29
9w,13w,
17w
12–15m
2m
30,
4m
30,
15m
30
2m,4m,
12–15m
2m,4m,
10–11m
2m,
4m,
6m,
12m
2m,4m,
6m,
12–15m
Polio
(IPV)
2m,3m,
4m,
16m
4,6y
2m,4m,
6m,1y,
6y,
14y
9w,13w,
17w
11–18m
10–11y
3m,4.5
m,
6m,2y,
6–7
y
2m,3m,
4m,18m,
6y
2m,4m,
6m,12–
15m,7y,
14y
2m,4m,
6m,18m,
6–7
y
2m,4m,
6,16m
31
5y3
2
2m,4m,
6m,12m,
6y,
9y
2m,4m,
10–11m,
5y,
12y
3m,
4–5
m,
6m,
12–24m
2m,
4m,
6m
32,
18m
32,
6y
2m,4m,
6–1
8m,
4–6
y
Rotavirus
6–2
4w
33
2m,4m
or
2m,4m,
6m
34
2m,4m,
or2m,
4m,
6m
34
Varicella
12–15m,
7y
12m
12–15m,
4–6
y
Influenza
annually
6–2
3m
(IIV)
2–1
8y(IIV
andLA
IV)
Men
ingococcal
11–12y,
16y
Immunization of high-risk pediatric populations Review
informahealthcare.com doi: 10.1586/14760584.2014.897615
Exp
ert R
evie
w o
f V
acci
nes
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
87.1
10.1
61.2
16 o
n 03
/22/
14Fo
r pe
rson
al u
se o
nly.

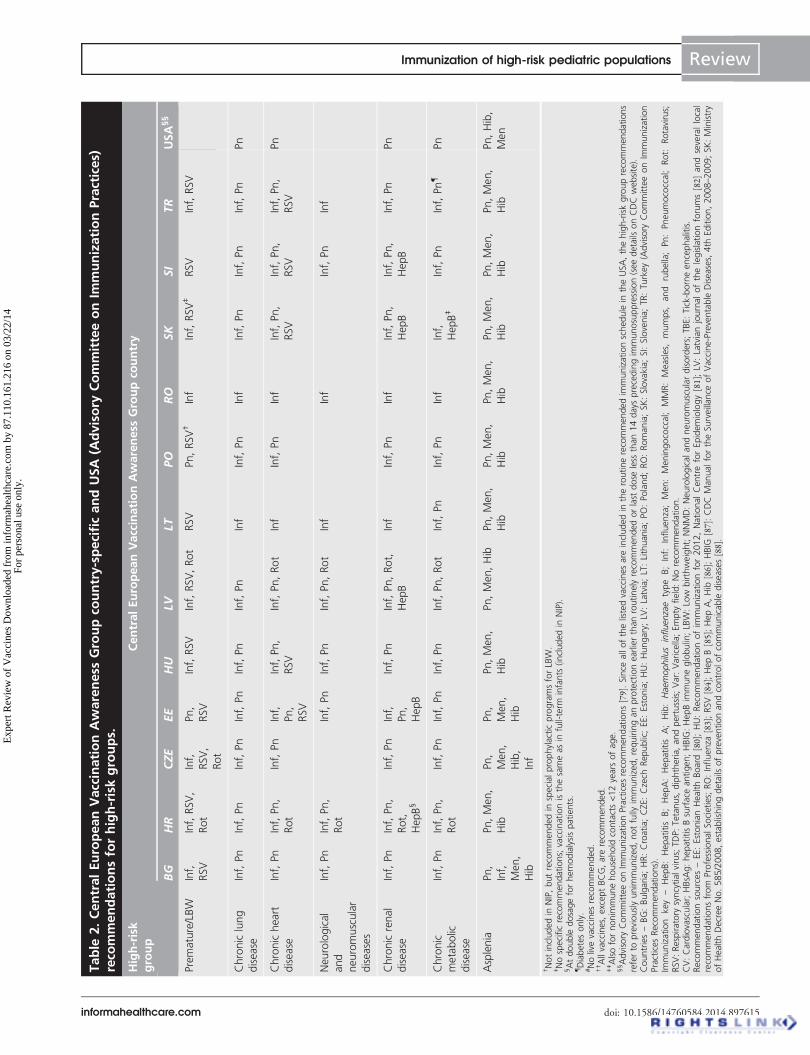
given in most CEVAG countries (except inthe Czech Republic and Slovakia). The ratio-nale for this practice is difficult to referenceappropriately. The BCG has an accepted rolein the prevention of disseminated tuberculosisinfection in children born in populationswith general annual TB incidence >40/100,000 [17]. Only Latvia (42 in 2011), Lith-uania (58.2 in 2011) and Romania (90.5 in2010) of the CEVAG countries have a higherincidence (data communicated by theCEVAG panel members). In the USA, onlychildren known to be exposed to persons withpulmonary TB are recommended to get BCG.It is not recommended for any particular med-ical condition including HIV infection [18]. Allpreterm and low birthweight infants shouldreceive the influenza vaccine at 6 months ofage preferably prior to, but also at any timeduring the influenza season [12]. The infantshould receive a second vaccine dose at aninterval of ‡4 weeks. Preterm infants are par-ticularly susceptible to respiratory syncytialvirus (RSV) due to their immature and vulner-able airways, immature immune system andthe incomplete transfer of maternal antibod-ies [19]. Since there is no available vaccine,passive immunization with monoclonalhumanized anti-RSV antibodies (palivizumab)is recommended. However, the gestation cut-off varies between countries. Being born pre-maturely or having a low birthweight is a riskfactor for severe rotavirus gastroenteritis [20],and the ACIP supports vaccination of preterminfants (<37 weeks’ gestation) with the sameschedule and precautions as full-terminfants [21]. Immunization recommendationsin CEVAG countries are summarizedin TABLE 2 and APPENDIX A (supplementary mate-rial can be found online at www.informa-healthcare.com/suppl/10.1586/14760584.2014.897615). US recommendations issued annu-ally by ACIP are included for comparison.
Children with chronic medicalconditionsChronic lung/pulmonary disease
Chronic lung disease in children is a risk fac-tor for severe influenza and pneumococcaldisease [22,23]. Lung diseases warrantingadministration of pneumococcal and influ-enza vaccines include bronchopulmonary dys-plasia (chronic lung disease of prematurity),cystic fibrosis and allergic asthma, especiallyif high dose inhaled corticosteroids or oral1
Rep
eatvaccinationto
bead
ministeredat7monthsifnoscar
andtuberculin
neg
ative;repeatvaccinationto
beadministeredat
7,11an
d17years
iftuberculin
neg
ative.
2Revaccinationin
tuberculin-neg
ativechildren.
3Recommen
ded
tonew
born
infants
ofim
migrantfamiliesin
last
5years
from
countrieswithahighprevalence
oftuberculosisandwhen
mothersare
treatedfortuberculosis.
4Minim
um
1yearafterthirddose.
5At2,4,6and16months–DTPw.
6dTvaccination(reduceddiphtheria
dose)recommendedat25years
ofageandthen
every
10years
thereafter;
dTis
usedroutinelyan
dreim
bursed
while
DTaPhas
beenrecommended
since
October2012,butis
notreim
bursed.
7DTaP-IPVadministered.
8DTaPisadministered.
9DTaPisadministered(reduceddiphtheria
andpertussisdose).
10Recommen
ded
every10years
thereafter;dTadministered.
11At14and19years
–dT.
12Recommen
ded
every10years
thereafter;dTfrom
14yearson,DTaPat
2,4,6,12months,4years
and6years.
13DTap+IPVadministeredat12years
ofage,dTvaccinationrecommen
dedevery
15years
thereafter.
146–1
8yearoldsreceiveDTaPandadultsreceivedT;
revaccinationgivenevery
10years.
15Onlyifunvaccinatedpreviously(catch-up);three-dose
sched
ule
(at0,1and6months).
16Hexavalentvaccine;
secondandthirddosesadministered‡1
month
afterprecedingdose
butwithin
firstyearoflife;
fourthdose
administered6monthsafterthirddose
andbefore
18monthsofage.
17Administeredat12years
ifchild
born
between1995an
d2003andnotpreviouslyvaccinated(catch-up).
18Administeredto
infants
ofHBsA
g-positive
mothersandto
motherswithunknownHBsA
gstatus:threedosesstartingwithin
12hpostpartum,seconddose
1month
laterandthirddose
6monthsafterfirstdose.
19Administeredasamonovaccineat
0–1
2hafterbirth
onlyto
new
bornsofHBsA
g-positive
mothersorto
motherswithanunknownHBsA
gstatus.
20Administeredto
infants
born
toHBsA
g-positive
mothers;athree-dose
primary
courseofhep
atitisBvaccinationisgivenat
birth
(upto
24hafterbirth),at3–5
weeksandat5–9
months.
21Obligatory
fornew
born
infants
ofHBsA
g-positive
mothers;administeredin
fourdoses(at0,1,2an
d12monthsofagesched
ule)startingwithin
12hpostpartum.
22Recommen
ded
(notman
datory)for2-year-old
childrenwholivein
poorsocialconditions.
