Controlling Viral Immuno-Inflammatory Lesions by Modulating ...

ORIGINAL COMMUNICATION
Identification of cortical lesions using DIR and FLAIR in earlystages of multiple sclerosis
Pierre Kolber1• Swantje Montag1
• Vinzenz Fleischer1• Felix Luessi1 •
Janine Wilting1• Joachim Gawehn2
• Adriane Groger1• Frauke Zipp1
Received: 13 February 2015 / Revised: 25 March 2015 / Accepted: 26 March 2015
� Springer-Verlag Berlin Heidelberg 2015
Abstract The use of non-routine MRI sequences such as
DIR has highlighted the role of gray matter (GM) pathol-
ogy in multiple sclerosis (MS). The aim of this study was to
assess the detection and relevance of cortical lesions (CLs)
using MRI in early (\5 years) MS patients. 3D DIR and
3D FLAIR images at 3T from 122 patients [93 relapsing–
remitting MS (RRMS), 29 clinically isolated syndrome
(CIS)] were scored for CLs by two blinded readers. Pa-
tients were divided into two groups depending on the
presence or absence of CLs. For FLAIR, 51 CLs were
identified, of which 13 were purely intracortical and 38
mixed CLs; for DIR, this was 60 in total and 16 and 44,
respectively. In both groups, there was no difference in GM
fraction. Neuropsychological testing was performed for a
subgroup of 66 patients. In 22.1 % of patients CLs were
identified. The number of CLs revealed an association with
lower working memory scores and semantical word flu-
ency. Overall, CLs imaged with 3D FLAIR and 3D DIR
sequences are found more frequently in RRMS patients
than CIS and may also be a correlate for mild neuropsy-
chological pathology.
Keywords Multiple sclerosis � Cortical lesions �Magnetic resonance imaging � Neuropsychological testing
Introduction
Multiple sclerosis (MS), one of the most common chronic
neuroinflammatory diseases and causes of disability in
young adults, is traditionally considered to be caused by
demyelination in white matter (WM); however, the role of
gray matter (GM) is becoming increasingly prominent.
Although described in anatomopathological studies over a
century ago [1], cortical pathology only recently returned
to the spotlight of MS research as a result of specialized
MRI sequences not used in clinical routine. With con-
ventional T2-weighted sequences, GM lesions are less
visible, but by nulling the signal from the CSF and WM,
double inversion recovery (DIR) allows better detection of
cortical lesions (CLs). Using this sequence, CLs have even
been reported to potentially precede demyelination of WM
[2–4], the neuroinflammatory [5] and neurodegenerative
[6] processes that characterize all MS phenotypes and
occur early in the disease [7]. However, controversy re-
mains about whether DIR should be adopted in MS clin-
ical routine [8–10]. Other specialized sequences such as
phase-sensitive inversion recovery (PSIR) have been
shown to offer improvements over DIR in evaluating
cortical pathology and offer complementary information
[11–13].
Recent studies indicate an association of CL with clin-
ical and cognitive impairment [14–19] in relapsing–
remitting (RRMS) and progressive MS patients. The aim of
this study was to evaluate the frequency and clinical impact
of CLs in patients early in the disease. To ensure an ac-
curate determination of CL load, we independently
A. Groger and F. Zipp contributed equally.
& Frauke Zipp
1 Department of Neurology, Neuroimaging Center (NIC) of the
Focus Program Translational Neuroscience (FTN),
University Medical Center of the Johannes Gutenberg-
University Mainz, Langenbeckstraße 1, 55131 Mainz,
Germany
2 Institute of Neuroradiology, University Medical Center of the
Johannes Gutenberg-University Mainz, Mainz, Germany
123
J Neurol
DOI 10.1007/s00415-015-7724-5

assessed both 3D DIR and 3D fluid-attenuated inversion
recovery (FLAIR) sequences, considering that they provide
complementary information [13, 20, 21] and were both
available as part of our standard MRI protocol for MS. This
was performed for a large cohort of CIS and early RRMS
patients and the results were then correlated against clinical
and cognitive measures.
Materials and methods
Patients
This retrospective, single-center analysis was performed on
122 patients (29 CIS, 93 RRMS) diagnosed using the
McDonald criteria [22] with a median age of 32 years
(18–63 years), female/male ratio of 2.3, median disease
duration of 1.7 years (0–5 years), median number of re-
lapses (NOR) of 2 (1–6) and median Expanded Disability
Status Scale (EDSS) [23] of 1.0 (0–4.0). At the time of
MRI, 37 patients were being treated with interferon-beta
(IFNb), 21 with glatiramer acetate (GA), 4 with oral im-
munomodulating drugs [teriflunomide (TF) or dimethyl
fumarate (DF)], 15 with monthly natalizumab infusions
(NA) and 45 subjects were not being treated (NT). Nine of
the 29 CIS patients converted to RRMS within 2 years of
diagnosis. Patients with a disease duration exceeding
5 years were not included to establish a cohort of early MS
patients. Other exclusion criteria were being under
18 years of age or having a chronic progressive form of
MS (SPMS, PPMS). Detailed demographic data are shown
in Table 1.
