Identity, Voice, Place - Australian Institute of Aboriginal and ...
114
Identity, Voice, Place. Krysinska, Martin & Sheehan, 2009. The University of Queensland. 1 Identity, Voice, Place Suicide Prevention for Indigenous Australians - a Social and Emotional Wellbeing Approach Krysinska, K., Martin, G. and Sheehan, N. The University of Queensland “The Mental Health of a Nation is judged by the care with which those most in need are assisted to regain control of their own lives”
-
Upload
khangminh22 -
Category
Documents
-
view
2 -
download
0
Transcript of Identity, Voice, Place - Australian Institute of Aboriginal and ...

Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
1
Identity, Voice, Place
Suicide Prevention for Indigenous Australians -
a Social and Emotional Wellbeing Approach
Krysinska, K., Martin, G. and Sheehan, N.
The University of Queensland
“The Mental Health of a Nation is judged by the care with which those most in need are
assisted to regain control of their own lives”
Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
2
© 2009 Centre for Suicide Prevention Studies, The University of Queensland.
This work is based on a redraft of a commission from
The Centre for Rural and Remote Mental Health Queensland.
CITATION
Krysinska, K., Martin, G. & Sheehan, N., 2009. Identity, Voice, Place: Suicide Prevention for
Indigenous Australians - A Social and Emotional Wellbeing Approach. The University of
Queensland.
ISBN
Cover
Fragment, ‘Bush Medicine Dreaming’, 2009. Janet Golder Kngwarreye
Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
3
TABLE OF CONTENTS
___________________________________________________________
Introduction 5
Executive Summary 6
Recommendations for Action and Investment in Suicide Prevention for Indigenous
Australians, based on a social and emotional wellbeing framework 11
The Review
Key Principles 19
Literature Review Strategy 21 Policy Review on Suicide Prevention, Mental Health and Social and
Emotional Wellbeing in Aboriginal and Torres Strait Islander Australians 22
Indigenous Suicide in Australia 35
Suicide in Indigenous peoples: An International Perspective 47
Searching for Solutions: Prevention of Suicide in Indigenous Australians 54
Social and Emotional Wellbeing and Suicide Prevention 59
Principles of Good Practice 75
References 81
Appendices
One: Glossary 97
Two: Acknowledgements 99
Three: Existing Suicide Prevention Programs for Indigenous Australians 100
Four: Training Programs for Indigenous Mental Health Workers 107
Five: Ethical Guidelines for Research 110

Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
4

Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
5
Introduction
The National Mental Health Plan 2003-2008 recognises that influences on mental health and
social and emotional wellbeing occur in the events and settings of everyday life. The
complex interplay of biological, psychological, social, environmental and economic factors at
the individual, family, community, national levels must be acknowledged and addressed if
we are to effectively promote and support population-based approaches to social
emotional, cultural and spiritual wellbeing. For Aboriginal and Torres Strait Islander people,
the concept of health and wellbeing is inextricably linked to a holistic understanding of life
itself.
This broader understanding of health is outlined in Ways Forward:
Aboriginal concept of health is holistic, encompassing mental health and physical,
cultural and spiritual health...This holistic concept does not merely refer to the ‘whole
body’ but is in fact steeped in the harmonised interrelations which constitute cultural
wellbeing.
The National Strategic Framework for Aboriginal and Torres Strait Islander People’s Mental
Health and Social and Emotional Wellbeing 2004-2009 reaffirms and expands upon the
concept of health as multi-dimensional and recognises the strengths, resilience and diversity
of Aboriginal and Torres Strait Islander communities. This is supported by the Cultural
Respect Framework for Aboriginal and Torres Strait Islander Health 2004-2009 which states
that recognition of cultural differences is essential if we are to deliver services to Aboriginal
and Torres Strait Islander people that do not compromise their legitimate cultural rights,
practices, values and expectations.
The determinants of Aboriginal and Torres Strait Islander social, emotional, cultural and
spiritual wellbeing are complex and reflect factors acting across the developmental
continuum at individual, family community and societal levels. Suicide in Indigenous
Australians is an equally complex issue, and a relatively new phenomenon. It occurs in
communities across Australia in a sporadic way and is difficult to predict at both the

Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
6
individual and community levels. As with other Indigenous societies across the world, it
appears that many of the approaches emerging from western research programs and
incorporated into programs designed to prevent suicide, either do not work for Indigenous
Australians, or are inappropriate when translated to Indigenous Australian communities.
This research reviewed all of the available research, literature, and relevant available
unpublished materials across a range of fields in an attempt to find solutions that might
work for Aboriginal and Torres Strait Islander communities. We also discussed the issues and
took advice from a large number of key informants both in Australia, but also in New
Zealand, Canada and the United States. The intent was to devise a framework for Indigenous
suicide prevention in Australia that might be relevant, acceptable, fundable, manageable,
and successful. As with many before us, we concluded that social, cultural, emotional, and
spiritual wellbeing as building blocks toward overall mental wellbeing are likely to be crucial
in reducing suicide in Indigenous Australians, and that social reform to help rediscover
Identity, Voice and Place, is likely to be more important than measures taken to improve
pathways to care.

Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
7
Executive Summary
1. This literature review is based on 9 Key Principles (see page Error! Bookmark not
defined.), consistent with existing Australian and International declarations,
frameworks, policy, plans and strategies (see page Error! Bookmark not defined.).
2. There is considerable rhetoric in the area of suicide prevention for Indigenous
Australians, but very little in the way of local evidence-based practice or practice-
based evidence to drive interventions.
3. Our recommendations derive from the best available evidence (both national and
international) in promotion of social and emotional wellbeing, and prevention of
suicide through early intervention in social, family, personal and biological
determinants along the trajectory to suicide. Recommendations will need
considerable goodwill and commitment to ensure translation into culturally
meaningful practice in diverse communities.
4. The estimated resident number of Indigenous Australians (June 2006) is 517,200
including 463,900 Aboriginal Australians, 33,100 Torres Strait Islander Australians and
20,200 people identifying as both Aboriginal and Torres Strait Islander, altogether
comprising 2.5% of the total population (ABS&AIHW, 2008).
5. Best available data indicate that overall mortality rates among Indigenous males and
females are almost three times higher than for non-Indigenous Australians, and there
is a 17-year gap between life expectancy at birth for Indigenous and non-Indigenous
males and females (59 v 77 yrs and 65 v 82 yrs respectively) (ABS&AIHW, 2008).
6. Among Indigenous Australian males, overall suicide rates are almost three times
higher than suicide rates for non-Indigenous Australian males, with biggest
differences in younger ages (ABS&AIHW, 2008). Suicide rates among Indigenous
Australian females aged 10-24 are five times the rate of other Australian females,
although in age groups 45-54 and over, suicide rates are similar or lower compared
to rates for non-Indigenous Australian females.
7. In 2000-02 suicide rates in Aboriginal and Torres Strait Islander Australians were
highest in remote areas of Australia (55 per 100,000), lower in inner and outer
regional areas (37 per 100,000 and 35 per 100,000; respectively) and lowest in major
Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
8
cities (16 per 100,000). Highest suicide rates were found in DOGIT communities (68
per 100,000) - twice the overall Indigenous Australian rate (30 per 100,000). Suicide
rates are lower in Torres Strait Islander Australians (18 per 100,000) (Partnerships
Queensland, 2006).
8. Of serious concern is the high and increasing rate of suicide among Indigenous
Australian children and adolescents (Commission for Children and Young People and
Child Guardian Queensland, 2007). In 2006-07, Aboriginal and Torres Strait Islander
Australian children and adolescents accounted for 39% youth suicide victims in
Queensland, despite comprising only 6% of the youth population.
9. The situation of Indigenous Australians looks grim even by comparison to other
Indigenous populations (Freemantle et al., 2007), and not much has changed since
1995 when Ring observed that “expectations for life for Indian populations in Canada
and the United States, and for the Maoris in New Zealand are at least 10 years more
than for Australian Aborigines, an enormous difference” (Ring, 1995; p. 228).
10. According to Kunitz (1994), the particularly bad mortality and morbidity status of
Aboriginal Australians can be traced back to two factors concerning how
governments have dealt with Native peoples across history: signing of treaties and
the level of responsibility for Indigenous affairs (see page 36 onwards).
11. Average expenditure on health for Aboriginal and Torres Strait Islander Australians is
$4,718 per capita, approximately 17% higher than for other Australians ($4,019).
However, this level of expenditure is not sufficient to match the needs related to
higher levels of morbidity (ABS&AIHW, 2008), nor the cost of delivery particularly to
rural and remote communities.
12. In our review of relevant policies and strategies, some include special cultural
considerations for Indigenous Australians, others provide direction, targets and
strategies for all Australians. Our view is that considerable affirmative action is
required to enable Indigenous Australians to reach equity with all other Australians.
In particular, affirmative action is necessary in the areas addressed, for instance,
under Outcome 6 of the Queensland Government Suicide Prevention Strategy (2003-
2008), the first 3 dot points of which state:
Engage Indigenous communities in identifying the cultural, historical and
spiritual factors which may influence suicide and suicidal behaviour;

Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
9
Promote approaches to enhance self-esteem and capacity to enable individuals
and communities to connect with a value system based on identity, place,
people and land;
Develop partnership approaches with communities to strengthen local
responses to complex issues, including drug and alcohol use, interpersonal
conflict, violence, and grief and loss1.
It appears from our discussions with key informants that there is still a long way to go
to achieve any of this.
13. We note with some dismay in our summation of the Australian literature on
Indigenous Australian suicide (page 41 onwards), our inability “at this time, to
identify empirical studies which could provide further evidence or a theoretical
framework to explain the protective impact of these factors and their application to
social and emotional wellbeing of Aboriginal and Torres Strait Islander Australians”. A
case can be made that when we develop protective programs against suicide for
Indigenous Australians, at this time we are using a mix of guesswork, a literature
replete with rhetoric, and translations from International literature. We acknowledge
there are a number of community driven Aboriginal Australian programs which
appear to be effective, but for which a culturally relevant research base still needs to
be confirmed.
14. Despite obvious and significant cultural, socio-economic and historical differences
between and within Indigenous populations in New Zealand, Canada and the United
States, in general, suicide rates and suicide risk are highest among young Indigenous
males; the age of Indigenous suicide deaths is decreasing; suicides tend to cluster,
and a significant role is played by alcohol in suicidal behaviour. Indigenous suicides
appear to have their roots in ‘collective despair’, related to persisting social
disadvantage, cultural and social exclusion and destruction of cultural continuity and
identity. Clearly these core themes must inform our understanding, as well as
preventive practice in Australia.
15. The majority of international suicide prevention programs in Indigenous communities
are either not well evaluated or are not reported in the published literature. A 2001
1 Each of these are known to be distal risk factors in the life trajectory to suicide

Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
10
review, in the United States, identified 9 programs, including 5 suicide-specific
programs, and 4 programs addressing related mental health and wellbeing issues,
such as alcohol and substance abuse, and teen pregnancy. There were disappointing
conclusions: “information on the effectiveness of suicide preventive intervention
programs among American Indians/Alaskan Native communities is scarce….
generalizability of the results is somewhat limited” (Middlebrook et al., 2001; p. 140).
A more recently published report Suicide among Aboriginal People in Canada
(Kirmayer et al., 2007) presents a more comprehensive and updated list of promising
suicide prevention programs with a focus on Aboriginal Canadian communities (see
page 46 onwards).
16. In searching for solutions to suicide in Indigenous Australians, it is better to build on
existing initiatives like those in Appendix Two, rather than wipe the slate clean and
pretend that the international literature that does exist has some magic formula that
can be transposed to the Australian environment.
17. Despite wide recognition and acknowledgment of the importance of Indigenous
holistic concepts of self, health, and social and emotional wellbeing, there is a lack of
consensus regarding its operationalisation and measurement (Kowal et al., 2007). In
addition, to date, there is a paucity of studies and program evaluations across
Australia to indicate which initiatives and frameworks are effective in development
of social and emotional wellbeing in Indigenous Australians.
18. There is clearly an urgent need for increased training of Indigenous Australians at all
levels of the Mental Health workforce to ensure a critical mass of workers steeped in
local culture and acceptable to local communities. We recommend the recently
published National Aboriginal and Torres Strait Islander Health Council document ‘A
blueprint for action: Pathways into the health workforce for Aboriginal and Torres
Strait Islander people’ which is relevant here (Commonwealth of Australia, 2008).

Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
11
Recommendations for Action and Investment in Suicide Prevention for Indigenous
Australians, based on a social and emotional wellbeing framework
To provide consistency with other current Australian and Frameworks and Strategies, we
have chosen to use the Mrazek and Haggerty (1994) Spectrum for Intervention focusing
mainly on Universal, Selective and Indicated areas; those areas most consistent with a
Population Health perspective on prevention.
Universal approaches
1. Toward equal opportunity
It is noticeable that many national and state documents refer to Aboriginal and Torres Strait
Islander “peoples”. On the one hand, this may properly identify people at higher health risk
than non-Indigenous Australians, but on the other hand may divide Aboriginal and Torres
Strait Islander Australians from other Australians and either create, or enhance possibilities
for, stigmatisation. We recommend the universal adoption in Government publications of
the terms ‘Indigenous Australians’, ‘Aboriginal Australians’, ‘Torres Strait Island Australians’,
or ‘Aboriginal and Torres Strait Island Australians’ (where appropriate2) to underscore the
fact that the original owners of our land are citizens of Australia3, and therefore entitled to
levels of health and social and emotional wellbeing applicable to all Australians.
2. Consensus and agreement on Recommendations for Action and Investment
To move toward a unified understanding of Indigenous Australian suicide, to gain
commitment to the Recommendations, and agreement on where Investment may be
targeted, a convocation (or ‘yarning’) process will need to be funded at different
community levels:
All identified Indigenous Australian groups and committees within Government and
the bureaucracy, with Commonwealth representative committees and groups who
work with and for Indigenous Australians;
2 In all subsequent text we use the term „Indigenous Australians‟ unless we seek to be more specific; we mean
no disrespect to anyone. Simply stated, we sought to reduce the number of words and make the text as readable
as possible. Where we quote from others who have used alternative terms, we retain their terminology. 3 Arabena (2006) has taken the debate around this issue much further in her model of a „Universal Citizen‟.
Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
12
Elders and/or broad senior representation from all recognisable communities and
groupings of Indigenous Australians. The venue or venues for this part of the
convocation process will have to be carefully considered to maximise commitment
from relevant parties, and there be a need for a series of meetings to confirm
agreement. The methods by which information is shared between member groups
must also be given serious consideration;
Representatives of those professions relevant to development of social and
emotional wellbeing and/or suicide prevention, and already involved in Indigenous
Australian communities, as well as representatives from all government and all
non-government organizations managing or developing relevant health or welfare
programs.
Proposed Outcomes:
1. Indigenous Australian commitment to the Recommendations
2. General agreement on where investment may be targeted
3. General agreement on what constitutes Aboriginal Australian Resilience
4. General agreement on an approach towards Suicide Prevention based on Social and
Emotional Wellbeing
5. General agreement on the specific steps to be taken.
3. Training for the Indigenous Australian Mental Health Workforce
There remain large disparities between Indigenous communities in terms of a trained mental
health workforce with the capacity to contribute locally to both building social and
emotional wellbeing, creating knowledge about signs of mental health problems and suicide
potential, and providing crisis care or access to care in their own community. Attempts to
build local capacity seem to be haphazard, and one community often does not know what is
happening elsewhere or what the possibilities are for training. In fact many key informants
were able to describe a local program, but did not know of programs being developed
elsewhere. There is a need for a critical mass of workers steeped in, and situated in, local
culture, and acceptable to local communities. We recommend:
Engagement of relevant workforce planning groups to review how to increase of
Indigenous Australians numbers at all levels of the Mental Health workforce, and
Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
13
That, as a priority, training programs become better coordinated across Australia.
Increased funding be provided to existing training programs to allow them to fill
known gaps and enhance the capacity of all communities to sustain mental health
and/or suicide prevention programs – whether these are about cultural, social
and emotional wellbeing or about greater awareness of mental health issues, and
pathways to care.
Development of funding formulae [for workforce needs] based on population
needs weighted for Aboriginal and Torres Strait Islander populations, rural and
remote locations and other relevant variables (Key Direction 30.2, Australian
Mental Health Plan).
Proposed Outcomes:
1. Sufficient Indigenous professional capacity to
1.1. sustain development and implementation of programs toward Social and Emotional
Wellbeing at the local level;
1.2. coordinate local training in Mental Health First Aid, ASIST, Drop the Rock and other
relevant programs where evaluation shows them to be effective;
1.3. provide relevant crisis management at the local level for suicidal people.
2. Sufficient local awareness of mental health systems and how these are accessed.
4. Mapping of Services
Based on our research and discussions with key informants, there remains a need for careful
mapping of suicide prevention and Social and Emotional Wellbeing development programs
in communities to clarify who funds what for whom, in which communities, who coordinates
the programs, and where capacity needs to be enhanced? This is a crucial exercise to
prioritise values, clarify duplication, and identify gaps where additional funding might be
appropriate and lead to solid outcomes. We recommend funding of a taskforce with capacity
to dialogue with Indigenous Australian communities and groupings to discover what
programs exist and where, how they are funded, how coordinated, and where there is
capacity to provide apparently successful programs in a culturally appropriate way to other
communities.
Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
14
Proposed Outcome:
A sufficient range of programs for each and every local community to enable
development of Social and Emotional Wellbeing, and the prevention of suicide.
5. Research
As we noted in the Executive Summary, a case can be made that when we develop
protective programs against suicide for Indigenous Australians, at this time we are using a
mix of guesswork, a literature replete with rhetoric, and translations from International
literature that may not provide best practice based on a sound evidence base about
Indigenous Australians. Our review demonstrates a clear need to contribute to improved
knowledge about which programs work in which communities, under what culturally
appropriate circumstances, with what initial resource development, and with what ongoing
funding to maintain community capacity to sustain programs and their evolution at the local
level.
We recommend provision of dedicated funding to a representative (Indigenous and non-
Indigenous Australian) expert group to explore and advise state wide and local programs on
culturally cogent and appropriate ways of working with communities to evaluate programs,
and more formally contribute to the specific knowledge base in Australia of what reduces
suicide and its precursors in Indigenous Australians and in their communities.
Further, we recommend funding a culturally appropriate program of research which pairs
Indigenous and non-Indigenous researchers to gain the best available evidence in the areas
of promotion, prevention and early intervention, specifically to drive relevant and culturally
situated and appropriate programs of prevention. This might include:
5.1 A review of potential impact of disturbances (e.g. incarceration) in the Indigenous
Australian family functioning and parenting skill to clarify whether a program of
improvement is needed, and how such a program could be developed and
implemented in a culturally appropriate manner.
5.2 In discussion with relevant Indigenous organisations, development of a number of
trial programs in the area of improving Social and Emotional Wellbeing, to determine
what impact this has on grief and loss issues, suicide, substance misuse, family

Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
15
violence, and child abuse. While increased funding to Aboriginal Controlled
Community Health Services may be an important direction to take, (see Action Area
4.1.2, National Strategic Framework for Aboriginal and Torres Strait Islander People’s
Mental Health and Social and Emotional Well Being 2004-2009), it is at this point in
our narrative unclear just which programs would provide the most benefit. Clearly
such trial programs would need to observe the criteria we have provided for ethical
practice in this area, and would gain from discussions with an expert group on
culturally appropriate evaluation if we are to contribute to the accepted knowledge
base in Australia.
5.3 Little research exists into trajectories to suicide in Indigenous Australians, particularly
in younger suicides. We do have some information from psychological autopsy of
recent young suicides in Queensland, as well as specific surveys from Western
Australia. There is an urgent need for a program of culturally sensitive research to
determine the pathways to suicide in young Indigenous Australians, specifically to
determine risk factors for suicide, protective factors against suicide, and key proximal
indicators, which might lead to evidence based programs of prevention and
intervention. Further to improved clarity about pathways, funding could be allocated
to salutogenic programs in schools, or other youth-focussed programs targeting
culturally appropriate changes in the pathways.
Proposed Outcome:
Clarification of specific points along the trajectory to suicide in young people, where
targeted funding might have some impact in reducing youth suicide rates in
Indigenous young Australians.
5.4 There remains a need to examine how methodologies which might be inherent in
knowledge systems (Emic) can be developed to, as it were, ‘hear the system speak’,
or allow the system to look at who they are. There is urgent need for work to define
how traditional forms of Emic knowledge can be translated in a culturally acceptable
manner, but also made available in a format that would be acceptable to ‘western’
science. If this could be achieved, it would be a valuable outcome in its own right, but

Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
16
would also assist the process of ongoing funding from relevant national and state
bodies.
Proposed Outcome:
Knowledge remains owned by communities, but an acceptable framework for
translation allows publication in national or international journals, which can turn the
rhetoric into the reality of funded, cogent and locally acceptable programs based, not
on opinion, but on evidence based practice as it is understood around the world.
Selective approaches
As previously noted, arguments can be mounted that discount Selective Prevention as being
in the area of population health strategy, or suggest it is the domain of state or local health
services. However, every Indigenous community can be said to be a group at increased risk
for suicide because of the history of Indigenous communities. Even small communities can
be considered for population-style universal strategies. We argue that both Selective
Prevention and Indicated Prevention demand a sufficient level of capacity on the ground,
relevant to each community, and as highly trained as possible. Item 3 under Universal
approaches then becomes crucial for success of these programs.
5.5 We recommend that:
All existing suicide prevention programs available in Indigenous Australian
communities be prioritised according to currently available evaluation and expert
consensus, and that additional funding be provided to:
o Ensure existing programs can survive and be sustained;
o Ensure successful programs are culturally adapted for other communities;
o Evaluate programs to the best of local ability, within culturally acceptable
parameters, and utilising evaluation expertise from existing experts in;
o Discuss implications of programs in detail at convocations (see above).
5.6 Several programs for which good evidence exists should be made available to every
Indigenous community, and could form the basis of work for local trained Aboriginal Health
Workers. For example:
Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
17
Mental Health First Aid (Kitchener & Jorm, 2006), and/or
ASIST (Applied Suicide Intervention Skills Training, Living Works).
5.7 From emerging evidence there is urgent need for culturally informed interventions
targeting Aboriginal Australian prison inmates and young Aboriginals in youth detention
centres; these could reduce suicide rates in these at-risk populations. Programs need to
provide careful transition back into communities with ongoing support of social and
emotional wellbeing. In addition, funding needs to be provided for programs to rebuild
understanding of culture, educational status, a sense of role and purpose, and transition
to meaningful work.
5.8 It is clear from the literature that alcohol and other substance abuse play a large role
in pathways to suicide, both for young people and for older suicides. There is a need for
programs developed specifically for community-based Indigenous young Australians in
the areas of awareness of risks and problems associated with abuse, and strategies for
changing behaviour. Funding should be made available to trial and evaluate programs -
which might be based in supporting developing resilience through awareness of culture
and improved identity or might lead to intervention in high risk young people who
currently abuse alcohol and other substances.
5.9 A corollary of the need for alcohol abuse reduction relates to Foetal Alcohol
Syndrome in Indigenous communities. Foetal Alcohol Syndrome (FAS) is the most
common preventable cause of mental retardation and is due to alcohol use in the first
trimester of pregnancy. FAS has long term implications for education, social relationships
and mental health problems, and burden on families and communities. Rates are said to
be 10 times higher in Indigenous communities. Heightened awareness, education and
Early Intervention reduce rates (Senate Select Committee on Regional and Remote
Indigenous Communities - September 20084).
4 http://www.aph.gov.au/senate/committee/indig_ctte/reports/2008/report1/c05.htm

Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
18
The Review
Key Principles
This Report is based on the following key principles from a review of the policy and
literature, as well as consultations with key informants judged to be expert in the field (see
from page 74 onwards for in-depth discussion):
1. Community Empowerment
2. Recognition of Human Rights, Transgenerational Trauma, Loss and Grief
3. Development of Individual, Family and Community Social and Emotional
Wellbeing
4. Acknowledgement and Recognition of Aboriginal and Torres Strait Islander
Diversity and Importance of the Local Context
5. Direct Involvement of Community Members and Development of Local
Workforce
6. Ensuring Program Sustainability and Organization Capacity
7. Evidence- or Theory-Base for Programs
8. Appropriate Program Evaluation
9. “Researching Ourselves Back to Life”
Overall, the principles involve a commitment to improve mental health status in Indigenous
Australians to eliminate any differences between their social and emotional wellbeing and
that of the rest of the Queensland population. The principles acknowledge the holistic and
relational concept of health (social, emotional, cultural, spiritual) so important in Aboriginal
and Torres Strait Islander culture, and are consistent with a wide range of existing policy and
other documents:
Universal Declaration of Human Rights (United Nations, 1948)
United Nations Declaration on the Right s of Indigenous Peoples (UN, 2008)
Prevention of Mental Disorders: Effective Interventions and Policy Options. Summary
Report (World Health Organization [WHO], 2004)
Promoting Mental Health: Concepts, Emerging Evidence, Practice (WHO, 2005a)
Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
19
Living Is For Everyone (LIFE) Framework: A Framework for Prevention of Suicide in
Australia (Commonwealth of Australia, 2007)
National Mental Health Plan 2003-2008 (Australian Health Ministers, 2003)
National Action Plan for Promotion, Prevention and Early Intervention for Mental
Health 2000 (Commonwealth Department of Health and Aged Care, 2000)
National Strategic Framework for Aboriginal and Torres Strait Islander Health 2003-
2013: Australian Government Implementation Plan 2007-2013 (Australian
Government Department of Health and Ageing, 2003)
National Strategic Framework for Aboriginal and Torres Strait Islander People’s
Mental Health and Social and Emotional Well Being 2004-2009 (National Aboriginal
and Torres Strait Islander Health Council, 2004a)
Values and Ethics: Guidelines for ethical conduct in Aboriginal and Torres Strait
Islander Health Research (National Health and Medical Research Council, 2003).
Keeping research on track: A guide for Aboriginal and Torres Strait Islander peoples
about health research ethics (National Health and Medical Research Council, 2005).
Guidelines for ethical research in Indigenous studies (Australian Institute of Aboriginal
and Torres Strait Islander Studies, 2000)
Reducing Suicide: The Queensland Government Suicide Prevention Strategy 2003-
2008 (Queensland Health, 2003a) and Reducing Suicide: Action Plan: Queensland
Government Suicide Prevention Strategy 2003-2008 (Queensland Health, 2003b)
Queensland Mental Health Policy Statement: Aboriginal and Torres Strait Islander
People (Queensland Health, 1996)
Queensland Plan for Mental Health 2007-2017 (Queensland Government, 2008)
It is important to recognise the particular place of the Ottawa Charter for Health Promotion
(WHO, 1986), adopted at the First International Conference on Health Promotion in 1986
and a basis for development of Jakarta Declaration on Leading Health Promotion into the
21st Century (WHO, 1997) and Bangkok Charter for Health Promotion in a Globalized World
(WHO, 2005b). Ottawa Charter defines health promotion as “the process of enabling people
to increase control over, and to improve, their health. To reach a state of complete physical,
mental and social wellbeing, an individual or group must be able to identify and to realize

Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
20
aspirations, to satisfy needs, and to change or cope with the environment. Health is,
therefore, seen as a resource for everyday life; not the objective of living. Health is a positive
concept emphasizing social and personal resources, as well as physical capacities. Therefore,
health promotion is not just the responsibility of the health sector, but goes beyond healthy
life-styles to wellbeing” (p. 1). Health promotion can be achieved through building healthy
public policy, creating supportive environments, strengthening community actions,
development of personal skills, appropriate reorientation of health services and moving into
the future.
The Charter indicated that health improvement requires a secure foundation in the
following prerequisites - Peace, Shelter, Education, Food, Income, A stable eco-system,
Sustainable resources, and Social justice and equity.
Literature search strategy
The Report is based upon review of literature regarding suicide and suicide prevention, and
other relevant material on mental health promotion in the context of social and emotional
wellbeing of Aboriginal people and Torres Strait Islanders in Australia, and in Indigenous
peoples in Canada, USA, and New Zealand. Review of literature on Aboriginal and Torres
Strait Islander Australians encompasses published articles (including reviews), funding body
reports and project reports where appropriate. Review of international literature is based
upon published review articles and major reports from Canada, USA, and New Zealand.
Published literature was searched through PubMed, PsycINFO, Australian Indigenous
HealthInfoNet, and Web of Science using the following keywords: “indigenous” OR
“aboriginal” OR “atsi” AND “indigenous suicide” OR “aboriginal suicide” OR “suicide
prevention” AND “australia*”. Lists of references of retrieved articles were searched to
identify further material. Unpublished literature, including community organisation reports,
project protocols and reports, workshop reports and conference proceedings were identified
through Internet search engines using key words listed above and accessed online. Other
material was identified through searches of online Aboriginal and Torres Strait Island health
bibliographies and research and public policy centres and Australian Government
departments. Additional published and/or unpublished resources were identified through
consultations with other Key Informants and Experts (see Appendix One).

Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
21

Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
22
Policy Review on Suicide Prevention, Mental Health and Social and Emotional Wellbeing in
Aboriginal and Torres Strait Islander Australians
This section provides a review of government policies and strategies related to suicide
prevention, mental health and social and emotional wellbeing in Indigenous Australians56
.
Some policies and strategies include special cultural considerations for Indigenous
Australians, others provide direction, targets and strategies for all Australians. Our overall
conclusion is that considerable affirmative action is required to enable Indigenous Australians
to reach equity with all other Australians.
Reducing Suicide: Queensland Government Suicide Prevention Strategy 2003-2008
(Queensland Health, 2003a) and Reducing Suicide: Action Plan: Queensland Government
Suicide Prevention Strategy 2003-2008 (Queensland Health, 2003b)
The Queensland Government Suicide Prevention Strategy recognises Indigenous
Queenslanders as a priority group for suicide prevention, including Indigenous people in
custody. The strategy identifies seven Outcome Areas, some with special considerations for
the Aboriginal populations (in particular, Outcome Six):
Outcome Area One: Enhanced community capacity to promote and maintain social,
emotional, cultural and spiritual wellbeing across the lifespan.
Outcome Area Two: A more knowledgeable community, able to take responsibility and
implement risk reduction strategies.
Outcome Area Three: Greater system-wide knowledge, capacity and skills to ensure
services are able to intervene early and respond effectively to suicide and suicidal
behaviour.
Outcome Area Four: Enhanced treatment and support services that are responsive to
people who are at high risk of suicide and suicidal behaviour.
Outcome Area Five: A coordinated system of care across sectors, between Departments,
services and individual providers.
5 Funding for the original review was provided by Health Promotion Queensland. The review could ultimately
benefit from inclusion of policies from other states of Australia. 6 In this section we have retained the original (although inconsistent) terminology in relation to Indigenous
Australians used in the documents we quote.

Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
23
Outcome Area Six: Service responses across the spectrum of interventions that are
culturally sensitive and consider the needs of Aboriginal and Torres Strait peoples,
including the following strategies:
Engage Indigenous communities in identifying the cultural, historical and spiritual
factors which may influence suicide and suicidal behaviour (Outcome Area One);
Promote approaches to enhance self-esteem and capacity to enable individuals and
communities to connect with a value system based on identity, place, people and
land (Outcome Area One);
Develop partnership approaches with communities to strengthen local responses to
complex issues, including drug and alcohol use, interpersonal conflict, violence, and
grief and loss (Outcome Areas Two, Three and Four);
Enhance primary health and mental health services for Indigenous peoples to
promote mental health and prevent mental illness (Outcome Areas Two and Three);
Improve access to specialist mental health services (Outcome Areas Four and Five);
Enhance the capacity of communities and front line workers to recognise and
respond to risk at the individual and community level (Outcome Areas Two, Three
and Four), and
Develop partnerships with Indigenous peoples to improve data collection, research
and evaluation and sharing of best practice approaches across communities and
sectors (Outcome Area Seven).
Outcome Area Seven: Evidence-based policy, program and service development.
COMMENT: Outcome Area One goes to the heart of this review. Together with Outcome
Area Two it informs and guides our recommendations on Actions needing to be taken.
Outcome Area Four evokes comments similar to those in our responses to the
Commonwealth of Australia (2008) Principles 3, 5, 6 and 7.
The overarching guiding principles underlying the Strategy (all applicable to suicide
prevention in Indigenous Australians) are presented in Table 1 (below).

Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
24
Table 1. Principles underlying Queensland Government Suicide Prevention Strategy
(Queensland Health, 2003a)
1. A focused and collaborative government approach.
2. Active partnership development across sectors.
3. A range of interventions and responses from a focus on wellbeing and prevention,
through to improved access to care and relevant services, to postvention.
4. Continuous learning, implementation of agreed best practice and further development of
the body of evidence.
5. Sustainable outcomes that build on existing infrastructure.
6. Culturally appropriate actions responsive to the needs of local communities.
7. Contextually sensitive and targeted actions that respond to particular needs of urban and
rural areas, and regional profiles.
8. Do no harm.
Queensland Mental Health Policy Statement: Aboriginal and Torres Strait Islander People
(Queensland Health, 1996)
The Policy Statement recognises Aboriginal and Torres Strait Islander people as a priority
group which calls for specific strategies to ensure equal access to appropriate mental health
services and to improve the standard of treatment provided there. The Policy identifies
seven Key Areas for action and recommends a number of strategies under each of the Areas:
Area One: Culturally appropriate service provision.
Area Two: Participation and partnership.
Area Three: Needs based criteria for service provision and resource allocation.
Area Four: Workforce planning and development.
Area Five: Information, monitoring and evaluation.
Area Six: Community education and support.
Area Seven: Across government approach to the provision of key social and
infrastructure services.

Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
25
Queensland Plan for Mental Health 2007-2017 (Queensland Government, 2008)
The Plan includes Aboriginal and Torres Strait Islander (ATSI) populations among high suicide
risk groups. The Plan supports strategies aiming to reduce suicide risk and mortality and
supports programs building individual and community resilience and capacity in the ATSI
populations (Priority One: Mental Health Promotion, Prevention and Early Intervention) and
aims to improve mental health services available to these populations, including
employment of ATSI mental health workers and supporting specialist hubs of expertise
(Priority Two: Integrating and Improving the Care System). “Improved capacity to respond to
the mental health needs of Aboriginal and Torres Strait Islander people” is among the Plan
outcomes envisaged for the year 2017.
COMMENT on Queensland Mental Health Policy Statement and Queensland Plan for Mental
Health 2007-2017
Area Four of the Policy Statement is relevant to comments made on the LiFE Framework
principles 3, 5, 6 and 7. There is a clearly a need to adopt a program of affirmative action. As
part of this we recommend review of the possibilities for training of Indigenous Australians
at all levels of the Mental Health workforce. Priority Two of the Plan cannot be achieved
without a critical mass of workers steeped in local culture and acceptable to local
communities.
Living Is For Everyone (LiFE) Framework: A Framework for Prevention of Suicide in Australia
(Commonwealth of Australia, 2007)
The current national framework for suicide prevention in Australia recognises Aboriginal and
Torres Strait Islander populations as a group at high risk of suicide. The framework indicates
six Action Areas with several special considerations for the Aboriginal and Torres Strait
Islander population:
Action Area One: Improving the evidence base and understanding of suicide prevention,
including application and continuing development of the research and evidence base for
suicide prevention in Aboriginal and Torres Strait Islander communities (Outcome 1.3).

Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
26
Action Area Two: Building individual resilience and the capacity for self-help, including
development and promotion of programs that enhance help-seeking in Aboriginal and
Torres Strait Islander communities (Outcome 2.2).
Action Area Three: Improving community strength, resilience and capacity in suicide
prevention.
Action Area Four: Taking a co-ordinated approach to suicide prevention.
Action Area Five: Providing targeted suicide prevention activities, including support for
interventions for groups identified as high risk, including men in Aboriginal and Torres
Strait Islander communities (Outcome 5.3).
Action Area Six: Implementing standards and quality in suicide prevention.
Although no special consideration for Aboriginal and Torres Strait Islander Australians is
provided in the principles and aims of the framework, these will clearly apply to all
Australians. All programs developed under the framework, including those targeting
Indigenous Australians should aim to build stronger individuals, families and communities,
increase individual and group resilience to traumatic events, and increase community
capacity to identify and respond to needs. They should support the individual and
community capability to respond quickly and appropriately, and to provide a coordinated
response and smooth transitions to and between care. The framework principles are
presented in Table 2.
Table 2. Principles underlying Living Is For Everyone (LiFE) Framework (Commonwealth of
Australia, 2007).
1. Suicide prevention is a shared responsibility across the community (including families and
friends), professional groups, and non-government and government agencies.
2. Activities should be designed and implemented to target and involve: the whole
population; specific communities and groups who are known to be at risk of suicide; and
individuals at risk.
3. Activities need to include access to clinical or professional treatment for those in crisis and
support for people who are recovering and getting back into life.
Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
27
4. Activities must be appropriate to the social and cultural needs of the groups or
populations being served.
5. Information, service and support need to be provided at the right time, when it can best
be received, understood and applied.
6. Activities need to be located at places and in environments where the target groups are
comfortable, and where the activities will reach and be accessible to those who most need
them.
7. Local suicide prevention activities must be sustainable to ensure continuity and
consistency of service.
8. Suicide prevention activities should either be, or aim to become, evidence-based,
outcome focused and independently evaluated.
9. Suicide prevention activities should first do no harm. Some activities that aim to protect
against suicide have the potential to increase suicide risk amongst vulnerable groups.
Activities need to respect the context, health, receptivity and needs of the person who is
feeling suicidal.
10. Activities need to be sensitive to the broader factors that may influence suicide risk – the
many social, environmental, cultural and economic factors that contribute to quality of life
and the opportunities life offers – and how these vary across different cultures, interest
groups, individuals, families and communities.
11. Services for people who are recognised as suicidal should reflect a multi-disciplinary
approach and aim to provide a safe, secure and caring environment.
COMMENT: Principle 1 creates complexity and confusion. Who coordinates programs
(funded at multiple levels) to ensure synergy and avoid duplication at the community level?
Careful mapping of programs in communities is needed to clarify who funds what for whom,
the coordination, duplication, and gaps requiring funding.
Principles 3, 5, 6 and 7 reflect problems for Indigenous communities resulting from
remoteness, isolation and relative inaccessibility. Funding provided on a per capita basis may
lead to many small communities missing out in terms of all four principles. A program of
affirmative action is needed to ensure all Indigenous Australian communities have access to
services which, while culturally appropriate, meet standards which can be expected by any
Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
28
Australian. A corollary is that there is a need for training programs providing a critical mass
of culturally relevant staff to communities.
National Mental Health Plan 2003-2008 (Australian Health Ministers, 2003)
The National Plan recommends that mental health care should be responsive to the
particular needs of Aboriginal and Torres Strait Islander consumers, families and carers, and
communities, and indicates the need for investment in the Aboriginal and Torres Strait
Islander health workforce. The plan acknowledges that mental health reforms must occur in
concert with other developments in the broader health sector. Among the 34 Outcomes and
Key Directions, several have special application to Aboriginal and Torres Strait Islander
Australians. These include:
Key Direction 3.4: Support antidiscrimination initiatives aimed at identifying and
combating the impact of racism on the wellbeing of the Aboriginal and Torres Strait
Islander people.
Key Direction 6.2: Promote activities aimed at reduction of risk factors and strengthening
of protective factors for suicidal behaviour for the general community and for groups of
high suicide risk, such as Aboriginal and Torres Strait Islander people.
Outcome 16: Improved access to services for Aboriginal and Torres Strait Islander people,
which encompass:
Key Direction 16.1: Include Aboriginal and Torres Strait Islander people in mental
health policy-making and planning.
Key Direction 16.2: Deliver mental health care through partnerships between mental
health services and Aboriginal and Torres Strait Islander-specific health service, with
Aboriginal and Torres Strait Islander people taking a lead role through the Social and
Emotional Wellbeing Framework Agreement Partnership Forums.
Key Direction 16.3: Facilitate access for Aboriginal and Torres Strait Islander people to
mental health services, which may include recognising the importance of early
intervention in the primary care setting, increasing outreach services, and improving
access to psychiatrists.
Key Direction 16.4: Improve the cultural appropriateness and safety of mental health
service options for Aboriginal and Torres Strait Islander people, through enhancing
knowledge of risk factors for Aboriginal and Torres Strait Islander people, improving
Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
29
cultural awareness for the mental health workforce, addressing workforce issues for
Aboriginal and Torres Strait Islander health and mental health workers, and
supporting community initiatives.
Key Direction 16.5: Improve linkages between mainstream mental health services
and general practitioners, and Aboriginal and Torres Strait Islander health services
and drug and alcohol services.
Key Direction 16.6: Support the implementation of the Social and Emotional
Wellbeing Framework, once agreed upon.
Key Direction 16.7: Drawing on the Social and Emotional Wellbeing Framework and
this Plan, support the development and implementation of State and Territory
Aboriginal and Torres Strait Islander Social and Emotional Wellbeing Plans.
COMMENT on Key Directions 16.2 and 16.3: An issue for discussion here relates to the place
of diagnosable mental illness in Indigenous Australians and whether this is of biological
origin (as with all other racial origins) social origin (given the marked level of social exclusion
which exists), or historical (related to long term traumatisation from results of the Stolen
Generation). Either way we recommend clarification of accessible and appropriate pathways
to care which, while culturally aware, do not use culture as a block to high quality rapidly
accessed psychiatric services where needed. This will foster Early Intervention in the context
of a whole population.
Outcome 22: Improved coordination between the mental health sector and other areas
of health, such as child and adolescent services, general adult services, aged care
services, drug and alcohol services and Aboriginal and Torres Strait Islander health
services which encompass:
Key Direction 22.2: Improve continuity of care between Aboriginal and Torres Strait
Islander health services and mental health services through local planning and
partnerships.
Key Direction 25.2: Include Aboriginal and Torres Strait Islander community,
consumer and carer representatives on appropriate committees through the
Aboriginal and Torres Strait Islander Framework Agreement Partnership Forums.
Key Direction 28.4: Support improvements in the effectiveness and quality of mental
health services, through the development of complementary outcome measure and
Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
30
instruments for specialist sectors and particular groups, such as Aboriginal and Torres
Strait Islander people.
Key Direction 29.1: Identify, monitor and disseminate information about effective
models of service and partnerships that improve service responsiveness to Aboriginal
and Torres Strait Islander people.
Key Direction 29.2: Improve the usage of Aboriginal and Torres Strait Islander
identifiers in health data collection.
Key Direction 30.2: Develop funding formulae based on population needs weighted
for Aboriginal and Torres Strait Islander populations, rural and remote locations and
other relevant variables.
Key Direction 33.5: Increase the proportion of Aboriginal and Torres Strait Islander
mental health workers within the mental health workforce and provide appropriate
support and career structures.
National Action Plan for Promotion, Prevention and Early Intervention for Mental Health
2000 (Commonwealth Department of Health and Aged Care, 2000)
The National Plan recognises the Aboriginal and Torres Strait Islander population as a
priority group for its initiatives across the lifespan and in coordination with initiatives for
related priority groups, for example people living in rural and remote areas. The Plan aims to
promote mental health, and prevent and reduce mental health problems and mental
disorders among Aboriginal and Torres Strait Islander peoples through reduced social
disadvantage, racism and oppression, mental health literacy, culturally appropriate
initiatives determined by local communities, community capacity to be resilient to adversity,
enhanced protective factors for mental health problems and mental disorders, reduces risk
factors for mental health problems and mental disorders, especially around issues of loss,
trauma, incarceration, violence and substance misuse, awareness of mainstream services of
the impact of cultural issues on the mental health of Aboriginal and Torres Strait Islander
peoples, and links between mainstream and Aboriginal Community Controlled Health
Services.
The Plan indicates six Outcome Indicators for all priority groups, including Aboriginal and
Torres Strait Islander people:
Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
31
Outcome Indicator One: Reduction of mental health problems and symptoms as these
relate to a range of symptomatic presentations and disorders, including anxiety,
depression, postnatal depression, substance misuse, conduct disorder and behavioural
disorders, suicide and self-harming behaviours, eating disorders, psychosis, and
dementia.
Outcome Indicator Two: Increased mental health, wellbeing, quality of life and resilience.
Outcome Indicator Three: Increased mental health literacy.
Outcome Indicator Four: Improved family functioning and parenting skills.
Outcome Indicator Five: Enhanced social support and community connectedness.
Outcome Indicator Six: Increased investment in evidence-based programs relevant to
promoting mental health and preventing and reducing mental health problems and
mental disorders by governments and non-government agencies.
The following outcome indicators are recommended specifically for Indigenous populations:
1. Reduced racism and discrimination for Aboriginal peoples and Torres Strait Islanders;
2. Improved capacity for Aboriginal and Torres Strait Islander communities to be self-
determining and resilient;
3. Reduced socioeconomic disadvantage, violence, incarceration, family separation,
substance misuse, depression and anxiety for the Aboriginal and Torres Strait Islander
communities, and
4. Reduced suicide and self-harm for Aboriginal and Torres Strait Islanders who are
incarcerated.
The Plan indicates eight Process Indicators for all priority groups:
Process Indicator One: Increased monitoring and surveillance of mental health problems,
mental disorders and risk and protective factors, including social and family functioning.
Process Indicator Two: The presence of evidence-based programs related to promotion,
prevention and early intervention for all priority groups.
Process Indicator Three: Increased early identification of mental health problems and
mental disorders and appropriate referral.
Process Indicator Four: Increased community education related to mental health.
Process Indicator Five: Increase in public policy and practices that promote mental health
in all relevant settings (including family, education, workplace, recreation, and
community).

Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
32
Process Indicator Six: Increased professional education and training.
Process Indicator Seven: Increased inter, intra, and multisectoral collaboration and
partnerships.
Process Indicator Eight: Increased mental health research and evaluation activities.
In addition, the following process indicators are recommended specifically for the Aboriginal
populations:
1. Aboriginal community ownership of programs;
2. Torres Strait Islander community ownership of programs;
3. Increase in culturally appropriate mental health promotion, prevention and early
intervention initiatives;
4. Joint planning between Aboriginal Community Controlled Health Services and
mainstream organizations;
5. Increase in Aboriginal peoples and Torres Strait Islanders professionally trained and
employed in health and education settings.
Of special interest is identification of Media as a key strategic group in the Plan. It recognises
how media present Indigenous Australians and communities impacts on non-Indigenous
prejudice and discrimination, and recommends a media strategy to promote positive
messages on social/cultural diversity, to reduce discrimination and prejudice.
COMMENT regarding Process Indicator Two: This is problematic in that our review and
discussion reveal that there is considerable rhetoric in this area, but very little in the way of
practice based evidence or evidence based practice to drive interventions. We recommend
culturally appropriate programs of research which paired Indigenous and non-Indigenous
researchers to gain best available evidence in the areas of promotion, prevention and early
intervention specifically to drive relevant and culturally appropriate programs of prevention
(Process Indicator Eight). In the context of this review, the aim of the Plan (while inclusive
and wordy) does cover the territory we have aimed to cover. Indicators Two and Three relate
to this document, and challenge us to understand the enormity of the task if we are to
realistically achieve the outcome.
Outcome Four: This is critical to SEWB of future Indigenous Australians. Review of the
complexity of Indigenous Australian family functioning and parenting skills would clarify how
these may be influenced in a culturally appropriate manner.

Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
33
National Strategic Framework for Aboriginal and Torres Strait Islander Health 2003-2013:
Australian Government Implementation Plan 2007-2013 (Australian Government
Department of Health and Ageing, 2007)
This is the second Implementation Plan against the National Strategic Framework for
Aboriginal and Torres Strait Islander Health 2003-2013 (National Aboriginal and Torres Strait
Islander Health Council, 2004b)7 which aims among other things to strengthen the service
infrastructure essential to improving access by Aboriginal peoples to health services and
responding to substance misuse, mental disorder, stress, trauma and suicide, and recognises
improving emotional and social heath and wellbeing with particular emphasis on addressing
mental health problems and suicide among its immediate priority areas for government
action.
COMMENT: The National Strategic Framework and Implementation Plan lay out the context
and content of what is necessary to improve Indigenous health. They underscore our
recommendations on a program of affirmative action to enhance services, and training for
long-term culturally appropriate service provision. Key Result Area Four in the
Implementation Plan is Social and Emotional Wellbeing.
National Strategic Framework for Aboriginal and Torres Strait Islander People’s Mental
Health and Social and Emotional Well Being 2004-2009 (National Aboriginal and Torres Strait
Islander Health Council, 2004a)
Two Key Strategic Directions, including relevant Action Areas of the framework are directly
applicable to suicide prevention in Aboriginal Australians:
Key Strategic Direction 1: Focus on children, young people, families and communities
Key Result Area 1.3: Responding to grief, loss, trauma and anger.
7 The first report back under the implementation plan of the National Strategic Framework is Aboriginal and
Torres Strait islander Health Performance Framework 2006 Report. Canberra: AGDHA. Available at:
http://www.dhs.vic.gov.au/pdpd/koori/downloads/healthperformanceframework_112006.pdf.
The latest report (Australian Government Department of Health and Ageing (2008). Aboriginal and Torres Strait
Islander Health Performance Framework. Report Summary. Canberra: AGDHA) will be released at the end of
2008.

Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
34
Action Area 1.3.6: Acknowledge and recognise the causes of individual and
community anger and provide effective programs to reduce the risk of violent
behaviour and self-harm.
Key Strategic Direction 4: Coordination of resources, programs, initiatives and
planning.
Key Result Area 4.1: Providing optimal funding and coordination in order to
improve Aboriginal and Torres Strait Islander mental health and social and
emotional wellbeing.
Action Area 4.1.2: Increase mainstream funding to Aboriginal Community
Controlled Health Services to operate mental health and social and emotional
wellbeing programs to respond to grief and loss issues, suicide, substance
misuse, family violence and child abuse.
COMMENT: While increased funding to Aboriginal Community Controlled Health Services
may be important (see Action Area 4.1.2, National Strategic Framework for Aboriginal and
Torres Strait Islander People’s Mental Health and Social and Emotional Wellbeing 2004-
2009), it is at this point in our narrative unclear just which programs would provide the most
benefit in providing mental health and social and emotional wellbeing programs to respond
to grief and loss issues, suicide, substance misuse, family violence and child abuse. We
would recommend discussion with Aboriginal Community Controlled Health Services to fund
trials in the area of improving social and emotional wellbeing, to see what impact this has on
grief and loss issues, suicide, substance misuse, family violence and child abuse. Clearly such
trial programs would need to observe criteria we have provided for ethical practice in this
area (see Appendix Two).
Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
35
Indigenous Suicide in Australia
Health and Welfare of Indigenous Australians
The estimated resident number of Indigenous Australians as at June 2006 was 517,200
people, including 463,900 Aboriginal people, 33,100 Torres Strait Islanders and 20,200
people identifying as both Aboriginal and Torres Strait Islander, altogether comprising 2.5%
of the total Australian population (Australian Bureau of Statistics & Australian Institute of
Health and Welfare [ABS&AIHW], 2008). Twenty eight percent (28%) of Indigenous
Australians (146,400 people) live in Queensland and they comprise 3.6% of the population of
the state (ABS&AIHW, 2008). Based on the Remoteness Area classification, 26% of
Indigenous Australians in Queensland live in major cities, 20% in inner regional areas, 32% in
outer regional areas, 8% in remote and 14% in very remote areas (ABS, 2007b).
Geographical location has an impact on health and welfare of Indigenous Australians.
The Baseline Report (Partnerships Queensland, 2006) shows differences between the status
of Aboriginal people living in major cities, inner and outer regional and remote/very remote
locations, and Torres Strait Islanders, including health factors, disability, cultural strength,
mortality, and family and community wellbeing. Overall, people living in Aboriginal Deed-of-
Grant-in-Trust (DOGIT) communities in Queensland face the most difficult conditions across
a range of health and welfare indicators, including non-fatal and fatal suicidal behaviour.
A detailed discussion of the welfare and health status of Aboriginal and Torres Strait
Islanders is beyond the scope of this Report. However, it should be noted that the Social
Justice Report 2005 (Aboriginal and Torres Strait Islander Social Justice Commissioner, 2005)
“detailed the poor state of Indigenous health and Indigenous health inequality as compared
to the rest of the population. It set out how the ‘right to health’ could guide government
action on Indigenous health, and recommended that all governments of Australia commit to
a campaign to achieve Indigenous health and life expectation equality within 25 years. In
order to achieve this goal, the report recommended that governments commit to achieving
equal access to primary health care and health infrastructure for Indigenous Australians
within 10 years” (Calma, 2007; p. S5).
To date “there is some evidence that ATSI people do not have the same level of
access to many health services as other Australians and this can adversely impact on their

Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
36
health outcomes. The relatively poor health status and high mortality and morbidity rates
among Indigenous Australians points to the need for more health services and a greater per
capita investment of health resources for this population.” (ABS&AIHW, 2008; p. 187). In
2004-05, the average expenditure on health goods and services for Aboriginal and Torres
Strait Islander Australians was $4,718 per capita, approximately 17% higher than the
expenditure for other Australians ($4,019). This level of expenditure is not sufficient to
match the needs of Aboriginal and Torres Strait Islander people, who have high levels of
morbidity and whose mortality rates are more than twice the rates for non-Indigenous
Australians (ABS&AIHW, 2008).
Mortality in Indigenous Australians
Considerable caution is required regarding mortality data (including suicide) of
Indigenous Australians. There are numerous problems with data quality and availability,
including identification of Aboriginal status, differences between States and Territories
regarding coronial procedures and data collection systems, and classification of the external
causes of mortality and morbidity (ABS&AIHW, 2008; Moller, 1996). In Queensland,
information on Aboriginal status of the deceased on death certificates has been required
only from January 1996 onwards and, prior to this, it was not possible to determine the
injury death rate in Aboriginal and Torres Strait Islander populations (Moller, 1996).
Available data indicate that overall mortality rates among Indigenous males and
females are almost three times higher than for non-Indigenous Australians, and there is a
17-year gap between life expectancy at birth for Indigenous and non-Indigenous males and
females (59 v. 77 years and 65 v. 82 years; respectively) (ABS&AIHW, 2008). The five leading
causes of death in Indigenous Australians are: (1) diseases of the circulatory system; (2)
injury; (3) neoplasms; (4) diabetes and other endocrine, metabolic and nutritional disorders,
and (5) respiratory diseases. Over the period of 2001-2005, external causes of mortality,
such as accidents, suicide and assaults represented 16% of all deaths among Indigenous
Australians (compared with 6% of deaths in the non-Indigenous population). In the same
period, Torres Strait Islander Australians were less likely to die from external causes
including injury (10%) than Indigenous Australians overall (16%); however, they were more
likely to die from cancer (21% versus 15%) (ABS&AIHW, 2008).

Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
37
Elevated mortality rates (including suicide) have also been reported in other
Indigenous populations worldwide, such as the Maori in New Zealand, American Indians and
Alaska Natives in the US, and the Aboriginal people in Canada (Freemantle, Officer,
McAullay, & Anderson, 2007; Hill, Barker, & Vos, 2007; Ring & Firman, 1998; Stevenson,
Wallace, Harrison, Moller, & Smith, 1998). Still, the situation of Indigenous Australians looks
grim even in comparison to other Indigenous populations (Freemantle et al., 2007), and not
much has changed since 1995 when Ring observed that “expectations for life for Indian
populations in Canada and the United States, and for the Maoris in New Zealand are at least
10 years more than for Australian Aborigines, an enormous difference. Maori adult death
rates are falling at a faster rate than for whites in New Zealand, and the gap in the
expectation of life between the United States Indians and the United States whites is now
only three years, whereas in Australia, the gap in the expectation of life between Aboriginal
communities and the total population in most states is the best part of 20 years” (Ring,
1995; p. 228).
The Indigenous peoples in Australia, New Zealand, the United States and Canada
share some similarities: they have been colonized by the British, exposed to genocide,
racism and discrimination, and currently are citizens of liberal Western democracies (Kunitz,
1994; Kunitz & Brady, 1995). At the same time, there have been differences regarding the
history of colonization and current social and political practices which can account for the
disparities in the health status among Indigenous groups. According to Kunitz (1994), the
particularly bad mortality and morbidity status of Aboriginal Australians can be traced back
to two factors concerning the ways governments have been dealing with the Native people
across history: signing of treaties and the level of responsibility for Indigenous affairs.
Although treaties signed by colonizing powers have been notoriously breached, at least they
gave Native peoples in New Zealand or the United States legitimization for claims for land,
reparation, and services. No such treaties have ever been signed in Australia.
Regarding the level of responsibility for Native people’s affairs, Kunitz (1994)
observed that “(…) no matter how difficult the relationship between the indigenous peoples
and the federal government, from the perspective of indigenous peoples it is still preferable
to control by state governments. Having state governments assume responsibility for native
affairs is not unlike using a fox to guard the chickens, for state governments have even more

Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
38
direct conflicts of interest over land rights than do federal governments” (p. 28). Again, in
Australia the responsibility has been mostly at the state/territory level.
Epidemiology of Indigenous Suicide
In 2001-05, suicide was the leading cause of death from external causes for Indigenous
Australian males (35% of such deaths), and the second leading external cause of death for
Indigenous Australian females (18% of deaths) (ABS&AIHW, 2008). Among Australian males,
the overall Indigenous suicide rate was almost three times higher than that suicide rate for
non-Indigenous males, with the biggest differences in the younger age groups of 0-24 and
25-34 years. The suicide rate among Indigenous Australian females aged 0-24 was five times
the rate of non-Indigenous females, and in age groups 45-54 and over the suicide rates were
similar or lower than the rates for non-Indigenous females.
In 2002-04 in Queensland, Indigenous Australian suicide accounted for approximately
6% of all suicide deaths (De Leo, Klieve, & Milner, 2006). The overall suicide rate in
Indigenous Queenslanders was almost twice that of non-Indigenous (25 per 100,000 v. 15
per 100.000; respectively) and the majority of Indigenous suicides (74%) were under the age
of 35 years. Highest rates were observed among males in the 15-24 and 25-34 years groups
(108 per 100,000 and 56 per 100,000; respectively); both almost three times higher than
corresponding rates for non-Indigenous males.
Regarding geographic location, in 2000-02 suicide rates in Aboriginal and Torres
Strait Islander Australians are highest in remote areas (55 per 100,000), lower in inner and
outer regional areas (37 per 100,000 and 35 per 100,000; respectively) and lowest in major
cities (16 per 100,000). Highest suicide rates were found in DOGIT communities (68 per
100,000) - twice the overall Indigenous Australian rate (30 per 100,000). Suicide rates are
lower in Torres Strait Islander Australians (18 per 100,000) (Partnerships Queensland, 2006).
Of special concern is the high and increasing number of suicides among Indigenous
Australian children and adolescents (Commission for Children and Young People and Child
Guardian Queensland, 2007). In 2006-07, 6 of the 19 children and young people who
completed suicide in Queensland were of Aboriginal or Torres Strait Islander origin, including
5 deaths in the 10–14 age group and 1 death in the 15–17 age group. The majority were
males (5 deaths). Aboriginal and Torres Strait Islander children and adolescents accounted

Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
39
for approximately a third of young suicide victims, despite comprising only 6% of the state
youth population. There was an increase in comparison with findings reported from the
period of 2005-06, where Aboriginal and Torres Strait Islander children accounted for 20% of
child suicides. In 2006-07 the rate of suicide among Indigenous Queensland children was
seven times greater than for non-Indigenous children (22 per 100,000 and 3 per 100,000;
respectively).
Hanging has been the most common method of Indigenous suicide and attempted
suicide in Queensland and across Australia since the mid-1980s (Boots et al., 2006; Cooke,
Cadden, & Margolius, 1995; Davidson, 2003; Hunter, Reser, Baird, & Reser, 1999; Kosky &
Dundas, 2000). In Queensland in 2002-04, hanging accounted for 90% Indigenous suicides
(De Leo et al., 2006). Indigenous suicides by hanging are of special concern due to easy
availability and high lethality of the method, and its acquired deep political and cultural
meaning linked to the Report of the Royal Commission into Aboriginal Deaths in Custody
(1991). There is a pattern of high risk for impulsive young Indigenous males under the
pressure of interpersonal problems and under the influence of alcohol, who choose this
common popular and culturally and politically meaningful method with a fatal or a non-fatal
result (Hunter et al., 1999).
One of the particular features of Indigenous Australian suicide is temporal clustering
of deaths in certain geographical areas and communities, a pattern reported in Queensland
(Hunter et al., 1999; Reser, 1989a) and in the Northern Territory (Hanssens, 2007a; 2007b;
Hanssens & Hanssens, 2007; Parker & Ben-Tovim, 2002). In the late 1990s, Hunter and his
colleagues (1999) examined the distribution of suicide through time in one of the Northern
Queensland communities and found an aggregation of suicide deaths, with gaps of several
years between the aggregates. The possible first cluster of three suicides in the span of as
many months occurred in 1986-1987, and a more significant and extensive cluster lasted
between June of 1991 and November of 1996 (17 suicides). The “epidemic-like” pattern of
Indigenous Australian suicide may be related to “the dense social and interpersonal
networks that exist within and between Aboriginal communities in the north (…). Once
established in a community’s consciousness, suicide becomes another possibility in a
behavioural repertoire, interacting with other constructive and destructive means of coping”
(Hunter et al., 1999; p. 78). However, in understanding Indigenous Australian suicide a
deeper understanding of social determinants may be required.
Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
40
Regarding non-fatal self-harm, Queensland Health hospital separation data for 2002-
03 and 2003-04 show that Aboriginal and Torres Strait Islanders were almost twice as likely
to be admitted to a hospital following an episode of self-harm than non-Indigenous people
(2.5 per 1000 v. 1.5 per 1000) (Partnerships Queensland, 2006). Aboriginal and Torres Strait
Islander Australians living in remote locations were at significantly higher risk than Aboriginal
and Torres Strait Islander Australians in major cities, inner and outer regional areas. People
living in the Torres Region had the lowest rates of hospital admission for self-harm, while
people in Aboriginal DOGITS had the highest admission rates.
The Western Australian Aboriginal Child Health Survey (Zubrick et al., 2005) showed
that 9% of Aboriginal girls and 4.1% of Aboriginal boys aged 12-17 made a suicide attempt in
the 12 months prior to the study. Suicidal ideation was almost twice as prevalent among
young females as among young males (20% v. 12%), an overall 16% of young people having
thoughts about ending their own life in the previous 12 months. Unfortunately, no
comparable data regarding suicidal ideation and attempts among young Indigenous
Queenslanders is currently available.
High suicide risk among Indigenous people in contact with the corrective system
warrants special attention, especially in the aftermath of the Royal Commission on
Indigenous Deaths in Custody (1991) which had a significant social and political impact on
the way Aboriginal suicide is perceived in Aboriginal communities and the mainstream
culture (Hunter 1989; Reser, 1989a, 1989b). The Royal Commission into Aboriginal Deaths in
Custody addressed the critical role that policing and incarceration play in Aboriginal and
Torres Strait Islander community life. A greater proportion of the Aboriginal and Torres Strait
Islander population are in prison or ex-prisoners, a group that is highly vulnerable to self
harm and suicide both inside jail and in the weeks after release (Cunneen, 1997).
The proportion of Indigenous Australians in the prison population is very high: in
2007 Indigenous prisoners comprised a quarter of the prison population in Australia (24%)
and in Queensland (26%) (ABS, 2007a). There are multiple reasons for the
overrepresentation of Aboriginal Australians in the inmate population, such as systemic bias
in policing and judicial systems, social and economic disadvantage, high rates of crime in the
communities, early contact with juvenile justice system and high rates of re-offending
(Coffey et al., 2004; Krieg, 2006; Weatherburn, Fitzgerald, & Hua, 2003), but a detailed
discussion of these issues is beyond the scope of this Report.
Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
41
The overall mortality and suicide rates of both Aboriginal and non-Aboriginal inmates
are high (Dalton, 1999) and suicide has been reported as a leading cause of death in
prisoners after release from jail, especially among Indigenous and non-Indigenous males
(Stewart, Henderson, Hobbs, Ridout, & Knuiman, 2004). Aboriginal adolescents in custody
are as likely as their non-Aboriginal fellows to attempt suicide, and given their over-
representation among people in custody they comprise a high risk group requiring special
attention (Lawlor & Kosky, 1992). Culturally-specific interventions targeting Aboriginal
inmates (Tongs, Chatfield, & Arabena, 2007) and Aboriginal youth in detention centres
(Letters & Stathis, 2004) could reduce the mortality rate in these at-risk populations.
Risk and Protective Factors for Indigenous Suicide
Despite the fact that suicide is currently a significant cause of death among Indigenous
Australians, there has been very little research looking at risk and protective factors for
Indigenous suicide. This section presents an overview of what is known about suicide in
Aboriginal and Torres Strait Australians; however, much of the literature on the subject
presents opinions and theoretical understandings of the subject rather than empirical data.
Moreover, due to the changing nature of Indigenous suicide, studies and analyses published
over a decade ago should be viewed with some caution. Aboriginal and Torres Strait
Australians are a diverse population regarding language and culture, historical experiences
(for example, mission times, DOGIT communities), levels of acculturation, living
arrangements and access to services, and current knowledge regarding suicidal behaviour
across a range of Aboriginal and Torres Strait peoples is practically non-existent, and
urgently required if we are to reduce current rates.
Historically, suicide was very rare in traditional Aboriginal and Torres Strait Islander
Australian societies, although recorded instances of Aboriginal suicide occurred first in the
times of colonial expansion and involved the suicides of women and their children who
threw themselves from cliffs to avoid capture by parties of white men (Coe 1989; Read 1988;
Salisbury & Gresser, 1971).
Available sources on Indigenous Australian suicide state that until the mid-1980s
suicide risk among Aboriginal and Torres Strait Islander people was very low or even non-
existent (Burvill, 1975; Eastwell, 1987; 1988; Jones, 1972; 1973; Jones & de Horne, 1973;
Kidson & Jones, 1968). For example, in Western Australia, Jones and de Horne (1973) found
Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
42
no suicide cases in a period of 10 years in a survey of a population of over 2,000 Indigenous
people. Eastwell (1988) in his study of recorded cases of death in Arnhem Land in Northern
Territory in 1957-1987 found two cases of suicide in a population of over 5,000 people.
Burvill’s (1975) study reported 18 cases of attempted suicide among Aboriginal people in
Perth in 1971-1972. According to the literature published at that time, the low incidence of
suicide could be attributed to high levels of support provided by extended families, existence
of culturally sanctioned outlets for hostility, external attribution of blame, and presence of
complex mourning rituals (Eastwell, 1985; Jones, 1972).
A dramatic increase in the incidence of suicide among Indigenous Australians started
in the 1980s. An analysis of mortality in Northern Territory in 1981-2002 showed that the
rates of suicide among Indigenous males increased by 800% (Measey, Li, Parker, & Wang,
2006) and in South Australia a 10-fold increase in Indigenous suicide was observed over the
period of 1981-1988 (Clayer & Czechowicz, 1991). In Western Australia, the proportion of
male deaths due to suicide increased almost 6-fold from, from 0.5% of all deaths in 1957 to
2.9% of all deaths in 1986 (Hunter, 1988a). In Queensland, Indigenous Australian suicide
rates have been approximately twice as high as the non-Indigenous suicide rates since 1990
(Baume, Cantor, & McTaggart, 1998; Cantor & Slater, 1997; De Leo & Evans, 2002; De Leo &
Heller, 2004; De Leo et al., 2006)8.
Hunter (1990a; 1991a; 2006) has proposed a socio-historical frame to explain the
increase in Indigenous suicide (especially in young males) observed since the mid-1980s.
According to his observations, “Aboriginal suicide was rare before the late 1980s, before
which it tended to be men in their third and fourth decades in non-remote areas. That
changed with the Royal Commission into Aboriginal Deaths in Custody, which investigated
deaths in detention, one-third of which were suicide. The intense media focus informed
constructions of hanging that fore-grounded oppression, associating ‘meaningfulness’ with
hanging. Since then, suicide has increased in the wider Aboriginal population, the highest
rates being teenage and young adult males, now increasingly in remote populations,
sometimes taking on ‘traditional’ meanings. But, the patterns continue to change. In the first
8 Statistical information should be treated with caution due to small Aboriginal and Torres Strait Islander
population numbers and relatively small numbers of suicide deaths, problems with identification of the
Aboriginal and Torres Strait Islander status and possible misclassification of some deaths, for instance,
accidental death instead of a suicide. Official suicide rates may actually under-report the incidence of
Indigenous suicide in Queensland and Australia.
Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
43
months of 2004, four children aged 12 and 13 died by hanging in four communities in Far
North Queensland. (…) Across Indigenous Australia the 1970s ushered in turbulent social
change that has been described as ‘deregulation’. This most immediately impacted young
adults for whom onerous controls were lifted, with entry into the cash economy through
welfare, and unrestricted access to alcohol. However, while discriminatory legislation was
revoked, other barriers, less tangible but robust, persisted, what has been called ‘cultural
exclusion’. (…) Suicide did not increase until the late 1980s - some fifteen years delayed (…).
These were teenagers and young adults – the children of that earlier generation exposed, as
young adults and new parents, to deregulation and its social consequences. The young
suicides were from the first generation to have been raised in that environment of
unremitting instability. Not only were they at risk of self-harm but also petrol-sniffing, sexual
abuse (as victims and perpetrators) and self-destructive confrontations with increasingly
reactionary authorities.” (Hunter, 2006; p. 9)9. [The original version of the quote was
extensively referenced. We refer the reader to the original].
Alcohol and cannabis abuse, impulsivity, and disruption of major interpersonal
relationships have been repeatedly identified as major triggering factors for Indigenous
suicide (Hanssens, 2007a; Hunter, 1988a, 1988b; 1991b; Parker & Ben-Tovim; 2002; Tatz,
2001). These factors seem to operate in a context of a “lifestyle of risk” or an elevated
potential for harm encompassing a range of risky behaviours, such as substance abuse, non-
suicidal self-harm and impersonal violence and “clearly, risk is elevated for those individuals,
particularly males from their teens through to the fourth decade of life, who are members of
communities in which suicide has become common - the best indicator is at a social or
community level, what *can be+ called the ‘community at risk’” (Hunter et al., 1999; p. 75).
The role of psychopathology and psychological factors in relation to suicide in
Indigenous Australians is not clear; there are some data to support the notion that
depression, psychosis, substance abuse and “classical” warning signs of suicide can be
detected in Indigenous victims of suicide. For example, an analysis of coronial records for
Indigenous and non-Indigenous suicide deaths in the Top End (Parker & Ben-Tovim, 2002)
9 Hunter (2006) has also observed that for the young Indigenous children “self-harm is no longer uncommon and
its visibility in remote communities exposes children – from other children wandering the streets with cans of
petrol, to violence to self and others, to threats, acts and representations of suicide. Indeed, among the child
hanging-deaths described earlier, all had been exposed. They belong to the first generation in which many
children‟s early development includes exposure to the threat or act of self-annihilation” (p. 9).
Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
44
showed that suicides in both populations were often preceded by expression of suicidal
intent, signs of abnormal behaviour such as depressed mood and aggression, alcohol abuse
and a formal diagnosis of mental illness.
The Western Australian Aboriginal Child Health Survey (Zubrick et al., 2005) identified
a range of risk factors for suicidal ideation in Aboriginal youth which resemble risk factors for
non-aboriginal children and adolescents, including history of exposure to family violence,
low self-esteem, significant emotional and behavioural difficulties, having friends who
attempted or thought about suicide, smoking cigarettes, using of marihuana and alcohol,
and exposure to racism. Depression, anxiety, poor coping with stress and problem solving
skills, as well as impulsivity, might increases the risk of suicide in Indigenous Australian
adolescents and young adults (Henderson, 2003; Westerman, 2002a).
Other studies, observations and discussions downplay the role of psychopathology
and psychological factors in Indigenous suicide, and instead focus on the impact of socio-
cultural and economic factors, both current and experienced by the Aboriginal and Torres
Strait Islander people in the past, such as genocide and racism (Tatz, 2001), trans-
generational trauma and the impact of “Stolen Generations” (Atkinson, 2002; Human Rights
and Equal Opportunity Commission, 1997), dependence of individuals and communities on
the welfare system (Hunter, 2006), and easy access to alcohol and other harmful substances
(Barber, Punt, & Albers, 1988; Hanssens, 2007a; Shore & Spicer, 2004). For example,
members of the “Stolen Generations” and their progeny are in high risk groups for a range of
conditions including mental illness, self-harm and suicide, and there are reports of
witnessing the suicides of children in institutions and work stations (Healey, 1998; Huggins,
1998; Kilroy, 2008; May, 1994; Robinson, 2008; Terszak, 2008). The utter disempowerment
experienced by people subjected to domination results in social illnesses described as
learned helplessness and lateral violence which result in ennui, hopelessness, self hatred,
addictions, family violence, depression, self harm and suicide (Briscoe, 2003; Copland, 2005;
Wesley-Esquimaux & Smolewski, 2004).
The destruction of Indigenous Australian culture has resulted in ongoing grief,
despair and confusion including the disruption of traditional gender roles (especially for
men), cultural values and pride, disruption of kinship networks and support systems, and
confusion of people forced to balance between two, often irreconcilable cultures. These
factors are very strongly linked to Aboriginal and Torres Strait Islander suicide (Adams &

Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
45
Danks, 2007; Reser, 1991; 2004). According to Tatz (2001), the dynamics and risk factors for
Indigenous Australian suicide are not comparable with those observed in the general
population in Australia or any other Western country, and “Aboriginal suicide is different.
(…) Aboriginal suicide has unique social and political contexts, and must be seen as a distinct
phenomenon” (Tatz, 2001; p. 10)10.
Very little has been written on protective factors for Aboriginal suicide in Australia.
As previously mentioned, early studies linked low suicide rates before the mid-1980s to
external attribution of blame, high levels of support provided by extended families,
effectiveness of culturally sanctioned outlets for hostility and complex mourning rituals
(Eastwell, 1985; Jones, 1972). Recently, Westerman and Vicary (2001) suggested a list of
protective factors for Indigenous youth suicide, including the role of temperament and
coping skills, family and external factors and positive contact with peers. According to the
Western Australian Aboriginal Child Health Survey (Zubrick et al., 2005), high household
occupancy level and living in extremely isolated locations might protect Indigenous
Australian children from developing significant emotional and behavioural difficulties. Sport
and recreation programs in Indigenous communities may strengthen social cohesion,
improve school attendance, and serve as powerful protective factors against juvenile crime,
substance abuse, violence and self-harm (Beneforti & Cunningham, 2002; Cunningham &
Beneforti, 2005). Traditional Aboriginal and Torres Strait Islander ceremonies and spirituality
also may have a potential to protect against suicide (McCoy, 2007; Tse, Lloyd, Petchkovsky,
& Manaia, 2005).
However we have been unable, at this time, to identify empirical studies that could
provide further evidence or a theoretical framework to explain the protective impact of
these factors and their application to social and emotional wellbeing of Aboriginal and
Torres Strait Islander Australians.
10
Publication of Tatz‟s book was followed by a series of polemics (e.g., Goldney, 2002; Reser, 2004) and such
an approach to Indigenous suicide seems quite controversial. On one hand, it rightly stresses the importance of
socio-cultural, political and historical factors, including the history of genocide and current racism and
discrimination, in aetiology of suicide in Indigenous Australians. On the other hand, it may contribute to
marginalisation of Indigenous suicide as a subject of scientific research and practical prevention initiatives, and
result in the denial of the role of individual risk factors, including depression, substance abuse, and lack of
resilience and problem-solving skills, which could become targets of effective interventions, including school-
based programs.

Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
46
Suicide in Indigenous Peoples: An International Perspective
Suicide in Indigenous Peoples in New Zealand, Canada and the United States
“Wherever there has been dispossession, we see in the disposed populations significant
damage in health, in education levels and in social wellbeing. And dispossession of one’s
land in not the only form of dispossession. Native peoples have been dispossessed of their
labour, language, culture, and religious beliefs as well. We are only beginning to
comprehend the consequences of what occurred long ago and still continues throughout the
world” (Bird, 2002; p. 1391). Indigenous people worldwide suffer from persistent social
disadvantage, inferior health status and high mortality, including suicide.
Despite obvious and significant cultural, socio-economic and historical differences
between and within Indigenous populations in New Zealand, Canada and the United States,
several recurring themes and patterns in suicide mortality and morbidity can be identified
and will be presented in this section. In general, suicide rates among Indigenous populations
are elevated in comparison to non-Indigenous populations in respective countries, suicide
risk is highest among young Indigenous males, age of Indigenous suicide deaths is decreasing
and suicides tend to cluster. There is a significant role of alcohol in suicidal behaviour in
Indigenous populations. Indigenous suicides have their roots in ‘collective despair’ related to
persistent social disadvantage, cultural and social exclusion and destruction of cultural
continuity and identity.
In New Zealand, suicide rates among the Maori are high, especially in the younger
age groups: young Maori males and females die of suicide at higher rates than their non-
Maori peers and Maori males have high rates of hospital admissions for suicide attempts.
The older age groups (over 45) are relatively protected against suicide and suicide is very
rare in Maori aged over 60 (Beautrais, Wells, McGee, & Oakley Browne, 2006; Beautrais &
Fergusson, 2006; Coupe, 2000).
In the United States, American Indians and Alaskan Natives of all ages have the
highest rates of violent death among all ethnic groups (31.4 per 100,000 in 2005) and suicide
is the second leading cause of death among the young American Indians in the 15-24 year
age group, and the third leading cause of death in the 10-14 year age group (LaFromboise &
Lewis, 2008). Suicide risk is especially high among American Indian and Alaska Native young

Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
47
males (Echohawk, 1997; 2006). Over the period of 1999-2003 in Alaska, suicide was the
leading cause of death among Alaska Natives aged 15-24 (Wexler, Bertone-Johnson, &
Fenaughty, 2008).
In Canada in 2000, the First Nation suicide rate was twice the overall Canadian rate
(24 per 100,000 v. 12 per 100,000; respectively) and from 1999 to 2003, the suicide rate in
Inuit regions averaged 135 per 100,000 - 10 times the national rate (Kirmayer et al., 2007).
Indigenous suicide in Canada is most prevalent among young people (mostly males), and in
2000, 22% of all youth deaths (10-19 year-olds) and 16% of all early adults deaths (20-44
year-olds) were due to suicide (Kirmayer et al., 2007).
Indigenous suicides often occur in clusters. A study of suicide in a South-western
American Indian tribe of 12,000 individuals found a cluster of seven suicide deaths and
attempts by hanging in the period of 40 days, all deaths among young people aged 13 to 28
years (Wissow, Walkup, Barlow, Reid, & Kane, 2001). Wilkie, Macdonald, and Hildahl (1998)
reported a suicide cluster in an isolated Canadian Manitoba First Nations community of
approximately 1,500 individuals where in period of three months, six young people aged 14
to 25 committed suicide and nineteen aged 12 to 23 attempted suicide (mostly by hanging).
Alcohol has been identified as a major risk factor for suicide in Indigenous people. In
Canada, a study on Indigenous suicide in British Columbia found that 74% of suicide victims
were intoxicated at time of death, and alcohol was detected in 80-90% of Indigenous people
in Alberta who died by suicide (Royal Commission on Aboriginal Peoples, 1995). In the
United States, American Indians have the highest prevalence of substance dependence and
abuse among the racial and ethnic groups (McFarland, Gabriel, Bigelow, & Walker, 2006) and
a study on suicide among American Indian decedents in New Mexico found alcohol in 69% of
suicide victims (May et al., 2002).
Individual risk factors, including psychopathology, alcohol and drug abuse, history of
childhood trauma, abuse and neglect, interpersonal problems and other negative life events,
hopelessness and inability to solve problems and cope with stress play an important role in
suicide in Indigenous peoples (e.g. Enns, Inayatulla, Cox, & Chayne, 1997; Kirmayer et al.,
2007; LaFromboise, Meddoff, Lee, & Harris, 2007; Strickland, Walsh, & Cooper, 2006). It is
impossible to consider Indigenous suicide without taking into consideration socio-historical
factors and issues of cultural identity and continuation in Maori (Beautrais et al., 2006;
Coupe, 2005; Skegg, Cox, & Broughton, 1995), American Indians and Alaska Natives

Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
48
(EchoHawk, 1997; LaFromboise & Meddoff, 2004) and the First Nation peoples in Canada
(Chandler & Lalonde; 1998; Leenaars, 2006).
Indigenous suicide and “collective despair, or collective lack of hope” (Royal
Commission on Aboriginal Peoples, 1995) has been related to persistent social disadvantage,
cultural and social exclusion (Hunter & Harvey, 2002; Hunter & Milroy, 2006), breadown of
cultural continuity (Chandler & Lalonde, 1998; Chandler & Lalonde, in press) and lack of
cultural identity (Coupe, 2005). Chandler and Lalonde (1998) applied the concept of cultural
continuity to explain the significant differences in incidence of youth suicide among different
groups of the First Nation people in Canada: “like other potential sources of continuity and
discontinuity, cultures too appear to be double-edged swords. At least when they tended to
outlive the people who populated them, cultures offered a more ‘mythic’ time-frame that
could be relied on to lend a certain age to things. (…) In other times and places, cultures
appear to be more a part of the problem than the solution. Certainly this appears to be the
case with the various cultures that make up BC’s *British Columbia+ First Nations. Here, in
addition to all those factors that ordinarily work to undermine cultures and promote their
‘natural’ deaths, the massed forces of government have also actively disassembled
aboriginal culture as an explicit matter of official policy” (Chandler & Lalonde, 1998; p. 7).
Figure 1. Community factors and suicide rate (per 100,000).
(Courtesy: Michael Chandler, University of British Columbia)
0
5
10
15
20
25
30
35
40
45
Self Govt Land
Claims
Education Health Cultural
Facil
Police/Fire * Women in
Govt
* Child
Services
PresentAbsent

Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
49
Apparently, communities’ efforts to rebuild, preserve or reconstruct their cultures by
taking control over important areas of life have a protective impact on youth suicide. In
British Columbia, Chandler and Lalonde (1998) found an inverse correlation between the
number of cultural continuity and identity indicators (including land claims, self-government,
community control over education system, health services, cultural facilities, police and fire
services) and suicide rates11 (Figure 1 and Figure 2).
Figure 2. Overall suicide rate (per 100,000) by number of community factors.
(Courtesy: Michael Chandler, University of British Columbia)
Suicide Prevention in Indigenous Peoples in New Zealand, Canada and the United States
There seems to be more research and published literature on suicide prevention in
Indigenous peoples outside Australia, especially in the United States and Canada, than about
suicide prevention for Aboriginal and Torres Strait Islander Australians. Nevertheless, the
11
An expert in suicide and suicide prevention in Indigenous Australians, Professor Ernest Hunter, has observed
that “several years ago one of the authors of the Canadian research (Chris LaLonde) came to Cairns (and to
Yarrabah) on sabbatical and we were interested to know if the research undertaken in British Columbia could be
replicated in Australia. In fact, it probably cannot. What passes as „control‟ in Indigenous Australia is of a very
different nature to the experience of Aboriginal Canadians. Pervasive welfare dependence, the demise of ATSIC,
the vulnerability of community controlled health services, the Commonwealth intervention in the Northern
Territory … all make clear that there are very significant limits to Indigenous control and autonomy in
Australia” (Hunter, in press).
0
5
10
15
20
25
30
35
40
45
0 1 2 3 4 5 6 7 8
Number of Factors Present
Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
50
knowledge regarding the effectiveness of interventions for the American Indians, Alaska
Natives and the Aboriginal Canadians is limited.
A comprehensive review of suicide prevention programs in communities of the
American Indians and Alaska Natives in the United States showed that many programs are
developed by the tribes themselves (Middlebrook, LeMaster, Beals, Novins, & Manson,
2001). The majority of programs are local grass-roots initiatives, informal and independent
of any centralised planning or control, and relatively few are evaluated and reported in the
published literature. The review identified nine programs, including five suicide-specific
programs12 and four programs addressing related mental health and wellbeing issues, such
as alcohol and drug abuse and teen pregnancy13. These programs in varying degrees
addressed the generic factors associated with suicide (i.e. stress, depression, and
hopelessness) and culture-specific factors relevant to Indigenous peoples, such as loss of
ethnic identity and cultural and spiritual development, cultural confusion and acculturation.
The review led to rather disappointing conclusions: “information on the effectiveness
of suicide preventive intervention programs among American Indians/Alaskan Native
communities is scarce. There are few descriptions of programs in the literature and even
fewer with any type of evaluation effort. (…) As a result of constraints or omissions [in
program design and implementation], the effectiveness of the programs cannot be
determined. In many cases, the reported effectiveness of the programs is impressionistic.
(…) Because many of the programs were developed for the particular communities in which
they were implemented, the generalizability of the results is somewhat limited; however,
core program components can be tailored to other AI/AN communities, because many of
the basic risk factors (e.g., age, family disruption, school conditions) cut across communities.
(…) The absence of formal proactive evaluation is indicative of the majority of AI/AN
programs that have been reported in the literature. As a result, programs may be
implemented that have not been shown to be effective for the AI/AN communities that they
are meant to help. The necessity of identifying programs proven to be effective is evident
when one considers the limited amount of funding available” (Middlebrook et al., 2001; p.
140).
12
Zuni Life-Skills Development Curriculum, Wind River Behavioral Health Program, Tohono O'odham
Psychology Service, Western Athabaskan „Natural Helpers‟ Program, and Indian Suicide Prevention Center. 13
Blue Bay Healing Centre, Acoma-Canoncito-Laguna Adolescent Health Program, Rainbow Lodge Alcohol
Recovery Program, and Positive Reinforcement in Drug Education Program.

Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
51
In Canada, the Advisory Group on Suicide Prevention (2003) found an absence of
rigorously evaluated studies and serious gaps in knowledge regarding effectiveness of
suicide prevention programs developed for Indigenous people. Based on an earlier review of
evidence (Kirmayer, Boothroyd, Laliberté, & Laronde Simpson, 1999), the report identified
twenty nine suicide prevention and mental health promotion programs developed
specifically for Aboriginal populations or modified to meet their needs. Nine of the
programs14 were recommended as “promising or particularly appropriate models for
Aboriginal communities who wish to use a pre-existing program” (Advisory Group on Suicide
Prevention, 2003; pp. 43-44).
A more recently published report Suicide among Aboriginal People in Canada
(Kirmayer et al., 2007) presents a more comprehensive and updated list of promising suicide
prevention programs with a focus on Aboriginal communities15. Each of these programs is
either (1) created or driven by the community or (2) adapted by the community in part or as
a whole or (3) intended to mobilize the community toward development or implementation
of own prevention initiatives. These programs are ongoing, wide-reaching, include an
evaluation component, and information about the programs is easily accessible via the
Internet or through contact organisations.
The Special Report on Suicide among Aboriginal People by the Canadian Royal
Commission on Aboriginal Peoples (1995) concluded that only “a comprehensive approach
to suicide prevention has any hope of changing the existing picture. A comprehensive
approach must include plans and programs at three levels of intervention: (1) those that
focus on building direct suicide crisis services, (2) those that focus on promoting broadly
preventive action through community development, and (3) those that focus on the long-
term needs of Aboriginal people, for self-determination, self-sufficiency, healing, and
reconciliation within Canada” (p. 75). The Canadian Advisory Group on Suicide Prevention
(2003) suggested a number of specific guidelines for Aboriginal suicide prevention programs,
14
Jicarilla Mental Health and Social Services Program, Community-Based Suicide Prevention Program,
Miyupimaatisiiuwin Wellness Curriculum, Let‟s Live!, Life Skills Training, Programme d‟entraide par les pairs
(Peer Support Program), Native Parenting Program, Family Workshop: Parents and Problems Parenting
Program, and Multimedia CD-ROM: Mauve. 15
Applied Suicide Intervention Skills Training (ASIST), 5-Day Suicide Prevention Training for Aboriginal
Communities, White Stone: Aboriginal Youth Suicide Prevention Training for Youth Educators, Community-
Based Suicide Prevention Program, Zuni Life Skills Development Curriculum, Jicarilla suicide prevention
program, and Northwest Territories Suicide Prevention Training.

Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
52
which seem highly relevant to suicide prevention and social and emotional wellbeing in
Aboriginal and Torres Strait Islander Australians, and thus are presented in Table 3.
Table 3. Guidelines for Aboriginal suicide prevention programs in Canada (Advisory Group on
Suicide Prevention, 2003).
1. Programs should be locally initiated, owned and accountable, embodying the norms and
values of the local/regional First Nations culture;
2. Suicide prevention should be the responsibility of the entire community, requiring
community support and solidarity among family, religious, political or other groups. There
should be close collaboration between health, social and education services;
3. A focus on the behaviour patterns of children and young people (up to their late 20s) is
crucial. This requires involvement of the family and the community;
4. The problem of suicide must be addressed from many perspectives, encompassing
biological, psychological, socio-cultural and spiritual dimensions of health and wellbeing;
5. Programs that are long-term in focus should be developed along with “crisis” responses;
6. Evaluation of the impact of prevention strategies is essential.
In New Zealand, the national suicide prevention strategy (Ministry of Health, 2008)
includes a Maori component and recommends implementation of culturally appropriate
initiatives aiming to reduce the incidence of suicide, especially among young people, and
increase health and wellbeing in the Maori population. Such initiatives should be tailored to
meet the needs and expectations of the Maori people and should be based on the concepts
of health (hauora) and support for Maori families to achieve maximum health and wellbeing
(whänau ora). Unfortunately, we were not able to identify any literature reporting on the
effectiveness of suicide prevention programs for the Maori population.

Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
53
Searching for Solutions: Prevention of Suicide in Indigenous Australians
As presented in detail earlier in this Report, suicide is a cause of significant loss of life in
Aboriginal and Torres Strait Islander communities across Australia, especially among young
males in their twenties and thirties, and over the last decade it has started to take its toll
among Indigenous children and adolescents. Suicide deaths in communities often take place
in public places, and due to the close-knit social structure of communities, the victims are
known to others. Suicides often happen in “waves” and against the background of other
premature deaths due to poor general health, accidents, and interpersonal violence,
including domestic violence. In the aftermath of a suicide, the communities are left with the
terrifying question “who will be next?”, feelings of guilt and inadequacy (“what’s wrong with
us”), and due to lack of services, are bereft of help and support to cope with grief and loss.
The risk of accepting suicide as a “normal reaction” to problems and an effective way of
expressing anger and emotionally “blackmailing” the environment, underscores the need for
postvention.
Despite the general agreement that “suicide among Indigenous Australians is a
problem” and “something has to be done”, there is a dearth of suicide prevention programs
for Indigenous Australians for which there are rigorous evaluations and evidence for
effectiveness (and for which there is accessible literature). The lack of programs and
evaluations is partly related to insufficient funding and resources, lack of services and
remoteness, but not knowing what should and could be done contributes to the confusion.
Cultural and historical differences between communities make it often impossible to use or
adapt programs developed in different locations. Suicide remains a cultural taboo subject in
some communities and this may stop people from opening the subject and seeking help.
Other communities actively seek help after suicide and appreciate the normalization of the
grieving experience offered by suicide prevention and postvention programs.
The Western (over)medicalised and (over)individualistic paradigm sees depression as
the major contributor to suicide and tends to focus on individual interventions and
treatments. However, Indigenous suicide prevention requires a broad approach and
understanding, including consideration of social, historical and political factors. Both
Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
54
reviewed literature and experts in the field stress that suicide prevention for Indigenous
Australians has to have a broad community and family focus.
A number of suicide prevention and social and emotional wellbeing programs
applicable to prevention of suicide have been initiated, developed and implemented either
by members of communities themselves or in collaboration with mainstream services and
organizations. Appendix 2 presents programs we were able to identify through the literature
search and through consultations with experts in the field. Some of the programs were
developed especially for Indigenous communities and individuals and used in a number of
communities (e.g., Family Wellbeing Empowerment Program, Toughin’ it out pamphlet).
Others are mainstream suicide prevention initiatives modified to suit the needs and
characteristics of Aboriginal and Torres Strait Islander people, for instance, Suicide
Awareness for Aboriginal Communities and Applied Suicide Intervention Skills Training
(ASIST). Some of the initiatives focus on suicide prevention and the aftermath of suicide
(e.g., Indigenous community suicide intervention forums, Healing Our Way self-help
resource) while others are more general and tackle a range of issues, including domestic
violence, substance abuse, boredom and lack of meaningful activities in the communities
(e.g., Family Wellbeing Empowerment Program). Mental Health First Aid (MHFA), a training
course for members of the public teaching them to recognise and give assistance in mental
health crisis situations has been recently adapted to serve Indigenous Australians, i.e.
Mental Health First Aid for Aboriginal and Torres Strait Islander Communities (Kanowski,
Kitchener, & Jorm, 2008). Given the promising MHFA outcomes and evaluations in the
general population (Kitchener & Jorm, 2006) and its great potential in improving social and
emotional wellbeing and preventing suicide in Indigenous Australians, the program is
mentioned here, although it is not listed in Appendix 2 - no published materials regarding its
implementation in Asutralian Indigenous communities were identified.
There is evidence of effectiveness available for some of the initiatives, either based on
anecdotal or clinical evidence from individuals or organisations that run the programs (e.g.
Suicide Awareness for Aboriginal Communities, ASIST) or from structured process evaluation
(e.g., Family Wellbeing Empowerment Program). In general; however, suicide prevention
initiatives for Indigenous Australians are plagued by the same evaluation dilemmas
regarding the type of evaluation (i.e. process v. outcome), outcome measures and
methodology, as programs run in the other populations in Australia and internationally.

Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
55
Despite a remarkable number of such initiatives in Australia (Headley et al., 2006; Robinson
et al., 2006) and in other countries (Beautrais et al., 2007; Goldsmith, Pellmar, Kleinman, &
Bunney, 2002), there is limited knowledge regarding their effectiveness.
Unfortunately, some prevention programs are implemented despite lack of any
evidence of their effectiveness and in some cases there are strong claims regarding
effectiveness of approaches which have never been properly evaluated or might even be
harmful, such as no-suicide contracts in clinical practice. On the positive side, the situation is
not totally bleak and some types of interventions designed for the general population or
selected high risk groups seem to be effective (at least in certain environments) (Beautrais et
al., 2007; Goldsmith et al., 2002; Mann et al., 2006). There is an overall consensus that
physician education in recognition and treatment of depression, the training of gatekeepers,
and limiting access to lethal means of suicide, have an impact on suicide rates. Restricted
availability of lethal means of suicide, such as guns, toxic substances, high bridges and rail
tracks, is frequently linked to significant reductions in overall suicide rates. For instance, in
the 1960s in Australia restriction of access to barbiturates was associated with a 23% decline
in suicide using this method without an increase in the use of other means (Oliver & Hetzel,
1972).
Other approaches to suicide prevention in the general population or in selected
groups at elevated suicide risk appear promising, although there is lack of strong scientific
evidence-base to unequivocally prove their effectiveness (Beautrais et al., 2007; Goldney,
1998). These include clinical interventions for people with a history of suicide attempts,
especially interventions aiming at improved treatment compliance and more efficient
follow-up. One aspect of this relates to antidepressant use; where increased prescribing of
selective serotonin reuptake inhibitors (SSRIs) has occurred, suicide rates have appeared to
fall. However, autopsy studies of people prescribed antidepressants and who later suicide,
often show a complete absence of antidepressants in the system prior to death, and recent
research has disputed the direct causal effect on suicide rates, noting that rates began to fall
prior to the onset of increased use of antidepressants (Reseland et al., 2006). Psychotherapy
and psychosocial treatments (eg Cognitive Behavioural Therapy or Dialectical Behavioural
Therapy) for mental disorders have also been shown to reduce suicidal behaviour (Brown et
al., 2005). Recent work suggests the impact of psychotherapy in community or population
studies could be the availability of psychotherapists (as a proxy for relevant healthcare

Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
56
services) in a community as much as the actual therapy (Kapusta et al., 2009). This work
may underpin our recommendation about developing a critical mass of Aboriginal mental
health workers in a community.
A wide range of general population and community-based programs, such as easy
access to crisis centres and counselling, public awareness and education, mental health
literacy programs, screening for depression and elevated suicide risk in educational and
primary care settings, school-based competency and skill enhancement programs, and
support for suicide survivors and communities bereaved by suicide also may lead to positive
outcomes; however, there is insufficient or contradictory data regarding their impact on
actual rates of suicide.
There is strong evidence linking media reports of suicide to increased suicide rates in
Australia (Pirkis et al., 2006) and internationally (Pirkis & Blood, 2001), and decreasing the
level of media reporting of suicides and encouraging a responsible covering of the subject is
a promising approach to suicide prevention (Fu & Yip, 2008; Mann et al., 2006).
Consequently, national or local guidelines for responsible coverage of suicide have been
developed internationally, including Australian “A resource for media professionals”
(Commonwealth Department of Health and Aged Care, 2004). The National Action Plan for
Promotion, Prevention and Early Intervention for Mental Health 2000 (Commonwealth
Department of Health and Aged Care, 2000) has also identified the Australian media as a key
strategic group and recommends national-level action to develop a media strategy to
promote positive messages around social and cultural diversity to reduce prejudice and
discrimination towards Indigenous Australians. Such initiatives could support suicide
prevention in Indigenous Australians.
One of the most effective, comprehensive, population-based, prevention programs is
the US Air Force suicide prevention initiative for active duty military personnel started in
1996 (Knox et al., 2003). This program aims at reducing suicide risk factors and enhancing
protective factors, including changing policies and social norms, proving awareness of
mental heath issues and reducing the stigma of help-seeking. Implementation of the
program in late 1990s was associated with a 33% decline in suicide rate as well as reductions
in levels of other related outcomes, such as accidental deaths, homicide and incidents of
domestic violence among the Air Force personnel. There are 11 sub-programs within this
program, and at this point it is not clear whether it is the help-seeking aspect or the

Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
57
resilience development aspects that are of more importance, or whether the total package is
necessary to create change.
This literature review began with the intent to consider the development (or
redevelopment) of social and emotional wellbeing as a way forward to reduce the possibility
of suicide in Indigenous Australian communities. Unfortunately, the evidence for large-scale
population approaches to building protective factors toward reducing suicidality, is still in its
early stages.
Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
58
Social and Emotional Wellbeing in Indigenous Australians
Suicide prevention is an integral part of the holistic view of physical and mental health and
social and emotional wellbeing of Indigenous Australians. The Indigenous concept of health
is multi-dimensional, embraces all aspects of living and points out the importance of survival
in harmony with the environment, including good relationships between families and
communities, strong culture, sense of trust, belonging, and participation, and healthy
relationships with the land (Grieves, 2007; Kowal, Guntorpe, & Bailie, 2007; Northern
Territory Aboriginal Health Forum Emotional and Social Wellbeing Working Party, 2003).
According to Kowal et al. (2007), “increase in interest in this area has been in response to
the efforts of Indigenous leaders to raise the profile of mental health/Emotional and Social
Wellbeing on the national policy agenda, through what has been called the Indigenous
Mental Health Movement” and “the term ‘Emotional and Social Wellbeing’ is currently the
term used within Aboriginal and Torres Strait Islander health policy to represent an area that
includes mental health” (p. 2). The National Aboriginal Health Strategy developed in 1989
with a significant input of Aboriginal and Torres Strait Islander people defined heath as:
“Not the physical wellbeing of the individual; but the social cultural wellbeing of the
whole community. This is a whole of life view and it includes a cyclical concept of life.
Health care services should strive to achieve the state where every individual is able to
achieve their full potential as human beings, and thus bring about the total wellbeing of
their community.” (National Aboriginal Health Strategy Working Party, 1989; p. X)
The seminal National Consultancy Report Ways Forward observed: “Aboriginal
people emphasised the strong relationship of mental health and wellbeing to physical health
and saw loss of mental wellbeing as contributing in a major way to the poor physical health
and health outcomes of Aboriginal people. There is much to suggest that this is indeed a
further significant and major contributor to the adverse and deteriorating state of the health
of Aboriginal people” (Swan & Raphael, 1995; p. 7). The document defined the concept of
Aboriginal and Torres Strait Islander health as:
“Holistic, encompassing mental health and physical, cultural and spiritual health. Land is
central to wellbeing. This holistic concept does not merely refer to the ‘whole body’ but in
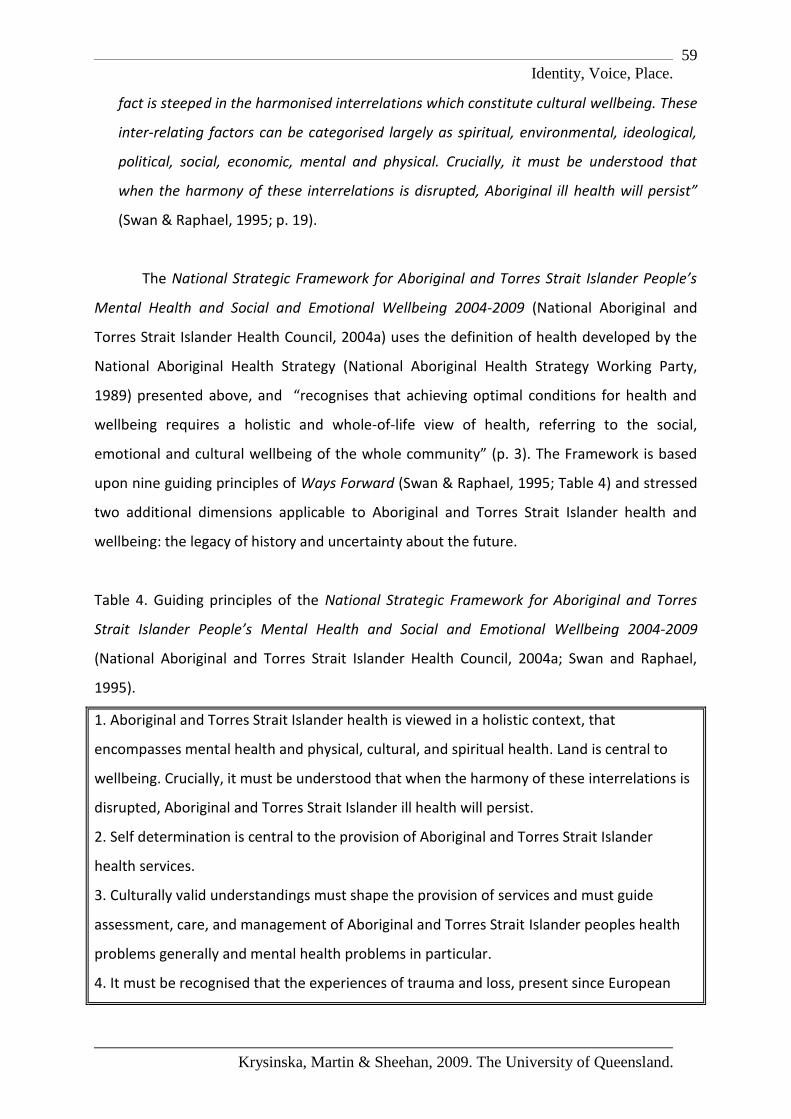
Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
59
fact is steeped in the harmonised interrelations which constitute cultural wellbeing. These
inter-relating factors can be categorised largely as spiritual, environmental, ideological,
political, social, economic, mental and physical. Crucially, it must be understood that
when the harmony of these interrelations is disrupted, Aboriginal ill health will persist”
(Swan & Raphael, 1995; p. 19).
The National Strategic Framework for Aboriginal and Torres Strait Islander People’s
Mental Health and Social and Emotional Wellbeing 2004-2009 (National Aboriginal and
Torres Strait Islander Health Council, 2004a) uses the definition of health developed by the
National Aboriginal Health Strategy (National Aboriginal Health Strategy Working Party,
1989) presented above, and “recognises that achieving optimal conditions for health and
wellbeing requires a holistic and whole-of-life view of health, referring to the social,
emotional and cultural wellbeing of the whole community” (p. 3). The Framework is based
upon nine guiding principles of Ways Forward (Swan & Raphael, 1995; Table 4) and stressed
two additional dimensions applicable to Aboriginal and Torres Strait Islander health and
wellbeing: the legacy of history and uncertainty about the future.
Table 4. Guiding principles of the National Strategic Framework for Aboriginal and Torres
Strait Islander People’s Mental Health and Social and Emotional Wellbeing 2004-2009
(National Aboriginal and Torres Strait Islander Health Council, 2004a; Swan and Raphael,
1995).
1. Aboriginal and Torres Strait Islander health is viewed in a holistic context, that
encompasses mental health and physical, cultural, and spiritual health. Land is central to
wellbeing. Crucially, it must be understood that when the harmony of these interrelations is
disrupted, Aboriginal and Torres Strait Islander ill health will persist.
2. Self determination is central to the provision of Aboriginal and Torres Strait Islander
health services.
3. Culturally valid understandings must shape the provision of services and must guide
assessment, care, and management of Aboriginal and Torres Strait Islander peoples health
problems generally and mental health problems in particular.
4. It must be recognised that the experiences of trauma and loss, present since European

Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
60
invasion, are a direct outcome of the disruption to cultural wellbeing. Trauma and loss of this
magnitude continues to have inter-generational effects.
5. The human rights of Aboriginal and Torres Strait Islander peoples must be recognised and
respected. Failure to respect these human rights constitutes continuous disruption to mental
health, (versus mental ill health). Human rights relevant to mental illness must be specifically
addressed.
6. Racism, stigma, environmental adversity and social disadvantage constitute ongoing
stressors and have negative impacts on Aboriginal and Torres Strait Islander peoples’ mental
health and wellbeing.
7. The centrality of Aboriginal and Torres Strait Islander family and kinship must be
recognised as well as the broader concepts of family and the bonds of reciprocal affection,
responsibility and sharing.
8. There is no singe Aboriginal and Torres Strait Islander culture or group, but numerous
groupings, languages, kinships, and tribes, as well as ways of living. Furthermore, Aboriginal
and Torres Strait Islander peoples may currently live in urban, rural or remote settings, in
urbanised, traditional, or other lifestyles, and frequently move between these ways of living.
9. It must be recognised that Aboriginal and Torres Strait Islander peoples have great
strengths, creativity and endurance and a deep understanding of the relationship between
human beings and their environments.
According to the Framework, “the first dimension is the historical context and its
legacy that underlies the high levels of morbidity and mortality in Aboriginal and Torres
Strait Islander communities and continues to contribute to the ongoing difficulty in
relationships and Reconciliation. The final dimension is the future uncertainty surrounding
the unresolved issues of land, control of resources, cultural security, the right of self-
determination and sovereignty, as these issues have been recognised as contributing to
health and wellbeing and reducing health inequalities in Aboriginal and Torres Strait Islander
peoples within the international arena” (National Aboriginal and Torres Strait Islander Health
Council, 2004a; p. 7).

Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
61
Grieves (2007) stressed that the Aboriginal wellbeing is “much more than a health
issue” and observed that “the term ‘wellbeing’ is an English term adopted to explain the
meaning of an Aboriginal concept that goes far beyond welfare. Unfortunately, the original
Indigenous concept is not adequately explained by the term ‘wellbeing’. Professor Judy
Atkinson16 has explained: “There is no word in Aboriginal languages for Health. The closest
words mean ‘wellbeing’ and wellbeing in the language of Nurwugen people of the Northern
Territory means ‘strong, happy, knowledgeable, socially responsible, to take a care,
beautiful, clean’, both in the sense of being within the Law and in the sense of being cared
for and that suggests to me that country and people and land and health and Law cannot be
separated. They are all One and it’s how we work with and respect each other and how we
work with and respect the country on which we live that will enable us to continue to live
across generations” (Grieves, 2007; p. 20).
These ways of thinking are difficult for the Western mind to grasp. Historically, we
have understood for thousands of years that a healthy mind exists in a healthy body (mens
sana in corpore sano) and lately health practitioners have grappled with health from a bio-
psycho-social perspective. However, this has very rarely included a spiritual dimension. The
strength of the connection to land (place) and to forefathers (family history) has not been
stressed even if the social dimension does include the family system (often limited in
western culture to the immediate family or at most three generations, and certainly not the
same as Aboriginal and Torres Strait Islander kinship).
The implications of these are that non-aboriginal health practitioners clearly need
extensive training in cultural awareness prior to working with Indigenous people, or in
Indigenous communities. Conversely, while this is a minimum requirement, a better long
term strategy is to train large numbers of Aboriginal and Torres Strait Islander people in
health development, recognition of health problems and disorders and treatment
approaches or management.
In some ways some of the early discussions on social and emotional wellbeing in
Indigenous Australians set up a situation for which there have been difficulties in finding
solutions. We cannot turn back the clock on colonisation, immigration and annexure,
genocide, “Stolen Generations”, and artificial community. It is important that as a nation, 16
“Healing Relationships between People and Country” an address given at the Wollumbin Dreaming Festival 2002.
Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
62
Australians have been able to say “Sorry” (February 13th, 2008) and it is to be hoped that this
can begin a process of reconciliation and healing, and genuinely begin actions towards
“Ways Forward”.
Despite wide recognition and acknowledgment of importance of the Indigenous
holistic concept (or perhaps an ‘extended’ conception) of health and social and emotional
wellbeing, there is lack of consensus regarding its operationalisation and measurement
(Kowal et al., 2007). To-date several tools have been developed or adapted to be applied to
the Indigenous people in Australia, including the Kessler Psychological Distress Scale (ABS,
2006), the Medical Outcome Short Form Health Survey/SF-36 (ABS, 2006), the Negative Life
Events Scale (Kowal et al., 2007), the Strengths and Difficulties Questionnaire (SDQ) (Zubrick
& Lawrence, 2006), the Westerman Aboriginal Symptom Checklist-Youth (Westerman,
2002b), and the Western Australian Aboriginal Child Health Survey (Zubrick & Lawrence,
2006).
Many of these tools were developed for use in a particular population, for example,
children and adolescents (e.g. Westerman, 2002b) and to measure selected dimensions of
wellbeing, for example, the impact of stressful life events (Kowal et al., 2007). There is a
continuing need to further develop (or adapt) holistic, reliable and culturally appropriate
measures, such as the Hua Oranga scale for mental health outcomes specifically in the
Maori population in New Zealand (Kingi & Durie, 2001). In the United States, there has been
an interesting attempt (Graham, 2002) to find connections between the American Indian
relational worldview perspective to wellness and healing (Cross, Earle, Echo-Hawk Solie, &
Manness, 2000) and the Western concept of reasons for living measured by the Reasons for
Living Questionnaire (Linehan, Goldstein, Nielsen, & Chiles., 1983) and the Reasons for Living
Inventory for Adolescents (Osman et al., 1998).
Unfortunately, to-date there is a paucity of studies and program evaluations across
Australia to indicate which initiatives and frameworks are effective in development of social
and emotional wellbeing in Indigenous Australians (and applicable to suicide prevention),
including projects addressing depression (Leggett & Krom, 2005; Thomson, Krom, Trevaskis,
Weissofner, & Leggett, 2005). A systematic review of international literature on mental
health promotion in Indigenous populations, including Aboriginal and Torres Strait Islanders,
Aboriginal Canadians, Americans Indians, Alaska Natives, and African Americans (Clelland,
Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
63
Gould, & Parker, 2007) identified a number of interventions17. These included programs
promoting mental health, mental health literacy, quality of life and resilience, initiatives
targeting increased social support and community connectedness, parenting and family
functioning skills programs, and initiatives aiming at reduction of racism, oppression and
discrimination.
The conclusions of the review were somewhat disappointing: due to scarcity of
published material and paucity of well-conducted evaluations, “it is problematic to draw
conclusions as to the efficacy of such interventions” (Clelland et al., 2007; p. 214). It was
quite clear; however, that to-date programs focusing on individuals outnumbered
interventions addressing the broader social and policy contexts and many of the programs
were community driven. Such initiatives involved Indigenous people in design and
implementation of programs to make them culturally relevant and appropriate and to
ensure the community control over the initiative.
Suicide Prevention and Social and Emotional Wellbeing in Indigenous Australians
Prevention of suicide in Indigenous Australians is closely related to the holistic concept of
health and wellbeing. Indigenous suicide has its origins in individual, family, community and
transgenerational risk factors as well as the challenging and difficult every-day living
conditions rooted in the historical and cultural trauma, including the history of genocide and
the on-going racism and discrimination. Only a holistic and comprehensive approach to
suicide prevention targeting a range of factors, including better services and care for
individuals, families and communities at risk of self-harm, community development and
empowerment, strengthening of Aboriginal and Torres Strait Islander culture and identity,
and healing of the individual and collective traumas and loss, can lead to positive outcomes
and save lives of Indigenous Australians.
17
The review included the Family Wellbeing Empowerment Program and Participatory Action Research
implemented in a number of Indigenous communities in Northern Queensland (Tsey et al. 2004a, 2004b, 2005,
2007). The project outcomes are promising: “the use of a long-term (10-year) community research strategy
focussing directly on empowerment has demonstrated the power of this approach to facilitate Indigenous
people‟s capacity to regain social and emotional wellbeing and begin to rebuild the social norms of their families
and community” (Tsey et al., 2007; p. S34). The description of the project and evaluation summary is presented
in Appendix Two.
Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
64
The on-going focus on problems in Indigenous communities, much fuelled by the
media (Hunter, 1990b; Sheehan, 2001), makes it too easy to forget that Indigenous
Australians are “exceptional survivors” (Merritt, 2007; p. 11)18. Moreover, “Aboriginal
society has much to teach the rest of the world about sharing, caring, and human
connections - about human survival and wellbeing. It is ironic that these 60,000 years of
collective wisdom with respect to mental health and human and ecosystem
interdependencies are ignored at the same time that biomedical health sciences are just
discovering the importance of supportive and caring connections between people” (Reser,
1991; p. 281).
This section of our Report identifies promising venues for suicide prevention in the
context of social and emotional wellbeing in Indigenous Australians which we identified
through the review of policies, literature and consultations with experts in the field. These
include (1) resilience in Indigenous Australians, (2) early development, family and school-
based interventions for Indigenous children and youth, (3) Indigenous Australian culture and
identity, and (4) development of Indigenous workforce and services.
Resilience in Indigenous Australians
Resilience can be defined as a dynamic process based on an interaction between risk and
protective factors, both internal and external to the individual, which modify the effects of
an adverse life event (Rutter, 1985; 1987) and the “personal qualities that enable an
individual to thrive in face of adversity” (Connor & Davidson, 2003; p. 76). Resilience is a
multidimensional individual characteristic which varies with time, age, gender, culture and
context; and it changes depending on life circumstances to which the individual is exposed
across the lifespan (Connor & Davidson, 2003). Resilience can be understood as an outcome,
i.e. the maintenance of social and functional competence and good mental health in face of
adversity, or as a process – how an individual adapts to the difficult conditions. Three broad
18
A conclusion of a study of wellbeing indicators for Native American children and youth seems highly
applicable to the Australian situation: “Native Americans are still discussed in the literature from a deficit and/or
problem perspective. (…) The citations that came up most often [in an Internet search] were generally terms
describing problems in the individual, family and/or community. Common topics (…) were alcoholism, suicide,
gangs, child abuse and neglect, child sexual abuse, violence, boarding school, drugs, substance abuse, homicide,
and poverty. Few, if any, strengths or positive indicators of behaviour were listed. It is time for this situation to
change and for strengths to be associated with Native Americans” (Goodluck, 2002; pp. 14-15). To paraphrase
the last sentence, “it is time for this situation to change and for strengths to be associated with Indigenous
Australians”.

Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
65
categories of factors strengthen personal resilience: individual (e.g., personal
communication skills, intelligence), social (e.g., supportive families), and societal (e.g., socio-
economic status, supportive communities) (Olsson, Bond, Burns, Vella-Brodrick, & Sawyer,
2003).
Resilience is frequently mentioned in the context of child and adolescent
development, mental health promotion, prevention and early intervention and suicide
prevention in both Indigenous and non-Indigenous Australians (Commonwealth Department
of Health and Aged Care, 2000; Commonwealth of Australia, 2007). To the best of our
knowledge, the concept of resilience has not been studied in the context of suicide
prevention and social and emotional wellbeing in Indigenous Australians, although it has
been applied to prevention of chronic offending in Indigenous youth (Zubrick & Robson,
2003). Merritt (2007) has even observed that “to date, the term resilience has been a
construct based on Western knowledge” and called for development of “an Indigenous
perspective on resilience” (p. 12). Moreover, “delving into what resilience is to Aboriginal
people is important, but that it should not preclude or divert attention from efforts to
address adversity. (…) Adversities arising from social justice and equality issues still need to
be addressed” (Merritt, 2007; p. 12).
Indigenous resilience was studied in the American Indians and Aboriginal Canadians,
especially in Indigenous adolescents (e.g. Burack, Blinder, Flores, & Fitch, 2007;
LaFromboise, Hoyt, Oliver, & Whitbeck, 2006; LaFromboise & Medoff, 2004). In Indigenous
populations the concept of resilience can be applied on both a community/nation level and
an individual/personal level. In the former understanding of the word, “resilience in the face
of adversity is not new to American Indian tribes [and other Indigenous peoples, including
Indigenous Australians]. They have survived genocidal practices directed toward them,
including a massive redistribution of people away from their homelands and the imposition
of the reservation system. They withstood drastic changes in sociopolitical, cultural, and
physical environments and the added stress from oppression and hostility. Through it all,
many were able to adapt and overcome adverse circumstances” (LaFrombiose et al., 2006;
p. 194).
On the individual level, Indigenous resilience can be understood as positive outcomes
in face of adversity (Connor & Davidson, 2003) or absence of problem behaviours, for
example substance abuse, and high levels of pro-social behaviour, such as good school

Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
66
performance (LaFrombiose et al., 2006). A study of resilience in American Indian adolescents
showed that a primary risk factor for low resilience was perceived discrimination and
protective factors came from multiple contexts, including family, community, and culture
(LaFrombiose et al., 2006). The high likelihood of pro-social outcomes was related to having
a warm and supportive mother, perceiving community support, and exhibiting higher levels
of enculturation, i.e. identification with American Indian culture, participation in traditional
activities, and traditional spiritual involvement.
It can be hypothesised that certain features of the traditional culture shared by
Indigenous Australians, the American Indians and the Aboriginal Canadians such as extended
family, spirituality, and participation in traditional activities can serve as protective factors
buffering against the negative consequences of adverse events on individual and community
levels and supporting individual resilience (Dudgeon & Oxenham, 1989; Daly & Smith, 2005;
Reser, 1991). An Australian study of self-harm among Indigenous and non-Indigenous sole
parent females in urban state housing (Radford et al., 1999) provides some support for this
hypothesis. Study results showed that Indigenous mothers were at lower risk of self-harm
than their non-Indigenous counterparts, and their higher resilience might be related to
greater family support and frequency of contact with relatives and “a stronger sense of
resistance to, and acquired toleration of, long-term, inter-generational oppression of various
kinds” (Radford et al., 1999; p. 83).
Early Development, Family and School-based Interventions for Indigenous Children and Youth
Families and schools seem to be the best settings for programs and interventions targeting
resilience and wellbeing in Indigenous Australian children and adolescents (Craven & Bodkin-
Andrews, 2006; Eckersley, Wierenga, & Wyn, 2006). There is accumulating evidence that
programs for pregnant women and parents of young children, especially nurse home visiting
programs, hold significant promise for improving children’s life-course trajectories and for
reducing development and health problems (Gluckman et al., 2005; Olds, Sadler, & Kitzman,
2007).
Hunter (2006) observed that “the effects of prenatal environmental factors (including
social adversity) on the development of diseases including diabetes and hypertension later in
life is well known. Similarly, from conception through infancy, neurological, cognitive,
affective and social development is an interactive process between a phase-sensitive

Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
67
evolving system and the environment. This includes the ‘embedding’ of experience in
biology through processes of selective activation and neural sculpting, and ‘reciprocal, co-
regulated emotional interactions’. Extensive developmental neurobiology research now also
informs our understanding of social gradients in health. Indeed, it has been noted that ‘the
effects of these early developmental processes can be observed in the health and
competence of populations’. Longitudinal studies demonstrate that failure to provide for
early phase specific needs is consequential for the later development of serious emotional
and behavioural problems, including violence” (pp. 9-10). [The original version of the quote
was extensively referenced. We refer the reader to the original].
The Australian study Footprints in Time: The Longitudinal Study of Indigenous
Children (LSIC)19 which commenced Wave 1 interviews in April 2008 aims to improve the
understanding of the diverse circumstances faced by Aboriginal and Torres Strait Islander
children, their families, and communities and to provide a better insight into how a child's
early years affect the way they develop and mature. Once completed, the study will provide
a valuable data resource which can be used by Australian governments, researchers, service
providers, parents and communities.
There are examples of promising school-based resilience enhancing, skill-building and
suicide prevention programs for Indigenous youth in Canada and the United States
(Kirmayer et al., 2007; LaFromboise & Lewis, 2008) and “youth skill-building programs have
been applied to diverse adolescent prevention programs, especially in school-based settings.
These programs have focused primarily on the enhancement of competence in youth
development work (e.g., self-regulation), as well as the reduction of at-risk behaviours and
the prevention of mental health problems. Outcome data from these prevention
interventions have been promising, especially when coupled with parent and family training
and support” (LaFromboise & Lewis, 2008; p. 346).
Indigenous Australian Culture and Identity
Destruction of culture and spirituality, and problems with identity and cultural continuation,
a legacy of centuries of colonisation and genocide, are among the most significant risk
factors for suicide and other indicators of social and emotional ill health in Indigenous
Australians (Tatz, 2001; Hunter, 1993), Maori in New Zealand (Coupe, 2005; Skegg et al.,
19
http://www.facsia.gov.au/internet/facsinternet.nsf/research/ldi-lsic_nav.htm

Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
68
1995), American Indians and Alaska Natives (Duran & Duran, 1995; Wexler, 2006) and
Aboriginal Canadians (Kral, 1998).
Simultaneously, as Brady (1995) has pointed out, there is a great potential of “culture
as treatment” and “culture in treatment”. The Indigenous culture and identity has an
enormous potential for strengthening the social and emotional wellbeing of Indigenous
Australians (Brady, 1995; Pattel, 2007; Tse et al., 2005), including prevention of suicide
(McCoy, 2007; Petchkovsky, Cord-Urdy, & Grant, 2007). Indigenous suicide prevention in
New Zealand (Coupe, personal communication, July 2008), Canada (e.g. Jacono & Jacono,
2008) and the United States (e.g. Garroutte et al., 2003) based on traditional cultural
knowledge and values underline the importance and high effectiveness of such an approach.
However, culture in mental health promotion and suicide prevention must not be treated in
a tokenistic way. Resnicow, Baranowski, Ahluwalla, and Braithwaite (1999) described two
dimensions of cultural sensitivity: the surface structure and deep structure. “Surface
structure involves matching intervention materials and messages to observable ‘superficial’
(thought nonetheless important) characteristics of a target population20. (…) The second
dimension, deep structure, has received less attention and can be more elusive. Deep
structure sensitivity requires understanding the cultural, social, historical, environmental
and psychological forces that influence the target health behaviour in the proposed target
population. Whereas surface structure generally increases the ‘receptivity’ or acceptance’ of
messages, deep structure conveys salience. Surface structure is a prerequisite for feasibility,
whereas deep structure determines the efficacy or impact of a program” (Resnicow et al.,
1999; pp. 11-12).
Aboriginal and Torres Strait Islander Australians need space to strengthen cultural
continuity and identity, and to develop and follow their own wellbeing pathways.
Strengthening of Indigenous Australian culture and identity can form a good basis for
universal social and emotional wellbeing and suicide prevention programs, as well as being
an outcome indicator for effectiveness of programs. The traditional Aboriginal and Torres
Strait Islander culture is imbued with natural protective and wellbeing factors, such as
20
“For audiovisual materials, surface structure may involve using people, places, language, music, food, product
brands, location and clothing familiar to, and proffered by, the target audience. Surface structure also includes
identifying what channels (e.g., media) and settings (e.g., churches, schools) are most appropriate for delivery of
messages and programs. With regards to cultural competence, or interpersonal sensitivity, this generally entails
using ethnically-matched staff to recruit participants as well as to deliver and evaluate programs” (Resnicow et
al., 1999; p. 11).
Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
69
kinship networks and traditional support systems, spirituality, loving, caring, and trust
(Reser, 1991). The Elders and traditional healers can play a very important role in
strengthening of social and emotional wellbeing in Indigenous Australians (Westerman,
2004).
A qualitative health study exploring the role of Indigenous ceremonies
(kanyirninpa/holding) in suicide prevention in desert communities in the southeast
Kimberley region of Western Australia (McCoy, 2004; 2007) showed that “the desert value of
kanyirninpa, especially as it is expressed across generations of men, offers one form of
protection against that relational and social isolation often noted at the time of self-harm. As
a social process, kanyirninpa protects young men because it is reflected in multiple and
supporting relationships across and within generations. This can be particularly valuable for
those who spend their teenage years, and sometimes beyond, exploring a high-risk pathway
of autonomy. (…) What the social process of kanyirninpa reveals, as does also the research
performed by Chandler [and Lalonde] with Native North Americans, is an important link
between self-continuity and cultural continuity” (McCoy, 2007; p. S66).
The first step in the journey to effect a social and emotional wellbeing program to
alleviate suicide and self-harm in Indigenous Australian communities is to stop
disempowering intrusion into these wounded social spaces The imposition of understanding
across cultures (however well intentioned) is based in a culturally embedded violence where
only one culture is proposed as possessing ameliorative value. Identity and wellbeing are
related and homeostatic features that differ greatly from culture to culture and from
individual to individual; such differences are not problematic they are integral and essential
to the nature of wellbeing. The imposition of common identity frameworks for wellbeing
such as those founded in conceptions of the ‘modern’ and ‘economic’ is an epistemic
violence that promotes divisive categorisation and risks further harm to communities and
individuals (Nangala, 2008; Spivac, 2003; Sheehan et al., in press).
Culture is best described as a process that constitutes a third party to all
engagements and an informative partner in all proposals. Therefore it is problematic to
objectify culture as a set of qualities, features or factors which can be quantified in terms of
similarity or difference then generically adjusted and broadly applied. Culture is a process
that accompanies and informs life. In Indigenous Knowledge terms each culture is a
companion to life for a group of people who live in a specific relationship to the landscape of
Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
70
that culture. This is often described as the holist nature of Aboriginal and Torres Strait
Islander culture. This is not accurate; however, because western conceptions of holism do
not apply well in this context. Aboriginal and Torres Strait Islander culture is better described
as a relational patterning culture, because effective social structures build productive
connections and generative separations into this whole through a knowledge management
device known as kinship. Kinship patterns the people into their place or Country through
instituting necessary and generative individuation into the social system. So Aboriginal and
Torres Strait Islander culture is not an open field; each step in culture and cultural renewal
must come from within the community charged with responsibility for these complex
connections give reciprocal life through their culture to their Country and themselves
(Nangala, 2008; Sheehan, 2004). Cultural approaches to social and emotional wellbeing
require the development of methodologies that hand over of power to know to those who
will experience the future of these communities.
Therefore, cultural solutions require the construction and maintenance of safe and
supporting social spaces where groups may examine reactivate and restore their own
understandings. In terms of the immense potential for violence, depression and self-harm in
Aboriginal and Torres Strait Islander social places such supporting social spaces are essential
because they may also afford individuals the psychic space required for positive self imaging
and the internal amelioration that only Aboriginal and Torres Strait Islander culture can
provide for Indigenous Australians. Clinicians and mental health professionals can be integral
to these spaces (Garvey, 2007; Oliver, 2004; Sue, Ivey & Pedersen, 1996).
Homeostasis is the tendency of a living organism to maintain a balance that is both
essential to and a feature of wellbeing. If we come to understand a community as a single
entity formed by the homeostatic patterning of relations between individuals who are
extended beings then we may perceive more effective and culturally relevant directions to
promote social and emotional wellbeing. From this Indigenous Knowledge perspective the
culture required to ameliorate conditions already exists as a process that is enfolded within
community life. Personal and group identities in Aboriginal places regardless of how they
may be distorted by social habitus or historic trauma transmission are essential everyday life
giving structures. These existing features are the only potent basis for the ameliorative
development of group and individual identity because they are the most generally
Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
71
acceptable and accessible avenues for finding a purpose in life for Aboriginal and Torres
Strait Islander people (Sheehan, 2004; Tatz, 2004).
The approach suggested here is not a definitive examination of the features of
Aboriginal and Torres Strait Islander identity as a basis for clinical or other health
intervention but a more relational context specific approach based on:
Activating group agency in Aboriginal and Torres Strait Islander places by providing
and sustaining a support framework that prompts cultural understanding to
articulate itself and become the primary agent in community and individual life.
Engaging this community life to construct and maintain social and psychic spaces
where effectively shared resolutions concerning future possibilities can be made.
Sustaining the conditions that will support and nurture the positive identities and
identifications that emerge from this group agency.
Lifelong education that builds on emergent strengths enhances the knowledge and
skills of Aboriginal and Torres Strait Islander people and empowers them to employ
these understandings to live well and contribute positively to their contemporary
contexts.
Programs that recognise and respond to the view that the identity most significant
for Aboriginal and Torres Strait Islander social and emotional wellbeing is one that
emerges from each group as it addresses and ameliorates its own context.
Evaluations that position all possible future programs as being responsible for
sustaining the pre-eminence of Aboriginal and Torres Strait Islander
cultural/community agency in Aboriginal community contexts.
In the contemporary Australian context the seven factors identified in Canadian
studies as critical to the elimination of self-harm in Aboriginal communities seem impossible
to achieve (Chandler & Lalonde, 1998; Tatz, 2004). Many Aboriginal communities live in
syndemic conditions where connections between social domination, marginalisation and
denial combine to ensure that stress, trauma, disease, lateral violence and poverty
culminate in pathogenic social conditions (Hammill, 2008). In these places Aboriginal and
Torres Strait Islander identity exists in a context where it is laden with trauma and engaged
in a constant and impossible struggle for positive self-imaginings. Such is the burden of
Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
72
these conditions at various times especially for Aboriginal men that suicide may be judged
to be the only rational and sovereign response available (Tatz, 2005).
The task of alleviating Aboriginal and Torres Strait Islander suicide requires that social spaces
be established that are free from the impositions of dominant culture where Aboriginal and
Torres Strait Islander identity has an opportunity to flourish and advance the inherent
resilience potential of unfettered cultural and social agency.
Development of Indigenous Workforce and Services
As mentioned earlier in this Report, despite the high morbidity and mortality of Indigenous
Australians, there is insufficient funding of health services serving this population and
numerous barriers in access to health care (ABS, 2004; 2006; ABS&AIHW, 2008). Due to
geographical remoteness, some of the Indigenous communities are exposed to “fly-in and
fly-out” contact with services; in such situations there is lack of relationship between service
providers and the community which contribute to frustration of community members and
high burnout rates in health workers. The point of entry of Indigenous Australians into
services, especially for mental health problems, is usually late and services focus more on
crisis intervention, instead of health promotion, prevention and early intervention (Hunter,
1995).
It is necessary to ensure good access to services for all Australians, including
appropriate and culturally safe services for Aboriginal and Torres Strait Islander staff and
clients (Australian Health Ministers’ Advisory Council, 2004), proper engagement of
Aboriginal clients in mental health services (Farrelly, 2008; Vicary & Andrews, 2001; Vicary &
Bishop, 2005; Westerman, 2004), and a deeper understanding of the impact of culture on
mental health problems and treatment (Durie, 2004; Hunter, 2008; Janca & Bullen; 2003;
Procter, 2005; Sheldon, 2001; Vicary & Westerman, 2004).
Simultaneously, while there is certainly room for service improvement, it is not the
quantity or quality of mental health services that is at the root of the tragedy, and the
solution is not ‘more of the same’ (Hunter, in press). According to Hunter (in press),
“improvements in the services for Indigenous Australians are necessary and should occur as
a matter of course in pursuit of social justice and equity. However, (…) without enabling
Indigenous control (not simply an Indigenous veneer or tokenistic platitudes, but Indigenous

Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
73
expertise and effective governance), program and project-based, service ‘solutions’,
regardless of sector, will only result in marginal gains”. Development of Indigenous
workforce and services is one of the venues for development of Indigenous control and
cultural continuity, which as Canadian experience has shown, can be related to lower suicide
risk (Chandler & Lalonde, 1998; Chandler & Lalonde, in press).
Currently, Aboriginal and Torres Strait Islander Australians are under-represented in
health-related occupations and in graduate courses in health (ABS&AIHW, 2008). In 2005-06,
despite comprising 1.9% of the general population over the age of 15 years, they
represented only 1% of people employed in the health sector and only 1% of all students
completing undergraduate courses in health- and welfare-related fields. Through search of
literature and consultations with experts in the field we were able to identify a number of
training programs for Indigenous mental health workers and services developed specifically
for Indigenous Australians (Appendix Three). A detailed review and evaluation of such
programs and services is beyond the scope of this Report; however, even a brief overview
can give the reader an idea about the directions of Indigenous mental health force and
service development and their outcomes (where information is available) in relation to social
and emotional wellbeing in Indigenous Australians

Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
74
Principles of Good Practice
This part of the Report presents Principles of Good Practice to guide practice in reviewing
and funding suicide prevention programs related to development of social and emotional
wellbeing in Indigenous Australians (Table 5). These guidelines are based on a review of the
literature (Aboriginal Deaths in Custody Counselling Project, 1994, Adams & Danks, 2007;
Advisory Group on Suicide Prevention, 2003; Clelland et al., 2007; Elliot-Farrelly, 2004;
Farrelly, 2007; Henderson; 2003; Martin, Krysinska, & Swannell, 2008; National Health and
Medical Research Council, 1996; Scougall, 1997; Stacey et al., 2007) and consultations with
experts in the field.
Table 5. Principles of Good Practice.
Principle One: Community Empowerment
Principle Two: Recognition of Human Rights, Transgenerational Trauma, Loss and Grief
Principle Three: Development of Individual, Family and Community Social and Emotional
Wellbeing
Principle Four: Acknowledgement and Recognition of Aboriginal and Torres Strait Islander
Diversity and Importance of the Local Context
Principle Five: Direct Involvement of Community Members and Development of Local
Workforce
Principle Six: Ensuring Program Sustainability and Organization Capacity
Principle Seven: Evidence- or Theory-Base for Programs
Principle Eight: Appropriate Program Evaluation
Principle Nine: “Researching Ourselves Back to Life”
Principle One - Community Empowerment
Working with Aboriginal and Torres Strait Islander communities needs to be based on
community consultation and involvement at every stage of the project. Members of the
community should “own the project”: the initiative for program implementation should
come from within the community and be based on the current needs identified by
Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
75
community members themselves. The community should decide how the program is
implemented and evaluated, based on direct involvement of community members and
development of local workforce (see Principle Five). Community members should be
empowered and gain confidence by being involved in the project instead of “being told what
to do (again)”. This principle can be summarised in words of a popular slogan “Nothing
About Us Without Us”.
Appendix Two presents ethical guidelines for conducting research and working with
Indigenous communities.
Principle Two - Recognition of Human Rights, Transgenerational Trauma, Loss and Grief
Working with Indigenous Australians requires recognition and acknowledgement of human
rights issues, transgenerational trauma, loss and grief, both in the historical context of
colonization and genocide (including the “Stolen Generations”), and in the current context of
social injustice, neglect and racism. These factors have a serious impact on the everyday life
in communities contributing to the prevalent feelings of disempowerment, hopelessness,
despair, negativism and resentment. The destruction of traditional Aboriginal and Torres
Strait Islander culture and social structure has frequently resulted in breaking down of
traditional support systems, undermining of male roles and leadership, rejection of cultural
and spiritual values, depression and anomie. Also, loss and grief related to (often premature)
deaths of community members and the intergenerational trauma seem to permeate many
communities.
Programs leading to positive outcomes in social and emotional wellbeing and suicide
prevention have to recognise and target both risk and protective factors in communities. The
risk factors plaguing Indigenous communities include poor health status, high premature
mortality, unemployment, and overcrowding, substance abuse, interpersonal and domestic
violence, and normalization of suicide. These risk factors are related to the general “lifestyle
of risk” stemming from historical factors mentioned above and perpetuated by current social
exclusion of Indigenous Australians. However, there seems to be a dialectic tension between
despair and strength in communities and Indigenous Australians (see Principle Three), and
focusing on the problems only can result in harmful negative labelling of Indigenous
Australians and internalised racism.

Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
76
Principle Three - Development of Individual, Family and Community Social and Emotional
Wellbeing
In the context of the harsh reality of everyday life for many Indigenous Australians, the
holistic concept of social and emotional wellbeing seems to be “pie in the sky”. However, it
has to stressed repeatedly that Indigenous Australians are exceptional survivors full of
resilience and strength and “a mental health promotion or social emotional wellbeing
approach, rather than a diagnostic or problem-based approach to suicide prevention, is
required to focus on support pathways, not just clinical pathways (…) communities respond
well to the positive approach of mental health promotion for suicide prevention when there
is a focus on resilience, coping strategies, wellbeing, and positive personal and cultural
identity” (Stacey et al., 2007; p. 251).
Social and emotional wellbeing and suicide prevention programs can be delivered
within a spectrum of interventions encompassing a wide range of mental health initiatives,
including universal, selective and indicated interventions (Commonwealth Department of
Health and Aged Care, 2000; Commonwealth of Australia, 2007). In the Indigenous context,
there should be enough resources and willingness to develop and implement a wide range
of programs ranging from community development and positive cultural identity, through
strengthening of families and development of resilience in children and young adults, to
crisis intervention and treatment. There should be a balance between interventions
addressing mental health issues and mental health promotion on individual and family
levels, and social and economic issues on the community level.
Principle Four - Acknowledgement and Recognition of Aboriginal and Torres Strait Islander
Diversity and Importance of the Local Context
“There is great diversity within Aboriginality. (…) although stereotypical views of Aborigines
have been perpetuated for a very long time, there is now a growing recognition of the
variations and diversity of Aboriginal peoples” (Dudgeon & Oxenham, 1989; p. 1). The
diversity mentioned here relates to different Aboriginal and Torres Strait Islander cultures
and languages, different social structures and dwelling places both in pre-colonisation and
post-colonisation periods. Social and emotional wellbeing and suicide prevention programs
not only have to be run in close collaboration with Indigenous Australians and communities
(see Principle One), but also have to acknowledge and allow for diversity and uniqueness

Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
77
and give special consideration for regional differences related to geographical location (i.e.,
rural, remote and urban setting). Services, organizations and programs must involve and fit
the community. Each setting is unique and understanding the “mind of a community”,
including its needs, dynamics and formal and informal organisation, requires time and trust.
Some programs can be easily adapted to work across a range of communities and settings;
other may require rethinking and changes, while others may be effective in one location and
population only.
Principle Five - Direct Involvement of Community Members and Development of Local
Workforce
As indicated under Principle One, communities should be involved in every stage of
development, implementation and evaluation of suicide prevention and social and
emotional wellbeing programs, including direct involvement of community members as
program facilitators and strengthening of local workforce as a target and an outcome of the
program. This should particularly include effective involvement of young people. Such
approach supports community development and empowers and strengthens the Indigenous
Australians by recognising and acknowledging their knowledge and skills, and giving them a
possibility of meaningful employment.
Often programs are initiated from within the community (“work from the heart”), by
people who see the need for change and start seeking support from other communities or
mainstream organisations. Community members frequently work as unpaid volunteers, but
many programs (such as “Drop the Rock”) encompass training, support and employment for
community workers. Such programs help to empower Indigenous Australians, both those
who act as trainers and facilitators and those in communities, including the elders, who are
happy to see Indigenous workers and leaders.
Training of Aboriginal and Torres Strait Islander mental health workers and other
professional workforce will help to achieve a critical mass of people who understand the
context and needs of Indigenous Australians and can help make a difference. Given the
deeply ingrained lack of trust of many Indigenous Australians in mainstream services and
organisations, including health services, the justice system and the police, involvement of
Aboriginal people in these areas may help to break the mistrust and increase their use.
There is also a necessity of ensuring cultural safety in service organisation and delivery and

Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
78
establishing effective partnerships between Indigenous and non-Indigenous health workers,
organisations, and communities based on mutual respect, support and recognition of
knowledge, skills, experience and cultural values.
Principle Six - Ensuring Program Sustainability and Organization Capacity
Low sustainability of projects and preponderance of short-term “pilot” projects is one of the
notorious problems plaguing Indigenous communities. There is need for sustainable
programs delivered by organizations with enough capacity to develop, implement and
evaluate the programs. “Negative effects of short-term funded projects that raise
expectations then end before their objectives can be realised. In order to build trust and gain
good community involvement, particularly in sensitive areas such as suicide prevention,
regions need access to dedicated, consistent, long-term resources. Resources are also
needed for strengthening workforce capacity within regions - both skills and positions
(particularly for Aboriginal workers) - to continue and extend initial work” (Stacey et al.,
2007; p. 252).
Principle Seven – Evidence - or Theory-Base for Programs
Best intention, anecdotal evidence and personal or organisational beliefs do not comprise a
sufficient base for development and implementation of suicide prevention and social and
emotional wellbeing programs for Indigenous Australians (see Principle Eight and Principle
Nine). Given the very limited evidence regarding effectiveness of interventions in Aboriginal
and Torres Strait Islander communities and the diversity of settings (see Principle Four), it
may be truly challenging to provide an evidence-base for some of the programs; however,
the suggested initiatives should be at least theory-based, including identification of risk and
protective factors, processes and outcomes relevant to the needs of the community.
Principle Eight - Appropriate Program Evaluation
Lack of evaluation of suicide prevention and social and emotional wellbeing programs in
Indigenous communities as well as in the mainstream populations is a well known problem
contributing to the lack of evidence-base mentioned above. Best intentions and enthusiasm
may not be sufficient to develop and implement effective programs, and there is a danger of
wasting financial and human resources on ineffective or even harmful programs. “Clearly,
action to prevent suicide cannot wait on definitive research. At the same time, there is an

Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
79
urgent need for evaluation research of intervention programs in Aboriginal communities,
since there is a real possibility that some well-intentioned interventions may do more harm
than good” (Kirmayer et al., 2007; p. 110).
Evaluation methodology, including the choice of realistically attainable and
measurable outcomes, should be culturally informed and appropriate, and decided upon
through the process of collaboration with the community. Usually it is not possible within
the timeframe of the program to evaluate its effectiveness through its impact on suicide
mortality and morbidity, i.e. the number of suicide deaths and attempts. Other more
intermediate outcomes may be more appropriate, such as increased involvement in
community initiatives aiming at improving social and emotional wellbeing, changes in the
environment, increased collective sense of control and empowerment, increased personal
skills and knowledge, positive changes in public policy, service organisation, delivery, and
utilization.
Principle Nine - “Researching Ourselves Back to Life”
Historically, as a consequence of abusive and culturally disrespectful studies, “research” has
become a “dirty word” for many Indigenous Australians and in many communities. Recently,
given the success of the Cooperative Research Centre for Aboriginal Health, many Aboriginal
and Torres Strait Islander organisations across the country have embraced research with
enthusiasm. Many universities have Aboriginal and Torres Strait Islander units, and the
National Health and Medical Research Council and Australian Research Council fund and
support Indigenous Australian researchers and postgraduate students. Some community
organisations fund their own researchers, foe example, Winnunga Nimmityjah Aboriginal
Health Service in the ACT. Torres Strait Islanders are setting up their own academy of
scholars and an academic journal.
Without the good knowledge and proper understanding of the causes and correlates
of Aboriginal and Torres Strait Islander suicide and the positive protective factors
strengthening social and emotional wellbeing, it is not possible to make any real progress
and to save lives. In the words of a Native Canadian Elder, “if we have been researched to
death, maybe it’s time we started researching ourselves back to life” (Castellano, 2004; p.
98). Culturally sensitive and appropriate, non-abusive research methodologies are being
developed, including Participatory Action Research, and Indigenous Australians are

Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
80
“researching themselves back to life” (Foster, Williams, Campbell, Davis, & Pepperill, 2006).
Such studies need further support and funding.

Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
81
References
Aboriginal and Torres Strait Islander Social Justice Commissioner (2005). Social Justice Report 2005. Sydney:
HREOC.
Aboriginal Deaths in Custody Counselling Project (1994). Reclaiming Our Stories, Reclaiming Our Lives.
Aboriginal Health Services, Keeping the Community Strong. Adelaide: SA Department of Human
Services.
Adams, M., & Danks, B. (2007). A positive approach to addressing Indigenous male suicide in Australia.
Aboriginal and Islander Health Worker Journal, 31, 28-31.
Advisory Group on Suicide Prevention (2003). Acting on What We Know: Preventing Youth Suicide in First
Nations: The Report of the Advisory Group on Suicide Prevention. Ottawa, ON: First Nations and Inuit
Health Branch, Health Canada.
Appleby, M., King, R., & Johnson, B. (1992). Suicide Awareness Training Manual. Narellan, NSW: Rose Education
Training and Consultancy.
Arabena, K. (2006). The Universal Citizen: An Indigenous citizenship framework for the Twenty First Century.
Australian Aboriginal Studies, 2, 36-46.
Atkinson, J. (2002). Trauma trails. Recreating song lines. The transgenerational effects of trauma in Indigenous
Australia. North Melbourne: Spinifex.
Australian Bureau of Statistics (2004). National Aboriginal and Torres Strait Islander Social Survey 2002. 4714.0.
Canberra: ABS.
Australian Bureau of Statistics (2006). National Aboriginal and Torres Strait Islander Health Survey 2004-05.
4715.0. Canberra: ABS.
Australian Bureau of Statistics (2007a). Prisoners in Australia. 4517.0. Canberra: ABS.
Australian Bureau of Statistics (2007b). Population distribution, Aboriginal and Torres Strait Islander Australians.
4705.0. Canberra: ABS.
Australian Bureau of Statistics & Australian Institute of Health and Welfare (2008). Health and Welfare of
Australia’s Aboriginal and Torres Strait Islander Peoples. Canberra: AIHW and ABS.
Australian Government Department of Health and Ageing (2003). National Strategic
Framework for Aboriginal and Torres Strait Islander Health 2003-2013: Australian Government
Implementation Plan 2007-2013. Canberra: Australian Government Department of Health and Ageing.
Australian Health Ministers (2003). National Mental Health Plan 2003-2008. Canberra:
Australian Government.
Australian Health Ministers’ Advisory Council (2004). Cultural Respect Framework for
Aboriginal and Torres Strait Islander Health 2004-2009. Adelaide: Department of
Health SA.
Australian Institute of Aboriginal and Torres Strait Islander Studies (2000). Guidelines for ethical research in
Indigenous studies. Canberra: AIATSIS.

Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
82
Barber, J.G., Punt, J., & Albers, J. (1988). Alcohol and power on Palm Island. Australian Journal of Social Issues,
23, 87-100.
Bartik, W., Dixon, A., & Dart, K. (2007). Aboriginal child and adolescent mental health: A rural worker training
model. Australasian Psychiatry, 15, 135-139.
Baume, P., Cantor, C., & McTaggart, P. (1998). Suicide in Queensland. A comprehensive study, 1990-1995.
Brisbane: Australian Institute for Suicide Research and Prevention, Griffith University.
Beautrais, A.L., & Fergusson, D.M (2006). Indigenous suicide in New Zealand. Suicide and
Life-Threatening Behavior, 10, 159-168.
Beautrais, A., Fergusson, D., Coggan, C., Collings, C., Doughty, C., Ellis, P. et al. (2007).
Effective strategies for suicide prevention in New Zealand: A review of the evidence. New Zealand
Medical Journal, 120, 1251.
Beautrais, A., Wells, J.E., McGee, M.A., & Oakley Browne, M.A. (2006). Suicidal behaviour
in Te Rau Hinengaro: The New Zealand Mental Health Survey. Australian and New
Zealand Journal of Psychiatry, 40, 896-904.
Beneforti, M., & Cunningham, J. (2002). Investigating Indicators for Measuring the Health And Social Impact of
Sport and Recreation Programs in Indigenous Communities. Darwin: Australian Sports Commission and
Cooperative Research Centre for Aboriginal and Tropical Health.
Bird, M.E. (2002). Health and Indigenous people: Recommendations for the next generation [Editorial].
American Journal of Public Health, 92, 1391-1392.
Boots, R.J., Joyce, C., Mullany, D.V., Anstey, C., Blackwell, N., Garrett, P.M., et al. (2006). Near-hanging as
presenting to hospitals in Queensland: Recommendations for practice. Anaesthesia and Intensive Care,
34, 736-745.
Brady, M. (1995). Culture in treatment, culture as treatment. A critical appraisal of developments in addiction
programs for Indigenous North Americans and Australians. Social Science and Medicine, 41, 1487-1498.
Brideson, T., & Kanowski, L. (2004). The struggle for systematic ‘adulthood’ for Aboriginal Mental Health in the
mainstream: The Djirruwang Aboriginal and Torres Strait Islander Mental Health Program. Australian e-
Journal for the Advancement of Mental Health, 3.
Bridge, S., Hanssens, L., & Santhanam, R. (2007). Dealing with suicidal thoughts in schools: Information and
education directed at secondary schools. Australasian Psychiatry, 15(Supplement), S58-S62.
Briscoe, G. (2003). Counting, health and identity: A history of Aboriginal health and demography in Western
Australia and Queensland 1900-1940. Canberra: Aboriginal Studies Press.
Burack, J., Blinder, A., Flores, H., & Fitch, T. (2007). Constructions and deconstructions of risk, resilience and
wellbeing: A model for understanding the development of Aboriginal adolescents. Australasian
Psychiatry, 15(Supplement), S18-S23.
Burvill, P.W. (1975). Attempted suicide in the Perth Statistical Division 1971-1972. Australian and New Zealand
Journal of Psychiatry, 9, 273-279.
Calma, T. (2007). Creating futures: Influencing the social determinants of mental health and wellbeing in rural,
Indigenous and Island peoples. Australasian Psychiatry, 15(Supplement), S5-S9.

Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
83
Cantor, C.H., & Slater, P.J. (1997). A regional profile of suicide in Queensland. Australian
and New Zealand Journal of Public Health, 34, 181-186.
Castellano, M.B. (2004). Ethics of Aboriginal research. Journal of Aboriginal Health, 1, 98-114.
Chandler, M.J., & Lalonde, C. (1998). Cultural continuity as a hedge against suicide in Canada’s First Nations.
Transcultural Psychiatry, 35, 191–219.
Chandler, M.J., & Lalonde, C. (in press). Transferring whose knowledge? Exchanging whose best practices? On
knowing about Indigenous knowledge and Aboriginal suicide. In D. Beavan, & J. White (Eds.).
Aboriginal policy research. London, ON: Althouse Press.
Clayer, J.R., & Czechowicz, A.S. (1991). Suicide by Aboriginal people in South Australia: Comparison with suicide
deaths in the total urban and rural populations. Medical Journal of Australia, 154, 683–685.
Clelland, N., Gould, T., & Parker, E. (2007). Searching for evidence: What works in
Indigenous mental health promotion? Health Promotion Journal of Australia, 18, 208-216.
Coe, M. (1989). Windradyne, a Wiradjuri Koorie. Canberra: Aboriginal Studies Press.
Coffey, C., Wolfe, R., Lovett, A.W., Moran, P., Cini, E., & Patton, G.C. (2004). Predicting
death in young offenders: A retrospective cohort study. Medical Journal of Australia, 181, 473-477.
Commission for Children and Young People and Child Guardian Queensland (2007). Annual Report: Deaths of
children and young people, Queensland, 2006–07. Brisbane: Commission for Children and Young
People and Child Guardian Queensland.
Commonwealth Department of Health and Aged Care (2000). National Action Plan for Promotion, Prevention
and Early Intervention for Mental Health 2000. Canberra: Mental Health and Special programs Branch,
Commonwealth Department of Health and Aged Care.
Commonwealth of Australia (2004). Reporting suicide and mental illness. A resource for media professionals.
Canberra: Commonwealth Department of Health and Aged Care.
Commonwealth of Australia (2007). Living Is For Everyone (LIFE) Framework: A Framework for Prevention of
Suicide in Australia. Canberra: Australian Government Department of Health and Ageing.
Commonwealth of Australia (2008). A Blueprint for Action: Pathways into the health workforce for Aboriginal
and Torres Strait Islander people. Canberra: Australian. Government Department of Health and Ageing.
Online at http://www.aida.org.au/pdf/Pathways.pdf
Connor, K.M., & Davidson, J.R.T. (2003). Development of a new resilience scale: The Connor-Davidson Resilience
Scale (CD-RISC). Depression and Anxiety, 18, 76-82.
Cooke, C.T., Cadden, G.A., & Margolius, K.A. (1995). Death by hanging in Western Australia. Pathology, 27, 268-
272.
Copland, M. (2005). Calculating Lives: The numbers and narratives of forced removals in Queensland 1859-1972.
Unpublished Doctoral thesis, School of Arts Media and Culture, Griffith University, Queensland.
Coupe, N.M. (2000). The epidemiology of Maori suicide in Aotearoa/New Zealand. South Pacific Journal of
Psychology, 12, 1-12.
Coupe, N.M. (2005) Whakamomori: Maori suicide prevention. Unpublished Doctoral thesis, Massey University
Palmerston North.
Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
84
Craven, R.C., & Bodkins-Andrews, G. (2006). New solutions for addressing Indigenous mental health: A call to
counselors to introduce the new positive psychology of success. Australian Journal of Guidance and
Counseling, 16, 41-54.
Cross, T. L., Earle, K. A., Echo-Hawk Solie, H., & Manness, K. (2000). Cultural strengths and challenges in
implementing a system of care model in American Indian communities. Systems of care: Promising
practices in children's mental health, 2000 Series, Volume I. Washington, DC: Center for Effective
Collaboration and Practice, American Institutes for Research.
Cunneen, C. (1997) The Royal Commission into Aboriginal Deaths in Custody: An overview of its establishment,
findings and outcomes. Canberra: Monitoring and Reporting Section, ATSIC.
Cunningham, J., & Beneforti, M. (2005). Investigating indicators for measuring the health and social impact of
sport and recreation programs in Australian Indigenous communities. International Review for the
Sociology of Sport, 40, 89-98.
Dalton, V. (1999). Death and dying in prison in Australia: National overview, 1980-1998. Journal of Law,
Medicine and Ethics, 27, 269-274.
Daly, A., & Smith, D., (2005). Indicators of risk to the wellbeing of Australian Indigenous children. Australian
Review of Public Affairs, 6, 39-57.
Davidson, J.A. (2003). Presentation of near-hanging to an emergency department in the Northern Territory.
Emergency Medicine, 15, 28-31.
De Leo, D., & Evans, R. (2002). Suicide in Queensland 1996-1998: Mortality rates and related data. Brisbane:
Australian Institute for Suicide Research and Prevention, Griffith University.
De Leo, D., & Heller, T. (2004). Suicide in Queensland 1999-2001: Mortality rates and related data. Brisbane:
Australian Institute for Suicide Research and Prevention, Griffith University.
De Leo, D., Klieve, H., & Milner, A. (2006). Suicide in Queensland 2002-2004: Mortality rates and related data.
Brisbane: Australian Institute for Suicide Research and Prevention, Griffith University.
Dudgeon, P., & Oxenham, D. (1989) The complexity of Aboriginal diversity: Identity and kindredness. Black
Voices, 5, 22-38.
Duran, E., & Duran, B. (1995). Native American postcolonial psychology. Albany, NY: State University of New
York Press.
Durie, M. (2004). Understanding health and illness: Research at the interface between science and indigenous
knowledge. International Journal of Epidemiology, 33, 1138-1143.
Eastwell, H.D. (1985). Psychological disorders among the Australian Aborigines. In C.T.H. Friedman, & R.A.
Faguet (Eds.). Extraordinary disorders of human behavior (pp. 229–257). New York: Plenum Press.
Eastwell, D. (1987). Did Aborigines take their own lives in the old times? Aboriginal Health Worker, 12, 29-31.
Eastwell, H.D. (1988). The low risk of suicide among the Yolngu of the Northern Territory: The traditional
Aboriginal pattern. Medical Journal of Australia, 148, 338-340.
EchoHawk, M. (1997). Suicide: The scourge of Native American People. Suicide and Life-Threatening Behavior,
27, 60-67.

Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
85
EchoHawk, M. (2006). Suicide prevention efforts in one area of Indian Health Service, USA. Suicide and Life-
Threatening Behavior, 10, 169-167.
Eckersley, R., Wierenga, A., & Wyn, J. (2006). Flashpoints & signposts: Pathways to success and wellbeing for
Australia’s young people. Carlton South: VicHealth.
Elliott-Farrelly, T. (2004). Australian Aboriginal suicide: The need for an Aboriginal suicidology. Australian e-
Journal for the Advancement of Mental Health, 3.
Enns, M.W., Inayatulla, M., Cox, B., & Chayne, L. (1997). Prediction of suicide intent in Aboriginal and non-
Aboriginal adolescent inpatients: A research note. Suicide and Life-Threatening Behavior, 27, 218–224.
Farrelly, T. (2007). Aboriginal suicide prevention: Community-specific research and Aboriginal control over
interpretation of data. Aboriginal and Islander Health Worker Journal, 31, 32-35.
Farrelly, T. (2008). The Aboriginal suicide and self-harm help-seeking quandary. Aboriginal and Islander Health
Worker Journal, 32, 11-15.
Foster, D., Williams, R., Campbell, D., Davis, V., & Pepperill, L. (2006). “Researching ourselves cack to life”: New
ways of conducting Aboriginal alcohol research. Drug and Alcohol Review, 25, 213-217.
Freemantle, J., Officer, K., McAullay, D., & Anderson, I. (2007). Australian Indigenous Health - Within an
International Context. Darwin: Cooperative Research Centre for Aboriginal Health.
Fu, K.W., & Yip, P.S. (2008).Changes in reporting of suicide news after the promotion of the WHO media
recommendations. Suicide and Life-Threatening Behavior, 38, 631-636.
Garroutte, E.M., Goldberg, J., Beals, J., Herrell, R., Manson, S.M., & the AI-SUPERPFP Team (2003). Spirituality
and attempted suicide among American Indians. Social Science and Medicine, 56, 1571-1579.
Garvey, D.C. (2007). Indigenous identity in contemporary psychology: dilemmas, developments, directions.
Melbourne: Cengage Learning.
Garvey, D (2008) A review of social and emotional wellbeing of Indigenous Australian peoples - considerations,
challenges and opportunities. Online at http://www.healthinfonet.ecu.edu.au/sewb_review
Gluckman, P.D., Hanson, M.A., Spencer, H.G., & Bateson, P. (2005). Environmental influences during
development and their later consequences for health and disease: implications for the interpretation
of empirical studies. Proceedings of the Royal Society, 272, 671-677.
Goldney, R.D. (1998). Suicide prevention is possible: A review of recent studies. Archives of Suicide Research, 4,
329-339.
Goldney, R.D. (2002). Is Aboriginal suicide different? A commentary on the work of Colin Tatz. Psychiatry,
Psychology and Law, 9, 257-259.
Goldsmith S.K., Pellmar, T.C., Kleinman, A.M., & Bunney, W.E. (2002). Programs for suicide prevention. In S.K.
Goldsmith, T.C. Pellmar, A.M. Kleinman, & W.E. Bunney (Eds.). Reducing suicide: A national imperative
(pp. 273-328). Washington, DC: National Academic Press.
Goodluck, C. (2002). Native American children and youth wellbeing indicators: A strengths Perspective. Portland,
OR: National Indian Child Welfare Association.
Graham, T.L.C. (2002). Using Reasons for Living to connect to American Indian healing traditions. Journal of
Sociology and Social Welfare, 29, 55-75.

Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
86
Grieves, V. (2007). Indigenous Wellbeing: A Framework for Governments’ Aboriginal Cultural Heritage Activities.
Sydney: NSW Department of Environment and Conservation.
Guttormsen T., Hoifodt T., Silvola K., & Burkeland O. (2003). Applied suicide intervention: An evaluation. Tidsskr
Nor Laegeforen, 123, 2284-2286.
Hammill, J. (2008). Human rights and human biology: The role of foetal programming and biological embedding
as an indicator for poor life outcomes. Seminar presentation, Centre for Chronic Diseases Research,
University of Queensland.
Hanssens, L. (2007a). Indigenous dreaming: How suicide in the context of substance abuse has impacted on and
shattered the dreams and reality of Indigenous Communities, Northern Territory, Australia. Aboriginal
and Islander Health Worker Journal, 31, 26-34.
Hanssens, L. (2007b). The search to identify contagion operating within suicide clusters in Indigenous
Communities, Northern Territory, Australia. Aboriginal and Islander Health Worker Journal, 31, 27-33.
Hanssens, L., & Hanssens, P. (2007). Research into clustering effect of suicide within Indigenous Communities,
Northern Territory, Australia. Aboriginal and Islander Health Worker Journal, 31, 6-11.
Harris, A., & Robinson, G. (2007). The Aboriginal Mental Health Worker Program: The challenge of supporting
Aboriginal involvement in mental health care in the remote community context. Australian e-Journal
for the Advancement of Mental Health, 6.
Headley, A., Pirkis, J., Merner, B., VandenHeuvel, A., Mitchell, P., Robinson, J. et al. (2006). A review of 156 local
projects funded under Australia’s National Suicide Prevention Strategy: Overview and lessons learned.
Australian e-Journal for the Advancement of Mental Health 5, 3.
Healey, K. (Ed.) (1998). The stolen generation. Balmain, NSW: Spinney Press.
Henderson, A. (2003). Report of the workshop on best practices in suicide prevention and the evaluation of
suicide prevention programs in the Arctic. Iqaluit, Nunavut: Dept. of Executive and Intergovernmental
Affairs. Evaluation and Statistics Division.
Hill, K., Barker, B., & Vos, T. (2007). Excess Indigenous mortality: Are Indigenous Australians more severely
disadvantaged that other Indigenous populations? International Journal of Epidemiology, 36, 580-589.
Huggins, J. (1998). Sister Girl: The writings of Aboriginal activist and historian Jackie Huggins. St Lucia, Qld: The
University of Queensland Press.
Human Rights and Equal Opportunity Commission (1997). Bringing Them Home: Report of the National Inquiry
into the Separation of Aboriginal and Torres Strait Islander Children from Their Families. Canberra:
Australian Government Publishing Service.
Hunter, E. (1988a). On Gordian knots and nooses: Aboriginal suicide in the Kimberley. Australian and New
Zealand Journal of Psychiatry, 22, 264-271.
Hunter, E. M. (1988b). Aboriginal suicides in custody: A view from the Kimberley. Australian and New Zealand
Journal of Psychiatry, 225, 273-282.
Hunter, E.M. (1989). Commissions and omissions: The wider context of Aboriginal suicides in custody. Medical
Journal of Australia, 151, 218-223.

Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
87
Hunter, E. (1990a). Using a socio-historical frame to analyses Aboriginal self-destructive behaviour. Australian
and New Zealand Journal of Psychiatry, 24, 191-198.
Hunter, E. (1990b). Images of violence in Aboriginal Australia. Aboriginal Law Bulletin, 2, 2-16.
Hunter, E. (1991a). Out of sights, out of mind – 2. Social and historical contexts of self-harmful behaviour among
Aborigines of remote Australia. Social Science and Medicine, 33, 661-667.
Hunter, E. M. (1991b). An examination of recent suicides in remote Australia: Further information from the
Kimberley. Australian and New Zealand Journal of Psychiatry, 25, 197-202.
Hunter, E. (1993). Aboriginal health and history: Power and prejudice in remote Australia. Melbourne,
Cambridge University Press.
Hunter, E. (1995). Is there a role for prevention in Aboriginal mental health? Australian Journal of Public Health,
19, 573-579.
Hunter, E. (2006). Back to Redfern: Autonomy and the 'middle E' in relation to Aboriginal health. Discussion
Paper Number 18. Canberra: Australian Institute of Aboriginal and Torres Strait Islander Studies.
Hunter, E. (2008). The Aboriginal tea ceremony: Its relevance to psychiatric practice. Australasian Psychiatry,
16, 130-132.
Hunter, E. (in press). Not quite enough: Service solutions or stagnation in Indigenous health. Arena).
Hunter, E., & Harvey, D. (2002). Indigenous suicide in Australia, New Zealand, Canada and the United States.
Emergency Medicine, 14, 14-23.
Hunter, E., & Milroy, H. (2006). Aboriginal and Torres Strait Islander suicide in context. Archives of Suicide
Research, 10, 141-157.
Hunter, E., Reser, J., Baird, M., & Reser, P. (1999). An analysis of suicide in Indigenous communities of North
Queensland: The historical, cultural and symbolic landscape. Canberra: Mental Health/Health Services
Development Branch, Commonwealth Department of Health and Aged Care.
Hunter, E., Travers, H., Gibson, J., & Campion, J. (2007). Bridging the triple divide: performance and innovative
multimedia in the service of behavioural health change in remote Indigenous settings. Australian
Psychiatry, 15(Supplement), S44-S48.
Jacono, J., & Jacono, B. (2008). The use of puppetry for health promotion and suicide prevention among
Mi'Kmaq youth. Journal of Holistic Nursing, 26, 50-55.
Janca, A., & Bullen, C. (2003). The Aboriginal concept of time and its mental health implications. Australasian
Psychiatry, 11(Supplement), S40-S44.
Jones, I.H. (1972). Psychiatric disorders among Aborigines of the Australian Western Desert. Social Science and
Medicine,6, 263-267.
Jones, I.H. (1973). Psychiatric disorders among Desert and Kimberley people. Australian Institute of Aboriginal
Studies, 3, 17-20.
Jones, I.H., & de Horne, D.J. (1973). Psychiatric disorders among Aborigines of the Australian Western Desert:
Further data and discussion. Social Science and Medicine, 7, 219–228.
Kanowski, L., Kitchener, B., & Jorm, A. (Eds.) (2008). Aboriginal and Torres Strait Islander Mental Health First Aid
Manual. Melbourne: ORYGEN Research Centre.

Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
88
Kapusta, N, Niederkrotenthaler, T, Etzersdorfer, E et al. (2009). Influence of psychotherapist density and
antidepressant sales on suicide rates. Acta Psychiatrica Scandinavica, 119: 236-242.
Kidson, M.A., & Jones, I.H. (1968). Psychiatric disorders among Aboriginals of the Australian Western Desert.
Archives of General Psychiatry, 19, 413–17.
Kilroy, K. (2008). Project Interview social and emotional wellbeing in Aboriginal communities. Musgrave Park
Aboriginal Cultural Centre. Brisbane
King, R., Appleby, M., & Brown, C. (1995). Suicide Awareness for Aboriginal Communities. Narellan, NSW: Rose
Education Training and Consultancy.
Kingi, T.K., & Durie, M. (2001). Hua Oranga: A Maori Mental Health Outcome Measure. Palmerston North:
Massey University, School of Maori Studies.
Kirmayer, L.J., Boothroyd, L.J., Laliberté, A., & Laronde Simpson, B. (1999). Suicide prevention and mental health
promotion in Native communities (No. 9). Montreal, QC: Culture and Mental Health Research Unit,
Institute of Community & Family Psychiatry, Sir Mortimer B. Davis-Jewish General Hospital.
Kirmayer, L.J., Brass, G.M., Holton, T.L., Paul, K., Simpson, C., & Tait, C. (2007). Suicide among Aboriginal Peoples
in Canada. Ottawa: Aboriginal Healing Foundation.
Kitchener, B. & Jorm, A. (2006). Mental health first aid training: Review of evaluation studies. Australian and
New Zealand Journal of Psychiatry, 40, 6–8.
Knox, K.L., Litts, D.A., Talcott, G.W., Feig, J.C., & Caine, E.D. (2003). Risk of suicide and related adverse outcomes
after exposure to a suicide prevention programme in the US Air Force: Cohort study. British Medical
Journal, 327, 1376-1378.
Kosky, R.J., & Dundas, P. (2000). Death by hanging: Implications for prevention of an important method of
youth suicide. Australian and New Zealand Journal of Psychiatry, 34, 836-841.
Kowal, E., Gunthorpe, W., & Bailie. R.S. (2007). Measuring emotional and social wellbeing in Aboriginal and
Torres Strait Islander populations: an analysis of a Negative Live Events Scale. International Journal for
Equity in Health, 6, 18.
Kral, M.J. (1998). Suicide and the internalisation of culture: Three questions. Transcultural Psychiatry, 35, 221-
233.
Krieg, A.S. (2006). Aboriginal incarceration: Health and social impacts. Medical Journal of Australia, 184, 534-
536.
Kunitz, S. (1994). Disease and social diversity: The European impact on the health of non-Europeans. New York:
Oxford University Press.
Kunitz, S.J., & Brady, M. (1995). Health care policy for Aboriginal Australians: The relevance of the American
Indian experience. Australian Journal of Public Health, 19, 549-558.
LaFromboise, T.D., & Lewis, H.A. (2008). The Zuni Life Skills Development Program: A school/community-based
suicide prevention intervention. Suicide and Life-Threatening Behavior, 38, 343-353.
LaFromboise, T. D., & Meddoff, L. (2004). Sacred spaces: The role of context in American Indian youth
development. In C. Clauss-Ehlers, & M. Weist (Eds.). Community planning to foster resilience in children
(pp. 45-63). New York: Kluwer Academics Publishers.

Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
89
LaFromboise, T. D., Hoyt, D.R., Oliver, L., & Whitbeck, L.B. (2006). Family, community, and school influences on
resilience among American Indian adolescents in the Upper Midwest. Journal of Community
Psychology, 34, 193-209.
LaFromboise, T. D., Meddoff, L., Lee, C.C., & Harris, A. (2007). Psychosocial and cultural correlates of suicidal
ideation among American Indian early adolescents on a North Plains Reservation. Research in Human
Development, 4, 119-143.
Laugharne, J., Glennen, M., & Austin, J. (2002). The ‘Maga Barndi’ mental health service for Indigenous people
in Western Australia. Australasian Psychiatry, 10, 13-17.
Lawlor, D., & Kosky, R. (1992). Serous suicide attempts among adolescents in custody. Australian and New
Zealand Journal of Psychiatry, 26, 474-478.
Leenaars, A. (2006). Suicide among Indigenous people: Introduction and call for action. Archives of Suicide
Research, 10, 103-115.
Leggett, N., & Krom, I. (2005). Programs and projects addressing depression and the social and emotional
wellbeing of Indigenous peoples. Perth: Australian Indigenous HealthInfoNet.
Letters, P., & Stathis, S. (2004). A mental health and substance abuse service for a youth detention centre.
Australasian Psychiatry, 12, 126-129.
Linehan, M.M., Goldstein, J.L., Nielsen, S.L., & Chiles, J.A. (1983). Reasons for staying alive when you are
thinking of killing yourself: The Reasons for Living Inventory. Journal of Consulting and Clinical
Psychology, 51, 276-286.
MacDonald, M. (1999). Suicide intervention training evaluation: A study of immediate and long term training
effects. Unpublished doctoral dissertation, Calgary, Alberta: The University of Calgary.
Mann, J.J., Apter, A., Bertolote, J., Beautrais, A., Currier, D., Haas, A. et al. (2006). Suicide prevention strategies:
A systematic review. Journal of American Medical Association, 26, 2064-2074.
Martin, G., Krysinska, K., & Swannell, S. (2008). The struggle to evaluate prevention programs. Australian e-
Journal for the Advancement of Mental Health, 7.
May, D. (1994). Aboriginal labour and the cattle industry: Queensland from white settlement to the present.
Melbourne, Vic: Cambridge University Press.
May, P.A., Van Winkle, N.M., Williams, M.B., McFeeley, P.J., DeBruyn, L.M., & Serna, P. (2002). Alcohol and
suicide among American Indians of New Mexico, 1980-1998. Suicide and Life-Threatening Behavior, 32,
240-255.
McCoy, B.F. (2004). Kanyirninpa: Health, masculinity and wellbeing of Desert Aboriginal men. Unpublished
Doctoral thesis, Centre for the Study of Health and Society, School of Population Health, The University
of Melbourne.
McCoy, B. (2007). Suicide and desert men: The power and protection of kanyirninpa (holding). Australasian
Psychiatry, 15(Supplement), S63-S67.
McFarland, B.H., Gabriel, R.M., Bigelow, D.A., & Walker, R.D. (2006). Organization and financing of alcohol and
substance abuse programs for American Indians and Alaska Natives. American Journal of Public Health,
96, 1469-1477.

Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
90
Measey, M.-A.L., Li, S.Q., Parker, R., & Wang, Z. (2006). Suicide in the Northern Territory, 1981-2002. Medical
Journal of Australia, 185, 315-319.
Merritt, S. (2007). An Aboriginal perspective on resilience: Resilience needs to be defined from an Indigenous
context. Aboriginal and Islander Health Worker Journal, 31, 10-12.
Middlebrook, D.L., LeMaster, P., Beals, J., Novins, D.K., & Manson, S.M. (2001). Suicide prevention in American
Indian and Alaska Native communities: A critical review of programs. Suicide and Life-Threatening
Behavior, 31, 132-149.
Ministry of Health (2008). New Zealand Suicide Prevention Action Plan 2008-2012: The Summary for Action.
Wellington: Ministry of Health.
Mitchell, S. (Ed.) (2005). Mental health and wellbeing: Small grants storybook. Adelaide: Australian Network for
Promotion, Prevention and Early Intervention for Mental Health (Auseinet).
Moller, J. (1996). Understanding national injury data regarding Aboriginal and Torres Strait Islander peoples.
Australian Injury Prevention Bulletin, 14. Adelaide: National Injury Surveillance Unit.
Mrazek P.J., & Haggerty, R.J. (1994). Reducing Risks for Mental Disorders: Frontiers for preventive intervention
research. Washington, DC: National Academy Press.
Nagel, T., & Thompson, C. (2006). Aboriginal mental health workers and the improving Indigenous mental
health service delivery model in the ‘Top End’. Australasian Psychiatry, 14, 291-294.
Nangala, S. (2008). Project Interview social and emotional wellbeing in Aboriginal communities.
National Aboriginal and Torres Strait Islander Health Council (2004a). National Strategic Framework for
Aboriginal and Torres Strait Islander People’s Mental Health and Social and Emotional Wellbeing 2004-
2009. Canberra: Australian Government.
National Aboriginal and Torres Strait Islander Health Council (2004b). National Strategic Framework for
Aboriginal and Torres Strait Islander Health 2003-2013. Canberra: AGDHAC.
National Aboriginal Health Strategy Working Party (1989). National Aboriginal Health Strategy. Canberra,
Australian Government Publishing Service.
National Health and Medical Research Council (1996). Promoting the health of Aboriginal and Torres Strait
Island communities [Rescinded]. Canberra: Commonwealth of Australia.
National Health and Medical Research Council (2003). Values and Ethics: Guidelines for Ethical Conduct in
Aboriginal and Torres Strait Islander Health Research. Canberra:Commonwealth of Australia.
National Health and Medical Research Council (2005). Keeping Research on Track: A guide for Aboriginal and
Torres Strait Islander peoples about health research ethics. Canberra: Commonwealth of Australia.
Norris, G., Parker, R., Beaver, C., & van Konkelenberg, J. (2007). Addressing Aboriginal mental health issues on
the Tiwi Islands. Australasian Psychiatry, 15, 310-314.
Northern Territory Aboriginal Health Forum Emotional and Social Wellbeing Working Party, (2003). NT
Aboriginal Emotional and Social Wellbeing Strategic Plan. Darwin, Northern Territory Government.
Olds, D.L., Sadler, L., & Kitzman, H. (2007). Programs for parents of infants and toddlers: Recent evidence from
randomized trails. Journal of Child Psychology and Psychiatry, 48, 355-391.

Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
91
Oliver, K. (2004) The colonization of psychic space: a psychoanalytic social theory of oppression. University of
Minnesota Press, London.
Oliver, R.G., & Hetzel, B.S. (1972). Rise and fall of suicide rates in Australia: Relation to sedative availability.
Medical Journal of Australia, 2, 919-923.
Olsson, C.A., Bond, L., Burns, J.M., Vella-Brodrick, D.A. & Sawyer, S.M. (2003). Adolescent resilience: A concept
analysis. Journal of Adolescence, 26, 1-11.
Osman, A., Downs, W.R., Koper, B.A., Barrios, F.X., Baker, M.T., Osman, J.R., et al. (1998). The Reasons for Living
Inventory for Adolescents (RFL-A): Development and psychometric properties. Journal of Clinical
Psychology, 54, 1063-78.
Parker, R., & Ben-Tovim, D.I. (2002). A study of factors affecting suicide in Aboriginal and ‘other populations in
the Top End of the Northern Territory through an audit of coronial records. Australian and New
Zealand Journal of Psychiatry, 36, 404-410.
Partnerships Queensland (2006). Baseline Report: Future Directions Framework for Aboriginal and Torres Strait
Islander Policy in Queensland 2005-2010. Brisbane: Department of Communities, Office for Aboriginal
and Torres Strait Islander Partnerships.
Pattel, N. (2007). Aboriginal families, cultural context and therapy. Counselling, Psychotherapy and Health, 3, 1-
24.
Patterson, D. (2000). Yarrabah Men’s Health Group. Aboriginal and Islander Health Worker, 24, 3.
Petchkovsky, L., Cord-Udy, N., & Grant, L. (2007). A post-Jungian perspective on 55 Indigenous suicides in
Central Australia; deadly cycles of diminished resilience, impaired nurturance, compromised
interiority; and possibility for repair. Australian e-Journal for Advancement of Mental Health, 6.
Pirkis, J., & Blood, R. W. (2001). Suicide and the media. A critical review. Canberra: Department of Health and
Aged Care.
Pirkis, J., Burgess, P.M., Francis, C., Blood, R.W., & Jolley, D.J. (2006). The relationship between media reporting
of suicide and actual suicide in Australia. Social Science and Medicine, 62, 2874-2886.
Procter, N.C. (2005). Parasuicide, self-harm and suicide in Aboriginal people in rural Australia: A review of the
literature with implications for mental health nursing practice. International Journal of Nursing
Practice, 11, 237-2341.
Queensland Government (2008). Queensland Plan for Mental Health 2007-2017. Brisbane: Queensland
Government.
Queensland Health (1996). Queensland Mental Health Policy Statement: Aboriginal and Torres Strait Islander
People. Brisbane: Queensland Government.
Queensland Health (2003a). Reducing Suicide: Queensland Government Suicide Prevention Strategy 2003–2008.
Brisbane: Queensland Government.
Queensland Health (2003b). Reducing Suicide: Action Plan: Queensland Government Suicide Prevention Strategy
2003-2008. Brisbane: Queensland Government.

Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
92
Radford, A.J., Brice, G.A., Harris, R., van der Byl, M., Monten, H., McNeece-Neeson, M., et al. (1999). The 'easy
street' myth: Self harm among Aboriginal and non-aboriginal female sole parents in urban state
housing. Australian and New Zealand Journal of Public Health, 23, 77-85.
Read, P. (1988) A hundred years war: The Wiradjuri people and the state. Sydney: Australian National
University Press.
Reseland, S., Bray, I., Gunnell, D., 2006. Relationship between antidepressant sales and secular trends in suicide
rates in the Nordic countries. British Journal of Psychiatry, 188: 354-8.
Reser, J.P. (1989a). Australian Aboriginal suicide deaths in custody: Cultural context and cluster evidence.
Australian Psychologist, 24, 325-324.
Reser, J.P. (1989b). Aboriginal deaths in custody and social construction: A response to the view that there is no
such thing as Aboriginal suicide. Australian Aboriginal Studies, 2, 43-50.
Reser, J.P. (1991). Aboriginal mental health: Conflicting cultural perspectives. In J. Reid, & P. Trompf (Eds.). The
health of Aboriginal Australia (pp. 218-291). Sydney: Harcourt Brace Jovanovich.
Reser, J.P. (2004). What does it mean that Aboriginal suicide is different? Differing cultures, accounts, and
idioms of distress in the context of indigenous youth suicide. Australian Aboriginal Studies, 2, 34-53.
Resnicow, K., Baranowski, T., Ahluwalla, J.S., & Braithwaite, R.L. (1999). Cultural
sensitivity in public health: Defined and demystified. Ethnicity and Disease, 9, 10-21.
Ring, I. (1995). An open letter to the President of the Public Health Association. Australian Journal of Public
Health, 19, 228-230.
Ring, I.T., & Firman, D. (1998). Reducing Indigenous mortality in Australia: Lessons from other countries.
Medical Journal of Australia, 169, 528-533.
Robinson, J., McGorry, P., Harris, M.G., Pirkis, J., Burgess, P., Hickie, I. et al. (2006). Australia’s National Suicide
Prevention Strategy: The next chapter. Australian Health Review, 30, 271-276
Robinson, S. (2008). Something like slavery: Queensland's Aboriginal child workers 1842-1945. North
Melbourne, Vic: Australian Scholarly Publishing.
Royal Commission into Aboriginal Deaths in Custody (1991). Final Report. Canberra: Australian Government
Publishing Service.
Royal Commission on Aboriginal Peoples (1995). Choosing Life: Special Report on Suicide among Aboriginal
People. Ottawa: Canada Communication Group.
Rutter, M. (1985). Resilience in the face of adversity. Protective factors and resistance to psychiatric disorder.
British Journal of Psychiatry, 147, 598-611.
Rutter, M. (1987). Psychosocial resilience and protective mechanisms. American Journal of Orthopsychiatry, 57,
316-331.
Salisbury, T., & Gresser, P. J. (1971). Windradyne of the Wiradjuri: Martial law at Bathurst in 1824. Sydney:
Wentworth Books.
Scougall, J. (1997). Giving voice: The conduct of evaluation research in Aboriginal contexts. Evaluation Journal of
Australasia, 9, 53-60.

Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
93
Sheehan, N. (2001). “Some call it culture”: Aboriginal identity and the imaginary moral centre. Social
Alternatives, 20, 29-33.
Sheehan, N. (2004). Indigenous Knowledge and Education: instigating relational education in a higher education
context. Unpublished Doctoral thesis, School of Education. University of Queensland.
Sheehan, N.W., Dunleavy, J., Cohen, T. & Mitchell, S. (in press). Denatured Spirit: Neo-colonial Social Design.
Sheldon, M. (2001). Psychiatric assessment in remote Aboriginal communities. Australian and New Zealand
Journal of Psychiatry, 35, 435-442.
Shore, J.H., & Spicer, P. (2004). A model for alcohol-mediated violence in an Australian Aboriginal community.
Social Science and Medicine, 58, 2509-2521.
Skegg, K., Cox, B., & Broughton, J. (1995). Suicide among New Zealand Maori: Is history repeating itself? Acta
Psychiatrica Scandinavica, 92, 453-459
Spivak, G.C. (2003) Death of a discipline. Columbia University Press, New York.
Stacey, K., Keller, N., Gibson, B., Johnson, R., Jury, L., Kelly, D., et al. (2007). Promoting mental health and
wellbeing in Aboriginal contexts: Successful elements of suicide prevention work. Health Promotion
Journal of Australia, 18, 247-254.
Stevenson, M.R., Wallace, L.J.D., Harrison, J., Moller, J., & Smith, R.J. (1998). At risk in two worlds: Injury
mortality among Indigenous people in the US and Australia, 1990-1992. Australian and New Zealand
Journal of Public Health, 22, 641-644.
Stewart, L.M., Henderson, C.J., Hobbs, M.S.T., Ridout, S.C., & Knuiman, M.W. (2004). Risk of death in prisoners
after release from jail. Australian and New Zealand Journal of Public Health, 28, 32-36.
Strickland, C.J., Walsh, E., & Cooper, M. (2006). Healing fractured families: Parents’ and elders’ perspectives on
the impact of colonization and youth suicide prevention in a Pacific Northwest American Indian Tribe.
Journal of Transcultural Nursing, 17, 5-12.
Sue, D. W., Ivey, A. E. & Pedersen, P. B. (1996) A theory of multicultural counselling and therapy. Pacific Grove,
CA: Brooks/Cole Pub. Co.
Swan, P., & Raphael, B. (1995). Ways Forward: National Consultancy Report On Aboriginal and Torres Strait
Islander Mental Health. Canberra, ACT: Australian Government Department of Health and Ageing.
Tatz, C. (2001). Aboriginal suicide is different: A portrait of life and self-destruction (No. 0855753714). Canberra:
Aboriginal Studies Press.
Tatz, C. (2004). Aboriginal, Maori and Inuit Youth Suicide: Avenues to Alleviation? Australian Aboriginal Studies,
2, 15-25.
Tatz, C. (2005). Aboriginal suicide is different: A portrait of life and self-destruction (2nd ed). Canberra:
Aboriginal Studies Press.
Terszak, M. R. (2008). Orphaned by the colour of my skin: a stolen generation story. Maleny, Qld: Verdant
House.
Thomson, N., Krom, I., Trevaskis, G., Weissofner, N., & Leggett, N. (2005). A scoping study of depression among
Indigenous peoples. Perth: Australian Indigenous HealthInfoNet.
Tierney, R.J. (1994). Suicide intervention training evaluation: A preliminary report. Crisis, 15, 70-76

Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
94
Tongs, J., Chatfield, H., & Arabena, K. (2007). The Winnunga Nimmityjah Aboriginal Health Service holistic
health care for prison model. Aboriginal and Islander Health Worker Journal, 31, 6-8.
Tse, S., Lloyd, C., Petchkovsky, L., & Manaia, W. (2005). Exploration of Australian and New Zealand Indigenous
people’s spirituality and mental health. Australian Occupational Therapy Journal, 52, 181-187.
Tsey, K., Patterson, D., Whiteside, M., Baird, L., Baird, B., & Tsey, K. (2004a). A micro
analysis of a participatory action research process with a rural Aboriginal men’s health group.
Australian Journal of Primary Health, 10, 64-71.
Tsey, K., Wenitong, M., McCalman, J., Baird, L., Patterson, D. Baird, B., et al. (2004b). A participatory action
research process with a rural Indigenous men’s group: Monitoring and reinforcing change. Journal of
Primary Health, 10, 130-136.
Tsey, K., Travers, H., Gibson, T., Whiteside, M., Cadet-James, Y., Haswell-Elkins, M., et al. (2005). The role of
empowerment through life skills development in building comprehensive primary health care systems
in Indigenous Australia. Australian Journal of Primary Care, 11, 16-25.
Tsey, K., Wilson, A., Haswell, M., Whiteside, M., McCalman, J., Cadet-James, Y., et al. (2007). Empowerment-
based research methods: A 10-year approach to enhancing Indigenous social and emotional wellbeing.
Australasian Psychiatry, 15 (Supplement), S34-S38.
Turley, B., & Tanney, B. (1998). SIFTA Evaluation Report. Melbourne: Lifeline Australia
United Nations (1948). Universal Declaration of Human Rights. Online at
http://www.un.org/Overview/rights.html
United Nations (2008). United Nations Declaration on the Rights of Indigenous Peoples. Online at
http://www.un.org/esa/socdev/unpfii/documents/DRIPS_en.pdf
Vicary, D., & Andrews, H. (2001). A model of therapeutic intervention with Indigenous
Australians. Australian and New Zealand Journal of Public Health, 25, 349-51.
Vicary, D., & Bishop, B.J. (2005). Western psychotherapeutic practice: Engaging Aboriginal people in culturally
appropriate and respectful ways. Australian Psychologist, 40, 8-19.
Vicary, D., & Westerman, T. (2004). "That's just the way he is": Some implications of Aboriginal mental health
beliefs. Australian e-Journal for the Advancement of Mental Health, 3.
Weatherburn, D., Fitzgerald, J., & Hua, J. (2003). Reducing Aboriginal over-representation in prison. Australian
Journal of Public Administration, 62, 65-73.
Wesley-Esquimaux, C. C., & Smolewski, M. (2004). Historic Trauma and Aboriginal Healing. Ontario: Aboriginal
Healing Foundation Ottawa.
Westerman, T.G. (2002a). Psychological interventions with Aboriginal people. Connect Magazine. Health
Department of Western Australian.
Westerman, T. (2002b). Westerman Aboriginal Symptom Checklist-Youth. Perth: Indigenous Psychological
Services.
Westerman, T. (2004). Engagement of Indigenous clients in mental health services: What role do cultural
differences play? Australian e-Journal for the Advancement of Mental Health, 3, 1–7.

Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
95
Westerman, T., & Vicary, D. (2001). Aboriginal youth suicide. In P. Dudgeon, D. Garvey, & H. Pickett (Eds.).
Working with Indigenous Australians: A handbook for psychologists (pp. 471–479). Perth: Gunada
Press.
Wexler, L.M. (2006). Inupiat youth suicide and culture loss: Changing community conversations for prevention.
Social Science and Medicine, 63, 2938-2948.
Wexler, L., Bertone-Johnson, E., & Fenaughty, A. (2008). Correlates of Alaska Native fatal and nonfatal suicidal
behaviors 1990-2001. Suicide and Life-Threatening Behavior, 38, 311-320.
Wilkie, C., Macdonald, S., & Hildahl, K. (1998). Community case study: Suicide cluster in a small Manitoba
community. Canadian Journal of Psychiatry, 43, 823–828.
Wissow, L.S., Walkup, J., Barlow, A., Reid, R., & Kane, S. (2001). Cluster and regional influences on suicide in a
Southwestern American Indian Tribe. Social Science and Medicine, 53, 1115-1124.
World Health Organization (1986). Ottawa Charter for Health Promotion. Geneva: WHO.
Online at http://www.who.int/hpr/NPH/docs/ottawa_charter_hp.pdf
World Health Organization (1997). Jakarta Declaration on Leading Health Promotion into the 21st
Century.
Geneva: WHO. Online at http://www.who.int/hpr/NPH/docs/jakarta_declaration_en.pdf
World Health Organization (2004). Prevention of Mental Disorders: Effective Interventions and Policy
Options. Summary Report. Geneva: WHO.
World Health Organization (2005a). Promoting Mental Health: Concepts, Emerging Evidence, Practice. Geneva:
WHO.
World Health Organization (2005b). Bangkok Charter for Health Promotion in a Globalized World. Geneva:
WHO. Online at http://www.who.int/healthpromotion/conferences/6gchp/hpr_050829_%20BCHP.pdf
Zubrick, S.R., & Lawrence, N. (2006). Research Paper: Testing the Reliability of a Measure of Aboriginal
Children's Mental Health. 1351.0.55.011. Canberra: Australian Bureau of Statistics.
Zubrick, S.R., & Robson, A. (2003). Resilience to offending in high-risk groups: Focus on Aboriginal youth.
Prepared for Criminology Research Council.
Zubrick, S., Silburn, S., Lawrence, D. Mitrou, F.G., Dalby, R.B., Blair, E., et al. (2005). Western Australian
Aboriginal Child Health Survey: The social and emotional wellbeing of Aboriginal children and young
people. Perth: Curtin University of Technology and Telethon Institute for Child Health Research
Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
96
Appendix One: Glossary
This Glossary has been compiled based on glossary of the Australian Network for Promotion,
Prevention and Early Intervention for Mental Health (Auseinet)21, glossaries of policy
documents reviewed in this Report, and Mrazek and Haggerty (1994).
Aboriginal: A person of Aboriginal descent who identifies as an Aboriginal and is accepted as
such by the community in which he or she lives.
Aboriginal and Torres Strait Islander health: Holistic concept, encompassing mental health
and physical, cultural and spiritual health, considering land to be central to wellbeing. This
holistic concept does not merely refer to the ‘whole body’ but in fact is steeped in the
harmonised interrelations which constitute cultural wellbeing. These inter-relating factors
can be categorised largely as spiritual, environmental, ideological, political, social, economic,
mental and physical. Crucially, it must be understood that when the harmony of these
interrelations is disrupted, Aboriginal ill health will persist.
Health: Health does not just mean the physical wellbeing of an individual, but refers to the
social, emotional and cultural wellbeing of the whole community. This is a whole-of-life view
and includes the cyclical concept of life-death-life. Health care services should strive to
achieve the state where every individual can achieve their full potential as human beings and
thus bring about the total wellbeing of their communities.
Holistic approach: A holistic approach to health incorporates a comprehensive approach to
service delivery and treatment where coordination of a client’s needs and total care takes
priority. It is an acknowledgement that economic and social conditions affect physical and
emotional wellbeing. Care therefore needs to take into account physical, environmental,
cultural, and spiritual factors for achieving social and emotional wellbeing.
Illness: An unhealthy condition of body or mind.
21
http://auseinet.com/glossary
Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
97
Indicated intervention: A preventive intervention targeted to high-risk individuals who are
identified as having minimal but detectable signs and symptoms foreshadowing mental
disorder but who do not meet DSM-IV diagnostic levels at the current time.
Indigenous: A person of Aboriginal and/or Torres Strait Islander descent who identifies as an
Aboriginal and/or Torres Strait Islander and is accepted as such by the community with
which he or she is associated.
Mental health: Capacity of the individual, the groups and the environment to interact with
one another in ways that promote subjective wellbeing, the optimal development and use of
mental abilities (cognitive, affective or emotional and relational), the achievements of
individual and collective goals consistent with the attainment and presentation of conditions
of fundamental equality. Mental health is incorporated into the holistic approach to health
care as defined in the definition of health.
Mental health promotion: A process aimed at changing environments (social, physical,
economic, educational and cultural) and enhancing the ‘coping’ capacity of communities,
families and individuals, by giving people the power, knowledge, skills and necessary
resources.
Prevention : Interventions that occur before the initial onset of a disorder
Protective factors: Capacities, qualities, environmental and personal resources that drive
individuals towards growth, stability, and health.
Resilience: Capacities within a person that promote positive outcomes, such as mental
health and wellbeing, and provide protection from factors that might otherwise place that
person at risk of adverse health outcomes. Factors that contribute to resilience include
personal coping skills and strategies for dealing with adversity, such as problem-solving,
good communication and social skills, optimistic thinking, and help-seeking.

Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
98
Risk factors: Factors such as biological, psychological, social and cultural agents that are
associated with suicide/suicide ideation. Risk factors can be defined as either distal (internal
factors, such as genetic or neurochemical factors) or proximal (external factors, such as life
events or the availability of lethal means - factors which can ‘trigger’ a suicide or suicidal
behaviour).
Selective intervention: A preventive intervention targeted at individuals or population
subgroup whose risk of developing mental disorders is significantly higher than average.
Self-injury: Deliberate damage of body tissue, often in response to psychosocial distress,
without the intent to die. Sometimes called non-suicidal self-injury, or self-harm.
Suicidal behaviour: Includes the spectrum of activities related to suicide and self-harm
including suicidal thinking, self-harming behaviours not aimed at causing death and suicide
attempts. Some writers also include deliberate recklessness and risk-taking behaviours as
suicidal behaviours.
Suicidal ideation: Thoughts about attempting or completing suicide.
Suicide: The act of purposely ending one’s life.
Suicide prevention: Actions or initiatives to reduce the risk of suicide among populations or
specific target groups.
Torres Strait Islander: A person of Torres Strait Islander descent who identifies as a Torres
Strait Islander and is accepted as such by the community in which he or she lives.
Universal intervention: A preventive intervention targeted to the general public or a whole
population group that has not been identified on the basis of individual risk.
Wellness: The quality or state of being in good health especially as an actively sought goal
Identity, Voice, Place.
Krysinska, Martin & Sheehan, 2009. The University of Queensland.
99
Appendix Two: Acknowledgements
Mick Adams, National Aboriginal Community Controlled Health Organisation
Diana Aitchison, Department of Health and Ageing, Qld
Jeff Allen, Health Promotion Queensland
Margaret Appleby, Rose Education, NSW
Kerry Arabena, Australian Institute of Aboriginal and Torres Strait Islander Studies
Mercy Baird, Yarrabah Community Support Group, Qld
Thomas Brideson, NSW Aboriginal Mental Health Workforce Program
Adrian Carson, Queensland Aboriginal and Islander Health Council
Nicolle Coupe, Ministry of Health, New Zealand
Mason Durie, Massey University, New Zealand
Bruce Gynther, Queensland Health, Mental Health
Leonore Hanssens, Charles Darwin University, NT
Caroline Harvey, Department of Health and Ageing, Qld
Melissa Haswell, University of Queensland
Graham Henderson, Australian Institute of Aboriginal and Torres Strait Islander Studies
Ernest Hunter, University of Queensland
Laurence Kirmayer, McGill University, Canada
Helen Klieve, Griffith University, Qld
Teresa LaFromboise, Stanford Center on Adolescence, Stanford University, USA
Janya McCalman, James Cook University, Qld
Helen Milroy, University of Western Australia
Katie Panaretto, Queensland Aboriginal and Islander Health Council
Pauline Peel, Department of Communities, Qld
Leon Petchkovsky, University of Queensland
Greg Pratt, Centre for Rural and Remote Mental Health, Qld
Cindy Shannon, University of Queensland, Qld
Ian Shochet, Queensland University of Technology
Joan Smith, Clinic Manager Bidgerdii Community Health Service, Qld
Yolandy Surawsky, Commission for Children and Young People and Child Guardian, Qld
Komla Tsey, James Cook University, Qld
Tracey Westerman, Indigenous Psychological Services, WA
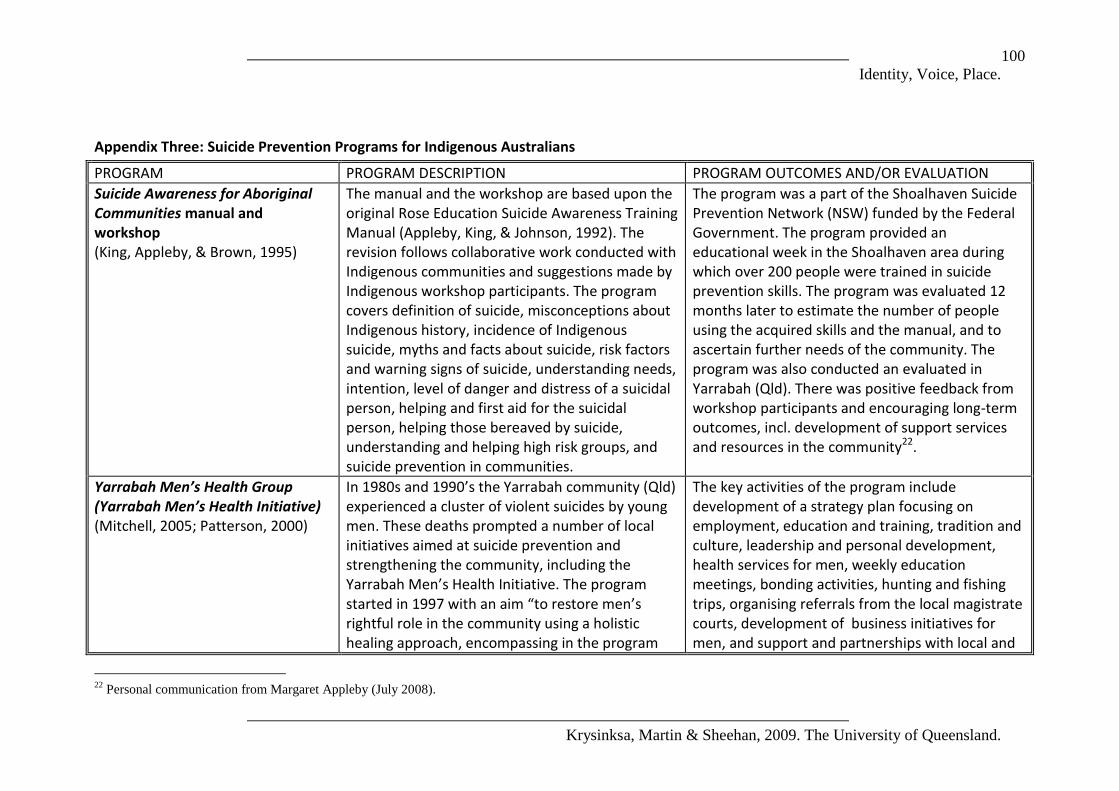
Identity, Voice, Place.
Krysinksa, Martin & Sheehan, 2009. The University of Queensland.
100
Appendix Three: Suicide Prevention Programs for Indigenous Australians
PROGRAM PROGRAM DESCRIPTION PROGRAM OUTCOMES AND/OR EVALUATION
Suicide Awareness for Aboriginal Communities manual and workshop (King, Appleby, & Brown, 1995)
The manual and the workshop are based upon the original Rose Education Suicide Awareness Training Manual (Appleby, King, & Johnson, 1992). The revision follows collaborative work conducted with Indigenous communities and suggestions made by Indigenous workshop participants. The program covers definition of suicide, misconceptions about Indigenous history, incidence of Indigenous suicide, myths and facts about suicide, risk factors and warning signs of suicide, understanding needs, intention, level of danger and distress of a suicidal person, helping and first aid for the suicidal person, helping those bereaved by suicide, understanding and helping high risk groups, and suicide prevention in communities.
The program was a part of the Shoalhaven Suicide Prevention Network (NSW) funded by the Federal Government. The program provided an educational week in the Shoalhaven area during which over 200 people were trained in suicide prevention skills. The program was evaluated 12 months later to estimate the number of people using the acquired skills and the manual, and to ascertain further needs of the community. The program was also conducted an evaluated in Yarrabah (Qld). There was positive feedback from workshop participants and encouraging long-term outcomes, incl. development of support services and resources in the community22.
Yarrabah Men’s Health Group (Yarrabah Men’s Health Initiative) (Mitchell, 2005; Patterson, 2000)
In 1980s and 1990’s the Yarrabah community (Qld) experienced a cluster of violent suicides by young men. These deaths prompted a number of local initiatives aimed at suicide prevention and strengthening the community, including the Yarrabah Men’s Health Initiative. The program started in 1997 with an aim “to restore men’s rightful role in the community using a holistic healing approach, encompassing in the program
The key activities of the program include development of a strategy plan focusing on employment, education and training, tradition and culture, leadership and personal development, health services for men, weekly education meetings, bonding activities, hunting and fishing trips, organising referrals from the local magistrate courts, development of business initiatives for men, and support and partnerships with local and
22
Personal communication from Margaret Appleby (July 2008).
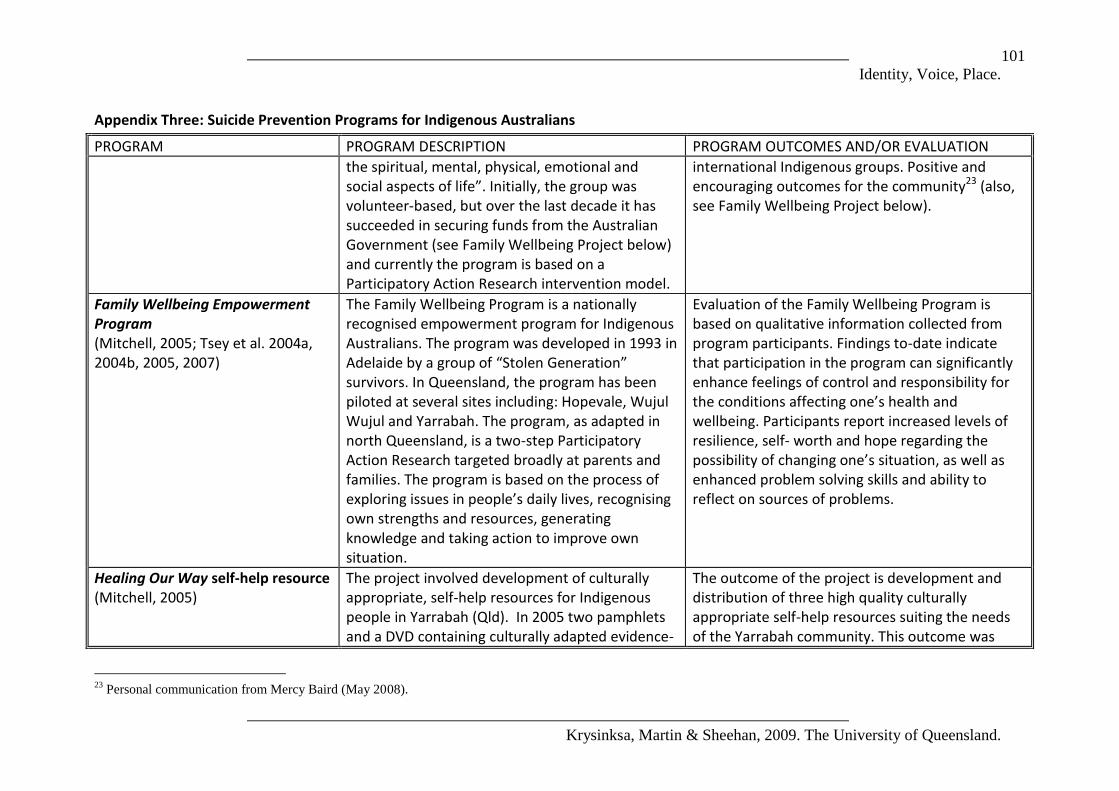
Identity, Voice, Place.
Krysinksa, Martin & Sheehan, 2009. The University of Queensland.
101
Appendix Three: Suicide Prevention Programs for Indigenous Australians
PROGRAM PROGRAM DESCRIPTION PROGRAM OUTCOMES AND/OR EVALUATION
the spiritual, mental, physical, emotional and social aspects of life”. Initially, the group was volunteer-based, but over the last decade it has succeeded in securing funds from the Australian Government (see Family Wellbeing Project below) and currently the program is based on a Participatory Action Research intervention model.
international Indigenous groups. Positive and encouraging outcomes for the community23 (also, see Family Wellbeing Project below).
Family Wellbeing Empowerment Program (Mitchell, 2005; Tsey et al. 2004a, 2004b, 2005, 2007)
The Family Wellbeing Program is a nationally recognised empowerment program for Indigenous Australians. The program was developed in 1993 in Adelaide by a group of “Stolen Generation” survivors. In Queensland, the program has been piloted at several sites including: Hopevale, Wujul Wujul and Yarrabah. The program, as adapted in north Queensland, is a two-step Participatory Action Research targeted broadly at parents and families. The program is based on the process of exploring issues in people’s daily lives, recognising own strengths and resources, generating knowledge and taking action to improve own situation.
Evaluation of the Family Wellbeing Program is based on qualitative information collected from program participants. Findings to-date indicate that participation in the program can significantly enhance feelings of control and responsibility for the conditions affecting one’s health and wellbeing. Participants report increased levels of resilience, self- worth and hope regarding the possibility of changing one’s situation, as well as enhanced problem solving skills and ability to reflect on sources of problems.
Healing Our Way self-help resource (Mitchell, 2005)
The project involved development of culturally appropriate, self-help resources for Indigenous people in Yarrabah (Qld). In 2005 two pamphlets and a DVD containing culturally adapted evidence-
The outcome of the project is development and distribution of three high quality culturally appropriate self-help resources suiting the needs of the Yarrabah community. This outcome was
23
Personal communication from Mercy Baird (May 2008).
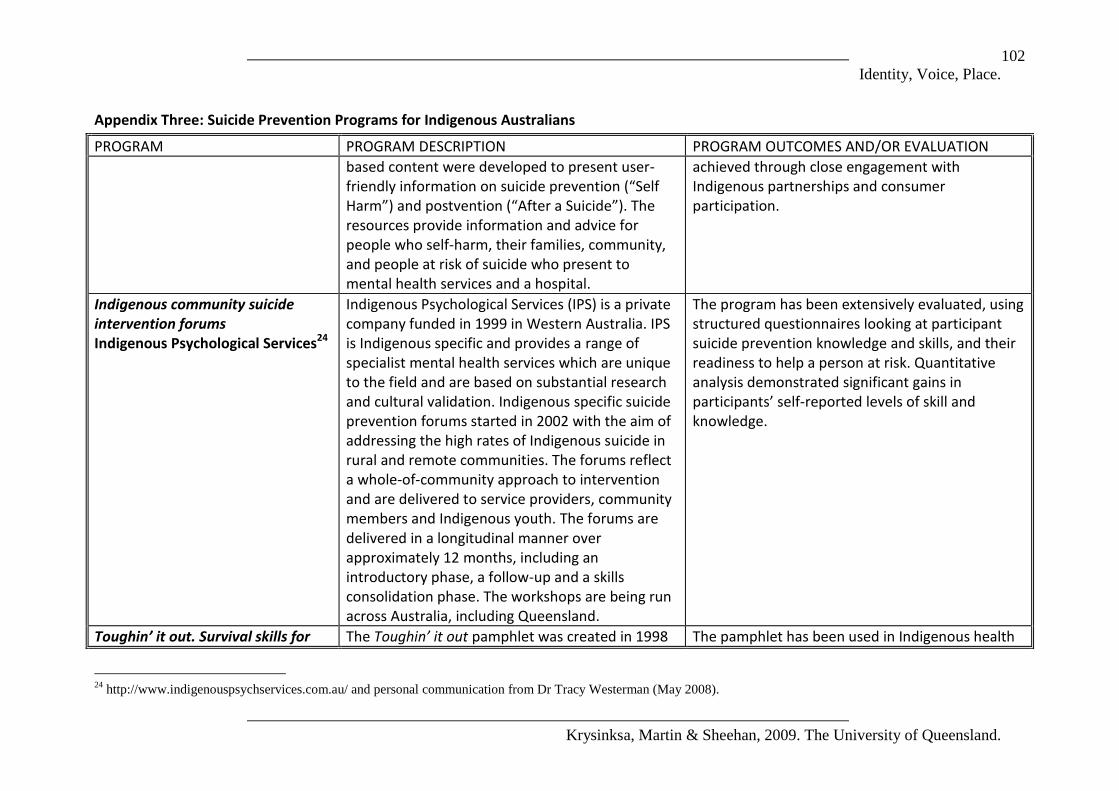
Identity, Voice, Place.
Krysinksa, Martin & Sheehan, 2009. The University of Queensland.
102
Appendix Three: Suicide Prevention Programs for Indigenous Australians
PROGRAM PROGRAM DESCRIPTION PROGRAM OUTCOMES AND/OR EVALUATION
based content were developed to present user-friendly information on suicide prevention (“Self Harm”) and postvention (“After a Suicide”). The resources provide information and advice for people who self-harm, their families, community, and people at risk of suicide who present to mental health services and a hospital.
achieved through close engagement with Indigenous partnerships and consumer participation.
Indigenous community suicide intervention forums Indigenous Psychological Services24
Indigenous Psychological Services (IPS) is a private company funded in 1999 in Western Australia. IPS is Indigenous specific and provides a range of specialist mental health services which are unique to the field and are based on substantial research and cultural validation. Indigenous specific suicide prevention forums started in 2002 with the aim of addressing the high rates of Indigenous suicide in rural and remote communities. The forums reflect a whole-of-community approach to intervention and are delivered to service providers, community members and Indigenous youth. The forums are delivered in a longitudinal manner over approximately 12 months, including an introductory phase, a follow-up and a skills consolidation phase. The workshops are being run across Australia, including Queensland.
The program has been extensively evaluated, using structured questionnaires looking at participant suicide prevention knowledge and skills, and their readiness to help a person at risk. Quantitative analysis demonstrated significant gains in participants’ self-reported levels of skill and knowledge.
Toughin’ it out. Survival skills for The Toughin’ it out pamphlet was created in 1998 The pamphlet has been used in Indigenous health
24
http://www.indigenouspsychservices.com.au/ and personal communication from Dr Tracy Westerman (May 2008).
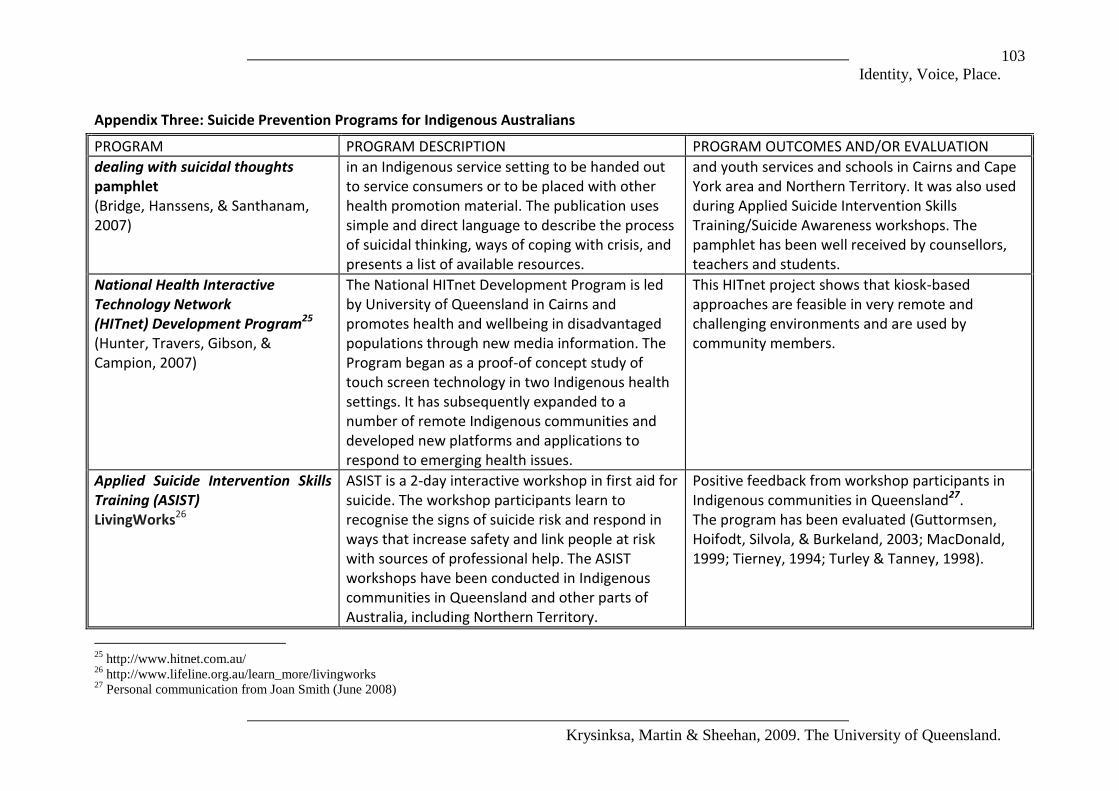
Identity, Voice, Place.
Krysinksa, Martin & Sheehan, 2009. The University of Queensland.
103
Appendix Three: Suicide Prevention Programs for Indigenous Australians
PROGRAM PROGRAM DESCRIPTION PROGRAM OUTCOMES AND/OR EVALUATION
dealing with suicidal thoughts pamphlet (Bridge, Hanssens, & Santhanam, 2007)
in an Indigenous service setting to be handed out to service consumers or to be placed with other health promotion material. The publication uses simple and direct language to describe the process of suicidal thinking, ways of coping with crisis, and presents a list of available resources.
and youth services and schools in Cairns and Cape York area and Northern Territory. It was also used during Applied Suicide Intervention Skills Training/Suicide Awareness workshops. The pamphlet has been well received by counsellors, teachers and students.
National Health Interactive Technology Network (HITnet) Development Program25 (Hunter, Travers, Gibson, & Campion, 2007)
The National HITnet Development Program is led by University of Queensland in Cairns and promotes health and wellbeing in disadvantaged populations through new media information. The Program began as a proof-of concept study of touch screen technology in two Indigenous health settings. It has subsequently expanded to a number of remote Indigenous communities and developed new platforms and applications to respond to emerging health issues.
This HITnet project shows that kiosk-based approaches are feasible in very remote and challenging environments and are used by community members.
Applied Suicide Intervention Skills Training (ASIST) LivingWorks26
ASIST is a 2-day interactive workshop in first aid for suicide. The workshop participants learn to recognise the signs of suicide risk and respond in ways that increase safety and link people at risk with sources of professional help. The ASIST workshops have been conducted in Indigenous communities in Queensland and other parts of Australia, including Northern Territory.
Positive feedback from workshop participants in Indigenous communities in Queensland27. The program has been evaluated (Guttormsen, Hoifodt, Silvola, & Burkeland, 2003; MacDonald, 1999; Tierney, 1994; Turley & Tanney, 1998).
25
http://www.hitnet.com.au/ 26
http://www.lifeline.org.au/learn_more/livingworks 27
Personal communication from Joan Smith (June 2008)