23Recommen
ded
since
October2012(National
program
forcervicalcarcinomaprevention);im
munizationisonvoluntary
basisandfully
reim
bursed
;three-dose
sched
ule.
24Three-dose
sched
ule.
25Notyetincluded
intheNIP,buttheRomanianMoHwillbeg
inasecondcampaignforvaccinationofschoolgirls(>12years,threedoses).
26Recommen
ded
(notman
datory)for12-year-old
girls,partially
reim
bursed.
27Administeredto
allunvaccinatedgirls,an
dgirlsonlyvaccinatedonce
previously.
28Notrequirediftw
opreviousdosesadministered.
29Minim
um
6monthsafterthirddose.
30Nonmandatory.
31Recommen
ded
inthefirstandsecondyearoflife–IPV,attheageof5years
oralpolio
vaccine,notreim
bursed.
32Oralpolio
vaccinead
ministeredconcomitantlywithDTaP.
33Recommen
ded
butnotreim
bursed.
34Two-orthree-dose
seriesdep
endingonwhichvaccineisused(RV1orRV5).
35Advisory
CommitteeonIm
munizationPracticesrecommendations[79].
Countries–BG:Bulgaria;HR:Croatia;CZE:
Czech
Rep
ublic;EE:Estonia;HU:Hungary;
LV:Latvia;LT:Lithuan
ia;PO:Poland;RO:Romania;SK
:Slovakia;SI:Slovenia;TR
:Tu
rkey(Advisory
CommitteeonIm
munization
PracticesRecommen
dations).
BCG:BacillusCalm
ette–Guerin;d:Days;DTaP:Diphtheria,tetanusan
dacellularpertussis;dT:
Diphtheria
andtetanus;
HBsA
g:HepatitisBsurface
antigen
;Hib:Haem
ophilusinfluenzaetypeb;IPV:Inactivatedpoliovirus
vaccine;
m:Months;MMR:Measles,mumpsandrubella;PCV:Pneumococcalconjugate
vaccine;T:
Tetanus;Empty
field:Norecommen
dation;w:Weeks;y:
Years.
Review Richter, Anca, Andre et al.
doi: 10.1586/14760584.2014.897615 Expert Rev. Vaccines
Exp
ert R
evie
w o
f V
acci
nes
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
87.1
10.1
61.2
16 o
n 03
/22/
14Fo
r pe
rson
al u
se o
nly.
Table
2.CentralEuropeanVaccinationAwareness
Groupco
untry-specificandUSA
(Advisory
CommitteeonIm
munizationPractices)
reco
mmendationsforhigh-riskgroups.
High-risk
group
CentralEuropeanVaccinationAwareness
Groupco
untry
BG
HR
CZE
EE
HU
LVLT
PO
RO
SK
SI
TR
USA§§
Premature/LBW
Inf,
RSV
Inf,RSV,
Rot
Inf,
RSV,
Rot
Pn,
RSV
Inf,RSV
Inf,RSV,Rot
RSV
Pn,RSV†
Inf
Inf,RSV‡
RSV
Inf,RSV
Chroniclung
disease
Inf,Pn
Inf,Pn
Inf,Pn
Inf,Pn
Inf,Pn
Inf,Pn
Inf
Inf,Pn
Inf
Inf,Pn
Inf,Pn
Inf,Pn
Pn
Chronicheart
disease
Inf,Pn
Inf,Pn,
Rot
Inf,Pn
Inf,
Pn,
RSV
Inf,Pn,
RSV
Inf,Pn
,Rot
Inf
Inf,Pn
Inf
Inf,Pn,
RSV
Inf,Pn,
RSV
Inf,Pn,
RSV
Pn
Neu
rological
and
neuromuscular
diseases
Inf,Pn
Inf,Pn,
Rot
Inf,Pn
Inf,Pn
Inf,Pn
,Rot
Inf
Inf
Inf,Pn
Inf
Chronicrenal
disease
Inf,Pn
Inf,Pn,
Rot,
HepB§
Inf,Pn
Inf,
Pn,
HepB
Inf,Pn
Inf,Pn
,Rot,
HepB
Inf
Inf,Pn
Inf
Inf,Pn,
HepB
Inf,Pn,
HepB
Inf,Pn
Pn
Chronic
metabolic
disease
Inf,Pn
Inf,Pn,
Rot
Inf,Pn
Inf,Pn
Inf,Pn
Inf,Pn
,Rot
Inf,Pn
Inf,Pn
Inf
Inf,
HepB‡
Inf,Pn
Inf,Pn{
Pn
Asplenia
Pn,
Inf,
Men,
Hib
Pn,Men,
Hib
Pn,
Men,
Hib,
Inf
Pn,
Men
,
Hib
Pn,Men
,
Hib
Pn,Men,Hib
Pn,Men,
Hib
Pn,Men,
Hib
Pn,Men,
Hib
Pn,Men,
Hib
Pn,Men,
Hib
Pn,Men,
Hib
Pn,Hib,
Men
†Notincluded
inNIP,butrecommended
inspecialprophylacticprogramsforLBW.
‡Nospecificrecommen
dations;vaccinationisthesameas
infull-term
infants
(included
inNIP).
§Atdouble
dosageforhem
odialysispatients.
{ Diabetes
only.
#Nolivevaccinesrecommended
.††Allvaccines,excep
tBCG,are
recommended.
‡‡Alsofornonim
munehousehold
contacts<12years
ofage.
§§Advisory
CommitteeonIm
munizationPracticesrecommen
dations[79].Since
allofthelistedvaccines
are
included
intheroutinerecommendedim
munizationsched
ule
intheUSA,thehigh-riskgrouprecommendations
referto
previouslyunim
munized,notfully
immunized,requiringanprotectionearlierthan
routinelyrecommen
ded
orlast
dose
less
than
14daysprecedingim
munosuppression(see
details
onCDCwebsite).
Countries–BG:Bulgaria;HR:Croatia;CZE:
Czech
Rep
ublic;EE:Estonia;HU:Hungary;
LV:Latvia;LT:Lithuan
ia;PO:Poland;RO:Romania;SK
:Slovakia;SI:Slovenia;TR
:Tu
rkey(Advisory
CommitteeonIm
munization
PracticesRecommen
dations).
Immunization
key
–HepB:Hepatitis
B;Hep
A:HepatitisA;Hib:Haemophilusinfluenzae
type
B;Inf:
Influenza;Men
:Men
ingococcal;
MMR:Measles,
mumps,
and
rubella;Pn:Pneumococcal;
Rot:
Rotavirus;
RSV
:Respiratory
syncytial
virus;TDP:Tetan
us,diphtheria,andpertussis;Var:Varicella;Empty
field:Norecommendation.
CV:Cardiovascular;HBsA
g:hep
atitisBsurface
antigen;HBIG:HepBim
muneglobulin;LBW:Low
birthweight;NNMD:Neurologicalandneu
romusculardisorders;TB
E:Tick-borneencephalitis.
Recommen
dationsources–EE:EstonianHealthBoard
[80];HU:Recommendationofim
munizationfor2012,National
Cen
treforEpidem
iology[81];LV
:Latvianjournalofthelegislationforums[82]
andseverallocal
recommen
dationsfrom
ProfessionalSo
cieties;RO:Influenza
[83];RSV
[84];HepB[85];HepA,Hib
[86];HBIG
[87]:CDCMan
ualfortheSu
rveillance
ofVaccine-Preventable
Diseases,4th
Edition,2008–2009;SK
:Ministry
ofHealthDecreeNo.585/2008,establishingdetails
ofpreventionandcontrolofcommunicable
diseases[88].
Immunization of high-risk pediatric populations Review
informahealthcare.com doi: 10.1586/14760584.2014.897615
Exp
ert R
evie
w o
f V
acci
nes
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
87.1
10.1
61.2
16 o
n 03
/22/
14Fo
r pe
rson
al u
se o
nly.

Table
2.CentralEuropeanVaccinationAwareness
Groupco
untry-specificandUSA
(Advisory
CommitteeonIm
munizationPractices)
reco
mmendationsforhigh-riskgroups(cont.).
High-risk
group
CentralEuropeanVaccinationAwareness
Groupco
untry
BG
HR
CZE
EE
HU
LVLT
PO
RO
SK
SI
TR
USA§§
Complement
deficien
cy
see#
Pn,Men
,
Hib
Pn,
Men,
Hib
Pn,Men,
Hib
Men
Pn
Men
Pn,Hib,
Men
HIV
infection
Inf,
Pn,
Men
,
Hib
††
Inf,Pn
Inf,Pn
Hep
B,
PnInf
Referral
to vaccine
centers
Inf
Pn
Inf
Inf,Pn
Inf,Pn
,
Hib,
HepA,
HepB
Inf,Pn
Hib
Organ
transplantation
Inf
Pn,
Hib,
Men
Hep
B,
PnInf
Referral
to vaccine
centers
Inf,HepA,
Men,Pn
Pn
Inf
Hep
BInf,Pn
Pn
Malignan
t
disease
Inf,
Pn,
HepB
Pn
Inf,
Pn,
Hep
B
Inf,Pn,
HepB
Pn,HepB
Inf,HepB
Pn,Var‡‡
Inf
Pn
Inf
Inf,Pn
Pn,Hib
Freq
uen
tblood
transfusions/
haemophilia
Inf,
HepB,
HepA
Inf,HepB
Inf,
HepB
Inf,
Hep
B
Inf,HepB
Inf,HepB
Inf,Hep
Pn
Inf,HepB
Inf,HepB
Inf,HepB,
HepA
Inf,HepB
HBsA
g-positive
mothers
HepB
HBIG
HepB
HBIG
HepB
HBIG
HepB
HBIG
HepB
HBIG
HepB
HBIG
Hep
B
HBIG
HepB,
HBIG
Hep
B
HBIG
Long-term
aspirin
therapy
Inf
Inf
Inf
Inf
Inf
Inf
Inf
Inf
Inf
Inf
Cochlear
implants
Pn
Pn
Pn
Pn
PnPn,Inf
Pn
Pn
Pn
Pn
†Notincludedin
NIP,butrecommendedin
specialprophylacticprogramsforLBW.