Table 1 Demographic data Variable Total (n = 122) CIS (n = 29) RRMS (n = 93) p value
Gender
Female (n) 85 18 67 0.308c
Male (n) 37 11 26 0.308c
Disease type
CIS (n) 29 – – –
RRMS (n) 93 – – –
Age (years)
Median (range) 31.75 (18–63) 32.50 (19–56) 30.50 (18–63) 0.691b
EDSS
Median (range) 1.0 (0.0–4.0) 1.0 (0.0–3.0) 1.5 (0.0–4.0) 0.389b
NOR
Median (range) 2 (1–6) 1 2 (1–6) \0.0001b,*
DD (years)
Median (range) 1.65 (0.00–5.00) 0.60 (0.00–4.00) 2.00 (0.00–5.00) \0.0001b,*
LV (ml)
Median (range) 1.82 (0.00–45.36) 1.27 (0.10–19.47) 2.05 (0.00–45.36) 0.127b
GMF
Mean ± SD 0.44 ± 0.03 0.44 ± 0.03 0.44 ± 0.03 0.837a
Therapy
Interferon-beta 37 9 28 0.924c
Glatiramer acetate 21 3 18 0.262c
Teriflunomide 2 1 1 0.380c
Dimethyl fumarate 2 0 2 0.426c
Natalizumab 15 0 15 0.026c,*
Other/none 45 16 29 0.019c,*
CIS clinically isolated syndrome, RRMS relapsing–remitting multiple sclerosis, GA? group of subjects
treated with glatiramer acetate, GA- group of subjects not treated with glatiramer acetate, CL? group with
cortical lesions, CL- group without cortical lesions, EDSS Expanded Disability Status Scale, DD disease
duration, NOR number of relapses, LV lesion volume, GMF gray matter fraction
* Statistically significanta Derived from t testb Derived from Mann–Whitney U testc Derived from Chi-square test
J Neurol
123

All patients gave their written informed consent to ex-
aminations before participating in this study, which was
approved by the local ethics committee and adhered to
institutional guidelines in accordance with the Declaration
of Helsinki.
For a subgroup of 66 of the patients, we also had results
from neuropsychological testing, including measurements
of information processing speed [Symbol Digit Modality
Test (SDMT), Trail Making Test (TMT-A)], working
memory [Paced Auditory Serial Addition Test (PASAT)],
visual short-term memory [block span of the Wechsler
Memory Scale-Revised (WMS-R)], learning and memory
[Verbal Learning and Memory Test (VLMT), with
VLMT_verbal for verbal learning, VLMT_global for
global learning and VLMT_longterm for longterm learning
capacity], alertness [Tests of Attentional Performance
(TAP)––subtest Alertness], cognitive flexibility (TMT-B)
and word fluency [Regensburger Word Fluency Test
(RWT), with RWT_lexical for lexical word fluency and
RWT_semantical for semantical word fluency]. Neu-
ropsychological data are given as z-scores.
MR image acquisition
All patients underwent an MRI examination. Measure-
ments were performed on a 3T MR scanner (Magnetom
Tim Trio, Siemens Healthcare, Erlangen, Germany) with a
32-channel head coil. The following sequences were used:
1. Sagittal 3D fluid-attenuated inversion recovery
(FLAIR): repetition time (TR) = 5000 ms, echo time
(TE) = 388 ms, inversion time (TI) = 1800 ms, turbo
factor = 141, echo train length = 848 ms, field of
view (FOV) = 256 9 256 mm2, matrix size = 256 9
256, slab thickness = 192 mm, voxel size = 1 9 1 9
1 mm3, optimized variable flip angle, band-
width = 781 Hz/Px.
2. Sagittal 3D double inversion recovery (DIR): repeti-
tion time (TR) = 7500 ms, echo time (TE) = 307 ms,
inversion time (TI) = 3000 ms, turbo factor = 216,
echo train length = 657 ms, field of view (FOV) =
256 9 256 mm2, matrix size = 256 9 256, slab
thickness = 192 mm, voxel size = 1 9 1 9 1 mm3,
optimized variable flip angle, bandwidth = 781 Hz/
Px.
3. Sagittal 3D T1-weighted magnetization prepared rapid
gradient echo (MP-RAGE): repetition time
(TR) = 1900 ms, echo time (TE) = 2.52 ms, inver-
sion time (TI) = 900 ms, field of view (FOV) =
256 9 256 mm2, matrix size = 256 9 256, slab
thickness = 192 mm, voxel size = 1 9 1 9 1 mm3,
flip angle = 9�, bandwidth = 170 Hz/Px.
Image analysis and group definition
Given that the sensitivity and specificity of DIR are low
[11, 21, 24, 25] (signal intensity variations or vessel hy-
perintensities) and possible misinterpretation is common if
used alone without other confirmatory sequences [21], we
used a second T2-weighted MR sequence, in this case 3D-
FLAIR, to confirm the presence of lesions. FLAIR se-
quences are well established in clinical practice for the
diagnosis of MS and T2-weighted sequences are included
in the revised McDonald criteria [22]. DIR and FLAIR
were viewed (in groups and several days apart to avoid any
bias) by two raters with respect to CL load, blinded to the
outcome of the other sequence and the clinical features of
the patients.
