
WHO_MNC_82.2_eng.pdf - WHO | World Health Organization
239
• WORLD HEALTH ORGANIZATION ORGANISATION MONDIALE DE LA SANTE School of Public Health University of Minnesota United States of America WHO/MNC/82.2 Appendix III Rev. 1 LABORATORY OF PHYSIOLOGICAL HYGIENE MINNESOTA HEART HEALTH PROGRAM MANUAL OF OPERATIONS The i$Sue of this document does not constitute formal' publication. It should not be reviewed, abstracted or quoted without the agreement of the World Health Organization. Authors alone are responsible for views expressed in signed articles. 1981-1982 Ce document ne constitue pas une publication. II ne doit faire I'objet d'aucun compte rendu QU resume ni d'aucune citation sans I'autorisation de ,'Organisation mondiale de la Sante. Les opinions exprimees dans les articles signes n'engagent Que leurs auteurs.
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of WHO_MNC_82.2_eng.pdf - WHO | World Health Organization

• WORLD HEALTH ORGANIZATION
ORGANISATION MONDIALE DE LA SANTE
School of Public Health University of Minnesota United States of America
WHO/MNC/82.2 Appendix III Rev. 1
LABORATORY OF PHYSIOLOGICAL HYGIENE
MINNESOTA HEART HEALTH PROGRAM
MANUAL OF OPERATIONS
The i$Sue of this document does not constitute formal' publication. It should not be reviewed, abstracted or quoted without the agreement of the World Health Organization. Authors alone are responsible for views expressed in signed articles.
1981-1982
Ce document ne constitue pas une publication. II ne doit faire I'objet d'aucun compte rendu QU
resume ni d'aucune citation sans I'autorisation de ,'Organisation mondiale de la Sante. Les opinions exprimees dans les articles signes n'engagent Que leurs auteurs.

WHO/MNC/82.2 Appendix III Rev. 1 page 2
TABLE OF CONTENTS
Project Overview 5
Design and Objectives 7
Criteria for Events 14
Clarifications for MHHP Coders and Abstractors 23
Tabular Presentation of MHHP Event Criteria 24
Morbidity and Mortality Flow 35
Morbidity Data Flow 36
Instruction for MRHP Abstracting Forms 40
~~/MHHP Personal Code Nos 41
Standardised and County Abbreviations 42
MHHP Hospital Code Nos. and Abstractor Assignments 43
Hospital Listing out of Twin City Metropolitan Area 44
Seven County Hospital Listing 46
Zip Codes for Minnesota Heart Survey 50
hospital Codes 1980 51
Discharge Diagnosis Indices 53
Hospital Codes (as listed in the Directory of Licensed and Certified Health Care Facilities 1980) 54
Abstracting Forms and Instructions
Form 02
Form 02
Form 04
Form 41
Form 04
Form 40
Form 40
Core Data Sheet
Instructions
MI Hospital Abstract
MI Abstract - Physician Review/Chest X-ray/Angiogram
MI Hospital Abstract - Instructions
Enzyme Values
Instructions
61
64
73
81
82
99
100
ECG Coding (su ary sheet) Form
Form 06
Form 06
Neurology
ctions
Form 21 y Report Abstract
Form 08 Death Certificate Abstract
Form 41 MI Abttract for Physician Review of Chest,X-rays and Coronary Angiography
! Death Certificate Abstract
Out of Hospital Death - Physician Information Form
Final Interview Status - Family Interview Information. I Mortality Surveillance
Family Interviet Information. Mortality Survei 11ance! - Ins tructions
,
Autopsy Report Abstract
Autopsy Report Abstract - Instructions
County Court House Information
Letters to Witn~sses
Data Collection - QU~lity Control
I Bethesda Lutheran HojPital
Hospital Diagno is Form. Pathology Report, Admittance Form Progress Notes. Nursing Notes i
Fairview Hospitals
Inpatient Admit Rehabilitation Progress Report Care charts, Pa Nurse's Notes, Lab. Record, E 1 Portable Chest
I
ing Record and Discharge Form, nit, History and Physican,
Intensive Care. Coronary ient's Progress Record, peech and Language Evaluation, ctro-cardiograph records. -ray reports
WHO/MNC/82.2 Appendix III Rev. 1 page 3
102
103
112
131
135
136
137
138
139
152
154
163
164
166
167
171
175-186
187-206
Wl:tO/MNC/82.2 Appendix III Rev. 1 page 4
Lakeview Hospital
Admittance Form, Diagnosis Sheet, Autopsy Repo~t Medical Report, X-ray Report, Consultation Reports, Respiratory Therapy Department Report, Periodic Rounds Record, Doctor's Order Sheets, Graphic Records, Patient Care, TreatmentsTeaching-Conferences, Accountability, Medication Record Sheet, Blood Pressure Chart, Nursing Data Base, Problem List, Nurse's Notes.

MINNESOTA HEART HEALTH PROGRAH
Henry Blackburn, M.D. Principai Investigator
Russell V. Luepker, M.D. Co-Principal Investigator and Project Director
A. Objectives
Thomas Kottke, M.D. Field Director Morbidity Surveillance
Laboratory of Physiological Hygiene School of Public Health University of Minnesota Minneapolis, Minnesota
PROJECT OVERVIEW
WHO/MNC/82.2 Appendix III Rev. 1 page 5
1. To continue to monitor Hinnesota mortality rates by causes and to begin to monitor morbidity in order to assess the changing burden of cardiovascular disease in the Twin Cities metropolitan community.
2. To estimate the extent to which changes in cardiovascular mortality rates are due to changes in disease incidence and/or case fatality,
3. To estimate the extent to which changes in mortality rates are related to and hence might be explained by changes in levels of risk factors and their associated behaviors and selected indicators of medical care.
4. To establish a model system for long-term surveillance and an ongoing system for the Twin Cities metropolitan area.
B. Specific Aims
1. Continued documentation of age-sex-race-area, cause-specific deaths in Minnesota from 1960 through 1990. follow change in mortality rates from cardiovascular disease and to examine change in competing causes of death.
2. Establishment for the years 1970~1990 of hospital morbidity data surveillance of myocardial infarction (XI) and cerebrovascular accident (eVA) to ascertain a) morbidity rates and b) fatality rates to determine how they contribute to the changing mortality rates.
3. Measurement of primary risk factors for HI and CVA (cigarette smoking, serum cholesterol levels, blood pressure levels, diet and physical activity) in serial cross-sectional samples of the Minn~sota population to examine temporal relationships of change in risk factors and change in morbidity and mortality.
4. Monitor trends in knowledge, attitudes and behavior related to risk factor levels, e.g. eating habits.

WHO/MNC/82.2 Appendix III Rev. 1 page 6
5. Examination of various methodological problems in surveillance of mortality, morbidity and risk factors and creation of a model long-term surveillance system.
6. Estimation of trends in the following indicators of medical care in the Twin Cities population for the years 1970-90. number of admissions to coronary care units; number of MI patients admitted alive following out-of-hospital resuscitation; number of coronary artery bypass graft operations.
C. Overview of Methods
1. Data will be gathered and in mind:
ed with the following hypotheses
a. The downward trends in coro cerebrovascular disease (C decreasing case-fatality ra incidence.
ary heart disease (CHD) and ) mortality can be explained by es and decreasing disease
b. Decreasing mortality, morbi ity and case-fatality from CHD and CVA are correlated with downward trends in the prevalence and population distribution of risk factors (elevated blood pressure, serum cholesterol, cigarette smoking, etc.), changes in their associated health ehavior and with improved medical care.
2. This will be accomplished as fo lows:
a. Mortality data in Twin Citi s metropolitan area (pop. approx. 2 million). will be obtained rom the State Health Department for
b.
the years 1960-1990.
Morbidity data will be hospital discharges in the and completed eVA for the
The ages to be considered are 30 through 74.
ned through surveillance of etropolitan area for acute HI ars 1970 -90.
mortality and morbidity analyses
c. The accuracy of both data s urces will be verified by validation of samples of' cases.
d. Trends in risk factors and related health behaviors will be measured in the metropo1ita annual surveys, 1980-1990.
population in four consecutive Ages surveyed are 20 through 74.
e. Trends in medical care indi ators (coronary care unit admisSions, successful out-of-ho pital resuscitations of MI cases coronary artery bypass oper tions) in the metropolitan population will be estimate from hospital statistiCS, record reviews and PSRO data for the years 1970 -90.

WHO/MNC/82.2 Appendix III Rev. 1 page 7
SECTION 2
DESIGN A~~ OBJECTI\~S
2.1
Minnesota Heart Health Program Objectives
The overall objectives of the Heart Health Pro~ram for cardiovascular diseases as stated in Section 1.3 are:
1. To develop, test. imolement and evaluate coordinated strategies of community-wide health education for behavioral change to reduce cardiovascular risk.
2. To increase community knowledge of cardiovascular risk factors.
3. To improve community behaviors related to population levels of risk factors.
4. To change levels of the known risk characteristics for heart and vascular diseases among the educated communities.
5. To modify specific eating and activity patterns, reduce blood lipids, weight, cigarette smoking and blood pressure level.
6 < To reduce incidence of premature disability and death from heart and vascular diseases in ~ucated communitie~.
7. To develop a vital resource of knowledge, skills, research and training in community approaches to prevention and health promotion.
In order to meet these objectives a specific strategy is designed tel develop and apply health education programs by techniques of community screening and referral for direct individual and group education, combined with mass communications, community organization, enhancement of prevention services and environmental change. and to demonstrate the feasibility and efficacy of these programs in free-livin~ educated communities compared to similar reference communities.
2.2
Pro15ram Design
2.2.1
Town Pairinl'(
Co~unity-wide prevention education and mass COffimunications are carried out in total populations defined by town boundaries. For each
WHO/MNC/82.2 Appendix III Rev. 1 page 8
communi ty chosen for the educa tion program, a similar community has been selected to serve as a comparison in which only surveillance is performed. The many changes in economic conditions, energy supply, changing lifestyles, concern for health, medical care, work status and other factors are not' highly predictable or controllable. The Minnesota Heart Heal th Pro~ram w11l control in part for these potential confounders' by the identification of reference communi ties alike in as many variahles as possible to the educated communities.
Three to'lo."n pairs will provide the population base of the program. Each town pair will include an educated town and a reference town, while systematic surveys of morbidity, mortali ty I risk factor status, and health beliefs and behavior will be conducted throughout the course of the program in both. The beginning of intervention in the educated towns will arrive sequentially at one year intervals. This staged introduction of the program is necessary for logistic reasons but defensible on the scientific grounds of repetitions and increased generalizability. Experience in the first educated town will also allow improvement of the education program prior to the beginning of intervention in the remaining educated towns.
The choice of several distinct town pairs is made for three reasons • First, sizeable populations are required to obtain sample sizes adequate to differentiate accurately morbidity and mortality changes from random variables. Second, intervention and comparison in several pairs is required to assess even minimally the generalizabili ty of resultSf· obtained. Use of criteria of consistency and temporality of change in addition to statistical significance will also strengthen the evaluation. Third, tmanticipated events within t'he program plan or extraneous. to ·it may occur in a single pair. potentially weakening the analysis. For example, industry shutciowns in one town of a pair could cause serious changes in population characteristics.
2.2.2
Community Selection Criteria
Community selection is based on three levels of criteria:
1. Primary criteria are basic characteris.tics requiring close matching critical to the study rlesiF:n. Included are the characteristics important to "success" plus the· comparability of endpoint measures:
a. Population size b. Geographic location c. Population in age of interest (25-74) d. Distribution of major risk indicators e. Hortality trends f. Migration rates
Laboratory of Physiological Hygiene (LPH) studies in the Twin Cities and in 'Western Hinnesota indicate no significant dif-
WHO/MNC/82.2 Appendix III Rev. 1 page 9
ferences in average levels of risk indicators between areas. Mortality rates by region in Minnesota are also quite similar between areas.
2. Secondary criteria are characteristics of importance to the educational program, but of less direct importance to the endpoint criteria:
a. Hospital and medical care base b. Industrial base c. Ethnic composition d. Educ~tion level of population e. Agricultural base f. Educational system g. Media characteristics h. Employment/unemployment characteristics i. Economic status j. Distance from Minneapolis
3. The final criteria are not easily quantified but ~ere considered when the town assignments were made:
a. Town receptivity b. Medical community receptivity c. Governmental receptivity d. Media availability e. Community organization potential.
2.2.3
Research and Program Evaluation
It will be possible to desc:-ibe and measure the effects of the educational program on the educated communities. The preventive effects of the program will be evaluated by tested epidemiological methods describing changes in morbidity, mortality and risk indicators. In addit.ion, health related behavior change will be both directly and unobtrusively evaluated.
Equally important to the demonstration is evaluation of the individual components of the educational program. The purposes of this evaluation are to tmderstand the nature and effect of individual strategies and to isolate the successful elements. There is a need for the rapid identification of. more and less successful strategies so that the former may be enhanced and the latter eliminated. Finally, new and innovative health education hypotheses will be formed and tested in the field setting to advance knowledge and deternine relevance and effect.
Other evaluation elenents include the collection of information related to costs, because co=unity based prevention efforts are new and their cost, relative to benefits, is tmknown.

WHO/MNC/82.2 Appendix III Rev. 1 page 10
2.2.3.1
Evaluation Activities
The Heart Health Program evaluation activities and their methods include morbidi t;y surveillance, mortali ty surveillance. risk factor surveys. screening panels. pilot proiec ts, unoht:-usi ve measures, rapid surveys. school surveys. anc cost analyses. Following is a brief description of each:
Mortality surveillance Irlll be performed in educated and reference communities and in the entire state. The obiective is to determine whether mortality rates change differentially in the educated towns. It is hypothesized that cardiovascular mortality in the educated towns will be lower at the end of the program relative to that experienced in comparison towns. The surveillance will be conducted by the systematic examination of death certificates t with validation of subsamples.
Morbidity surveillance Irlll be performed in all educated and reference towns. The objective is to determine whether differential TiDrbidity rates occur in communities exposed to the educational program. It is hypothesized that by the end of the education progra:n, cardiovascular disease morbidity will be lower in the educated towns, relative to observed morbidity in the reference towns. This evaluation will be carried out through systematic analysis of hospital data.
The risk factor survey will be performed in each educated and reference town, using randomly generated population samples. Survey activity in all tow-us \'''ill be1i\in the first year of the program anc will be designed to assess pre-education risk factor clistributions. knowledge. attitudes, beliefs and values related to health behavior, intentions regarding future health behavior, anc self-reports of health-related behavior. The population survey will be repeated annually. The objective is to determine whether risk and related characteristics change differentially in educated towns. By the end of the education pro~ral!l. risk factor levels should be lowered and beliefs and behavior altered in line with the educational message, more so in the educated than in the reference towns.
All persons who participate at the Reart Health Education Centers Irll1 be randomly assigned to one of eight follow-up screening panels in each town. Subsamples of each panel will be re-surveyed once during the ret:laining period of the study. The ob,iective of this study is to assess the effects of screening and subsequent direct education in the educated towns. This survey is restricted to the educated towns as an education prORrat:l is not conducted in the reference towns.
Pilot ts will be conducted in educated and non-Heart Health Program communities to test new strategies and procedures, although much pilot testin2 of strategies and procedures has alredy been accomplished and some is under way. This pilot activity will be con-
WHQ/MNC/82,2 1\ppendu I II Rev. 1 page 11
centra ted during the first year of the program but ;.rill also continue in succeeding years.
Throughout the term of the education program occasional rapid surveys will be conducted by telephone, mail, or direct interview, with the ob;ective of obtaining prompt feedback on the effect of specific educational strategies. The ob~ective is to rapidly determine the effect of any Single strategy, so it may be altered, improved. or discontinued. These rapid surveys will be conducted in the educated towns only.
Subgroup surveys will be conducted throughout the pro~ram on subsets of randomly selected individuals from a population subgroup. The object.ive is to assess the effect of individual programs, such as the youth education p,rogram, or the health professional education programs, in the educated towns.
Unobtrusive assessments of co=unity health behavior will be rr:tade in the educated and reference co=unities throughout the proJect. These will include measures of medication prescriptions, fO'od and -cigarette sales, and the recording of other community health and major'nonhealth events. The objective is to provide additional information, from a different data source, related to health behavior.
Cost data, including medical-related costs and Heart Health Program costs ;.rill be collected in each community for later program cost analysis evaluation.
2.2.3.2
Evaluation of th~ Education Process
Hultiple methods and a special working group is dedicated to the task of evaluating the intervention process. Many small and medium size evaluation projects ;.rill be carried out (approximately SO/year) and will also review the risk factor and unobtrusive measures data. The evaluation goals are: 1) to examine each major education strategy and attempt separation of effects of the individual components; 2) to identify ef fecti ve education strategies and strengthen them, and to identify ineffective st:-ategies and eliminate or alter them; and 3) to increase understanding of health-related behavior by testing alternative strategies aimed at modification of specific behaviors.
Evaluation will be made of both the principal object.ives in the areas of smoking, eating pattern, high hlood pressure and physical activity. and the individual methods of mass media, community organizations, education center and health professional, adult and youth ,education. Several methods ;.rill be utilized in this task including the annual risk factor surveys, screening panels, pilot projects, rapid surveys and subgroup surveys.

WHO/MNC/82.2 Appendix III Rev. 1 page 12
2.2.4
Risk Factor Change Analyses
Risk factor reduction is anticipated from the education program in the educated communities. That change will precede reductions of morbidity and mortality related to the education program. Risk factor distribution and distributions of relevant antecedent behavior and unobtrusive measures of risk will be obtained from survey samples. These form the data base for analysis of risk factor change and evaluations for strategy adjustment in the study.
To enhance ~owledge or risk factor change throughout the study period, surveillance will be carried out in each reference. and educated tOl.l'n in each year of the study. The survey in years zero and one will be under "control" or baseline conditions in all towns. In year 2 the survey will be under control conditions in five towns and intervention conditions in one. In year 3 the survey will be under control conditions in four towns, under intervention in two towns; in year 4 under maintenance intervention conditions in two towns, initial intervention in one, and control in three. The surveys for years 5-8 will be under maintenance intervention conditions in three towns and under control conditions in three towns.
Limiting attention to mean levels of risk factors, the assumption that Beart Health Program efforts are the predominant cause of risk factor change leads to a re~mlt where there is 11 ttle change in the risk or education characteristic during control years or the later years ofthe study, but large changes in the first two years of the study in each cOillIDunity. The model suggested will be used to infer that the program is not working a~ anticipated and whether or not the comparison cOillIDunities are relatively unaffected by risk factor change.
It is proposed to survey a probability sample annually from each communi ty of total sample size 500, a new sample being drawn each year. This sampling method is chosen over a cohort survey because persons in the cohort are likely to be affected by the frequent survey, probably in the direction of making more changes than the general population. This would ~ive an over-estimate of the program effect. In addition, cohorts are relatively hard to follow and dropout is a problem, whereas cross-sectional samples are not affected by screening or dropout hut require larger sample sizes. One exception to crosssectional samples is a proposition to resurvey all persons with elevated blood pressure for their blood pressure and medication status one year after initial identification. About Rn persons per year per town are estimated. In identifying these persor.s, efforts will Le taken to minimize the effect of screening without avoiding the ethical obligation for referral by specified criteria.
The risk factor or knowledge levels between any year and baseline will be compared. Typically, the nUl:lber in the sample each year will be 500 for a single community pair or 1500 for all educated communities
WHO/MNC/82.2 Appendix III Rev~ 1 page 13
comoared to all comparison communities. In the case of larger coemunities the use of a two-year baseline period may be iustified, in which case the number used would be as much as 3000 for hase1ine and 1500 for a single year baseline. Such larger samples may be subdivided according to other characteristics and subgroups of interest (male ys female; young vs old).
~ore complex analyses will be carried out using least squares models. Even with sample sizes lieited for subgroup analysis, differential aspects of the Heart Health Program can be examined and evaluated for s ta tis tical signi ficance USing regression modeling. wi th some added power at the expense of added modeling assumptions. Data can also be pooled across years of education to increase power. This technique would be particularly effective in the situation in which the risk level achieves 'a maximum drop, then remains stable for a period of time.

WHO/MNC/82.2 Appendix III Rev. 1 page 14
CRITERIA FOR EVENTS
The events will be classified as definite, possible, and no event.
I. Fatal Coronary Events
A. Definite Fatal Myocardial Infarction (MI) (Dx Code 01)
la. Definite myocardial infarction within 4 weeks of death by MHHP criteriaj
-OR-
lb. Acute myocardial infarction diagnosed by autopsy.
B. Definite Sudden Death Due to Coronary Heart Disease (CHD) (Dx Code 02)
1. Death witnessed as occurring within one hour after the onset of severe cardiac symptoms (ischemic cardiac pain =-see below, shortness of breath, fainting) or within ~ hour after the subject having last been seen without symptoms.
-AND-
2. No documentation of definite acute Ml within 4 weeks prior to death by MHHP criteria. (See below for criteria for definite MI).
-AND-
3. No known non-atherosclerotic or non-cardiac-atherosclerotic process that was probably lethal according to death certificate, autopsy report, hospital records or physician report.
C. Definite Fatal Heart Disease (Dx Code 03)
1. Death certificate with consistent underlying or immediate cause(s) (ICD-9 codes 410-414) or hospital record with any mention of ICD9CM 410-414. (Medical certification of cause of death, Part I a, b or c.)
-AND-
2. No documentation by MHHP criteria of definite acute MI within 4 weeks prior to death.
3.
4.
-AND-
MHHP criteria for sudden death not met.
-AND-
No known non-atherosclerotic or non-cardiac atheroscLerotic process or event that was probably lethal according to death certificate, autopsy report, hospital records or physican records.
-AND-
Sa. Previous history of HI according to relative, physican or hospital records; old MI on autopsy; or definite, or possible MI by MHHP record

-OR-
WHQ!MNC/82~2 Appendi~ III Rev, 1 page 15
5b. Autopsy reporting severe atherosclerotic coronary artery disease or old MI without acute myocardial infarction. (> 50% proximal narrowing of two major vessels or > 75% proximal narrowing of one major vessel if anatomic details given.)
-OR-
5c. Rapid death:
Death occurring greater than one and less than or equal to 24 hours after the onset of severe cardiac symptoms or subject having last been seen without symptoms.
D. Possible Fatal CHD (Dx Code 08)
1. No documentation by ~rnHP criteria of definite acute HI within 4 weeks prior to death.
-AND-
2. No documentation by MHHP criteria of definite sudden death.
-AND-
3. No documentation by MHHP criteria of definite fatal CHD.
-AND-
4. Death certificate with consistent underlying or immediate cause (ICD-9 Codes 410-414,427,429,798,799) or hospital record with any mention of ICD9CM 410-414.
-AND-
5. No known non-atherosclerotic or non-cardiac atherosclerotic process that was probably lethal according to death certificate, autopsy report, hospital records, or physician records.
II. Nonfatal Myocardial Infarction
A. Definite (Ox Code 04)
1. Evolving diagnostic ECG
2. Diagnostic ECG and abnormal enzymes.
3. Prolonged cardiac pain and abnormal enzymes.
B. Possible -, hospital discharge diagnosis 410-411 or one or more of the following categories using the stated definitions below: (Dx Code 10)
1. Equivocal enzymes and equivocal ECG (with or without pain).
2. Equivocal enzymes and diagnostic ECG (no pain).
3. Abnormal enzymes and other ECG (no pain).

WHO/MNC/82.2 Appendix III Rev. 1 page 16
4. Abnormal enzymes and equivocal ECG (no pain).
5. Abnormal enzymes alone (no pain, ECG absent).
6. Prolonged cardiac pain and equivocal enzymes (ECG absent).
7. Prolonged cardiac pain and equivocal ECG (enz;rmes incomplete).
8. Prolonged cardiac pain and diagnostic ECG (equivocal or incomplete enzymes)
9. Prolonged cardiac pain alone .(ECG and enzymes incomplete) • , 10. Prolonged cardiac pain, , other' ECG, equivocal enzymes.
li. Prolonged cardiac pain, 'other' ECG, incomplete enzymes.
DEFINITIONS
Prolonged cardiac pain: When it is characterized by pain with the f0110wing characteristics.
ECG
(a) occurring anywhere in the anterior chest, left arm or jaw which may also involve the back, shoulder, right a~, or abdomen on one or both sides,
(b) duration of more than 20 minutes.
(c) no definite non-cardiac cause of chest pain (all cases of non-cardiac chest pain to be reviewed by physicians' panel).
(a) Evolving diagnostic ECG - an evolving pattern on serial ECGs of a diagnostic ECG:
(An evolving pattern of changes (appearance or disappearance within lead groups: anterior (VI-VS); lateral (1, aVL, V6); inferior (II, III, aVF» established the infarct as acute. Two or more ECG recordings during the hospitalization are needed for this classification.
1) No Q code in one ECG record followed by a record with a diagnostic Q code Vtinn. code 1-1-1 through 1-2-5 plus 1-2-7).
-Oll-
2) An equivocal Q code (Minn. code 1-2-8 or any 1-3 code) and no major ST segment depression in one ECG record followed by a-record wi th a diagnostic Q code PLUS a ST segment (Minn. code 4-1, or 4-2).
-OR-
3) An equivocal Q code and no ST segment elevation in one ECG record followed by a record with a diagnostic Q code PLUS an ST segment elevation (Minn. code 9-2). -

-OR-
WJ;iO/MNC/82.2 Appendix III Rev~ 1 page 17
4) An equivocal Q code and no major T wave inversion in one ECG record followed by a record witha diagnostic Q code PLUS a major! wave inversion (Minn. code 5-1 or 5-2). -
-OR-
5) No Q code and neither 4-1 nor 4-2 followed by a record with an equivocal Q code plus a 4-1 or a 4-2.
-QR-,
6) No Q code and no 9-2 followed by a record with an equivocal Q-code plus a 9-2.
-OR-
7) No Q code and neither 5-1 nor 5-2 followed by a record with an equivocal Q code plus a 5-1 or a 5-2.
(b) Diagnostic ECG: 1) Minnesota code 1-1-1 through 1-2-5 and 1-2-7 for Q and QS patterns
-OR-
2) Minnesota code 9-2 for ST segment elevation PLUS any T wave depression item coded 5-1 or 5-2.
(None of the above T-wave depression items can be used in the presence of ventricular conduction defects).
(c) Equivocal ECG: 1) Q and QS pattern 1-2-8 through 1-3-6
-OR-
2) ST junction (J) and segment depression 4-1 through 4-3
-OR-
3) T-wave items 5-1 through 5-3
-OR-
4) ST segment e1~vatlon ite~ 9-2
(d) Other ECG: all other findings, including normal.
(e) Uncodable ECG
1) Missing lead.
2) Baseline drift greater than 1 in 20, if it obscures ST-T wave.
3) Muscle tremor artifact giving more than 2 mm peak-to-peak oscillation.
4) Other technical errors making Q-wave measurement impossible, such as extreme lack of centering, or marked clipping.
(f) Absent ECG: No EeG available for coding.
The ECG series will be assigned the highest category for which criteria are met, i.e. evolving diagnostic> diagnostic> equivocal> other.

WHO/MNC/82.2 Appendix III Rev. 1 page 18
CARDIAC ENZYMES
Enzymes will be considered for the category of "abnormal" only if the upper limit of normal for the laboratory making the determination is recorded for the enzymes(s) used to make the diagnosis, and:
a. CPK-HB and total CPK have been measured within 12 hours of admission or onset of acute event, whichever is later.
-OR-
b. total CPK has been measured and one of LDH or SCOT has been measur~d within 72 hours of admission or onset of acute event, whichever is later.
Enzymes are "abnormal" if:
1. CPK-HB has been measured and is "present" (If hospital uses criteria of "present" and "absent") or at least twice the upper limits of normal (if hospital uses quantitative criteria) and total CPK is at least twice the upper limits of normal.
-OR-
2. total CPK has been measured and is at least twice the upper limits of normal and either LDII or SCOT has been measured and is at least tvlice the upper limits of normal.
Enzymes will be considered for the category of "equivocal" only if the upper limit of normal for the laboratory making the determination is recorded for the enzyme(s) used to ~ake the diagnosis.
Enzymes are ~equivocal" if:
1. CPK-HB and total CPK have been measured wi thin 72 hours of adclission or onset of acute event and CPK-HB is above the upper limits of normal but less than twice the upper limits of normal for laboratories giving quantitative values or "present" for laboratories giving qualitative values but in either case total CPK is less than twice the upper limits of normal.
-OR-
2. at least one of CPK,LDH or SCOT has been measured within 72 hours of admission or onset of acute event and is above the upper limits of normal, and the criteria for "abnormal" enzymes are not met.
-OR-
3. Enzymes (CPK-~lB. CPK, SCOT or LDH) are "abnormal", as defined above, but there is a non-ischemic cause present (defibrillation, surgery. liver disease, injections, etc.).
Enzymes are "normal" if:
they meet criteria for consideration as "abnormal" or "equivocal" but criteria for these categories are not met.
Enzymes are "incomplete" if:
they do not meet criteria for consideration as "abnormal" or "equivocal."
Ill. Primary Cardiac Arrest with Successful Resuscitation
A. DEFINITE (Dx Code 07)
1. Ischemic arrest
WHO!I1NC/82~2 Appendi~ III Rev~ 1 page 19
(a) Sudden cardiovascular (absent pulse) and pulmonary (absent spontaneous respiration) collapse with successful resuscitation
-AND-(b) Ventricular fibrillation or asystole reported on resuscitation ECG
-AND-(c) ECG's, enzymes and history necessary for diagnosis of "definite" or
"possible" MI collected. "Definite" and "possible" HI by MHHP criteria have been excluded
-AND-(d) No known non-atherosclerotic or non-cardiac atherosclerotic acute
or chronic process or event that would have been probably lethal -AND-
(e) History of previous HI -AND-
( f) Subsequent documentation of significant CliO (but not acute HI) during same hospitalization (coronary angiography showing > 50% proximal narrowing of 2 or more major vessels, or > 757. proxilual of 1 or more major vessels, old HI on ECG - Minnesota Codes 1-1; 1-2).
2. Primary Arrhythmia (without ischemia)
(a) Sudden cardiovascular (absent pulse) and pulmonary (a~sent spontaneous respiration) collapse with resuscitation
-AND-(b) Ventricular fibrillation or asystole reported on resuscitation ECG
-AND-(c) ECG's. enzymes and history necessary for diagnosis of "definite" or
"possible" HI collected. "Definite" and "possible" HI by MHHP criteria have been excluded
-AND-(d) No known non-atherosclerotic or non-cardiac atherosclerotic acute
or chronic process or event that would have been probably lethal -AND-
(e) No history of previous MI. -AND-
(f) Subsequent documentation of no significant CHD during same hospitalization (absence of both> 50% proximal narrowing of 2 or more or > 75% proximal narrowing of 1 or more major vessels on coronary angiography)
3. Non-Specific {insufficient information to classify as ischemic or primary arrhythmia}.
(a) Sudden cardiovascular (absent pulse) and pulmonary (absent spontaneous respiration) collapse with resuscitation.
-AND-(b) Ventricular fibrillation or asystole reported on resuscitation ECG.
-AND-(c) ECG' s. enzymes and history necessary for diagnosis of "definite" or
"possible" HI collected. "Definite" and "possible" HI by MHHP criteria have been excluded.
-AND-(d) No known non-atherosclerotic or non-cardiac atherosclerotic acute
or chronic process or event that would have been probably lethal.

WHO/MNC/82.2 Appendix III Rev. 1 page 20
B. Possible (Dx Code 12)
1. Apparent sudden cardiovascular and pulmonary collapse with resuscitation as with "definite primary cardiac arrest"
-AND-
2. Lack of documentation for ventricular fibrillation or asystole during resuscitation
-AND-
3. Definite HI by r-llillP criteria has not been diagnosed for this event.
-AND-
4. No known nonatherosclerotic or non-cardiac atherosclerotic acute or chronic process or event that would have been probably lethal.
IV. Fatal Stroke
A. Definite (Dx Code 05)
lao Cerebral infarction or helnorrhage diagnosed at autopsy
-AND-
lb. No history of atrial flutter or fibrillation; myocardial infarction in the preceding 2 months; mitral stenosis or other source for cardiac thromboembolus or paradoxical embolus; no hypercoagulable state/hemorrhage, other disease process or event such as brain tunor, subdural hematoma, subarachnoid hemorrhage, meLabolic disorder or peripheral lesion that could cause localizing neurological deficit or coma - according to death certificate, autopsy, hospital records or physician records.
-OR-
2a. History of rapid onset « 48 hours from onse t to time of admission or maximum acute neurologic deficit) of localizing neurologic deficit and/or change in state of consciousness.
-AND-
2b. Documentation of localizing neurologic deficit by unequivocal physician or laboratory finding within 6 weeks.of death with> 24 hour duration of objective physician findings.
-AND-
2c. See list under lb above.
B. Possible (Dx Code 09)
1. Death certificate with consistent underlying or immediate cause (lCD-9, Codes 431-437).
-AND-
2. No evidence at autopsy examination of the brain, if performed, of any disease process other than cerebral infarction or hemorrhage that could cause localizing neurological signs. (See lb above.)

V. Nonfatal Stroke
A. Definite (Dx Code 06)
WHQ/MNC/82.2 Appendi~ III Rev, 1 page 21
1. History of rapid onset « 48 hours from onset to time of admission or maximum acute neurologic deficit) of localizing neurologic deficit and/or change in state of consciousness.
-AND-
2. Documentation of localizing neurologic deficit by unequivocal physician or laboratory finding within 6 weeks of onset with> 24 hour duration of objective physician findings.
-AND":'
3. No history of atrial flutter or fibrillation; myocardial infarction in the preceding two months; mitral stenosis or other source for cardiac thromboembolus, or paradoxical embolus; hypercoagulable state; hemorrhage; brain tumor; subdural hematoma; subarachnoid hemorrhage; metabolic disorder; or peripheral lesion that could cause localizing neurological deficit or coma according to hospital records.
B. Possible (Dx Code 11)
la. History of rapid onset « 48 hours from onset to time of admission or maximum acute neurologic deficit) of localizing neurologic deficit and/or change in state of consciousness.
-AND-
lb. Documentation of localizing neurologiC deficit by unequivocal physiCian or laboratory finding within 6 weeks of onset with> 24 hour duration of objective physician findings.
-OR-lc. Discharge diagnoses with consistent primary or secondary codes
(ICD-9-Ct1 Codes 431, 432, 434, 436, 437) -AND-
2. No evidence by unequivocal physician or laboratory findings of any other disease process or event caUSing focal brain deficit or coma other than cerebral infarction or hemorrhage (N.B. definite evidence of systemic arterial embolism to other organs is required as proof of cardiac or paradOXical thromboembolism) according to hospital records.
MHHP Criteria for Events
Unequivocal Laboratory Findings
1. A CAT scan shOWing no definite findings of any disease process or event causing focal brain deficit or coma other than cerebral infarction or hemorrhage.
-AND-
2a. sho\.ing focal art!a of decreased or normal attenuation consistent with with cerebral infarct
-OR-
2b. showing focal increased attenuation consistent with intracerebral hemorrhage.
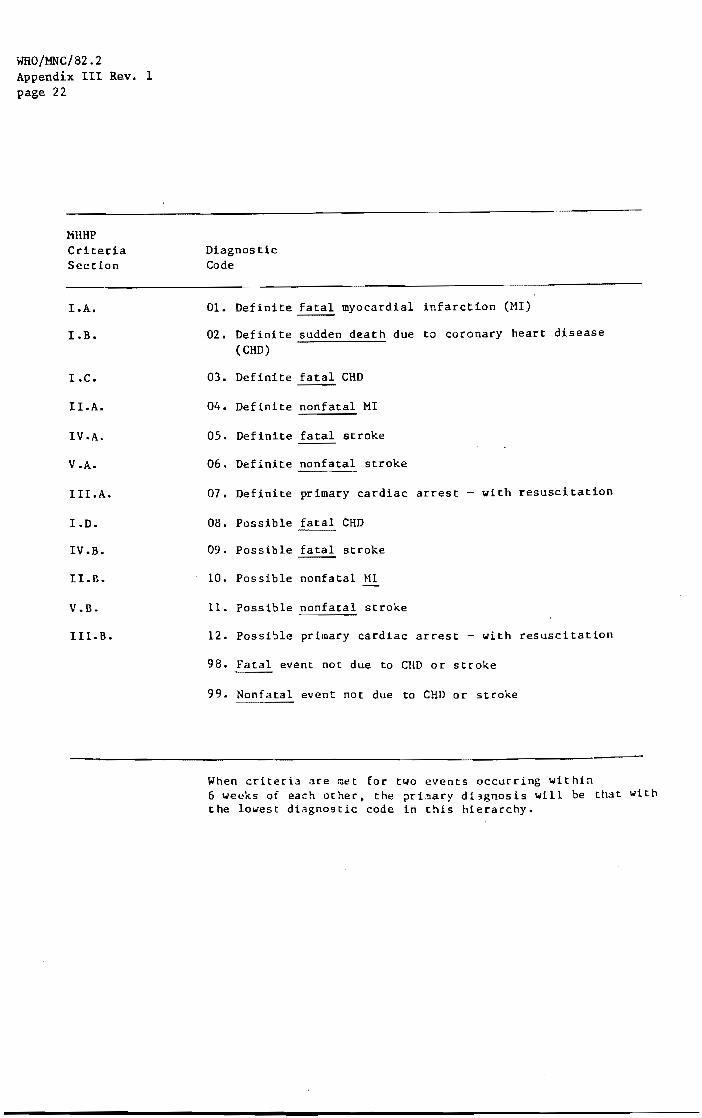
WHO/MNC/82.2 Appendix III Rev. 1 page 22
MHHP Criteria Section
I.A.
LB.
I.C.
ILA.
IV.A.
V.A.
IILA.
LD.
IV.B.
I LB.
V.B.
III.B.
Diagnostic Code
Ol. Definite fatal myocardial
02. Definite sudden death due (eHD)
03. Definite fatal CHD
04. Definite nonfatal MI
05. Definite fatal stroke
06. Definite nonfatal stroke
infarction (MI)
to coronary heart disease
07. Definite primary cardiac arrest - with resuscitation
OS. Possible fatal eHD
09. Possible fatal stroke
10. Possible nonfatal HI
11. Possible nonfatal stroke
12. Possible primary cardiac arrest - with resuscitation
9S. ~ event not due to CIlO or stroke
99. Nonfatal event not due to CHO or stroke
When criteria are met for two events occurring within 6 weeks of each other, the ?ri~ary dl~gnosis will be that with the lowest diagnostic code in this hierarchy.
Clarifications fot;" MHHP Coders. and Abstractors
WHO/MNC/82.2 Appendix III Rev. 1 page 23
Rules when using the Hinnesota Code:
1. 4-codes are independent of 5-codes (4's without 5's)
2. QS pattern in lead I 1-1-1; QS pattern in lead V6 1-1-1
3. New code for abstractors 1-1-6 QS pattern when initial R-wave is present in adjacent lead to the right on chest, in any of leads V2. V3. V4, V5, V6·
4. Do not code 4-4 or 5-4's.
5. Although MHHP is limited to Q, 4, 5, 9-2, 6-1, 6-8. 7-4, 8-2 and and 9-8 codes, the suppressions from the rlinnesota Code book should be applied for any other code that affects a coding procedure. (Example: 3-2 suppresses 1-2-8. It is not coded for MHHP but the suppression is still in effect. Put the reason for the HHHP suppression (Le., "3-2 suppresses 1-2-8") in the "Uncoded Leads" column.
6. When a QRS > 0.12 sec., determine if it is a 7-1-1. 7-2-1 or a 7-4. Then apply the suppressions for that specific code. Record 7-4 regardless of which 7-code it is.
7. If there are any questions on coding, call Denise Hesselroth.
Rules for the special codes in the ECG category:
1. Evolving Diagnostic deals in lead groups. If more than one code is needed, they have to occur in the same lead group.
2. Diagnostic can occur on any ECG. in the same lead group. Example:
The criteria does not have to occu~ 5-2 lead II; 9-2 lead V5'

WHO/MNC/82.2 Appendix III Rev. 1 page 24
TABULAR PRESENTATION OF
MINNESOTA HEART HEALTH PROGRAM (MHHP) EVENT CRITERIA
INTRODUCTION - The Minnesota Heart Health Program Event Criteria divide events into 12 cardiovascular disease (CVD) events--four fatal coronary events (definite fatal myocardial infarction, definite sudden death due to coronary heart disease (CHD) , definite fatal CHD, and possible fatal CHD), two levels of non-fatal MI ('possible' and 'definite' non-fatal MI), two levels of primary cardiac arrest with successful resuscitation ('definite' and'possible'), twv levels of fatal stroke ('definite' and'possible' fatal stroke), and two levels of non-fatal stroke ('definite' and'possible' non-fatal stroke). Each CVD event is assigned a code number for ordering the hierarchy of events occuring within six weeks of each other (codes 01-12), and fatal events not due to CVD are assigned code 98 and non-CVD events not associated with death are assigned code 99.
Some of the criteria categories require definition of other criteria categories or of subcategories (i.e., ECG and cardiac enzyme data) that do not appear in the list of final diagnoses. For example, the test for a fatal coronary heart disease (CHD) requires first testing for non-fatal MI; and testing for a non-fatal MI requires categorization of ECG and enzyme data.
Table 1 presents the fourteen categories of final diagn.osis, their hierarchical codes and the table number that explains how the diagnostic elements are applied to assign a final diagnosis. Tables 2 through 8 present the rules for categorizing the data into each of the diagnostic categories and subcategories. The tables are in order of expected application.

waO/MNC/82.2 Appendix III Rev. 1 page 25
Table 1 - The 14 MHHP final diagnoses, their hierarchical levels for assigning diagnosis when two events occur within a six-week time period, and the table numbers for determining final diagnosis (if two or more events occur within six weeks of each other, diagnosis is event with lowest code number)
NON-FATAL CORONARY HEART DISEASE EVENTS (table 4)
Definite non-fatal MI (Code 04)
Possible non-fatal MI (Code 10)
FATAL CORONARY ~ DISEASE EVENTS (table, 5)
Definite fatal myocardial infarction (MI) (Code 01)
Definite sudden death due to coronary heart disease (CHD) (Code 02)
Definite fatal CHD (Code 03)
Possible fatal CHD (Code 08)
PRIMARY CARDIAC ARREST EVENTS (table 6)
Definite pri~ary cardiac arrest with resuscitation (Code 07)
Possible primary cardiac arrest with resuscitation (Code 12)
FATAL STROKE EVENTS (table 7)
Definite fatal stroke (Code 05)
Possible fatal stroke (Code 09)
NON-FATAL STROKE EVENTS (table 8)
Definite non-fatal stroke (Code 06)
Possible non-fatal stroke (Code 11)
NON-CVD EVENTS
Fatal event not due to CVD (Code 98)
Non-fatal non-CVD event (Code 99)

WHO/MNC/82.2 Appendix III Rev. 1 page 26
Table 2 - Criteria for Categorizing Cardiac Enzymes
(To be applied if case has target or screening MI codes)
DIAGNOSTIC ELEMENT
Total CPK and CPK-MB measured
-or-Total CPK and one of SGOT or LDH measured (1)
At least one measurement of total CPK > 2 times ULN* and CPK-MB 'present' or > 2 times ULN (2)
-or-At least one measurement of total CPK > 2 times ULN and at least one measurement of SGOT or LDH > 2 times ULN (2)
All measurements < ULN
Other cause for enzyme (3,4) elevation present
DIAGNOSTIC CATEGORY abnormal equivocal normal
+ + +
+ +
+
+ +
Key: + = must be present; + may be present but not essential; - = must be not present
* upper limits of normal
incomplete
+
+
(1) only measurements within 72 hours of admission or acute event, whtchever is later, are considered in categorizing the enzyme data
(2) If another cause of enzyme elevation is present, the enzyme valup. is treated as being between one and 2 times ULN, not> 2 times ULN
(3) Enzyme patterns which would otherwise be categorized as 'abnormal' are categorized as 'equivocal' in the presence of another cause of enzyme elevation
(4) Conditions other than myocardial infarction which cause elevations of ' serum enzymes
[From: Wallach J. Interpretation of diagnostic tests. 2nd Ed. Boston; Little, Brown and Co, 1974.J

ICD9 Codes Description
191,198.3,225.0, 237.5,239.6 cerebral neoplasm
415.1 434.9 570-3
pulmonary infarction cerebral infarction liver disease
Raises SGOT
ICD9 Codes
574-6 577 593.81 791.3 863 990
ICD9 Codes Description Raises LDH
ICD9 'COdes
428.0 36 070,571,573
281.0
ICD9 Codes
429.0 359.0,359.1 710.4 791.3
800-869, 880-897, 922-929
congestive heart failure cardiovascular surgery hepatitis
pernicious anemia (untreated)
Description
myocarditis muscular dystrophy polymyositis myoglobinuria
muscle trauma
140-239 710.3-710.9,728.0 415.1
580-593
Raises CPK
ICD9 Codes
345.3 244.9 434.9 641-676 01-86.9 99.1-99.2 99.6
.
WHO/MNC/82.2 Appendix III Rev. 1 page 27
Description
cholecystitis acute pancreatitis renal infarction myoglobinuria intestinal injury irradiation injury
Description
malignant tumors muscle diseases pulmonary embolus and infarction renal disease€
Description
st~tus epilepticus hypothyroidism brain infarction partuition post-operative state injection defibrillation
Table 3 - Criteria for categorizing electrocardiographic data
(To be applied if case has target or screening MI codes; the diagnostic category is defined by the presence or absence of the diagnostic elements
DIAGNOSTIC CATEGORY Evolving Diagnostic
Diagnostic Equivocal Other
DIAGNOSTIC ELEMENTS
At least 2 EeG's
Evolving Q-wave pattern (1)
Stationary diagnostic Q-waves (2)
-or-ST elevation (3) and major T-wave inversion (4)
Equivocal Q-waves (5) -or-
any ST depression (6) -or-
any T-wave inversion (7) --or-
ST elevation (3)
+ + + +
+
+ +
+ + +
-------------------------------------------------------------------------Key: + must be present; ~ may be present but not essential;
- = must be n~t present

WHO/MNC/82.2 Appendix III Rev. 1 page 28
(1) An evolving Q-wave pattern includes at least 2 ECG's with:
(2)
(3)
(4 )
(5)
(6)
(7)
No Q code in a lead group in one ECG followed by an ECG with a diagnostic Q code (1-1-1 through 1-2-5 or 1-2-7) in the same lead group (lead groups are: V1-V5; I. aVL. V6; and II, III aV·F). or
An equivocal Q code 0-2-6, 1-2-8. or any 1-3-x) and no major ST segment depression (4-1 or 4-2) in a lead group in one ECG followed by an ECG with a diagnostic Q code PLUS major ST segment depression in the same lead group. or
An equivocal Q code and no ST segment elevation (9-2) in a lead group in one ECG followed by an ECG with a diagnostic Q-code PLUS an ST segment elevation in the same lead group. or
An equivocal Q code and no major T-wave inversion (5-1 or 5-2) itl a lead group in one ECG followed by an ECG with a diagnostic Q-code PLUS major T-wave inversion in the same lead group. or
No Q-code and no major ST segment depression in a lead group in one ECG followed by an ECG with an equivocal Q-code and major'ST segment depression, or
No Q-code and no ST segment elevation in a lead group in one ECG followed by an ECG with an equivocal Q-code and ST segment elevation. or
No Q-code and no major T-wave inversion in a lead group in one ECG followed by an ECG with an equivocal Q-code and major T-wave inver-sion"
Codes 1-1-1 through 1-2-5 and 1-2-7
Code 9-7-
Codes 5-1 and 5-2
Codes 1-2-6, 1-2-8. and any 1-3-x
4-1. 4-2, and 4-3
5-1. 5-2, and 5-3
Note: A lead is uncodable (not coded) if any of the following are present: Missing record; baseline drift greater than 1:20 or if it obscures the ST-T wave; muscle tremor artifact giving more than 2 mm peak-to-peak oscillation; other tedm' ical errors making Q-wave measurement impossible such as extreme lack of centering or marked clipping of the complex; QRS ).012 sec; pacemaker stimulated complex; complete AV block; ventricular tachycardia or asystole. Any and all pathological findings in a lead group are recorded for that lead group; that is, even if one or more leads in a group are uncodable, the remaining leads are coded.

(1)
WHO/MNC/82.2 Appendix III Rev. 1 page 29
Table 4 - Diagnostic Criteria for Non-fatal Myocardial Infarction ------------------------------------------------------------------------------(To be applied if case has target or screening MI codes)
Diagnosis is found in cell defined by the level of pain, ECG category and enzyme category
PAIN (1) , NO PAIN , , ,.
ENZYMES (2) , ENZYMES abn. equiv incorop normal ,. abn. equiv incomp normal
,- , ,. , ,. ,. , ---- ----,. ,. , , , ,. , , , , , 04 ,. 04 , 04 , 04 'iEvolving diagnostic ,. 04 , 04 , 04 , 04 , , , , ,- , ,. , , , , , ,. ,. ,. , , , , , ,. , 04 ,. 10 , 10 ,. 99 , Diagnostic ,. 04 ,. 10 , 99 , 99 ,
'l ,. , , , , , ,. , , ,. , , ,. , , , , , ,. , 04 ,- 10 ,. 10 , 99 ,. Equivocal ,. 10 ,. 10 ,. 99 , 99 ,. ,. ~I ,. , ,. ,. ,. , , , , ,. ,. , , Absent, ,. ,. , ,. , ,. 04 ,. 10 , 10 , 99 'i Uncodable or , 10 , 99 , 99 , 99 , , ,- , , , 'Other t , ,. , , ,
ELECTROCARDIOGRAM (3)
------------------------------------------------------------~-------------------~ 04=DEFINITE MI 10=POSSIBLE MI (conditional on MI screening codes being present on discharge) 99=NO MI
Pain: (a) occurring anywhere in the anterior chest, left arm or jaw which may also involve the back, should, right arm, or abdomen on one or both sirles, and (b) with a duration of more than 20 minutes or if duration is not defi-ned, for which the patient sought medical care after taking nitroglycerin or calcium blockers.
(2) See table 2 enzyme for categorization rules
(3) See table 3 for ECG categorization rules

WHO/MNC/82.2 Appendix III Rev. 1 page 30
Table 5 - Diagnostic Criteria for Fatal Coronary Heart Disease (CHD) Events ----------------------------------------------------------------------------
Death certificates are excluded from analysis if decedent is outside age range or if cause of death (Medical certification of cause of deatn, Part I a,b, or c) lists accident, homicide or suicide, other trauma, chronic obstructive pulmonary disease, cancer, cirrhosis of liver, or rheumatic heart disease without mention of atherosclerotic heart or vascular disease,
The diagnostiC'. category is defined by the presence or absence of the diagnostiC elements DIAGNOSTIC CATEGORY
DIAGNOSTIC ELEMENTS
Definite MI (1) -or-
Acute MI on Autopsy
Sudden Death (2)
History of Previous Mi (3)
-or-
Definite Fatal MI (Code 01)
+
+
Autopsy reporting severe CAD (4) +
-or-Rapid death (5)
Death Certificate + with 410-414
Probably lethal non-atheroscler- + otic or non-cardiac athero-;;:;clerotic cause of. deatn oresent (6)
Defini te Sudden Death Due to CHD
(Code 02)
+
+
+
Definite Fatal CHD (Code 03)
+
Possible Fatal CHD (Code 08)
+*
Key: + ~ must be present; + = may be present but not required; must be documented to be absent or documentation of absenCr or presence lacking
(1) within 4 weeks of death and oeeting MHHP criteria for MI (see table 4) (2) death within 1 hour of developing symptoms or being found dead within 1 hour of being
seen without symptoms (3) any source of information acceptable (4) > 50% proximal narrowing of :;: or core major vessels or )75% proximal
narrowing of one or more major vessels (5) death between 1 and 24 hours of developing symptoms or being found dead within 1 hour of being seen without symptoms * Any of 427,429,798 or 799 also qualifies death for possible fatal CHD
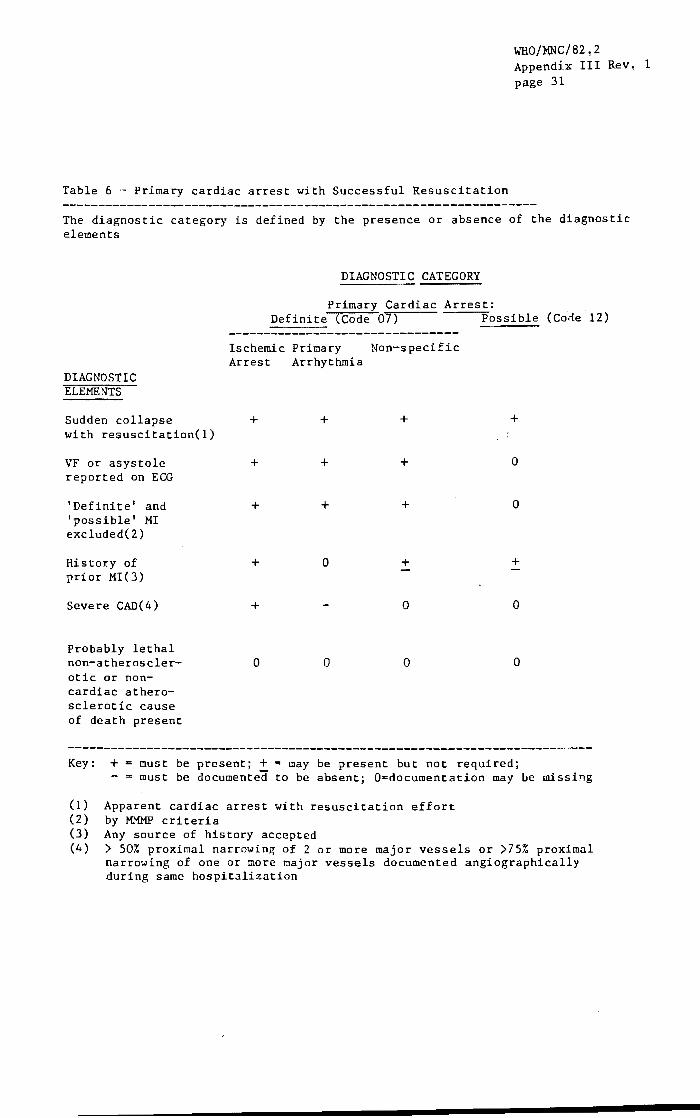
Table 6 ,~ Primary cardiac arrest with Successful Resuscitation
WHO/XNC/82,2 Appendix III Rev. 1 page 31
The diagnostic category is defined by the presence or absence of the diagnostic elements
DIAGNOSTIC CATEGORY
Primary Cardiac Arrest: Definite <Code 07) Possible (Cone 12)
DIAGNOSTIC ELEMENTS
Sudden collapse with resuscitation(l)
VF or asystole reported on ECG
'Definite' and 'possible' MI excluded(2)
Histo:r:y of prior MI(3)
Severe CAD(4)
Probably lethal non-atherosclerotic or noncardiac atherosclerotic cause of death present
Ischemic Primary Non-specific Arrest Arrhythmia
+ + + +
+ + + o
+ + + o
+ o + +
+ o o
o o o o
Key: + must be present; + = may be present but not required; - ,. must be documented to be absent; O=documentation ma.y be missing
(1) Apparent cardiac arrest with resuscitation effort (2) by MMMP criteria (3) Any source of history accepted (4) > 50% proximal narrowing of 2 or more major vessels or >75% proximal
narrowing of one or more major vessels documented angiographically during same hospitalization

WHO/MNC/82.2 Appendix III Rev. 1 page 32
Table 7 - Diagnostic Criteria for Non-fatal Stroke
Diagnosis is found in cell defined by correct combination of neurological event and non-stroke cause for the event
NON-STROKE CAUSE PRESENT? definite (1) possible (2) not present
N .. .: .. , , E definite (3) .. 99 , 11 , 06 , U , , , , R , , , , 0 , , , ,
possible (4) .. 99 , 11 1 11 , E , , , , V , , , , E , , , , N no event , 99 'I 99 , 99 , T , , , , ? , , , , Key: 06 = Definite non-fatal stroke; 11 = Possible non-fatal stroke;
99 = No CVD event ----.... -.-------~~~-~----------."" -----------~---....... -----..... _._----- - ...... -~-.. , -_ ......... _----_ ....
0) 'Detinite' causes of non-fatal focal neurological deficit'or coma
ICD9 Code
140-208 and 235-239
250 251 345.3 430 432.0 432.1 444 444 572.2 586
Description
brain tumor and (possible) metastasis
diabetic coma hypoglycemic coma epileptic coma subarachnoid hemorrhage epidural hematoma subdural hematoma peripheral (systemic) embolism paradoxical thromboembolism hepatic coma uremic coma

WHO/MNC/82.2 Appendix III Rev. 1 page 33
September 7, 1982 Page 11
(2) 'Possible' causes of non-fatal focal neurological deficit or coma
ICD9 Code Description
276 disorders of fluid, electrolyte and acid-base balance
286.6 286 350-359 394 410-411 427.31 427.32 459.0 88.41 88.57
disseminated intravascular coagulation coagulation defect peripheral neuropathy mitral stenpsis myocardial infarction atrial fibrillation atrial flutter hemorrhage carotid angiography coronary angiography left ventriculography 88.53, 88.54
(3) History of rapid onset «48 hours from onset to time of admission or maximum acute neurological deficit) of localizing neurological deficit and/or change in state of consciousness, and; documentation of localizing neurological deficit or change in state of consciousness by unequivocal physician or laboratory findings within 6 weeks of onset with> 24 hour duration of objective physical findings. Unequivocal laboratory findings are defined as a CAT scan showing: 1. no definite findings of any disease process or event causing focal brain deficit or coma other than cerebral infarction; and 2a. a focal area of decreased or normal attenuation consistent with cerebral infarct or 2b. a focal area of increased attenuation consistent with intra-cerebral hemorrhage.
(4) One or more of ICD9 Codes 431, 432, 434, or 436 present.

WHO/MNC/82.2 Appendix III Rev. 1 page 34
WHO/MNC/82.?
Table 8 - Diagnostic Criteria for Fatal Stroke
Diagnosis is found in cell defined by correct cocbination of neurological event and non-stroke cause for the event
NON-STROKE CAUSE PRESENT? definite (1) possible (2) not present
N , 'J 'I , E definite (3) , 98 , 09 , 05 , U , , 'I , R • 0 , :------------':-------------':-------------, , 'I ,
possible (4) , 98 , 09 , 09 , E , , " V , E 'I
, _________ , 'I , '/ , 'I
N no event , 98 'I 98 'I 98 , T , , , , ? , _____ , , 'I
Key: 05 = Definite fatal stroke; 09 = Possible fatal stroke; 98 = No fatal CVD event
(1) evidence at autopsy examination of the brain, if performed, of any disease process other than cerebral infarction or cerebral hemorrhage that could cause localizing neurological deficit.
(2) use list for 'possible' and 'definite' non-fatal non-stroke causes of neurological event in Table 6 as criteria for 'possible non-stroke cause of fatal neurological event'.
(3) A. Cerebral infarction or cerebral hemorrhage diagnosed at autopsy; -or-
B. History of rapid onset «48 hours from onset to time of admission, maximum neurological deficit or death) of localizing neurological deficit and/or change in state of consciousness, and documentation of localizing neurological deficit by unequivocal physician or laboratory findings within 6 weeks of death with> 24 hours duration of unequivocal physician findings or findings leading to death.
(4) One or more of ICD9 Codes 431, 432, 433, 434, 435, 436, 437 present
(mhhpcrit.wps)

Morbidity and Mortality Flow - MHHP
Hosp.
T CPHA Tape
Hosp. Data
~,-------,-Tar_--",-ltry - Hosp·l
(target criteria)
(copy of assg'n)
Labels for folders
Work
~rts
Complete Folders
/
(corrections, Status)
1------,1- -~~ECG /---1 Log Ins - Hosp. ~
:i~ 1 Review Reports
* death within 24 hours and no enzymes
** Hasp. within 6 wks of death
file?)
MNDH DC's
\ <I
WHO/MNC/82.2 Appendix III Rev. 1 page 35
L, Gatewood 30/9/82
SDDH DC's
J next-af-kin
NDDH DC's
I Selection Int.
Labels for folders
~Death Lists~
Death certlficates
ICD Coding
L Log Outs - Int.
__ Data Entry
work~ LI ts
~ Complete Folders
(Corrections, Status)
(copy of assg'n)
I--___ -.-_I,n,t,. _,j: :
~ Reports. MD
Review
rCD
COding(?\

WHO/MNC/82.2 Appendix III Rev. 1 page 36
I. SA}IPLE SELECTION
MORBIDITY OATA FLm.,
A. Selection of Hospital Charts
The selection of medical records is determined by the hospital medical record number and the MI and STROKE diagnosis codes recorded in a patient's hospital chart. This information may be obtained from computer tapes provided by the hospital or the examination of hospital records by clerical staff.
}yGl B. Morbidity Log Files \~t.D
The hospital code, medical record number, ~ex, age, date of discharge, length of stay in the hospital and the MI and/or STROKE diagnosis codes are entered on a computer log uSing computer tapes or keypunched hospital record information. Each medical record number is assigned an MHHP 10 number and abstractor code number. Information concerning patient eligibility and data form completion is updated to the Morbidity Log file by Data Control personnel upon receipt of abs.tracted hospital charts.
C. Data Identification
The MHHP ID number consists of nine digits. The first character is an alpha character designating city. The second and third characters indicate year, the fourth character is the numerical city code, the fifth digit is the quality control identifier and the last five characters are a sequential number identifying the chart.
H City
City codes - M=t1ankato W==Hinona
Year - 80, 81, etc.
Area codes - l==Mankato 2==Winona
80 Year Area
o Q.C.
00001 Sequence
B=B1oomington F,=Rosevi1le
3=Bloomington 4=Rosevi 11e
Quality Control - 0=Non-qua1ity control l=Quality Control
Sequence Number - 00001,00002, etc.
D. Identification Labels
S=Sioux Fa11s F=Fargo
5=Rosevi11e 6=Fargo
Using the computer log infornation, identification labels are generated for each hospital chart. Two "selection" labels are printed listing the MHHP 10 number and log file information and twenty -10" labels are printed listing the MHHP 10 nu~ber.
E. Hospital Listings
A computer listing will accompany the folders assigned to an abstractor. The computer listing will contain the name of the
WHo/MNC/82~2 Appendix ur Rev, 1 pa,ge. 37
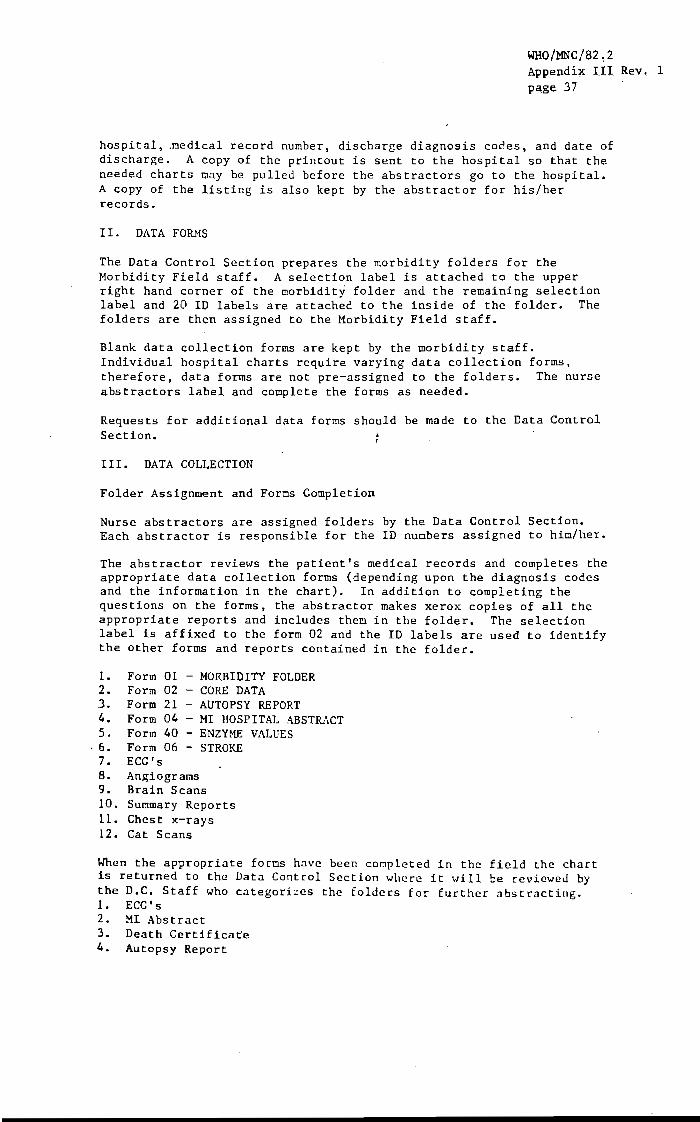
hospital, .oedical record number, discharge diagnosis codes, and date of discharge. A copy of the printout is sent to the hospital so that the needed charts may be pulled before the abstractors go to the hospital. A copy of the listing is also kept by the abstractor for his/her records.
II. DATA FORMS
The Data Control Section prepares the morbidity folders for the Morbidity Field staff. A selection label is attached to the upper right hand corner of the morbidity folder and the remaining selection label and 20 10 labels are attached to the inside of the folder. The folders are then assigned to the Morbidity Field staff.
Blank data collection forms are kept by the morbidity staff. Individual hospital charts require varying data collection forms, therefore, data forms are not pre-assigned to the folders. The nurse abstractors label and complete the forms as needed.
Requests for additional data forms should be made to the Data Control Section.
III. DATA COLLECTION
Folder Assignment and Forms Completion
Nurse abstractors are assigned folders by the Data Control Section. Each abstractor is responsible for the 10 nuobers assigned to him/her.
The abstractor reviews the patient's medical records and completes the appropriate data collection forms (depending upon the diagnosis codes and the information in the chart). In addition to completing the questions on the forms, the abstractor makes xerox copies of all the appropriate reports and includes them in the folder. The selection label is affixed to the form 02 and the 10 labels are used to identify the other forms and reports contained in the folder.
1. Form 01 - MORBIDITY FOLDER 2. Form 02 - CORE DATA 3. Form 21 - AUTOPSY REPORT 4. Form 04 - MI HOSPITAL ABST&\CT 5. Form 40 - ENZYME VALUES
. 6. Form 06 - STROKE 7. ECG's 8. Angiograms 9. Brain Scans 10. Summary Reports 11. Chest x-rays 12. Cat Scans
When the appropriate forms have been completed in the field the chart is returned to the Data Control Section wllcre it will be reviewed by the D.C. Staff who categorL::es the folders for further abstracting. 1. ECG's 2. MI Abstract 3. Death Certificaee 4. Autopsy Report

WHO/MNC/82.2 Appendix III Rev. 1 page 38
IV. VISUAL EDITING BY MORBIDITY STAFF
Before sending a folder to Data Control, it should be checked to make sure all of the for~s indicated on the folder checklist are contained in the folder, that the appropriate forns and reports have been completed, and that the questionnaires have been completed properly.
Completed folders should be shipped to Data Control at least once a week. A monthly report will be prepared by the Data Control Section indicating the ID's given to the l10rbidity staff and those returned to the Data Control Section.
VI. DATA PROCESSING
A. Morbidity Log File
When the folders are returned to the LPH Data Control Section they are logged on the Morbidity Log file and the forms are visually edited and batched.
B. Visual Editing, Keying, and Computer Editing
Folders which have missing information will be returned to th~ Morbidity Section for completion. ,
Folders will fall into three categories; INELIGIBLE, ALIVE, and DEAD.
If the patient chart is INELIGIBLE the ineligibility status is entered on the log file. Data forms are not completed for INELIGIBLE charts.
ALIVE folders are divided into STROKES (06) and HI'S (04). The 06's are visually edited and sent directly to keying. Form 04's are divided into two groups; folders which must have further abstracting (eg. HI abstract,ECG coding) before being sent to keying; folders \.hich do not need further abstracting and are sent directly to keying.
DEAD folders are divided into: "waiting for death certificate or autopsy" and "received death certificate or autopsy". Once they have passed from the "waiting to the "received" category, they are processed in the same manner as the ALIVE folders.
Folders with forms requiring further abstracting "ill be separated into . categories and sent to the various coding sections. Coding stations
will be provided in the Data Control Section for coding personnel (MD abstracting, ECG coding, Death Certificate and Autopsy coding)
C. Filing After the forms have been computer edited they will be filed back into the patient folders.
D. Masterfiles
The final step of the editing process will be to add the edited forms to the morbidity masterfiles and return the charts to the ':lo~bidity ~Section.