‡Nospecificrecommendations;vaccinationisthesameas
infull-term
infants
(included
inNIP).
§Atdouble
dosageforhem
odialysispatients.
{ Diabetesonly.
#Nolivevaccinesrecommended.
††Allvaccines,exceptBCG,are
recommen
ded
.‡‡Alsofornonim
munehousehold
contacts<12years
ofag
e.§§Advisory
CommitteeonIm
munizationPracticesrecommendations[79].Since
allofthelistedvaccines
are
includedin
theroutinerecommen
ded
immunizationsched
ule
intheUSA,thehigh-riskgrouprecommen
dations
referto
previouslyunim
munized,notfully
immunized,requiringan
protectionearlierthan
routinelyrecommended
orlast
dose
less
than
14daysprecedingim
munosuppression(seedetailsonCDCweb
site).
Countries–BG:Bulgaria;HR:Croatia;CZE:Czech
Rep
ublic;EE:
Estonia;HU:Hungary;
LV:Latvia;LT:Lithuania;PO:Po
land;RO:Roman
ia;SK:Slovakia;SI:Slovenia;TR:Turkey(Advisory
CommitteeonIm
munization
PracticesRecommendations).
Immunization
key
–HepB:Hep
atitis
B;HepA:Hepatitis
A;Hib:Haem
ophilusinfluenzae
type
B;Inf:
Influenza;Men
:Men
ingococcal;
MMR:Measles,
mumps,
and
rubella;Pn:Pneumococcal;Rot:
Rotavirus;
RSV
:Respiratory
syncytialvirus;TDP:Tetanus,diphtheria,andpertussis;Var:Varicella;Empty
field:Norecommendation.
CV:Cardiovascular;HBsA
g:hep
atitisBsurface
antigen
;HBIG:Hep
Bim
muneglobulin;LBW:Low
birthweight;NNMD:Neurologicalan
dneu
romusculardisorders;TBE:Tick-borneencephalitis.
Recommendationsources–EE:EstonianHealth
Board
[80];HU:Recommendationofim
munizationfor2012,National
CentreforEpidemiology[81];LV
:Latvianjournal
ofthelegislationforums[82]
andseverallocal
recommen
dationsfrom
ProfessionalSocieties;RO:Influenza
[83];RSV
[84];Hep
B[85];HepA,Hib
[86];HBIG
[87]:CDCMan
ual
fortheSurveillance
ofVaccine-Preventable
Diseases,4th
Edition,2008–2
009;SK
:Ministry
ofHealthDecreeNo.585/2008,establishingdetails
ofpreventionan
dcontrolofcommunicab
lediseases[88].
Review Richter, Anca, Andre et al.
doi: 10.1586/14760584.2014.897615 Expert Rev. Vaccines
Exp
ert R
evie
w o
f V
acci
nes
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
87.1
10.1
61.2
16 o
n 03
/22/
14Fo
r pe
rson
al u
se o
nly.

corticosteroid therapy are required [24]. The ACIP recommendsroutine pneumococcal vaccination of all children from 2 to59 months and an additional dose for immunocompetent chil-dren aged up to 71 months with comorbidities includingchronic lung disease [23]. Additionally, children in this groupaged ‡2 years are recommended to receive one dose ofPPSV23 ‡8 weeks after the last PCV dose [23]. The ACIP alsorecommends that vaccine efforts should focus on individuals athigher risk of influenza-related complications including thosewith chronic lung disease. However, they should not receivethe live attenuated influenza vaccine [22]. Most European coun-tries (all CEVAG countries) identify high-risk groups, regard-less of age, as primary influenza vaccination targets [25].
Chronic heart/cardiovascular disease
Children with significant chronic heart disease are at increased riskof infections, complications and death from influenza and pneu-mococcal disease [22,23]. Specific cardiovascular conditions that maybe indications for immunization include congenital heart diseasewith significant shunting, cyanosis, valvular disease, cardiomyopa-thy and congestive heart failure. The ACIP classifies children withchronic heart disease as having an underlying comorbidity that isan indication for pneumococcal vaccination [23] and children<18 years with heart disease as a high-risk group for influenza [22].Rotavirus immunization is recommended in some countries dueto frequent hospitalization and increased exposure to nosocomialgastroenteritis [26]. Additionally, infants with symptomatic cardiacdisease are at increased risk of complicated RSV bronchiolitis [19,27].Passive immunization with palivizumab can reduce the number ofRSV hospitalizations [27] and is usually recommended in infantswith hemodynamically significant congenital heart disease duringthe first year of life and second RSV season [28].
Children with neurological & neuromuscular diseases
Individuals with neurological and neuromuscular disease(NNMD) are at higher risk of developing influenza-related com-plications [6,29]. These conditions include disorders of the brain,spinal cord, peripheral nerve and muscle, such as cerebral palsy,congenital brain and/or spinal cord malformations, ischemic andhemorrhagic brain injury, epilepsy, intellectual disability, moder-ate-to-severe developmental delay, muscular dystrophy or spinalcord injury. Children with these conditions often have compro-mised respiratory function, frequent pulmonary aspirations andthe inability to handle secretions, which are further exacerbatedby influenza infection and resulting pneumonia [28]. However,during 2005, the ACIP updated its recommendation to includechildren with NNMD (cognitive dysfunction; spinal cordpathology; seizure disorder) [30]. In a study evaluating childrenhospitalized with community-acquired influenza, those withNNMD had the highest risk of respiratory failure [31].
Chronic kidney disease/renal failure & nephrotic syndrome
Children with chronic kidney disease (e.g., glomerular disorders,especially with significant proteinuria; on chronic immunosup-pressants; end-stage renal disease; dialysis and renal transplant
patients) are at increased risk of infection from vaccine-preventable diseases, but also have reduced immunologicalresponsiveness to certain vaccines [32]. These patients shouldreceive all routine immunizations, except for those on immuno-suppressants who should not receive live vaccines (rotavirus;MMR; varicella; live attenuated influenza vaccine) [32,33]. There-fore, MMR and varicella vaccines should ideally be administeredbefore immunosuppressants. In the USA, in children with end-stage renal disease, only 32% received influenza vaccine and 13%received pneumococcal vaccine [34]. This population shouldreceive pneumococcal, influenza and HepB vaccines [32,34].Patients with chronic renal failure are at particular risk of HepBinfection [35]; therefore, antibody levels should be monitoredannually and additional doses given if anti-HBs antibody levelsare <10 mIU/ml after a three-dose schedule [31,32].
Chronic metabolic diseases (including diabetes & obesity)
Insulin-dependent diabetes mellitus can increase vulnerability toinfections, including influenza and pneumonia, which tend tobe more severe than in the general population [36]. Diabeticpatients are three-times more likely to be hospitalized or diefrom influenza-related complications [37]. The main immuniza-tions recommended for diabetic patients include those againstinfluenza, pneumococcal disease and HepB [38].
In adults, obesity (BMI ‡30) and morbid obesity (BMI‡40) are independently associated with an increased risk ofrespiratory hospitalizations, intensive care admission and deathfrom influenza [39,40]. Annual influenza vaccinations are recom-mended [40,41]. Data in the pediatric age group are missing.
Children with inherited metabolic disease also have a high-risk of infection [41,42]. Glycogen storage disease type IB isregularly associated with neutropenia, predisposing patients topurulent skin and respiratory infections including pneumococ-cal disease.
Immunocompromised childrenImmunocompromised patients are a heterogeneous populationwith special immunization requirements. Immunocompromis-ing conditions are divided into two groups: primary (congeni-tal) or secondary (due to comorbidity, immunosuppressants orHIV infection).
Immunocompromised children are at increased risk of infec-tion, for example, pneumococcal [23], influenza [22]. Vaccine rec-ommendations depend on the degree of immunosuppression andsusceptibility to infection [43]. In general, live vaccines are contra-indicated in immunocompromised patients in which replicationof vaccine strains can be enhanced and induce serious disease [44].However, all asplenic, neutropenic and complement-deficientpatients can receive live attenuated vaccines. Inactivated or com-ponent vaccines pose no risk to immunocompromised popula-tions although they may be unable to mount a protectiveimmune response. Nevertheless, immunocompromised patientsshould be differentiated according to their specific risk and thenature of their immune defect and immunized appropriately togain at least partial immunity.