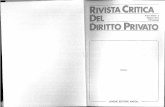
For scoring, both raters followed the international
criteria proposed by Geurts et al. [21]. CLs were classi-
fied by their topographic location (infra- and supratento-
rial lesions) (Fig. 1c) and their relation to the cortical
band (purely intracortical lesions or mixed white–gray
matter lesions). Intracortical lesions were confined ex-
clusively to the cortical ribbon, and did not encompass
any subcortical WM (Fig. 1a, b); mixed cortical lesions
were defined as lesions that overlap both the cortical
ribbon and the WM (Fig. 1d). Patients were positively
scored for CL (CL?) if both raters identified lesions in
both scans, and otherwise negatively scored (CL-). The
number of patients with CLs as well as the total number
of CLs was counted.
MRI post-processing
For lesion and tissue segmentation, the statistical parameter
mapping (SPM8) software (http://www.fil.ion.ucl.ac.uk/
spm) with lesion segmentation toolbox (LST) (http://www.
applied-statistics.de/lst.html) and VBM8 toolbox (http://
dbm.neuro.uni-jena.de/vbm/) was used.
First, using LST, 3D FLAIR images were co-registered
to 3D MP-RAGE images and bias corrected. After partial
volume estimate (PVE) label estimation, lesion segmenta-
tion was performed with an optimal threshold value
(j = 0.1) for the lesion growth algorithm [26]. Subse-
quently, the filled MP-RAGE images were segmented into
GM, WM, and cerebrospinal fluid (CSF). With regard to
measuring brain atrophy [27, 28], GM results were asses-
sed as fractions of total brain volume.
Statistics
Statistical analysis was performed using SPSS Statistics,
Version 22.0 (IBM, Chicago, Illinois, United States of
America). The Kolmogorov–Smirnov test was used to
J Neurol
123

verify a normal distribution of data. Means with standard
deviations (SD) as well as medians with ranges were cal-
culated. Between-group differences of demographic and
MRI features were evaluated with the t test, Mann–Whit-
ney U test and Chi-square test, respectively. The Spearman
rank and Pearson correlation tests were used to determine
correlations between the variables. The significance level
was set to p \ 0.05.
Results
Using DIR images, we identified 27 patients with C1 CL,
representing 22.1 % of our cohort. In total, 60 CL (16 in-
tracortical, 44 mixed lesions) were counted (Table 2).
After using FLAIR images, we confirmed the 27 subjects
with CLs. However, only 51 lesions were counted, of
which 13 were purely intracortical and 38 mixed CLs.
These 27 patients were defined as the group positively
scored for CLs (CL?).
We detected most CLs in supratentorial GM, with 49
CLs in DIR (35 mixed and 14 intracortical) and 41 CLs in
FLAIR (32 mixed and 9 intracortical). In infratentorial
GM, DIR and FLAIR images revealed a similar number of
CLs (11 and 10, respectively) (Table 2). Altogether, with
FLAIR images we were able to detect 85 % of the CLs
seen in DIR.
Clinical data (disease duration, number of relapses,
EDSS, gender and comorbidities) as well as GMF and LV
did not differ between CL? and CL- (Table 1). We found
clear differences between the number of patients with and
without CLs being treated with GA (p = 0.035) and also
between those with the CIS phenotype (p = 0.006). Fur-
ther, the number of CLs (counted in DIR or in FLAIR
images) did not correlate with these clinical and MRI data
(Table 3).
Fig. 1 Examples of cortical
lesions. a Intracortical lesion
(DIR left, FLAIR right). b U-
shaped cortical lesion in DIR
(sagittal view left, axial view
right). c Infratentorial cortical
lesion (DIR left, FLAIR right).
d Mixed gray–white matter
lesion in DIR
J Neurol
123

Ta
ble
2C
ort
ical
lesi
on
sco
rin
g:
freq
uen
cyo
fco
rtic
alle
sio
ns
inea
rly
ph
ase
of
the
dis
ease
Cla
ssifi
cati
on
DIR
scre
enin
gA
fter
inte
r-re
ader
con
firm
atio
n(F
LA
IRan
dD
IR)
To
tal
(n=
12
2)
CIS
(n=
29
)
RR
MS
(n=
93
)
pv
alu
ea,c
GA
?
(n=
21
)
GA
-
(n=
10
1)
pv
alu
ea,d
To
tal
(n=
12
2)
CIS
(n=
29
)
RR
MS
(n=
93
)
pv
alu
ea,c
GA
?
(n=
21
)
GA
-
(n=
10
1)
pv
alu
ea,d
Les
ion
count
(num
ber
of
CL
)
ST
mix
edC
L35
629
0.3
99
035
0.0
32*
32
230
0.0
53
032
0.0
38*
ST
intr
acort
ical
CL
14
311
0.7
81
113
0.5
12
91
80.3
56
09
0.1
57
ITm
ixed
CL
91
80.6
71
09
0.2
54
60
60.4
28
06
0.5
17
ITin
trac
ort
ical
CL
20
20.4
28
11
0.2
17
40
30.2
58
13
0.6
76
Tota
lle
sion
count
60
10
50
0.2
51
258
0.0
99
51
348
0.0
07*
150
0.0
33*
Cla
ssifi
cati
on
DIR
scre
enin
gA
fter
inte
r-re
ader
con
firm
atio
n(F
LA
IRan
dD
IR)
To
tal
(n=
12
2)
CIS
(n=
29
)
RR
MS
(n=
93
)
pv
alu
eb,c
GA
?