MORBIDITY SURVEILLANCE ID LABEL
WHO/MNC/82.2 Appendi~ III Rev_ 1
'page 39
PATIENT STATUS
D 04 MI
ELIGIBLE
1 DEAD
20 ALIVE
3D NOT FOUND
o 02 CORE DATA
INELIGIBLE
1 D AGE
2 0 ZIP CODE
3 0 SAMPLE SELECTION CODE
4 DISCHARGE DATE
5 D DUPLICATE
o 20 DEATH CERTIFICATE ABSTRACT
[J Death Certificate
o 21 AUTOPSY REPORT ABSTRACT
[J Autopsy Repoft
D 06 STROKE
o 40 ENZYME VALUES
[J 41 PHYSICIAN REVIEW
D Summary Reports (Discharge or Death Summary)
[J Chest X-rays CD o Coronary Angiogracs CD
o 42 ECG CODING SHEET
[J ECG's OJ
[J Cerebral Angiograms
[J Cardiac Angiograms
o Brain Scans
[J CAT/EMI Scans
OJ OJ OJ OJ

WHO/MNC/82.2 Appendix III Rev. 1 page 40
General Instructions:
INSTRUCTIONS FOR MHllP ABSTRACTING FORMS (07/06/82)
1. Use black felt-tip pen Do not use pencil.
2. Write legibly.
3. Two types of boxes are used:
A. Small boxes are to be marked with an x as shown: L~ Use a black felt tip pen, and ~~p the x within the box.
B. Large boxes are to be marked with the appropriate letter or number. Draw horizontal lines through boxes that are not applicable. Keep numbers and letters within boxes.
EXAMPLES: n I I
or W or I I I I I I Third Name/Title .
C. Not recorded box is to be marked'with an x when information is not recorded, not sure, missing from chart, not done or unknown. If there Is no box draw a horizontal line through the boxes as shown below.
EXA.>.fPLES: G! Not --t!---,r--+-Recorded
I I I 4. Comple te only appropriate boxes. E. g.. record minutes / times OR "Not recorded
in chart." Do not fill in both.
5. When an error is made, cross out the error with a single horizontal line through the entire box or set of boxes. Write the correction just above or as near as possible. Do not in any way obliterate (black out, erase) any data that has been written in, correct or not.
6. Be sure to follow correct skip patterns.
7. Before beginning to fill out any of these forms, read quickly through the following: face sheet, emergency report, ambulance report, problem list, physician admitting note, and discharge summary. This should take about 5-10 minutes. Then begin completing the forms. So~e items can be done from memory, or you should remember approximately where in the chart to find the needed information. It is helpful to use paper clips or strips of paper to identify these pages in the chart.
In answering most questions you will have the choice of "Yes". "No" and not recorded "NR". "Yes" or "No" will be marked only if there is no doubt due to information in the hospital record. If nothing is written down which definitely answers the question, "NR" should be circled.

WHO/MNC/82.2 Appendi~ III Rev. 1 pa,ge 41
~mp/MHHP Personal Code Numbers
(08/25/82)
Person Code Num er Person Code Number
Rosalie Seibel R.N. (inactive) 011 Charlotte Herman, R.N.(inactive)012 Jane Edmondson R.N. (inactive) 013 Deborah HcGuire R.N. 014 K.C. Jenkins R.N. 015 Judy Broeker (inactive) 016 R. Gillum, M.D. 017 T. Kottke, M.D. 018 R. Prineas, M.D. 019 R. Luepker, M.D. 020 Sue Mendesh (inactive) 021 Masako Katoh (inactive) 022 Jim Huber 023 Isabelle Fertey 024 Cheryl Bernstein R.N.(inactive) 025 Leah Hillesheim R.N. (inactive) 026 Cynthia Jurgensen R.N. 027
June Lofgren R.N. (inactive) Ruth Whitlock R.N. Debra Dykins (inactive) John Che (inactive) Dale Moss Wendy Adams R.N. (inactive') PHRED (computer) Kathleen Mullen R.N. (inactive) Adjudicated Diagnosis Bernice McCullough Cindy Royce (inactive) Carol Thompson (inactive) Fran Galle, R.N. Stephen Mascioli, M.D. Michelle Paul (inactive) Steve Norgaard Aaron Folsom, M.D. John Kipp, M.D. Peg Wedell
028 029 040 041 042 043 044 045 046 047 048 049 056 069 070 073 076 077 092

WHO/MNC/82.2 Appendix III Rev. 1 page 42
AV
BLVD
CIR
CTR
cn RD
CT
COVE
CVE
DR
E
HWY
LN
LK
MALL
MPLS
MN
N
PKY
Anoka
Carver
Dakot:a
Avenue
Boulevard
Circle
Center
County Road
Court
Cove
Curve
Drive
East
Highway
Lane
Lake
Mall
Minneapolis
Minnesota
North
Parkway
An
Ca
Da
Hennepin He
STANDARDIZED ABBREVIATIONS
-PL- Place
PT Point
RGE Ridge
RD Road
R Route
RR Rural Route
RFD Rural Free
S South
SQ Square
ST Street
TR Trial
TR Terrace
TRL CT Trailer Court
VA 'Valley
WAY Way
W tves t:
COUNTY ABBREVIATIONS
Ramsey RA
Scott: Sc
Washington Ua
WllQ/l1NC/82~2 Append~ II~ Rev, 1 p~ge. 43
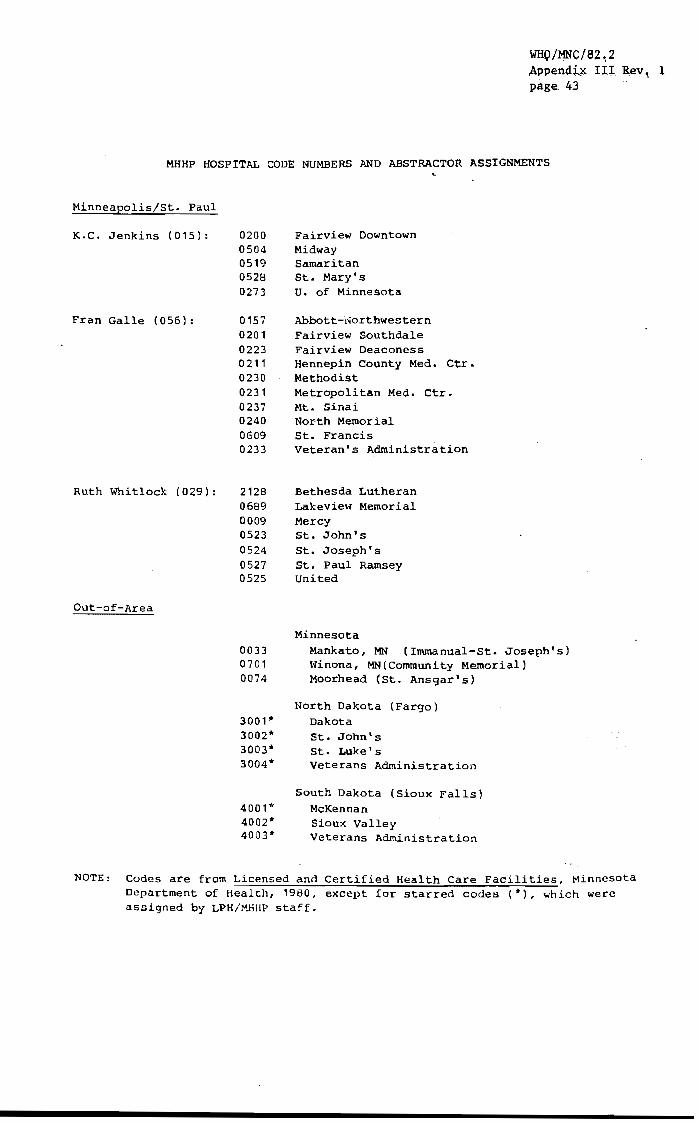
MHHP HOSPITAL CODE NUMBERS AND ABSTRACTOR ASSIGNMENTS
Minneapolis/St. Paul
K.C. Jenkins (015):
Fran Galle (056):
Ruth Whitlock (029):
Out-of-Area
0200 0504 0519 0528
Fairview Downtown Midway Samaritan St. Mary's
0273 U. of Minnesota
0157 0201 0223 0211 0230 0231 0237 0240 0609 0233
2128 0689 0009 0523 0524 0527
Abbott-Northwestern Fairview Southdale Fairview Deaconess Hennepin County Med. Ctr. Methodist Metropolitan Med. Ctr. Mt. Sinai North Memorial St. Francis Veteran's Administration
Bethesda Lutheran Lakeview Memorial Mercy St. John's St. Joseph's St. Paul Ramsey
0525 United
0033 0701 0074
3001* 3002* 3003* 3004*
4001* 4002* 4003*
Minnesota Mankato, MN (Inunanual-St. Joseph's) Winona, MN(Community Memorial) Moorhead (St. Ansgar's)
North Dakota (Fargo) Dakota St. John's St. Luke's Veterans Administration
South Dakota (Sioux Falls) McKennan Sioux Valley Veterans Administration
NOTE: Codes are from Licensed and Certified Health Care Facilities, Minnesota Department of Health, 1980, except for starred codes (*), which were assigned by LPH/t-'.HIIP staff.

WHO/MNC/82.2 Appendix ,III Rev. 1 page 44
In-State Hospitals
:Hankato
HOSPITAL LISTING
01;"1' OF TinN CITY METROPOLITAN ARE..t.
I~anua1-St. Joseph's Hospital 325 Gordon Blvd. r~nkato, MN 56001
Pres. Donald Stordahl CS Dr. R.W. Kearney, J~
CC Dr. R.W. Reissen (507) 625-4031 ·CN None
Winona
Community Memorial Hospital Convalescant & Rehabilitation Unit
855 Mankato Ave. t.anona, !>IN 55987 (507) 454-3650
Out-oi-State Hosoitals
Dakota Hospital 1720 University Dr. Fargo, ND 58103 (701) 2,80-4100
St. John's Hospital 510 4th St. So. Fargo, ND 58103 (701) 232-3331
St. Luke's Hospital 5th St. at Mills Ave. Fargo, ND 58122 (701) 280-'5000
V. A. Hosp ita1 Elm St. and 21st. Ave. N. Fargo, ND 58102 (701) 232-3241
DMR Bonnie Doering
Adm. CS CC CN DMR
Roger L. Metz Dr. J.V. Testor Dr. Edin None Haizie Myers
Pres. D.D. l.Jightman (Mr.) C'S fr. E. P. \~enz CC Dr. Houghton CN Dr. Grossman DXR Peggy Sullivan
Adm. CS CC CN DHR
Adm. CS CC CN DMR
Dir. CS CC CN DXR
Robert Wolter Dr. C. }1. Hunter None None
'Mary Jen Hagen
A.J. Finn1.e (Mr.) Dr. Rogert Jordheim Dr. Matt Ehlen Dr. Ryan Harrington Mary Jen Hagen
Francis E. GO,thman Dr. Michael J. Kelly' Dr. Gopal Das Dr. Roger Brumback Jill Domenichetti

Moorhead
St. Ansgar Hospital 715 N. 11th St. Moorhead, MN 56560 (218) 299-2220
Sioux Falls
McKennan Hospital 800 E. 21st St. Sioux Falls, SD 57105 (605) 339-8000
Sioux Valley Hospital 1100 S. Euclid Ave. Sioux Falls, SD 57105 (605) 336-3440
Veteran's Hospital 2501 W. 22nd St. Sioux Falls, SD 57105 (605) 336-3230
WHO/MNC/82.2 Appendix III Rev. 1 page 45
Adm. Lloyd Smith CS Dr. John Thomas CC Dr. Ladwit CN None DMR Joan Miska
Exec. Dir. Henry J. Morris CS Dr. V.V. Volin CC Dr. E.W. Sanderson CN None DMR Roger C. Paavola CAss't
Debra Bylund (Sup •• MR.)
Adm. CS CC CN DMR
Dir. CS CC CN DMR
Lyle Schroeder Dr. Richard Frieff Dr. Larry Solberg (*) None Derrold Hofer (Mr.)
Dexter Dix Dr. George Wyatt Dr. Robert Talley Dr. George Flora Kent Simoni!:,
* Dr. Solberg is the Cardiologist for the North Central Heart Insti~ute, which is affiliated with the Sioux Valley Hospital.
Pres. President Dir. Director Ad!:l. Adoinistrator CS Chief of Staff CC Chief of Cardiology C, Chief of Neurology DMR Director of Medical Records
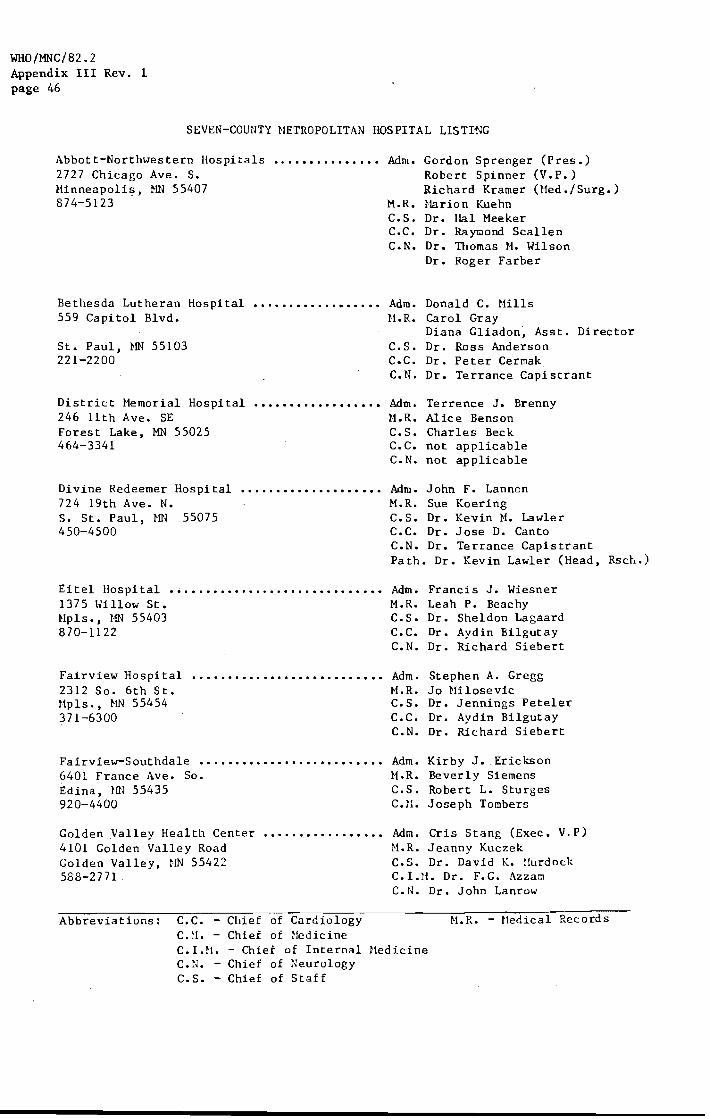
WHO/MNC/82.2 Appendix III Rev. 1 page 46
SEVEN-COUNTY HETROPOLITAN HOSPITAL LISTING
Abbott-Northwestern Hospitals 2727 Chicago Ave. S. Hinneapo1i~, .t--IN 55407 874-5123
••••••••••••••• Adm. Gordon Sprenger (Pres.) Robert Spinner (V.P.) Richard Kramer (tled./Surg.)
M.R. Narion Kuehn
Bethesda Lutheran Hospital •••••••••••••••••• 559 Capitol Blvd.
St. Paul, ~rn 55103 221-2200
District Memorial Hospital 246 11th Ave. SE Forest Lake. MN 55025 464-3341
Divine Redeemer Hospital 724 19th Ave. N. S. St. Paul, HN 55075 450-4500
Eitel lIospital .~ ••••••••••••••••••••.••••••• 1375 \Ullow St. Npls •• t·rn 55403 870-1122
C.S. Dr. Hal Meeker C.C. Dr. Raymond Scallen C.N. Dr. Thomas tt. Wilson
Dr. Roger Farber
Adm. Donald C. Hills H.R. Carol Gray
Diana Gliadon', Asst. Director C.S. Dr. Ross Anderson C.C. Dr. Peter Cermak C.N. Dr. Terrance Capistrant
Adm. ~l.R.
C.S. C.C. C.N.
Terrence J. Brenny Alice Benson Charles Beck not applicable not applicable
Adm. John F. Lannon M.R. Sue Koering C.S. Dr. Kevin H. Lawler C.C. Dr. Jose D. Canto C.N. Dr. Terrance Capistrant Pa th. Dr. Kevin Lawler (Head, Rsct,.)
Adm. Francis J. Wiesner M.R. Leah P. Beachy C.S. Dr. Sheldon Lagaard C.C. Dr. Aydin Bilgutay C.N. Dr. Richard Siebert
Fairview Hospital 2312 So. 6th St. Hpls •• HN 55454 371-6300
•..•.•..••....•••••••••.••• Adm. Stephen A. Gregg
Fairview-Southdale ••••• ~ •....•••..•••••.•••• 6401 France Ave. So. Edina, UN 55435 920-4400
Golden Valley Health Center •••••••.••••••••• 4101 Golden Valley Road Golden Valley. HN 55422 588-2771
Abbreviations: C.C. - Chief of Cardiology C. tl. - Chief of ~1edicine
M.R. Jo Nilosevic C.S. Dr. Jennings Peteler C.C. Dr. Aydin Bilgutay C.N. Dr. Richard Siebert
Adm. H.R. C.S. C.H.
Kirby J. Erickson Beverly Siemens Robert L. Sturges Joseph Tombers
Adm. Cris Stang (Exec. V.P) H.R. Jeanny Kuczek C.S. Dr. David K. !!urdock C.l.tl. Dr. F.G. Azzam C. N. Dr. John La nrow
H.R. - Uedical Records
C.I.M. - Chief of Internal Medicine C.N. - Chief of ~eurology C.S. - Chief of Staff
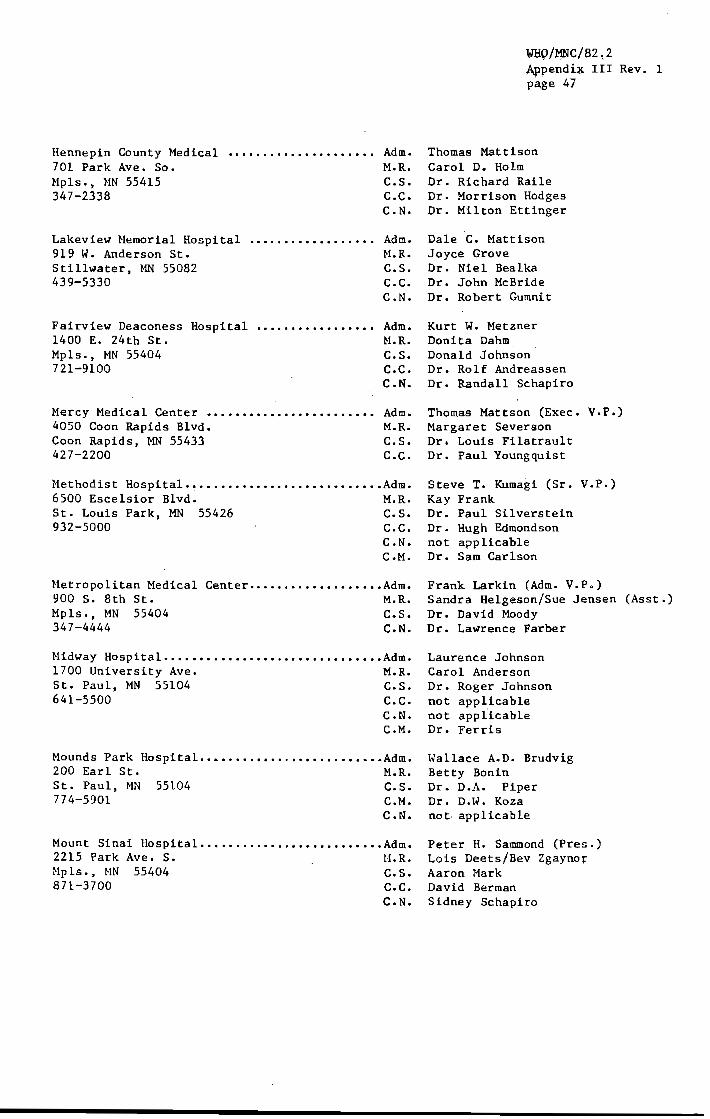
Hennepin County Medical 701 Park Ave. So. Mpls., NN 55415 347-2338
Lakeview I'lemorial Hospi tal 919 W. Anderson St. Stillwater, MN 55082 439-5330
. . . . . . . . . . . . . . . . . .
Adm. M.R. C.S. C.C. C.N.
Adm • H.R. C.S. C.C.
WHQ/:t1NC/82~2 ~ppendi~ III Rev. 1 pa,ge 47
Thomas Mattison Carol D. Holm Dr. Richard Raile Dr. Morrison Hodges Dr. Milton Ettinger
Dale e. Mattison Joyce Grove Dr. Niel Bealka Dr. John McBride
C.N. Dr. Robert Gumnit
Fairview Deaconess Hospital ••••••••••••••••• 1400 E. 24th St. Mpls., MN 55404 721-9100
Hercy Medical Center •••••••••••••••••••.•••• 4050 Coon Rapids Blvd. Coon Rapids, NN 55433 427-2200
Adm. M.R. e.s. e.c. e.N.
Adm. M.R. C.S. C.C.
l-'lethodist Hospital. ~ ...... .................... Adm. 6500 Escelsior Blvd. M.R. St. Louis Park, MN 55426 C.S. 932-5000 C.C.
C.N. C.M.
Metropolitan Medical Center .••••.••••••••••••• Adm. 900 S. 8th St. M.R. Mpls., MN 55404 C.S. 347-4444 e.N.
~lidway Hospital ••••.•••••.........••••••••..•• Adm. 1700 University Ave. M.R. St. Paul, MN 55104 C.S. 641-5500 C.C.
C.N. C.M.
Mounds Park Hospital •••..•..••••..••••••••.••• Adm. 200 Earl St. H.R. St. Paul, MN 55104 C.S. 774-5901 C.M.
C.N.
Mount Sinai Hospital ••..•.•.•......••..••••••• Adm. 2215 Park Ave. S. H.R. Mpls., MN 55404 C.S. 871-3700 e.c.
C.N.
Kurt W. Metzner Donita Dahm Donald Johnson Dr. Rolf Andreassen Dr. Randall Schapiro
Thomas Mattson (Exec. V.P.) Margaret Severson Dr. Louis Filatrault Dr. Paul Youngquist
Steve T. Kumagi (Sr. V.P.) Kay Frank Dr. Paul Silverstein Dr. Hugh Edmondson not applicable Dr. Sam Carlson
Frank Larkin (Adm, V.P.) Sandra Helgeson/Sue Jensen (Asst.) Dr. David Moody Dr. Lawrence Farber
Laurence Johnson Carol Anderson Dr. Roger Johnson not applicable not applicable Dr. Ferris
Hallace A.D. Brudvig Betty Bonin Dr. D.A. Piper Dr. D.l\,. Koza not, applicable
Peter H. Sammond (Pres.) Lois Deets/Bev Zgaynor Aaron Mark David Berman Sidney Schapiro

WHO/MNC/82.2 Appendix III Rev. 1 page 48
North Memorial Medical 3220 Lowry Ave. NO. Hpls., HN 55422 588-0618
Queen of Peace ••••••.•••.•.••••••.••••••••.• 301 Second St. S.E. New Prague, ~m 56071 758-4431
Adm. H.R. C.S. C.C. C.N.
Vance C. DeHong (Pres.) Harilyn Galazen Dr. Hilliam R. Scott Dr. John Hanior Dr. Bruce Norbac k
C. IoU. Dr. Gary Hanovich
Adm. Sister Jean Juenemann H.R. Sister Catherine Hclnnis C.S. Dr. Roger Hallgren Cons. Card.: Dr. Richard Nelson
Regina Hemorial Hospital Nininger Road
.. ' •.•••......••••••• Mm. John Junkman Natalia Schiller Dr. James Noreen not applicable not applicable
Hastings, MN 55033 437-3121
Samaritan Hospital 1515 Charles Ave. St. Paul, HN 55104 645-9111
Sanford Hemorial Hospital 913 Hain St. Farmington, 11N 55024 463-7825
St. Francis Hospital 325 W. 5th St. So. Shakopee, lIN 55379 445-2322
St. John's Hospital 403 Haria Ave. St. Paul, HN 55106 228-3600
St. Joseph's Hospital 69 tJ. Exchange St. St. Paul, }m 55102 291-3000
. . . . . . . . . . . . . . . . . . . . . . .
H.R. C.S. C.C. C.N.
Adm. M.R. C.S. C.C. C.N.
Adm. H.R. Prim.
Adm. H.R. C.S. C.C. C.N.
Erick Sande Bernadine Prusak Dr. John Benton not applicable not applicable
James Elmslie Arlene Judd Phys. Dr. Murray Hunter
Riverside Clinic
Sister Agnes Otting {Exec. D1.',', Rick Schreck Dr. Barry Bershaw Dr. Narriane Kanning Dr. Charlotte Lee
Pres. Gerald J. HcCarthy M.R. Anne Voss Tegen C.S. Dr. Harold Broman C.C Dr. Thomas J. Sharkey C.N. Dr. Richard Foreman
Adm • H.R. C.S. C.H.
Lawrence T. Suess ~larlene Johnson Dr. Richard Carley Dr. David Bartsch
St. Nary's Hospital •.•.•.••••. f' •••••••••••• Adm. Sister Nary }ladonna (Pres.) Connie Brown 2414 So. 7th St. M.R.
Hpls., MN 55454 C.S. 338-2229 C.~I.
Dr. Patrick J. Barrett John Hiddlebrook
C. N. Lou! se Town
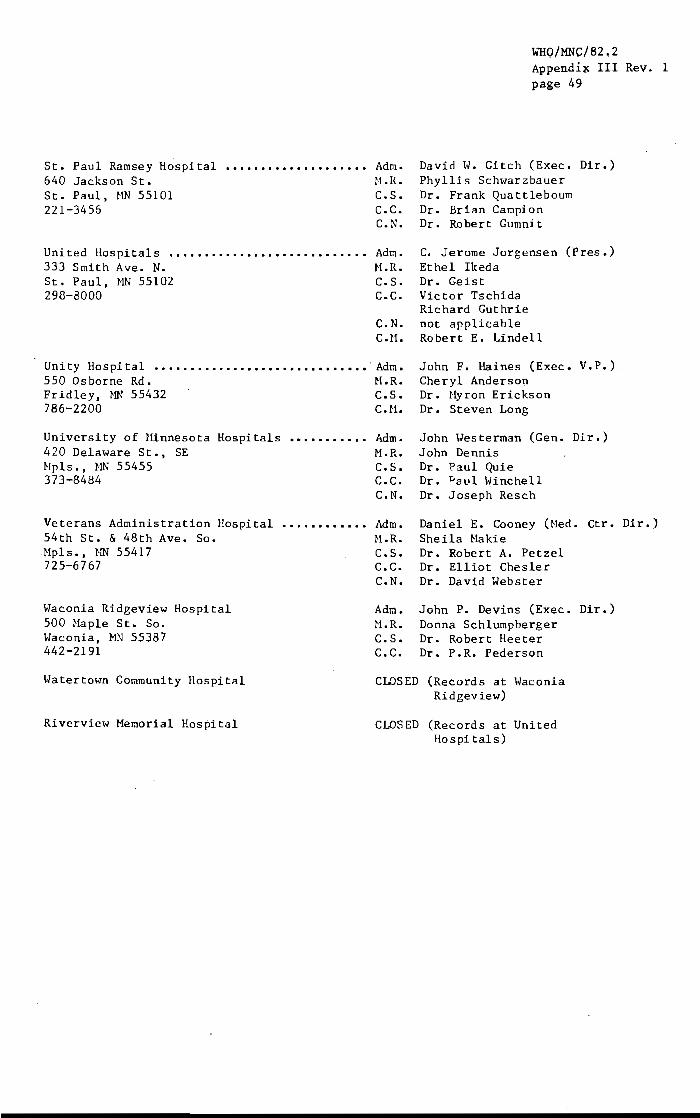
St. Paul Ramsey Hospi tal 640 Jackson St. St. Paul, tiN 55101 221-3456
United Ilospitais •••••••••••••••••••••••••••• 333 Smith Ave. N. St. Paul, }lli 55102 298-8000
Unity Hospital •••••••••••••••••••••••••••••• 550 Osborne Rd. Fridley, }lli 55432 786-2200
University of Hinnesota Hospitals ••••••••••• 420 Delaware St., SE Hpls., HN 55455 373-8484
Veterans Administration Hospital 54th St. & 48th Ave. So. Hpls., HN 55417 725-6767
Waconia Ridgeview Hospital 500 Haple St. So. Waconia, MN 55387 442-2191
Watertown Community Hospital
Riverview Hemorial Hospital
Adm. H.R. C.S. C.C. C.N.
Adm. H.R. C.S. C.C.
WHO/MNC/82.2 Appendi~ III Rev~ 1 page 49
David W. Gitch (Exec. Dir.) Phyllis Schwarzbauer Dr. Frank Quattleboum Dr. Brian Campion Dr. Robert Gumnit
C. Jerome Jorgensen (Pres.) Ethel Ikeda Dr. Geist Victor Tschida Richard Guthrie
C.N. not applicable C.H. Robert E. Lindell
Adm. H.R. C.S. C.tt.
Adm. M.R. C.S. C.C. C.N.
Adm. H.R. C.S. C.C.
John F. Haines (Exec. Cheryl Anderson Dr. Hyron Erickson Dr. Steven Long
V.P.)
John Uesterman (Gen. Dir.) John Dennis Dr. l'aul Quie Dr. Pa.ul Winchell Dr. Joseph Resch
Daniel E. Cooney (Ned. Ctr. Dir.) Sheila Hakie Dr. Robert A. Petzel Dr. Elliot Chesler
C.N. Dr. David Webster
Adm. John P. Devins (Exec. Dir. ) H.R. Donna Schlumpberger C.S. Dr. Robert Heeter C.C. Dr. P.R. Pederson
CLOSED (Records at ivaconia Ridgeview)
CLOSED (Records at United Hospi tals)

WHO/MNC/82.2 Appendix III Rev. 1
page 50
ZIP CODES FOR MINNESOTA HEART SURVEY
Minnesota
Bloomington.
Roseville, Haplewood. North St. Paul ••••
Mankato • • • North Manka to
Moorhead
Winona •
North Dakota
Fargo
South Dakota
Sioux Falls
55420 55431 55435 55437
55109 55113 55117 55119
.56001
• 56560
55987
58102 58103
.57102 57103 57104 57105 57106 57107

Seven County Area:
Abbott-Northwestern Bethesda Lutheran Fairview Deaconess Fairview Downtown Fairview Southdale Hennepin County Medjcal Center Lakeview Memorial Mercy Medical Center Methodist Metropolitan Medical Center Midway Mount Sinai North Memorial Medical Center Samaritan St. Francis
St. John's St. Joseph's St. Mary's St. Paul-Ramsey United University of Minnesota Veterans Administration
WHO/MNC/82.2 Appendix III Rev. 1 page 51
HOSPITAL CODES 1980
0242
2128 0223 0200 0201 0211 0689 0009 0230 0231 0504 0237 0240 0519 0609
0523 0524 0528 0527 0525 0273 0233
Out-of-Area:
Minnesota
Mankato (Irnrnanuel-St. Joseph's) Winona (Community Memorial) Moorhead (St. Ansgar's)
North Dakota (Fargo)
Dakota St~ John's St. Luke's
Veterans Administration
South Dakota (Sioux Falls)
McKennan Sioux Valley Veterans Administration
0033 0701 0074
3001* 3002" 300.3*
3004 1
4001" 4002;-400:<'-
NOTE~ Codes are from Licensed and Certified Health Care Facilities, Minnesota Department of Health, 1978, except for starred codes (*), which we:ce assigned by LPH/MHHP staff.
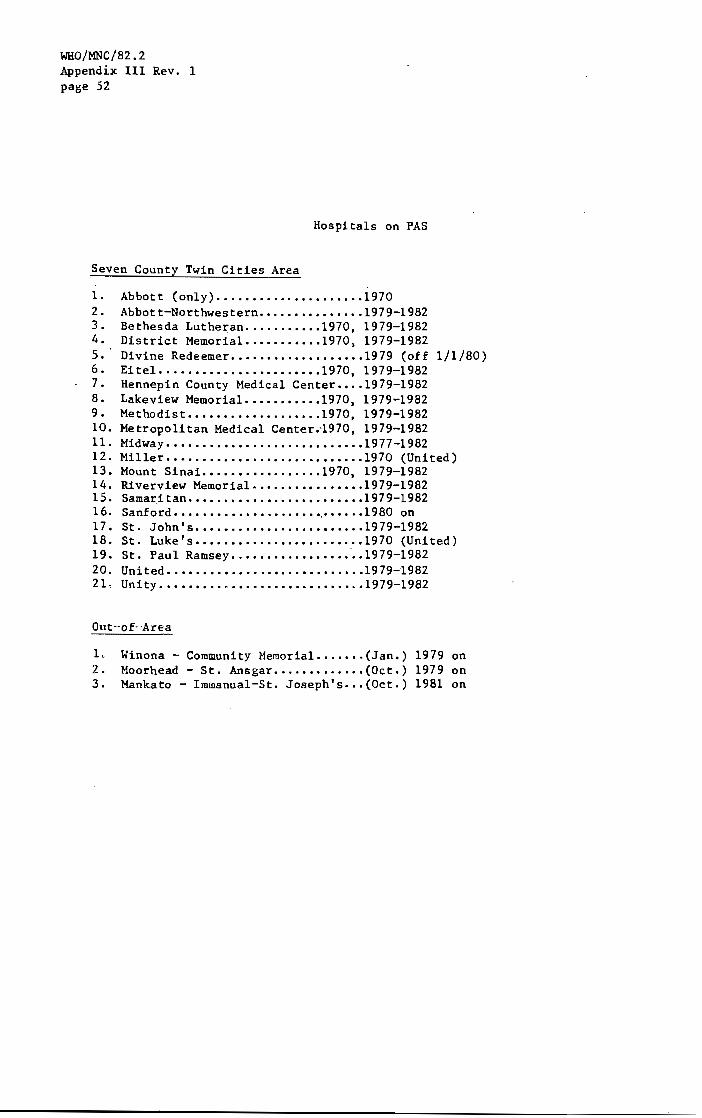
WHO/MNC/82.2 Appendix III Rev. 1 page 52
Seven County Twin Cities Area
Hospitals on PAS
1. Abbott (only) ••••••••••••••••••••• 1970 2. Abbott-Northwestern .•••••••••••••• 1979-1982 3. Bethesda Lutheran •••••••.••• 1970. 1979-1982 4. District Memoria1 ••••••••••• 1970. 1979-1982 5. Divine Redeemer ••••••••••••••••••• 1979 (off 1/1/80) 6. Eitel ••••••••••••••••••••••• 1970. 1979-1982 7. Hennepin County Medical Center •••• 1979-1982 8. Lakeview Memorial ••••••••••• 1970. 1979-1982 9. Methodist ••••••••••••••••••• 1970. 1979-1982 10. Metropolitan Medical Center.'1970, 1979-1982 11. Midway •••••••••••••••••••••••••••• 1977-1982 12. Miller •••••••••••••••••••••••••••• 1970 (United) 13. Mount Sinai •••••••••••.••••• 1970. 1979-1982 14. Riverview Memoria1 •••••••••••••••• 1979-1982 15. Samaritan ••••••••••••••••••••••••• 1979-1982 16. Sanford •••••••••••••••••••••.•••••• 1980 on 17. St. John's •••••••••••••••••••••••• 1979-1982 18. St. Luke's •••••••••••••••••••••••• 1970 (United) 19. St. Paul Ramsey ••••••.••.••••••••• 1979-1982 20. United •.•••••••••••••••••••••••••• 1979-1982 210 Unity •••••••••••••••••••••••••.••• 1979-1982
Out-of' A"cea
1. Winona - Community Memorial ••••••• (Jan.) 1979 on 2. Moorhead - St. Ansgar ••••••••••••• (Oct.) 1979 on 3. Mankato - I~nanual-St. Joseph's •.• (Oct.) 1981 on
DISCHARGE DIAGNOSIS INDICES
MHHP Hospitals on PAS (1980, 1981, 1982):
WHO/MNC/82~2 Appendi~ III Rev, 1 page 53
In 1980 HMMP contracted with CPHA in Ann Arbor, Michigan, to purchace a tape of discharge diagnosis index information covering the time period January 1, 1980 through December 31, 1980 and including the hospitals listed below (1-11). A copy of the contract and the tapes are on file in the LPH data center in Unit A. It was necessary to have each hospital administrator sign a contract as well. These signed contracts are on file in Room 87, Stadium Gate 20.
l. Abbott-Northwestern
2. Bethesda Lutheran
3. Hennepin County Medical Center
4. Lakeview }olemorial
5. Methodist
6. Metropolitan Medical Center
7. Mount Sinai
8. Samaritan
9. St. John's
10. St. Paul Ramsey
11. United
12. Mankato (On PAS in October 1981)
13. Moorhead (Not on MMMP PAS Tape 1980)
14. tUnona ( " ")

(OOll " I (0I!!l r.:-: I «(>011 HA..Ml . NIIMI SIAn Sl ... " (tl'l (ny (OUU,O <In (0",. .. •
... u\ hEr COOli I . ""'" I KlI./lA! ________________ ~~Il~.~I\_~~C~I"~~----------------Ll~I~.I~I~~~~~---------------J~~.I-~_4~~,---------------J~~+-~-t
1l1NNl:SOTA
~ I~ Mt T RiIIll MilTON
nlG STONl DtUl EARlII 1j!\I;WII .
JCJ~~fJ:l 'ASS tHlrPfwA CIIISAr.O ClllY Cl f Mil A T (1\
ClinK CUT HlNWono C!',Ow \IING
~~IJ)lJ 111)(,1:
OflUGLIlS ~I\I\ I Mill T , Ill/III O!: FRI: I:lIOI'\N r.LlUnf~lf
&f~~ir lUI IHJUS TON IIUnOIlP 0 I SIIIH 1
ITASCA JIlClcsnN KArlftlll't K"~IIIYOIII 1(J TTS{JN
KnutlllCHING lllC QUI PAAU, LAKE LIII(f, Of TH£ IIOOOS LC SUEUIt
27 HINNESOTA
~. 1.1 NCOlN ~ LYCJt-0115 /'.C LEOD orll MAli I\C.-:eN OO? MARSHALL
011 ~AI\T11\ .' 013 Mr.r:Kr:/l
lm0l!o MIlLr: LACS Cll IIllRnlSCN ~ ,IItIWI:Il
02 1 HUIlilll Y 023 NICCLLt::r
, . OZ 5 11011 U: S on tlOf\I',I\N O~ 'J OLliS TF.D
031 CTTEn TAIL on r~NNlI\GTON O:i;i PINE till PIP[SlCNt: [On PULK
0'01 POI'~_ O'.)~' 0"5 ~t:l) lllJ(e 0't1 nf:Il\iOCn O~? I<ENVlllt;
~Pt.Cf: ,!a.OI i;OC K O!j~; t:CSfAU 0; 7 :;r lOUtS 059 ~oTfJ
or.1 StU! RIJt:RNE Ob1l SIIHGY o(,!> 5HAIlII:S 0(.7 SlECf.E O{'9 SHVE/lS
011 SIll F1' 07:1 tUOD 015 1I\ftV!:IISE 017 liAOJlSIIA 01? wADENA
t.\~()\Q 037· 'lA;C~~'i)(±t 'v Ih"3 ~{\.~C~) o',q <;)Catr 0 /39
~'~l~ r\~ I)\~\'V 053 I' \ ~ f\C\ n v;;\l.l:/\- 1.;1 ~ I '
(~'flOk(fq 003
'.) : , I'
21 ~INNESOTA
onl 'IllS (tA Oil'} • ~1SHIN(;Taql. no!> 'n' TONIlAtI OU" WILKIN OU9 :OrlONA
091 If'II CHr O'}) HllOi! /I(OleINE 095'
. 0'17 O'J9
101 10l 10!> 101 10'1
III II)
'" II:; 111 119
~ 12 " III 12?
1.11 IH l)~ L 'IJ
~ HI I'd 1'. ~. 11,' lIt'}
1'>1 1 s·" 155 lnl 159
Uf,
,2 III NN[;SOlA 1.
Hoi Mill 0010 m J\li~HS 0020 ADOLPH OOlf,
1l.1 IIURIAN OOJO II> ? IIf lON oo~o
171 All CllAII~CHING 00',) 113 ~I 1KII'I oo:.()
IIKeLeY /"' OO(,Q • AUlANY 0010
AlllEIITA OOUO
IIlOGRT HA OO?O Alnt:ATVllU 0100 IIlO~N 0110 A L1H1 I Gil 01.10 ALCXMW'IIA (1)0
AlIIH UIID OIH AU'IIA OHO ALTUr.A \ 01)0 AL VMIl\OO 0160 AlVl/oon
, 0161
ARI,OY 0110 MH;(1fr/\ 01 n IIIJr.US 011e.. IINIII\NOIlLE o H\O
AIm"'" , 01?0
IIPI'LHCI'I 0100 III'Pll: YALLl:.Y • OlOl Meo OlIU /lIIDEN IlIlL S • Oll) IIRcnE 0210
, 111\ LI f\,'; TOI'\ 0230
" ASIIIIY Ol~O
115M1V 0250 II lI,lI TEk ono IIUOUUON 0210
IIURORA 02uo AUSTIN 0190 AveCA 0)00 AVON OliO bAOOI TT 0)15
,"
, -~ -
-. 't;I>~ '---- ' \l)'t;I (I'\.,.,,*,- , OQ't;I 0 -: 11> 11>_
V1g.~ +:- r" n
101 ~-0", CO
III H N H .
10\ H N
In ~ (!l
0/1 <: . 001 OH I-'
l\~ 1\1
OH 111 O~ 1 LH 0\1
Ol~ au 1b1 no, 061,
oil 1)1 119 111 001
IH on Q~l III OU1
Hl UH 1l~ 06 OOS
IH 0'11 101 H5 lH

lUAU
"I NNC SOU
lAr.KUS ) AOr.el! ~At.l n .~u~
UlATON
Gt,ll c.LUn Hf.ICHVllLE UA"",UII OAA~HT U~'1T
SAffLE LAKE u.uCfln AXHR d~YI'ORT u [A·~SLEY
D q
" .\
d h a D 8
U J U h ft
(lY(k MY (Aym tRHK curt. fJOU Ll(;~AOt:
flU PLIlINE HlFtllESHR rltcCHfSHR El L HI GHAII II IM/ll
UYlhl r~ II\J 1 fH/I l~l OICT fll~\lI1
ftllllil (lhEl IcrlOW Ie. fllllS /CFORK
IC tllKf 11I(;!IA'\ L~KE liCl!uAL f IHI~IOOO ItO ISLANe
I coou ~lAn ellT
2.1
ono 0330 0140 03'.5 0350
0352 0)60 OllO 0300 0390
0400 ()I. 10 0420 0430 0""0
0',',9 O'.~O 0'.60 OHO 0',00
0490 0498 0490 0500 0510
0520 OHO 0~40 05',2 1>550
0560 o~no
0500 0590 0(,00
06'10 06Z0
• 0627 0630 0640
I (con ItAMI I HAle :0,"'"'''' CITT
KIN/oII:$OTA 2.1
021 UISCAY 0650 13> ill WIIBI I< O('b:! 02.'1 :II X;\y 0662. 027 I)LI\(/(O\:CK : 0610 063 !lLAINE ! 0(,11
061 OLhlNI: 0611 021 OLOIIKESl , 0612 017 (}LCCIlIIiGTCN 0675 051 OLOOMlt>G PRARIE' 06(10 all BLUF. UR1H 0690
111 DLUl'nCN 0700 071 [lOCK 0110 OJ5 IJONr.ARDS 0715 163 UORUP 0719 011 (lOVEY 0120
"
075 ::IOw5TIlI t-;G j
• orH 133 OOWLUS 0130 1',1 .10YO 01',' . 067 lIOY RIVER 0'150 1'.5 I>RAIIAH CHi)
139 tlRATN(RO 0770 0'.9 ')RA ,,(Ii • iJ77" 151 :1P,AI'o'OCN 0100 013 OPECKEI\RIDGE 019() 119 IlIIBSTER 0000
127 flRI CEL YN 0010 007 :IRI !'IStt-; • 0013 021 110lIlT 01114 057 IIROOKlYN CHTEP. 01120 1:> 1 I\ROOKl YN PIIRK ,. 01121
153 .IROOK PAIlK 0830 (103 :lIlOCKS 0030 105 [JkO[KS1ON 00',0 071 a~(j('TEN OR5) 061 llROhERVJ US 00(.0
1"1 llnO\(N~DALE OU70 0)) ,IROkNS VALLEY 0000 071 :lRCIIN 5VIl LE 0090 163 llROIINTGN 0900 lZ9 {\RU~O ,0910
I coon NAAII I COCiC$ NAI,II IlAII CIIY (OUfHOW tOV·tl" UAll (IN (<1\1"'"
ilINtlt:SOTA 2 KINtlESOTA 27
~6S BUCK KilN 091.0 091 CLAM eI lY 1230 023 131 ~UHIILO, 0930 ln CLAREIiCNT 1240 0)9 V.l ;IUFFALO LAKE 09'.0 129 CLARISSA 1250 153 001 OUItL 0950 131 CLARKF I flO lZ60 113 DO) ;lUR/IS VIllE 0956 031 CLARKS GROVE U10 047
123 IlUnTnUIi 091.0 153 CLEAllllROGK 1280 029 067 OUTTERFIeLO 0910 165 CLEAR ur.e U?O 1',1 p~3 ,WRON 0900 109 CL(;M\WATEI\ 1300 111 1',7 ALEDONIA 0990 055 CLEMENTS 1310 127 ~Hl •• \LL AwAY 1000 005 CLEVELAND 1320 079
III ALUMET 1010 041 CLIMAX 1330 119 )?~ :flMllrtiOGE 10Z0 OS'} (ll NTON 1l't0 011 019 :AHPDtu' 1030 167 C.UTIlERAll 1350 111 101 ~AHP RIPLEY U S ARHY • 1035 097 ClCNTARF 1360 151 061 'ANUY 1040 173 CLCOUET 1370 0.7
0(,1 : MlNON FAllS 1050 01.9 CODOEN 1300 01$ ,,'H -/lllrON 1060 O'.~ (OI1A SSET 13'.10 061 P13 :ANYtlN 1065 137 ((KATO 1'.00 171 121 • AI\L05 1010 01,1 COlO 5PRINC 11, 10 l',5 )!i9 :Mll TON 10110 011 COLERAIIiE 1~20 001
())S IIRVER 1090 01? COllEGEVILLE 1428 HS 025 .A55 LAKE. 1100 Oll COLOGNE 1',)0 019, 0',1 'ASTLE ROCK 110) on COLUI<O I A IITS 1'.1,0 003 167 :EOAR 1100 003 CO}lFRE T 1/.50 015 105 ~r:o"ll CROVE • 11 0') on COHFflEY 1450 033
H) C(OAR MILLS 1110 093 CC/ISTOCI( 1'>60 027 131 K;(NT Ell (I TY 1120 025 CONGER . 1"70 047 137 HHERVlllE 1130 003 COCK 14no 137 053 CE'flON 11',0 091 COOLE Y 14"0 061, )53 CHAMPLIN 11S0 OS3 C.OUN RAPIDS 1',92 003
115 CHANDlER 1160 101 CORc.onAN 14?6 053 : 125 WII/IIIIA:>SEN 1170 019 CORRELL 1500 Oil 137 CliIlSKA 11110 019 COSHOS 1510 093 1'.5 CIlAr fl flO 11'}0 01'.5 COrTAGE CROVE 1517 163 l!JJ "II/If r IltO 1190 109 conON 1518 1)7
J9" CIII CK/IHAW BeliCH 1193 021 COrTONI/Oeo 1520 003 15S ClllSAUl CITY 1200 025 COURTlIIND 1530 103 )5(; CHlSIlULIi 1210 137 eflllNE LAICE 1$)5 137 OUS CNOK to 1220 II, <J CRCMItELl !Sit 0 017 11S C1RCLE PINES 1225 003 CROOKSTOk 1550 119

IIAItIJ
IIINHI:SOU
'RIIShY UflHLAKE CIIHTf.L 'ilL Vf.R , I)ltk IE
CUSHING , C o o
\'YIJNA
o o o o n
YIUlS IIKCTA AL'lO
AL rr .... AtIOnE A1!1If.1l S HflJl'-All 11111
OAS~H o o o o
o o o Q
J
o o I)
cO
/)
n u 1\ o
o Q
1.1 o /)
AI/SCN AYH'IlI AY Tf,~ tEl'I'''VrN
HI< necK Hi! RIVER HfI\.(I('IO ~ t;~AfF
ELj\NO
EL AVAN nH rLin ClllolOOD [NIIAJI
f~~IS(l~ lMllSON EIlT H,.Olf LAKES EXHR
IL "WUII 1..:01.1": ,un III ONALOSON U~INHL Y UMAN
I coon I HAil (IN (0.",,,,,,,,
;:1
15«.0 on 151.5 on 1 ~10 O~D 1~15 1)1 15110 101
1 !ill 5 097 1 !>90 0)5 luOO III 160!i 16 'l 1/.06 059
lltlO 111 1620 12'1 11>30 151 1640 1t,5 11,:;0 O'}l
1660 0'.1,1 16 '10 07) H.1l0 0:0 lhllO lH 1690 OS)
1100 111 1110 0(,1 Ina 015 lHO 1~1 11'.0 17.1
ll!iO 0',) 1755 033 17'.0 ll1 1110 163 111)0 115
1790 Ot,9 1190 1)1 11100 111 IntO 005 lnzo O??
1'I~0 027 10',0 03? 10S0 069 I1l60 l'.? 1870 1(,1
I coo'\ HAMI I u.n (In ""."1'\
MI/UiLSOTA 21
1l01\$':T 101S OS'/ IUVUl 1/100 10')
,1OVIl,\Y 160;0 10 I 1H1f. 5I1A'H I (J'/!i 1';') vUL UTtI 1900 1)7
IlUlICNT 1910 iSS IHJp.;CA S 1'120 131 OUN!lr.I: 1')0 10!; liUNh~ L L 1 'l',O 0'11 SAGAU 1945 on
f;AGLF. DeNa 1?50 153 cAGlf lAKE I?M) Oll "AS T GflANO FORKS lno 11 I) rAST GI!LL L Me 1'/00 () 21 liAS T De TIItL 1961 00)
1'1\ Sl LAKE 19UJ 001 LASlON 1 ?'}O OH U;II(, lOOO 113 clltl;, PItAIRlE looa 053 cOtN VollUY ,010 0')3
"rJC N VALLEY 2010 11.5 lIlGt:l1TCN I.O~O 111 WINA lOlO OH t:F1'1F. ;;0'.0 Old eGAN • 20'." 037
EITlfN 1.0S0 OS5 aDA ~060 It.·] HODII LAKE lO'11l O!)l nGIN ;>OUO 151 H IlADElli 20')0 111
HIIO lIO) 11') ELK RIVER ll1l) vt! F.LK1UN lll!J Q 'J? lll(NGAlE 11 J(I 1',1 ~LlS}/OnTH 21'.0 I"!>
€LII(\,UE l150 on HIlC.Rc'
111
(') 0'13
~LI10SA • !170 l't5 flY 21 cI:J lJ7 H YSIAN 2190 01')
I coon Nil/,ll I COOlS IIAMI r 11AI'{ r \,." Ctrr CO·"Nfl" (IN (.).;;.011
I1INHfSOTA 2 HI NIII, SOlA 27
U1UARtHlSS 21') 9 131 F r.UNTr.1 Ii 2',')0 045
(;IULY ll,),) OJ:' F()XIIOI1E 2500 I (,1
ttl/IUNS 220,) 0', '/ fRANKLIN 252u 12'/
(llilARD l210 fil I'IlAIiI<!.lN Z jZ2 1J1
,,!lSK INS 2220 11'1 HlA:;a;R 2530 1Jl
t:SKO 2225 011 fRAlH 25',0 OOS ~S$IG .. 222'1 015 rRHIlO~N lS',5 0;1
l.:.Ill 10 2120 ll? fllEEI'URT ~~~O 145
"'UN 2230 015 I'RIDLEY Z~60 oal (;vM;SVILlE 2240 0',1 fRG:HI;~A' 2~b5 04?
I
f;VFl ETil 2250 131 FRGST z~10 0'.)
l:x(.tLS Wit 2260 0:; J FULOA 2~UO 101
nOTA 2210 10') fUNKLEY 2590 007 FA l[,fflJ( 2200 12" GARDEN C.UY 25911 013 ~ AI RII.W I:N • Z2U:; 1', S GfII\f'lHO 2600 OH
Fj\II-./WIlIT 22'10 0')1 GAI\III SCN 21>10 035
I' AL CIIIlI liE' GIlTS 2)00 10 GfIIlV 1 N l6ltl 00)
FtIIll OAUL T 2)10 1.11 GAIlY 26)0 101
F "'\~II N t: TUt-! 020 Oj7 GAYLeR-O 2(1'10 I'. ) FMlllaL 2)JO 121 GClI lAKE 2<0'42 III
HnEI~,\L UM' 2)'.0 O;~ 1 GENf:VA 2/t~0 0'.1
Fa TON l)!JO OJ! I GENOLA 2/,<00 on F[I\I;US flll.LS ;!:IM) 111 (,E(IIG!! It'-N 2610 021
F~'l Till, 2.H0 119 G'iHN 201c) 1)1
FIFTY LAKU • lJl'. O)!> GHENT 26/J0 oa)
r: INLAND Z:nS 015 Gl0BO" 21.1)0 143 FINLAYSON ZJOO 11> GILDEn'!' ;noo 131
rHIlt;ft 2390 11') GillIAN 2701 009
fUNSlllJRG 1',00 091 r.lI:NCU~ 2710 00; • nUll, • 7.'00$ 101 t;Ll:NVILLE .2120 O'tl
HllfJOlIlJll1) 1'.10 u1 GlUllfO(.O 2130 121
HIiltl:NC.1.. 2'.20 003 GLYNllUN Z 1'.0 027
r-PLI:Y 2'dO 00'] I;UlOHI VlIlL€Y lno 05J
I'lW.\IlA 2,,',0 0 /.1 I;ONVICIt 2160 029
f.OI1IlES Ziti,'. 1.11 GOl:OllU~ I.HO v~9
!'IlI1ES T ;.4'( e .. 2'.!JO 16:1 GOf:OJlIOGf 2100 III
HIIlCSoWN 2.',(,0 ()*)!.J r.UtO lI1UWI:R 2.7')0 au !'OIIT 11II'LlY li,/a 03:' t;O()!Jvlt:1I 2UOO 169
HJIIT ~N~Ll IlliG 2't °15 0~3 r.unOON 2001 0·t,7
F(,~STUlll 2',00 11? GRAtHUN • 2801 017

- H.UIJ
IIHlNESOTA
r.u.(£VILLE CIIM:A{IA GRA',O IIAIIAJ$ ,.ANO II fA COW r,~MIU POP. TAC £
CRANO RAPIDS It~ AllOY C~ANITE FALLS CtlANIH FALLS CKAIICF.R
c KASSTOH CHI (IIUUSH CRHltf IflO GM((N ISLE /;RU/lIlALO
tRHNIIOOO C G HY [AGLE Wl,lf CITY
'"Y(;U " Ii 'UlLY
r; UTItRI £ 1.\r.1( (It SACK IADLEY IALll(K IHIU
IAL STAO /MIUURG 1;,IIfL IMHlllNO IAIII'TON
/~NCUCK IM,try FALLS I
It I
1/
.'NOV(R 'ANIII,I(it \N;I(A
II .\ltlllNC IAPllillCK AU ~lJNY II
I II IAllp 1 S ... llANO
I COOlS ,
r "."~ ••• ' 21
011 on
. U oH 2O't0 .o·}') 2UU OH
2850 Ob1 7U% 0!i'J 2U(,0 023 20(,0 173
• 21)65 ()I,5
21110 0(,5 2BIl0 115 2006 OSJ "U90 HJ 2'100 I~ ~
2'.lM 053 2910 153 2no 09) 2'130 089 :l9~0 119
,')47 051 2950 OZl 2960 101 :/ no 009 l'lOO 0(,')
2990 107 JOOO 019 '3003 053 3~10 In l020 037
lO)O 14'1 )040 17) 11150 05) 1050 1ll ]060 01 :;
)070 091 3000 133 3090 (}It!;
lIOU 02 S 3110 041
I coou N.UU
I "'U C1I.
iii NNUiOTA 27
!If. sru:es H2O "A 511 f,.t;S .. 'H2O IIA TI'I HU II \0 IIAIIICK H.l~
IIAWll Y JI '.0
IIAYF! flD , 'n ~o i1l\ YI .. \ItD .H60 II~HL "UN J170 IIt.CTOR Jlu(J IIClllElUERG )190
Il(NOCRSON nov tll'NUll J (K S )710 II (till II U /" ')l20 IlfNtdl\G ,'12 )U
II0illiurE Jl'.O
II(RMN )250 11((10/1 LAICE nw IIr \.llT )210 IUDUINe 3280 HILL ClTY 3:190
IlIlUlhII ))00 HillS ..IHO lUll TOP J) 1't III tlCKLEY '))20 IIINlS ))1',
HI TTEIlDAl )330 tlOFFHhtl HIt<)
HUKAtI 33!i0 IWL 0 II\CFCPO 3)(,0
'WlLA"O 3310
IIOLLANDALE :))00 IIOLlC.AY ))90 'IOL T 3',00 IIOPI' 3',01 !lOrY-INS HI0
IIQUSTCN , 3',20 lIOVlA"O J',2! lIU~I\(tO LAKE )',30 IlIl'Yl LAKES )'13? IlU~IIARD • 3'.)5
I coarl I coon HAMI H.v.II
~ JlAU (IIr (0"''''11 ., ... 11 (Wi (ovurt
MINNeSOTA 2' HINN~SOlA 2
tJJ1 HUGO 3','.0 1<.3 KENYUN nbO 0~9 H., flU/WOLtH 3'.50 0t.9 K(IlKIIUYEN J770 lSI 117 IIUNILI Y l~!i~ 0'.) K(HIHCK HUO 115 Obi IIIHC,"r;~o.'1 )4<.0 OilS Kf.TTLE I\ly"R .lI?O 017 all II~. EN lHO III Kll:ST(1l 3UOO 043
o ,I'} IIwrrCNOENce l<Hl 053 KILKENNY lOla 019 Old I;WUS • l'<1', 011 KI H()ALL 31120 1',5 113 l:>IeER • lH5 0(,1 KIIIORAE 3030 105 12'1- INrtltNATJONAL FALLS 3'000 oli KWllc Y 31)',0 131 01'1 INY[II GROYE HE/GllrS Jlt90 0)1 KLOSSNER 4 33'tZ 103
1 ',3 1111'1" 3S00 101 KNIFE RI\'ER lOH 015 UBI J I!IIN 3500 131 LA CRE SCENT 3650 055 10/ I"ONTON l5'20 0)5 LAFAYUrE )660 103 III ISAUHLA 3~2S OJ~ LAI(£ OCN10N JU'10 oui 115 I'.MIT I 3,530 O~~ LAKE 8t10l\SON 3unu 0<'9
O~I I~LAIlD VJeIl 3550 011 LAKE Cl TV 3890 157 0(,] ISU: l%O O? S LAKE cn Y5TAL HOD 013 153 IYANlIlIE 3570 001 LAKE Ellie 3910 163 131 JACKSCII 3500 063 LAKEFIfLU J'lLO 063 001 JACOOSUN • 35'03 001 LAJ(E G EOPGE 3935 051
091 JANESVILLe 3590 161 LAKE HENRY 3'HO 1"5 l.n JASPER 1600 111 LAKE Illl)fRT 3945 035 00) JASPeR li-OO 133 LAKE I TA.sCA 3946 029 liS HfFms J(,10 DB LAKElANO 391,9 Ib3 00'1 J [NK INS l620 O)~ LAKELAND S/lOR:.:s :>950 I<'l
027 JCIINSON 3630 011 LAKE lIll/AN 3960 061 051 Jult!)AN 36~0 139 LAKE PARK 3970 005 055 KM-IOIYOHI 3(,50 061 LAKE ST CROIX !lEACH ~ 391(, 163 1 ',5 1(,\N~RANl I .. 36!it:. UJ LAK~VILLE )9'JO 031 111 KARLSTArJ 36bO 06') LAKE WILSON "000 101
01,7 KAsuTA 3670 079 lAl-lnrR lOti ~010 1:/7 1';1 K:'SSON 3600 039 LA/mILLE '.015 149 ;
(JU'l KHWATlN 3690 Obi LAIiCASHR 1.0 20 06') l',7 KfUllIl'R 3700 00'1 LANDFAll "025 Ib3 OS) Kr.llOG(; J710 15'/ LAN~ Silune "OJO 045
055 KF.LL Y LAKE 3115 131 LANS' NG 4035 0'19 011 K t:NN 1:0'( 3120 069 LAPOR re 4040 057 1"11 KCNN€TIi 3730 133 LA PRAIRIE 4050 01.01 1)'1 KtNSINGTO'" 31',0 U',l LA SALLE ',abO 11.:; OS1 KlOtH :USa 161 LASTRUP "070 Q'I1