Identity, Voice, Place.
Krysinksa, Martin & Sheehan, 2009. The University of Queensland.
104
Appendix Three: Suicide Prevention Programs for Indigenous Australians
PROGRAM PROGRAM DESCRIPTION PROGRAM OUTCOMES AND/OR EVALUATION
Increasing the Capacity of Local Counsellors “Drop the Rock” Royal Flying Doctor Service of Australia (Qld)28
The program is based on engagement of local services to assist clients experiencing social and emotional wellbeing and mental health difficulties in the five Cape York Peninsula communities (Kowanyama, Pormpuraaw, Aurukun, Lockhart River and Coen). The project aims to enhance local and visiting social and emotional wellbeing (mental health) services by developing or increasing the capacity of local community counsellors to provide basic counselling, support and liaison between clients and visiting services. The community counsellor positions work with visiting mental health personnel engaged in community development initiatives addressing social and emotional wellbeing (mental health) issues by focusing on local strategies. The trainee community counsellors undertake a Certificate 4 in Mental Health (non-clinical) through the Far North Queensland TAFE - an additional subject has been incorporated into the course which looks at the impact of historical events upon current Aboriginal and Torres Strait Islander culture and communities.
The program is ongoing.
Learning from the experts: Building bridges to implement successful life
A suicide prevention and education project targeting Aboriginal communities in Far North and
The program is ongoing.
28
Information obtained from Australian Government Department of Health and Ageing, Queensland State Office

Identity, Voice, Place.
Krysinksa, Martin & Sheehan, 2009. The University of Queensland.
105
Appendix Three: Suicide Prevention Programs for Indigenous Australians
PROGRAM PROGRAM DESCRIPTION PROGRAM OUTCOMES AND/OR EVALUATION
promotion and suicide prevention expertise across Aboriginal communities Centre for Rural and Remote Mental Health Queensland Ltd. in partnership with James Cook University, University of Southern Queensland, University of Queensland; AISRAP, Griffith University29
South West Queensland involving five key projects: (1) establishing Men's support groups in Yarrabah, Hope Vale, Kowanyama, Dalby and Goondir, (2) delivery of the Family Wellbeing Program in Kowanyama, Hope Vale, Dalby and Yarrabah and Lotus Glen Correctional Facility, (3) collection, organisation and analysis of stories from Far North Qld communities and Dalby, (4) implementation of touch-screen kiosks in Hopevale, Dalby, and Lotus Glen and Cleveland Detention Centre and (5) collection, collation and communication of information on community health (injuries, suicides, mental health, alcohol, school attendance etc) in an empowering way.
Something Better Queensland Police-Citizens Youth Welfare Association30
The project aims to assist and support young people in Aboriginal communities of Wujal Wujal, Napranum, Hope Vale and Mapoon (Qld) that are at risk of suicide by providing them with exposure to sporting activities outside of their community by a suitably trained and dedicated local Indigenous person.
The program is ongoing.
Napranum Life Promotion Queensland Police-Citizens Youth Welfare Association31
The project aims to assist and support young people in the Aboriginal communities of Napranum, that are at risk of suicide by providing
The program is ongoing.
29
Ibid. 30
Ibid. 31
Ibid.

Identity, Voice, Place.
Krysinksa, Martin & Sheehan, 2009. The University of Queensland.
106
Appendix Three: Suicide Prevention Programs for Indigenous Australians
PROGRAM PROGRAM DESCRIPTION PROGRAM OUTCOMES AND/OR EVALUATION
them with a range of programs including a Breakfast Program, Homework Program, Scouts Program, Parenting Program and a Resume Program - provision of materials and computer access to enable participants to complete resumes.
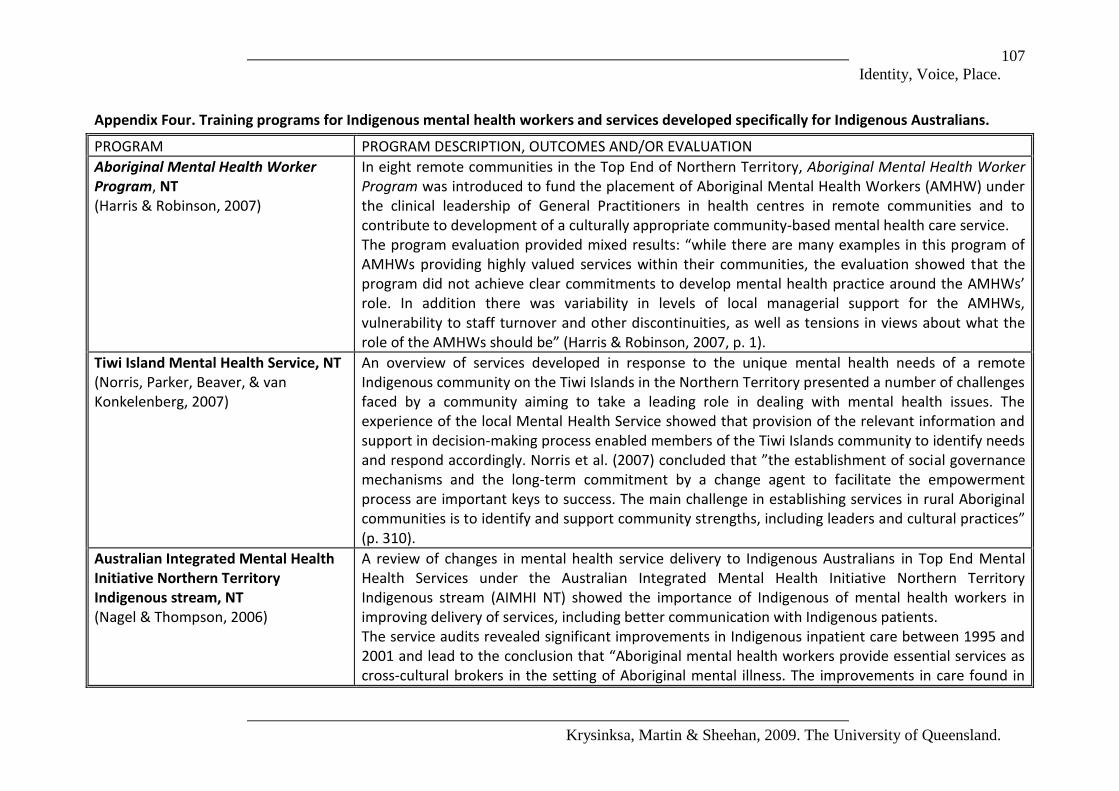
Identity, Voice, Place.
Krysinksa, Martin & Sheehan, 2009. The University of Queensland.
107
Appendix Four. Training programs for Indigenous mental health workers and services developed specifically for Indigenous Australians.
PROGRAM PROGRAM DESCRIPTION, OUTCOMES AND/OR EVALUATION
Aboriginal Mental Health Worker Program, NT (Harris & Robinson, 2007)
In eight remote communities in the Top End of Northern Territory, Aboriginal Mental Health Worker Program was introduced to fund the placement of Aboriginal Mental Health Workers (AMHW) under the clinical leadership of General Practitioners in health centres in remote communities and to contribute to development of a culturally appropriate community-based mental health care service. The program evaluation provided mixed results: “while there are many examples in this program of AMHWs providing highly valued services within their communities, the evaluation showed that the program did not achieve clear commitments to develop mental health practice around the AMHWs’ role. In addition there was variability in levels of local managerial support for the AMHWs, vulnerability to staff turnover and other discontinuities, as well as tensions in views about what the role of the AMHWs should be” (Harris & Robinson, 2007, p. 1).
Tiwi Island Mental Health Service, NT (Norris, Parker, Beaver, & van Konkelenberg, 2007)
An overview of services developed in response to the unique mental health needs of a remote Indigenous community on the Tiwi Islands in the Northern Territory presented a number of challenges faced by a community aiming to take a leading role in dealing with mental health issues. The experience of the local Mental Health Service showed that provision of the relevant information and support in decision-making process enabled members of the Tiwi Islands community to identify needs and respond accordingly. Norris et al. (2007) concluded that ”the establishment of social governance mechanisms and the long-term commitment by a change agent to facilitate the empowerment process are important keys to success. The main challenge in establishing services in rural Aboriginal communities is to identify and support community strengths, including leaders and cultural practices” (p. 310).
Australian Integrated Mental Health Initiative Northern Territory Indigenous stream, NT (Nagel & Thompson, 2006)
A review of changes in mental health service delivery to Indigenous Australians in Top End Mental Health Services under the Australian Integrated Mental Health Initiative Northern Territory Indigenous stream (AIMHI NT) showed the importance of Indigenous of mental health workers in improving delivery of services, including better communication with Indigenous patients. The service audits revealed significant improvements in Indigenous inpatient care between 1995 and 2001 and lead to the conclusion that “Aboriginal mental health workers provide essential services as cross-cultural brokers in the setting of Aboriginal mental illness. The improvements in care found in

Identity, Voice, Place.
Krysinksa, Martin & Sheehan, 2009. The University of Queensland.
108
PROGRAM PROGRAM DESCRIPTION, OUTCOMES AND/OR EVALUATION
this file audit coincide with the commencement of employment of Aboriginal mental health workers in the inpatient unit. The AIMHI consultation reveals broad support for employment of more Aboriginal mental health workers in the Top End” (Nagel & Thompson, 2006; p. 291).
Maga Barndi Unit, WA (Laugharne, Glennen, & Austin, 2002)
In Western Australia, a two-year pilot project of delivery of culturally sensitive psychiatric services (Maga Barndi Unit) resulted in a marked increase in service utilisation by local Aboriginal people. Over the project period, the Unit was able to establish a significant local patient base and the majority of the Indigenous patients had not previously accessed mainstream mental health services. The success of the project was related to its location within an Indigenous controlled health centre with good access to Indigenous health workers, as well as a flexible assertive community management approach. According to Laugharne et al. (2002), “it is particularly encouraging that the total number of admissions of Aboriginal people with psychiatric diagnoses to Geraldton Regional Hospital was reduced by 58% in the second year of the project. In addition, we believe that through assertive community follow-up we prevented several patients with serious mental illness having to be transferred to the nearest available “gazetted” beds in Perth and all the associated problems that go with such a procedure” (p. 16).
Aboriginal and Torres Strait Islander Child and Adolescent Mental Health Traineeship Program, NSW (Bartik, Dixon, & Dart, 2007)
The Aboriginal and Torres Strait Islander Child and Adolescent Mental Health Traineeship Program was established in New South Wales in collaboration between Hunter New England Area Health Service (HNEAHS), Hunter New England Aboriginal Mental Health (HNEAMH) and the Department of Psychological Medicine at the Children’s Hospital at Westmead (CHW) with guidance and input from additional collaborators. The program encompasses employment of a child and adolescent mental health worker under professional support and supervision of HNEAHS, a mentoring program provided through HNEAMH, a clinical education and supervision program conducted through the Department of Psychological Medicine, CHW, and formal academic studies in Aboriginal Mental Health. The initial feedback has been positive and shows the program is a promising venue for training of Aboriginal and Torres Strait Islander child and adolescent mental health workers.
Djirruwang Aboriginal and Torres Strait Islander Mental Health Program, NSW (Brideson & Kanowski, 2004)
Te Djirruwang Aboriginal and Torres Strait Islander Mental Health Program delivers a three-year Bachelor of Health Science (Mental Health) Degree with exit points at Degree, Diploma and Certificate levels. The Program commenced in November 1993 and is restricted to Aboriginal and Torres Strait Islander people.
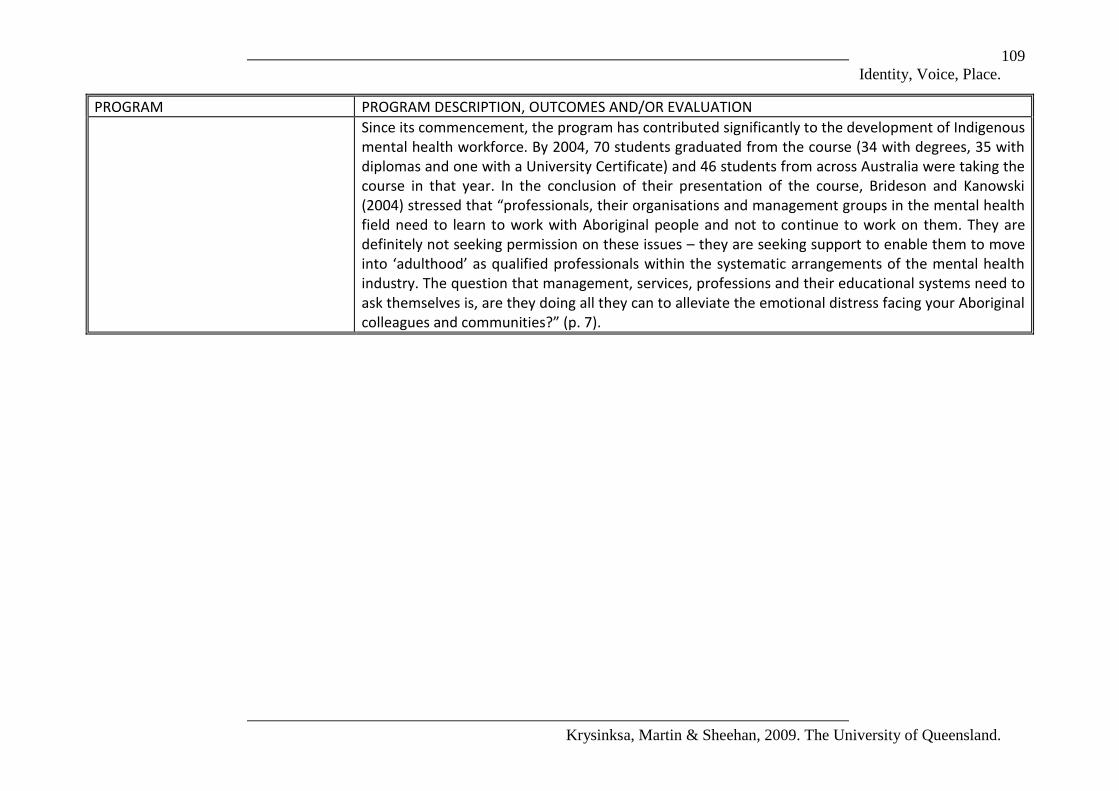
Identity, Voice, Place.
Krysinksa, Martin & Sheehan, 2009. The University of Queensland.
109
PROGRAM PROGRAM DESCRIPTION, OUTCOMES AND/OR EVALUATION
Since its commencement, the program has contributed significantly to the development of Indigenous mental health workforce. By 2004, 70 students graduated from the course (34 with degrees, 35 with diplomas and one with a University Certificate) and 46 students from across Australia were taking the course in that year. In the conclusion of their presentation of the course, Brideson and Kanowski (2004) stressed that “professionals, their organisations and management groups in the mental health field need to learn to work with Aboriginal people and not to continue to work on them. They are definitely not seeking permission on these issues – they are seeking support to enable them to move into ‘adulthood’ as qualified professionals within the systematic arrangements of the mental health industry. The question that management, services, professions and their educational systems need to ask themselves is, are they doing all they can to alleviate the emotional distress facing your Aboriginal colleagues and communities?” (p. 7).
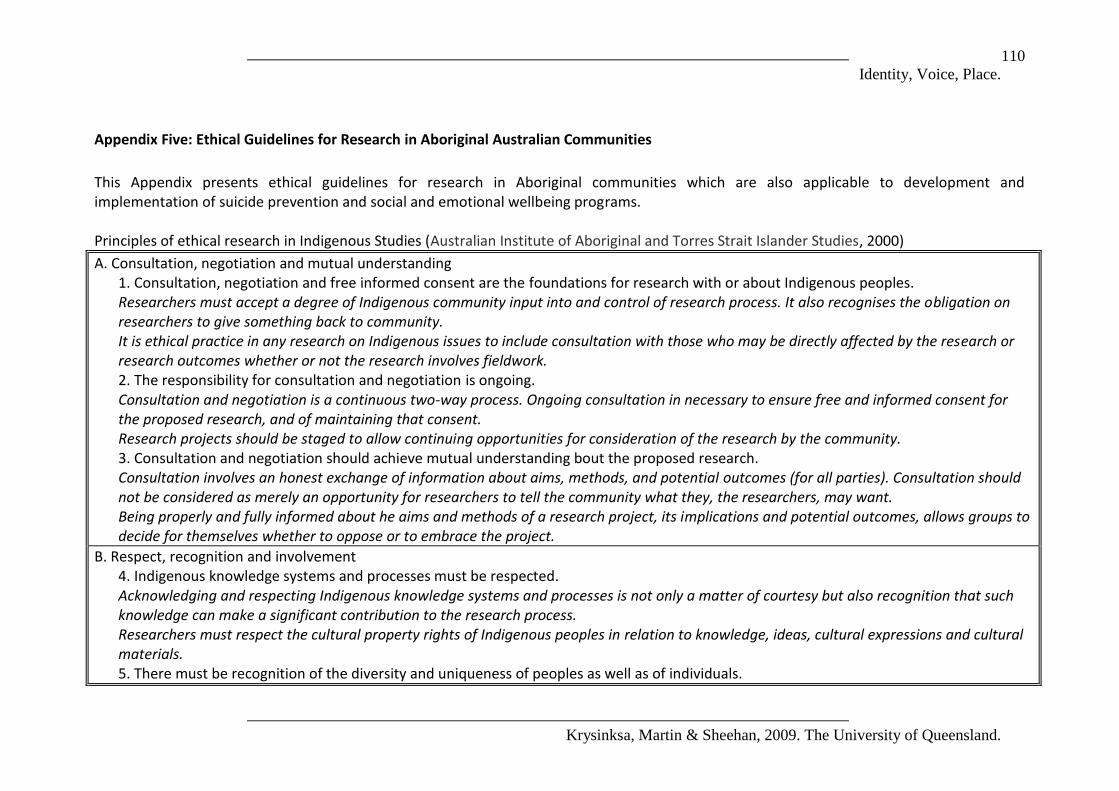
Identity, Voice, Place.
Krysinksa, Martin & Sheehan, 2009. The University of Queensland.
110
Appendix Five: Ethical Guidelines for Research in Aboriginal Australian Communities
This Appendix presents ethical guidelines for research in Aboriginal communities which are also applicable to development and implementation of suicide prevention and social and emotional wellbeing programs. Principles of ethical research in Indigenous Studies (Australian Institute of Aboriginal and Torres Strait Islander Studies, 2000)
A. Consultation, negotiation and mutual understanding 1. Consultation, negotiation and free informed consent are the foundations for research with or about Indigenous peoples. Researchers must accept a degree of Indigenous community input into and control of research process. It also recognises the obligation on researchers to give something back to community. It is ethical practice in any research on Indigenous issues to include consultation with those who may be directly affected by the research or research outcomes whether or not the research involves fieldwork. 2. The responsibility for consultation and negotiation is ongoing. Consultation and negotiation is a continuous two-way process. Ongoing consultation in necessary to ensure free and informed consent for the proposed research, and of maintaining that consent. Research projects should be staged to allow continuing opportunities for consideration of the research by the community. 3. Consultation and negotiation should achieve mutual understanding bout the proposed research. Consultation involves an honest exchange of information about aims, methods, and potential outcomes (for all parties). Consultation should not be considered as merely an opportunity for researchers to tell the community what they, the researchers, may want. Being properly and fully informed about he aims and methods of a research project, its implications and potential outcomes, allows groups to decide for themselves whether to oppose or to embrace the project.
B. Respect, recognition and involvement 4. Indigenous knowledge systems and processes must be respected. Acknowledging and respecting Indigenous knowledge systems and processes is not only a matter of courtesy but also recognition that such knowledge can make a significant contribution to the research process. Researchers must respect the cultural property rights of Indigenous peoples in relation to knowledge, ideas, cultural expressions and cultural materials. 5. There must be recognition of the diversity and uniqueness of peoples as well as of individuals.
Identity, Voice, Place.
Krysinksa, Martin & Sheehan, 2009. The University of Queensland.
111
Research in Indigenous studies must show an apperception of the diversity of Indigenous peoples, who have different languages, cultures, histories and perspectives. It is also important to recognise the diversity of individuals and groups within those communities. 6. The intellectual and cultural property rights of Indigenous peoples must be respected and preserved. Indigenous cultural and intellectual property rights are part of the heritage that exists in the cultural practices, resources and knowledge systems of Indigenous peoples, and that are passed on by them in expressing their cultural identity. Indigenous intellectual property is not static and extends to things that may be created based on that heritage. It is a fundamental principle of research to acknowledge the sources of information and those who have contributed to the research. 7. Indigenous researchers, individuals and communities should be involved in research as collaborators. Indigenous communities and individuals have a right to be involved in any research project focussed upon them and their culture. Participants have the right to withdraw from the project at any time. Research on Indigenous issues should also incorporate Indigenous perspectives and this is often effectively achieved by facilitating more direct involvement in the research.
C. Benefits, outcomes and agreement 8. The use of, and access to, research results should be agreed. Indigenous peoples make a significant contribution to research by providing knowledge, resources or access to data. That contribution should be acknowledged by providing access to research results and negotiating rights in the research at an early stage. The community’s expectations, the planned outcomes, and access to research results should be in agreement. 9. A researched community should benefit from, and not be disadvantaged by, the research project. Research in Indigenous studies should benefit Indigenous peoples at a local level, and more generally. A reciprocal benefit should accrue for their allowing researchers often intimate access to their personal and community knowledge. 10. The negotiation of outcomes should include results specific to the needs of the researched community. Among the tangible benefits that a community should be able to expect from a research project is the provision of research results in a form that is useful and accessible. 11. Negotiation should result in a formal agreement for the conduct of a research project, based on good faith and free and informed consent. The aim of the negotiation process is to come to a clear understanding, which results in a formal agreement (preferably written), about research intentions, methods and potential results. The establishment of agreements and protocols between Indigenous peoples and researchers is an important development in Indigenous studies.
Identity, Voice, Place.
Krysinksa, Martin & Sheehan, 2009. The University of Queensland.
112
Good faith negations are those that have involved a full and frank disclosure of all available information and that were entered into with honest view to reaching an agreement. Free and informed consent means that agreement must be obtained free of duress or pressure and fully cognisant of the details, and risks of the proposed research. Informed consent of the people as a group, as well as individuals within that group, is important.

Identity, Voice, Place.
Krysinksa, Martin & Sheehan, 2009. The University of Queensland.
113
Values relevant to health research ethics (National Health and Medical Research Council, 2003; 20005).
1. Reciprocity: A mutual obligation exists among members of the ATSI families and communities to achieve an equitable distribution of resources, responsibility and capacity and to achieve cohesion and survival of the social order. This mutual obligation extends to the land, animals and other natural elements and features. In contemporary settings the value of reciprocity continues in various forms, and may vary between locations. Examples include redistribution of income, benefits from the air, land and sea, and the sharing of other resources, such as housing.
Inclusion: Inclusion, the basis for mutual obligation, describes the degree of equitable and respectful engagement with ATSI peoples, their values and cultures in the proposed research. Benefit: Benefit in this context describes the establishment or enhancement of capacities, opportunities or outcomes that advance the interests of the ATSI peoples and that are valued by them.
2. Respect: Respect for human dignity and worth as a characteristic of relationships between people, and in the way individuals behave, is fundamental to a functioning and moral society. Within ATSI cultures respect is reinforced by and in turn strengthens dignity. A respectful relationship induces trust and co-operation. Strong culture is a personal and collective framework built on respect and trust that promotes dignity and recognition.
Respect of people and their contribution: Respect acknowledges the individual and collective contribution, interests and aspirations of the ATSI peoples, researchers and other partners in the research process. Minimising difference blindness: Respectful research relationships acknowledge and affirm the rights of people to have different values, norms and aspirations. Those involved in research should recognise and minimise the effect of difference blindness through all stages of the research process. Consequences of research: Researchers need to understand that research has consequences for themselves and others, the importance of which might not be immediately apparent. This should be taken into account through all stages of the research process.
3. Equality: One of the values expressed by the ATSI peoples and cultures is the equal value of people. One of the ways it is reflected is a commitment to distributive fairness and justice. Equality affirms ATSI people’s right to be different.
Valuing knowledge and wisdom: ATSI peoples value their collective memory and shared experience as a resource and inheritance. Researchers who fail to appreciate or ignore ATSI people’s knowledge and wisdom may misinterpret data or meaning, may create mistrust, otherwise limit quality or may overlook a potentially important benefit of research. Equality of partners: Ethical research processes treat all participants as equal notwithstanding that they may be different. In the absence of equal treatment, trust among researcher funders, researchers, host institutions, ATSI communities and other stakeholders is not possible. Without such trust ethical research is undermined. The distribution of benefit: The distribution of benefit stands as a fundamental test of equality. If the research process delivers benefit in

Identity, Voice, Place.
Krysinksa, Martin & Sheehan, 2009. The University of Queensland.
114
greater proportion to one partner in the initiative than other partners, the distribution of benefit may be seen as unequal.
4. Responsibility: Central to ATSI societies and cultures is the recognition of core responsibilities. These responsibilities include these to the country, kinship bonds, caring of others and the maintenance of harmony and balance within and between the physical and spiritual realms. A key responsibility within this framework is to do no harm, including avoiding having an adverse impact on others’ abilities to comply with their responsibilities. As well, one person’s responsibilities may be shared with others so that they will also be held accountable.
Doing no harm: There is a clear responsibility for researchers to do no harm to ATSI individuals and communities and also to those things that they value. Accountability: Researchers and participating communities need to establish processes to ensure researchers’ accountability to individuals, families, and communities, particularly in relation to the cultural ad social dimensions of ATSI life.
5. Survival and protection: ATSI peoples continue to act o protect their cultures and identity from erosion by colonisation and marginalisation. A particular feature of ATSI cultures and their efforts has been the importance of a collective identity. This collective bond reflects and draws strength from the values base of the ATSI peoples and cultures.
Importance of values based solidarity to ATSI peoples: ATSI vigorously oppose the assimilation, integration or subjugation of their values and will defend them against perceived or actual encroachment. Researchers must be aware of the history and the continuing potential for research to encroach ion these values. Respect for social cohesion: The importance of the personal and collective bond within ATSI communities and its critical function in their social lives. Commitment to cultural distinctiveness: The cultural distinctiveness of ATSI peoples is highly valued by them. Within the scope if these guidelines, researchers must find ways of working that d not diminish the right to the assertion or enjoyment of that distinctiveness.
6. Spirit and integrity: This is an overarching value that binds all others into a coherent whole. It has two components. The first about the continuity between past, current and future generations. The second is about behaviour, which maintains the coherence of ATSI values and cultures. Any behaviour that diminishes any of the previous five values could not be described as having integrity.
Motivation and action: This means that researchers must approach the conduct of the research in ATSI communities with respect for the richness and integrity of the cultural inheritance of past, current and future generations, and of the links which bind the generations together. Intent and process: Negotiations with ATSI communities will need to exhibit credibility in intent and process. In many circumstances this will depend not only on being able to demonstrate that the proposal is in keeping with these guidelines, but also on the behaviours and perceived integrity of the proponents of research.