(n=
21
)
GA
-
(n=
10
1)
pv
alu
eb,d
To
tal
(n=
12
2)
CIS
(n=
29
)
RR
MS
(n=
93
)
pv
alu
eb,d
GA
?
(n=
21
)
GA
-
(n=
10
1)
pv
alu
eb,d
Subje
ctco
unt
(num
ber
of
subje
cts
wit
hC
1C
L)
ST
mix
edC
L19
316
0.3
74
c0
19
0.0
31
c, *
18
117
0.0
49
c, *
018
0.0
36
c, *
ST
intr
acort
ical
CL
10
28
0.7
70
c1
90.5
28
c9
18
0.3
54
c0
90.1
55
c
ITm
ixed
CL
61
50.6
75
c0
60.2
52
c2
02
0.4
26
c0
30.5
16
c
ITin
trac
ort
ical
CL
20
20.4
26
c1
10.2
16
c4
04
0.2
56
c1
20.6
75
c
Tota
lsu
bje
ctco
unt
27
423
0.2
15
c2
25
0.1
26
c27
126
0.0
06
c, *
126
0.0
35
c, *
CIS
clin
ical
lyis
ola
ted
syn
dro
me,
RR
MS
rela
psi
ng
–re
mit
tin
gm
ult
iple
scle
rosi
s,G
A?
gro
up
of
sub
ject
str
eate
dw
ith
gla
tira
mer
acet
ate,
GA
-g
rou
po
fsu
bje
cts
no
ttr
eate
dw
ith
gla
tira
mer
acet
ate,
CL
cort
ical
lesi
on
,S
Tsu
pra
ten
tori
al,
ITin
frat
ento
rial
*S
tati
stic
ally
sig
nifi
can
ta
Der
ived
fro
mS
pea
rman
ran
kte
stb
Der
ived
fro
mC
hi-
squ
are
test
cS
tati
stic
alsi
gn
ifica
nce
eval
uat
ion
for
com
par
iso
nb
etw
een
ph
eno
typ
ed
Sta
tist
ical
sig
nifi
can
ceev
alu
atio
nfo
rco
mp
aris
on
bet
wee
ntr
eatm
ent
typ
e
J Neurol
123

Table 3 Group comparison (CL? vs CL-): clinical impact of cortical lesions in early phase of the disease
Variable CL? (n = 27) CL- (n = 95) p value Correlation with number of CL
in CL? group
p value
Gender
Female (n) 16 69 0.182c
Male (n) 11 26 0.182c
Disease type
CIS (n) 1 28 0.006c,*
RRMS (n) 26 67 0.006c,*
Age (years)
Median (range) 32.90 (19–63) 31.10 (18–63) 0.953b
EDSS
Median (range) 1.0 (0.0–3.5) 1.5 (0.0–4.0) 0.227b -0.301 0.127
NOR
Median (range) 2 (1–6) 1 (1–5) \0.0001b,* -0.163 0.416
DD (years)
Median (range) 2.00 (0.00–5.00) 1.60 (0.00–5.00) 0.269b 0.312 0.114
LV (ml)
Median (range) 2.05 (0.24–32.99) 1.66 (0.00–45.36) 0.246b 0.133 0.509
GMF
Mean ± SD 0.45 ± 0.04 0.44 ± 0.03 0.805a 0.038 0.850
Therapy
Interferon-beta 10 27 0.390c
Glatiramer acetate 1 20 0.035c,*
Teriflunomide 0 2 0.447c
Dimethyl fumarate 1 1 0.338c
Natalizumab 4 11 0.651c
Other/none 11 34 0.638c
Cognitive tests (n = 66) CL? (n = 18) CL- (n = 46) p value Correlation with number of CL p value
TAP
Mean ± SD, n 0.09 ± 0.59, 18 0.00 ± 0.90, 46 0.647a 0.085 0.738
SDMT
Mean ± SD, n -0.61 ± 1.33, 18 -0.19 ± 1.03, 45 0.268a 0.462 0.054
PASAT
Median (range), n -0.17 (-3.00 to 1.31), 18 -0.14 (-3.00 to 1.31), 46 0.321b 0.495 0.037*
WMS-R
Median (range), n 0.15 (-1.30 to 1.50), 18 0.20 (-2.00 to 2.40), 44 0.950b 0.096 0.706
VLMT_verbal
Median (range), n -0.37 (-2.23 to 1.99), 18 0.12 (-1.62 to 2.23), 45 0.062b 0.294 0.236
VLMT_global
Mean ± SD, n -0.21 ± 0.99, 18 0.18 ± 0.90, 45 0.140a 0.134 0.597
VLMT_longterm
Median (range), n -0.34 (-4.57 to 0.83), 18 0.23 (-2.57 to 1.43), 45 0.088b 0.209 0.406
TMT_A
Median (range), n -0.48 (-2.50 to 2.20), 18 -0.23 (-11.11 to 1.63), 46 0.585b 0.310 0.210
TMT_B
Median (range), n -0.10 (-2.50 to 1.20), 18 0.16 (-3.00 to 2.30), 46 0.988b 0.165 0.514
J Neurol
123

In the subgroup of 66 patients (18 CL? and 48 CL-) for
whom we had neuropsychological test results, all z-scores
were in the same range as those of healthy controls, indi-
cating that there was no cognitive impairment. No differ-
ences between the CL? and CL- groups were found in the
results of the cognitive tests (Table 1). In the CL? group, a
significant correlation was found between the total number
of CLs in FLAIR and the RWT semantic word fluency
(p = 0.035), as well as with the PASAT working memory
(p = 0.037) (Table 3).