Immunization of high-risk pediatric populations Review
informahealthcare.com doi: 10.1586/14760584.2014.897615
Exp
ert R
evie
w o
f V
acci
nes
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
87.1
10.1
61.2
16 o
n 03
/22/
14Fo
r pe
rson
al u
se o
nly.

Whenever possible, patients from these groups should havetheir protection tested by a surrogate marker, typically serumantibody titer to the vaccinal pathogen. The correlation maynot always be perfect. In some instances, for example asplenia,titers against Streptococcus pneumoniae sertoypes and Hib mayhave to be higher than in healthy population for adequate pro-tection [45]. Some of the cutoffs proposed for protective anti-body thresholds are: Hib 1.0 mg/ml 3–4 weeks followingthe initial series, S. pneumoniae 1.3 mg/ml at 3–4 weeks, Neisse-ria meningitidis 2.0 mg/ml at 3–4 weeks, tetanus 0.15 IU/ml3–4 weeks following initial series [46]. Polio neutralizing anti-bodies, influenza hemagglutinin inhibition, hepatitis A andHepB antibodies have also been utilized [47]. Response to vacci-nation may also be used in order to assess a child’simmunocompetence [45,46].
Asplenia
Children with anatomical or functional asplenia are at increasedrisk of bacterial sepsis (overwhelming postsplenectomy infec-tion) [48,49]. People without a functional spleen are particularlysusceptible to infection with encapsulated bacteria (e.g., N.meningitidis, Hib and particularly S. pneumoniae) due to loss ofsplenic phagocytic function [50]. Vaccination against pneumo-coccal, meningococcal, Hib and influenza vaccinations isrecommended [49].
Children with complement deficiency
Classical and alternative complement pathway defects renderthe patient exceptionally prone to infection due to encapsulatedbacteria, primarily S. pneumoniae, H. influenzae, N. meningitidisand Enterobacteriaceae [51]. Children with defects in properdinor membrane attack complex are highly susceptible to infec-tions by N. meningitidis. Although very rare, patients with thesedefects are universally recommended to receive the widest possi-ble coverage against pneumococcal, Hib and meningococcaldisease.
HIV infection
Although pediatric HIV infection can be managed withHAART, vaccine-preventable diseases still cause significantmorbidity and mortality in this population [52]. Despite theHIV-associated immune system impairment, vaccinationagainst infectious diseases remains one of the most effectivepreventive strategies. HIV-infected children should receivepneumococcal, Hib, meningococcal, influenza and MMR vac-cines [53]. Children on HAART respond to revaccination eventhough some may not achieve long-term immunity [54]. S.pneumoniae is the most common invasive bacterial pathogen inHIV-infected children [53], who have a 40-fold increased risk ofIPD. Consequently, despite <1% of children under 5 years ofage being HIV positive, they constitute approximately 10% ofall annual deaths from S. pneumoniae [53,55,56]. HIV-positivechildren are also at a higher risk for varicella, Herpes zoster andmeasles complications [53]. Due to the limited safety, immuno-genicity and efficacy data in these individuals, varicella and
MMR vaccination should only be considered if the child is notseverely immunocompromised (i.e., CD4+ T-lymphocyte count‡15%) [53]. Postvaccination testing for HepB is recommendeddue to the potentially impaired humoral response; if anti-HBslevels are <10 mIU/ml, then revaccination with a second three-dose series is recommended [53]. All HIV-positive childrenshould have individually tailored immunizations, adjusted fordisease stage, HIV viral load and CD4+ count.
Organ transplantation
Infectious diseases, including vaccine-preventable infections, arethe leading cause of morbidity and mortality in bone marrowand solid-organ transplant recipients [57]. Post-transplant immu-nosuppression and decreased antibody production increase sus-ceptibility to infectious diseases and associated life-threateningcomplications in transplant recipients, regardless of prior vacci-nation status [57]. Once stabilized, transplant patients should, inprinciple, continue to receive routine inactivated vaccinesaccording to local NIPs [58]. Hematopoietic stem cell transplant(HSCT) recipients are at increased risk of vaccine-preventablediseases because antibody titers decline 1–4 years post-trans-plant, if they are not revaccinated [59]. All HSCT recipients arerecommended to receive pneumococcal, Hib, meningococcalconjugate, DTaP, inactivated influenza and inactivated poliovaccines post-transplant [60]. PCV and influenza vaccines can begiven 3–6 and 4–6 months post-HSCT, respectively [60]. Othernonlive vaccines can be started 6–12 months post-transplant.Live vaccines, such as MMR and varicella, should be adminis-tered 2 years post-transplantation, if the patient is adequatelyimmunocompetent [59]. Therefore, when possible, a childshould receive all possible missed or indicated vaccinations pre-transplantation and <3 weeks prior to immunosuppression [58].Following solid-organ transplantation, live vaccines remaincontraindicated including MMR. Starting at 2–6 months post-transplant, the child should be evaluated for booster and addi-tional inactivated vaccines (commonly influenza, pneumococcaland meningococcal) [45].
Malignant disease
Children with malignant disease have a higher risk of acquir-ing vaccine-preventable diseases and developing complica-tions. Immunosuppressive treatment and the malignantdisease itself adversely affect the immunity established byprior vaccination. Children who receive immunosuppressivecancer therapy will benefit from immunization; however,safety and reduced vaccine responsiveness should be takeninto consideration [61]. As a general rule, these children cancontinue to receive routine inactivated vaccines according tolocal NIPs during the stable phases of disease, but shouldnot receive live vaccines [58]. After completing their treat-ment, these children should be re-evaluated for booster dosesof previously administered vaccines [62] and additional pro-tection starting ‡3 months postchemotherapy and ‡6months post-anti-B-cell monoclonal antibodies for inacti-vated vaccines [45].
Review Richter, Anca, Andre et al.
doi: 10.1586/14760584.2014.897615 Expert Rev. Vaccines
Exp
ert R
evie
w o
f V
acci
nes
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
87.1
10.1
61.2
16 o
n 03
/22/
14Fo
r pe
rson
al u
se o
nly.

Children on medical immunosuppression
This group includes children with chronic inflammatory diseasesof various organs receiving systemic corticosteroids, cytostaticagents (e.g., methotrexate, cyclophosphamide), biologic therapy(e.g., anti-TNF therapy) and monoclonal antibodies (e.g., rituxi-mab). In the CEVAG countries, it has not been singled out as aspecific high-risk group, perhaps due to lack of centralized care (asopposed to the organ transplant and cancer group). Additionally,the immunization problems are compounded by the fear of puta-tive flare-ups of the underlying disease related to vaccines [63]. Thevaccination problems in these children are left to individual incen-tives of the subspecialist and/or primary care physicians. Thesepatients, especially the ones on anti-TNF therapy, are inordinatelysusceptible to pneumococcal, influenza and human papillomavi-rus infections [64]. They should receive all the inactivated vaccineslisted in the NIPs plus conjugated pneumococcal and meningo-coccal, inactivated influenza and hepatitis A no less than 4 weeksprior to the planned immunosuppression. If vaccines are givenduring the period of treatment, then they should be delivered dur-ing remission. Live vaccines should not be given during any lowor high level of active immunosuppresion [45]. Immunization willhave no effect if given during treatment with drugs that selectivelyeliminate B cells (rituximab). BCG in general should not begiven, and Kawasaki disease is a strict contraindication to BCGbecause of a high rate (50%) of severe local reactions [65].
Children who require frequent blood transfusions
Patients with bleeding disorders have an increased risk of infec-tion due to previous and potential exposure to blood prod-ucts [66]. The WHO states that individuals who frequentlyrequire blood or blood products are possible targets for HepBcatch-up vaccination [35]. Children with bleeding disordersshould also receive subcutaneously administered vaccines due tothe risk of hematoma formation [66].
Other risk groupsInfants born to HepB surface antigen-positive mothers
These infants are universally recognized as high risk due to ver-tical transmission from mother to child (70–90%, if themother is HepB surface antigen [HBsAg] and HBeAg positive)and associated high likelihood of chronic infection (90% ofthose infected) [67]. Whether HepB vaccination is universal atbirth, or later, all infants of HBsAg-positive mothers shouldalso receive HepB immune globulin within 12 h postpartum.The administration of HepB immune globulin is particularlyimportant in this high-risk group as the timing of the nextHepB dose in the NIP varies between countries. HBsAg shouldbe tested on umbilical cord blood, and infants should also betested for HBsAg and antibody to HBsAg (anti-HBs) 1 monthafter completion of at least three doses of HepB series andagain at 9–18 months [57].
Long-term aspirin (salicylates) therapy
Reye’s syndrome is a very rare but potentially fatal disease inchildren that causes encephalopathy and fatty degeneration of
the liver. It affects children who are on long-term aspirin ther-apy and have a varicella or influenza virus infection [68]. Reye’ssyndrome is now particularly rare since aspirin is no longerroutinely given to children and due to the availability of diag-nostic tools to detect congenital errors of mitochondrial fattyacid oxidation. Children aged 0.5–18 years on long-term aspi-rin should receive the influenza vaccine [22]. Furthermore, theunderlying cardiovascular condition for which aspirin is pre-scribed is also an indication for influenza vaccination. Varicellavaccination should also be recommended.
