ICOPE Physician Manual - WHO | World Health Organization
180
i Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of ICOPE Physician Manual - WHO | World Health Organization
i
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)

Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
ii
i
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
Integrated Care for Older People
A manual for primary care physicians(Facilitator’s Guide)

Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
ii
Title: Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
ISBN: 978-92-9022-754-0
© World Health Organization 2021
Some rights reserved. This work is available under the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 IGO licence (CC BY-NC-SA 3.0 IGO; https://creativecommons.org/licenses/by-nc-sa/3.0/igo).
Under the terms of this licence, you may copy, redistribute and adapt the work for non-commercial purposes, provided the work is appropriately cited, as indicated below. In any use of this work, there should be no suggestion that WHO endorses any specific organization, products or services. The use of the WHO logo is not permitted. If you adapt the work, then you must license your work under the same or equivalent Creative Commons licence. If you create a translation of this work, you should add the following disclaimer along with the suggested citation: “This translation was not created by the World Health Organization (WHO). WHO is not responsible for the content or accuracy of this translation. The original English edition shall be the binding and authentic edition”.
Any mediation relating to disputes arising under the licence shall be conducted in accordance with the mediation rules of the World Intellectual Property Organization (http://www.wipo.int/amc/en/mediation/rules/).
Suggested citation. Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide). New Delhi: World Health Organization, Regional Off ice for South-East Asia; 2021. Licence: CC BY-NC-SA 3.0 IGO.
Cataloguing-in-Publication (CIP) data. CIP data are available at http://apps.who.int/iris.
Sales, rights and licensing. To purchase WHO publications, see http://apps.who.int/bookorders. To submit requests for commercial use and queries on rights and licensing, see http://www.who.int/about/licensing.
Third-party materials. If you wish to reuse material from this work that is attributed to a third party, such as tables, figures or images, it is your responsibility to determine whether permission is needed for that reuse and to obtain permission from the copyright holder. The risk of claims resulting from infringement of any third-party-owned component in the work rests solely with the user.
General disclaimers. The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of WHO concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted and dashed lines on maps represent approximate border lines for which there may not yet be full agreement.
The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or recommended by WHO in preference to others of a similar nature that are not mentioned. Errors and omissions excepted, the names of proprietary products are distinguished by initial capital letters.
All reasonable precautions have been taken by WHO to verify the information contained in this publication. However, the published material is being distributed without warranty of any kind, either expressed or implied. The responsibility for the interpretation and use of the material lies with the reader. In no event shall WHO be liable for damages arising from its use.
Printed in India
iii
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
Foreword v
Background and objectives of the training programme vii
Part I: Planning and preparation 1
Section 1: Introduction to the training programme 3
Section 2: Designing the structure and content of the training programme 9
Section 3: Training methodologies 13
Section 4: Assessment of trainees 21
Section 5: Inviting participants and other contributors 25
Section 6: Planning for the training programme 27
Section 7: Evaluation methods for the training programme 29
Part II: Guidelines for conducting the individual modules 31
Session: Health of the older people and geriatric medicine 37
Session: Integrated care for older people (ICOPE) 38
Session: Functional assessment in older people 39
Session: ICOPE based screening of intrinsic capacities and functional status 40
Session: Health promotion and disease prevention in old age 43
Session: Cardiovascular system 45
Session: Respiratory system 46
Session: Endocrine system 47
Session: Hypertension and diabetes mellitus management in old age 48
Contents
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
iv
Session: Digestive system 50
Session: Musculoskeletal system 51
Session: ICOPE based locomotive capacity assessment and management 52
Session: Genitourinary system 56
Session: Neurological diseases of old age 57
Session: Brain ageing and cognitive impairment 58
Session: ICOPE-based cognitive capacity assessment and management 59
Mini-Cog - Cognitive assessment tool 61
Session: Mental health in old age 64
Session: ICOPE-based psychological capacity assessment and management 65
Session: Sensory system 68
Session: ICOPE-based sensory assessment and management 69
Session: Cancer and palliative care 72
Session: Elder abuse 73
Session: Long-term care and caregivers’ issues 74
Annexure 1: Sample questionnaire for pre- and post-training knowledge assessment 75
Annexure 2: ICOPE care pathways 81
Annexure 3: WHO simple eye chart 89
Annexure 4: PowerPoint presentation slides 91

v
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
Foreword
Populations across the WHO South-East Asia Region are ageing. Whereas in 2010 older people accounted for 8% of the Region’s population, by 2017 they accounted for 9.8%. This number will continue to rise, with older people expected to make up 13.7 percent of the population by 2030 – or 289 million people – and a significant 20.3% by 2050. Though the proportion of older people in the Region is projected to remain below global levels, the speed of the Region’s demographic transition is faster.
To ensure all older people can access quality health services, health workers must be equipped to provide dedicated care to older people. WHO’s 2021-2030 “Decade of Healthy Ageing” is clear: all countries must focus on ensuring the human resources necessary for integrated care. To do this, pre-service and in-service training for health workers, especially at the primary health care level, is crucial.
This manual is designed to help primary health care physicians in the Region provide the health services required for older people. The manual has 16 modules, each of them addressing a specific area of care. The contents are in line with the ICOPE (Integrated Care for Older People) approach to old age care, which proposes evidence-based recommendations for health care professionals to prevent, slow or reverse declines in the physical and mental capacities of older people.
By adopting and implementing the manual, policymakers and administrators will help ensure primary health care in the Region can meet the challenges of today and prepare for the challenges of tomorrow. WHO stands committed to supporting Member States in the Region as together we strive to achieve health for all at all ages.
Dr Poonam Khetrapal SinghRegional Director
WHO South-East Asia Region

Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
vi
vii
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
Background and objectives of the training programme
IntroductionThis manual is an instruction guide for facilitators to provide competence-based training to primary care physician (PCP) for integrated care of older people. The training is intended to assist the physician to learn and improve upon their skills to screen, assess as well as manage various physical, psychological as well as social aspects of old age care.
Facilitators are required to consult both the Facilitator’s Guide and the Trainee’s Manual while training participants through interactive presentations, group discussions, role plays etc. The Facilitator’s Guide contains detailed training methodologies, structure of the individual training sessions and guidelines for assessment of trainees. The Trainee’s Handbook contains diff erent modules to assist trainees with step-by-step learning of various aspects of old age care. Training resources are based on the “Integrated Care for Older People” (ICOPE) manual for primary care physicians which will be the primary reference book for trainees. Henceforth, the book will be referred to as WHO Guidance book (WGB) in this document. Facilitators should be conversant with the contents of the WHO Guidance book since all the modules in the Trainee’s Handbook are linked to the corresponding chapters and the practice sheets in the practice guidelines.
Overall aimThe overall aim is to orient PCP to the special characteristics of older people and to appropriate approaches to addressing their health needs and problems. This will strengthen the abilities of PCP to respond to older people more eff ectively and with greater sensitivity. It is expected that the training programme will significantly contribute to building national and regional capacity on older people health and development.
Training objectivesThe training module has been designed in a comprehensive manner to provide a holistic approach to short term human resource development with focus on in-service PCP, who provide care to older people in diff erent levels of health-care facilities. The information on old age care contained in these modules is meant to be incorporated into the everyday clinical practice of PCP. The training package will be useful for the knowledge as well as skill enhancement of the PCP. The training is expected to improve the approach to issues of old age and act as a
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
viii
stimulant for the holistic care of which will ultimately improve their quality of life. The objectives include both knowledge enhancement and skills development. After completion of the training, trainees will be able to:
» Perform screening of intrinsic capacity.
» Perform assessment of intrinsic capacity and functional status.
» Provide preventive, promotive, curative as well as rehabilitative services to the older people based on the available resources.
» Ensure appropriate follow-up of older people.
Knowledge-based objectivesBy the end of the training, trainees will be able to:
» Describe the important concepts in geriatrics and gerontology.
» Describe the alteration in pharmacological properties with ageing.
» Describe the physical, psychological as well as social aspects of ageing and their clinical implications.
» Management of common morbidities of old age comprehensively.
Skill-based objectivesBy the end of the training, trainees will be able to:
» Perform the screening as well as assessment of intrinsic capacities as well as functional status in older people.
» Provide preventive, promotive as well as rehabilitative services to older people presenting in primary care centres.
» Manage common morbidities of old age with the available resources.
» Manage the caregiver burden syndrome.
» Conduct follow-up of the older person after the management of morbidity.
» Provide counselling for appropriate referral.
Intended benefi ciariesThis manual is intended for the licensed physicians working in the primary health care facility, The training module has been designed in a comprehensive manner to provide a holistic approach to short term human resource development with focus on in-service physician, who provide care to older people in diff erent levels of health care facilities. The information on old age care
ix
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
contained in these modules is meant to be incorporated into the everyday clinical practice of physician. The training package will be useful for the knowledge as well as skill enhancement of the physician. The training is expected to improve the approach to old age health and act as a stimulant for the holistic care to enhance quality of life through an integrated plan.
Expected outcomesIt is expected that primary care physicians who participate in the training programme will:
» Become more knowledgeable about the characteristics of older people and of diff erent aspects of older people health and health related issues.
» Become more sensitive to the needs of older peoples.
» Be better equipped with facts and figures to argue for increased investment in older people health and development.
» Be better able to provide health services to older peoples that respond to their needs and are sensitive to their preferences.
» Have prepared a personal plan indicating the changes they will make in their work.
» The training programme is not intended to equip physicians with specific clinical or counselling skills in older people’s health care. In practical terms, it will provide participants with ideas and practical tips to two key questions:
» What do I as a primary care physician need to know and do diff erently if the older person who walks into my clinic is aged 60 years, rather than six or 36?
» How could I help other influential people in my community to understand and respond better to the needs and problems of older peoples?
Components of the Facilitator’s GuideThe training programme is designed to be implemented mainly in a programme context. It is intended to be a dynamic and interactive programme in which facilitators actively engage the participants in the teaching/learning process. A range of teaching and learning methods has been carefully selected to enable this to happen in an eff ective manner. This Facilitator’s Guide provides essential information to the organizers and facilitators to plan and implement the training programme.
Aims of the Facilitator’s Guide» To provide information on planning and preparing for the programme.
» To provide an overview of the teaching and learning methods used in the programme.
» To give detailed instructions for conducting individual modules.
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
x
Components of the Facilitator’s GuideThe guide consists of two parts:
» Part I. Planning and preparing
» Part II. Guidelines for conducting individual modules
Part I: Planning and preparingPart I is organized in seven sections as follows
Section I » Introduction: Provides an overview on the content of the programme
Section II» Designing the structure and content of the training programme and methodologies
Section III» Training methodologies
Section IV» Assessment of trainee
Section VInviting participants and other contributors: Provides suggestions on inviting the participants and other contributors to the training programme, with specific suggestions on:
» Drawing on the expertise of specialists
» Planning a formal opening ceremony
» Involving older peoples.
Section VI» Planning of the training programme
Section VIIEvaluation methods for a training programme, providing an overview of programme evaluation methods:
» To measure the participants’ reactions
» To measure changes in the participants’ knowledge
xi
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
» To measure changes in the participants’ practice
» Follow-up questionnaire
Part II: Guideline for conducting the individual module/ training programme Part II includes the module schedule and the “step-by-step instructions” to run each of the sessions. It also includes all the support materials needed to run the module, such as slides with accompanying talking points, flip charts and their contents, and case-study materials with notes on issues that they raise. Finally, it includes tips for you to help you respond to questions that may be raised by participants, identifies matters that may be sensitive and about how to deal with them.
Module 1: Integrated care for older people (ICOPE)
Module 2: Functional assessment of older adults
Module 3: Health promotion and disease prevention in old age
Module 4: Cardiovascular system
Module 5: Respiratory system
Module 6: Digestive system
Module 7: Endocrine system
Module 8: Musculoskeletal system
Module 9: Genitourinary system
Module 10: Neurological diseases of old age
Module 11: Brain ageing and cognitive impairment
Module 12: Mental health
Module 13: Sensory system
Module 14: Cancer and palliative care
Module 15: Elder abuse
Module 16: Long-term care and caregiver issues

Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
xii
1
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
Part I: Planning and preparation

Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
2
3
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
Introduction to the training programme
1SECTION
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
4
Contents of the training programmeThe training programme consists of core modules which have been developed according to the need; it is necessary for all participants in the training programme to go through the core modules. This is because they cover the essential topics that will equip the participants with the knowledge and understanding they need to achieve the overall aims of the Programme.
Trainee’s profi leThis training is intended for the physicians [completed undergraduate degree e.g. Bachelor of Medicine and Bachelor of Surgery (MBBS) or equivalent] working in the primary health care facility.
Facilitator’s profi leFacilitators should have adequate knowledge and skills in the concerned subjects. They should undergo training of trainers to be conversant with objectives, methodologies, session plans and the training materials. It is preferable that facilitators have training in training technology. They should be conversant with the management of medical issues of older adults in their respective countries/region. The facilitator should preferably be a geriatrician with a Master’s degree in geriatric medicine or an internist/general practitioner with some formal training in geriatric medicine.
Course coordinatorOne of the facilitators will be designated as course coordinator whose responsibilities will be as follows:
» check the audio-visual system for proper functioning
» check availability of all training aids
» ensure that sessions are conducted as per schedule
» introduce the course
» oversee administrative aspects including record maintenance
» check for general facilities like running water, washrooms, power back-up, refreshments etc.
» check functioning of all equipment
» check availability of adequate number of instruments and adequate number of consumables, including those required for simulation sessions.
Batch size of trainees and number of facilitatorsThe total number of trainees should be 25–30 per batch. The number of facilitators per batch should be at least four.
5
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
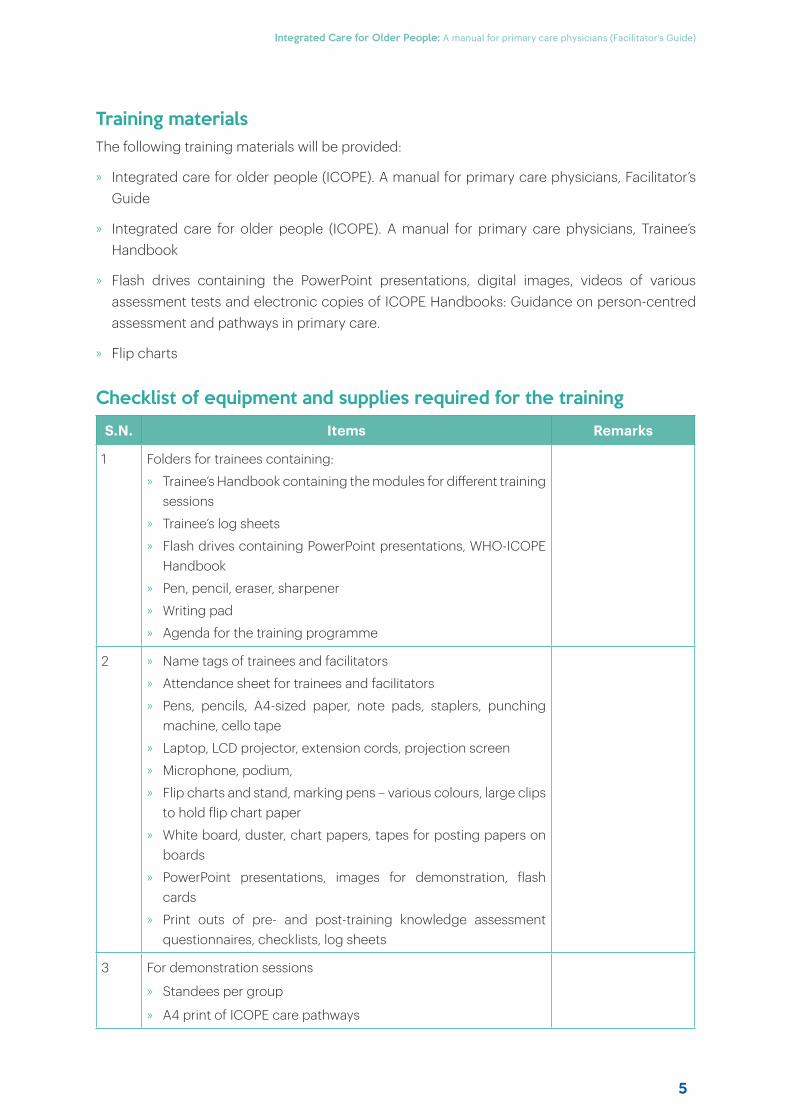
Training materialsThe following training materials will be provided:
» Integrated care for older people (ICOPE). A manual for primary care physicians, Facilitator’s Guide
» Integrated care for older people (ICOPE). A manual for primary care physicians, Trainee’s Handbook
» Flash drives containing the PowerPoint presentations, digital images, videos of various assessment tests and electronic copies of ICOPE Handbooks: Guidance on person-centred assessment and pathways in primary care.
» Flip charts
Checklist of equipment and supplies required for the training
S.N. Items Remarks
1 Folders for trainees containing:
» Trainee’s Handbook containing the modules for diff erent training sessions
» Trainee’s log sheets
» Flash drives containing PowerPoint presentations, WHO-ICOPE Handbook
» Pen, pencil, eraser, sharpener
» Writing pad
» Agenda for the training programme
2 » Name tags of trainees and facilitators
» Attendance sheet for trainees and facilitators
» Pens, pencils, A4-sized paper, note pads, staplers, punching machine, cello tape
» Laptop, LCD projector, extension cords, projection screen
» Microphone, podium,
» Flip charts and stand, marking pens – various colours, large clips to hold flip chart paper
» White board, duster, chart papers, tapes for posting papers on boards
» PowerPoint presentations, images for demonstration, flash cards
» Print outs of pre- and post-training knowledge assessment questionnaires, checklists, log sheets
3 For demonstration sessions
» Standees per group
» A4 print of ICOPE care pathways
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
6
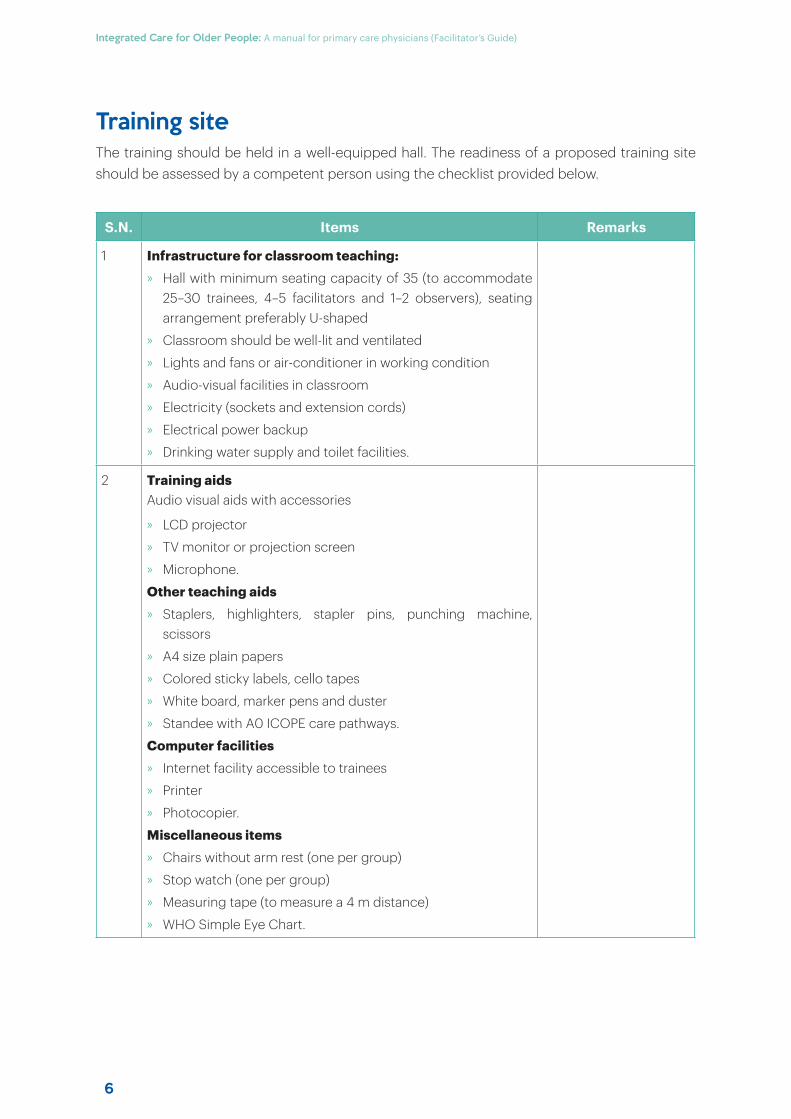
Training siteThe training should be held in a well-equipped hall. The readiness of a proposed training site should be assessed by a competent person using the checklist provided below.
S.N. Items Remarks
1 Infrastructure for classroom teaching:» Hall with minimum seating capacity of 35 (to accommodate
25–30 trainees, 4–5 facilitators and 1–2 observers), seating arrangement preferably U-shaped
» Classroom should be well-lit and ventilated
» Lights and fans or air-conditioner in working condition
» Audio-visual facilities in classroom
» Electricity (sockets and extension cords)
» Electrical power backup
» Drinking water supply and toilet facilities.
2 Training aidsAudio visual aids with accessories
» LCD projector
» TV monitor or projection screen
» Microphone.
Other teaching aids» Staplers, highlighters, stapler pins, punching machine,
scissors
» A4 size plain papers
» Colored sticky labels, cello tapes
» White board, marker pens and duster
» Standee with A0 ICOPE care pathways.
Computer facilities» Internet facility accessible to trainees
» Printer
» Photocopier.
Miscellaneous items» Chairs without arm rest (one per group)
» Stop watch (one per group)
» Measuring tape (to measure a 4 m distance)
» WHO Simple Eye Chart.
7
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
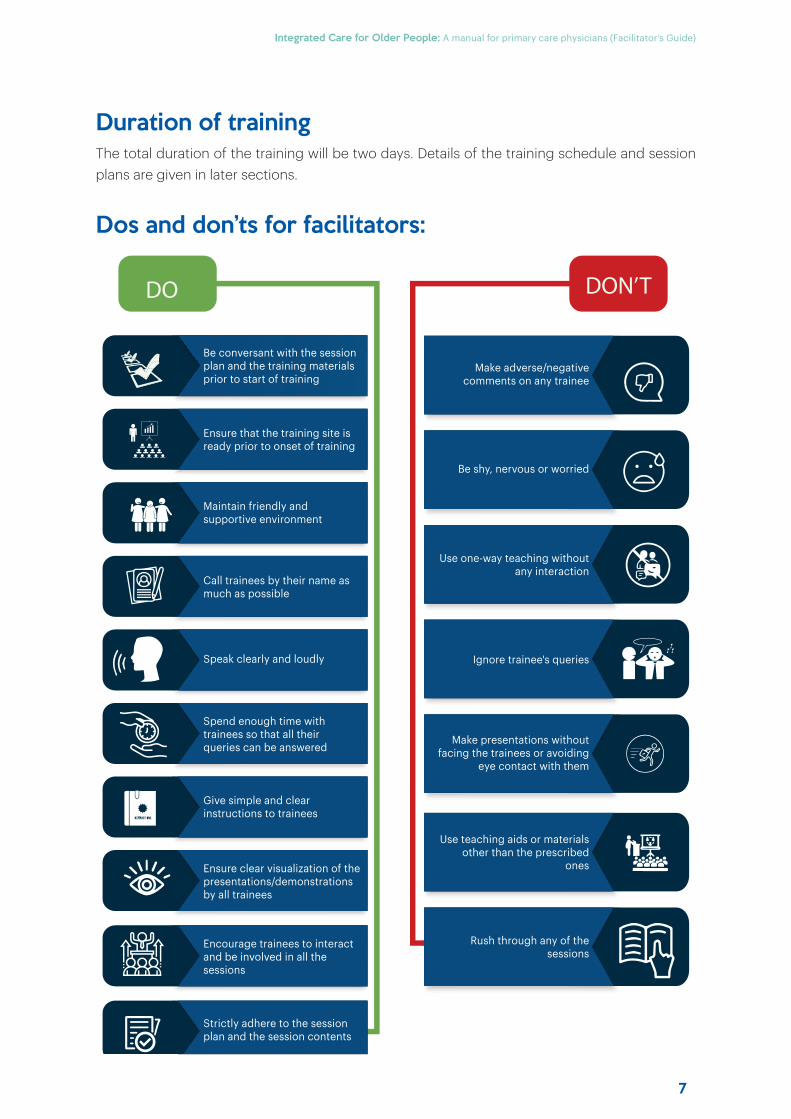
Duration of trainingThe total duration of the training will be two days. Details of the training schedule and session plans are given in later sections.
Dos and don’ts for facilitators:
DO DON’T
Be conversant with the session plan and the training materials prior to start of training
Make adverse/negative comments on any trainee
Be shy, nervous or worried
Use one-way teaching without any interaction
Make presentations without facing the trainees or avoiding
eye contact with them
Ensure that the training site is ready prior to onset of training
Maintain friendly and supportive environment
Call trainees by their name as much as possible
Speak clearly and loudly
Spend enough time with trainees so that all their queries can be answered
Give simple and clear instructions to trainees
Ensure clear visualization of the presentations/demonstrations by all trainees
Encourage trainees to interact and be involved in all the sessions
Strictly adhere to the session plan and the session contents
Use teaching aids or materials other than the prescribed
ones
Rush through any of the sessions
Ignore trainee's queries

Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
8
9
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
Designing the structure and content of the training programme
2SECTION
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
10
This section contains the information you will need for developing the content and structure of the programme. There is flexibility in the structure and duration of the programme, together with a choice of health issues/topics (optional modules) to include. Given this modular structure, it is possible to adapt the programme to any context.
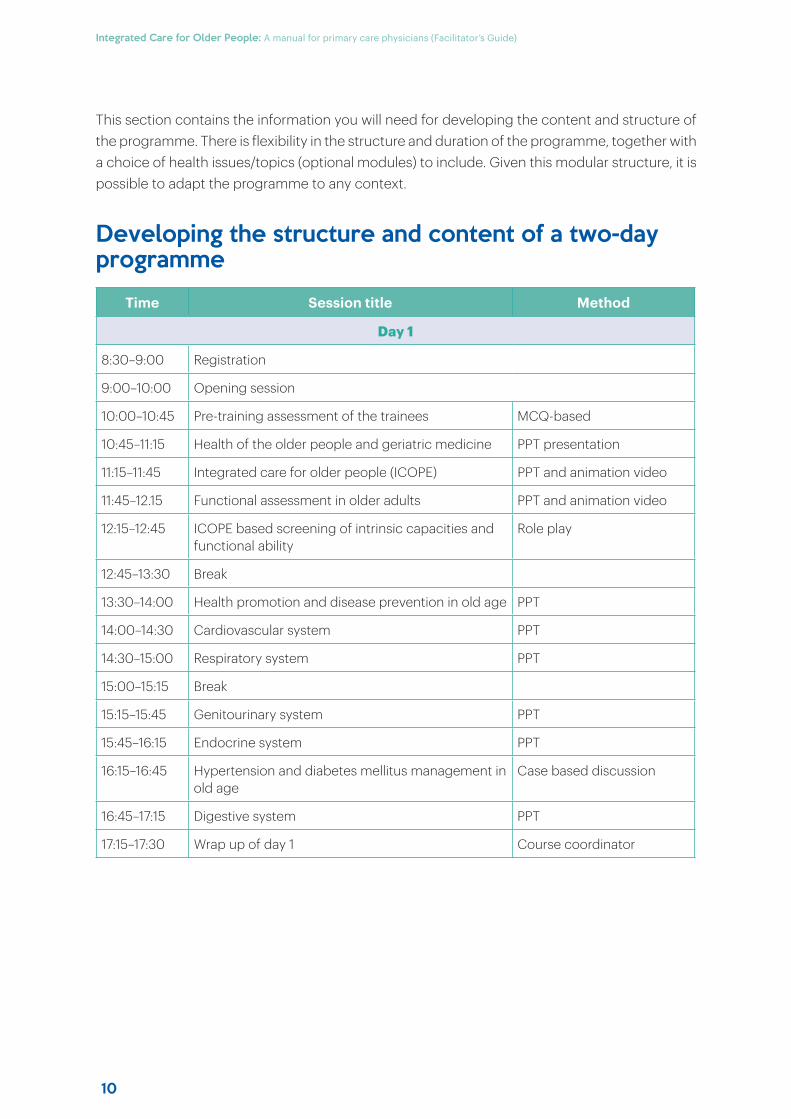
Developing the structure and content of a two-day programme
Time Session title Method
Day 1
8:30–9:00 Registration
9:00–10:00 Opening session
10:00–10:45 Pre-training assessment of the trainees MCQ-based
10:45–11:15 Health of the older people and geriatric medicine PPT presentation
11:15–11:45 Integrated care for older people (ICOPE) PPT and animation video
11:45–12.15 Functional assessment in older adults PPT and animation video
12:15–12:45 ICOPE based screening of intrinsic capacities and functional ability
Role play
12:45–13:30 Break
13:30–14:00 Health promotion and disease prevention in old age PPT
14:00–14:30 Cardiovascular system PPT
14:30–15:00 Respiratory system PPT
15:00–15:15 Break
15:15–15:45 Genitourinary system PPT
15:45–16:15 Endocrine system PPT
16:15–16:45 Hypertension and diabetes mellitus management in old age
Case based discussion
16:45–17:15 Digestive system PPT
17:15–17:30 Wrap up of day 1 Course coordinator
11
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
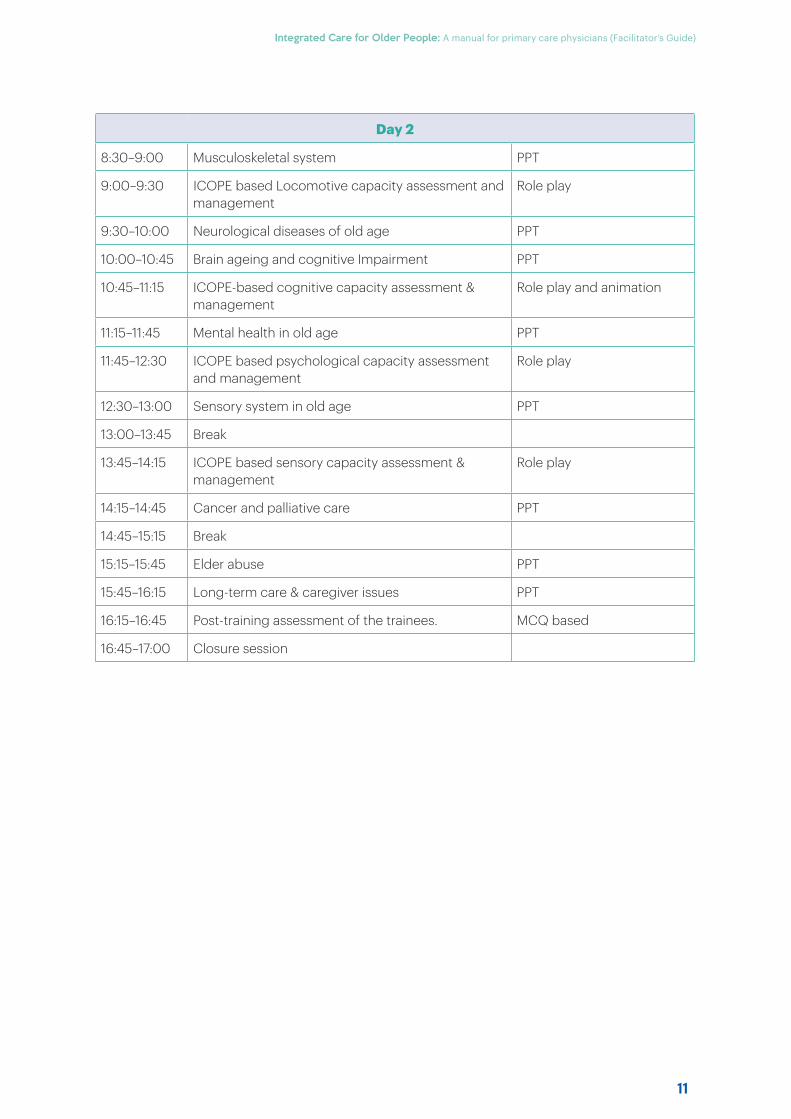
Day 2
8:30–9:00 Musculoskeletal system PPT
9:00–9:30 ICOPE based Locomotive capacity assessment and management
Role play
9:30–10:00 Neurological diseases of old age PPT
10:00–10:45 Brain ageing and cognitive Impairment PPT
10:45–11:15 ICOPE-based cognitive capacity assessment & management
Role play and animation
11:15–11:45 Mental health in old age PPT
11:45–12:30 ICOPE based psychological capacity assessment and management
Role play
12:30–13:00 Sensory system in old age PPT
13:00–13:45 Break
13:45–14:15 ICOPE based sensory capacity assessment & management
Role play
14:15–14:45 Cancer and palliative care PPT
14:45–15:15 Break
15:15–15:45 Elder abuse PPT
15:45–16:15 Long-term care & caregiver issues PPT
16:15–16:45 Post-training assessment of the trainees. MCQ based
16:45–17:00 Closure session

Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
12
13
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
Training methodologies
3SECTION
ainmethodologies
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
14
Introduction The training on “Integrated care for older people” (ICOPE) involves knowledge development through interactive presentations and skill enhancement through facilitated group learning activities and clinical sessions. Training sessions should be conducted as per a predetermined schedule, and adherence to this schedule is important for timely and eff icient conduct of the sessions. Facilitators should meet daily after all the sessions are over to review the day’s activities and plan for the next day’s training and to ensure availability of all training materials and teaching aids. All facilitators should agree about each other’s’ roles and responsibilities prior to the start of the training.
Role of facilitatorsLearn in an active way, equal relationship between participants and those who run the programme when working with other facilitators. It is important that everyone agrees before the programme starts about the facilitator’s roles and responsibilities and who is responsible for which sessions. It is a good idea for facilitators to change their roles so that the participants can experience a change of style and voice.
It would be useful to stress to the participants that they must decide what is useful and important to them and their work. You are not supposed to tell anyone what to do; you can only advise them and give the support and the space to make up his or her own mind. The programme requires range of methods and approaches like short mini lectures to conduct role plays, stimulating problem-solving exercises in small groups.
Ground rules for participatory learning
Treating everyone with respect at all times, irrespective of cultural, age or sex diff erences
Ensuring and respecting confidentiality