Discussion
Patient-based studies with the goal of translating ex-
perimental findings to the clinic are necessary to advance
the understanding and treatment of multiple sclerosis [29].
Among other challenges facing research of this disease is
that the meaning and processes of neuronal compartment
pathology are still not fully understood [30]. One approach
to address this gap in our knowledge is to employ MRI
sequences such as DIR that are not routinely used in
clinical practice to unravel the overall role of GM pathol-
ogy in the disease [31]. CLs are difficult to detect, but have
been reported to be associated with disability and a more
severe disease course [32]. Studies have shown that CLs
are present in early stages of MS [2], but that their im-
portance increases with disease progression (EDSS) [15].
However, both the frequency and specific role of these
lesions are still under debate. These studies have focused
on small or rather heterogeneous cohorts, including various
disease phenotypes and patients across the whole course of
the disease. Our study aimed to evaluate the frequency and
clinical impact of CLs in a large disease cohort consisting
of only RRMS and CIS patients in very early stages of the
disease, namely less than 5-year disease duration.
The most common type of CL is located on the subpial
layer of the cortex [33, 34] and often can only be seen
postmortem or with magnetic field strengths greater than
3T [13]. Also, different MR sequences can affect the
identification of lesions, with some juxtacortical lesions
assigned in FLAIR images being interpreted as mixed GM/
WM lesions in DIR due to poor definition of lesion
boundaries [11] (Fig. 2). Artifacts due to magnetic field
inhomogeneities or vessel hyperintensities are further
causes of misinterpretation. Additionally, even when fol-
lowing the international recommendations on lesion scor-
ing, an agreement of only 19 % of the CLs scored was
reached between experts [21], so that DIR, despite its
sensitivity for CL scoring, may have a rather low speci-
ficity. To ensure reliable findings [24, 25] and to minimize
any false positives resulting from artifacts in DIR images,
two blinded readers viewed both 3D DIR and 3D FLAIR
images to assess them for the presence of CLs; only in
cases where the readers were in consensus were the pa-
tients defined as having CLs. The use of additional T2- or
T1-weighted MRI sequences to classify a cortical lesion
[13, 35] follows current recommendations [21] and has also
been discussed recently in smaller studies [36].
In 122 patients (93 RRMS, 29 CIS) with a median dis-
ease duration of 1.5 years, we detected CLs in 22.1 % of
the patients (28.0 % RRMS, 3.4 % CIS). We did not find
major clinical differences between patients with and
without cortical lesions, suggesting that these lesions may
be less frequent in early stages of RRMS than previously
thought [15, 17, 32]. In the neuropsychological analysis
Table 3 continued
Cognitive tests (n = 66) CL? (n = 18) CL- (n = 46) p value Correlation with number of CL p value
RWT_lexical
Median (range), n -0.15 (-2.50 to 1.50), 18 0.25 (-1.60 to 1.60), 44 0.629b 0.233 0.352
RWT_semantical
Mean ± SD, n -0.43 ± 1.03, 17 -0.32 ± 0.90, 41 0.678a 0.514 0.035*
CIS clinically isolated syndrome, RRMS relapsing–remitting multiple sclerosis, GA ? group of subjects treated with glatiramer acetate, GA -
group of subjects not treated with glatiramer acetate, CL ? group with cortical lesions, CL - group without cortical lesions, EDSS Expanded
Disability Status Scale, DD disease duration, NOR number of relapses, LV lesion volume, GMF gray matter fraction, TAP tests of attentional
performance, SDMT Symbol Digit Modality Test for information processing speed, PASAT Paced Auditory Serial Addition Test, WMS-
R Wechsler Memory Scale-Revised, VLMT_verbal Verbal Learning and Memory Test for verbal learning, VLMT_global Verbal Learning and
Memory Test for global learning, VLMT_longterm Verbal Learning and Memory Test for longterm learning capacity, TMT_A Trail Making Test
for information processing speed, TMT_B Trail Making Test for cognitive flexibility, RWT_lexical Regensburger Word Fluency Test for lexical
word fluency, RWT_semantical Regensburger Word Fluency Test for semantical word fluency
* Statistically significanta Derived from t testb Derived from Mann–Whitney U testc Derived from Chi-square test
J Neurol
123

performed on a subgroup of 66 patients, we found a cor-
relation between the number of CLs and the semantic word
fluency (RWT), as well as working memory (PASAT),
suggesting that GM pathology in MS starts with structural
or functional alterations in the left frontal lobe of the brain.