Children with cochlear implants
Children with cochlear implants are at greater risk of bacterialmeningitis and have a >30-fold higher incidence of pneumo-coccal meningitis than the general population [69]. Infants andchildren who are candidates for cochlear implants shouldreceive pneumococcal and Hib conjugate vaccines and annualinfluenza immunization [70]. Children should receive PCV orPPSV23 at least 2 weeks before surgery [23]. Physicians shouldbe aware that, despite available recommendations, this pediatricgroup may not be optimally protected as pneumococcal guide-lines for high-risk children are regarded as complicated and dif-ficult to interpret [71]. For example, in the UK, 54% ofchildren with cochlear implants are not optimally immunizedbefore surgery and 75% require further immunizations [71].
Children living in endemic TBE areas
Tick-borne encephalitis (TBE) is a viral zoonotic disease trans-mitted to humans via ticks or unpasteurized dairy products.Most cases present with influenza-like symptoms, while 10% canlead to inflammation of the meninges, brain or spinal cord [72].The incidence of TBE varies considerably between countries andregions. In areas that are highly endemic (‡5 cases/100,000 popu-lation), the WHO recommends that immunization be offered toall age groups including children [73]. TBE is highly endemic insome Central European countries, and CEVAG strongly recom-mends universal TBE vaccination in children >1 year of age insuch areas [66]. For countries with a low risk of TBE, the vaccineshould be offered to children >10 years of age and to those travel-ling to endemic areas [74].
Current immunization recommendations for all high-riskgroups in each CEVAG country are presented in TABLE 2 andAPPENDIX A.
CEVAG guidance statementPhysicians, healthcare workers and families of infants and chil-dren need to be made aware of the infectious diseases relevantto each high-risk category. Physicians should take a broad andrational approach to immunization, as delineated in this paper,when advising patients on their exposure risks and the need toget vaccinated. In particular, for immunocompromised chil-dren, the extent of immunosuppression should be consideredand recommendations should be made on an individual basis.This can best be achieved through multidisciplinary approachinvolving the primary care physician, treating subspecialist,
Immunization of high-risk pediatric populations Review
informahealthcare.com doi: 10.1586/14760584.2014.897615
Exp
ert R
evie
w o
f V
acci
nes
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
87.1
10.1
61.2
16 o
n 03
/22/
14Fo
r pe
rson
al u
se o
nly.

clinical immunologist and vaccine expert. Every effort shouldbe made to administer vaccines prior to immunosuppressivetreatment. Details concerning the immunization of individualpatients in this group are beyond the scope of this paper; theyare amply discussed elsewhere [45].
The risks need to be better defined by the epidemiologicservices of each country. CEVAG suggests adopting mandatorydisease reporting of vaccine-preventable diseases and broadeningthe case definition to include all relevant cases, regardless ofclinical presentation.
The CEVAG group high-risk immunization recommendationsare summarized in TABLE 3. Influenza and pneumococcal vaccinesshould be recommended for most high-risk groups includingthose with chronic lung, heart, metabolic and renal diseases. Allvaccines routinely recommended for full-term infants should begiven to premature and low birthweight infants; this includesinfluenza, pneumococcal conjugate, Hib, DTaP, HepB, rotavirusand poliovirus vaccines. This risk group should additionallyreceive RSV prophylaxis. Children who are immunocompromisedare also recommended to receive immunization for most infec-tious diseases, unless the specific vaccine is contraindicated.Human papillomavirus is not specifically recommended for anyof the high-risk groups in the CEVAG countries.
The CEVAG panel strongly feels thatall high-risk children should receive fullmandatory NIP vaccinations unless medi-cally contraindicated. Reliance on herdimmunity due to high NIP coverage acrossmost CEVAG countries should not be theargument to avoid NIP vaccines.
Expert commentaryWith an increasing number of vaccinesgaining approval in Europe, immunizationschedules are becoming more complex. Anin-depth understanding of both vaccinesand associated infectious diseases is impor-tant to ensure that the right people receivethe right vaccines. To allow this, there aretwo general approaches to immunization:universal administration of all vaccines toa predefined age group and target high-risk populations. Although universalimmunization is effective in reducing dis-ease burden and can result in herd immu-nity, individual risks and circumstancesshould also be considered.
Evaluation of current high-risk recom-mendations in CEVAG countries hasrevealed a broad consensus as to whichhigh-risk groups should receive particularvaccinations. In most CEVAG countries,influenza vaccination is broadly recom-mended across all pediatric risk groupsincluding children with malignancy or
immunodeficiency. Recommendations for other vaccines, suchas those against pneumococcal and meningococcal disease, areless consistent although there is general agreement on whichgroups are at high risk from these infections. The availability ofconjugate vaccines has extended the indications for pneumococ-cal disease prevention beyond the time-honored conditions ofasplenia and complement deficiencies; however, these stillremain the principal indications for meningococcal vaccination.
Immunization recommendations for risk groups with definedcomorbidities are fairly consistent across CEVAG countries.However, recommendations for conditions with heterogeneouspopulations, such as immunocompromised children, are lessconsistent. The heterogeneity of this population means that theexisting guidelines may not be applicable to all conditions [61].Furthermore, immunocompromised children may not receiveroutine immunizations as a result of lack of efficacy and safetydata in this group [75]. However, all killed vaccines are generallysafe and live vaccines can be given depending on the extent ofthe suppression and time elapsed since therapy [45]. Indirectprotection of high-risk children should be secured by increasingimmunity in household and other close contacts of the child,especially healthcare workers. These should be up to date withall mandatory vaccines and additionally receive inactivated
Table 3. Central European Vaccination Awareness Group consensusof recommended immunizations for high-risk groups.
High-risk group Recommended immunizations
Premature and low birthweight babies All routine immunizations plus RSV, Rot, Inf
Chronic lung disease Pn, Inf, RSV (<1–2 years old)
Chronic heart disease Pn, RSV (<1–2 years old), Inf
NNMD Inf
Chronic renal disease Pn, Inf, HepB
Chronic metabolic disease Pn, Inf, TD, HepB
Immunocompromised (general) Pn, Inf, Men
Asplenia Pn, Men, Hib, Inf
Complement deficiency Pn, Hib, Men
HIV infection Pn, Men, Hib, Inf, MMR, Var
Organ transplantation Inf, Pn, MMR†, Var†, HepA (prior to liver
transplantation)
Frequent blood transfusions HepB, HepA, Inf
Malignant disease Pn, Inf
Long-term aspirin therapy Inf, Var (before aspirin is started)
Cochlear implants Pn, Hib, Inf
Newborns of HBsAg-positive mothers HepB, HBIG
†Live vaccines should be taken before immunosuppressive treatment.Immunization key:HepB: Hepatitis B; HepA: Hepatitis A; Hib: Haemophilus influenzae type b; Inf: Influenza; Men: Meningococcal;MMR: Measles, mumps, and rubella; Pn: Pneumococcal; Rot: Rotavirus; RSV: Respiratory syncytial virus;TBE: Tick-borne encephalitis; TDP: Tetanus, diphtheria and pertussis; Var: Varicella.HBsAg: Hepatitis B surface antigen; HBIG: HepB immune globulin; NNMD: Neurological and neuromuscular disorders.
Review Richter, Anca, Andre et al.
doi: 10.1586/14760584.2014.897615 Expert Rev. Vaccines
Exp
ert R
evie
w o
f V
acci
nes
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
87.1
10.1
61.2
16 o
n 03
/22/
14Fo
r pe
rson
al u
se o
nly.

influenza, pneumococcal, inactivated polio, MMR, varicellaand rotavirus vaccines if needed/indicated. MMR strains arenot transmitted in human contact. Rotavrius may be excretedin stools, but transmission to contacts has not been reported.For varicella, no specific precautions are needed unless the vac-cine recipient develops a rash, in which case, direct contactshould be avoided until the rash resolves. Attenuated oral poliovaccine should not be given to contacts of immunocompro-mised children [45,76].
Children with neurological conditions are one of the threegroups (the others being chronic heart and lung disease) thatare particularly at risk of severe influenza [77,78]. Children withNNMDs are overlooked in some CEVAG countries as thereare recommendations for influenza and pneumococcal immuni-zation in eight and six of CEVAG countries, respectively. Evenwhen such recommendations exist for a particular risk group,they may be overlooked due to the complexity of care for thesechildren and a lack of understanding of the vaccine contraindi-cations. Furthermore, frequent hospitalization may result inmissed doses.
There have been several published studies highlighting thegeneral lack of optimal immunization of these high-riskgroups [32,71]. Reasons for this may include the lack of efficacyand safety data, in particular for immunocompromised popula-tions [65]. Inadequate vaccination of solid-organ transplantpatients is a common problem worldwide, and a standardizedapproach to vaccination of solid-organ transplant patients istherefore required.
It is also apparent that the supporting evidence for vaccina-tion of individual high-risk groups with comorbidities is lim-ited. This is due in part to the lack of epidemiological data forcertain conditions [3]. As a general rule, high-risk patientsemerge as candidate groups for immunization from retrospec-tive analyses unless the condition is very common, such as dia-betes [3], or the association of an underlying condition andadverse outcome of an infection is difficult to oversee (e.g.,obesity, neurological disorder and influenza) [78]. There alsoappears to be a lack of European morbidity and mortality datafor individual high-risk groups. Such data are available for theUSA but not for most of Europe. As a result, the burden ofpreventable infectious diseases in these risk groups may beunderestimated leading to a lack of awareness. Discussing theaffected risk groups should in turn help raise awareness andincrease reporting of infectious diseases in children at high risk.