15
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
Drawing on the expertise of others, both co-facilitators and participants, in diff icult situations
Asking for critical feedback on what you do and treating that feedback with respect, so that others
see the fairness of your behaviour
Agreeing that every time a facilitator or resource person makes a presentation or leads a session, another facilitator will be responsible for keeping an eye on the time and informing the speaker of this
From the start when and how the facilitators and specialist contributors will work together, how to
give feedback – both positive and negative
Criteria for selecting the training programme facilitatorsHaving two or three facilitators for a programme, exposes the participants to diff erent styles. The facilitators can also change roles between the main facilitator and co-facilitator.
Content areas of the modules on older peoples’ health issuesBelow you will find information on the teaching methods used in the modules. Each module (independently of a number of formal sessions) has four main components:
» Introductory
» Input
» Participatory
» Concluding.
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
16
Introductory component: Module introductionThis opening session sets the stage for the module. It allows you to share with the participants the overall aim and objectives of the module and any special remarks about it. Participants will also have an opportunity to complete the spot checks for that module.
Input component: Mini lecture(s) and module handoutA mini lecture provides an opportunity for eff iciently providing participants with the basic information that they need. For each mini lecture, some of the following resources are available:
» Slides on global aspects of the health issue – you will need to make your own slides on regional and country specific information;
» Handouts (reading material containing information to complement what is provided during the module);
» Additional references are usually listed at the end of the handout of each module.
In every module, there are a few mini lectures distributed across the sessions, to provide inputs on diff erent aspects of the health issue covered.
Clear presentation and structure
Good visual aids
Clear and comprehensible language
The effectiveness of the mini-lectures can be increased by ensuring the following:
17
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
The session will be more eff ective when the presentation (PPT) made is brief and addresses the key issues about the health issue, with particular reference to the local situation. It would be a good idea to allow adequate time for questions and discussion in plenary. Ask participants to review the handout and questions in small groups, and then discuss their findings in plenary. Distribute the handout at the start of the session. Allow adequate time for this and for plenary discussion of the questions in the handout – or for specific issues raised by the participants.
Participatory component: Various participatory methods to explore the topic in more depthThis training programme includes a balanced mix of methods order to maximize the participants’ interaction and benefit. Few points are listed below:
» Filtering the points participants make as you write them up on a flip chart.
» Small group work ensures that every participant has an opportunity to contribute to the discussion and to work through the thought processes for him/herself. Each facilitator is able to trouble-shoot problems, re-focus the discussion, and respond to questions.
Relevant and interesting content
Relevant examples
Room for comments from participants
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
18
Visualization in participatory programmes (VIPP)Cards of diff erent sizes, colours and shapes should be used to show linkages between ideas and areas of consensus and disagreement. Rules for VIPP card-writing are:
» Write only one idea per card
» Write a maximum of three lines on each card
» Use key words
» Write large letters in both upper and lower case
» Write legibly
» Use diff erent sizes, shapes and coloured cards to creatively structure the results of discussions
» Follow the colour code established by the facilitator for diff erent categories of ideas to put down their responses to a question, the question asked be clear and unambiguous.
The use of cards enables the responses to be organized in a logical way and to show areas of consensus and disagreement allows all participants the opportunity to express themselves. VIPP methods are also used to evaluate how participants feel the programme is progressing and more information is provided in the section on evaluation methods. In this case, long sheets of plain wrapping paper can be obtained and prepared in advance. This would include cutting them in diff erent sizes and shapes needed for VIPP exercises.
Brainstorming/buzz groups It helps quickly generate ideas which can be used as a basis for later discussion. This technique is often used at the beginning of a session the responses are usually written on a flip chart or on VIPP cards, which at a later stage can be organized to show the themes that emerged from the exercise. Once this has been done, the ideas can be examined and discussed. It is important to decide in advance why you want the participants to brainstorm and what you will go on to do. Your initial brainstorming question should be clear and unambiguous. About 10 to 15 minutes is right, and make sure that everyone has the opportunity to contribute.
Role playIt provides an opportunity for the expression of emotions which cannot be achieved through discussion alone. Given the limited time available for each role play – only 3–5 minutes – it can illustrate both the problems and the ways of dealing with them. For example:
» The facilitators and/or participants can use role play to demonstrate “bad practice” or “model good practice”. A problem-identification tool, in which everyone in the role play is familiar with the scenario and role play the diff iculties it illustrates. Again, this would normally occur in plenary, although small groups could also use it to develop their problem identification skills.
19
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
» A means to practise clinical or counselling skills, or problem-solving role play for skills practice is best undertaken in groups of three, working in groups of three enables each person, in turn, to practise health-worker skills. “Real” situations relevant to them by asking participants to write a “diff icult moment” on the card; the cards are then displayed on the wall or read aloud by the facilitator, maintaining anonymity.
» Begin by asking the group to think about what they, as health-care providers (not the older peoples), would find most diff icult when dealing with older peoples on the particular health issue. Ask them to focus on the interaction with an older people, or the family, rather than on abstract issues. Typical examples might be an older people who is:
• Too anxious to speak
• Angry or ashamed, and so unwilling to be there
• Afraid of a clinical examination
• With family who will not let him/her speak freely to the health-care provider.
Let the group select one or two such diff iculties to illustrate typical problems faced in dealing with older people, and ways to overcome such diff iculties. Ask for volunteers to play the roles in the chosen situation, explaining exactly what the health-care provider’s task is: to illustrate bad practice as part of a problem-solving exercise or work on good practice. In any case, explain that they will be expected to demonstrate a “typical” reaction, not an ideal one. Ask the volunteers to choose a name, age and sex. Start the first role play with the arrival of the older people to see how he or she is greeted by the health-care provider. Let the role play run for 3–5 minutes. The facilitator should observe, especially, what the healthcare provider does or says that makes a diff erence in the way the elderly reacts, what kind of “body language” is used by both health-care provider and elderly, what attitude the healthcare provider displays towards the adolescent and any family members, and any diff iculties the health-care provider experiences.
Afterwards, ask the role players to stay where they are until the discussion is over. Be sure to thank and praise the role players, and then ask them to come out of their roles, i.e. say who they really are. Explain to the group that this is important to diminish the surprisingly powerful eff ect role plays can have on the players afterwards. Next, ask that comments be focused on what happened in the role play, not on general issues that can be taken up later. Begin by asking each of the role players how they felt in the role (in addition to what they thought). When they have finished, ask the group for their reactions. If necessary, refer to any behaviour that was significant and ask people to comment on it. Demonstrate that you expect people to give helpful positive and negative feedback. When the group has finished commenting, go back to the role players to give them the “last word”.
Running the fi rst role play sessionAlthough the participants should have the maximum opportunity for role playing, they may feel less inhibited if the facilitator begins by very briefly demonstrating bad practices
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
20
Intervening if a role play becomes diffi cultOccasionally, it may happen that someone involved in a role play becomes deeply emotional. Please do all you can to reassure the participants that they must go no further than they feel comfortable, and they are free to stop and come out of the role at any time. the facilitator requires tact, empathy and acute observation.
Case studiesEach case study should contain set of questions. Always remember to allow the participants suff icient time for read and answer questions, which are put directly to the participants, or provided to them in a “task sheet”. Devise a list of “good” and “bad” health-care practices based on the case studies. Ask each group to write up their agreed points on a flip chart and report their findings in plenary. Ask each group in turn for one point of feedback and write this up on a flip chart. Repeat the process until no one has anything more to add.
Guided discussionsFollowing the group work, it is likely that most participants will have in mind a range of ideas for change when they return to their work situation.
» Initially ask them to work alone, or in pairs or small groups, or even (if there is little time remaining) in plenary. After working alone or in pairs, the participants might move on to a bigger group to pull together ideas before finally sharing them in plenary.
» Separate tasks for each pair or small group it also provides an opportunity for each group to challenge, alter or aff irm the solutions of others.
» Your role is to facilitate proper discussion by the whole group. This requires a careful balance between intervening and “taking a back seat”, noting on a flip chart or cards the main points as they occur, asking open-ended questions and directing the discussion.
» Draw out contributions from the shy or more silent participants can state their views, experiences and worries honestly and without fear of disapproval the group to summarize the main points that arise, or do this yourself.
Concluding component: Module reviewIt is important, at the end of each module, to summarize the key points brought out in the plenary discussion and group work. It is also necessary to go back to the module’s objectives and ask the participants to say whether they feel that these have been fully met. The section on evaluation methods gives some good examples of how you can obtain feedback.
21
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
Assessment of trainees
4SECTION
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
22
Introduction Assessment of trainees is an essential component of training that helps in assessing if trainees have achieved the desired levels of knowledge and skills. The purpose of assessment is to analyse gaps in both training and learning processes.
It is recommended that the assessment of trainees be carried out in two phases:
a) Pre-training assessment, and
b) Post-training assessment.
The purpose of the pre-training assessment is to understand focused training needs and determine areas that require improvement. It helps to monitor progress towards achieving training objectives more eff ectively and eff iciently.
Final assessment helps to assess how eff ective training eff orts have been in enhancing the knowledge and related skills of trainees and to what extent the objectives of the training have been achieved. It also helps to determine how competently trainees would be able to provide integrated care to the older people when they return to their own place of work. The process of assessment includes knowledge assessment to be conducted in the classroom using assessment questionnaires having multiple-choice questions.
Guidelines for conducting knowledge assessment
PreparationKeep the following ready for knowledge assessment in the classroom:
» Copies of the assessment questionnaire – you may use the sample questionnaire given in this manual or develop your own set of MCQs based on the sample MCQs given at the end of each module.
» Print outs of knowledge assessment matrix (Box 4.1).
» Flip charts, stand and marker pens
How to conduct the knowledge assessment?» Inform trainees about the purpose of the assessment (pre or post, as appropriate).
» Brief them on the components of the knowledge assessment process and the order in which each component would be reviewed. (Trainees may be informed about the purpose of the assessment and the process to be followed a day prior to allow them to be prepared).
» Distribute the assessment questionnaire comprising 20 questions to all trainees and explain how to tick the correct responses.
23
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
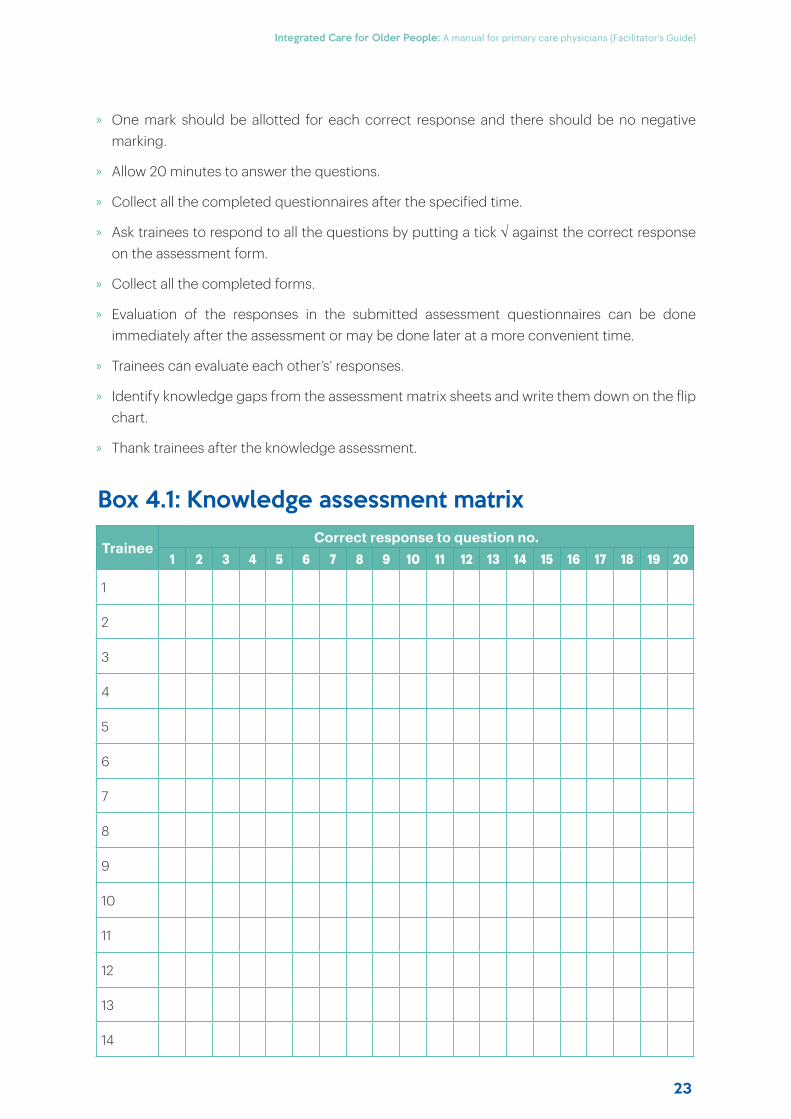
» One mark should be allotted for each correct response and there should be no negative marking.
» Allow 20 minutes to answer the questions.
» Collect all the completed questionnaires after the specified time.
» Ask trainees to respond to all the questions by putting a tick against the correct response on the assessment form.
» Collect all the completed forms.
» Evaluation of the responses in the submitted assessment questionnaires can be done immediately after the assessment or may be done later at a more convenient time.
» Trainees can evaluate each other’s’ responses.
» Identify knowledge gaps from the assessment matrix sheets and write them down on the flip chart.
» Thank trainees after the knowledge assessment.
TraineeCorrect response to question no.
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20
1
2
3
4
5
6
7
8
9
10
11
12
13
14
Box 4.1: Knowledge assessment matrix
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
24
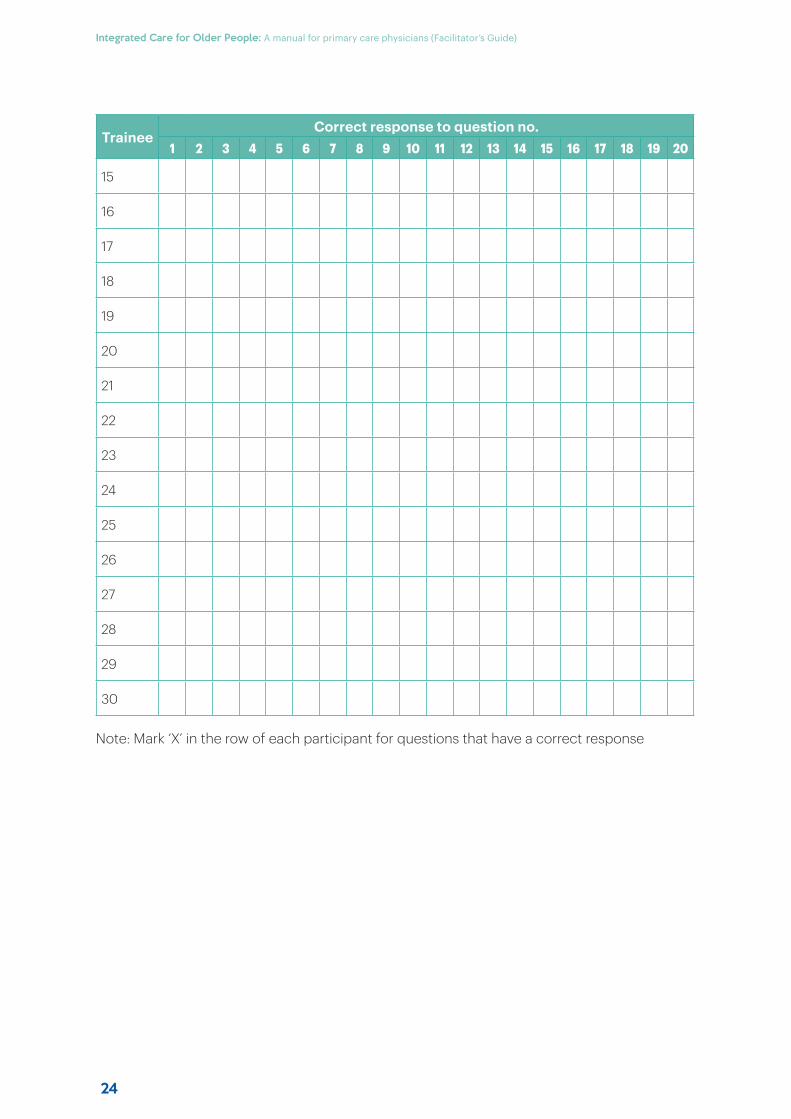
TraineeCorrect response to question no.
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
Note: Mark ‘X’ in the row of each participant for questions that have a correct response
25
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
Inviting participants and other contributors
5SECTION
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
26
Selection of participantsIt would be useful to invite physicians from diff erent specialities. This would enhance the opportunity for information-sharing and networking during the programme, and for post-programme collaboration. As part of your preparation for the training program, we would like you to spend some time thinking through the questions given below please jot down some notes and bring them with you to the programme.
» For what kind of health issues do older peoples come to you or are brought to you?
» What challenges have you faced, if any, when dealing with elderly and their families?
» What diff iculties do you think elderly might face in using health services?
» What else would you like to know about elderly health?
Its purpose is to prepare participants for the training programme, by asking them to reflect on their current work with older people. Potential candidates should be invited one to two weeks in advance of the programme. A useful way to deal with this in the context of the training programme is to invite a small group of older people to participate throughout the programme. It is advised to invite an appropriate group of local older people, perhaps from a community group of elders, to participate in the programme. It is important to have both male and female older people represented. Once they are selected, it is necessary to meet them before the programme and introduce them to their roles during the programme. Some suggestions are given below.
Before the programmeExplain the themes and purpose of the training programme and how they could contribute. Reinforce their important contribution as equal participants in the programme, regardless of their background.
During the programmeThe facilitation team (of 2–3 individuals maximum) should encourage them to participate in small group discussions and activity to provide an adolescent perspective on key issues.
Drawing on the expertise of specialistsOnce the programme structure has been decided and the health issues and problems selected, the facilitation team should decide which resource individuals to be invited. We advise that some time is spent reading the rest of these preparation notes and the selected health issue modules so that you can be clear about the role that these specialists could play; for example, a psychiatrist for mental health or a nutritionist for healthy eating add strength to training.
27
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
Planning for the training programme
6SECTION
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
28
Training programme organizers and facilitators will need to address the proposed items in the preparation and planning in advance of the programme. We recommend that a small group of 2–3 individuals form a planning group, review the proposed list below, and distribute responsibilities 6–8 weeks before the training programme.
Programme preparation and planning checklist
4–6 weeks before the programme» Training programme structure and agenda
» Selection of participants
» Accommodation, meals and coff ee breaks
» Programme facility
» Photocopying and computers
» Programme equipment and tools
» Participants’ tools
» Notify participants of the course objectives, dates and venue
» Start gathering relevant local data on elderly health and development.
Two weeks before the course» Make photocopies of programme agenda, local data, support materials
» Make transparencies out of the slides files or just have them ready for PPT
» Prepare VIPP cards or alternatives
» Check that the needed pieces of equipment are available.
One week in advance of the course» Confirm that those invited to the formal opening ceremony can attend
» Confirm that the participants can all attend
» Confirm venue and accommodation arrangements
» Confirm catering arrangements
» Check the programme meeting room/facility
» Greet the participants who have arrived early.
Planning a formal opening ceremonyWhen planning a formal opening, there should be backup speaker/s for opening ceremony. The speakers should be advised to keep to time and a break should be arranged after the opening to compensate for any loss of time and adhere to the theme of the programme.
29
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
Evaluation methods for the training programme
7SECTION
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
30
Evaluation methods should be quick and easy to use and to obtain immediate feedback. Using them will provide the following information:
» Evidence of how the programme has aff ected the participants.
» Facilitators can see where the programme has been less eff ective, which means you can try to address the reasons for that in the future.
» Future support for the training programme will be easier because you can show that you can evaluate the results or, even better, because you can show the positive eff ect of a previous programme.
» Participants’ reactions to the programme changes in participants’ attitude and knowledge changes in participants’ practice.
Evaluation methods to measure participants’ reactions to the programmeWe have included three ways of keeping in touch with how the participants experience the programme on a daily basis as it goes on. By getting their early reactions you will be able to make changes immediately, rather than receiving complaints at the end of the programme when it is too late to respond to them.
The mood meterAs its name suggests, the mood meter allows you to get a sense of the group’s mood as it changes during the programme. Put the mood meter in an accessible location but one that is not in a busy place like a corridor. Use the mood meter as a means of tracking the group’s feelings about how the programme is proceeding, and as a starting point for discussion.
Discussion groupsFacilitator can hold a discussion group with a small group of interested persons. Ask about five participants if they are willing to talk about the session, and let them discuss a small number of questions.
» How do you feel about this module?
» Which sessions worked best?
» Which sessions did not work well?
» What could we have done diff erently?
» What did you get out of the module?
Please remember that the point of such a discussion is for you to hear the participants’ opinions.Try not to talk much yourself, and listen to criticism without becoming defensive. There is no need to respond directly to any criticism.
31
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
Part II: Guidelines for conducting the individual modules
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
32
IntroductionThe training comprises sessions of classroom-based trainings (lectures and demonstration of skills). A standard session plan has been included in the document. The timing of the classroom sessions may be re-arranged at times convenient for the facility where the training is organized.
Classroom trainingClassroom training has been structured in the form of 11 modules. Each module starts with an overview that refers to the chapter and sections of the WHO Guidance book on which that particular module is based. The module contains a discussion of key points and the list of relevant group learning activities. The checklists for clinical skills trainings are also included in the module where appropriate. The topics in each module are arranged in a logical sequence and it is recommended that facilitators follow the given sequence during teaching.
Training assessmentThe pre-training assessment is to be conducted on Day 1 before the classroom teaching starts and final assessment on Day 2 after the completion of the modules. The assessment process comprises assessment knowledge.
Distribution of sessions and fl ow of events
Day 1Opening sessionSession length: 60 minutes
» Welcome trainees to the session.
» Display a slide showing the overall objectives of the training. Explain the objectives.
» Self-introduction of facilitators and trainees:
Explain to the trainees that a few minutes will be spent on introduction of facilitators and trainees.
For the introduction of facilitators and trainees, write the following points on a flip chart:
Your name
Place where you currently work
A few words about the organization you work for
Nature of your work
You and your co-facilitators should introduce yourselves first, based on the points listed on the flip chart.
Ask each trainee to introduce himself or herself briefly based on the same points.
» Inform trainees about the ground rules (show as a slide and explain).
33
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
Ground rules for trainees
Adhere to the training schedule according to session plans
Maintain an attendance record for certification by the facilitator
Go through the subjects discussed during various sessions in the WHO ICOPE nursing manual at the end of the day, for better understanding and discussion with the facilitator
Attend all clinical sessions according to the schedule
Participate in group activities according to the session plan
Complete the specified number of worksheets during each clinical session, and get them certified by the facilitator
Ensure and respect the privacy and rights of clients in the examination rooms
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
34
» Inform trainees about the available facilities (refreshment, toilets, computers, internet facility)
» Inform them about reimbursement of expenses and names of the support staff providing secretarial assistance.
» Display a slide showing the contents of the folder given to the trainees and ask them to verify.
» Explain the parts of the training package.
» Divide trainees into smaller groups as per the instructions given in box below for group learning activities.
» Discuss the overall session plan: Show the agenda of the training in a slide (modify session time according to local needs).
» Discuss how to use the Trainee’s Handbook:
Ask trainees to take out the Trainee’s Handbook from the folder.
Ask them to open the page for Module 5, so they can see the structure of a sample module.
Display the slide on the structure of a sample module.
Explain that each module presents key information to complement the materials in the corresponding chapter of the WHO Guidance book. Trainees are required to be well-versed with the contents of the chapter before they attend clinical sessions.
» List trainee’s expectations:
Put up a flip chart with the heading “Expectations”.
Ask each participant to mention at least one expectation. Note it on the flip chart.
At the end, discuss how expectations will be addressed during the training.
35
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
DO DON’T
Reach the training venue at least 15 minutes before the session starts each day
Cross-talk among your-selves during teaching
sessions
Use mobile phones, or do anything to distract your colleagues during
training sessions
Hesitate to ask questions
Make racist orgender-biased comments
Eat in the classrooms
Put your mobile phones on silent mode
Be familiar with training sessions and training materials provided
Get to know your group members and stay with your allocated group, during group activities
Listen carefully to the instructions given by facilitators for the clinical sessions
Be respectful of each other and considerate to fellow colleagues
Interact with facilitators as and when required, and get doubts cleared
Display the slide listing dos and don’ts instructions for trainees and discuss.
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
36
How to conduct pre-training knowledge assessment?
» Prepare a set of multiple choice questions (MCQs) from the sample MCQs listed in the appendix of facilitator’s manual before commencement of the training.
» Distribute question sheets to trainees and explain how to tick correct responses.
» Allow 15 to 20 minutes for trainees to answer questions.
» Evaluate responses immediately after the pre-test using the knowledge assessment matrix or on another convenient time on Day 1. Ask your fellow facilitators for help, if necessary.
» Facilitator will prepare a quiz with five questions and explain how to respond.
» Identify knowledge gaps from the assessment matrix and share them with other facilitators. This need not be shared with trainees at this point of time.
» Participants have to give five suggestions about the training and five take-home messages after every session.
37
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
Session: Health of the older people and geriatric medicine
Method: PowerPoint presentation
Session length: 30 minutes
» PowerPoint presentation: 20 minutes
» Question/Answer and Discussion: 10 minutes.
Welcome trainees to the session.
Display the slide with learning objectives of the module as given below.
Explain the learning objectives to trainees; by the end of this module; they will be able:
To understand the health of older people and geriatric medicine
To understand important concepts and principles of geriatric medicine
To understand comprehensive geriatric assessment
To understand the role of primary care physicians in old age care.
» Project the presentation on “Chapter 2: Health of the older people and geriatric medicine”.
» Discuss the contents of the slides.
» Ask trainees if they have any questions or doubts. List these on the flip chart.
» Respond to questions and doubts.
» Thank the group at the end of the session.
Key points for discussion
» Health challenges in old age
» Normative changes of ageing vis-á-vis pathological states
» Important concepts in geriatric medicine
» Concept of frailty syndrome and sarcopenia
» Concept of acute care in old age
» Stereotypes of ageing
» Concept of Comprehensive geriatric assessment
» Geriatric history taking and physical examination
» Role of the primary care physician in care of older adults
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
38
Session: Integrated care for older people (ICOPE)
Method: PowerPoint presentation and animation video
Session length: 30 minutes
» PowerPoint presentation: 20 minutes
» Animation video: 5 minutes
» Question/answer and discussions: 5 minutes
Welcome trainees to the session.
Display the slide with learning objectives of the module as given below.
Explain the learning objectives to trainees; by the end of this module, they will be able:
To understand integrated care for older people
To learn to measure the intrinsic capacity of an older adult
To learn about the concept of ICOPE person-centred and care pathways.
» Project the presentation on “Module 1: Integrated care for older people”.
» Discuss the contents of the slides.
» Ask trainees if they have any questions or doubts. List these on the flip chart.
» Respond to questions and doubts.
» Thank the group at the end of the session.
Key points for discussion
» Introduction to ICOPE approach
» Concept of intrinsic capacity and its various domains
» WHO ICOPE intrinsic capacity screening tool
» Generic pathways of ICOPE strategy
39
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
Session: Functional assessment in older people
Method: PowerPoint presentation and animation video
Session length: 30 minutes
» PowerPoint presentation: 20 minutes
» Animation video: 5 minutes
» Question/answer and discussions: 5 minutes
Welcome trainees to the session.
Display the slide with learning objectives of the module as given below.
Explain the learning objectives to trainees; by the end of this module, they will be able:
To understand the relevance of good functional status in older patients
To learn to use tools for the assessment of functional status.
» Project the presentation on “Module 2: Functional assessment in older people”.
» Discuss the contents of the slides.
» Ask trainees if they have any questions or doubts. List these on the flip chart.
» Respond to questions and doubts.
» Thank the group at the end of the session.
Key points for discussion
» Introduction to functional assessment
» Concept of basic, instrumental and advanced activities of daily living
» Clinical implications of functional status
» Commonly used scales for functional assessment and the interpretation of scores
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
40
Session: ICOPE based screening of intrinsic capacities and functional status
Method: Role play
Session length: 30 minutes
» Role play: 20 minutes
» Question/answer and discussions: 10 minutes
Divide the trainees into proportionate groups (maximum 10 in each).
Scene: The facilitator to appoint a trainee to act as an older person coming to the OPD for periodic
follow-up for diabetes mellitus for the last one year having diff iculty in walking because of balance issues and a history of fall in the bathroom one month ago. He/she also needs support of his/her family members while bathing.
One of the trainees will act as an assessor.
The assessor will make the following enquiries:
a) Chief complaints: (For what the older person has come to the primary health centre)
b) History of presenting complaints: (Detailed elaboration of the complaints)
c) History of geriatric syndromes: (Enquiry into falls, incontinence, memory issues, depressive symptoms, etc.)
d) Past history: (Transient ischaemic attacks, strokes, acute coronary syndromes, syncope, tuberculosis etc.)
e) Socioeconomic history: (Family support, financial handling, employment/engagement)
f) History of addiction: (Smoking/chewing tobacco, alcoholism)
g) History of treatment/drugs
h) History of vaccination: (Adult vaccination: influenza, pneumococcal vaccines etc.)
41
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
42
The assessor will do the general physical examination including vitals.
The assessor will do the relevant systemic examination:
a) Cardiovascular examination
b) Nervous system examination
c) Other relevant system-based examination.
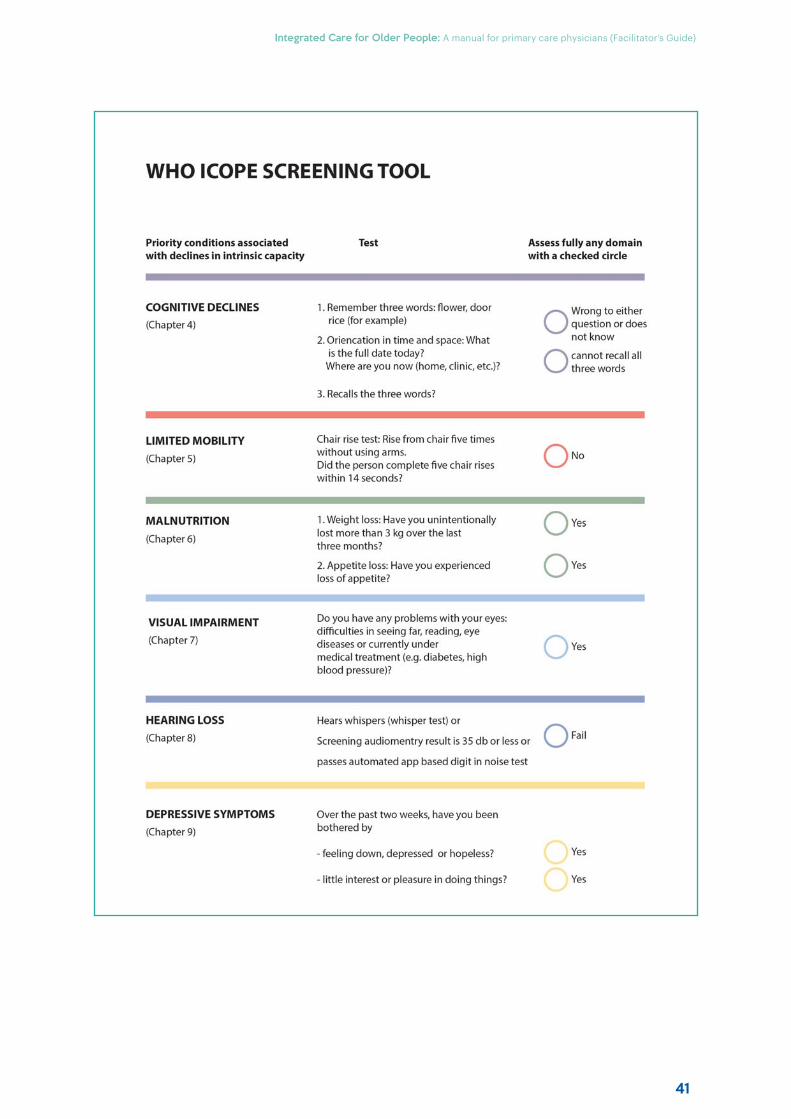
The assessor will carry out screening of the intrinsic capacities based on WHO Intrinsic Capacity Screening Questionnaire.
The assessor will inform the observer trainee about the positive screening in the locomotor domain.
The assessor will inform the observer trainees that a detailed assessment of locomotor ability will be required based on ICOPE strategies.
Total scoreThe accessor will summarize the findings of the assessment of the intrinsic capacity and
the functionality in this individual to the trainees.
The facilitator will ask the other trainees about their comments on the role play.
The facilitator will give feedback.
The facilitator will respond to the questions and doubts of the trainees.
The facilitator will thank the actors as well as the other trainees.
43
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
Session: Health promotion and disease prevention in old age
Method: PowerPoint presentation
Session length: 30 minutes
» PowerPoint presentation: 20 minutes
» Question/answer and discussions: 10 minutes
Welcome trainees to the session.
Display the slide with learning objectives of the module as given below.
Explain the learning objectives to trainees; the end of this module, they will be able:
To assess the general status of older adults in terms of health promotion
To enumerate strategies for health promotion among older people
To enumerate strategies for disease prevention in old age.
» Project the presentation on “Module 3: Health promotion and disease prevention in old age“
» Discuss the contents of the slides.
» Ask trainees if they have any questions or doubts. List these on the flip chart.
» Respond to questions and doubts.
» Thank the group at the end of the session.
Key points for discussion
» Health promotion strategies:
Nutrition:
Importance
Assessment of nutritional status in older people using MNA
Nutritional management based on MNA
Nutritional advice for older adults
Continue
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
44
Exercise:
Importance
Types of physical activity
WHO recommendation for physical activity
Social support and social interaction
» Disease prevention strategies:
Prevention of use of tobacco products and prevention of alcoholism
Screening for disease prevention
Vaccination
Prevention of polypharmacy and principle of prescribing in older people
Continue
45
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
Session: Cardiovascular system
Method: PowerPoint presentation
Session length: 30 minutes
» PowerPoint presentation: 20 minutes
» Question/answer and discussions: 10 minutes
Welcome trainees to the session.
Display the slide with learning objectives of the module as given below.
Explain the learning objectives to trainees; the end of this module, they will be able:
To enumerate age-related changes which occur in the cardiovascular system
To enumerate common cardiovascular diseases and strategies to screen and manage
To develop short-term and long-term care plans.
Project the presentation on “Module 4: Cardiovascular system”.
Discuss the contents of the slides.
Ask trainees if they have any questions or doubts. List these on the flip chart.
Respond to questions and doubts.
Key points for discussion
» Age-related changes in the cardiovascular system
» Primary prevention of cardiovascular diseases
» Common cardiovascular problems of old age; diagnosis and management
Hypertension
Acute coronary syndrome
Dizziness and syncope
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
46
Session: Respiratory system
Method: PowerPoint presentation
Session length: 30 minutes
» PowerPoint presentation: 20 minutes
» Question/answer and discussions: 10 minutes
Welcome the trainees to the session.
Display the slide with learning objectives of the module as given below.
Explain the learning objectives to trainees; the end of this module, they will be able:
To enumerate age-related changes which occur in the respiratory system
To enumerate common respiratory diseases
To develop screening strategies and care plans for these conditions.
Project the presentation on “Module 5: Respiratory System”.
Discuss the contents of the slides.
Ask trainees if they have any questions or doubts. List these on the flip chart.
Respond to questions and doubts.
Key points for discussion
» Age-related changes in the respiratory system
» Common respiratory problems of old age; diagnosis and management
Community acquired pneumonia: symptoms, severity assessment
Tuberculosis
Chronic obstructive pulmonary disease
Lung cancer
47
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
Session: Endocrine system
Method: PowerPoint presentation
Session length: 30 minutes
» PowerPoint presentation: 20 minutes
» Question/answer and discussions: 10 minutes
Welcome trainees to the session.
Display the slide with learning objectives of the module as given below.
Explain the learning objectives to trainees; the end of this module, they will be able:
To enumerate the normal age-related changes in the endocrine system
To develop care plans for older patients with diabetes mellitus
To identify thyroid disease among older patients and develop care plans.
Project the presentation on “Module 7: Endocrine system”
Discuss the contents of the slides.
Ask trainees if they have any questions or doubts. List these on the flip chart.
Respond to questions and doubts.
Key points for discussion
» Age related changes in the endocrine system
» Common endocrine problems of old age; diagnosis and management
Diabetes mellitus, Hypoglycemia and Hyperglycemic hyperosmolar state
Hypothyroidism
Hyperthyroidism
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
48
Session: Hypertension and diabetes mellitus management in old age
Method: Case-based discussion
Session length: 30 minutes
» Divide the trainee into proportionate groups (maximum 10 in each)
» Initiate discussion among the trainee in the group based on the similar case scenario.
Example of case scenarioA 70-year-old hypertensive male (on daily Amlodipine 5 mg) is brought to your primary health centre/clinic by his son for routine evaluation.
Q1. What are the other relevant enquiries for history taking?i. Past history
ii. Socioeconomic history
iii. Dietary history
iv. Medication history
v. History of geriatric syndrome
vi. Functionality
On further enquiry, the patient complained of history of fall in bathroom three months ago. He did not suff er any injury, but he had a fear of fall.
Q2. How will you proceed for further physical examination?i. Vitals: BP in sitting position 150/90 mmHg and standing 155/90 mmHg
ii. General: Bilateral pedal oedema
iii. Systemic examination: normal
Q3. How will you assess ICOPE based intrinsic capacity in this patient?On using ICOPE screening test, cognitive impairment present.
Q4. What will you do next?Mini-Cog: Normal.