HAM.
IIINNESOTA
LlllOlR.MLE LHI' LIIKE L E ClNHR L ~Nc.nY L(ONARU
l(ON IOA5 L EOtA LE IIOY LESHR PRAII\IE LE SU(UI\
l L L L L
L L l l l
L L l L L
L L L L L
L l L l l
l L II 11 11
(1IISTOH (III S'" ILL E ex II,G TON IlYflAL£ IIIOSTIIOM
I~:O LAKES IS"OHE ITtmtrlU I THE (IIIIAOA IYTU f·\lLS
I TTLl fllf\K ItTlt IIMIAIS IlIHN ONUUN OIIG OEAtH
OllG tIIK E ONG PRA IR IE ()I,GV ILL E ON S(lAl E OP.ETTO
rUISOURC (,~PY
Ue,AlI UT SCN UV~I\IIE
YlE YIID CGP.IITII CGP.CGOR (INTOSH
I f('f)l~ --, I '!AIl (flY 10"'"
2"1
',oeo lZ) ',ono III ~O?O 07') ',loa 11? ',110 02 ?
4120 IH 4123 10~ 4130 0')9 ',1',0 oo~ ., 4150 0"19
1,160 169 ',1'/0 1C,~
'1115 003 ',117 031 '.1 no 025
410'. 00) " I?D 10 :J ~100 U?J ',205 123 ',lIO O? 1
',220 011
• ',222 07~ ',225 011 ',Z26 oJ', 7 ',2)0 121
',l',O 053 ',2 ~o 153 ',7.60 021 ',210 131 ',200 lJ53
',2?0 07) 'dOO 12L ',HO 121 ',31~ 031 '0320 133
4330 0')9 4331 003 1.]'tO 001 10350 001 '0360 119
I conn IIAM. --. r ".1\ CHY ('""''''
Mll\'NESOrA 21
"CI( I NLF.Y '.310 1H M~O~L ',)00 v',5 "AOELIA ',390 165 .~~O I seN ''',a" (J73
.'1 A 0 I seN LAKE ',',10 01)
MAG Ilau A '142:) 1.13 1'/111 ~(/\EN ',',30 001 Mil TOI'IF.OI 'l't',:1 163 11M110)'A 1,'.',1 all IMKINEN It/.I,~ 137
11/1NCIIFST£A " ',',50 0',7 MAtHlIl T T 1114 O[IICII ~',70 0.'\ ~j IMI\KIITO ',',DO Oil :-1MIlOPVlll( II/IJ!) OJ? ,~APlE GI\OVE ,,',?!i 053
11APlE LAKE 4500 111 IlAPlr: PllIlN ',510 O!'jJ 'MPlUCN t,5Z0 OIJ IIAP LE VIE W ',~30 099 MIIP L £)'COO 45)6 IZ)
"ARVl E ',Si,O 0('1 l1ARr.~LL 1.~/t~ 0('1 MAli I E TTII ',550 07) MIIIIINE ON Sf CliO IX ',561 163 IIARKVILlE _ 1,566 115
lIAR SIIHl ',5111 003 MX • ',~""5 01.1 11o\YER ',500 01? ~IIYI\III\D '.590 02) /lIIHPPA ',600 1:.1
HEIlOOkL~NDS 'oC,10 1)1 I1UlfUHD 'tI,2l1 l'tI IoI[OICII\'E LAXE ',(,)0 O'l3 ME I R!: GROVE ',(,'.0 1', 'j MelROSE 1.6~O I"'~
IoIEII~HCA ~I,(,O \59 II[NOOTA 4610 PJ7 1If:IWOTA IIElGHTS ',61} OH liE II H'R ',6UO 11? I\~R 10(;N ',605 1101
~r-COO" L (0011
NAMI NNAI 1u.'1 (I'T f.!o',·,h r 1,.tI em l('v"rr
/lINN~SOTA Z' IIINNESUIA n
~UIIII FlnU 1,606 OJ!> linSON 5050 0',1
:11 OUL E Ill ... Ell 410':10 OU,) ~iF.HSTII~ND 5060 III
HI[SVllLE ',f,?3 0)1 "" T r l/IKc 506'. 131
,~ ILACA 1,70U 095 NE VI S 5010 on
MILAN 4110 023 141:11 AUOUPN 5000 1't3
MILLERVILLE '.720 041 NEil DR IGlilON 5070 123
~\Ill V III E It130 151 NE"FCLnH 5100 001/
11/ L ROY ',7'.0 121 NE" G~n/l~NY SilO 019
lilL T aNA ','/50 041 11(1/ !tUPE 5113 053
II I NNE APULI 5 4160 O~) r.E 1/ lUI\OCN ~ll0 067
:ilNNE I SKA 4710 15'/ NEW I\IIIU(~ r ~ DO 139 1\lI/NUIT A ',lOll 001 NOl /lUNI til ~ I',U 1'05
:11 NNl SUT II CITY 4190 169 NE kPOr. T 5l~0 163
II INN[ SOT II LAKE ',uou 01) liE 1/ PIIAGUE ~I('O 01')
11Itlrl(SOTIl lME ',000 0',) N(II 1',IAt;U[ 5160 I J'J
'1INNCTONKA ~O10 0'3 /lEW II I lliLIIND 51'(0 161 II INllll IJrlKIl ,O(IICII ',0 1:1 05) Nl k TillER !:IluO Oll '1ILPIIII ',OlO 071 IlEk Ul/I !> 1')0 01' :-1UNTlvIOE~ 1,040 023 NE" YU,lK HilLS ~200 III ,\UNTGU:-1ERY '1050 0,(') NltUllH ~Z10 10J
'10NT ICU,LO ',~I,O I'll NIWUI. S • H15 001
,'!UNT 11iiS (; ',n 10 I'll III tLS ... IllE !i220 II?
'\UUIIIIt;AO ~noo 021 "IMUo HJO I~?
~tjOS( LAKE ',090 011 NI SSIIII SZ40 OJ5
~URII I.?OO 065 NODI liE , !>24', 169
, 'WIIGAN Hl0 121 NOP(;I\I NG 52',5 131
~ORkIS 4930 I'.? NCR(ROSS 5250 051
IIOIIR I STaliN "9',0 131 1101\111 ,!II liNCH 5260 Ol5 IlImT(tN '.?50 17.9 IWIIlllflElD 5270 131
:-1UTllY '.960 O'JI NOR TIl IIA r-KA TO 5200 (0) "
111,UND ',910 05) NOIITII DIlKS ~ZO/t III
IIllliNIJ~ "'1[11 '.'l7', 12 J NOIIIIIUII( ~2')0 071
IIIJUNT A I N IRON '.?Oo 131 /1011 TIl R E OIlUOO 5300 lZ1 1oIr:\JlHIlIN lllKIi ',??,' on IIlJll TIIlIOP SHO 0?1
.'IUllOuCK 5000 151 14011111 Sf PAUL 5J20 12J
11YRTI, E 5010 0',1 NOIIIIOOU 5330 019 N~SIIUIl -, 5020 167 CAKOIIL[ • 5334 16J NASIIIlAUK !iOJO 0(.1 NOYlS 5335 061/
rMS~1I1l 5040 on 01lK I UAI\'O 53J6 017 IIIIYrllllWIIU5H 50'15 007 OIlKLAND 5Hl 041,
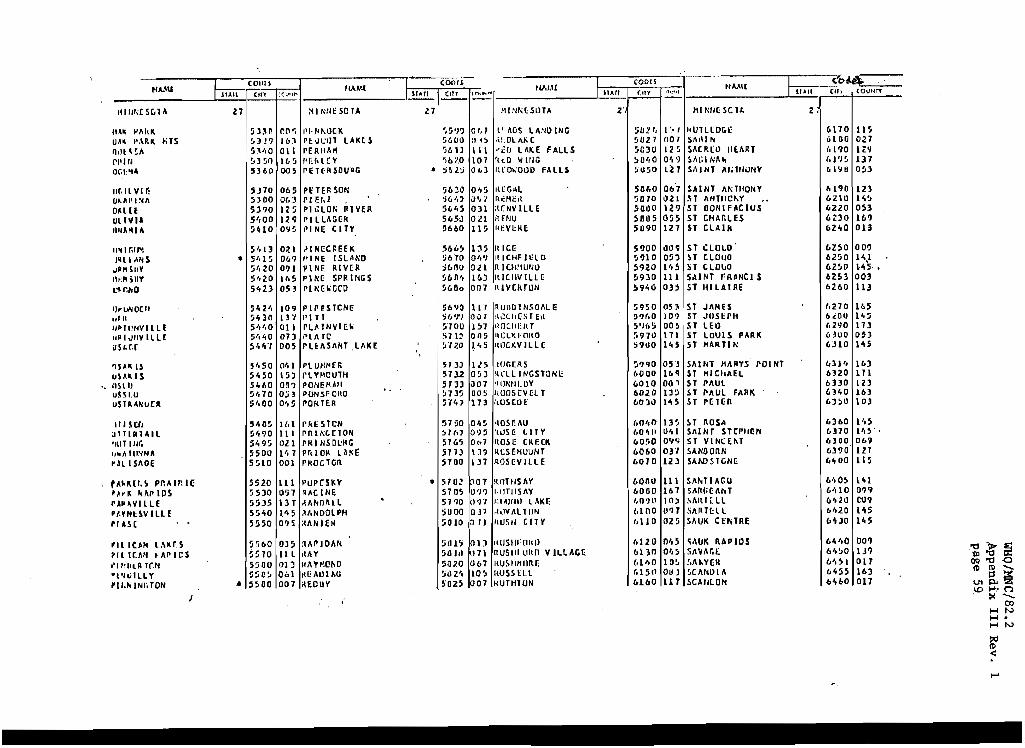
H .... IU
111111,;CS[,TA
lI~k "'~I'I\ UA\ ,'UK liTS n,!t\~A PI'1fj Or.PI~
ufollVI r: O~AnINIl
OHU OLIVIA UIlM\I~
1I~1r.11'\
l~lI.\N So
.I'" SUY I.JlsnV L",m"o
,,~ liN oe II .1.11 I~ Il!NV III E '" 1 <illY J L L( o
'I U
SLr.r
SAl<. IS Hka
'. I 1St IJ u u
SHU STA "'.:oCR
IIISCfI ITIRTAIL
I\IT IN'" I_A III~NA
r , ~ , r
" ,
All SIIOE
A~lUh~ Pr. ... Ir.U; A-II. "flP IDS A'''VILLE '.YIII:$V 1 lU r AS(
IlleMI l.\KB Il I r.MI • III' I C S 1"illR Tr.N t'1~ILLY
II." IN/a ON
T COlli I
lUll (In
27
5l:\n ~3J? ~:;\/iO
!.tJ ~o 5360
SJ70 5)00 5.,.,0 5',00 5~10
5',13 .. 5'.15 !i'.20 5'.20 5423
5"2', !;t,30 5','.0 !i /,1,0 54""(
~'.SO 5't50 St,60 ~/t70
S',OO
!.i40!:t ~',90 S49~ SSOU S!j10
5520 5530 !.i5JS 5540 5550
~~60 5:070 5:iOU ~:;o~ .. 5500
IIAA'J:
" cOOr!
:C~I,", lIArI (1fT
:0 NtlE SO TA Z7
O(\'i I'I,III\OCK 'i5'J? 16) PbH.:tll lAKe S %01) all rERWIK 'It> l)
I t.. ~ I'U,U:V '>bZO oos I'EHRSOUPG • :i6z:i
065 PE TEll. SON ~bJtJ 0(.;1 PI EI,Z ,)6'1' 125 pl"tO" AIVER 56',!) 129 1'1 LlIIG~R 565;) O'l!i I'INE CITY 5660
Oll i'INcC~EEK '6b!> 0&9 1'1 HE I SlM<O %70 091 !'INr: RIVeR :i61lQ Il,S PINe SPRINGS !:abO', 053 I'II'lCIlGC'D 5600
109 PI peSTCN!? 56'J0 13 "( 1'\ TT ,6 'l')
011 l'L/dNIlIr:1l nOD 01) PLIITC Sll::'> 005 I'UIlSII/jT lllKE ~'I7.()
0'11 rLUMHfl: 5133 15) f'l VP-ICUUI 5732 06? PONEMAH
" S133
O~) PONSFQIIO ~135 Olt !.i POlt1ER 5741
)1.1 1'f<1i STCII ~l:;O
1\1 pnlt.;(.nON !>H., 021 PKINSDl:ItG ; 5165 1',7 prdOll lAIC!: !i1n 001 !'KOCTGR SlOO
111 I'UP(Sk'l' • ,'O;! 0')7 RACINE 57 OS 131 AM;OAll
. 51?0
1" 5 ilI.NOOlPH :;000 095 ;{II/I IEII !i010
OlS :lIlPIOIIN 5dl? III KAY 5111,1 013 HIIVI((!I\O ~a7.0
0 ... 1 ~cAUl 1>1; 51J2.4 007 ilEOUV ~02!i
."-1.11 I cootS
IIMII I ~O~
1"1,,..,-1 I I All (tty "'l"'. r " .. , (U, CO",,,"
IIINI'\UOrll Z' tlll'\//(SC 11. 2,
01.1 .t' ADS \.IINO ING SO;! f, I ~. / HUTLlOr.l: 6110 II' " I~ .<I,OI.I\I(C !1HZ '/ (101 St.,11 II 61110 021 III re!) l AK E FALL S SC30 12 ~ SAC 1\(0 /tEIIR T (,11)0 H'i 107 lItO '1/ WG )0',0 0'19 ~A(;IN"" /.l')S 137 (),,3 f\~OIiOOO FALLS ~U!Jo lil S,\ I NT M;1II\)N'I' 111'1 Ii OS3
045 II(GAl 5060 06'7 SAINT III'\TliONV 6190 lZl u" I n~HE,~ ~1I10 1121 !iT MITfICI\Y " 611lU H~ Oll ;t(NVIllE 5000 129 ST OONIF/tCIUS 6220 053
Oll R£NU 5805 OB ST CHAr-lES 6DO 1(1)
115 1(f.V!.:RE 51190 127 ST CLAlk 62'00 013
135 IlICr: 5900 009 ST l:LOI .. O' 6250 009 O/.fJ ItICHFI~LO ~910 05) H c.LouO 62!10 1'.,1 OZl nl('H~IUNO 5920 !'oS liT c.LOIJO 6250 1"5 • I!oJ f\lCIIV ILlC ~930 111 SAINT .'R_Nel S 6253 003 007 f\lVCI\TON 5940 03:> Sf IlILAIRE 6260 113
117 I'I.'JIIQ I NSOIIL e ~950 05) Sf JIIMES (.270 165 001 ,~.:!tl'(S T e,t ~'J()O 10? n JUSEPH I>dlO 145 1)1 <WCHEIlT ~')(.!; OO!> 5T Ull (,290 III Oll~ 1I0Ll~rOftO ~,970 171 Sf lOUtS PJlAK (dOO on 1'.5 IWCKV ILL £: ~9UO IH Sf tlARTl1'l 6310 145
115 IOGr:RS !i?90 (5) SIlINT tlllAYS rOINT 63F. 16) O~) ~ ell I NGSTONE 6000 169 Sf MIChAEl. 6320 171 007 '11)1'\111;0'1' 6010 01) ~ Sf PIIUl 6330 123 oos I(oosrva T 6020 1)5 ST PIlUl "ARK 6340 163 173 ['US tOE (,0)11 lH ST ""un 6J!>O 10.)
0'. !i 'IOSr:IIU (.0 /,1) 13~, loT 1I.0S-' 6360 1',5 09!J I!USE tHY (00"" 0"1 Sill NT StrPIU!N UTO I', ~' . 0 .. 7 1I0S" CKHK 60:;0 0'1'1 ST VINCEI\T 6300 06~
13' I\LHHUUNT 6060 03" SANOORN 6390 121 137 I~OS(V lLLE 6010 123 SAWSTGNI: (,~OO 115
P07 !{OTlISIlY 6000 111 5111.1 IJIGO MO~ 141 0')9 '.fITlISIlY 6060 161 SJII«; ~ "" T C,HO 0'1'1
o ?'I ':1'1/1111 l AK~ 1.0')0 10:' SIIfHHL 6420 CO?
0.1'1 ;(,lY III TIIN t.100 un SJ\I\THl 1>',20 145
PII IIUSII CITV I,UO 025 SAUK CEtilnE MJO 1<\5
IlD ,wsw' nit Il (,1.21) OItS ~"IIK RAP lOS 6~',O DO? 171 nUSl1i UlHl V ILlller: 6130 Ql,5 SIIVllr.£, 6't!>0 1J9
067 IlUSllllnnr: (,1',0 10~ !.J\I,YER bit!> 1 017
10~ I(USS tl.L t.l5 II OUJ ~CIINDI II 6~55 163
007 IlUTHTON 6160 117 SCAULO/i tot, 60 017

HAM,
KIN/IUlIU
Sf-Iall'r. nCR $l.uOk Til HI'[KA SIOMi S/l,HI:~
S~,\l(urti!
SIIU,lY SII£,,:lllP.N SHEVLIN " SW)I(~VI£W
SllrllCIIUOD ~II VIII OAY SIL\!O C • ..IfK S Il V \:1', LAKl SKYLINE
SLAYlml HUPY rYf. $,111 ItSK I StlOC"VILL E SOl "AY
SOI/IIAN \l.illill IIAYl:N ~ I hlUWAll FAllS SOUTH $1 PAUL SPltlll.
Srr.INGI'IELC SPIIIHG C:\CVE S .. kItIC IlIll Sl'~ ute. LAKE PARK S"" Hie LAk£ PAkK
PI't I PIG lAKE S/,I:INC lllKI: SI'~ INr. PA,IK $"'\ IIlG VALlCY s
s S S
UIIAH LAKE
lACY TAkU,FIElO TANTON
STAl'llS S TAJlOUeK
I (0011
I StAll (flY '(\\".'"
,27
(,~(,~, 0'\1 (,410 lZl ("1110 159 64?0 III 6)00 02 S
6Sl0 13') 6520 101 6!JJO 091 65',0 029 "HZ 123
65',) 05)
"'~' OH 1)5'", 111 65!JO on ~; 65:;1 Olj
(,SUO 101 6~10 015 6~nO 00)7 c..~tJ/t ('0) 4~'10 001
65')~ In (,I) au 111 6610 011 £620 037 66~0 067
6650 015 661,0 055 6670 1'.5 6671 00) 6(.72 UJ
• 6(.7) 059 .. 661't 061 1.>675 OS) 6(,00 O'.S (,,,90 061
6100 025 ('105 or,? 6700 OI,'! 6710 I~J 6720 121
(COt.! ruM.!.
(IIY ,'(\ •• ,,1">"
HI "NfSCTA 27
5 Tl' I: ,,/ (,'t')0 13.) :; Tt PlIfN 1.11',0 OD? STE\JIIIT ';/:iO OU~ STEh4RTVllLE (,760 109 STILLIIAHR 6710 16]
S TOI;I< TeN 6700 169 STCr(o~", 67')0 on STRANO~U!ST 6UOO 009 Sill 4 nlCONA 6010 13S S TURGEOII LAlI:~ (,620 115
SIJNBll~G .
MIl'> 06'1 Su.'~r-I SII LAM: 1\010 o :J'I ~,l<',"VILLe (11)0 0')7 5"11 lAI(A • btU;! 001 rllCCN ITE ('0',0 061
1"'~A~IICK 01l5J 001 1hOPI i>llbO 099 1,\UN10N (,910 Ot);! lAYlO~S FALLS MilO OU TI:NNr;y ,,11'10 1/'., If;NSTRJI« (,')00 00'1 1111 U' 111 VEil FAllS 69 \ol 11J 1II01'SC" 6?'0 OU TINTAH (93) I5!i 101' IE 6?15 OJI
TlJl'o;KA BAY 6'1'" OH lr.HR 6*}5(' 117 l.lACY· u'H.) iI'l) lRAll f,'/('',; 11'1 TrtlllONT 69/,1 0'11
lROIIl<lIlO (,?~n 0.', TIIOSKY l.f}f]) lit InUI':I\N 7000 (1'/1
TU:lTlE RlvrR 1() 1~ OO{ rwl G '{01:; lJ7
TW!N CITIES AI RPORT • 'IOU 051 II1IN lAI<~S 7019 047 1111/\ VALLEY 7.12) I.17 THO IIAlIl/DRS 10,10 o t) rnclI lO',i) ~lIl
coon (oe" ttAM' I $1011 t;Ovw"
flAMl I IIAII (If' cO\ltln ('1'1
lilNNESOTA 2' III NNE SeTA 2'
VLUI 7050 01..1 ~hUllU~ 7',20 OUl U:;OUP.lIDOD 70(,0 111 "AlI~UY 11030 I'll UPSALA 7070 01)7 ;:AYlA TA '14',0 053
UIlIlANK 70'00 111 l<.E I.lSTF. 1\ 7't ',3 131
UT leA '/090 16'J linCH ,1447 O',?
VAONAIS HEIGHTS 7096 III l,nCGM!: '{',50 0?1 VtllOI 71 os O~I hHU '1460 0'.1 nF.(;AS 7110 III hF.NOELl 7',10 05l V~IlH!LLIOIi 7120 031 \.ESTO!\C',OK 7',110 Oll VERNDALE 7lJO 1S'i liE Sf C ONeOl\1) 7',90 OJ'}
vr;rtNoN C~,'IT(I\ '11',0 01:! ).c$lI'Orlr I~,OO 111 VI:STIl 1150 127 "r:n 5T PAUL. 1:>10 on V lelO1\1A n('o 019 t.OT UNIIjN H2O 153 VIKING 1110 01)', •• tIlLIlN 1!)JO :I',S VILLARO 11 00 121 I<IIEAlOI\ 1.5'tO U5
VINING 1190 1 i 1 ktlll'llOl T 7!i',1i 01.1 III1,C INIA 1200 1)'1 ~tll H 1l1!1I!! lAKI: 1!>50 12l IIAOASIIA 7210 157 1.111 IE fJlllill '(:;55 005 1{.\OIlSSU H2O 121 IotlllElICC.1l • 7')51 0',,)
4i1CIlN III 7lJO ,119 I.IUlcll 7)(,0 \)(.:.1
~AI)HIII 72',0 I !i') Ifllll,P.N1E 7)'/0 16l I-IMIKON 7Z: .. ) O'}!J hI III JI liS 75UO 011 ~,11 Ie I'AI\I( '17.(,0 1/• ~ AIUM"II "?O ot.7 ;f,\LI.lOllf 7270 H,I kJUON RIVEI' 7600 11~ WlIlK(f( 7280 021 liJllIONT 7610 10~
ilAlIIUT GROVE 7Z?1l ll7 WilTON Ib~O 001
\.fflLTERS noo 043 HNOOM 1i>JO OJl
"'Jllfll"~ 7Jl{) 09'} 1011 NC,(II l6'.0 119 IIMlA,'1IN(iO 1320 OIo'} 1001 NN[OAGC 16~0 O',l .. ANIlA nJ') 127 IfINONA " 7660 169
1oI~II...,ftSI<A 1))5 1:\ ~, "IN~rr:n 7670 0115 '~flIHIA '1::l'.O 0101 1001 "rllf\(,p 11>00 1'.]
tillkltrN n~.o Oil? HINTON 1(,')0 137 WM,HlAO 73(,0 1.1:. hlRT • 7693 061 iI.ISLCA 'f310 H.I kOlf LAKE 7700 OOli
'U.~KIStt 'IlH 007 t:Cl VEil ION 7HO 167 "
WATI:IlTOWN '1300 01'} liOr.OllU;lY • 7716 16l wATIRVILlE 7HO 019 WllfOO 1I.KF. 7120 113 WATKINS 7',00 O?l hOW S Hit: I< 7140 117 IIA1SUN 7 /tlO 023 hORTIIIl<GTON 7750 lOS
jlllt t:SIlAll '?f(.0 011 Vllf.ur 1770 017 lIn.nfF noo 0'.5 IIVl'H It.G 71.,0 0::' YOUNG AM(RICA 7000 019
l(ill'U 7010 061 L III 1014 1'H Z IMI1f1UIAH 111l!! 14l l UlIIIRO fAll S 7820 lS 7 11J1I.IROTA 70)0 0',9

CORE DATA
FORM 02
LPH/MHHP-MORB 02(1-3) 1/82 Ver. 1
WHO/MNC/82.2 Appendix III Rev. 1 page 61
Record 01 12
IDCODE 1.. 29
1. ID LABEL
2. Abstractor ID Code I I I I
30
3. Date Abstracted:

WHO/MNC/82.2 Appendix III Rev. 1 page 62
4. Medical Record Number I I I I I I I I [lJ 39 (From Hospital Chart)
ADMISSION DISCHARGE
5. DATE, rn,m,m 1+ 9 5}-L-l s!---l---l
7. DATE, m,OJ,m s}-JL-l 61 6}-L-l
6. rn rn 24 HOUR
TIME: s}-L-l :h---l--l CLOCK
PATIENT INFORMATION
8.1 I I I I I I I I I I I I I I I I I I • .1" I I IT ii I I I I 1100
H 3 FIRST NAME 91+ HI
95 105
skip Reaord 02 IDeODE 12
1.. 29
11. L I JJ ill 12U I LJJl J.1J 11 Jill I I I I 13.~ ~ :~i I I I I
3 tt LOT 56 NUMBER 55
I 114J I I I I I I I I I I I I I I 115m 61 CITY 76 STATE
l6~ I I I I I 17. I I I I 78 ZIP CODE COUNTY 83 CODE
18. BIRTHDATE: rnrnrn 19.
86 88 ~O
20. MARITAL STATUS: 21. ETHNIC STATUS
102
10 Harried
2 0 Separated
3D Divorced
40 Widowed
5 0 Never Harried
103
1 0 Whi te Caucasian
2 0 Black/Negro
3[] Asian/Pacific Islander
4 [J American Indian/Native American
50 Hispanic
6 0 Single (no other data 6 0 Other , _______ _ available)
7 0 NOT RECORDED IN CHART 7 0 NOT RECORDED IN CHART 10 .. 105
skip

WHO/MNC/82.2 Appendix III Rev. 1 page 63
Record 03 12
22. DISCHARGE DIAGNOSIS CODES PHYSICIAN'S DISCHARGE DIAGNOSIS IDCODE
~J[ I I IOJ :01 I II.rn
"2
~ 01 t--t-I -+---tl I OJ s ..
~ 01 t---t--I -t--tl I OJ 66
tOI--+-l I -t--tl l.rn 78
bOllllOJ ___ _ 36
dOITDOJ ----411
fOt---t-1 I-t--tJ IOJ ___ _ 60
h 0 It--t-I -t--tl I OJ 30111 !OJ
11'+
tell I I I OJ lOITD OJ
1'+ 29
102 105 skip Record 04
mO OJ n IIIIOJ ------- 12
mCODE 3u ------- 14 29
) Olt---t--l-+---tl I OJ pOI I I I OJ ----
23. OPERATIONS & PROCEDURES CODES
Patient status on DISCHARGE
10 ALIVE
2 0 DEAD --+ ATTACH AtrrOPS'l REPORT ABSTRACT (if autopsy was performed)
25. Did the patient die in the Emergency Room?
95 10 YES 20 NO 30 NOT RECORDED 96 105
skip
I

WHO/MNC/82.2 Appendix III Rev. 1 page 64
1-----1 I COl'll': Cl'.Th. I I 02 1
L 1
1. 1D Number: This number will be generated by the computer, and a label on which
the number is printed will be put at the top of the first page of each section of the form by the abstractor. For example: Form 02-1; 04-1; etc., until you run out of labels, then write in the number and enclose it in a box. Be sure to write and box in the number on all photocopies.
2. Abstractor Personal Code Number:
The abstractor/validator/interviewer/coder must fill in his/her per-' sonal code number. (See Personal Code Number sheet).
3. Date Abstracted
Use all six boxes, begin' . h n1ng W1t the ~nth in the first two boxes, day in the next two, and year in the 1 ast two. Use a "leading, zero" if necessary, as shown in this example:
5.
6.
January 6, 1925 1----,1-1 I 1 I ~ 11,_0 -'--.6-11 ;1,----::...2 ...c......::5~
4. Medical Record
ADMISSION
MONTH DAY YEAR
DATE: ~90] ~ 10] ~ JTI TIME: 51=0 :DJ 24 HOUR
CLOCK
1 1 1 1--1 1 1 [TI Number 1
39 (From Hospital Chart)
DISCHARGE
7. DATE: rrtrr:Lrn 59 61 63
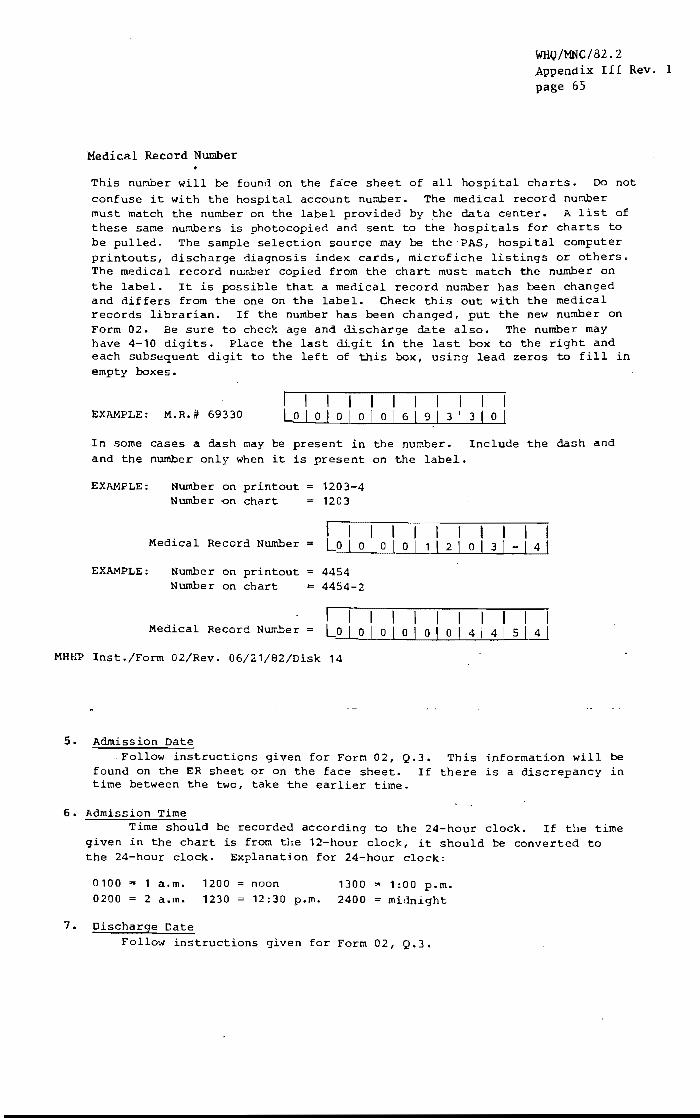
Medical Record Number
WHQ/MNC/82,2 Appendix III Rev. I page 65
This number will be found on the face sheet of all hospital charts. Do not confuse it with the hospital account number. The medical record number must match the number on the label provided by the data center. A list of these same numbers is photocopied and sent to the hospitals for charts to be pulled. The sample selection source may be the-PAS, hospital computer printouts, discharge diagnosis index cards, microfiche listings or others. The medical record nur.~er copied from the chart must match the number on the label. It is possible that a medical record number has been changed and differs from the one on the label. Check this out with the medical records librarian. If the number has been changed, put the new number on Form 02. Be sure to check age and discharge date also. The number may have 4-10 digits. Place the last in the last box to the right and each subsequent digit to the left of this box, using lead zeros to fill in empty boxes.
EXAMPLE: M.R.# 69330 I I I I Lo \ 0 I 0 \ 0
\ I I I 06\9131310
In some cases a dash may be present in the number. Include the dash and and the number only when it is present on the label.
EXAMPLE:
EXAMPLE:
Number on printout Number -on chart
Medical Record Number
Number on printout Number on chart
Medical Record Number =
1203-4 1203
I I I I I I 1 I I I I Lo I 0 1 0 1 0 1 1 \ 2 I 0 \ 3 I - \ 4 1
4454 4454-2
I I I I I I I I I I Lo I 0 I 0 I 0 I 0 I 0 I 4 I 4 \ 5 I 4
MHrW Inst./Form 02/Rev. 06/21/82/Disk 14
5. Admission Date Follow instructions given for Form 02, Q.3. This information will be
found on the ER sheet or on the face sheet. If there is a discrepancy in time between the two, take the earlier time.
6. Admission Time Time should be recorded according to the 24-hour clock. If the time
given in the chart is from the 12-hour clock, it should be converted to the 24-hour clock. Explanation for 24-hour clock:
0100 0200
1 a.m. 1200 2 a.m. 1230
7. Discharge Date
noon 1300 12 :30 p.m. 2400
1 :00 p.m. midnight
Follow instructions given for Form 02, Q.3.
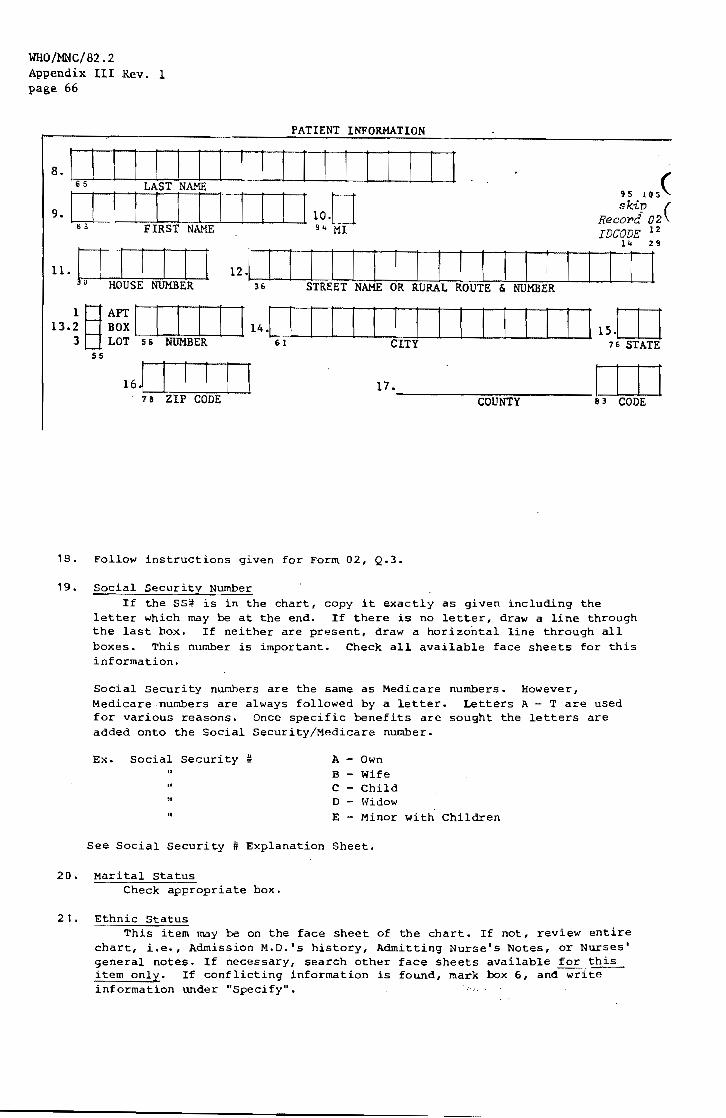
WHO/MNC/82.2 Appendix III Rev. 1 page 66
PATIENT INFORMATION
8. 16 I I I ! I I I I ! I I I I I I I I I 9. [ 'I [ [r Ii 1 [ [ [ 110.0
til FIRST NAL'1E 94 HI
95 IOS(
skip ( RecoT'd 02 . IDCODE 12
n.! [ [ [ [ [ [ 12.[ I I I 1 [ I 1 I I 1 I I I [ 1 I I'i r U HOUSE NUMBER 36 STREET NAME OR RURAL ROUTE & NUMBER
13.~ p!~ I I ! ! 3 ti LOT S 6 NUMBER
SS
! ! 14.1 I I I I ! I I 1 ! I ! I I I 115.[0 6 1 CITY 7 G STATE
16.' I I ! ! I 78 ZIP CODE
17._~_1111 COUNTY 83 CODE
18. Follow instructions given for Form 02, Q.3.
19. Social Security Number If the SS~ is in the chart, copy it exactly as given including the
letter which may be at the end. If there is no letter, draw a line through the last box. If neither are present, draw a horizontal line through all boxes. This number is important. Check all available face sheets for this information.
Social Security numbers are the same as Medicare numbers. However, Medicare.numbers are always followed by a letter. Letters A - T are used for various reasons. Once specific benefits are sought the letters are added onto the Social Security/11edicare number.
Ex. Social Security a A - Own 1T
B - Wife
" C - Child o - \ .. idow
" E - Minor with Children
See Social Security. # Explanation Sheet.
20. Marital Status Check appropriate box.
21. Ethnic Status This item may be on the face sheet of the chart. If not, review entire
chart, i.e., Admission M.D.'s history, Admitting Nurse'S Notes, or Nurses' general notes. If necessary, search other face sheets available for this item only. If conflicting information is found, mark box 6, and write information under "Specify".
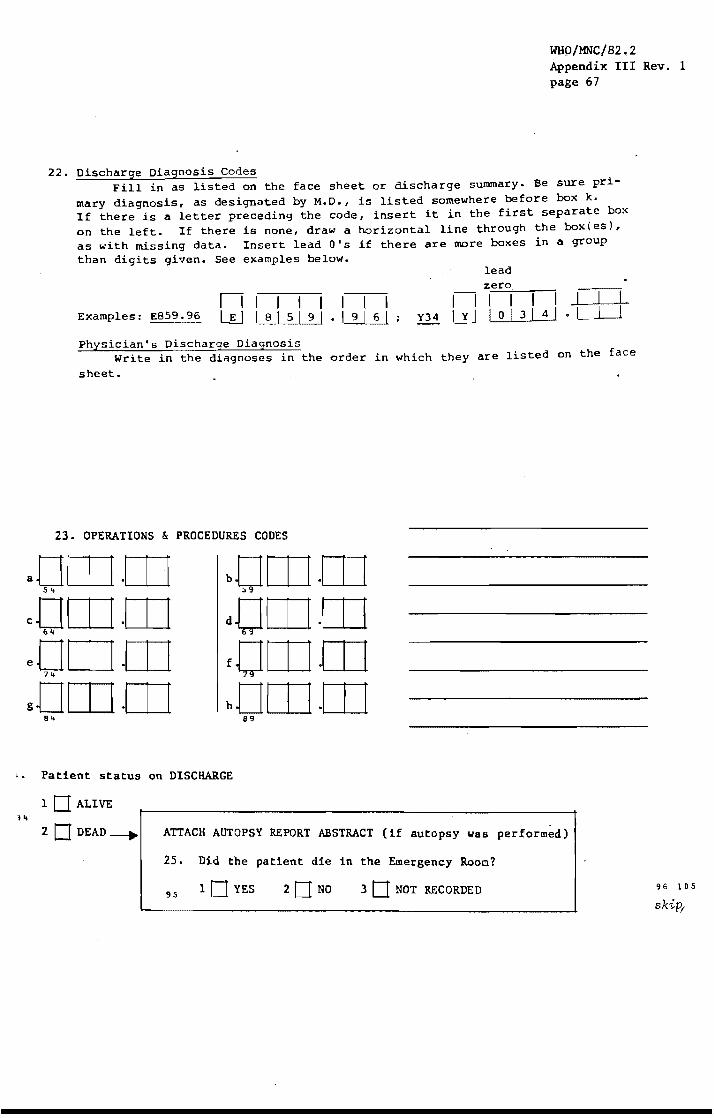
WHO/MNC/82.2 Appendix III Rev. 1 page 67
22. Discharge Diagnosis Codes Fill in as listed on the face sheet or discharge summary. Be sure pri
mary diagnosis, as designated by M.D., is listed somewhere before box k. If there is a letter preceding the code, insert it in the first separate box on the left. If there is none, draw a horizontal line through the box{es), as with missing data. Insert lead O's if there are more boxes in a group than digits given. See examples below.
nil I I I I I Examples: E859. 96 L~ I 8 1 5 I 9 I • I 9 I 6 I
lead zero
I-I I I 1 I J.1---L--1-Y34 W I 0 I 3 I 4 1 • ,--I --'----'
Physician's Discharge Diagnosis Write in the diagnoses in the order in which they are listed on the face
sheet.
23. OPERATIONS & PROCEDURES CODES
I. Patient status on DISCHARGE
1 0 ALIVE
20 DEAD--+ ATTACH AUTOPSY REPORT ABSTRACT (if autopsy was performed)
25. Did the patient die in the Emergency Room?
95 10 YES 20NO 3 0 NOT RECORDED 96 105
skiPI
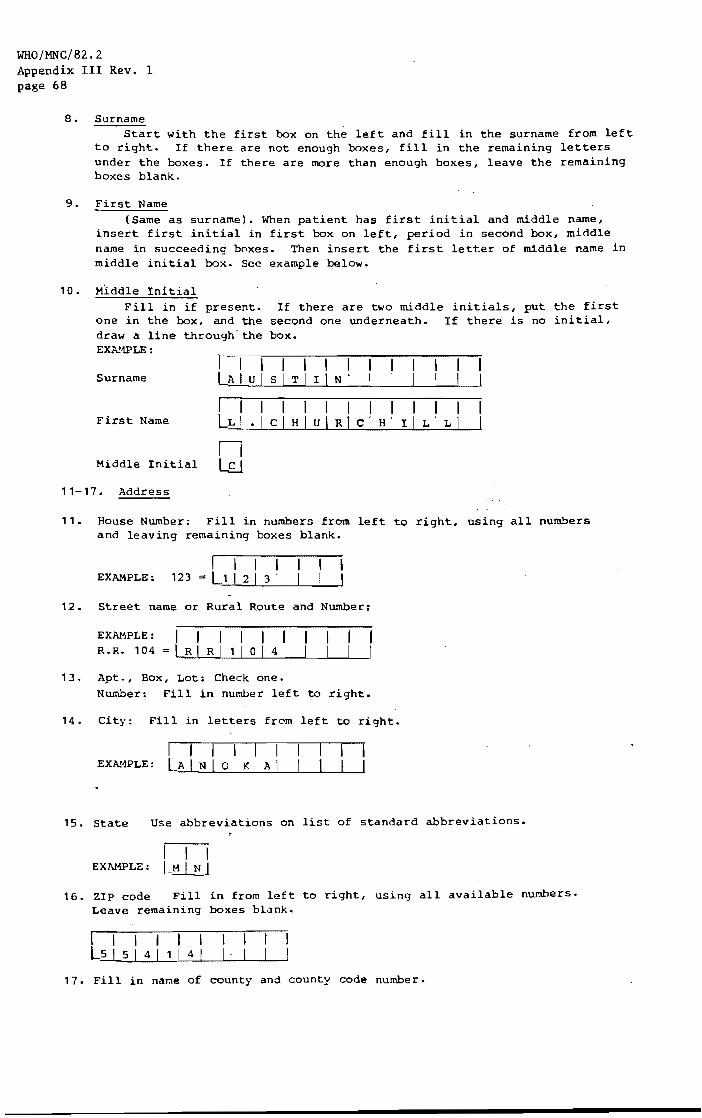
WHO/MNC/82.2 Appendix III Rev. 1 page 68
8. Surname Start with the first box on the left and fill in the surname from left
to right. If there are not enough boxes, fill in the remaining letters under the boxes. If there are more than enough boxes, leave the remaining boxes blank.
9. First Name
10.
(Same as surname). When patient has first initial and middle name, insert first initial in first box on left, period in second box, middle name in succeeding boxes. Then insert the first letter of middle name in middle initial box. See example below.
Middle Initial Fill in if present.
one in the box, and the draw a line through'the EXA.'1PLE:
If there are two middle initials, put the first second one underneath •. If there is no initial, box.
I I I I I I I I Surname LA I u I SiT I liN I I
I I I I I I I I I I I I First Name LL I • I C I H I u I RIc 1 H 1 I I L ILl
n Middle Initial lfJ
11-17. Address
11. House Number: Fill in numbers from left to right, using all numbers and leaving remaining boxes blank.
I I I I EXAMPLE: 123 = L~1-,-1...;;2;;...1L...;::..3 ...J..l_'---L--1
12. Street name or Rural Route and Number:
EXAMPLE: I I I I I I R.R. 104 = LR I R I 1 I 0 I 4 I
13. Apt., Box, Lot: Check one. Number: Fill in number left to right.
14. City: Fill in letters from left to right.
I I I I I I EXA?1PLE: LA I N I 0 I K I A I
15. State Use abbreviations on list of standard abbreviations.
I I I EXAMPLE: L~
16. ZIP code Fill in from left to right, using all available numbers. Leave remaining boxes blank.
I I I I I I I L5 I 5 I 4 I 1 I 4 I I '
17. Fill in name of county and county code number.

WHO/MNC/82.2 Appendix III Rev \ 1 page 69
rnrnrn 18. BIRTHDATE: 19. SOCIAL SECURITY NUMBER I I I I 1-[0-111 11-0
92 86 88 ~o
20. MARITAL STATUS: 21. ETHNIC STATUS
102
10 Married
2 0 Separated
3 0 Divorced
40 Widowed
5 0 Never Married
103
1 0 Whi te Caucasian
2 0 Black/Negro
3 0 Asian/Pacific Islander
4 0 American Indian/Native American
sO Hispanic
6 0 Single (no other data 6 0 Other , _________ _ available)
7 0 NOT RECORDED IN CHART 7 0 NOT RECORDED IN CHART 10 .. 105
skip
Record O~ l:
22. DISCHARGE DIAGNOSIS CODES PKYSICIAN'S DISCHARGE DIAGNOSIS IDCODE
O[]-IJ.[o cOl II 1.[0
.. 2
eOr I I 1.[0 s'+
gOI I I 1.[0 66 ,
i01111 78
k011 I 1.[0 90
mOllllCO 3u
001 I I I
bOil I 1.[0 36
dOli I 1.[0 .. ~
EOI I I 1.[0 60
h
_____________________ 102 lOS
skip ______________ Recop~i
______________ TDCOr-, I' ,

WHO/MNC/82.2 Appendix III Rev. 1 page 70
23. Operations and Procedures Codes Fill in as listed on the face sheet or discharge summary.
See instructions for Form 02, Q.22.
24. Patient Status on Discharge Check appropriate box. If dead, attach autopsy report abstract (if
autopsy was performed) and answer Form 02, Q.25.
25. Did the patient die in the emergency room? Check the appropriate box.
CORE DATA
FORM 02
LPH/~HH.P-MORB 02(1-3) 1/82 Ver. 1
1. ID LABEL
2. Abstractor ID Code
WHO/MNC/82.2 Appendix III Rev. 1
page 71
Record 01 12
IDCODr }'I 29
[OJ 30
3. Date Abstracted:
~------------------------------
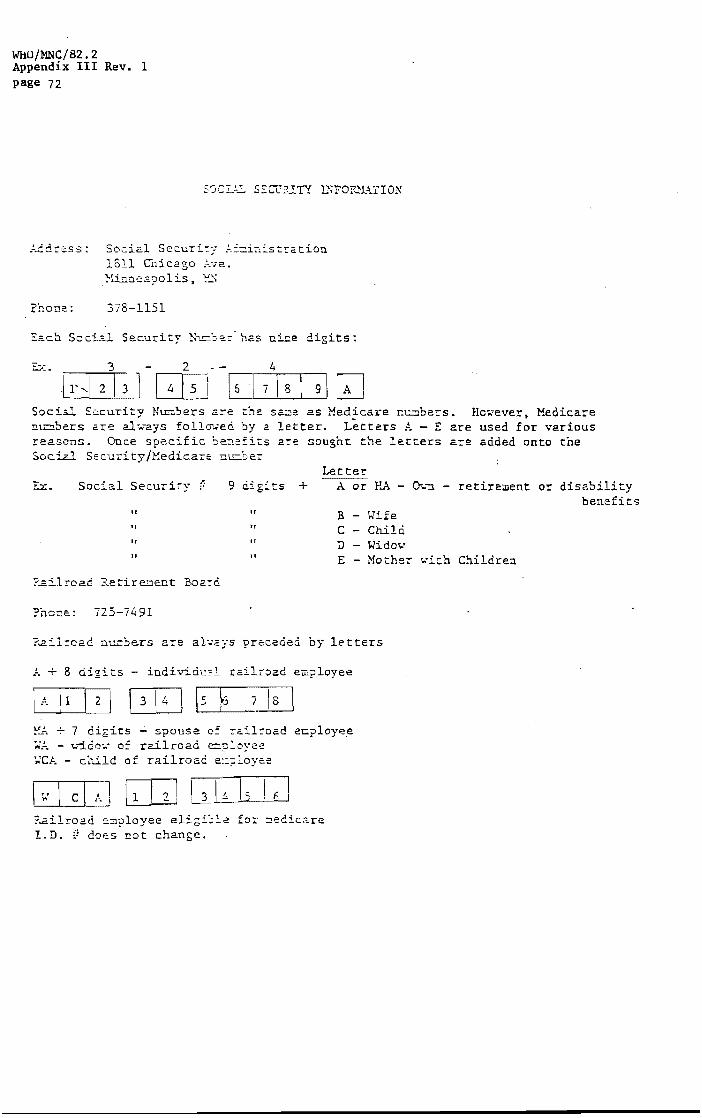
WHO/MNC/82.2 Appendix III Rev. 1 page 72
,~dress: Social Security ~~~i~~stration 1811 Cnicago 01e. 'H.inne2.polis, 1:'_"
?hone. : 378-1151
Each SociD Se.curity 't:.":.!:::';) has nine digits:
'E:>: • 3 2
b',·1 2 13 J [iliJ Social Security Nunbers are the sa.;::,e as Medical'e ut:.:::lbers. However. Medicare n~bers are al~ays follvwed by a letter. Letters A - E are used for various reasons. Once specific be~efits are sought the letters are added onto the Social Securi ty /1-~edicare nu::.ber
Let Ex. Social Security f: 9 ts + A or HA -
II It B - wife " " C - Child It .. D - Widow If II E - Mother
P~ilroad Retirement Board
?hone: 725-7491
?-ailroac! nu.:;:,:'er5 are al','aY5 preceded by let ters
A + 8 digits - iudivici~ railroad e~?loyee
!:,_!., + 7 digits - spouse 0: .ai1:-oad ecployee ~A - w~do~ of railroad ~?loyee ~CA - child of railroae. e::?loyee
?...ai1road ~:::J?loyee eligi';le for: ::edicare I.D. 0 does not change.
D-.. "';l - retirement or dis.?,bility benefits
r.-'"ich Children

1. ID LABEL
MI HOSPITAL ABSTRACT
FORM 04
LPK/MHHP-MORB 04(1-8) 1/82 Ver. 1
WHO/MNC/82.2 Appendix III Rev. 1 page 73
Record 01 12
IDCODE 11. 29

WHO/MNC/82.2 Appendix III Rev. 1 page 74
2. Give a brief narrative description of the acute event that led to admission or occurred during this hospitalization. (Include the time sequence and course of symptoms)
3. Is there a history of previous HI?
10 YES iii- 4. How long before admission was the last HI? (CHECK ONE ONLY)
30 20NO 1 0 Less than 4 weeks 40 Hore than 8 weeks
30NOT RECORDED
n 20 6 weeks or less 5 0 NOT RECORDED
30 8 weeks or less
5. Was the patient hospitalized for this last HI?
32 1 DYES 20NO 3 0 NOT RECORDED
YES NO
6. Is there a history of stroke previous to this admission?33 10 20
7. Is there a history of coronary bypass surgery? 3<t 10 20
8. Is there a hiotory of angina pectoris which began more than 8 weeks before this admission? 35 10 20
9. Is there a history of hypertension? 36 10 20
10. Was the patient on a digitalis drug at the time of hospital 10 20 admission? 37
NOT RECORDED
3D
3D
3D
3D
3D

WHO/MNC/82.2 Appendix III Rev. 1 page 75
YES NO ll. Is there a history of previous cardiac arrest with
10 20 resuscitation? 38
12. Was the patient transported in an ambulance? 39 10 20
13. Was the patient admitted to a CCU/ICU? 40 10 20
14. Was BP obtainable at first attempted measurement? 4 1 10 20
15. First recorded blood pressure and heart rate (not during CPR):
A.rTf I, rrr1 NOT 10 RECORDED s. i"fiAT NOT
10 RECORDED 4a
IF ONLY SYSTOLIC BLOOD PRESSURE WAS RECORDED ENTER 999 UNDER DIASTOLIC
49
16. Where was the above blood pressure and heart rate measured?
1 0 Ambulance
5j 20 ER
3D Medical Unit
4 0 NOT RECORDED
S2
The following questions apply to the acute illness that led to and/or developed or recurred during the current hospitalization. This includes events in the last 6 weeks or since the last hospital discharge. whichever is shorter.
17. Was this an elective admission?
1 0 YES ___ -1 ••
20NO
30NOT RECORDED
18. What was the reason for this admission?
a. 1 0 Transfer from anothe-r hospital 5S
b. 1 0 Coronary angiography S6
c. 1 0 Coronary surgery 57
d. 1 0 Other cardiac problem sa
e. 1 0 Other non-cardiac problem 59
-NOT RECORDED
3D
3D
3D
3D
60 75
skip

WHO/MNC/82.2 Appendix III Rev. 1 page 76
19. Was there an acute eptsode(s) of discomfoct or pain anywhece in the ante~ior chest. left arm or jaw, which may also have involved the back, shoulder, right arm or abdomen on one or both sides?
30
1 0 YES----tI- 20. Record date and tilue of onset of pain:
20NO A. IT I wrn 1 0 :~~O'DE~· rn OJ 1 0 :~ORDEO
31 3j 35 37 38 ~O 42 21. Was onset of pain in the hospital?
lO YES 20NO 30 NOT RECORDED
22. Did this pain include the anterior chest?
.... 10 YES 20NO 3D NOT RECORDED
23. Prior to receiving medical attention, did the patient take nitrates or calcium blockers over and above the fixed dosage regiment? (i.e. took "prn" medication)
.. 5
10 YES _____
20NO
30NOT RECORDED
~
24. Did the patient seek emergency medical care because the pain was not relieved by the nitrates or calcium blockers or because the pain kept returning?
46 10 YES 3 0 NOT RECORDED
25. Did any of the pain episodes last longer than 20 minutes?
10 YES _____ 26. Were enzymes measured within 72 hours. of the most recent of these episodes?
.. 7 20NO 10 YES 20NO 3 0 NOT RECORDED
48
30NOT 27. What was the date. time and duration of RECORDED the most recent episode?
MONTH DAY YEAR
CIJ/PJ/DJ 10NOT A.
~s RECORDED
hTI:hTI 24 hour B. clock 1 Po NOT
o RECORDED
DJhrUJmin. lONOT
C. 65 RECORDED 61 3
28. What was the duration of the longest episode?
DJhrOJmin. 10 NOT
" 70 RECORDED
b6 bH
ReeuY'd 02 12
[UCODg 14 29
71 75
skip

29.
"!rC
36.
WHO/MNC/82.2 Appendix III Rev. 1 page 77
Reaor-d 03
Was there out-of-hospital collaps~ with closed chest massage and/or cardioversion (CPR) since last hospital discharge or within 6 we~ks of this admission, whichever
l:l
Is shorter? IDCODE ~ ______________________________________________________________ ~,14 29
1 0 Y8S .. 2 0 NO
3 0 NOT RECO RDED
30.
31-
Estimated date wwrrI 31 0 0 Locat ion of collapse: 1 0 Home 2 Work 3 Other
37 32. CPR was administered by:
1 0 Bystander
20 M.D.
30 Ambulance attendant, EMT, Fire, or Police 40 Other, specify ________________________________ _
5 0 NOT RECORDED
33. Was DC countershock given (cardioversion)?
39 1 0 YES 20 NO 30 NOT RECORDED
34. Was cardiac rhyti~h=m~d=o~c~u=m~e~n~te~d~? ____________________________ _,
1 0 YES __ -I .... 35. What abnormal rhythm was documented? .... (CHECK ALL THAT APPLY)
20 NO 41 a. 1 0 Ventricular fibrillation (VF)
3 0 NOT 42 b. 1 0 Atrial flutter RECORDED
,,3 c. 10 Atrial fibrillation (AF)
4" d. 1 0 Ventricular tachycardia (VT)
45 e. lD Asystole
"" to 1 0 Complete AV block (3° HB)
4 I g. 1 0 Other,
Was closed chest massage or cardioversion successfully administered during this hospitalizatiol.?~. __ (~i~.~e~.~r~e~s~u~l~t~e~d~i~n_p~a~t~i~e~n~t~be~i~n~g~d~i~s~c~h~a~r~ge~d~a~l~i~v~e~)~.~ ____________ ~
1 0 YES ----. 37. Where was CPR administered? (CHECK ALL THAT APPLY)
,,9 a. lOOn ward/CCU/ICU 20 NO 5 u b. lOIn emergency room 3D NOT
RECORDED 5 1 c. lOOt her, spec ify _________________________ _
38. Was DC countershock (cardioversion) ever given during this hospitalization~
~ 2 1 0 YES 2 0 NO 3 0 NOT RECORDED
39. Was cardiac rhylhm documented at time of any cardioversion?
lO YES ____ -I ...... 40. What abnormal rhythm was documented? .... (CHECK ALL THAT APPLY)
:.3 20 NO
3D NOT RECORDI-:D
S4
55
56
57
5 a
59
60
a.
b.
c.
d.
e.
to
g.
1 0 Ventricular fibrillation (VF)
1 0 Atrial flutter
1 0 Atrial fibrillation (AF)
1 0 Ventricular tachycardia (VT)
1 0 Asystole
1 0 Complete AV block (3° HB)
1 0 Other,
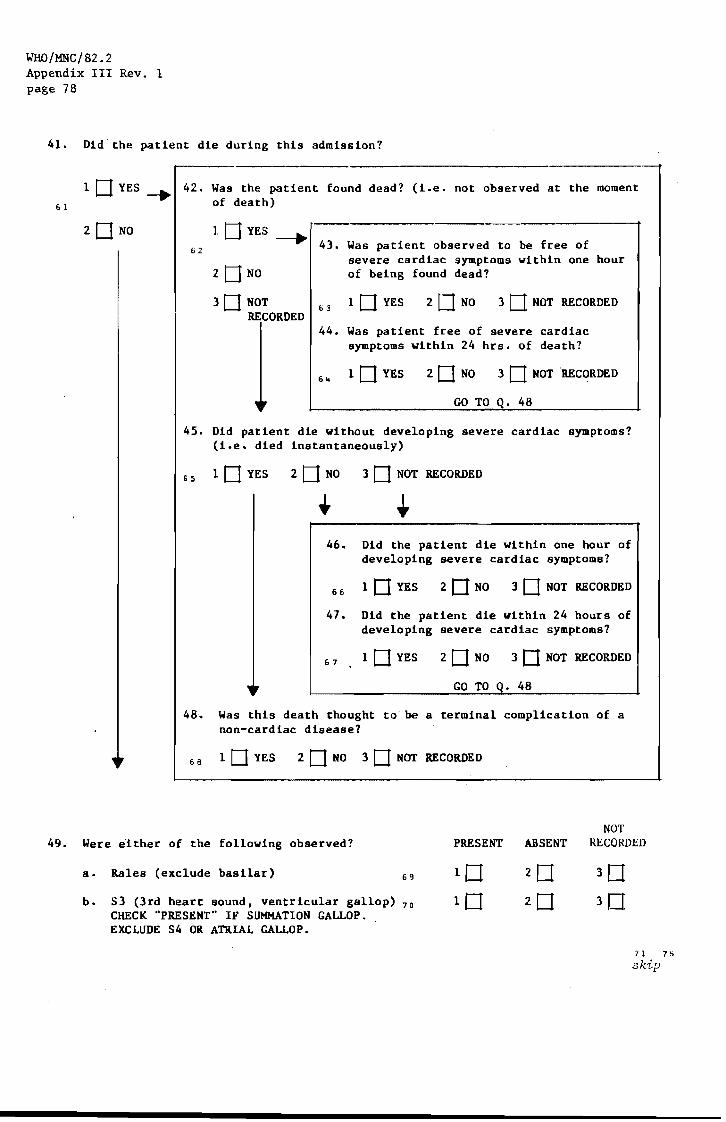
WHO/MNC/82.2 Appendix III Rev. 1 page 78
41.
6 1
Did-the patient die during this admission?
1 c=t YES ~ 42. Was the patient found dead? (i.e. not observed at the moment of death)
2 c=t NO 62
1 c=t YES ---.. 43. Was patient observed to be free of
severe cardiac symptoms within one hour 2 c=t NO of being found dead?
3 c=t NOT RECORDED
63 1 c=t YES 20NO 30 NOT RECORDED
44. Was patient free of severe cardiac symptoms within 24 hrs. of death?
1 c=t YES 2 c=t NO 3 c=t NOT RECORDED
GO TO Q. 48
45. Did patient die without developing severe cardiac symptoms? (i.e. died instantaneously)
65 1 c=t YES 2 c=t NO 3 c=t NOT RECORDED
46. Did the patient die within one hour of developing severe cardiac symptoms?
66 1 c=t YES 2 c=t NO 3 c=t NOT RECORDED
47. Did the patient die within 24 hours of developing severe cardiac symptoms?
67 1 c=t YES 2 c=t NO 3 c=t NOT RECORDED
GO TO Q. 48
48-. Was this death thought to be a terminal complication of a non-cardiac disease?
68 1 c=t YES 2 c=t NO 3 c=t NOT RECORDED
49. Were either of the following observed? PRESENT ABSENT NOT
RECORDED
a. Rales (exclude basilar) 69
b. S3 (3rd heart sound, ventricular gallop) 70
CHECK "PRESENT" IF SUMMATION GAlJ..OP. EXCLUDE S4 OR ATRIAL GALLOP.
n 75 skip

WHO/MNC/82.2 Appendix III Rev. 1 page 79
50. Was there evidence of a stroke during this hospitalization, within 6 weeks of this event or since last hospital discharge whichever is shorter?
- 1 DYES
zONa
_____ ...... COMPLETE FORM 06
3D NOT RECORDED
51. Were ECG's recorded?
1 0 YES _____ ...,.., .. INCLUDE COPIES OF ALL TRACINGS
31 20NO
3 0 NOT RECORDED
52. Was a coronary angiography performed?
lOYES ____ • .,
20NO
3 0 NOT RECORDED
32 []j/m/IT] 33 3~ 37
1 0 NOT RECORDED
53. Date of procedure:
,,9
Record 04 12
IDCODE I" 29
INCLUDE A COpy OF THE CORONARY ANGIOGRAPHY REPORT
54. Has patient had any surgical procedures this admission?
1 DYES~ 55. Dates of Procedures:
2 DNa
57. Status of Chest X-rays (check one)
1 0 X:-rays not done
59 2 0 Reports not present
56. Specify procedures:
3 0 All reports say "no change" and refer to other admissions
4 0 Not all films read as "normal"
50 All films read as "normal"
(XEROX'ALL COPIES OF CHEST X-RAYS)
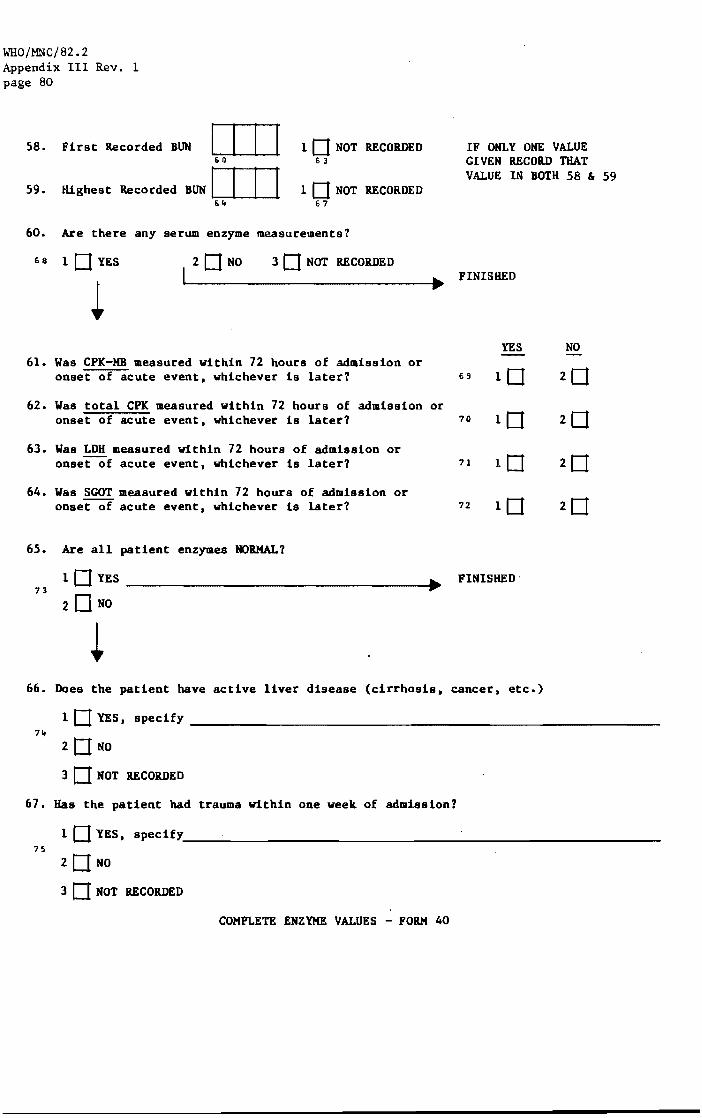
WHO/MNC/82.2 Appendix III Rev. 1 page 80
58. First Recorded BUN I 59. Highest Recorded BUN I
61l
6,.
I I I IDNOT Ii 3
I I I IDNOT 67
60. Are there any serum enzyme measurements?
RECORDED
RECORDED
68 10 YES I
2DNO 3 0 NOT RECORDED
61. Was CPK-MB measured within 72 hours of admission or onset of acute event, whichever is later?
62. Was total CPK measured within 72 hours of admission or onset of acute event, whichever is later?
63. Was LDH measured within 72 hours of admission or onset of acute event, whichever is later?
64. Was SCOT measured within 72 hours of admission or onset of acute event, whichever is later?
65. Are all patient enzymes NORMAL?
73 IDYES
2DNO
IF ONLY ONE VALUE GIVEN RECORD THAT VALUE IN BOTH 58 &
FINISHED
YES NO
69
70
71
72 20
FINISHED·
66. Does the patient have active liver disease (cirrhosis, cancer, etc.)
59
I DYES, specify ____________________________________________________________ _
74
20NO
3 0 NOT RECORDED
67. Has the patient had trauma within one week of admission?
I DYES, specify ____________________________________________________________ ___
75
20NO
3 0 NOT RECORDED
COMPLETE ENZYME VALUES - FORM 40

7a.
b.
c •
M I A B S T RAe T
1 0 CHEST X-RAYS 30
1 0 CORONARY ANGIOGRAPHY 3 I
CHEST X-RAYS
Excludes both )50% proximal narrowing of 2 or more and )75% proximal narrowing of any major vessels.
Documents either )507. proximal narrowing of 2 or more and )75% proximal narrowing of any major vessels.
Neither "I" or "2" above
. L-_______________________________________ __
LPH/MHHP-MORB 41(1-1) 1/82 Ver. 1
38
WHO/MNC/82.2 Appendix III Rev. 1 page 81
ID LABEL
20
Record 01 12
IDCODE 14 2 '3
39 40
skip
l !
WHO/MNC/82.2 Appendix 111 Rev. 1 page 82
MI
1. 10 LABEL
HOSPITAL "ABSTRACT
FORM 04
LPH/MHHP-MORB 04(1-8) 1/82 Ver. 1
Record (; i
IDCODE 14 2
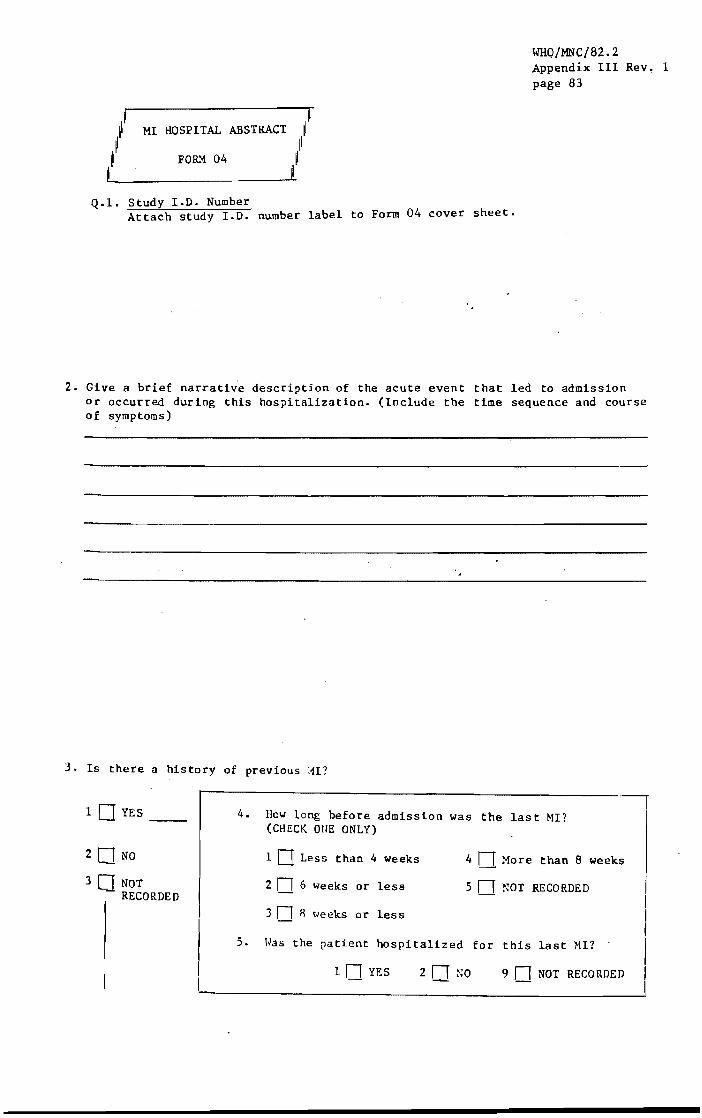
WHO/MNC/82~2 Appendix III Rev, 1 page 83
MI HOSPITAL ABSTRACT
FO&'1 04
Q.l. Study 1.0. Number Attach study 1.0. number label to Form 04 cover sheet.
2. Give a brief narrative description of the acute event that led to admission or occurred during this hospitalization. (Include the time sequence and course of symptoms)
3. Is there a history of previous tlI?
1 DYES __
20 NO
30 NOT RECORDED
I L
4. How long before admission was the last MI? (CHECK OUE ONLY)
1 [J Less than 4 weeks
2 n 6 weeks or less
3 n 8 t ... eeks or less
4 n More than 8 weeks
5 n NOT RECORDED
5. Was the patient hospitalized for this last HI? .
1 n YES 2 n NO 9 n NOT RECORDED

WHO/MNC/82.2 Appendix III Rev. 1 page 84
Q.2. Narrative The purpose of the narrative is to describe the specific circumstances surrounding the event that precipitated the patient's admission to the hospital. Using direct quotes from the hospital chart whenever possible, this description must include: 1. the location and duration of pain 2. any medication given to relieve the pain and how long (minutes/hours)
until pain was relieved 3. if the patient died during this hospitalization, explain your answers
to Q.42-48.
In addition, if you feel your responses to any of these questions misses an important aspect of the case, add this to the narrative. If the physician' s discharge summary covers all of the above; it is still necessary to include items 1-4 above and attach 'eopy of discharge death summary to form 04. If conflicting information is recorded in two or more of the sources, choose the information from the source according to the order listed below.
l. 2. 3. 4. 5. 6.
Resident/Intern Attending PhYSician Neurology Consultant ER Physician Nurse
(If unable to determine titles among names given, ask Medical Records for assistance.)
Other (List medical students under "Other".)
Focus on first "acute episode" of chest pain or discomfort (a crushing y
band-like pressure or heaviness on chest) lasting more than 20 minutes Mention other cardiac symptoms such as shortness of breath, palpitatior!a, dizinessj past fainting, ankle swellf.ng. etc., but do not elaborate on these latter symptoms. Pertinent past historical information on physician's findings, tests, etc. prior to admission may be noted briefly. If there are several acute events, be sure to record information for each event 0
Q.3. Is there a history of previous MI?
Take information from the history of the resident or intern, if any, the attending physician, the cardiovascular consultant, the ER physician, nursing notes, or medical student, in that order. "History" r.efers to information from the patient and his family. A "Q" wave noted in the progress notes is not sufficient to constitute an MI. If conflicting information is recorded in two or more sources, choose the informatioa from the source according to the order listed above (Q.2). (See following example.)