Adherence to the recommendations presented in this papermay help raise awareness among physicians of the infectious dis-eases relevant to their subspecialty and ensure that their patientsreceive all appropriate immunizations. However, cost remains anissue. Although the CEVAG countries reimburse the cost of vac-cinations included in the NIP, additional immunization mustoften be paid for by parents who in many cases cannot afford it.Detailed knowledge of the rationale for delivering specific vacci-nations is required for high-risk groups, but clear and transparentguidelines for each individual condition would ensure that thesepopulations receive the appropriate vaccines.
Five-year viewIn many countries with moderate or modest Gross NationalProduct, high-risk groups are targeted for vaccination to avoidlarge scale, universal immunization costs. In some cases, placingvaccines on the list for high-risk groups allow for future intro-duction into the NIP. This is likely to be the case with immu-nization against pneumococcal disease, and it is foreseeable thatthis vaccine will be included in the NIP soon after it has beenintroduced for high-risk groups. However, even if vaccines dobecome included in the NIP, CEVAG recommendationsshould remain in place as it is unlikely that universal immuni-zation will cover all age groups and circumstances includingthose who become severely immunocompromised and requirerevaccination. With improved disease monitoring and reportingthroughout Europe, it is likely that the risk factors involved foreach infectious disease will be increasingly understood and therecommendations can be refined and revised accordingly.
Acknowledgements
All authors were actively involved in the selection and review of all con-
tent and had full editorial control during the writing of the manuscript.
Financial & competing interests disclosure
D Richter has received honoraria for lectures on vaccines and respiratory
drugs from GlaxoSmithKline (GSK) Croatia, MSD Idea Inc. Croatia,
Pfizer and Medoka (representing Sanofi Pasteur). I Anca has been the
principal investigator in clinical studies supported by GSK, Apogepha and
Ferring. The author has also been a scientific consultant to GSK, Wyeth
Lederle, Teva, AstraZeneca and Nestle and has received sponsorship from
GSK, Pfizer and Nestle to attend scientific meetings. M Bakir has received
sponsorship for scientific meetings from GSK, Wyeth Lederle, sanofi aventis
and Merck Sharp & Dohme (MSD). R Chlibek has received lecture fees
and sponsorship to attend scientific meetings from GSK, Sanofi Pasteur
and Pfizer and has been principal investigator in clinical trials sponsored
by GSK. M Cizman has received honoraria for lectures on vaccine use
from GSK, Pfizer and MSD. A Mangarov has been a scientific consultant
to GSK, Aventis Pasteur, Pfizer, Danone and Solvay Pharma and has
received sponsorship from these companies to attend scientific meetings. Z
Meszner is a consultant to Pfizer, GSK, MSD, Sanofi Pasteur, Novartis
and Baxter on vaccination issues and has also received travel grants. M
Pokorn has received lecture fees from GSK Slovenia, speaker fees from
GSK and has received sponsorship from GSK and PharmaSwiss Slovenia
to attend scientific meetings. R Prymula is a member of advisory boards
for GSK, MSD, Pfizer, Baxter and Aventis Pasteur and has received
research grants and honoraria from GSK, Pfizer, Baxter, Aventis Pasteur
and Novartis. P Simurka has received consulting fees and lecture fees from
GSK, Pfizer and MSD. E Tamm has received sponsorship from GSK and
PharmaSwiss to attend scientific meetings. G Tesovic has received sponsor-
ship from GSK, MSD, PharmaSwiss, and Pfizer to attend scientific meet-
ings. I Urbancıkova has been a scientific consultant to GSK and Pfizer
and has received lecture fees from GSK, Pfizer, MSD and Novartis and
sponsorship from GSK, Pfizer and Sanofi Pasteur to attend scientific meet-
ings. V Usonis has been the principal investigator in clinical studies sup-
ported by GSK, Novartis and Pfizer. The author has also been a scientific
consultant to Aventis Pasteur, Baxter, GSK, Merck and Pfizer and has
Immunization of high-risk pediatric populations Review
informahealthcare.com doi: 10.1586/14760584.2014.897615
Exp
ert R
evie
w o
f V
acci
nes
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
87.1
10.1
61.2
16 o
n 03
/22/
14Fo
r pe
rson
al u
se o
nly.

received sponsorship from these companies to attend scientific meetings. J
Wysocki has been principal investigator in clinical trials sponsored by
GSK, Wyeth, Pfizer and Novartis. The author has also received sponsor-
ship from GSK, Pfizer and Wyeth to attend scientific congresses. D Zavad-
ska has received lecture fees from GSK, Sanofi Pasteur and Abbott and
has received sponsorship from GSK and Baxter to attend scientific meet-
ings. F Andre and N Salman have no competing interests. The authors
have no other relevant affiliations or financial involvement with any
organization or entity with a financial interest in or financial conflict
with the subject matter or materials discussed in the manuscript apart
from those disclosed.
Preparation of this report was supported by an educational grant from
GlaxoSmithKline, Novartis and Pfizer.
Writing assistance was utilized in the production of this manuscript.
Editorial assistance was provided by C Combs and Wells Healthcare Com-
munications Ltd.
Key issues
• High-risk groups are defined as those who are more susceptible to vaccine-preventable diseases and their complications, and include
those with underlying chronic diseases or comorbidities and those at increased risk of exposure to vaccine-preventable diseases.
• High-risk groups therefore require additional immunization recommendations and strategies to ensure maximum protection.
• Physicians, healthcare workers and families of infants and children need to be made aware of the infectious diseases relevant to each
high-risk category.
• Neonates, infants and very young children remain the principal targets of most universal national immunization programmes (NIPs)
because of the high risk of morbidity and mortality at this young age.
• Preterm and low birthweight babies are at even higher risk of complications and morbidity from vaccine-preventable diseases and
should receive all routine vaccines including rotavirus and influenza, as well as respiratory syncytial virus prophylaxis.
• Vaccines against influenza, pneumococcus and rotavirus are currently the most commonly recommended for pediatric high-risk groups
across Central European Vaccination Awareness Group countries.
• Children with cochlear implants are at increased risk of bacterial meningitis (pneumococcal in particular) and should receive
pneumococcal, Haemophilus influenzae type b and influenza vaccines.
• Immunizations for immunocompromised children should be individually tailored according to their specific condition, disease stage and
level of immunosuppression.
• Limited financial resources and lack of consistent surveillance systems may explain the practice of limited targeting of high-risk groups
with vaccines that are included in NIPs in many countries.
• The decision to include a vaccine-preventable disease in the NIP could be greatly facilitated by making the disease notifiable and
gathering sound evidence from surveillance.
• Expanded immunization initiatives should help prevent the disproportionate morbidity and mortality that can occur when high-risk
pediatric populations contract vaccine-preventable diseases.
References
Papers of special note have been highlighted as:
• of interest
•• of considerable interest
1. Hebert CJ, Hall C, Odoms LN. Lessons
learned and applied: what the 20th century
vaccine experience can teach us about
vaccines in the 21st century. Hum Vaccin
Immunother 2012;8(5):560-8
• Excellent review of the impact of
vaccination in children with useful
tabular presentation of the reduction in
infectious diseases following mass
vaccination in the 20th century.
2. Global Public Health Achievements Team,
CDC. Corresponding contributor: ram
Koppaka. Ten Great Public Health
Achievements – Worldwide, 2001–2010.
MMWR 2011;60(24):812-18
3. Nicoll A, Ciancio B, Tsolova S, et al. The
scientific basis for offering seasonal influenza
immunization to risk groups in Europe.
Euro Surveill 2008;13:43
4. CEVAG. Available from: www.cevag.org
5. McGraw-Hill Concise Dictionary of
Modern Medicine. The McGraw-Hill
Companies; Inc, New York; 2002
6. Sachedina N, Donaldson LJ. Paediatric
mortality related to pandemic influenza
A H1N1 infection in England:
an observational population-based study.
Lancet 2010;376(9755):1846-52
7. Altmann M, Fiebig L, Soyka J, et al. Severe
cases of pandemic (H1N1) 2009 in
children, Germany. Emerg Infect Dis 2011;
17(2):186-92
8. Blumental S, Huisman E, Cornet MC,
et al. Pandemic A/H1N1v influenza
2009 in hospitalized children: a multicenter
Belgian survey. BMC Infect Dis
2011;11:313
9. Vaccine European New Integrated
collaboration Effort. Vaccine influenza
vaccination survey in EU/EEA. Seasonal
influenza vaccination survey in EU/EEA,
influenza season 2009–10. Available from:
http://venice.cineca.org/Final_Seasonal_
Influenza_Vaccination_Survey_2010.pdf
[Last accessed 23 August 2012]
10. WHO. Vaccines against influenza WHO
position paper – Nov 2012. Week
Epidemiol Rec 2012;47(87):461-76
11. Davis RL, Rubanowice D, Shinefield HR,
et al. Immunization levels among premature
and low-birth-weight infants and risk factors
for delayed up-to-date immunization status.