49
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
Q5. How will you assess functionality in this patient?Katz activities of daily living: Normal.
On routine investigations, random blood sugar was 110 mg/dl. The patient was advised to get serum thyroid stimulating hormone (TSH) and serum creatinine tested and to follow up with the reports.
Q6. How will you manage the issue of pedal oedema and increased BP in this patient?The patient will be advised to stop Amlodipine 5 mg; to start Hydrocholrthiazide 12.5 mg in the morning; and visit for follow up assessment after 2 weeks.
Q7. After two weeks, the patient comes back with reports and TSH of 1.8 milli-international units per litre and creatinine of 0.6mg/dl with BP of 140/90 mmHg. Pedal oedema subsided. He has improvement in overall quality of life. What will you advise him now?He will be advised to continue Hydrocholrthiazide as before and restrict salt in food.
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
50
Session: Digestive system
Method: PowerPoint presentation
Session length: 30 minutes
» PowerPoint presentation: 20 minutes
» Question/answer and discussions: 10 minutes
Welcome trainees to the session.
Display the slide with learning objectives of the module as given below.
Explain the learning objectives to trainees; the end of this module, they will be able:
To enumerate the age-related changes in the digestive system
To enumerate common diseases of the digestive system among older patients
To screen for common disease conditions and develop care plans.
Project the presentation on “Module 6: Digestive system”.
Discuss the contents of the slides.
Ask trainees if they have any questions or doubts. List these on the flip chart.
Respond to questions and doubts.
Key points for discussion
» Age-related changes in the digestive system
» Common disorders of the digestive system:
Compromised oral health
Hiatus hernia and gastro-oesophageal reflux
Gastropathy and gastric ulcers
Cancers of the gastrointestinal tract
Constipation
Diarrhoea
Red flag signs and symptoms of gastrointestinal system
51
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
Session: Musculoskeletal system
Method: PowerPoint presentation
Session length: 30 minutes
» PowerPoint presentation: 20 minutes
» Question/answer and discussions: 10 minutes
Welcome trainees to the session.
Display the slide with learning objectives of the module as given below.
Explain the learning objectives to trainees; the end of this module, they will be able:
To enumerate normal age-related changes in the musculoskeletal system
To enumerate common musculoskeletal disorders of older patients
To identify common musculoskeletal diseases and develop care plans.
Project the presentation on “Module 8: Musculoskeletal system”
Discuss the contents of the slides.
Ask trainees if they have any questions or doubts. List these on the flip chart.
Respond to questions and doubts.
Distribution of sessions and fl ow of events
Day-2
Key points for discussion
» Age-related changes in the bones, muscles and joints
» Locomotor capacity in older adults: Screening, assessment and management using ICOPE care pathways
» Common disorders of the musculoskeletal system:
Osteoarthritis
Osteoporosis
Falls and fractures
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
52
Session: ICOPE based locomotive capacity assessment and management
Method: Role play
Session length: 30 minutes
» Role play: 20 minutes
» Question/answer and discussions: 10 minutes
Material required:
ICOPE-A manual for primary care physicians
A chair of appropriate height without arm rest
A measuring tape
A stop-watch.
The facilitator will measure and mark spot a distance of 4 metres on the floor before the session.
» Divide the trainee into proportionate groups (maximum 10 in each).
Scene:
The facilitator to designate a trainee to act as an older person coming to the OPD of the primary health centre for periodic follow up for hypertension for last one year with diff iculty in walking because of imbalance and a history of fall in the bathroom one month ago. Now, he needs help from a family member while going to the toilets or while taking bath.
» One of the trainees will act as an assessor.
» The assessor will make the following enquiries:
Chief complaints
History of presenting complains
History of geriatric syndrome
Past history
Family history
Socioeconomic history
History of addiction
History of treatment/drugs
History of vaccination
53
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
» The assessor will do the general physical examination including vitals.
» The assessor will do the systemic examination:
Cardiovascular examination
Nervous system examination
Other relevant system-based examination
» The assessor will carry out screening of the intrinsic capacities based on WHO Intrinsic Capacity Screening Questionnaire:
The actor can do chair-rise only for four times in 14 seconds.
» The assessor will inform the trainees about the positive screening in the locomotor domain.
» The assessor will inform the trainees that a detailed assessment of the locomotor ability will be based on ICOPE strategies.
» The assessor will summarize the findings of the assessment of the intrinsic capacity and the functionality in this individual to the trainees.
» As screening is positive for losses, the assessor should assess the patient’s mobility using the short physical performance battery (SPPB).
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
54
Note: Please refer to WHO ICOPE Screening Tool on page 41
Short physical performance battery (SPPB):
The actor could do the following:
a) Balance test: Could stand side-by-side for more than 10 seconds (1 point)
Could stand semi-tandem for 4 seconds only (0 points)
Couldn’t attempt tandem stand at all (0 points)
b) Gait speed test: Could walk 4 metres in 7 seconds only (2 points)
c) Chair rises test: Took 15 seconds to rise from chair 5 times (2 points)
Total score: 1+0+0+2+2= 5
» The facilitator now asks the observer trainees about their comments on the act.
» The facilitator gives his/her feedback on the assessment techniques.
» The facilitator explains to the trainees that,
As the older person displays “limited mobility” on SPPB:
» Advise multimodal exercise with close supervision:
strength/resistance training
aerobic/cardiovascular training
balance training
flexibility training.
» Advice for physiotherapy.
» Advice for increasing protein intake.
» Manage hypertension as an associated condition in this patient.
» Polypharmacy: Review medications that can interfere with balance e.g. sedatives, diuretics.
» Evaluate for osteoarthritis and consider pain management.
» Assess and manage the person’s social and physical environments to reduce risk of falls.
» The facilitator will respond to the questions and doubts of the trainees.
» The facilitator will thank the actors as well as the other trainees.
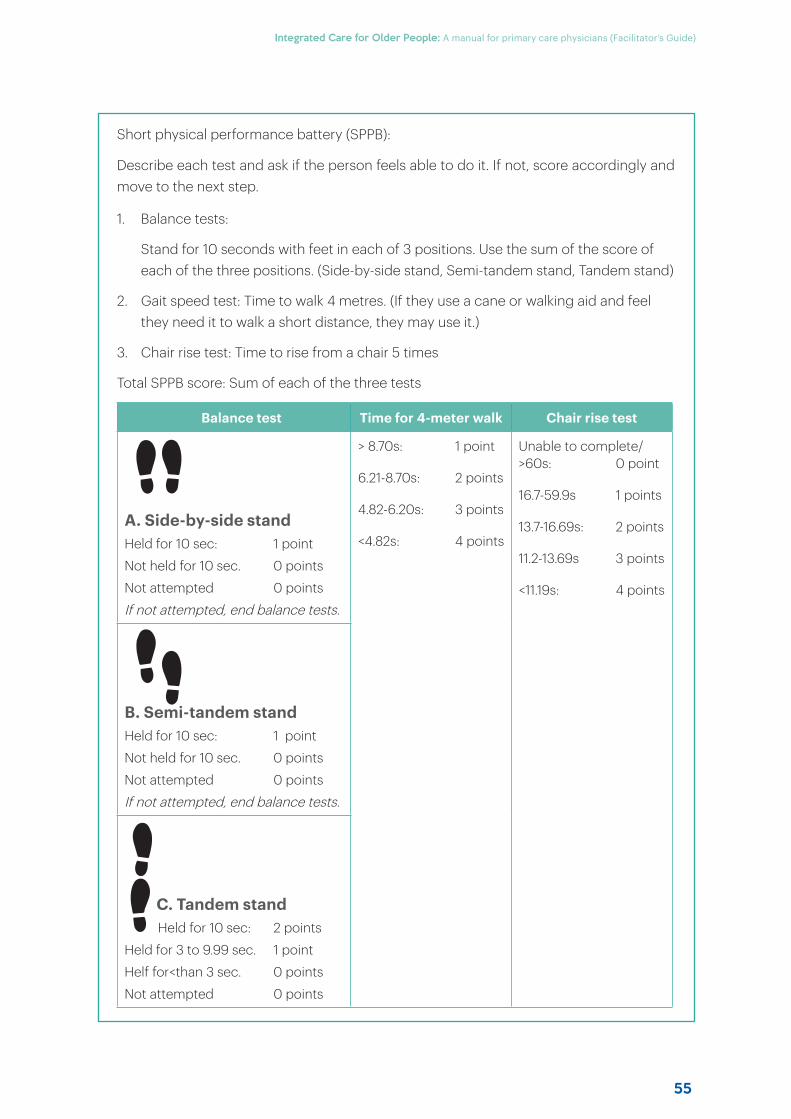
55
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
Short physical performance battery (SPPB):
Describe each test and ask if the person feels able to do it. If not, score accordingly and move to the next step.
1. Balance tests:
Stand for 10 seconds with feet in each of 3 positions. Use the sum of the score of each of the three positions. (Side-by-side stand, Semi-tandem stand, Tandem stand)
2. Gait speed test: Time to walk 4 metres. (If they use a cane or walking aid and feel they need it to walk a short distance, they may use it.)
3. Chair rise test: Time to rise from a chair 5 times
Total SPPB score: Sum of each of the three tests
Balance test Time for 4-meter walk Chair rise test
A. Side-by-side standHeld for 10 sec: 1 point
Not held for 10 sec. 0 points
Not attempted 0 points
If not attempted, end balance tests.
> 8.70s: 1 point
6.21-8.70s: 2 points
4.82-6.20s: 3 points
<4.82s: 4 points
Unable to complete/>60s: 0 point
16.7-59.9s 1 points
13.7-16.69s: 2 points
11.2-13.69s 3 points
<11.19s: 4 points
B. Semi-tandem standHeld for 10 sec: 1 point
Not held for 10 sec. 0 points
Not attempted 0 points
If not attempted, end balance tests.
C. Tandem stand Held for 10 sec: 2 points
Held for 3 to 9.99 sec. 1 point
Helf for<than 3 sec. 0 points
Not attempted 0 points
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
56
Session: Genitourinary system
Method: PowerPoint presentation
Session length: 30 minutes
» PowerPoint presentation: 20 minutes
» Question/answer and discussions: 10 minutes
Welcome trainees to the session.
Display the slide with learning objectives of the module as given below.
Explain the learning objectives to trainees; the end of this module, they will be able:
To enumerate normal age-related changes in the genitourinary system
To enumerate common health problems of genitourinary system and develop care plans.
Project the presentation on Module 9: “Genitourinary system diseases of old age”.
Discuss the contents of the slides.
Ask trainees if they have any questions or doubts. List these on the flip chart.
Respond to questions and doubts.ha
Key points for discussion
» Age-related changes in the genitourinary system
» Common diseases of the nervous system and their diagnosis and management
Urinary incontinence
Urinary tract infection
Benign prostatic hypertrophy
57
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
Session: Neurological diseases of old age
Method: PowerPoint presentation
Session length: 30 minutes
» PowerPoint presentation: 20 minutes
» Question/answer and discussions: 10 minutes
Welcome the trainees to the session.
Display the slide with learning objectives of the module as given below.
Explain the learning objectives to trainees; the end of this module, they will be able:
To enumerate normal age-related changes in the nervous system
To diagnose stroke; and learn its management strategy and understand the need for timely referral
To detect Parkinson’s disease and understand referral and management.
Project the presentation on “Module 10: Neurological diseases of old age”
Discuss the contents of the slides.
Ask trainees if they have any questions or doubts. List these on the flip chart.
Respond to questions and doubts.r-ol
Key points for discussion
» Age-related changes in the nervous system
» Common diseases of the nervous system and their diagnosis and management
Stroke
Parkinson’s disease
Essential tremor
Delirium
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
58
Session: Brain ageing and cognitive impairment
Method: PowerPoint presentation
Session length: 30 minutes
» PowerPoint presentation: 20 minutes
» Question/answer and discussions: 10 minutes
Welcome trainees to the session.
Display the slide with learning objectives of the module as given below.
Explain the learning objectives to trainees; the end of this module, they will be able:
To enumerate age-related changes in cognition
To screen and identify cognitive impairment
To assess and develop care plans for older patients with dementia.
Discuss the contents of the slides.
Project the presentation on “Module 11: Brain ageing and cognitive impairment”
Key points for discussion
» Age-related changes in cognition
» Diff erences between age-related memory changes and cognitive impairment
» Dementia: types and clinical manifestation
» Role of primary care physicians on dementia evaluation and management
Discuss the contents of the slides.
Ask trainees if they have any questions or doubts. List these on the flip chart.
Respond to questions and doubts.
59
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
Session: ICOPE-based cognitive capacity assessment and management
Method: Role play and animation video
Session length: 30 minutes
» PowerPoint presentation: 20 minutes
» Question/answer and discussions: 5 minutes
» Animation video: 5 minutes
Divide the trainee into proportionate groups (maximum 10 in each)
Case scenario:
One of the trainees to act as an older person coming to the OPD with his/her spouse with recurrent episodes of forgetfulness while going for fetching household stuff in the nearby shops and occasionally overshooting his/her way back to her house. He/he has been dependent on his/her spouse for putting on clothes and bathing.
» One of the trainees will act as an assessor.
» The assessor will make the following enquiries:
a. Chief complaints
b. History of presenting complaints
c. History of geriatric syndrome
d. Past history
e. Family history
f. Socioeconomic history
g. History of addiction
h. History of treatment/drugs
» The assessor will do the general physical examination including vitals.
» The assessor will do the systemic examination:
a. Nervous system examination
b. Cardiovascular examination
c. Other relevant system-based examination
» The assessor will carry out screening of the intrinsic capacities based on WHO Intrinsic Capacity Screening Questionnaire.
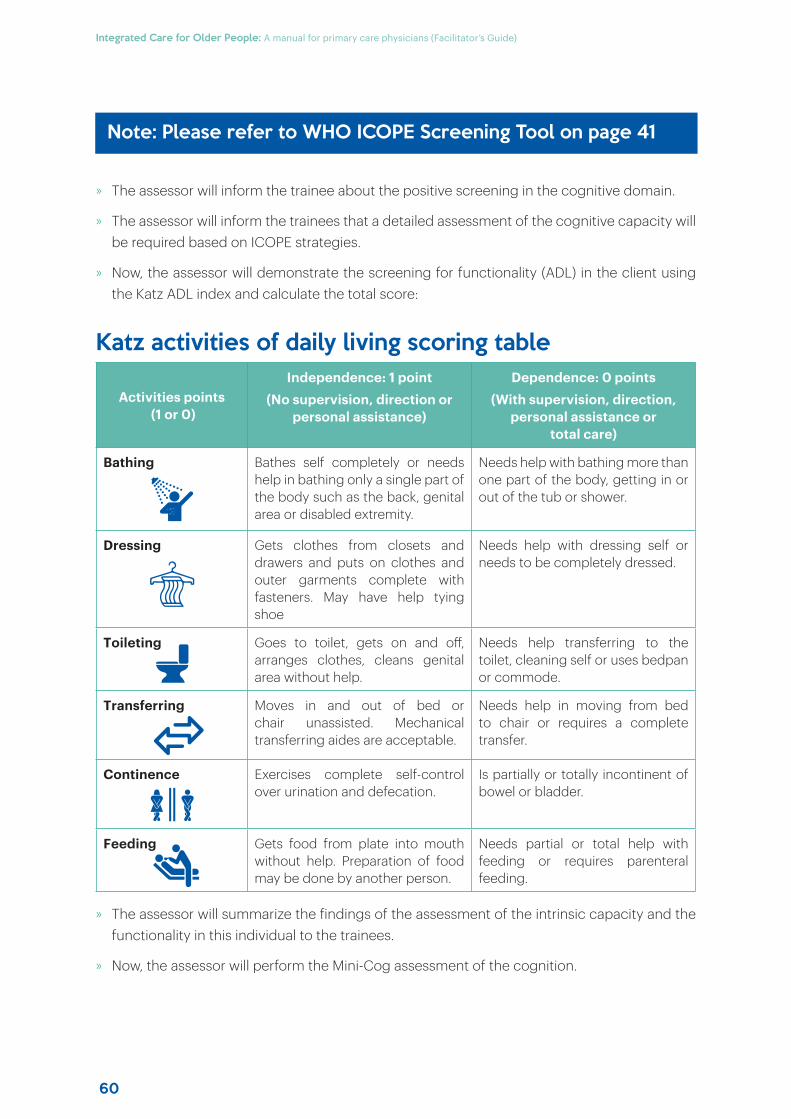
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
60
» The assessor will inform the trainee about the positive screening in the cognitive domain.
» The assessor will inform the trainees that a detailed assessment of the cognitive capacity will be required based on ICOPE strategies.
» Now, the assessor will demonstrate the screening for functionality (ADL) in the client using the Katz ADL index and calculate the total score:
Katz activities of daily living scoring table
Activities points (1 or 0)
Independence: 1 point(No supervision, direction or
personal assistance)
Dependence: 0 points (With supervision, direction,
personal assistance or total care)
Bathing Bathes self completely or needs help in bathing only a single part of the body such as the back, genital area or disabled extremity.
Needs help with bathing more than one part of the body, getting in or out of the tub or shower.
Dressing Gets clothes from closets and drawers and puts on clothes and outer garments complete with fasteners. May have help tying shoe
Needs help with dressing self or needs to be completely dressed.
Toileting Goes to toilet, gets on and off , arranges clothes, cleans genital area without help.
Needs help transferring to the toilet, cleaning self or uses bedpan or commode.
Transferring Moves in and out of bed or chair unassisted. Mechanical transferring aides are acceptable.
Needs help in moving from bed to chair or requires a complete transfer.
Continence Exercises complete self-control over urination and defecation.
Is partially or totally incontinent of bowel or bladder.
Feeding Gets food from plate into mouth without help. Preparation of food may be done by another person.
Needs partial or total help with feeding or requires parenteral feeding.
» The assessor will summarize the findings of the assessment of the intrinsic capacity and the functionality in this individual to the trainees.
» Now, the assessor will perform the Mini-Cog assessment of the cognition.
Note: Please refer to WHO ICOPE Screening Tool on page 41
61
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
Mini-Cog - Cognitive assessment tool
Step 1: Three word registrationSay any three unrelated words to the person. Then ask him/her to repeat the words. If the person is unable to repeat the words after three attempts, move on to Step 2 (clock drawing).
Step 2: Clock drawingAsk the person to draw a clock by putting all the numbers in the correct positions in an already pre-printed circle. When that is completed, ask the person to set the hands to 10 past 11 (11:10). Repeat instructions as needed as this is not a memory test. Move to Step 3 if the clock is not complete within three minutes.
Step 3: Three word recallAsk the person to recall the three words you stated in Step 1. Record the person’s answers.
Scoring:
Word recall
(0-3 points)
Points: 1 point for each word spontaneously recalled without clues
Clock draw
(0 or 2 points)
Points: Normal clock = 2 points (all numbers placed in the correct sequence and approximately correct position)
Inability or refusal to draw a clock (abnormal) = 0 points
Total score …….................
points
Total score = Word recall score + Clock draw score
A cut point of <3 has been validated for dementia screening.
» Now, the facilitator will inform the trainee that the diagnosis of ‘pseudo-dementia’ secondary to depression or delirium should be ruled out before considering the diagnosis of ‘dementia’ in this patient.
(Refer to the module on Mental Health in Older People.)
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
62
» The facilitator should inform the trainees that associated medical issues should be identified.
Onset of symptoms associated with head injury, stroke, or altered consciousness
Clinical history of goitre, slow pulse, dry skin (hypothyroidism)
History of sexually transmitted infection, including HIV/AIDS.
» The facilitator should teach the trainee that the following symptoms should be enquired for any “behavioural and psychological symptoms of dementia (BPSD)”.
Agitation
Personality change
Abnormal eating behaviour
Wandering
Mood disorder, depression
Anxiety, phobias, fear
Restlessness
Hallucinations, delusions
Aggression, shouting, rage, violence
Dis-inhibition
Compulsive behaviour
Hypersexuality
Repeating stories and statements
Hoarding
Resisting care
Psychosis
Screaming
Taking clothes off in inappropriate places
Smearing faecal matter.
» The facilitator should now inform the trainees about evaluating for the needs of carers.
Is the carer having diff iculty coping with and experiencing strain?
Does the carer feel depressed?
Is the carer incurring loss of income and additional expenses because of care needs?
» The facilitator should inform the trainees that the management of dementia symptoms, depends on the presence or absence of BPSD.
63
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
A. Dementia without BPSD:
Provide the carers with basic education on the nature and progression of the illness.
Encourage carers to conduct interventions to improve cognitive functioning.
Promote independence, functioning and mobility.
Refer to a specialist for the diagnosis of Alzheimer’s and other dementia subtypes.
B. Dementia with BPSD:
Follow the management steps for dementia without BPSD.
Start quetiapine 25 mg once a day. Gradually increase to 25 mg twice daily.
If the BPSD are not controlled with the above dose, refer the patient to a specialist.
» The facilitator will inform the trainees about conducting follow-ups in such patients.
Assess for improvement, and review adherence, adverse drug reactions and dosing.
Review the psychosocial interventions.
Evaluate the patient for comorbidities.
Review basic activity of daily living (BADL) and instrumental activity of daily living (IADL) dependence.
Review for safety risks and recommend appropriate modification of behaviour if the disease has progressed (limit driving, cooking, etc.).
Review for new BPSD or symptoms of depression: refer to a specialist.
» Ask trainees if they have any questions or doubts. List these on the flip chart.
» Respond to questions and doubts.
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
64
Session: Mental health in old age
Method: PowerPoint presentation
Session length: 30 minutes
» PowerPoint presentation: 20 minutes
» Question/answer and discussions: 10 minutes
Welcome trainees to the session.
Display the slide with learning objectives of the module as given below.
Explain the learning objectives to trainees; by the end of this module; they will be able:
To enumerate the common stresses of old age
To enumerate the social and cultural barriers to seeking mental health services
To identify common mental health problems and develop care plans.
Project the presentation on “Module 12: Mental health in old age”.
Discuss the contents of the slides.
Ask trainees if they have any questions or doubts. List these on the flip chart.
Respond to questions and doubts.
Key points for discussion
» Common stresses of old age
» Barriers to accepting mental health problems in old age
» Sleep and sleep hygiene in older adults
» Depression and its management
» Generalized anxiety disorder
65
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
Session: ICOPE-based psychological capacity assessment and management
Method: Role play
Session length: 30 minutes
» Role play: 20 minutes
» Question/answer and discussions: 10 minutes
Divide the trainee into proportionate groups (maximum 10 in each)
Case scenario:
The facilitator to ask one of the trainees to act as an older male coming to the OPD with his wife with the following complaints:
Increasing tiredness while performing regular works x 3 weeks
Doesn’t like going out of his house x 2 weeks
Cries easily x 2 weeks
» The facilitator to ask one of the trainees to act as an assessor.
» The assessor will make the following enquiries:
a. Chief complaints
b. History of presenting complaints
c. History of geriatric syndromes
d. Past history
e. Family history
f. Socioeconomic history
g. History of addiction
h. History of treatment/drugs
» The assessor will do the general physical examination including vitals.
» The assessor will do the systemic examination:
a. Nervous system examination
b. Cardiovascular examination
c. Other relevant system-based examination
» The assessor will carry out screening of the Intrinsic capacities based on WHO Intrinsic Capacity Screening Questionnaire:
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
66
» The assessor will inform the trainee about the positive screening in the psychological/depressive domain.
» The assessor will inform the trainees that a detailed assessment of the psychological capacity will be required based on ICOPE strategies.
Total score» The assessor will summarize the findings of the assessment of the intrinsic capacity and the
functionality in this individual to the trainees.
» Now the assessor would follow the following steps for the screening, assessment and management of depression in the actor:
Step 1. Screening for depressionThe assessor will ask the actor, over the past two weeks, have you been:
feeling down, depressed or hopeless?
losing interest or pleasure in doing things?
The actor responds as losing interest in the things that were once pleasurable previously. The assessor informs the other trainees that the screening is positive for depression.
Step 2. As the answer to one of the questions is “Yes”, the assessor performs an assessment of mood, using the following set of questions.
Step 3. The assessor should rule out other conditions resembling/exacerbating depression which include:
Anaemia
Malnutrition
Hypothyroidism
Mood changes from substance use
Side-eff ects of medications, e.g. steroids.
Step 4. The assessor should assess for history of maniaTake the patient’s history from the caregiver, asking whether the patient suff ered from several of the following symptoms simultaneously, for at least one week, and severely enough to interfere significantly with work and social activities, or requiring hospitalization or confinement:
Elevation of mood and/or irritability
Decreased need for sleep
Increased activity, feeling of increased energy, increased talkativeness or rapid speech
67
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
Impulsive or reckless behavior, such as excessive spending, making important decisions without planning and sexual indiscretion
Loss of normal social inhibitions resulting in inappropriate behaviors
Being easily distracted
Unrealistically inflated self-esteem.
(The caregiver tells that the patient doesn’t have the above symptoms, the diagnosis of a depressive episode in bipolar disorder is unlikely.)
Step 5. Management of depressionThe assessor should take the following steps for the management of depression:
Educate the patient and the family members on depression.
Ask the person’s carers to keep and monitor the medications, and to follow up frequently to prevent overdose of any medication.
Consider prescribing an antidepressant (if a specialist’s support is not available).
Selective serotonin reuptake inhibitors(SSRIs) are the first-choice antidepressants. Amitriptyline needs to be avoided in older adults. Use a low dose of benzodiazepine (Clonazepam 0.25 mg once a day) with the antidepressant for a maximum of two weeks to prevent rebound anxiety.
Antidepressants take at least a week or two to demonstrate gradual benefit. Medications should never be stopped just because the person experiences some improvement. Anti-depressants usually need to be continued for at least 9–12 months after the resolution of symptoms.
Table. Medications for management of depression
Medication Dosage Side-eff ects Contraindications
Fluoxetine Start at 10 mg/day, increase to 20 mg after 1 week
Common for all: sedation, insomnia, headache, dizziness, gastrointestinal disturbances, sexual dysfunction
Serious: Bleeding abnormalities in those using aspirin or other NSAIDs, hyponatremia
Avoid combination with warfarin (may increase risk of bleeding), may increase levels of tricyclic antidepressants, anti-psychotics, and beta-blockers, may cause QT prolongation in susceptible individuals
Escitalopram Start at 5 mg/day. Increase to 10 mg after 1 week
Sertraline Start at 25 mg/day, increase to 50 mg/day after 1 week
» Ask trainees if they have any questions or doubts. List these on the flip chart.
» Respond to questions and doubts.
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
68
Session: Sensory system
Method: PowerPoint presentation
Session length: 30 minutes
» PowerPoint presentation: 20 minutes
» Question/answer and discussion: 10 minutes
Welcome trainees to the session.
Display the slide with learning objectives of the module as given below.
Explain the learning objectives to trainees; by the end of this module; they will be able:
To describe the normal age-related changes in the sensory system and their implications
To identify the common problems in the sensory system and develop care plans.
Project the presentation on “Module 13: Sensory system”.
Discuss the contents of the slides.
Ask trainees if they have any questions or doubts. List these on the flip chart.
Responds to questions and doubts.
Key points for discussion
» Age-related changes in sensory system: skin, eyes and ears
» Pressure ulcers: Risk factors and management
» Cataract: Diagnosis and management
» Glaucoma
» Hearing loss in old age: Assessment and management
69
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
Session: ICOPE-based sensory assessment and management
Method: Role play
Session length: 30 minutes
» Role play: 20 minutes
» Question/answer and discussions: 10 minutes
» Additional materials required: WHO Simple eye chart (Annexure 3)
Divide the trainee into proportionate groups (maximum 10 in each).
Case scenario:
The facilitator will act as an older person visiting OPD for periodic follow up for diabetes mellitus. For last 1 year she has increasing diff iculty in reading newspaper. Similarly, she also has been complaining of diff iculty in hearing for past few years. She can do all the daily activities by herself and doesn’t require support of his family members for daily activities.
» The trainee will act as an assessor.
» The assessor will make the following enquiries:
a. Chief complaints
b. History of presenting complaints
c. History of geriatric syndrome
d. Past History
e. Family history
f. Socioeconomic history
g. History of addiction
h. History of treatment/drugs
i. History of vaccination
» The assessor will do the general physical examination including vitals.
» The assessor will carry out screening of the intrinsic capacities based on WHO Intrinsic Capacity Screening Questionnaire:
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
70
» The assessor will inform the trainee about the positive screening in the sensory domain (both hearing and vision).
» The assessor will inform the trainees that a detailed assessment of the sensory capacity will be required based on ICOPE strategies.
» Look into the actor’s eyes: If there are changes such as red eyes, secretions, scars, ongoing pain, intolerance to sunlight or a cataract, an eye care professional (ophthalmologist, optometrist) should examine the person.
Check for distance vision» The assessor will check the distance vision of the actor using WHO Simple eye chart.
» Demonstrate close to the person how to do the E test by showing the direction the Es point.
1. Test with the four small Es at 3 metres.
Vision is normal (6/18 or better) if the direction of at least ¾ small Es can be seen.
2. If not able to see at least 3 of the small Es, test with large Es at 3 metres.
If the Es are seen, vision is 6/60.
3. If not able to see at least 3 of the large Es, test with the large Rs at 1.5 metres.
If at least 3 out of 4 large Es are seen, vision is 3/30.
Check for near visionThe assessor will check the distance vision of the actor using WHO Simple eye chart. Demonstrate close to the person how to do the E test by showing the direction the Es point.
1. Let the actor hold the near vision test card as close as he/she wants. Test from the largest to the smallest Es. At least 3 out of 4 must be correct in each line before testing the next.
2. If only the largest size (N48) can be seen, refer for a comprehensive eye and vision examination and specialized eye care.
3. The medium size (N20) is similar to the print in large-print books. The smallest size (N8) is similar to print in newspaper.
Note: Please refer to WHO ICOPE Screening Tool on page 41
71
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
Check for hearing: Whisper test: The following are the steps of the whisper test.
1. Stand about an arm’s length away behind and to the side of the person.
Ask the person or an assistant to close off the opposite ear by pressing on the tragus.
2. Breathe out and then softly whisper several words. Use any common, unrelated words.
Ask the person to repeat the words. If the person repeats the words and you are sure that he/she can hear you clearly, then the person is likely to have normal hearing in this ear.
3. Repeat the same with the other ear.
» The facilitator should inform the trainees that, if the person fails the screening test, he/she should be referred to a specialist for further management.
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
72
Session: Cancer and palliative care
Method: PowerPoint presentation
Session length: 30 minutes
» PowerPoint presentation: 20 minutes
» Case study: 5 minutes
» Question/answer and discussions: 5 minutes
Welcome the trainees to the session.
Display the slide with learning objectives of the module as given below.
Explain the learning objectives to trainees, by the end of this session, trainees will be able:
To enumerate the peculiarities of cancer in old age
To enumerate the alarm signs for cancer in old age
To enumerate the role of primary care physicians in palliative care.
Project the presentation on “Module 14: Cancer and palliative care”.
Discuss the contents of the slides.
Ask trainees if they have any questions or doubts. List these on the flip chart.
Respond to questions and doubts
Key points for discussion
» Cancer and its delay in diagnosis in old age
» Alarm signs and symptoms for cancer
» Role of primary care physicians in management of cancer in the community
» Palliative care and its components
» Control of cancer pain and WHO analgesic ladder
73
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
Session: Elder abuse
Method: PowerPoint presentation and case study
Session length: 30 minutes
» PowerPoint presentation: 20 minutes
» Case study: 5 minutes
» Question/answer and discussions: 5 minutes
Welcome the trainees to the session.
Display the slide with learning objectives of the module as given below.
Explain the learning objectives to trainees, by the end of this session, trainees will be able:
To define elder abuse and explain its various forms
To understand the signs and symptoms of elder abuse.
Project the presentation on “Module 15: Elder abuse”
Discuss the contents of the slides.
Ask trainees if they have any questions or doubts. List these on the flip chart.
Respond to questions and doubts.
Case scenarioA 84-year-old man was brought to the hospital by the neighbours with shortness of breath due to pneumonia. He appeared malnourished and was unable to walk due to extreme pain. He was unable to eat or go to the toilet. On careful examination doctor noted multiple bruises in the body. On detailed enquiry from the patient it was noted that family members were abusing him for his property.
Q.1 What are the signs of abuse?
Q2 Role of physician in tackling this issue
Key points for discussion
» Definition of elder abuse and its various types
» Risk factors for abuse, its signs and symptoms
» Management of elder abuse by a primary care physician.
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
74
Session: Long-term care and caregivers’ issues
Method: PowerPoint presentation and case study
Session length: 30 minutes
» PowerPoint presentation: 20 minutes
» Case study: 5 minutes
» Question/answer and discussions: 5 minutes
Welcome the trainees to the session.
Display the slide with learning objectives of the module as given below.
Explain the learning objectives to trainees; by the end of this session, trainees will be able:
To understand the concepts of long-term care and its various forms
To understand the issues related to the caregiving.
Project the presentation on “Module 16: Long-term care and caregivers’ issues”.
Discuss the contents of the slides.
Ask trainees if they have any questions or doubts. List these on the flip chart.
Case studyAfter seeking follow-up advice for an 84-year-old man with moderately severe dementia in the Memory Clinic, the 45-year-old daughter-in-law visited the memory clinic with complaints of anxiety, lack of motivation, irritability and suicidal ideation for the last three months. On detailed enquiry it was noted that the father-in-law was having several behavioural symptoms such as aggressive behaviour, over-eating and going out from home.
Q1. What is the diagnosis? How to mitigate caregiver stress in elderly suff ering from dementia? What is the role of primary care physician in this scenario?
Q2: What are the features of caregiver stress in this scenario?
Key points for discussion
» Define long-term care and its various models
» Issues related to care-giving
» Role of primary care physicians in managing caregiver stress syndrome.
75
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
Annexure 1:Sample questionnaire for pre- and post-training knowledge assessment
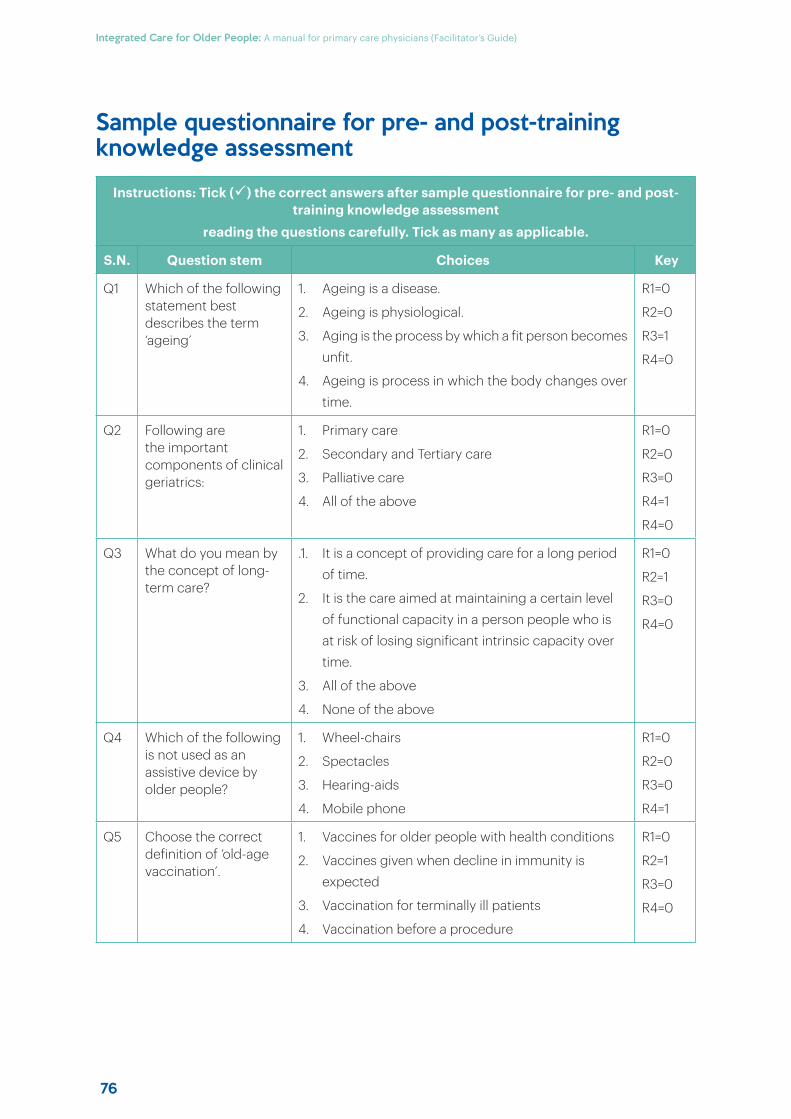
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
76
Sample questionnaire for pre- and post-training knowledge assessment
Instructions: Tick () the correct answers after sample questionnaire for pre- and post-training knowledge assessment
reading the questions carefully. Tick as many as applicable.
S.N. Question stem Choices Key
Q1 Which of the following statement best describes the term ‘ageing’
1. Ageing is a disease.
2. Ageing is physiological.
3. Aging is the process by which a fit person becomes unfit.
4. Ageing is process in which the body changes over time.
R1=0
R2=0
R3=1
R4=0
Q2 Following are the important components of clinical geriatrics:
1. Primary care
2. Secondary and Tertiary care
3. Palliative care
4. All of the above
R1=0
R2=0
R3=0
R4=1
R4=0
Q3 What do you mean by the concept of long-term care?
.1. It is a concept of providing care for a long period of time.
2. It is the care aimed at maintaining a certain level of functional capacity in a person people who is at risk of losing significant intrinsic capacity over time.
3. All of the above
4. None of the above
R1=0
R2=1
R3=0
R4=0
Q4 Which of the following is not used as an assistive device by older people?
1. Wheel-chairs
2. Spectacles
3. Hearing-aids
4. Mobile phone
R1=0
R2=0
R3=0
R4=1
Q5 Choose the correct definition of ‘old-age vaccination’.
1. Vaccines for older people with health conditions
2. Vaccines given when decline in immunity is expected
3. Vaccination for terminally ill patients
4. Vaccination before a procedure
R1=0
R2=1
R3=0
R4=0
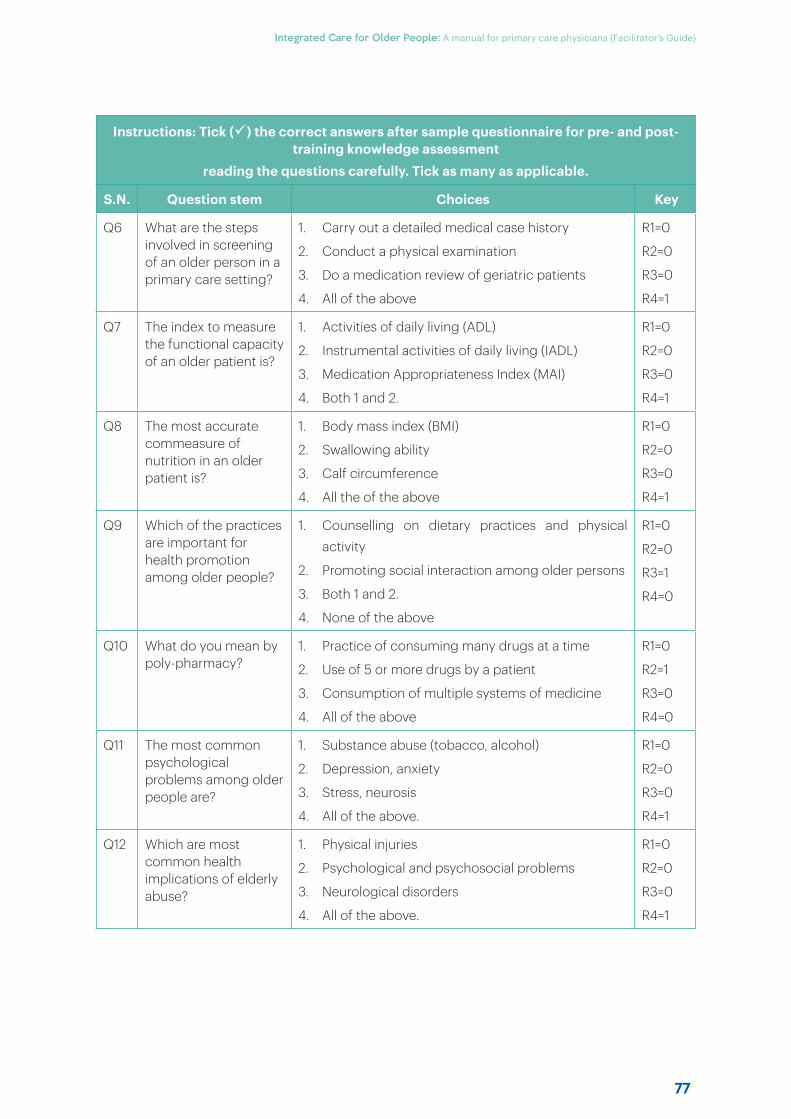
77
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
Instructions: Tick () the correct answers after sample questionnaire for pre- and post-training knowledge assessment
reading the questions carefully. Tick as many as applicable.
S.N. Question stem Choices Key
Q6 What are the steps involved in screening of an older person in a primary care setting?
1. Carry out a detailed medical case history
2. Conduct a physical examination
3. Do a medication review of geriatric patients
4. All of the above
R1=0
R2=0
R3=0
R4=1
Q7 The index to measure the functional capacity of an older patient is?
1. Activities of daily living (ADL)
2. Instrumental activities of daily living (IADL)
3. Medication Appropriateness Index (MAI)
4. Both 1 and 2.
R1=0
R2=0
R3=0
R4=1
Q8 The most accurate commeasure of nutrition in an older patient is?
1. Body mass index (BMI)
2. Swallowing ability
3. Calf circumference
4. All the of the above
R1=0
R2=0
R3=0
R4=1
Q9 Which of the practices are important for health promotion among older people?
1. Counselling on dietary practices and physical activity
2. Promoting social interaction among older persons
3. Both 1 and 2.
4. None of the above
R1=0
R2=0
R3=1
R4=0
Q10 What do you mean by poly-pharmacy?
1. Practice of consuming many drugs at a time
2. Use of 5 or more drugs by a patient
3. Consumption of multiple systems of medicine
4. All of the above
R1=0
R2=1
R3=0
R4=0
Q11 The most common psychological problems among older people are?
1. Substance abuse (tobacco, alcohol)
2. Depression, anxiety
3. Stress, neurosis
4. All of the above.
R1=0
R2=0
R3=0
R4=1
Q12 Which are most common health implications of elderly abuse?
1. Physical injuries
2. Psychological and psychosocial problems
3. Neurological disorders
4. All of the above.
R1=0
R2=0
R3=0
R4=1
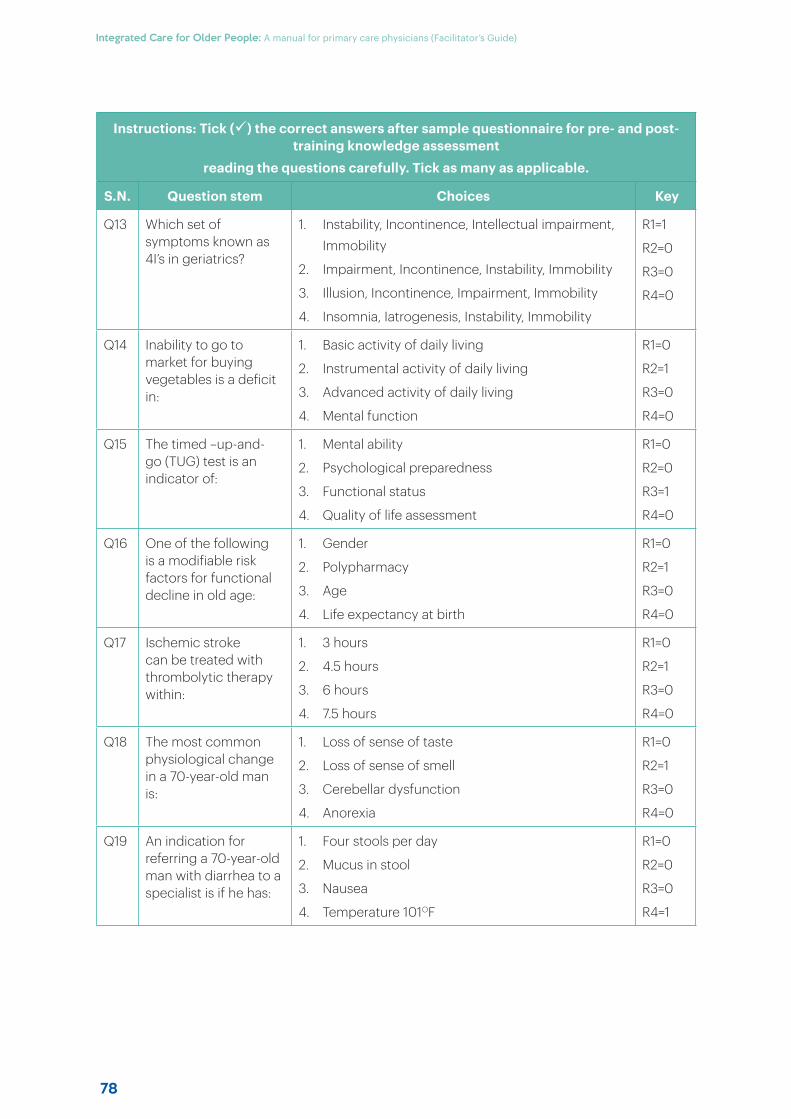
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
78
Instructions: Tick () the correct answers after sample questionnaire for pre- and post-training knowledge assessment
reading the questions carefully. Tick as many as applicable.
S.N. Question stem Choices Key
Q13 Which set of symptoms known as 4I’s in geriatrics?
1. Instability, Incontinence, Intellectual impairment, Immobility
2. Impairment, Incontinence, Instability, Immobility
3. Illusion, Incontinence, Impairment, Immobility
4. Insomnia, Iatrogenesis, Instability, Immobility
R1=1
R2=0
R3=0
R4=0
Q14 Inability to go to market for buying vegetables is a deficit in:
1. Basic activity of daily living
2. Instrumental activity of daily living
3. Advanced activity of daily living
4. Mental function
R1=0
R2=1
R3=0
R4=0
Q15 The timed –up-and-go (TUG) test is an indicator of:
1. Mental ability
2. Psychological preparedness
3. Functional status
4. Quality of life assessment
R1=0
R2=0
R3=1
R4=0
Q16 One of the following is a modifiable risk factors for functional decline in old age:
1. Gender
2. Polypharmacy
3. Age
4. Life expectancy at birth
R1=0
R2=1
R3=0
R4=0
Q17 Ischemic stroke can be treated with thrombolytic therapy within:
1. 3 hours
2. 4.5 hours
3. 6 hours
4. 7.5 hours
R1=0
R2=1
R3=0
R4=0
Q18 The most common physiological change in a 70-year-old man is:
1. Loss of sense of taste
2. Loss of sense of smell
3. Cerebellar dysfunction
4. Anorexia
R1=0
R2=1
R3=0
R4=0
Q19 An indication for referring a 70-year-old man with diarrhea to a specialist is if he has:
1. Four stools per day
2. Mucus in stool
3. Nausea
4. Temperature 101OF
R1=0
R2=0
R3=0
R4=1
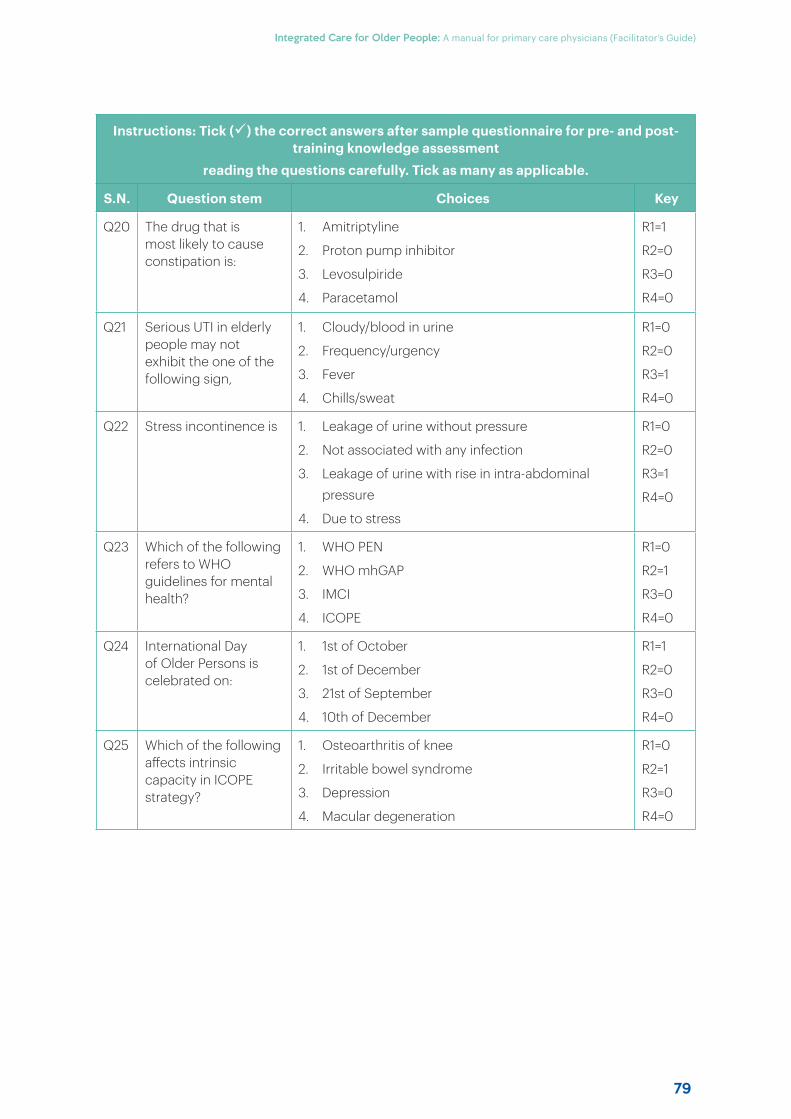
79
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
Instructions: Tick () the correct answers after sample questionnaire for pre- and post-training knowledge assessment
reading the questions carefully. Tick as many as applicable.
S.N. Question stem Choices Key
Q20 The drug that is most likely to cause constipation is:
1. Amitriptyline
2. Proton pump inhibitor
3. Levosulpiride
4. Paracetamol
R1=1
R2=0
R3=0
R4=0
Q21 Serious UTI in elderly people may not exhibit the one of the following sign,
1. Cloudy/blood in urine
2. Frequency/urgency
3. Fever
4. Chills/sweat
R1=0
R2=0
R3=1
R4=0
Q22 Stress incontinence is 1. Leakage of urine without pressure
2. Not associated with any infection
3. Leakage of urine with rise in intra-abdominal pressure
4. Due to stress
R1=0
R2=0
R3=1
R4=0
Q23 Which of the following refers to WHO guidelines for mental health?
1. WHO PEN
2. WHO mhGAP
3. IMCI
4. ICOPE
R1=0
R2=1
R3=0
R4=0
Q24 International Day of Older Persons is celebrated on:
1. 1st of October
2. 1st of December
3. 21st of September
4. 10th of December
R1=1
R2=0
R3=0
R4=0
Q25 Which of the following aff ects intrinsic capacity in ICOPE strategy?
1. Osteoarthritis of knee
2. Irritable bowel syndrome
3. Depression
4. Macular degeneration
R1=0
R2=1
R3=0
R4=0

Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
80
81
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
Annexure 2:ICOPE care pathways
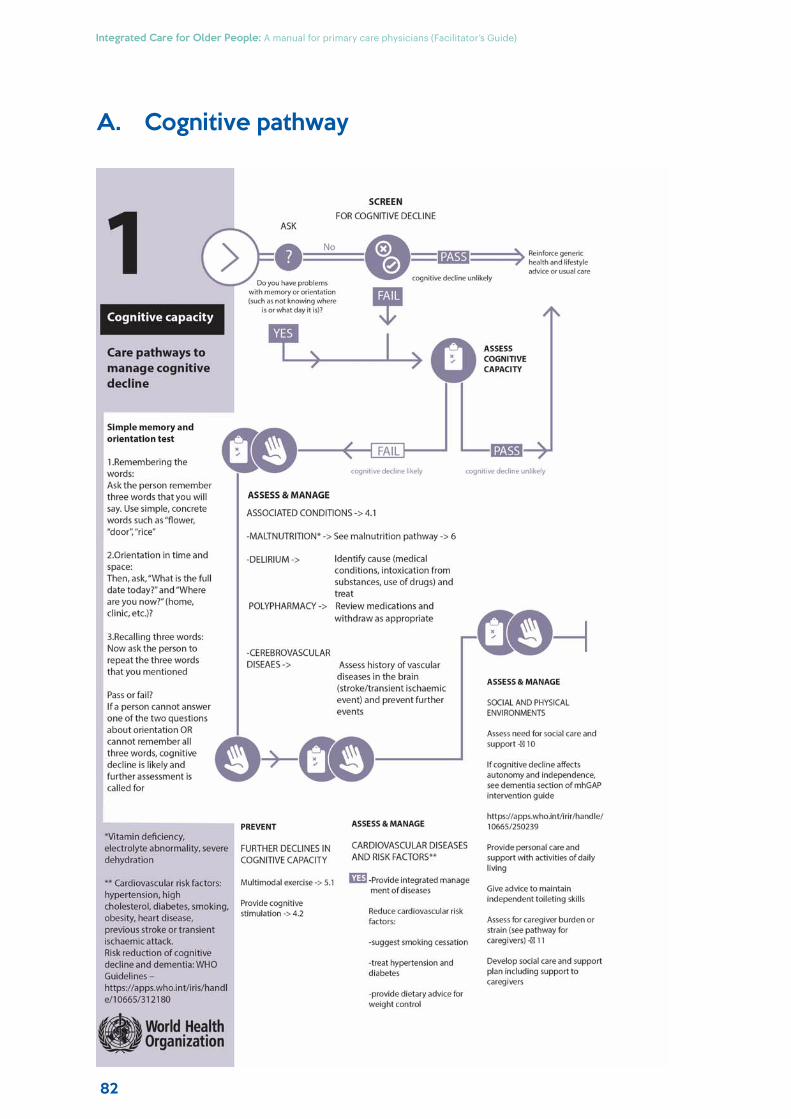
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
82
A. Cognitive pathway
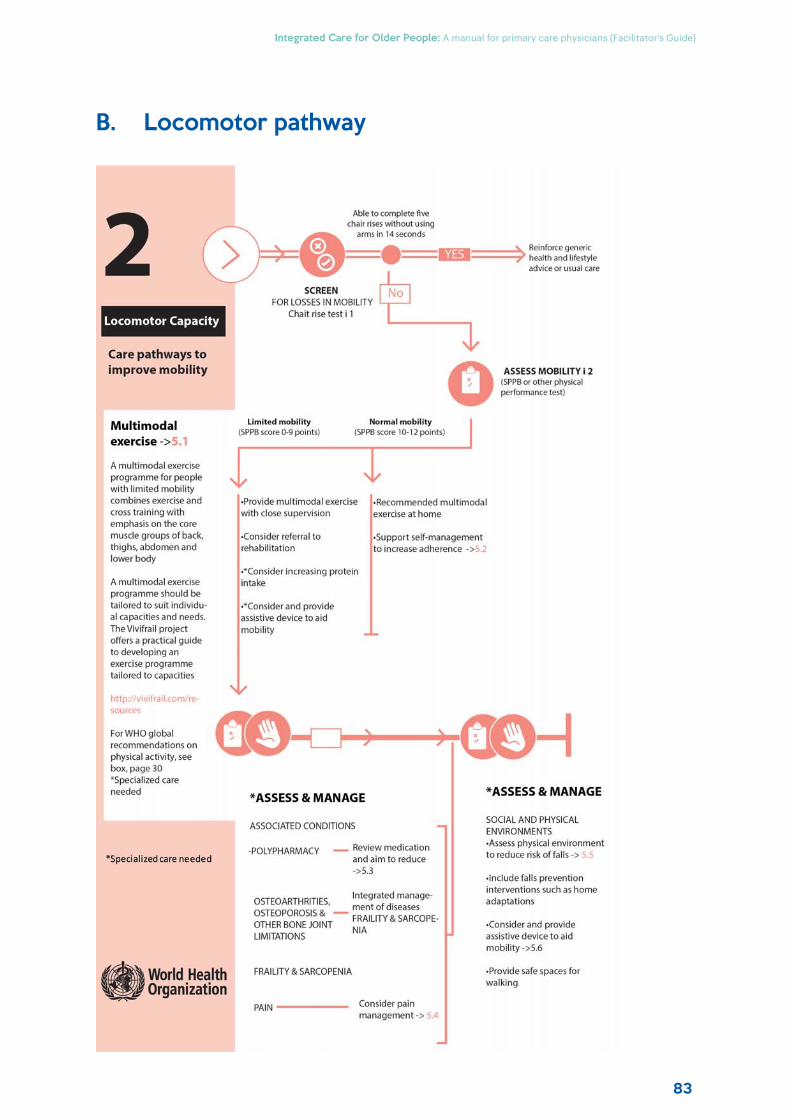
83
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
B. Locomotor pathway
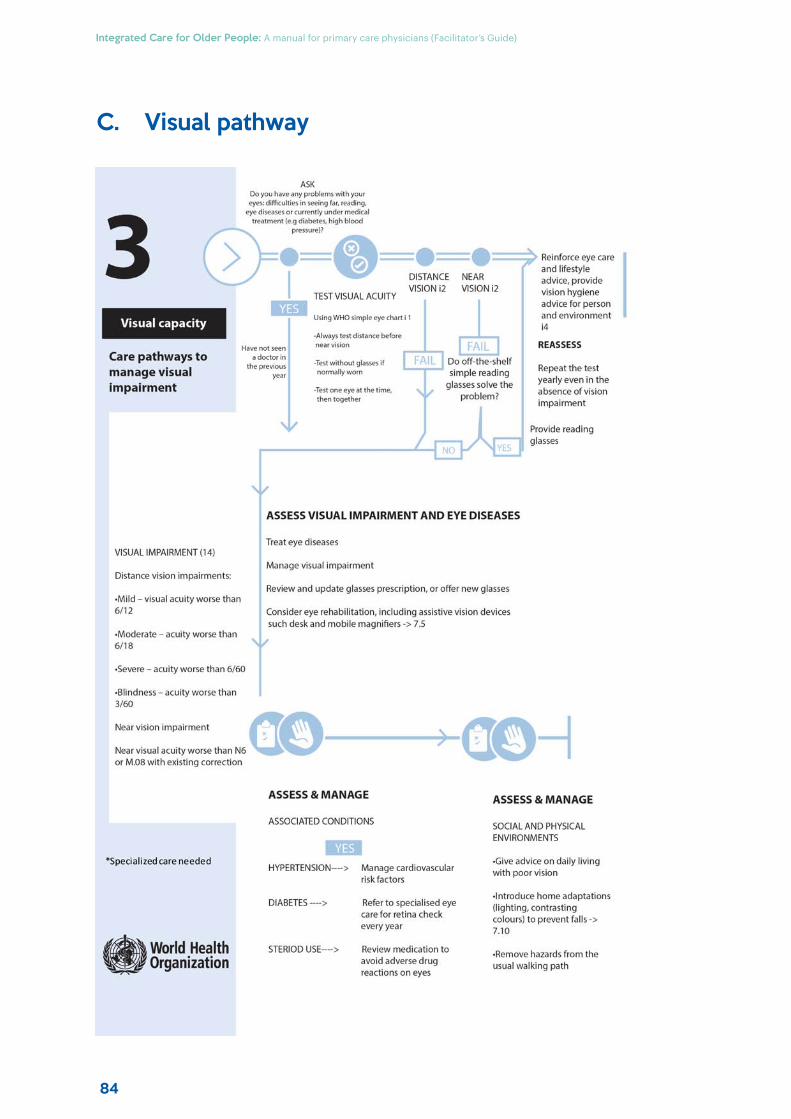
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
84
C. Visual pathway
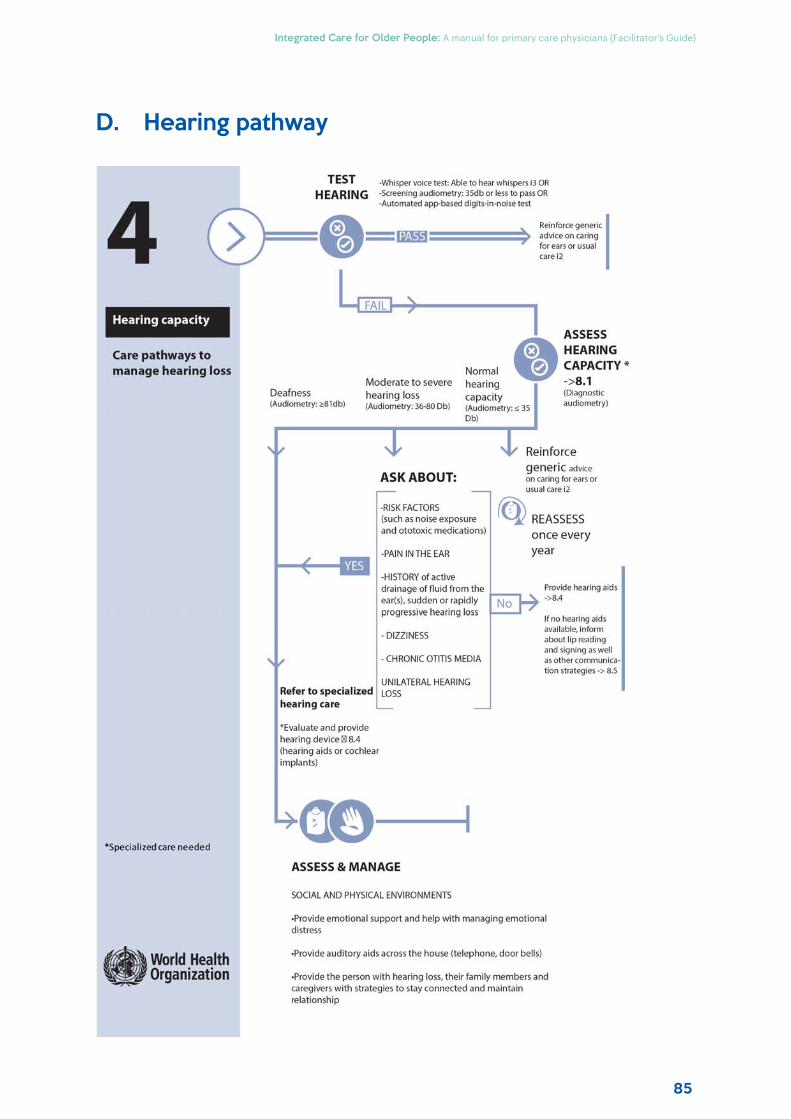
85
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
D. Hearing pathway
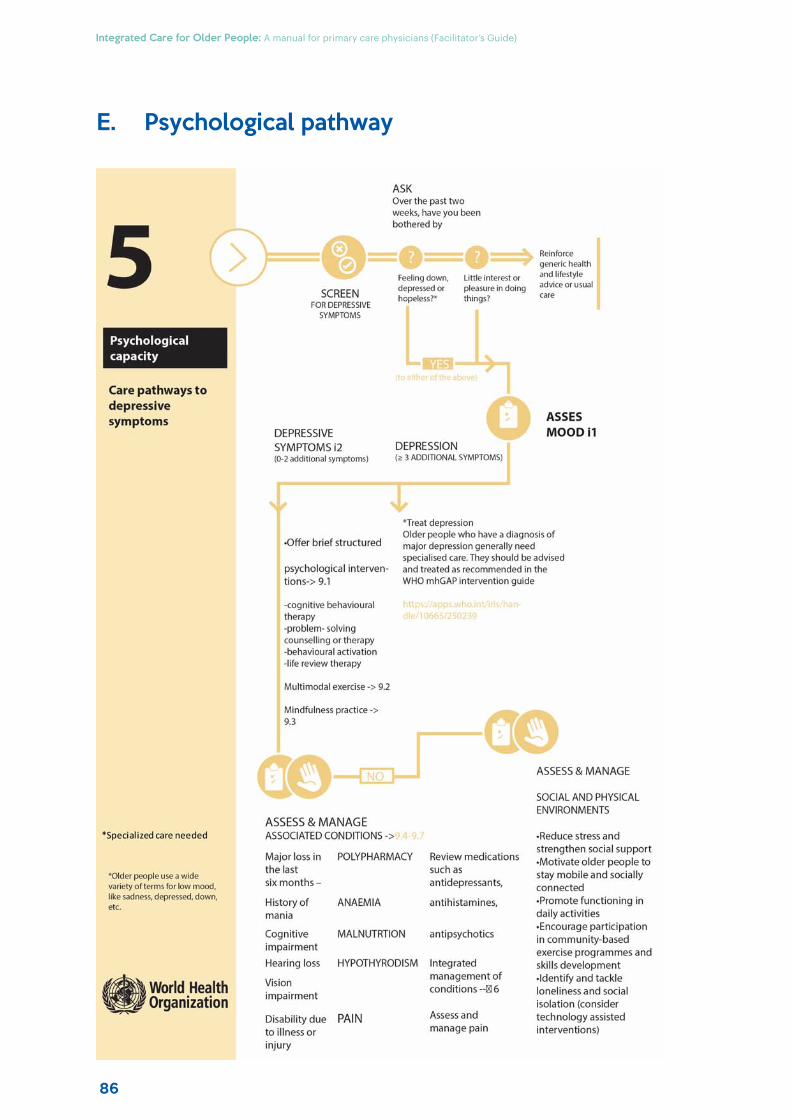
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
86
E. Psychological pathway
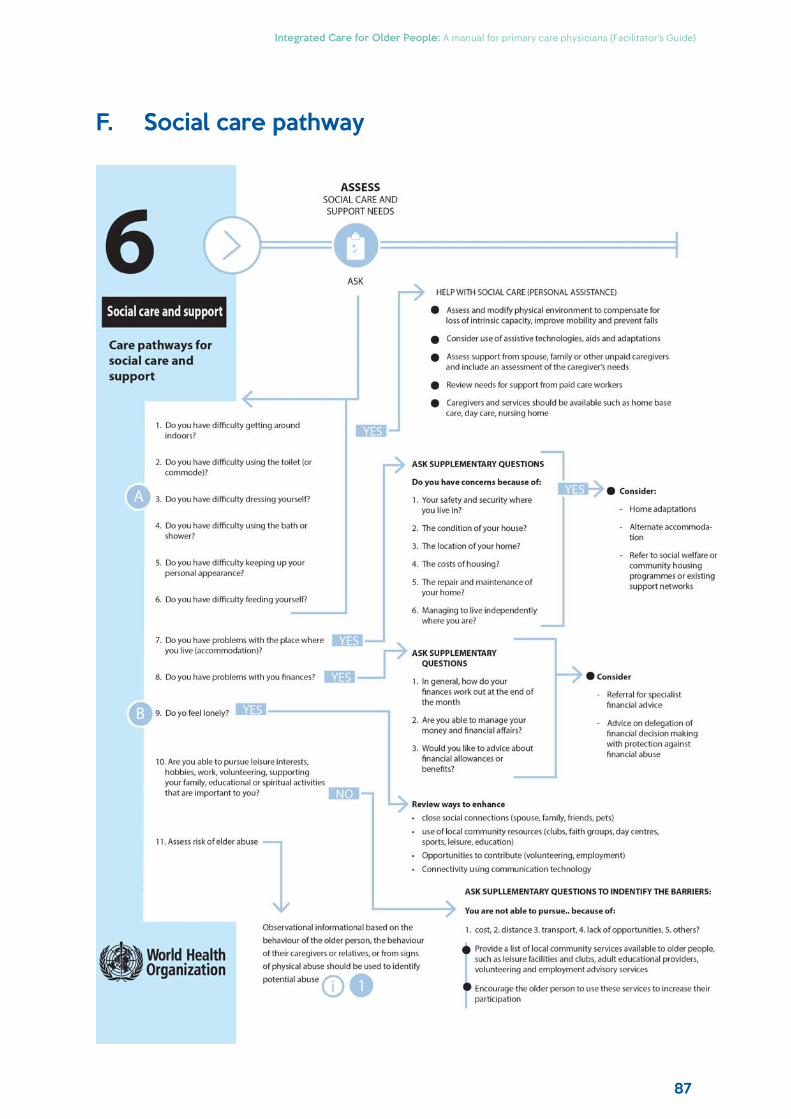
87
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
F. Social care pathway

Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
88
89
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
Annexure 3:WHO simple eye chart
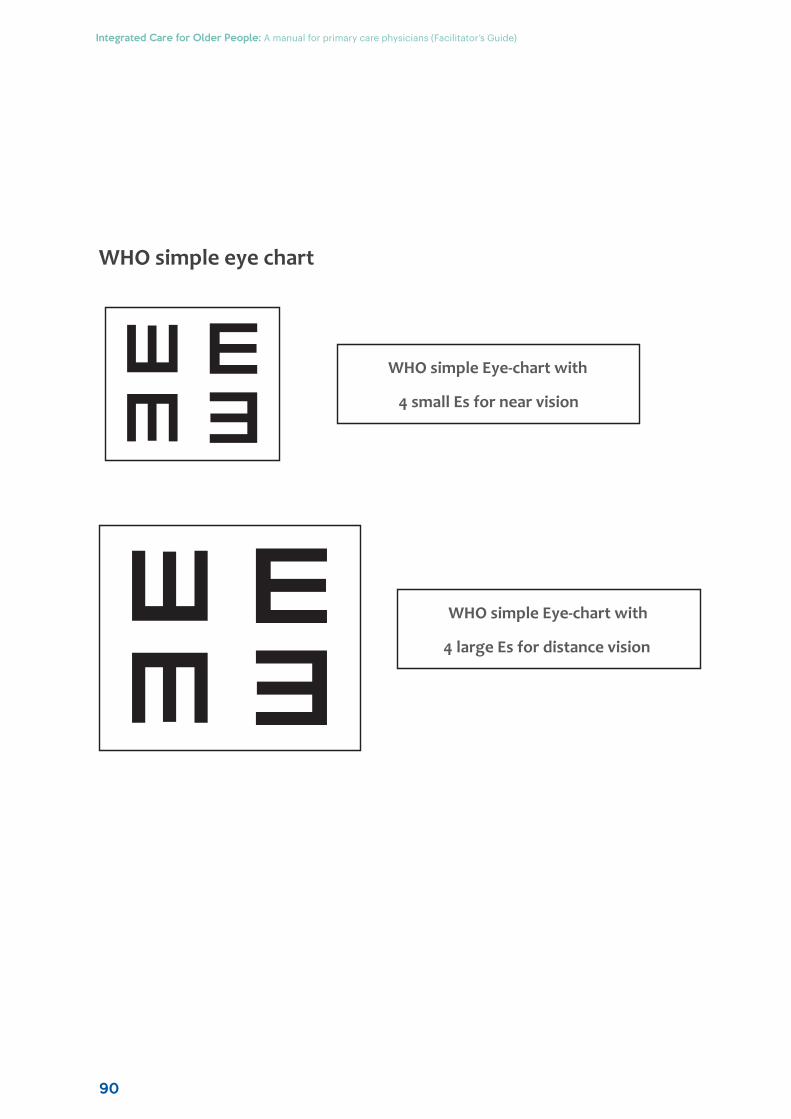
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
90
WHO simple eye chart
WHO simple Eye-chart with
4 small Es for near vision
WHO simple Eye-chart with
4 large Es for distance vision
91
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
Annexure 4:PowerPoint presentation slides
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
92
Talking points
Module 1: Integrated care for older people (ICOPE)
Slide 1:
In this module, we will discuss about a new way of managing an older patient with complex health problems.
Slide 2:
This module, has three learning objectives. Read them out explaining each point from reference manual.
Slide 3:
The new ICOPE approach of WHO reflects a community-based strategy. This approach will help to reorient health and social services towards a person-centered and coordinated model of care to support optimization of functional ability for older people to face the environmental challenges.
IIntegrated care for older people (ICOPE)
Module - 1
• To define the concepts of integrated care of older people• To learn measurement of intrinsic capacity of older people• To learn the concept of person-centered care through ICOPE
pathways
Learning Outcomes
ICOPE reflects a community-based approach that will help tore-orient health and social services towards a more person-centered and coordinated model of care that supportsoptimising functional ability for older people.
ICOPE approach
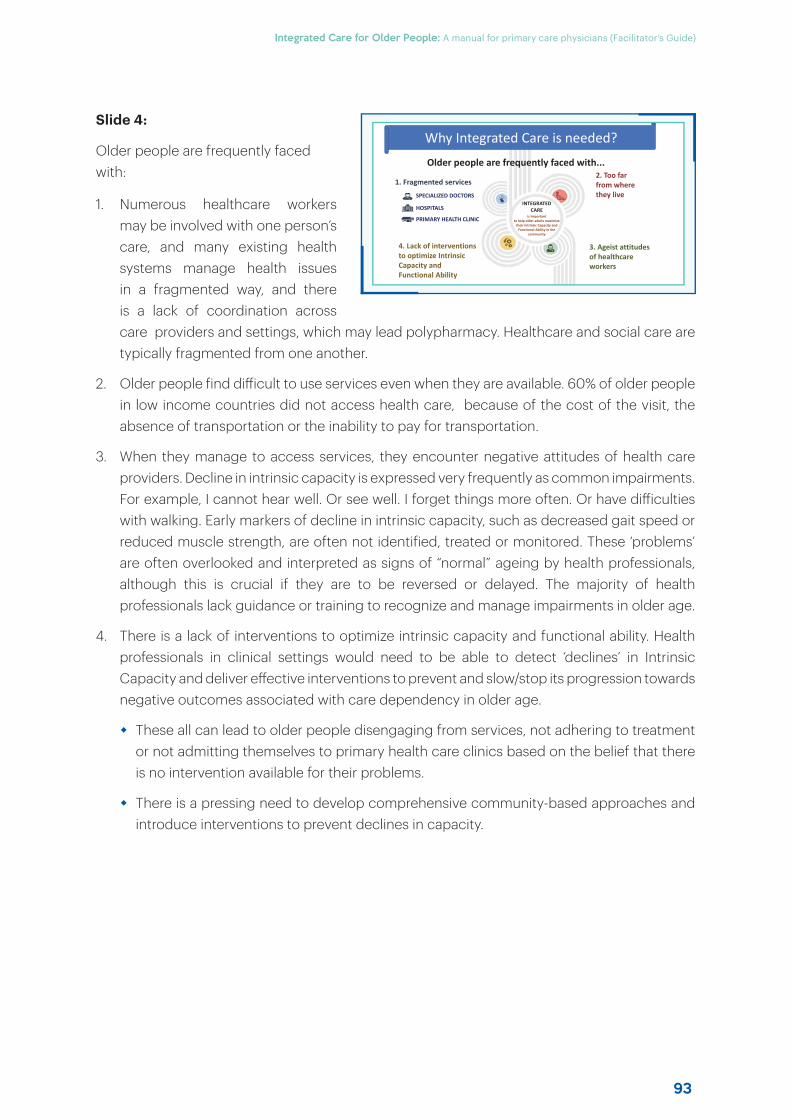
93
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
Slide 4:
Older people are frequently faced with:
1. Numerous healthcare workers may be involved with one person’s care, and many existing health systems manage health issues in a fragmented way, and there is a lack of coordination across care providers and settings, which may lead polypharmacy. Healthcare and social care are typically fragmented from one another.
2. Older people find diff icult to use services even when they are available. 60% of older people in low income countries did not access health care, because of the cost of the visit, the absence of transportation or the inability to pay for transportation.
3. When they manage to access services, they encounter negative attitudes of health care providers. Decline in intrinsic capacity is expressed very frequently as common impairments. For example, I cannot hear well. Or see well. I forget things more often. Or have diff iculties with walking. Early markers of decline in intrinsic capacity, such as decreased gait speed or reduced muscle strength, are often not identified, treated or monitored. These ‘problems’ are often overlooked and interpreted as signs of “normal” ageing by health professionals, although this is crucial if they are to be reversed or delayed. The majority of health professionals lack guidance or training to recognize and manage impairments in older age.
4. There is a lack of interventions to optimize intrinsic capacity and functional ability. Health professionals in clinical settings would need to be able to detect ‘declines’ in Intrinsic Capacity and deliver eff ective interventions to prevent and slow/stop its progression towards negative outcomes associated with care dependency in older age.
These all can lead to older people disengaging from services, not adhering to treatment or not admitting themselves to primary health care clinics based on the belief that there is no intervention available for their problems.
There is a pressing need to develop comprehensive community-based approaches and introduce interventions to prevent declines in capacity.
INTEGRATED CARE
is important to help older adults maximize
their Intrinsic Capacity and Functional Ability in the
community
1. Fragmented services2. Too far from where they live
3. Ageist attitudes of healthcare workers
4. Lack of interventions to optimize Intrinsic Capacity and Functional Ability
SPECIALIZED DOCTORS
HOSPITALS
PRIMARY HEALTH CLINIC
Older people are frequently faced with...
Why Integrated Care is needed?
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
94
Slide 5:
Here are the principles of ICOPE person-centered care.
The aim is to maximize intrinsic capacity and functional ability.
» It is essential older person is involved in decision making and goal setting and those goals are set and prioritized according to the person’s value, needs and preferences and then develop the personalized care plans
» Opportunities to involve the communities in supporting care must be explored. Multicomponent interventions, should be delivered at home and in the community. Such as strength and resistance exercise, oral supplemental nutrition, home adaptation to prevent falls, and cognitive stimulation
» Assessment and management should involve multi-disciplinary health and social care workers
» Support for self-management includes providing older people with information, skills and tools, respecting their autonomy and abilities to direct their own care (mAgeing)
» Supporting caregivers includes to provide basic information about the older person’s health conditions and training to develop practical skills, and explore opportunities to involve communities and neighborhood
» Strong referral pathways to specialized care are important such as geriatric care, acute acre in case of unforeseen events, and palliative care. Furthermore, regular follow up is essential, as it promotes early detection of changes in functional status.
Slide 6:
The concept of Intrinsic capacity was launched by WHO in World Report on Ageing and Health which defines the healthy ageing focuses on the goal of maintaining functional ability, across the life course. There are two key words related to healthy ageing concept: intrinsic capacity and functional ability. WHO defines intrinsic capacity as a combination of individuals physical and mental capacities. Functional ability is the Combination and interaction of intrinsic capacity with the environment a person inhabits
Support caregivers
Support for self-management
Multidisciplinary care teams
Community-level and home-based interventions
Person-centered assessment & personalized care plans
Maximize intrinsic capacity and functional ability
Ensure referral and follow up
What is ICOPE person-centered care?
Combination of all the physical and mental capacities of an individualDOMAINS OF INTRINSIC CAPACITY
Intrinsic Capacity (IC)
95
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
For example, my visual acuity is low which is my intrinsic capacity, but with contract lenses or glasses, my functional ability for vision is fine.
As people age, their intrinsic capacity become more chronic and complex. Multimorbidity – the presence of multiple chronic conditions at the same time – is increasingly prevalent with age. The health and social needs of older people are typically complex and long-term. There are limitations of traditional models of care.
• Assess the domain associated with loss of intrinsic capacity in greaterdepth.
• Understand the life of the older person – conventional history-takingwith a thorough understanding of the person’s life, values, priorities andpreferences regarding his/her health and its management
• Assess and manage the underlying diseases – assess the underlyingchronic illnesses and assess for polypharmacy
• Assess the patient’s needs for social care support (home, institution).
Steps for person-centered assessment
Slide 7:
Person centered assessment is a modification of the existing way of assessing an older patient. Read out each point and discuss with examples if possible.
Slide 8:
The first step in person centered approach is screening; which in case of ICOPE has been put in diff erent domains.
Slide 9:
If a person cannot answer one of the two questions about the orientation,
OR
cannot remember all three words; this is considered abnormal and step 2 assessment is required.
ICOPE SCREENING
ASK• Do you have problems with memory and orientation?
or1. Remember three words: flower, door, rice 2. Orientation in time and space: What is the full date
today?Where are you now (home, clinic, etc)?
3. Recalls the three words?
A person who cannot answer one of two questions about the orientation OR cannot remember all three words Go To Step 2
Cognitive decline: Step 1
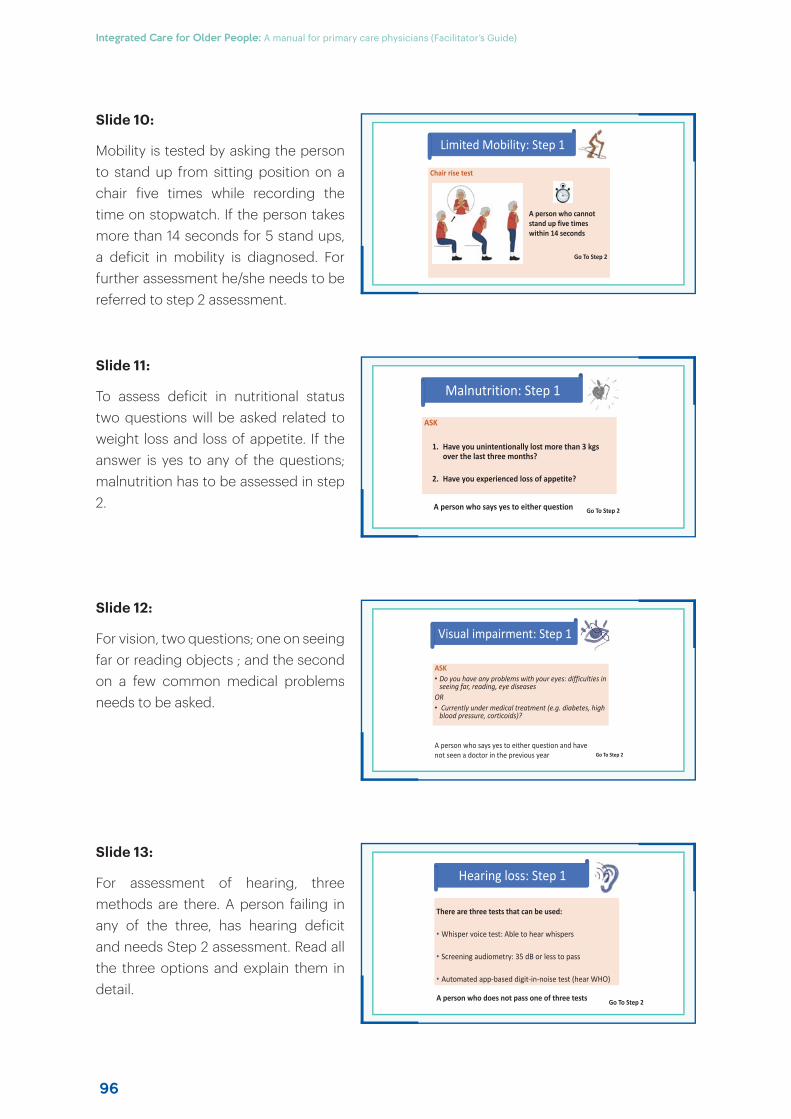
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
96
Slide 10:
Mobility is tested by asking the person to stand up from sitting position on a chair five times while recording the time on stopwatch. If the person takes more than 14 seconds for 5 stand ups, a deficit in mobility is diagnosed. For further assessment he/she needs to be referred to step 2 assessment.
Slide 11:
To assess deficit in nutritional status two questions will be asked related to weight loss and loss of appetite. If the answer is yes to any of the questions; malnutrition has to be assessed in step 2.
Slide 12:
For vision, two questions; one on seeing far or reading objects ; and the second on a few common medical problems needs to be asked.
Slide 13:
For assessment of hearing, three methods are there. A person failing in any of the three, has hearing deficit and needs Step 2 assessment. Read all the three options and explain them in detail.
Chair rise test
A person who cannot stand up five times within 14 seconds
Go To Step 2
Limited Mobility: Step 1
ASK
1. Have you unintentionally lost more than 3 kgs over the last three months?
2. Have you experienced loss of appetite?
A person who says yes to either question Go To Step 2
Malnutrition: Step 1
ASK• Do you have any problems with your eyes: difficulties in
seeing far, reading, eye diseasesOR• Currently under medical treatment (e.g. diabetes, high
blood pressure, corticoids)?
A person who says yes to either question and have not seen a doctor in the previous year Go To Step 2
Visual impairment: Step 1
There are three tests that can be used:
• Whisper voice test: Able to hear whispers
• Screening audiometry: 35 dB or less to pass
• Automated app-based digit-in-noise test (hear WHO)
A person who does not pass one of three tests Go To Step 2
Hearing loss: Step 1
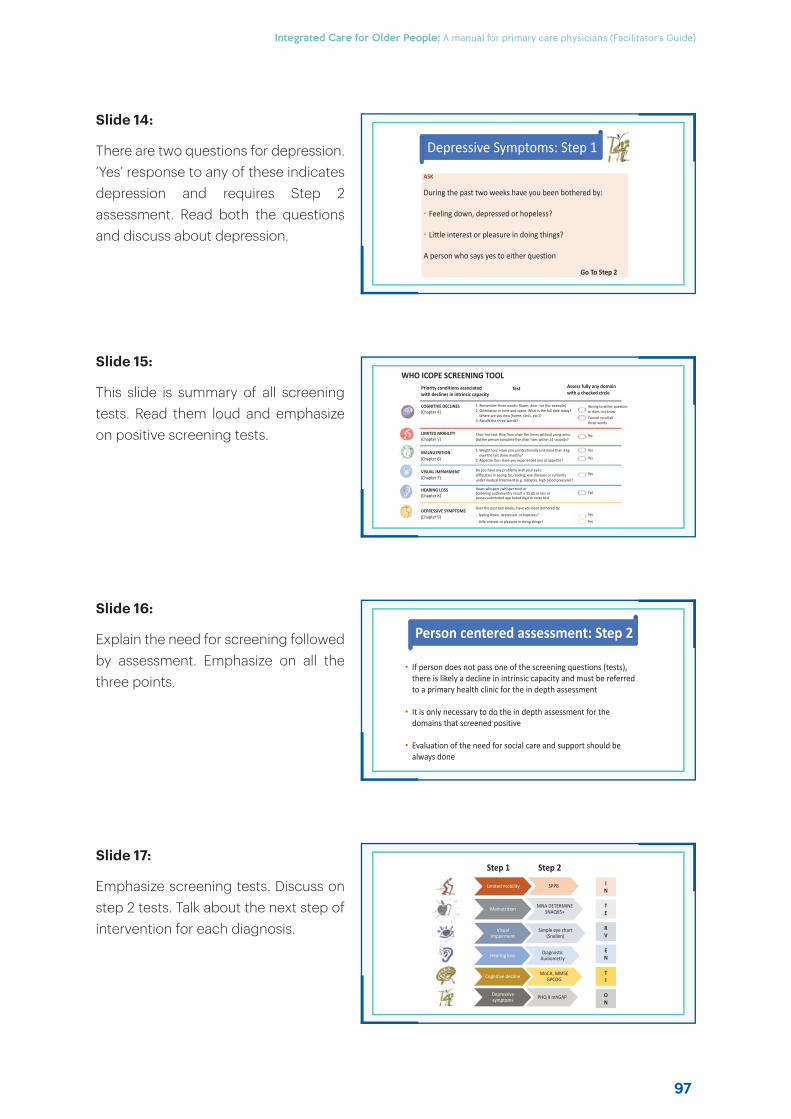
97
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
Slide 14:
There are two questions for depression. ‘Yes’ response to any of these indicates depression and requires Step 2 assessment. Read both the questions and discuss about depression.
Slide 15:
This slide is summary of all screening tests. Read them loud and emphasize on positive screening tests.
Slide 16:
Explain the need for screening followed by assessment. Emphasize on all the three points.
Slide 17:
Emphasize screening tests. Discuss on step 2 tests. Talk about the next step of intervention for each diagnosis.
ASK
During the past two weeks have you been bothered by:
• Feeling down, depressed or hopeless?
• Little interest or pleasure in doing things?
A person who says yes to either question
Go To Step 2
Depressive Symptoms: Step 1
WHO ICOPE SCREENING TOOLPriority conditions associatedwith declines in intrinsic capacity
Test Assess fully any domainwith a checked circle
COGNITIVE DECLINES(Chapter 4)
1. Remember three words: flower, door rice (for example)2. Orientation in time and space: What is the full date today?
Where are you now (home, clinic, etc.)?3. Recalls the three words?
Wrong to either question or does not knowCannot recall all three words
LIMITED MOBILITY(Chapter 5)
Chair rise test: Rise from chair five times without using arms.Did the person complete five chair rises within 14 seconds?
No
MALNUTRITION(Chapter 6)
1. Weight loss: Have you unintentionally lost more than 3 kg over the last three months?
2. Appetite loss: Have you experienced loss of appetite?
Yes
Yes
VISUAL IMPAIRMENT(Chapter 7)
Do you have any problems with your eyes:difficulties in seeing far, reading, eye diseases or currently under medical treatment (e.g. diabetes, high blood pressure)?
Yes
HEARING LOSS(Chapter 8)
Hears whispers (whisper test) or Screening audiomentry result is 35 db or less or passes automated app based digit in noise test
Fail
DEPRESSIVE SYMPTOMS(Chapter 9)
Over the past two weeks, have you been bothered by
- feeling down, depressed or hopeless?
- little interest or pleasure in doing things?
Yes
Yes
• If person does not pass one of the screening questions (tests), there is likely a decline in intrinsic capacity and must be referred to a primary health clinic for the in depth assessment
• It is only necessary to do the in depth assessment for the domains that screened positive
• Evaluation of the need for social care and support should be always done
Person centered assessment: Step 2
Limited mobility SPPB
Malnutrition MNA DETERMINE SNAQ65+
Visual impairment
Simple eye chart (Snellen)
Hearing loss Diagnostic Audiometry
Cognitive decline MoCA, MMSE GPCOG
Depressive symptoms PHQ 9 mhGAP
IN
TE
EN
RV
TI
ON
Step 1 Step 2
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
98
Slide 18:
Explain each step with examples.
Slide 19:
Explain each step with examples. Some points may not be culturally/socially adaptable in your country. Give their alternative if possible.
Generic care pathway
No loss of intrinsic capacity
Reinforce generic health and lifestyle advice or usual careSTEP 1
SCREEN
STEP 2PERSON-CENTRED ASSESSMENT IN PRIMARY CARE
ASSESS IN GREATER DEPTHFor conditions associated with loss in intrinsic capacity
ASSESS & MANAGEUnderlying diseases
ASSESS & MANAGESocial and physical
environment
STEP 3DEVELOP PERSONALIZED CARE PLAN
STEP 5ENGAGE COMMUNITIES AND SUPPORT CAREGIVERS
STEP 4ENSURE REFERRAL PATHWAY AND MONITORING OF THE CARE PLAN WITH LINKS TO SPECIALIZED GERIATRIC CARE
ScreenFor losses in intrinsic capacity
in the community
ASSESS SOCIAL CARE AND SUPPORT NEEDS
Social care and support
Care pathways for social care and support
ASK
1. Do you have difficulty getting around indoors?
2. Do you have difficulty using the toilet (or commode)?
3. Do you have difficulty dressing yourself?4. Do you have difficulty using the bath or
shower?5. Do you have difficulty keeping up your
personal appearance?6. Do you have difficulty feeding yourself?
7. Do you have problems with the place where you live (accommodation)?
8. Do you have problems with you finances?
9. Do yo feel lonely?
10. Are you able to pursue leisure interests, hobbies, work, volunteering, supporting your family, educational or spiritual activities that are important to you?
11. Assess risk of elder abuse
Observational informational based on the behaviourof the older person, the behaviour of their caregivers or relatives, or from signs of physical abuse should be used to identify potential abuse
HELP WITH SOCIAL CARE (PERSONAL ASSISTANCE) • Assess and modify physical environment to compensate for loss of intrinsic capacity, improve mobility and prevent falls• Consider use of assistive technologies, aids and adaptations• Assess support from spouse, family or other unpaid caregivers and include an assessment of the caregiver’s needs• Review needs for support from paid care workers • Caregivers and services should be available such as home base care, day care, nursing home
ASK SUPPLEMENTARY QUESTIONSDo you have concerns because of: 1. Your safety and security where you
live in?2. The condition of your house?3. The location of your home?4. The costs of housing?5. The repair and maintenance of your
home?6. Managing to live independently
where you are?
Consider: − Home adaptations− Alternate
accommodation− Refer to social welfare or
community housing programmes or existing support networks
Consider− Referral for specialist financial advice − Advice on delegation of financial
decision making with protection against financial abuse
ASK SUPPLEMENTARY QUESTIONS1. In general, how do your
finances work out at the end of the month
2. Are you able to manage your money and financial affairs?
3. Would you like to advice about financial allowances or benefits?
Review ways to enhance• close social connections (spouse, family, friends, pets)• use of local community resources (clubs, faith groups, day centres, sports, leisure, education)• Opportunities to contribute (volunteering, employment) • Connectivity using communication technology
ASK SUPLLEMENTARY QUESTIONS TO INDENTIFY THE BARRIERS:You are not able to pursue.. because of: 1. cost, 2. distance 3. transport, 4. lack of opportunities, 5. others? Provide a list of local community services available to older people, such as leisure facilities and clubs, adult educational providers, volunteering and employment advisory servicesEncourage the older person to use these services to increase their participation
Care pathways for Social care and support
99
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
Talking points
Module 2: Functional assessment of older people
Slide 1:
The core content of assessment of an older person revolves around functional assessment. In this module the concept and practice of functional assessment will be discussed.
Slide 2:
At the end of this module, trainees will be able to enumerate the relevance of conserved functional status and will be able to carry out its assessment.
Slide 3:
Define functional status as provided in the slide and discuss its clinical significance.
Slide 4:
ADLs indicate their importance in life process. While BADLs are the most essential AADLs provide meaning to life.
FFunctional assessment of older people
Module - 2
• To enumerate the relevance of good functional status in older
patients
• To carry out assessment of functional status.
Learning objectives
• It is a measure of the overall impact of an individual's health in the
context of his or her environment and social support network.
• It reflects the ability of an individual to perform the physical and
social tasks necessary for their usual activities and roles.
Functional status
The most commonly used measures of function evaluate the following
three levels of activity of daily life:
• Basic activities of daily living (BADLs)
• Instrumental activities of daily living (IADLs)
• Advanced activities of daily living (AADLs).
Commonly used measures of function
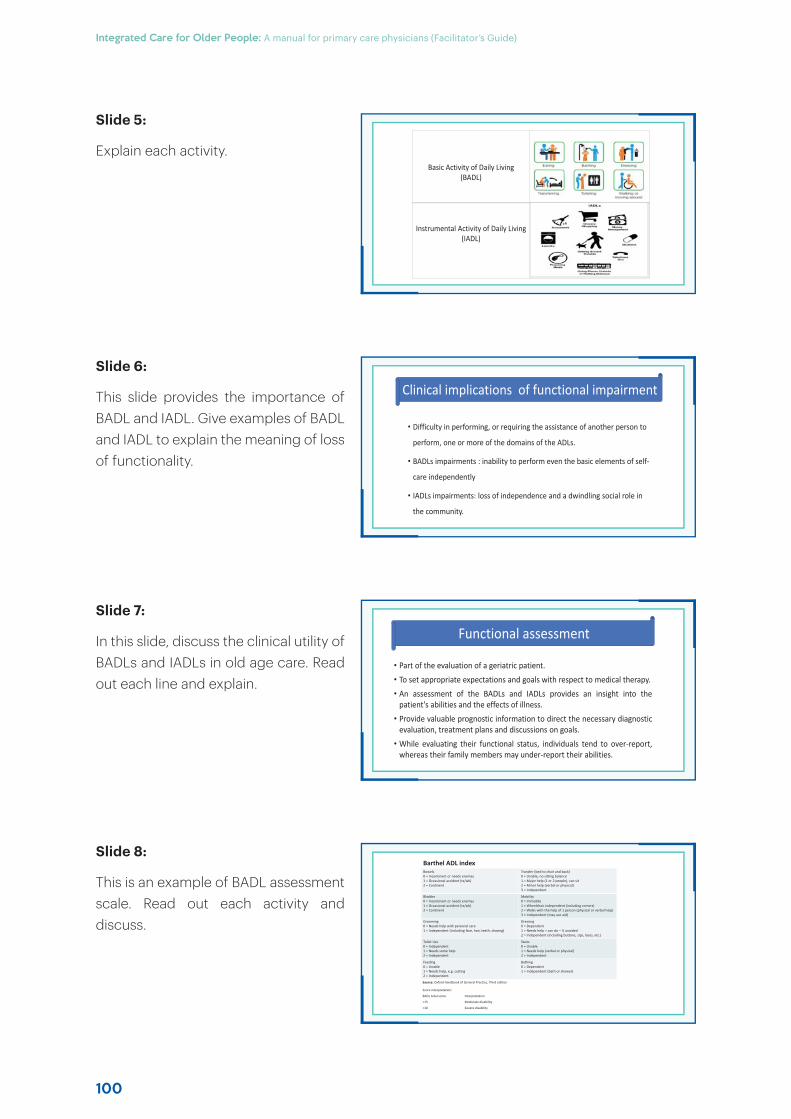
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
100
Slide 5:
Explain each activity.
Slide 6:
This slide provides the importance of BADL and IADL. Give examples of BADL and IADL to explain the meaning of loss of functionality.
Slide 7:
In this slide, discuss the clinical utility of BADLs and IADLs in old age care. Read out each line and explain.
Slide 8:
This is an example of BADL assessment scale. Read out each activity and discuss.
Basic Activity of Daily Living (BADL)
Instrumental Activity of Daily Living (IADL)
• Difficulty in performing, or requiring the assistance of another person to
perform, one or more of the domains of the ADLs.
• BADLs impairments : inability to perform even the basic elements of self-
care independently
• IADLs impairments: loss of independence and a dwindling social role in
the community.
Clinical implications of functional impairment
• Part of the evaluation of a geriatric patient.
• To set appropriate expectations and goals with respect to medical therapy.
• An assessment of the BADLs and IADLs provides an insight into thepatient's abilities and the effects of illness.
• Provide valuable prognostic information to direct the necessary diagnosticevaluation, treatment plans and discussions on goals.
• While evaluating their functional status, individuals tend to over-report,whereas their family members may under-report their abilities.
Functional assessment
Barthel ADL indexBowels0 = Incontinent or needs enemas1 = Occasional accident (tx/wk)2 = Continent
Transfer (bed to chair and back)0 = Unable, no sitting balance1 = Major help (1 or 2 people), can sit2 = Minor help (verbal or physical)3 = Independent
Bladder0 = Incontinent or needs enemas1 = Occasional accident (tx/wk)2 = Continent
Mobility0 = Immobile1 = Wheelchair independent (including comers)2 = Walks with the help of 1 person (physical or verbal help)3 = Independent (may use aid)
Grooming0 = Needs help with personal care1 = Independent (including face, hair, teeth, shaving)
Dressing0 = Dependent1 = Needs help = can do – ½ unaided2 = Independent (including buttons, zips, laces, etc.)
Toilet Use0 = Independent1 = Needs some help2 = Independent
Stairs0 = Unable1 = Needs help (verbal or physical)2 = Independent
Feeding0 = Unable1 = Needs help, e.g. cutting2 = Independent
Bathing0 = Dependent1 = Independent (bath or shower)
Source: Oxford Handbook of General Practice, Third edition
Score interpretation:
BADL total score Interpretation
<15 Moderate disability
<10 Severe disability
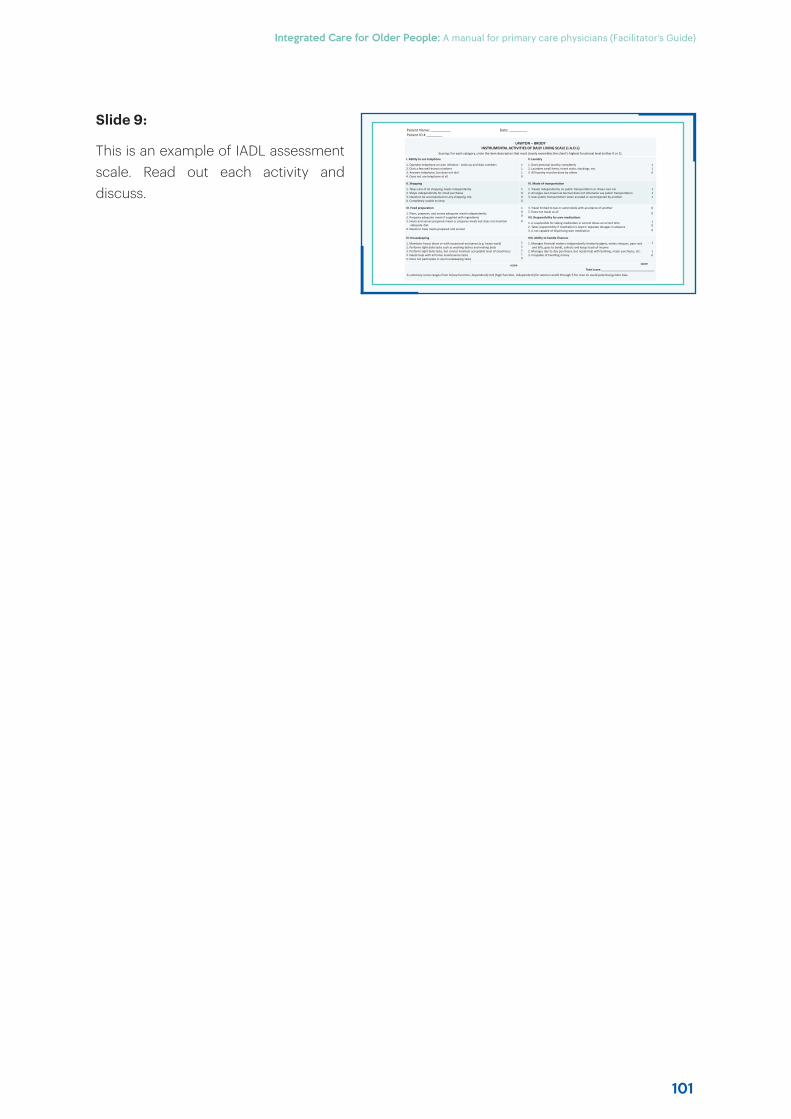
101
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
Slide 9:
This is an example of IADL assessment scale. Read out each activity and discuss.
LAWTON – BRODYINSTRUMENTAL ACTIVITIES OF DAILY LIVING SCALE (I.A.D.L)
Scoring: For each category, circle the item description that most closely resembles the client’s highest functional level (either 0 or 1).
I. Ability to use telephone
1. Operates telephone on own initiative - looks up and dials numbers 2. Dials a few well-known numbers 3. Answers telephone, but does not dial 4. Does not use telephone at all
1110
V. Laundry
1. Does personal laundry completely 2. Launders small items, rinses socks, stockings, etc. 3. All laundry must be done by others
110
II. Shopping
1. Takes care of all shopping needs independently 2. Shops independently for small purchases 3. Needs to be accompanied on any shopping trip 4. Completely unable to shop
1000
VI. Mode of transportation
1. Travels independently on public transportation or drives own car 2. Arranges own travel via taxi but does not otherwise use public transportation 3. Uses public transportation when assisted or accompanied by another
111
III. Food preparation
1. Plans, prepares, and serves adequate meals independently 2. Prepares adequate meals if supplied with ingredients 3. Heats and serves prepared meals or prepares meals but does not maintain
adequate diet 4. Needs to have meals prepared and served
100
0
4. Travel limited to taxi or automobile with assistance of another 5. Does not travel at all
VII. Responsibility for own medications
1. Is responsible for taking medication in correct doses at correct time 2. Takes responsibility if medication is kept in separate dosages in advance 3. Is not capable of dispensing own medication
0
0
100
IV. Housekeeping
1. Maintains house alone or with occasional assistance (e.g. heavy work) 2. Performs light daily tasks such as washing dishes and making beds 3. Performs light daily tasks, but cannot maintain acceptable level of cleanliness 4. Needs help with all home maintenance tasks 5. Does not participate in any housekeeping tasks
11110
VIII. Ability to handle finances
1. Manages financial matters independently (makes budgets, writes cheques, pays rent and bills, goes to bank), collects and keeps track of income
2. Manages day-to-day purchases, but needs help with banking, major purchases, etc. 3. Incapable of handling money
1
10
score score
Total score:_________________________________
A summary score ranges from 0 (low function, dependent) to 8 (high function, independent) for women and 0 through 5 for men to avoid potential gender bias.
Patient Name: __________ Date: _________Patient ID # ________
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
102
Talking points
Module 3: Health promotion and disease prevention in old age
Slide 1:
The Primary Care Physician has an important role in the health system as the most eff ective health educator. Health can improve and diseases can be prevented as each. In this module various strategies for health promotion and diseases prevention will be discussed.
Slide 2:
At the end of this module, the trainees will be carrying out health promotion and disease prevention interventions in older population.
Slide 3:
Define health promotion and discuss each of the clauses: enabling, control and improve.
Slide 4:
Discuss each of the three engagements with examples.
HHealth promotion and disease pprevention in old age
Module - 3
• To enumerate strategies for health promotion among olderpeople.
• To enumerate strategies for disease prevention in old age.
Learning Objectives
“Health promotion is the process of enabling people to increase
control over, and to improve their health”.
Health Promotion
Health Promotion
Strategies
Health Promotion Strategies
Health Promotion Strategies
Exercise
Social Support
and Social Interaction
Nutrition
103
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
Slide 5:
Discuss age related changes in gastrointestinal tract that aff ects nutrition. Read out each point and discuss.
Slide 6:
This slide provides information on impact of poor nutrition on various aspects of body structure and function. Discuss each point.
Slide 7:
This slide provides a practical strategy for nutritional assessment and management.
Slide 8:
This slide provides management strategy as per mini nutritional assessment.
Food is less palatable than before due to changes in taste and smell
Lack of teeth, gum problems and ill-fitting dentures make eating painful
The appetite decreases due to lack of exercise, loneliness, depression, chronic debilitating disease, confusion, forgetfulness, side-eff ects of drugs, alcohol and smoking
Age Related Changes
MNA Score Interpretation Management strategy
12-14 Normal Nutritional Status Reinforce generic health and lifestyle advice or usual care
8-11 At risk of malnutrition • Offer dietary advice• Consider Oral Supplemental Nutrition (OSN) if unable
to improve food intake• Monitor weight closely• Consider Multimodal exercise
0-7 Malnourished • Refer to a dietician/nutritionist if available• Nutritional Intervention necessary• Give OSN with increase protein intake (400-600
Kcal/day)• Offer dietary advice• Monitor weight closely
Mini-Nutritional Assessment and Management
Weight Loss
Protein Energy Malnutrition
Sarcopenia
Frailty
Physical Dependence
Premature DeathConsequences of Malnutrition
1. Screen for vitality/malnutrition using ICOPE screening questionnaireHave you unintentionally lost more than 3 Kgs over the last 3 months? Yes/ No
Have you experienced loss of appetite? Yes/NoIf any of the answer is yes: proceed to 2
2. Detailed Assessment of nutritional status using Mini-Nutritional Assessment (MNA)®
(Refer to annexure 2D for details)
3. Management of the older adult as per the result of MNA score
Role of primary care physicians in nutritional assessment
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
104
• Eating nutritious and easily digestive diet and have access to food that is tasty and easy to prepare
• Protein requirements for older people:
Condition Protein requirement
Healthy older person 1-1.2 g/kg/day
Recovering from weight loss, acute illness or injury
Up-to 1.5 g/kg/day
Older patient with pressure sore
High protein diet (Contains 25% of calories as protein)
• Calorie requirements
Condition Calorie Requirement
Healthy Ambulant older person 30-35 kcal/kg/day
Bedbound older person 25-30 kcal/kg/day
Dietary Advice for Older People
A food pyramid for the elderly
Sweets and fats in
moderation
Milk, yogurt, cheese 3 portions
Vegetables 3 portions
Wholemealis better
Water and liquids 8 glasses
Calcium, vitamin D, vitamin B12, Wholemeal
Fish meat legumes 2 portions
Fruit 2 portions
Cereals and tubers 6 portons
• Evaluate the social interaction of the elderly and promote such interaction.
• Social support and the strengths and abilities of the family and community are important for the promotion of health, as well as the prevention and treatment of disease and disability.
• It help to promote the mental health of older people and prevent mental ill health.
• People who are isolated have an increased risk of mortality from several causes.
Social support and social interaction
• Ageing causes a progressive decline in the power, strength and
endurance of the skeletal and cardiac musculature.
• Older people should perform at least 30 minutes of moderate-
intensity aerobic physical activity per day throughout the week.
Exercise
• Strength/Resistive: Squats, lunges, sit-to-stand exercises
• Aerobic/cardiovascular: fast walking, cycling
• Balance Training: standing on one leg at a time, walking heel to toe in straight line
• Flexibility Training: Stretching exercise, Yoga
Type of Exercises
Slide 9:
This slide provides detailed dietary advice to be carried out by a dietician if available. General advice by the physician can be on the basis of food pyramid provided on the slide.
Slide 10:
This slide provides information on exercises for older people. Discuss in detail.
Slide 11:
This slide provides information on various types of exercises for older people. Discuss in detail.
Slide 12:
Read out and discuss in detail with examples.
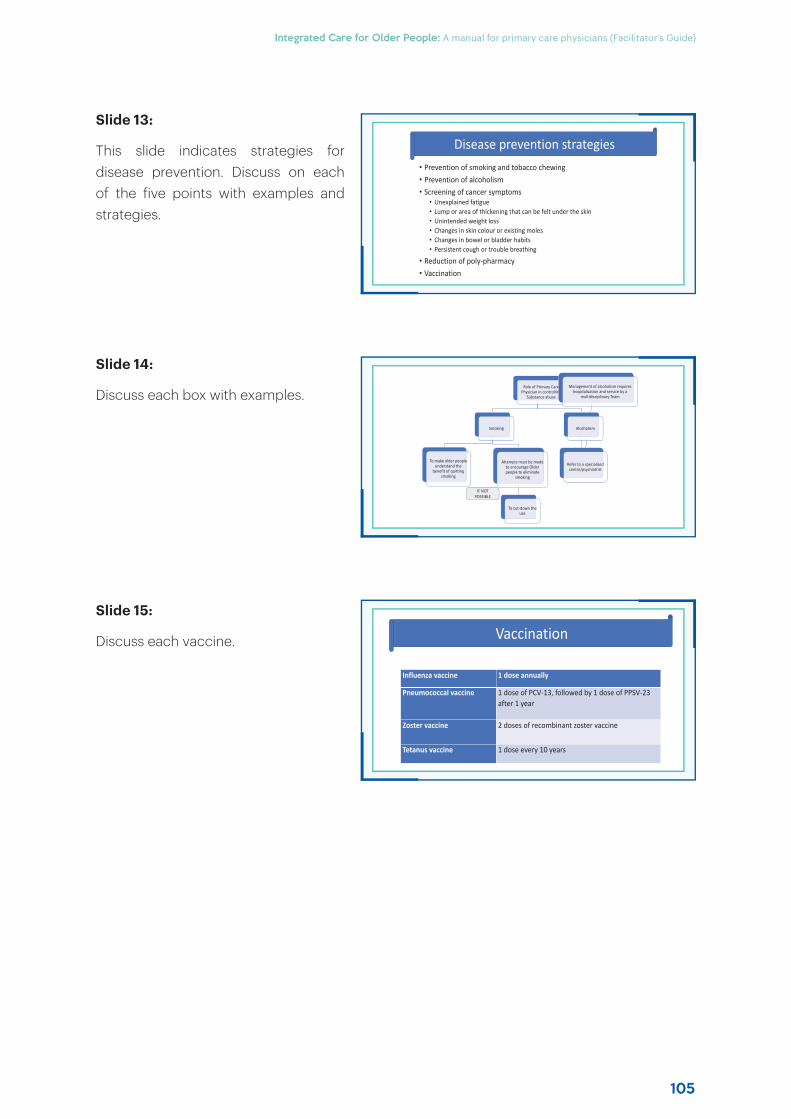
105
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
• Prevention of smoking and tobacco chewing• Prevention of alcoholism• Screening of cancer symptoms
• Unexplained fatigue• Lump or area of thickening that can be felt under the skin• Unintended weight loss• Changes in skin colour or existing moles• Changes in bowel or bladder habits• Persistent cough or trouble breathing
• Reduction of poly-pharmacy• Vaccination
Disease prevention strategies
Role of Primary Care Physician in controlling
Substance abuse
Smoking
To make older people understand the
benefit of quitting smoking
Attempts must be made to encourage Older people to eliminate
smoking
To cut-down the use
Alcoholism
Refer to a specialized centre/psychiatrist
Management of alcoholism requires hospitalization and service by a
multidisciplinary Team
IF NOT POSSIBLE
Influenza vaccine 1 dose annually
Pneumococcal vaccine 1 dose of PCV-13, followed by 1 dose of PPSV-23 after 1 year
Zoster vaccine 2 doses of recombinant zoster vaccine
Tetanus vaccine 1 dose every 10 years
Vaccination
Slide 13:
This slide indicates strategies for disease prevention. Discuss on each of the five points with examples and strategies.
Slide 14:
Discuss each box with examples.
Slide 15:
Discuss each vaccine.
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
106
Talking points
Module 4: Cardiovascular system
Slide 1:
Cardiovascular diseases are commonest causes of physician consultation with serious illness, hospitalization and death. Every physician must be aware of management of hypertension, acute coronary syndrome and heart failure.
Slide 2:
At the end of this module, the trainee should be able to provide basic management for common heart diseases.
Slide 3:
Discuss these age related changes with examples of outcome.
Slide 4:
Discuss the slide in detail about each box with examples.
CCardiovascular system
Module - 4
• To enumerate age-related changes which occur in the cardiovascular system.
• To enumerate common cardiovascular diseases and strategies to screen.
• To develop short-term and long-term care plans.
Learning objective
• Decrease in cardiac reserve capacity• Decreased β-adrenergic responsiveness• Increase in arterial stiffness • Baroreceptor responses are blunted• Changes in conduction system
Age related changes in cardio vascular system
WHO/ISH risk
prediction charts
Healthy Diet
Physical Activity
Control Diabetes Mellitus
Control Hypertens
ion
Control Tobacco
use
WHO/ISH Risk prediction charts
Indicate 10-year risk of a fatal or nonfatalmajor cardiovascular event (myocardialinfarction or stroke), according to age,sex, blood pressure, smoking status, totalblood cholesterol and presence orabsence of diabetes mellitus for 14 WHOepidemiological sub-regions.
Primary prevention of cardiovascular diseases
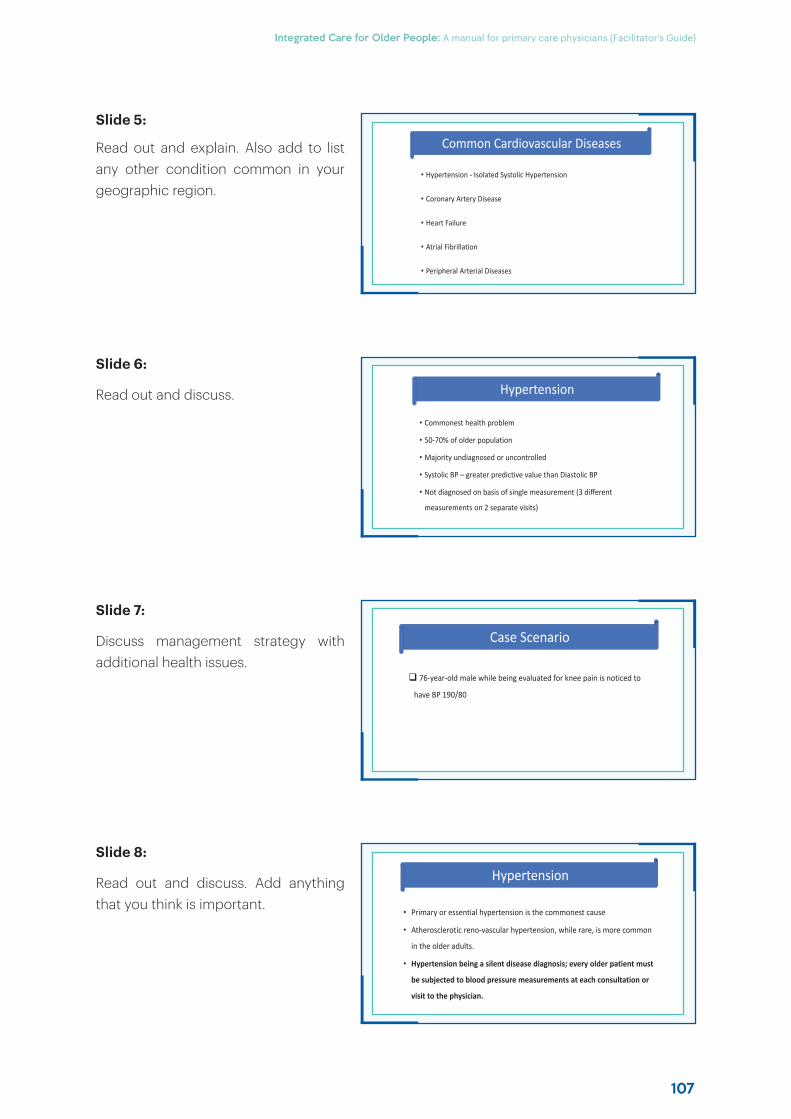
107
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
Slide 5:
Read out and explain. Also add to list any other condition common in your geographic region.
Slide 6:
Read out and discuss.
Slide 7:
Discuss management strategy with additional health issues.
Slide 8:
Read out and discuss. Add anything that you think is important.
• Hypertension - Isolated Systolic Hypertension
• Coronary Artery Disease
• Heart Failure
• Atrial Fibrillation
• Peripheral Arterial Diseases
Common Cardiovascular Diseases
• Primary or essential hypertension is the commonest cause
• Atherosclerotic reno-vascular hypertension, while rare, is more common
in the older adults.
• Hypertension being a silent disease diagnosis; every older patient must
be subjected to blood pressure measurements at each consultation or
visit to the physician.
Hypertension
• Commonest health problem
• 50-70% of older population
• Majority undiagnosed or uncontrolled
• Systolic BP – greater predictive value than Diastolic BP
• Not diagnosed on basis of single measurement (3 different
measurements on 2 separate visits)
Hypertension
76-year-old male while being evaluated for knee pain is noticed to
have BP 190/80
Case Scenario
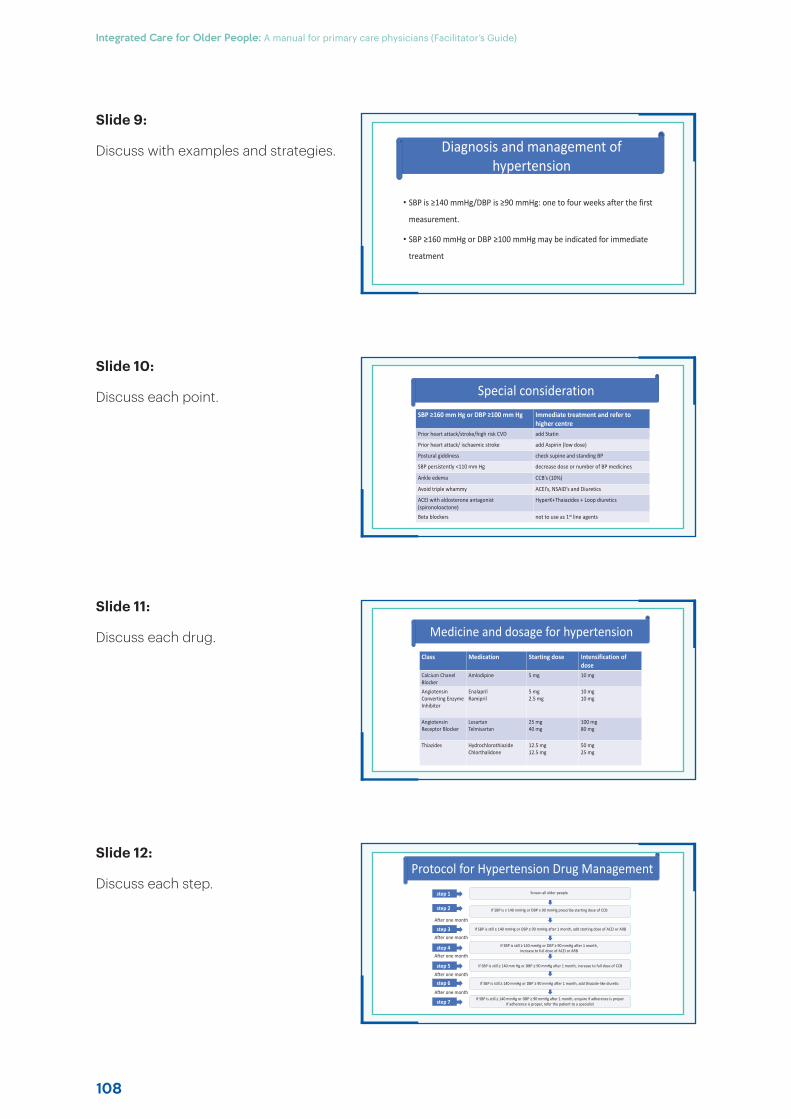
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
108
• SBP is ≥140 mmHg/DBP is ≥90 mmHg: one to four weeks after the first
measurement.
• SBP ≥160 mmHg or DBP ≥100 mmHg may be indicated for immediate
treatment
Diagnosis and management of hypertension
Protocol for Hypertension Drug ManagementScreen all older people
If SBP is ≥ 140 mmHg or DBP ≥ 90 mmHg prescribe starting dose of CCB
If SBP is still ≥ 140 mmHg or DBP ≥ 90 mmHg after 1 month, add starting dose of ACEI or ARB
If SBP is still ≥ 140 mmHg or DBP ≥ 90 mmHg after 1 month, increase to full dose of ACEI or ARB
If SBP is still ≥ 140 mm Hg or DBP ≥ 90 mmHg after 1 month, increase to full dose of CCB
If SBP is still ≥ 140 mmHg or DBP ≥ 90 mmHg after 1 month, add thiazide-like diuretic
If SBP is still ≥ 140 mmHg or DBP ≥ 90 mmHg after 1 month, enquire if adherence is proper If adherence is proper, refer the patient to a specialist
step 2
After one month
After one month
step 1
step 3
step 4
step 5
step 6
step 7
After one month
After one month
After one month
SBP ≥160 mm Hg or DBP ≥100 mm Hg Immediate treatment and refer to higher centre
Prior heart attack/stroke/high risk CVD add Statin
Prior heart attack/ ischaemic stroke add Aspirin (low dose)
Postural giddiness check supine and standing BP
SBP persistently <110 mm Hg decrease dose or number of BP medicines
Ankle edema CCB’s (10%)
Avoid triple whammy ACEI’s, NSAID’s and Diuretics
ACEI with aldosterone antagonist (spironoloactone)
HyperK+Thaiazides + Loop diuretics
Beta blockers not to use as 1st line agents
Special consideration
Class Medication Starting dose Intensification of dose
Calcium Chanel Blocker
Amlodipine 5 mg 10 mg
Angiotensin Converting Enzyme Inhibitor
EnalaprilRamipril
5 mg2.5 mg
10 mg10 mg
Angiotensin Receptor Blocker
LosartanTelmisartan
25 mg40 mg
100 mg80 mg
Thiazides Hydrochlorothiazide Chlorthalidone
12.5 mg 12.5 mg
50 mg 25 mg
Medicine and dosage for hypertension
Slide 9:
Discuss with examples and strategies.
Slide 10:
Discuss each point.
Slide 11:
Discuss each drug.
Slide 12:
Discuss each step.
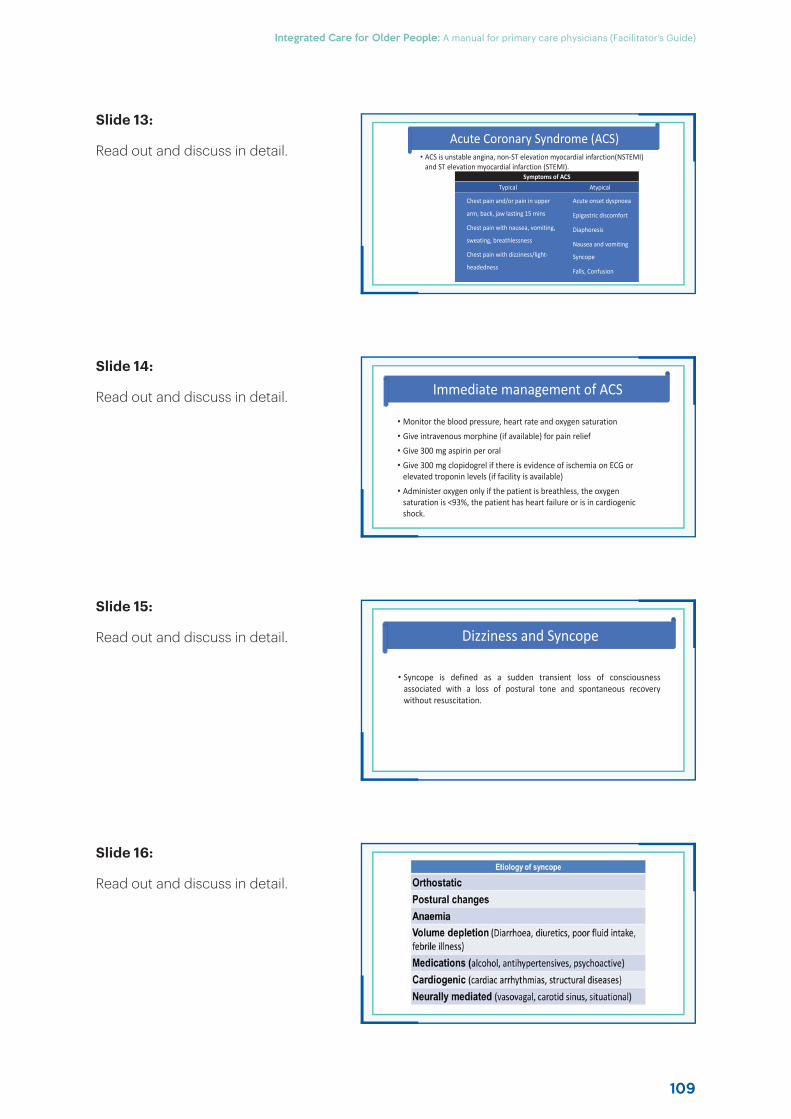
109
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
• ACS is unstable angina, non-ST elevation myocardial infarction(NSTEMI) and ST elevation myocardial infarction (STEMI).
Symptoms of ACSTypical Atypical
Chest pain and/or pain in upper
arm, back, jaw lasting 15 mins
Chest pain with nausea, vomiting,
sweating, breathlessness
Chest pain with dizziness/light-
headedness
Acute onset dyspnoea
Epigastric discomfort
Diaphoresis
Nausea and vomiting
Syncope
Falls, Confusion
Acute Coronary Syndrome (ACS)
• Monitor the blood pressure, heart rate and oxygen saturation
• Give intravenous morphine (if available) for pain relief
• Give 300 mg aspirin per oral
• Give 300 mg clopidogrel if there is evidence of ischemia on ECG or elevated troponin levels (if facility is available)
• Administer oxygen only if the patient is breathless, the oxygen saturation is <93%, the patient has heart failure or is in cardiogenic shock.
Immediate management of ACS
• Syncope is defined as a sudden transient loss of consciousnessassociated with a loss of postural tone and spontaneous recoverywithout resuscitation.
Dizziness and Syncope
Slide 13:
Read out and discuss in detail.
Slide 14:
Read out and discuss in detail.
Slide 15:
Read out and discuss in detail.
Slide 16:
Read out and discuss in detail.
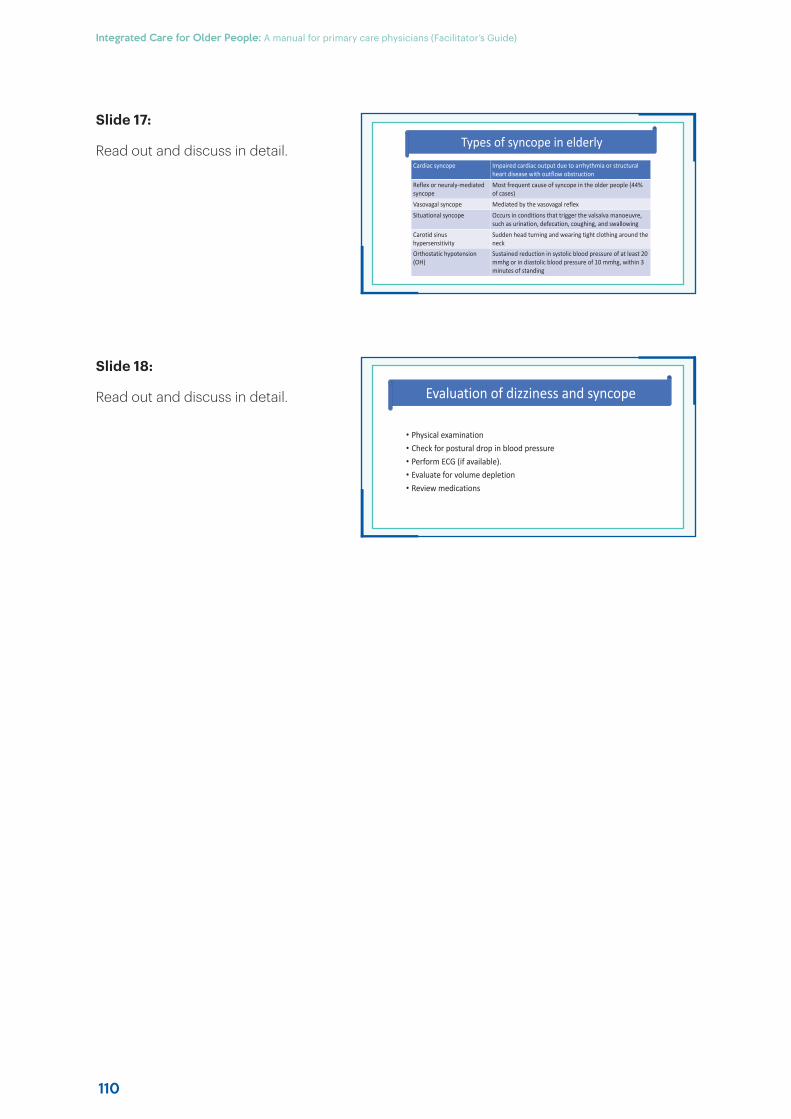
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
110
Cardiac syncope Impaired cardiac output due to arrhythmia or structural heart disease with outflow obstruction
Reflex or neuraly-mediated syncope
Most frequent cause of syncope in the older people (44% of cases)
Vasovagal syncope Mediated by the vasovagal reflex
Situational syncope Occurs in conditions that trigger the valsalva manoeuvre, such as urination, defecation, coughing, and swallowing
Carotid sinus hypersensitivity
Sudden head turning and wearing tight clothing around the neck
Orthostatic hypotension (OH)
Sustained reduction in systolic blood pressure of at least 20mmhg or in diastolic blood pressure of 10 mmhg, within 3 minutes of standing
Types of syncope in elderly
• Physical examination• Check for postural drop in blood pressure• Perform ECG (if available).• Evaluate for volume depletion• Review medications
Evaluation of dizziness and syncope
Slide 17:
Read out and discuss in detail.
Slide 18:
Read out and discuss in detail.
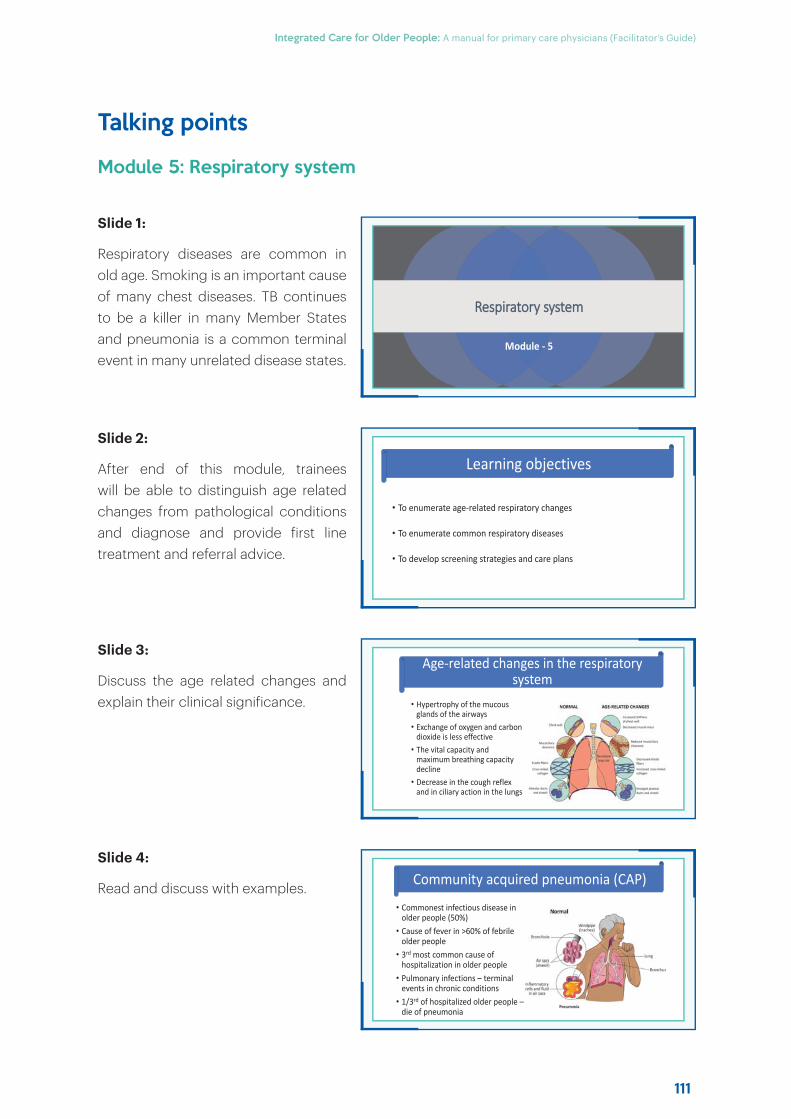
111
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
Talking points
Module 5: Respiratory system
Slide 1:
Respiratory diseases are common in old age. Smoking is an important cause of many chest diseases. TB continues to be a killer in many Member States and pneumonia is a common terminal event in many unrelated disease states.
Slide 2:
After end of this module, trainees will be able to distinguish age related changes from pathological conditions and diagnose and provide first line treatment and referral advice.
Slide 3:
Discuss the age related changes and explain their clinical significance.
Slide 4:
Read and discuss with examples.
RRespiratory system
Module - 5
• To enumerate age-related respiratory changes
• To enumerate common respiratory diseases
• To develop screening strategies and care plans
Learning objectives
• Hypertrophy of the mucous glands of the airways
• Exchange of oxygen and carbon dioxide is less effective
• The vital capacity and maximum breathing capacity decline
• Decrease in the cough reflex and in ciliary action in the lungs
Age-related changes in the respiratory system
• Commonest infectious disease in older people (50%)
• Cause of fever in >60% of febrile older people
• 3rd most common cause of hospitalization in older people
• Pulmonary infections – terminal events in chronic conditions
• 1/3rd of hospitalized older people –die of pneumonia
Community acquired pneumonia (CAP)
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
112
Slide 5:
Read and discuss atypical features.
Slide 6:
Read and discuss each box.
Slide 7:
Discuss each of the points in detail.
Slide 8:
Discuss the x-rays.
AAtypical Features of PPneumonia in EElderly
• Confusion, incontinence, immobility
• Signs of inflammation like fever, tachycardia and leucocytosis may be absent
• Progression and resolution of pneumonia are slower – prolonged hospitalization
Cavitary lung lesion
Diffused puffy opacity in B/L lungs
Tuberculosis
Assessment of severity and prognosis of pneumonia in Older people
EEmpirical Treatment of Pneumonia
Site Precondition Empirical regimen
OPD: Previously healthy patient who has had no antibiotics in previous 3 months
Azithromycin 500 mg orally, once a day for 5 days or doxycycline 100 mg orally, twice a day for 5 days
Has comorbidities such as chronic heart, lung, liver or renal disease, diabetes mellitus, alcoholism, malignancies, asplenia, immunosuppressing medications or conditions, or has had antibiotics within previous 3 months
(Amoxycillin-clavulanate 625 mg orally, three times a day or Cefuroxime 500 mg orally, twice a day) + Azithromycin 500 mg orally, once a day for 5-7 days
IPD Non-ICUInjection Ceftriaxone 1 g intravenous twice daily + Azithromycin 500 mg orally or intravenous, once daily for 5-7 days
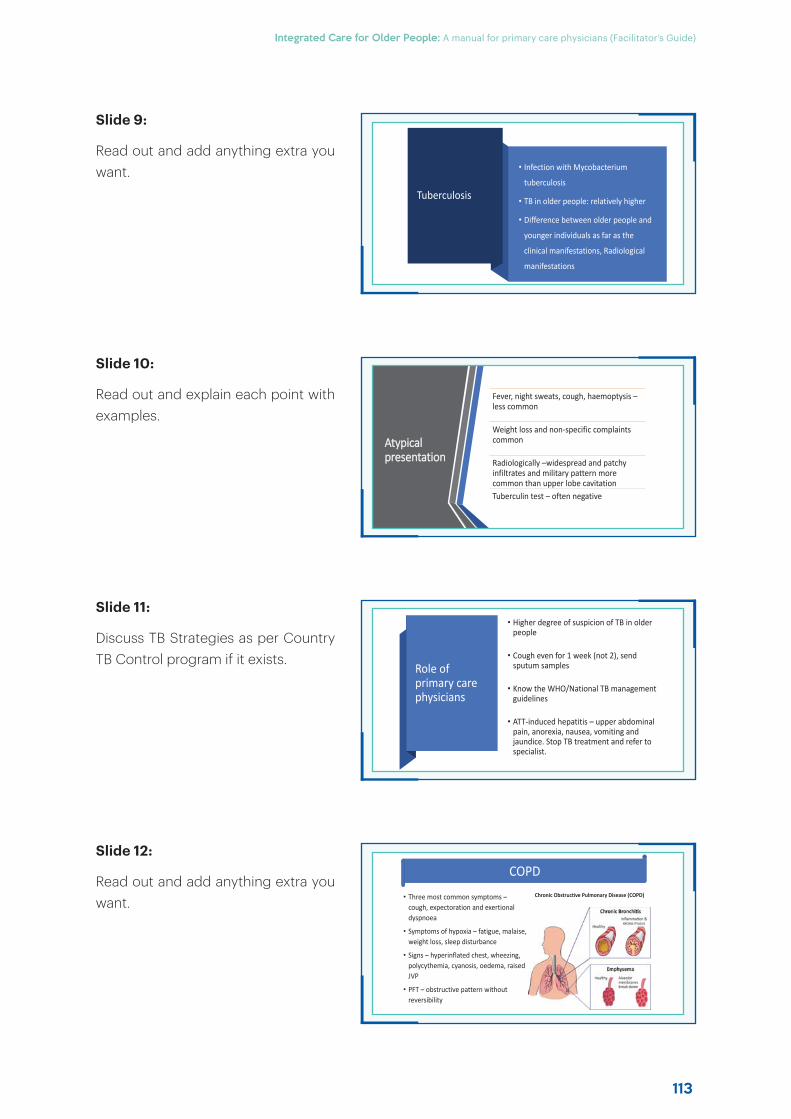
113
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
Slide 9:
Read out and add anything extra you want.
Slide 10:
Read out and explain each point with examples.
Slide 11:
Discuss TB Strategies as per Country TB Control program if it exists.
Slide 12:
Read out and add anything extra you want.
Tuberculosis
• Infection with Mycobacterium
tuberculosis
• TB in older people: relatively higher
• Difference between older people and
younger individuals as far as the
clinical manifestations, Radiological
manifestations
COPDChronic Obstructive Pulmonary Disease (COPD)• Three most common symptoms –
cough, expectoration and exertional dyspnoea
• Symptoms of hypoxia – fatigue, malaise, weight loss, sleep disturbance
• Signs – hyperinflated chest, wheezing, polycythemia, cyanosis, oedema, raised JVP
• PFT – obstructive pattern without reversibility
Atypical ppresentation
Fever, night sweats, cough, haemoptysis –less common
Weight loss and non-specific complaints common
Radiologically –widespread and patchy infiltrates and military pattern more common than upper lobe cavitationTuberculin test – often negative
Role of primary care physicians
• Higher degree of suspicion of TB in older people
• Cough even for 1 week (not 2), send sputum samples
• Know the WHO/National TB management guidelines
• ATT-induced hepatitis – upper abdominal pain, anorexia, nausea, vomiting and jaundice. Stop TB treatment and refer to specialist.
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
114
Slide 13:
Read out and add anything extra you want.
Slide 14:
Read out and add anything extra you want.
Slide 15:
Read out and add anything extra you want.
Slide 16:
Discuss in detail.
Management
• Inhalers – provide instructions and demonstrate proper technique
• Re-check technique at each visit • Long-acting beta-agonists (LABAs):s
(Salmaterol, Formoterol) and Long-acting muscarinic antagonist (LAMA) (tiotropium) preferred over SABA’s and SAMA’s (Salbutamol, Ipratropium)
• Long-term oxygen therapy (LTOT)
Role of pprimary care physicians
• Manage stable COPD with appropriate therapy
• Educate on proper inhaler technique
• Encourage smoking cessation
• Administer vaccines
• Prescribe LTOT, if needed
• Recommend apt physical activity and diet
• Apt referral
Management
• Start single LAMA or LABA and escalate as per symptoms
• Theophylline not recommended; if has to be given then sustained release preparations preferred
• Exacerbation despite LAMA and/or LABA –inhaled corticosteroids
• Drugs for primary pulmonary hypertension not recommended
• Smoking cessation• Influenza and pneumococcal vaccination• Pulmonary rehabilitation
Long term ooxygen therapy iindications
• SPO2 on Room Air ≤85% twice over a 3 week period
• SPO2 on Room Air ≤88% with pulmonary hypertension
• Cor pulmonale or polycythaemia (haematocrit >55%)
115
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
Lung cancer
• Commonest cancer among older people men worldwide
• 95% related to cigarette smoking
• Older patients present at advanced stage
• Refer to higher centre on clinical suspicion
Lung cancer
The diagnostic evaluation of lung cancer in old age should aim both at tissue diagnosis and operability from the anatomical as well as functional points of view.
The primary care physician should refer the patient to an appropriate centre on the basis of the X-ray and clinical suspicion.
Slide 17:
Read out and add anything extra you want.
Slide 18:
Read out and add anything extra you want.
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
116
Talking points
Module 6: Digestive system
Slide 1:
Symptoms related to gastrointestinal tract are extremely common among older patients in primary care. Further digestive tract dysfunction can lead to malnutrition and its accompanying health problems.
Slide 2:
After end of this module, trainees will be able to distinguish age related changes from pathological conditions and diagnose and provide first line treatment and referral advice.
Slide 3:
Read out and discuss their clinical implications.
Slide 4:
Read out and discuss their clinical implications.
DDigestive system
Module - 6
• To enumerate the age-related changes in the digestive system
• To enumerate common diseases of the digestive system in older patients
• To screen common disease conditions and develop care plans.
Learning outcomes
• Loss of teeth• Atrophy of the oral mucosa• Loss of taste buds• Decline in salivary secretion• Weakness of the muscles involved in mastication• Disturbed swallowing mechanism • Bacterial overgrowth in the small intestine• Decline in Liver volume, blood flow and perfusion
Age-related changes in the digestive system
AGE RELATED CHANGES IN DIGESTIVE SYSTEMLiverAltered Drug Metabolism
Risk of Drug interactions
Gallbladder/Biliary TreeCholelithiasis
Small BowelAltered Drug Metabolism
Mucosal Immunity IgA plasma cell migration
Anal SphincterInternal Sphincter muscle thicknessInternal Sphincter Pressure
External Sphincter Connective Tissue
OropharynxImpaired Neuromuscular Coordination
DysphagiaAspiration
EsophagusUES pressureUES relaxationSecondary peristalsis
[ Exocrine Secretion]
ColonDelayed Transit
Mucosal Proliferation
StomachLES pressureEmptying of LiquidsCytoprotectionPancreas
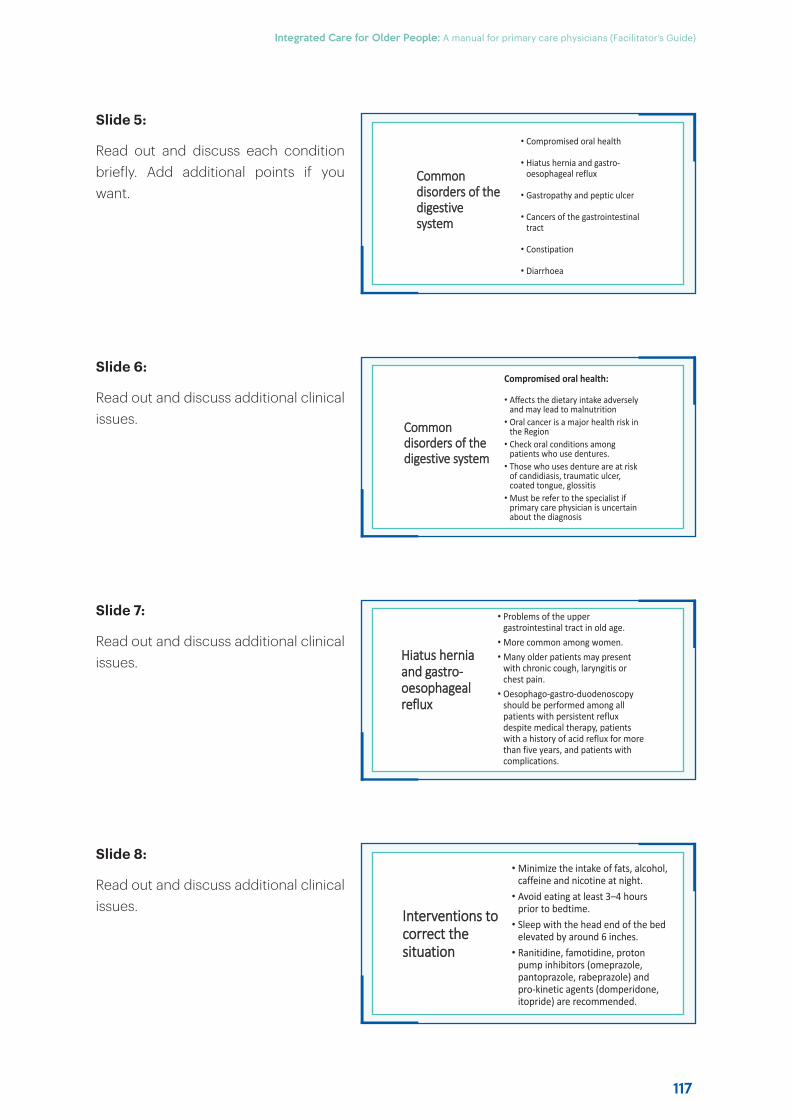
117
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
Common ddisorders of the digestive ssystem
• Compromised oral health
• Hiatus hernia and gastro-oesophageal reflux
• Gastropathy and peptic ulcer
• Cancers of the gastrointestinal tract
• Constipation
• Diarrhoea
Interventions to ccorrect the situation
• Minimize the intake of fats, alcohol, caffeine and nicotine at night.
• Avoid eating at least 3–4 hours prior to bedtime.
• Sleep with the head end of the bed elevated by around 6 inches.
• Ranitidine, famotidine, proton pump inhibitors (omeprazole, pantoprazole, rabeprazole) and pro-kinetic agents (domperidone, itopride) are recommended.
Common ddisorders of the digestive system
Compromised oral health:
• Affects the dietary intake adversely and may lead to malnutrition
• Oral cancer is a major health risk in the Region
• Check oral conditions among patients who use dentures.
• Those who uses denture are at risk of candidiasis, traumatic ulcer, coated tongue, glossitis
• Must be refer to the specialist if primary care physician is uncertain about the diagnosis
Hiatus hernia aand gastro-ooesophagealreflux
• Problems of the upper gastrointestinal tract in old age.
• More common among women.• Many older patients may present
with chronic cough, laryngitis or chest pain.
• Oesophago-gastro-duodenoscopy should be performed among all patients with persistent reflux despite medical therapy, patients with a history of acid reflux for more than five years, and patients with complications.
Slide 5:
Read out and discuss each condition briefly. Add additional points if you want.
Slide 6:
Read out and discuss additional clinical issues.
Slide 7:
Read out and discuss additional clinical issues.
Slide 8:
Read out and discuss additional clinical issues.
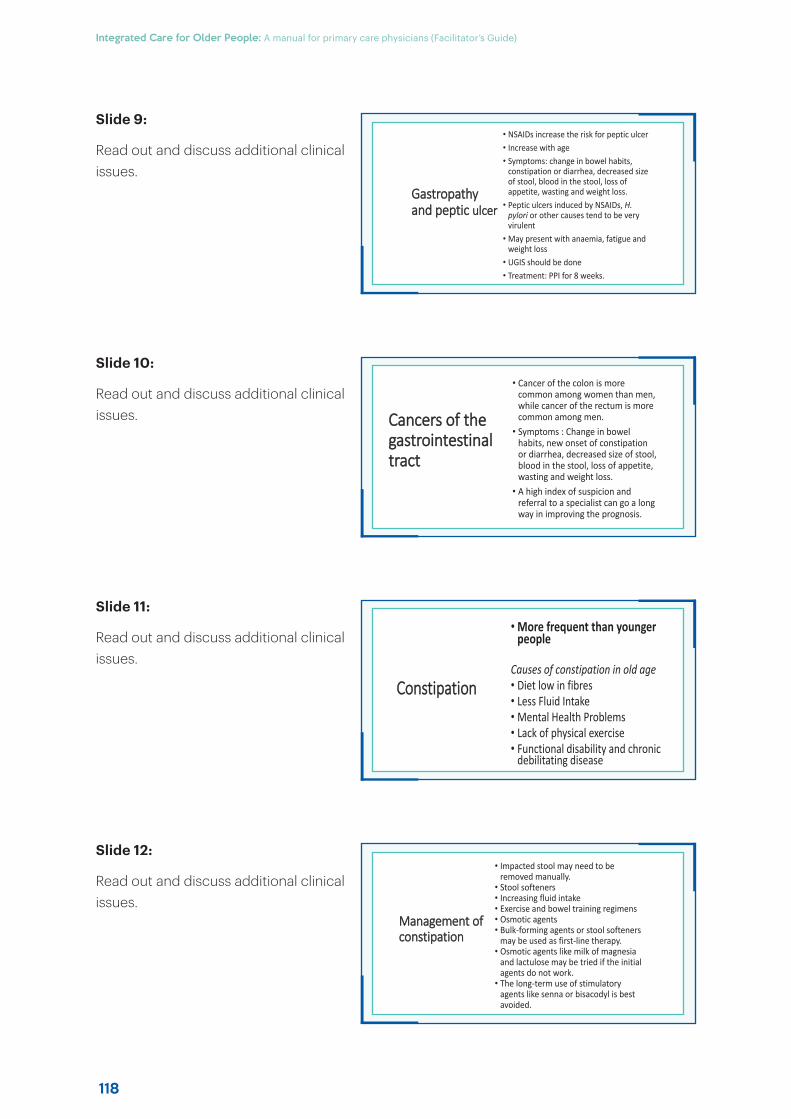
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
118
Gastropathy aand peptic ulcer
• NSAIDs increase the risk for peptic ulcer• Increase with age• Symptoms: change in bowel habits,
constipation or diarrhea, decreased size of stool, blood in the stool, loss of appetite, wasting and weight loss.
• Peptic ulcers induced by NSAIDs, H. pylori or other causes tend to be very virulent
• May present with anaemia, fatigue and weight loss
• UGIS should be done• Treatment: PPI for 8 weeks.
Management of cconstipation
• Impacted stool may need to be removed manually.
• Stool softeners• Increasing fluid intake• Exercise and bowel training regimens• Osmotic agents• Bulk-forming agents or stool softeners
may be used as first-line therapy.• Osmotic agents like milk of magnesia
and lactulose may be tried if the initial agents do not work.
• The long-term use of stimulatory agents like senna or bisacodyl is best avoided.
Cancers of the ggastrointestinal tract
• Cancer of the colon is more common among women than men, while cancer of the rectum is more common among men.
• Symptoms : Change in bowel habits, new onset of constipation or diarrhea, decreased size of stool, blood in the stool, loss of appetite, wasting and weight loss.
• A high index of suspicion and referral to a specialist can go a long way in improving the prognosis.
Constipation
• More frequent than younger people
Causes of constipation in old age• Diet low in fibres• Less Fluid Intake • Mental Health Problems • Lack of physical exercise• Functional disability and chronic
debilitating disease
Slide 9:
Read out and discuss additional clinical issues.
Slide 10:
Read out and discuss additional clinical issues.
Slide 11:
Read out and discuss additional clinical issues.
Slide 12:
Read out and discuss additional clinical issues.
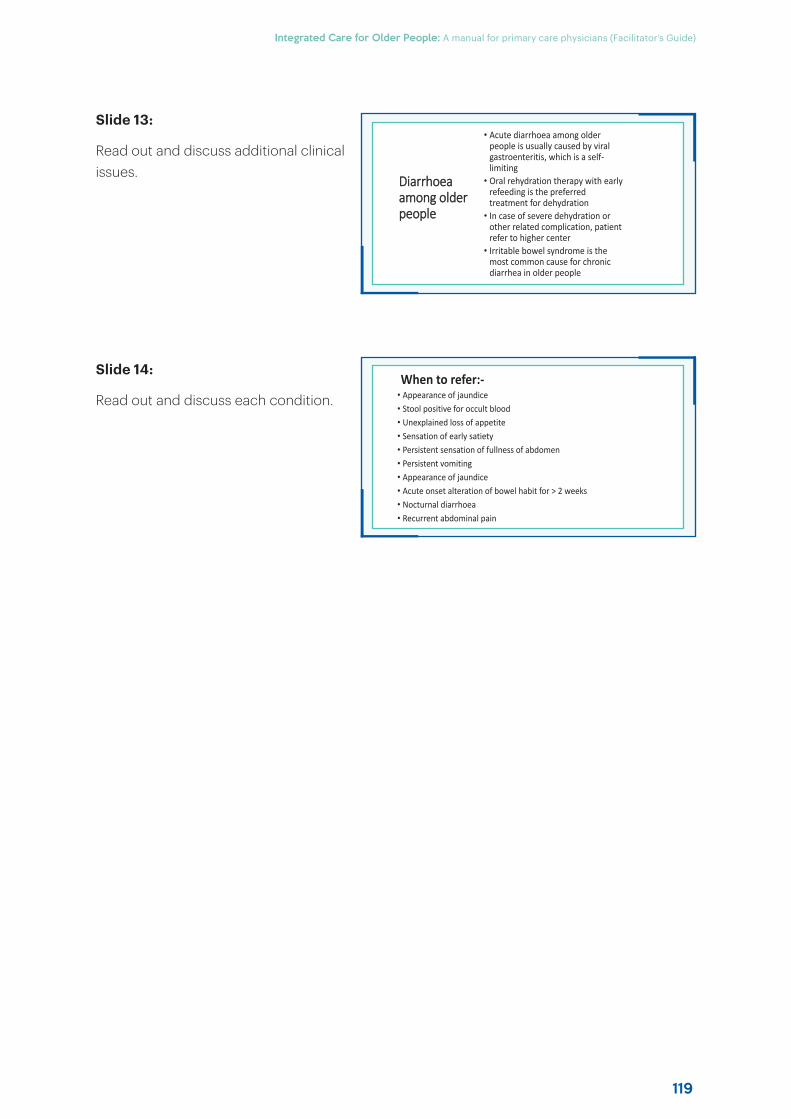
119
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
Diarrhoea aamong older people
• Acute diarrhoea among older people is usually caused by viral gastroenteritis, which is a self-limiting
• Oral rehydration therapy with early refeeding is the preferred treatment for dehydration
• In case of severe dehydration or other related complication, patient refer to higher center
• Irritable bowel syndrome is the most common cause for chronic diarrhea in older people
• Appearance of jaundice• Stool positive for occult blood• Unexplained loss of appetite• Sensation of early satiety• Persistent sensation of fullness of abdomen• Persistent vomiting• Appearance of jaundice• Acute onset alteration of bowel habit for > 2 weeks• Nocturnal diarrhoea• Recurrent abdominal pain
When to refer:-
Slide 13:
Read out and discuss additional clinical issues.
Slide 14:
Read out and discuss each condition.
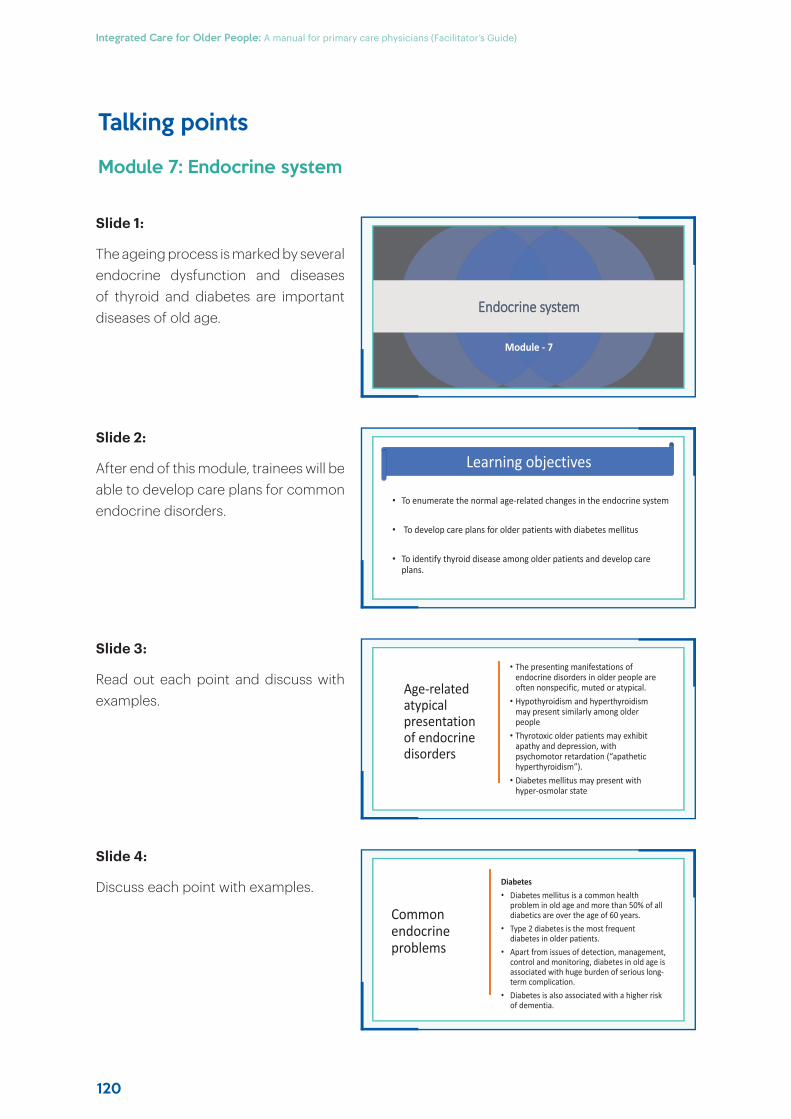
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
120
Talking points
Module 7: Endocrine system
Slide 1:
The ageing process is marked by several endocrine dysfunction and diseases of thyroid and diabetes are important diseases of old age.
Slide 2:
After end of this module, trainees will be able to develop care plans for common endocrine disorders.
Slide 3:
Read out each point and discuss with examples.
Slide 4:
Discuss each point with examples.
EEndocrine system
Module - 7
• To enumerate the normal age-related changes in the endocrine system
• To develop care plans for older patients with diabetes mellitus
• To identify thyroid disease among older patients and develop care plans.
Learning objectives
Age-related atypical presentation of endocrine disorders
• The presenting manifestations of endocrine disorders in older people are often nonspecific, muted or atypical.
• Hypothyroidism and hyperthyroidism may present similarly among older people
• Thyrotoxic older patients may exhibit apathy and depression, with psychomotor retardation (“apathetic hyperthyroidism”).
• Diabetes mellitus may present with hyper-osmolar state
Common endocrine problems
Diabetes• Diabetes mellitus is a common health
problem in old age and more than 50% of all diabetics are over the age of 60 years.
• Type 2 diabetes is the most frequent diabetes in older patients.
• Apart from issues of detection, management, control and monitoring, diabetes in old age is associated with huge burden of serious long-term complication.
• Diabetes is also associated with a higher risk of dementia.
4
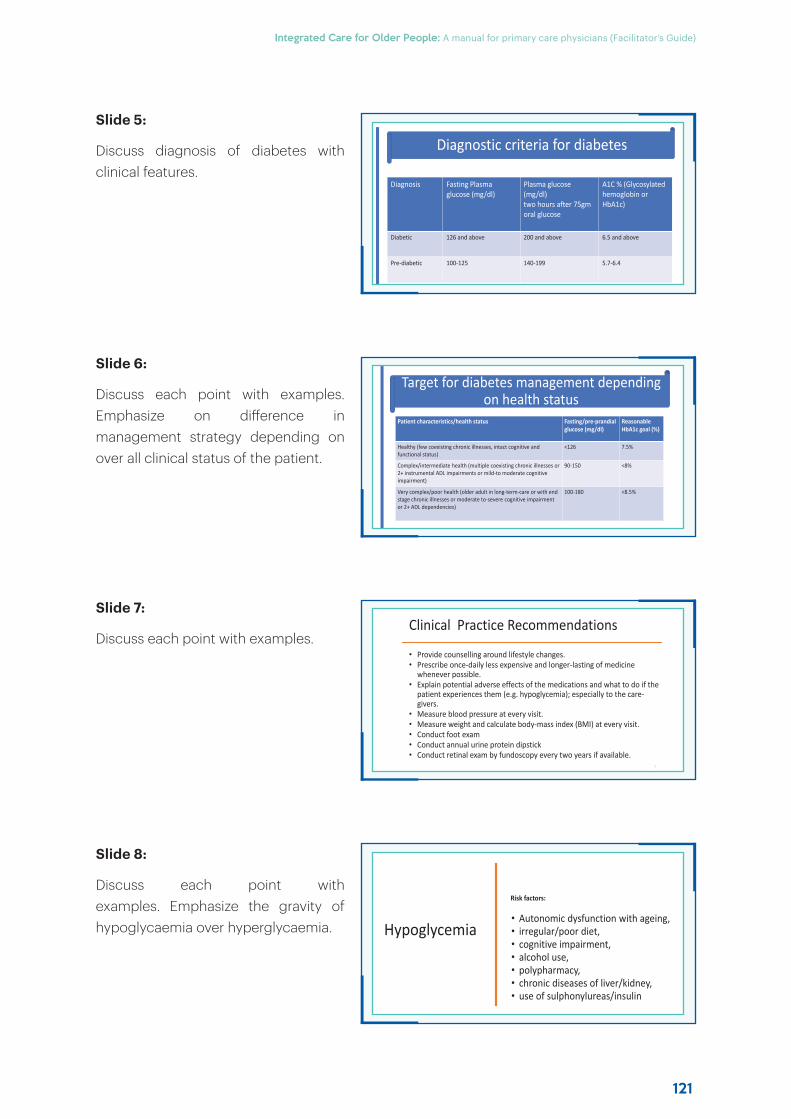
121
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
Diagnostic criteria for diabetes
Diagnosis Fasting Plasma glucose (mg/dl)
Plasma glucose (mg/dl)two hours after 75gmoral glucose
A1C % (Glycosylatedhemoglobin or HbA1c)
Diabetic 126 and above 200 and above 6.5 and above
Pre-diabetic 100-125 140-199 5.7-6.4
Hypoglycemia
Risk factors:
• Autonomic dysfunction with ageing, • irregular/poor diet, • cognitive impairment, • alcohol use, • polypharmacy, • chronic diseases of liver/kidney, • use of sulphonylureas/insulin
Target for diabetes management depending on health status
Patient characteristics/health status Fasting/pre-prandial glucose (mg/dl)
ReasonableHbA1c goal (%)
Healthy (few coexisting chronic illnesses, intact cognitive andfunctional status)
<126 7.5%
Complex/intermediate health (multiple coexisting chronic illnesses or 2+ instrumental ADL impairments or mild-to moderate cognitive impairment)
90-150 <8%
Very complex/poor health (older adult in long-term-care or with end stage chronic illnesses or moderate to-severe cognitive impairment or 2+ ADL dependencies)
100-180 <8.5%
Clinical Practice Recommendations
• Provide counselling around lifestyle changes.• Prescribe once-daily less expensive and longer-lasting of medicine
whenever possible. • Explain potential adverse effects of the medications and what to do if the
patient experiences them (e.g. hypoglycemia); especially to the care-givers.
• Measure blood pressure at every visit. • Measure weight and calculate body-mass index (BMI) at every visit. • Conduct foot exam • Conduct annual urine protein dipstick• Conduct retinal exam by fundoscopy every two years if available.
7
Slide 5:
Discuss diagnosis of diabetes with clinical features.
Slide 6:
Discuss each point with examples. Emphasize on diff erence in management strategy depending on over all clinical status of the patient.
Slide 7:
Discuss each point with examples.
Slide 8:
Discuss each point with examples. Emphasize the gravity of hypoglycaemia over hyperglycaemia.
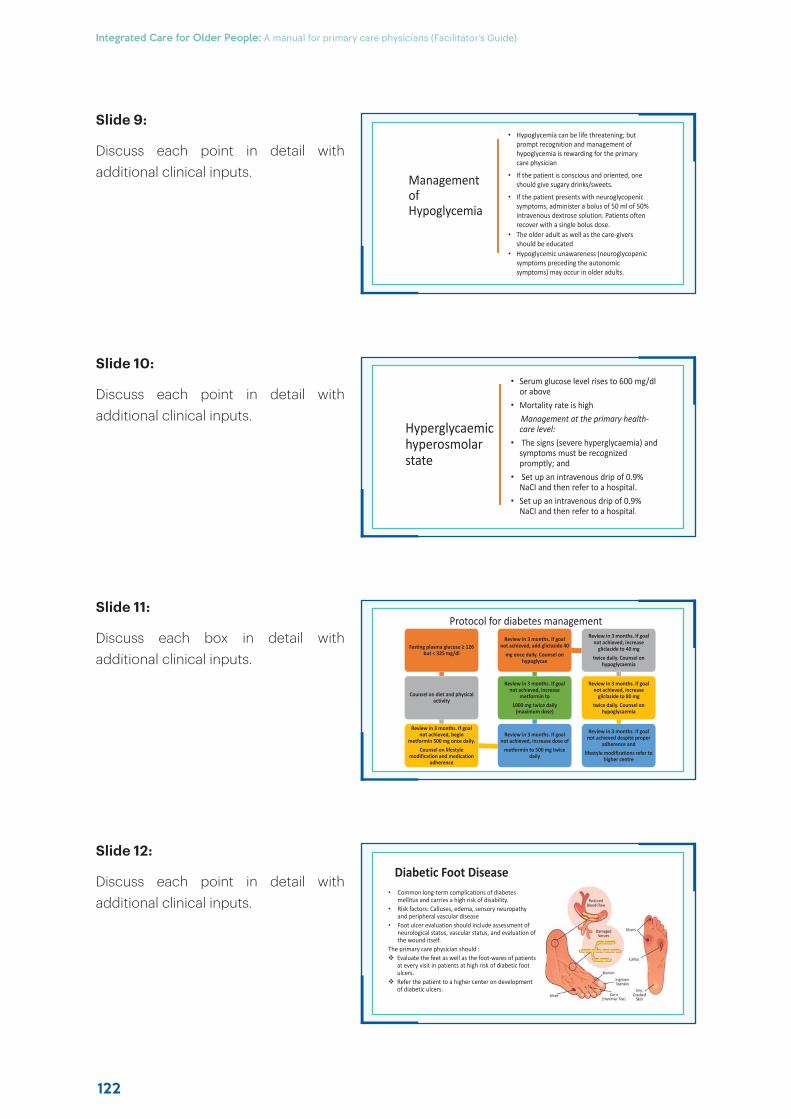
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
122
Management of Hypoglycemia
• Hypoglycemia can be life threatening; but prompt recognition and management of hypoglycemia is rewarding for the primary care physician
• If the patient is conscious and oriented, one should give sugary drinks/sweets.
• If the patient presents with neuroglycopenic symptoms, administer a bolus of 50 ml of 50% intravenous dextrose solution. Patients often recover with a single bolus dose.
• The older adult as well as the care-givers should be educated
• Hypoglycemic unawareness (neuroglycopenic symptoms preceding the autonomic symptoms) may occur in older adults.
• Common long-term complications of diabetes mellitus and carries a high risk of disability.
• Risk factors: Calluses, edema, sensory neuropathy and peripheral vascular disease
• Foot ulcer evaluation should include assessment of neurological status, vascular status, and evaluation of the wound itself.
The primary care physician should :Evaluate the feet as well as the foot-wares of patients at every visit in patients at high risk of diabetic foot ulcers.Refer the patient to a higher center on development of diabetic ulcers.
Diabetic Foot Disease
Hyperglycaemic hyperosmolar state
• Serum glucose level rises to 600 mg/dl or above
• Mortality rate is highManagement at the primary health-care level:
• The signs (severe hyperglycaemia) and symptoms must be recognized promptly; and
• Set up an intravenous drip of 0.9% NaCI and then refer to a hospital.
• Set up an intravenous drip of 0.9% NaCI and then refer to a hospital.
Protocol for diabetes management
Fasting plasma glucose ≥ 126 but < 325 mg/dl
Counsel on diet and physical activity
Review in 3 months. If goal not achieved, begin
metformin 500 mg once daily.Counsel on lifestyle
modification and medication adherence
Review in 3 months. If goal not achieved, increase dose of
metformin to 500 mg twice daily
Review in 3 months. If goal not achieved, increase
metformin to1000 mg twice daily
(maximum dose)
Review in 3 months. If goal not achieved, add gliclazide 40
mg once daily. Counsel on hypoglycae
Review in 3 months. If goal not achieved, increase
gliclazide to 40 mgtwice daily. Counsel on
hypoglycaemia
Review in 3 months. If goal not achieved, increase
gliclazide to 80 mgtwice daily. Counsel on
hypoglycaemia
Review in 3 months. If goal not achieved despite proper
adherence andlifestyle modifications refer to
higher centre
Slide 9:
Discuss each point in detail with additional clinical inputs.
Slide 10:
Discuss each point in detail with additional clinical inputs.
Slide 11:
Discuss each box in detail with additional clinical inputs.
Slide 12:
Discuss each point in detail with additional clinical inputs.
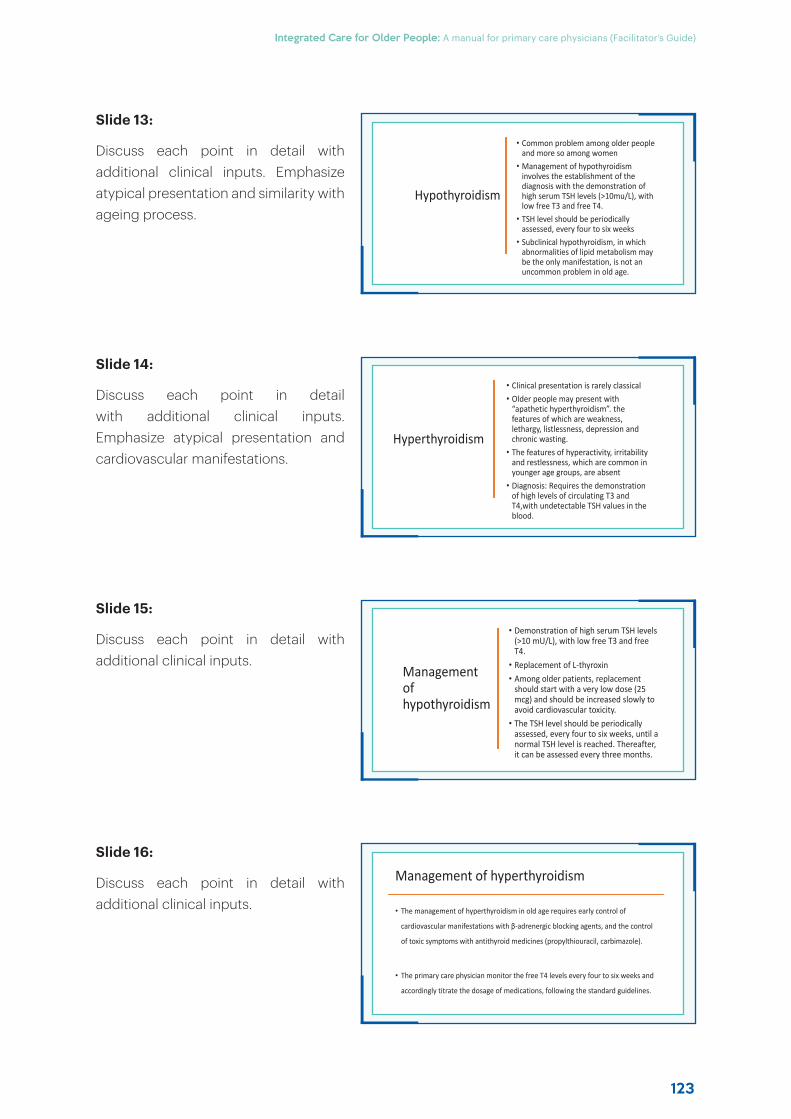
123
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
Hypothyroidism
• Common problem among older people and more so among women
• Management of hypothyroidism involves the establishment of the diagnosis with the demonstration of high serum TSH levels (>10mu/L), with low free T3 and free T4.
• TSH level should be periodically assessed, every four to six weeks
• Subclinical hypothyroidism, in which abnormalities of lipid metabolism may be the only manifestation, is not an uncommon problem in old age.
Management of hyperthyroidism
• The management of hyperthyroidism in old age requires early control of
cardiovascular manifestations with β-adrenergic blocking agents, and the control
of toxic symptoms with antithyroid medicines (propylthiouracil, carbimazole).
• The primary care physician monitor the free T4 levels every four to six weeks and
accordingly titrate the dosage of medications, following the standard guidelines.
Hyperthyroidism
• Clinical presentation is rarely classical• Older people may present with
“apathetic hyperthyroidism”. the features of which are weakness, lethargy, listlessness, depression and chronic wasting.
• The features of hyperactivity, irritability and restlessness, which are common in younger age groups, are absent
• Diagnosis: Requires the demonstration of high levels of circulating T3 and T4,with undetectable TSH values in the blood.
Management of hypothyroidism
• Demonstration of high serum TSH levels (>10 mU/L), with low free T3 and free T4.
• Replacement of L-thyroxin • Among older patients, replacement
should start with a very low dose (25 mcg) and should be increased slowly to avoid cardiovascular toxicity.
• The TSH level should be periodically assessed, every four to six weeks, until a normal TSH level is reached. Thereafter, it can be assessed every three months.
Slide 13:
Discuss each point in detail with additional clinical inputs. Emphasize atypical presentation and similarity with ageing process.
Slide 14:
Discuss each point in detail with additional clinical inputs. Emphasize atypical presentation and cardiovascular manifestations.
Slide 15:
Discuss each point in detail with additional clinical inputs.
Slide 16:
Discuss each point in detail with additional clinical inputs.
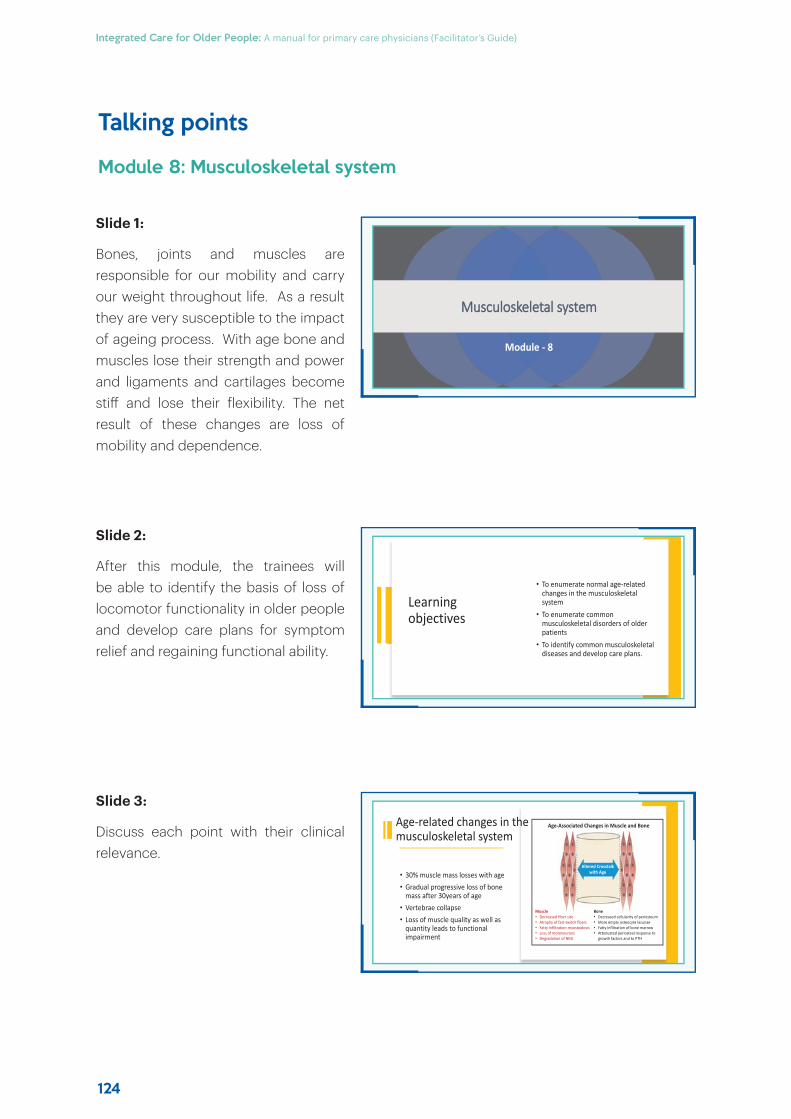
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
124
Talking points
Module 8: Musculoskeletal system
Slide 1:
Bones, joints and muscles are responsible for our mobility and carry our weight throughout life. As a result they are very susceptible to the impact of ageing process. With age bone and muscles lose their strength and power and ligaments and cartilages become stiff and lose their flexibility. The net result of these changes are loss of mobility and dependence.
Slide 2:
After this module, the trainees will be able to identify the basis of loss of locomotor functionality in older people and develop care plans for symptom relief and regaining functional ability.
Slide 3:
Discuss each point with their clinical relevance.
MMusculoskeletal system
Module - 8
Learning objectives
• To enumerate normal age-related changes in the musculoskeletal system
• To enumerate common musculoskeletal disorders of older patients
• To identify common musculoskeletal diseases and develop care plans.
• 30% muscle mass losses with age • Gradual progressive loss of bone
mass after 30years of age• Vertebrae collapse • Loss of muscle quality as well as
quantity leads to functional impairment
Age-related changes in the musculoskeletal system
Altered Crosstalk with Age
Muscle• Decreased fiber size• Atrophy of fast-twitch fibers• Fatty infiltration-myosteatosis• Loss of motoneurons• Degradation of NMJ
Bone• Decreased cellularity of periosteum• More empty osteocyte lacunae• Fatty infiltration of bone marrow• Attenuated periosteal response to
growth factors and to PTH
Age-Associated Changes in Muscle and Bone
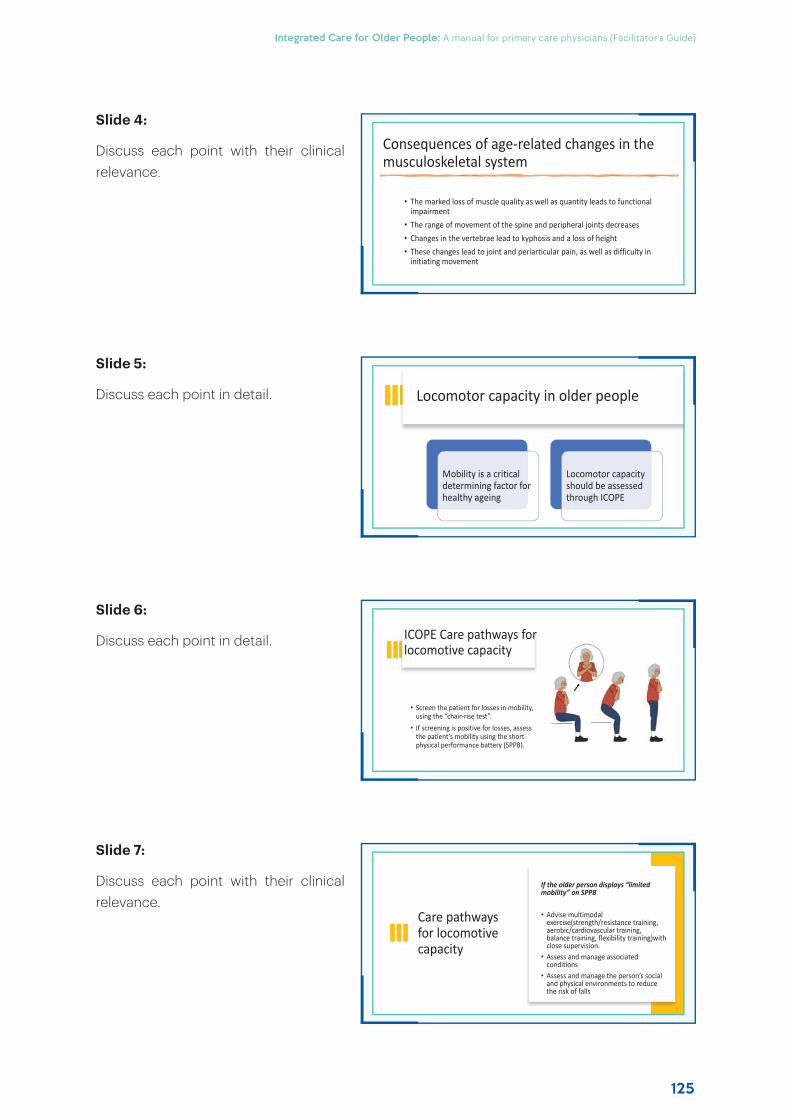
125
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
Consequences of age-related changes in the musculoskeletal system
• The marked loss of muscle quality as well as quantity leads to functional impairment
• The range of movement of the spine and peripheral joints decreases • Changes in the vertebrae lead to kyphosis and a loss of height• These changes lead to joint and periarticular pain, as well as difficulty in
initiating movement
Care pathways for locomotive capacity
If the older person displays “limited mobility” on SPPB
• Advise multimodal exercise(strength/resistance training, aerobic/cardiovascular training, balance training, flexibility training)with close supervision.
• Assess and manage associated conditions
• Assess and manage the person’s social and physical environments to reduce the risk of falls
Locomotor capacity in older people
Mobility is a critical determining factor for healthy ageing
Locomotor capacity should be assessed through ICOPE
ICOPE Care pathways for locomotive capacity
• Screen the patient for losses in mobility, using the “chair-rise test”.
• If screening is positive for losses, assess the patient’s mobility using the short physical performance battery (SPPB).
Slide 4:
Discuss each point with their clinical relevance.
Slide 5:
Discuss each point in detail.
Slide 6:
Discuss each point in detail.
Slide 7:
Discuss each point with their clinical relevance.
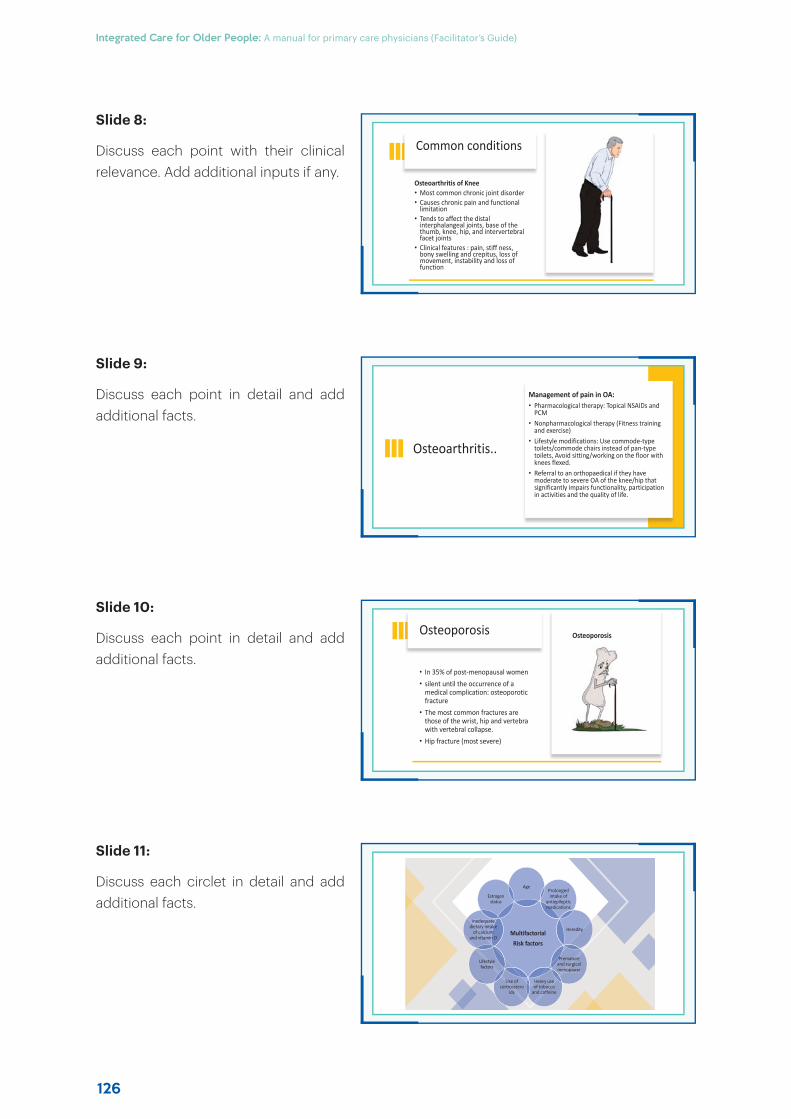
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
126
Slide 8:
Discuss each point with their clinical relevance. Add additional inputs if any.
Slide 9:
Discuss each point in detail and add additional facts.
Slide 10:
Discuss each point in detail and add additional facts.
Slide 11:
Discuss each circlet in detail and add additional facts.
Common conditions
Osteoarthritis of Knee• Most common chronic joint disorder• Causes chronic pain and functional
limitation• Tends to affect the distal
interphalangeal joints, base of the thumb, knee, hip, and intervertebral facet joints
• Clinical features : pain, stiff ness, bony swelling and crepitus, loss of movement, instability and loss of function
Multifactorial Risk factors
AgeProlonged intake of
antiepileptic medications
Heredity
Premature and surgical menopause
Heavy use of tobacco
and caffeine
Use of corticostero
ids
Lifestyle factors
Inadequate dietary intake
of calcium and vitamin D
Estrogen status
Osteoarthritis..
Management of pain in OA: • Pharmacological therapy: Topical NSAIDs and
PCM• Nonpharmacological therapy (Fitness training
and exercise)• Lifestyle modifications: Use commode-type
toilets/commode chairs instead of pan-type toilets, Avoid sitting/working on the floor with knees flexed.
• Referral to an orthopaedical if they have moderate to severe OA of the knee/hip that significantly impairs functionality, participation in activities and the quality of life.
Osteoporosis
• In 35% of post-menopausal women• silent until the occurrence of a
medical complication: osteoporotic fracture
• The most common fractures are those of the wrist, hip and vertebra with vertebral collapse.
• Hip fracture (most severe)
Osteoporosis
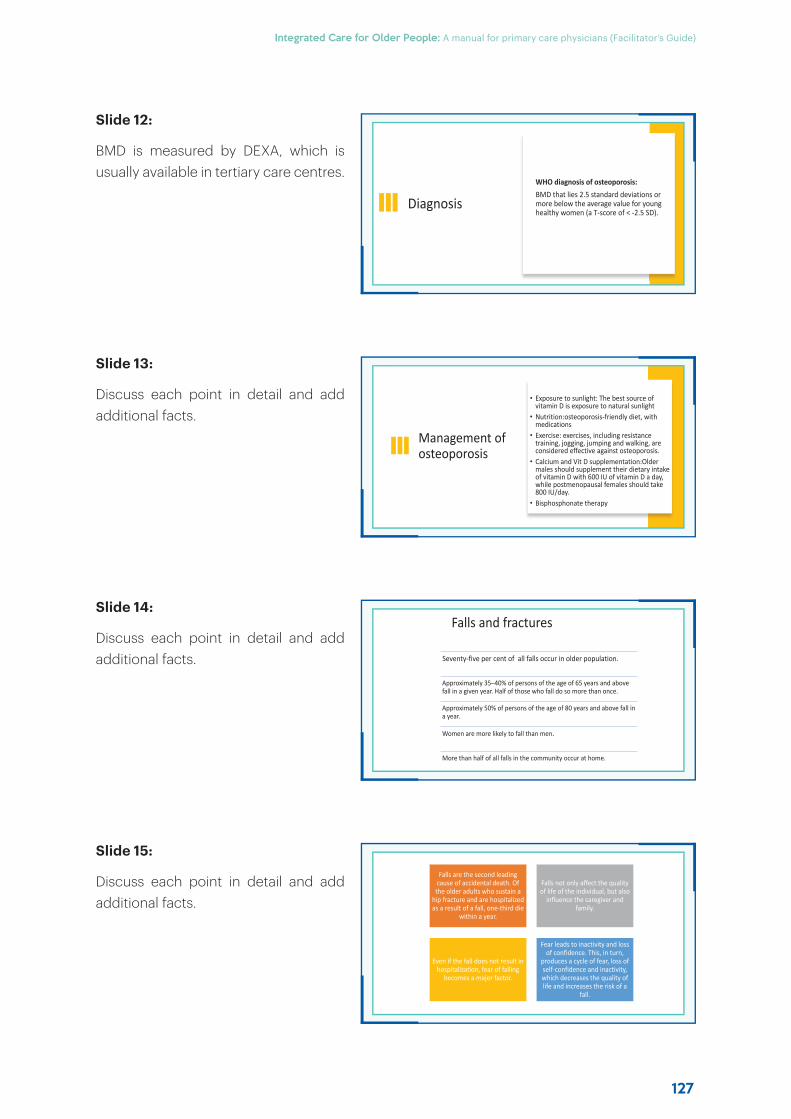
127
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
Slide 12:
BMD is measured by DEXA, which is usually available in tertiary care centres.
Slide 13:
Discuss each point in detail and add additional facts.
Slide 14:
Discuss each point in detail and add additional facts.
Slide 15:
Discuss each point in detail and add additional facts.
Diagnosis
WHO diagnosis of osteoporosis:BMD that lies 2.5 standard deviations or more below the average value for young healthy women (a T-score of < -2.5 SD).
Falls are the second leading cause of accidental death. Of
the older adults who sustain a hip fracture and are hospitalized as a result of a fall, one-third die
within a year.
Falls not only affect the quality of life of the individual, but also
influence the caregiver and family.
Even if the fall does not result in hospitalization, fear of falling
becomes a major factor.
Fear leads to inactivity and loss of confidence. This, in turn,
produces a cycle of fear, loss of self-confidence and inactivity, which decreases the quality of life and increases the risk of a
fall.
Management of osteoporosis
• Exposure to sunlight: The best source of vitamin D is exposure to natural sunlight
• Nutrition:osteoporosis-friendly diet, withmedications
• Exercise: exercises, including resistance training, jogging, jumping and walking, are considered effective against osteoporosis.
• Calcium and Vit D supplementation:Older males should supplement their dietary intake of vitamin D with 600 IU of vitamin D a day, while postmenopausal females should take 800 IU/day.
• Bisphosphonate therapy
Seventy-five per cent of all falls occur in older population.
Approximately 35–40% of persons of the age of 65 years and above fall in a given year. Half of those who fall do so more than once.
Approximately 50% of persons of the age of 80 years and above fall in a year.
Women are more likely to fall than men.
More than half of all falls in the community occur at home.
Falls and fractures
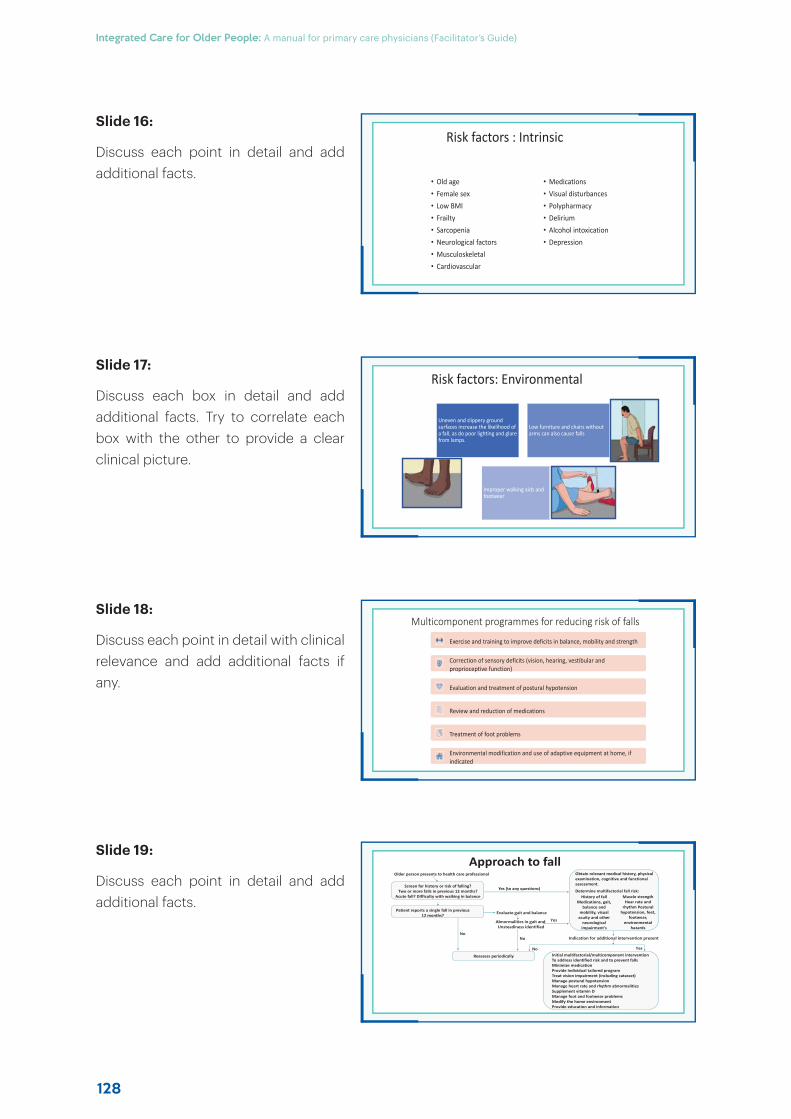
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
128
Risk factors : Intrinsic
• Old age• Female sex• Low BMI• Frailty• Sarcopenia• Neurological factors• Musculoskeletal• Cardiovascular
• Medications• Visual disturbances• Polypharmacy• Delirium • Alcohol intoxication• Depression
Approach to fallOlder person presents to health care professional
Screen for history or risk of falling?Two or more falls in previous 12 months?
Acute fall? Difficulty with walking in balance
Patient reports a single fall in previous12 months?
Obtain relevant medical history, physical examination, cognitive and functional assessment.
Determine multifactorial fall risk:History of fall
Medications, gait, balance and
mobility, visual acuity and other
neurological impairment's
Muscle strength Hear rate and
rhythm Postural hypotension, feet,
footwear, environmental
hazards
Yes (to any questions)
Evaluate gait and balance
NoIndication for additional intervention present
Reassess periodically
Abnormalities in gait and Unsteadiness identified
No
No
Yes
Yes
Initial multifactorial/multicomponent interventionTo address identified risk and to prevent fallsMinimize medicationProvide individual tailored programTreat vision impairment (including cataract)Manage postural hypotensionManage heart rate and rhythm abnormalitiesSupplement vitamin DManage foot and footwear problemsModify the home environmentProvide education and information
Risk factors: Environmental
Uneven and slippery ground surfaces increase the likelihood of a fall, as do poor lighting and glare from lamps.
Low furniture and chairs without arms can also cause falls
Improper walking aids and footwear
Exercise and training to improve deficits in balance, mobility and strength
Correction of sensory deficits (vision, hearing, vestibular and proprioceptive function)
Evaluation and treatment of postural hypotension
Review and reduction of medications
Treatment of foot problems
Environmental modification and use of adaptive equipment at home, if indicated
Multicomponent programmes for reducing risk of falls
Slide 16:
Discuss each point in detail and add additional facts.
Slide 17:
Discuss each box in detail and add additional facts. Try to correlate each box with the other to provide a clear clinical picture.
Slide 18:
Discuss each point in detail with clinical relevance and add additional facts if any.
Slide 19:
Discuss each point in detail and add additional facts.
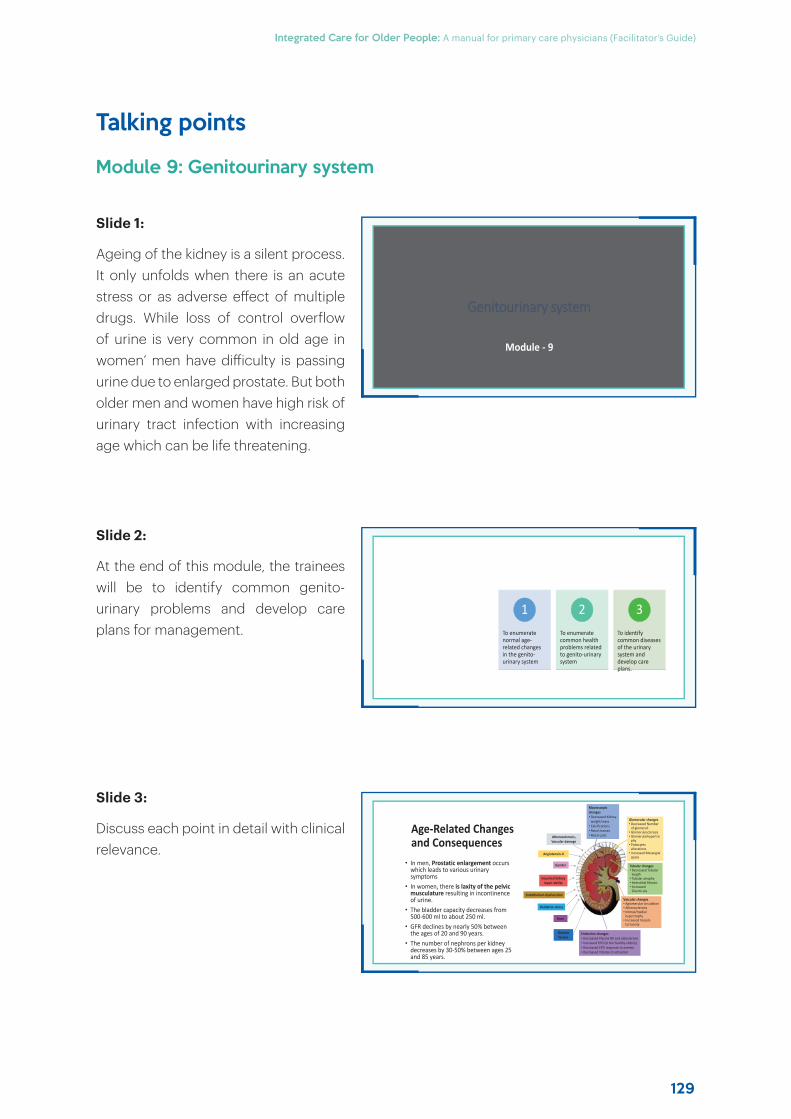
129
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
Talking points
Module 9: Genitourinary system
Slide 1:
Ageing of the kidney is a silent process. It only unfolds when there is an acute stress or as adverse eff ect of multiple drugs. While loss of control overflow of urine is very common in old age in women’ men have diff iculty is passing urine due to enlarged prostate. But both older men and women have high risk of urinary tract infection with increasing age which can be life threatening.
Slide 2:
At the end of this module, the trainees will be to identify common genito-urinary problems and develop care plans for management.
Slide 3:
Discuss each point in detail with clinical relevance.
GGenitourinary system
Module - 9
Learning outcomes To enumerate
normal age-related changes in the genito-urinary system
1To enumerate common health problems related to genito-urinary system
2To identify common diseases of the urinary system and develop care plans.
3
Age-Related Changes and Consequences
• In men, Prostatic enlargement occurs which leads to various urinary symptoms
• In women, there is laxity of the pelvic musculature resulting in incontinence of urine.
• The bladder capacity decreases from 500-600 ml to about 250 ml.
• GFR declines by nearly 50% between the ages of 20 and 90 years.
• The number of nephrons per kidneydecreases by 30-50% between ages 25 and 85 years.
Macroscopic changes• Decreased Kidney
weight/mass• Calcifications• Renal masses• Renal cysts
Glomerular changes• Decreased Number
of glomeruli• Glomerulosclerosis• Glomerularhypertro
phy• Podocytes
alterations• Increased Mesangial
space
Tubular changes• Decreased Tubular
length• Tubular atrophy• Interstitial fibrosis• Increased
Diverticula
Vascular changes• Agiomerular circulation• Atherosclerosis• Intimal/medial
hypertrophy• Increased Vessels
tortuosity
Atherosolerosis, Vascular damage
Angiotensin-II
Gender
Impaired kidney repair ability
Endothelium dysfunction
Oxidative stress
Race
Genetic factors
Endocrine changes• Decreased Plasma RA and aldosterone• Increased EPO (in the healthy elderly)• Decreased EPO response to anemia• Decreased Vitamin-D activation
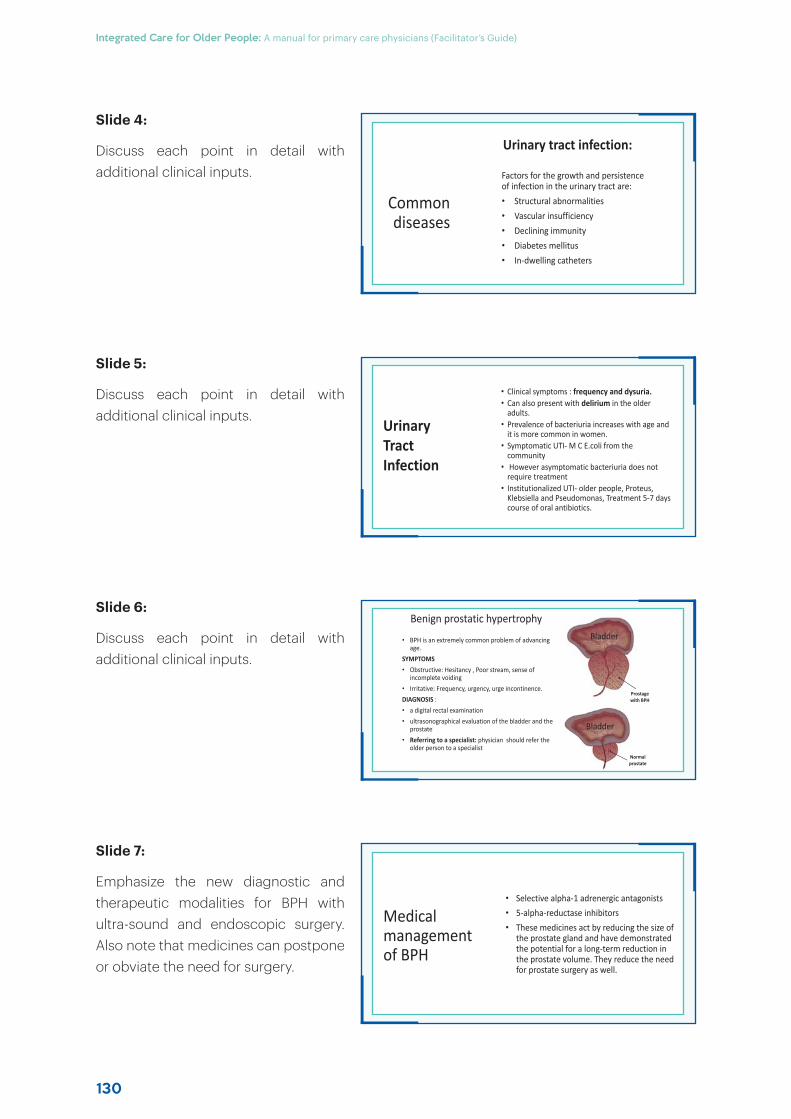
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
130
Common diseases
Factors for the growth and persistence of infection in the urinary tract are:• Structural abnormalities• Vascular insufficiency• Declining immunity• Diabetes mellitus• In-dwelling catheters
Urinary tract infection:
Medical management of BPH
• Selective alpha-1 adrenergic antagonists• 5-alpha-reductase inhibitors• These medicines act by reducing the size of
the prostate gland and have demonstrated the potential for a long-term reduction in the prostate volume. They reduce the need for prostate surgery as well.
• Clinical symptoms : frequency and dysuria.• Can also present with delirium in the older
adults.• Prevalence of bacteriuria increases with age and
it is more common in women. • Symptomatic UTI- M C E.coli from the
community• However asymptomatic bacteriuria does not
require treatment• Institutionalized UTI- older people, Proteus,
Klebsiella and Pseudomonas, Treatment 5-7 days course of oral antibiotics.
Urinary Tract Infection
Benign prostatic hypertrophy
• BPH is an extremely common problem of advancing age.
SYMPTOMS• Obstructive: Hesitancy , Poor stream, sense of
incomplete voiding• Irritative: Frequency, urgency, urge incontinence.DIAGNOSIS : • a digital rectal examination• ultrasonographical evaluation of the bladder and the
prostate• Referring to a specialist: physician should refer the
older person to a specialist
Bladder
Normal prostate
Bladder
Prostagewith BPH
Slide 4:
Discuss each point in detail with additional clinical inputs.
Slide 5:
Discuss each point in detail with additional clinical inputs.
Slide 6:
Discuss each point in detail with additional clinical inputs.
Slide 7:
Emphasize the new diagnostic and therapeutic modalities for BPH with ultra-sound and endoscopic surgery. Also note that medicines can postpone or obviate the need for surgery.
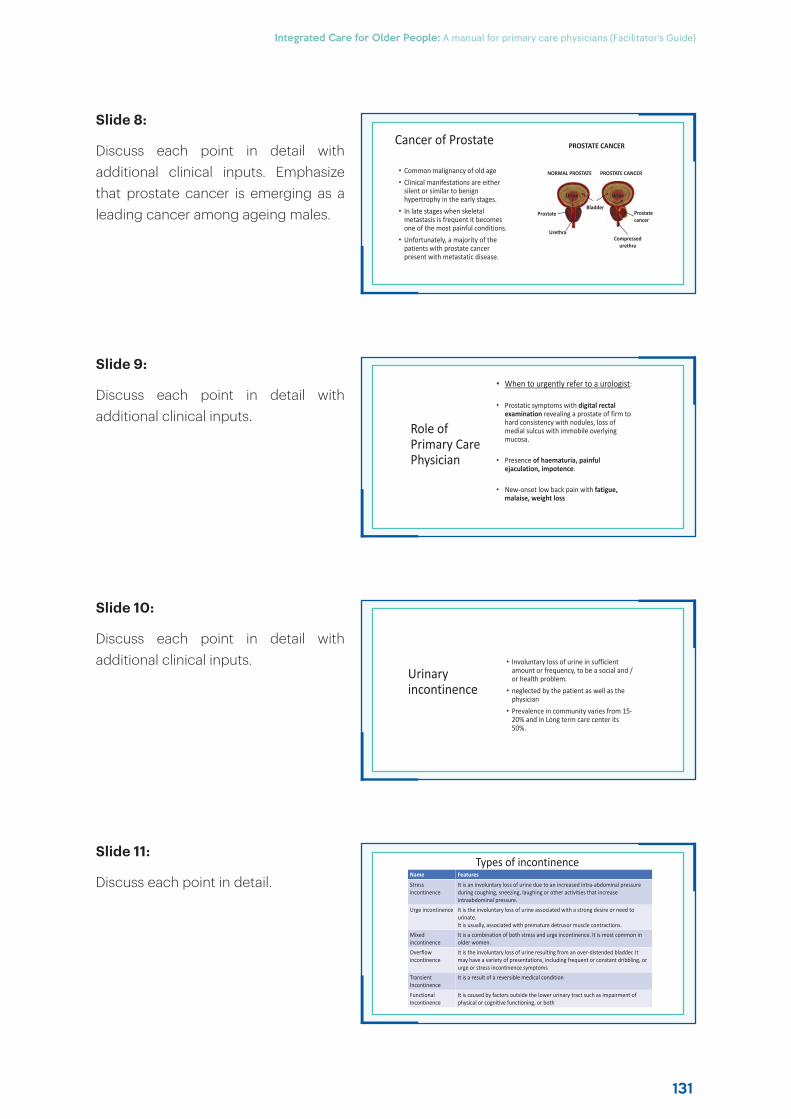
131
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
Cancer of Prostate
• Common malignancy of old age• Clinical manifestations are either
silent or similar to benign hypertrophy in the early stages.
• In late stages when skeletal metastasis is frequent it becomes one of the most painful conditions.
• Unfortunately, a majority of the patients with prostate cancer present with metastatic disease.
PROSTATE CANCER
NORMAL PROSTATE PROSTATE CANCER
Urine
Prostate cancer
Compressed urethra
Bladder
Urine
Prostate
Urethra
Types of incontinenceName Features
Stress incontinence
It is an involuntary loss of urine due to an increased intra-abdominal pressureduring coughing, sneezing, laughing or other activities that increaseintraabdominal pressure.
Urge incontinence It is the involuntary loss of urine associated with a strong desire or need to urinate.It is usually, associated with premature detrusor muscle contractions.
Mixed incontinence
It is a combination of both stress and urge incontinence. It is most common inolder women.
Overflow incontinence
It is the involuntary loss of urine resulting from an over-distended bladder. Itmay have a variety of presentations, including frequent or constant dribbling, orurge or stress incontinence symptoms
Transient Incontinence
It is a result of a reversible medical condition
Functional Incontinence
It is caused by factors outside the lower urinary tract such as impairment ofphysical or cognitive functioning, or both
Role of Primary Care Physician
• When to urgently refer to a urologist:
• Prostatic symptoms with digital rectal examination revealing a prostate of firm to hard consistency with nodules, loss of medial sulcus with immobile overlying mucosa.
• Presence of haematuria, painful ejaculation, impotence.
• New-onset low back pain with fatigue, malaise, weight loss
Urinary incontinence
• Involuntary loss of urine in sufficient amount or frequency, to be a social and / or health problem.
• neglected by the patient as well as the physician
• Prevalence in community varies from 15-20% and in Long term care center its 50%.
Slide 8:
Discuss each point in detail with additional clinical inputs. Emphasize that prostate cancer is emerging as a leading cancer among ageing males.
Slide 9:
Discuss each point in detail with additional clinical inputs.
Slide 10:
Discuss each point in detail with additional clinical inputs.
Slide 11:
Discuss each point in detail.
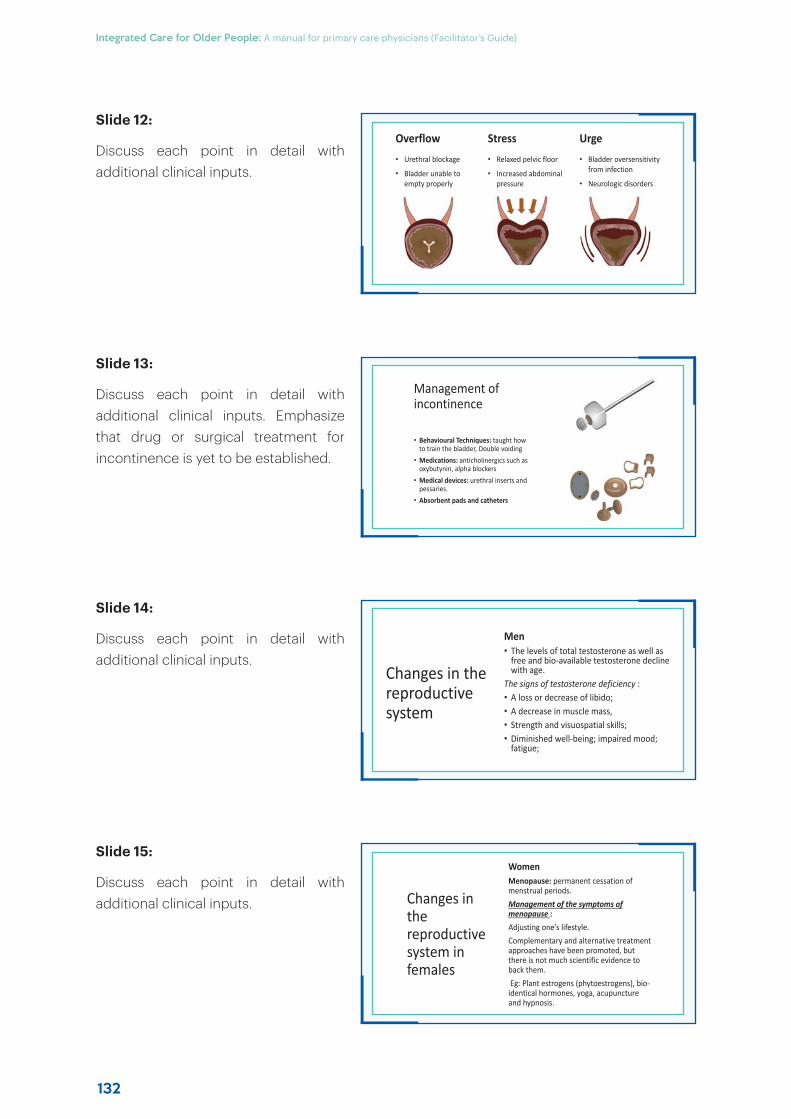
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
132
Overflow
• Urethral blockage
• Bladder unable to empty properly
Stress
• Relaxed pelvic floor
• Increased abdominal pressure
Urge
• Bladder oversensitivity from infection
• Neurologic disorders
Changes in the reproductive system in females
Women Menopause: permanent cessation of menstrual periods.Management of the symptoms of menopause :Adjusting one’s lifestyle.Complementary and alternative treatment approaches have been promoted, but there is not much scientific evidence to back them.Eg: Plant estrogens (phytoestrogens), bio-identical hormones, yoga, acupuncture and hypnosis.
Management of incontinence
• Behavioural Techniques: taught how to train the bladder, Double voiding
• Medications: anticholinergics such as oxybutynin, alpha blockers
• Medical devices: urethral inserts and pessaries.
• Absorbent pads and catheters
Changes in the reproductive system
Men• The levels of total testosterone as well as
free and bio-available testosterone decline with age.
The signs of testosterone deficiency :• A loss or decrease of libido; • A decrease in muscle mass, • Strength and visuospatial skills; • Diminished well-being; impaired mood;
fatigue;
Slide 12:
Discuss each point in detail with additional clinical inputs.
Slide 13:
Discuss each point in detail with additional clinical inputs. Emphasize that drug or surgical treatment for incontinence is yet to be established.
Slide 14:
Discuss each point in detail with additional clinical inputs.
Slide 15:
Discuss each point in detail with additional clinical inputs.
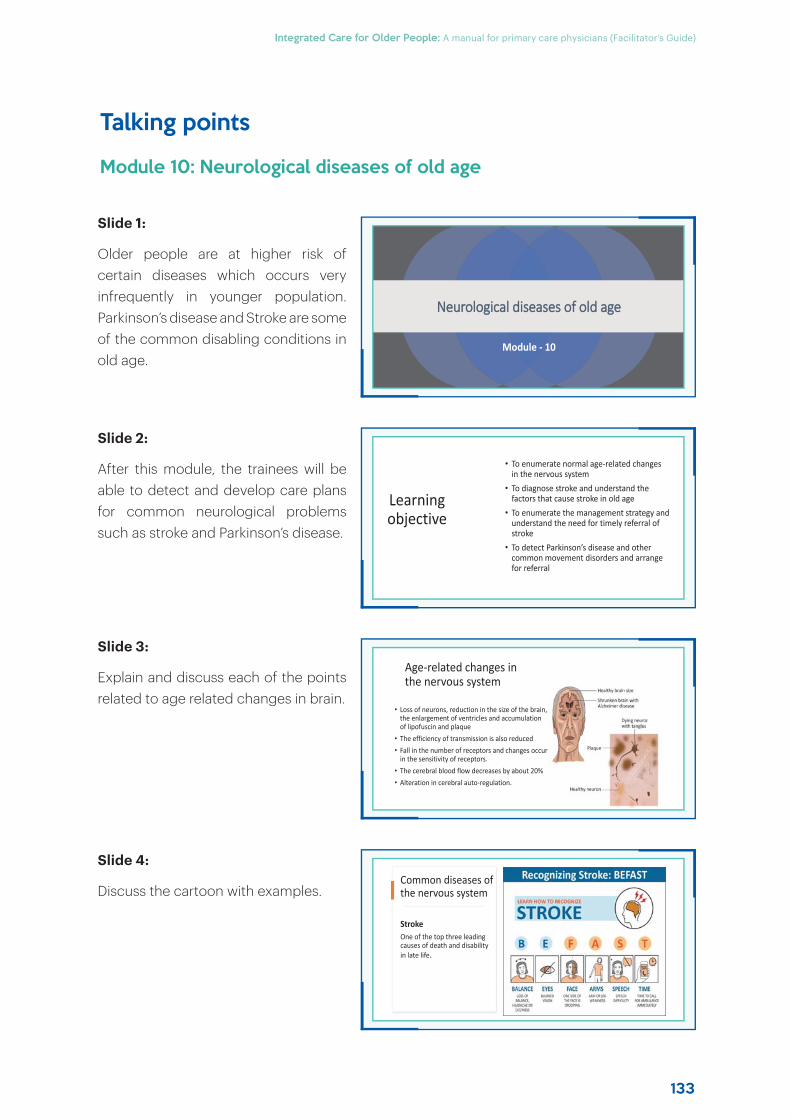
133
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
Talking points
Module 10: Neurological diseases of old age
Slide 1:
Older people are at higher risk of certain diseases which occurs very infrequently in younger population. Parkinson’s disease and Stroke are some of the common disabling conditions in old age.
Slide 2:
After this module, the trainees will be able to detect and develop care plans for common neurological problems such as stroke and Parkinson’s disease.
Slide 3:
Explain and discuss each of the points related to age related changes in brain.
Slide 4:
Discuss the cartoon with examples.
NNeurological diseases of old age
Module - 10
Learning objective
• To enumerate normal age-related changes in the nervous system
• To diagnose stroke and understand the factors that cause stroke in old age
• To enumerate the management strategy and understand the need for timely referral of stroke
• To detect Parkinson’s disease and other common movement disorders and arrange for referral
Age-related changes in the nervous system
• Loss of neurons, reduction in the size of the brain, the enlargement of ventricles and accumulation of lipofuscin and plaque
• The efficiency of transmission is also reduced• Fall in the number of receptors and changes occur
in the sensitivity of receptors.• The cerebral blood flow decreases by about 20% • Alteration in cerebral auto-regulation.
Common diseases of the nervous system
StrokeOne of the top three leading causes of death and disability in late life.
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
134
Clinical manifestations
• Numbness or weakness of face, arm or leg, especially on one side of the body
• Confusion, trouble speaking or understanding• Trouble seeing with one or both eyes• Trouble walking, dizziness, loss of balance or coordination• Severe headache with no known cause
Idiopathic Parkinson’s Disease
• Parkinson’s disease (PD) is an insidious and asymmetric disease with a progressive course.
• Causes severe disability and all treatment strategies provide only limited relief
Role of primary care physicians in stroke management
Recognize the above-mentioned symptoms and refer to a specialist centre immediatelyRecognize
Help in post-stroke rehabilitation to minimize disabilities after the patient is discharged from hospital
Help in
Help in secondary prevention of strokeHelp in
Post-stroke rehabilitation
A multidisciplinary activity which focuses on problem-solving and educating the patient on the disability. The basic principles of rehabilitation :• Documentation of the impairment
and disabilities• Maximization of independence and
minimization of dependency. • Should address several sequelae
which affect the patient’s quality of life
Slide 5:
Explain and discuss each of the points related to stroke.
Slide 6:
Explain and discuss each of the points related to stroke management.
Slide 7:
Explain and discuss each of the points related to stroke rehabilitation.
Slide 8:
Explain and discuss each of the points related to Parkinson’s disease.
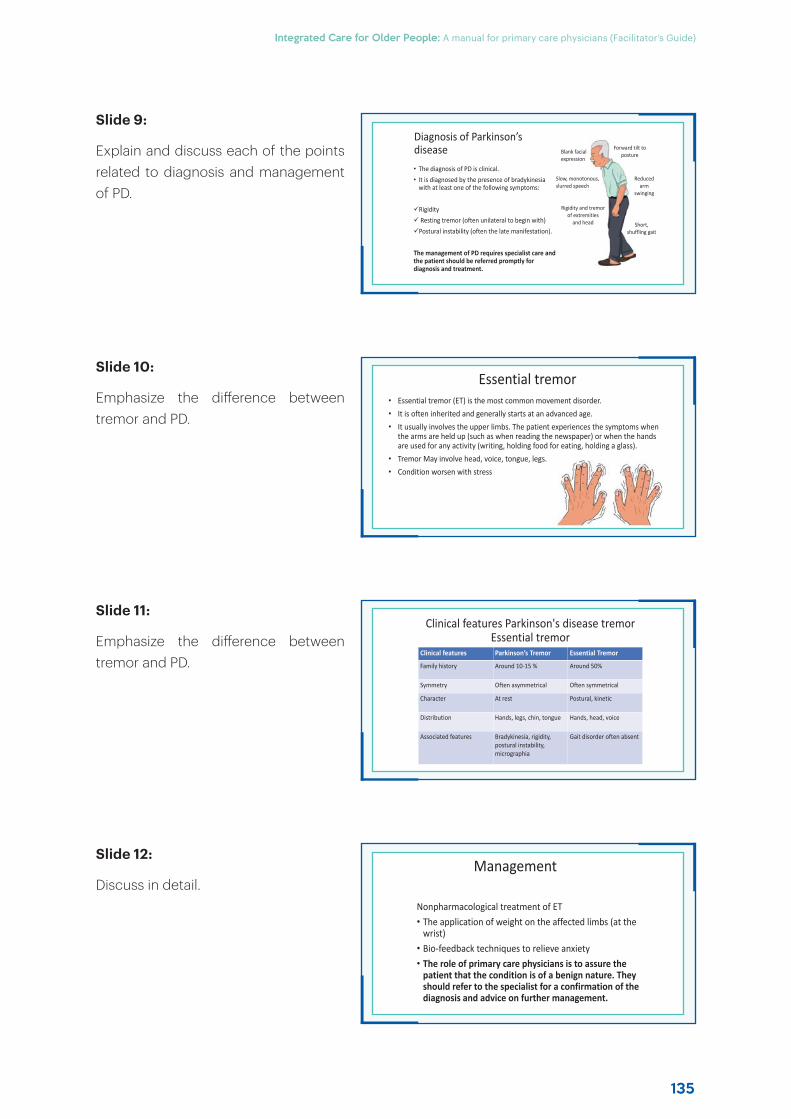
135
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
Diagnosis of Parkinson’s disease Forward tilt to
posture
Reduced arm
swinging
Short, shuffling gait
Blank facial expression
Slow, monotonous, slurred speech
Rigidity and tremor of extremities
and head
• The diagnosis of PD is clinical. • It is diagnosed by the presence of bradykinesia
with at least one of the following symptoms:
RigidityResting tremor (often unilateral to begin with)Postural instability (often the late manifestation).
The management of PD requires specialist care and the patient should be referred promptly for diagnosis and treatment.
Management
Nonpharmacological treatment of ET • The application of weight on the affected limbs (at the
wrist) • Bio-feedback techniques to relieve anxiety• The role of primary care physicians is to assure the
patient that the condition is of a benign nature. They should refer to the specialist for a confirmation of the diagnosis and advice on further management.
Essential tremor• Essential tremor (ET) is the most common movement disorder.• It is often inherited and generally starts at an advanced age.• It usually involves the upper limbs. The patient experiences the symptoms when
the arms are held up (such as when reading the newspaper) or when the hands are used for any activity (writing, holding food for eating, holding a glass).
• Tremor May involve head, voice, tongue, legs.• Condition worsen with stress
Clinical features Parkinson's disease tremor Essential tremor
Clinical features Parkinson’s Tremor Essential Tremor
Family history Around 10-15 % Around 50%
Symmetry Often asymmetrical Often symmetrical
Character At rest Postural, kinetic
Distribution Hands, legs, chin, tongue Hands, head, voice
Associated features Bradykinesia, rigidity, postural instability, micrographia
Gait disorder often absent
Slide 9:
Explain and discuss each of the points related to diagnosis and management of PD.
Slide 10:
Emphasize the diff erence between tremor and PD.
Slide 11:
Emphasize the diff erence between tremor and PD.
Slide 12:
Discuss in detail.
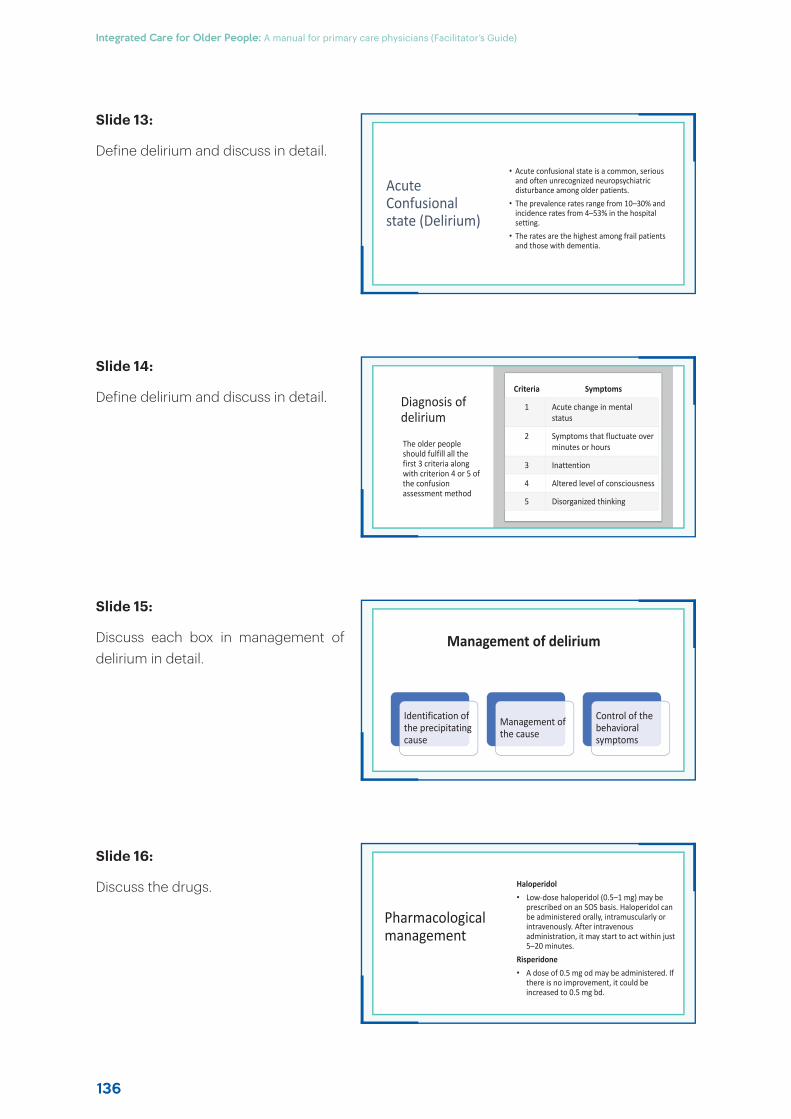
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
136
Acute Confusional state (Delirium)
• Acute confusional state is a common, serious and often unrecognized neuropsychiatric disturbance among older patients.
• The prevalence rates range from 10–30% and incidence rates from 4–53% in the hospital setting.
• The rates are the highest among frail patients and those with dementia.
Pharmacological management
Haloperidol• Low-dose haloperidol (0.5–1 mg) may be
prescribed on an SOS basis. Haloperidol can be administered orally, intramuscularly or intravenously. After intravenous administration, it may start to act within just 5–20 minutes.
Risperidone• A dose of 0.5 mg od may be administered. If
there is no improvement, it could be increased to 0.5 mg bd.
Diagnosis of delirium
The older people should fulfill all the first 3 criteria along with criterion 4 or 5 of the confusion assessment method
Criteria Symptoms
1 Acute change in mental status
2 Symptoms that fluctuate over minutes or hours
3 Inattention
4 Altered level of consciousness
5 Disorganized thinking
Management of delirium
Identification of the precipitating cause
Management of the cause
Control of the behavioral symptoms
Slide 13:
Define delirium and discuss in detail.
Slide 14:
Define delirium and discuss in detail.
Slide 15:
Discuss each box in management of delirium in detail.
Slide 16:
Discuss the drugs.
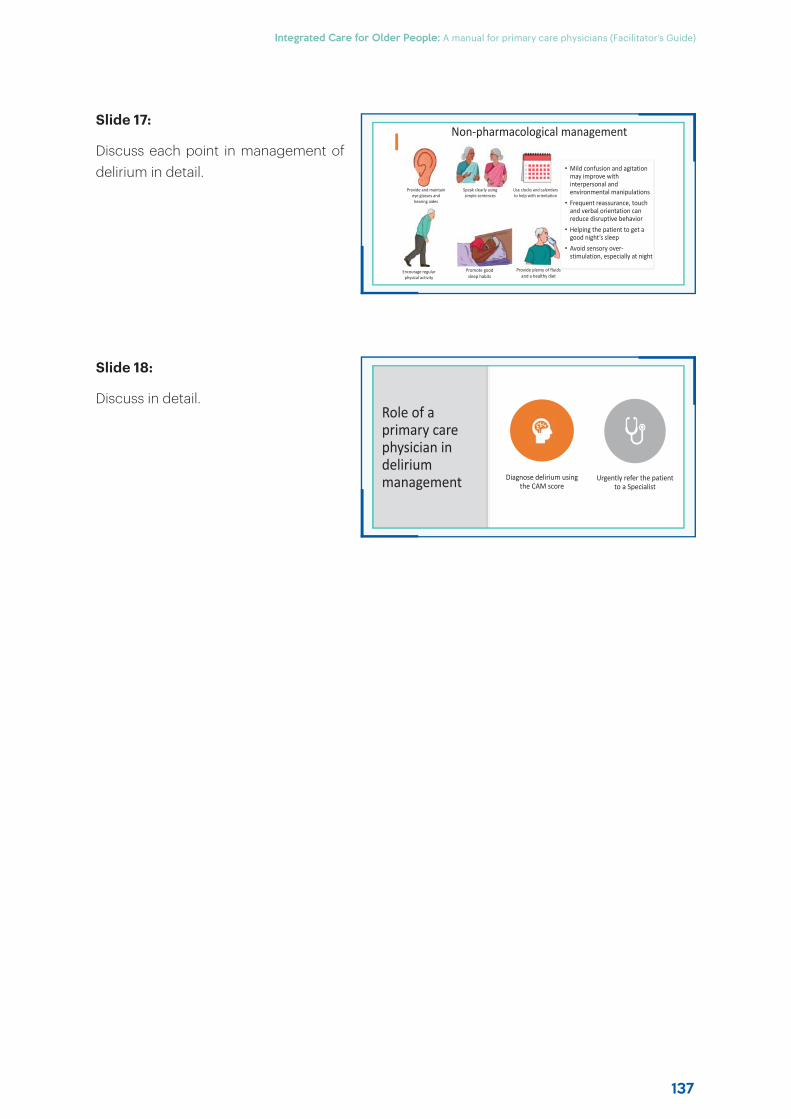
137
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
Non-pharmacological management
• Mild confusion and agitation may improve with interpersonal and environmental manipulations
• Frequent reassurance, touch and verbal orientation can reduce disruptive behavior
• Helping the patient to get a good night’s sleep
• Avoid sensory over-stimulation, especially at night
Provide and maintain eye glasses and hearing aides
Speak clearly using simple sentences
Use clocks and calendars to help with orientation
Encourage regular physical activity
Promote good sleep habits
Provide plenty of fluids and a healthy diet
Role of a primary care physician in delirium management Diagnose delirium using
the CAM scoreUrgently refer the patient
to a Specialist
Slide 17:
Discuss each point in management of delirium in detail.
Slide 18:
Discuss in detail.
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
138
Talking points
Module 11: Brain ageing and cognitive impairment
Slide 1:
Like all organs, our brain also ages; becomes smaller in size and less eff icient in functioning. As a result several finer functioning of the brain declines. In this session we will discuss issues related to ageing brain and its clinical implications.
Slide 2:
After this module, the trainee will be able to recognise eff ects ageing on brain in a clinical context and develop care plans for its management.
Slide 3:
Discuss all the points in detail.
Slide 4:
Discuss all phrases in the statement in detail.
BBrain Ageing and Cognitive Impairment
Module - 11
Learning objectives
• To enumerate age-related changes in cognition
• To screen for and identify cognitive impairment
• To assess and develop care plans for older patients with dementia
Age-related changes in cognition
If the age-related changes in the brain are excessive, it leads to significant functional impairment, termed as ‘cognitive impairment’
Cognitive decline is manifested as increasing forgetfulness, loss of attention and a reduced ability to solve problems
DDeclines in cognitive can be minimized and reversed by a healthier llifestyle, cognitive stimulation and social engagement.