YES
WHO/MNC/82.2 Appendix III Rev. 1 page 85
NO Nat'
RECORDED
6. Is there a history of stroke previous to this admission?
7. Is there a history of coronary bypass surgery?
8. Is there a history of angina pectoris which began more than 8 weeks before this admission? 211
--1 "J L....!
EXAMPLE: History states: "Patient awoke yesterday with chest pain.
prior history of heart disease or stroke. hospital after three hours of pain.
There is no He came to
Answers 3. No to Q.3-19 6. No
7- No 8. No 9. NR
10. NR li. NR 17. No 19. Yes
8. Mst-ler "Yes" if the history includes any of the following:
1. the statement that the patient has "angina" or "angina pectoris".
2. the statement that the patient takes nitroglycerine or calcium blockers for chest pain.
3. The statement (or an equivalent) that the patient has any of the following symptoms: "substernal pressure, pain, tightness, or burning distress precipitated by exercise or excitement. or both, and is relieved by rest and/or nitroglycerine" and appears to have been present for 4 or more weeks prior to admission.
Answer "No" if the history explicitly states that the patient has "no history of angina", or "no history of angina pectoris".
Answer UNo" if the patient has developed angina-like symptoms (see 3 above) in 4 weeks or less prior to the acute event.
Answer "NR" if none of the above criteria for "Yes"/"No" responses apply. (These criteria are adapted from the ~~yo Clinic criteria. )
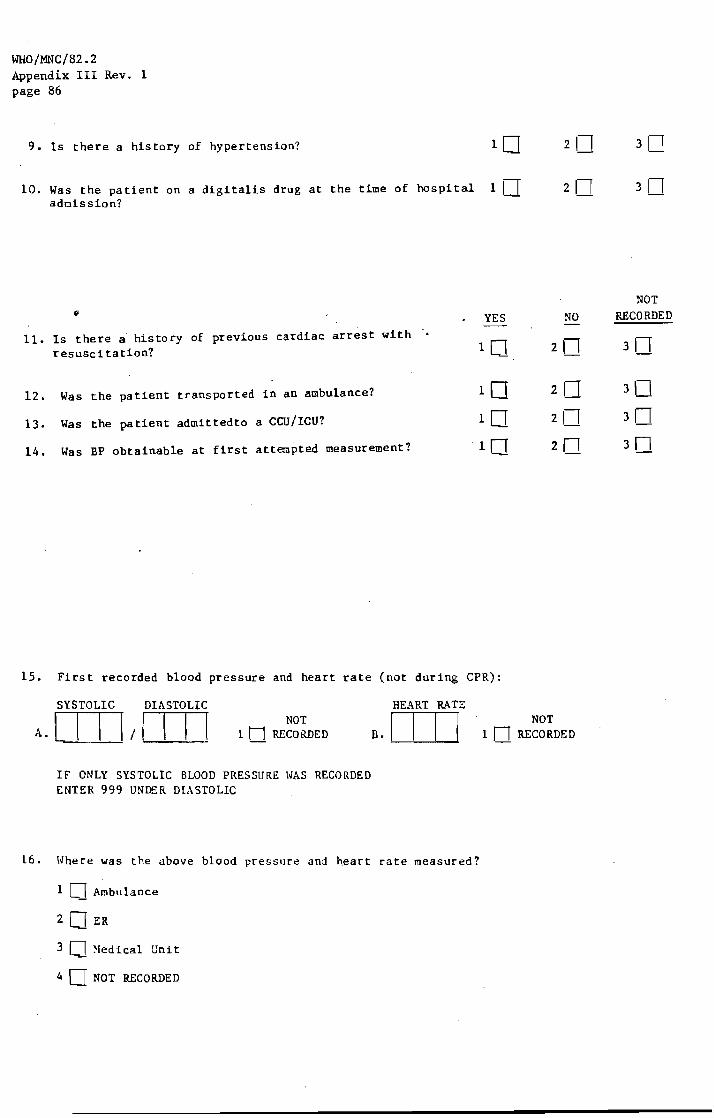
WHO/MNC/82.2 Appendix III Rev. 1 page 86
9. Is there a history of hypertension? 1 0
10. Was the patient on a digitalis drug at the time of hospital 1 D admission?
{I YES
11. Is there a history of previous cardiac arrest with . resusci tation? 10
12. Was the patient transported in an ambulance? 10 13. Was the patient admittedto a Cm/ICU? 10 14. Was BP obtainable at first attempted measurement? 10
15. First recorded blood pressure and heart rate (not during CPR):
SYSTOLIC DIASTOLIC HEART RATE NOT
NO
2n
2n 211 2n
NOT A. [I I \/1 I I [ 1 n RECORDED a.1 I I I 1 n RECORDED
IF ONLY SYSTOLIC BLOOD PRESSURE \O/AS RECORDED ENTER 999 UNDER DIASTOLIC
16. \o/here was the above blood pressure and heart rate measured?
1 0 Ambulance
20 ER
3 0 :-Iedical Unit
4 0 NOT RECORDED
NOT RECORDED
311
30 3n 3n
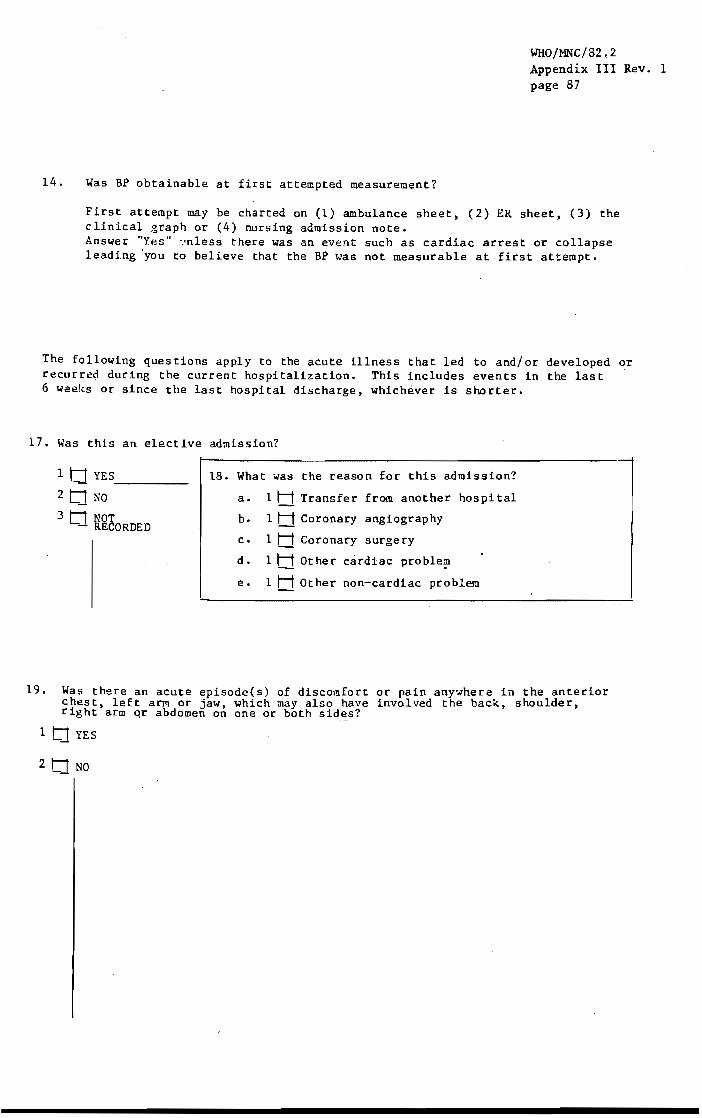
14. Was BP obtainable at first attempted measurement?
WHO/MNC/82,2 Appendix III Rev. 1 page 87
First attempt may be charted on (1) ambulance sheet, (2) ER sheet, (3) the clinical graph or (4) nursing admission note. Answer "Yes" 1.'nless there was an event such as cardiac arrest or collapse leading 'you to believe that the BP was not measurable at first attempt.
The following questions apply to the acute illness that led to and/or developed or recurred during the current hospitalization. This includes events in the last 6 weeks or since the last hospital discharge, whichever is shorter.
17. Was this an elective admission?
1 tJ YES ___ _ 18. What was the reason for this admission?
2 tJ NO a. 1 H Transfer from another hospital
3 tJ ~~eORDED b. 1 H Coronary angiography
c. 1 H Coronary surgery
d. 1 H Other cardiac proble?
e. 1 H Other non-cardiac problem
19. Was there an acute episode(s) of discomfort or pain anywhere in the anterior chest, left arm or jaw, which may also have involved the back, shoulder, right arm qr abdomen on one or both sid~s?
1 t1 YES
2 tJ NO

WHO/MNC/82.2 Appendix III Rev. 1 page 88
17. Elective Admission
Defined as any admission for a non-acute event. (E.g., repeated angina-patient admitted for stabilization of medication, or for coronary angiography). If an admission is through the ER, it is probably not elective.
19. If "Yes", answer Q.20-28. If "No" or "NR", go to Q.29. Record first "acute episode" of chest pain or discomfort, (a crushing, band-like pressure on chest) lasting more than 20 minutes. If there are several acute events (i.e., events occurring in-hospital), be sure to record information for each event in Q.2 (Narrative) using Q.19-28 as guidelines.
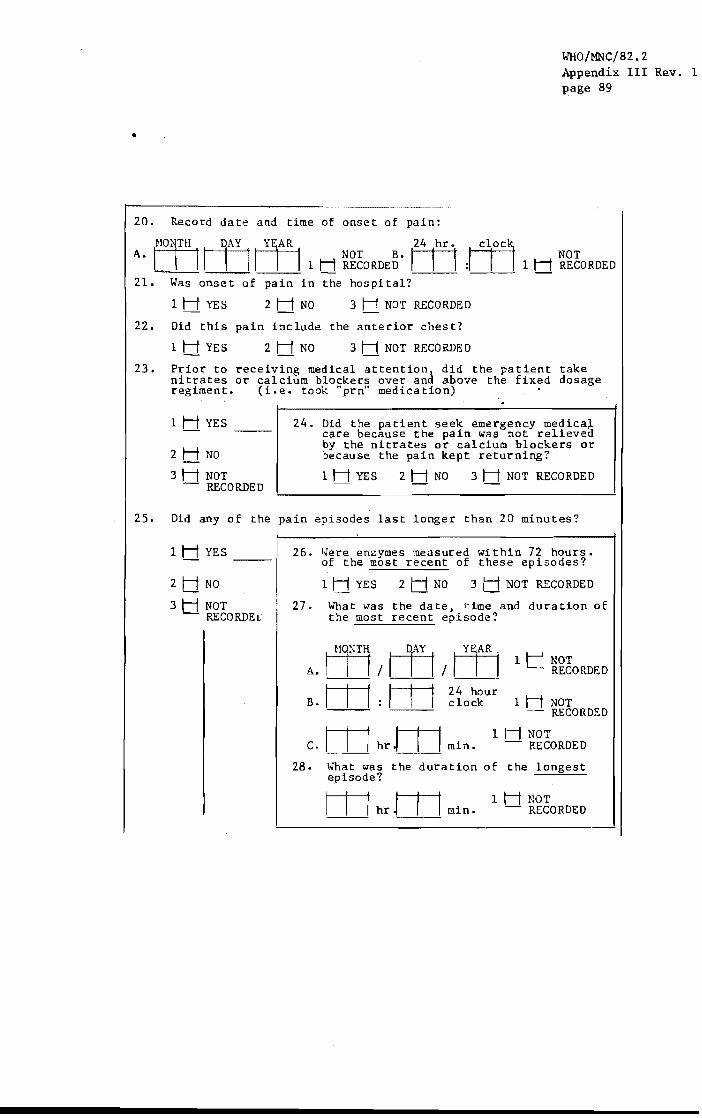
..
WHO/MNC/82.2 Appendix III Rev. 1 page 89
20. Record dat~ and time of onset of pain:
(OyH I DAY mAR 24 hr. A. t---f-=-t NOT B. m
I I I 1 H RECORDED "~ NOT I I I 1 H RECORDED
21. Was onset of pain in the hospital?
1 H YES 2 H NO 3 NOT RECORDED
22. Did this pain include the anterior chest?
1 H YES 2 H NO 3 H NOT RECOP~ED
23. Prior to receiving medical attention, did the patient take nitrates or calcium blockers over and above the fixed dosage regiment. (i.e. took "prn" medication)
1 H YES
2 H NO
3H NOT - RECORDED
24. Did the patient seek emergency medica~ care because the pain was not relieved by the nitrates or calcium blockers or because the pain kept returning?
1 H YES 2 H NO 3 H NOT RECORDE 0
25. Did any of the pain episodes last longer than 20 minutes?
1 H YES
2 t:1 NO
3 H NOT - RECORDE(;
26. l.Jere enzymes measured within 72 hours. of the most recent of these episodes?
1 H YES 2 H NO 3 H NOT RECORDED
27. What was the date, time and duration of the most recent episode?
\HTT1/m/m 1 NOT
A. RECORDED
B. m : lit ~io~~ur 1 H NOT - RECORDED
m m 1 1---1 NOT C. hr min. - RECORDED
28. Imat was the duration of the longest episode?
m m IHNaT hr min. - RECORDED
'----'---'

WHO/MNC/82.2 Appendix III Rev. 1 page 90
20. A. Record date of continuous episode of chest pain leading to admission
B. Record time chest pain began. Estimate clock time based on time of admission and any other statements in record. according to the 24-hour clock.
Time should be recorded
Explanation for 24-hour clock:
0100 0200
1 a.m. 2 a.m.
1200 1230
noon 12:30 p.m.
1300 = 1:00 p.m. 2400 = midnight
Record time only if enough data is available to make a reasonable estimate. Otherwise, record 9999=NR.
25. It is most crucial to attempt an accurate estimate if the pain lasted more than 20 minutes. If there were repeated episodes of pain of relatively short duration, record the length of the last episode prior to admission, and indicate the intermittent nature of symptoms in the narrative summary (Q.2). Answer "NR" if it is not possible to determine how long the pain lasted.
27. The most recent episode is the one that precipitated the patient's admission to the hospital or occurred within the hospital. Refer to history, physical examination and physician's progress notes for this information. Date is Q.27a. Time pain began is Q.27b and duration of pain is Q.27c.
28. The longest episode is from the moment - the patient first developed symptoms to when the pain was first relieved.

29.
WHO/MNC/82.2 Appendix III Rev. 1 page 91
Was there out-of-hospital collapse , .. ith closed chest massage and/or cardioversion (CPR) since last hospital discharge or within 6 weeks of this admission, whichever is shorter?
1 LJ YES ---
2 LJ NO
3 L I NOT - RECORDED
. i 31. Location of collapse: 1 Ll Home 2 I_I Work 3 I_I Other
32. CPR was administered by:
11_1 Bystander
21_1 M.D.
3 I_I Ambulance attendant, EMT, Fire, or Police
4 I_lather, specify ______________________________ __
5 '_I NOT RECORDED
33. Was DC countershock given (cardioversion)?
11_' YES 2' __ ' NO 3 I 'NOT RECORDED
34. Was cardiac rhy lllIl documented?
11_' YES __
21 __ ' NO
31 I NOT - RECORDED
35. What abnormal rhythm was documented (CHECK ALL THAT APPLi')
a. 1 '_I Ventricular fibrillation (VF)
b. 1 I_I Atrial flutter
c. 1 '_I Atrial fibrillation (AF)
d. 1 I_I Ventricula.r tachycardia (VT)
e. 1 ,_, Asystole
£. 1 ,_, Complete AV block (30 liB)
g. 1 LJ Other, __________ _

WHO/MNC/82.2 Appendix III Rev. 1 page 92
29. If "Yes", answer Q.30-35. If "No" or "NR", go to Q.36. Q.29 refers to an out-of-hospital occurence only, i.e., it would be answered "Yes" if a patient collapsed at work, had a cardiac arrest in the ambulance enroute to the hospital and CPR was administered at that time. Cardiovascular collapse is defined as a loss of consciousness with the apparent cessation of respiration and pulse. Cardiopulmonary resuscitation (CPR) is defined as electrical cardioversion for V-tach or V-fib and/or external cardiac massage by chest compression, combined with artificial ventilation by mouth-tomouth, bag/mask-to-mouth, or other means. A bystander is someone who initiates CPR immediately on the scene. A physician or other health professional with the patient in a non-professional capacity at the time would be counted as a bystander.
30-35. Refer to the following sources of information: emergency room notes, hospital admission notes, ambulance sheet (usually pink, sometimes to be located outside the patient chart).
ward notes, physician's progress notes, CPR or cardiac Refer to ER, ICU/CCU, arrest sheets.
35. If answered "Yes", check all items for a-f. These refer to the rhythm immediately surrounding CPR administration. "Other" (g) can be anything othel than Q.35a-e, including normal.

WHO/MNC/82.2 Appendix III Rev. 1 page 93
36. l,zas closed chest massage or cardioversion successfully administered during this hospitalizatio? (i.e. resulted in patlent being discharged alive).
1 LJ YES
2 LJ NO
3 U ~~tORDED
37. Where was CPR administered? (CHECK ALL THAT APPLy)
a. 1 1 __ 1 On ward/CCU/ICU
b. 1 I_i In emergency room
c. 1 I_I Other, spect
38. Was DC countershock (cardioversion) ever given during this hospitalization?
11_1 YES 21_1 NO 3 I_I NOT RECO RDE D
39. Has cardiac rhy hm documented at time of any cardioversion
11_'1 YES __
21_1 NO
3 U NOT RECORDED
40. Hhat abnormal rhyt h;n was documented? (CHECK ALL THAT APPLY)
a. 1 I_I Ventricular fibrillation (VF)
b. 1 I_I Atrial flutter
c. 1 I_I Atrial fibrillation (AF)
d. 1 U Ventricular tachycardia (VT)
e. 1 I_I Asystole
f. 1 1 __ 1 Complete AV block (3 0 HBj
f. 11_1 Other, __________ .
~1. Did the patient die during this admission?
1 tJ YES
2 t1 NO
42. T,zas the patient found dead? (I.e. not observed at the momenr of death)
1 HYES_ ~------------------------------43. Was patient observed to be free of
severe cardiac symptoms within one hour of .being found dead? 2 H NO
3 NOT 1 H YES 2 1-1 NO 3 H NOT RECORDED
TRDED 44. l,zas patient free of severe cC'rdiac symptoms within 24 hrs. of death?
1 H YES 2 H NO 3 H NOT RECO RDE D
GO TO Q. 48
45. Did patient die without developing severe cardiac symptoms? (i.e. died instantaneously)
1 H YES 2H NO
I 3 1-1 NOT RECORDED
1 1------------------"--------
46.
47.
Did the patient die within one hour JE developing severe cardiac symptoms?
1 H YES 2 1-1 :W 3 1-1 NOT RECO R[)E D
Did the patient di.e within 24 hours of developing severe cardiac symptoms?
1 t:1 YES 2 II ~W 3 t:1 NOT RECORDED
GO TO Q. 48
48. Was this de3th thou,:}ht to be a ter:ni:1al cQ!:Ipl1cation of 3 non-cardiac disease.
1 H Y£S 2 H ~O 3 H NOT RECORDED

WHO/MNC/82.2 Appendix III Rev. 1 page 94
36. Check appropriate box. Refer to ER, ICU!CCU, ward notes, CPR or cardiac arrest sheets. Answer "yes" only if the patient received CPR. at any time in-hospital and was alive at discharge.
EXAMPLE: CPR administered twice in-hospital.
37-40.
41-48,
Patient died in-hospital.
No CPR in-hospital. Patient alive at discharge.
CPR administered 5 times in-hospital. Patient alive at discharge.
Follow instructions for Form 04, Q.30-35.
ANSWER: No
ANSWER: No
ANSWER: Yes
If the patient died during this admission, refer to the physician's progress notes, the nurse's notes and the discharge summary for this i.nformatior\.