Centers for Disease Control and Prevention
Vaccine Safety Datalink Group. JAMA
1999;282(6):547-53
Review Richter, Anca, Andre et al.
doi: 10.1586/14760584.2014.897615 Expert Rev. Vaccines
Exp
ert R
evie
w o
f V
acci
nes
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
87.1
10.1
61.2
16 o
n 03
/22/
14Fo
r pe
rson
al u
se o
nly.

12. Saari TN. Immunization of preterm and
low birth weight infants. American
Academy of Pediatrics Committee on
Infectious Diseases. Pediatrics 2003;
112(1 Pt 1):193-8
13. Esposito S, Fumagalli M, Principi N.
Immunogenicity, safety and tolerability of
vaccinations in premature infants. Expert
Rev Vaccines 2012;11(10):1199-209
•• Theory and practice of immunization of
preterm infants with evidence-based
recommendations in favor of vaccinating
even very low birthweight children.
14. D’Angio CT. Active immunization of
premature and low birth-weight infants:
a review of immunogenicity, efficacy, and
tolerability. Paediatr Drugs 2007;9(1):17-32
15. D’Angio CT, Heyne RJ, Duara S, et al.
Immunogenicity of trivalent influenza
vaccine in extremely low-birth-weight,
premature versus term infants. Pediatr Infect
Dis J 2011;30(7):570-4
16. Negrete-Esqueda L, Vargas-Origel A.
Response to Bacillus Calmette-Guerin
vaccine in full-term and preterm infants.
Am J Perinatol 2007;24(3):183-9
17. Pilger D, Nguipdop-Djomo P, Abubakar I,
et al. BCG vaccination in England since
2005: a survey of policy and practice. BMJ
Open 2012;2:e001303
18. Prevention of disseminated TB by BCG: the
role of BCG vaccine in the prevention and
control of tuberculosis in the United States.
A joint statement by the Advisory Council
for the Elimination of Tuberculosis and the
Advisory Committee on Immunization
Practices. MMWR Recomm Rep 1996;45:
1-18
19. Sommer C, Resch B, Simoes EA. Risk
factors for severe respiratory syncytial virus
lower respiratory tract infection. Open
Microbiol J 2011;5:144-54
20. Huppertz H, Salman N, Giaquinto C. Risk
Factors for Severe Rotavirus Gastroenteritis.
Pediatr Infect Dis J 2008;27:S11-19
21. Cortese MM, Parashar UD. Prevention of
rotavirus gastroenteritis among infants and
children: recommendations of the Advisory
Committee on Immunization Practices
(ACIP). MMWR Recomm Rep 2009;
58(RR-2):1-25
22. Fiore AE, Uyeki TM, Broder K, et al.
Prevention and control of influenza with
vaccines: recommendations of the Advisory
Committee on Immunization Practices
(ACIP), 2010. MMWR Recomm Rep
2010;59(RR-8):1-62
23. Nuorti JP, Whitney CG. Prevention of
pneumococcal disease among infants and
children - use of 13-valent pneumococcal
conjugate vaccine and 23-valent
pneumococcal polysaccharide vaccine -
recommendations of the Advisory
Committee on Immunization Practices
(ACIP). MMWR Recomm Rep 2010;
59(RR-11):1-18
24. James KM, Peebles RS Jr, Hartert TV.
Response to infections in patients with
asthma and atopic disease:
an epiphenomenon or reflection of host
susceptibility? J Allergy Clin Immunol
2012;130(2):343-51
25. Usonis V, Anca I, Andre F, et al. Central
European Vaccination Advisory Group
(CEVAG) guidance statement on
recommendations for influenza vaccination
in children. BMC Infect Dis 2010;10:168
26. Meszner Z, Anca I, Andre F, et al.
Rotavirus vaccination in central Europe. J
Pediatr Gastroenter Nutritr 2013;56:586-96
27. Alexander PM, Eastaugh L, Royle J, et al.
Respiratory syncytial virus
immunoprophylaxis in high-risk infants
with heart disease. J Paediatr Child Health
2012;48(5):395-401
28. Armstrong C. AAP Updates Guidelines on
Immunoprophylaxis for RSV Infection;
2010. Available from: www.aafp.org/afp/
2010/0901/p542.pdf [Last accessed from
29 October 2012]
29. Centers for Disease Control and Prevention
(CDC). Influenza-associated pediatric deaths
– United States, September 2010-August
2011. MMWR 2011;60(36):1233-8
• In-depth analysis of pediatric influenza
mortality due to pandemic H1N1 virus
with definition of risk factors.
30. Harper SA, Fukuda K, Uyeki TM, et al.
Prevention and control of influenza.
Recommendations of the Advisory
Committee on Immunization Practices
(ACIP). MMWR Recomm Rep 2005;
54(RR-8):1-40
31. Keren R, Zaoutis TE, Bridges CB, et al.
Neurological and neuromuscular disease as a
risk factor for respiratory failure in children
hospitalized with influenza infection. JAMA
2005;294(17):2188-94
32. Neu AM. Immunizations in children with
chronic kidney disease. Pediatr Nephrol
2012;27(8):1257-63
33. Fivush BA, Neu AM. Immunization
guidelines for pediatric renal disease. Semin
Nephrol 1998;18(3):256-63
34. CDC. Guidelines for Vaccinating Kidney
Dialysis Patients and Patients with Chronic
Kidney Disease; 2006. Available from:
www.cdc.gov/diabetes/pubs/pdf/
CKD_vaccination.pdf [Last accessed
26 September 2012]
35. WHO Hepatitis B position paper. Week
Epidemiol Rec 2006;40(84):405-20
36. Shepherd JE, Grabenstein JD.
Immunizations for high-risk populations.
J Am Pharm Assoc (Wash) 2001;41(6):
839-49.quiz 923-5
37. CDC Diabetes and Flu: what do you need
to know and do. Available from: www.cdc.
gov/diabetes/news/flu.htm [Last accessed
24 August 2012]
38. Advisory Committee on Immunization
Practices. Recommended adult
immunization schedule: united States, 2012.
Ann Intern Med 2012;156(3):211-17
39. Kwong JC, Campitelli MA, Rosella LC.
Obesity and respiratory hospitalizations
during influenza seasons in Ontario,
Canada: a cohort study. Clin Infect Dis
2011;53(5):413-21
40. Jain S, Chaves SS. Obesity and influenza.
Clin Infect Dis 2011;53(5):422-4
41. Kwok R. Vaccines: the real issues in vaccine
safety. Nature 2011;473(7348):436-8
42. Klein NP, Aukes L, Lee J, et al. Evaluation
of immunization rates and safety among
children with inborn errors of metabolism.
Pediatrics 2011;127(5):e1139-46
43. American Academy of Pediatrics. Red Book:
2012 Report of the Committee on
Infectious Diseases. Pickering LK, ed. 29th
ed. American Academy of Pediatrics, Elk
Grove Village, IL; 2012
44. Recommendations of the Advisory
Committee on Immunization Practices
(ACIP): use of vaccines and immune
globulins for persons with altered
immunocompetence. MMWR Recomm
Rep 1993;42(RR-4):1-18
45. Rubin LG, Levin MJ, Ljungman P, et al.
2013;IDSA Clinical Practice Guideline for
Vaccination of the Immunocompromised
Host. Clin Infect Dis 2014;58(3):e44-e100
•• This is the most up to date and detailed
guideline for implementing immunization
in the immunocompromised host.
46. Orange JS, Ballow M, Stiehm ER, et al.
Use and interpretation of diagnostic
vaccination in primary immunodeficiency:
a working group report of the Basic and
Clinical Immunology Interest Section of the
American Academy of Allergy, Asthma &
Immunology. J Allergy Clin Immunol
2012;130:S1-24
Immunization of high-risk pediatric populations Review
informahealthcare.com doi: 10.1586/14760584.2014.897615
Exp
ert R
evie
w o
f V
acci
nes
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
87.1
10.1
61.2
16 o
n 03
/22/
14Fo
r pe
rson
al u
se o
nly.

47. Abraham RS. Relevance of antibody testing
in patients with recurrent infections. J
Allergy Clin Immunol 2012;130:558-9.
e1-e6
48. Pebody RG, Hippisley-Cox J, Harcourt S,
et al. Uptake of pneumococcal
polysaccharide vaccine in at-risk populations
in England and Wales 1999-2005.
Epidemiol Infect 2008;136(3):360-9
49. Price VE, Dutta S, Blanchette VS, et al.
The prevention and treatment of bacterial
infections in children with asplenia or
hyposplenia: practice considerations at the
Hospital for Sick Children, Toronto.