In a study on CL and WM lesions in a pediatric form of MS
[37], investigators found that CL volume and GM volume
were the same in both cognitively impaired and cognitively
preserved children, but that WM volume was significantly
decreased in patients with cognitive deficits. However, in
recent studies on adults with MS [17, 18], GM pathology
[38] has been associated with a bad cognitive outcome,
which is in agreement with our findings.
Interestingly, we note that fewer subjects treated with
GA were scored positively for CL and had a lower CL
count than those receiving other therapies. However, fur-
ther studies with more subjects must be performed to
conclude whether this finding might be of significance.
In contrast to earlier studies, we observed fewer CLs
than expected. Calabrese et al. [14] reported that 64 % of
RRMS patients with a disease duration up to 13 years
(mean disease duration of 5 years) and mean EDSS of 2
exhibited CLs as identified by 1.5T MRI, and 36 % of CIS
patients with mean disease duration of 0.8 years and EDSS
of 1.2 (up to 3.5). We found only 28 % of patients had CLs
in the RRMS group with a median disease duration of less
than 2 years and not exceeding 5 years and identified only
3 % having CLs in our group of CIS patients, whose dis-
ease duration did not exceed 4 years. These differences
could be due to the shorter disease duration of our cohort as
well as the different methodologies employed (2D FLAIR
and 2D DIR at 1.5T versus 3D FLAIR and 3D DIR at 3T;
different voxel size).
Based on the results presented here, we agree with
Chard et al. [9].that the identification of CLs with DIR is
not yet suitable to allow clear-cut conclusions concerning
disease severity or overall ‘‘neurodegeneration’’ in clinical
practice.
Although the use of DIR is relatively widespread, this
study shows that it remains of limited value in the de-
tection of CLs in MS. This finding is in line with other
studies [11, 24, 25] and the current recommendations
[21], which specify that DIR should be used with other
T1- or T2-weighted MRI sequences to assure reliable
findings. 3D FLAIR at 3T has a similar contrast for
cortical lesions and a higher signal-to-noise ratio than
DIR. Furthermore, DIR is very time consuming and has a
high specific absorption rate. Therefore, for high-field
MRI, it seems that 3D-FLAIR might be the best sequence
to study cortical pathology lesion [13, 35]. The more
recently used PSIR sequence permits better detection of
CLs than DIR, which may further make the utility of DIR
sequences less relevant [11, 12]. Although it has been
previously reported that the number of CLs increases over
time and that there is an association with disability in MS,
in our early cohort we found no correlation between CLs
and EDSS or NOR. However, a correlation was found
between the number of CLs and changes in cognitive
function in word fluency and working memory, suggest-
ing that cognitive functions are the first to be altered by
GM pathology. Furthermore, a recent report on RIS pa-
tients identified 40 % as having CLs using DIR [39],
which in light of the difference we observed between CIS
and RRMS CL frequency must be interpreted either as a
different underlying pathology or erroneous CL identifi-
cation using DIR images alone.
A limitation of our study is the cross-sectional design as
well as detailed neuropsychological testing being available
for only a subgroup of patients. Further prospective in-
vestigations focusing on early phase MS patients including
a detailed analysis of the lesion distribution should increase
our knowledge of the early disease.
In conclusion, using 3D DIR and 3D FLAIR images in
CIS and RRMS, we present evidence that CLs, although
already present, are less common in early phases of the
disease than previously expected. Despite a clear difference
between CIS and MS, no relation with other parameters
such as GMF, which characterizes the neuronal compart-
ment, or with disease severity was detected at this early
disease stage, indicating that the presence and number of
CLs may not be a relevant indicator of early neurodegen-
eration in MS.
Fig. 2 Juxtacortical lesion
scored as a mixed gray–white
matter lesion. The DIR image is
shown in the left panel and the
FLAIR in the right
J Neurol
123

Acknowledgments F.Z. is grateful for financial support from the
German Multiple Sclerosis Competence Network (KKNMS, Project
B7.3) funded by the Federal Ministry for Education and Research
(BMBF).
Conflicts of interest Pierre Kolber reports no conflicts of interest
and financial disclosures. Swantje Montag reports no conflicts of in-
terest and financial disclosures. Dr. Vinzenz Fleischer reports no
conflicts of interest and financial disclosures. Dr. Felix Lussi reports
no conflicts of interest and financial disclosures. Janine Wilting re-
ports no conflicts of interest and financial disclosures. Dr. Joachim
Gawehn reports no conflicts of interest and financial disclosures. Dr.
Adriane Groger reports no conflicts of interest and financial disclo-
sures. Dr. Frauke Zipp has received research grants from Teva, Merck
Serono, Novartis and Bayer as well as consultation funds from Teva,
Merck Serono, Novartis, Bayer Healthcare, Biogen Idec Germany,
ONO, Genzyme, Sanofi-Aventis and Octapharma. Her travel com-
pensation has been provided for by the aforementioned companies.
Ethical standard All patients gave their written informed consent
to examinations before participating in this study, which was ap-
proved by the local ethics committee and adhered to institutional
guidelines in accordance with the Declaration of Helsinki.