WHO/MNC/82.2 Appendix III Rev. 1 page 95
49. Were either of the following observed? PRESENT ABSENT
a. Rales (exclude basilar)
b. 83 (3rd heart sound, ventricular gallop) CHECK "PRESENT" IF SUNNATIO~1 GALLOP EXCLUDE S4 OR ATRIAL GALLOP.
10 10
50. Was there evidence of a stroke during this hospitalization, within 6 weeks of this event or since last hospital discharge whichever is shorter?
I t:1 YES
2 t:r NO
3 tI NOT RECORDED
COHPLETE FORt1 06
51. Were ECG's recorded?
1 tI YES _____ _ INCLUDE COPIES OF ALL TRACINGS
~ tI NO
3 tI NOT RECORDED
52. Was a coronary angiography performed?
1 tJ YES ------2 C1 NO
3 tJ NOT RECORDED
I
m/l--Tl/m 1 H NOT RECO REDE D
INCLUDE A COpy OF THE CORONARY ANGIOGRAPHY REPORT
53. Date of procedure:
54. Has patient had any surgical procedures this admission?
1 t:r YES
2 tr NO
55. Dates of Procedures:
~~~ a. Ll.J / I I I I Ll.J b.mlmlm c.mlmllll
57. Status of Chest X-rays (check one)
X-rays not done
Reports not present
56. Specify procedures:
--------------------------------~ __ J
All reports say "no change" and refer to other ad~i8sions
~ot at 1 films read as "nonal"
All films read as "nor1:<11"
(XEROX ALL COPlr:S OF CH~:ST X-RAYS)

WHO/MNC/82.2 Appendix III Rev. I page 96
50. Refer to physician's admitting note. If answered "Yes", complete Form 06.
51. If answered "Yes", attach all tracings for each acute event. Photocopy mounted 12-lead ECG's only. An attempted 12-lead is counted as a 12-lead ECG. Do not photocopy tracings from exercise stress tests unless no other ECG is available, in which case only the resting. preexercise tracing should be copied. If there are multiple acute cardiac events in-hospital. include all ECG's for each event.
52. If answered "Yes", attach photocopy and answer Q.53. If M.D. mentions a~giogram in progress notes or elsewhere in chart, but there is no spec1fic date listed and notation that an angiogram was done and there is no report, check N.R.
57. Check one box only. If box tl 4 is checked ("not all films read. as normal"), photocopy all chest X-rays and attach to form.
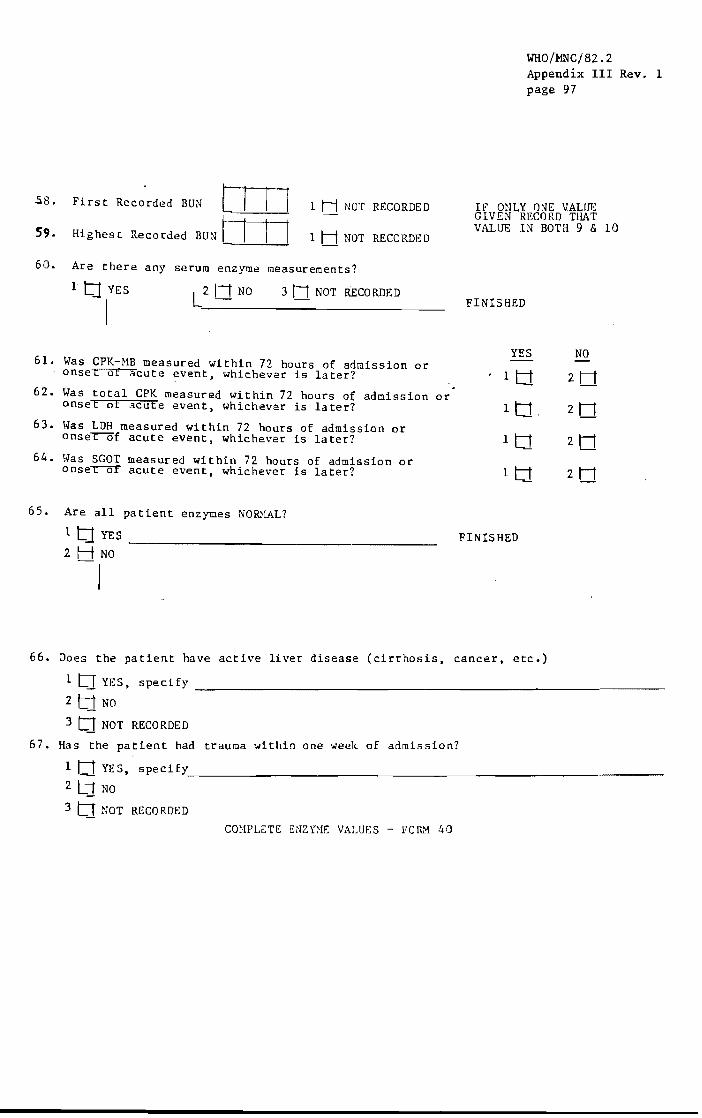
.5.8.
59.
Fi rs t Recorded BUN [I I I Highest Recorded BUN I I I I
1 H NOT RECORDED
1 H NOT RECORDED
60. Are there any serum enzyme measurements?
3 NOT RECORDED
61. Was CPK-MB measured within 72 hours of admission or onset of acute event, whichev2r is later?
62. Was total CPK measured within 72 hours of admission or onset of acute event, whichever is later?
63. \.\Tas LDH measured Within 72 hours .of admission or onse~f acute event, whichever is later?
64. \vas SGOT measured within 72 hours of admission or onse~ acute event, whichever is later?
65. Are all patient enzymes NOID1AL?
1 tI YES ________________ _
2 H NO
-I
WHO/MNC/82.2 Appendix III Rev. 1 page 97
IF ONLY ONE VALUE GIVEN RECORD THAT VALUE IN BOTH 9 & 10
FINISHED
YES NO
FINISHED
66. Does the patient have active liver disease (cirrhosis, cancer, etc.)
1 tJ YES, specify _______________________ ~--_
2 t1 NO
3 t:J NOT RECORDED
67. Has the patient had trauma < .. ithin one week. of admission?
1 t1 YES, specify, ___________________________________________________________ __
2 t1 NO
3 t:I NOT RECORDED
cmlPLETE ENZnlE VALUES - FOlt.'1 40

WHO/MNC/82.2 Appendix III Rev. 1 page 98
58-59. Record the first and highest BUN values obtained during this hospitalization. Refer to lab sheet and ER sheet for these values. If only one BUN was obtained, record this value in boxes for Q.58-59.
60. If answered "Yes", complete Q.61-67 and Enzyme Values - Form 40. If answered "No" or "NR", you are finished.
61-64 Refer to lab sheets or lab reports. The enzymes ?re CPK-MB, total CPK, total LDH, and SGOT. Total CPK = MB+MM+BB. '9PK synonyms are CK, CKI. If any of these have been measured within 72 hours of admission or onset of the acute event, whichever is later, answer "Yes", and' go to Q.65. Answer "No" if lab sheet is missing, or if lab values were measured after 72 hours of admissIon or onset of acute event, whichever is later. For further information on eyzyme values, see instructions for Form 40: Enzyme Values.
65. Refer to the hospital's established normal values listed in the chart or obtainable from the hospital lab to determine if the patient's values are within normal range. If answer to Q.65 is "Yes", you are finished.
If there are any abnormal patient enzyme values, complete Q.66-67 and complete Enzyme Values - Form 40. See instructions for Form 40~ Enzyme Values.

WHO/MNC/82.2 Appendix III Rev. 1 page 99
E N Z Y MEV A L U E S FORM 40
Pe(}DX'd OJ 12
1. =:.....::=-=.
2. =:.....::=-=.
3. RANGE SET 3
CHART A - LABORATORY STANDARDS
PRESENT/POSITIVE - 7777 TRACE ~ 7777
ABSENT/NEGATIVE - 6666
LOW I 30
HIGH 1 46
CHART B - PATIENT'S VALUES
1D LABEL
-L------------------------fRecord 02 RECORD ALL ENZYMES IN FIRST 24 HOURSA AND THE HIGHEST READINGS FOR EACH OF THE NEXT 3 DAYS FOLLOWING
AN ACUTE EVENT. PLACE THE APPROPRI TE RANGE SET NUMBER IN THE BOX ON THE RIGHT.
A. B. C. D. E. RANGE RANGE RANGE RANGE
MONTH DAY HOUR CPK-MB SET TOTAL CPK SET SGOT SET TOTAL LOR SET
4. gJ[[l QJrn IJ I I IQ I~J I I IQ 14J I 1 l~l1531 1 I [el 5. rn[[l rnrn I I I 1 10 1 I 1 1 1 I I I I 10 I I I I I
12
IDCODE 14 2. 9
6. " rn riJrn ': 0 ': 0 ': q I:) [ [I i~ig~;'03 rn rnrn I I I I 10 I 1 I I 10 1~1--&.-1 -I---lD 0 IDCCDE 12
30 3~ 38 42 43 47 48 ,2 53 57 14 2.9
7.
8. rnrn rnrn 1 I 1 I 10 1 I 1 1 10 I I I 0 I 1 I 1 10 '0 62 66 70 71 75 76 60 OJ 65
9. rnDJ rnrn 1 1 I I 10 I 1 I 1 10 [ I I 0 I I 1 10 114 145 86 9U g~ 98 99 103 10~ 108 109 113
10. OJrn OJ 0 I) I 1 10 I.) I Q 1'3 1 I 10 IDCODE 7: 11 OJ cprn b 0 IJ I I 10 7 Q 181 I 1 10
14 29
12: OJDJ OJDJ I) I I 10 I) I I 10 [oJ I I 10 los 1 I IW 13. OJDJ rn [) I 1 10 I) I I 10 [) 1 I IW L7 I I In 142145 h-rl skip
'llhmJlP-Moa.B 40(1-1) 1/82 Ver. 1
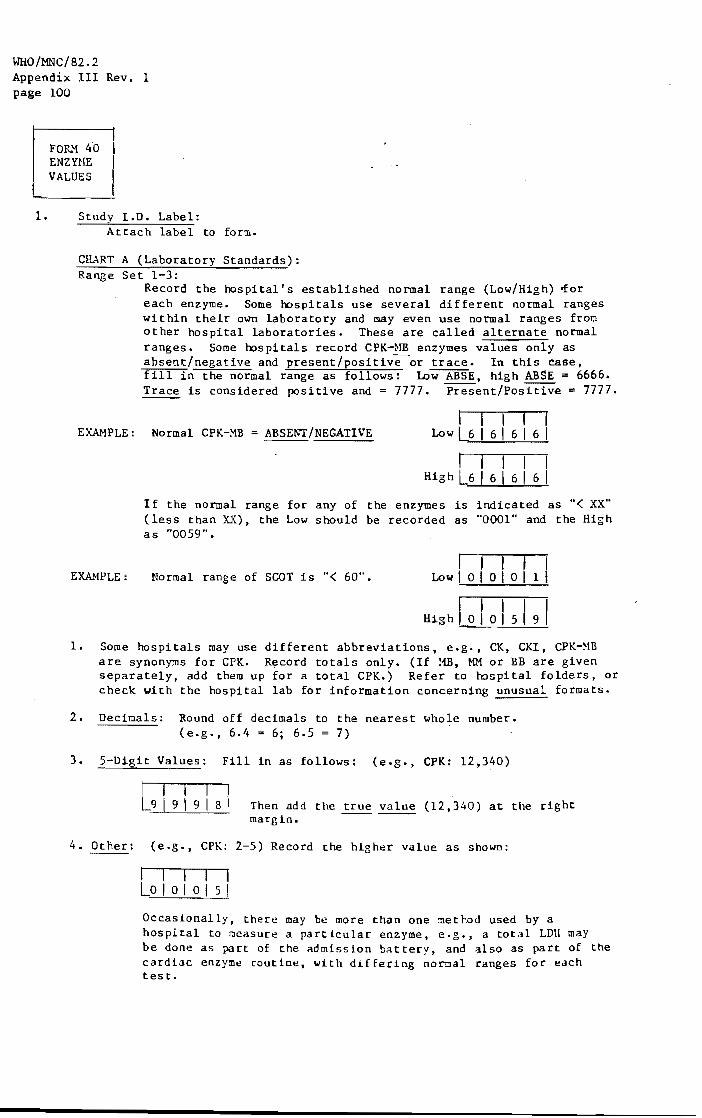
WHO/M.NC/82.2 Appendix III Rev. 1 page 100
FOR}l 4'0 ENZYHE VALUES
L~ __ ~ 1. Study 1.0. Label:
Attach label to form.
CHART A (Laboratory Standards): Range Set 1-3:
Record the hospital's established normal range (Low/High) ~or each enzyme. Some hospitals use several different normal ranges within their own laboratory and may even use normal ranges from other hospital laboratories. These are called alternate normal ranges. Some hospitals record CPK-}lB enzymes values only as absent/negative and present/positive or trace. In this case, fill in the normal range as follows: Low ABSE, high ABSE = 6666. Trace is considered positive and = 7777. Present/Positive = 7777.
EXAMPLE: Normal CPK-MB ABSENT/NEGATIVE I I I I I
Low L6 I 6 I 6 I 6 I
EXM1PLE:
I I I I I High L6 I 6 I 6 I 6 I
If the normal range for any of the enzymes is indicated as "< XX" (less than X.X), the Low should be recorded as "0001" and the High as "0059".
Normal range of SGOT is "< 60". I I I I I
Low I 0 I 0 I 0 I 1 I
I I I I I High I 0 I 0 I 5 I 9
1. Some hospitals may use different abbreviations, e.g •• CK, CKI, CPK-HB are synonyms for CPK. Rt;!cord totals only. (If HB, MM or BB are given separately, add them up for a total CPK.) Refer to hospital folders. or check with the hospital lab for information concerning unusual formats.
2. Decimals: Round off decimals to the nearest whole number. (e.g., 6.4 .. 6; 6.5 = 7)
3. 5-Digit Values: Fill in as follows: (e.g., CPK: 12,340)
[I I I I 91919181 Then add the true value (12,340) at the right
margin.
4. Other: (e.g., CPK: 2-5) Record the higher value as shown:
I I I I I Lo I 0 I 0 I 5 I
OccaSionally, there may be more than one ::lethod used by a hospital to r:leasure a particular enzyme, e.g., a total LOll may be done as part of the admission battery, and also as part of the cardiac enzy~e routine, with differing normal ranges for each test.

WHO/MNC/82~2 ,Appendi:x: I n Rev. 1 page 101
FO~1 40 ENZY~IE
VALUES
4-13. CHART B (Patient's Values):
4.
Record all patient's enzymes in first 24 hours. Also include the highest reading for each of the 3 days after each acute event. Place the appropriate range set number in the last box on the right.
Month/Day: Use "leading zeroes", if necessary.
Hour: Record time according lu the 24-hour clock. If the time given in the chart is from the 12-hour clock, it should be converted to the 24-hour clock.
EXAMPLE: 0100 0200
1 a.m. 2 a.m.
1200 1230
noon 12:30 p.m.
1300 2400
1:00 p.m. lIlidnight
Refer to the lab sheet or lab report for patient values.
NOTE: There is a difference between CPK-}1B and total CPK. Be sure to fill in the appropriate values beneath the proper heading and to use totals when indicated under headings D. and F.
NOTE: If some enzymes are not measured at a given time, draw a line through boxes corresponding to enzymes not measured. See below.
C H ART B (PATIENT'S VALUES) A. B. C. RANGE I D. RANGE I E. RANGE I F. RAt~GE
MONTH DAY HOUR CPK-NB SET 1 TOTAL CPK SET 1 SGOT SET 1 TOTAL LDH SET
[~ ~ 1:0 I Q a ~ Q I 1=1=1=1i l-=r I I Q ~ ~ a nr I l=1iii r:r I I l=1ii=1 0
Range Set: Fill in corresponding range set number from Chart A (1,2,or 3). (See instructions for Chart A.
Use as many Form 40's as necessary, and attach to HI Form 04.

ECG C~G FORM 1-------------,
MMMP 1.0.# I ______ .--1 Abstractor# ____ Date Coded ___ _ ------- -
CRJibG ~de-.S 1 4 5 9-2 Uncoded leads 10mm. Date
l~AYL, ~tJ~ V1-V5 I,AVL, II,AVF V2-V5 I,AY1, II,AVF V2-V5 I,t,~_, 11,111, V1-V5 ±.25 V6 V6 V6 AVF Ireason and leadl*~
-
! I
--
---
--- ----r---
---'--------
ECG Category: _Evolving diagnostic _Diagnostic ._Equivocal _Other -
*.1 = yes 2=no
-t*Reasons for uncodable complexes: Complete A-V block 16-11 Artificial pacemaker 16-81 QRS >.12 ' 11-41 Asystole or V. fib. (8-21 Technical problems 19-81
I
Lead numbering: 1=01 11-02 11.=03 'AVL=04 Ji"f: .".n'=t
.V1=11, V2=12, etc. present in alilead9 =33
LPH-MMMP (1/81) 18-1
Examplel w"lndering baseline in lead V6 .I".l1i hn Q-R 11~
I

1. ID LABEL
STROKE HOSPITAL ABSTRACT
FORM 06
LPH/MHHP-MORB 06(1-9) 1/82 Ver. 1
WHO/MNC/82.2 Appendix III Rev. 1 page 103
Reoord O~ 1 ;
IDCODE 1.. 2 ~
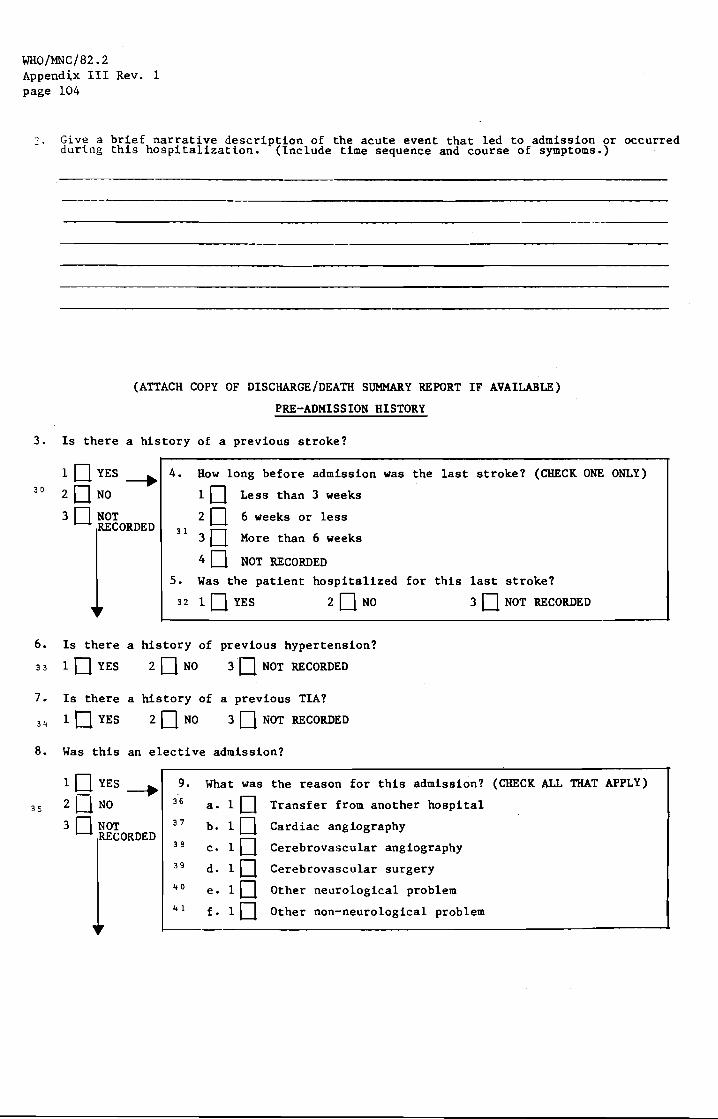
WHO/MNC/82.2 Appendix III Rev. 1 page 104
o - . Give a brief narrative description of the acute event that led to admission or occurred during this hospitalization. (Include time sequence and course of symptoms.)
---------------------
(ATTACH COpy OF DISCHARGE/DEATH SUMMARy REPORT IF AVAILABLE)
PRE-ADMISSION HISTORY
3. Is there a history of a previous stroke?
30
6.
33
7.
34
8.
3S
1 0 YES -----. 4. How long before admission was the last stroke? (CHECK ONE ONLY)
20 NO
30 NOT
10 Less than 3 weeks
CORDED 20 6 weeks or less
31 3D More than 6 weeks
40 NOT RECORDED
5. Was the patient hospitalized for this last stroke?
32 1 0 YES 20 NO 30 NOT RECORDED
Is there a history of previous hypertension?
10 YES 20NO 3D NOT RECORDED
Is there a history of a previous TIA?
10 YES 20NO 3D NOT RECORDED
Was this an elective admission?
10 YES ~ 9. What was the reason for this admission? (CHECK ALL THAT APPLY)
2 UNO 36 a. 10 Transfer from another hospital
3D NOT 37 b. 10 Cardiac angiography CORDED
10 38 c. Cerebrovascular angiography 39 d. 10 Cerebrovascular surgery .. 0 e. 10 Other neurological problem .. 1 f- lO Other non-neurological problem
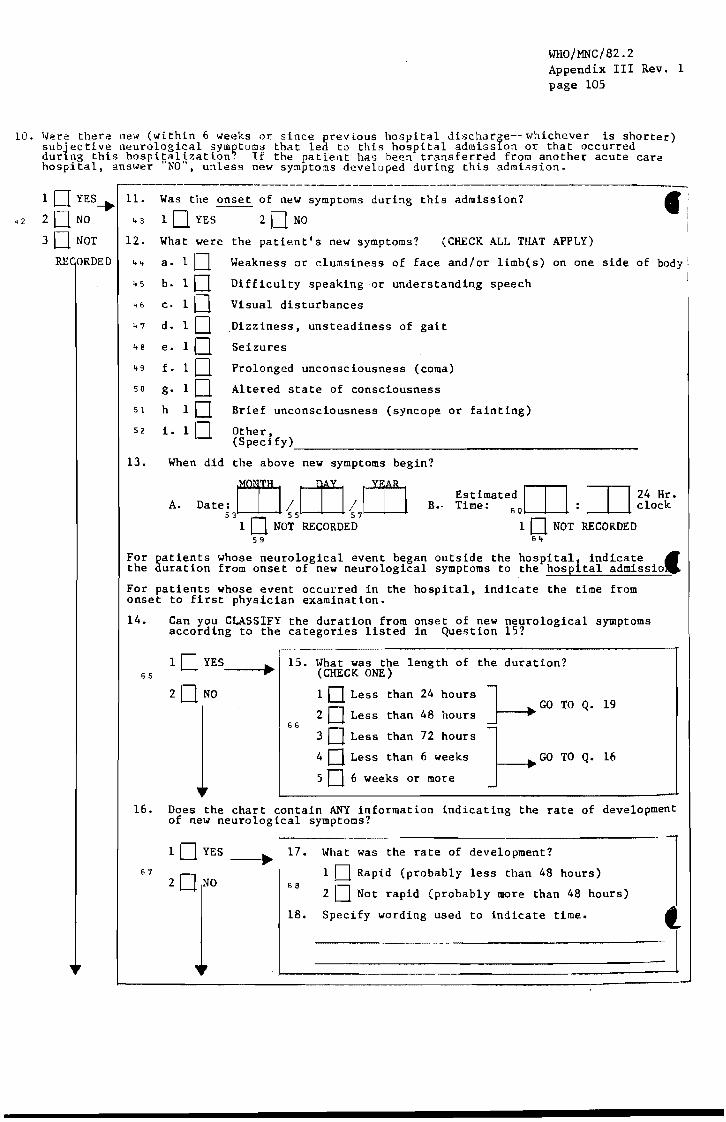
10.
WHO/MNC/82.2 Appendix III Rev. 1 page 105
\~ere there new (within 6 weeks or since previous hospital discharlSe-- whichever is shorter) subjective neurological 5ym~toms that led to this hospital admisslon or that occurred durlng this hospitalization. If the patient has been transferred from another acute care hospital, answer "NO", unless new symptoms developed during this admission.
;------------------------- -------------------1 D YES-.. 11. Was the onset of new symptoms during this admission? f ~
42. 2 0 NO 43 1 0 YES 2 0 NO
3D NOT 12. What were the patient's new symptoms? (CHECK ALL THAT APPLY)
RE ORDED 44 a. 10 Weakness or clumsiness of face and/or limb(s) on one side of body
45
46
47
48
"9 50
51
S2
13.
b. 10 Difficulty speaking ·or understanding speech
c. 10 Visual disturbances
d. 10 Dizziness, unsteadiness of gait
e. 10 Seizures
f. 10 Prolonged unconsciousness (coma)
g. 10 Altered state of consciousness
h 10 Brief unconsciousness (syncope or fainting)
i- 10 Other (Specify)
When did the above new symptoms begin?
A. Date:W/W/W 53 55 57
B.· Estimated OJ OJ 24 Hr. Time: 60 : clock
1 0 NOT RECORDED 59
1 0 NOT RECORDED 6 ..
For patients whose neurological event began outside the hospital indicate ~ the duration from onset of new neurological symptoms to the hospital admissiolJ
For patients whose event occurred in the hospital, indicate the time from onset to first physician examination.
14. Can you CLASSIFY the duration from onset of new neurological symptoms according to the categories listed in Question 15?
65 10 yES __ .....
20 NO
15. \.J'hat was the length of the duration? (CHECK ONE)
66
1 0 Less than 24 hours
2 0 Less than 48 hours
3 0 Less than 72 hours
4 0 Less than 6 weeks
5 0 6 weeks or more
J---. GO TO Q. 19
:;::
1--". GO TO Q. 16
-16. Does the chart contain ANY information indicating the rate of development
of new neurological symptoms?
67
10 YES __ .... 17.
20 NO 68
What was the rate of development?
1 0 Rapid (probably less than 48 hours)
2 0 Not rapid (probably more than 48 hours)
18. Specify wording used to indicate time. t I

WHO/MNC/82.2 Appendix III Rev. 1 page 106
PHYSICIAN'S EXAM FINDINGS
J-9 Did a physician document a new localizing neurological deficit (within 6 weeks or since previous hospital discharge) whichever is shorter) or did a CAT SCAN indicate definite or probable cereDral infarction or nemorrhage without other pathology?
69 1 [] YES 2[] NO
• 20. Can you CLASSIFY the length of time from symptom onset to physician exam in hospital according to the categories listed in Question 2l?
70 1 DYES
2 DNO
__ ....... 21.
71
What was the length of time from symptom onset?
1 [] Less than 72 hours
2 0 Less than 3 weeks
3 0 Less than 6 weeks
4 0 6 weeks or more GO TO Q. 25
22. Does the chart contain any information indicating the length of time from symptom onset to physician exam?
l[]YES~ 23. What was the length of time from symptom onset? 72 1 0 Probably less than 6 weeks
73
20 NO 2 0 ProbablY 6 weeks or more
24. Specify wording used to indicate length of time
25. \Jhat was the conclusion from the pupil examination'? (abnormal • "constricted" or "dilated" or "unresponsive to light") (CHECK ONE)
1 D Both normal
2 [] One abnormal (anisocoria)
74 3 D Both abnormal
4 [] Physician not sure/cannot determine
5 [J NOT EXAMINED (NR)
26. What was the conclusion from the Plantar (Babinski) reflex examination? (Abnormal" "positive". "up-going toe". ~·extensor". or "present") (CHECK ONE)
1 [] Normal both sides
2 [] Abnormal one side
3 [J Abnormal both sides
4 [] "Equivocal" one or both sides
5 [J NOT EXAMINED (NR)
76 85
skip

WHO/MNC/82.2 Appendix III Rev. 1 page 107
27. What was the patient's level of consciousness? (CHECK ONE) R{v~oY'd 02
12
IDCODE
1 [] Comatose (unresponsive to pain, voice, or other stimuli) 1 ~ 2;
2 [] Unconscious but responsive to pain or other noxious stimuli
30 3 [] Conscious, but with abnormality of consciousness or orientation
4 [J Normal, conscious and oriented
5 [] NOT RECORDED
28. What were the motor function findings? Each item refers to the body region indicated or any parts thereof.
UNAFFECTED AFFECTED 0 BUT CAN BE M VIW TOTALLY NOT
(NORMAL) BY PATIENT PARALYZED RECORDED
a. Left Arm 31 l[] 2[] 3[] 4[] b. Right Arm 32 l[] 2[] 30 4[J c. Left Leg 33 l[] 2[] 3[] 4[] d. Right Leg 3" l[] 2[] 3[] 4[] e. Left Face 35 l[J 2[] 3[] 40 f- Right Face 36 10 2[] 3[] 40
29. Did the patient have any of the following neurological deficits? (SEE MANUAL FOR DEFINITIONS)
YES NO NOT RECORDED
a. Aphasia 37 10 20 3[] b. Apraxia 38 l[] 20 3[] c. Dysarthria 39 l[] 20 30 d. Visual field defects 10 2[] 3[]
.. 0 e. Other .. 1 l[] 2[] 3[]
specifl:
30. Was the patient's temperature recorded on this admission (ER/WARD!CCU)?
42 10 YES-..
2DNO
31. What was this first temperature recorded in the hospital after onset of symptoms?
I I 1 I 0 "7~ O[]: ~ 43
(Indicate farenheit or centigrade)
32. How was this temperature obtained?
48 lD Oral 2 0 Rectal 3 [] Axillary 4 [] NOT RECORDED

WHO/MNC/82.2 Appendix III Rev. 1 page 108
33. Was the blood pressure recorded on this admission (ER/WARD/ICU)?
1 0 YES ______ .... 34.
2°f What was the first blood pressure reading recorded in the hospital after onset of symptoms?
35. Can you CLASSIFY the duration of new objective findings of localizing neurological deficit according to the categories listed in Question 36?
10 YES ... 36 . What was the duration of the objective deficit from first physician documentation until last? (CHECK ONE) 56
2U 0 10 Less than 1 hour
20 Less than 24 hours 57
3D 48 Less than hours
40 Less than 72 hours
50 72 hours or 1IIOre
GO TO Q. 37
37. Does the chart contain any information indicating duration of deficit or coma?
58 1 0 YES _____ _. ...
20 NO
38. What was the duration?
1 0 Transient (probably 24 hours or less) S9
2 0 Prolonged (probably 1IIOre than 24 hours)
39. Specify wording used to indicate duration.
40. Was the patient discharged alive?
1 0 YES ______ .......
2D!o 60
GO TO QUESTION 43
41. Did death occur within 6 weeks of first documentation of deficit?
lDYES ___________ ~r---------------------------------------, 42. What was the duration from first physician
2 0 NO documentation to death? (CHECK ONE) 6 J
10 Less than 24 hours
62 20 Less than 48 hours
30 Less than 72 hours
40 72 hours or more
50 Unknown
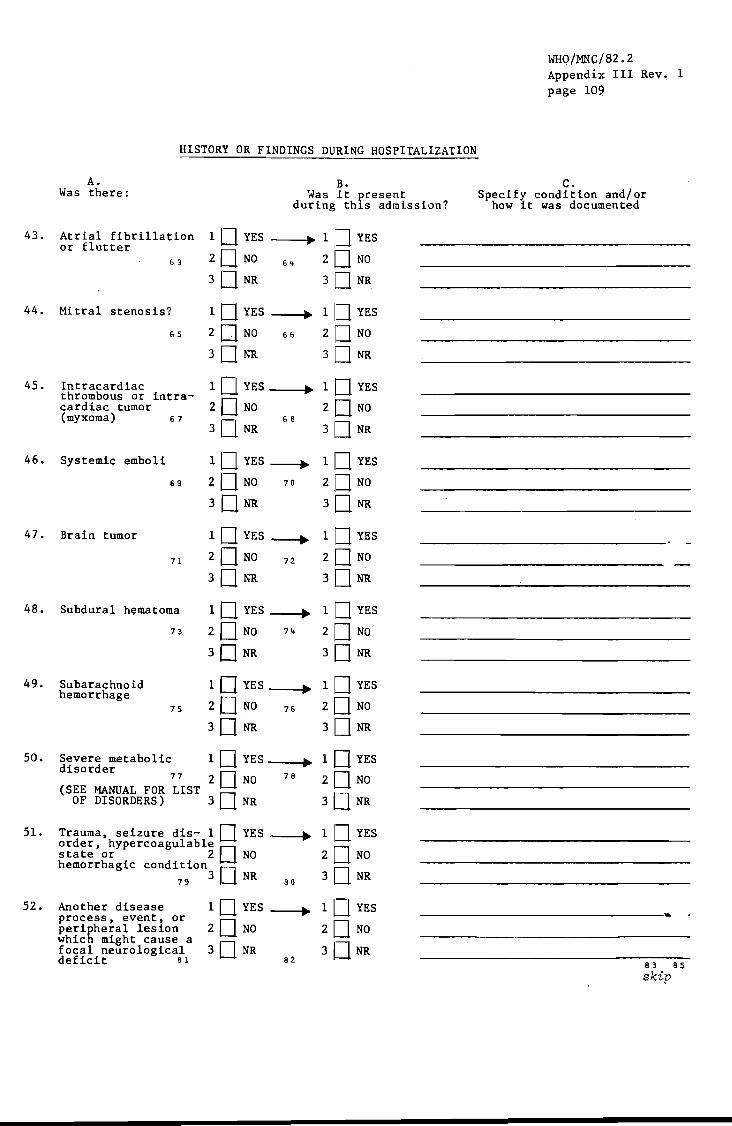
43.
44.
45.
46.
47.
48.
49.
50.
51-
52.
HISTORY OR FINDINGS DURING HOSPITALIZATION
A. B. Was there: Was it ?resent
during th1s admission?
Atrial fibrillation 1 0 YES ~ 1 IJ. YES or flutter
20 NO 20 NO 63 64
3D NR 3 D NR
Mitral stenosis? 1 0 YES ~ 1 [] YES
65 2 DNO 66 20 NO
3 D NR 3 D NR
Intracardiac 1 0 YES • 1 0 YES thrombous or intra-
20 NO 2 DNO cardiac tumor (myxoma) 67
3D NR 68
3 D NR
Systemic emboli 1 0 YES ----. 1 0 YES
69 20 NO 70 20 NO
3 DNR 30NR
Brain tumor 1 0 YES---+ 1 0 YES
71 2 DNO 72 20 NO
3D NR 3DNR
Subdural hematoma 1 DYES---+ 1 0 YES
73 2 D NO 7'+ 2 D NO
3DNR 3D NR
Subarachnoid 1 0 YES • 1 DYES hemorrhage
20 NO 20 NO 75 76
3 D NR 3D NR
Severe metabolic 1 0 YES ~ 1 0 YES disorder
77 2 D NO 78 2 DNO (SEE MANUAL FOR LIST
3 D NR 3D NR OF DISORDERS)
Trauma, seizure dis- 1 0 YES ---+ 1 [] YES order, hypercoagulable []
2 D NO state or 2 NO hemorrhagic condition 0
3D NR 79 3 NR 80
Another disease 1 0 YES ----. 1 0 YES process, event, or
2 D NO 20 NO peri~heral lesion whic might cause a
3D NR 3DNR focal neurological deficit 81 82
WHQ/MNC/82.2 Appendix III Rev, 1 page 109
c. Specify condition and/or
how it was documented
83
skip 85

WHO/MNC/82.2 Appendix III Rev. 1 page 110
53. Was there any evidence (e.g. history, prior to this admission or during this
1 [] YES, COMPLETE FO~~ 04
2 [] NO
'[]JrOT RECORDED
physical, or laboratory) of an MI within 8 weeks hospital1zation?
Record 03 12
IDCODE 14 2'.1
54. Was there a spinal tap?
10 YES ---1 ••
20 0
55. What was the result of the spinal tap? (CHECK ONE)
10 CLEAR AND COLORLESS l s~gf~Y I I I I I I 20 BLOOD IN SPINAL TAP J--'" .... 3'""":3....1--+-~-+--...,. 3 0 "GROSSLY BLOODY" -
32
56. Were there other abnormal CSF findings? 10 YES ,specify ____________________ _
38 20 NO
3 0 NOT RECORDED
57. Was there cerebral angiography?
39
10 YES __ .....
20 NO
ATTACH COPIES OF CEREBRAL ANGIOGRAPHIES
58. Did it precede the neurological deficit?
40
10 YES--+
20 0
59.
41
By how many hours did the angiography precede the event? (CHECK ONE)
1 0 Less than 24 hours
2 0 Less than 48 hours
3 0 Less than 72 hours
4 0 72 hours or more
60. Was there cardiac angiography?
42 10 YES ---1 ...
20 NO 61.
43
ATTACH COPIES OF CARDIAC ANGIOGRAPHIES
Did it precede the neurological deficit?
10 YES --JI-2[] 0
62. By how many hours did the angiography precede the event? (CHECK ONE)
1 0 Less than 24 hours
2 0 Less than 48 hours
3 [] Less than 72 hours
4 [] 72 hours or more
63. l-las there a radionuclide brain scan?
1 0 YES __ -I •• ATTACH COPIES OF TEST REPORTS
2 [] NO
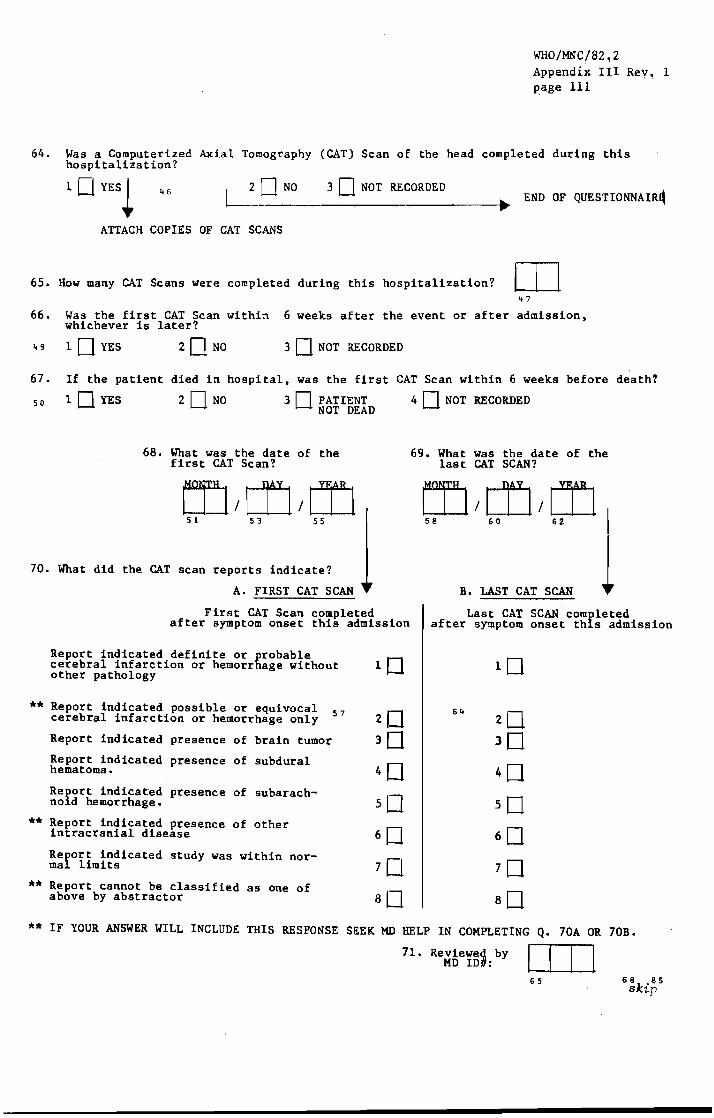
WHo/MNC/82~2
Appendix III ReY1 1 page 111
64. Was a Computerized Axial Tomography (CAT) Scan of the head completed during this hospitalization?
1 0 YES~ L ONO 3 0 NOT RECORDED ~ END OF QUESTIONNAIR~
ATTACH COPIES OF CAT SCANS
65. How many CAT Scans were completed during this hospitalization? OJ .. 7
66. Was the first CAT Scan within 6 weeks after the event or after admission, whichever is later?
49 10 YES 20NO 3 0 NOT RECORDED
67. If the patient died in hospital, was the first CAT Scan within 6 weeks before death?
50 1 0 YES 2 0 NO 3 0 PATIENT 4 0 NOT RECORDED NOT DEAD
68. What was the date of the first CAT Scan?
69. What was the date of the last CAT SCAN?
70. What did the CAT scan reports indicate?
**
**
**
A. FIRST CAT SCAN
First CAT Scan completed after symptom onset this admission
Report indicated definite or probable cerebral infarction or hemorrhage without other pathology
Report indicated possible or equivocal cerebral infarction or hemorrhage only 57
Report indicated presence of brain tumor
Report indicated presence of subdural hematoma.
Refort indicated presence of subarach-no d hemorrhage.
Report indicated presence intracranial disease
of other
Re~ort indicated study was within nor-ma limits
Report cannot be classified above by abstractor
a's one of
20
3D 40 50 60 70
aD
B. LAST CAT SCAN
Last CAT SCAN completed after symptom onset this admission
** IF YOUR ANSWER WILL INCLUDE THIS RESPONSE SEEK MD HELP IN COMPLETING Q. 70A OR 70B.
71. Re~fie¥~~:by I I I I 65 68 85
skip

WHO/MNC/82.2 Appendix III Rev. 1 page 112
1. lD LABEL
STROKE HOSPITAL ABSTRACT
FORM 06
Reco'f'd C I
IDCODE )1, 2

I' II CVA HOSPITAL ABSTRACT ~
I~ II STROKE ,I II , FORH 06
j
" Q.l. Study I.D. Number Attach study I.D. number label to cover sheet of Form 06.
WHO/MNC/82.2 Appendix III Rev. 1 page 113
2. Give a brief narrative qescription of the acute event that led to admission or occurred during this hospitalization. (Include time sequence and course of symptoms.)
(ATTACH COpy OF DISCHARGE/DEATH SUHMARY REPORT IF AVAILABLE)
PRE-ADMISSION HISTORY
, 3. Is there a history of a previous stroke?-
6.
7.
lUYES_ 4.
2 UNO
H10UW Ilong before admission was the last stroke? (CHECK ONE ONLY) l Less than 3 weeks
3 LJ N~CORDED 2 I_I 6 weeks or less I
Is there a
1 U YES
Is there a
1 LJ YES
More than 6 weeks 3U 41_1 NR
5. Was the patient hospitalized for this last stroke?
1 I_I YES 21_1 NO 3 I_I NOT RECORDED
history of previous hypertension?
2 UNO 3 I_I NOT RECORDED
history of a previous TIA?
21_1 NO 31_1 NOT RECORDED
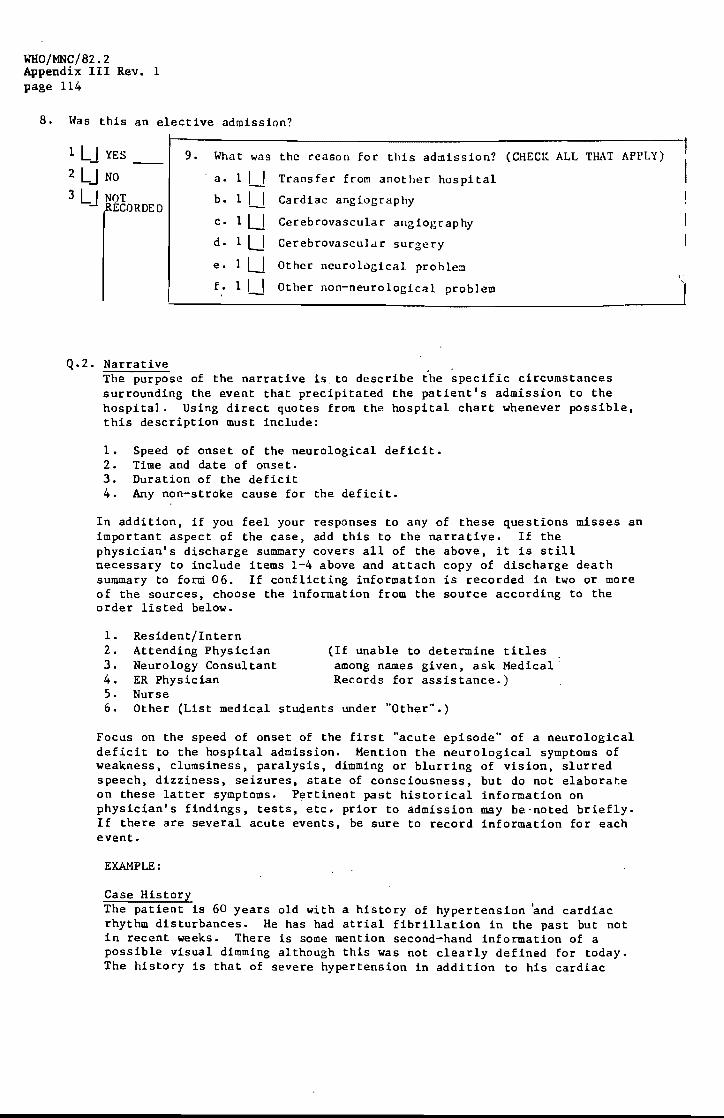
WHO/MNC/82.2 Appendix III Rev. 1 page 114
8. Has this an elective admission?
1 LJ YES_
2 LJ NO
3 LJ NOT RECORDED
Q.2. Narrative
9. What was
a. 1 I_I b. 1 I_I c. 1U d. 1U
e. lU
f. 1 U
the reason for this admission? (CHECK ALL THAT APPLY)
Transfer from another hospital
Cardiac angiography
Cerebrovascular angiography
Cerebrovasculd r sur~ery
Other neurological problem
Other non-neurological problem
The purpose of the narrative is to describe the specific circumstances surrounding the event that precipitated the patient's admission to the hospital. Using direct quotes from the hospital chart whenever possible, this description must include:
1. Speed of onset of the neurological deficit. 2. Time and date of onset. 3. Duration of the deficit 4. Any non-stroke cause for the deficit.
In addition, if you feel your responses to any of these questions misses an important aspect of the case, add this to the narrative. If the physician's discharge summary covers all of the above, it is still necessary to include items 1-4 above and attach copy of discharge death summary to form 06. If conflicting information is recorded in two or more of the sources, choose the information from the source according to the order listed below.
1-2. 3. 4. 5. 6.
Resident/Intern Attending Physician Neurology Consultant ER Physician Nurse Other (List medical
(If unable to determine titles _ among names given, ask Medical' Records for assistance.)
students under "Other".)
Focus on the speed of onset of the first "acute episode" of a neurological deficit to the hospital admission. Mention the neurological symptoms of weakness, clumsiness, paralysis, dimming or blurring of vision, slurred speech, dizziness, seizures, state of consciousness, but do not elaborate on these latter symptoms. Pertinent past historical information on physician's findings, tests, etc. prior to admission may be-noted briefly. If there are several acute events, be sure to record information for each event.
EXAMPLE:
Case History The patient is 60 years old with a history of hypertension 'and cardiac rhythm disturbances. He has had atrial fibrillation in the past but not in recent weeks. There is some mention second-hand information of a possible visual dimming although this was not clearly defined for today. The history is that of severe hypertension in addition to his cardiac
\'
'I

~'HO/:MNC/ 82.2 Appendix III Rev. 1 page 115
rhythm disturbances, but no history of prior CVAs. Yesterday he was found in the home with left-sided weakness and admitted in this state. It was not certain how long the patient was lying on the floor of his home. He had been well the evening before. It may hav-e been hours or very suddenly.
An appropriate summary of the central points of our example case would include:
1. Speed: "He had been well the evening before." "Yesterday (11/7/80) he was found in the home with left-sided weakness and admitted in this state ...
2. Time and date of onset: Sometime during night or morning before admission. "It may have been hours or very suddenly." Definitely less than 24 hours before admission (11/7/80).
3. Duration of deficit: Discharge summary (12/23/80) states "No real improvement in his neurological status". Essentially unchanged after 44 days of hospitalization.
4. Any non-stroke cause for the deficit: "He has had atrial fibrillation in the past but not in recent weeks."
Q.3-l8 Pre-Admission History This information may be found in the history of the resident or intern, if any, the attending physician, the neurology consultant, the ER physician, nursing notes, medical students, in that order. "History" refers to information from the patient and his family.
SY~WTOMS ARE COMPLAINTS EXPRESSED BY THE PATIENT OR RELAYED BY PATIENT'S FAMILY/FRIENDS. SIGNS ARE PHYSICAL FINDINGS THAT C&~ BE OBSERVED BY A SECOND PARTY.
Q.3. Is there a history of previous stroke? This refers to events preceding the present acute illness and hospitalization. Synonyms for "stroke" may include some of the following: Intracranial hemorrhage, cerebral thrombosis, cerebral artery occlusion, cerebral infarction, apoplexy, cerebrovascular accident, cerebral seizure. intracerebral hemorrhage. rupture of blood vessel in brain. Answer "Yes" if one or more of the sources listed above makes explicit mention of previous "stroke" (or synonym). Answer "No" if absence of stroke is explicitly mentioned. Otherwise, answer "NR". This information is needed to distinguish first events from recurrent events in subsequent data analysis. If answer to Q. 6 is "Yes", answer Q. 7 and Q. 8. If answer is "No" or "NR" go to Q.9.
Q.4-5 How long before admission was the last stroke? If the phrase "old stroke" appears, but no specific date is given in the chart, check "More than 6 weeks". This information is needed to distinguish a new from a recurrent stroke. Check the lowest number possible.
Q.7. Is there a history of a previous TIA? (Transient ischemic attack) Synonyms for "TIA" may include: acute cerebrovascular insufficiency. spasm of cerebral arteries. insufficiency of basilar. carotid, or vertebral arteries.

WRO/MNC/82.2 Appendix III Rev. 1 page 116
10.
Q.8. Was this an elective admission? An elective admission is defined here as one that is scheduled in advance at the convenience of physician and patient, rather than an admission brought on urgently by the patient's acute symptoms. Generally, a non-elective admission will be through the ER or directly from a doctor's office. A transfer from another hospital is arbitrarily defined as elective regardless of the circumstances. (In this case, mark 9a.)
Q.9. What was the reason for the admission? "Cardiac angiography" includes coronary arteriography and ventriculography. "Cerebrovascular angiography" includes the carotid arteries.
Here there new (within 6 weeks or s.ince previous hospi tal dlscharge--whichl!ver is short.;. subjective neurological symptoms that led to this hospital admission or that occurred during this hospitalization? If the patient has been transferred from another acute car' hospi tal, answer "NO", unless new symptoms developed during this admission.
1 LJ YES_ 11.
Z LJ NO
3 LJ NOT 12.
RE RDED
13.
Was the onset of new symptoms during this admission?
11_1 YES 21_1 NO
What were the patient's new symptoms? (CHECK ALL THAT APPLY)
a. 11_1 Weakness or clumsiness of. face and/or limb(s) on one side of
b. 11_1 Difficulty speaking or understanding speech
c. 11_1 Visual disturbances
d. 11_1 Dizziness, uns teadiness of gait
e. 11_1 Seizures
f- lU Prolonged unconsciousness (coma)
g. 11_1 Altered state of consciousness
h 1U Brief unconsciousness (syncope or fainting)
i. 11_1 Other, (Spec1.fy)
When did the above new symptom s begin?
A. Date: W I jY1 B.
Estimated W W 24 Time: : clo
1 1_' NOT RECORDED 1 '_I NOT RECORDED
Q. to. h'crc there new (within 6 weej(s or ::;inCl! pr!:!vious hospital discharge, whichever is shorter.) subjective neuro1ogi.cal symptoms that led to this hospital admission or that occurred during this hospitalization? nlis refers to subjective symptoms described by· the patient, or observations made by the family or a friend, if the patient was unable to talk. A transfer from another hospital is considered a discharge and read-
."" mission. Thus, any symptoms occurring before discharge from prior hospitalization would not be considered "new". For example, if a patient is transferred after admission to another hospital, answer "No" unless new symptoms developed during this admission.
Q.ll-13. These questions refer only to new symptoms as defined in Q.lO instructions.
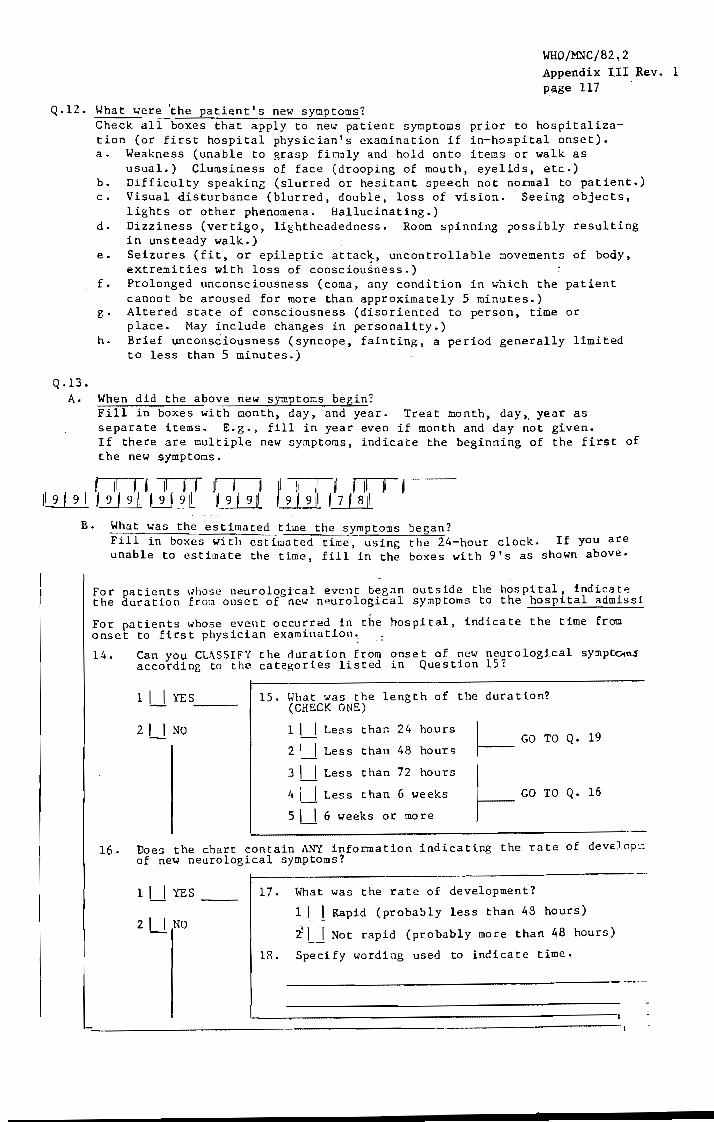
WHO/MNC/82,2 Appendix III Rev. 1 page 117
Q.12. What were ~he patient's new symptoms?
Q.13 •
Check all boxes that apply to new patient symptoms prior to hospitalization (or first hospital physician's examination if in-hospital onset). a. Weakness (unable to grasp firmly and hold onto items or walk as
usual.) Clumsiness of face (drooping of mouth, eyelids, etc.) b. Difficulty speaking (slurred or hesitant speech not normal to patient.) c. Visual disturbance (blurred, double, loss of vision. Seeing objects,
lights or other phenomena. Hallucinating.) d. Dizziness (vertigo, lightheadedness. Room spinning possibly resulting
in unsteady walk.) e. Seizures (fit, or epileptic attack, uncontrollable ~ovements of body,
extremities with loss of consciou~ness.) f. Prolonged unconsciousness (coma, any condition in .... hich the patient
cannot be aroused for more than approximately 5 minutes.) g. Altered state of consciousness (disoriented to person, time or
place. May include changes in personality.) h. Brief unconsciousness (syncope, fainting, a period generally limited
to less than 5 minutes.)
A. When did the above new symptoms begin? Fill in boxes with month, day, and year. Treat month, day,. year as separate items. E.g., fill in year even if month and day not given. If there are multiple new symptoms, indicate the beginning of the first of the new symptoms.
t II I j II " jl 9 I 911 I 9 j 911 I 9 ! 911 jl II II j , II
9 I 9 II I 7 , 8 II
B. What was the estimated time the symptoms began? Fill in boxes with estimated time, using the 24-hour clock. If you are unable to estimate the time, fill in the boxes with 9's as shown above.
For patients 111105e neurological event began outside the hospital, indicat,,! the duration frO!" onset of new neurological symptoms to the hospital admissi
For patients whose event occurred in the hospital, indicate the time from onset to first physician examinatIon. :
14. Can you CLASSIFY the duration from onset of new neurological sympto'"1\S according to the categories listed in QuestIon 15?
16.
11_1 YES __
21_' NO
15. What was the length of the duration? (CHECK ONE)
1 1 __ 1 Less than 24 hours
2 1 __ 1 Less than 48 hours
3 1 __ 1 Less than 72 hours
4 Less than 6 weeks
51 __ 1 6 weeks or more
~ GO TO Q. 19
~ GO TO Q. 16
Does the chart contain ANY information indicatIng the rate of deveJ.(lp~1 of new neurological symptoms?
11_1 YES
21_1 NO
17. 'fuat was the rate of development?
1 1 __ 1 Rapid (probably less than 48 hours)
t Not rapid (probably more than 48 hours)
18. Speci fy wording used to indica te time.

WHO/MNC/82.2 Appendix III Rev. I
page 118
Q.14-l8. The purpose of these questions is to determine how rapidly the symptoms developed. Interval from onset of neurological symptoms to hospital admission (or to first physician examination if onset in hospital) is what we are looking for here. Since this interval is rarely given exactly in a chart, we are looking for the closest estimation possible.
Q.14. Can you classify the time from onset to hospital admission (or peak severity if in hospital) of neurological symptoms according to the categories listed in Q.l5? If answer is "Yes" check appropriate box. If answer is "No", go to Q.16.
Q.15. What was the length of the duration (time from onset to admission)? Check appropriate box using the lowest number possible. Go to Q.19.
EXAMPLE (Symptoms):
History states: The patient is 60 years old with a history of hypertension and cardiac rhythQ disturban~es. He has had atrial fibrillation in the past but not in recent weeks. There is some mention second-hand information of a possible visual dimming although this was not clearly defined for today. The history is that of severe hypertension in addition to his cardiac rhythm disturbances, but no history of prior CVAs. Yesterday he was found in the home with left-sided weakness and admitted in this state. It was not certain how long the patient was lying on the floor of his home. He had been well the evening before. It may have been hours or very suddenly.
Answers to Q. 10-15: 10. 11. 12. DA. UB. 14. 15.
Yes No Check a. and c. NOT RECORDED NOT RECORDED Yes "Less than 24 hours"
Q.16. Does the chart contain ANY information indicating the duration (time of onset to admission) of the neurological symptoms? If you are unable to classify the length of time into one of the time frames given in Q.15, you might be able to pick out clues from the chart which tell you, in general terms, whether the time from peak to onset was rapid (probably less than 48 hours) or ~.ot (probably more than 48 hours). If answer to Q.16. is "Yes" answer Q. and 18. If answer is "No" go to Q.19.
Q.18. Specify wording used to indicate time. Write down the exact words from the chart leading you to believe the symptoms were of rapid or not rapid onset.

PHYSICIAN'S EXAH FINDINGS
w'HO/MNC/82.2 Appendix III Rev. 1 page 119
19. Did a physician document a nC\<I localizing neurological deficit? (wi thin 6 \~eeks or since previous hospi tal discharge, whichever is shorter) or did a CAT SCfu~ indicate definite or probable cerebral infarction or OelDorrhage wi thout other pathology?
1 LJ YES 2 I_I NO 3 I_I NR L~ __________________ _ GO TO PAGE 7 Q. 43
HISTORY OF FbOINGS DURING HOSPITALIZATIO::
20. Can you CLASSIFY the length of time from symptom onset to physician exam in hospital according to the categories listed in Question 2l?
1 LJ YES
2 LJ NO
21. What was the length of
1 I_I Less than 72 hours
2 U Less than 3 weeks
31_1 Less than 6 weeks
41_1 6 weeks or more
time from symptom onset?
GO TO Q. 25
22. Does the chart contain any information indicating the length of 'time from symptom onse t to physician exam?
1 LJ YES 23. What was the length of time from symptom onset?
1 I_I Probably less than 6 weeks
2 LJ NO 2 I_I Probably 6 weeks or more
24. Specify wording used to indicate leng th of
25. \fuat was the conclusion from the pupil examination? (abnormal or "unresponsive to light") (CHECK ONE)
1 L-l Both normal
2 L-l One abnormal (anisocoria)
3 L-l Both abnormal
4 L-l Physician not sure/cannot determine
5 L-l NOT EXAMINED (NR)
time
"constricted" or "dilate
26. '.'hat was the conclusion fro:l the Plantar (Babinski) r~flex examination? (Abnormal = "positive", "up-going toe", "extensor", or "present") (CHECK ONE)
1 L-l Normal both sidcs
2 L-l Abnormal one side
3 LJ Abnormal both sides
4 LJ "Equi vocal" one or both sides
5 LJ NOT E~~I~ED (NR)
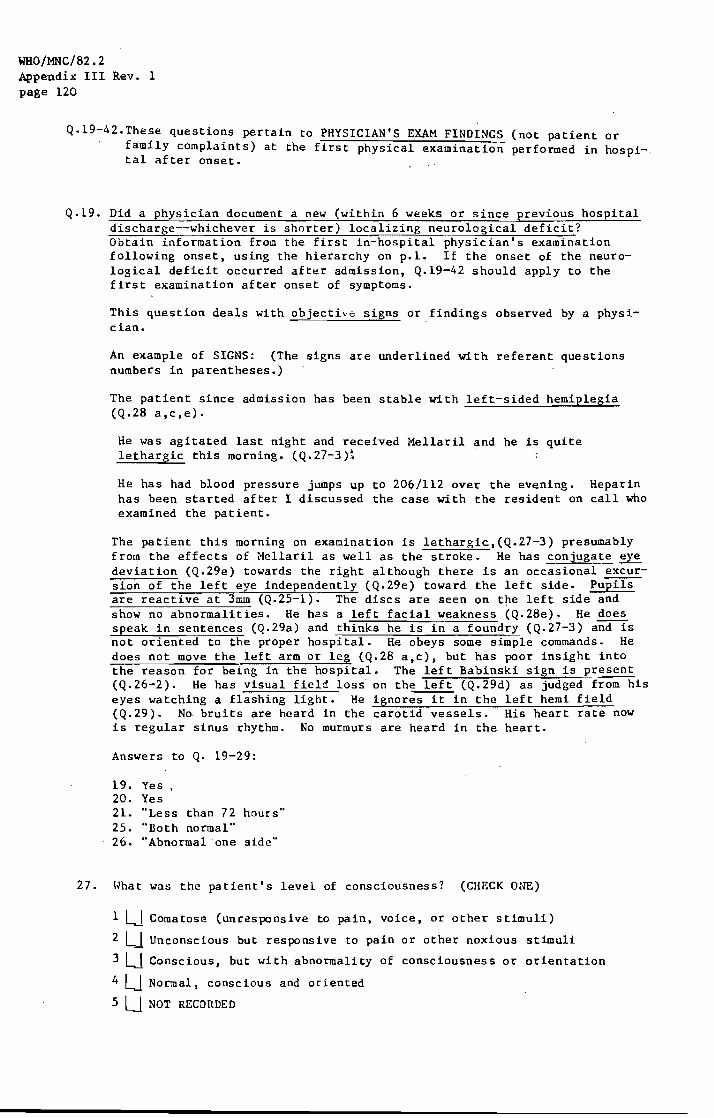
WHO/MNC/82.2 Appendix III Rev. 1 page 120
Q.19-42.These questions pertain to PHYSICIAN'S EXAM FINDINGS (not patient or family complaints) at the first physical examination performed in hospital after onset.
Q.19. Did a physician document a new (within 6 weeks or since previous hospital discharge--whichever is shorter) localizing neurological deficit? Obtain information froQ the first in-hospital physician's examination following onset, using the hierarchy on p.1. If the onset of the neurological deficit occurred after admission, Q.19-42 should apply to the first examination after onset of symptoms.
This question deals with objective signs or findings observed by a physician.
An example of SIGNS: (The signs are underlined with referent questions numbers in parentheses.)
The patient since admission has been stable with left-sided hemiplegia (Q.28 a,c,e).
He was agitated last night and received Mellaril and he is quite lethargic this morning. (Q.27-3)t
He has had blood pressure jumps up to 206/112 over the evening. Heparin has been started after I discussed the case with the resident on call who examined the patient.
The patient this morning on examination is lethargic,(Q.27-3) presumably from the effects of Hellaril as well as the stroke. He has conjugate eye deviation (Q.2ge) towards the right although there is an occasional ~sion of the left eye independently (Q.2ge) toward the left side. Pupils are reactive at 3mm (Q.25-1). The discs are seen on t~e left side and show no abnormalities. He has a left facial weakness (Q.28e). He does speak in sentences (Q.29a) and thinks he is in a foundry (Q.27-3) and is not oriented to the proper hospital. He obeys some simple commands. He does not move the left arm or leg (Q.28 a,c), but has poor insight into the reason for being in the hospital. The left Babinski sign is present (Q.26-2). He has visual field loss on the left (Q.29d) as judged from his eyes watching a flashing light. He ignores it in the left hemi field (Q. 29). No bruits are heard in the carotid vessels. His heart rate now is regular sinus rhythm. No murmurs are heard in the heart.
Answers to Q. 19-29:
19. Yes 20. Yes 21. "Less than 72 hours .. 25. "Both normal" 26. "Abnormal one side"
27. \yhat was the patient's level of consciousness? (CHECK ONE)
1 L-J Comatose (unresponsive to pain, voice, or other stimuli)
2 LJ Unconscious but responsive to pain or other noxious stimuli
3 LJ Conscious, but with abnormality of consciousness or orientation
4 LJ Normal, conscious and oriented
5 U NOT RECORDED

WHO/~C/82.2 Appendix III Rev, 1 page 121
28. l-lhat were the motor function findings? Each item refers to the body region indicated 0
any parts thereof.
29.
AFFECTED, BUT TOTALLY NOT UNAFFECTED CAN BE MOVED
(NORK<\L) BY PATIENT PAR.U YZED RECORDED
a. Left Arm 1 LJ 21_1 31_1 41_1
b. Right Arm 1 LJ 21_1 31_1 41_1
c. Left Leg 1 LJ 21_1 31_1 41_1
d. Right Leg 1 LJ 21_1 31_1 41_1
e. Left Face lU 2U 3U 4U
f. Right Face 1 LJ 21_1 31_1 4U
Did the pa tient have any of the following neurological deficits? (SEE Mk~UAL FOR DEyr 'I:
a.
b.
c.
d.
e.
YES NO NOT RECORDED
Aphasia 1 LJ 21_1 31_' Apraxia 1 LJ 21_1 31_1
Dysarthria 1 LJ 21_1 31_1
Visual field defects 1 LJ 21_1 31_1 Other lU _21_' 31_1
specify:
:l7. "Conscious but with ahuonualit.· or consciousness ..
28. a.3. b.l. c.3. d.l. e.2. f.1.
29. a. No. b. NOT c. NOr d. Yes e. Yes
RECORDED RECORDED
Specify: Not oriented to place. Poor insight into reason for being in hospital. Also, conjugate eye deviation with excursion of left eye independently.
Q.20-24. The purpose of these questions is to determine how long the subjective symptoms of a neurologic deficit were present prior to the first physician examination.
Q.22-23. Does the chart contain any general information indicating the length of time from symptom onset to physiCian exam? If you cannot answer Q.2l with the information provided in the chart, you might be able to pick out clues from the chart which indica-te whether the onset of symptoms was RECENT (Probably less than 6 weeks) or OLD (probably more than 6 weeks).

WHO/MNC/82.2 Appendix III Rev. 1 page 122
q.24. Specify wording used to indicate length of time. Wrice down exact words used in the chart that led you to the assumption ~ither trlat symptoms we.re "probably less than six weeks" or "probably more than six weeks".
Q.2:S-34. Babinski reflex (Abnormal = "positive", "up-going toe", "extensor", or "present". Pupil examination (Abnormal = "constrict'ed" or "dilated" or "unresponsive to light".
Q.Z7. What was the patient's level of consciousness? 1. Comatose (unresponsive to pain, voice or any stimuli) 2. Unconscious but responsive to pain or other noxious stimuli 3. Conscious, but with abnormality of consciousness or orientation.
This might be disorientation to person, place, or time; lethargy; or somnolence.
4. Normal, conscious and oriented to person, time and place.
If insufficient information is present to distinguish between comatose 'I' and unconscious '2', and the patient clearly has more than a minor disturbance of consciousness, check '2', Do not check 'NR',
EXAMPLE: A man is found unconscious and admitted to the hospital. He is described as not responding to voice, but his response to other stimuli is not noted. Thus, it is not possible to distinguish between coma '1' and unconscious '2', but is clearly not conscious '3' or '4'. So, the proper response is 'Z'. Unconscious, but responsive to pain or other noxious stimuli.
Q.2S. What were the motor function findings'! For comatose patients check "Totally paralyzed" (3).
Motor function is ability to move muscles. If "Paresis" is used, check '2', "Affected. but can be moved by patient". If "Plegia" is used, check '3', "Totally paralyzed".
Q.29 Did fhe patient have any of the following neurol02ical deficits?
30. Was the patient's temperature recorded on this ad~ission?
I LJ YES
2 U NO
What was this first temperature recorded in the hospital after onset of symptoms? '.
l I I I 1 __ 1 1 I_I 0 F . (Indicate farenheit or centigrade)
zl_lo C
3Z. How was this temperature obtained?
1 I I Oral 2 I I Rectal 3 Ll Axillary 4 I_I NR
33 •. Has the blood pressure recorded on this admission (ER!I..TARD!ICU)?
1 LJ YES ______ _
2 LJ NO
34. What was the first blood pressure reading recorded in the hospital after onset of symptoms?

35.
WHO/MNC/82,2 Appendix III Rev .. 1 page 123
Can you CLASSIFY the duration of new objective findings of localizing neurological defic according to the categories listed in Question 36?
1 LJ YES _____ _
2 LJ NO
~------------------------------------36. What was the duration of the objective deficit from
first physician documentation until last? (CHECK ONE)
1 LJ ~ess than 1 hour
2 1 __ 1 Less than 24 hours
3 1 __ 1 Less than 48 hours
4 1 __ 1 Less than 72 hours
5 I_I 72 hours or more
GO TO Q. 37
37. Does the chart contain any information indicating duration of deficit or coma?
1 LJ YES _____ _ 38. What was the duration?
2 UNO I Ll Transient (pronably 24 hours or less)
2 LJ Prolonged (probably more than 24 hours)
39. Specify wording used to indicate duration.
40. Was the patient discharged alive ----------------------I LJ YES ____ ~ __ _ co TO QUESTION 43
2 LJro
41. Did death occur within 6 weeks of first documentation of deficit?
1 LJ YES _____ _
2 LJ NO 42. What was the duration ;rom first p'~)sician
docur.l~ntation to death. (CHECK O,.,~
IU Less than 24 hours
21_1 Less than 48 hours
3U Less than 72 hours
4U 72 hours or lllore
5U Unknown
Visual field defects involve the inability to perceive an object which would be visible if visual fields were normal.
(See Neurology Terms sheet for definitions for a. - c.)
Q.30-34. Record first temperature and blood pressure taken during this admission following onset of symptoms. Assume oral temperature if not designated otherwise.
Q.35. Can you CLASSIFY the duration of new objective findings of localizing neurological deficits according to the categories listed in Q.37? The purpose of this question is to determine, as accurately as possible, the duration of the deficit. Precise durations usually will not be present but we need your best estimate.
WHO/MNC/82.2 Appendix III Rev. 1 page 124
Q,38. What was the duration? If the chart does not supply information adequate to select one of the time frames given in Q.36, you might be able to determine, if the duration was TRANSIENT or PROLONGED. TRANSIENT is defined as 'probably 24 hours or less' PROLONGED is defined as 'probably more than 24 hours'.
Q.39. Specify wording used to indicate duration. Write down the exact words used ip the chart that led you to the assumptiun that the duration was TRANSIENT or PROLONGED.
Q.40. If patient was alive at discharge, go to Q.43.
Q<41 Did death occur within 6 weeks of first documentation of deficit? If the patient died in the hospital, did death occur within 6 weeks of first objective physician documentation of deficit? This question only applies if the patient died in the hospital.

WHO/MNC/82,2 Appendix III Rev. 1 page 125
HISTORY OR FINDINGS DURING HOSPITALIZATION
43.
44.
45.
46.
47.
A. {"as there:
Atrial fibrillation or flutter
Mitral stenosis?
Intracardiac thrombous or intracardiac tumor (myxoma)
Sys temic emboli
1 U YES
2 LJ NO
3 LJ :-;R
1 U YES
2 UNO
3 U NR
1 YES
2 U NO
3 U NR
1 U YES
2 UNO
3 U NR
2 LJ NO
3 LJ NR
48. Subdural hematoma 1 U YES
2 UNO
3 LJ NR
49.
50.
Subarachnoid heraorrhage
Severe metabolic disorder
(SEE MANUAL FOR OF DISORDERS)
1 U YES
2 LJ NO
3 LJ NR
1 U YES
. 2 L 1 1\0 LIST -
3 U NR
51. Trauma, seizure dis- 1 U YES order, hypercoagulable state or 2 U NO
52.
hemorrhagic condition L 3 J NR
Another disease process, event, or peripheral lesion which might cause a focal neurological defIcit
1 U YES
2 U :\0
3 U ~R
B. Was it present
during thIs admission?
1 I_I YES
21_1 NO
31_1 NR
1 I_I YES
21_1 NO
3 _I I NR
11_1 YES
21_1 NO
3 U NR
11_1 YES
21_1 NO
3 NR
1 I I YF.!,; - '_I ......... ~
21_1 NO
31_1 NR
C. Specify condition and/or
how it was documented
11_1 YES
21_1 NO
31_1 NR
-------------------,
11_1 YES
2 UNO
31_1 NR
11_1 YES
21_' NO
31_1 NR
11_1 YES
21_1 NO
31_1 NR
11_1 YES
21_1 NO
3' I NR
WHO/MNC/82.2 Appendix III Rev. 1 page 126
Q.43-53. Pertain to HISTORY OR FINDINGS DURING HOSPITALIZATION. These questions attempt to detect non-cerebral thrombosis and hemorhage causes of neurological deficits. Whenever the question "Was it present during this admission?" is asked, check appropriate box and go on to next appropriate questions. For the questions "How was it documented?" record specific information from chart indicating presence of the condition during the current admission. EXAHPLES: ECG report said "atrial fibrillation". (Q.43.C.) MD says "murmur of mitral stenosis on physical exam". (Q.44.C.)
If not mentioned in physical exam by physician, check "N:R". Q.46. Were there systemic emboli?
Systemic emboli are emboli to the systemic arterial circulation, i.e., limbs, brain, kidney; they are to be distinguished from pulmonary emboli, which go to pulmonary circulation i.e., lungs only. So a renal embolus, or a femoral artery embolus is a systemic embolus. The origin of systemic emboli may be the heart. If a "paradoxical embolus" (a systemic embolus arising "paradoxically" from the ~ystemic veins and travelling through a septal defect in the heart) is noted in the chart, check Q.46 "Yes".
Q.47. Was there a brain tumor? Synonyms include neoplasm of brain, glioma, meningioma, pituitary adenoma, metastasis to brain.
Q.48. Was there a subdural hematoma: A synonym would be a subdural hemorrhage. Note: Extradural or epidut'al hemorrhage should be indicated in Question 51. These are usually acute and associated with trauma.
Q.49. Was there a subarachnoid hemorrhage? Synonyms include meningeal hemorrhage, ruptured berry aneurysm, ruptured (congenital) cerebral aneurysm.
Q .50. Was there a severe metabolic disorder? '(SEE Mk'mAL FOR LIST OF DISORDERS). Check "Yes" only if disorder was severe enough to cause altered consciousness, unconsciousness or coma. Examples of a severe disorder would include diabetes (with hyperglycemia, hypoglycemia, or abnormal blood sugar), renal failure, septicemia, hypocalcemia, hypercalcemia, hypomagnesemia, hypokalemia, or hypothyroidism. Metabolic disorder.s resembling strokes with coma could include acute drug intoxications or overdoses with barbituates, tranquilizers, pain killers, narcotics, etc., prolonged hyperglycemia in a diabetic on insulin, terminal kidney failure, etc.

53.
WHO/!1NC/82.2 Appendix III Rev, I page 127
Q.51. Was there trauma, seizure disorder, hypercoagulable state, or hemmorhagic disorder?
of trauma include disc disease, carpal tunnel syndrome, compartment syndrome, lumbar strain, or blunt trauma to the head, spinal column. Hypercoagulable states would include promyelocytic leukemia or other blood conditions specifically termed hypercoagulable by a physician. Hemorrhagic conditions could include therapeutic overdose of anticoagulant drugs such as heparin, coumadin, warfarin, antiplatelet drugs; blood diseases leading to defects in blood clotting such as thrombocytopenia, leukemia, aplastic anemia; liver disease, Vitamin K deficiency and anti-coagulation therapy. Hemorrhagic conditions may also be side effects of the use of anticancer drugs which destroy the bone marroW'. You may also see the term "hemorrhagic diathesis" which means a tendency to bleed. Examples of seizure disorders would be epilepsy or myoclonus, tonic-clonic seizures, petit mal or grand mal seizures. Toxin exposures including fumes, chemicals, or poisonous plants would also fit this category. Any co-eXisting chronic life-threatening condition that the patient may have should be listed if a stroke occurs in this setting.
Q.52. Was there a disease process, event or peripheral lesion present which might cause a focal neurological deficit? Examples of a diseas~ process are sarCOidosis, vasculitis, Parkinsonism, hemiballismus,' rheumatic fever, meningitis, encephalitis, Guillain-Barre syndrome, multiple sclerosis, amyotrophic lateral sclerosis, polyarteritis nodosa. Examples of peripheral neuropathy include Bell's Palsy, Erb's Palsy, ulnar palsy, fractures, injury or tumor affecting the peripheral nl.::r-...ous system.
\~as there any evidence (e.g. history, physical, or laboratory) of an HI within 8 wee:ts prior to this admission or during this hospitalization?
1 LJ YES, COHPLETE FORH 04
2 LJ NO
3 LJ rWT RECORDED
54. ~as there a spinal tap?
1 LJ YES
2 LJ NO
55. Hhat was the result of the spinal tap? (CHECK ONE)
1 CLEAR A.t~D COLORLESS ~SPECIFY I I I I I 2 U BLOOD IN
REC'S SPINAL TAP
31_1 "GROSSLY BLOODY"
56. Were there other abnormal CSF findings?
lU YES ,specify
21.J NO
3 U NOT RECORDED

WHO/MNC/82.2 Appendix III Rev. 1 page 128
57. Was there cerebral angiography?
~--------------------------------~ 1 LJ YESc __ _ ATTACH COPIES OF CEREBRAL ANGIOGRAPHI~S
2 LJ NO 58. Did it precede the neurological deficit? ~
11 __ 1 YES 59. By hOI" many hours did the angiography precede the event? (CHECK ONE)
21_1 NO
60. \las there cardiac angiography?
1 1 __ 1 Less than- 24 hours
2 1 __ 1 Less than 48 hours
3 1 __ 1 Less than 72 hours
4 1 __ 1 72 hours or more
1 LJ YES __ _
2 LJ NO
ATTACH COPIES OF CARDIAC ANGIOGRAPHIES
61. Did it precede the neurological deficit?
1 U YES_
2 UNO
63. Ilas there a rad lonuclide brai:! scan:
62.
1 U YES ___ ATTACH COPES OF TEST REPORTS
2 U NO
Q.54. Was there a spinal tap?
By hOI-; many hours did the angiography preced~ the event? (ClIECK ON~:)
1 U Less than 24 hours
2 U Less than 48 hours
3 I_I Less than 72 hours
4 I_I 72 hours or mor<'!
A synonym for "spinal tap" may be Lumbar Puncture (LP). Spinal tap results will usually be recorded in the progress notes, but in some hospitals may be on a separate sheet. Results of spinal fluid analYSis often appear in the laboratory sheets. If there is no indication of a spinal tap, check "No" or "NR" and go to Q.57.
Q.55. What was the result of the spinal tap? (CHECK ONE). This question deals with the finqings of the CSF (cerebral spinal fluid). Th~ purpose of this question is to obtain information about non-stroke conditions and about cerebral hemorrhage. If more than one tube of fluid was obtained, report findings of last tube. If more than one finding is reported, use the first one done. If more than 5 boxes are used, chec~ grossly bloody (Form 06, Q.55-3).
Normal cerebrospinal fluid (CSF) is clear and colorless with no RBe or P~lli and < 3 lymphocytes. If Q.54 is "Yes", answer Q.55. Xanthochromic means "yellowish in color." "Traumatic tap" results in blood from surrounding tissues contaminating the sample. Check "Other" and specify if these words were used.
'--

Q.57. Was there cerebral angiography?
WHO/MNC/82.2 ,Appendi)t III Rev. 1 page 129
Attach copies of reports. Synonyms for "cerebral angiography" may include the following: cerebral arteriogram, carotid angiogram/arteriogram, vertebral or basilar or posterior circulation angiogram/arteriogram, and four vessel study.
Q.60. Was there cardiac angiography? Attach copies of reports. Synonyms include arteriography or aortic arch, angiocardiography, coronary arteriography, pulmonary angiography.
Q.63. Was there a brain scan? Synonyms for "brain scan" that we may see include: Radionucleide brain scan, Technetium brain scan, Perfusion brain scan, Isotope brain scan, Isotope flow studies, and Nuclear flow studies. Attach copy of report.
04. ',hiS a Computerized Axial To;~ogr'lphy (CAr) S.::an or the head compl.ctea during this_ hospitalization?
1 LJ YES I 21_1 NO 3 U NOT RECO ROE D END OF QUESTIOUNAIRE
ATTACH COPIES OF CAT SC&~S
65. Ho\,> many CAT Scans \.ere completed during this hospitalization? w 66. l.fas the first CAT Scan within 6 weeks after the event or after admiSSion,
Whichever is later?
1 LJ YES 21_1 NO 3\_1 NOT RECORDED
67. If the patient died in hospital, was the first CAT Scan within 6 weeks before death?
1 LJ YES 2 UNO 3 \_1 fleF~~ID 4 1_1 NO~ RECORDED

WHO/MNC/82.2 Appendix III Rev. 1 page 130
68. '~hat was the date of the first CAT Scan?
69. ~~hat was the date of the 1a s t GAT SCA.N?
NONTH DAY YEAR
W/W/W
70. \~hat did the CAT scan reports indicate?
**
**
**
**
A. FIRST CAT SCAN B. LAST CAT SCAN
First CAT Scan completed after symptom onset this admission?
Last CAT SCAN com(,leted after symptom onset th~s admission
Report indicated definite or probable cerebral infarction or hemorrhage without other pathology
Report indicated possible or equivocal cerebral infarction or hemorrhage only
Report indicated presence of brain tumor.
Report indicated hematoma.
presence of subdural
Retort indicated presence of subarach-no d hemorrhage.
Repo rt indicated presence intracranial disease
of other
Rc10rt indicated study was within nor-ma limits.
Report cannot be classified as one of above by abstractor.
IF YOUR ANSHER iHLL I:-iCLUDE THIS RESPO;:S£
lU
2U 3U
4 LJ
5 LJ
6U
7 LJ
sU SEEK MD
21_1 31_1
41_1
51_1
61_1
71~
sU HELP I~ COMPLETl~G Q. 70A OR 70B.
71. Reviewed by L I I I HD 1U:,1:
Q.64. Was a Computerized Axial Tomography (CAT) Scan of the head completed during this hospitalization? EHI and ACTA are synonyms for CAT scan. If answer is "Yes", answer Q.65-70.B.· If answer is "NO" or "NR", END OF QUESTIONNAIRE.
Q.65. How many CAT Scans were completed during this hospitalization? Fill in the appropriate number. (99 - NR)
NOTE: Attach copies of CAT scans.
Q.70. What did the first CAT Scan completed after symptom onset during this admission indicate? (CHECK TO SEE THAT Q.20-39 ARE COHPLETED EVEN IF THERE WAS NO PHYSICIAN DOCmlENTATION OF A NEW LOCALIZING ~~UROLOGICAL DEFICIT.) The abstractor is to read the CAT Scan report(s) and assign one or more of the 8 categories listed. If you check starred response~ (boxes 2,6 or 8) seek M.D. assistance to complete Q.70.A/B. Possible synonyms for "cerebral infarction" are as follows: cerebral ischemic lesion, ischemic infarct, cerebral thrombosis, cerebral artery occlusion. Possible synonyms for "cerebral hemorrhage" are as follows: hemorrhage: basilar, bulbar, cerebellar, cerebral, cerebromeningeal, cortical, internal ca~sule, intrapontine, pontine, subcortical, or ventr.icular hemorrhagt, rupture of blood vessel in brain.

NEUROLOGY TERMS
Acalculia: loss of ability to do math reckoning
WHQ/:MNC/82.2 Appendi~ III Rey~ 1 page 131
Adiadochokinesia: inability to perform rapidly alternating movements
Agraphia: inability to write
Alexia or Visual aphasia: loss of ability to understand written word
auditory - lack of comprehension of spoken word jargon or pharaphasia - words may be fluent but inappropriate amnesic - loss of memory of special words with hesitant and
fragmentary speed nominal aphasia (anomia, dysnomia) - loss of ability to name objects semantic aphasia - loss of meaning of words syntactic aphasia - loss of correct grammatical construction
Analgesia: loss of pain
Anisocoria: inequality of the diameter of pupils
Anopsia: disuse of vision (does not include blindness or weak ·sight)
Anosmia: loss of smell
Aphasia: inability to express oneself properly through speech or loss of verbal comprehension
Apraxia: Inability to perform certain movements without loss of motor power, sensation, or coordination
Astereognosis: loss of ability to recognize common objects.by touching and handling them with eyes closed
Ataxia: muscular incoordination, especially when voluntary muscular movements are attempted
!abinski reflex: on plantar stimulation large toe extends upwatd on invol ved side
Ballism: wild, flinging movements of limbs
Brui blowing sound over aneurysm or murmur
Bulbar palsy: involvement of brain stem
Choreiform movements: .quick, jerky. purposeless, unsustained involuntary movements jumping from 1 muscle group to another (gen. limbs and face) chorea-like
Choroid plexus: tuft of dilated vessels which project into ventricles; forms spinal fluid
spasm wi til rapidly alternating rigidity, relaxation
Conjugate movement: extraocular muscles participate in binocular movement with precise integration of movement of 2 eyes
cerebrospinal fluid

WHO/MNC/82.2 Appenciix III Rev. 1 page 132
Diplopia: double vision
Dizziness: sensation of unsteadiness with feeling of movement in head
Dysaphia: dullness of the sense of touch
Dysarthria: Difficult and defective speech due to impairment of the tongue or other muscles essential to speech
Dysesthesia: spontaneously occurring unpleasant cutaneous sensation (burn, tickle, etc.)
Dysphagia: difficulty in swallowing
Dysphonia: difficulty with phonation
Dysstasia: difficulty in standing
Dyssynergia: failure of muscular coordination
Dystaxia: partial ataxia
Dystonia: slow, long sustained twisting activity - gen. of trunk
EOH: extraocular musculature
Fasciculations: irregular, inconstant, isolated contractions of fiber bundles within a muscle
Flaccid: weak, lax, soft
Hemiparesis: involving half of body (weakness)
Hemiplegia: paralysis half side of body
Hoffman sign: finger reflex - contraction of thumb and/or fingers when distant phalanx of middle finger (hand prone and relaxed) forcibly flexed by examiner
Holme's sign: excessive flexion rebound after muscle extension pressure released
Homonomous hemianopsia: impairment of half field of vision on lesion side
Homonymous hemianopsia: impairment of half field of vision side opposite lesion
Hypalgesia: decreased pain, diminished sensitivity to pain
Hypesthesia: decreased tactile sensibility
Ipsilateral: situation on or pertaining to same side
LP: lumbar puncture
~~: moves all extremities
Meninges: membranes covering brain
dura - thick outer layer pia - innermost layer - wrapped around brain arachnoid - middle ~~~~rane - vasculAr l~ver
of each eye on

~lyoclonus: clonic spasm of muscle or group of muscles
WHO/MNC/82~2 Appendi~ III Rev, 1 page 133
Hyotonus: persistence of muscle contraction after stimulation has ceased
Neurological deficit: the absence of normal functioning of any nerve pathway, motor or sensory (Focal neurological deficit applies only if the deficit is one-sided and localized (confined to one side, one extremity, or one organ system)
Nystagmus: oscillating movements of the eye
Oriented oriented to person, time, place
Paraplegia: paralysis of legs and lower part of body - both in motion and sensation
Paresthesia: unpleasant cutaneous sensation result froo contact with object
Parosmia: any disease or perversion of the sense of smell
PERL: pupils equal, react to light
P}!&R: physical medicine and rehab
Proprioception: deep s~nsation
Ptosis: dropping of upper eyelid
Quadriplegia: paralysis of all four limbs
Reflexes: N normal reaction 1+ slightly hyperactive~ 2+ markedly increased unsustained clonus 3+ one that shows sustained clonus 1- reflex slightly decreased 2- reflex markedly decreased 3- = reflex absent except on reinforcement o = reflex cannot be obtained at all
Romberg sign: patient unable to stand with feet placed close together and eyes closed
Scotoma: a blind or partially blind area in visual field
Scotomata: optic nerve lesion producing impaired vision in one eye only
Snout reflex: mouth puckers when chin tapped
Spastic: muscles stiff, movements awkward (of the nature of or characterized by spasm)
Syncope: faint, swoon
Synergistic: working together
Tic doulouroux: trifacial neuralgia
Tinnitus: ringing sound in ear
WHO/MNC/82.2 Appendix III Rev. 1 page 134
Trapezii: shoulder muscles
Tremors: involuntary movements resulting in rhythmic movement of a joint
Triplegia: hemiplegia with paralysis of one limb on opposite side
Vertigo: abnormal sense of movement
Visual field: the area within which c~jects may be seen when the eye is fixed. See homonomous hemianopsia, synonym. Visual field cut.

FORM CODE 21 AUTOPSY REPORT ABSTRACT
WHO/MNC/82.2 Appendix III Rev. 1 page 135
1. Study I.D. Number: Attach label here.
2. Report Status: Check appropriate box.
3-8. Cerebral Disease:
o
Check appropriate box.
Q.3. Answer "yes" if the autopsy report states that there was a "recent" cerebral infarct or if it specifies 6 weeks or less prior to death. Answer "no" if the autopsy includes the head but does not specify a recent infarct. Answer "NR" if the head was not autopsied. HOWEVER, if the autopsy states that the infarct was caused by an embolism, Q.3 should be answered "no" and Q.6 "Yes".
Q.4. Answer "yes" if the autopsy states that there was a "recent" cerebral hemorrhage or if it specifies 6 weeks or less prior to death. Answer "no" if the autopsy includes the head, but does not specify a recent hemorrhage. Answer "NR" if the head was not autopsied.
Q.5. This includes "old" CI and CH or events specified to have occurred more than 6 weeks prior to death.
Q.6. Some of the items to be included under "Yes" are subarachnoid hemorrhage; atherosclerosis of cerebral arteries; atherosclerosis of pre-cerebral arteries, carotid arteries, or vertebral arteries; and cerebral infarct due to embolism as mentioned under Q.3,
Q.7. Self-explanatory.
Q.8. Examples are cerebral degeneration, atrophy, Alzheimer's disease, etc.
23. Operations and Procedures Codes . Fill in as listed on the face sheet or discharge summary.
See instructions for Form 02, Q.22.
24. Patient Status on Discharge Check appropriate box. If dead, attach autopsy report abstract (if
autopsy was performed) and answer Form 02, Q.25.
25. Did the patient die in the emergency room? Check the appropriate box.

WHO/MNC/82.2 Appendix III Rev. 1 page 136
FORB 03 DEATH CERTIFICATE ABSTRACT
TO BE ABSTRACTED BY NOSOLOGIST
la. Study I.D. Number Label: Attach label to form.
lb. Abstractor Personal Code Number: Fill in Abstracxor Personal Code Number.
2. Death Certificate 1.0. Number: Refer to top right-hand corner of death certificate. Fill in digits
from left to right, starting with first box on left, The first three digits of every number must be "122" OUnnesota State code). The fourth and fifth digits are for year. or death. The remaining six digits are the certificate identifier.
3. County of Death: See County Code List.
4. Date of Death: Record month, day and year of death •. Use "leading zeroes" if necessary.
Refer to top line of death certificate.
5. Time of Death: Refer to either 23a or 23b on death certificate. If this time is
marked as "found", fill in 9999. Time should be recorded according to the 24-hour clock. If the time given on the certificate is from the 12-hour clock, it should be converted to the 24-hour clock.
EXAt'1PLE: 01 00 0200
1 a.m. 2 a.m.
1200 1230
noon 12:30 p.m.
l300 2400
1: 00 p.m. midnight
6. Check appropriate box. Refer to 7d on death certificate for this information. Answer "Yes" if person was DOA at the hospital.
7-8. Primary/Secondary Causes of Death: Rccord the nosologist's red code numbers from the death certificate in
the appropriate boxes. The underlined code number is the primary cause of death to be recorded in boxes for Q.7. Secondary causes of .de.:lth are to be recorded in boxes for Q.8.
9. Check appropriate box.
10. Check appropriate box.
11. Check appropriate box. Refer to 21a. on death certificate.
12. Death Certified by: ,
A signature under 23c. on the death certificate is the physician. (Check box til). A si;;nature under 2Jd. is the r.1Cdical eX<lf!1iner or coroner. (Check box #2).

FORM 41
MI ABSTRACT FOR PHYSICIAN REVIEW OF CHEST X-RAYS
AND CORONARY ANGIOGRAPHY
WHO/MNC/82.2 Appendix III Rev. 1 page 137
NOTE: A Form 41 must be completed by a physician for any Form 04 having photocopies of chest X-rays and/or coronary angiograms attached to it.
It is the abstractor's reponsibi1ity to attach the appropriate study label to Form 41 and forward Form 41 along with photocopies of chest Xrays and/or coronary angiograms to the appropriate LPH physician for completion. When Form 41 is completed, the abstractor is to forward Form 04, Form 41 and Form 40 as a complete set to data processing.

WHo/MNC/82.2 Appendix III Rev. 1 page 138
DEATH CERTIFICATE ABSTRACT
3.
4.
(ATTACH COpy OF DEATH CERTIFICATE)
2. ( I I I 1 I I I I I I I 30 DEATH CERTIFICATE ID NUMBER
Date of []]MONTH []]DAY []]YEAR Death: I I
.. 5
24 hour clock
1. ID LABEL
5.
S1
Death certified by:
1 0 Physician
2 0 Med ical Examiner
3D Coroner
4 0 NOT RECORDED
6. County of I 1 1 I Residence: ___ ~_
7. Where was the death certificate completed:
1 0 Minnesota
2 0 Another state
!r.. 3 0 Another country
4 0 NOT RECORDED
S6
S2
8. Where did the patient die:
10 Dead on Arrival
20 Hospital
3 0 Nursing Home
4 0 Other institution
50 Home
Reaord 01 12
IDCODE 1.. 29
-6DOther,specify ______________________ __
7 [] NOT RECORDED
9. Was an autopsy performed? 1 0 YES .. GO TO Q. 10
2 [] NO l FINISHED
3 0 NOT RECORDED J--+ 57
10. UNDERLYING CAUSE OF DEATH 11. SECONDARY CAUSES OF DEATH
011110 a.OI I I 1.0 63
b.OI I I 1.0 58
68
c.pIIIID 12. Were there more than three secondary causes of death listed?
78 1 [] YES 2 [] NO 3 [] NOT RECORDED IN CHART skip
79 110
--------------------------------------------------------------------------~ ~PH/MHHP-MORB 20(1-1) 1/82 Ver. 1

I. D. Nu..."'iber
OUT-DF-HOSPITAL DEATH PHYSICIAN INFORMATION FORM
WllO/MNC/82.2 Appendix III Rev. 1 page 139
. Case Source [::=J
... '*' ** '*'**** ......... +*** ****'* ****'*'***** * .......... **'*** ... ** ... + ... ** ... ****** ... * *************** ... **.****
DECEDENT 'S NA!1E ____________ -'-__ _ Da te of Birth
Date 0= Death Age
Add=ess . City
PHYSICIANS'S NAME Phone ---------------------------------------------~---------------------------------------------------
DATE OF FOR~ COMPLETION (mo/day/yr)
1. How long befo:::e death did yot: last see the decedent?
2. Did you witness the death?
No
Yes- If yes, what we:::e ~~e ci:::cumstances? Speci!ically, did the decedent have any SUInptomS p::: io::: to death a.l1d for ho ... · long/ (e.g. dyspnea, 30 n.inutesl
3. Did t.":Ie decedent have a..'1Y of the following?
APP ROY..IID.TE D~.TE OF DIAGNOSIS DIAGNOSIS NO YES .l-IONTH YEAR
Coronary Fieart disease 0 0 OJ OJ Myocardial infarctio:'l 0 0 OJ [I]
Anc;i.'1a pecto::: is 0 0 OJ OJ Othe::: cardiovascular disease 0 0 OJ OJ Specil.'y:
Hype:::-tension 0 0 OJ OJ Cereb:::ovascul a::: disease 0 0 IT] IIi Ce:::ebr ov as cul a:: accider:-:; 0 0 OJ IT]
LPH-~~~P (07/1/80) 10-1

WHO/MNC/82.2 Appendix III Rev. 1 page 140
I. D. Nu.cber
DIAGNOSIS
Tra."lsient ischemic attack
Diabetes mellitus
Cancer (specify site)
Chronic brcachitis cr emphysema
Cirrhosis a::: al cohol PFcblem
Mental .illness
Ot..~e= fatal 0::: serious co:'lditio:'l
NO
D 0 0
0
0 [J
0
APPROXIMATE DATE OF DIArnOSIS YES MONTH YEl-.R·
0 OJ OJ 0 CIJ OJ 0 OJ OJ
0 ITJ rn 0 IT] rn 0 IT] OJ 0 IT] [I]
-'. Was this patient being treatec fo:: an illness during the 30 days p:do:: to death?
No Yes -specify ____________________________________________________________ __
Unkno;..'n
s. Was this patient taki.l'lg' any medicatiCJ:'l.S du=inS the 30 days p::-ior to his/her d.eath?
No Yes Unknown
If yes, please check those which apply below:
Digital is Nit::-ogl ycer in
Diuretics Sedatives
LPE-Y..""_~P (07/1/80.) 10-2
Antihypertensives
Other I specify

FINAL INTERVIEH STATUS
1 § Completed Interview 2 Interview Refused 3 Not able to contact
MIDHEST HEART SURVEY FAHILY INTERVIEH INFORMATION
HORTAILITY SURVEILLANCE
ID LABEL
WHO/M;NC/82.2 Appendix III Rev. 1 page 141
DATE LETTER SENT TO INFO~~NT
INTERVIEW SCHEDULED FOR:
1 B IN PERSON 2 TELEPHONE
INTERVIEW CQ}lPLETED:
Time Interview begun:
CD OJ 24 hr. : clock
Time Interview ended:
OJ IT! 24 hr.
L clock
~----------------------------------------
CALL RECORD
DAY I INT'W ID/I
I
DATE TIHE COMMENTS I
I I
I I I
I
I ,
I
LPH/l1HHP-HORB 009 (1-12) 8/82 Ve r.. 1

WHO/MNC/82.2 Appendix III Rev. 1 page 142
1. [ 11J 1J.,LJ NUR I I 2. NAHE OF DECEASED
ID LABEL
11111111111111011111111111111111 Title First Name HI LAST ~.!E
3. LAST KNOl-lN ADDRESS:
1 1 1 I 1 I 1 I 1 1 I 1 1 1 1 1 1 1 I 1 I I I 1·1 I I 1 1 I I Address
I I I I I I I I I I 1 II I I I I 1 1 I j I I I 1 I I I I I I City/State Zip Code
Month Day Year
4a. Date of Death OJ OJ [I] 4b. Time of Death CD : rn ; B ~~
s. NAME OF RESPONDENT
I I ! II 1 I I I I 1 1 I 101 I I 1 I I I 1 I I I I 1 I I I ,-Title First Name HI LAST ::\A}!E
6. ADDRESS:
I 1 I I I I I I I I I I 1 I I 1 I I I I I I I I 1 I 1 I I IJ Address
I I I I I I I 1 I I I I I I I I I I I II! I I I 1 I I 1 I I City/State Zip Code
rTTl rTTl r---r---11 I I~I I ~ ~onc ~umber 7. Relationship to deceased: 1 0 Spouse
20 Child
3 0 Other rda tive
40 Other, specify __ _
LPH/~HHP-MORB 009(2-12) 8/82 Ver. 1

Ffu~ILY INTERVIEW INFO~~TION
WHO/MNC/82.2 Appendix III Rev. 1 page 143
This is calling from the University of Hinnesota about the letter that you received from us concerning our heart disease and stroke study. We'd like to get some more information concerning the illness and death of This ~nvo1ves a 15 to 30 minute interview over the phone, now if you have time, or would nother time be better? Could you start by telling me if he/she had a long-term illness,
or was the death a very sudden event?
(THIS QUESTION WILL USUALLY START THE INFORMANT GIVI~G THE SERIES OF EVENTS. BE SURE TO GET DATES OF THE EVENTS k~D A TI~TABLE FOR THE DAY OF DEATH).
OTHER PROBES HIGHT INCLUDE: Could you tell me something about the changes in 's condition which led to his/her death? What occurred that indicated that something was seriously wrong?
NARRATIVE:
LPH/MHHP HORB 009(3-12) 8/82 Ver. 1

WHO/MNC/82.2 Appendix III Rev. 1 page 144
NARRATIVE:
LPII/:-1HI!P-XORB 009 (3-12) 9/82 Ve r. 1
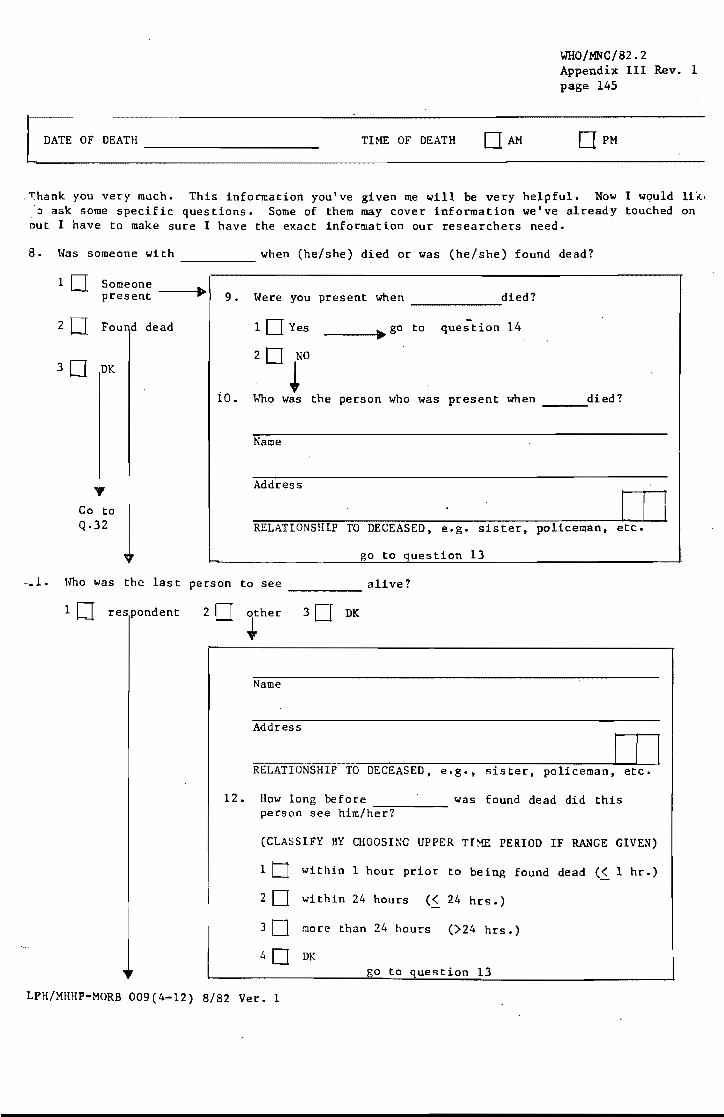
WHO/MNC/82.2 Appendix III Rev. 1 page 145
[ DATE OF DEATH __________ _ TIME OF DEATH
~hank you very much. This information you've given me will be very helpful. Now I would likl o ask some specific questions. Some of them may cover information we've already touched on
out I have to make sure I have the exact information our researchers need.
8. l.;ras someone with when (he/she) died or was (he/she) found dead? -----1 Someone
present ---I~~
2 0 Fou d dead
3D DK
Go to Q.32
9. l.;rere you present when died?
iO.
10 Yes
20 NO
~
------~ go to question 14
----I .......
lfuo was the person who was present when ___ died?
Name
Address
I I I RELATIONSHIP TO DECEASED, e.g. sister, policeman, etc.
go to question 13
-_1. lfuo was the last person to see alive?
1 0 res pondent
-----20 other
~ 3D DK
Name
Address
I / I RELATIONSHIP TO DECEASED, e.g., sister, policeman, etc.
12. How long before was found dead did this person see him/h-e-r~?----
(CLASSIFY BY CHOOSING UPPER TI~ PERIOD IF R&~GE GIVEN)
1 tJ within 1 hour prior to being found dead (~ 1 hr.)
2 0 within 24 hours (~24 hrs.)
3 [J ~ore than 24 hours (>24 hrs.)
40 DK go to question 13
LPH/MHHP-MORB 009(4-12) 8/82 Ver. 1

WHO/MNC/82.2 Appendix III Rev. 1 page 146
13. \.Jhen did you last see alive? (CLASSIFY BY CHOOSING UPPER TI~~ PERIOD IF RANGE GIVEN)
1 0 wi thin 1 hour prior to death/being found dead (5. 1 hr.)
2 [] wi thin 24 hours prior to death/being found dead (5. 24 hrs.)
3 tJ more than 24 hours prior to death/being found dead () 24 hrs.)
40 DK
14. \.Jas conscious and able to communicate at any time ••• (CLASSIFY BY CHOOSING UPPER TH~ PERIOD IF RANGE GIVEN)
10 within 1 hour prior to death (5. 1 hr.)
2 [] within 24 hours prior to death (s. 24 hrs.)
3 [] No, continuously unconscious for more than 24 hours prior to death () 24 hrs.)
4 [] DK
Next we would like to ask you about some specific conditions or symptoms that may or may not have experienced around the time of death. By a symptom we mean a feeling or occurence so strong that it makes an individual stop or change what (he/she) is doing. Sometimes ill people have symptoms, sometimes they don't. By "around the time of death" we mean the period after which first seemed to become ill and never returned to his/her usual state of health. I want to ask you about 's experience.
Did develop any (sympto:n) to the extent that (he/she) had to stop or change what (he/she) was doing?
A. Symptoms at the time of death:
15. Chest pain or discomfort
10 Yes
20 No
3D DK
C. How long prior to (death/bei found dead) did (symptom) ma'
stop or change ~--;--,...-
B. Was the symptom: (his/her) activities?
1 D New
2 D Something he/ she had had before
3D DK
1 D < 5 minutes
205. 1 hr.
3 0 s.24 hrs.
40 )24 hrs.
50 DK D. How did 's behavior change
16. Pres sure on chest
---
10 Yes
20 No
30 OK
1 D New
2 D Something he/ she had had before
3 D OK
D. How did's behavior change ----
10 < 5 minutes
20 < 1 hr.
3 D s.24 hrs.
40)24 hrs.
50 OK
I
I !

WHO/MNC/82.2 Appendix III Rev. 1 page 147
.' . Did develop any (symptom) to the extent that (he/she) had to stop or change what (he/she) was doing?
A. Symptoms at the time of death:
C. How long prior to (death/bein found dead) did (symptom) mak ...".,..-,--....,.,.._~ s top or change
B. Was the symptom: (his/her) activities?
-, . Shortness of breath
10 Yes
20 No
3DDK
10 New
20 Something he/she had had before
3DOK
D. How did • s behavior change ----
18. Fainting, passing out, or loss of consciousness
D. How did
19. Palpitations (pounding in the ches t)
10 Yes
20 No
3DOK
's behavior
10 Yes
20 No
30 OK
10 New
20 Something he/she had had before
3D DK
change
10 New
2 0 Something he/ she had had before
3D DK
D. How did ____ ·s behavior change
20. Marked or 10 Yes 10 New increased fatigue, tiredness or 20 Something he/she weakness 20 No had had before
3D OK 3D DK
D. How did 's behavior change
LPH ~HHP-MORB (6-12) 8 82 Ver. 1
1 0 < 5 minutes
20.5. 1 hr.
3 0 .5. 24 hrs.
40 >24 hrs.
50 DK
1 0 < 5 minutes
20.5. 1 hr.
3D.5. 24 hrs.
40>24 hrs.
5 DDK
1 0 < 5 minutes
20 S 1 hr.
3 D S 24 hrs.
40 >24 hrs.
50 DK
1 0 < 5 minutes
20 S 1 hr.
3D S' 24 hrs.
40 >24 hrs.
50 DK
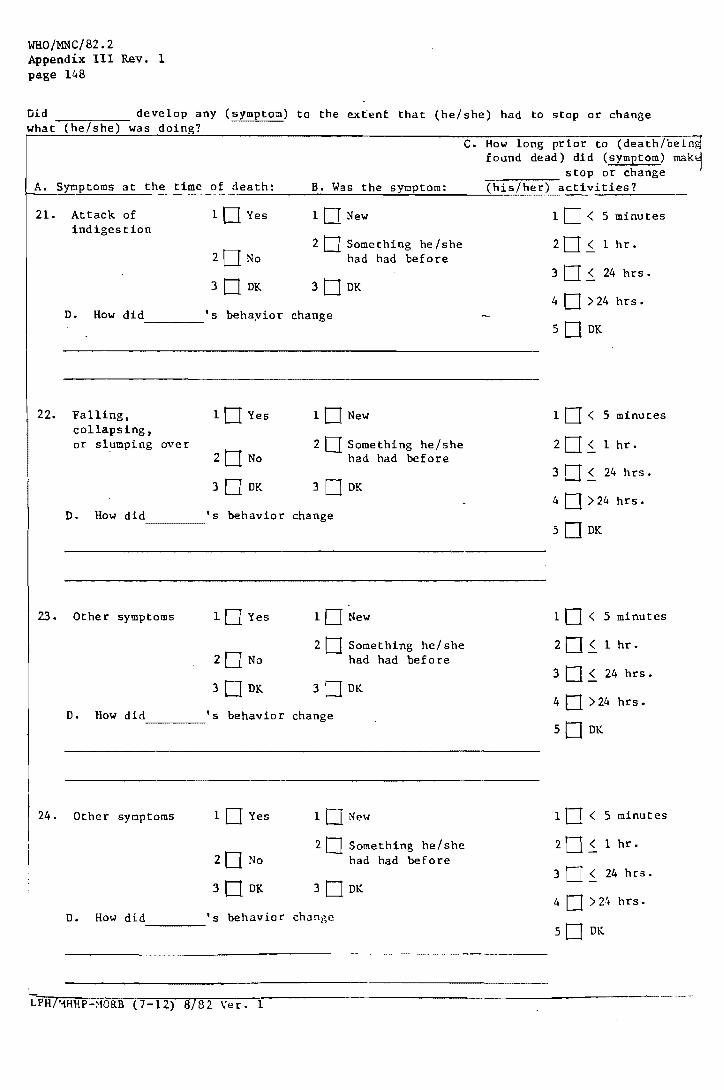
WHO/MNC/82.2 Appendix III Rev. 1 page 148
Did ____ ~---- develop any (symptom) to the extent that (he/she) had to stop or change what (he/she) was doing?
C. How long prior to (death/bein found dead) did (symptom) mak
A. Symptoms at the time of death: B. Was the symptom:
21- Attack of 10 Yes 10 New indigestion
20 Something he/she 20 No had had before
30 OK 3D OK
O. How did 's behayior change ----
22. Falling, collapsing, or slumping over
D. How did
23. Other symptoms
10 Yes
20 No
30 OK
's behavior
lO Yes
20 No
3DOK
10 New
20 Something he/she had had before
30 OK
change
10 New
2 0 Something he/ she had had before
3DOK
O. How did 's behavior change -----
24. Other symptoms 10 Yes
20 No
3D OK
10 New
20 Something he/she had had before
3D OK
O. How did 's behavior change c ______ __
LPHI~HHP-MORB (7-12) 8/82 Ver. 1
stop or change -::-:--:--;-:---;---(his/her) activities?
1 0 < 5 minutes
20s. 1 hr.
3 0 ~ 24 hrs.
4 D >24 hrs.
5 D OK
10 < 5 minutes
2D~ 1 hr.
3D~ 24 hrs.
4 D >24 hrs.
50 OK
10 < 5 minutes
2 0 ~ 1 hr.
3 D S. 24 hrs.
4 D >24 hrs.
50 OK
10 < 5 minutes
2 0 ~ 1 hr.
3 0 ~ 24 hrs.
40>24hrs.
50 OK
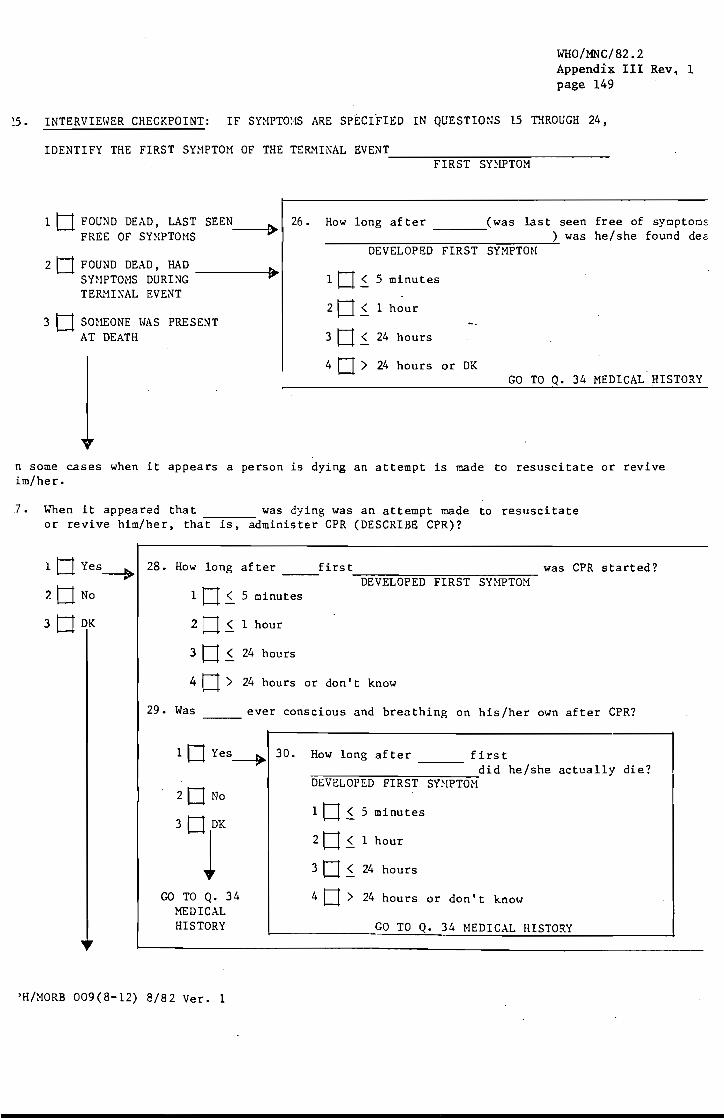
WHO/MNC/82.2 Appendi~ III Rev. 1 page 149
~5. INTERvIEtmR CHECKPOINT: IF SY~IPTO:·IS ARE SpECIFIED IN QUESTIO~JS 15 THROUGH 24,
IDENTIFY THE FIRST SY~IPTOM OF THE TER...'1.INAL EVENT ------~F~I~R~S~T~S~Y~~~W~T~O~M~---------
1 t1 FOUND DEAD, LAST SEEN~ 26. How long after (was last seen free of sympton~ FREE OF SY:WTOMS ) was he/she found de~
DEVELOPED FIRST SYMPTOH 2 tl FOUND DEAD, HAD
~ ltI~ SY~IPTOHS DURING 5 minutes TER}!INAL EVENT
20~ 1 hour 3 D SQ}IEONE HAS PRESENT
AT DEATH 3tI~ 24 hours
4 tI > 24 hours or DK GO TO Q. 34 MEDICAL HISTORY
n some cases when it appears a person is dying an attempt is made to resuscitate or revive im/her.
7. When it appeared that was dying was an attempt made to resuscitate ----:----
or revive him/her, that is, administer CPR (DESCRIBE CPR)?
1. tl Yes-----.
? t1 No
3 tl DK
28. How long after first was CPR started?
1 tl ~ 5 minutes DEVELOPED FIRST SY}~TOM
2tI~ 1 hour
3tI~ 24 hours
4 tJ > 24 hours or don't know
29. Was ever conscious and breathing on his/her own after CPR?
1 0 Yes~ 30.
20 No
3 tJ DK
1 GO TO Q.34
MEDICAL HISTORY
How long after first -------, ==~~~~~~~~~~~did he/she actually die? I DEVELOPED FIRST SY~IPTON
1 tI ~ 5 minutes
2 tI ~ 1 hour
3 tI ~ 24 hours
4 tI > 24 hours or don't knotl
GO TO Q. 34 HEDICAL HISTORY
'H/MORB 009(8-12) 8/82 Ver. 1

WHO/MNC/82.2 Appendix III Rev. 1 page 150
31. In the last few moments that (you/observer) saw did he/she show any signs of life, that is, appear to be breathing or moving? ----
10 Yes 32. How long after first did he/she actually die DEVELOPED FIRST SYMPTOM /'
20 No 1 0 ~ 5 minutes
20~ 1 hour 30 DK
1 30~ 24 hours
40> 24 hours or don't know
33. How long after first did he/she last show signs of life?
1 0 ~ 5 minutes
2 0 ~ 1 hour
3 0 ~ 24 hours
DEVELOPED FIRST SYMPTOM
4 0 > 24 hours or don t t know
MEDICAL HISTORY
34. Was a resident of a nursing home at the time of (his/her) death? -------
10 YES -+ Name of nursing home
20 NO
3D r Addr s
35. Was (he/she) confined to bed at any time within the two weeks prior to death? (that is, had to spend more than half of (his/her) waking hours in bed)
10 YES--. 36. How long had he/she been confined to bed?
20 NO 10 (2 days
3tJ DK 20 (1 wk
30 <2 wks
40 <4 wks
50 <6 wks
60 > 6 wks
70 DK
~PH/MHHP-MORB (9-12) 8/82 Ver. 1

WHQ/~c/82,2 AppendiJe Ul. Rev ~ 1 page 151
37. Had _____ had Njor surgery at any t.ime within the 4 weeks prior to death?
10 YES--.. 38.
20 NO
30 r At any time after surgery was (he/she) able to resume his/her usual level of daily activities?
10 YES
20 NO
30 DK
39. In the past, had ever had a heart attack for which (he/she) was in the hospital for a week or more?
10 YES 20 NO 3 UDK
40. In the past, had for a week or more?
ever had a stroke for which (he/she) was in the hospital -::-----
10 YES 2 NO 3 U DK
41. In the year prior to 's death, did a doctor ever tell that he/she had the following or did the doctor treat for any of these conditions?
YES NO DK A. angina pectoris or heart pains? •••••••••••••••••••
(ANSHER "YES" IF DECEDENT HAS TAKING NITRATES) 10 20 30
B abdominal aneurysm (bulging of the aorta)? •••••••• 10 20 3D c. congestive heart failure? ......................... . 10 2U 3U D. high blood pressure? ..••.•••.....••..•••.••...•••. 10 20 30 E. cancer? ...........•................••...•....••... 10 2U 3U F. emphysema or chronic lung disease? •••••••••••••••• 10 2U 3U G. cirrhosis of the liver (liver failure)? ••••••••••• 10 20 3D H. diabetes? ................................................. . 10 20 3 I. kidney failure requiring dialysis? •••••••••••••••• 10 20 3D J. myocarditis, cardiomyopathy or inflamation
of the heart tnuscle? ................................. . 10 20 3D K. rheumatic heart disease which limited activities?. 10 20 30 L. mitral valve prolapse? ••••.....••••••.•••••••••••• 10 20 3D M. Other, heart related probL~ms, .•.•••..•••••••••••••
specify ________________ __ 10 20 3D
L.PH/HHIIP-MORB 009(10- L2) 8/82 Ver. 1

WI:10/MNC/82.2 Appendix III Rev. 1 page 152
42. Thinking back, in the year prior to and then discharged?
. "s death was (he/she) in the hospi tal -----
1 0 YES
20 NO
30 DK
LIST HOST RECENT VISIT FIRST Date of admittance
43. VISIT 1 mrnrn Reason
44. VISIT 2
Reason
45. VISIT 3 DJDJ[[] Reason
46. VISIT 4
Reason
47. Total number of hospitalizations in the past year
Name of Hospital
rn lODK
48. Did have a regular physician? (PHYSICIAN WITH THE HOST INFOR}1ATION -----10 YES 20 NO
ABOUT ) 30DK
49. Did (he/she) see this or any other physician within one year prior to death?
10 YES 20 NO 30 DK
(IF EITHER 48 OR 49 IS YES - OBTAIN:)
Physician's name: _____________________________________________________________ _
Practice/Clinic:
Address:
Physician's name: ________________ __
Practice/Clinic:
Address:
LPH/~HHP-MORB 009(11-12) 8/82 Ver. 1

WHO/MNC/82.2 Appendix III Rev. 1 page 153
50. Would it be alright with you if r sent a short questionnaire to the doctor. and also requested some information from the hospital (or nursing home, or both)?
1 t1 YES ~ I will send you a permission form to sign and then mail back to me in an envelope I'll enclose. You should
2 t1 NO receive it withi::1 a few days.
51. Is there anything else about 's death that you feel may be important to add?
52.
-----
1 t1 YES~ INCLUDE THIS INFOR.'1..f;TION IN THE NARRATIVE
2 t1 NO
Is there anyone else who would be able to provide us with more information regarding the the circumstances of 's death? (SPECIFY NAME, ADDRESS, TELEPHO~~ ~~MBER) 1 tI YES 2 tJ NO 3 t1 DK
I (
11) II I I I J-LLLLL 1..JI I I I III I I II I I I I I I I I , I I ! [ , ! , ! I I ! I I I I I I I I ! I I I I I I
Address
[ r I I [ I I I I I I , I I I I I I I I I I I I I I I I I I I City/State Zip Code
[ I I II ! I I I Area Code Telephone Number Relationship to deceased
ASK IF THEY HAVE ANY QUESTIONS OF YOU. THANK RESPONDENT.
RELIABILITY OF INFOR.~NT REG~~rNG EVENTS SURROUNDING DEATH
53. Did the respondent frequently contradict himself YES NO or give information that he/she would have no way of knowing? 1 [J 20
54. Did the respondent seem to be reluctant to answer questions & thus might not have given all the 1 [J 2 t1 information the interviewer would wish to know?
55. On the basis of these questions, give your rating of reliability of the interview.
1 t1 GOOD 2 t1 FAIR 30 POOR
I I I I iDCODE
56. INTERVIE~~R'S ~~
LPH/:·mHP-MORB 009( 12-12) 8/8~ Ver. 1

WHO/MNC/82.2 Appendix III Rev. 1 page 154
MIDt-JEST HEART SURVEY F~~ILY INTERVIEW INFORMATION
MORTALITY SURVEILLANCE

WHO/MNC/82.2 Appendix III Rev. 1 page 155
The Family Interview Information questionnaire will be attempted for every out of hospital death selected for I1HHP Mortali ty Surveillance.
For Pre-test and training each interviewer will complete at least 3 interviews prior to certification evaluation.
Final Interview Status is to be checked when no more effort will be made on this assignment (ie., the Interview has been completed satisfactorily, a respondent has given a final refusal or the interviewer has exhausted all efforts to contact an informant).
ID Label - The label with the ID number assigned will be attached.
Date Letter Sent - This form should be prepared the day the letters are mailed to the informants. The first attempt to reach the informant should be made within 5 days of mailing the letter.
Interview Schedule - If when you reach the informant and an appointment is made for an interview at a later date enter the date and time.
Interview Completed - Enter the date
Call Record - Keep track of every effort to reach the appropriate respondent on the Call Record form. Use this to check that you are trying to reach people on a variety of days and times. Include in the comments section any messages or information you get that may help in contacting the informant (ie., "back from vacation 8/16," works nights", etc.). Enter your ID number in the space provided. Since different interviewers may try to contact a respondent at different times it is important to know who wrote which comments.
Complete 1-4 before telephoning. This information can be obtained from the death certificate. Print in Block Capital letters using black ball point pen.
5-6 In order to determine who can provide the most accurate information about a death (ie., who should be the respondent) the interviewer should check the death certificate. Every death certificate 'lists an informant. This is usually a relative of the deceased. If a relative is not the informant the Interviewer can contact the deceased's last known address to obtain the name of a relative.
7 Double check the relationship of the respondent to the deceased with the respondent. This can be done at any time during the interview.

WHO/MNC/82.2 Appendix III Rev. 1 page 156
SPECIAL INSTRUCTIONS FOR THE NARRATIVE
In certain instances, particularly in sudden or unwitnessed deaths, it may be necessary to ask additional questions in order to clarify the actual cause of death. Given below are some follow-up questions that should be used to make sure that all necessary information is obtained.
The Narrative is the key to providing information about an out of hospital death. The major points to remember are:
1. Record information verbatim (ie., in the respond~nts own words) as much as possible. We are after the R's perceptions not the interviewers. A great deal of meaning can hinge on a choice of terms or phrases.
2. Get the sequence of events and the time intervals between them. 3. Get as much detail as possible about the period following the onset of final
illness. Listed below are some follow-up questions to ask if certain situations are mentioned.
IF HE COLLAPSED
IF ALCOHOL IS MENTIONED
IF HE COHPLAlNED OF PAIN
IF TROUBLE WITH EYES
IF SEDENTARY OR IMHOBILIZED
Was he conscious? Did he make any sound? Was vomiting or sputum present? Did skin color change? Did he fall forward or back? Did he fall from a standing or seated
position? Was he perspiring heavily? Was there shortness of breath? Was he eating?
Was there any bleeding? Was he drinking that day? How much? Was that unusual?
Where was the pain? What did he do about it? Did anything seem to relieve it? If he lay down, was it in bed? Dressed
or undressed?
Did he compL,'!.in of dimness, blurred or double vision?
Did he complain of feeling weak, dizzy, or faint?
Did he have difficulty with speech or memory?
Had there been broken bones or surgery? Was he unable to walk?
4. It is best to have a notebook for note-taking as you are interviewing. The Narrative should then be written out on the page provided as soon as possibla af ter the interview takes place.
5. As is suggested in the Introduction to Hortality Interviewing, it is helpful to tape record each interview. This should be done \.1ith all pretest interviews to get the interviewer used to the recording procedure and devise ways to use it efficiently to get all the p~rtainent details.

WHO/MNC/82.2 Appendix III Rev. 1 page 157
After the narraLive the series of specific quesions is provided to 1) get more detail that might have been missed in the narrative and 2) put the most pertinent facts in a format that can be analyzed by the computer.
Thus the information about the onset of death will be in two places on the same questionnaire; one a free form narrative that will allow the respondent to give the details in the way that is most comfortable for him/her, the second in an arrangement that will make the information more accessible for data processing.
Because the second phase of this form is a repeat of the first the interviewer must read the introduction at the top of the page that explains this to the respondent.
Whenever the interviewer comes to a question that was discussed in the course of. the narrative it is to be read as worded. The interviewer can add a reference to the information in the narrative.
ie., "You touched on this before-----?" "You mentioned that Mrs .. Smith's brother ..... ?"
Where ever a blank line is provided insert the deceased's name or relationship to the respondent.
ie., "Mr. Smith" "Your husband"
DO NOT use overly familiar terms such as first names
Questions 8-13 are asked to determine who had the closest contact to the deceased just prior to death. In some cases this may mean that additional interviews may provide more information.
Q: 8
Q: 9
Q: 10
Q: 11
We want to know if there was a witness to the moment of death. If a spouse says his/her partner died during the night and was dead when the respondent awoke, record that as "found dead" but write a note in the margin describing the situation. However, if the respondent was awakened by the agonal event, e.g., a groan or gasp, the respondent is considered to be present at death.
For someone to be counted as "present" at the time of death they must have been in the same room and awake or have heard a noise(s) associated with the agonal event (ie., if the husband died in the bedroom when the wife was in the kitchen, and had found her husband dead and heard no noise, she was NOT present at the time of death). However, if she heard a nOise, went in and found her husband dead, she was present.
If anyone else witnessed the death we want to have as much information about them as possible since we may need to contact them for information.
If a subject was found dead we want to know who was the last person to see him/her alive. Again we want as much identification as possible of someone who had contact with the deceased prior to death.

WHO/MNC/82.2 Appendix III Rev. 1 page 158
Q: 12 In order to assess the validity of information provided we need to know how close to the time of death or discovery of death the person had contact with the decedent. The shortest time interval volunteered is to be checked.
This also applies to questions 13 and 14, and 15-24.
If the respondent gives a time range, chose the upper limit of the interval the one that includes the entire range.
Examples: 1. John Smith says 15 minutes Check III
2. Jane Doe says between an hour and an hour and a half Check #2
3. Jack Jones says somewhere between 45 minutes and an hour and one half Check 12
4. ~1rs. Nelson says the day before yes terday Check. 13
Q: 13 Even if another individual witnessed the death we want to know how soon prior to death the respondent saw the deceased. We'll use this to assess the accuracy of the information in the interview.
Q: 8-13 Two separate facts must be established in the interview: First, if the decedent was found dead or was oserved at the time of death. Second, if the interviewee was present at the time of death. The 2 x 2 table presents the logic of the question flow.
DECEDENT FOUND DEAD
Yes No
Yes 8, 11, 13 8, 9 Interviewee present at the time of death 8, 11, 13, 8, 10, 13
Q: 14
No
We want to know if the subject was able to communicate (and thus report symptoms or problems) at any point 24 hours prior to death.
Ask the question as a YES/NO reading each of the choices in turn. At whatever point the R says YES put an X in that box and go to the next
-question.
If a subject was only conscious and communicating for a short while during the time period it still qualifies as a YES and should be X'ed.
If the R says NO to both A and B double check by asking C.
"You mean that was unconscious continually for more than 24 hours prior to death?" If the R agrees that that was so X C.
. SYMPTOMS Q:l5-24
WHO/MNC/82.2 Appendix III Rev. 1 page 159
We are interested in finding out if the subject exhibited or complained of any symptoms that are associated with heart disease. Every respondent will be asked the specific list of symptoos. In most cases this information will have been mentioned in the narrative so the interviewer can make references to that when asking these symptoms.
We want to introduce the respondent to what we mean by a symptom before asking about the specific ones we're concerned about. For our purpose a symptom is defined as an event that is severe enough to make the subject stop or change his/her activity. If no sy~ptoms were present we would call it an instantaneous death.
If the respondent was aware of deceased's symptoms we want to know within what time frame these developed prior to death.
For the first two symptoms ask the triggering question in its entirety.
"Did ____ develop any (symptoms) ••• "
It must be clear to the respondent that in order for the symptom to be considered present it must have resulted in a stopping or changing of activity.
If the respondent asks, this change may be subtle (stopped reading a book and just stared off into space) or dramatic (had to stop jogging because of chest pain).
The respondent has to be the judge of whether a change occurred.
If the respondent answers "NO" to the presence of a symptom go on to the next one.
If a symptom was present, ask B, C, and D.
B We want to know if this was the first time that the deceased experienced or complained of this problem or if it was a chronic condition (something that he/she had had before). If the respondent answers don't know X the DK box.
C It's very important that we get the specific time frame for each symptom. Read questions C in its entirety for at least the first 3 times so it is clear to the respondent what is being asked.
D In the respondent's own words we want to know how the deceased's behavior or activities changed, ie., what had he/she been doing and what he/she did after the symptom appeared.
If man~ of these symptoms are mentioned you may not need to keep repeating the questions, the respondent will pick up on the pattern.
Be sure to check if any other symptoms (besides the ones listed) were present and get the details on them.

WHO/MNC/82.2 Appendix III Rev. 1 page 160
Q: 25-36 The time period we are concerned about is the period between onset of symptoms and death. Read the introduction. A cardiovascular collapse is defined as the loss of consciousness with the apparent cessation of respiration and pulse. 'Sudden' means collapse within an hour of first becoming 111. Be sure to distinguish "can't decide" from "don't know."
Q: 27-31 We want to knOlo/' where this happened to evaluate the type of medical help that could have been provided the victim.
Q: 28
We want to double check if the conditions that would necessitate CPR ,were present.
Describe CPR to all respondentb.
CPR is helping a person to start breathing again after they have stopped by 1) blowing directly into their mouth in a rhythmic fashion (mouth to mouth resusitation) and 2) applying pressure on the chest to get the heart started (pumping blood).
This can be done by one or two people.
A bystander is someone who initiates CPR immediately on the scene. A physician or other health professional with the patient in a nonprofessional capacity at the time would be counted as a bystander, health professional.
Q: 29-30 If the respondent says he/she is uncertain of the amount of time ask them to give their best estimate. If still unable to answer check DK.
Q: 31
Q: 32
For all deaths we want to know if the deceased was taken to a hospital or not. The type of emergency vehicle used will indicate the level of care the subject could have received. Describe the different types of transportation units to the respondent:
Paramedic (Advance Life Support) This is usually printed on the side of the vehicle. The staff usually have machinery and equipment to help a patient and can use it and drugs and start IV's while taking the patient to the hospital.
Ambulance (Basic Life Support) If it only says ambulance on the vehicle it is likely to be Basic Life Support. Staff can do CPR and have oxygen tanks but do not have advanced equipment or drugs at their disposal. Police and fire department units are Basic Life Support.
Records from nursing homes will be obtained if the deceased had been a resident.
Obtain a complete name and address (including zip code) if possible. If any information is missing you will have to look it up after the interview.
Q: 33-34 He want to know if any illness or symptoms kept the deceased confined to bed. Enter the number of days or number of weeks if known.
For example, if the decedent spent 5 days in bed the week prior to death, 33 would be 'yes' and 34 would be '(I wk'. If the decedent had spent 6 weeks in bed but was up and about in the week prior to death, 33 would be 'yes' and 34 would be ') 6 wks'. If the decedent was confined to bed for any length of time-more than two weeks prior to death, 33 would be 'no' and the interviewer would skip to 35.

WHO/MNC/82.2 Appendix III Rev. 1 page 161
Q: 35-36 Because effects of surgery could have influenced a death we want to know if the decedent had had major surgery within a month prior to death. Major surgery is when person receives general anesthesia and is hospitalized for about a week or more.
If YES we want to know whether or not the subject had been able to resume his/her usual level of daily activities. We've used the example of return to work but since many s~bjects may have been retired that will not apply in all cases, so stress "return to usual activities".
Q: 37-38 We want to k~ow if subjects had had a previous heart attack or stroke.
Q: 39
Q: 56
The subject must have been hospitalized for a week or more in order for us to accept event as a true heart attack or stroke.
Read the list of medical conditions and X the appropriate box. If the respondents have questions or difficulties with the terms write that down in the margins (we know we have to have more clarification about some of these terms and the doctors will be providing that).
If a respondent answers that they do not know what a term is make a note of that so we can separate those from the "don't know if the person had it but does not know what it is."
Did you notice or did her/she experience chronic shortness of breath, that is have difficulty breathing While walking up stairs or short distances, other than while exercising. Do not confuse myocarditis with pericarditis. If respondent answered "inflamation of sac around the heart" it was not myocarditis but pericarditis.
This question is necessary to determine if there were other heart related disease that the decedent may have had or ones that may shed a different light on the decedents condition at time of death.
By asking if a doctor ever told the decedent he had a condition, we are making it easier for the respondent to be more accurate and for the interviewer to run thru the diseases without lengthy technical definition or descriptions of the di~eases. The respondent's memory is being jogged, by the exact words, so repeat the disease and if they hesitate too long, or can't remember X OK.
We do not want the respondent's judgments as to the decedents medical problems, we want information that can be verified by a physician.
For example:
"He drank like a fish. He must have had cirrhosis of the liver!"
The interviewer should repeat the question did a doctor tell him he had cirrhosis of the liver or did he treat him for the condition.
If the resondent says "He was told ten years ago that he had cirrhosis," ask, "Did a doctor in the last year tell him that he had cirrhosis," The conditions listed hereare serious chronic conditions, and if an old diagnosis is correct, the decedent will most likely have been followed or treated by a doctor for the condition within the last year.

WHO/MNC/82.2 Appendix III Rev. 1 page 162
Q: 40-45 In order to get complete medical records we want to know about any hospital admissions within a year prior to the subjects death.
There is no minimum stay. Any admission (even as an out-patient) is counted.
Try to get the date of admission even if it is a "best guess". This will be needed in order to obtain hospital records.
The name and city of the hospital is also necessary for obtaining records.
Also obtain the reason that the subject was admitted to the hospital.
Enter the total number of hospitalizations in the past year.
Q: 46-47 If the respondent reports that the deceased had a regular physician or had been seen by a physician in the past year we want to know his/her name and address in order to contact for a physician interview or access to records.
Any type of medical doctor "counts".
Q: 48-50 It may be necessary to do an additional selling job here. Stress the importance of the information the respondent has given you as well as the added benefit that can be derived from an interview with a doctor and/or information from hospitals and nursing homes. Most people will have no objections to providing this. Be sure you make clear that a stamped envelope will be provided so completing this request will take little additional effort on their part.
In terminating the interview we want to give the respondents an opportunity to add anything they think may be important. If they do have something significant to say this can be added to the notes for the narrative and incorporated when the full narrative is written out.
Q: 50 This is another effort to find out if there may be someone else we should interview. If someone else is given make sure to get full information on how to contact this person.
Q: 51-54 Each interviewer should give his/her assessment on the reliability of the interview information. Check YES or NO to the three questions (by "giving information he/she would have no way of knowing" we mean thi:lgs like if the respondent describes the deceased's behavior and appearance the last few minutes of life but were unobserved).
The responses to items 67 and 68 will be looked over by the editors before the questionnaire information is entered in the computor. In the case of multiple interviews about one subject. this may be used to detemine which information will take precedence.
Before closing the conversation with the respondent you must let him/her know there is a chance they may be recontacted on a validity check. Read the following explanation.
Thank you very much for your help. We appreciate all the information you have given us. It will be very helpful to our study.
Because this is the start of a large research project we will be recontacting a small percentage of those who participated. Therefore we may be recontacting you to ask some additional questions or to verify the accuracy of my report.
This effort is to make sure that all the interviewers ask the questions in the same way. As you know, this is very important for the accuracy of research projects.
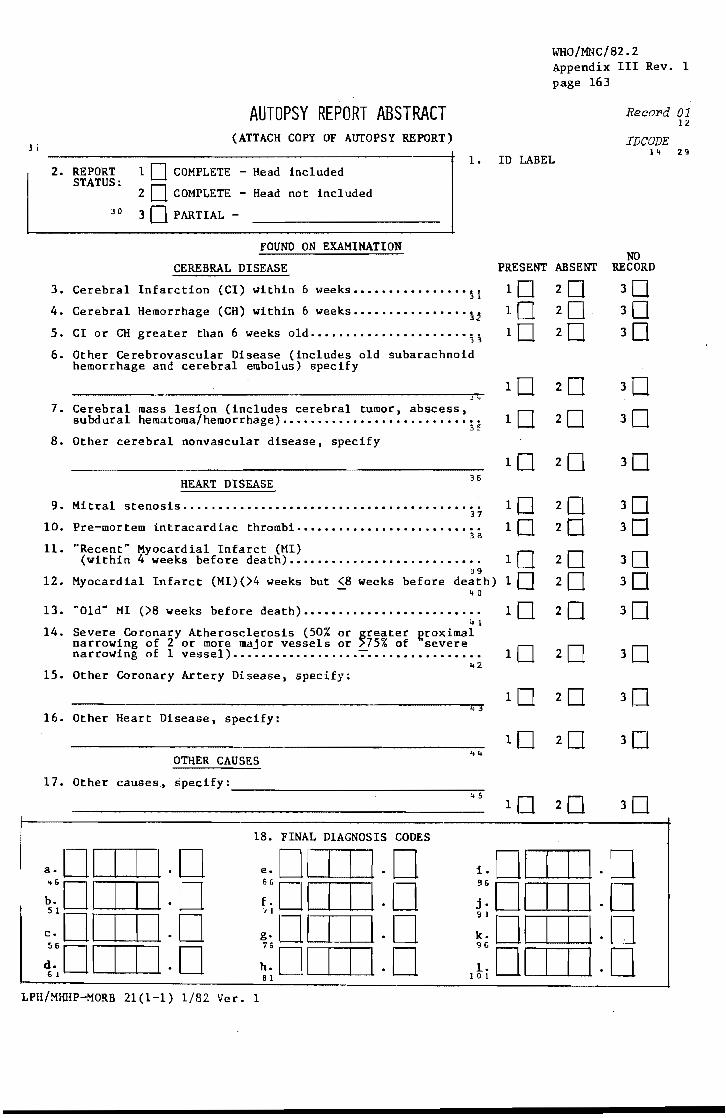
J I
2. REPORT STATUS:
AUTOPSY REPORT ABSTRACT (ATTACH COPY OF AUTOPSY REPORT)
1 0 COMPLETE - Head inc1 uded
2 0 COMPLETE - Head not included
30 PARTIAL -
FOUND ON EXAMINATION
CEREBRAL DISEASE
3. Cerebral Infarction (CI) within 6 weeks •••••••••••••••• ~i
4. Cerebral Hemorrhage (CH) within 6 weeks •••••••••••••••• ~~
5. CI or CH greater than 6 weeks old •••••••••••••••••••••• 3~
6. Other Cerebrovascular Disease (includes old subarachnoid hemorrhage and cerebral embolus) specify
j,
7. Cerebral mass lesion (includes cerebral tumor, abscess, subdural hematoma/hemorrhage) ••••••••••••••••••••••••••••
35
8. Other cerebral nonvascular disease, specify
HEART DISEASE 36
9. Mitral stenosis ...................•.........•••.•........ 37
10. Pre-mortem tntracardiac thrombi •••••••••••••••••••••••••• 38
11. "Recent" Myocardial Infarct (MI) (within 4 weeks before death) •••••••••••••••••••••••••••
39 12. Myocardial Infarct (MI)(>4 weeks but (8 weeks before death)
~ 0
13. "Old" MI (>8 weeks before death) ••••••••••••••••••••••••• .. 1
14. Severe Coronary Atherosclerosis (50% or greater Rroximal narrowing of 2 or more major vessels or )75% of severe narrowing of 1 vessel) •••••••••••••••••• 7 •••.••.•...•••••
15. Other Coronary Artery Disease, specify:
16. Other Heart Disease, specify:
OTHER CAUSES
17. Other causes~ specify:
.. 2
~ ..
------------------------------~4~5
18. FINAL DIAGNOSIS CODES
WHO/MNC/82.2 Appendix III Rev. 1 page 163
ID LABEL
Reco:l'd 01 12
IDCODE l~ 29
NO PRESENT ABSENT RECORD
2 0 2 0
2 0 2 0 2 0 2 0 2 0
e.OI I I 1.0 :,~ 01 I I I· 0 g·OI I I \.0 ~~Ol 1 I 1.0
i. 01 I I 1.0 ;: 01 I I 1.0 :~DI I I 1.0
1;: 01 I I 1.0 81
LPH/MHHP-MORB 21(1-1) 1/82 Ver. 1

WHO/MNC/82.2 Appendix III Rev. 1 page 164
FOID-I CODE 21 AUTOPSY REPORT ABSTRACT
9-17. Heart Disease
Q. 9. Self-explanatory.
Q.IO. Answer "Yes" if any mention of pre-mortem intracardiac thrombi in the left atrium or left ventricle.
Q .11. This question should be a.n~wered "yes" if the autopsy mentions a "recent", "acute", "early", "evolving" MI, or if it states an MI occurred 4 weeks or less prior to death. Anser "no" if the autopsy does not specify that there were signs of a recent infarc"t. Answer "NR" if the heart was not autopsied.
Q.12. Answer "Yes" if report indicates the HI occurred within 8 weeks, but was not "acute" or definitely within 4 weeks.
Q.13. This should be answered "Yes" if the autopsy states:there was an "old" infarct or an infarct greater than 8 weeks old. Answer "no" if the heart was autopsied, but no mention was made of an old MI. Answer "NR" if the heart was not autopsied.
Q.14. Coronary atherosclerosis should be called "severe" if the autopsy states it is "severe", or if the autopsy says there is a 50% or greater proximal narrowing of 2 or more major vessels, or 75% or greater narrowing of one vessel. The major arteries are:
1. right coronary artery (RCA) 2. left main segment of the left coronary artery (LeA) 3. left anterior descending artery (LAD) 4. left circumflex branch of the left coronary artery (LCF)
If the 50% or greater narrowing is in the segment of the left coronary artery before it branches (Q.14, item 2 above), this counts as 2 major arteries.
Q.15. This question is answered "Yes" if there is any other coronary atherosclerosis than that labelled "severe" in Q.1!. Also for any other type of coronary artery disease, e.g. congenital, traumatic.
Q .16. After "Specify" list any heart disease on the autopsy report not covered by Q.1l-Q.15. Record any codes on autopsy report in boxes for Q.1S.
Q.17. After "Specify" list any non-heart, non-cerebral disease on the autopsy report. Record any codes on autopsy report in boxes for Q .1S.
Q.18. Fill in final diagnosis code(s} by nosologist when avaIlable.
HORTALITY
A. Nosologist coding of death certificates to rCD9 Revision
WHO/MNC/82.2 Appendix III Rev. 1 page 165
In order to maximize cooparability between countries and over time, all death certificates should be coded to at least three and preferably four digits for underlying cause of death. The t1anual of the International Statistical Classification of Diseases, Injuries, and Causes of Death, Volume 1 contains the WHO nosological protocol for the 9th rCD revision (~ledical CertH ica tion and Rules for Classification, pages 699 to 743.
B. Validation of hospitalized strokes, MI's and in-hospital deaths
Validation of in-hospital deaths {yill be based on the hospital record history, ECGs, serum enzyme and death certificate data. In the case that the patient died before adequate data could be collected, the death should be treated as an out-of-hospital death: The next-of-kin or another informant should be contacted to gather as much information as possible about the events preceding the death and the validation will be based on this interview plus the death certificate information.
C. Validation of out-of-hospital deaths
All study-area death certificates should be reviewed quarterly or semiannually. Death certificates that are ineligible because the decedent was outside the age range can be excluded imwediately, and those deaths that are clearly due to trauma (e.g., contain a sequence of events including accident, homicide, or suicide), chronic obstructive pulmonary disease, cancer, cirrhosis of the liver, or rheumatic heart disease without mention of atherosclerotic heart or vascular disease can also be excluded. However, if an atherosclerotic condition is mentioned in the sequence of events or if the cause of death is not attributed to one of the conditions listed above, the cause of death should be validated.
Validation is based on interview of the decedent's next-of-kin or another informant and any available medical records. The interview should establish the circumstances surrounding the decedent's death. Medical records for the period within a minimum of 28 days of death should also be examined for information that may elucidate the circumstances leading to the death.
WHO/MNC/82.2 Appendix III Rev. 1 page 166
COUNTY COURT HOUSE INFORMATION 7/16/82
1. Anoka County Court House 325 E. Main Street Anoka
2. Carver County Court House 600 E. 4th Street Chaska
3. Dakota Government Center 1560 Highway 55 Hastings, MN
4. Hennepin County - Suburban Govt. Cr., Licensing Dept. Downtown Minneapolis
Hennepin County - City Mpls. Public Health Dept. 250 So. 4th St. Minneapolis
5. Ramsey County - Suburban County Court House, 12th Fl. 4th and Wabasha Streets Downtown St. Paul
Ramsey County - City City Health Dept. 555 Cedar St. St. Paul
6. Scott County Court House 428 So. Holmes St. Shakopee
7. Washington County Near Hwy 212, off N. Osgood St. Stillwater
Contact
Phone: 421-4760
Helen Therres Clerk of Courts Phone: 448-3435
Phone: 437-3191
Mary Ann Melberg Licensing Dept. Phone: 348-8240
Virginia Bryone Clerk of Courts Office, Rm 1215 Phone: 292-6544 Dept. Head: Fran Reese (292-6544)
Grace Selinski Vital Statistics, Main Floor Phone: 227-7741 Dept. Head: ~.;m. Timms, Ex.34
Doni Miles Clerk of Courts Phone: 445-7750
Rosemary Pozzini Vital Records Phone: 439-3220
~l
Dear v3:
WHO/MNC/82.2 Appendix III Rev. 1 page 167
I am writing on behalf of the Minnesota Heart Survey to ask for your help in our study, which is designed to measure the rates of heart disease and stroke in the Twin Cities metropolitan area. Your name is given on the death certificate of ~, who passed away on v7. In a few days an interviewer will be contacting you by phone to further explain the Survey and to ask a few medical questions. The information we need will be used for statistical purposes only, and will remain strictly confidential. It will contribute to our efforts to better understand heart disease and stroke and prevent their occurrence in the future. If you would like additional information before we contact you, please feel free to call K.C. Jenkins, R.N., Supervisor, at 376-8220 between 9:00 a.m. and 4:00 p.m.
Sincerely,
Thomas E. Kottke, M.D. Field Director Minnesota Heart Survey
TK/bg

WHO/MNC/82.2 Appendix III Rev. 1 page 168
UNIVERSITY OF MINNESOTA Laboratory of Physiological Hygiene TWIN CITIES School of Public Health
Stadium Gate 27
Dear
611 Beacon Street S,E. Minneaoolis, Minnesota 55455
Thank you very much for taking part in the Minnesota Heart Survey. The information you have given us will be most helpful to the doctors who are working on this study.
In the interview we asked if you would be willing to sign a permission for release of information form. Enclosed is the permission form for your signature and a pre-stamped envelope.
Please return the form to us at your earliest convenience.
Thank you.
Sincerely,
Thomas E. Kottke, M.D. Field Director Minnesota Heart Survey
TEK;.ssj

PERNISSION FOR
RELEASE OF INFORMATION
WijQ/MNC/82~2 Appendix III Rev. 1 page 169
I hereby authorize persons engaged in the Minnesota Heart Survey
to gain access to the medical records on ---------------------as was previously discussed over the phone.· These records will be
revie~.;red only for research purposes. no names ~.;rill be kept with
medical data. and none of the information will be released to any
individual other than the research team. This authorization
applies to hospital charts, nursing home charts, physician's office
records and autopsy report as applicable.
Date of death:
Date
Relationship to Deceased
t-litnessed by
LPH-~ffiHP (9/10/82) 1l-1

WHO/MNC/82.2 Appendix III Rev. 1 page 170
REQUEST FOR rnFORl-lATION
TO:
(Hospi:::al)
RE:
(Name)
(Social Security h~~er)
(Birt::date)
(Date of Death)
Pleas~ orovide the following recorcs for any a~~ssion within a year of death:
1. Hospital.a~ission hist9ry and physical examination 2. Hospital discharge s~ary 3. Laboratory reports 4. All electrocardiograms 5. Computerized axial tomography (CAT. CT) scan reports 6. Brain scan reports 7. Autopsy report
A COpy .OF THE CO~SE~7 FORM FOR RELEASE .OF n,FORY~TION
IS ENCLOSED ALONG IHTH A.~ ADDRESSED STAMPED ENVELOPE
FOR YOUR CONVENIENCE. THANK YOU FOR YOUR COOPERATION.
LPH-~~~P (02/80) 12-1
DATA COLLBCT IO~l
Quali ty Control
Forms/guidelines
WHO/MNC/82.2 Appendix III Rev. 1 page 171
In a longitudinal study such as the ~ffiHP, multiple observers over time or
change in the manner a single observer interprets data threatens the stability
of the observations. A set of clear and concise data collection forms is the
single most important intervention for insuring the collect.ion of complete.
stable and accurate data. The forms should be developed to reflect the criteria
and a center should budget enough time to create and test multiple drafts. One
test of the adequacy of the forms is to have a "naive" observer interpret the
forms using the printed guidelines. To the extent that they can do this with
sufficient accuracy to satisfy the investigators, the forms are adequate.
When developing questions, one particular problem that will arise is the use
of adjustives and adverbs as modifiers; they usually only provide the illusion
of concise definition. For example, in the question, "Was there a recent
myocardial infarction?", "recent" implies different intervals to different
people and will lead to inconsistent data recording. Therefore, it is suggested
that either the modifier be dropped altogether to include all myocardial infarc-
tions or an explicit interval, for example, 28 days, be used in its place.
A second problem is asking questions with multiple contingencies: for
example, if the ques tion, "Did the pa tient receive cardioversion for ventricular
fibrillation?" is asked, and the abstractor responds with "Don't know" or "Not
recorded", it is not clear for analysis whether the patient was cardioverted and
the reason was unknown, or whether there was no record onC! way or the other
about the cardioversion itself. To avoid this problem, the question should be
divided into two separate questions: Le., "Did the patient receive
WHO/MNC/82.2 Appendix III Rev. 1 page 172
cardiovcrsion?", and. if tile (llls' .. er if "Yes", then ask, "Was the cardioverslon
for ventricular fibrillation?"
When preparing the guidelines for forms completion, those data elements
which become labelled "self-explanatory" should be examined closely. It is our
experience that the "self-explanatory" items usually involve implicit assump-
tions of meaning, and if the implicit assumptions are not made explicit, they
create severe problems with reliability.
Hospital record abstracting
When training observers for the abstraction of hospital records it is more
important to focus on the accurate completion of the forms rather than On the
understanding of cardiovascular disease in general. A set of test records
should be developed offering a broad range of examples and problems likely to be
encountered by the abstractor. These records can be used both to train the
abstractors and for abstractor recertification every three to four months.
The goal of the quality control effort is to detect and eliminate bias and
errors. Bias, for example, appears when an abstractor answers "No" rather than
"Not Recorded" to the question, "Was there a history of previous myocardial
infarction?" even if no mention is made either way in the chart and the
abstracting rules say that the chart must have an explicit statement about the
presence or absence of a prior MI for the abstractor to answer "Yes" or "No".
Errors will ap~ear in the demographic data. and because large numbers of such
data are collected from each chart, only a few charts need to be reviewed to
detect unacceptable error rates.
Approximately one of thirty to one of fifty records should be reabstracted
by a second observer to check for bias and unacceptable error rates on the part
of the abstractor.

Death certificate validation - interview of witnesses
WHO/MNC/82.2 Appendix III Rev. 1 page 173
The ideal interviewer for this job is one who has had experience in inter-
viewing but is not a health professional. The health professional is avoided to
prevent the preconceptions which they bring with them onto a job. Interviewer
training should begin with a review of basic interviewing techniques and with
tapes of interviews which demonstrate these skills. Elizabeth Kubler-Ross'
book: On Death and Dying may also be assigned to acquaint the interviewer with
the grieving process and to help them understand that the interview will not
cause unnecessary grief or emotional trauma to the respondent.
Role playing is also a helpful exercise. The trainee knows only the death
certificate diagnOSis and interviews the supervisor who has a scenario of the
events surrounding the death of interest. If more than one interviewer is being
trained, the other trainees can observe the session and participate in the
discussion at the end of the interview.
It is also helpful to record the interviewer's voice during actual inter-
views. These are then reviewed with the supervisor to detect leading questions
or missed opportunities for follow-up of leads given by the subject. Although
it only contains the voice of the interviewer, this tape will also help the
interviewer reconstruct the interview from his or her notes.
Faulty interviewing technique can generally be divided into the use of
leading questions and the failure to probe into indefinite answers. To avoid
leading questions, the interviewer should be taught to use general rather than
specific probes. For example, when trying to establish whether the decedent
became short of breath before he died. rather than asking, "Did you husband
become short of breath before he died?", the interviewer can ask, "Could you
describe your husband's breathing for me?"
A lack of adequate probing, on the other hand, leads to the collection of
uninterpretable data. E.g •• , Respondent states, "His breathing got real funny

WHO/MNC/82.2 Appendix III Rev. 1 page 174
just bt!fore he died", and the intervi..!wcr fails to try to define "funny". In
this case, "funny" has no explicit meaning, so the interviewer should probe with
the question, "I"m not sure I understand exactly what you mean by "funny".
Could you describe this for me.
Re-interview can also be used as a quality control procedure. At the end of
the interview, the interviewer simply asks permission for the study to call the
respondent back if clarifications are needed. The respondent will probably
agree, and a sample of respondents can be re-interviewed by the supervisor at a
later date.

WHO/MNC/82.2 Appendix III Rev. 1 page 175
--Ui1iESDAWmSWf HOSPITAL , .': IRWIN BROTHER 10 033;;7
____ ~--~9~~~---------... ..,... ..... _00-
:~: CHABT cOPY ~~
HIt leu
.::
PROV. DIAG •
GROSSKI\N CHEV SALES "&AIl1.8'1' •• U'I'lva
BETIV WIFE _U'I'IYC ADD .....
-CERE8RAL VASCULAR ACCIDENT ... INAL DIAGNOSIS
MLATIOH.HIP
I
---------------------------------------.------_._- --- -
"ae. W
-------+=-~~~--=---=--------.------.--.--.-.. ----.-----
----~~-~-~(~<.-=nJ~=~--~-~~--
-: COMpLICATIONS
OPERATIONS AND I OR DIAGNOSIIC PRO~_E_DU_RE
7t--=-;-. ----_~-:-.----~ ... ------.-------------
-~. -- __ J ----- 11;;t.
----~-DISCHARGE SUMMARY U'I!.OV'''I!.D ON AL.L. CASES IN HOSPITAL..' HOURS ."'0 OVERt
---------------------_._----------- --.-- - -_ ...
----. --- .. ------
~ ...... -.0.
420 459
SAME
NONE Tl'H 0' , ...
SUB IC
COOE NO.
WHO/MNC/82.2 Appendix III Rev. 1 page 176
,,~'~JiOSPn'At: 1lD.una:n 01' PA1'I!otoGT
~tiU&e _____________________________ 7_C ___ O_~_~_3_g_7 __________ __
Pathologillt!... ___ .:..:A~. 'II,;.;,.;;.. • ...,;W:.:.;a;:;.t:;.;e;;..;r;;..;s:..l:,....;;.:M"".D::;.;.,. _____________ Autopsy No A 70-80
Physician O. Tveten, M.D. Hospilal No 420 459
" Patlan!...1 _---: ____ ---'=---__ _ ,----Age.A ___ 46_--""Se'''-____ -I
Date, Hour - Death'--,;;.o9/'-1_8-'-/_70 _____ ~AuIOpsY--'"'9'--1'-'6-'--7-0----___1 ,Mortuary, __________ ~B~ewt~h~e~s~d~a~Mo~~u~e _______________ _;
Clinical Data:
Specimens preserved
EX'IERNAL EXAMlNAnah The body is that of a well developed and well nourished 46 y~!r old ~=l~. There is nc jaY~~ice or ~ema. The
scalp and body hair is normal in amounts and distribution. There are no abnormalities of the eyes, ears, nose, or mouth. No nodes are palpable. There is a well healed stump following amputation many years ago of the right a~. There is a recent incision at the site of a right carotid artery angiogram.
INTERNAL EXAMINAnON. The subcutaneous fat is 3 cm. in thickness. The peri-toneal surfaces are smooth ann shiny and there is no
fluid present. The liver is 2 cm. below the midportion of the right costal margin. The pleural surfaces are free of adhesions and there is no fluid. The perl. cardium is normal. The pulmonary artery is patent. The heart weighs approximately 350 grams •. There are no abnormalities of the ventricles. ~e valves are normal. The auricular appendages and atria are normal. The for~.~n ovale is closed" The coronary vessels show very minimal arteriosclerosis •
.. There is no evidence of myocardial infarction or fibrosis. The lungs are re) a;tlvely'light and fluffy. There isa minimal amount of frothy fluid in the bronchi. The vessels are patent. ·The liver weighs 1700 grams. The outer surfaces are smooth. The cut surfaces are unremarkable. The portal vein, hepatic vessels, gall bladder and bile ducts are normal. The spleen, pancreas, adr~nals and kidneys are grossly normal. The bladder and pAostate are grossly normal. No gastro-intestinal tr~ct abnormalities are noted. The thyroid is normal. The scalp anc! calva:r!.~ .. show no abnormalities. The dura is bulging; the brain is swollen and presses against the cranial cavity. Gross configurations of the brain are aften indistinct due to massive edema; the brain is markedly softened and difficult to remove intact due to almost total infarction of the brain. The brain stem is likewise softened. The cut surfaces show a massive hemorrhage throughout the mid-brain and Pons. The vessels at the base of the brain are gros~ly unremarkable. The right carotid artery is occluded but it is not dissected to further examine the site of obstruction; fluid can easily be injected through the left carotid artery and the vertebral arteries. Hemorrhage compresses the aqueduct. The ventricles are slightly dilateo.
MICROSCOPIC. Sections through the mid~brain show dif!use hemorrhage and scattered irregular areas of acute infarction. Vessels are
engorged and show beginning exudation of neutrophll Sl there is no vascul it! s.
The lungs show evidence of chronic bronchitis and ~ilj ch:-:Jnic interstitial in fldllr'llati on. There is scarring ¥>out SC:"lt'
bronchioles and some of the adjacent septal walls are slightly thickened ard contain a light infiltrate of chronic inflammatory cells. In adoition. there is
70 33(:7
WHO/MNC/82.2 Appendix III Rev. 1 page 177
It 70-80
.superimposed on this an acute infl:al'Jlllatory reaction with neutrophils present in ,SOM bronchioles and in the immediately adjacent pulmonary parenchyma appearlng ·tobe the beginning of a broncho-pneumonia.
Sec~ions of the liver show some acute passive changes of central lobular congestion. There is prominence of some sinusoidal lining
cells that contain dark rounded granules of pigment. Whether or not this indicates previous inflammation within the liver is not clear; there is no acute 1nflamation in the liver.
Scattered throughout the renal cortex are small irregular areas of condensation of renal parenchyma in which the glomeruli have been
destroyed and are now hyalin rounded structures. Such areas also shOW a mild to moderate infiltrate of lymphocytes. Sorne glomeruli are slightly hypercellular but this does not appear to be a glomerulitis but probably represents an old inactive chronic pyelonephritis.
Sections of other organs examined are essentially histologically normal.
CONCLUSION. 1. Massive hemorrhage within mid-brain and Pons.
, ... 2. Swelling and softening of cerebral hemispheres. . - .
3. Lungs, chronic bronchitis and inter-sti tial infl'lJMlatory changes.
4. Lungs, acute bronchitis and beginning foci of brJncho-pneumonia.
,- '---"") i 1.-.; l' ~~~A._·· A.W. waters, M.D.
Pathologist
AW/ms

WHO/MNC/82.2 Appendix III Rev. 1 page 178
• ~. ~v'A J ~-~..., -rt....i.. ,t:... ,.,. r .....-t;....,.. c,~ 'f..A..&--....-1,.. ..... ........:
r i
Doctor
TOTAL
.It. L .. ·~ --:.1. '" I.~~K .~..1 ... T .; , ""'- r'\! ~ '", .' ••• • ~ ... C I "'''
WHO/MNC/82.2 Appendix III Rev. 1 page 179
~~~' .... ~'. lJM'" '."~' "'-"!f.'f/:' .• '. . .. " "'1 .. 1',- ',0;, .'~+ .. ft· • __ _ ., .' o. ...." .... ,,, .• :!"'420"'4~9"; ~)'" ., ,~-, ."Jr.",,,,;f,
~~~ __ ij;,,;Ml~.I" ~~1~ 4i~. r~;;;:'; tiloaJi ~,II~';';" ' ';)~;l/Ij (.:;,/1,'3 Rj . ,'. ~ft.'§t~~t;:Ii)ii'i"1n'\Y1tti·:ia·hhtory;Qf app'f'X1qat4>1 Y' 2' da;~' of:yomitlo~~ he';idacb"; \M~~~~rS~~!~91~M ~8dfallen out of tha car d(,ur at tJClme. ,. Was apf!,.:Clllq with. !~bhl-\'i1fR' 'eI!rlythi S I7'prol.oa' boweyer toward 6AM b .. laPSed $ ota !Income! OY'O" u ~Jlnd::hact.~qat,betln rt!Gpoosiw slnc~. . . '. ",,:.' ~. .' 1:.: '.
)' ----------------------------------;,ptiS!:'WIlICr,J HISIClH, Fair)" good. He bas b,i1 CA cf to? rlqbt c.re pu,,'1
:~&pprodlf.ate1y 10 yeilrs ago. '''! ' .', .• ~.-
--~------~.~~~--------------------------------------------------------'.ittorc.A&. .. lew.. of .• .~TOaY.'..-.,., ,Seeal HI5Iml. ftWo,., .";'
EAl.!I! I,;, 3
!-.".J . ~~~'~AIIif~:':':-' -----------------------------------------'m"," IUllln
: ..... ~ -_. :."tw,..... '; ...... y HlSTOU
::cKJ ...... n"a1' snt .. c IIWII.
-'" . - ., ~--: ...... -.... ,.-...... :-. --........... ---.,.... ....... ..
-..1-. ..... ---,,"SIC:.\1 •
. !XAMIIA YiOM ' ..... .. - ... ' OlJftU4 '.$It ... '\..,. .... .,.te·· ,I'll" ..... " MOle
!:;";n.;,, . ... cs .~.~
:ateSY ,
.... All-aL_
. iriSIn' M_ ..
5bI'T .... ' .. ........ ...... Loc_ro. In ... ",,, III'V.OL(K,tCA&.
PH'{3tCr',L <: .<t\~H'IAIIO'-!: '1"-v-als; lan mal!'. U;"jC ;"joe:, us. 'ri. C:yeSl 1ilat"'d aoj fixc". :-k> -jilr.a3- to :1i.S.',',1 :1. r I :1r(-,. ,f
·-.;-.a·....a.
Itv-:. rU:1',u?cn2\Ci r·~·v ala or. ~r;:sj iJr ,;5urn 4 5 •
Chest: cl"'ar ill+.);uJ:1 :-,e is hiv;)oJ ,': ,-,n'" ;)J:it":1esil.:l',. 1 c~,ain stc.i<,.>s Q*<at".L)_L wit:t jeep s:\i.ri:'l3 SI'U,':!:> r~v~alL):) s(.:;r ,fJ >t)i:·"".·,~·! ()~ ".:;J:.tio Ie
.H"art: :1;--rmal si:'lu:; 'n.,t:}.11. :1"di;)it·c C.UrIT.L.;S .• :r;,o'"u1i'- ~)'c .n • AO.-jl-.rr.t?n: s •. ft. n" Jo:'ii~lit·,", r:a5Si.'~.
~:e.:k: 3\.;021.'. 10 'lefinit'" tig:ltn"s;; f MU;C' -~, Cl(u,,".ities "cgativ'!, t!.(ce;>t fr.r :h~ a.HC"";)Ce :>f t~.", :i~:-.: I::;' it ':.:1-: U;>.)··: f"moral l .. y-l •
DlAI'.HOHIC ''''IIUIOM '/ •
DA1l lC-!7·7C
3.
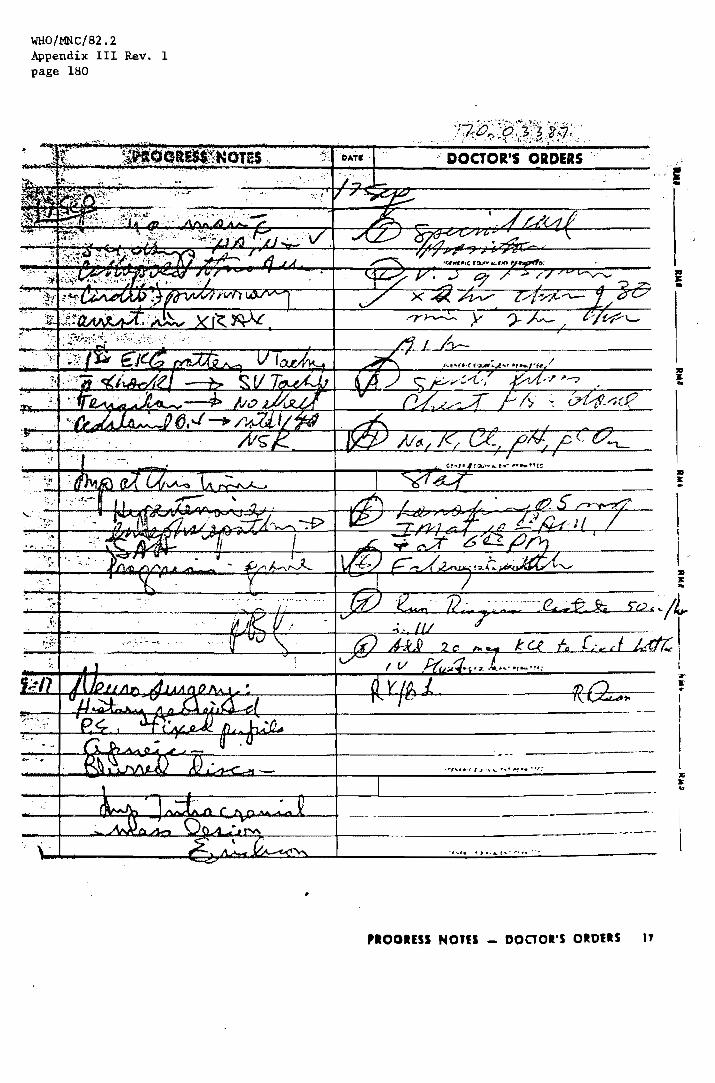
WHO/MNC/82.2 Appendix III Rev. 1 page 180
.' DOCTOR'S ORDERS
lIS J: •
lIS J: ..
~·~------~~~-*~~~~~~~~~~4
~+---------~--~---~~~~~~~~~~~~I
t ..•
----~--~--~~--~----------~--~--~-------------------------------
__ -+-____ ..JUI .... I.oC.II::;;L--.i~!!o'I ...... 4L.::..;...----_+--------------------.--~ ) ..... t .. • .~i". ' ..
/I
'.OOIESS Nons _ DOCTOR'S OROttS .,
I ;r a: ..
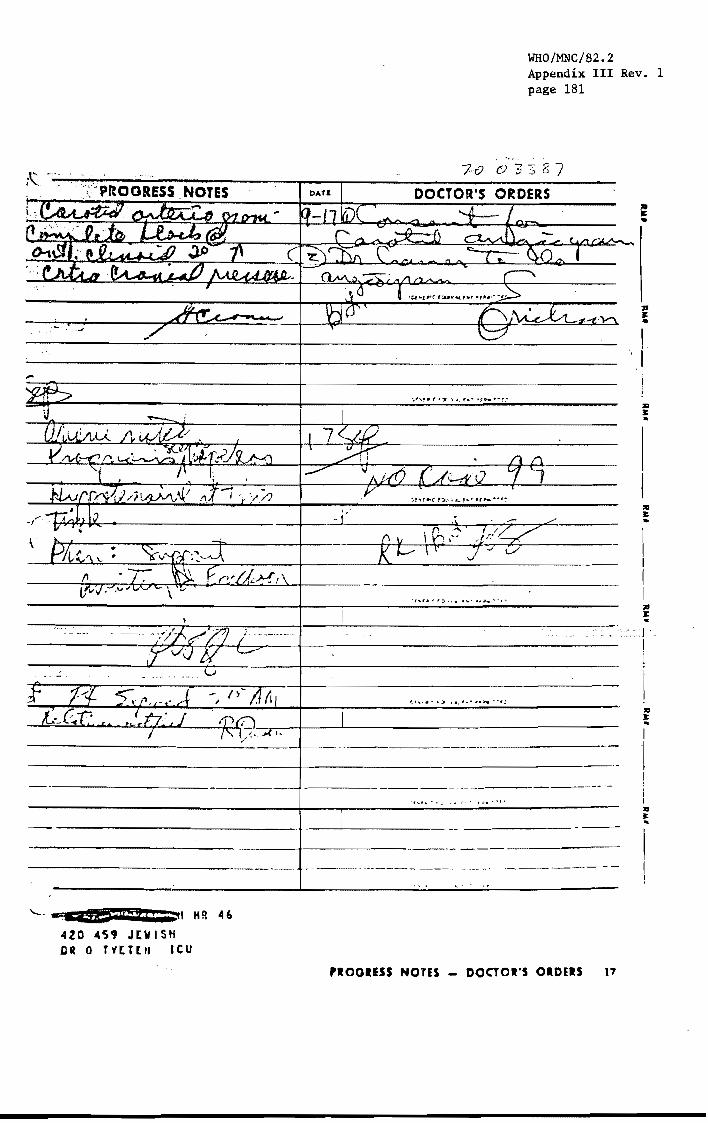
-----------------
WHO/MNC/82.2 Appendix III Rev. 1 page 181
.~ .'
7-0 03::; '6 "7
DOCTOR'S ORDERS
-+-------~------
--~-------- ~- ._-------- --- -
:III J: .
:III J: .. I
I I
! , I I lQ J: ..
·-------------------------------f-------------------------------
"--- .• %\15>: 4# Iii j ;ttl H R 046
420 4'59 JEWISH DR 0 T1tHIi leu
----- ._---_.-
,IOOIESS NOTES _ DOClOI'S OloElS t7

WHO/MNC/82.2 Appendix III Rev. 1 page 182
. " .'.,
.....
,,' '. ,'_,RUOilT OF' RADIOLOGIST
..;i.~H~j..;:~.;,;:~t;>(1:~~~~:·:~~~':J$t~·.:~~·.~/~!: 'Z:.~ _.' -' . _
·'::N~'FfA$(:;1~fletr:coftKtly,tbm:. q,pea=8to b •• aignlf1cmt shift' of ;~t#.i'f' ':it~ntj·~~:nd;;.:uf~e{'left. by CPP1'O:d.mately 8 IS. to !l 1 C3. ,lb. l'esal:lda t .' ':~A;~d:~at" ,p:'OCd.r.tDt vasculz =eking& but 1I1tn I'lO 8:pec1flc ,
~£ "".~_, ,.~~f~:~J"<'-'"' " , ~~i~ft;lh~li~'.!a':EialG'gcd~' :031190. in tIle per1h11m' :t"C9ion 1. seen i~~~~§t~t~tii'~ur.; :edcma. '~: JI:) 1'""""= peripherel COf)fiOl1dat!OA, ia :;·~~e·~)';· .," , - .' ' , ...
:)~f"!~1;~~.~~I.:m..~if~ectlon of c~~ast into"the right COIIIIIlOQ Cal'aUd ;, ~"';'-~1!I'::111':J\~M,W'bo .• block of the flow of contrast ~t the anterior .~ __ ."~~. ~,~C~3i:;~~(~bo~~1ght condatmtw1tb-tho he!!Cdynsc block, 8econdary ""'!'~lfUltk~l.y.:'ln=,o.Md"lct1'IC1'udal pzoeSIUl'G. nae cl1Gtr1bution of utemDl ~;~~ •. Ouotld · ...... 10 end middle merdngeal vea •• ls it quit. marked. t/PtlWt4j-.11~daGlrQn.t1'at.:ftO 519~f1cant fll11r.g of any iDtncranlal vea.eh .. ~. "'. '~ .. " .. -' -':-" '
~:t~$,mb~::;nSi'e:trn~o .block, anterior cl1nold proca.t tKondary to increased )i:5:1~.c~wAl:~PiE".l'tW.~/,:",:;" -', '; '.' J. /" . -.' .t ";,~-:-'-" - - ,'"
, .;f-
~,
-,
____ ~a=1~en=-a.~~Cr~e&==er~.~M~.~~ ___________ M6
9=17-70 .... __ d~~ ____ _
'0

70 l/33E7
WHO/MNC/82.2 Appendix III Rev. 1 page 183
~ .. ' .. ~~'~i~!l:.::'tz-'2;::· Z!la:;; « Adml"ed;~:' (hn.-IJ&---a '-.L..- '" /","..ctiOft CMdr list:
~;;~'~~~~I_ ~ .7:LY<~;~:" q,.: .IlhaeJ - (wa:/:ui M1~~. ~ IA 1--fti j; 1\ S;;IIOI c:cnI. (j .7 I' OC.ili'9 119«1"-' ---
~~;~ ____ ~a'_-k:.-,.l_.'-J-~.:::,-__ Othe, Protth •• M:. 41 ·4/ir-·".l.LL Prlvileg<ft ____ _ HI' ~,
'8,.. ____________ T~ ___________ Weigh' ___ Height ____ _
"StoMtMnlregon:iil'G reo$Ol'l palient it odmltted and hit g .. """,1 condi,ion.
>,~ lz~1 - <1 ,,l,'lLd.f' --I-- tJt.~ {: dLt~ / rAk
Uri .... spec. ___ _
Las, ChM'
,,-... ,------Sid_as ____ _
P'II- 119«1 .... _-_
"~'-------------------------------------------------------------------------
/t;- you 0" any special medication CIt diet beforCl you co ... e 10 th .. h0>9;1012 _______________________ _
'-:fOU hove any all"'9;"'? _/;L..4._7 ("':--.:.'--___________________________________ _
. Do 'IOU ho ... any part;cular food hob it. or probl ...... that will off .. cl you. hosp;101 izotion? ______ .< ___ •• _______ -_
) .. , I' Do you hove any difFiculty ,1 .. C!9.ng'?-__ ...... ...:·;.....,.. ____ _
1);;.;;t;~o'.;dilfi~.;i,y-wiih·eli,;;i;;;..;iion?'·8<>w.11 _ .• _-_ .. _ .. ~)_. :...' .... t _______ _____
Do you toka 101lOttv ... 'e<Ojularly? ____ ..L.J....... ..... _______ . (If y .... whot?) __________________ _
Anyrpec:ial 'eq .... ~I' (TV, No s...d.irt,J. visiton, ~onoe Calls, Cor .. you would I;k .. ~ _____________________ _
. I
.~: ...... LJ.2, .l rr,..: ...... .7: .. >..1... ~_".~(X . ..:..~ 1
2. Ski ... (roth, I>< ... i .... ope ... or_ •• or oth ... i""gvla, •• ; .. tl _/~wr:it:. _------'r.:c.;.;" .... ,...;'t..L~ ... ~ ... '....:LL.j\· :.. ~ ' •.. : 1lJ'.': •
--------.--... Sp.uh _______ _ H_ring ______ _ Sight. _ _______ . Cia .....
·5. SftoCldiM" .. hen up (if all_ed) ____________________ _
, ) l..::" • ...:'. -'.-:.._ ~_ ;..-':......_--
~--l."' ..• "
Mti lE!;l*I.u"P' C::' .1=,, __ .• 420 459 Jtv I SH OM 0 U[lUI leu ADMITTING NURSING NOTES 20

WHO/MNC/82.2 Appendix III Rev. 1 page 184
' ..
>OAT&- ~c '1-/Z- 70 J.)qy ibplt;U ,'.4.1 ...... .1.
i'o<rt p.o. or P.P .. A. ~. P. w.,
,':'HOUR • • I) • • 112
I F. j ... .. , t-
106"
! ., . .. : IDS'
I r
'f- Ig - '/ V
A ~ P U,
• • 11 • • JI:
104' ~
I
I
w IDl" , c:= ~ 102" -< a:
~ w t>.
101" 0 ... 100'
99" NORM;"I
98
97
P'a.J:se '5 (;1 tll-M:l /()
R.,piralions I').' I;,i L:l /"-B,P. * It}. j,.t.. ~'" Me1llht6 WI ·~_,. .... 1 \::,. 1..9-"
OOCTORS ~~_O~ fD_R , 'j lY. VISIT - - ~""-. ,.' . ( ,; ~__ I:JJ
Diet
AM.PM Co,,, I i fI (/'v'
MS, em. S 11".1. g~ ':: nrrAKL 11·7 7·3 J·ll
Orol r,9f Z~-
Ot,,1 0 l:t I V, /~ T:>lol.
Bicod
TOTAL 2( r" n:T ;.KE It~('C:·
OUTPUT, i j.7 I 1·3 I l·i I
Urlr.e - ~/7.,:>T -[me ...
TOTAL 24 "'t 0'·-....,.·-. ., l t ~. ~ !?j-
S;::4-:-Jr.\oe-r.~
S!OGI~
120 4S, JEWISH Ok 0 T., [H" leu
5l: r ! I ,)?-!
, r . , r !
/""
- - - - -- - - - -
s p:.:. 11 ~, 7·3
:3 .)7.;
:: .:'~U
.. j I • j
i ~~ I
~;,.
i·· -
i
I
- --
.~;>-'.
3·! 1
J.; •
. l(i (J :2 3 f?7-
.-A. U. PM. A 101. , \4 AM P M.
• • 12 . • " • • ., • • I I, . • 12 • ! • .,
- .- .-
~-~
.. -+-~
_ .• --1--
----: I ~
; : , I ! I ,
I ! ; I I i I I ! i
I T
- - - - - - - - - - - - - - - - - .. .. ,- -- - - - - - - - - - - - - - .. -
..
I I i S f,.:. .... ~- S ~,.;\ ;" - : ;'t 1. :": -. - ~"
i ;·7 i .J 3 .. ' .. ;," '~J i 3·.; - I ".J I 3. !
I I I
-.- -----
,., I " .. ' I ].: . "
, : I 1 .. • I ': : J.: . ._- .-I i i I ,--
._--- !------_.--.-- ....... - -~--.. -
----_._- - --- ---
.a ... " GRAPHlC SHIrr 11

~:'1~r7;"7 ·o·~,: .
", <''"' . -.
"'"'''+.''' ~ ./ .~ '!1 v~ ,;.; ""}( i; IrQ f; f D tf /' ~~.,.i~· Ill) \0 1\\ J)) J:}- '('T ~/ ~ r· i···.
''',210 "':4 :>, ~ ..," ~2dO
~.~.~
::10; ", .. - : 230
<r:J.O "
. 210
'a ",'., . . '1'PO \~': . III)
Ji'O
leo lSO
Ie
130 ......-1.21) i/' " ,/
:
no ,f .; j
•• -It .... ;-- I--- .,/ '100' I . .- I
fO .; '.
f
" ._ V . II)
.t 1 '1 I,
i'O \ .... 1/\ 1\
eo
** I
=m I 30 !
20 :g YO I I
rt- S~ I
'fA 7\)/ ,. II'L ~f! ~;[ S~ ..;, ~-' (.:J -'
I"~ .). 1'- . j'# ,
~), ;. " ... - ,~
',,,",
VJT AL SIGN GRAPH
'1~ .~ q (()
I "
~.
.... ~,
- : ......
~ '-. " !, '-' I - ! , -, f
.r',
- 1"1 ~
'-- ,,; .
. .... "'. "-"(
~ ! J .' -.1
.;;: ~ .', ~ ~ I
-..::
I
• i
.: , . " ;
, .-t-. J
, i'l., I f"D II -L w
'~ .-'"
I;). . ~ r; o...j r_
It, ().t( \~
, ~
.\ ;, t'
f--
_.
-,' I"
,~ . ,.
WHO/MNC/82.2 Appendix III Rev. 1 page 185
.VITAL SIGN GRAPH
:l
=l - J
I ,
Et=
188
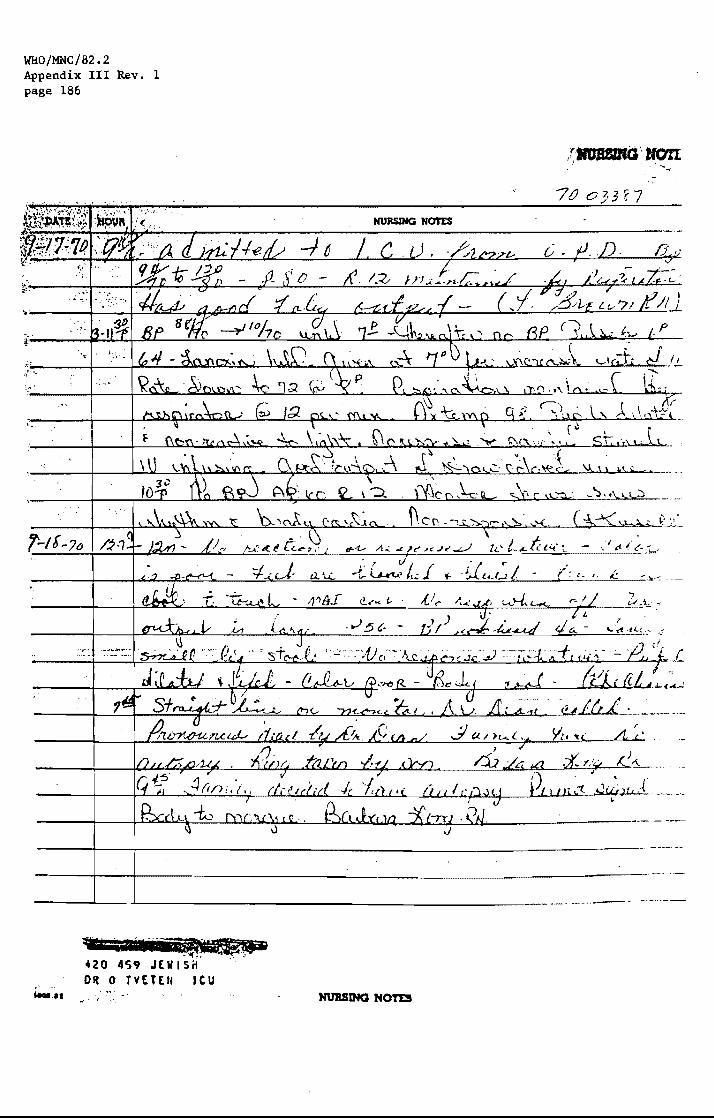
WI:10/MNC/82.2 Appendix III Rev. 1 page 186
. " '; .. ~,.
('-I[-?o
w:···;-~ D'll -':If,: " .. :'
420 4S9 JElllSif Oil 0 TVETEI4 leu .! ......
-~~--.-- -- _._-
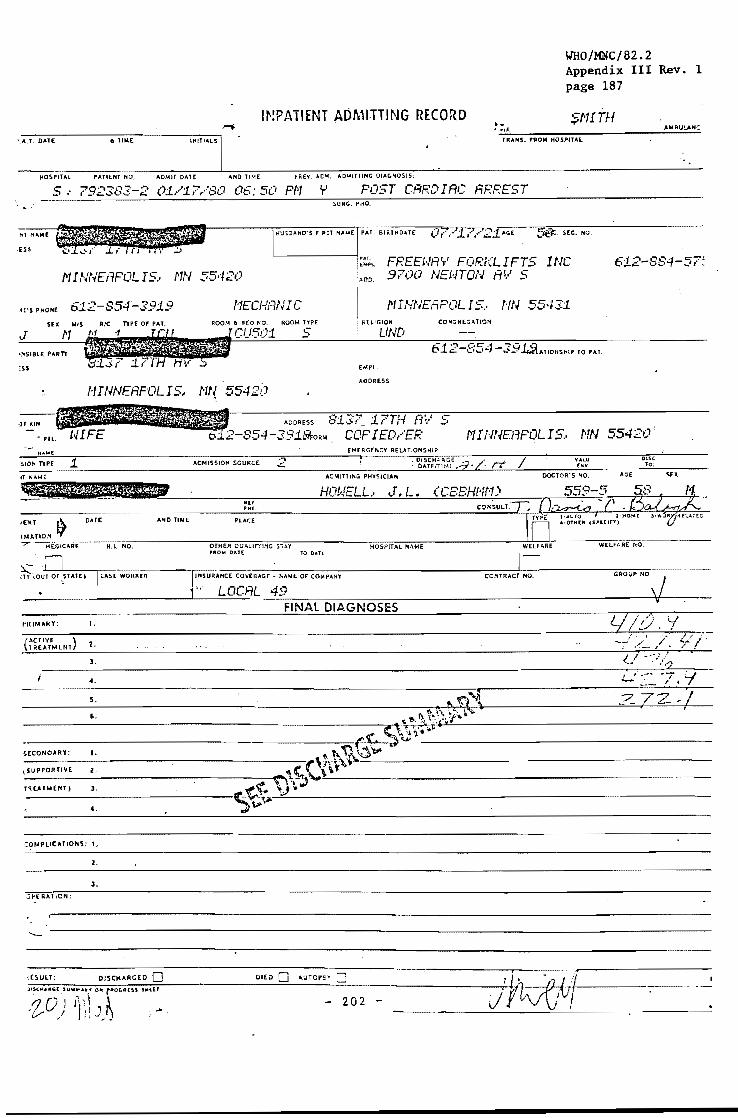
INPATIENT ADMITTING RECORD
WHO/MNC/82.2 Appendix III Rev. 1 page 187
J""'f. '-'~,T-.~O'~T7E---------.~TI~N7E--------~IN~IT~"-L~S
SNITH TRA"!. fROM HOSPITAl
HOSP1TAl PATIENT HO, ADMIT DATE ANOJIME PREVo ACl<!'. AO"'ITIIN(; 0IAGNO$15:
5., 792383:-2 01/1.7,··S() 06: 50 PN II POST CARDIAC ARREST
1'1 INNEr/POL IS .•
612-854~3919 MIS AIC TYPE Of PAT,
SURG. PRO.
HUSBANO'S rlRST NAME PAl. BIRTHDAT( SEC. NO.
NEC/-fFINIC ROOM I. SED NO. ROOM TYPE
5
FREEHAr' FORKLIFTS INC 9700 NENTON All 5
I N I NNEAPOL 15.. /'IN 554:];1 I ~H.lGION COPiGREGA nON
. UND -39L:lLAt,Ot,SHtP TO PAT.
EMPL
612-SS4-57~
NINNEAF"OLI5.. Nf{ 55421) I.OORESS
-J' !UN
C.TE ANO TiME
H.I. NO.
CASE WORKER
"itIMAHY: I-
(.'TI"E ) T REATM[l/T 2.
3.
~. ---_ ..... 5.
6.
SiAl TO o,a,n
iNSURANCE COVEOAGE - NAME Of COMPANY
LOCAL 4:9 FINAL DIAGNOSES
NINNEFlPOLIS .. NN 55420
CONTRACT NO, GROVP 140.
LI/o. i I j .,,) .' "-. '.:..,
.. ~~ "7 .f Z ,,1 ~ I'. P,,"", ''''. ---------------------~=_,f_-=:::....:'_I_--
'I'> ~ \ •. ,~.~ ...
'.' 'To" ;;"'il" ( ... ~ .. ' .. ;.. --------------------------------=~~~~-----------------------------
~ '1\ 1; \) 'tr' r\r\\~'.\.:=---------------------
~(CONOARY; I.
,SUPPORTIVE Z.
TUATMEliT I J.
~,
---------------------------~\~~\,~-----------------------------------------------------------------~~~~~~~-~---------------------------------------------
1.
2.
3 .
.)jo<[RATION;
--..;..
,UULT; DISCHARGED 0 OlEO 0 ,urop~v 0
- 202

WRO/MNC/82.2 Appendix III Rev. 1 page 188
1'1 I NNEAPOL IS.. NN 55420 FF:E.£NH'r' FOf:KLIFr5 INC 9700 NHJTON AV S
f'11 NN£APOL IS., N
L'r'LE H HE I N£CK£ 813? 17TH RV'S
NJNNEAl-'OLIS .. . NN 55420
, TT
"fIlT MEOS.-
Y\ffrJ!.-, ORY .. EX .. M,,. .. T'ON:
alUUD"SMt,. 10 ".rl£1n
p
612-854-:"~91 <A<£
612-884-si5. ROUG.' 'N,,, 5NJ TH f""( 0 J) 4VTO I) "OM' 1) \!ton atl..u{O
""10 "!iTS.
5ti9-.~~;~AIl HONELL.. \.T. L. UflRR"L 'HTS.
<' CBBHN"Co..,,,o ) (p L/ ~ ~o~ r-
IHS. CO~(lI.G( ""M( (;1' .:0 ..... LOCAL 49
, .. ou' 00.
, ....
IttVl;(J", ~ TO .suIiSCAlii

WriO/MNC/82.2 Appendix III Rev. 1 page 189
C':: 1'lctropolitan Hedical (en. Rehab. Unit
FAIRVIEW HOSPITALS
ROOM NO.
:JeTOR John Howell, M.D. CASE NO. 792383-2
Admitted: 1/17/80 Discharged:
PLEASE INCLUDE: 1. Peninc"l H&P Findings 2. Pertinent L~b &. X·ray 3. Hosp'tal Course/med·surg 4. Dischnrge Recommendations
+ mads, prognosis 5. Final DJagnosis
This 58 year old forklift mechanic and businessman was admitted to Fain,iel'l Southdale Hospital on 1/17/80 by the rescue squad. He had a sudden syncopal episode at home and was given cardiopulmonary resuscitation. The rescue squad found that he \'1as in.ventricular fibrillation and he was defibrillated. He was brought to Fairviev/ Southdale Hospital. It I"as felt during subsequent vlol'kup that he had an acute myocardial infarct.
This was based on serial enzyme changes. His past history did include a Type IV hyperlipoproteinemia and presumable myocardial infarct in 1969 and abnormal EKG thereafter. Some two years ago he had been thought to have some tntnsient ischemic attacks and for a time was on some anticoagulant and/or Persantine. His course in Fairvie'l Hospital initially was complicated by some pulmonary 1'ales and. positive culture of Hemophilus influenza, so he I'/as given some I.H. Penicillin and this did not prove to be an ongoing problem.
Over the next several days in the hospital he was in and out of various ectopic beats and rhythm disturbances with rr.ultiple PVC's and some supl'aventricular tachycardia. Lidocaine \'las not effective but these I'/ere controlled l'iell by Digitalis and Inderal. ~oley catheter was inserted.
__ ~her features of this man's admitting physical exam revealed a chronic furunculosis over the occipital area for vlhich he had been seen by dennatologist.
This man's hospital course was stable over the following week and then on the night of 1/24/80 he sustained an acute cerebrovascular accident l'/ith right hemiplegia and aphasia. He vias seen in consultation by neul'ologist. It was felt that the pathological process vias most likely an embolic phenomena from the heart in viel'l of the recent myoc.ardial infarct. He was treated I'lith Decadron and Heparin. He subsequently regained his sense abilities but demonstrated some aphasia and the right ann and right leg hemiparesis. For a time he had a Foley catheter but pulled this out himself and subsequently vias able to void by himself.
LABORATORY ~JORK: Initial hgb. 14.9, I'/hite count 14.200. UA had 1+ albumen and 2+ glucose and a repeat UA on 1/26/80 \'las negative. Initial SMA 12 showed the follovling abnonnalities: Cholesterol 305, glucose 359, triglycerides 388. Initial SGOT was 37 but on two consecutive days rose to 80 and then to 77. Initial creatinine kinase 1-18 l'/as two units and the follo\'Jing da'y l'laS 45 and the next day vias 18. Repeat blood sugars on 2/2/80 shm'led fasting values of 106 mg.%. It l'/as not felt that the diabetes vias a significant problem. T4 and T3 uptake I'/ere normal. Urea nitrogen was nonnal. Serum electrolytes l'/ere normal on 2/2/80 \"/itll a sodium of 135, potassium ;1.2. Chest x-ray lias clear on 1/20/30. Prio)' chest x-rays on 1/17 and 1/18/80 showed som:! pulmonary congestion suggesti~;J congestive failure. EKG on 1/17/80 shOl'/ed nyocardial irritability, LBBG. some evidence of left ventriculal" hypertrophy . .... llol"lup EKG shO\'/ed persistent abnor.;:alities on 2/1/80. Tile pattern suggested
anteroseptal infarct of indetenr.inate age I'/ith nonspecif~c T "/ave abnonnalities _~ negative T waves in 1 AVL, V4, V5, and V6.
The patient's BP over the last several hospital days ranged arou~d 110 to 120 systolic .1nC 60-70 diastolic. He has been arebl"ile over the last several cays and his only
'24 Aev, 11/71 DISCHARGE SUMMARY REPORT ;'-'c::mtinc;ed--

WhO/MNC/82.2 Appendix III Rev. 1 page 190
)CTOR John Howell, M.D.
Admitted:
PLEASE INCLUDE, 1. Penmenl H&P Findings 2. Pertinent L3b & X-ray 3. Hospital Course/med-surg ~. Discharge Recommendations
+ meds. prognosis 5. Final Diagnosis
FAIRVIEW HOSPITALS
ROOM NO.
CASE NO.
Ou.charged:
Continued from page 1
;;]edications have been Inderal 10 mg. q.i .d., Procainamide Penicillin 300,000 units o.i.d., Digoxin .25 mg. daily, and ~umadin 5 mg. daily. He has been on 1% HydroCortisone and Bacitracin ointment bi.d. to his scalp lesions.
ransfer date to MMC is to be 2/6/80.
-ransfer dismissal diagnosis: 1. Acute myocardial infarct, 1/17/80. 2. Ventricular fibrillation and subsequent cardiac
an'hythmias associated \vith myocardial infarcL 3. Acute cerebrovascular accident secondary to
arteriolar embolus vlith result in right hemi paresis and aphasia, occurring on 1/24/80.
4. Underlying Type IV hyperli?oprcteinemia.
ISPOSITION: This man will be seen over the next several weeks at the rehab unit HtK and I will f0l1C1-1 him there.
;HN Hm'lEll, M.D./skr 2/7 /80
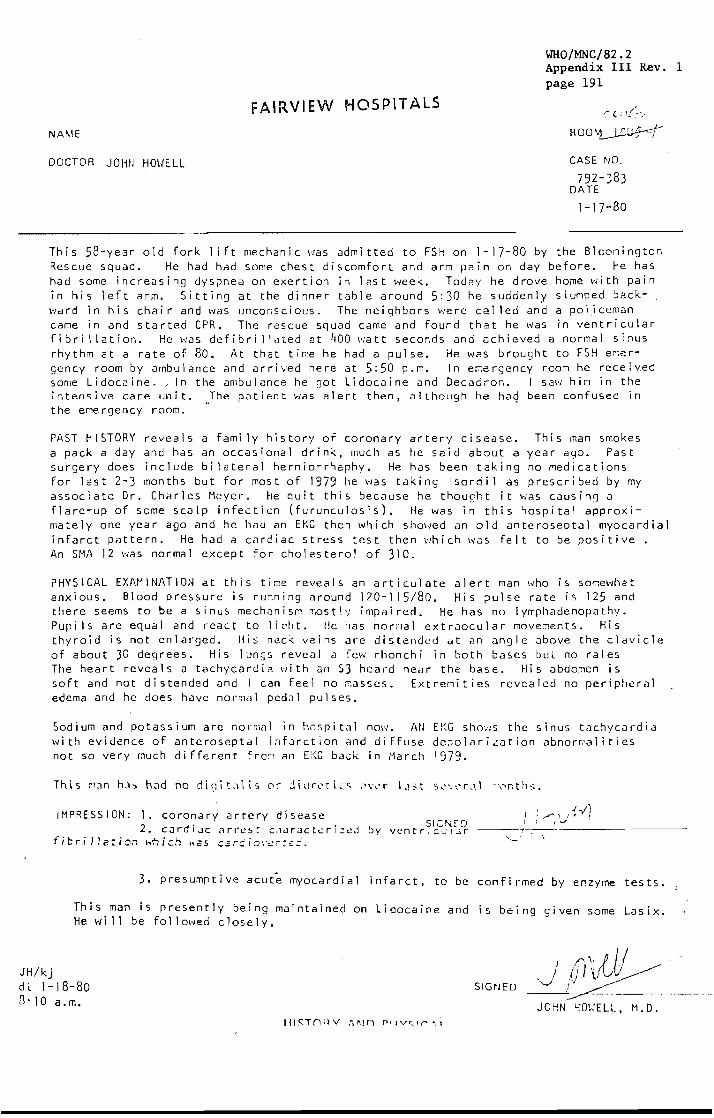
FAIRVIEW HOSPITALS
WHO/MNC/82.2 Appendix III Rev. 1 page 191
NAME
" (, If~:,
ROO~~
DOCTOR JOHN HO\JELL CASE NO,
792-383 DATE
1-17-80
This 58-year old fork 1 ift mechanic was admitted to FSH on 1-1 80 by the Bloomington Rescue squad. He had had some chest discomfort and arm pain on day before. He has had some increasing dyspnea on exertion in last week. Today he drove home with pain in his left arm. Sitting at the dinner table around 5:30 he suddenly slumped back-., ward in his chair and was unconscious. The neighbors were called and a policeman came in and started CPR. The rescue squad came and found that he Ivas in ventricular fibri 1lation. He was defibri llated at 400 watt seconds and achieved a normal sinus rhythm at a rate of 80. At that time he had a pul se. He was brought to FSH emergency room by ambulance and arrived here at 5:50 p.r,. In e~ergency rOO:7l he received some Lidocaine. ,in the ambulance he got Lidocaine and Decadron. I saI'l him in the intensive care unit. The patient was alert then, although he ha~ been confused in the emergency room.
PAST HISTORY reveals a fami ly history of coronary artery disease. This man smokes a pack a day and has an occasional drink, much as he said about a year ago. Past surgery does include bilateral herniorrhaphy. He has been taking no medications for last 2-3 months but for most of 1979 he VJas taking Isordil as prescribed by my associate Dr. Charles Meyer. He quit this because he thought it was causing a flare-up of some scalp infection (furunculosis). He was in this hospital approximately one year ago and he had an EKG then which showed an old anteroseptal myocardial infarct pattern. He had a cardiac stress test then which was felt to be positive. An SMA 12 was normal except for cholesterol of 310.
PHYSICAL EXAMINATiON at this time reveals an articulate alert man who is somewhat anxious. Blood pressure is running around 120-115/80. His ?ulse rate Is 125 and there seems to be a sinus mechanisM mostly Impaired. He has no lymphadenopathy. Pupl Is are equal and react to light. He has normal extraocular movements. His thyroid is not enlarged. His neck veins arc distended at an angle above the cldvicle of about 30 degrees. His lungs revea.1 a fe\" rhonchi in both bases but no rales The heart reveals a tachycardia with an 53 heard near the base. His abdomen is
jH/kj
soft and not distended and I can feel no masses. Extrenities revealed no peripheral edema and he does have normal pedal pulses.
Sodium and potassium are norn,al in hospital nOl·/. AN E!-~G shO":s the sinus tachycardia with evidence of anteroseptal infarction and di ffuse de~olarization abnormalities not so very much different frc~ an EKG back in March 1979.
IMPRESSION: 1. coronary artery disease 2. cardL:lc ar,"est choract..::ri::eJ by vent
ficrilJaticn ),,'hich ;,25 c.ar:;'io'.'er:e;:' ..
3. presumptive acute myocardial infarct, to be confirmed by enzyme tests.
This man is presently being maintained on Lidocaine and is being given some Lasix. He wi 11 be follolved closely.
dt 1-18-80 B· lOa. m.
SIGNED

WHO/MNC/82.2 Appendix III Rev. 1 page 192
DATE PROOLEM NU~.16"R
FAIRVIE'N HOSPITALS
. : .~~
"
--I------------------~------------.-----.----
{ /' ;-1:. / f 1'1 i . ---~---+_---------~c~-~~f~----~-----~-----------·- ------
/4 lJ, ,_,_".d· c.,/j, 10.~ -.1; .-;'f,:'. J .. /', /L,----~---i--------------------------------------
I r --"
I //'_ i ~ ______ v_,,_
/ ---------~-----------------------------------------
'\ -
PROGRESS REPORT l-C('15 (12-/~j

, .. ri J1 'J ;:~. ~'J.
cn.J. L. iiU.H:L1 .. 01-11-30 50 M
DATE PROOLH.1 NUMBER
-----4-----+-----------
;r'.
; ,
DLS
WHO/MNC/82.2 Appendix III Rev. 1 page 193
FAIRVIE.\MDHOSP1T,~LS ':';41" -.;)
(vi k fa,..,..... -z:;-~ &-<.:./ __ .
L/ L L j /-:'&-:Gft- • S ,-r M0
I
---;~----+---::,....------;-.......--:-----------------.~-------.. ~ (;)At"fi-l-C C l/A-
i : r\ ,,1[ ~----~----~------------.-.----------------------------.r\:!l-~~/~7"-.-~~
. PROGRESS REPORT Ie>' ~= . • .... ..l~.

WHO/MNC/82.2 Appendix III Rev. 1 page 194
F;\I RVIEWUROSPIT ALS
1{ 1.1 A
12M 1 2 3 4 5 6 'i 8 9 10 11 12 2 J 4 5 6 7 8 9 10 ll P
/'J - yl,,----I=~1--:t.::-~~-' :-:_; __ ~~ __ ,--I -:-\_==\-:-.:::-:::--:--'--T-~'-' -~-=; .:----: :_-_."",+----. ,--, ;,:=~:~,.,-,---,--.--- --,
140
130
106 1 __ I_I ___ :--=':;~---:-~:~:-- :-:-_____ ,~;--:':T:::-=l':--:--':---=-.-- ____ . :--;--1 105 -:-::":'l=:-=:-'-'--' • -- ,-----. __ .::,-l:=:t_-:-~L==;~=::___ ,---- -'."-
-i' '-i:--:- L -"~:---,.-,---.. :;.:::?»:----,--__ ., -:::=:-";-'-:::-.:=-:~-. -, ,-==1---::::.+-- . .., ;,r!"'; t-~-
120 '---.... -... ,-;--. '-.-~-.--;.-- --,:,._::(-"-'-':P'--1----- ---, ---,--. -. !:=1~,,-
110 10) .----------,·---r----t -~'-----,I---,l-q;V .. -=== .--- ... _-- ----,;
ICO 102 +-
101 f--
so 100
70 ... --- ------t---- ,-.-- r---.,--'----------+- ~'"'.-
.--.--- -,,--. -.-~-----. ·-----'-1--' .--.----!-=1:.:::=~~ ~--b--- .--'..
.=:=-::-:: :.~=-·_t:::_-=-._+_ L __ ~ .. -- .: •. ,: ---I --i-
60
50 .:--. .-:~I_-::::-:j ~:::::r=.::r.:-·-:--=-t- --'-=-.,
CVP I · .: ~I (-Total IrHoke _-"'--..!...""::" ___ ,_
ORAL INTAKE
11·7
MISC.
7·3 Towl Output __ "',-' -"-S_·L=-, ___ __ 5 I
3·11 Dildy Weight ______ , __
6 24 he Or.11 Defecation _______ _
7 }(( 1,(" 24 hr. IV <-' , / (
8 24 hr
UIH1C
9 OUT PUTS --
T,Tuhe
)
---------~,------------------+---~----~------------------,------------------, 10
11 ) (l· 11-7 11·7
7-3 7·3 _._ ... 3-11 3·1 i
24 hr, 24 h.-,
C ... iiic SU"'"
11·7 , 1·7
! 73
3 11
'.J ! 311
--------.~----- ------:-1 hr ;"\ I" --_._--------'--'-'-'--------------:...:...:.:;..-------::llt:\t r:"l~S:i
I 1,7 II i
7,3
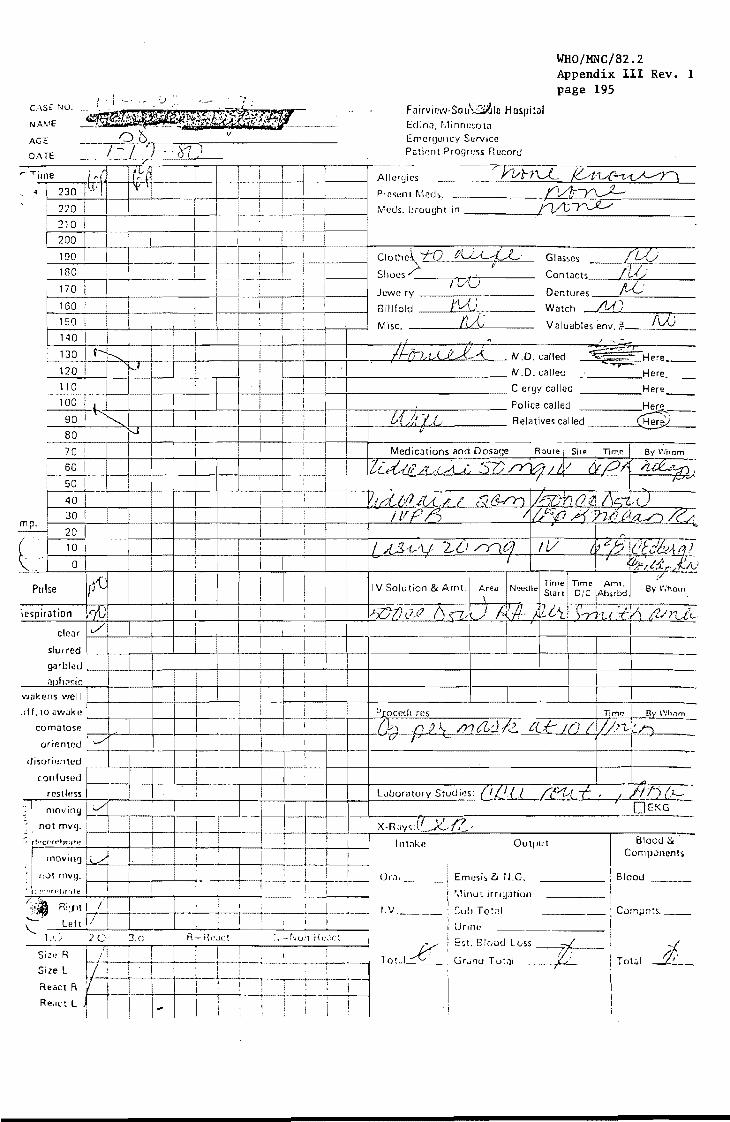
0/\ oj
AGE
O/\TE I-I ~1l
.---rime Ikfi-~ I I I I i
. ~ I 230 I ~, • I I I ! ,
220 I i I i 210 i I H 200 i i I ; ! 190 I I i I
180 I I I , i 170
, I I i I I
160 I I I I . I , 150 I I I ! ! I 140 I I I I I
130 I~ I I I !
120 I f.-I I i I I I I !
110 I ! ! I I I
100 j I I I ! : , 90 i ~ I i i I ; ! ;
80 I \'..I I I i 70 ! I I I i I i I 60 I i I I
•
50 I
m I :
40 I I . : I I 30 I I I P ~ 20 I ! I I
l.· 10 I ; I I I I
oj I I
lire I i
) i
I I
Pulse I ! I
)cspiration kiJI I ! I i ,
I ,
clear ,/1 i I I j
- ! slUffed I i g<Jrblilu I i ;}lJh:!~ir. I I I I
I
"'ilkens well I I I
I j I :off. 10 "wake I
comatOSf! I [ I
orienwu ,,.,/ I I !
disorien led ! I 1 "
.. .;...-
can fused I I
r--"" i I (estl~,ss I
il "'''''''m -+-1-- I I
1-' not mV9. -L
:: ~!"cer"t)f."f" f : i I ! ! I
I rnOllln~ 1(,.) , : I I i I 'I
I ,
I ! I : I ,:;)t 1ll119. ,
, ~: ~ " '~rl'br:l t t' I 1 i
~lt Ri'/ll I I I I
;~-.-Left 1/ :
! i \...
1.' . .1 2C 3r R-F{""ct 1'.UIl H, .. ,\c~
Silt) R
~ , I I ,
Size L :
React R j i I J
React L J, I : ! I 1 I
WHO/MNC/82.2 Appendix III Rev. 1 page 195
Filirvir,w·Soll~lc HOSllil<l1 EdinJ, r.linn(:~,otil Emcr9cllcy Service Puticnt Progress Record
Allergies J:J/rJU Kd'y~-=:l Present Meds. ~ Meds. brought in .LkYf~
ie~~() fU,A-L-L Glasses jLV Shoes /' Contacts lUi Jcwelry
/VU Dentures IvL'
Billfold FVu Watch {],A)
Mise, IVe Valuables env. Ii- fVJ I . /' -. ....
I/-./h, '/ (.f! A:_-k M.D. called
M.D. called .".,.--' Here_
Clergy called
Police called Here
&t IILL Relatives called ~ ~'
Medications and Dos<J!;e Route I Site Time By \~;hom
Zi..lt:...lr? /1 ,·LA..( <\7)~ ~/ -.t.v!21, ;u:1!~~-: f F""""
V1dLi'J[{LI ,-;;r3-rY1~1JO~ = / LF]?/) lit ~f) X'n /2:./
If A~'lf W me} IV (~~ "'1/ I i ;l:i'- f.j
i , j ;r." I :~ r:e.:'-.I.:. ' Time: TIme Am!.
I V Solu lion & AmI. A;ea N~ecll~ St,Ht' ole IAbsrbd By Whom
lJ:Z,77cUZ rJU/!"') f~lf· Af.,i'L! S-y',t(:=ty) I'JrLiL I
!
I --
Procedures T;M~ I By Whom
i);) () ) \ /?]j,Z.:J /2- ter/() (I un,,!(,~ y;t----, '= I
~ :~
/'7; /') (I..-' LJuorat,ory Studies: CL'(,I itrt,( i , OEKG
X.Rays(1 .' 17 x.., i~'
Inwke Output I Blood 8<' Components
! B!ood 01'':)1_, Emesis lt il.G. ---I
: r'll~lnu~ irrigation , !
I.V. ___ ! Sui> To:::! : Compn:s, __
: Urine I -_. __ . ,
Tot.JI"':::::b"
! Est. 8!(,od LvS~ i Gr~n(j T wtJI ( ' __ Tot;,1 1,-_
!

Wl:tO/MNC/82.2 Appendix III Rev. 1 page 196
FAI RVI EW.S0~r~DALE HOSPITAL
P/,TIENT PROGRESS R.ECORO
H7tRGENCY SERVICE NURSES NOTES ONLY . . --~--~------------------~
lte

,TE TIME
,Personal Belongings:
NURSE'S OElSERVATIOi'lS
WHO/MNC/82.2 Appendix III Rev. 1 page 197
I'. ". ; W<ltcn n::,\ ; Ring; (Describe) II. 'l', __ -+ ____ ~~----------~l~~~.'----------~-~------------------~.~--------------------------------__ _ GIJS$CS
Dentures: Upper [:lL'') ; lower t 1 '.1 I ",.. t . ....., ; Partial
Miscellaneous (list) ~_: r - (I I __ -+ __ ----~--------------------~L-~(~~~'~'~-L,~C~----------------------------------------______ ___ Valuables Stub -- Staple Stub Here -
Medications Brought In: Rx Number and Name
isposi ,
Vel ied 01 by: --+----r---------~~~--------------------------"'.- ---,
Verified on Transfer by: Sign. ------ Date/Sign, - 1 Dat~ __ ---~----+-------------------------------~----------+-----------------------
~'V1-'1'~ ,I.,V) l?/\ J Verified on Discharge by:
'yJ 0 0 "
,- i---+-------------------------------------------Chief Complaint:
Patient's Stated Reason for Admission:
~~----I----------------------------------------------------·-------· Health History;
--4---~~-------------------------------------------------------------- .. /, .,t7.f<'_-/~ ,{/'·Lf2i.:_/~"·· ",t;;: Cit' ~ re,; ""1' ,0(i,·./.,( ('f>'~ Z:<;,C~:""-/-'-'-'-:I----"_
Patient's Other Health Problems ina Treatment: ./' 7
c)/ -I~ L (('1 d, J/';,._"-' _______________________ ~------- ...
------------_.-'gics '7 J (, III /,., I (I' Oth~r:
,
ing I' !
, ___ -, __________ ~!~/~(.~_/ ____________ ~'i _______ . __ ~~_.'. ___ ~i~(.~/~-~.=-:., ___ _ -
____ t_P_ed_'_a_tr_ic_ia_n_o_r_Fa_m_il·_I_P_h_Y_,'_C,_~1_n:_~ __ ,~ .. ~L-~!'~_'~~ _____________ ~ _____ ~ __ ~ ________ ~--_______ -------_-
I
/.
.,., f'\.-,.." ... c: '''''t'' " r-. • ~ I (" (' • ,.... ". ..,.. r- .... ,. ,.. ... "... .. • __
.-:- -,,'''. ,..:.-.------./ ., j>J ,"'-Z (;/l ',.-'~

WHO/MNC/82.2 Appendix III Rev. 1 page 198
.' ,I ,/
OF 00
Fairview Hospital
2312 South Sixth Street. Minneapolis, Minn. 55454
Room: 7733 Doctor: Howell/Davis Date of Eval~~tion: 2/4/80
SPEECH Al';D LAKGUAGr: E\',\LUATIO)l
Mr. _ was seen for evaluation of his speech and language skills at the request of Dr. Thomas Davis ~hile he was a patient in Fairview-Southdale Hospital.
Mr. was admitted to Fairview Southda1e Hospital on January 17, 1980, following a cardiac arrest. Upon admission he \.;as aphasic and had right-sided weakness. Mr. has a family history of coronary artery disease. Medical information on his chart revealed that in 1971 Hr. was admitted to Fairvietv-Southdale Hospital with let::-sided paresthesia and slurred speech. An angiogram administered at that ti::\e sho'.;ed "both internal carotid arteries have atherosclerotic plaques near their origin - more narrowi~gof the lumen of the left internal carotid than the right". l'1r. ; was discharged from the hospital and continued to work as a fork-lift operator u~ti1 his present hospitalization.
The }!innesota Test for Differential Diagnosis of Aphasia was administered. Test findings are as follows.
AUDITORY DISTURBA..NCES: Hr. \IIas only able to recognize objects named by the examiner \IIith 45;~ accuracy. He could not recogr:ize letters or identify items named serially. He answered 5 out of 12 comprehension questions accurately. For exa;nple, he erred on qL:esticns such as "Do apples groH on trees?"; "Are there seven days in a week?" He was able to follow most simple test directions. He had difficulty repeating sentences. His responses were usually jargon.
SPEECH A:\D LA~GUAGE DISTl'RBA,,'lCES: He was able to ioitate gross movements of the tongue and oake rapid alternating movements of the oral musculature. He was able to repeat words without errors in articulation. He was able to complete some automatic tasks such as counting a~d naming the days of the week in order, however, he failed to grasp the di~ections for completing sentences. He does use SO::le automatic phrases whe::t conversing, i.e., "Don't ask me that". He could not na~;le
most objects accurately because of perseveration errors and also because of jargon. He could not ansl.er most s:i:~ple questions. It is interestin~ th3t he gave correct responses to the first ite::: on each test, ho\,ever, his responses to the rer.:::tining items in each area were incorrect.
VlsrAL-~·!OTOR. AND ..... RITI:\C DIS:TR!L\::C::S: There was evidence of visual-motor perceptt:al deficits in his copies of Greek letters and reproduction of a \,.I\eel. He has no functional .... riting skills. Ee coul.': print his first nar,e but !H! could not In'ite .;ords to -dictatioCi. He ceul;;:: print letters to dictation ~::d .... rite the nll~lbers 'Ol~e through five. He reversed 50=e n~nbcrs and letters.

- 2
OF 00
WHO/MNC/82.2 Appendix III Rev. 1 page 199
Fairview Hospital
2312 South S;xth Street, Minneapolis, Minn, 55454
Mr. was mildly restless on occasion. He was cooperative. Perseveration was noted on all language tasks.
SL~'~L;"'RY: Test findings are conpati';;le with left henispt-=re involvenent characterized by reduced auditory comprehensior:, \,lOrd find problef.1s, and reduced word recognitio:-. skills. However, some right hemisphere involvement was also noted because of visualmotor perceptual deficits. Prognosis is guarded due to a lack of neurophysiological stabilization. He \Jould benefit from speech and language therapy geared toward increasing his skills. in auditory and reading comprehens~on and oral expression.
If I may be of further in interpreting these test rindings, please call.
(7 ) .7 /:'
4.u~-"v l'u/Y'--1;?l-"- ,-'-Susan }!eneghel Speech & Language Pathologist
CC: Chart T. Davis, M.D.
21,::;400> Rev. 3·78

WHO/MNC/82.2 Appendix III Rev. 1 page 200
U .f:.l t..l t1 Yl ... 1
GI
l/lli': . ..., IIi lied 1/1~/M.)
I/llj/bu l/l'flbu i/J'fIHU
~ ~-' ,.~ p . ';
()UUrl,
IUd.: " IU:J4:,'
. lULl.':" IU')'\1'0
PI (1
11\ Ul
11 j 7/00 6uur'" 11 c' c. I ~l; 1 J 2.1/, v t Ii 51 ~,_, 1/~S/':''.J
l'! clUe leu 1ii 2/,,!c./'jl.l
~1
i.: 1 iJl q' Ul 'J 1
11 1., 1 "~'lJ
11 I ~ 1'< L'
1/1-·/~tI
11 1 ~ 1 i' J
i/l"·/t:li..1
II 1,,,\ I ~u
7ut' ,\;'. IUl·r.!¥' 1'.11';, .; 1:)'.11.'"
I w"",·: If";U.:4 "
7.)1 !.\ 'v'
"JUI' ,'; /.jell. '; I !JIll",
1 " " I 1 1 1 I C l) ,... \; l;t-''''
111 '11 r' oJ ,(.y J h r '
l u· ';: .-::
FAIRVI~W .HOSPIT ALS
LABORATORY RECORD
l'> t. , i f\ (,-.;\ Sf , .
l.,. , ... ; t. ,', r ,,1 , .. ;,t , ~,,'t.,i I !\ I ;',1\ ;)t
l' C .\ t. .. , I 1\ I ,,~ ;)1:.
:'4; \.---·tt'.. r l'\ 1'" f,$;;. ~, l .. t" r I\L·:~,::'t
" ~;1. 1.it:.;St ':' \.jL A,IJ:; t (;, '.;1. ~·L ;';St. , \;:L ,:Cl.dt
".'
;;1 __ \..iC.J~.:
'.:iU.ILi.;::'t;:.
~S.'-t-r:.~
L ,. .. I. ...
. ":,'1
.'. d H.¥\
'''t> t": ;"'! .. ,~
.i !
L,)n"'l Lt't1-C: U;j1- .) L;)!'-'~
U'r;-., L·)., fl.ll '\L
._.1 '" ~.·l/) IldU .. _. ~t .. lt It .... ,,~:· ... ~~._#·: o"J.1 J).I"!'.·S~·~·.-''''' ,.I S
1'. : I II llt"U 01 hit''' 111 11 l.r:·I.;v Iv! 1.1'" y 1 1 I 1 11 ':)tJ 7 (.~; .. ) 1\ .... I
1<1 11 1 II "'" ~U'J""~"
J I c.1 •. 'U/~:': f":"'C;: i It h .
H' c./~"'Ir< .1 it;'JI~"~
Ib i/: '-\ I"'l I f.':t;;·
1',;, c: I·. :t Illi. II," fit
1 "j 1 I 17/1\\.' .",( rJt#·-.
1 '. 21 tJt!.1 ~:.; i i • ..' ~#; I~ :';-
p. 11 1 II '::'u ? :;; !~"
fOl!'" 11 ~S<l8
,;.' ,:, J ,
t, .') i.',; r -:, :;,;,-.• 1
T ; ~ 1 }' \",
I .' j (: L
I 7 ~r 1
1 \
.;!- L ., \.1~, L, -,
, .' , ,:
t'~'d 1 t. i !;
it !:.' ll:t.<:-
I
;!" I ".'\ t.
l , !. \ t \., '.: •• '.
1 1 ,-.1_ ;ut-.;·
iJ' [ )
- 216 -
CLINICAl lAB REPORT /<It' )-:.:, .:
Oc/Ub/80
2/jo :-Abt
!l7 I • tJ • 2 I.u.
qob I .l! • LIS 1. u.
2'11 1. U. 18 I.u.
~.iJ t'lGlfAL
359 '''Gz 130 "-'G% 1111 I"G .~ ISU ~H; ~~
106 1"'i"J.
110 1·1\j ~
c2 '4 2d 4 c2 4 1 1 4 1 I X
130 0"11 T ~
d 7 Ur·l r s 15'" UNiT:'
tyPE:. I v
5.1 ~1G z:
!l7 Ui~ J r s dO U, .. 11 S 17 U,lIT:;
0.1:1 br.~~
.5. I IU ~. 2. .··c ~;'y.
j"1 • It ;;.
U rlG~ 21 i-Ii; i;
tl2/u61 f~U

7 9 ~ 3 3 3 - 2 ~ :. L'i~.!:.
dl j'U 11 i'11 tl Ii::. ~U. i on • .). : .• :!lYl.2LL
01-1J-~O 58 M DLS
CAflO-6
WHO/MNC/82.2 Appendix III Rev. 1 page 201
Fairview- Southdale Hospital 640} FrilJlCe Ave. So .. Minneapolis, MlflnCSol<l 55435
LEGEND URINE MICROSCOPIC REPORT:
Indicates Report Below N · Neutrophils % HHC,'.IPr WIJC/HPF. CASl ~iI.yr
@ Int"c~tes Outsi(!c of 95% Confidence Limits L · L ymphocyles % Ot.:t.:f\·,~" LL$~; Itll\N4 LESS rHI\N ~ LES5 ,. IAN ,
Hgh, Hemoglohin: gms % M · Monocytes % 1+ 4,8 5,20 1,5 RBC, Red Cell Count: millions/mm) E · Eosinophils 0' 2+ 8,30 20·50 5,10 70
ESR, Erythrocyte Sedimentation Rate:mm/hr, B ' Basophils % 3+ 3/4 Field 3/4 Field 10,30 Hct . Hematocrit % 4+ Packed Field Packed Field Packed Field
BLOOD Exr:::CTED VALUES
BLOOD ICont'd)
Acid P'tase ... , ...... , ......... UP to 5.0 K.A. lInits Prostatic Fraction ............ . up to 2.0 K.A. units Alk. P·tase .. , •.... , ... , . 25 1001.U.
Children IUp to Ane 15) .. .50·280 LU Alpha· Antitrypsin ... , ... , . . . . . . 180 244 mg % Amylase ,...... . . up to 187 "nits Bicarbonate .. ,........... . ... 22 . 30 meq/L
Bilirubin .. , , .. l' lip In .3. rnH ~1,',
. . .. . • . . . . . . . . . . . . . .. Total UP to 1.6 mg % SSP ..............•............. , Less than S% in 4S' Calcium .. , ................. . Chloride ..... .
"Cholesterol .......•.......
. 8.8 to 106 mg % . .96 . 106 meqlL
150·250 mg % 120·165mg% Complement ..•......... , ......... .
C02 Content .......... , , .
CPK .. '" ..•. , ...... " .. .
CPK· MB.
23 31 meqiL . Male 4 . 55 I.U.
Female 4 ·35 I.U. Chilorcn 4·55 I.U.
... Less than 15 LU. Creatinine ...•......•.............. O.S . 1.5 m9 % Electrophoresis - Albumin ............. 3.3 . 4.7 Gm %
tt. ,Globulin ........ . ...... 0.1 .0.3 Gm % tt I . Globulin ................... 0.4 . 0.9 Gm %
fJ . Globulin ,:.,.: ..... , .... '., ..... 0.7 ' 1.2 Gm % "I ·Globulin ,·.- .. ·.·,· ......... ;· ... 0.6.1AGm%
•• Fibrino']cn ...•...... , • . . . . . • . . .. . 200· .100 m!) % Gamma G ...••..... , •.•....•. , .... 700· 1600 mg %
··G •• amma A •.•..••.•.•......•.•...•. 50.450 m!) % Gamma M •.•••.•••••••.. , ••....••. 50. 250 mg % Glucose ••. , •..........••......... 70· 110 mg % Glutamyl Transpcptidase .......... Female 5·24 I.U.
• . . . • • . . , .. Mall! 8 . 37 LU. Haptoglobin ... , ..... , ............. 40 . 170 mg % Iron ....................... , ..... GO· 140 mc.!) ~:. Iron Binding Capacity ................. 250·380 meg % Iron Saturation Inuex . . .... 25 50% Lact.c ACid (PI~'ma) .•.. , .. , ... , ..... 9 20 I.i'l ~~ LOH . . . . . . . . . . .. "" to 90 LU.
Chliuren (up to Age 101. . , ....... U[1 to 100 I.U. M.lgnclillm .,'...... 1.5·2.4 mcqfL OsmOlality ..•. ,....... . ... 275 . 300 mos/Kg Oxygen Saturation ................... 9~ . 98":'
pCO~ (Arterial) . . . . . • . . 32 ·40 "'m HU
pCOl (Venous) ... J.) .4', r.1m Hg
pH (Arte"al) ....... , . . . . . . 7 .33 . 7..1.' pH (Venousl . . . . 7.3G 7 .. 3
·Phosphorus ...... . 2.6 ~ 5 I1HJ % Potass.um. . . . . . .. 3S . 5 5 meq'L Prote.n: TOT AL. . . 5 8 G'n
Globulin
.: HHJher values .In ch.lldren Lower value, In children
21·9953
,\ G rt.~o 1·2.2
SGOT .........•.... up to 40 I.U. SGPT ' ..... ,........... . Male UP to 24 I.U.
Sodium Triglycerides.
Female UP to 17 I.U. . ................. 134· 144 meqlL
........•...... 40 . 150 mg ~o
Urea Ni trogen ..
Uric Acid .....•..
. ......... 8·22 mg %
. •. " .... M: 3·8 mg %
T3 Uptake. T4 .. , .. .
. . . . . . . . . . • . . . . . . . F: 2 ·7 m9 .~
35-45",
FTI (I71 ..... . 4.5·13mcg'. 1.58·5.85
URINE
Addis COU'1lS per cay: Up to 5,000 casts Up to 500.000 rbc's Up to 1,000.000 wbc's & Ep. cells
Amylase ...•......... , UP to 600 units/2 hrs . Amylase .. , ....•.•.. ,. UP to 6000 units!24 hrs.
Calcium ....... up to 250 mgs/24 hrs. Chloride ........ 50 . 260 meq/L Creat. Clearance ........... 70 . 130 mllmin.
Glucose ..........•.. ,. up to 0.5 Gm/day Phosphorus ............. 0.1 . 1.0 Gm/day Potassium ............... 40 . 120 meq/L
Protein ......••••••..•.. less than 0,2 gm(dav Sodium ,.;,., ...•.. : .. 40 . 250 meq/L UriC Acid ...••..•.....•. 200 . 500 mgiday Urobilinogen ..•••..•.. Maleup to 2 E. units/2 hrs.
Female up to 1.5 E. units / 2 hrs. O,molJlity . 300·1100 mos'Kg MISCELLANEOUS
CSF PrOlein ..... , ....... 15·50 mg .... CSF Glucose ........ , ...• 40.80 mg 0 .•
Glill> Stool Urobitinoqen ..... 100·300 E.U.ll00 Gm Ieee; Stool U,obilllWgCIl .......... up to 250 ",y/d.IY Swe;,t Chloride. . ... up to 50 meq/L HEI\'ATOLOGY
ASO T,ter .. . . , ..... Adults up to 50 Todo un'ts . .. , . , ... Children up to 250 ,\od<l units
flIe~d",'I T.me (h'vl ..••... 2·7 ",intltes Clot RetractIon ....... , ... 40· 65%/hr. Cord Hcmn,)lohin . , ... 13.5·21.0 Gm -, MCV .. 82.94 p' MCH .......... . .. 27 . 32 Il J.!o ,
MCHC . • .. 32 . 38 % P.T.T. 25.<10 ",con.!s Platekt ... 100.000· 350.000 ',"'m 3
RC1.cCI;ocy;c Count .... 0.5· 1.5% Sedtmef1tJtlon Rate .... Female IIp to 20
M~:e 1Ir'i to 15 13 . 70 ,econ,!s

WHO/MNC/82.2 Appendix III Rev. 1 page 202
42073
Nome
Rete 120 sinus'tachycardia
FAIRVIEW HOSPITALS
Age 58 Address 8137 17th Ave So .
PR Interyol .16 QR S Interval .08
i Dia9nosis:There are numerous ectopic beats of apparently multifocal ongln. The QRS complexEjs
show left bundle branch block and increased voltage of S in V2. The ST segments are depressed in V5,6. T waves are inverted in V5,6. Similar changes in 1,AVL,
IMPRESSION: ABNORMAL EKG with myocardial irritability, left bundle branch block, some evidence for left ventricular hypertrophy, and ischemia as vlell. Compared to 3-12-79, the myocardial irritability has developed, and the voltage of S in V2,3 has increased.
Lead 1
Lead 2
Lf'ad 3
210025 (REV. 3·Ge,
r; a a /' /! n Oil {)',: .. '"' ctLV';o . .;.!-. ~}1 tV/=? ,I M.D.
EL ECTR8 CARD:OGR,\PH RECORD
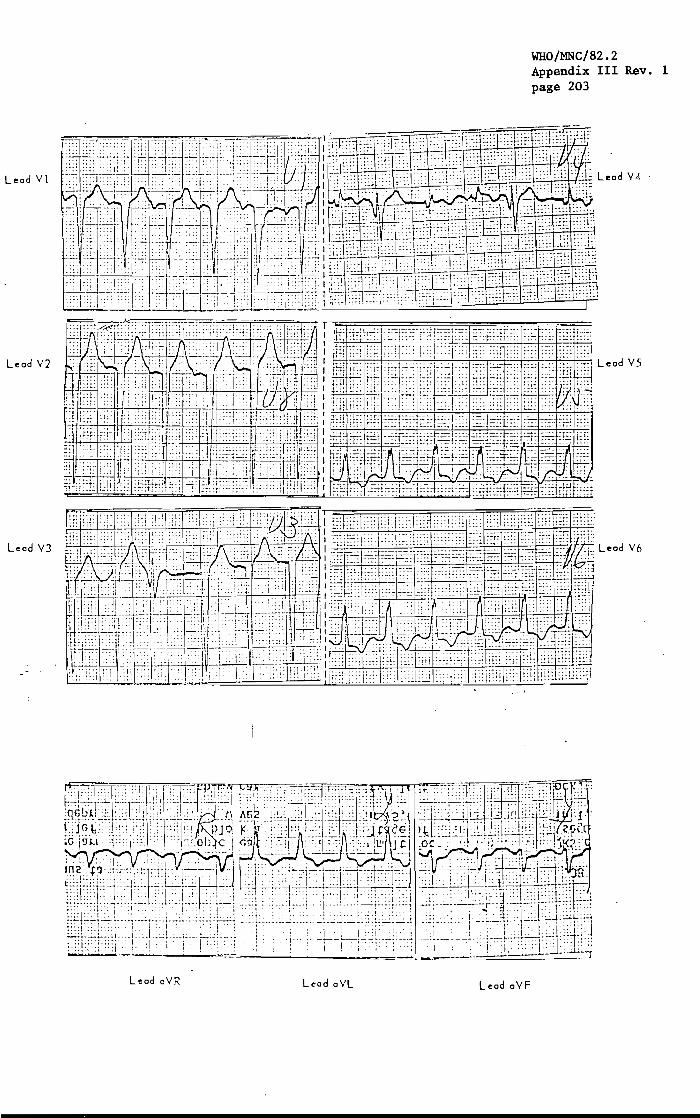
LeedY!
Leed Y2
Leed Y3
Leed eYR Leed eYL Leed eYF
WHO/MNC/82.2 Appendix III Rev. 1 page 203

WHO/MNC/82.2 Appendix III Rev. 1 page 204
8::83 ~4B~
8137 11th Ave. S. Dr. J. Howell 1-17-80
Dale of Ex('mrnolion 1-17 -80
PORTABLE CHEST
FAIRVIH't-SOUTIIQAU BOSPIT.u EDINA, MINNESOT A
58
. Ii ll./ .. ~ r. L .. \:' -
Rm ~I~
Film was taken in AP projection.
Monitoring electrodes \'/ere present overlYing the chest. The
heart is moderately enlarged. There appears to be some mild
bilateral pulmonary vascular congestion co~patible with mild
cardiac decompensation. No appreciable pleural reaction is
seen. Bony structures are unremarkable.
CONCLUSION: Cardiomegaly and mild pulmonary \li:'~cular con-
gestion compatible with mild conqestive failure"
Jf4:ln

. ,.;..:.
:-:1-18-'80 _t.,
PORTABLE CHE~T " .".
" ....... .
F" If;V I n'l·sn U i H D;HE 1105 PIT i\,C
Rm
-',.EDINA, MINNESOTA ",',
313'/ ITni /WE. . DR.J.L.flOWELL
2
'01-17-BO 58 M DLS :.~ :,' ': ~', " ,... ... ~ ....... -.-
CARD-6
WHO/MNC/82.2 Appendix III Rev. 1 page 205
',.', .
CAFlO-6
' .. ': .
. - l~"
.; . ,
" .. .. ; ~
", ,~ompa r~s_~ n 1-17 -80. .' " , ,
,'The '~'~r~'t' '; s' ~n 1 arged. "The; nte'rs t it i a 1 rna rk i!1 9S' are prornin~nt -";~'~'.:; ~t~ ~~;:;'~'''-~iJ~ E:·;'·~i}·~~ {~.\~:-~. : : ,- - " *~ .' :>': L :";' , 'throiighout,both lung fields 'suggesting early .failure., The" ',:
.':>'::':a~;~'~::;~:h:~~':~h;as not changed in th,e o.ne-day interval. ,,',' .... - . .,~ ~ .. "'- ~ ;:.~;._:.:; -' ':.: .... ~"' .. ,
"'If.' .... , "'. .J:::-,A.
'.~ ". ','
'::~" :. - .. ,~.:~ # .... ; • .': • '. ,,,,'
:~ !>~., ' .• - .; • .,. :;c., ... . '. ~ .... :.~:":, ' ..

WHO/MNC/82.2 Appendix III Rev. 1 page 206
792-383 .. . ,
.-~ 8137 17th Avenue South
. Dr.~J.L. Howell., 1-2D-BO.
_,,",,;,'('_, ·.c· _ ,.
Dale of Exominoti.~~ .. ~· ..• 1,:'<20·~BO .;". ..::: .. -
. . '.': ~ : -"". ~' . " .
'PORTABLE CHEST ••••• #.
_ .. ',
Frol:lV I,~;i -SOUT U!} AU U 0 SPIT tl( EDINA, MINN ESOT A
58 yrs.
Rm CARD-6
-_ £ a r d a c .~ 1 z e 'i s not c han 9 e d a p pre cia b 1 y fro m the stu d y of 1 - 1 8 - B 0 , ;- '.-";--.' ,"
'The .lung fields appear clear at this time. The remainder of the
chest; s·u nc hanged from the p rev/ ou S study .
. JDH:c';b
X-RAY REPORT. (PAGE ni

COVEH SII£::ET-IlOSPITAL ABSTRACT
lao Study 1.0. Number: 30
LABEL
WHO/MNC/82,2 Appendix III Rev. 1 page 207
t.... f.,.·t·\!:- .t.>- \...1: ........ - - l L • ...; •• \. .... ;' , /' .. ',' :
1 /Hospital Chart 33,2 ' Death Certificate IDcode·
2. ~a§se Source: Record ?;
5 Other, specifY _____ --l 1 .. 2( 21 29
lb. AbstractorJ I I I *******************************************************************************
ski;;:
3. Surname: f~.I.I·1 1 r=: I· 1 II I I 4. Third flame I 1 I I (Jr,Sr,I):. _ _ _
3 .. ..7
6. Middle 1nitial:
7. Social Security Nunber: 13 h I + II ~ I /1 13/'110 I / til 62 &5 67 71
*8. Birthdate:
72 7" 76
0iJ ffi II I lsi (Ho) (Day) (Yr)
9. Address:
att: Lfl (I ITI 7e- House Nunber
c. l § Apt. 302 Box
3 Lot
_ .- :-~"""5 1
e.1 ;M!;d County
" 53
£./ /ll rli State
l 1
6.. 66' 68
*10. Admission Date: 0lJ l~iL~ I/[ zlo I ( Ho ) ( Da y ) ( Y r )
71; "
11210 I *11. Discharge Date: r:~[~~ 1
(Ho) (Day) (Yr)
12. HospLtal Code: [QL.:...-1.._L..!-!
13. Date Abstracted: ~ / ~ /~ Ulo) (Day) (Yr)
LPH-:J:L'IP (9-79) 01-2 Version 11 (01/08/81) Disk 13-D
61
103 110
ski;
8 6 II."
ski;;
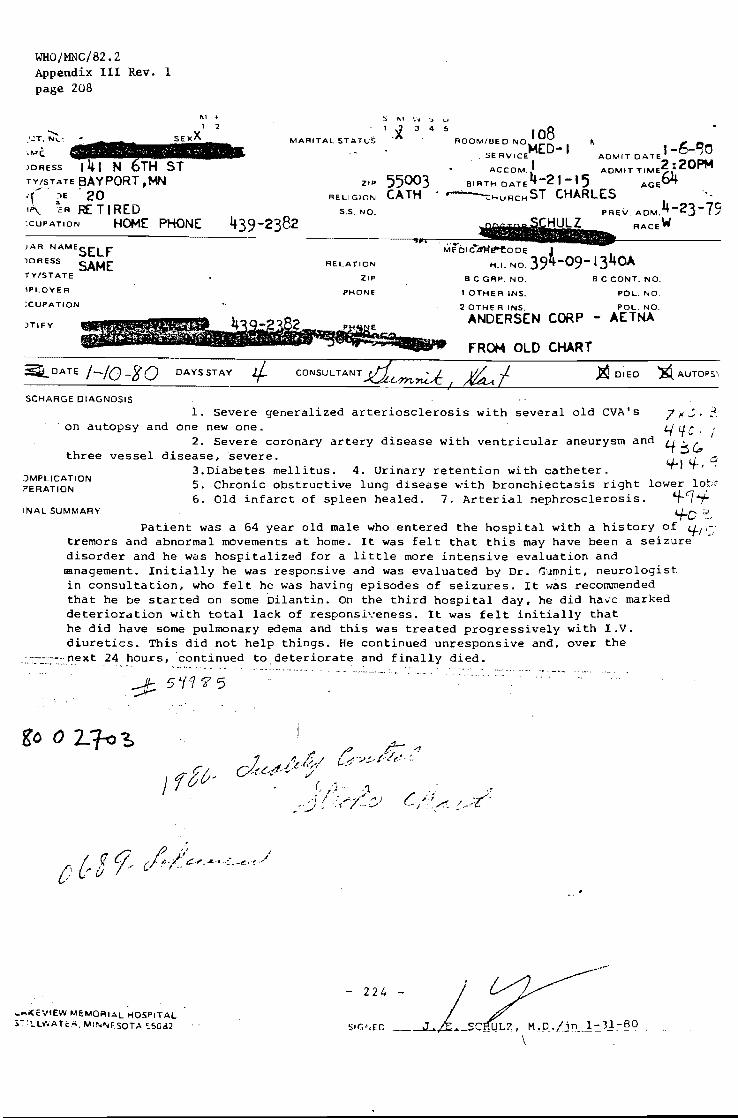
WHO/MNC/82.2 Appendix III Rev. 1 page 208
,""c;. )DRESS , I N ST TV/STATE BAYPORT ,MN I(';E . 20 11'\ ;OR F£ TI RED
MARITAL STATVS
ZIP
RELIGION
S.S. NO.
S 1\, \':\1 ::> u
'.'1.. ;} 4 !) ROOM/OED NO 108 " SERVICE
MED- 1 ADMIT DATE t -26-"PM)O
ACCOM I ADMIT TJME2: 0 55003 BIRTH DATE 4-21-' 5 AGE64 CATH • ~HuRcHST CHARLES
:CUPATION HOME PHONE PREY. ADM. 4-23-79
RACEW
JAR. NAMESELf )DRESS SAME TY/STATE
'PLOYER
:CUPATION
JTlFY
RELATION
ZIP
PHONe
B C GRP. NO.
1 OTHER INS.
2 OTHER INS.
ANDERSEN CORP
FROM OLO CHART
B C CONT. NO.
POL. NO.
POL. NO.
AETNA
:iiiDATE /-/0-80 DAYS STAY CONSULTANT ~ DIED E. AUTOPS',
SCHARGE DIAGNOSIS
1. Severe generalized arteriosclerosis with several old CVA's on autopsy and one new one.
2. Severe coronary artery disease with ventricular aneurysm and three vessel disease, severe.
3.Diabetes mellitus. 4. Urinary retention with catheter.
7i'';'~ 4LfC# "/ 4:sc" 4-1 't., 9
)MPLICATION ?ERATION S. Chronic obstructive lung disease ""ith bronchiectasis right lower lobt
. LI Clt'LJ.. 6. Old infarct of spleen healed. 7. Arterial nephroscleros1s. .- t INAL SUMMARY '+C :::~
Patient was a 64 year old male who entered the hospital with a history of '+/':; tremors and abnormal movements at home. It was felt that this may have been a seizure disorder and he was hospitalized for a little more intensive evaluation and mmagement. Initially he was responsive and was evaluated by Dr. GUll\nit, neurologist in consultation, who felt he was having episodes of seizures. It was recommended that he be started on some Dilantin. On the third hospital day, he did have marked deterioration with total lack of responsh-eness. It was felt initiallY that he did have some pulmonary edema and this was treated progressively with I.V. diuretics. This did not help things. He continued unresponsive and, over the
::·::-::::-.::-.::next 24 hours,continued to. deteriorate and finally died .
...... i<E\lIEW MEMORIAL HOSPITAL ~-·!..LI"'ATc",. MIII.f\jESOTA ':.50d2

AUTOPSY REPORT
Patient: ...... ~ .. p't<" ..........
Time of death: 7:47 P. M., 1/10/80
Place of death: lakeview Memorial Hospital, Stillwater, MN
Phys I ci an: Dr. Schlfl z
Autopsy permission granted by:
Time of autopsy: 9:00 A. M., 1/11/80
Place of autopsy: Simonet Mortuary, Stillwater, MN
Pathologist: Dr. Johnson
GROSS AUTOPSY DESCRIPTION • r
EXTERNAL EXAMINATION:
WHO/MNC/82.2 Appendix III Rev. 1 page 209
lA-80-1
The body is that of a well-developed, well-nourished, adult, white male appearing to be older than the stated age of 64 years. The body has been previously arterIally embalmed and there is marked loss of pigment of the skin of the face and upper body secondary to vitiligo. There is marked edema of the dependent parts, and the skin of the legs is discolored. There are a few small crusted ulceratlons( on the legs.
INTERNAL EXAMINATION: ,
On opening the body, the abdominal fat measures 1.5 cm. in. thickness. The. abdomen contains approximately 1500 cc. of amber fluid with some fibrin clots. There are adhesions around the spleen and the gallbladder. The abdominal organs are In their normal relation one to another. The appendix Is present and normal. The I iver extends ~ cm. below the xiphoid process and 2 cm. below the costal margin in the right mid-clavicular line. The diaphragm arches to the right third intercostal space and the left fifth rib. On opening the chest, the right pleural cavity Is obliterated by dense fibrous adhesions. The heart is pulled slightly to the right, and the left lung Is adherent to the anterior lateral wall by two string adheslons< The left pleural cavity is dry.
Heart: The heart Is markedly dilated but not enlarged. The coronary arteries are extremely atherosclerotic with essentially no lumen in any of the coronary arteries. The mitral and tricuspid rings appear to be slightly dilated, but the valves appear functional. There is an old healed myocardial infarct anterior-laterally at the apex with ventricular aneurysm and old organized neurothrombus,overlying the endocardial aspect of the infarct. The myocardium is a deep red-brown in color, faIrly firm in consistency. There is no evidence of recent myocardial Infarct.' The atrial and auricular appendages show nothing of note on gross examination. The foramen ovale Is closed. The root of the aorta shows marked atherosclerosis with ulceration.
lungs: The right .lung is enclosed in thick fibrous pleura. After removal, the pleura measures from 2 to 5 mm. in thickness. The bronchi contain a frothy, yellowish material. The lung is approximatel~ one-third the usual size. The cut

WHO/MNC/82.2 Appendix III Rev. 1 page 210
"A~"~ft-_ -2. .
s'urfac~ I s dry and the bronchi ~n the lower lobe ~ed and the bronchial walls are markedly thickened. They contain a yellowish, somewhat mucoid, material. The left lung is more nearly of usual size. It is rubbery in consistency and the cut surface is fairly dry. There is no evidence of consolidation or tumor.
Liver: The liver is of usual size. The surface is sl ightly granular and the edges are slightly rounded. The cut surface shows marked excess of blood and fluid, and there is definite darkening of the centers of the lobules.
Spleen: The spleen is approximately three times normal size. There is marked perisp'l'emi~"and there is an. old healed infarct on the superior aspect. The cut sUl;.faceshows the pulp to be mal-kedly firm.
Pancreas and Adrenal Glands: The pancreas shows nothing of note on gross examination. The adrenal glands show thinning of the cortex.
Kidneys: The kidneys are of usual size and configuration. The capsule strips with some difficulty leaving a granular brown surface. The cut surface shows a marked excess of blood and fluid, and the cortical-medullary junction is obscured. The cortices measure approximately 5 mm. in thickness. The pelves, ureters, and bladder show nothing of note on gross examination.
Gastrointestinal Tract: The gastrointestinal tract shows a marked bluish-red discoloration with swelling in the first portion of the duodenum. This has the appearance of possible hemangioma or mucosal hemorrhage. The gastrointestinal tract otherwise shows nothing of note on gross examination.
Abdominal Aorta: The abdominal aorta consists of a fusiform aneurysm extending from the diaphragm to the pelvic rim and measuring up to 15 cm. in diameter. On section, it contains mostly plaque material.
Organs of the Neck: The pharynx, larynx and trachea show nothing of note on gross examination. The thyroid shows the left lobe to be absent. The Isthmus is much
:Iarger than usual and the right lobe appears to be essentially normal.
Head: On opening the head, the scalp and calvarium show nothing of note on gross examination. The brain is of usual size and configuration. The vessels at the base of the brain show marked atherosclerosis. There is a small area of encephalomalacia in the cortex in the left occipital area. The brain will be cut later and the brain diagnosis will also be dictated later.
GROSS IMPRESSION:
1. Marked generalized atherosclerosis. A. Fusiform abdominal aortic aneurysm.
2. Marked coronary atherosclerosis of all three coronary vessels.
3. Old healed apical. arterio-septal, myocardial infarct with aortic aneurysm and organized neurothrombus.
q. Chronic obstructive pulmonary disease, bronchiectasis of the right lower lobe.
5. Chronic fibrous pleuritis with obliteration of the right pleural cavity.

WHO/MNC/82.2 Appendix III Rev. 1 page 211
Autopsy Report - 3 - ....... -, ... "
6 . .,...,,_.' .... , .. ,t, of the I' spleen and kl·dneys. . Acute and chronic congestion Iver,
7. Old healed infarct of the spleen.
8. Possible arterio and arteriolonephrosclerosis.
9. Possible hemangioma of the first portion of the duodenum.
10. Congenital absence of the left lobe of the thyroid.
11. Ascites.
12. Vitiligo, pronounced on the face.
13. Dependent edema, marked.
1/11/80
Autopsy Report
GROSS BRAIN DESCRIPTION:
The brain is of usual size and configuration except for a small area of old encephalomalacia in the left occiput measuring up to 1.2 cm. in greatest dimension. The vessels at the base of the brain show marked atherosclerosis with extreme narrowing of lumina. On section of the cerebrum, there are mUltiple old healed infarcts with encephalomalacia in the right cerebral hemisphere involving the head of the caudate nucleus and adjacent white matter, the thalmus, the internal capsule, the lentiform nucleus, the claustrum, and enlarging the left lateral ventricle. There is a third healed infarct in the posterior portion of the occipital lobe and involving the gray and white matter at the tail of the lateral ventricle. There appears to be a rather small, recent infarct with some cystic degeneration in the right lentiform nucleus which measures 1.5 by 0.8 by 0.7 em. Section of the cerebellum, pons, and medulla shovi nothing of note on gross examination.
GROSS IMPRESSION: •
Cerebral arteriosclerosis, severe, with old mUltiple infarcts and encephalo-malacia of the right cerebellar hemisphere and of a recent infarct involving the left lentiform nucleus.
~~~~ 1/16/80
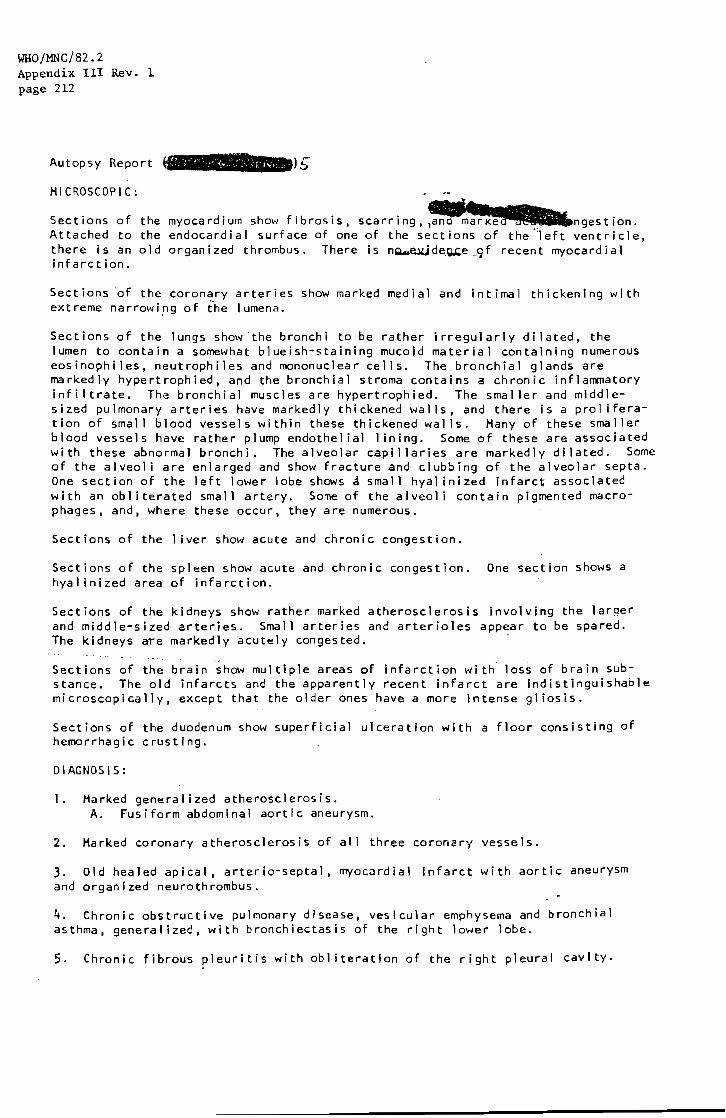
WHO/MNC/82.2 Appendix III Rev. 1 page 212
Autopsy Report
MICROSCOPIC: .
Sections of the myocardium show fibrosis, scarring, ~ngestion. Attached to the endocardial surface of one of the sections of the~eft ventricle, there is an old organized thrombus. There is nQ.u~de,~e,9f recent myocardial infarction.
Sections of the coronary arteries show marked medial and intimal thickening with ext reme narrowi.ng of i'he I umena.
Sections of the lungs show 'the bronchi to be rather irregularly dilated, the lumen to contain a somewhat blueish-staining mucoid material containing numerous eosinophiles, neutrophiles and mononuclear cells. The bronchial glands are markedly hypertrophied, and the bronchial stroma contains a chronic inflammatory infiltrate. Th~ bronchial muscles are hypertrophied. The smaller and middlesized pulmonary arteries have markedly thickened walls, and there is a proliferation of small blood vessels within these thickened walls. Many of these smaller blood vessels have rather plump endothelial I ining. Some of these are associated with these abnormal bronchi. The alveolar capillaries are markedly dilated. Some of the alveoli are enlarged and show fracture and clubbing of the alveolar septa. One section of the left lower lobe shows a small hyal inized infarct associated with an obliterated small artery. Some of the alveol i contain pigmented macrophages, and, where these occur, they are numerous.
Sections of the I iver show acute and chronic congestion.
Sections of the spleen show acute and chronic congestion. One section shows a hyalinized area of infarction.
Sections of the kidneys show rather marked atherosclerosis involving the larger and middle-sized arteries. Small arteries and arterioles appear to be spared. The kidneys are markedly acutely congested.
Sections of the brain show multiple areas of infarction with loss of brain substance. The old infarcts and the apparently recent infarct are Indistinguishable microscopically, except that the older ones have a more intense gl iosis.
Sections of the duodenum show superficial ulceration with a floor consisting of hemorrhagic crusting.
DIAGNOSiS:
I. Marked generalized atherosclerosis. A. Fusiform abdominal aortic aneurysm.
2. Marked coronary atherosclerosis of all three coronary vessels.
3. Old healed apical, arterio-septal, myocardial Infarct with aortic aneurysm and organized neurothrombus.
4. Chronic obstructive pulmonary disease, vesicular emphysema and bronchial asthma, generalized, with bronchiectasis of the right lower lobe.
5. Chronic fibrous pleuritis with obliteration of the right pleural cavity.