Pediatr Blood Cancer 2006;46(5):597-603
50. Castagnola E, Fioredda F. Prevention of
life-threatening infections due to
encapsulated bacteria in children with
hyposplenia or asplenia: a brief review of
current recommendations for practical
purposes. Eur J Haematol 2003;71(5):
319-26
51. Pettigrew HD, Teuber SS, Gershwin ME.
Clinical significance of complement
deficiencies. Ann NY Acad Sci 2009;1173:
108-23
52. Menson EN, Mellado MJ, Bamford A,
et al. Guidance on vaccination of
HIV-infected children in Europe. HIV Med
2012;13(6):333-6; e1-14
53. Mofenson LM, Brady MT, Danner SP,
et al. Guidelines for the Prevention and
Treatment of Opportunistic Infections
among HIV-exposed and HIV-infected
children: recommendations from CDC, the
National Institutes of Health, the HIV
Medicine Association of the Infectious
Diseases Society of America, the Pediatric
Infectious Diseases Society, and the
American Academy of Pediatrics. MMWR
Recomm Rep 2009;58(RR-11):1-166
54. Sutcliffe CG, Moss WJ. Do children
infected with HIV receiving HAART need
to be revaccinated? Lancet Infect Dis 2010;
10(9):630-42
55. O’Brien KL, Wolfson LJ, Watt JP, et al.
Burden of disease caused by Streptococcus
pneumoniae in children younger than
5 years: global estimates. Lancet 2009;
374(9693):893-902
56. Nunes MC, Madhi SA. Safety,
immunogenicity and efficacy of
pneumococcal conjugate vaccine in
HIV-infected individuals. Hum Vaccin
Immunother 2012;8(2):161-73
57. Genc G, Ozkaya O, Aygun C, et al.
Vaccination status of children considered for
renal transplants: missed opportunities for
vaccine preventable diseases. Exp Clin
Transplant 2012;10(4):314-18
58. Abzug MJ. Vaccination in the
immunocompromised child: a probe of
immune reconstitution. Pediatr Infect Dis J
2009;28(3):233-6
59. Centers for Disease Control and Prevention.
Epidemiology and prevention of
vaccine-preventable diseases. Atkinson W,
Wolfe S, Hamborsky J, eds. 12th ed.,
second printing. Public Health Foundation,
Washington DC; 2012
60. Guidelines for preventing infectious
complications among hematopoietic cell
transplant recipients: a global perspective.
Bone Marrow Transplant 2009;44(8):
453-558
61. Shetty AK, Winter MA. Immunization of
children receiving immunosuppressive
therapy for cancer or hematopoietic stem
cell transplantation. Ochsner J 2012;12(3):
228-43
62. Patel SR, Ortin M, Cohen BJ, et al.
Revaccination of children after completion
of standard chemotherapy for acute
leukemia. Clin Infect Dis 2007;44(5):
635-42
63. Ravelli A, Martini A. Juvenile idiopathic
arthritis. Lancet 2007;369:767-78
64. Heijstek MW, Ott de Bruin LM, Borrow R
, et al. Vaccination in paediatric patients
with auto-immune rheumatic diseases:
a systemic literature review for the European
League against Rheumatism: evidence-based
recommendations. Autoimmun Rev
2011;11:112-22
65. Bijl M, Agmon-Levin N, Dayer J-M, et al.
Vaccination of patients with auto-immune
inflammatory rheumatic diseases requires
careful benefit-risk assessment. Autoimmun
Rev 2012;11:572-6
•• Concise and evidence-based directions
how to go about vaccinating children
with autoimmune and rheumatic diseases.
66. Makris M, Conlon CP, Watson HG.
Immunization of patients with bleeding
disorders. Haemophilia 2003;9(5):541-6
67. CDC Hepatitis B. The Pink Book.
Available from: www.cdc.gov/vaccines/pubs/
pinkbook/downloads/hepb.pdf [Last
accessed 30 November 2012]
68. Belay ED, Bresee JS, Holman RC, et al.
Reye’s syndrome in the United States from
1981 through 1997. N Engl J Med 1999;
340(18):1377-82
69. Reefhuis J, Honein MA, Whitney CG,
et al. Risk of bacterial meningitis in children
with cochlear implants. N Engl J Med
2003;349(5):435-45
70. Rubin LG, Papsin B. Cochlear implants in
children: surgical site infections and
prevention and treatment of acute otitis
media and meningitis. Pediatrics 2010;
126(2):381-91
71. Andrew M, Robert H, David S. Optimizing
pneumococcal vaccination for paediatric
cochlear implant recipients using the
cochlear implant pneumococcal vaccination
flowchart. Cochlear Implants Int 2012;
13(4):193-6
72. Kistner-Griffin E, Brune CW, Davis LK,
et al. Parent-of-origin effects of the
serotonin transporter gene associated with
autism. Am J Med Genet B Neuropsychiatr
Genet 2011;156(2):139-44
73. WHO. Summary of WHO position papers
– recommended routine immunizations for
children. Available from: www.who.int/
immunization/policy/Immunization_
routine_table2.pdf [Last accessed 23 August
2012]
74. Zavadska D, Anca I, Andre F, et al.
Recommendations for tick-borne
encephalitis vaccination from the Central
European Vaccination Awareness Group
(CEVAG). Hum Vaccin Immunother 2013;
9:2
75. Casswall TH, Fischler B. Vaccination of the
immunocompromised child. Expert Rev
Vaccines 2005;4(5):725-38
76. General recommendations on
immunization. Recommendations of the
advisory committee on immunization
practices (ACIP). MMWR Recomm Rep
2011;60(RR-2):3-61
•• Traditionally complete, practice oriented
and evidence-based recommendations for
professionals involved in immunization.
77. Blanton L, Peacock G, Cox C, et al.
Neurologic disorders among pediatric deaths
associated with the 2009 pandemic
influenza. Pediatrics 2012;130(3):390-6
78. Cox CM, Blanton L, Dhara R, et al. 2009;
Pandemic influenza A (H1N1) deaths
among children – United States,
2009-2010. Clin Infect Dis 2011;
52(Suppl 1):S69-74
79. CDC Vaccine Recommendations of the
ACIP. Available from: www.cdc.gov/
vaccines/hcp/acip-recs/index.html
80. Terviseamet Health Board. Available from:
www.terviseamet.ee/nakkushaigused/
vaktsineerimine/immuniseerimiskava-valised-
vaktsiinid.html
81. Oek. Available from: www.oek.antsz.hu
Review Richter, Anca, Andre et al.
doi: 10.1586/14760584.2014.897615 Expert Rev. Vaccines
Exp
ert R
evie
w o
f V
acci
nes
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
87.1
10.1
61.2
16 o
n 03
/22/
14Fo
r pe
rson
al u
se o
nly.

82. Likumi. Available from: www.likumi.lv/
[Last accessed January 2013]
83. Asociatia Medicilor de Familie Mures.
Available from: www.amfms.ro
84. Ministry of Health. Available from: www.
ms.gov.ro
85. Centrul National de Supraveghere si
Control al Bolilor Transmisibile. Available
from: www.insp.gov.ro/cnscbt
86. Vaccinnet Romania. Available from: www.
vaccinnet.ro
87. DSP Cluj. Available from: www.dspcluj.ro
88. Urad verejneho zdravotnıctva Slovenskej
republiky. Available from: www.uvzsr.sk
Affiliations
Darko RichterDepartment of Paediatrics, University Hospital Centre, Zagreb, Croatia
Ioana AncaUniversity of Medicine and Pharmacy ‘Carol Davila’ Bucharest – Institute for Motherand Child Care, Bucharest, Romania
Francis E AndreChaussee de Huy, 136, 1325-Chaumont-Gistoux, Belgium
Mustafa BakirDepartment of Pediatrics, Division of Pediatric Infectious Diseases, MarmaraUniversity School of Medicine, Istanbul, Turkey
Roman ChlibekFaculty of Military Health Sciences, University of Defence, Hradec Kralove, CzechRepublic
Milan CizmanDepartment of Infectious Diseases, University Medical Centre, Ljubljana, Slovenia
Atanas MangarovInfectious Diseases Hospital, Sofia, Bulgaria
Zsofia MesznerNational Institute of Child Health, Budapest, Hungary
Marko PokornDepartment of Infectious Diseases, University Medical Centre, Ljubljana, Slovenia
Roman PrymulaFaculty of Military Health Sciences, University of Defence, Hradec Kralove, CzechRepublicandUniversity Hospital, Hradec Kralove, Czech Republic
Nuran SalmanDivision of Infectious Disease and Clinical Microbiology, University of Istanbul,Istanbul, Turkey
Pavol SimurkaUniversity of Trencin, Pediatric Clinic, Faculty Hospital, Trencın, Slovakia
Eda TammChildren’s Clinic of Tartu University Hospital, Tartu, Estonia
Goran TesovicPaediatric Infectious Diseases Department, University of Zagreb, School of Medicine,Zagreb, Croatia
Ingrid UrbancıkovaDepartment of Paediatric Infectious Diseases, Children’s Faculty Hospital, Kosice,Slovakia
Vytautas UsonisFaculty of Medicine, Clinic of Children’s Diseases, Vilnius University, Vilnius,Lithuania
Jacek WysockiDepartment of Preventive Medicine, Poznan University School of Medical Sciences,Poznan, Poland
Dace ZavadskaDepartment of Pediatrics, Riga Stradins University, Riga, Latvia
Immunization of high-risk pediatric populations Review
informahealthcare.com doi: 10.1586/14760584.2014.897615
Exp
ert R
evie
w o
f V
acci
nes
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
87.1
10.1
61.2
16 o
n 03
/22/
14Fo
r pe
rson
al u
se o
nly.