139
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
Differences between normal age-related memory changes and cognitive impairment/dementia
Normal age-related memory changes Symptoms suggestive of cognitive impairment/dementia
Able to function independently and pursue normal activities, despite occasional memory lapses
Difficulty performing simple tasks and forgetting how to do things that one has done many times in the past
Able to recall and describe incidents of forgetfulnessUnable to recall or describe specific instances in which memory loss caused problems
May pause to remember directions, but does not get lost in familiar places
Gets lost or disoriented even in familiar places, unable to follow directions
Occasional difficulty finding the right word, but no trouble holding a conversation
Words are frequently forgotten, misused or garbled; repetitive in conversation
Judgment and decision-making ability intactTrouble making choices; poor judgment or socially inappropriate behavior
Clinical manifestations of dementia
Cognitive and other problems in dementia
• Memory loss• Poor concentration• Visuospatial difficulties• Speech and language defects• Inability to recognize self and others• Seizures• Disturbances of gait
Behavioural and psychological problems
• Agitation• Personality change• Abnormal eating behaviour• Wandering• Mood disorder, depression• Anxiety, phobias, fear
DementiaDementia is an acquired brain syndrome characterized by a decline in the previous level of cognitive functioning. It is associated with impairment in two or more cognitive domains, such as memory, executive functions, attention, language, social cognition and judgment, psychomotor speed and visuo-perceptual or visuospatial abilities.
Domains of dementia
Executive Functioning
Attention
Language
Visual-Spatial
Perception
Memory
Aetiology of dementia
Irreversible causes Reversible causes
Degenerative disease
• Alzheimer’s dementia• Dementia with Lewy bodies• Frontotemporal dementia• Parkinson’s-associated
dementia
Vascular • multi-infarct dementia• lacunar infarct• small vessel disease.
Infective • AIDS dementia complex• Creutzfeldt–Jakob disease.
Reversible Causes
Vitamin
deficiencies
Subdural haematoma
CNS tumours
Hypo
thyroidism
Obstructive sleep
apnoea
Side-effects of
medication
Slide 5:
Discuss age related brain changes and their clinical correlates with explanation.
Slide 6:
Define dementia and explanation the deficits domain wise as demonstrated in the diagram.
Slide 7:
Discuss the causes. Emphasize the reversible causes such and on investigations required to exclude them such as brain imaging, thyroid h\function test, vitamin B12 levels etc.
Slide 8:
Discuss in detail with examples.
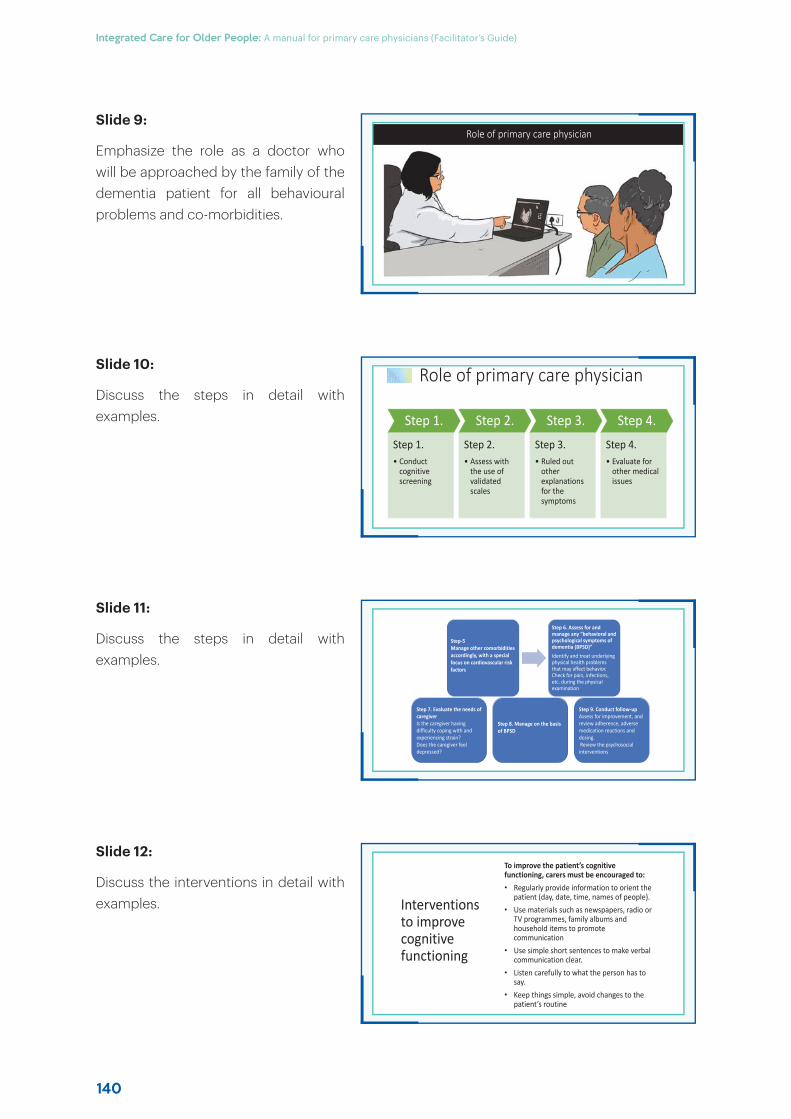
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
140
Role of primary care physician
Interventions to improve cognitive functioning
To improve the patient’s cognitive functioning, carers must be encouraged to:
• Regularly provide information to orient the patient (day, date, time, names of people).
• Use materials such as newspapers, radio or TV programmes, family albums and household items to promote communication
• Use simple short sentences to make verbal communication clear.
• Listen carefully to what the person has to say.
• Keep things simple, avoid changes to the patient’s routine
Role of primary care physician
Step 1.
Step 1.• Conduct
cognitive screening
Step 2.
Step 2.• Assess with
the use of validated scales
Step 3.
Step 3.• Ruled out
other explanations for the symptoms
Step 4.
Step 4.• Evaluate for
other medical issues
Step-5Manage other comorbidities accordingly, with a special focus on cardiovascular risk factors
Step 6. Assess for and manage any “behavioral and psychological symptoms of dementia (BPSD)”
Identify and treat underlying physical health problems that may affect behavior. Check for pain, infections, etc. during the physical examination
Step 7. Evaluate the needs of caregiverIs the caregiver having difficulty coping with and experiencing strain?Does the caregiver feel depressed?
Step 8. Manage on the basis of BPSD
Step 9. Conduct follow-upAssess for improvement, and review adherence, adverse medication reactions and dosing.Review the psychosocial interventions
Slide 9:
Emphasize the role as a doctor who will be approached by the family of the dementia patient for all behavioural problems and co-morbidities.
Slide 10:
Discuss the steps in detail with examples.
Slide 11:
Discuss the steps in detail with examples.
Slide 12:
Discuss the interventions in detail with examples.
141
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
Carer support
• Assess the impact providing care on the Carer’ needs to ensure that they have the support and resources necessary for their family life, employment, social activities and health.
• Acknowledge that it can be extremely frustrating and stressful to take care of people with dementia.
• Carer need to be encouraged to respect the dignity of people with dementia and avoid hostility towards, or neglect of, them.
• Encourage Carer to seek help if they are experiencing difficulty or strain in caring for their loved one.
• Provide the Carer with training and support in specific skills, e.g. managing difficult behaviour, if necessary. It would be most effective to elicit active participation, e.g. role play.
Slide 13:
Read each point and discuss in detail.

Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
142
Talking points
Module 12: Mental health
Slide 1:
Older people have multiple stresses arising out of their life situation as well as the social environment in which they live. In addition the likelihood of developing dementia also increases with age. Multiple co-morbidities also contribute to poor mental health. Assessing mental health issues during routine consultation and addressing them through non-pharmacological or pharmacological strategies; or referral to specialist for complexity of the clinical problem.
Slide 2:
At the end of this module, trainees will be able address mental health issues of old age with diagnosis and care planning.
Slide 3:
Enumerate the stress of old age listed in the slide with examples and discuss.
MMental Health
Module - 12
Learning objectives
• To enumerate the common stresses of old age
• To enumerate the social and cultural barriers to seeking mental health services
• To identify common mental health problems among older patients and develop care plans
Common stresses that older people have to cope with
Widowhood and the death of other significant friends and relatives• Caregiver stress• Fear of death• Financial difficulties
• Loss of independence• Changes in living arrangements and previous roles• Social isolation
• Chronic diseases
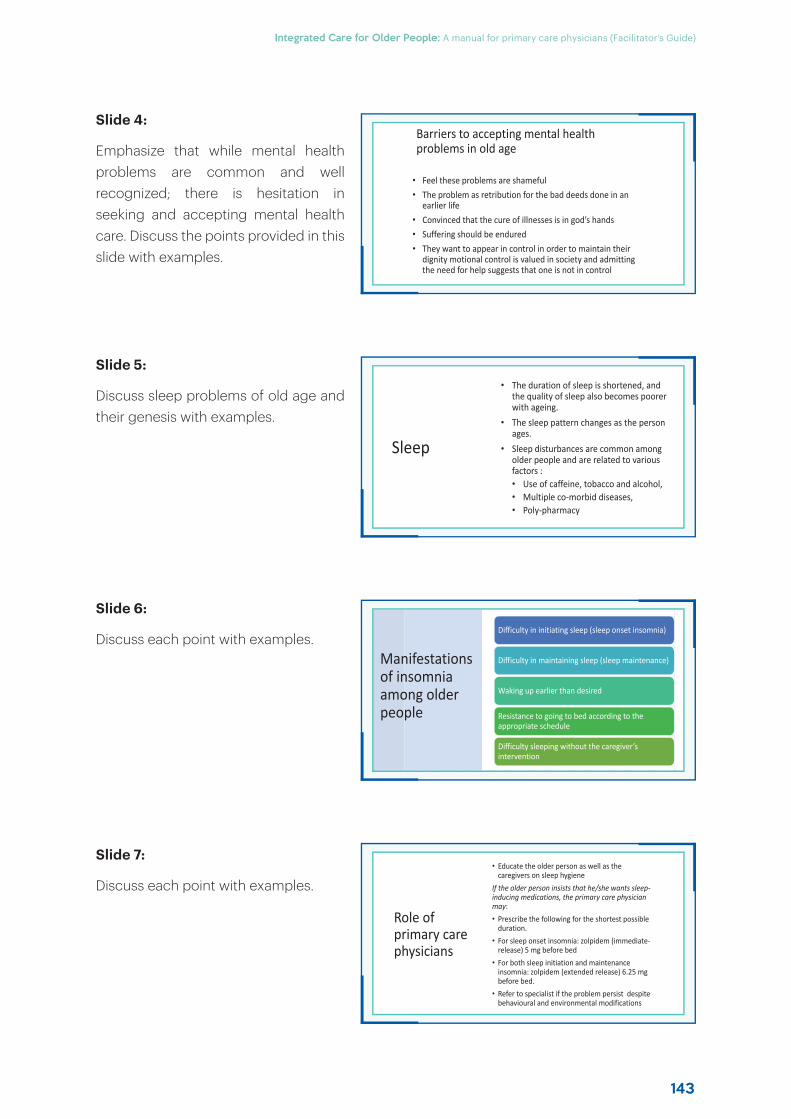
143
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
Barriers to accepting mental health problems in old age
• Feel these problems are shameful• The problem as retribution for the bad deeds done in an
earlier life• Convinced that the cure of illnesses is in god’s hands• Suffering should be endured• They want to appear in control in order to maintain their
dignity motional control is valued in society and admitting the need for help suggests that one is not in control
Role of primary care physicians
• Educate the older person as well as the caregivers on sleep hygiene
If the older person insists that he/she wants sleep-inducing medications, the primary care physician may:• Prescribe the following for the shortest possible
duration.• For sleep onset insomnia: zolpidem (immediate-
release) 5 mg before bed
• For both sleep initiation and maintenance insomnia: zolpidem (extended release) 6.25 mg before bed.
• Refer to specialist if the problem persist despite behavioural and environmental modifications
Sleep
• The duration of sleep is shortened, and the quality of sleep also becomes poorer with ageing.
• The sleep pattern changes as the person ages.
• Sleep disturbances are common among older people and are related to various factors :• Use of caffeine, tobacco and alcohol, • Multiple co-morbid diseases,• Poly-pharmacy
Manifestations of insomnia among older people
Difficulty in initiating sleep (sleep onset insomnia)
Difficulty in maintaining sleep (sleep maintenance)
Waking up earlier than desired
Resistance to going to bed according to the appropriate schedule
Difficulty sleeping without the caregiver’s intervention
Slide 4:
Emphasize that while mental health problems are common and well recognized; there is hesitation in seeking and accepting mental health care. Discuss the points provided in this slide with examples.
Slide 5:
Discuss sleep problems of old age and their genesis with examples.
Slide 6:
Discuss each point with examples.
Slide 7:
Discuss each point with examples.
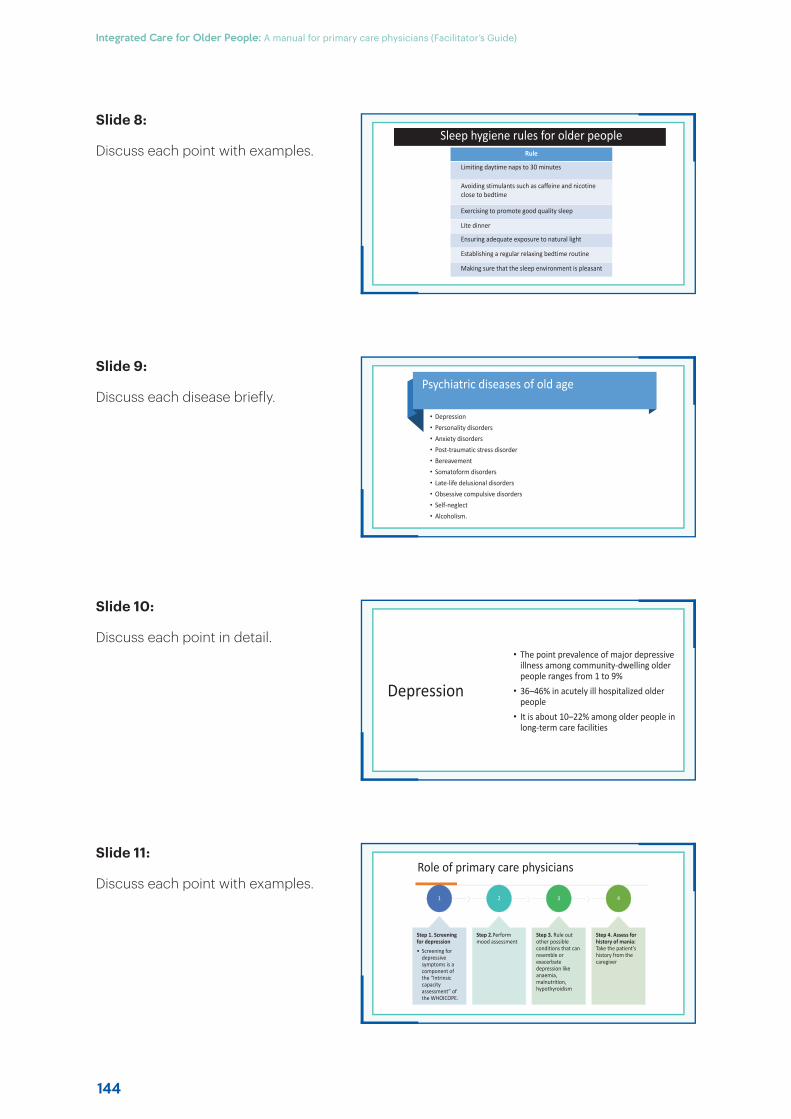
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
144
Sleep hygiene rules for older peopleRule
Limiting daytime naps to 30 minutes
Avoiding stimulants such as caffeine and nicotine close to bedtime
Exercising to promote good quality sleep
Lite dinner
Ensuring adequate exposure to natural light
Establishing a regular relaxing bedtime routine
Making sure that the sleep environment is pleasant
Role of primary care physicians
1
Step 1. Screening for depression• Screening for
depressive symptoms is a component of the “Intrinsic capacity assessment” of the WHOICOPE.
2
Step 2.Perform mood assessment
3
Step 3. Rule out other possible conditions that can resemble or exacerbate depression like anaemia, malnutrition, hypothyroidism
4
Step 4. Assess for history of mania: Take the patient’s history from the caregiver
Psychiatric diseases of old age
• Depression• Personality disorders• Anxiety disorders• Post-traumatic stress disorder • Bereavement• Somatoform disorders• Late-life delusional disorders• Obsessive compulsive disorders• Self-neglect• Alcoholism.
Depression
• The point prevalence of major depressive illness among community-dwelling older people ranges from 1 to 9%
• 36–46% in acutely ill hospitalized older people
• It is about 10–22% among older people in long-term care facilities
Slide 8:
Discuss each point with examples.
Slide 9:
Discuss each disease briefly.
Slide 10:
Discuss each point in detail.
Slide 11:
Discuss each point with examples.
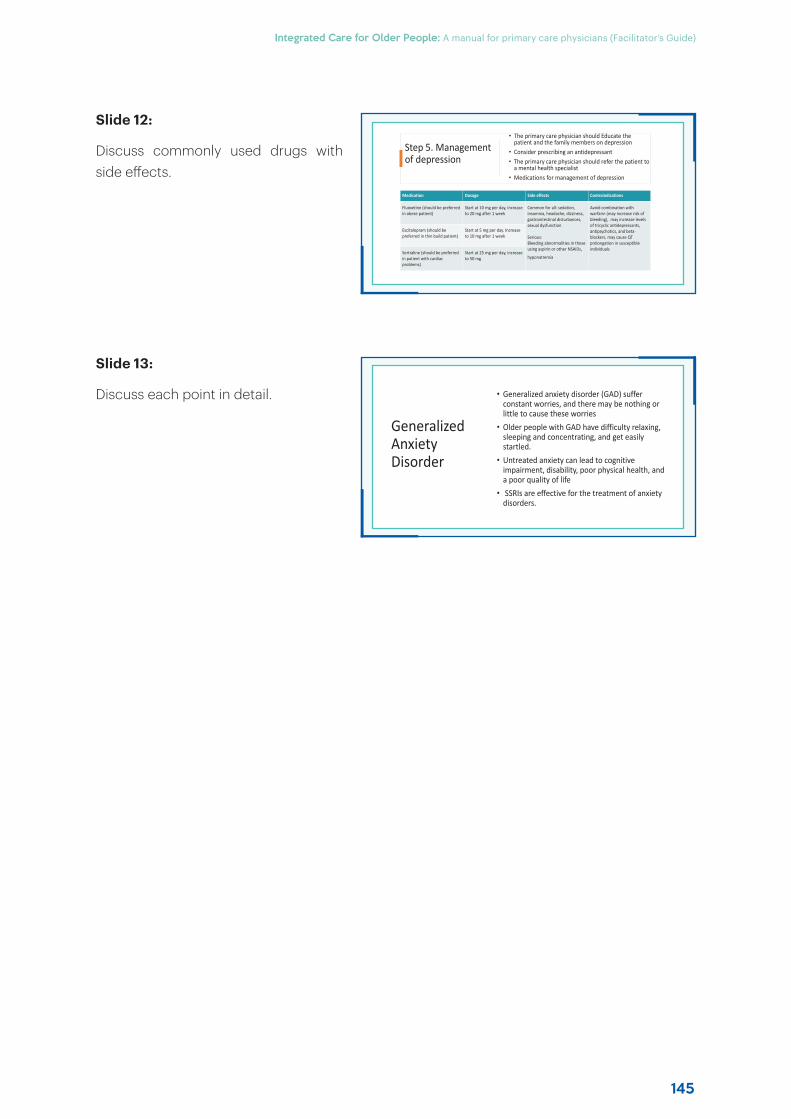
145
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
Step 5. Management of depression
• The primary care physician should Educate the patient and the family members on depression
• Consider prescribing an antidepressant• The primary care physician should refer the patient to
a mental health specialist• Medications for management of depression
Medication Dosage Side effects Contraindications
Fluoxetine (should be preferred in obese patient)
Start at 10 mg per day, increase to 20 mg after 1 week
Common for all: sedation, insomnia, headache, dizziness, gastrointestinal disturbances, sexual dysfunction
Serious: Bleeding abnormalities in those using aspirin or other NSAIDs,
hyponatremia
Avoid combination with warfarin (may increase risk of bleeding), may increase levels of tricyclic antidepressants, antipsychotics, and beta-blockers, may cause QTprolongation in susceptible individuals
Escitalopram (should be preferred in thin build patient)
Start at 5 mg per day. Increase to 10 mg after 1 week
Sertraline (should be preferred in patient with cardiac problems)
Start at 25 mg per day, increase to 50 mg
Generalized Anxiety Disorder
• Generalized anxiety disorder (GAD) suffer constant worries, and there may be nothing or little to cause these worries
• Older people with GAD have difficulty relaxing, sleeping and concentrating, and get easily startled.
• Untreated anxiety can lead to cognitive impairment, disability, poor physical health, and a poor quality of life
• SSRIs are effective for the treatment of anxiety disorders.
Slide 12:
Discuss commonly used drugs with side eff ects.
Slide 13:
Discuss each point in detail.
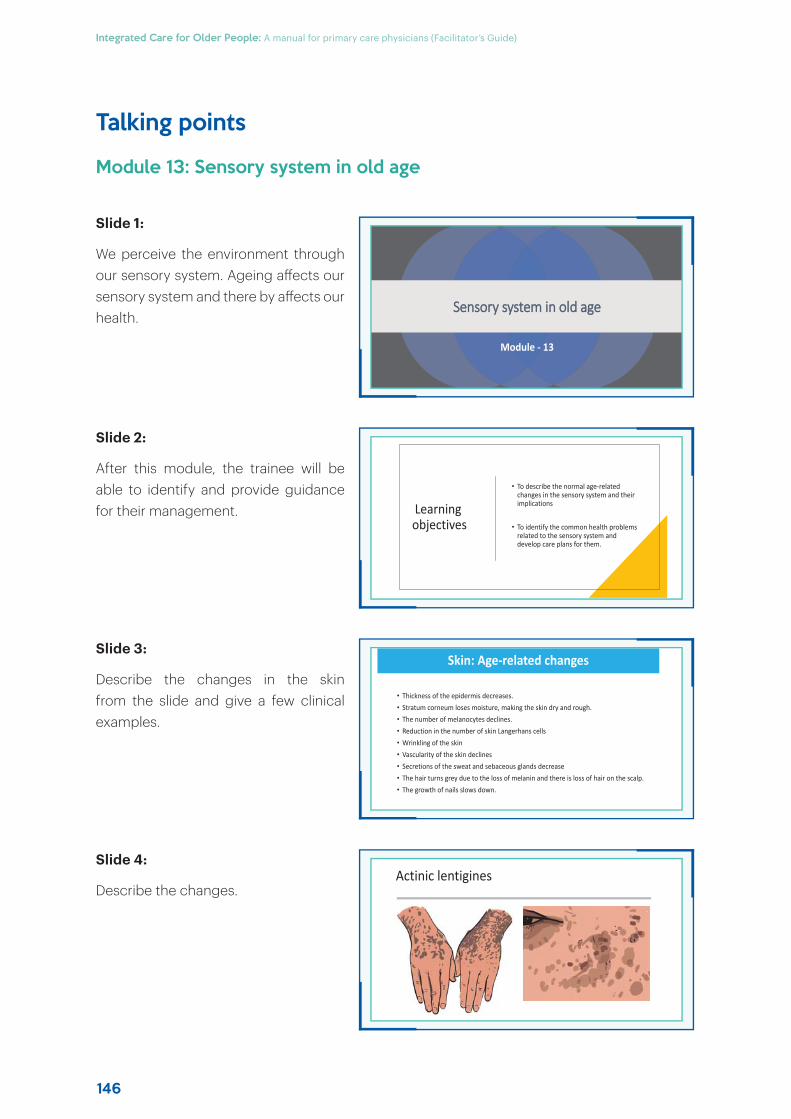
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
146
Talking points
Module 13: Sensory system in old age
Slide 1:
We perceive the environment through our sensory system. Ageing aff ects our sensory system and there by aff ects our health.
Slide 2:
After this module, the trainee will be able to identify and provide guidance for their management.
Slide 3:
Describe the changes in the skin from the slide and give a few clinical examples.
Slide 4:
Describe the changes.
SSensory system in old age
Module - 13
Learning objectives
• To describe the normal age-related changes in the sensory system and their implications
• To identify the common health problems related to the sensory system and develop care plans for them.
Skin: Age-related changes
• Epidermis and dermis, change with advancing age.
• Thickness of the epidermis decreases. • Stratum corneum loses moisture, making the skin dry and rough. • The number of melanocytes declines. • Reduction in the number of skin Langerhans cells• Wrinkling of the skin• Vascularity of the skin declines• Secretions of the sweat and sebaceous glands decrease• The hair turns grey due to the loss of melanin and there is loss of hair on the scalp. • The growth of nails slows down.
Actinic lentigines
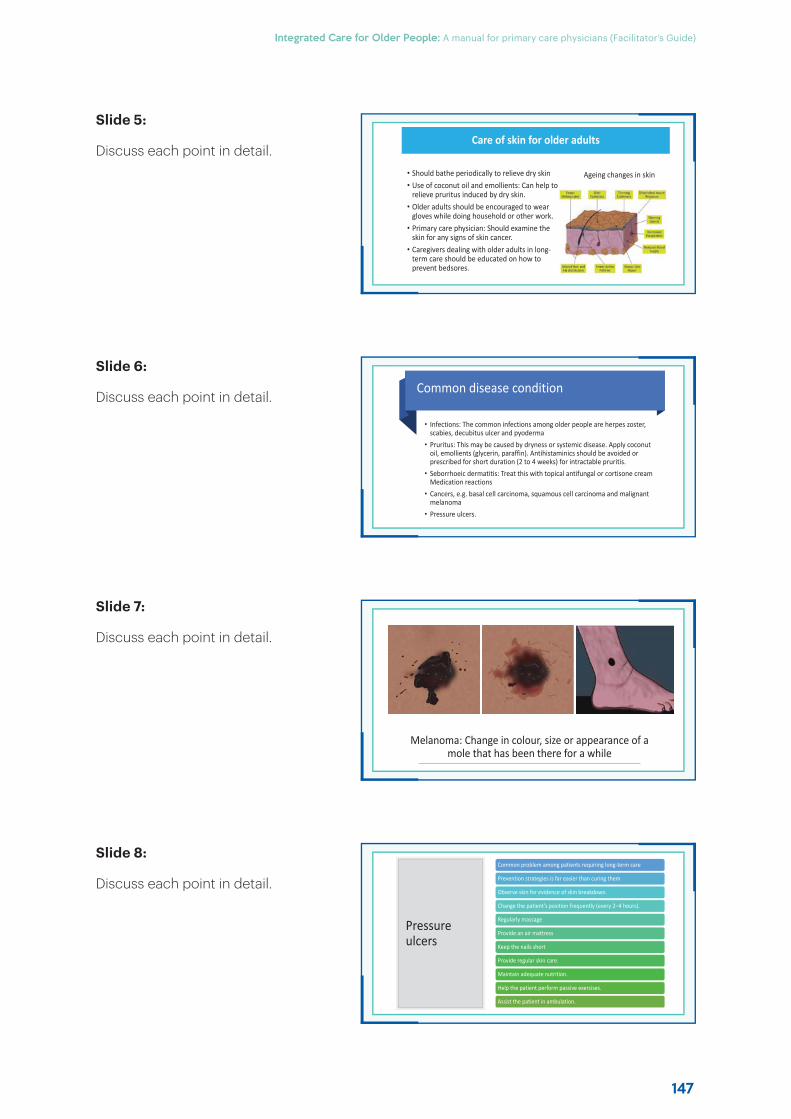
147
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
Care of skin for older adults
• Should bathe periodically to relieve dry skin• Use of coconut oil and emollients: Can help to
relieve pruritus induced by dry skin.• Older adults should be encouraged to wear
gloves while doing household or other work.• Primary care physician: Should examine the
skin for any signs of skin cancer.• Caregivers dealing with older adults in long-
term care should be educated on how to prevent bedsores.
Ageing changes in skin
Pressure ulcers
Common problem among patients requiring long-term care
Prevention strategies is far easier than curing them
Observe skin for evidence of skin breakdown.
Change the patient’s position frequently (every 2–4 hours).
Regularly massage
Provide an air mattress
Keep the nails short
Provide regular skin care.
Maintain adequate nutrition.
Help the patient perform passive exercises.
Assist the patient in ambulation.
Common disease condition
• Infections: The common infections among older people are herpes zoster, scabies, decubitus ulcer and pyoderma
• Pruritus: This may be caused by dryness or systemic disease. Apply coconut oil, emollients (glycerin, paraffin). Antihistaminics should be avoided or prescribed for short duration (2 to 4 weeks) for intractable pruritis.
• Seborrhoeic dermatitis: Treat this with topical antifungal or cortisone cream Medication reactions
• Cancers, e.g. basal cell carcinoma, squamous cell carcinoma and malignant melanoma
• Pressure ulcers.
Melanoma: Change in colour, size or appearance of a mole that has been there for a while
Slide 5:
Discuss each point in detail.
Slide 6:
Discuss each point in detail.
Slide 7:
Discuss each point in detail.
Slide 8:
Discuss each point in detail.
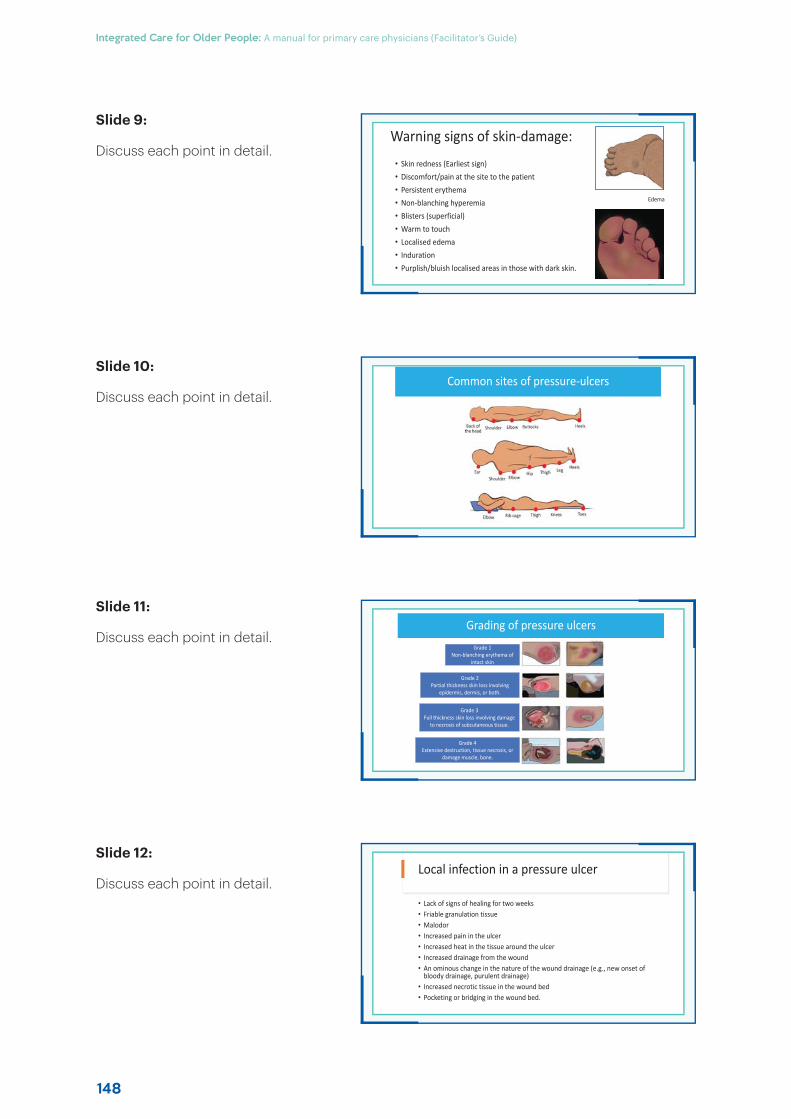
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
148
Warning signs of skin-damage:
• Skin redness (Earliest sign)• Discomfort/pain at the site to the patient• Persistent erythema • Non-blanching hyperemia• Blisters (superficial)• Warm to touch• Localised edema • Induration • Purplish/bluish localised areas in those with dark skin.
Bli t
Edema
Local infection in a pressure ulcer
• Lack of signs of healing for two weeks• Friable granulation tissue • Malodor • Increased pain in the ulcer • Increased heat in the tissue around the ulcer • Increased drainage from the wound • An ominous change in the nature of the wound drainage (e.g., new onset of
bloody drainage, purulent drainage)• Increased necrotic tissue in the wound bed• Pocketing or bridging in the wound bed.
Common sites of pressure-ulcers
Grading of pressure ulcers
Grade 1Non-blanching erythema of
intact skin
Grade 2Partial thickness skin loss involving
epidermis, dermis, or both.
Grade 3Full thickness skin loss involving damage
to necrosis of subcutaneous tissue.
Grade 4Extensive destruction, tissue necrosis, or
damage muscle, bone.
Slide 9:
Discuss each point in detail.
Slide 10:
Discuss each point in detail.
Slide 11:
Discuss each point in detail.
Slide 12:
Discuss each point in detail.
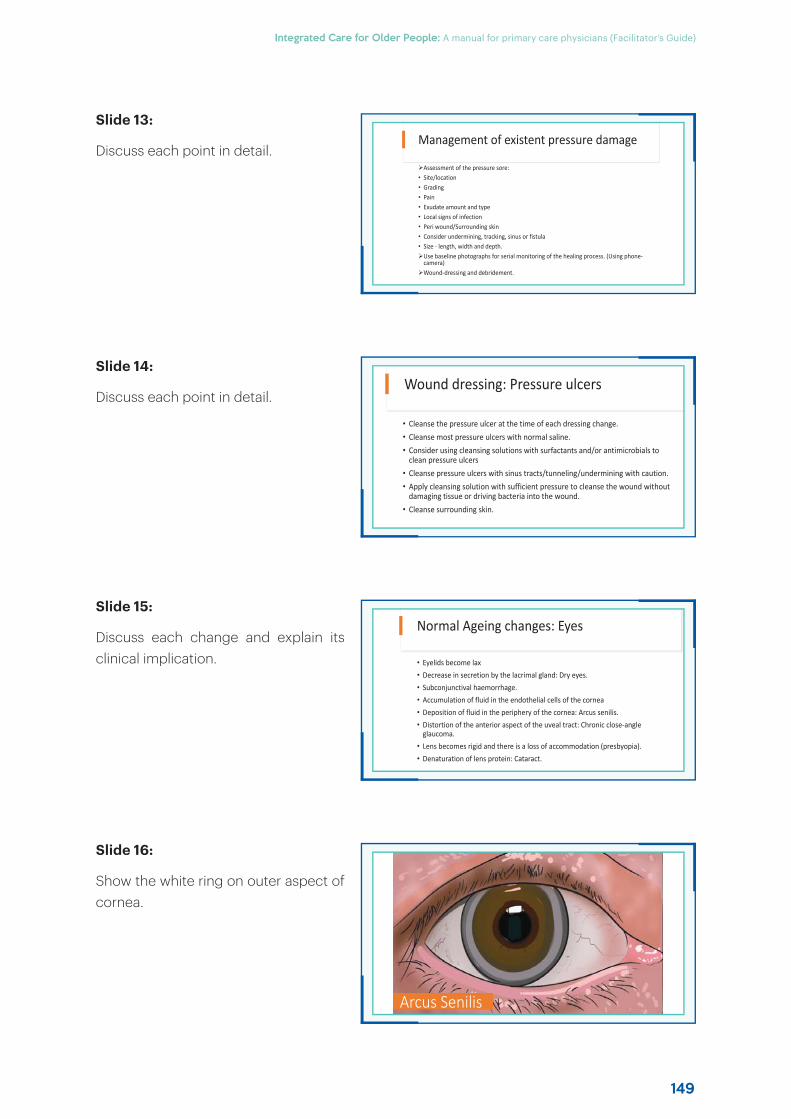
149
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
Management of existent pressure damage
Assessment of the pressure sore:• Site/location • Grading• Pain • Exudate amount and type • Local signs of infection• Peri wound/Surrounding skin• Consider undermining, tracking, sinus or fistula• Size - length, width and depth.
Use baseline photographs for serial monitoring of the healing process. (Using phone-camera)Wound-dressing and debridement.
Arcus Senilis
Wound dressing: Pressure ulcers
• Cleanse the pressure ulcer at the time of each dressing change.• Cleanse most pressure ulcers with normal saline.• Consider using cleansing solutions with surfactants and/or antimicrobials to
clean pressure ulcers • Cleanse pressure ulcers with sinus tracts/tunneling/undermining with caution.• Apply cleansing solution with sufficient pressure to cleanse the wound without
damaging tissue or driving bacteria into the wound.• Cleanse surrounding skin.
Normal Ageing changes: Eyes
• Eyelids become lax• Decrease in secretion by the lacrimal gland: Dry eyes.• Subconjunctival haemorrhage. • Accumulation of fluid in the endothelial cells of the cornea• Deposition of fluid in the periphery of the cornea: Arcus senilis.• Distortion of the anterior aspect of the uveal tract: Chronic close-angle
glaucoma.• Lens becomes rigid and there is a loss of accommodation (presbyopia). • Denaturation of lens protein: Cataract.
Slide 13:
Discuss each point in detail.
Slide 14:
Discuss each point in detail.
Slide 15:
Discuss each change and explain its clinical implication.
Slide 16:
Show the white ring on outer aspect of cornea.
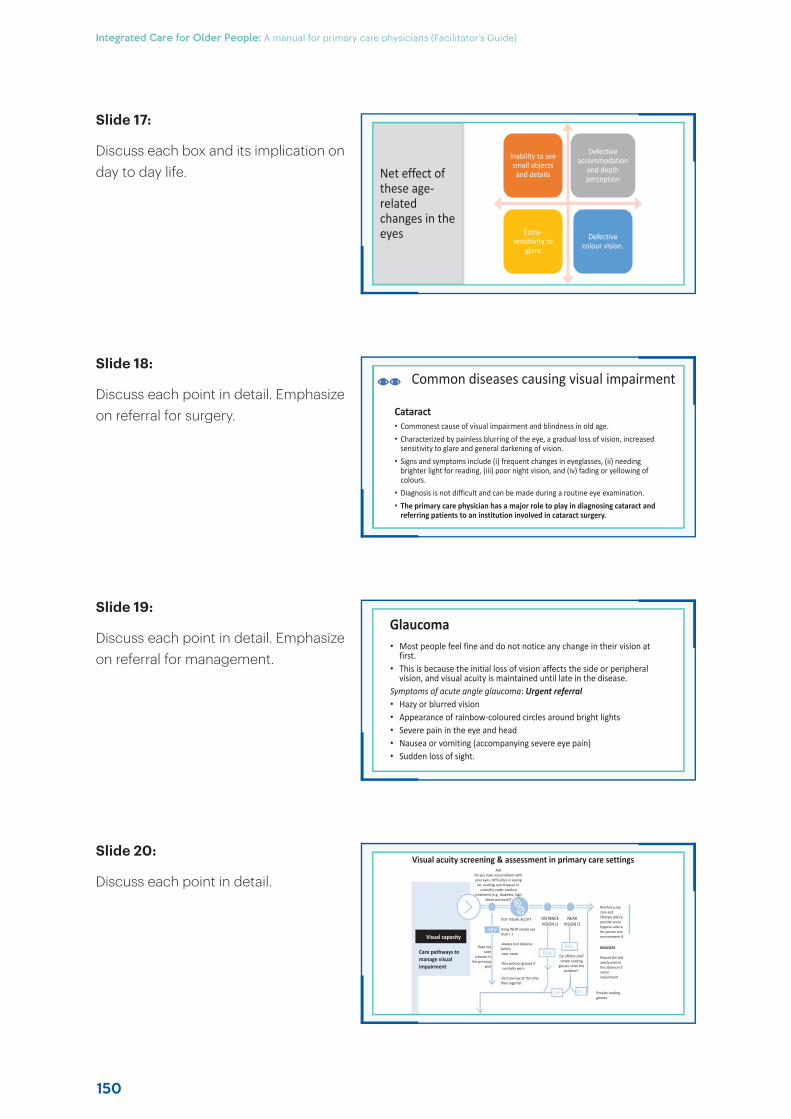
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
150
Net effect of these age-related changes in the eyes
Inability to see small objects and details
Defective accommodation
and depth perception
Extra-sensitivity to
glare
Defective colour vision.
Visual acuity screening & assessment in primary care settingsASK
Do you have any problems with your eyes: difficulties in seeing
far, reading, eye diseases or currently under medical
treatment (e.g., diabetes, high blood pressure)?
Have not seen
a doctor inthe previous
year
TEST VISUAL ACUITY
Using WHO simple eye chart i 1
-Always test distance beforenear vision
-Test without glasses if normally worn
-Test one eye at the time, then together
DISTANCEVISION i2
NEARVISION i2
Reinforce eye care and lifestyle advice, provide vision hygiene advice for person and environment i4
REASSESS
Repeat the test yearly even in the absence of vision impairment
Provide readingglasses
Do off-the-shelfsimple reading
glasses solve theproblem?
Visual capacity
Care pathways tomanage visualimpairment
Common diseases causing visual impairment
Cataract• Commonest cause of visual impairment and blindness in old age.• Characterized by painless blurring of the eye, a gradual loss of vision, increased
sensitivity to glare and general darkening of vision. • Signs and symptoms include (i) frequent changes in eyeglasses, (ii) needing
brighter light for reading, (iii) poor night vision, and (iv) fading or yellowing of colours.
• Diagnosis is not difficult and can be made during a routine eye examination. • The primary care physician has a major role to play in diagnosing cataract and
referring patients to an institution involved in cataract surgery.
Glaucoma• Most people feel fine and do not notice any change in their vision at
first.• This is because the initial loss of vision affects the side or peripheral
vision, and visual acuity is maintained until late in the disease. Symptoms of acute angle glaucoma: Urgent referral• Hazy or blurred vision• Appearance of rainbow-coloured circles around bright lights• Severe pain in the eye and head • Nausea or vomiting (accompanying severe eye pain)• Sudden loss of sight.
Slide 17:
Discuss each box and its implication on day to day life.
Slide 18:
Discuss each point in detail. Emphasize on referral for surgery.
Slide 19:
Discuss each point in detail. Emphasize on referral for management.
Slide 20:
Discuss each point in detail.
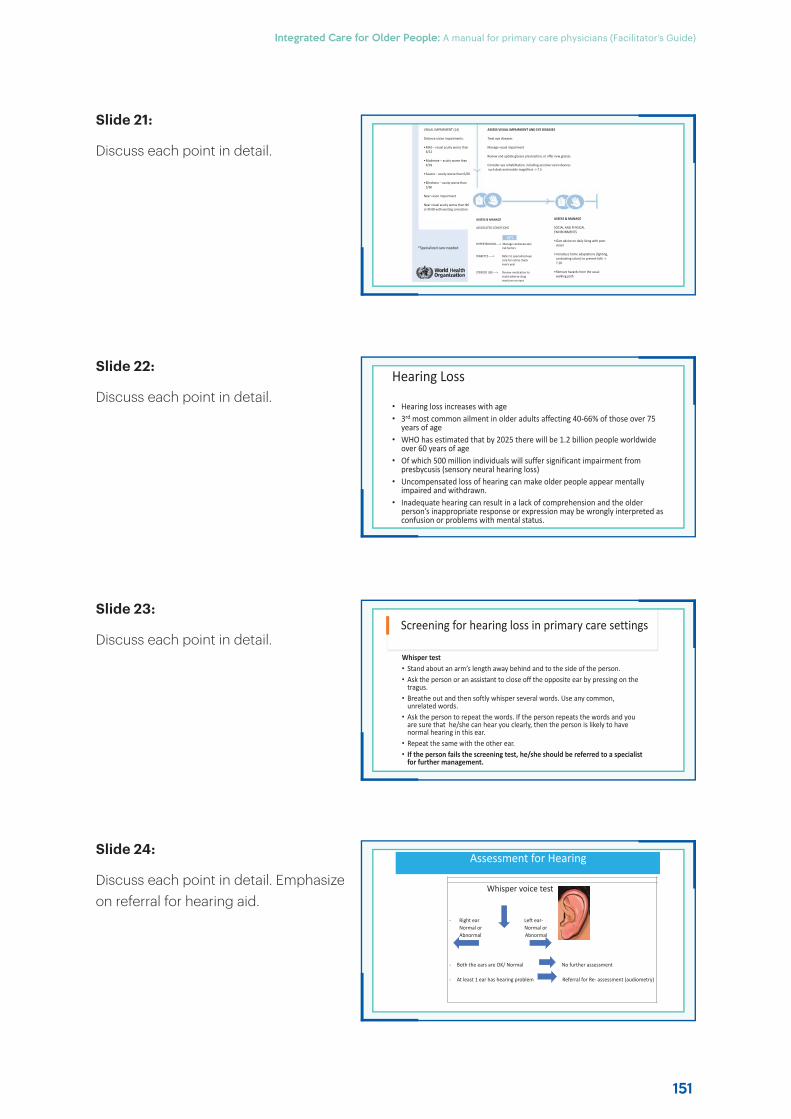
151
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
VISUAL IMPAIRMENT (14)
Distance vision impairments:
•Mild – visual acuity worse than 6/12
•Moderate – acuity worse than 6/18
•Severe – acuity worse than 6/60
•Blindness – acuity worse than 3/60
Near vision impairment
Near visual acuity worse than N6or M.08 with existing correction
ASSESS VISUAL IMPAIRMENT AND EYE DISEASES
Treat eye diseases
Manage visual impairment
Review and update glasses prescription, or offer new glasses
Consider eye rehabilitation, including assistive vision devicessuch desk and mobile magnifiers -> 7.5
ASSESS & MANAGE
ASSOCIATED CONDITIONS
HYPERTENSION----> Manage cardiovascularrisk factors
DIABETES ----> Refer to specialized eyecare for retina checkevery year
STEROID USE----> Review medication toavoid adverse drugreactions on eyes
ASSESS & MANAGE
SOCIAL AND PHYSICAL ENVIRONMENTS
•Give advice on daily living with poor vision
•Introduce home adaptations (lighting, contrasting colors) to prevent falls -> 7.10
•Remove hazards from the usual walking path
*Specialized care needed
Assessment for Hearing
Whisper voice test
- Right ear Left ear-Normal or Normal orAbnormal Abnormal
- Both the ears are OK/ Normal No further assessment
- At least 1 ear has hearing problem Referral for Re- assessment (audiometry)
Hearing Loss
• Hearing loss increases with age• 3rd most common ailment in older adults affecting 40-66% of those over 75
years of age• WHO has estimated that by 2025 there will be 1.2 billion people worldwide
over 60 years of age• Of which 500 million individuals will suffer significant impairment from
presbycusis (sensory neural hearing loss)• Uncompensated loss of hearing can make older people appear mentally
impaired and withdrawn.• Inadequate hearing can result in a lack of comprehension and the older
person’s inappropriate response or expression may be wrongly interpreted as confusion or problems with mental status.
Screening for hearing loss in primary care settings
Whisper test • Stand about an arm’s length away behind and to the side of the person.• Ask the person or an assistant to close off the opposite ear by pressing on the
tragus.• Breathe out and then softly whisper several words. Use any common,
unrelated words.• Ask the person to repeat the words. If the person repeats the words and you
are sure that he/she can hear you clearly, then the person is likely to have normal hearing in this ear.
• Repeat the same with the other ear.• If the person fails the screening test, he/she should be referred to a specialist
for further management.
Slide 21:
Discuss each point in detail.
Slide 22:
Discuss each point in detail.
Slide 23:
Discuss each point in detail.
Slide 24:
Discuss each point in detail. Emphasize on referral for hearing aid.

Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
152
Talking points
Module 14: Cancer and palliative care
Slide 1:
Age is a strong risk factor for cancer. Cancer is the second most common cause of death among older people. However, most of these patients in low and middle income countries are diagnosed at an advanced stage of disease when definitive or curative treatment is not possible. Older cancer patients are thus in great need of palliative care. This module will provide a comprehensive account of cancer in old age useful for primary care physicians.
Slide 2:
After this module, the trainees will be able to provide initial treatment and referral to older patients with cancer and manage the terminal phase with palliation of distressful symptoms.
Slide 3:
Discuss about facts of cancer in old age. Read all points and discuss with examples.
CCancer and palliative care
Module - 14
Learning objectives
• To enumerate the peculiarities of cancer in old age
• To enumerate the alarm signs for cancer in old age
• To enumerate the role of primary care physicians in palliative care
Introduction
• Cancer is the second most common non-communicable disease in old age.
• It is one of the five common causes of death in old age and among the top three causes of death in old age all over the world.
• In developed societies, 55–60% of all cancers and 70% of all cancer deaths occur after the age of 65 years.
153
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
Causes for delay in diagnosis
• People are not particularly interested in screening for cancer.
• There is a lack of awareness of the problem.
• Older patients are usually under-treated due to a widely prevalent misconception that they are less eligible for surgery and they tolerate radiotherapy and chemotherapy poorly.
Palliative care
“An approach that improves the quality of life of patients and their families facing the problem associated with life-threatening illness, through the prevention and relief of suffering by means of early identification and impeccable assessment and treatment of pain and other problems, physical, psychosocial and spiritual.”- WHO
The majority of adults in need of palliative care have chronic diseases, such as cardiovascular diseases (38.5%), cancer (34%), chronic respiratory diseases (10.3%), HIV-AIDS (5.7%) and diabetes (4.6%)
Signs and symptoms of suspected malignancy
General signs Changes specific to certain cancersContinuous feverFatigueUnexplained weight lossLoss of appetitePainSkin changes
Changes in bladder and bowel habitsNon healing sores White patches in the mouth or on tongueUnusual bleeding or dischargeLump in any part of the body.Indigestion or difficulty in swallowingRecent change in warts or moles Nagging cough or hoarseness of voice
Role of primary care physician in management of cancer in the community
• Screening for cancer and detecting cancer at an early stage
• Referring the patient to a specialized unit involved in the management of cancer addressing pre-treatment health issues
• Detecting and managing comorbidities, and making the necessary referrals
• Detecting and managing post-treatment health problems
• Providing palliative care• Providing care in the terminal stage
Slide 4:
Read all points and discuss with examples.
Slide 5:
Read all points and discuss with examples.
Slide 6:
Read all points and discuss with examples.
Slide 7:
Define palliative care with emphasis on each of the phrases. Point out the co-morbidities. Discuss their clinical impact.
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
154
Components of palliative carePhysical care needs Anemia
Pain (all types) Drowsiness or sedation
Gastrointestinal problems (constipation, nausea, vomiting, dry mouth, mucositis, diarrhea)
Sweating
Respiratory problems (dyspnoea, cough) Psychological/emotional needs
Delirium Psychological distress
Wounds, ulcers, skin rash and skin lesions Anxiety, Depression
Insomnia Suffering of family or caregivers
Fatigue Spiritual needs and existential distress
Anorexia Bereavement problems of caregivers
Principles governing the use of morphine in advanced cancer
• Use when a weak opioid and an NSAID are no longer adequate.
• Continue to prescribe an NSAID, unless there is a major contraindication.
• Administer by mouth• Administer regularly by the clock, with
additional doses (as needed) or rescue doses
• Titrate the dose according to the individual’s need
• Anticipate and treat vomiting and constipation
• Monitor the response.• Use adjuvant analgesics or nondrug
treatments if the response remains poor
Role of Primary Care Physician
• Identify sources of support and the resources available
• Develop and implement a care plan based on the patient’s needs
• Provide care in the last weeks/days of life
• Facilitate the availability of and access to medications (especially opioids)
• Identify the psychosocial/spiritual needs of the professionals providing care (including yourself)
Control of cancer pain
The WHO analgesic ladder
Type of drugs Non-opioid+ adjuvant
Mild opioid+ non-opioid+ adjuvant
Strong opioid+non-opioid+adjuvant
Examples ParacetamolNSAIDS
CodeineTramadol
MorphineFentanylMethadone
Slide 8:
Read all points and discuss their importance with examples. Discuss on their management.
Slide 9:
Read all points and discuss their importance with examples.
Slide 10:
Discuss pain management as a part of palliative care in detail.
Slide 11:
Discuss the slide in detail. Also talk about availability of morphine in your country.