References
1. Sander M (1898) Hirnrindenbefunde bei multipler Sklerose.
Monatschrift Psychiatrie Neurol IV:427–436
2. Calabrese M, Gallo P (2009) Magnetic resonance evidence of
cortical onset of multiple sclerosis. Mult Scler 15:933–941
3. Coebergh JA, Roosendaal SD, Polman CH, Geurts JJ, van Wo-
erkom TC (2010) Acute severe memory impairment as a pre-
senting symptom of multiple sclerosis: a clinical case study
with 3D double inversion recovery MR imaging. Mult Scler
16:1521–1524
4. Popescu BF, Bunyan RF, Parisi JE, Ransohoff RM, Lucchinetti
CF (2011) A case of multiple sclerosis presenting with inflam-
matory cortical demyelination. Neurology 76:1705–1710
5. Lucchinetti CF, Popescu BF, Bunyan RF, Moll NM, Roemer SF,
Lassmann H, Bruck W, Parisi JE, Scheithauer BW, Giannini C,
Weigand SD, Mandrekar J, Ransohoff RM (2011) Inflammatory
cortical demyelination in early multiple sclerosis. N Engl J Med
365:2188–2197
6. Bo L, Vedeler CA, Nyland H, Trapp BD, Mork SJ (2003) In-
tracortical multiple sclerosis lesions are not associated with in-
creased lymphocyte infiltration. Mult Scler 9:323–331
7. Kutzelnigg A, Lucchinetti CF, Stadelmann C, Bruck W,
Rauschka H, Bergmann M, Schmidbauer M, Parisi JE, Lassmann
H (2005) Cortical demyelination and diffuse white matter injury
in multiple sclerosis. Brain 128:2705–2712
8. Calabrese M, De Stefano N (2014) Cortical lesion counts by
double inversion recovery should be part of the MRI monitoring
process for all MS patients: yes. Mult Scler 20:537–538
9. Chard D (2014) Cortical lesion counts by double inversion re-
covery should be part of the MRI monitoring process for all MS
patients: no. Mult Scler 20:539–540
10. Rovira A, Auger C (2014) Cortical lesion counts by double in-
version recovery should be part of the MRI monitoring process
for all MS patients: commentary. Mult Scler 20:541–542
11. Sethi V, Muhlert N, Ron M, Golay X, Wheeler-Kingshott CA,
Miller DH, Chard DT, Yousry TA (2013) MS cortical lesions on
DIR: not quite what they seem? PLoS One 8:e78879
12. Sethi V, Yousry TA, Muhlert N, Ron M, Golay X, Wheeler-
Kingshott C, Miller DH, Chard DT (2012) Improved detection of
cortical MS lesions with phase-sensitive inversion recovery MRI.
J Neurol Neurosurg Psychiatry 83:877–882
13. Tallantyre EC, Morgan PS, Dixon JE, Al-Radaideh A, Brookes
MJ, Morris PG, Evangelou N (2010) 3 Tesla and 7 Tesla MRI of
multiple sclerosis cortical lesions. J Magn Reson Imaging
32:971–977
14. Calabrese M, Agosta F, Rinaldi F, Mattisi I, Grossi P, Favaretto
A, Atzori M, Bernardi V, Barachino L, Rinaldi L, Perini P, Gallo
P, Filippi M (2009) Cortical lesions and atrophy associated with
cognitive impairment in relapsing–remitting multiple sclerosis.
Arch Neurol 66:1144–1150
15. Calabrese M, Poretto V, Favaretto A, Alessio S, Bernardi V,
Romualdi C, Rinaldi F, Perini P, Gallo P (2012) Cortical lesion
load associates with progression of disability in multiple sclero-
sis. Brain 135:2952–2961
16. Calabrese M, Rocca MA, Atzori M, Mattisi I, Bernardi V,
Favaretto A, Barachino L, Romualdi C, Rinaldi L, Perini P, Gallo
P, Filippi M (2009) Cortical lesions in primary progressive
multiple sclerosis: a 2-year longitudinal MR study. Neurology
72:1330–1336
17. Damasceno A, Damasceno BP, Cendes F (2014) The clinical
impact of cerebellar grey matter pathology in multiple sclerosis.
PLoS One 9:e96193
18. Papadopoulou A, Muller-Lenke N, Naegelin Y, Kalt G, Bendfeldt
K, Kuster P, Stoecklin M, Gass A, Sprenger T, Radue EW,
Kappos L, Penner IK (2013) Contribution of cortical and white
matter lesions to cognitive impairment in multiple sclerosis. Mult
Scler 19:1290–1296
19. Roosendaal SD, Moraal B, Pouwels PJ, Vrenken H, Castelijns JA,
Barkhof F, Geurts JJ (2009) Accumulation of cortical lesions in
MS: relation with cognitive impairment. Mult Scler 15:708–714
20. Geurts JJ, Pouwels PJ, Uitdehaag BM, Polman CH, Barkhof F,
Castelijns JA (2005) Intracortical lesions in multiple sclerosis:
improved detection with 3D double inversion-recovery MR
imaging. Radiology 236:254–260
21. Geurts JJ, Roosendaal SD, Calabrese M, Ciccarelli O, Agosta F,
Chard DT, Gass A, Huerga E, Moraal B, Pareto D, Rocca MA,
Wattjes MP, Yousry TA, Uitdehaag BM, Barkhof F (2011)
Consensus recommendations for MS cortical lesion scoring using
double inversion recovery MRI. Neurology 76:418–424
22. Polman CH, Reingold SC, Banwell B, Clanet M, Cohen JA,
Filippi M, Fujihara K, Havrdova E, Hutchinson M, Kappos L,
Lublin FD, Montalban X, O’Connor P, Sandberg-Wollheim M,
Thompson AJ, Waubant E, Weinshenker B, Wolinsky JS (2011)
Diagnostic criteria for multiple sclerosis: 2010 revisions to the
McDonald criteria. Ann Neurol 69:292–302
23. Kurtzke JF (1983) Rating neurologic impairment in multiple
sclerosis: an expanded disability status scale (EDSS). Neurology
33:1444–1452
24. Chen JT, Pirko I (2011) MS cortical lesion or not? Double in-
version recovery MRI reveals some answers and uncertainties.