. Autopsy Report - 6
'6. Acute and ch,QIit[Jt&ngestio,?,!';'M the liver, spleen and kidneys.
7. Old healed infa
8. Arterionephrosclerosis.
WHO/MNC/82,2 App~dil.:t IU Rev, 1 page. 213
9. Superficial stress ulceration of the first portion of the duodenum. -.
10. Congenital absence of the left lobe of the thyroid.
11. Ascites.
12. Vitiligo, pronounced on the face.
13. Dependent edema, marked.
14. Multiple old arteriosclerotic infarcts with encephalomalacia of the left cerebral hemisphere.
15. Recent Infarct of the left lentiform nucleus.
~~ 1/24/80
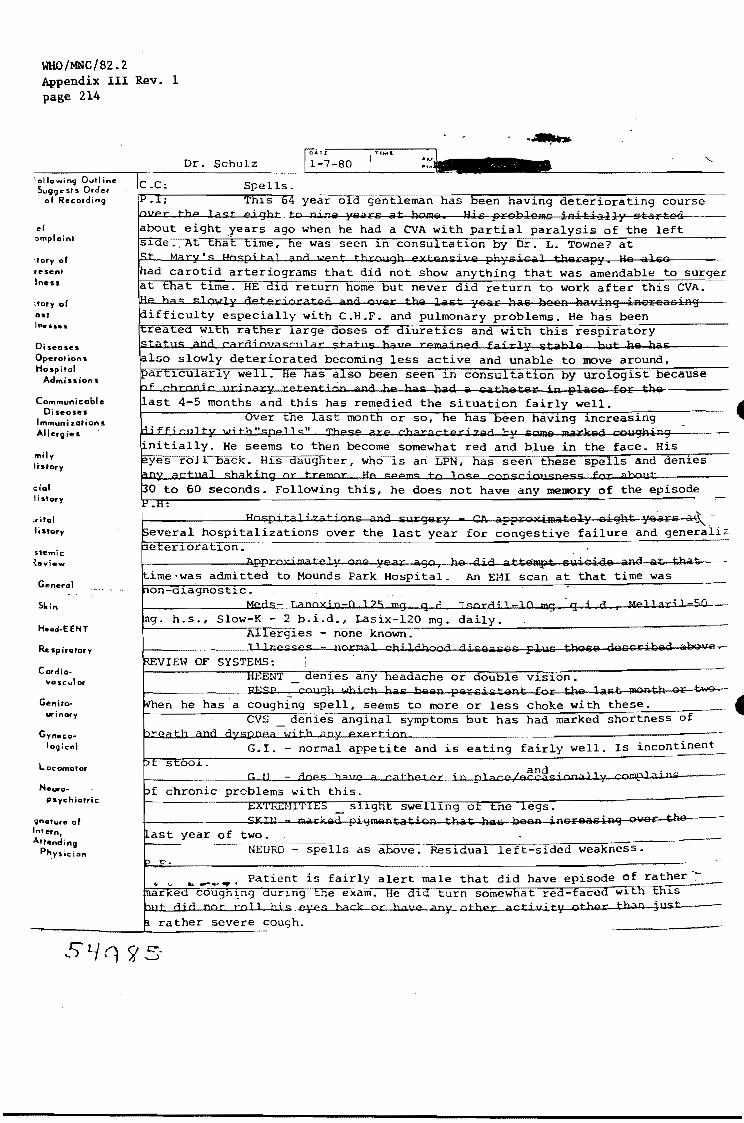
WHO/MNC/82.2 Appendix III Rev. 1 page 214
:ollowing Outl in" Su99" 01S Order
01 Recording
el ""'plaint
:tory 01 resent Iness
. tory 01 ost
Diseases Operotions Hospital
Admissions
Communicable Oiseoses
Immunizations Allergies
"lily lislOry
dol Ii story
;rital iistory
sternie ~eview
General
Hud·EENT
R .. spirotory
Cordia· vas-cutor
Genitourinory
G yn• co-logica'
Locomotor
N ..... o-psychiatric
'gnQtur. of In'ern, Altending
Physician
C.C:
Dr. Schulz ~Ar< 1-7-80
gentleman has been having deteriorating course
partial paralysis of the left seen 1n consu tat10n by Dr. L. Towne? at
anything that was amendable to surger did return to work after this CVA .
and pulmonary problems. He has been 1uret1cs and with this respiratory
deteriorated becoming less active and unable to move around, . He een seen 1n consultat1on by urologist because
situation fairly well. as been haV1ng increasing
1--
become somewhat red and b.1ue in the face. His ~~~~~r-~~~-U~~r.-.~k~~~~~ 1S an LPN, has seen these spells and denies
Following this, he does not have any memory of the episode.
.. ' ~-hospitalizations over the last year for congestive failure and generali~
to Mounds Park Hospital. An EHI scan at that time was
- 2 b.i.d., Lasix-120 mg. daily. - none known.
crma] cbi 1 ahcca giGs_GSG pll;ls Ul96S QesoribsQ aOOvev-
v1s10n.
coughing spell, seems to more or less choke with these. 1---------""'''''-=---:;d.:e:-:n==--1i:· es anginal symptoms but has had marked shortness of
is eating fairly well. Is incontinent
chronic problems with this,
9ver the ast year of two.
NEURO - spells as above. Res1dual left-sided weakness.
Patient is fairly alert male that did have episode of rather ',:. __ ~~~~~~~~~~~~~~~-ce~x~am. He d1d turn somewhat red-faced w1th th1S
ck or balte any other actillity other th)O just