155
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
Talking points
Module 15: Elder abuse
Slide 1:
Older persons are easy targets for abuse and violence as they do not have physical strength to retaliate. This is a universal phenomenon and occurs in every society in various forms. Though it is not a direct health issue, the health care worker is in a most suitable position to detect it.
Slide 2:
After this module, the trainee will be able to detect elder abuse and prepare plans to prevent it.
Slide 3:
Read out the definition and discuss each of the phrases in detail with examples.
EElder Abuse
Module - 15
Learning Objectives
•To enumerate the concept and health consequences of elder abuse
•To enumerate measures to prevent elder abuse
WHO defines elder abuse as "a single, or repeatedact, or lack of appropriate action, occurring withinany relationship where there is an expectation oftrust which causes harm or distress to an olderperson".
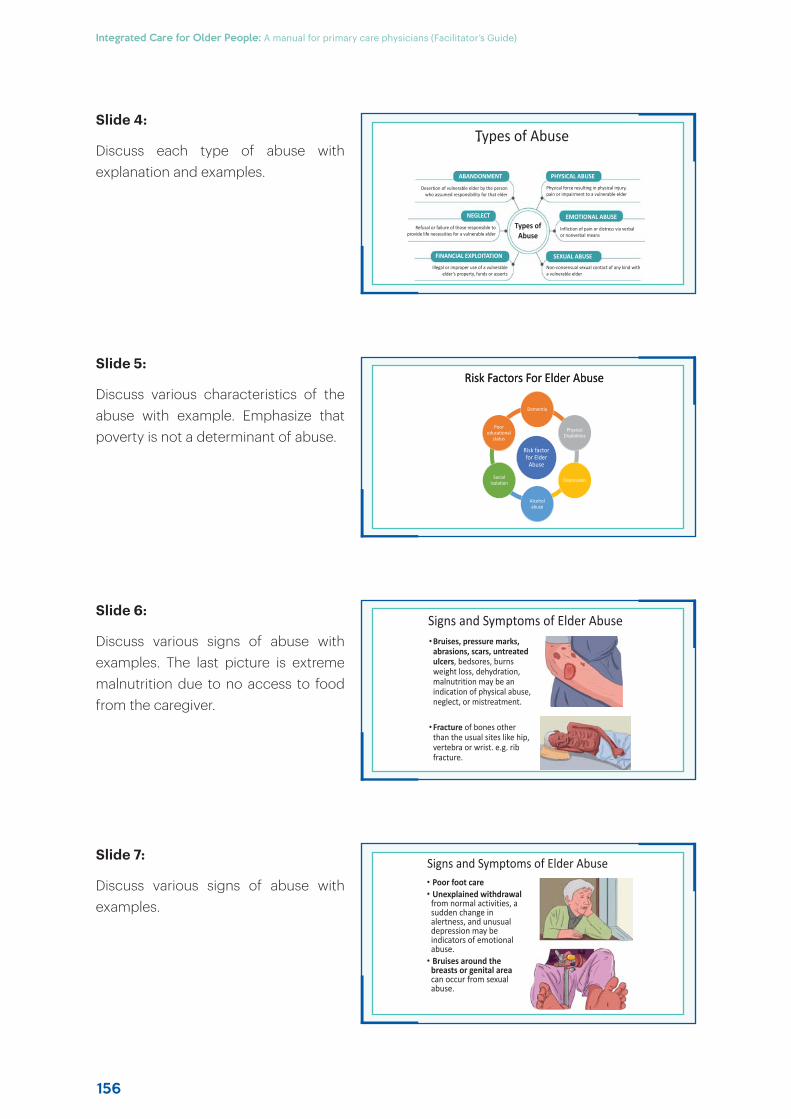
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
156
Types of Abuse
ABANDONMENT
NEGLECT
FINANCIAL EXPLOITATION
PHYSICAL ABUSE
EMOTIONAL ABUSE
SEXUAL ABUSE
Desertion of vulnerable elder by the person who assumed responsibility for that elder
Refusal or failure of those responsible to provide life necessities for a vulnerable elder
Illegal or improper use of a vulnerable elder’s property, funds or asserts
Physical force resulting in physical injury, pain or impairment to a vulnerable elder
Infliction of pain or distress via verbal or nonverbal means
Non-consensual sexual contact of any kind with a vulnerable elder
a
Types of Abuse
Signs and Symptoms of Elder Abuse• Poor foot care• Unexplained withdrawal
from normal activities, a sudden change in alertness, and unusual depression may be indicators of emotional abuse.
• Bruises around the breasts or genital area can occur from sexual abuse.
Risk Factors For Elder AbuseRisk Factors For Elder Abuse
Risk factor for Elder
Abuse
Dementia
Physical Disabilities
Depression
Alcohol abuse
Social Isolation
Poor educational
status
Signs and Symptoms of Elder Abuse•Bruises, pressure marks,
abrasions, scars, untreated ulcers, bedsores, burns weight loss, dehydration, malnutrition may be an indication of physical abuse, neglect, or mistreatment.
•Fracture of bones other than the usual sites like hip, vertebra or wrist. e.g. rib fracture.
Slide 4:
Discuss each type of abuse with explanation and examples.
Slide 5:
Discuss various characteristics of the abuse with example. Emphasize that poverty is not a determinant of abuse.
Slide 6:
Discuss various signs of abuse with examples. The last picture is extreme malnutrition due to no access to food from the caregiver.
Slide 7:
Discuss various signs of abuse with examples.
157
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
Signs and Symptoms of Elder Abuse• Bedsores, unattended medical needs, poor hygiene,
and unusual weight loss are indicators of possible neglect.
• Behavior such as belittling, threats and other uses of power and control by spouses are indicators of verbal or emotional abuse.
• Strained or tense relationships, frequent arguments between the caregiver and older person are also signs.
• Changes in personality or behavior in the elders
Management and prevention of abuse
•The management of the abuse of elders requires the involvement of multidisciplinary team like nurse, doctors, physiotherapist, counselor, social worker.
•The physician should use tact and discretion while dealing with the problem.
Management and prevention of abuse
The steps involved are:• Assessment of the older
person’s physical and mental capacity
• Counselling of the abuser• Documentation, liaison and
interaction with other professionals
• Admission to sheltered accommodation, such as an old age home or nursing home, if the abuse cannot be prevented
Slide 8:
Discuss various signs of abuse with examples.
Slide 9:
Discuss strategies for prevention and management with examples.
Slide 10:
Discuss strategies for prevention and management with examples.
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
158
Slide 1:
At some point of time or the other, many older people will lose their autonomy and independence; and will be dependent for activities of daily living. This dependence can be for variable period of time. While caring for short periods is usually managed by the caregivers without much problem, providing care for long period of time is a major challenge for the family and the health and social welfare system.
Slide 2:
After the end of this module, trainees will be able to conceptualize long-term care, its components and the challenges associated with it.
Slide 3:
In this slide, define long-term and explain its components. Discuss the profile of caregivers and their characteristics with examples.
Slide 4:
Discuss the social issues in care-giving. Describe the profile of care receiver with various health problems.
Talking points
Module 16: Long-term care and caregiver issues
LLong--tterm care and caregiver issues
Module - 16
Learning objectives
• To enumerate the concept of long-term care
• To enumerate need for long-term care• To enumerate the issues related to
caregiving
Introduction
Long-term care covers activities undertaken by people to ensure that individuals with, or at risk of, a significant ongoing loss of intrinsic capacity can maintain a level of functional ability consistent with their basic rights
• Among family caregivers, 72% are women, one-third are over the age of 65 years and one-third are in poor health themselves, suffering from unrecognized caregiver stress.
Introduction
There has been an increasing demand for formal care due to:• Migration of the younger generation• Trend towards nuclear families and break-
up of joint families• Rapid increase in the older population• Severe disability resulting from the
complications of rising non-communicable diseases
• Increase in the prevalence of neurodegenerative diseases
• Living alone without any surviving caregiver.
159
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
Goals of Institutional care
• Are actively recuperating or being rehabilitated• Have substantial physical dependencies• Have primarily severe cognitive losses• Are receiving terminal care• Are in a permanent vegetative state.• Institutional residents
Role of primary care physicians
• To handle agitated, demented or delirious patients
• Assess gait disorders and balance in all the older patients
• Develop a preliminary plan for the management of all patients, including those presenting with functional deficits.
• The plan should include adaptive interventions and involve interdisciplinary team members
• PCP should know about home safety assessment and eliminating hazards in the home including those related to falls
Types of care giving
Non institutional care• Various models of cost-effective health-care
delivery systems for long-term home-or community-based care are in use.
• Assisted living services
• Day care centers
• Telehealth
• Home hospice care
Institutional careIn the West, nursing homes have emerged as the touchstone of institutional long-term care.
They are an important part of the health-care delivery system for frail older people.
Slide 5:
In this slide, the role of primary care physician will be discussed. Read out each point with examples and discuss in detail.
Slide 6:
There are two types of setting for long-term care: institutions of long-term care and home and community sites. Discuss each of these sites with examples.
Slide 7:
In this slide, discuss types of care receivers in institutional care in detail with examples.
Slide 8:
In this slide, discuss types of care receivers in institutional care from length of stay point of view. Discuss in detail with examples.
Institutional residents
Institutional residents may be of the following kinds:
Short stayers (1–6 months)• Terminally ill• In need of short-term rehabilitation
• Medically unstable or suffering from subacute illness.
Long stayers (6 months to years)• Primarily cognitively impaired• Primarily physically impaired• Both physically and cognitively impaired.
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
160
Supporting the caregiver
• Maintain her/his physical and mental health• Avoid the development of an abusive situation• Reduce the risk of institutionalization• Promote a good quality of life for the entire family
Caregiving
• Older people with physical or cognitive disability require continuous care from formal or informal caregiver.
• Caregiver Burden: Long-term care of a frail and physically dependent older person causes the caregiver to feel a variety of stresses, such as physical, emotional, social and financial
• The caregiver is usually the “hidden patient” and the health-care worker must direct some attention towards his/her needs
Assessment of caregiver stress
• The older person’s capacity to care for himself/herself
• The type of care required by the older person (feeding, dressing, bathing, toilet)
• The amount of extra time the caregiver needs to spend on caring for the older person
• Arrangements for rest and relaxation for the caregiver
• Resources and support systems available to the caregiver• Vague physical health-related complaints by a caregiver, which should make
one suspect that he/ she needs more assistance at home.
Slide 9:
In this slide, discuss challenges of care giving and problems of caregivers.
Slide 10:
In this slide, discuss about assessment of caregiver stress. Read out each point and discuss in detail.
Slide 11:
In this slide, discuss ways and means of supporting the caregiver with examples.
Slide 12:
Discuss the role of primary care physician. Read out each point with examples.
Role of the primary care physician
• Educate the caregiver and the family members on ways to recognize danger signs in the person receiving care
• Teach the caregivers at home about the prevention of complications, such as bedsores, aspiration pneumonitis, catheter-related infections and deep-vein thrombosis
• Consult a psychiatrist, as psychiatrist services are very important in organizing day hospitals, day-care centres and centres for seniors that provide engagement and food
• Should be involved in outpatient and inpatient care for the investigation of major problems

161
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
Talking points
Chapter 2: Health of older people and geriatric medicine
Slide 1:
I welcome you all to this training program on health and health care in old age. The program will include presentations on various aspects of health. Disease and disabilities of old age and strategies to manage them. In this discussion, we will discuss various concepts in geriatrics or old age medicine.
Slide 2:
There are four learning objectives of this session. These include diseases and disabilities of old age, concepts and principle of geriatric medicine; comprehensive geriatric assessment; and role of primary care physician in old age care.
Slide 3:
Define old age; the impact of ageing on body and mind and age cut off by UN agencies. Impress that the 60 year cut off is to ensuring uniformity in policy formulation for support and services. The cut off s are not indicator of health status or retirement policy.
HHealth of Older People and GGeriatric Medicine
Chapter-2
Learning objectives
To enumerate diseases and disabilities of
old age;
To enumerate important
concepts and principles of
geriatric medicine;
To carry out comprehensive
geriatric assessment;
and
To enumerate the role of
primary care physicians in old
age care
Introduction
• Ageing "accruing maturity with the passage of time". It begins with conception and continues throughout life, until death.
• With ageing, a deterioration occurs in the functional, emotional, socioeconomic and cognitive areas.
• The cut-off of “60 years” has been accepted by all UN agencies, keeping in mind the needs of the developing countries, where the life expectancy may not be as high as in the developed countries.

Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
162
Health challenges in old age• The origin of the diseases of old age can be
conceptualized in three broad formats:Biological decline,
Lifestyle-related,
Environmental exposure.
• Besides the conditions mentioned, older peoplesuffer from complex medical conditions called“geriatric syndromes”
• Chronic noncommunicable diseases (NCD) arecommon among older people. According toWHO, NCDs are the leading cause of death in theworld, accounting for over 71% of all deaths
Osteoarthritis
Hypertension
Diabetes
Dementia and Parkinson’s
disease
Chronic Obstructive Pulmonary
Disease
Ischaemic
Heart disease
Cataract
Common diseases of old age
Normative changes of ageing vis-á-vis pathological states
• Normal age-related changes should be distinguished from pathological changes that may be taking place because of exposure to various health risks.
• Normative changes are gradual and are difficult to perceive initially
• Pathological changes make their presence felt by various symptoms and signs.
Normal adult
Adaptive factorsChaperones, Growth Factors, anti-apoptotic proteins, antioxidant enzymes, neurogenesis and synaptogenesis, DNA repair
Balance between AdaptiveAnd Accelerating factors
Accelerating factorsCardiovascular risk, stress, depression, obesity, genetic predisposition, early life experiences
Therapeutic approachesHerbs, diet with antioxidant supplementation and calorie
restrictions, proper lifestyle, stem cells, molecular targeting, hormonal
interventions
Normal aged
Pathological
Geriatric Medicine
• Geriatric Medicine : A branch of medicine that concerns itself with the ageing process; the prevention, diagnosis and treatment of health-care problems in the aged; and the social and economic conditions that affect the health care of the older people.
• Goal of geriatric medicine: Maximize the positive aspects of ageing, delaying the onset of chronic disease and maximizing function despite the disease
• The key strategies are: To break down the complex issues into multiple simple problems, and to address them individually in terms of diagnostic tests, therapeutic interventions or rehabilitation.
Slide 4:
Speak on origin of non-communicable diseases from the three format with examples: Biological decline- cataract, sensory neural deafness; prostate enlargement; Lifestyle - related - hypertension, diabetes, heart disease; and Environmental exposure: cancer; COPD. Discuss about multiple diseases leading to multiple disabilities and complex symptoms termed as geriatric syndromes. Emphasize on NCDs as important health problems in old age in terms of burden of care requirement and death.
Slide 5:
In this slide, discuss about distinction between normative changes of ageing and pathological states.
Slide 6:
Discuss about geriatric medicine here as provided in this slide.
163
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
Important concepts in Geriatric Medicine
Ageing does not produce an abrupt decline in organ function, but disease may cause.
Older people and their caregivers often fail to recognize certain symptoms as abnormal.
Multiple pathology or concurrence of diseases is common.
Functional loss is a common pathway for most clinical problems in older people especially those over the age of 75 years.
Atypical presentation of disease poses another challenge in the case of older patients.
Multiple small abnormalities in many organ systems produce significant clinical abnormality and, when corrected, the overall effect is gratifying.
Adverse consequences of diseases are more frequent among older patients
Risk factors
Constitutional factors
Ageing
Lifestyle
Chronic health conditions
Living conditions
Body protein contentThermoregulationInsulin resistance
ImmunityInfections
Axial muscular tonus Masticator force
Venous flow
Osteopenia/fractures
Mobility impaired gait falls
Endurance
Physical performance
DisabilityPoor quality of lifeNursing home admissionMortality
Sarcopenia Frailty Poor outcomes
Care Costs
• It is progressive and generalized loss of skeletal muscle mass and strength
• Sarcopenia is the most important cause of frailty in older persons.
• Mechanism of Sarcopenia:
Sarcopenia
Frailty syndrome
A physiologic syndrome characterized by decreased reserve and resistance to stressors, resulting from cumulative decline across multiple physiologic systems, and causing vulnerability to adverse outcomes” (Linda Fried et al. 2003).
Frailty syndrome
Frailty syndrome is associated with • An increased risk of mortality, irrespective of the morbidity or intervention• Directly proportional to the prevalence of geriatric syndromes• An increased prevalence of falls, hip fractures, functional impairment and
hospitalization• Predicts adverse outcomes related to renal transplantation, general surgery (elective
and emergency), cardiac surgery and many other forms of interventions• Likely to increase the potential for medicine interactions and adverse effects• Increased mobilization of health-care resources• Increased caregiver burden.
Slide 7:
Read out and discuss about each of the concepts with adequate examples.
Slide 8:
Explain the concept of frailty.
Slide 9:
Discuss each bullet point.
Slide 10:
Define this entity to health professionals.
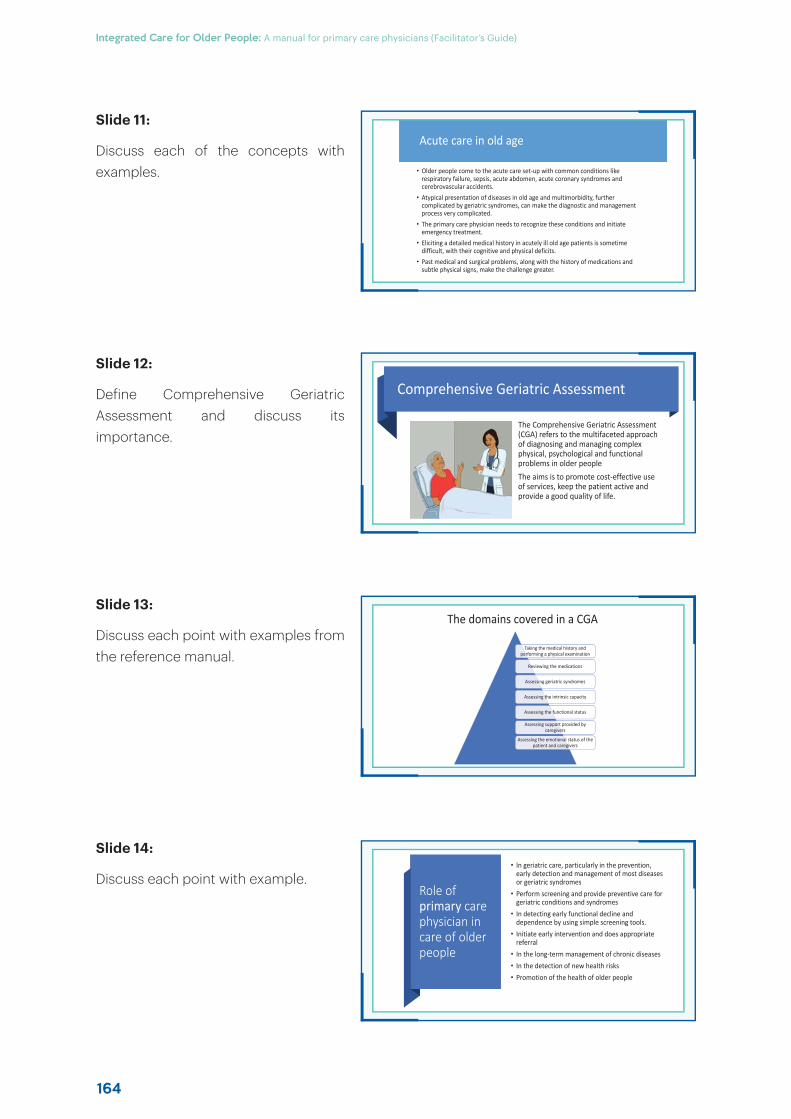
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
164
Acute care in old age
• Older people come to the acute care set-up with common conditions like respiratory failure, sepsis, acute abdomen, acute coronary syndromes and cerebrovascular accidents.
• Atypical presentation of diseases in old age and multimorbidity, further complicated by geriatric syndromes, can make the diagnostic and management process very complicated.
• The primary care physician needs to recognize these conditions and initiate emergency treatment.
• Eliciting a detailed medical history in acutely ill old age patients is sometime difficult, with their cognitive and physical deficits.
• Past medical and surgical problems, along with the history of medications and subtle physical signs, make the challenge greater.
Role of primary care physician in care of older people
• In geriatric care, particularly in the prevention, early detection and management of most diseases or geriatric syndromes
• Perform screening and provide preventive care for geriatric conditions and syndromes
• In detecting early functional decline and dependence by using simple screening tools.
• Initiate early intervention and does appropriate referral
• In the long-term management of chronic diseases• In the detection of new health risks • Promotion of the health of older people
Comprehensive Geriatric Assessment
The Comprehensive Geriatric Assessment (CGA) refers to the multifaceted approach of diagnosing and managing complex physical, psychological and functional problems in older peopleThe aims is to promote cost-effective use of services, keep the patient active and provide a good quality of life.
The domains covered in a CGA
Taking the medical history and performing a physical examination
Reviewing the medications
Assessing geriatric syndromes
Assessing the intrinsic capacity
Assessing the functional status
Assessing support provided by caregivers
Assessing the emotional status of the patient and caregivers
Slide 11:
Discuss each of the concepts with examples.
Slide 12:
Define Comprehensive Geriatric Assessment and discuss itsimportance.
Slide 13:
Discuss each point with examples from the reference manual.
Slide 14:
Discuss each point with example.

165
Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)

Integrated Care for Older People: A manual for primary care physicians (Facilitator’s Guide)
166