Neurology 76:412–413
25. Simon B, Schmidt S, Lukas C, Gieseke J, Traber F, Knol DL,
Willinek WA, Geurts JJ, Schild HH, Barkhof F, Wattjes MP
(2010) Improved in vivo detection of cortical lesions in multiple
sclerosis using double inversion recovery MR imaging at 3 Tesla.
Eur Radiol 20:1675–1683
26. Schmidt P, Gaser C, Arsic M, Buck D, Forschler A, Berthele A,
Hoshi M, Ilg R, Schmid VJ, Zimmer C, Hemmer B, Muhlau M
(2012) An automated tool for detection of FLAIR-hyperin-
tense white-matter lesions in Multiple Sclerosis. Neuroimage
59:3774–3783
27. Chard DT, Parker GJ, Griffin CM, Thompson AJ, Miller DH
(2002) The reproducibility and sensitivity of brain tissue volume
measurements derived from an SPM-based segmentation
methodology. J Magn Reson Imaging 15:259–267
J Neurol
123

28. Rudick RA, Fisher E, Lee JC, Simon J, Jacobs L (1999) Use of
the brain parenchymal fraction to measure whole brain atrophy in
relapsing–remitting MS. Multiple Sclerosis Collaborative Re-
search Group. Neurology 53:1698–1704
29. Roep BO, Buckner J, Sawcer S, Toes R, Zipp F (2012) The
problems and promises of research into human immunology and
autoimmune disease. Nat Med 18:48–53
30. Siffrin V, Vogt J, Radbruch H, Nitsch R, Zipp F (2010) Multiple
sclerosis—candidate mechanisms underlying CNS atrophy.
Trends Neurosci 33:202–210
31. Zipp F, Gold R, Wiendl H (2013) Identification of inflammatory
neuronal injury and prevention of neuronal damage in multiple
sclerosis: hope for novel therapies? JAMA Neurol 70:1569–1574
32. Calabrese M, De Stefano N, Atzori M, Bernardi V, Mattisi I,
Barachino L, Morra A, Rinaldi L, Romualdi C, Perini P, Battistin
L, Gallo P (2007) Detection of cortical inflammatory lesions by
double inversion recovery magnetic resonance imaging in pa-
tients with multiple sclerosis. Arch Neurol 64:1416–1422
33. Bo L, Vedeler CA, Nyland HI, Trapp BD, Mork SJ (2003)
Subpial demyelination in the cerebral cortex of multiple sclerosis
patients. J Neuropathol Exp Neurol 62:723–732
34. Kutzelnigg A, Lassmann H (2005) Cortical lesions and brain
atrophy in MS. J Neurol Sci 233:55–59
35. Kilsdonk ID, de Graaf WL, Soriano AL, Zwanenburg JJ, Visser F,
Kuijer JP, Geurts JJ, Pouwels PJ, Polman CH, Castelijns JA, Lui-
jten PR, Barkhof F, Wattjes MP (2013) Multicontrast MR imaging
at 7T in multiple sclerosis: highest lesion detection in cortical gray
matter with 3D-FLAIR. Am J Neuroradiol 34:791–796
36. Vural G, Keklikoglu HD, Temel S, Deniz O, Ercan K (2013)
Comparison of double inversion recovery and conventional
magnetic resonance brain imaging in patients with multiple
sclerosis and relations with disease disability. Neuroradiol J
26:133–142
37. Rocca MA, De Meo E, Amato MP, Copetti M, Moiola L, Ghezzi
A, Veggiotti P, Capra R, Fiorino A, Pippolo L, Pera MC, Falini
A, Comi G, Filippi M (2014) Cognitive impairment in paediatric
multiple sclerosis patients is not related to cortical lesions. Mult
Scler
38. Rovaris M, Filippi M, Minicucci L, Iannucci G, Santuccio G,
Possa F, Comi G (2000) Cortical/subcortical disease burden and
cognitive impairment in patients with multiple sclerosis. Am J
Neuroradiol 21:402–408
39. Giorgio A, Stromillo ML, Rossi F, Battaglini M, Hakiki B,
Portaccio E, Federico A, Amato MP, De Stefano N (2011) Cor-
tical lesions in radiologically isolated syndrome. Neurology
77:1896–1899
J Neurol
123
Copyright © 2022 FDOKUMEN