..
WBO/l'lNC/82,2 Append:j.~ r.u Rey, 1 Pi\~e 21,5
HEENT pupils are somewhat constricted. "Tympanic membranes and throat • are clear. NECK - no palpable masses. LUNGS rales bilaterally - more pronounced also audible over the chest. HEART tachycardia with no murmur. ABDOMEN somewhat voluntarily rigid making EXTREHITIES _ slight puffiness of the lower calf tenderness. SKIN - deep pigmentation around the face.
on the right side. WHEEZES
it difficult to evaluate. legs and complains of some
NEURO residual left sided weakness with positive Babinski on the left. Slight-hyper-reflexia on the left.
IMPRESSION:
disease.
jn 1-7-80-
1. Spells - questionable seizure disorder or epoxic episodes. 2. Old CVA with probable general cerebral arteriovascular
3. Severe congestive 4. Diabetes mellitus 5. Urinary retention 6. Deep pigmentation
heart failure with marked cardiomegaly, stabl in the past. with catheter in place. of the face of questionable etiology.
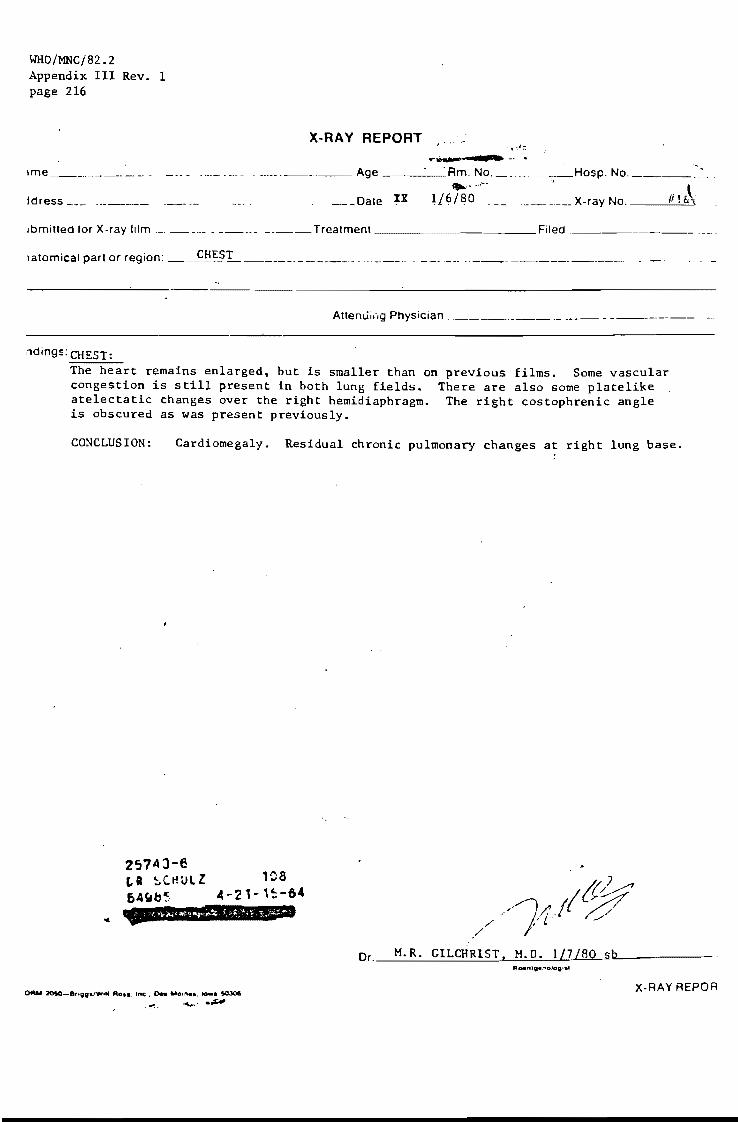
WHO/MNC/82.2 Appendix III Rev. 1 page 216
X-RAY REPORT 1'".a.- ••
_. ___ . _______ Age ____ ·l1m. NO. ____ ·_Hosp. No. _____ .-- . ... ,.... -,
____ Date IX 1./6/80 . ___ _______ X-ray No. __ --I:..-;=-'
Jbmitted for X-ray film ____ •... _ ____ Treatment _____ _ Filed . ____________ .
1atomical part or region: ___ ~::.:. -------------. -_ .. _-------
Attenui,',g Physiclan ___________ ._
ndings: CHEST: The heart remains enlarged, but is smaller than on previous films. Some vascular congestion is still present in both lung fields. There are also some platelike atelectatic changes over the right hemidiaphragm. The right costophrenic angle is obscured as was present previously.
CO~CLUSlON: Cardiomegaly. Residual chronic pulmonary changes at right lung base.
2574J-e La ~C~UlZ ~A~6~
108 4-21-'~-&.
OFtu 2O!IO-8r'99VW ... Rot I. Inc. Dea "ol"el. to.. 50.301 ........ ~
/ ./
Dr. M. R. GILCHRIST. M. D. l/7.1MLs.hIL __ ---
X-RAY REPOR
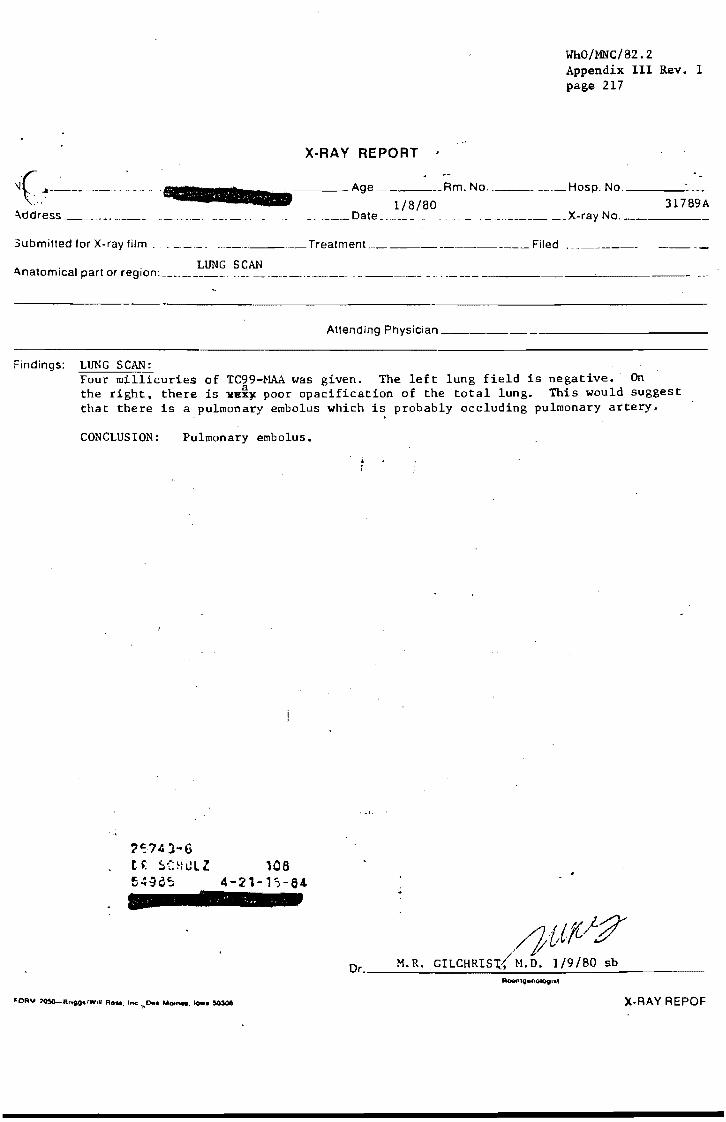
WhO/MNC/82.2 Appendix III Rev. 1 page 217
X-RA Y REPORT
'J( A------------- -=--=-_____ Age _____ Am. No __________ Hosp. No. ___ _
_ ____ ~Date 1/8/80 31789A
~ddress __ ._. __ . _. __ __ ~ . __ • _________ X-ray No. _. _______ .
3ubmilled for X-ray lifm. _ __ ___ _ . _______ Trealment ____________ ~~_ Filed
1\ t . I - LUNG SCAN .. na omlca parlor region: _________ _ -- -------- - ------- ._ ... -- --- ------
Attending Physician _______ _
Findings: LUNG SCAN: Four millicuries of TC99-NAA was given. The left lung field is negative. On the right. there is ~e~~ poor opacification of the total lung. This would suggest that there is a pulmonary embolus which is probably occluding pulmonary artery.
CONCLUSION: Pulmonary embolus.
?~74l-6
t~ 5(H~lZ 108 54~Q5 4-21-1,-64
//}{,lfi!:7 O M. R. GILCHRIS~ N.D. 1/9/80 sb r. ___________ ~ ___ ~~ _________ _
X-RAY REPOF

WHO/MNC/82.2 Appendix III Rev. 1 page 218
" '"" cc: Dr. Hart
SBH LZ
PATIENT: II-
Date __ ~~~~~ ____________ ___
Patient a 64 year old white male with a history of a right hemispheral CVA on 9 July 1974, admitted at this time by Dr. Schulz because of episodes of apparent loss of consciousr.ess in the last month. History obtained from he and his family suggest that these episodes tend to occur after coughing spells and often occur while he is eating. His daughter relates that he see~s to stop ventilating, turns red, and eyes roll back and he is unresponsive for a matter of 30 seconds to 1 minute and then begins ventilaifng again then becomes responsive with no postictal state. There have been no convulsive movements noted or symptoms suggestive of posterior circulation problems. The patient does relat~ that he notices difficulty breathing, numbness in hands and some racing of his heart at the time of these episodes. P.H: • Illnesses - CVA in 'July 1974. Angiogram dorie at that time showed an occluded right internal carotid artery at its origin and collateral filling of the left anterior cerebral EEG's inJuly 1974 and December 1977 showed some swelling over the right hemisphere. 1977-patient hospitalized here for questionable posterior circulation insufficiencj and was put on Coumadin for a time without apparent improvement in symptoms. 197!i-hospitalized here with right lower lobe pneumonia and subsequent right ple(, i. effusion. Patient attempted suicide by carbon monoxide inhalation. February 1979 - hospitalized here with C.H.F. Lung scan at that time did not suggest pulmonary emboli. MEDICATIONS Digoxin-0.125 mg.q:d.', LalE;ix-120 mg., Isordil-lO mg. q.i.d., Slow-K - ~ b.i.d. ALLERGIES none' DIET regular ALCOHOL - occasional. FAMILY MEDICAL HISTORY:
SMOKING ,occasional in the past but never heavy~
Both parents died of CVA'S. Otherwise non-contributory. REVIEW OF SYSTEMS.:' -no~ ,done PULSE 110, regular. B.P. 108/80 ALERT older male, with an obvious Cheynne-Stoke respiratory pattern. SKIN - few crusted lesions over the pretibial surface. LYMPH - lxl cm. rubbery mobile node in the right supraclavicular area. HEENT Pupils small but equal and reactive. Fundi not well seen secondary to myosis. Upper plate. . NECK - so~ewhat decreased range of motion. No goiter. CHEST rales at the right base. CARDIOVASCULAR regular rhythm, no JVD. No murmur, S-r or gallop. Questionable f:ioft 5-3. ABDOMEN - distende and firm. Diastasis recti. Liver approximately 14 cm. by
percussion but do not feel good edge. No oA'.J7? .. IIC1l1llMblii.'.lif .... 1I1 BACK 1+ presacral edema,' lSi EXTREMITIES pulses absent below the femorals. Trace lower extremity edema t~· he knbes. No-synovitis. NEUROLOGIC spa'stic left upper extremity. left knee jerk slightly greater the right, Normal Babinski's signs. Positive Hoffman's on the right.
than
GENITALIA mild swelling of the prepuce. RECTAL_not done. (OVER)

L 2 • HEHOGLOBIN- 13.2 SED RATE - 35
',' UA 4+ albumin, 13 to 18 wbc' s.
WJ;lO/MNC/82.2 Appendix III Rev. 1 page 219
CHEST X RAY - gross cardiomegaly. Bibasilar alveolar infiltrates which appear to be chronic, right lower lobe pleural changes which also appear to be chronic. EKG - IVCD. Old anteroseptal H.I. Intra-atrial conduction defect. Decreased voltage. Arterial blood gases - pH-7.50, P02-53. PC02-22. PC03-16. TSH-done in the office recently was 13 which was slightly elevated. T-4-6.4. Alk. p'tase-96. Albumin-3.l. Bilirubin-l.9.
ASSESSMENT: 1. Apparent syncopal episodes - no good history of the common causes of syncope such as seizures, arrhythmias or posterior circulation problems. Would wonder if these episodes are not a primary ventilation disturbance secondary to the patient' Cheynne-Stokes respiration which is likely secondary to diffuse bihemispheral arteriosclerotic disease. Patient's blood gases suggest a marked alveolar/arterial oxygen ~~ ___ and it might also be that during the apneic phase of his respirations, his hypoxemia becomes quite severe ~ that he has a seoondary bradycardia. The etiology of his hypoxemia is unclear bat may be merely secondary to a respiratory apraxia with marked ventilation p~fusion in ?v#??.-.mismatching. Pulmonary emboli. would certainly be another consideration. 2. ALbuminuria - no obvious cause - may be secondary to nephrosclerosis. 3. Slightly elevated TSH.
Suggests early hypothyroidism. With his vitiligo, this may be an ~ phenomenon. 4. Cardiomegaly - apparently on the basis of ischemic cardiomyopathy. No gross congestive heart failure at this time .
. PLAN: 1. Consider lung scan. 2. Consider Holter monitor. 3. Quantitate albuminiuria. 4. Discuss case with neurologist.
jn 1-7-80
_S1--t~ {/HART, H.D.
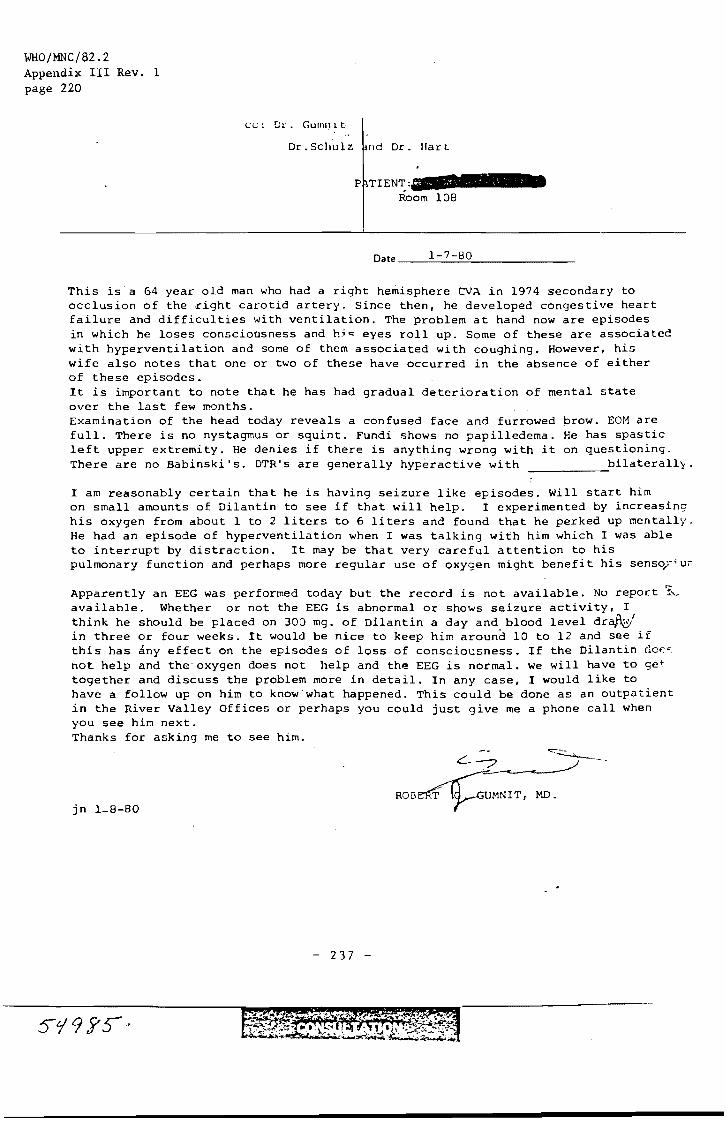
WHO/MNC/82.2 Appendix III Rev. 1 page 220
cc: Dt' _ GUIIlIl i t,
Dr _ Schulz nd Dr. liar t
P TrENT: Room 108
Date 1-7-80
This is"a 64 year old man who had a right hemisphere eVA in 1974 3econdary to occlusion of the right carotid artery_ Since then, he developed congestive heart failure and difficulties with ventilation. The problem at hand now are episodes in which he loses consciousness and hj~ eyes roll up. Some of these are associated with hyperventilation and some of them associated with coughing. However, his wife also notes that one or two of these have occurred in the absence of either of these episodes. It is important to note that he has had gradual deterioration of mental state over the last few months.
brow. EOM are He has spastic on questioning.
bilaterally.
Examination of the head today reveals a confused face and furrowed full. There is no nystagmus or squint. Fundi shows no papilledema. left upper extremity. He denies if there is anything wrong with it There are no Babinski's. DTR's are generally hyperactive with ------I am reasonably certain that he is having seizure like episodes. Will start him on small amounts of Dilantin to see if that will help_ I experimented by increasing his oxygen from about 1 to 2 liters to 6 liters and found that he perked up mentally. He had an episode of hyperventilation when I was talking with him which I was able to interrupt by distraction. It may be that very careful attention to his pulmonary function and perhaps more regular use of oxygen might benefit his senso)';uu
Apparently an EEG was performed today but the record is not available. No report 1~ available. Whether or not the EEG is abnormal or shows seizure activity, I think he should be placed on 300 mg. of Dilantin a day and blood level dr~ in three or four weeks. it would be nice to keep him around 10 to 12 and see if this has any effect on the episodes of loss of consciousness. If the Dilantin dcf"<, not help and the oxygen does not help and the EEG is normal. we will have to get together and discuss the problem more in detail. In any case, I would like to have a follow up on him to know'what happened. This could be done as an outpatient in the River Valley Offices or perhaps you could just give me a phone call when you see him next. Thanks for asking me to see him.
jn 1_8-80
- 237 -
RESPIRATORY THERAPY DEPARTMENT
PERIODIC ROUNDS RECORD ,"
. .-
, 2"''-'4 J ." -€ r p ... ,
, -'. '!"Ll e·.: s; c.
WHO/MNC/82.2 Appendix III Rev. 1 page 221
. lOa
,
4- 2 1-11: 6 .: - 4
place in chart after service is stopped STAMP PATIENT INFORMATION HERE
O .. TE COMMENjlt_ d.NITtAL
IlllJrit n::J \'f!r' 1) ie) ','J \J L .. '\,,\.,,/) • .) (' ~,,-~~"1\.A '.e ( <..J ~~ pry\. SlOP " ; ';1. r; /' ,
services 2) "'- STOP / 3) STOP
12 am
4am
8am
12 pm .~ --liUt: [..> 4 pm I~~ [. 'l .j \':A (~ A"--:t\. . \A;c.. u~'t LJ....P ~ "--J ~-d. Pm \""'.-1 WP
I 8pm V \ , i/ '-..
12 am ,
4 am
7/ Yo 8am ..,- O"L &~~<JiL. /1 J-~~. . C2 ~ I
12 pm ,
4 pm
8 pm
12 am
,.~ J/l~ 4am
() 8 am - /.l~ I' A.--YL-J~~ &-., , ;;;:tAu ~~. J"'~.z, ~ ~ 12 pm ,Y
4 pm
8pm , 12 am
4 am
11cj!;( (.' 8am - 0,;1 fY/'I /I 1~£Lh LYU -:Iti<..d O. Y?Z a ~ii ..... _-12 pm P'
.'--4 pm
8pm
12am
4 am --8am
12 pm
4 pm
8pm
12 am
4 am
8am .-r-12 pm . 4 pm
I--
8pm
12 am
o4am
8 am
12 pm . I --4pm I - --.-
~ ,-I

WHO/MNC/82.2 Appendix III Rev. 1 page 222
E & TIME Ptog ..... of Co ... , S'fmptom.~ COMplicotiQn,_ Conl'"'ltot'on.~ Condition on OilchOfge
\:-. .' "
-------4~~--~~~~--~~~~--~~------------------~--~----~------------~ -
cot Ions, COP"\$ultottOnS, ition on Otu:norge
Wlio/!iNc/82~2 A:ppendb: IlJ Rey. 1 page 223
.," -.".,.,..,."., ....

WHO/MNC/82.2 Appendix III Rev. 1 page 224
~, .., ..
IME Frog'."
-.
(P SCHULl loe ~~~8~ 4-21-'~-64
ions, Cond~tion on Di.chorge
t
WHO/MNC/82.2 Appendix III Rev. 1 page 225
WHO/MNC/82.2 Appendix III Rev. 1 page 226
00 NOT USE THIS SHEET UNLESS A REO NUMBER SHqWS
.TE&TIME DOCTOR!. ORDER!. & TREATMENT
2~743-6
Or. ~ClltJLZ 106 5498S 4-21-15-6.
CHART copy
rE 8. TIME
LAKEVIEW MEMORIAL HOSPITAL Stillwater. Minn.
DO NOT USE THIS SHEET UNLESS A RED NUMBER SHOWS
DOCTORS ORDERS 4. TREATMENT
WHO/MNC/82.2 Appendix III Rev. 1 page 227
-.' ----'---------------r-----------------------
~'S7·~:-6
tlo: ~Ut:.slZ ~_S'f,:-
106 4-Z1-1':::-64
,
WHO/MNC/82.2 Appendix III Rev. 1 page 228
LAKEVIEW MEMORIAL-HOSPITAL Stillwater. Minn.
DO NOT USE THIS SHEET UNLESS A RED NUMBER SHOWS
E &. TIME DOCTORS ORDERS a. TREATMENT
~------------------------------------------------~
~!:li ~l-f
(P !.:':tilill 108 ~49~~ 4-11-'~-64 "'iJtI $t? 3f!!l1t.Lt.iS iRE CHART copy

~::llal Day
PO Day
Hour 01 D~~ FO
140 1060
130 1040
SO 960
.. ~ ..
LAKEVIEW MEMORIAL HOSPITAL 919 W. ANDERSON STREET
STILLWATER, MINNESOTA 55082
/ - 9 -90 3 ... ..1
WHo/mC/82.2 Appendix III Rev. 1 page 229
GRAPHIC RECORD
lit<, I I)' -I I I
-
, Jspiratior.s .)~ '~lJ ~ :j~ R~ '11 Y:::.~ ,
Blood Systolic: itO li~ ~~ Pressure
Diastolic: 70 bO 1~
J"'?"'YfLC R~ Ao T t "IH ) 1 () iOg'l) ,::l."IO'&- 0
lover)
(~ ~(~vLZ iC8 ~.3~8;:;, 4-:1<(;.-64
';po=1iIIIW1!:m9¥iiS'Jt

WHO/MNC/82.2 Appendix III Rev. 1 page 230
PATIENT CARE-TREATMENTS-TEACHING-CONFERENCES-ACCOUI\11At.:HLlI '(
:TlON TIME AND INITIALS
Ie 1- (0- ~n j-, 7- fto /-E'-pn /- 9-80 th --- f-}:Le--J S h/l/v-fJ ~ 1!tJ~ ~tivity 1,· 7 C'lecd- c;.1~d II"'I .
"j..Bd U U
-"-
7·3 lldm,'5Slhr'l /~clu'/ro- BeN UlOJA ~(1~o.rt (!/o-.J ( • nMV1J ~~
3·11 1\ '\
;.;" 'J! """'" t ~ "l~r ~ , I " r . it"" ... 1\ .' <.l '--'..Air 6."~ . ct\(ti ~LI
. '1~L II'/}. / " o')j l' (f',., .fir><. ;, ,Jit~l fZf>.'" //-7 1?:~i;~ ~. ''J:;'''' ~Q'-'~ .7 nn :-> .. "il. If o~ ,<:l "" 1 ~ 3- '\ ,
:,:.f''1J11
. '/ -wY '1
t ,,-;'.4 .J, ., 1.JiK .1f" ~ ~ I, tPJf ~ 3·11 -'", o' I /.1 li/· 7 1---1- o-tw.... (' <II.~ r / ... 4-~~f ',<' .
'f; ( .~::. ljSJ.) 't;
\ rf·'ti. ' i ,,,f . . I ,
~ \ ... , . /
/ (' ·tt rL .. ~,
":\~~).) .J vi- ".J'. ' ,,',- ;'_l
-.:. ,\ ~ . I -:fi (t 7 :''''l «,.----'1 ...
. -,~"
/,
d..st.P . t!&.~R..
_ ..... "
Tp.achm!i
Conferences
'. Accountahil,ty 11·7 n ' --?', d, Jd: . ... ·n .' .n L_ L ' )' -..... L'I .• .1 11:,).:L:.1 f.)~)
I/-)o-lffj~ P(1kZ~-
B~ -:
~,
.£d'f..uiF
~1.:":;'-' ~ ; -711kt 1·)/,
.&-t
.r ... ·lt) --
-
--~t-· J ' ~6."'U;-~";
7·3( JI.!VlUli tJJi.J) £. -R) t ~~; Wu,,7li.~:L. /A~r' C;Vr/p fUr 1':&)11" " Y/' . . '
3·11 l ":, . U. • \ I I, .... \
,v ) .. ; . .,
.'1> .. i1" .. :.' t I- , • , .* • • J , .", • .I'.~, • I • ,I '" .' I.,; •
Medication date date date
Dose, Frequency, Route
WHO/MNC/82.2 Appendix III Rev. 1 page 231
Discharge Date _____ _ Chart Copy
date date date date Total
.{'I
I fHAf~ gO ~~ (111)-- ~
U
Iln.<\ 't I~Df1\a lO\
~fj
c!)OD)'Y\.-)-. 1" iJ • u
::PJ wl{ \-\tPHR',;) Q. ~~~k
[: : •• ::, j. '- L 1 1 t) e ~ .. ; :"l ; . ..: - ;- 1 ~ ~ - 6 4 .~.
1,1
-- -
!
At the ."d of 7 days Of at dis<:ha'9'" .. nd COpy 10 Ph .. ,m.cy. i
I • ........... ATlrHd Ql"rnp.D SHEET
WHO/MNC/82.2 Appendix III Rev. 1 page 232
311 3 1-hs_l
PATlEN! 1 ""IE AGE 1 -AOOM PATI£NT HO. "0. OUf; . .. :
"'UTI! '''SURANCE CLAIM "0. _____ .. ___ ._ ATT£NOI"G PHYSIC.A,. PHON [
DATE
HOUR I~ 11.'-, ;I
W' +1 B.P. · , ,
240 ' . .
230 :
T I .
220
210
200
~L I : 190 I-
180
I-170 c:
1-7- c: I
160 C
e II. C
ISO
~ (/ (/ l! 1.c0 C
" I - r. 'no : (
: : c c 120
a 110 ...:. . .
1I · . 100 · -· - . 90 .
10 :-.---- , : I ~ L: 10 : : ~l < ., . '-· - .
" .
H4-' 50 · ., ~ ...... .
! ~ : F:R: '-.., ~
.") ..... ? .'"' 1--L . . .
t:::""~; ~lh.' 't U ..;.;v 108 I I ..x. .
1 ~ J' ~ 4-?'-'~-64

-
WHO/MNC/82.2 Appendix III page 233
Rev. 1
LAKEVIEW MEMORIAL HOSPITAL
'Jte _' _'_:---!.I_-_'..,(~;..;-;G",',,_. --,80.:..,,,,,0_ Time 01 Interview ~Cf/f'l How arrived _--Lt.G4t.::yJ"-f~:";".l...C: __ ~'_· -._....,.-_____ ---,-__ ronunci.lliol1 Wan, t~ tCY beaddrttssed as __ .f.Jl'.I.(J~~1'J,.d1"'1o::1·'~:':::/=---_______ _
,dmitted from_--,C~2a""Y:":";LJ!..J ,,,,,.~t""':'r.aL'':'''':''·--7/./.,,,I-,-,-____ Accompanied by ~~ '. :. ! '. Oc~upation _________ .,.-_ 1)ltts 7. , .PJven to rela)ivc;>l.N.ame) Safe __ ' _
",~i9I1S: T <J? P--FL,~ R~BP 1!JJ-/.lQWt. /!j'2.:r"!- Chair;( Standing ____ _
.troduction to or cXIJlanation of: Articles with Patient: Check: Yes No Yes No ---
ivilelWS ,>j' Upper Denture X de rails & bed controls ..... Lower Denture X V Radio cost '. V Loose bridge ~'
lone V Partial plate :r ) band v Ring , Jthroom-towels,' etc. v Watch )r
rine spec. v Glasses .Y
gnal Cord >/ Contact Lenses )f
Hearing Aid ~
JHent Medications: Artificial Eye ;-
limb ~' . Other ..
Crutches :'<
Walker .' Cane I-Brace " )M1eelchair ) . . -'\:~.~(:{ Disposition of Meds: ___________ _
"tlirth Control Pjll~
,'.' "'.'
FOOd~~.tls.-li~~~~i~~~"~~m-----------------------------________ _ .' J",t'+-
" /1:{ "/,~,,
B/wel and blad~er habit~: Last 8.M. ,,Does anythin~ help? ________________ _
I .~ .' ,i (' I I .'i ";' ,: I a' ,J/ I' .) /. /I " (/' .:..", .) ... \ ,: I /t' ,,'. I. ,- " (. i ' " . ' /
Sleep habits: Do you take anything for sleep? -It ,f,! ..'?, • Do you get up at night? i!.:. ' Why? ..;u ...... ·:..; ..; .. .:..i..t.:.I:..-:...r .... /_.I~."f_;j'-I-__., ...:. .. ~ . ... ~, . f' 141 f' )' '. j"
5, Smoking: Yes or No_....r;,;.;.:/t.:.:,! __ How much __ --______ _
Are you bothered by smoke? __ ~iL··:.. • .:.,""',-i-----------
~':.7Ij-r,
~; ·~I.l . ~:;r, ~ :;,:.. '.; it - ;~ , - ~ ': - (j .1
, over , NURSING OAT A BASE
250 - .-
WHO/MNC/82.2 Appendix III Rev. 1 page 234
Reason for hospitalization, precipitating factors, initial observations. W.hat type of treatment did you and
your 9octor plan for? / /' ~, h ' •• , •
,i . I .. , ,-l •. .. ....... ",' ,. /", (',
".1 /; /
I ~II' ,'';'/ \: ... I
" ,. .. "/ -'," \ //.> .j II I. .. I 'l • .... : .',:. ,'Jr..<> J. <..(,. /.. .. ', / - ,,(:
Past hospitalizations: When - Why ~ Any spef!ial memories?
<~I".',I '71 (JIlt (II./TI/;If.1..1 /'I,.JI,/~ ... J
z .., ,";/
/~J / _..--.'.. ....
Do you have any difficulties other than present illness for which you are being treated?
I ,-' llJ '- t II J ,.;1 , ./ .,./ !,J./.--J
.j ,. 7 I '. I,'"
/ , .. .' ~'i.." ~-'!j. ) ..... :... '
Significant personal family and planning neeqed. -!-
~ . . <7 11/(1_)/
Ii /.,.,. , , . " c'" '"
social factors
{I 1
(relatives, friends, legal guardian, etc.) ( ') i
. ./_I.~!' I j :) !,r _ ~.,<! / .; '-1 '.') e / ' . . 1
Special discharge
f ) I // (,-1
--------------------------------------------~,
. /, . ,- ~, / ." , .
'"j I':' ','
I) I 1-.... 1, 1,-, .. .14 \.
1·--~--------~)~----7/~· ------------____________________ ~--------~ Y 7 -
'" i 3. ~ 4. ~
, r Admitting Nurse _...:......:......._ .. ..:.'--....:...-.-:.......t......:.._:--.:.....-----
Infor~ant

WHO/MNC/82.2 Appendix III Rev. 1 page 235
......... ...,..:. ---~-------.----PROBLEIf OOAL NURSING PLAN 1111:
--- -_._-------
-- .- .. ---~ ~.-., ... _---_._---..
-------
- - .- --____ .I--_______ ~L:L-..J.-~..;II...:.-----_; +<'-£. _ H _._ ... _____ • ____ _ ---------t---.---.------.. ---------. ,
~.- ----------+--~----..:.---I---------_t_-::-. -- -;---"..-----I--------~I__--------t__-.. -
-- ------------1---------4-----------1-
. - ... - . ., .- ... --..,...- .. _---. . ' ..
.. _- "'---_. - ................... - - ----- ----_ .. __ ... _. ' .... -- ' .
________ ---.-..f-------.. _ .. _·.0_ .--
---~--------------4~--------------~----------------r_-
2C.7t.-~-6
L~ :ChLlZ ~O~ ~~ye~ 4-21-;:-·4

WHO/MNC/82.2 Appendix III Rev. 1 page 236
•..
- .......... - ,.7"_ ............ , •• "
NURSE'S NOTES
NURSE'S NOTES
rA - and Time
--------+ . --_ ... _ ... --_ ... __ ..
NURSE'S' NOTES
WHO/MNC/82.2 Appendix III Rev. 1 page 237
~ ________ ROOM NO ____ ' __
Nurse-s Name
~'" --- .. ---.-~-: ..... -: ..• --------- ---. -----. --- _ ... _--------!----¥-,--- ~.-- _ .. -------1
I
• PI . •• NURSE'S NOTES
p.
WHO/MNC/82.2 Appendix III Rev. 1 page 238
Jlt! allu T ,01.,
. -f!f"""f9'\ 12." 8'''GGS tkt~ Mo." ... '0-. ~O:)06. ".~,,,,T{O'" V S A
NURSE'S'NOTES
DOCTOR. -- .. - ;,. ... ROOM NO. ~ __ _
NURSE'S NOTES
NUR9E'9NOTE9
WHO/MNC/82.2 Appendix III Rev. 1 page 239
:;""-''!!!!III !!!!!!"_....:.;.------~.--.---.~---- DOCTOR ---~--------- ROOM NO. -----
Nurse's Name
,.
--------f-------.---.-- ----------- ----- .-----,
------+---------- ----------------- -'--.-------------.--.. -----t--
-----+----- ----------------------
_----f----------------- --- --.- .------.-.
-------_._- ... _---
-~-- ----- -
'.nl ... ·• I, .... 1, ~,. NURSE'S NOTES
===




















